Using Cognitive Mapping to Understand Problems Experienced by Family Caregivers of Persons with...
10
Journal of Clinical Psychology in Medical Settings, Vol. 11, No. 3, September 2004 ( C 2004) Using Cognitive Mapping to Understand Problems Experienced by Family Caregivers of Persons With Severe Physical Disabilities Richard M. Shewchuk, 1,4 Patricia A. Rivera, 2 Timothy R. Elliott, 2 and Alice M. Adams 3 Individuals who provide ongoing care for family members who have a chronic disease or disability are likely to encounter a wide array of problems that can compromise their own health and their ability to function effectively in a caregiving role. Structured focus group meetings were conducted to elicit a comprehensive list of the problems that caregivers expe- rienced during their first year of providing care to a person with a severe physical disability. A separate group of caregivers ( N = 60) individually sorted problems into piles based on their similarity and assigned relative importance to each problem. The aggregated data were an- alyzed with multidimensional scaling and hierarchical cluster analysis. Results indicated that caregivers cognitively organize problems along three dimensions: I. Centeredness–caregiver versus patient-oriented; II. Relationship Demands–physical versus emotional; and III. Care- giver Burden–time versus emotional. Additionally, 6 clusters of substantively similar prob- lems were identified and prioritized in terms of personal relevance: Basic Needs (lowest); Perceived Constraints; Caregiver Challenges; Patient Resentment; Patient Withdrawal; and Pa- tient Intrapsychic Adjustment (highest). Further examination of the organization of problems identified by caregivers should provide important insights about the experience of caregivers and how more targeted interventions can be developed to address their specific needs. KEY WORDS: cognitive mapping; rehabilitation; caregiving; spinal cord injury. The health care landscape in the United States has undergone many dramatic changes in the past 20 years. Rising health care costs have led to public and private initiatives aimed at curbing the rate of in- crease, including capitated payment mechanisms, care coordination efforts, and shortened lengths of stay in hospitals. At the same time, the aging of the pop- ulation, the increasing prevalence of chronic condi- tions, and a shortage of nursing personnel have placed 1 Department of Health Services Administration, University of Alabama at Birmingham, Birmingham, Alabama. 2 Department of Psychology, University of Alabama at Birming- ham, Birmingham, Alabama. 3 Department of Health Science, Armstrong Atlantic University, Savannah, Georgia. 4 Correspondence should be addressed to Richard M. Shewchuk, Department of Health Services Administration, University of Alabama at Birmingham, 1675 University Blvd. (Webb 560), Birmingham, Alabama 35294-3361. increased burdens on the health care system (Donelan et al., 2002). Chronic health conditions are the major cause of illness, disability, and death in the United States, accounting for 68% of all health care expenditures, and representing perhaps the greatest single chal- lenge facing our health care system (Frank, 1997). In 1995, nearly 100 million Americans were living with one or more chronic conditions, costing more than $503 billion in health care expenditures. By 2050, those numbers are expected to increase to 167 million people with chronic conditions, costing $906 billion (Institute for Health and Aging, UCSF, 1996). Despite the evidence of the need for a greater emphasis on the care and management of chronic health conditions, the health care system remains primarily focused on acute care and the treatment of episodic illness (Shewchuk & Elliott, 2000). The 141 1068-9583/04/0900-0141/0 C 2004 Springer Science+Business Media, Inc.
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Using Cognitive Mapping to Understand Problems Experienced by Family Caregivers of Persons with...
Journal of Clinical Psychology in Medical Settings, Vol. 11, No. 3, September 2004 ( C© 2004)
Using Cognitive Mapping to Understand Problems Experienced by FamilyCaregivers of Persons With Severe Physical Disabilities
Richard M. Shewchuk,1,4 Patricia A. Rivera,2 Timothy R. Elliott,2 and Alice M. Adams3
Individuals who provide ongoing care for family members who have a chronic disease ordisability are likely to encounter a wide array of problems that can compromise their ownhealth and their ability to function effectively in a caregiving role. Structured focus groupmeetings were conducted to elicit a comprehensive list of the problems that caregivers expe-rienced during their first year of providing care to a person with a severe physical disability. Aseparate group of caregivers (N = 60) individually sorted problems into piles based on theirsimilarity and assigned relative importance to each problem. The aggregated data were an-alyzed with multidimensional scaling and hierarchical cluster analysis. Results indicated thatcaregivers cognitively organize problems along three dimensions: I. Centeredness–caregiverversus patient-oriented; II. Relationship Demands–physical versus emotional; and III. Care-giver Burden–time versus emotional. Additionally, 6 clusters of substantively similar prob-lems were identified and prioritized in terms of personal relevance: Basic Needs (lowest);Perceived Constraints; Caregiver Challenges; Patient Resentment; Patient Withdrawal; and Pa-tient Intrapsychic Adjustment (highest). Further examination of the organization of problemsidentified by caregivers should provide important insights about the experience of caregiversand how more targeted interventions can be developed to address their specific needs.
KEY WORDS: cognitive mapping; rehabilitation; caregiving; spinal cord injury.
The health care landscape in the United Stateshas undergone many dramatic changes in the past20 years. Rising health care costs have led to publicand private initiatives aimed at curbing the rate of in-crease, including capitated payment mechanisms, carecoordination efforts, and shortened lengths of stay inhospitals. At the same time, the aging of the pop-ulation, the increasing prevalence of chronic condi-tions, and a shortage of nursing personnel have placed
1Department of Health Services Administration, University ofAlabama at Birmingham, Birmingham, Alabama.
2Department of Psychology, University of Alabama at Birming-ham, Birmingham, Alabama.
3Department of Health Science, Armstrong Atlantic University,Savannah, Georgia.
4Correspondence should be addressed to Richard M. Shewchuk,Department of Health Services Administration, University ofAlabama at Birmingham, 1675 University Blvd. (Webb 560),Birmingham, Alabama 35294-3361.
increased burdens on the health care system (Donelanet al., 2002).
