






Bahasa
Halaman
Hukum


Homozygosity of MSH2 c.1906G?C germline mutationis associated with childhood colon cancer, astrocytomaand signs of Neurofibromatosis type I
Helen Toledano Æ Yael Goldberg Æ Inbal Kedar-Barnes Æ Hagit Baris ÆRinnat M. Porat Æ Chen Shochat Æ Dani Bercovich Æ Eli Pikarsky ÆIsraela Lerer Æ Isaac Yaniv Æ Dvorah Abeliovich Æ Tamar Peretz
Published online: 20 December 2008
� Springer Science+Business Media B.V. 2008
Abstract Hereditary non-polyposis colorectal cancer is a
cancer predisposition syndrome known to be caused by
heterozygous germline mutations in DNA mismatch repair
genes (MMR) most commonly hMLH1, hMSH2, hMSH6.
Heterozygous mutations in one of these genes confer an
increased risk, mainly for colon and endometrial cancer.
Recently, several publications identified that biallelic
mutations in the MMR genes are associated with a more
severe phenotype, including childhood malignancies and
signs of neurofibromatosis type I (NF1). We report on a non-
consanguineous Ashkenazi Jewish family with two affected
siblings with features of NF1, colon cancer and astrocytoma
at age 13 and 14. Their mother developed endometrial
cancer at age 54. Their father had leukoplakia of the vocal
cords with a family history of pancreatic cancer. Molecular
and pathology studies were done on the tumor tissue and on
genomic DNA of family members. Tumor testing demon-
strated a high degree of microsatellite instability (MSI
analysis), expression of MLH1 and absence of expression of
both MSH2 and MSH6 proteins. A biallelic c.1906G [ C
(p.A636P) mutation in the hMSH2 gene was detected in the
blood of one affected child. Parental genetic testing showed
that each parent was heterozygote for the mutation. The
c.1906G [ C mutation is a founder mutation in the Ashke-
nazi Jewish population. To our knowledge this is the first
report of homozygosity for this founder mutation.
Keywords HNPCC, NF1 � Ashkenazi � Bi-allelic �MMR � MSI � MSH2
Abbreviations
AC Amsterdam criteria
CCS Childhood cancer syndrome
CRC Colorectal cancer
DHPLC Denaturing high performance liquid
chromatography
HNPCC Hereditary non-polyposis colorectal cancer
IHC Immunohistochemistry
MLPA Multiplex ligase dependent probe amplification
MMR Mismatch repair
MMR-
D
Mismatch repair deficiency
MSI Microsatellite instability
NF1 Neurofibromatosis type 1
H. Toledano and Y. Goldberg contributed equally to the paper.
H. Toledano � I. Yaniv
Schneider Children’s Medical Center of Israel and Sackler
Faculty of Medicine, Tel Aviv University, Tel Aviv, Israel
Y. Goldberg (&) � T. Peretz
Sharett Institute of Oncology, Hadassah-Hebrew University
Medical Center, P.O. Box 12000, 91120 Jerusalem, Israel
e-mail: [email protected]
I. Kedar-Barnes � H. Baris
The Raphael Recanati Genetic Institute Rabin Medical Center,
Beilinson Hospital, Petah Tikva, Israel
R. M. Porat � E. Pikarsky
Department of Pathology, Hadassah-Hebrew University Medical
Center, Jerusalem, Israel
C. Shochat � D. Bercovich
The Human Molecular Genetics & Pharmacogenetics lab,
Migal - Galilee Bio-Technology Center, Kiryat-Shmona, Israel
I. Lerer � D. Abeliovich
Department of Human Genetics, Hadassah-Hebrew University
Medical Center, Jerusalem, Israel
D. Bercovich
Tel Hai Academic College, Tel Hai, Israel
123
Familial Cancer (2009) 8:187–194
DOI 10.1007/s10689-008-9227-3

Introduction
Hereditary non-polyposis colorectal cancer (HNPCC) is an
autosomal dominant inherited condition known to be
associated with a predisposition to several malignancies,
mainly colorectal cancer (CRC) and endometrial cancer.
