







Bahasa
Halaman
Hukum


The debridement of chronic wounds:a systematic review
M BradleyN CullumT Sheldon
HTAHealth Technology Assessment NHS R&D HTA Programme
Health Technology Assessment 1999; Vol. 3: No. 17 (Pt 1)
Review

How to obtain copies of this and other HTA Programme reports.An electronic version of this publication, in Adobe Acrobat format, is available for downloading free ofcharge for personal use from the HTA website (http://www.hta.ac.uk). A fully searchable CD-ROM isalso available (see below).
Printed copies of HTA monographs cost £20 each (post and packing free in the UK) to both public andprivate sector purchasers from our Despatch Agents.
Non-UK purchasers will have to pay a small fee for post and packing. For European countries the cost is£2 per monograph and for the rest of the world £3 per monograph.
You can order HTA monographs from our Despatch Agents:
– fax (with credit card or official purchase order) – post (with credit card or official purchase order or cheque)– phone during office hours (credit card only).
Additionally the HTA website allows you either to pay securely by credit card or to print out yourorder and then post or fax it.
Contact details are as follows:HTA Despatch Email: [email protected]/o Direct Mail Works Ltd Tel: 02392 492 0004 Oakwood Business Centre Fax: 02392 478 555Downley, HAVANT PO9 2NP, UK Fax from outside the UK: +44 2392 478 555
NHS libraries can subscribe free of charge. Public libraries can subscribe at a very reduced cost of £100 for each volume (normally comprising 30–40 titles). The commercial subscription rate is £300 per volume. Please see our website for details. Subscriptions can only be purchased for the current orforthcoming volume.
Payment methods
Paying by chequeIf you pay by cheque, the cheque must be in pounds sterling, made payable to Direct Mail Works Ltdand drawn on a bank with a UK address.
Paying by credit cardThe following cards are accepted by phone, fax, post or via the website ordering pages: Delta, Eurocard,Mastercard, Solo, Switch and Visa. We advise against sending credit card details in a plain email.
Paying by official purchase orderYou can post or fax these, but they must be from public bodies (i.e. NHS or universities) within the UK.We cannot at present accept purchase orders from commercial companies or from outside the UK.
How do I get a copy of HTA on CD?
Please use the form on the HTA website (www.hta.ac.uk/htacd.htm). Or contact Direct Mail Works (seecontact details above) by email, post, fax or phone. HTA on CD is currently free of charge worldwide.
The website also provides information about the HTA Programme and lists the membership of the variouscommittees.
HTA

The debridement of chronic wounds:a systematic review
M Bradley1*
N Cullum2
T Sheldon3
1 NHS Centre for Reviews and Dissemination, University of York, UK2 Centre for Evidenced Based Nursing, University of York, UK3 York Health Policy Group, University of York, UK
*Corresponding author
Competing interests:none declared
Published September 1999
This report should be referenced as follows:
Bradley M, Cullum N, Sheldon T. The debridement of chronic wounds: a systematic review.Health Technol Assess 1999;3(17 Pt 1).
Health Technology Assessment is indexed in Index Medicus/MEDLINE and Excerpta Medica/EMBASE. Copies of the Executive Summaries are available from the NCCHTA web site(see overleaf).

NHS R&D HTA Programme
The overall aim of the NHS R&D Health Technology Assessment (HTA) programme is toensure that high-quality research information on the costs, effectiveness and broader impact
of health technologies is produced in the most efficient way for those who use, manage and workin the NHS. Research is undertaken in those areas where the evidence will lead to the greatestbenefits to patients, either through improved patient outcomes or the most efficient use of NHS resources.
The Standing Group on Health Technology advises on national priorities for health technologyassessment. Six advisory panels assist the Standing Group in identifying and prioritising projects.These priorities are then considered by the HTA Commissioning Board supported by theNational Coordinating Centre for HTA (NCCHTA).
This report is one of a series covering acute care, diagnostics and imaging, methodology,pharmaceuticals, population screening, and primary and community care. It was identified as a priority by the Pharmaceutical Panel and funded as project number 93/29/01.
The views expressed in this publication are those of the authors and not necessarily those of theStanding Group, the Commissioning Board, the Panel members or the Department of Health.The editors wish to emphasise that funding and publication of this research by the NHS shouldnot be taken as implicit support for the recommendations for policy contained herein. Inparticular, policy options in the area of screening will be considered by the National ScreeningCommittee. This Committee, chaired by the Chief Medical Officer, will take into account theviews expressed here, further available evidence and other relevant considerations.
Reviews in Health Technology Assessment are termed ‘systematic’ when the account of the search,appraisal and synthesis methods (to minimise biases and random errors) would, in theory, permitthe replication of the review by others.
Series Editors: Andrew Stevens, Ruairidh Milne and Ken SteinEditorial Assistant: Melanie Corris
The editors have tried to ensure the accuracy of this report but cannot accept responsibility forany errors or omissions. They would like to thank the referees for their constructive commentson the draft document.
ISSN 1366-5278
© Crown copyright 1999
Enquiries relating to copyright should be addressed to the NCCHTA (see address given below).
Published by Core Research, Alton, on behalf of the NCCHTA.Printed on acid-free paper in the UK by The Basingstoke Press, Basingstoke.
Copies of this report can be obtained from:
The National Coordinating Centre for Health Technology Assessment,Mailpoint 728, Boldrewood,University of Southampton,Southampton, SO16 7PX, UK.Fax: +44 (0) 1703 595 639 Email: [email protected]://www.hta.nhsweb.nhs.uk

Health Technology Assessment 1999; Vol. 3: No. 17 (Pt 1)
List of abbreviations .................................... i
Executive summary ..................................... iii
1 Introduction .................................................. 1Mechanical debridement ............................... 1Non-mechanical debridement ...................... 2
2 Methods ......................................................... 3Literature search ............................................ 3Study selection and data extraction .............. 3Data synthesis ................................................. 3Assessment of outcome measures ................. 3
3 Results ............................................................ 7Debriding agents versus traditional or control therapy ............................................... 7Comparisons between debriding agents ....... 9Cost-effectiveness ............................................ 9
4 Discussion ...................................................... 19
5 Conclusions ................................................... 23Implications for policy ................................... 23Recommendations for research .................... 23
Acknowledgements ...................................... 25
References ..................................................... 27
Appendix 1 MEDLINE search strategy ....... 31
Appendix 2 CINAHL and EMBASE search strategy ................................................. 33
Appendix 3 Additional databases searched .......................................................... 35
Appendix 4 Expert advisory panel .............. 37
Appendix 5 Quality assessment ................... 39
Appendix 6 Summary of studies ................. 41
Health Technology Assessment reportspublished to date .......................................... 71
Health Technology Assessment panel membership ........................................ 75
Contents


Health Technology Assessment 1999; Vol. 3: No. 17 (Pt 1)
i
List of abbreviations
C comparator*
I intervention*
CI confidence interval
CRD Centre for Reviews and Dissemination
ES effect size
F female*
HTA Health Technology Assessment
ITT intention-to-treat
M male*
NS not significant*
OR odds ratio
RCT randomised controlled trial
SD standard deviation*
SEM standard error of the mean*
* Used only in tables and figures


Health Technology Assessment 1999; Vol. 3: No. 17 (Pt 1)
iii
BackgroundA wide variety of debridement methods andproducts are available, all of which have diverseproperties, costs and levels of acceptability. There is currently wide variation in their use and a lack ofconsensus on how to treat specific wound types.
Objectives
• To summarise the evidence for the relativeeffectiveness and cost-effectiveness of differentdebriding agents on wound healing.
• To identify areas for future research.
Methods
Data sourcesA range of electronic databases and several woundcare journals were searched; organisations, manu-facturers, researchers and healthcare professionalsconcerned with wound care were contacted foradditional trials. The reference sections of obtainedstudies were also searched for further trials.
Inclusion criteriaStudies were considered for inclusion if they wererandomised controlled trials (RCTs), published orunpublished, that assessed the effectiveness of arecognised debriding agent as identified by anexpert panel, and assessed patients with chronicnon-healing wounds (pressure sores, leg ulcers,sinuses and surgical wounds healing by secondaryintention). Studies were only included if they used aquantifiable and objective measure of healing rate.
Data synthesisFor each trial an odds ratio and/or effect size was cal-culated for all objective outcomes. Where possible theanalysis was performed on an intention-to-treat basis,and 95% confidence intervals were included when suf-ficient detail to allow their calculation was provided.
Results
Forty-seven reports describing 35 RCTs wereidentified that met the inclusion criteria.
InterventionsThe following interventions were identified asagents that would be used primarily for wounddebridement.
• Dextranomer polysaccharide beads or paste• Cadexomer iodine polysaccharide beads
or paste• Hydrogels• Enzymatic agents• Adhesive zinc oxide tape• Surgery or sharp debridement• Larval (maggot) therapy.
Other interventions that are believed to have adebriding function, such as hydrocolloid dressingsand antibiotics/antiseptics, were not included inthis review as debridement was not the primaryreason for their application.
No RCTs were found that evaluated the effective-ness of surgical debridement, larval therapy, or thatcompared debridement with no debridement.
Dextranomer polysaccharide beads or pasteversus traditional or control treatmentNine trials met the inclusion criteria, five of whichfound a statistically significant difference betweentreatments: three favoured dextranomer poly-saccharide, and two favoured traditional treatment.
Cadexomer iodine polysaccharide versustraditional or control treatmentNine trials met the inclusion criteria, of whichthree had a statistically significant result thatfavoured cadexomer iodine polysaccharide.
Hydrogels versus traditional or control treatmentOnly one trial out of four that compared ahydrogel with a traditional or control treatmentfound a statistically significant difference betweentreatments, which suggested a small benefit from treatment with a hydrogel dressing compared with a hydrocolloid dressing.
Enzymatic agents versus traditional or control treatmentNone of the five trials in this category showed astatistically significant outcome in favour of eithertreatment for wound closure. In fact, one trial
Executive summary

Executive summary
iv
showed an increase in wound size with both theenzyme collagenase and the control treatment;however, the increase was significantly less in theenzyme-treated group.
Adhesive zinc oxide tape versus traditionaltreatmentA single trial meeting the inclusion criteria showed that adhesive zinc oxide tape was moreeffective in eradicating or reducing by more than50% the necrotic area of diabetic foot ulcers than a hydrocolloid dressing.
Cadexomer iodine polysaccharide versus otherdebriding agentsTwo trials were comparisons with dextranomerpolysaccharide and one trial was a comparison with a hydrogel. None of the trials had statisticallysignificant results.
Dextranomer versus other debriding agentsFour RCTs comparing dextranomer polysaccharidewith another debriding agent included two trialswith enzyme formulations, namely collagenase andstreptokinase/streptodornase, and two trials usinga hydrogel as the comparator. Only one of the twocomparisons with a hydrogel showed a statisticallysignificant benefit associated with the hydrogel.
Hydrogel versus hydrogelA single trial was found. There was no statisticallysignificant difference between the two treatments.
Enzymatic agent versus enzymatic agentOne trial that compared the enzyme preparationstreptokinase/streptodornase with the enzymetrypsin was included in the review. No statisticallysignificant difference between the two treatmentswas found.
Cost-effectivenessCost-effectiveness has not been thoroughly assessedin studies of debriding agents. The unit cost foreach treatment is stated in some studies, and a fewcontain further details on other important vari-ables, such as nursing time or number of dressingchanges. However, no study provides sufficientdetail from which a reliable cost-effectivenessanalysis can be constructed.
Conclusions
No studies were found that compared debridementwith no debridement and without these studies it is
unclear whether wound debridement is a beneficialprocess that expedites healing.
There is insufficient evidence to promote the use of one debriding agent over another. There was only a single comparison between twodebriding agents that produced a significant result (hydrogel significantly reduced necroticwound area compared with dextranomerpolysaccharide paste).
Implications for policyThere is little evidence to identify which agents are the most effective. Pending the availability ofimproved data on relative effectiveness, otherconsiderations, such as cost-minimisation, mayreasonably guide decisions on the use of debriding agents.
Recommendations for researchMuch of the research is of poor quality, and direct comparisons are few. In the trials reviewed,sample sizes were rarely sufficient to detectclinically important effects, and poor baselinecomparability frequently confounded outcomemeasures. Several important messages can beidentified for future studies.
• Recruitment numbers should be based on asample size calculation.
• The proportion of wounds healed should beused as an objective outcome measure. Wherehealing rates are based on wound area, both thepercentage and absolute change in area shouldbe given.
• Experimental groups should be comparable at baseline.
• Baseline data and intervention details shouldalways include a thorough description of how the patients were nursed and report the use of concurrent treatments, including secondary dressings.
• Comparisons between debriding agents are required and should use agents that are recommended for wounds of a similar nature.
• Assessment should be blind to treatment.• Survival rate analysis should be adopted for
all studies that assess wound healing.• All RCTs should be published.• Detailed cost-effectiveness analyses should be
seen as a priority for future trials.• The frequent use of surgical debridement
and the increasing interest in larval therapyindicate that RCTs in these areas are needed.

Health Technology Assessment 1999; Vol. 3: No. 17 (Pt 1)
1
Wound healing is an efficient and naturalprocess that normally requires no special
treatment. However, chronic non-healing woundscan occur when there is some underlying factorpreventing healing, and in such cases interventionis considered necessary. For example, pressuresores are initially acute wounds caused by ischaemicdeath of tissue due to excessive pressure and willusually heal readily when pressure is relieved andthe blood supply restored. However, in certainpatients, particularly the elderly and persons withlow mobility, it may not be easy to resolve thesecausative factors and chronic wounds can develop.
A characteristic of most chronic wounds is anaccumulation of devitalised tissue and cellularexudate at the outer surface. These products resultfrom a restriction of nutrients to the damagedepithelium and form either a dry, hard eschar or, as in the case of deep moist wounds, a slough thatfrequently hardens on the outside with exposure to the air. The accumulation of these products in the wound bed is generally regarded, though not experimentally proven, to prevent or delaygranulation and epithelialisation. The removal of this tissue by a process termed debridement istherefore thought to facilitate healing.1
Although the clinical evidence in support ofdebridement is lacking, treatment is regarded as a necessity for patient acceptability and for the prevention of infection:2 moist slough ismalodorous and visually repugnant, and providesan ideal culture medium for pathological organ-isms. The treatment of infection with topicalprophylactic antibiotics is often unsuccessful in sloughy wounds as the active agent is unable to penetrate and diffuse through the necroticdebris. Debridement will remove this barrier and may thereby assist in the treatment of infection.
Although many products used during the treat-ment of a wound may have a debriding function,only a few are commonly used specifically for this purpose. Despite having diverse properties,costs and levels of acceptability, these specificdebriding agents can broadly be classified asmechanical or non-mechanical interventions (Table 1 ).
Mechanical debridementSurgical or sharp debridement has been practisedfor several centuries and is still commonplacetoday. The technique is simple, requiring only the use of sterile scissors or a scalpel, but it doesrequire some degree of skill to avoid aggravatingthe wound. It is considered that sharp debridementis best suited to wounds where there is a cleardistinction between healthy and devitalised tissueand where a patient is unlikely to experiencesignificant pain.2
Bio-surgery, which exploits the feeding behaviourof certain insect larvae, has an equally long medicalhistory and is presently enjoying a resurgence ofinterest.3 Sterile maggots (fly larvae) are consideredideal debriders, having a ferocious appetite fornecrotic material while actively avoiding newlyformed healthy tissue.4 Maggots are placed directlyonto the affected area and held in place by a close-net-dressing.5 These animals may also perform anantimicrobial role that is beneficial for woundhealing, as the antibacterial agent allotoxin isactively excreted from the maggot’s body.2 Evi-dence for clinical effectiveness is restricted to casereports and expert opinion; it remains untested by randomised controlled trials (RCTs).
Wet-to-dry debridement is used infrequently in theUK but is common in many European countriesand the USA. The wound is soaked in saline tomoisten hard material before the application of a moist gauze pad over the affected area. As thedevitalised tissue drys it re-hardens and becomes
Chapter 1
Introduction
TABLE 1 Classification of debriding agents2
Mechanical Non-mechanical debridement debridement
Surgery (scalpel) Polysaccharide beads or paste (dextranomer,
Wet-to-dry dressings cadexomer iodine)(saline gauze)
Enzymatic agents Bio-surgery (maggot larvae) (streptokinase/
streptodornase,trypsin, collagenase)
Hydrogels

Introduction
2
attached to the gauze, when the dressing ischanged the adhered material is pulled free.6
This method is less discriminating than thosepreviously discussed, removing both healthy andgranulating tissue from the wound bed. Patients are known to experience pain, and newly formedepithelial tissue may be significantly damaged.7
Non-mechanical debridement
Non-mechanical techniques have becomeincreasingly popular for wound cleansing. Thesetreatments are usually easy to apply and may haveadditional properties that are beneficial for woundhealing. Such interventions include enzymes,hydrogels and specific chemical formulations, such as cadexomer iodine and dextranomer.
Several different enzyme preparations are available that digest slough and necrotic tissue. In the UK, only the formulation containingstreptokinase and streptodornase (VaridaseTopical®, Wyeth Laboratories) is licensed for use.8 This enzyme aggressively digests the proteinsfibrin, collagen and elastin which are commonlyfound in the necrotic exudate of a wound.9
Other enzymatic debriding agents are available and used internationally; these include trypsin and collagenase.
Dextranomer polysaccharide is supplied asanhydrous, porous beads with a diameter of 0.1–0.3 mm or as a paste. The beads are highlyhydrophilic and rapidly absorb exudate from anecrotic sloughy mass. Prostaglandins, hormonesand other relatively small molecules enter thematrix of the beads, while larger particles such asbacteria and wound debris become concentrated at the surface of the dextranomer layer. When the beads are changed by washing with saline the absorbed and trapped necrotic material is removed.10
Cadexomer iodine is similar to dextranomer,consisting of small spherical beads that are
hydrophilic in nature. The beads are made from amodified starch infused with iodine at a concentra-tion of 0.9%. Absorption of fluid from the woundresults in a slow controlled displacement of iodinefrom the matrix, which acts as a bactericidal agent.10
The slow and consistent release of iodine overcomesthe problem of iodine inactivation by protein ab-sorption in the wound. The antibacterial property,biodegradability and high rate of fluid absorptiondistinguish cadexomer iodine from dextranomer.
Hydrogels are a group of agents that were pri-marily developed as debriding agents. These gelsare biologically inert and have a significant watercontent. They complement the body’s naturaldebriding process by providing an advantageousenvironment for autolysis, while still acting topreserve living healthy tissue.2 The hydrogel isusually applied directly into the wound bed andheld in place by a non-adherent dressing. Once the gel is fully hydrated it is unable to absorb thecopious quantities of exudate that are released bysome wounds. For this reason hydrogels are oftenused in conjunction with a highly absorbent dress-ing. In addition to the amorphous gel, hydrogelsare also available in a sheet form. Several types of hydrogel are available manufactured underdifferent trade names (Intrasite® Gel, Smith &Nephew Healthcare Ltd; Sterigel®, Seton Health-care Group plc; Granugel®, CovaTec UK Ltd).
In clinical practice there is wide variation in the use of debriding agents and no consensus on whichagent is most appropriate for each type of wound.11
As a result, many clinicians combine debridingagents in a dual or triple therapy in an attempt to maximise healing rates, but such measures areuntested and are not endorsed by manufacturers.This review, commissioned by the NHS HealthTechnology Assessment (HTA) Programme,attempts to summarise the evidence to date for the relative effectiveness and cost-effectiveness ofthese different interventions and to identify thegaps in our research knowledge. In this way it ishoped that clinical practice may better reflect the results of scientific research.

Health Technology Assessment 1999; Vol. 3: No. 17 (Pt 1)
3
Literature searchA systematic review of primary research wasundertaken using the NHS Centre for Reviews and Dissemination (CRD) structured guidelines.12
Nineteen electronic databases of medical literaturewere searched up to October 1997 using a sensitivesearch strategy designed in collaboration with aninformation specialist in CRD (appendices 1–3).This was supplemented by a handsearch of fivespecialist wound care journals, twelve conferenceproceedings and systematic reviews held on theNHS CRD Database of Abstracts of Reviews ofEffectiveness (DARE). The bibliographies of allretrieved and relevant publications were searchedfor further studies. Companies with an interest inwound care products were approached for un-reported trials. An advisory panel of experts inwound management, established to comment on the review as it progressed, were also asked toidentify any additional trials (appendix 4). Rele-vant economic studies were identified by addingeconomic-related search terms to those used in thesearch for clinical trials. Authors of trials publishedafter 1985 were contacted and asked to providedetails of any trial-based economic evaluations.
Study selection and data extractionRetrieved studies were assessed by a single reviewerfor relevance to this review, and decisions on finalinclusion were checked by a second reviewer;disagreements were resolved through discussion.Trials, irrespective of date, language and publi-cation status, were included if they were human-based RCTs, which evaluated the efficacy of arecognised debriding agent in relation to woundhealing and had an outcome measure that wasconsidered an objective measure of healing. Where study details were lacking the authors were invited to provide further information.
Many treatments commonly used in woundmanagement may have a debriding function; only a few, however, are specifically used for thispurpose. An expert panel was consulted to identifythose treatments that they believed were primarilyused for debridement. The panel identified
the following interventions as debriding agents:dextranomer polysaccharide, cadexomer iodinepolysaccharide, hydrogels, various enzymaticagents, adhesive zinc oxide tape, surgery and larval therapy. Other interventions such as hydro-colloid dressings and antibiotics/antiseptics werenot considered by the panel to be debriding agentsas debridement may occur only as a secondaryfunction following their application rather thanbeing the primary reason for their use.
Data from included trials were extracted by a single reviewer into data extraction tables and thenchecked independently by a second reviewer.
Data synthesis
For each trial an odds ratio (OR) and/or effect size (ES) was calculated for all objective outcomes.Where possible the analysis was performed on anintention-to-treat (ITT) basis and 95% confidenceintervals (CIs) were included when sufficient detailto allow their calculation was provided. The resultsfrom each study were plotted onto graphs, andindividual study details are presented in structuredtables containing information relevant to studyvalidity. Heterogeneity between studies indicatedthat pooling of results would be inappropriate.Studies varied in duration of follow-up, nature ofthe comparator treatment, wound types, settingand baseline comparability of patient groups.
Assessment of outcome measures
A single standard outcome measure for woundhealing does not exist. Both objective and subjec-tive measures are widely used by researchers butlittle effort has been made to determine the validity of these measurements.
Most subjective outcomes, such as estimates ofoedema, erythema, granulation, pus and debris, are unlikely to be measured consistently betweenwounds. Unless assessment is blinded to treatmentallocation, subjective outcomes are likely to resultin significant biases. For example, in one trialcadexomer iodine was judged by visual assessmentto be more effective than dextranomer, but a later
Chapter 2
Methods

Methods
4
assessment of quantitative planimetric resultsindicated that there was no difference between thetwo treatments.13 This appears to be a characteristicfeature of research in this area; subjective measure-ments almost invariably overestimate the relativeeffectiveness of the experimental treatment com-pared with objective measures in the same trial.
Objective measures of debridement are usuallybased on wound area. Planimetry, often aided bycomputer assessment, is the most frequently usedtool for calculating wound area, though othermethods, such as the measurement of wounddiameter or the weight of a celluloid tracing drawnaround the area of the wound, are also used.
Measurements of wound volume are infrequentlyreported in the literature. These methods are oftencumbersome and their accuracy has not been suffi-ciently demonstrated.14 Computerised image ana-lysis may in the future, as the equipment becomesmore affordable and portable, prove to be a usefultechnique for the assessment of wound volume.15
However, even though objective measures reduceor eliminate subjective biases and reduce randommeasurement errors, they have certain inherentbiases if the patients being compared have woundswith different baseline size.
A change in wound area is often expressed as thepercentage change, which unlike the absolutechange in area, takes into account the initial size of the wound. For two wounds healing at the samelinear rate (as measured by diameter reduction),percentage area calculations will show a largerchange for a small wound than a big wound. Theconverse is true when the absolute change in area is measured, as for any unit reduction in woundradius a bigger area reduction will occur for a largewound. This has important consequences for thevalidity of trial results, where there is poor com-parability in initial wound size at baseline betweenthe treatment groups. This is illustrated in Table 2.
In large trials, random allocation should ensurethat the mean wound size and variance in eachgroup are similar. In a small trial, random allo-cation is unlikely to result in an even distribution of wound sizes. This problem will persist in smalltrials, even when the average wound size appears to be comparable between groups, because thedistribution of wound sizes about the mean is likelyto differ. This is illustrated in Table 3.
In a trial where there is poor comparabilitybetween groups for wound size at baseline, and the
outcome is based on the change in area, the resultcan only be considered valid if it is obtained eitheragainst the anticipated direction of the bias forwound size, or where percentage area change andabsolute area change are in the same direction. Ifbaseline data are not given then it is not possible todetermine the direction of bias and the validity ofthe result cannot be assessed.
The change in area of a wound also assumes alinear rate of healing or at least a predictable rate.However, this may not always be the case, with somewounds enlarging prior to healing while othersinitially decrease rapidly in size before experi-encing a slower rate of healing. For this reasoncomplete healing is seen as the most valuableoutcome in studies of wound healing. Unfortun-ately, to follow all wounds to complete healing canrequire an extended period of follow-up that is notideal for most studies, where financial resourcesand time are limited. For this reason many studies
TABLE 2 Percentage and absolute measures of wound healingcan give different results for relative effectiveness
Group A Group B
Baseline mean area (cm2) 50 60
Follow-up mean area (cm2) 35 43
Mean of % reduction in area 30 28
Mean absolute reduction in area (cm2) 15 17
Using % change, wounds in group A appear to have healedmore rapidly than those in group B. The converse is true whenthe outcome is expressed as absolute change in wound area
TABLE 3 Groups with similar means may have differentdistributions
Group C Group D
Wound size at baseline (cm2) 10, 10, 30, 30 4, 4, 4, 70
Mean area (cm2) 20 20.5
Standard deviation (SD) 11.5 33
Groups C and D have approximately the same mean area. If both groups of wounds heal at the same rate (thetreatments are equally effective) it could be expected that thethree small wounds in group D will heal before those in groupC.Therefore measuring outcome based on the number ofwounds healed within a certain time period will be biased.Similarly, the percentage change in area will appear greater in group D, while the absolute change in area will appeargreater in group C

Health Technology Assessment 1999; Vol. 3: No. 17 (Pt 1)
5
in the literature report changes in wound sizerather than complete healing.
Despite the potential for the objective outcomesdiscussed to be biased by differences in wound
size at baseline or by the variability of healing rate between wounds, they remain the most reliable assessment of wound healing as theyreduce the bias of the assessor, which cannot be estimated.


Health Technology Assessment 1999; Vol. 3: No. 17 (Pt 1)
7
Atotal of 47 RCTs met the review inclusioncriteria. Twelve studies (26%) had a shared
data set with another publication, and of these: two contained interim results later published in full,16,17 three were reproduced as paperspresented at international conferences,18–20 one was presented at an international conference and later published as a drug company bulletin,21
six studies were repeat publications of resultspreviously published in other journals,22–27 two of which22,23 were identical to a previouslypublished paper,28 except for a change in the first author. Where duplication occurred andsufficient detail could not be extracted from asingle publication, the studies were pooled andincorporated to represent a single trial entry. In total, 35 individual trials from the 47 relevant publications were identified for inclusion.
The majority of trials had methodologicalweaknesses (appendix 5, Table 4 ). Fewer than 10% of studies reported an a priori estimate of the number of participants required to havesufficient power to detect a clinically importanteffect as statistically significant. It was rare for a trial to have more than 50 patients in each arm, and typically fewer than 30 wereincluded. Twenty-six per cent reported that the outcome had been assessed by someone blind to treatment allocation. Appropriate patient characteristics were recorded by treatment group in 90% of studies, but ulcer size at baseline was reported in only 62%.Withdrawals occurred in most trials and wererecorded by group and cause in 72% of trials where it was appropriate, but less than one fifth performed an ITT analysis. Seventy-four per cent of trials clearly stated the inclusion criteria for patients to the trial, but informationthat indicated whether or not that participants had been truly randomised to alternativetreatments was given in only 37%.
Figures 1–7 show the OR and/or ES calculated from the results for each of the included studies.Where possible, ITT analysis has been used; where such analysis was inappropriate the sample size used in the calculation is given in parentheses.
Debriding agents versus traditional or control therapy Twenty-eight trials compared a recogniseddebriding agent with a traditional or controltherapy. The definition and nature of traditionaltherapy varied widely between trials. In many trials,a single traditional treatment was not used in thecomparative group, in extreme cases a differenttreatment regimen was used for each patient in the control group. The absence of a singlestandard comparator makes interpretation of the results across studies difficult.
Dextranomer polysaccharide versustraditional or control treatment Nine RCTs met the inclusion criteria (Figure 1;appendix 6, Table 5). Four trials showed astatistically significant result, three of whichfavoured treatment with dextranomer poly-saccharide,29–31 and one which favoured treatment with calcium alginate dressings.32
In an additional trial, the author’s own statis-tical analysis indicated a significant improve-ment for those wounds treated with a collagen sponge dressing when compared withdextranomer.33 However, insufficient data were available to test the analysis further. The remaining four trials had statisticallyinsignificant results.34–37
Trials of dextranomer polysaccharide versustraditional or control treatment can be groupedinto categories which are defined by the nature of the comparative therapy.
Dextranomer polysaccharide versus EusolTwo small studies compared dextranomer poly-saccharide with Eusol; both were unable to detect a statistical difference between the treatments.35,36
The study by Nasar and Morley36 was confoundedby the switching of treatment for three wounds that were considered to be healing slowly from the Eusol group to the dextranomer group. These patients were excluded from the analysisbecause of the bias that was hence introduced. In this same study, the cost of materials for average treatment time was calculated, and showed that Eusol was 1.6 times more costly than dextranomer.
Chapter 3
Results

Results
8
Dextranomer polysaccharide versus saline soaks Saline soaks were evaluated against dextranomerpolysaccharide in two trials, which were bothconducted over a 2-week period.31,34
The trial by Eriksson and co-workers34 found nostatistically significant difference between thetreatments for the percentage of ulcers healed by50% or 25%. The trial by Sawyer and co-workers,31
however, found a statistically significant effect infavour of dextranomer beads for the healing ofvenous leg ulcers. Despite the absence of baselinedata in this latter trial it is unlikely that such a large difference in healing rates between the twotreatments could be explained merely in terms ofpoor group matching at baseline.
Dextranomer polysaccharide versus othertraditional or control therapiesOne study found that dextranomer poly-saccharide beads were significantly more effective than povidone-iodine for the treat-ment of venous leg ulcers.29 However, high dropout rates were reported, which could have introduced a bias. Dextranomer poly-saccharide beads have also been found to be more effective when compared with antiseptic/antibiotic treatments.30 This is in contrast to a small study comparing dextranomer poly-saccharide beads with an air dried combination of sugar and egg white, which did not find astatistically significant difference between the two treatments.37
Dextranomer polysaccharide paste was out-performed by calcium alginate dressings for the healing of pressure sores over an 8-weekperiod.32 These results were statistically signifi-cant despite a bias that favoured the smaller sores in the dextranomer polysaccharide group.
Insufficient data were provided to determine the CIs required to test statistical significance in a study that compared dextranomer beads with a collagen sponge dressing.33 However, theauthor’s own analysis suggested a statisticallysignificant reduction in healing time occurred with the collagen sponge dressings.
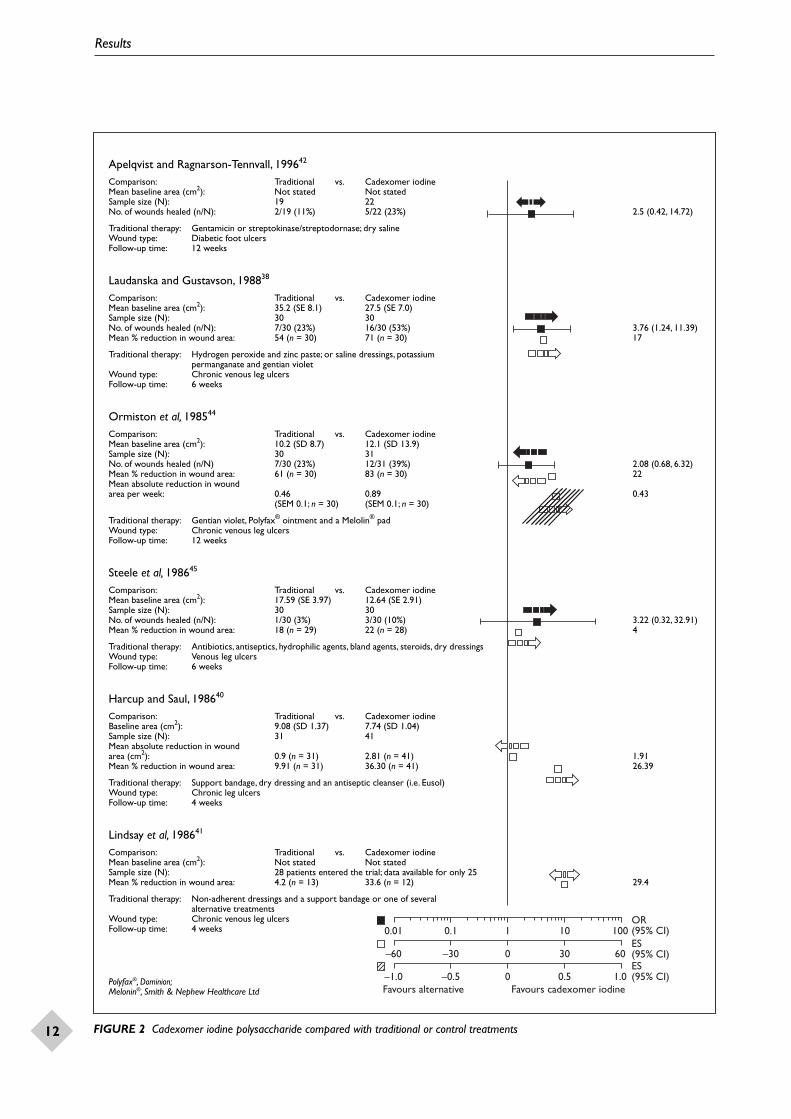
Cadexomer iodine polysaccharide versustraditional or control treatment Nine RCTs compared cadexomer iodinepolysaccharide with a traditional or control therapy (Figure 2 ; appendix 6, Table 6 ). Three trials (five papers) had a statistically significantresult favouring treatment with cadexomer
iodine polysaccharide when compared withhydrogen peroxide and zinc paste,38 hydrogenperoxide or potassium permanganate,22,23,28
and mechanical debridement by wet-to-drydressings.39 However, high withdrawal rates22,23,28
and inappropriate movement of some patientsbetween groups during the trial39 may haveintroduced confounding factors, which would have implications for the validity of these results.
In two trials the authors own statistical analysisindicated that cadexomer iodine resulted in a significant reduction in wound size whencompared to traditional dressing regimes.40,41
However, in both studies the papers providedinsufficient information for CIs to be calcu-lated which prevented further analysis in this review.
The remaining trials comparing a traditionaltreatment with cadexomer iodine polysaccharidewere unable to detect a statistically significant effect in favour of either treatment.42–45 This may have been a consequence of small sample size or a reflection of the diversity of traditionaltherapies evaluated in a single trial. In one trial, 12 of the 13 patients in the traditional group were treated with a variant on the basic standard therapy.41
Hydrogels versus traditional or control treatment Four trials were included that compared a hydrogel with a traditional or control treatment(Figure 3; appendix 6, Table 7 ).46–49 Only one ofthese trials showed a statistically significant differ-ence between treatments. In this comparison ahydrogel dressing showed a small improvement in the number of wounds healed when compared with a hydrocolloid dressing.46
Enzyme treatments versus traditional or control treatment Only one of the five trials included in the reviewshowed a statistically significant difference be-tween an enzymatic debriding agent (collagenase) and a control treatment (Figure 4; appendix 6, Table 8 ).50 However, the wounds in this trial actually increased in size and the predicted bias was in the direction of enzymatic treatment.Despite the majority of trials showing a trend infavour of enzyme treatment, statistical significancecould not be demonstrated. All the trials in thiscategory suffered from small sample size;9,37,51,52
only one of the included studies had more than 15 patients in each arm.52

Health Technology Assessment 1999; Vol. 3: No. 17 (Pt 1)
9
Adhesive zinc oxide tape versus traditional treatmentIn a single trial an adhesive zinc oxide tape wascompared with a hydrocolloid dressing for thetreatment of necrotic diabetic foot ulcers (appen-dix 6, Table 9 ).53 The adhesive zinc oxide tape wasmore effective in eradicating or reducing necroticarea than the hydrocolloid dressing (OR = 4.44;95% CI: 1.34, 14.70). Treatment was discontinuedin nine patients (four from the adhesive zinc oxidetape group and five from the hydrocolloid dressinggroup) due to a significant increase in necroticarea (> 100%). Common adverse effects seen in both groups were maceration of skin edges, pain and oedema.
Comparisons between debriding agentsNine trials were identified that directly comparedtwo debriding agents. Seven trials compared eitherdextranomer polysaccharide or cadexomer iodinepolysaccharide with another debriding agent, onetrial compared two enzyme treatments, and afurther trial was a comparison between hydrogels.
Cadexomer iodine polysaccharideversus other debriding agentsThree RCTs were included that comparedcadexomer iodine polysaccharide with anotherdebriding agent (Figure 5; appendix 6, Table 10 ).Dextranomer polysaccharide13,54 was the com-parator in two trials and a hydrogel was used in the third trial.55 None of the trials showed astatistically significant effect, and in two the pointestimate of relative effectiveness was close to the line of no effect.13,55
Dextranomer polysaccharide versusother debriding agents Four RCTs were included that compared dextra-nomer polysaccharide with another debridingagent (Figure 6; appendix 6, Table 11 ). Two trialswere comparisons with enzyme formulations(collagenase or streptokinase/streptodornase), and two were comparisons with a hydrogel.
Both hydrogel trials attempted to recorddebridement directly by employing an outcomemeasure based on wound cleansing (the reductionin area of necrotic tissue covering the woundbed).56,57 The study by Colin and co-workers56
failed to find a statistically significant effect for100% cleansing. However, the smaller study byThomas and Fear57 found a large statistically sig-nificant effect in favour of the hydrogel. Although
the treatments used in both studies appear to have been similar, it is likely that the formulation of Intrasite used by Colin was a modification of that employed by Thomas and Fear. Interestingly,in the latter study, treatment was continued beyondthe 14-day follow-up period in a selected group ofpatients. After 28 days, a further four wounds werefully cleansed in the dextranomer polysaccharidegroup, compared with no additional successes inthe hydrogel group. This may suggest that over alonger period the results in this trial would havereflected those reported by Colin and co-workers.
A non-significant benefit was found in favour of dextranomer polysaccharide when comparedwith the enzyme collagenase, this benefit wasrecorded against the direction of wound size bias.37 In the only other trial to compare dextra-nomer polysaccharide with an enzyme preparation(streptokinase/streptodornase), no differencebetween the treatments was found.58
Hydrogel versus hydrogelOnly one study made a direct comparison be-tween two hydrogels (Intrasite Gel and Granugel) (Figure 7; appendix 6, Table 12 ).59 This trial found no statistically significant difference between thegroups after 21 days treatment. The total cost fortreatment per person from baseline to final assess-ment was calculated to be £43.25 for Granugel and £40.25 for Intrasite, while the average cost per 10 cm2 reduction in area was £8.59 and £13.38,respectively. The data appear to indicate that treat-ment with Granugel may be more cost-effectivethan with Intrasite. However, this is misleading asthe analysis is based on absolute changes in ulcersize. The Granugel group had larger ulcers atbaseline, suggesting that this group was more likelyto experience larger changes in absolute ulcer area.
Enzyme versus enzyme Only one RCT directly compared two enzymaticagents (Figure 8; appendix 6, Table 13 ).60 Nostatistically significant difference was foundbetween wounds treated with streptokinase/streptodornase and those treated with trypsin.
Cost-effectiveness
Cost-effectiveness has not been thoroughly assessedin studies of debriding agents. The unit cost for eachtreatment is stated in some studies, and a few con-tain further details on other important variables,such as nursing time or number of dressing changes.However, no study provides sufficient detail for areliable cost-effectiveness analysis to be constructed.

