Precision medicine/personalized medicine: a critical analysis ...

Int. J. Biomedical Engineering and Technology, Vol. 16, No. 3, 2014 223
Copyright © 2014 Inderscience Enterprises Ltd.
Using IS/IT to support the delivery of Chinese medicine: a Chinese medicine clinic management system
Catherine Han Lin* and Siddhi Pittayachawan School of Business IT and Logistics, RMIT University, Melbourne, Australia Email: [email protected] Email: [email protected] *Corresponding author
Angela Wei Hong Yang School of Health Sciences, RMIT University, Melbourne, Australia Email: [email protected]
Nilmini Wickramasinghe School of Business IT and Logistics, RMIT University, Melbourne, Australia and Epworth HealthCare, 89 Bridge Road, Richmond, VIC 3121, Australia Email: [email protected]
Abstract: OECD countries today are focusing on ways to incorporate IS/IT to facilitate superior healthcare delivery. However, studies of IS/IT implementations for Chinese Medicine (CM) practice are very limited. We analyse western medicine (WM) and CM diagnosis and treatment processes and find that these clinical processes share some similarities. Hence, we contend that by implementing IS/IT system solutions, CM practice can also enjoy similar benefits from IS/IT as WM. This paper serves to identify a role for IS/IT in assisting CM clinic key processes as well as identify key IT investment portfolio components of such IS/IT solutions.
Keywords: IS/IT healthcare; information systems; clinical management systems; medicine management system; Chinese medicine.
Reference to this paper should be made as follows: Lin, C.H., Pittayachawan, S., Yang, A.W.H. and Wickramasinghe, N. (2014) ‘Using IS/IT to support the delivery of Chinese medicine: a Chinese medicine clinic management system’, Int. J. Biomedical Engineering and Technology, Vol. 16, No. 3, pp.223–243.

224 C.H. Lin et al.
Biographical notes: Catherine Han Lin is a Teacher at RMIT University. She worked in the IS/IT profession for more than 20 years with international companies such as Mobil Oil, Hawker De Havilland, ANZ, and Telstra in various positions including System Analyst, BI/BA, ICT Manager, and IS/IT Lecturer. Her research interest include: information systems, information management, health informatics, IS/IT in complementary and alternative medicine especially Chinese medicine. She was involved in research collaboration/activities with Infineon Technology (Australia) on green energy projects. She is currently working on various health IT research projects at Epworth healthcare and RMIT University.
Siddhi Pittayachawan is a Senior Lecturer in the School of Business IT and Logistics, RMIT University. He earned his PhD addressing trust issues in online shopping. His research interests include information systems and supply chain management, especially on trust, e-commerce, BYOD, information security behaviour, measurement, sustainable consumption, and business education. He is specialised in research design and methodologies. He has collaborated actively with academics in several other disciplines such as information management, health informatics, and Chinese medicine. He has been invited to run several advanced statistical workshops in Australia and Thailand.
Angela Wei Hong Yang has been teaching, researching and practicing Chinese medicine for nearly 20 years. Her research specialty is to investigate the quality, safety and effectiveness of Chinese medicine, particularly Chinese herbal medicine, for the ageing population and those with chronic diseases (e.g. diseases of immune system and endocrine system). Her research expertise includes the development of systematic reviews and clinical trials as well as instruments for quality assessment of Chinese medicine studies. She is also specialising in using the interdisciplinary approach (e.g. information systems) to promote, manage and analyse Chinese medicine knowledge.
Nilmini Wickramasinghe is the inaugural Epworth Chair Health Information Management, researches and teaches within the information systems domain with particular focus on developing suitable models, strategies and techniques grounded in various management disciplines to facilitate more effective design, development and implementation of IS/IT solutions to effect superior, patient centric healthcare delivery. She collaborates with leading scholars at various premier healthcare organisations throughout Australasia, USA and Europe. She is well published with more than 300 referred scholarly articles, more than ten books, numerous book chapters, an encyclopaedia and a well established funded research track record.
1 Introduction
Using Information Systems/Information Technology (IS/IT) applications and solutions in the practice of Western Medicine (WM) has become more and more common nowadays (Lin et al., 2013; Wickramasinghe and Schaffer, 2010). It has been discussed deeply and widely in the literature that IS/IT can support superior WM delivery (ibid). However, healthcare is not restricted only to WM. In the 21st century, we are witnessing an increased global trend of treatments in Complementary and Alternative Medicine (CAM) (Lu et al., 2004). More than 80% of the world’s population rely on herbal medicine

Using IS/IT to support the delivery of Chinese medicine 225
(WHO, 2013). In Australia, the number of visits to CAM practitioners in 2004–2005 reached 69.2 million, while the number of visits to WM practitioners was 69.3 million in the same period (Xue et al., 2007). World Health Organization (WHO) has a clear plan and vision to gradually integrate CAM to WM; this is stated in its 2014–2023 strategy (Lin et al., 2014; WHO, 2013). Since IS/IT has been implemented in many areas of healthcare (e.g. hospitals, insurance companies and laboratories) and will be continually deployed with advanced technology, it is vital that CAM IS/IT developments are studied and enhanced for the preparation of this integration.
Chinese Medicine (CM) is one of the most popular CAM practices today (Lukman et al., 2007). It is considered by many patients to have fewer side effects and complications as compared to WM (Shi and Lu, 2006). CM is also seen as having more effective treatment to the root of the disease and is good for the overall health of patients (Chi, 1994). Moreover, Chinese herbs like ginseng (or RenShen) are widely sold and used by many western physicians, while many WM practitioners have taken courses in Chinese acupuncture (Kaptchuk, 2000). Despite the rapid growth in the embracement of CM, research and study into the role of IS/IT implementations to support and enable CM practices has not been discussed much in the literature. To address this void, this paper reports on a research in progress that serves to focus on investigating the potential of using IS/IT tools and techniques to assist CM clinics and thereby support enhancing the delivery of CM practices. In particular, how can IS/IT be used and incorporated into the delivery of CM in its clinics daily processes?
2 Background
2.1 Why IS/IT can facilitate superior healthcare delivery
Voluminous data and information permeate medical clinics and hospitals. Processing these data manually is one of the reasons for inefficient, ineffective and costly healthcare (Wickramasinghe and Schaffer, 2010). Hence, IS/IT systems which coordinate organisational tasks, provide information at the point of care, reduce clinical and hospital cost and support quality healthcare delivery are being embraced (Lenz and Reichert, 2007). The advantages of using such IS/IT solutions are summarised as follows.
1 Facilitate delivery of care: care can be delivered to people who are located in remote areas. For example, doctors may use telemedicine equipment like tele-radiology and tele-surgery to diagnose and treat patients (Hojabri and Manafi, 2012).
2 Improve quality of care: IT can help provide easier and safer access to patient data including laboratory results, therapeutic procedures, medication administration, clinic notes and billing (Austin and Boxerman, 2003). This results in informed-based diagnosis, acceleration of communication and reduction in medical errors (COCIR, 2012).
3 Reduce cost and save time: healthcare information can be accessed faster. This reduces the issue of staff shortage as well as increases efficiency. Clinical and administrative costs can be reduced by avoiding the duplication of medical examinations and unnecessary visits. For example, by embracing cloud technology,

