







Bahasa
Halaman
Hukum

REVIEW ARTICLEpublished: 29 January 2013
doi: 10.3389/fendo.2013.00003
Community-based physical activity interventions fortreatment of type 2 diabetes: a systematic review withmeta-analysisRonald C. Plotnikoff 1*, Sarah A. Costigan1, Nandini D. Karunamuni 2 and David R. Lubans1
1 Priority Research Centre in Physical Activity and Nutrition, University of Newcastle, Callaghan, NSW Australia2 Faculty of Physical Education and Recreation, University of Alberta, Edmonton, AB, Canada
Edited by:Catherine Chan, University of Alberta,Canada
Reviewed by:Mini R. Abraham, Overland ParkMedical Specialists, USAJohan H. Jendle, Karlstad CentralHospital, Sweden
*Correspondence:Ronald C. Plotnikoff , PriorityResearch Centre in Physical Activityand Nutrition, Advance TechnologyCentre, Level 3, The University ofNewcastle, University Drive,Callaghan, NSW 2308, Australia.e-mail: [email protected]
Evidence suggests engaging in regular physical activity (PA) can have beneficial outcomesfor adults with type 2 diabetes (TD2), including weight loss, reduction of medication usageand improvements in hemoglobin A1c (HbA1c)/fasting glucose. While a number of clinical-based PA interventions exist, community-based approaches are limited. The objective ofthis study is to conduct a systematic review with meta-analysis to assess the effective-ness of community-based PA interventions for the treatment of TD2 in adult populations.A search of peer-reviewed publications from 2002 to June 2012 was conducted acrossseveral electronic databases to identify interventions evaluated in community settings.Twenty-two studies were identified, and 11 studies reporting HbA1c as an outcome mea-sure were pooled in the meta-analysis. Risk of bias assessment was also conducted. Thefindings demonstrate community-based PA interventions can be effective in producingincreases in PA. Meta-analysis revealed a lowering of HbA1c levels by −0.32% [95% CI−0.65, 0.01], which approached statistical significance (p < 0.06). Our findings can guidefuture PA community-based interventions in adult populations diagnosed with TD2.
Keywords: type two diabetes, physical activity, community-based intervention, treatment, HbA1c
INTRODUCTIONThe estimated global prevalence of diabetes in 2010 was 6.4%(equating to ∼285 million adults). Type two diabetes (T2D) hascontributed to the majority of these cases (Shaw et al., 2010).T2D is largely related to weight gain associated with a combina-tion of low physical activity (PA) levels and a consumption of anenergy dense diet (Nolan et al., 2011). Evidence suggests engagingin regular PA can have beneficial outcomes for adults with T2D(Sigal et al., 2007), including improved self-management of T2D,weight loss, increased fitness, reduction of medication usage andimprovements in HbA1c/fasting glucose (Church et al., 2010).
Researchers have investigated a variety of PA interventionstrategies to encourage individuals with T2D to be more active.One such strategy is supervised facility-based exercise training,which has potential to improve glycemic control and other car-diovascular risk factors (Sigal et al., 2007; Balducci et al., 2010;Church et al., 2010). However, these programs are often resource-intensive, only available in metropolitan areas, and their long-termsustainability is indeterminate.
Other strategies to promote PA in T2D adults includeindividual-based approaches such as medication use and behav-ior change. These strategies have become increasingly common,with information on diet, exercise, and medication generally pro-vided by health care professionals (e.g., GP, pharmacist, specialist).However, encouraging individuals with T2D to adopt behaviormodification during short visits to their GP, is challenging. Theseself-management approaches also have modest efficacy in the short
term,and long-term assessments are often very limited (Plotnikoff,2006). Further, these types of interventions can be “out of reach”for individuals with a low-income, low education, lack of access tocare, and cultural and linguistic barriers.
On the other hand, community-based approaches may helpimprove self-management of T2D by addressing barriers encoun-tered in both facility-based approaches and individual-basedapproaches. For example, community-based interventions candeliver culturally appropriate health education which can improveself-care compliance and adherence to self-management prac-tices (Two Feathers et al., 2005; Vachon et al., 2007). Further,community-based interventions can be more cost-effective andpractical, may have better long-term effectiveness, and the poten-tial to reach a large proportion of individuals who are in most needof treatment (Two Feathers et al., 2005; Plotnikoff, 2006; Vachonet al., 2007).
The objective of this paper is to conduct a systematic reviewwith meta-analysis to assess the effectiveness of community-based,PA interventions for the treatment of T2D in adult populations.The meta-analysis focused on interventions that assessed changesin hemoglobin A1c (HbA1c) as an outcome measure. This reviewincludes interventions that employ community-based approaches(e.g., community centers, local facilities, community-based edu-cators), rather than those delivered in workplace or traditionalclinical settings. To the best of our knowledge, this is the first sys-tematic review to examine the efficacy of community-based PAapproaches for treatment of T2D in adults.
www.frontiersin.org January 2013 | Volume 4 | Article 3 | 1

Plotnikoff et al. Community-based physical activity interventions
METHODSSEARCH STRATEGY AND DATA SOURCESStudies published in peer-reviewed journals were identified bytwo authors (SAC & NK) through a structured electronic databasefrom January 2002 until June 2012 in CINAHL, Web of Science,Scopus, and Medline. The following search strings were used: (PAOR exercise) AND (Type two diabetes OR Type 2 Diabetes ORT2D) AND (Intervention OR Program) AND Community. Thesestrings were further limited to subjects 18+ years and English lan-guage. In the first stage of the literature search, titles, and abstractsof identified articles were checked for relevance and additionalarticles known to the authors were assessed for possible inclusion.In the second stage, full-text articles were retrieved and consid-ered for inclusion. In the final stage, the reference lists of retrievedfull-text articles were searched for additional studies.
STUDY SELECTION CRITERIAQuantitative community-based PA interventions for treatment ofT2D were included in this review. Interventional studies were con-sidered for inclusion. Studies were eligible for inclusion if they:(1) included participants 18+ years; (2) employed a PA basedintervention [i.e., studies were classified by proportion of theintervention which was PA based (i.e., ≥50%)]; (3) employedcommunity-based approaches (e.g., community centers, localfacilities, community-based educators; (4) implemented strategiesfor treating existing cases of T2D (e.g., increased PA, weight loss,reduction of medication usage, improvements in HbA1c); and (5)were quantitative studies.
Studies not included in this review consist of publicationswhich: (1) examined children or adolescents (aged < 18 years); (2)were non-interventional; (3) had an intervention that was not atleast 50% focused on PA; (4) did not include strategy for < 50%of the total intervention; (5) were conducted in traditional clinicalsettings; (6) employed preventative measures to adults at risk ofT2D (i.e., cases of pre-diabetes); (7) used qualitative studies; and(8) were conference abstracts, dissertations, theses, and articlespublished in non-peer-reviewed journals.
DATA EXTRACTIONInitially, articles were assessed for eligibility by a single reviewer(SAC) based on the study title. After this initial cull, study abstractswere assessed by two authors (SAC & NK) independently in anunblinded standardized manner. Findings were compared and dif-ferences were resolved by consensus or by a third author (RCP).Specific study characteristics were identified and extracted by twoauthors (SAC & NK). These characteristics included the countryof origin, study-design, size/source of study population, details ofthe PA intervention and community components of the study (seeTable 1).
SYNTHESIS OF RESULTSMeta-analysis was conducted for studies that reported their effecton HbA1c using RevMan version 5.1 [The Nordic Cochrane Cen-tre, The Cochrane Collaboration, Copenhagen, Denmark; ReviewManager (RevMan), 2011]. As recommended by the CochraneCollaboration, post-test means (i.e., Less et al., 2009; Plotnikoffet al., 2010, 2012; Piette et al., 2011) or change scores (i.e.,
Goldhaber-Fiebert et al., 2003; Dunstan et al., 2006; Engel andLindner, 2006; Brooks et al., 2007; Davies et al., 2008; Skoro-Kondza et al., 2009; Plotnikoff et al., 2011) and their SD were usedin the analysis. One study compared multiple treatment groupswith a single control group (n= 1), to avoid double counting, thesample size of the control group was divided by two. All data wereconsidered continuous and therefore the mean difference (MD)with 95% confidence intervals was used to determine effect mea-sures. Statistical heterogeneity was examined via Chi-squared andthe I2-Index tests. A guide to the interpretation of heterogeneitybased on the I2-Index is as follows: 0–40% might not be impor-tant; 30–60% may represent moderate heterogeneity; 50–90% mayrepresent substantial heterogeneity; and 75–100% considerableheterogeneity (Deeks et al., 2008).
RISK OF BIASRisk of bias was assessed using a nine-item checklist tool adaptedfrom the Consolidated Standards of Reporting Trials (CONSORT)statement and previous reviews (van Sluijs et al., 2007; Younget al., 2012). The following items were assessed: (1) baselineresults reported separately for each group; (2) randomizationclearly described and adequately completed; (3) dropout≤ 20%for≤6 months follow-up and≤30% for >6 months follow-up; (4)assessor blinding; (5) intention-to-treat analysis; (6) confoundersaccounted for in analyses; (7) summary results presented andestimated effect sizes and precision estimates; (8) power calcula-tion reported and study adequately powered; and (9) an objectivemeasure of PA was used.
Each item was scored as“present”(X),“absent”(×), or“unclearor inadequately described” (?). Depending on the study-design,some items were not applicable (n/a). Unweighted sum totals werecalculated for each study using a predefined scoring system (X= 1|×= 0 | ?= 0 | n/a= 0). Low risk of bias studies were regarded asthose with a 8–9, a moderate risk of bias presented scores of 4–7,high risk of bias scored 0–3.
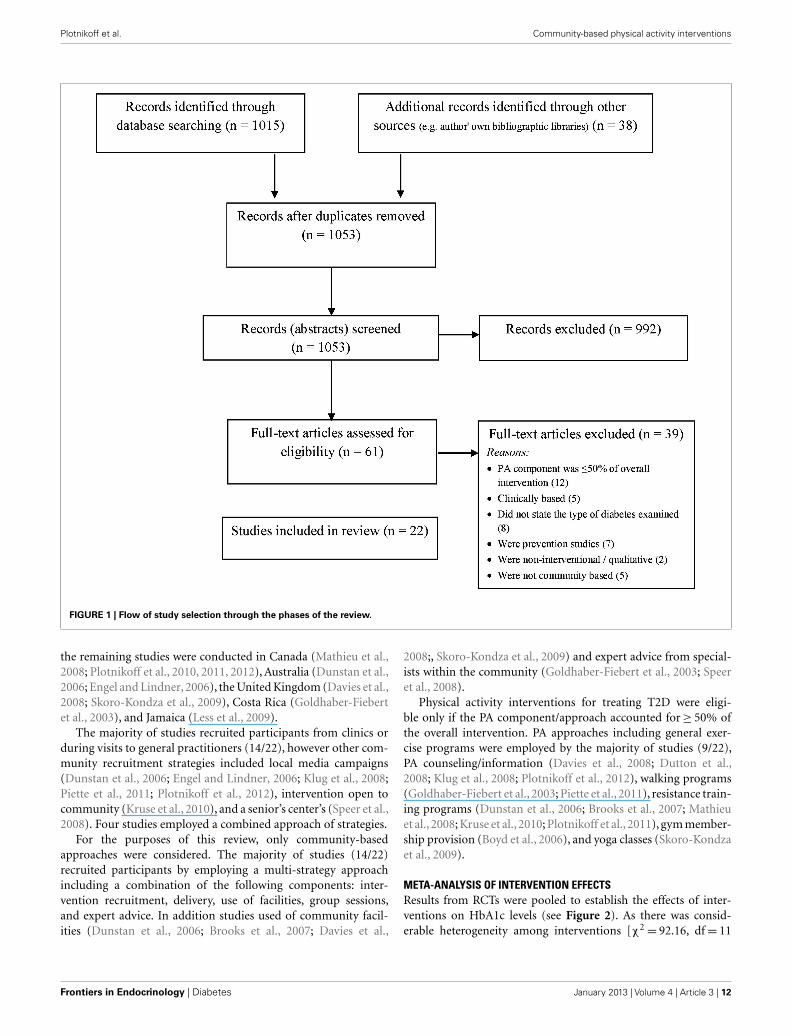
RESULTSDESCRIPTION OF STUDIESFigure 1 describes the progress through the stages of study selec-tion. The electronic database search strategy provided 1015 refer-ences; 38 additional records were identified through other sources.About 1053 records were screened based on titles and abstracts,and of these 992 records were excluded. The remaining 61 recordswere assessed as full-text articles. Of these 61 studies, 39 did notmeet eligibility criteria. The remaining 22 studies were includedin our review (see Figure 1).