Results
10
–40 –20 0 20 40
0.01 0.1 1 10 100
Favours alternative Favours Dextranomer
OR(95% CI)ES(95% CI)
Goode et al, 197935
Comparison: Traditional vs. DextranomerMean baseline area (cm2): Not stated Not statedSample size (N): 10 10No. of wounds healed without secondary closure (n/N): 1/10 (10%) 1/10 (10%) 1.00 (0.05, 18.32)
Traditional therapy: EusolWound type: Surgical wounds (bowel or appendicectomy)Follow-up time: Until healed or ready for secondary suture
Nasar and Morley, 198236
Comparison: Traditional vs. DextranomerMean baseline area (cm2): Not stated Not statedSample size (N): 9 9No. of wounds reduced by > 25%,clean and granulating (n/N): 5/9 (56%) 6/9 (67%) 1.6 (0.24, 10.81)
Traditional therapy: Eusol Wound type: Pressure soresFollow-up time: Until wound was clean and granulating
Sawyer et al, 197931
Comparison: Traditional vs. DextranomerMean baseline area (cm2): Not stated Not statedSample size (N): 31 35No. of wounds healed (n/N): 3/19 (16%) 15/18 (83%) 26.70 (4.639, 153.29)
Traditional therapy: Saline soaks, or mechanical debridement where indicatedWound type: Venous leg ulcersFollow-up time: 3 weeks
Eriksson et al, 198434
Comparison: Traditional vs. DextranomerMean baseline area (cm2): Not stated Not statedSample size (N): 27 26No. of wounds reduced by > 50% (n/N): 6/27 (19%) 2/26 (8%) 0.29 (0.05, 1.60)No. of wounds reduced by 25% or more (n/N): 21/27 (78%) 24/26 (92%) 3.43 (0.62, 18.85)
Traditional therapy: Saline soaksWound type: Venous leg ulcersFollow-up time: 2 weeks
Groenewald, 198029
Comparison: Traditional vs. DextranomerBaseline area (cm2): < 6 cm2: 7 ulcers 7 ulcers
6–12 cm2: 21 ulcers 20 ulcers> 12 cm2: 22 ulcers 23 ulcers
Sample size (N): 50 50No. of wounds healed (n/N): 2/50 (4%) 11/50 (22%) 6.77 (1.42, 32.38)No. of wounds reduced by 50–100% (n/N): 7/50 (14%) 24/50 (48%) 5.67 (2.14, 15.00)
Traditional therapy: Povidone-iodine, zinc oxide, and gauzeWound type: Venous leg ulcersFollow-up time: 3 weeks
FIGURE 1 Dextranomer polysaccharide compared with traditional or control treatments. Study results are presented as OR and/or ES enclosed by their 95% CI. An arrow by a trial indicates that the results were biased by poor comparability between groups for woundsize at baseline; the direction of the arrow suggests which intervention was favoured by this bias. Convergent arrows suggest that thegroups were reasonably comparable for wound size, while divergent arrows indicate that the bias could not be determined from the data presented

Health Technology Assessment 1999; Vol. 3: No. 17 (Pt 1)
11
–40 –20 0 20 40
0.01 0.1 1 10 100
Favours alternative Favours Dextranomer
OR(95% CI)ES(95% CI)
Sayag et al, 199632
Comparison: Traditional vs. DextranomerMean baseline area (cm2): 20.1 (SD 12.9) 16.1 (SD 12.5)Sample size (N): 47 45No. of wounds reduced by 40–100% (n/N): 35/47 (74%) 19/45 (42%) 0.25 (0.10, 0.61)No. of wounds reduced by > 75% (n/N): 15/47 (32%) 6/45 (13%) 0.33 (0.11, 0.94)
Traditional therapy: Calcium alginate dressing Wound type: Pressure soresFollow-up time: Until the wound reached 40% of its original size or on completion
of 8 weeks’ treatment
Garcia et al, 198430
Comparison: Traditional vs. DextranomerMean baseline area (cm2): Not stated Not statedSample size (N): 22 22Mean % reduction in wound area: 85.2 93.1 7.9 (2.27, 15.53)
(SD 10.8; n = 22) (SD 7.4; n = 22)Mean % reduction in wound circumference: 70.1 80.0 9.9 (–2.70, 22.50)
(SD 20.8; n = 22) (SD 20.6; n = 22)
Traditional therapy: Potassium permanganate and hypertonic saline or antibiotic ointments Wound type: Secondary perimalleolar ulcersFollow-up time: 3 weeks
Parish and Collins, 197937
Comparison: Control vs. DextranomerMean baseline area (cm2): 5.76 20.25Sample size (N): 9 14No. of wounds healed (n/N): 0/9 (0%) 6/14 (43%) 14.53 (0.71, 298.23)
Traditional therapy: Sugar and egg white Wound type: Pressure soresFollow-up time: 4 weeks
Palmieri, 199233
Comparison: Traditional vs. DextranomerMean baseline area (cm2): Not stated Not statedSample size (N): 24 24Mean no. of days to healing for leg ulcers: 36 (n = 6) 60 (n = 6) –24Mean no. of days to healing for pressure sores: 20 (n = 6) 47 (n = 6) –27
Traditional therapy: Collagen sponge Wound type: Leg ulcers and pressure soresFollow-up time: Until all wounds had healed
FIGURE 1 contd Dextranomer polysaccharide compared with traditional or control treatments. Study results are presented as OR and/orES enclosed by their 95% CI. An arrow by a trial indicates that the results were biased by poor comparability between groups for wound sizeat baseline; the direction of the arrow suggests which intervention was favoured by this bias. Convergent arrows suggest that the groups werereasonably comparable for wound size, while divergent arrows indicate that the bias could not be determined from the data presented
Results
12
–60 –30 0 30 60
0.01 0.1 1 10 100
Favours alternative Favours cadexomer iodine
OR(95% CI)ES(95% CI)ES (95% CI)–1.0 –0.5 0 0.5 1.0
Apelqvist and Ragnarson-Tennvall, 199642
Comparison: Traditional vs. Cadexomer iodineMean baseline area (cm2): Not stated Not statedSample size (N): 19 22No. of wounds healed (n/N): 2/19 (11%) 5/22 (23%) 2.5 (0.42, 14.72)
Traditional therapy: Gentamicin or streptokinase/streptodornase; dry salineWound type: Diabetic foot ulcersFollow-up time: 12 weeks
Laudanska and Gustavson, 198838
Comparison: Traditional vs. Cadexomer iodineMean baseline area (cm2): 35.2 (SE 8.1) 27.5 (SE 7.0)Sample size (N): 30 30No. of wounds healed (n/N): 7/30 (23%) 16/30 (53%) 3.76 (1.24, 11.39)Mean % reduction in wound area: 54 (n = 30) 71 (n = 30) 17
Traditional therapy: Hydrogen peroxide and zinc paste; or saline dressings, potassium permanganate and gentian violet
Wound type: Chronic venous leg ulcersFollow-up time: 6 weeks
Ormiston et al, 198544
Comparison: Traditional vs. Cadexomer iodineMean baseline area (cm2): 10.2 (SD 8.7) 12.1 (SD 13.9)Sample size (N): 30 31No. of wounds healed (n/N) 7/30 (23%) 12/31 (39%) 2.08 (0.68, 6.32)Mean % reduction in wound area: 61 (n = 30) 83 (n = 30) 22Mean absolute reduction in wound area per week: 0.46 0.89 0.43
(SEM 0.1; n = 30) (SEM 0.1; n = 30)
Traditional therapy: Gentian violet, Polyfax® ointment and a Melolin® padWound type: Chronic venous leg ulcersFollow-up time: 12 weeks
Steele et al, 198645
Comparison: Traditional vs. Cadexomer iodineMean baseline area (cm2): 17.59 (SE 3.97) 12.64 (SE 2.91)Sample size (N): 30 30No. of wounds healed (n/N): 1/30 (3%) 3/30 (10%) 3.22 (0.32, 32.91)Mean % reduction in wound area: 18 (n = 29) 22 (n = 28) 4
Traditional therapy: Antibiotics, antiseptics, hydrophilic agents, bland agents, steroids, dry dressingsWound type: Venous leg ulcersFollow-up time: 6 weeks
Harcup and Saul, 198640
Comparison: Traditional vs. Cadexomer iodineBaseline area (cm2): 9.08 (SD 1.37) 7.74 (SD 1.04)Sample size (N): 31 41Mean absolute reduction in wound area (cm2): 0.9 (n = 31) 2.81 (n = 41) 1.91Mean % reduction in wound area: 9.91 (n = 31) 36.30 (n = 41) 26.39
Traditional therapy: Support bandage, dry dressing and an antiseptic cleanser (i.e. Eusol)Wound type: Chronic leg ulcersFollow-up time: 4 weeks
Lindsay et al, 198641
Comparison: Traditional vs. Cadexomer iodineMean baseline area (cm2): Not stated Not statedSample size (N): 28 patients entered the trial; data available for only 25Mean % reduction in wound area: 4.2 (n = 13) 33.6 (n = 12) 29.4
Traditional therapy: Non-adherent dressings and a support bandage or one of several alternative treatments
Wound type: Chronic venous leg ulcersFollow-up time: 4 weeks
Polyfax®, Dominion;Melonin®, Smith & Nephew Healthcare Ltd
FIGURE 2 Cadexomer iodine polysaccharide compared with traditional or control treatments

Health Technology Assessment 1999; Vol. 3: No. 17 (Pt 1)
13
–60 –30 0 30 60
0.01 0.1 1 10 100
Favours alternative Favours cadexomer iodine
OR(95% CI)ES(95% CI)ES(95% CI)–1.0 –0.5 0 0.5 1.0
Moberg et al, 198343
Comparison: Traditional vs. Cadexomer iodineMean baseline area (cm2): 12.4 (SEM 4.3) 9.6 (SEM 1.8)Sample size (N): 19 19Mean absolute reduction in wound area (cm2): 2.5 2.9 0.4 (–3.05, 3.85)
(SEM 1.1; n = 18) (SEM 1.3; n = 16)Mean % reduction in wound area: 9.6 30.9 21 (–5.83, 48.43)
(SD 31; n = 18) (SD 46; n = 16)
Traditional therapy: Saline dressings, enzymatic agents, non-adhesive dressings Wound type: Pressure soresFollow-up time: 3 weeks
Skog et al, 1983;23 Hillström, 1988;22 Troëng et al, 198328
Comparison: Control vs. Cadexomer iodineMean baseline area (cm2): 34.0 (SEM 5.7) 20.1 (SEM 4.4)Sample size (N): 45 50Mean % change in wound area: +5 –34 39 (8.16, 69.84)
(SEM 15; n = 36) (SEM 5; n = 38)
Traditional therapy: Dilute hydrogen peroxide or potassium permanganate and a non-adherent dressing
Wound type: Chronic venous leg ulcersFollow-up time: 6 weeks
Holloway et al, 198939
Comparison: Traditional vs. Cadexomer iodineMean baseline area (cm2): 11.2 20.1Median baseline area (cm2): 9.75 (range, 3–37) 10.7 (range, 0.6–136.0)Sample size (N): 37 38 Mean absolute reduction in wound area per week (cm2): 0.41 0.95 0.54 (0.19, 0.90)
(SEM 0.13; n = 27) (SEM 0.12; n = 27)Mean reduction in wound area per week vs. baseline circumference (cm2/wk/cm2): 0.03 0.04 0.01 (–0.02, 0.04)
(SEM 0.01; n = 27) (SEM 0.01; n = 27)
Traditional therapy: Wet-to-dry dressings and saline-soaked gauze Wound type: Venous leg ulcersFollow-up time: 24 weeks
FIGURE 2 contd Cadexomer iodine polysaccharide compared with traditional or control treatments

Results
14
–100 –50 0 50 100
0.01 0.1 1 10 100
Favours alternative Favours hydrogel
OR(95% CI)ES(95% CI)ES(95% CI)10 5 0 5 10
Darkovich et al, 199046
Comparison: Traditional vs. Hydrogel (Biofilm®)Mean baseline area (cm2): 9.2 (range, 0.4–64) 11.0 (range, 0.2–100)Sample size: 63 60No. of wounds healed (n/N): 15/63 (24%) 26/60 (43%) 2.45 (1.13, 5.30)Mean % reduction in wound area: 40 68 28Mean absolute reduction in wound area (cm2): 3.7 (n = 63) 7.5 (n = 60) 3.8
Traditional therapy: DuoDerm®
Wound type: Pressure soresFollow-up time: 60 days
Brown-Etris et al, 199647
Comparison: Traditional vs. Hydrogel (Transorbent®)Mean baseline area (cm2): Not stated Not statedSample size: 63 77No. of wounds healed (n/N)37/63 (59%) 39/77 (51%) 0.72 (0.37, 1.41)Mean absolute reduction in wound area:
stage II sores (2–30 cm2): 2.3 (n = 12) 3.6 (n = 12) 1.3
stage III sores (2–30 cm2): 5.2 (n = 36) 6.3 (n = 42) 1.1
stage III sores (31–80 cm2): 4.3 (n = 2) 24.5 (n = 3) 20.2
Traditional therapy: DuoDermWound type: Pressure soresFollow-up time: 10 weeks
Lum et al, 199648
Comparison: Traditional vs. Hydrogel (Intrasite)Mean baseline area (cm2): 18.6 36.3
(range, 1.0–72.5) (range, 1.5–160)Sample size (patients): 3 5Mean absolute change reduction in wound area (cm2): +1.9 (n = 3) –20.4 (n = 5) 22.3Mean % reduction in wound area: +10 (n = 3) –56 (n = 5) 66
Traditional therapy: Saline alone or with eusol where the wound was infectedWound type: Pressure soresFollow-up time: 8 weeks
Mulder et al, 199349
Comparison: Control vs. Hydrogel (Clearsite®)Mean baseline area (cm2): Not stated Not statedSample size (N): 21 20Mean % reduction in wound area per week (cm2): 5.1 8 2.9 (–6.45, 12.25)
(SD 14.8; n = 21) (SD 14.8; n = 20)Median % reduction in wound area per week (cm2): 7.0 (n = 21) 5.6 (n = 20) –1.4
Control treatment: Saline soaksWound type: Pressure soresFollow-up time: 8 weeks
Comparison: Traditional vs. Hydrogel (Clearsite)Mean baseline area (cm2): Not stated Not statedSample size (N): 20 20Mean % reduction in wound area per week (cm2) 3.3 8 4.7 (–11.55, 20.95)
(SD 32.7; n = 20) (SD 14.8; n = 20) Median % reduction in wound area per week (cm2) 7.4 (n = 20) 5.6 (n = 20) –1.8
Traditional therapy: DuoDermWound type: Pressure soresFollow-up time: 8 weeks
Biofilm®, Braun Biotrol;Transorbent®, Braun Medical;Duoderm®, UK equivalent Granuflex, ConvaTec Ltd;Clearsite®, New Dimensions in Medicine
FIGURE 3 Hydrogels compared with traditional or control treatments

Health Technology Assessment 1999; Vol. 3: No. 17 (Pt 1)
15
–200 –100 0 100 200
0.01 0.1 1 10 100
Favours alternative Favours enzyme
OR(95% CI)ES(95% CI)
Westerhof et al, 198752
Comparison: Control vs. Enzyme (Elase®)Mean baseline area (cm2): 20.2 (range, 2–48) 25.7 (range, 2–273)Sample size (N): 17 16No. of wounds sucessfully grafted or healed (n/N): 6/17 (35%) 11/16 (69%) 4.03 (0.94, 17.23)
Mean baseline area (cm2): 22.3 (range, 3–48) 14.9 (range, 2–48)Sample size (N): 8 6No. of complex wounds successfully grafted or healed (n/N): 3/8 (38%) 3/6 (50%) 1.67 (0.20, 14.27)
Mean baseline area (cm2): 18.1 (range, 2–40) 36.4 (range, 3–273)Sample size (N): 9 10No. of venous ulcers successfully grafted or healed (n/N): 3/9 (33%) 8/10 (80%) 8.00 (1.00, 64.00)
Control: Placebo (freeze-dried powder, no active ingredients)Wound type: Leg ulcers Follow-up time: Until ulcers ready for grafting
Lee and Ambrus, 197550
Comparison: Control vs. Enzyme (Santyl®)Mean baseline volume (cm3): 1.25 (SD 1.62) 15.44 (SD 19.92)Sample size (N): 11 17Mean % increase in wound volume: 13.14 78.79 65.65 (1.72, 129.58)
(SD 49.8; n = 11) (SD 94.6; n = 17)
Control therapy: Placebo (heat-inactivated enzyme)Wound type: Pressure soresFollow-up time: 4 weeks
Gordon, 197551
Comparison: Control vs. Enzyme (Chymacort®)Mean baseline area (cm2): 14.5 (SD 22.13) 15.82 (SD 19.67)Sample size (N): 9 10No. of wounds healed (n/N): 0/9 (0%) 2/10 (20%) 5.59 (0.23, 133.71)Mean absolute reduction in ulcer area (cm2): 6.1 10.5 4.40 (–9.92, 18.72)
(SD 13.2; n = 8) (SD 15.0; n = 10)Mean % change in wound size +47 –71.8 118.80 (–50.20, 287.50)
(SD 252.8; n = 8) (SD 22.5; n = 10)
Control therapy: Hydrocortisone and neomycin palitateWound type: Leg ulcers Follow-up time: 6 weeks
Ågren and Strömberg, 19859
Comparison: Traditional vs. Enzyme (Varidase) Mean baseline area (cm2): 5.8 4.2
(range, 1.2–26.0) (range, 1.2–18.2)Sample size (N): 14 14Median % change in wound area: –2.4 (n = 14) +18.7 (n = 11) –21.1
Traditional therapy: Zinc oxide dressingWound type: Pressure soresFollow-up time: 8 weeks
Parish and Collins, 197937
Comparison: Traditional vs. Enzyme (Santyl) Mean baseline area (cm2): 5.76 10.24Sample size (n/N): 9 11No. of wounds healed (n/N): 0/9 (0%) 1/11 (9%) 2.71 (0.098, 75.05)
Traditional therapy: Sugar and egg whiteWound type: Pressure soresFollow-up time: 4 weeks
Elase®, manufacturer unknown;Santyl®, Knoll Pharmaceutical Co;Chymacort®, Armour Pharmaceutical Company Ltd
FIGURE 4 Enzymatic agents compared with traditional or control treatments

Results
16
–20 –10 0 10 20
0.1 0.2 1 5 10
Favours alternative Favours cadexomer iodine
OR(95% CI)ES(95% CI)
for median
for range
Tarvainen, 198854
Comparison: Dextranomer vs. Cadexomer iodineMean baseline area (cm2): Not stated Not statedSample size (N): 13 14No. of wounds healed (n/N): 2/13 (15%) 7/14 (50%) 5.50 (0.88, 34.48)
Wound type: Leg ulcersFollow-up: 8 weeks
Moss et al, 198713
Comparison: Dextranomer vs. Cadexomer iodineMean baseline area (cm2): 25.5 (SD 29.5) 19.7 (SD 19.8)Sample size (N): 21 21Mean % reduction in wound area: 3 (CI: 4, –9; n = 21) 4 (CI: 5, –14; n = 21) 1 (–10.28, 12.28)
Wound type: Venous leg ulcersFollow-up: 6 weeks
Stewart and Leaper, 198755
Comparison: Hydrogel (Scherisorb®) vs. Cadexomer iodineMedian baseline area (cm2): 2.6 2.8
(range, 0.4–74.4) (range, 0.2–50.5)Sample size (N): 49 46No. of wounds healed (n/N): 14/49 (29%) 14/46 (30%) 1.09 (0.45, 2.64)
Wound type: Leg ulcers of mixed aetiologyFollow-up: 10 weeks
Scherisorb®, presently Intrasite Gel
FIGURE 5 Cadexomer iodine polysaccharide compared with other debriding agents

Health Technology Assessment 1999; Vol. 3: No. 17 (Pt 1)
17
–30 –15 0 15 30
0.01 0.1 1 10 100
Favours alternative Favours dextranomer
OR(95% CI)ES(95% CI)
Colin et al, 199656
Comparison: Hydrogel (Intrasite) vs. DextranomerBaseline area: 4 cm2: 15 ulcers 18 ulcers
4–13 cm2: 25 ulcers 25 ulcers > 13 cm2: 27 ulcers 25 ulcers
Sample size (N): 67 68No. of wounds 100% cleansed (n/N): 13/67 (19%) 14/68 (21%) 1.08 (0.46, 2.51)No. of wounds 75–100% cleansed (n/N): 33/67 (49%) 29/68 (43%) 0.77 (0.39, 1.51)Median % reduction in wound area: 35 7 –28
(range,–185–+91; (range, –340–+98;n = 53) n = 43)
Median % reduction in non-viable tissue: 74 (range, –103–+100; 62 (range, –340–+100; –12
n = 53) n = 43)
Wound type: Pressure soresFollow-up time: 3 weeks
Thomas and Fear, 199357
Comparison: Hydrogel (Intrasite) vs. DextranomerMean baseline (cm2): 22.2 (SD 23.4) 15.6 (SD 16.2)Sample size (N): 21 20 No. of wounds fully cleansed (n/N): 8/20 (40%) 1/20 (5%) 0.08 (0.01, 0.71)
Wound type: Pressure soresFollow-up time: 2 weeks
Parish and Collins, 197937
Comparison: Enzyme (Santyl) vs. DextranomerMean baseline (cm2): 10.24 20.25Sample size (N): 11 14 No. of wounds healed (n/N): 1/11 (9%) 6/14 (43%) 7.50 (0.74, 75.72)
Wound type: Pressure soresFollow-up time: 4 weeks
Hulkko et al, 198158
Comparison: Enzyme (Varidase) vs. DextranomerMean baseline (mm): Not stated Not statedSample size (N): 13 18Mean % reduction in wound diameter: 11.9 (n = 12) 14.5 (n = 15) 2.6Mean absolute reduction in wound diameter (mm): 9.8 (n = 12) 9.3 (n = 15) 0.5
Wound type: Venous ulcersFollow-up time: 2 weeks
FIGURE 6 Dextranomer polysaccharide compared with other debriding agents

Results
18
–10 –5 0 5 10
0.01 0.1 1 10 100
Favours Intrasite Favours Granugel
OR(95% CI)ES(95% CI)
Gibson, 199559
Comparison: Hydrogel (Intrasite) vs. Hydrogel (Granugel)Mean baseline area (cm2): 18.7 24.9Sample size (N): 32 30Mean % reduction in wound area after 21 days: 10 (n = 32) 14 (n = 30) 4Mean % reduction in slough area after 21 days: 32 (n = 32) 37 (n = 30) 5Median absolute reduction in wound area (cm2) after 7 days: 0.54 (n = 32) 0.74 (n = 30) 0.2Median absolute reduction in slough area after 7 days (cm2): 1.12 (n = 32) 1.51 (n = 30) 0.4
Wound type: Leg ulcersFollow-up time: 3 weeks
FIGURE 7 Comparison between hydrogels
–10 –5 0 5 10
0.01 0.1 1 10 100
Favours Trypure Favours Varidase
OR(95% CI)ES(95% CI)
Hellgren, 198360
Comparison: Enzyme (Trypure®) vs. Enzyme (Varidase)Mean baseline area (cm2): Not stated Not statedSample size (N): 19 21No. of wounds fully cleansed (n/N): 5/19 (26%) 13/21 (62%) 3.58 (0.90, 14.16)Mean % granulated area at 14 days: 56 (n = 16) 60 (n = 21) 4
Wound type: Leg ulcersFollow-up time: 3 weeks
Trypure®, Novo Laboratories
FIGURE 8 Comparison between enzyme treatments

Health Technology Assessment 1999; Vol. 3: No. 17 (Pt 1)
19
There are no RCTs comparing debridementwith no debridement. A limited number of
trials have employed an inert or placebo com-parison, but the extent to which even secondarydressings contribute to wound healing is unclear.Given the multi-faceted way that topical debridingagents are thought to work, the obvious study toanswer the question of whether debridement is a necessity for wound healing would be a com-parative evaluation of surgical, or sharpdebridement with no debridement.
The majority of trials investigated debridement of either pressure sores or venous ulcers and forthese wounds the debriding agent generally showeda benefit over traditional or control treatments.However, without conclusive evidence that debride-ment is an important procedure for wound healing,it is not possible to determine whether the benefitover traditional treatment is a true assessment ofeffectiveness, or a consequence of harm induced by the traditional therapies.
Although evidence in the form of RCTs is lacking,many clinicians believe that debridement facilitateswound closure by removing necrotic tissue that actsas a barrier to new tissue growth. This suggests thatif debridement really does aid wound closure thenthe effectiveness of a debriding agent should bemeasured by an outcome based on wound healing.Even though the debriding agent is not necessarilyused throughout the entire healing process anoutcome measure based on healing remains validas long as both comparison groups follow a similarschedule of nursing care after the debridementperiod. In this way, any difference in healing ratesbetween groups can be attributed to the debridingagent used. Some researchers however, haveattempted to estimate the effectiveness of theseagents by measuring the degree of debridementexpressed as the percentage area of wound coveredin necrotic material. This measurement may not be a reliable indication of treatment effect as theextent of debridement does not appear to havebeen scientifically validated as a surrogate or proxy measure of wound healing.
The results reported in many of the includedstudies are biased by a lack of comparabilitybetween the groups for wound size at baseline.
The underlying bias is frequently in the directionof the treatment effect, suggesting that the studyresults should be viewed cautiously. A statisticallysignificant study result favouring one treatmentover another can only be considered valid if it isobtained either: against the anticipated direction of the bias for wound size, or where percentagearea change and absolute area change are in thesame direction. When baseline data are not givenfor wound size it is not possible to estimate thedegree of bias, and in the absence of otherindicators, validity of the trial result should be considered doubtful.
Analysis of studies where patients received atraditional or control therapy in the comparisonarm indicates that the validity of the outcomemeasure, according to baseline comparability, was doubtful in about 70% of the trials. In theremaining 30%, where wound size bias was unlikely to have affected the outcome measure, the OR or ES was in the direction of the debridingagent in over 88% of cases, though only two studiesobtained statistical significance. In other wordsthose studies with the most reliable results indicatethat treatment with a known debriding agent isfavourable to traditional or control therapy.
Analysis by intervention type suggests that bothdextranomer polysaccharide and cadexomer iodinepolysaccharide may improve wound healing whencompared with a traditional or control therapy.However, evidence for the use of hydrogels orenzymatic agents in preference to traditional orcontrol treatment is less convincing as, with theexception of one trial,46 these debriding agents did not show a statistically significant improvementin wound closure. The lack of evidence for theeffectiveness of enzymatic agents suggests thatcareful consideration should be given to thecontinued use of streptokinase/streptodornase,given that its topical application is known to inducethe production of anti-streptokinase antibodies,which could theoretically put patients at risk ifgiven streptokinase immediately following amyocardial infarction.61
In drawing these conclusions on effectiveness it is necessary to bear in mind that many of thetraditional treatments employed as comparators
Chapter 4
Discussion

Discussion
20
are no longer used in clinical practice, and somemay even have a detrimental effect on healing. Thisimplies that relative effectiveness, as recorded inmany of the trials, may be an over-estimate of whatwe might expect to obtain in a similar trial today.
Recently, there have been several non-systematicnarrative reviews in nursing-orientated publi-cations, which have suggested that hydrogels are the non-mechanical debridement agent ofchoice.2,62 In terms of scientific evidence, such a statement can only be supported by trials thatdirectly compare two or more debriding agents;such trials, however, are relatively rare in theliterature and are generally of poor quality. Usingthe criteria previously described, around 40% ofcomparisons between debriding agents had a validresult, but only one trial found a statistically signifi-cant difference between treatments.57 The smallnumber of reliable trials and the diversity of com-parisons implies that there is insufficient evidenceto promote the use of one debriding agent overanother on the basis of effectiveness alone.
In wound care research it is not uncommon for trials to be associated with funding from thepharmaceutical industry. This may in part explainthe lack of direct comparisons between different,commercially important debriding agents. Apharmaceutical company is unlikely to be willing to compare its product with that of a competitor if the product has only shown marginal benefitsover traditional or control treatments.
A pooled estimate of effectiveness for each debrid-ing agent has not been calculated; to do so wouldbe inappropriate considering the heterogeneousnature of the studies and the potential biases due to differences in wound size at baseline. Poolingwould compound these biases and result in an over-estimate of effectiveness, particularly consideringthe likely influence of publication bias favouringpositive outcomes. If similar trials reported bothabsolute and percentage reductions in ulcer sizethen a pooled estimate could be calculated for eachof the outcomes, which would provide a reasonableestimate of effectiveness. Unfortunately, this is rarelythe case and where sufficient details are providedthere are other differences between studies, such as wound type, follow-up time, the presence of other underlying conditions such as ischaemia, and the variability of traditional treatments within a single comparison group which make combiningresults inappropriate.
A multiplicity of traditional therapies are frequentlyemployed in the same trial to act as a comparator
with a single debriding agent. Although it could be argued that this reflects typical clinical practiceit makes interpretation of the results very difficult.It is likely that within such a varied group oftraditional treatments there will be considerablevariation in effectiveness. It is possible also that one of these treatments may be equally, if not more effective, than the debriding agent underevaluation, but that its beneficial effect is maskedby the other less effective treatments within thegroup. It is also possible that treatment care mayvary depending on the care givers familiarity witheach of the traditional treatments employed. This is less likely to be an issue in the application of a homogeneous debriding agent.
Different debriding agents may be more appro-priate for different types of wound because themode of action employed by each agent to facili-tate wound healing differs. For example, twostudies compared the same hydrogel with dextra-nomer polysaccharide for the treatment of pres-sure sores.56,57 Dextranomer polysaccharide isthought to actively absorb water and necroticmaterial from the wound bed, whereas thehydrogel is believed to liquefy the wound andmaintain a moist environment that facilitates auto-debridement.57 Clearly these two agents work in very different ways and their effectiveness is likely to depend on the type of wound to whichthey are applied. Dextranomer polysaccharide isthen recommended for the treatment of moist,yellow sloughy wounds, while a hydrogel, althougha generalist agent, is recommended particularly for dry necrotic wounds.10 Comparisons betweendebriding agents should then take into account the local nature of the wound under examinationwhen assessing effectiveness.
The categories used in this review to groupdebridement interventions could be misleadingbecause they may mask pharmaceutical develop-ments. For example, the formulation of IntrasiteGel has changed over time, and that used in a trialin the late 1980s is unlikely to be the same as thatused in the early 1990s. The vehicle used for atreatment may also vary. For example, dextranomerpolysaccharide can be applied as either beads or asa paste with polyethylene glycol, and the nature ofthis vehicle may have consequences for effective-ness. Considering all dextranomer polysaccharidetrials together does not take into account thesepotential differences. However, only by groupingthese interventions under broad categories can a general overview of effectiveness be gained, andas the data are not statistically pooled erroneousinterpretations are avoided. In addition, both

Health Technology Assessment 1999; Vol. 3: No. 17 (Pt 1)
21
clinicians and patients alike are primarilyconcerned with whether a treatment works rather than its mode of action. If the subtledifferences identified between products in thelaboratory do not translate into improved woundhealing rates in clinical practice, then there is little benefit in discussing differences in product formulation.
Quality assessment indicates that most studiesincluded in the review have methodological flawsthat affect their validity. In general, the RCTs aretoo small to ensure that wounds of different sizesare equally allocated to both experimental groups.This suggests that most trials will be subject to abias at baseline. Most trials had a short follow-up,which mitigates against the outcome of the numberof wounds healed. Studies that employ such anoutcome measure should analyse the data using‘survival analysis’, which takes into account bothwhether and when a wound healed; in this way it isa more efficient method for estimating the rate ofhealing. Many of the studies also excluded sick,debilitated or confused patients and those withdiseases that affect healing, such as diabetes andrheumatoid arthritis. These are the very patientswhose wounds tend to be chronic and are there-fore the most likely to be prescribed debridingagents in practice. In general then, the patientsenrolled into a trial are a highly selected group and are unlikely to be representative of the thoseencountered in clinical practice.
Subjective outcome measures such as degrees of oedema, erythema, granulation, pus and debrisare frequently recorded by authors, but are notconsidered in this review. These outcomes are more susceptible to bias as the assessor may have an unconscious preference for one of the treat-ments. Analysis of subjective outcomes nearlyalways produced a statistically significant result in favour of the experimental treatment. Similarly,other variables that are likely to influence treat-ment choice such as pain, comfort and quality of life issues, are not addressed in this reviewbecause the outcome measures employed had
not been validated and were likely to result inmisleading information.
Larval (maggot) therapy has had a long history,and is enjoying a resurgence of interest in the UK.4 However, evidence for effectiveness remainsrestricted to case reports and anecdotal articles;there is presently no research evidence to supportclaims of effectiveness. Considering the highprofile of this intervention, clinical trials, partic-ularly RCTs, are urgently required.
Publication bias appears to be present in debride-ment studies with the majority of trials favouringthe debriding agent under evaluation. This may bea reflection of commercial interests in many of theincluded trials. Even if a debriding agent was effec-tive, one would expect by chance to get occasionalresults from studies that found in favour of thealternative treatment, particularly because of thesmall sample size of the RCTs, giving moreopportunity for chance variation.
Future trials that assess wound healing need to be larger in terms of patient numbers than themajority of those reviewed here. The design ofsmaller trials could be improved by the use ofmatched or stratified randomisation to ensurecomparability between treatment groups atbaseline: patients should be stratified based onwound type and size at baseline and these group-ings should then be randomised to treatment. Ifpatients have been matched for wound size andtype then matched pairs analysis should be used toanalyse the data. But even with this type of designthe trial still needs to be large enough to ensurecomparability for other features and confoundingfactors, such as age or duration of the wound.
Planned and future studies would also benefit from the inclusion of a detailed cost-effectivenessanalysis. Several reports included in this reviewdetailed the costs incurred during the trial period,but unfortunately none of the studies providedsufficient detail for a reliable cost-effectivenessanalysis to be constructed.


