The Returned Spirit (Gui Ling) of Traditional Chinese Medicine
Upload
khangminh22Category
view
4download
0




SHORT COMMUNICATION
Journal of Evolution of Medical and Dental Sciences/ Volume 1/ Issue 3/ July- Sept 2012
Page 69
USE OF TRADITIONAL MEDICINE IN FEVER
Purabi Phukan
1. Associate Professor, Department of Community Medicine, Srinivasa Institute of Medical Sciences and Research
Centre, Mangalore- 574146
CORRESPONDING AUTHOR:
Dr Purabi Phukan,
Associate Professor,
Department of Community Medicine,
Srinivasa Institute of Medical Sciences and Research Centre,
Mangalore- 574146,
Karnataka, India.
Email ID- [email protected]
INTRODUCTION:
Malaria is the most common cause of fever in India and is an age old problem in India
claiming thousands of life over the years 1,2. WHO launched its first ever comprehensive traditional
Medicine strategy in 2002 strategy to assist countries to gather and preserve knowledge on such
practices with the hope to develop a good database for finding antimalarial properties in future in
wake of drug resistance. Majority of the rural and tribal in rural areas have vast store of knowledge
and practice of traditional medicines as it is cheaper and easily accessible to them 3 4 5. Traditional
Medicine often becomes the first source of treatment for these communities. The WHO estimated
that 80% of the world’s population use botanical medicines for their primary health care needs,
malaria treatment inclusive6. The current study was therefore undertaken with an objective to find
out the knowledge and practices of traditional medicines among rural and tribal communities for
fever and the factors influencing such practices.
KEY WORDS: Malaria, Traditional Medicine, Fever, Ethnopharmacology
MATERIAL & METHODS:
A community based cross-sectional study was undertaken from June 2009 to May 2010 in
Rani Community Development Block which is the Rural Field practice area of Gauhati Medical
College, Assam. The Block has 96 villages with total population of 86,539 and literacy rate is 66.8%
(2001 Census). The block has 18% tribal population residing in 36 villages.
Considering expected frequency as 50%, by using Epi Info Version 7 sample size was
calculated to be 300 (95% confidence level, confidence limits of 5.65%). To get a representative
population, the households were selected by Proportionate Probability Stratified Random Sampling
technique from 16 villages. The 16 villages together formed a uniform composition, firstly in terms
of tribal and non-tribal study subjects and secondly in terms of easier and more difficult access to
health services. Stratification was done based WHO Protocols and methods of malaria situation
analysis 6. Head of the household was interviewed and data was collected in a pre-tested and
predesigned proforma regarding socio-demographic characteristics, knowledge and practices of

SHORT COMMUNICATION
Journal of Evolution of Medical and Dental Sciences/ Volume 1/ Issue 3/ July- Sept 2012
Page 70
traditional medicines in fever and in known malaria, factors influencing their use. Also the herbs
and plants that are used was identified and recorded. However the pharmacological property of
these plants and herbs are out of the scope of this study and review of Botanical Plants literature
was done to find out available data on its use and medicinal properties. Statistical Analysis of the
data was subjected to descriptive analysis and Epi Info Version7.
RESULTS:
The Socio demographic profile of the study population is shown in Table 1. Among the 150
tribal and 150 non-tribal households visited it was found that literacy level of head of the
household was 82.7% and 92.6% respectively, with total literacy rate of 87.7%. According to
occupation of the head of the families it was found that majority are cultivators (51.2%) among the
tribal and businessman (40.7%) among the non-tribal communities and 24 % and 12.6% of the
tribal and non-tribal families are living below poverty line (income less than Rs 228.9 per capita per
month at 1993-94 prices). The respondents belonged to the age group of 19 -59 years, of which,
among the tribal 61.4% are males and 38.6% are females while among the non-tribal respondents,
72% are males and 28% are females. Majority of the tribal respondents belonged to Hindu (82.4%)
and rest were Christian (21.3%) whereas among the non-tribal respondents majority were Hindu
(86%) and the rest Muslim (14%).
Table 2 shows that knowledge and practice of traditional medicine. Out of the 300
households visited only 49 (16.3%) households knew of traditional medicines used in fever. Out of
these 49 households, majority, 38 (25.3%) belonged to the tribal community while 11 (7.3%)
belonged to non-tribal community. However, out of the 49 households, only 8 (5.3%) of the tribal
households and 3 (2%) of the non-tribal households are currently involved in collection and
preparation and distribution of the medicine prepared from the herbs. The names of the herbs and
plants used and the mode of preparation and administration was demonstrated and explained by
them.
The remaining 251 (83.7%) of the respondents did not have any faith in traditional
medicines for treatment of malaria and they neither had any knowledge of these remedies. Further,
it must be mentioned that although use of traditional medicines was reported by 49 households, it
is usually used as an initial management; if fever does not improve in next 2-3 days then they opt
for allopathic medicines.
Table 3 shows the common factors influencing the practice of traditional medicines for
fever. However, 40 (81.6%) respondents, 32 (84.2%) tribal and 8 (72.7%) non-tribal respondents
said they would also prefer to use traditional medicines as an adjunct to antimalarials if diagnosed
as malaria fever.
In this study 6 botanical plants that are practiced in the study area were identified and
recorded. Table 4 shows the different plants and herbs that were identified. These are Murraya
koenijii, Vitex negundo, Centella asiatica, Azadiracta indica, Ocimum sanctum/Ocimum basilicum
and a plant known as Tupurilata or Panipanta locally (scientific name unknown) are identified to be
used for treatment of fever and malaria as home remedy.
It was found that in case of the plant Tupurilata (local name), it was made into a thin paste
mixed with coconut oil and is applied over the scalp of infants and young children with high fever
when parents fear to giving allopathic medicines because they believe them to be having adverse

SHORT COMMUNICATION
Journal of Evolution of Medical and Dental Sciences/ Volume 1/ Issue 3/ July- Sept 2012
Page 71
side effects. The other plants and herbs like Narasingha, Pasotia are grinded together applied on
scalp or body to get relief from headache and bodyache associated with fever. Whereas Manikmoni,
Neem and Tulsi taken orally in the treatment of persistent fever for young children as well as adults
by grinding and mixing them together and making a decoction and taken orally to get relief from
fever.
DISCUSSION:
The results of this study revealed that knowledge of traditional medicines was present only
in 49 (16.3%) of the respondents while only 11 (3.6%) practiced it in their homes recently. Similar
result was found in another study where 2.1% of the tribal community used local herbs for
treatment of malaria7. This value is comparatively less than the findings in other studies in Assam
where initial treatment through traditional healer (Vaidya) was found in 39.2% 8. The remaining
97% of the respondents did not have any knowledge about these traditional medicines used nor
believed that they can be helpful in malaria treatment.
The decreasing knowledge and practice of traditional medicines may be due to increased
malaria awareness campaigns in recent years and also due to high literacy rate of the study
population.
However in this study none of the respondents said that they will depend solely on TM if
fever is known to be due to malaria which is a positive finding in this study. After initial home
management if fever does not improve in 2-3 days than they opt for allopathic treatment from
doctor. This shows that access to early diagnostic facility would prevent the morbidity and
mortality that occurs due to delay in diagnosis. The factors like severity of fever, associated
symptoms of jaundice, infants and young children with persistent fever and fever in elderly people
and fear of side effects of the antipyretics and anti-malarials influenced the use of traditional
medicine. They are of the opinion that these medicines are safer to give to infants rather than
antimalarials as they seen side effects after using these. Similar finding was observed in Nigeria9.
Affordability of medicines was not a factor as they were aware of the free antimalarials available at
the health center.
Regarding the medicinal value of the plants used it was found that some of them indeed
were found to be having some benefit in treatment of fever and even in malaria.
Ocimum sanctum, locally known as “Tulosi” was found to be having many properties
including antipyretic and anti-malarial activity against P. falciparum and P vivax 10, 11, 12.
Similar use for fever and cough was also found in Arunachal Pradesh among Khamti tribes
in Lohit District13 and in rural area of Tamil Nadu14. In another study insecticidal property of tulsi
was also found15.
Azadirachta indica, locally known as “neem” was also found to exhibit antimalarial activity
by inhibiting the growth of P. falciparum 16and even against drug resistant strains of P. falciparum 17, 18.
Vitex negundo, locally known a “pasotia” meaning five leaved plant, Ayurveda it is called
nirgundi and in the west known as Chastetree, has proved to be useful in fever, spleen enlargement
and convulsion14 and in malaria19. Besides this it was also found to have insecticidal and pesticidal
properties by other studies 20, 21, 22.

SHORT COMMUNICATION
Journal of Evolution of Medical and Dental Sciences/ Volume 1/ Issue 3/ July- Sept 2012
Page 72
Centella asciatica, locally known as “manikmoni”, was also found to be useful malarial fever 23, 24, 25.
Murraya koenigii, locally known as “Narasingha” in this study area was also found to be
having anti-inflammatory property and hepatoprotective26.
A study in Africa has shown that traditional medicine can reduce 1 million malaria deaths.
In rural Tanzania a study about traditional Masai medicine showed 48% children already had
knowledge about these plants which have been preserved in the UN database for future reference27.
“Tupurilata” was not found in any database and it is a new plant found in this study which needs to
be studied. B N Prakash, a researcher with the foundation for the revitalization of Local Health
Tradition, based in Bangalore found Guduchi (Tinospore coeditdia) to have shown to reduce
malaria related deaths by 5 to 10 times.
CONCLUSION:
The study indicates that knowledge and practices regarding traditional medicines for
malaria or fever has significantly declined in the study population. The study indicates that delay in
malaria diagnosis may be one of the causes of depending on traditional medicine which can be
improved by making easier access to early diagnosis. That the use of traditional medicines does
more damage than good does not hold good in the current scenario when many studies did reveal
their usefulness. But certain remedies which have not been tested for efficacy is not encouraged so
vigorous research on the efficacy of traditional plants on malaria treatment should be carried out to
ascertain their usefulness. Ethno-pharmacological studies are encouraged to determine the
usefulness these traditional remedies, as few of these were found to be having some anti-malarial
property. The commonly used plants are brought out in this study along with their use. For this
purpose a book called “Traditional medicines and plants and malaria” by Merlin Wilcox, Gerard
Bodeker and Phillipe Rasanova provides guidelines on how to conduct such studies.
TM practice is an established health care system in India and is fast growing importance in
the western world. India can therefore contribute immensely for development and research for
alternative malaria treatment.
ACKNOWLEDGEMENT:
I thank, Dr R Sarma, Professor, Department of Community Medicine, Gauhati Medical
College, for her guidance pertaining to this work. I also would like to thank Ms. M Baruah, Lecturer
Botany, Arya Vidyapeeth College and Dr N D Bendegeri, Professor and Head, Department of
Community Medicine, KBNIMS for providing their valuable suggestions in preparation of this paper
for publication.
REFERENCES:
1. (Dhiman RC, Pillai CR, Subbaroa SK. Investigation of malaria outbreak in Bahraich district,
Uttar Pradesh. Malaria Research Center (ICMR), Delhi, India. Indian J of Med. Res. May 2001;
113:186-91.
2. C D Alert. Some important outbreaks of malaria in India during 2000. Jan 2001; 5:1.
3. WHO. Traditional Medicine Strategy 2003-2005. Geneva. Document: WHO/EDM/TRM/
2002.1.

SHORT COMMUNICATION
Journal of Evolution of Medical and Dental Sciences/ Volume 1/ Issue 3/ July- Sept 2012
Page 73
4. Pulok K. Mukherjee and Atul Wahile. Integrated approaches towards drug development
from Ayurveda and other Indian system of medicines. Journal of Ethnopharmacology; 2006;
103: 25–35.
5. Merlin Willcox. Traditional herbal medicines for malaria. BMJ. 2004; 329 (7475):1156
6. Protocols and methods for malaria situation analysis. WHO, HIV/AIDS, Tuberculosis,
Malaria. Roll Back Malaria. July 2003. Trial Edition. Pg.1-88. (WHO/HTM/RBM/ 2003.47)
7. V Soan, Gyan Chand. Proceedings of National Symposium on Tribal Health. Knowledge,
Attitude and Practices towards Malaria in Tribal Community of Baigachak Area, Dindori
District (MP), Pg-75-78 (http://www.rmrct.org/files_rmrc_web/centre's_publications/
NSTH_06/NSTH06_9.V.Soan.pdf)
8. Chaturvedi HK, Mahanta J and Pandey A. Treatment-seeking for febrile illness in north-east
India: an epidemiological study in the malaria endemic zone. Malaria Journal.
17 December 2009; 8:301 (doi:10.1186/1475-2875-8-301)
9. Erhun W O, Agbani E.O and Adesanya S.O. Malaria Prevention: Knowledge, Attitude and
Practice in a Southwestern Nigerian Community. African Journal of Biomedical Research;
2005; 8: 25 - 29.
10. Pandey BP, Anita. In: Economic Botany; 1990. p. 294 (Published by Chand and Company
Ltd., Ramnagar, New Delhi.
11. P. Prakash and Neelu Gupta. Therapeutic uses of Ocimum sanctum Linn. (TULSI) with a note
on Eugenol and its pharmacological action: A Short Review. Indian J Physiol Pharmacol
2005; 49 (2): 125–131
12. Savitri Godhwani, J.L. Godhwani and D.S. Vyas. Ocimum sanctum: An experimental study
evaluating its anti-inflammatory, analgesic and antipyretic activity in animals. Journal of
Ethnopharmacology. November 1987; 21(2): 153-163
13. Hui Tag, AK Das, Hari Loyi. Anti-inflammatory palnts used by Khamti tribes in Lohit District
of Auranachal Pradesh, India. Natural Product Radiance. 2007; 6(4):334-340.
14. Chellaiah Muthu, Muniappan Ayyanar, Nagappan Raja and Savarimuthu Ignacimuthu.
Medicinal plants used by traditional healers in Kancheepuram District of Tamil Nadu, India.
Journal of Ethnobiology and Ethnomedicine; 2006, 2:43 doi:10.1186/1746-4269-2-43).
(available online at: http://www.ethnobiomed.com/content/2/1/43)
15. Ocimum sanctum. The Indian home remedy. In: Current Medical Scene, March-April 1992;
(Edited and published by S. Rajeshwari, Cipla Ltd., Bombay Central, Bombay.
16. Rochanakij, S., Thebtaranonth, Y., Yenjal, C. H. and Yuthavong, Y. Nimbolide, a constituent of
Azadirachta indica inhibits Plasmodium falciparum in culture. Southeast Asian J. Trop. Med.
Public Health; 1985; 16: 66–72.
17. Kausik Biswas, Ishita Chattopadhyay, Ranajit K Banerjee and Uday Bandopadhyay.
Biological activities and medicinal properties of neem (Azadirachta indica). Curent Science;
82(11):1336-1345.
18. Badani, L., Deolankar, R. P., Kulkarni, M. M., Nagsampgi, B. A. and Wagh, U. V. Biological
activities and medicinal properties of neem. Indian J. Malariol.; 1987; 24: 111–117.
19. agnus-castus.co.uk. [homepage]. Agnus castus (Vitex negundo). (available from
http://www.herb-agnus-castus.co.uk)

SHORT COMMUNICATION
Journal of Evolution of Medical and Dental Sciences/ Volume 1/ Issue 3/ July- Sept 2012
Page 74
20. Vishal R Tandon. Review article: Medicinal Uses and biological properties of Vitex negundo.
NISCAIR Online Periodicals Repositories (NOPR). 2005; 4 (3): 162-165.
21. Hebbalkar DS, Hebbalkar GD, Sharma RN, Joshi VS, Bhat VS. Mosquito repellent activity of
oils from Vitex negundo Linn. leaves. Indian J Med Research; 1992; 95:200–203.
22. Krishnan Kannathasan & Annadurai Senthilkumar & Manivachagam Chandrasekaran &
Venugopalan Venkatesalu. Differential larvicidal efficacy of four species of Vitex against
Culex quinquefasciatus larvae. Parasitol Res; 2007; 101:1721–1723.
23. Nima D. Namsaa, M. Mandal and S. Tangjang. Anti-malarial herbal remedies of northeast
India, Assam: An ethnobotanical survey. Journal of Ethnopharmacology. Article. In Press-
Corrected Proof. 2010).
24. Sakshi Singh, Asmita Gautam, Abhimanyu Sharma and Amla Batra. Centella asiatica (L.): A
plant with immense medical potential but threatened. International Journal of
Pharmaceutical Sciences Review and Research. 2010; 4(2). Article 003 (Available online at
www.globalresearchonline.net).
25. Rahmatullah Mohammad, Ferdausi Dilara, Mollik Haque Ariful Md., Jahan Rownak,
Chowdhury H. Majeedul, Haque Mozammel Wahid, A survey of medicinal plants used by
Kavirajes of Chalna Area, Khulna District, Bangladesh. Afr. J. Trad. 2010; 7(2): 91-97
26. Bitterroot restoration [homepage]. Herbal Medicine> Medicinal Plants-Murraya koenijii.
27. IRIN: AFRICA: Turning to traditional medicines in fight against malaria. [Homepage]. IRIN:
The humanitarian news and analysis. A service of the UN Office for the co-ordination of
Humanitarian Affairs). (available at: http://www.irinnews.org)

SHORT COMMUNICATION
Journal of Evolution of Medical and Dental Sciences/ Volume 1/ Issue 3/ July- Sept 2012
Page 75

SHORT COMMUNICATION
Journal of Evolution of Medical and Dental Sciences/ Volume 1/ Issue 3/ July- Sept 2012
Page 76
* fisherman, silkworm rearing, selling household produce like betel nuts and vegetables,
agricultural labourer, income from house rent and income from pension.
Table 1. Socio-demographic profile of the study population
Socio demographic Tribal (150) Non-tribal (150) Total (300)
profile No. (%) No. (%) No. (%)
Religion
Hindu 118 (78.7%) 129 (86%) 247 (82.4%)
Muslim - - 21 (14%) 21 (14%)
Christian 32 (21.3%) - - 32 (21.3%)
Sex
Male 92 (61.4%) 108 (72%) 200 (66.7%)
Female 58 (38.6%) 42 (28%) 100 (33.3%)
Age range (years)
19-28 15 (10.0%) 9 (6.0%) 24 (8.0%)
29-38 44 (29.2%) 49 (32.7%) 93 (31.0%)
39-48 52 (34.8%) 52 (34.8%) 104 (34.7%)
49-58 28 (18.8%) 26 (17.3%) 54 (18.0%)
>59+ 11 (7.2%) 14 (9.2%) 25 (8.4%)
Education Level
Illiterate 26 (17.3%) 11 (7.4%) 37 (12.4%)
Primary School 56 (37.3%) 35 (23.3%) 91 (30.4%)
High School 44 (29.3%) 57 (38.0%) 101 (33.7%)
HSCL passed 16 (10.7%) 21 (14.0%) 37 (12.4%)
HS passed & above 8 (5.4%) 26 (17.3%) 34 (11.4%)
Occupation
Cultivator 77 (51.2%) 47 (31.3%) 124 (41.3%)
Daily wage earner 62 (41.3%) 19 (12.7%) 81 (27%)
Skilled labour 5 (3.3%) 2 (1.3%) 7 (2.3)
Service 26 (17.3%) 37 (24.7%) 63 (21%)
Business 10 (6.6%) 61 (40.7%) 71 (23.7%)
Others* 17 (11.3%) 8 (5.3%) 25 (8.4%)

SHORT COMMUNICATION
Journal of Evolution of Medical and Dental Sciences/ Volume 1/ Issue 3/ July- Sept 2012
Page 77
Table 2. Head of household having knowledge and practice of traditional medicine in fever
Traditional
Medicine
Tribal
(n=150)
Non-tribal
(n=150)
Total
(N=300)
No. % No. % No. %
Current knowledge Yes 38 25.3 11 7.3 49 16.3
No 112 74.7 139 92.7 251 83.7
Practicing within household Yes 8 5.3 3 2 11 3.6
No 142 94.7 147 98 289 96.3
Table 3: Reason for use of traditional medicines in fever
Variables Tribal
(n=38)
Nontribal
(n=11)
Total
(N=49)
Very high fever in young children 29 76.3 2 18.1 31 63.3
Fever associated with jaundice 10 26.3 2 18.1 12 24.5
Fear of side effects of allopathic drugs 20 52.6 10 90.9 30 61.2
Use side by side with allopathic treatment 32 84.2 8 72.7 40 81.6
Side effects of Antimalarials drugs 20 52.6 10 90.9 30 61.2
Fever in Elderly with poor physical status 10 26.3 4 36.4 14 28.6
*Multiple responses

SHORT COMMUNICATION
Journal of Evolution of Medical and Dental Sciences/ Volume 1/ Issue 3/ July- Sept 2012
Page 78
Table 4- Showing information collected about the botanical plants used.
Local name Scientific name Parts of plants
used.
Mode of use
Panipanta/
Tupurilata
Unknown leaf is the useful
part.
Leaf is made to a thin paste, after
mixing with oil and applied to the
scalp
Narasingha Murraya koenijia leaf and stem Leaves are eaten directly or by
boiling in water and making a paste
Pasotia Vitex negundo leaf
Leaves are eaten directly as
vegetable or boiled and thin paste
made
Manikmoni Centella asiatica leaf A paste of the leaves are made and
given empty stomach.
Mahaneem Azadiracta indica leaves, stem and
roots
Boiled in water and the water is
given to drink
Tulsi Ocimum sanctum/
Ocimum basilicum
leaves Leaves are eaten directly.

CASE REPORT
Journal of Evolution of Medical and Dental sciences/ Volume 1/ Issue 3/ July- Sept 2012 Page 79
UNUSUAL LOCATION OF CYSTICERCOSIS LESION PRESENTATION
Dr. V. Geeta, Dr. Parimla Devi, Dr. A. Sirisha, Dr. Rama Devi, Dr. Jijiya Bai, Dr. Shravan Kumar
1. Assistant Professor, Department of Pathology, Gandhi Medical College, Secunderabad-6
2. Associate Professor, Department of Pathology, Gandhi Medical College, Secunderabad-6
3. Assistant Professor, Department of Pathology, Gandhi Medical College, Secunderabad-6
4. Assistant Professor, Department of Pathology, Gandhi Medical College, Secunderabad-6
5. Professor and HOD, Department of Pathology, Gandhi Medical College, Secunderabad-6
6. Professor, Department of Pathology, Gandhi Medical College, Secunderabad-6
CORRESPONDING AUTHOR:
Dr. V. Geeta,
Assistant Professor,
Department of Pathology,
Gandhi Medical College,
Secunderabad-6
Email ID- [email protected]
INTRODUCTION:
Cysticercosis in humans is exclusively caused by larvae of T.solium which have predilection
for skeletal muscle, eyes, and central nervous system. In literature head and neck manifestations of
Cysticercosis is reported as soft tissue swellings at sub mental area, cheek as well as tongue1-4.
Cysticercosis presenting as a nodule or mass on neck is a very rare occurance5. The diagnosis was
usually made on Histo pathologic examination. The ensuing clinical disorder is named after the
organism at this larval stage, cysticercosis cellulose Larva of pork tapeworm Taenia solium.
KEY WORDS: Cysticercosis, T.solium
CASE HISTORY:
A 21 years male presented with a painless solitary nodular swelling on right side of the
upper neck of 2 years duration. The nodule was gradually increasing in size, associated with
anxiety, easy fatigability, palpitations, decreased appetite and weight loss.
Local examination revealed 2 x 2 cm round, smooth swelling present on right side of neck at the
level of Thyroid cartilage and anterior to the upper 1/3rd of sternocleido mastoid muscle and on
palpation the swelling is cystic, non tender, firm in consistency, not moving with deglutition and on
protrusion of tongue.
Skin over the swelling was non pinchable. No local rise in temperature. Swelling was mobile
both horizontally and vertically, not attached to the underlying muscle. General and systematic
examination within normal limits.
Clinical Diagnosis made was
1) Benign cystic swelling of right neck.

CASE REPORT
Journal of Evolution of Medical and Dental sciences/ Volume 1/ Issue 3/ July- Sept 2012 Page 80
2) Sebaceous cyst
3) Lipoma
4) TB lymph node
5) Aberrant thyroid
6) Salivary gland
FNAC: S/o ‘?’ necrotic lymph node, complex cyst or parasitic cyst.
U/S: S/o ‘?’ necrotic lymph node
Excision of the cyst was done and sent for HPE
The Histopathologic examination revealed ‘Cysticercosis Cellulose’ characterized by a scolex
and epithelium lined by tortuous body and continuous with outer cystic layer. Cyst enclosed by a
fibrous capsule infiltrated with lymphocytes, plasma cells and eosinophils. Figure.1
The post operative period was uneventful.
DISCUSSION:
Taenia solium passes its life cycle in two hosts. The definitive host is human who harbors
the adult worm and intermediate host in pig which harbors the larval stage. The adult worm lives in
the small intestine of man. Usually one adult worm is present which lives for years. It is about 3
meters long with proglotids, the gravid segments with about 50000 eggs in each gravid segment.
The worm sheds gravid segments laden with eggs in the stools which infect pigs on reaching the
alimentary canal of the intermediate host penetrate the gut wall and reach systemic circulation and
are lodged in different organs and muscles. They develop in to larvae referred as cysticercosis
Human being are infected through eating under cooked contaminated pork or infected vegetables.
Adult worms shed gravid segment laden with eggs in the stool, which re infect pigs. Thus
completing the cycle. Autoinfection of man may occur by contaminated fingers or by reversal of
peristaltic movements of intestine, the gravid segments are thrown back to the stomach and larvae
disseminate throughout the body via Arterio Venous Channels and lymphatics encysting in
subcutaneous tissue, striated muscle, brain and ocular tissue6.
Cysticercosis manifestations are different and depend on the location in the body and also
number of cysticercosis of a particular site and associated inflammatory response. 87%
cysticercosis cases – presents as solitary or multiple subcutaneous nodules on the trunk, upper
arm, neck, tongue, face and breast has been reported in this order of frequency.
In many patients involvement of central nervous system in the form of neuro Cysticercosis is
diagnosed when multiple cystic ring enhancing parenchymal lesions has been detected on CT Scan7.
We are not reporting this case because of its unusual site of presentation, but also the importance of
histopathologic examination is emphasized since neither the clinical examination nor history
suggested the diagnosis other than a benign lesion.

CASE REPORT
Journal of Evolution of Medical and Dental sciences/ Volume 1/ Issue 3/ July- Sept 2012 Page 81
Photo micrographs showing cystic lesion containing parts of parasite and the cystic wall containing
granulation tissue with inflammatory reaction.
REFERENCES:
1. Kinnman J, Chi CH, Park JH. Cysticercosis in Otolaryngology. Arch Otolaryngol 1976;
102:144-7
2. Beaver PC, Jung RC, Cupp EW. Clinical Parasitology, 9 th edition. Philadelphia: Lea & Febiger,
1984.
3. Jain RK, Gupta OP, Aryya NC. Cysticercosis of the tongue. J Laryngol Otol 1989; 103:1227-8
4. Gupta SC and Gupta SC. Cysticercosis of the tongue. Ear Nose Throat J 1995;74:174-8

CASE REPORT
Journal of Evolution of Medical and Dental sciences/ Volume 1/ Issue 3/ July- Sept 2012 Page 82
5. Cysticercosis of the neck-a report of unusual case. Danai Tanechpongfamb, dept.of oto rhino
laryngeology; Pathum thani Hospital, Journal of Medicine and health sciences, faculty of
medicine, srinakharin wirat university, Vol. 12, No.2, Aug-2005.
6. Park K. Epidemiology of Communicable diseases. In: Park K. Park's Textbook of Preventive
and Social Medicine. 16 th ed. New Delhi: M/s Banarsidas Bhanot Publishers, 2000; 229.
7. Smiti S, Sripathi H and Naik L. Unusual location of cysticercosis lesions in soft tissue –
Report of three cases. Ind J Radiol Imag 2003;13:157-8

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences / Volume 1 / Issue 3 / July- Sept 2012 Page 83
CLINICO– EPIDEMIOLOGICAL PROFILE OF ROAD TRAFFIC INCIDENTS
ADMITTED AT A TERTIARY CARE HOSPITAL IN GARHWAL-
UTTARAKHAND
Sumeet Dixit, Praveen K. Tyagi, Amit K. Singh, Sudhir K. Gupta, Nidhi Malik
1. Dr. Sumeet Dixit, Assistant professor, Department of Community Medicine, VCSGGMSRI– Srinagar, Pauri– Garhwal
(Uttarakhand)
2. Dr. Praveen K. Tyagi, Assistant professor, Department of General Surgery, VCSGGMSRI– Srinagar, Pauri– Garhwal
(Uttarakhand)
3. Dr. Amit K. Singh, Associate professor, Department of Community Medicine, VCSGGMSRI– Srinagar, Pauri– Garhwal
(Uttarakhand)
4. Dr. Sudhir K. Gupta, Associate professor, Department of Community Medicine, VCSGGMSRI– Srinagar, Pauri– Garhwal
(Uttarakhand)
5. Miss Nidhi Malik, Demonstrator, Department of Community Medicine, VCSGGMSRI– Srinagar, Pauri– Garhwal
(Uttarakhand)
CORRESPONDING AUTHOR:
Dr. Amit K. Singh,
Associate Professor,
(Community Medicine),
VCSG Govt. Medical College,
Srinagar – Garhwal, Uttarakhand,
India– 246174.
Email ID- [email protected]
ABSTRACT:
BACKGROUND: The magnitude of Road traffic incidents and fatalities in India is alarming. In 2009,
4.22 lakh road traffic incidents and 1.27 lakh road traffic fatalities were reported. These numbers
translate into one road accident every minute and one road accident death every four minutes
METHODS: The study (based on Jorgensen and Abane model, 1999) was conducted over a period
of one year during April 2011 to March 2012, among 136 victims (including 33 drivers) of road
traffic incidents coming to Veer Chandra Singh Garhwali government medical college, Srinagar,
Garhwal. RESULTS: 136 victims including 33 drivers were interviewed who were brought to the
causality in the aforesaid period. 23 people were brought dead. There is clustering of cases from the
month of August to October when compared to other months of year. 40% of drivers were
drunk/or using some other substance at the time of accident. Only 12.1% of drivers were using seat
belts at the time of accident. 57.6% were having driving license and 54.5% were either refractive
error or hearing impairment or both. Human error, High speed, Lack of sleep, effect of Alcohol and
mechanical fault of vehicle were reasons of accident as told by the drivers CONCLUSIONS: During
August to October there is clustering of cases. This period coincides with “Char Dham Yatra” and
rainy season both. Special efforts should be done during this period. Strong vigilance of drivers for

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences / Volume 1 / Issue 3 / July- Sept 2012 Page 84
alcohol use, presence of driving license, compulsory use of seat belts, and premedical checkup for
refractive errors may prove valuable and morbidity and mortality can be minimized.
KEY WORDS: Road Traffic Incident, Determinants, Hilly region
INTRODUCTION:
Road traffic incidents which are generally unintended and preventable are a common risk
every day to life that can happen to almost every one, anywhere. The problem of road traffic
incident is increasingly becoming a threat to public health and national development in many
developing countries. Road traffic incidents contribute to poverty by causing deaths, injuries,
disabilities, grief, lost of productivity and material damages. Road traffic incidents are the most
frequent causes of injury-related deaths world wide1. According to the World Report on Road
Traffic Injury Prevention2 traffic accidents account for about 3000 daily fatalities worldwide.
Statistical projections show that during the period between 2000 and 2020, fatalities related to
traffic incidents will decrease with about 30% in high income countries. The opposite pattern is
expected in developing countries, where traffic accidents are expected to increase at a fast rate in
the years to come. In developing countries the trend has reached an alarming state, but very little
attention is paid to the problem3. There is evidence that using minimum safety standards, crash
worthiness improvement in vehicles, seatbelts use laws and reduced alcohol use can substantially
reduce deaths on the road4. The magnitude of Road traffic incidents and fatalities in India is
alarming. In 2009, 4.22 lakh road traffic incidents and 1.27 lakh road traffic fatalities were
reported5.These numbers translate into one road incident every minute and one road incident
death every four minutes. However, this is an underestimate, as not all injuries are reported to the
police5. Hilly regions are prone for RTA and there are very few number of studies in such areas.
Therefore this study is under taken to identify the clinic – epidemiological profile of Road traffic
incidents amongst patients admitted at Base hospital, Srinagar - Garhwal and to assess the factors
associated with the causation of the same.
METHODOLOGY:
A model for traffic incident as inspired by the ecological model of a disease was developed
by Jorgensen and Abane (1999)6 who made a heuristic adjustment of this basic model to suit road
traffic accident analysis. The model is characterized by three main components:
1. The vehicle (corresponding to the vector in disease ecology) which describes vehicles into
its composition, age, technical conditions and safety equipments like seat belts in a car.
2. The environment, comprising the road system and the wider physical and built up
environment. The physical environment splits further into different aspects such as;
Daylight and climate (weather conditions and road conditions), Spatial conditions
(arrangements and Macro structures), Settlement pattern (Urban or rural / sparse or
populated area), situation of areas of residence and working areas, Principle of traffic
separation, topography and road constructions qualities.
3. The behavior of the population; including its characteristics such as age and sex ratio as
well as attitudes and general traffic behavior. And it goes further into driving behavior,
driving experience, driving style, risk compensation and risk driving (influence of alcohol
and drugs).

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences / Volume 1 / Issue 3 / July- Sept 2012 Page 85
Superimposed on this model is a system of traffic laws, regulations and mode of enforcement
designed to ensure that the population adheres to the controls and regulations so as to maintain
some level of road safety i.e. traffic rules (speed restrictions, road signs), speed controls and
convictions for various road traffic offences6. Based on this model this cross sectional study was
done with the help a pretested questionnaire, in a tertiary care hospital in Garhwal. All cases of RTA
coming to the tertiary care hospital during March 2011 to February 2012 were included in the
study. Questions were asked for assessing various risk factors as per the above said model and data
entry was done on excel and analyzed thereafter.
ETHICAL CONSIDERATIONS:
Ethical clearance from institutional review board/ institutional ethical committee was taken
for the study. Written consent was sought from the all respondents. They were informed about the
nature and the purpose of the survey.
RESULTS:
During the study period a total of 136 individuals came for the medical assistance (Figure-
1).117 were males 19 were females. Out of them 33 were drivers of the vehicle, which got the
accident. The number of brought dead persons because of Road Traffic Incidents, in the aforesaid
period was 23. Out of the brought dead individuals 5 were drivers of the vehicle. Maximum number
of morbidity because of RTI is evident in the month of December. There is clustering of cases from
the month of August to October when compared to other months of year (Figure-1).
Most of the drivers were literate. Out of 33 drivers interviewed only 3 (9%) were illiterate.
Nearly 40% of drivers were drunk/or using some other substance at the time of accident.50% of
drivers were >40 years of age. 15.8% of drivers were less than 20 years of age. Most of the drivers
(51.5%) who met the accident were having driving experience of >5 years. 12.1% of drivers were
having driving experience of less than 1 year. Only 12.1% of drivers were using seat belts at the
time of incident. 57.6% were having driving license and 54.5% were either refractive error or
hearing impairment or both. Most of the respondents told that it was mistake of other drivers
which led to the accident. High speed, Lack of sleep, effect of Alcohol and mechanical fault of vehicle
were other reasons of accident as told by the drivers (Table-2). 78% of victims were brought to the
hospital with help of 108 helpline service. Rest 22 % were came either by themselves or by other
people (Figure-1).

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences / Volume 1 / Issue 3 / July- Sept 2012 Page 86
Figure -1: Monthly distribution of RTI cases
Figure-2: Mode of transfer to the hospital
310
27
15 12 92
41
4 7 5
117
1 0 0 1 2 0 2 29
0 0 2
19
410
28
1712 11
4
50
4 7 7
136
0
20
40
60
80
100
120
140
160
No
of
case
s
Year- Month
Distribution of cases monthwise
Male
Female
Total
78%
15%
6%
1%
Mode of transfer to the hospital
108 helpline
Other people
self
other

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences / Volume 1 / Issue 3 / July- Sept 2012 Page 87
Table-1: Clinico-epidemiological profile of RTI cases
*Human error: wrongful U-turn by other vehicle , Wrongful overtaking by un-coming vehicle
**Mechanical fault: break failure, burst tyre, and locked steering mechanism
Maximum number (47.8%) of RTI morbidity was because of polytrauma associated. And
upper limb injury was least responsible for the mortality.50% of accidents took place in the evening
Drivers interviewed Yes % age
Education(n=33)
Illiterate 03 9.1
Up to 5th std 13 39.4
5-12 th std 16 48.4
Graduate/Post graduate 01 3.1
Age(n=38,
Including the
brought dead
drivers)
<20 years 6 15.8
20-40 years 13 34.2
>40 years 19 50
Alcohol /other substance use at the time of accident( n=33) 13 39.4
Driving experience
( n=33)
<1 year 4 12.1
1-5 years 12 36.4
>5 years 17 51.5
Seat belt use( n=33) 4 12.1
Driving license( n=33) 19 57.6
Refractive error /Hearing impairment / both( n=33) 18 54.5
Cause as told by
driver( Multiple
answers could
be given)
Mistake of others/Human error*( n=33) 23 69.7
More speed 14 42.4
Lack of sleep 11 33.3
Alcohol use 09 27.3
Mechanical fault of the vehicle** 09 27.3
Others including environmental
conditions
04 12.1

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences / Volume 1 / Issue 3 / July- Sept 2012 Page 88
hours. 72.7% of vehicles were older than 5 years of age. Fall from hill was the mode of accident in
most of the cases and the mortality and severe injuries were also more in fall from hillside, followed
by accident from the sides and head on collision.
Table -2: Epidemiological profile of RTI cases
DISCUSSION:
Maximum number of Morbidity because of RTI is evident in the month of December. It was
fall of a bus, from the hill side leading to higher toll in mortality and morbidity in month of
December. There is clustering of cases from the month of August to October when compared to
other months of year. “Char dham yatra” which lead to sudden increase in number of vehicles on
hillside and heavy rainy season both coincides with this period. These can be contributing factor for
such clustering of cases. Most of the drivers were literate. Out of 33 drivers interviewed only 3 (9%)
were illiterate. Substance use including drinking behavior was noticed in 39% of the drivers at the
Variable Number % age
Injury( n=136) Involved head 20 14.7
Upper limb 14 10.3
Lower limb 21 15.5
Abdomen 16 11.7
Multiple / polytrauma 65 47.8
Time of accident(N=38) 12pm -6 pm 14 36.8
6pm-9pm 19 50.0
9pm-6am 02 5.3
6am- 12 pm 03 7.9
Age of the vehicle(N=33) <5 years 09 27.3
>5 years 24 72.7
Type of
collision/accident(N=38)
Head on 04 10.5
From behind 02 5.3
From sides 07 18.4
Fall from hill 18 47.4
Other 07 18.4

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences / Volume 1 / Issue 3 / July- Sept 2012 Page 89
time of accident. Experienced drivers (>5 years) met the accident in maximum number.
Overconfidence leading to recklessness can be the reasons for such happening. 77.9% drivers were
not using seat belt at the time of accident and when asked for the driving license only 42.4% could
not produce the same. 50% of drivers who met the accident were >40 years of age. In the elderly
visual impairment prevents adequate visual function, which may be responsible for the accident.
When examined, 54.5% were having either refractive error or hearing impairment or both. A study,
which examined the association between visual impairment and RTI among 1,428 drivers seen at
the accident and emergency department of a hospital in the United Arab Emirates, also identified
visual impairment to be significant risk factors7. Likewise Davidson in his examination of the
interrelationship between British drivers’ visual abilities, age and RTI histories found strongest
positive association between RTI variables and visual disabilities, among older drivers8. Most of the
respondents told that it was mistake of other drivers which led to the accident. High speed, Lack of
sleep, effect of Alcohol and mechanical fault of vehicle were other reasons of accident as told by the
drivers. Study by Asogwa et al9 showed that commercial drivers drive for hours without sleep and
food, until fatigue inevitably sets in and a crash may be the end result. Effect of alcohol or other
substances was also substantiated by Lemoineet al10. Maximum number (47.8%) of RTI morbidity
was because of polytrauma associated. And upper limb injury was least responsible for the
mortality. This is in contrast to the study by Biswas G11 who cited that the maximum (56.4%)
injuries were found on head and neck, followed by thorax (54.5%) and abdomen (44.5%). Other
studies12,13 also showed a high incidence of head injuries in their studies. 50% of accidents took
place in the evening hours. Fall from hill was the mode of accident in most of the cases and the
mortality and severe injuries were also maximum in such mode of accident followed by accident
from the sides and head on collision.
CONCLUSION:
During “Char Dham Yatra” period and rainy seasons there is clustering of cases. Special
efforts should be done during this period. Strong vigilance of drivers for alcohol use, presence of
driving license, compulsory use of seat belts, premedical checkup for refractive errors, must be
ensured. The role of 108 helpline14 cannot be ruled out and strengthening of this service can be of
paramount importance. All These measures may prove valuable and morbidity and mortality can be
minimized.
ACKNOWLEDGEMENT:
The author acknowledges medical social workers of department of community medicine,
Veer Chandra singh Garhwali govt. medical college, Srinagar, Garhwal for their work and support in
the study. The author also acknowledges the respondents who formed the building blocks for the
study.
REFERENCES:
1. Astrom, J. S, Kent, M.P. and Jovin, R. D. (2006) Signatures of Four Generations of Road Safety
Planning in Nairobi City, Kenya In: Journal of Eastern African Research and Development.
Vo. l20, pp. 186-201.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences / Volume 1 / Issue 3 / July- Sept 2012 Page 90
2. Peden, M. (Ed), (2004), World Report on Road Traffic Injury Prevention. World Health
Organisation, Geneva.
3. Odero, W., Garner, P. and Zwi, A. (1997). Road traffic injuries in the developing countries: a
comprehensive review of epidemiological studies. Journal of Tropical Medicine and
International Health. 2(5), 445-460.
4. Leon, S.R. (1996).Reducing death on the Road.The effects of minimum safety standards,
Unpublicised crash test, seat belts and alcohol. Am J Public Health; 86(1):31-3.
5. Road Accidents in India, 2009. Transport Research Wing, Ministry of Road Transport &
Highways, Government Of India, New Delhi.
6. Jorgensen, S. H., and Abane, A. M. (1999). A comparative study of urban traffic accidents in
developing and developed countries: Empirical observations and problems from Trondheim
(Norway) and Accra (Ghana). Bulletin of Ghana Geographical Association. No. 21, 113-128.
7. Bener A, Ahmad MF, El-Tawil MS, Al- Bakre S. Visual impairment and motor vehicle
accident. Middle East Journal of Emergency Medicine. 2004; 4: 1-9
8. Davidson PA. Inter-relationships between British drivers’ visual abilities, age and road
accident histories. Opthalmic and Physiological Optics. 1985; 5:195-204.
9. Asogwa SE. Kola nut and road traffic accidents in Nigeria. American Journal of Public Health.
1978; 68:1228.
10. Lemoine P, Ohayon M. Abuse of psychotropic drugs during driving. Encephale. 1996; 22:1-6.
11. Biswas G, Verma SK, Sharma JJ, Aggarwal NK. Pattern of Road Traffic Accidents in North
East Delhi. Journal of Forensic Medicine & Toxicology.2003; 20(1):27-32.
12. Sahdev P, Laeque MD, Singh B and Dogra TD. Road Traffic Accidents in Delhi, causes, injury
pattern and incidence of preventable deaths. Accid Anal Prev 1994; 26:12-18.
13. Salgado MSL, Colombage SM. Analysis of fatalities in road accidents. For Sci Int .1998;
36:91-96.
14. In Uttarakhand, Emergency helpline Number “108″ to tackle disaster calls, complaints.
Available at http://www.indiahillstoday.com/2010/10/12/in-uttarakhand-emergency-
helpline-number-108-to-tackle-disaster-calls-complaints/

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences / Volume 1 / Issue 3 / July- Sept 2012 Page 91
A STUDY ON EVALUATION OF APPROPRIATE USAGE OF FRESH FROZEN
PLASMA (FFP)
Dr. V. Geeta, Dr. I. Srilakshmi, Dr. A. Krishnayya, Dr. Lakshmi, Dr. Poornima, Dr. O. Shravan Kumar,
Dr. P. Jijiya Bai
1. Assistant Professor, Department of Pathology, Gandhi Medical College, Secunderabad, AP.
2. Assistant Professor, Department of Pathology, Gandhi Medical College, Secunderabad, AP.
3. Assistant Professor, Department of Pathology, Gandhi Medical College, Secunderabad, AP.
4. Blood bank Medical Officer, Gandhi Medical College, Secunderabad, AP.
5. Post Graduate Student, Department of Pathology, Gandhi Medical College, Secunderabad, AP.
6. Professor & HOD, Department of Pathology, Gandhi Medical College, Secunderabad, AP.
CORRESPONDING AUTHOR-
Dr. V. Geeta,
Assistant Professor,
Department of Pathology,
Gandhi Medical College,
Secunderabad, AP.
Email id- [email protected]
ABSTRACT:
The term FFP refers to the fluid portion of 1 unit of human blood that has been centrifuged,
separated & frozen solid at -18°C or colder within 8hrs of collection. The indications for transfusing
FFP are very limited, as it can cause unpredictable adverse reactions. A retrospective study of FFP
transfusion was carried out at the blood bank-Gandhi Medical College for a period of 6 months; i.e
January 2011–July 2011 for various indications. We evaluated 840 patients who received 1534
units of FFP and classified them as appropriate, clinically appropriate and inappropriate. In our
study appropriate and clinically appropriate transfusions of FFP were about 61%- a good
proportion of FFP transfusions were justified but 39% were of without any appropriate indication.
KEY WORDS: Fresh Frozen Plasma, Centrifugation, Adverse Reactions
INTRODUCTION:
The use of FFP has increased due to multiple factors, possibly increased acceptance of the
concept of component therapy.FFP contains the labile as well as stable components of the
coagulation , fibrinolytic & complement system; the proteins(that maintain oncotic pressure &
modulate immunity) and fats, carbohydrates & minerals are present in concentrations similar to
those in circulation. The most labile coagulation factors are preserved for 1 yr if FFP is kept at -30°
C or below. The FFP should be administered as soon as possible after thawing & in any event within
12 hrs if kept at 2-6°C.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences / Volume 1 / Issue 3 / July- Sept 2012 Page 92
Contents of 1 unit of FFP prepared from 450ml of whole blood
Plasma : 175-230ml
All Coagulation Factors : 1 i.u/ml of each factor including factors V
& VIII)
Fibrinogen : 200-400 mgm
INDICATIONS OF FFP:
� Active bleeding,
� Liver diseases
� Disseminated intravascular coagulation (DIC)
� Thrombotic Thrombocytopenic Purpura (TTP)
� Coagulopathy in massive transfusion
� Familial Factor V deficiency
� Deficiency of Factors II, VII, IX, X
� Antithrombin III deficiency
� Congenital or Acquired coagulation factor deficiency1
DOSAGE OF FFP:
About 10ml/Kg body wt. Post transfusion assessment of levels of APTT, PT & fibrinogen is
done for monitoring the effect of FFP2. Plasma should be ABO compatible with the recipient blood.
AIMS & OBJECTIVES:
Evaluation of appropriate usage of FFP in a period of 6 months (January 2011- June 2011)
in Gandhi Hospital.
MATERIALS & METHOD:
A Retrospective study was conducted at Gandhi Hospital Blood bank for a period of
6months (January 2011-june 2011). We evaluated 840 patients, who received 1534 units of FFP &
classified them as 1.Appropriate; 2.Inappropriate; 3. Clinically appropriate.
Table: 1- SEX RATIO (M: F ratio- 1:1.5)
SEX MALE FEMALE TOTAL
No. of patients 382 458 840
% 45.5% 54.5% 100%
Table: 2- AGE GROUP
AGE
GROUP
JAN FEB MARCH APRIL MAY JUNE TOTAL JAN
0-20 33 35 36 34 28 56 222 26.7%
21-40 71 44 49 68 74 91 397 21-40
41-60&
ABOVE
31 39 30 25 24 62 211 31

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences / Volume 1 / Issue 3 / July- Sept 2012 Page 93
Table: 3- Guidelines-British Committee for Standard Hematology3
SNO CLINICAL
CONDITIONS
TOTAL
REQUIREMENT
APPROPRI
ATE
CLINICALY
APPROPRIATE
INAPPROP
RIATE
%
1. Liver Diseases 152 ---- 152 ---- 18%
2. DIC 84 ---- 84 ---- 10%
3. Hemophilia 168 168 ---- ---- 20%
4. Sepsis + Burns 168 60 ---- 108 20%
5. Cardiac
surgeries
168 ---- ---- 168 20%
6. Snakebite 80 50 ---- 30 9.5%
7. Others 20 ---- ---- ---- 2.5%
8. Total 840 278 236 306
Table: 4- Total patients-840 ; Total units-1534
BLOOD
GROUP
O+ve B+ve AB+ve A+ve O-ve A-ve B-ve AB-ve
No. of
Patients
338 227 48 168 13 6 20 2
Percentage 40.9
%
27.3
%
5.9% 20% 1.7% 0.9% 2.8% 0.5%
RESULTS:
• Total patients who received FFP are 840, out of which males were 382 and females we 558
(table:1)
• Age group ranging from 0-20 years constitute 26.4%; 21-40 years 47.2%; 41-60 years
26.2% (table:2)
• Depending upon the conditions patients received FFP have been divided into 8 groups
according to the guidelines provided by British Committee for Standard Hematology3
(table:3)
• Out of 840 patients, conditions like liver diseases, disseminated intravascular coagulation
are clinically appropriate (where there is active bleeding leading to coagulopathy) and
hemophilia, sepsis, burns, rheumatic heart diseases, snake bite and shock are considered to
be appropriate (the term appropriate is limited to the treatment of coagulation protein
deficiency, for which specific factor concentrates are un available or undesirable)-(table:3)
• No.of units of FFP transfused are 1534 in six months period. Of this 40.9% are transfused to
O positive blood group (table: 4).
DISCUSSION:
� FFP is efficacious for treatment of Deficiencies of factors II, V, VII, IX, X & XI.
� Reversal of warfarin effects: Patients who are anticoagulated with warfarin are deficient in
functional vitamin K dependent coagulation factors II, VII, IX, X as well as protein C & S. FFP
can be used to achieve immediate hemostasis.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences / Volume 1 / Issue 3 / July- Sept 2012 Page 94
� Massive Blood Transfusion: In patients with documented blood clotting abnormalities,
prolonged APTT, INR after huge blood loss requiring 4 or more units of packed red cells-
FFP is commonly recommended.
� FFP can be used as a source of Antithrombin III in patients who are deficient of this
inhibitor & undergoing surgery or who require heparin for the treatment of thrombosis.
� FFP useful in infants with secondary immunodeficiency associated with severe protein
losing enteropathy, FFP can be used as a source of immunoglobulin for children & adults
with human immunodeficiency.
� FFP is used in treatment of Thrombotic thrombocytopenic purpura.
ASSOSIATED RISKS:
• Anaphylactoid reactions
• Alloimmunisation
• Transfusion related acute lung injury (TRALI): antibodies against the patients granulocytes
may cause leucocyte aggregation in pulmonary vessels leading to TRALI4
• Increase in infections
• Excess usage-Hypervolemia & cardiac failure (The guidelines set by British Committee for
Standard Hematology was followed in our study). 3
Approximately 60% FFP used are inappropriate according to Kakkar et al 5, but clinically
apparent cases like liver diseases, coronary bypass surgeries reduced the inappropriate usage to
28%. Severe liver disease6, 7, 8 is one of the most common clinical indications for transfusion of FFP.
Patients with liver diseases have several abnormalities that can lead to bleeding like coagulopathy,
Disseminated Intravascular Coagulation (DIC), Thrombosis. According to Consten et al9 & LA
Harker et al10 in cardiac surgery 11 post operative bleeding due to residual effects of heparin may be
corrected with transfusion of FFP.
CONCLUSION:
In our study appropriate & clinically appropriate transfusions of FFP were about 61%. It is
desirable that educational programmes be arranged for doctors regarding appropriate usage of
FFP.
Blood bank associations & Hematologists should more firmly adhere to the guidelines.
In our institution 61%, a good proportion of FFP transfusions were justified and 39% were
used without any appropriate indications.
ACKNOWLEDGEMENT:
I extend my special thanks to all the technical staff off blood bank and the personnel of
record room of Gandhi Hospital for helping me in collecting the necessary data.
REFERENCES:
1. NIH consensus conference: Fresh frozen plasma: indications and risk JAMA1985; 253:551-
3.
2. Snyder AJ, Gotschall JL and Menitove JE. Why is fresh frozen plasma transfused?
Transfusion1986; 26:107-12.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences / Volume 1 / Issue 3 / July- Sept 2012 Page 95
3. British Committee for standards in Hematology, blood transfusion Task force. Guidelines for
the use of Fresh frozen plasma, cryoprecipitate and cryo supernatant.TransfusionMed1992;
2:57-63.
4. Nordhagen R, Conradi M, Dromtort SM. Pulmonary reaction associated with transfusion of
plasma containing anti-Vb. VOXSANG. 1986; 5:`102-8 (Pubmed)
5. Kakkar N, Kaur R and Dhanoa J. Improvement in fresh frozen plasma transfusion practice:
results of an outcome audit. Transfus Med 2004; 14231-5.
6. Schofield WN, Rubin GL and Dean MG. Appropriateness of platelet, fresh frozen plasma and
cryoprecipitate transfusion in New South Wales public hospital. Med J Aust 2003; 178:117-
21.
7. Spector I, Corn M and Ticktin HE. Effect of plasma transfusion on the prothrombin time and
clotting factors in liver disease. Eng J Med 1966; 275: 1032-7.
8. Mannucci PM, Franchi F, Dioguardi N. Correction of abnormal coagulation in chronic liver
disease by combined use of fresh frozen plasma and prothrombin complex concentrates.
Lancet 1976; 2: 542-5.
9. Consten E, Henny CP, Eijsman L, Donglemant DA, Van Oers MH. The routine use of fresh
frozen plasma in operations with coronary bypass surgery is not justified. J thorac
Cardiovasc Surg 1996; 112:162-7.
10. LA Harker, TW Malpass, HE Branson, EA 2d Hessel and SJ Slichter. Mechanism of abnormal
bleeding in patients undergoing coronary bypass surgeries. Acquired transient platelet
dysfunction associated with selective Alpha granule release. Blood 1980; 56: 824-34.
11. Wilhelmi M, Franke U, Cohmert T, Weber P, Kaukemuller J, Fisher S, et al. Coronary artery
by pass grafting surgery with out the routine application of blood products: Is it feasible?
Eur J Cardiothorac Surg 2001; 19: 657-61

CASE REPORT
Journal of Evolution of Medical and Dental Sciences / Volume 1 / Issue 3 / July- Sept 2012
Page 96
PALATAL PLEOMORPHIC ADENOMA WITH FLORID SQUAMOUS METAPLASIA: A
POTENTIAL DIAGNOSTIC PITFALL
Abdul Hakeem Attar, Mandakini B. T, Azhar Fatima
1. Assistant Professor, Department of Pathology, KBN Institute of Medical Sciences, Gulbarga, Karnataka
2. Assistant Professor, Department of Pathology, KBN Institute of Medical Sciences, Gulbarga, Karnataka
3. Lecturer, Unanai College
CORRESPONDING AUTHOR:
Dr Abdul Hakeem Attar,
C/o Abdul Azeem Attar,
Shameem Masala,
Attar Gazar, Gulbarga.
Email id- [email protected]
ABSTRACT:
Pleomorphic adenoma is the most common benign tumor occurring in the major
and minor salivary glands. We report a case of pleomorphic adenoma with extensive
squamous metaplasia in the palate of a 20 year old man. The dimensions of the tumor were
3x2x2cm. More than 75% 0f the epithelial element in the tumor was composed of sheets of
squamous cells, with multiple keratin filled cysts. This case illustrates that pleomorphic
adenoma with squamous metaplasia presents a potential for misinterpretation as
mucoepidermoid carcinoma and squamous cell carcinoma. We discuss the various pitfalls
and the features that are helpful in distinguishing between these lesions.
KEY WORDS: Pleomorphic adenoma, Squamous metaplasia
INTRODUCTION:
Pleomorphic adenoma is the most common benign tumor occurring in the major or
minor salivary glands. [1] The tumor is characterized by epithelial and modified
myoepithelial elements intermingled with tissue of mucoid, myxoid or chondroid
appearance. It has a wide spectrum of morphological patterns, [2] squamous cells, oncocytes,
sebaceous cells, bone, adipose tissue and crystalline materials can be found in the tumor.
We report a benign salivary gland tumor with a predominant and extensive squamous
component. The features are those of a pleomorphic adenoma with florid squamous
metaplasia. This case illustrates the difficulty of making a correct diagnosis in the initial
tissue specimen and we discuss the diagnostic pitfalls of this pathological entity.
CASE PRESENTATION (CLINICAL DETAILS):
A 20 year old patient presented with complaint of swelling in the oral cavity since
two years. The swelling was painless and progressively increasing in size .Physical
examination showed a firm nodule of 4x4cm in diameter on the left side of the hard palate
and anterior part of soft palate.

CASE REPORT
Journal of Evolution of Medical and Dental Sciences / Volume 1 / Issue 3 / July- Sept 2012
Page 97
CYTOLOGICAL FINDINGS:
Fine needle aspiration was done and demonstrated some clusters of squamous cells,
with some of the cells showing keratinizing cytoplasm .Also seen some clusters of cells with
features suggestive of glandular differentiation .Differential diagnosis of well differentiated
squamous cell carcinoma & pleomorphic adenoma was made .
GROSS / HISTOPATHOLOGICAL FINDINGS:
Surgical resection was done. Gross specimen comprised of well circumscribed, well
encapsulated mass, grey white in color and measured 3x3x2cm .No cystic area, hemorrhage
or necrosis was seen .Histological examination showed a well encapsulated tumor more
than 75% of epithelial element in the tumor was composed of squamous cells with multiple
keratin filled cysts. The rest of areas showed features of conventional pleomorphic
adenoma.
DISCUSSION:
Histological diversity is the hallmark of pleomorphic adenoma. [3] Histological
patterns vary considerably between different parts of same tumor. [3] Focal squamous
metaplasia is found in about 25% of pleomorphic adenoma. Rarely focal squamous
metaplasia is reported. [4] Squamous metaplasia is commonly associated with repair
following infarction and necrosis of the salivary gland. In the present case necrosis was not
seen and squamous cells were detected in FNA biopsy as well as in the resection specimen.
squamous metaplasia has been noted in non-neoplastic entities like chronic sialadenitis,
necrotizing sialometaplasia, lymphothelial cysts occurring in the vicinity of salivary gland .
Potential for misdiagnosis of pleomorphic adenoma as mucoepidermoid carcinoma and
squamous cell carcinoma have been reported. In our case also the features misinterpreted
as mucoepidermoid & squamous cell carcinoma. To avoid misinterpretation of pleomorphic
adenoma with squamous metaplasia as mucoepidermoid carcinoma on cytology, a close
scrutiny for fragments of chondromyxoid stroma – a characteristic feature for pleomorphic
adenoma. In our case also on reviewing the slides again after histological diagnosis we could
find occasional tiny fragments of stroma . Also keratinization especially of the extracellular
type is rare in mucoepidermoid carcinoma. How ever even if the features diagnostic of
pleomorphic adenoma are identified, the differential diagnosis may still includes a
mucoepidermoid carcinoma arising in a preexisting pleomorphic adenoma.
CONCLUSION:
We have reported a case of palatal pleomorphic adenoma with florid squamous
metaplasia and with potential pitfalls in the diagnosis.
ACKNOWLEDGEMENT:
The work was indeed a mammoth task to accomplish and would not have been
possible without active co-operation, constant strategic support and encouragement by our

CASE REPORT
Journal of Evolution of Medical and Dental Sciences / Volume 1 / Issue 3 / July- Sept 2012
Page 98
beloved – PRESIDENT- (Khaja Bandanawaz Institute of Medical Sciences)—DR.SYED SHAH
KHUSRO HUSSAINI.
REFERENCES:
1. Spiro RH. Salivary neoplasms : overview . Head Neck Surg 1986; 8 :177-84
2. Waldron CA. Mixed Tumor ( pleomorphic adenoma ) and myoepithelioma. In : Ellis
GL, Auclair PL, Gnepp PR. Eds . Surgical pathology of salivary glands. Philadelphia :
Saunders , 1999; 165-86
3. Das DK. Anim JT. Pleomorphic adenoma of salivary glands. Cytopathology 2005 : 16:
65-70
4. Lam KY, Ng IOL, Chan GSW. Palatal pleomorphic adenoma with florid squamous
metalasia . J Oral Pathol Med. 1998; 27: 407-10.

CASE REPORT
Journal of Evolution of Medical and Dental Sciences / Volume 1 / Issue 3 / July- Sept 2012
Page 99
Fig 1- Photograph showing swelling in the palate
Fig 2- Gross photograph showing well circumscribed tumor

CASE REPORT
Journal of Evolution of Medical and Dental Sciences / Volume 1 / Issue 3 / July- Sept 2012
Page 100
Fig 3- Photomicrograph showing squamous cells with keratin pearls. (H&E, 400X)

CASE REPORT
Journal of Evolution of Medical and Dental Sciences / Volume 1 / Issue 3 / July- Sept 2012
Page 101
Fig 4- Photomicrograph showing conventional pleomorphic adenoma (H&E, 400X)

CASE REPORT
Journal of Evolution of Medical and Dental Sciences/Volume 1/Issue 3/July- Sept 2012 Page 102
CUTANEOUS NECROTISING VASCULITIS – THERAPEUTIC FACT-A CASE
REPORT
Dr Kiran. D. R, Dr Palaniswamy
1. Associate Professor, Department of General Medicine, Karuna Medical College, Vilayodi, Chittur, Palghat,
Kerala.
2. Professor, Department of General Medicine, Karuna Medical College, Vilayodi, Chittur, Palghat, Kerala.
CORRESPONDING AUTHOR:
Dr. Kiran D R.,
Associate Professor,
Department of Medicine,
Karuna Medical College, Vilayodi,
Chittur, Palghat, Kerala.
Email id- [email protected]
ABSTRACT: INTRODUCTION: Mixed connective tissue disorder, unlike other connective tissue
disorders have a milder course. MTCD with only necrotizing cutaneous vasculitis without organ
damage respond well to Immunosuppresents and Steroids. CASE REPORT: Middle aged Young
lady presented with multiple non healing large pressure sores and multiple nonblanchable
purpuric lesions. She was bedridden, anaemic and with significant weight loss. All her major
organ functions were normal. Her U1 RNP Antibody is positive and Skin Biopsy showed
positive direct fluorescent test for IgG. She responded well to immunosuppresants and steroids.
CONCLUSION: This patient who presented with MTCD, with predominant necrotizing
cutaneous vasculitis and without major organ involvement showed good recovery and
responded well to cyclophosphamide pulse therapy, daily azathioprine and good wound care.
KEY WORDS: Necrotising Vasculitis, MCTD, U1 RNP Antibody, Immunosuppresants
INTRODUCTION:
Vasculitis is not a disease but rather a disease process (from Merck manual).Here we
came across a MCTD with predominant necrotizing vasculitis involving only skin .This is been
reported so as to stress the fact that MTCD , unlike other connective tissue disorders has milder
course and necrotizing vasculitis confined to skin do well with immunosuppresives, steroids
and good wound care 5.
CASE REPORT:
Female patient aged 34 year old, presented with weight loss( more than 10%), lethargy
and multiple non healing open ulcers associated with necrotic base over pressure bearing areas
predominantly confined to extensor areas of limbs of one year duration. She had intermittent,
moderate grade fever without cough and rashes. She was bed ridden due to sever nonhealing
disabling ulcers over the pressure bearing areas and joint contractures.
On examination, Patient is thin built and poorly nourished.
Multiple non blanchable purpuric lesions, multiple depigmented lesions on face and loss of scalp
hair.
Pallor present, Febrile, Tachycardia present.
Systemic examination– Normal.

CASE REPORT
Journal of Evolution of Medical and Dental Sciences/Volume 1/Issue 3/July- Sept 2012 Page 103
Investigations: Hb 6gm/dl, WBC -8200, Eosinophils increased, Platelet count- 80,000, ESR-110,
CRP elevated,
LFT and RENAL FUNCTION: Normal
Urine Routine: Normal, No albumin or microscopic Haematuria
ECG: WNL
Echo: No pericardial fluid, EF – 60%, Normal Function.
PFT: Normal curve, No features of interstitial pattern.
Chest X Ray: CP angles free and normal, lung parenchyma normal, No Infiltrates.
USG Abdomen: NO Organomegaly, pelvis normal.
Stool examination: No occult blood.
CT brain: Normal study.
NCS: Normal.
Ophthalmological Examination: Visual Aquity-6/6, Fundus –Normal.
ANA positive, RA Factor negative
ANCA negative, U1 RNP Antibody positive,
Skin Biopsy – direct fluorescent test positive for IgG, Complements were normal ,
HIV 1&2 negative, Hepatitis B & C Negative.
Diagnosis of MCTD was made with above findings.
TREATMENT GIVEN:
Patient was started with steroids, monthly pulse therapy of Cyclophosphamide and daily
2mg of Azathioprine. Other general conditions maintained with blood transfusion and
supportive care. Wounds were been taken care of by debridement and allowed them to go for
healing by secondary intention. Some of the wounds healed in one setting, but others required
2-3 attempts. Finally in six months duration all wounds healed well and now patient is
ambulatory, self dependant with only Azathioprine daily.
ACKNOWLEDGEMENT:
I take this opportunity to extend my sincere thanks and indebtedness to all those
persons and dignitaries who helped me to complete this work.
It gives pleasure to express my sense of gratitude to my professor Dr Palaniswamy for
his guidance, encouragement and constant source of inspiration during case management.
Above all I thank the Almighty for the successful completion of this work.
DISCUSSION:
MCTD also known as Sharp’s syndrome an undifferentiated connective tissue disease.
MCTD a combined feature of scleroderma, myositis, SLE and Rheumatoid Arthritis (with some
source adding polymyositis, dermatomyositis and inclusion body myositis) and is thus
considered as overlap syndrome. MCTD commonly causes joint swelling, malaise, Raynaud’s
phenomenon, Sjogren’s syndrome, muscle inflammation and sclerodactyly. Distinguishing lab
characteristics are positive speckled ANA and an anti U1RNP antibody. It is associated with HLA
DR-41.
Vasculitis induced injury to blood vessel may lead to increased vascular permeability,
vessel weakening that cause aneurysm formation, haemorrhage and intimal proliferation,
thrombosis that result in obstruction and local ischemia2. It is critical to distinguish vasculitis
occurring as a primary autoimmune disorder from vasculitis secondary to infection, drugs,
malignancy or connective tissue disease such as SLE/ RA. Much of the diagnostic work up in a

CASE REPORT
Journal of Evolution of Medical and Dental Sciences/Volume 1/Issue 3/July- Sept 2012 Page 104
patient with suspected vasculitis is directed at excluding secondary causes that can mimic
vasculitis3.
Immunoglobulin finding may be helpful in diagnosing MTCD. Indirect Immuno
fluroscent test – Presence high titre of IgG against U1RNP as the only autoantibody support
MTCD. The fluroscent auto nuclear antibody test typically reveals a speckled pattern of staining
on HEP-2 substrate. Recent studies revealed that antibody directed to an appropriate specific
epitop on 70 kd are specifically associated with MTCD than other anti 70 k antibody. Direct
Immuno fluroscent test- Performed on lesional skin of patients with MTCD, this may reveal
epidermal nuclear IgG staining. The staining is thought to be related to high titres U1RNP
antibody in the patient seen. In some cases Lupus Band test may be positive (linear deposition
of Ig, Fibrin and/or compliment components present at the basement membrane) 4.
Treatment option includes corticosteroids, Immunosuppressive drugs to reduce the
inflammation. Cyclophosphamide may be in severe vasculitis. Dramatic remission seen in
patient with alternate day corticosteroid treatment with continuation of cyclophosphamide.
Later corticosteroid was discontinued. Mean duration of remission was 22 months. No patient
showed recurrence of disease during treatment with cytotoxic agents5. IV cyclophosphamide is
better than oral and recommended at least six months. Substitution of Azathioprine after
remission with cyclophosphamide did not increase the rate of relapse.
Newer treatment approach includes deoxysperagualin, achieved a high rate of disease
remission and permitted prednisolone reduction. Other newer Immunosuppresives are
Leflunamide, TNF antagonists – Infliximab and ENBREL. Colchicine not that much effective in
skin va sculitis, but some showed improvement. Development of plasma exchange including
semi specific immunoabsorption with L-tryptophan or Protein A columns to remove ANCA
without depletion of non Ig plasma proteins and appear of comparable efficacy to plasma
exchange6.
CONCLUSION:
MCTD, although called as overlap syndrome, here we came across MCTD without major
organ involvement, without associated other connective tissue diseases. Predominant
presentation was confined to skin as necrotizing cutaneous vasculitis. The disease here showed
a chronic disabling course which provided enough time to treat with Pulse cyclophosphamide
therapy, daily Azathioprine and good wound care. MCTD without predominant organ
dysfunction and confined to skin manifestation as a good prognosis with regular treatment than
the systemic vasculitis or MCTD with other connective diseases, which has mixed results to the
regular treatment.
REFERENCES:
1 Aringer M, Steiner G, Smolen JS (Aug-03). “Does MCTD exist? Yes.” Rheumatic disease clinical
North America. 31(3): 411-29.
2 Mandell BF, Hoffman G.S. Differrentiating the Vasculitis. Rheumatic disease clinical North
America (1994); 20:409-42.
3 Hunder G. Vasculitis Diagnosis and therapy. Am. J Med: 1996; 100(22):375-455
4 H Ihn, K Yamane, N Yazawa, M Kuba, M Fujimoto, S Sato, K Kikuchi and K Tamaki; Distribution
of antigen specificity of Anti U1RNP antibody in patient with systemic sclerosis. Clinical
Experimental Immunology(1999)117(2);383-387.
5 FauciAS,Katz P,Haynes BF, Wolf SM:Cyclophosphamide therapy for sever necrotizing
vasculitis(1979) vol 301:235- 238.

CASE REPORT
Journal of Evolution of Medical and Dental Sciences/Volume 1/Issue 3/July- Sept 2012 Page 105
6 Jayne D (2000)Evidence based treatment of systemic vasculitis. Rheumatology(Oxford)
39:585-595.
ABBREVIATIONS:
MCTD: Mixed Connective Tissue Disease
HLA: Human Leucocyte Antigen
SLE: Systemic Lupus Erythematosis
RA: Rheumatoid Arthritis
RNP: Ribosomal Neucleo Protein
ANA: Anti Nuclear Antibody
ANCA: Anti Nuclear Cytoplasmic Antibody
Post Treatment- Healed cutaneous Vasculitis on face, Post Healed Hypopigmented Lesion

CASE REPORT
Journal of Evolution of Medical and Dental Sciences/Volume 1/Issue 3/July- Sept 2012 Page 106
PLASMA CELL LEUKEMIA- LIGHT CHAIN SECRETORY TYPE, WITH
PRIMARY AMYLOIDOSIS
Dr Kiran. D. R, Dr Palaniswamy
1. Associate Professor, Department of General Medicine, Karuna Medical College, Vilayodi, Chittur, Palghat,
Kerala.
2. Professor, Department of General Medicine, Karuna Medical College, Vilayodi, Chittur, Palghat, Kerala.
CORRESPONDING AUTHOR:
Dr. Kiran D R.,
Associate Professor,
Department of Medicine,
Karuna Medical College, Vilayodi,
Chittur, Palghat, Kerala.
Email id- [email protected]
ABSTRACT:
INTRODUCTION: Secondary PCL (Plasma Cell Leukemia), arising from multiple myeloma is
aggressive and rare variant of multiple myeloma. It is known that AL (Amyloid Light Chain)
type of Amyloidosis is primary amyloidosis occurring in multiple myeloma. Attempt to report
this case of secondary PCL of light chain secretory type with primary amyloidosis. Emphasis
given to this report is so as to highlight the helpful prognostic tools in this rare variety.
CASE REPORT: 60 year old female presenting with Hepatosplenomegaly, severe anemia,
bleeding manifestations and fever. She had pancytopenia with ESR of 170. Peripheral smear
showed plenty of plasma cells >20% and bone marrow biopsy showed mature to immature
plasma cells, plenty in number. Skull X ray showing multiple punched out lesions.
Electrophoresis was normal, abdominal wall fat stained positive for Congo Red and Serum Free
Light Chain Assay was positive. Diagnosed as PCL of light chain secretory type. CONCLUSION:
PCL itself, high plasma cell labeling index, increased LDH, increased serum
β2microglobulin,renal indices like increased serum creatinine, organomegaly, non secretory
variety-all carry bad prognostic signs.
KEY WORDS: PCL, Primary Amyloidosis, Light chain, Punched out bone lesions
INTRODUCTION:
It is known that incidence of PCL is <1 / million cases and 2% of multiple myeloma1. It is
an aggressive and rare presentation of multiple myeloma2. It has features of acute leukemia and
multiple myeloma.PCL usually arises from myeloma having IgD or IgE as M component. PCL,
arising from pre existing multiple myeloma of light chain secretory type associated with AL
(Amyloid Light chain) type of Amyloidosis is very rare. Since there are no large trials on
treatment of patients with PCL, we here make an attempt report this case.
CASE REPORT:
A 60 years old female patient presented with history of fever and epistaxis of one month
duration. On examination she was Febrile, having tachycardia and pallor. She had no
generalized lymphadenopathy but had moderate Hepatosplenomegaly. She had sternal
tenderness.