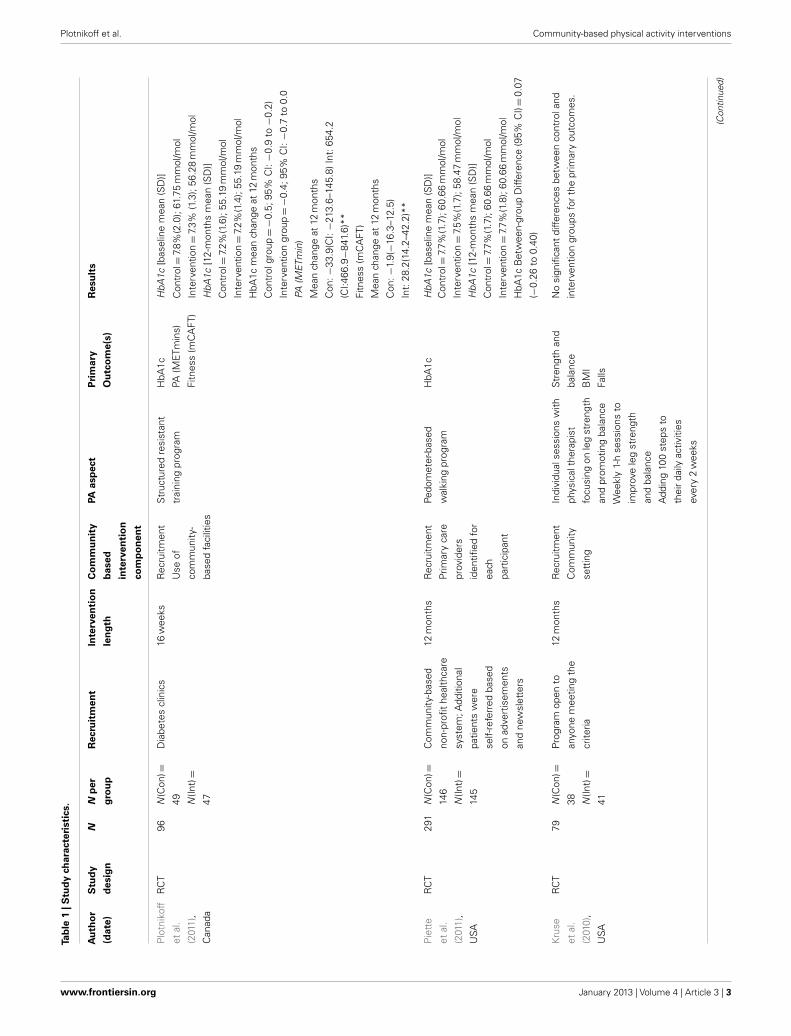
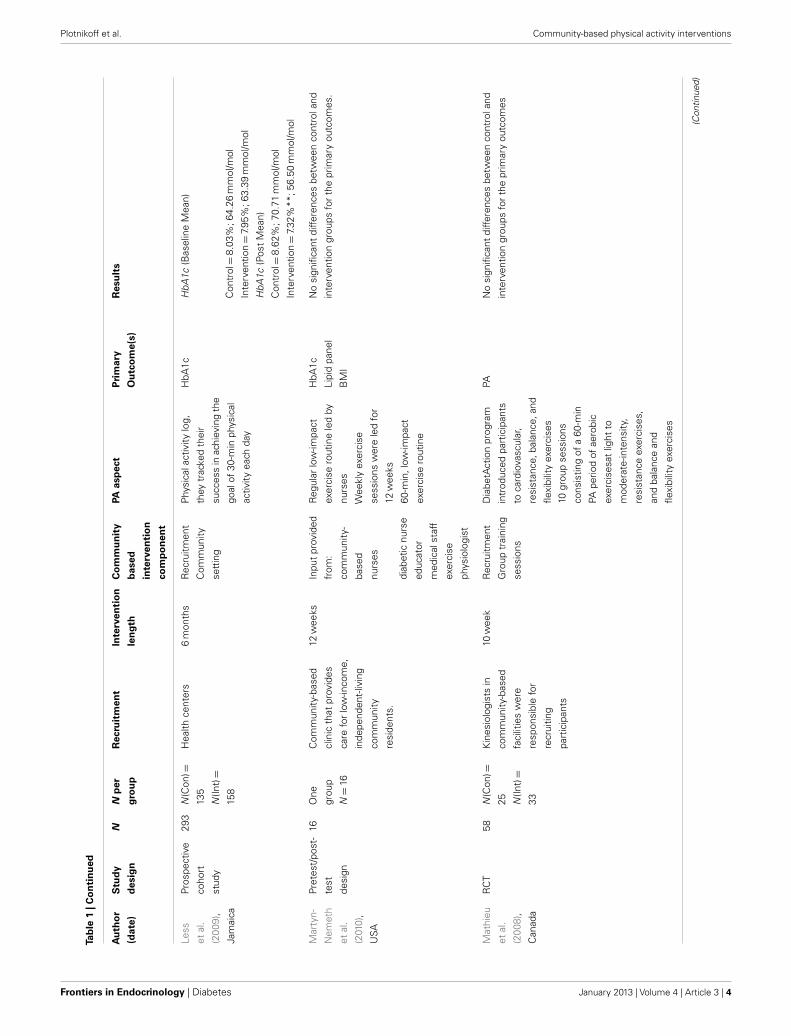
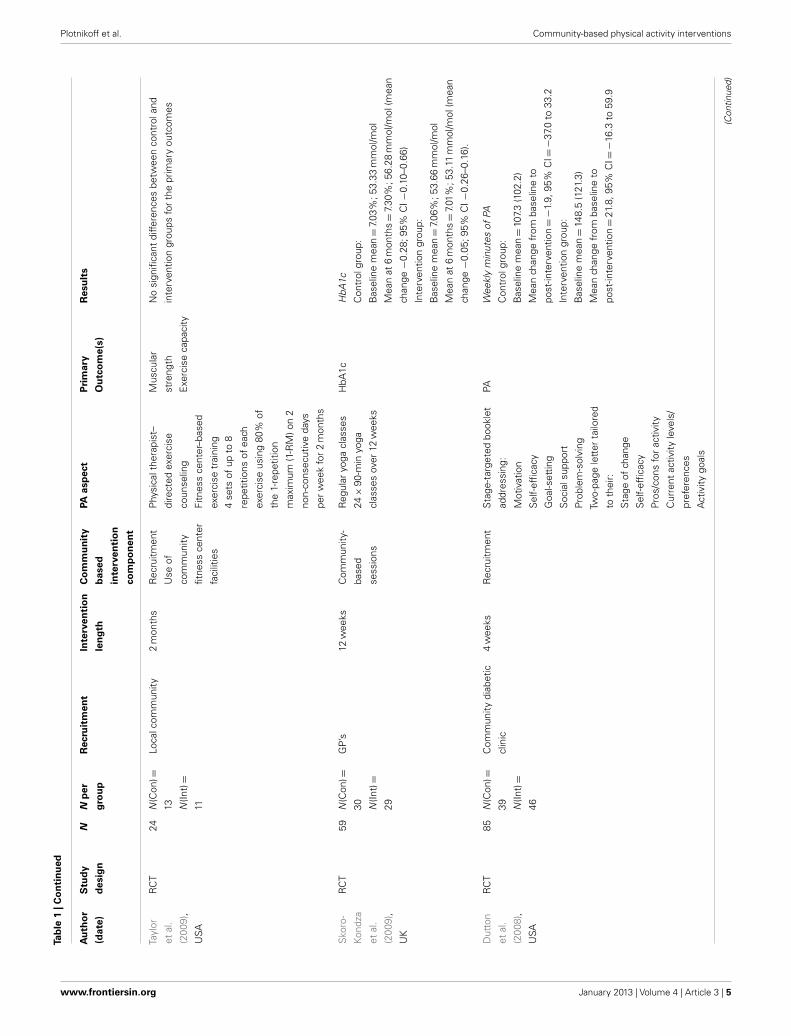
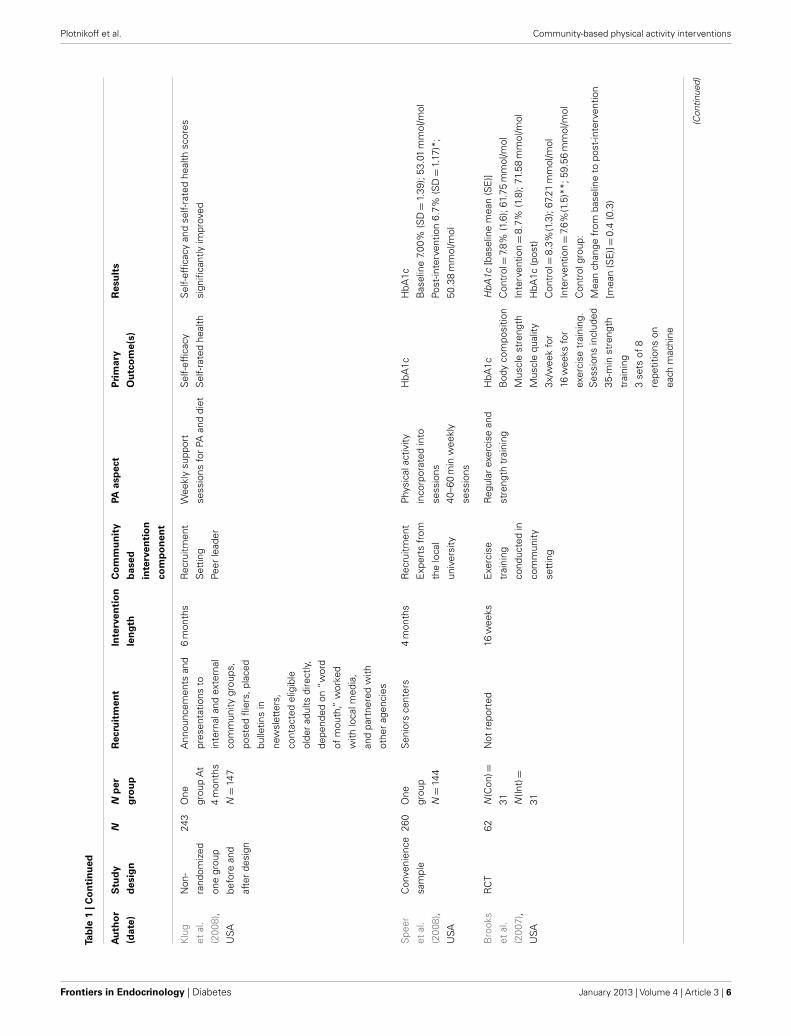
STUDY CHARACTERISTICSTable 1 reports selected characteristics of all eligible studies. Oursearch identified 22 studies that examined community-based PAinterventions for treatment of T2D, of which a PA component of≥50% of the overall intervention was employed.
Most studies (16/22, 73%) employed a RCT design. The activeintervention periods ranged from 4 weeks (Dutton et al., 2008)to 24 months (Brandon et al., 2003). Study populations rangedfrom 19 (Martyn-Nemeth et al., 2010) to 652 (Davies et al., 2008).Most of the studies were conducted in the United States (12/20),
Frontiers in Endocrinology | Diabetes January 2013 | Volume 4 | Article 3 | 2
Plotnikoff et al. Community-based physical activity interventions
Tab
le1
|Stu
dy
char
acte
rist
ics.
Au
tho
r
(dat
e)
Stu
dy
des
ign
NN
per
gro
up
Rec
ruit
men
tIn
terv
enti
on
len
gth
Co
mm
un
ity
bas
ed
inte
rven
tio
n
com
po
nen
t
PAas
pec
tP
rim
ary
Ou
tco
me(
s)
Res
ult
s
Plo
tnik
off
etal
.
(201
1),
Can
ada
RC
T96
N(C
on)=
49 N(In
t)=
47
Dia
bete
scl
inic
s16
wee
ksR
ecru
itmen
t
Use
of
com
mun
ity-
base
dfa
cilit
ies
Str
uctu
red
resi
stan
t
trai
ning
prog
ram
HbA
1c
PA(M
ETm
ins)
Fitn
ess
(mC
AFT
)
HbA
1c[b
asel
ine
mea
n(S
D)]
Con
trol=
7.8%
(2.0
);61
.75
mm
ol/m
ol
Inte
rven
tion=
7.3%
(1.3
);56
.28
mm
ol/m
ol
HbA
1c[1
2-m
onth
sm
ean
(SD
)]
Con
trol=
7.2%
(1.6
);55
.19
mm
ol/m
ol
Inte
rven
tion=
7.2%
(1.4
);55
.19
mm
ol/m
ol
HbA
1cm
ean
chan
geat
12m
onth
s
Con
trol
grou
p=−
0.5;
95%
CI:−
0.9
to−
0.2)
Inte
rven
tion
grou
p=−
0.4;
95%
CI:−
0.7
to0.
0
PA(M
ETm
in)
Mea
nch
ange
at12
mon
ths
Con
:−33
.9(C
I:−
213.
6–14
5.8)
Int:
654.
2
(CI:4
66.9−
841.
6)**
Fitn
ess
(mC
AFT
)
Mea
nch
ange
at12
mon
ths
Con
:−1.
9(−
16.3
–12.
5)
Int:
28.2
(14.
2–42
.2)*
*
Pie
tte
etal
.
(201
1),
USA
RC
T29
1N
(Con
)=
146
N(In
t)=
145
Com
mun
ity-b
ased
non-
profi
the
alth
care
syst
em;A
dditi
onal
patie
nts
wer
e
self-
refe
rred
base
d
onad
vert
isem
ents
and
new
slet
ters
12m
onth
sR
ecru
itmen
t
Prim
ary
care
prov
ider
s
iden
tified
for
each
part
icip
ant
Pedo
met
er-b
ased
wal
king
prog
ram
HbA
1cH
bA1c
[bas
elin
em
ean
(SD
)]C
ontr
ol=
7.7%
(1.7
);60
.66
mm
ol/m
ol
Inte
rven
tion=
7.5%
(1.7
);58
.47
mm
ol/m
ol
HbA
1c[1
2-m
onth
sm
ean
(SD
)]
Con
trol=
7.7%
(1.7
);60
.66
mm
ol/m
ol
Inte
rven
tion=
7.7%
(1.8
);60
.66
mm
ol/m
ol
HbA
1cB
etw
een-
grou
pD
iffer
ence
(95%
CI)=
0.07
(−0.
26to
0.40
)
Kru
se
etal
.
(201
0),
USA
RC
T79
N(C
on)=
38 N(In
t)=
41
Prog
ram
open
to
anyo
nem
eetin
gth
e
crite
ria
12m
onth
sR
ecru
itmen
t
Com
mun
ity
sett
ing
Indi
vidu
alse
ssio
nsw
ith
phys
ical
ther
apis
t
focu
sing
onle
gst
reng
th
and
prom
otin
gba
lanc
e
Str
engt
han
d
bala
nce
BM
I
Falls
No
sign
ifica
ntdi
ffere
nces
betw
een
cont
rola
nd
inte
rven
tion
grou
psfo
rth
epr
imar
you
tcom
es.
