
Colleges Affiliated to Bangalore University, Bangalore for the ...
Upload
christuniversityCategory
view
0download
0
Article
Women Caregivers of Persons with Brain Tumour: A Psychosocial Needs Assessment in a Tertiary Care Hospital in Bangalore
Anekal C. Amaresha1
N. Krishna Reddy1
Atiq Ahmed2
Diana Ross3
Julian A. J. Arthur1
Abstract
The diagnosis of a brain tumour poses severe challenges to patients as well as their caregivers. As caregivers, women play an important role.
Indian Journal of Gender Studies22(1) 41–62
© 2015 CWDSSAGE Publications
sagepub.in/home.navDOI: 10.1177/0971521514556944
http://ijg.sagepub.com
Corresponding author:Anekal C. Amaresha, Ph.D Scholar, Department of Psychiatric Social Work, National Institute of Mental Health and Neurosciences (NIMHANS), Hosur Road, Bangalore, Karnataka, India 560029.E-mail: [email protected]
1Department of Psychiatric Social Work, National Institute of Mental Health and Neurosciences (NIMHANS), Bangalore, Karnataka, India.2Department of Social Work, Central University of Rajasthan, Ajmer, Rajasthan, India.3The Richmond Fellowship Post Graduate College for Psycho-Social Rehabilitation, Bangalore, Karnataka, India.
at Bobst Library, New York University on May 10, 2015ijg.sagepub.comDownloaded from

42 Indian Journal of Gender Studies 22(1)
However, most of the literature on brain tumours has failed to empha-sise the invaluable services of women caregivers, and their psychosocial needs have been overlooked. The current study aims to highlight this neglected aspect. Thirty women caregivers were selected through pur-posive sampling and their needs were assessed using a semi-structured questionnaire under five heads such as, professional service needs, informational needs, psychological/emotional needs, personal and spir-itual needs and social support needs. It was found that some of their needs were unmet, especially their psychological/emotional and infor-mational needs. Thus, gender-specific interventions are recommended across neuro-oncological settings.
Keywords
Brain tumour, women caregivers, psychosocial needs
Introduction
A brain tumour occurs when there is a growth of abnormal and uncon-trolled cells in the brain (Hill et al., 2002). It is a life-threatening illness, which causes significant disruption in the functioning of a person. Patients have multifaceted physiological and psychosocial needs, which include:
1. Managing their physical, behavioural and cognitive deterioration. 2. Undergoing surgery, radiation or chemotherapy. 3. Continuation of medication. 4. Coping with the adverse consequences of the illness. 5. Ensuring support from family and the health care team.
In most cases, the exact cause of a brain tumour is unknown. It can occur at any age. Men are more prone to developing cancerous (malignant) tumours than women. The most common symptoms are headaches, seizures or fits, nausea or vomiting, impairments in speech, vision or hearing, difficulties in balancing or walking, changes in mood, personality, or inability to concentrate, disturbances in memory, numb-ness or tingling in the arms or legs, fatigue, etc. (Hill et al., 2002). Diagnosis is made through a combination of neurological examinations,
at Bobst Library, New York University on May 10, 2015ijg.sagepub.comDownloaded from
Amaresha et al. 43
brain imaging and biopsy. The choice of treatment and prognosis of the condition depends mainly on the type and grade of brain tumour, its location in the brain, its size, age and the general health status of the patient. A multi-disciplinary team approach involving neurologists, clinical psychologists, oncologists and other professionals such as physiotherapists, occupational therapists and social workers, etc., is fol-lowed. The primary treatment options are surgery, radiation therapy and chemotherapy. Patients with a cancerous brain tumour, live for at least five years after being diagnosed. Those with benign brain tumours sur-vive longer. However, any tumour can be life threatening because it compresses the brain tissue and other structures inside the skull. The survival rates tend to be greater for younger patients.
It has been reported that a considerable proportion of brain tumour patients and their caregivers are referred for psychiatric consultation for psychological disturbances followed by increased levels of stress (Sherwood et al., 2004). Holistic care should include systematic under-standing of the psychosocial issues of the patient and the caregiver, and psychosocial interventions for the affected person and her/his family caregiver with mainstream treatment modalities.
Psychosocial Issues of Caregivers
Caregivers report high levels of stress and poor physical and emotional health, as well as career sacrifices, economic burden and workplace dis-crimination (DesRoches et al., 2002). In addition to stress, acting as a caregiver has been associated with psychiatric disorders such as panic disorder, depression, posttraumatic stress disorder and generalised anxi-ety disorder (Chentsova-Dutton et al., 2000; Vanderwerker et al., 2005). It is evident that even after treatment for the brain tumour is complete, stressors and challenges persist, requiring families to adjust to a ‘new normal’ state of daily life that include further social, emotional and finan-cial stress (Oeffinger et al., 2004; Van Dongen-Melman et al., 1998). Hence, the diagnosis of a brain tumour negatively affects the quality of life of the primary caregivers (Fox and Lantz, 1998).
Active information seeking is one of the important ways of coping for both patients and caregivers (Strang and Strang, 2001). Janda and colleagues (2006) recommended that both caregivers and patients need to understand the disease and its repercussions, and in particular,
at Bobst Library, New York University on May 10, 2015ijg.sagepub.comDownloaded from
44 Indian Journal of Gender Studies 22(1)
caregivers need extended access to information and clear answers to their queries. In a 2011 study, the majority of the caregivers reported their need for information about the illness, supportive care and guidance in dealing with their own psychological disturbances (Parvataneni et al., 2011). Caregivers need help in accessing other welfare services available for patients and caregivers, meeting other caregivers with similar problems, balancing work and family life and dealing with financial difficulties (ibid., 2011).
Women as Caregivers
The literature shows that the majority of caregivers of any illness are women, which is evident from the ‘National Long-Term Care Survey and Informal Caregivers Survey’ done in the USA. This particular survey has shown that two-thirds of caregivers were women (Wolff and Kasper, 2006). Even Indian studies on caregivers of the elderly (Brinda et al., 2014; Gupta et al., 2009), caregivers of dementia and Alzheimer’s disease (Dias et al., 2008; Pattanayak et al., 2010; Shaji et al., 2009), and caregivers of psychiatric patients (Kumar et al., 2014; Talwar and Matheiken, 2010), show that the majority of caregivers are women.
Often, women caregivers perform roles that are ignored, unpaid and inimical to their emotional and physical health (Robinson and Thurnher, 1979; Wright, 1983). Research on the psychosocial issues of caregivers of brain tumour patients describes the issues of caregivers in general and to the best of our knowledge it has not focused on studying women’s psychosocial needs or on the priceless services they provide (psychosocial needs are defined as any professional, informational or emotional needs felt by the caregivers in accessing care and treatment for their relatives with brain tumour).