Chronic health conditions are the major causeof illness, disability, and death in the United States,accounting for 68% of all health care expenditures,and representing perhaps the greatest single chal-lenge facing our health care system (Frank, 1997).In 1995, nearly 100 million Americans were livingwith one or more chronic conditions, costing morethan $503 billion in health care expenditures. By2050, those numbers are expected to increase to167 million people with chronic conditions, costing$906 billion (Institute for Health and Aging, UCSF,1996).
Despite the evidence of the need for a greateremphasis on the care and management of chronichealth conditions, the health care system remainsprimarily focused on acute care and the treatmentof episodic illness (Shewchuk & Elliott, 2000). The
141
1068-9583/04/0900-0141/0 C© 2004 Springer Science+Business Media, Inc.
142 Shewchuk, Rivera, Elliott, and Adams
combination of these trends has resulted in increaseddemands being placed on persons with chronic healthconditions and their family members and otherinformal caregivers who support them (Hoffman,Rice, & Sung, 1996). In 1998, approximately onequarter of American adults reported having providedcare for an ill, disabled, or aged family memberor friend during the previous year (Donelan et al.,2002). For many caregivers, these tasks require asubstantial time commitment: 20% of caregiversprovide full-time or constant care, 37% providehighly intensive care, and 41% have been servingas caregivers for 5 years of more (Donelan et al.,2002). The value of caregiving services providedby family caregivers—usually without any financialcompensation—is estimated to be $257 billion (Levit,Smith, Cowan, Lazenby, & Martin, 2001).
A considerable amount of research has been con-ducted on the costs incurred by and burdens placedon family members of persons living with chronicconditions, providing valuable insights into the ex-periences they encounter in their caregiving careers(Aneshensel, Pearlin, Mullan, Zarit, Whitlatch, 1995)(Pearlin, Mullan, Semple, & Skaff, 1990). Collec-tively, the research provides ample evidence that care-givers are at an increased risk for problems withdistress, depression, and well-being, as well as theirphysical health (for reviews, see Schulz et al., 1997;Schulz & Quittner, 1998). Descriptive studies haveshown that caregivers of people with physical dis-ability experience more distress than noncaregivers(e.g., Weitzenkamp, Gerhart, Charlifue, Whiteneck,& Savic, 1997), and are more likely to report having aserious or chronic illness or disability (Donelan et al.,2002). Caregivers are particularly susceptible to inter-related problems with physical health, anxiety, and de-pression over the first year of their caregiving career,and these outcomes are sensitive to changes in so-cial support experienced by the caregiver (Shewchuk,Richards, & Elliott, 1998).
Longitudinal studies indicate that caregivers areat risk for disruptions in cardiovascular and immunefunctioning (Vitaliano, 1997) and wound healing(Kiecolt-Glaser, Marucha, Malarkey, Mercado, &Glaser, 1995), and that their psychological and phys-ical problems may be exacerbated as they neglecttheir own health needs (Burton, Newsom, Schulz,Hirsch, & German, 1997). Elderly caregivers whohave a history of chronic illness and are themselvesexperiencing caregiver stress have a 64% higher mor-tality rate than their non-caregiving peers (Schulz &Beach, 1999).
Still, much remains unknown about the prob-lems encountered by caregivers and caregivers’ per-ceptions of their experiences. For instance, the effectsof caregiving are by no means uniform, as evidencedby the varying levels of distress seen in those who havebeen subjected to similar caregiving demands. Manystudies now acknowledge that caregiver adjustmentmay be influenced by myriad individual differencesand environmental variables (Elliott & Shewchuk,2002). Paradoxically, some research shows that a num-ber of caregivers may not experience any appreciabledegree of elevated distress, and may, in fact, derive asense of well-being and personal meaning in provid-ing care (Donelan et al., 2002; Kramer, 1997; Miller& Lawton, 1997). Additionally, although there is aclear consensus that family caregiving is not a staticevent or a single behavior, but is instead a complexdynamic process that unfolds over time, the observeddifferential patterns of experiences between differentcaregivers or within the same caregiver over time arenot well understood (Shewchuk & Elliott, 2000)
Thus, it is not surprising that the analysis ofnon-time-order data contributes to findings in whichthe “explained variance in physical and psychologicaloutcomes has remained relatively modest” (Thoits,1995, p. 68). Although theoretical models that definevariables and specify relationships in an a priorifashion may show statistical associations betweencontextual variables (such as demographic charac-teristics, type of disability, or type of relationshipbetween the caregiver and the recipient) and out-comes, they do little to reveal the inner workings ofthe caregiving experience.
In order to gain a better understanding of the dif-ferent experiential journeys that individual caregiversnegotiate over their careers and the “black box” be-tween characteristics and outcomes, and to promotea more participatory ethic in service delivery to per-sons who live with chronic health conditions, we mustacknowledge caregivers as experts on the “realitiesof their daily lives” (Mechanic, 1998, p. 284). Further-more, if we are to develop programs to assist fam-ily caregivers, it is imperative that we understand theunique problems and concerns as they experience andidentify them (Elliott, 2002). Effective program andpolicy development for family caregivers and theircare recipients may be realized when these peopleare involved in health care partnerships in which theycan exercise some degree of choice, control, input,and direction in the delivery of services (Kosciulek,2000). Qualitative assessment devices can help us un-derstand the experience, needs, and solutions from the

Cognitive Mapping 143
perspective of caregivers so that relevant and strate-gic programs and services might ensue (Elliott, 2002).Qualitative methods are uniquely suited to this taskbecause they can be used to help people identify, ar-ticulate, and prioritize the problems they encounterin ways that can help us develop programs and un-derstand needs that may not be readily apparent tothese consumers (Kurylo, Elliott, & Shewchuk, 2001;Shewchuk, Franklin, Harrington, Davies, & Windle,2004).
This paper describes a card-sort approach,used in a community problem-solving interven-tion, designed to uncover the critical dimensionsof the caregiving experience from the perspective ofthe caregivers themselves, rather than from that of theresearchers. These methods allow the richness of thecaregivers’ experiences to emerge, illuminating pat-terns and underlying structures in a way that is likelyto be hindered by more traditional methods in whichthe researchers’ assumptions and a priori specifica-tions constrain analysis. These findings can then beemployed to empirically operationalize the ways thatcaregivers represent a variety of problems, formingthe basis for screening devices and programmatic in-terventions that are specifically targeted toward dif-ferent groups of caregivers.