226 C.H. Lin et al.
the Swedish Red Cross was able to save 20% on their IT operating costs. This action led to freeing 25% of people’s time to focus on more strategic tasks, better supporting the core missions of the organisation (Microsoft, 2011).
4 Support better management and monitoring: patients learn how to control and manage their diseases correctly with the help of online disease management systems. Features like ‘ask a physician’ or nurse online assist patients to take control of their disease rather than solely relying on a doctor (Ball and Lillis, 2001).
5 Provide decision support: Clinical Decision Support (CDS) systems can give automatic alerts and warnings to physicians. For instance, a community hospital in USA used a computerised alert system to target 37 drug-specific adverse reactions. They detected opportunities to prevent injury at a rate of 64 per 1000 admissions; 44% of the true positive alerts had not been recognised by the physician (Bates, 2000). Thus, there is strong evidence in the literature to show that IS/IT can provide and enable superior healthcare delivery.
2.2 Chinese Medicine (CM)
CM began in China thousands of years ago at the time when Chinese philosophy, astronomy and literature were developed to maturity (Liao, 2011). At that time, key individuals gained experiences in how to deal with human diseases by natural methods, such as acupuncture, Qigong (mind controlling) and herbs (Wang et al., 1999). Further, many of these individuals began to summarise these practices and thereby developed a theory based on their philosophical and social knowledge which in turn formed the origins of CM (Wang et al., 1999). Succinctly, CM follows two philosophies: (1) a homeostasis perspective that focuses on the integrity of human body, and emphasises the close relationship between human body and its social and natural environment and (2) a dynamic balance perspective with an emphasis on the movement in the integrity (Lu et al., 2004). Table 1 summarises the key aspects of CM. As can be seen from this table, CM is different and distinct from western medical practice but also perhaps even more heavily reliant on tacit knowledge and expertise of the practitioner, a point made more apparent when we look at the processes involved with CM diagnosis.
Table 1 CM five elements
Five elements
Five Zang (principal)
organs
Five Fu organs
Five sense organs
Five body tissues
Five passions
Five fluids
Five pulses
Wood Liver Gall bladder
Eyes Tendons Anger Tears Taut
Fire Heart Small intestine
Tongue Vessels Joy Sweat Surging
Earth Spleen Stomach Lips Muscles Thought/anxiety
Saliva Moderate
Metal Lung Large intestine
Nose Skin and hair
Sorrow Nasal discharge
deep and thin
Water Kidney Urinary bladder
Ears Bones Fear/fright Spittle Deep
Source: Adopted from Liu and Liu (2009, p.23)

Using IS/IT to support the delivery of Chinese medicine 227
2.2.1 CM diagnosis
CM practitioners use four basic methods for diagnosis: inspection, auscultation and olfaction, enquiring and palpation (Huang and Chen, 2007; Zhao et al., 1994). Diagnosis and treatments are based on an overall analysis of the patient’s symptoms and signs. This process is called ‘bian zheng’ (differentiation of syndrome). ‘Bian’ means discrimination or classification, while ‘zheng’ means syndrome (Zhao et al., 1994). Inspection begins with the physician understanding and predicting the pathological changes of internal organs by observing abnormal changes in the patient’s vitality, colour, appearance, secretions and excretions (Huang and Chen, 2007). The second method, auscultation and olfaction, includes listening and smelling. The physician listens to the patient’s voice, breathing, coughing and sounds emanating from the internal organs. Ear and stethoscope may also be applied in this process (ibid). A patient’s ‘stinky’ smell, for example, usually indicates heat syndromes, while foul and sour smells imply retention of food (ibid). Enquiring is about getting information from a patient about his/her disease condition. Examples of common enquiries are chills and fever, perspiration, appetite and thirst, and pain (ibid). Regarding palpation, the physician would put his/her first three fingers on the radial artery of a patient’s wrist. A trained and skilled physician can detect over 30 different pulse qualities (e.g. floating, sunken, weak and bounding) on each of the 12 pulses (Zhu and Wang, 2011). The pulse qualities help the physician to identify the condition of the related organs. These four approaches are used in combination in every diagnosis and cannot be separated or omitted (Zhu and Wang, 2011). A correct diagnosis can only be made based on a comprehensive and systematic analysis of a patient’s condition.
CM treatments can include any of the following: Chinese herbs (i.e. leaves, seeds, roots, flowers, fruits, minerals and animal products), acupuncture and moxibustion, tuina (Chinese remedial massage), cupping, qigong and taichi, and diet therapy (Xue and O’Brien, 2003). All treatments aim to increase human body’s resistance to diseases and prevention by improving the inter-connections among self-controlled systems (Lu et al., 2004).
3 Literature review
Healthcare is one of the most complicated systems in our society today. It has many dimensions and involves many parties that need to collaborate in order to deliver a quality care to a patient, such as clinical/hospital administrations, physicians, specialists, nurses, radiologic technology technicians, psychologists, lab technicians, financial clerks, insurance companies and department of health of the country. It is unarguably important that knowledge is captured and created from all parties and participants. It is equally important that all this knowledge is made available to all others in order to deliver quality healthcare to a patient at the point of need. Research has shown that KM can increase performance, develop partnership, evaluate risks, organise management and enhance economic value (Morr and Subercaze, 2010). With proper KM tools and techniques, knowledge can be formalised, shared, structured and organised so that organisation knowledge assets will not be lost. A human mind can only obtain limited information and knowledge. A WM physician must be aware of hundreds of medical references, biological tests, thousands of imagery tests and surgical interventions (Wickramasinghe

228 C.H. Lin et al.
et al., 2006). Additionally, they must know the medicines’ potential effects and prices. KM helps healthcare professionals to focus on acquisition, knowledge storage and retrieval, as well as other activities such as learning, strategic planning and decision-making (ibid).
As mentioned earlier, CM is based on ancient wisdom and philosophies that were tested and refined over centuries. It contains enormous knowledge and information that any CM practitioners must have. From its unique diagnosis methods, treatments, multi-ingredient prescriptions and acupuncture to yin–yang inner system balance (Lu et al., 2004; Liu and Liu, 2009). This takes years of learning and practice. It is said that patients favour older and experienced physicians because they have more knowledge and effective methods of treatments (Hesketh and Zhu, 1997). It is important that the unique tacit and explicit knowledge of CM is effectively managed and used for great purposes. Thus, we will incorporate KM focus on the design and development of a suitable CM clinic management system.
3.1 Knowledge Management (KM)
KM is a process of continually managing knowledge of all kinds to meet existing and emerging needs, to identify and exploit acquired knowledge assets and to develop new opportunities (Quintas et al., 1997). KM is about designing and implementing processes, tools, structures, systems and culture to facilitate knowledge capture, sharing and reuse to enhance organisational performance (Gottschalk, 2005).
Integral to KM is, of course, the knowledge construct. Nonaka (1994, p.14) notes that “knowledge is created and organised by a flow of information, anchored on the commitment and belief of its holder”. Goodson (2005, p.148) refers to knowledge as an “insight, experience, and creativity that exist within people expressed through explicit and tacit communication events”. Polanyi (1966) further categorised knowledge into two types: tacit and explicit. Tacit knowledge is gained from experience and ‘by doing’. It is accumulated through an individual’s experience, actions, ideas or values he or she embraces (ibid). This type of knowledge is very hard to express and formalise; hence, it is also difficult to share with others. Explicit knowledge, in contrast, can be expressed in words, numbers and diagrams; hence, it is easier to be captured, used and shared (ibid). Organisations must be aware that these two types of knowledge are equally important.
The form of the knowledge can be changed in several ways. In particular, Nonaka et al. (1998) defined key transformations as the following: tacit to tacit through socialisation; tacit to explicit through externalisation; explicit to tacit through internalisation; and explicit to explicit through combination. This process is known as the knowledge spiral (Nonaka et al., 1998). When people share experiences, such as a master passing on his or her knowledge to the apprentice through apprenticeship, tacit knowledge can be transferred to tacit (ibid). Through a combination or conversion, explicit knowledge can be edited and systemised into more complex sets of explicit knowledge (ibid). This usually happens in a formal learning of facts (Nonaka et al., 1998; Rao 2005). Tacit knowledge is transferred to explicit knowledge that can be understood by the others through the use of metaphors and analogies (Nonaka et al., 1998; Wickramasinghe, 2013). Wickramasinghe et al. (2006) use this in a healthcare context and explain, for example, that a surgeon answers the questions of why he does a particular procedure in a certain way. The tacit knowledge of the surgeon is captured and