Wee
kly
1-h
sess
ions
to
impr
ove
leg
stre
ngth
and
bala
nce
Add
ing
100
step
sto
thei
rda
ilyac
tiviti
es
ever
y2
wee
ks
(Con
tinue
d)
www.frontiersin.org January 2013 | Volume 4 | Article 3 | 3
Plotnikoff et al. Community-based physical activity interventions
Tab
le1
|Co
nti
nu
ed
Au
tho
r
(dat
e)
Stu
dy
des
ign
NN
per
gro
up
Rec
ruit
men
tIn
terv
enti
on
len
gth
Co
mm
un
ity
bas
ed
inte
rven
tio
n
com
po
nen
t
PAas
pec
tP
rim
ary
Ou
tco
me(
s)
Res
ult
s
Less
etal
.
(200
9),
Jam
aica
Pros
pect
ive
coho
rt
stud
y
293
N(C
on)=
135
N(In
t)=
158
Hea
lthce
nter
s6
mon
ths
Rec
ruitm
ent
Com
mun
ity
sett
ing
Phy
sica
lact
ivity
log,
they
trac
ked
thei
r
succ
ess
inac
hiev
ing
the
goal
of30
-min
phys
ical
activ
ityea
chda
y
HbA
1cH
bA1c
(Bas
elin
eM
ean)
Con
trol=
8.03
%;6
4.26
mm
ol/m
ol
Inte
rven
tion=
7.95
%;6
3.39
mm
ol/m
ol
HbA
1c(P
ost
Mea
n)
Con
trol=
8.62
%;7
0.71
mm
ol/m
ol
Inte
rven
tion=
7.32
%**
;56.
50m
mol
/mol
Mar
tyn-
Nem
eth
etal
.
(201
0),
USA
Pret
est/
post
-
test
desi
gn
16O
ne
grou
p
N=
16
Com
mun
ity-b
ased
clin
icth
atpr
ovid
es
care
for
low
-inco
me,
inde
pend
ent-
livin
g
com
mun
ity
resi
dent
s.
12w
eeks
Inpu
tpr
ovid
ed
from
:
com
mun
ity-
base
d
nurs
es
Reg
ular
low
-impa
ct
exer
cise
rout
ine
led
by
nurs
es
Wee
kly
exer
cise
sess
ions
wer
ele
dfo
r
12w
eeks
60-m
in,l
ow-im
pact
exer
cise
rout
ine
HbA
1c
Lipi
dpa
nel
BM
I
No
sign
ifica
ntdi
ffere
nces
betw
een
cont
rola
nd
inte
rven
tion
grou
psfo
rth
epr
imar
you
tcom
es.
diab
etic
nurs
e
educ
ator
med
ical
staf
f
exer
cise
phys
iolo
gist
Mat
hieu
etal
.
(200
8),
Can
ada
RC
T58
N(C
on)=
25 N(In
t)=
33
Kin
esio
logi
sts
in
com
mun
ity-b
ased
faci
litie
sw
ere
resp
onsi
ble
for
recr
uitin
g
part
icip
ants
10w
eek
Rec
ruitm
ent
Gro
uptr
aini
ng
sess
ions
Dia
betA
ctio
npr
ogra
m
intr
oduc
edpa
rtic
ipan
ts
toca
rdio
vasc
ular
,
resi
stan
ce,b
alan
ce,a
nd
flexi
bilit
yex
erci
ses
PAN
osi
gnifi
cant
diffe
renc
esbe
twee
nco
ntro
land
inte
rven
tion
grou
psfo
rth
epr
imar
you
tcom
es
10gr
oup
sess
ions
cons
istin
gof
a60
-min
PApe
riod
ofae
robi
c
exer
cise
sat
light
to
mod
erat
e-in
tens
ity,
resi
stan
ceex
erci
ses,
and
bala
nce
and
flexi
bilit
yex
erci
ses
(Con
tinue
d)
Frontiers in Endocrinology | Diabetes January 2013 | Volume 4 | Article 3 | 4
Plotnikoff et al. Community-based physical activity interventions
Tab
le1
|Co
nti
nu
ed
Au
tho
r
(dat
e)
Stu
dy
des
ign
NN
per
gro
up
Rec
ruit
men
tIn
terv
enti
on
len
gth
Co
mm
un
ity
bas
ed
inte
rven
tio
n
com
po
nen
t
PAas
pec
tP
rim
ary
Ou
tco
me(
s)
Res
ult
s
Tayl
or
etal
.
(200
9),
USA
RC
T24
N(C
on)=
13 N(In
t)=
11
Loca
lcom
mun
ity2
mon
ths
Rec
ruitm
ent
Use
of
com
mun
ity
fitne
ssce
nter
faci
litie
s
Phy
sica
lthe
rapi
st–
dire
cted
exer
cise
coun
selin
g
Fitn
ess
cent
er–b
ased
exer
cise
trai
ning
Mus
cula
r
stre
ngth
Exe
rcis
eca
paci
ty
No
sign
ifica
ntdi
ffere
nces
betw
een
cont
rola
nd
inte
rven
tion
grou
psfo
rth
epr
imar
you
tcom
es
4se
tsof
upto
8
repe
titio
nsof
each
exer
cise
usin
g80
%of
the
1-re
petit
ion
max
imum
(1-R
M)o
n2
non-
cons
ecut
ive
days
per
wee
kfo
r2
mon
ths
Sko
ro-
Kond
za
etal
.
(200
9),
UK
RC
T59
N(C
on)=
30 N(In
t)=
29
GP
’s12
wee
ksC
omm
unity
-
base
d
sess
ions
Reg
ular
yoga
clas
ses
24×
90-m
inyo
ga
clas
ses
over
12w
eeks
HbA
1cH
bA1c
Con
trol
grou
p:
Bas
elin
em
ean=
7.03
%;5
3.33
mm
ol/m
ol
Mea
nat
6m
onth
s=
7.30
%;5
6.28
mm
ol/m
ol(m
ean
chan
ge−
0.28
;95%
CI−
0.10
–0.6
6)
Inte
rven
tion
grou
p:
Bas
elin
em
ean=
7.06
%;5
3.66
mm
ol/m
ol
Mea
nat
6m
onth
s=
7.01
%;5
3.11
mm
ol/m
ol(m
ean
chan
ge−
0.05
;95%
CI−
0.26
–0.1
6).
Dut
ton
etal
.
(200
8),
USA
RC
T85
N(C
on)=
39 N(In
t)=
46
Com
mun
itydi
abet
ic
clin
ic
4w
eeks
Rec
ruitm
ent
Sta
ge-t
arge
ted
book
let
addr
essi
ng:
PAW
eekl
ym
inut
esof
PA
Con
trol
grou
p:
Bas
elin
em
ean=
107.
3(1
02.2
)
Mea
nch
ange
from
base
line
to
post
-inte
rven
tion=−
1.9,
95%
CI=−
37.0
to33
.2
Inte
rven
tion
grou
p:
Bas
elin
em
ean=
148.
5(1
21.3
)
Mea
nch
ange
from
base
line
to
post
-inte
rven
tion=
21.8
,95%
CI=−
16.3
to59
.9
Mot
ivat
ion
Sel
f-ef
ficac
y
Goa
l-set
ting
Soc
ials
uppo
rt
Prob
lem
-sol
ving
Two-
page
lett
erta
ilore
d
toth
eir:
Sta
geof
chan
ge
Sel
f-ef
ficac
y
Pros
/con
sfo
rac
tivity
Cur
rent
activ
ityle
vels
/
pref
eren
ces
Act
ivity
goal
s
(Con
tinue
d)
www.frontiersin.org January 2013 | Volume 4 | Article 3 | 5
Plotnikoff et al. Community-based physical activity interventions
Tab
le1
|Co
nti
nu
ed
Au
tho
r
(dat
e)
Stu
dy
des
ign
NN
per
gro
up
Rec
ruit
men
tIn
terv
enti
on
len
gth
Co
mm
un
ity
bas
ed
inte
rven
tio
n
com
po
nen
t
PAas
pec
tP
rim
ary
Ou
tco
me(
s)
Res
ult
s
Klu
g
etal
.
(200
8),
USA
Non
-
rand
omiz
ed
one
grou
p
befo
rean
d
afte
rde
sign
243
One
grou
pA
t
4m
onth
s
N=
147
Ann
ounc
emen
tsan
d
pres
enta
tions
to
inte
rnal
and
exte
rnal
com
mun
itygr
oups
,
post
edfli
ers,
plac
ed
bulle
tins
in
new
slet
ters
,
cont
acte
del
igib
le
olde
rad
ults
dire
ctly
,
depe
nded
on“w
ord
ofm
outh
,”w
orke
d
with
loca
lmed
ia,
and
part
nere
dw
ith
othe
rag
enci
es
6m
onth
sR
ecru
itmen
t
Set
ting
Peer
lead
er
Wee
kly
supp
ort
sess
ions
for
PAan
ddi
et
Sel
f-ef
ficac
y
Sel
f-ra
ted
heal
th
Sel
f-ef
ficac
yan
dse
lf-ra
ted
heal
thsc
ores
sign
ifica
ntly
impr
oved
Spe
er
etal
.
(200
8),
USA
Con
veni
ence
sam
ple
260
One
grou
p
N=
144
Sen
iors
cent
ers
4m
onth
sR
ecru
itmen
t
Exp
erts
from
the
loca
l
univ
ersi
ty
Phy
sica
lact
ivity
inco
rpor
ated
into
sess
ions
HbA
1cH
bA1c
Bas
elin
e7.
00%
(SD=
1.39
);53
.01
mm
ol/m
ol
Post
-inte
rven
tion
6.7%
(SD=
1.17
)*;
50.3
8m
mol
/mol
40–6
0m
inw
eekl
y
sess
ions
Bro
oks
etal
.
(200
7),
USA
RC
T62
N(C
on)=
31 N(In
t)=
31
Not
repo
rted
16w
eeks
Exe
rcis
e
trai
ning
cond
ucte
din
com
mun
ity
sett
ing
Reg
ular
exer
cise
and
stre
ngth
trai
ning
HbA
1cH
bA1c
[bas
elin
em
ean
(SE
)]
Bod
yco
mpo
sitio
nC
ontr
ol=
7.8%
(1.6
);61
.75
mm
ol/m
ol
Mus
cle
stre
ngth
Inte
rven
tion=
8.7%
(1.8
);71
.58
mm
ol/m
ol
Mus
cle
qual
ityH
bA1c
(pos
t)
3x/w
eek
for
16w
eeks
for
exer
cise
trai
ning
.
Con
trol=
8.3%
(1.3
);67
.21
mm
ol/m
ol
Inte
rven
tion=
7.6%
(1.5
)**;
59.5
6m
mol
/mol
Con
trol
grou
p:
Mea
nch
ange
from
base
line
topo
st-in
terv
entio
n
[mea
n(S
E)]=
0.4
(0.3
)
Ses
sion
sin
clud
ed
35-m
inst
reng
th
trai
ning
3se
tsof
8
repe
titio
nson
each
mac
hine
(Con
tinue
d)
Frontiers in Endocrinology | Diabetes January 2013 | Volume 4 | Article 3 | 6
Plotnikoff et al. Community-based physical activity interventions
Tab
le1
|Co
nti
nu
ed
Au
tho
r
(dat
e)
Stu
dy
des
ign
NN
per
gro
up
Rec
ruit
men
tIn
terv
enti
on
len
gth
Co
mm
un
ity
bas
ed
inte
rven
tio
n
com
po
nen
t
PAas
pec
tP
rim
ary
Ou
tco
me(
s)
Res
ult
s
Trai
ning
inte
nsity
durin
gw
ks1–
8
wer
e60
–80%
of
base
line
1-re
petit
ion
max
imum
(1-R
M),
and
durin
gw
ks
10–1
4w
ere
70–8
0%of
mid
-stu
dy1-
RM
Inte
rven
tion
grou
p:
Mea
nch
ange
from
base
line
topo
st-in
terv
entio
n
[mea
n(S
E)]=−
1.0
(0.2
)
Sig
nific
ant
chan
gesc
ore
diffe
renc
esfo
rth
e
inte
rven
tion
grou
pvs
.con
trol
son
uppe
rbo
dy
mus
cle
stre
ngth
,low
erbo
dym
uscl
est
reng
th,
Who
le-b
ody
lean
tissu
em
ass,
Mus
cle
qual
ity,T
ype
1an
dTy
pe2
mus
cle
fire
area
Dun
stan
etal
.
(200
6),
Aus
tral
ia
RC
T57
N(h
ome
trai
n-
ing)=
26
N(c
ente
r
trai
n-
ing)=
27
Rec
ruite
dfr
omth
e
clin
ics
ofth
e
Inte
rnat
iona
l
Dia
bete
sIn
stitu
te
and
bya
loca
lmed
ia
cam
paig
n.
12m
onth
sC
omm
unity
fitne
ssce
nter
faci
litie
sus
ed
Res
ista
nce
trai
ning
prog
ram
2da
ys/w
eek
HbA
1cH
bA1c
Hom
egr
oup:
Bas
elin
em
ean=
7.5%
(0.5
);58
.47
mm
ol/m
ol
Cen
ter
grou
p:
Bas
elin
em
ean=
7.8%
(0.9
);61
.75
mm
ol/m
ol
Hom
egr
oup:
Mea
nch
ange
from
base
line:
M(S
D):−
0.1(
1.1)
Cen
ter
grou
p:
Mea
nch
ange
from
base
line:
M(S
D):−
0.4(
1.0)
**
Low
-inte
nsity
stat
iona
ry
cycl
ing
plus
stre
tchi
ng
exer
cise
san
d45
min
of
high
inte
nsity
resi
stan
cetr
aini
ng
Goa
lwas
toac
hiev
e
betw
een
75an
d85
%of
the
curr
ent
1-R
M.T
hree
sets
ofei
ght
repe
titio
ns
wer
epe
rfor
med
for
all
exer
cise
s
Boy
d
etal
.
