
Which drug is effective and safe for acute malaria in pregnancy? Reviewing the evidence
13
DRUG DEVELOPMENT RESEARCH 71:56–68 (2010) Research Overview Which Drug is Effective and Safe for Acute Malaria in Pregnancy? Reviewing the Evidence Rose McGready 1– 3 and Franc - ois Nosten 1– 3 1 Shoklo Malaria Research Unit, Mae Sot, Thailand 2 Mahidol-Oxford Tropical Medicine Research Unit (MORU), Faculty of Tropical Medicine, Mahidol University, Bangkok, Thailand 3 Centre for Tropical Medicine, Nuffield Department of Clinical Medicine, University of Oxford, Oxford, United Kingdom Strategy, Management and Health Policy Enabling Technology, Genomics, Proteomics Preclinical Research Preclinical Development Toxicology, Formulation Drug Delivery, Pharmacokinetics Clinical Development Phases I-III Regulatory, Quality, Manufacturing Postmarketing Phase IV ABSTRACT During pregnancy, a woman living or travelling in a malaria endemic area is more at risk of contracting the disease and developing a severe infection and dying than a non-pregnant woman. Despite this increased morbidity and mortality in pregnancy, there are almost no studies on which to base recommendations on the use of antimalarial drugs in this vulnerable group. This is because, paradoxically, the emphasis is often put on the safety of the unborn child rather than that of the infested mother. As a result of this neglect, tens of thousands of pregnant women (and their fetuses) are dying every year of a very preventable and treatable infection. In recent years, some trials have been conducted, especially in areas of high resistance in Plasmodium falciparum in South East Asia. The results show that quinine plus clindamycin is the treatment of choice in the first trimester, while artemisinin treatment should be used in the second and third trimesters in the treatment of uncomplicated malaria. For severe malaria, parenteral artesunate is the treatment of choice. However these studies have also shown that the pharmacokinetic properties of most antimalarials are altered during gestation and that the doses used in non-pregnant adults are often not adapted to pregnancy. Urgent efforts are required to optimize the treatment of malaria in pregnancy. Drug Dev Res 71:56–68, 2010. r 2009 Wiley-Liss, Inc. Key words: malaria; P. falciparum; pregnancy INTRODUCTION The aim of this review is to provide up-to-date information on the efficacy and safety of antimalarials used for treatment (not prophylaxis) of malaria in pregnancy (MIP), based on published evidence. There are few or no studies for most of the drugs used for the treatment of tropical infections in pregnancy, and only few or no evidence-based recommendations [White et al., 2008]. While prompt and effective treatment is now recognized as essential and far outweighs the risk of having malaria parasites in a pregnant woman’s body, there are remarkably few studies of antimalarial drugs in pregnancy [Nosten et al., 2007]. Of over 500 antimalarial drug trials conducted between 1966 and December 2006, only 31 evaluated antimalarial treatments (including intermittent preventive treatments) in pregnant women, and 14 of these were from a single centre [Myint et al., 2004]. Most of what is know about chloroquine use in pregnancy comes from research on autoimmune disease in pregnancy [Costedoat-Chalumeau et al., DDR Published online in Wiley InterScience (www.interscience.wiley. com). DOI: 10.1002/ddr.20348 Correspondence to: Rose McGready, Shoklo Malaria Research Unit, PO Box 46, Mae Sot, Tak, Thailand, 63110. E-mail: [email protected] c 2009 Wiley-Liss, Inc.
-
Upload
shoklo-unit -
Category
Documents
-
view
4 -
download
0
Transcript of Which drug is effective and safe for acute malaria in pregnancy? Reviewing the evidence
DRUG DEVELOPMENT RESEARCH 71:56–68 (2010)
Research Overview
Which Drug is Effective and Safe for Acute Malariain Pregnancy? Reviewing the Evidence
Rose McGready1– 3� and Franc-ois Nosten1– 3
1Shoklo Malaria Research Unit, Mae Sot, Thailand2Mahidol-Oxford Tropical Medicine Research Unit (MORU), Faculty of Tropical Medicine,
Mahidol University, Bangkok, Thailand3Centre for Tropical Medicine, Nuffield Department of Clinical Medicine, University of Oxford,
Oxford, United Kingdom
Strategy, Management and Health Policy
Enabling
Technology,
Genomics,
Proteomics
Preclinical
Research
Preclinical Development
Toxicology, Formulation
Drug Delivery,
Pharmacokinetics
Clinical Development
Phases I-III
Regulatory, Quality,
Manufacturing
Postmarketing
Phase IV
ABSTRACT During pregnancy, a woman living or travelling in a malaria endemic area is more at riskof contracting the disease and developing a severe infection and dying than a non-pregnant woman.Despite this increased morbidity and mortality in pregnancy, there are almost no studies on which to baserecommendations on the use of antimalarial drugs in this vulnerable group. This is because, paradoxically,the emphasis is often put on the safety of the unborn child rather than that of the infested mother. As aresult of this neglect, tens of thousands of pregnant women (and their fetuses) are dying every year of a verypreventable and treatable infection. In recent years, some trials have been conducted, especially in areasof high resistance in Plasmodium falciparum in South East Asia. The results show that quinine plusclindamycin is the treatment of choice in the first trimester, while artemisinin treatment should be used inthe second and third trimesters in the treatment of uncomplicated malaria. For severe malaria, parenteralartesunate is the treatment of choice. However these studies have also shown that the pharmacokineticproperties of most antimalarials are altered during gestation and that the doses used in non-pregnant adultsare often not adapted to pregnancy. Urgent efforts are required to optimize the treatment of malaria inpregnancy. Drug Dev Res 71:56–68, 2010. r 2009 Wiley-Liss, Inc.
Key words: malaria; P. falciparum; pregnancy
INTRODUCTION
The aim of this review is to provide up-to-dateinformation on the efficacy and safety of antimalarialsused for treatment (not prophylaxis) of malaria inpregnancy (MIP), based on published evidence. Thereare few or no studies for most of the drugs used for thetreatment of tropical infections in pregnancy, and onlyfew or no evidence-based recommendations [White et al.,2008]. While prompt and effective treatment is nowrecognized as essential and far outweighs the risk ofhaving malaria parasites in a pregnant woman’s body,there are remarkably few studies of antimalarial drugs inpregnancy [Nosten et al., 2007]. Of over 500 antimalarial
drug trials conducted between 1966 and December 2006,only 31 evaluated antimalarial treatments (includingintermittent preventive treatments) in pregnant women,and 14 of these were from a single centre [Myint et al.,2004]. Most of what is know about chloroquine usein pregnancy comes from research on autoimmunedisease in pregnancy [Costedoat-Chalumeau et al.,
DDR
Published online in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/ddr.20348
�Correspondence to: Rose McGready, Shoklo MalariaResearch Unit, PO Box 46, Mae Sot, Tak, Thailand, 63110.E-mail: [email protected]
�c 2009 Wiley-Liss, Inc.
2003; Ostesen, 1994; Parke, 1988; Parke and West, 1996]and for quinine from its historical use [Dilling andGemmell, 1929; Maxwell, 1908]. Sulphadoxine-pyri-methamine has been widely advocated in pregnancywithout ever knowing the efficacy or until recently thepharmacokinetic properties of this drug in pregnantwomen [Green et al., 2007; Nyunt et al., 2009].
Measuring the efficacy of antimalarial drugs inpregnancy differs in a very important way from non-pregnant studies in that Plasmodium falciparum has theability to sequester in the placenta. In a recentlyconducted randomized controlled trial with artemisininsin pregnancy on the Thai-Burmese border, one third ofPCR-confirmed drug failures occurred after day 42 offollow-up, and as late as day 98. This has been reportedpreviously in Asia [Brockman et al., 1999; McGready et al.,2000] and Africa [Kalilani et al., 2007]. Treatment trials inpregnancy require a longer period of follow-up and abroader approach than treatment trials in non-pregnantpatients as two hosts are essentially under study. Thesample size of randomized controlled treatment trials ofmalaria are usually determined by the difference betweenthe expected efficacy of the trial drug and that of thecomparator. However, these trials are often underpoweredto describe safety in the mothers and their infants.
BACKGROUND
Malaria is the most important parasitic infectionin humans and in pregnancy is detrimental to both themother and fetus. The protozoan parasites, Plasmo-dium falciparum, P. vivax, P. malariae, P. ovale andrarely P. knowlesi are transmitted by the bite of asporozoite-bearing female anopheline mosquito.P. falciparum causes greater morbidity (maternal andfetal), principally low birth weight and anaemia, andmortality than non-falciparum infections [Desai et al.,2007]. After a period of pre-erythrocytic developmentin the liver, the blood-stage infection, which causes thedisease, begins. Parasitic invasion of the erythrocyteconsumes hemoglobin and alters the red cell mem-brane allowing it to cytoadhere (or stick) inside thesmall blood vessels of brain, kidneys, and other affectedorgans. P. falciparum–infected red cells may alsoadhere to uninfected red cells to form rosettes.Cytoadherence and rosetting of falciparum malariainterfere with microcirculatory flow and metabolism ofvital organs. The hallmark of malaria in pregnancy isparasites sequestered in the placenta. Sequesteredparasites evade the host defence mechanisms of splenicprocessing and filtration. Sequestration is not knownto occur in the benign malarias due to P. ovale andP. Malariae but is suspected in P. vivax.
In pregnancy the adverse effects of malariainfection arise from two main processes. The first is
from systemic infection, comparable to the effects ofany severe febrile illness in pregnancy, which causesmaternal/fetal mortality, abortion, stillbirth, and pre-mature delivery. The second is the parasitisation itself,which results in fetal growth restriction and low birthweight, maternal/fetal anemia, interaction with HIV,and susceptibility of the infant to malaria.
Lack of premunition, i.e., the degree of naturalacquired host immunity to malaria, or malaria-specificimmunity, results in the accumulation of parasites andinflammatory cells in the placenta, leading to pooroutcomes for both mother and baby, and in the case ofnon-immune women, pregnancy increases the risk ofsevere disease and death. A recent review of the burdenof MIP estimates that about 1 in 4 women in Sub-Saharan Africa in areas of stable transmission havemalaria at the time of delivery [Desai et al., 2007].Ideally, malarial infection (parasitation) during preg-nancy should be prevented but failing this (an increasingproblem due to drug resistance) prompt diagnosis andeffective treatment will prevent potentially fatal out-comes and reduce morbidity in mothers and infants.