Health Technology Assessment 1999; Vol. 3: No. 17 (Pt 1)
23
There is some, if limited, evidence to suggestthat the use of a specific debriding agent is
beneficial for wound healing when compared with certain traditional or control treatments. In contrast, there is little or no evidence to suggestthat one debriding agent is more effective than any other.
Implications for policy
As the benefits shown over traditional or controltreatments are at best marginal, the choice ofwhich debriding process to adopt should perhapsbe based on the relative cost of the treatments,unless clinical experience suggests otherwise.There is little reliable research evidence to suggest that the more expensive agents should be used in preference to some of the less costlyones. However, this decision should not be basedon the net cost of each treatment as this does nottake into account important variables, such as thenumber of dressing changes required, coverage of the wound area, or nursing time. The financialcost of a treatment can only be determined fromstudies designed specifically to address this issueand this should be seen as a priority for future research.
Recommendations for research
Much of the research into wound debridement is of poor quality and direct comparisons are few.In those trials reviewed, sample sizes were rarelysufficient to detect clinically important effects, and poor baseline comparability frequentlyconfounded outcome measures. Several importantmessages can be identified for future studies.
• Recruitment numbers should be based on an a priori sample size calculation, though this maybe complicated by the lack of trials on which tobase such a calculation.
• The proportion of wounds healed should beused as an objective outcome measure. Wherehealing rates are based on wound area both thepercentage and absolute change in area shouldbe given.
• Experimental groups should be comparable at baseline. In small RCTs, randomisation alonewill not achieve comparability; in such situationspatients should be paired by baseline character-istics and then the individuals of each pair ran-domised to treatment. However, with particularlysmall groups, pairing of patients is still unlikelyto ensure that all risk factors (known and un-known) are distributed equally between thegroups, and hence, large sample size should still be the ultimate goal.
• Baseline data and intervention details shouldalways include a thorough description of how the patients were nursed and the use of concurrent treatments including secondary dressings.
• Comparisons between debriding agents arerequired and should use agents that arerecommended for wounds of a similar nature.
• Assessment should be blind to treatment.• Survival rate analysis should be adopted for
all studies that assess wound healing.• All RCTs should be published.• Detailed cost-effectiveness analyses should be
seen as a priority for future trials.• RCTs of both surgical and larval debridement
have not been performed. The frequent use of surgical debridement and the increasinginterest in the larval therapy indicate that these trials are needed.
Chapter 5
Conclusions


Health Technology Assessment 1999; Vol. 3: No. 17 (Pt 1)
25
This review was commissioned by the NHS R&D HTA programme. The authors are
indebted to Julie Glanville and Alison Fletcher for assistance with the search, location andcollection of literature. We are also grateful
to our expert panel (appendix 4) for their helpful comments on the review protocol and draft report. The report also benefited greatly from comments received from the HTA referees.
Acknowledgements


Health Technology Assessment 1999; Vol. 3: No. 17 (Pt 1)
27
1. US Department of Health and Human Services.Treatment of pressure ulcers. Clinical PracticeGuidelines 1994;15:47.
2. Bale S. A guide to wound debridement. J WoundCare 1997;6(4):179–82.
3. Thomas S, Jones M, Shutler S, Jones S. Using larvaein modern wound management. J Wound Care1996;5(2 Suppl):60–9.
4. Sherman RA, Wyle F, Vulpe M. Maggot therapy for treating pressure ulcers in spinal cord injurypatients. J Spinal Cord Med 1995;18(2):71–4.
5. Thomas S, Jones M, Shutler S, Andrews A. All you need to know about maggots – larval therapy.Nurs Times 1996;92(46):63–4.
6. Thomas S. Wound management and dressings.London: The Pharmaceutical Press, 1990.
7. Longe RL. Current concepts in clinicaltherapeutics: pressure sores. Clin Pharmacol1986;5(8):669–81.
8. British National Formulary. British MedicalAssociation and the Royal Pharmaceutical Society of Great Britain, 1998:35.
9. Ågren MS, Strömberg HE. Topical treatment ofpressure ulcers. A randomized comparative trial ofVaridase and zinc oxide. Scand J Plast Reconstr Surg1985;19(1):97–100.
10. Thomas S. A handbook of surgical dressings.Bridgend: The Surgical Materials TestingLaboratory, 1992.
11. Thomas S. Nurses’ knowledge of dressings.Community Outlook 1993;3(10):21–2.
12. NHS Centre for Reviews and Dissemination.Undertaking systematic reviews of research oneffectiveness. University of York, 1996;Report 4.
13. Moss C, Taylor AE, Shuster S. Comparison ofcadexomer iodine and dextranomer for chronicvenous ulcers. Clin Exp Dermat 1987;12(6):413–18.
14. Brown-Etris MB, Pribble J, LaBrecque J. Evaluationof two wound measurement methods in a multi-center, controlled study. Ostomy Wound Manage1994;40(7):44–8.
15. Frantz RA, Johnson D. Stereophotography andcomputerised image analysis: a three dimensionalmethod of measuring wound healing. Wounds1992;4:58–64.
16. Fear M, Thomas S. Wound cleansing properties of Debrisan and Scherisorb gel: interim results of a clinical trial. Proceedings of the 1st EuropeanConference on Advances in Wound Management.London: Macmillan Ltd, 1992;1:162–4.
17. Sawyer PN, Dowbak G, Sophie Z, Feller J, Cohen L.A preliminary report of the efficacy of Debrisan(dextranomer) in the debridement of cutaneousulcers. Surgery 1979;85(2):201–4.
18. Apelqvist J, Ragnarson-Tennvall G, Persson U. Acomparative trial between Iodosorb and standardtreatment of deep diabetic ulcers including anevaluation of cost-effectiveness. Proceedings of the3rd European Conference on Advances in WoundManagement. 1993;3:126.
19. Colin D, Kurring PA, Quinlan D, Yvon C. The clinicalinvestigation of an amorphous hydrogel comparedwith a dextranomer paste dressing in the manage-ment of sloughy pressure sores. Proceedings of the5th European Conference on Advances in WoundManagement. London: Macmillan Ltd, 1996;5:151–5.
20. Mulder GD. A prospective controlled randomizedstudy of the efficacy of Clearsite, DuoDERM, and wet-to-dry gauze dressing in the management of pressureulcers. Proceedings of the 2nd European Conferenceon Advances in Wound Management. 1992;2:45.
21. ConvaTec. Management of leg ulcers and pressuresores. Company Bulletin. Uxbridge: Convatec1996;1–4.
22. Hillström L. Iodosorb compared to standardtreatment in chronic venous leg ulcers – a multi-center study. Acta Chir Scand 1988;544 (Suppl):53–6.
23. Skog E, Arnesjö B, Troëng T, Gjöres JE, Bergljung L,Gundersen J, et al. A randomized trial comparingcadexomer iodine and standard treatment in theout-patient management of chronic venous ulcers.Br J Dermatol 1983;109(1):77–83.
24. Eriksson G, Eklund AE, Kallings LO. The clinicalsignificance of bacterial growth in venous leg ulcers.Scand J Infect Dis 1984;16(2):175–80.
25. Groenewald JH. The treatment of varicose stasisulcers: a controlled trail. Schweiz Rundsch Med Prax1981;70(28):1273–8.
26. Leaper DJ, Stewart AJ. A comparative trial ofScherisorb gel and cadexomer iodine: problems ofcommunity-based trials involving chronic leg ulcers.In: Turner TD, Schmidt RJ, Harding KG, editors.Advances in wound management. Chichester: Wiley, 1986:121–6.
References
References
28
27. Sawyer PN, Sophie Z, Dowback G, Cohen L, Feller J.New approaches in the therapy of the peripheralvascular ulcer. Angiology 1978;29(9):666–74.
28. Troëng T, Skog E, Arnesjö B, Gjöres JE, Bergljung L,Gundersen J, et al. A randomised multicentre trial to compare the efficacy of cadexomer iodine andstandard treatment in the management of chronicvenous ulcers in out-patients. In: Fox JA, Fisher H,editors. Cadexomer iodine. Stuttgart: FK Schattaüer,1983:43–50.
29. Groenewald JH. An evaluation of dextranomer as a cleansing agent in the treatment of the post-phlebitic stasis ulcer. S Afr Med J 1980;57(20):809–15.
30. Garcia HG, Cobian RR, Martin JR, Konaizeh S,Rahola JG. The effect on the reparation process of dextranomer (Debrisan) in perimalleolar ulcersdue to chronic venous insufficiency. Clin Trials J1984;21(3):121–34.
31. Sawyer PN, Hague S, Reddy K, Sophie Z, Feller J.Wound healing effects of Debrisan on varicose,postoperative, decubitus, and sickle-cell ulcers inman. Vasc Surg 1979;13:251–6.
32. Sayag J, Meaume S, Bohbot S. Healing properties of calcium alginate dressings. J Wound Care1996;5(8):357–62.
33. Palmieri B. Heterologous collagen in woundhealing: a clinical study. Int J Tissue React1992;14(Suppl):21–5.
34. Eriksson G, Eklund AE, Lidén S, Zetterquist S.Comparison of different treatments of venous legulcers: a controlled study using stereophoto-grammetry. Curr Ther Res 1984;35:678–84.
35. Goode AW, Glazer G, Ellis BW. The cost-effectiveness of Dextranomer and Eusol in thetreatment of infected surgical wounds. Br J ClinPract 1979;33:325–8.
36. Nasar MA, Morley R. Cost-effectiveness in treatingdeep pressure sores and ulcers. Practitioner1982;226:307–10.
37. Parish LC, Collins E. Decubitus ulcers: acomparative study. Cutis 1979;23(1):106–10.
38. Laudanska H, Gustavson B. In-patient treatment ofchronic varicose venous ulcers. A randomized trialof cadexomer iodine versus standard dressings. J Int Med Res 1988;16(6):428–35.
39. Holloway GA, Jr, Johansen KH, Barnes RW, PierceGE. Multicenter trial of cadexomer iodine to treatvenous stasis ulcer. West J Med 1989;151(1):35–8.
40. Harcup JW, Saul PA. A study of the effect ofcadexomer iodine in the treatment of venous leg ulcers. Br J Clin Pract 1986;40(9):360–4.
41. Lindsay G, Latta D, Lyons KGB, Livingstone ED,Thomson W. A study in general practice of theefficacy of cadexomer iodine in venous leg ulcerstreated on alternate days. Acta Therapeut1986;12:141–7.
42. Apelqvist J, Ragnarson-Tennvall G. Cavity foot ulcers in diabetic patients: a comparative study of cadexomer iodine ointment and standardtreatment. Acta Derm Venereol 1996;76:231–5.
43. Moberg S, Hoffman L, Grennert ML, Holst A. Arandomized trial of cadexomer iodine in decubitusulcers. J Am Geriatr Soc 1983;31(8):462–5.
44. Ormiston MC, Seymour MT, Venn GE, Cohen RI,Fox JA. Controlled trial of Iodosorb in chronicvenous ulcers. Br Med J 1985;291(6491):308–10.
45. Steele K, Irwin G, Dowds N. Cadexomer iodine inthe management of venous leg ulcers in generalpractice. Practitioner 1986;230(1411):63–8.
46. Darkovich SL, Brown-Etris M, Spencer M. Biofilmhydrogel dressing: a clinical evaluation in thetreatment of pressure sores. Ostomy WoundManagement 1990;29:47–60.
47. Brown-Etris M, Fowler E, Papen J, Stanfield J, HarrisA, Tintle T, et al. Comparison and evaluation of theperformance characteristics, usability and effective-ness on wound healing of Transorbent versusDuoDerm CGF. Proceedings of the 5th EuropeanConference on Advances in Wound Management.London: Macmillan Ltd, 1996;5:151–5.
48. Lum CC, Cheung W, Chow PM, Woo J, Hui E, OrKH. Comparative study of pressure sore manage-ment. 1996 unpublished report provided by theauthor. (Conference abstract also available: LumCC, Cheung W, Chow PM, Woo J, Hui E, Or KH.Use of a hydrogel in pressure sore management. Arandomised controlled clinical trial. Proceedings of the 5th European Conference on Advances inWound Management. London: Macmillan Ltd,1996;5:283.)
49. Mulder GD, Altman M, Seeley JE, Tintle T.Prospective randomized study of the efficacy ofhydrogel, hydrocolloid, and saline solution-moistened dressings on the management ofpressure ulcers. Wound Repair Regeneration1993;1(4):213–18.
50. Lee LK, Ambrus JL. Collagenous therapy fordecubitus ulcers. Geriatrics 1975;30(5):91–8.
51. Gordon B. The use of topical proteolytic enzymes in the treatment of post-thrombotic leg ulcers. Br J Clin Pract 1975;29(6):143–6.
52. Westerhof W, Jansen FC, de Wit FS, Cormane RH.Controlled double-blind trial of fibrinolysin-desoxyribonuclease (Elase®) solution in patientswith chronic leg ulcers who are treated beforeautologous skin grafting. J Am Acad Dermatol1987;17(1):32–9.

Health Technology Assessment 1999; Vol. 3: No. 17 (Pt 1)
29
53. Apelqvist J, Larsson J, Stenström A. Topicaltreatment of necrotic foot ulcers in diabeticpatients: a comparative trial of DuoDerm andMeZinc. Br J Dermatol 1990;123:787–92.
54. Tarvainen K. Cadexomer iodine (Iodosorb)compared with dextranomer (Debrisan) in thetreatment of chronic leg ulcers. Acta Chir ScandSuppl 1988;544:57–9.
55. Stewart A J, Leaper DJ. Treatment of chronic leg ulcers in the community: a comparative trial of Scherisorb and Iodosorb. Phlebologie1987;2:115–21.
56. Colin D, Kurring PA, Quinlan D, Yvon C. Managingsloughy pressure sores. J Wound Care 1996;5(10):444–6.
57. Thomas S, Fear M. Comparing two dressings forwound debridement. J Wound Care 1993;2(5):272–4.
58. Hulkko A, Holopainen YV, Orava S, Kangas J,Kuusisto P, Hyvarinen E, et al. Comparison of dextra-nomer and streptokinase-streptodornase in thetreatment of venous leg ulcers and other infectedwounds. Ann Chir Gynaecol 1981; 70(2):65–70.
59. Gibson B. A cost effectiveness comparison of two gels in the treatment of sloughy leg ulcers.Advanced Wound Care Symposium. April 1995; San Diego, USA.
60. Hellgren L. Cleansing properties of stabilizedtrypsin and streptokinase-streptodornase in necroticleg ulcers. Eur J Clin Pharmacol 1983;24(5):623–8.
61. Bux M, Baig MK, Rodrigues E, Armstrong D, Brown A. Antibody response to topicalstreptokinase. J Wound Care 1997;6(2):70–3.
62. Collier M. Hydrogels and their practical use inwound debridement. Community Nursing Notes1997;13:3–5.


Health Technology Assessment 1999; Vol. 3: No. 17 (Pt 1)
31
MEDLINE has been searched for RCTs from1966 to October 1997 using a mixture of free
text terms and MEDLINE search headings:
Wound infection Pilonidal cyst Wounds and injuries Wound healing Leg ulcer Varicose ulcer Skin ulcer Decubitus
The MEDLINE search strategy used is as follows:
decubitus ulcer/ or foot ulcer/ leg ulcer/ or varicose ulcer/ pilonidal cyst/ skin ulcer/ diabetic foot/ ((plantar or diabetic or heel or venous or stasis orarterial) adj ulcer$).tw. ((decubitus or foot or diabetic or ischaemic orpressure) adj ulcer$).tw. ((pressure or bed) adj sore$).tw. ((pilonidal adj cyst) or (pilonidal adj sinus) orbedsore$).tw. ((diabetic adj foot) or (cavity adj wound)).tw. ((varicose or leg or skin) adj ulcer$).tw. (decubitus or (chronic adj wound$)).tw. ((sinus adj wound$) or (cavity adj wound$)).tw.
or/1-13
debridement/ or biological dressings/ orbandages/ occlusive dressings/ or clothing/ or woundhealing/ antibiotics/ or growth substances/ or platelet-derived growth factor/ fibroblast growth factor/ or electrical stimulationtherapy.ti,ab,sh. lasers/ or nutrition/ or surgery/ or surgery,plastic/ surgical flaps/ or skin transplantations/ orhomeopathy/ or homeopathic/ acupuncture therapy/ or acupuncture/ oralternative medicine/ alternative medicine/ or massage/ or iloprost/ or alginates/
zinc/ or zinc oxide/ or ointments/ or anti-infective agents/ dermatologic agents/ or colloids/ or cushions/ or wheelchairs/ beds/ or wound dressings/ (debridement or dressing$ or compress$ or cream$ or (growth adj factor$)).tw. (pressure-relie$ or (recombinant adj protein$) or bandag$ or stocking$).tw. (antibiotic$ or (electric adj therapy) or laser$ ornutrition$ or surg$).tw. (homeopath$ or acupunture or massage orreflexology or ultrasound).tw. (iloprost or alginate$ or zinc or paste$ orointment$ or hydrocolloid$).tw. ((compression adj therapy) or (compression adjbandag$) or wrap$).tw. (bed$ or mattress$ or wheelchair$ or (wheel adjchair) or cushion$).tw. ((wound adj dressing$) or vitamin$ or bind$ orgauze$ or heals or healing).tw. (diet or lotion$ or infect$ or reduc$ or (wound adjhealing)).tw. (treat$ or prevent$ or epidemiol$ or aetiol$ oretiol$ or therap$ or prevalence or incidence).tw.
or/15–35 14 and 36
random allocation/ or randomized controlledtrials/ controlled clinical trials/ or clinical trials phase I/or clinical trials phase II/ clinical trials phase III/ or clinical trials phase IV/ or clinical trials overviews/ single-blind method/ or double-blind method/ publication bias/ or review/ or review, academic/ review tutorial/ or meta-analysis/ or systematicreview/ ((random$ adj controlled adj trial$) or(prospective adj random$)).tw. ((random adj allocation) or random$ or (clinicaladj trial$) or control$).tw. ((standard adj treatment) or compar$ or single-blind$ or double-blind$).tw. (blind$ or placebo$ or systematic$ or (systematicadj review)).tw. (randomized controlled trial or clinical trial).pt. orcomparative study.sh.
Appendix 1
MEDLINE search strategy
Appendix 1
32
or/38-48 37 and 49 limit 50 to human
burns/ or wounds, gunshot/ or corneal ulcer/ orexp dentistry/ peptic ulcer/ or duodenal ulcer/ or stomachulcer/
((peptic adj ulcer) or (duodenal adj ulcer) ortraum$).tw. ((aortocaval adj fistula) or (arteriovenous adjfistula)).tw. (bite adj wound$).tw.
or/52–56 51 not 57

Health Technology Assessment 1999; Vol. 3: No. 17 (Pt 1)
33
Other databases that have been searched forRCTs are:
EMBASE [to October 1997] CINAHL (Cumulative Index of Nursing and Allied Health Literature) [to April 1997]
The CINAHL search strategy used is as follows:
pressure ulcer/ or foot ulcer/ or leg ulcer/ or skin ulcer/ diabetic foot/ or diabetic neuropathies/ diabetic angiopathies/ or diabetes mellitus/co pilonidal cyst/ or surgical wound infection/ ((plantar or diabetic or heel or venous or stasis or arterial) adj ulcer$).tw. ((decubitus or foot or diabetic or ischaemic orpressure) adj ulcer$).tw. ((pressure or bed) adj sore$).tw. ((pilonidal adj cyst) or (pilonidal adj sinus) orbedsore).tw. ((diabetic adj foot) or (cavity adj wound)).tw. ((varicose or leg or skin) adj ulcer$).tw. (decubitus or (chronic adj wound$)).tw. ((sinus adj wound$) or (cavity adj wound$)).tw.
or/1–12
debridement/ or biological dressings/ or occlusivedressings/ (bandages.ti,sh,ab,it. and “Bandages andDressings”/) or compression garments/ or antibiotics/ electric stimulation/ or Laser Surgery/ or lasers/thlasers/ or Nutrition Care (Saba HHCC)/ or diettherapy/ or Nutrition Therapy (Iowa NIC)/ surgery, reconstructive/ or surgery, plastic/ orsurgical flaps/ surgical stapling/ or skin transplantation/ oralternative therapies/ acupuncture/ or massage/ or zinc/ or ointments/ antiinfective agents, local/ or antibiotics/ ordermatologic agents/ dermatology nursing/ or colloids/ or beds nadmattresses/ flotation beds/ or wheelchairs/ orpositioning:wheelchair/ or positioning:therapy/ patient positioning/ or positioning/ or woundcare/ or wound healing/
(debridement or dressing$ or compress$ orcream$).tw. ((growth adj factor$) or pressure relie$ or(recombinant adj protein$) or bandag$).tw. (stocking$ or antibiotic$ or (electric adj therapy)or laser$ or nutrition$ or surg$).tw. (iloprost or alginate$ or zinc or paste$ orointment$ or hydrocolloid$).tw. ((compression adj therapy) or (compression adjbandag$) or wrap$).tw. (bed$ or mattress$ or wheelchair$ or (wheel adjchair) or cushion$).tw. ((wound adj dressing$) or vitamin$ or bind$ orgauze$ or heals or healing).tw. (diet or lotion$ or infect$ or reduc$ or etiol$ or(wound adj healing)).tw. (treat$ or prevent$ or epidemiol$ or aetiol$ ortherap$ or prevalence or incidence).tw. “Bandages and dressings”/ or skin transplantation/or homeopathy/ or ointments/ or “beds andmattresses”/
or/14–34 13 and 35
clinical trials/ or single-blind studies/ or double-blind studies/ control group/ or placebos/ or meta analysis/ ((random$ adj clinical adj trial$) or (prospectiveadj random$)).tw. ((random adj allocation) or random$ or controlledclinical trial$ or control).tw. (comparison group$ or (standard adj treatment) orcompar$).tw. (single-blind$ or (single adj blind) or double-blindor (double adj blind)).tw. (blind$ or placebo$ or systematic or (systematic adjreview)).tw. (meta analysis or meta-analysis).tw. or (trials or trialor prospective).tw. (clinical trials).sh. or (comparative studies).sh .
or/37–45 36 and 46
burns/ or wounds, gunshot/ or corneal ulcer/ orexp dentistry/ peptic ulcer/ or duodenal ulcer/ ((peptic adj ulcer) or (duodenal adj ulcer) ortrauma).tw.
Appendix 2
CINAHL and EMBASE search strategy

Appendix 2
34
(burn$ or (gunshot adj wound$) or (corneal adjulcer) or dentist$ or (bite adj wound)).tw. or/48–51
47 not 52

Health Technology Assessment 1999; Vol. 3: No. 17 (Pt 1)
35
ISI Science Citation Index (on BIDS)
BIOSIS (on Silver Platter)
British Diabetic Association Database
CINAHL (on OVID CD-ROM)
CISCOM, the database of the Reseach Council for Complementary Medicine
Cochrane Database of Systematic Reviews (CDSR)
Cochrane Wounds Group Specialised Trials Register
Current Research in Britain (CRIB)
Database of Abstract of Reviews of Effectiveness(DARE)
Dissertation Abstracts
DHSS Data (on Knight-Ridder Datastar)
EconLit
EMBASE (on Knight-Ridder Datastar)
Index to Scientific and Technical Proceedings(searched on BIDS)
MEDLINE (on OVID CD-ROM)
National Research Register (to locate ongoingresearch in NHS)
NHS Economic Evaluation Database (NHS CRD)
Royal College of Nursing Database (CD-ROM)
System for Information on Grey Literature inEurope (SIGLE – on Blaise Line)
Appendix 3
Additional databases searched


Health Technology Assessment 1999; Vol. 3: No. 17 (Pt 1)
37
Dr Mary Bliss, Consultant Geriatrician, Departmentof Medicine for the Elderly, Homerton Hospital,Homerton Row, London E9 6SR, UK.
Professor Nick Bosanquet, Imperial College Schoolof Medicine, Department of General Practice,Norfolk Place, London W2 1PG, UK.
Professor Andrew Boulton, Department ofMedicine, Manchester Royal Infirmary, OxfordRoad, Manchester M13 9WL, UK.
Dr Richard Bull, Department of Dermatology,Homerton Hospital, Homerton Row, London E9 6SR, UK.
Mr Michael Callam, Department of VascularSurgery, Bedford Hospital, South Wing, KempstonRoad, Bedford MK42 9DJ, UK.
Mrs Carol Dealey, Research Fellow, UniversityHospital Birmingham NHS Trust, Department ofNursing, Queen Elizabeth Medical Centre,Edgbaston, Birmingham B15 2TH, UK.
Professor Peter Friedmann, Dermatology Unit,University Medicine, Level F, Centre Block (Mail Point 825), Southampton General Hospital,Tremona Road, Southampton SO16 6YD, UK.
Mr Brian Gilchrist, Department of Nursing Studies,King’s College London, Cornwall House Annexe,Waterloo Road, London SE1 8TX, UK.
Dr Keith Harding, Director, Wound HealingResearch Unit, University of Wales College ofMedicine, University Department of Surgery, Heath Park, Cardiff CF4 4XN, UK.
Deborah Hofman, Dermatology Department,Churchill Hospital, Headington, Oxford OX3 7LJ, UK.
Vanessa Jones, Educational Facilitator, WoundHealing Research Unit, University Department of Surgery, Heath Park, Cardiff CF4 4XN, UK.
Dr Christina Lindholm, Nattarövägen 42, S-132 34 SaltsjöBoo, Sweden.
Dr Raj Mani, Southampton University HospitalsTrust, Medical Physics Department, Level D, Centre Block, Southampton SO9 4XY, UK.
Andrea Nelson, Department of Health Studies,University of York, Heslington, York YO1 5DD, UK.
Dr Steve Thomas, Director, Surgical MaterialsTesting Laboratory, Bridgend General Hospital,Bridgend, Mid Glamorgan, UK.
Dr Ewan Wilkinson, Liverpool Health Authority,Hamilton House, 24 Pall Mall, Liverpool L3 6AL, UK.
Appendix 4
Expert advisory panel


Health Technology Assessment 1999; Vol. 3: No. 17 (Pt 1)
39
Appendix 5
Quality assessment
TABLE 4 Quality assessment of RCTs of debridement
Study Inclusion Total no. A priori Random- Appropriate Blinded Appropriate With- ITT and exclu- of wounds sample size isation baseline outcome outcome drawals† analysission criteria [arms] calculation procedure characteristics assessment measuresstated stated reported*
Ågren and Strömberg, ✗ 28 patients [2] ✗ ✔ ✔c ✗ ✔ ✔a ✗19859
Apelqvist et al, 199053 ✔ 44 patients [2] ✗ ✗ ✔c ✔ ✔ ✔a ✗
Apelqvist and Tennvall, ✔ 41 [2] ✗ ✔ ✗ ✔ ✔ ✔b ✗199642
Brown-Etris et al, ✔ 140 [2] ✗ ✗ ✔ ✔ ✔ ✔b ✗199647
Colin et al, 199656 ✔ 135 [2] ✔ ✗ ✔c ✗ ✔ ✔a ✔
Darkovich et al, 199046 ✔ 123[2] ✗ ✗ ✔c ✗ ✔ ✔a ✗
Eriksson et al, 198434 ✔ 53 [2] ✗ ✗ ✔ ✗ ✔ N/A N/A
Garcia et al, 198430 ✔ 44 [2] ✗ ✗ ✔ ✗ ✔ N/A N/A
Gibson, 199559 ✗ 62 [2] ✗ ✗ ✔c ✗ ✔ ✗ ✗
Goode et al, 197935 ✗ 20 [2] ✗ ✔ ✔ ✗ ✔ N/A N/A
Gordon, 197551 ✗ 19 [2] ✔ ✗ ✔c ✔ ✔ ✔a ✗
Groenewald, 198029 ✗ 100 [2] ✗ ✗ ✔c ✗ ✔ ✔a ✗
Harcup and Saul, 198640 ✔ 72 [2] ✗ ✗ ✔c ✗ ✔ ✔a ✔
Hellgren, 198360 ✔ 40 [2] ✗ ✗ ✔ ✔ ✔ ✔a ✗
Holloway et al, 198939 ✔ 75 [2] ✗ ✗ ✔c ✗ ✔ ✔a ✗
Hulkko et al, 198158 ✗ 31 [2] ✗ ✗ ✔ ✗ ✔ ✔b ✗
Laudanska and Gustavson, 198838 ✔ 60 [2] ✗ ✗ ✔c ✗ ✔ ✔b ✗
Lee and Ambrus, 197550 ✗ 28 [2] ✗ ✗ ✔c ✗ ✔ ✔a ✗
Lindsay et al, 198641 ✔ 28 [2] ✗ ✗ ✔ ✗ ✔ ✔a ✗
Lum et al, 199648 ✔ 20 [2] ✗ ✔ ✔c ✗ ✔ ✔a ✗
Moberg et al, 198343 ✔ 38 patients [2] ✗ ✗ ✔c ✔ ✔ ✔a ✗
Moss et al, 198713 ✔ 42 [2] ✗ ✗ ✔c ✗ ✔ ✔b ✗
Mulder et al, 199349 ✔ 64 patients [3] ✗ ✔ ✔ ✗ ✔ ✔b ✗
Nasar and Morley, 198236 ✔ 18 [2] ✗ ✗ ✗ ✔ ✔ ✔a ✗
✔ = Yes; ✗ = No; N/A = not appropriate (no withdrawals)* Baseline characteristics: ✔ = one or more appropriate characteristics stated (but not initial wound size); ✔c = initial wound size stated† Withdrawals: ✔a = reported by group and with reason; ✔b = withdrawals but not reported by group or reason not given; ✗ = withdrawals not reported
continued

Appendix 5
40
TABLE 4 contd Quality assessment of RCTs of debridement
Study Inclusion Total no. A priori Random- Appropriate Blinded Appropriate With- ITT and exclu- of wounds sample size isation baseline outcome outcome drawals† analysission criteria [arms] calculation procedure characteristics assessment measuresstated stated reported*
Ormiston et al, 198544 ✔ 61 [2] ✗ ✔ ✔c ✔ ✔ ✔a ✔
Palmieri, 199233 ✔ 48 [2] ✗ ✗ ✔ ✗ ✔ N/A N/A
Parish and Collins, ✗ 34 [3] ✗ ✗ ✔c ✗ ✔ N/A N/A197937
Sawyer et al, 197931 ✗ 37 [2] ✗ ✔ ✗ ✗ ✔ N/A N/A
Sayag et al, 199632 ✔ 92 [2] ✔ ✔ ✔c ✗ ✔ ✔a ✔
Skog et al, 1983;23 ✔ 95 [2] ✗ ✗ ✔c ✗ ✔ ✔a ✗Hillström, 1988;22
Troëng et al, 198328
Steele et al, 198645 ✔ 60 [2] ✗ ✔ ✔c ✗ ✔ ✔a ✗
Stewart and Leaper, ✔ 95 [2] ✗ ✔ ✔c ✗ ✔ ✔a ✗198755
Tarvainen, 198854 ✔ 27 [2] ✗ ✔ ✔ ✗ ✔ ✔a ✗
Thomas and Fear, 199357 ✔ 40 patients [2] ✗ ✔ ✔c ✗ ✔ ✔a ✔
Westerhof et al, 198752 ✔ 33 [2] ✗ ✔ ✔c ✔ ✔ ✔b ✗
✔ = Yes; ✗ = No; N/A = not appropriate (no withdrawals)* Baseline characteristics: ✔ = one or more appropriate characteristics stated (but not initial wound size); ✔c = initial wound size stated† Withdrawals: ✔a = reported by group and with reason; ✔b = withdrawals but not reported by group or reason not given; ✗ = withdrawals not reported

Health Technology Assessment 1999; Vol. 3: No. 17 (Pt 1)
41
Appendix 6
Summary of studies

Appendix 6
42 TAB
LE 5
Dex
trano
mer
pol
ysac
char
ide
vers
us tr
aditi
onal
or
cont
rol t
reat
men
ts
Stud
y an
d de
sign
Incl
usio
n/ex
clus
ion
crit
eria
Inte
rven
tion
det
ails
Bas
elin
e ch
arac
teri
stic
sR
esul
ts
Wit
hdra
wal
sC
omm
ents
Deb
risan
®,P
harm
acia
Upj
ohn
cont
inue
d
Erik
sson
et a
l,198
434
Swed
en
Wou
nd ty
pe:
Veno
us le
g ul
cers
.
Met
hod
of r
ando
misa
tion:
Not
sta
ted.
Obj
ectiv
e ou
tcom
e:A
rea
and
volu
me
mea
sure
dby
ste
reop
hoto
gram
met
ricex
amin
atio
n.
Sett
ing
and
leng
th
of tr
eatm
ent:
Trea
ted
over
a
2-w
eek
perio
d.
Incl
usio
n cr
iteria
:O
utpa
tient
s w
ith v
enou
s le
g ul
cers
.
Excl
usio
n cr
iteria
:D
iabe
tes
mel
litus
;man
ifest
arte
rial i
nsuf
ficie
ncy;
clin
ical
pict
ure
of e
rysip
elas
or
cellu
litis.
Befo
re c
omm
ence
men
t th
e ge
nera
l hea
lth o
f all
part
icip
ants
and
the
stat
e of
veno
us a
nd a
rter
ial p
erip
hera
lci
rcul
atio
n w
ere
eval
uate
d.A
pre
ssur
e in
dex
ankl
e/ar
m o
fle
ss th
an 0
.75
was
con
sider
edpa
thol
ogic
al a
nd a
s su
ch a
nex
clus
ion
crite
ria.
Trea
tmen
t:I:
Dex
tran
omer
pol
ysac
char
ide
bead
s (D
ebris
an®) m
ixed
with
ster
ilise
d gly
cero
l and
cov
ered
with
gau
ze.T
he d
ress
ing
was
chan
ged
ever
y da
y fo
r th
e fir
stw
eek
and
ever
y se
cond
day
for
the
seco
nd w
eek,
n =
26.
C:S
teril
ised
gauz
e so
aked
in
0.9%
(w/v
) sod
ium
chl
orid
e in
wat
er.T
he g
auze
was
moi
sten
edre
gula
rly th
roug
h th
e da
y,n
= 27
.
Prio
r to
the
initi
al tr
eatm
ent a
ndat
the
star
t of t
he s
econ
d w
eek
oftr
eatm
ent,
all u
lcer
s w
ere
bath
edfo
r 15
min
in w
ater
con
tain
ing
1 m
l/l o
f 3%
(w/v
) pot
assiu
mpe
rman
gana
te.C
rust
and
deb
risw
ere
rem
oved
.
Mea
n w
ound
are
a (c
m2 ):
Not
sta
ted.
Oth
er c
hara
cter
istic
s:A
ll gr
oups
Mea
n ag
e (y
ears
):70
.1M
:F r
atio
:1:
3.1
Mea
n du
ratio
n (m
onth
s):
No
deta
ils
Both
gro
ups
com
para
ble
for
all
back
grou
nd c
hara
cter
istic
s ex
cept
elev
ated
blo
od g
luco
se le
vels
and
ahi
stor
y of
pre
viou
s th
rom
bosis
(bot
h th
ese
fact
ors
are
nega
tivel
yco
rrel
ated
with
ulc
er h
ealin
g):
Hig
hH
istor
y of
gluc
ose
leve
lsth
rom
bosis
I:8%
16%
C:
30%
38%
Num
ber
of w
ound
s de
crea
sed
in
% a
rea:
> 50
5025
I:2
814
C:
65
10
Num
ber
of w
ound
s in
crea
sed
in
% a
rea:
> 50
5025
I:0
11
C:
03
3
Num
ber
of w
ound
s de
crea
sed
in
% v
olum
e:>
5050
25I:
46
11C
:9
16
Num
ber
of w
ound
s in
crea
sed
in
% v
olum
e:>
5050
25I:
02
3C
:0
56
No
stat
istic
al d
iffer
ence
bet
wee
n th
e tw
o tr
eatm
ents
was
foun
d.
No
with
draw
als.
Pain
as
judg
ed b
y th
e pa
tient
sho
wed
a r
educ
tion
in th
e I (
dext
rano
mer
) gro
up(p
< 0.
05).
Cha
nges
in a
rea
wer
e fo
und
to b
e hi
ghly
cor
rela
ted
with
bac
kgro
und
varia
bles
:el
evat
ed g
luco
se le
vels
resu
lted
in s
low
er h
ealin
g as
did
a h
istor
y of
pre
viou
sth
rom
bosis
.
Bact
eria
l flo
ra r
emai
ned
unch
ange
d th
roug
hout
the
stud
y irr
espe
ctive
of
trea
tmen
t.
Gar
cia
et a
l,198
430
Spai
n
Wou
nd ty
pe:
Seco
ndar
y pe
rimal
leol
arul
cers
.
Met
hod
of r
ando
misa
tion:
Not
sta
ted.
Obj
ectiv
e ou
tcom
e:A
rea
and
circ
umfe
renc
e of
the
wou
nd m
easu
red
by p
lani
met
ry.
Sett
ing
and
leng
th o
ftr
eatm
ent:
Hos
pita
l and
com
mun
ity-b
ased
tria
l ov
er a
3-w
eek
perio
d.
Incl
usio
n cr
iteria
:Pa
tient
s w
ith s
econ
dary
perim
alle
olar
ulc
ers
and
chro
nic
veno
us in
suffi
cien
cy
Excl
usio
n cr
iteria
:Pa
tient
s no
t sub
mitt
ed fo
rsu
rgic
al tr
eatm
ent.
Trea
tmen
t:I:
Dex
tran
omer
pol
ysac
char
ide
bead
s (D
ebris
an),
n =
22.
C:P
otas
sium
per
man
gana
te 1
/500
0an
d hy
pert
onic
sal
ine
or a
ntib
iotic
oint
men
ts,n
= 2
2.
Mea
n w
ound
are
a:N
ot s
tate
d.
Oth
er c
hara
cter
istic
s:A
ll gr
oups
Mea
n ag
e (y
ears
):56
.5M
:F r
atio
:2.
2:1
Mea
n du
ratio
n (m
onth
s):
164
33 p
atie
nts
requ
ired
hosp
italis
atio
nw
hile
the
rem
aini
ng n
ine
coul
d be
tr
eate
d as
out
-pat
ient
s.
% r
educ
tion
in m
ean
area
of w
ound
afte
r 3
wee
ks:
I:93
.1%
(7.4
SD
;n =
22)
C:8
5.2%
(10.
8 SD
;n =
22)
(p<
0.01
;Stu
dent
’s t-t
est)
% r
educ
tion
in m
ean
circ
umfe
renc
eaf
ter
3 w
eeks
:I:
80.0
% (2
0.6
SD;n
= 2
2)C
:70.
1% (2
0.8
SD;n
= 2
2)
(p>
0.05
,NS;
Stud
ent’s
t-te
st)
No
with
draw
als
repo
rted
.I (
dext
rano
mer
) doe
s no
tin
duce
con
tact
der
mat
itis,
ecze
ma
or a
llerg
ic r
eact
ions
.
Stat
istic
al s
igni
fican
ce is
grea
ter
1 an
d 2
wee
ks a
fter
the
initi
atio
n of
trea
tmen
t(fo
r ar
ea p
< 0
.001
;for
circ
umfe
renc
e p
< 0.
05).

Health Technology Assessment 1999; Vol. 3: No. 17 (Pt 1)
43TAB
LE 5
con
td D
extra
nom
er p
olys
acch
arid
e ve
rsus
trad
ition
al o
r co
ntro
l tre
atm
ents
Stud
y an
d de
sign
Incl
usio
n/ex
clus
ion
crit
eria
Inte
rven
tion
det
ails
Bas
elin
e ch
arac
teri
stic
sR
esul
ts
Wit
hdra
wal
sC
omm
ents
cont
inue
d
Goo
de e
t al,1
97935
UK
Wou
nd ty
pe:
Surg
ical
wou
nds.
Met
hod
of r
ando
misa
tion:
Seal
ed e
nvel
opes
.
Obj
ectiv
e ou
tcom
e:Ti
me
to s
econ
dary
wou
ndcl
osur
e.Ea
ch w
ound
was
phot
ogra
phed
at t
he s
tart
,du
ring
and
at th
e en
d of
trea
tmen
t.
Sett
ing
and
leng
th
of tr
eatm
ent:
Hos
pita
lised
sur
gica
lpa
tient
s.Tr
eatm
ent w
asco
ntin
ued
until
it w
asco
nsid
ered
app
ropr
iate
tocl
ose
the
wou
nd.
Incl
usio
n cr
iteria
:Pa
tient
s w
ho d
evel
oped
wou
ndin
fect
ions
afte
r an
app
endi
cec-
tom
y or
bow
el s
urge
ry.
Excl
usio
n cr
iteria
:N
ot s
tate
d.
Trea
tmen
t:I:
Dex
tran
omer
pol
ysac
char
ide
bead
s (D
ebris
an) w
ere
appl
ied
dire
ctly
into
the
wou
nd to
a d
epth
of 0
.5 c
m,fo
llow
ed b
y a
light
pac
k.D
extr
anom
er w
as a
pplie
d tw
ice
daily
,n =
10.
C:E
usol
and
par
affin
soa
ked
ribbo
n ga
uze
dres
sings
cha
nged
twic
e da
ily,n
= 1
0.
All
othe
r nu
rsin
g pr
oced
ures
wer
eid
entic
al fo
r bo
th g
roup
s.
Mea
n w
ound
are
a (c
m2 ):
Not
sta
ted.
Oth
er c
hara
cter
istic
s:I
CM
ean
age
(yea
rs):
52.9
50.9
M:F
rat
io:
1:0.
41:
0.7
Wou
nds:
App
endi
cect
omy
67
Para
med
ian
43
Del
ayed
prim
ary
sutu
re4
6W
ound
abs
cess
64
All
wou
nds
wer
e ei
ther
hea
vily
cont
amin
ated
at o
pera
tion
and
left
open
for
delay
ed p
rimar
y su
ture
(ten
pat
ient
s),o
r th
ose
whi
chw
ere
clos
ed p
rimar
ily a
nd s
ubse
-qu
ently
dev
elop
ed a
n ab
sces
s th
atre
quire
d th
e re
mov
al o
f sut
ures
and
drai
nage
(ten
pat
ient
s).
Num
ber
of w
ound
s he
aled
with
out
seco
ndar
y cl
osur
e:I:
1/10
(10%
)C
:1/1
0 (1
0%)
Mea
n tim
e an
d ra
nge
(day
s) to
seco
ndar
y cl
osur
e:I:
8.1
(ran
ge,5
–28;
n =
10)
C:1
.6 (r
ange
,6–2
2;n
= 10
)(p
< 0.
05;M
ann-
Whi
tney
U-T
est)
Ther
e w
ere
now
ithdr
awal
s.Th
ree
patie
nts
in th
e C
gro
up(E
usol
) con
tinue
d to
hav
ese
rious
disc
harg
es fo
r up
to
5 da
ys a
fter
wou
nd c
losu
re.
This
did
not o
ccur
in th
e I
(dex
tran
omer
) gro
up.
Wou
nd h
ealin
g w
as th
epr
inci
pal f
acto
r pr
even
ting
disc
harg
e fro
m h
ospi
tal;t
hose
trea
ted
with
I ha
d a
shor
ter
hosp
ital s
tay
by a
med
ian
of2.
2 da
ys.
The
auth
or s
tate
s th
at th
ehi
gh c
ost o
f I is
com
pens
ated
by th
e sa
ving
from
sho
rter
hosp
ital s
tay.

