
Targeted EV to Deliver Chemotherapy to Treat Triple-Negative ...
Upload
independentCategory
view
3download
0
International Journal of Nursing Studies 48 (2011) 100–120
Review
What support can community mental health nurses deliver to carersof people diagnosed with schizophrenia? Findings from a reviewof the literature
Sheena H. Macleod a,*, Lawrie Elliott b, Richard Brown c
a School of Nursing and Midwifery, University of Dundee, 11 Airlie Place, Dundee, Tayside DD1 4 HJ, Scotland, UKb Centre for Integrated Healthcare Research, School of Nursing, Midwifery, and Social Care, Edinburgh Napier University,
Comely Bank Campus, 13 Crewe Road South, Edinburgh, Scotland, UKc University of Dundee, Dundee, Scotland, UK
A R T I C L E I N F O
Article history:
Received 11 November 2009
Received in revised form 14 July 2010
Accepted 4 September 2010
Keywords:
Burden
Carer
Mental health nurses
Schizophrenia
Support
A B S T R A C T
Objectives: The purpose of this review was to determine the nature of support that mental
health nurses could deliver to carers of people diagnosed with schizophrenia. The aim was
to identify approaches that could be delivered within community practice to reduce
burden and increase knowledge, mental health and coping.
Questions addressed: What effect did support have on carer burden and other needs? What
were the key elements of effective support? What effective supports could mental health
nurses deliver within practice?
Design: This review covers the international scientific literature published between 1980
and 2008.
Data sources: Searches were made of electronic databases relevant to nursing. All papers,
published in English, were assessed. Hand searches of review papers and references were
also carried out. Sixty-eight studies were included.
Study appraisal and synthesis: Only comparative studies providing a quantitative
assessment of carer outcomes were included. Findings were synthesised in narrative
format and grouped by intervention type.
Results: Of the 68 emerging studies, 12 (18%) directly included nurses in delivering the
intervention and 16 (24%) included nurses as part of a multidisciplinary team. There is fairly
robust evidence that education improves carer knowledge of schizophrenia. There is,
however, little evidence that it addresses more substantive areas such as burden, coping or
mental health. Supportive family education moves beyond information giving by developing
coping. As might be expected these approaches can reduce burden. More intensive
programmes such as behavioural family therapy aim to address stressful relationships which
commonly occur in families of people diagnosed with schizophrenia. These programmes are
particularly effective in reducing burden and can also improve mental health. Community
support such as intensive outreach is also effective in reducing burden. Finally, there is some
evidence that mutual support groups reduce burden and improve coping.
Conclusions: Research on effective support for carers of people diagnosed with
schizophrenia is emerging. Although findings were mixed, there was some evidence
supporting a range of approaches that mental health nurses could offer to carers. There is,
however, still a need for pragmatic studies to determine the extent that these approaches
can be delivered within nursing practice.
� 2010 Elsevier Ltd. All rights reserved.
Contents lists available at ScienceDirect
International Journal of Nursing Studies
journal homepage: www.elsevier.com/ijns
* Corresponding author.
E-mail address: [email protected] (S.H. Macleod).
0020-7489/$ – see front matter � 2010 Elsevier Ltd. All rights reserved.
doi:10.1016/j.ijnurstu.2010.09.005

S.H. Macleod et al. / International Journal of Nursing Studies 48 (2011) 100–120 101
What is already known about the topic?
� A
substantial number of people diagnosed with schizo-phrenia are supported to remain in the community byinformal carers such as family or friends. � P roviding such support can result in carer burden,mental health problems, stress and loneliness
� T he nature of support that mental health nurses couldoffer to meet the needs of these carers is uncertain.
What this paper adds
� T
he current review synthesised the research evidence onthe impact of support on the burden and needs reportedby carers of people diagnosed with schizophrenia. � It identified potentially effective approaches that couldbe delivered by mental health nurses to meet the supportneeds of carers of people diagnosed with schizophrenia.
� R esearch gaps include the theoretical underpinnings andfocus of new programmes, the use of convenientrecruitment strategies, lack of assessment of the facil-itators and barriers to implementation in practice andthe low number of studies from developing countries.
1. Background
With a prevalence rate of around 1.1% of adults, about51 million people worldwide have been diagnosed withschizophrenia (WHO, 2005, 2006). Not all will have anenduring form of the condition. Within Europe, around 14–24% develop chronic symptoms, 53% have residualsymptoms and 29% recover. This indicates that manypeople diagnosed with schizophrenia will experiencerelapse or chronic impairment and may require long-termsupport (Warner, 1997).
Over the last 50 years advances in mental health carehave enabled a growing number of people to be cared for incommunity rather than hospital settings (WHO, 2007).There is, however, great variability in community mentalhealth care across the world. In 2005, community servicesexisted in 68% of countries (WHO, 2005). Currently, theWHO European Region supports the development ofcommunity services for people diagnosed with mentallyillness within the 42 member states (WHO, 2008a), and theWorld Organisation of Family Doctors (WONCA) supportthis globally (WHO, 2008b).
Non-professional carers represent a substantial part ofthe health economy in most countries (Lefley, 1997). Theyare often parents, partners, siblings or friends and are highlycommitted and often driven by a sense of social duty for thepeople they care for. Providing such support, however, canbe demanding, isolating and exhausting for carers and mayresult in mental health problems, stress and loneliness(Doran et al., 2003; Saunders, 2003). Carers may also have tocope with public stigma and professional ignorance of theirneeds (Corrigan and Miller, 2004). The effects of caring havebeen widely studied and include burden, difficulty in copingand managing, impaired health, and low satisfaction withservices (Ruane et al., 2004).
Reports indicate that these negative effects can startearly in the caring process (Tennakoon et al., 2001). As
such, there are powerful health, social and economicreasons to support carers to maintain their own wellbeing.In line with many countries, UK health policies acknowl-edge this and require health and social care professionalsincluding nurses to provide support. The type of support,however, is not well defined and legal requirement to do sofocus solely on assessing carers’ needs (Department ofHealth, 2008, 2009). Furthermore, it is uncertain how thiscould be achieved for carers of people diagnosed withschizophrenia (Arksey et al., 2002; Arksey, 2003).
A key question therefore, and one not answered bypolicy, is which type of support might be of benefit tocarers who look after someone diagnosed with schizo-phrenia? The academic literature acknowledges that keysituational variables mediate the level of burden experi-enced. These include the carer’s informal support system,coping strategies, their relationship with the patient andprofessional support (Platt, 1985; Baronet, 1999). Weknow that lack of social support contributes to carerburden and there is some evidence that it buffers stressand is related to improved carer outcomes (Magliano et al.,2003; McCarty and McMahon, 2003). As a result, a numberof support interventions are based on stress-coping andsocial support theories (Dow and McDonald, 2003).
In addition, caring can also provide a source ofsatisfaction (Nolan and Lundh, 1999) and satisfactionhas been positively correlated with improved access toservices (Chen and Greenberg, 2004), and reduced burdenand distress (Budd et al., 1998). In particular, distress canbe reduced through collaborative relationships withservice providers (McCann and Baker, 2001). Thus thereappears to be a growing body of evidence which, ifsynthesised could indicate which types of interventionmight be of benefit to carers of people diagnosed withschizophrenia.
Although training, titles and experiences of nurses vary,mental health nursing is well established in manycountries and it could be argued that as a professionnurses are well placed to offer carer support (Tilley andRyan, 2000; WHO, 2007). A review of UK communitymental health nurses indicates that they can effectivelydeliver a range of interventions to people diagnosed withschizophrenia and their families (Curran and Brooker,2007). A major concern, however, is the extent to whichnurses do so in practice (Fadden, 1997; Magliano et al.,2006). A review of psychosocial interventions reported byBrooker (2001) concluded that even after training, deliverywithin nursing practice was limited. This is supported in areview of psycho-education reported by McFarlane et al.(2003). Relatively few RCTs are carried out on nursingpractice and those that are commonly report difficultieswithin community mental health settings (Taylor, 2003;Pawson et al., 2005).
Although systematic reviews have been carried out onsupport intervention categories such as psycho-educationthese do not include other forms of support and theirprimary focus is on carers in general. To our knowledgethere is no review of the international literature whichprovides evidence of which type of interventions are mosteffective to support carers of people diagnosed withschizophrenia, particularly those which could be offered

S.H. Macleod et al. / International Journal of Nursing Studies 48 (2011) 100–120102
by nurses. Also, within the international literature there islimited research on the roles and functions of nurses in thesupport of carers of people diagnosed with schizophreniain practice (Gall et al., 2003; Elsom et al., 2007). As such, itis unclear what carer related outcomes could realisticallybe improved through professional support and wheremental health nurses might contribute to this.
To summarise, people diagnosed with schizophreniarepresent a key group internationally who experiencechronic mental health problems. It is also likely that asubstantial number are being cared for in the communityby informal carers such as family or friends. This can placeadditional burden on carers, some of which results instress. Thus, mental health policies in many countriesstrongly encourage services to offer carer support. How-ever, the nature of that support is not well defined and anylegal requirement, such as that in the UK, does not gobeyond assessing carer’s needs. There is a growing body ofevidence which suggests that interventions may improvecarer outcomes, but as yet, a synthesis of this evidence hasnot been undertaken for carers who look after someonediagnosed with schizophrenia. This is particularly so forinterventions which could be provided by communitymental health nurses who may be well placed to offer suchsupport. This review addresses these issues in that itreviews the research literature, published between 1980and 2008, on the effect of support based interventions onthe needs of carers of people diagnosed with schizo-phrenia. The aim was to determine effective approachesthat could be delivered by community mental healthnurses in practice.
Three key questions were explored:
1. W
hat effect did support have on carer burden and otherneeds?2. W
hat were the key elements of effective support? 3. W hat effective supports could mental health nursesdeliver within practice?
2. Method
This review differs from a systematic review in two ways.First, searches were made of key electronic databases whichwere thought to be relevant to nursing, that is, theycontained papers which evaluated the evidence of inter-ventions which may be suited to nurses or conducted bynurses. This means not all available databases weresearched which in turn may mean that some papers weremissed. Second, we sought to include intervention studieswhich had comparative designs and did not restrict these toRCTs. That is, studies which assessed outcomes before andafter interventions even if the comparison was restricted toa single sample follow-up. Thus strict adherence to onedesign was not used to select or deselect studies.
Papers in the English language between 1980 and 2008were assessed. 1980 was selected as the time whenrelevant carer outcomes began to be reported in theliterature (Schene et al., 1994; Loukissa, 1994). Searcheswere made of key electronic databases. The sources were:CINAHL (1982–2008), MEDLINE (1980–2008), EMBASE(1988–2008), PsycINFO (1980–2008), Web of Knowledge –
Social Sciences Citation Index (1980–2008) and TheCochrane Library (1999–2008). Key journals, such asSchizophrenia Bulletin and websites such as MIND wereidentified and reviewed for relevant articles. Cross Search(Nursing and Midwifery) was carried out to identifymissing studies meeting the review criteria. Cross Searchprovided a single interface that simultaneously searchedmultiple sources. Reference lists of identified articles werehand searched to identify further relevant studies. We alsoincluded the individual studies identified from reviewsthat were relevant to the subject area that did not appear inour search of single study papers.
2.1. Search criteria
The population was defined as adult carers of peoplediagnosed with schizophrenia. Applying the PICO format(CRD, 2009) the search employed the following key terms(along with related terms).
Population – carer, caregiver, family, schizophrenia.Interventions and comparators – psychosocial, educa-
tion, day care, mutual support, community, mental healthservices.
Outcomes – knowledge, coping and managing, mentaland physical health. Our reasons for choosing theseoutcomes was based on our understanding of the mainprinciples upon which carer interventions were based thatis to raise awareness of schizophrenia, help carers copewith and manage caring, and in some instances improvetheir own physical health and wellbeing.
Papers containing the following designs were included.The taxonomy was derived from the CRD (2009).
� R
andomised controlled studies: Random assignment withcontrol and follow up. � Q uasi-experimental studies: Studies not achieving genu-ine randomisation or allocation concealment.
� N on-randomised controlled studies: Studies comparingtwo or more interventions and non random allocation.
� B efore and after studies: Comparison of a single sample.Papers were required to report on a quantitativeevaluation of support for carers of people diagnosed withschizophrenia, and include relevant outcomes (burden,knowledge, health, coping and managing). Data reportedfor more than one group or more than one time pointwas required. The guidance provided within the Con-solidated Standards of Reporting Trials (CONSORT)statement is used to discuss randomised designs (Alt-man, 1996), and the Transparent Reporting of Non-randomised Designs (TREND) statement for non-rando-mised designs (Don et al., 2004). The PRISMA statementfor reporting reviews of healthcare interventions is alsoacknowledged (Moher et al., 2009). Although RCTs couldbe considered the ideal design for evaluating carersupport, they can be difficult to apply within health caresettings (Victoria et al., 2004). Some approaches are alsoeasier to evaluate using this design than others (Deeks etal., 2003). As a result non-randomised designs are widelyused to evaluate health interventions and are, therefore,included within this review.

S.H. Macleod et al. / International Journal of Nursing Studies 48 (2011) 100–120 103
Differences in means were used to evaluate summarymeasures. The risk of bias within and across studies wasassessed. Studies failing to report power calculations,reporting low numbers and/or the use of non-validatedoutcome measures, variability in interventions and out-come measures used across studies were identified as apotential risks. While supports can comprise a singleapproach such as education, they predominantly comprisea package of interventions. Such packages are regarded ascomplex interventions (Gotzche, 1989), and defining theiractive elements can be difficult. In order to determine thepossible mechanisms for the success, or otherwise, ofapproaches CRD (2009) guidelines propose that evalua-tions should include the theoretical basis of interventionsand we sought to include this as part of our assessment.
The review excluded qualitative evaluations andarticles not reporting relevant outcomes. Child carerswere also excluded as it was acknowledged that they couldhave different support needs from adults.
3. Results
Data searches were carried out by (SM) and checked bya second researcher (LE). Statistical guidance was providedby DB. Initial database searching using the key terms‘‘carer’’ and ‘‘schizophrenia’’ (and related terms) yieldedthousands of hits. Fig. 1 provides a flow diagram of dataretrieved through different stages of the review. As can beseen, relevant websites and review papers were alsosearched for studies. The search was refined in a series ofstages using each of the outcomes and then each of theinterventions (refined to 1708 papers). As a result of thisprocess 545 potentially relevant articles were identified. Ofthese, 396 were rejected as they were descriptive,quantitative or did not report relevant outcomes. Inparticular, a large body of literature reporting ExpressedEmotion did not meet the review criteria. The search[()TD$FIG]
Source: Moher et al 2009
Studies identified from database searches n=1,661 Studies identified from Websites n=5 34 reviews identified and references searched n= 42 Total = 1,708
Potentially relevant studies identified from initial screening (n=545)
Studies not meeting relevant criteria excluded and duplicate reports removed (n=396)
Full texts assessed for eligibility (n= 149)
Studies excluded (n=81)
No quantitative data reported n= 43 Data reported for mixed diagnostic groups n= 31 Data reported for one group at one time point only n= 7
Studies included (n= 68)
Education n= 10 Supportive family education n= 13 Family interventions n = 29 Community support services n= 9 Mutual support groups n= 4 Day care services n= 3
Fig. 1. Flow diagram of data retrieved at each stage of the review.
yielded 149 potentially relevant studies. After full assess-ment, 81 of these were rejected and 68 were included.Studies were rejected for either of the following reasons.
� N
o quantitative data reported for relevant outcomes. � D ata reported for mixed diagnostic groups. � D ata reported for one group at one time point only.Appendix 1 provides an example of the search strategyusing MEDLINE to demonstrate the use of the search termsand limits.
Summary findings are reported according to the author,year, country and the PICO format (CRD, 2009) (Tables 1–6). A key to the abbreviations used for outcome measures isprovided as Appendix 2. Interventions include a broad,overlapping range of approaches with no formally agreedsystem for categorising these. For the purpose of thisreview, studies were grouped as: education, supportivefamily education, family interventions, community sup-port services, mutual support groups and day care services.