METHODS
A literature search was performed using Medline(1983–2009). The keywords used were ‘‘malaria,’’‘‘severe malaria,’’ ‘‘P. falciparum,’’ ‘‘P. vivax,’’ ‘‘chloro-quine-resistant P. vivax,’’ ‘‘pregnancy,’’ ‘‘treatment,’’‘‘antimalarials,’’ ‘‘amodiquine,’’ ‘‘quinine,’’ ‘‘artemisi-nins,’’ ‘‘artesunate,’’ ‘‘mefloquine,’’ ‘‘chloroquine,’’ ‘‘ma-larone,’’ ‘‘clindamycin,’’ ‘‘artemether-lumefantrine,’’‘‘dihyroartemisinin-piperaquine,’’ ‘‘atovaquone-progua-nil,’’ ‘‘suphodoxine-pyrimethamine,’’ ‘‘malaria mortal-ity,’’ and ‘‘maternal mortality.’’ Nearly all of thepreceding words were used in combinations with thekeyword ‘‘pregnancy,’’ e.g., ‘‘P. falciparum’’ and ‘‘preg-nancy.’’ Reference lists of the articles identified werehand-searched for additional articles. Other sourcesincluded: malaria treatment guidelines from the UK,Centre for Disease Control (CDC), World HealthOrganisation (WHO), and Shoklo Malaria ResearchUnit (SMRU), as well as websites for malaria,travellers, and pregnancy. Where possible, recommen-dations are based on, and explicitly linked to, theevidence that supports them. Overall, there were 10randomized controlled trials (RCT) on the treatment ofP. falciparum in pregnancy [Bounyasong, 2001; Keuteret al., 1990; McGready et al., 2000, 2001b, 2005, 2008;Naing et al., 1988; Nosten et al., 1993; Sowunmi et al.,1998; Tagbor et al., 2006] and one on severe malariathat did not exclude pregnant women [Dondorp et al.,2005], 13 pharmacokinetic studies [Abdelrahim et al.,2007; Green et al., 2007; Massele et al., 1997;McGready et al., 2003b,c, 2006a,b; Na-Bangchang
57MALARIA TREATMENT IN PREGNANCY
Drug Dev. Res.

et al., 1994, 2005; Nosten et al., 1990; Nyunt et al.,2009; Phillips et al., 1986; Wangboonskul et al., 1993],and treatment and prevention trials that were observa-tional or descriptive.
PITFALLS IN TREATMENT OF UNCOMPLICATED MIP
Accidental exposure in the first trimester toantimalarials can be minimized by practising basic(essential) prescription procedures. Woman of child-bearing age should be asked if they could be pregnantbecause most of the commonly used antimalarialsshould not be prescribed in the first trimester. Thisshould be clearly explained. Where there is doubt,confirmation by urine pregnancy testing is helpful.Similar enquiries should be made to every patientregarding allergy. The diagnosis of malaria in pregnancy,as in non-pregnant patients, relies on microscopic (thecurrent gold standard) examination of thick and thinblood films for parasites, or the use of rapid diagnostictests that detect specific parasite antigens. An experi-enced microscopist can detect 15 parasites/mL of bloodin a thick film (well below the pyrogenic densitythreshold of symptoms in non-pregnant patients) usingsimple Field’s stain or Giemsa stain [Nosten et al., 2007].However, malaria in pregnancy is associated withdeleterious effects even at parasite densities below thelimit of detection of microscopy or rapid diagnostic tests.A negative test by microscopy is still compatible with atotal parasite biomass of 108 parasites that will bedeleterious to the mother and the fetus. In immunewomen, peripheral thick films can be negative whenthere are parasites in the placenta but these are onlydetectable at delivery when it is far too late to doanything about it. This means that the diagnosis ofmalaria in pregnancy is more difficult than in non-pregnant patients. In a febrile patient, 3 negative malariasmears (smear interval of 12–24 h) almost certainly rulesout malaria as the cause of fever but patients who mayhave taken prophylaxis that can suppress the parasitae-mia below the level of microscopic detection (totalbiomass 108 parasites) need to be taken into account.
Treatment response in the presence of resistanceto antimalarial drugs depends on the grade ofresistance and the immune response of the patient.At low levels of resistance, the patient may appear to bebetter for some weeks before symptoms recur. When adrug fails to suppress circulating parasitaemia, thepatient symptoms will fail to be resolved by treatmentand the risk of morbidity and mortality is high [Priceet al., 2004; Roper et al., 2003; Wernsdorfer, 1994;White, 1999]. Logically, this means that a woman with abreakthrough episode of malaria whilst on prophylaxisshould not be treated with the same drug, wherealternative treatment is available. Similarly, a woman
with parasite reappearance following treatment is bestnot treated with the same antimalarial again. Evidencesupporting this was documented while treating womenin an area with high levels of multidrug-resistant strainsof P. falciparum (MDR-Pf) in descriptive studiespublished 10 years ago [McGready and Nosten,1999]. In the early years of artemisinin use inpregnancy on the Thai-Burmese border, artesunatewas reserved for women with multiple treatmentfailures. The standard treatments of quinine andmefloquine were favoured as first- and second-linetreatment under the assumption that more was knownabout their safety in pregnancy than on the effects ofartemisinin. Women with a third reappearance weretreated with an artemisinin derivative as a last resort.Retreatment, compared to primary treatment inpregnancy, with quinine and mefloquine, resulted in anear doubling of the failure rates (Table 1).
This evidence has been further verified inpregnancy with PCR genotyping data in a recentlypublished trial of artemisinin-based combination therapy[McGready et al., 2008]. The PCR confirmed failurerates of women who entered the study with a PCRconfirmed failure of a previous episode rather than asnovel or primary infections, were significantly higherwith the use of 3 days of artemether-lumefantrine: 26.1(12–40.8; 95% CI)% compared to 7 days of artesunatemonotherapy: 8.9 (0–21.2)%, P 5 0.034.
The following drugs should not be given inpregnancy: primaquine, which is associated withneonatal hemolysis and methemoglobinaemia; tetracy-cline/doxycycline, which can cause dental discolourationand maternal hepatoxicity with large parenteral doses;and halofantrine, which should not be used because ofsignificant and potentially fatal cardiotoxicity.
In any case of MIP, treatment with antimalarialsshould not be delayed regardless of whether thewoman has symptoms or not. Even asymptomatictreated episodes (even a single episode) are associatedwith a reduction of birth weight and anemia. This istrue for falciparum [Nosten et al., 1991] and vivax[Nosten et al., 1999a].
THE OBJECTIVES OF TREATMENT
The objective of treatment of uncomplicatedmalaria is to cure the infection to prevent diseaseprogression and reduce morbidity [WHO, 2006]. Inendemic areas, there is the public health goal ofreducing the transmission of infection to others andpreventing the emergence and spread of resistance toantimalarials. The prophylactic effect of antimalarials isan important consideration in pregnancy as preventioncan reduce the number of parasitemic episodes and,
58 MCGREADY AND NOSTEN
Drug Dev. Res.
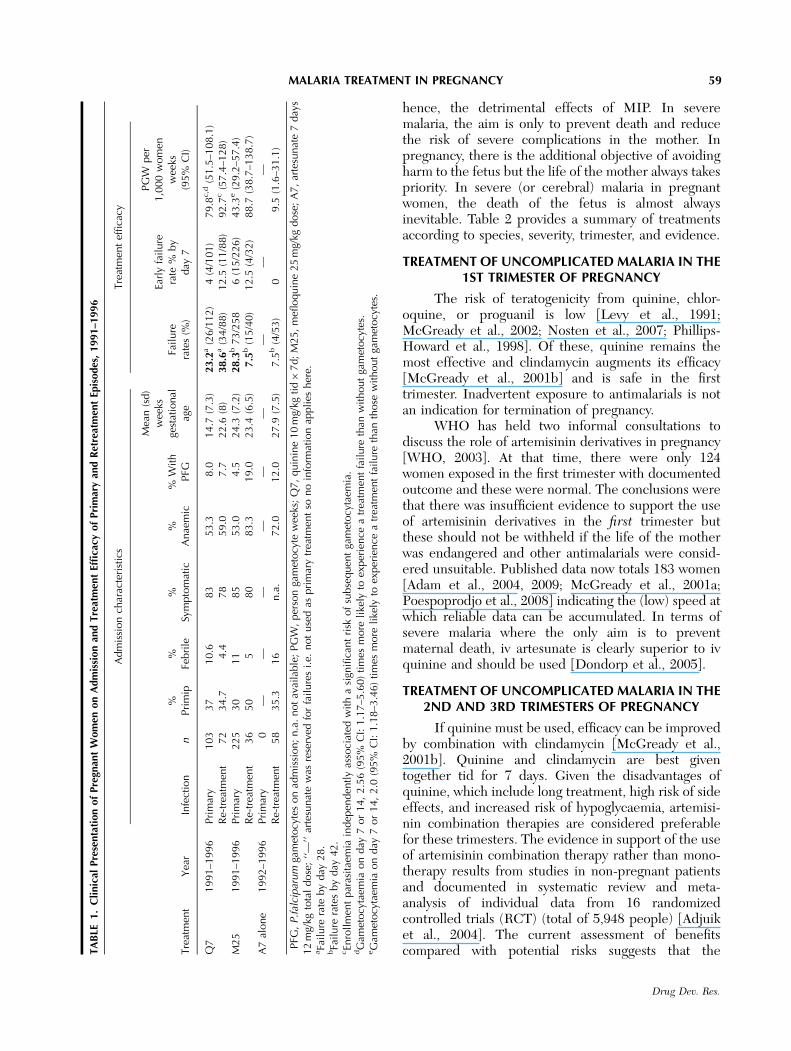
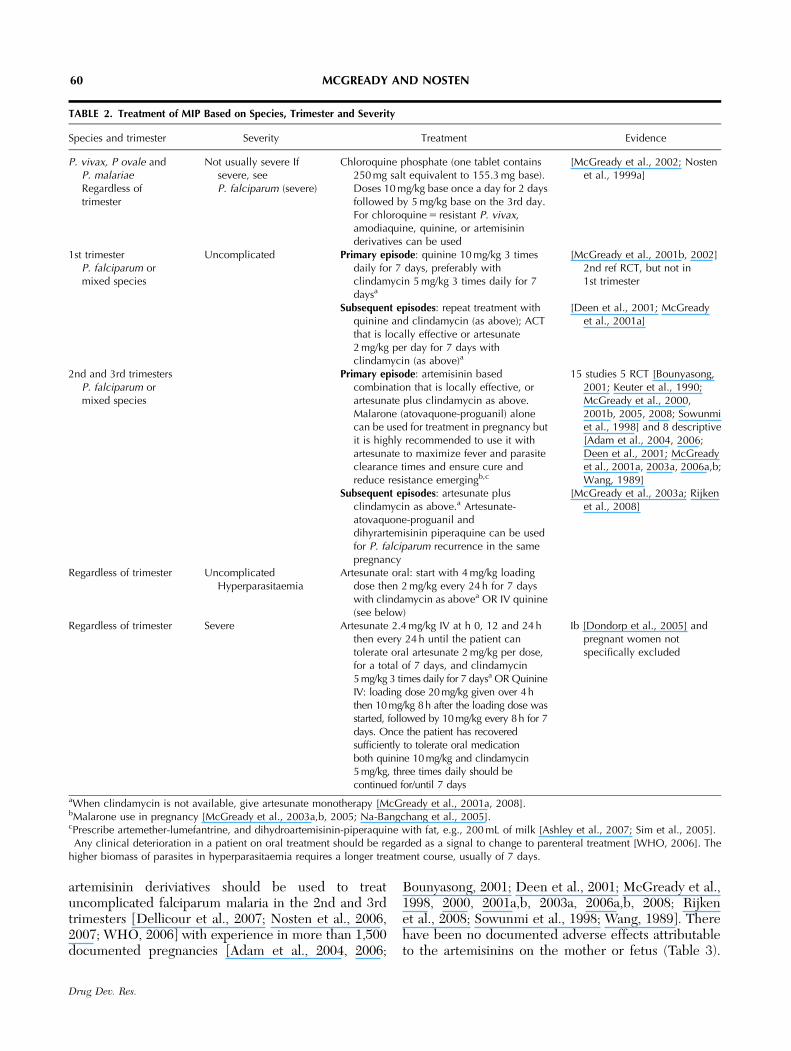
hence, the detrimental effects of MIP. In severemalaria, the aim is only to prevent death and reducethe risk of severe complications in the mother. Inpregnancy, there is the additional objective of avoidingharm to the fetus but the life of the mother always takespriority. In severe (or cerebral) malaria in pregnantwomen, the death of the fetus is almost alwaysinevitable. Table 2 provides a summary of treatmentsaccording to species, severity, trimester, and evidence.