Other malignancies such as ovarian, gastric, small intes-
tine, pancreas, bile duct, urinary tract and brain tumors
have also been associated with HNPCC [1, 2]. Typically,
affected individuals with HNPCC present with cancer in
the fourth or fifth decade but in some families the pre-
sentation may be in the third decade or later in the sixth
decade [2]. Germline and somatic mutations in the MMR
genes have been implicated in HNPCC and in 15–20% of
sporadic CRC [1, 3]. In HNPCC, defined by the presence of
a MMR gene mutation, mutations in hMLH1 and hMSH2
account for approximately 90% of cases, hMSH6 for 10%
and hPMS2 accounts for less than 5% [4].
Biallelic mutations in the MMR genes lead to a dis-
tinctive syndrome, characterized by hematological
malignancies, tumors of brain and bowel early in child-
hood, often associated with signs of neurofibromatosis type
1 (NF1). This syndrome has been referred to as childhood
cancer syndrome (CCS) [5] and mismatch repair deficiency
syndrome (MMR-D) [6]. In 1999, Wang et al. were the first
to describe the association between compound heterozy-
gous mutation in MLH1 gene, early onset extracolonic
cancers and signs of NF1 [7]. Menko et al. described a
child with multiple cafe-au-lait spots (CLS), oligodendro-
glioma and rectal cancer who was homozygous for a
mutation in hMSH6 gene [8]. Kruger et al. [9] reported on
six children from two consanguineous families with a
homozygous PMS2 mutation, who suffered from glioblas-
toma, colorectal cancer, lymphoma and other HNPCC-
associated tumors at early ages. Kruger et al. also reviewed
reports of 43 individuals with biallelic MMR germline
mutations in 23 different families. Brain tumors occurred in
most families, followed by hematological malignancies and
intestinal tumors [9]. All affected individuals with CCS had
clinical features characteristic of NF1: either CLS, or CLS
and axillary freckling. The median age of tumor onset was
9 years, ranging from 1 to 24 years.
Mouse knockouts for all MMR genes have been gen-
erated [10–12]. When comparing the tumor spectra of these
homozygous mouse models to the spectrum of humans
with biallelic mutations it becomes clear that they are
similar in terms of frequent lymphoma development and
relatively low abundance of gastrointestinal tumors. A
difference is that brain tumors are very rare and neurofi-
bromas and CLS are absent in mouse MMR knockouts. In
Msh2 deficient mice there is an increasing rate of somatic
mutations in genes associated with tumorigenesis [13].
Knockout mutants of the three major MMR genes in
zebrafish mimic distinct features of the human disease and
are complementary to mouse models. They develop pre-
dominantly, neurofibromas/malignant peripheral nerve
sheath tumors at low frequencies [14].
Several mutations in HNPCC have been described as
founder mutations in certain populations; two founder
mutations in the MLH1 gene account for 63% of all dele-
terious mutations identified in HNPCC families in the
Finnish population [15]. The MSH2 c.1906G [ C mutation
was initially described by Yuan et al. in an Ashkenazi
Jewish family that fulfilled the Amsterdam criteria for the
clinical diagnosis of HNPCC [16]. This finding was con-
firmed by Foulkes et al. [17]. The mutation results in a
substitution of alanine to proline at codon 636 (A636P) in
the MSH2 protein, associated with an alteration in MSH2
Crystal structure. Foulkes et al. [17] found that all CRC
tumors, from carriers of the mutation, were MSI-H and
were negative for the expression of both MSH2 and MSH6
proteins in all tumors examined by IHC studies. This
finding could be explained by the fact that MSH2 and
MSH6 form a functional complex-MutSa, as a result
MSH2 loss often causes concurrent loss of MSH6.
The MSH2 c.1906G [ C mutation was examined in a
population-based series of Ashkenazi Jews with colorectal
cancer and shown to be rare (0.44%), yet highly penetrant;
In a combined consecutive series from Israel, New York
and Toronto, the A636P mutation was found in 8 of 1,345
(0.59%) Ashkenazi Jewish CRC cases versus 0 of 1,588
healthy Ashkenazi Jewish controls [17]. It has been
reported that 20–30% of Ashkenazi Jewish families that
fulfill Amsterdam criteria carry this mutation [18, 19].
Hereby, we describe a family with two siblings who
died from cancer in childhood. One was affected with
features of NF1 and astrocytoma and the other sibling with
features of NF1, astrocytoma and CRC. Genetic studies for
HNPCC done on one sibling found that he was homozy-
gous for a c.1906G [ C (A636P) mutation in the MSH2
gene. Both parents were found to be heterozygous for the
mutation. None of them come from a family that complies
with the Amsterdam Criteria, or fulfills the Bethesda
guidelines.