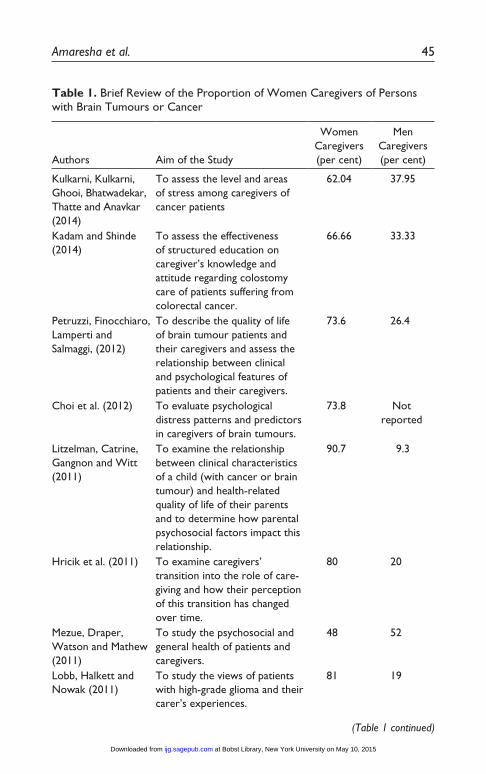
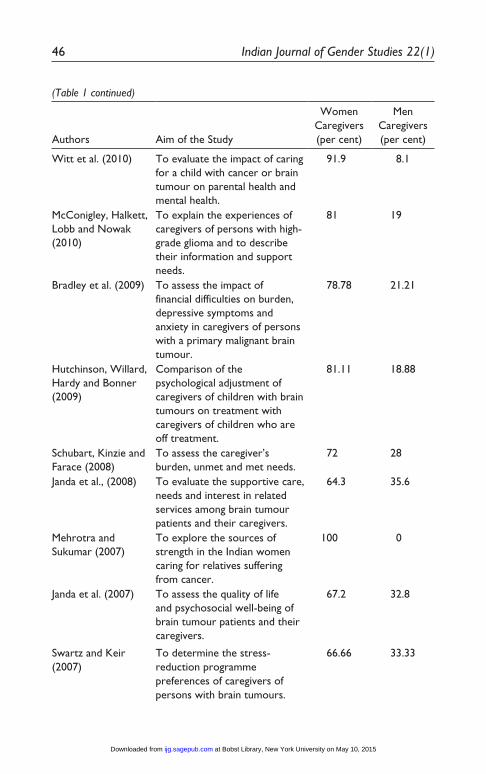
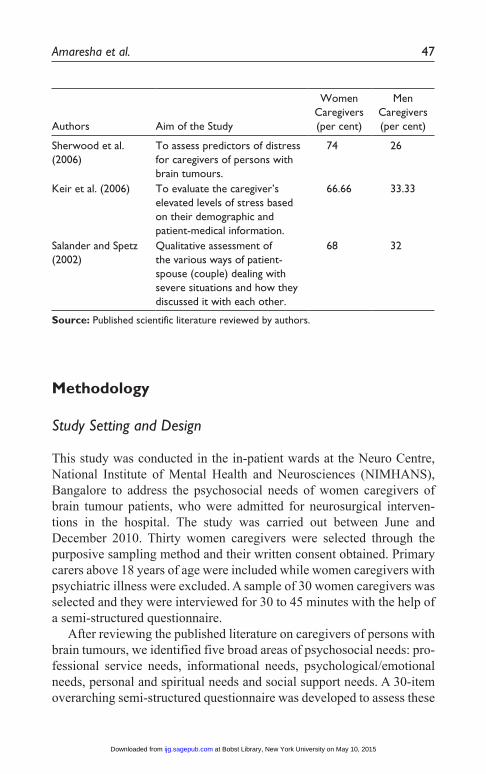
As depicted in Table 1, the proportion of women caregivers is greater than men caregivers across countries, ranging from 48 to almost 92 per cent. There is a dearth of literature on the psychosocial needs of women caregivers of brain tumour patients in India. The current study attempts to assess the needs of women caregivers of such patients being treated in a government run tertiary care hospital in Bangalore, Karnataka.
at Bobst Library, New York University on May 10, 2015ijg.sagepub.comDownloaded from
Amaresha et al. 45
Table 1. Brief Review of the Proportion of Women Caregivers of Persons with Brain Tumours or Cancer
Authors Aim of the Study
Women Caregivers (per cent)
Men Caregivers (per cent)
Kulkarni, Kulkarni, Ghooi, Bhatwadekar, Thatte and Anavkar (2014)
To assess the level and areas of stress among caregivers of cancer patients
62.04 37.95
Kadam and Shinde (2014)
To assess the effectiveness of structured education on caregiver’s knowledge and attitude regarding colostomy care of patients suffering from colorectal cancer.
66.66 33.33
Petruzzi, Finocchiaro, Lamperti and Salmaggi, (2012)
To describe the quality of life of brain tumour patients and their caregivers and assess the relationship between clinical and psychological features of patients and their caregivers.
73.6 26.4
Choi et al. (2012) To evaluate psychological distress patterns and predictors in caregivers of brain tumours.
73.8 Not reported
Litzelman, Catrine, Gangnon and Witt (2011)
To examine the relationship between clinical characteristics of a child (with cancer or brain tumour) and health-related quality of life of their parents and to determine how parental psychosocial factors impact this relationship.
90.7 9.3
Hricik et al. (2011) To examine caregivers’ transition into the role of care-giving and how their perception of this transition has changed over time.
80 20
Mezue, Draper, Watson and Mathew (2011)
To study the psychosocial and general health of patients and caregivers.
48 52
Lobb, Halkett and Nowak (2011)
To study the views of patients with high-grade glioma and their carer’s experiences.
81 19
(Table 1 continued)
at Bobst Library, New York University on May 10, 2015ijg.sagepub.comDownloaded from
46 Indian Journal of Gender Studies 22(1)
Authors Aim of the Study
Women Caregivers (per cent)
Men Caregivers (per cent)
Witt et al. (2010) To evaluate the impact of caring for a child with cancer or brain tumour on parental health and mental health.
91.9 8.1
McConigley, Halkett, Lobb and Nowak (2010)
To explain the experiences of caregivers of persons with high-grade glioma and to describe their information and support needs.
81 19
Bradley et al. (2009) To assess the impact of financial difficulties on burden, depressive symptoms and anxiety in caregivers of persons with a primary malignant brain tumour.
78.78 21.21
Hutchinson, Willard, Hardy and Bonner (2009)
Comparison of the psychological adjustment of caregivers of children with brain tumours on treatment with caregivers of children who are off treatment.
81.11 18.88
Schubart, Kinzie and Farace (2008)
To assess the caregiver’s burden, unmet and met needs.
72 28
Janda et al., (2008) To evaluate the supportive care, needs and interest in related services among brain tumour patients and their caregivers.
64.3 35.6
Mehrotra and Sukumar (2007)
To explore the sources of strength in the Indian women caring for relatives suffering from cancer.
100 0
Janda et al. (2007) To assess the quality of life and psychosocial well-being of brain tumour patients and their caregivers.
67.2 32.8
Swartz and Keir (2007)
To determine the stress-reduction programme preferences of caregivers of persons with brain tumours.