TREATMENT OF UNCOMPLICATED MALARIA IN THE1ST TRIMESTER OF PREGNANCY
The risk of teratogenicity from quinine, chlor-oquine, or proguanil is low [Levy et al., 1991;McGready et al., 2002; Nosten et al., 2007; Phillips-Howard et al., 1998]. Of these, quinine remains themost effective and clindamycin augments its efficacy[McGready et al., 2001b] and is safe in the firsttrimester. Inadvertent exposure to antimalarials is notan indication for termination of pregnancy.
WHO has held two informal consultations todiscuss the role of artemisinin derivatives in pregnancy[WHO, 2003]. At that time, there were only 124women exposed in the first trimester with documentedoutcome and these were normal. The conclusions werethat there was insufficient evidence to support the useof artemisinin derivatives in the first trimester butthese should not be withheld if the life of the motherwas endangered and other antimalarials were consid-ered unsuitable. Published data now totals 183 women[Adam et al., 2004, 2009; McGready et al., 2001a;Poespoprodjo et al., 2008] indicating the (low) speed atwhich reliable data can be accumulated. In terms ofsevere malaria where the only aim is to preventmaternal death, iv artesunate is clearly superior to ivquinine and should be used [Dondorp et al., 2005].
TREATMENT OF UNCOMPLICATED MALARIA IN THE2ND AND 3RD TRIMESTERS OF PREGNANCY
If quinine must be used, efficacy can be improvedby combination with clindamycin [McGready et al.,2001b]. Quinine and clindamycin are best giventogether tid for 7 days. Given the disadvantages ofquinine, which include long treatment, high risk of sideeffects, and increased risk of hypoglycaemia, artemisi-nin combination therapies are considered preferablefor these trimesters. The evidence in support of the useof artemisinin combination therapy rather than mono-therapy results from studies in non-pregnant patientsand documented in systematic review and meta-analysis of individual data from 16 randomizedcontrolled trials (RCT) (total of 5,948 people) [Adjuiket al., 2004]. The current assessment of benefitscompared with potential risks suggests that theT
AB
LE1.
Cli
nic
alPre
senta
tion
of
Pre
gnan
tW
om
enon
Adm
issi
on
and
Tre
atm
ent
Effi
cacy
of
Pri
mar
yan
dR
etre
atm
ent
Epis
odes
,1991–1
996�
Adm
issi
on
char
acte
rist
ics
Tre
atm
ent
effica
cy
Tre
atm
ent
Yea
rIn
fect
ion
n%
Pri
mip
%Fe
bri
le%
Sym
pto
mat
ic%
Anae
mic
%W
ith
PFG
Mea
n(s
d)
wee
ksge
stat
ional
age
Fail
ure
rate
s(%
)
Earl
yfa
ilure
rate
%by
day
7
PG
Wper
1,0
00
wom
enw
eeks
(95%
CI)
Q7
1991–1
996
Pri
mar
y103
37
10.6
83
53.3
8.0
14.7
(7.3
)23.2
a(2
6/1
12)
4(4
/101)
79.8
c,d
(51.5
–108.1
)R
e-tr
eatm
ent
72
34.7
4.4
78
59.0
7.7
22.6
(8)
38.6
a(3
4/8
8)
12.5
(11/8
8)
92.7
c(5
7.4
–128)
M25
1991–1
996
Pri
mar
y225
30
11
85
53.0
4.5
24.3
(7.2
)28.3
b73/2
58
6(1
5/2
26)
43.3
e(2
9.2
–57.4
)R
e-tr
eatm
ent
36
50
580
83.3
19.0
23.4
(6.5
)7.5
b(1
5/4
0)
12.5
(4/3
2)
88.7
(38.7
–138.7
)A
7al
one
1992–1
996
Pri
mar
y0
——
——
——
——
—R
e-tr
eatm
ent
58
35.3
16
n.a
.72.0
12.0
27.9
(7.5
)7.5
b(4
/53)
09.5
(1.6
–31.1
)
� PFG
,P.f
alci
par
um
gam
etocy
tes
on
adm
issi
on;
n.a
.not
avai
lable
;PG
W,
per
son
gam
etocy
tew
eeks
;Q
7,
quin
ine
10
mg/
kgtid�
7d;
M25,
mefl
oquin
e25
mg/
kgdose
;A
7,
arte
sunat
e7
day
s12
mg/
kgto
tal
dose
;‘‘—
’’ar
tesu
nat
ew
asre
serv
edfo
rfa
ilure
si.
e.not
use
das
pri
mar
ytr
eatm
ent
sono
info
rmat
ion
appli
esher
e.aFa
ilure
rate
by
day
28.
bFa
ilure
rate
sby
day
42.
cEn
rollm
ent
par
asit
aem
iain
dep
enden
tly
asso
ciat
edw
ith
asi
gnifi
cant
risk
of
subse
quen
tga
met
ocy
taem
ia.
dG
amet
ocy
taem
iaon
day
7or
14,
2.5
6(9
5%
CI:
1.1
7–5
.60)
tim
esm
ore
like
lyto
exper
ience
atr
eatm
ent
fail
ure
than
wit
hout
gam
etocy
tes.
eG
amet
ocy
taem
iaon
day
7or
14,
2.0
(95%
CI:
1.1
8–3
.46)
tim
esm
ore
like
lyto
exper
ience
atr
eatm
ent
fail
ure
than
those
wit
hout
gam
etocy
tes.
59MALARIA TREATMENT IN PREGNANCY
Drug Dev. Res.