CASE REPORT
Journal of Evolution of Medical and Dental Sciences/Volume 1/Issue 3/July- Sept 2012 Page 107
INVESTIGATIONS:
WBC count – 1, 22,000
Hb-2.8mg/dl
Platelet count – 80,000
ESR- 170
Renal and Liver function tests are normal
Serum calcium: 12 mg/dl
Serum uric acid: normal
Serum LDH: 310u/L
Serum β2 microglobulin: 3.1mg/L
Serum Electrophoresis showed no M band
Serum Free Light Chain Assay: detected
Urine Bence Jones protein: Negative
Peripheral Smear Report: RBC showed hypochromia and anisocytosis. Neutrophils were
decreased in number. A large number of plasma cells were seen .Immature and abnormal
plasma cells were seen in plenty. A good number of binucleated plasma cells also seen.
Immature cells exceeded 20%. Platelets grossly decreased in number.
Bone Marrow Aspiration Report: Hypercellularmarrow.RBC precursors were reduced in
number and were normopoietic. Granulocytic precursors were also reduced in number. Each
field showed sheets of plasma cells. Many of the plasma cells were atypical. Some of them were
rounded, some had nuclear abnormalities and some were binucleated. A large number of
plasma blasts were also seen. Megakaryocytes were reduced in number.
Flow Cytometry of Bone Marrow Aspirate: Showed intense positivity for CD 38 and the
presence of cytoplasmic kappa light chains.
Abdominal fat stained positive for Congo Red.
Skull X-ray showed multiple punched out lesions.
Our patient was diagnosed to have primary PCL – light chain type with Primary Amyloidosis,
based on peripheral smear, bone marrow and flow cytometric analysis.
Treatment: Patient was given supportive treatment. Prednisolone and Melphelan were started.
Patient expired in two months after diagnosis.
DISCUSSION:
Plasma cell leukemia is a lymphoproliferative disorder. It is a rare monoclonal
neoplasm having B lymphocyte lineage. It is one of the aggressive human neoplasms accounting
for 2-4% of all cases of plasma cell diseases3. Rarity of PCL can be accessed from the fact that at
M.D. Anderson cancer centre, 27 patients with PCL were seen in 20 year period whereas at
Policlinico-Sanmateo in Italy, 15 cases were seen in 15 years, both representing 2-5% of total
cases of multiple myeloma seen at these centers. Incidence of PCL is less than 1 case per million
population1. Presentation may be primary, secondary – evolving from an existing case of
multiple myeloma as part of the terminal phase of the disease or denova. Sixty to seventy
percent cases are primary. PCL is of two types, Secretory and non-secretory. No M protein is
detected in the non secretory type of PCL4.
WHO criteria to diagnose PCL are - Plasma cells constitute more than 20% of cells in the
peripheral blood with an absolute plasma cell count of more than 2 X 109 / litre.
Lab findings: There is overlap between cells of multiple myeloma and Primary PCL. PCL plasma
cells more frequently express the CD 20 antigen than those of multiple myeloma and they often

CASE REPORT
Journal of Evolution of Medical and Dental Sciences/Volume 1/Issue 3/July- Sept 2012 Page 108
lack CD 56 antigen which is present on the majority of myeloma cells. CD 56 is important in
anchoring plasma cells to bone marrow stroma and its expression is associated with poor
prognosis. CD 28 is more frequently expressed on malignant plasma cells in secondary than in
primary PCL. Acquisition of CD 28 is associated with increased proliferative rate and disease
progression. PCL is derived from terminally differentiated B cells and the malignant cells stain
positive for mature B cell markers (CD38 and PCA1, Prostate Cancer Antigen 1)5.
In 80% of PCL patients, using FISH (Flourescent In Situ Hybridisation) technique- losses in long
arm of chromosome 13 (13 Q) and deletion of one of the homologous chromosome 13
(Monosomy 13). In 80% of cases, loses on chromosome 16 also occur. Overexpression of
PRAD1/cyclinD1 (Parathyroid associated Neoplasia gene) also present (help in controlling cell
cycle). PCL is more frequent in light chain (Bence Jones’s protein) or IgD myeloma and less in
IgA or IgG myeloma. Hypercalcaemia and increased LDH are known bad prognostic signs of
disease 6. PCL is an extremely aggressive disease with no standard treatment regimen so far
due to the rarity of the disease. Median survival is 2-8 months, prognosis is very poor.
Regimens includes MP, (Melphelan, Prednisolone) VAD (Vincristine, Doxorubicin,
Dexamethasone) TD (Thalidomide, Dexamethasone) VBAP (Vincristine, Carmustine,
Adriamycin, Prednisolone) 7. Case reports regarding long time survival after autologous bone
marrow transplantation or stem cell transplantation also exists but again there is no long term
prospective data on a large number of patients. We presented this case for its rarity.
CONCLUSION:
PCL itself has aggressive course, short survival time, high plasma cell labeling index,
expression of CD 28, Cyclin, PRAD 1 indicate high proliferation. Lytic bone lesion is more
common in multiple myeloma than PCL. Biochemical parameters like increased serum
creatinine, LDH, Serum β2microglobulin and calcium have poor prognosis. Amyloidosis
associated multiple myeloma indicate tumor burden. Non secretory variety has got bad
prognosis. So above mentioned prognostic tools may help to judge the severity of the tumour
burden in a PCL case and act accordingly
ABBREVIATIONS:
PCL: Plasma Cell Leukemia
LDH: Lactate Dehydrogenase
CD: Cluster Differentiating
AL: Amyloid Light
ACKNOWLEDGEMENT:
I take this opportunity to extend my sincere thanks and indebtedness to all those
persons and dignitaries who helped me to complete this work.
It gives me pleasure to express my sense of gratitude to my Professor Dr Palaniswamy,
for their guidance, encouragement and constant source of inspiration during case management.
Above all I thank the Almighty for the successful completion of this work.
CASE REPORT
Journal of Evolution of Medical and Dental Sciences/Volume 1/Issue 3/July- Sept 2012 Page 109
Skull X Ray PA view- Showing punched out lesions
Skull X Ray Lateral view- Showing punched out lesions
REFERENCES:
1. Kosma MA, Gale RP. Plasma Cell Leukemia.SeminHaematology 1987.24; 202-8
2. DimopoulasMA,PalumboA,DelasalleKB,AlexanianR.Primary Plasma Cell leikamia.Br
Journal Hematol 1994;88;754-9.
3. Chan SM, George T, Cherry AM,Medeiras BC(2009) Complete remission of primary PCL
Bortezomito, Doxorubicin and Dexamethasone; a case report; cases 12: 1186/1757-
1626-2.
4. ShindoT,Yumoto Y, Yoshida M, Okuda T; Non Secretory Primary Plasma Cell Leukemia
successfully treated with VAD and MP therapy.RhinshoKetsueki; 2002;43; 107-11
5. Badhe BA, Basu D, Toe P Ch,Dutta TK, Ghotekar LH; Plasma Cell Leukemia; a case report.
Indian Journal Pathology Microbiology 2003; 46; 484-7.
6. Voutsadakis IA; Plasma Cell Leukemia. Hama 2000; 3:82-9.
7. Suzuki M, Kawauchi K, Sugiyama H, Yasuyama M, Watanabe H. Primary Plasma Cell
Leukemia; a case report of successful responder to a combination of Vincristine,
Doxorubicin and Dexamethasone. ActaHematol 1989; 82:95-7.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/ Volume 1/ Issue 3/ July- Sept 2012 Page 110
ANTI-CONVULSANT ACTIVITY OF GANAXOLONE ALONE AND IN
COMPARISON WITH STANDARD ANTI-EPILEPTIC DRUGS IN
RODENT MODELS
Mr. S.K. Subhani Basha, Dr .B. L. Kudagi, Dr. R. Pravin Kumar
1. Tutor, Department of Pharmacology, Narayana Medical College, Nellore.
2. Professor & H.O.D., Department of Pharmacology, Narayana Medical College, Nellore.
3. PG Student, Department of Pharmacology, Narayana Medical College, Nellore.
CORRESPONDING AUTHOR:
Dr .B. L. Kudagi,
Professor & H.O.D.,
Department of Pharmacology,
Narayana Medical College,
Nellore.
Email ID- [email protected]
ABSTRACT:
BACKGROUND: Presently, treatment of epilepsy with standard anti-epileptic drugs is
associated with a number of shortcomings inviting us to study newer agents that would
overcome these problems or search for the drugs or substances, which would enhance the
efficacy or reduce the dose or toxicity of these standard anti-epileptic drugs. Ganaxolone
(GNX) (3α-hydroxy-3β-methyl-5α-pregnan-20-one), a synthetic analog of the endogenous
neurosteroid allopregnanolone and a positive allosteric modulator of GABAA receptors, may
represent a new treatment approach for epilepsy. AIM: To evaluate the effect of Ganaxolone
on maximal electroshock (MES) induced and Pentylenetetrazol (PTZ) induced convulsions
and also their effect in combination with conventional antiepileptic drugs (CAEDs).
MATERIAL AND METHODS: Wister strain albino rats weighing 200-250 gm were used.
Effects of Ganaxolone (5 &10 mg/kg) alone and in combination with standard drugs were
studied in MES and PTZ induced seizure models. Abolition of tonic hind limb extension was
an index of anticonvulsant activity in MES, while for PTZ seizures; failure to observe clonus
for 5sec duration for 30min was the index. Following that, percentage inhibition was
calculated. STATISTICS: ANOVA followed by Newman-Keuls Multiple Comparison Test was
used for analysis of data between the groups. RESULTS: In MES seizures, significant anti-
epileptic activity was observed with 10mg of Ganaxolone compared to control group but
has less activity when compared to that of Phenobarbitone. In PTZ induced convulsions, the
anti-epileptic effect of Sodium Valproate was higher than Ganaxolone, but both were
statistically significant as compared to control. In PTZ-induced seizures, augmented effects
were obtained when Ganaxolone was combined with sodium valproate i.e. 55%.
CONCLUSIONS: The results provide a lead for potential benefit of adding Ganaxolone to
Sodium Valproate in the treatment of epilepsy, which needs to be explored further.
KEYWORDS: Seizures, Ganaxolone, Phenobarbitone, Sodium Valproate, Pentylenetetrazol,
Hydoxypropyl-β-Cyclodextrin, GABA.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/ Volume 1/ Issue 3/ July- Sept 2012 Page 111
INTRODUCTION:
Epilepsy is a common and chronic neurological disorder characterized by apparently
unprovoked recurrent paroxysmal events or seizures that are associated with a sudden
alteration in motor activity and behavior, with or without alteration in conscious
awareness. The alteration in state is the result of an abnormal and excessive hyper
synchronous firing within a group of epileptic neurons in the brain1. Epilepsy affects
around 50 million people worldwide and the majority of people with epilepsy (70%) have
a good prognosis if they receive appropriate treatment. The prevalence of active epilepsy is
roughly in the range of 5–10 per 1000 people2. Epilepsy's approximate annual incidence
rate is 40–70 per 100,000 in industrialized countries and 100–190 per 100,000 in
resource-poor countries; socioeconomically deprived people are at higher risk. In
industrialized countries the incidence rate decreased in children but increased among the
elderly during the three decades prior to 2003, for reasons not fully understood. Epilepsy's
lifetime prevalence is relatively high because most patients either stop having anti-epileptic
drugs or (less commonly) die3.
In about two-thirds of all patients affected with epilepsy, seizures are well
controlled with currently available anti-epileptic drugs, while in the remainder seizures are
refractory to treatment. Moreover, many of the existent anti-epileptic agents produce many
undesirable side-effects including drowsiness, mental dullness, nausea, ataxia, paresthesia,
hematologic changes, hirsutism, weight gain, hypertrophy of gums and congenital
malformations. For these reasons, new antiepileptic drugs are needed to improve seizure
control and decrease side-effect profile4.
At the neuronal level, seizure activity often occurs when glutamatergic excitatory
neurotransmission overrides GABA-mediated inhibition. Therefore, glutamatergic and
GABAergic systems are rational targets for antiepileptic drug development5. Pharmacological
manipulations leading to increased levels of GABA (by inhibition of GABA degradation or
reuptake) and/or positive allosteric modulation of the GABA receptor complex are among
the approaches that have been used to facilitate inhibitory GABAergic neurotransmission6.
Ganaxolone (3α-hydroxy-3β-methyl-5α-pregnan-20-one), the 3β-methyl analog of the
progesterone metabolite allopregnanolone, is the first synthetic neurosteroid related agent
to be evaluated in man for the drug treatment of epilepsy, which is now undergoing phase-
III clinical trials7. Ganaxolone, like Allopregnanolone, acts as a powerful positive
allosteric modulator of GABAA receptors, resulting in enhanced neural inhibition8.
Hence, the present study was undertaken to determine whether Ganaxolone alone or
along with standard antiepileptic drugs could provide superior seizure control in maximal
electroshock (MES) induced and Pentylenetetrazol (PTZ) induced convulsions as compared
to CAEDs.
MATERIALS & METHODS:
ANIMALS:
Wister strain albino rats weighing between 200-250gms were used, for this study.
The animals were obtained from the central animal house of Narayana Medical College,

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/ Volume 1/ Issue 3/ July- Sept 2012 Page 112
Nellore. They were housed in standard polypropylene cages. The animals were excluded if the
weight of rats were below 200gms and if they had any visible diseases. The animals are
maintained under standard laboratory conditions (12:12 hr light: dark cycles and
temperature 250C ± 10C with free access to food and water ad libitum. All the experiments
were carried out around the same time each day. All the experimental procedures and
protocols were reviewed and approved by the Institutional Animal Ethics Committee (IAEC)
of the institute, with protocol number 12/2010/NMC.
CHEMICALS & DRUGS:
All standard chemicals used in this study were of analytical grade. Pure form of
Ganaxolone & Hydoxypropyl-β-Cyclodextrin were obtained from Sigma chemicals. Stock
solutions of Ganaxolone for injection were made in 40% Hydoxypropyl-β-Cyclodextrin in
water. By itself, β-cyclodextrin at concentrations as high as 50% failed to affect seizures.
ASSESSMENT OF ANTICONVULSANT ACTIVITY:
GROUPING:
To study the anti-epileptic activity of Ganaxolone, two models namely MES induced
convulsions and Pentylenetetrazol induced convulsions in rats were used. Each model
consists of five groups, each group containing 6 animals.
Groups were divided as follows,
Group I (Control group) was treated with 40% (w/v) Hydoxypropyl-β-Cyclodextrin 4ml/kg
body weight.
Group II received Ganaxolone at a dose of 5 mg/kg body weight.
Group III received Ganaxolone at a dose of 10 mg/kg body weight.
Group IV received standard drug (Phenobarbitone 20mg/kg – MES, Sodium Valproate
200mg/kg – PTZ seizures).
Group V received Ganaxolone at 5 mg/kg body weight and standard drug.
Separate groups of animals were used for different models and all the groups
received the drugs intraperitonially at different sites throughout the experiment.
Concentration of drugs were so adjusted that all the animals in the group received the
same volume of preparation throughout the study. All the drugs were given 30 min prior
to the induction of convulsions.
MES SEIZURE METHOD9:
Anticonvulsant activity of Ganaxolone was tested for MES seizure by inducing
convulsions with an electroconvulsiometer. In this method, electrical stimulation was
applied via clipped-ear electrodes (moistened with saline solution before each application)
which delivered a constant current of 150mA current for 0.2 seconds. Abolition of hind limb
tonic extension was taken as an index of anticonvulsant activity10. Parameters observed
were time for onset and duration of tonic hind limb extension (THE).
CHEMICALLY INDUCED SEIZURES9:

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/ Volume 1/ Issue 3/ July- Sept 2012 Page 113
Pentylenetetrazol is a tetrazol derivative with consistent convulsive effect in a larger
number of animal species like mice, rats, cats, primates etc. It is believed to act by
antagonizing the inhibitory GABAergic neurotransmission10. This model was used to screen
the anti-epileptic efficacy of Ganaxolone against petit mal epilepsy as Ganaxolone also acts
through GABA-A receptor modulator mechanism.
Rats were injected with Pentylenetetrazol (70 mg/kg, i.p) 30 minutes after test drug
and standard drug (Sodium Valproate – 200mg/kg) and the occurrence of the first
generalized clonus (repeated clonic seizures of the fore and hind limb lasting over 5sec.
with an accompanying loss of righting reflex) or jerky movements were recorded during
individual observation for 30 min.
STATISTICAL ANALYSIS:
The data was collected in case record forms and then entered into excel
spreadsheet 2007. Statistical analysis was performed using Microsoft Excel – 2007 and
Sigma Graph pad prism version-5 USA. Data was described as Mean ± Standard deviation.
One way ANOVA followed by Newman-Keuls Multiple Comparison Test was used for
analysis of data between the five groups. For all inferential statistical tests a two tailed P
value of less than 0.05 was considered significant.
RESULTS:
EFFECT OF GANAXOLONE ON TONIC HIND LIMB EXTENSION IN MES:
Tonic hind limb extension was completely abolished in group IV (treated with
Phenobarbitone) and group V (combination of Ganaxolone and Phenobarbitone). Percentage
inhibition of duration of tonic hind limb extension increased with the use of Ganaxolone
10mg/kg up to 50% and were 100% for group IV and V. MES induced convulsions
blocking activity of Ganaxolone 10mg/kg was extremely significant (p<0.001) when
compared to that of control but it was less effective when compared to Phenobarbitone.
The combination of Ganaxolone + Phenobarbitone has a similar / superior MES induced
convulsions blocking activity compared to that of Phenobarbitone alone.
EFFECT OF GANAXOLONE ON PTZ INDUCED SEIZURES:
The onset of jerky movements in PTZ induced convulsions were significantly
delayed by Ganaxolone 10mg/kg (p<0.001) as compared to the control. Percentage
inhibition of duration of jerky movements with 10 mg of Ganaxolone was 37.5% and it was
45% for sodium valproate, whereas as the combination of Ganaxolone + Sodium Valproate
(group V) further decreased the duration of jerky movements up to 55%, implying that PTZ
induced convulsions blocking activity of Sodium Valproate was more than that of
Ganaxolone, but both were statistically significant. The combination of Ganaxolone and
Sodium Valproate has a superior PTZ induced convulsions blocking activity compared to
that of Sodium Valproate alone.
DISCUSSION:

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/ Volume 1/ Issue 3/ July- Sept 2012 Page 114
The present study was aimed at evaluating the effect of Ganaxolone on maximal
electroshock (MES) induced and Pentylenetetrazol (PTZ) induced convulsions and also
their effect in combination with conventional antiepileptic drugs (CAEDs) using animal
models.
Ganaxolone (GNX) is the synthetic analog of allopregnanolone (3α, 5α-P ) it belongs
to a class of compounds referred to as neurosteroids that have been termed “epalons”
which has been presumed to possess sedative, anxiolytic, and anticonvulsant effects11.
Maximal electric shock induced convulsions is a suitable test for evaluating anti-
epileptic properties of drugs, because it is the best-validated preclinical test that predicts
drugs effective against generalized seizures of the tonic–clonic (grand mal) type.
In our study, we demonstrated significant anti-epileptic activity with 10mg of
Ganaxolone compared to control group but has less activity when compared to that of
Phenobarbitone but both were statistically significant. Using this model, Virinder Nohria et
al. (2007) reported that, although Ganaxolone effectively blocked tonic seizures induced by
maximal electroshock in mice (ED50 of 29.7 mg/kg, i.p.), it did so at doses that produced
ataxia on the rotorod ( mean toxic dose, TD50, of 33.4mg/kg, i.p.)12. Same results were
observed by Richard B. Carter et al (1997), who also reported that Ganaxolone was less
potent against MES (ED50 of 29.7 mg/kg i.p.) than sodium valproate, resulting in protective
indices of 1.1, as opposed to 1.9 for valproate9.
We also evaluated the anti-epileptic activity of Ganaxolone using Pentylenetetrazol
induced convulsions model, as this test is used for screening of drugs effective in petit mal
epilepsy or absence seizures. By analyzing our results we like to state that PTZ induced
convulsions blocking activity of Ganaxolone was slightly less than that of Sodium Valproate.
Our study was supported my Richard B. Carter et al (1997), who also reported that
Ganaxolone produced potent anticonvulsant effects with PTZ induced convulsions, with an
i.p. ED50 of 4.3 mg/kg in mice and 7.8 mg/kg in rats. Ganaxolone was also active after oral
administration in rats, with an ED50 of 21.0 mg/kg. The profile of anticonvulsant activity
obtained for Ganaxolone is similar in many respects to that of the clinically used reference
agent valproate. Ganaxolone is superior to valproate, however, in its ability to increase the
seizure threshold for i.v. PTZ infusion at nonataxic doses9.
Also, Marjolein Beekman et al (1998) concluded that the neuroactive steroid
Ganaxolone is superior to a host of standard antiepileptic agents (Diazepam, Clonazepam,
Valproic acid, Ethosuximide, Phenobarbitone) in controlling the behavioral disturbances that
result from both acute PTZ administration and a regimen of PTZ that induces seizure
kindling. Although much less potent than Ganaxolone, Phenobarbital was the drug that most
closely mirrored Ganaxolone in its anti-PTZ effects13 .
Furthermore, Virinder Nohria et al (2007) also reported that Ganaxolone was
effective against clonic convulsions induced by subcutaneous Pentylenetetrazol
administration in mice and rats (ED50 values of 4.3 and 7.8 mg/kg i.p., respectively). He
also stated that PTZ-induced seizures in rats did not develop tolerance to chronic treatment
with Ganaxolone12.
MES-induced tonic extension can be blocked by drugs that inhibit voltage dependent
Na + channels, such as phenytoin, carbamazepine, and valproate (Macdonald and Kelly,1995;

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/ Volume 1/ Issue 3/ July- Sept 2012 Page 115
Rogawski and Porter, 1990; White, 1997), as well as by drugs that block glutamatergic
excitation mediated by the N-methyl-D-aspartate receptor, such as felbamate (McCabeet al.,
1993; Subramaniam et al., 1995; White et al., 1995). In contrast, clonic seizures induced by
PTZ can be blocked by drugs that reduce T-type Ca++ currents, such as ethosuximide
(Coulter et al., 1989), and drugs that enhance GABA-A receptor mediated inhibitory
neurotransmission, such as benzodiazepines, phenobarbital and perhaps valproate and
felbamate (Macdonald and Kelly, 1995; Rogawski and Porter, 1990; White, 1997)9.
Ganaxolone exhibits anticonvulsant activity to PTZ and to a lesser extent against
MES induced convulsions. Ganaxolone increased the seizure threshold before attaining a
dose sufficient to produce ataxia on the rota rod. The ability of Ganaxolone to both elevate
seizure threshold and block i.p. PTZ induced seizures can be attributed to its modulatory
effect on GABA-A neurotransmission. Whether this effect contributes to its ability to block
MES induced tonic extension is not known, but that is likely, because there is at present
no experimental evidence to suggest that Ganaxolone blocks voltage-dependent Na+ channels
or N-methyl-D-aspartate receptors.
Ganaxolone inhibits binding of the GABA-A chloride channel ligand and enhanced
binding of the benzodiazepine site ligand and the GABA site ligand. Electrophysiological
recordings showed that nanomolar concentrations of GNX potentiated GABA-evoked chloride
currents in Xenopus oocytes expressing human GABA-A receptor subunits α1, β2, γ2L, but
direct activation of chloride flux occurred only at micromolar concentrations14,15.
The unique potency and efficacy of Ganaxolone against PTZ induced convulsions have
several implications. First, these anti-epileptic effects of Ganaxolone in PTZ induced
convulsions appear to be predictive of the potency and efficacy of Ganaxolone against absence
seizures as it compares favorably with that of valproate. The results provide a lead for
potential benefit of adding Ganaxolone to Sodium Valproate in the treatment of epilepsy,
which needs to be explored further. Second, Ganaxolone may provide additional benefit in the
treatment of epilepsy by controlling anxiety, mood changes and other behavioral alterations
associated with preseizure activity. Finally, Ganaxolone may represent a novel treatment
approach to the clinical control of epilepsy.
CONCLUSION:
Overall, Ganaxolone is a high-affinity, stereo selective, positive allosteric modulator of
GABA-A receptors that exhibits potent, broad-spectrum anti-epileptic activity. The present
study supports clinical evaluation of Ganaxolone as an anti-epileptic medication with
potential therapeutic utility in the treatment of generalized, absence seizures as well as
simple and complex partial seizures, alone or as an add on drug with the conventional anti-
epileptic drugs to reduce their dose / adverse effects.
ACKNOWLEDGEMENTS:
The authors are thankful to the staffs and PGs of Narayana Medical College, Nellore
and Sigma Aldrich.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/ Volume 1/ Issue 3/ July- Sept 2012 Page 116
Table 1: Antiepileptic effect of Ganaxolone alone and in combination with Phenobarbitone
on Maximal Electric Shock (MES) induced seizures in rats
Table 2: Antiepileptic effect Ganaxolone alone and in combination with Sodium Valproate on
PTZ induced seizures in rats
S.No Group & Dose
(mg/kg i.p )
Mean time for
onset of THE
in secs
Mean time duration of
THE in secs.
Percentage
inhibition of
duration of THE
1. Control 2.7±0.52 7±0.63 ----
2. Phenobarbitone - 20 0** 0** 100
3. Ganaxolone - 5 3.5± 0.55* 6±0.89* 14.29
4. Ganaxolone - 10 6±0.63** 3.5±0.55** 50
5. Ganaxolone 5 +
Phenobarbitone - 10 0** 0** 100
** - p<0.001 compared to control , * - p<0.01compared to control ,
THE – Tonic Hind limb Extension
S.
N
o
Group & Dose
(mg/kg bw )
Onset of mean time
for jerky movements
in min.
Mean time
duration of jerky
movements in min.
Percentage
inhibition of
duration of jerky
movements
1. Control 1.8±0.34 40±4.1 ------
2. Sodium Valproate – 200 8.9±1.3** 22±1.8** 45
3. Ganaxolone - 5 4.4±0.86** 33±1.2** 17.5
4. Ganaxolone - 10 7.8±0.88** 25±1.5** 37.5
5. Ganaxolone 5 +
Sodium Valproate – 200 9.5±0.7** 18±1.2** 55
** - p<0.001 compared to control

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/ Volume 1/ Issue 3/ July- Sept 2012 Page 117
ANTICONVULSANT ACTIVITY OF GANAXOLONE ON PTZ SEIZURES

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/ Volume 1/ Issue 3/ July- Sept 2012 Page 118
REFERENCES:
1. Fisher RS, Van Emde Boas W, Blume W, et al. Epileptic seizures and epilepsy:
definitions proposed by the International League Against Epilepsy (ILAE) and the
International Bureau for Epilepsy (IBE). Epilepsia 2005;46(4):470-2.
2. "Epilepsy". World Health Organization. January 2009. Retrieved January 5, 2012.
3. Sander JW. The epidemiology of epilepsy revisited. Curr Opin Neurol 2003; 16: 165-70.
4. Maciej Gasior, Richard B Carter, Steven R Goldberg, Jeffrey M Witkin. Anticonvulsant
and behavioral effects of neuroactive steroids alone and in conjunction with Diazepam.
J Pharmacol Exp Ther 1997; 282: 543-553.
5. Bradford H F. Glutamate, GABA and epilepsy. Progress in Neurobiol 1995; 47:477–511.
6. Macdonald R L, Olsen RW. GABAA receptor channels. Annu. Rev. Neurosci. 1994; 17:
569–602.
7. Nohria V, Giller E. Ganaxolone. Neurotherapeutics 2007;4:102–105.
8. Rogawski MA, Reddy DS. Neurosteroids: endogenous modulators of seizure
susceptibility. In: Rho JM, Sankar R, Cavazos JE, editors. Epilepsy: scientific
foundations of clinical practice. New York: Marcel Dekker; 2004. P.319–355.
9. Carter RB, Wood PL, Wieland S, Hawkinson JE, Belelli D, Lambert JJ, et al.
Characterization of the anticonvulsant properties of Ganaxolone (CCD 1042; 3-alpha-
hydroxy-3-beta-methyl-5-alpha-pregnan-20-one), a selective, high-affinity, steroid
modulator of the gamma-aminobutyric acid (A) receptor. J Pharmacol Exp Ther
1997;280:1284-95.
10. Mittal R. Antiepileptics. In: Gupta SK, editor. Drug Screening Methods. 1st ed. New
Delhi: Jaypee Brothers Medical Publishers; 2009. P. 408-9.
11. Gee K.W. Epalons as anticonvulsants: actions mediated by the GABA-A receptor
complex. Proc West Pharmacol Soc 1996; 39: 55-60.
12. Virinder Nohria, Earl Griller. Ganaxolone. Neurotherpeutics: The Journal of the
American society for Experimental Neurotherpeutics 2007; 4(1): 102-5.
13. Marjolein Beekman, Jesse T Ungard, Maciej Gasior, Richard B Carter, Durk Dijkstra,
Steven R Goldberg, et al. Reversal of behavioral effects of Pentylenetetrazol by the
Neuroactive Steroid Ganaxolone. JPET 1998; 284(3): 868-77.
14. Liptakova S, Velisek L, Veliskova J, Moshe SL. Effect of Ganaxolone on flurothyl seizures
in developing rats. Epilepsia 2000; 41:788–93.
15. Kaminski RM, Livingood MR, Rogawski MA. Allopregnanolone analogs that positively
modulate GABA receptors protect against partial seizures induced by 6-Hz electrical
stimulation in mice. Epilepsia 2004; 45: 864–67.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/ Volume 1/ Issue 3/ July-Sept 2012 Page 119
SERUM MAGNESIUM AS A MARKER OF DIABETIC COMPLICATIONS Dr Mirza Sharif Ahmed Baig1, Dr Mohd Shamshuddin2 Dr K L Mahadevappa 3, Dr Abdul Hakeem
Attar1 Dr Abdul Kayyum Shaikh1
1. Department of Biochemistry, KBN Institute of Medical Sciences, Gulbarga.
2. Department of Biochemistry, Al Ameen Institute of medical Sciences, Bijapur.
3. Department of Biochemistry, KempeGowda Institute of Medical Sciences, Bangalore.
CORRESPONDING AUTHOR:
Dr Mirza Sharif Ahmed Baig,
Plot No. 109,
Macca Colony, Ring Road,
Gulbarga- 04,
Karnataka.
Email id- [email protected]
Ph- 0091 9916039995
ABSTRACT:
Type 2 diabetes has become a leading cause of morbidity and mortality world over.
Magnesium homeostasis has been hypothesized to be a link between insulin resistance type 2
diabetes mellitus, hypertension and CAD. This study was under taken to evaluate the relationship
between serum magnesium and diabetes mellitus without and with complications. We found
significantly low levels of serum magnesium in patients with DM when compared to control.
Further significantly low levels of serum magnesium were found in patients with diabetic
complications when compared with diabetic patients without complications. Hence it is concluded
that the lower levels of serum magnesium may have a bearing on the complication and morbidity in
patients of DM, and estimation of serum levels of magnesium may be helpful to monitor the severity
of complications in diabetic patients.
KEY WORDS: Coronary Artery Disease, Diabetes Mellitus, Diabetic Retinopathy, Hypomagnesemia.
INTRODUCTION:
Magnesium, the fourth most common cation in the body, has been the recent focus of much
clinical and scholarly interest. Previously underappreciated, this ion is now established as a central
electrolyte in a large number of cellular metabolic reactions, including DNA and protein synthesis,
neurotransmission, and hormone receptor binding. It is a component of GTPase and a cofactor for
Na+/ K +-ATPase, adenylate cyclase, and phosphofructokinase.
Magnesium is a cofactor in more than 300 cellular enzymatic systems and has a key role in
cellular metabolism, the recognition that Mg deficiency or excess may be associated with significant
clinical consequences has resulted in an increased interest in the utility of serum Mg
measurement(1). Magnesium is an important intracellular cation that is distributed into three
major compartments: mineral phase of bones (65%), intracellular space (34%) and extracellular
fluid (1%) (2).

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/ Volume 1/ Issue 3/ July-Sept 2012 Page 120
In several studies reduced magnesium concentrations have been observed in diabetic adults
(3-7).
The interrelationships between magnesium and carbohydrate metabolism have regained
considerable interest over the last few years. The association between diabetes mellitus and
hypomagnesaemia is compelling for its wide ranging impact on diabetic control and complications.
Magnesium depletion has been linked to the development of retinopathy (8). The etiology of
hypomagnesiamea cannt be clearly explained and serum magnesium levels have been shown to be
inversely related to the severity of diabetes (9). Hypomagnesaemia has been linked to poor
glycemic control, coronary artery diseases, hypertension, and diabetic neuropathy and foot
ulcerations (10).
Hence this work was undertaken to evaluate the relationship between serum magnesium
and diabetes mellitus without and with complications.
MATERIAL AND METHODS:
The present study was carried out in the Department of Biochemistry KBN Institute of
Medical Sciences and KBNTGH Gulbarga, and KempeGowda Institute of Medical Sciences,
Bangalore. Clearance was obtained from the institutional ethical committee.
The study was carried out on 30 age and sex matched healthy controls and 60 type 2
diabetic patients who attended the outpatient and inpatient department of KempeGowda Institute
of Medical Sciences, Bangalore during the year 2007-2008.A total 60 patients of type 2 diabetes
mellitus between 40 – 70 years, which were divided into following groups.
Control group: Included 30 healthy, age and sex matched individuals.
Group I: Included 30 patients of type 2 diabetes without complications.
Group II: Included 30 patients of type 2 diabetes with proven complications, like CAD,
retinopathy and neuropathy.
The diagnosis of type 2 diabetes mellitus was established with the recommended criteria’s
of American diabetes Association.
Inclusion Criteria: Patients in the age group of 40–70 years with type 2 diabetes without
and with proven complications, like CAD, neuropathy and retinopathy were selected.
Exclusion Criteria: Patients with recent infectious disease, immunological disorders, taking
diuretics and magnesium containing antacids, malabsorption syndrome, chronic diarrhea, renal
failure, pancreatitis, alcoholism, liver diseases, tuberculosis and thyrotoxicosis were excluded from
the study.
Informed consent was taken from patient and control subjects. A pre-structured and pre-
tested proforma was used to collect the data. Baseline data including age and sex, detailed medical
history including conventional risk factors, clinical examinations and relevant investigations
including ECG, echocardiogram, nerve conduction test, fundoscopy etc were included as part of the
methodology.
Fasting venous blood samples were collected from cases and controls and the samples were
centrifuged, serum was separated and stored at 40C. Serum magnesium was estimated by Calmagite
dye method (11) by using auto-analyzer (A25Biosystem). Magnesium reacts with the blue dye,
calmagite, in alkaline medium to form red colored complex which is measured at 530-550nm. The
intensity of the color formed is directly proportional to the amount of magnesium in the sample.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/ Volume 1/ Issue 3/ July-Sept 2012 Page 121
Protein interference and dye precipitation are avoided including the 9-ethylene oxide adduct of p-
nonylphenol (Bion NE9) and Polyvinyl pyrrolidone (Bion pup). Calcium interference is avoided by
preferential combination with EDTA and heavy metal interference is prevented by Potassium
cyanide. The reference range for serum magnesium concentration does not vary significantly for
age or sex and is closely maintained within a range of 1.7-2.4mg/dl.
PPBS were estimated 2 hours after breakfast. Urine sample was analyzed for protein and
sugar.
STATISTICAL METHODS:
Student `t’ test /Chi-square test has been used to find the significance of homogeneity of
study characteristics between three groups of patients. Analysis of variance has been used to find
the significance of study parameters between three groups. Results were expressed as mean + SD.
Probability values of P< 0.05 were considered to indicate statistical significance.
STATISTICAL SOFTWARE:
SPSS 15.0, Stata 8.0, MedCalc 9.0.1 and Systat 11.0 were used for the analysis of the data and
Microsoft word and Excel have been used to generate graphs, tables etc.
RESULTS:
Results of the present study showed significant low values of serum magnesium (P<0.001)
in patients of DM without complications when compared with controls. Further significant low
values of serum mg (P<0.001) were found in patients of DM (Table 1 & Fig 1) with complications
when compared with control.
DISCUSSION:
The magnesium ion has been shown to play an important role in the metabolism of
carbohydrates by activating various enzyme systems and helping insulin for its action. In this study
it was observed that the mean serum magnesium level was statistically significantly low (P<0.001)
in Diabetic patients without and with complications when compared with controls. This indicates
the association of hypomagnesaemia with diabetes mellitus. These results are in accordance with
the observation of Tosiello L (12), Kao WH (13), and Chamber E C (14). In our study, serum
magnesium level in cases with diabetic complications (1.29 + 0.31) was much lower than those
without complications (1.61 + 0.41).
We also noted that in subjects with diabetic complications serum magnesium levels were
much lower when compared to diabetics without complications. Hatwal A et al, Andrea Corsenello
et al and Rodriguez Moran M et al have found similar results in patients with diabetic
complications. Ishrath Kareem et al found that serum magnesium levels in patients with diabetic
retinopathy were significantly lowered compared to patients without retinopathy (15). Aradhana
Sharma et al also found that serum magnesium levels were significantly lowered in patients with
diabetic complications when compared to diabetic patients without complications (16).
In our opinion the release of insulin caused by a glucose challenge is partly dependent on
adequate magnesium. Insulin, via its interaction with ligand activated tyrosine protein kinase
associated receptors, initiates a cascade of biochemical interactions that result in several

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/ Volume 1/ Issue 3/ July-Sept 2012 Page 122
physiological, biochemical and molecular events that are involved in carbohydrate, lipid and
protein metabolism (17). Although the binding of insulin to its receptor does not appear to be
altered by magnesium status, the ability of insulin once bound to receptor to activate tyrosine
kinase is reduced in hypomagnesaemia states (18). As a result reduced peripheral glucose uptake
and oxidation are often noted in subjects with hypomagnesaemia. Decrements in the enzymatic
activities of several metabolic pathways are seen in DM patients as a result of the relative
magnesium deficiency (19).
The exact cause of diabetic hypomagnesaemia is still unknown but an increased urinary loss
of magnesium may contribute to it. Hypomagnesaemia has been reported to occur at an increased
frequency among patients with type 2 diabetes compared with their counter parts without
diabetes. Despite numerous reports linking hypomagnesaemia to chronic diabetic complications,
attention to this issue is poor among clinicians. The precise mechanism for development of
microvascular changes is not fully understood, it is possible that hypomagnesaemia inhibits
prostacyclin receptor function producing an imbalance between prostacyclin and thromboxane
effect which has marked atherogenic potential which is responsible for microvascular
complications.
Thus we conclude that the estimation of serum magnesium levels is helpful to monitor the
severity of complications in type 2 diabetes and also be useful for proper medical intervention.
Hence further studies on serum magnesium levels and on oral supplementation to prevent
late complications of diabetes will be interesting and helpful.
Table 1: Serum Magnesium in the three study groups
Study
parameters Controls
DM without
complications
DM with
Complications
Sr.Mg /dl 2.17±0.35 1.61±0.41** 1.29±0.31**
Results are presented in Mean ± SD P < 0.001 highly significant
Fig 1: Serum Magnesium in the three study groups
0
0.5
1
1.5
2
2.5
3
Controls DM without complications
DM with complications
Sr. M
g (m
g/dl
)

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/ Volume 1/ Issue 3/ July-Sept 2012 Page 123
REFERENCES:
1. Elin R. J.Assement of magnesium status. Clin Chem 1987; 33:1965 – 1970.
2. Gums J G. Clinical significance of magnesium: A review. Drug Intell Clin Pharm 1987; 21:
240 – 246.
3. Maltezos E,Papazoglou D, Exiara T, Kambouromiti G, Antonoglou C. Serum magnesium
levels in non diabetic offspring of patients with type 2 diabetes mellitus. Diabetes Nutr
Metab 2004; 17:12 – 16.
4. Mc Nair P, Christiansen C, Madshad S. Hypomagnesaemia a risk factor in diabetic
retinopathy. Diabetes 1978; 27:961 – 965.
5. Mather H M, Nisbet J A, Bruton G H. Hypomagnesaemia in diabetes. Clin Chem Acta
1979; 95:235 – 242.
6. Fuji S, Tekemura T, Wada M, Akai T, Okurr k m. Magnesium levels in plasma ,
erythrocyte and urine in patients with diabetes mellitus. Horn Metab Res 1982; 14: 161
– 162.
7. Johansson G, Danielsson B G, Ljunghalls, Wibell L. Evidence for a disturbed magnesium
metabolism in diabetes mellitus. Magnesium 1982; 3:178 – 180.
8. Ceriella A, Giugliano D, Dellorurso P, Passariello. Hypomagnesaemia in relation to
diabetic retinopathy. Diabetic Care. 1982; 5:558 – 559.
9. Hamid Nasri, Hamid Raza Baradaran. Lipids in association with serum magnesium in
diabetes mellitus patients. Bratisl Lek Listy.2008;109(7):302-306
10. Pham PC, Pham PM, Pham SV et al .Hypomagnesaemia in patients with type 2 diabetes
.Clin Am Soc Nephrol 2007;2:366-73.
11. Gindler EM, Heth DA. Colorimeter determination with bound “Calmagite” of magnesium
in human blood serum. Clin Chem 1971; 17:662.
12. Tosiello L. Hypomagnesaemia and diabetes mellitus. A review of clinical implications.
Arch Intern Med 1996; 156(1):1143 – 1148.
13. Kao W H. Serum and dietary magnesium and the risk for type 2 diabetes mellitus. The
Atherosclerosis risk in communities study. Arch Intern Med 1999; 159(8):2151 – 2159.
14. Chambers EC, Heshkas, Gallagherd.Serum magnesium and type 2 diabetes in African
Americans and Hispanics a Newyork Cohort. J Am Coll Nutr. 2006; 25:509 – 513.
15. Ishrat Kareem, Jaweed SA. Bardapurkar JS et al. Study of magnesium, glycosylated
hemoglobin and lipid profile in diabetic retinopathy. Indian Journal of Clinical
Biochemistry, 2004; 19(2);124-127.
16. Aradhana Sharma, Surekha Dabla, RP Agarwal et al. Serum magnesium; An early
predictor of course and complications of diabetes mellitus. J Indian Med Assoc
2007;105:16-20.
17. Lefebvre P J, Scheen A J. Improving the action of insulin. Clin Invest Med 1995; 18:342 –
347.
18. Suarez A. Decreased insulin sensitivity in skeletal muscle of hypomagnesaemia rats.
Diabetologia 1993; 36:A82.
19. Laughlin M R, Thompson D. The regulatory rule for magnesium in glycolytic flux of the
human erythrocyte. J Biol Chem 1996; 271: 28977 – 83.

CASE REPORT
Journal of Evolution of Medical and Dental Sciences/ Volume 1/ Issue 3/ July-Sept 2012 Page 124
LUPUS VULGARIS: - AN UNUSUAL FACIAL INVOLVMENT
Mandakini. B. T, Hakeem. A, Zennath. B
1. Assistant Professor, Department of Pathology, KBN Institute of Medical Sciences, Gulbarga.
2. Assistant Professor, Department of Pathology, KBN Institute of Medical Sciences, Gulbarga.
3. Associate Professor, Department of Pathology, KBN Institute of Medical Sciences, Gulbarga.
CORRESPONDING AUTHOR:
Dr Mandakini. B. Tenglr,
C/O Dr. Srinivas,
H. No. 1-888/1, Shastri Nagar,
Gulbarga- 04, Karnataka,
Email id- [email protected],
Ph- 0091 9844586236.
ABSTRACT:
BACKGROUND: Primary infection with tuberculosis occurs only rarely on the skin. The lesions of
Lupus vulgaris are usually found on the head or neck. The skin of and around the nose is
frequently involved. But, we report a rare case, where a 36 years’ old male patient presented with
a Lupus vulgaris lesion over the upper part of the cheek, near the outer canthus of the right eye, of
9 years’ duration. Histopathological examination showed granulomatous infiltration, with caseous
necrosis. Mantoux test was positive. The lesion showed marked improvement on antituberculous
treatment. We want to emphasize that histopathological examination has diagnostic value in
Lupus vulgaris.
KEYWORDS: Lupus vulgaris, facial skin, granuloma, caseation necrosis.
INTRODUCTION:
There is a resurgence of tuberculosis everywhere because of a combination of factors
including immigration from endemic countries, HIV pandemic, poverty, etc. as a result,
tuberculosis remains a clinical and diagnostic problem[1].
Lupus vulgaris is the most common morphological variant of cutaneous tuberculosis
accounting for approximately 59% of cases of cutaneous tuberculosis in India. [4, 6, 10].
Cutaneous tuberculosis forms a small proportion of extrapulmonary tuberculosis [3, 7].It has
been shown that Lupus vulgaris is the most common form in adults. [3, 8].
In India, the sites of predilection are the buttocks and trunk [3, 9].
We report a rare case of Lupus vulgaris affecting facial skin.
CASE REPORT:
A 36 year’s old male patient presented with history of a chronic progressive non- healing
lesion on the upper part of the right cheek, near the outer canthus of the eye, of 9 year’s
duration. Clinical examination revealed a well-demarcated, irregularly bordered, reddish-brown
patch, containing deep-seated nodules, each about 1mm. in diameter, with central area of
atrophy and scarring (fig-1).

CASE REPORT
Journal of Evolution of Medical and Dental Sciences/ Volume 1/ Issue 3/ July-Sept 2012 Page 125
Topical antibacterial, antifungal and steroid ointments were tried earlier, but there was
no response.
Clinical diagnosis of Granuloma annulare was made, and Lupus vulgaris was the
differential diagnosis. There was no pervious history of tuberculosis, either pulmonary or extra-
pulmonary. There was no regional lymphadenopathy, and systemic examination showed no
abnormalities. There was no similar family history Routine hematological examination revealed
lymphocytosis and raised ESR-80mm. Mantoux test was positive. Biochemical investigations like
random blood sugar, TB-IgG/IgM (slide method), VDRL, HIV, serum creatinine, and serum urea
levels were within normal limits. Chest X-ray was done which showed bronchitis with no
evidence suggestive of tuberculosis.
Histopathological study of the punch biopsy from the edge of the lesion revealed normal
epidermis, and the dermis showed tuberculoid granulomas consisting of epithelioid histiocytes,
Langhans giant cells surrounded by lymphocytes, with slight central caseation necrosis. Tissue
sections were negative for Acid fast bacilli.
DISCUSSION:
Infection of the skin and subcutis by Mycobacterium tuberculosis occurs by three routes;
1) By direct inoculation into the skin.
2) By hematogenous spread from an internal lesion.
3) From an underlying tuberculous lymph node by direct extension (causing
scrofuloderma).[1]
Mycobacterium bovis, atypical Mycobacteria and the BCG Vaccine can cause tuberculosis
involving the skin [5]. The diagnosis of cutaneous tuberculosis is challenging and requires the
correlation of clinical finding with diagnostic testing. [5] The determinants of what happens in
tuberculosis infection, includes, the virulence of the organism, the size of the inoculum, the
route of infection, and the immune status of the patient. The lesions of Lupus vulgaris are
usually found on the head and neck. The lesion in our case was a well-demarcated, reddish-
brown patch, containing deep-seated nodules, each about 1mm in diameter, with central area
of atrophy and scarring. The diagnosis in this case was based on histopathological study of the
biopsy of the lesion, which showed typical granulomatous tubercles with epithelioid cells,
Langhans giant cells and a mono-nuclear inflammatory infiltrate (fig-3&4). Caseation necrosis
was seen (fig-5) and AFB Negative
The patient was administered antitubercular therapy and the lesion resolved completely
in 6 months and 2 year follow-up shows no recurrence. (Fig-2).
Lupus vulgaris is completely curable as has been seen in the present case. The
consequences of failing to make an early diagnosis can be disastrous for the patients, as the
progression of the disease can lead to necrosis, destruction of bones and cartilage leading to
permanent deformity [4, 6, 9, and 10].
The special test like polymerase chain reaction (PCR) for TB can be done to substantiate
the diagnosis or wherever the histopathology is inconclusive [4, 6, 9, and 10].

CASE REPORT
Journal of Evolution of Medical and Dental Sciences/ Volume 1/ Issue 3/ July-Sept 2012 Page 126
Fig 01 Fig 02
Fig 03 Fig 04
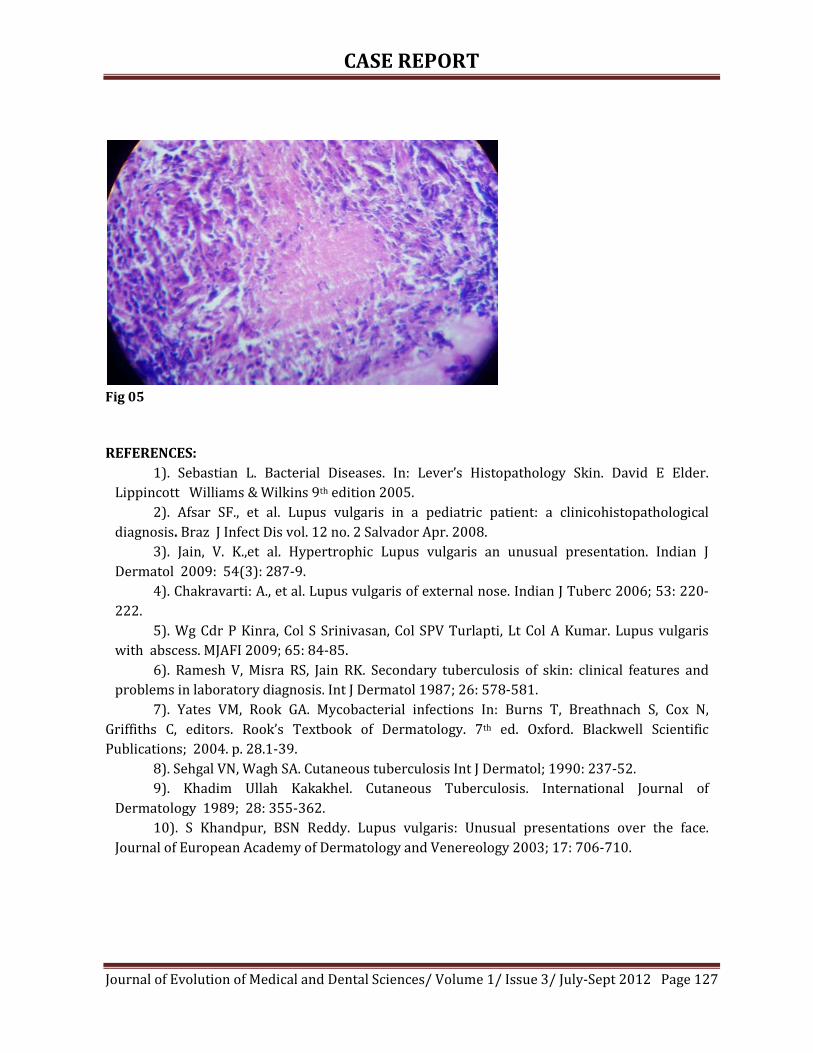
CASE REPORT
Journal of Evolution of Medical and Dental Sciences/ Volume 1/ Issue 3/ July-Sept 2012 Page 127
Fig 05
REFERENCES:
1). Sebastian L. Bacterial Diseases. In: Lever’s Histopathology Skin. David E Elder.
Lippincott Williams & Wilkins 9th edition 2005.
2). Afsar SF., et al. Lupus vulgaris in a pediatric patient: a clinicohistopathological
diagnosis. Braz J Infect Dis vol. 12 no. 2 Salvador Apr. 2008.
3). Jain, V. K.,et al. Hypertrophic Lupus vulgaris an unusual presentation. Indian J
Dermatol 2009: 54(3): 287-9.
4). Chakravarti: A., et al. Lupus vulgaris of external nose. Indian J Tuberc 2006; 53: 220-
222.
5). Wg Cdr P Kinra, Col S Srinivasan, Col SPV Turlapti, Lt Col A Kumar. Lupus vulgaris
with abscess. MJAFI 2009; 65: 84-85.
6). Ramesh V, Misra RS, Jain RK. Secondary tuberculosis of skin: clinical features and
problems in laboratory diagnosis. Int J Dermatol 1987; 26: 578-581.
7). Yates VM, Rook GA. Mycobacterial infections In: Burns T, Breathnach S, Cox N,
Griffiths C, editors. Rook’s Textbook of Dermatology. 7th ed. Oxford. Blackwell Scientific
Publications; 2004. p. 28.1-39.
8). Sehgal VN, Wagh SA. Cutaneous tuberculosis Int J Dermatol; 1990: 237-52.
9). Khadim Ullah Kakakhel. Cutaneous Tuberculosis. International Journal of
Dermatology 1989; 28: 355-362.
10). S Khandpur, BSN Reddy. Lupus vulgaris: Unusual presentations over the face.
Journal of European Academy of Dermatology and Venereology 2003; 17: 706-710.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 128
Epidemiology of Needle-Stick Injuries in Mangalore Dr. Prakash. K. P
1. Assistant Professor, Department of Community Medicine, Kasturba Medical College. Mangalore.
CORRESPONDING AUTHOR:
Dr. Prakash K.P, Kurubarahalli Patel,
PES Medical College,
Kuppam– 517425, AP, India,
Email id- [email protected],
Ph- 0091 9686448868.
ABSTRACT:
BACKGROUND: Health care workers (HCWs) are always at greater risk of infection by needle-
stick injuries (NSIs) owing to their greater handling of sharps in various situations. OBJECTIVE:
The main objective was to review the epidemiology of NSIs among HCWs, and describe the
circumstances under which these injuries occurred. METHODS: A questionnaire based, cross
sectional study was done during the month of January 2008 at 3 Kasturba Medical College
(KMC) institutions, Mangalore. The data was computed and analyzed using SPSS statistical
package. RESULTS: During the study period 272 HCWs were self administered
questionnaire/interviewed and 102 HCWs reported (37.5%) incidents of injuries with needles
during the past 12 months. Doctors were the most frequent victims (64.7%), followed by waste
disposal staff (25.5%) and Nurses (7.8%). More than 50% of the victims had more than 3 pricks
in the last 12 months. Hospital wards and operation theatre were the major locations of needle-
stick incidents (31.4% each). Most commonly, injuries occurred during suturing (41.1%) and
when using solid bore or suturing needle (47.1%). Majority of them neither reported the injury
(60.8%) nor received post-exposure prophylaxis (70.6%). Patient tested sero-negative was the
major reason for not reporting the injury. Government hospital staff and waste disposal staff
had significantly higher chance of NSI when compared to their counterparts. Conclusions: The
study re-emphasized the importance of continued educational and prevention programmes for
HCWs in the prevention of needle-stick injuries.
KEYWORDS: Epidemiology, Needle-stick injuries, Health care workers, Mangalore.
INTRODUCTION:
Many infections including blood-borne viruses such as Human Immuno-deficiency Virus
(HIV), hepatitis B and C can be transmitted by exposure to infected blood or other body fluid via
an accidental inoculation injury (1). Health care workers (HCWs) who are exposed to needles
during clinical and non-clinical activities are at increased risk of acquiring needle-stick injuries
(NSIs) (2).
Accidental NSIs are an occupational hazard for HCWs. According to a global estimation,
16,000 Hepatitis C (HCV), 66,000 Hepatitis B (HBV) and 1000 cases of HIV may have occurred
worldwide in the year 2000 among HCWs through their exposure to NSI’s (3). In Germany,
about 500,000 needle-stick injuries occur annually among HCWs (4). More than 100,000 and
600,000 to 800,000 injuries annually have been reported in UK hospitals and in USA
respectively (5, 6). About half of these injuries go unreported (7-9,). Data from the EPINet

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 129
system suggest that approximately 28 needle-stick injuries/100 beds/year occur in US hospitals
(10).
Hollow-bore needles are most frequently implicated with the transmission of blood-
borne pathogens because the blood remaining inside the bore of the needle after use contains a
larger volume of organisms than the relatively small amount remaining on the outside of a solid
bore needle, such as the suturing needle (11). The activities associated with the majority of NSI
include withdrawing blood, recapping of needles, administering injections, inappropriate
disposal of needles, and missing the target while attempting to transfer blood or other body
fluids from syringes to specimen tubes or culture bottles (12).
Following a NSI with infected blood, transmission of the 3 principal viruses, HIV, HCV
and HBV occurs in 0.3, 3 and 30% of cases, respectively (13). Although the risk of infection
following a single NSI is very small, “universal precautions” and immunization against HBV may
reduce the risk of injury, infection and illness (14).
In general, only a few studies have been published on NSI from developing countries,
(15-17) although more than 90% of NSI occur in developing countries (18). Published data from
India (19-22) and in our institutions are limited, therefore, the present study was undertaken to
study the epidemiology of NSI in HCWs in the Kasturba Medical College (KMC) institutions, and
describe the circumstances under which these injuries occurred.
MATERIALS AND METHODS:
The study was conducted in the 3 KMC institutions (KMC Hospital (Attavar),
Government Wenlock and Lady Goschen Hospital) in Mangalore. Convenience non-random
samples of 372 HCW’s were self administered/interviewed using a pretested Performa. The
Performa was a self administered questionnaire that was completed by the HCW’s. The ancillary
staffs were interviewed and the questionnaire was filled by the trained medical students. The
assessment of data was done using modified methods established by World Health Organization
(WHO) (23).
The study was conducted during the month of January 2008. The target population was
HCWs in KMC institutions including doctors (staff, postgraduate students and Inters), nurses,
and waste disposal staff. The working definition of needle-stick injuries used was injuries
caused by hollow–bore needles such as hypodermic needles, blood collection needles,
intravenous (IV) stylets and needles used to connect parts of IV delivery systems (12). Data
collected from the Performa include: age, gender, details of the incident which included the type
of needlestick device and the circumstances under which the injury occurred. Additionally,
questions related to awareness as well as basic steps in management of injuries were also
included. The data also included was hepatitis B immune status, HIV and hepatitis B serologic
markers, the job category and place of work of the injured HCWs. Prevalence calculation was
according to, HCW who had at least 1 NSI during the last 12 months. The data was computed in
a Microsoft Excel 5.0 spreadsheet and statistically analyzed using the Statistical Package for the
Social Sciences (SPSS Inc, Chicago, IL, USA). Proportions were calculated and chi-square test was
used to test the significance and p value <0.05 was considered as significant at 95% confidence
interval.
RESULTS:
A total of 272 HCW’s were involved in the study. The basic characteristics of the study
population are shown in Table1. Of the 272, majority of them were in the age group of 25-34

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 130
years (51.5%), females (64%), doctors (57.4%) and from KMC, Attavar Hospital (42.6%). The
mean age and standard deviation of study subjects was 32.1±9.2 years. Almost 80% of HCW’s
had received hepatitis B vaccine, although only 75.3% had 3 complete doses. Fifty-four persons
(19.8%) received no immunization.
AWARENESS:
Nearly, 10% of the HCWs had no knowledge and 24% had partial knowledge about the
diseases transmitted through needle stick injuries. Approximately, 72% of them were aware of
the presence of written policy. Notably, 24% of the study subjects were not aware about the
correct disposal of sharps.
Approximately 37.5% (102/272) of the study subjects reported that they had at least
one NSI during the last 12 months. Needle-stick injuries and circumstances in which these
injuries occurred are depicted in table 2. Doctors were the most frequent victims (66/102 -
64.7%), followed by waste disposal staff (26/102 - 25.5%) and Nurses (8/102 - 7.8%).
Proportionately Waste disposal staff (26/42 - 61.9%), Doctors (66/156 - 42.3%) and Nurses
(8/62 – 7.8%) were the most common occupation among the NSI candidates. Alarmingly more
than 50% of the NSI’s had more than 3 pricks in the last 12 months. Nearly 63% of the injuries
occurred during suturing or during disposal of sharp objects. Solid bore or suturing needle was
the most common device causing the injury (47.1%). The most common cause of NSI was
accidental (45.1%) (Not preventable) followed by restless patient (17.6%) and rushed (11.8%)
or fatigued (11.8%). Surprisingly 60.8% of them who had NSI did not report to the authorities
even though majority (80%) of them said that they would report if they had a NSI and only
29.4% of the injured received post exposure prophylaxis. The common reason for not reporting
the injury was patient tested sero-negative. Only four (3 HBV and 1 HIV) of the patients on
whom the needle was used tested positive and in nearly 51% (52/102) of the patients disease
status was not know. Thirty two (31.4%) of NSI occurred in hospital wards, 32 (31.4%) in the
operation theatre, 18 (17.6%) in the waste disposal center (figure 1).
Government hospital staff had significantly higher chance of NSI (X2 = 8.05, p=0.01,
df=2) and waste disposal staff had significantly higher chance when compared to their
counterparts (X2 = 13.9, p=0.01, df=2) (Table 3)
DISCUSSION:
Needle-stick injuries are the most frequent occupational hazard affecting health care
workers, and the most life-threatening. This cross sectional study involved a total of 272 study
subjects among them 102 needle-stick injuries was reported. In this study the rate of NSIs being
0.42/doctor/year, 0.13/nurse/year, 0.62/waste-disposal staff/year was higher when compared
to a study in Saudi Arabia (0.06 /doctor/year and 0.11/nurse/year) (24) and lesser (0.57
/doctor/year and 0.83/nurse/year) when compared to a study in USA (25).
In our study, 37.5% (prevalence) of participant HCW’s had sustained at least one needle-
stick injury in the last 12 months, which is comparable to a study in Germany (31.4%) (4) and in
India (34.8%) (19). However, the reported prevalence was more than double in an Indian study
(80.1%) (26). Twelve months is a long period leading to bias which is a limitation in the study.
Nursing assistants are at high risk for NSIs because of their nature of work. Studies from Saudi
Arabia (65.8% and 19.2%) (24), Ireland (49.5% and 28.5%) (27) and in USA (40% and 28%)
(28) reported that the NSIs were more frequent among nurses than doctors, whereas doctors
reported frequent NSIs in Indian studies (19-22) including our study. This is probably because

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 131
in most of the Indian hospitals Junior/Senior resident doctors and Interns are more commonly
involved in clinical procedures. This wide variation in prevalence and proportions in various
studies could be due to underreporting (7-9), and/or different study methodologies (24). The
highest rate (26/42 - 61.9%) among waste disposal staff can be attributed to unsafe methods of
waste disposal and collection.
In this study, hospital wards and operation theatre were the common places of NSIs
(31.4% each). Similar observations were made in Saudi Arabia (45.1% - hospital wards, 16.9% -
OT) and Scotland (53% - hospital wards, 16% - OT) (24) (29).
The proportion of medical staff who reported to the authorities after a NSI was 20.0% in
our study. The main reason for not reporting in our study was patient tested sero-negative.
Other possible explanation may be that some doctors are inclined to self-assess and not report
such injuries, thus contributing to the apparent lower reporting of NSIs (29). Historically,
suboptimal (under-reporting) reporting of incidents can introduce bias in studies on self-
reported injuries. (30). Some researchers have shown that the rate of under-reporting among
doctors, especially among those frequently exposed to HIV-infected blood (31).
Some of the circumstances in which the injuries in various studies occurred are
compared in table 4 with the present study.
Continuing medical education (CME) programs for HCWs including health education
program for waste disposal staffs need to be conducted by the infection control department to
increase the awareness about the prevention and management of NSI’s because of proven
positive impact of intervention educational programmes (32). Hepatitis B vaccination of all at
risk HCWs in our institutions (23.4% never received). It is recommended by the CDC that all at-
risk HCWs be vaccinated against HBV infection (33). When the results of the study were
reported to the authorities, they were surprised and promised to take appropriate necessary
action.
In conclusion, Needle-stick injuries is a major concern in our institutions especially
government hospitals. The study re-emphasized the importance of continued medical
educational and prevention programmes for HCWs especially health education for waste
disposal staff in the prevention of needle-stick injuries. Mandatory reporting, laboratory testing,
post exposure prophylaxis (HBV) are some of the administrative measures (Accidental
Inoculation Policy) that needs to be taken to reduce the prevalence of NSIs in our institutions.
ACKNOWLEDGEMENT
The author is grateful for the assistance of the medical students in conducting the study.
All the HCWs who participated in the study and who supported in conducting this study are
acknowledged.
CONFLICT OF INTEREST:
None declared.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 132
Table1. Socio-demographic characteristics of the study subjects at the KMC institutions,
Mangalore. (N=272)
Characteristics Numbers Percent (%)
Age:
<25 46 16.9
25-34 140 51.5
35-44 54 19.8
≥ 45 32 11.8
Gender:
Male 98 36
Female 174 64
Hospital:
KMC, Attavar 116 42.6
Govt. Wenlock 96 35.3
Lady Goschen 60 22.1
Occupation:
Doctors 156 57.4
Nurses 62 22.8
Lab Technicians 12 4.4
Waste disposal staff 42 15.4
Table2. Distributions of NSI’s according to the circumstances in which the injuries
occurred
Situation (N=102) Numbers Percent (%)
Injection related 18 17.6
Re-capping needles 8 7.8
Suturing 42 41.1
During disposal 22 21.6
IV-line related, canula 4 4.0
Accidental exposure 8 7.8
Device (N=102)
Hypodermic needles 12 11.8
Blood collection needles 12 11.8
IV stylets 6 5.9
Sharps related to IV delivery system 4 3.9
Solid bore/suturing needle 48 47.1
Don’t know 20 19.6
Cause of injury (N=102)
Rushed 12 11.8

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 133
Fatigued 12 11.8
Lack of skills 4 3.9
Restless patient 18 17.6
Lack of assistance 10 9.8
Not preventable 46 45.1
Reasons for not reporting (N=62)
It takes too much time 0 0
No benefit in reporting 10 16.1
Did not want to know the results 0 0
Stigma of having had a NSI 0 0
Not mandatory to report 18 29
Patient was tested sero-negative 34 54.8
Table3. Occurrence of needle-stick injuries in 3 different hospitals and among staff
Hospital (N=102): Yes No X2
KMC, Attavar 28 88 8.05,
p=0.01,
df=2
Govt. Wenlock 48 48
Lady Goschen 26 34
Occupation (N=100):
Doctors 66 90 13.9,
p=0.01,
df=2
Nurses 8 54
Waste disposal staff 26 16
Note: Laboratory technicians were excluded in the comparison because only 2of 12 reported
NSI
Table4. Comparison of NSI’s according to the circumstances in which the injuries
occurred
REFERENCES Present
Study 26 24 19 20 21
Situation
During Suturing 41.1 20.3 41.7 29.4* 62* 58.1*
Recapping
needles 7.8 39 29 30.4 6.3 14.8
Device Used
Solid bore/
suturing needle 47.1 33 15.1 30.5 19.2 20.9
Cause of injury
Restless patient 17.6 12 8 - - -
Not preventable 45.1 - - 10.9 - -
Fatigue 11.8 - - 50.4 - -
ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 134
Note: All the numbers are percentage unless specified
* During clinical procedures including suturing
- Particular information not available
REFERENCES
1. Parkside Health. Policy for the prevention and management of accidental inoculation
injuries.TrustPolicies 200 2001; Page3. Available at
http://www.brentpct.nhs.uk/doxpixandgragix/ICC9PolicyforthePreventionandManagementofA
ccidentalInoculationInjuries.doc. Accessed on 20-11-2010.
2. Tarantola A, Golliot F, Astagneau P, Fleury L, Brucker G. Blood and Body Fluids
Exposure Surveillance Taskforce. Occupational blood and body fluids exposures in HCWs: four-
year surveillance from the Northern France network. Am J Infect Control 2003; 31:357-63.
3. Pruss-Ustun A, Rapiti E, Hutin Y. Estimation of the global burden of disease
attributable to contaminated sharps injuries among health-care workers. Am J Ind Med 2005;
48(6):482–90.
4. Wicker S, Jung J, Allwinn R, Gottschalk R, Rabenau HF. Prevalence and prevention of
needlestick injuries among health care workers in a German university hospital. Int Arch Occup
Environ Health 2008; 81(3):347-54.
5. World Health Organization (WHO). Nursing Matters fact sheets. ICN on Preventing
Needlestick Injuries. July 2000. Available from http://www.who.int/occupational_health/
activities/2icnneed.pdf Accessed latest on 01-12-2010.
6. Henry K, Campbell S. Needlestick/sharps injuries and HIV exposures among health
care workers: national estimates based on a survey of U.S. hospitals. Minn Med 1995; 78:1765-
68.
7. Rodriguez EB, Moruno AJR, Dona JAC, Pujolar AE, Fernandez FJL. Underreporting of
percutaneous exposure accidents in a teaching hospital in Spain. Clin Perform Qual Health Care
1999; 7:88–91.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 135
8. Centers for Disease Control and Prevention (CDC). Evaluation of safety devices for
preventing percutaneous injuries among health-care workers during phlebotomy procedures -
Minneapolis-St.Paul, New York City, and San Francisco, 1993–1995. MMWR 1997; 46(2):21-5.
9. Osborn EHS, Papadakis MA, Gerberding JL. Occupational exposures to body fluids
among medical students. A seven year longitudinal study. Ann Intern Med 1999; 130(1):45-51.
10. International Health Care Worker Safety Center, University of Virginia. US. Exposure
prevention information network (EPINet) Sharps Injury and Blood and Body Fluid Exposure
Surveillance Research Group. Sharps Injury and Blood and Body Fluid Exposure Report for 2007.
August 2009. Available from http://www.healthsystem.virginia.edu/internet/epinet/EPINet -
2007-rates.pdf Accessed latest on 01-11-2010.
11. Occupational Safety and Health Administration (OSHA). Safer Needle Devices: Protecting
Health Care Workers 1997. Available from http://www.thebody.com/content/art5947.html.
Accessed latest on 06-12-2010
12. National Institute for Occupational Safety and Health (NIOSH). Preventing needle
stick injuries in health care setting. November 1999; Publication No. 2000-108. Available from
http://www.cdc.gov/niosh/docs/2000-108/pdfs/2000-108.pdf. Accessed latest on 18-11-
2010.
13. Leasa Benson. Accidental Inoculation Injury - Guidance for healthcare professionals on
dealing with needle-stick injuries to members. NHS Manchester Infection Control Committee report,
Document Reference CICT001 April 2007; Page 6. Available from
http://www.manchester.nhs.uk/document.../AccidentalInnoculationInjuryCommunitySettingN
ov08.doc Accessed latest on 8-11-2010.
14. Centers for Disease Control and Prevention (CDC). Universal Precautions for
prevention of HIV, HBV and other blood borne pathogens in health care settings. MMWR 1988;
37: 377-88.
15. Gumodoka B, Favot I, Berege ZA, Dolmans WM. Occupational exposure to the risk of
HIV and health care workers in Mwanza Region, United Republic of Tanzania. Bull World Health
Org 1997; 75: 133-40.
16. Vong S, Perez JF, Sok S, Som S, Goldstein S, Hutin Y, Tulloch J. Rapid assessment of
injection practices in Cambodia, 2002. BMC Pub Health 2005; 5: 56-62.
17. Memish ZA, Almuneef M, Dillon J. Epidemiology of needle sticks and sharps injuries
in a tertiary care center in Saudi Arabia. Am J Infec Control 2002; 30: 234-41.
18. World Health Organization (WHO). Safe Injection Global Network, Health Care Worker
Safety, Aide-Memoire for a Strategy to Protect Health Care Workers from infection from blood
borne virus. 2003; WHO/BCT/03.11. Available from http://www.who.int/injection_safety/
toolbox/en/AM_HCW_Safety_EN.pdf. Accessed latest on 20-11-2010.
19. Sharma R, Rasania S, Verma A, Singh S. Study of prevalence and response to needle
stick injuries among health care workers in a tertiary care hospital in Delhi, India. Indian J
Community Med 2010; 35(1):74-7.
20. Salelkar S, Motghare DD, Kulkarni MS, Vaz FS. Study of needle stick injuries among
health care workers at a tertiary care hospital. Indian J Public Health. 2010; 54(1):18-20.
21. Jayanth ST, Kirupakaran H, Brahmadathan KN, Gnanaraj L, Kang G. Needle stick
injuries in a tertiary care hospital. Indian J Med Microbiol 2009; 27(1):44-7.
22. Rele M, Mathur M, Turbadkar D. Risk of needle stick injuries in health care workers -
a report. Indian J Med Microbiol. 2002; 20(4):206-7.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 136
23. World Health Organization (WHO). Injection practices: Rapid assessment and
responseguide; October 2002. Available from
http://www.who.int/injection_safety/toolbox/en/RARG.pdf. Accessed latest on 20-10-2010.
24. Saulat J. Epidemiology of needle-stick injuries among health care workers in a
secondary care hospital in Saudi Arabia. Ann Saudi Med 2005; 25(3):233-38.
25. Stotka JL, Wong ES, Williams DS, Stuart CG, Markowitz SM. An analysis of blood and
body fluid exposures sustained by house officers, medical students, and nursing personnel on
acute-care general medical wards: a prospective study. Infect Control Hosp Epidemiol 1991;
12:583–90.
26. Muralidhar S, Singh PK, Jain RK, Malhotra M, Bala M. Needle stick injuries among
health care workers in a tertiary care hospital of India. Indian J Med Res 2010; 131:405-10.
27. O’Connell T, Hayes B. Occupational sharps injuries in a Dublin teaching hospital. Ir
Med J. 2005; 96(5): 143-5.
28. Shah SM, Silverstein B, Bonauto D, Foley M, Kalat J. Needlestick Injuries among health
care workers in Washington State, 1996–2000. Safety and Health Assessment and Research for
Prevention, (SHARP), Washington State Department of Labor and Industries, Technical Report
Number 64-04-2003. Available from http://www.lni.wa.gov/Safety/Research/files/Needle
Stick.pdf. Accessed latest on 1-12-2010.
29. National Health Services (NHS), Scotland. Needlestick injuries: sharpen your
awareness: Report of the Short Life Working Group on needlestick injuries in the NHS Scotland.
Available from http://www.scotland.gov.uk/Resource/Doc/158726/0043078.pdf. Accessed
latest on 02-12-2010.
30. Hamory BH. Underreporting of needle stick injuries in a university hospital. Am J
Infect Control 1983; 11: 174-177.
31. Mangione CM, Gerberding JL, Cummings SR. Occupational exposure to HIV:
frequency and rates of under-reporting of percutaneous and mucocutaneous exposure by
medical house staff. Am J Med 1991; 90: 85-90.
32. Richard VS, Kenneth J, Ramaprabha P, Kirupakaran H, Chandy GM. Impact of
introduction of sharps containers and of education programmes on the pattern of needle stick
injuries in a tertiary care centre in India. J Hosp Infect. 2001; 47(2):163-5.
33. Centers for Disease Control and Prevention (CDC). Immunization of health care
workers. MMWR 1997; 46 (RR-18): 1-42

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/ Volume 1/ Issue 3/ July-Sept 2012 Page 137
ROLE OF PLATELET TRANSFUSIONS IN DENGUE HEMORRHAGIC FEVER-
6 MONTHS REPORT
Dr. V. Geeta, Dr. Bheeshma, Dr. I. Srilakshmi, Dr.Ramya, Dr. Yashoda, Dr. Jijiya Bai.
1. Assistant Professor, Department of Pathology, Gandhi Medical College, Secunderabad.
2. Assistant Professor, Department of Pathology, Gandhi Medical College, Secunderabad.
3. Assistant Professor, Department of Pathology, Gandhi Medical College, Secunderabad.
4. Post Graduate, Department of Pathology, Gandhi Medical College, Secunderabad.
5. Medical Officer-Blood bank, Department of Pathology, Gandhi Medical College, Secunderabad.
6. Professor & Head, Evaluator, Department of Pathology, Gandhi Medical College, Secunderabad.
CORRESPONDING AUTHOR:
Dr. V. Geetha,
Assistant Professor of Pathology,
Gandhi Medical College,
Secunderabad, Andhra Pradhesh,
Email id- [email protected],
Ph- 0091 09849450199.
ABSTRACT:
BACKGROUND: Allogenic platelet transfusion plays a major role in the management of
thrombocytopenia. The study includes details of platelet transfusion over a period of 6 months
from January-2011 to June-2011 at blood bank of Gandhi Hospital. Total number of patients who
received were 487 and proportionate use of total units of RDP (Random Donor Platelets) issued
from blood bank were as follows; dengue hemorrhagic fever (38%) and remaining for acute
leukemia (12%), Aplastic anemia (10%), sepsis (10%), DIC (Disseminated Intravascular
Coagulation) (10%), cardiac surgery (10%). In dengue hemorrhagic fever, correlation of platelet
count with platelet transfusion and platelet increment have been evaluated.
KEYWORDS: Thrombocytopenia, RDP, DIC, Aplastic anemia.
AIM: To evaluate the role of platelet transfusion in dengue hemorrhagic fever.
INTRODUCTION:
Dengue infection is usually a benign syndrome caused by an arthropod born virus. Dengue
fever and dengue hemorrhagic fever have emerged as a global public health problem in recent
decades. The South East Asian Countries such as India, Indonesia and Thailand are at the highest
risk of dengue accounting for nearly half of the global risk.
Dengue hemorrhagic fever (DHF) and dengue shock syndrome (DSS) are life threatening
clinical manifestations1. The mechanisms of hemorrhagic manifestations of DHF/DSS are not well
understood. The suggested factors contributing to bleeding include thrombocytopenia,
coagulopathy and vasculopathy and Suggested mechanisms for thrombocytopenia include:
1) Maturational arrest of megakaryocyte production in the bone marrow
2) Platelet destruction by the virus it self
3) DIC

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/ Volume 1/ Issue 3/ July-Sept 2012 Page 138
The world health organization manual and text books of pediatrics and infectious diseases
recommend infusion of fresh whole blood, fresh frozen plasma and/or platelet concentrates2.
Theoretically the risk of spontaneous bleeding becomes significant at a platelet count of <20 X
107/ml.
MATERIALS AND METHODS:
A retrospective study was conducted in the blood bank of Gandhi Hospital for a period of 6
months from 1st Jan to 31st June 2011. Total no. of patients received platelet transfusion is 487
and total units of RDPs given are 1116. Patients clinical data, platelet count and platelet
transfusion given to them were analyzed.
RESULTS:
Total no. of patients received platelet transfusion is 487 and total units of RDPs given are
1116 (Table.1), with males numbering 223 and females 264.
Age Group January February March April May June Total
0-10 16 17 10 21 27 38 129
11-20 10 25 30 17 07 22 111
21-30 16 7 28 15 19 25 110
31-40 4 11 6 18 07 13 59
> 41 12 10 9 9 13 15 68
Grand total 487
Blood group wise distribution of platelet transfusion is as follows
� B+ve: 180
� O+ve: 178
� A+ve: 161
� AB+ve: 37
� O-ve: 8
� B-ve: 14
Distribution of platelet transfusion by diseases wise are (Fig.1)
Dengue confirmed patients - 38% (186)
Acute leukemias (ALL + AML) - 12% (58)
A plastic anemia -10% (49)
Sepsis -10% (49)
DIC -10% (49)
Cardiac patients -10% (49)
Others -10% (49)
Total 489

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/ Volume 1/ Issue 3/ July-Sept 2012 Page 139
Majority of Dengue patients belonged to B+ve and O+ve Blood groups, most common age
group is between 11 to 20 years (46%) and females outnumbered males at 101 Vs 85.
During the study period 186 patients had positive serology (IgM or IgG) to dengue fever
by ELISA method. Fever was the most common clinical presentation associated with headache,
myalgia, vomiting, and diarrhea. Platelet count less than 10,000 / cumm noted in 20 patients
(10.7%).
< 10,000 - 20 patients 10.7%
11-20,000 - 36 patients 19.35%
21-40,000 - 50 patients 26.88% - Moderate Risk
41-1 lakh - 80 patients 43% - Low Risk
Most of the patients received platelet transfusion recovered completely and were
discharged with 2-5 transfusions. The platelet count had picked up considerably. Guidelines for
platelet transfusions in dengue hemorrhagic fever as follows:
INDICATIONS:
Prophylactic transfusions (in a non bleeding patient) with Platelet count < 20 X 109/L
Therapeutic transfusions (in a bleeding patient)
1) Significant active clinical bleeding with platelet count < 50 X 109 / L.
2) DIC
DISCUSSION:
Dengue viruses belonging to the genus flavi virus of family flaviviridae has antigentically
four distinct serotype DEN-1, DEN-2, DEN-3 and DEN-4. The virus is transmitted to the human
being by the bite of infected Aedes Egypti Mosquito and few other members of Aedes species.
Dengue virus causes a broad spectrum of illness ranging from mild undifferentiated fever to
classical dengue fever, DHF, DSS.
Our study showed majority of dengue cases were children and adolescents in the age
group of 10-20. Chaunsumrit et al also noted high percentage of dengue cases in age group of 10-
14 years3. In contrast Ayyub et al and Lye et al noted adult preponderance in age group of 20-40
yrs4, 5.
Thrombocytopenia is a common problem in dengue. In our study thrombocytopenia was
found in all most all the confirmed cases of dengue which was equal when compared with findings
of Makroo et al and Chairulfatah et al (84.88% and 83% respectively)6, 7 .
In our study bleeding occurred significantly more often in patients with thrombocytopenia
most often in patients with platelet count less than 20,000 / cumm which is similar to Shivbalan et
al. but chairulfatah et al found significant bleeding with platelet count less than 15,000 / cumm8, 7.
In our study high risk patient: platelet count < 20,000-30%. Moderate risk: 27% (21,000-40,000)
and Low risk: 43% (40,000-1 lakh)
According to Makroo et al all Hospitalized patients with dengue with high risk should be
given platelet transfusion6.
High Risk

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/ Volume 1/ Issue 3/ July-Sept 2012 Page 140
Dengue, 38%
Acute Leukemia, 12%
A Plastic Anemia, 10%
Sepsis, 10%
DIC, 10%
Cardiac, 10%
Others, 10%
Moderate risk patient can be given platelet transfusion if associated hemorrhagic
manifestations are present. Low risk patients can be managed with IV fluids and supportive
therapy. But in our study prophylactic transfusion of platelet given to 43% of low risk patients.
Most of the patients (99%) who received platelet transfusion recovered completely were
monitored for increment of platelet count after 2-3 transfusion at the time of discharge the
platelet count was above 1 lakh / cumm. Besides platelet transfusion FFP and PRP also
transfused.
Death occurred in 3% of patients due to complications like septicemia and severe bleeding
with multi organ failure belonged to age group of 31-40.
CONCLUSION:
All Hospitalized dengue patients can be categorized into high, moderate and low risk
patients based on platelet count at the time of Hospitalization. High risk patient should be given
priority and platelet transfusion accordingly. In our study the outcome is good with 97% recovery
of dengue patients with platelet transfusion and supportive therapy this clearly emphasizes the
role of platelet transfusion in the management of dengue patients.
Figure 1: Proportionate recipients of platelet transfusion
REFERENCES:
1. Directorate of health services, Management of Dengue Fever/DHF/DSS. Guidelines for
indoor patients, 2005:4
2. World Health Organization (2009) Dengue: guidelines for diagnosis, treatment, prevention
and control. World Health Organization, Geneva, pp 40–41.
3. Chuansumrit A, Phimolthares V, Tardtong P et al (2000) transfusion requirements in
patients with dengue hemorrhagic fever. Southeast Asian J Trop Med Public Health 31:10-
14
4. Ayyub M, Khazindar AM, Lubbad EH et al (2006) Characteristics of dengue in a large
public hospital, Jeddah, Saudi Arabia. J Ayub Medical coll Abbottabad 18:9-13
ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/ Volume 1/ Issue 3/ July-Sept 2012 Page 141
5. Lye DC, Lee VJ, Sun Y, Leo YS (2009) Lack of efficacy of prophylactic platelet transfusion
for severe thrombocytopenia in adults with acute uncomplicated dengue infection . Clin
Infecct Dis 48:1262-1265
6. Makroo RN Raina V, Kumar P, Kanth RK (2007) Role of platelet transfusion in the
management of dengue pts in a tertiary care hospital. Asian J Trans Sci 1:4-7
7. Chairulfatah A, Setibudi D, Agoes R, Colebunder R (2003) Thrombocytopenia and platelet
transfusion in dengue. Haemorrhagic fever and dengue shock syndrome.WHO Dengue Bull
27:141- 143
8. Shivabalan S, Anandanathan K, Balasubramaniyan S, Dutta N, Amalraj E; predictors of
spontaneous dengue, Indian J Ped. 2004; 71:33-6 (Pubmed)

REVIEW ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 142
DRUG COMPLIANCE AND ADHERENCE TO TREATMENT Dr. T. Manmohan, Dr. G. Sreenivas, Dr. V.V. Sastry, Dr. E. Sudha Rani, Dr. K. Indira,
Dr. T. Ushasree.
1. Associate Professor, Department of Pharmacology. Gandhi Medical College, Secunderabad.
2. Assistant Professor, Department of Community Medicine. Gandhi Medical College, Secunderabad.
3. Professor, Department of Community Medicine. Gandhi Medical College, Secunderabad.
4. P.G. Student, Department of Pharmacology. Gandhi Medical College, Secunderabad.
5. Professor, Department of Pharmacology. Gandhi Medical College, Secunderabad.
6. Professor & Head, Evaluator, Department of Pharmacology. Gandhi Medical College, Secunderabad.
CORRESPONDING AUTHOR:
Dr. Tepoju Manmohan,
Gandhi Medical College,
Secunderabad, AP,
Email id- [email protected],
Ph- 0091 09346935968.
ABSTRACT:
BACKGROUND: In spite of any number of medicines will not be of use unless patient takes’
them. After diagnosing the disease, the next most important step is to follow the instructions of
physician in terms of treatment. The doctor’s responsibility does not end with writing
prescription, assuming patient will adhere to it. He/she should cross check the behavior of
patient for drug compliance and see that patient follows it and get the benefit.
Non compliance is the main barrier for the effective delivery of the medical care. This
will have greater implications on the economic burden on the country in terms of frequent
hospitalization, use of expensive medicines in case of relapse due to non adherence.Though the
terms compliance and adherence are used synonymously, they differ in the delivery of quality of
the medicare as the former implicates the passive following of the physician instruction, while
in the later, patient actively participates in the development of the treatment plan, which will
improves outcome of the treatment. Adherence is the preferred term over compliance by WHO.
KEYWORDS: Adherence; compliance; concordance; non compliance; non adherence; treatment
INTRODUCTION: Significant advances have been made in understanding etiology of disease
states, and development of new therapeutic agents made it possible to cure or provide
symptomatic control. However, in many circumstances, drugs are not being used in the manner
conducive to optimal benefit and safety. Efforts to maintain or improve health, fall short of the
goals considered attainable, and has been attributed to patient’s noncompliance or partial
compliance.
Medication compliance (taking one’s medicine as prescribed) is a major concern as it
prevents hospitalization up to 5.5% and increase deaths by 8.48-fold to medication errors. Cost
and poor understanding of the directions for the treatment are major barriers in completing
treatment. WHO (World Health Organization) has estimates that only 50% of people complete
long-term therapy for chronic illnesses as prescribed1.
Half of all prescriptions for drugs to be taken on an ongoing basis are either not
completed or are never filled in the first place due to cognitive issues, depression or physical
problems 2-3. Medication for asymptomatic conditions is most likely not to be taken casually,

REVIEW ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 143
else land up with devastating problems over a period of time, especially with conditions like
diabetes, high blood pressure or high cholesterol1. A report from the American heart association
reveals that nearly 60 percent of patients whenever taking five or more medicines gets confused
while taking them.
TYPES OF PATIENTS: Based on the acceptance of diagnosis and treatment initiation,
patients are categorized into four types
1.NON COMPLIERS: Those who do not accept diagnosis and need treatment.
2.PARTIAL COMPLIERS: Those who accept diagnosis and treatment but cannot fulfill
the recommended actions sufficiently to reach targeted improvements in their health.
3.OVER COMPLIERS: Those who take recommended actions in excess of targeted
improvements (These patients are rare).
4.ADEQUATE COMPLIERS: Those who follow health advice adequately to improve or
control their disorder.
TYPES OF MEDICATION-TAKING BEHAVIOR:
COMPLIANCE: It is the conscious effort to use drugs in the manner prescribed, it is the extent to
which all individuals’ behavior coincides with medical & health advice. Understanding how
medication should be used, with sufficient positive motivation, and intentions, looking at the
perceived self benefit and positive outcome. , it can also apply to other situations such as
medical device use, self care, self-directed exercises, or therapy sessions.
ADHERENCE: The extent to which a person takes medication as prescribed. WHO defines
adherence as “The extent to which a person’s behavior, corresponds with agreed
recommendations from a health care professional”. Concept of adherence is broadly viewed as
related to instructions concerning medicine intake, use of medical device, diet, exercise, life
style changes, rest and return for scheduled appointments4-7.
CONCORDANCE: Consultative and consensual course of therapy partnership between the
consumer and their doctor. Concordance is the process by which a patient and clinician make
decisions together about treatment8.
PERSISTENCE: A person’s ability to continue medical advice for the intended course, which
may range from few days to life long.
However the preferred terminology remains a matter of debate. In some cases,
concordance is used to refer specifically to patient adherence to a treatment regimen that is
designed collaboratively by the patient and physician, to differentiate it from adherence to a
physician only prescribed treatment regimen5-8, despite the ongoing debate, adherence is the
preferred term for the WHO1, the American pharmacists association9 and the US National
Institutes of Health Adherence Research Network8,10, and is important for optimum therapeutic
outcome which improves patient’s quality of life.
Concordance also refers to a current UKNHS (United Kingdom National Health
Services) initiative to involve the patient in the treatment process to improve compliance 11, 12.
Here patient is informed about their condition and treatment options, they are involved with
the treatment team in decision making process and partially responsible for monitoring and
reporting back to the team1.

REVIEW ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 144
Non-compliance is a major obstacle to the effective delivery of health care. Estimates
from the WHO indicate that about 50% of patients with chronic diseases living in developed
countries do not follow treatment recommendations1, 13. Non-compliance means not following
the directions for treatment due to irrational behavior or willful ignoring of instructions leading
to increased morbidity, treatment failures, exacerbation of disease, more frequent physician
visits, increased hospitalizations and even death (Fig.1) 6, 14, 15.
(Fig.1: TYPES OF MEDICATION TAKING BEHAVIOR)
PRESCRIBED REGIME FOR ENTIRE PERIOD
FULLY COMPLIANT
FULLY PERSISTANT
PARTIALLY COMPLIANT
NON-PERSISTANT (STOPPED THERAPY BEFORE COURSE)
NON COMPLIANT & NON-PERSISTENT
NON PERSITENT, NON-ACCEPTANCE (NOT STARTED THERAPY)
The most common situations associated with non adherence are
� Failure to have the prescription dispensed or renewed, not refilling
prescriptions for chronic diseases states, not obtaining refills at appropriate
intervals, 25% don’t fill new prescriptions16-18 ,
� Omission of doses most common type of non compliance and more likely to
occur when a medication is to be administered at frequent intervals. Increased
frequency cause more interruption of normal routine, or work schedule,
especially in poly pharmacy or when treatment is needed with an extended
period of time. Few patients cannot identify their own medications 18,19.
� Errors of dosage, like giving instructions in measures of tea spoon (measure
range from 5ml. to 15ml.) and not following administration of medicines at night
time if patient falls into sleep etc., where dose of administration is incorrect20.
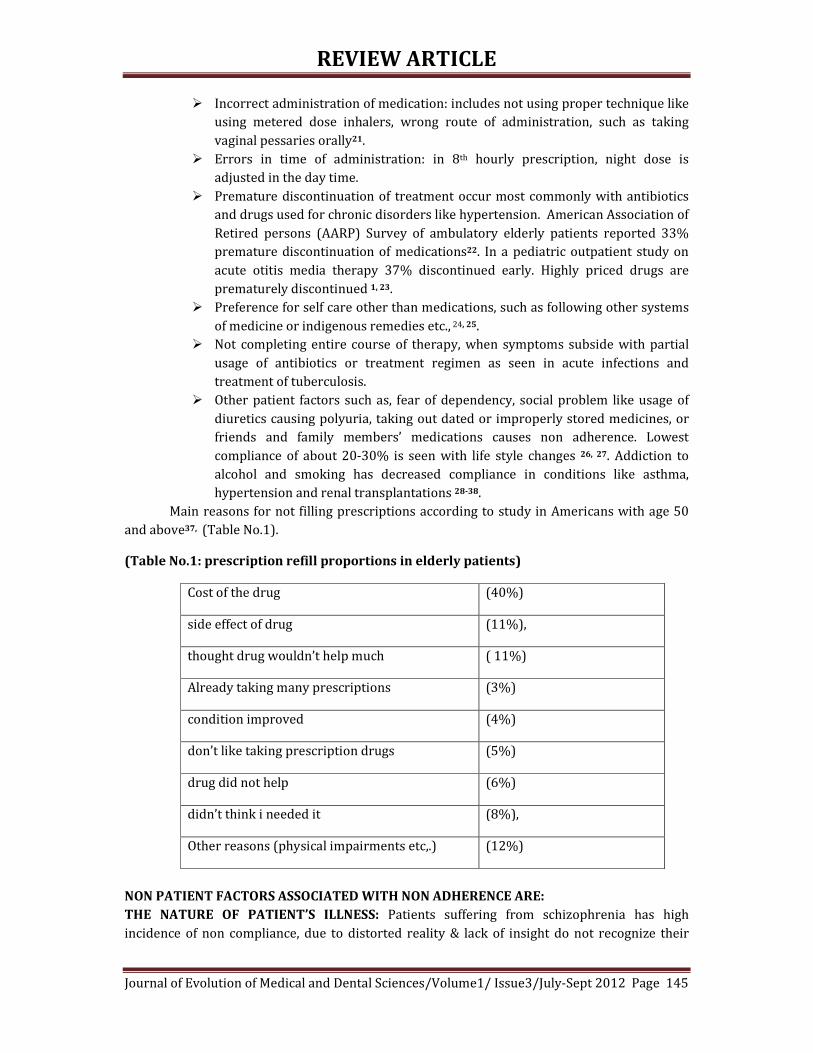
REVIEW ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 145
� Incorrect administration of medication: includes not using proper technique like
using metered dose inhalers, wrong route of administration, such as taking
vaginal pessaries orally21.
� Errors in time of administration: in 8th hourly prescription, night dose is
adjusted in the day time.
� Premature discontinuation of treatment occur most commonly with antibiotics
and drugs used for chronic disorders like hypertension. American Association of
Retired persons (AARP) Survey of ambulatory elderly patients reported 33%
premature discontinuation of medications22. In a pediatric outpatient study on
acute otitis media therapy 37% discontinued early. Highly priced drugs are
prematurely discontinued 1, 23.
� Preference for self care other than medications, such as following other systems
of medicine or indigenous remedies etc., 24, 25.
� Not completing entire course of therapy, when symptoms subside with partial
usage of antibiotics or treatment regimen as seen in acute infections and
treatment of tuberculosis.
� Other patient factors such as, fear of dependency, social problem like usage of
diuretics causing polyuria, taking out dated or improperly stored medicines, or
friends and family members’ medications causes non adherence. Lowest
compliance of about 20-30% is seen with life style changes 26, 27. Addiction to
alcohol and smoking has decreased compliance in conditions like asthma,
hypertension and renal transplantations 28-38.
Main reasons for not filling prescriptions according to study in Americans with age 50
and above37, (Table No.1).
(Table No.1: prescription refill proportions in elderly patients)
Cost of the drug (40%)
side effect of drug (11%),
thought drug wouldn’t help much ( 11%)
Already taking many prescriptions (3%)
condition improved (4%)
don’t like taking prescription drugs (5%)
drug did not help (6%)
didn’t think i needed it (8%),
Other reasons (physical impairments etc,.) (12%)
NON PATIENT FACTORS ASSOCIATED WITH NON ADHERENCE ARE:
THE NATURE OF PATIENT’S ILLNESS: Patients suffering from schizophrenia has high
incidence of non compliance, due to distorted reality & lack of insight do not recognize their

REVIEW ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 146
illness and need for treatment. Similarly in chronic disorders like hypertension, tuberculosis
etc., same pattern is observed 39.
THERAPEUTIC REGIME: Multiple drug therapy like 5-6 prescribed drugs13, 40-42 taking at
different timings ,taking tablets with same color, size and shape cause more confusion43 and
skip doses. Technical difficulty in using inhalers44-50.
DURATION OF TREATMENT: Compliance is inversely proportional to duration of treatment27,
51, 52. In a study of long term therapy, low compliance is observed as in bronchial asthma (50%)
and hypertension (50-70%) 53-60.
FREQUENCY: Increased frequency of drug administration causes more disruption of normal
routine or work schedule, hence many patients forget or inconvenienced or embarrassed. In one
of the study, compliance has improved from 59% on 8thhourly regimen to 84% with once a day
regimen 61-67
ADVERSE EVENTS: Events are like deterrents; in a study on elderly patients 40% experienced
side effects of this 20% stopped medications and in this only 18-19% informed their physicians
about discontinuation22. In one of the survey, over 60% are noncompliant due to adverse
events. Some drugs like Anti-Hypertensive agents, Anti depressants or Anti psychotics cause
sexual dysfunction which is frequently implicated for non compliance. 68-82
TASTE OF MEDICATION: Can be the cause for noncompliance especially in children.
Failure to comprehend the importance of therapy, as patient has limited knowledge
about the illness, become non compliant if beliefs and expectations are not met with. Poor
understanding of instructions also contributes to non compliance83, 84. Non compliance in elder
age group is due to2, 13, 33, 40, 41, 85 & 86
• Adverse effects,
• Increased, or decreased sensitivity to drugs,
• Frequent change of prescriptions( prescription cascade),
• Living alone,
• Lack of social support system,
• Difficulty in opening the medication container that has flip off type of lid
• Going to pharmacist/chemist due to physical problems like (osteoarthritis)
• Cognitive impairment,
• Impaired mobility or dexterity,
• Swallowing problems,
• Financial issues like, Low income and high cost of medications,
• Everyday inconvenience in carrying and taking of medicines.
CONSEQUENCES OF NON COMPLIANCE: Drugs do not work if people do not take them 87. Non-
compliance is a major obstacle to the effective delivery of health care. National Council on
Patient Information and Education designated it as America’s other drug problem88, 89. Under
use is very common, depriving the patient of anticipated therapeutic benefits and resulting in
progressive worsening of the condition or increased complications as in hypertension. overuse

REVIEW ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 147
of medication is also common, where in patients increase dose or frequency of medications
anticipating extra benefit or quick action and remission of symptoms and some times it can be
an extra dose due to forgetfulness as in elderly age groups, causing increased adverse reactions,
leading to unnecessary use of medical resources such as
� Physician Consultations
� Emergency Department visits,90
� Unnecessary additional laboratory tests and
� Treatments which are preventable
(Table No. 2: Consequences of non adherence to treatment in elderly patients39, 91-93)
Cause Proportion of hospitalization
due to non compliance 10-33%9
inability to self-administer 23% of nursing home admissions
Studies on HIV/AIDS have revealed higher viral loads in patients with 10- days drug
holiday or 20% of missed doses of Anti retroviral agents, who are otherwise had nearly
undetectable viral loads94. Non compliance with anti psychotics in schizophrenia had relapses
with violent behavior. Similarly in Epileptics unexpected deaths are due to low the4rapeutic
concentrations of antiepileptic drugs95. Deaths in transplant patients who have waited for years
to get donor organ are because of organ rejection resulting from noncompliance in using
immunosuppressants96
Low rates of adherence to therapies for asthma, diabetes, and hypertension are thought
to contribute substantially to the human morbidity, mortality and economic burden of those
conditions1, 14. In asthma non-compliance incidence is 28-70% worldwide, increasing the risk of
acute severe asthmatic attacks requiring hospitalization. Non compliance to Anti Hypertensive
agents is very common even in developed countries, and it is the main cause for hypertension
related complications like heart diseases and strokes. In united States, it is estimated that drug
related morbidity & mortality expenditure exceeded $177.4 billions97
Compliance rates are often high or over estimated in a formal clinical trial but drops off
in a "real-world" setting. In a study, compliance rate for statins is 97% at the beginning, and
dropped to 50% after six months98.
ASSESSMENT TOOLS FOR MEDICATION ADHERENCE: Detection of non compliance is as
important as diagnosis of a medical condition Compliance or non compliance is not stable; it
may change over time, necessitating regular use of detection methods to measure the behavior
as part of assessment for therapeutic efficacy99.
Structured interviews using highly skilled and refined techniques, like Morisky scale which is
validated scale estimating the risk of medication non-adherence, is cited in numerous articles since
1986 used for many different disease such as, hypertension, hyperlipidemia, asthma and HIV.