(200
6),
USA
Non
-
rand
omiz
ed
one
grou
p
befo
rean
d
afte
rde
sign
48O
ne
grou
p
N=
35
Rec
ruite
dan
d
refe
rred
by
phys
icia
ns,
phys
icia
ns
assi
stan
ts,a
dvan
ce
nurs
epr
actit
ione
rs
12m
onth
sPa
rtne
rshi
p
betw
een
a
com
mun
ity
heal
thce
nter
s
toim
prov
e
acce
ssto
exer
cise
for
low
-inco
me
patie
nts
with
type
2
diab
etes
3m
onth
YM
CA
mem
bers
hip
exer
cise
clas
ses
twic
e
per
wee
kla
stin
gup
to
12m
onth
s
HbA
1cH
bA1c
Blo
odpr
essu
reB
asel
ine:
8.6%
;70.
49m
mol
/mol
Post
-inte
rven
tion:
6.9%
*;51
.91
mm
ol/m
ol
LDL
Blo
odpr
essu
re
Bas
elin
esy
stol
ic:1
30m
mH
g
Post
-inte
rven
tion:
126
mm
Hg
Bas
elin
edi
asto
lic:7
9m
mH
g
Post
-inte
rven
tion
dias
tolic
:75
mm
Hg*
LDL
Bas
elin
e:11
6m
g/dL
Post
-inte
rven
tion:
99m
g/dL
*
(Con
tinue
d)
www.frontiersin.org January 2013 | Volume 4 | Article 3 | 7
Plotnikoff et al. Community-based physical activity interventions
Tab
le1
|Co
nti
nu
ed
Au
tho
r
(dat
e)
Stu
dy
des
ign
NN
per
gro
up
Rec
ruit
men
tIn
terv
enti
on
len
gth
Co
mm
un
ity
bas
ed
inte
rven
tio
n
com
po
nen
t
PAas
pec
tP
rim
ary
Ou
tco
me(
s)
Res
ult
s
Wei
ght
HD
L
Bas
elin
e:41
mg/
dL
Post
-inte
rven
tion:
44m
g/dL
Wei
ght
Bas
elin
e:21
8lb
Post
-inte
rven
tion:
206
lb
Eng
el
and
Lind
ner
(200
6),
Aus
tral
ia
RC
T57
N(c
oach
ing
only
)=28
Loca
lmed
ia
cam
paig
n
6m
onth
sR
ecru
itmen
t
Gro
up
coac
hing
sess
ions
Gro
upco
achi
ng
sess
ions
HbA
1c
Blo
odpr
essu
re
BM
I
PA Fitn
ess
(shu
ttle
run)
HbA
1c
Coa
chin
gon
lygr
oup:
N(P
edo-
met
er)=
22
Pedo
met
erus
e
valu
esof
betw
een
6000
and
8500
step
s
per
day
(hea
lthy
olde
r
adul
ts)a
ndbe
twee
n
3500
and
5500
step
s
per
day
(old
erad
ults
)
Bas
elin
em
ean=
7.70
%(1
.39)
;60.
66m
mol
/mol
Mea
nch
ange
from
base
line
to
post
-inte
rven
tion=−
0.2(
1.1)
Pedo
met
ergr
oup:
Bas
elin
em
ean=
7.14
%(0
.98)
;54.
54m
mol
/mol
Mea
nch
ange
from
base
line
to
post
-inte
rven
tion=
0.02
(1.0
)
Syst
olic
bloo
dpr
essu
re
Pedo
met
er
Mea
nch
ange
from
base
line=
2.4
(18.
3)
Coa
chin
g=
–2.9
(14)
Dia
stol
icbl
ood
pres
sure
Mea
nch
ange
from
base
line
Pedo
met
er=
1.6
(9.9
)
Coa
chin
g=
–4.1
(9.9
)
BM
I
Mea
nch
ange
from
base
line
Pedo
met
er=
–0.7
(2.3
)
Coa
chin
g=
–0.7
(1.5
)
Fitn
ess
Mea
nch
ange
from
base
line
Pedo
met
er=
65(1
02)
Coa
chin
g=
49(7
2)
(Con
tinue
d)
Frontiers in Endocrinology | Diabetes January 2013 | Volume 4 | Article 3 | 8
Plotnikoff et al. Community-based physical activity interventions
Tab
le1
|Co
nti
nu
ed
Au
tho
r
(dat
e)
Stu
dy
des
ign
NN
per
gro
up
Rec
ruit
men
tIn
terv
enti
on
len
gth
Co
mm
un
ity
bas
ed
inte
rven
tio
n
com
po
nen
t
PAas
pec
tP
rim
ary
Ou
tco
me(
s)
Res
ult
s
Two
Feat
hers
etal
.
(200
5),
USA
Non
-
rand
omiz
ed
one
grou
p
befo
rean
d
afte
rde
sign
91O
ne
grou
p
N=
91
Hea
lthca
resy
stem
s
inde
troi
t
5m
onth
sLo
cally
base
d
com
mun
ity
resi
dent
mee
tings
Som
em
eetin
gs
focu
sed
onin
crea
sing
PAto
impr
ove
patie
nts
self-
man
agem
ent
of
diab
etes
HbA
1cH
bA1c
Bas
elin
e:8.
4%(S
D=
2.3)
;68.
31m
mol
/mol
Post
-inte
rven
tion:
7.6%
(SD=
1.9)
*;
59.5
6m
mol
/mol
Bra
ndon
etal
.
(200
3),
USA
RC
T31
N(C
on)=
15 N(In
t)=
16
Vete
rans
affa
irs
diab
etic
clin
ic,a
com
pute
rized
rese
arch
cent
er
data
base
,loc
al
diab
etic
clin
ics,
and
seni
orce
nter
s,an
d
byw
ord
ofm
outh
24m
onth
sR
ecru
itmen
tR
egul
artr
aini
ngfo
r
24m
onth
s
Mob
ility
Str
engt
h-hi
pfle
xors
Com
mun
ityPA
faci
litie
s
3se
ssio
nspe
rw
eek
Str
engt
hC
ontr
ol:0
.38(
0.07
)S
tren
gth
trai
ning
was
com
plet
edon
an
11-s
tatio
nN
autil
us
mac
hine
.The
subj
ects
com
plet
ed3
sets
of
8–12
repe
titio
nspe
r
exer
cise
.The
inte
nsity
was
50,6
0,an
d70
%
for
sets
1,2,
and
3,
resp
ectiv
ely.
Eac
h1-
h
sess
ion
cons
iste
dof
50m
inof
stre
ngth
-tra
inin
g
exer
cise
san
d10
min
of
war
m-u
p,fle
xibi
lity,
and
cool
-dow
nex
erci
ses
Inte
rven
tion:
0.44
(0.1
2)
Mob
ility
-tim
edup
and
go:
Con
trol
:8.3
(1.0
)
Inte
rven
tion:
7.6(
1.8)
Ther
ew
asa
grou
p×
time
effe
ctas
the
Inte
rven
tion
grou
pin
crea
sed
31.4
%(p
<.0
01)i
nst
reng
thfo
ral
l
mus
cle
grou
psaf
ter
the
first
6m
onth
s,an
dth
e
stre
ngth
gain
sw
ere
reta
ined
at24
mon
ths.
Ther
e
was
also
agr
oup×
time
effe
ctfo
rm
obili
tyas
perf
orm
ance
incr
ease
d8.
6an
d9.
8%(p
<03
2an
d
p<
0.03
1)fo
rth
efir
st6
and
12m
onth
s,
resp
ectiv
ely,
but
decr
ease
dto
4.6%
abov
e
base
line
atth
een
dof
the
inte
rven
tion.
Gol
dhab
er-
Fieb
ert
etal
.
(200
3),
Cos
ta
Ric
a
RC
T75
N(C
on)=
28 N(In
t)=
33
Com
mun
ityG
P’s
12w
eeks
Inte
rven
tion
clas
ses
cond
ucte
dby
:
Nut
ritio
nist
s
Loca
l
volu
ntee
rs
/lead
ers
60m
inw
alki
nggr
oup
sess
ions
thre
etim
es
per
wee
kfo
r12
wee
ks
HbA
1c
BM
I
Wei
ght
Fast
ing
plas
ma
gluc
ose
Ser
umlip
ids
Blo
odpr
essu
re
HbA
1c
Con
trol
grou
p:
Bas
elin
em
ean=
8.6%
(3.9
);70
.49
mm
ol/m
ol
Mea
nch
ange
from
base
line:−
0.4(
2.3)
Inte
rven
tion
grou
p:
Bas
elin
em
ean=
8.6%
(3.7
);70
.49
mm
ol/m
ol
Mea
nch
ange
from
base
line:−
1.8(
2.3)
**
Sig
nific
ant
decr
ease
sin
wei
ght,
BM
I,an
dfa
stin
g
plas
ma
bloo
dgl
ucos
efo
rin
terv
entio
nvs
.con
trol
grou
p
(Con
tinue
d)
www.frontiersin.org January 2013 | Volume 4 | Article 3 | 9
Plotnikoff et al. Community-based physical activity interventions
Tab
le1
|Co
nti
nu
ed
Au
tho
r
(dat
e)
Stu
dy
des
ign
NN
per
gro
up
Rec
ruit
men
tIn
terv
enti
on
len
gth
Co
mm
un
ity
bas
ed
inte
rven
tio
n
com
po
nen
t
PAas
pec
tP
rim
ary
Ou
tco
me(
s)
Res
ult
s
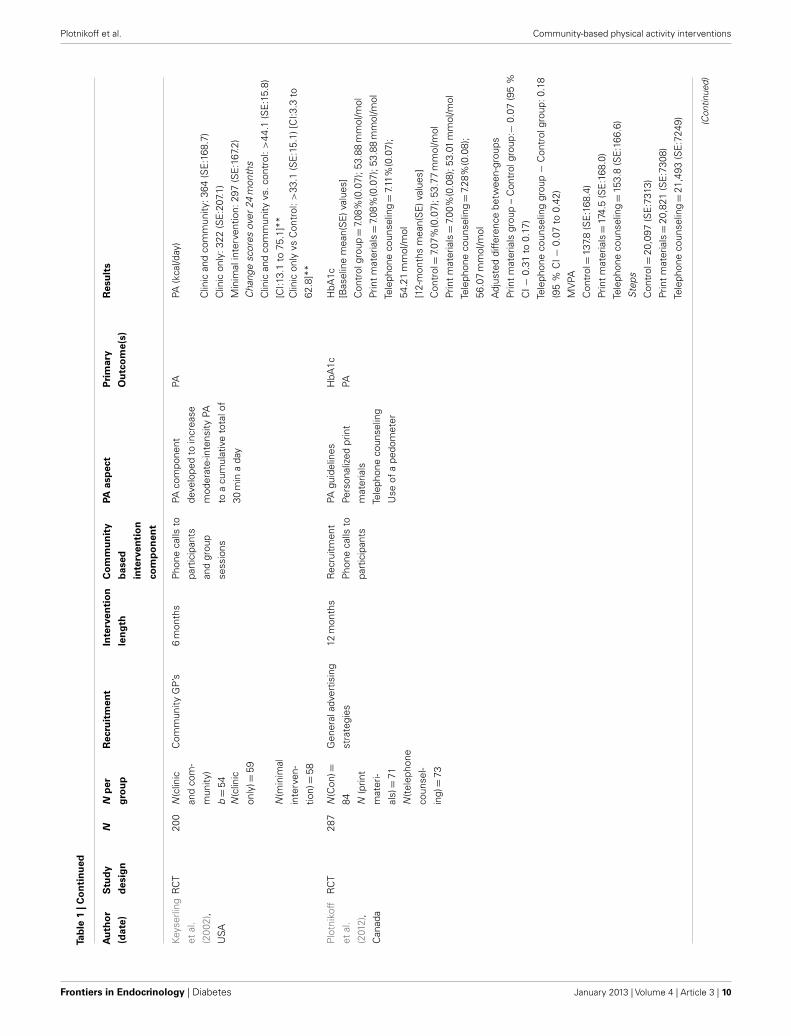
Keys
erlin
g
etal
.
(200
2),
USA
RC
T20
0N
(clin
ic
and
com
-
mun
ity)
b=
54
Com
mun
ityG
P’s
6m
onth
sP
hone
calls
to
part
icip
ants
and
grou
p
sess
ions
PAco
mpo
nent
deve
lope
dto
incr
ease
mod
erat
e-in
tens
ityPA
toa
cum
ulat
ive
tota
lof
30m
ina
day
PAPA
(kca
l/day
)
Clin
ican
dco
mm
unity
:364
(SE
:168
.7)
Clin
icon
ly:3
22(S
E:2
07.1
)
N(c
linic
only
)=59
Min
imal
inte
rven
tion:
297
(SE
:167
.2)
Cha
nge
scor
esov
er24
mon
ths
Clin
ican
dco
mm
unity
vs.c
ontr
ol:>
44.1
(SE
:15.
8)
[CI:1
3.1
to75
.1]*
*N
(min
imal
inte
rven
-
tion)=
58
Clin
icon
lyvs
Con
trol
:>33
.1(S
E:1
5.1)
[CI:3
.3to
62.8
]**
Plo
tnik
off
etal
.