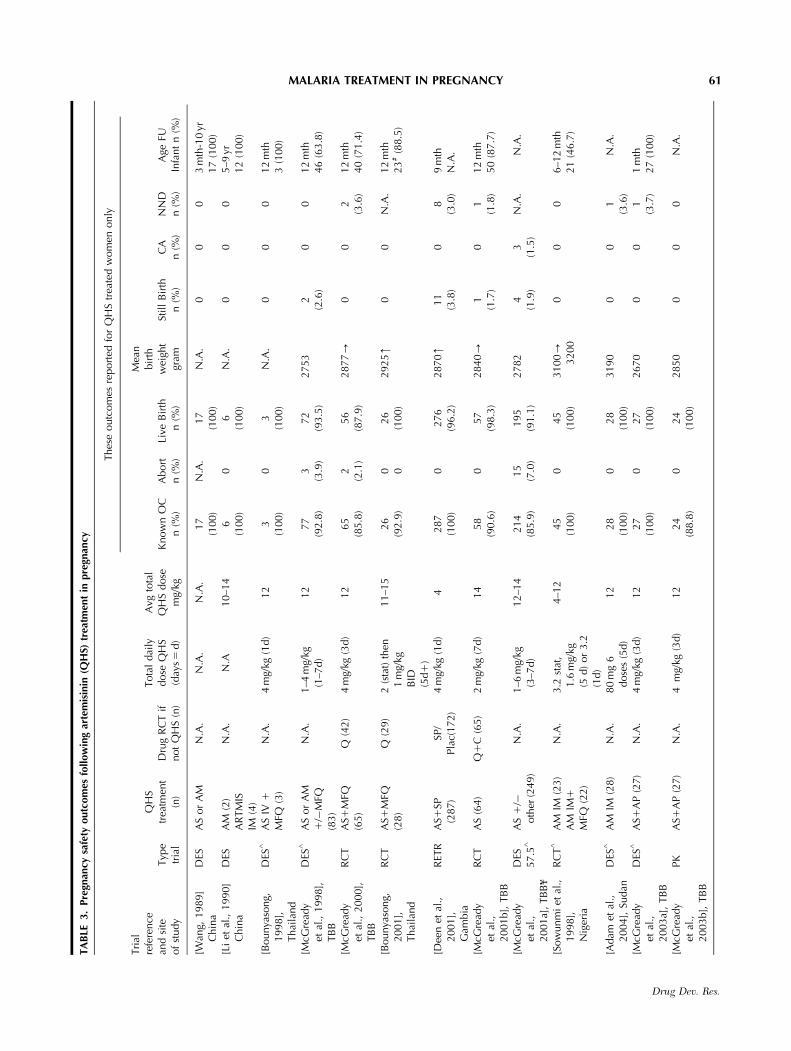
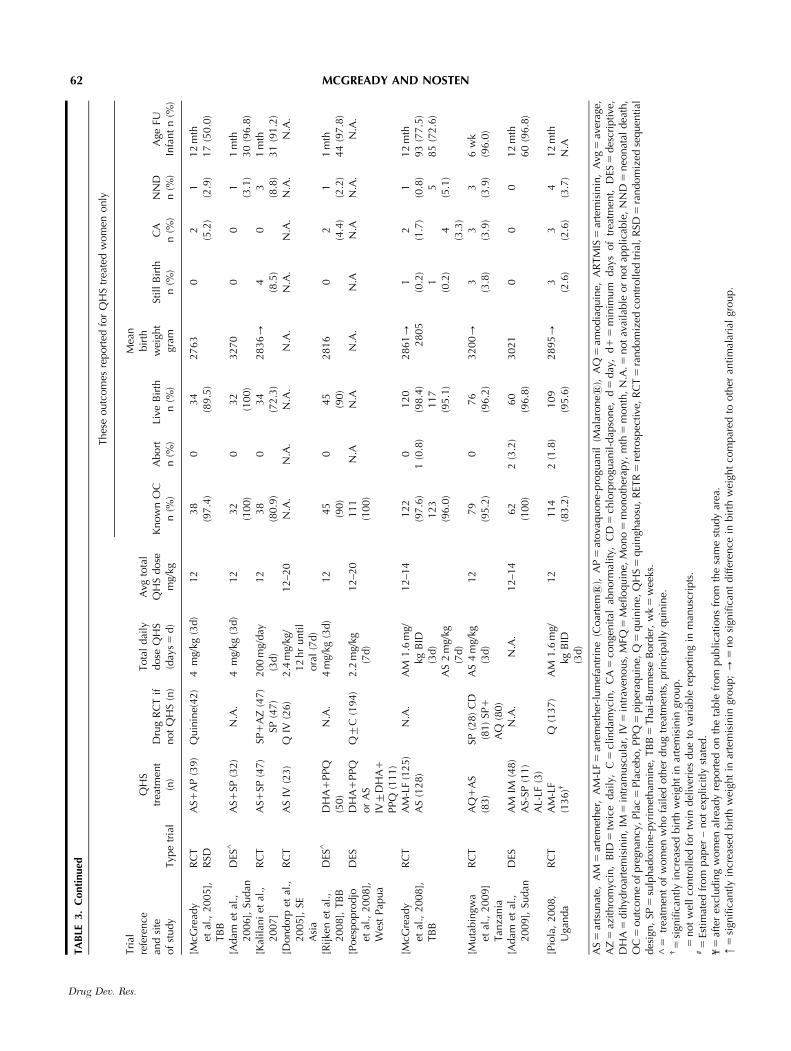
artemisinin deriviatives should be used to treatuncomplicated falciparum malaria in the 2nd and 3rdtrimesters [Dellicour et al., 2007; Nosten et al., 2006,2007; WHO, 2006] with experience in more than 1,500documented pregnancies [Adam et al., 2004, 2006;
Bounyasong, 2001; Deen et al., 2001; McGready et al.,1998, 2000, 2001a,b, 2003a, 2006a,b, 2008; Rijkenet al., 2008; Sowunmi et al., 1998; Wang, 1989]. Therehave been no documented adverse effects attributableto the artemisinins on the mother or fetus (Table 3).
TABLE 2. Treatment of MIP Based on Species, Trimester and Severity�
Species and trimester Severity Treatment Evidence
P. vivax, P ovale andP. malariaeRegardless oftrimester
Not usually severe Ifsevere, seeP. falciparum (severe)
Chloroquine phosphate (one tablet contains250 mg salt equivalent to 155.3 mg base).Doses 10 mg/kg base once a day for 2 daysfollowed by 5 mg/kg base on the 3rd day.For chloroquine 5 resistant P. vivax,amodiaquine, quinine, or artemisininderivatives can be used
[McGready et al., 2002; Nostenet al., 1999a]
1st trimesterP. falciparum ormixed species
Uncomplicated Primary episode: quinine 10 mg/kg 3 timesdaily for 7 days, preferably withclindamycin 5 mg/kg 3 times daily for 7daysa
[McGready et al., 2001b, 2002]2nd ref RCT, but not in1st trimester
Subsequent episodes: repeat treatment withquinine and clindamycin (as above); ACTthat is locally effective or artesunate2 mg/kg per day for 7 days withclindamycin (as above)a
[Deen et al., 2001; McGreadyet al., 2001a]
2nd and 3rd trimestersP. falciparum ormixed species
Primary episode: artemisinin basedcombination that is locally effective, orartesunate plus clindamycin as above.Malarone (atovaquone-proguanil) alonecan be used for treatment in pregnancy butit is highly recommended to use it withartesunate to maximize fever and parasiteclearance times and ensure cure andreduce resistance emergingb,c
15 studies 5 RCT [Bounyasong,2001; Keuter et al., 1990;McGready et al., 2000,2001b, 2005, 2008; Sowunmiet al., 1998] and 8 descriptive[Adam et al., 2004, 2006;Deen et al., 2001; McGreadyet al., 2001a, 2003a, 2006a,b;Wang, 1989]
Subsequent episodes: artesunate plusclindamycin as above.a Artesunate-atovaquone-proguanil anddihyrartemisinin piperaquine can be usedfor P. falciparum recurrence in the samepregnancy
[McGready et al., 2003a; Rijkenet al., 2008]
Regardless of trimester UncomplicatedHyperparasitaemia
Artesunate oral: start with 4 mg/kg loadingdose then 2 mg/kg every 24 h for 7 dayswith clindamycin as abovea OR IV quinine(see below)
Regardless of trimester Severe Artesunate 2.4 mg/kg IV at h 0, 12 and 24 hthen every 24 h until the patient cantolerate oral artesunate 2 mg/kg per dose,for a total of 7 days, and clindamycin5mg/kg 3 times daily for 7 daysa OR QuinineIV: loading dose 20 mg/kg given over 4hthen 10mg/kg 8h after the loading dose wasstarted, followed by 10mg/kg every 8h for 7days. Once the patient has recoveredsufficiently to tolerate oral medicationboth quinine 10mg/kg and clindamycin5mg/kg, three times daily should becontinued for/until 7 days
Ib [Dondorp et al., 2005] andpregnant women notspecifically excluded
aWhen clindamycin is not available, give artesunate monotherapy [McGready et al., 2001a, 2008].bMalarone use in pregnancy [McGready et al., 2003a,b, 2005; Na-Bangchang et al., 2005].cPrescribe artemether-lumefantrine, and dihydroartemisinin-piperaquine with fat, e.g., 200 mL of milk [Ashley et al., 2007; Sim et al., 2005].�Any clinical deterioration in a patient on oral treatment should be regarded as a signal to change to parenteral treatment [WHO, 2006]. Thehigher biomass of parasites in hyperparasitaemia requires a longer treatment course, usually of 7 days.
60 MCGREADY AND NOSTEN
Drug Dev. Res.
TA
BLE
3.
Pre
gnan
cysa
fety
outc
om
esfo
llow
ing
arte
mis
inin
(QH
S)tr
eatm
ent
inpre
gnan
cy
Thes
eoutc
om
esre
port
edfo
rQ
HS
trea
ted
wom
enonly
Tri
alre
fere
nce
and
site
of
study
Typ
etr
ial
QH
Str
eatm
ent
(n)
Dru
gR
CT
ifnot
QH
S(n
)
Tota
ldai
lydose
QH
S(d
ays
5d)
Avg
tota
lQ
HS
dose
mg/
kgK
now
nO
Cn
(%)
Abort
n(%
)Li
veB
irth�
n(%
)
Mea
nbir
thw
eigh
tgr
amSt
ill
Bir
thn
(%)
CA
n(%
)N
ND
n(%
)A
geFU
Infa
nt
n(%
)
[Wan
g,1989]
Chin
aD
ESA
Sor
AM
N.A
.N
.A.
N.A
.17
(100)
N.A
.17
(100)
N.A
.0
00
3m
th-1
0yr
17
(100)
[Li
etal
.,1990]
Chin
aD
ESA
M(2
)A
RTM
ISIM
(4)
N.A
.N
.A10–1
46
(100)
06
(100)
N.A
.0
00
5–9
yr12
(100)
[Bounya
song,
1998],
Thai
land
DES
^A
SIV
1
MFQ
(3)
N.A
.4
mg/
kg(1
d)
12
3(1
00)
03
(100)
N.A
.0
00
12
mth
3(1
00)
[McG
read
yet
al.,
1998],
TB
B
DES
^A
Sor
AM
1/�
MFQ
(83)
N.A
.1–4
mg/
kg(1
–7d)
12
77
(92.8
)3
(3.9
)72
(93.5
)2753
2(2
.6)
00
12
mth
46
(63.8
)
[McG
read
yet
al.,
2000],
TB
B
RC
TA
S1M
FQ(6
5)
Q(4
2)
4m
g/kg
(3d)
12
65
(85.8
)2
(2.1
)56
(87.9
)2877-
00
2(3
.6)
12
mth
40
(71.4
)
[Bounya
song,
2001],
Thai
land
RC
TA
S1M
FQ(2
8)
Q(2
9)
2(s
tat)
then
1m
g/kg
BID
(5d
1)
11–1
526
(92.9
)0 0
26
(100)
2925m
00
N.A
.12
mth
23
#(8
8.5
)
[Dee
net
al.,
2001],
Gam
bia
RET
RA
S1SP
(287)
SP/
Pla
c(172)
4m
g/kg
(1d)
4287
(100)
0276
(96.2
)2870m
11
(3.8
)0
8(3
.0)
9m
thN
.A.
[McG
read
yet
al.,
2001b],
TB
B
RC
TA
S(6
4)
Q1
C(6
5)
2m
g/kg
(7d)
14
58
(90.6
)0
57
(98.3
)2840-
1(1
.7)
01
(1.8
)12
mth
50
(87.7
)
[McG
read
yet
al.,
2001a]
,TB
Bf
DES
57.5
^A
S1
/�oth
er(2
49)
N.A
.1–6
mg/
kg(3
–7d)
12–1
4214
(85.9
)15
(7.0
)195
(91.1
)2782
4(1
.9)
3(1
.5)
N.A
.N
.A.
[Sow
unm
iet
al.,
1998],
Nig
eria
RC
T^
AM
IM(2
3)
AM
IM1
MFQ
(22)
N.A
.3.2
stat
,1.6
mg/
kg(5
d)
or
3.2
(1d)
4–1
245
(100)
045
(100)
3100-
3200
00
06–1
2m
th21
(46.7
)
[Adam
etal
.,2004],
Sudan
DES
^A
MIM
(28)
N.A
.80
mg
6dose
s(5
d)
12
28
(100)
028
(100)
3190
00
1(3
.6)
N.A
.