3.1. Education
Educational interventions take many forms and aredelivered either individually or through groups. Educationcan be professionally, or non-professionally, led with varieddurations and methods. Methods include lectures, bookletsor audio-visual presentations. The theoretical basis is that anunderstanding of schizophrenia and its management will bebeneficial for the carer, although apart from knowledgeother benefits are not often specified (Kazarin andVanderheyden, 1992). Ten studies are reviewed in thiscategory (Table 1). Interventions are delivered by specialistresearcher/clinicians except in one study where it wasdelivered by nurses as part of a team (Stengard, 2003), andone study where it was delivered by nurses experienced inthe intervention (Li and Arthur, 2005).
The impact of educational interventions on burden waslimited. Five studies report mixed findings. Only one quasi-experimental study reported reduced distress following 4–6 h of education (Smith and Birchwood, 1987). No effect onstress was reported in the remaining four studies (Cozolinoet al., 1988; Smith and Birchwood’s, 1987; Sidley et al.,1991; Stengard, 2003).
As could be expected the interventions had a favourableimpact on carer’s knowledge. Of the ten studies onereported no knowledge gain following a single (3 h) session(Cozolino et al., 1988) while the remaining nine reportedincreased carer knowledge about schizophrenia and itsmanagement following more than one educational session.One non-randomised controlled study assessed the impactof education on somatic symptoms, anxiety, insomnia,social dysfunction and severe depression and reported noimprovement (Stengard, 2003).
3.1.1. Critical conclusions
Educational programmes are fairly short in durationand aim to improve carer’s knowledge of schizophrenia.They generally achieve this aim but there is little evidencethat they address more substantive areas of caring such asimproving coping, reducing burden or improving health

Table 1
Reported effect of education n = 10.
Authors Intervention Effective elements, framework,
intensity and outcome measure
Delivered by Effects
Merinder et al. (1999).
Denmark RCT n = 46
Family Education
Comparison: Standard services
8 taught sessions on schizophrenia and its
management, early warning signs and legal issues
(Framework – Merinder et al., 1999) (KOS)
1 year follow up
Group Leaders Improves knowledge p< 0.05
Li and Arthur (2005).
China RCT n = 101
Family and Patient Education
Comparison: Standard care
Education while patient in hospital (8 h with patient
and 36 h with family) and 6 h following discharge
(for both together) (Framework: Li and Arthur,
2005) (KASI)
Nurses experienced in
the intervention
Improves knowledge
p< 0.01
Smith and Birchwood (1987).
UK n = 40
Birchwood et al. (1992).
UK Quasi Experimental n = 62
Education Package
Comparison: Postal Booklet’s
Education� 6 h. Seminar group format plus 4 booklets
about schizophrenia and its management. Emphasis
can be given to symptom management and package
extended to address carer misconceptions and quality
of life issues (Framework – Smith and Birchwood,
1987) (KSQ, SRT, FDS). 6 month follow up
Specialist
researcher/clinician
Improves knowledge p< 0.001,
fear and distress p< 0.01 but
no effect on health
Stengard (2003).
Finland Non-random
allocation n = 191
Education: Oral
Comparison: Video
Education� 8 sessions about schizophrenia and its
management. including support services or video
programme� 6 lectures (3 h) (Framework -Stengard,
2003) (KT and BS-developed for study, GHQ)
Nurses as part of the
mental health team
Improves knowledge p< 0.01,
but no effect on burden or health
Sidley et al. (1991).
UK Pilot n = 18
Education package Comparison:
Modified educational package
4 educational booklets about schizophrenia and its
management – posted to carers at 1week intervals
or an educational video (Framework – Smith and
Birchwood, 1987) (KASI, KSQ, FDS)
Specialist researcher/
clinician
Improves knowledge p< 0.001,
but no effect on distress or burden
Barrowclough et al. (1987). UK
Single sample n = 24
Information Booklet 2 information booklets with a one week interval.
Worked through with clinicians and questions
answered (Framework – Barrowclough et al.,
1986) (KASI)
Specialist researcher/
clinician
Improves knowledge p< 0.001
Cazzullo et al. (1989).
Italy Single sample n = 17
Education Group Education and discussion group about schizophrenia
and its management. 24 h (Framework Cazzullo et al.,
1989) (KI)
Specialist researcher/
clinician
Improves knowledge
p< 0.001
Cozolino et al. (1988). USA
Quasi Experimental pre-post
with a 2 month delay n = 36
Single education session
Comparison: Control group
Single (3 h) education session. Semi-formal didactic
presentation (Framework Snyder and Liberman,
1981) (KSU, RSS)
Specialist researcher/
clinician
Does not improve health and
information was not retained
at 2 months.
Orhagen and d’Elia (1992).
Sweden. Single sample. n = 47
Multi-family Education programme Six, 2 h, structured educational sessions with unstructured
participant socialisation (Framework – Orhagen and d’Elia,
1992) (KST, FDS)
Specialist researcher/
clinician
Increased knowledge was
associated with decreased
burden p< 0.05
S.H.
Ma
cleod
eta
l./Intern
atio
na
lJo
urn
al
of
Nu
rsing
Stud
ies4
8(2
01
1)
10
0–
12
01
04

Table 2
Reported effect of supportive family education n = 13.
Authors Intervention Effective elements, framework, intensity and outcome
measure
Delivered by Effects
Zhang et al. (1998b)
China RCT n = 1048
Psycho-education group plus
standard services
Comparison Standard services
Lectures on schizophrenia, its management, family self-help
and promotion of carer health (14 h) and 5 group discussions
(Framework – Zhang et al., 1998a) Over 2 years plus standard
services (FBIS at 6, 12 and 24 months)
Nurse or psychiatrist Improves knowledge and
burden p< 0.01, but no
effect on health
Rotondi et al. (2005)
USA RCT n = 21
Web-based psycho education
Comparison: standard care
On-line group therapy and education about schizophrenia,
its management, library resource, problem solving and
e-mail response to questions.(Frameworks; Web-resource –
Rotondi et al., 2005) Therapy group -Manuals of Anderson
et al. (1986) and McFarlane et al. (1999) (DRD)
Experienced
researcher/clinician
Improves stress p< 0.05
Bradley et al. (2006)
Australia RCT n = 50
Multi Family
Psycho-education Group
Comparison: Psycho-education
Multifamily Psycho-education group (Framework –
McFarlane et al., 1999). Education and support
about schizophrenia and its management.
26 sessions over 1 year (FBIS)
Multidisciplinary group
excluding nurses
Improves burden
p< 0.001
Gutierrez-Maldonado and
Caqueo-Urizar (2007)
Chile RCT n = 45
Multi Family
Psycho-education Group
Comparison: Meetings with staff
Multifamily Psycho-education group (Framework –
McFarlane et al., 1999). Education and support about
schizophrenia and its management. 20 sessions (ZBI)
Psychologists Improves burden
p< 0.001
So et al. (2006) China
RCT n = 45
Group psycho-education� 9 h
Comparison –Waiting list
Psycho education– (Framework – So et al., 2006).
Knowledge about schizophrenia, its management,
relapse and stress, with role play and rehearsal of
skills. Six sessions over 9 h (ECI, GHQ)
Psychologist Improves knowledge
p< 0.01 but no effect on
health, burden, coping
Chan et al. (2008)
China RCT n = 73
Psycho-education group 10 sessions delivered over 3 months based on the Early
Psychosis Prevention and Intervention Centre (EPPIC)
handbook. Focus on education about schizophrenia
and its management, recovery, legal issues and early
warning signs (Framework –Chan et al., 2008) (FBIS)
Nurse trained in the
intervention
Improves burden p< 0.05
and self efficacy p< 0.001
Comparison: Standard care
Abramowitz and
Coursey (1989) USA
Non-random allocation n = 48
Education/Support Group.
Comparison: Waiting list matched.
Education and support utilising 3 coping strategies.
Problem solving, handling stress and social support.
2 h (Framework – Abramowitz and Coursey, 1989) (STAI)
Group leader Improves anxiety p< 0.005,
distress p< 0.001
Sota et al. (2008) Japan
Non-random
allocation n = 110
Family psycho-education
Comparison of 2, 5 and 9 sessions
Framework – Sota et al. (2008). 2 sessions = 2-3 families
given 4 h of education about schizophrenia, recovery and
relapse using 2 videos produced by the National Alliance
for the mentally Ill and NAMI and a pamphlet. 5 sessions.
Large group education about schizophrenia supported
with a different video followed by supportive group
therapy� 10 h. 9 sessions. Large group given 9 h of
education about schizophrenia and its management
followed by 10 h of group therapy (KASI)
Psychiatrists and social
workers
Improves knowledge p< 0.05
Hugen (1993) USA
Single sample n = 22
Educational Workshop Education about schizophrenia and its management,
coping skills and role of support groups� 7 h over
1 day (Framework – Mixed) (KASI)
Social worker-clinicians Improves knowledge
p< 0.05
S.H.
Ma
cleod
eta
l./Intern
atio
na
lJo
urn
al
of
Nu
rsing
Stud
ies4
8(2
01
1)
10
0–
12
01
05
Ta
ble
2(C
on
tin
ued
)
Au
tho
rsIn
terv
en
tio
nE
ffe
ctiv
ee
lem
en
ts,
fra
me
wo
rk,
inte
nsi
tya
nd
ou
tco
me
me
asu
re
De
liv
ere
db
yE
ffe
cts
Ca
ssid
ye
ta
l.(2
00
1)
Ire
lan
dS
ing
lesa
mp
len
=1
01
Ed
uca
tio
nP
rog
ram
me
We
ek
lyp
sych
o-e
du
cati
on
gro
up
s(1
4h
).T
ea
chin
ga
nd
dis
cuss
ion
ab
ou
t:sc
hiz
op
hre
nia
,it
sm
an
ag
em
en
t,b
urd
en
,
cop
ing
an
da
cce
ssin
gse
rvic
es.
Fra
me
wo
rk–
Ca
ssid
y
et
al.
(20
01
).P
lus
rea
din
gm
ate
ria
la
da
pte
dfr
om
Mo
ser
et
al’
s‘‘E
du
cati
on
al
Fam
ily
Th
era
py
’’fo
r
sch
izo
ph
ren
ia(1
99
4)
(KS
Q)
Ex
pe
rie
nce
dth
era
pis
ts
No
Imp
rov
es
kn
ow
led
ge
p<
0.0
01
0
Ya
ma
gu
chi
et
al.
(20
06
)
Jap
an
,S
ing
lesa
mp
len
=4
6
Gro
up
psy
cho
-ed
uca
tio
nLe
ctu
res
an
dd
iscu
ssio
na
bo
ut
sch
izo
ph
ren
ia,
be
ha
vio
ur
ma
na
ge
me
nt
an
dp
rob
lem
solv
ing
.4�
2h
sess
ion
so
ve
r
2m
on
ths
(Fra
me
wo
rk–
Ya
ma
gu
chi
et
al.
,2
00
6)
(FB
DS
,S
TA
I)
Mu
ltid
isci
pli
na
ryg
rou
p
incl
ud
ing
nu
rse
s
Imp
rov
es
sub
ject
ive
bu
rde
n
an
da
nx
iety
p<
0.0
01
Be
rko
wit
ze
ta
l.(1
99
0)
UK
RC
Tn
=2
1
Ed
uca
tio
np
lus
are
lati
ve
sg
rou
p
Co
mp
ari
son
:E
du
cati
on
plu
s
fam
ily
the
rap
y
4le
ctu
res
cov
eri
ng
sch
izo
ph
ren
iaa
nd
its
ma
na
ge
me
nt.
De
liv
ere
din
ap
ers
on
al
wa
yto
two
rela
tiv
es
at
ati
me
inth
ere
lati
ve
so
wn
ho
me
ov
er
2w
ee
ks
(4h
).P
lus
a
rela
tiv
es
gro
up
(KI-
mo
difi
ed
)
Sp
eci
ali
stre
sea
rch
er/
clin
icia
n
No
be
twe
en
gro
up
dif
fere
nce
sin
kn
ow
led
ge
.
Win
efi
eld
an
dH
arv
ey
(19
95
)
als
ose
eW
ine
fie
lde
ta
l.,
19
98
Au
stra
lia
Ma
tch
ed
con
tro
lsn
=3
6
Dis
cuss
ion
gro
up
Co
mp
ari
son
:
Ma
tch
ed
gro
up
Ag
rou
pp
rog
ram
me
of
ex
pe
rtp
rese
nta
tio
ns,
dis
cuss
ion
an
d
soci
al
sup
po
rt.
8se
ssio
ns
(Fra
me
wo
rkW
ine
fie
lda
nd
Ha
rve
y,
19
95
)(P
OM
S)
Cli
nic
al
psy
cho
log
ist
Ina
de
qu
ate
sta
tist
ica
l
po
we
rre
po
rte
d.
S.H. Macleod et al. / International Journal of Nursing Studies 48 (2011) 100–120106
outcomes. Thus, the effects on more long terms goals suchas reducing burden or improving mental or physical healthshould not be expected. Of the ten studies in this categorysix were randomised controlled trials which compared theintervention with a control over time. Great variability wasobserved in study quality. Only Li and Arthur (2005) andStengard (2003) reported adequate sample sizes (althoughStengard used a non-validated scale). The comparativescope of these studies suggests a fairly robust evidencebase that education improves carer knowledge. Nursesdelivered education in two studies, but there is nothingfrom the remaining studies to indicate that they should beexcluded from doing so.
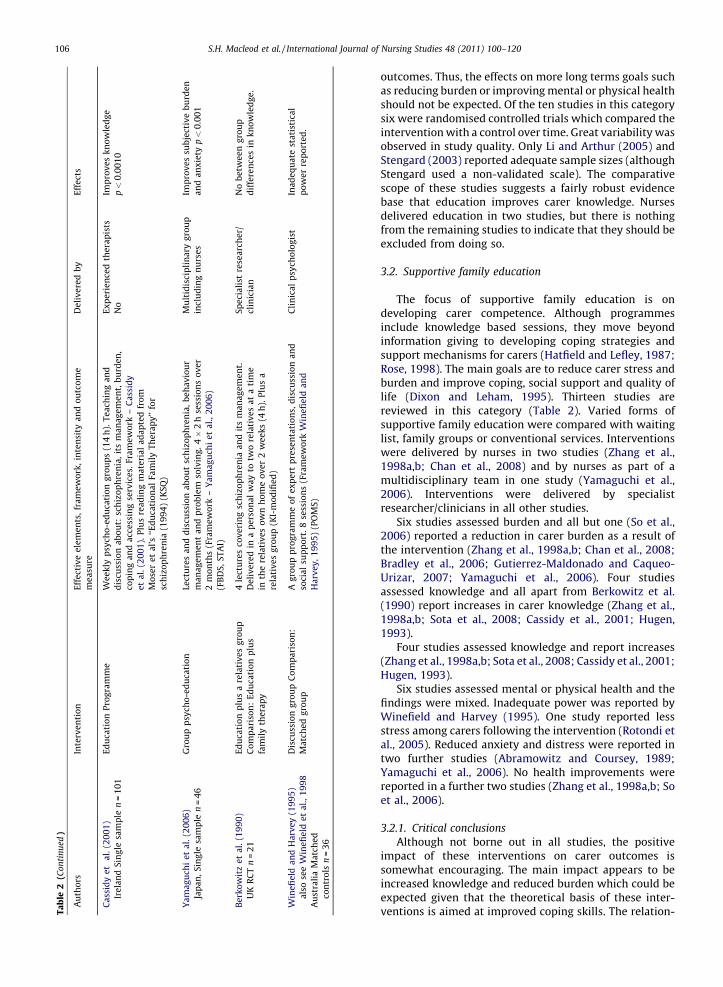
3.2. Supportive family education
The focus of supportive family education is ondeveloping carer competence. Although programmesinclude knowledge based sessions, they move beyondinformation giving to developing coping strategies andsupport mechanisms for carers (Hatfield and Lefley, 1987;Rose, 1998). The main goals are to reduce carer stress andburden and improve coping, social support and quality oflife (Dixon and Leham, 1995). Thirteen studies arereviewed in this category (Table 2). Varied forms ofsupportive family education were compared with waitinglist, family groups or conventional services. Interventionswere delivered by nurses in two studies (Zhang et al.,1998a,b; Chan et al., 2008) and by nurses as part of amultidisciplinary team in one study (Yamaguchi et al.,2006). Interventions were delivered by specialistresearcher/clinicians in all other studies.