66.66 33.33
(Table 1 continued)
at Bobst Library, New York University on May 10, 2015ijg.sagepub.comDownloaded from
Amaresha et al. 47
Authors Aim of the Study
Women Caregivers (per cent)
Men Caregivers (per cent)
Sherwood et al. (2006)
To assess predictors of distress for caregivers of persons with brain tumours.
74 26
Keir et al. (2006) To evaluate the caregiver’s elevated levels of stress based on their demographic and patient-medical information.
66.66 33.33
Salander and Spetz (2002)
Qualitative assessment of the various ways of patient-spouse (couple) dealing with severe situations and how they discussed it with each other.
68 32
Source: Published scientific literature reviewed by authors.
Methodology
Study Setting and Design
This study was conducted in the in-patient wards at the Neuro Centre, National Institute of Mental Health and Neurosciences (NIMHANS), Bangalore to address the psychosocial needs of women caregivers of brain tumour patients, who were admitted for neurosurgical interven-tions in the hospital. The study was carried out between June and December 2010. Thirty women caregivers were selected through the purposive sampling method and their written consent obtained. Primary carers above 18 years of age were included while women caregivers with psychiatric illness were excluded. A sample of 30 women caregivers was selected and they were interviewed for 30 to 45 minutes with the help of a semi-structured questionnaire.
After reviewing the published literature on caregivers of persons with brain tumours, we identified five broad areas of psychosocial needs: pro-fessional service needs, informational needs, psychological/emotional needs, personal and spiritual needs and social support needs. A 30-item overarching semi-structured questionnaire was developed to assess these
at Bobst Library, New York University on May 10, 2015ijg.sagepub.comDownloaded from
48 Indian Journal of Gender Studies 22(1)
psychosocial needs along with socio-demographic details of women car-egivers such as age, education, occupation, marital status, domicile, fam-ily type and relationship with the patient. The participants’ responses to questions on needs were recorded as ‘required and not available’, ‘required and available’, ‘not required and available’ and ‘not required and not available’. The English version of this questionnaire was trans-lated into the local vernacular Kannada.
Socio-demographic Details of the Sample
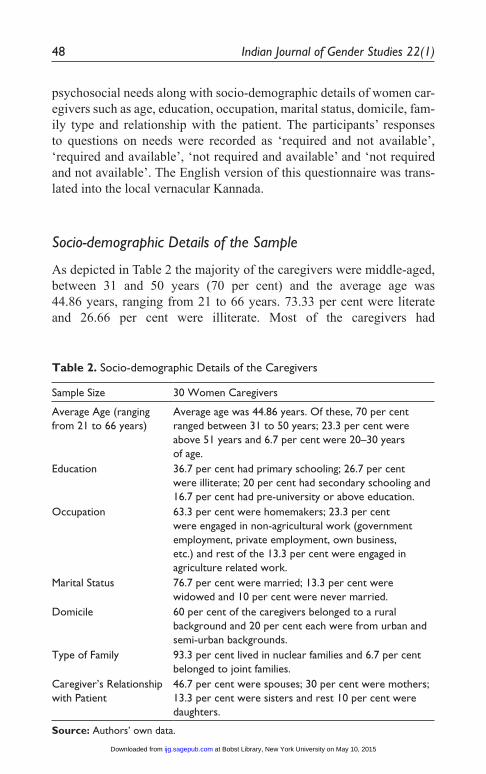
As depicted in Table 2 the majority of the caregivers were middle-aged, between 31 and 50 years (70 per cent) and the average age was 44.86 years, ranging from 21 to 66 years. 73.33 per cent were literate and 26.66 per cent were illiterate. Most of the caregivers had
Table 2. Socio-demographic Details of the Caregivers
Sample Size 30 Women Caregivers
Average Age (ranging from 21 to 66 years)
Average age was 44.86 years. Of these, 70 per cent ranged between 31 to 50 years; 23.3 per cent were above 51 years and 6.7 per cent were 20–30 years of age.
Education 36.7 per cent had primary schooling; 26.7 per cent were illiterate; 20 per cent had secondary schooling and 16.7 per cent had pre-university or above education.
Occupation 63.3 per cent were homemakers; 23.3 per cent were engaged in non-agricultural work (government employment, private employment, own business, etc.) and rest of the 13.3 per cent were engaged in agriculture related work.
Marital Status 76.7 per cent were married; 13.3 per cent were widowed and 10 per cent were never married.
Domicile 60 per cent of the caregivers belonged to a rural background and 20 per cent each were from urban and semi-urban backgrounds.
Type of Family 93.3 per cent lived in nuclear families and 6.7 per cent belonged to joint families.
Caregiver’s Relationship with Patient
46.7 per cent were spouses; 30 per cent were mothers; 13.3 per cent were sisters and rest 10 per cent were daughters.
Source: Authors’ own data.
at Bobst Library, New York University on May 10, 2015ijg.sagepub.comDownloaded from
Amaresha et al. 49
primary schooling (36.7 per cent) and the majority were housewives (63.3 per cent). Of the caregivers, 76.7 per cent were married. Most of the participants belonged to nuclear families (93.3 per cent) and hailed from rural Bangalore (60 per cent).
Needs of the Women Caregivers
Professional Service Needs
The majority of cancer, palliative care or neuro-surgery settings in India do not have multi-disciplinary teams to offer multi-disciplinary services to address the psychosocial needs of either patients or caregiv-ers, especially women caregivers. The current study was conducted in a tertiary care hospital where such services are available. Here the multi-disciplinary team consists of neurosurgeons, nurses, clinical psy-chologists and psychiatric social workers; and for the referral services, the hospital has super specialised neurology and psychiatry units with allied departments for clinical as well as laboratory investigations. This multi-disciplinary team and its services were reflected in the women caregivers’ need for professional services.
Caregivers wish to meet healthcare professionals for discussions about their patients, and wish to get counselling services. They also expect reassurance and respect from them, since they undergo emotional turmoil during hospitalisation and even after discharge. Provision of such services facilitates an effective treatment process, decision making and helps caregivers to cope with the traumatic experience.
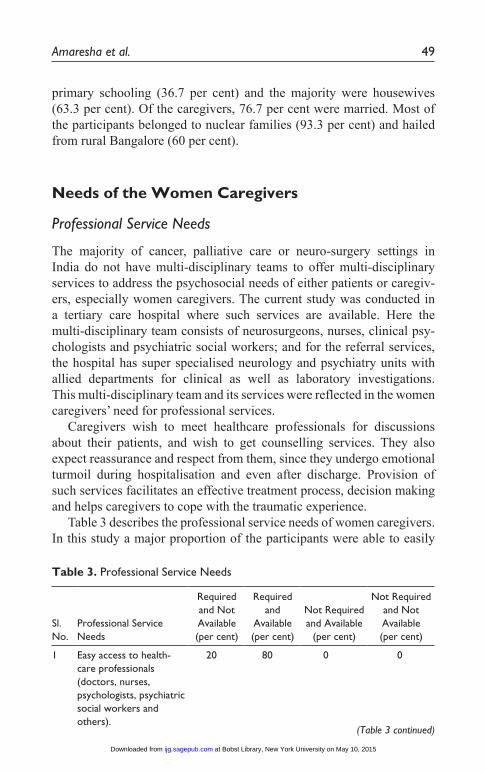
Table 3 describes the professional service needs of women caregivers. In this study a major proportion of the participants were able to easily
Table 3. Professional Service Needs
Sl. No.