[McG
read
yet
al.,
2003a]
,TB
B
DES
^A
S1A
P(2
7)
N.A
.4
mg/
kg(3
d)
12
27
(100)
027
(100)
2670
00
1(3
.7)
1m
th27
(100)
[McG
read
yet
al.,
2003b],
TB
B
PK
AS1
AP
(27)
N.A
.4
mg/
kg(3
d)
12
24
(88.8
)0
24
(100)
2850
00
0N
.A.
61MALARIA TREATMENT IN PREGNANCY
Drug Dev. Res.
TA
BLE
3.
Conti
nued
Thes
eoutc
om
esre
port
edfo
rQ
HS
trea
ted
wom
enonly
Tri
alre
fere
nce
and
site
of
study
Typ
etr
ial
QH
Str
eatm
ent
(n)
Dru
gR
CT
ifnot
QH
S(n
)
Tota
ldai
lydose
QH
S(d
ays
5d)
Avg
tota
lQ
HS
dose
mg/
kgK
now
nO
Cn
(%)
Abort
n(%
)Li
veB
irth�
n(%
)
Mea
nbir
thw
eigh
tgr
amSt
ill
Bir
thn
(%)
CA
n(%
)N
ND
n(%
)A
geFU
Infa
nt
n(%
)
[McG
read
yet
al.,
2005],
TB
B
RC
TR
SDA
S1A
P(3
9)
Quin
ine(
42)
4m
g/kg
(3d)
12
38
(97.4
)0
34
(89.5
)2763
02
(5.2
)1
(2.9
)12
mth
17
(50.0
)
[Adam
etal
.,2006],
Sudan
DES
^A
S1SP
(32)
N.A
.4
mg/
kg(3
d)
12
32
(100)
032
(100)
3270
00
1(3
.1)
1m
th30
(96.8
)[K
alil
ani
etal
.,2007]
RC
TA
S1SP
(47)
SP1
AZ
(47)
SP(4
7)
200
mg/
day
(3d)
12
38
(80.9
)0
34
(72.3
)2836-
4(8
.5)
03
(8.8
)1
mth
31
(91.2
)[D
ondorp
etal
.,2005],
SEA
sia
RC
TA
SIV
(23)
QIV
(26)
2.4
mg/
kg/
12
hr
unti
lora
l(7
d)
12–2
0N
.A.
N.A
.N
.A.
N.A
.N
.A.
N.A
.N
.A.
N.A
.
[Rijke
net
al.,
2008],
TB
BD
ES^
DH
A1
PPQ
(50)
N.A
.4
mg/
kg(3
d)
12
45
(90)
045
(90)
2816
02
(4.4
)1
(2.2
)1
mth
44
(97.8
)[P
oes
popro
djo
etal
.,2008],
Wes
tPap
ua
DES
DH
A1
PPQ
or
AS
IV7
DH
A1
PPQ
(111)
Q7
C(1
94)
2.2
mg/
kg(7
d)
12–2
0111
(100)
N.A
N.A
N.A
.N
.AN
.AN
.A.
N.A
.
[McG
read
yet
al.,
2008],
TB
B
RC
TA
M-L
F(1
25)
AS
(128)
N.A
.A
M1.6
mg/
kgB
ID(3
d)
AS
2m
g/kg
(7d)
12–1
4122
(97.6
)123
(96.0
)
01
(0.8
)120
(98.4
)117
(95.1
)
2861-
2805
1(0
.2)
1(0
.2)
2(1
.7)
4(3
.3)
1(0
.8)
5(5
.1)
12
mth
93
(77.5
)85
(72.6
)
[Muta
bin
gwa
etal
.,2009]
Tan
zania
RC
TA
Q1
AS
(83)
SP(2
8)
CD
(81)
SP1
AQ
(80)
AS
4m
g/kg
(3d)
12
79
(95.2
)0
76
(96.2
)3200-
3(3
.8)
3(3
.9)
3(3
.9)
6w
k(9
6.0
)
[Adam
etal
.,2009],
Sudan
DES
AM
IM(4
8)
AS-
SP(1
1)
AL-
LF(3
)
N.A
.N
.A.
12–1
462
(100)
2(3
.2)
60
(96.8
)3021
00
012
mth
60
(96.8
)
[Pio
la,
2008,
Uga
nda
RC
TA
M-L
F(1
36)y
Q(1
37)
AM
1.6
mg/
kgB
ID(3
d)
12
114
(83.2
)2
(1.8
)109
(95.6
)2895-
3(2
.6)
3(2
.6)
4(3
.7)
12
mth
N.A
AS
5ar
tsunat
e,A
M5
arte
met
her
,A
M-L
F5
arte
met
her
-lum
efan
trin
e(C
oar
tems
),A
P5
atova
quone-
pro
guan
il(M
alar
ones
),A
Q5
amodia
quin
e,A
RTM
IS5
arte
mis
inin
,A
vg5
aver
age,
AZ
5az
ithro
myc
in,
BID
5tw
ice
dai
ly,
C5
clin
dam
ycin
,C
A5
conge
nit
alab
norm
alit
y,C
D5
chlo
rpro
guan
il-d
apso
ne,
d5
day
,d
15
min
imum
day
sof
trea
tmen
t,D
ES5
des
crip
tive
,D
HA
5dih
ydro
arte
mis
inin
,IM
5in
tram
usc
ula
r,IV
5in
trav
enous,
MFQ
5M
efloquin
e,M
ono
5m
onoth
erap
y,m
th5
month
,N
.A.5
not
avai
lable
or
not
applica
ble
,N
ND
5neo
nat
aldea
th,
OC
5outc
om
eofpre
gnan
cy,Pla
c5
Pla
cebo,PPQ
5pip
eraq
uin
e,Q
5quin
ine,
QH
S5
quin
ghao
su,R
ETR
5re
trosp
ecti
ve,R
CT
5ra
ndom
ized
contr
oll
edtr
ial,
RSD
5ra
ndom
ized
sequen
tial
des
ign,
SP5
sulp
had
oxi
ne-
pyr
imet
ham
ine,
TB
B5
Thai
-Burm
ese
Bord
er,
wk
5w
eeks
.^
5tr
eatm
ent
of
wom
enw
ho
fail
edoth
erdru
gtr
eatm
ents
,pri
nci
pal
lyquin
ine.
y5
sign
ifica
ntly
incr
ease
dbir
thw
eigh
tin
arte
mis
inin
group.
�5
not
wel
lco
ntr
olled
for
twin
del
iver
ies
due
tova
riab
lere
port
ing
inm
anusc
ripts
.#
5Es
tim
ated
from
pap
er–
not
expli
citl
yst
ated
.f
5af
ter
excl
udin
gw
om
enal
read
yre
port
edon
the
table
from
publi
cati
ons
from
the
sam
est
udy
area
.m
5si
gnifi
cantl
yin
crea
sed
bir
thw
eigh
tin
arte
mis
inin
group;-
5no
sign
ifica
nt
dif
fere
nce
inbir
thw
eigh
tco
mpar
edto
oth
eran
tim
alar
ial
group.
62 MCGREADY AND NOSTEN
Drug Dev. Res.

The choice of the partner drug for an artemisininderivative relies on it being independently effective andhaving a different mode of action to artemisinin[Chawira et al., 1987; Curtis and Otoo, 1986; Peters,1969, 1987, 1990; White et al., 1999]. Artemisinin and itsderivatives are rapidly eliminated. When given incombination with rapidly eliminated and slow-actingcompounds (e.g., clindamycin), a 7-day treatment courseis required; but when given in combination with a slowlyeliminated antimalarial (e.g., piperaquine or meflo-quine), shorter courses (3 days) of treatment areeffective. In pregnancy, the choice of combinationpartner is difficult. Mefloquine has been associated withan increased risk of stillbirth in Thailand [Nosten et al.,1999b] but not in Malawi [Steketee et al., 1996a,b], thesafety of pyronaridine is unknown, and the othercandidates are lost to resistance: sulphadoxine-pyri-methamine and amodiaquine. The data on fixed andnon-fixed ACT remain sparse for the moment but trialsare in progress. Artemether-lumefantrine, dihyroartemi-sinin-piperaquine [Poespoprodjo et al., 2008; Rijkenet al., 2008], and artesunate-atovaquone-proguanil[McGready et al., 2003a,b, 2005] are better toleratedthan quinine and result in faster fever and parasiteclearance times but they must be given with fat [Ashleyet al., 2007; Sim et al., 2005]. The sub-optimal efficacy[McGready et al., 2008] and lower drug concentration[McGready et al., 2006a] of artemether-lumefantrine inpregnancy suggest it is not suitable for use in areascomplicated by a high level of MDR P. falciparum.Pharmacokinetic modelling suggests higher dosing willlead to improved cure rates [Tarning et al., 2009] but nostudies have examined this yet. What does this mean inpractice? If artemether-lumefantrine is the only anti-malarial available in the hospital, then it can beprescribed but higher cure rates are likely to be achievedwith 7 days of artesunate (or quinine) and clindamycin.
Sulphadoxine-pyrimethamine and atovaquone-proguanil are not recommended for treatment inpregnancy if they have been given for prophylaxis.Although chloroquine and sulphadoxine-pyrimetha-mine are recognized as failing treatments, they stillappear in randomized controlled treatment trials. Inthe Gambia, chloroquine, sulphadoxine-pyrimethamine(SP), amodiaquine, or amodiaquine plus sulphadoxine-pyrimethamine were used in randomized trials to treatparasitaemic pregnant women in the 2nd and 3rdtrimester. Chloroquine and SP failed to reach the 95%cure rates recommended by WHO to accept a drug asefficacious [WHO, 2006]. PCR-corrected parasitologi-cal failure by day 28 was 14, 11, 3, and 0% in thewomen assigned chloroquine, sulphadoxine-pyrimetha-mine, amodiaquine, and amodiaquine plus sulpha-doxine-pyrimethamine, respectively (Po0.0001). The
unacceptably low 28-day cure rate with SP was notmentioned in the discussion. There were no major toxicside effects although minor side-effects were moreoften reported on day 3 by those women treated withamodiaquine (86%) or amodiaquine plus sulphadoxine-pyrimethamine (90%) than those receiving sulphadox-ine-pyrimethamine (48%). In Tanzania, 1,433 womenwere screened and 272 were randomized to one offour study arms: sulfadoxine-pyrimethamine, chlorpro-guanil-dapsone, SP1amodiaquine, or amodiaquine1
artesunate. The day-28 PCR confirmed failure rateswere 18% for CD, 1% for SP1AQ, and 4.5% forAQ1AS. The high failure rates for monotherapy wereacknowledged. Chlorproguanil-dapsone is no longer indevelopment because of the risk of severe hemolysis.