Appendix 6
44 TAB
LE 5
con
td D
extra
nom
er p
olys
acch
arid
e ve
rsus
trad
ition
al o
r co
ntro
l tre
atm
ents
Stud
y an
d de
sign
Incl
usio
n/ex
clus
ion
crit
eria
Inte
rven
tion
det
ails
Bas
elin
e ch
arac
teri
stic
sR
esul
ts
Wit
hdra
wal
sC
omm
ents
cont
inue
d
Gro
enew
ald,
1980
29
Sout
h A
fric
a
Wou
nd ty
pe:
Veno
us le
g ul
cers
.
Met
hod
of r
ando
misa
tion:
Not
sta
ted.
Obj
ectiv
e ou
tcom
e:Th
e ci
rcum
fere
nce
of
the
wou
nd w
as m
easu
red
by a
mill
imet
re o
verla
y.A
pho
togr
aph
was
take
n at
eac
h vi
sit.
Sett
ing
and
leng
th
of tr
eatm
ent:
Hos
pita
l clin
ic.P
atie
nts
trea
ted
for
21 d
ays
and
asse
ssed
dai
ly b
y tw
oin
depe
nden
t inv
estig
ator
s.
Incl
usio
n cr
iteria
:O
utpa
tient
s w
ith p
ost-
phle
bitic
stas
is le
g ul
cers
.
Excl
usio
n cr
iteria
:N
ot s
tate
d.
Trea
tmen
t:I:
Dex
tran
omer
pol
ysac
char
ide
(Deb
risan
) bea
ds w
ere
pour
eddi
rect
ly o
nto
the
ulce
r su
rfac
e to
form
a la
yer
at le
ast 2
–3 m
m th
ick.
A m
ultil
ayer
gau
ze p
ad w
as u
sed
to c
over
the
ulce
r an
d ke
pt in
plac
e by
a s
tand
ard
gauz
e ba
ndag
e,n
= 50
.
C:P
ovid
one-
iodi
ne o
intm
ent w
assw
abbe
d on
to th
e ul
cer
and
apr
essu
re b
anda
ge a
pplie
d.Th
ew
hole
foot
and
low
er le
g w
ere
boun
d w
ith a
zin
c ox
ide-
impr
eg-
nate
d ga
uze
band
age,
n =
50.
The
ulce
rs a
nd s
urro
undi
ng
leg
area
in b
oth
grou
ps w
ere
initi
ally
was
hed
with
a s
oft b
rush
ina
povi
done
-iodi
ne s
olut
ion,
befo
rebe
ing
tem
pora
rily
cove
red
with
gauz
e sw
abs
soak
ed in
Eus
olso
lutio
n.
In th
e pr
esen
ce o
f Pse
udom
onas
infe
ctio
n 0.
25%
ace
tic a
cid
solu
tion
was
app
lied.
The
surr
ound
ing
skin
was
pai
nted
with
tinc
ture
of
met
hiol
ate.
In th
e pr
esen
ce o
fco
mm
only
occ
urrin
g fu
ngal
infe
ctio
ns o
f the
sur
roun
ding
ski
nar
ea,a
n ap
prop
riate
ant
ifung
alag
ent w
as a
pplie
d.W
here
the
sur-
roun
ding
ski
n w
as e
czem
atou
s,flu
cino
line
oint
men
t was
app
lied.
Wou
nd s
ize:
IC
< 6
cm:
77
6–12
cm
:20
21>
12 c
m:
2322
Oth
er c
hara
cter
istic
s: IC
Mea
n ag
e (y
ears
):N
ot s
tate
dM
:F r
atio
:1:
3.5
1:4.
6M
ean
dura
tion
(mon
ths)
:N
ot s
tate
d
Dep
th o
f ulc
er:
Shal
low
2029
Dee
p30
21
Raci
al d
istrib
utio
n (%
):W
hite
2322
Col
oure
d26
25Bl
ack
13
The
num
ber
of a
ffect
ed r
ight
and
left
legs
wer
e al
mos
t equ
al in
eac
hof
the
two
grou
ps.
The
sam
ples
wer
e sh
own
to b
ere
pres
enta
tive
of th
e ov
eral
l clin
icpo
pula
tion.
Redu
ctio
n in
wou
nd s
ize a
t 21
days
:I
C0%
:8
2610
%:
21
25%
:1
150
%:
62
75%
:7
310
0%:
112
Mea
n tim
e to
hea
ling:
I:4.
44 w
eeks
(n =
35)
C:5
.32
wee
ks (n
= 35
)(p
< 0.
05)
30 p
atie
nts,
15 in
each
gro
up w
ere
not i
nclu
ded
in th
efin
al a
naly
sis.T
hese
patie
nts
wer
etr
eate
d su
rgic
ally
afte
r th
e w
ound
was
dee
med
to b
ecl
ean
(e.g
.by
skin
graf
ting)
.
Five
add
ition
alpa
tient
s dr
oppe
dou
t of t
he tr
ial a
ndw
ere
repl
aced
toke
ep th
e gr
oup
num
ber
at 5
0.
(Rea
sons
for
thes
ew
ithdr
awal
s ar
e no
tst
ated
.)
Of 3
0 I (
dext
rano
mer
)pa
tient
s co
mpl
aini
ng o
f pai
n,20
sho
wed
impr
ovem
ent
with
in 2
4 hr
,one
afte
r 3
days
and
one
afte
r 10
day
s.In
the
rem
aini
ng e
ight
pat
ient
s th
epa
in in
itial
ly w
orse
ned
befo
reim
prov
ing.
Of t
he 3
5 C
pat
ient
sco
mpl
aini
ng o
f pai
n,se
ven
impr
oved
afte
r 24
hr,
thre
eaf
ter
3 da
ys,a
nd s
ix a
fter
7 da
ys.In
13
the
pain
wor
sene
d be
fore
impr
ovin
g,in
two
patie
nts
the
pain
leve
lre
mai
ned
unch
ange
d,an
d in
four
the
pain
wor
sene
dw
ithou
t im
prov
ing
late
r.

Health Technology Assessment 1999; Vol. 3: No. 17 (Pt 1)
45TAB
LE 5
con
td D
extra
nom
er p
olys
acch
arid
e ve
rsus
trad
ition
al o
r co
ntro
l tre
atm
ents
Stud
y an
d de
sign
Incl
usio
n/ex
clus
ion
crit
eria
Inte
rven
tion
det
ails
Bas
elin
e ch
arac
teri
stic
sR
esul
ts
Wit
hdra
wal
sC
omm
ents
cont
inue
d
Nas
ar a
nd M
orle
y,19
8236
UK
Wou
nd ty
pe:
Pres
sure
sor
es.
Met
hod
of r
ando
misa
tion:
Not
sta
ted.
Obj
ectiv
e ou
tcom
e:W
ound
are
a w
as m
easu
red
usin
g ce
llulo
id s
quar
es a
ndth
e en
tire
wou
ndph
otog
raph
ed.
End
poin
t was
rea
ched
whe
n th
e w
ound
was
cle
anan
d gr
anul
atin
g an
d ap
pear
-ed
to b
e le
ss th
an 2
5% it
sor
igin
al s
ize (=
hea
led)
.
Sett
ing
and
leng
th
of tr
eatm
ent:
Hos
pita
l-bas
ed tr
ial.
Ass
essm
ents
wer
e m
ade
ever
y 3
days
by
an in
de-
pend
ent o
bser
ver
and
aph
otog
raph
take
n on
ce a
wee
k.Tr
eatm
ent w
asco
ntin
ued
until
the
wou
ndre
ache
d th
e en
d po
int,
orfo
r a
max
imum
of 9
4 da
ys.
Incl
usio
n cr
iteria
:Pa
tient
s w
ith d
eep
pres
sure
sore
s of
app
roxi
mat
ely
simila
rsiz
e.
Excl
usio
n cr
iteria
:U
rinar
y tr
act i
nfec
tion.
Trea
tmen
t:I:
Dex
tran
omer
pol
ysac
char
ide
(Deb
risan
) app
lied
as a
stif
f pas
tetw
ice
daily
for
the
first
3 d
ays
and
daily
ther
eafte
r,n
= 9.
C:E
usol
and
par
affin
pac
ks w
ere
appl
ied
to th
e w
ound
and
dres
sings
wer
e ch
ange
d th
ree
times
dai
ly fo
r th
e fir
st 3
day
s an
dth
erea
fter
twic
e da
ily.M
elol
indr
essin
gs w
ere
used
thro
ugho
uthe
ld in
pla
ce b
y m
icro
pore
tape
.Asa
vlon
sac
het w
as u
sed
each
tim
eth
e dr
essin
g w
as c
hang
ed,n
= 9
.
Prio
r to
initi
atio
n of
the
tria
l all
hard
ened
slo
ughs
wer
e cu
t off
and
all p
atie
nts
wer
e nu
rsed
on
a la
rge
cell
rippl
e m
attr
ess.
The
only
con
-cu
rren
t the
rapy
was
ultr
avio
let
light
app
lied
to 1
2 sq
uare
inch
es
of s
kin
to p
rodu
ce fi
rst d
egre
eer
ythe
ma
with
the
sore
mas
ked
from
the
ultr
avio
let r
ays.
Mea
n w
ound
are
a:N
ot s
tate
d.
Oth
er c
hara
cter
istic
s:I
CM
ean
age
(yea
rs):
83.2
77.4
M:F
rat
io:
Not
sta
ted
Mea
n du
ratio
n (m
onth
s):
Not
sta
ted
Ana
emia
,hyp
oalb
umin
aem
ia,
hypo
vita
min
osis,
and
high
blo
odur
ea w
ere
corr
ecte
d if
pres
ent.
Scru
pulo
us c
ontr
ol o
f dia
betic
patie
nts
was
ens
ured
.Pat
ient
s w
ithur
inar
y in
cont
inen
ce w
ere
cath
eter
ised.
Pres
sure
sor
es w
ere
mos
tly o
n th
efo
ot o
r he
el in
bot
h gr
oups
.
Num
ber
of w
ound
s at
tain
ing
the
end
poin
t:I:
6/9
(67%
) C
:5/9
(56%
)
Mea
n tim
e to
rea
ch e
nd p
oint
:I:
39.3
day
sC
:62
days
I:Thr
ee w
ound
s.Tw
o du
e to
pat
ient
deat
h;on
e as
are
sult
of p
atie
ntdi
scom
fort
.
C:F
our
wou
nds.
One
due
to p
atie
ntde
ath;
thre
esw
itche
d to
dext
rano
mer
(tw
oaf
ter
16 d
ays
and
one
afte
r 48
day
s).
Wou
nds
trea
ted
with
C(E
usol
) wer
e ob
serv
ed to
be
asso
ciat
ed w
ith a
rise
inbl
ood
urea
to 1
1 m
mol
/l.
Cos
t of m
ater
ials
calc
ulat
edfo
r ea
ch tr
eatm
ent f
orav
erag
e tr
eatm
ent t
ime
inth
at g
roup
.C tr
eatm
ent w
as1.
6 tim
es m
ore
cost
ly th
an I.
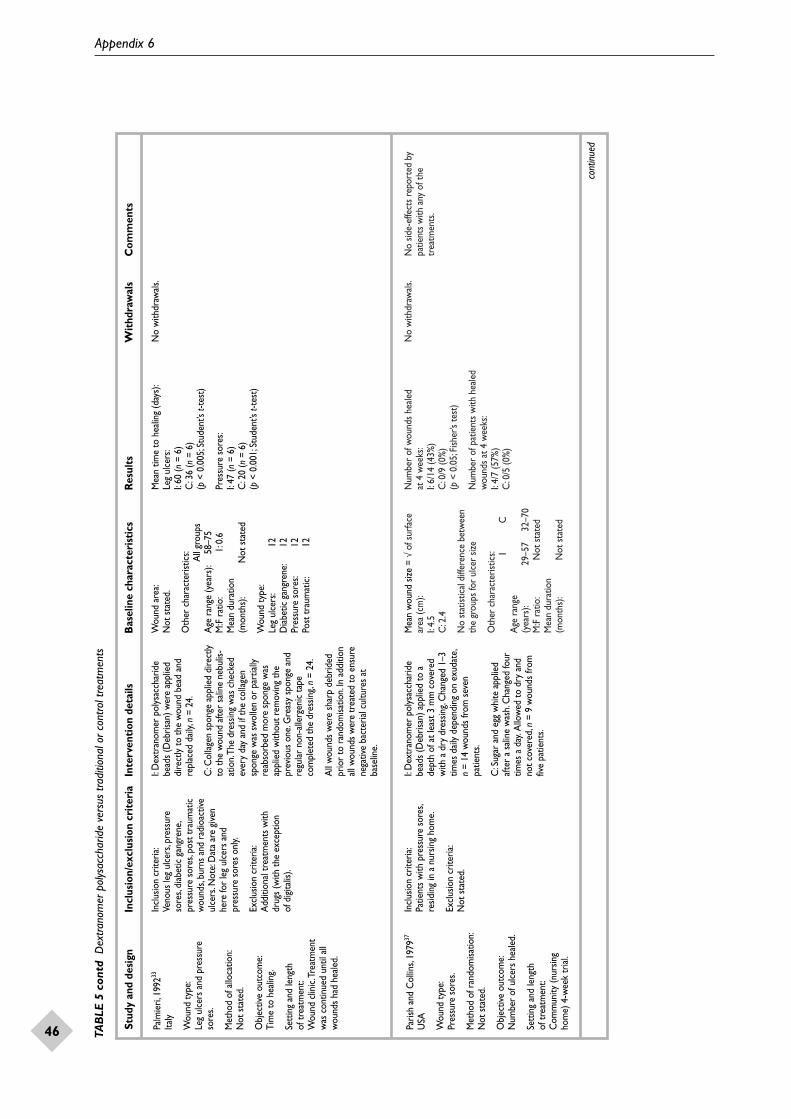
Appendix 6
46 TAB
LE 5
con
td D
extra
nom
er p
olys
acch
arid
e ve
rsus
trad
ition
al o
r co
ntro
l tre
atm
ents
Stud
y an
d de
sign
Incl
usio
n/ex
clus
ion
crit
eria
Inte
rven
tion
det
ails
Bas
elin
e ch
arac
teri
stic
sR
esul
ts
Wit
hdra
wal
sC
omm
ents
cont
inue
d
Palm
ieri,
1992
33
Italy
Wou
nd ty
pe:
Leg
ulce
rs a
nd p
ress
ure
sore
s.
Met
hod
of a
lloca
tion:
Not
sta
ted.
Obj
ectiv
e ou
tcom
e:Ti
me
to h
ealin
g.
Sett
ing
and
leng
th
of tr
eatm
ent:
Wou
nd c
linic
.Tre
atm
ent
was
con
tinue
d un
til a
llw
ound
s ha
d he
aled
.
Incl
usio
n cr
iteria
:Ve
nous
leg
ulce
rs,p
ress
ure
sore
s,di
abet
ic g
angr
ene,
pres
sure
sor
es,p
ost t
raum
atic
wou
nds,
burn
s an
d ra
dioa
ctive
ulce
rs.N
ote:
Dat
a ar
e gi
ven
here
for
leg
ulce
rs a
nd
pres
sure
sor
es o
nly.
Excl
usio
n cr
iteria
:A
dditi
onal
trea
tmen
ts w
ith
drug
s (w
ith th
e ex
cept
ion
of d
igita
lis).
I:D
extr
anom
er p
olys
acch
arid
ebe
ads
(Deb
risan
) wer
e ap
plie
ddi
rect
ly to
the
wou
nd b
ead
and
repl
aced
dai
ly,n
= 24
.
C:C
olla
gen
spon
ge a
pplie
d di
rect
lyto
the
wou
nd a
fter
salin
e ne
bulis
-at
ion.
The
dres
sing
was
che
cked
ever
y da
y an
d if
the
colla
gen
spon
ge w
as s
wol
len
or p
artia
lly
reab
sorb
ed m
ore
spon
ge w
asap
plie
d w
ithou
t rem
ovin
g th
epr
evio
us o
ne.G
reas
y sp
onge
and
regu
lar
non-
alle
rgen
ic ta
peco
mpl
eted
the
dres
sing,
n =
24.
All
wou
nds
wer
e sh
arp
debr
ided
prio
r to
ran
dom
isatio
n.In
add
ition
all w
ound
s w
ere
trea
ted
to e
nsur
ene
gativ
e ba
cter
ial c
ultu
res
atba
selin
e.
Wou
nd a
rea:
Not
sta
ted.
Oth
er c
hara
cter
istic
s: All
grou
psA
ge r
ange
(yea
rs):
58–7
5M
:F r
atio
:1:
0.6
Mea
n du
ratio
n (m
onth
s):
Not
sta
ted
Wou
nd ty
pe:
Leg
ulce
rs:
12D
iabe
tic g
angr
ene:
12Pr
essu
re s
ores
:12
Post
trau
mat
ic:
12
Mea
n tim
e to
hea
ling
(day
s):
Leg
ulce
rs:
I:60
(n=
6)
C:3
6 (n
= 6)
(p<
0.00
5;St
uden
t’s t-
test
)
Pres
sure
sor
es:
I:47
(n=
6)
C:2
0 (n
= 6)
(p<
0.00
1;St
uden
t’s t-
test
)
No
with
draw
als.
Paris
h an
d C
ollin
s,19
7937
USA
Wou
nd ty
pe:
Pres
sure
sor
es.
Met
hod
of r
ando
misa
tion:
Not
sta
ted.
Obj
ectiv
e ou
tcom
e:N
umbe
r of
ulc
ers
heal
ed.
Sett
ing
and
leng
th
of tr
eatm
ent:
Com
mun
ity (n
ursin
g ho
me)
4-w
eek
tria
l.
Incl
usio
n cr
iteria
:Pa
tient
s w
ith p
ress
ure
sore
s,re
sidin
g in
a n
ursin
g ho
me.
Excl
usio
n cr
iteria
:N
ot s
tate
d.
I:D
extr
anom
er p
olys
acch
arid
ebe
ads
(Deb
risan
) app
lied
to a
dept
h of
at l
east
3 m
m c
over
edw
ith a
dry
dre
ssin
g.C
hang
ed 1
–3tim
es d
aily
dep
endi
ng o
n ex
udat
e,n
= 14
wou
nds
from
sev
enpa
tient
s.
C:S
ugar
and
egg
whi
te a
pplie
daf
ter
a sa
line
was
h.C
hang
ed fo
urtim
es a
day
.Allo
wed
to d
ry a
ndno
t cov
ered
,n =
9 w
ound
s fro
mfiv
e pa
tient
s.
Mea
n w
ound
size
= √
of s
urfa
cear
ea (c
m):
I:4.
5 C
:2.4
No
stat
istic
al d
iffer
ence
bet
wee
nth
e gr
oups
for
ulce
r siz
e
Oth
er c
hara
cter
istic
s: IC
Age
ran
ge
(yea
rs):
29–5
732
–70
M:F
rat
io:
Not
sta
ted
Mea
n du
ratio
n (m
onth
s):
Not
sta
ted
Num
ber
of w
ound
s he
aled
at
4 w
eeks
:I:
6/14
(43%
)C
:0/9
(0%
)(p
< 0.
05;F
isher
’s te
st)
Num
ber
of p
atie
nts
with
hea
led
wou
nds
at 4
wee
ks:
I:4/
7 (5
7%)
C:0
/5 (0
%)
No
with
draw
als.
No
side-
effe
cts
repo
rted
by
patie
nts
with
any
of t
hetr
eatm
ents
.
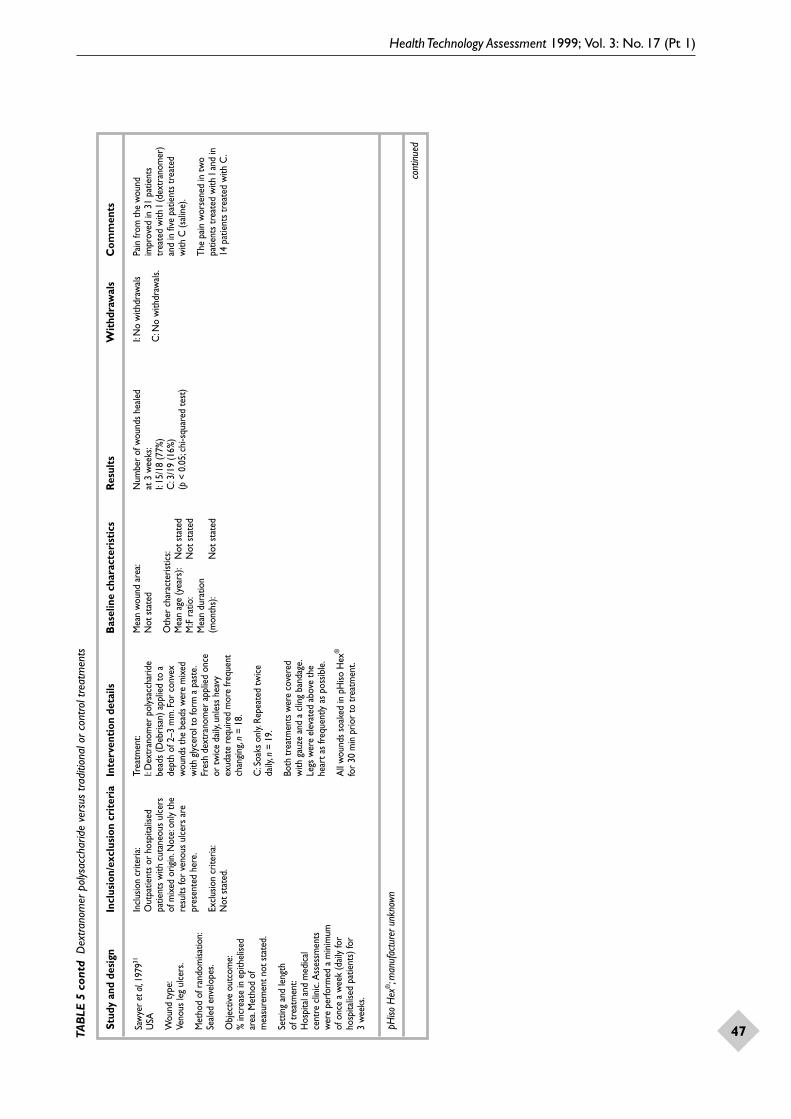
Health Technology Assessment 1999; Vol. 3: No. 17 (Pt 1)
47TAB
LE 5
con
td D
extra
nom
er p
olys
acch
arid
e ve
rsus
trad
ition
al o
r co
ntro
l tre
atm
ents
Stud
y an
d de
sign
Incl
usio
n/ex
clus
ion
crit
eria
Inte
rven
tion
det
ails
Bas
elin
e ch
arac
teri
stic
sR
esul
ts
Wit
hdra
wal
sC
omm
ents
pHiso
Hex
®;m
anuf
actu
rer u
nkno
wn
cont
inue
d
Saw
yer
et a
l,197
931
USA
Wou
nd ty
pe:
Veno
us le
g ul
cers
.
Met
hod
of r
ando
misa
tion:
Seal
ed e
nvel
opes
.
Obj
ectiv
e ou
tcom
e:%
incr
ease
in e
pith
elise
dar
ea.M
etho
d of
mea
sure
men
t not
sta
ted.
Sett
ing
and
leng
th
of tr
eatm
ent:
Hos
pita
l and
med
ical
ce
ntre
clin
ic.A
sses
smen
tsw
ere
perfo
rmed
a m
inim
umof
onc
e a
wee
k (d
aily
for
hosp
italis
ed p
atie
nts)
for
3 w
eeks
.
Incl
usio
n cr
iteria
:O
utpa
tient
s or
hos
pita
lised
patie
nts
with
cut
aneo
us u
lcer
s of
mix
ed o
rigin
.Not
e:on
ly th
ere
sults
for
veno
us u
lcer
s ar
epr
esen
ted
here
.
Excl
usio
n cr
iteria
:N
ot s
tate
d.
Trea
tmen
t:I:
Dex
tran
omer
pol
ysac
char
ide
bead
s (D
ebris
an) a
pplie
d to
ade
pth
of 2
–3 m
m.F
or c
onve
xw
ound
s th
e be
ads
wer
e m
ixed
with
gly
cero
l to
form
a p
aste
.Fr
esh
dext
rano
mer
app
lied
once
or tw
ice
daily
,unl
ess
heav
yex
udat
e re
quire
d m
ore
frequ
ent
chan
ging
,n =
18.
C:S
oaks
onl
y.Re
peat
ed tw
ice
daily
,n =
19.
Both
trea
tmen
ts w
ere
cove
red
with
gau
ze a
nd a
clin
g ba
ndag
e.Le
gs w
ere
elev
ated
abo
ve th
ehe
art a
s fre
quen
tly a
s po
ssib
le.
All
wou
nds
soak
ed in
pH
iso H
ex®
for
30 m
in p
rior
to tr
eatm
ent.
Mea
n w
ound
are
a:N
ot s
tate
d
Oth
er c
hara
cter
istic
s:M
ean
age
(yea
rs):
Not
sta
ted
M:F
rat
io:
Not
sta
ted
Mea
n du
ratio
n (m
onth
s):
Not
sta
ted
Num
ber
of w
ound
s he
aled
at
3 w
eeks
:I:
15/1
8 (7
7%)
C:3
/19
(16%
) (p
< 0
.05;
chi-s
quar
ed te
st)
I:N
o w
ithdr
awal
s
C:N
o w
ithdr
awal
s.
Pain
from
the
wou
ndim
prov
ed in
31
patie
nts
trea
ted
with
I (d
extr
anom
er)
and
in fi
ve p
atie
nts
trea
ted
with
C (s
alin
e).
The
pain
wor
sene
d in
two
patie
nts
trea
ted
with
I an
d in
14 p
atie
nts
trea
ted
with
C.

Appendix 6
48 TAB
LE 5
con
td D
extra
nom
er p
olys
acch
arid
e ve
rsus
trad
ition
al o
r co
ntro
l tre
atm
ents
Stud
y an
d de
sign
Incl
usio
n/ex
clus
ion
crit
eria
Inte
rven
tion
det
ails
Bas
elin
e ch
arac
teri
stic
sR
esul
ts
Wit
hdra
wal
sC
omm
ents
Algo
steril
®,L
es L
abor
ator
ies B
roth
ier (n
ow m
anuf
actu
red
by B
eiers
dorf
UKLt
d)* Ya
rkon
y GM
,et a
l.Cla
ssific
ation
of p
ress
ure
ulce
rs.A
rch
Der
mat
ol 1
990;
126:
1218
–19.
Saya
g et
al,1
99632
Fran
ce
Wou
nd ty
pe:
Pres
sure
sor
es.
Met
hod
of r
ando
misa
tion:
Seal
ed e
nvel
opes
.
Obj
ectiv
e ou
tcom
e:A
rea
of w
ound
mea
sure
dby
pla
nim
etry
,dig
itise
dtw
ice
and
the
area
cal
cu-
late
d by
com
pute
r.The
mea
n of
the
two
valu
es w
asus
ed to
det
erm
ine
indi
vid-
ual w
ound
are
a.A
pho
to-
grap
h w
as ta
ken
of e
ach
wou
nd a
t eve
ry e
valu
atio
n.
Sett
ing
and
leng
th
of tr
eatm
ent:
A m
ultic
entr
e tr
ial b
ased
at 2
0 ce
ntre
s (1
7 sp
ecia
l-isi
ng in
the
care
of e
lder
lype
ople
and
thre
e in
derm
atol
ogy)
.Ass
ess-
men
ts w
ere
mad
e on
aw
eekl
y ba
sis b
y th
e sa
me
rese
arch
er a
t eac
hce
ntre
.Tre
atm
ent w
aste
rmin
ated
whe
n th
ew
ound
rea
ched
40%
of
the
initi
al a
rea,
or a
fter
am
axim
um o
f 8 w
eeks
.
Incl
usio
n cr
iteria
:Pa
tient
s ag
ed ≥
60 h
ospi
talis
edfo
r ≥
8 w
eeks
,with
a p
ress
ure
sore
gra
ded
III o
r IV
(* Yark
ony’s
clas
sific
atio
n) a
nd s
urfa
ce
area
from
5–1
00 c
m2 .
Excl
usio
n cr
iteria
:M
ore
than
hal
f the
tota
l ulc
erar
ea h
ad g
ranu
latin
g tis
sue;
wou
nd c
over
ed b
y ne
crot
icpl
aque
;act
ive in
fect
ion
requ
iring
loca
l or
syst
emic
ant
ibio
ticth
erap
y;se
vere
ren
al fa
ilure
;hee
lul
cers
whe
n co
mbi
ned
with
end
-st
age
arte
riopa
thy
of th
e lo
wer
limbs
;rec
eivi
ng r
adio
ther
apy
orcy
toto
xic
ther
apy.
Trea
tmen
t:I:
Dex
tran
omer
pol
ysac
char
ide
past
e (D
ebris
an) a
pplie
d to
ade
pth
of 3
mm
ove
r th
e w
ound
surf
ace,
n =
45.
C:C
alci
um a
lgin
ate
dres
sings
(Algo
ster
il®) a
pplie
d di
rect
ly
on to
wou
nd to
cov
er th
e en
tire
area
,n =
47.
In b
oth
grou
ps a
ste
rile
gauz
e w
asap
plie
d as
a s
econ
dary
dre
ssin
g.N
o ot
her
loca
l tre
atm
ents
wer
eus
ed e
xcep
t for
sal
ine
solu
tion
the
use
of w
hich
was
not
res
tric
ted.
Dre
ssin
gs w
ere
insp
ecte
d an
dch
ange
d da
ily o
r at
leas
t eve
ry
4 da
ys d
epen
ding
on
the
degr
ee
of e
xuda
te.
Mea
n w
ound
are
a (c
m2 ):
I:16
.1 (1
2.5
SD)
C:2
0.1
(12.
9 SD
)
Oth
er c
hara
cter
istic
s:I
CM
ean
(SD
) ag
e (y
ears
):80
.4 (9
.1)
81.9
(8.9
)M
:F r
atio
:1:
2.8
1:2.
9M
ean
(SD
) du
ratio
n (m
onth
s):
3.0
(3.2
)3.
5 (3
.8)
Wou
nd g
rade
:III
3033
IV15
14
No
signi
fican
t diff
eren
ce b
etw
een
the
two
grou
ps (S
tude
nt’s
t-tes
t).
Whe
re p
atie
nts
had
mul
tiple
wou
nds
only
one
was
sel
ecte
d fo
r st
udy.
Pres
sure
sor
es w
ere
loca
ted
onth
e sa
crum
,isch
ium
,tro
chan
ter
and
heel
s.
Mea
n w
ound
are
a re
duct
ion
per
wee
k (c
m2 ):
I:0.
27 (3
.21
SD)
C:2
.39
(3.5
4 SD
) (p
= 0.
0001
;Stu
dent
’s t-t
est)
Mea
n w
ound
are
a re
duct
ion
per
wee
k us
ing
the
data
from
onl
y th
ose
patie
nts
reac
hing
≥40
% (c
m2 ):
I:2.
15 (3
.60
SD)
C:3
.55
(2.1
8 SD
) (p
= 0.
0004
;Stu
dent
’s t-t
est)
Num
ber
of w
ound
s w
ith >
75%
redu
ctio
n in
are
a:1:
6/45
(13%
)C
:15/
47 (3
2%)
Num
ber
of p
ress
ure
sore
s w
ith
≥40
% r
educ
tion
in a
rea:
I:19
/45
(42%
)C
:35/
47 (7
4%)
(p=
0.00
2;Fi
sher
’s ex
act t
est)
Cum
ulat
ive c
urve
s of
the
num
ber
of p
atie
nts
reac
hing
40%
red
uctio
ndi
ffere
d sig
nific
antly
(p=
0.00
02Lo
gran
k te
st) b
etw
een
the
grou
ps,
with
a m
edia
n of
4 w
eeks
in C
and
8
wee
ks in
I.
I:22
With
draw
als:
deat
h (n
= 6)
;ad
vers
e ev
ent
(n=
1);
dete
riora
tion
or s
tagn
atio
n of
ulc
er a
fter
4 w
eek
(n=
15).
C:T
en w
ithdr
awal
s:de
ath
(n=
5);
tran
sfer
(n=
2);
dete
riora
tion
ofhe
alth
(n=
1);
dete
riora
tion
or s
tagn
atio
n of
ulce
r af
ter
4 w
eek
(n=
2).
All
wer
e in
clud
ed in
the
analy
sis a
nd fe
ww
ere
cons
ider
ed to
have
impr
oved
at
the
last
eva
luat
ion.
End
poin
t dat
aw
ere
not a
vaila
ble
for
one
patie
nt in
Cdu
e to
adm
issio
n to
a sp
ecia
l car
e un
it.
On
aver
age
the
num
ber
ofdr
essin
g ch
ange
s pe
r w
eek
was
sim
ilar:
4.28
(1.4
9 SD
)fo
r C
and
4.5
2 (1
.42
SD)
for
I.
8% o
f the
C p
atie
nts
and
33%
of I
patie
nts
expe
rienc
edad
vers
e ef
fect
s.