Professional Service Needs
Required and Not Available (per cent)
Required and
Available (per cent)
Not Required and Available
(per cent)
Not Required and Not Available (per cent)
1 Easy access to health-care professionals (doctors, nurses, psychologists, psychiatric social workers and others).
20 80 0 0
(Table 3 continued)
at Bobst Library, New York University on May 10, 2015ijg.sagepub.comDownloaded from
50 Indian Journal of Gender Studies 22(1)
Sl. No.
Professional Service Needs
Required and Not Available (per cent)
Required and
Available (per cent)
Not Required and Available
(per cent)
Not Required and Not Available (per cent)
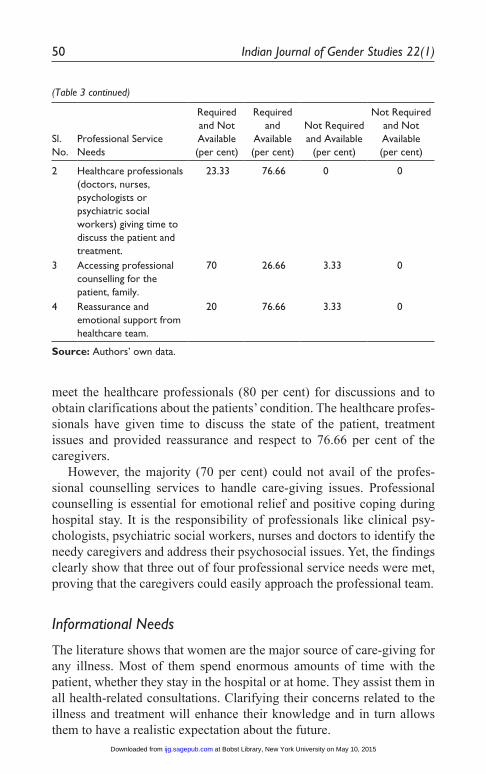
2 Healthcare professionals (doctors, nurses, psychologists or psychiatric social workers) giving time to discuss the patient and treatment.
23.33 76.66 0 0
3 Accessing professional counselling for the patient, family.
70 26.66 3.33 0
4 Reassurance and emotional support from healthcare team.
20 76.66 3.33 0
Source: Authors’ own data.
meet the healthcare professionals (80 per cent) for discussions and to obtain clarifications about the patients’ condition. The healthcare profes-sionals have given time to discuss the state of the patient, treatment issues and provided reassurance and respect to 76.66 per cent of the caregivers.
However, the majority (70 per cent) could not avail of the profes-sional counselling services to handle care-giving issues. Professional counselling is essential for emotional relief and positive coping during hospital stay. It is the responsibility of professionals like clinical psy-chologists, psychiatric social workers, nurses and doctors to identify the needy caregivers and address their psychosocial issues. Yet, the findings clearly show that three out of four professional service needs were met, proving that the caregivers could easily approach the professional team.
Informational Needs
The literature shows that women are the major source of care-giving for any illness. Most of them spend enormous amounts of time with the patient, whether they stay in the hospital or at home. They assist them in all health-related consultations. Clarifying their concerns related to the illness and treatment will enhance their knowledge and in turn allows them to have a realistic expectation about the future.
(Table 3 continued)
at Bobst Library, New York University on May 10, 2015ijg.sagepub.comDownloaded from
Amaresha et al. 51
Table 4. Informational Needs
Sl. No.
Informational Needs of the Caregivers
Required and Not Available (per cent)
Required and
Available (per cent)
Not Required
and Available (per cent)
Not Required and Not Available (per cent)
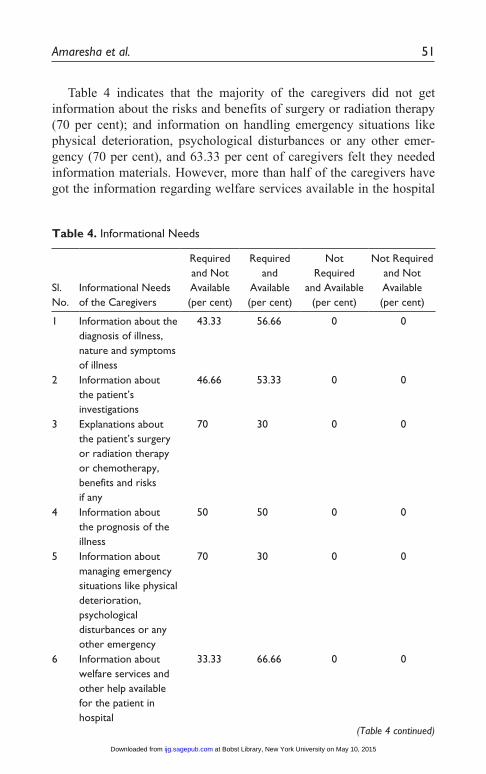
1 Information about the diagnosis of illness, nature and symptoms of illness
43.33 56.66 0 0
2 Information about the patient’s investigations
46.66 53.33 0 0
3 Explanations about the patient’s surgery or radiation therapy or chemotherapy, benefits and risks if any
70 30 0 0
4 Information about the prognosis of the illness
50 50 0 0
5 Information about managing emergency situations like physical deterioration, psychological disturbances or any other emergency
70 30 0 0
6 Information about welfare services and other help available for the patient in hospital
33.33 66.66 0 0
Table 4 indicates that the majority of the caregivers did not get information about the risks and benefits of surgery or radiation therapy (70 per cent); and information on handling emergency situations like physical deterioration, psychological disturbances or any other emer-gency (70 per cent), and 63.33 per cent of caregivers felt they needed information materials. However, more than half of the caregivers have got the information regarding welfare services available in the hospital
(Table 4 continued)
at Bobst Library, New York University on May 10, 2015ijg.sagepub.comDownloaded from
52 Indian Journal of Gender Studies 22(1)
(Table 4 continued)
Sl. No.