Materials and methods
Patient data
The proband, a 14-year-old boy, presented with a two-
month history of fatigue, mild weight loss, falls, intermit-
tent melena and fresh blood per rectum. A blood count
revealed hemoglobin of 7.7 g/dl with microcytic indices.
Past history was remarkable for the fact that since child-
hood he had been noted to have multiple CLS on the skin.
188 H. Toledano et al.
123

He was presumed to have NF1 and had been seen inter-
mittently in an NF clinic. Brain MRI studies 2 years earlier
reportedly showed changes in the temporal region consis-
tent with the diagnosis of NF1. On examination at the
pediatric day center he appeared pale, thin and unwell. He
had torticollis and ataxia.
A family history of a brother who had died of a
malignant brain tumor was reported. The clinical exami-
nation and his family history prompted an immediate MRI
of the brain which revealed two separate lesions. One was
in the temporal area—this had been present on the MRI
from 2 years previously but was considerably enlarged and
the other was a large lesion in the pons with an appearance
of a diffuse brainstem glioma that had not been evident on
the previous MRI (Fig. 1a). He underwent resection of the
temporal lesion only and pathology revealed a fibrillary
astrocytoma (grade II).
He then had a gastrointestinal workup for the anemia,
which included an upper GI endoscopy and a barium study
of the small bowel that were reported as normal. However,
colonoscopy revealed a large mass in the rectum 3 cm from
the anal sphincter and there were 20–30 polyps throughout
the large bowel of different sizes and biopsies were taken.
Pathology revealed the polyps to be tubulo-villous adeno-
mata and the rectal mass was a well differentiated
adenocarcinoma. Tumor markers CEA and CA19-9 were
normal. MRI demonstrated involvement of the peri-rectal
fat and PET-CT showed uptake in the mass and several of
the polyps but not in the lymph nodes and there was no
evidence of distant metastases.
In view of the average 1 year life expectancy following
diagnosis of a brain stem glioma there was debate
regarding the management of the rectal tumor. However,
longer than average survival has been described for glio-
mas in some genetic conditions such as Turcot syndrome
and after discussion with the family it was decided to start
aggressive management of his rectal tumor. Since imme-
diate surgery for the rectal mass would have involved
permanent loss of sphincter function, initial chemo-radia-
tion with the hope of shrinking the tumor and performing
sphincter-sparing surgery at a later date was attempted. At
the same time, he began suffering from increasing right-
sided weakness and falls and MRI showed increased size of
the brain stem lesion so that he received radiation therapy
simultaneously to the brain and rectum. Imaging studies
performed 6 weeks after completion of radiation showed
an improvement in the brain lesion but increase in size of
the rectal mass, making sphincter sparing surgery impos-
sible. Since colonic polyposis is a premalignant condition
and some of his polyps were already large and positive on
the PET scan he underwent panproctocolectomy with
permanent ileostomy. Pathology confirmed adenocarci-
noma of the rectum without lymph node involvement and
approximately 100 polyps in the large bowel.
Post-operatively he received adjuvant chemotherapy for
the rectal tumor with the FOLFOX regimen but had early
relapse at the rectal stump 2 months post-operatively. He
received second line therapy with FOLFIRI and Avastin
but by 11 months post diagnosis he was suffering from
intractable rectal pain as well as neurological deterioration
and he died at 1 year following the diagnosis.
At the time of his diagnosis with two concurrent tumors
and the death of their previous son, increasing family anxiety
prompted referral to genetic counseling. Physical examina-
tion by the geneticist revealed: head circumference 51 cm
(\2%), multiple CLS scattered over the body of which 21
were between 15 and 55 mm in diameter and multiple
smaller spots. There was inguinal and axillary freckling.