REVIEW ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 148
Compliance or non compliance is not stable; it may change over time, necessitating
regular use of detection methods to measure the behavior as part of assessment for therapeutic
efficacy99.
As such there are no gold standards for Assessment for medication adherence; the ideal
detection would measure compliance at the time and place of medication taking event. Direct
observation of the patient would come closest to providing this ideal measure of adherence.100.
Indirect methods of monitoring compliance other than Electronic event monitoring (EEM) are;
o Pill counts,
o Medication refill records,
o Patient self report,
o Structured interviews using highly skilled and refined techniques,
o Change in weight of meter dose inhaler canisters, ,
o Medication event monitoring using computer are most commonly
used.
o
Pill count is often used in clinical trials, it measures the difference between the dosage
units initially dispensed and number remaining on return visit or unscheduled home visit, but
pill dumping and medication discard misrepresents compliance101, 102
Structured interviews using highly skilled and refined techniques, like Morisky scale
which is validated scale estimating the risk of medication non-adherence, is cited in numerous
articles since 1986 used for many different disease such as, hypertension, hyperlipidemia,
asthma and HIV. It is a structured four item self reported adherence measure that addresses
barriers to compliance and permit health care provider to reinforce positive adherence
behavior 103
Sometimes achievement of treatment goals are used as a measure for compliance, like
normal blood pressure in hypertensive, normal blood glucose levels in diabetics, after
eliminating “ tooth brush effect” (like people brushing their teeth before seeing a dentist) where
patients load up medication just before their return visit to physician. Electronic event
monitoring is a recent and reliable computerized compliance monitoring, here medication
container cap is housed with microprocessor which records date and time of opening the cap
and data can be retrieved by connecting the micro processor to computer, the disadvantage
being no data is provided regarding actual amount of drug taken, It helps when supplemented
with other methods of measurements104.
Direct methods to measure adherence is by using biological markers and tracer
compounds like measurement of glycosylated hemoglobin which provides objective assessment
of metabolic control in preceding three months in Diabetics. Small amounts of tracer
compounds with long half- lives, like Phenobarbital or digoxin are added to the medications and
these tracers are measured in biological fluids.
Therapeutic drug levels monitoring in biological fluids is another direct method of
compliance assessment but draw backs are individual pharmacokinetic variations, and tooth
brush effect invalidate this type of measurement as data do not provide timing of doses10

REVIEW ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 149
(Table: 3 Comparison of different methods for the measurement of adherence)
DIRECT METHODS INDIRECT METHODS
They are more sensitive and specific They are less sensitive and specific
They are direct pharmacologic indicators of
medication adherence
Tooth brush effect can not be ruled out
Limitations:
i) Legal and ethical issues
ii) Individual pharmaco-kinetic
variations of drugs
They are better measure of detection if two
different indirect methods are used and
correlated;
Eg: Pill count and electronic event monitoring
device.
HOW TO IMPROVE COMPLIANCE/ADHERENCE: Effective ways to help people follow
medication regimes could have far larger effects on health than any other treatment”-Haynes et
al. 2005106. Patient should be evaluated before changing therapeutic regimen as non adherence
is most common missed diagnosis.
Demographic factors such as age, marital status, sex, race, income, occupation, number
of dependents, intelligence, level of education, or personality type have been shown to be
marginally related to noncompliance107-111. Based on behavioral principles patient-centered
compliance models are described, taking into consideration of socio behavioral determinants112
which includes health belief models and health decision models , former is related to a
preventive health behavior and latter focusing more on health decisions which combines the
health belief model and patient preferences with comprehensive cognitive behavioral and
affective components for advocated behavior5, 113, 114.
Patient prerequisites for adherence:
� Understand diagnosis and potential impact
� Believe that treatment will be beneficial
� Treatment favors benefit over cost
� Confidence in health care practitioners
Patient factors for improved compliance include:
� Quick relief of symptoms � Becomes quickly ill without therapy � Treatment involving expensive procedure � Recurrence if treatment is stopped � Increased disability as a consequence with out treatment
HEALTH BELIEFS: To achieve compliance patient should believe that, he/she actually have
illness which is diagnosed, and with treatment, severity of condition is reduced. Patient
education & counseling should be designed to encourage health beliefs115-118.
Patient physician interaction also affects compliance or adherence. Patient who has
respect towards treating physician and is well known, giving information, assurance and
psychological support, showing empathy, improves compliance or adherence. The interaction
should be a negotiation between two active and equal participants with goal/strategy “to put ill

REVIEW ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 150
at ease”.119-124. As recommended by NCPIE (National Council for Patient Information and
Education) physician should respond to patient’s queries regarding treatment and other related
topics.
IDENTIFICATION OF RISK FACTORS FOR NON COMPLIANCE: As it is difficult to identify a non
coplier, every patient is assumed a potential defaulter 125. By recognizing individuals who are at
risk, treatment is planned with simplest regimen compatible with patient’s normal activities,
such as avoiding expensive medicines, unnecessary medication, using long acting formulations
and combination medications, to decrease frequency of administration
Prescribing low cost medicines as high cost medicine prescription fill rates are low, even if
they buy reluctant to use entire prescribed quantity. Medication-flavoring formulary system
developed about three dozen flavors, to overcome taste problems in medications especially in
children
In cases with mental illness discuss with patients or family members regarding delayed onset
of therapeutic effects, and the need for prolonged treatment by prescribing medicines with
least side effects.
With physical disabilities such as visual impairment, communicate with patient verbally or
use tape record instructions, increase font size or color code medication bottles, advise pre-
measure and pre-cut medications. With hearing impaired patients the problem is solved by
using interpreter, or speaking to better ear using regular voice volume and lip movement with
eye contact maintained, repeat instructions when necessary, supplement with written
information, and turn up hearing aids2-3
In cases with reduced mobility and dexterity advise patients to store medications in easily
accessible location, using pre-cut, pre-measured medications or easy open tops that are easy to
administer. Foiled backed wrappers are avoided in patients with arthritis or tremors. Wherever
difficulty in swallowing is seen use alternative dosing formulations like liquids, trans-dermal
patches, crushable tablets or capsules that can be opened and mixed with soft foods.
DEVELOPMENT OF TREATMENT PLAN: Hippocrates: “decisions to deviate, un aware of
physician intentions keep watch also on the fault of patients which often makes them lie about
the taking of things prescribed”. Develop a simple plan on individual basis, involving patient in
deciding treatment with minimal inconvenience and overcome forgetfulness by timing doses
corresponding to regular activities in patient’s daily schedule. Do not write twice or thrice a day
instead of writing time in am/pm. in instructions44, 126
Health literacy is the degree to which individuals have the capacity to obtain, process
and understand basic health information and services needed to make appropriate health
decisions (world health organization, 2003)127. Patients with low health literacy were reported
to be less compliant with their therapy128. Written instructions and pictograms on medicine
labels has proven to be effective in improving patient’s compliance129.
PATIENT EDUCATION: Best way to improve compliance. Decide what information is necessary
for about illness and treatment130. Too much details/inappropriate presentation of adverse
events may alarm patient & decrease compliance. Involve patient in decision-making process.
Make patient understand benefits of treatment and importance of compliance without using
complex technical terms. Patient is asked to repeat the instructions. Encourage patients to ask
REVIEW ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 151
questions. Patient education regarding asymptomatic hypertension, glaucoma, asthma, and
diabetes mellitus removes non adherence 64.
PHYSICIANS FACTORS: Asking few questions, occasional eye contact not understanding
language spend little time, giving large information in short time, lack of concern also effect
compliance131.
Physicians liability for non compliance is often over looked as they prefer pointing
deficiencies of the patients rather than themselves. Physician’s compliance is the extent to
which the behavior of doctor fulfills their professional duty like not being ignorant, adopting
new advances when they are sufficiently proved, writing prescription accurately and legibly,
warning patients about side effects or adverse effects, and counseling them to use medicines
effectively and safely.132-136
ORAL COMMUNICATIONS: Oral communication / counseling in a room with privacy137 and
free of distractions to give patient an opportunity to raise questions- supplemented by written
instructions. Studies indicate that counseling has improved adherence in hypertensive
patients138. Compliance clinics run by Pharmacists in western countries have improved
adherence by reducing hospitalizations when pre & post clinics are compared139, 140.
WRITTEN COMMUNICATION: Write timings and supplementary information regarding illness
& treatment, especially for acute conditions (e.g. antibiotics) compared to chronic conditions141.
One way communication is disadvantageous with illiterate. In a study 42% patients unable to
comprehend instructions142. So combine both oral and written and encourage patient to put
questions.
AUDIO VISUAL AIDS: help in visualizing the nature of illness, how a medicine has to be
administered eg; metered dose inhalers and how they act. Many health care professionals are
using very effectively by placing them in waiting room or consultation room and answering
questions patients may have.
CONTROLLED THERAPY: Hospitalized patients are entrusted to self medicate before
discharge, under direct supervision of health care professionals so that latter; can identify
situations that undermine compliance that are corrected by answering questions 143
Special programs and devices: In some situations highly structured programs are
developed to improve compliance eg; behaviorally oriented program for training medication
management skills in schizophrenia patients which increased compliance from 63% to
81%.Similar programs are needed for vision and hearing impairment subjects by producing
prescription labels in Braille, and hearing aids respectively.
PATIENT MOTIVATION: For achieving optimum benefit, information is provided to the patient
in a manner that is not coercive, threatening or demeaning, by counseling, providing written
materials, supplying cues for appropriate behavior. Cues may be verbal or non verbal in latter
case using special packaging or reminders, Negotiable physician- patient interaction 123 with
respect and positive attitude, and realistic appraisal of the circumstances ,or development of
contracts 144,145 or paying incentives in the form of monitory and non monitory like gifts,
vouchers etc., to achieve agreed upon treatment goals.146,147 Mass programs like sterilization

REVIEW ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 152
and immunization, wherein patients are positively motivated by beneficiaries and neighbors
also improve compliance 3,148
TIME COMMITMENT: Patients may not be able to take time off work for treatment; as a
shorter traveling time between residence and healthcare facilities could enhance patient’s
compliance. Housewives more compliant to therapy they adapt well to clinic appointment times
and treatment 3, 149-151.
COMPLIANCE AIDS: The accuracy and specificity of information on the label of prescription
container and Auxiliary labels that provide additional information regarding the use,
precautions, and storage of medicines also help in improving adherence.
Medication Calendars and Drug Reminder Charts are designed and developed to assist
self administration of drugs by patients. Special medication container like 28- compartment
(MEDISET) container are designed to help patient organize their medications on weekly basis. fig
Specially designed caps for prescription container like The Prescript Time Cap; containing
digital time piece display time and date of last dose taken. They are effective in improving
adherence by patients who forgets doses or who are confused by the complexity of regimen.
Medication packaging also influence the patients adherence. Compliance Packs are
developed which are pre-packed units, which provides one treatment cycle of medication in a
ready to use package152. New dosage forms are developed to overcome non adherence due to
increased frequency, in the form of long acting and controlled release preparations. Similarly
Trans- dermal drug- delivery systems also permits less frequency of drug administration.
MONITORING THERAPY: 1. Self Monitoring-Patient should be appraised of the importance of
monitoring their own treatment and assume personal responsibility of adherence to treatment.
Pharmacist or physician monitoring. “.brown bag program was conducted by NCPIE
&The Administration on ageing in which patients are encouraged to put all their medicines in a
bag for personalized medicine review in geriatrics.
D.O.T (directly observed therapy.153-154 It is the ideal way to monitor therapy, especially
in cases of prolonged drug intake.
“French saying- 5 centuries back about patient care “To care sometimes, to restore often,
and to comfort always”
Summary: Valuable resources like time, effort and expenses put on diagnosis of illness
with the aim of developing treatment plan for cure, control or increased survival are not
achieved, unless patient complies to treatment. Non adherence is responsible for missed
diagnosis, treatment failures and changing prescriptions with more potent, expensive and toxic
drugs.
Adherence to medication is not routinely measured in clinical practice, for reasons as
busy practice and depriving patients on close attention and monitoring therapy are not
acceptable155. The highest priority should be given for patients adherence problems.
Improved adherence benefits every body (patient, physician, pharmaceuticals,
pharmacist & community). For patient there will be increased efficacy and safety of treatment
and decreased physician and hospital visits. For pharmacist increased recognition and respect
for advise and services. Pharmaceuticals by manufacturing drugs suitable to the patients need,
like blister pack, increase sales of drugs. Finally society at large and health care system gets
benefit as a result of few problems with non compliance.

REVIEW ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 153
REFERENCES
1. WHO Library Cataloguing-in-Publication Data. Adherence to long-term therapies:
evidence for action.ISBN 92 4 154599 2 (NLM classification:W 85);
2. Okuno J, Yanagi H, Tomura S. Is cognitive impairment a risk factor for poor compliance
among Japanese elderly in the community? Eur J Clin Pharmacol. 2001; 57:589–94.
[PubMed]
3. Hernandez-Ronquillo L, Tellez-Zenteno JF, Garduno-Espinosa J, et al. Factors associated
with therapy noncompliance in type-2 diabetes patients. Salud Publica Mex. 2003;
45:191–7. [PubMed
4. Aronson.JK-2007; Compliance, concordance, adherence; Br.J.Clinical Pharmacology, 63
(4), 383-384.
5. Tilson HH (2004). "Adherence or compliance? Changes in terminology". Ann
Pharmacother 38 (1):161–2.doi:10.1345/aph.1D207. PMID 14742813Osterberg>L,
Blaschke (2005); “Adherence to medication” N.Eng.J.Med-353 (5), 487-97.
6. Osterberg L, Blaschke T (2005). "Adherence to Medication". N Engl J Med 353 (5): 487–
97.doi:10.1056/NEJMra050100.PMID 16079372
7. Bell JS, Airaksinen MS, Lyles A, Chen TF, Aslani P (2007). "Concordance is not
synonymous with compliance or adherence". Br J Clin Pharmacol 64 (5): 710–
1. doi:10.1111/j.1365-2125.2007.02971_1.x. . PMID 17875196
8. Office of Behavior and Social Sciences Research. "Adherence Research Network".
U.S. National Institutes of Health. Retrieved 12 May 2010
9. "Enhancing Patient Adherence: Proceedings of the Pinnacle Roundtable Discussion". APA
Highlights Newsletter. October 2004
10. Ngoh LN (2009). "Health literacy: a barrier to pharmacist-patient communication and
medication adherence". J Am Pharm Assoc (2003) 49 (5): e132–46; quiz e147–
9.doi:10.1331/JAPhA.2009.07075.PMID 19748861.
11. National Institute for Health and Clinical Excellence. [3 March 2008]. Medicines
Concordance (Involving Patients in Decisions about Prescribed Medicines) Available
athttp://guidance.nice.org.uk/page.aspx?o=267072
12. Elliott RA, Marriott JL (2009)."Standardized assessment of patients' capacity to manage
medications: a systematic review of published instruments". BMC Geriatr 9:
27. doi:10.1186/1471-2318-9-27. .PMID 19594913.
13. Murray MD, et al.DICP 1986; 20:146.
14. Bond WS, Hussar DA. Detection methods and strategies for improving medication
compliance. Am J Hosp Pharm. 1991;48:1978–88. [PubMed-rept
15. Svarstad BL, Shireman TI, Sweeney JK. Using drug claims data to assess the relationship
of medication adherence with hospitalization and costs. Psychiatr Serv. 2001;52:805–11.
[PubMed]
16. "Dosing and compliance?". Bandolier117: Figure 1. November 2003
17. Norton M. (Reuters Health)Many patients may not fill their prescriptions.
(2010), [1]Accessed May 12, 2010
18. Schering Report, , XVIII, 1996
19. Primary non compliance in a Singapore poly clinic, Singapore Med. J 1999, Nov; 40
(11):691-3
20. Mattar ME, et al, J.Pediatr.1975; 18:137

REVIEW ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 154
21. De Tullio PL, Corson ME. Am J Hosp.Pharm,1987; 44:1802
22. Prescription drugs:survey of consumer use, attitudes & behavior. Washington, DC: AARP,
1984.
23. Robinson B. Drug topics, 1987; 131(Feb.16):37.
24. Shah NR, Hirsch AG, Zacker C, Taylor S, Wood GC, Stewart WF (February 2009)."Factors
associated with first-fill adherence rates for diabetic medications: a cohort study". J Gen
Intern Med 24 (2): 233–7.doi:10.1007/s11606-008-0870-z. .PMID 19093157
25. Shah NR, Hirsch AG, Zacker C, et al. (April 2009). "Predictors of first-fill adherence for
patients with hypertension". Am. J. Hypertens. 22 (4): 392–6.doi:10.1038/ajh.2008.367.
.PMID 19180061.
26. Tebbi CK, Cummings KM, Zevon MA, et al. Compliance of pediatric and adolescent cancer
patients. Cancer. 1986; 58:1179–84. [PubMed
27. DiMatteo MR. Social support and patient adherence to medical treatment: a meta-
analysis. Health Psychol. 2004;23:207–18. [PubMed]
28. Degoulet P, Menard J, Vu HA, et al. Factors predictive of attendance at clinic and blood
pressure control in hypertensive patients. Br Med J (Clin Res Ed) 1983;287:88–93.
29. Shea S, Misra D, Ehrlich MH, et al. Correlates of nonadherence to hypertension treatment
in an inner-city minority population. Am J Public Health. 1992;82:1607–12. [PMC free
article] [PubMed
30. Turner J, Wright E, Mendella L, et al. Predictors of patient adherence to long-term home
nebulizer therapy for COPD. Chest. 1995; 108:394–400. [PubMed]
31. Leggat JE, Jr, Orzol SM, Hulbert-Shearon TE, et al. Noncompliance in hemodialysis:
predictors and survival analysis. Am J Kidney Dis. 1998; 32:139–45. [PubMed
32. Kyngas H, Lahdenpera T. Compliance of patients with hypertension and associated
factors. J Ad Nurs. 1999;29:832–9.
33. Kim YS, Sunwoo S, Lee HR, et al. Determinants of non-compliance with lipid-lowering
therapy in hyperlipidemic patients. Pharmacoepidemiol Drug Saf. 2002;11:593–600.
[PubMed]
34. Ghods AJ, Nasrollahzadeh D. Noncompliance with immunosuppressive medications after
renal transplantation. Exp Clin Transplant. 2003;1:39–47. [PubMed]
35. Yavuz A, Tuncer M, Erdogan O, et al. Is there any effect of compliance on clinical
parameters of renal transplant recipients? Transplant Proc. 2004;36:120–1. [PubMed]
36.
36. Balbay O, Annakkaya AN, Arbak P, et al. Which patients are able to adhere to tuberculosis
treatment? A study in a rural area in the northwest part of Turkey. Jpn J Infect Dis.
2005;58:152–8. [PubMed]
37. Cooper C, Carpenter I, Katona C, et al. The AdHOC study of older adults’ adherence to
medication in 11 countries. Am J Geriatr Psychiatry. 2005;13:1067–76. [PubMed
38. Fodor GJ, Kotrec M, Bacskai K, et al. Is interview a reliable method to verify the
compliance with antihypertensive therapy? An international central-European study. J
Hypertens. 2005;23:1261–6. [PubMed
39. Feinstein S, Keich R, Becker-Cohen R, et al. Is noncompliance among adolescent renal
transplant recipients inevitable? Pediatrics. 2005;115:969–73.
40. Kyngas H, Lahdenpera T. Compliance of patients with hypertension and associated
factors. J Ad Nurs. 1999;29:832–9.

REVIEW ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 155
41. Medications,due to polypharmacy,(williams a, manias e and walker r. interventions to
improve medication adherence in people with multiple chronic conditions: a systematic
review. journal of advanced nursing. february 2008:1-12.
42. GotzschePC.Controlled Clin Trials 1989;10:31.
43. Kroenke K.Am. J Med 19855;79:149
44. Feder R. N, Eng.J Med, 1978; 298:463
45. Kelloway JS, Wyatt RA, Adlis SA. Comparison of patients’ compliance with prescribed oral
and inhaled asthma medications. Arch Intern Med. 1994;154:1349–52. [PubMed]
46. Nichols-English G, Poirier S. Optimizing adherence to pharmaceutical care plans. J Am
Pharm Assoc. 2000;40:475–85.
47. Bender BG, Bender SE. Patient-identified barriers to asthma treatment adherence:
responses to interviews, focus groups, and questionnaires. Immunol Allergy Clin N Am.
2005;25:107–30
48. Horne R, Weinman J. Patients’ beliefs about prescribed medicines and their role in
adherence to treatment in chronic physical illness. J Psychosom Res. 1999;47:555–67.
[PubMed
49. Patal RP, Taylor SD. Factors affecting medication adherence in hypertensive patients. Ann
Pharmacother. 2002;36:40–5. [PubMed]
50. Grant RW, Devita NG, Singer DE, et al. Polypharmacy and medication adherence in
patients with type 2 diabetes. Diabetes Care. 2003;26:1408–12. [PubMed]
51. Iihara N, Tsukamoto T, Morita S, et al. Beliefs of chronically ill Japanese patients that lead
to intentional non-adherence to medication. J Clin Pharm Ther. 2004;29:417–24.
[PubMedrept-ref91
52. Factors influencing compliance-length of time treatment-an integrative review of patient
medication compliance from 1990-1998”wood &graythe online journal of knowledge
synthesis for nursing,vol7,document number 1 January 14, 2000
53. Combs D L, et al. Ann Intern Med. 199; 112:397
54. Sabaté E, editor. Adherence to long-term therapies: evidence for action. Geneva: World
Health Organization; 2003.
55. Gascon JJ, Sanchez-Ortuno M, Llor B, et al. Treatment Compliance in Hypertension Study
Group. Why hypertensive patients do not comply with the treatment: results from a
qualitative study. Fam Pract. 2004;21:125–30. [PubMed]
56. Farmer KC, Jacobs EW, Phillips CR. Long-term patient compliance with prescribed
regimens of calcium channel blockers. Clin Ther. 1994;16:316–26. [PubMed]
57. Frazier PA, Davis-Ali SH, Dahl KE. Correlates of noncompliance among renal transplant
recipients. Clin Transplant. 1994;8:550–7. [PubMed
58. Medication adherence: Finding solutions to a costly medical problem-Gottlieb,Drug
benefit trends 12(6) 57-62,2000
59. Dhanireddy KK, Maniscalco J, Kirk AD. Is tolerance induction the answer to adolescent
non-adherence? Pediatr Transplant. 2005;9:357–63. [PubMed]
60. Combs DL, O’Brien RJ, Geiter LJ, et al. Compliance with tuberculosis regimes: results from
USPHS therapy trial 21. Am Rev Respir Dis. 1987;135:A138.
61. International Union Against Tuberculosis Committee on Prophylaxis. Efficacy of various
durations of isoniazid preventive therapy for tuberculosis: five years of follow-up in the
IUAT trial. Bull World Health Organ. 1982;60:556–64.

REVIEW ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 156
62. Kass MA, Meltzer DW, Gordon M, et al. Compliance with topical pilocarpine treatment.
Am J Ophthalmol. 1986;101:515–23. [PubMed]
63. Cockburn J, Gibberd RW, Reid AL, et al. Determinants of non-compliance with short term
antibiotic regimens. Br Med J (Clin Res Ed) 1987;295:814–8.
64. Cramer JA, Mattson RH, Prevey ML, et al. How often is medication taken as prescribed? A
novel assessment technique. JAMA. 1989;261:3273–7. [PubMed]
65. Eisen SA, Miller DK, Woodward RS, et al. The effect of prescribed daily dose frequency on
patient medication compliance. Arch Intern Med. 1990;150:1881–4. [PubMed]
66. Sung JC, Nichol MB, Venturini F, et al. Factors affecting patient compliance with
antihyperlipidemic medications in an HMO population. Am J Manag Care. 1998;4:1421–
30. [PubMed]
67. Claxton AJ, Cramer J, Pierce C. A systematic review of the associations between dose
regimens and medication compliance. Clin Ther. 2001;23:1296–310. [PubMed]
68. Iskedjian M, Einarson TR, MacKeigan LD, et al. Relationship between daily dose frequency
and adherence to antihypertensive pharmacotherapy: evidence from a meta-analysis.
Clin Ther. 2002;24:302–16. [PubMed
69. Hoagland AC, et al. AMJ Clin Oncol, 1983; 6:239
70. Spagnoli A, Ostino G, Borga AD, et al. Drug compliance and unreported drugs in the
elderly. J Am Geriatr Soc. 1989;37:619–24. [PubMed
71. Shaw E, Anderson JG, Maloney M, et al. Factors associated with noncompliance of patients
taking antihypertensive medications. Hosp Pharm. 1995;30:201–3.
72. Buck D, Jacoby A, Baker GA, et al. Factors influencing compliance with antiepileptic drug
regimes. Seizure. 1997;6:87–93. [PubMed]
73. Dusing R, Weisser B, Mengden T, et al. Changes in antihypertensive therapy-the role of
adverse effects and compliance. Blood Press. 1998;7:313–5. [PubMed]
74. Hungin AP, Rubin G, O’Flanagan H. Factors influencing compliance in long-term proton
pump inhibitor therapy in general practice. Br J Gen Pract. 1999;49:463–4. [PMC free
article] [PubMed]
75. Kiortsis DN, Giral P, Bruckert E, et al. Factors associated with low compliance with lipid-
lowering drugs in hyperlipidemic patients. J Clin Pharm Ther. 2000;25:445–51
76. Linden M, Gothe H, Dittmann RW, et al. Early termination of antidepressant drug
treatment. J Clin Psychopharmacol. 2000;20:523–30. [PubMed]
77. Dietrich AJ, Oxman TE, Burns MR, et al. Application of a depression management office
system in community practice: a demonstration. J Am Board Fam Pract. 2003;16:107–14;
78. Grant RW, Devita NG, Singer DE, et al. Polypharmacy and medication adherence in
patients with type 2 diabetes. Diabetes Care. 2003;26:1408–12. [PubMed]
79. Loffler W, Kilian R, Toumi M, et al. Schizophrenic patients’ subjective reasons for
compliance and noncompliance with neuroleptic treatment. Pharmacopsychiatry.
2003;36:105–12 .
80. Helene Levens Lipton;”Elderly patients and their pills: The role of compliance in safe and
effective drug use”. Pride Institute Journal of long Term Home Health Care 8,no.1
(winter1989):26-31
81. Kaplan RC, Bhalodkar NC, Brown EJ, Jr, et al. Race, ethnicity, and sociocultural
characteristics predict noncompliance with lipid-lowering medications. Prev Med.
2004;39:1249–55. [PubMed]
82. O’Donoghue MN. Compliance with antibiotics. Cutis. 2004;73(Suppl 5):30–2. [PubMed

REVIEW ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 157
83. Christensen DB. Drug-taking compliance: a review and synthesis. Health Serv Res.
1978;13:171–87. [PMC free article
84. NorrelSE,et al. Am J Hosp Pharm 1984; 41: 1183
85. Ballard DB. Am j Health-System Pharm 1996; 53 1962
86. Chizzola PR, Mansur AJ, da Luz PL, et al. Compliance with pharmacological treatment in
outpatients from a Brazilian cardiology referral center. Sao Paulo Med J. 1996;114:1259–
64. [PubMed]
87. Nikolaus T, Kruse W, Bach M, et al. Elderly patients’ problems with medication. An in-
hospital and follow-up study. Eur J Clin Pharmacol. 1996;49:255–9. [PubMed]
88. Koop CE.Proc Symp Natl Pharm Council 1984;1.
89. National Council On Patient Information and Education (NCPIE) “Advancing Precription
Medicine Compliance: New Paradigms, New Practices”. December 1994
90. Maronda RF, et al.Med Care;1989; 27: 1159
91. Drug related visits to the emergency department:”how big is the problem?” patel &peter,
pharmacotherapy,22(7):915-923,2002
92. Einarson TR. Ann Pharmacother 1993; 27: 832
93. Col N,et al.Arch Intern Med 1990; 150: 841
94. Strandberg LR.Am Health Care Assoc J 1984; 10 (7) :20
95. Vogel M. Pharmacy Today 1997; 3: 8.
96. Bowerman DL, et al. J Forensic Sci 1978; 23: 522.
97. Rovelli M, et al.Transplant Proc 1989; 21: 833 Bond WS, Hussar DA. Detection methods
and strategies for improving medication compliance. Am J Hosp Pharm. 1991;48:1978–
88. [PubMed]
98. Journal of the American pharmaceutical association 41 (2): 192-199,2001
99. "Patient Compliance with statins".Bandolier. 2004
100. R. Brian, Haynes, et al, “How to detect & manage low patient compliance in chronic
illness”, Geriatrics 355 (1980) : 91-97.
101. Cohn, DL, et al. Ibid 407.
102. Rudd P, et al. Clin Pharmacol Ther 1989; 46: 169.
103. Pullar T, et al. Ibid 163.
104. Morisky--de, green lw, levine dw. concurrent and predictive validity of a self-reported
measure of medication, adherence. medical care 1986;24:67-74
105. Rudd P, et al. Clin Pharmacol Ther 1990; 48: 676
106. Kossoy AF, et al. J Allergy Clin Immunol 1989; 84: 60.
107. Haynes RB, Montague P, Oliver T, et al. Interventions for helping patients to follow
prescriptions for medications. Cochrane Database tr
108. De Geest S, Borgermans L, Gemoets H, et al. Incidence, determinants, and consequences
of subclinical noncompliance with immunosuppressive therapy in renal transplant
recipients. Transplantation. 1995;59:340–7. [PubMed]
109. McLane CG, Zyzanski SJ, Flocke SA. Factors associated with medication noncompliance
in rural elderly hypertensive patients. Am J Hypertens. 1995;8:206–9. [PubMed]
110. Lorenc L, Branthwaite A. Are older adults less compliant with prescribed medication
than younger adults? Br J Clin Psychol. 1993;32:485–92. [PubMed]
111. Sirey JA, Bruce ML, Alexopoulos GS, et al. Stigma as a barrier to recovery: Perceived
stigma and patient-rated severity of illness as predictors of antidepressant drug
adherence. Psychiatr Serv. 2001;52:1615–20. [PubMed

REVIEW ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 158
112. Wild MR, Engleman HM, Douglas NJ, et al. Can psychological factors help us to determine
adherence to CPAP? A prospective study. Eur Respir J. 2004;24:461–5. [PubMed
113. Svartad BL. NARD J 1986; Feb: 75.
114. Rosestock IM. Milkbank Mem Fund Q 1966; 55(Jul): 94.
115. Becker MH, et al. Med Care 1977; 15(Suppl 5): 27
116. Barnes L, Moss-Morris R, Kaufusi M. Illness beliefs and adherence in diabetes mellitus: a
comparison between Tongan and European patients. N Z Med J. 2004;117:U743.
[PubMed
117. Bosley CM, Fosbury JA, Cochrane GM. The psychological factors associated with poor
compliance with treatment in asthma. Eur Respir J. 1995;8:899–904. [PubMed
118. Apter AJ, Boston RC, George M. Modifiable barriers to adherence to inhaled steroids
among adults with asthma: it’s not just black and white. J Allergy Clin Immunol.
2003;111:1219–26. [PubMed]
119. Sloan JP, Sloan MC. An assessment of default and non-compliance in tuberculosis control
in Pakistan. Trans R Soc Trop Med Hyg. 1981;75:717–8. [PubMed
120. Stromberg A, Brostrom A, Dahlstrom U, et al. Factors influencing patient compliance
with therapeutic regimens in chronic heart failure: A critical incident technique analysis.
Heart Lung. 1999;28:334–41. [PubMed]
121. Moore PJ, Sickel AE, Malat J, et al. Psychosocial factors in medical and psychological
treatment avoidance: the role of the doctor-patient relationship. J Health Psychol.
2004;9:421–33. [PubMed]
122. Gonzalez J, Williams JW, Jr, Noel PH, et al. Adherence to mental health treatment in a
primary care clinic. J Am Board Fam Pract. 2005;18:87–96. [PubMed
123. Lawson VL, Lyne PA, Harvey JN, et al. Understanding why people with type 1 diabetes
do not attend for specialist advice: a qualitative analysis of the views of people with
insulin-dependent diabetes who do not attend diabetes clinic. J Health Psychol.
2005;10:409–23. [PubMed]
124. Benarde MA, Mayerson EW. JAMA 1978; 239: 1413.
125. . Geiseler PJ, Nellson KE, Cripsen RG. Am Rev Respir Dis 1987; 135:3.2-8
126. Porter AMW. Br Med J 1969; 1: 218
127. Guidelines ror prescribers: By American Pharmaceutical Association/American Society
of Internal Medicine (March 1976)
128. Vasnik JJ, Aliotta SL, DeLor B. Medication adherence: factors influencing compliance with
prescribed medication plans. Case Manager. 2005;16:47–51. [PubMed
129. Butterworth JR, Banfield LM, Iqbal TH, et al. Factors relating to compliance with a
gluten-free diet in patients with coeliac disease: comparison of white Caucasian and
South Asian patients. Clin Nutr. 2004;23:1127–34. [PubMed
130. Dowse R, Ehlers M. Medicine labels incorporating pictograms: do they influence
understanding and adherence? Patient Educ Couns. 2005;58:63–70. [
131. PubMed Rubin RR. Adherence to pharmacologic therapy in patients with type 2 diabetes
mellitus. Am J Med. 2005;118:27s–34s. [PubMed
132. Lim TO, Ngah BA. The Mentakab hypertension study project. Part II – why do
hypertensives drop out of treatment? Singapore Med J. 1991;32:249–51. [PubMed
133. Haynes RB, Taylor DW, Sackett DL, et al. Can simple clinical measurements detect
patient noncompliance? Hypertension. 1980;2:757–64. [PubMed]

REVIEW ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 159
134. Norman SA, Marconi KM, Schezel GW, et al. Beliefs, social normative influences, and
compliance with antihypertensive medication. Am J Prev Med. 1985;1:10–7. [PubMed]
135. Olubodun JOB, Falase AO, Cole TO. Drug compliance in hypertensive Nigerians with and
without heart failure. Int J Cardiol. 1990;27:229–34. [PubMed
136. Milas NC, Nowalk MP, Akpele L, et al. Factors associated with adherence to the dietary
protein intervention in the Modification of Diet in Renal Disease Study. J Am Diet Assoc.
1995;95:1295–300. [PubMed]
137. Thomas LK, Sargent RG, Michels PC, et al. Identification of the factors associated with
compliance to therapeutic diets in older adults with end stage renal disease. J Ren Nutr.
2001;11:80–9. [PubMed]
138. Gannon K. Drug Topics 1990;134(July 9): 13
139. McKenney JM, et al. Circulation 1973; 48: 1104
140. Monson R, et al. Arch Intern Med 1981; 141: 1441.
141. Cable GL, et al. Contemp Pharm Pract 1982; 5: 38.
142. Tebbi CK. Treatment compliance in childhood and adolescence. Cancer. 1993;71:3441–
9. [PubMed
143. Williams MV, et al. JAMA 1995; 274: 1677
144. Remington IX Edn. Clinical Pharmacology, Chapter115; Pg.1966-76.
145. Dunbar JM, Agros WS. Comprehensive Handbook of Behavioral Medicine, vol 3. In
Ferguson JM, Taylor CB, eds. New York: Spectrum, 1980, p 328
146. Eraker SA, et al. Ann Intern Med 1984; 100: 258.
147. Giuffrida A, Torgerson. Should we pay, BMJ.1997 (sept 20) 315 (7110) 703-707
148. AID-Incentives. Public Health Rep. 1994 (July-Aug) 109 (4): 548-554
149. Spikmans FJ, Brug J, Doven MM, et al. Why do diabetic patients not attend appointments
with their dietitian? J Hum Nutr Diet. 2003;16:151–8. [PubMed]
150. Siegal B, Greenstein SJ. Compliance and noncompliance in kidney transplant patients:
cues for transplant coordinators. Transpl Coord. 1999;9:104–8.
151. Neal RD, Hussain-Gambles M, Allgar VL, et al. Reasons for and consequences of missed
appointments in general practice in the UK: questionnaire survey and prospective review
of medical records. BMC Fam Pract. 2005;6:47. [PMC free article] [PubMed]
152. Chuah SY. Factors associated with poor patient compliance with antituberculosis
therapy in Northwest Perak, Malaysia. Tubercle. 1991;72:261–4. [PubMed]
153. Smith DL, Am Pharm 1989;NS29(2):42
154. Alpert PL Munaiff SS et al, A Prospective study of tuberculosis and Human
immunodeficiency Virus Infection: Clinical manifestations and factors associated with
survival, Clin. Inf. Dis. 1997; 24; 661-668
155. Alwood K, Kernly J,Moore-Rice k, et al; Effectiveness of Supervised, Intermittent therapy
for Tuberculosis in HIV-Infected Patients, AIDS 1994; 8: 1103-8

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012. Page 160
INTERESTING LESIONS OF BONE MARROW WITH SPECIAL REFERENCE
TO METASTASIS.
Dr. I. Sreelakshmi, Dr. P. Sunethri, Dr. B. Bheeshma, Dr. V. Geetha, Dr. P. Jijiya bai, Dr. O. Shravan
Kumar, Dr. M. Anjani Devi, Dr. K. Ramakrishna Reddy.
1. Assistant Professor, Department of Pathology. Gandhi Medical College, Hyderabad.
2. Assistant Professor, Department of Pathology. Gandhi Medical College, Hyderabad.
3. Associate Professor, Department of Pathology. Gandhi Medical College, Hyderabad.
4. Assistant Professor, Department of Pathology. Gandhi Medical College, Hyderabad.
5. Professor & Head of Department, Department of Pathology. Gandhi Medical College, Hyderabad.
6. Professor, Department of Pathology. Gandhi Medical College, Hyderabad.
7. Post Graduate, Department of Pathology. Gandhi Medical College, Hyderabad.
8. Post Graduate, Department of Pathology. Gandhi Medical College, Hyderabad.
CORRESPONDING AUTHOR:
Dr. I. Sreelakshmi,
Gandhi Medical College,
Musheerabad, Secunderabad, AP,
Email id- [email protected],
Ph- 0091 09346371707.
ABSTRACT:
BACKGROUND: Bone marrow examination is a commonly used diagnostic modality in the
evaluation of hemato-oncological disorders and in patients with malignancies of visceral organs
to detect metastasis. This study reviews clinical, hematological and pathological data of
interesting cases with bone marrow involvement. Out of 490 bone marrow aspirations
performed during a period of 4 years, 5 cases show metastatic carcinomatous deposits which
included adenocarcinomas(3), squamous cell carcinoma(1) and neuroendocrine tumour(1),
Non-Hodgkins lymphomas(2), storage disorder(2), granulomatous lesions(1), gelatinous
transformation(1). Fever, generalized weakness, loss of appetite and loss of weight were the
main symptoms. Anemia and pancytopenia were the main hematological findings. Dry tap was a
significant finding in bone marrow aspiration in cases of metastatic cancers.
KEYWORDS : Bone Marrow Biopsy, Dry tap, Metastasis Cancer.
INTRODUCTION: Bone marrow examination is used commonly in evaluation of myeloid or
lymphoid haematological malignancies, suspected storage disorders, plasma cell neoplasms, to
detect infections & reactive changes, metastasis in patients with cancer of visceral organs &
staging of tumors. Most common tumors that metastasize to bone in adults are prostrate, breast
& lung cancer and in children neuroblastoma, rhabdomyosarcoma, Ewing’s sarcoma &
Retinoblastoma.
Infiltration of marrow is suspected in unexplained haematological abnormalities, fever
of unknown origin, failure to thrive in infants, bone pains & pathologic fractures, hot spots in
PET CT and hypercalcemia, increased alkaline phosphatase.
We studied clinical, hematological, pathological data of interesting cases with bone
marrow involvement.
MATERIALS AND METHODS: A total of 490 bone marrow aspirations performed between
2008- 2011 were analyzed. A total of 19 bone marrow aspirations, followed by biopsy were
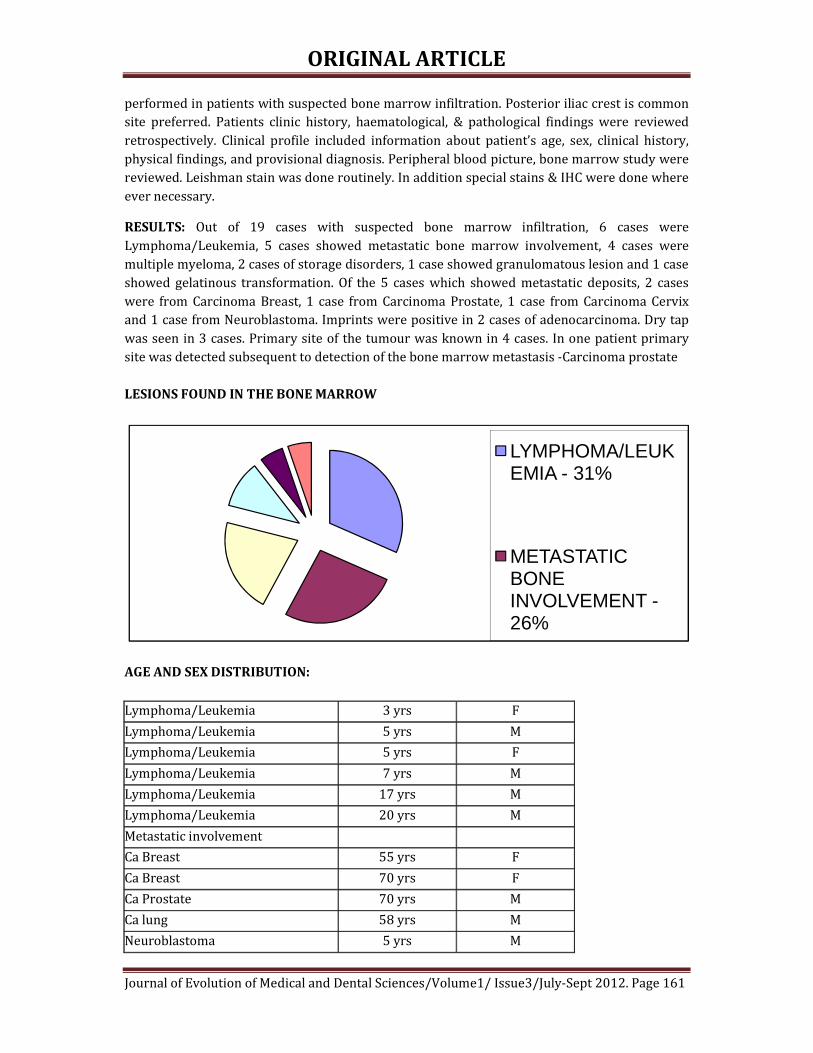
ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012. Page 161
performed in patients with suspected bone marrow infiltration. Posterior iliac crest is common
site preferred. Patients clinic history, haematological, & pathological findings were reviewed
retrospectively. Clinical profile included information about patient’s age, sex, clinical history,
physical findings, and provisional diagnosis. Peripheral blood picture, bone marrow study were
reviewed. Leishman stain was done routinely. In addition special stains & IHC were done where
ever necessary.
RESULTS: Out of 19 cases with suspected bone marrow infiltration, 6 cases were
Lymphoma/Leukemia, 5 cases showed metastatic bone marrow involvement, 4 cases were
multiple myeloma, 2 cases of storage disorders, 1 case showed granulomatous lesion and 1 case
showed gelatinous transformation. Of the 5 cases which showed metastatic deposits, 2 cases
were from Carcinoma Breast, 1 case from Carcinoma Prostate, 1 case from Carcinoma Cervix
and 1 case from Neuroblastoma. Imprints were positive in 2 cases of adenocarcinoma. Dry tap
was seen in 3 cases. Primary site of the tumour was known in 4 cases. In one patient primary
site was detected subsequent to detection of the bone marrow metastasis -Carcinoma prostate
LESIONS FOUND IN THE BONE MARROW
AGE AND SEX DISTRIBUTION:
Lymphoma/Leukemia 3 yrs F
Lymphoma/Leukemia 5 yrs M
Lymphoma/Leukemia 5 yrs F
Lymphoma/Leukemia 7 yrs M
Lymphoma/Leukemia 17 yrs M
Lymphoma/Leukemia 20 yrs M
Metastatic involvement
Ca Breast 55 yrs F
Ca Breast 70 yrs F
Ca Prostate 70 yrs M
Ca lung 58 yrs M
Neuroblastoma 5 yrs M
LYMPHOMA/LEUKEMIA - 31%
METASTATIC BONE INVOLVEMENT -26%

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012. Page 162
Multiple Myeloma 62 yrs M
Multiple Myeloma 64 yrs M
Multiple Myeloma 68 yrs M
Multiple Myeloma 57 yrs M
Storage disorders 3 yrs M
Storage disorders 9 m F
Granulamtous lesions 35 yrs M
Gelatinous transformation 40 yrs M
CLINICAL DETAILS
SYMPTOMS
Generalized weakness
NO. OF CASES
19
% OF CASES
100%
Loss of weight & loss of appetite 16 84%
Bone pain 10 52%
Fever 9 47%
Low back pain 8 42%
Organomegaly 7 36%
Lymphadenopathy 6 31%
HEMATOLOGICAL PROFILE
PERIPHERAL SMEAR FINDING
Anaemia
NO. OF CASES
19
% OF CASES
100%
Thrombocytopenia 12 63%
Pancytopenia 8 42%
Leucopenia 7 36%
Leucoerythroblastic picture 6 31%
Dry tap 3 15%
Rouleaux formation 3 15%

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012. Page 163
IMPRINT – LYMPHOMA ALCIAN-PAS POSITIVITY ON IMPRINTS
BMB: METASTATIC DEPOSITS FROM PROSTATE IHC-ER-POSITIVE IN BREAST METS TO BONE
MARROW
ROULEAUX FORMATION - MULTIPLE MYELOMA IMPRINTS OF BM- MULTIPLE MYLOMA

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012. Page 164
EPITHELOID CELLS – GRANULOMA GELATINOUS TRANSFORMATION OF BM
DISCUSSION : Bone marrow examination is very useful in the evaluation of hemato-oncological
disorders. Common findings in the peripheral blood - leucoerythroblastic blood picture,
Pancytopenia, rouleaux formation. Bone marrow aspirates and trephine biopsies are sensitive
techniques for detecting bone marrow pathology. Trephine biopsy is more sensitive than bone
marrow aspiration and sensitivity is increased by performing bilateral biopsies or by obtaining
a single large biopsy.
In adolescent individuals who were eventually diagnosed with Lymphoma/leukemia,
they initially showed pancytopenia with occasional atypical cells in the peripheral smear. Dry
tap was seen in both the cases. Imprint smears from bone marrow biopsy showed that the
marrow was packed with blasts.
Renal failure, low back pain and male predominance was common in all the cases of
multiple myeloma. All the four cases showed elevated levels of serum creatinine.
Marrow infiltration may be focal or diffuse. Reticulin and collagen fibrosis are commonly
present in bone marrow with metastasis. Fibrosis is more in case of greater degree of marrow
infiltration. Marked fibrosis is most common in carcinoma of breast, stomach, prostate, lung.
Marked fibrosis causes pancytopenia, chemotherapeutic drugs causes haemotoxicity, all these
carries bad prognosis. The two primary sites whose identification is most important because of
their sensitivity to hormonal therapy are breast and prostate. The presence of bone marrow
metastasis is helpful in detecting hormonal receptor status when it was not done on primary
tumour.
In children spleenic aspirate is supplementary to bone marrow aspiration in
identification of storage disorders. Neuroblastoma metastasis to bone marrow is very rare in
children less than one year age.
CONCLUSION: Bone marrow aspiration and trephine biopsy are effective and cheap methods of
evaluating various pathological lesions, more useful especially in visceral tumours
metastasizing to bone marrow. Bone marrow examination is indicated when there is significant
probability of identifying lesion which would affect the treatment of primary lesion. Bone
marrow examination itself sometimes gives clue to primary pathology. Imaging techniques like
radionucleide bone scan MRI, CT are usually less effective when compared to bone marrow
examination.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012. Page 165
REFERENCES:
1. Singh G, Krause JR, Breit feld V (1977) Bone marrow examination for metastatic tumor,
Cancer 40:2317-2321.
2. Finkelstein JZ, Ekert H, ISSACSH, Higgins G (1970) Bone marrow metastases in children
with solid tumors. Amj Dis child 119:49-52.
3. Moid F, Depalma L (2005) comparison of relative value of bone marrow aspirater and
bone marrow trephine biopsies in the diagnosis of solid tumors metastasis and
Hodgkins Lymphoma. Institutional experience and literature review Arch Pathol Lab
Med 129:497-501.
4. Gangadeep Kaur, Metastatic bone marrow tumors: study of nine cases and review of the
literature J Blood Disorder Transfus 2011, 2:3.
5. Saadettin Kilickap, Bone marrow metastasis of solid tumors: Clinicopathological
evaluation of 73 cases: Turkish journal of cancer.
6. Atac B, Lawrence C, Goldberg SN, metastatic tumor: the complementary role of the
marrow aspinate and biopsy. Amj Med SCi, 1991; 302:211-213.
7. Nanda A, Basus, Marwaha N. Bone marrow trephine biopsy as an adjunct to
bonemarrow aspiration. J Assoc physicians India, 2002:50:893-895.
8. Bearden JD, Ratkin GA, Coltman CA Comparison of the diagnostic value of bone marrow
biopsy and bone marrow aspiration in neoplastic disease. J clin pathol. 1974:27:738-
740.
9. Bone marrow pathology, fourth edition B.J. Bain, D.M. Clark and B.S. Wilkins (c) 2010
Barbara.j. Bain, David M. Clark, Bridget S. Wilkins ISBN:978-1-405-16825-0.
10. Jonsson U, Rundles RW (1951) tumor metastases in bone marrow: Blood 6:16-25.
11. Papac RJ (1994) bone marrow metastases-A review cancer 74:2403-2413.
12. Savage RA. Hoffman GC, Shakar K (1978) Diagnostic problems involved in detection of
metastatic neoplasms by bone marrow aspinate compared with needle biopsy Amj Clin
Pathol 70:623-627.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 166
CORRELATION BETWEEN BIOFILM FORMATION OF UROPATHOGENIC
ESCHERICHIA COLI AND ITS ANTIBIOTIC RESISTANCE PATTERN. Dr. SarojGolia, Dr. Vivek Hittinahalli, Dr. Sujatha K Karjigi, Dr. K. Mallika Reddy.
1. Professor & HOD, Department of Microbiology, Dr. B.R. Ambedkar Medical College. 2. Associate Professor, Department of Microbiology, Dr. B.R. Ambedkar Medical College.
3. Post Graduate, Department of Microbiology, Dr. B.R. Ambedkar Medical College. 4. Post Graduate, Department of Microbiology, Dr. B.R. Ambedkar Medical College.
CORRESPONDING AUTHOR:
Dr. Vivek Hittinahalli, Dr B R Ambedkar Medical College, Kadugondanhalli, Bangalore-45, Email id- [email protected], Ph- 0091 07760984581. ABSTRACT
BACKGROUND: Microorganisms growing in multilayered cell clusters embedded in a matrix of extracellular polysaccharide (slime) which facilitates the adherence of these microorganisms to biomedical surfaces and protect them from host immune system and antimicrobial therapy. There are various methods to detect biofilm production like Tissue Culture Plate (TCP) ,Tube method (TM) ,Modified Congo Red Agar Method (MCRA),bio luminescent assay ,piezoelectric sensors and fluorescent microscopic examination. OBJECTIVES : This study was conducted to compare three methods for the detection of biofilms and compare with antibiotic sensitivity pattern, in uropathogenic Escherichia coli. METHOD: This study was carried out at the Department of Microbiology Dr. B. R. Ambedkar Medical College from Dec 2011 to June 2012. Total number of 107 clinical Escherichia coli isolates were randomly selected from all age groups were subjected to biofilm detection methods and their antibiotic resistance pattern was compared. Isolates were identified by standard phenotypic methods. Biofilm detection was tested by TCP, TM and MCRA methods . Antibiotic susceptibility test of uropathogenic E coli was performed using Kirby –Bauer disc diffusion method according to CLSI guidelines.
RESULTS: From the total of 107 clinical isolate 74 (69.1 %) isolates showed biofilm formation by all the TCP, TM, CRP methods. Biofilm forming isolates from catheter associated UTI showed drug resistance to more than 6 drugs. Only 2(13.3%) isolates from Asymptomatic UTI showed biofilm by TM & MCRA methods & were sensitive all drugs. Biofilm forming isolates from symptomatic UTI showed mixed drug resistance pattern.
CONCLUSION: We conclude from our study that biofilm formation is more common in catheterized patients. TCP method is more quantitative and reliable method for the detection of biofilm forming micro-organisms as compared to TM and MCRA methods. So TCP method can be recommended for screening of biofilm as virulence marker in drug resistant E coli isolates. KEY WORDS: Escherichia coli, Biofilm, Drug Resistance, Congo Red Agar, Tissue Culture Plate
ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 167
INTRODUCTION: E coli accounts for 70 to 95% of urinary tract infections1,13 Bacteria follow ascending route of infections in 90% of urinary tract infections. These are primarily derived from fecal flora of the host, but haematogenic infections do occur. Virulence factors like adhesins, toxins , lipo polysaccharides , iron acquisition , presence of capsule, or serum resistance , determine the uropathogenicity of E.coli strains. Adhesion to epithelial cells of urogenital bacteria is generally accepted as being essential for Uropathogenic bacteria because otherwise the bacteria would be washed out rapidly. In 100% E.coli isolates from pyelonephritis patients & 17% E.coli isolates from Asymptomatic bacteriuria, pap (pili associated pyelonephritis ) was a significant virulence factor. Uropathogenic E.coli (UPEC) can also express a fimbrial adhensins like AFA I , AFA III , which are encoded by gene clusters.
UPEC can invade and colonise the bladder epithelium establishing a urinary tract reservoir allowing an explanation of recurrent UTI that does not necessarily involve reinfection via the Gastrointestinal tract.1,10
Biofilm is an aggregate of micro-organism in which the cells are irreversibly attached to substratum or to each other. They are embedded in a matrix of extra cellular polymeric substances (EPS) in which they have produced and exhibit an altered phonotype with respect to growth rate and gene transcription2,3
Availability of key nutrients, chemotaxis towards surface, motility of bacteria, surface adhesins and presence of surface bacteria are some factors which influences biofilm formation.4 The bacteria enclosed within the biofilm are extremely resistant to treatment. This may be because the drug concentration obtained may be insufficient in certain areas of the film. The bacteria located at the base of the biofilm are metabolically inactive and are thus resistant to certain antibiotics and possess active antibiotic degradation mechanism that contribute to avoid the accumulation of an effective drug concentration.19
So in this study we screened 107 non Repetitive Clinical urinary Isolates of E.coli received in Department of Microbiology Dr. B.R. Ambedkar Medical college by conventional microbiological methods& were subjected to various methods of detections of biofilm production .These include Tissue Culture Plate (TCP)method,5 Tube method(TM) 6,Modified Congo Red Agar method(MCRA) 7.
The samples received by patients were also divided into three groups namely catheter associated infection, Asymptomatic bacteriuria and Symptomatic bacteriuria. The antibiotic susceptibility test was carried out by Kirby Bauer Disc diffusion Technique on Mueller Hinton agar. OBJECTIVE: Evaluation of different detection methods of biofilm formation of uropathogenic E.coli and their drug susceptibility pattern. MATERIALS AND METHODS:
PLACE AND DURATION OF THE STUDY: The prospective study was conducted at the Department of Microbiology, Dr. B.R. Ambedkar Medical College from Dec 2011 to June 2012 . INCLUSION CRITERIA: Pure growth of Escherichia coli isolates were randomly selected from all age groups.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 168
E coli isolated from significant bacteriuria, in urine samples of catheterized patients, antenatal cases ,UTI complicated by urinary obstruction, antibiotic therapy, recurrent infections, chronic prostatitis were selected. EXCLUSION CRITERIA; Insignificant bacteriuria, mixed growth & any other organism showing significant growth .
SELECTION OF THE ISOLATES : Total number of 107 urine E coli isolates were subjected to biofilms detection methods. The urine samples of patients were divided into three groups namely – Catheter associated infections, Symptomatic bacteriuria, and Asymptomatic bacteriuria.
The organisms were identified by conventional microbiological methods. The antibiotic susceptibility test was carried out by Kirby Bauer Disc diffusion method
using reference strain of positive biofilm producer E.coli ATCC-25922. Statistical method used was linear correlation. TISSUE CULTURE PLATE METHOD5,8:
The organisms isolated from fresh agar plates were inoculated in Brain Heart Infusion(BHI) with 2% sucrose incubated for 24hrs at 37O c in stationary conditions. Broth was diluted 1:100 with fresh medium. Individual wells of sterile polystyrene 96 well flat bottom culture plate well were filled with 200ul aliquots of diluted cultures. Only medium served as control to check sterility and nonspecific binding of media.9
The TCP were incubated for 24hrs at 370 c. After incubation contents of each well was gently removed by taping the plates. The wells were washed four times with 0.2ml of phosphate buffer saline (PBS pH 7.2) to remove free floating planktonic bacteria. Biofilms formed by adherent ‘sessile’ organisms in plate were fixed with sodium acetate (2%) and stained with crystal violet (0.1%w/v) for one minute. Excess stain was rinsed off by thorough washing with deionized water and plates were kept for drying. Adherent E.coli cells usually formed biofilm on all side wells and were uniformly stained with crystal violet. Optical Density (OD) of stained adherent bacteria was determined with a micro ELISA auto reader (model 680, Bio rad) at wavelength of 570 nm (OD 570nm). These OD values were considered as index of bacteria adhering to surface and forming biofilms.8
Experiment was performed in triplicate and repeated three times, the data was then averaged and standard deviation was calculated. To compensate for background absorbance, OD readings from sterile medium, fixation and dye were averaged and subtracted from all test values. The mean OD value obtained from media control well was deducted from all test values. Classification of Bacteria Adherence:
We classified based on OD values obtained for individual strains of E.coli, but moderate biofilm forming isolates are taken as biofilm forming isolates.
Mean OD value Adherence Biofilm formation
< 0.120 Non Non/weak
0.120-0.240 Moderate Moderate
0.240 Strong High

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 169
Table no 1; Detection of biofilm formation by mean OD values
Negative OD <0.120
Strong positive OD > 0.240
Fig 1 Detection of biofilm formation by mean OD values.
TUBE METHOD : A quantitative assessment of biofilm formation was determined as previously described by Christensen et al BHI with2% sucrose was inoculated with loopful of microorganisms from overnight culture plates incubated for 24hrs at 37 c. Tubes were decanted and washed with PBS and dried tubes were stained with crystal violet 0.1%. Excess stain was removed and tubes were washed with deionized water Tubes were then dried inverted position and observed for biofilm formation.
Biofilm formation was considered positive when visible film lined the wall and bottom of the tube ring formation at the liquid interface was not indicative of biofilm formation, and interpreted as positive (tube 1) as negative(tube2) . Experiments were performed in triplicate and repeated three times.8 but moderate biofilm forming isolates are taken as biofilm forming isolates
Figure 2 . Tube 1 showing strong biofilm formation. Tube 2 negative for biofilm
production.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 170
MODIFIED CONGO RED AGAR METHOD (CRA): Freeman et al15 had described an alternative method of screening biofilm formation by E coli isolates. In this study we use modified Congo red agar for biofilm formation. In vitro slime production ability on the published Congo red agar by Freeman et al (1989) in diffuse black pigment in the agar with growth of black pigmented colonies but pigmentation decreased with time. In the present study the modified Congo red agar (MCRA) was optimized to get strong black pigmentation at 48hrs incubation and then for 2-4 days room temperature. Black colored colonies with dry crystalline consistency interpreted- as positive biofilm producing strains. Red coloured colonies- interpreted as negative for biofilm production
Table 2; composition of Congo red agar.
fig 3 Congo red agar plate showing biofilm formation a) dry crystalline colonies-positive
for biofilm, b)red colored colonies-negative for biofilm
Antibiotic susceptibility test of biofilm producing bacteria was done on Mueller Hinton agar using the following antibiotic discs12:
Norfloxacin, Nitrofurantoin, Ceftizoxime,ceftazidime, Amoxyclavulanic acid, Cotrimoxazole, Ampicillin ,Amikacin Imipenem,Tetracycline.
All the antibiotic disc were obtained from the Himedia. E coli ATCC 25922 were used as positive control and susceptibility testing was performed by using the Kirby Bauer Disc Diffusion Technique according CLSI guidelines.
RESULTS: Among 107 patients 65 were males and 42 were females. From the total of 107 clinical isolates 74( 69.1 %) isolates showed biofilm formation by all the TCP,TM,CRP methods. Among 67 catheter associated UTI ,60 (89.5%)isolates produced biofilm by all the three methods .
Composition /Litter Congo Red Agar Modified Congo red agar
Congo red 0.8g 0.4g
Sucrose 36g -
Glucose - 10g
BHAI 52g -
BAB-2 - 40g
Water 100ml 1000ml

ORIGINAL
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/
Among Asymptomatic bacteriuria out of 15 isolates none produced biofilm by TCP method.
2(13.3%) produced biofilm&13(86.6%) were non biofilm producer by TM &MCRA meth
Among symptomatic UTI complicated from urinary obstructions, antibiotic therapy, recurrent infections, chronic site of infections(chronic prostatitis or stones) , 14(56%) were biofilm producers by TCPmethod,12(48%) by TM method,18(72%) by MCRA metin table3 & chart 3.
Table no 3 Above table shows percentage of
&its correlation with patient’s condition
CHART NO 1 : ABOVE CHART SHOWS PERCENTAGE OF BIOFILM & NON BIOFILM FORMING
E.COLI ISOLATES & ITS CORRELATION WITH PATIENT’S CONDITION.
0102030405060
bio
film
Bio
film
nonbiofilm
nonbiofilmbiofilmNonbiofm
TCP TM MCRA
E coli isolated from
TCP
biofilm
nonbiofilm
Catheter associated infection (n=67)
60(89.5%) 7(10.44%)
Asymptomatic bacteriuria (n=15)
0 15
Symptomatic bacteriuria (n=25)
14(56%) 11(44%)
ORIGINAL ARTICLE
of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012
Among Asymptomatic bacteriuria out of 15 isolates none produced biofilm by TCP method.
2(13.3%) produced biofilm&13(86.6%) were non biofilm producer by TM &MCRA meth
Among symptomatic UTI complicated from urinary obstructions, antibiotic therapy, infections, chronic site of infections(chronic prostatitis or stones) , 14(56%) were
biofilm producers by TCPmethod,12(48%) by TM method,18(72%) by MCRA method, as shown
Table no 3 Above table shows percentage of biofilm & non biofilm forming E.coli
with patient’s condition.
CHART NO 1 : ABOVE CHART SHOWS PERCENTAGE OF BIOFILM & NON BIOFILM FORMING
ISOLATES & ITS CORRELATION WITH PATIENT’S CONDITION.
biofilmNonbiofm
MCRA
Catheter associated
infection (n=67)
Asymptomatic bacteriuria
(n=15)
Symptomatic bacteriuria
(n=25)
TM MCRP
nonbiofilm
Biofilm
Nonbiofilm
biofilm
7(10.44%) 60(89.5%) 7(10.44%) 60(89.5%)
15 2(13.3%) 13(86.6%) 2(13.3%)
11(44%) 12(48%0 13(52%) 18(72%)
Sept 2012 Page 171
Among Asymptomatic bacteriuria out of 15 isolates none produced biofilm by TCP method.
2(13.3%) produced biofilm&13(86.6%) were non biofilm producer by TM &MCRA method .
Among symptomatic UTI complicated from urinary obstructions, antibiotic therapy, infections, chronic site of infections(chronic prostatitis or stones) , 14(56%) were
hod, as shown
E.coli isolates
CHART NO 1 : ABOVE CHART SHOWS PERCENTAGE OF BIOFILM & NON BIOFILM FORMING
Nonbiofm
60(89.5%) 7(10.44%)
2(13.3%) 13(86.6%)
18(72%) 7(28%)
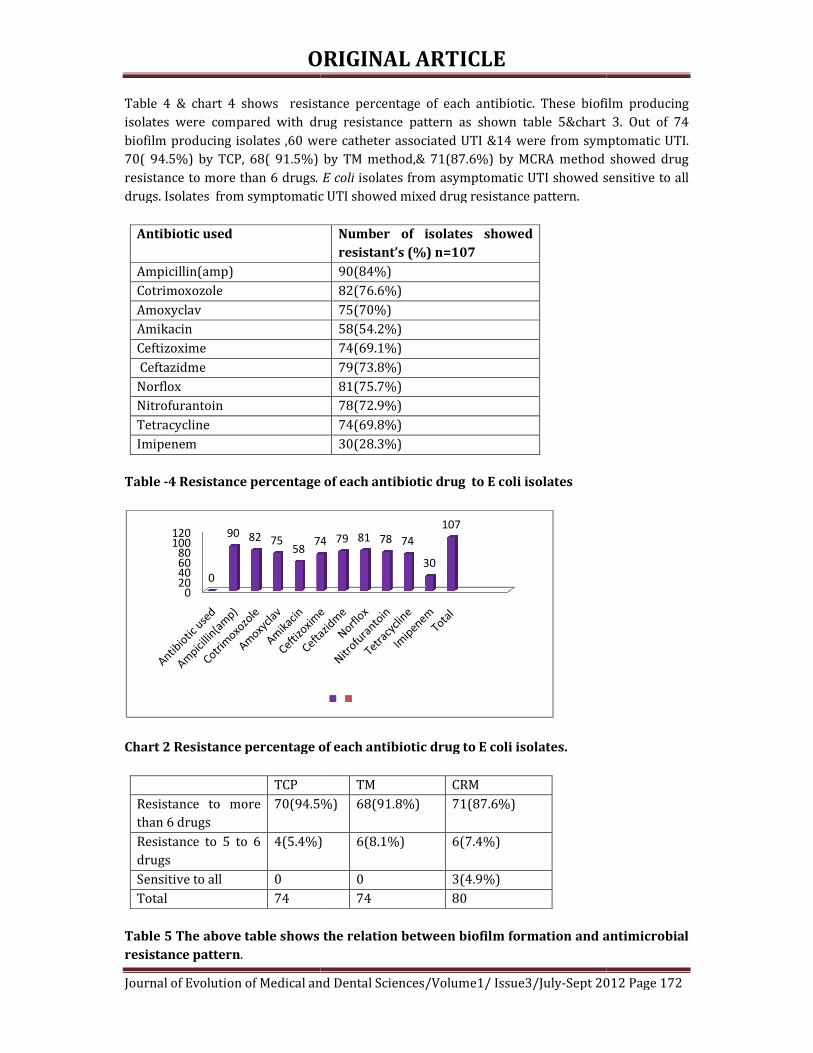
ORIGINAL
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/
Table 4 & chart 4 shows resistance percentage of each antibiotic. These biofilm producingisolates were compared with drug resistance pattern as shown table 5&chart 3. Out of 74 biofilm producing isolates ,60 were catheter associated UTI &14 were from symptomatic UTI. 70( 94.5%) by TCP, 68( 91.5%) by TM method,& 71(87.6%) by MCRA method showedresistance to more than 6 drugs. E coli
drugs. Isolates from symptomatic UTI showed mixed drug resistance pattern.
Antibiotic used
Ampicillin(amp)
Cotrimoxozole
Amoxyclav
Amikacin
Ceftizoxime
Ceftazidme
Norflox
Nitrofurantoin
Tetracycline
Imipenem
Table -4 Resistance percentage
Chart 2 Resistance percentage of each antibiotic drug to E coli isolates.
TCP
Resistance to more than 6 drugs
70(94.5%)
Resistance to 5 to 6 drugs
4(5.4%)
Sensitive to all 0
Total 74
Table 5 The above table shows the relation between biofilm formation and antimicrobial
resistance pattern.
020406080
100120
0
90 82 7558
74
ORIGINAL ARTICLE
of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012
Table 4 & chart 4 shows resistance percentage of each antibiotic. These biofilm producingisolates were compared with drug resistance pattern as shown table 5&chart 3. Out of 74 biofilm producing isolates ,60 were catheter associated UTI &14 were from symptomatic UTI. 70( 94.5%) by TCP, 68( 91.5%) by TM method,& 71(87.6%) by MCRA method showed
. E coli isolates from asymptomatic UTI showed sensitive to all drugs. Isolates from symptomatic UTI showed mixed drug resistance pattern.
Number of isolates showed
resistant’s (%) n=107
90(84%)
82(76.6%)
75(70%)
58(54.2%)
74(69.1%)
79(73.8%)
81(75.7%)
78(72.9%)
74(69.8%)
30(28.3%)
4 Resistance percentage of each antibiotic drug to E coli isolates
Chart 2 Resistance percentage of each antibiotic drug to E coli isolates.
TM CRM
70(94.5%) 68(91.8%) 71(87.6%)
4(5.4%) 6(8.1%) 6(7.4%)
0 3(4.9%)
74 80
Table 5 The above table shows the relation between biofilm formation and antimicrobial
74 79 81 78 74
30
107
Sept 2012 Page 172
Table 4 & chart 4 shows resistance percentage of each antibiotic. These biofilm producing isolates were compared with drug resistance pattern as shown table 5&chart 3. Out of 74 biofilm producing isolates ,60 were catheter associated UTI &14 were from symptomatic UTI. 70( 94.5%) by TCP, 68( 91.5%) by TM method,& 71(87.6%) by MCRA method showed drug
isolates from asymptomatic UTI showed sensitive to all
Table 5 The above table shows the relation between biofilm formation and antimicrobial

ORIGINAL
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/
Chart 3The relation between biofilm formation and antimicrobial resistance pattern
Antibiotics
Catheter associated infection N=60
Ampicillin(amp) 60
Cotrimoxozole 60
Amoxyclav 58
Amikacin 50
Ceftizoxime 60
Ceftazidme 60
Norflox 60
Nitrofurantoin 60
Tetracycline 60
Imipenem 24
Table 5 The above table shows correlation between antibiotic resistance pattern with
patient’s condition & biofilm formation. (N=number of biofilm positive isolates).
Chart 4 The above chart shows correlation between patient’s condition ,biofilm
formation & antibiotic resistance pattern. N=number of biofilm positive isolates.
DISCUSSION: Bacterial adhesion has long been considered as virulence factor contributing to infection associated with catheter and other including medical devices.There are two possible explanations for the ability of materials . The first and the bacterial production of polysaccharide slime, the second one is the presence of adhesins for the host matrix proteins that are absorbed on to the biomedical surface.15
There are various methods for biofilm detection
0
Resistance to more than 6 drugs
Resistance to 5 to 6 drugs
Sensitive to all
Total
CRM
ORIGINAL ARTICLE
of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012
Chart 3The relation between biofilm formation and antimicrobial resistance pattern
Catheter associated infection
Symptomatic bacteriuria N=14
Non biofilm Forming Isolates N =33.
14 16
14 8
12 5
8 0
14 0
14 5
14 7
14 4
14 0
6 0
Table 5 The above table shows correlation between antibiotic resistance pattern with
patient’s condition & biofilm formation. (N=number of biofilm positive isolates).
shows correlation between patient’s condition ,biofilm
formation & antibiotic resistance pattern. N=number of biofilm positive isolates.
Bacterial adhesion has long been considered as virulence factor contributing to catheter and other including medical devices.13
There are two possible explanations for the ability of E coli species to colonies artificial materials . The first and the bacterial production of polysaccharide slime, the second one is the
sins for the host matrix proteins that are absorbed on to the biomedical
There are various methods for biofilm detection5,6,7.
20 40 60 80 100
CRM TM TCP
Sept 2012 Page 173
Chart 3The relation between biofilm formation and antimicrobial resistance pattern
Table 5 The above table shows correlation between antibiotic resistance pattern with
patient’s condition & biofilm formation. (N=number of biofilm positive isolates). shows correlation between patient’s condition ,biofilm
formation & antibiotic resistance pattern. N=number of biofilm positive isolates.
Bacterial adhesion has long been considered as virulence factor contributing to
species to colonies artificial materials . The first and the bacterial production of polysaccharide slime, the second one is the
sins for the host matrix proteins that are absorbed on to the biomedical

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 174
In this study we evaluated 107 isolates from urine samples by three screening methods for their ability to form biofilms .
In our study we found that the majority of biofilm producing bacteria was form catheterised patients (89.5%) similarly , Donlan 2,3 reported in his study the association of biofilm producing bacteria with urinary catheters. In our study we performed TCP and TM by addition of 2% sucrose to BHI broth. Sugar supplementations is essential for biofilm formation 8.This was reported by studies conducted by Mathur T et all.
In modified TCP method extended incubation for 24hrs could lead to a better discrimination between moderate and non- biofilm producing isolates17. This was also observed in our study.
Biofilm exhibits more resistance to broad Spectrum antibiotics20. This supports that biofilm adds to the virulence profile of microorganism’s biofilm production. 16 The Tube method correlates well with TCP test for strong biofilm production but it was difficult to discriminate between weak and biofilm negative isolates due to the variability is observed results by different observers so in agreement with previous report Tube test cannot be recommended as a general screening test to identify biofilm producing isolates.18
CONCLUSION: By this study we conclude that biofilm forming microorganisms show resistance to many drugs. TM method showed 74 isolates as biofilm formers ,TCP method also showed 74 isolates as biofilm formers but MRCA showed 80 isolates as biofilm formers .Only 74 isolates that showed biofilm formation correlated with patients condition and antibiotic resistance pattern ,by this 6 isolates were false positive by MRCA method .TCP and TM method are more reliable for detection of biofilm formation ,when correlated with patient’s clinical condition and drug resistance pattern of biofilm forming isolates TM method is more subjective ,differs with different observers, so TCP method is more reliable and accurate among all , as CRA method showed false positive. Our study concludes TCP method is better method for screening of biofilm formation as virulence marker in drug resistant E coli isolates. REFERENCES:
Book. 1)Topley And Wilsos 10th edition, bact vol 2;p1379-1380. Journals. 2)Donlan RM(2001).Biofilms and device associated infections.Emerg.infect Dis 7:277-281. 3)DonlanRM,costerton w.Biofilms:survival mechanisms of clinically relevant Microorganisms,clin Microbiol Rev 2002;15(2);167-93. 4)Thomas D,Day F.Biofilmformation by plant associated bacteria.Ann Rev Microbiol2007;61:401-22. 5)Christensen GD,simpsonWA Younger JAet al.Adherance of coagulase negative staphylococci to plastic tissue cultures ;a qualitative model for the adherence of staphylococci to medical devices J Clin Microbiol 1995;22:996 -1006. 6) Christensen GD,simpsonWA.Bisno AL, BeacheyEH Adherance of slime producing strains of staphylococcus epidermidis to smooth surfaces.InfectImmune 1982;37:318 -26. 7) Freeman DJ, Falkiner FR and Keane CT (1989). New method for detecting slime production by coagulase negative staphylococci. Journal of Clinical Pathology., 42 (8): 872-874. 8)T Mathure et al ijmm aug 19 2011, ip;27.7.49.6

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 175
9)Quantification of biofilm in microtiter plates: Overview of testing conditions and practical recommendations for assessment of biofilm production by staphylococci Stepanović, S., Vuković, D., Hola, V., Bonaventura, G.D., Djukić, S., Ćirković, I., Ruzicka, F.APMIS. 2007; 115(8): 891-899[Pubmed] 10) Stickler DJ (2005) Urinary catheters: ideal sites for the development of biofilm communities. 11)Stickler DJ, Young R, Jones G, Sabubba NA, and Morris NS (2003) Why are Foley catheters so vulnerable to www.sgm.ac.uk/pubs/micro_today/pdf/020505.pdf. Microbiology Today, Feb: 22-25.. 12) Makie & McCartney practical medical microbiology, 14th ed., Churchill Livingstone In., New York 131-149. 13)Madbhusharma, Aparna,Sarita, DOI:10.4103/0377-4929,48960. 14) Montanaro L, Arciola CR, Borsetti E, Brigotti M, and Baldassarri L (1998) A polymerase chain reaction (PCR) method for the identification of collagen adhesin gene (cna) in Staphylococcus-induced prosthesis infections. New Microbiol 21: 359–363. 15)Montanaro L, Arciola CR, Borsetti E, Brigotti M, and Baldassarri L (1998) A polymerase chain reaction (PCR) method for the identification of collagen adhesin gene (cna) in Staphylococcus-induced prosthesis infections. New Microbiol 21: 359–363. 16) Salwa S. Seif El-Din et al Journal of American Science, 2011;7(1) 17) Ludwicka A, Switalski LM, Lundin A, Pulverer G, Wadstrom T. Bioluminescent assays for measurement of bacterial attachment to polyethylene. J Microbiol Methods1985;4:169-77 18) Christensen GD, Simpson WA, Bisno AL, Beachey EH. Adherence of slime-producing strains of Staphylococcus epidermidis to smooth surfaces. Infect Immun1982;37:318-26 19)Anderson GG.Palermo JJ,Roth R,Heuser J, Hultgren SJ.Intracellular bacterial Biofilm- like pods in urinary tract infection.science 2003;301:105-7. 20)Suman E,J Jose,S Varghese,MS Kotian aug 19 2011,IP;27.7.49.6

CASE REPORT
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012. Page 176
RETROPERITONEAL HYDATD CYST: A RARE PRESENTATION
Dr. Siddesh. Basavaraj. Sirwar, Dr. Amrutha. Swati. Indupalli, Dr. Subhanulla P.
1. Professor, Department of Microbiology. Khajabanda Nawaz Institute of Medical Sciences, Gulbarga. 2. Associate Professor, Department of Community Medicine, Khajabanda Nawaz Institute of Medical Sciences. 3. Professor, Department of Surgery, Khajabanda Nawaz Institute of Medical Sciences, Gulbarga.
CORRESPONDING AUTHOR:
Dr. Siddesh. Basavaraj. Sirwar, Mathru Nilaya, Plot No: 11, Siddeshwara Colony, Old Jewargi Road, Gulbarga -02, Karnataka, Email id- [email protected], Ph- 0091 09448320166 / 09902536576. ABSTRACT: Primary retro peritoneal hydatid cyst is extremely rare and only occasional case reports have appeared since first reported this entity in 1958. We report this rare case from KBN Hospital Gulbarga Karnataka diagnosis confirmed post operatively. Mass approached through greater sac which revealed a single cavity in retroperitonium containing enormous number of typical cyst of 2-5cms diameter occupying sub hepatic, epigastria, umbilical and left lumbar regions extending to pelvis. It was never expected that such enormous 2970 cysts would be recovered. Hence, suspicion and ruling out hydatid cyst in every case of retroperitoneal cystic swelling especially in endemic areas, and a careful search for hydatid cysts in other uncommon sites should be cogitated. KEY WORDS: Hydatid Cyst, Retro Peritoneum. INTRODUCTION: Hydatid disease is a parasitic infestation by a tapeworm of the genus Echinococcus. Hydatid cysts are a manifestation of infection at the larval stage of Echinococcus granulosus. Human echinococcosis is a zoonotic infection transmitted by dogs in livestock raising areas.
Developing countries with poor hygiene, where sheep and cattle are raised are high-risk areas of acquiring this disease. Hydatid disease (Echinococcus granulosus) is endemic in the Middle East as well as other parts of the world, Africa, South America, New Zealand, Australia, Turkey and Southern Europe including India1-3, Foci of hydatid disease also exists in India where the highest prevalence is reported in Andhra Pradesh and Tamil Nadu than in other parts of the country4.
Echinococcus granulosus causes cystic echinococcosis in humans. This relatively benign parasitic disease is characterized by slowly growing cysts most commonly in the liver(accounting for 50-70% of cases), followed by the lungs(20-30%), and less frequently the spleen, kidneys, heart, bones, central nervous system, and other organs5.
The annual incidence of hydatid disease has been reported to be 18 to 20 cases per 100.000 inhabitants6. Retroperitoneal localization of hydatid cyst is unusual7 here we are reporting a case of primary retroperitoneal hydatid cyst with unusual number which is a very rare presentation.
CASE REPORT: A female aged 35 year presented with history of abdominal discomfort and distension of 1 year duration, loss of appetite, fever on and off for 3 months. On examination patient looked pallor. There was no jaundice, no edema, vital signs were, pulse 76/min, blood

CASE REPORT
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012. Page 177
pressure was 110/70 mmHg and mild fever (990F). Chest auscultation revealed normal breath sounds and heart sounds. On Local Examination of abdomen there was diffuse distension confined to upper abdomen, left flank and lower pelvis. Very soft, non tender mass felt more like fluid but no shifting dullness. Borders were indistinct.
INVESTIGATIONS: Hemoglobin-9.5gm%, Hypochromic, normocytic anemia, blood cell count 11.500/mm3, Eosinophil count 550/mm3, erythrocyte sedimentation rate 35 mm/h. The chest and abdominal ultra sound showed normal liver, spleen, kidneys and multiple cystic lesions in the peritoneal cavity occupying upper abdomen, left flank and parts of pelvis. Explorative laparotomy was done through upper midline incision Fig -1 .Liver, spleen, kidneys and peritoneum showed no cysts. Lesion appeared to be more posterior. Mass approached through greater sac which revealed a single cavity in retroperitonium containing enormous number of typical cyst of 2-5cms diameter occupying sub hepatic, epigastria, umbilical and left lumbar regions extending to pelvis . A total of 2970 cysts were delivered Fig-2. Examination of contents of cysts in laboratory revealed numerous hooklets, scolices, many pus cells. Histopathological examination also confirmed the diagnosis. ELISA test was positive for both Ig.M, and Ig.G Echinococcus. DISCUSSION: Hydatid disease in human is one of the oldest diseases known to mankind. Hydatid cysts in humans and animals have been known since Roman times, but, as was true for the other tapeworms, the relationship between the larval cyst and the adult worm was not suspected until the eighteenth century. E. granulosus was described as a separate species in 1850, and its life cycle was worked out with feeding experiments in 18638. Echinococcus granulosus, which commonly has a sheep–dog cycle, but which may also infect goats, cattle, swine, and camels, is the most likely to infect human beings. Human echinococcosis occurs primarily in sheep rearing areas. Dogs ingest cysts in the offal of dead sheep and pass eggs in their feces. Humans acquire the eggs from a dog's fur or from contaminated food or water. The adult worm lives in the proximal small bowel of the definitive host, attached by hooklets to the mucosa. Eggs are released into the host’s intestine and excreted in the feces. Humans may become intermediate hosts through contact with a definitive host (usually a domesticated dog) or ingestion of contaminated water or vegetables. The ovum loses its protective layer as it is digested in the duodenum. Once the parasitic embryo passes through the intestinal wall to reach the portal venous system or lymphatic system, the liver acts as the first line of defense and is therefore the most frequently involved organ. Secondary involvement due to hematogenous dissemination may be seen in almost any anatomic location9. Cysts holding 2 or more liters of fluid and larvae can grow for years in the liver, lungs, brain, or other organs and exert enough mechanical pressure to cause grave or fatal consequences8. The vast majority of abdominal and pelvic cysts are considered to be secondary to prior hepatic involvement following spontaneous rupture or surgical inoculation. Isolated primary retroperitoneal location is exceptional. Haemotagenous or lymphatic spread could account for a solitary retroperitoneal lesion10,11. Dow12 waddle13 had favored air borne transmission and direct implantation of the embryo in the bronchial mucosa, which is another possible mode of entry. This raises the possibility of an embryo of the parasite entering a venule after penetrating the bronchial mucosa and reaching the left side of the heart to involve other sites and thus bypassing the lung. But this remains largely theoretical and needs to be proved14. Preoperative diagnosis is difficult to make unless circumlinear calcification is seen in the plain x-ray of the abdomen. The diagnosis was missed

CASE REPORT
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012. Page 178
clinically as it was provisionally diagnosed retroperitoneal or peritoneal mass. However after ultra sound examination and during surgery, the possibility of hydatid cyst was considered but it was never expected that such enormous cysts would be recovered. Necessary precautions were taken during the excision and marsupialisation of the entire huge cyst cavity and washed with scolicidal (hypertonic saline) solutions. The rupture will result in anaphylactic shock or systemic metastasis. So the treatment of choice is surgical and complete removal of the cyst is the gold standard but its feasibility is related to the location of the cyst. Hence, one must have a high index of suspicion and rule out hydatid cyst in every case of retroperitonel cystic swelling especially in endemic areas. A careful search for hydatid cysts in other organs of abdomen including liver should be made because secondary retroperitoneal hydatids may out number primary retroperitoneal Hydatids.
FIGURES
Figure1: showing the surgical approach by Explorative laprotomy through upper midline incision to the cyst.
Figure2: Showing unusual number of isolated retro peritoneum Hydatid Cyst.