Informational Needs of the Caregivers
Required and Not Available (per cent)
Required and
Available (per cent)
Not Required
and Available (per cent)
Not Required and Not Available (per cent)
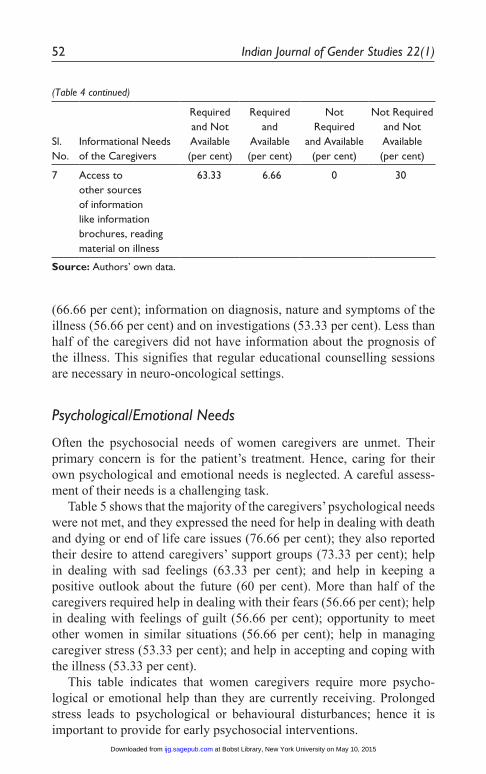
7 Access to other sources of information like information brochures, reading material on illness
63.33 6.66 0 30
Source: Authors’ own data.
(66.66 per cent); information on diagnosis, nature and symptoms of the illness (56.66 per cent) and on investigations (53.33 per cent). Less than half of the caregivers did not have information about the prognosis of the illness. This signifies that regular educational counselling sessions are necessary in neuro-oncological settings.
Psychological/Emotional Needs
Often the psychosocial needs of women caregivers are unmet. Their primary concern is for the patient’s treatment. Hence, caring for their own psychological and emotional needs is neglected. A careful assess-ment of their needs is a challenging task.
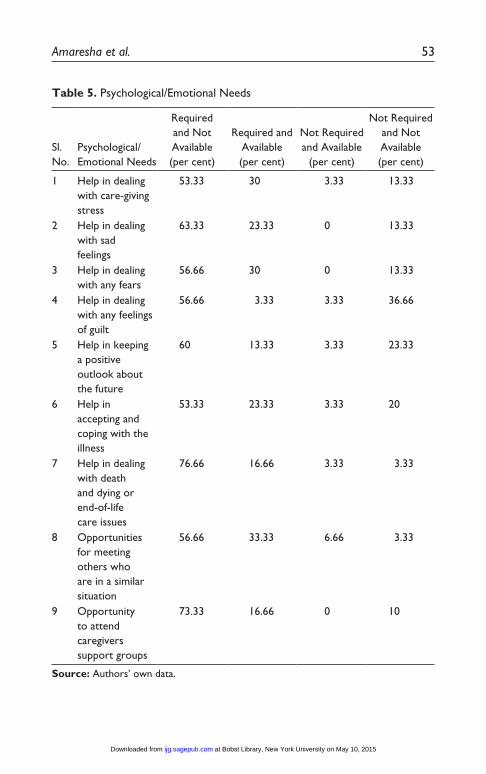
Table 5 shows that the majority of the caregivers’ psychological needs were not met, and they expressed the need for help in dealing with death and dying or end of life care issues (76.66 per cent); they also reported their desire to attend caregivers’ support groups (73.33 per cent); help in dealing with sad feelings (63.33 per cent); and help in keeping a positive outlook about the future (60 per cent). More than half of the caregivers required help in dealing with their fears (56.66 per cent); help in dealing with feelings of guilt (56.66 per cent); opportunity to meet other women in similar situations (56.66 per cent); help in managing caregiver stress (53.33 per cent); and help in accepting and coping with the illness (53.33 per cent).
This table indicates that women caregivers require more psycho- logical or emotional help than they are currently receiving. Prolonged stress leads to psychological or behavioural disturbances; hence it is important to provide for early psychosocial interventions.
at Bobst Library, New York University on May 10, 2015ijg.sagepub.comDownloaded from
Amaresha et al. 53
Table 5. Psychological/Emotional Needs
Sl. No.
Psychological/Emotional Needs
Required and Not Available (per cent)
Required and Available (per cent)
Not Required and Available
(per cent)
Not Required and Not Available (per cent)
1 Help in dealing with care-giving stress
53.33 30 3.33 13.33
2 Help in dealing with sad feelings
63.33 23.33 0 13.33
3 Help in dealing with any fears
56.66 30 0 13.33
4 Help in dealing with any feelings of guilt
56.66 3.33 3.33 36.66
5 Help in keeping a positive outlook about the future
60 13.33 3.33 23.33
6 Help in accepting and coping with the illness
53.33 23.33 3.33 20
7 Help in dealing with death and dying or end-of-life care issues
76.66 16.66 3.33 3.33
8 Opportunities for meeting others who are in a similar situation
56.66 33.33 6.66 3.33
9 Opportunity to attend caregivers support groups
73.33 16.66 0 10
Source: Authors’ own data.
at Bobst Library, New York University on May 10, 2015ijg.sagepub.comDownloaded from
54 Indian Journal of Gender Studies 22(1)
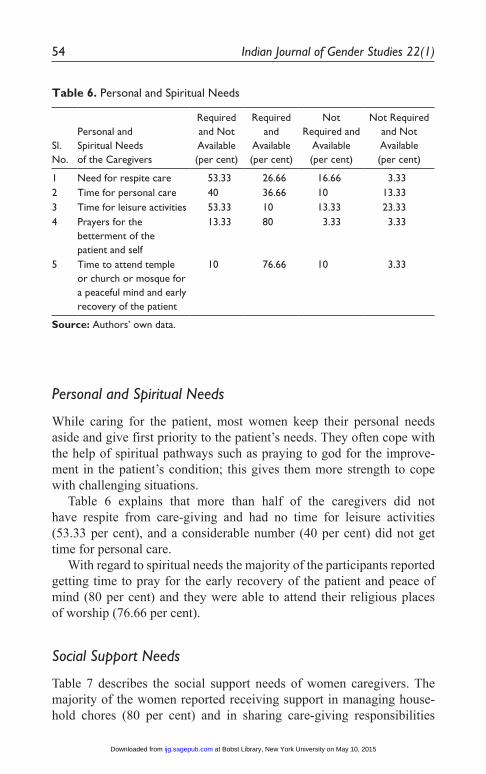
Personal and Spiritual Needs
While caring for the patient, most women keep their personal needs aside and give first priority to the patient’s needs. They often cope with the help of spiritual pathways such as praying to god for the improve-ment in the patient’s condition; this gives them more strength to cope with challenging situations.
Table 6 explains that more than half of the caregivers did not have respite from care-giving and had no time for leisure activities (53.33 per cent), and a considerable number (40 per cent) did not get time for personal care.
With regard to spiritual needs the majority of the participants reported getting time to pray for the early recovery of the patient and peace of mind (80 per cent) and they were able to attend their religious places of worship (76.66 per cent).
