






Bahasa
Halaman
Hukum

8/10/2019 Insufisiensi Vena Kronik Ka Jadeh
1/39
INSUFISIENSI VENAKRONIK
disusun oleh:Intan Maulinar
Pembimbing:
dr. Yopie A. Habibie, Sp.BTKV
8/10/2019 Insufisiensi Vena Kronik Ka Jadeh
2/39
8/10/2019 Insufisiensi Vena Kronik Ka Jadeh
3/39
Epidemiologi
5-30% pada populasi dewasaWanita : pria = 3 : 1
8/10/2019 Insufisiensi Vena Kronik Ka Jadeh
4/39
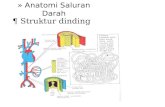
Anatomi
8/10/2019 Insufisiensi Vena Kronik Ka Jadeh
5/39
Etiologi
Insufisiensi vena kronik yang kongenital ( present since birth )
Terdapat kelainan dimana katup yang seharusnya terbentuk di suatusegmen ternyata tidak terbentuk sama sekali (aplasia, avalvulia), ataupembentukannya tidak sempurna (displasia), berbagai malformasi vena,dan kelainan lainnya.
Insufisiensi vena kronik yang primer ( undetermined etiology )
Kelemahan intrinsik dari dinding katup, yaitu terjadi daun katup yang terlalupanjang (elongasi) atau daun katup menyebabkan dinding vena menjaditerlalu lentur tanpa sebab yang diketahui. Keadaan daun katup yangpanjang melambai (floppy, rebundant) sehingga penutupan tidak sempurnayang mengakibatkan terjadinya katup tidak dapat menahan aliran balik,sehingga aliran vena menjadi retrograd atau refluks.
Insufisiensi vena kronik yang sekunder ( associated with post-thrombotic,
traumatic )
8/10/2019 Insufisiensi Vena Kronik Ka Jadeh
6/39
Faktor Resiko
Penambahan Usia
Jenis Kelamin
Family history of venous disease
Berdiri terlalu lama
Increased body mass indexSmoking
Inaktivitas fisik
Lower extremity trauma
Prior venous thrombosis (superficial or deep)
Hereditary conditions
High estrogen states
Pregnancy 2.
http://howmanyarethere.net/wp-content/uploads/2012/10/healthy_pregnancy_image.jpghttp://www.trauma.org/archive/cases/images/classic013b.jpghttp://www.osteoarthritisblog.com/category/about-knee-osteoarthritis/page/2/http://www.medimanage.com/my-worries/articles/have-digestion-problems-heres-why.aspxhttp://uhaweb.hartford.edu/IKEACHUMB/8/10/2019 Insufisiensi Vena Kronik Ka Jadeh
7/39
Patofisiologi
Refluks
CVI merupakan akibat dari disfungsi katup-katup vena yangmenyebabkan aliran darah vena yang anterograd untukmengalir dalam dua arah, yaitu secara antegrad dan
retrograde, sehingga terjadi refluks darah dalam pembuluhdarah (vena).
Hal ini menyebabkan vena tidak saja menerima darah yangdipompa dari ventrikel kiri, tetapi juga aliran darah daridalam pembuluh darah yang gagal dipompa ke atrium kanan(atau dari aliran vena yang tidak efisien)
Pembuluh darah vena berfungsi mengalirkan darah dariseluruh tubuh kembali ke jantung. Untuk mencapai jantung,darah pada vena tungkai harus mengalir ke arah atas. Otot
otot tungkai harus berkontraksi untuk memeras darah padavena tersebut. Vena memiliki katu satu arah untuk
8/10/2019 Insufisiensi Vena Kronik Ka Jadeh
8/39
CVI terjadi jika katup ini mengalami kerusakan sehingga darah yang dipompa kembali ke arahbawah dan tertumpuk sehingga tekanan dalamvena meningkat. Kerusakan katup dapat terjadiakibat proses penuaan, duduk atau berdiridalam jangka waktu lama, atau penurunanmobilitas tungkai.ObstruksiSumbatan pada vena profunda tungkai ( deepvein thrombosis , DVT), dapat akut maupunkronis
Kombinasi
8/10/2019 Insufisiensi Vena Kronik Ka Jadeh