CASE REPORT
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012. Page 179
REFERENCES:
1. Goel MC, Agarwal MR, Misra A.: Percutaneous drainage of renal hydatid cyst: early results and follow-up.:Br J Urol: 1995; 75: 724—8.
2. Altinors N, Senveli E, Donmez T, Bavbek M, Kars Z, Sanli M.; Management of problematic intracranial hydatid cysts;. Infection 1995; 23: 283—7.
3. Brown RA, Millar AIW, Steiner Z, Krige JEJ, Burkimsher D, Cywes S.; Hydarid cyst of the pancreas: a case report in a child. Eur J Pediatr Surg; 1995; 5:121—4.
4. Reddy CRRM. Epidemiology of hydatid disease in Kurnool.Ind; J Med Res; 1968; 56:1205-20. 5. Kammerer WS, Schantz PM.; Echinococcal disease. Infect DisClin North Am 1993; 7:605-18. 6. Özdemir N., Akal M., Kutlay H., Yavuzer Ș. Chest Wall Echinoccocosis. Chest, 1994, 105 :
1277-9. 7. Hatipog Lu A. R, Coșkun Í, Karakaya K, Íbiș C. Retroperitoneal Localization of Hydatid Cyst
Disease. Hepato-Gastroenterology, 2001, 48 : 1037-9 8. Patterson, K David, “ Echnicoccosis (Hydatidosis)” The Cambridge World History of Human
Disease. Ed. Kenneth F.Kiple. Cambridge University Press 1993. Cambridge Histories Online. Cambridge University Press 11 September 2012 DOI: 10.1017/CHOL9780521332866.105.
9. Pedrosa I, Saiz A, Arrazola L, Ferreiros J, Pedrosa CS. “Hydatid disease: radiologic and pathologic features and complications.” RadioGraphics 2000;20:795-817
10. Elton C., Lewis M., Jourdan M. H. Unusual site of hydatid disease. Lancet, 1999, 355 : 2132. 11. Balık I. A. A.,Celebi F., Bașog˘LU M, Oren,D, Yıldırgan.I, Atmanalp.S.S.: Intra-abdominal
extrahepatic echinococcosis. Surg Today, 2001,31:881-4. 12. Dow HR Hydatid disease it’s pathology, diagnosis and treatment 1st edition, 1928, 304-315 13. Waddle.N; pulmonary hydatid disease. Aust.N.Z.J Surg, 1950,19:273-78. 14. SekarNN, Madhavan KK, Yadav RV, Katariya RN: Primary retroperitoneal hydatid cyst (A
report of three cases & review of the literature): J. Post grad Med.1982: 28:112-48.

REVIEW ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 180
EPIDEMIOLOGY, PREVENTION & CONTROL OF RABIES IN INDIA-
A REVIEW STUDY. Dr. Pranab Jyoti Bhuyan.
1. Assistant Director (Public Health) Department of Health, National Centre for Disease Control, Coonoor
branch, Coonoor.
CORRESPONDING AUTHOR:
Dr. P.J. Bhuyan,
NCDC, Coonoor branch.
Coonoor-643101.
The Nilgiris, Tamil Nadu,
Email id- [email protected],
Ph- 0091 09442181442.
ABSTRACT: Rabies is a zoonotic disease and its magnitude of problem is underestimated due to
lack of surveillance. In spite of hundred percent fatality, the optimistic view is that it is totally
and absolutely preventable with the aid of effective post-exposure prophylaxis. It is prevalent
mainly in the developing countries like Africa and Asia. Wild carnivorous animals act as
reservoir and domestic/peridomestic warm blooded animals transmit the virus to the human
population. It is popularly known as “Hydrophobia” in human and children are at particularly
risk. More than 3.3 billion people live in regions where rabies is enzootic. Dog bite is the
principal mode of infection in India and lower limb is the most common site of injury. Ineffective
surveillance, shortage of TCV and Immunoglobulin manufacturer and its high cost, peoples
ignorance of first aid measures after bite and the importance of compliance of PEP, uncontrolled
street dog population etc. are the key issues which should be addressed to tackle this problem.
KEYWORDS: Tissue culture vaccine (TCV), Ministry of Health (MOH), Nervous tissue vaccine
(NTV), Post exposure prophylaxis (PEP), Upper limb (U.limb) and Lower limb (L.limb).
INTRODUCTION: This is an infectious disease, also known as hydrophobia caused by Lyssa
virus type I, characterized by acute and profound dysfunction of CNS, nearly always terminating
in the death of the host. All warm blooded mammals are susceptible particularly carnivorous
such as dogs, cats, jackals and wolves and transmitted to man by bites or licks of rabid animals1.
Due to complete absence of any successful medical treatment for clinical rabies and the horrific
nature of the disease, most rabies victims die at home rather than being admitted to a hospital
in abysmal conditions. These circumstances add to the notorious lack of surveillance data
underestimating the health implications of rabies lead many high ranking decision makers in
public health and animal health to perceive rabies as a rare disease of human resulting from a
bite of an uneconomically important animal (dog). Therefore, rabies usually falls between two
stools and is not dealt with appropriately either by MOH or M.O. Agriculture 2.
INDIA: It is endemic in every state of India except Andaman Nicobar Island & Lakshadeep 3.
Some clinico-epidemiological studies are available in India which recorded the types of animal
bite, sites of injury, mode of transmission, usage of PEP etc. NTV has been banned since 2004
due to its life threatening complication and the current cell culture vaccine is quite safe and
effective.

REVIEW ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 181
1. MAGNITUDE OF PROBLEM, TREND AND TYPES OF ANIMALS BITE: B.K.Kathuria 4
reported cases of animal rabies from different states of India during the period of 1949-67.
Though the reporting was not regular and uniform, he summarized some important data. In
1967, majority cases of animal rabies were reported from West Bengal (59.89%) whereas 57%
dogs, 38% cattle, followed by Punjab (14.7%) whereas 22% dogs, 55% cattle. The types of the
laboratory positive cases were- dogs (59.72%), Horse & donkey (14.58%), cattle (13.19%),
buffalo (8.33%), Cat (2%), camel (1.38%) and mongoose (0.69%).
The figure 1 has shown the hydrophobia cases as reported from different states from
1956 to 1969-(including nil reporting and under reporting). The peak of the curve signifies that
most of the state reported during that period which indicates lack of reporting in non-peak
period. Admitted cases of rabies from 41 teaching hospitals of India were 247(1965) and
252(1966) 5.
Sarma S.M et.al6 studied rabies in animal with laboratory diagnostic done. The
endemicity of rabid dog was apparent from 78 rabid dog detected out of 83 rabid animals
during the period of July 1982 to June 1983. An increase of rabies in dog was observed from
October 1983 to may 1984 subsequent to detection of rabies in jackals.
Rasina S.K et.al 7 found that 83.7% cases were bitten by dog among which 21.8% was pet dog,
followed by monkey (8.2%) and cat (8.2%).
Acc. to WHO 8, India officially reported 30,000 human rabies deaths (an estimated figure
which remained constant since 1990) and it accounts to 60% of global report of 50,000 deaths
annually. Due to lack of any surveillance and proper reporting there is no report on current
situation of rabies in India. Hence, at the behest of WHO & GOI, APCRI, a registered society was
entrusted this task of doing a National Rabies survey in 2003. The burden and clinico-
epidemiological profiles are clear as per findings of APCRI/WHO study on rabies in India, the
incidence of animal bite is 1.7% with frequency 1 per sec and out of 17 million people only 3
million receive PEP. Incidentally, rabies positivity was reported very rarely in rats, rabbits and
bandicoots, total dog population 28 million; annual man day lost for animal bite 38 million.
The biting animal mainly responsible for human rabies death was dog (96.2%) of which
majority strays (75.2%) followed by pet (11.1%), wild (3.5%); cat accounted for 1.7% of deaths.
The status of biting animal was unknown (46.4%) or killed (28.5%) or dead (23%) and
surprisingly in 2.1% cases it was reported as alive by surviving household members. This might
be that either the people were observing the wrong animal or had forgotten trivial bite by a
rabid animal in the past.
Ichhpujani R.L et al9found that dog bites caused maximum morbidity (92%), followed by
monkey (3.2%), cat (1.8%), fox (0.4%) etc. Most bites were unprovoked (64.3%) by stray
animals (64.7%). Analysis of 192 cases of rabies, from two centres, revealed that dog bites
caused maximum mortality (96.9%).
2. AGE & SEX DISTRIBUTION: Rao Bhanu L.N, Kalaselvan 10studied that main victims were
adults-83.80% and predominantly males (84.42%) affected. Rasina S.K. et.al 7found that the
commonest age group was 6-25 yrs(82.4%). According to WHO & GOI, APCRI survey in 2003 8,
235 Deaths Were investigated at household level by a medical team. Majority of human rabies
were adults (64.7%), men (71.1%) and were from poor income levels (87.6%). Ichhpujani R.L et
al 9 in the study, 72.4% victims were males and 47.5% were children in age group of 2-18 years.
Nearly 40% were children below 15 years of age group and 78.6% were males indicating that it
is an exposure related disease.

REVIEW ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 182
3. TYPES OF INJURY: (Fig:2) Rao Bhanu L.N, Kalaselvan 10 found type bites i.e Class III -59.81%,
II-37.7%. RasinaS.K et.al 7studied the common categories of bite were-class II (54.4%) followed
by class I (31.3%) and class III (14.3%). The 78.9% cases completed PEP and the common sites
of bite were U.limb (40.1%) followed by L.limb (36.7%). In the study of WHO & GOI, APCRI
(2003)8, the commonest sites of injury were - lower limb (56.2%) followed by upper limb
(20.9%), hands (17%) and then the head and face (11.5%). Ichhpujani R.L et al (2008)9 found
that 63% had category III exposure as per WHO classification.
4. TREATMENT AFTER BITES: After bite, some people have the practice of washing the wound
with soap-45.6% but other harmful practices are not uncommon like application of chilly
powder (29%), oil (24.5%), turmeric powder (10.9%) etc7. WHO & GOI, APCRI (2003) 8, 39.5%
had wound clean and 47.9% received ARV and even those who had received it mostly had
incomplete/irregular/delayed treatment. The use of RIG was very low (2.1%). In 85% cases,
IP < 6 months; mean IP was lowest (42days) in bites on head & face and highest (107 & 108
days) in those on upper limb (excluding hands) and lower limbs. About 45.3% of victims had
resorted to indigenous treatment like-magico religious followed by herbal therapy, red chili
powder. Ichhpujani R.L et al 9 studied that before coming to ARCs 58.5% people had washed the
wound with water/soap or water alone. Some of the bite victims (10.8%) also applied chillies,
salt, turmeric powder, lime, snuff powder, paste of leaves, acid, ash given by Peer
Baba(magician) etc.
5. RABIES CONTROL IN DOG: A WHO expert consultation meeting on Rabies has identified
mass immunization as single most effective tool for dog rabies control whereas dog culling
alone is ineffective 11. Studies have shown that, in general, 80-90% of the dog population is
accessible for vaccination, thus confirming that the concept of controlling rabies through mass
vaccination is a sound one 12. It has also been recommended the use of oral vaccine as a
complimentary measure in dog in addition to i.m or s.c route. In the light of this oral rabies
vaccine strain, ORA-DPC would offer a major opportunity for rabies control. Better part with
ORA-DPC is that the strain elicits seroconversion too unlike other attenuated rabies vaccine
strains, could be a good indicator to monitor the vaccinated animal in the field as always regd.
by WHO 13. In the majority of industrialized countries, human rabies is under control, mainly
due to oral vaccination of wild animal, mandatory parenteral vaccination of domestic animal
and easy access to modern cell culture vaccine, immunoglobulin for PEP, whereas these are in
short supply & their high cost often prevent their use by those most in need for those product.
In India, Animal Welfare Board of India (AWBI) had successfully implemented Animal Birth
Control (ABC) Programmes among stray dogs in various places including Chennai 14.
6. CONCLUSION: Rabies is a hidden but neglected public health problem in India which affects
mostly the people of lower socio-economic group. Being a zoonotic disease, it cannot be
eradicated but elimination or control is possible with primary health care approach like-
availability of post-exposure prophylaxis, refreshment of recent guideline of PEP, re-exposure
and drop-out management to physicians & medical students; evaluation of technical feasibility
at peripheral level of intradermal route before implementation. Transmission chain will be
broken if herd of at least 75-80% of dog population is immunized on a sustained basis. Recently,
IDSP has introduced its surveillance in the reporting format.

REVIEW ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 183
*Fig 1. shows the cases of hydrophobia as reported from different states of India.
Fig-2: shows frequency of Class III bites. Source: Rao Bhanu L.N, Barman S (2000-01 &
2001-02).
REFERENCE:
1. Park K. Rabies- Park’s Textbook of Preventive and Social Medicine 2007; 19: 226-34.
2. WHO Bulletin “Human & animal rabies” Dec , 2008.
3. Seghal and Bhatia R (1985) rabies: Current Status and proposed control programme in India,
NICD, 22 Shamnath Marg, Delhi-54.
4. Kathuria B.K. Studies on rabies-its epizootology and diagnosis. Journal of Comm. Disease
1970; 2: 1-4.
5. Prakash S. Rabies in and around Delhi. J.C.Disease 1970; 2,69-75.
6. Sarma S.M, Sarmah S.B, Saxena SN. Surveillance of Rabies in animals in north India.
J.Com.Disease 1986; 18(1):9-12.
Cases of hydrophobia in diff. states.
0
200
400
600
800
1000
1200
56 57 58 59 60 61 62 63 64 65 66 67 68
Years
No
s. o
f ca
ses.
Frequency of ClassIII bites.
0
500
1000
1500
2000
2500
3000
3500
4000
1995 96 97 98 99 2000April
Years.
Fre
qu
ency
.
Total animal bite cases.
Adult-ClassIII bite.
Child-ClassIII bite.

REVIEW ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 184
7. Rasnia S.K, Bhalla S, Khanekar J, Pathi S, Matta S, Singh S. Post exposure management of
animal bite attending a P.H.C of Delhi, J. Com. Disease 2004; 36(3),195-198.
8. APCRI, Assessing burden of rabies in India: WHO National Multicentric Rabies Survey, 2003
9. Ichhpujani R.L, Chhabra M, Mittal V, Singh J, Bharadwaj M, Bhattacharya D, Pattanik SK,
Balakrishnan N et al. –Epidemiology of Animal bites and Rabies cases in India-A Multicentric
study. J.Commun.Dis. 40(1) 2008:27-36.)
10. Rao Bhanu L.N, Kalaselvan J. Epidemiology of Rabies-16 years study at PIIC-Annual Report,
2000-02, 57-60.
11. WHO Techn. Report Series,1973,No 52315.WHO Expert Consultation on Rabies: first report.
Geneva, WHO Technical Report Series, No. 931.
12. The work of WHO. 1986-87,176.
13. Bhubaneswari A, Kilari S, Visser N, Goovarerts D. Oral rabies vaccine, ORA-DPC: Dose
finding studies confirms vaccine efficacy in challenge experiments. APRICON Souvenir, 2009,
17-18.
14. The Hindu, September, 2010, 3. WHO Expert Consultation on Rabies: first report. Geneva,
WHO Technical Report Series, No. 931.

ORIGINAL CASE SERIES STUDY
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 185
BENEFICIARIES VIEW POINT AND FACTORS INFLUENCING INDUCED
ABORTIONS IN A RURAL COMMUNITY OF WEST BENGAL. Dr. Debabrata Mallik. Dr. Ranadeb Biswas, Dr. S. Kole, Dr. Manob Dhar, Madhulina Mallik.
1. Assistant Professor, Department of Community Medicine, Bankura Sammilani Medical College. 2. Professor & Head, Department of Community Medicine, AIIH & PH, Kolkata.
3. Assistant Professor, Department of Community Medicine, Bankura Sammilani Medical College.
4. Medical Officer, Department of Community Medicine, AIIH & PH, Kolkata.
CORRESPONDING AUTHOR,
Dr. Debabrata Mallik,
1483, R N Tagore Road.
Dum Dum, Kol-77.
E-mail: [email protected],
Ph: 09433657571.
ABSTRACT:
BACKGROUND: Study of induced abortion in India by considering the complete birth history of
women is lacking. Induced abortion is associated with high mortality and morbidity in India.
OBJECTIVES: The objectives of the study were to find out the Induced abortions ratio and to
identify certain characteristics like perception, health care seeking behavior and the
motivational factors for such an act. METHODS: An exploratory type of investigation (a
retrospective case series study) was carried out among 46 acceptors of induced abortion in a
rural community of west Bengal, between September, 11 to February 12. RESULTS: The ratio of
induced abortions was 20.62 per year per 1000 women of reproductive age group. 89% belongs
to Hindu and 93% of them were married. Unplanned pregnancy (43.47%) and financial problem
(21.73 %) were the main reasons for acceptance of induced abortions. About 71 % of induced
abortions were carried out by qualified person in hospital set up. CONCLUSION: Eventually
induced abortions are increasing universally and several traditional methods are also found to
be life threatening. So exploration of induced abortions is important aspect and explores the
point for entry of further research.
KEY WORDS: Abortion, motivation, unplanned pregnancy, unqualified persons.
INTRODUCTION: Although abortion services in India were liberalized more than three decades
ago, access to safe services remains limited for the vast majority of women. The results
highlights that a host of factors, notably lack of awareness of the legality of abortion services;
limited access to safe services; poor quality of services; and gender roles and norms, lead
women to seek services from untrained providers. In the Indian context, where the preference
for sons is particularly strong, the practice of second trimester sex-selective abortions is
becoming widespread, and thereby also placing women at risk of undergoing unsafe abortion1.
The introduction of new technologies and legislation is expected to make safe abortion services
more accessible. However, the challenge remains in effectively implementing these measures.
An overwhelming proportion of induced abortions (6.7 million annually as per indirect
estimate1) take place in unauthorized centers, which provide abortion services of varying
degrees of safety2. At the same time, in recent years significant changes in the abortion scenario
have been taking place in the country, which have had wide ramifications. Official figures report
that about 0.6 million induced abortions take place annually inIndia2.27 Given that only

ORIGINAL CASE SERIES STUDY
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 186
approximately 10%of abortions are conducted by qualified providers in approved
institutions,28 and that abortions taking place at registered facilities are grossly under-
reported,1, this represents only a fraction of the total number of induced abortions taking place
in the country. Indirect estimates for the year 1991, using parameters arrived at on the basis of
small-scale study conducted in 1966, project the number of induced abortions annually at 6.7
million3.All the Countries in the World underestimate this abortion is much more than
spontaneous due to medical reasons, victims of sex behaviors, rape etc4.Despite the fact that, in
India these induced abortion is legalized under certain condition & facilities but evidently the
quantum of induced abortion are not matching with the such records of the Governments &
private organizations because widespread of unqualified & untrained practitioners are very
much prevalent in rural & urban society5.Among all these contraceptive failure is a unique
example of falsification & gateway of criminal abortion by the unqualified & untrained
personnel & maiming the lives of the victims due to lack of protocol of maintenance of asepsis. .
The hidden cost of contraception–such as shame, command, resistance from seniors & loss of
social prestige are the prime concern in a country where the number of children count the
prosperity of rural couple by acquiring human manpower6. Scientific advancement made these
treatment behaviors as gender specific to avoid much more harassment of life events of a girl
child. In view of ever increasing priority, quantity, context & coverage of RCH services across the
country but this induced abortion is quite paradoxical7. Needless to say that the mortality
declines of newborn & early child hood are spectacular & reduction of maternal death also
convincingly decline. Therefore to safeguard the health of the mothers & newborn it is
imperative to focus couples own perceptions & compulsions & there by appropriate modalities
for reversal of the trends should also be looked into8.
MATERIALS AND METHODS: It was an exploratory type of investigation for seeking
information regarding induced abortions to acquire certain characteristics. The study was
conducted at Diarrah village with a population of 2230 (2011 census), under Singur block at the
district of Hooghly, West Bengal. Ethical consideration was undertaken from the All India
Institute of Hygiene & public Health. The duration of the study was six months from Sep 11 –
Feb 12. Last five years records of the acceptors of induced abortions were verified from the
Singur BPHC after obtaining informed written consent from the BMOH. From the records a
check list of Diarrah village was prepared which include address of the acceptors of induced
abortions. Similar type of check list was also prepared from the Two Quack practitioners’ after
obtaining informed written consent assuming full confidentiality. Total 53 acceptor’s addresses
were framed for obtaining information. After the questionnaire was finalized, informed written
consent was taken from the Formal Leaders (Gram Panchayat) of the Community. Then the
entire clients were interviewed with the predesigned open ended questionnaire after obtaining
the written consent with assured full confidentiality. Out of 53 acceptors of induced abortion 7
were absent so the total study subjects were 46.
RESULTS: It was noted that total number of population of the study village was 2230 (2011
census) of which total number of women of reproductive age groups (15-45) were 446 (20% of
total population). The study revealed that total number of induced abortion during last 5 years
was 46.And the average induced abortion per year was 46/5=9.2. So the inducedabortion rate
per year per 1000 of women of Reproductive age group was 9.2 #1000/446 =20.62.From the
study it was noted that majority of study subjects 54.3 %( 25) belongs to younger age groups i.e.

ORIGINAL CASE SERIES STUDY
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 187
15-24 yrs. About 89.1% (41) belongs to Hindu community. 97.4% (43) acceptors of induced
abortion were married. About 67%respondent’s percapita incomes were bellow or equal to
Rs.350. Regarding literacy status only 15 % were illiterate rest of the accepters were literate.
Out of 43 married clients about 88% (38) were getting married before the age of 18 years &
majority (95.34%) gave birth within 2 years of marriage. About 80% acceptors birth spacing
was less than 2 years. It was noted from the study that about83% (36) have 2-3 children but a
considerable 16% have 4-5 children. Majority of the abortion was done 73% (34) within 2-3
month of age of the foetus. Regarding their contraceptive practice 44% (19) did not practice any
methods of contraception while rest of the acceptors practices other methods of contraception.
On enquired about the reason of such an act it was noted that 43% (20) induced abortion was
unwanted pregnancy followed by financial ground 20% & contraceptive failure 19%
respectively. Most the abortion were conducted 71% by the qualified doctors at health center.
But only 28% were conducted by the unqualified personals at their chambers. On enquired
about the reasons of their preference of act for the unqualified persons about 43% (20) replied
that maintained confidentiality was their prime concern. Other important reasons were less
harassment which constitutes about 21%. Besides those monitory problems, less time required
resistance from seniors were others reasons of less priority.
DISCUSSION: The retrospective qualitative survey was include both married and unmarried
women and the data was collected both the Govt. Hospital and untrained practitioners so the
induced abortion ratio was to some extent high.Similar findings were found in NFHS survey for
induced abortion (1998-99)9&DLHS survey (iii) GOI. (2007-08).10The study explore that
women’s age, unplanned and unwanted pregnancy, less acceptance of contraceptive methods,
financial reasons number of living children’swere the major determinants of induced abortion.
Similar findings was also found in a rural community of Maharastra (A cohort
study).11&Tamilnadu (Rabindran &Balasubramanian,2004)12The study explore that maintained
confidentiality, less harassment and less time requirement were another determinants for
accepting abortion of untrained personnel.
CONCLUSION: Traditional practitioners & untrained or ill-trained M.B.B.S practitioners, widely
perform abortion in the rural community. The complications at their hands are frequent & often
serious. Assurances of keeping secrecy attract the ignorant rural people to them. Contraceptive
acceptance is far from the requirement & sterilization acceptance is far from the requirement
acceptance is poor & often late. Repeated & early child birth, inadequate spacing, high parity
along with financial & other relevant problems need availability of M.T.P side by side with
contraceptives & sterilization in the years ahead. Rural people need awareness about the
problem of population expansion, the needs & benefits of contraceptive & sterilization & the
dangers of illegal abortions. Simultaneous publicity about M.T.P services needs to be promoted.
A comprehensive guideline thus evolved from this abortion may be replicated in several socio
economic classes & regions. Instead of indiscriminant intervention, a logical solution locally
derived agreed upon & sharing that benefit will definitely be rewarding. Last of course not the
least, that the exploration of induced abortion is important as it opens some important aspect &
explore the point of entry for further research.
ACKNOWLEDGEMENTS: We are grateful to the Director of AIIH&PH, Kolkata whose support
and guidance has been critical for conduction of the study. We are also indebted toMr.Madan

ORIGINAL CASE SERIES STUDY
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 188
Das and Mr.SukantaPandit for providing us necessary help in conducting the study. We also
extend our gratitude to the staffs of Singur BPHC and the community people through which
information were collected.
Table-1: Socio demographic characteristics of the Acceptors of Induced abortion (n=46)
Table: 2 Obstetric pattern of the Study subjects.
Socio demographic character Number Percentage
Age in years
15-24
25-34
35-44
Religion
Hindu
Muslim
Marital status
Married
unmarried
Per capita income
<350
=
>350
=
Literacy status
Primary
Secondary
Higher Secondary
Graduation
Illiterates
25
18
3
41
5
43
3
31
15
19
10
8
2
7
54.3
39.1
6.5
89.1
10.9
97.4
6.6
67.4
32.6
41.4
21.7
17.4
4.3
15.2

ORIGINAL CASE SERIES STUDY
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 189
Variables numbers percentages
Age at marriage(n=43)
<18 yrs.
First child birth <2 yrs.
Spacing <2yrs
<3yrs
No of living children 2-3
4-5
Month of abortion
1-1/2
2
2-1/2
3
>3
Contraceptive acceptance. (n=43)
Safe periods
Condom
Cup-T
OC
Nil
Sterilization
38
41
34
9
36
7
8
11
14
9
4
5
6
7
4
19
2
88.37
95.34
79.06
20.94
83.72
16.28
17.4
23.9
30.4
19.6
8.7
11.6
13.9
16.3
9.3
44.2
4.6
Table: 3 Reasons for acceptance of induced abortions.
Variables Numbers percentages #
Reasons
Financial/for well being
Unplanned pregnancy
Forced by husband
Contraceptive failure
10
20
4
9
21.7
43.4
8.7
19.5

ORIGINAL CASE SERIES STUDY
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 190
# --- Multiple responses possible
REFERENCES:
Unmarried
Performers
Qualified personals
Unqualified personals
Place of abortion.
Hospitals
Chambers of unqualified
personnel’s
Reasons for acceptance
By Unqualified personals
Maintained confidentiality
Less harassment
Monitory problems
Less time required
To avoid so many test &
Conditions by the Govt.
setup.
Resistance from seniors
To take Govt. facilities
3
33
13
33
13
20
10
4
5
3
4
6.5
71.7
28.3
71.7
28.3
43.4
21.7
8.7
10.9
6.5
8.7

ORIGINAL CASE SERIES STUDY
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 191
1. Chhabra, R. and S.C. Nuna. 1994. Abortion inIndia: An Overview. New Delhi:
VeeremdraPrinters.
2. Government of India (GOI). 2002. The MedicalTermination of Pregnancy (Amendment) Bill
(BillNo. XXXV).
3. Mallik, R. 2002. India -Recent Developments Affecting Women’s Reproductive Rights. Centre
for Health and Gender Equity (CHANGE).
4. Ministry of Health and Family Welfare (MOHFW).2003. Notification, Medical Termination of
Pregnancy Rules.http://mohfw.nic.in/MTP%20Rules.htm
5. Ministry of Health and Family Welfare (MOHFW).2000. National Population Policy, 2000. New
Delhi: Government of India.
6. Oomman, N. and B.R. Ganatra. 2002. Sexselection: The systematic elimination of
girls.Reproductive Health Matters, 10(19): 184-88.
7. Government of India (GOI). 2003. The Pre-NatalDiagnostic Techniques (Regulation and
Prevention of Misuse) Amendment Act (Act. No. 14).
8. Coyaji, K. 2002. Medical Abortion. Paper
9.M.Barsharani.Correlates of Spontaneous and Induced Abortion in India: An Investigation using
a Nationwide Large Scale Survey Data.
http://paa2011.princeton.edu/download.aspx?submissionId=111333.
10. PallikadavnathS,William Stones R. opportunites and choices programme working paper;
21;2005.
11. www.biomedcentral.com/1471-2458/12/543.
12.Rabindran TKS&Balasubramanian P, Yes to No Abortion.2004; 12: 88-99

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 192
THE MICROBIOLOGICAL PROFILE OF VENTILATOR ASSOCIATED
PNEUMONIA. Dr. Poonam C. Sharma, Dr. S. S. Raut, Dr. S. R. More, Dr. V. S. Rathod, Dr. V. M. Gujar.
1. Post Graduate Student, Department of Microbiology, Dr. Shankar Rao Chavan Government Medical College &
Sri Guru Gobind Singhji Memorial Hospital, Nanded. 2. Professor & Head of Department, Department of Microbiology, Dr. Shankar Rao Chavan Government
Medical College & Sri Guru Gobind Singhji Memorial Hospital, Nanded.
3. Associate Professor, Department of Microbiology, Dr. Shankar Rao Chavan Government Medical College &
Sri Guru Gobind Singhji Memorial Hospital, Nanded.
4. Assistant Professor, Department of Microbiology, Dr. Shankar Rao Chavan Government Medical College &
Sri Guru Gobind Singhji Memorial Hospital, Nanded.
5. Assistant Professor, Department of Microbiology, Dr. Shankar Rao Chavan Government Medical College &
Sri Guru Gobind Singhji Memorial Hospital, Nanded.
CORRESPONDING AUTHOR,
Dr. Poonam Chanderlal Sharma,
501, Abhilasha Mahal Co. Op. Hsg. Scty,
Opp. Bhatia Hospital, Ulhasnagar Dist.
Thane, Maharashtra- 421005
E-mail: [email protected],
Ph: 08888096033.
ABSTRACT: BACKGROUND- Nosocomial infections (NI) are responsible for increased
morbidity and mortality in hospitalized patients. Hospital acquired pneumonia is the
second most common nosocomial infection. AIM : To isolate and identify the organisms
causing Ventilator associated pneumonia and to know their resistance pattern. METHOD :
We conducted the study in the Intensive Care Unit of our Hospital over a period of one
year. All patients on mechanical ventilation for more than 48 hours were included in this
study. The pathogens were identified based on the standard bacteriological procedures
including Gram's stain, colony morphology on Blood agar, MacConkey agar and SDA and
biochemical reactions. FINDINGS- 50 out of 128 samples were culture positive, the
incidence being 39.06%. Out of 50 cases, 33(45.2%) were males & 17(30.9%) were
females. 50% of the cases ventilated for respiratory cause developed VAP while only
20.8% of the cases ventilated for non-respiratory cause developed VAP. Out of 50 cases,
20(40%) were early onset VAP cases, while 30(60%) were late onset VAP cases.
CONCLUSION : P. aeruginosa was the predominant organism isolated followed by E.coli
with maximum sensitivity to Imipenem.
KEYWORDS: Ventilator associated pneumonia, Pseudomonas aeruginosa, Imipenem.
INTRODUCTION: Ventilator associated pneumonia(VAP) is defined as pneumonia occurring
after 48 hours of endotracheal intubation and initiation of mechanical ventilation. VAP is
categorized as early onset VAP which occurs within four days of endotracheal intubation
whereas late onset VAP occurs after four days of endotracheal intubation. Early onset
VAP is caused by Str. pneumoniae, H. influenza, Moraxella catarrhalis, MSSA, etc. While
Late onset VAP is caused by P. aeruginosa, Acinetobacter, Enterobacter species, MRSA,
etc. VAP is frequently polymicrobial and Gram negative bacilli are the predominant
organisms isolated.[3]

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 193
CLINICAL DIAGNOSTIC CRITERIA FOR VAP ARE:
Clinical suspicion of pneumonia with a new or progressive chest radiographic infiltrates
after 48 hours of patient’s mechanical ventilation and one of the following
Fever >38.3oC
Leukocytosis > 12000/cmm or leukopenia < 4000/cmm
Purulent respiratory secretions with gram stain demonstration of bacteria and
polymorphs
Cultures with growth >105 cfu/ml [3]
AIM: To isolate and identify the organisms causing Ventilator associated pneumonia and
to know their resistance pattern.
METHODS:
SETTING AND SUBJECTS: We conducted the study in the Intensive Care Unit of our
hospital over a period of one year from 1st July 2011 to 30th June 2012. All patients on
mechanical ventilation for more than 48 hours were included in this study. Patients with
pneumonia prior to mechanical ventilation or within 48 hours of mechanical ventilation
were excluded.
STUDY DESIGN AND DATA COLLECTION: From each patient the following data was
collected- Name, age, sex, primary diagnosis, date of admission in the hospital and ICU.
The patients fulfilling both the clinical and microbiological criteria were diagnosed to be
suffering from VAP. Microbiological criteria included positive Gram stain (>10
polymorphonuclear cells/ low power field and ≥1 bacteria/ oil immersion field with or
without the presence of intracellular bacteria). Clinical criteria included modified Clinical
Pulmonary Infection Score (CPIS) > 6

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 194
IDENIFICATION OF VAP PATHOGENS: The pathogens were identified based on the
standard bacteriological procedures including-
- Gram’s stain
- Colony morphology on Blood agar , MacConkey agar and SDA
- Biochemical reactions. [10]
FINDINGS
INCIDENCE: 50 out of 128 samples were culture positive, the incidence being 39.06%
Characterisics of the patients-
Incidence in males and females- Table I
Incidence differences due to various causes of ventilation- Table II
Incidence due to early onset and late onset pneumonia- Table III
DISCUSSION: The incidence of VAP in our study was 39.06% which was similar to a
study conducted by Shalini et. al.(35.78%) and Rakshit et. al.[4][8] In males incidence of
VAP was 45.2% and that in females was 30.9% which was similar to the study
conducted by Gadani et. al.[11] 40% of cases were early onset VAP and 60% were late
onset VAP which tallies to other studies conducted by Chastre et. al. and Kollef et. al.[5][6]
Incidence in patients ventilated for respiratory cause was 50% and that due to non-
respiratory cause was 20.83%, which co-relates to the study conducted by Akash Deep et.
al.[7] Pseudomonas was the predominant organism in our study (31.48%) similar to that
conducted by Joseph et. al. (21.3%) and Gadani et. al. (43.24%)[9][11]
CONCLUSION: Pseudomonas aeruginosa was the predominant micro organism isolated
with maximum resistance to Tobramycin. E. coli was the second most common micro
organism with maximum resistance to Ampicillin. While both were 100% sensitive to
Imipenem. Microbiologial surveillance facilitates the monitoring of changes of dominant
micro- organisms and antibiotic susceptibilities helping in the decision of empirical
treatment regimes and as a result, selecting the right antibiotics.
ACKNOWLEDGEMENTS : Staff of Microbiology Department and Medicine Department,
Study patients.
FUNDING: None
TABLE I:
Gender No. of VAP
cases
No. of cases in
whom VAP
absent
Total no. of
cases
Male 33 (45.2%) 40 (54.8%) 73 (100%)
Female 17 (30.9%) 38 (69.1%) 55 (100%)
Χ2 =2.69
P value > 0.1 (not significant)

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 195
TABLE II
Cause of
ventilation
No. of VAP
cases
No. of cases in
whom VAP
absent
Total no. of
cases
Respiratory cause 40 (50%) 40 (50%) 80 (100%)
Non respiratory
cause
10 (20.8%) 38 (79.2%) 48 (100%)
Χ2 =10.72
P value <0.01 (highly significant)
TABLE III
Duration of ventilation No. of VAP cases Total no. of cases
Early onset 20 (40%) 50 (100%)
Late onset 30 (60%) 50 (100%)
Χ2 =4
P value < 0.05 (significant)
FIGURE 1 Causative Agents-
31.48%
16.67%14.81%
12.96%
9.26%
3.70%1.85% 1.85%1.85%1.85%
3.70%
0.00%
5.00%
10.00%
15.00%
20.00%
25.00%
30.00%
35.00%

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 196
FIGURE 2
Resistance Pattern of P. aeruginosa-
FIGURE 3
Resistance Pattern of E. coli
CONFLICT OF INTEREST: None
48%
33%
26%22%
5%
0%0%
10%
20%
30%
40%
50%
60%
95%
67%
50% 50%
20%
0%0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Ampicillin Cefazolin Tobramycin Amikacin Gentamicin Imipenem

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 197
REFERENCES:
1) Steven M. Koenig and Jonathon D. Truwit Ventilator-Associated Pneumonia:
Diagnosis, Treatment, and Prevention. PubMed Central Clin Microbiol Rev. October 2006;
19(4): 637–657.
2 ) Bailey & Scott’s Diagnostic Microbiology Eleventh Edition, Mosby Inc. Betty A. Forbes,
Daniel F. Sahm, Alice S. Weissfeld ISBN 0-323-01678-2
3) Girish L. Dandagi Nosocomial pneumonia in critically ill patients Lung India Jul-Sep
2010; 27(3)
4) Rakshit P, Nagar V S, Deshpande A K Incidence, clinical outcome, and risk stratification
of ventilator-associated pneumonia- a prospective cohort study. Indian J Crit Care Med
2005 9(4): 211-216
5) Chastre J and Fagon J Y Ventilator associated pneumonia. Am J Respir Crit Care Med
2002 165: 867-903.
6) Kollef M H Ventilator-associated pneumonia. A multivariate analysis. JAMA 1993; 270:
1965-1970.
7) Akash Deep, R. Ghildiyal, S. Kandian and N. Shinkre Clinical and Microbiological Profile
of Nosocomial infection in the PICU. Indian Pediatrics 2004 41: 1238-1246
8) Shalini S, Kranthi K, Gopalkrishna Bhat K Microbiological profile of infections in ICU. J
of Clinical and Diagnostic Research 2010 4: 3109-3112
9) Noyal Mariya Joseph, Sujatha Sistla, Tarun Kumar Dutta, Ashok Shankar Badhe,
Subhash Chandra Parija. Incidence and risk factors of VAP. J Infect Dev Ctries 2009
3(10): 771-777
10) Mackie & McCartney Practical Medical Microbiology. J. G. Collee, A. G. Fraser, B. P.
Marmion, A. Simmons. Churchill Livingstone, Fourteenth Edition, ISBN 0 443 049068
11) Gadani H, Vyas A, Kar A K. A study of ventilator-associated pneumonia: Incidence,
outcome, risk factors and measures to be taken for prevention. Indian J Anaesth 2010;
54:535-40.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 198
BACTERIOLOGICAL PROFILE OF CELL PHONES OF HEALTHCARE
WORKERS AT TERTIARY CARE HOSPITAL. Dr. Chinjal A. Panchal, Dr. Mitesh N. Kamothi, Dr. Sanjay J. Mehta,
1. Post Graduate Student, Department of Microbiology, C.U. Shah Medical College & Hospital, Surendranagar. 2. Assistant Professor, Department of Microbiology, C.U. Shah Medical College & Hospital, Surendranagar.
3. Professor & Head, Department of Microbiology, C.U. Shah Medical College & Hospital, Surendranagar.
CORRESPONDING AUTHOR,
Dr. Chinjal Arvindbhai Panchal, C. U. Shah Medical College and Hospital, Surendranagar – 363001, E-mail: [email protected], Ph: 09898576504.
ABSTRACT: BACKGROUND AND OBJECTIVES: Cell phones are increasingly used by healthcare
workers. They can harbour potential bacterial pathogens and can become an exogenous source
of nosocomial infections. Aim of this study was to identify microbial colonisation and their
antimicrobial sensitivity; from cell phones used by healthcare workers.
MATERIALS AND METHODS: A total of 100 samples were collected from cell phones of
clinical and para-clinical staff and non-medical personnel. Specimens were collected and
subjected to culture and sensitivity as per the standard guidelines.
RESULTS: Bacterial species were isolated from 65 (65%) out of total 100 samples. Coagulase
Negative Staphylococcus (42) was the most commonly isolated organism. Isolates included
Methicillin resistant Staphylococcus aureus (10), Methicillin sensitive Staphylococcus aureus
(3), Bacillusspp(15), Pseudomonas spp(4),Moraxella spp(2), E. coli (1), Klebsiella spp (1) and
Acinetobacterspp (1).
CONCLUSION: The carriage rate of bacterial isolates was higher in the clinical staff (92%)
in comparison to para-clinical staff (56%) and non-medical personnel (20%). Cell phones
may serve as potential source of nosocomial infections.
KEYWORDS: Bacterial pathogens, Multidrug resistance, Healthcare workers, Nosocomial
infections
INTRODUCTION: The global system for mobile telecommunication (GSM) was established in
1982 in Europe with a view of providing and improving communication network. Cell phones
have become one of the most indispensable accessories of professional and social
life.1Today,India has 500million Cell phone users. Cell phones increase the speed of
communication and contact within health care institutions, making health care delivery more
efficient; hence, Cell phones are increasingly used by healthcare workers.2Cell phones are
frequently used in hospital wards, casualty, laboratories, ICUs and operation theatres.3However,
Cell phones which are seldom cleaned and often touched during or after the examination of
patients without hand washing, can harbour various potential pathogens and become an
exogenous source of nosocomial infections for hospitalized patients.4Nosocomial infections are
important problem in all hospitals. These infections are increasing day-by-day and can affect
rate of mortality and morbidity. In this study, Cell phones of non-medical personnel were also
included as it represents an environment of community. Therefore bacterial isolates from Cell
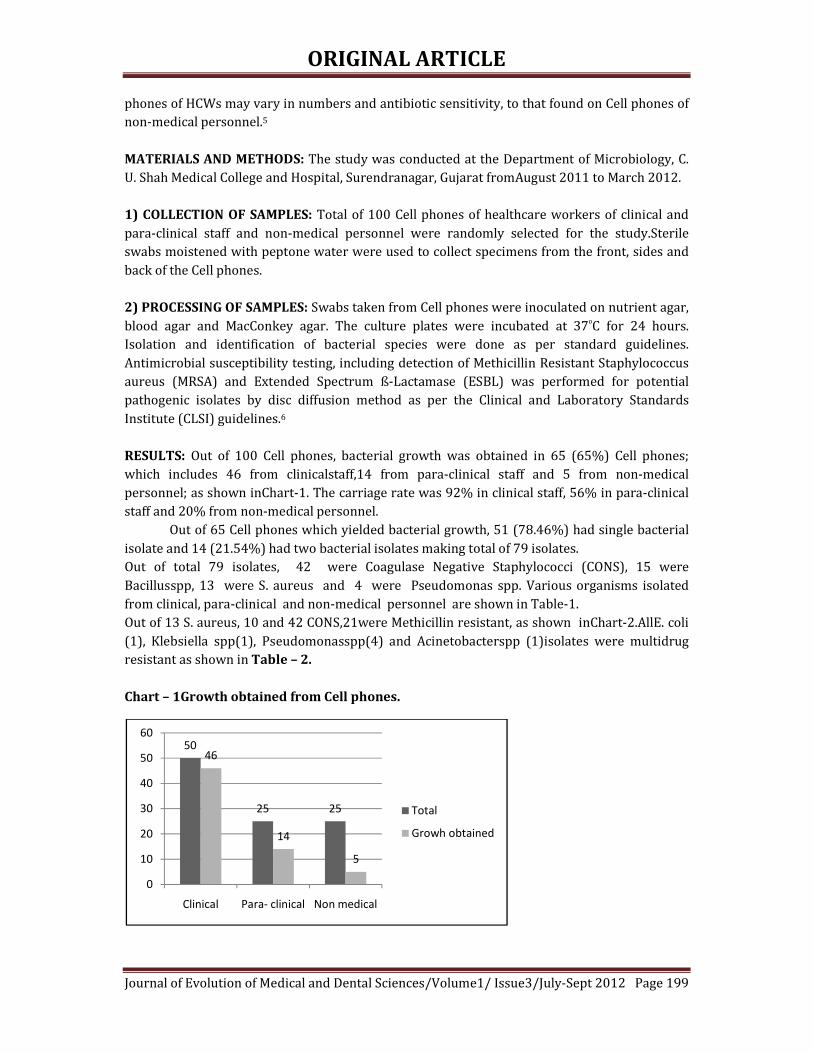
ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 199
phones of HCWs may vary in numbers and antibiotic sensitivity, to that found on Cell phones of
non-medical personnel.5
MATERIALS AND METHODS: The study was conducted at the Department of Microbiology, C.
U. Shah Medical College and Hospital, Surendranagar, Gujarat fromAugust 2011 to March 2012.
1) COLLECTION OF SAMPLES: Total of 100 Cell phones of healthcare workers of clinical and
para-clinical staff and non-medical personnel were randomly selected for the study.Sterile
swabs moistened with peptone water were used to collect specimens from the front, sides and
back of the Cell phones.
2) PROCESSING OF SAMPLES: Swabs taken from Cell phones were inoculated on nutrient agar,
blood agar and MacConkey agar. The culture plates were incubated at 37⁰C for 24 hours.
Isolation and identification of bacterial species were done as per standard guidelines.
Antimicrobial susceptibility testing, including detection of Methicillin Resistant Staphylococcus
aureus (MRSA) and Extended Spectrum ß-Lactamase (ESBL) was performed for potential
pathogenic isolates by disc diffusion method as per the Clinical and Laboratory Standards
Institute (CLSI) guidelines.6
RESULTS: Out of 100 Cell phones, bacterial growth was obtained in 65 (65%) Cell phones;
which includes 46 from clinicalstaff,14 from para-clinical staff and 5 from non-medical
personnel; as shown inChart-1. The carriage rate was 92% in clinical staff, 56% in para-clinical
staff and 20% from non-medical personnel.
Out of 65 Cell phones which yielded bacterial growth, 51 (78.46%) had single bacterial
isolate and 14 (21.54%) had two bacterial isolates making total of 79 isolates.
Out of total 79 isolates, 42 were Coagulase Negative Staphylococci (CONS), 15 were
Bacillusspp, 13 were S. aureus and 4 were Pseudomonas spp. Various organisms isolated
from clinical, para-clinical and non-medical personnel are shown in Table-1.
Out of 13 S. aureus, 10 and 42 CONS,21were Methicillin resistant, as shown inChart-2.AllE. coli
(1), Klebsiella spp(1), Pseudomonasspp(4) and Acinetobacterspp (1)isolates were multidrug
resistant as shown in Table – 2.
Chart – 1Growth obtained from Cell phones.
50
25 25
46
14
5
0
10
20
30
40
50
60
Clinical Para- clinical Non medical
Total
Growh obtained

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 200
Table – 1 Distribution of bacterial isolates
Organism Clinical Para - clinical Non medical Total
CONS 29 (69.04%)
11 (26.19%)
2 (4.76%)
42
Bacillus sp. 10 (66.67%)
1 (6.66%)
4 (26.67%)
15
S. aureus 10 (76.92%)
3 (23.08%)
0 13
Pseudomonas sp.
4 (100%)
0 0 4
Moraxella sp. 2 (100%)
0 0 2
Acinetobacter sp.
1 (100%)
0 0 1
Klebsiella sp. 1 (100%)
0 0 1
E. coli 1 (100%)
0 0 1
Total 58
(73.42%)
15
(18.99%)
6
(7.59%)
79
Chart – 2 Methicillin resistance among Staphylococcus species
Table - 2Percentage incidence of antibiotic sensitivity of bacterial isolates
Organism Total AS BA CH RC TE GM CX CF
CONS 42
38 (90.48%)
23 (54.76%)
33 (78.57%)
28 (66.67%)
30 (71.42%)
32 (76.19%)
21 (50%)
16 (38.09%)
S. aureus 13 11 (84.62%)
5 (38.46%)
5 (38.46%)
7 (53.85%)
7 (53.85%)
9 (69.23%)
3 (23.08%)
3 (23.08%)
Pseudomonas
spp
4 2 (50%)
1 (25%)
1 (25%)
1 (25%)
- 3 (75%)
1 (25%)
-
Moraxella
spp
2 1 (50%)
1 (50%)
1 (50%)
1 (50%)
- 1 (50%)
- -
Klebsiella spp 1 1 (100%)
- 1 (100%)
1 (100%)
- 1 (100%)
- -
E. coli 1 1 (100%)
1 (100%)
1 (100%)
1 (100%)
- 1 (100%)
- -
Acinetobacter
spp
1 1 (100%)
- - 1 (100%)
1 (100%)
1 (100%)
- -
13
42
10
21
0
10
20
30
40
50
S.aureus CONS
Nu
mb
er
of
org
an
ism
s
Organisms
Total
Methicillin Resistant

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 201
AS – Ampicillin/ Sulbactum,CH – Chloramphenicol,TE – Tetracycline,CX –Cefoxitn,
BA – Cotrimoxazole,RC – Ciprofloxacin,GM – Gentamycin,CF - Ceftiaxone
DISCUSSION: The study shows that bacterialpathogensarepresent oncellphones. The carriage
rate of bacterial isolates was 65 %, which was higher in clinical (92%) staff than in para-
clinical (56%) staff and non- medical personnels (20%). Similar pattern was observed by
Arora U. et al 2. Table-3 shows carriage ratesof bacterial isolates oncellphones reported by
various authors.Bacterial isolates from cellphones of HCWs were varying in their numbers and
antibioticsensitivity, to that found on cellphones of non-medical personnels.
Coagulase NegativeStaphylococci(CONS)were found to be the most common colonizing organisms in the present study. Similar pattern have been reported by different authors as shown inTable-4. Many bacterial pathogens isolated from cellphones of healthcare workers were also multidrug
resistant. 21(50%) Coagulase NegativeStaphylococciand 10 (76.92%)S. aureuswere methicillin
resistant.All E. coli, Klebsiella spp, PseudomonassppandAcinetobactersppwerealsomultidrug
resistant.
Table –3 Comparison of carriage rate with other studies
Study Organisms
isolated
Clinical Para -
clinical
Non-
medical
Kabir O. et al – 2009 (1) 62.00% 15.30% - 66.45% Arora U. et al - 2009(2) 40.62% 44.78% 37.77% - Jayachandra T. et al - 2011(3) 84.30% - - - Jayalakshmi J. et al - 2008(7) 91.67% 90.40% 93.30% - Bhat S.- 2011(8) 98.50% - - - Datta P. – 2009 (9) 59.60% - - 10.00% Present study 65.00% 92.00% 56.00% 20.00%
Table – 4 Comparison of CONS carriage rate with other studies
Study CONS
Kabir O. et al – 2009 (1) 42.70% Arora U. et al – 2009 (2) 27.55% Jayalakshmi J. et al-2008 (7) 47.16% Bhat S. et al-2011 (8) 21.78% Fatma U. et al – 2009 (10) 58.96% Present study 53.16%
CONCLUSION: The overall carriage rate of Cell phones was found to be 65% in the present
study. It was higher in the clinical staff (92%) as compared to para-clinical staff (50%) and non-
medical personnel 20 (20%). Cell phones harboured potential pathogens, which included
multidrug resistant strains.
Restriction of Cell phones seems impractical, prevention of nosocomial pathogens is important,
use of antibacterial agents to clean Cell phones and strict adherence to infection control
measures like hand washing and good hygienic practice can reduce the risk of spread of
nosocomial pathogens.3,9

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 202
ACKNOWLEDGMENT: We are sincerely thankful to the Dean, Dr. H. H. Agravat and
Superintendent Dr. K.G. Patel of C.U. Shah Medical College& Hospital for their permission to
carry out this study.
REFERENCES:
1) Kabir O, Audu D, Olabisi O, Akitoye O. The potential roleof mobile phones in spread of
bacterial infections.JinfectDevCtries2009; 3(8):628-32.
2) Arora U, Pushpa D, Chadha A, Malhotra S. Cell phones amodernstayhouse for bacterial
pathogens. JK Science2009;11(3):127-9.
3) Jayachandra T, LakshmiprasannaT, Venkateswar A. Astudy on isolation and
identificationofbacteria causing nosocomial infections on mobile phones of health care
workers. CalicutMedical Journal 2011; 9(1):1-6.
4) SrikanthP, Rajaram E,Sudharsanam S, Lakshmanan A, UmamaheswariS, Kalyani J. The
mobile phone in a tropical setting – emerging threat for infection control. Sri
Ramachandra Journal of Medicine 2009;2(2):18-20
5) Chawla K, Mukhopadhayay C, Gurung B, Bhate P, Bairy I. Bacterial ‘Cell’ Phones: Do
cell phones carry potential pathogens?Online J Health AlliedScs.2009; 8(1):8-12.
6) Clinical and Laboratory Standards Institute. Performance standard for antimicrobial
susceptibility testing;20thinformational supplementM100-S20,Vol 30 No 1. Clinical and
Laboratory Standards Institute, Wayne,PA, USA; 2010.
7) Jayalakshmi J, Appalaraju B, Usha. Cell phonesas reservoirs of nosocomial pathogens. J
AssocPhy India 2008;56:388-9.
8) Bhat S, Hegde S, Salian S. Potential of mobile phones to serve as a reservoir in spread of
nosocomial pathogens. Online JHealth AlliedScs. 2011;10(2):14-20.
9) Datta P, Rani H,ChanderJ, Gupta V. Bacterial Contamination of Mobile Phones of
HealthCare Workers. Ind J Med Microbiol 2009; 27(3):279-81.
10) Ulger F, Esen S, Dilek A, Yanik K, Gunaydin M, Leblebicioglu H. Are we aware how
contaminated our mobile phones with nosocomial pathogens?Annals of Microbiology
and Antimicrobials2009,8:7.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 203
STUDY OF HEMATOLOGICAL PARAMETERS AMONG NEONATES
ADMITTED WITH NEONATAL JAUNDICE. Dr. Amar Shah, Dr. C. K Shah, Dr. Venu Shah.
1. Assistant Professor, Department of Pathology, Pramukhswami Medical College, Karamsad, Anand, Gujrat.
2. Professor, Department of Pathology, Smt. NHL Medical College, Ahmedabad.
3. Assistant Professor, Department of Community Medicine, GCS Medical College, Ahmedabad.
CORRESPONDING AUTHOR,
Dr. Amar Shah,
Pramukhswami Medical College,
Karamsad, Anand, Gujarat,
E-mail: [email protected], Ph: 09909927725.
ABSTRACT: INTRODUCTION: Jaundice is most common problem faced by neonates in the first
week of life. Although physiological jaundice is more frequent as compared to pathological
jaundice it is very important to differentiate between the two as pathological jaundice may lead
to kernicterus and subsequently brain damage. There are various modalities of investigations
e.g. Serum bilirubin, Direct and indirect coomb’s test, Blood group, G-6PD deficiency,
reticulocyte count by which we can reach at diagnosis. Treatment is also dependent upon the
amount of serum bilirubin and various other laboratory investigations. Thus laboratory workup
is very important for diagnosis and prevention of neonatal hyperbilirubinemia in newborn.
With this background present study was conducted to study the clinico- pathological profile
among infants with neonatal hyperbilirubinemia. METHODOLOGY: A prospective study was
carried out for the duration of 1 year in one of the teaching hospitals. RESULTS: Altogether 63
babies were enrolled in the study. Male babies out numbered the female (58.7% vs.
41.3%).Mean age of the study population was 2.97 days with standard deviation of 1.2 days.
Percentage of Pre-term babies was 30.1. Neonates having low birth weight were 17(26.9%).
Physiological jaundice constituted (40)62% cases of Neonatal hyperbilirubinemia. ABO
incompatibility was the commonest cause of pathological jaundice followed by septicemia.
Statistically significant rise in the serum bilirubin was noted in pathological jaundice as
compared to physiological jaundice. C-reactive protein (CRP) was found to be positive in all the
cases of septicemia. Direct and indirect Coomb’s test was positive in all the cases with Rh
incompatibility. CONCLUSION: Neonatal hyperbilirubinemia is associated with various other
clinical morbidities. Causes of hyperbilirubinemia should be investigated comprehensively. ABO
and Rh typing should be done along with Coombs Test, reticulocyte count and G6PD screening.
KEY WORDS: neonates, hyperbilirubinemia, hematological parameters.
INTRODUCTION: Neonatal hyperbilirubinemia is a very common condition in newborn
sometimes leading to kernicterus causing brain damage. There are various conditions, both
physiological and pathological leading to hyperbilirubinemia in newborn. Neonatal
hyperbilirubinemia, defined as a total serum bilirubin level above 5 mg per dL (86 µmol per L),
is a frequently encountered problem in developed as well as developing countries. Although up
to 60 percent of term newborns have clinical jaundice in the first week of life, few have
significant underlying disease.1 It is very important for pathologists and pediatricians to
differentiate the physiological and pathological causes of hyperbilirubinemia. Treatment is

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 204
dependent upon the amount of serum bilirubin and various other laboratory investigations. So
there is very important role of the pathologist in this condition to classify the neonatal
hyperbilirubinemia.
The most common cause of neonatal hyperbilirubinemia in India is physiological
jaundice. Various other conditions in decreasing order are preterm infant, blood group
incompatibility, Neonatal septicemia, G-6PD deficiency, cephalhematoma, drug induced, RBC
membrane disorders and many others.
Though the history and clinical presentation of the newborn plays a major role, the
laboratory plays an important role in diagnosing the cause of hemolysis in is also helpful in
diagnosing antenatally by amniocentesis and other recent available modality thereby
preventing the hemolytic sequel in newborn. There are various modalities of investigations e.g.
Direct and indirect coomb’s test, Blood group, G-6PD deficiency, reticulocyte count by which we
can reach at diagnosis. Thus laboratory workup is very important for diagnosis and prevention
of neonatal hyperbilirubinemia in newborn. With this background present study was conducted
to study the laboratory profile among infants with neonatal hyperbilirubinemia admitted to the
hospital.
OBJECTIVES:
1. To study different causes of neonatal hyperbilirubinemia
2. To study laboratory profile of neonatal hyperbilirubunemia
MATERIAL AND METHODS: A prospective cross sectional study on neonatal
hyperbilirubinemia was conducted at one of the teaching institutes of Ahmedabad. Infants
admitted with significant neonatal jaundice in first week of life are included in the study.
Significant Jaundice was defined as total serum bilirubin exceeding 15mg/dl or even between 5
mg/dl and 15 mg/dl within 24 hour of birth or the same persisting beyond one week of life.
Total 63 such cases of newborn were admitted during the study period of August 2007 to
October2008.Written informed consent were taken from the guardian of neonates. Detailed
history of baby and mother was taken. Following investigations were done in all cases.
BLOOD GROUP (ABO/RH) OF MOTHER, FATHER AND BABY: The blood grouping was done
by using known antisera with slide and tube methods
SERUM BILIRUBIN ESTIMATION OF BABY: It has been done on auto analyzer by Diazo
method of Pearlman and lee.
COMPLETE BLOOD COUNT WITH PERIPHERAL SMEAR EXAMINATION: It included
haemoglobin, total count, different count, band cells, peripheral smear examination and
reticulocyte count.
DIRECT AND INDIRECT COOMB’S TEST OF BABY AND MOTHER RESPECTIVELY
RETICULOCYTE COUNT: Reticulocytes count has been done by stain –Briliant cresyl blue.
TEST FOR G-6-PD DEFICIENCY: Test for G-6-PD deficiency has been carried out by using SPAN
Diagnostic Reagent Kit from the red cell hemolysate.
C-REACTIVE PROTEIN OF BABY: has been carried out by Latex agglutination method
Data was entered and analyzed by using appropriate statistical software. t test was used as a
test of significance to find out the probability value.
RESULTS AND OBSERVATION: The present study includes 63 cases of newborn admitted in
one of the tertiary care institutes. Various laboratory investigations of neonatal jaundice were

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 205
carried out. Out of 63 neonates, almost two thirds (63.5%) were 2 to 3 days old. Mean age of the
neonates was 2.97 days with standard deviation of 1.2 days. 37(58.7%) were male while
26(41.3%) were females. Percentage of Pre-term babies was 30.1. Neonates having low birth
weight were 17(26.9%). (Table 1) Physiological jaundice constituted (40) 62% cases of
Neonatal hyperbilirubinemia. ABO incompatibility was the commonest cause of pathological
jaundice and Septicemia is second commonest cause of pathological jaundice. (Table 2) Among
half of the cases (33, 52.4%) range of serum total bilirubun was found between 15 and 19.9
mg/dl. 5(7.9%) were having the serum total bilirubin more than 25 mg/dl.(Figure 1)
Hemoglobin level was lowest (12.1 gm %) in Rh incompatibility. Highest level of serum bilirubin
was found in Rh Incompatibility whereas highest level of reticulocytes was noted in G-6PD
Deficiency. Pre-term and low birth weight babies were having higher levels of serum total
bilirubin but the difference was not significant (P>0.05) (Table 3) The rise in serum bilirubin
level was found to be more in pathological jaundice as compare to physiological jaundice.
Difference was significant statistically with p value of <0.05. (Table 4) Direct Coomb’s test and
Indirect Coomb’s test were found to be positive in all case in Rh incompatibility while they were
positive in 77% of cases in ABO incompatibility. (Table 5) In cases of septicemia CRP was found
to be positive in 100% of cases. CRP was found to be positive in a few cases of ABO
incompatibility (22.2%) and physiological jaundice (5%). (Table 6)
DISCUSSION: Study included 63 cases of Neonatal hyperbilirubinemia cases. Mean age of the
neonates was 2.97 ±1.2 days. Among them 37(58.7%) were male while 26(41.3%) were
females. In the study of Choudhury Habibur Rasul2 male-to-female ratio among the neonatal
jaundice cases was 1.3:1 and mean age at the appearance of jaundice was 4.5±2.3days. Neonatal
hyperbilirubinemia was more common in male babies as compared to female babies in two
different studies done by Mantani et al 3(62% vs. 38%) and Sharma et al 4(1.3:1)
In present study, percentage of Pre-term (<37 weeks) babies was 30.1 and neonates
having low birth weight (<2.5 kg) were 17(26.9%). In the study of Nepal D et al5 LBW babies
constituted 19.2%. Where as in the study of Choudhury Habibur Rasul2 42% patients with
neonatal jaundice had low birth weight and 37% were preterm.
In our study out of 63, 40(62%) cases were diagnosed as having physiological jaundice
by while others were having ABO incompatibility (15%), Rh incompatibility(8%),
septicemia(12%) and G-6 PD deficiency(3%). In the study of Nepal D et al5 they noted that
clinical sepsis as defined by WHO criteria was found in 86.3% of babies. Nearly 1/3rd (32.9%)
babies were ABO incompatible and 4.1% babies were Rh incompatible. Choudhury Habibur
Rasul et al2 mentioned that Physiological jaundice was most common and was diagnosed in
114(26.7%) cases. In their study Prematurity (20.9%) and sepsis (17.6%) were also
major causes of jaundice. C. N. Onyearugha6 concluded in their study that septicaemia followed
by prematurity were the leading aetiological factors of neonatal jaundice. Joshi et al7 reported
that in Septicemia, ABO incompatibility, Rh incompatibility were observed in 36.36%, 31.8%,
4.54% cases of neonatal jaundice respectively.G-6 PD deficiency was there in 3 percent of cases
in present study. Singhal et al reported almost similar finding (G-6 PD deficiency in 5% of cases)
in their study.8
In present study mean Hb level was 14.2+/- 1.7 gm/dl with range of 10-18gm/dl.
Similar findings were noted in the study carried out by Joshi et al7. The findings of their study
showed Mean Hb level of 13.87+/- 3.59gm/dl with a range of 8– 19.4 gm/dl.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 206
In any infant, 24 hours old any jaundice is considered pathologic and requires evaluation. This
evaluation should minimally include a serum bilirubin and workup for hemolytic disease.
Guidelines for therapy depend upon the serum concentration of bilirubin and the patient’s age.
Also serum bilirubin is most important investigation to judge severity and management of
patient. In present study serum bilirubin was highest in ABO incompatibility and Rh
Incompatibility. Among half of the cases (52.4%) range of serum total bilirubun was found
between 15 and 19.9 mg/dl. Same results were observed in the study of Nepal D et al5. They
mentioned that maximum number (67.1%) of infants' peak serum bilirubin fell in the range of
15-19.9 mg/dl.
DCT and ICT were positive in 100% cases of Rh incompatibility while in ABO
incompatibility they were found to be positive in 77% of cases. The reason for this difference
may have been that “A” and “B” antigens are weaker antigens and the distance between a/b
antigen sites on the fetal red cells as compared to adult red cells is more. In all cases of
septicemia CRP was positive in present study. It is an acute phase reactant; is synthesized by the
liver and it becomes positive after any inflammation. It is a very reliable indicator.
To conclude, most of the cases were having idiopathic jaundice although septicemia and
ABO-Rh incompatibility were not exceptional. Peak serum bilirubin levels were found to be
more among the pathological jaundice. Also prematurity and low birth weight were having
higher levels of s. bilirubin. Special care must be given to them in order to avoid future
complications of hyperbilirubinemia
ACKNOWLEDGEMENT: We are thankful to parents/guardians of all the neonates for their
cooperation while carrying out the study.
TABLE-1 Demographic profile of Neonatal Hyperbilirubinemia cases
Variables No. Percentage
Age (in Days)
1 5 7.9
2 19 30.2
3 21 33.3
4 13 20.6
5 2 3.2
6 2 3.2
7 1 1.6
Sex
Female 26 41.3
Male 37 58.7
Gestational Age
Pre-Term 19 30.1
Term 44 69.9
Birth weight
Normal 46 73.1
LBW 17 26.9
TABLE-2 Etiology wise distribution of Neonatal Hyperbilirubinemia
Etiology No. Of Cases Percentage
Physiological Jaundice 40 62
Suspected ABO Incompatibility 09 15

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 207
Septicemia 08 12
Rh Incompatibility 04 08
G-6PD deficiency 02 03
Total 63 100
TABLE-3 Mean level of Hemoglobin, Serum bilirubin and Reticulocyte count in Neonatal
hyperbilirubinemia
Etiology Mean Hb
(gm %)
Mean serum
Bilirubin level
(mg/dl)
Mean
Reticulocyte
count (%)
Physiological
Jaundice 14.8 15.5 2.53
ABO
Incompatibility 14.2 19.6 3.77
Rh Incompatibility 12.1 18 5.5
Septicemia 12.6 20.2 4.6
G-6PD deficiency 13.7 19.2 6
TABLE-4 Mean Serum bilirubin value: physiological Vs Pathological Neonatal Jaundice
Neonatal Jaundice Mean Level of S. Bilirubin(mg/dl) t- value P value
Physiological(n=40) 15.4± 2.8
4.6 <0.05 Pathological(n=23) 19.5± 4.1
TABLE-5 Result of Coomb’s test in Rh and ABO incompatibility
DCT ICT
+ve -ve Total +ve -ve Total
Rh
incompatibility
4 (100%) 0 4 4 (100%) 0 4
ABO
incompatibility
7(77%) 2(23%) 9 7(77%) 2(23%) 9
TABLE-6 Result of C - reactive protein in Neonatal Septicemia
Etiology CRP positive
n(%)
Total No. of Cases
Septicemia 08 (100) 08
Physiological
Jaundice
02(5) 40
ABO
Incompatibility
02(22.2) 09
Rh Incompatibility 00(00) 04
G-6PD deficiency 00(00) 02

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 208
Figure: 1 Level of serum total bilirubin (mg/dl) among the neonatal jaundice cases
REFERENCES:
1. American Academy of Pediatrics. Report of the committee on infectious disease
(Redbook).Elk Grove Village III: AAP, 24th Ed.1997, p5054.
2. Choudhury Habibur Rasul, Md Abul Hasan, Farhana Yasmin. Outcome of Neonatal
Hyperbilirubinemia in a Tertiary Care Hospital in Bangladesh Malaysian J Med Sci. Apr-
Jun 2010; 17(2): 40-44
3. Mantani M, Patel A, Renge R, Kulkarni H. Prognostic value of direct bilirubin in Neonatal
Hyperbilirubinemia. Indian J Pediatr 2007; 79: 819-22.
4. Sharma P, Chhangani NP, Meena KR, Jora R, Sharma N, Gupta BD. Brainstem Evoked
Response Audiometry (BAER) in neonates with hyperbilirubinemia. Indian J Pediatr
2006; 73: 413-16.
5. Nepal D, Banstola D, Dhakal AK ,Mishra U, Mahaseth C Clinico-Laboratory Profile and
Immediate Outcomes of Hyperbilirubinemic Babies Admitted in Kanti Children
Hospital Journal of Nepal Paediatric Society; January-June, 2010/Vol 30/Issue 1
6. C. N. Onyearugha, B. N. Onyire and H. A. A. Ugboma. Neonatal jaundice: Prevalence and
associated factors as seen in Federal Medical Centre Abakaliki, Southeast Nigeria.
Journal of Clinical Medicine and Research Vol. 3(3) pp. 40-45, March 2011
7. Joshi BD, Singh R, Mahato D and Prasad R. Clinico-Laboratory Profile of Neonatal
Hyper-bilirubinemia in Term Babies at B.P. Koirala Institute of Health Sciences
(BPKIHS), Dharan, Nepal. Journal of Nepal Health Research Council Vol. 2 No. 2 October
2004
8. Singhal PK, Singh M, Paul VK, Deorari AK, Ghorpade MG. Spectrum of neonatal
hyperbilirubinemia: An analysis of 454 cases. Indian Pediatr 1992; 29: 319-325.
27.0
52.4
12.77.9
0.0
10.0
20.0
30.0
40.0
50.0
60.0
<15 15-19.9 20-24.9 >25
Per
cent
age
Levels of serum total bilirubin (mg/dl )

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 209
ESBL DETECTION: PREVALENCE & COMPARISON WITH NEW CRITERIA Dr. Ashwini Manhas, Dr. Prerna Aggarwal, Dr. Manju Bala, Dr. Satish Gupte.
1. Assistant Professor, Department of Microbiology, Giansagar Medical College, Patiala (Punjab).
2. Associate Professor, Department of Microbiology, Giansagar Medical College, Patiala (Punjab).
3. Assistant Professor, Department of Microbiology, Giansagar Medical College, Patiala (Punjab).
4. Professor, Department of Microbiology, Giansagar Medical College, Patiala (Punjab).
CORRESPONDING AUTHOR
Dr. Ashwini Manhas
Giansagar Medical College,Ramnagar,
Rajpura,Dist. Patiala (Punjab) Pin code-140601
E-mail: [email protected],
Ph: 09888473208.
ABSTRACT: AIM: To study the prevalence of ESBL producing organisms in our area both by
phenotypic method and latest CLSI breakpoints. Effect of change in break points on predicting
ESBL was also studied. MATERIAL & METHODS: Successive clinical isolates were tested by
phenotypic assay and zone diameters compared by Kirby Bauer’s disc diffusion method.
RESULTS: Total 231 clinical isolates were studied of which 81.8% were ESBL producers.
Cefotaxime had high sensitivity (97.91%), specificity (97.43%) and positive predictive value
(99.47%). Cefpodoxime had strikingly 100% specificity and positive predictive value but a very
poor negative predictive value. Aztreonam had a very high sensitivity (99.4%) and negative
predictive value (97.61%) CONCLUSION: Cefotaxime was found to be the most appropriate
antibiotic when used as single agent.
KEYWORDS: ESBL, Double Disc Synergy Test, Drug Resistance
INTRODUCTION: Since their first description more than twenty years ago, pathogens
producing extended-spectrum β- lactamases (ESBLs) have become an increasing cause of
clinical concern for several reasons1-3. First, systemic infections due to ESBL-producing
Enterobacteriaceae are associated with adverse clinical outcomes. Second, initially restricted to
certain, these enzymes have spread globally and their prevalence varies geographically. Third,
primarily characterized in limited bacteria such as Escherichia coli and Klebsiella spp., ESBLs
have been spreading and reaching other genera, principally Enterobacter and Proteus spp.
Finally, besides the growing species diversity, ESBL phenotypes have become more complex
due to the production of multiple enzymes including inhibitor-resistant ESBL variants, plasmid-
borne AmpC, production of ESBLs in AmpC - producing bacteria, production of ESBLs in KPC-
producing bacteria, enzyme hyperproduction and porin loss1-4.
A strong relationship exists between third-generation cephalosporin use and acquisition
of an ESBL producing strain5. Other antibiotic classes associated with infections due to ESBL-
producing organisms include quinolones, trimethoprim-sulphamethoxazole, aminoglycosides
and metronidazole.6 In some centers from India as many as 86 percent of Klebsiellae have been
found to be ESBL producers7.
Despite Clinical and Laboratory Standard Institute’s (CLSI) recommendations 6,8 that
clinical microbiology laboratories perform specialized tests for detection of ESBLs, many of
them make no effort to detect ESBL production or are ineffective at doing so. In India there is no
regulation regarding performance and reporting of ESBL isolates from various hospitals and

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 210
clinical laboratories. Many laboratories lack sufficient expertise to identify and report ESBLs.
There is a need for simple yet effective methodologies which can be routinely used for
monitoring the prevalence of ESBL producing organisms.
The most common method of testing for extended spectrum β-lactamases (ESBLs) is
screening for reduced susceptibility to cefpodoxime/ cefotaxime/ ceftriaxone/ ceftazidime/
aztreonam followed by phenotypic confirmatory testing by demonstrating a synergistic effect
between an indicator cephalosporin and a β-lactamase inhibitor i.e., clavulanic acid 9,10. The
sensitivity of screening for ESBLs can vary depending on the type of antimicrobial agent
tested.11, 12 According to Clinical Laboratory Standards Institute (CLSI) M100-S13 guidelines,10
use of more than one of the five indicator cephalosporins suggested for screening improves the
sensitivity of ESBL detection. Some studies have reported that if it should be necessary to rely
on a single screening antibiotic, cefpodoxime or ceftazidime is the recommended antibiotic for
ESBL detection in Klebsiella spp.11, 12 Phenotypic methods are easier to perform as compared to
genotypic and at the same time they are indicative of gene expression. If criteria for ESBL
detection could be incorporated in routine susceptibility testing the detection and
interpretation would become simpler.
So a study was planned to estimate the prevalence of ESBL producing organisms in our
area both by phenotypic method and latest CLSI breakpoints. The isolates studied belonged to
family Enterobacteriacae.
MATERIALS & METHODS: The study was conducted in Giansagar Medical College and Hospital
which is a 600 bedded tertiary care hospital. A prospective study on successive clinical isolates
of family enterobacteriacae was undertaken. All isolates were screened for ESBL production by
Kirby- Bauer’s disc diffusion method demonstrating reduced susceptibility to cefpodoxime (30
μg), cefotaxime (30μg), ceftazidime (30 μg), and aztreonam (30 μg). Cut-off zone sizes as an
indicator of potential ESBL producer for K. pneumoniae, K. oxytoca & E. coli were ≤ 27 mm for
cefotaxime, ≤ 22 mm for ceftazidime, ≤ 27 mm for aztreonam and ≤17 mm for cefpodoxime. For
P. mirabilis the zone size cut offs were cefotaxime ≤ 27 mm, ceftazidime ≤ 22 mm, aztreonam ≤
27 mm and cefpodoxime ≤ 22 mm. Escherichia coli ATCC 25922 & Klebsiella pneumoniae ATCC
700603 (ESBL positive) were used as quality control for ESBL detection.
Phenotypic confirmatory test was performed for confirmation. The combined disk
method was used to confirm the presence of ESBL on all the isolates of enterobacteriacae family
by placing a disk of ceftazidime (30 μg) and ceftazidime (30 μg)/ clavulanic acid (10 μg) besides
cefotaxime (30 μg) and cefotaxime (30 μg)/ clavulanic acid (10 μg) on a Mueller-Hinton agar
plate as recommended by CLSI. A ≥ 5 mm increase in zone diameter for either antimicrobial
agent tested in combination with clavulanic acid vs its zone when tested alone was considered
ESBL producer. CLSI has reviewed the interpretation criteria as shown in Table 2.18 If new
interpretation criteria are being used then the screening test need not be performed. Penicillins,
cephalosporins and aztreonam should be reported as found on susceptibility testing without
altering susceptibility status as recommended earlier.
RESULTS: Altogether 231 clinical isolates were studied. The most prevalent isolate was E. coli
(78.3%) followed by Klebsiella spp.(12.1%), Proteus mirabilis (4.3%), Citrobacter spp. (2.1%) &
others (Table 1). Overall ESBL producers were 81.8% and ESBL non producers were 18.2%.
Outpatient clinics contributed to 65 isolates of total 231 isolates. Amongst them the prevalence
of ESBLs was 75.38% (49/65). From inpatients 166 isolates were obtained amongst which the
prevalence of ESBLs was 84.34% (140/166) (Table 3).