(201
2),
Can
ada
RC
T28
7N
(Con
)=
84 N(p
rint
mat
eri-
als)=
71
N(t
elep
hone
coun
sel-
ing)=
73
Gen
eral
adve
rtis
ing
stra
tegi
es
12m
onth
sR
ecru
itmen
t
Pho
neca
llsto
part
icip
ants
PAgu
idel
ines
Pers
onal
ized
prin
t
mat
eria
ls
Tele
phon
eco
unse
ling
Use
ofa
pedo
met
er
HbA
1c
PA
HbA
1c[B
asel
ine
mea
n(S
E)v
alue
s]
Con
trol
grou
p=
7.08
%(0
.07)
;53.
88m
mol
/mol
Prin
tm
ater
ials=
7.08
%(0
.07)
;53.
88m
mol
/mol
Tele
phon
eco
unse
ling=
7.11
%(0
.07)
;
54.2
1m
mol
/mol
[12-
mon
ths
mea
n(S
E)v
alue
s]
Con
trol=
7.07
%(0
.07)
;53.
77m
mol
/mol
Prin
tm
ater
ials=
7.00
%(0
.08)
;53.
01m
mol
/mol
Tele
phon
eco
unse
ling=
7.28
%(0
.08)
;
56.0
7m
mol
/mol
Adj
uste
ddi
ffere
nce
betw
een-
grou
ps
Prin
tm
ater
ials
grou
p–
Con
trol
grou
p:−
0.07
(95
%
CI−
0.31
to0.
17)
Tele
phon
eco
unse
ling
grou
p−
Con
trol
grou
p:0.
18
(95
%C
I−0.
07to
0.42
)
MV
PA
Con
trol=
137.
8(S
E:1
68.4
)
Prin
tm
ater
ials=
174.
5(S
E:1
68.0
)
Tele
phon
eco
unse
ling=
153.
8(S
E:1
66.6
)
Ste
ps
Con
trol=
20,0
97(S
E:7
313)
Prin
tm
ater
ials=
20,8
21(S
E:7
308)
Tele
phon
eco
unse
ling=
21,4
93(S
E:7
249) (C
ontin
ued)
Frontiers in Endocrinology | Diabetes January 2013 | Volume 4 | Article 3 | 10
Plotnikoff et al. Community-based physical activity interventions
Tab
le1
|Co
nti
nu
ed
Au
tho
r
(dat
e)
Stu
dy
des
ign
NN
per
gro
up
Rec
ruit
men
tIn
terv
enti
on
len
gth
Co
mm
un
ity
bas
ed
inte
rven
tio
n
com
po
nen
t
PAas
pec
tP
rim
ary
Ou
tco
me(
s)
Res
ult
s
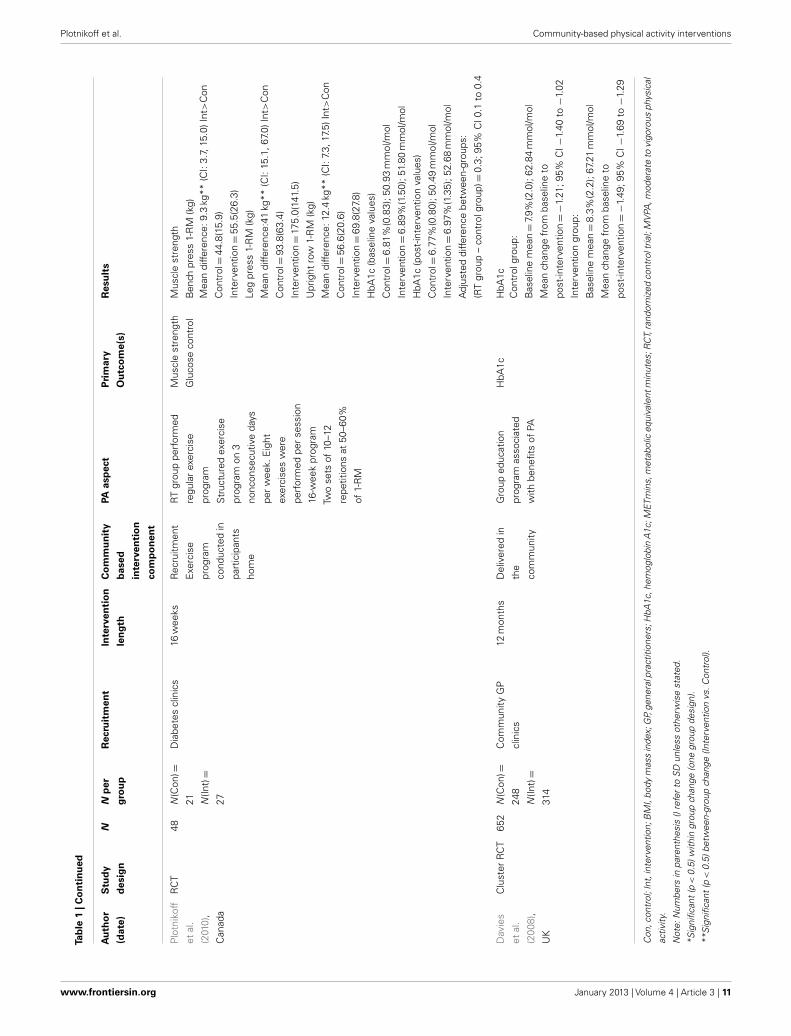
Plo
tnik
off
etal
.
(201
0),
Can
ada
RC
T48
N(C
on)=
21 N(In
t)=
27
Dia
bete
scl
inic
s16
wee
ksR
ecru
itmen
t
Exe
rcis
e
prog
ram
cond
ucte
din
part
icip
ants
hom
e
RT
grou
ppe
rfor
med
regu
lar
exer
cise
prog
ram
Mus
cle
stre
ngth
Glu
cose
cont
rol
Mus
cle
stre
ngth
Ben
chpr
ess
1-R
M(k
g)
Str
uctu
red
exer
cise
prog
ram
on3
nonc
onse
cutiv
eda
ys
per
wee
k.E
ight
exer
cise
sw
ere
perf
orm
edpe
rse
ssio
n
16-w
eek
prog
ram
Two
sets
of10
–12
repe
titio
nsat
50–6
0%
of1-
RM
Mea
ndi
ffere
nce:
9.3
kg**
(CI:
3.7,
15.0
)Int
>C
on
Con
trol=
44.8
(15.
9)
Inte
rven
tion=
55.5
(26.
3)
Leg
pres
s1-
RM
(kg)
Mea
ndi
ffere
nce:
41kg
**(C
I:15
.1,6
7.0)
Int>
Con
Con
trol=
93.8
(63.
4)
Inte
rven
tion=
175.
0(14
1.5)
Upr
ight
row
1-R
M(k
g)
Mea
ndi
ffere
nce:
12.4
kg**
(CI:
7.3,
17.5
)Int
>C
on
Con
trol=
56.6
(20.
6)
Inte
rven
tion=
69.8
(27.
8)
HbA
1c(b
asel
ine
valu
es)
Con
trol=
6.81
%(0
.83)
;50.
93m
mol
/mol
Inte
rven
tion=
6.89
%(1
.50)
;51.
80m
mol
/mol
HbA
1c(p
ost-
inte
rven
tion
valu
es)
Con
trol=
6.77
%(0
.80)
;50.
49m
mol
/mol
Inte
rven
tion=
6.97
%(1
.35)
;52.
68m
mol
/mol
Adj
uste
ddi
ffere
nce
betw
een-
grou
ps:
(RT
grou
p–
cont
rolg
roup
)=0.
3;95
%C
I0.1
to0.
4
Dav
ies
etal
.
(200
8),
UK
Clu
ster
RC
T65
2N
(Con
)=
248
N(In
t)=
314
Com
mun
ityG
P
clin
ics
12m
onth
sD
eliv
ered
in
the
com
mun
ity
Gro
uped
ucat
ion
prog
ram
asso
ciat
ed
with
bene
fits
ofPA
HbA
1cH
bA1c
Con
trol
grou
p:
Bas
elin
em
ean=
7.9%
(2.0
);62
.84
mm
ol/m
ol
Mea
nch
ange
from
base
line
to
post
-inte
rven
tion=−
1.21
;95%
CI−
1.40
to−
1.02
Inte
rven
tion
grou
p:
Bas
elin
em
ean=
8.3%
(2.2
);67
.21
mm
ol/m
ol
Mea
nch
ange
from
base
line
to
post
-inte
rven
tion=−
1.49
;95%
CI−
1.69
to−
1.29
Con
,con
trol
;Int
,int
erve
ntio
n;B
MI,
body
mas
sin
dex;
GP,
gene
ralp
ract
ition
ers;
HbA
1c,h
emog
lobi
nA
1c;M
ETm
ins,
met
abol
iceq
uiva
lent
min
utes
;RC
T,ra
ndom
ized
cont
rolt
rial;
MV
PA,m
oder
ate
tovi
goro
usph
ysic
al
activ
ity.
Not
e:N
umbe
rsin
pare
nthe
sis
()re
fer
toS
Dun
less
othe
rwis
est
ated
.
*Sig
nific
ant
(p<
0.5)
with
ingr
oup
chan
ge(o
negr
oup
desi
gn).
**S
igni
fican
t(p
<0.
5)be
twee
n-gr
oup
chan
ge(In
terv
entio
nvs
.Con
trol
).
www.frontiersin.org January 2013 | Volume 4 | Article 3 | 11
Plotnikoff et al. Community-based physical activity interventions
FIGURE 1 | Flow of study selection through the phases of the review.
the remaining studies were conducted in Canada (Mathieu et al.,2008; Plotnikoff et al., 2010, 2011, 2012), Australia (Dunstan et al.,2006; Engel and Lindner, 2006), the United Kingdom (Davies et al.,2008; Skoro-Kondza et al., 2009), Costa Rica (Goldhaber-Fiebertet al., 2003), and Jamaica (Less et al., 2009).
The majority of studies recruited participants from clinics orduring visits to general practitioners (14/22), however other com-munity recruitment strategies included local media campaigns(Dunstan et al., 2006; Engel and Lindner, 2006; Klug et al., 2008;Piette et al., 2011; Plotnikoff et al., 2012), intervention open tocommunity (Kruse et al., 2010), and a senior’s center’s (Speer et al.,2008). Four studies employed a combined approach of strategies.
For the purposes of this review, only community-basedapproaches were considered. The majority of studies (14/22)recruited participants by employing a multi-strategy approachincluding a combination of the following components: inter-vention recruitment, delivery, use of facilities, group sessions,and expert advice. In addition studies used of community facil-ities (Dunstan et al., 2006; Brooks et al., 2007; Davies et al.,
2008;, Skoro-Kondza et al., 2009) and expert advice from special-ists within the community (Goldhaber-Fiebert et al., 2003; Speeret al., 2008).