Six studies assessed burden and all but one (So et al.,2006) reported a reduction in carer burden as a result ofthe intervention (Zhang et al., 1998a,b; Chan et al., 2008;Bradley et al., 2006; Gutierrez-Maldonado and Caqueo-Urizar, 2007; Yamaguchi et al., 2006). Four studiesassessed knowledge and all apart from Berkowitz et al.(1990) report increases in carer knowledge (Zhang et al.,1998a,b; Sota et al., 2008; Cassidy et al., 2001; Hugen,1993).
Four studies assessed knowledge and report increases(Zhang et al., 1998a,b; Sota et al., 2008; Cassidy et al., 2001;Hugen, 1993).
Six studies assessed mental or physical health and thefindings were mixed. Inadequate power was reported byWinefield and Harvey (1995). One study reported lessstress among carers following the intervention (Rotondi etal., 2005). Reduced anxiety and distress were reported intwo further studies (Abramowitz and Coursey, 1989;Yamaguchi et al., 2006). No health improvements werereported in a further two studies (Zhang et al., 1998a,b; Soet al., 2006).
3.2.1. Critical conclusions
Although not borne out in all studies, the positiveimpact of these interventions on carer outcomes issomewhat encouraging. The main impact appears to beincreased knowledge and reduced burden which could beexpected given that the theoretical basis of these inter-ventions is aimed at improved coping skills. The relation-
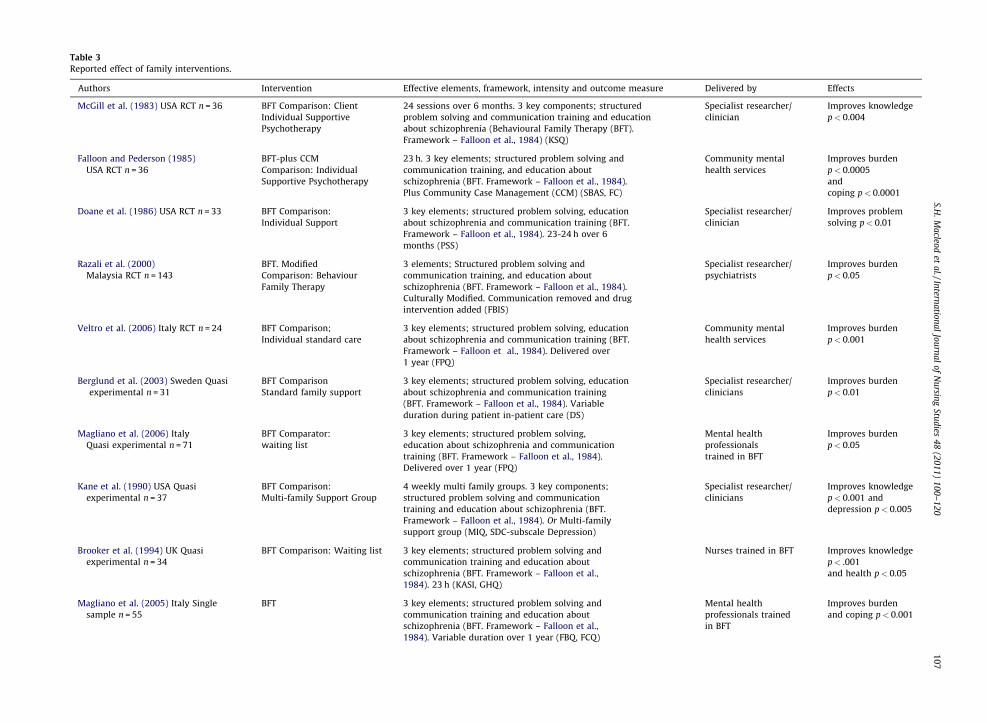
Table 3
Reported effect of family interventions.
Authors Intervention Effective elements, framework, intensity and outcome measure Delivered by Effects
McGill et al. (1983) USA RCT n = 36 BFT Comparison: Client
Individual Supportive
Psychotherapy
24 sessions over 6 months. 3 key components; structured
problem solving and communication training and education
about schizophrenia (Behavioural Family Therapy (BFT).
Framework – Falloon et al., 1984) (KSQ)
Specialist researcher/
clinician
Improves knowledge
p< 0.004
Falloon and Pederson (1985)
USA RCT n = 36
BFT-plus CCM
Comparison: Individual
Supportive Psychotherapy
23 h. 3 key elements; structured problem solving and
communication training, and education about
schizophrenia (BFT. Framework – Falloon et al., 1984).
Plus Community Case Management (CCM) (SBAS, FC)
Community mental
health services
Improves burden
p< 0.0005
and
coping p< 0.0001
Doane et al. (1986) USA RCT n = 33 BFT Comparison:
Individual Support
3 key elements; structured problem solving, education
about schizophrenia and communication training (BFT.
Framework – Falloon et al., 1984). 23-24 h over 6
months (PSS)
Specialist researcher/
clinician
Improves problem
solving p< 0.01
Razali et al. (2000)
Malaysia RCT n = 143
BFT. Modified
Comparison: Behaviour
Family Therapy
3 elements; Structured problem solving and
communication training, and education about
schizophrenia (BFT. Framework – Falloon et al., 1984).
Culturally Modified. Communication removed and drug
intervention added (FBIS)
Specialist researcher/
psychiatrists
Improves burden
p< 0.05
Veltro et al. (2006) Italy RCT n = 24 BFT Comparison;
Individual standard care
3 key elements; structured problem solving, education
about schizophrenia and communication training (BFT.
Framework – Falloon et al., 1984). Delivered over
1 year (FPQ)
Community mental
health services
Improves burden
p< 0.001
Berglund et al. (2003) Sweden Quasi
experimental n = 31
BFT Comparison
Standard family support
3 key elements; structured problem solving, education
about schizophrenia and communication training
(BFT. Framework – Falloon et al., 1984). Variable
duration during patient in-patient care (DS)
Specialist researcher/
clinicians
Improves burden
p< 0.01
Magliano et al. (2006) Italy
Quasi experimental n = 71
BFT Comparator:
waiting list
3 key elements; structured problem solving,
education about schizophrenia and communication
training (BFT. Framework – Falloon et al., 1984).
Delivered over 1 year (FPQ)
Mental health
professionals
trained in BFT
Improves burden
p< 0.05
Kane et al. (1990) USA Quasi
experimental n = 37
BFT Comparison:
Multi-family Support Group
4 weekly multi family groups. 3 key components;
structured problem solving and communication
training and education about schizophrenia (BFT.
Framework – Falloon et al., 1984). Or Multi-family
support group (MIQ, SDC-subscale Depression)
Specialist researcher/
clinicians
Improves knowledge
p< 0.001 and
depression p< 0.005
Brooker et al. (1994) UK Quasi
experimental n = 34
BFT Comparison: Waiting list 3 key elements; structured problem solving and
communication training and education about
schizophrenia (BFT. Framework – Falloon et al.,
1984). 23 h (KASI, GHQ)
Nurses trained in BFT Improves knowledge
p< .001
and health p< 0.05
Magliano et al. (2005) Italy Single
sample n = 55
BFT 3 key elements; structured problem solving and
communication training and education about
schizophrenia (BFT. Framework – Falloon et al.,
1984). Variable duration over 1 year (FBQ, FCQ)
Mental health
professionals trained
in BFT
Improves burden
and coping p< 0.001
S.H.
Ma
cleod
eta
l./Intern
atio
na
lJo
urn
al
of
Nu
rsing
Stud
ies4
8(2
01
1)
10
0–
12
01
07
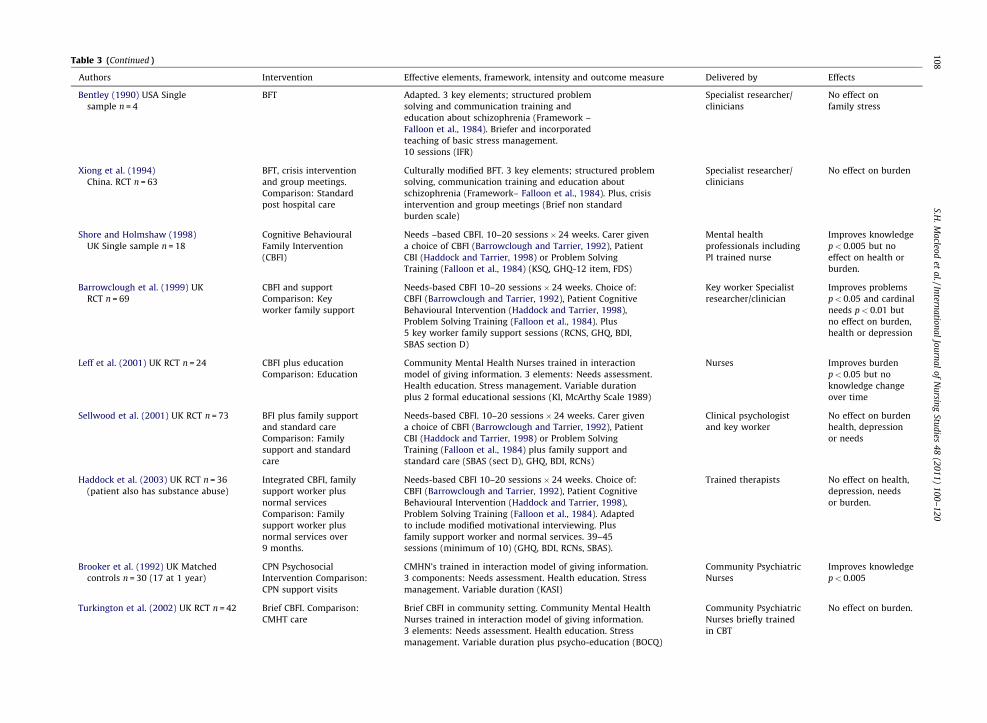
Table 3 (Continued )
Authors Intervention Effective elements, framework, intensity and outcome measure Delivered by Effects
Bentley (1990) USA Single
sample n = 4
BFT Adapted. 3 key elements; structured problem
solving and communication training and
education about schizophrenia (Framework –
Falloon et al., 1984). Briefer and incorporated
teaching of basic stress management.
10 sessions (IFR)
Specialist researcher/
clinicians
No effect on
family stress
Xiong et al. (1994)
China. RCT n = 63
BFT, crisis intervention
and group meetings.
Comparison: Standard
post hospital care
Culturally modified BFT. 3 key elements; structured problem
solving, communication training and education about
schizophrenia (Framework– Falloon et al., 1984). Plus, crisis
intervention and group meetings (Brief non standard
burden scale)
Specialist researcher/
clinicians
No effect on burden
Shore and Holmshaw (1998)
UK Single sample n = 18
Cognitive Behavioural
Family Intervention
(CBFI)
Needs –based CBFI. 10–20 sessions� 24 weeks. Carer given
a choice of CBFI (Barrowclough and Tarrier, 1992), Patient
CBI (Haddock and Tarrier, 1998) or Problem Solving
Training (Falloon et al., 1984) (KSQ, GHQ-12 item, FDS)
Mental health
professionals including
PI trained nurse
Improves knowledge
p< 0.005 but no
effect on health or
burden.
Barrowclough et al. (1999) UK
RCT n = 69
CBFI and support
Comparison: Key
worker family support
Needs-based CBFI 10–20 sessions� 24 weeks. Choice of:
CBFI (Barrowclough and Tarrier, 1992), Patient Cognitive
Behavioural Intervention (Haddock and Tarrier, 1998),
Problem Solving Training (Falloon et al., 1984). Plus
5 key worker family support sessions (RCNS, GHQ, BDI,
SBAS section D)
Key worker Specialist
researcher/clinician
Improves problems
p< 0.05 and cardinal
needs p< 0.01 but
no effect on burden,
health or depression
Leff et al. (2001) UK RCT n = 24 CBFI plus education
Comparison: Education
Community Mental Health Nurses trained in interaction
model of giving information. 3 elements: Needs assessment.
Health education. Stress management. Variable duration
plus 2 formal educational sessions (KI, McArthy Scale 1989)
Nurses Improves burden
p< 0.05 but no
knowledge change
over time
Sellwood et al. (2001) UK RCT n = 73 BFI plus family support
and standard care
Comparison: Family
support and standard
care
Needs-based CBFI. 10–20 sessions� 24 weeks. Carer given
a choice of CBFI (Barrowclough and Tarrier, 1992), Patient
CBI (Haddock and Tarrier, 1998) or Problem Solving
Training (Falloon et al., 1984) plus family support and
standard care (SBAS (sect D), GHQ, BDI, RCNs)
Clinical psychologist
and key worker
No effect on burden
health, depression
or needs
Haddock et al. (2003) UK RCT n = 36
(patient also has substance abuse)
Integrated CBFI, family
support worker plus
normal services
Comparison: Family
support worker plus
normal services over
9 months.
Needs-based CBFI 10–20 sessions� 24 weeks. Choice of:
CBFI (Barrowclough and Tarrier, 1992), Patient Cognitive
Behavioural Intervention (Haddock and Tarrier, 1998),
Problem Solving Training (Falloon et al., 1984). Adapted
to include modified motivational interviewing. Plus
family support worker and normal services. 39–45
sessions (minimum of 10) (GHQ, BDI, RCNs, SBAS).
Trained therapists No effect on health,
depression, needs
or burden.
Brooker et al. (1992) UK Matched
controls n = 30 (17 at 1 year)
CPN Psychosocial
Intervention Comparison:
CPN support visits
CMHN’s trained in interaction model of giving information.
3 components: Needs assessment. Health education. Stress
management. Variable duration (KASI)
Community Psychiatric
Nurses
Improves knowledge
p< 0.005
Turkington et al. (2002) UK RCT n = 42 Brief CBFI. Comparison:
CMHT care
Brief CBFI in community setting. Community Mental Health
Nurses trained in interaction model of giving information.
3 elements: Needs assessment. Health education. Stress
management. Variable duration plus psycho-education (BOCQ)
Community Psychiatric
Nurses briefly trained
in CBT
No effect on burden.
S.H.