Using IS/IT to support the delivery of Chinese medicine 229
can be used and made available for the others. Explicit to tacit occurs as conversion of new explicit to tacit knowledge of individuals (Nonaka et al., 1998). Examples of this are on-the-job-training, simulations and experiments (ibid).
It is important to note that knowledge do not transfer automatically by itself (Nonaka et al., 1998). Socialisation, externalisation, internalisation and combination (ibid) involve participants’ interaction, cooperation, collaboration, reflection and management (ibid). It is equally important to note that knowledge transformation is not a one-way street. Tacit knowledge can be transferred to explicit, and the newly formed explicit knowledge can be transferred to either tacit or explicit knowledge. Hence, managing knowledge and knowledge transfer is important. Wickramasinghe et al. (2006) illustrated the generation of these two types of knowledge during the healthcare process. We would like to take a step further here to show the transfer of knowledge through some examples. Moreover, we identify the involvements of IS/IT in these processes in Table 2.
Table 2 Healthcare knowledge transfer
Healthcare process
Knowledge transfer
Example IS/IT involvement
Symptoms Explicit to tacit
A medically well-educated (self-educated) patient may claim that he/she is suffering from diabetes (explicit), as some of the symptoms he/she has experienced closely match the disease (tacit).
A patient is medically well educated by browsing medical information on the internet. This medical information was prepared and made available for the public with the use of IT.
Primary diagnosis
Explicit to explicit
A doctor listens and records the patient’s symptoms (explicit) and diagnoses the patient’s illness is diabetes (explicit).
A doctor records the patient’s symptoms through an electronic device. Patient’s records are stored at the clinic level or as an EMR which can be accessed nationally.
Referral Tacit to tacit
A doctor will ask (tacit) the patient to undergo a set of tests or refer him to a specialist (tacit).
An electronic referral letter can be generated and sent to a specialist or laboratory for testing with details of testing items.
Second opinion
Explicit to explicit/ tacit to explicit
The test results will show some data and/or information (explicit) to confirm if the patient is diabetic (explicit). A specialist may find that the patient has additional illness (tacit) and further tests may be required (explicit).
Test results are updated automatically through electric medical equipment. These results are transferred to the doctor or specialist electronically.
Confirmation Explicit to tacit/tacit to tacit
All test results (explicit) confirm the patient’s illnesses (explicit). A specialist confirms the original diagnosis from the doctor (tacit to tacit).
Confirmation of a patient’s illness is recorded in patient’s file or EMR.
3.2 Problems and challenges of CM
Today CM clinics still operate its clinical activities manually (Lin et al., 2013). Many CM practitioners use their first language to record patients’ syndromes and treatments (ibid). This creates language difficulties to others. It is also hard to implement standards,

230 C.H. Lin et al.
and to encourage an internationally recognised and registered practice. A patient’s medical record can come in many forms, including films, images, telegraphs and Electronic Medical Record (EMR). CM doctors found it difficult to store these crucial evidences in analysing and diagnosing the patient without proper and adequate technology and equipment.
As an ancient treatment to human diseases, CM today has a huge collection of herbs and medical equipments. Managing these medicines and equipments manually is a continuous resource- and space-demanding task for the CM clinics. Capturing and transforming the voluminous information and knowledge in Chinese herbs, acupuncture, syndromes and treatments to an IS/IT system is another major challenge. Research has attempted to build and transfer this tremendous knowledge to a knowledge-based system which can be retrieved online or through intranet. Dasherb has an herb database that contains lists of common Chinese herbal medicines that can be searched by their Latin names, English names and Pinyin names (a pronunciation of Chinese characters) (Dasherb, 2013). Complementary and Alternative Healing University (CAHU), California, has developed a comprehensive online dictionary of Chinese herbs. Each herb is explained in detail including its pharmaceutical name; botanical name; Japanese, Korean and Cantonese pronunciations; distribution of the herb; properties (characteristics); channels (meridians) entered; medical functions; actions and indications; chemical ingredients; recommended dosage; samples of formulae, toxicity and cautions (CAHU, 2013). A similar development has been done in Australia; the Chinese Medicine Portal (CMP) is an online CM knowledge pool where information and clinical data can be retrieved and accessed (Yang et al., 2009). Some CM expert systems and applications are developed for certain diseases or particular treatments. For example, an expert in Chinese acupuncture system can assist physicians on acupuncture prescription, needle insertion position and acupuncture points’ usage (Lam et al., 2012). These developments have few limitations:
1 They are incomprehensive. Most developments and resources only include limited or small amount of Chinese herbs with no or limited resources in Chinese acupuncture or vice versa (Yang et al., 2009).
2 They are not an IS/IT system solution for CM clinics and practitioners to handle their key daily processes.
3 There are no standards and compliances to government regulations and assessments.
4 There are no system functions and features on clinic medicine and supply management.
5 There is a limitation on system integration. Most expert systems and applications are designed as a stand-alone with limited integration with others.
In this research, we propose that the solution lies in the design and development of a Chinese Medicine Clinic Management System (CMCMS). The idea of such a system is to help CM clinics and practitioners in their key daily processes and activities in managing medicine and supplies.
3.3 CM diagnosis and treatment processes
In order to develop a suitable CMCMS, it is first necessary to map the processes that take place in CM clinics. This is done in Figure 1.