METHODS
Participants
Participants included 11 men (M age = 47 years,SD = 5.93 years) and 49 women (M age = 41.73 years,SD = 9.46 years) who were assuming the role of care-giver for a family member who had recently incurred aspinal cord injury (SCI) and who were participating inan SCI inpatient rehabilitation program. The prepon-derance of women identified as caregivers in this sam-ple is reflective of the number of women who assumecaregiving roles for family members. The sample wascomprised of 38 Caucasian and 22 African Americanindividuals. Parents (n = 26) and spouses (n = 23)were over represented in the sample. Other caregiversincluded sisters (n = 5), adult children (n = 4), andbrothers (n = 2) of the patient. Of the care recipients,31 had complete lesions to the cord and 29 had incom-plete lesions; 28 of these persons had paraplegia, 29had tetraplegia, and three had either spinal stenosisor cauda equina.
As patients were admitted to the SCI inpatientrehabilitation program, admitting staff asked familymembers to identify who would be most likely to
assume responsibility for providing daily assistanceand care to the patient following discharge. Thisperson would then be available to participate ininpatient therapies and learn self-care regimens.These identified caregivers were then approachedby a trained research staff member and asked toparticipate in Project FOCUS, a program developedto provide ongoing, home-based education to familycaregivers of persons with SCI (cf. Kurylo, Elliott,& Shewchuk, 2001). Of the 85 people approached,60 agreed to participate and provided informedconsent; 20 persons were ineligible for a variety ofreasons (e.g., minimal involvement as a caregiver,unable to read materials, unstable relationship withpatient, etc.). Fifteen caregivers were eligible forthe study but declined to participate for personalreasons. There were no apparent systematic reasonsfor refusal into the study. Persons who agreed toparticipate in Project FOCUS were seen individuallyand administered measures of social problem-solvingabilities, depression, personal health, and general dis-tress. Half of the participants were randomly assignedto the experimental group of Project FOCUS, andhalf were randomly assigned to the control group.However, as part of the assessment process, bothgroups completed the two card-sort tasks describedbelow. This group of 60 caregivers comprised the firstwave of participants in Project FOCUS.
Procedure
Two card-sort activities, an unforced card sortand a forced card sort, were employed to investi-gate the ways in which participants cognitively orga-nize problems related to their caregiving roles. Bothcard-sort activities used identical sets of 24 cards,with each card containing a single statement reflect-ing some aspect or problem of the caregiving expe-rience. These statements were generated during anearlier phase of research through the use of nominalgroup technique (NGT) sessions to identify and ratethe specific problems experienced by caregivers ofpersons with severe physical disabilities (described inElliott & Shewchuk, 2002). The use of multiple NGTsessions, in which each subsequent session providedmarginally fewer additional statements, ensured thatwe collected a representative list of statements aboutcaregivers’ experiences.
Participants were asked first to complete the un-forced card-sort activity. The caregivers were asked toexamine the deck of 24 cards and divide the cards intodifferent stacks based on their perceived similarity
144 Shewchuk, Rivera, Elliott, and Adams
(Brown, 1986; Stephen, 1985). Caregivers were in-structed to use as many or as few stacks as they wished,and to move cards into different stacks until they weresatisfied with how the cards were arranged. Caregiverswere asked to provide a name for each stack to encour-age them to think about how the individual statementscontained within each stack overlap or share similarcharacteristics.
The data from the unforced card sort were col-lected to form an individual co-occurrence matrix foreach participant. The individual co-occurrence ma-trices were then aggregated across all participantsto form a group co-occurrence matrix. This matrixindicated the number of times each statement wassorted together with other statements, and, as such,the group’s overall perception of the similarity for anypair of statements.
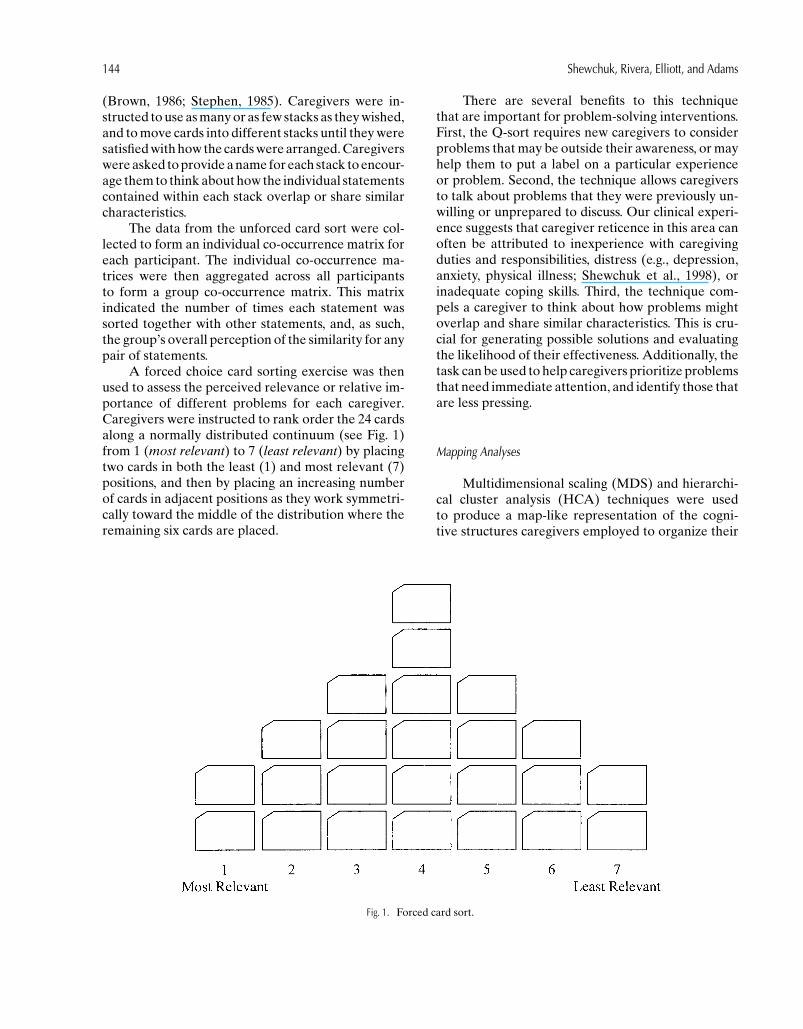
A forced choice card sorting exercise was thenused to assess the perceived relevance or relative im-portance of different problems for each caregiver.Caregivers were instructed to rank order the 24 cardsalong a normally distributed continuum (see Fig. 1)from 1 (most relevant) to 7 (least relevant) by placingtwo cards in both the least (1) and most relevant (7)positions, and then by placing an increasing numberof cards in adjacent positions as they work symmetri-cally toward the middle of the distribution where theremaining six cards are placed.