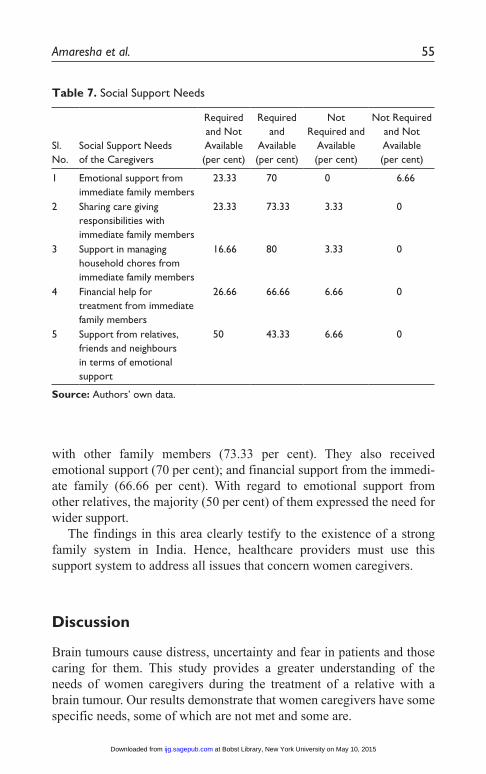
Social Support Needs
Table 7 describes the social support needs of women caregivers. The majority of the women reported receiving support in managing house-hold chores (80 per cent) and in sharing care-giving responsibilities
Table 6. Personal and Spiritual Needs
Sl. No.
Personal and Spiritual Needs of the Caregivers
Required and Not Available (per cent)
Required and
Available (per cent)
Not Required and
Available (per cent)
Not Required and Not Available (per cent)
1 Need for respite care 53.33 26.66 16.66 3.33 2 Time for personal care 40 36.66 10 13.33 3 Time for leisure activities 53.33 10 13.33 23.33 4 Prayers for the
betterment of the patient and self
13.33 80 3.33 3.33
5 Time to attend temple or church or mosque for a peaceful mind and early recovery of the patient
10 76.66 10 3.33
Source: Authors’ own data.
at Bobst Library, New York University on May 10, 2015ijg.sagepub.comDownloaded from
Amaresha et al. 55
Table 7. Social Support Needs
Sl. No.
Social Support Needs of the Caregivers
Required and Not Available (per cent)
Required and
Available (per cent)
Not Required and
Available (per cent)
Not Required and Not Available (per cent)
1 Emotional support from immediate family members
23.33 70 0 6.66
2 Sharing care giving responsibilities with immediate family members
23.33 73.33 3.33 0
3 Support in managing household chores from immediate family members
16.66 80 3.33 0
4 Financial help for treatment from immediate family members
26.66 66.66 6.66 0
5 Support from relatives, friends and neighbours in terms of emotional support
50 43.33 6.66 0
Source: Authors’ own data.
with other family members (73.33 per cent). They also received emotional support (70 per cent); and financial support from the immedi-ate family (66.66 per cent). With regard to emotional support from other relatives, the majority (50 per cent) of them expressed the need for wider support.
The findings in this area clearly testify to the existence of a strong family system in India. Hence, healthcare providers must use this support system to address all issues that concern women caregivers.
Discussion
Brain tumours cause distress, uncertainty and fear in patients and those caring for them. This study provides a greater understanding of the needs of women caregivers during the treatment of a relative with a brain tumour. Our results demonstrate that women caregivers have some specific needs, some of which are not met and some are.
at Bobst Library, New York University on May 10, 2015ijg.sagepub.comDownloaded from
56 Indian Journal of Gender Studies 22(1)
Women Caregivers’ Unmet Needs
In this study the majority of the women caregivers admitted in their responses that they required emotional help in dealing with death and dying issues, care-giving stress, acceptance of the illness and negative emotions such as sadness, guilt and fear. These findings are in con- sonance with other published studies on patients and caregivers of persons suffering with a brain tumour (Cornwell et al., 2012; Parvataneni et al., 2011). McMillan et al. (2006) conducted a study on coping skills and interventions for caregivers of cancer patients, which proved effective in improving the quality of life, reducing the burden caused by patients’ symptoms, and care-giving tasks. Hence this kind of structured caregiver skill-training interventions can be replicated for women caregivers in end-of-life care situations.
Our research has shown that a good majority of the women caregivers wanted to get information on the consequences of the surgery or radia-tion therapy and to acquire skills to deal with any emergencies that could occur. This is one of the most important needs to be addressed to prepare women caregivers to tackle post-surgery and post-discharge episodes. Similar needs were also found in the study done by Janda et al. (2006), where they identified six major needs, including the need for information about the illness, coping with uncertainty, practical help to prepare for post discharge long-term care, support to deal with social stigma and support to discuss the prognosis of the illness. These needs were addressed by Cashman et al. (2007) in their study about the impact of an educational programme on caregivers of brain tumour patients based on their pre-assessed needs. The results of the Cashman et al. (2007) study highlighted the fact that an increase in the acquisition of knowledge and understanding about the brain tumour helped to reduce anxiety and improved self-esteem immediately after the programme. This strongly suggests the need for providing educational interventions especially for women caregivers in neuro-oncology settings.
The majority of the women caregivers in this study expressed the need for ongoing caregiver support groups, where they can meet and share information about the illness and share their emotional difficulties. This kind of support group programme will help women caregivers to find solutions in their day-to-day hassles/glitches in care-giving and provide emotional support. This need has been addressed in the study conducted by Parvataneni et al. (2011), where they provided insights into the caregiver’s psychosocial problems and highlighted improved services for brain tumour patients and their caregivers. A 1996 study evaluated a supportive care intervention for carers of patients with brain
at Bobst Library, New York University on May 10, 2015ijg.sagepub.comDownloaded from
Amaresha et al. 57
tumour, finding it to be successful in improving well-being among carers (Horowitz et al., 1996).
The current study revealed that women caregivers were in dire need of respite from care-giving roles. The provision of respite is based on the assumption that temporary relief from care-giving will reduce caregiver stress and possibly enhance the ability of care-giving. Willingness to use respite care facilities was found in a study investigated by Huang et al. (2009). In this study women caregivers also expressed that they need time for themselves, for personal care and leisure activities. Unless healthcare professionals explore these issues they will remain unnoticed. Hence, there is a great need for professional attention to provide neces-sary psychosocial support for women caregivers in this kind of setting. However, countries like India lack the services of ancillary healthcare professionals such as trained psychologists and social workers (Saxena et al., 2006) which is a barrier to addressing the psychosocial issues being discussed here. It is necessary to provide necessary professional help to women caregivers.
Concluding Remarks
The need to have easy access to healthcare providers, discussions on the patient’s treatment, basic information about the diagnostic investi- gations, prognosis, and information on welfare benefits has been empha-sised by several studies (Cornwell et al., 2012; Janda et al., 2006; Parvataneni et al., 2011). The current study has recognised that some if not all of the significant needs of women caregivers were met in the set-ting of our research. For the rest, the majority of the women caregivers coped with the help of spiritual practices, such as praying and visiting religious places, where they prayed for the improvement of the patient as well as for themselves. The majority of the women received primary social support from their immediate families. A 2012 study found that good social support will reduce the caregiver burden (Shieh et al., 2012). Healthcare professionals should address the needs of caregivers highlighted in this study but too often overlooked.