Using IS/IT to support the delivery of Chinese medicine 231
Figure 1 CM patient diagnosis and treatment processes (see online version for colours)
2.0 CM Consultation and Diagnosis (Bian Zheng)
Inspection Auscultation & Olfaction
Inquiring Palpation
Observing abnormal changes ( colour, appearance, secretions, excretions)
Listening ( voice, breathing, coughing, sounds) Smelling
Inquiring patient disease condition
Identify pulses
3.0 CM Treatments
Herbs ( leaves, seeds, roots, flowers, fruits, minerals and animal products
Acupuncture, Moxibustion
Tuina, Cupping, Qigong, Taichi
Diet therapy
1.0 Register
2.0 CM Consultati
on and Diagnosis
3.0 CM Treatment
s
Patient
In these processes, after consultation and diagnosis, a CM doctor may give the patient a treatment plan: the patient is given Chinese herbal medicine and/or other kinds of treatments; the patient may be referred to a specialist for more specialised treatments or be transferred to a hospital for emergency care. It is very common that the doctor asks the patient to come back for a subsequent treatment.
The CM processes in Figure 1 are a close match to WM clinics. A typical western physician clinic patient process is analysed and modelled by Swisher et al. (2001). It includes registration, check-in, examination (including pre-examination and post-examination), exit interview and checkout (Swisher et al., 2001). In the registration process, a patient interacts with a clinical staff prior to treatment. During check-in, the clinical staff spends time with the patient collecting initial medical information before examination. Next a physician collects more extensive medical information from the patient (pre-examination) if necessary, diagnoses the patient and prescribes treatments (examination); additional medical information is collected if any (post-examination). A physician performs the final consultation and diagnosis in the exit interview process. At checkout, a patient may interact with the clinical staff before exiting the clinic (ibid). Comparing the above-mentioned processes, Swisher’s registration process matches 1.0 process in Figure 1. The check-in and examination processes match process 2.0. Swisher’s post-examination is the same as process 3.0 in Figure 1. Instead of having an exit interview and checkout, we realise that the processes can flow back and be repeated for some patients. This may suggest that CM clinics can expect as much benefit from the proposed IS/IT solution as we are now witnessing when IS/IT solutions are applied to WM clinics.
The differences between CM and WM clinics are, however, in the methods of diagnosis, ingredients in the medicine, the treatment approaches as well as the amount of and reliance on expert tacit knowledge. A study on a group of six people with stomach pain who were diagnosed by a WM doctor and then by a CM physician has shown a significant difference. Based on the knowledge and theory of western medicine practice of analysing that has a tendency to narrow the diagnosis to an underlying entity, the western medicine doctor used upper gastrointestinal X-rays or endoscopy by means of a fiberscope and diagnosed all the six patients as having peptic ulcer disease (Kaptchuk, 2000). According to the western medicine doctor, all the six patients suffered from the same disorder, and they were given the same prescription (ibid). However, the CM physician found the differences in each patient, diagnosed six different syndromes and
232 C.H. Lin et al.
prescribed six different herbal formulas (ibid). The CM physician’s expert knowledge and comprehensive analysis of each patient’s unique health condition revealed the differences in diagnoses and treatments between the two. Therefore, implementing any existing WM IS/IT systems and/or applications to CM clinic processes and activities will not be appropriate. It may result in problems and possible system failures.
4 Medicine clinical system environment and portfolio
Despite the differences between CM and WM, developing unique CM clinic management system cannot be isolated and separated from its practice environment and connections with WM. The ultimate goal is to achieve WHO’s vision of having CM and WM practices alongside each other (Lin et al., 2014; WHO, 2013). So while creating and studying for a suitable CMCMS for CM, clinics should also consider and integrate the developments and systems that are currently employed in other sectors of healthcare. Based on Figure 1, the following IS/IT involvements are identified.
When a patient schedules or walks into a CM clinic for treatment, the patient triggers the registration process. A scheduling resources or facilities system manages booking or scheduling of all care provider resources and identifies conflicts with other appointments for patients. This system is usually a part of the Patient Administration System (PAS) which administers patients’ personal information, admission, discharge and transfer (COCIR, 2012).
EMR information systems: the purpose of this system is to record and host information of patients’ electronic files. EMR includes data and information such as demographics, medical history, medication and allergies, immunisation status, lab test results and radiology images (Hannan, 1996).
Medical Document Management (MDM) information system: MDM manages and supports different electronic patient medical documents and files (Mitamura, 2010). These files contain data and information such as scanned PDF files, care episodes, test results, diagnoses and referrals. Functions of MDM include computer-assisting document/file entry, indexing, administration, file/document storage, access/retrieval and archiving (ibid).
Clinical Knowledge Management (CKM) and CDS system: CKM is a repository which contains codified knowledge such as a practical set of rules and guidelines derived from experts (Wyatt, 2001). CKM often comes together with CDS, as it is the back-end database on which CDS depends or from where it gets references. CDS is a program assisting healthcare professionals and physicians with decision-making tasks by linking dynamic individual patient health observations (ibid). In CM, when a CKM like the CMP is available, it can assist CM practitioners in checking/ confirming a Chinese herb’s toxicity and cautions, hence making better decisions on the amount of usage of such herbs.
Finance and Accounting Systems (FAS): this refers to patient billing, insurance claims and cost accounting (COCIR, 2012). This system is usually a built-in PAS either directly or indirectly through EMR. The system can assist the clinical staff to find a medical procedure, diagnosis, treatment and their prices with codes to optimise billing and reimbursement.
Using IS/IT to support the delivery of Chinese medicine 233
Human Resources Management (HRM) system manages the clinic personnel. This includes clinic staff planning, staff details and scheduling, employee time and attendance, and payroll and controlling (COCIR, 2012). Stock Management System (SMS) assists in planning, implementing and controlling all movements and storages of materials and inventory from point of origin to point of consumption. Functions of SMS are ordering purchase, stock management, materials management and supplier management/sourcing (ibid).
Although some of the above systems can be stand-alone systems, most of the above sub-systems are built-in or connected with others. An integration to support the exchange, processing and storage of information and knowledge in between these systems is essential. Security is an important aspect in the design of a suitable CMCMS. Key areas to consider should include protecting patient and health information through access control and passwords, encryption and firewalls; system backup, archive and recovery; and database security with authorisation.
4.1 Analysis of the current CMCMS environment
Improvements start with knowing the current situation, the standard or benchmark and finding the gap between the current and the to-be (Wickramasinghe et al., 2006). Most countries around the world, except China, consider CM as a CAM and do not regulate and subsidise CM in their healthcare system (Lin et al., 2013). IT developments in CM in most countries are very limited; manual system is still very common in most CM clinics (ibid). In this study, we identify a few common CMCMS from different countries: SmartTCM, Australia; TCM Herbalist, Israel; TCM Organiser, Canada; and Shen Professional, Venezuela. Their functions, features and limitations are compared and summarised below.
Language. All four CMCMS include both English and Chinese. Shen Professional allows additional choices of Spanish, German and Portuguese (http://www. shenprofessional.com). Australia is a multicultural and large immigrant country (Jupp, 2002). Therefore, CM practice must include a much wider range of languages such as Vietnamese, Korean, Italian, Greek and various Indian dialects, which are not possible in Smart TCM (Smart TCM, 2014). When using the Chinese language, it is important to know that it contains two components: Pinyin and the character system. Pinyin, like English letters, is used for pronunciation and has four tones. The same Pinyin with different tone means totally different things and results in different Chinese characters. In this aspect, it is a major disadvantage that TCM Herbalist uses Pinyin but without tones and characters (http://www.tcmherbalist.com). This can be very confusing to the user, which can result in wrong prescriptions.
Multi-user and access. All four CMCMS have versions for two user-level password securities and backups with extra cost on every additional level after the first. TCM Organiser has three user-level accesses including administrator, physician and dispenser (TCM Organiser, 2014).
Multi system, devise and discipline management. Although CM and acupuncture are covered by all four systems, only TCM Herbalist covers massage and other CAM disciplines. All four CMCMS include sub-systems such as patient management system (include booking and patient personal records), patient medical record, prescription management and assistance, and reports and document management. TCM Organiser has