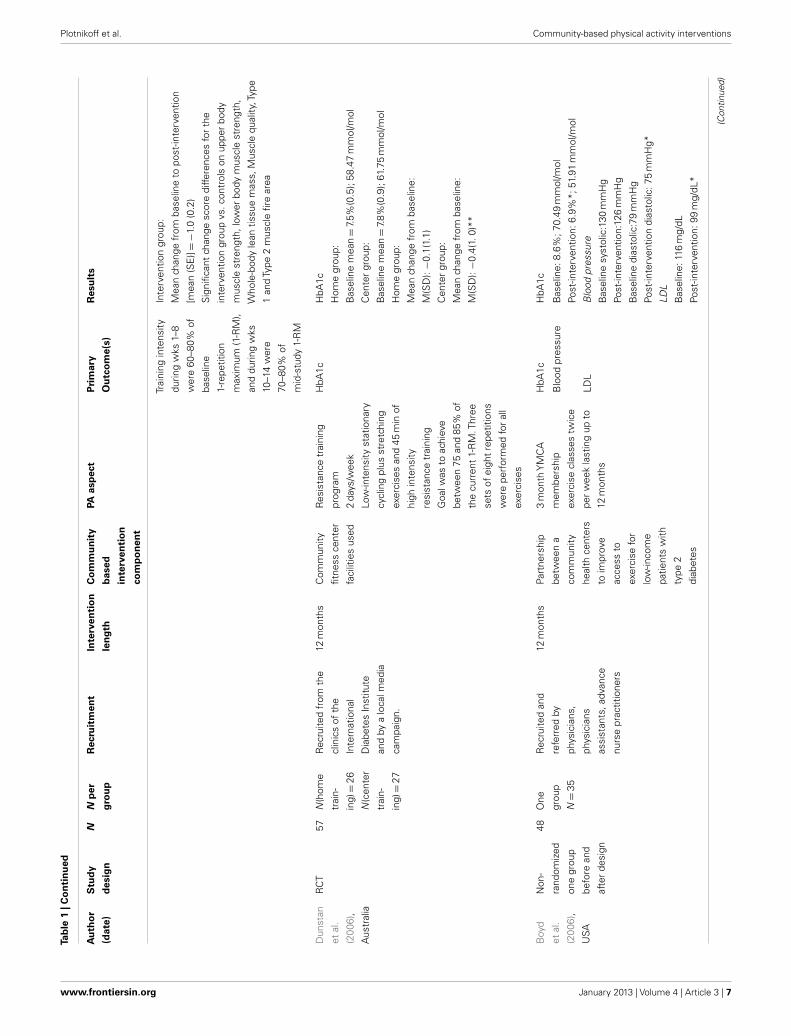
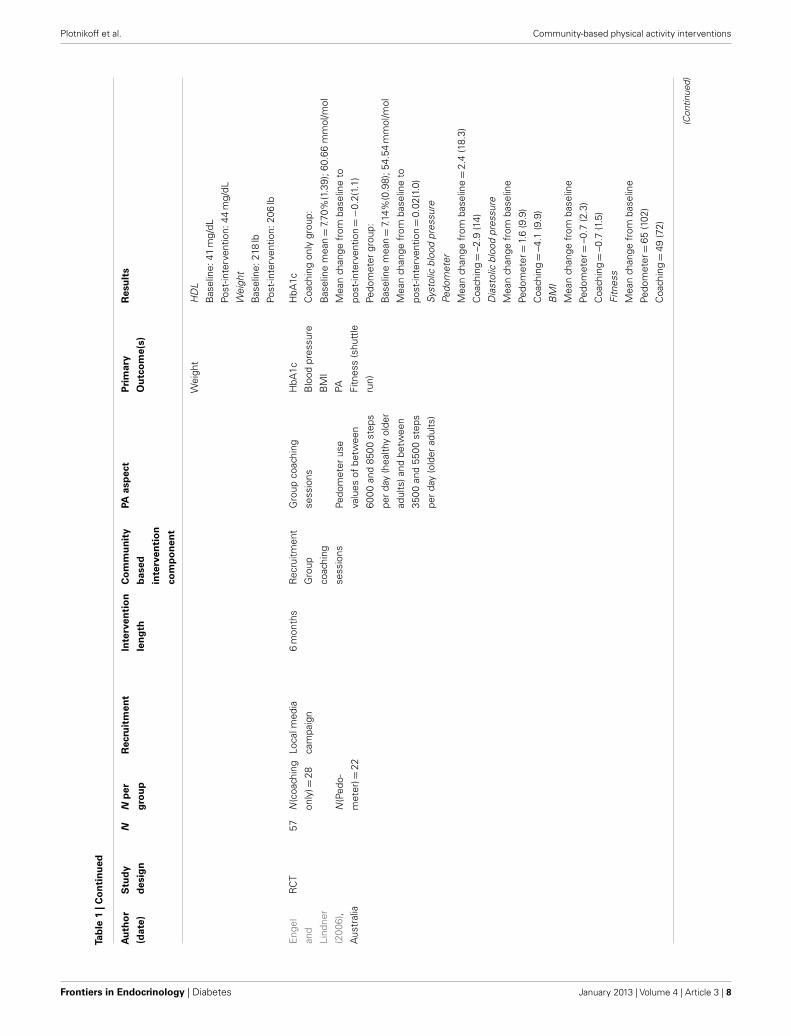
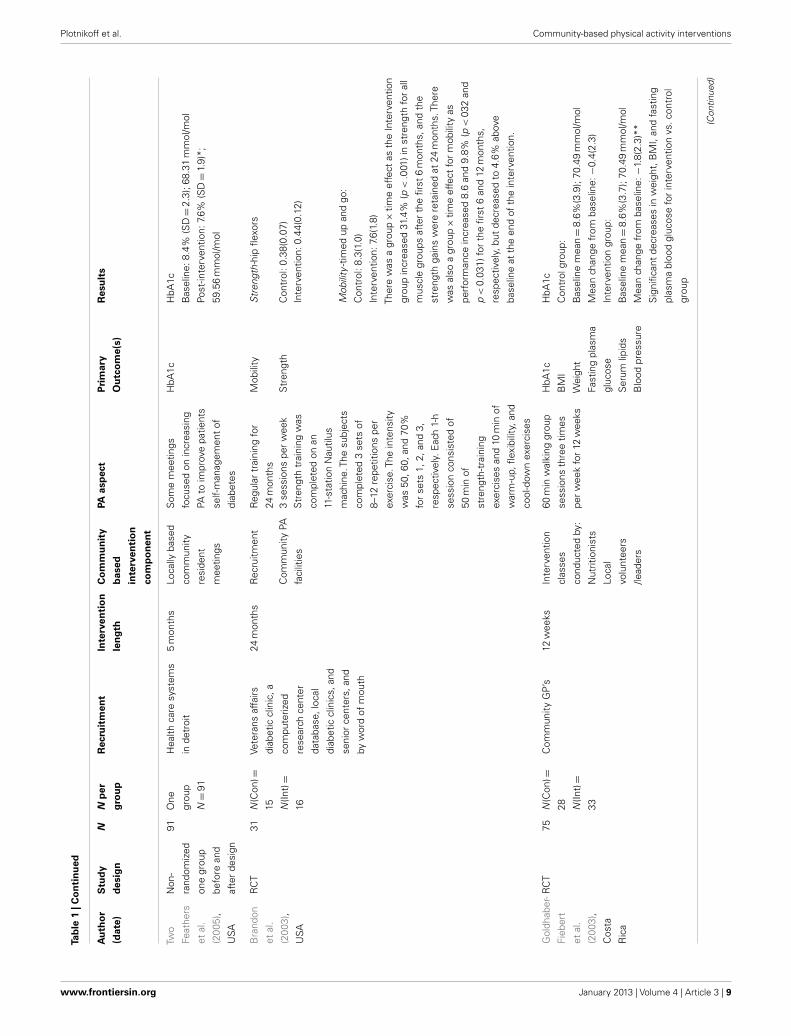
Physical activity interventions for treating T2D were eligi-ble only if the PA component/approach accounted for≥ 50% ofthe overall intervention. PA approaches including general exer-cise programs were employed by the majority of studies (9/22),PA counseling/information (Davies et al., 2008; Dutton et al.,2008; Klug et al., 2008; Plotnikoff et al., 2012), walking programs(Goldhaber-Fiebert et al., 2003; Piette et al., 2011), resistance train-ing programs (Dunstan et al., 2006; Brooks et al., 2007; Mathieuet al., 2008; Kruse et al., 2010; Plotnikoff et al., 2011), gym member-ship provision (Boyd et al., 2006), and yoga classes (Skoro-Kondzaet al., 2009).
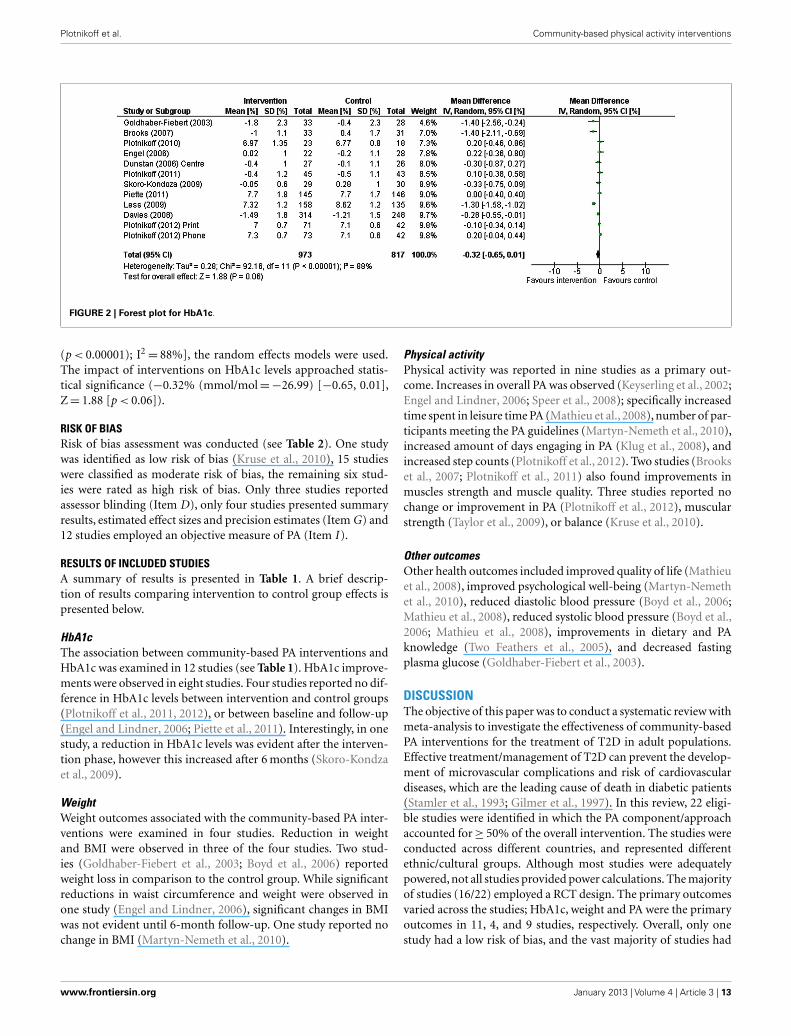
META-ANALYSIS OF INTERVENTION EFFECTSResults from RCTs were pooled to establish the effects of inter-ventions on HbA1c levels (see Figure 2). As there was consid-erable heterogeneity among interventions [χ2
= 92.16, df= 11
Frontiers in Endocrinology | Diabetes January 2013 | Volume 4 | Article 3 | 12
Plotnikoff et al. Community-based physical activity interventions
FIGURE 2 | Forest plot for HbA1c.
(p < 0.00001); I2= 88%], the random effects models were used.
The impact of interventions on HbA1c levels approached statis-tical significance (−0.32% (mmol/mol=−26.99) [−0.65, 0.01],Z= 1.88 [p < 0.06]).
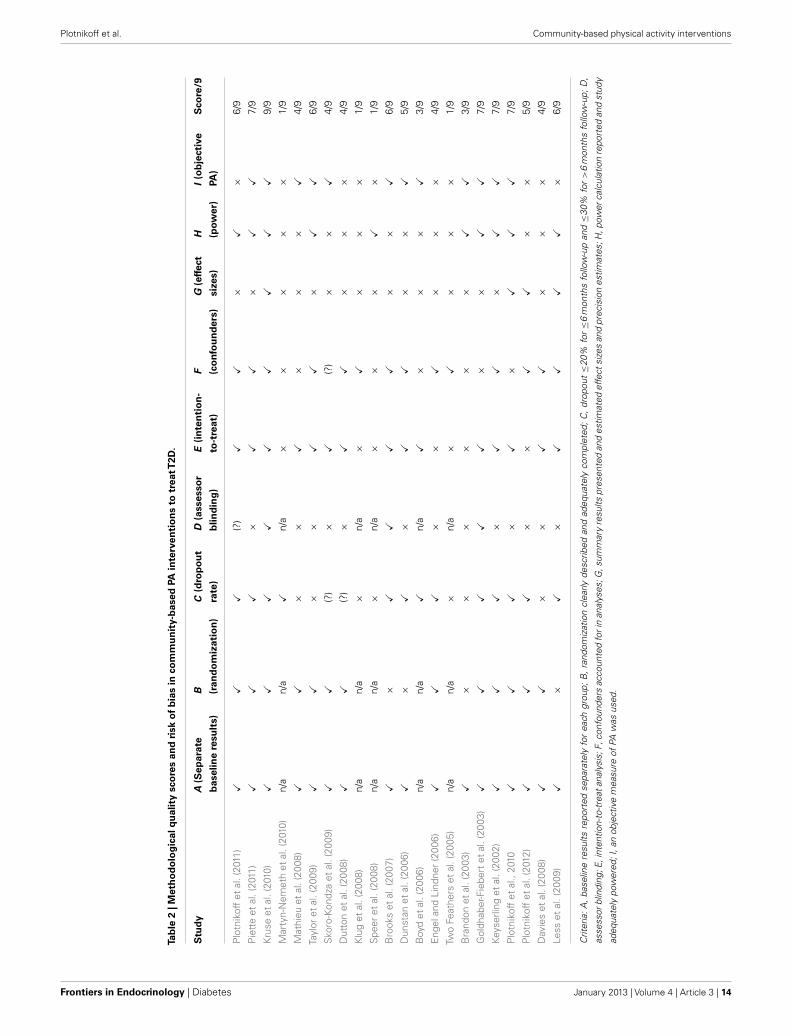
RISK OF BIASRisk of bias assessment was conducted (see Table 2). One studywas identified as low risk of bias (Kruse et al., 2010), 15 studieswere classified as moderate risk of bias, the remaining six stud-ies were rated as high risk of bias. Only three studies reportedassessor blinding (Item D), only four studies presented summaryresults, estimated effect sizes and precision estimates (Item G) and12 studies employed an objective measure of PA (Item I ).
RESULTS OF INCLUDED STUDIESA summary of results is presented in Table 1. A brief descrip-tion of results comparing intervention to control group effects ispresented below.
HbA1cThe association between community-based PA interventions andHbA1c was examined in 12 studies (see Table 1). HbA1c improve-ments were observed in eight studies. Four studies reported no dif-ference in HbA1c levels between intervention and control groups(Plotnikoff et al., 2011, 2012), or between baseline and follow-up(Engel and Lindner, 2006; Piette et al., 2011). Interestingly, in onestudy, a reduction in HbA1c levels was evident after the interven-tion phase, however this increased after 6 months (Skoro-Kondzaet al., 2009).
WeightWeight outcomes associated with the community-based PA inter-ventions were examined in four studies. Reduction in weightand BMI were observed in three of the four studies. Two stud-ies (Goldhaber-Fiebert et al., 2003; Boyd et al., 2006) reportedweight loss in comparison to the control group. While significantreductions in waist circumference and weight were observed inone study (Engel and Lindner, 2006), significant changes in BMIwas not evident until 6-month follow-up. One study reported nochange in BMI (Martyn-Nemeth et al., 2010).
Physical activityPhysical activity was reported in nine studies as a primary out-come. Increases in overall PA was observed (Keyserling et al., 2002;Engel and Lindner, 2006; Speer et al., 2008); specifically increasedtime spent in leisure time PA (Mathieu et al., 2008), number of par-ticipants meeting the PA guidelines (Martyn-Nemeth et al., 2010),increased amount of days engaging in PA (Klug et al., 2008), andincreased step counts (Plotnikoff et al., 2012). Two studies (Brookset al., 2007; Plotnikoff et al., 2011) also found improvements inmuscles strength and muscle quality. Three studies reported nochange or improvement in PA (Plotnikoff et al., 2012), muscularstrength (Taylor et al., 2009), or balance (Kruse et al., 2010).