Recommendations and Implications of the Study
1. Inclusion of women caregivers in the treatment process. Most of the time women are ignored in the treatment process and decision
at Bobst Library, New York University on May 10, 2015ijg.sagepub.comDownloaded from
58 Indian Journal of Gender Studies 22(1)
making with regard to patient care. Generally, clinicians prefer to disclose information about the diagnosis, prognosis and treatment to male family members whose concerns alone are taken into consideration. Since women are the primary caregivers, they should be included in the treatment process to help them understand the situation better, so that they can give the patient improved care.
2. Understanding psychosocial issues of women caregivers. It is obvious that patient care is the first preference of clinicians and even family members prefer that. The psychosocial issues of women caregivers are overlooked due to the over-emphasis on patient care as they rarely get the opportunity to reveal their con-cerns. Hence special attention is required to understand these silent sufferers.
3. Training professionals. Primary health care providers such as doctors often have hectic clinical responsibilities and have less time to address such issues. There is a dearth of trained professionals such as clinical psychologists and social workers in these settings. Hence, recruitment of dedicated counsellors is required to handle women caregiver’s issues. Postgraduate courses such as nursing, psychology, social work and other courses should train students to deal with the problems of women caregivers in medical settings so that the necessary human resources can be drawn from among them to meet this urgent need.
4. Case management. Research has shown that a proportion of caregiv- ers of patients with a brain tumour suffer from psychiatric disorders themselves. This requires individual attention in terms of psycho-logical therapy or counselling. Case management should involve a comprehensive, holistic approach, which can offer tailor-made individual need-based interventions for women caregivers.
5. Support groups. These are empirically proven therapeutic interven-tions for caregivers in distress. Such groups facilitate the ventilation of inner feelings such as fear, sadness, guilt, grief, self-imposed stigma; information-sharing among group members regarding the nature of the illness, treatment and prognosis; dealing with caregiver issues; patient management skills; coping with the illness; problem solving and enhancing the support network among caregivers. Such groups are cost effective and provide the necessary psychosocial support for women caregivers.
6. Identifying and utilising the strengths in women caregivers. Although life-threatening illnesses pose significant challenges and cause severe stress, burden and emotional problems, some women
at Bobst Library, New York University on May 10, 2015ijg.sagepub.comDownloaded from

Amaresha et al. 59
caregivers quickly adapt to the troubles and face them with determi-nation. Available strengths in terms of life skills and having strong social support could ease the suffering caused by the patient’s illness. Viewing women as a source of strength and addressing their abilities will help them in overcoming unexpected adversities.
7. Research. As women caregivers play a vital role in the treatment of any illness, future research should give more importance to a com-prehensive understanding of their concerns, which may be different from those of male caregivers. Gender-specific interventions would help in addressing the specific needs of women caregivers and their significant problems.
The results of this study may change the attitude of health care professionals in neuro-oncology settings towards such caregiver issues and provide valuable insights in developing the necessary organi- sational policy level changes to improve the quality of life of women caregivers.
References
Bradley, S., Sherwood, P., Kuo, J., Kammerer, C., Gettig, E., Ren, D., et al. (2009). Perceptions of economic hardship and emotional health in a pilot sample of family caregivers. Journal of Neuro-Oncology, 93(3), 333–342.
Brinda, E.M., Rajkumar, A.P., Enemark, U., Attermann, J., & Jacob, K. (2014). Cost and burden of informal caregiving of dependent older people in a rural Indian community. BMC Health Service Research, 14(1), 207.
Cashman, R., Bernstein, L.J., Bilodeau, D., Bovett, G., Jackson, B., Yousefi, M., et al. (2007). Evaluation of an educational program for the caregivers of persons diagnosed with a malignant glioma. Canadian Oncology Nursing Journal, 17(1), 6–15.
Chentsova-Dutton, Y., Shuchter, S., Hutchin, S., Strause, L., Burns, K., & Zisook, S. (2000). The psychological and physical health of hospice caregivers. Annals of Clinical Psychiatry, 12(1), 19–27.
Choi, C.W., Stone, R., Kim, K., Ren, D., Schulz, R., Given, C., et al. (2012). Group-based trajectory modeling of caregiver psychological distress over time. Annals of Behavioral Medicine, 44(1), 73–84.
Cornwell, P., Dicks, B., Fleming, J., Haines, T.P., & Olson, S. (2012). Care and support needs of patients and carers early post-discharge following treatment for non-malignant brain tumour: Establishing a new reality. Supportive Care in Cancer, 20(10), 2595–2610.
DesRoches, C., Blendon, R., Young, J., Scoles, K., & Kim, M. (2002). Caregiving in the post-hospitalisation period: Findings from a national survey. Nursing Economics, 20(5), 216–221, 224.
at Bobst Library, New York University on May 10, 2015ijg.sagepub.comDownloaded from

60 Indian Journal of Gender Studies 22(1)
Dias, A., Dewey, M.E., D’Souza, J., Dhume, R., Motghare, D.D., Shaji, K.S., et al. (2008). The effectiveness of a home care program for supporting caregivers of persons with dementia in developing countries: A randomised controlled trial from Goa, India. PLoS One, 3(6), e2333.
Fox, S., & Lantz, C. (1998). The brain tumor experience and quality of life: A qualitative study. Journal of Neuroscience Nursing, 30(4), 245–252.
Gupta, R., Rowe, N., & Pillai, V.K. (2009). Perceived caregiver burden in India: Implications for social services. Affilia, 24(1), 69–79.
Hill, C.I., Nixon, C.S., Ruehmeier, J.L., & Wolf, L.M. (2002). Brain tumours. Physical Therapy, 82(5), 496–502.
Horowitz, S., Passik, S.D., & Malkin, M.G. (1996). In sickness and in health. Journal of Psychosocial Oncology, 14(2), 43–56.
Hricik, A., Donovan, H., Bradley, S.E., Given, B.A., Bender, C.M., Newberry, A., et al. (2011). Changes in caregiver perceptions over time in response to providing care for a loved one with a primary malignant brain tumor. Oncology Nursing Forum, 38(2), 149–155.
Huang, H.L., Shyu, Y.I., Chang, M.Y., Weng, L.C., & Lee, I. (2009). Willingness to use respite care among family caregivers in Northern Taiwan. Journal of Clinical Nursing, 18(2), 191–198.
Hutchinson, K.C., Willard, V.W., Hardy, K.K., & Bonner, M.J. (2009). Adjustment of caregivers of pediatric patients with brain tumors: A cross-sectional analysis. Psycho-Oncology, 18(5), 515–523.
Janda, M., Eakin, E.G., Bailey, L., Walker, D., & Troy, K. (2006). Supportive care needs of people with brain tumours and their carers. Supportive Care in Cancer, 14(11), 1094–1103.
Janda, M., Steginga, S., Langbecker, D., Dunn, J., Walker, D., & Eakin, E. (2007). Quality of life among patients with a brain tumor and their carers. Journal of Psychosomatic Research, 63(6), 617–623.
———. (2008). Unmet supportive care needs and interest in services among patients with a brain tumor and their carers. Patient Education and Coun-seling, 71(2), 251–258.
Kadam, A., and Shinde, M.B. (2014). Effectiveness of structured education on caregiver’s knowledge and attitude regarding colostomy care. International Journal of Science and Research, 3(4), 586–593.