234 C.H. Lin et al.
a better accounting system which handles some extra accounting functions like split bills, tax and insurance calculation (TCM Organiser, 2014). TCM Organiser can be used on multiple devices such as PC, Mac, USB and tablets, while the other three CMCMS are restricted to PC and laptops.
Clinic medicine and supply management. This system is not available in SmartTCM, TCM Herbalist and Shen Professional. Limited basic herbal package, row herbs and clinic product usage reports can be generated in TCM Organiser. However, it is far from a complete medicine and supply management system which can handle ordering and reorder, medicine used by dates and other inventory control functions such as the following: indicating the number of times that inventory cycles, cost of the on-hand items and forecasting. Extensive literature search suggests that this system is not included in most of the existing CM clinical management systems (Lin et al., 2013).
These features may not seem to be must-haves to some clinics, but they are necessary when CM and WM are integrated. As the two types of medical practices become more and more integrated and practiced alongside each other, it is our contention that it will be even more necessary that CM be practiced like WM in all hospitals and clinics with many users and devices. Further, CM should also be accessible by many medical modular management systems and disciplines.
4.2 IT investment portfolio and collaboration
Effective IT investments and portfolios should constantly match the underlying business strategy (Weill and Aral, 2006; Weill and Ross, 2009). Planned ongoing use of interlocking business practices and competencies collectively gain superior value from IT investments (ibid). These well-designed, well-understood and transparent IT investments or portfolios attract many IT assets and returns (ibid). An important consideration concerns what allocation of IT should be followed to support infrastructure, transaction, information and strategic needs (ibid). The average IT investments of companies according to a study by Weill and Aral (2006) show the following percentages: 46% infrastructure, 26% transaction, 17% information and 11% strategic needs. With this in mind, it is, however, important to focus on how technology is used rather than technology itself, as different IT investments deliver different values and returns (Weill and Aral, 2006; Weill and Ross, 2009). IT infrastructure is the foundation and it is shared across multiple business units or functional areas (ibid). It is mainly aimed at providing a flexible base for future business initiatives or reducing long-term IT costs through standardisation and consolidation (ibid). Transactional investments’ primary purposes are reduction of the cost of goods sold and increasing the output for the same cost (ibid), e.g. a digitised company’s repetitive transaction. Informational investments provide information for purposes such as accounting, reporting, compliance, communication or analysis, which deliver company profits. Strategic investments help stimulate innovation and thus position an organisation for growth (ibid). The above categorisations provide estimate proportions for an IT investment; however, there are other things one should investigate on before starting an IT project or portfolio. These include an analysis of the current IT environment, identification of where IT investments are applied and what changes should be considered (Weill et al., 2012).
Using IS/IT to support the delivery of Chinese medicine 235
4.3 CMCMS IT investment portfolio
4.3.1 Infrastructure
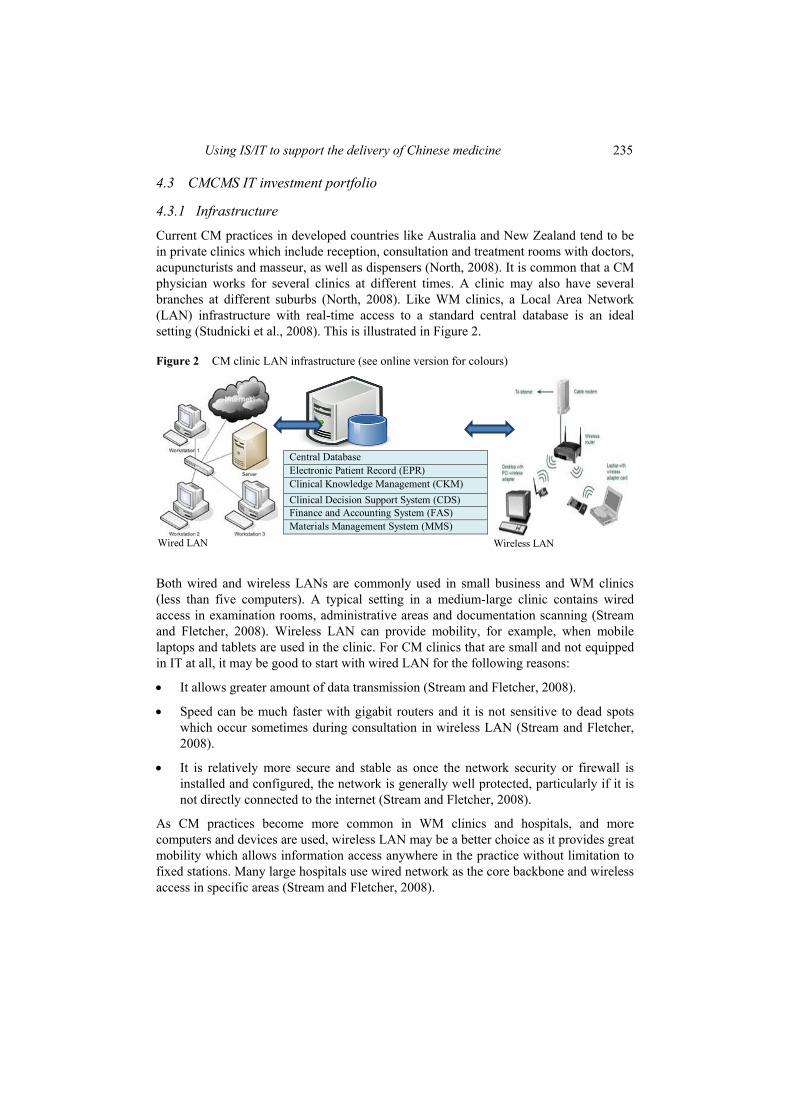
Current CM practices in developed countries like Australia and New Zealand tend to be in private clinics which include reception, consultation and treatment rooms with doctors, acupuncturists and masseur, as well as dispensers (North, 2008). It is common that a CM physician works for several clinics at different times. A clinic may also have several branches at different suburbs (North, 2008). Like WM clinics, a Local Area Network (LAN) infrastructure with real-time access to a standard central database is an ideal setting (Studnicki et al., 2008). This is illustrated in Figure 2.
Figure 2 CM clinic LAN infrastructure (see online version for colours)
Wired LAN
Central Database Electronic Patient Record (EPR)Clinical Knowledge Management (CKM)
Clinical Decision Support System (CDS)Finance and Accounting System (FAS)Materials Management System (MMS)
Wireless LAN
Both wired and wireless LANs are commonly used in small business and WM clinics (less than five computers). A typical setting in a medium-large clinic contains wired access in examination rooms, administrative areas and documentation scanning (Stream and Fletcher, 2008). Wireless LAN can provide mobility, for example, when mobile laptops and tablets are used in the clinic. For CM clinics that are small and not equipped in IT at all, it may be good to start with wired LAN for the following reasons:
It allows greater amount of data transmission (Stream and Fletcher, 2008).
Speed can be much faster with gigabit routers and it is not sensitive to dead spots which occur sometimes during consultation in wireless LAN (Stream and Fletcher, 2008).
It is relatively more secure and stable as once the network security or firewall is installed and configured, the network is generally well protected, particularly if it is not directly connected to the internet (Stream and Fletcher, 2008).
As CM practices become more common in WM clinics and hospitals, and more computers and devices are used, wireless LAN may be a better choice as it provides great mobility which allows information access anywhere in the practice without limitation to fixed stations. Many large hospitals use wired network as the core backbone and wireless access in specific areas (Stream and Fletcher, 2008).

236 C.H. Lin et al.
4.3.2 Transaction
Transactional IT investment has been consistently linked to improve performance as its main purpose is to process the basic and often repeated transactions in an organisation with the replacement of computer technology; hence, it helps reduce cost (Weill and Ross, 2009). For example, in CM clinics, material management (including CM, equipment and other clinical supplies) is a repetitive and resource-demanding task. The quality of CM varies by a range of parameters, which include location source, age, production process, authentication, company standards, etc. All this information must be available to assist in diagnosis and treatment, as it directly affects patients’ health. It also needs to be managed for ordering and re-ordering purposes. If a certain medicine is flagged as bad or dangerous, it should not be ordered for prescription and it should have an alert message to support the CDS. Managing the ordering can shorten the waiting period as reordering can be triggered as soon as a reminder appears when stock is close to running out. This ensures no overstocking and shortages of medicines for prescriptions.
4.3.3 Information & strategy
Medical workers are heavily engaged with knowledge and information; hence, it is very important to invest in information systems which provide the support and control for decision-making, communication and quick and quality information at the point of care (Lin et al., 2013). Literature search has shown a lot of evidences that medical supply and inventory management is one of the important areas of healthcare delivery (Xu et al., 2011). Effective medical supply management systems can reduce medical cost and ensure quality (ibid). It is ideal that these systems develop and follow one universal standard and regulation to avoid different versions and confusion. They should also be placed at a centre point or pool where information can be shared and accessed by different healthcare providers at real-time with security protection.
Strategically and ideally, all CM should be integrated to WM so that both medicines can be practiced alongside to take the best of each and compensate for the potential weaknesses in each of them. The reality is this may take quite a long time as every country’s situation is different. However, knowing the destination and goal gives all countries guidance in planning strategic IT investments. Research shows that it is usually safer, less costly and has a higher chance of success by implementing the change in one module or level gradually (Weill and Ross, 2009).
5 Discussion
5.1 WM medicine management system
Current medicine supply management systems and Enterprise Resource Planning (ERP) systems in WM hospitals and clinics are not the best fit for healthcare services (Botta and Pierre, 2006). Some of the reasons are the following:
Healthcare institutions are complex, multi-functional, information-intensive organisations (Lin et al., 2013). Hospitals and clinics process large volumes of data generated by diverse systems in clinics, laboratories, pharmacies, material warehouses