Health Technology Assessment 1999; Vol. 3: No. 17 (Pt 1)
49TAB
LE 6
Cad
exom
er io
dine
pol
ysac
char
ide
vers
us tr
aditi
onal
or
cont
rol t
reat
men
ts
Stud
y an
d de
sign
Incl
usio
n/ex
clus
ion
crit
eria
Inte
rven
tion
det
ails
Bas
elin
e ch
arac
teri
stic
sR
esul
ts
Wit
hdra
wal
sC
omm
ents
Iodo
sorb
®,S
mith
& N
ephe
w H
ealth
care
Ltd
;Jelon
et®,S
mith
& N
ephe
w H
ealth
care
Ltd
* W
agne
r FW
.The
dys
vasc
ular
foot
:a sy
stem
for d
iagn
osis
and
treat
men
t.Fo
ot A
nkle
198
1;2:
64–1
22.
cont
inue
d
Ape
lqvi
st a
nd Te
nnva
ll,19
9642
Swed
en
Wou
nd ty
pe:
Dia
betic
foot
ulc
ers.
Met
hod
of r
ando
misa
tion:
Com
pute
r al
loca
tion.
Stra
ti-fic
atio
n w
as p
erfo
rmed
on
size
and
type
of w
ound
(Wag
ner
grad
e I–
II).
Obj
ectiv
e ou
tcom
e:A
rea
of w
ound
det
erm
ined
by p
hoto
grap
hing
wou
nds
agai
nst a
gra
duat
ed s
cale
.Th
e m
axim
um le
ngth
and
max
imum
wid
th w
ere
mul
-tip
lied
toge
ther
to c
alcu
late
the
area
.In
addi
tion
the
num
ber
of w
ound
s he
aled
was
rec
orde
d.
Sett
ing
and
leng
th
of tr
eatm
ent:
Ope
n co
ntro
lled
tria
l with
blin
ded
phot
o-ev
alua
tion.
Patie
nts
wer
e tr
eate
dei
ther
at h
ome
or o
nvi
sitin
g an
out
patie
nt c
linic
.A
sses
smen
ts w
ere
mad
e at
1,4,
8 an
d 12
wee
ks.
Incl
usio
n cr
iteria
:C
auca
sian
outp
atie
nts
> 40
yea
rs o
ld w
ith p
revi
ously
know
n di
abet
es m
ellit
us.A
llw
ound
s w
ere
exud
atin
g an
dbe
low
the
ankl
e (W
agne
r gr
ade
I–II* ) w
ith a
n ul
cer
area
> 1
cm
2
and
a sy
stol
ic to
e pr
essu
re
> 30
mm
Hg
or a
sys
tolic
ank
lepr
essu
re >
80
mm
Hg.
Excl
usio
n cr
iteria
:W
ound
s >
25 c
m2 ;p
atie
nts
with
a de
ep a
bsce
ss;o
steo
mye
litis
orga
ngre
ne (W
agne
r gr
ade
III–I
V);
patie
nts
unde
rgoi
ng th
yroi
dgl
and
inve
stig
atio
n;pa
tient
sun
likel
y to
adh
ere
to th
e st
udy
prot
ocol
.
In p
atie
nts
with
sev
eral
wou
nds,
only
the
larg
est w
ound
mee
ting
the
sele
ctio
n cr
iteria
was
chos
en.
Trea
tmen
t:I:
Cad
exom
er io
dine
pol
ysac
-ch
arid
e oi
ntm
ent (
Iodo
sorb
®) w
asch
ange
d on
ce d
aily
for
the
first
wee
k an
d th
en d
aily
or
ever
yse
cond
or
third
day
ther
eafte
rac
cord
ing
to th
e de
gree
of
exud
atio
n,n
= 22
.
C:G
enta
mic
in s
olut
ion
(80
mg/
ml)
was
give
n tw
ice
daily
whe
re c
ellu
litis
was
pre
sent
.St
rept
odor
nase
/ str
epto
kina
se(V
arid
ase T
opic
al) w
as u
sed
for
moi
st n
ecro
tic le
sions
and
cha
nged
twic
e da
ily.D
ry s
alin
e ga
uze
was
used
as
an a
bsor
ptive
dre
ssin
g an
dch
ange
d on
ce o
r tw
ice
daily
acco
rdin
g to
exu
datio
n,n
= 19
.
Wou
nds
wer
e cl
eane
d w
ith s
teril
esa
line
prio
r to
dre
ssin
g in
acc
ord-
ance
with
the
man
ufac
ture
rsgu
idel
ines
.Dre
ssin
gs w
ere
appl
ied
by r
egul
ar h
ealth
care
nur
ses.
For
both
trea
tmen
ts w
hen
the
ulce
rs h
ad s
topp
ed e
xuda
ting,
Vase
line
gauz
e (Je
lone
t®) w
as u
sed.
Foot
wea
r of
pat
ient
s w
asco
rrec
ted
or s
peci
al fo
otw
ear
prov
ided
to r
elie
ve p
ress
ure.
Ora
lan
tibio
tics
wer
e gi
ven
in c
ase
ofsig
ns o
f inf
ectio
n.
Mea
n w
ound
are
a (c
m2 ):
Not
sta
ted.
Oth
er c
hara
cter
istic
s:M
ean
age
(yea
rs):
Not
sta
ted
M:F
rat
io:
Not
sta
ted
Mea
n du
ratio
n (m
onth
s):
Not
sta
ted
Num
ber
of w
ound
s he
aled
:I:
5/22
(23%
)C
:2/1
9 (1
1%)
I:Fi
ve w
ithdr
awal
sC
:One
with
draw
al
Two
patie
nts
wer
eex
clud
ed fr
om th
ean
alysis
due
tovi
olat
ion
of in
clu-
sion
crite
ria (s
ize
> 25
cm
2an
d/or
ulce
r ty
pe,W
agne
rIII
).Tw
o pa
tient
sw
ere
excl
uded
beca
use
of h
ospi
tal-
isatio
n (o
ne fo
rm
yoca
rdia
l inf
arc-
tion,
one
beca
me
febr
ile a
nd la
ter
died
),th
ese
hosp
italis
atio
nsw
ere
not a
ssoc
iate
dw
ith tr
eatm
ent.
One
pat
ient
was
excl
uded
for
non-
com
plia
nce
with
trea
tmen
t.O
neot
her
patie
nt w
asex
clud
ed b
ecau
seof
insu
ffici
ent d
ata.
35 p
atie
nts
rem
aine
d fo
rcl
inic
al e
valu
atio
n.
Mea
n w
eekl
y co
st w
as 9
03SE
K fo
r I a
nd 1
421
SEK
for
C,
of w
hich
the
maj
or p
art w
asco
sts
for
staf
f and
tran
spor
tatio
n re
late
d to
frequ
ency
of d
ress
ing
chan
ges.
No
adve
rse
reac
tions
wer
ere
cord
ed w
ith e
ither
trea
tmen
t.
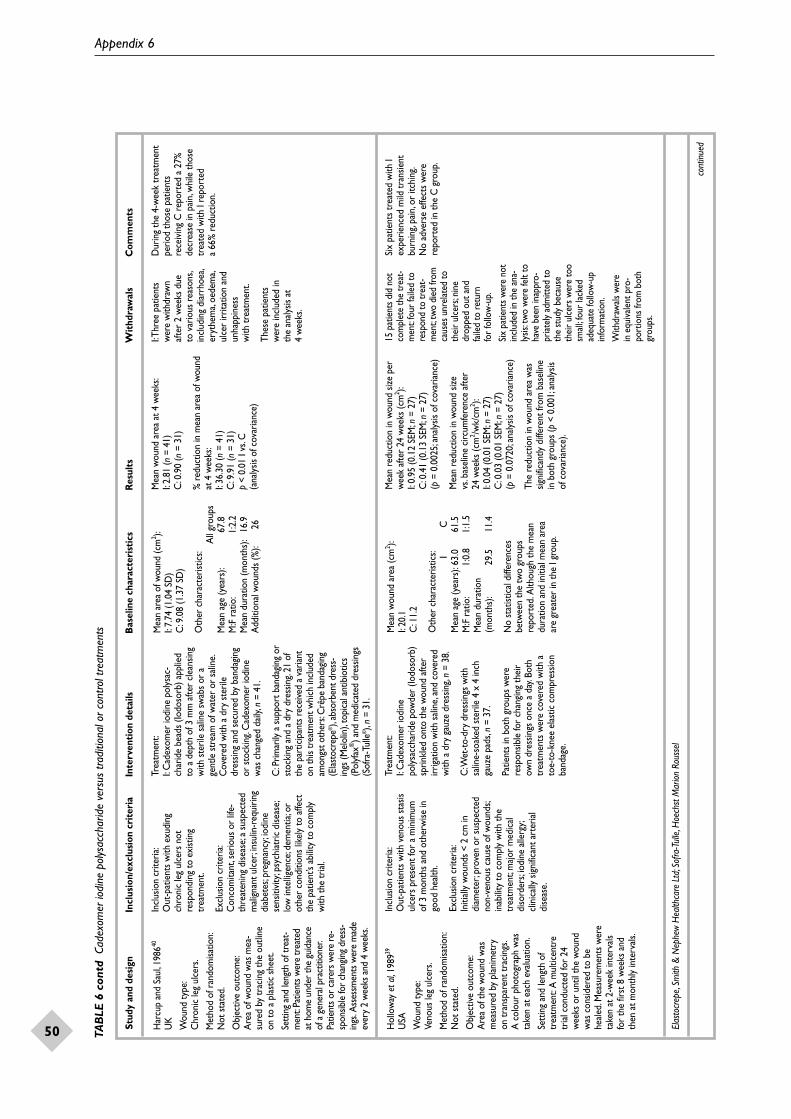
Appendix 6
50 TAB
LE 6
con
td C
adex
omer
iodi
ne p
olys
acch
arid
e ve
rsus
trad
ition
al o
r co
ntro
l tre
atm
ents
Stud
y an
d de
sign
Incl
usio
n/ex
clus
ion
crit
eria
Inte
rven
tion
det
ails
Bas
elin
e ch
arac
teri
stic
sR
esul
ts
Wit
hdra
wal
sC
omm
ents
Elas
tocr
epe,
Smith
& N
ephe
w H
ealth
care
Ltd
;Sof
ra-T
ulle
,Hoe
chst
Mar
ion R
ouss
el
cont
inue
d
Har
cup
and
Saul
,198
640
UK
Wou
nd ty
pe:
Chr
onic
leg
ulce
rs.
Met
hod
of r
ando
misa
tion:
Not
sta
ted.
Obj
ectiv
e ou
tcom
e:A
rea
of w
ound
was
mea
-su
red
by tr
acin
g th
e ou
tline
on to
a p
last
ic s
heet
.
Sett
ing
and
leng
th o
f tre
at-
men
t:Pa
tient
s wer
e tr
eate
dat
hom
e un
der
the
guid
ance
of a
gen
eral
prac
titio
ner.
Patie
nts o
r ca
rers
wer
e re
-sp
onsib
le fo
r ch
angin
g dr
ess-
ings
.Ass
essm
ents
wer
e m
ade
ever
y 2
wee
ks a
nd 4
wee
ks.
Incl
usio
n cr
iteria
:O
ut-p
atie
nts
with
exu
ding
chro
nic
leg
ulce
rs n
otre
spon
ding
to e
xist
ing
trea
tmen
t.
Excl
usio
n cr
iteria
:C
onco
mita
nt,s
erio
us o
r lif
e-th
reat
enin
g di
seas
e;a
susp
ecte
dm
alig
nant
ulc
er;in
sulin
-req
uirin
gdi
abet
es;p
regn
ancy
;iodi
nese
nsiti
vity
;psy
chia
tric
dise
ase;
low
inte
llige
nce;
dem
entia
;or
othe
r co
nditi
ons
likel
y to
affe
ctth
e pa
tient
’s ab
ility
to c
ompl
yw
ith th
e tr
ial.
Trea
tmen
t:I:
Cad
exom
er io
dine
pol
ysac
-ch
arid
e be
ads
(Iodo
sorb
) app
lied
to a
dep
th o
f 3 m
m a
fter
clea
nsin
gw
ith s
teril
e sa
line
swab
s or
age
ntle
str
eam
of w
ater
or
salin
e.C
over
ed w
ith a
dry
ste
rile
dres
sing
and
secu
red
by b
anda
ging
or s
tock
ing.
Cad
exom
er io
dine
was
cha
nged
dai
ly,n
= 41
.
C:P
rimar
ily a
sup
port
ban
dagin
g or
stoc
king
and
a d
ry d
ress
ing.
21 o
fth
e pa
rtic
ipan
ts re
ceive
d a
varia
nton
this
trea
tmen
t whi
ch in
clud
edam
ongs
t oth
ers:
Crê
pe b
anda
ging
(Elas
tocr
epe®
),ab
sorb
ent d
ress
-in
gs (M
elol
in),
topi
cal a
ntib
iotic
s(P
olyf
ax®) a
nd m
edic
ated
dre
ssin
gs(S
ofra
-Tul
le®),
n =
31.
Mea
n ar
ea o
f wou
nd (c
m2 ):
I:7.
74 (1
.04
SD)
C:9
.08
(1.3
7 SD
)
Oth
er c
hara
cter
istic
s:A
ll gr
oups
Mea
n ag
e (y
ears
):67
.8M
:F r
atio
:1:
2.2
Mea
n du
ratio
n (m
onth
s):
16.9
Add
ition
al w
ound
s (%
):26
Mea
n w
ound
are
a at
4 w
eeks
:I:
2.81
(n=
41)
C:0
.90
(n=
31)
% r
educ
tion
in m
ean
area
of w
ound
at 4
wee
ks:
I:36
.30
(n=
41)
C:9
.91
(n=
31)
p <
0.01
I vs
.C
(ana
lysis
of c
ovar
ianc
e)
I:Thr
ee p
atie
nts
wer
e w
ithdr
awn
afte
r 2
wee
ks d
ueto
var
ious
rea
sons
,in
clud
ing
diar
rhoe
a,er
ythe
ma,
oede
ma,
ulce
r irr
itatio
n an
dun
happ
ines
s w
ith tr
eatm
ent.
Thes
e pa
tient
sw
ere
incl
uded
inth
e an
alysis
at
4 w
eeks
.
Dur
ing
the
4-w
eek
trea
tmen
tpe
riod
thos
e pa
tient
sre
ceiv
ing
C r
epor
ted
a 27
%de
crea
se in
pai
n,w
hile
thos
e tr
eate
d w
ith I
repo
rted
a
66%
red
uctio
n.
Hol
low
ay e
t al,1
98939
USA
Wou
nd ty
pe:
Veno
us le
g ul
cers
.
Met
hod
of r
ando
misa
tion:
Not
sta
ted.
Obj
ectiv
e ou
tcom
e:A
rea
of th
e w
ound
was
mea
sure
d by
pla
nim
etry
on
tran
spar
ent t
raci
ngs.
A c
olou
r ph
otog
raph
was
take
n at
eac
h ev
alua
tion.
Sett
ing
and
leng
th o
ftr
eatm
ent:
A m
ultic
entr
etr
ial c
ondu
cted
for
24w
eeks
or
until
the
wou
ndw
as c
onsid
ered
to b
ehe
aled
.Mea
sure
men
ts w
ere
take
n at
2-w
eek
inte
rval
sfo
r th
e fir
st 8
wee
ks a
ndth
en a
t mon
thly
inte
rval
s.
Incl
usio
n cr
iteria
:O
ut-p
atie
nts
with
ven
ous
stas
isul
cers
pre
sent
for
a m
inim
um
of 3
mon
ths
and
othe
rwise
ingo
od h
ealth
.
Excl
usio
n cr
iteria
:In
itial
ly w
ound
s <
2 cm
indi
amet
er;p
rove
n or
sus
pect
edno
n-ve
nous
cau
se o
f wou
nds;
inab
ility
to c
ompl
y w
ith th
etr
eatm
ent;
maj
or m
edic
aldi
sord
ers;
iodi
ne a
llerg
y;cl
inic
ally
sig
nific
ant a
rter
ial
dise
ase.
Trea
tmen
t:I:
Cad
exom
er io
dine
poly
sacc
harid
e po
wde
r (Io
doso
rb)
sprin
kled
ont
o th
e w
ound
afte
rirr
igat
ion
with
sal
ine,
and
cove
red
with
a d
ry g
auze
dre
ssin
g,n
= 38
.
C:W
et-t
o-dr
y dr
essin
gs w
ithsa
line-
soak
ed s
teril
e 4
x 4
inch
gauz
e pa
ds,n
= 3
7.
Patie
nts
in b
oth
grou
ps w
ere
resp
onsib
le fo
r ch
angi
ng th
eir
own
dres
sings
onc
e a
day.
Both
trea
tmen
ts w
ere
cove
red
with
ato
e-to
-kne
e el
astic
com
pres
sion
band
age.
Mea
n w
ound
are
a (c
m2 ):
I:20
.1C
:11.
2
Oth
er c
hara
cter
istic
s: IC
Mea
n ag
e (y
ears
):63
.061
.5M
:F r
atio
:1:
0.8
1:1.
5M
ean
dura
tion
(mon
ths)
:29
.511
.4
No
stat
istic
al d
iffer
ence
s be
twee
n th
e tw
o gr
oups
re
port
ed.A
lthou
gh th
e m
ean
dura
tion
and
initi
al m
ean
area
ar
e gr
eate
r in
the
I gro
up.
Mea
n re
duct
ion
in w
ound
size
per
wee
k af
ter
24 w
eeks
(cm
2 ):I:
0.95
(0.1
2 SE
M;n
= 2
7)C
:0.4
1 (0
.13
SEM
;n =
27)
(p=
0.00
25;a
naly
sis o
f cov
aria
nce)
Mea
n re
duct
ion
in w
ound
size
vs
.bas
elin
e ci
rcum
fere
nce
afte
r 24
wee
ks (c
m2 /w
k/cm
2 ):I:
0.04
(0.0
1 SE
M;n
= 2
7)C
:0.0
3 (0
.01
SEM
;n =
27)
(p=
0.07
20;a
naly
sis o
f cov
aria
nce)
The
redu
ctio
n in
wou
nd a
rea
was
signi
fican
tly d
iffer
ent f
rom
bas
elin
e in
bot
h gr
oups
(p<
0.00
1;an
alysis
of
cov
aria
nce)
.
15 p
atie
nts d
id n
otco
mpl
ete
the
trea
t-m
ent:
four
faile
d to
resp
ond
to tr
eat-
men
t;tw
o di
ed fr
omca
uses
unr
elat
ed to
thei
r ul
cers
;nin
edr
oppe
d ou
t and
faile
d to
retu
rn
for
follo
w-u
p.Si
x pa
tient
s wer
e no
tin
clude
d in
the
ana-
lysis:
two
wer
e fe
lt to
have
bee
n in
appr
o-pr
iatel
y ad
mitt
ed to
the
stud
y be
caus
eth
eir
ulce
rs w
ere
too
small
;four
lack
edad
equa
te fo
llow
-up
info
rmat
ion.
With
draw
als w
ere
in e
quiva
lent
pro
-po
rtio
ns fr
om b
oth
grou
ps.
Six
patie
nts
trea
ted
with
Iex
perie
nced
mild
tran
sient
burn
ing,
pain
,or
itchi
ng.
No
adve
rse
effe
cts
wer
ere
port
ed in
the
C g
roup
.

Health Technology Assessment 1999; Vol. 3: No. 17 (Pt 1)
51TAB
LE 6
con
td C
adex
omer
iodi
ne p
olys
acch
arid
e ve
rsus
trad
ition
al o
r co
ntro
l tre
atm
ents
Stud
y an
d de
sign
Incl
usio
n/ex
clus
ion
crit
eria
Inte
rven
tion
det
ails
Bas
elin
e ch
arac
teri
stic
sR
esul
ts
Wit
hdra
wal
sC
omm
ents
cont
inue
d
Laud
ansk
a an
d G
usta
vson
,19
8838
Pola
nd
Wou
nd ty
pe:
Veno
us le
g ul
cers
.
Met
hod
of r
ando
misa
tion:
Not
sta
ted.
Obj
ectiv
e ou
tcom
es:
The
wou
nd p
erim
eter
was
draw
n on
to a
tran
spar
ency
and
the
area
cal
cula
ted
bypl
anim
etry
.The
num
ber
ofw
ound
s he
aled
was
reco
rded
.
Sett
ing
and
leng
th
of tr
eatm
ent:
6-w
eek
tria
l.Mea
sure
-m
ents
take
n at
0,1
,2,
4 an
d 6
wee
ks.
Incl
usio
n cr
iteria
:H
ospi
talis
ed p
atie
nts
with
chro
nic
veno
us u
lcer
s th
at h
adre
siste
d ou
tpat
ient
trea
tmen
t for
mor
e th
an 3
mon
ths.
Excl
usio
n cr
iteria
:W
ound
s <
2 cm
;iodi
nese
nsiti
vity
;sev
ere
perip
hera
lar
teria
l dise
ase.
Trea
tmen
t:I:
Cad
exom
er io
dine
pow
der
(Iodo
sorb
) app
lied
daily
in a
3–
4 m
m la
yer,
cove
red
with
a li
ght
elas
tic b
anda
ge,n
= 3
0.
C:D
ilute
hyd
roge
n pe
roxi
de a
ndzin
c pa
ste
(in a
dditi
on s
alin
edr
essin
gs,d
ilute
pot
assiu
m p
er-
man
gana
te a
nd G
entia
n vi
olet
wer
e ap
plie
d) c
over
ed w
ith a
ligh
tel
astic
ban
dage
,n =
30.
All
patie
nts
wer
e gi
ven
com
plet
ebe
d re
st fo
r 6
wee
ks.
Mea
n w
ound
are
a (c
m2 ):
I:27
.5 (7
.0 S
E)C
:35.
2 (8
.1 S
E)
(p>
0.05
;Stu
dent
’s t-t
est)
Oth
er c
hara
cter
istic
s: IC
Mea
n ag
e (y
ears
):64
.863
.5M
:F r
atio
:1:
0.8
1:1.
5M
ean
dura
tion
(mon
ths)
:19
.115
.0
No
stat
istic
al d
iffer
ence
bet
wee
nth
e tw
o gr
oups
.
Det
ails
are
only
ava
ilabl
e fo
r 60
of t
he 6
7 pa
rtic
ipan
ts in
itial
lyra
ndom
ised
to tr
eatm
ent.
Mea
n %
red
uctio
n in
wou
nd a
rea
at6
wee
ks:
I:71
% (n
= 30
)C
:54%
(n=
30)
(p<
0.01
;Stu
dent
’s t-t
est)
Both
trea
tmen
ts w
ere
signi
fican
tlydi
ffere
nt fr
om b
asel
ine.
(p<
0.05
;W
ilcox
on m
atch
ed p
airs
)
Num
ber
of u
lcer
s he
aled
or
shal
low
at 6
wee
ks:
I:16
/30
(53%
)C
:7 /
30 (7
%)
Four
with
draw
als
befo
re th
e fir
stas
sess
men
t:th
ree
due
to s
ocia
l rea
s-on
s an
d on
e du
e to
card
iac
failu
re.
Thre
e pa
tient
sw
ere
with
draw
naf
ter
com
plet
ing
the
tria
l.One
inea
ch g
roup
was
excl
uded
due
tola
rge
ulce
r ar
ea(t
en ti
mes
that
of
the
mea
n ul
cer
area
).The
third
patie
nt h
ad r
heu-
mat
oid
arth
ritis
whi
ch in
terfe
red
with
ass
essm
ent.
30 p
atie
nts
in e
ach
grou
p co
mpl
eted
the
tria
l.
App
licat
ion
of I
resu
lted
inm
ore
pain
than
with
C.
Seru
m c
once
ntra
tions
of
prot
ein-
boun
d io
dine
incr
ease
with
I tr
eatm
ent.
But t
here
isno
dist
urba
nce
of th
yroi
dfu
nctio
n.
Five
pat
ient
s on
I co
mpl
aine
dof
stin
ging
.

Appendix 6
52 TAB
LE 6
con
td C
adex
omer
iodi
ne p
olys
acch
arid
e ve
rsus
trad
ition
al o
r co
ntro
l tre
atm
ents
Stud
y an
d de
sign
Incl
usio
n/ex
clus
ion
crit
eria
Inte
rven
tion
det
ails
Bas
elin
e ch
arac
teri
stic
sR
esul
ts
Wit
hdra
wal
sC
omm
ents
cont
inue
d
Lind
say
et a
l,198
641
UK
Wou
nd ty
pe:
Veno
us le
g ul
cers
.
Met
hod
of r
ando
misa
tion:
Not
sta
ted.
Obj
ectiv
e ou
tcom
e:A
rea
of th
e w
ound
was
trac
ed o
nto
a pl
astic
she
etan
d m
easu
red.
Sett
ing
and
leng
th o
ftr
eatm
ent:
Patie
nts
trea
ted
at h
ome
unde
r th
e gu
idan
ceof
a g
ener
al pr
actit
ione
r.Pa
tient
s or
car
ers
wer
ere
spon
sible
for
chan
ging
dres
sings
.Ass
essm
ents
w
ere
mad
e ev
ery
2 w
eeks
for
4 w
eeks
.
Incl
usio
n cr
iteria
:O
ut-p
atie
nts
with
chr
onic
veno
us le
g ul
cers
and
not
resp
ondi
ng to
exi
stin
gtr
eatm
ent.
Excl
usio
n cr
iteria
:C
onco
mita
nt s
erio
us o
r lif
e-th
reat
enin
g di
seas
e,su
spec
ted
mal
igna
nt c
hang
e in
the
ulce
r;in
sulin
-dep
ende
nt d
iabe
tes;
preg
nanc
y;io
dine
sen
sitiv
ity;
psyc
hiat
ric d
iseas
e;ve
ry lo
win
telli
genc
e;de
men
tia;a
ny o
ther
cond
ition
that
mig
ht a
ffect
the
patie
nts
abili
ty to
com
ply
with
the
cond
ition
s of
the
tria
l.
Trea
tmen
t:28
pat
ient
s en
tere
d th
e tr
ial,b
utal
loca
tion
betw
een
the
grou
ps
was
not
sta
ted.
I:C
adex
omer
iodi
ne p
owde
r(Io
doso
rb) a
pplie
d to
a d
epth
of
not l
ess
than
3 m
m a
fter
clea
nsin
gw
ith s
teril
e sa
line
swab
s,or
age
ntle
str
eam
of w
ater
or
salin
e.C
over
ed w
ith a
dry
ste
rile
dres
s-in
g an
d se
cure
d by
ban
dagi
ng o
rst
ocki
ng.T
he d
ress
ing
was
ch
ange
d on
alte
rnat
e da
ys.
C:P
rimar
ily a
non
-adh
eren
tdr
essin
g pl
us s
uppo
rt b
anda
ging
or
sto
ckin
g.Th
e dr
essin
g w
asch
ange
d on
alte
rnat
e da
ys.T
wel
veof
the
part
icip
ants
rec
eive
d a
varia
nt o
n th
is tr
eatm
ent w
hich
incl
uded
am
ongs
t oth
ers:
Crê
peba
ndag
ing
(Ela
stoc
repe
),ab
sorb
ent
dres
sings
(Mel
olin
),Po
vido
neio
dine
and
med
icat
ed d
ress
ings
(Sof
ra-T
ulle
).
Mea
n w
ound
are
a:N
ot s
tate
d.
Oth
er c
hara
cter
istic
s:A
ll gr
oups
Mea
n ag
e (y
ears
):66
.7M
:F r
atio
:A
ll fe
mal
eM
ean
dura
tion
(mon
ths)
:20
.1N
o.of
pat
ient
s w
ithad
ditio
nal u
lcer
s:11
Mea
n %
red
uctio
n in
wou
nd a
rea
at4
wee
ks:
I:33
.6 (n
= 12
)C
:4.2
(n=
13)
(p <
0.0
05 I
vs.C
;ana
lysis
of
varia
nce)
.
I:O
ne p
atie
nt w
asw
ithdr
awn
afte
r 2
wee
ks d
ue to
an
alle
rgic
rea
ctio
n.
C:O
ne p
atie
nt w
asw
ithdr
awn
afte
r 4
wee
ks o
n th
edi
scov
ery
of p
eri-
pher
al v
ascu
lar
dise
ase.
The
resu
lts
are
base
d on
25
patie
nts
sugg
estin
gth
ere
was
a fu
rthe
rw
ithdr
awal
,pro
b-ab
ly in
the
I gro
up.
Mea
n w
ound
dur
atio
n w
as
20 m
onth
s so
a r
educ
tion
of33
% in
onl
y 4
wee
ks o
n I i
sim
pres
sive.
How
ever
,no
data
are
give
n of
oth
er m
easu
res
that
may
hav
e be
en e
mpl
oyed
to r
educ
e w
ound
size
.
Mob
erg
et a
l,198
343
Swed
en
Wou
nd ty
pe:
Pres
sure
sor
es.
Met
hod
of r
ando
misa
tion:
Not
sta
ted.
Obj
ectiv
e ou
tcom
e:Pe
rimet
er o
f the
wou
ndw
as tr
aced
and
the
area
calc
ulat
ed b
y pl
anim
etry
or
mea
sure
men
t of t
helo
nges
t dia
met
er.
Sett
ing
and
leng
th
of tr
eatm
ent:
3-w
eek
tria
l.
Incl
usio
n cr
iteria
:H
ospi
talis
ed p
atie
nts
with
pres
sure
sor
es.
Excl
usio
n cr
iteria
:C
onfir
med
or
susp
ecte
dm
alig
nanc
ies,
mor
ibun
d,io
dine
sens
itivi
ty,p
sych
iatr
ic il
lnes
s,se
vere
pso
riasis
,any
oth
ercr
iteria
that
mig
ht m
ake
apa
tient
uns
uita
ble
for
a cl
inic
al tr
ial o
r un
able
to
give
info
rmed
con
sent
.
Trea
tmen
t:I:
Cad
exom
er io
dine
pol
ysac
-ch
arid
e po
wde
r (Io
doso
rb)
appl
ied
daily
to a
dep
th o
f 3 m
m.
Rem
oved
by
runn
ing
wat
er
salin
e or
wet
sw
ab,n
= 1
9.
C:S
tand
ard
trea
tmen
t was
var
i-ab
le.I
t inc
lude
d:sa
line
dres
sings
,en
zym
e-ba
sed
debr
idin
g ag
ents
,an
d no
n-ad
hesiv
e dr
essin
gs,n
= 1
9.
All
patie
nts
wer
e su
bjec
t to:
atte
ntio
n to
nut
ritio
n;im
prov
e-m
ent o
f hyg
iene
;rem
oval
of
pres
sure
by
usin
g de
cubi
tus
mat
tres
ses,
turn
ing
the
patie
ntev
ery
2 or
3 h
rs,a
nd o
ptim
alm
obili
satio
n.
Mea
n w
ound
are
a (c
m2 ):
I:9.
6 (1
.8 S
EM)
C:1
2.4
(4.3
SEM
)
Oth
er c
hara
cter
istic
s: IC
Mea
n ag
e (y
ears
):72
.680
.1M
:F r
atio
:1:
4.3
1:2.
6M
ean
dura
tion
(mon
ths)
:6.
26.
2
Valu
es a
re o
nly
avai
labl
e fo
r th
epa
tient
s no
t with
draw
n fro
m th
est
udy.
Mea
n de
crea
se in
are
a of
wou
nd
at 3
wee
ks:
I:2.
9 (1
.3 S
EM;n
= 1
6)
C:2
.5 (1
.1 S
EM;n
= 1
8)(p
< 0.
05 fo
r bo
th tr
eatm
ents
whe
nco
mpa
red
with
bas
elin
e;co
rrel
ated
t-tes
t or
Fish
er’s
exac
t tes
t).
% r
educ
tion
in m
ean
area
of
wou
nd a
t 3 w
eeks
:I:
30.9
% (4
6 SD
;n =
16)
C:1
9.6%
(31
SD;n
= 1
8)
(p<
0.02
;cor
rela
ted
t-tes
t or
Fish
er’s
exac
t tes
t)
I:Thr
eew
ithdr
awal
s.Tw
opa
tient
s fe
lt th
eyw
ere
gett
ing
wor
sean
d on
e ha
d sk
inirr
itatio
n an
doe
dem
a ar
ound
asa
cral
ulc
er a
ndch
ose
not t
oco
ntin
ue.
C:O
ne w
ithdr
awal
whe
re th
e w
ound
had
grow
n an
d th
epa
tient
was
mov
edto
ano
ther
hos
pita
l.
I cau
sed
thre
e pa
tient
s to
expe
rienc
e sm
artin
g af
ter
appl
icat
ion,
one
patie
nt h
adm
inor
ski
n irr
itatio
n an
dan
othe
r ha
d an
exa
cerb
atio
nof
pso
riasis
.
Ove
rall
pain
as
a re
sult
of th
ew
ound
was
sig
nific
antly
less
inpa
tient
s tr
eate
d w
ith I.
I was
eas
y to
app
ly a
ndre
mov
e.

Health Technology Assessment 1999; Vol. 3: No. 17 (Pt 1)
53TAB
LE 6
con
td C
adex
omer
iodi
ne p
olys
acch
arid
e ve
rsus
trad
ition
al o
r co
ntro
l tre
atm
ents
Stud
y an
d de
sign
Incl
usio
n/ex
clus
ion
crit
eria
Inte
rven
tion
det
ails
Bas
elin
e ch
arac
teri
stic
sR
esul
ts
Wit
hdra
wal
sC
omm
ents
ABPI
,ank
le br
achi
al p
ress
ure
inde
x
cont
inue
d
Orm
iston
et a
l,198
544
UK
Wou
nd ty
pe:
Veno
us le
g ul
cers
.
Met
hod
of r
ando
misa
tion:
Seal
ed e
nvel
opes
.
Obj
ectiv
e ou
tcom
es:
Perim
eter
of t
he w
ound
was
draw
n on
to a
tran
spar
ency
and
the
area
calc
ulat
ed b
ypl
anim
etry
.The
wou
nd w
asals
o ph
otog
raph
ed.T
henu
mbe
r of
wou
nds h
eale
dw
as re
cord
ed.
Sett
ing
and
leng
th
of tr
eatm
ent:
12-w
eek
tria
l.Pat
ient
s w
ere
asse
ssed
at r
egul
arin
terv
als.
Afte
r 12
wee
kspa
tient
s w
ere
allo
wed
tocr
oss-
over
.
Incl
usio
n cr
iteria
:O
ut-p
atie
nts
with
chr
onic
veno
us le
g ul
cers
per
sistin
g fo
rat
leas
t 3 m
onth
s.
Excl
usio
n cr
iteria
:U
lcer
s of
non
-ven
ous
aetio
logy
,pe
riphe
ral v
ascu
lar
dise
ase
(ABP
I < 0
.7),
poor
com
plia
nce
expe
cted
due
to c
onco
mita
ntph
ysic
al o
r m
enta
l disa
bilit
y,tr
avel
ling
prob
lem
s.
Alm
ost a
ll pa
tient
s se
lect
edw
ere
able
to d
ress
and
ban
dage
thei
r ow
n ul
cers
.
I:C
adex
omer
iodi
nepo
lysa
ccha
ride
pow
der
(Iodo
sorb
),3–
5 m
m d
eep
and
cove
red
with
aga
uze
pad,
n =
31.
C:G
entia
n vi
olet
,follo
wed
by
topi
cal a
ntib
iotic
s (P
olyf
ax) a
pplie
din
a g
ener
ous
layer
,and
cov
ered
with
a n
on-a
dher
ent p
ad (M
elol
in),
n =
30.
Each
dre
ssin
g w
as c
over
ed w
ith a
crêp
e ba
ndag
e an
d a
cott
on c
rêpe
band
age.
Mea
n w
ound
are
a (c
m2 ):
I:12
.1 (1
3.9
SD)
C:1
0.2
(8.7
SD
)
Oth
er c
hara
cter
istic
s: IC
Mea
n ag
e (y
ears
):67
.370
.3M
:F r
atio
:1:
1.3
1:2.
6M
ean
dura
tion
(mon
ths)
:45
.915
.9
Base
line
data
was
onl
y gi
ven
for
30 o
f the
31
patie
nts
trea
ted
with
I (s
ee w
ithdr
awal
s).
% r
educ
tion
in m
ean
area
of w
ound
at 1
2 w
eeks
:I:
83%
(n=
30)
C:6
1% (n
= 30
) (p
< 0.
02;S
tude
nt’s
t-tes
t).
Redu
ctio
n in
mea
n ar
ea p
er w
eek
over
12
wee
ks (c
m2 ):
I:0.
89 (0
.1 S
EM;n
= 3
0)C
:0.4
6 (0
.1 S
EM;n
= 3
0)
(p<
0.00
01;S
tude
nt’s
t-tes
t).
Both
trea
tmen
ts a
re s
tatis
tical
lydi
ffere
nt fr
om b
asel
ine
(p <
0.0
01;
analy
sis o
f cov
aria
nce)
.
Num
ber
of u
lcer
s he
aled
afte
r 12
wee
ks:
I:12
/31
(39%
)C
:7/3
0 (2
3%)
(p>
0.05
;chi
-squ
ared
ana
lysis
)
I:O
ne p
atie
nt w
asad
mitt
ed to
hosp
ital f
or s
urge
ry,
and
had
inap
prop
riate
lydr
esse
d ul
cers
(thi
spa
tient
was
excl
uded
from
the
base
line
data
set)
.Tw
o fu
rthe
rpa
tient
s w
ere
with
draw
n:on
edi
ed o
f a p
erfo
rate
dul
cer
and
the
othe
rha
d di
fficu
lty in
rem
ovin
g I f
rom
the
ulce
r.The
se tw
opa
tient
s w
ere
incl
uded
in th
ean
alysis
.
C:N
o w
ithdr
awal
s.
Patie
nts
wer
e ab
le to
adeq
uate
ly b
anda
ge th
eir
own
wou
nds.
Two
patie
nts
had
diffi
culty
rem
ovin
g I a
nd th
ree
patie
nts
com
plai
ned
of s
tingi
ng a
nditc
hing
.
Pain
was
ass
esse
d on
a s
cale
of 0
–100
by
the
indi
vidu
alpa
tient
.Pai
n w
as p
erce
ived
to b
e sim
ilar
in b
oth
grou
ps.
Two
patie
nts
on C
and
five
on
I dev
elop
ed e
czem
a,pu
ritis
ora
rash
.

Appendix 6
54 TAB
LE 6
con
td C
adex
omer
iodi
ne p
olys
acch
arid
e ve
rsus
trad
ition
al o
r co
ntro
l tre
atm
ents
Stud
y an
d de
sign
Incl
usio
n/ex
clus
ion
crit
eria
Inte
rven
tion
det
ails
Bas
elin
e ch
arac
teri
stic
sR
esul
ts
Wit
hdra
wal
sC
omm
ents
Salvs
trum
pa®,m
anuf
actu
rer u
nkno
wn
cont
inue
d
Skog
et a
l,198
3;23
Hill
strö
m,1
988;
22
Troë
ng e
t al,1
98328
Swed
en
Wou
nd ty
pe:
Leg
ulce
rs.
Met
hod
of r
ando
misa
tion:
Not
sta
ted.
Obj
ectiv
e ou
tcom
e:A
rea
of th
e w
ound
was
mea
sure
d by
plan
imet
ry,o
rby
mea
surin
g th
e gr
eate
stdi
amet
ers.
All
wou
nds
wer
e ph
otog
raph
ed a
gain
sta
rule
r sc
ale a
t eac
has
sess
men
t.
Sett
ing
and
leng
th
of tr
eatm
ent:
A m
ultic
entr
e tr
ial i
n te
nce
ntre
s.A
sses
smen
ts w
ere
mad
e af
ter
1,2,
4 an
d 6
wee
ks a
t whi
ch p
oint
the
tria
l was
term
inat
ed.
Incl
usio
n cr
iteria
:O
ut-p
atie
nts
with
chr
onic
infe
cted
leg
ulce
rs th
at fa
iled
tore
spon
d to
cur
rent
trea
tmen
ts.
Excl
usio
n cr
iteria
:U
lcer
s w
ith d
iam
eter
s sm
alle
rth
an 2
cm
and
are
as le
ss th
an
3 cm
2 ;hist
ory
of io
dine
sens
itivi
ty;p
erip
hera
l ar
teria
l dise
ase.
Trea
tmen
t:I:
Cad
exom
er io
dine
pol
ysac
-ch
arid
e po
wde
r (Io
doso
rb) a
pplie
dto
a d
epth
of a
ppro
x.3
mm
afte
rw
ashi
ng in
run
ning
wat
er,a
ndco
vere
d w
ith a
dry
dre
ssin
g,n
= 50
.
C:E
ach
day
ulce
rs w
ere
clea
ned
with
dilu
te h
ydro
gen
pero
xide
or
dilu
te p
otas
sium
per
man
gana
tean
d no
n-ad
here
nt d
ress
ings
wer
eap
plie
d.Pa
raffi
n-im
preg
nate
ddr
essin
gs w
ere
mos
t com
mon
lyus
ed,b
ut s
alin
e dr
essin
gs a
nd
blan
d oi
ntm
ents
wer
e oc
casio
nally
used
.In
case
of d
iffic
ultie
s th
eph
ysic
ian
was
abl
e to
mod
ify
the
trea
tmen
t.O
ther
ther
apie
sus
ed in
clud
ed:S
alvs
trum
pa®,
mer
brom
ine
and
syst
emic
antib
iotic
s,n
= 45
.
In b
oth
grou
ps d
urin
g th
e fir
st
few
day
s w
hen
exud
ate
was
hea
vyth
e dr
essin
gs c
ould
be
chan
ged
twic
e da
ily,b
ut fo
r th
e re
mai
nder
of th
e tr
ial t
his
was
sel
dom
nece
ssar
y an
d dr
essin
gs w
ere
chan
ged
daily
.
All
patie
nts
wer
e tr
eate
d w
ithco
mpr
essio
n ba
ndag
es a
pplie
d by
a n
urse
eith
er a
t the
clin
ic o
r at
hom
e.So
me
patie
nts
wer
e tr
aine
dto
cha
nge
thei
r ow
n ba
ndag
es
(n-v
alue
s gi
ven
are
for
patie
nts
rem
aini
ng a
fter
with
draw
als)
.
Mea
n w
ound
are
a (c
m2 ):
I:20
.1 (4
.4 S
EM)
C:3
4.0
(5.7
SEM
)
Oth
er c
hara
cter
istic
s:I
CM
ean
(SEM
) age
(y
ears
):68
.1
72.1
(1
.99)
(3.5
4)M
:F r
atio
:1:
2.8
1:3.
5M
ean
(SEM
) du
ratio
n (m
onth
s):
26.5
22.2
(1
8.3)
(1
4.3)
Wou
nd ty
pe:
Veno
us37
30O
ther
16
Dep
th o
f ulc
er:
Dee
p11
12Su
perf
icia
l26
23Ve
ry s
uper
ficia
l1
1
No
signi
fican
t diff
eren
ce b
etw
een
the
two
grou
ps.
Base
line
deta
ils a
re o
nly
avai
labl
efo
r th
e 74
pat
ient
s co
mpl
etin
g th
e tr
ial f
rom
the
orig
inal
95
ran
dom
ised.
Mea
n %
cha
nge
in w
ound
are
a af
ter
6 w
eeks
(cm
2 ):I:
–34%
(5 S
EM;n
= 3
8)C
:+5%
(15
SEM
;n =
36)
(p<
0.02
;Wilc
oxon
mat
ched
pai
rssig
ned-
rank
s te
st,t
wo-
sided
).
I:Fo
ur p
atie
nts
did
not m
eet t
he s
elec
-tio
n cr
iteria
;one
deve
lope
d a
rash
;tw
o to
ok h
olid
ays;
two
had
beta
-ha
emol
ytic
Str
epto
-co
ccus
infe
ctio
n;tw
o ha
d m
issin
gin
form
atio
n;an
don
e ex
perie
nced
recu
rren
ce o
f ul
cer
pain
.
C:T
hree
pat
ient
sdi
d no
t mee
t the
sele
ctio
n cr
iteria
;fo
ur h
ad b
eta-
haem
olyt
ic S
trep
to-
cocc
us in
fect
ion;
one
deve
lope
dsq
uam
ous
cell
carc
inom
a ;a
nd
one
expe
rienc
ed
a dr
amat
ic in
crea
sein
ulc
er s
ize.
One
pat
ient
on
C a
nd fo
uron
I co
mpl
aine
d of
pai
n on
appl
icat
ion
of th
e dr
essin
g.Th
is su
bsid
ed 3
0–60
min
late
r.
One
pat
ient
dev
elop
ed a
ra
sh in
the
I gro
up,b
ut te
sts
show
ed th
at th
is w
as d
ue to
coal
tar
deriv
ative
s an
d no
tth
e tr
eatm
ent.
Ano
ther
patie
nt in
this
grou
p ac
quire
dan
itch
aro
und
the
ulce
rw
hich
sub
sided
afte
r 2
wee
ks.
Thyr
oxin
e,tr
i-iod
othy
roni
ne,
seru
m th
yrox
ine
bind
ing
prot
ein
and
thyr
oid
inde
x di
d no
t cha
nge
signi
fican
tlyov
er th
e st
udy
perio
d.