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 211
TABLE 1: Species distribution
Species No. of isolates ESBL producers
Escherichia coli 181 (78.3%) 150 (82.8%)
Klebsiella species 28(12.1%) 22 (78.5%)
Proteus mirabilis 10 (4.3%) 8(80%)
Citrobacter species 5 (2.1%) 5(100%)
Serratia species 4 (1.7 %) 3(75%)
Enterobacter
species
1 (0.4%) 1 (100%)
Morganella
morganii
1 (0.4%) 1(100%)
Salmonella typhi 1(0.4%) 0(0%)
TABLE 2: Revised CLSI zone diameter (in mm)
Sensitive Intermediate Resistance
Cefotaxime ≥26 23-25 ≤22
Ceftazidime ≥21 18-20 ≤17
Aztreonam ≥21 18-20 ≤17
Cefpodoxime ≥21 18-20 ≤17
TABLE 3: In patient & outpatient distribution
Isolates ESBL producers Non ESBL
producers
Out patient 65 49 (75.38%) 16 (24.61%)
In patient 166 140 (84.34%) 26 (15.66%)
Total 231 189 (81.80%) 42(18.18%)
TABLE 4: Comparison of old and new CLSI criteria for ESBL detection
Sensitivity Specificity Positive
predictive value
Negative
predictive value
Old
criteria
New
criteria
Old
criteria
New
criteria
Old
criteria
New
criteria
Old
criteria
New
criteria
Cefotaxime 97.91% 97.91% 97.43% 97.43% 99.47% 99.47% 90.47% 90.47%
Ceftazidime 91.45% 95.72% 78.12% 77.27% 96.29% 94.7% 59.52% 80.95%
Aztreonam 89.9% 99.4% 91.3% 66.12% 98.94% 88.88% 50% 97.61%
Cefpodoxime 96.89% 82.17% 94.73% 100% 99.94% 100% 85.71% 2.38%
The species distribution of ESBLs amongst the various isolates was as shown in Table 1. Using
phenotypic methods the highest number of ESBLs was contributed by E. coli followed by
Klebsiella spp. and Proteus mirabilis. Citrobacter spp. though had only 5 isolates but alarmingly
all of them were ESBL producers. The drugs that were tested for ESBL production were
cefotaxime, aztreonam, ceftazidime & cefpodoxime. We also compared the zone diameters

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 212
according to old and current CLSI criteria to see if a single drug was better predictor of ESBL
activity when used in the absence of ESBL phenotypic assay.
The effect of change in CLSI criteria on predicting ESBL production is shown in Table 4.
For cefotaxime the sensitivity, specificity, positive predictive value and negative predictive
value was 97.91%, 97.43%, 99.47% & 90.47% respectively. Upon testing with ceftazidime the
sensitivity was 95.72% and positive predictive value was 94.7%. A fall in specificity (77.27%)
and negative predictive value (80.95%) was observed. With ceftazidime 182 isolates were
confirmed ESBL producers, 25 were ESBL non producers and 24 were doubtful. Out of these
isolates 17 were later found to be non ESBL producers and 7 were ESBL producers. With
aztreonam 187 isolates were confirmed ESBL producers, 21 were non ESBL producers and 23
were doubtful. Of these 23, 21 isolates were found to be non ESBL producers but 2 were ESBL
producers. Aztreonam showed improved sensitivity (99.4%) and negative predictive value
(97.61%) but reduced specificity (66.12%) and positive predictive value (88.88%). For
cefpodoxime the current criteria resulted in 100% specificity and positive predictive value but a
poorer sensitivity (82.17%) and negative predictive value (2.38%).
DISCUSSION: ESBL producing bacteria have become quite prevalent in Indian hospitals and
community. Different studies from India have quoted variable ESBL detection rates. According
to multicentric SMART study conducted in Asia Pacific region during the year 2007 ESBL rates
in India for E. coli, Klebsiella pneumoniae, and Klebsiella oxytoca were 79.0%, 69.4%, and
100%, respectively13. Another study found ESBL producing E. coli increase from 40 per cent in
2002 to 61 per cent in 2009, with a significant (P<0.05) rise in resistance to cefotaxime (75 to
97%). This study also found the resistance directly related to high antibiotic usage.14 A study
from central India reports the incidence of 69% and 41% ESBL producing isolates of E. coli and
Klebsiella pneumoniae respectively.15 Another study from Vellore in South India found 50.29 %
of inpatients and 45.86 % of outpatients harboring ESBL producers.16 A study from
Northwestern India found ESBL production as 23.83% in E. coli strains and 8.69% in Klebsiella
strains17. We observed that 81.8% of clinical isolates were ESBL producers. From outpatient
clinics the reporting of ESBL producers was 75.38% whereas from inpatient clinics it was
84.34%.
Though ESBLs are prevalent in our hospitals and community they are not specifically
reported by Microbiology labs. For certain reasons there is also a wide variability in prevalence
reporting of ESBLs. The possible factors could be different geographical locations, variable
proficiency levels of microbiology trained technical staff, different antibiotic cut offs being used,
different guidelines being followed (as they differ between different infectious diseases unions
throughout the world) and different techniques being used for ESBL detection.
In developing countries like India it is desirable to incorporate both ESBL detection and
antimicrobial susceptibility testing. Different drugs have been used to detect ESBLs but no
single antibiotic has been perfect at ruling -in or -out an ESBL producer. CLSI has recently
changed the breakpoints of for aztreonam, cefotaxime and ceftazidime for routine testing.
Criteria for cefotaxime to be used for ESBL detection have remained unchanged. With
high sensitivity, specificity and positive predictive value it remains the best drug for ESBL
detection. Ceftazidime has remained almost equally sensitive and specific as old criteria with
improvement in negative predictive value from 59.52% to 80.95% with almost sustained
sensitivity, specificity and positive predictive value. Aztreonam had shown improved sensitivity

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 213
from 89.9% to 99.4% but reduction in specificity from 91.3% to 66.12%. Its positive predictive
value drops from 98.94% to 88.88% with significant increase in negative predictive value to
97.61%. Therefore, to improve the interpretation aztreonam remains additional preferred agent
besides cefotaxime. Cefpodoxime has shown reduced sensitivity from 96.89% to 82.17% with
sustained improvement in specificity and positive predictive value to 100%. The most striking
observation was a very poor negative predictive value. This will result in need to perform
additional confirmatory tests if used as single agent.
Overall we found that cefotaxime was the single most appropriate antibiotic for
predicting ESBL production. Cefpodoxime can be considered a good agent due to high specificity
and positive predictive value. However, it has a very poor negative predictive value. Therefore,
no single agent can be recommended for predicting ESBL production.
CLSI has so far not given any specific criteria with the use of above mentioned four
antibiotics for detecting ESBLs while performing routine susceptibility testing. At the same time
it recommends that with the current criteria antibiotics should be reported as observed on
susceptibility testing. Earlier it recommended the reporting of all drugs as resistant when it was
observed as resistant to any one drug of the four. These guidelines are based on PK/PD analysis.
More clinical studies are needed to support the current recommendation which is based
on PK/PD measurements of the above mentioned drugs. Therapeutic failure or success of
antibiotic therapy when one drug is sensitive and other resistant in vitro needs to be studied in
parallel with clinical outcome of cases.
To conclude, cefotaxime was found to be the most appropriate drug when used as single
agent with both old as well as current criteria. Adding Aztreonam to the interpretation
improves the detection of ESBL. The current criteria definitely reduce the need for ESBL
screening test due to increased sensitivity and negative predictive value with at least three out
of four antibiotics. However, the need for using more than one drug for predicting ESBL activity
continues to be there as before.
ACKNOWLEDGEMENT: “We are thankful to the Management & Principal, Giansagar Medical
College, Patiala for approving and facilitating the study.”
REFERENCE:
1. Kim YK, Pai H, Lee HJ, Park SE, Choi EH, Kim J, Kim JH, Kim EC. Bloodstream infections by
extended-spectrum beta-lactamase-producing Escherichia coli and Klebsiella
pneumoniae in children: epidemiology and clinical outcome. Antimicrob Agents
Chemother 2002;46 : 1481- 1491.
2. Schwaber MJ, Navon-Venezia JS, Kaye KS, Ben-Ami R, Schwartz D, Carmeli Y. Clinical and
economic impact of bacteremia with extended-spectrum-{beta}-lactamase-producing
Enterobacteriaceae. Antimicrob Agents Chemother 2006; 50: 1257-1262.
3. Perez F, Endimiani A, Hujer KM, Bonomo RA. The continuing challenge of ESBLs. Curr
Opin Pharmacol 2007; 7: 459-469.
4. Tsakris A, Poulou A, Themeli-Digalaki K, Voulgari E, Pittaras T, Sofianou D, Pournaras S,
Petropoulou D. Use of boronic acid disk tests to detect extended spectrum beta-

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 214
lactamases in clinical isolates of KPC carbapenemase-possessing Enterobacteriaceae. J
Clin Microbiol 2009; 47: 3420- 3426
5. Lautenbach E, Patel JB, Bilker WB, Edelstein PH, Fishman NO. Extended-spectrum beta-
lactamase-producing Escherichia coli and Klebsiella pneumoniae: risk factors for
infection and impact of resistance on outcomes. Clin Infect Dis 2001; 32: 1162-71.
6. Paterson DA, Bonomo RA. Extended-spectrum b-lactamases: a clinical update. Clin
Microbiol Rev 2005; 18: 657-86.
7. Jain A, Mondal R. Prevalence & antimicrobial resistance pattern of extended spectrum
beta-lactamase producing Klebsiella spp. isolated from cases of neonatal septicemia.
Indian J Med Res 2007; 125: 699-700.
8. Clinical and Laboratory Standards Institute. Performance standards for antimicrobial
susceptibility testing. 13th Informational Supplement. Wayne, Pennsylvania. CLSI
Document M100-S13: 2003.
9. Sturenburg E, Mack D. Extended spectrum beta-lactamases: implications for the clinical
microbiology laboratory, therapy, and infection control. J infect 2003; 47 : 273 -95.
10. Clinical and Laboratory Standards Institute. Performance standards for antimicrobial
susceptibility testing; 16th Informational Supplement; Wayne, Pennsylvania. CLSI
Document M100-S16; 2006.
11. MacKenzie FM, Miller CA, Gould IM. Comparison of screening methods for TEM- and
SHV-derived extended spectrum beta-lactamase detection. Clin Microbiol Infect 2002; 8:
715-24.
12. Ho PL, Tsang DN, Ho M, Yuen KY. Comparison of screening methods for detection of
extended spectrum beta-lactamases and their prevalence among Escherichia coli and
Klebsiella species in Hong Kong. APIMS 2000; 108: 237-40.
13. Hawser SP, Bouchillon SK, Hoban DJ, Badal RE, Hsueh PR, Paterson DL, et al. Emergence
of high levels of extended-spectrum-ß-lactamase-producing gram-negative bacilli in the
Asia-Pacific region: data from the Study for Monitoring Antimicrobial Resistance Trends
(SMART) program, 2007. Antimicrob Agents Chemother. 2009; 53: 3280–4
14. Datta S, Wattal C, Goel N, Oberoi JO, Raveendran R and Prasad KJ. A ten year analysis of
multi-drug resistant blood stream infections caused by Escherichia coli & Klebsiella
pneumoniae in a tertiary care hospital. Indian J Med Res. 2012 June; 135(6): 907–912
15. Pathak A, Marothi Y, Kekre V, Mahadik K, Macaden R, Lundborg CS. High prevalence of
extended-spectrum β-lactamase-producing pathogens: results of a surveillance study in
two hospitals in Ujjain, India. Infect Drug Resist. 2012;5:65-73
16. Sankar S, Narayanan H, Kuppanan S, Nandagopal B. Frequency of extended-spectrum β-
lactamase (ESBL)-producing Gram-negative bacilli in a 200-bed multi-specialty hospital
in Vellore district, Tamil Nadu, India. Infection. 2012 Aug;40(4):425-9
17. Sood S, Gupta R. Antibiotic resistance pattern of community acquired uropathogens at a
tertiary care hospital in jaipur, rajasthan. Indian J Community Med. 2012 Jan;37(1):39-
44
18. Clinical and Laboratory Standards Institute. Performance standards for antimicrobial
susceptibility testing; 21st Informational Supplement; Wayne, Pennsylvania. CLSI
Document M100-S21; 2011.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 215
PREDICTION OF OUTCOME OF PATIENTS WITH PERFORATION
PERITONITIS ON THE BASIS OF APACHE-II SCORING SYSTEM Dr. S. K. Katiyar, Dr. S. K. Gahlot.
1. Assistant Professor, Department of Surgery, Rama Medical College Hospital & Research Centre, Kanpur.
2. Assistant Professor, Department of Anesthesiology, Major S.D. Singh Memorial Medical College & Hospital,
Farrukhabad.
CORRESPONDING AUTHOR
Dr. S. K. Katiyar
M.S., FIAGES,
675, Singhpur Kanpur-208017,
E-mail: [email protected],
Ph: 09415044878
ABSTRACT: Peritonitis is the inflammation of the peritoneum and is most commonly due to
localized or generalized infection. It is most common surgical emergency in India. Most common
causes in India are perforated gastric /duodenal ulcer. Any type of peritonitis can be very
serious and life threatening if not evaluated and treated properly. Prognosis in peritonitis is
decisively influenced by the health status of the patients at beginning of treatment. Accurate
prediction of the outcome of the disease can initially be made on the basis of the prognostic
scoring systems, currently several scoring systems are employed.
The APACHE prognostic scoring system for measuring severity of illness in critically ill
patients was developed in 1981 by William A Knaus1. APACHE - II introduced in 1985 was a
simplified modification of original APACHE. APACHE - II was further refined to APACHE - III in
1991. It is important for surgeons to develop at least a rudimentary knowledge of scoring
system for perforation peritonitis, as it will play an increasing role to explain the prognosis of
the disease. Aims & objectives of study are to predict the outcome of the patients with
perforation peritonitis on the basis of APACHE - III scoring system. This study was conducted on
72 patients, admitted to emergency ward of Rama Medical college hospital & Research centre,
Mandhana Kanpur, who were diagnosed as cases of perforation peritonitis from January 2009 –
January 2011. All the patients were evaluated according to APACHE - III scoring system within
24 hours of admission. All the patients admitted in emergency ward initially examined clinically
then required investigations were done. Total APACHE III score range for (0-299). Patients with
lower scores have more favourable prognosis than patients with higher scores. Thus it was
concluded from this study that patients with low scores have favourable outcome as compared
to patients with high scores.
KEYWORDS: Peritonitis, APACHE, Prognosis, Outcome.
INTRODUCTION: Peritonitis is the inflammation of the peritoneum and is most commonly due
to localized or generalized infection. Currently Peritonitis is organized into three divisions
based upon the source and nature of microbial contamination.
1. Primary peritonitis is diffuse bacterial infection without loss of integrity of GI tract, and
is most commonly caused by Streptococcus pneumonia.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 216
2. Secondary peritonitis occurs due to acute peritoneal inflammation resulting from GI
tract perforation , infected pancreatic necrosis, perforations of other infected viscera e.g.
hepatic abscess or pyometra and penetrating abdominal injuries.
3. Tertiary peritonitis develops following treatment failure of secondary peritonitis.
Peritonitis is most common surgical emergency in India. Most common causes in India are
perforated gastric /duodenal ulcer followed by appendicitis, GIT perforation due to blunt
trauma, typhoid fever and tuberculosis.
Signs and symptoms of peritonitis are-
1. Severe pain in abdomen and worsened by movement
2. Abdominal distention
3. Board like rigidity
4. Fever and chills
5. Nausea and vomiting
6. Inability to pass flatus & faeces
7. Low BP
8. Limited urine output
Any type of peritonitis can be very serious and life threatening if not evaluated and treated
properly.
Prognosis in peritonitis is decisively influenced by the health status of the patients at
beginning of treatment accurate prediction of the outcome of the disease can initially be made
on the basis of the prognostic scoring systems, currently several scoring systems are employed.
The APACHE prognostic scoring system for measuring severity of illness in critically ill
patients was developed in 1981 by William A Knaus1, Statistical detail on the predictive power
of APACHE was published in 1983, which showed that by using estimated equation to forecast
death rates for independent data, APACHE allowed accurate estimates of death rates for groups
of patients.
APACHE - II introduced in 1985 was a simplified modification of original APACHE. The
APACHE - II scores consisted of three parts –
1. 12 acute physiological variables (0-60) points
2. Age (0-6) points
3. Chronic health status (0-5) points
The probability of death can be calculated from the individual APACHE - II total scores (0-71)
points. APACHE - II scores has received far more attention in the literature than any other
prognostic model. APACHE - II was further refined to APACHE - III in 1991, Five new variables –
1. Blood urea nitrogen
2. Urine output
3. Serum bilirubin,
4. Serum albumin
5. Glucose
It is important for surgeons to develop at least a rudimentary knowledge of scoring
system for perforation peritonitis, as it will play an increasing role to explain the prognosis of
the disease.
Aims & objectives of study are to predict the outcome of the patients with perforation
peritonitis on the basis of APACHE - III scoring system.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 217
MATERIAL AND METHODS: This study was conducted on 72 patients, admitted to emergency
ward of Rama Medical college hospital & Research centre, Mandhana Kanpur, who were
diagnosed as cases of perforation peritonitis from January 2009 –January 2011. All the patients
were evaluated according to APACHE - III scoring system within 24 hours of admission.
All the patients admitted in emergency ward initially examined clinically then required
investigations were done.
• Plain x-ray abdomen
1. Erect view
2. Supine view
• USG whole abdomen
• Aspiration of peritoneal fluid
The following acute physiological parameters of APACHE III scoring system were assessed and
recorded at the time of admission-
1. Pulse rate
2. Respiratory rate
3. Mean arterial pressure (mm of Hg)
4. Temperature ( 0C)
5. Urine out put ( 24 hr ).
6. Hematocrit (%)
7. White blood cell count
8. Serum sodium (mmol./L)
9. Serum creatinine (mg/dl)
10. Serum albumin (g/dl)
11. Serum bilirubin (mg/dl)
12. Blood urea nitrogen (mg/dl)
13. Blood sugar (mg/dl)
14. Arterial pH
15. Oxygenation (PaO2 in mm of Hg with FiO2 <0.05)
16. Glasgow coma score
These values were scored in accordance to the APACHE III chart scoring for abnormally
high or low range. Zero score represents a normal value. These parameters represent Acute
physiology Score.
(A) Acute Physiology score (0-252)
1. Pulse rate 0 – 17
2. Mean B.P. 0 – 23
3. Temperature 0 – 20
4. Respiratory rate 0 – 18
5. PaO2 /AaDO2 0 - 15 / 0 - 14
6. Hematocrit 0 - 3
7. WBC 0 - 19
8. Creatinine 0 - 10
9. Urine output 0 - 15
10. BUN 0 - 12
11. Sodium 0 - 4

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 218
12. Albumin 0 - 11
13. Bilirubin 0 - 16
14. Glucose 0 - 9
15. pH 0 - 12
16. GCS 0 – 48
(B) Age points (0-24)
1 < 44 0
1 45 – 59 5
1 60 - 64 11
1 65 – 69 13
1 70 – 74 16
1 75 – 84 17
1 > 85 24
(C) Chronic health points (0-23)
1. None 0
2. Cirrhosis 4
3. Immunosupression 10
4. Leukemia/multiple myeloma 10
5. Metastatic cancer 11
6. Lymphoma 13
7. Hepatic failure 16
8. AIDS 23
APACHE III Score = (A) + (B) +(C)
= 252 +24 + 23
= 299
Total APACHE III score range for (0-299)
RESULTS:
TABLE –I
CAUSES OF PERFORATION PERITONITIS ( n = 72)
SI.
No.
Cause
Patients
Male
Female
1. Gastric / Duodenal
40 55% 35 87.5% 5 12.5%
2. Small bowel
Perforation
15 20.8% 9 60%
6 40%
3. Colon perforation 2 2.7% 1 50%
1 50%
4. Appendicular
Perforation
3 4.1% 2 66%
1 33%
5. Gall bladder
Perforation
2 2.7% 0 0% 2 100%
6. Blunt abdominal
Trauma
8 11% 6 75%
2 2.5%
7. Stab injury
Abdomen
1 1.3% 1 100%
0 0%

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 219
8. Firearm injury
Abdomen
1 1.3% 1 100% 0 0%
TABLE – II
DISTRIBUTION OF PATIENTS WITH POST OPERATIVE COMPLICATION ACCORDING TO
APACHE - III SCORE
SI. No.
APACHE III
Score
No.of
Cases
Wound
Infection
Septicemia Burst
Abdomen
Fecal
fistula
1.
0 - 30 35 9 1 3 0
2.
31 – 60 25 6 2 5 2
3.
> 60 12 3 5 3 0
TABLE – III
DISTRIBUTION OF PATIENTS WITH OUTCOME ACCORDING TO APACHE – III SCORE
SI.
No.
APACHE
III score
No. of
patients
Survived Expired LAMA Observed
Mortality
1.
0 – 30 35 33 1 1 2.8%
2.
31 – 60 25 22 2 1 8%
3.
>60 12 7 5 0 41.6%
TABLE – IV
COMPARISON OF OBSERVED AND PREDICTED MORTALITY
SI.
No.
APACHE
III score
No. of patients Expired Mortality
Observed
predicted
1. 0 - 30
35 1 2.8% 7.5%
2. 31 – 60 25 2 8%
25.2%
3. > 60 12 5 41.6%
42.6%
DISCUSSION: Perforation peritonitis is a frequently encountered surgical emergency in tropical
countries like India. In majority of cases presentation to hospital is late with well established
generalized peritonitis with purulent / faecal contamination and varying degree of septicemia.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 220
Clinical presentation of patients varied according to site of perforation. Abdominal distension
was found in 84% along with vomiting in 50% and constipation in 60% cases. 15% patients
were in shock at the time of admission. Only 64% patients had evidence of pneumoperitoneum
on chest X- ray done in erect posture.
The most elaborate study on APACHE III prognostic system and the risk prediction has
been conducted by knaus et al 2, where they prospectively collected data on 17,440 medical /
surgical ICU patients and found that a 5 points increase in APACHE III score ( range 0 – 299 ) is
independently associated with a statistically significant increase in the relative risk of hospital
death. We categorised patients into 3 groups according to APACHE – III score of 30 points each
and found an increase in the mortality risk as the scores increased from < 30 to > 60.
Perforations of proximal gastrointestinal tract are more common than of distal gastrointestinal
tract as has been noted in earlier studies from India70 , which is in sharp contrast to studies
form developed countries like United States71 and Japan72
Rajender Singh Jhobta et al3 in their study concluded that most common cause of
perforation was perforated dupdenal ulcer (57%) followed by appendicitis (11%) and blunt
trauma (9.1%). These findings are similar to present study in which most common cause of
perforation was gastric / duodenal ulcer (55%), blunt trauma (8%) and appendicitis (3%). A
study done by Mathkere LR et al4 also showed perforation of peptic ulcer was most common
cause of peritonitis (64%). Not only the site but the etiological factors also show a wide
geographical variation. Khanna et al5 from Varanasi studied 204 consecutive patients of
gastrointestinal perforation and found that over half (100 cases ) were due to typhoid. Duodenal
ulcer (58), appendicitis (9), amoebiasis (8) and tuberculosis (4). These figures show the
importance of infection and infestation in third word. At the other end of spectrum, Noon et al6
from Texas studied 430 patients of gastrointestinal perforations and found 2010 cases to be due
to penetrating trauma. This shows the importance of trauma in developed countries.
The mean length of hospital stay was 13 days. For survivors mean length of stay was
17.8 days as comparable to 18 days in the study by Bohnen et al7. The study by Adesunkanmi et
al8 showed an incidence of postoperative complications of 42.4% similar to present study with
an incidence of 54% patients having higher APACHE – III score had higher incidence of
postoperative complications. In this series, the major cause of postoperative morbidity were
wound infection (25%), wound dehiscence (15.2%), septicemia (11%) and faceal fistula (2.7%)
as compared to series by Rajender Singh Jhobta et al9 in their study wound infection rate was
(25%), wound dehiscence (9%) and septicemia (18%). Markgrof R et al51 done a
showed that hospital morality rate was higher than predicted for APACHE III
score > 60 is 41.6% as compared to predicted mortality rate of 42.5%.
CONCLUSION: All the patients were evaluated according to APACHE –III scoring system within
24 hours of admission. Age is a significant factor contributing to survival. Majority of survivors
belong to age group 20- 60 yrs. In this series, male patients were 55 (76%) and female patients
were 17 (23%). Mortality was higher in females (23.5%) as compared to male (7.2%). Most
common cause of perforation peritonitis was gastric / duodenal perforations (55%) followed by
small bowel perforations (20%), blunt abdominal trauma (11%), appendicular perforation
(4%), colon perforation (2.7%), gall bladder perforation (2.7%), stab injury abdomen (1.3%)
and firearm injury abdomen (1.3%). Most of the patients (72%) were managed with primary
repair of perforations. Mean duration of hospital stay is 13 days. Major causes of postoperative
complications were wound infection (25%), wound dehiscence (15%), septicemia (8%) and

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 221
faecal fistula (2.7%). Patients with lower scores have more favourable prognosis than patients
with higher score. Observed mortality rate was 41.6% in the group with APACHE –III score of
>60, which was comparable to predicted mortality of 42.6%.
Thus it was concluded from this study that patients with low scores have favourable
outcome as compared to patients with high scores. And APACHE III score, as measured before
the treatment of perforation peritonitis, correlates significantly with the outcome of disease
with respect to both morbidity and mortality.
REFERENCES:
I. W.A. Knaus. APACHEs The development of a quality assurance system based on
prognosis: Milestones and personal reflections. Arch Surg 137 (2002), pp. 37 –
41.
II. Kanus W.A., Wagner D.P: Individual patients decision. Chaper 6, Crit Care Med.
17 : S204 – 209.
III. Rajender Singh Jhobta, Ashok Kumar Attri, Robin Kaushik, Rajeev Sharma and
Anupam Jhobta : Spectrum of perforation peritonitis in India – review of 504
consecutive cases. World Journal of Emergency Surgery 2006, 1 : 26.
IV. Mathikere Lingaish Ramachandra, Beellary Jagadesh, Sathees BC Chandra :
Clinical study and management of secondary peritonitis due to perforated hollow
viscous. Arc Med Sci. 2007 ; 3, 1: 61-68.
V. Khanna AK, Mishra MK : Typhoid perforation of the gut. Postgraduate Medical
Journal 1984, 60 : 523.
VI. Noon GP, Beall AC, Jorden GL : clinical eveluation of peritoneal irrigation with
antibiotic solution. Surgery 1967, 67 : 73.
VII. Bohnen JM, Mustard RA, Oxhalm SE, Schouten BD: APACHE II score and
abdominal sepsis. Arch Surg. 1988; 123 : 225 - 229.
VIII. Adesunkanmi ARK, Badmus TA, Fadiora FO, Agbakwuru EK: Generalised
peritonitis secondary to typhoid ileal perforation : Assessment of senerity using
modified APACHE II score. Indian J Surg 2005; 67 : 29 – 33.
IX. MR Capoor, D Nair, MS Chintamani, J Khanna, P Aggarwal, D Bhatnagar : Role of
enteric fever in Ileal perforations: An overstated problem in tropics ? Indian J
Med Microbiol 2008 ; 26 : 54 - 57.
X. A. Horiuchi, y. Watanable, T. Doi, K. Sato, S. Yukumi, M. Yashida, Y. Yamamoto, H.
Sugishita, K. Kawachi : Evaluation of prognostic factors and scoring in colonic
perforation. World J Gastroenterol 2007; 13(23): 3228 – 3231.
XI. A.Y. Ukewenya, Ilyasu Muhammad and P.T. Nmadu: Assessing severity of
intraabdominal infections ; the value of APACHE II scoring system. Nigerian
Journal of Surgical Research, Vol 8, No. 1-2, 2006, pp. 24-29.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 222
ALTERATIONS OF SERUM ENZYMES IN PROTEIN ENERGY
MALNUTRITION Dr. A. K. Tadas, Dr. A. N. Jadhao, Dr. S. A. Tadas.
1. Associate Professor, Department of Biochemistry, Government Medical College, Nagpur. 2. Junior Resident, Department of Biochemistry, Government Medical College, Nagpur.
3. Assistant Professor, Department of Physiology, Government Medical College, Nagpur.
CORRESPONDING AUTHOR,
Dr. A.K. Tadas,
437 A, Hanuman Nagar,
Nagpur – 440009,
E-mail: [email protected],
Ph: 09423100663.
ABSTRACT: OBJECTIVES: To study the correlation of serum enzymes (alkaline phosphatase,
aspartate aminotransferase, alanine aminotransferase, amylase) abnormalities in protein
energy malnutrition and to assess their clinical significance. MATERIAL AND METHOD: 30
cases of PEM admitted to the pediatric wards of Government Medical College and Hospital,
Nagpur were studied from 5 Jan 2011 to 15 August 2011. 30 age and sex matched controls were
selected from children of normal weight for age attending OPD or wards. All the clinical details,
along with the relevant clinical history were noted. Venous blood sample was collected for
estimation of alkaline phosphatase, aspartate aminotransferase, alanine aminotransferase, and
amylase. RESULTS AND OBSERVATIONS: Patients with PEM had reduced serum alkaline
phosphatase. Amylase was found to be reduced in kwashiorkor while it remained unchanged in
marasmus. Increase in aspartate aminotransferase, alanine aminotransferase was found in PEM.
Serum amylase in kwashiorkor is lower than marasmus. DISCUSSION: In patients with PEM, we
found higher levels of AST and ALT ,as there is increased tissue breakdown in PEM to
metabolise the amino acids released by protein catabolism, the process of transamination is
enhanced leading to increased activity of related enzymes AST and ALT. Reduced serum
Alkaline phosphatase may be due to impairment of protein synthesis. Many of these
alternations of enzymes may be due to metabolic readjustment resulting from protein
deficiency.
KEY WORDS: Protein Energy Malnutrition, Enzymes, Alanine Aminotransferase, Aspartate
aminotransferase,Alkaline phosphatase,Amylase.
INTRODUCTION: The World Bank estimates that after Bangladesh, India is ranked 2nd in
number of children suffering from malnutrition (in 1998), where 47% of the children exhibit a
degree of malnutrition. The prevalence of underweight children in India is among the highest in
the world, and is nearly double that of Sub-Saharan Africa with dire consequences for mobility,
mortality, productivity and economic growth1. The UN estimates that 2.1 million Indian children
die before reaching the age of 5 every year – four every minute – mostly from preventable
illnesses such as diarrhoea, typhoid, malaria, measles and pneumonia. Every day, 1,000 Indian
children die because of diarrhoea alone1. According to the 1991 census of India, it has around
150 million children, constituting 17.5% of India's population, who are below the age of 6 years.
Enzymes being proteins, disturbances in their functions and levels in the body are
expected to occur in PEM of any severity 2. Our aim is to determine if any biochemical

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 223
parameters could be helpful in early diagnosis of PEM and to understand the correlation of
abnormalities of serum enzymes (alkaline phosphatase, aspartate aminotransferase, alanine
aminotransferase, amylase) in protein energy malnutrition and to assess their clinical
significance.
METHODS: The study was carried out in 60 children of six months to five years of age of both
sexes. Group A includes 30 children suffering from various grades of PEM were selected as
experimental group and excludes hepatobiliary and other disease by history, physical
examination and investigations i.e. serum bilirubin and ultrasonography of abdomen.. Group B
includes 30 age and sex matched healthy children. The exclusion criteria for group A was
children suffering from any systemic disease other than PEM, but minor association like
diarrhoea, cough and cold was included in the study .Protocol of study had been accepted by
the Ethical Committee. After taking the informed consent from the mothers and guardians they
were asked a pre-coded questionnaire to collect data related to the study.
By aseptic precautions 5 ml of blood was drawn from patient’s dorsal hand or wrist vein
and collect with a smaller gauge needle (22g or 23g) .Serum was separated immediately by
centrifugation at 3000 rpm for 10 min. Estimation of enzyme was carried out immediately
METHODS: Enzymes were estimated by kinetic method.
ALKALINE PHOSPHATASE BY KIT METHOD8
PRINCIPLE: Alkaline phosphatase cleaves p-nitrophenyl phosphate (p-Npp) into p-nitrophenol
and phosphate. p-nitrophenol is a yellow colour compound in alkaline medium and absorbs
light at 405nm.The rate of increase in absorbance at 405 nm is proportional to alkaline
phosphatase activity in specimen.
p-nitrophenyl phosphate � p-nitrophenol + phosphate
ASPARTATE AMINOTRANSFERASE(AST) BY KIT METHOD9
PRINCIPLE:- L-Asparate + α-ketoglutarate AST Oxaloacetate + L-Glutamate
Oxaloacetate + NADH + H+ MDH L-Malate + NAD+
This conversion of NADH to NAD+ is proportional to the concentration of AST in serum and is
measured at 340 nm, as rate of decrease in absorbance.
ALANINE AMINOTRANSFERASE(ALT) BY KIT METHOD10
PRINCIPLE:-SGPT catalses the transfer of amino group from L-alanine to 2-oxoglutarate with
the formation of pyruvate and L-glutarate.The pyruvate so formed is allowed to react with
NADH to produce L-lactate.The rate of this reactioin is monitored by an indicator reaction
coupled with LDH(lactate dehydrogenase) in the presence of NADH.The oxidation of NADH in
this reaction is measured as a decrease in the absorbance of NADH at340nm,which is
proportional to SGPT activity
L-alanine + 2-oxoglutarate ALT pyruvate + L-glutamate
Pyruvate + NADH LDH L-actetate + NADH
AMYLASE BY KIT METHOD11
PRINCIPLE: Amylase test involves use of a chromogenic substrate Gal G2 –α CNP (2-chloro -4-
nitrophenyl linked with galactosylmaltosid).The direct action of amylase with this substrate
results in the release of more than 90% of 2-chloro -4-nitrophenol, which can be monitored by

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 224
kinectic assay at 405 nm.The increase in absorbance is directly proportional to the amylase
activity in sample.
Gal G2 –α CNP α- amylase CNP + Gal G2
STATISTICAL ANALYSIS
� Data was analysed using primer software..
� The values were quoted in the form of mean ± standard deviation.
Statistical analysis of the result was done by unpaired student “t”-test.
� The p value (p< 0.05) was used to find the significance.
RESULTS: In our study, the mean values of transaminases (ALT&AST) levels were significantly
increased in PEM than in controls ( table I).
Table I .Comparision of ALP, AST and ALT Between group A (PEM) and Group B (Control)
Enzyme (units) Group A PEM ( N =30 )
.Mean ± SD
Group B CONTROL ( N =30 )
.Mean ± SD
P value
ALP (IU/L)
6.77*** ± 0.23 12.82 ± 0.27
<0.001
AST(IU/L)
73.43*** ± 2.73 31.83 ± 1.16
<0.001
ALT(IU/L)
82.96*** ± 2.11 29.43 ± 0.90
<0.001
The mean values of Alkaline phosphatase leve(ALP) was significantly higher in PEM than
controls shown in table I.
Table II. Comparison of serum amylase between group A (Kwashiorkor) and Group B
(Control)
Kwashiorkor
Enzyme (units) PEM ( N =17) CONTROL ( N =17 ) P value
AMYLASE (U/L) 47.64*** ± 10.97 80.17 ± 9.04 <0.001
The mean values of serum amylase was significantly higher in kwashiorkor than controls ( table
II).
Table III. Comparision of serum amylase between group A (marasmus) and Group B
(Control)
Marasmus
Enzyme (units) PEM ( N =13) CONTROL ( N =13 ) P value
AMYLASE (U/L) 79.30**± 7.66 81± 6.97 >0.05
The mean value of serum amylase was significantly higher in marasmus than controls ( table
III).

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 225
DISCUSSION: In our study, serum AST and ALT levels in PEM were significantly higher than that
of controls. Similar findings were reported by Kumari R et al 2 that the mean serum values of
aspartate aminotransferase, alanine aminotransferase in patients with PEM were significantly
higher than the controls. Similerly our findings also mimics with study conducted by McLean
AEM 3 in his study he showed that the activity of alanine aminotransferase in serum was
increased, and that greater the value greater was the mortality. Our finding also resembles with
Rao A et al 4 in their study, the aminotransferase elevated. Our study also coinside with
Karmacharya K et al5 .It is suggested that the moderate rise in aminotransferases found in
PEM is not due to damage to the liver. There is increased metabolism of amino acids released
from increased tissue breakdown. Thus process of transamination is enhanced leading to
increased activity of ALT and AST 13.
Serum alkaline phosphatase level in PEM was significantly lowered than controls.
Similar findings were reported by Karmacharya K5,Singh R.S et al7 and Schwartz R6 In PEM,
lowering of serum values of ALP could be explained on the basis of generalized protein
deficiency leading to impaired synthesis. Failure of bone growth may also contribute to the
lowering ALP value14.
Serum amylase in kwashiorkor was lower than marasmus.The low levels of amylase in
serum are accompanied by a reduced output of pancreatic enzymes into the gut, as pancreas is
the first organ to get damaged leading to degeneration and atrophy12.
CONCLUSION: The present study shows that any type of PEM can be associated with alteration
in levels of serum enzymes. Many of these abnormalities are probably due to metabolic
readjustment resulting from PEM. The ultimate practical objective of the enzyme studies which
have been described is to help in the management of PEM, as it is often supposed that this is a
practical problem for which new scientific knowledge is not needed.
Above mentioned view is a superficial. We are faced with the possibility that 'marginal
malnutrition' in childhood may cause a permanent impairment, and yet we cannot recognize or
define this 'marginal malnutrition' with any precision. But this can be done with the enzyme
studies described above.
REFERENCES:
I. 1."World Bank Report". Source: The World Bank (2009).
http://web.worldbank.org/WBSITE/EXTERNAL/COUNTRIES/SOUTHASIAEXT/
0,,contentMDK:20916955~pagePK:146736~piPK:146830~theSitePK:223547,0
0.html. Retrieved 2009-03-13. "World Bank Report on Malnutrition in India"
II. Kumari R., Rao Y.N., Talukdar B. et.al., Serum Enzyme Abnormalities in Protein
Energy Malnutrition, Indian Pedtr 1993;30:469-473.
III. McLean AEM. Heptic Failure in Malnutrition. Lancet 1962,2; 1292-1294.
IV. Rao A., Cherian A., Onuora C.U. Suvarnabai P.C. Serum Amonitransferases and r-
glutamyl transferase in Protein Energy Malnutrition. Trop Geogr Med. 1985,
37:11-14.
V. Karmacharya K, Islam MN, Role of Serum Alanine Aminotransferase Aspartate
Aminotransferase and Alkaline Phosphatase in Early Detection of Protein Energy

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 226
VI. Malnutrition, J. Nepal Paediatr. Soc. Vol 27, No. 2.
VII. Schwartz R. Alkaline Phosphatase Activity in Kwashiorkor, Journal Clin Path
1956, 9:333
VIII. Singh R.S, Agrawal S.P. & Dikshit S.K., Serum Enzymes in Nutritional Muscular
Wasting. Ind J. Pedtr. 1972, 39:299: 383-388.
IX. 8.Autozyme new alkaline phosphatase enzymatic, manufactured by Accurex
Biomedical private limited, Thane, India. Kit.
X. 9.Autozyme new aspartate aminotransferase enzymatic, manufactured by
Accurex Biomedical private limited, Thane, India. Kit.
XI. Autozyme alanine aminotransferase enzymatic, manufactured by Accurex
Biomedical private limited, Thane, India. Kit.
XII. Autozyme infinite amylase enzymatic, manufactured by Accurex Biomedical
private limited, Thane, India. Kit.

CASE REPORT
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 227
CLEAR CELL MYOEPITHELIAL CARCINOMA OF OROPHARYNX : A CASE
REPORT Dr. Adil S. A. K, Dr. G. Nataraju, Dr. Ravi Kumar T.
1. Assistant Professor, Department of Pathology, Mysore Medical College & Research Institute, Mysore.
2. Professor, Department of Pathology, Mysore Medical College & Research Institute, Mysore.
3. Post Graduate Student, Department of Pathology, Mysore Medical College & Research Institute, Mysore.
CORRESPONDING AUTHOR
Dr. S.A.K. Adil,
# 259, 5th Main,
Bannimantap, ‘C’ Layout, Mysore, E-mail: [email protected], Ph: 09019691259.
ABSTRACT: Myoepitheliomas are rare neoplasms. We present a case of clear cell myoepithelial
carcinoma arising from submucosal minor salivary glands of oropharynx.The significance of this
lesion is that it is a recent entity1,2 and it shares morphological similarities with many
neoplasms that pose a challenge in the diagnosis.
It has to be distinguished from benign myoepitheliomas and neoplasms with
predominantly clear cells like mucoepidermoid carcinoma, clear cell carcinoma, acinic cell
carcinoma, metastatic renal cell carcinoma etc. Imaging studies were unremarkable and
immunohistochemistry was crucial for the diagnosis.
KEYWORDS: Myoepithelial Carcinoma- clear cell variant, minor salivary gland, Oropharynx.
INTRODUCTION: Primary myoepithelial tumors in oral cavity are rare neoplasms.1 Clinically,
they commonly present as painless mass.
Clear cell myoepithelial carcinoma is very rare and it is recently considered as a separate
tumour entity2.Awareness of this lesion is important as the differential diagnosis of this lesion
can be extensive. These neoplasms diagnostically require evidence of myoepithelial
differentiation.
In this report, we present a rare case of clear cell myoepithelial carcinoma arising from
minor salivary glands in oropharynx.
CASE HISTORY: A 75-year-old male, presented with difficulty in swallowing not associated
with pain since one month. No history of known malignant diseases was present. Clinical
examination revealed a proliferative growth of 4x3 cm in the oropharynx on the posterior
pharyngeal wall.X-ray chest and ultrasonographic study of abdomen was found to be normal.
PATHOLOGICAL FINDINGS: Grossly, the specimen consisted of an irregular brown bit of tissue
measuring 1x0.5 cms. Cut section was grey white. The entire tissue was taken for processing.
Microscopically the sections showed a neoplasm comprising of monomorphic population of
clear cells arranged in solid nodules separated by fibrous septa. These cells contain abundant
amount of cytoplasm and bland nucleus, which was central to eccentrically placed.Occasional
cells showed granular eosinophilic cytoplasm.The neoplasm showed invasion into the adjacent
stroma.Necrosis was not evident and mitotic figures were rare. Immunohistochemical studies

CASE REPORT
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 228
confirmed the nature of the tumor. The cells showed immunopositivity for cytokeratins, p63, S-
100 and caldesmon.
DISCUSSION: Myoepithelial carcinoma has been recently recognised as a separate tumour
entity1,2.. Clear cell variant of myoepithelial carcinoma is comparatively much rarer than other
variants and only few cases have been reported in literature.
It has a wide age distribution ranging from 14-86yrs1 and is usually encountered in the
parotid gland, nasopharynx, paranasal sinus, nasal cavity and breast. Clinically, they usually
present as painless mass.
The neoplasm exhibits a wide spectrum of cytomorphologic features and the tumour
cells often are spindled, stellate, epithelioid, plasmacytoid (hyaline), or, occasionally, vacuolated
With signet ring like appearance.1,5.
Clear cell tumours are a challenge to diagnosis as variety of lesions have similar
morphological features. Myoepithelial carcinoma can be distinguished from benign
myoepithelial tumours by invasion of the neoplasm into the adjacent stroma1, which was
evident in our case.
The neoplasm showed monomorphic population of clear cells similar to clear cell-rich
salivary gland tumors which include mucoepidermoid carcinoma, pleomorphic adenoma, acinic
cell carcinoma, clear cell carcinoma.
Mucoepidermoid carcinoma consists of mucin containing cells, squamous cells, and
intermediate cells. Pleomorphic adenoma is identified by the distinct chondro/fibromyxoid
stroma and acinic cell carcinoma and clear cell carcinoma stain negatively for myoepithelial
markers.
Imaging studies were undertaken to exclude any renal mass.
Immunohistochemistry plays a critical role in the diagnosis of this tumour.
Cytokeratin expression indicated the epithelial nature of this neoplasm and the
myoepithelial markers p63, caldesmon and S-100 which were positive in our case,confirmed the
diagnosis as myopithelial carcinoma.
Literature search reveals the therapy options for this lesion are conservative excision
with a margin of uninvolved tissue or radiation and chemotherapy which also has resulted in a
significant shrinkage of the tumour.5, 6, 7.
CONCLUSION: Clear cell myoepithelial carcinoma can share morphological features with
various clear cell entities and pathologists should be aware of this lesion.
New immunohistochemical markers for myoepithelial cells which are crucial for
accurate diagnoses of this neoplasm are p63, and caldesmon along with S-100.

CASE REPORT
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 229
fig1 Malignant cells with clear cytoplasm
and bland nucleus(H & E,X 40)
Fig 3- Tumor cells showing cytoplasmic
positivity for cytokeratin
immunostain(X 20)
5- Tumor cells showing cytoplasmic
positivity for caldesmon immunostain(X
10)
Fig 2- Malignant cells infiltrating into
stroma(H & E,X 20)
Fig 4- Tumor cells showing nuclear
positivity for p63 immunostain(X 20)
6- Tumor cells showing variable nuclear
and cytoplasmic light intensity stain in
myoepithelial cells for S- 100 (X 40)
REFERENCES:
I. Barnes L, Eveson J. W, Reichart P, and Sidransky D. World Health Organization
Classification of Tumours. Pathology and Genetics of Head and Neck Tumours,
IARC Press, Lyon, France, 2005.p242-243
II. Wang B,Brandwein M, Gordon R, Robinson R, Urken M, Zarbo R J. Primary
Salivary Clear Cell Tumors-A Diagnostic Approach. Arch Pathol Lab Med. 2002;

CASE REPORT
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 230
Vol126 (6):676-685
III. Savera A T, Sloman A, Huvos A G, Klimstra D S. Myoepithelial carcinoma of the
salivary glands: a clinicopathologic study of 25 cases. Am J Surg Pathol. 2000; vol
24(6):761-74.
IV. Fletcher.C.D.M. Diagnostic pathology of tumors, 2ndedition, Vol.1, London;
Churchill Livingstone, 2000.p250-251
V. Rosai.J.Rosai and Ackerman's Surgical Pathology.9thedition.Vol 1
India;Elsevier, 2011.p888-89
VI. Ren J,Liu Z,Liu X,Li Y,Zhang X , Li Z,Yang Y,Yang Y,Chen Y,Jiang S Primary
myoepithelial carcinoma of palate. World J Surg Oncol.2011; 9:104
doi10.1186/1477-7819-9-104.
VII. Mills S.E,Carter.D,Greenson.K.J,Oberman.A.H, Reutar.V,Stoler.M.H.Sternbergs
Diagnostic Surgical Pathology.Vol 2.U.S.A.Lippincott Williams &Wilkins.2004.pp 943-944.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 231
A COMMUNITY BASED STUDY ON INFANT AND YOUNG FEEDING
PRACTICES IN A RURAL AREA OF KARNATAKA. Dr. Sharvanan Udayar E. Dr. Angadi M. M, Dr. Rekha Udgiri, Dr. Santosh Patil D.
1. Assistant Professor, Department of Community Medicine, PES Institute of Medical Science and Research,
Kuppam. 2. Professor & HOD, Department of Community Medicine, BLDEU’s Shri B. M. Patil Medical College, Bijapur.
3. Professor, Department of Community Medicine, Shri. B. M. Patil Medical College, Bijapur.
4. Assistant Professor, Department of Community Medicine, Shri B. M. Patil Medical College, Bijapur.
CORRESPONDING AUTHOR:
Dr. Sharvanan. E,
PES Institute of Medical Science and Research,
Kuppam, Chittoor Dist, Andhra Pradesh-517425,
E-mail: [email protected],
Ph: 09618292770/08095515455.
ABSTRACT: BACKGROUND: Adequate nutrition during infancy and early childhood is critical
to the development of children’s full human potential. OBJECTIVE: The main objective was to
assess the Infant and Young Child Feeding (IYCF) practices and associated socio demographic
variables among children aged less than two years in rural areas METHODS: A community
based, cross sectional descriptive study was done during Sept 09-Aug 2010 which is the rural
field practice area of Shri. B. M. Patil Medical College SBMPMC. The data was computed and
analyzed using SPSS statistical package (version 13.0). RESULTS: During the study period 264
mothers of infants and young children interviewed with the questionnaire and 159 out of 264
had received prelacteal feeds (males 64 % and females56.3 %). Illiterate mothers (69.7%)
practiced more prelacteal feeding than the literate mothers (54.6%). 36% received exclusive
breast feeding for a period six months. Majority of the illiterate mothers were practicing early
(31.4%) and delayed weaning (32.5%).Poor socioeconomic status, illiteracy, birth spacing and
cultural beliefs had significant effect on infant and young children feeding practices.
CONCLUSIONS: The study re-emphasized the need for conducting continued infant and child
feeding intervention programmes especially for the mother during antenatal and postnatal
checkups.
KEY WORDS: Exclusive breast feeding, Weaning, Infant and Young children.
INTRODUCTION: Adequate nutrition during infancy and early childhood is critical to the
development of children’s full human potential. Poor Infant and Young Child Feeding (IYCF)
practices, coupled with high rates of infectious diseases, are the proximate causes of
malnutrition during the first two years of life. The second half of an infant’s first year is an
especially vulnerable time, when breast milk alone is no longer sufficient to meet his or her
nutritional requirements and complementary feeding should start1. Of the 19 million infants in
the developing world who have low birth weight (< 2,500 grams), 8.3 million are in India. This
means that approximately 43 per cent of all the world’s infants who are born with a low birth
weight are born in India. Malnutrition is an underlying cause in up to 50 per cent of all under-
five deaths. About 55 million, or one-third, of the world’s underweight children under age five
live in India.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 232
Children need complementary foods in addition to breast milk from the age of six
months. In India, common problems include the provision of poor quality complementary foods,
insufficient amounts of complementary foods, insufficient breastfeeding, detrimental feeding
practices, and contamination of complementary food and feeding utensils. In addition, if
complementary foods are given too early or too frequently, they displace breast milk, which is of
higher nutritional value than other foods. Various social, economic and cultural factors in rural
areas will also influence the IYCF practices2.
The timely introduction of complementary feeding can prevent almost 6% of under-five
mortality. It was estimated that, if 90% of infants are covered with a package of intervention to
protect, promote, and support the optimal IYCF practices, almost one-fifth of overall under-five
mortality can be averted. The World Health Organization (WHO) and other various
international agencies recommended exclusive breastfeeding for the first six months of life with
early initiation and continuation of breastfeeding for two years or more together with
nutritionally-adequate, safe, age-appropriate complementary feeding starting at six months3.
With this background, the present study was undertaken to assess the IYCF practices and
associated socio demographic variables among children aged less than two years in rural areas
of Bijapur, District, Karnataka.
METHODS: A community-based, cross-sectional descriptive study was conducted in Shivanagi
during Sept 09-Aug 2010 which is the rural field practice area of Shri B.M.Patil Medical College,
situated 27km away from Bijapur and has population of 7060.4A house to house survey was
done and mothers with children aged less than two years were included in the study. Those who
were not permanent residents and not willing to participate were excluded and Modified
B.G.Prasad socioeconomic classification5 was used classifying socioeconomic status.
ETHICS: The Institutional Ethics Committee of the Shri B.M.Patil Medical College approved the
study.
STATISTICS: Analysis was done using the SPSS software (version 13.0), Simple proportions
were calculated for each IYCF practice. The differences in the feeding practices and
sociodemographic variables if any were noted using chi-square test.
RESULTS: In the present study 264 infants and young children up to 2 years were studied of
whom 136 were males and 128 were females.159 out of 264 had received prelacteal feeds
(males 64 % and females 56.3%).Illiterate mothers (69.7%) practiced more prelacteal feeding
than the literate mothers (54.6%) and the observed difference according to education of the
mother was not statistically significant in our study (p=0.015). 53.3% of nuclear families
were giving more prelacteal than three generation (62%) and joint family (63%) (Table1).
However the difference in type of family and prelacteal practices was not
statistically significant in our study (p=0.38). The study also found that the practice of prelacteal
feeding was more prevalent in lower socioeconomic group than in higher class and this
difference was found to be statistically significant(P<0.001).
Only 36% received exclusive breast feeding for a period six months and less than half of
the infants and young children belonged to Hindu and Muslim families received exclusive breast
feeding, literate mothers (41.9%) were more aware about it as compared to illiterate
mothers(26.3%).Statistically significant difference was observed according to socioeconomic

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 233
status and exclusive breastfeeding (p<0.001).Similarly with the birth interval (p=0.07) (Table
2).
With respect to weaning, majority of the illiterate mothers were practicing early
(31.4%) and delayed weaning (32.5%).Only literate mothers (56.9%) initiated it at the age of 6
months as per the WHO guidelines5. Poor socioeconomic status (p=0.001) and birth interval
(p=0.002) also had an effect on initiation of weaning.
DISCUSSION: In our study more than half of the infants and young children had received
prelacteal feeds and it was high in children with illiterate mothers belonging to poor
socioeconomic status and most important reason for this was family customs and relatives
advice. Similar findings were observed in a study by Devang raval6 (2001) in which 61.9% of
infants had received prelacteal feeds. According to NFHS-3 report7 (2005-2006) 57% newborns
received prelacteal feeds (57.3% male and 57% female) and 67.5% of the illiterate mothers
gave prelacteal feeds. Saurav et al8(2003) also reported similar findings.
Exclusive breastfeeding by mothers as derived from our study is much lower than the
values reported by Devang raval6, Chatterjee Saurav et al8 and however this when compared to
study by Vyas Shaili et al 9 in rural areas of Uttarakhand was much higher. This may be because
of the low literacy levels and customs and many of the mothers gave reasons as insufficient
breast milk and could not able to feed during illness.
Majority of the mothers practiced early and delayed weaning and this trend observed
higher among illiterate mothers. The findings from the present study clearly highlights the
importance of educating the women on infant and child feeding practices and the knowledge
may be imparted even at the school or college level. The Government of India recommends that
children should be exclusively breastfed for the first six months of life (that is, they should be
given only breast milk with no other liquids or food). There are many reasons for
recommending exclusive breastfeeding for the first six months. First, breast milk is nutritionally
superior to other liquids and solid foods. Second, when a child consumes other liquids and solid
foods, the intake of breast milk is reduced, which in turn decreases the mother’s supply of milk.
Third, feeding young infants liquids and solid foods increases their exposure to pathogens,
putting them at greater risk of contracting diarrhoeal disease. There is also need for conducting
infant and child feeding intervention programmes especially for the mother during antenatal
and postnatal checkups.
Practices such as early or delayed inititation of weaning should be discouraged and
women organizations need to be associated for active dissemination of information on infant
and child feeding practices to educationally deprived women.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 234
Table 1: Distribution of Prelacteal feed practices in infants and young children (n=264).
Parameters
Prelacteal
feed given n=159
percent (60.3%)
Prelacteal
feed not given
n=105 percent
(30.7%)
Chi
square
Gender
Male136 (51.8)
Female128 (48.2)
87 (64.0)
72 (56.3)
49(36.0)
56(43.7)
Chi
sq.:1.61
p=0.2
Religion
Hindu 236 (89.7)
Muslim28 (10.3)
147(62.3)
12(43.0)
89(37.7)
16(57.0)
Chi
sq.:3.99
p=0.04
Education
of Mother
Illiterate99 (37.5)
Literate165 (62.5)
57(69.7)
82(54.6)
42(30.3)
83(45.4)
Chi sq.:
1.6
p>0.5
Type of Family
Nuclear 62 (23.5)
3gene 105 (40.0)
Joint 97 (36.5)
33(53.0)
65(62.0)
61(63.0)
29(47.0)
40(38.0)
36(37.0)
Chi sq.:
1.68
p=0.43
Socio
Economical class
Class I 7 (2.90)
Class II 7 (2.9)
Class III 66 (25.10)
Class IV 89 (33.75)
Class V 95 (35.40)
2(28.6)
6(85.8)
23(34.9)
63(70.8)
65(68.4)
5(71.4)
1(14.2)
43(65.1)
26.(29.2)
30(31.6)
Chi
sq: 24.64
p<0.001

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 235
Table 2: Distribution of exclusivebreastfeeding practices in infants and young
children (n=264).
Parameters
EBF given
n=95 percent
(36.0%)
EBF not given
n=169 percent
(64.0%)
Chi square
Gender
Male136 (51.8)
Female128 (48.2)
40(29.4)
55(42.3)
96(70.6)
73(57.7)
Chi sq.:5.4
p=0.02
Religion
Hindu 236 (89.7)
Muslim28 (10.3)
87(36.9)
8(28.6)
149(63.1)
20(71.4)
Chi sq.:0.68
p=0.38
Education
of Mother
Illiterate99 (37.5)
Literate165 (62.5)
29(26.3)
66(41.9)
70(73.7)
99(58.1)
Chi sq.: 3.06
P=0.07
Type of Family
Nuclear 62 (23.5)
3gene 105 (40.0)
Joint 97 (36.5)
24(38.7)
32(30.5)
39(40.2)
38(61.3)
73(69.5)
58(59.8)
Chi sq.: 2.33
p=0.31
Socio
Economical class
Class I 7 (2.90)
Class II 7 (2.9)
Class III 66 (25.10)
Class IV 89 (33.75)
Class V 95 (35.40)
2(28.5)
5(71.4)
38 (57.6)
23 (25.9)
29(30.6)
5(71.5)
2(28.6)
28(42.4)
66(74.1)
66(69.4)
Chi sq: 19.9
p<0.001
Birth interval
<1yr 45 (17.3)
1-2 yr 143(54.3)
>3yrs 76(28.4)
28(62.2)
51(35.7)
34(44.8)
17(37.8)
92(64.3)
42(55.2)
Chi sq: 10.0
p=0.007
ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 236
REFERENCES:
I. Improving Complementary Feeding Practices: A Review of Evidence from South Asia .
Evidence review series march 2008; Available from
http://www.intrahealth.org/~intrahea/files/media/maternal-neonatal-and-childrens-
healthfamily-planning/ER_Brief_CF%202.pdf.
II. Cooperative for Assistance and Relief Everywhere(CARE). Infant and Young Child
Feeding Practices. Collecting and Using Data: A Step-by-Step Guide.2010.Available from
http://windowofopp.files.wordpress.com/2010/12/final-iycf-guide-iycf-practices.pdf.
III. Apurba S, Dipta KM, Tanmay KP, Asit BS, Nirmal KM, Akhil BB. Infant and Young Child
feeding Practices in Bankura District, West Bengal, India. J Health Popul Nutr
2010Jun;28(3):294-299.
IV. Govt.of India (2001).Census of India 2001, Provisional Population Totals, Paper-1 of
2001.
V. Insurance worker volume XLVII, No.12, Dec 2008 and Insurance worker volume XLVIII
No. 10, Oct 2009.
VI. World Health Organization (WHO). Maternal, newborn, child and adolescent health:
Indicators for assessing infant and young child feeding practices – part I: definition;
2008.
Availablefromhttp://www.who.int/maternaments/9789241596664/en/l_child_adolesc
ent/docu.Accessed latest on 28-08-2012.
VII. Devang R, Jankar DV, Singh MP. A study of breast feeding practices among infants
living in slums of Bhavnagar city, Gujarat, India. healthline Jul-Dec 2011; 2(2):73-82.
VIII. National Family Health Survey 2005-2006 (NFHS-3). Mumbai: International Institute of
Population Sciences.Available from: http://www.nfhsindia.org.
IX. Chatterjee Saurav , Saha Sandhita: A study on KP of mothers regarding infant feeding
and nutritional status of Under 5 children attending immunization clinic of Medical
college 2008.Avalable from http://www.ispub.com/journal/the-internet-journal-of-
nutrition-and-wellness/archives.html.Accessed latest on 29-08-2012.
X. Vyas S, Sharma P, Kandpal S D, Semwal J, Srivastava A, Nautiyal V. A community based
study on breastfeeding practices in a rural area of Uttarakhand. National J Commuity
Med Apr-jun2012;3(2):283-287.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 237
ATHEROGENIC INDEX OF PLASMA IN MYOCARDIAL INFARCTION IN
RURAL POPULATION OF MARATHWADA REGION
Dr. Ganesh D Ghuge, Dr. Rahul Zine.
1. Associate Professor, Department of Biochemistry, Rural Medical College, Loni, Ahmednagar, Maharashtra.
2. Assistant Professor, Department of Biochemistry, Indian Institute of Medical Sciences and Research, Jalna,
Maharashtra.
CORRESPONDING AUTHOR
Dr. Ganesh D Ghuge, Associate Professor, Department of Biochemistry,
Rural Medical College, Loni, Taluka- Rahata,
District- Ahmednagar, Maharashtra 413736.
E-mail: [email protected],
Ph: 91-9850694964, 91-7588846300.
ABSTRACT: BACKGROUND: Extensive research work by mankind over several decades has
concluded that cure as well as the treatment of CAD is very difficult hence attention towards
prevention of such ischemic events is of utmost importance. METHODS: The present study was
conducted with an aim to study the Atherogenic Index and various lipid levels of plasma in
Acute Myocardial Infarction (AMI) and to compare lipid profile and Atherogenic Index of plasma
in the patients of Myocardial Infarction with healthy controls. RESULTS: A total of 150acute
Myocardial Infarction (AMI) patients for the study were selected from the Medicine Ward, ICU,
and OPD. Normal healthy person of matched number, age and sex of the study group were used
as control. Serum cholesterol, TGVLDLc, LDLc and AIP were significantly higher in AMI patients
as compared. CONCLUSION: Atherogenic Index of plasma is very useful research tool to assess
the effect of risk factors pertaining cardiovascular diseases.
KEYWORDS: Atherogenic index, lipid profile, myocardial infarction, triglycerides.
INTRODUCTION: Coronary Artery diseases (CAD) are the most frequent cause of death in
developing country like India (1). Extensive research work by mankind over several decades
has concluded that cure as well as the treatment of CAD is very difficult hence attention towards
prevention of such ischemic events is of utmost importance. The famous Framingham study
firmly established cholesterol as an important risk factor for CAD and now we have a clear
perception of the inter-relationship between serum lipids, Atherosclerosis & Ischemic Heart
Disease (IHD) (2). Therefore research laboratories have made conflicting claims to the helpful
serum lipid level predictor for detecting and managing IHD with emphasis on the measurement
of levels of serum cholesterol, lipoproteins and Triglycerides. The Atherogenic index of plasma
defined as log (TG / HDLc) has recently been proposed as a marker of plasma atherogenicity
(3). It is increased in people at higher risk of CAD .Tan et al used the AIP, calculated as log (TG /
HDLc) with TG and HDLc expressed in molar concentration(4). Value of AIP corresponds closely
to those of esterification rate in apo-B-lipoprotein – depleted plasma and to lipoprotein particle
size. AIP reflects the delicate metabolic interactions within the whole lipoprotein complex (3).
The present study was conducted with an aim to study the Atherogenic Index and various lipid
levels of plasma in Acute Myocardial Infarction (AMI) and to compare lipid Profile and
Atherogenic Index of plasma in the patients of Myocardial Infarction with healthy controls.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 238
MATERIALS AND METHODS: The present study was conducted in Department of
Biochemistry, S R T R Medical College Ambejogai, Maharashtra, India. A total of 150 Acute
Myocardial Infarction (AMI) patients for the study were selected from the Medicine Ward, ICU,
and OPD. Normal healthy person of matched number, age and sex of the study group were used
as control.
COLLECTION OF SAMPLE: The fasting blood sample was obtained in plain bulb from the study
group and control group from antecubital vein with all aseptic precaution.
ESTIMATION OF LIPID PROFILE: The blood samples collected from the study and control
group were estimated for lipid profile by a routine biochemical Kits methods using ERBA Chem
5+ Semi-automated machine. Estimation of Serum Cholesterol was done by (Enzymatic)
Dynamic extended stability CHOD – PAP method, End point with Lipid clearing agent. Serum
HDL cholesterol was estimated by Phosphotungstic Acid Method, End Point. Estimation of
Serum Triglyceride was done by Dynamic extended stability End point with Lipid clearing agent,
Trinder Method. VLDLc and LDLc are calculated parameters and they calculated using
Friedwald’s Formula, TG/5 where TG is less than 400 mg/dl, LDLc was calculated as : TC -
(HDLc + VLDLc) these two are calculated parameters. AIP calculated as log (TG/HDLc) when
expressed in molar concentration. Conversion factor for Cholesterol –mg% X 0.026 = mmol/lt.
Conversion factor for Triglyceride - mg% X 0.0113 = mmol/lt (Glycerol phosphate oxidase).
RESULT: As shown in table 1 Serum cholesterol, TG, VLDLc, LDLc and AIP were significantly
higher in AMI patients as compared to controls while HDLc was significantly lower in AMI
patients as compared to controls.
DISCUSSION: The coronary atherosclerosis is the major cause of IHD, which is chief single cause
of death both in developed and developing countries. Early diagnosis of coronary
atherosclerosis can reduce the mortality and morbidity. There are several biochemical ratios
indicating the risk of atherosclerosis. Gaziano et al reported that the ratio of triglyceride to
HDLc was a strong predictor of MI (5). As the search for the risk factor responsible for the CAD
goes on many ratio of the lipid have been described as better predictor of CAD. These ratios are
total cholesterol / HDLc, LDLc / HDLc and HDLc2 / HDLc3. Result of the Lipid Research Clinics
Prevalence Study showed that the ratio of Total Cholesterol / HDLc was better predictor of CAD
(6). Tan et al found AIP to be a suitable and statically reliable for evaluating the atherogenicity
index (4). Although an independent, inverse relationship between HDLc and cardiovascular risk
has been demonstrated beyond any doubt. TG has also been proposed to be a major
determinate of cholesterol esterification / Transfer and HDL remodeling in human plasma (7).
Fraction etherification rate of cholesterol and ratio of TG / HDLc are powerful predictor of
positive finding on coronary angiography (8) .The plasma parameter of log ( TG / HDLc ) as an
atherogenic index has correlation with lipoprotein particle size and esterification rate in apo B –
lipoprotein depleted plasma ( FER HDL ) (5). There is a high significant association between
FER HDL and AIP, suggesting that AIP reflects the delicate metabolic interaction with in the
whole lipoprotein complex (9). AIP provides information about the atherogenicity of plasma.
Application of AIP to data from earlier trials may offer new insights. The authors, Tan et al
should be complimented for evaluating this Atherogenic Index to test it’s significance and
statistical reliability in a large study with 1669 Diabetic patients (10). Nwagha and Ikekpeazy
also reported AI of plasma as an useful predictor of cardiovascular risk among postmenopausal

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 239
women in Enugu, Nigeria (11). They found AIP to be a suitable reliable. AIP may be an
important tool for analyzing the results of clinical trials. The association of TGs and HDLc in this
simple ratio theoretically reflects the balance risk and protective lipoprotein forces, and both
TGs and HDLc are widely measured and available (12, 13).
CONCLUSION: Atherogenic Index of plasma can now easily measured in humans and is very
useful research tool to assess the effect of risk factors. Although AIP assumes to play a
predominant role in evaluation of AMI and developing coronary atherosclerosis, more research
is needed on measurement of AIP to be used as clinically useful tool.
Table.1 Lipid profile and Atherogenic index of plasma in patients with AMI and controls.
Parameter Healthy Control AMI Cases
Total cholesterol 145.24 ± 25.42* 232.04 ± 65.23*
Triglyceride 123.94 ± 39.38 * 206.44 ± 101.10 *
HDLc 51.12 ± 8.45* 30.50 ± 8.01*
VLDLc 24.67 ± 8.11* 40.08 ± 20.36*
LDLc 91.54 ± 26.41* 161.10 ± 61.00*
AIP 0.470 ± 0.308* 0.24 0.30*
* indicates p < 0.05.
ƢƢƢƢ All values were expressed in mg/dl ± SD Number of subjects is 50. While calculating AIP
values were expressed in mmol/lt.
REFERENCES:
1. Kundu S C, Bhattachajee T D: Profile in Myocardial Infarction among the rail road
workers I Eastern India a 6 year study. Indian H Journal. 1982; 34:151-155.
2. National Cholesterol Education Programme Expert Panel: Expert Panel report on
detection, evaluation and treatment of high blood cholesterol in adults. Arch. Inter. Med.
1988; 148: 36-69.
3. Dobiáová M, Frohlich J. The plasma parameter log (TG/HDL-C) as an atherogenic index:
correlation with lipoprotein particle size and esterification rate in apoB-lipoprotein-
depleted plasma (FERHDL). Clin Biochem 2001; 34:583-588.
4. Tan MH, Johns D, Glazer NB. Pioglitazone reduces atherogenic index of plasma in
patients with type 2 diabetes. Clin Chem 2004; 50:1184-1188.
5. Gaziano JM, Hennekens CH, O’Donnell CJ, Breslow JL, Buring JE. Fasting triglycerides,
high-density lipoprotein, and risk of myocardial infarction. Circulation 1997; 96:2520-
2525.
6. Dobiáová M, Stíbrná J, Pritchard PH, Frohlich J. Cholesterol esterification rate in plasma
depleted of very low and low density lipoproteins is controlled by the proportion of
HDL2 and HDL3 subclasses: study in hypertensive and normal middle-aged and
septuagenarian men. J Lipid Res 1992; 33: 1411-1418.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 240
7. Frohlich J, Dobiáová M. Fractional esterification rate of cholesterol and ratio of
triglycerides to HDL-cholesterol are powerful predictors of positive findings on
coronary angiography. Clin Chem 2003; 49:1873-1880.
8. Dobiáová M, Ralová K, Rauchová H, Vohnout B, Ptáková K, Frohlich J. Atherogenic
lipoprotein profile in families with and without history of early myocardial infarction;
fractional esterification rate of cholesterol in plasma depleted of apoB lipoproteins
(FERHDL) and logarithmically transformed ratio of triglycerides to HDL-cholesterol.
Physiol Res 2001; 50: 1-8.
9. Dobiáová M. Atherogenic Index of Plasma [Log (Triglycerides/HDL-Cholesterol)]:
Theoretical and Practical Implications. Clin. Chem 2004; 50: 1113-1115.
10. Lehto S, Ronnemaa T, Pyorala K, Laakso M. Cardiovascular risk factors clustering with
endogenous hyperinsulinaemia predict death from coronary heart disease in patients
with type II diabetes. Diabetologia 2000; 43:148-155.
11. Nwagha UI, Ikekpeazy EJ. Atherogenic index of plasma as useful predictor of
cardiovascular risk among postmenopausal women in Enugu, Nigeria. Afr. Health Sci
2010; 10(3):248-252.
12. Hokanson JE, Austin MA. Plasma triglyceride level is a risk factor to cardiovascular
disease independent of high-density lipoprotein cholesterol level: a meta-analysis of
population based prospective studies. J Cardiovasc Risk 1996; 3:213-219.
13. Guérin M, Le Goff W, Lassel TS, Van Tol A, Steiner G, Chapman MJ. Proatherogenic role of
elevated CE transfer from HDL to VLDL1 and dense LDL in type 2 diabetes. Arterioscler
Thromb Vasc Biol 2001; 21:282-289.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 241
SPECIES DISTRIBUTION AND ANTIFUNGAL SUSCEPTIBILITY PROFILE
OF CANDIDA SPECIES ISOLATED FROM BLOOD STREAM INFECTIONS Sachin C. Deorukhkar, Dr. Santosh Saini.
1. Assistant Professor and PhD Student, Department of Microbiology, Rural Medical College, Loni,
Ahmednagar, Maharashtra.
2. Professor and Head, and PhD guide, Department of Microbiology, Rural Medical College, Maharashtra.
CORRESPONDING AUTHOR
Sachin C Deorukhkar,
Assistant Professor, Department of Microbiology,
Rural Medical College, Loni, Taluka- Rahata,
District- Ahmednagar, Maharashtra 413736.
E-mail: [email protected],
Ph: 91-9545181908, 91-9850775564.
ABSTRACT: BACKGROUND: Candidemia remains as one of the major cause of morbidity and
mortality in health care setting. Over the last two decades, the proportion of blood stream
infection (BSI) due to non-albicans Candida (NAC) species has increased. Several NAC spp. are
inherently resistant to commonly used antifungal drugs. The increased isolation rates of NAC
spp. and a gradual shift in the antifungal susceptibility profile underlines the need of early and
accurate diagnosis of infecting Candida spp. along with antifungal susceptibility testing for
selecting the most appropriate antifungal agent for therapy. AIM: The Aim of the present study
was to investigate the distribution pattern of Candida spp. isolated from candidemia patients
and evaluate its antifungal susceptibility pattern. SETTING AND DESIGN: The present study
was conducted in the department of Microbiology for a period of six years (January 2006 to
December 2011) which included, 194 Candida spp. isolated from the cases of candidemia.
MATERIALS AND METHODS: Candida isolates were speciated by conventional techniques and
HiCandida identification kit. Antifungal susceptibility test was performed using two disc
diffusion methods. Clinical details and risk factors were recorded and analyzed. RESULTS AND
CONCLUSIONS: Isolation of NAC spp. was significantly higher than Candida albicans. The most
important risk factor associated with candidemia was intensive care unit stay, followed by
diabetes and HIV infection. Azole resistance was more in NAC species as compared to C.
albicans. The early and accurate diagnosis of infecting Candida spp. along with antifungal
susceptibility testing plays a pivotal role in preventing morbidity and mortality associated with
Candida BSI. Disc diffusion technique for antifungal susceptibility using glucose methylene blue
Mueller- Hinton (GM-MH) agar was found to be simple, cost effective and sufficiently accurate
for the routine testing of antifungal susceptibility of Candida spp. in resource constrained
microbiology laboratories.
KEY WORDS: Candidemia, Candida albicans, NAC species, antifungal resistance
INTRODUCTION: Candida blood stream infection (BSI) has become a major problem in tertiary
care hospital worldwide 1. Despite some improvement in fungal BSI diagnosis during recent
years, diagnosis of candidemia remains difficult 2. Candidemia has been associated with many
risk factors like long- term hospitalization, antibiotic therapy, use of intravascular catheters, and
underlying diseases like diabetes and malignancy. Although Candida albicans continues to be

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 242
the most common cause of Candidal BSI, the epidemiology of species causing candidemia is
changing. Recent longitudinal studies have detected an increase proportion of BSI by non-
albicans Candida (NAC) species 3, 4.
Importantly many NAC spp. have decreased susceptibility to antifungal agents.
Specifically C. krusei and C. glabrata demonstrate decreased susceptibility to fluconazole 5. The
changing epidemiology of Candida BSI has generated concern about the emergence of azole
drug resistance and its clinical relevance.
Clinicians now depend on identification of Candida to the species level in order to
optimize the selection of antifungal agents allowing them to provide the best possible patient
care 6. Therefore there is a need for continuous surveillance to monitor trends in incidence,
species distribution and antifungal drug susceptibility profiles of Candida BSI.
The Clinical and Laboratory Standards Institute (CLSI) (previously National Committee
for Clinical Laboratory Standards (NCCLS)) after collaborative efforts with various laboratories
has recommended an in-vitro standardized macro broth dilution antifungal susceptibility
testing technique for yeasts 7. CLSI has recommended alternative techniques like ATB fungus,
API, Vitek and disc diffusion to address issues in different laboratories. These methodologies
give reproducible results.8 Disc diffusion procedure appears to be generally acceptable as a
simple, in house standardized procedure for antifungal susceptibility of yeasts 9.
The present study was carried out in a rural tertiary care hospital with an aim to
determine the distribution of Candida spp. isolated from the cases of candidemia and to
compare the efficacy of yeast nitrogen base with glucose (YNBG) media and glucose methylene
blue Mueller- Hinton (GM-MH) agar for the antifungal susceptibility testing of Candida isolates.
MATERIALS AND METHODS: The present study is part of a PhD thesis and was approved by
the Institutional Ethics Committee (Registration No.FN.32/2010). A total 194 Candida spp.
isolated from the blood of patients was included in the study.
The culture was considered true candidemia only when Candida spp. was isolated from
at least two blood culture samples or from a clinically significant single blood culture sample
among hospitalized patients 10. Patient's demographic features such as age, sex, ward, date of
admission, underlying illness, various associated risk factors like presence of urinary catheter,
respiratory ventilation, central line insertion, duration of antibiotic therapy and antifungal
prophylaxis if any, were recorded and analyzed.
SPECIES IDENTIFICATION: Speciation of Candida isolates was done by conventional
techniques and colony colour on Chrom agar 11 Hicandida identification kit (Himedia
Laboratories Pvt. Ltd Mumbai, India) was used for the identification of isolates which could not
be identified by conventional techniques.
ANTIFUNGAL AGENTS: The antifungal agents used were amphotericin B (10 µg), fluconazole
(25 µg), and itraconazole (10µg). Antifungal discs were procured from Himedia Laboratories
Pvt. Ltd Mumbai, India.
ANTIFUNGAL SUSCEPTIBILITY TESTS:
Antifungal susceptibility tests were performed using 2 disc diffusion methods.
1. Yeast Nitrogen base with glucose (YNBG) media.
2. Glucose methylene blue Mueller- Hinton (GM-MH) agar.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 243
ANTIFUNGAL SUSCEPTIBITY TESTING USING YNBG MEDIA:9 YNBG media was prepared
using yeast nitrogen base 10g and glucose 10g, dissolved in 100ml of distilled water and filter
sterilized. Susceptibility test against azoles was performed with addition of 1.5% L-asparagine
to YNBG media. YNBG media mixed with 2% sterile Difco agar (Difco, USA) was poured into 9cm
diameter Petri dishes. Inoculum size of 106 Candida cells/ml was inoculated in one half with the
control strain (C. kefyr Y/16). The cell density was spectrophotometrically adjusted to 0.5
McFarland standard. Inoculation was done by swabbing from the edge of the plate to the centre
using a sterile swab. Discs were placed in the centre of the control and test organism with the
help of sterile forceps. After incubation of the plate at 370C for 48 hours the diameter of
inhibition was read.
The result of the disc diffusion method was interpreted according to the following
criteria: test strain was considered sensitive when the zone diameter was ≥ 80% of the zone
diameter of control strain; intermediate when the zone diameter was < 80% but there was
visible zone of the inhibition; resistant, when there was no zone of inhibition.
2. BY USING GM-MH AGAR: Mueller-Hinton (MH) agar was solidified after addition of 2%
glucose and 0.5ug of methylene blue. Inoculum was prepared by picking five distinct colonies of
approximately 1mm from 24 hours old culture grown on Sabouraud's dextrose agar (SDA).
Colonies were suspended in 5ml of sterile 0.85% saline. This suspension was vortexed to adjust
the turbidity yielding 1x106-5x106 cells/ml and streaked on the entire surface of GM-MH agar.
The antifungal disc was placed 24mm apart from each other. The plates were incubated at 37oC
for 24 hours. If insufficient growth was observed after 24 hours the plates were read after 48
hours. Zone diameters were interpreted as per the approved CLSI /NCCLS (M44-A) guidelines 12. The quality control test was performed by using C. parapsilosis (ATCC 22019), C. krusei
(ATCC 6258), and C. albicans (ATCC 90028).
RESULTS: Between January 2006 to December 2011, out of 4984 blood culture samples
processed in Department of Microbiology, Candida spp. were isolated from the blood culture of
194 patients. Male predominance was noted in our study (n=126/194) 64.9%. Candidemia was
common in more than 50 years age group in males (n=58/126) 46.03%, whereas in females it
was with 0-10 years age group (n=22/68) 32.35% (Figure.1). The most important risk factor
associated with candidemia was ICU stay (49\194) 25.25%, followed by diabetes (40\194)
20.61% and HIV infection (38\194) 19.58% (Figure.2). In this study predominant isolates were
NAC spp. C. albicans was isolated from 78 (40.2%) cases. Among the NAC species, C. tropicalis, C.
glabrata and C. krusei were the major isolates. (Figure.3). All 194 isolates recovered were tested
for antifungal susceptibility by using YNGB medium and GM-MH agar. Their pattern of
resistance is summarized in Table 1. NAC spp. showed more resistance to antifungal agents as
compared to C. albicans.
DISCUSSION: In the last twenty years, various factors like the AIDS epidemic, increase in the
number immunosuppressive therapy recipients and the use of long term antibiotic therapy
have altered the epidemiology of invasive mycoses in general and of candidemia in particular.
Candida spp. is the fourth most common pathogens isolated from the blood of hospitalized
patients13. More recently, NAC spp. has been recovered with increasing frequency. Linked with
this is a recent increase in treatment failure of these infections to standard antifungal therapy,
largely due to the emergence of drug resistance in fungi.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 244
In our study the Candida spp. were isolated from 3.9% of total blood cultures processed
in the Department of Microbiology. Lot of variation in the prevalence and incidence of
candidemia have been reported from India. Kumar et al14 from South India reported an
incidence rate of 5.7% for candidemia among children with onco-haematological malignancies.
Verma et al 15 reported an incidence rate of 1.61% whereas, Xess et al 16 found a prevalence rate
of 6% for candidemia. A study by Sahni et al 17 from Maulana Azad Medical College, New Delhi,
found an incidence rate of 6.9% for Candida spp.
The age and sex distribution of the patients in our study correlates with the observation
of other researchers like Verma et al 15 and Hajjeh et al 18. The importance of risk factors analysis
cannot be over emphasized for infection like candidemia so that preventive measures and
prophylactic therapy can be initiated for patients at risk. Many studies have established
independent risk factors for candidemia on the basis of multivariate analyses. The ICU stay
followed by diabetes and HIV infection was the major risk factors responsible for candidemia in
our study. This was also an observation of other researchers like, Shivaprakasha et al 10, Verma
et al 15and Sandven et al 19. This might be because of severely ill and immunocompromised
patients being cared for in the unit with most of them being on life support systems. Wenzel and
Gennings 20 and Shorr et al 21 have tried to develop risk assessment strategies and calculate
“Candida scores” to predict the true risk of disease in patients admitted in ICU. Candida risk
scores may help clinician to rule out candidemia and to identify the patients at high risk of
developing Candida BSI in the hospital stay. Al- Attas et al 22 have reported high Candida spp.
colonization in diabetic patients compared to control subjects. Isolates colonizing diabetic
patients have also been found to show a greater degree of resistance to antifungal agents than
strains isolated from control subjects.
Our study also underlines the importance of HIV infection as factor contributing to
candidemia. In the United State the proportion of candidemia cases varied from 10% to 15% 23.
The contribution of HIV infection as a predisposing risk factor for candidemia is further
emphasized by a report from Italy, where Candida spp. was the third most common cause of
blood stream infections in HIV patients 24. From India Chowta et al 25 also reported HIV as one of
the major predisposing risk for candidemia. The duration of hospital stay, antibiotic prophylaxis
and treatment, level of immunosuppression, presence of other opportunistic infection and other
clinical types of candidiasis increases the risk of candidemia in HIV infected patients.
The emergence of new species Candida as potential pathogens is a reflection of the
changing scenario in medicine since 1960s. More than 17 species of Candida have been
implicated in human infections till date. However, the list of new species continues to grow. The
use of automated identification system in addition to conventional methods and increase in the
number of HIV infected patients can explain this fact. The incidence of BSI caused by NAC spp.
was higher than C. albicans at our hospital. Among the NAC spp., C. tropicalis followed by C.
glabrata and C. krusei predominately caused BSI. A number of international surveillance
programs like ARTEMIS Antifungal Surveillance Study conducted in 127 health-care centres in
39 countries have documented increased prevalence of NAC species like C. tropicalis and C.
parapsilosis 26.
Epidemiological studies from India reports C. tropicalis as aetiological agent in as many as
67-90% cases of candidemia. Shivprakasha et al 10 found C. tropicalis to be the most common
isolate from candidemia patients. Other workers have also documented the similar observation 16. The increased use of fluconazole has been determined to be the major reason for
predominance of C. tropicalis over C. albicans.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 245
C. glabrata has emerged as an important opportunistic pathogen worldwide. It is the
second most common yeast isolated as part of normal flora and its role as a pathogen has only
been recognized in the past few decades. Trick et al 27reported a considerable increase in the
incidence in the rate of isolation of C. glabrata from BSI patients. There is concern over an
increase in azole resistance among strains of C. glabrata.
With the increased incidence of candidemia and the growing number of antifungal
agents, laboratory aids to guide in the selection of antifungal therapy have gained greater
attention. The standardized broth micro dilution method is expensive, laborious and
cumbersome for use in clinical microbiology laboratories. Recently, a disc diffusion method has
been approved by CLSI for antifungal susceptibility testing of yeast.
In the present study we performed disc diffusion method for antifungal susceptibility
testing of Candida isolates. In our study Fluconazole resistance was noted in 19.07% of Candida
isolates, 11.9% showed resistance to itraconazole and 4.63% of Candida isolates showed
resistance to amphotericin B. In India, there is lack of multicentric studies regarding antifungal
susceptibility pattern. Goel et al 28 and Capoor et al 29 reported less incidence of resistance to
fluconazole. On the other hand, workers like Kumar et al 14, Kothari et al 30 and Gupta et al 31
reported high incidence of resistance to fluconazole.
The resistance to fluconazole is of great concern because it is the most common azole
used for treatment of disseminated candidiasis including candidemia. It is available in both
intravenous and oral formulation with high bioavailability and is more cost effective than other
antifungal agents. Although Amphotericin B is effective against most strains of Candida species,
it is not the first choice for the treatment of candidemia because of nephrotoxicity associated
with it. Itraconazole is used for treatment of mucosal candidiasis 32. Studies regarding its role in
treatment of candidemia are less. In a study by Kothari et al 30 24% of Candida isolates were
resistant to itraconazole.
In the present investigation, resistance to antifungal agents was observed more in NAC
spp. as compared to C. albicans. Fluconazole resistance was high in C. tropicalis and C. glabrata.
Itraconazole resistance was more in C. tropicalis. Amphotericin B resistance was higher in C.
glabrata isolates. Other researchers have also documented high antifungal resistance among
NAC spp as compared to C. albicans 1, 3.
We have compared the efficacy of YNBG medium and GM-MH agar for the antifungal
susceptibility testing of Candida isolate. Trailing phenomena around the zone margin were
infrequent and minimal on the GM-MH agar. Zone edges with this method were frequently
definite and clear, facilitating the measurement of zone sizes and minimizing subjectivity in
zone size measurements. The occurrence of the macrocolonies near the center of the clear zone
was also less with this method. The methylene blue in this medium stained the Candida colony
facilitating the identification. Our study showed that there is less variation in the result of GM-
MH agar and YNBG medium. Therefore GM-MH agar can be recommended as simple, cost
effective and sufficiently accurate medium for the routine testing of antifungal susceptibility of
Candida spp.
To conclude, the spectrum of Candida BSI has shifted dramatically from C. albicans to
NAC spp. Hence, it is essential that an early and accurate diagnosis be made of infecting species
of Candida, since each species varies markedly in susceptibility to the currently used antifungal
drugs. It is imperative that antifungal susceptibility testing be carried out routinely in the
laboratory. This will aid the clinician in timely institution of the appropriate and accurate

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July
antifungal drug to be used and will restrict the empirical use of antifungal
commonly done today.
Figure 1. Age and sex distribution of candidemia patients.
Figure 2. Risk factors predisposing
0
20
40
60
80
100
120
140
0-10 years
11-20 years
26
5
22
6
38
15
12
8
8
86
6 4
ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012
antifungal drug to be used and will restrict the empirical use of antifungal agents, as being
sex distribution of candidemia patients.
Figure 2. Risk factors predisposing Candidemia.
21-30 years
31-40 years
41-50 years
>50 years
Total
413
20
58
126
4 9 12 15
68
Male Female
49
40
ICU stay
Diabetes
HIV infection
Urinary catheter
Ventilator
Renal failure
Central line
Neonate
Malignancy
surgery in last 3 months
Dialysis
Sept 2012 Page 246
agents, as being

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 247
Figure 3. Species distribution of Candida isolates obtained from candidemia patients.
Table 1 Comparison of antifungal resistance pattern of Candida isolates using YNBG
medium and GM-MH agar.
Isolate Total Amphotericin B Fluconazole Itraconazole
YNBG GM-MH YNBG GM-MH YNBG GM-MH
C. albicans 78 02 02 07 07 04 03
C. tropicalis 52 02 02 19 19 20 21
C. glabrata 27 05 04 08 08 05 05
C. krusei 20 - - 02 02 02 02
C. guilliermondii 10 - - 01 01 01 01
C. parapsilosis 05 - - - - - -
C. dubliniensis 02 - - - - - -
REFERENCES:
1. Tortorano AM, Biraghi E, Astolfi A, Ossi C, Tejada M, Farina C et al. European
confederation of Medical Mycology (ECMM) prospective survey of candidaemia:
report from one Italian region. J Hosp Infect 2002;51:297-304.
2. Gudlaugsson O, Gillespie S, Lee K, Vande BJ, Hu J, Messer S, et al. Attributable
mortality of nosocomial candidemia, revisited. Clin Infect Dis 2003;37:1172-
1177.
3. Almirante B, Rodriguez D, Park B J, Cuenca-Estrella, Planes AM, Almela M et al.
Epidemiology and predictors of mortality in the cases of Candida bloodstream
infection: results from population-based surveillance, Barcelona, Spain, from
78
52
27
20
105
2
C. albicans
C. tropicalis
C. glabrata
C. krusei
C. guilliermondii
C. parapsilosis
C. dubliniensis

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 248
2002 to 2003. J Clin Microbiol 2005;43:1829-1835.
4. Pfaller M, Diekema D. Role of Sentinel Surveillance of Candidemia: trends in
species distribution and antifungal susceptibility. J. Clin. Microbiol
2002;40:3551-3557.
5. Iwata K. Drug resistance in human pathogenic fungi. Eur J Epidemiol 1992;
8:407-421.
6. Horvarth L, Hospenthal D, Murray C, Dooley D. Direct isolation of Candida spp.
from blood cultures on chromogenic medium on CHROMagar Candida. J Clin
Microbiol 2003;41:2629-2632.
7. National Committee for Clinical Laboratory Standards. Reference method for
broth dilution antifungal susceptibility testing for yeasts: Proposed standard
M27-P (National committee for Clinical Laboratory Standards, Villanova, Pa)
1992;12:No.25.
8. Khan S, Singhal S, Mathur T, Upadhyay DJ, Rattan A. Antifungal susceptibility
testing method for resource constrained laboratories. Indian J Med Microbiol
2006;24:171-176.
9. Chakrabarti A, Ghosh A, Kanta A, Kumar P. In Vitro antifungal susceptibility of
Candida. Indian J Med Res 1995;102:13-19.
10. Shivaprakasha S, Radhakrishnan K, Karim P. Candida spp. other than Candida
albicans: A major cause of fungaemia in a tertiary care centre. Indian J Med
Microbiol 2007;25:405-407.
11. Sachin CD, Ruchi K, Santosh S. In vitro evaluation of proteinase, phospholipase
and haemolysin activities of Candida species isolated from clinical specimens. Int
J Med Biomed Res 2012; 1:153-157.
12. National Committee for Clinical Laboratory Standards. Methods for antifungal
disk diffusion susceptibility testing of yeasts. Approved guidelines M-44A.
Wayne, PA: NCCLS;2004.
13. Berrounae Y, Herwalat l, Pfaller. Trends in antifungal use and epidemiology of
nosocomial yeast infection in a university hospital. J Clin Microbiol 1999;37:531-
537.
14. Kumar CP, Sundarajan T, Menon T, Venkatadesikalu M. Candidiosis in children
with onco-hematological studies in Chennai, South India. Jpn J Infect Dis
2005;58:218-221.
15. Verma AK, Prasad KN, Singh M, Dixit AK, Ayyagari A. Candidaemia in patients of a
tertiary health care hospital from north India. Indian J Med Res 2003;117:122-
128.
16. Xess I, Jain N, Hasan F, Mandal P, Banerjee U. Epidemiology of candidemia in a
tertiary care centre of North India: 5-year study. Infection 2007;35:256-259.
17. Sahni V, Agarwal SK, Singh NP, Anuradha S, Sikdar S, Wadhwa A. Candidemia-An
Under-recognized nosocomial infection in Indian Hospitals. J Assoc Physicians
India 2005;53:607-611.
18. Hajjeh RA, Sofair AN, Harrison LH, Lyon GM, Arthington-Skaggs BA, Mirza SA et
al. Incidence of bloodstream infections due to Candida species and In Vitro
susceptibilities of isolates collected from 1998 to 2000 in a population-based
active surveillance program. J Clin Microbiol.2004;42:1519-1527.
19. Sandven P, Bevanger L, Digranes A, Gaustad P, Haukland HH, Steinbakk M.
Constant low rate of fungaemia in Norway, 1991 to 1996. The Norwegian Yeast
Study Group. J .Clin. Microbiol. 1998;36:3455-3459.
20. Wenzel RP, Gennings C. Bloodstream infections due to Candida species in

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 249
intensive care unit: Identifying especially high-risk patients to determine
prevention strategies. Clin Infect Dis 2005; 41:S389-S393.
21. Shorr AF, Tabak YP, Johannes RS, Sun X, Splading J, Kollef MH. Candidemia on
presentation to the hospital: Development and validation of a risk score. Crit
Care 2009 (13: 1-10.doi:10.1186/cc8110.
22. Al-Attas SA, Amro SO. Candidial colonisation, strain diversity and antifungal
susceptibility among adult diabetic patients. Ann Saudi Med 2010;30:101-108.
23. Kao AS, Brandt ME, Pruitt WR, Conn LA, Perkins BA, Stephens DS et al. The
Epidemiology of candidemia in Two United States Cities: Results of a population-
based active surveillance. Clin Infect Dis 1999;29:1164-1170.
24. Petrosilo N, Viale P, Nicastri E, Arici C, Bombana E, Caeila A, et al. Nosocomial
blood stream infections among human immunodeficiency virus infected patients:
Incidence and risk factors. Clin Infect Dis 2002;34:677-685.
25. Chowta MN, Adhikari P, Rajeev A, Shenoy AK. Study of risk factors and
prevalence of invasive candidiasis in a tertiary care hospital. Indian J Crit Care
Med 2007;11:67-73.
26. Pfaller MA, Diekema DJ, Rinaldi MG, Barnes R, Hu B, Veselov AV. Results from the
ARTEMIS DISK Global antifungal surveillance study: A 6.5-year analysis of
susceptibilities of Candida and other yeasts species to fluconazole and
voriconazole by standardized disk diffusion testing. J Clin Microbiol
2005;43:5848-5859.
27. Trick WE, Fridkin SK, Edwards JR, Hajjeh RA, Gaynes RP. Secular trends of
hospital-acquired candidemia among intensive care unit patients in the United
States during 1989-1999. Clin Infect Dis 2002;35:627-630.
28. Goel N, Ranjan PK, Agarwal R, Chaudhary U, Sanjeev N. Emergence of
nonalbicans Candida in neonatal septicemia and antifungal susceptibility:
Experience from tertiary care centre. J Lab Physicians 2009;1:53-55.
29. Capoor MR, Nair D, Deb M, Verma PK, Srivastava L, Aggarwal P. Emergence of
non-albicans Candida and antifungal resistance in a tertiary care hospital. Jpn J
Infect Dis 2005;58:344-348.
30. Kothari A, Sagar V. Epidemiology of Candida Bloodstream Infection in a Tertiary
Care Institute in India. Indian J Med Microbiol 2009;27:171-172.
31. Gupta N, Mittal N, Sood P, Kumar S, Kaur R, Mathur MD. Candidemia in neonatal
intensive care unit. Indian J Pathol Microbiol 2001;44:45-48.
32. Pappas PG, Kauffman CA, Andens D, Benjamin DK, Calandra TF, Edwards JE.
Clinical practice guidelines for the management of candidiasis: 2009 Update by
infectious diseases society of America. Clin Infect Dis 2009;48:503-535.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 250
ASSESSMENT OF UMBILICAL CORD BLOOD IRON AND TIBC LEVELS IN
NEONATES OF ANAEMIC MOTHERS Dr. Durdana Sayeed, Dr. Ghouse M Ali, Dr. Arshiya Masood Osmani, Dr. Rohini N.
Dr. MD. Siddique Ahmed Khan.
1. Assistant Professor, Department of Biochemistry, Dr. VRK Women’s Medical College & Allied Hospitals,
Hyderabad.
2. Professor and HOD, Department of Biochemistry, Dr. VRK Women’s Medical College & Allied Hospitals,
Hyderabad.
3. Assistant Professor, Department of Biochemistry, Dr. VRK Women’s Medical College & Allied Hospitals,
Hyderabad.
4. Assistant Professor, Department of Biochemistry, Dr. VRK Women’s Medical College & Allied Hospitals,
Hyderabad.
5. Associate Professor, Department of Biochemistry, Dr. VRK Women’s Medical College & Allied Hospitals,
Hyderabad.
CORRESPONDING AUTHOR
Dr. Durdana Sayeed,
H.NO-10-1-128/1/2/E,
”ALIMANOR” MASAB TANK,
Hyderabad. AP-500028,
E-mail: [email protected],
Ph: 9848502341/9866226286.
ABSTRACT: The most common cause of anaemia in pregnancy is Iron deficiency which can
affect the newborns. This study was done to compare the serum Iron & Total Iron Binding
Capacity (TIBC) levels in the 20 newborns of non–anaemic and anaemic mothers each.
Results showed that Haemoglobin % was significantly lower (P≤ 0.001) in newborns of anaemic
mothers. Serum Iron levels did not show any significant difference (P = 0.1) & TIBC levels were
significantly higher (P≤ 0.01) in newborns of anaemic mothers as compared to newborns of
non- anaemic mothers.
KEYWORDS: Umbilical Cord blood, Iron deficiency anaemia, pregnancy, Serum Iron, S. TIBC.
INTRODUCTION: Anaemia is one of the most common conditions prevalent in our country. The
most common cause of anaemia in pregnancy is Iron deficiency.
WHO defines anaemia in pregnancy when Hb % is ≤ 11 gm/dl1.
Hb % ≤ 11 gm/dl especially in late pregnancy should be considered abnormal and due to Iron
deficiency rather than due to hypovolemia of pregnancy2.
The mean Hb level in cord blood is 13.5 – 20.5 gm/dl and Hb % ≤ 14 gm/dl at birth is
considered abnormal2.
AIM: This study was done to compare the Haemoglobin, serum Iron & TIBC levels in 20
newborns of non-anaemic mothers and anaemic mothers each.
MATERIALS & METHODS: The study done by the approval of ethical committee of Dr.
VRKWMC, Teaching Hospital & Research Centre. The study group is comprised of 20 pregnant
women without anaemia and their 20 newborns (Group I). The control group included 20
pregnant women with anaemia (Hb levels < 10 gm/dl) and their 20 newborns (Group II). Cord

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 251
blood was collected from the newborns’ end of the umbilical cord within 5 minutes of the
delivery.
FOR ESTIMATION OF HAEMOGLOBIN – We followed Cyanmethaemoglobin method3.
FOR ESTIMATION OF SERUM IRON & TIBC – We followed Dipyridyl method4.
The instrument used was Spectrophotometer (Elico sl 159).
RESULTS:
TABLE I-SHOWING Hb, IRON AND TIBC LEVELS IN NEWBORNS OF NON-ANAEMIC
MOTHERS (GROUP I)
Hb in gm% S. Fe in ugm% TIBC ugm%
MEAN 14.7 107.5 256.3
S. D +/_ 0.91 30.61 114.04
S.E +/_ 0.2 6.84 25.4
TABLE II – SHOWING Hb, IRON and TIBC LEVELS IN NEW BORNS OF ANAEMIC MOTHERS
(GROUP II)
Hb in gm% S. Fe in ugm% TIBC ugm%
MEAN 12.6 99.7 301.45
S.D +/_ 0.96 34 56.31
S.E +/_ 0.22
TABLE III – COMPARISSION of Hb, IRON AND TIBC LEVELS B/W GROUPS I & II
Hb in gm% S. Fe in ugm% TIBC ugm%
t-value 6.93 0.76 1.59
p-value < 0.001 = 0.1 ≤0.01
Df 38 38 38
The stastical analysis done was done using SAS Version of software.
Newborns of anaemic mothers showed
I. Significantly lower levels of Hb(P<0.001) when compared to newborns of non anaemic
mothers.
II. Serum Iron did not show any significant difference (P = 0.1).
III. Serum TIBC levels were significantly higher (P ≤0.01) in
New borns of anaemic mothers as compared to new borns of non- anaemic mothers.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 252
DISCUSSION: In our study comparison of newborns of non-anaemic and anaemic mothers
showed
� Haemoglobin of Group I is 14.7gm% and that of Group II is 12.6gm % with p value
(<0.001).
� Serum Iron showed Group I is 107.5µgm/dl and that of Group II is 99.7 µgm/dl with p
value (=0.1).
� Serum TIBC of Group I is 256.3 µgm/dl and that of Group II is 301.45 µgm/dl with p (≤
0.01).
A significant difference in all parameters except SERUM IRON reflects the metabolic demands
created by the foetus for erythropoiesis and foetus draws its full requirement from the mother.
Iron deficiency anaemia in mother is considered as a risk factor for Iron deficiency in infancy 5,6
Chitra Upadhyaya et al7 , found that there was a significant decrease in Hb% in the new borns of
anaemic groups when compared to the newborns of nonanaemic mothers. Similarly serum iron
levels was also having a significant difference .Where as in our study there is no significant
difference in serum iron levels.
TABLE IV – COMPARISSION B/W REFERENCE STUDY & OUR STUDY
NEWBORNSOFANAEMIC
MOTHERS
Hb in gm% S.IRON(µgm/dl) TIBC(µgm/dl)
REFERENCE STUDY 14.9 108.0 288.9
OUR STUDY 14.7 107.5 256.3
NEWBORNS OF NON-
ANAEMIC MOTHERS
REFERENCE STUDY 13.1 76.7 332.8
OUR STUDY 12.6 99.7 301.45
CONCLUSION: Compared to previous study7, our study shows that serum iron does not show
any significant difference in the newborns of non-anaemic and anaemic mothers,whereas Hb &
TIBC showing significant difference.
In the socio-economic conditions of our country , people are scared of nutritional deficiency for
the newborn children. But it has been observed in our study that the newborns of anaemic
mothers have no iron deficiency inspite of being born to anaemic mothers.
LIMITATIONS OF THE STUDY:
i) Samples for study has to be collected only from those cases which are
delivered before noon, because S.iron levels show a diurnal variation-S.iron
levels decline by almost 50% from 8:00 to 14:00 hours.
ii) Sample collection from umbilical cord fails, if there is delay in drawing the
sample.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 253
ACKNOWLEDGMENT: We are extremely thankful to Dr. SARIB RASOOL KHAN – Managing
Director DR. V R K WMC, Teaching Hospital & Research Centre and Allied Hospitals, for
providing all the facilities for the research work.
Our sincere thanks to Dr. SIKANDER HUSSAIN – Professor –Dept. of Physiology for the
cooperation.
REFERENCES:
1. Saraiya.Rao.Chatterjee,Principles of Obs and Gyn forPGs , 2nd edition pg-33.
2. Williams, Obstetrics-21st Edn.
3. Harold Varley, Practical Clinical Biochemistry, 4th Edn ,pg no.585.
4. Harold Varley, Practical Clinical Biochemistry, 4th Edn. pg no. 472.
5. Kilbride, J., Baker,T.G., Parapia, L.A.,Khoury,S.A..Shuqaidef , S.W., & Jerwood, D.Anaemia
During Pregnancy as a Risk Factor for Iron Defeciency Anaemia in infancy. Int J
Epidemiol (1999) 28: 461- 468 .
6. J. Colomer, C. colomer ,D. Gutierrez, A. Jubert A. Nolosaco, J. Donat,
R.Fernandez- Delgado, F. Donat and C. Alavarez- Dardet. Anaemia During Pregnancy as
a Risk Factor for Infant Iron Deficiency. Paediatric & Perinatal Epidemiology 1990,4
(2).196 – 204.
7. Chitra Upadhyaya et al, Serum Iron, copper & Zinc status in Maternal & Cord blood, IJCB
, 2004, 48 – 52.