Using IS/IT to support the delivery of Chinese medicine 237
and administrations (ibid). It requires specialised applications, developed by many different vendors, which need to communicate with each other. Additionally, integration problems also occur with applications built in-house and off-the-shelf software packages that are used in different departments and operation areas. Therefore, an absolute homogeneous information system platform is not the best option for a complex and dynamic business environment such as healthcare (Stefanou and Andreas, 2006).
Use of different units of measurements of drug doses among ERP system stakeholders such as pharmacy, clinics and hospitals (Stefanou and Andreas, 2006). From Figure 1, we know there are many forms of CM treatment. Each medicine is measured with a different tool and in a different way. Inconsistencies and variations will result in medical errors, which can lead to loss of life.
There still is an IT acceptance issue for some physicians. This is more of the case with new solutions and system updates. One of the reasons behind these updates is organisation product development and profit (Botta and Pierre, 2006). Many ERP vendors adopt the strategy of implementing core business functions first to their customers, then sale the updated system versions as separate products (ibid). However, this leads to misunderstandings between the physicians themselves, nurses, pharmacists and suppliers (ibid). In Australia, since the majority of CM practitioners are still using the manual system (Lin et al., 2013), IT awareness and acceptance margin is relatively larger than WM doctors. To avoid misunderstandings, a study of a suitable system is necessary to reduce frequent system changes and updates after implementation.
5.2 CM Medicine Management System (CMMS)
The updated documentation and inventory of CM consists of 500–600 species of commonly used medicines based on the Chinese National Corporation of Traditional & Herbal Medicine database, published by Science Press, Beijing, in 1994–1995 (Sheng-Ji, 2001). Additionally, in Chinese clinics, many different sizes of acupuncture needles are used for different purposes. Managing the vast amount of CM medicine inventory is an essential but labour-intensive task to the CM clinics; however, there is no suitable CMMS available currently (Lin et al., 2013). Furthermore, the following aspects are also important reasons of developing a suitable CMMS:
System success factors: IS/IT project and portfolio implementation success factors have been widely discussed in the literature (Xue et al., 2005). Despite the technical issues, context-related factors such as business environment and culture must be seriously considered (ibid). As mentioned earlier, most clinical management systems (including medicine and supply management) are designed and developed for WM. They are crafted and customised to suit the WM environment and practice. Simply adopting and using these systems for CM has a great potential of implementation failure. Examples of this can be found in the attempt by SAP and Oracle in 1988–1990 to take the Chinese ERP market (ibid). CM practice has its unique knowledge, methods and treatments. A CMMS must be designed and created for this specific business environment.
238 C.H. Lin et al.
Single drug vs. multi-ingredient prescription: WM often offers single-drug treatments, while CM offers mixed ingredient prescriptions and treatments (Li et al., 2008). A typical herb prescription contains over five medicines, with each in different amounts (Kaptchuk, 2000). Each patient has his/her unique prescription; the combination of the herbs and their quantity/amount make a big difference (ibid). This makes it more complicated in managing and tracking the medicine in stock.
Quality: CM quality refers to a range of parameters which include location source, age, production process, authentication, company standards, etc. All this information must be available to assist in diagnosis/treatment usages as it directly affects patients’ health. It also needs to be managed for ordering and reordering purposes. If a certain medicine is flagged as bad or dangerous, it should not be ordered for prescription, and it should have an alert message to support the CDS. Quality is a golden thread in connecting with the patients. A well-known top CM clinic’s reputation relies on its physicians’ knowledge, skills and experience as well as the medicine quality and its efficacy.
Control: managing the ordering can shorten the waiting period as reordering can be triggered as soon as a reminder appears when supply is close to running out of stock. This ensures no overstocking or shortage of medicines for prescriptions. The forecasting on patient visiting pattern and disease pattern will help the clinic to predict what medicine should be ordered, in what amount and in what season.
Cost: quality and control on medicine and supplies lead to saving time and money. With the installation of CMMS, clinical resources will be better managed and used, and thus reduce cost. Human errors such as omitting/forgetting to reorder will also be reduced.
5.3 Conceptual model
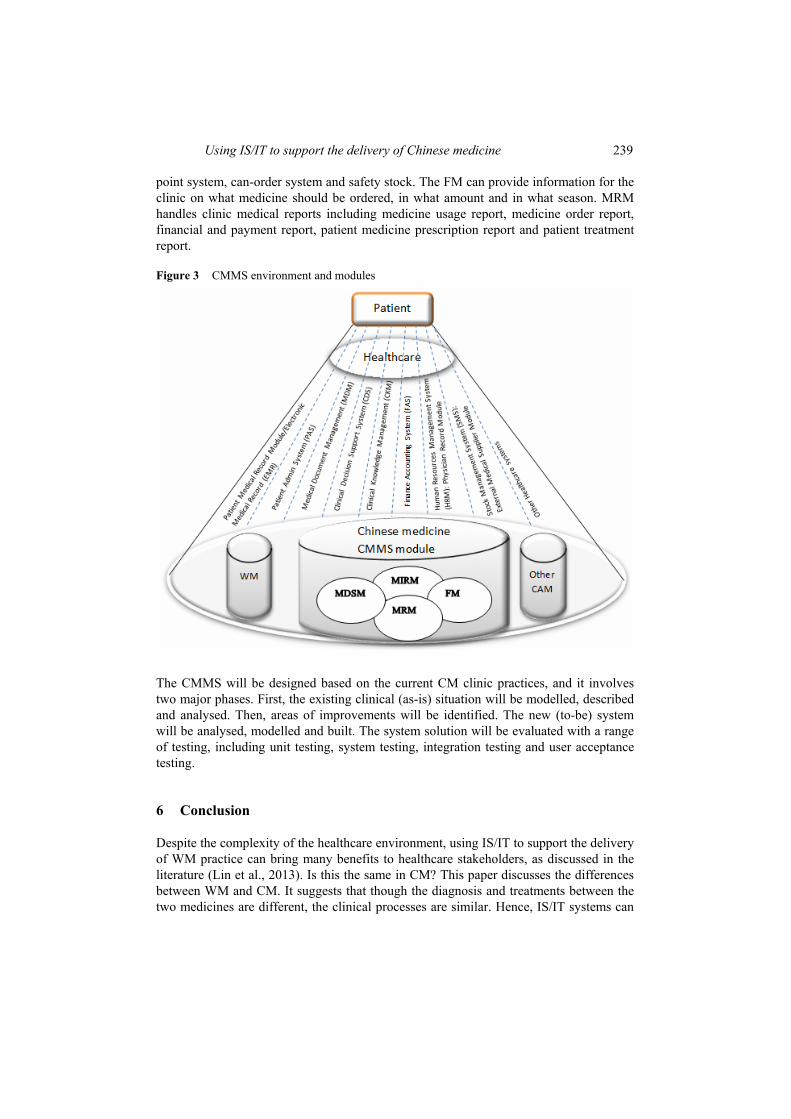
Earlier in this paper, we have identified some of the most common clinical management systems that can be developed and implemented in CM clinics. The CMMS in this study is a sub-system. Figure 3 illustrates the environment, the players, the components and the integration of the development of the Chinese medicine system with other sectors and systems of healthcare. In this figure, the primary driver/player is the patient. That is because without the patient, none of the services are necessary regardless of WM or CM. Therefore, all activities, systems and healthcare sectors share a fundamental goal: deliver quality and effective healthcare services to patients at point of care.
When the patient is in need of care, he/she can trigger any of the components in Figure 3: WM, CM and/or other CAM. Ideally, the listed systems and modules under healthcare can be shared and information can be accessed and used across sectors. The broken line/link has the indication of communication and integration. Under the Chinese medicine CMMS, there are few internal modules. They are Medicine Item Record Module (MIRM), Medicine Decision Support Module (MDSM), Forecast Module (FM) and Medicine Reports Module (MRM). The MIRM contains detailed information about medicine items including item name, category, item model, location at the clinic, vendor, manufacturer, reorder level, stock level, discontinued comments, transaction number, quantity, current on-hand quantity, transaction type and payment information. The MDSM can support demand analysis, point of use, economic order quantity, reorder
Using IS/IT to support the delivery of Chinese medicine 239
point system, can-order system and safety stock. The FM can provide information for the clinic on what medicine should be ordered, in what amount and in what season. MRM handles clinic medical reports including medicine usage report, medicine order report, financial and payment report, patient medicine prescription report and patient treatment report.
Figure 3 CMMS environment and modules
The CMMS will be designed based on the current CM clinic practices, and it involves two major phases. First, the existing clinical (as-is) situation will be modelled, described and analysed. Then, areas of improvements will be identified. The new (to-be) system will be analysed, modelled and built. The system solution will be evaluated with a range of testing, including unit testing, system testing, integration testing and user acceptance testing.
6 Conclusion
Despite the complexity of the healthcare environment, using IS/IT to support the delivery of WM practice can bring many benefits to healthcare stakeholders, as discussed in the literature (Lin et al., 2013). Is this the same in CM? This paper discusses the differences between WM and CM. It suggests that though the diagnosis and treatments between the two medicines are different, the clinical processes are similar. Hence, IS/IT systems can