Asymmetrical facies (right [ left) was evident. Neurologi-
cal examination was normal except for mild imbalance
exhibited on tandem walk test only. Ophthalmological
evaluation excluded Lisch nodules but bilateral retinal
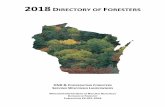
Fig. 1 MRI of brain tumor. a MR T2 weighted sagittal image of the
brain at diagnosis. Hyperintensity of the pons and medulla is seen,
compatible with a brain stem tumor. b, c MR T1 weighted fat
suppressed axial image of the lower pelvis post Gadolinium injection.
b At diagnosis: irregular thickening of the rectal wall is seen,
indicative of tumoral involvement. 10 months post diagnosis. c Local
recurrence is evident: a large necrotic mass is seen between the
sacrum and the bladder
Homozygosity of MSH2 c.1906G?C Ashkenazi mutation 189
123

hyperpigmentation raised the possibility of congenital
hypertrophy of the retinal pigment epithelium (CHRPE).
Targeted physical examination of his family members
included paternal head circumference of 54.4 cm (25%),
maternal head circumference of 52 cm (2%). No CLS were
observed on his father’s and mother’s dermal examination.
His healthy siblings had one CLS each.
Family history
The proband was the youngest of four siblings: two
apparently healthy siblings and another brother who was
diagnosed with anaplastic astrocytoma and NF1 features
and died at the age of 13. During the proband’s treatment
his father received radiation for severe, progressive lar-
yngeal leukoplakia and his mother was diagnosed age 54
with endometrial carcinoma and underwent a hysterec-
tomy. A paternal grandfather had been diagnosed with
pancreatic cancer at age 61 and died soon after. All living
first-degree relatives had a colonoscopy that was reported
as normal (Fig. 2).
Tumor testing
Tumor tissue was obtained from archived paraffin blocks.
Normal and pathological tissue of the colon were differen-
tially marked on the slide. DNA extraction from the paraffin
embedded tissues was performed as described [20]. DNA
was extracted from peripheral blood lymphocytes using the
QIAGEN DNA Isolation kit (QIAGEN, Germany).
MSI analysis was performed by a fluorescence-based
PCR method as described [21]. PCR products were ana-
lyzed on ABI Sequencer (3100) using GeneScan and
Genotyper software (PE Applied Biosystems).
Immunohistochemistry analysis
Five micro meter paraffin sections were de-waxed and
hydrated through graded ethanols, antigen retrieval was
done either with 20 mM citrate buffer pH 6.0 (hMSH2) or
with Borg Decloaker (Biocare Medical) pH 9.5 (hMLH1
and hMSH6) in a pressure cooker (Biocare Medical).
Slides were incubated with the indicated primary antibody,
diluted 1:50 in CAS-Block (Zymed) for overnight at 48C,
washed with Optimax (biogenex), incubated with MACH 3
Mouse HRP Polymer (Biocare Medical) and developed
with DAB. Normal cells showing strong nuclear staining
for the MMR proteins were used as an internal positive
control. Mouse monoclonal antibodies used were: hMLH1:
clone G168-15; hMSH2: clone FE11; hMSH6: clone BC/
44 from Biocare Medical.
DHPLC homozygous mutations screening
Mutation testing of the MMR genes was performed using a
combination of DHPLC and semiquantitative fluorescent
multiplex–PCR analysis. To identify homozygous muta-
tions, 10 ll PCR product of wild-type DNA, and 10 ll
PCR product of sample DNA were mixed 1:1 and dena-
tured at 95�C. This enabled detection of homozygous
Fig. 2 An abbreviated pedigree
of the reported family: Squaresmales; circles females; diagonalbars deceased; black mini-squares cancer; MSH2/
MSH2—homozygous for the
c.1906C [ G mutation;
w/w—wild-type for mutation;
w/MSH2 heterozygous for
mutation
190 H. Toledano et al.
123

mutations by formation of a heteroduplex [22]. All exonic
fragments of each gene, including intron junctions, were
amplified individually. PCR and DHPLC (WAVE, Trans-
genomic Inc., Omaha, NE) were preformed as described
previously [18, 23].
Testing for the Ashkenazi Jewish mutation
The c.1906G [ C was tested by allele specific amplifica-
tion as described in [18]. PCR conditions: 94�C—20 min;
35 cycles of 94�C—30 s; 61�C—1 min; 72�C—1 min;
final extension 20 min—72�C. PCR products run on 3%
NuSieve-Agarose gel (FMC-CAMBREX) in TBE buffer,
stained with ethidium bromide and visualized under UV
illumination.