Keir, S., Guill, A., Carter, K., Boole, L., Gonzales, L., & Friedman, H. (2006). Differential levels of stress in caregivers of brain tumor patients-observations from a pilot study. Supportive Care in Cancer, 14(12), 1258–1261.
Kulkarni, P., Kulkarni, P., Ghooi, R., Bhatwadekar, M., Thatte, N., & Anavkar, V. (2014). Stress among care givers: The impact of nursing a relative with cancer. Indian Journal of Palliative Care, 20(1), 31–39.
Kumar, C.N., Suresha, K.K., Thirthalli, J., Arunachala, U., & Gangadhar, B.N. (2014). Caregiver burden is associated with disability in schizo-phrenia: Results of a study from a rural setting of south India. Inter- national Journal of Social Psychiatry. first published on June 19, 2014 as doi:10.1177/0020764014537637
at Bobst Library, New York University on May 10, 2015ijg.sagepub.comDownloaded from
Amaresha et al. 61
Litzelman, K., Catrine, K., Gangnon, R., & Witt, W. (2011). Quality of life among parents of children with cancer or brain tumors: The impact of child characteristics and parental psychosocial factors. Quality of Life Research, 20(8), 1261–1269.
Lobb, E.A., Halkett, G.K., & Nowak, A.K. (2011). Patient and caregiver perceptions of communication of prognosis in high grade glioma. Journal of Neuro-Oncology, 104(1), 315–322.
McConigley, R., Halkett, G., Lobb, E., & Nowak, A. (2010). Caring for someone with high-grade glioma: A time of rapid change for caregivers. Palliative Medicine, 24(5), 473–479.
McMillan, S.C., Small, B.J., Weitzner, M., Schonwetter, R., Tittle, M., Moody, L., et al. (2006). Impact of coping skills intervention with family caregivers of hospice patients with cancer: A randomized clinical trial. Cancer, 106(1), 214–222.
Mehrotra, S., and Sukumar, P. (2007). Sources of strength perceived by females caring for relatives diagnosed with cancer: An exploratory study from India. Supportive Care in Cancer, 15(12), 1357–1366.
Mezue, W.C., Draper, P., Watson, R., & Mathew, B.G. (2011). Caring for patients with brain tumor: The patient and care giver perspectives. Nigerian Journal of Clinical Practice, 14(3), 368–372.
Oeffinger, K.C., Mertens, A.C., Hudson, M.M., Gurney, J.G., Casillas, J., Chen, H., et al. (2004). Health care of young adult survivors of childhood cancer: A report from the Childhood Cancer Survivor Study. The Annals of Family Medicine, 2(1), 61–70.
Pattanayak, R.D., Jena, R., Tripathi, M., & Khandelwal, S.K. (2010). Assessment of burden in caregivers of Alzheimer’s disease from India. Asian Journal of Psychiatry, 3(3), 112–116.
Parvataneni, R., Polley, M.-Y., Freeman, T., Lamborn, K., Prados, M., Butowski, N., et al. (2011). Identifying the needs of brain tumor patients and their caregivers. Journal of Neuro-Oncology, 104(3), 737–744.
Petruzzi, A., Finocchiaro, C.Y., Lamperti, E., & Salmaggi, A. (2012). Living with a brain tumor: Reaction profiles in patients and their caregivers. Supportive Care in Cancer, 21(4), 1105–1111.
Robinson, B., & Thurnher, M. (1979). Taking care of aged parents: A family cycle transition. The Gerontologist, 19(6), 586–593.
Salander, P., & Spetz, A. (2002). How do patients and spouses deal with the serious facts of malignant glioma? Palliative Medicine, 16(4), 305–313.
Saxena, S., Sharan, P., Garrido, M., & Saraceno, B. (2006). World Health Organization’s mental health atlas 2005: Implications for policy develop- ment. World Psychiatry, 5(3), 179–184.
Schubart, J.R., Kinzie, M.B., & Farace, E. (2008). Caring for the brain tumor patient: Family caregiver burden and unmet needs. Neuro-Oncology, 10(1), 61–72.
at Bobst Library, New York University on May 10, 2015ijg.sagepub.comDownloaded from
62 Indian Journal of Gender Studies 22(1)
Shaji, K.S., George, R.K., Prince, M.J., & Jacob, K.S. (2009). Behavioral symptoms and caregiver burden in dementia. Indian Journal of Psychiatry, 51(1), 45–49.
Shieh, S.C., Tung, H.S., & Liang, S.Y. (2012). Social support as influencing primary family caregiver burden in Taiwanese patients with colorectal cancer. Journal of Nursing Scholarship, 44(3), 223–231.
Sherwood, P., Given, B., Given, C., Schiffman, R., Murman, D., & Lovely, M. (2004). Caregivers of persons with a brain tumor: A conceptual model. Nursing Inquiry, 11(1), 43–53.
Sherwood, P.R., Given, B.A., Given, C.W., Schiffman, R.F., Murman, D.L., Lovely, M. et al. (2006). Predictors of distress in caregivers of persons with a primary malignant brain tumor. Research in Nursing & Health, 29(2), 105–120.
Strang, S., & Strang, P. (2001). Spiritual thoughts, coping and ‘sense of coherence’ in brain tumour patients and their spouses. Palliative Medicine, 15(2), 127–134.
Swartz, J.J., & Keir, S.T. (2007). Program preferences to reduce stress in caregivers of patients with brain tumors. Clinical Journal of Oncology Nursing, 11(5), 723–727.
Talwar, P., & Matheiken, S.T. (2010). Caregivers in schizophrenia: A cross cultural perspective. Indian Journal of Psychological Medicine, 32(1), 29–33.
Van Dongen-Melman, J.E., Van Zuuren, F.J., & Verhulst, F.C. (1998). Experiences of parents of childhood cancer survivors: A qualitative analysis. Patient Education and Counseling, 34(3), 185–200.
Vanderwerker, L.C., Laff, R.E., Kadan-Lottick, N.S., McColl, S., & Prigerson, H.G. (2005). Psychiatric disorders and mental health service use among caregivers of advanced cancer patients. Journal of Clinical Oncology, 23(28), 6899–6907.
Witt, W., Litzelman, K., Wisk, L., Spear, H., Catrine, K., Levin, N. et al. (2010). Stress-mediated quality of life outcomes in parents of childhood cancer and brain tumor survivors: A case-control study. Quality of Life Research, 19(7), 995–1005.
Wolff, J.L., & Kasper, J.D. (2006). Caregivers of frail elders: Updating a national profile. The Gerontologist, 46(3), 344–356.
Wright, F. (1983). Single careers: Employment, housework and caring. In J. Finch & D. Groves (Eds), A labour of love: Women, work, and caring (pp. 89–105). London: Routledge and Kegan Paul.
at Bobst Library, New York University on May 10, 2015ijg.sagepub.comDownloaded from
Copyright © 2022 FDOKUMEN




