240 C.H. Lin et al.
be developed and implemented in CM clinics in assisting its daily clinical activities. In this paper, IT investment portfolio portions are studied and a CMCMS development model is analysed and proposed. Currently existing CMCMS systems are identified and the advantages and disadvantages of the systems are discussed. These findings provide valuable inputs for designing a suitable CMCMS. The importance of system integration is addressed in this paper. CMCMS and its sub-systems are inter-linked and information is shared between the internal and the external modules. This paper provides a literature analysis for developing a suitable CMCMS and its sub-systems. It also offers a platform for designing and creating a CMMS, which is proposed as the next step in this research.
Reference
Austin, C.J. and Boxerman, S.B. (2003) Information Systems For Healthcare Management, Health Administration Press, Chicago, IL.
Ball, M.J. and Lillis, J. (2001) ‘E-health: transforming the physician/patient relationship’, International Journal of Medical Informatics, Vol. 61, No. 1, pp.1–10.
Bates, D.W. (2000) ‘Using information technology to reduce rates of medication errors in hospitals’, British Medical Journal, Vol. 320, No. 7237, pp.788–791.
Botta, G.V. and Pierre, A.M. (2006) ‘An investigation into the use of ERP systems in the service sector’, International Journal of Production Economics, Vol. 99, No. 1, pp.202–221.
Chi, C. (1994) ‘Integrating traditional medicine into modern health care systems: examining the role of Chinese medicine in Taiwan’, Social Science & Medicine, Vol. 39, No. 3, pp.307–321.
COCIR (European Coordination Committee of the Radiological, Electromedical and Healthcare IT Industry) (2012) COCIR eHealth Toolkit: Contributing to the European Digital Agenda, 2nd ed. Available online at: http://www.cocir.org/site/fileadmin/Publications_2011/ehealth_ toolkit_link2.pdf (accessed on 27 July 2014).
CAHU (Complementary and Alternative Healing University) (2013) Dictionary of Chinese herbs. Available online at: http://alternativehealing.org/Chinese_herbs_dictionary_original_copy.htm (accessed on 27 July 2014).
Dasherb (2013) Dasherb herb database. Available online at: http://www.dasherb.com/database/ index.html (accessed on 27 July 2014).
Goodson, B. (2005) ‘Ready for take-off: knowledge management infrastructure at EasyJet’, in Rao, M. (Ed.): Knowledge Management Tools and Techniques Practitioners and Experts Evaluate KM Solutions, Elsevier, Burlington, MA, pp.147–154.
Gottschalk, P. (2005) Strategic Knowledge Management Technology, Idea Group Publishing, Hershey, PA.
Hannan, T.J. (1996) ‘Electronic medical records’, in Hovenga, E., Kidd, M. and Cesnik, B. (Eds): Health Informatics: An Overview, Churchill Livingstone, South Melbourne, pp.133–148.
Hesketh, T. and Zhu, W.X. (1997) ‘Traditional Chinese medicine: one country, two systems’, British Medical Journal, Vol. 315, pp.115–117.
Hojabri, R. and Manafi, M. (2012) ‘Impact of using telemedicine on knowledge management in healthcare organisations: a case study’, African Journal of Business Management, Vol. 6, No. 4, pp1604–1613.
Huang, M.J. and Chen, M.Y. (2007) ‘Integrated design of the intelligent web-based Chinese medical diagnostic system (CMDS): systematic development for digestive health’, Expert Systems with Applications, Vol. 32, No. 2, pp.658–673.
Jupp, J. (2002) From White Australia to Woomera: The Story of Australian Immigration, Cambridge University Press, Cambridge.
Using IS/IT to support the delivery of Chinese medicine 241
Kaptchuk, T.J. (2000) Chinese Medicine: The Web That Has No Weaver, 2nd Rev. ed., Rider, London.
Lam, C.F.D., Leung, K.S., Heng, P.A., Lim, C.E.D. and Wong, F.W.S. (2012) ‘Chinese acupuncture expert system (CAES): a useful tool to practice and learn medical acupuncture’, Journal of Medical Systems, Vol. 36, No. 3, pp.1883–1890.
Lenz, R. and Reichert, M. (2007) ‘IT support for healthcare processes: premises, challenges, perspectives’, Data & Knowledge Engineering, Vol. 61, No. 1, pp.39–58.
Li, W.F., Jiang, J.G. and Chen, J. (2008) ‘Chinese medicine and its modernization demands’, Archives of Medical Research, Vol. 39, No. 2, pp.246–251.
Liao, Y.Q. (2011) Traditional Chinese Medicine, Cambridge University Press, Cambridge.
Lin, C.H., Yang, A.W.H., Pittayachawan, S. and Wickramasinghe, N. (2013) ‘Using IS/IT to support the delivery of Chinese medicine: the design of a Chinese medicine clinic system’, Proceedings of the 24th Australasian Conference on Information Systems, 4–6 December, Melbourne, Australia, pp.1–10.
Lin, C.H., Yang, A.W.H., Pittayachawan, S., Vogel, D. and Wickramasinghe, N. (2014) ‘Investigating the possibility for IS/IT to support the delivery of Chinese medicine’, Proceedings of the 1st AIS-Journals Joint Author Workshop in ECIS, 7 June, Tel Aviv, Israel.
Liu, Z.W., and Liu, L. (2009) Essentials of Chinese Medicine, Springer, Berlin.
Lu, A.P., Jia, H.W., Xiao, C. and Lu, Q.P. (2004) ‘Theory of traditional Chinese medicine and therapeutic method of diseases’, World Journal of Gastroenterology, Vol. 10, No. 13, pp.1854–1856.
Lukman, S., He, Y. and Hui, S.C. (2007) ‘Computational methods for traditional Chinese medicine: a survey’, Computer Methods and Programs in Biomedicine, Vol. 88, No. 3, pp.283–294.
Microsoft (2011) Manifesto for a e-healthier Europe. Available online at: http://www.microsoft. com/nl-be/healthcare/knowledge-centre/microsoft-manifesto-for-a-e-healthier-europe.aspx (accessed on 27 July 2014).
Mitamura, Y. (2010) Electronic Document Management System, Medical Information System, Method for Printing Sheet of Chart Paper, and Sheet of Chart Paper, U.S. Patent No. 7,654,463.
Morr, C.E. and Subercaze, J. (2010) Handbook of Research on Developments in E-Health and Telemedicine: Technological and Social Perspectives, IGI Global, Hershey, PA.
Nonaka, I. (1994) ‘A dynamic theory of organisational knowledge creation’, Organisation Science, Vol. 5, No. 1, pp.14–37.
Nonaka, I., Reinmoeller, P. and Senoo, D. (1998) ‘Management focus: the “ART” of knowledge: systems to capitalize on market knowledge’, European Management Journal, Vol. 16, No. 6, pp.673–684.
North, N. (2008) Immigrant Doctors Practising Non-Western Medicine: A Study of Self-Employed Immigrant Chinese and Indian Doctors Practising Non-Biomedical Traditions of Medicine, New Settlers Programme, Massey University, Palmerston North, New Zealand.
Polanyi, M. (1966) ‘The logic of tacit inference’, Philosophy, Vol. 41, No. 155, pp.1–18.
Quintas, P., Lefrere, P. and Jones, G. (1997) ‘Knowledge management: a strategic agenda’, Long Range Planning, Vol. 30, No. 3, pp.385–391.
Rao, M. (2005) Knowledge Management Tools and Techniques Practitioners and Experts Evaluate KM Solutions, Elsevier Butterworth-Heinemann, Burlington, MA.
Sheng-Ji, P. (2001) ‘Ethnobotanical approaches of traditional medicine studies: some experiences from Asia’, Pharmaceutical Biology, Vol. 39, No. 1, pp.74–79.
Shi, J. and Lu, L. (2006) ‘Traditional Chinese medicine in treatment of opiate addiction’, Acta Pharmacologica Sinica, Vol. 27, No. 10, pp1303–1308.