Fig. 1. Forced card sort.
There are several benefits to this techniquethat are important for problem-solving interventions.First, the Q-sort requires new caregivers to considerproblems that may be outside their awareness, or mayhelp them to put a label on a particular experienceor problem. Second, the technique allows caregiversto talk about problems that they were previously un-willing or unprepared to discuss. Our clinical experi-ence suggests that caregiver reticence in this area canoften be attributed to inexperience with caregivingduties and responsibilities, distress (e.g., depression,anxiety, physical illness; Shewchuk et al., 1998), orinadequate coping skills. Third, the technique com-pels a caregiver to think about how problems mightoverlap and share similar characteristics. This is cru-cial for generating possible solutions and evaluatingthe likelihood of their effectiveness. Additionally, thetask can be used to help caregivers prioritize problemsthat need immediate attention, and identify those thatare less pressing.
Mapping Analyses
Multidimensional scaling (MDS) and hierarchi-cal cluster analysis (HCA) techniques were usedto produce a map-like representation of the cogni-tive structures caregivers employed to organize their

Cognitive Mapping 145
perceptions of problems they encountered duringtheir caregiving responsibilities. The data obtainedfrom each caregiver’s unforced card-sort assessmentwere used to produce a 24 × 24 co-occurrence matrixthat indicated how often each problem was sorted to-gether with all other problems. Problems that are per-ceived as more similar are sorted together more fre-quently than those perceived as dissimilar. The indi-vidual co-occurrence matrices were then aggregatedto form a proximity matrix that indicated how care-givers, as a group, viewed the “perceptual distances”between each pair of problems. The group proximitymatrix (i.e., perceived distances) was analyzed by us-ing an alternating least squares (ALSCAL) nonmetricMDS procedure. MDS techniques essentially attemptto map or model the similarities among perceptual ob-jects in terms of a dimensional representation that iscommensurate with the decisional criteria that indi-viduals use in completing the sorting task.
In this study, this procedure mapped the similari-ties among sorted problems in terms of a geometricalrepresentation. Each problem can be identified as apoint on the map that shows where it is located rel-ative to other problems. Pairs of perceptually similarproblems (i.e., those sorted together frequently intothe same piles) are represented by points that are rela-tively closer on the map than problems that are viewedas perceptually dissimilar.
Within the MDS space, points are arranged alongorthogonal axes or dimensions that are assumed torepresent criteria that caregivers use in making de-cisions about how cards should be sorted. These di-mensions, then, provide some understanding of theunderlying or latent structure inherent in the reporteddata, and convey meaning about the primary distinc-tions that caregivers made in thinking about prob-lems. A qualitative interpretation of the MDS solu-tion involved examining the clustering of points atthe extreme edges of each dimension, and informalhypotheses for why the problems represented by op-posing points are perceived as different.
The adequacy of an MDS solution is determinedby assessing its representational accuracy and inter-pretability of as well as the goodness-of-fit relativeto its dimensional structure. An objective criterionthat is evaluated to determine the fit of a model isthe level of error (i.e., distortion) in the map, or the“stress” that results from the discrepancies betweenthe actual proximities data and the modeled repre-sentation of those data. Specific goodness-of-fit crite-ria (i.e., S-Stress and RSQ values) that indicate thelevel of correspondence between the observed simi-
larities of the perceived problems (i.e., data producedfrom the card-sort tasks) and the estimates of thosesimilarities as indicated by the map of interpoint dis-tances between pairs of problems are provided bymost MDS programs to evaluate the validity of amapped solution.
As a general rule, the level of error (S-Stress) fora derived model is inversely related to the numberof dimensions specified. Thus, an improvement in theoverall fit of any MDS model always can be achievedby specifying additional dimensions. Consequently, atrade-off must be achieved between the dimensionalcomplexity of a model and its overall fit.
Further insight into the meaning of the proxim-ity data was obtained by subjecting the coordinatesfrom the MDS solution (i.e., the values that definethe position of each problem on each dimension inthe multidimensional space) to a hierarchical clusteranalysis using Ward’s method. Generally, MDS anal-yses provide an understanding of perceptual data byuncovering the latent structure used in organizing per-ceptions and by representing the relative ordering ofthese perceptions along dimensions of more or less.Cluster analysis adds to this understanding by assign-ing various perceptions to exclusive membership cat-egories. In the present study, a hierarchical clusteringapproach was employed to identify coherent groupsof similarly perceived problems in terms of their clus-ter membership. When MDS and HCA proceduresare combined to examine the same proximity data,it is possible to observe how the dimensions of themap reflect both the ordering of the clusters and theordering of individual items within each cluster.
Although these procedures are computationallysophisticated, they are not based on statistical theory.Consequently the validity of a cognitive map is notstrictly sample size dependent, but instead, is a func-tion of the representational adequacy of the stimuliincluded in the sorting task as well as the participantswho complete the sorts.
RESULTS
Multidimensional Scaling
Solutions were obtained for models that includedbetween one and six dimensions. A three-dimensionalALSCAL MDS solution provided a relatively betterfit to the data than did a two-dimensional solution asjudged by a substantially lower stress score (0.133 vs.0.217), and a greater proportion of variance that was
146 Shewchuk, Rivera, Elliott, and Adams
accounted for by the mapped distances (R2 = 0.879vs. 0.780). Moreover, relative to a four-dimensionalsolution, the axes of the three-dimensional solutionwere more easily interpretable.