Health Technology Assessment 1999; Vol. 3: No. 17 (Pt 1)
55TAB
LE 6
con
td C
adex
omer
iodi
ne p
olys
acch
arid
e ve
rsus
trad
ition
al o
r co
ntro
l tre
atm
ents
Stud
y an
d de
sign
Incl
usio
n/ex
clus
ion
crit
eria
Inte
rven
tion
det
ails
Bas
elin
e ch
arac
teri
stic
sR
esul
ts
Wit
hdra
wal
sC
omm
ents
Stee
le e
t al,1
98645
UK
Wou
nd ty
pe:
Veno
us le
g ul
cers
.
Met
hod
of r
ando
misa
tion:
Rand
om n
umbe
r ta
ble.
Obj
ectiv
e ou
tcom
es:
The
wou
nd p
erim
eter
was
draw
n on
to a
tran
spar
ency
and
the
area
cal
cula
ted
byco
mpu
ter
plan
imet
ry.
Num
ber
of w
ound
s he
aled
was
also
rec
orde
d.
Sett
ing
and
leng
th
of tr
eatm
ent:
Patie
nts
recr
uite
d fro
mpr
imar
y ca
re p
ract
ices
.Si
x-w
eek
tria
l.M
easu
rem
ents
take
n at
0,2,
4 an
d 6
wee
ks.
Incl
usio
n cr
iteria
:O
ut-p
atie
nts
with
ven
ous
leg
ulce
rs p
rese
nt fo
r m
ore
than
3
mon
ths,
and
larg
er th
an 2
cm
2 .
Excl
usio
n cr
iteria
:A
rter
ial d
iseas
e,di
abet
es,
rheu
mat
oid
arth
ritis,
neur
o-lo
gica
l dise
ase,
conn
ectiv
e tis
sue
dise
ase,
and
ongo
ing
hosp
ital
trea
tmen
t.
Trea
tmen
t:I:
Cad
exom
er io
dine
pol
y-sa
ccha
ride
pow
der
(Iodo
sorb
),co
vere
d w
ith g
auze
,n =
30.
C:A
var
iety
of a
gent
s w
ere
used
incl
udin
g:an
tibio
tics,
antis
eptic
s,hy
drop
hilic
age
nts,
blan
d ag
ents
,st
eroi
ds a
nd d
ry d
ress
ings
.All
trea
tmen
ts w
ere
cove
red
with
gauz
e,n
= 30
.
Dre
ssin
gs c
hang
ed th
ree
times
aw
eek.
All
patie
nts
wor
e cr
êpe
band
ages
.
Mea
n w
ound
are
a (m
m2 ):
I:12
64 (2
91 S
EM)
C:1
759
(397
SEM
)(p
= 0.
32;s
tatis
tical
met
hod
not s
tate
d).
Oth
er c
hara
cter
istic
s: IC
Mea
n ag
e (y
ears
):69
.573
.4M
:F r
atio
:1:
2.5
1:2.
6M
ean
dura
tion
(mon
ths)
:16
.616
.3
No
stat
istic
al d
iffer
ence
s be
twee
nth
e tw
o gr
oups
.
Dat
a ar
e on
ly a
vaila
ble
for
57 o
fth
e 60
par
ticip
ants
.
% r
educ
tion
in m
ean
area
of w
ound
sat
6 w
eeks
:I:
22%
(n=
28)
C:1
8% (n
= 29
)(p
= 0.
31;c
hi-s
quar
ed a
naly
sis)
Num
ber
of w
ound
s he
aled
at
6 w
eeks
:I:
3/30
(10%
)C
:1/3
0 (3
%)
I:2
C:1
With
draw
als
due
toho
spita
l adm
issio
nan
d la
ck o
fco
oper
atio
n.
Pain
dire
ctly
afte
r ap
plic
atio
nw
as m
ore
com
mon
for
I.
Day
-to-
day
pain
was
sim
ilar
inbo
th g
roup
s af
ter
6 w
eeks
’tr
eatm
ent.

Appendix 6
56 TAB
LE 7
Hyd
roge
l dre
ssin
gs v
ersu
s tra
ditio
nal o
r co
ntro
l tre
atm
ents
Stud
y an
d de
sign
Incl
usio
n/ex
clus
ion
crit
eria
Inte
rven
tion
det
ails
Bas
elin
e ch
arac
teri
stic
sR
esul
ts
Wit
hdra
wal
sC
omm
ents
cont
inue
d
Brow
n-Et
ris e
t al,1
99647
USA
Wou
nd ty
pe:
Pres
sure
sor
es.
Met
hod
of r
ando
misa
tion:
Not
sta
ted;
stra
tific
atio
noc
curr
ed a
ccor
ding
tosu
rfac
e ar
ea a
nd s
tage
.
Obj
ectiv
e ou
tcom
e:A
rea
redu
ctio
n as
sess
ed
by g
ravi
met
ric p
lani
met
ryw
ith w
ound
trac
ing
onto
plas
tic fi
lm a
nd p
hoto
-gr
aphy
.Ind
epen
dent
ana
lysis
by b
iost
atist
ical
ana
lysis
firm
.Cha
nge
in le
vel o
fw
ound
mar
gin
unde
r-m
inin
g as
sess
ed.
Sett
ing
and
leng
th
of tr
eatm
ent:
A m
ultic
entr
e tr
ial.
Part
icip
atio
n w
as u
ntil
10 w
eeks
,or
whe
n tr
eat-
men
t cha
nge
was
indi
cate
dor
the
wou
nd h
eale
d,w
hich
ever
cam
e fir
st.
Incl
usio
n cr
iteria
:Pa
tient
s >
18 y
ears
with
one
or
mor
e pr
essu
re s
ores
.Sta
ge II
,III
or IV
onl
y.W
ound
size
bet
wee
n2
cm a
nd 8
0 cm
2an
d <
1 cm
deep
;clin
ical
ly n
on-in
fect
ed;
esch
ar-fr
ee,w
ith ≥
75%
gra
nu-
latio
n ba
se w
ith fi
xed
wou
ndm
argi
ns;a
dequ
ate
nutr
ition
alin
take
by
mou
th tu
be o
rhy
pera
limen
tatio
n.
Excl
usio
n cr
iteria
:St
age
I sor
es o
r St
age
IV
sore
s w
ith e
xpos
ed te
ndon
or
bone
;wou
nd s
ize <
2 c
m2
or
> 80
cm
2 ,or
> 1
cm d
eep;
wou
nds
cove
red
with
nec
rotic
esch
ar o
r ne
crot
ic w
ound
bas
eco
ntai
ning
> 2
5% s
loug
h;di
agno
sis o
r su
spic
ion
ofos
teom
yelit
is at
stu
dy w
ound
site;
carc
inom
atos
is;or
sig
ns o
rsy
mpt
oms
of w
ound
clin
ical
infe
ctio
n;in
adeq
uate
nut
ritio
nal
inta
ke;s
inus
trac
t,tu
nnel
ling
or >
0.5
cm
of w
ound
mar
gin
unde
rmin
ing.
I:H
ydro
gel d
ress
ing
(Tra
nsor
bent
),n
= 77
.
C:H
ydro
collo
id d
ress
ing
(Duo
derm
CG
F),n
= 6
3.
Eval
uatio
n to
ok p
lace
wee
kly,
dres
sing
chan
ges
occu
rred
eve
ry
7 da
ys o
r m
ore
frequ
ently
.
Mea
n w
ound
are
a:N
ot s
tate
d
Oth
er c
hara
cter
istic
s:A
ll gr
oups
Mea
n ag
e (y
ears
):70
M:F
rat
io1:
1 IC
Dur
atio
n (m
onth
s):
< 1
23%
31%
1–3
38%
49%
4–
6 10
%14
%7–
12
13 %
2%>
12
16%
4%
Loca
tion:
Sacr
um33
%37
%Tr
ocha
nter
17%
26%
Hee
l 16
%18
%Isc
hium
16
%13
%M
alle
olus
10
%4%
Spin
e 6%
2%K
nee
0%2%
Num
ber
of w
ound
s he
aled
at
10
wee
ks:
I:39
/77
(51%
)C
:37/
63 (5
9%)
Redu
ctio
n in
mea
n ar
ea o
f wou
nds
at 1
0 w
eeks
:St
age
II so
res
(2–3
0 cm
2 ):I:
3.6
cm2
(n=
12)
C:2
.3 c
m2
(n=
12) (
NS)
Stag
e II
sore
s (2
–30
cm2 ):
I:6.
3 cm
2(n
= 42
)C
:5.2
cm
2(n
= 36
) (N
S)
Stag
e III
sor
es (3
1–80
cm
2 ):I:
24.5
cm
2(n
= 3)
C:4
.3 c
m2
(n=
2) (N
S)
Insu
ffici
ent d
ata
wer
e av
aila
ble
for
analy
sis o
f the
sub
grou
ping
s:St
age
II (3
1–80
cm
2 ) St
age
IV (2
–30
cm2 )
Stag
e IV
31–
80 c
m2 )
19 r
ando
mise
dpa
tient
s w
ere
not
incl
uded
in th
ean
alysis
as
they
did
not c
ompl
ete
the
first
3 w
eeks
of t
hest
udy,
or m
issed
two
or m
ore
sequ
entia
l wee
kly
visit
s.
No
signi
fican
t diff
eren
ces
incl
inic
al w
ound
infe
ctio
n,od
our,
or d
ress
ing
chan
ges/
wee
k.

Health Technology Assessment 1999; Vol. 3: No. 17 (Pt 1)
57TAB
LE 7
con
td H
ydro
gel d
ress
ings
ver
sus
tradi
tiona
l or
cont
rol t
reat
men
ts
Stud
y an
d de
sign
Incl
usio
n/ex
clus
ion
crit
eria
Inte
rven
tion
det
ails
Bas
elin
e ch
arac
teri
stic
sR
esul
ts
Wit
hdra
wal
sC
omm
ents
cont
inue
d
Dar
kovi
ch e
t al,1
99046
USA
Wou
nd ty
pe:
Pres
sure
sor
es.
Met
hod
of r
ando
misa
tion:
Not
sta
ted.
Obj
ectiv
e ou
tcom
es:
Perim
eter
of t
he w
ound
was
trac
ed a
nd in
som
eca
ses
phot
ogra
phed
tode
term
ine
size.
The
num
ber
of w
ound
s he
aled
was
al
so r
ecor
ded.
Sett
ing
and
leng
th
of tr
eatm
ent:
Max
imum
60-
day
tria
l unl
ess
wou
nd h
eale
d,pa
tient
disc
harg
ed o
r w
ithdr
awn
by c
linic
ian.
Mea
sure
men
tsta
ken
at e
ach
dres
sing
chan
ge o
r at
leas
t wee
kly
inte
rval
s.
Incl
usio
n cr
iteria
:Pa
tient
s in
acu
te c
are
faci
litie
san
d nu
rsin
g ho
mes
with
sta
ge I
or II
pre
ssur
e so
res
ulce
rs
(size
> 2
cm
2 ).
Excl
usio
n cr
iteria
:Rec
eivi
ngra
diat
ion
ther
apy;
infe
ctio
n,sin
us tr
acts
or
fistu
las
in th
ew
ound
;a b
lood
sug
ar le
vel
> 18
0 m
g/dl
;no
impr
oved
nutr
ition
al s
tatu
s.
I:H
ydro
gel d
ress
ing
(Bio
film
),n
= 60
wou
nds.
C:H
ydro
collo
id d
ress
ings
(Duo
derm
),n
= 63
wou
nds.
All
wou
nds
wer
e in
itial
ly c
lean
sed
with
hyd
roge
n pe
roxi
de a
nd s
alin
e.Pa
tient
s w
ith a
n oi
ly s
kin
wer
ede
grea
sed
to a
llow
for
a 1.
25 in
chad
hesio
n be
lt ar
ound
the
wou
nd.
Alth
ough
this
was
not
mai
ntai
ned
whe
re th
e w
ound
was
> 2
0 cm
2 ,in
stea
d ut
ilisin
g 4
x 4
inch
dres
sings
.
Dre
ssin
gs w
ere
usua
lly c
hang
edev
ery
3–4
days
and
was
hed
insa
line
befo
re r
eapp
licat
ion.
All
patie
nts
lay o
n th
e sa
me
type
of
pres
sure
-red
ucin
g m
attr
esse
s.
Mea
n ar
ea o
f pre
ssur
e so
re (c
m2 ):
I:11
.0 (0
.2–1
00 r
ange
)C
:9.2
(0.4
– 64
ran
ge)
Oth
er c
hara
cter
istic
s: All
grou
psM
ean
age
(yea
rs):
75
(ran
ge,3
0–98
)M
:F r
atio
:1:
1.6 I
CRa
tio o
f gra
de
I:II u
lcer
s:1:
1.3
1:1.
6Se
rum
alb
umin
(g
m/d
l):2.
82.
7N
o.of
sta
ge I
wou
nds:
2731
No.
of s
tage
II w
ound
s:35
36
Ther
e w
as a
sig
nific
ant d
iffer
ence
betw
een
the
age
of p
atie
nts
in
the
acut
e ca
re s
ettin
g (6
9 ye
ars)
and
the
exte
nded
car
e fa
cilit
ies
(83
year
s).
Mea
n w
ound
are
a at
60
days
(cm
2 ):I:
3.5
C:5
.5
Mea
n re
duct
ion
in w
ound
are
a at
60
days
(cm
2 ):I:
7.5
(68%
red
uctio
n)C
:3.7
(40%
red
uctio
n)
Num
ber
of w
ound
s he
aled
at
60
days
:I:
26/6
0 (4
3%)
C:1
5/63
(24%
)
Mea
n tr
eatm
ent d
ays:
I:12
C:1
1.3
I:O
ne p
atie
nt w
asex
clud
ed b
ecau
seth
e w
ound
enl
arge
dby
> 1
0% p
er d
ay.
One
pat
ient
was
excl
uded
bec
ause
the
wou
ndde
crea
sed
by
> 25
% p
er d
ay.
C:T
hree
pat
ient
sw
ere
excl
uded
beca
use
thei
rw
ound
s en
larg
ed
by >
10%
per
day
.O
ne p
atie
nt w
asex
clud
ed b
ecau
seth
e w
ound
decr
ease
d by
>
25%
per
day
.
Patie
nts
appe
ared
to p
refe
r I
(hyd
roge
l) be
caus
e of
the
lack
of o
dour
,cus
hion
ing
and
light
ness
.
The
gel l
ayer
in C
(hyd
ro-
collo
id) w
as fo
und
to d
egra
deea
sily
whi
ch n
eces
sitat
edm
echa
nica
l cle
ansin
g of
the
wou
nd,w
hich
dam
aged
the
heal
ing
tissu
e lay
ers.

Appendix 6
58 TAB
LE 7
con
td H
ydro
gel d
ress
ings
ver
sus
tradi
tiona
l or
cont
rol t
reat
men
ts
Stud
y an
d de
sign
Incl
usio
n/ex
clus
ion
crit
eria
Inte
rven
tion
det
ails
Bas
elin
e ch
arac
teri
stic
sR
esul
ts
Wit
hdra
wal
sC
omm
ents
Alle
vyn®
,Sm
ith &
Nep
hew
Hea
lthca
re L
td
cont
inue
d
Lum
et a
l,199
6(u
npub
lishe
d)48
Hon
g Ko
ng
Wou
nd ty
pe:
Pres
sure
sor
es.
Met
hod
of r
ando
misa
tion:
Patie
nts
with
an
odd
adm
issio
n nu
mbe
r w
ere
assig
ned
to th
e co
ntro
lgr
oup,
thos
e w
ith a
n ev
ennu
mbe
r w
ere
assig
ned
toth
e tr
eatm
ent g
roup
.
Obj
ectiv
e ou
tcom
e:W
ound
size
was
mea
sure
d.In
add
ition
the
time
spen
tby
nur
sing
staf
f and
cos
t of
pha
rmac
eutic
als
was
mon
itore
d.
Sett
ing
and
leng
th
of tr
eatm
ent:
Post
-acu
te h
ospi
tal.
Trea
tmen
t pro
gres
sion
was
mon
itore
d w
eekl
y an
d a
final
ass
essm
ent
was
mad
e af
ter
8 w
eeks
,co
mpl
ete
heal
ing,
disc
harg
e or
dea
th.
Incl
usio
n cr
iteria
:H
ospi
talis
ed p
ost a
cute
pat
ient
sag
ed ≥
65 y
ears
with
pre
ssur
eso
res.
Excl
usio
n cr
iteria
:Pr
essu
re s
ores
≤1
cm2 ;g
rade
Iso
res;
patie
nts
cons
ider
ed fo
rsu
ppor
tive
care
onl
y;pa
tient
sre
quiri
ng a
ntim
icro
bial
age
nts
for
man
agem
ent o
f sys
tem
icin
fect
ion
from
pre
ssur
e so
res;
patie
nts
(or
care
rs) d
id n
ot g
iveco
nsen
t for
the
stud
y.
Trea
tmen
t:I:
Hyd
roge
l dre
ssin
g (In
tras
ite
Gel
) cov
ered
with
a h
ydro
phili
cpo
lyur
etha
ne fo
am d
ress
ing
(Alle
vyn®
),n
= 12
wou
nds
from
five
pat
ient
s.
C:T
he s
ore
was
cle
anse
d w
ith a
freq
uenc
y de
pend
ent
on th
e am
ount
of d
ischa
rge
(for
unin
fect
ed s
ores
cle
ansin
g w
aspe
rform
ed b
y sa
line
only
whi
le
for
infe
cted
sor
es c
lean
sing
was
perfo
rmed
with
1 /2Eu
sol f
or a
tm
ost t
hree
tim
es a
day
follo
wed
by
rinsin
g w
ith s
alin
e),n
= 8
wou
nds
from
five
pat
ient
s.
All
patie
nts
rece
ived
the
sam
ege
nera
l tre
atm
ent w
hich
incl
uded
:ba
thin
g at
leas
t on
alte
rnat
e da
ys;
turn
ing
ever
y 2
hrs
(7 a
m–1
1 pm
)an
d ev
ery
3 hr
s (1
1 pm
–7 a
m);
give
n at
leas
t 1.5
litr
es o
f flu
id
per
day
unle
ss c
ontr
aind
icat
ions
exist
ed;n
utrit
iona
l sup
port
and
mon
itorin
g;vi
tam
ins
only
to b
egi
ven
if ev
iden
ce o
f def
icie
ncy;
anti-
mic
robi
al a
gent
s on
ly to
be
give
nw
ith e
vide
nce
of s
yste
mic
sep
sis.
Mea
n w
ound
are
a (c
m2)
:I:
36.3
(ran
ge,1
.5–1
60)
C:1
8.6
(ran
ge,1
.0–7
2.5)
Oth
er c
hara
cter
istic
s:I
CM
ean
age
(yea
rs):
8078
.4M
:F r
atio
:1:
41:
1.5
Mea
n du
ratio
n (m
onth
s):
Not
sta
ted
No
stat
istic
ally
sig
nific
ant
diffe
renc
e be
twee
n th
e tw
o gr
oups
was
rep
orte
d.
Mea
n siz
e of
pre
ssur
e so
re a
t fin
alas
sess
men
t (cm
2 ):I:
15.9
(p=
0.02
)C
:20.
5 (p
= 0.
87)
(p=
0.94
;Wilc
oxon
sig
n te
st o
rM
ann-
Whi
tney
ran
k su
m te
st w
ere
used
for
stat
istic
al a
naly
sis)
Mea
n %
cha
nge
in w
ound
are
a at
final
ass
essm
ent:
I:–5
6%C
:+10
%
Cos
t of l
ocal
trea
tmen
t (H
K$)
:I
CN
ursin
g tim
e:78
516
58Ph
arm
aceu
tical
ite
ms:
1884
280
Trea
tmen
t with
I w
as s
tatis
tical
ly le
ssex
pens
ive th
an tr
eatm
ent w
ith C
.
I:N
o w
ithdr
awal
s.
C:T
wo
patie
nts
died
from
pneu
mon
ia.
Estim
ated
man
pow
erre
quire
d fo
r ge
nera
l car
e w
as5.
8 an
d 2.
72 h
r/da
y/pa
tient
,w
ith le
ss ti
me
used
in th
etr
eatm
ent a
rm (p
= 0.
046)
.
The
aver
age
dura
tion
of s
tay
was
4.8
day
s in
the
I (H
ydro
-ge
l) gr
oup
and
6.4
days
in th
eC
(sta
ndar
d tr
eatm
ent)
gro
up(p
= 0.
15;N
S).

Health Technology Assessment 1999; Vol. 3: No. 17 (Pt 1)
59TAB
LE 7
con
td H
ydro
gel d
ress
ings
ver
sus
tradi
tiona
l or
cont
rol t
reat
men
ts
Stud
y an
d de
sign
Incl
usio
n/ex
clus
ion
crit
eria
Inte
rven
tion
det
ails
Bas
elin
e ch
arac
teri
stic
sR
esul
ts
Wit
hdra
wal
sC
omm
ents
Mul
der
et a
l,199
349
USA
Wou
nd ty
pe:
Pres
sure
sor
es.
Met
hod
of r
ando
misa
tion:
Com
pute
r al
loca
tion.
Obj
ectiv
e ou
tcom
es:
The
wou
nd p
erim
eter
was
trac
ed o
n to
a tr
ansp
aren
cyan
d th
e ar
ea d
eter
min
ed
by c
ompu
ter
analy
sis.I
nad
ditio
n th
e la
rges
t len
gth,
wid
th a
nd d
epth
of e
ach
wou
nd w
as m
easu
red
and
a ph
otog
raph
take
n at
ea
ch a
sses
smen
t.
Sett
ing
and
leng
th
of tr
eatm
ent:
A m
ultic
entr
e tr
ial a
t thr
eein
depe
nden
t site
s.A
sses
s-m
ents
of w
ound
size
wer
em
ade
wee
kly
for
8 w
eeks
or u
ntil
the
wou
nd w
ashe
aled
.Whe
re p
ossib
le,
each
pat
ient
was
eva
luat
edby
the
sam
e in
vest
igat
orth
roug
hout
the
tria
l.Effo
rts
wer
e m
ade
to s
tand
ardi
seob
serv
atio
ns b
etw
een
inve
stig
ator
s.
Incl
usio
n cr
iteria
:In
-pat
ient
s an
d ou
t-pa
tient
s w
ithst
age
II an
d III
pre
ssur
e so
res.
Sore
s ≥
1.5
cm x
0.5
cm
and
≥
10 c
m x
10
cm w
ere
incl
uded
.Pa
tient
s w
ere
≥18
yea
rs a
nd
had
a lif
e ex
pect
ancy
of a
t le
ast 2
mon
ths.
Excl
usio
n cr
iteria
:St
age
IV w
ound
s or
thos
e w
ithte
ndon
,bon
e,ca
psul
e,or
fasc
iaex
posu
re;p
regn
ancy
;che
mo-
ther
apy;
prio
r w
ound
infe
ctio
n;ex
tens
ive u
nder
min
ing
of th
eul
cer
(> 1
cm
);AID
S;pa
tient
sre
ceiv
ing
> 10
mg
ofco
rtic
oste
roid
s.
Trea
tmen
t:I:
Hyd
roge
l dre
ssin
g (C
lear
site)
,ch
ange
d tw
ice
a w
eek,
n =
23.
C1:
Hyd
roco
lloid
dre
ssin
g(D
uoD
erm
),ch
ange
d tw
ice
aw
eek,
n =
20.
C2:
Salin
e so
lutio
n an
d m
oist
ened
gauz
e,ch
ange
d th
ree
times
a d
ay,
n =
21.
Dre
ssin
gs w
ere
chan
ged
eith
er b
yth
e pa
tient
or
the
care
give
r,af
ter
they
had
rec
eive
d ap
prop
riate
inst
ruct
ions
.
67 p
atie
nts
wer
e en
rolle
d in
to
the
tria
l;dat
a w
ere
analy
sed
for
only
64.
Mea
n w
ound
are
a (c
m2 ):
Not
sta
ted.
Oth
er c
hara
cter
istic
s: IC
1C
2
Mea
n ag
e (y
ears
):56
.763
.157
.2M
:F r
atio
:1:
3.6
1:5.
61:
9.5
Wou
nd s
tage
:II:
89
5III
:14
1318
Race
(pat
ient
s):
Blac
k:4
36
Whi
te:
1716
14H
ispan
ic:
11
0
No
stat
istic
ally
sig
nific
ant
diffe
renc
es b
etw
een
the
thre
egr
oups
was
rep
orte
d.
Mea
n %
red
uctio
n in
wou
nd a
rea
per
wee
k:I:
8 (1
4.8
SD)
C1:
3.3
(32.
7 SD
)C
2:5.
1 (1
4.8
SD)
(p>
0.05
;non
-par
amet
ric te
st)
Med
ian
% r
educ
tion
in w
ound
are
ape
r w
eek:
I:5.
6C
1:7.
4C
2:7.
0(p
> 0.
05;n
on-p
aram
etric
test
)
Thre
e pa
tient
sw
ere
not e
valu
able
and
thei
r da
ta a
reno
t pre
sent
ed in
the
base
line
char
acte
ristic
s.
I:Thr
ee p
atie
nts
wer
e om
itted
from
the
final
ana
lysis
.N
o re
ason
s w
ere
give
n fo
r th
ese
with
draw
als.
C1:
No
with
draw
als.
C2:
No
with
draw
als.
One
pat
ient
in th
e C
1tr
eatm
ent g
roup
(hyd
ro-
collo
id) h
ad m
ild ir
ritat
ion,
and
anot
her
had
min
orse
nsiti
vity
to th
e C
1 dr
essin
g.
One
cas
e of
infla
mm
atio
noc
curr
ed in
the
I (hy
drog
el)
grou
p,an
d an
othe
r pa
tient
had
exco
riatio
n w
hich
was
poss
ibly
rela
ted
to I.
Ther
e w
ere
no a
dver
sere
actio
ns to
C2
(sal
ine)
.

Appendix 6
60 TAB
LE 8
Enz
yme
prep
arat
ions
ver
sus
tradi
tiona
l or
cont
rol t
reat
men
ts
Stud
y an
d de
sign
Incl
usio
n/ex
clus
ion
crit
eria
Inte
rven
tion
det
ails
Bas
elin
e ch
arac
teri
stic
sR
esul
ts
Wit
hdra
wal
sC
omm
ents
cont
inue
d
Ågr
en a
nd S
tröm
berg
,19
859
Swed
en
Wou
nd ty
pe:
Pres
sure
sor
es.
Met
hod
of r
ando
misa
tion:
Patie
nts
cons
ecut
ively
mat
ched
in p
airs
(for
wha
tno
t sta
ted)
.Eac
h m
embe
rof
the
pair
was
ran
dom
lyal
loca
ted
to o
ne o
f the
tw
o tr
eatm
ents
.
Obj
ectiv
e ou
tcom
e:W
ound
are
a w
as tr
aced
and
the
size
mea
sure
d by
plan
imet
ry.A
pho
togr
aph
was
take
n at
eac
has
sess
men
t.
Sett
ing
and
leng
th
of tr
eatm
ent:
Sing
le-b
lind
tria
l for
8
wee
ks.O
ne o
f the
auth
ors
was
res
pons
ible
fo
r m
easu
ring
all t
hew
ound
s at
wee
kly
inte
rval
s.A
n in
depe
nden
t sur
geon
from
ano
ther
hos
pita
las
sess
ed th
e ph
otog
raph
s.
Incl
usio
n cr
iteria
:El
derly
in-p
atie
nts
and
out-
patie
nts
with
one
or
mor
ene
crot
ic p
ress
ure
sore
s.
Excl
usio
n cr
iteria
:N
ot s
tate
d.
Trea
tmen
t:I:
Stre
ptok
inas
e/st
rept
odor
nase
enzy
me
prep
arat
ion
(Var
idas
eTo
pica
l) ap
plie
d to
a s
teril
e ga
uze
com
pres
s.D
ress
ings
cha
nged
tw
ice
daily
,n =
14.
C:Z
inc
oxid
e (4
00 m
g Z
nO/c
m2 )
appl
ied
to a
ste
rile
gauz
eco
mpr
ess.
Dre
ssin
gs c
hang
ed
once
dai
ly,n
= 14
.
All
dres
sings
wer
e se
cure
d w
ithpo
rous
acr
ylic
-bas
ed ta
pes.
Whe
rem
ultip
le w
ound
s ex
isted
they
wer
eal
l tre
ated
uni
form
ly,bu
t onl
y th
ela
rges
t was
mon
itore
d.
Prio
r to
trea
tmen
t loo
sely
atta
ched
nec
rotic
mat
eria
l was
rem
oved
,but
no
surg
ical
deb
ride-
men
t was
per
form
ed th
erea
fter.
No
patie
nts
rece
ived
antib
iotic
s.N
ursin
g ca
re fo
llow
ed it
s us
ual
proc
edur
e.
Med
ian
wou
nd a
rea
(cm
2 ):I:
4.2
(ran
ge,1
.2–1
8.2)
C
:5.8
(ran
ge,1
.2–2
6.0)
Oth
er c
hara
cter
istic
s:I
CM
edia
n ag
e (y
ears
):86
81M
:F r
atio
:1:
3.7
1:1.
8D
iabe
tes
mel
litus
(n):
45
% m
edia
n ch
ange
in w
ound
are
a at
final
ass
essm
ent:
I:+1
8.7%
C:–
2.4%
I:Thr
ee p
atie
nts
wer
e w
ithdr
awn
beca
use
ofun
succ
essfu
ltr
eatm
ent.
In o
ne
of th
ese
patie
nts
a sk
in r
eact
ion
occu
rred
on
the
heel
afte
r 3
wee
ksof
trea
tmen
t.In
anot
her
patie
ntne
cros
is de
velo
ped
to 8
x its
orig
inal
size.
In th
e th
irdpa
tient
Pse
udo-
mon
as a
erug
inos
ain
fect
ion
deve
lope
daf
ter
6 w
eeks
.
C:N
o w
ithdr
awal
s
All
with
draw
als
wer
e in
clud
ed in
the
analy
sis.
I (en
zym
e) w
as a
ssoc
iate
dw
ith a
n in
crea
se in
wou
ndsiz
e.Th
is m
ay b
e du
e to
exce
ssive
wou
nd d
ebrid
e-m
ent,
or in
hibi
tion
of ti
ssue
grow
th b
y th
e en
zym
e.