Ma
cleod
eta
l./Intern
atio
na
lJo
urn
al
of
Nu
rsing
Stud
ies4
8(2
01
1)
10
0–
12
01
08
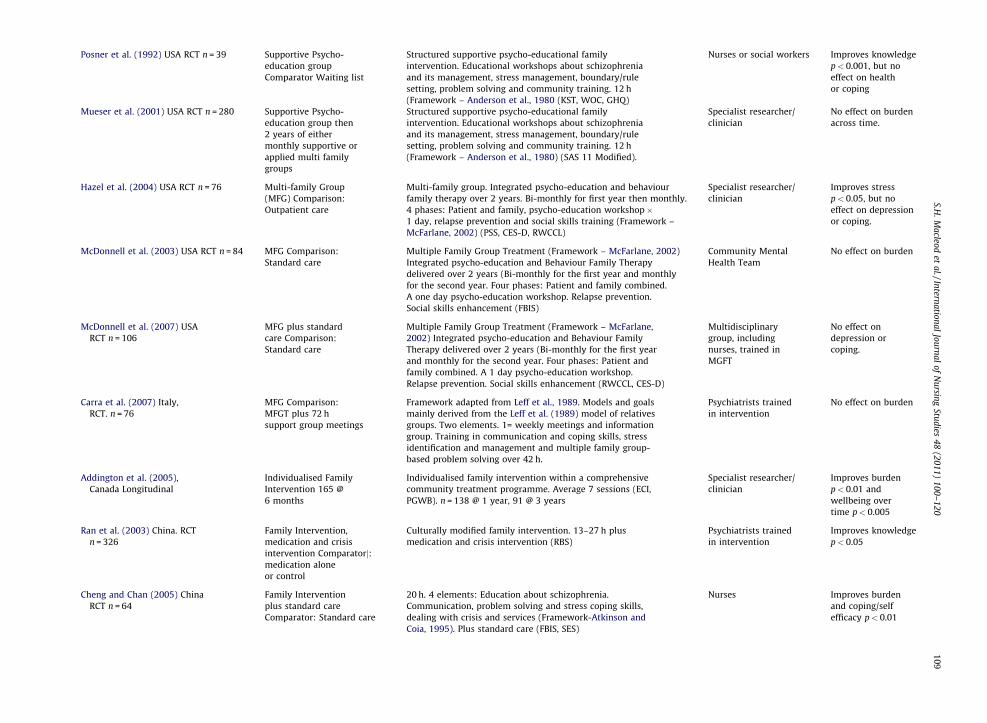
Posner et al. (1992) USA RCT n = 39 Supportive Psycho-
education group
Comparator Waiting list
Structured supportive psycho-educational family
intervention. Educational workshops about schizophrenia
and its management, stress management, boundary/rule
setting, problem solving and community training. 12 h
(Framework – Anderson et al., 1980 (KST, WOC, GHQ)
Nurses or social workers Improves knowledge
p< 0.001, but no
effect on health
or coping
Mueser et al. (2001) USA RCT n = 280 Supportive Psycho-
education group then
2 years of either
monthly supportive or
applied multi family
groups
Structured supportive psycho-educational family
intervention. Educational workshops about schizophrenia
and its management, stress management, boundary/rule
setting, problem solving and community training. 12 h
(Framework – Anderson et al., 1980) (SAS 11 Modified).
Specialist researcher/
clinician
No effect on burden
across time.
Hazel et al. (2004) USA RCT n = 76 Multi-family Group
(MFG) Comparison:
Outpatient care
Multi-family group. Integrated psycho-education and behaviour
family therapy over 2 years. Bi-monthly for first year then monthly.
4 phases: Patient and family, psycho-education workshop�1 day, relapse prevention and social skills training (Framework –
McFarlane, 2002) (PSS, CES-D, RWCCL)
Specialist researcher/
clinician
Improves stress
p< 0.05, but no
effect on depression
or coping.
McDonnell et al. (2003) USA RCT n = 84 MFG Comparison:
Standard care
Multiple Family Group Treatment (Framework – McFarlane, 2002)
Integrated psycho-education and Behaviour Family Therapy
delivered over 2 years (Bi-monthly for the first year and monthly
for the second year. Four phases: Patient and family combined.
A one day psycho-education workshop. Relapse prevention.
Social skills enhancement (FBIS)
Community Mental
Health Team
No effect on burden
McDonnell et al. (2007) USA
RCT n = 106
MFG plus standard
care Comparison:
Standard care
Multiple Family Group Treatment (Framework – McFarlane,
2002) Integrated psycho-education and Behaviour Family
Therapy delivered over 2 years (Bi-monthly for the first year
and monthly for the second year. Four phases: Patient and
family combined. A 1 day psycho-education workshop.
Relapse prevention. Social skills enhancement (RWCCL, CES-D)
Multidisciplinary
group, including
nurses, trained in
MGFT
No effect on
depression or
coping.
Carra et al. (2007) Italy,
RCT. n = 76
MFG Comparison:
MFGT plus 72 h
support group meetings
Framework adapted from Leff et al., 1989. Models and goals
mainly derived from the Leff et al. (1989) model of relatives
groups. Two elements. 1= weekly meetings and information
group. Training in communication and coping skills, stress
identification and management and multiple family group-
based problem solving over 42 h.
Psychiatrists trained
in intervention
No effect on burden
Addington et al. (2005),
Canada Longitudinal
Individualised Family
Intervention 165 @
6 months
Individualised family intervention within a comprehensive
community treatment programme. Average 7 sessions (ECI,
PGWB). n = 138 @ 1 year, 91 @ 3 years
Specialist researcher/
clinician
Improves burden
p< 0.01 and
wellbeing over
time p< 0.005
Ran et al. (2003) China. RCT
n = 326
Family Intervention,
medication and crisis
intervention Comparatorj:medication alone
or control
Culturally modified family intervention. 13–27 h plus
medication and crisis intervention (RBS)
Psychiatrists trained
in intervention
Improves knowledge
p< 0.05
Cheng and Chan (2005) China
RCT n = 64
Family Intervention
plus standard care
Comparator: Standard care
20 h. 4 elements: Education about schizophrenia.
Communication, problem solving and stress coping skills,
dealing with crisis and services (Framework-Atkinson and
Coia, 1995). Plus standard care (FBIS, SES)
Nurses Improves burden
and coping/self
efficacy p< 0.01
S.H.
Ma
cleod
eta
l./Intern
atio
na
lJo
urn
al
of
Nu
rsing
Stud
ies4
8(2
01
1)
10
0–
12
01
09
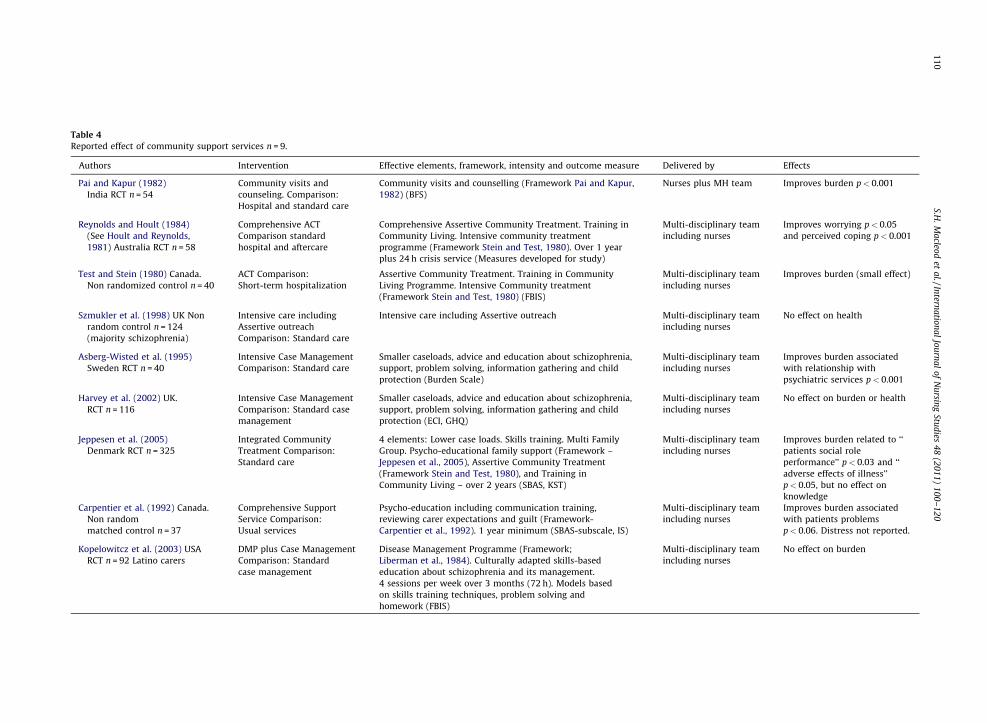
Table 4
Reported effect of community support services n = 9.
Authors Intervention Effective elements, framework, intensity and outcome measure Delivered by Effects
Pai and Kapur (1982)
India RCT n = 54
Community visits and
counseling. Comparison:
Hospital and standard care
Community visits and counselling (Framework Pai and Kapur,
1982) (BFS)
Nurses plus MH team Improves burden p< 0.001
Reynolds and Hoult (1984)
(See Hoult and Reynolds,
1981) Australia RCT n = 58
Comprehensive ACT
Comparison standard
hospital and aftercare
Comprehensive Assertive Community Treatment. Training in
Community Living. Intensive community treatment
programme (Framework Stein and Test, 1980). Over 1 year
plus 24 h crisis service (Measures developed for study)
Multi-disciplinary team
including nurses
Improves worrying p< 0.05
and perceived coping p< 0.001
Test and Stein (1980) Canada.
Non randomized control n = 40
ACT Comparison:
Short-term hospitalization
Assertive Community Treatment. Training in Community
Living Programme. Intensive Community treatment
(Framework Stein and Test, 1980) (FBIS)
Multi-disciplinary team
including nurses
Improves burden (small effect)
Szmukler et al. (1998) UK Non
random control n = 124
(majority schizophrenia)
Intensive care including
Assertive outreach
Comparison: Standard care
Intensive care including Assertive outreach Multi-disciplinary team
including nurses
No effect on health
Asberg-Wisted et al. (1995)
Sweden RCT n = 40
Intensive Case Management
Comparison: Standard care
Smaller caseloads, advice and education about schizophrenia,
support, problem solving, information gathering and child
protection (Burden Scale)
Multi-disciplinary team
including nurses
Improves burden associated
with relationship with
psychiatric services p< 0.001
Harvey et al. (2002) UK.
RCT n = 116
Intensive Case Management
Comparison: Standard case
management
Smaller caseloads, advice and education about schizophrenia,
support, problem solving, information gathering and child
protection (ECI, GHQ)
Multi-disciplinary team
including nurses
No effect on burden or health
Jeppesen et al. (2005)
Denmark RCT n = 325
Integrated Community
Treatment Comparison:
Standard care
4 elements: Lower case loads. Skills training. Multi Family
Group. Psycho-educational family support (Framework –
Jeppesen et al., 2005), Assertive Community Treatment
(Framework Stein and Test, 1980), and Training in
Community Living – over 2 years (SBAS, KST)
Multi-disciplinary team
including nurses
Improves burden related to ‘‘
patients social role
performance’’ p< 0.03 and ‘‘
adverse effects of illness’’
p< 0.05, but no effect on
knowledge
Carpentier et al. (1992) Canada.
Non random
matched control n = 37
Comprehensive Support
Service Comparison:
Usual services
Psycho-education including communication training,
reviewing carer expectations and guilt (Framework-
Carpentier et al., 1992). 1 year minimum (SBAS-subscale, IS)
Multi-disciplinary team
including nurses
Improves burden associated
with patients problems
p< 0.06. Distress not reported.
Kopelowitcz et al. (2003) USA
RCT n = 92 Latino carers
DMP plus Case Management
Comparison: Standard
case management
Disease Management Programme (Framework;
Liberman et al., 1984). Culturally adapted skills-based
education about schizophrenia and its management.
4 sessions per week over 3 months (72 h). Models based
on skills training techniques, problem solving and
homework (FBIS)
Multi-disciplinary team
including nurses
No effect on burden
S.H.
Ma
cleod
eta
l./Intern
atio
na
lJo
urn
al
of
Nu
rsing
Stud
ies4
8(2
01
1)
10
0–
12
01
10
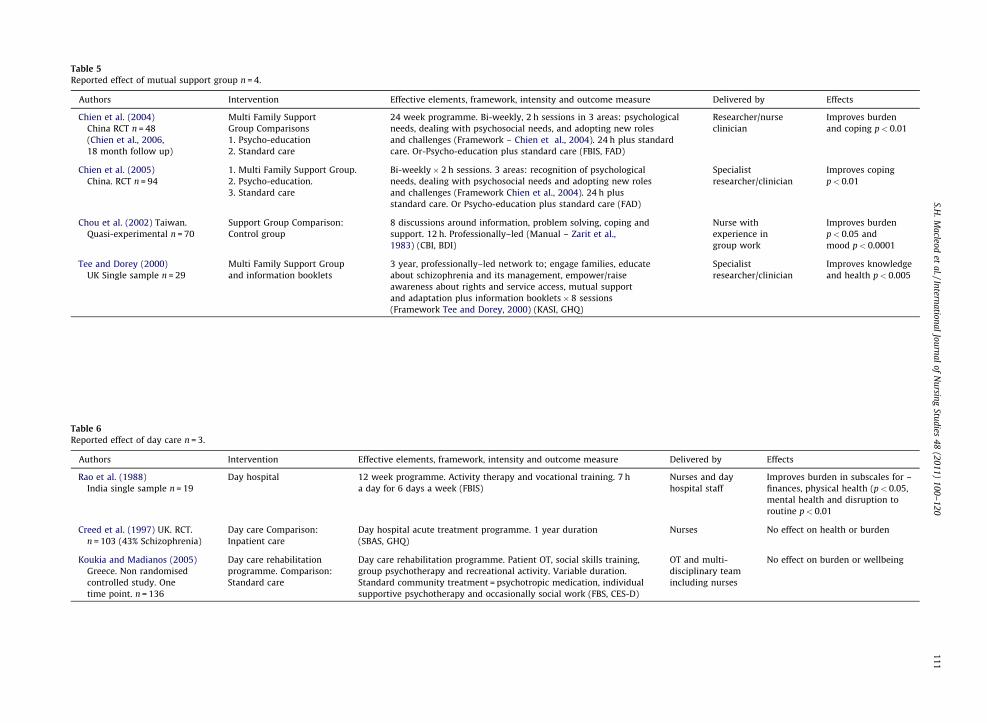
Table 5
Reported effect of mutual support group n = 4.
Authors Intervention Effective elements, framework, intensity and outcome measure Delivered by Effects
Chien et al. (2004)
China RCT n = 48
Multi Family Support
Group Comparisons
24 week programme. Bi-weekly, 2 h sessions in 3 areas: psychological
needs, dealing with psychosocial needs, and adopting new roles
and challenges (Framework – Chien et al., 2004). 24 h plus standard
care. Or-Psycho-education plus standard care (FBIS, FAD)
Researcher/nurse
clinician
Improves burden
and coping p< 0.01
(Chien et al., 2006,
18 month follow up)
1. Psycho-education
2. Standard care
Chien et al. (2005)
China. RCT n = 94
1. Multi Family Support Group.
2. Psycho-education.
3. Standard care
Bi-weekly� 2 h sessions. 3 areas: recognition of psychological
needs, dealing with psychosocial needs and adopting new roles
and challenges (Framework Chien et al., 2004). 24 h plus
standard care. Or Psycho-education plus standard care (FAD)
Specialist
researcher/clinician
Improves coping
p< 0.01
Chou et al. (2002) Taiwan.
Quasi-experimental n = 70
Support Group Comparison:
Control group
8 discussions around information, problem solving, coping and
support. 12 h. Professionally–led (Manual – Zarit et al.,
1983) (CBI, BDI)
Nurse with
experience in
group work
Improves burden
p< 0.05 and
mood p< 0.0001
Tee and Dorey (2000)
UK Single sample n = 29
Multi Family Support Group
and information booklets
3 year, professionally–led network to; engage families, educate
about schizophrenia and its management, empower/raise
awareness about rights and service access, mutual support
and adaptation plus information booklets� 8 sessions
(Framework Tee and Dorey, 2000) (KASI, GHQ)
Specialist
researcher/clinician
Improves knowledge
and health p< 0.005
Table 6
Reported effect of day care n = 3.
Authors Intervention Effective elements, framework, intensity and outcome measure Delivered by Effects
Rao et al. (1988)
India single sample n = 19
Day hospital 12 week programme. Activity therapy and vocational training. 7 h
a day for 6 days a week (FBIS)
Nurses and day
hospital staff
Improves burden in subscales for –
finances, physical health (p< 0.05,
mental health and disruption to
routine p< 0.01
Creed et al. (1997) UK. RCT.
n = 103 (43% Schizophrenia)
Day care Comparison:
Inpatient care
Day hospital acute treatment programme. 1 year duration
(SBAS, GHQ)
Nurses No effect on health or burden
Koukia and Madianos (2005)
Greece. Non randomised
controlled study. One
time point. n = 136
Day care rehabilitation
programme. Comparison:
Standard care
Day care rehabilitation programme. Patient OT, social skills training,
group psychotherapy and recreational activity. Variable duration.