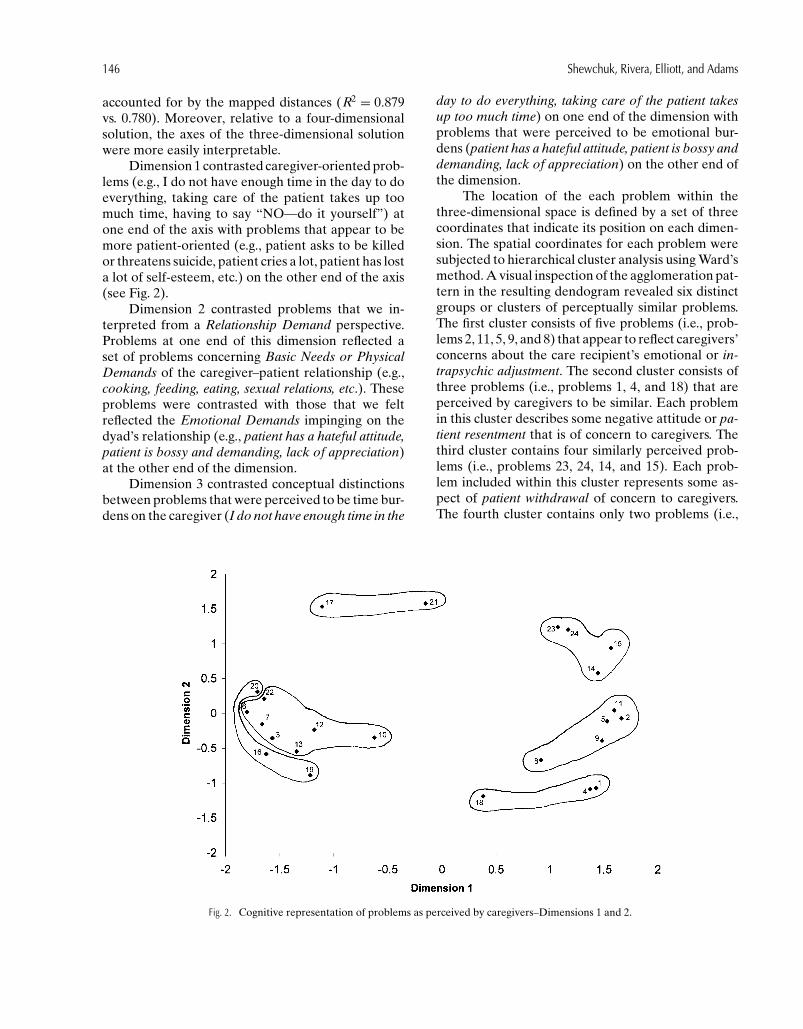
Dimension 1 contrasted caregiver-oriented prob-lems (e.g., I do not have enough time in the day to doeverything, taking care of the patient takes up toomuch time, having to say “NO—do it yourself”) atone end of the axis with problems that appear to bemore patient-oriented (e.g., patient asks to be killedor threatens suicide, patient cries a lot, patient has losta lot of self-esteem, etc.) on the other end of the axis(see Fig. 2).
Dimension 2 contrasted problems that we in-terpreted from a Relationship Demand perspective.Problems at one end of this dimension reflected aset of problems concerning Basic Needs or PhysicalDemands of the caregiver–patient relationship (e.g.,cooking, feeding, eating, sexual relations, etc.). Theseproblems were contrasted with those that we feltreflected the Emotional Demands impinging on thedyad’s relationship (e.g., patient has a hateful attitude,patient is bossy and demanding, lack of appreciation)at the other end of the dimension.
Dimension 3 contrasted conceptual distinctionsbetween problems that were perceived to be time bur-dens on the caregiver (I do not have enough time in the
Fig. 2. Cognitive representation of problems as perceived by caregivers–Dimensions 1 and 2.
day to do everything, taking care of the patient takesup too much time) on one end of the dimension withproblems that were perceived to be emotional bur-dens (patient has a hateful attitude, patient is bossy anddemanding, lack of appreciation) on the other end ofthe dimension.
The location of the each problem within thethree-dimensional space is defined by a set of threecoordinates that indicate its position on each dimen-sion. The spatial coordinates for each problem weresubjected to hierarchical cluster analysis using Ward’smethod. A visual inspection of the agglomeration pat-tern in the resulting dendogram revealed six distinctgroups or clusters of perceptually similar problems.The first cluster consists of five problems (i.e., prob-lems 2, 11, 5, 9, and 8) that appear to reflect caregivers’concerns about the care recipient’s emotional or in-trapsychic adjustment. The second cluster consists ofthree problems (i.e., problems 1, 4, and 18) that areperceived by caregivers to be similar. Each problemin this cluster describes some negative attitude or pa-tient resentment that is of concern to caregivers. Thethird cluster contains four similarly perceived prob-lems (i.e., problems 23, 24, 14, and 15). Each prob-lem included within this cluster represents some as-pect of patient withdrawal of concern to caregivers.The fourth cluster contains only two problems (i.e.,

Cognitive Mapping 147
problems 17 and 21) that are perceived as alike. Bothproblems in this cluster reflect some basic needs thatcaregivers have as concerns. The fifth cluster consistsof three issues that caregivers perceive as similar (i.e.,problems 16, 19, and 20). These problems overlap per-ceptually in terms of the various caregiver challengesthat they present. The sixth and largest cluster in-cludes seven perceptually related problems (i.e., prob-lems 10, 12, 3, 7, 13, 6, and 22). The problems groupedwithin this cluster represent a set of perceived con-straints that impinge on caregivers’ time. The results ofthe hierarchical cluster analysis are superimposed onthe multidimensional scaling maps (see Figs. 2 and 3).