THE PROBLEM WITH QUININE
Quinine is almost universally relied upon as thefall-back treatment for malaria in pregnancy. However,quinine has significant side-effects, principally cinch-onism and hypoglycaemia [Nosten et al., 2007] and thisfrequently leads to failure of the 7-day treatmentcourse due to non-compliance [Bunnag et al., 1996;Denis, 1998; Fungladda et al., 1998; Lasserre, 1989;White, 1998]. For this reason, directly observedtherapy for each dose of quinine [Abdel-Hameed,2001; Fungladda et al., 1998] is advisable.
VOMITING ANTIMALARIALS AND PREGNANCY
Vomiting is a known side-effect of quinine [Bolandet al., 1985; Phillips-Howard and Wood, 1996; Whiteet al., 1982] and mefloquine [Palmer et al., 1993; terKuile et al., 1995] and is associated with antimalarialtreatment failure [White, 1998]. If the woman vomitsrepeatedly within the first hour after treatment,consideration should be given to the use of parenteraltreatment. Antipyretics can control the fever and anantimetic can control nausea and vomiting [Matok et al.,2009] although there are no studies of their efficacy inmalaria in pregnancy [WHO, 2006]. Vomiting in the firsthalf hour after requires readministration of the fulltreatment dose. Further vomiting is a definite indicationfor parenteral treatment.
TREATMENT OF SEVERE MALARIA IN PREGNANCY
Treatment of severe malaria in pregnancy is amedical emergency and ideally patients should beadmitted to an intensive care facility without delay.Antimalarial drugs recommended to treat severemalaria in pregnancy are artesunate iv, artemetherim, and parenteral quinine. Artesunate and artemetherare faster acting and do not cause hypoglycaemia. In arandomised trial, where pregnant women were not
63MALARIA TREATMENT IN PREGNANCY
Drug Dev. Res.

excluded, iv artesunate (2.4 mg/kg initial dose and at12 h, followed by 2.4 mg/kg qd) reduced mortality inAsian adults by 35% compared with iv quinine[Dondorp et al., 2005]. Artemether im can also beused to treat severe malaria but absorption is lesspredictable than that of artesunate, especially inpatients with cardiovascular collapse. When artemetherand artesunate are not available, parenteral quininewith a loading dose (20 mg/kg) is recommended.Quinine frequently causes hyperinsulinemia and hy-poglycemia in pregnant women that can be profoundand intractable [Davis et al., 1994; Looareesuwan et al.,1985; White et al., 1983]. Artesunate has not achievedGMP certification, but it has received the OrphanMedicinal Drug Designation from the EuropeanMedicines Agency (www.emea.europa.eu/pdfs/human/comp/opinion/48693207en.pdf) and may be obtainedfrom IDIS Pharma (www.idispharma.com). Treatmentshould commence with parenteral quinine if there willbe a delay in acquiring injectable artesunate. Compli-cations of severe malaria should be managed accordingto WHO malaria treatment guidelines [WHO, 2006].
TREATMENT OF P. vivax: CHLOROQUINE-SENSITIVEAND -RESISTANT
At least for P. vivax, the adverse effects ofinfection, maternal anaemia, and low-birth weight aresimilar but not as severe as infection with P. falciparum[Nosten et al., 1999a; Poespoprodjo et al., 2008; Singhet al., 1998]. It is not unreasonable to assume P. ovaleand P. malariae would have similar adverse effects asP. vivax in pregnancy but there are no data to supportthis. The fever of P. vivax is associated with prematurelabour and as for P. falciparum requires prompttreatment and effective antimalarials.
Evidence from non-pregnant patients has demon-strated that chloroquine-resistant P. vivax should betreated in the same way as chloroquine-resistantP. falciparum. [Baird et al., 1991; Poespoprodjo et al.,2008; Pukrittayakamee et al., 2001; Ratcliff et al.,2007a,b]. Artemisinin-based combination therapies(except artesunate-sulphadoxine pyrimethamine) are,therefore, indicated [WHO, 2006]. Women in the firsttrimester of pregnancy should be treated with quinine.Severe P. vivax malaria can be treated with parenteralquinine or artesunate [Tjitra et al., 2008]. Primaquineused to treat liver stages of P. vivax crosses the placentaand is absolutely contraindicated in pregnancy.
PHARMACOKINETIC STUDIES OF ANTIMALARIALSIN PREGNANCY
An essential determinant of drug efficacy is thepresence of the drug in the blood circulation (or itsmetabolites) for a duration and at a concentration
sufficient to eliminate all parasites. There are very fewstudies of the pharmacokinetics of antimalarials duringpregnancy [Ward et al., 2007]. Most of those publishedare from Karen pregnant women on the Thai-Burmeseborder. These studies have shown that the disposition ofmost antimalarials is altered during pregnancy[McGready et al., 2003b,c, 2006a,b; Nosten et al.,1990]. This is explained either by the physiologicalchanges induced by gestation (increase in the volume ofdistribution, and in the glomerular filtration, reduction ofthe intestinal transit and the gastric emptying), orhormonal changes that impact on the functions of theliver cytochromes. Artesunate (and its metabolite DHA),artemether, lumefantrine, and atovaquone all have lowerplasma concentrations during pregnancy as comparedwith non-pregnant patients. Proguanil bio-transformationinto the active cycloguanil is impaired by pregnancy.These changes translate into lower parasitologicalefficacy of the drugs when given to pregnant women.Recently, the kinetics of SP were reported and it appearsthat this drug has been used and recommended for manyyears at a suboptimal dose [Green et al., 2007; Nyuntet al., 2009]. There is an urgent need for information inthe kinetics of mefloquine, quinine, and other drugsin different populations as genetic factors could result indifferences in the dispositions of these drugs. It is criticalthat information be obtained on the relationship betweenday-7 blood levels and efficacy in treatment (and forIPTp) for mefloquine, piperaquine, and lumefantrineand between venous and capillary sampling, as it may notbe the same as in non-pregnant patients due to alteredphysiology. Interactions with ARVs must also be studiedas the two infections often coexist [Nosten et al., 2006].
CONCLUSIONS
What is the Best Drug for Treatment of Malariain Pregnancy?
This question has no single correct answer.Efficacy depends upon the country of origin of thewoman, the use of antimalarial prophylaxis, theinfecting species and country of origin where malariawas acquired, whether the patient is under treatmentfor a primary or recrudescent infection, the severity ofmalaria, the gestational age of the pregnancy, and thehistory of drug allergies in the patient. In mostresource-poor settings, the final choice is likely to relyon drug availability and cost. Progress in antimalarialdrug trials in pregnancy is slow because the emphasis isoften on the safety for the fetus and this translates intoa long period of follow-up in the first year of life. Inparts of the world where women are infected withmultidrug-resistant strains of P. falciparum, the choiceof antimalarials is severely restricted. Until now, there
64 MCGREADY AND NOSTEN
Drug Dev. Res.
is no safe, efficacious, and affordable 3-day treatmentfor pregnant women. Compliance with 7-day regimensis poor. The fixed ACTs including dihyroartemisinin-piperaquine and mefloquine-artesunate are the mostlikely candidate drugs for this indication assumingartesunate does not also fall to resistance.
REFERENCES
Abdel-Hameed AA. 2001. Malaria case management at thecommunity level in Gezira, Sudan. Afr J Med Med Sci 30(Suppl):43–46.
Abdelrahim II, Adam I, Elghazali G, Gustafsson LL, Elbashir MI,Mirghani RA. 2007. Pharmacokinetics of quinine and itsmetabolites in pregnant Sudanese women with uncomplicatedPlasmodium falciparum malaria. J Clin Pharm Ther 32:15–19.
Adam I, Elwasila E, Mohammed Ali DA, Elansari E, Elbashir MI.2004. Artemether in the treatment of falciparum malaria duringpregnancy in eastern Sudan. Trans R Soc Trop Med Hyg 98:509–513.
Adam I, Ali DM, Abdalla MA. 2006. Artesunate plus sulfadoxine-pyrimethamine in the treatment of uncomplicated Plasmodiumfalciparum malaria during pregnancy in eastern Sudan. Trans RSoc Trop Med Hyg 100:632–635.
Adam I, Elhassan EM, Omer EM, Abdulla MA, Mahgoub HM,Adam GK. 2009. Safety of artemisinins during early pregnancy,assessed in 62 Sudanese women. Ann Trop Med Parasitol103:205–210.
Adjuik M, Babiker A, Garner P, Olliaro P, Taylor W, White N. 2004.Artesunate combinations for treatment of malaria: meta-analysis.Lancet 363:9–17.
Ashley EA, Stepniewska K, Lindegardh N, Annerberg A, Kham A,Brockman A, Singhasivanon P, White NJ, Nosten F. 2007. Howmuch fat is necessary to optimize lumefantrine oral bioavail-ability? Trop Med Int Health 12:195–200.
Baird JK, Basri H, Purnomo, Bangs MJ, Subianto B, Patchen LC,Hoffman SL. 1991. Resistance to chloroquine by Plasmodiumvivax in Irian Jaya, Indonesia. Am J Trop Med Hyg 44:547–552.
Boland ME, Roper SM, Henry JA. 1985. Complications of quininepoisoning. Lancet 1:384–385.
Bounyasong S. 2001. Randomized trial of artesunate and mefloquinein comparison with quinine sulfate to treat P. falciparum malariapregnant women. J Med Assoc Thai 84:1289–1299.
Brockman A, Paul RE, Anderson TJ, Hackford I, Phaiphun L,Looareesuwan S, Nosten F, Day KP. 1999. Application of geneticmarkers to the identification of recrudescent Plasmodiumfalciparum infections on the northwestern border of Thailand.Am J Trop Med Hyg 60:14–21.
Bunnag D, Karbwang J, Na-Bangchang K, Thanavibul A,Chittamas S, Harinasuta T. 1996. Quinine-tetracycline for multi-drug resistant falciparum malaria. Southeast Asian J Trop MedPublic Health 27:15–18.
Chawira AN, Warhurst DC, Robinson BL, Peters W. 1987. Theeffect of combinations of qinghaosu (artemisinin) with standardantimalarial drugs in the suppressive treatment of malaria in mice.Trans R Soc Trop Med Hyg 81:554–558.