Standard community treatment = psychotropic medication, individual
supportive psychotherapy and occasionally social work (FBS, CES-D)
OT and multi-
disciplinary team
including nurses
No effect on burden or wellbeing
S.H.
Ma
cleod
eta
l./Intern
atio
na
lJo
urn
al
of
Nu
rsing
Stud
ies4
8(2
01
1)
10
0–
12
01
11
S.H. Macleod et al. / International Journal of Nursing Studies 48 (2011) 100–120112
ship between coping skills and burden is neatly summedup to two studies. One reported increased self-efficacy anda reduction in burden in carers (Chan et al., 2008) and theother reported no difference in coping between carers inthe intervention and controls and no reduction in burden(So et al., 2006).
Two of the four randomised control studies reportingreduced burden used the same burden scale (Zhang et al.,1998b; Chan et al., 2008). A lack of any standard measure ofburden leads to difficulty in making direct comparisonswith the other studies and also in generating meaningfulstatistical synthesis across these studies. These problemsare exacerbated by studies which use different statisticaltechniques to report outcomes or studies providingextremely cursory data (Abramowitz and Coursey, 1989;Yamaguchi et al., 2006).
Furthermore, there was a relatively wide range ofintervention components across the studies. For examplethe following components were delivered in the fourrandomised controlled studies reporting reduced burden:Lectures and group discussions (Zhang et al., 1998a,b),multi-family psycho-education group work (Bradley et al.,2006; Gutierrez-Maldonado and Caqueo-Urizar, 2007) andan educational package about schizophrenia and itsmanagement (Chan et al., 2008). Thus it is difficult todetermine the most successful components from thesestudies or to be prescriptive about what might be deliveredin future interventions.
3.3. Family interventions
Family interventions have been extensively studiedsince the 1970s. Although differing in method and design,they share a common set of assumptions (Lam, 1991). Abiological basis for schizophrenia and the stress vulner-ability model of Zubin and Spring (1977) are acknowledgedand the seminal work of Brown in the 1960s led to a socialfocus and the development of the concept of ExpressedEmotion (EE) (1986). EE provides a measure of familystress (Brown and Rutter, 1966). High EE family’sexperience more burden than low EE families (Scazufcaand Kuipers, 1996). There are a number of highlystructured and distinct family interventions comprisingof a core set of elements. Most interventions combinebiological and social components. A key biologicalcomponent is compliance with medication. Social compo-nents include communication and problem solving train-ing, education and increasing social networks (Leff et al.,1976; Falloon et al., 1984; Ruane et al., 2004). The two mostcommon forms of family intervention are behaviouralfamily therapy (BFT) developed by Falloon et al. (1984) andcognitive behavioural family therapy (CBFT) (Barrow-clough et al., 1998).
Family interventions represent the largest group ofstudies and include twenty-nine studies, of which, nine-teen were randomised controlled trials (Table 3). A range offamily interventions were assessed alongside a number ofcontrols including client supportive psychotherapy, groupsupport, waiting list and standard care. Interventions aredelivered by mental health nurses in eight studies and bynurses as part of a mental health team in five.
Nineteen studies assessed carer burden. The strongestevidence was for twenty-three hours or more of Falloon etal.’s (1984) behavioural family therapy (BFT) where areduction in burden was reported in favour of theintervention in three randomised controlled trials (Falloonand Pederson, 1985; Razali et al., 2000; Veltro et al., 2006).When quasi-experimental studies are included, thenumber of trials reporting a favourable effect on burdenfrom BFT rises to five (Berglund et al., 2003; Magliano et al.,2006). There was less support for cognitive behaviouralfamily interventions (CBFI) where five out of six trialsreported no change in carer burden (Shore and Holmshaw,1998; Barrowclough et al., 1999; Sellwood et al., 2001;Haddock et al., 2003; Turkington et al., 2002). Only onetrial reported reduced burden following variable durationsof CBFI (Leff et al., 2001). This study, however, appeared toemploy low numbers. There was no evidence of an effecton burden among other family approaches except thatdesigned by Atkinson and Coia (1995) which consisted ofeducation, communication problem solving, coping skills,dealing with crises and services and reported in arandomised controlled trial by Cheng and Chan (2005).
Three studies reported improved coping in favour of theintervention, two based on BFT (Falloon and Pederson,1985; Magliano et al., 2005) and one on Atkinson andCoia’s (1995) framework (Cheng and Chan, 2005). Fourrandomised controlled studies reported no difference incoping (Posner et al., 1992; Szmukler et al., 1996;McFarlane et al., 1999; Hazel et al., 2004; McDonnell etal., 2007).
Eight studies reported knowledge gains which weremaintained for up to one year. Effective interventionsconsisted of BFT (McGill et al., 1983; Turkington et al.,2002; Kane et al., 1990; Brooker et al., 1994) CBFI (Shoreand Holmshaw, 1998); group psycho education (Posner etal., 1992) psychosocial intervention (Brooker et al., 1992)and culturally modified family intervention (Ran et al.,2003)
Twelve studies assessed health and report mixedfindings. Three studies reported improved health in favourof the intervention. Reduced depression (Kane et al., 1990)and general health (Brooker et al., 1994) were reportedfollowing BFT, and improved wellbeing was reportedfollowing an individualized family intervention (Adding-ton et al., 2005).
3.3.1. Critical discussion
The most studied intervention was that of behaviourfamily therapy (12/29 studies). Most report improvementsin either knowledge or burden and some improvements inthe mental health of carers were also noted. Cognitivebehavioural family therapy was less effective in reducingcarer burden and mental health and there is equivocalevidence for the success of other types of familyinterventions. Interestingly, the control interventionsvaried considerably in the BFT studies ranging from nointervention (waiting list) standard care or other forms offamily support. This acts to strengthen the findings in thatBFT is likely to be more beneficial to families than otheractive interventions. Nevertheless the sample sizes in moststudies (including BFT) are rather small (circa 30) which

S.H. Macleod et al. / International Journal of Nursing Studies 48 (2011) 100–120 113
may mean some studies were probably underpowered. Aspreviously stated, family interventions have a long historyin terms of clinical development and formal assessmentand as a result there are signs of increasingly sophisticateddesigns including follow-ups of up to 3 years (Addington etal., 2005). This history is not apparent in other forms offamily intervention, but this should not be interpreted as asign that BFT for example out performs other interven-tions.
3.4. Community support services
Community care policies have led to a range ofcommunity services for people diagnosed with schizo-phrenia (Weinberg and Huxley, 2000). Communityapproaches include case management, assertive outreach,community visits and daily living programmes. Marshalland Lockwood (1998) identify two distinct types ofapproach; Assertive Community Treatment (outreach,lower case loads and intensive support) and Clinical CaseManagement (case managers organising communityservices). However some interventions have a mixedapproach or use alternative interventions such as homecounseling (Mueser et al., 1998, 2001). Nine studies werereviewed in this category. All supports are delivered bymultidisciplinary teams that include nurses (Table 4)
Seven studies assessed carer burden and five reportreduced burden as a result of assertive communitytreatment (Test and Stein, 1980; Jeppesen et al., 2005)clinical case management (Asberg-Wisted et al., 1995)home counseling (Pai and Kapur, 1982) and multidisci-plinary support (Carpentier et al., 1992).
One randomised controlled study reported no signifi-cant knowledge gains following an integrated approach(ACT, psycho-education and MFG) compared with stan-dard services (Jeppesen et al., 2005).
Two randomised controlled studies reported no healthimprovements following intensive management and asser-tive outreach (Szmukler et al., 1998), or intensive comparedwith standard case management (Harvey et al., 2002).
Only one study assessed coping and reported improvedworrying and coping following more than a year ofcomprehensive ACT plus a 24 h crisis service (Reynoldsand Hoult, 1984). This study however, used a non-validated outcome measure developed for the study.
3.4.1. Critical discussion
It is difficult to disentangle the more active elements ofcommunity support services from those which are perhapsless effective. However there is some evidence that moreintensive support in the form of outreach or home visitsand low case loads will result in reduced carer burden. Thisis likely to be more expensive and thus perhaps lessattractive to service managers seeking to reduce costs.Interventions which were theoretically based showed thegreatest promise. For example four of the five studieswhich demonstrated a favourable effect on burden werebased on theoretical approaches including that developedby Stein and Test (1980), Pai and Kapur (1982), Carpentieret al. (1992) and Jeppesen et al. (2005). Nurses wereinvolved in delivering all of the interventions and thus
these interventions appear to be suited to nurses incommunity settings. A variety of burden measures wereused and sample sizes of circa 50 or under were used in fiveof the nine studies. However despite the relatively lowsample sizes statistically significant differences in burdenwere evident.
3.5. Mutual support groups
Carer support groups date from 1963 (Katschnig andKonieczna, 1989). Since this time numerous professionaland non-professional mutual support groups (MSG) haveemerged. These groups differ in relation to the level ofsupport, education and theoretical underpinnings (Wuer-ker, 2000). These might include role development (Chien etal., 2004) developing a sense of empowerment and controlor improving social support (Tee and Dorey, 2000). Fourstudies were including in this category. Interventions weredelivered by specialist researchers in all apart from onestudy (Chou et al., 2002) (Table 5).
Reduced burden was reported in one randomisedcontrolled study based on Chein’s role development model(Chien et al., 2004), and one quasi-experimental studyZarit et al.’s (1983) framework which encouraged problemsolving, coping and social support (Chou et al., 2002).Knowledge gains were reported in a single sample studyfollowing eight MSG sessions plus information booklets(Tee and Dorey, 2000).Two studies reported healthimprovements. Reduced depression was reported follow-ing twelve hours of Zarit et al.’s (1983) MSG framework(Chou et al., 2002) and improved general health wasreported following MSG plus information booklets (Teeand Dorey, 2000).
Increased coping was reported in two randomisedcontrolled studies following 24 hours of MSG (Chien et al.,2004, 2005).
3.5.1. Critical discussion
Despite its relatively long history there were only fourstudies included in the review which reported impact ofmutual support groups on carer outcomes. Compare thiswith family interventions which have been running over asimilar time period but have almost 30 published outcomestudies. Interestingly all four mutual support groups weredelivered by professionals, including nurses, and this raisesthe question about the possible effects of carer run groupswhich indicates a gap in the literature on this subject. Themajority of studies rejected from this category employedmixed diagnostic groups. This aside there was some, iflimited, evidence that MSG improved burden, mood,health, coping and knowledge.
3.6. Day care services
Day care services typically provide supervised andstructured programmes for the patient and in doing so mayprovide respite for the carer (Creed et al., 1997; Catty et al.,2007). Three studies were included in the review. Allincluded nurses in the delivery of these services (Table 6).
There was limited evidence that day care reducedburden. One single sample study reported improvements

S.H. Macleod et al. / International Journal of Nursing Studies 48 (2011) 100–120114
in burden following a twelve week active therapy andvocational training programme for people diagnosed withschizophrenia in India (Rao et al., 1988). No reductions inburden or health were reported for similar programmes ina randomised controlled study in the UK (Creed et al.,1997), or in a non-randomised controlled study in Greece(Koukia and Madianos, 2005). Although the focus of daycare programmes is on the patient they can provide respitefor carers.
3.6.1. Critical discussion
There was no evidence that day care significantlyimpacted on carer burden or health. Only Rao et al. (1988)reported subscale reductions in burden. In terms of qualitythis single sample study employed a convenient sample,very low numbers (n = 19) and a high drop out. It is worthnoting that some carers reported returning to work and afinancial payment was made to study participants thatcould contribute to the subscale reduction in burden forreduced financial burden reported by carers.
4. Discussion
While varying in quality, studies included within thisreview indicate potentially effective approaches and thatsome of these can be delivered by mental health nurses(Table 7). There is fairly robust evidence that carereducation programmes improve knowledge about schizo-phrenia, however there is little evidence that thisaddresses more substantive areas of caring such asimproved coping, reduced burden or improved health.Other interventions such as supportive family educationmove beyond information giving by providing socialsupport and developing coping strategies. As might beexpected these interventions are able to reduce carerburden and distress and increase self efficacy. Moreintensive programmes such as behavioural family therapyaim to address stressful relationships which commonlyoccur in families where a member is diagnosed withschizophrenia. These programmes are particularly effec-tive in reducing carer burden and in some instancesimproving the carer’s coping and mental health. Commu-nity based support such as intensive outreach whencombined with low case loads is also effective in reducingcarer burden and increasing coping. There is someevidence that mutual support groups reduce carer burdenand improve coping. Finally there is minimal evidence thatday care for those diagnosed with schizophrenia reducescarer burden or improves health and coping
These findings support and update existing reviews,which incidentally also report mixed findings. A meta-analysis of family interventions (Cuijpers, 1999) reportedmoderate effects on distress, patient–carer relationshipand family functioning for more than twelve sessions.Barbato and d’Avanzo (2000), however, concluded thattheir effectiveness on outcomes were weakly supported.Dixon and Leham (1995) reported modest evidence thatfamily interventions improved well-being. An update ofthis review, concluded that benefits were unclear and thatcritical components still had to be identified (Dixon et al.,2000). Education and supportive family education tend to
be included together within reviews. Kazarin and Van-derheyden (1992) and Pekkala and Merinder (2004)reported inconclusive effects on burden. A meta analysis(1980–1998) of community treatments reported byZiguras and Stuart (2000) concluded that, from a limitednumber of studies, Assertive Community Treatment andCommunity Management were associated with improvedburden.
There is, however, support from the studies included inthe present review of the importance of a theoreticalfoundation for an intervention. For example supportivefamily education attempts to move beyond informationgiving by developing carers’ coping skills which in turnshould reduce carer burden. This relationship wasdemonstrated in one study where the intervention worked(Chan et al., 2008) and was not observed in another studywhere the intervention failed (So et al., 2006). There is alsoa strong theoretical foundation to family therapy, notablythe work of Brown (1986) on expressed emotion. Familytherapy aims to help the family identify and tackle thesource of expressed emotion and if successful should leadto reduced carer burden and improved mental health.Other interventions such as community support addelements of management theory particularly in terms ofreducing case load and improving the relationshipbetween services and carers (Asberg-Wisted et al.,1995). Interestingly mutual support groups remainedrelatively ineffective in reducing carer burden. This issurprising given that these may have a natural appeal tocarers, however as Chien and Norman (2009) indicates in arecent review of the international literature there is a weaktheoretical base for this type of programme. There waslittle evidence to link the theoretical basis of day care withcarer outcomes, and this was also relatively ineffective inreducing carer burden.
A key question is whether nurses are able to deliver theeffective interventions. Of the 68 studies included, 12 (18%)were delivered solely by nurses and 16 (24%) included nursesas part of a multidisciplinary team. The remaining studiesemployed researchers or therapists or provided little detailon who delivered the intervention. The extent that nurseswere involved in delivery also varied across approaches; 1%for education, 25% for supportive family education andmutual support groups, 32% for family interventions and100% community support and day care services. Thus, apartfrom education based interventions there is substantialevidence that nurses are capable of delivering all of theprogrammes described in this review. With respect toeducational interventions these are probably the moststraight forward of all to deliver and thus should fall withinthe capability of most nurses.