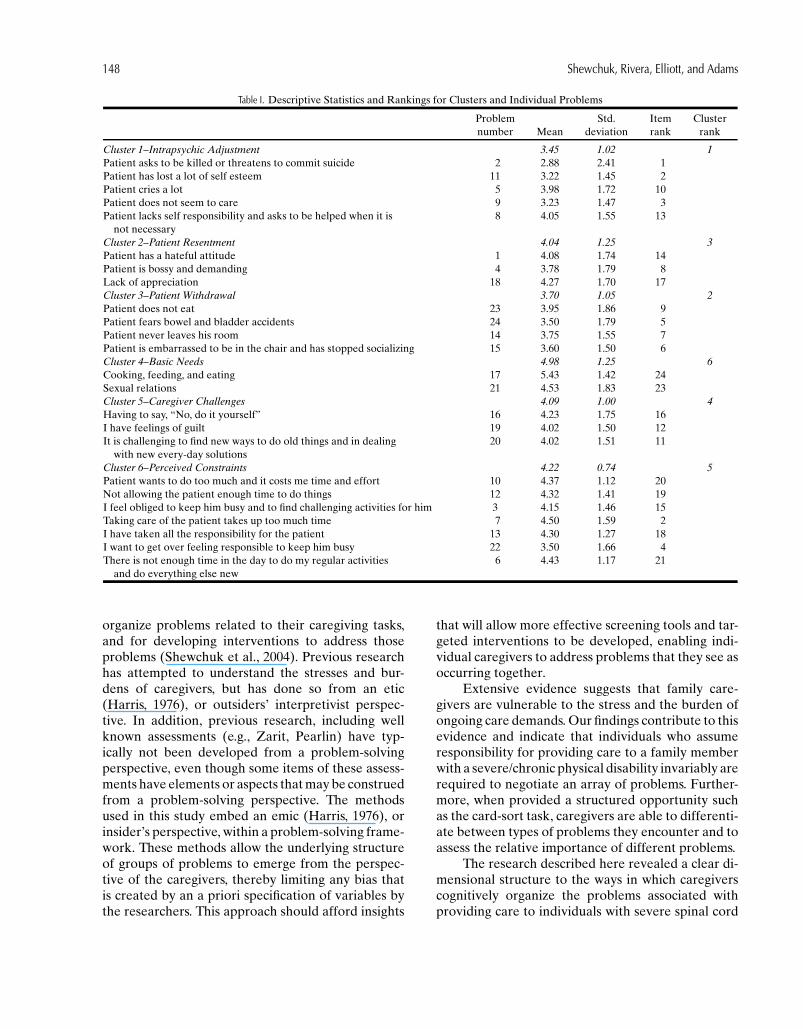
The relative importance ascribed to each prob-lem was assessed with the forced Q-sort task. Eachproblem was given a numerical value that reflected itsrelative position in the forced sort distribution (i.e., 1– most important to 7 – least important). The averagecluster importance was then obtained by calculatingthe mean value of perceived importance for all prob-lems included within a specified cluster. The mean andthe rank ordering of importance ratings for individualproblems and the six problem clusters are presentedin Table I. The three most important perceived prob-lems of caregivers in this study were: (1) Patient asksto be killed or threatens to commit suicide (M = 2.88,SD = 2.41); (2) Patient has lost a lot of self-esteem
Fig. 3. Cognitive representation of problems as perceived by caregivers–Dimensions 1 and 3.
(M = 3.22, SD = 1.45); and (3) Patient does not seemto care (M = 3.23, SD = 1.47). All three problemswere contained in the Intrapsychic Adjustment clus-ter which, not surprisingly, was perceived as the mostimportant cluster (M = 3.45, SD = 1.02). In orderof perceived importance, this cluster was followedby Patient Withdrawal (M = 3.70, SD = 1.05), PatientResentment (M = 4.04, SD = 1.25), Caregiver Chal-lenges (M = 4.09, SD = 0.962), Perceived Constraints(M = 4.22, SD = 0.74), and finally, Basic Needs (M =4.98, SD = 1.25). Pairwise comparisons indicated thatthe Intrapsychic Adjustment cluster was perceivedas significantly more important (p < .05) than theCaregiver Challenges, Perceived Constraints, and theBasic Needs clusters. Moreover, Patient Resentmentwas deemed significantly more important than BasicNeeds (p < .05); Patient Withdrawal was rated signif-icantly (p < .05) more important than Basic Needsand Perceived Constraints; and Caregiver Challengeswas rated significantly (p < .05) more important thanBasic Needs (see Fig. 3).
DISCUSSION
Cognitive mapping holds considerable poten-tial for understanding the ways in which individuals
148 Shewchuk, Rivera, Elliott, and Adams
Table I. Descriptive Statistics and Rankings for Clusters and Individual Problems
Problem Std. Item Clusternumber Mean deviation rank rank
Cluster 1–Intrapsychic Adjustment 3.45 1.02 1Patient asks to be killed or threatens to commit suicide 2 2.88 2.41 1Patient has lost a lot of self esteem 11 3.22 1.45 2Patient cries a lot 5 3.98 1.72 10Patient does not seem to care 9 3.23 1.47 3Patient lacks self responsibility and asks to be helped when it is 8 4.05 1.55 13
not necessaryCluster 2–Patient Resentment 4.04 1.25 3Patient has a hateful attitude 1 4.08 1.74 14Patient is bossy and demanding 4 3.78 1.79 8Lack of appreciation 18 4.27 1.70 17Cluster 3–Patient Withdrawal 3.70 1.05 2Patient does not eat 23 3.95 1.86 9Patient fears bowel and bladder accidents 24 3.50 1.79 5Patient never leaves his room 14 3.75 1.55 7Patient is embarrassed to be in the chair and has stopped socializing 15 3.60 1.50 6Cluster 4–Basic Needs 4.98 1.25 6Cooking, feeding, and eating 17 5.43 1.42 24Sexual relations 21 4.53 1.83 23Cluster 5–Caregiver Challenges 4.09 1.00 4Having to say, “No, do it yourself” 16 4.23 1.75 16I have feelings of guilt 19 4.02 1.50 12It is challenging to find new ways to do old things and in dealing 20 4.02 1.51 11
with new every-day solutionsCluster 6–Perceived Constraints 4.22 0.74 5Patient wants to do too much and it costs me time and effort 10 4.37 1.12 20Not allowing the patient enough time to do things 12 4.32 1.41 19I feel obliged to keep him busy and to find challenging activities for him 3 4.15 1.46 15Taking care of the patient takes up too much time 7 4.50 1.59 2I have taken all the responsibility for the patient 13 4.30 1.27 18I want to get over feeling responsible to keep him busy 22 3.50 1.66 4There is not enough time in the day to do my regular activities 6 4.43 1.17 21
and do everything else new
organize problems related to their caregiving tasks,and for developing interventions to address thoseproblems (Shewchuk et al., 2004). Previous researchhas attempted to understand the stresses and bur-dens of caregivers, but has done so from an etic(Harris, 1976), or outsiders’ interpretivist perspec-tive. In addition, previous research, including wellknown assessments (e.g., Zarit, Pearlin) have typ-ically not been developed from a problem-solvingperspective, even though some items of these assess-ments have elements or aspects that may be construedfrom a problem-solving perspective. The methodsused in this study embed an emic (Harris, 1976), orinsider’s perspective, within a problem-solving frame-work. These methods allow the underlying structureof groups of problems to emerge from the perspec-tive of the caregivers, thereby limiting any bias thatis created by an a priori specification of variables bythe researchers. This approach should afford insights
that will allow more effective screening tools and tar-geted interventions to be developed, enabling indi-vidual caregivers to address problems that they see asoccurring together.