242 C.H. Lin et al.
Smart TCM (2014) Smart Chinese medicine clinic record management system. Available online at: http://www.smarttcm.com/index-E.html (accessed on 27 July 2014).
Stefanou, C.J. and Andreas, R. (2006) ‘ERP integration in a healthcare environment: a case study’, Journal of Enterprise Information Management, Vol. 19, No. 1, pp.115–130.
Stream, G. and Fletcher, J. (2008) ‘Demystifying computer networks for small practices’, Family Practice Management, Vol. 15, No. 1, pp.25–28.
Studnicki, J., Berndt, D.J. and Fisher, J.W. (2008) Using Information Systems for Public Health Administration, Public Health Administration: Principles for Population-Based Management, 2nd ed., Jones and Bartlett Publishers, Sudbury, MA.
Swisher, J.R., Jacobson, S.H., Jun, J.B. and Balci, O. (2001) ‘Modeling and analyzing a physician clinic environment using discrete-event (visual) simulation’, Computers & Operations Research, Vol. 28, No. 2, pp.105–125.
TCM Organiser (2014) TCM Organiser: clinic management system – a complete solution to manage a Chinese medicine and acupuncture clinic. Available online at: http://www. tcmsoftware.ca/english/default_frame.htm (accessed on 27 July 2014).
Wang, Z.G., Chen, P. and Xie, P.P. (1999) History and Development of Traditional Chinese Medicine, Science Press, Beijing.
Weill, P. and Aral, S. (2006) ‘Generating premium returns on your IT investments’, Sloan Management Review, Vol. 47, No. 2, pp.39–48.
Weill, P. and Ross, J.W. (2009) It Savvy: What Top Executives Must Know to Go from Pain to Gain, Harvard Business Press, Boston, MA.
Weill, P., Subramani, M. and Broadbent, M. (2012) ‘Building IT infrastructure for strategic agility’, MIT Sloan Management Review, Vol. 44, pp.57–66.
Wickramasinghe, N. (2013) ‘Implicit and explicit knowledge assets in healthcare’, in Bali, R., Troshani, I., Goldberg, S. and Wickramasinghe, N. (Eds): Pervasive Health Knowledge Management, Springer, New York, pp.15–26.
Wickramasinghe, N. and Schaffer, J.L. (2010) Realizing Value Driven Patient Centric Healthcare through Technology, IBM Centre for The Business of Government, Washington, DC.
Wickramasinghe, N., Geisler, E. and Schaffer, J.L. (2006) ‘Realising the value proposition for healthcare by incorporating KM strategies and data mining techniques with the use of information and communication technologies’, International Journal of Healthcare Technology and Management, Vol. 7, No. 3, pp.303–318.
WHO (World Health Organisation) (2013) WHO traditional medicine strategy: 2014–2023. Available online at: http://www.who.int/medicines/publications/traditional/trm_strategy14_ 23/en/ (accessed 27 July 2014).
Wyatt, J.C. (2001) ‘Management of explicit and tacit knowledge’, Journal of the Royal Society of Medicine, Vol. 94, No. 1, pp.6–9.
Xu, E., Marek W. and Deborah B.B. (2011) ‘Development of an integrated medical supply information system’, Enterprise Information Systems, Vol. 5, No. 3, pp.385–399.
Xue, C.L, Zhang, A.L., Lin, V., Costa, C.D. and Story, D.F. (2007) ‘Complementary and alternative medicine use in Australia: a national population-based survey’, The Journal of Alternative and Complementary Medicine, Vol. 13, No. 6, pp.643–650.
Xue, C.C. and O’Brien, K.A. (2003) ‘Modalities of Chinese medicine’, in Leung, P.C., Xue, C.C. and Cheng, Y.C. (Eds): A Comprehensive Guide to Chinese Medicine, World Scientific Publishing, River Edge, NJ, pp.19–46.
Xue, Y., Liang, H., Boulton, W.R. and Snyder, C.A. (2005) ‘ERP implementation failures in China: case studies with implications for ERP vendors’, International Journal of Production Economics, Vol. 97, No. 3, pp.279–295.

Using IS/IT to support the delivery of Chinese medicine 243
Yang, A.W., Allan, G., Li, C.G. and Xue, C.C. (2009) ‘Effective application of knowledge management in evidence-based Chinese medicine: a case study’, Evidence-based Complementary and Alternative Medicine, Vol. 6, No. 3, pp.393–398.
Zhao, Y.K., Tsursui, T., Endo, A., Minato, K. and Takahashi, T. (1994) ‘Design and development of an expert system to assist diagnosis and treatment of chronic hepatitis using traditional Chinese medicine’, Informatics for Health and Social Care, Vol. 19, No. 1, pp.37–45.
Zhu, B. and Wang, H.C. (2011) Basic Theories of Traditional Chinese Medicine, Jessica Kingsley Publishers, London.
Copyright © 2022 FDOKUMEN