We acknowledge however that nurses may have to betrained to deliver more intensive interventions such asfamily support, family therapy and community support.These types of interventions often require the nurse towork intensively with carers over a longer time period.This in turn requires low case loads, see for examplecommunity support, and thus are fairly resource intensive.Brooker (2001) and Brooker and Brabban (2004) note thateven when nurses are trained to deliver carer interventionsfew go on to deliver these in practice. One review of the
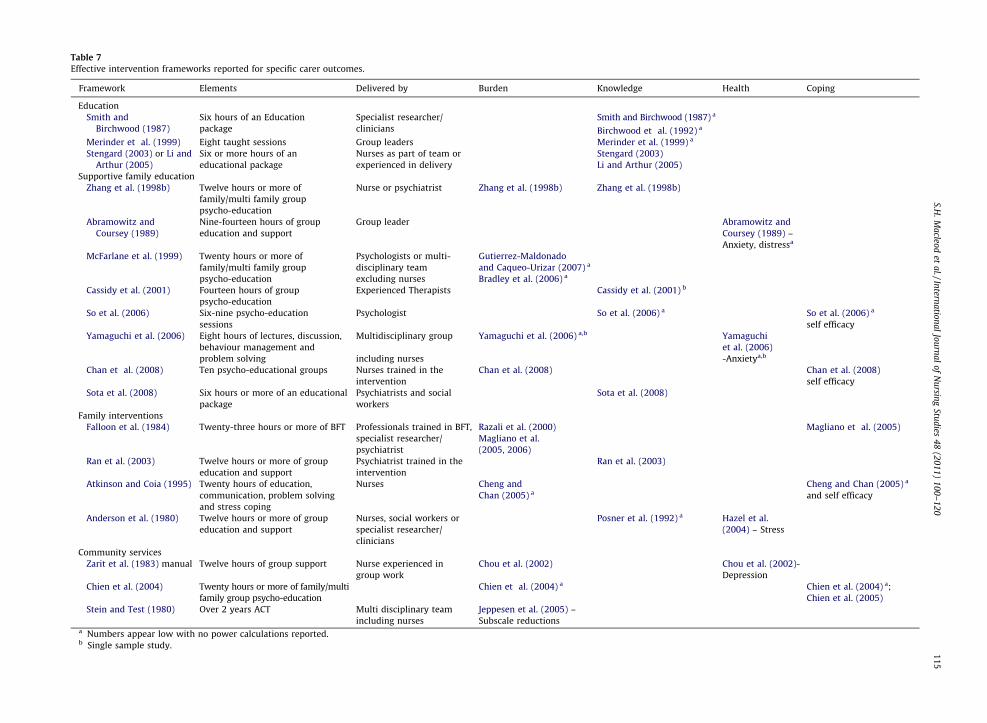
Table 7
Effective intervention frameworks reported for specific carer outcomes.
Framework Elements Delivered by Burden Knowledge Health Coping
Education
Smith and
Birchwood (1987)
Six hours of an Education
package
Specialist researcher/
clinicians
Smith and Birchwood (1987) a
Birchwood et al. (1992) a
Merinder et al. (1999) Eight taught sessions Group leaders Merinder et al. (1999) a
Stengard (2003) or Li and
Arthur (2005)
Six or more hours of an
educational package
Nurses as part of team or
experienced in delivery
Stengard (2003)
Li and Arthur (2005)
Supportive family education
Zhang et al. (1998b) Twelve hours or more of
family/multi family group
psycho-education
Nurse or psychiatrist Zhang et al. (1998b) Zhang et al. (1998b)
Abramowitz and
Coursey (1989)
Nine-fourteen hours of group
education and support
Group leader Abramowitz and
Coursey (1989) –
Anxiety, distressa
McFarlane et al. (1999) Twenty hours or more of
family/multi family group
psycho-education
Psychologists or multi-
disciplinary team
excluding nurses
Gutierrez-Maldonado
and Caqueo-Urizar (2007) a
Bradley et al. (2006) a
Cassidy et al. (2001) Fourteen hours of group
psycho-education
Experienced Therapists Cassidy et al. (2001) b
So et al. (2006) Six-nine psycho-education
sessions
Psychologist So et al. (2006) a So et al. (2006) a
self efficacy
Yamaguchi et al. (2006) Eight hours of lectures, discussion,
behaviour management and
problem solving
Multidisciplinary group
including nurses
Yamaguchi et al. (2006) a,b Yamaguchi
et al. (2006)
-Anxietya,b
Chan et al. (2008) Ten psycho-educational groups Nurses trained in the
intervention
Chan et al. (2008) Chan et al. (2008)
self efficacy
Sota et al. (2008) Six hours or more of an educational
package
Psychiatrists and social
workers
Sota et al. (2008)
Family interventions
Falloon et al. (1984) Twenty-three hours or more of BFT Professionals trained in BFT,
specialist researcher/
psychiatrist
Razali et al. (2000)
Magliano et al.
(2005, 2006)
Magliano et al. (2005)
Ran et al. (2003) Twelve hours or more of group
education and support
Psychiatrist trained in the
intervention
Ran et al. (2003)
Atkinson and Coia (1995) Twenty hours of education,
communication, problem solving
and stress coping
Nurses Cheng and
Chan (2005) a
Cheng and Chan (2005) a
and self efficacy
Anderson et al. (1980) Twelve hours or more of group
education and support
Nurses, social workers or
specialist researcher/
clinicians
Posner et al. (1992) a Hazel et al.
(2004) – Stress
Community services
Zarit et al. (1983) manual Twelve hours of group support Nurse experienced in
group work
Chou et al. (2002) Chou et al. (2002)-
Depression
Chien et al. (2004) Twenty hours or more of family/multi
family group psycho-education
Chien et al. (2004) a Chien et al. (2004) a;
Chien et al. (2005)
Stein and Test (1980) Over 2 years ACT Multi disciplinary team
including nurses
Jeppesen et al. (2005) –
Subscale reductionsa Numbers appear low with no power calculations reported.b Single sample study.
S.H.
Ma
cleod
eta
l./Intern
atio
na
lJo
urn
al
of
Nu
rsing
Stud
ies4
8(2
01
1)
10
0–
12
01
15

S.H. Macleod et al. / International Journal of Nursing Studies 48 (2011) 100–120116
international evidence on the uptake of family interven-tions raises the interesting possibility that these types ofprogrammes may not be acceptable to families because ofthe substantial investment of time and commitmentrequired (Mairs and Bradshaw, 2005). Thus perhaps akey question for nurses is reaching a decision on the type ofsupport which is both acceptable to and effective forcarers. To that one might also introduce the issue of costs.Interestingly none of the studies included in this reviewevaluated the economic impact of these interventions andthis highlights a gap in the available scientific evidence.
There is of course the fundamental issue of whethermental health services across the globe are in a position tooffer support to carers. As indicated in the introductionapproximately 30% of countries do not offer communitybased mental health services and thus are unlikely toengage with carers in a home setting. This is likely to be inthe less economically developed countries. Indeed most ofthe studies included in this review were from the UK,America, Australia, Italy, Denmark, Sweden and Finlandalthough there was a growing number of studies fromChina, Malaysia and India.
This raises the issue of the structural configuration ofmental health services per se (including hospital basedservices) and whether such structures are predisposed tocarer engagement. Evidence suggests not. For exampleSimpson (2005) points to structural difficulties, such as theimpact of case loads and other ‘duties’ which preventedmental health nurses in England from adopting a widercare co-ordinating role. Bee et al. (2008) point to thestructural issues and focus of care which led to poor nurse-patent and carer (our emphasis) interactions in hospitalsettings. Goodwin and Happell (2006) go further andcriticize policies which prioritise the rights of the patientover those of the carer and which prevent mental healthnurses from fully engaging with carers. There is also thevexed issue of compulsory treatment which may focusmore on containing risks than meeting the needs of serviceusers and their carers (O’Brien et al., 2009).
There is the need to address these issues and in doing somake carers more visible in nursing policy and practice.This could be achieved by involving carers in policymaking, service provision and indeed the training ofnurses. For example in a review of the internationalliterature on user and carer involvement in professionaltraining Repper and Breeze (2007) suggest that this willrequire personal commitment and motivation on behalf ofpractitioners as well as strategic and organisationalcommitment. Otherwise the commitment may at bestbe highly localized and at worst appear partonising, Thusin order for nurses to provide effective supports to carers itis important to secure engagement not only from theindividual practitioners but also at organisational levelwhich includes managerial and strategic buy-in.
4.1. Evidence base
Although the studies included in this review represent awide range of designs most studies reporting an effect arebased on randomised or quasi-randomised designs. This isencouraging. Table 7 presents the results of these studies.
While most studies provided details of the intervention,few included adequate details about comparators. This isparticularly problematic within studies comparing theintervention with standard services. This point is raised inBurns and Catty’s (2002) editorial on service structures andis an extremely important issue as there is a growingawareness that carer’s needs could be shaped by the waythat mental health services are provided to people diagnosedwith schizophrenia (Magliano et al., 1998; Roick et al., 2007).Consequently there is merit in distinguishing the parts of anintervention that are dedicated to resolving problems whichare relevant to the carer from those which are relevant to theperson who is diagnosed with schizophrenia.
The majority of studies recruited convenient samples byfirst identifying patients who were diagnosed with schizo-phreniaand thencontactingcarers.Thismaymeanthatsomecarers were missed, particularly where contact was lost withthe patient. In addition, carers were not screened for theseverity of burden or distress. These can vary over the courseof a caring career and thus could affect the differences in keyoutcomes reported across studies. Thus, in the field ofgerontology, Zarit et al. (2003) proposed that recruitment ofcarers should be based on the presence and severity ofintended outcomes. A related issue was that key outcomessuch as burden were measured over a number of studiesusing a variety of scales (Appendix 2). As such, it was notknown whether these measure the ‘‘same’’ carer experi-ences.
5. Conclusions
Research on effective nurse-led support of carers ofpeople diagnosed with schizophrenia is emerging. Thisreview identified potentially effective approaches thatmental health nurses could deliver to help reduce carerburden and improve knowledge, coping and mental health. Acombination of education, mutual support and copingstrategies delivered within an intensive community pro-gramme could effectively reduce carer burden and improvehealth and coping.Nurses couldalso deliver support tocarerswithinstructuredintensiveprogrammessuchasbehaviouralfamily therapy, and these appear to be associated withgreater improvement. Nurses, however, would requiretraining and sufficient time to deliver more intensiveprogrammes to carers. Future research is also required toimprove understanding of the extent that nurses coulddeliver these programmes within their current practice.
6. Recommendations
� T
his review highlights a number of gaps in the evidencebase for effective mental health nurse support for carersof people diagnosed with schizophrenia. There is a needto clarify the theoretical basis of any new interventionand therefore the selection of appropriate outcomes toensure that these can be realistically achieved throughinterventions. � A clear need emerged for studies which examine thebarriers and facilitators in delivering support withinnursing practice and which focus on both practitionersand health systems.

S.H. Macleod et al. / International Journal of Nursing Studies 48 (2011) 100–120 117
� P
ractitioners and researchers need to distinguish theelements of an intervention which are carer focused,patient focused or both. Related to this is the need toprovide more detail on any interventions that may beused as comparators. � C arers should be recruited based on the presence andseverity of intended outcomes and interventions need toinclude carers who may be out of contact with mentalhealth services.
� It would be encouraging to see more research fromdeveloping countries
� T here is the need to assess the economic impact of carersupport interventions.
Conflict of interest. None declared.
Appendix 1 and 2. Supplementary data
Supplementary data associated with this article can be
found, in the online version, at doi:10.1016/j.ijnurstu.
2010.09.005.
References
Abramowitz, I.A., Coursey, R.D., 1989. Impact of an educational supportgroup on family participants who take care of their schizophrenicrelatives. Journal of Consulting and Clinical Psychology 57 (2), 232–236.
Addington, J., McCleery, A., et al., 2005. Three-year outcome of familywork in an early psychosis program. Schizophrenia Research 79 (1),107–116.
Altman, D.G., 1996. Better reporting of randomized controlled trials: theCONSORT statement. British Medical Journal 313, 570–571.
Anderson, C.M., Hogarty, G.E., et al., 1980. Family treatment of adultschizophrenic patients: a psychoeducational approach. Schizophre-nia Bulletin 6 (3), 490–505.
Anderson, C.M., et al., 1986. Schizophrenia and the family. A practitioner’sguide to psychoeducation and management. Guilford Press, New York.
Arksey, H., et al., 2002. Services to Support Carers of People with MentalHealth Problems: Literature Review Report. Social Policy ResearchUnit, York.
Arksey, H., 2003. Scoping the field: services for carers of people withmental health problems. Health and Social Care in the Community 11(4), 335–344.
Asberg-Wisted, A., Cressell, T., et al., 1995. Two-year outcome of teambased intensive case management for patients with schizophrenia.Psychiatric Services 46, 1263–1266.
Atkinson, J.M., Coia, D., 1995. Families Coping with Schizophrenia. APractitioners Guide to Family Groups. John Wiley & Sons, Chichester.
Barbato, A., d’Avanzo, B., 2000. Family interventions in schizophrenia andrelated disorders: a critical review of clinical trials. Acta PsychiatricaScandanavica 102 (2), 81–97.
Baronet, A.M., 1999. Factors associated with caregiving burden in mentalillness: a critical review of the literature. Clinical Psychology Review19 (7), 819–841.
Barrowclough, C., Tarrier, N., 1985. Family Questionnaire. Manchester.Barrowclough, C., Tarrier, N., et al., 1986. Information for Relatives about
Schizophrenia. Warrington North-West Fellowship, Warrington.Barrowclough, C., Tarrier, N., et al., 1987. Assessing the functional value of
relatives’ knowledge about schizophrenia. A preliminary report. Brit-ish Journal of Psychiatry 151, 1–8.
Barrowclough, C., Tarrier, N., 1992. Families of Schizophrenic Patients. ACognitive-Behavioural Intervention. Chapman and Hall, London.
Barrowclough, C., Marshall, M., et al., 1998. Assessing relatives’ needsfor psychosocial interventions in schizophrenia: a relative versionof the Cardinal Needs Schedule (RCNS). Psychological Medicine 28,531–542.
Barrowclough, C., Tarrier, N., et al., 1999. Randomised controlled effec-tiveness trial of a needs-based psychosocial intervention service forcarers of people with schizophrenia. British Journal of Psychiatry 174,505–511.
Bech, P., 1993. Rating Scales for Psychopathology, Health Status andQuality of Life. Springer-Verlag, New York.
Beck, A.T., Steer, R.A., 1987. The BDI Manual. SAP Corporation, SanAntonio.
Bee, P., Playle, J., Lovall, K., Barnes, P., Gray, R., Keeley, P., 2008. Service userviews and expectations of UK registered mental health nurses: asystematic review of the empirical research. International Journal ofNursing Studies 45, 442–457.
Bentley, K.J., 1990. An evaluation of family-based intervention withschizophrenia using single-system research. British Journal of SocialWork 20, 101–116.
Berglund, N., Vahlne, J.Q., et al., 2003. Family intervention in schizo-phrenia—impact on family burden and attitude. Social Psychiatry andPsychiatric Epidemiology 38 (3), 116–121.
Berkowitz, R., Eberlein-Fries, R., et al., 1984. Educating relatives aboutschizophrenia. Schizophrenia Bulletin 10 (3), 418–429.
Berkowitz, R., Shavit, N., et al., 1990. Educating relatives of schizophrenicpatients. Social Psychiatry and Psychiatric Epidemiology 25, 216–220.
Benson, P., 1994. Deinstitutionalisation and family caretaking of theseriously mentally ill. The policy context. International Journal ofLaw and Psychiatry 17 (2), 119–138.
Birchwood, M., Smith, J., et al., 1992. Specific and non-specific effects ofeducational intervention for families living with schizophrenia. Acomparison of three methods. British Journal of Psychiatry 160,806–814.
Bradley, G.M., et al., 2006. Multiple-family group treatment for English-and Vietnamese-speaking families living with schizophrenia. Psy-chiatric Services 57 (April (4)), 521–530.
Brooker, C., Barrowclough, C., et al., 1992. Evaluating the impact oftraining community psychiatric nurses to educate relatives aboutschizophrenia. Journal of Clinical Nursing 1, 19–25.
Brooker, C., Falloon, I.R.H., et al., 1994. The outcome of training commu-nity psychiatric nurses to deliver psychosocial intervention. BritishJournal of Psychiatry 165, 222–230.
Brooker, C., 2001. A decade of evidence-based training for work withpeople with serious mental health problems: progress in the devel-opment of psychosocial interventions. Journal of Mental Health 10(1), 17–31.
