






Bahasa
Halaman
Hukum

7/28/2019 3.Kuliah Endokrin I UWK
1/32
Survey of Some Human
Endocrine Glands
7/28/2019 3.Kuliah Endokrin I UWK
2/32
Endocrine organs
7/28/2019 3.Kuliah Endokrin I UWK
3/32
Central Roles of the
Hypothalamus and Pituitary
7/28/2019 3.Kuliah Endokrin I UWK
4/32
7/28/2019 3.Kuliah Endokrin I UWK
5/32
Pituitary Dwarfism
7/28/2019 3.Kuliah Endokrin I UWK
6/32
Gigantism and Acromegaly
7/28/2019 3.Kuliah Endokrin I UWK
7/32
7/28/2019 3.Kuliah Endokrin I UWK
8/32
7/28/2019 3.Kuliah Endokrin I UWK
9/32
7/28/2019 3.Kuliah Endokrin I UWK
10/32
Action of Steroid Hormones
7/28/2019 3.Kuliah Endokrin I UWK
11/32
Action of Peptide Hormones
7/28/2019 3.Kuliah Endokrin I UWK
12/32
7/28/2019 3.Kuliah Endokrin I UWK
13/32
7/28/2019 3.Kuliah Endokrin I UWK
14/32
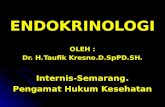
Thyroid Gland P618-623
located over trachea
inferior to larynx
Hormones:
Thyroid hormoneCalcitonin
F16.7
7/28/2019 3.Kuliah Endokrin I UWK
15/32
anterior
pituitary
paraventricular
nucleus
Hypothalamus
Anterior Pituitary
Thyroid gland
TRH+
+
TSH
Thyroid
-
T4, T3
-
SRIF
7/28/2019 3.Kuliah Endokrin I UWK
16/32
Follicle epithelial cell
Thyroidfollicle Thyroidfollicle
Thyroidfollicle
Synthesis and secretion
EC Space Follicle Lumen
7/28/2019 3.Kuliah Endokrin I UWK
17/32
Oxidization and organification
TPO
TPO
I-
apical membrane
Thyroid peroxidase:Oxidation
Incorporation into thyroglobulin
Monoiodotyrosine
Diiodotyrosine
Coupling of MIT and DIT
within TG to form T3 and T4
Reabsorption of TG into follicle cellProteolysis: release of T3, T4
SecretionPeripheral conversion of T
4to T
3
Regulated by TSH
7/28/2019 3.Kuliah Endokrin I UWK
18/32
7/28/2019 3.Kuliah Endokrin I UWK
19/32
7/28/2019 3.Kuliah Endokrin I UWK
20/32
7/28/2019 3.Kuliah Endokrin I UWK
21/32
7/28/2019 3.Kuliah Endokrin I UWK
22/32
Cli i l f th id
7/28/2019 3.Kuliah Endokrin I UWK
23/32
Clinical uses of thyroid
hormoneLevothyroxine (synthetic T
4
)
Drug of choice for routine replacement therapy
Identical to endogenous T4 and converted to T3
Long half-life allows once daily oral administration
Liothyronine (synthetic T3)
Rapid absorption, shorter T1/2
spiking, uneven blood levels, transient action
Frequent dosing required
Use limited to situations requiring rapid response
7/28/2019 3.Kuliah Endokrin I UWK
24/32
Hyperthyroidism (thyrotoxicosis)
Characterized by: Increased cardiac output Nervousness
Muscle weakness Increased BMR
Hyperglycemia Hypocholesterolemia
Weight loss
Graves' disease:
Most common form of hyperthyroidism
Thyroid-stimulating immunoglobulins (TSIg) interact with theTSH receptor, activate the thyroid
Symptoms: Diffuse goiter
Exophthalmus - protruding eyes, mucopolysaccharideinfiltration of the extraocular tissue
Other signs of hyperthyroidism (above)
7/28/2019 3.Kuliah Endokrin I UWK
25/32
Hypothyroidism
Characterized by:
decreased cardiac output slow mental function muscle fatigue hypoglycemia decreased body temperature
Causes: Primary hypothyroidism: Hashimoto's autoimmune thyroiditis radiation damage thyroidectomy iodine deficiency autosomal defects in hormone synthesis idiopathic
Secondary hypothyroidism
7/28/2019 3.Kuliah Endokrin I UWK
26/32
HypothyroidismMyxedema:
Onset of hypothyroidism in the adult Named for characteristic thickening of subcutaneous tissue
caused by deposition of mucopolysaccharides
Once thought to be due to increased mucus ("myx")formation
Cretinism: Onset in infancy
Usually due to thyroid dysgenesis
Impaired physical growth Impaired brain growth and myelination
Mental retardation
7/28/2019 3.Kuliah Endokrin I UWK
27/32
Adverse effects
Nervousness Hypertension
Vomiting and diarrhea
Increased sensitivity to heat Impaired reproductive function
Cardiotoxicity
Iatrogenic hyperthyroidism
Especially in the elderly
Arrhythmias
Shortness of breath
7/28/2019 3.Kuliah Endokrin I UWK
28/32
Contraindications to T4
therapyUse with caution in presence of:
Adrenal insufficiency: increases cortisol turnover
Coumarin anticoagulants: increases catabolism of
clotting factors
Diabetes mellitus: increases insulin requirement
Stimulates gluconeogenesis and glycogenolysis
Cardiovascular disease: initiate therapy slowly, monitor
closely because of effects on the heart
7/28/2019 3.Kuliah Endokrin I UWK
29/32
Thionamides: Clinical usesGraves' hyperthyroidism:
100 to 600 mg propylthiouracil/day in divided doses or10 to 40 mg methimazole /day as single dose
Reduce dose for maintenance
Continue for 6 months or longer, until remission
Propylthiouracil: also partially inhibits T4 T3 May be used when fast action is desired
Methimazole: longer duration of action
Suitable for once daily dosing
Propylthiouracil indicated for hyperthyroidism duringpregnancy
Use minimum dose that controls symptoms
7/28/2019 3.Kuliah Endokrin I UWK
30/32
Thionamides: Clinical uses
Following radioiodine treatment:
To achieve euthyroid status until effects ofradiation are observed
Prior to subtotal thyroidectomy:
Euthyroid status improves response tosurgical stress
7/28/2019 3.Kuliah Endokrin I UWK
31/32
Thionamides: Adverse effects
Skin rashes Agranulocytosis (in 0.3 % of patients) -
reversible upon discontinuation
Arthralgia and myalgia Hepatic abnormalities
necrosis (propylthiouracil)
cholestatic jaundice (methimazole)
7/28/2019 3.Kuliah Endokrin I UWK
32/32
Most common treatment in U.S. Radioactive T1/2: 8 days
Rapidly and efficiently trapped by the thyroid
Dose is determined by preliminary uptake test
Adjusted for complete or partial destruction ofthyroid with no injury to adjacent tissue
Adjunctive therapy:
-adrenergic blocking agents (propanolol) or
Ca2+ channel antagonists (verapamil)
For relief of symptoms (tachycardia, hypertension,arrhythmias) until euthyroid
Radioactive iodine (131I)
Copyright © 2022 FDOKUMEN