Health Technology Assessment 1999; Vol. 3: No. 17 (Pt 1)
61TAB
LE 8
con
td E
nzym
e pr
epar
atio
ns v
ersu
s tra
ditio
nal o
r co
ntro
l tre
atm
ents
Stud
y an
d de
sign
Incl
usio
n/ex
clus
ion
crit
eria
Inte
rven
tion
det
ails
Bas
elin
e ch
arac
teri
stic
sR
esul
ts
Wit
hdra
wal
sC
omm
ents
cont
inue
d
Gor
don,
1975
51
UK
Wou
nd ty
pe:
Leg
ulce
rs.
Met
hod
of r
ando
misa
tion:
Not
sta
ted.
Obj
ectiv
e ou
tcom
e:W
ound
are
a w
as e
stim
ated
by m
easu
ring
the
two
larg
est d
iam
eter
s an
dm
ultip
lyin
g to
geth
er.E
ach
wou
nd w
as p
hoto
grap
hed.
Sett
ing
and
leng
th o
ftr
eatm
ent:
Patie
nts
atte
nd-
ing
a cl
inic
for
leg
ulce
rtr
eatm
ent.
Ass
essm
ents
wer
e m
ade
at w
eekl
yin
terv
als
for
6 w
eeks
.
Incl
usio
n cr
iteria
:Pa
tient
s w
ith le
g ul
cers
cons
ider
ed to
be
post
-th
rom
botic
.
Excl
usio
n cr
iteria
:N
ot s
tate
d.
Trea
tmen
t:C
:For
mul
atio
n A
–
hydr
ocor
tison
e ac
etat
e an
dne
omyc
in p
alita
te,n
= 9
.
I:Fo
rmul
atio
n B
(Chy
mac
ort)
.Th
is tr
eatm
ent w
as th
e sa
me
asfo
rmul
atio
n A
but
with
the
addi
tion
of th
e pa
ncre
atic
enz
ymes
chym
otry
psin
and
tryp
sin in
the
prop
ortio
n of
1:6
,n=
10.
All
wou
nds
wer
e co
vere
d w
ith a
non-
adhe
rent
dre
ssin
g;a
tube
gauz
e;an
abs
orbe
nt g
auze
dre
ssin
gpa
d ov
er th
e w
ound
are
a;an
dfin
ally
a 4
-inch
crê
pe b
anda
geap
plie
d fro
m th
e to
es to
the
knee
Dre
ssin
gs w
ere
chan
ged
at th
ecl
inic
.Pat
ient
s w
ere
inst
ruct
ed n
otto
inte
rfere
with
dre
ssin
gs a
nd to
rem
ain
fully
am
bula
nt.
App
roxi
mat
e m
ean
wou
nd
area
(cm
2 ):C
:14.
50 (2
2.13
SD
)I:
15.8
2 (1
9.67
SD
)
Oth
er c
hara
cter
istic
s: All
grou
psM
ean
age
(yea
rs):
61M
:F r
atio
:1:
9.5
Ther
e w
as n
o st
atist
ical
diff
eren
cebe
twee
n th
e tw
o gr
oups
with
resp
ect t
o th
e gi
ven
base
line
char
acte
ristic
s.
App
roxi
mat
e m
ean
wou
nd a
rea
at 6
wee
ks:
C:8
.40
(9.7
9 SD
)I:
5.37
(7.8
2 SD
)(C
vs.
base
line,
p<
0.05
;I v
s.ba
selin
e,p
< 0.
01;s
tatis
tical
test
met
hod
not s
tate
d)
Num
ber
of w
ound
s he
aled
afte
r 6
wee
ks:
C:0
/9 (0
%)
I:2/
10 (2
0%)
C:O
ne p
atie
ntde
faul
ted
afte
r th
e fir
st w
eek
oftr
eatm
ent a
nd
was
exc
lude
d fro
mth
e an
alysis
.
I:N
o w
ithdr
awal
s.
Pain
cau
sed
by tr
eatm
ent w
asin
suffi
cien
t to
caus
ew
ithdr
awal
in e
ither
gro
up.
Lee
& A
mbr
us,1
97550
USA
Wou
nd ty
pe:P
ress
ure
sore
s.
Met
hod
of r
ando
misa
tion:
Not
sta
ted.
Obj
ectiv
e ou
tcom
e:Tw
odi
amet
ers o
f the
wou
ndm
easu
red
and
a co
lour
phot
ogra
ph ta
ken.
In a
dditi
ona
volu
me
mou
ld w
as m
ade
with
Jeltr
ate
or K
err
No.
1,an
d th
e vo
lum
e de
term
ined
by w
ater
disp
lacem
ent.
Sett
ing
and
leng
th o
f tre
at-
men
t:Se
ttin
g no
t sta
ted.
Patie
nts
wer
e tr
eate
d fo
r 4
wee
ks o
r un
til c
ompl
ica-
tions
dev
elop
ed o
r th
epa
tient
die
d.M
easu
rem
ents
whe
re ta
ken
wee
kly
and
onco
mpl
etio
n of
the
stud
y.
Incl
usio
n cr
iteria
:Pa
tient
s w
ith a
dvan
ced
pres
sure
sor
es.
Excl
usio
n cr
iteria
:N
ot s
tate
d.
Trea
tmen
t:I:
Col
lage
nase
enz
yme
prep
arat
ion
(San
tyl)
appl
ied
at 2
50 u
nits
per
gram
of w
hite
pet
rola
tum
,n =
17.
C:P
lace
bo (h
eat-
inac
tivat
ed S
anty
l)ap
plie
d in
the
sam
e pr
opor
tions
as
for
I,n
= 11
.
Befo
re a
pplic
atio
n of
eith
ertr
eatm
ent t
he w
ound
was
was
hed
with
ste
rile
salin
e (p
H 7
.5).
Each
appl
icat
ion
was
app
lied
once
da
ily to
eac
h w
ound
unl
ess
mor
efre
quen
t cle
ansin
g w
as r
equi
red
beca
use
of c
onta
min
atio
n fro
min
cont
inen
ce o
f urin
e,fa
eces
or
bot
h.
All
wou
nds
wer
e co
vere
d w
ith a
ster
ile g
auze
pad
.
Mea
n w
ound
are
a (c
m2 ):
Not
sta
ted.
Mea
n w
ound
vol
ume
(cm
3 ):I:
15.4
4 (1
9.92
SD
)C
:1.2
5 (1
.62
SD)
Oth
er c
hara
cter
istic
s:A
ll gr
oups
Mea
n ag
e (y
ears
):67
.6 (1
3.7
SD)
M:F
rat
io:
1:2.
7
Base
line
wou
nd v
olum
e is
signi
fican
tly d
iffer
ent b
etw
een
grou
ps (p
< 0.
01).
11 p
atie
nts
with
28
adva
nced
pres
sure
sor
es w
ere
incl
uded
inth
e st
udy.
All
had
chro
nic
dise
ase
and
wer
e in
poo
r ph
ysic
al c
on-
ditio
n.Fo
ur h
ad n
eopl
astic
dise
ase;
four
had
ath
eros
cler
otic
hea
rtdi
seas
e or
had
a c
ereb
rova
scul
arac
cide
nt,o
r bo
th;t
wo
had
Park
in-
son’s
dise
ase;
and
one
had
afe
mor
al n
eck
frac
ture
.
Mea
n %
cha
nge
in w
ound
vol
ume
at c
ompl
etio
n of
the
tria
l:I:
+13.
14 (5
9.8
SD)
C:+
78.7
9 (9
4.6
SD)
(Pre
ssur
e so
res
in b
oth
grou
psin
crea
sed
in s
ize.)
I:Pa
tient
s w
ere
rem
oved
from
da
y 6
to d
ay 3
0(t
erm
inat
ion
of
the
tria
l).
C:P
atie
nts
wer
ew
ithdr
awn
from
da
y 3
to d
ay 1
0.N
o pa
tient
in th
isgr
oup
cont
inue
d to
be
trea
ted
afte
r10
day
s.
One
wou
nd tr
eate
d w
ith I
(enz
yme)
exp
erie
nced
mild
blee
ding
and
a b
urni
ngse
nsat
ion.
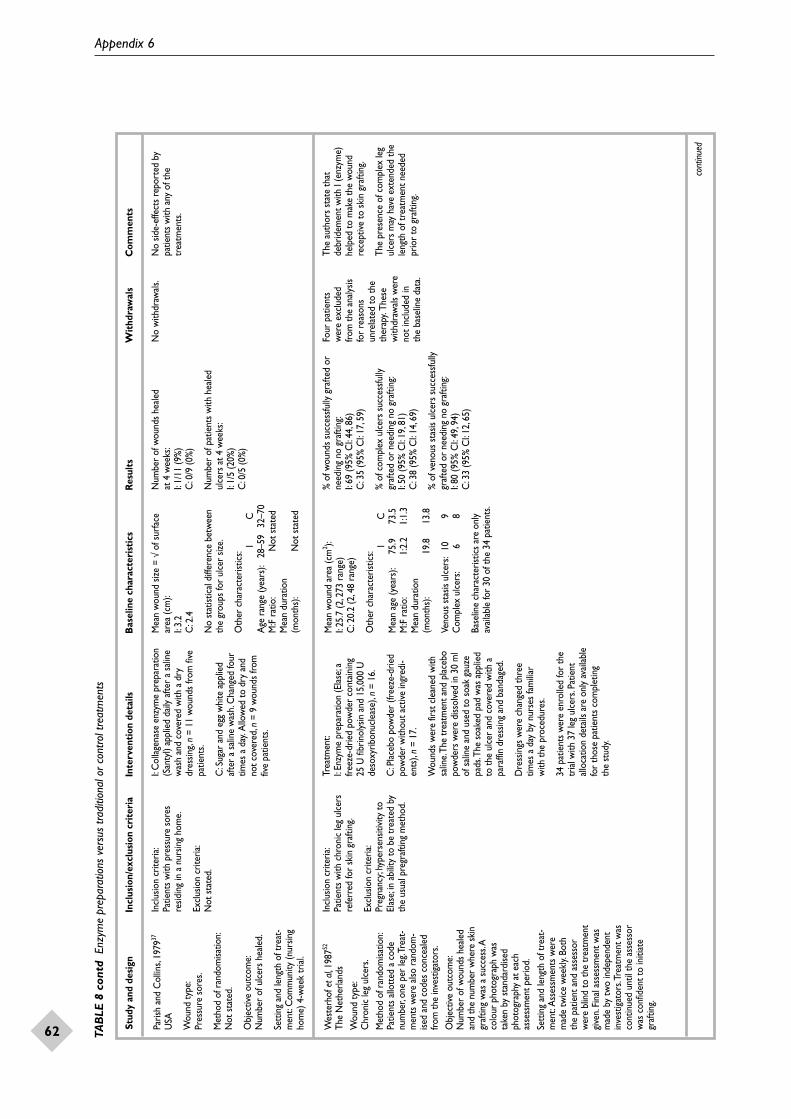
Appendix 6
62 TAB
LE 8
con
td E
nzym
e pr
epar
atio
ns v
ersu
s tra
ditio
nal o
r co
ntro
l tre
atm
ents
Stud
y an
d de
sign
Incl
usio
n/ex
clus
ion
crit
eria
Inte
rven
tion
det
ails
Bas
elin
e ch
arac
teri
stic
sR
esul
ts
Wit
hdra
wal
sC
omm
ents
cont
inue
d
Paris
h an
d C
ollin
s,19
7937
USA
Wou
nd ty
pe:
Pres
sure
sor
es.
Met
hod
of r
ando
misa
tion:
Not
sta
ted.
Obj
ectiv
e ou
tcom
e:N
umbe
r of
ulc
ers
heal
ed.
Sett
ing
and
leng
th o
f tre
at-
men
t:C
omm
unity
(nur
sing
hom
e) 4
-wee
k tr
ial.
Incl
usio
n cr
iteria
:Pa
tient
s w
ith p
ress
ure
sore
sre
sidin
g in
a n
ursin
g ho
me.
Excl
usio
n cr
iteria
:N
ot s
tate
d.
I:C
olla
gena
se e
nzym
e pr
epar
atio
n(S
anty
l) ap
plie
d da
ily a
fter
a sa
line
was
h an
d co
vere
d w
ith a
dry
dres
sing,
n =
11 w
ound
s fro
m fi
vepa
tient
s.
C:S
ugar
and
egg
whi
te a
pplie
daf
ter
a sa
line
was
h.C
hang
ed fo
urtim
es a
day
.Allo
wed
to d
ry a
ndno
t cov
ered
,n =
9 w
ound
s fro
mfiv
e pa
tient
s.
Mea
n w
ound
size
= √
of s
urfa
cear
ea (c
m):
I:3.
2 C
:2.4
No
stat
istic
al d
iffer
ence
bet
wee
nth
e gr
oups
for
ulce
r siz
e.
Oth
er c
hara
cter
istic
s:I
CA
ge r
ange
(yea
rs):
28–5
932
–70
M:F
rat
io:
Not
sta
ted
Mea
n du
ratio
n (m
onth
s):
Not
sta
ted
Num
ber
of w
ound
s he
aled
at
4 w
eeks
:I:
1/11
(9%
)C
:0/9
(0%
)
Num
ber
of p
atie
nts
with
hea
led
ulce
rs a
t 4 w
eeks
:I:
1/5
(20%
)C
:0/5
(0%
)
No
with
draw
als.
No
side-
effe
cts
repo
rted
by
patie
nts
with
any
of t
hetr
eatm
ents
.
Wes
terh
of e
t al,1
98752
The
Net
herla
nds
Wou
nd ty
pe:
Chr
onic
leg
ulce
rs.
Met
hod
of r
ando
misa
tion:
Patie
nts
allo
tted
a c
ode
num
ber,
one
per
leg.
Trea
t-m
ents
wer
e al
so r
ando
m-
ised
and
code
s co
ncea
led
from
the
inve
stig
ator
s.O
bjec
tive
outc
ome:
Num
ber
of w
ound
s he
aled
and
the
num
ber
whe
re s
kin
graf
ting
was
a s
ucce
ss.A
colo
ur p
hoto
grap
h w
asta
ken
by s
tand
ardi
sed
phot
ogra
phy
at e
ach
asse
ssm
ent p
erio
d.Se
ttin
g an
d le
ngth
of t
reat
-m
ent:
Ass
essm
ents
wer
em
ade
twic
e w
eekl
y.Bo
thth
e pa
tient
and
ass
esso
rw
ere
blin
d to
the
trea
tmen
tgi
ven.
Fina
l ass
essm
ent w
asm
ade
by tw
o in
depe
nden
tin
vest
igat
ors.
Trea
tmen
t was
cont
inue
d un
til th
e as
sess
orw
as c
onfid
ent t
o in
itiat
egr
aftin
g.
Incl
usio
n cr
iteria
:Pa
tient
s w
ith c
hron
ic le
g ul
cers
refe
rred
for
skin
gra
fting
.
Excl
usio
n cr
iteria
:Pr
egna
ncy;
hype
rsen
sitiv
ity to
Elas
e;in
abi
lity
to b
e tr
eate
d by
the
usua
l pre
graf
ting
met
hod.
Trea
tmen
t:I:
Enzy
me
prep
arat
ion
(Ela
se;a
freez
e-dr
ied
pow
der
cont
aini
ng
25 U
fibr
inol
ysin
and
15,
000
Ude
soxy
ribon
ucle
ase)
,n =
16.
C:P
lace
bo p
owde
r (fr
eeze
-drie
dpo
wde
r w
ithou
t act
ive in
gred
i-en
ts),
n =
17.
Wou
nds
wer
e fir
st c
lean
ed w
ithsa
line.
The
trea
tmen
t and
pla
cebo
pow
ders
wer
e di
ssol
ved
in 3
0 m
lof
sal
ine
and
used
to s
oak
gauz
epa
ds.T
he s
oake
d pa
d w
as a
pplie
dto
the
ulce
r an
d co
vere
d w
ith a
para
ffin
dres
sing
and
band
aged
.
Dre
ssin
gs w
ere
chan
ged
thre
etim
es a
day
by
nurs
es fa
mili
ar
with
the
proc
edur
es.
34 p
atie
nts
wer
e en
rolle
d fo
r th
etr
ial w
ith 3
7 le
g ul
cers
.Pat
ient
allo
catio
n de
tails
are
onl
y av
aila
ble
for
thos
e pa
tient
s co
mpl
etin
g th
e st
udy.
Mea
n w
ound
are
a (c
m2 ):
I:25
.7 (2
,273
ran
ge)
C:2
0.2
(2,4
8 ra
nge)
Oth
er c
hara
cter
istic
s:I
CM
ean
age
(yea
rs):
75.9
73.5
M:F
rat
io:
1:2.
21:
1.3
Mea
n du
ratio
n (m
onth
s):
19.8
13.8
Veno
us s
tasis
ulc
ers:
109
Com
plex
ulc
ers:
68
Base
line
char
acte
ristic
s ar
e on
lyav
aila
ble
for
30 o
f the
34
patie
nts.
% o
f wou
nds
succ
essfu
lly g
rafte
d or
need
ing
no g
rafti
ng:
I:69
(95%
CI:
44,8
6)C
:35
(95%
CI:
17,5
9)
% o
f com
plex
ulc
ers
succ
essfu
llygr
afte
d or
nee
ding
no
graf
ting:
I:50
(95%
CI:
19,8
1)C
:38
(95%
CI:
14,6
9)
% o
f ven
ous
stas
is ul
cers
suc
cess
fully
graf
ted
or n
eedi
ng n
o gr
aftin
g:I:
80 (9
5% C
I:49
,94)
C:3
3 (9
5% C
I:12
,65)
Four
pat
ient
s w
ere
excl
uded
from
the
analy
sisfo
r re
ason
sun
rela
ted
to th
eth
erap
y.Th
ese
with
draw
als
wer
eno
t inc
lude
d in
th
e ba
selin
e da
ta.
The
auth
ors
stat
e th
atde
brid
emen
t with
I (e
nzym
e)he
lped
to m
ake
the
wou
ndre
cept
ive to
ski
n gr
aftin
g.
The
pres
ence
of c
ompl
ex le
gul
cers
may
hav
e ex
tend
ed th
ele
ngth
of t
reat
men
t nee
ded
prio
r to
gra
fting
.

Health Technology Assessment 1999; Vol. 3: No. 17 (Pt 1)
63TAB
LE 9
Zin
c ox
ide
tape
ver
sus
tradi
tiona
l tre
atm
ent
Stud
y an
d de
sign
Incl
usio
n/ex
clus
ion
crit
eria
Inte
rven
tion
det
ails
Bas
elin
e ch
arac
teri
stic
sR
esul
ts
Wit
hdra
wal
sC
omm
ents
MeZ
inc®
,Moln
lycke
Hea
lth C
are
Ape
lqvi
st e
t al,1
99053
Swed
en
Wou
nd ty
pe:
Dia
betic
foot
ulc
ers.
Met
hod
of r
ando
misa
tion:
Not
sta
ted.
Obj
ectiv
e ou
tcom
es:
Are
a of
nec
rotic
tiss
uem
easu
red
and
a co
lour
phot
ogra
ph ta
ken.
Asu
cces
sful o
utco
me
was
whe
n th
e ne
crot
ic a
rea
had
redu
ced
by 5
0% o
r m
ore.
Eval
uatio
ns w
ere
blin
ded.
Sett
ing
and
leng
th o
ftr
eatm
ent:
Out
patie
nt c
linic
.A
sses
smen
ts w
ere
mad
ew
eekl
y fo
r 5
wee
ks.
Incl
usio
n cr
iteria
:Pa
tient
s w
ith n
ecro
tic d
iabe
ticfo
ot u
lcer
s (s
uper
ficia
l ful
lth
ickn
ess
skin
ulc
er b
elow
ank
lean
d w
ith s
ysto
lic to
e pr
essu
reab
ove
45 m
mH
g or
abs
ence
of
cuta
neou
s er
ythe
ma;
ulce
rsbe
twee
n 1–
25 c
m2
in a
rea
with
> 50
% o
f are
a co
vere
d w
ithdr
y/w
et n
ecro
tic ti
ssue
).Whe
reth
ere
was
mor
e th
an o
ne u
lcer
the
larg
est w
as c
hose
n.
Excl
usio
n cr
iteria
:Po
sitive
pat
ch te
st;c
linic
al s
igns
of c
ellu
litis;
ulce
rs w
here
the
appl
icat
ion
of th
ese
dres
sings
was
inap
prop
riate
.
Trea
tmen
t:I:A
dhes
ive z
inc
oxid
e ta
pe(M
eZin
c®),
n =
22.
C:H
ydro
collo
id d
ress
ing
(Duo
Der
m),
n =
22.
All
patie
nts
wer
e of
fere
d th
e sa
me
addi
tiona
l tre
atm
ent:
the
foot
w
ear
was
cor
rect
ed a
nd e
xter
nal
pres
sure
on
the
ulce
r re
lieve
d.U
lcer
s w
ere
clea
ned
with
ste
rile
salin
e an
d dr
esse
d ac
cord
ing
toth
e m
anuf
actu
rers
gui
delin
es.
Dre
ssin
gs w
ere
chan
ged
daily
for
the
first
wee
k an
d ev
ery
3 da
ysaf
terw
ards
.
No
surg
ical
deb
ridem
ent w
asal
low
ed.
Mea
n w
ound
are
a (c
m2 ):
I:2.
2 (1
,10.
5 SD
)C
:2.2
(0.9
,20.
4 SD
)
Mea
n ne
crot
ic a
rea
of w
ound
(cm
2 ):I:
1.5
(0.5
,10.
5 SD
)C
:1.6
(0.9
,19.
2 SD
)
Oth
er c
hara
cter
istic
s:I
CM
ean
age
(yea
rs):
6362
M:F
rat
io:
1:1.
21:
0.5
Mea
n du
ratio
n (y
ears
) of d
iabe
tes:
2219
Insu
lin:
1718
Syst
olic
toe
pres
sure
(mm
Hg)
:66
68Sy
stol
ic a
nkle
pr
essu
re (m
mH
g):
104
114
Num
ber
of w
ound
s re
duce
d by
50
% o
r m
ore
at 5
wee
ks:
I:14
/21
(67%
)C
:6/2
1 (2
9%)
Mea
n %
cha
nge
in w
ound
are
a at
5 w
eeks
:I:
60%
red
uctio
n (n
= 18
)C
:5%
incr
ease
(n=
17)
I:Fo
ur p
atie
nts
beca
use
of >
50%
incr
ease
in a
rea
ofne
crot
ic ti
ssue
,as
soci
ated
pai
n an
doe
dem
a or
sig
ns o
fce
llulit
is.
C:F
ive p
atie
nts
beca
use
of >
50%
incr
ease
in a
rea
ofne
crot
ic ti
ssue
,as
soci
ated
pai
n an
doe
dem
a or
sig
ns o
fce
llulit
is.
Com
mon
adv
erse
effe
cts
wer
e se
en in
bot
h gr
oups
whi
ch w
ere
usua
lly m
acer
-at
ion
of th
e sk
in e
dges
.
The
com
plia
nce
of p
atie
nts
was
rep
orte
d as
exc
elle
nt.

Appendix 6
64 TAB
LE 1
0 C
adex
omer
iodi
ne p
olys
acch
arid
e ve
rsus
oth
er d
ebrid
ing
agen
ts
Stud
y an
d de
sign
Incl
usio
n/ex
clus
ion
crit
eria
Inte
rven
tion
det
ails
Bas
elin
e ch
arac
teri
stic
sR
esul
ts
Wit
hdra
wal
sC
omm
ents
cont
inue
d
Mos
s et
al,1
98713
UK
Wou
nd ty
pe:
Veno
us le
g ul
cers
.
Met
hod
of r
ando
misa
tion:
Not
sta
ted.
Obj
ectiv
e ou
tcom
es:
The
wou
nd p
erim
eter
w
as d
raw
n on
to p
oly-
then
e sq
uare
s an
d th
e ar
ea c
alcu
late
d by
com
pute
r pl
anim
etry
.Th
e nu
mbe
r of
wou
nds
heal
ed w
as a
lso r
ecor
ded.
Sett
ing
and
leng
th
of tr
eatm
ent:
6-w
eek
tria
l.Mea
sure
-m
ents
take
n at
0,2
,4
and
6 w
eeks
.Afte
r 6
wee
kspa
tient
s w
ere
allo
wed
to
cro
ss-o
ver.
Incl
usio
n cr
iteria
:O
ut-p
atie
nts
with
unr
espo
nsive
veno
us le
g ul
cers
for
> 3
mon
ths.
Patie
nts
with
ischa
emic
ven
ous
insu
ffici
ency
wer
e in
clud
ed.
Excl
usio
n cr
iteria
:N
ot s
tate
d
56 p
atie
nts
wer
e re
crui
ted
and
obse
rved
on
a va
riety
of
stan
dard
trea
tmen
ts.T
hose
not
impr
ovin
g af
ter
6 w
eeks
wer
ead
mitt
ed to
the
tria
l (n
= 43
).
I:C
adex
omer
iodi
nepo
lysa
ccha
ride
pow
der
(Iodo
sorb
),n
= 21
.
C:D
extr
anom
er p
olys
acch
arid
ebe
ads
(Deb
risan
),n
= 21
.
Both
age
nts
wer
e co
vere
d w
ith a
non-
adhe
sive
pad,
cott
on-w
ool
wad
ding
,sto
ckin
ette
and
a fi
rmel
astic
ban
dage
.
If ba
cter
ial i
nfec
tion
occu
rred
a
2-w
eek
cour
se o
f ora
l ant
ibio
tics
was
allo
wed
.
Med
ian
wou
nd a
rea
(cm
2 ):I:
19.7
(19.
8 SD
)C
:25.
5 (2
9.5
SD)
Oth
er c
hara
cter
istic
s:I
CM
edia
n ag
e (y
ears
):70
68M
:F r
atio
:1:
3.5
1:4.
2M
edia
n du
ratio
n (m
onth
s):
7561
Ischa
emia
:6
5
No
stat
istic
al d
iffer
ence
s be
twee
nth
e tw
o gr
oups
.Dat
a ar
e on
lyav
aila
ble
for
42 o
f the
43
patie
nts.
% r
educ
tion
in m
ean
wou
nd a
rea
at 6
wee
ks:
I:4
(95%
CI:
5,–1
4)C
:3 (9
5% C
I:4,
–9)
(p>
0.05
;tw
o sa
mpl
e t-t
est)
No
signi
fican
t cha
nge
in w
ound
siz
e fro
m b
asel
ine
over
6 w
eeks
(pai
red
t-tes
t).
Num
ber
of w
ound
s he
aled
at
6 w
eeks
:I:
0/21
(0%
)C
:0/2
1 (0
%)
One
pat
ient
was
with
draw
n fro
m
the
tria
l at w
eek
4be
caus
e of
poo
rco
mpl
ianc
e.D
ata
are
only
ava
ilabl
efo
r th
e 42
pat
ient
sre
mai
ning
for
the
6-w
eek
trea
tmen
tpe
riod.
The
antib
acte
rial p
rope
rtie
sof
I (c
adex
omer
pol
ysac
-ch
arid
e) w
ere
of li
ttle
adva
ntag
e in
the
trea
tmen
t of
res
istan
t chr
onic
leg
ulce
rs.
Stew
art a
nd L
eape
r,19
8755
UK
Wou
nd ty
pe:
Leg
ulce
rs.
Met
hod
of r
ando
misa
tion:
Com
pute
r al
loca
tion.
Obj
ectiv
e ou
tcom
e:N
umbe
r of
wou
nds
heal
ed.
Sett
ing
and
leng
th
of tr
eatm
ent:
10-w
eek
tria
l.Mea
sure
-m
ents
take
n w
eekl
y fo
r 6
wee
ks a
nd th
en o
nce
at 8
and
10
wee
ksth
erea
fter.
Incl
usio
n cr
iteria
:O
ut-p
atie
nts
with
leg
ulce
rs o
fva
rious
aet
iolo
gies
.
Excl
usio
n cr
iteria
:rec
eivi
ngst
eroi
ds,c
ytot
oxic
s,or
antib
iotic
s;po
or n
utrit
iona
lst
atus
;abn
orm
al th
yroi
dfu
nctio
n;un
able
to g
ive
info
rmed
con
sent
.
I:C
adex
omer
iodi
nepo
lysa
ccha
ride
pow
der
(Iodo
sorb
)ap
plie
d to
a d
epth
of 3
mm
,n =
46.
C:H
ydro
gel d
ress
ing
(Sch
eriso
rb/In
tras
ite) a
pplie
d to
a d
epth
of 5
mm
,n =
49.
Both
trea
tmen
ts w
ere
cove
red
with
gau
ze,a
non
-adh
eren
t dre
ss-
ing
and
padd
ing.
A c
rêpe
ban
dage
,or
for
thos
e w
ith a
ven
ous
ulce
r a
Tubi
grip
sto
ckin
g w
ere
supp
lied
ifth
e pa
tient
agr
eed
to w
ear
them
.
Med
ian
wou
nd a
rea
(cm
2 ):I:
2.8
(ran
ge,0
.2–5
0.5)
C:2
.6 (r
ange
,0.4
–74.
4)(p
> 0.
05;M
ann-
Whi
tney
U te
st).
Oth
er c
hara
cter
istic
s:I
CM
ean
age
(yea
rs):
7077
M:F
rat
io:
1:1.
41:
2.8
Mea
n du
ratio
n (m
onth
s):
12.0
24.0
No
stat
istic
al d
iffer
ence
s be
twee
nth
e gr
oups
with
the
exce
ptio
n of
age
(p<
0.01
;Man
n-W
hitn
ey
U te
st).
Num
ber
of w
ound
s he
aled
at
10
wee
ks:
I:14
/46
(30%
)C
:14/
49 (2
9%)
(p>
0.05
;chi
-squ
ared
ana
lysis
).
I:13
pat
ient
s.
C:1
1 pa
tient
s.
Thre
e pa
tient
s di
ed;
18 w
ere
with
draw
nby
req
uest
;tw
o ha
dal
lerg
ies;
one
was
lost
to fo
llow
-up.
Both
age
nts
wer
e sim
ilar
for
dres
sing
time
and
pain
expe
rienc
ed b
y th
e pa
tient
.
Cos
t for
one
wee
k of
trea
tmen
t per
per
son:
I:£4
.68
C:£
3.33
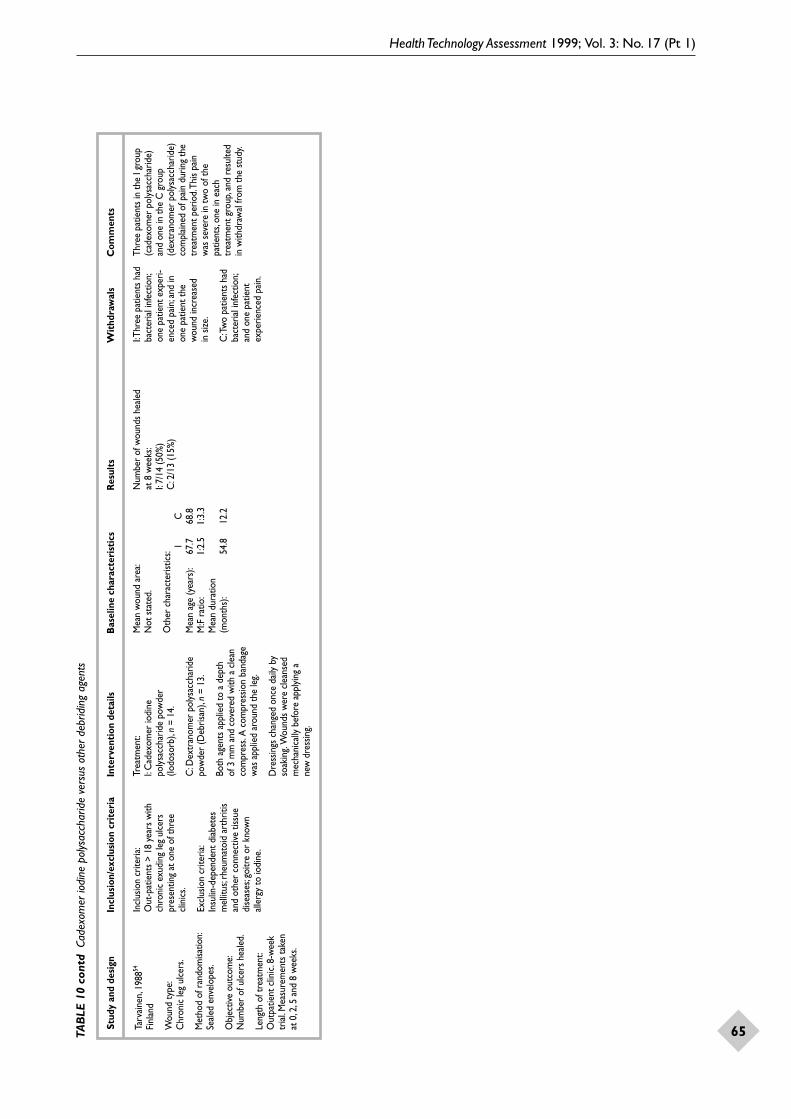
Health Technology Assessment 1999; Vol. 3: No. 17 (Pt 1)
65TAB
LE 1
0 co
ntd
Cad
exom
er io
dine
pol
ysac
char
ide
vers
us o
ther
deb
ridin
g ag
ents
Stud
y an
d de
sign
Incl
usio
n/ex
clus
ion
crit
eria
Inte
rven
tion
det
ails
Bas
elin
e ch
arac
teri
stic
sR
esul
ts
Wit
hdra
wal
sC
omm
ents
Tarv
aine
n,19
8854
Finl
and
Wou
nd ty
pe:
Chr
onic
leg
ulce
rs.
Met
hod
of r
ando
misa
tion:
Seal
ed e
nvel
opes
.
Obj
ectiv
e ou
tcom
e:N
umbe
r of
ulc
ers
heal
ed.
Leng
th o
f tre
atm
ent:
Out
patie
nt c
linic
.8-w
eek
tria
l.Mea
sure
men
ts ta
ken
at 0
,2,5
and
8 w
eeks
.
Incl
usio
n cr
iteria
:O
ut-p
atie
nts
> 18
yea
rs w
ithch
roni
c ex
udin
g le
g ul
cers
pres
entin
g at
one
of t
hree
clin
ics.
Excl
usio
n cr
iteria
:In
sulin
-dep
ende
nt d
iabe
tes
mel
litus
;rhe
umat
oid
arth
ritis
and
othe
r co
nnec
tive
tissu
edi
seas
es;g
oitr
e or
kno
wn
alle
rgy
to io
dine
.
Trea
tmen
t:I:
Cad
exom
er io
dine
poly
sacc
harid
e po
wde
r (Io
doso
rb),
n =
14.
C:D
extr
anom
er p
olys
acch
arid
epo
wde
r (D
ebris
an),
n =
13.
Both
age
nts
appl
ied
to a
dep
th
of 3
mm
and
cov
ered
with
a c
lean
com
pres
s.A
com
pres
sion
band
age
was
app
lied
arou
nd th
e le
g.
Dre
ssin
gs c
hang
ed o
nce
daily
by
soak
ing.
Wou
nds
wer
e cl
eans
edm
echa
nica
lly b
efor
e ap
plyi
ng a
ne
w d
ress
ing.
Mea
n w
ound
are
a:N
ot s
tate
d.
Oth
er c
hara
cter
istic
s:I
CM
ean
age
(yea
rs):
67.7
68.8
M:F
rat
io:
1:2.
51:
3.3
Mea
n du
ratio
n (m
onth
s):
54.8
12.2
Num
ber
of w
ound
s he
aled
at
8 w
eeks
:I:
7/14
(50%
)C
:2/1
3 (1
5%)
I:Thr
ee p
atie
nts
had
bact
eria
l inf
ectio
n;on
e pa
tient
exp
eri-
ence
d pa
in;a
nd in
one
patie
nt th
ew
ound
incr
ease
d in
size
.
C:T
wo
patie
nts
had
bact
eria
l inf
ectio
n;an
d on
e pa
tient
expe
rienc
ed p
ain.
Thre
e pa
tient
s in
the
I gro
up(c
adex
omer
pol
ysac
char
ide)
and
one
in th
e C
gro
up(d
extr
anom
er p
olys
acch
arid
e)co
mpl
aine
d of
pai
n du
ring
the
trea
tmen
t per
iod.
This
pain
was
sev
ere
in tw
o of
the
patie
nts,
one
in e
ach
trea
tmen
t gro
up,a
nd r
esul
ted
in w
ithdr
awal
from
the
stud
y.

Appendix 6
66 TAB
LE 1
1 D
extra
nom
er p
olys
acch
arid
e ve
rsus
oth
er d
ebrid
ing
agen
ts
Stud
y an
d de
sign
Incl
usio
n/ex
clus
ion
crit
eria
Inte
rven
tion
det
ails
Bas
elin
e ch
arac
teri
stic
sR
esul
ts
Wit
hdra
wal
sC
omm
ents
cont
inue
d
Col
in e
t al,1
99656
Fran
ce
Wou
nd ty
pe:
Pres
sure
sor
es.
Met
hod
of r
ando
misa
tion:
Not
sta
ted.
Obj
ectiv
e ou
tcom
e:Pe
rcen
tage
red
uctio
n in
area
of n
on-v
iabl
e tis
sue
(wou
nd a
rea
x (%
yel
low
+
% b
lack
tiss
ue) x
1/1
00).
Phot
ogra
phs
wer
e ta
ken
at th
e in
itial
and
fina
las
sess
men
t.
Sett
ing
and
leng
th
of tr
eatm
ent:
Ope
n,m
ultic
entr
e,m
ulti-
natio
nal,p
aral
lel g
roup
tria
l.Si
x di
ffere
nt c
entr
es w
ere
invo
lved
with
app
roxi
mat
ely
equa
l num
bers
of p
atie
nts
in e
ach
tria
l.Ass
essm
ents
wer
e m
ade
ever
y 7
days
until
the
wou
nd w
ascl
eans
ed o
r on
the
com
plet
ion
of 2
1 da
ys.
Incl
usio
n cr
iteria
:M
ale
and
fem
ale
patie
nts
≥16
yea
rs w
ith p
ress
ure
sore
s pr
esen
t in
any
area
that
need
ed c
lean
sing.
Excl
usio
n cr
iteria
:Pr
egna
ncy,
imm
unod
efic
ienc
y,cl
inic
al in
fect
ion
of th
e w
ound
,ha
rd b
lack
esc
har
cove
ring
mor
eth
an 2
0% o
f the
wou
nd,d
iabe
tes,
inab
ility
to fo
llow
the
dem
ands
of th
e pr
otoc
ol in
for
any
reas
on,n
on-c
onse
ntin
g pa
tient
s.
Trea
tmen
t:I:
Dex
tran
omer
pol
ysac
char
ide
past
e (D
ebris
an),
n =
68.
C:H
ydro
gel d
ress
ing
(Intr
asite
Gel
),n
= 67
.
The
two
inte
rven
tions
wer
eap
plie
d in
acc
orda
nce
with
the
man
ufac
ture
rs’ i
nstr
uctio
ns.A
nab
sorb
ent p
last
ic fi
lm d
ress
ing
(Mel
olin
) was
use
d as
a s
tand
ard-
ised
seco
ndar
y dr
essin
g fo
r bo
thtr
eatm
ents
.
Whe
re a
pat
ient
had
mor
e th
anon
e w
ound
onl
y th
e la
rges
t was
eval
uate
d in
the
tria
l.Oth
erw
ound
s w
ere
trea
ted
with
the
sam
e ra
ndom
ised
dres
sing
if th
isw
as c
onsid
ered
app
ropr
iate
by
the
clin
ical
inve
stig
ator
.
Wou
nd a
rea:
IC
< 4
cm2
1815
4–13
cm
225
25>
13 c
m2
2527
Non
-via
ble
tissu
e ar
ea: I
C<
3 cm
218
153–
9 cm
227
24>
9 cm
223
28
Oth
er c
hara
cter
istic
s:I
CM
edia
n ag
e (y
ears
)81
79M
:F r
atio
1:1
1:1.
4
Sore
dur
atio
n:<
1 m
onth
22
241–
3 m
onth
s35
28>
3 m
onth
s11
15
Sore
gra
de:
11
02
1016
345
384
1213
Aut
hors
sta
te g
roup
s w
ere
wel
lm
atch
ed.A
ll pa
tient
s ga
ve w
ritte
nco
nsen
t and
wer
e ca
pabl
e of
part
icip
atin
g in
the
tria
l.
Med
ian
% r
educ
tion
in w
ound
are
aat
21
days
:I:
7 (–
340,
98%
ran
ge)
C:3
5 (–
185,
91%
ran
ge)
(p=
0.03
;Wilc
oxon
Ran
k Su
m te
st).
Num
ber
of w
ound
s by
deg
ree
ofcl
eans
ing
at 2
1 da
ys:
IC
100%
1413
75–9
9%15
2050
–74%
1312
25–4
9%6
90–
25%
75
Det
erio
rate
d13
8
Ove
rall
med
ian
% r
educ
tion
in
non-
viab
le ti
ssue
at 2
1 da
ys:
I:62
(–34
0,10
0 ra
nge)
C:7
4 (–
103,
100
rang
e)(p
= 0.
20;W
ilcox
on R
ank
Sum
test
)
I:19
lost
to fo
llow
-up
,tw
o di
ed,fo
urad
vers
e re
actio
ns(o
ne r
elat
ed to
pa
in o
n ap
plic
atio
nof
the
agen
t,no
deta
ils o
n th
e ot
her
thre
e).
C:1
1 lo
st to
fo
llow
-up,
two
died
,and
one
adve
rse
reac
tion.
Five
adv
erse
eve
nts
wer
ere
port
ed,o
ne in
the
C g
roup
(hyd
roge
l) an
d fo
ur in
the
Igr
oup
(dex
tran
omer
pol
ysac
-ch
arid
e).T
he o
nly
one
con-
sider
ed to
be
dres
sing
rela
ted
was
pai
n re
port
ed b
y on
epa
tient
in th
e I g
roup
.
C w
as fo
und
to b
e ea
sier
toap
ply
and
rem
ove
than
the
I.C
was
also
foun
d to
be
asso
ciat
ed w
ith le
ss p
ain.