CASE REPORT
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 254
ENTEROCOCCAL BRAIN ABSCESS OF OTOGENIC ORIGIN: A CASE
REPORT
Dr. K. Vidyasagar, Dr. R. Ravikumar. Dr. Nupur Pruthi.
1. Non-PG Senior Resident, Department of Neuromicrobiology, NIMHANS, Hosur Road, Bangalore.
2. Professor and Head, Department of Neuromicrobiology, NIMHANS, Hosur Road, Bangalore.
3. Assistant professor, Department of Neurosurgery, NIMHANS, Hosur Road, Bangalore
CORRESPONDING AUTHOR
Dr. R. Ravikumar MD,
Professor and Head, Department of Neuromicrobiology,
NIMHANS, Hosur Road, Bangalore-560029,
E-mail: [email protected],
Ph: 09448073965.
ABSTRACT: Various aerobic and anaerobic bacteria have been reported as causative agents of
brain abscess but only a few cases of enterococcal brain abscesses have been reported. We
report a case of enterococcal brain abscess of otogenic origin in a 35 year old male who was
known case of chronic suppurative otitis media (CSOM) and cholesteotoma of the right ear. The
abscess material culture yielded an isolate which was identified as Enterococcus faecium by
standard biochemical reaction. The isolate was sensitive to penicillin, ampicillin, gentamicin,
vancomycin, ofloxacin, lincomycin, and cloxacillin.
KEY-WORDS: Brain abscess, Enterococcus faecium, Computerized tomography
INTRODUCTION: Despite the advent of modern neurosurgical techniques, new antibiotics and
new powerful imaging technologies, brain abscess remains a potentially fatal central nervous
system (CNS) infection.1-4Brain abscess is a relatively uncommon infection with an incidence of
0.3-1.3/100,000 persons per year 1. Most of these cases occur in association with the
predisposing conditions such as otitis media, sinusitis, or presence of pyogenic infections in
other parts of the body. Dental infections are associated with around 2% of the brain abscesses.2
The causative pathogens of bacterial brain abscess vary with time period, geographic
distribution, age, underlying medical and/or surgical conditions and mode of infection. A large
number of Gram positive cocci, Gram negative aerobic bacilli, anaerobes and Mycobacterium
tuberculosis have been reported as the causative agents of bacterial brain abscess.1-4The
commonest organisms causing brain abscess following an otogenic source include
Staphylococcus aureus, Streptococcus pneumoniae, H. influenzae, Escherichia.coli, Proteus and
Pseudomonas species. Very few studies have reported Enterococcus species as one of the
causative agents of brain abscesses2-4.
We report a rare case of enterococcalbrain abscess of otogenic origin in a 35 years old
male which was managed successfully with surgical drainage and antibiotics.
CASE HISTORY: A 35-year old male patient presented to the Department of Neurosurgery with
three days of headache, giddiness and vomiting. The patient was a known case of CSOM and
cholesteotoma of right ear for the past three years having ear discharge and ear pain. The
patient underwent radical mastoidectomy with excision of cholesteotoma. On third post op day

CASE REPORT
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 255
patient developed headache, vomiting and giddiness with blurring of vision with no h/o fever,
seizures or limb weakness. At time of admission patient was conscious, had no fever and neck
stiffness. Neurological examination revealed left hemi paresis with grade two power, bilateral
papilledema, nystagmus and right cerebellar dysfunction. Cardiovascular, respiratory and
abdominal examinations were found to be normal.
His white blood cell (WBC) count was 13000/mm3 with 70% neutrophils. The
erythrocyte sedimentation rate (ESR) was 10mm/hr. Biochemical parameters were within
normal limits. CT of brain showed right cerebro-pontine angle cistern enhancing lesion with
loculation of size 4.4 × 3.5 × 3.0 cm2 with mass effect on fourth ventricle. Intracranial mass or
abscess was suspected as the probable diagnosis and craniotomy was performed and excision of
right cerebro-pontine angle abscess with EVD placement was done. Abscess material was
processed in the lab. Gram stain of the smear showed plenty of pus cells and Gram positive cocci
in pairs and short chain along with Gram negativebacilli. ZN stain showed no acid fast bacilli.
Abscess material was cultured on blood agar, MacConkey agar, thioglycollate broth and
anaerobic blood agar aerobically and anaerobically. A culture was also put up in LJ medium.
Culture yielded a bacterium which was identified as Enterococcus faecium by standard
biochemical reactions)6.
LJ medium showed no growth after eight weeks of incubation. The isolate was sensitive
to penicillin, ampicillin, gentamicin, vancomycin, ofloxacin, lincomycin and cloxacillin by disc
diffusion method. Patient was treated with iv ampicillin, iv gentamicin and metronidazole iv for
3 weeks. After three weeks of antibiotic therapy he was discharged without any neurological
deficit. The patient on follow up visits was doing well with no residual neurological deficit and
marked improvement in the radiological findings on a follow-up CT scan(fig1 B&C).

CASE REPORT
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 256
DISCUSSION: There have been many advances with respect to the diagnosis and management
of brain abscess, resulting in a corresponding increase of survival rates. However its incidence is
high, approximately 5% per million people, and the number of immuno-deficient hosts having
high risk of opportunistic infections might be increasing. This disease continues to be one of the
most common neurosurgical diseases[1-5].
Regarding portal of entry, brain abscess is almost always secondary to a focus of
suppuration elsewhere in the body or may develop either by a contiguous focus of infection,
head trauma or hematogenous spread from a distant focus.1-5 Thus the predisposing factors for
the development of brain abscess include infections of the middle ear, mastoid, paranasal
sinuses, orbit, face, scalp penetrating skull injury, intracranial surgery including insertion of
ventriculo-peritoneal shunts5-6.
A previous study conducted by Malik et al.6from Mumbai showed that in 47 cases of
brain abscess, the primary focus of infection could be established in 37 cases (78.7%) and
otogenic source was the commonest in 34% cases.
Another prospective study of pattern of brain abscess reported from India7 showed
chronic suppurative otitis media to be the commonest predisposing factor in 48% of patients.
The location and number of abscesses depends upon the predisposing factors. The temporal
abscess and the cerebellum are the commonest sites following otogenic source as observed in
the present case. The list of bacteria causing brain abscesses is very large. It includes Gram
negative aerobic bacilli like Klebsiella pneumoniae, Pseudomonas aeruginosa, Escherichia coli,
Salmonella species, Proteus species, Klebsiella oxytoca, Haemophilus influenzae, Pasturella
species, Vibrio cholerae non 01; Gram positive bacteria like Staphylococcus aureus, other
Staphylococcus species, Streptococcus pneumoniae, Enterococcus species, Viridans
streptococci, other Streptococcal species. The anaerobic organisms reported are Bacteroides
species, Fusobacterium species, Peptostreptococcus and Propionibacterium species.1-4
The commonest organisms causing brain abscess following an otogenic source include
Staphylococcus aureus, Streptococcus pneumoniae, H. influenzae, Escherichia.coli, Proteus and
Pseudomonas species.1-7 Very few studies have reported Enterococcus species as one of the
causative agents of brain abscesses in India.
Kurien et al.2in 1993 reported Enterococcus faecalis as one of the causative agents of
brain abscesses in India, while studying 153 cases of brain abscesses.
In the year 2002, Park et al.4from Korea reported a case of otogenic brain abscess due to
Enterococcusfaecium.
A recent case report from India by Mohanty et al. 3 in the year 2005 reported a brain
abscess due to Enterococcus avium in a 19-year-old man with chronic otitis media since
childhood.
Enterococcus faecalis and Enterococcus faecium are responsible for most enterococcal
infections in humans, while Enterococcus gallinarum, Enterococcus avium and Enterococcus
casseliflavus are not frequently reported8.Enterococciare clearly unusual etiological agents of
brain abscess, and they account for 0.3–4% of reported cases of brain abscess9.Based on a
clinical spectrum of symptoms and findings, enterococcal brain abscess can be found in two
clinical forms postoperative and spontaneous. Postoperative brain abscess appears as a
nosocomial infection usually associated with neurosurgical procedures and shunt devices10. Our
patient had CSOM and also underwent radical mastoidectomy with excision of cholesteotoma
which was considered as risk factors for his enterococcal brain abscess. For most clinical
microbiological laboratories, the primary method of identifying Enterococcus species strains

CASE REPORT
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 257
relies on phenotypic characterization [10]. The treatment of enterococcal brain abscess includes
administration of appropriate antibiotics that have in vitro activity against the strain, and can
efficiently penetrate the cerebrospinal fluid, in addition to the elimination of the predisposing
factors if necessary10.
We would like to stress that a high index of suspicion, timely diagnostic support by CT
scan, surgical intervention and vigorous antimicrobial therapy are crucial for better outcome.
REFERENCES:
1. Lu CH, Chang WN, Lin YC, Tsai NW, Liliang PC, Su TM, et al. Bacterial brain abscess:
microbiological features, epidemiological trends, therapeutic outcomes. QJM. 2002;
95:501–09.
2. Kurien M, Job A, Mathew J, Chandy M. Otogenic intracranial abscess. Concurrent
craniotomy and mastoidectomy- Changing trends in a developing country. Arch
Otolaryngol Head Neck Surg. 1998; 124:1353–56.
3. Mohanty S, Dhawan B, Kapil A, Das BK, Pandey P, Gupta A. Brain abscess due to
Enterococcus avium. Am J Med Sci. 2005; 329:161–62.
4. Park SY, Min JH, Ryu JW, Ko YS. Enterococcal otogenic brain abscess. Korean J
Otolaryngol Head Neck Surg. 2002; 45:1188–92.
5. Sung DJ, Ealaan K, Chang YL, Kim IS, Son EIK, Kim DW, et al. Clinical features and
surgical treatment of brain abscess. J Korean Neurosurg Soc. 2007; 41:391–96.
6. Malik S, Joshi SM, Kandoth PW, Vengsarkar US. Experience with brain abscesses.
Indian Pediatr. 1994; 31:661–66.
7. Lakshmi V, Rao RR, Dinkar I. Bacteriology of brain abscess--observations on 50
cases. J Med Microbiol. 1993; 38:187–90.
8. Sood S, Malhotra M, Das BK, Kapil A. Enterococcal infections & antimicrobial
resistance. Indian J Med Res. 2008; 128: 111-21.
9. Kurup A, TeeW, Loo I, Lin R. Infection of central nervous system by motile
Enterococcus: First case report. J Clin Microbiol.2001; 39:820-22.
10. Murray BE.The life and times of the Enterococcus. ClinMicrobiol Rev.1990;3: 46-65.

CASE REPORT
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 258
MYOFIBROBLASTIC SARCOMA: A CASE REPORT Dr. Rithesh. K. B, Dr. Nandesh Shetty, Dr. Sumukh. M, Dr. Ashish Shetty. Dr. Raghavendra. P
1. Assistant Professor, Department of OMFS, A. J. Institute of Dental Sciences, Kuntikana, Mangalore.
2. Head of the Department, Department of OMFS, A. J. Institute of Dental Sciences, Kuntikana, Mangalore.
3. Post Graduate Student, Department of OMFS, A. J. Institute of Dental Sciences, Kuntikana, Mangalore.
4. Assistant Professor, Department of OMFS, A. J. Institute of Dental Sciences, Kuntikana, Mangalore.
5. Assistant Professor, Department of Pedodontics, A. J. Institute of Dental Sciences, Kuntikana, Mangalore.
CORRESPONDING AUTHOR
Dr. Sumukh. M,
Dept. of Oral & Maxillofacial Surgery,
A. J. Institute of Dental Sciences, N.H 17,
Kuntikana, Mangalore-575004,
E-mail: [email protected],
Ph: 09886809202.
ABSTRACT: Myofibroblastic Sarcoma is a rare or uncommon neoplasm characterized by
myofibroblastic proliferation. The tumour may present as single or multiple nodules of soft
tissue, bone, or internal organs. When encountered in the jaws, the lesions exhibit clinical and
radiographic features suggestive of several odontogenic and non-odontogenic neoplasms.
Myofibroblastic Sarcoma of the jaws are usually well-demarcated, but sometimes can be poorly
delineated or infiltrated that may result in misdiagnosis and mistreatment1. A painless,
enlarging mass is the most common clinical presentation, but a definitive diagnosis requires
both histopathological and immunohistochemical analyses. In this paper we are going to discuss
a case of 64 years old male with Myofibroblastic Sarcoma of left side of face. The patient
underwent excision of the lesion in toto with reconstruction of the floor of the orbit using
prolene mesh.
KEYWORDS: Myofibroblastic Sarcoma, Myofibroma, Maxilla, Alveolus, Floor of Orbit, Prolene
mesh.
INTRODUCTION: Defining neoplastic Myofibroblastic Sarcoma (MS) as a distinct entity was
controversial. With increasing case reports, it became clear that Myofibroma was a distinct
entity in soft tissue sarcomas. Even though only low-grade Myofibroma was classified as a
distinct entity in the newly published World Health Organization classification of soft tissue
tumours, intermediate- and high-grade Myofibroma cases were documented in the literature.
Some cases of MYOFIBROBLASTIC SARCOMA were easy to misdiagnose as reactive lesions
because of the common existence of myofibroblasts in reactive granuloma. In addition, the
frequent exhibition of bland cytologic features in MYOFIBROBLASTIC SARCOMA is an important
factor in persuading pathologists toward a benign diagnosis. MYOFIBROBLASTIC SARCOMA,
especially low-grade MYOFIBROBLASTIC SARCOMA, is easily confused with myofibroblasts
composing nodular fasciitis because of their morphologic similarity and the overlapping
immunophenotype.
MYOFIBROBLASTIC SARCOMA is a common mesenchymal neoplasm that occurs most
frequently in the uterus and gastrointestinal tract. The occurrence of primary
MYOFIBROBLASTIC SARCOMA in the oral soft tissues or jawbones is very unusual. 1) Only 31
cases have been reported in the literature.2) Among cases of oral soft tissue MYOFIBROBLASTIC

CASE REPORT
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 259
SARCOMA, six arose in the cheek, five in the gingiva, five in the tongue and the remainder were
located in the floor of the mouth, soft palate, hard palate, mandibular alveolar mucosa, posterior
maxillary soft tissue and maxillary sinus. Among the jawbone lesion cases, six occurred in the
mandible and four in the maxilla2.
This paper discusses an unusual case of primary MYOFIBROBLASTIC SARCOMA of the
oral cavity, which arose in the maxillary buttress and had the growth pattern of a polyp.
DESCRIPTION OF CASE: A 64-year-old Male patient visited the Department of Oral & Maxillo-
facial Surgery at A. J. Institute of Dental Sciences, Mangalore with the chief complaint of a
swelling over the left side of the face region since 2 months duration. Swelling was insidious in
onset, initially small in size and associated with pain which was mild in intensity and continuous
type. Extent
Anteriorly: Left lateral aspect of the nose.
Posteriorly: 3 cm in front of the tragus.
Superiorly: Infraorbital rim
Inferiorly: Line joining corner of the mouth to tragus of the ear on the left side.
Size: 5 cm x 4 cm.
Patient had previously visited a dentist with complaints of pain and swelling and
underwent extraction of the two upper left molars as they were mobile. After extraction
swelling rapidly increased in size to its present size. Pain was moderate type and not subsiding
with medications. Patient is hypertensive and is on medication. On examination bucco-palatal
expansion was noted in the upper left molar region and 1st premolar region. Physical
examination revealed a firm swollen region, which showed tenderness, pain at palpation.
Surface was smooth, irregular in shape with ill defined margin with normal overlying skin.
Gingival swellings extended from the left maxillary canine to the 3rd molar. However, the patient
had not experienced any symptoms. On radiographic examination an extensive radiolucent
lesion with sclerotic borders was revealed above the left maxillary canine and molar region.
Root resorption of involved teeth was observed with grade III mobility of the 2nd and 3rd molar
teeth for which patient was treated with extraction and Incision & Drainage was done for the
swelling as the swelling was believed to be a periodontal abscess. On cross-sectional view of
occlusal projection expansion of buccal and palatal cortical bone of the maxilla with partial
resorption of buccal cortical bone was observed. Skin over the swelling was normal in
appearance but stretched. Obliteration of the nasolabial fold was seen. Watery discharge was
seen from the left eye.
Provisional diagnosis was Peripheral Ossifying Fibroma, Fibrosarcoma, Osteosarcoma.
Incisional biopsy was performed under local anaesthesia with adrenaline (1:200000) and the
sample was sent to Department of oral pathology for histopathological examination.
Histopathological examination suggested the lesion to be Osteosarcoma (Chondroblastic
Variant).
Patient was admitted in our hospital and all the necessary blood investigations were
carried out along with ECG, ECHO, Chest X ray and C. T. Scan of the Head. After obtaining a
medical clearance, the patient was taken up for Tumour excision under general anesthesia.
Reconstruction of the orbital floor was done using prolene mesh which was suture using 3.0
vicryl. Intra orally suturing was done using 3.0 vicryl and skin suturing using 5.0 prolene. The
excised tumour was then sent for histopathological examination.
Furthermore, patient was advised for therapeutic radiotherapy.

CASE REPORT
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 260
HISTO PATHOLOGICAL ASSESSMENT: Sections show a cellular spindle cell tumour arranged
in intersecting fascicles and slight swirling striform and whorl-like pattern. The tumour cells are
spindly to lump to stellate shaped showing mild pleomorphism, with vesicular nucleus some
showing conspicuous nucleolus and ill-defined pale eosinophilic cytoplasm. Focal nuclear
hyperchromasia is also seen. The stroma is myxoid at places and contains many thin walled
dilated and congested blood vessels. Large ares of hemorrhage are also seen in the studied
sections. Mitosis is low. A sparse chronic inflammatory infiltrate is also seen. Tumor tissue is
seen infiltrating the surgical resected margin.
Histological features are suggestive of low grade malignant SPINDLE CELL SARCOMA.
Immunohistochemistry for further evaluation and confirmation of histopathological changes
(CD34, S- 100 CD 99, Desmin, Actin).
IMMUNOPHENOTYPING REPORT:
SMA : Positive in some of the tumour cells.
Desmin : Negative in tumour cells.
S-100 : Negative in tumour cells.
CD99 : Negative in tumour cells.
CD34 : Negative in tumour cells.
IMPRESSION: With above features, Myofibroblastic Sarcoma has to be considered.
DISCUSSION: Myofibroblasts are modified fibroblasts, which can occur in normal tissues (e.g.
periodontal ligaments), reparative granulation tissue and reactive soft-tissue lesions. The cause
of Myofibroma is presently unknown. A number of authors have suggested that the tumors are
inherited in an autosomal dominant or alternatively in an autosomal recessive trait. However,
its low familial incidence suggests that there are probably factors other than genetics that play
an important role in the cause of this disease7.They are, however, also a principal cell type in
benign and malignant soft-tissue tumours. Myofibroblasts are spindle-shaped or stellate cells
with ovoid pale nucleus and distinct nucleolus. The cytoplasm is usually amphophilic and there
are indistinct cell borders. Ultrastructurally, myofibroblasts can be distinguished from
fibroblasts and smooth muscle cells by the findings of indentation of nucleus, presence of
peripheral or subplasmalemmal bundles of thin cytoplasmic filaments, termed stress fibres, and
a distinctive cell-stromal attachment termed fibronexus4. Myofibroblastic Sarcoma is a well
defined malignant tumour composed of myofibroblasts. It can occur at any age with slight male
predominance; the tumour size varies from 1.5 cm to 17 cm. MYOFIBROBLASTIC SARCOMA can
arise in soft tissues of various anatomic sites, including extremities, trunk (e.g. retroperitoneum,
breast and heart) and genital tract, but there is a predilection for the head and neck region. Oral
cavity (especially tongue, cheek and gingiva), nasal cavity, salivary glands and bones (e.g.
maxilla and mandible) can be affected. Grossly, most cases were described as firm, gray-white
coloured tumours with ill-defined margins. Histologically, the tumour cells show diffuse
fascicular or storiform growth pattern and they infiltrate surrounding tissues (e.g. skeletal
muscle). The cytological and ultrastructural characteristics of neoplastic cells are consistent
with myofibroblasts (described above). Increased mitotic activity of tumour cells and tumour
necrosis is associated with more aggressive behaviour of MYOFIBROBLASTIC SARCOMA5.
Tumour cells in MYOFIBROBLASTIC SARCOMA show a variable immunophenotype: actin
positive/desmin negative, actin negative/desmin positive, and actin positive/desmin positive
CASE REPORT
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 261
cases. In addition, neoplastic cells can express fibronectin, calponin, CD 34, CD 99 and CD 117,
whereas S-100 protein, epithelial markers and h-caldesmon are negative. MYOFIBROBLASTIC
SARCOMA is usually a tumour of low grade malignancy, prone to local recurrence (about 30% in
general), even after many years5. However, metastases to lungs have been also reported.
Therefore, close clinical follow-up of the patient is mandatory. Differential diagnosis of
MYOFIBROBLASTIC SARCOMA includes reactive myofibroblastic lesions, benign
myofibroblastic lesions and other Myofibroblastic Sarcomas. In these cases,
immunohistochemistry is not helpful and the differential diagnosis is based on careful
examination of the slides stained with hematoxylin-eosin. On the other hand, many
histogenetically different spindle-cell tumours can be distinguished from MYOFIBROBLASTIC
SARCOMA using immunohistochemistry. Nodular fasciitis is a rapidly growing lesion,
histologically with variable cellularity and myxoid stroma. It is less cellular and uniform than
MYOFIBROBLASTIC SARCOMA. Although mitoses can be present, the cells lack nuclear atypia,
which is usually present in MYOFIBROBLASTIC SARCOMA. Fibromatoses are composed of
uniform, collagen-producing myofibroblasts without nuclear pleomorphism. Inflammatory
myofibroblastic tumour (IMT) is histologically characterized by fasciitis-like, fascicular and
sclerosing areas with a prominent chronic inflammatory infiltrate with numerous plasma cells.
In addition, anaplastic lymphoma kinase (ALK) can be immunohistochemically detected in 30–
40% of Inflammatory myofibroblastic tumours6. The inflammatory infiltration in the presented
case of MYOFIBROBLASTIC SARCOMA was, however, due to tumour ulceration. High grade
Myofibroblastic Sarcoma is often difficult to distinguish from other high grade sarcomas. This
diagnosis should be established in those cases, where the presence of myofibroblasts is
confirmed by electronmicroscopy. Histogenetically different spindle-cell tumours can be
distinguished from MYOFIBROBLASTIC SARCOMA using immuno-histochemistry. Spindle-cell
carcinoma shows positivity for cytokeratins, fibrosarcoma is SMA negative, leiomyosarcoma has
a different microscopic appearance and shows desmin and h-caldesmon positivity. Spindle-cell
rhabdomyosarcoma shows SCMA positivity, angiosarcoma shows positivity for endothelial
markers (e.g. F VIII, CD 31 and CD 34) and malignant peripheral nerve sheath tumour shows at
least focal positivity for S-100 protein. In summary, MYOFIBROBLASTIC SARCOMA is a well-
defined myofibroblastic malignancy with predilection for head and neck region, which is prone
to local recurrency, rather than metastasing. For the diagnosis, a careful examination of
routinely stained slides is crucial. Immunohistochemistry can be useful in differential diagnosis
from some other spindle cell lesions and tumours. Electronmicroscopic examination can
support the diagnosis of MYOFIBROBLASTIC SARCOMA by proving the origin of tumour cells.
LEGENGS:
1. Frontal pre -operative photograph.
2. Birds eye view pre – operative photograph.
3. Intra oral lesion pre – operative photograph.
4. Intra operative photograph after excision of the lesion.
5. Excised lesion in toto.
6. Frontal view Post operative photograph.
7. Birds eye view Post operative photograph.
8. Histopathology Photograph.
9. C. T. Scan Pre opertive sub mento vertex view.
10. Occlual Radiograph

CASE REPORT
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 262

CASE REPORT
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 263
ACKNOWLEDGEMENTS:
Our sincere gratitude to Dr. Vinay Kumar Hegde, General Practitioner, Moodbidri, Dr. Aravind,
Consultant Pathologist, A. J. Hospital & Research Hospital, Mangalore and Department of Oral
Pathology, A. J. Institute of Dental Sciences, Mangalore.
REFERENCES:
1. Chiu-Kwan Poon and Po-Cheung Kwan. Myofibroma of the Mandible: A Case Report.
Chin J Oral Maxillofac Surg 16: 156-165, September 2005.
2. Hideki Mizutani, Iwai Tohnai, Makoto Yambe and Minoru Veda. LEIOMYOSARCOMA OF
THE MAXILLARY GINGIVA: A CASE REPORT. Nagoya J. Med. Sci. 165 - 170, 1995.
3. Nada O. Binmadi, Harold Packman, John C. Papadimitriou and Mark Scheper Oral
Inflammatory Myofibroblastic Tumor: Case Report and Review of Literature. The Open
Dentistry Journal, 2011, 5, 66-70.
4. Eyden, B. P.: The fibronexus in reactive and tumoral myofibroblasts: further
characterisation by electron microscopy. Histol. Histopathol., 16, 2001, s. 57–70.
5. Mentzel, T., Dry, S., Katenkamp, D., Fletcher, C. D.: Low-grade myofibroblastic sarcoma:
analysis of 18 cases in the spectrum of myofibroblastic 1tumors. Am. J. Surg. Pathol., 22,
1998, s. 1228–1238.
6. Li, X. Q., Hisaoka, M., Shi, D. R., Zhu, X. Z., Hashimoto, H.: Expression of anaplastic
lymphoma kinase in soft tissue tumors: an immunohistochemical and molecular study of
249 cases. Hum.1 Pathol., 35, 2004, s. 711–721.
7. Jin-Soo Kim, Sung-Eun Kim, Jae-Duk Kim. Myofibroma of the mandible: A case report.
Korean Journal of Oral and Maxillofacial Radiology 2006; 36 : 211-5.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sep 2012 Page 264
INDIRECT BONDING WITH NEW TRANSFER TRAY - LIGHT TRAY
Dr. R. Satish, Dr. T. Srinivasan, Dr. R. Suresh, Dr. Sujith sivarajan
1. Associate Professor, Department of Orthodontics, Adhiparasakthi Dental College and Hospital.
Melmaruvathur, Tamil Nadu.
2. Reader, Department of Orthodontics, Adhiparasakthi Dental College and Hospital. Melmaruvathur, Tamil
Nadu.
3. Senior lecturer, Department of Orthodontics, Adhiparasakthi Dental College and Hospital. Melmaruvathur,
Tamil Nadu.
4. Senior lecturer, Department of Orthodontics, Adhiparasakthi Dental College and Hospital. Melmaruvathur,
Tamil Nadu.
CORRESPONDING AUTHOR
Dr. R. Satish,
Adhiparasakthi Dental College and Hospital,
Melmaruvathur, Kanchipuram District,
Tamilnadu, India-603319,
E-mail: [email protected], Ph: 91 09444183900
ABSTRACT: BACKGROUND: Indirect bonding is a technique in which orthodontic brackets are
transferred from dental casts onto the dentition using a transfer tray. The aim of this paper is to
describe a simple and efficient procedure of indirect bonding. The transfer tray used here is
Light tray (Ivoclar), light polymerised resin composite special tray material, which is used to
fabricate customized trays for fixed and removable implant-restorations. This light tray has
many advantages when compared with similar trays for indirect bonding.
KEYWORDS: Indirect bonding, light tray
INTRODUCTION: Traditional bracket placement involves hand placing each bracket directly in
the mouth. Accurate direct bracket placement is very difficult for even the most experienced
orthodontist. Indirect bonding has been an exciting advancement in orthodontics. It has great
benefit to the patient as it improves patient comfort, reduces the amount of time in the dental
chair, improves the accuracy of bracket placement, and reduces treatment time. Indirect
Bonding of brackets using light-curing transfer trays,(Fig.1), has several advantages like easy
mouldable, fast and easy working, accurate adaptation, stability of shape immediately after
polymerization and excellent elastic memory. Light trays can be cured by Light curing unit for 3
minutes or exposing to direct day light for 5 minutes.
Fig .1 Light Tray.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sep 2012 Page 265
LABORATARY PROCEDURE: The indirect bonding technique starts by taking impressions of
the patient teeth. The impressions are used to make a stone model of the teeth, (Fig.2). The
brackets are secured to the stone model with water soluble glue (fevi stick,Fig.3). Use wax to
block and prevent adapting light tray in to the bracket wings and slots. Adapt the Light tray over
the brackets mounted on the patient cast from labial to lingual surface. Trim the excess tray
material with a wax knife, (Fig.4). Light cure the tray for 4 minutes, (Fig.5). Soak the working
model with the custom transfer tray in warm water for a minimum of one hour to dissolve
water soluble glue from the bracket base and release the custom tray from the model.
Fig.2. Model with markings of Bracket Position.
Fig.3 The brackets are fixed with water soluble glue.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sep 2012 Page 266
Fig.4. Adaptation of Light tray over the brackets.
Fig.5. Light curing the Light tray.
Fig.6. Light tray with the brackets.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sep 2012 Page 267
CLINICAL APPLICATION: Apply bonding agent and light cure adhesive on the brackets in
transfer tray. Etch the teeth and apply the bonding agent. Keep a dry field. Place the tray in the
mouth and the adhesive part of the tray pressed on to the teeth with fingers. Light cure the
adhesive for 20 seconds for each bracket, (Fig.7). Remove the tray and cure all the brackets for
10 seconds. Remove any excess adhesive from the teeth surface, (Fig.8).
Fig .7. Light tray with brackets on the teeth
Fig .8. After the removal of the light tray
CONCLUSION: Indirect bonding offers many advantages combined with safety, especially the
exact positioning of brackets. One of the main problems, however, is their transfer to the mouth
with precision and sufficient adhesion. Currently, there are various transfer trays for indirect
bonding available—opaque, translucent silicone-based polymer, and thermoplastic transfer
devices. The technique described in this article serves to simplify tray fabrication. This is
accomplished by using Light tray. The Light tray is easier to adapt, stability of shape
immediately after polymerization, excellent elastic memory, easy to trim, less bulky, easy to
transfer than other types, extremely cheap and cost effective. Light tray- transfer trays offer an
accurate bracket positioning and hence it could be treated as one of the preferable methods of
bracket placement.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sep 2012 Page 268
REFERENCES:
1. Gottlieb, E.L.; Nelson, A.H.; and Vogels, D.S.III: 1996 JCO Study of Orthodontic
Diagnosis and Treatment Procedures, Part I: Results and trends. J. Clin. Orthod.
30:615-630, 1996.
2. White, L.W.: An expedited indirect bonding technique. J. Clin. Orthod. 35: 36-41,
January 2001.
3. Bishara, S.E.; Gordan, V.V.; VonWald, L; Olson, M.E.: Effect of an acidic primer on
shear bond strength of orthodontic brackets, Am. J. Orthod. and Dentofacial
Orthop. 114: 243-247, September 1998.
4. Miles PG: Indirect bonding with a flowable light-cured adhesive. J Clin Orthod
36:646, 2002
5. Sondhi A. Effective and efficient indirect bonding: The Sondhi
6. method. Semin Orthod ;13:43-57 2007

BRIEF COMMUNICATION
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sep 2012 Page 269
MODIFIED PERIODONTAL EXPLORER FOR EXPANSION SCREW
ACTIVATION
Dr. T. Srinivasan, Dr. R. Satish, Dr. R. Suresh, Dr. Sujith Sivarajan
1. Reader, Department of Orthodontics, Adhiparasakthi Dental College and Hospital. Melmaruvathur, Tamil
Nadu.
2. Associate Professor, Department of Orthodontics, Adhiparasakthi Dental College and Hospital.
Melmaruvathur, Tamil Nadu.
3. Senior lecturer, Department of Orthodontics, Adhiparasakthi Dental College and Hospital. Melmaruvathur,
Tamil Nadu.
4. Senior lecturer, Department of Orthodontics, Adhiparasakthi Dental College and Hospital. Melmaruvathur,
Tamil Nadu.
CORRESPONDING AUTHOR
Dr. T. Srinivasan,
Adhiparasakthi Dental College and Hospital,
Melmaruvathur, Kanchipuram District,
Tamilnadu, India-603319,
E-mail: [email protected], Ph: 91 09841611886.
INTRODUCTION: Accidents with expansion screw activation keys are reported in the
literature1,2. A simple method to prevent such accident is to use a modified periodontal explorer
as a key for expansion screw activation. A no.17 periodontal explorer (fig 1) is cut at its first
terminal bend (fig 2). The second section is bent more vertically to the long axis of the shaft (fig
3). This part which is tapered and stiff enough to activate the screw is tried extra orally into the
screw. It is further trimmed in such a way that only a mm of instrument can project through the
screw hole (fig 4). Now a safe key for activating the maxillary expansion screw is ready to use
(fig 5). Once the patient’s parent or guardian successfully repeat the activation procedure in
office, the instrument can be given to them for home use.

BRIEF COMMUNICATION
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sep 2012 Page 270

BRIEF COMMUNICATION
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sep 2012 Page 271
REFERENCES:
1. Nazif MM, Ready MA. Accidental swallowing of orthodontic expansion key: report of two
cases. ASDC J Dent child 1983; 50:126-127
2. Sfondrini MF, Cacciafesta V, Lena A. Accidental ingestion of a rapid palatal expander. J
Clin Orthod 2003; 37: 201-202

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sep 2012 Page 272
INCIDENTAL RADIOGRAPHIC FINDINGS AND THEIR RESTORATIVE
IMPLICATIONS R. Sridevi, Sai Laxman Bharadwaj B, R. Thirumalai Prabhu
1. Senior lecturer, Department of Prosthodontics, Adhiparasakthi Dental College and Hospital. Melmaruvathur,
Tamil Nadu.
2. Intern, Department of Orthodontics, Adhiparasakthi Dental College and Hospital. Melmaruvathur, Tamil
Nadu.
3. Intern, Department of Orthodontics, Adhiparasakthi Dental College and Hospital. Melmaruvathur, Tamil
Nadu.
CORRESPONDING AUTHOR
Dr. R. Sridevi,
A-11, Laxmi Apartments,
Meenambal ST, Melmaruvathur, ,
Tamilnadu, India,
E-mail: [email protected], Ph: 91 09952363999.
ABSTRACT: Radiographs are an irreplaceable diagnostic tool, especially in dealing with
dentofacial hard tissues. Guidelines like the ALARA require professionals to limit the number of
radiographs prescribed to patient, thereby minimizing radiation dose. On the other hand, for
prosthetic evaluation, a latest radiograph has the potential to uncover new findings that can
alter the treatment planning sequence or affect the outcome of the planned treatment. This
review article discusses ten such radiographs. The significant findings in each radiograph have
been highlighted and treatment protocols tailored to the same. The aim of this article is to help
the reader adopt a meticulous approach and a keen eye for detecting problems, and emphasizes
the efficacy of radiographs in patient evaluation for restorative care.
KEYWORDS: Incidental, Findings, Treatment, Interpretation
INTRODUCTION: Dental clinics here in our country are teeming with patients keeping dental
personnel on a tight schedule. Efficient practice in this scenario demands a good balance
between speed, time management and prescribing what is needed and best for the patient.
Frequently patients present for prosthetic rehabilitation with radiographs taken during
previous treatment sittings and we often avoid prescribing a new one. Considering the
possibility of incidental findings, it is wise practice to prescribe a new radiograph during
abutment evaluation. This additional measure avoids unnecessary failures and the need for
prosthetic retreatment like the removal and re-fabrication of fixed bridges which can cause
considerable damage to both tooth structure and the patients’ wallet.
All the radiographs reviewed here, presented to the Prosthodontic clinic in our
institution for rehabilitation. A thorough perusal of this article will tell us how, and bring to
light a multitude of possibilities and occurrences during diagnostic radiography; for what the
mind does not know, the eyes do not see!

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue
Radiograph 1 – RESIDUAL ROOT FRAGMENT
Fracture of a root during exodontia, particularly long,divergent ones is a common
complication 1. The edentulous area in this radiograph reveals the presence of a root fragment
following extraction of the maxillary left second premolar. This incidental finding is familiar
even with novice dental practitioners and cannot be missed. The fragment in thi
more than 5mm in length.
Current guidelines suggest that a root fragment of up to 5mm can be left in situ in a
healthy patient provided there is no evidence of apical pathology
Radiograph 2 – ADJACENT TOOTH PATHOLOGY
In endodontic practice, pulp sensibility testing of the tooth in question is corroborated
with the response of control teeth which are usually adjacent teeth. These tests are indirect and
subject to false positive and false negative readings
interpretation of radiographic findings are an invaluable adjunct to pulp sensibility testing.
In the above radiograph, exposed to evaluate 26 for crown placement, a periapical lesion was
identified in relation to 25. Clinical exami
Class I composite filling, tenderness to percussion and poor response to electric pulp testing
when compared to the contra lateral 15. Endodontic treatment of 25 prior to restoration of 26
was considered prudent to avoid patient discomfort and minimize the number of prosthetic
visits.
ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sep 2012
RESIDUAL ROOT FRAGMENT
Fig 1
Fracture of a root during exodontia, particularly long,divergent ones is a common
. The edentulous area in this radiograph reveals the presence of a root fragment
following extraction of the maxillary left second premolar. This incidental finding is familiar
even with novice dental practitioners and cannot be missed. The fragment in this radiograph is
Current guidelines suggest that a root fragment of up to 5mm can be left in situ in a
healthy patient provided there is no evidence of apical pathology2.
ADJACENT TOOTH PATHOLOGY
Fig 2
endodontic practice, pulp sensibility testing of the tooth in question is corroborated
with the response of control teeth which are usually adjacent teeth. These tests are indirect and
subject to false positive and false negative readings3. In such cases, careful evaluation and
interpretation of radiographic findings are an invaluable adjunct to pulp sensibility testing.
In the above radiograph, exposed to evaluate 26 for crown placement, a periapical lesion was
identified in relation to 25. Clinical examination was positive for the presence of an occlusal
Class I composite filling, tenderness to percussion and poor response to electric pulp testing
when compared to the contra lateral 15. Endodontic treatment of 25 prior to restoration of 26
prudent to avoid patient discomfort and minimize the number of prosthetic
2012 Page 273
Fracture of a root during exodontia, particularly long,divergent ones is a common
. The edentulous area in this radiograph reveals the presence of a root fragment
following extraction of the maxillary left second premolar. This incidental finding is familiar
s radiograph is
Current guidelines suggest that a root fragment of up to 5mm can be left in situ in a
endodontic practice, pulp sensibility testing of the tooth in question is corroborated
with the response of control teeth which are usually adjacent teeth. These tests are indirect and
careful evaluation and
interpretation of radiographic findings are an invaluable adjunct to pulp sensibility testing.
In the above radiograph, exposed to evaluate 26 for crown placement, a periapical lesion was
nation was positive for the presence of an occlusal
Class I composite filling, tenderness to percussion and poor response to electric pulp testing
when compared to the contra lateral 15. Endodontic treatment of 25 prior to restoration of 26
prudent to avoid patient discomfort and minimize the number of prosthetic

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue
Radiograph 3 – MISSED ROOTS
The root canal treated tooth approximating the maxillary right first molar in this
radiograph shows clear evidence of two
The case notes for the patient under reference reveal that this tooth was designated as
15. However, obtaining the past dental history elicits extraction of the upper second premolars
for orthodontic purposes. A maxillary firs
palatal roots, whereas a maxillary second premolar has a single root with a single canal
effect the tooth in question was a first premolar and was scheduled for orthograde retreatment.
This radiograph is significant for two other findings
1. The orientation dot has been positioned mesio
2. The restorative margin in the first premolar is at the level of the interdental bone
distally due to tipping. Adjunctive periodontal therapy is imminent to ensure healthy
placement of crown margins for long
Radiograph 4 – CORONAL SEAL
1
2
ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sep 2012
Fig 3
The root canal treated tooth approximating the maxillary right first molar in this
radiograph shows clear evidence of two root outlines (white arrows)
The case notes for the patient under reference reveal that this tooth was designated as
15. However, obtaining the past dental history elicits extraction of the upper second premolars
for orthodontic purposes. A maxillary first premolar has two canals one each in buccal and
palatal roots, whereas a maxillary second premolar has a single root with a single canal
effect the tooth in question was a first premolar and was scheduled for orthograde retreatment.
h is significant for two other findings
The orientation dot has been positioned mesio-apical instead of mesio-occlusal
The restorative margin in the first premolar is at the level of the interdental bone
distally due to tipping. Adjunctive periodontal therapy is imminent to ensure healthy
placement of crown margins for long-term success.
CORONAL SEAL
Fig 4
2012 Page 274
The root canal treated tooth approximating the maxillary right first molar in this
The case notes for the patient under reference reveal that this tooth was designated as
15. However, obtaining the past dental history elicits extraction of the upper second premolars
t premolar has two canals one each in buccal and
palatal roots, whereas a maxillary second premolar has a single root with a single canal 4. In
effect the tooth in question was a first premolar and was scheduled for orthograde retreatment.
occlusal
The restorative margin in the first premolar is at the level of the interdental bone
distally due to tipping. Adjunctive periodontal therapy is imminent to ensure healthy

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue
Hermetic apical seal for eras has been considered the gold standard for endodontic
success. Contemporary concepts stress that both the coronal and apical seal play an equal role
in determining the same. Coronal seal refers to the protection rendered
restoration (direct or indirect). If the coronal seal is not intact, leakage through the dentinal
tubules can establish reinfection within three months in the canal system leading to failure
The temporary restoration shown in the r
portion adequately. Though marginal discrepancies can be detected clinically on facial and
lingual aspects, the presence and extent of such defects in the approximal regions are detected
with relative ease and precision on radiographs during follow
in this radiograph is a victim of proximal (distal) under preparation and an over contoured
crown (arrow).The necessary adjustments have to done and the crown has to be replaced at
earliest.
Radiograph 5 – ROOT FRACTURE
This is a pretreatment radiograph for a maxillary anterior diastema closure.
Transverse root fractures can occur in the coronal, middle and apical third. Apical third
fractures are usually asymptomatic,
approach for treatment6.
Apical root fractures are by and large detected on radiographs as depicted here in tooth 22.
Prosthetic treatment planning for such teeth involves
1. Eliciting the history of trauma
2. Thorough sensibility testing for all the teeth in the segment
3. Adjuvant endodontic therapy where mandatory
4. In case these teeth are to be used as fixed partial denture abutments, it should be borne
in mind that there is an effective reduction in pericemental area available for support,
especially in a weak abutment like the lateral incisor.
ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sep 2012
Hermetic apical seal for eras has been considered the gold standard for endodontic
success. Contemporary concepts stress that both the coronal and apical seal play an equal role
in determining the same. Coronal seal refers to the protection rendered by a post endodontic
restoration (direct or indirect). If the coronal seal is not intact, leakage through the dentinal
tubules can establish reinfection within three months in the canal system leading to failure
The temporary restoration shown in the radiograph does not seal and cover the coronal
portion adequately. Though marginal discrepancies can be detected clinically on facial and
lingual aspects, the presence and extent of such defects in the approximal regions are detected
precision on radiographs during follow-up visits. Also, the restored tooth
in this radiograph is a victim of proximal (distal) under preparation and an over contoured
crown (arrow).The necessary adjustments have to done and the crown has to be replaced at
ROOT FRACTURE
Fig 5
This is a pretreatment radiograph for a maxillary anterior diastema closure.
Transverse root fractures can occur in the coronal, middle and apical third. Apical third
fractures are usually asymptomatic, exhibit no mobility and advocate a wait and watch
Apical root fractures are by and large detected on radiographs as depicted here in tooth 22.
Prosthetic treatment planning for such teeth involves
Eliciting the history of trauma
Thorough sensibility testing for all the teeth in the segment
Adjuvant endodontic therapy where mandatory
In case these teeth are to be used as fixed partial denture abutments, it should be borne
effective reduction in pericemental area available for support,
especially in a weak abutment like the lateral incisor.
2012 Page 275
Hermetic apical seal for eras has been considered the gold standard for endodontic
success. Contemporary concepts stress that both the coronal and apical seal play an equal role
by a post endodontic
restoration (direct or indirect). If the coronal seal is not intact, leakage through the dentinal
tubules can establish reinfection within three months in the canal system leading to failure 5.
adiograph does not seal and cover the coronal
portion adequately. Though marginal discrepancies can be detected clinically on facial and
lingual aspects, the presence and extent of such defects in the approximal regions are detected
up visits. Also, the restored tooth
in this radiograph is a victim of proximal (distal) under preparation and an over contoured
crown (arrow).The necessary adjustments have to done and the crown has to be replaced at the
This is a pretreatment radiograph for a maxillary anterior diastema closure.
Transverse root fractures can occur in the coronal, middle and apical third. Apical third
exhibit no mobility and advocate a wait and watch
Apical root fractures are by and large detected on radiographs as depicted here in tooth 22.
In case these teeth are to be used as fixed partial denture abutments, it should be borne
effective reduction in pericemental area available for support,

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sep 2012 Page 276
Radiograph 6 – CYSTIC LESIONS
Fig 6
Fig 7
Cystic lesions in the jaws are generally incidental findings on radiographs. The extent
and the nature of the lesion determine the prognosis. Henceforth, it is wise to subject these
lesions to histopathological examination before harping on a treatment plan for the patient.
The periapical radiograph and the ortho-pantomograph are those of two different
patients. The anterior maxillary lesion in the periapical (Fig 6) revealed a residual cyst. The
right mandibular posterior lesion in the panoramic view (Fig 7) turned out to be an odontogenic
keratocyst.
Significance – Residual cyst can expand and interfere with the fit of a prosthesis7, and
the presence of this multilocular odontogenic keratocyst presents an absolute contraindication
to implant placement or immediate replacement with fixed bridges owing to their aggressive
behavior and high recurrence rate 8. The residual cyst has to be thoroughly enucleated and
following the period of healing definitive prosthesis can be fabricated. As far as the Gorlins cyst
goes, it demands radical treatment and an extended follow up period to ensure complete
regression of the lesion before any form of definitive rehabilitation is planned.
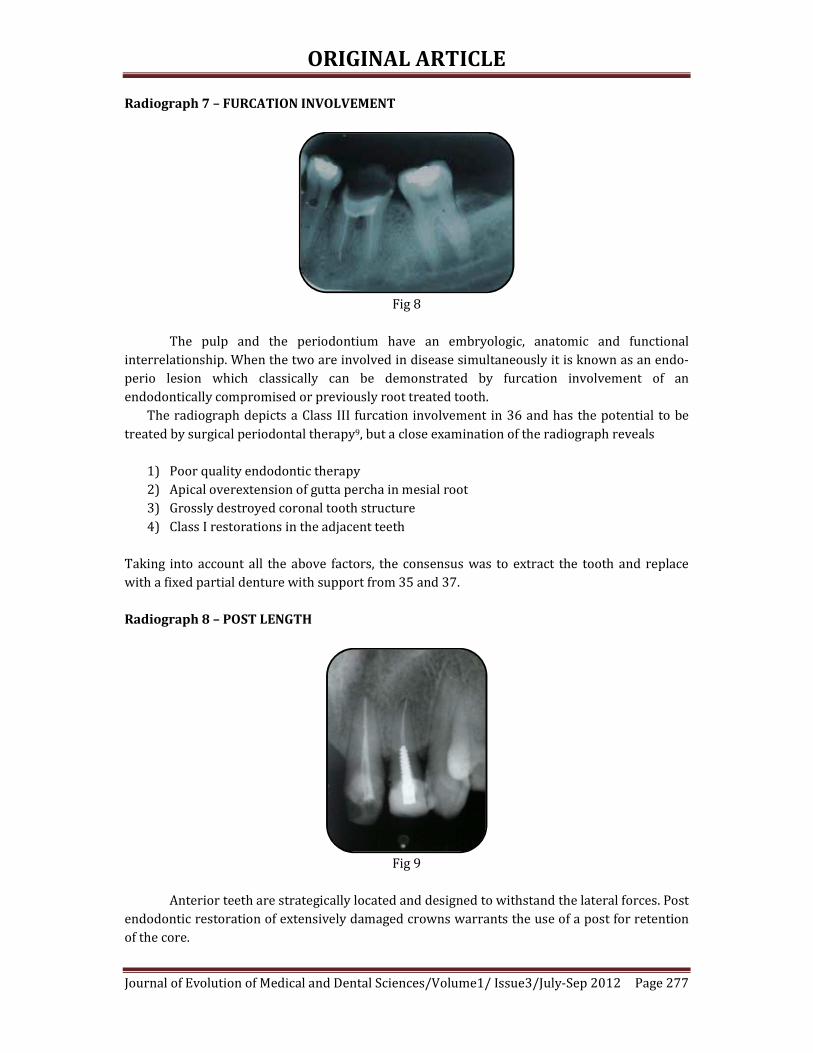
ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sep 2012 Page 277
Radiograph 7 – FURCATION INVOLVEMENT
Fig 8
The pulp and the periodontium have an embryologic, anatomic and functional
interrelationship. When the two are involved in disease simultaneously it is known as an endo-
perio lesion which classically can be demonstrated by furcation involvement of an
endodontically compromised or previously root treated tooth.
The radiograph depicts a Class III furcation involvement in 36 and has the potential to be
treated by surgical periodontal therapy9, but a close examination of the radiograph reveals
1) Poor quality endodontic therapy
2) Apical overextension of gutta percha in mesial root
3) Grossly destroyed coronal tooth structure
4) Class I restorations in the adjacent teeth
Taking into account all the above factors, the consensus was to extract the tooth and replace
with a fixed partial denture with support from 35 and 37.
Radiograph 8 – POST LENGTH
Fig 9
Anterior teeth are strategically located and designed to withstand the lateral forces. Post
endodontic restoration of extensively damaged crowns warrants the use of a post for retention
of the core.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sep 2012 Page 278
In selecting posts for anterior teeth, it is vital that the post should be long enough to satisfy
clinical requirements without jeopardizing the root integrity10. The standard parameters are11,
1) The post should be 2/3rd the length of the root
2) The length of the post can also equal the coronal length of the tooth
3) The post should extend into one half the length of the root embedded in its supporting
bone.
In this patient the core in 22 is supported by a screwed post that does not extend to the
adequate depth. The bone levels are well below normal and the post stops at the level of
alveolar support. Short, stiff posts transfer forces to the unsupported root extending above the
alveolus and can cause root fracture11. It was decided to use only the central incisor 21 as a
terminal abutment to restore the edentulous area and follow up on the prognosis of the lateral
incisor.
Radiograph 9 – ANKYLOSED TOOTH
Fig 10
The patient presented for single unit restoration of root canal treated 26.
Accidental finding includes ankylosed maxillary left second premolar as evident in the absence
of a distinct periodontal ligament space, definitive pulp canals and chamber and infraoccluded
position.
Ankylosis is a pathologic fusion of the cementum or dentin of a tooth root to the alveolar
bone12. Adults, with their slower rate of replacement resorption may retain an ankylosed tooth
for many years with minimal treatment or minor cosmetic modifications13. At present, there are
no guidelines in the dental literature for the treatment of ankylosis14. The parameters that
influence treatment in this case include
1) Adult presentation and diagnosis of ankylosis
2) Mild infraocclusion
3) Considerable rotation and misplaced proximal contacts which necessitates pulp therapy
before preparation for full coverage restorations.
4) An adjacent root treated molar
Therefore, it was decided to restore the molar with a full metal coverage crown combined with a
minimal preparation onlay restoration on 25 to restore function.
CONCLUSION: A patient’s radiograph is an indicator of both past and current disease
experience. Dental professionals should aim at absorbing as much information as possible from

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sep 2012 Page 279
a given radiograph, for, this information may possess the power to reroute our original
treatment plan in lieu of the patient’s best interests.
An incidental finding is one that accompanies and does not constitute the major reason
for exposing the radiograph. Majority of these findings can be attributed to iatrogenic causes
except for pathologies like cysts and fractures. Timely identification of these errors can best
avoid irreversible damage to the dentition.
REFERENCES :
1. Peterson. Ellis. Hupp. Tucker: Ch 11 Prevention and management of surgical
complication in Contemporary oral and maxillofacial surgery, 4 ed, Pg 221-237
2. Abhay N Dhatarkar: Ch 13 in Exodontia Practice 1ed, Pg 129 – 134
3. V Gopikrishna et al; Assessment of pulp vitality – A review. International Journal of
Pediatric Dentistry 2009, Vol 19: 3-15.
4. T.R Pitt Ford, Ch 3 in Endodontics- Problem Solving In Clinical Practice, Pg 33-35
5. B A Begotka et al, The importance of coronal seal following root canal treatment.
Virginia Association Dental Journal, 1996, Oct-Dec, 73(4); 8-10
6. J.O Andreasen and F.M Andresen: Ch 12 Root fractures in Text Book and Color Atlas of
Traumatic Injuries to the teeth 4ed, pg 337-371
7. Cawson and Odell: Cysts of the jaws in Essentials of Oral Pathology and Medicine 7ed,
Pg 102-128
8. Nakamura et al: Marsupilization of Odontogenic Keratocysts – Long term follow up
analysis of the effect and changes in growth characteristics, Oral Surgery Oral Medicine
Oral Pathology Radiology Endodontology, 2002 Vol 94: 543-553.
9. Murray Arlin, Oral Health 1987 Vol 77(5): 29-34
What this article tells us?
To always consider the possibility of spotting pathologies on
routine radiography
Why is it important?
The preservation of that which remains is of utmost importance
than the meticulous replacement of that which has been lost.
How can we identify them?
A thorough knowledge combined with adequate experience
Where to learn these skills from?
Practice is the key.
It is the onus of every practitioner to keep himself up-to-date on
changing trends in treatment planning and diagnosis and apply
them on a daily basis.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sep 2012 Page 280
10. Goodacre CJ et al: The Prosthodontic Management of Endodontically treated teeth – A
literature review II – Maintaining the apical seal, Journal of Prosthetic Dentistry 4:51,
1995
11. Stephen Cohen, Ch 21 Restoration of Endodontically treated teeth in Pathways of the
Pulp, Pg 786 – 821
12. William Biederman et al, Etiology and treatment of tooth ankylosis, American Journal of
Orthodontics, Vol 48(9): 670–684
13. Ebeleseder KA, Friehs S, et al, A study of replanted permanent teeth in different age
groups. Endod Dent Traumatol 14(6):274-8, 1998
14. Moffat MA et al , Intentional surgical repositioning of ankylosed permanent maxillary
incisor Dental Traumatology 2002; 18: 222–226



SHORT COMMUNICATION
Journal of Evolution of Medical and Dental Sciences/ Volume 1/ Issue 3/ July- Sept 2012
Page 69
USE OF TRADITIONAL MEDICINE IN FEVER
Purabi Phukan
1. Associate Professor, Department of Community Medicine, Srinivasa Institute of Medical Sciences and Research
Centre, Mangalore- 574146
CORRESPONDING AUTHOR:
Dr Purabi Phukan,
Associate Professor,
Department of Community Medicine,
Srinivasa Institute of Medical Sciences and Research Centre,
Mangalore- 574146,
Karnataka, India.
Email ID- [email protected]
INTRODUCTION:
Malaria is the most common cause of fever in India and is an age old problem in India
claiming thousands of life over the years 1,2. WHO launched its first ever comprehensive traditional
Medicine strategy in 2002 strategy to assist countries to gather and preserve knowledge on such
practices with the hope to develop a good database for finding antimalarial properties in future in
wake of drug resistance. Majority of the rural and tribal in rural areas have vast store of knowledge
and practice of traditional medicines as it is cheaper and easily accessible to them 3 4 5. Traditional
Medicine often becomes the first source of treatment for these communities. The WHO estimated
that 80% of the world’s population use botanical medicines for their primary health care needs,
malaria treatment inclusive6. The current study was therefore undertaken with an objective to find
out the knowledge and practices of traditional medicines among rural and tribal communities for
fever and the factors influencing such practices.
KEY WORDS: Malaria, Traditional Medicine, Fever, Ethnopharmacology
MATERIAL & METHODS:
A community based cross-sectional study was undertaken from June 2009 to May 2010 in
Rani Community Development Block which is the Rural Field practice area of Gauhati Medical
College, Assam. The Block has 96 villages with total population of 86,539 and literacy rate is 66.8%
(2001 Census). The block has 18% tribal population residing in 36 villages.
Considering expected frequency as 50%, by using Epi Info Version 7 sample size was
calculated to be 300 (95% confidence level, confidence limits of 5.65%). To get a representative
population, the households were selected by Proportionate Probability Stratified Random Sampling
technique from 16 villages. The 16 villages together formed a uniform composition, firstly in terms
of tribal and non-tribal study subjects and secondly in terms of easier and more difficult access to
health services. Stratification was done based WHO Protocols and methods of malaria situation
analysis 6. Head of the household was interviewed and data was collected in a pre-tested and
predesigned proforma regarding socio-demographic characteristics, knowledge and practices of

SHORT COMMUNICATION
Journal of Evolution of Medical and Dental Sciences/ Volume 1/ Issue 3/ July- Sept 2012
Page 70
traditional medicines in fever and in known malaria, factors influencing their use. Also the herbs
and plants that are used was identified and recorded. However the pharmacological property of
these plants and herbs are out of the scope of this study and review of Botanical Plants literature
was done to find out available data on its use and medicinal properties. Statistical Analysis of the
data was subjected to descriptive analysis and Epi Info Version7.
RESULTS:
The Socio demographic profile of the study population is shown in Table 1. Among the 150
tribal and 150 non-tribal households visited it was found that literacy level of head of the
household was 82.7% and 92.6% respectively, with total literacy rate of 87.7%. According to
occupation of the head of the families it was found that majority are cultivators (51.2%) among the
tribal and businessman (40.7%) among the non-tribal communities and 24 % and 12.6% of the
tribal and non-tribal families are living below poverty line (income less than Rs 228.9 per capita per
month at 1993-94 prices). The respondents belonged to the age group of 19 -59 years, of which,
among the tribal 61.4% are males and 38.6% are females while among the non-tribal respondents,
72% are males and 28% are females. Majority of the tribal respondents belonged to Hindu (82.4%)
and rest were Christian (21.3%) whereas among the non-tribal respondents majority were Hindu
(86%) and the rest Muslim (14%).
Table 2 shows that knowledge and practice of traditional medicine. Out of the 300
households visited only 49 (16.3%) households knew of traditional medicines used in fever. Out of
these 49 households, majority, 38 (25.3%) belonged to the tribal community while 11 (7.3%)
belonged to non-tribal community. However, out of the 49 households, only 8 (5.3%) of the tribal
households and 3 (2%) of the non-tribal households are currently involved in collection and
preparation and distribution of the medicine prepared from the herbs. The names of the herbs and
plants used and the mode of preparation and administration was demonstrated and explained by
them.
The remaining 251 (83.7%) of the respondents did not have any faith in traditional
medicines for treatment of malaria and they neither had any knowledge of these remedies. Further,
it must be mentioned that although use of traditional medicines was reported by 49 households, it
is usually used as an initial management; if fever does not improve in next 2-3 days then they opt
for allopathic medicines.
Table 3 shows the common factors influencing the practice of traditional medicines for
fever. However, 40 (81.6%) respondents, 32 (84.2%) tribal and 8 (72.7%) non-tribal respondents
said they would also prefer to use traditional medicines as an adjunct to antimalarials if diagnosed
as malaria fever.
In this study 6 botanical plants that are practiced in the study area were identified and
recorded. Table 4 shows the different plants and herbs that were identified. These are Murraya
koenijii, Vitex negundo, Centella asiatica, Azadiracta indica, Ocimum sanctum/Ocimum basilicum
and a plant known as Tupurilata or Panipanta locally (scientific name unknown) are identified to be
used for treatment of fever and malaria as home remedy.
It was found that in case of the plant Tupurilata (local name), it was made into a thin paste
mixed with coconut oil and is applied over the scalp of infants and young children with high fever
when parents fear to giving allopathic medicines because they believe them to be having adverse

SHORT COMMUNICATION
Journal of Evolution of Medical and Dental Sciences/ Volume 1/ Issue 3/ July- Sept 2012
Page 71
side effects. The other plants and herbs like Narasingha, Pasotia are grinded together applied on
scalp or body to get relief from headache and bodyache associated with fever. Whereas Manikmoni,
Neem and Tulsi taken orally in the treatment of persistent fever for young children as well as adults
by grinding and mixing them together and making a decoction and taken orally to get relief from
fever.
DISCUSSION:
The results of this study revealed that knowledge of traditional medicines was present only
in 49 (16.3%) of the respondents while only 11 (3.6%) practiced it in their homes recently. Similar
result was found in another study where 2.1% of the tribal community used local herbs for
treatment of malaria7. This value is comparatively less than the findings in other studies in Assam
where initial treatment through traditional healer (Vaidya) was found in 39.2% 8. The remaining
97% of the respondents did not have any knowledge about these traditional medicines used nor
believed that they can be helpful in malaria treatment.
The decreasing knowledge and practice of traditional medicines may be due to increased
malaria awareness campaigns in recent years and also due to high literacy rate of the study
population.
However in this study none of the respondents said that they will depend solely on TM if
fever is known to be due to malaria which is a positive finding in this study. After initial home
management if fever does not improve in 2-3 days than they opt for allopathic treatment from
doctor. This shows that access to early diagnostic facility would prevent the morbidity and
mortality that occurs due to delay in diagnosis. The factors like severity of fever, associated
symptoms of jaundice, infants and young children with persistent fever and fever in elderly people
and fear of side effects of the antipyretics and anti-malarials influenced the use of traditional
medicine. They are of the opinion that these medicines are safer to give to infants rather than
antimalarials as they seen side effects after using these. Similar finding was observed in Nigeria9.
Affordability of medicines was not a factor as they were aware of the free antimalarials available at
the health center.
Regarding the medicinal value of the plants used it was found that some of them indeed
were found to be having some benefit in treatment of fever and even in malaria.
Ocimum sanctum, locally known as “Tulosi” was found to be having many properties
including antipyretic and anti-malarial activity against P. falciparum and P vivax 10, 11, 12.
Similar use for fever and cough was also found in Arunachal Pradesh among Khamti tribes
in Lohit District13 and in rural area of Tamil Nadu14. In another study insecticidal property of tulsi
was also found15.
Azadirachta indica, locally known as “neem” was also found to exhibit antimalarial activity
by inhibiting the growth of P. falciparum 16and even against drug resistant strains of P. falciparum 17, 18.
Vitex negundo, locally known a “pasotia” meaning five leaved plant, Ayurveda it is called
nirgundi and in the west known as Chastetree, has proved to be useful in fever, spleen enlargement
and convulsion14 and in malaria19. Besides this it was also found to have insecticidal and pesticidal
properties by other studies 20, 21, 22.

SHORT COMMUNICATION
Journal of Evolution of Medical and Dental Sciences/ Volume 1/ Issue 3/ July- Sept 2012
Page 72
Centella asciatica, locally known as “manikmoni”, was also found to be useful malarial fever 23, 24, 25.
Murraya koenigii, locally known as “Narasingha” in this study area was also found to be
having anti-inflammatory property and hepatoprotective26.
A study in Africa has shown that traditional medicine can reduce 1 million malaria deaths.
In rural Tanzania a study about traditional Masai medicine showed 48% children already had
knowledge about these plants which have been preserved in the UN database for future reference27.
“Tupurilata” was not found in any database and it is a new plant found in this study which needs to
be studied. B N Prakash, a researcher with the foundation for the revitalization of Local Health
Tradition, based in Bangalore found Guduchi (Tinospore coeditdia) to have shown to reduce
malaria related deaths by 5 to 10 times.
CONCLUSION:
The study indicates that knowledge and practices regarding traditional medicines for
malaria or fever has significantly declined in the study population. The study indicates that delay in
malaria diagnosis may be one of the causes of depending on traditional medicine which can be
improved by making easier access to early diagnosis. That the use of traditional medicines does
more damage than good does not hold good in the current scenario when many studies did reveal
their usefulness. But certain remedies which have not been tested for efficacy is not encouraged so
vigorous research on the efficacy of traditional plants on malaria treatment should be carried out to
ascertain their usefulness. Ethno-pharmacological studies are encouraged to determine the
usefulness these traditional remedies, as few of these were found to be having some anti-malarial
property. The commonly used plants are brought out in this study along with their use. For this
purpose a book called “Traditional medicines and plants and malaria” by Merlin Wilcox, Gerard
Bodeker and Phillipe Rasanova provides guidelines on how to conduct such studies.
TM practice is an established health care system in India and is fast growing importance in
the western world. India can therefore contribute immensely for development and research for
alternative malaria treatment.
ACKNOWLEDGEMENT:
I thank, Dr R Sarma, Professor, Department of Community Medicine, Gauhati Medical
College, for her guidance pertaining to this work. I also would like to thank Ms. M Baruah, Lecturer
Botany, Arya Vidyapeeth College and Dr N D Bendegeri, Professor and Head, Department of
Community Medicine, KBNIMS for providing their valuable suggestions in preparation of this paper
for publication.
REFERENCES:
1. (Dhiman RC, Pillai CR, Subbaroa SK. Investigation of malaria outbreak in Bahraich district,
Uttar Pradesh. Malaria Research Center (ICMR), Delhi, India. Indian J of Med. Res. May 2001;
113:186-91.
2. C D Alert. Some important outbreaks of malaria in India during 2000. Jan 2001; 5:1.
3. WHO. Traditional Medicine Strategy 2003-2005. Geneva. Document: WHO/EDM/TRM/
2002.1.

SHORT COMMUNICATION
Journal of Evolution of Medical and Dental Sciences/ Volume 1/ Issue 3/ July- Sept 2012
Page 73
4. Pulok K. Mukherjee and Atul Wahile. Integrated approaches towards drug development
from Ayurveda and other Indian system of medicines. Journal of Ethnopharmacology; 2006;
103: 25–35.
5. Merlin Willcox. Traditional herbal medicines for malaria. BMJ. 2004; 329 (7475):1156
6. Protocols and methods for malaria situation analysis. WHO, HIV/AIDS, Tuberculosis,
Malaria. Roll Back Malaria. July 2003. Trial Edition. Pg.1-88. (WHO/HTM/RBM/ 2003.47)
7. V Soan, Gyan Chand. Proceedings of National Symposium on Tribal Health. Knowledge,
Attitude and Practices towards Malaria in Tribal Community of Baigachak Area, Dindori
District (MP), Pg-75-78 (http://www.rmrct.org/files_rmrc_web/centre's_publications/
NSTH_06/NSTH06_9.V.Soan.pdf)
8. Chaturvedi HK, Mahanta J and Pandey A. Treatment-seeking for febrile illness in north-east
India: an epidemiological study in the malaria endemic zone. Malaria Journal.
17 December 2009; 8:301 (doi:10.1186/1475-2875-8-301)
9. Erhun W O, Agbani E.O and Adesanya S.O. Malaria Prevention: Knowledge, Attitude and
Practice in a Southwestern Nigerian Community. African Journal of Biomedical Research;
2005; 8: 25 - 29.
10. Pandey BP, Anita. In: Economic Botany; 1990. p. 294 (Published by Chand and Company
Ltd., Ramnagar, New Delhi.
11. P. Prakash and Neelu Gupta. Therapeutic uses of Ocimum sanctum Linn. (TULSI) with a note
on Eugenol and its pharmacological action: A Short Review. Indian J Physiol Pharmacol
2005; 49 (2): 125–131
12. Savitri Godhwani, J.L. Godhwani and D.S. Vyas. Ocimum sanctum: An experimental study
evaluating its anti-inflammatory, analgesic and antipyretic activity in animals. Journal of
Ethnopharmacology. November 1987; 21(2): 153-163
13. Hui Tag, AK Das, Hari Loyi. Anti-inflammatory palnts used by Khamti tribes in Lohit District
of Auranachal Pradesh, India. Natural Product Radiance. 2007; 6(4):334-340.
14. Chellaiah Muthu, Muniappan Ayyanar, Nagappan Raja and Savarimuthu Ignacimuthu.
Medicinal plants used by traditional healers in Kancheepuram District of Tamil Nadu, India.
Journal of Ethnobiology and Ethnomedicine; 2006, 2:43 doi:10.1186/1746-4269-2-43).
(available online at: http://www.ethnobiomed.com/content/2/1/43)
15. Ocimum sanctum. The Indian home remedy. In: Current Medical Scene, March-April 1992;
(Edited and published by S. Rajeshwari, Cipla Ltd., Bombay Central, Bombay.
16. Rochanakij, S., Thebtaranonth, Y., Yenjal, C. H. and Yuthavong, Y. Nimbolide, a constituent of
Azadirachta indica inhibits Plasmodium falciparum in culture. Southeast Asian J. Trop. Med.
Public Health; 1985; 16: 66–72.
17. Kausik Biswas, Ishita Chattopadhyay, Ranajit K Banerjee and Uday Bandopadhyay.
Biological activities and medicinal properties of neem (Azadirachta indica). Curent Science;
82(11):1336-1345.
18. Badani, L., Deolankar, R. P., Kulkarni, M. M., Nagsampgi, B. A. and Wagh, U. V. Biological
activities and medicinal properties of neem. Indian J. Malariol.; 1987; 24: 111–117.
19. agnus-castus.co.uk. [homepage]. Agnus castus (Vitex negundo). (available from
http://www.herb-agnus-castus.co.uk)
SHORT COMMUNICATION
Journal of Evolution of Medical and Dental Sciences/ Volume 1/ Issue 3/ July- Sept 2012
Page 74
20. Vishal R Tandon. Review article: Medicinal Uses and biological properties of Vitex negundo.
NISCAIR Online Periodicals Repositories (NOPR). 2005; 4 (3): 162-165.
21. Hebbalkar DS, Hebbalkar GD, Sharma RN, Joshi VS, Bhat VS. Mosquito repellent activity of
oils from Vitex negundo Linn. leaves. Indian J Med Research; 1992; 95:200–203.
22. Krishnan Kannathasan & Annadurai Senthilkumar & Manivachagam Chandrasekaran &
Venugopalan Venkatesalu. Differential larvicidal efficacy of four species of Vitex against
Culex quinquefasciatus larvae. Parasitol Res; 2007; 101:1721–1723.
23. Nima D. Namsaa, M. Mandal and S. Tangjang. Anti-malarial herbal remedies of northeast
India, Assam: An ethnobotanical survey. Journal of Ethnopharmacology. Article. In Press-
Corrected Proof. 2010).
24. Sakshi Singh, Asmita Gautam, Abhimanyu Sharma and Amla Batra. Centella asiatica (L.): A
plant with immense medical potential but threatened. International Journal of
Pharmaceutical Sciences Review and Research. 2010; 4(2). Article 003 (Available online at
www.globalresearchonline.net).
25. Rahmatullah Mohammad, Ferdausi Dilara, Mollik Haque Ariful Md., Jahan Rownak,
Chowdhury H. Majeedul, Haque Mozammel Wahid, A survey of medicinal plants used by
Kavirajes of Chalna Area, Khulna District, Bangladesh. Afr. J. Trad. 2010; 7(2): 91-97
26. Bitterroot restoration [homepage]. Herbal Medicine> Medicinal Plants-Murraya koenijii.
27. IRIN: AFRICA: Turning to traditional medicines in fight against malaria. [Homepage]. IRIN:
The humanitarian news and analysis. A service of the UN Office for the co-ordination of
Humanitarian Affairs). (available at: http://www.irinnews.org)

SHORT COMMUNICATION
Journal of Evolution of Medical and Dental Sciences/ Volume 1/ Issue 3/ July- Sept 2012
Page 75

SHORT COMMUNICATION
Journal of Evolution of Medical and Dental Sciences/ Volume 1/ Issue 3/ July- Sept 2012
Page 76
* fisherman, silkworm rearing, selling household produce like betel nuts and vegetables,
agricultural labourer, income from house rent and income from pension.
Table 1. Socio-demographic profile of the study population
Socio demographic Tribal (150) Non-tribal (150) Total (300)
profile No. (%) No. (%) No. (%)
Religion
Hindu 118 (78.7%) 129 (86%) 247 (82.4%)
Muslim - - 21 (14%) 21 (14%)
Christian 32 (21.3%) - - 32 (21.3%)
Sex
Male 92 (61.4%) 108 (72%) 200 (66.7%)
Female 58 (38.6%) 42 (28%) 100 (33.3%)
Age range (years)
19-28 15 (10.0%) 9 (6.0%) 24 (8.0%)
29-38 44 (29.2%) 49 (32.7%) 93 (31.0%)
39-48 52 (34.8%) 52 (34.8%) 104 (34.7%)
49-58 28 (18.8%) 26 (17.3%) 54 (18.0%)
>59+ 11 (7.2%) 14 (9.2%) 25 (8.4%)
Education Level
Illiterate 26 (17.3%) 11 (7.4%) 37 (12.4%)
Primary School 56 (37.3%) 35 (23.3%) 91 (30.4%)
High School 44 (29.3%) 57 (38.0%) 101 (33.7%)
HSCL passed 16 (10.7%) 21 (14.0%) 37 (12.4%)
HS passed & above 8 (5.4%) 26 (17.3%) 34 (11.4%)
Occupation
Cultivator 77 (51.2%) 47 (31.3%) 124 (41.3%)
Daily wage earner 62 (41.3%) 19 (12.7%) 81 (27%)
Skilled labour 5 (3.3%) 2 (1.3%) 7 (2.3)
Service 26 (17.3%) 37 (24.7%) 63 (21%)
Business 10 (6.6%) 61 (40.7%) 71 (23.7%)
Others* 17 (11.3%) 8 (5.3%) 25 (8.4%)

SHORT COMMUNICATION
Journal of Evolution of Medical and Dental Sciences/ Volume 1/ Issue 3/ July- Sept 2012
Page 77
Table 2. Head of household having knowledge and practice of traditional medicine in fever
Traditional
Medicine
Tribal
(n=150)
Non-tribal
(n=150)
Total
(N=300)
No. % No. % No. %
Current knowledge Yes 38 25.3 11 7.3 49 16.3
No 112 74.7 139 92.7 251 83.7
Practicing within household Yes 8 5.3 3 2 11 3.6
No 142 94.7 147 98 289 96.3
Table 3: Reason for use of traditional medicines in fever
Variables Tribal
(n=38)
Nontribal
(n=11)
Total
(N=49)
Very high fever in young children 29 76.3 2 18.1 31 63.3
Fever associated with jaundice 10 26.3 2 18.1 12 24.5
Fear of side effects of allopathic drugs 20 52.6 10 90.9 30 61.2
Use side by side with allopathic treatment 32 84.2 8 72.7 40 81.6
Side effects of Antimalarials drugs 20 52.6 10 90.9 30 61.2
Fever in Elderly with poor physical status 10 26.3 4 36.4 14 28.6
*Multiple responses

SHORT COMMUNICATION
Journal of Evolution of Medical and Dental Sciences/ Volume 1/ Issue 3/ July- Sept 2012
Page 78
Table 4- Showing information collected about the botanical plants used.
Local name Scientific name Parts of plants
used.
Mode of use
Panipanta/
Tupurilata
Unknown leaf is the useful
part.
Leaf is made to a thin paste, after
mixing with oil and applied to the
scalp
Narasingha Murraya koenijia leaf and stem Leaves are eaten directly or by
boiling in water and making a paste
Pasotia Vitex negundo leaf
Leaves are eaten directly as
vegetable or boiled and thin paste
made
Manikmoni Centella asiatica leaf A paste of the leaves are made and
given empty stomach.
Mahaneem Azadiracta indica leaves, stem and
roots
Boiled in water and the water is
given to drink
Tulsi Ocimum sanctum/
Ocimum basilicum
leaves Leaves are eaten directly.

CASE REPORT
Journal of Evolution of Medical and Dental sciences/ Volume 1/ Issue 3/ July- Sept 2012 Page 79
UNUSUAL LOCATION OF CYSTICERCOSIS LESION PRESENTATION
Dr. V. Geeta, Dr. Parimla Devi, Dr. A. Sirisha, Dr. Rama Devi, Dr. Jijiya Bai, Dr. Shravan Kumar
1. Assistant Professor, Department of Pathology, Gandhi Medical College, Secunderabad-6
2. Associate Professor, Department of Pathology, Gandhi Medical College, Secunderabad-6
3. Assistant Professor, Department of Pathology, Gandhi Medical College, Secunderabad-6
4. Assistant Professor, Department of Pathology, Gandhi Medical College, Secunderabad-6
5. Professor and HOD, Department of Pathology, Gandhi Medical College, Secunderabad-6
6. Professor, Department of Pathology, Gandhi Medical College, Secunderabad-6
CORRESPONDING AUTHOR:
Dr. V. Geeta,
Assistant Professor,
Department of Pathology,
Gandhi Medical College,
Secunderabad-6
Email ID- [email protected]
INTRODUCTION:
Cysticercosis in humans is exclusively caused by larvae of T.solium which have predilection
for skeletal muscle, eyes, and central nervous system. In literature head and neck manifestations of
Cysticercosis is reported as soft tissue swellings at sub mental area, cheek as well as tongue1-4.
Cysticercosis presenting as a nodule or mass on neck is a very rare occurance5. The diagnosis was
usually made on Histo pathologic examination. The ensuing clinical disorder is named after the
organism at this larval stage, cysticercosis cellulose Larva of pork tapeworm Taenia solium.
KEY WORDS: Cysticercosis, T.solium
CASE HISTORY:
A 21 years male presented with a painless solitary nodular swelling on right side of the
upper neck of 2 years duration. The nodule was gradually increasing in size, associated with
anxiety, easy fatigability, palpitations, decreased appetite and weight loss.
Local examination revealed 2 x 2 cm round, smooth swelling present on right side of neck at the
level of Thyroid cartilage and anterior to the upper 1/3rd of sternocleido mastoid muscle and on
palpation the swelling is cystic, non tender, firm in consistency, not moving with deglutition and on
protrusion of tongue.
Skin over the swelling was non pinchable. No local rise in temperature. Swelling was mobile
both horizontally and vertically, not attached to the underlying muscle. General and systematic
examination within normal limits.
Clinical Diagnosis made was
1) Benign cystic swelling of right neck.

CASE REPORT
Journal of Evolution of Medical and Dental sciences/ Volume 1/ Issue 3/ July- Sept 2012 Page 80
2) Sebaceous cyst
3) Lipoma
4) TB lymph node
5) Aberrant thyroid
6) Salivary gland
FNAC: S/o ‘?’ necrotic lymph node, complex cyst or parasitic cyst.
U/S: S/o ‘?’ necrotic lymph node
Excision of the cyst was done and sent for HPE
The Histopathologic examination revealed ‘Cysticercosis Cellulose’ characterized by a scolex
and epithelium lined by tortuous body and continuous with outer cystic layer. Cyst enclosed by a
fibrous capsule infiltrated with lymphocytes, plasma cells and eosinophils. Figure.1
The post operative period was uneventful.
DISCUSSION:
Taenia solium passes its life cycle in two hosts. The definitive host is human who harbors
the adult worm and intermediate host in pig which harbors the larval stage. The adult worm lives in
the small intestine of man. Usually one adult worm is present which lives for years. It is about 3
meters long with proglotids, the gravid segments with about 50000 eggs in each gravid segment.
The worm sheds gravid segments laden with eggs in the stools which infect pigs on reaching the
alimentary canal of the intermediate host penetrate the gut wall and reach systemic circulation and
are lodged in different organs and muscles. They develop in to larvae referred as cysticercosis
Human being are infected through eating under cooked contaminated pork or infected vegetables.
Adult worms shed gravid segment laden with eggs in the stool, which re infect pigs. Thus
completing the cycle. Autoinfection of man may occur by contaminated fingers or by reversal of
peristaltic movements of intestine, the gravid segments are thrown back to the stomach and larvae
disseminate throughout the body via Arterio Venous Channels and lymphatics encysting in
subcutaneous tissue, striated muscle, brain and ocular tissue6.
Cysticercosis manifestations are different and depend on the location in the body and also
number of cysticercosis of a particular site and associated inflammatory response. 87%
cysticercosis cases – presents as solitary or multiple subcutaneous nodules on the trunk, upper
arm, neck, tongue, face and breast has been reported in this order of frequency.
In many patients involvement of central nervous system in the form of neuro Cysticercosis is
diagnosed when multiple cystic ring enhancing parenchymal lesions has been detected on CT Scan7.
We are not reporting this case because of its unusual site of presentation, but also the importance of
histopathologic examination is emphasized since neither the clinical examination nor history
suggested the diagnosis other than a benign lesion.