9/39
Manifestasi Klinis
ASYMPTOMATICSUPERFICIAL VENOUS DILATATION
Telangiectasis (intradermal)
Reticular veins (subdermal)
8/10/2019 Insufisiensi Vena Kronik Ka Jadeh
10/39
VARICOSE VEINS (subcutaneous)
8/10/2019 Insufisiensi Vena Kronik Ka Jadeh
11/39
Leg edema
8/10/2019 Insufisiensi Vena Kronik Ka Jadeh
12/39
8/10/2019 Insufisiensi Vena Kronik Ka Jadeh
13/39
Skin changesHyperpigmentation
8/10/2019 Insufisiensi Vena Kronik Ka Jadeh
14/39
Skin changesStasis dermatitis
8/10/2019 Insufisiensi Vena Kronik Ka Jadeh
15/39
Skin changesCorona phlebectatica
a. venous cups (veins)
b. telangiectasisc. reticular veins
d. stasis spots(capillaries)
8/10/2019 Insufisiensi Vena Kronik Ka Jadeh
16/39
Lipodermatosclerosisa form of panniculitis just above the ankles
8/10/2019 Insufisiensi Vena Kronik Ka Jadeh
17/39
Venous stasis ulceration
8/10/2019 Insufisiensi Vena Kronik Ka Jadeh
18/39
8/10/2019 Insufisiensi Vena Kronik Ka Jadeh
19/39
CLASSIFICATION OF VEINDISEASECEAP an international consensus conference initiated the Clinical-Etiology-Anatomy-
Pathophysiology classification.
C 0 no evidence of venous disease.C 1 telangiectasias/reticular veins.C 2 varicose veins.C 3 edema associated with vein disease.C 4a pigmentation or eczema.C 4b lipodermatosclerosis.
C 5 healed venous ulcer.C 6 active venous ulcer.E c congenitalE p primary venous disease.E s secondary venous disorder.E n not specified.
A s superficial veins. A d deep veins. A p perforating veins. A n not specified.P r venous reflux.P o venous obstruction.P n not specified.
8/10/2019 Insufisiensi Vena Kronik Ka Jadeh
20/39
Diagnosis
AnamnesisPemeriksaan fisikInspection dan palpation may reveal visualevidence for CVI Pemeriksaan penunjang
8/10/2019 Insufisiensi Vena Kronik Ka Jadeh
21/39
8/10/2019 Insufisiensi Vena Kronik Ka Jadeh
22/39
Pemeriksaan Penunjang
Venous Duplex Imaging Photoplethysmography (PPG) Air Plethysmography (APG)
8/10/2019 Insufisiensi Vena Kronik Ka Jadeh
23/39
VENOUS DOPPLER ULTRASOUNDEvaluate for deep and superficial venousthrombosis.Evaluate for incompetent veins withsignificant reflux disease.Evaluate for incompetent perforatingveins and tributaries.
8/10/2019 Insufisiensi Vena Kronik Ka Jadeh
24/39
Tata Laksana
8/10/2019 Insufisiensi Vena Kronik Ka Jadeh
25/39
LEG ELEVATION heart level for 30 minutes 3-4 timesdaily improves micro-circulation reduces edema, andpromotes healing of venous ulcers.
EXERCISE daily walking and simple ankle flexionexercises.
Conservative Management
8/10/2019 Insufisiensi Vena Kronik Ka Jadeh
26/39
Compression therapy Compression bandages elastic or non-elastic
with single or multi-layers.
8/10/2019 Insufisiensi Vena Kronik Ka Jadeh
27/39
Compression stockings
8/10/2019 Insufisiensi Vena Kronik Ka Jadeh
28/39
CLASS PRESSURE LEVEL OF
SUPPORT
INDICATION CEAP
OTC 40 mmHg Extra firm Lymphedema. NA
8/10/2019 Insufisiensi Vena Kronik Ka Jadeh
29/39
MANAGEMENT OF CVI SKINCARE
Skin cleansing wash with a mild non-soapcleanser (e.g. Dove, Olay, Caress).Emollients provides a film of oil to lubricate
the skin (e.g. Vaseline, Lubriderm, Aveeno).Barrier preparations physically blockchemical irritants and moisture (e.g. Zinc
oxide, Vaseline ).Topical corticosteroids often used to treatstasis dermatitis.