Costedoat-Chalumeau N, Amoura Z, Duhaut P, Huong du LT,Sebbough D, Wechsler B, Vauthier D, Denjoy I, Lupoglazoff JM,Piette JC. 2003. Safety of hydroxychloroquine in pregnantpatients with connective tissue diseases: a study of one hundred
thirty-three cases compared with a control group. ArthritisRheum 48:3207–3211.
Curtis CF, Otoo LN. 1986. A simple model of the build-up ofresistance to mixtures of anti-malarial drugs. Trans R Soc TropMed Hyg 80:889–892.
Davis TM, Suputtamongkol Y, Spencer JL, Wilson SG, Mekhton S,Croft KD, White NJ. 1994. Glucose turnover in pregnant womenwith acute malaria. Clin Sci (Lond) 86:83–90.
Deen JL, von Seidlein L, Pinder M, Walraven GE, Greenwood BM.2001. The safety of the combination artesunate and pyrimetha-mine-sulfadoxine given during pregnancy. Trans R Soc Trop MedHyg 95:424–428.
Dellicour S, Hall S, Chandramohan D, Greenwood B. 2007. The safetyof artemisinins during pregnancy: a pressing question. Malar J 6:15.
Denis MB. 1998. Improving compliance with quinine1tetracyclinefor treatment of malaria: evaluation of health education interven-tions in Cambodian villages. Bull World Health Org 76(Suppl 1):43–49.
Desai M, ter Kuile FO, Nosten F, McGready R, Asamoa K,Brabin B, Newman RD. 2007. Epidemiology and burden ofmalaria in pregnancy. Lancet Infect Dis 7:93–104.
Dilling JW, Gemmell AA. 1929. A preliminary investigation of foetaldeaths following quinine induction. J Obstet Gynaecol 36:352–366.
Dondorp A, Nosten F, Stepniewska K, Day N, White N. 2005.Artesunate versus quinine for treatment of severe falciparummalaria: a randomised trial. Lancet 366:717–725.
Fungladda W, Honrado ER, Thimasarn K, Kitayaporn D,Karbwang J, Kamolratanakul P, Masngammueng R. 1998.Compliance with artesunate and quinine1tetracycline treatmentof uncomplicated falciparum malaria in Thailand. Bull WorldHealth Org 76(Suppl 1):59–66.
Green MD, van Eijk AM, van Ter Kuile FO, Ayisi JG, Parise ME,Kager PA, Nahlen BL, Steketee R, Nettey H. 2007. Pharmaco-kinetics of sulfadoxine-pyrimethamine in HIV-infected anduninfected pregnant women in Western Kenya. J Infect Dis196:1403–1408.
Kalilani L, Mofolo I, Chaponda M, Rogerson SJ, Alker AP, Kwiek JJ,Meshnick SR. 2007. A randomized controlled pilot trial ofazithromycin or artesunate added to sulfadoxine-pyrimethamineas treatment for malaria in pregnant women. PLoS ONE 2:e1166.
Keuter M, van Eijk A, Hoogstrate M, Raasveld M, van de Ree M,Ngwawe WA, Watkins WM, Were JB, Brandling-Bennett AD.1990. Comparison of chloroquine, pyrimethamine and sulfa-doxine, and chlorproguanil and dapsone as treatment forfalciparum malaria in pregnant and non-pregnant women,Kakamega District, Kenya. Br Med J 301:466–470. URL: http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=2207399
Lasserre R. 1989. The treatment of multiresistant falciparummalaria in Southeast Asia. Bull Soc Pathol Exot Filiales 82:94–100.
Levy M, Buskila D, Gladman DD, Urowitz MB, Koren G. 1991.Pregnancy outcome following first trimester exposure tochloroquine. Am J Perinatol 8:174–178.
Li GQ, Guo XB, Jin R, Wang ZC, Jian HX, Li ZY. 1990. Clinicaltrials on qinghaosu and its derivatives. China: Guangzhou Collegeof Traditional Chinese Medicine.
Looareesuwan S, Phillips RE, White NJ, Kietinun S, Karbwang J,Rackow C, Turner RC, Warrell DA. 1985. Quinine and severefalciparum malaria in late pregnancy. Lancet 2:4–8.
65MALARIA TREATMENT IN PREGNANCY
Drug Dev. Res.
Massele AY, Kilewo C, Aden Abdi Y, Tomson G, Diwan VK,Ericsson O, Rimoy G, Gustafsson LL. 1997. Chloroquine bloodconcentrations and malaria prophylaxis in Tanzanian womenduring the second and third trimesters of pregnancy. Eur J ClinPharmacol 52:299–305.
Matok I, Gorodischer R, Koren G, Sheiner E, Wiznitzer A, Levy A.2009. The safety of metoclopramide use in the first trimester ofpregnancy. N Engl J Med 360:2528–2535.
Maxwell JP. 1908. The use of quinine during pregnancy, labour andthe puerperium. J Trop Med Hyg 11:191–194.
McGready R, Nosten F. 1999. The Thai-Burmese border: drugstudies of Plasmodium falciparum in pregnancy. Ann Trop MedParasitol 93(Suppl 1):S19–S23.
McGready R, Cho T, Cho JJ, Simpson JA, Luxemburger C,Dubowitz L, Looareesuwan S, White NJ, Nosten F. 1998.Artemisinin derivatives in the treatment of falciparum malaria inpregnancy. Trans R Soc Trop Med Hyg 92:430–433.
McGready R, Brockman A, Cho T, Cho D, van Vugt M,Luxemburger C, Chongsuphajaisiddhi T, White NJ, Nosten F.2000. Randomized comparison of mefloquine-artesunate versusquinine in the treatment of multidrug-resistant falciparum malariain pregnancy. Trans R Soc Trop Med Hyg 94:689–693.
McGready R, Cho T, Keo NK, Thwai KL, Villegas L, Looareesuwan S,White NJ, Nosten F. 2001a. Artemisinin antimalarials in pregnancy:a prospective treatment study of 539 episodes of multidrug-resistantPlasmodium falciparum. Clin Infect Dis 33:2009–2016.
McGready R, Cho T, Samuel, Villegas L, Brockman A, van Vugt M,Looareesuwan S, White NJ, Nosten F. 2001b. Randomizedcomparison of quinine-clindamycin versus artesunate in thetreatment of falciparum malaria in pregnancy. Trans R Soc TropMed Hyg 95:651–656.
McGready R, Thwai KL, Cho T, Samuel, Looareesuwan S,White NJ, Nosten F. 2002. The effects of quinine and chloroquineantimalarial treatments in the first trimester of pregnancy. Trans RSoc Trop Med Hyg 96:180–184.
McGready R, Keo NK, Villegas L, White NJ, Looareesuwan S,Nosten F. 2003a. Artesunate-atovaquone-proguanil rescue treat-ment of multidrug-resistant Plasmodium falciparum malaria inpregnancy: a preliminary report. Trans R Soc Trop Med Hyg97:592–594.
McGready R, Stepniewska K, Edstein MD, Cho T, Gilveray G,Looareesuwan S, White NJ, Nosten F. 2003b. The pharmacoki-netics of atovaquone and proguanil in pregnant women with acutefalciparum malaria. Eur J Clin Pharmacol 59:545–552.
McGready R, Stepniewska K, Seaton E, Cho T, Cho D, Ginsberg A,Edstein MD, Ashley E, Looareesuwan S, White NJ, Nosten F. 2003c.Pregnancy and use of oral contraceptives reduces the biotransforma-tion of proguanil to cycloguanil. Eur J Clin Pharmacol 59:553–557.
McGready R, Ashley EA, Moo E, Cho T, Barends M, Hutagalung R,Looareesuwan S, White NJ, Nosten F. 2005. A randomizedcomparison of artesunate-atovaquone-proguanil versus quinine intreatment for uncomplicated falciparum malaria during preg-nancy. J Infect Dis 192:846–853.
McGready R, Stepniewska K, Lindegardh N, Ashley EA, La Y,Singhasivanon P, White NJ, Nosten F. 2006a. The pharmacoki-netics of artemether and lumefantrine in pregnant women withuncomplicated falciparum malaria. Eur J Clin Pharmacol62:1021–1031.
McGready R, Stepniewska K, Ward SA, Cho T, Gilveray G,Looareesuwan S, White NJ, Nosten F. 2006b. Pharmacokinetics
of dihydroartemisinin following oral artesunate treatment ofpregnant women with acute uncomplicated falciparum malaria.Eur J Clin Pharmacol 62:367–371.
McGready R, Tan SO, Ashley EA, Pimanpanarak M,Viladpai-nguen J, Phaiphun L, Wustefeld K, Barends M,Laochan N, Keereeharoen L, and others. 2008. A randomizedcontrolled trial of artemether-lumefantrine versus artesunate forthe treatment of uncomplicated Plasmodium falciparum malariain pregnancy in north-west Thailand. PLoS Med 5.
Mutabingwa TK, Muze K, Ord R, Briceno M, Greenwood BM,Drakeley C, Whitty CJ. 2009. Randomized trial of artesunate1
amodiaquine, sulfadoxine-pyrimethamine1amodiaquine, chlor-proguanal-dapsone and SP for malaria in pregnancy in Tanzania.PLoS ONE 4:e5138.
Myint HY, Tipmanee P, Nosten F, Day NP, Pukrittayakamee S,Looareesuwan S, White NJ. 2004. A systematic overview ofpublished antimalarial drug trials. Trans R Soc Trop Med Hyg98:73–81.
Na Bangchang K, Davis TM, Looareesuwan S, White NJ,Bunnag D, Karbwang J. 1994. Mefloquine pharmacokinetics inpregnant women with acute falciparum malaria. Trans R Soc TropMed Hyg 88:321–323.
Na-Bangchang K, Manyando C, Ruengweerayut R, Kioy D,Mulenga M, Miller GB, Konsil J. 2005. The pharmacokineticsand pharmacodynamics of atovaquone and proguanil for thetreatment of uncomplicated falciparum malaria in third-trimesterpregnant women. Eur J Clin Pharmacol 61:573–582.
Naing T, Win H, Nwe YY. 1988. Falciparum malaria and pregnancy:relationship and treatment response. Southeast Asian J Trop MedPublic Health 19:253–258.
Nosten F, Karbwang J, White NJ, Honeymoon, Na Bangchang K,Bunnag D, Harinasuta T. 1990. Mefloquine antimalarial prophy-laxis in pregnancy: dose finding and pharmacokinetic study. Br JClin Pharmacol 30:79–85.