Other outcomesOther health outcomes included improved quality of life (Mathieuet al., 2008), improved psychological well-being (Martyn-Nemethet al., 2010), reduced diastolic blood pressure (Boyd et al., 2006;Mathieu et al., 2008), reduced systolic blood pressure (Boyd et al.,2006; Mathieu et al., 2008), improvements in dietary and PAknowledge (Two Feathers et al., 2005), and decreased fastingplasma glucose (Goldhaber-Fiebert et al., 2003).
DISCUSSIONThe objective of this paper was to conduct a systematic review withmeta-analysis to investigate the effectiveness of community-basedPA interventions for the treatment of T2D in adult populations.Effective treatment/management of T2D can prevent the develop-ment of microvascular complications and risk of cardiovasculardiseases, which are the leading cause of death in diabetic patients(Stamler et al., 1993; Gilmer et al., 1997). In this review, 22 eligi-ble studies were identified in which the PA component/approachaccounted for≥ 50% of the overall intervention. The studies wereconducted across different countries, and represented differentethnic/cultural groups. Although most studies were adequatelypowered, not all studies provided power calculations. The majorityof studies (16/22) employed a RCT design. The primary outcomesvaried across the studies; HbA1c, weight and PA were the primaryoutcomes in 11, 4, and 9 studies, respectively. Overall, only onestudy had a low risk of bias, and the vast majority of studies had
www.frontiersin.org January 2013 | Volume 4 | Article 3 | 13
Plotnikoff et al. Community-based physical activity interventions
Tab
le2
|Met
ho
do
log
ical
qu
alit
ysc
ore
san
dri
sko
fb
ias
inco
mm
un
ity-
bas
edPA
inte
rven
tio
ns
totr
eatT
2D.
Stu
dy
A(S
epar
ate
bas
elin
ere
sult
s)
B (ran
do
miz
atio
n)
C(d
rop
ou
t
rate
)
D(a
sses
sor
blin
din
g)
E(i
nte
nti
on
-
to-t
reat
)
F (co
nfo
un
der
s)
G(e
ffec
t
size
s)
H (pow
er)
I(o
bje
ctiv
e
PA)
Sco
re/9
Plo
tnik
off
etal
.(20
11)
XX
X(?
)X
X×
X×
6/9
Pie
tte
etal
.(20
11)
XX
X×
XX
×X
X7/
9
Kru
seet
al.(
2010
)X
XX
XX
XX
XX
9/9
Mar
tyn-
Nem
eth
etal
.(20
10)
n/a
n/a
Xn/
a×
××
××
1/9
Mat
hieu
etal
.(20
08)
XX
××
X×
××
X4/
9
Tayl
oret
al.(
2009
)X
X×
×X
X×
XX
6/9
Sko
ro-K
ondz
aet
al.(
2009
)X
X(?
)×
X(?
)×
×X
4/9
Dut
ton
etal
.(20
08)
XX
(?)
×X
X×
××
4/9
Klu
get
al.(
2008
)n/
an/
a×
n/a
×X
××
×1/
9
Spe
eret
al.(
2008
)n/
an/
a×
n/a
××
×X
×1/
9
Bro
oks
etal
.(20
07)
X×
XX
XX
××
X6/
9
Dun
stan
etal
.(20
06)
X×
X×
XX
××
X5/
9
Boy
det
al.(
2006
)n/
an/
aX
n/a
X×
××
X3/
9
Eng
elan
dLi
ndne
r(2
006)
XX
X×
×X
××
×4/
9
Two
Feat
hers
etal
.(20
05)
n/a
n/a
×n/
a×
X×
××
1/9
Bra
ndon
etal
.(20
03)
X×
××
××
×X
X3/
9
Gol
dhab
er-F
iebe
rtet
al.(
2003
)X
XX
XX
××
XX
7/9
Keys
erlin
get
al.(
2002
)X
XX
×X
X×
XX
7/9
Plo
tnik
off
etal
.,20
10X
XX
×X
×X
XX
7/9
Plo
tnik
off
etal
.(20
12)
XX
X×
×X
X×
×5/
9
Dav
ies
etal
.(20
08)
XX
××
XX
××
×4/
9
Less
etal
.(20
09)
X×
X×
XX
XX
×6/
9
Crit
eria
:A,
base
line
resu
ltsre
port
edse
para
tely
for
each
grou
p;B
,ra
ndom
izat
ion
clea
rlyde
scrib
edan
dad
equa
tely
com
plet
ed;
C,
drop
out≤
20%
for≤
6m
onth
sfo
llow
-up
and≤
30%
for>
6m
onth
sfo
llow
-up;
D,
asse
ssor
blin
ding
;E,i
nten
tion-
to-t
reat
anal
ysis
;F,c
onfo
unde
rsac
coun
ted
fori
nan
alys
es;G
,sum
mar
yre
sults
pres
ente
dan
des
timat
edef
fect
size
san
dpr
ecis
ion
estim
ates
;H,p
ower
calc
ulat
ion
repo
rted
and
stud
y
adeq
uate
lypo
wer
ed;I
,an
obje
ctiv
em
easu
reof
PAw
asus
ed.
Frontiers in Endocrinology | Diabetes January 2013 | Volume 4 | Article 3 | 14

Plotnikoff et al. Community-based physical activity interventions
a moderate risk of bias. Overall, this review demonstrates thatcommunity-based interventions utilizing a large PA componentcan be effective in treating T2D in terms of decreasing HbA1c lev-els, reducing weight (including BMI and waist circumference) andincreasing PA levels.
Eleven of the studies that reported HbA1c as an outcome mea-sure were pooled in the meta-analysis. Meta-analysis revealedcommunity-based PA interventions contribute to a lowering ofHbA1c by−0.32% (−26.99 mmol/mol) which approached statis-tical significance effect (p= 0.06). The results of the meta-analysesmay have indeed been stronger than what has been provided inthis report, as the control groups in three of the studies used in themeta-analysis (i.e., Dunstan et al., 2006; Engel and Lindner, 2006;Plotnikoff et al., 2011) received a greater intervention dose than“true controls” receiving no intervention and/or those receiving“standard practice.”
It is interesting to note that in a meta-analyses of 14 clini-cally based exercise trials in the T2D population, Boulé et al.(2001) reported exercise training decreased HbA1c by −0.66%(−30.71 mmol/mol) which is considered to significantly decreasethe clinical risk of diabetes complications in this population. Smallchanges in HbA1c may still be important from a public healthperspective, considering small changes at the individual levelcan translate to substantial changes within the population if thechanges are distributed across the entire target (T2D) population.Health promotion experts advocate that practical, low/minimalintensity interventions that might not have large clinical effects,but can be delivered to large numbers of participants, are morelikely to have a broader health impact (Tunis et al., 2003).
A variety of factors may have contributed to the limited changein HbA1c observed in the meta-analysis. A floor effect may haveoccurred in several studies because individuals may have had well-controlled diabetes at baseline. Some studies employed inclusioncriteria, where only individuals with high HbA1c levels at baselinewere admitted. The ADAPT study (Plotnikoff et al., 2012), one ofthe larger studies in this review that reported no impact on HbA1c,had a relatively low baseline level of HbA1c.
Different methods used to recruit individuals into the studiesmay also have had an impact on outcomes. Several of the studies inthis review had participant recruitment in the form of advertising(as employed by 6 of 22 studies). It is possible those who respond topublic advertising (e.g., media campaigns) may be a biased groupwho are more active and take “better care” of themselves. Thereis evidence that individuals who volunteer to participate in thesetypes of studies are healthier on average compared to those whodo not voluntarily participate in studies (Plotnikoff et al., 2008;Rosal et al., 2011).
Adherence to intervention studies may have also played a role.For example, a study conducted by Skoro-Kondza et al. (2009),included in this review, report a very low adherence resulting frommotivational barriers to program attendance. Also it is possiblethat individuals who are most in need of intervention treatmentdo not adhere to programs. For example, in the ADAPT study,Plotnikoff et al. (2012), found that many dropouts initially had lowlevels of PA, and it was also individuals most needy of PA inter-ventions that did not participate in the full length of the study.Future research should examine strategies to reach and encourage
inactive individuals who are genuinely in need of interventions toparticipate in research studies.
There was considerable heterogeneity in terms of the differ-ent intervention strategies used to promote PA. Some techniquesincluded structured group education programs, yoga classes, tele-phone counseling, YMBA membership, motivational techniques,providing multi-gym apparatus for home use and the use of laydiabetes facilitators. For adults with T2D, studies have shown bet-ter metabolic outcomes when interventions focus exclusively onPA compared to strategies that encompass multiple diabetes carebehaviors (Conn et al., 2007). However, this difference was notobserved in our review.
Considering that this review examined interventions thatused≥ 50% PA component, other factors of the program besidesPA may also have influenced HbA1c levels in participants, such aschanges in diet and sitting time. Fourteen of the 22 studies hada dietary component and/or measured dietary changes. However,studies have shown when diet and exercise approaches were com-bined, the effect on HbA1c was similar to the effect of exercisealone (Boulé et al., 2001). Further, no studies included the pro-motion of reducing sitting time behavior. Future studies shouldinclude strategies to promote the reduction of this sedentary activ-ity given its negative impact on metabolic health (van der Ploeget al., 2012).
In the set of studies reviewed, five studies (Dunstan et al.,2006; Brooks et al., 2007; Mathieu et al., 2008; Kruse et al., 2010;Plotnikoff et al., 2011) incorporated resistance training mode ofactivity either as the main focus of the intervention or as part of theintervention. Resistance training has been recognized as a usefultherapeutic tool for the treatment of a number of chronic diseasesand has been demonstrated as safe and efficacious for elderly andobese individuals (Eves and Plotnikoff, 2006). Resistance traininghas the potential for increasing muscle strength, lean muscle mass,and bone mineral density, which could enhance functional statusand glycemic control.
It is generally accepted that behavior change programs for PAthat are theoretically grounded are more efficacious/effective thana theoretical strategies (Biddle et al., 2007). In the reviewed stud-ies, six studies had interventions based in social-cognitive theories,or interventions that were tailored based on theories. Differenttheoretical frameworks utilized include Social Ecological Model,Health Belief Model, Theory of Planned Behavior, and Social-Cognitive Theory. In this regard, it should be noted that thereare limited PA theory-based, long-term studies with large samplestargeting the adult T2D population. Few studies have exploredthe mechanisms of behavior change in community-based inter-ventions for individuals with T2D. One notable exception is theADHERES study (Plotnikoff et al., 2010) which reported in a sec-ondary analysis that RT planning strategies mediated the effect ofthe intervention on RT behavior (Lubans et al., 2011). Researchersare encouraged to operationalize their interventions and test thehypothesized mediators of behavior change.
In this review, 10 studies reviewed employed self-report mea-sures for PA, and 12 studies employed objective measures.Although assessing objective measures of PA may not always be fea-sible in community-based interventions, objective measurementtechniques using recent technologies such as accelerometers and
www.frontiersin.org January 2013 | Volume 4 | Article 3 | 15

Plotnikoff et al. Community-based physical activity interventions
pedometers as well as GPS devices wherever possible should beused to assess levels of PA given the over-reporting in self-reportPA measures.
In terms of study follow-up, the maximum followed-up timewas 2 years (Brandon et al., 2003). In the literature, there is gener-ally limited information on long-term outcomes of interventions,and sharp declines in intervention benefits after a few months havealso been observed (Deakin et al., 2005). Future studies need toinvestigate the effectiveness of interventions to produce long-termchange in PA levels, and how effectiveness could be sustained byusing strategies such as booster sessions following interventions tofacilitate longer-term behavior change.
Considering that the studies included in this review representa variety of ethnic groups (Mexican, Latino, Caucasian, African-American), a range of age groups (ages 52 to 73), and were 64%female, study findings are perhaps by and large generalizable. How-ever, the variability between the economic and health status ofcountries included in this review (for example, USA and Canadavs. Jamaica and Costa Rica), must also be considered in the inter-pretation of the study’s results. In the meta-analysis, we did notconduct additional analyses to investigate intervention featuresthat may moderate intervention effectiveness (e.g., mode of deliv-ery, objective PA vs. self-report PA, age, sex) due to the relativelyfew number of studies that qualified for the analysis. Further stud-ies which collect such information could be useful to inform thedevelopment of future research and interventions. As the numberof trials of community-based interventions to increase PA grows,future research should attempt to isolate the impact of specificintervention features on PA change as well as implement highquality study-designs that will allow such investigations.
In terms of a health economical aspect, there is evidence oflower health care utilization and costs in T2D individuals whomeet minimum PA guidelines (Plotnikoff et al., 2008). Otherstudies have shown community-based programs that target PAappear to be cost-effective for individuals with diabetes (Jacobs-van der Bruggen et al., 2007; Roux et al., 2008). Community-basedapproaches to increase PA have the potential to improve program
adherence by using intervention strategies that directly addressfactors such as socio-economic, psychological, social, and culturalelements (Rosal et al., 2011). Although resource-intensive, clin-ical approaches can be effective. Future research may considerthe combination of clinical and community-based approaches tomaximize treatment effects.
Strengths of the study include being the first study, to ourknowledge, to meta-analyze solely on community-based interven-tions to increase PA. Studies representative of a variety of culturalgroups from different countries is an additional strength. Limi-tations include the difficulty in generalizing the contribution ofmulti-component interventions, and the relatively small numberof studies that were included in the meta-analysis. The reviewedstudies have moderate levels of risk bias in the methodologicalquality which should also be considered in the interpretation ofthese findings. Future community-based trials should be method-ologically more rigorous. Publication bias of studies should alsobe taken into consideration when interpreting the results of thismeta-analysis. Studies that do not find statistically significantresults may not be published either due to authors’ not attempt-ing to publish or journals not accepting the article for publica-tion, and therefore, this meta-analysis should be interpreted withcaution.