CASE REPORT
Journal of Evolution of Medical and Dental sciences/ Volume 1/ Issue 3/ July- Sept 2012 Page 81
Photo micrographs showing cystic lesion containing parts of parasite and the cystic wall containing
granulation tissue with inflammatory reaction.
REFERENCES:
1. Kinnman J, Chi CH, Park JH. Cysticercosis in Otolaryngology. Arch Otolaryngol 1976;
102:144-7
2. Beaver PC, Jung RC, Cupp EW. Clinical Parasitology, 9 th edition. Philadelphia: Lea & Febiger,
1984.
3. Jain RK, Gupta OP, Aryya NC. Cysticercosis of the tongue. J Laryngol Otol 1989; 103:1227-8
4. Gupta SC and Gupta SC. Cysticercosis of the tongue. Ear Nose Throat J 1995;74:174-8

CASE REPORT
Journal of Evolution of Medical and Dental sciences/ Volume 1/ Issue 3/ July- Sept 2012 Page 82
5. Cysticercosis of the neck-a report of unusual case. Danai Tanechpongfamb, dept.of oto rhino
laryngeology; Pathum thani Hospital, Journal of Medicine and health sciences, faculty of
medicine, srinakharin wirat university, Vol. 12, No.2, Aug-2005.
6. Park K. Epidemiology of Communicable diseases. In: Park K. Park's Textbook of Preventive
and Social Medicine. 16 th ed. New Delhi: M/s Banarsidas Bhanot Publishers, 2000; 229.
7. Smiti S, Sripathi H and Naik L. Unusual location of cysticercosis lesions in soft tissue –
Report of three cases. Ind J Radiol Imag 2003;13:157-8

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences / Volume 1 / Issue 3 / July- Sept 2012 Page 83
CLINICO– EPIDEMIOLOGICAL PROFILE OF ROAD TRAFFIC INCIDENTS
ADMITTED AT A TERTIARY CARE HOSPITAL IN GARHWAL-
UTTARAKHAND
Sumeet Dixit, Praveen K. Tyagi, Amit K. Singh, Sudhir K. Gupta, Nidhi Malik
1. Dr. Sumeet Dixit, Assistant professor, Department of Community Medicine, VCSGGMSRI– Srinagar, Pauri– Garhwal
(Uttarakhand)
2. Dr. Praveen K. Tyagi, Assistant professor, Department of General Surgery, VCSGGMSRI– Srinagar, Pauri– Garhwal
(Uttarakhand)
3. Dr. Amit K. Singh, Associate professor, Department of Community Medicine, VCSGGMSRI– Srinagar, Pauri– Garhwal
(Uttarakhand)
4. Dr. Sudhir K. Gupta, Associate professor, Department of Community Medicine, VCSGGMSRI– Srinagar, Pauri– Garhwal
(Uttarakhand)
5. Miss Nidhi Malik, Demonstrator, Department of Community Medicine, VCSGGMSRI– Srinagar, Pauri– Garhwal
(Uttarakhand)
CORRESPONDING AUTHOR:
Dr. Amit K. Singh,
Associate Professor,
(Community Medicine),
VCSG Govt. Medical College,
Srinagar – Garhwal, Uttarakhand,
India– 246174.
Email ID- [email protected]
ABSTRACT:
BACKGROUND: The magnitude of Road traffic incidents and fatalities in India is alarming. In 2009,
4.22 lakh road traffic incidents and 1.27 lakh road traffic fatalities were reported. These numbers
translate into one road accident every minute and one road accident death every four minutes
METHODS: The study (based on Jorgensen and Abane model, 1999) was conducted over a period
of one year during April 2011 to March 2012, among 136 victims (including 33 drivers) of road
traffic incidents coming to Veer Chandra Singh Garhwali government medical college, Srinagar,
Garhwal. RESULTS: 136 victims including 33 drivers were interviewed who were brought to the
causality in the aforesaid period. 23 people were brought dead. There is clustering of cases from the
month of August to October when compared to other months of year. 40% of drivers were
drunk/or using some other substance at the time of accident. Only 12.1% of drivers were using seat
belts at the time of accident. 57.6% were having driving license and 54.5% were either refractive
error or hearing impairment or both. Human error, High speed, Lack of sleep, effect of Alcohol and
mechanical fault of vehicle were reasons of accident as told by the drivers CONCLUSIONS: During
August to October there is clustering of cases. This period coincides with “Char Dham Yatra” and
rainy season both. Special efforts should be done during this period. Strong vigilance of drivers for

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences / Volume 1 / Issue 3 / July- Sept 2012 Page 84
alcohol use, presence of driving license, compulsory use of seat belts, and premedical checkup for
refractive errors may prove valuable and morbidity and mortality can be minimized.
KEY WORDS: Road Traffic Incident, Determinants, Hilly region
INTRODUCTION:
Road traffic incidents which are generally unintended and preventable are a common risk
every day to life that can happen to almost every one, anywhere. The problem of road traffic
incident is increasingly becoming a threat to public health and national development in many
developing countries. Road traffic incidents contribute to poverty by causing deaths, injuries,
disabilities, grief, lost of productivity and material damages. Road traffic incidents are the most
frequent causes of injury-related deaths world wide1. According to the World Report on Road
Traffic Injury Prevention2 traffic accidents account for about 3000 daily fatalities worldwide.
Statistical projections show that during the period between 2000 and 2020, fatalities related to
traffic incidents will decrease with about 30% in high income countries. The opposite pattern is
expected in developing countries, where traffic accidents are expected to increase at a fast rate in
the years to come. In developing countries the trend has reached an alarming state, but very little
attention is paid to the problem3. There is evidence that using minimum safety standards, crash
worthiness improvement in vehicles, seatbelts use laws and reduced alcohol use can substantially
reduce deaths on the road4. The magnitude of Road traffic incidents and fatalities in India is
alarming. In 2009, 4.22 lakh road traffic incidents and 1.27 lakh road traffic fatalities were
reported5.These numbers translate into one road incident every minute and one road incident
death every four minutes. However, this is an underestimate, as not all injuries are reported to the
police5. Hilly regions are prone for RTA and there are very few number of studies in such areas.
Therefore this study is under taken to identify the clinic – epidemiological profile of Road traffic
incidents amongst patients admitted at Base hospital, Srinagar - Garhwal and to assess the factors
associated with the causation of the same.
METHODOLOGY:
A model for traffic incident as inspired by the ecological model of a disease was developed
by Jorgensen and Abane (1999)6 who made a heuristic adjustment of this basic model to suit road
traffic accident analysis. The model is characterized by three main components:
1. The vehicle (corresponding to the vector in disease ecology) which describes vehicles into
its composition, age, technical conditions and safety equipments like seat belts in a car.
2. The environment, comprising the road system and the wider physical and built up
environment. The physical environment splits further into different aspects such as;
Daylight and climate (weather conditions and road conditions), Spatial conditions
(arrangements and Macro structures), Settlement pattern (Urban or rural / sparse or
populated area), situation of areas of residence and working areas, Principle of traffic
separation, topography and road constructions qualities.
3. The behavior of the population; including its characteristics such as age and sex ratio as
well as attitudes and general traffic behavior. And it goes further into driving behavior,
driving experience, driving style, risk compensation and risk driving (influence of alcohol
and drugs).

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences / Volume 1 / Issue 3 / July- Sept 2012 Page 85
Superimposed on this model is a system of traffic laws, regulations and mode of enforcement
designed to ensure that the population adheres to the controls and regulations so as to maintain
some level of road safety i.e. traffic rules (speed restrictions, road signs), speed controls and
convictions for various road traffic offences6. Based on this model this cross sectional study was
done with the help a pretested questionnaire, in a tertiary care hospital in Garhwal. All cases of RTA
coming to the tertiary care hospital during March 2011 to February 2012 were included in the
study. Questions were asked for assessing various risk factors as per the above said model and data
entry was done on excel and analyzed thereafter.
ETHICAL CONSIDERATIONS:
Ethical clearance from institutional review board/ institutional ethical committee was taken
for the study. Written consent was sought from the all respondents. They were informed about the
nature and the purpose of the survey.
RESULTS:
During the study period a total of 136 individuals came for the medical assistance (Figure-
1).117 were males 19 were females. Out of them 33 were drivers of the vehicle, which got the
accident. The number of brought dead persons because of Road Traffic Incidents, in the aforesaid
period was 23. Out of the brought dead individuals 5 were drivers of the vehicle. Maximum number
of morbidity because of RTI is evident in the month of December. There is clustering of cases from
the month of August to October when compared to other months of year (Figure-1).
Most of the drivers were literate. Out of 33 drivers interviewed only 3 (9%) were illiterate.
Nearly 40% of drivers were drunk/or using some other substance at the time of accident.50% of
drivers were >40 years of age. 15.8% of drivers were less than 20 years of age. Most of the drivers
(51.5%) who met the accident were having driving experience of >5 years. 12.1% of drivers were
having driving experience of less than 1 year. Only 12.1% of drivers were using seat belts at the
time of incident. 57.6% were having driving license and 54.5% were either refractive error or
hearing impairment or both. Most of the respondents told that it was mistake of other drivers
which led to the accident. High speed, Lack of sleep, effect of Alcohol and mechanical fault of vehicle
were other reasons of accident as told by the drivers (Table-2). 78% of victims were brought to the
hospital with help of 108 helpline service. Rest 22 % were came either by themselves or by other
people (Figure-1).

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences / Volume 1 / Issue 3 / July- Sept 2012 Page 86
Figure -1: Monthly distribution of RTI cases
Figure-2: Mode of transfer to the hospital
310
27
15 12 92
41
4 7 5
117
1 0 0 1 2 0 2 29
0 0 2
19
410
28
1712 11
4
50
4 7 7
136
0
20
40
60
80
100
120
140
160
No
of
case
s
Year- Month
Distribution of cases monthwise
Male
Female
Total
78%
15%
6%
1%
Mode of transfer to the hospital
108 helpline
Other people
self
other

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences / Volume 1 / Issue 3 / July- Sept 2012 Page 87
Table-1: Clinico-epidemiological profile of RTI cases
*Human error: wrongful U-turn by other vehicle , Wrongful overtaking by un-coming vehicle
**Mechanical fault: break failure, burst tyre, and locked steering mechanism
Maximum number (47.8%) of RTI morbidity was because of polytrauma associated. And
upper limb injury was least responsible for the mortality.50% of accidents took place in the evening
Drivers interviewed Yes % age
Education(n=33)
Illiterate 03 9.1
Up to 5th std 13 39.4
5-12 th std 16 48.4
Graduate/Post graduate 01 3.1
Age(n=38,
Including the
brought dead
drivers)
<20 years 6 15.8
20-40 years 13 34.2
>40 years 19 50
Alcohol /other substance use at the time of accident( n=33) 13 39.4
Driving experience
( n=33)
<1 year 4 12.1
1-5 years 12 36.4
>5 years 17 51.5
Seat belt use( n=33) 4 12.1
Driving license( n=33) 19 57.6
Refractive error /Hearing impairment / both( n=33) 18 54.5
Cause as told by
driver( Multiple
answers could
be given)
Mistake of others/Human error*( n=33) 23 69.7
More speed 14 42.4
Lack of sleep 11 33.3
Alcohol use 09 27.3
Mechanical fault of the vehicle** 09 27.3
Others including environmental
conditions
04 12.1
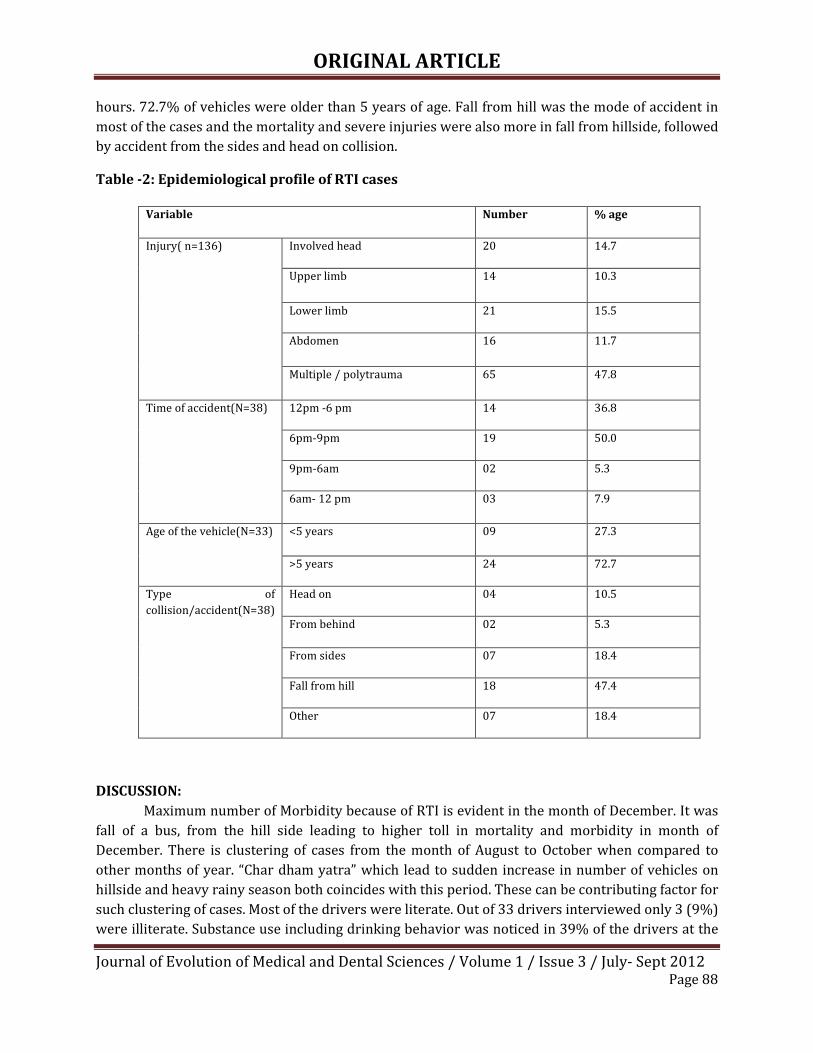
ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences / Volume 1 / Issue 3 / July- Sept 2012 Page 88
hours. 72.7% of vehicles were older than 5 years of age. Fall from hill was the mode of accident in
most of the cases and the mortality and severe injuries were also more in fall from hillside, followed
by accident from the sides and head on collision.
Table -2: Epidemiological profile of RTI cases
DISCUSSION:
Maximum number of Morbidity because of RTI is evident in the month of December. It was
fall of a bus, from the hill side leading to higher toll in mortality and morbidity in month of
December. There is clustering of cases from the month of August to October when compared to
other months of year. “Char dham yatra” which lead to sudden increase in number of vehicles on
hillside and heavy rainy season both coincides with this period. These can be contributing factor for
such clustering of cases. Most of the drivers were literate. Out of 33 drivers interviewed only 3 (9%)
were illiterate. Substance use including drinking behavior was noticed in 39% of the drivers at the
Variable Number % age
Injury( n=136) Involved head 20 14.7
Upper limb 14 10.3
Lower limb 21 15.5
Abdomen 16 11.7
Multiple / polytrauma 65 47.8
Time of accident(N=38) 12pm -6 pm 14 36.8
6pm-9pm 19 50.0
9pm-6am 02 5.3
6am- 12 pm 03 7.9
Age of the vehicle(N=33) <5 years 09 27.3
>5 years 24 72.7
Type of
collision/accident(N=38)
Head on 04 10.5
From behind 02 5.3
From sides 07 18.4
Fall from hill 18 47.4
Other 07 18.4

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences / Volume 1 / Issue 3 / July- Sept 2012 Page 89
time of accident. Experienced drivers (>5 years) met the accident in maximum number.
Overconfidence leading to recklessness can be the reasons for such happening. 77.9% drivers were
not using seat belt at the time of accident and when asked for the driving license only 42.4% could
not produce the same. 50% of drivers who met the accident were >40 years of age. In the elderly
visual impairment prevents adequate visual function, which may be responsible for the accident.
When examined, 54.5% were having either refractive error or hearing impairment or both. A study,
which examined the association between visual impairment and RTI among 1,428 drivers seen at
the accident and emergency department of a hospital in the United Arab Emirates, also identified
visual impairment to be significant risk factors7. Likewise Davidson in his examination of the
interrelationship between British drivers’ visual abilities, age and RTI histories found strongest
positive association between RTI variables and visual disabilities, among older drivers8. Most of the
respondents told that it was mistake of other drivers which led to the accident. High speed, Lack of
sleep, effect of Alcohol and mechanical fault of vehicle were other reasons of accident as told by the
drivers. Study by Asogwa et al9 showed that commercial drivers drive for hours without sleep and
food, until fatigue inevitably sets in and a crash may be the end result. Effect of alcohol or other
substances was also substantiated by Lemoineet al10. Maximum number (47.8%) of RTI morbidity
was because of polytrauma associated. And upper limb injury was least responsible for the
mortality. This is in contrast to the study by Biswas G11 who cited that the maximum (56.4%)
injuries were found on head and neck, followed by thorax (54.5%) and abdomen (44.5%). Other
studies12,13 also showed a high incidence of head injuries in their studies. 50% of accidents took
place in the evening hours. Fall from hill was the mode of accident in most of the cases and the
mortality and severe injuries were also maximum in such mode of accident followed by accident
from the sides and head on collision.
CONCLUSION:
During “Char Dham Yatra” period and rainy seasons there is clustering of cases. Special
efforts should be done during this period. Strong vigilance of drivers for alcohol use, presence of
driving license, compulsory use of seat belts, premedical checkup for refractive errors, must be
ensured. The role of 108 helpline14 cannot be ruled out and strengthening of this service can be of
paramount importance. All These measures may prove valuable and morbidity and mortality can be
minimized.
ACKNOWLEDGEMENT:
The author acknowledges medical social workers of department of community medicine,
Veer Chandra singh Garhwali govt. medical college, Srinagar, Garhwal for their work and support in
the study. The author also acknowledges the respondents who formed the building blocks for the
study.
REFERENCES:
1. Astrom, J. S, Kent, M.P. and Jovin, R. D. (2006) Signatures of Four Generations of Road Safety
Planning in Nairobi City, Kenya In: Journal of Eastern African Research and Development.
Vo. l20, pp. 186-201.
ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences / Volume 1 / Issue 3 / July- Sept 2012 Page 90
2. Peden, M. (Ed), (2004), World Report on Road Traffic Injury Prevention. World Health
Organisation, Geneva.
3. Odero, W., Garner, P. and Zwi, A. (1997). Road traffic injuries in the developing countries: a
comprehensive review of epidemiological studies. Journal of Tropical Medicine and
International Health. 2(5), 445-460.
4. Leon, S.R. (1996).Reducing death on the Road.The effects of minimum safety standards,
Unpublicised crash test, seat belts and alcohol. Am J Public Health; 86(1):31-3.
5. Road Accidents in India, 2009. Transport Research Wing, Ministry of Road Transport &
Highways, Government Of India, New Delhi.
6. Jorgensen, S. H., and Abane, A. M. (1999). A comparative study of urban traffic accidents in
developing and developed countries: Empirical observations and problems from Trondheim
(Norway) and Accra (Ghana). Bulletin of Ghana Geographical Association. No. 21, 113-128.
7. Bener A, Ahmad MF, El-Tawil MS, Al- Bakre S. Visual impairment and motor vehicle
accident. Middle East Journal of Emergency Medicine. 2004; 4: 1-9
8. Davidson PA. Inter-relationships between British drivers’ visual abilities, age and road
accident histories. Opthalmic and Physiological Optics. 1985; 5:195-204.
9. Asogwa SE. Kola nut and road traffic accidents in Nigeria. American Journal of Public Health.
1978; 68:1228.
10. Lemoine P, Ohayon M. Abuse of psychotropic drugs during driving. Encephale. 1996; 22:1-6.
11. Biswas G, Verma SK, Sharma JJ, Aggarwal NK. Pattern of Road Traffic Accidents in North
East Delhi. Journal of Forensic Medicine & Toxicology.2003; 20(1):27-32.
12. Sahdev P, Laeque MD, Singh B and Dogra TD. Road Traffic Accidents in Delhi, causes, injury
pattern and incidence of preventable deaths. Accid Anal Prev 1994; 26:12-18.
13. Salgado MSL, Colombage SM. Analysis of fatalities in road accidents. For Sci Int .1998;
36:91-96.
14. In Uttarakhand, Emergency helpline Number “108″ to tackle disaster calls, complaints.
Available at http://www.indiahillstoday.com/2010/10/12/in-uttarakhand-emergency-
helpline-number-108-to-tackle-disaster-calls-complaints/

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences / Volume 1 / Issue 3 / July- Sept 2012 Page 91
A STUDY ON EVALUATION OF APPROPRIATE USAGE OF FRESH FROZEN
PLASMA (FFP)
Dr. V. Geeta, Dr. I. Srilakshmi, Dr. A. Krishnayya, Dr. Lakshmi, Dr. Poornima, Dr. O. Shravan Kumar,
Dr. P. Jijiya Bai
1. Assistant Professor, Department of Pathology, Gandhi Medical College, Secunderabad, AP.
2. Assistant Professor, Department of Pathology, Gandhi Medical College, Secunderabad, AP.
3. Assistant Professor, Department of Pathology, Gandhi Medical College, Secunderabad, AP.
4. Blood bank Medical Officer, Gandhi Medical College, Secunderabad, AP.
5. Post Graduate Student, Department of Pathology, Gandhi Medical College, Secunderabad, AP.
6. Professor & HOD, Department of Pathology, Gandhi Medical College, Secunderabad, AP.
CORRESPONDING AUTHOR-
Dr. V. Geeta,
Assistant Professor,
Department of Pathology,
Gandhi Medical College,
Secunderabad, AP.
Email id- [email protected]
ABSTRACT:
The term FFP refers to the fluid portion of 1 unit of human blood that has been centrifuged,
separated & frozen solid at -18°C or colder within 8hrs of collection. The indications for transfusing
FFP are very limited, as it can cause unpredictable adverse reactions. A retrospective study of FFP
transfusion was carried out at the blood bank-Gandhi Medical College for a period of 6 months; i.e
January 2011–July 2011 for various indications. We evaluated 840 patients who received 1534
units of FFP and classified them as appropriate, clinically appropriate and inappropriate. In our
study appropriate and clinically appropriate transfusions of FFP were about 61%- a good
proportion of FFP transfusions were justified but 39% were of without any appropriate indication.
KEY WORDS: Fresh Frozen Plasma, Centrifugation, Adverse Reactions
INTRODUCTION:
The use of FFP has increased due to multiple factors, possibly increased acceptance of the
concept of component therapy.FFP contains the labile as well as stable components of the
coagulation , fibrinolytic & complement system; the proteins(that maintain oncotic pressure &
modulate immunity) and fats, carbohydrates & minerals are present in concentrations similar to
those in circulation. The most labile coagulation factors are preserved for 1 yr if FFP is kept at -30°
C or below. The FFP should be administered as soon as possible after thawing & in any event within
12 hrs if kept at 2-6°C.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences / Volume 1 / Issue 3 / July- Sept 2012 Page 92
Contents of 1 unit of FFP prepared from 450ml of whole blood
Plasma : 175-230ml
All Coagulation Factors : 1 i.u/ml of each factor including factors V
& VIII)
Fibrinogen : 200-400 mgm
INDICATIONS OF FFP:
� Active bleeding,
� Liver diseases
� Disseminated intravascular coagulation (DIC)
� Thrombotic Thrombocytopenic Purpura (TTP)
� Coagulopathy in massive transfusion
� Familial Factor V deficiency
� Deficiency of Factors II, VII, IX, X
� Antithrombin III deficiency
� Congenital or Acquired coagulation factor deficiency1
DOSAGE OF FFP:
About 10ml/Kg body wt. Post transfusion assessment of levels of APTT, PT & fibrinogen is
done for monitoring the effect of FFP2. Plasma should be ABO compatible with the recipient blood.
AIMS & OBJECTIVES:
Evaluation of appropriate usage of FFP in a period of 6 months (January 2011- June 2011)
in Gandhi Hospital.
MATERIALS & METHOD:
A Retrospective study was conducted at Gandhi Hospital Blood bank for a period of
6months (January 2011-june 2011). We evaluated 840 patients, who received 1534 units of FFP &
classified them as 1.Appropriate; 2.Inappropriate; 3. Clinically appropriate.
Table: 1- SEX RATIO (M: F ratio- 1:1.5)
SEX MALE FEMALE TOTAL
No. of patients 382 458 840
% 45.5% 54.5% 100%
Table: 2- AGE GROUP
AGE
GROUP
JAN FEB MARCH APRIL MAY JUNE TOTAL JAN
0-20 33 35 36 34 28 56 222 26.7%
21-40 71 44 49 68 74 91 397 21-40
41-60&
ABOVE
31 39 30 25 24 62 211 31

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences / Volume 1 / Issue 3 / July- Sept 2012 Page 93
Table: 3- Guidelines-British Committee for Standard Hematology3
SNO CLINICAL
CONDITIONS
TOTAL
REQUIREMENT
APPROPRI
ATE
CLINICALY
APPROPRIATE
INAPPROP
RIATE
%
1. Liver Diseases 152 ---- 152 ---- 18%
2. DIC 84 ---- 84 ---- 10%
3. Hemophilia 168 168 ---- ---- 20%
4. Sepsis + Burns 168 60 ---- 108 20%
5. Cardiac
surgeries
168 ---- ---- 168 20%
6. Snakebite 80 50 ---- 30 9.5%
7. Others 20 ---- ---- ---- 2.5%
8. Total 840 278 236 306
Table: 4- Total patients-840 ; Total units-1534
BLOOD
GROUP
O+ve B+ve AB+ve A+ve O-ve A-ve B-ve AB-ve
No. of
Patients
338 227 48 168 13 6 20 2
Percentage 40.9
%
27.3
%
5.9% 20% 1.7% 0.9% 2.8% 0.5%
RESULTS:
• Total patients who received FFP are 840, out of which males were 382 and females we 558
(table:1)
• Age group ranging from 0-20 years constitute 26.4%; 21-40 years 47.2%; 41-60 years
26.2% (table:2)
• Depending upon the conditions patients received FFP have been divided into 8 groups
according to the guidelines provided by British Committee for Standard Hematology3
(table:3)
• Out of 840 patients, conditions like liver diseases, disseminated intravascular coagulation
are clinically appropriate (where there is active bleeding leading to coagulopathy) and
hemophilia, sepsis, burns, rheumatic heart diseases, snake bite and shock are considered to
be appropriate (the term appropriate is limited to the treatment of coagulation protein
deficiency, for which specific factor concentrates are un available or undesirable)-(table:3)
• No.of units of FFP transfused are 1534 in six months period. Of this 40.9% are transfused to
O positive blood group (table: 4).
DISCUSSION:
� FFP is efficacious for treatment of Deficiencies of factors II, V, VII, IX, X & XI.
� Reversal of warfarin effects: Patients who are anticoagulated with warfarin are deficient in
functional vitamin K dependent coagulation factors II, VII, IX, X as well as protein C & S. FFP
can be used to achieve immediate hemostasis.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences / Volume 1 / Issue 3 / July- Sept 2012 Page 94
� Massive Blood Transfusion: In patients with documented blood clotting abnormalities,
prolonged APTT, INR after huge blood loss requiring 4 or more units of packed red cells-
FFP is commonly recommended.
� FFP can be used as a source of Antithrombin III in patients who are deficient of this
inhibitor & undergoing surgery or who require heparin for the treatment of thrombosis.
� FFP useful in infants with secondary immunodeficiency associated with severe protein
losing enteropathy, FFP can be used as a source of immunoglobulin for children & adults
with human immunodeficiency.
� FFP is used in treatment of Thrombotic thrombocytopenic purpura.
ASSOSIATED RISKS:
• Anaphylactoid reactions
• Alloimmunisation
• Transfusion related acute lung injury (TRALI): antibodies against the patients granulocytes
may cause leucocyte aggregation in pulmonary vessels leading to TRALI4
• Increase in infections
• Excess usage-Hypervolemia & cardiac failure (The guidelines set by British Committee for
Standard Hematology was followed in our study). 3
Approximately 60% FFP used are inappropriate according to Kakkar et al 5, but clinically
apparent cases like liver diseases, coronary bypass surgeries reduced the inappropriate usage to
28%. Severe liver disease6, 7, 8 is one of the most common clinical indications for transfusion of FFP.
Patients with liver diseases have several abnormalities that can lead to bleeding like coagulopathy,
Disseminated Intravascular Coagulation (DIC), Thrombosis. According to Consten et al9 & LA
Harker et al10 in cardiac surgery 11 post operative bleeding due to residual effects of heparin may be
corrected with transfusion of FFP.
CONCLUSION:
In our study appropriate & clinically appropriate transfusions of FFP were about 61%. It is
desirable that educational programmes be arranged for doctors regarding appropriate usage of
FFP.
Blood bank associations & Hematologists should more firmly adhere to the guidelines.
In our institution 61%, a good proportion of FFP transfusions were justified and 39% were
used without any appropriate indications.
ACKNOWLEDGEMENT:
I extend my special thanks to all the technical staff off blood bank and the personnel of
record room of Gandhi Hospital for helping me in collecting the necessary data.
REFERENCES:
1. NIH consensus conference: Fresh frozen plasma: indications and risk JAMA1985; 253:551-
3.
2. Snyder AJ, Gotschall JL and Menitove JE. Why is fresh frozen plasma transfused?
Transfusion1986; 26:107-12.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences / Volume 1 / Issue 3 / July- Sept 2012 Page 95
3. British Committee for standards in Hematology, blood transfusion Task force. Guidelines for
the use of Fresh frozen plasma, cryoprecipitate and cryo supernatant.TransfusionMed1992;
2:57-63.
4. Nordhagen R, Conradi M, Dromtort SM. Pulmonary reaction associated with transfusion of
plasma containing anti-Vb. VOXSANG. 1986; 5:`102-8 (Pubmed)
5. Kakkar N, Kaur R and Dhanoa J. Improvement in fresh frozen plasma transfusion practice:
results of an outcome audit. Transfus Med 2004; 14231-5.
6. Schofield WN, Rubin GL and Dean MG. Appropriateness of platelet, fresh frozen plasma and
cryoprecipitate transfusion in New South Wales public hospital. Med J Aust 2003; 178:117-
21.
7. Spector I, Corn M and Ticktin HE. Effect of plasma transfusion on the prothrombin time and
clotting factors in liver disease. Eng J Med 1966; 275: 1032-7.
8. Mannucci PM, Franchi F, Dioguardi N. Correction of abnormal coagulation in chronic liver
disease by combined use of fresh frozen plasma and prothrombin complex concentrates.
Lancet 1976; 2: 542-5.
9. Consten E, Henny CP, Eijsman L, Donglemant DA, Van Oers MH. The routine use of fresh
frozen plasma in operations with coronary bypass surgery is not justified. J thorac
Cardiovasc Surg 1996; 112:162-7.
10. LA Harker, TW Malpass, HE Branson, EA 2d Hessel and SJ Slichter. Mechanism of abnormal
bleeding in patients undergoing coronary bypass surgeries. Acquired transient platelet
dysfunction associated with selective Alpha granule release. Blood 1980; 56: 824-34.
11. Wilhelmi M, Franke U, Cohmert T, Weber P, Kaukemuller J, Fisher S, et al. Coronary artery
by pass grafting surgery with out the routine application of blood products: Is it feasible?
Eur J Cardiothorac Surg 2001; 19: 657-61

CASE REPORT
Journal of Evolution of Medical and Dental Sciences / Volume 1 / Issue 3 / July- Sept 2012
Page 96
PALATAL PLEOMORPHIC ADENOMA WITH FLORID SQUAMOUS METAPLASIA: A
POTENTIAL DIAGNOSTIC PITFALL
Abdul Hakeem Attar, Mandakini B. T, Azhar Fatima
1. Assistant Professor, Department of Pathology, KBN Institute of Medical Sciences, Gulbarga, Karnataka
2. Assistant Professor, Department of Pathology, KBN Institute of Medical Sciences, Gulbarga, Karnataka
3. Lecturer, Unanai College
CORRESPONDING AUTHOR:
Dr Abdul Hakeem Attar,
C/o Abdul Azeem Attar,
Shameem Masala,
Attar Gazar, Gulbarga.
Email id- [email protected]
ABSTRACT:
Pleomorphic adenoma is the most common benign tumor occurring in the major
and minor salivary glands. We report a case of pleomorphic adenoma with extensive
squamous metaplasia in the palate of a 20 year old man. The dimensions of the tumor were
3x2x2cm. More than 75% 0f the epithelial element in the tumor was composed of sheets of
squamous cells, with multiple keratin filled cysts. This case illustrates that pleomorphic
adenoma with squamous metaplasia presents a potential for misinterpretation as
mucoepidermoid carcinoma and squamous cell carcinoma. We discuss the various pitfalls
and the features that are helpful in distinguishing between these lesions.
KEY WORDS: Pleomorphic adenoma, Squamous metaplasia
INTRODUCTION:
Pleomorphic adenoma is the most common benign tumor occurring in the major or
minor salivary glands. [1] The tumor is characterized by epithelial and modified
myoepithelial elements intermingled with tissue of mucoid, myxoid or chondroid
appearance. It has a wide spectrum of morphological patterns, [2] squamous cells, oncocytes,
sebaceous cells, bone, adipose tissue and crystalline materials can be found in the tumor.
We report a benign salivary gland tumor with a predominant and extensive squamous
component. The features are those of a pleomorphic adenoma with florid squamous
metaplasia. This case illustrates the difficulty of making a correct diagnosis in the initial
tissue specimen and we discuss the diagnostic pitfalls of this pathological entity.
CASE PRESENTATION (CLINICAL DETAILS):
A 20 year old patient presented with complaint of swelling in the oral cavity since
two years. The swelling was painless and progressively increasing in size .Physical
examination showed a firm nodule of 4x4cm in diameter on the left side of the hard palate
and anterior part of soft palate.

CASE REPORT
Journal of Evolution of Medical and Dental Sciences / Volume 1 / Issue 3 / July- Sept 2012
Page 97
CYTOLOGICAL FINDINGS:
Fine needle aspiration was done and demonstrated some clusters of squamous cells,
with some of the cells showing keratinizing cytoplasm .Also seen some clusters of cells with
features suggestive of glandular differentiation .Differential diagnosis of well differentiated
squamous cell carcinoma & pleomorphic adenoma was made .
GROSS / HISTOPATHOLOGICAL FINDINGS:
Surgical resection was done. Gross specimen comprised of well circumscribed, well
encapsulated mass, grey white in color and measured 3x3x2cm .No cystic area, hemorrhage
or necrosis was seen .Histological examination showed a well encapsulated tumor more
than 75% of epithelial element in the tumor was composed of squamous cells with multiple
keratin filled cysts. The rest of areas showed features of conventional pleomorphic
adenoma.
DISCUSSION:
Histological diversity is the hallmark of pleomorphic adenoma. [3] Histological
patterns vary considerably between different parts of same tumor. [3] Focal squamous
metaplasia is found in about 25% of pleomorphic adenoma. Rarely focal squamous
metaplasia is reported. [4] Squamous metaplasia is commonly associated with repair
following infarction and necrosis of the salivary gland. In the present case necrosis was not
seen and squamous cells were detected in FNA biopsy as well as in the resection specimen.
squamous metaplasia has been noted in non-neoplastic entities like chronic sialadenitis,
necrotizing sialometaplasia, lymphothelial cysts occurring in the vicinity of salivary gland .
Potential for misdiagnosis of pleomorphic adenoma as mucoepidermoid carcinoma and
squamous cell carcinoma have been reported. In our case also the features misinterpreted
as mucoepidermoid & squamous cell carcinoma. To avoid misinterpretation of pleomorphic
adenoma with squamous metaplasia as mucoepidermoid carcinoma on cytology, a close
scrutiny for fragments of chondromyxoid stroma – a characteristic feature for pleomorphic
adenoma. In our case also on reviewing the slides again after histological diagnosis we could
find occasional tiny fragments of stroma . Also keratinization especially of the extracellular
type is rare in mucoepidermoid carcinoma. How ever even if the features diagnostic of
pleomorphic adenoma are identified, the differential diagnosis may still includes a
mucoepidermoid carcinoma arising in a preexisting pleomorphic adenoma.
CONCLUSION:
We have reported a case of palatal pleomorphic adenoma with florid squamous
metaplasia and with potential pitfalls in the diagnosis.
ACKNOWLEDGEMENT:
The work was indeed a mammoth task to accomplish and would not have been
possible without active co-operation, constant strategic support and encouragement by our

CASE REPORT
Journal of Evolution of Medical and Dental Sciences / Volume 1 / Issue 3 / July- Sept 2012
Page 98
beloved – PRESIDENT- (Khaja Bandanawaz Institute of Medical Sciences)—DR.SYED SHAH
KHUSRO HUSSAINI.
REFERENCES:
1. Spiro RH. Salivary neoplasms : overview . Head Neck Surg 1986; 8 :177-84
2. Waldron CA. Mixed Tumor ( pleomorphic adenoma ) and myoepithelioma. In : Ellis
GL, Auclair PL, Gnepp PR. Eds . Surgical pathology of salivary glands. Philadelphia :
Saunders , 1999; 165-86
3. Das DK. Anim JT. Pleomorphic adenoma of salivary glands. Cytopathology 2005 : 16:
65-70
4. Lam KY, Ng IOL, Chan GSW. Palatal pleomorphic adenoma with florid squamous
metalasia . J Oral Pathol Med. 1998; 27: 407-10.

CASE REPORT
Journal of Evolution of Medical and Dental Sciences / Volume 1 / Issue 3 / July- Sept 2012
Page 99
Fig 1- Photograph showing swelling in the palate
Fig 2- Gross photograph showing well circumscribed tumor

CASE REPORT
Journal of Evolution of Medical and Dental Sciences / Volume 1 / Issue 3 / July- Sept 2012
Page 100
Fig 3- Photomicrograph showing squamous cells with keratin pearls. (H&E, 400X)
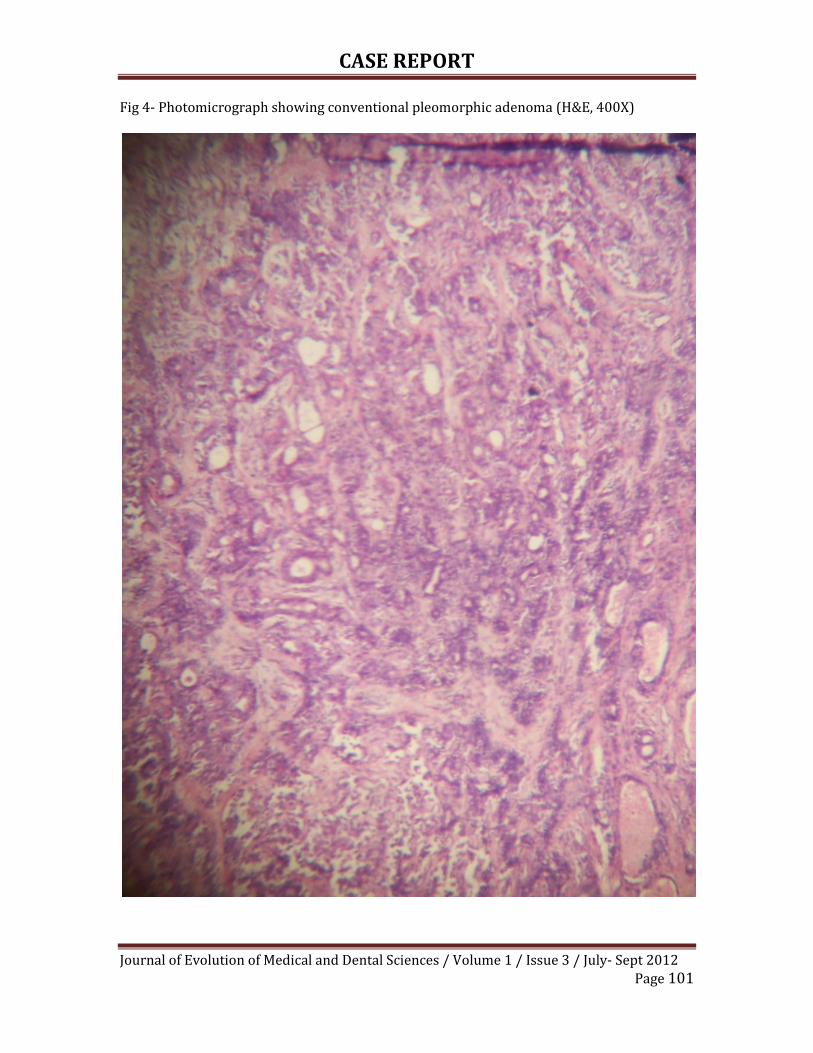
CASE REPORT
Journal of Evolution of Medical and Dental Sciences / Volume 1 / Issue 3 / July- Sept 2012
Page 101
Fig 4- Photomicrograph showing conventional pleomorphic adenoma (H&E, 400X)

CASE REPORT
Journal of Evolution of Medical and Dental Sciences/Volume 1/Issue 3/July- Sept 2012 Page 102
CUTANEOUS NECROTISING VASCULITIS – THERAPEUTIC FACT-A CASE
REPORT
Dr Kiran. D. R, Dr Palaniswamy
1. Associate Professor, Department of General Medicine, Karuna Medical College, Vilayodi, Chittur, Palghat,
Kerala.
2. Professor, Department of General Medicine, Karuna Medical College, Vilayodi, Chittur, Palghat, Kerala.
CORRESPONDING AUTHOR:
Dr. Kiran D R.,
Associate Professor,
Department of Medicine,
Karuna Medical College, Vilayodi,
Chittur, Palghat, Kerala.
Email id- [email protected]
ABSTRACT: INTRODUCTION: Mixed connective tissue disorder, unlike other connective tissue
disorders have a milder course. MTCD with only necrotizing cutaneous vasculitis without organ
damage respond well to Immunosuppresents and Steroids. CASE REPORT: Middle aged Young
lady presented with multiple non healing large pressure sores and multiple nonblanchable
purpuric lesions. She was bedridden, anaemic and with significant weight loss. All her major
organ functions were normal. Her U1 RNP Antibody is positive and Skin Biopsy showed
positive direct fluorescent test for IgG. She responded well to immunosuppresants and steroids.
CONCLUSION: This patient who presented with MTCD, with predominant necrotizing
cutaneous vasculitis and without major organ involvement showed good recovery and
responded well to cyclophosphamide pulse therapy, daily azathioprine and good wound care.
KEY WORDS: Necrotising Vasculitis, MCTD, U1 RNP Antibody, Immunosuppresants
INTRODUCTION:
Vasculitis is not a disease but rather a disease process (from Merck manual).Here we
came across a MCTD with predominant necrotizing vasculitis involving only skin .This is been
reported so as to stress the fact that MTCD , unlike other connective tissue disorders has milder
course and necrotizing vasculitis confined to skin do well with immunosuppresives, steroids
and good wound care 5.
CASE REPORT:
Female patient aged 34 year old, presented with weight loss( more than 10%), lethargy
and multiple non healing open ulcers associated with necrotic base over pressure bearing areas
predominantly confined to extensor areas of limbs of one year duration. She had intermittent,
moderate grade fever without cough and rashes. She was bed ridden due to sever nonhealing
disabling ulcers over the pressure bearing areas and joint contractures.
On examination, Patient is thin built and poorly nourished.
Multiple non blanchable purpuric lesions, multiple depigmented lesions on face and loss of scalp
hair.
Pallor present, Febrile, Tachycardia present.
Systemic examination– Normal.

CASE REPORT
Journal of Evolution of Medical and Dental Sciences/Volume 1/Issue 3/July- Sept 2012 Page 103
Investigations: Hb 6gm/dl, WBC -8200, Eosinophils increased, Platelet count- 80,000, ESR-110,
CRP elevated,
LFT and RENAL FUNCTION: Normal
Urine Routine: Normal, No albumin or microscopic Haematuria
ECG: WNL
Echo: No pericardial fluid, EF – 60%, Normal Function.
PFT: Normal curve, No features of interstitial pattern.
Chest X Ray: CP angles free and normal, lung parenchyma normal, No Infiltrates.
USG Abdomen: NO Organomegaly, pelvis normal.
Stool examination: No occult blood.
CT brain: Normal study.
NCS: Normal.
Ophthalmological Examination: Visual Aquity-6/6, Fundus –Normal.
ANA positive, RA Factor negative
ANCA negative, U1 RNP Antibody positive,
Skin Biopsy – direct fluorescent test positive for IgG, Complements were normal ,
HIV 1&2 negative, Hepatitis B & C Negative.
Diagnosis of MCTD was made with above findings.
TREATMENT GIVEN:
Patient was started with steroids, monthly pulse therapy of Cyclophosphamide and daily
2mg of Azathioprine. Other general conditions maintained with blood transfusion and
supportive care. Wounds were been taken care of by debridement and allowed them to go for
healing by secondary intention. Some of the wounds healed in one setting, but others required
2-3 attempts. Finally in six months duration all wounds healed well and now patient is
ambulatory, self dependant with only Azathioprine daily.
ACKNOWLEDGEMENT:
I take this opportunity to extend my sincere thanks and indebtedness to all those
persons and dignitaries who helped me to complete this work.
It gives pleasure to express my sense of gratitude to my professor Dr Palaniswamy for
his guidance, encouragement and constant source of inspiration during case management.
Above all I thank the Almighty for the successful completion of this work.
DISCUSSION:
MCTD also known as Sharp’s syndrome an undifferentiated connective tissue disease.
MCTD a combined feature of scleroderma, myositis, SLE and Rheumatoid Arthritis (with some
source adding polymyositis, dermatomyositis and inclusion body myositis) and is thus
considered as overlap syndrome. MCTD commonly causes joint swelling, malaise, Raynaud’s
phenomenon, Sjogren’s syndrome, muscle inflammation and sclerodactyly. Distinguishing lab
characteristics are positive speckled ANA and an anti U1RNP antibody. It is associated with HLA
DR-41.
Vasculitis induced injury to blood vessel may lead to increased vascular permeability,
vessel weakening that cause aneurysm formation, haemorrhage and intimal proliferation,
thrombosis that result in obstruction and local ischemia2. It is critical to distinguish vasculitis
occurring as a primary autoimmune disorder from vasculitis secondary to infection, drugs,
malignancy or connective tissue disease such as SLE/ RA. Much of the diagnostic work up in a

CASE REPORT
Journal of Evolution of Medical and Dental Sciences/Volume 1/Issue 3/July- Sept 2012 Page 104
patient with suspected vasculitis is directed at excluding secondary causes that can mimic
vasculitis3.
Immunoglobulin finding may be helpful in diagnosing MTCD. Indirect Immuno
fluroscent test – Presence high titre of IgG against U1RNP as the only autoantibody support
MTCD. The fluroscent auto nuclear antibody test typically reveals a speckled pattern of staining
on HEP-2 substrate. Recent studies revealed that antibody directed to an appropriate specific
epitop on 70 kd are specifically associated with MTCD than other anti 70 k antibody. Direct
Immuno fluroscent test- Performed on lesional skin of patients with MTCD, this may reveal
epidermal nuclear IgG staining. The staining is thought to be related to high titres U1RNP
antibody in the patient seen. In some cases Lupus Band test may be positive (linear deposition
of Ig, Fibrin and/or compliment components present at the basement membrane) 4.
Treatment option includes corticosteroids, Immunosuppressive drugs to reduce the
inflammation. Cyclophosphamide may be in severe vasculitis. Dramatic remission seen in
patient with alternate day corticosteroid treatment with continuation of cyclophosphamide.
Later corticosteroid was discontinued. Mean duration of remission was 22 months. No patient
showed recurrence of disease during treatment with cytotoxic agents5. IV cyclophosphamide is
better than oral and recommended at least six months. Substitution of Azathioprine after
remission with cyclophosphamide did not increase the rate of relapse.
Newer treatment approach includes deoxysperagualin, achieved a high rate of disease
remission and permitted prednisolone reduction. Other newer Immunosuppresives are
Leflunamide, TNF antagonists – Infliximab and ENBREL. Colchicine not that much effective in
skin va sculitis, but some showed improvement. Development of plasma exchange including
semi specific immunoabsorption with L-tryptophan or Protein A columns to remove ANCA
without depletion of non Ig plasma proteins and appear of comparable efficacy to plasma
exchange6.
CONCLUSION:
MCTD, although called as overlap syndrome, here we came across MCTD without major
organ involvement, without associated other connective tissue diseases. Predominant
presentation was confined to skin as necrotizing cutaneous vasculitis. The disease here showed
a chronic disabling course which provided enough time to treat with Pulse cyclophosphamide
therapy, daily Azathioprine and good wound care. MCTD without predominant organ
dysfunction and confined to skin manifestation as a good prognosis with regular treatment than
the systemic vasculitis or MCTD with other connective diseases, which has mixed results to the
regular treatment.
REFERENCES:
1 Aringer M, Steiner G, Smolen JS (Aug-03). “Does MCTD exist? Yes.” Rheumatic disease clinical
North America. 31(3): 411-29.
2 Mandell BF, Hoffman G.S. Differrentiating the Vasculitis. Rheumatic disease clinical North
America (1994); 20:409-42.
3 Hunder G. Vasculitis Diagnosis and therapy. Am. J Med: 1996; 100(22):375-455
4 H Ihn, K Yamane, N Yazawa, M Kuba, M Fujimoto, S Sato, K Kikuchi and K Tamaki; Distribution
of antigen specificity of Anti U1RNP antibody in patient with systemic sclerosis. Clinical
Experimental Immunology(1999)117(2);383-387.
5 FauciAS,Katz P,Haynes BF, Wolf SM:Cyclophosphamide therapy for sever necrotizing
vasculitis(1979) vol 301:235- 238.

CASE REPORT
Journal of Evolution of Medical and Dental Sciences/Volume 1/Issue 3/July- Sept 2012 Page 105
6 Jayne D (2000)Evidence based treatment of systemic vasculitis. Rheumatology(Oxford)
39:585-595.
ABBREVIATIONS:
MCTD: Mixed Connective Tissue Disease
HLA: Human Leucocyte Antigen
SLE: Systemic Lupus Erythematosis
RA: Rheumatoid Arthritis
RNP: Ribosomal Neucleo Protein
ANA: Anti Nuclear Antibody
ANCA: Anti Nuclear Cytoplasmic Antibody
Post Treatment- Healed cutaneous Vasculitis on face, Post Healed Hypopigmented Lesion

CASE REPORT
Journal of Evolution of Medical and Dental Sciences/Volume 1/Issue 3/July- Sept 2012 Page 106
PLASMA CELL LEUKEMIA- LIGHT CHAIN SECRETORY TYPE, WITH
PRIMARY AMYLOIDOSIS
Dr Kiran. D. R, Dr Palaniswamy
1. Associate Professor, Department of General Medicine, Karuna Medical College, Vilayodi, Chittur, Palghat,
Kerala.
2. Professor, Department of General Medicine, Karuna Medical College, Vilayodi, Chittur, Palghat, Kerala.
CORRESPONDING AUTHOR:
Dr. Kiran D R.,
Associate Professor,
Department of Medicine,
Karuna Medical College, Vilayodi,
Chittur, Palghat, Kerala.
Email id- [email protected]
ABSTRACT:
INTRODUCTION: Secondary PCL (Plasma Cell Leukemia), arising from multiple myeloma is
aggressive and rare variant of multiple myeloma. It is known that AL (Amyloid Light Chain)
type of Amyloidosis is primary amyloidosis occurring in multiple myeloma. Attempt to report
this case of secondary PCL of light chain secretory type with primary amyloidosis. Emphasis
given to this report is so as to highlight the helpful prognostic tools in this rare variety.
CASE REPORT: 60 year old female presenting with Hepatosplenomegaly, severe anemia,
bleeding manifestations and fever. She had pancytopenia with ESR of 170. Peripheral smear
showed plenty of plasma cells >20% and bone marrow biopsy showed mature to immature
plasma cells, plenty in number. Skull X ray showing multiple punched out lesions.
Electrophoresis was normal, abdominal wall fat stained positive for Congo Red and Serum Free
Light Chain Assay was positive. Diagnosed as PCL of light chain secretory type. CONCLUSION:
PCL itself, high plasma cell labeling index, increased LDH, increased serum
β2microglobulin,renal indices like increased serum creatinine, organomegaly, non secretory
variety-all carry bad prognostic signs.
KEY WORDS: PCL, Primary Amyloidosis, Light chain, Punched out bone lesions
INTRODUCTION:
It is known that incidence of PCL is <1 / million cases and 2% of multiple myeloma1. It is
an aggressive and rare presentation of multiple myeloma2. It has features of acute leukemia and
multiple myeloma.PCL usually arises from myeloma having IgD or IgE as M component. PCL,
arising from pre existing multiple myeloma of light chain secretory type associated with AL
(Amyloid Light chain) type of Amyloidosis is very rare. Since there are no large trials on
treatment of patients with PCL, we here make an attempt report this case.
CASE REPORT:
A 60 years old female patient presented with history of fever and epistaxis of one month
duration. On examination she was Febrile, having tachycardia and pallor. She had no
generalized lymphadenopathy but had moderate Hepatosplenomegaly. She had sternal
tenderness.

CASE REPORT
Journal of Evolution of Medical and Dental Sciences/Volume 1/Issue 3/July- Sept 2012 Page 107
INVESTIGATIONS:
WBC count – 1, 22,000
Hb-2.8mg/dl
Platelet count – 80,000
ESR- 170
Renal and Liver function tests are normal
Serum calcium: 12 mg/dl
Serum uric acid: normal
Serum LDH: 310u/L
Serum β2 microglobulin: 3.1mg/L
Serum Electrophoresis showed no M band
Serum Free Light Chain Assay: detected
Urine Bence Jones protein: Negative
Peripheral Smear Report: RBC showed hypochromia and anisocytosis. Neutrophils were
decreased in number. A large number of plasma cells were seen .Immature and abnormal
plasma cells were seen in plenty. A good number of binucleated plasma cells also seen.
Immature cells exceeded 20%. Platelets grossly decreased in number.
Bone Marrow Aspiration Report: Hypercellularmarrow.RBC precursors were reduced in
number and were normopoietic. Granulocytic precursors were also reduced in number. Each
field showed sheets of plasma cells. Many of the plasma cells were atypical. Some of them were
rounded, some had nuclear abnormalities and some were binucleated. A large number of
plasma blasts were also seen. Megakaryocytes were reduced in number.
Flow Cytometry of Bone Marrow Aspirate: Showed intense positivity for CD 38 and the
presence of cytoplasmic kappa light chains.
Abdominal fat stained positive for Congo Red.
Skull X-ray showed multiple punched out lesions.
Our patient was diagnosed to have primary PCL – light chain type with Primary Amyloidosis,
based on peripheral smear, bone marrow and flow cytometric analysis.
Treatment: Patient was given supportive treatment. Prednisolone and Melphelan were started.
Patient expired in two months after diagnosis.
DISCUSSION:
Plasma cell leukemia is a lymphoproliferative disorder. It is a rare monoclonal
neoplasm having B lymphocyte lineage. It is one of the aggressive human neoplasms accounting
for 2-4% of all cases of plasma cell diseases3. Rarity of PCL can be accessed from the fact that at
M.D. Anderson cancer centre, 27 patients with PCL were seen in 20 year period whereas at
Policlinico-Sanmateo in Italy, 15 cases were seen in 15 years, both representing 2-5% of total
cases of multiple myeloma seen at these centers. Incidence of PCL is less than 1 case per million
population1. Presentation may be primary, secondary – evolving from an existing case of
multiple myeloma as part of the terminal phase of the disease or denova. Sixty to seventy
percent cases are primary. PCL is of two types, Secretory and non-secretory. No M protein is
detected in the non secretory type of PCL4.
WHO criteria to diagnose PCL are - Plasma cells constitute more than 20% of cells in the
peripheral blood with an absolute plasma cell count of more than 2 X 109 / litre.
Lab findings: There is overlap between cells of multiple myeloma and Primary PCL. PCL plasma
cells more frequently express the CD 20 antigen than those of multiple myeloma and they often

CASE REPORT
Journal of Evolution of Medical and Dental Sciences/Volume 1/Issue 3/July- Sept 2012 Page 108
lack CD 56 antigen which is present on the majority of myeloma cells. CD 56 is important in
anchoring plasma cells to bone marrow stroma and its expression is associated with poor
prognosis. CD 28 is more frequently expressed on malignant plasma cells in secondary than in
primary PCL. Acquisition of CD 28 is associated with increased proliferative rate and disease
progression. PCL is derived from terminally differentiated B cells and the malignant cells stain
positive for mature B cell markers (CD38 and PCA1, Prostate Cancer Antigen 1)5.
In 80% of PCL patients, using FISH (Flourescent In Situ Hybridisation) technique- losses in long
arm of chromosome 13 (13 Q) and deletion of one of the homologous chromosome 13
(Monosomy 13). In 80% of cases, loses on chromosome 16 also occur. Overexpression of
PRAD1/cyclinD1 (Parathyroid associated Neoplasia gene) also present (help in controlling cell
cycle). PCL is more frequent in light chain (Bence Jones’s protein) or IgD myeloma and less in
IgA or IgG myeloma. Hypercalcaemia and increased LDH are known bad prognostic signs of
disease 6. PCL is an extremely aggressive disease with no standard treatment regimen so far
due to the rarity of the disease. Median survival is 2-8 months, prognosis is very poor.
Regimens includes MP, (Melphelan, Prednisolone) VAD (Vincristine, Doxorubicin,
Dexamethasone) TD (Thalidomide, Dexamethasone) VBAP (Vincristine, Carmustine,
Adriamycin, Prednisolone) 7. Case reports regarding long time survival after autologous bone
marrow transplantation or stem cell transplantation also exists but again there is no long term
prospective data on a large number of patients. We presented this case for its rarity.
CONCLUSION:
PCL itself has aggressive course, short survival time, high plasma cell labeling index,
expression of CD 28, Cyclin, PRAD 1 indicate high proliferation. Lytic bone lesion is more
common in multiple myeloma than PCL. Biochemical parameters like increased serum
creatinine, LDH, Serum β2microglobulin and calcium have poor prognosis. Amyloidosis
associated multiple myeloma indicate tumor burden. Non secretory variety has got bad
prognosis. So above mentioned prognostic tools may help to judge the severity of the tumour
burden in a PCL case and act accordingly
ABBREVIATIONS:
PCL: Plasma Cell Leukemia
LDH: Lactate Dehydrogenase
CD: Cluster Differentiating
AL: Amyloid Light
ACKNOWLEDGEMENT:
I take this opportunity to extend my sincere thanks and indebtedness to all those
persons and dignitaries who helped me to complete this work.
It gives me pleasure to express my sense of gratitude to my Professor Dr Palaniswamy,
for their guidance, encouragement and constant source of inspiration during case management.
Above all I thank the Almighty for the successful completion of this work.

CASE REPORT
Journal of Evolution of Medical and Dental Sciences/Volume 1/Issue 3/July- Sept 2012 Page 109
Skull X Ray PA view- Showing punched out lesions
Skull X Ray Lateral view- Showing punched out lesions
REFERENCES:
1. Kosma MA, Gale RP. Plasma Cell Leukemia.SeminHaematology 1987.24; 202-8
2. DimopoulasMA,PalumboA,DelasalleKB,AlexanianR.Primary Plasma Cell leikamia.Br
Journal Hematol 1994;88;754-9.
3. Chan SM, George T, Cherry AM,Medeiras BC(2009) Complete remission of primary PCL
Bortezomito, Doxorubicin and Dexamethasone; a case report; cases 12: 1186/1757-
1626-2.
4. ShindoT,Yumoto Y, Yoshida M, Okuda T; Non Secretory Primary Plasma Cell Leukemia
successfully treated with VAD and MP therapy.RhinshoKetsueki; 2002;43; 107-11
5. Badhe BA, Basu D, Toe P Ch,Dutta TK, Ghotekar LH; Plasma Cell Leukemia; a case report.
Indian Journal Pathology Microbiology 2003; 46; 484-7.
6. Voutsadakis IA; Plasma Cell Leukemia. Hama 2000; 3:82-9.
7. Suzuki M, Kawauchi K, Sugiyama H, Yasuyama M, Watanabe H. Primary Plasma Cell
Leukemia; a case report of successful responder to a combination of Vincristine,
Doxorubicin and Dexamethasone. ActaHematol 1989; 82:95-7.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/ Volume 1/ Issue 3/ July- Sept 2012 Page 110
ANTI-CONVULSANT ACTIVITY OF GANAXOLONE ALONE AND IN
COMPARISON WITH STANDARD ANTI-EPILEPTIC DRUGS IN
RODENT MODELS
Mr. S.K. Subhani Basha, Dr .B. L. Kudagi, Dr. R. Pravin Kumar
1. Tutor, Department of Pharmacology, Narayana Medical College, Nellore.
2. Professor & H.O.D., Department of Pharmacology, Narayana Medical College, Nellore.
3. PG Student, Department of Pharmacology, Narayana Medical College, Nellore.
CORRESPONDING AUTHOR:
Dr .B. L. Kudagi,
Professor & H.O.D.,
Department of Pharmacology,
Narayana Medical College,
Nellore.
Email ID- [email protected]
ABSTRACT:
BACKGROUND: Presently, treatment of epilepsy with standard anti-epileptic drugs is
associated with a number of shortcomings inviting us to study newer agents that would
overcome these problems or search for the drugs or substances, which would enhance the
efficacy or reduce the dose or toxicity of these standard anti-epileptic drugs. Ganaxolone
(GNX) (3α-hydroxy-3β-methyl-5α-pregnan-20-one), a synthetic analog of the endogenous
neurosteroid allopregnanolone and a positive allosteric modulator of GABAA receptors, may
represent a new treatment approach for epilepsy. AIM: To evaluate the effect of Ganaxolone
on maximal electroshock (MES) induced and Pentylenetetrazol (PTZ) induced convulsions
and also their effect in combination with conventional antiepileptic drugs (CAEDs).
MATERIAL AND METHODS: Wister strain albino rats weighing 200-250 gm were used.
Effects of Ganaxolone (5 &10 mg/kg) alone and in combination with standard drugs were
studied in MES and PTZ induced seizure models. Abolition of tonic hind limb extension was
an index of anticonvulsant activity in MES, while for PTZ seizures; failure to observe clonus
for 5sec duration for 30min was the index. Following that, percentage inhibition was
calculated. STATISTICS: ANOVA followed by Newman-Keuls Multiple Comparison Test was
used for analysis of data between the groups. RESULTS: In MES seizures, significant anti-
epileptic activity was observed with 10mg of Ganaxolone compared to control group but
has less activity when compared to that of Phenobarbitone. In PTZ induced convulsions, the
anti-epileptic effect of Sodium Valproate was higher than Ganaxolone, but both were
statistically significant as compared to control. In PTZ-induced seizures, augmented effects
were obtained when Ganaxolone was combined with sodium valproate i.e. 55%.
CONCLUSIONS: The results provide a lead for potential benefit of adding Ganaxolone to
Sodium Valproate in the treatment of epilepsy, which needs to be explored further.
KEYWORDS: Seizures, Ganaxolone, Phenobarbitone, Sodium Valproate, Pentylenetetrazol,
Hydoxypropyl-β-Cyclodextrin, GABA.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/ Volume 1/ Issue 3/ July- Sept 2012 Page 111
INTRODUCTION:
Epilepsy is a common and chronic neurological disorder characterized by apparently
unprovoked recurrent paroxysmal events or seizures that are associated with a sudden
alteration in motor activity and behavior, with or without alteration in conscious
awareness. The alteration in state is the result of an abnormal and excessive hyper
synchronous firing within a group of epileptic neurons in the brain1. Epilepsy affects
around 50 million people worldwide and the majority of people with epilepsy (70%) have
a good prognosis if they receive appropriate treatment. The prevalence of active epilepsy is
roughly in the range of 5–10 per 1000 people2. Epilepsy's approximate annual incidence
rate is 40–70 per 100,000 in industrialized countries and 100–190 per 100,000 in
resource-poor countries; socioeconomically deprived people are at higher risk. In
industrialized countries the incidence rate decreased in children but increased among the
elderly during the three decades prior to 2003, for reasons not fully understood. Epilepsy's
lifetime prevalence is relatively high because most patients either stop having anti-epileptic
drugs or (less commonly) die3.
In about two-thirds of all patients affected with epilepsy, seizures are well
controlled with currently available anti-epileptic drugs, while in the remainder seizures are
refractory to treatment. Moreover, many of the existent anti-epileptic agents produce many
undesirable side-effects including drowsiness, mental dullness, nausea, ataxia, paresthesia,
hematologic changes, hirsutism, weight gain, hypertrophy of gums and congenital
malformations. For these reasons, new antiepileptic drugs are needed to improve seizure
control and decrease side-effect profile4.
At the neuronal level, seizure activity often occurs when glutamatergic excitatory
neurotransmission overrides GABA-mediated inhibition. Therefore, glutamatergic and
GABAergic systems are rational targets for antiepileptic drug development5. Pharmacological
manipulations leading to increased levels of GABA (by inhibition of GABA degradation or
reuptake) and/or positive allosteric modulation of the GABA receptor complex are among
the approaches that have been used to facilitate inhibitory GABAergic neurotransmission6.
Ganaxolone (3α-hydroxy-3β-methyl-5α-pregnan-20-one), the 3β-methyl analog of the
progesterone metabolite allopregnanolone, is the first synthetic neurosteroid related agent
to be evaluated in man for the drug treatment of epilepsy, which is now undergoing phase-
III clinical trials7. Ganaxolone, like Allopregnanolone, acts as a powerful positive
allosteric modulator of GABAA receptors, resulting in enhanced neural inhibition8.
Hence, the present study was undertaken to determine whether Ganaxolone alone or
along with standard antiepileptic drugs could provide superior seizure control in maximal
electroshock (MES) induced and Pentylenetetrazol (PTZ) induced convulsions as compared
to CAEDs.
MATERIALS & METHODS:
ANIMALS:
Wister strain albino rats weighing between 200-250gms were used, for this study.
The animals were obtained from the central animal house of Narayana Medical College,

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/ Volume 1/ Issue 3/ July- Sept 2012 Page 112
Nellore. They were housed in standard polypropylene cages. The animals were excluded if the
weight of rats were below 200gms and if they had any visible diseases. The animals are
maintained under standard laboratory conditions (12:12 hr light: dark cycles and
temperature 250C ± 10C with free access to food and water ad libitum. All the experiments
were carried out around the same time each day. All the experimental procedures and
protocols were reviewed and approved by the Institutional Animal Ethics Committee (IAEC)
of the institute, with protocol number 12/2010/NMC.
CHEMICALS & DRUGS:
All standard chemicals used in this study were of analytical grade. Pure form of
Ganaxolone & Hydoxypropyl-β-Cyclodextrin were obtained from Sigma chemicals. Stock
solutions of Ganaxolone for injection were made in 40% Hydoxypropyl-β-Cyclodextrin in
water. By itself, β-cyclodextrin at concentrations as high as 50% failed to affect seizures.
ASSESSMENT OF ANTICONVULSANT ACTIVITY:
GROUPING:
To study the anti-epileptic activity of Ganaxolone, two models namely MES induced
convulsions and Pentylenetetrazol induced convulsions in rats were used. Each model
consists of five groups, each group containing 6 animals.
Groups were divided as follows,
Group I (Control group) was treated with 40% (w/v) Hydoxypropyl-β-Cyclodextrin 4ml/kg
body weight.
Group II received Ganaxolone at a dose of 5 mg/kg body weight.
Group III received Ganaxolone at a dose of 10 mg/kg body weight.
Group IV received standard drug (Phenobarbitone 20mg/kg – MES, Sodium Valproate
200mg/kg – PTZ seizures).
Group V received Ganaxolone at 5 mg/kg body weight and standard drug.
Separate groups of animals were used for different models and all the groups
received the drugs intraperitonially at different sites throughout the experiment.
Concentration of drugs were so adjusted that all the animals in the group received the
same volume of preparation throughout the study. All the drugs were given 30 min prior
to the induction of convulsions.
MES SEIZURE METHOD9:
Anticonvulsant activity of Ganaxolone was tested for MES seizure by inducing
convulsions with an electroconvulsiometer. In this method, electrical stimulation was
applied via clipped-ear electrodes (moistened with saline solution before each application)
which delivered a constant current of 150mA current for 0.2 seconds. Abolition of hind limb
tonic extension was taken as an index of anticonvulsant activity10. Parameters observed
were time for onset and duration of tonic hind limb extension (THE).
CHEMICALLY INDUCED SEIZURES9:

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/ Volume 1/ Issue 3/ July- Sept 2012 Page 113
Pentylenetetrazol is a tetrazol derivative with consistent convulsive effect in a larger
number of animal species like mice, rats, cats, primates etc. It is believed to act by
antagonizing the inhibitory GABAergic neurotransmission10. This model was used to screen
the anti-epileptic efficacy of Ganaxolone against petit mal epilepsy as Ganaxolone also acts
through GABA-A receptor modulator mechanism.
Rats were injected with Pentylenetetrazol (70 mg/kg, i.p) 30 minutes after test drug
and standard drug (Sodium Valproate – 200mg/kg) and the occurrence of the first
generalized clonus (repeated clonic seizures of the fore and hind limb lasting over 5sec.
with an accompanying loss of righting reflex) or jerky movements were recorded during
individual observation for 30 min.
STATISTICAL ANALYSIS:
The data was collected in case record forms and then entered into excel
spreadsheet 2007. Statistical analysis was performed using Microsoft Excel – 2007 and
Sigma Graph pad prism version-5 USA. Data was described as Mean ± Standard deviation.
One way ANOVA followed by Newman-Keuls Multiple Comparison Test was used for
analysis of data between the five groups. For all inferential statistical tests a two tailed P
value of less than 0.05 was considered significant.
RESULTS:
EFFECT OF GANAXOLONE ON TONIC HIND LIMB EXTENSION IN MES:
Tonic hind limb extension was completely abolished in group IV (treated with
Phenobarbitone) and group V (combination of Ganaxolone and Phenobarbitone). Percentage
inhibition of duration of tonic hind limb extension increased with the use of Ganaxolone
10mg/kg up to 50% and were 100% for group IV and V. MES induced convulsions
blocking activity of Ganaxolone 10mg/kg was extremely significant (p<0.001) when
compared to that of control but it was less effective when compared to Phenobarbitone.
The combination of Ganaxolone + Phenobarbitone has a similar / superior MES induced
convulsions blocking activity compared to that of Phenobarbitone alone.
EFFECT OF GANAXOLONE ON PTZ INDUCED SEIZURES:
The onset of jerky movements in PTZ induced convulsions were significantly
delayed by Ganaxolone 10mg/kg (p<0.001) as compared to the control. Percentage
inhibition of duration of jerky movements with 10 mg of Ganaxolone was 37.5% and it was
45% for sodium valproate, whereas as the combination of Ganaxolone + Sodium Valproate
(group V) further decreased the duration of jerky movements up to 55%, implying that PTZ
induced convulsions blocking activity of Sodium Valproate was more than that of
Ganaxolone, but both were statistically significant. The combination of Ganaxolone and
Sodium Valproate has a superior PTZ induced convulsions blocking activity compared to
that of Sodium Valproate alone.
DISCUSSION:

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/ Volume 1/ Issue 3/ July- Sept 2012 Page 114
The present study was aimed at evaluating the effect of Ganaxolone on maximal
electroshock (MES) induced and Pentylenetetrazol (PTZ) induced convulsions and also
their effect in combination with conventional antiepileptic drugs (CAEDs) using animal
models.
Ganaxolone (GNX) is the synthetic analog of allopregnanolone (3α, 5α-P ) it belongs
to a class of compounds referred to as neurosteroids that have been termed “epalons”
which has been presumed to possess sedative, anxiolytic, and anticonvulsant effects11.
Maximal electric shock induced convulsions is a suitable test for evaluating anti-
epileptic properties of drugs, because it is the best-validated preclinical test that predicts
drugs effective against generalized seizures of the tonic–clonic (grand mal) type.
In our study, we demonstrated significant anti-epileptic activity with 10mg of
Ganaxolone compared to control group but has less activity when compared to that of
Phenobarbitone but both were statistically significant. Using this model, Virinder Nohria et
al. (2007) reported that, although Ganaxolone effectively blocked tonic seizures induced by
maximal electroshock in mice (ED50 of 29.7 mg/kg, i.p.), it did so at doses that produced
ataxia on the rotorod ( mean toxic dose, TD50, of 33.4mg/kg, i.p.)12. Same results were
observed by Richard B. Carter et al (1997), who also reported that Ganaxolone was less
potent against MES (ED50 of 29.7 mg/kg i.p.) than sodium valproate, resulting in protective
indices of 1.1, as opposed to 1.9 for valproate9.
We also evaluated the anti-epileptic activity of Ganaxolone using Pentylenetetrazol
induced convulsions model, as this test is used for screening of drugs effective in petit mal
epilepsy or absence seizures. By analyzing our results we like to state that PTZ induced
convulsions blocking activity of Ganaxolone was slightly less than that of Sodium Valproate.
Our study was supported my Richard B. Carter et al (1997), who also reported that
Ganaxolone produced potent anticonvulsant effects with PTZ induced convulsions, with an
i.p. ED50 of 4.3 mg/kg in mice and 7.8 mg/kg in rats. Ganaxolone was also active after oral
administration in rats, with an ED50 of 21.0 mg/kg. The profile of anticonvulsant activity
obtained for Ganaxolone is similar in many respects to that of the clinically used reference
agent valproate. Ganaxolone is superior to valproate, however, in its ability to increase the
seizure threshold for i.v. PTZ infusion at nonataxic doses9.
Also, Marjolein Beekman et al (1998) concluded that the neuroactive steroid
Ganaxolone is superior to a host of standard antiepileptic agents (Diazepam, Clonazepam,
Valproic acid, Ethosuximide, Phenobarbitone) in controlling the behavioral disturbances that
result from both acute PTZ administration and a regimen of PTZ that induces seizure
kindling. Although much less potent than Ganaxolone, Phenobarbital was the drug that most
closely mirrored Ganaxolone in its anti-PTZ effects13 .
Furthermore, Virinder Nohria et al (2007) also reported that Ganaxolone was
effective against clonic convulsions induced by subcutaneous Pentylenetetrazol
administration in mice and rats (ED50 values of 4.3 and 7.8 mg/kg i.p., respectively). He
also stated that PTZ-induced seizures in rats did not develop tolerance to chronic treatment
with Ganaxolone12.
MES-induced tonic extension can be blocked by drugs that inhibit voltage dependent
Na + channels, such as phenytoin, carbamazepine, and valproate (Macdonald and Kelly,1995;

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/ Volume 1/ Issue 3/ July- Sept 2012 Page 115
Rogawski and Porter, 1990; White, 1997), as well as by drugs that block glutamatergic
excitation mediated by the N-methyl-D-aspartate receptor, such as felbamate (McCabeet al.,
1993; Subramaniam et al., 1995; White et al., 1995). In contrast, clonic seizures induced by
PTZ can be blocked by drugs that reduce T-type Ca++ currents, such as ethosuximide
(Coulter et al., 1989), and drugs that enhance GABA-A receptor mediated inhibitory
neurotransmission, such as benzodiazepines, phenobarbital and perhaps valproate and
felbamate (Macdonald and Kelly, 1995; Rogawski and Porter, 1990; White, 1997)9.
Ganaxolone exhibits anticonvulsant activity to PTZ and to a lesser extent against
MES induced convulsions. Ganaxolone increased the seizure threshold before attaining a
dose sufficient to produce ataxia on the rota rod. The ability of Ganaxolone to both elevate
seizure threshold and block i.p. PTZ induced seizures can be attributed to its modulatory
effect on GABA-A neurotransmission. Whether this effect contributes to its ability to block
MES induced tonic extension is not known, but that is likely, because there is at present
no experimental evidence to suggest that Ganaxolone blocks voltage-dependent Na+ channels
or N-methyl-D-aspartate receptors.
Ganaxolone inhibits binding of the GABA-A chloride channel ligand and enhanced
binding of the benzodiazepine site ligand and the GABA site ligand. Electrophysiological
recordings showed that nanomolar concentrations of GNX potentiated GABA-evoked chloride
currents in Xenopus oocytes expressing human GABA-A receptor subunits α1, β2, γ2L, but
direct activation of chloride flux occurred only at micromolar concentrations14,15.
The unique potency and efficacy of Ganaxolone against PTZ induced convulsions have
several implications. First, these anti-epileptic effects of Ganaxolone in PTZ induced
convulsions appear to be predictive of the potency and efficacy of Ganaxolone against absence
seizures as it compares favorably with that of valproate. The results provide a lead for
potential benefit of adding Ganaxolone to Sodium Valproate in the treatment of epilepsy,
which needs to be explored further. Second, Ganaxolone may provide additional benefit in the
treatment of epilepsy by controlling anxiety, mood changes and other behavioral alterations
associated with preseizure activity. Finally, Ganaxolone may represent a novel treatment
approach to the clinical control of epilepsy.
CONCLUSION:
Overall, Ganaxolone is a high-affinity, stereo selective, positive allosteric modulator of
GABA-A receptors that exhibits potent, broad-spectrum anti-epileptic activity. The present
study supports clinical evaluation of Ganaxolone as an anti-epileptic medication with
potential therapeutic utility in the treatment of generalized, absence seizures as well as
simple and complex partial seizures, alone or as an add on drug with the conventional anti-
epileptic drugs to reduce their dose / adverse effects.
ACKNOWLEDGEMENTS:
The authors are thankful to the staffs and PGs of Narayana Medical College, Nellore
and Sigma Aldrich.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/ Volume 1/ Issue 3/ July- Sept 2012 Page 116
Table 1: Antiepileptic effect of Ganaxolone alone and in combination with Phenobarbitone
on Maximal Electric Shock (MES) induced seizures in rats
Table 2: Antiepileptic effect Ganaxolone alone and in combination with Sodium Valproate on
PTZ induced seizures in rats
S.No Group & Dose
(mg/kg i.p )
Mean time for
onset of THE
in secs
Mean time duration of
THE in secs.
Percentage
inhibition of
duration of THE
1. Control 2.7±0.52 7±0.63 ----
2. Phenobarbitone - 20 0** 0** 100
3. Ganaxolone - 5 3.5± 0.55* 6±0.89* 14.29
4. Ganaxolone - 10 6±0.63** 3.5±0.55** 50
5. Ganaxolone 5 +
Phenobarbitone - 10 0** 0** 100
** - p<0.001 compared to control , * - p<0.01compared to control ,
THE – Tonic Hind limb Extension
S.
N
o
Group & Dose
(mg/kg bw )
Onset of mean time
for jerky movements
in min.
Mean time
duration of jerky
movements in min.
Percentage
inhibition of
duration of jerky
movements
1. Control 1.8±0.34 40±4.1 ------
2. Sodium Valproate – 200 8.9±1.3** 22±1.8** 45
3. Ganaxolone - 5 4.4±0.86** 33±1.2** 17.5
4. Ganaxolone - 10 7.8±0.88** 25±1.5** 37.5
5. Ganaxolone 5 +
Sodium Valproate – 200 9.5±0.7** 18±1.2** 55
** - p<0.001 compared to control

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/ Volume 1/ Issue 3/ July- Sept 2012 Page 117
ANTICONVULSANT ACTIVITY OF GANAXOLONE ON PTZ SEIZURES

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/ Volume 1/ Issue 3/ July- Sept 2012 Page 118
REFERENCES:
1. Fisher RS, Van Emde Boas W, Blume W, et al. Epileptic seizures and epilepsy:
definitions proposed by the International League Against Epilepsy (ILAE) and the
International Bureau for Epilepsy (IBE). Epilepsia 2005;46(4):470-2.
2. "Epilepsy". World Health Organization. January 2009. Retrieved January 5, 2012.
3. Sander JW. The epidemiology of epilepsy revisited. Curr Opin Neurol 2003; 16: 165-70.
4. Maciej Gasior, Richard B Carter, Steven R Goldberg, Jeffrey M Witkin. Anticonvulsant
and behavioral effects of neuroactive steroids alone and in conjunction with Diazepam.
J Pharmacol Exp Ther 1997; 282: 543-553.
5. Bradford H F. Glutamate, GABA and epilepsy. Progress in Neurobiol 1995; 47:477–511.
6. Macdonald R L, Olsen RW. GABAA receptor channels. Annu. Rev. Neurosci. 1994; 17:
569–602.
7. Nohria V, Giller E. Ganaxolone. Neurotherapeutics 2007;4:102–105.
8. Rogawski MA, Reddy DS. Neurosteroids: endogenous modulators of seizure
susceptibility. In: Rho JM, Sankar R, Cavazos JE, editors. Epilepsy: scientific
foundations of clinical practice. New York: Marcel Dekker; 2004. P.319–355.
9. Carter RB, Wood PL, Wieland S, Hawkinson JE, Belelli D, Lambert JJ, et al.
Characterization of the anticonvulsant properties of Ganaxolone (CCD 1042; 3-alpha-
hydroxy-3-beta-methyl-5-alpha-pregnan-20-one), a selective, high-affinity, steroid
modulator of the gamma-aminobutyric acid (A) receptor. J Pharmacol Exp Ther
1997;280:1284-95.
10. Mittal R. Antiepileptics. In: Gupta SK, editor. Drug Screening Methods. 1st ed. New
Delhi: Jaypee Brothers Medical Publishers; 2009. P. 408-9.
11. Gee K.W. Epalons as anticonvulsants: actions mediated by the GABA-A receptor
complex. Proc West Pharmacol Soc 1996; 39: 55-60.
12. Virinder Nohria, Earl Griller. Ganaxolone. Neurotherpeutics: The Journal of the
American society for Experimental Neurotherpeutics 2007; 4(1): 102-5.
13. Marjolein Beekman, Jesse T Ungard, Maciej Gasior, Richard B Carter, Durk Dijkstra,
Steven R Goldberg, et al. Reversal of behavioral effects of Pentylenetetrazol by the
Neuroactive Steroid Ganaxolone. JPET 1998; 284(3): 868-77.
14. Liptakova S, Velisek L, Veliskova J, Moshe SL. Effect of Ganaxolone on flurothyl seizures
in developing rats. Epilepsia 2000; 41:788–93.
15. Kaminski RM, Livingood MR, Rogawski MA. Allopregnanolone analogs that positively
modulate GABA receptors protect against partial seizures induced by 6-Hz electrical
stimulation in mice. Epilepsia 2004; 45: 864–67.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/ Volume 1/ Issue 3/ July-Sept 2012 Page 119
SERUM MAGNESIUM AS A MARKER OF DIABETIC COMPLICATIONS Dr Mirza Sharif Ahmed Baig1, Dr Mohd Shamshuddin2 Dr K L Mahadevappa 3, Dr Abdul Hakeem
Attar1 Dr Abdul Kayyum Shaikh1
1. Department of Biochemistry, KBN Institute of Medical Sciences, Gulbarga.
2. Department of Biochemistry, Al Ameen Institute of medical Sciences, Bijapur.
3. Department of Biochemistry, KempeGowda Institute of Medical Sciences, Bangalore.
CORRESPONDING AUTHOR:
Dr Mirza Sharif Ahmed Baig,
Plot No. 109,
Macca Colony, Ring Road,
Gulbarga- 04,
Karnataka.
Email id- [email protected]
Ph- 0091 9916039995
ABSTRACT:
Type 2 diabetes has become a leading cause of morbidity and mortality world over.
Magnesium homeostasis has been hypothesized to be a link between insulin resistance type 2
diabetes mellitus, hypertension and CAD. This study was under taken to evaluate the relationship
between serum magnesium and diabetes mellitus without and with complications. We found
significantly low levels of serum magnesium in patients with DM when compared to control.
Further significantly low levels of serum magnesium were found in patients with diabetic
complications when compared with diabetic patients without complications. Hence it is concluded
that the lower levels of serum magnesium may have a bearing on the complication and morbidity in
patients of DM, and estimation of serum levels of magnesium may be helpful to monitor the severity
of complications in diabetic patients.
KEY WORDS: Coronary Artery Disease, Diabetes Mellitus, Diabetic Retinopathy, Hypomagnesemia.
INTRODUCTION:
Magnesium, the fourth most common cation in the body, has been the recent focus of much
clinical and scholarly interest. Previously underappreciated, this ion is now established as a central
electrolyte in a large number of cellular metabolic reactions, including DNA and protein synthesis,
neurotransmission, and hormone receptor binding. It is a component of GTPase and a cofactor for
Na+/ K +-ATPase, adenylate cyclase, and phosphofructokinase.
Magnesium is a cofactor in more than 300 cellular enzymatic systems and has a key role in
cellular metabolism, the recognition that Mg deficiency or excess may be associated with significant
clinical consequences has resulted in an increased interest in the utility of serum Mg
measurement(1). Magnesium is an important intracellular cation that is distributed into three
major compartments: mineral phase of bones (65%), intracellular space (34%) and extracellular
fluid (1%) (2).