8/10/2019 Insufisiensi Vena Kronik Ka Jadeh
30/39
MANAGEMENT OF CVI -MEDICATIONS
Pentoxifylline more effective for complete or partialulcer healing.Stanozolol an anabolic steroid that stimulatesfibrinolysis and improves lipodermatosclerosis andpossibly ulcer healing.Escin (horseshoe chestnut) 50mg twice daily reducesleg volume and edema. It stimulates the release of Fseries prostaglandins which induce venoconstriction,decreasing the permeability of vessel walls to lowmolecular proteins, water, and electrolytes.
8/10/2019 Insufisiensi Vena Kronik Ka Jadeh
31/39
MANAGEMENT OF CVI VENOUSSTASIS ULCERS
Surgical debridement used to removedevitalized tissue.Enzymatic agents used to break downnecrotic tissue (e.g. Santyl).Growth factors synthesized by many celltypes such as platelets, neutrophils, andepithelial cells (e.g. Regranex).
Bioengineered tissue
used for a variety ofnon-healing ulcers (e.g. Apligraf, Dermagraft).Skin grafting an option for non-healing ulcers.
8/10/2019 Insufisiensi Vena Kronik Ka Jadeh
32/39
MANAGEMENT OF CVI VENOUSSTASIS ULCERS
Dressings depend upon the ulcer characteristics,frequency of dressing changes, and cost.-Occlusive dressings may be fully occlusive(impermeable to gases and liquids) or semi-impermeable (impermeable to liquids and partiallypermeable to gases and water vapor).It stimulates collagen synthesis, angiogenesis, andspeeds reepithelialization.-Low adherent gauze dressings frequent changes butinexpensive.-Hydrogels and alginate dressings are highly absorbentto handle heavily exudative ulcers, while hydrocolloidscan help with wound debridement and skin protection.-Silver can be incorporated if the ulcer is infected.
8/10/2019 Insufisiensi Vena Kronik Ka Jadeh
33/39
MANAGEMENT OF CVI -SCLEROTHERAPY
Chemical irritants injected to close unwantedveins. Preparations include liquid and foam. It isused primarily in the treatment of
telangiectasias, reticular veins, and smallvaricose veins.These substances cause endothelial damage bytheir actions as either osmotic or detergentagents. Osmotic agents achieve their effect bydehydrating endothelial cells through osmosis.Detergents are surface active agents whichdamage the endothelium by interfering with cellmembrane lipids. 8.
8/10/2019 Insufisiensi Vena Kronik Ka Jadeh
34/39
MANAGEMENT OF CVI -SCLEROTHERAPY
DETERGENT AGENTS- Sodium tetradecyl sulfate- Polidocanol
OSMOTIC AGENTS- Hypertonic saline- Glycerin
8/10/2019 Insufisiensi Vena Kronik Ka Jadeh
35/39
MANAGEMENT OF CVI ABLATIONTHERAPY
Indications patients with persistentsigns/symptoms of venous disease after aminimum of 3 months of medical therapy (e.g.compression) and documented reflux (e.g.>0.5 seconds of reflux GSV).
Absolute contraindications acute DVT orphlebitis and pregnancy.
8/10/2019 Insufisiensi Vena Kronik Ka Jadeh
36/39
MANAGEMENT OF CVI RADIOFREQUENCY ENDOVENOUS
ABLATION THERAPY
Radiofrequency devices generate a high
frequency alternating current for which theenergy heats the adjacent vein walls to theprobe which alters the protein structure of thevein effecting its closure.Superficial veins include Great SaphenousVein, Small Saphenous, and incompetentperforator veins.
MANAGEMENT OF CVI
8/10/2019 Insufisiensi Vena Kronik Ka Jadeh
37/39
MANAGEMENT OF CVI ENDOVENOUS LASER ABLATIONTHERAPY
Lasers emit a single, coherent wavelength of light.Laser therapy of venous structures is based uponthe concept of selective photothermolysis (ie,selective thermal confinement of light induceddamage). Vein wall injury is mediated directly byabsorption of photon energy by the vein wall andindirectly by thermal convection from steambubbles, and from heated blood.Superficial veins include Great Saphenous Vein,
Small Saphenous Vein, incompetent perforator
8/10/2019 Insufisiensi Vena Kronik Ka Jadeh
38/39
Surgical Treatment
- Vein ligation/stripping- Phlebectomy- Valve reconstruction- Open or endoscopic perforator ligation.
8/10/2019 Insufisiensi Vena Kronik Ka Jadeh
39/39
Terima Kasih
Top Related
Copyright © 2022 FDOKUMEN