Results
Tumor analysis
IHC
Immunostaining with antibodies against MLH1, MSH2 and
MSH6 was performed on tumor samples derived from the
proband, 14-year-old boy and from the mother. Immuno-
staining of the adenocarcinoma of the rectum from the
14-year-old patient shows nuclear staining for MLH1 both
in the tumor and in the normal cells (Fig. 3a) indicating the
retained protein, whereas the adenocarcinoma cells show
loss of nuclear staining for MSH2 and MSH6 (Fig. 3b, c).
Interestingly, the normal cells were also devoid of nuclear
staining for MSH2. The mother’s endometrial adenocar-
cinoma showed a similar pattern of loss of MSH2 and
MSH6 staining, with retained MLH1 staining as demon-
strated in Fig. 3d–i.
MSI (child, mother)
both tumors showed high degree of MSI in DNA extracted
from tumor tissue (Fig. 4) and showed microsatellite sta-
bility in DNA extracted from peripheral leukocytes, as
shown in Fig. 4. As can be seen, no difference in the pat-
tern of stability was seen between the heterozygote and the
homozygote samples.
Molecular analysis
Based on the results obtained from tumor testing, we tested
DNA from peripheral leukocytes. Genetic studies on the
Fig. 3 Immunostaining with antibodies against MLH1, MSH2 and
MSH6: Positive staining with antibodies against MSH2 and MSH6 is
represented by the presence of nuclear brown staining. Thick arrowsindicate tumor cells. Arrow heads indicate internal positive control
cells, either stromal or epithelial. Sections of moderately differentiated
adenocarcinoma of the rectum (a–c) show retained nuclear staining for
MLH1 (a) and loss of MSH2 and MSH6 staining (b, c). Endometrial
tissue with positive MLH1 staining in normal (d) and tumor cells (e) but
negative MSH2 and MSH6 staining in tumor nuclei (g, i)
Homozygosity of MSH2 c.1906G?C Ashkenazi mutation 191
123

proband revealed a homozygous c.1906G [ C germline
mutation in the hMSH2 gene (Fig. 5). Both parents were
found to be carriers of a heterozygous mutation. The pro-
band’s sister did not carry the mutation and a living brother
was found to be a healthy carrier for the mutation (Fig. 2).
Discussion
We report two siblings from a non-consanguinous Ashkenazi
family who present with CCS due to biallelic inheritance of
the Ashkenazi c.1906G [ C founder mutation in the MSH2
gene. Both had features of NF1, one died from Astrocytoma,
and the other had colon cancer and Astrocytoma at age 13 and
14, respectively. Their mother developed endometrial cancer
at age 54. Their father had leukoplakia of the vocal cords with
a family history of pancreatic cancer. Neither of the parental
families fulfilled the Amsterdam Criteria.
In contrast to the well-known phenotype caused by
heterozygous MMR gene mutations, little is known about
the phenotype of the very rare biallelic MMR mutation
carriers. Until recently, less than 100 carriers with biallelic
Fig. 4 DHPLC and direct sequencing of the homozygote son and
heterozygote mother. Screening for mutations in the MSH2 gene by
the DHPLC and direct sequencing of PCR fragments with abnormal
chromatograms in comparison to wild-type demonstrates the exis-
tence of a homozygous mutation (A636P). a, b The homozygous
mutation (son) was detected by mixing the patient PCR products with
a wild-type PCR (1:1) before denaturation and reaniling (b). cHeterozygous DNA (mother) was detected by regular screening of
PCR products after denaturation and reaniling
Fig. 5 MSI analysis by the
BAT25 marker in peripheral
blood and tumor tissue from
heterozygote mother and
homozygous son. The pattern
of stability in the blood and the
pattern of instability in tumor
is similar
192 H. Toledano et al.
123

MMR germline mutations have been reported (reviewed in
[9]). Only two families with mutations in the MSH2 gene
were reported [24, 25]. To our knowledge there have been
no previous reports of homozygosity for the Ashkenazi
c.1906G [ C founder mutation in the MSH2 gene.
The clinical phenotype of the affected brothers raised
the diagnosis of CCS. However, given the clinical pre-
sentation of a brain tumor and multiple colonic polyps
([100) suggesting Turcot syndrome, a blood sample of the
proband was sent for sequencing of the APC gene.
Sequencing of exon 1–14 and 3,000 bases from the 50 of
exon 15 did not reveal any mutations (data not shown).