Extensive evidence suggests that family care-givers are vulnerable to the stress and the burden ofongoing care demands. Our findings contribute to thisevidence and indicate that individuals who assumeresponsibility for providing care to a family memberwith a severe/chronic physical disability invariably arerequired to negotiate an array of problems. Further-more, when provided a structured opportunity suchas the card-sort task, caregivers are able to differenti-ate between types of problems they encounter and toassess the relative importance of different problems.
The research described here revealed a clear di-mensional structure to the ways in which caregiverscognitively organize the problems associated withproviding care to individuals with severe spinal cord

Cognitive Mapping 149
injuries. Multidimensional scaling analyses indicatedthat a three-dimensional model provided the best fitfor the data. The three dimensions along which care-givers categorize problems are depicted in two cog-nitive maps, representing the geographic placementof 24 problems in a three-dimensional space. Thefirst dimension contrasted caregiver-centered prob-lems and patient-centered problems. The second di-mension contrasted problems related to basic needsor physical demands with problems reflecting emo-tional demands. The third dimension contrasted timeburdens with emotional burdens on the caregiver.Each of the dimensions provides a clear delineation ofproblems along its continuum, with no interminglingof problems.
In addition, six distinct clusters of problems werederived from the data. Each cluster consisted of twoor more problems that were perceived by the care-givers to be similar to each other. The identified clus-ters were: (1) emotional or intrapsychic adjustment(5 problems); (2) patient resentment or negative at-titudes (3 problems); (3) patient withdrawal (4 prob-lems); (4) basic needs (2 problems); (5) caregiver chal-lenges (3 problems); and (6) perceived constraints (7problems).
The clusters were rated by the caregivers in termsof their perceived importance. Each of the threehighest rated clusters (emotional needs or intrapsy-chic adjustment, patient withdrawal, and patient re-sentment/negative attitudes) was more closely alignedwith care recipient or patient-oriented issues ratherthan caregiver-oriented issues (Dimension 1), andwith emotional issues rather than basic or physicalneeds (Dimension 2). The cluster with the highest per-ceived importance was related to the emotional needsor intrapsychic adjustment of the care recipients totheir condition. This cluster contained the three mostimportant problems overall (patient asks to be killedor threatens to commit suicide, patient has lost a lot ofself-esteem, and patient does not seem to care), whichserved as a conceptual anchor for the cluster. The im-portance rating for this cluster was significantly higherthan for the clusters reflecting problems with care-giver challenges, constraints, or basic needs.
The next three most important clusters, pa-tient withdrawal, patient resentment/negative atti-tudes, and caregiver challenges, were also rated assignificantly more important than the basic needscluster. This suggests that interventions should bemore focused on helping caregivers develop skills andstrategies to address patient-centered emotional is-sues, since failure to negotiate these various demands
and problems may be harmful to the well-being of thecaregiver (Haley et al., 1996; Shewchuk et al., 1998)as well as to the care recipient (Elliott & Shewchuk,2002).
Limitations
The specific context of this study—caregivers ofpersons with severe physical disabilities—limits thegeneralizability of the findings to other caregivinggroups (e.g., caregivers of persons with Alzheimers,mental illness, cystic fibrosis, or cancer). However, webelieve that the process employed in this study wouldbe useful in uncovering and understanding the under-lying structure of problems and concerns of any groupof caregivers.
Future Directions
A number of questions arise from the presentstudy that offer directions for future research. Onepossible avenue of investigation concerns the designand structure of the interventions to address the prob-lems experienced by caregivers. Should the differ-ent clusters of problems be addressed with differenttypes of problem solving interventions, for exam-ple skills training versus attitude-based interventions?Are there systematic effects that carry over from ad-dressing one set of problems to another set of prob-lems, that is, does developing a more positive orien-tation toward one set of problems generalize to othertypes of problems? There is also a need to address thetemporal structure of problem-solving interventions.How should they be staged? Are there advantagesto varying the sequence in which different types ofproblems are addressed?
Further investigation is also needed to determineif the caregiver problems uncovered here are general-izable to other types of caregivers, for example, thoseproviding care for people with Alzheimers, mental ill-ness, cystic fibrosis, or cancer. Are there dimensionsor meta-structures that characterize the general care-giving experience? Longitudinal studies are neededto reveal the dynamics of the caregiving dimensionsover time. To what degree are the problems experi-enced by caregivers enduring or resistant to change?Are there different stages or cycles of the caregivers’careers or the care recipients’ conditions in which dif-ferent dimensions emerge or dominate? Finally, fur-ther study is needed to determine how the dimensionsoperationalized in this study relate to other measures

150 Shewchuk, Rivera, Elliott, and Adams
known to be related to the caregiving experience, suchas depression, anxiety, or physical symptoms.