Nosten F, ter Kuile F, Maelankirri L, Decludt B, White NJ. 1991.Malaria during pregnancy in an area of unstable endemicity.Trans R Soc Trop Med Hyg 85:424–429.
Nosten F, ter Kuile F, Thwai KL, Maelankirri L, White NJ. 1993.Spiramycin does not potentiate quinine treatment of falciparummalaria in pregnancy. Trans R Soc Trop Med Hyg 87:305–306.
Nosten F, McGready R, Simpson JA, Thwai KL, Balkan S, Cho T,Hkirijaroen L, Looareesuwan S, White NJ. 1999a. Effects ofPlasmodium vivax malaria in pregnancy. Lancet 354:546–549.
Nosten F, Vincenti M, Simpson J, Yei P, Thwai KL, de Vries A,Chongsuphajaisiddhi T, White NJ. 1999b. The effects ofmefloquine treatment in pregnancy. Clin Infect Dis 28:808–815.
Nosten F, McGready R, d’Alessandro U, Bonell A, Verhoeff F,Menendez C, Mutabingwa T, Brabin B. 2006. Antimalarial drugsin pregnancy: a review. Curr Drug Saf 1:1–15.
Nosten F, McGready R, Mutabingwa T. 2007. Case management ofmalaria in pregnancy. Lancet Infect Dis 7:118–125.
Ostesen M. 1994. Optimisation of antirheumatic drug treatment inpregnancy. Clin Pharmacokinet 27:486–503.
Palmer KJ, Holliday SM, Brogden RN. 1993. Mefloquine. A reviewof its antimalarial activity, pharmacokinetic properties andtherapeutic efficacy. Drugs 45:430–475.
Parke A. 1988. Antimalarial drugs and pregnancy. Am J Med85:30–33.
66 MCGREADY AND NOSTEN
Drug Dev. Res.
Parke A, West B. 1996. Hydroxychloroquine in pregnant patientswith systemic lupus erythematosus. J Rheumatol 23:1715–1718.
Peters W. 1897. Chemotherapy and drug resistance in malaria.London: Academic Press.
Peters W. 1969. Drug resistance in malaria: a perspective. Trans RSoc Trop Med Hyg 63:25–45.
Peters W. 1990. The prevention of antimalarial drug resistance.Pharmacol Ther 47:499–508.
Phillips-Howard PA, Wood D. 1996. The safety of antimalarial drugsin pregnancy. Drug Saf 14:131–145.
Phillips-Howard PA, Steffen R, Kerr L, Vanhauwere B,Schildknecht J, Fuchs E, Edwards R. 1998. Safety of mefloquineand other antimalarial agents in the first trimester of pregnancy.J Travel Med 5:121–126.
Phillips RE, Looareesuwan S, White NJ, Silamut K, Kietinun S,Warrell DA. 1986. Quinine pharmacokinetics and toxicity inpregnant and lactating women with falciparum malaria. Br J ClinPharmacol 21:677–683.
Piola P. 2008. Artemether Lumefantrine for the treatment of malariain the 2nd and 3rd trimester pregnancy: a trial from Uganda. Am JTrop Med Hyg 79:107.
Poespoprodjo JR, Fobia W, Kenangalem E, Lampah DA, Warikar N,Seal A, McGready R, Sugiarto P, Tjitra E, Anstey NM, and others.2008. Adverse pregnancy outcomes in an area where multidrug-resistant plasmodium vivax and Plasmodium falciparum infectionsare endemic. Clin Infect Dis 46:1374–1381.
Price RN, Uhlemann AC, Brockman A, McGready R, Ashley E,Phaipun L, Patel R, Laing K, Looareesuwan S, White NJ, andothers. 2004. Mefloquine resistance in Plasmodium falciparumand increased pfmdr1 gene copy number. Lancet 364:438–447.
Pukrittayakamee S, Clemens R, Chantra A, Nontprasert A,Luknam T, Looareesuwan S, White NJ. 2001. Therapeuticresponses to antibacterial drugs in vivax malaria. Trans R SocTrop Med Hyg 95:524–528.
Ratcliff A, Siswantoro H, Kenangalem E, Maristela R, Wuwung RM,Laihad F, Ebsworth EP, Anstey NM, Tjitra E, Price RN. 2007a.Two fixed-dose artemisinin combinations for drug-resistantfalciparum and vivax malaria in Papua, Indonesia: an open-labelrandomised comparison. Lancet 369:757–765.
Ratcliff A, Siswantoro H, Kenangalem E, Wuwung M, Brockman A,Edstein MD, Laihad F, Ebsworth EP, Anstey NM, Tjitra E, andothers. 2007b. Therapeutic response of multidrug-resistantPlasmodium falciparum and P. vivax to chloroquine andsulfadoxine-pyrimethamine in southern Papua, Indonesia. TransR Soc Trop Med Hyg 101:351–359.
Rijken MJ, McGready R, Boel ME, Barends M, Proux S,Pimanpanarak M, Singhasivanon P, Nosten F. 2008. Dihydroarte-misinin-piperaquine rescue treatment of multidrug-resistantPlasmodium falciparum malaria in pregnancy: a preliminaryreport. Am J Trop Med Hyg 78:543–545.
Roper C, Pearce R, Bredenkamp B, Gumede J, Drakeley C,Mosha F, Chandramohan D, Sharp B. 2003. Antifolate anti-malarial resistance in southeast Africa: a population-basedanalysis. Lancet 361:1174–1181.
Sim IK, Davis TM, Ilett KF. 2005. Effects of a high-fat meal on therelative oral bioavailability of piperaquine. Antimicrob AgentsChemother 49:2407–2411.
Singh N, Saxena A, Chand SK, Valecha N, Sharma VP. 1998. Studieson malaria during pregnancy in a tribal area of central India
(Madhya Pradesh). Southeast Asian J Trop Med Public Health29:10–17.
Sowunmi A, Oduola AM, Ogundahunsi OA, Fehintola FA,Ilesanmi OA, Akinyinka OO, Arowojolu AO. 1998. Randomisedtrial of artemether versus artemether and mefloquine for thetreatment of chloroquine/sufadoxine-pyrimethamine-resistant fal-ciparum malaria during pregnancy. J Obstet Gynaecol 18:322–327.
Steketee RW, Wirima JJ, Slutsker L, Khoromana CO, Heymann DL,Breman JG. 1996a. Malaria treatment and prevention inpregnancy: indications for use and adverse events associated withuse of chloroquine or mefloquine. Am J Trop Med Hyg 55:50–56.
Steketee RW, Wirima JJ, Slutsker L, Roberts JM, Khoromana CO,Heymann DL, Breman JG. 1996b. Malaria parasite infectionduring pregnancy and at delivery in mother, placenta, andnewborn: efficacy of chloroquine and mefloquine in rural Malawi.Am J Trop Med Hyg 55(1 Suppl):24–32.
Tagbor H, Bruce J, Browne E, Randal A, Greenwood B,Chandramohan D. 2006. Efficacy, safety, and tolerability ofamodiaquine plus sulphadoxine-pyrimethamine used alone or incombination for malaria treatment in pregnancy: a randomisedtrial. Lancet 368:1349–1356.
Tarning J, McGready R, Lindegardh N, Ashley EA, Pimanpanarak M,Kamanikom B, Annerberg A, Day NPJ, Stepniewska K,Singhasivanon P, and others. 2009. Population pharmacokineticsof lumefantrine in pregnant women treated with artemether-lumefantrine for uncomplicated P. falciparum malaria. Anti-microbial Agents Chemother 53:3837–3846.
ter Kuile F, Luxemburger C, Nosten F, Thwai KL,Chongsuphajaisiddhi T, White NJ. 1995. Predictors of mefloquinetreatment failure: a prospective study of 1590 patients withuncomplicated falciparum malaria. Trans R Soc Trop Med Hyg89:660–664.
Tjitra E, Anstey NM, Sugiarto P, Warikar N, Kenangalem E,Karyana M, Lampah DA, Price RN. 2008. Multidrug-resistantPlasmodium vivax associated with severe and fatal malaria: aprospective study in Papua, Indonesia. PLoS Med 5:e128.
Wang TY. 1989. Follow-up observation on the therapeutic effectsand remote reactions of artemisinin (Qinghaosu) and artemetherin treating malaria in pregnant woman. J Tradit Chin Med9:28–30.
Wangboonskul J, White NJ, Nosten F, ter Kuile F, Moody RR,Taylor RB. 1993. Single dose pharmacokinetics of proguanil andits metabolites in pregnancy. Eur J Clin Pharmacol 44:247–251.
Ward SA, Sevene EJ, Hastings IM, Nosten F, McGready R. 2007.Antimalarial drugs and pregnancy: safety, pharmacokinetics, andpharmacovigilance. Lancet Infect Dis 7:136–144.
Wernsdorfer WH. 1994. Epidemiology of drug resistance in malaria.Acta Trop 56:143–156.
White NJ. 1998. Why is it that antimalarial drug treatments do notalways work? Ann Trop Med Parasitol 92:449–458.
White NJ. 1999. Antimalarial drug resistance and combinationtherapy. Phil Trans R Soc Lond B Biol Sci 354:739–749.
White NJ, Looareesuwan S, Warrell DA, Warrell MJ, Bunnag D,Harinasuta T. 1982. Quinine pharmacokinetics and toxicity incerebral and uncomplicated Falciparum malaria. Am J Med73:564–572.
White NJ, Warrell DA, Chanthavanich P, Looareesuwan S,Warrell MJ, Krishna S, Williamson DH, Turner RC. 1983. Severe
67MALARIA TREATMENT IN PREGNANCY
Drug Dev. Res.

hypoglycemia and hyperinsulinemia in falciparum malaria.N Engl J Med 309:61–66.
White NJ, Nosten F, Looareesuwan S, Watkins WM, Marsh K,Snow RW, Kokwaro G, Ouma J, Hien TT, Molyneux ME, andothers. 1999. Averting a malaria disaster. Lancet 353:1965–1967.
White NJ, McGready RM, Nosten FH. 2008. New medicines fortropical diseases in pregnancy: catch-22. PLoS Med 5:e133.
WHO. 2003. Assessment of the safety of artemisinin compounds inpregnancy. World Health Organization. Report nr WHO/CDS/MAL/2003.1094.
WHO. 2006. WHO guidelines for the treatment of malaria. Geneva:World Health Organization. Report nr WHO/HTM/MAL 2006/1108. Available at http://www.who.int/malaria/docs/TreatmentGuidelines2006.pdf.
68 MCGREADY AND NOSTEN
Drug Dev. Res.




