Overall, our findings demonstrate community-based PA inter-ventions can be effective for increasing PA and decreasing HbA1clevels. The change in HbA1c was clinically significant in the meta-analysis. Producing even small effects can be meaningful at a‘population level’ for adults living with T2D. As the number oftrials of community-based interventions to increase PA grows inthe future, the findings of this meta-analysis will need to be repli-cated, and intervention features and elements that may moderateintervention effectiveness can be further investigated.
ACKNOWLEDGMENTSRonald C. Plotnikoff is supported by a senior research fellow-ship salary award from the National Health and Medical ResearchCouncil (NHMRC), Australia.
REFERENCESBalducci, S., Zanuso, S., Nicolucci, A.,
De Feo, P., Cavallo, S., Cardelli, P.,et al. (2010). Effect of an inten-sive exercise intervention strategy onmodifiable cardiovascular risk fac-tors in subjects with type 2 diabetesmellitus: a randomized controlledtrial: the Italian diabetes and exer-cise study (IDES). Arch. Intern. Med.170, 1794–1803.
Biddle, S. J. H., Hagger, M. S., Chatzis-arantis, N. L. D., and Lippke,S. (2007). “Theoretical frameworksin exercise psychology,” in Hand-book of Sport Psychology, 3rdEdn, eds G. Tenenbaum and R.C. Eklund (New York: Wiley),537–559.
Boulé, N. G., Haddad, E., Kenny, G. P.,Wells, G. A., and Sigal, R. J. (2001).Effects of exercise on glycemic con-trol and body mass in type 2 diabetes
mellitus: a meta-analysis of con-trolled clinical trials. JAMA 286,1218–1227.
Boyd, S. T., Scott, D. M., and Augus-tine, S. C. (2006). Exercise for low-income patients with diabetes. Dia-betes Educ. 32, 385–393.
Brandon, L., Gaasch, D. A., Boyette,L. W., and Lloyd, A. M. (2003).Effects of long-term resistive train-ing on mobility and strength inolder adults with diabetes. J. Geron-tol. A Biol. Sci. Med. Sci. 58,M740–M745.
Brooks, N., Layne, J. E., Gordon, P.L., Roubenoff, R., Nelson, N. E.,and Castaneda-Sceppa, C. (2007).Strength training improves musclequality and insulin sensitivity in his-panic older adults with type 2 dia-betes. Int. J. Med. Sci. 4, 19–27.
Church, T. S., Blair, S. N., andCocreham, S. (2010). Effects of
aerobic and resistance training onhemoglobin A1c levels in patientswith type 2 diabetes. JAMA 302,2253–2262.
Conn, V., Hafdahl, A., Mehr, D.,LeMaster, J. W., Brown, S. A.,and Nielsen, P. J. (2007). Meta-bolic effects of interventions toincrease exercise among adults withtype 2 diabetes. Diabetologia 50,913–921.
Davies, M. J., Heller, S., Skinner, T.C., Campbell, M. J., Carey, M. E.,Cradock, S., et al. (2008). Effective-ness of the diabetes education andself-management for ongoing andnewly diagnosed (DESMOND) pro-gramme for people with newly diag-nosed type 2 diabetes: cluster ran-domised controlled trial. BMJ 336,491–495.
Deakin, T., McShane, C., Cade, J., andWilliams, R. (2005). Group based
training for self-management strate-gies in people with type 2 dia-betes. Cochrane Database Syst. Rev.2, CD003417.
Deeks, J. J., Altman, D. G., andBradburn, M. J. (2008). “Statisti-cal methods for examining hetero-geneity and combining results fromseveral studies in meta-analysis,” inSystematic Reviews in Health Care:Meta-Analysis in Context, 2nd Edn,Chap. 15, eds M. Egger, G. D. Smith,and D. G. Altman (London: BMJPublishing Group), doi: 10.1002/9780470693926.
Dunstan, D. W., Vulikh, E., Owen,N., Jolley, D., Shaw, J., and Zim-met, P. (2006). Communitycenter–based resistance train-ing for the maintenance ofglycemic control in adults withtype 2 diabetes. Diabetes Care 29,2586–2591.
Frontiers in Endocrinology | Diabetes January 2013 | Volume 4 | Article 3 | 16

Plotnikoff et al. Community-based physical activity interventions
Dutton, G. R., Provost, B. C., Tan, F., andSmith, D. (2008). A tailored print-based physical activity interventionfor patients with type 2 diabetes.Prev. Med. 47, 409–411.
Engel, L., and Lindner, H. (2006).Impact of using a pedometer on timespent walking in older adults withtype 2 diabetes. Diabetes Educ. 32,98–107.
Eves, N. D., and Plotnikoff, R. C. (2006).Resistance training and type 2 dia-betes. Diabetes Care 29, 1933–1941.
Gilmer, T. P., O’Connor, P. J., Man-ning, W. G., and Rush, W. A. (1997).The cost to health plans of poorglycemic control. Diabetes Care 20,1847–1853.
Goldhaber-Fiebert, J. D., Goldhaber-Fiebert, S. N., Tristán, M. L., andNathan, D. M. (2003). Random-ized controlled community-basednutrition and exercise interventionimproves glycemia and cardiovascu-lar risk factors in type 2 diabeticpatients in rural Costa Rica. DiabetesCare 26, 24–29.
Jacobs-van der Bruggen, M. A., Bos,G., Bemelmans, W. J., Hoogenveen,R. T., Vijgen, S. M., and Baan, C.A. (2007). Lifestyle interventions arecost-effective in people with differ-ent levels of diabetes risk: resultsfrom a modeling study. DiabetesCare 30, 128–134.
Keyserling, T. C., Samuel-Hodge, C.D., Ammerman, A. S., Ainsworth,B. E., Henríquez-Roldán, C. F.,Elasy, T. A., et al. (2002). Arandomized trial of an interven-tion to improve self-care behaviorsof African-American women withtype 2 diabetes. Diabetes Care 25,1576–1583.
Klug, C. D., Toobert, D. J., and Fogerty,M. (2008). Healthy changes™for liv-ing with diabetes. Diabetes Educ. 34,1053–1061.
Kruse, R. L., LeMaster, J. W., and Mad-sen, R. W. (2010). Fall and bal-ance outcomes after an interventionto promote leg strength, balance,and walking in people with diabeticperipheral neuropathy: “feet first”randomized controlled trial. Phys.Ther. 90, 1568–1579.
Less, L. A., Ragoobirsingh, D., Morri-son, E. Y., Boyne, M., and John-son, P. A. (2009). A preliminaryreport on an assessment of acommunity-based intervention fordiabetes control in adults withtype 2 diabetes. Fam. Pract. 27,i46–i52.
Lubans, D. R., Plotnikoff, R. C., Jung,M., Eves, N., and Sigal, R. (2011).Testing mediator variables in a resis-tance training intervention for obeseadults with type 2 diabetes. Psychol.Health 27, 1388–1404.
Martyn-Nemeth, P. A., Vitale, G. A., andCowger, D. R. (2010). A culturallyfocused exercise program in hispanicadults with type 2 diabetes. DiabetesEduc. 36, 258–267.
Mathieu, M., Brochu, M., and Béliveau,L. (2008). Diabetaction: changes inphysical activity practice, fitness, andmetabolic syndrome in type 2 dia-betic and at-risk individuals. Clin. J.Sport Med. 18, 70–75.
Nolan, C. J., Damm, P., and Prentki, M.(2011). Type 2 diabetes across gen-erations: from pathophysiology toprevention and management. Lancet378, 169–181.
Piette, J. D., Richardson, C., Himle, J.,Duffy, S., Torres, T., Vogel, M., etal. (2011). A randomized trial oftelephonic counseling plus walkingfor depressed diabetes patients. Med.Care 49, 641–648.
Plotnikoff, R. (2006). Physical activ-ity in the management of diabetes:population-based perspectives andstrategies. Can. J. Diabetes 30, 52–62.
Plotnikoff, R. C., Eves, N., Jung, M.,Sigal, R. J., Padwal, R., and Karuna-muni, N. (2010). Multicomponent,home-based resistance training forobese adults with type 2 diabetes: arandomized controlled trial. Int. J.Obes. 34, 1733–1741.
Plotnikoff, R. C., Karunamuni, N.,Courneya, K., Sigal, R., Johnson,J., and Johnson, S. (2012). TheAlberta diabetes and physical activ-ity trial (adapt): a randomized trialevaluating theory-based interven-tions to increase physical activity inadults with type 2 diabetes. Ann.Behav. Med. doi: 10.1007/s12160-012-9405-2. [Epub ahead of print].
Plotnikoff,R. C.,Karunamuni,N., John-son, J., Kotovych, M., and Sven-son, L. (2008). Health-related behav-iours in adults with diabetes: asso-ciations with health care utilizationand costs. Can. J. Public Health 99,227–231.
Plotnikoff, R. C., Pickering, M., Glenn,N., Doze, S., Reinbold-Matthews,M., McLeod, L., et al. (2011). Theeffects of a supplemental, theory-based physical activity counselingintervention for adults with type2 diabetes. J. Phys. Act. Health 8,944–954.
Rosal, M. C., Ockene, I. S., Restrepo, A.,White, M. J., Borg, A., Olendzki, B.,et al. (2011). Randomized trial of aliteracy-sensitive, culturally tailoreddiabetes self-management interven-tion for low-income latinos. DiabetesCare 34, 838–844.
Roux, L., Pratt, M., Tengs, T., Yore,M., Yanagawa, T., Van Den Bos, J.,et al. (2008). Cost effectiveness ofcommunity-based physical activityinterventions. Am. J. Prev. Med. 35,578–588.
Shaw, J. E., Sicree, R. A., and Zimmet,P. Z. (2010). Global estimates of theprevalence of diabetes for 2010 and2030. Diabetes Res. Clin. Pract. 87,4–14.
Sigal, R. J., Tai, S., Gadelrab, R., Drince-vic, D., and Greenhalgh, T. (2007).Effects of aerobic training, resistancetraining, or both on glycemic con-trol in type 2 diabetes: a randomizedtrial. Ann. Intern. Med. 147, 357–369.
Skoro-Kondza, L., Tai, S., Gadelrab,R., Drincevic, D., and Greenhalgh,T. (2009). Community based yogaclasses for type 2 diabetes: anexploratory randomised controlledtrial. BMC Health Serv. Res. 9:33.doi:10.1186/1472-6963-9-33
Speer, E. M., Reddy, S., Lommel, T.S., Fischer, J. G., Stephens, H.,Park, S., et al. (2008). Diabetesself-management behaviors and a1cimproved following a community-based intervention in older adults inGeorgia senior centers. J. Nutr. Elder.27, 179–200.
Stamler, J., Vaccaro, O., Neaton, J. D.,and Wentworth, D. (1993). Diabetes,other risk factors, and 12-yr cardio-vascular mortality for men screenedin the multiple risk factor interven-tion trial. Diabetes Care 16, 434–444.
Taylor, J. D., Fletcher, J. P., and Tiarks, J.(2009). Impact of physical therapist–directed exercise counseling com-bined with fitness center–based exer-cise training on muscular strengthand exercise capacity in people withtype 2 diabetes: a randomized clini-cal trial. Phys. Ther. 89, 884–892.
Tunis, S. R., Stryer, D. B., and Clancy,C. M. (2003). Practical clinical tri-als: increasing the value of clinicalresearch for decision making in clin-ical and health policy. JAMA 290,1624–1632.
Two Feathers, J., Kieffer, E. C.,Palmisano, G., Anderson, M.,Sinco, B., Janz, N., et al. (2005).Racial and ethnic approachesto community health (REACH)
detroit partnership: improvingdiabetes-related outcomes amongAfrican American and Latinoadults. Am. J. Public Health 95,1552–1560.
Vachon, G. C., Ezike, N., Brown-Walker,M.,Chhay,V.,Pikelny, I., and Pender-graft, T. B. (2007). Improving accessto diabetes care in an inner-city,community-based outpatient healthcenter with a monthly open-access,multistation group visit program. J.Natl. Med. Assoc. 99, 1327–1336.
van der Ploeg, H., Chey, T., Korda,R., Banks, E., and Bauman, A.(2012). Sitting time and all-causemortality risk in 222 497 Aus-tralian adults. Arch. Intern. Med. 172,494–500.
van Sluijs, E. M., McMinn, A. M., andGriffin, S. J. (2007). Effectiveness ofinterventions to promote physicalactivity in children and adolescents:systematic review of controlled tri-als. BMJ 335, 703.
Young, M. D., Morgan, P. J., Plotnikoff,R. C., Callister, R., and Collins, C.E. (2012). Effectiveness of male-only weight loss and weight lossmaintenance interventions: a sys-tematic review with meta-analysis.Obes. Rev. 13, 393–408.
Conflict of Interest Statement: Theauthors declare that the research wasconducted in the absence of any com-mercial or financial relationships thatcould be construed as a potential con-flict of interest.
Received: 27 September 2012; paperpending published: 22 October 2012;accepted: 07 January 2013; publishedonline: 29 January 2013.Citation: Plotnikoff RC, Costigan SA,Karunamuni ND and Lubans DR(2013) Community-based physical activ-ity interventions for treatment of type2 diabetes: a systematic review withmeta-analysis. Front. Endocrin. 4:3. doi:10.3389/fendo.2013.00003This article was submitted to Frontiersin Diabetes, a specialty of Frontiers inEndocrinology.Copyright © 2013 Plotnikoff, Costigan,Karunamuni and Lubans. This is anopen-access article distributed under theterms of the Creative Commons Attribu-tion License, which permits use, distrib-ution and reproduction in other forums,provided the original authors and sourceare credited and subject to any copy-right notices concerning any third-partygraphics etc.
www.frontiersin.org January 2013 | Volume 4 | Article 3 | 17
Top Related
Copyright © 2022 FDOKUMEN