Though the proband presented with features of NF1, the
lack of suggestive family history and some features that did
not support this diagnosis (small head circumference, no
neurofibromas, and presence of multiple colonic polyps)
did not support this diagnosis. The age of onset of malig-
nancies, the presence of the features of NF1 in both siblings
and their absence in both parents, supported the diagnosis
of CCS, but the absence of a suggestive family history did
not corroborate the diagnosis. However, this is in line with
previous reports of biallelic MMR gene mutation carriers;
all had features of NF1, mostly multiple CLS, but seldom
fulfilled the NIH diagnostic criteria for NF1. Interestingly,
an absence of significant family history has been reported
in cases of CCS; Kruger et al. have already reported that
family history does not seem to be a good predictor for
identifying CCS, while the early onset of hematological
malignancies, brain or intestinal tumors together with signs
of NF1 identified CCS in 80% (20 out of 25) of families
with biallelic MMR gene germline mutation carriers [9].
It has been suggested that the NF1 gene is an early target
in embryogenesis of carriers of biallelic MMR gene
mutations. Puisieux reports that the NF1 gene appears to be
a preferential mutational target [26]. This is further sup-
ported by Wang et al. [27], showing a higher rate of
mutations in the NF1 gene in highly unstable human cell
lines and tumors, and in Mlh1 knockout mice compared to
MMR-sufficient tissue. Still, the link between these two
syndromes or the common features is yet to be clarified.
Patients carrying a homozygous deletion of an MMR
gene have a different spectrum of tumors than that of
heterozygotes; specifically, these patients have a higher
occurrence of nervous system tumors. While we cannot
definitely explain this different phenotype we would like to
suggest two possible explanations that should be further
explored: 1. The window of opportunity hypothesis—it is
possible that some tumors can only develop if the initiating
mutation occurs up to a certain time point in life. If this is
the case, than it is clear why homozygotes will be more
susceptible to such tumors. 2. The non-cell autonomous
effect hypothesis—it has been shown that mast cells
lacking one allele of NF1 play an important role in the
pathogenesis of plexiform neurofibromas in patients with
NF1 in a non-cell autonomous way through the secretion of
factors that facilitate the growth of tumor cells. It is possible
that in homozygotes for MMR genes the microenviron-
mental deficiency plays a similar role in the tumors unique
for this syndrome.
We identified MSI-H in the tumor tissues from the pro-
band and a stable pattern in leukocyte DNA. Stable pattern in
non-neoplastic cells is in line with other reports [28, 29] and
with some knockout models of the MMR genes. However,
some others report MSI in non tumoral cells [7] confirming
the constitutional defect in DNA MMR. It has been sug-
gested that the different results may be explained by the lack
of clonal populations in the peripheral blood sample, or
from the relative advantage of stable cells in the normal
tissue.
A characteristic phenomenon of HNPCC tumors is loss
of nuclear expression of MMR proteins detectable by
immunohistochemical procedures [30, 31]. Indeed, IHC for
MSH2 expression performed in both examined tumors,
(namely the proband’s colorectal tumor and the mother’s
endometrial adenocarcinoma), exhibited clear loss of
MSH2 expression (Fig. 3). Our results, that tumor cells
harboring the missense A636P mutation show absence of
MSH2 protein by immunohistochemical analysis, are in
agreement with the data reported by Foulks et al. [17].
While the correlation between the absence of MSH2
staining and the pathogenicity of the missense mutation is
notable, the fact that a single amino acid substitution in
MSH2 protein results in both distortion of the antigenic site
and MMR function loss may indicate that the mutated
protein is unstable. Testing recombinant MSH2-A636P
protein for MMR efficiency by in vitro assay showed a
complete loss of function [32]. A636 is a non-conserved
residue adjacent to a conserved region near the ATP-DNA
binding region. Therefore, another suggested explanation
for the functional loss is that an inflexible adenosine to
proline substitution may cause steric hindrance which not
only changes the antibody recognition site, but also alters
an otherwise conserved region in the protein and possibly,
interferes with its function.
The MSH2 c.1906G [ C mutation was shown to be
relatively rare among unselected Ashkenazi CRC patients,
yet highly penetrant [33]; surprisingly, none of the parental
families in our pedigree fulfilled the AC, and hardly
comply with the Bethesda guidelines. Of note, we and
others have previously reported few Ashkenazi families
with this mutation that also did not even comply with the
Bethesda guidleines [18].
The incidence of the c.1906G [ C founder mutation is
estimated to be very low in the Ashkenazi population.