Brooker, C., Saul, C., et al., 2003. Is training in psychosocial interventionsworthwhile? Report of a psychosocial intervention trainee follow-upstudy. International Journal of Nursing Studies 40 (7), 731–747.
Brooker, C., Brabban, A., 2004. Measured Success: A Scoping Review ofEvaluated Psychosocial Interventions Training for Work with Peoplewith Serious Mental Health Problems. NIMHE/Trent WDC.
Brown, G.W., 1986. Expressed emotion and life events in schizophreniaand depression. Interview, Journal of Psychosocial Nursing 24 (7),31.
Brown, G.W., Rutter, M.L., 1966. The measurement of family activitiesand relationships. A methodological study. Human Relations 19,241–263.
Budd, R.J., Oles, G., et al., 1998. The relationship between coping style andburden in the carers of relatives with schizophrenia. Acta PsychiatricaScandanavica 98, 304–309.
Burns, T., Catty, J., 2002. Mental health policy and evidence: potentialsand pitfalls. Psychiatric Bulletin 26, 324–327.
Carpentier, N., Lesage, A., et al., 1992. Burden of care of families not livingwith young schizophrenic relatives. Hospital and Community Psy-chiatry 43 (1), 38–43.
Carra, G., Montomoli, C., et al., 2007. Family interventions for schizo-phrenia in Italy: randomized controlled trial. European Arch. Psy-chiatry Clinical Neuroscience 257, 23–30.
Cassidy, E., Hill, S., et al., 2001. Efficacy of a psychoeducational inter-vention in improving relatives’ knowledge about schizophrenia andreducing rehospitalisation. European Psychiatry 16 (8), 446–450.
Catty, J.S., Burns, Z., et al., 2007. Day centres for severe mental illness.Cochrane Database of Systematic Reviews. Issue 1. Art. No. CD001710.DOI: 10: Pub 2. Cochrane Collaboration, Oxford.
Cazzullo, C., Bertrando, P., et al., 1989. The efficacy of an informationgroup intervention for relatives of schizophrenics. International Jour-nal of Social Psychiatry 35 (4), 313–323.
Chan, S.W., et al., 2008. Evaluation of a psychoeducation program forChinese clients with schizophrenia and their family caregivers.Patient Education and Counseling, doi:10.1016/j.pec.2008.08.028.
Chen, F.P., Greenberg, J.S., 2004. A positive aspect of caregiving: theinfluence of social support on caregiving gains for family membersof relatives with schizophrenia. Community Mental Health Journal 40(5), 423–435.
Cheng, L., Chan, S., 2005. Psycho-education program for Chinese familycarers of members with schizophrenia. Western Journal of NursingResearch 27 (5), 585–599.
S.H. Macleod et al. / International Journal of Nursing Studies 48 (2011) 100–120118
Chien, W., Norman, I., et al., 2004. A randomized controlled trial of amutual support group for family caregivers of patients with schizo-phrenia. International Journal of Nursing Studies 41, 637–649.
Chien, W., Chan, S., et al., 2006. Effects of a mutual support group forfamilies of Chinese people with schizophrenia: 18 month follow-up.British Journal of Psychiatry 189, 41–49.
Chien, W.T., Chan, S., et al., 2005. Mutual support multiple-family groupintervention for Chinese families of patients with schizophrenia.Psychiatric Services 55, 1276–1284.
Chien, W.T., Norman, I., 2009. The effectiveness and active ingredients ofmutual support groups for family caregivers of people with psychoticdisorders: a literature review. International Journal of Nursing Stu-dies 46, 1604–1623.
Chou, K., Liu, S., et al., 2002. The effects of support groups on caregivers ofpatients with schizophrenia. International Journal of Nursing Studies39 (7), 713–722.
Cochrane, R., 1980. A comparative evaluation of the Symptom Rating Testand the Langner 22-item Index for use in epidemiological surveys.Psychological Medicine 10, 115–124.
Cozolino, L.J., Goldstein, et al., 1988. The impact of education aboutschizophrenia on relatives varying in expressed emotion. Schizophre-nia Bulletin 14 (4), 675–687.
Corrigan, P.W., Miller, F.E., 2004. Shame, blame, and contamination: areview of the impact of mental illness stigma on family members.Journal of Mental Health 13 (December (6)), 537–548.
C.R.D., 2009. Systematic reviews. CRD’s guidance for undertaking reviewsin health care. Centre for Reviews and Dissemination (CRD), Univer-sity of York, January.
Creed, F., Mbaya, et al., 1997. Cost effectiveness of day and inpatientpsychiatric treatment: results of a randomised controlled trial. BritishMedical Journal 314 (7091), 1381–1385.
Cuijpers, P., 1999. The effects of family interventions on relatives’ burden:a meta-analysis. Journal of Mental Health 8 (3), 275–285.
Curran, J., Brooker, C., 2007. Systematic review of interventions deliveredby UK mental health nurses. International Journal of Nursing Studies44 (3), 479–509.
Deeks, J.J., et al., 2003. Evaluating non-randomised intervention studies.Health Technology Assessment. 7 (27) NHS R&D HTA programme.
Derogatis, L., Lipman, R., et al., 1974. The Hopkins Symptom Checklist(HSCL): a self-report symptom inventory. Behavioural Science 19,1–15.
Department of Health, 2008. National Carers’ Strategy: Carers at the Heartof 21st-Century Families and Communities. DoH, London.
Department of Health, 2009. Commissioning for Carers. DoH, London.Dixon, L., Leham, A.F., 1995. Family interventions for schizophrenia.
Schizophrenia Bulletin 21 (4), 631–643.Dixon, L., et al., 2000. Therapists’ contacts with members of persons with
severe mental illness in a community treatment program. PsychiatricServices 51, 1449–1451.
Doane, J.A., Goldstein, M.J., et al., 1986. The impact of individual andfamily treatment on the affective climate of families of schizophrenia.British Journal of Psychiatry 148, 279–287.
Don, C., et al., 2004. Improving the reporting quality of nonrandomizedevaluations of behavioural and public health interventions: theTREND statement. American Journal of Public Health 94 (3), 361–366.
Doran, T., Drever, F., Whitehead, M., 2003. Health of young and elderlyinformal carers: analysis of UK census data. British Medical Journal327 (December), 1388.
Dow, B., McDonald, J., 2003. Social support or structural change? Socialwork theory and research on care-giving. Australian Social Work 56(3), 197–208.
Dupuy, H.J., 1984. In: Wenger, N.K., Matteson, M.E., Furberg, C.D., Elin-son, J. (Eds.), The Psychological General Well-being (PGWB) Index.Assessment of Quality of Life in Clinical Trials of CardiovascularTherapies. Le Jacq, New York, pp. 170–183.
Elsom, S., Elsom, S., et al., 2007. Exploring the expanded practice roles ofcommunity mental health nurses. Issues in Mental Health Nursing 28(4), 413–429.
Epstein, N.B., Baldwin, L.M., et al., 1983. The McMaster Family Assess-ment Device. Journal of Marital and Family Therapy 9, 171–180.
Fadden, G.B., 1984. The Relatives of Patients with Depressive Disorders: ATypology of Burden and Strategies of Coping. Institute of Psychiatry.London, University of London.
Fadden, G., Bebbington, P., et al., 1987. The burden of care. The impact offunctional psychiatric illness on the patient’s family. British Journal ofPsychiatry 150, 285–292.
Fadden, G., 1997. Implementation of family interventions in routineclinical practice following staff training programs: a major causefor concern. Journal of Mental Health 6 (6), 599–612.
Falloon, I.R.H., Boyd, C.B., et al., 1984. Family Care of Schizophrenia.Guilford Press, New York.
Falloon, I.R.H., Pederson, J., 1985. Family management in the prevention ofmorbidity of schizophrenia: the adjustment of the family unit. BritishJournal of Psychiatry 147, 156–163.
Falloon, I.R.H., Magliano, L., et al., 1996. The stress of caring for disablingmental disorders in a home-based rehabilitation service. Journal ofNervous and Mental Disorders 184, 381–384.
Folkman, S., Lazarus, R.S., 1985. If it changes it must be a process: a studyof emotion and coping during the stages of a college examination.Journal of Personality and Social Psychology 48, 150–170.
Gall, S., Atkinson, J., et al., 2003. Supporting carers of people diagnosedwith schizophrenia: evaluating change in nursing practice followingtraining. Journal of Advanced Nursing 41 (3), 295–305.
Goodwin, V., Happell, B., 2006. Conflicting agendas between consumersand carers: the perspectives of carers and nurses. InternationalJournal of Mental Health Nursing 15, 135–143.
Goldberg, D.P., Williams, P., 1988. A User’s Guide to the General HealthQuestionnaire. W. NFER, Nelson.
Gotzche, P.C., 1989. Methodology and overt and hidden bias in reports of196 double blind trials of non steroidal, anti-inflammatory drugs inrheumatoid arthritis. Controlled Clinical Trials 10, 31–56.
Greenberg, J.S., Seltzer, M.M., et al., 1993. Aging parents of adults withdisabilities: the gratifications and frustrations of later-life caregiving.Gerontologist 33, 542–550.
Gutierrez-Maldonado, J., Caqueo-Urizar, A., 2007. Effectiveness of a psy-cho-educational intervention for reducing burden in Latin Americanfamilies of patients with schizophrenia. Quality of Life Research 16(5), 739–747.
Haddock, G., Tarrier, N., 1998. In: Tarrier, N., Wells, A., Haddock, G.(Eds.), Assessment and Formulation in the Cognitive BehaviouralTreatment of Psychosis. Treating Complex Cases: The CognitiveBehavioural Therapy Approach. Wiley, pp. 155–175.
Haddock, G., Barrowclough, C., et al., 2003. Cognitive-behavioural ther-apy and motivational intervention for schizophrenia and substancemisuse. British Journal of Nursing 183, 418–426.
Harvey, E.J., Burns, T., et al., 2002. The effect of intensive case manage-ment on relatives of patients with severe mental illness. PsychiatricServices 53 (12), 1580–1585.
Hatfield, A.B., Lefley, H.P., 1987. In: Hatfield, A.B., Lefley, (Eds.), Families ofthe Mentally Ill. Coping and Adaptation. Casell, London, pp. 60–64.
Hatfield, A.B., 1994. Family education: theory and practice. New Direc-tions in Mental Health Services 12, 62–63.
Hazel, N.A., McDonnell, M.G., et al., 2004. Impact of multiple-familygroups for outpatients with schizophrenia on caregivers’ distress andresources. Psychiatric Services 55 (1), 35–41.
Hoult, H.J., Reynolds, I., 1981. A controlled study of psychiatric hospitalversus community treatment—the effect on relatives. Australian andNew Zealand Journal of Psychiatry 15, 323–328.
Hudson, W., Acklin, J., et al., 1980. Assessing discord in family relation-ships’. Social Work Research and Abstracts 16, 21–29.
Hugen, B., 1993. The effectiveness of a Psychoeducational Support Serviceto families of persons with a Chronic Mental Illness. Research onSocial Work Practice 3 (2), 137–154.
Illfield, F.W., 1976. Further validation of a psychiatric index in a normalpopulation. Psychological Reports 39, 1215–1228.
Jeppesen, P., Petersen, L., et al., 2005. Integrated treatment of first-episode psychosis: effect of treatment on family burden. BritishJournal of Psychiatry 187, s85–s90.
Kane, C.F., DiMartino, E., et al., 1990. A comparison of short-termpsychoeducational and support groups for relatives coping withchronic schizophrenia. Archives of Psychiatric Nursing IV (6), 343–353.
Katschnig, H., Konieczna, T., 1989. What works in work with relatives?—ahypothesis. British Journal of Psychiatry 155 (Suppl. 5), 144–150.
Kazarin, S.S., Vanderheyden, D.A., 1992. Family education of relatives ofpeople with psychiatric disability: a review. Psychosocial Rehabilita-tion Journal 15 (3), 67–84.
Kelner, R., Sheffield, B., 1973. A self-rating scale of distress. PsychologicalMedicine 3, 88–100.
Kopelowitcz, A., Zarate, R., et al., 2003. Disease management in Latinoswith Schizophrenia: a family-assisted, skills training approach. Schi-zophrenia Bulletin 29 (2), 211–227.
Koukia, E., Madianos, M.G., 2005. Is psychosocial rehabilitation of schizo-phrenic patients preventing family burden? A comparative study.Journal of Psychiatric and Mental Health Nursing 12, 415–422.
Lam, D., 1991. Psychosocial family intervention in schizophrenia: areview of empirical studies. Psychological Medicine 21, 423–441.
Leff, J., et al., 1976. Schizophrenia and the sensitivity of the familyenvironment. Schizophrenia Bulletin 2, 566–574.
S.H. Macleod et al. / International Journal of Nursing Studies 48 (2011) 100–120 119
Leff, J., Berkowitz, R., et al., 1989. A trial of family therapy v. a relativesgroup for schizophrenia. British Journal of Psychiatry 154, 58–66.
Leff, J., Sharpley, M., et al., 2001. Training community psychiatric nursesin schizophrenia family work: a study of clinical and economic out-comes for patients and relatives. Journal of Mental Health 10 (2), 189–197.
Lefley, H.P., 1997. Synthesizing the family caregiving studies: implica-tions for service planning, social policy, and further research. FamilyRelations 46 (4), 443–450.
Li, Z., Arthur, D., 2005. Family education for people with schizophrenia inBeijing, China. British Journal of Psychiatry 187, 339–345.
Liberman, R.P., Falloon, I.R.H., et al., 1984. Multiple family therapy forschizophrenia: a behavioural problem solving approach. PsychosocialRehabilitation Journal 7 (4), 60–77.
Loukissa, D.A., 1994. Concepts and models for the study of caregivers’burden. Journal of Psychiatric and Mental Health Nursing 1, 151–156.
Magliano, L., Guarneri, M., 1996. A new questionnaire assessingcoping strategies in relatives of patients with schizophrenia: devel-opment and factor analysis. Acta Psychiatrica Scandanavia 94, 224–228.
Magliano, L., Fadden, G., et al., 1998. Burden on the families of patientswith schizophrenia: results of the BIOMED 1 study. Social Psychiatryand Psychiatric Epidemiology 33, 405–412.
Magliano, L., Fiorillo, A., et al., 2003. The effect of social network onburden and pessimism in relatives of patients with schizophrenia.American Journal of Orthopsychiatry 73 (3), 302–309.
Magliano, L., Fiorillo, A., et al., 2005. Effectiveness of a psychoeducationalintervention for families of patients with schizophrenia: preliminaryresults of a study funded by the European Commission. World Psy-chiatry 4 (1), 45–49.
Magliano, L., et al., 2006. Patient functioning and family burden in acontrolled real-world trial of family psychoeducation for schizophre-nia. Psychiatric Services 57 (12), 1784–1791.
Mairs, H., Bradshaw, T., 2005. Implementing family intervention follow-ing training: what can the matter be? Journal of Psychiatric andMental Health Nursing 12, 488–494.
Marshall, M., Lockwood, A., 1998. Assertive community treatment forpeople with severe mental disorders. (Cochrane review) Issue 4.Oxford, Update software. Cochrane Library.
McCann, T.V., Baker, H., 2001. Mutual relating: developing interpersonalrelationships in the community. Journal of Advanced Nursing 34 (4),530–537.
McCarty, C.A., McMahon, R.J., 2003. Mediators in the relationshipbetween maternal depressive symptoms and child internalizingand disruptive behaviour disorders. Journal of Family Psychology17 (4), 545–556.
McCarthy, B., Kuipers, L., et al., 1989. Counselling relatives of the long-term adult mentally ill. Evaluation of the impact on relatives andpatients. British Journal of Psychiatry 154, 768–775.
McDonnell, M., Short, R.A., et al., 2003. Burden in schizophrenia care-givers: impact of family psychoeducation and awareness of patientsuicidality. Family Process 42 (1), 91–103.