Health Technology Assessment 1999; Vol. 3: No. 17 (Pt 1)
67TAB
LE 1
1 co
ntd
Dex
trano
mer
pol
ysac
char
ide
vers
us o
ther
deb
ridin
g ag
ents
Stud
y an
d de
sign
Incl
usio
n/ex
clus
ion
crit
eria
Inte
rven
tion
det
ails
Bas
elin
e ch
arac
teri
stic
sR
esul
ts
Wit
hdra
wal
sC
omm
ents
cont
inue
d
Hul
kko
et a
l,198
158
Finl
and
Wou
nd ty
pe:
Veno
us le
g ul
cers
.
Met
hod
of r
ando
misa
tion:
Not
sta
ted.
Obj
ectiv
e ou
tcom
e:Lo
nges
t and
sho
rtes
tdi
amet
ers
of e
ach
wou
ndw
ere
mea
sure
d,th
e pr
o-du
ct o
f whi
ch w
as u
sed
as a
mea
sure
of w
ound
siz
e.W
ound
s w
ere
also
phot
ogra
phed
at e
ach
asse
ssm
ent.
Sett
ing
and
leng
th
of tr
eatm
ent:
Hos
pita
l-bas
ed tr
ial.
Ass
essm
ents
wer
e m
ade
at 7
and
14
days
.
Incl
usio
n cr
iteria
:In
-pat
ient
s w
ith v
enou
s le
gul
cers
.
Excl
usio
n cr
iteria
:N
ot s
tate
d.
Trea
tmen
t:I:
Dex
tran
omer
pol
ysac
char
ide
bead
s (D
ebris
an) i
n a
glyce
rinpa
ste
(rat
io 4
:1) a
pplie
d to
the
wou
nd in
a la
yer
at le
ast 3
mm
thic
k.Th
e w
ound
was
cov
ered
with
a d
ry s
teril
e co
mpr
ess.
Dre
ssin
gs w
ere
rem
oved
by
rinsin
gw
ith w
ater
or
salin
e irr
igat
ion
Dre
ssin
gs w
ere
chan
ged
twic
e a
day
and
dext
rano
mer
was
app
lied
to o
nly
moi
st w
ound
s,n
= 18
.
C:S
trep
toki
nase
/str
epto
dorn
ase
enzy
me
prep
arat
ion
(Var
idas
eTo
pica
l).O
ne a
mpu
le w
as d
ilute
dw
ith 2
0 m
l of p
hysio
logi
cal s
alin
e.Th
e so
lutio
n w
as e
ither
pla
ced
dire
ctly
ont
o th
e w
ound
or
ast
erile
com
pres
s w
as s
oake
d in
the
solu
tion
prio
r to
app
licat
ion.
A w
ater
proo
f she
et w
as p
lace
d on
top
of th
e co
mpr
ess.
App
li-ca
tions
wer
e ch
ange
d tw
ice
daily
,n =
13.
All
hard
nec
rosis
was
exc
ised
from
wou
nds
in b
oth
grou
ps b
efor
eco
mm
ence
men
t of t
he tr
ial.
Mea
n w
ound
size
:N
ot s
tate
d.
Oth
er c
hara
cter
istic
s:I
CM
edia
n ag
e (y
ears
):68
.865
.1M
:F r
atio
Not
sta
ted
Ulc
er d
urat
ion:
< 1
mon
th1
11–
12 m
onth
s8
6>
12 m
onth
s9
6
All
wou
nds
wer
e ex
udin
g an
dm
any
of th
em w
ere
also
nec
rotic
.
Mea
n re
duct
ion
in w
ound
size
at
14
days
(mm
):I:
9.3
C:9
.8
Mea
n %
red
uctio
n in
wou
nd s
ize a
t14
day
s:I:
14.5
C:1
1.9
(NS)
I:Thr
ee p
atie
nts
wer
e w
ithdr
awn,
nore
ason
s gi
ven.
C:T
reat
men
t was
inte
rrup
ted
betw
een
the
day
7an
d da
y 14
in o
nepa
tient
bec
ause
of
pain
.
No
adve
rse
effe
cts
wer
ere
port
ed in
pat
ient
s tr
eate
dw
ith I
(dex
tran
omer
poly
sacc
harid
e).T
wo
patie
nts
in th
e C
gro
up (e
nzym
e)ex
perie
nced
pai
n,an
d in
one
it w
as s
ever
e.
One
wou
nd tr
eate
d w
ith I
incr
ease
d in
size
.The
re w
asno
size
incr
ease
rep
orte
d in
the
C g
roup
.
Paris
h an
d C
ollin
s,19
7937
USA
Wou
nd ty
pe:
Pres
sure
sor
es.
Met
hod
of r
ando
misa
tion:
Not
sta
ted.
Obj
ectiv
e ou
tcom
e:N
umbe
r of
wou
nds
heal
ed.
Sett
ing
and
leng
th
of tr
eatm
ent:
Com
mun
ity (n
ursin
g ho
me)
4-w
eek
tria
l.
Incl
usio
n cr
iteria
:Pa
tient
s w
ith p
ress
ure
sore
s,re
sidin
g in
a n
ursin
g ho
me.
Excl
usio
n cr
iteria
:N
ot s
tate
d
Trea
tmen
t:I:
Dex
tran
omer
pol
ysac
char
ide
bead
s (D
ebris
an) a
pplie
d to
ade
pth
of a
t lea
st 3
mm
cov
ered
with
a d
ry d
ress
ing.
Cha
nged
1–3
times
dai
ly d
epen
ding
on
exud
ate,
n =
14 w
ound
s fro
m s
even
patie
nts.
C:C
olla
gena
se e
nzym
epr
epar
atio
n (S
anty
l) ap
plie
d da
ilyaf
ter
a sa
line
was
h an
d co
vere
dw
ith a
dry
dre
ssin
g,n
= 11
wou
nds
from
five
pat
ient
s.
Mea
n w
ound
size
= √
of s
urfa
cear
ea (c
m):
I:4.
5C
:3.2
No
stat
istic
al d
iffer
ence
bet
wee
nth
e gr
oups
for
wou
nd s
ize.
Oth
er c
hara
cter
istic
s:I
CA
ge r
ange
(yea
rs)
29–5
728
–59
M:F
rat
io:
Not
sta
ted
Mea
n du
ratio
n (m
onth
s):
Not
sta
ted
Num
ber
of w
ound
s he
aled
at
4 w
eeks
:I:
6/14
(43%
)C
:1/1
1 (9
%)
Num
ber
of p
atie
nts
with
hea
led
wou
nds
at 4
wee
ks:
I:4/
7 (5
7%)
C:1
/5 (2
0%)
No
with
draw
als
No
side-
effe
cts
repo
rted
by
patie
nts
with
any
of t
hetr
eatm
ents
.

Appendix 6
68 TAB
LE 1
1 co
ntd
Dex
trano
mer
pol
ysac
char
ide
vers
us o
ther
deb
ridin
g ag
ents
Stud
y an
d de
sign
Incl
usio
n/ex
clus
ion
crit
eria
Inte
rven
tion
det
ails
Bas
elin
e ch
arac
teri
stic
sR
esul
ts
Wit
hdra
wal
sC
omm
ents
Thom
as a
nd F
ear,
1993
57
UK
Wou
nd ty
pe:
Pres
sure
sor
es.
Met
hod
of r
ando
misa
tion:
Com
pute
r-gen
erat
edra
ndom
isatio
n co
de.
Obj
ectiv
e ou
tcom
e:Th
e nu
mbe
r of
wou
nds
fully
cle
anse
d.C
lean
sing
was
det
erm
ined
by
mea
surin
g th
e %
of t
otal
wou
nd a
rea
cove
red
in s
loug
h.
Sett
ing
and
leng
th
of tr
eatm
ent:
2-w
eek
tria
l.Afte
r 14
day
sth
ose
wou
nds
show
ing
no im
prov
emen
t wer
ew
ithdr
awn
whi
le th
ere
mai
ning
wou
nds
wer
efo
llow
ed fo
r a
furt
her
14 d
ays.
Incl
usio
n cr
iteria
:H
ospi
talis
ed p
atie
nts
with
gr
ade
3 or
4 p
ress
ure
sore
s.Th
e w
ound
s ha
d to
be
cove
red
or p
artia
lly c
over
ed w
ithye
llow
/bro
wn
sloug
h.
Excl
usio
n cr
iteria
:A
ge <
16
year
s,in
sulin
-de
pend
ent d
iabe
tes,
imm
uno-
supp
ress
ion,
preg
nanc
y,ce
llulit
isan
d re
dnes
s of
the
surr
ound
ing
tissu
e (in
dica
tive
of in
fect
ion)
.
Trea
tmen
t:I:
Dex
tran
omer
pol
ysac
char
ide
bead
s (D
ebris
an) m
ade
into
apa
ste
with
pol
yeth
ylen
e gly
col 6
00an
d w
ater
.The
pas
te w
as a
pplie
dto
a d
epth
of 1
0 m
m o
ver
a lay
erof
pol
yam
ide
net,
n =
20.
C:H
ydro
gel d
ress
ing
(Intr
asite
Gel
) app
lied
to a
dep
th o
f 5 m
m.
Cov
ered
with
a p
erfo
rate
d pl
astic
film
abs
orbe
nt d
ress
ing
held
inpl
ace
with
tape
or
a ba
ndag
e,n
= 20
.
Dre
ssin
gs w
ere
chan
ged
asre
quire
d,an
d th
e w
ound
cle
anse
dw
ith s
alin
e be
fore
rea
pplic
atio
n.
Mea
n w
ound
are
a (c
m2 ):
I:15
.6 (1
6.2
SD;r
ange
1.5
–68.
9)C
:22.
2 (2
3.4
SD;r
ange
,2.6
–91.
4)
% w
ound
are
a co
vere
d in
slo
ugh:
I:75
.3 (2
2.4
SD;r
ange
,20–
100)
C:7
3.5
(29.
7 SD
;ran
ge,2
0–10
0)
Oth
er c
hara
cter
istic
s:I
C
Mea
n ag
e (y
ears
):81
.083
.5M
:F r
atio
:1:
5.7
1:3.
8Ra
tio o
f gra
de
3:4
ulce
rs5.
7:1
3.8:
1
Valu
es a
re o
nly
give
n fo
r 39
of t
he40
pat
ient
s en
terin
g th
e tr
ial.
Num
ber
of w
ound
s cl
eans
ed
at 1
4 da
ys:
I:1/
20 (5
%)
C:8
/20
(40%
)(p
= 0.
008;
Fisc
her’s
exa
ct te
st)
Afte
r 14
day
s al
l ulc
ers
wer
ere
asse
ssed
.Wou
nds
show
ing
noev
iden
ce o
f deb
ridem
ent w
ere
clas
sed
as fa
ilure
s an
d w
ithdr
awn.
The
rem
aini
ng w
ound
s w
ere
follo
wed
for
anot
her
14 d
ays.
Add
ition
al w
ound
s cl
eans
ed a
fter
follo
w-u
p at
28
days
:I1
:4/2
0 (o
vera
ll –
5/20
;25%
)C
:0/2
0 (o
vera
ll –
8/20
;40%
)
Up
to 1
4 da
ys:
I:th
ree
beca
use
ofdi
fficu
lty in
app
lyin
gth
e dr
essin
g.C
lass
ed a
s fa
ilure
sin
the
resu
lts.
C:o
ne p
atie
ntbe
caus
e th
e ca
sere
port
form
s w
ere
misl
aid.
Up
to 2
8 da
ys:
With
draw
als
occu
rred
ove
r th
efo
llow
-up
perio
dle
avin
g fo
ur p
atie
nts
in th
e C
gro
up a
ndtw
o pa
tient
s in
the
I gro
up.
C (h
ydro
gel)
had
to b
ech
ange
d m
ore
frequ
ently
th
an I
(dex
tran
omer
poly
sacc
harid
e).
How
ever
,eve
n w
ith fr
eque
ntdr
essin
g th
e co
st o
f the
C p
erpa
tient
was
less
than
for
the
I.
Mea
n co
st p
er p
atie
nt:
I:£4
4.70
C:£
22.6
0(N
B.O
nly
succ
esse
s co
sted
not f
ailu
res)

Health Technology Assessment 1999; Vol. 3: No. 17 (Pt 1)
69TAB
LE 1
2 H
ydro
gel d
ress
ings
ver
sus
hydr
ogel
dre
ssin
gs
Stud
y an
d de
sign
Incl
usio
n/ex
clus
ion
crit
eria
Inte
rven
tion
det
ails
Bas
elin
e ch
arac
teri
stic
sR
esul
ts
Wit
hdra
wal
sC
omm
ents
Gib
son,
1995
59
UK
Wou
nd ty
pe:
Leg
ulce
rs.
Met
hod
of r
ando
misa
tion:
Not
sta
ted.
Obj
ectiv
e ou
tcom
es:
Wou
nd a
rea,
and
the
area
of w
ound
cov
ered
inslo
ugh.
Sett
ing
and
leng
th
of tr
eatm
ent:
A m
ultic
entr
e pa
ralle
l tria
lco
nduc
ted
for
21 d
ays
orun
til th
e w
ound
was
cons
ider
ed to
be
clea
nsed
.M
easu
rem
ents
wer
e ta
ken
at 0
,10
and
21 d
ays
orw
hen
the
wou
nd w
as c
lean
.
Incl
usio
n cr
iteria
:Pa
tient
s w
ith s
loug
hy le
g ul
cers
(> 1
0% s
urfa
ce a
rea
of w
ound
cove
red
in s
loug
h).
Excl
usio
n cr
iteria
:N
ot s
tate
d.
Trea
tmen
t:I:
Hyd
roge
l dre
ssin
g (G
ranu
gel),
n =
30.
C:H
ydro
gel d
ress
ing
(Intr
asite
Gel
),n
= 32
.
Both
hyd
roge
ls w
ere
cove
red
with
eith
er a
n ab
sorb
ent p
last
ic fi
lmdr
essin
g (M
elol
in) o
r a
knitt
edvi
scos
e dr
essin
g (T
ricot
ex).
Dre
ssin
gs w
ere
chan
ged
daily
.
Mea
n w
ound
are
a (c
m2 ):
I:24
.9C
:18.
7
Oth
er c
hara
cter
istic
s:I
CM
ean
age
(yea
rs):
7776
M:F
rat
io:
1:2.
31:
3.5
Year
s sin
ce fi
rst
ulce
r:8
4
88%
of p
atie
nts
wer
e tr
eate
d in
the
com
mun
ity.
Med
ian
redu
ctio
n in
wou
nd a
rea
over
a 7
-day
per
iod
(cm
2 ):I:
0.74
4C
:0.5
40(p
= 0.
62;W
ilcox
on R
ank
Sum
test
)
Med
ian
redu
ctio
n in
slo
ugh
over
a
7-da
y pe
riod
(cm
2 ):I:
1.51
1C
:1.1
18(p
= 0.
25;W
ilcox
on R
ank
Sum
test
)
% r
educ
tion
in m
ean
area
of w
ound
afte
r 21
day
s:I:
14C
:10
(p=
0.35
8;W
ilcox
on R
ank
Sum
test
)
% r
educ
tion
in m
ean
area
of u
lcer
cove
red
in s
loug
h af
ter
21 d
ays:
I:37
C:3
2
Not
sta
ted.
Tota
l cos
ts fo
r tr
eatm
ent p
erpe
rson
from
bas
elin
e to
fina
las
sess
men
t are
:£43
.25
for
Ian
d £4
0.25
for
C.
Both
pro
duct
s w
ere
repo
rted
to b
e sa
fe a
nd c
onve
nien
t to
use
.
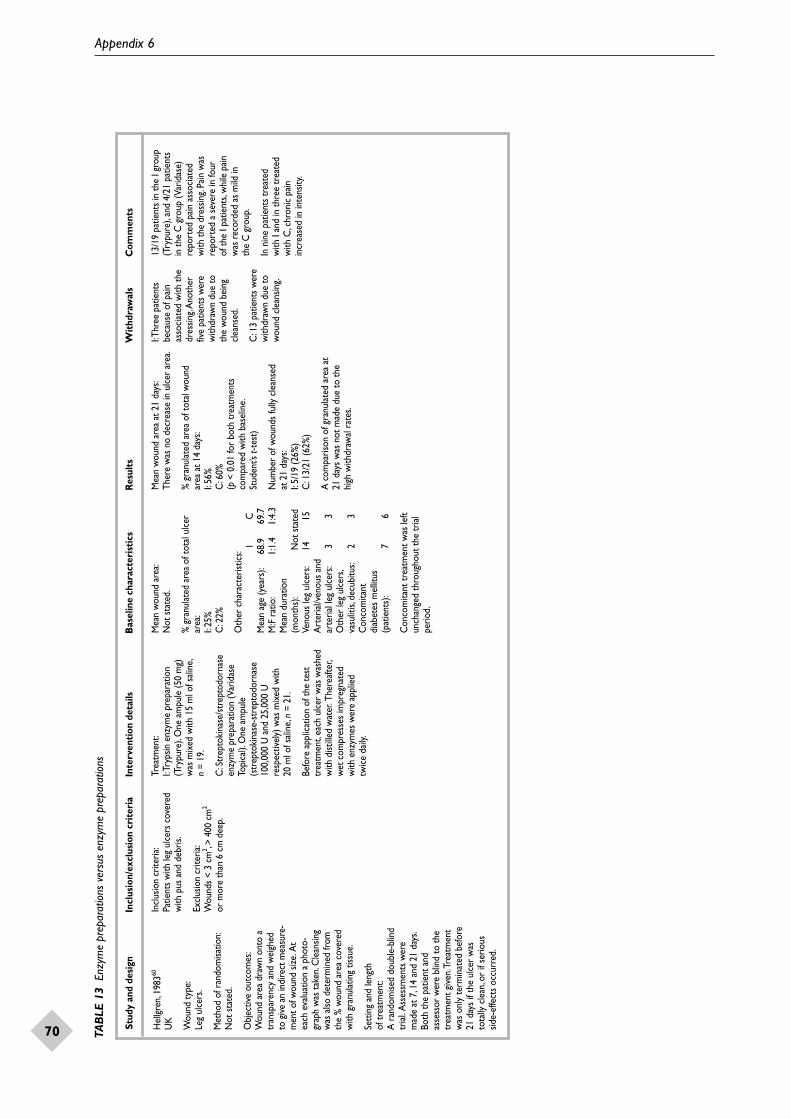
Appendix 6
70 TAB
LE 1
3 E
nzym
e pr
epar
atio
ns v
ersu
s en
zym
e pr
epar
atio
ns
Stud
y an
d de
sign
Incl
usio
n/ex
clus
ion
crit
eria
Inte
rven
tion
det
ails
Bas
elin
e ch
arac
teri
stic
sR
esul
ts
Wit
hdra
wal
sC
omm
ents
Hel
lgre
n,19
8360
UK
Wou
nd ty
pe:
Leg
ulce
rs.
Met
hod
of r
ando
misa
tion:
Not
sta
ted.
Obj
ectiv
e ou
tcom
es:
Wou
nd a
rea
draw
n on
to a
tran
spar
ency
and
wei
ghed
to g
ive a
n in
dire
ct m
easu
re-
men
t of w
ound
size
.At
each
eva
luat
ion
a ph
oto-
grap
h w
as ta
ken.
Cle
ansin
gw
as a
lso d
eter
min
ed fr
omth
e %
wou
nd a
rea
cove
red
with
gra
nula
ting
tissu
e.
Sett
ing
and
leng
th
of tr
eatm
ent:
A r
ando
mise
d do
uble
-blin
dtr
ial.
Ass
essm
ents
wer
em
ade
at 7
,14
and
21 d
ays.
Both
the
patie
nt a
ndas
sess
or w
ere
blin
d to
the
trea
tmen
t give
n.Tr
eatm
ent
was
onl
y te
rmin
ated
bef
ore
21 d
ays
if th
e ul
cer
was
tota
lly c
lean
,or
if se
rious
side-
effe
cts
occu
rred
.
Incl
usio
n cr
iteria
:Pa
tient
s w
ith le
g ul
cers
cov
ered
with
pus
and
deb
ris.
Excl
usio
n cr
iteria
:W
ound
s <
3 cm
2 ,> 4
00 c
m2
or m
ore
than
6 c
m d
eep.
Trea
tmen
t:I:T
ryps
in e
nzym
e pr
epar
atio
n(T
rypu
re).
One
am
pule
(50
mg)
was
mix
ed w
ith 1
5 m
l of s
alin
e,n
= 19
.
C:S
trep
toki
nase
/str
epto
dorn
ase
enzy
me
prep
arat
ion
(Var
idas
eTo
pica
l).O
ne a
mpu
le(s
trep
toki
nase
-str
epto
dorn
ase
100,
000
U a
nd 2
5,00
0 U
resp
ectiv
ely)
was
mix
ed w
ith
20 m
l of s
alin
e,n
= 21
.
Befo
re a
pplic
atio
n of
the
test
trea
tmen
t,ea
ch u
lcer
was
was
hed
with
dist
illed
wat
er.T
here
afte
r,w
et c
ompr
esse
s im
preg
nate
d w
ith e
nzym
es w
ere
appl
ied
twic
e da
ily.
Mea
n w
ound
are
a:N
ot s
tate
d.
% g
ranu
late
d ar
ea o
f tot
al u
lcer
area
:I:
25%
C:2
2%
Oth
er c
hara
cter
istic
s:I
CM
ean
age
(yea
rs):
68.9
69.7
M:F
rat
io:
1:1.
41:
4.3
Mea
n du
ratio
n (m
onth
s):
Not
sta
ted
Veno
us le
g ul
cers
:14
15A
rter
ial/v
enou
s an
d ar
teria
l leg
ulc
ers:
33
Oth
er le
g ul
cers
,va
sulit
is,de
cubi
tus:
23
Con
com
itant
di
abet
es m
ellit
us
(pat
ient
s):
76
Con
com
itant
trea
tmen
t was
left
unch
ange
d th
roug
hout
the
tria
lpe
riod.
Mea
n w
ound
are
a at
21
days
:Th
ere
was
no
decr
ease
in u
lcer
are
a.
% g
ranu
late
d ar
ea o
f tot
al w
ound
area
at 1
4 da
ys:
I:56
%C
:60%
(p<
0.01
for
both
trea
tmen
tsco
mpa
red
with
bas
elin
e.St
uden
t’s t-
test
)
Num
ber
of w
ound
s fu
lly c
lean
sed
at 2
1 da
ys:
I:5/
19 (2
6%)
C:1
3/21
(62%
)
A c
ompa
rison
of g
ranu
late
d ar
ea a
t21
day
s w
as n
ot m
ade
due
to th
ehi
gh w
ithdr
awal
rat
es.
I:Thr
ee p
atie
nts
beca
use
of p
ain
asso
ciat
ed w
ith th
edr
essin
g.A
noth
erfiv
e pa
tient
s w
ere
with
draw
n du
e to
the
wou
nd b
eing
clea
nsed
.
C:1
3 pa
tient
s w
ere
with
draw
n du
e to
wou
nd c
lean
sing.
13/1
9 pa
tient
s in
the
I gro
up(T
rypu
re),
and
4/21
pat
ient
s in
the
C g
roup
(Var
idas
e)re
port
ed p
ain
asso
ciat
ed
with
the
dres
sing.
Pain
was
repo
rted
a s
ever
e in
four
of
the
I pat
ient
s,w
hile
pai
n w
as r
ecor
ded
as m
ild in
th
e C
gro
up.
In n
ine
patie
nts
trea
ted
with
I an
d in
thre
e tr
eate
dw
ith C
,chr
onic
pai
nin
crea
sed
in in
tens
ity.

Health Technology Assessment 1999; Vol. 3: No. 17 (Pt 1)
75
Health Technology Assessment panel membership
This report was identified as a priority by the Pharmaceutical Panel.
Professor John Farndon,University of Bristol*
Professor Senga Bond, University of Newcastle-upon-Tyne
Professor Ian Cameron, Southeast Thames Regional Health Authority
Ms Lynne Clemence, Mid-Kent Health Care Trust
Professor Cam Donaldson, University of Aberdeen
Professor Richard Ellis, St James’s University Hospital,Leeds
Mr Ian Hammond, Bedford & Shires Health & Care NHS Trust
Professor Adrian Harris, Churchill Hospital, Oxford
Dr Gwyneth Lewis, Department of Health
Mrs Wilma MacPherson, St Thomas’s & Guy’s Hospitals,London
Dr Chris McCall, General Practitioner, Dorset
Professor Alan McGregor, St Thomas’s Hospital, London
Professor Jon Nicholl, University of Sheffield
Professor John Norman,University of Southampton
Professor Michael Sheppard,Queen Elizabeth Hospital,Birmingham
Professor Gordon Stirrat, St Michael’s Hospital, Bristol
Dr William Tarnow-Mordi,University of Dundee
Professor Kenneth Taylor,Hammersmith Hospital, London
Acute Sector Panel
continued
Past members
Chair: Professor Francis H Creed,University of Manchester
Professor Clifford Bailey,University of Leeds
Ms Tracy Bury, CharteredSociety of Physiotherapy
Professor Collette Clifford,University of Birmingham
Dr Katherine Darton, M.I.N.D.
Mr John Dunning, Papworth Hospital, Cambridge
Mr Jonathan Earnshaw,Gloucester Royal Hospital
Mr Leonard Fenwick, Freeman Group of Hospitals,Newcastle-upon-Tyne
Professor David Field, Leicester Royal Infirmary
Ms Grace Gibbs, West Middlesex UniversityHospital NHS Trust
Dr Neville Goodman, Southmead Hospital Services Trust, Bristol
Professor Mark P Haggard, MRC
Professor Robert Hawkins, University of Manchester
Dr Duncan Keeley, General Practitioner, Thame
Dr Rajan Madhok, East Riding Health Authority
Dr John Pounsford, Frenchay Hospital, Bristol
Dr Mark Sculpher, University of York
Dr Iqbal Sram, NHS Executive,North West Region
Current members
Professor Michael Maisey, Guy’s & St Thomas’s Hospitals,London*
Professor Andrew Adam, Guy’s, King’s & St Thomas’sSchool of Medicine & Dentistry,London
Dr Pat Cooke, RDRD, Trent Regional Health Authority
Ms Julia Davison, St Bartholomew’s Hospital,London
Professor MA Ferguson-Smith,University of Cambridge
Dr Mansel Hacney, University of Manchester
Professor Sean Hilton, St George’s Hospital Medical School, London
Mr John Hutton, MEDTAP International Inc.,London
Professor Donald Jeffries, St Bartholomew’s Hospital,London
Dr Ian Reynolds, Nottingham Health Authority
Professor Colin Roberts, University of Wales College of Medicine
Miss Annette Sergeant, Chase Farm Hospital, Enfield
Professor John Stuart, University of Birmingham
Dr Ala Szczepura, University of Warwick
Mr Stephen Thornton, Cambridge & Huntingdon Health Commission
Dr Jo Walsworth-Bell, South Staffordshire Health Authority
Diagnostics and Imaging Panel
Past members
Chair: Professor Mike Smith,University of Leeds
Dr Philip J Ayres, Leeds Teaching Hospitals NHS Trust
Dr Paul Collinson, Mayday University Hospital,Thornton Heath
Dr Barry Cookson, Public Health LaboratoryService, Colindale
Professor David C Cumberland,University of Sheffield
Professor Adrian Dixon, University of Cambridge
Mr Steve Ebdon-Jackson,Department of Health
Mrs Maggie Fitchett,Association of Cytogeneticists,Oxford
Dr Peter Howlett, Portsmouth Hospitals NHS Trust
Professor Alistair McGuire, City University, London
Dr Andrew Moore, Editor, Bandolier
Dr Peter Moore, Science Writer, Ashtead
Professor Chris Price, London Hospital MedicalSchool
Dr William Rosenberg,University of Southampton
Dr Gillian Vivian, Royal Cornwall Hospitals Trust
Dr Greg Warner, General Practitioner,Hampshire
Current members
* Previous Chair

Health Technology Assessment panel membership
76
continued
Professor Anthony Culyer,University of York *
Professor Michael Baum, Royal Marsden Hospital
Dr Rory Collins, University of Oxford
Professor George Davey-Smith,University of Bristol
Professor Stephen Frankel,University of Bristol
Mr Philip Hewitson, Leeds FHSA
Mr Nick Mays, King’s Fund, London
Professor Ian Russell, University of York
Dr Maurice Slevin, St Bartholomew’s Hospital,London
Professor Charles Warlow,Western General Hospital,Edinburgh
Methodology Panel
Past members
Chair: Professor Martin Buxton,Brunel University
Professor Doug Altman, Institute of Health Sciences,Oxford
Dr David Armstrong, Guy’s, King’s & St Thomas’sSchool of Medicine & Dentistry, London
Professor Nick Black, London School of Hygiene & Tropical Medicine
Professor Ann Bowling,University College LondonMedical School
Dr Mike Clarke, University of Oxford
Professor Michael Drummond,University of York
Dr Vikki Entwistle, University of Aberdeen
Professor Ewan Ferlie, Imperial College, London
Professor Ray Fitzpatrick,University of Oxford
Professor Jeremy Grimshaw,University of Aberdeen
Dr Stephen Harrison, University of Leeds
Mr John Henderson, Department of Health
Professor Richard Lilford, Regional Director, R&D, West Midlands
Professor Theresa Marteau,Guy’s, King’s & St Thomas’sSchool of Medicine &Dentistry, London
Dr Henry McQuay, University of Oxford
Dr Nick Payne, University of Sheffield
Professor Margaret Pearson,NHS Executive North West
Professor David Sackett, Centre for Evidence BasedMedicine, Oxford
Dr PAG Sandercock, University of Edinburgh
Dr David Spiegelhalter, Institute of Public Health,Cambridge
Professor Joy Townsend,University of Hertfordshire
Current members
Professor Michael Rawlins,University of Newcastle-upon-Tyne*
Dr Colin Bradley, University of Birmingham
Professor AlasdairBreckenridge, RDRD,Northwest Regional Health Authority
Ms Christine Clark, Hope Hospital, Salford
Mrs Julie Dent, Ealing, Hammersmith &Hounslow Health Authority,London
Mr Barrie Dowdeswell, Royal Victoria Infirmary, Newcastle-upon-Tyne
Dr Tim Elliott, Department of Health
Dr Desmond Fitzgerald, Mere, Bucklow Hill, Cheshire
Professor Keith Gull, University of Manchester
Dr Keith Jones, Medicines Control Agency
Dr John Posnett, University of York
Dr Tim van Zwanenberg, Northern Regional Health Authority
Dr Kent Woods, RDRD, Trent RO, Sheffield
Pharmaceutical Panel
Past members
Chair: Professor Tom Walley,University of Liverpool
Dr Felicity Gabbay, Transcrip Ltd
Mr Peter Golightly, Leicester Royal Infirmary
Dr Alastair Gray, Health Economics ResearchUnit, University of Oxford
Professor Rod Griffiths, NHS Executive West Midlands
Mrs Jeanette Howe, Department of Health
Professor Trevor Jones, ABPI, London
Ms Sally Knight, Lister Hospital, Stevenage
Dr Andrew Mortimore,Southampton & SW HantsHealth Authority
Mr Nigel Offen, Essex RiversHealthcare, Colchester
Mrs Marianne Rigge, The College of Health, London
Mr Simon Robbins, Camden & Islington Health Authority, London
Dr Frances Rotblat, Medicines Control Agency
Dr Eamonn Sheridan, St James’s University Hospital,Leeds
Mrs Katrina Simister, Liverpool Health Authority
Dr Ross Taylor, University of Aberdeen
Current members
* Previous Chair

Health Technology Assessment 1999; Vol. 3: No. 17 (Pt 1)
77
Dr Sheila Adam, Department of Health*
Professor George Freeman,Charing Cross & WestminsterMedical School, London
Dr Mike Gill, Brent & HarrowHealth Authority
Dr Anne Ludbrook, University of Aberdeen
Professor Theresa Marteau, Guy’s, King’s & St Thomas’sSchool of Medicine & Dentistry, London
Professor Catherine Peckham,Institute of Child Health,London
Dr Connie Smith, Parkside NHS Trust, London
Ms Polly Toynbee, Journalist
Professor Nick Wald, University of London
Professor Ciaran Woodman,Centre for CancerEpidemiology, Manchester
Population Screening Panel
Past members
Chair: Professor Sir John Grimley Evans, Radcliffe Infirmary, Oxford
Ms Stella Burnside, Altnagelvin Hospitals Trust,Londonderry
Mr John Cairns, University of Aberdeen
Professor Howard Cuckle,University of Leeds
Dr Carol Dezateux, Institute of Child Health,London
Dr Anne Dixon Brown, NHS Executive, Anglia & Oxford
Professor Dian Donnai, St Mary’s Hospital, Manchester
Dr Tom Fahey, University of Bristol
Mrs Gillian Fletcher, National Childbirth Trust
Dr JA Muir Gray, Institute of Health Sciences,Oxford
Professor Alexander Markham, St James’s University Hospital, Leeds
Dr Ann McPherson, General Practitioner, Oxford
Dr Susan Moss, Institute of Cancer Research
Dr Sarah Stewart-Brown, University of Oxford
Current members
Professor Angela Coulter, King’s Fund, London*
Professor Martin Roland,University of Manchester*
Dr Simon Allison, University of Nottingham
Professor Shah Ebrahim, Royal Free Hospital, London
Ms Cathy Gritzner, King’s Fund, London
Professor Andrew Haines, RDRD, North Thames Regional Health Authority
Dr Nicholas Hicks, Oxfordshire Health Authority
Mr Edward Jones, Rochdale FHSA
Professor Roger Jones, Guy’s, King’s & St Thomas’sSchool of Medicine & Dentistry, London
Mr Lionel Joyce, Chief Executive, Newcastle CityHealth NHS Trust
Professor Martin Knapp, London School of Economics & Political Science
Professor Karen Luker, University of Liverpool
Dr Fiona Moss, Thames Postgraduate Medical& Dental Education
Professor Dianne Newham, King’s College London
Professor Gillian Parker, University of Leicester
Dr Mary Renfrew, University of Oxford
Primary and Community Care Panel
Past members
Chair: Dr John Tripp, Royal Devon & ExeterHealthcare NHS Trust
Mr Kevin Barton, East London & City Health Authority
Professor John Bond,University of Newcastle-upon-Tyne
Dr John Brazier, University of Sheffield
Ms Judith Brodie, Age Concern, London
Mr Shaun Brogan, Daventry & South NorthantsPrimary Care Alliance
Mr Joe Corkill, National Association for Patient Participation
Dr Nicky Cullum, University of York
Professor Pam Enderby,University of Sheffield
Mr Andrew Farmer, Institute of Health Sciences,Oxford
Professor Richard Hobbs,University of Birmingham
Professor Allen Hutchinson,University of Sheffield
Dr Phillip Leech, Department of Health
Dr Aidan Macfarlane,Oxfordshire Health Authority
Professor David Mant, Institute of Health Sciences,Oxford
Dr Chris McCall, General Practitioner, Dorset
Dr Robert Peveler, University of Southampton
Professor Jennie Popay,University of Salford
Ms Hilary Scott, Tower Hamlets Healthcare NHS Trust, London
Dr Ken Stein, North & East Devon Health Authority
Current members
continued
* Previous Chair

Health Technology Assessment panel membership
78
National Coordinating Centre for Health Technology Assessment, Advisory Group
Chair: Professor John Gabbay, Wessex Institute for Health Research & Development
Professor MikeDrummond, Centre for Health Economics, University of York
Ms Lynn Kerridge, Wessex Institute for HealthResearch & Development
Dr Ruairidh Milne, Wessex Institute for HealthResearch & Development
Ms Kay Pattison, Research & DevelopmentDirectorate, NHS Executive
Professor James Raftery, Health Economics Unit, University of Birmingham
Professor Ian Russell,Department of Health Sciences & Clinical Evaluation, University of York
Dr Ken Stein, North & East Devon Health Authority
Professor Andrew Stevens, Department of Public Health & Epidemiology, University of Birmingham
Current members
Dr Paul Roderick, Wessex Institute for HealthResearch & Development
Past member

Professor Ian Russell, Department of Health Sciences & Clinical Evaluation, University of York*
Professor David Cohen, Professor of Health Economics, University of Glamorgan
Mr Barrie Dowdeswell, Chief Executive, Royal Victoria Infirmary,Newcastle-upon-Tyne
Dr Michael Horlington, Head of Corporate Licensing,Smith & Nephew GroupResearch Centre
Professor Martin Knapp, Director, Personal SocialServices Research Unit, London School of Economics & Political Science
Professor Theresa Marteau, Director, Psychology & Genetics Research Group, Guy’s, King’s & St Thomas’s School ofMedicine & Dentistry, London
Professor Sally McIntyre, MRC Medical Sociology Unit,Glasgow
Professor David Sackett, Centre for Evidence Based Medicine, Oxford
Dr David Spiegelhalter, MRC Biostatistics Unit, Institute of Public Health,Cambridge
Professor David Williams, Department of Clinical Engineering, University of Liverpool
Dr Mark Williams, Public Health Physician, Bristol
* Previous Chair
HTA Commissioning Board
Past members
Chair: Professor Charles Florey,Department of Epidemiology &Public Health, NinewellsHospital & Medical School,University of Dundee
Professor Doug Altman, Director of ICRF/NHS Centrefor Statistics in Medicine,Oxford
Professor John Bond,Professor of Health ServicesResearch, University ofNewcastle-upon-Tyne
Mr Peter Bower, Independent Health Advisor, Newcastle-upon-Tyne
Ms Christine Clark, Honorary Research Pharmacist, Hope Hospital, Salford
Professor Shah Ebrahim,Professor of Epidemiology of Ageing, University of Bristol
Professor Martin Eccles, Professor of Clinical Effectiveness, University of Newcastle-upon-Tyne
Dr Mike Gill, Director of Public Health &Health Policy, Brent & HarrowHealth Authority
Dr Alastair Gray, Director, Health EconomicsResearch Centre, University of Oxford
Professor Mark Haggard,MRC Institute of Hearing Research
Dr Jenny Hewison, Senior Lecturer, Department of Psychology,University of Leeds
Professor Sir Miles Irving (Programme Director),Professor of Surgery, University of Manchester, Hope Hospital, Salford
Professor Alison Kitson, Director, Royal College of Nursing Institute
Dr Donna Lamping, Senior Lecturer, Department ofPublic Health, London Schoolof Hygiene & Tropical Medicine
Professor Alan Maynard, Professor of Economics,University of York
Professor Jon Nicholl, Director, Medical Care Research Unit, University of Sheffield
Professor Gillian Parker, Nuffield Professor ofCommunity Care, University of Leicester
Dr Tim Peters, Reader in Medical Statistics,Department of Social Medicine,University of Bristol
Professor Martin Severs, Professor in Elderly Health Care, Portsmouth University
Dr Sarah Stewart-Brown,Director, Institute of Health Sciences, University of Oxford
Professor Ala Szczepura, Director, Centre for Health Services Studies, University of Warwick
Dr Gillian Vivian,Consultant, Royal CornwallHospitals Trust
Professor Graham Watt, Department of General Practice, Woodside Health Centre,Glasgow
Professor Kent Woods,Regional Director of R&D NHS Executive, Trent
Dr Jeremy Wyatt, Senior Fellow, Health & Public Policy, School of PublicPolicy, University College, London
Current members

Copies of this report can be obtained from:
The National Coordinating Centre for Health Technology Assessment,Mailpoint 728, Boldrewood,University of Southampton,Southampton, SO16 7PX, UK.Fax: +44 (0) 1703 595 639 Email: [email protected]://www.hta.nhsweb.nhs.uk ISSN 1366-5278
Health Technology Assessm
ent 1999;Vol.3:No.17 (Pt 1)
Debridem
ent of chronic wounds
Top Related
Copyright © 2022 FDOKUMEN