Accordingly the chance of such an event to occur is very
rare. But, it is important that children, who have multiple
Homozygosity of MSH2 c.1906G?C Ashkenazi mutation 193
123

tumors and CLS, will be tested for the possibility of
biallelic MMR mutations [34]. One should be aware of the
occurrence of this syndrome also among non-consanguin-
eous families, given the presence of a founder mutation.
Acknowledgments This work was supported, in part, by the Israeli
Cancer Association, and by the Levinace Friedl foundation.
References
1. Lynch HT, Smyrk TC, Watson P et al (1993) Genetics, natural
history, tumor spectrum, and pathology of hereditary nonpolyp-
osis colorectal cancer: an updated review. Gastroenterology
104:1535–1549
2. Vasen HF, Wijnen JT, Menko FH et al (1996) Cancer risk in
families with hereditary nonpolyposis colorectal cancer diag-
nosed by mutation analysis. Gastroenterology 110:1020–1027.
doi:10.1053/gast.1996.v110.pm8612988
3. Peltomaki P, Vasen HF (1997) Mutations predisposing to
hereditary nonpolyposis colorectal cancer: database and results of
a collaborative study. The International Collaborative Group on
Hereditary Nonpolyposis Colorectal Cancer. Gastroenterology
113:1146–1158. doi:10.1053/gast.1997.v113.pm9322509
4. Boland CR (2000) Molecular genetics of hereditary nonpolyposis
colorectal cancer. Ann N Y Acad Sci 910:50–59. discussion 59–61
5. De Vos M, Hayward BE, Picton S et al (2004) Novel PMS2
pseudogenes can conceal recessive mutations causing a distinc-
tive childhood cancer syndrome. Am J Hum Genet 74:954–964.
doi:10.1086/420796
6. Scott RH, Mansour S, Pritchard-Jones K et al (2007) Medullo-
blastoma, acute myelocytic leukemia and colonic carcinomas in a
child with biallelic MSH6 mutations. Nat Clin Pract Oncol
4:130–134. doi:10.1038/ncponc0719
7. Wang Q, Lasset C, Desseigne F et al (1999) Neurofibromatosis
and Early Onset of Cancers in hMLH1-deficient Children. Cancer
Res 59:294–297
8. Menko FH, Kaspers GL, Meijer GA et al (2004) A homozygous
MSH6 mutation in a child with cafe-au-lait spots, oligodendro-
glioma and rectal cancer. Fam Cancer 3:123–127. doi:
10.1023/B:FAME.0000039893.19289.18
9. Kruger S, Kinzel M, Walldorf C et al (2008) Homozygous PMS2
germline mutations in two families with early-onset haematologi-
cal malignancy, brain tumours, HNPCC-associated tumours, and
signs of neurofibromatosis type 1. Eur J Hum Genet 16:62–72.
doi:10.1038/sj.ejhg.5201923
10. de Wind N, Dekker M, Berns A et al (1995) Inactivation of the
mouse Msh2 gene results in mismatch repair deficiency, meth-
ylation tolerance, hyperrecombination, and predisposition to
cancer. Cell 82:321–330. doi:10.1016/0092-8674(95)90319-4
11. Reitmair AH, Schmits R, Ewel A et al (1995) MSH2 deficient
mice are viable and susceptible to lymphoid tumours. Nat Genet
11:64–70. doi:10.1038/ng0995-64
12. Reitmair AH, Redston M, Cai JC et al (1996) Spontaneous
intestinal carcinomas and skin neoplasms in Msh2-deficient mice.