ACKNOWLEDGMENTS
This study was supported by a grant fromthe National Center for Injury Prevention andControl and the Disabilities Prevention Pro-gram, National Center for Environmental Health(grant number R49/CCR412718-01), and by Grant#R49/CCR403641, USDHHS, Centers for DiseaseControl and Prevention, National Center for InjuryPrevention and Control to the University of Alabamaat Birmingham. Its contents are solely the responsi-bility of the authors and do not necessarily representthe official views of the funding agency.
REFERENCES
Aneshensel, C. S., Pearlin, L. I., Mullan, J. T., Zarit, S. H., &Whitlatch, C. J. (1995). Profiles in caregiving: The unexpectedcareer. San Diego, CA: Academic Press.
Brown, S. R. (1986). Q technique and method: Principles andprocedures. In W. D. Berry & M. S. Lewis-Beck (Eds.), Newtools for social scientists: Advances in application and researchmethods (pp. 57–76). Beverley Hills, CA: Sage.
Burton, L. C., Newsom, J., Schulz, R., Hirsch, C., & German, P.(1997). Preventive health behaviors among spousal caregivers.Preventive Medicine, 26, 162–169.
Donelan, K., Hill, C. A., Hoffman, C., Scoles, K., Feldman, P. H.,Levine, C., et al. (2002). Challenged to care: Informal care-givers in a changing health system. Health Affairs, 21(4), 222–231.
Elliott, T. (2002). Defining our common ground to reach new hori-zons. Rehabilitation Psychology, 47, 131–143.
Elliott, T., & Shewchuk, R. (2002). Using the nominal group tech-nique to identify the problems experienced by persons livingwith severe physical disabilities. Journal of Clinical Psychologyin Medical Settings, 9, 65–76.
Frank, R. G. (1997). Lessons from the great battle: Health carereform 1992–1994. Archives of Physical Medicine and Reha-bilitation, 78, 120–124.
Haley, W. E., Roth, D. L., Coleton, M. I., Ford, G. R., West, C. A. C.,Collins, R. P., et al. (1996). Appraisal, coping, and social sup-port as mediators of well-being in Black and White family care-givers of patients with Alzheimer’s disease. Journal of Consult-ing and Clinical Psychology, 64, 121–129.
Harris, M. (1976). History and significance of the emic/etic distinc-tion. Annual Review of Anthropology, 5, 329–350.
Hoffman, C., Rice, D., & Sung, H. (1996). Persons with chronicconditions: Their prevalence and costs. JAMA, 276, 1473–1479.
Institute for Health and Aging, University of California, SanFrancisco. (1996). Chronic care in America: A 21st century chal-lenge. Princeton, NJ: Robert Wood Johnson Foundation.
Kiecolt-Glaser, J. K., Marucha, P. T., Malarkey, W. B., Mercado,A. M., & Glaser, R. (1995). Slowing of wound healing by psy-chological stress. The Lancet, 346, 1194–1196.
Kosciulek, J. F. (2000). Implications of consumer direction for dis-ability policy development and rehabilitation service delivery.Journal of Disability Policy Studies, 11, 82–89.
Kramer, B. J. (1997). Gain in the caregiving experience: Where arewe? What’s next? The Gerontologist, 37, 218–232.
Kurylo, M., Elliott, T., & Shewchuk, R. (2001). FOCUS on the fam-ily caregiver: A problem-solving training intervention. Journalof Counseling and Development, 79, 275–281.
Levit, K., Smith, C., Cowan, C., Lazenby, H., & Martin, A. (2002).Inflation spurs health spending in 2000. Health Affairs, 21, 172–181.
Mechanic, D. (1998). Public trust and initiatives for new health carepartnerships. The Milbank Quarterly, 76, 281–302.
Miller, B., & Lawton, M. (1997). Symposium: Positive aspects ofcaregiving. The Gerontologist, 37, 216–217.
Pearlin, L. I., Mullan, J. T., Semple, S. J., & Skaff, M. M. (1990).Caregiving and the stress process: An overview of conceptsand their measures. The Gerontologist, 30, 583–594.
Schulz, R., & Beach, S. R. (1999). Caregiving as a risk factor formortality: The caregiver health effects study. JAMA, 282, 2215–2220.
Schulz, R., Newsom, J., Mittelmark, M., Burton, L., Hirsch, C., &Jackson, S. (1997). Health effects of caregiving: The caregiverhealth effects study. Annals of Behavioral Medicine, 19, 110–116.
Schulz, R., & Quittner, A. L. (1998). Caregiving for children andadults with chronic conditions: Introduction to the special is-sue. Health Psychology, 17, 107–111.
Shewchuk, R., & Elliott, T. (2000). Family caregiving in chronicdisease and disability: Implications for rehabilitation psychol-ogy. In R. G. Frank & T. Elliott (Eds.), Handbook of rehabil-itation psychology (pp. 553–563). Washington, DC: AmericanPsychological Association Press.
Shewchuk, R., Franklin, F. A., Harrington, K. H., Davies, S. L., &Windle, M. (2004). Using cognitive mapping procedures to de-velop a community-based family intervention. American Jour-nal of Health Behavior, 28, 43–53.
Shewchuk, R., Richards, J. S., & Elliott, T. (1998). Dynamicprocesses in health outcomes among caregivers of pa-tients with spinal cord injuries. Health Psychology, 17, 125–129.
Stephen, T. D. (1985). Q-METHODOLOGY in communicationscience: An introduction. Communication Quarterly, 33, 133–208.
Thoits, P. A. (1995). Stress, coping, and social support processes:Where are we? What next? [Special issue]. Journal of Healthand Social Behavior, 53–79.
Vitaliano, P. P. (Ed.). (1997). Physiological and physical concomi-tants of caregiving: Introduction to the special issue. Annals ofBehavioral Medicine, 19, 75–77.
Weitzenkamp, D. A., Gerhart, K. A., Charlifue, S. W., Whiteneck,G. G., & Savic, G. (1997). Spouses of spinal cord injury sur-vivors: The added impact of caregiving. Archives of PhysicalMedicine and Rehabilitation, 78, 822–827.




