McDonnell, M.G., et al., 2007. Clinician integrity in multiple familygroups. Psychometric properties and relationship with schizophre-nia client and caregiver outcomes. Cognitive Therapy Research 31,785–803.
McGill, C.W., Falloon, I.R.H., et al., 1983. Family educational interventionin the treatment of schizophrenia. Hospital and Community Psychia-try 34 (10), 934–938.
McFarlane, W.R., Deakins, S.M., et al., 1999. Psychoeducational GroupTreatment Manual. New York State Psychiatric Institute, BiosocialTreatment Division, New York.
McFarlane, W.R., 2002. Multiple Family Groups in the Treatment of SeverePsychiatric Disorders. Guilford, New York.
McFarlane, W.R., Dixon, W.R., et al., 2003. Family psychoeducation andschizophrenia: a review of the literature. Journal of Marital andFamily Therapy 29, 223–245.
McNair, D.M., Lorr, M., et al., 1971. Manual: Profile of Mood States(POMS). Educational and Industrial Testing Service, San Diego.
Merinder, L.B., Viuff, A.G., et al., 1999. Patient and relative education incommunity psychiatry: a randomised controlled trial regarding itseffectiveness. Social Psychiatry and Psychiatric Epidemiology 34 (6),287–294.
Moher, D., et al., 2009. Preferred reporting items for systematic reviewsand meta-analysis: the PRISMA statement. British Medical Journal339, 332–336.
Mueser, K.T., Webb, C., et al., 1996. Family burden of schizophrenia andbipolar disorder: perceptions of relatives and professionals. Psychia-tric Services 47, 507–511.
Mueser, K.T., Bond, G.R., et al., 1998. Models of community care for severemental illness: a review of research on case management. Schizo-phrenia Bulletin 24 (1), 37–74.
Mueser, K.T., Sengupta, A., et al., 2001. Family treatment and medicationdosage reduction in schizophrenia: effects on patient social function-ing, family attitudes, and burden. Journal of Consulting and ClinicalPsychology 69 (1), 3–12.
Nolan, M., Lundh, U., 1999. Satisfactions and coping strategies of familycarers. British Journal of Community Nursing 4 (9), 470–475.
Novak, M., Guest, C., 1989. Caregiver response to Alzheimer’s disease.International Journal of Aging and Human Development 28 (1), 67–79.
O’Brien, J.A., McKenna, B., Kydd, R., 2009. Compulsory community mentalhealth treatment: a literature review. International Journal of NursingStudies 46, 1245–1255.
Orhagen, T., d’Elia, S., 1992. Multifamily educational intervention inschizophrenia. 1: Does it have any effect? Nordic Journal of Psychia-try 46, 3–12.
Pai, S.P., Kapur, R.L., 1981. The burden on the family of a psychiatricpatient: development of an interview schedule. British Journal ofPsychiatry 138, 332–335.
Pai, S., Kapur, R.L., 1982. Impact of treatment intervention on therelationship between dimensions of clinical psychopathology,social dysfunction and burden on the family. Psychological Medi-cine 12 (3), 651–658.
Pasamanick, B., Scarpitti, F., et al., 1967. Schizophrenics in the Commu-nity. Appleton-Century-Crofts, New York.
Pawson, R., Greenhalgh, T., et al., 2005. Realist review—a new method ofsystematic review designed for complex policy interventions. Journalof Health Services Research Policy 10 (Supplement 1) S1:21–S1:32.
Pearlin, L.I., Schooler, C., 1978. The structure of coping. Journal of Healthand Social Behaviour 19 (March), 2–21.
Pekkala, E., Merinder, L., 2004. Psychoeducation for schizophrenia –Cochrane review. Cochrane Library, Issue 2, Update Software. Oxford.
Platt, S.D., Weyman, A., et al., 1980. The Social Behaviour AssessmentSchedule (SBAS). Rationale, contents, scoring and reliability of a newinterview schedule. Social Psychiatry 15, 43–55.
Platt, S.D., Weyman, A., et al., 1983. The Social Behaviour AssessmentSchedule (SBAS). Windsor, NFER-Nelson.
Platt, S.D., 1985. Measuring the burden of psychiatric illness on thefamily. An evaluation of some rating scales. Psychological Medicine15, 383–393.
Posner, C.M., Wilson, K.G., et al., 1992. Family psychoeducational supportgroups in schizophrenia. American Journal of Orthopsychiatry 62 (2),206–218.
Potaznik, Nelson, 1984. Stress and social support: the burden experiencedby the family of a mentally ill person. American Journal of CommunityPsychology 12 (5), 589–607.
Radloff, L.S., 1977. The CES-D scale: a self-report depression scale forresearch in the general population. Applied Psychology Measurement1, 385–401.
Ran, M.S., Xiang, M.Z., et al., 2003. Effectiveness of psychoeducationalintervention for rural Chinese families experiencing schizophrenia: arandomised controlled trial. Social Psychiatry and Psychiatric Epide-miology 38 (2), 69–75.
Rao, K., Barnabas, I.P., et al., 1988. Family burden in chronic schizophre-nia: the role of the day hospital. Indian Journal of PsychologicalMedicine 11 (2), 131–135.
Reynolds, W., Hoult, H.J., 1984. The relatives of the mentally ill. Acomparative trial of community-oriented and hospital-oriented psy-chiatric care. Journal of Nervous and Mental Disease 172 (8), 480–489.
Ruane, D., Kuipers, E., et al., 2004. Expressed emotion at first-episodepsychosis. Investigating a carer appraisal model. British Journal ofPsychiatry 184, 321–326.
Razali, S., Hasanah, C., et al., 2000. Psychosocial interventions for schizo-phrenia. Journal of Mental Health 9 (3), 283–289.
Reinhard, S., Gubman, G., et al., 1994. Burden Assessment Scale forfamilies of the seriously mentally ill. Evaluation and Program Plan-ning 17 (3), 261–269.
Repper, J., Breeze, J., 2007. User carer involvement in the training andeducation of health professions: a review of the literature. Interna-tional Journal of Nursing Studies 44, 511–519.
Roick, C., et al., 2007. Burden on caregivers of people with schizophrenia:comparison between Germany and Britain. British Journal of Psychia-try 190, 333–338.
Rose, L., 1998. Benefits and limitations of professional family interven-tions. Archives of Psychiatric Nursing 11 (3), 140–147.
Rotondi, A.J., Haas, G.L., et al., 2005. A clinical trial to test the feasibility ofa telehealth psychoeducational intervention for persons with schizo-
S.H. Macleod et al. / International Journal of Nursing Studies 48 (2011) 100–120120
phrenia and their families: intervention and 3 month findings. Reha-bilitation Psychology 50 (4), 325–336.
Saunders, J.C., 2003. Families living with severe mental illness: a literaturereview. Issues in Mental Health Nursing 24 (2), 175–198.
Scazufca, M., Kuipers, E., 1996. Links between expressed emotion andburden of care in relatives of patients with schizophrenia. BritishJournal of Psychiatry 168, 580–587.
Schene, A.H., Tessler, R.C., et al., 1994. Instruments measuring family orcaregiver burden in severe mental illness. Social Psychiatry andPsychiatric Epidemiology 29, 228–240.
Schene, A.H., vanWijngaarden, B., et al., 1998. Family caregiving inschizophrenia: domains and distress. Schizophrenia Bulletin 24,609–618.
Schooler, C., Hogarty, G.E., et al., 1979. In: Hargreaves, W.A., Atkisson,C.C., Sorenson, J.E. (Eds.), Social Adjustment Scale 11 (SAS-11).Resource Materials for Community Mental Health Program Evalua-tions. National Institute of Mental Health, Rockville MD, pp. 290–303.
Sellwood, W., Barrowclough, C., et al., 2001. Needs-based cognitive-behavioural family intervention for carers of patients suffering fromschizophrenia: 12 month follow-up. Acta Psychiatrica Scandinavica104 (5), 346–355.
Sherman, M.D., 2006. Updates and five-year evaluation of the S.A.F.E.program: a family psychoeducational program for serious mentalillness. Community Mental Health Journal 42 (April (2)), 213–219.
Shore, L., Holmshaw, J., 1998. What can carers do? Mental Health Care 2(2), 67–69.
Sidley, G.L., Smith, J., et al., 1991. Is it ever to late to learn? Informationprovision to relatives of long-term schizophrenia sufferers. Beha-vioural Psychotherapy 19, 305–320.
Simpson, A., 2005. Community psychiatric nurses role and the care co-ordinator role: squeezed to provide ‘limited nursing’. Journal ofAdvanced Nursing 52 (6), 689–699.
Smith, J.V., Birchwood, M.J., 1987. Specific and non-specific effects ofeducational intervention with families living with a schizophrenicrelative. British Journal of Psychiatry 150, 645–652.
Snyder, K., Liberman, R.P., 1981. Family assessment and intervention withschizophrenics at risk for relapse. In: Goldstein, M.J. (Ed.), NewDevelopments in Interventions with Families of Schizophrenics. Jos-sey Bass, San Fransisco, pp. 49–60.
So, H.W., Chen, E.Y.H., Chan, R.C.K., et al., 2006. Efficacy of a briefIntervention for carers of people with first-episode psychosis: awaiting list controlled study. Hong Kong Journal of Psychiatry 16,92–100.
Sota, S., Shimodera, S., et al., 2008. Effect of a family psychoeducationalprogram on relatives of schizophrenia patients. Psychiatry and clin-ical Neurosciences 62 (4), 379–385.
Stengard, E., 2003. Educational intervention for the relatives of schizo-phrenia patients in Finland. Nordic Journal of Psychiatry 57 (4),271–277.
Stein, L.I., Test, M.A., 1980. Alternatives to mental hospital treatment: 1.Conceptual model, treatment program, and clinical evaluation.Archives of General Psychiatry 37, 392–397.
Szmukler, G., Burgess, P., et al., 1996. Caring for relatives with seriousmental illness: the development of the Experience of CaregivingInventory. Social Psychiatry and Psychiatric Epidemiology 31, 137–148.
Szmukler, G., Wykes, T., et al., 1998. Care-giving and the impact on carersof a community mental health service. PRISM psychosis study 6.British Journal of Psychiatry 173, 399–403.
Sun, Y., 1994. A study of the family functioning of families with aschizophrenic patient. Unpublished Masters of Social Work Thesis.Cited in Chien et al. 2004. Department of Social Work. SAR China. TheChinese University of Hong Kong.
Taylor, M., 2003. Public Policy in the Community. MacMillan, Basingstoke,Palgreave.
Tee, S., Dorey, T., 2000. Families and schizophrenia. Mental Health Nur-sing 20 (2), 10–13.
Tennakoon, L.D., Fannon, D.G., et al., 2001. Experience of caregiving: aprospective follow-up study among the relatives of first-episodepsychotic clients. Schizophrenia Research 49, 277–278.
Tessler, R.C., Fisher, G., et al., 1991. Conceptualising and Measuring theBurden of Caregiving Families of the Severely Mentally Ill. Social &Demographic Research Institute, University of Massachusetts.
Test, M.A., Stein, L.I., 1980. Alternatives to mental hospital treatment. 111.Social cost. Archives of General Psychiatry 37, 409–412.
Tilley, S., Ryan, D., 2000. Reviewing the literature constructing the field:accounting for the CPN in practice and research. Journal of MentalHealth 9 (6), 589–604.
Turkington, D., Kingdon, D., et al., 2002. Effectiveness of a brief cognitive-behavioural therapy intervention in the treatment of schizophrenia.British Journal of Psychiatry 180, 523–527.
Veltro, F., Magliano, L., et al., 2006. Randomised controlled trial of abehavioural family intervention: 1 year and 11 year follow up.Epidemiologia e Psichiatria Sociale 15 (1), 44–51.
Victoria, C.G., Habicht, J.P., Bryce, J., 2004. Evidence-based public health;moving beyond randomized controlled trials. American Journal ofPublic Health 94, 400–4005.
Vitaliano, P., Russo, J., et al., 1985. he ways of coping checklist: revisionand psychometric properties. Multivariate Behaviour Research 20,3–26.
Warner, R., 1997. Recovery from schizophrenia. Psychiatric and politicaleconomy. New York, Routledge.
Warner, T., Skidmore, D., et al., 2000. Implication of current mental healthpolicy for the practice and education of the mental health workforce.Mental Health Care 4 (2), 48–52.
Weinberg, A., Huxley, P., 2000. An evaluation of the impact of voluntarysector family support workers on the quality of life of carers ofschizophrenia sufferers. Journal of Mental Health 9 (5), 495–503.
WHO, 2005. Mental Health Atlas. World Health Organisation, Geneva,Switzerland.
WHO, 2006. The World Health Report 2006. Working Together for Health.World Health Organisation, Geneva, Switzerland.
WHO, 2007. Atlas: Nurses in Mental Health 2007. World Health Organi-sation, Geneva, Switzerland.
WHO, 2008a. Policies and Practices for Mental Health in Europe. WHOPress. Regional Office for Europe, Geneva, Switzerland.
WHO, 2008b. Integrating Mental Health into Primary Health Care. AGlobal Perspective. World Organisation of Family Doctors (WONCA)World Health Organisation Press, Geneva, Switzerland.
Winefield, H.R., Barlow, J., et al., 1998. Responses to support groups forfamily caregivers in schizophrenia: who benefits from what? Aus-tralian and New Zealand Journal of Mental Health Nursing 7 (3), 103–110.
Winefield, H., Harvey, E.J., et al., 1992. Social support and psychologicalwell-being in young adults: the Multidimensional support Scale.Journal of Personality Assessment 58, 198–210.
Winefield, H., Harvey, E.J., 1995. Tertiary prevention in mental healthcare. Effects of group meetings for family caregivers. Australian andNew Zealand Journal of Psychiatry 29, 139–145.
Wuerker, A.K., 2000. The family and schizophrenia. Issues in MentalHealth Nursing 21 (1), 127–141.
Xiong, W., Phillips, M., et al., 1994. Family-based intervention for schizo-phrenic patients in China: a randomised controlled trial. BritishJournal of Psychiatry 165, 239–247.
Yamaguchi, H., Takahashi, A., et al., 2006. Direct effects of short-termpsychoeducational intervention for relatives of patients with schizo-phrenia in Japan. Psychiatry and Clinical Neuroscience 60 (5), 590–597.
Zarit, S.H., Orr, N.K., et al., 1983. Working with Families of DementiaVictims: A Treatment Manual. Human Development Services,Washington. DC.
Zarit, S.H., Orr, N.K., Zarit, J.M., 1985. The Hidden Victims of Alzheimer’sDisease: Families Under Stress. New York University Press, New York.
Zarit, S.H., Leitsch, S.A., 2001. Developing and evaluating communitybased intervention programs for Alzheimer’s patients and theircaregivers. Aging and Mental Health 5 (Supplement 1), S84–S98.
Zarit, S.H., et al., 2003. The validities of research findings: The case ofinterventions with caregivers. Alzheimer’s Care Quarterly 4, 216–228.
Zhang, M., Schwarger, R., 1995. Measuring optimistic self-beliefs, Chi-nese adaptation of the General Self Efficacy Scale. Psychologia 38,174–181.
Zhang, M., Gittleman, M., et al., 1998a. Group psychoeducation ofrelatives of schizophrenic patients: two-year experiences. Psychiatryand Clinical Neurosciences 52 (Suppl.), S344–S347.
Zhang, M., He, Y., et al., 1998b. Group psychosocial education for relativesof schizophrenic patients in the community: a three year experience.Hong Kong Journal of Psychiatry 8 (1), 33–37.
Ziguras, S.J., Stuart, G.W., 2000. A meta-analysis of the effectiveness ofmental health case management over 20 years. Psychiatric Services51 (11), 1410–1421.
Zubin, J., Spring, B., 1977. Vulnerability: a new view of schizophrenia.Journal of Abnormal Psychology 86, 103–126.
Copyright © 2022 FDOKUMEN




