Cancer Res 56:3842–3849
13. Sohn KJ, Choi M, Song J et al (2003) Msh2 deficiency enhances
somatic Apc and p53 mutations in Apc ± Msh2-/- mice. Car-
cinogenesis. 24(2):217–224
14. Feitsma H, Kuiper RV, Korving J et al (2008) Zebrafish with
mutations in mismatch repair genes develop neurofibromas and
other tumors. Cancer Res 68(13):5059–5066. doi:10.1158/
0008-5472.CAN-08-0019
15. Nystrom-Lahti M, Kristo P, Nicolaides NC et al (1995) Founding
mutations and Alu-mediated recombination in herediatry colon
cancer. Nat Med 1:1203–1206. doi:10.1038/nm1195-1203
16. Yuan ZQ, Wong N, Foulkes WD et al (1999) A missense
mutation in both hMSH2 and APC in an Ashkenazi Jewish
HNPCC kindred: implications for clinical screening. J Med Genet
36:790–793
17. Foulkes WD, Thiffault I, Gruber SB et al (2002) The founder
mutation MSH2*1906G ? C is an important cause of hereditary
nonpolyposis colorectal cancer in the Ashkenazi Jewish popula-
tion. Am J Hum Genet 71:1395–1412. doi:10.1086/345075
18. Goldberg Y, Porat RM, Kedar I et al (2008) Mutation spectrum in
HNPCC in the Israeli population. Fam Cancer (Apr):4
19. Vasen HF, Mecklin JP, Khan PM et al (1991) The International
Collaborative Group on Hereditary Non-Polyposis Colorectal
Cancer (ICG-HNPCC). Dis Colon Rectum 34:424–425. doi:
10.1007/BF02053699
20. Banjerjee SK, Maldisi WF, Weston AP et al (1995) Microwave-
based DNA extraction from paraffin-embedded tissue for PCR
amplification. Biotechniques 18(5):768–773
21. Fujita M, Enomoto T, Yoshino K et al (1995) Microsatellite
instability and alterations in the hMSH2 gene in human ovarian
cancer. Int J Cancer 64(6):361–366. doi:10.1002/ijc.2910640602
22. Shlush LI, Behar DM, Zelazny A et al (2002) Molecular epide-
miological analysis of the changing nature of a meningococcal
outbreak following a vaccination campaign. J Clin Microbiol
40(10):3565–3571. doi:10.1128/JCM.40.10.3565-3571.2002
23. Bercovich D, Beaudet AL (2003) Denaturing high-performance
liquid chromatography for the detection of mutations and poly-
morphisms in UBE3A. Genet Test Fall 7(3):189–194
24. Bougeard G, Charbonnier F, Moerman A et al (2003) Early onset
brain tumor and lymphoma in MSH2-deficient children. Am J
Hum Genet 72:213–216. doi:10.1086/345297
25. Whiteside D, McLeod R, Graham G et al (2002) A homozygous
germ-line mutation in the human MSH2 gene predisposes to hae-
matological malignancy and multiple. Cancer Res 62:352–362
26. Puisieux A (1999) HNPCC syndrome, microsatellite instability and
NF1 gene alteration (French). Bull Cancer Oct Rev 86(10):812–814
27. Wang Q, Montmain G, Ruano E et al (2003) Neurofibromatosis
type 1 gene as a mutational target in a mismatch repair-deficient
cell type. Hum Genet 112:117–123
28. Agostini M, Tibiletti MG, Lucci-Cordisco E et al (2005) Two
PMS2 mutations in a Turcot syndrome family with small bowel
cancers. Am J Gastroenterol 100(8):1886–1891. doi:10.1111/
j.1572-0241.2005.50441.x
29. Hegde MR, Chong B, Blazo ME et al (2005) A homozygous
mutation in MSH6 causes Turcot syndrome. Clin Cancer Res
11(13):4689–4693
30. Leach FS, Polyak K, Burrell M et al (1996) Expression of the
human mismatch repair gene hMSH2 in normal and neoplastic
tissues. Cancer Res 56(2):235–240
31. Thibodeau SN, French AJ, Roche PC et al (1996) Altered
expression of hMSH2 and hMLH1 in tumors with microsatellite
instability and genetic alterations in mismatch repair genes.
Cancer Res 56(21):4836–4840
32. Ollila S, Sarantaus L, Kariola R et al (2006) Pathogenicity of
MSH2 missense mutations is typically associated with impaired
repair capability of the mutated protein. Gastroenterology
131(5):1408–1417. doi:10.1053/j.gastro.2006.08.044
33. Guillem JG, Moore HG, Palmer C et al (2004) A636P testing in
Ashkenazi Jews. Fam Cancer 3(3–4):223–227. doi:10.1007/
s10689-004-0899-z
34. Poley JW, Wagner A, Hoogmans MM et al (2007) Rotterdam
Initiative on Gastrointestinal Hereditary Tumors. Biallelic
germline mutations of mismatch-repair genes: a possible cause
for multiple pediatric malignancies. Cancer 109(11):234
194 H. Toledano et al.
123
Top Related
Copyright © 2022 FDOKUMEN