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/ Volume 1/ Issue 3/ July-Sept 2012 Page 120
In several studies reduced magnesium concentrations have been observed in diabetic adults
(3-7).
The interrelationships between magnesium and carbohydrate metabolism have regained
considerable interest over the last few years. The association between diabetes mellitus and
hypomagnesaemia is compelling for its wide ranging impact on diabetic control and complications.
Magnesium depletion has been linked to the development of retinopathy (8). The etiology of
hypomagnesiamea cannt be clearly explained and serum magnesium levels have been shown to be
inversely related to the severity of diabetes (9). Hypomagnesaemia has been linked to poor
glycemic control, coronary artery diseases, hypertension, and diabetic neuropathy and foot
ulcerations (10).
Hence this work was undertaken to evaluate the relationship between serum magnesium
and diabetes mellitus without and with complications.
MATERIAL AND METHODS:
The present study was carried out in the Department of Biochemistry KBN Institute of
Medical Sciences and KBNTGH Gulbarga, and KempeGowda Institute of Medical Sciences,
Bangalore. Clearance was obtained from the institutional ethical committee.
The study was carried out on 30 age and sex matched healthy controls and 60 type 2
diabetic patients who attended the outpatient and inpatient department of KempeGowda Institute
of Medical Sciences, Bangalore during the year 2007-2008.A total 60 patients of type 2 diabetes
mellitus between 40 – 70 years, which were divided into following groups.
Control group: Included 30 healthy, age and sex matched individuals.
Group I: Included 30 patients of type 2 diabetes without complications.
Group II: Included 30 patients of type 2 diabetes with proven complications, like CAD,
retinopathy and neuropathy.
The diagnosis of type 2 diabetes mellitus was established with the recommended criteria’s
of American diabetes Association.
Inclusion Criteria: Patients in the age group of 40–70 years with type 2 diabetes without
and with proven complications, like CAD, neuropathy and retinopathy were selected.
Exclusion Criteria: Patients with recent infectious disease, immunological disorders, taking
diuretics and magnesium containing antacids, malabsorption syndrome, chronic diarrhea, renal
failure, pancreatitis, alcoholism, liver diseases, tuberculosis and thyrotoxicosis were excluded from
the study.
Informed consent was taken from patient and control subjects. A pre-structured and pre-
tested proforma was used to collect the data. Baseline data including age and sex, detailed medical
history including conventional risk factors, clinical examinations and relevant investigations
including ECG, echocardiogram, nerve conduction test, fundoscopy etc were included as part of the
methodology.
Fasting venous blood samples were collected from cases and controls and the samples were
centrifuged, serum was separated and stored at 40C. Serum magnesium was estimated by Calmagite
dye method (11) by using auto-analyzer (A25Biosystem). Magnesium reacts with the blue dye,
calmagite, in alkaline medium to form red colored complex which is measured at 530-550nm. The
intensity of the color formed is directly proportional to the amount of magnesium in the sample.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/ Volume 1/ Issue 3/ July-Sept 2012 Page 121
Protein interference and dye precipitation are avoided including the 9-ethylene oxide adduct of p-
nonylphenol (Bion NE9) and Polyvinyl pyrrolidone (Bion pup). Calcium interference is avoided by
preferential combination with EDTA and heavy metal interference is prevented by Potassium
cyanide. The reference range for serum magnesium concentration does not vary significantly for
age or sex and is closely maintained within a range of 1.7-2.4mg/dl.
PPBS were estimated 2 hours after breakfast. Urine sample was analyzed for protein and
sugar.
STATISTICAL METHODS:
Student `t’ test /Chi-square test has been used to find the significance of homogeneity of
study characteristics between three groups of patients. Analysis of variance has been used to find
the significance of study parameters between three groups. Results were expressed as mean + SD.
Probability values of P< 0.05 were considered to indicate statistical significance.
STATISTICAL SOFTWARE:
SPSS 15.0, Stata 8.0, MedCalc 9.0.1 and Systat 11.0 were used for the analysis of the data and
Microsoft word and Excel have been used to generate graphs, tables etc.
RESULTS:
Results of the present study showed significant low values of serum magnesium (P<0.001)
in patients of DM without complications when compared with controls. Further significant low
values of serum mg (P<0.001) were found in patients of DM (Table 1 & Fig 1) with complications
when compared with control.
DISCUSSION:
The magnesium ion has been shown to play an important role in the metabolism of
carbohydrates by activating various enzyme systems and helping insulin for its action. In this study
it was observed that the mean serum magnesium level was statistically significantly low (P<0.001)
in Diabetic patients without and with complications when compared with controls. This indicates
the association of hypomagnesaemia with diabetes mellitus. These results are in accordance with
the observation of Tosiello L (12), Kao WH (13), and Chamber E C (14). In our study, serum
magnesium level in cases with diabetic complications (1.29 + 0.31) was much lower than those
without complications (1.61 + 0.41).
We also noted that in subjects with diabetic complications serum magnesium levels were
much lower when compared to diabetics without complications. Hatwal A et al, Andrea Corsenello
et al and Rodriguez Moran M et al have found similar results in patients with diabetic
complications. Ishrath Kareem et al found that serum magnesium levels in patients with diabetic
retinopathy were significantly lowered compared to patients without retinopathy (15). Aradhana
Sharma et al also found that serum magnesium levels were significantly lowered in patients with
diabetic complications when compared to diabetic patients without complications (16).
In our opinion the release of insulin caused by a glucose challenge is partly dependent on
adequate magnesium. Insulin, via its interaction with ligand activated tyrosine protein kinase
associated receptors, initiates a cascade of biochemical interactions that result in several

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/ Volume 1/ Issue 3/ July-Sept 2012 Page 122
physiological, biochemical and molecular events that are involved in carbohydrate, lipid and
protein metabolism (17). Although the binding of insulin to its receptor does not appear to be
altered by magnesium status, the ability of insulin once bound to receptor to activate tyrosine
kinase is reduced in hypomagnesaemia states (18). As a result reduced peripheral glucose uptake
and oxidation are often noted in subjects with hypomagnesaemia. Decrements in the enzymatic
activities of several metabolic pathways are seen in DM patients as a result of the relative
magnesium deficiency (19).
The exact cause of diabetic hypomagnesaemia is still unknown but an increased urinary loss
of magnesium may contribute to it. Hypomagnesaemia has been reported to occur at an increased
frequency among patients with type 2 diabetes compared with their counter parts without
diabetes. Despite numerous reports linking hypomagnesaemia to chronic diabetic complications,
attention to this issue is poor among clinicians. The precise mechanism for development of
microvascular changes is not fully understood, it is possible that hypomagnesaemia inhibits
prostacyclin receptor function producing an imbalance between prostacyclin and thromboxane
effect which has marked atherogenic potential which is responsible for microvascular
complications.
Thus we conclude that the estimation of serum magnesium levels is helpful to monitor the
severity of complications in type 2 diabetes and also be useful for proper medical intervention.
Hence further studies on serum magnesium levels and on oral supplementation to prevent
late complications of diabetes will be interesting and helpful.
Table 1: Serum Magnesium in the three study groups
Study
parameters Controls
DM without
complications
DM with
Complications
Sr.Mg /dl 2.17±0.35 1.61±0.41** 1.29±0.31**
Results are presented in Mean ± SD P < 0.001 highly significant
Fig 1: Serum Magnesium in the three study groups
0
0.5
1
1.5
2
2.5
3
Controls DM without complications
DM with complications
Sr. M
g (m
g/dl
)

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/ Volume 1/ Issue 3/ July-Sept 2012 Page 123
REFERENCES:
1. Elin R. J.Assement of magnesium status. Clin Chem 1987; 33:1965 – 1970.
2. Gums J G. Clinical significance of magnesium: A review. Drug Intell Clin Pharm 1987; 21:
240 – 246.
3. Maltezos E,Papazoglou D, Exiara T, Kambouromiti G, Antonoglou C. Serum magnesium
levels in non diabetic offspring of patients with type 2 diabetes mellitus. Diabetes Nutr
Metab 2004; 17:12 – 16.
4. Mc Nair P, Christiansen C, Madshad S. Hypomagnesaemia a risk factor in diabetic
retinopathy. Diabetes 1978; 27:961 – 965.
5. Mather H M, Nisbet J A, Bruton G H. Hypomagnesaemia in diabetes. Clin Chem Acta
1979; 95:235 – 242.
6. Fuji S, Tekemura T, Wada M, Akai T, Okurr k m. Magnesium levels in plasma ,
erythrocyte and urine in patients with diabetes mellitus. Horn Metab Res 1982; 14: 161
– 162.
7. Johansson G, Danielsson B G, Ljunghalls, Wibell L. Evidence for a disturbed magnesium
metabolism in diabetes mellitus. Magnesium 1982; 3:178 – 180.
8. Ceriella A, Giugliano D, Dellorurso P, Passariello. Hypomagnesaemia in relation to
diabetic retinopathy. Diabetic Care. 1982; 5:558 – 559.
9. Hamid Nasri, Hamid Raza Baradaran. Lipids in association with serum magnesium in
diabetes mellitus patients. Bratisl Lek Listy.2008;109(7):302-306
10. Pham PC, Pham PM, Pham SV et al .Hypomagnesaemia in patients with type 2 diabetes
.Clin Am Soc Nephrol 2007;2:366-73.
11. Gindler EM, Heth DA. Colorimeter determination with bound “Calmagite” of magnesium
in human blood serum. Clin Chem 1971; 17:662.
12. Tosiello L. Hypomagnesaemia and diabetes mellitus. A review of clinical implications.
Arch Intern Med 1996; 156(1):1143 – 1148.
13. Kao W H. Serum and dietary magnesium and the risk for type 2 diabetes mellitus. The
Atherosclerosis risk in communities study. Arch Intern Med 1999; 159(8):2151 – 2159.
14. Chambers EC, Heshkas, Gallagherd.Serum magnesium and type 2 diabetes in African
Americans and Hispanics a Newyork Cohort. J Am Coll Nutr. 2006; 25:509 – 513.
15. Ishrat Kareem, Jaweed SA. Bardapurkar JS et al. Study of magnesium, glycosylated
hemoglobin and lipid profile in diabetic retinopathy. Indian Journal of Clinical
Biochemistry, 2004; 19(2);124-127.
16. Aradhana Sharma, Surekha Dabla, RP Agarwal et al. Serum magnesium; An early
predictor of course and complications of diabetes mellitus. J Indian Med Assoc
2007;105:16-20.
17. Lefebvre P J, Scheen A J. Improving the action of insulin. Clin Invest Med 1995; 18:342 –
347.
18. Suarez A. Decreased insulin sensitivity in skeletal muscle of hypomagnesaemia rats.
Diabetologia 1993; 36:A82.
19. Laughlin M R, Thompson D. The regulatory rule for magnesium in glycolytic flux of the
human erythrocyte. J Biol Chem 1996; 271: 28977 – 83.

CASE REPORT
Journal of Evolution of Medical and Dental Sciences/ Volume 1/ Issue 3/ July-Sept 2012 Page 124
LUPUS VULGARIS: - AN UNUSUAL FACIAL INVOLVMENT
Mandakini. B. T, Hakeem. A, Zennath. B
1. Assistant Professor, Department of Pathology, KBN Institute of Medical Sciences, Gulbarga.
2. Assistant Professor, Department of Pathology, KBN Institute of Medical Sciences, Gulbarga.
3. Associate Professor, Department of Pathology, KBN Institute of Medical Sciences, Gulbarga.
CORRESPONDING AUTHOR:
Dr Mandakini. B. Tenglr,
C/O Dr. Srinivas,
H. No. 1-888/1, Shastri Nagar,
Gulbarga- 04, Karnataka,
Email id- [email protected],
Ph- 0091 9844586236.
ABSTRACT:
BACKGROUND: Primary infection with tuberculosis occurs only rarely on the skin. The lesions of
Lupus vulgaris are usually found on the head or neck. The skin of and around the nose is
frequently involved. But, we report a rare case, where a 36 years’ old male patient presented with
a Lupus vulgaris lesion over the upper part of the cheek, near the outer canthus of the right eye, of
9 years’ duration. Histopathological examination showed granulomatous infiltration, with caseous
necrosis. Mantoux test was positive. The lesion showed marked improvement on antituberculous
treatment. We want to emphasize that histopathological examination has diagnostic value in
Lupus vulgaris.
KEYWORDS: Lupus vulgaris, facial skin, granuloma, caseation necrosis.
INTRODUCTION:
There is a resurgence of tuberculosis everywhere because of a combination of factors
including immigration from endemic countries, HIV pandemic, poverty, etc. as a result,
tuberculosis remains a clinical and diagnostic problem[1].
Lupus vulgaris is the most common morphological variant of cutaneous tuberculosis
accounting for approximately 59% of cases of cutaneous tuberculosis in India. [4, 6, 10].
Cutaneous tuberculosis forms a small proportion of extrapulmonary tuberculosis [3, 7].It has
been shown that Lupus vulgaris is the most common form in adults. [3, 8].
In India, the sites of predilection are the buttocks and trunk [3, 9].
We report a rare case of Lupus vulgaris affecting facial skin.
CASE REPORT:
A 36 year’s old male patient presented with history of a chronic progressive non- healing
lesion on the upper part of the right cheek, near the outer canthus of the eye, of 9 year’s
duration. Clinical examination revealed a well-demarcated, irregularly bordered, reddish-brown
patch, containing deep-seated nodules, each about 1mm. in diameter, with central area of
atrophy and scarring (fig-1).

CASE REPORT
Journal of Evolution of Medical and Dental Sciences/ Volume 1/ Issue 3/ July-Sept 2012 Page 125
Topical antibacterial, antifungal and steroid ointments were tried earlier, but there was
no response.
Clinical diagnosis of Granuloma annulare was made, and Lupus vulgaris was the
differential diagnosis. There was no pervious history of tuberculosis, either pulmonary or extra-
pulmonary. There was no regional lymphadenopathy, and systemic examination showed no
abnormalities. There was no similar family history Routine hematological examination revealed
lymphocytosis and raised ESR-80mm. Mantoux test was positive. Biochemical investigations like
random blood sugar, TB-IgG/IgM (slide method), VDRL, HIV, serum creatinine, and serum urea
levels were within normal limits. Chest X-ray was done which showed bronchitis with no
evidence suggestive of tuberculosis.
Histopathological study of the punch biopsy from the edge of the lesion revealed normal
epidermis, and the dermis showed tuberculoid granulomas consisting of epithelioid histiocytes,
Langhans giant cells surrounded by lymphocytes, with slight central caseation necrosis. Tissue
sections were negative for Acid fast bacilli.
DISCUSSION:
Infection of the skin and subcutis by Mycobacterium tuberculosis occurs by three routes;
1) By direct inoculation into the skin.
2) By hematogenous spread from an internal lesion.
3) From an underlying tuberculous lymph node by direct extension (causing
scrofuloderma).[1]
Mycobacterium bovis, atypical Mycobacteria and the BCG Vaccine can cause tuberculosis
involving the skin [5]. The diagnosis of cutaneous tuberculosis is challenging and requires the
correlation of clinical finding with diagnostic testing. [5] The determinants of what happens in
tuberculosis infection, includes, the virulence of the organism, the size of the inoculum, the
route of infection, and the immune status of the patient. The lesions of Lupus vulgaris are
usually found on the head and neck. The lesion in our case was a well-demarcated, reddish-
brown patch, containing deep-seated nodules, each about 1mm in diameter, with central area
of atrophy and scarring. The diagnosis in this case was based on histopathological study of the
biopsy of the lesion, which showed typical granulomatous tubercles with epithelioid cells,
Langhans giant cells and a mono-nuclear inflammatory infiltrate (fig-3&4). Caseation necrosis
was seen (fig-5) and AFB Negative
The patient was administered antitubercular therapy and the lesion resolved completely
in 6 months and 2 year follow-up shows no recurrence. (Fig-2).
Lupus vulgaris is completely curable as has been seen in the present case. The
consequences of failing to make an early diagnosis can be disastrous for the patients, as the
progression of the disease can lead to necrosis, destruction of bones and cartilage leading to
permanent deformity [4, 6, 9, and 10].
The special test like polymerase chain reaction (PCR) for TB can be done to substantiate
the diagnosis or wherever the histopathology is inconclusive [4, 6, 9, and 10].

CASE REPORT
Journal of Evolution of Medical and Dental Sciences/ Volume 1/ Issue 3/ July-Sept 2012 Page 126
Fig 01 Fig 02
Fig 03 Fig 04

CASE REPORT
Journal of Evolution of Medical and Dental Sciences/ Volume 1/ Issue 3/ July-Sept 2012 Page 127
Fig 05
REFERENCES:
1). Sebastian L. Bacterial Diseases. In: Lever’s Histopathology Skin. David E Elder.
Lippincott Williams & Wilkins 9th edition 2005.
2). Afsar SF., et al. Lupus vulgaris in a pediatric patient: a clinicohistopathological
diagnosis. Braz J Infect Dis vol. 12 no. 2 Salvador Apr. 2008.
3). Jain, V. K.,et al. Hypertrophic Lupus vulgaris an unusual presentation. Indian J
Dermatol 2009: 54(3): 287-9.
4). Chakravarti: A., et al. Lupus vulgaris of external nose. Indian J Tuberc 2006; 53: 220-
222.
5). Wg Cdr P Kinra, Col S Srinivasan, Col SPV Turlapti, Lt Col A Kumar. Lupus vulgaris
with abscess. MJAFI 2009; 65: 84-85.
6). Ramesh V, Misra RS, Jain RK. Secondary tuberculosis of skin: clinical features and
problems in laboratory diagnosis. Int J Dermatol 1987; 26: 578-581.
7). Yates VM, Rook GA. Mycobacterial infections In: Burns T, Breathnach S, Cox N,
Griffiths C, editors. Rook’s Textbook of Dermatology. 7th ed. Oxford. Blackwell Scientific
Publications; 2004. p. 28.1-39.
8). Sehgal VN, Wagh SA. Cutaneous tuberculosis Int J Dermatol; 1990: 237-52.
9). Khadim Ullah Kakakhel. Cutaneous Tuberculosis. International Journal of
Dermatology 1989; 28: 355-362.
10). S Khandpur, BSN Reddy. Lupus vulgaris: Unusual presentations over the face.
Journal of European Academy of Dermatology and Venereology 2003; 17: 706-710.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 128
Epidemiology of Needle-Stick Injuries in Mangalore Dr. Prakash. K. P
1. Assistant Professor, Department of Community Medicine, Kasturba Medical College. Mangalore.
CORRESPONDING AUTHOR:
Dr. Prakash K.P, Kurubarahalli Patel,
PES Medical College,
Kuppam– 517425, AP, India,
Email id- [email protected],
Ph- 0091 9686448868.
ABSTRACT:
BACKGROUND: Health care workers (HCWs) are always at greater risk of infection by needle-
stick injuries (NSIs) owing to their greater handling of sharps in various situations. OBJECTIVE:
The main objective was to review the epidemiology of NSIs among HCWs, and describe the
circumstances under which these injuries occurred. METHODS: A questionnaire based, cross
sectional study was done during the month of January 2008 at 3 Kasturba Medical College
(KMC) institutions, Mangalore. The data was computed and analyzed using SPSS statistical
package. RESULTS: During the study period 272 HCWs were self administered
questionnaire/interviewed and 102 HCWs reported (37.5%) incidents of injuries with needles
during the past 12 months. Doctors were the most frequent victims (64.7%), followed by waste
disposal staff (25.5%) and Nurses (7.8%). More than 50% of the victims had more than 3 pricks
in the last 12 months. Hospital wards and operation theatre were the major locations of needle-
stick incidents (31.4% each). Most commonly, injuries occurred during suturing (41.1%) and
when using solid bore or suturing needle (47.1%). Majority of them neither reported the injury
(60.8%) nor received post-exposure prophylaxis (70.6%). Patient tested sero-negative was the
major reason for not reporting the injury. Government hospital staff and waste disposal staff
had significantly higher chance of NSI when compared to their counterparts. Conclusions: The
study re-emphasized the importance of continued educational and prevention programmes for
HCWs in the prevention of needle-stick injuries.
KEYWORDS: Epidemiology, Needle-stick injuries, Health care workers, Mangalore.
INTRODUCTION:
Many infections including blood-borne viruses such as Human Immuno-deficiency Virus
(HIV), hepatitis B and C can be transmitted by exposure to infected blood or other body fluid via
an accidental inoculation injury (1). Health care workers (HCWs) who are exposed to needles
during clinical and non-clinical activities are at increased risk of acquiring needle-stick injuries
(NSIs) (2).
Accidental NSIs are an occupational hazard for HCWs. According to a global estimation,
16,000 Hepatitis C (HCV), 66,000 Hepatitis B (HBV) and 1000 cases of HIV may have occurred
worldwide in the year 2000 among HCWs through their exposure to NSI’s (3). In Germany,
about 500,000 needle-stick injuries occur annually among HCWs (4). More than 100,000 and
600,000 to 800,000 injuries annually have been reported in UK hospitals and in USA
respectively (5, 6). About half of these injuries go unreported (7-9,). Data from the EPINet

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 129
system suggest that approximately 28 needle-stick injuries/100 beds/year occur in US hospitals
(10).
Hollow-bore needles are most frequently implicated with the transmission of blood-
borne pathogens because the blood remaining inside the bore of the needle after use contains a
larger volume of organisms than the relatively small amount remaining on the outside of a solid
bore needle, such as the suturing needle (11). The activities associated with the majority of NSI
include withdrawing blood, recapping of needles, administering injections, inappropriate
disposal of needles, and missing the target while attempting to transfer blood or other body
fluids from syringes to specimen tubes or culture bottles (12).
Following a NSI with infected blood, transmission of the 3 principal viruses, HIV, HCV
and HBV occurs in 0.3, 3 and 30% of cases, respectively (13). Although the risk of infection
following a single NSI is very small, “universal precautions” and immunization against HBV may
reduce the risk of injury, infection and illness (14).
In general, only a few studies have been published on NSI from developing countries,
(15-17) although more than 90% of NSI occur in developing countries (18). Published data from
India (19-22) and in our institutions are limited, therefore, the present study was undertaken to
study the epidemiology of NSI in HCWs in the Kasturba Medical College (KMC) institutions, and
describe the circumstances under which these injuries occurred.
MATERIALS AND METHODS:
The study was conducted in the 3 KMC institutions (KMC Hospital (Attavar),
Government Wenlock and Lady Goschen Hospital) in Mangalore. Convenience non-random
samples of 372 HCW’s were self administered/interviewed using a pretested Performa. The
Performa was a self administered questionnaire that was completed by the HCW’s. The ancillary
staffs were interviewed and the questionnaire was filled by the trained medical students. The
assessment of data was done using modified methods established by World Health Organization
(WHO) (23).
The study was conducted during the month of January 2008. The target population was
HCWs in KMC institutions including doctors (staff, postgraduate students and Inters), nurses,
and waste disposal staff. The working definition of needle-stick injuries used was injuries
caused by hollow–bore needles such as hypodermic needles, blood collection needles,
intravenous (IV) stylets and needles used to connect parts of IV delivery systems (12). Data
collected from the Performa include: age, gender, details of the incident which included the type
of needlestick device and the circumstances under which the injury occurred. Additionally,
questions related to awareness as well as basic steps in management of injuries were also
included. The data also included was hepatitis B immune status, HIV and hepatitis B serologic
markers, the job category and place of work of the injured HCWs. Prevalence calculation was
according to, HCW who had at least 1 NSI during the last 12 months. The data was computed in
a Microsoft Excel 5.0 spreadsheet and statistically analyzed using the Statistical Package for the
Social Sciences (SPSS Inc, Chicago, IL, USA). Proportions were calculated and chi-square test was
used to test the significance and p value <0.05 was considered as significant at 95% confidence
interval.
RESULTS:
A total of 272 HCW’s were involved in the study. The basic characteristics of the study
population are shown in Table1. Of the 272, majority of them were in the age group of 25-34

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 130
years (51.5%), females (64%), doctors (57.4%) and from KMC, Attavar Hospital (42.6%). The
mean age and standard deviation of study subjects was 32.1±9.2 years. Almost 80% of HCW’s
had received hepatitis B vaccine, although only 75.3% had 3 complete doses. Fifty-four persons
(19.8%) received no immunization.
AWARENESS:
Nearly, 10% of the HCWs had no knowledge and 24% had partial knowledge about the
diseases transmitted through needle stick injuries. Approximately, 72% of them were aware of
the presence of written policy. Notably, 24% of the study subjects were not aware about the
correct disposal of sharps.
Approximately 37.5% (102/272) of the study subjects reported that they had at least
one NSI during the last 12 months. Needle-stick injuries and circumstances in which these
injuries occurred are depicted in table 2. Doctors were the most frequent victims (66/102 -
64.7%), followed by waste disposal staff (26/102 - 25.5%) and Nurses (8/102 - 7.8%).
Proportionately Waste disposal staff (26/42 - 61.9%), Doctors (66/156 - 42.3%) and Nurses
(8/62 – 7.8%) were the most common occupation among the NSI candidates. Alarmingly more
than 50% of the NSI’s had more than 3 pricks in the last 12 months. Nearly 63% of the injuries
occurred during suturing or during disposal of sharp objects. Solid bore or suturing needle was
the most common device causing the injury (47.1%). The most common cause of NSI was
accidental (45.1%) (Not preventable) followed by restless patient (17.6%) and rushed (11.8%)
or fatigued (11.8%). Surprisingly 60.8% of them who had NSI did not report to the authorities
even though majority (80%) of them said that they would report if they had a NSI and only
29.4% of the injured received post exposure prophylaxis. The common reason for not reporting
the injury was patient tested sero-negative. Only four (3 HBV and 1 HIV) of the patients on
whom the needle was used tested positive and in nearly 51% (52/102) of the patients disease
status was not know. Thirty two (31.4%) of NSI occurred in hospital wards, 32 (31.4%) in the
operation theatre, 18 (17.6%) in the waste disposal center (figure 1).
Government hospital staff had significantly higher chance of NSI (X2 = 8.05, p=0.01,
df=2) and waste disposal staff had significantly higher chance when compared to their
counterparts (X2 = 13.9, p=0.01, df=2) (Table 3)
DISCUSSION:
Needle-stick injuries are the most frequent occupational hazard affecting health care
workers, and the most life-threatening. This cross sectional study involved a total of 272 study
subjects among them 102 needle-stick injuries was reported. In this study the rate of NSIs being
0.42/doctor/year, 0.13/nurse/year, 0.62/waste-disposal staff/year was higher when compared
to a study in Saudi Arabia (0.06 /doctor/year and 0.11/nurse/year) (24) and lesser (0.57
/doctor/year and 0.83/nurse/year) when compared to a study in USA (25).
In our study, 37.5% (prevalence) of participant HCW’s had sustained at least one needle-
stick injury in the last 12 months, which is comparable to a study in Germany (31.4%) (4) and in
India (34.8%) (19). However, the reported prevalence was more than double in an Indian study
(80.1%) (26). Twelve months is a long period leading to bias which is a limitation in the study.
Nursing assistants are at high risk for NSIs because of their nature of work. Studies from Saudi
Arabia (65.8% and 19.2%) (24), Ireland (49.5% and 28.5%) (27) and in USA (40% and 28%)
(28) reported that the NSIs were more frequent among nurses than doctors, whereas doctors
reported frequent NSIs in Indian studies (19-22) including our study. This is probably because

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 131
in most of the Indian hospitals Junior/Senior resident doctors and Interns are more commonly
involved in clinical procedures. This wide variation in prevalence and proportions in various
studies could be due to underreporting (7-9), and/or different study methodologies (24). The
highest rate (26/42 - 61.9%) among waste disposal staff can be attributed to unsafe methods of
waste disposal and collection.
In this study, hospital wards and operation theatre were the common places of NSIs
(31.4% each). Similar observations were made in Saudi Arabia (45.1% - hospital wards, 16.9% -
OT) and Scotland (53% - hospital wards, 16% - OT) (24) (29).
The proportion of medical staff who reported to the authorities after a NSI was 20.0% in
our study. The main reason for not reporting in our study was patient tested sero-negative.
Other possible explanation may be that some doctors are inclined to self-assess and not report
such injuries, thus contributing to the apparent lower reporting of NSIs (29). Historically,
suboptimal (under-reporting) reporting of incidents can introduce bias in studies on self-
reported injuries. (30). Some researchers have shown that the rate of under-reporting among
doctors, especially among those frequently exposed to HIV-infected blood (31).
Some of the circumstances in which the injuries in various studies occurred are
compared in table 4 with the present study.
Continuing medical education (CME) programs for HCWs including health education
program for waste disposal staffs need to be conducted by the infection control department to
increase the awareness about the prevention and management of NSI’s because of proven
positive impact of intervention educational programmes (32). Hepatitis B vaccination of all at
risk HCWs in our institutions (23.4% never received). It is recommended by the CDC that all at-
risk HCWs be vaccinated against HBV infection (33). When the results of the study were
reported to the authorities, they were surprised and promised to take appropriate necessary
action.
In conclusion, Needle-stick injuries is a major concern in our institutions especially
government hospitals. The study re-emphasized the importance of continued medical
educational and prevention programmes for HCWs especially health education for waste
disposal staff in the prevention of needle-stick injuries. Mandatory reporting, laboratory testing,
post exposure prophylaxis (HBV) are some of the administrative measures (Accidental
Inoculation Policy) that needs to be taken to reduce the prevalence of NSIs in our institutions.
ACKNOWLEDGEMENT
The author is grateful for the assistance of the medical students in conducting the study.
All the HCWs who participated in the study and who supported in conducting this study are
acknowledged.
CONFLICT OF INTEREST:
None declared.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 132
Table1. Socio-demographic characteristics of the study subjects at the KMC institutions,
Mangalore. (N=272)
Characteristics Numbers Percent (%)
Age:
<25 46 16.9
25-34 140 51.5
35-44 54 19.8
≥ 45 32 11.8
Gender:
Male 98 36
Female 174 64
Hospital:
KMC, Attavar 116 42.6
Govt. Wenlock 96 35.3
Lady Goschen 60 22.1
Occupation:
Doctors 156 57.4
Nurses 62 22.8
Lab Technicians 12 4.4
Waste disposal staff 42 15.4
Table2. Distributions of NSI’s according to the circumstances in which the injuries
occurred
Situation (N=102) Numbers Percent (%)
Injection related 18 17.6
Re-capping needles 8 7.8
Suturing 42 41.1
During disposal 22 21.6
IV-line related, canula 4 4.0
Accidental exposure 8 7.8
Device (N=102)
Hypodermic needles 12 11.8
Blood collection needles 12 11.8
IV stylets 6 5.9
Sharps related to IV delivery system 4 3.9
Solid bore/suturing needle 48 47.1
Don’t know 20 19.6
Cause of injury (N=102)
Rushed 12 11.8

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 133
Fatigued 12 11.8
Lack of skills 4 3.9
Restless patient 18 17.6
Lack of assistance 10 9.8
Not preventable 46 45.1
Reasons for not reporting (N=62)
It takes too much time 0 0
No benefit in reporting 10 16.1
Did not want to know the results 0 0
Stigma of having had a NSI 0 0
Not mandatory to report 18 29
Patient was tested sero-negative 34 54.8
Table3. Occurrence of needle-stick injuries in 3 different hospitals and among staff
Hospital (N=102): Yes No X2
KMC, Attavar 28 88 8.05,
p=0.01,
df=2
Govt. Wenlock 48 48
Lady Goschen 26 34
Occupation (N=100):
Doctors 66 90 13.9,
p=0.01,
df=2
Nurses 8 54
Waste disposal staff 26 16
Note: Laboratory technicians were excluded in the comparison because only 2of 12 reported
NSI
Table4. Comparison of NSI’s according to the circumstances in which the injuries
occurred
REFERENCES Present
Study 26 24 19 20 21
Situation
During Suturing 41.1 20.3 41.7 29.4* 62* 58.1*
Recapping
needles 7.8 39 29 30.4 6.3 14.8
Device Used
Solid bore/
suturing needle 47.1 33 15.1 30.5 19.2 20.9
Cause of injury
Restless patient 17.6 12 8 - - -
Not preventable 45.1 - - 10.9 - -
Fatigue 11.8 - - 50.4 - -

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 134
Note: All the numbers are percentage unless specified
* During clinical procedures including suturing
- Particular information not available
REFERENCES
1. Parkside Health. Policy for the prevention and management of accidental inoculation
injuries.TrustPolicies 200 2001; Page3. Available at
http://www.brentpct.nhs.uk/doxpixandgragix/ICC9PolicyforthePreventionandManagementofA
ccidentalInoculationInjuries.doc. Accessed on 20-11-2010.
2. Tarantola A, Golliot F, Astagneau P, Fleury L, Brucker G. Blood and Body Fluids
Exposure Surveillance Taskforce. Occupational blood and body fluids exposures in HCWs: four-
year surveillance from the Northern France network. Am J Infect Control 2003; 31:357-63.
3. Pruss-Ustun A, Rapiti E, Hutin Y. Estimation of the global burden of disease
attributable to contaminated sharps injuries among health-care workers. Am J Ind Med 2005;
48(6):482–90.
4. Wicker S, Jung J, Allwinn R, Gottschalk R, Rabenau HF. Prevalence and prevention of
needlestick injuries among health care workers in a German university hospital. Int Arch Occup
Environ Health 2008; 81(3):347-54.
5. World Health Organization (WHO). Nursing Matters fact sheets. ICN on Preventing
Needlestick Injuries. July 2000. Available from http://www.who.int/occupational_health/
activities/2icnneed.pdf Accessed latest on 01-12-2010.
6. Henry K, Campbell S. Needlestick/sharps injuries and HIV exposures among health
care workers: national estimates based on a survey of U.S. hospitals. Minn Med 1995; 78:1765-
68.
7. Rodriguez EB, Moruno AJR, Dona JAC, Pujolar AE, Fernandez FJL. Underreporting of
percutaneous exposure accidents in a teaching hospital in Spain. Clin Perform Qual Health Care
1999; 7:88–91.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 135
8. Centers for Disease Control and Prevention (CDC). Evaluation of safety devices for
preventing percutaneous injuries among health-care workers during phlebotomy procedures -
Minneapolis-St.Paul, New York City, and San Francisco, 1993–1995. MMWR 1997; 46(2):21-5.
9. Osborn EHS, Papadakis MA, Gerberding JL. Occupational exposures to body fluids
among medical students. A seven year longitudinal study. Ann Intern Med 1999; 130(1):45-51.
10. International Health Care Worker Safety Center, University of Virginia. US. Exposure
prevention information network (EPINet) Sharps Injury and Blood and Body Fluid Exposure
Surveillance Research Group. Sharps Injury and Blood and Body Fluid Exposure Report for 2007.
August 2009. Available from http://www.healthsystem.virginia.edu/internet/epinet/EPINet -
2007-rates.pdf Accessed latest on 01-11-2010.
11. Occupational Safety and Health Administration (OSHA). Safer Needle Devices: Protecting
Health Care Workers 1997. Available from http://www.thebody.com/content/art5947.html.
Accessed latest on 06-12-2010
12. National Institute for Occupational Safety and Health (NIOSH). Preventing needle
stick injuries in health care setting. November 1999; Publication No. 2000-108. Available from
http://www.cdc.gov/niosh/docs/2000-108/pdfs/2000-108.pdf. Accessed latest on 18-11-
2010.
13. Leasa Benson. Accidental Inoculation Injury - Guidance for healthcare professionals on
dealing with needle-stick injuries to members. NHS Manchester Infection Control Committee report,
Document Reference CICT001 April 2007; Page 6. Available from
http://www.manchester.nhs.uk/document.../AccidentalInnoculationInjuryCommunitySettingN
ov08.doc Accessed latest on 8-11-2010.
14. Centers for Disease Control and Prevention (CDC). Universal Precautions for
prevention of HIV, HBV and other blood borne pathogens in health care settings. MMWR 1988;
37: 377-88.
15. Gumodoka B, Favot I, Berege ZA, Dolmans WM. Occupational exposure to the risk of
HIV and health care workers in Mwanza Region, United Republic of Tanzania. Bull World Health
Org 1997; 75: 133-40.
16. Vong S, Perez JF, Sok S, Som S, Goldstein S, Hutin Y, Tulloch J. Rapid assessment of
injection practices in Cambodia, 2002. BMC Pub Health 2005; 5: 56-62.
17. Memish ZA, Almuneef M, Dillon J. Epidemiology of needle sticks and sharps injuries
in a tertiary care center in Saudi Arabia. Am J Infec Control 2002; 30: 234-41.
18. World Health Organization (WHO). Safe Injection Global Network, Health Care Worker
Safety, Aide-Memoire for a Strategy to Protect Health Care Workers from infection from blood
borne virus. 2003; WHO/BCT/03.11. Available from http://www.who.int/injection_safety/
toolbox/en/AM_HCW_Safety_EN.pdf. Accessed latest on 20-11-2010.
19. Sharma R, Rasania S, Verma A, Singh S. Study of prevalence and response to needle
stick injuries among health care workers in a tertiary care hospital in Delhi, India. Indian J
Community Med 2010; 35(1):74-7.
20. Salelkar S, Motghare DD, Kulkarni MS, Vaz FS. Study of needle stick injuries among
health care workers at a tertiary care hospital. Indian J Public Health. 2010; 54(1):18-20.
21. Jayanth ST, Kirupakaran H, Brahmadathan KN, Gnanaraj L, Kang G. Needle stick
injuries in a tertiary care hospital. Indian J Med Microbiol 2009; 27(1):44-7.
22. Rele M, Mathur M, Turbadkar D. Risk of needle stick injuries in health care workers -
a report. Indian J Med Microbiol. 2002; 20(4):206-7.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 136
23. World Health Organization (WHO). Injection practices: Rapid assessment and
responseguide; October 2002. Available from
http://www.who.int/injection_safety/toolbox/en/RARG.pdf. Accessed latest on 20-10-2010.
24. Saulat J. Epidemiology of needle-stick injuries among health care workers in a
secondary care hospital in Saudi Arabia. Ann Saudi Med 2005; 25(3):233-38.
25. Stotka JL, Wong ES, Williams DS, Stuart CG, Markowitz SM. An analysis of blood and
body fluid exposures sustained by house officers, medical students, and nursing personnel on
acute-care general medical wards: a prospective study. Infect Control Hosp Epidemiol 1991;
12:583–90.
26. Muralidhar S, Singh PK, Jain RK, Malhotra M, Bala M. Needle stick injuries among
health care workers in a tertiary care hospital of India. Indian J Med Res 2010; 131:405-10.
27. O’Connell T, Hayes B. Occupational sharps injuries in a Dublin teaching hospital. Ir
Med J. 2005; 96(5): 143-5.
28. Shah SM, Silverstein B, Bonauto D, Foley M, Kalat J. Needlestick Injuries among health
care workers in Washington State, 1996–2000. Safety and Health Assessment and Research for
Prevention, (SHARP), Washington State Department of Labor and Industries, Technical Report
Number 64-04-2003. Available from http://www.lni.wa.gov/Safety/Research/files/Needle
Stick.pdf. Accessed latest on 1-12-2010.
29. National Health Services (NHS), Scotland. Needlestick injuries: sharpen your
awareness: Report of the Short Life Working Group on needlestick injuries in the NHS Scotland.
Available from http://www.scotland.gov.uk/Resource/Doc/158726/0043078.pdf. Accessed
latest on 02-12-2010.
30. Hamory BH. Underreporting of needle stick injuries in a university hospital. Am J
Infect Control 1983; 11: 174-177.
31. Mangione CM, Gerberding JL, Cummings SR. Occupational exposure to HIV:
frequency and rates of under-reporting of percutaneous and mucocutaneous exposure by
medical house staff. Am J Med 1991; 90: 85-90.
32. Richard VS, Kenneth J, Ramaprabha P, Kirupakaran H, Chandy GM. Impact of
introduction of sharps containers and of education programmes on the pattern of needle stick
injuries in a tertiary care centre in India. J Hosp Infect. 2001; 47(2):163-5.
33. Centers for Disease Control and Prevention (CDC). Immunization of health care
workers. MMWR 1997; 46 (RR-18): 1-42

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/ Volume 1/ Issue 3/ July-Sept 2012 Page 137
ROLE OF PLATELET TRANSFUSIONS IN DENGUE HEMORRHAGIC FEVER-
6 MONTHS REPORT
Dr. V. Geeta, Dr. Bheeshma, Dr. I. Srilakshmi, Dr.Ramya, Dr. Yashoda, Dr. Jijiya Bai.
1. Assistant Professor, Department of Pathology, Gandhi Medical College, Secunderabad.
2. Assistant Professor, Department of Pathology, Gandhi Medical College, Secunderabad.
3. Assistant Professor, Department of Pathology, Gandhi Medical College, Secunderabad.
4. Post Graduate, Department of Pathology, Gandhi Medical College, Secunderabad.
5. Medical Officer-Blood bank, Department of Pathology, Gandhi Medical College, Secunderabad.
6. Professor & Head, Evaluator, Department of Pathology, Gandhi Medical College, Secunderabad.
CORRESPONDING AUTHOR:
Dr. V. Geetha,
Assistant Professor of Pathology,
Gandhi Medical College,
Secunderabad, Andhra Pradhesh,
Email id- [email protected],
Ph- 0091 09849450199.
ABSTRACT:
BACKGROUND: Allogenic platelet transfusion plays a major role in the management of
thrombocytopenia. The study includes details of platelet transfusion over a period of 6 months
from January-2011 to June-2011 at blood bank of Gandhi Hospital. Total number of patients who
received were 487 and proportionate use of total units of RDP (Random Donor Platelets) issued
from blood bank were as follows; dengue hemorrhagic fever (38%) and remaining for acute
leukemia (12%), Aplastic anemia (10%), sepsis (10%), DIC (Disseminated Intravascular
Coagulation) (10%), cardiac surgery (10%). In dengue hemorrhagic fever, correlation of platelet
count with platelet transfusion and platelet increment have been evaluated.
KEYWORDS: Thrombocytopenia, RDP, DIC, Aplastic anemia.
AIM: To evaluate the role of platelet transfusion in dengue hemorrhagic fever.
INTRODUCTION:
Dengue infection is usually a benign syndrome caused by an arthropod born virus. Dengue
fever and dengue hemorrhagic fever have emerged as a global public health problem in recent
decades. The South East Asian Countries such as India, Indonesia and Thailand are at the highest
risk of dengue accounting for nearly half of the global risk.
Dengue hemorrhagic fever (DHF) and dengue shock syndrome (DSS) are life threatening
clinical manifestations1. The mechanisms of hemorrhagic manifestations of DHF/DSS are not well
understood. The suggested factors contributing to bleeding include thrombocytopenia,
coagulopathy and vasculopathy and Suggested mechanisms for thrombocytopenia include:
1) Maturational arrest of megakaryocyte production in the bone marrow
2) Platelet destruction by the virus it self
3) DIC

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/ Volume 1/ Issue 3/ July-Sept 2012 Page 138
The world health organization manual and text books of pediatrics and infectious diseases
recommend infusion of fresh whole blood, fresh frozen plasma and/or platelet concentrates2.
Theoretically the risk of spontaneous bleeding becomes significant at a platelet count of <20 X
107/ml.
MATERIALS AND METHODS:
A retrospective study was conducted in the blood bank of Gandhi Hospital for a period of 6
months from 1st Jan to 31st June 2011. Total no. of patients received platelet transfusion is 487
and total units of RDPs given are 1116. Patients clinical data, platelet count and platelet
transfusion given to them were analyzed.
RESULTS:
Total no. of patients received platelet transfusion is 487 and total units of RDPs given are
1116 (Table.1), with males numbering 223 and females 264.
Age Group January February March April May June Total
0-10 16 17 10 21 27 38 129
11-20 10 25 30 17 07 22 111
21-30 16 7 28 15 19 25 110
31-40 4 11 6 18 07 13 59
> 41 12 10 9 9 13 15 68
Grand total 487
Blood group wise distribution of platelet transfusion is as follows
� B+ve: 180
� O+ve: 178
� A+ve: 161
� AB+ve: 37
� O-ve: 8
� B-ve: 14
Distribution of platelet transfusion by diseases wise are (Fig.1)
Dengue confirmed patients - 38% (186)
Acute leukemias (ALL + AML) - 12% (58)
A plastic anemia -10% (49)
Sepsis -10% (49)
DIC -10% (49)
Cardiac patients -10% (49)
Others -10% (49)
Total 489

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/ Volume 1/ Issue 3/ July-Sept 2012 Page 139
Majority of Dengue patients belonged to B+ve and O+ve Blood groups, most common age
group is between 11 to 20 years (46%) and females outnumbered males at 101 Vs 85.
During the study period 186 patients had positive serology (IgM or IgG) to dengue fever
by ELISA method. Fever was the most common clinical presentation associated with headache,
myalgia, vomiting, and diarrhea. Platelet count less than 10,000 / cumm noted in 20 patients
(10.7%).
< 10,000 - 20 patients 10.7%
11-20,000 - 36 patients 19.35%
21-40,000 - 50 patients 26.88% - Moderate Risk
41-1 lakh - 80 patients 43% - Low Risk
Most of the patients received platelet transfusion recovered completely and were
discharged with 2-5 transfusions. The platelet count had picked up considerably. Guidelines for
platelet transfusions in dengue hemorrhagic fever as follows:
INDICATIONS:
Prophylactic transfusions (in a non bleeding patient) with Platelet count < 20 X 109/L
Therapeutic transfusions (in a bleeding patient)
1) Significant active clinical bleeding with platelet count < 50 X 109 / L.
2) DIC
DISCUSSION:
Dengue viruses belonging to the genus flavi virus of family flaviviridae has antigentically
four distinct serotype DEN-1, DEN-2, DEN-3 and DEN-4. The virus is transmitted to the human
being by the bite of infected Aedes Egypti Mosquito and few other members of Aedes species.
Dengue virus causes a broad spectrum of illness ranging from mild undifferentiated fever to
classical dengue fever, DHF, DSS.
Our study showed majority of dengue cases were children and adolescents in the age
group of 10-20. Chaunsumrit et al also noted high percentage of dengue cases in age group of 10-
14 years3. In contrast Ayyub et al and Lye et al noted adult preponderance in age group of 20-40
yrs4, 5.
Thrombocytopenia is a common problem in dengue. In our study thrombocytopenia was
found in all most all the confirmed cases of dengue which was equal when compared with findings
of Makroo et al and Chairulfatah et al (84.88% and 83% respectively)6, 7 .
In our study bleeding occurred significantly more often in patients with thrombocytopenia
most often in patients with platelet count less than 20,000 / cumm which is similar to Shivbalan et
al. but chairulfatah et al found significant bleeding with platelet count less than 15,000 / cumm8, 7.
In our study high risk patient: platelet count < 20,000-30%. Moderate risk: 27% (21,000-40,000)
and Low risk: 43% (40,000-1 lakh)
According to Makroo et al all Hospitalized patients with dengue with high risk should be
given platelet transfusion6.
High Risk

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/ Volume 1/ Issue 3/ July-Sept 2012 Page 140
Dengue, 38%
Acute Leukemia, 12%
A Plastic Anemia, 10%
Sepsis, 10%
DIC, 10%
Cardiac, 10%
Others, 10%
Moderate risk patient can be given platelet transfusion if associated hemorrhagic
manifestations are present. Low risk patients can be managed with IV fluids and supportive
therapy. But in our study prophylactic transfusion of platelet given to 43% of low risk patients.
Most of the patients (99%) who received platelet transfusion recovered completely were
monitored for increment of platelet count after 2-3 transfusion at the time of discharge the
platelet count was above 1 lakh / cumm. Besides platelet transfusion FFP and PRP also
transfused.
Death occurred in 3% of patients due to complications like septicemia and severe bleeding
with multi organ failure belonged to age group of 31-40.
CONCLUSION:
All Hospitalized dengue patients can be categorized into high, moderate and low risk
patients based on platelet count at the time of Hospitalization. High risk patient should be given
priority and platelet transfusion accordingly. In our study the outcome is good with 97% recovery
of dengue patients with platelet transfusion and supportive therapy this clearly emphasizes the
role of platelet transfusion in the management of dengue patients.
Figure 1: Proportionate recipients of platelet transfusion
REFERENCES:
1. Directorate of health services, Management of Dengue Fever/DHF/DSS. Guidelines for
indoor patients, 2005:4
2. World Health Organization (2009) Dengue: guidelines for diagnosis, treatment, prevention
and control. World Health Organization, Geneva, pp 40–41.
3. Chuansumrit A, Phimolthares V, Tardtong P et al (2000) transfusion requirements in
patients with dengue hemorrhagic fever. Southeast Asian J Trop Med Public Health 31:10-
14
4. Ayyub M, Khazindar AM, Lubbad EH et al (2006) Characteristics of dengue in a large
public hospital, Jeddah, Saudi Arabia. J Ayub Medical coll Abbottabad 18:9-13

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/ Volume 1/ Issue 3/ July-Sept 2012 Page 141
5. Lye DC, Lee VJ, Sun Y, Leo YS (2009) Lack of efficacy of prophylactic platelet transfusion
for severe thrombocytopenia in adults with acute uncomplicated dengue infection . Clin
Infecct Dis 48:1262-1265
6. Makroo RN Raina V, Kumar P, Kanth RK (2007) Role of platelet transfusion in the
management of dengue pts in a tertiary care hospital. Asian J Trans Sci 1:4-7
7. Chairulfatah A, Setibudi D, Agoes R, Colebunder R (2003) Thrombocytopenia and platelet
transfusion in dengue. Haemorrhagic fever and dengue shock syndrome.WHO Dengue Bull
27:141- 143
8. Shivabalan S, Anandanathan K, Balasubramaniyan S, Dutta N, Amalraj E; predictors of
spontaneous dengue, Indian J Ped. 2004; 71:33-6 (Pubmed)

REVIEW ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 142
DRUG COMPLIANCE AND ADHERENCE TO TREATMENT Dr. T. Manmohan, Dr. G. Sreenivas, Dr. V.V. Sastry, Dr. E. Sudha Rani, Dr. K. Indira,
Dr. T. Ushasree.
1. Associate Professor, Department of Pharmacology. Gandhi Medical College, Secunderabad.
2. Assistant Professor, Department of Community Medicine. Gandhi Medical College, Secunderabad.
3. Professor, Department of Community Medicine. Gandhi Medical College, Secunderabad.
4. P.G. Student, Department of Pharmacology. Gandhi Medical College, Secunderabad.
5. Professor, Department of Pharmacology. Gandhi Medical College, Secunderabad.
6. Professor & Head, Evaluator, Department of Pharmacology. Gandhi Medical College, Secunderabad.
CORRESPONDING AUTHOR:
Dr. Tepoju Manmohan,
Gandhi Medical College,
Secunderabad, AP,
Email id- [email protected],
Ph- 0091 09346935968.
ABSTRACT:
BACKGROUND: In spite of any number of medicines will not be of use unless patient takes’
them. After diagnosing the disease, the next most important step is to follow the instructions of
physician in terms of treatment. The doctor’s responsibility does not end with writing
prescription, assuming patient will adhere to it. He/she should cross check the behavior of
patient for drug compliance and see that patient follows it and get the benefit.
Non compliance is the main barrier for the effective delivery of the medical care. This
will have greater implications on the economic burden on the country in terms of frequent
hospitalization, use of expensive medicines in case of relapse due to non adherence.Though the
terms compliance and adherence are used synonymously, they differ in the delivery of quality of
the medicare as the former implicates the passive following of the physician instruction, while
in the later, patient actively participates in the development of the treatment plan, which will
improves outcome of the treatment. Adherence is the preferred term over compliance by WHO.
KEYWORDS: Adherence; compliance; concordance; non compliance; non adherence; treatment
INTRODUCTION: Significant advances have been made in understanding etiology of disease
states, and development of new therapeutic agents made it possible to cure or provide
symptomatic control. However, in many circumstances, drugs are not being used in the manner
conducive to optimal benefit and safety. Efforts to maintain or improve health, fall short of the
goals considered attainable, and has been attributed to patient’s noncompliance or partial
compliance.
Medication compliance (taking one’s medicine as prescribed) is a major concern as it
prevents hospitalization up to 5.5% and increase deaths by 8.48-fold to medication errors. Cost
and poor understanding of the directions for the treatment are major barriers in completing
treatment. WHO (World Health Organization) has estimates that only 50% of people complete
long-term therapy for chronic illnesses as prescribed1.
Half of all prescriptions for drugs to be taken on an ongoing basis are either not
completed or are never filled in the first place due to cognitive issues, depression or physical
problems 2-3. Medication for asymptomatic conditions is most likely not to be taken casually,
REVIEW ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 143
else land up with devastating problems over a period of time, especially with conditions like
diabetes, high blood pressure or high cholesterol1. A report from the American heart association
reveals that nearly 60 percent of patients whenever taking five or more medicines gets confused
while taking them.
TYPES OF PATIENTS: Based on the acceptance of diagnosis and treatment initiation,
patients are categorized into four types
1.NON COMPLIERS: Those who do not accept diagnosis and need treatment.
2.PARTIAL COMPLIERS: Those who accept diagnosis and treatment but cannot fulfill
the recommended actions sufficiently to reach targeted improvements in their health.
3.OVER COMPLIERS: Those who take recommended actions in excess of targeted
improvements (These patients are rare).
4.ADEQUATE COMPLIERS: Those who follow health advice adequately to improve or
control their disorder.
TYPES OF MEDICATION-TAKING BEHAVIOR:
COMPLIANCE: It is the conscious effort to use drugs in the manner prescribed, it is the extent to
which all individuals’ behavior coincides with medical & health advice. Understanding how
medication should be used, with sufficient positive motivation, and intentions, looking at the
perceived self benefit and positive outcome. , it can also apply to other situations such as
medical device use, self care, self-directed exercises, or therapy sessions.
ADHERENCE: The extent to which a person takes medication as prescribed. WHO defines
adherence as “The extent to which a person’s behavior, corresponds with agreed
recommendations from a health care professional”. Concept of adherence is broadly viewed as
related to instructions concerning medicine intake, use of medical device, diet, exercise, life
style changes, rest and return for scheduled appointments4-7.
CONCORDANCE: Consultative and consensual course of therapy partnership between the
consumer and their doctor. Concordance is the process by which a patient and clinician make
decisions together about treatment8.
PERSISTENCE: A person’s ability to continue medical advice for the intended course, which
may range from few days to life long.
However the preferred terminology remains a matter of debate. In some cases,
concordance is used to refer specifically to patient adherence to a treatment regimen that is
designed collaboratively by the patient and physician, to differentiate it from adherence to a
physician only prescribed treatment regimen5-8, despite the ongoing debate, adherence is the
preferred term for the WHO1, the American pharmacists association9 and the US National
Institutes of Health Adherence Research Network8,10, and is important for optimum therapeutic
outcome which improves patient’s quality of life.
Concordance also refers to a current UKNHS (United Kingdom National Health
Services) initiative to involve the patient in the treatment process to improve compliance 11, 12.
Here patient is informed about their condition and treatment options, they are involved with
the treatment team in decision making process and partially responsible for monitoring and
reporting back to the team1.

REVIEW ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 144
Non-compliance is a major obstacle to the effective delivery of health care. Estimates
from the WHO indicate that about 50% of patients with chronic diseases living in developed
countries do not follow treatment recommendations1, 13. Non-compliance means not following
the directions for treatment due to irrational behavior or willful ignoring of instructions leading
to increased morbidity, treatment failures, exacerbation of disease, more frequent physician
visits, increased hospitalizations and even death (Fig.1) 6, 14, 15.
(Fig.1: TYPES OF MEDICATION TAKING BEHAVIOR)
PRESCRIBED REGIME FOR ENTIRE PERIOD
FULLY COMPLIANT
FULLY PERSISTANT
PARTIALLY COMPLIANT
NON-PERSISTANT (STOPPED THERAPY BEFORE COURSE)
NON COMPLIANT & NON-PERSISTENT
NON PERSITENT, NON-ACCEPTANCE (NOT STARTED THERAPY)
The most common situations associated with non adherence are
� Failure to have the prescription dispensed or renewed, not refilling
prescriptions for chronic diseases states, not obtaining refills at appropriate
intervals, 25% don’t fill new prescriptions16-18 ,
� Omission of doses most common type of non compliance and more likely to
occur when a medication is to be administered at frequent intervals. Increased
frequency cause more interruption of normal routine, or work schedule,
especially in poly pharmacy or when treatment is needed with an extended
period of time. Few patients cannot identify their own medications 18,19.
� Errors of dosage, like giving instructions in measures of tea spoon (measure
range from 5ml. to 15ml.) and not following administration of medicines at night
time if patient falls into sleep etc., where dose of administration is incorrect20.

REVIEW ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 145
� Incorrect administration of medication: includes not using proper technique like
using metered dose inhalers, wrong route of administration, such as taking
vaginal pessaries orally21.
� Errors in time of administration: in 8th hourly prescription, night dose is
adjusted in the day time.
� Premature discontinuation of treatment occur most commonly with antibiotics
and drugs used for chronic disorders like hypertension. American Association of
Retired persons (AARP) Survey of ambulatory elderly patients reported 33%
premature discontinuation of medications22. In a pediatric outpatient study on
acute otitis media therapy 37% discontinued early. Highly priced drugs are
prematurely discontinued 1, 23.
� Preference for self care other than medications, such as following other systems
of medicine or indigenous remedies etc., 24, 25.
� Not completing entire course of therapy, when symptoms subside with partial
usage of antibiotics or treatment regimen as seen in acute infections and
treatment of tuberculosis.
� Other patient factors such as, fear of dependency, social problem like usage of
diuretics causing polyuria, taking out dated or improperly stored medicines, or
friends and family members’ medications causes non adherence. Lowest
compliance of about 20-30% is seen with life style changes 26, 27. Addiction to
alcohol and smoking has decreased compliance in conditions like asthma,
hypertension and renal transplantations 28-38.
Main reasons for not filling prescriptions according to study in Americans with age 50
and above37, (Table No.1).
(Table No.1: prescription refill proportions in elderly patients)
Cost of the drug (40%)
side effect of drug (11%),
thought drug wouldn’t help much ( 11%)
Already taking many prescriptions (3%)
condition improved (4%)
don’t like taking prescription drugs (5%)
drug did not help (6%)
didn’t think i needed it (8%),
Other reasons (physical impairments etc,.) (12%)
NON PATIENT FACTORS ASSOCIATED WITH NON ADHERENCE ARE:
THE NATURE OF PATIENT’S ILLNESS: Patients suffering from schizophrenia has high
incidence of non compliance, due to distorted reality & lack of insight do not recognize their

REVIEW ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 146
illness and need for treatment. Similarly in chronic disorders like hypertension, tuberculosis
etc., same pattern is observed 39.
THERAPEUTIC REGIME: Multiple drug therapy like 5-6 prescribed drugs13, 40-42 taking at
different timings ,taking tablets with same color, size and shape cause more confusion43 and
skip doses. Technical difficulty in using inhalers44-50.
DURATION OF TREATMENT: Compliance is inversely proportional to duration of treatment27,
51, 52. In a study of long term therapy, low compliance is observed as in bronchial asthma (50%)
and hypertension (50-70%) 53-60.
FREQUENCY: Increased frequency of drug administration causes more disruption of normal
routine or work schedule, hence many patients forget or inconvenienced or embarrassed. In one
of the study, compliance has improved from 59% on 8thhourly regimen to 84% with once a day
regimen 61-67
ADVERSE EVENTS: Events are like deterrents; in a study on elderly patients 40% experienced
side effects of this 20% stopped medications and in this only 18-19% informed their physicians
about discontinuation22. In one of the survey, over 60% are noncompliant due to adverse
events. Some drugs like Anti-Hypertensive agents, Anti depressants or Anti psychotics cause
sexual dysfunction which is frequently implicated for non compliance. 68-82
TASTE OF MEDICATION: Can be the cause for noncompliance especially in children.
Failure to comprehend the importance of therapy, as patient has limited knowledge
about the illness, become non compliant if beliefs and expectations are not met with. Poor
understanding of instructions also contributes to non compliance83, 84. Non compliance in elder
age group is due to2, 13, 33, 40, 41, 85 & 86
• Adverse effects,
• Increased, or decreased sensitivity to drugs,
• Frequent change of prescriptions( prescription cascade),
• Living alone,
• Lack of social support system,
• Difficulty in opening the medication container that has flip off type of lid
• Going to pharmacist/chemist due to physical problems like (osteoarthritis)
• Cognitive impairment,
• Impaired mobility or dexterity,
• Swallowing problems,
• Financial issues like, Low income and high cost of medications,
• Everyday inconvenience in carrying and taking of medicines.
CONSEQUENCES OF NON COMPLIANCE: Drugs do not work if people do not take them 87. Non-
compliance is a major obstacle to the effective delivery of health care. National Council on
Patient Information and Education designated it as America’s other drug problem88, 89. Under
use is very common, depriving the patient of anticipated therapeutic benefits and resulting in
progressive worsening of the condition or increased complications as in hypertension. overuse
REVIEW ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 147
of medication is also common, where in patients increase dose or frequency of medications
anticipating extra benefit or quick action and remission of symptoms and some times it can be
an extra dose due to forgetfulness as in elderly age groups, causing increased adverse reactions,
leading to unnecessary use of medical resources such as
� Physician Consultations
� Emergency Department visits,90
� Unnecessary additional laboratory tests and
� Treatments which are preventable
(Table No. 2: Consequences of non adherence to treatment in elderly patients39, 91-93)
Cause Proportion of hospitalization
due to non compliance 10-33%9
inability to self-administer 23% of nursing home admissions
Studies on HIV/AIDS have revealed higher viral loads in patients with 10- days drug
holiday or 20% of missed doses of Anti retroviral agents, who are otherwise had nearly
undetectable viral loads94. Non compliance with anti psychotics in schizophrenia had relapses
with violent behavior. Similarly in Epileptics unexpected deaths are due to low the4rapeutic
concentrations of antiepileptic drugs95. Deaths in transplant patients who have waited for years
to get donor organ are because of organ rejection resulting from noncompliance in using
immunosuppressants96
Low rates of adherence to therapies for asthma, diabetes, and hypertension are thought
to contribute substantially to the human morbidity, mortality and economic burden of those
conditions1, 14. In asthma non-compliance incidence is 28-70% worldwide, increasing the risk of
acute severe asthmatic attacks requiring hospitalization. Non compliance to Anti Hypertensive
agents is very common even in developed countries, and it is the main cause for hypertension
related complications like heart diseases and strokes. In united States, it is estimated that drug
related morbidity & mortality expenditure exceeded $177.4 billions97
Compliance rates are often high or over estimated in a formal clinical trial but drops off
in a "real-world" setting. In a study, compliance rate for statins is 97% at the beginning, and
dropped to 50% after six months98.
ASSESSMENT TOOLS FOR MEDICATION ADHERENCE: Detection of non compliance is as
important as diagnosis of a medical condition Compliance or non compliance is not stable; it
may change over time, necessitating regular use of detection methods to measure the behavior
as part of assessment for therapeutic efficacy99.
Structured interviews using highly skilled and refined techniques, like Morisky scale which is
validated scale estimating the risk of medication non-adherence, is cited in numerous articles since
1986 used for many different disease such as, hypertension, hyperlipidemia, asthma and HIV.

REVIEW ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 148
Compliance or non compliance is not stable; it may change over time, necessitating
regular use of detection methods to measure the behavior as part of assessment for therapeutic
efficacy99.
As such there are no gold standards for Assessment for medication adherence; the ideal
detection would measure compliance at the time and place of medication taking event. Direct
observation of the patient would come closest to providing this ideal measure of adherence.100.
Indirect methods of monitoring compliance other than Electronic event monitoring (EEM) are;
o Pill counts,
o Medication refill records,
o Patient self report,
o Structured interviews using highly skilled and refined techniques,
o Change in weight of meter dose inhaler canisters, ,
o Medication event monitoring using computer are most commonly
used.
o
Pill count is often used in clinical trials, it measures the difference between the dosage
units initially dispensed and number remaining on return visit or unscheduled home visit, but
pill dumping and medication discard misrepresents compliance101, 102
Structured interviews using highly skilled and refined techniques, like Morisky scale
which is validated scale estimating the risk of medication non-adherence, is cited in numerous
articles since 1986 used for many different disease such as, hypertension, hyperlipidemia,
asthma and HIV. It is a structured four item self reported adherence measure that addresses
barriers to compliance and permit health care provider to reinforce positive adherence
behavior 103
Sometimes achievement of treatment goals are used as a measure for compliance, like
normal blood pressure in hypertensive, normal blood glucose levels in diabetics, after
eliminating “ tooth brush effect” (like people brushing their teeth before seeing a dentist) where
patients load up medication just before their return visit to physician. Electronic event
monitoring is a recent and reliable computerized compliance monitoring, here medication
container cap is housed with microprocessor which records date and time of opening the cap
and data can be retrieved by connecting the micro processor to computer, the disadvantage
being no data is provided regarding actual amount of drug taken, It helps when supplemented
with other methods of measurements104.
Direct methods to measure adherence is by using biological markers and tracer
compounds like measurement of glycosylated hemoglobin which provides objective assessment
of metabolic control in preceding three months in Diabetics. Small amounts of tracer
compounds with long half- lives, like Phenobarbital or digoxin are added to the medications and
these tracers are measured in biological fluids.
Therapeutic drug levels monitoring in biological fluids is another direct method of
compliance assessment but draw backs are individual pharmacokinetic variations, and tooth
brush effect invalidate this type of measurement as data do not provide timing of doses10

REVIEW ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 149
(Table: 3 Comparison of different methods for the measurement of adherence)
DIRECT METHODS INDIRECT METHODS
They are more sensitive and specific They are less sensitive and specific
They are direct pharmacologic indicators of
medication adherence
Tooth brush effect can not be ruled out
Limitations:
i) Legal and ethical issues
ii) Individual pharmaco-kinetic
variations of drugs
They are better measure of detection if two
different indirect methods are used and
correlated;
Eg: Pill count and electronic event monitoring
device.
HOW TO IMPROVE COMPLIANCE/ADHERENCE: Effective ways to help people follow
medication regimes could have far larger effects on health than any other treatment”-Haynes et
al. 2005106. Patient should be evaluated before changing therapeutic regimen as non adherence
is most common missed diagnosis.
Demographic factors such as age, marital status, sex, race, income, occupation, number
of dependents, intelligence, level of education, or personality type have been shown to be
marginally related to noncompliance107-111. Based on behavioral principles patient-centered
compliance models are described, taking into consideration of socio behavioral determinants112
which includes health belief models and health decision models , former is related to a
preventive health behavior and latter focusing more on health decisions which combines the
health belief model and patient preferences with comprehensive cognitive behavioral and
affective components for advocated behavior5, 113, 114.
Patient prerequisites for adherence:
� Understand diagnosis and potential impact
� Believe that treatment will be beneficial
� Treatment favors benefit over cost
� Confidence in health care practitioners
Patient factors for improved compliance include:
� Quick relief of symptoms � Becomes quickly ill without therapy � Treatment involving expensive procedure � Recurrence if treatment is stopped � Increased disability as a consequence with out treatment
HEALTH BELIEFS: To achieve compliance patient should believe that, he/she actually have
illness which is diagnosed, and with treatment, severity of condition is reduced. Patient
education & counseling should be designed to encourage health beliefs115-118.
Patient physician interaction also affects compliance or adherence. Patient who has
respect towards treating physician and is well known, giving information, assurance and
psychological support, showing empathy, improves compliance or adherence. The interaction
should be a negotiation between two active and equal participants with goal/strategy “to put ill

REVIEW ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 150
at ease”.119-124. As recommended by NCPIE (National Council for Patient Information and
Education) physician should respond to patient’s queries regarding treatment and other related
topics.
IDENTIFICATION OF RISK FACTORS FOR NON COMPLIANCE: As it is difficult to identify a non
coplier, every patient is assumed a potential defaulter 125. By recognizing individuals who are at
risk, treatment is planned with simplest regimen compatible with patient’s normal activities,
such as avoiding expensive medicines, unnecessary medication, using long acting formulations
and combination medications, to decrease frequency of administration
Prescribing low cost medicines as high cost medicine prescription fill rates are low, even if
they buy reluctant to use entire prescribed quantity. Medication-flavoring formulary system
developed about three dozen flavors, to overcome taste problems in medications especially in
children
In cases with mental illness discuss with patients or family members regarding delayed onset
of therapeutic effects, and the need for prolonged treatment by prescribing medicines with
least side effects.
With physical disabilities such as visual impairment, communicate with patient verbally or
use tape record instructions, increase font size or color code medication bottles, advise pre-
measure and pre-cut medications. With hearing impaired patients the problem is solved by
using interpreter, or speaking to better ear using regular voice volume and lip movement with
eye contact maintained, repeat instructions when necessary, supplement with written
information, and turn up hearing aids2-3
In cases with reduced mobility and dexterity advise patients to store medications in easily
accessible location, using pre-cut, pre-measured medications or easy open tops that are easy to
administer. Foiled backed wrappers are avoided in patients with arthritis or tremors. Wherever
difficulty in swallowing is seen use alternative dosing formulations like liquids, trans-dermal
patches, crushable tablets or capsules that can be opened and mixed with soft foods.
DEVELOPMENT OF TREATMENT PLAN: Hippocrates: “decisions to deviate, un aware of
physician intentions keep watch also on the fault of patients which often makes them lie about
the taking of things prescribed”. Develop a simple plan on individual basis, involving patient in
deciding treatment with minimal inconvenience and overcome forgetfulness by timing doses
corresponding to regular activities in patient’s daily schedule. Do not write twice or thrice a day
instead of writing time in am/pm. in instructions44, 126
Health literacy is the degree to which individuals have the capacity to obtain, process
and understand basic health information and services needed to make appropriate health
decisions (world health organization, 2003)127. Patients with low health literacy were reported
to be less compliant with their therapy128. Written instructions and pictograms on medicine
labels has proven to be effective in improving patient’s compliance129.
PATIENT EDUCATION: Best way to improve compliance. Decide what information is necessary
for about illness and treatment130. Too much details/inappropriate presentation of adverse
events may alarm patient & decrease compliance. Involve patient in decision-making process.
Make patient understand benefits of treatment and importance of compliance without using
complex technical terms. Patient is asked to repeat the instructions. Encourage patients to ask

REVIEW ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 151
questions. Patient education regarding asymptomatic hypertension, glaucoma, asthma, and
diabetes mellitus removes non adherence 64.
PHYSICIANS FACTORS: Asking few questions, occasional eye contact not understanding
language spend little time, giving large information in short time, lack of concern also effect
compliance131.
Physicians liability for non compliance is often over looked as they prefer pointing
deficiencies of the patients rather than themselves. Physician’s compliance is the extent to
which the behavior of doctor fulfills their professional duty like not being ignorant, adopting
new advances when they are sufficiently proved, writing prescription accurately and legibly,
warning patients about side effects or adverse effects, and counseling them to use medicines
effectively and safely.132-136
ORAL COMMUNICATIONS: Oral communication / counseling in a room with privacy137 and
free of distractions to give patient an opportunity to raise questions- supplemented by written
instructions. Studies indicate that counseling has improved adherence in hypertensive
patients138. Compliance clinics run by Pharmacists in western countries have improved
adherence by reducing hospitalizations when pre & post clinics are compared139, 140.
WRITTEN COMMUNICATION: Write timings and supplementary information regarding illness
& treatment, especially for acute conditions (e.g. antibiotics) compared to chronic conditions141.
One way communication is disadvantageous with illiterate. In a study 42% patients unable to
comprehend instructions142. So combine both oral and written and encourage patient to put
questions.
AUDIO VISUAL AIDS: help in visualizing the nature of illness, how a medicine has to be
administered eg; metered dose inhalers and how they act. Many health care professionals are
using very effectively by placing them in waiting room or consultation room and answering
questions patients may have.
CONTROLLED THERAPY: Hospitalized patients are entrusted to self medicate before
discharge, under direct supervision of health care professionals so that latter; can identify
situations that undermine compliance that are corrected by answering questions 143
Special programs and devices: In some situations highly structured programs are
developed to improve compliance eg; behaviorally oriented program for training medication
management skills in schizophrenia patients which increased compliance from 63% to
81%.Similar programs are needed for vision and hearing impairment subjects by producing
prescription labels in Braille, and hearing aids respectively.
PATIENT MOTIVATION: For achieving optimum benefit, information is provided to the patient
in a manner that is not coercive, threatening or demeaning, by counseling, providing written
materials, supplying cues for appropriate behavior. Cues may be verbal or non verbal in latter
case using special packaging or reminders, Negotiable physician- patient interaction 123 with
respect and positive attitude, and realistic appraisal of the circumstances ,or development of
contracts 144,145 or paying incentives in the form of monitory and non monitory like gifts,
vouchers etc., to achieve agreed upon treatment goals.146,147 Mass programs like sterilization

REVIEW ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 152
and immunization, wherein patients are positively motivated by beneficiaries and neighbors
also improve compliance 3,148
TIME COMMITMENT: Patients may not be able to take time off work for treatment; as a
shorter traveling time between residence and healthcare facilities could enhance patient’s
compliance. Housewives more compliant to therapy they adapt well to clinic appointment times
and treatment 3, 149-151.
COMPLIANCE AIDS: The accuracy and specificity of information on the label of prescription
container and Auxiliary labels that provide additional information regarding the use,
precautions, and storage of medicines also help in improving adherence.
Medication Calendars and Drug Reminder Charts are designed and developed to assist
self administration of drugs by patients. Special medication container like 28- compartment
(MEDISET) container are designed to help patient organize their medications on weekly basis. fig
Specially designed caps for prescription container like The Prescript Time Cap; containing
digital time piece display time and date of last dose taken. They are effective in improving
adherence by patients who forgets doses or who are confused by the complexity of regimen.
Medication packaging also influence the patients adherence. Compliance Packs are
developed which are pre-packed units, which provides one treatment cycle of medication in a
ready to use package152. New dosage forms are developed to overcome non adherence due to
increased frequency, in the form of long acting and controlled release preparations. Similarly
Trans- dermal drug- delivery systems also permits less frequency of drug administration.
MONITORING THERAPY: 1. Self Monitoring-Patient should be appraised of the importance of
monitoring their own treatment and assume personal responsibility of adherence to treatment.
Pharmacist or physician monitoring. “.brown bag program was conducted by NCPIE
&The Administration on ageing in which patients are encouraged to put all their medicines in a
bag for personalized medicine review in geriatrics.
D.O.T (directly observed therapy.153-154 It is the ideal way to monitor therapy, especially
in cases of prolonged drug intake.
“French saying- 5 centuries back about patient care “To care sometimes, to restore often,
and to comfort always”
Summary: Valuable resources like time, effort and expenses put on diagnosis of illness
with the aim of developing treatment plan for cure, control or increased survival are not
achieved, unless patient complies to treatment. Non adherence is responsible for missed
diagnosis, treatment failures and changing prescriptions with more potent, expensive and toxic
drugs.
Adherence to medication is not routinely measured in clinical practice, for reasons as
busy practice and depriving patients on close attention and monitoring therapy are not
acceptable155. The highest priority should be given for patients adherence problems.
Improved adherence benefits every body (patient, physician, pharmaceuticals,
pharmacist & community). For patient there will be increased efficacy and safety of treatment
and decreased physician and hospital visits. For pharmacist increased recognition and respect
for advise and services. Pharmaceuticals by manufacturing drugs suitable to the patients need,
like blister pack, increase sales of drugs. Finally society at large and health care system gets
benefit as a result of few problems with non compliance.

REVIEW ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 153
REFERENCES
1. WHO Library Cataloguing-in-Publication Data. Adherence to long-term therapies:
evidence for action.ISBN 92 4 154599 2 (NLM classification:W 85);
2. Okuno J, Yanagi H, Tomura S. Is cognitive impairment a risk factor for poor compliance
among Japanese elderly in the community? Eur J Clin Pharmacol. 2001; 57:589–94.
[PubMed]
3. Hernandez-Ronquillo L, Tellez-Zenteno JF, Garduno-Espinosa J, et al. Factors associated
with therapy noncompliance in type-2 diabetes patients. Salud Publica Mex. 2003;
45:191–7. [PubMed
4. Aronson.JK-2007; Compliance, concordance, adherence; Br.J.Clinical Pharmacology, 63
(4), 383-384.
5. Tilson HH (2004). "Adherence or compliance? Changes in terminology". Ann
Pharmacother 38 (1):161–2.doi:10.1345/aph.1D207. PMID 14742813Osterberg>L,
Blaschke (2005); “Adherence to medication” N.Eng.J.Med-353 (5), 487-97.
6. Osterberg L, Blaschke T (2005). "Adherence to Medication". N Engl J Med 353 (5): 487–
97.doi:10.1056/NEJMra050100.PMID 16079372
7. Bell JS, Airaksinen MS, Lyles A, Chen TF, Aslani P (2007). "Concordance is not
synonymous with compliance or adherence". Br J Clin Pharmacol 64 (5): 710–
1. doi:10.1111/j.1365-2125.2007.02971_1.x. . PMID 17875196
8. Office of Behavior and Social Sciences Research. "Adherence Research Network".
U.S. National Institutes of Health. Retrieved 12 May 2010
9. "Enhancing Patient Adherence: Proceedings of the Pinnacle Roundtable Discussion". APA
Highlights Newsletter. October 2004
10. Ngoh LN (2009). "Health literacy: a barrier to pharmacist-patient communication and
medication adherence". J Am Pharm Assoc (2003) 49 (5): e132–46; quiz e147–
9.doi:10.1331/JAPhA.2009.07075.PMID 19748861.
11. National Institute for Health and Clinical Excellence. [3 March 2008]. Medicines
Concordance (Involving Patients in Decisions about Prescribed Medicines) Available
athttp://guidance.nice.org.uk/page.aspx?o=267072
12. Elliott RA, Marriott JL (2009)."Standardized assessment of patients' capacity to manage
medications: a systematic review of published instruments". BMC Geriatr 9:
27. doi:10.1186/1471-2318-9-27. .PMID 19594913.
13. Murray MD, et al.DICP 1986; 20:146.
14. Bond WS, Hussar DA. Detection methods and strategies for improving medication
compliance. Am J Hosp Pharm. 1991;48:1978–88. [PubMed-rept
15. Svarstad BL, Shireman TI, Sweeney JK. Using drug claims data to assess the relationship
of medication adherence with hospitalization and costs. Psychiatr Serv. 2001;52:805–11.
[PubMed]
16. "Dosing and compliance?". Bandolier117: Figure 1. November 2003
17. Norton M. (Reuters Health)Many patients may not fill their prescriptions.
(2010), [1]Accessed May 12, 2010
18. Schering Report, , XVIII, 1996
19. Primary non compliance in a Singapore poly clinic, Singapore Med. J 1999, Nov; 40
(11):691-3
20. Mattar ME, et al, J.Pediatr.1975; 18:137

REVIEW ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 154
21. De Tullio PL, Corson ME. Am J Hosp.Pharm,1987; 44:1802
22. Prescription drugs:survey of consumer use, attitudes & behavior. Washington, DC: AARP,
1984.
23. Robinson B. Drug topics, 1987; 131(Feb.16):37.
24. Shah NR, Hirsch AG, Zacker C, Taylor S, Wood GC, Stewart WF (February 2009)."Factors
associated with first-fill adherence rates for diabetic medications: a cohort study". J Gen
Intern Med 24 (2): 233–7.doi:10.1007/s11606-008-0870-z. .PMID 19093157
25. Shah NR, Hirsch AG, Zacker C, et al. (April 2009). "Predictors of first-fill adherence for
patients with hypertension". Am. J. Hypertens. 22 (4): 392–6.doi:10.1038/ajh.2008.367.
.PMID 19180061.
26. Tebbi CK, Cummings KM, Zevon MA, et al. Compliance of pediatric and adolescent cancer
patients. Cancer. 1986; 58:1179–84. [PubMed
27. DiMatteo MR. Social support and patient adherence to medical treatment: a meta-
analysis. Health Psychol. 2004;23:207–18. [PubMed]
28. Degoulet P, Menard J, Vu HA, et al. Factors predictive of attendance at clinic and blood
pressure control in hypertensive patients. Br Med J (Clin Res Ed) 1983;287:88–93.
29. Shea S, Misra D, Ehrlich MH, et al. Correlates of nonadherence to hypertension treatment
in an inner-city minority population. Am J Public Health. 1992;82:1607–12. [PMC free
article] [PubMed
30. Turner J, Wright E, Mendella L, et al. Predictors of patient adherence to long-term home
nebulizer therapy for COPD. Chest. 1995; 108:394–400. [PubMed]
31. Leggat JE, Jr, Orzol SM, Hulbert-Shearon TE, et al. Noncompliance in hemodialysis:
predictors and survival analysis. Am J Kidney Dis. 1998; 32:139–45. [PubMed
32. Kyngas H, Lahdenpera T. Compliance of patients with hypertension and associated
factors. J Ad Nurs. 1999;29:832–9.
33. Kim YS, Sunwoo S, Lee HR, et al. Determinants of non-compliance with lipid-lowering
therapy in hyperlipidemic patients. Pharmacoepidemiol Drug Saf. 2002;11:593–600.
[PubMed]
34. Ghods AJ, Nasrollahzadeh D. Noncompliance with immunosuppressive medications after
renal transplantation. Exp Clin Transplant. 2003;1:39–47. [PubMed]
35. Yavuz A, Tuncer M, Erdogan O, et al. Is there any effect of compliance on clinical
parameters of renal transplant recipients? Transplant Proc. 2004;36:120–1. [PubMed]
36.
36. Balbay O, Annakkaya AN, Arbak P, et al. Which patients are able to adhere to tuberculosis
treatment? A study in a rural area in the northwest part of Turkey. Jpn J Infect Dis.
2005;58:152–8. [PubMed]
37. Cooper C, Carpenter I, Katona C, et al. The AdHOC study of older adults’ adherence to
medication in 11 countries. Am J Geriatr Psychiatry. 2005;13:1067–76. [PubMed
38. Fodor GJ, Kotrec M, Bacskai K, et al. Is interview a reliable method to verify the
compliance with antihypertensive therapy? An international central-European study. J
Hypertens. 2005;23:1261–6. [PubMed
39. Feinstein S, Keich R, Becker-Cohen R, et al. Is noncompliance among adolescent renal
transplant recipients inevitable? Pediatrics. 2005;115:969–73.
40. Kyngas H, Lahdenpera T. Compliance of patients with hypertension and associated
factors. J Ad Nurs. 1999;29:832–9.

REVIEW ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 155
41. Medications,due to polypharmacy,(williams a, manias e and walker r. interventions to
improve medication adherence in people with multiple chronic conditions: a systematic
review. journal of advanced nursing. february 2008:1-12.
42. GotzschePC.Controlled Clin Trials 1989;10:31.
43. Kroenke K.Am. J Med 19855;79:149
44. Feder R. N, Eng.J Med, 1978; 298:463
45. Kelloway JS, Wyatt RA, Adlis SA. Comparison of patients’ compliance with prescribed oral
and inhaled asthma medications. Arch Intern Med. 1994;154:1349–52. [PubMed]
46. Nichols-English G, Poirier S. Optimizing adherence to pharmaceutical care plans. J Am
Pharm Assoc. 2000;40:475–85.
47. Bender BG, Bender SE. Patient-identified barriers to asthma treatment adherence:
responses to interviews, focus groups, and questionnaires. Immunol Allergy Clin N Am.
2005;25:107–30
48. Horne R, Weinman J. Patients’ beliefs about prescribed medicines and their role in
adherence to treatment in chronic physical illness. J Psychosom Res. 1999;47:555–67.
[PubMed
49. Patal RP, Taylor SD. Factors affecting medication adherence in hypertensive patients. Ann
Pharmacother. 2002;36:40–5. [PubMed]
50. Grant RW, Devita NG, Singer DE, et al. Polypharmacy and medication adherence in
patients with type 2 diabetes. Diabetes Care. 2003;26:1408–12. [PubMed]
51. Iihara N, Tsukamoto T, Morita S, et al. Beliefs of chronically ill Japanese patients that lead
to intentional non-adherence to medication. J Clin Pharm Ther. 2004;29:417–24.
[PubMedrept-ref91
52. Factors influencing compliance-length of time treatment-an integrative review of patient
medication compliance from 1990-1998”wood &graythe online journal of knowledge
synthesis for nursing,vol7,document number 1 January 14, 2000
53. Combs D L, et al. Ann Intern Med. 199; 112:397
54. Sabaté E, editor. Adherence to long-term therapies: evidence for action. Geneva: World
Health Organization; 2003.
55. Gascon JJ, Sanchez-Ortuno M, Llor B, et al. Treatment Compliance in Hypertension Study
Group. Why hypertensive patients do not comply with the treatment: results from a
qualitative study. Fam Pract. 2004;21:125–30. [PubMed]
56. Farmer KC, Jacobs EW, Phillips CR. Long-term patient compliance with prescribed
regimens of calcium channel blockers. Clin Ther. 1994;16:316–26. [PubMed]
57. Frazier PA, Davis-Ali SH, Dahl KE. Correlates of noncompliance among renal transplant
recipients. Clin Transplant. 1994;8:550–7. [PubMed
58. Medication adherence: Finding solutions to a costly medical problem-Gottlieb,Drug
benefit trends 12(6) 57-62,2000
59. Dhanireddy KK, Maniscalco J, Kirk AD. Is tolerance induction the answer to adolescent
non-adherence? Pediatr Transplant. 2005;9:357–63. [PubMed]
60. Combs DL, O’Brien RJ, Geiter LJ, et al. Compliance with tuberculosis regimes: results from
USPHS therapy trial 21. Am Rev Respir Dis. 1987;135:A138.
61. International Union Against Tuberculosis Committee on Prophylaxis. Efficacy of various
durations of isoniazid preventive therapy for tuberculosis: five years of follow-up in the
IUAT trial. Bull World Health Organ. 1982;60:556–64.

REVIEW ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 156
62. Kass MA, Meltzer DW, Gordon M, et al. Compliance with topical pilocarpine treatment.
Am J Ophthalmol. 1986;101:515–23. [PubMed]
63. Cockburn J, Gibberd RW, Reid AL, et al. Determinants of non-compliance with short term
antibiotic regimens. Br Med J (Clin Res Ed) 1987;295:814–8.
64. Cramer JA, Mattson RH, Prevey ML, et al. How often is medication taken as prescribed? A
novel assessment technique. JAMA. 1989;261:3273–7. [PubMed]
65. Eisen SA, Miller DK, Woodward RS, et al. The effect of prescribed daily dose frequency on
patient medication compliance. Arch Intern Med. 1990;150:1881–4. [PubMed]
66. Sung JC, Nichol MB, Venturini F, et al. Factors affecting patient compliance with
antihyperlipidemic medications in an HMO population. Am J Manag Care. 1998;4:1421–
30. [PubMed]
67. Claxton AJ, Cramer J, Pierce C. A systematic review of the associations between dose
regimens and medication compliance. Clin Ther. 2001;23:1296–310. [PubMed]
68. Iskedjian M, Einarson TR, MacKeigan LD, et al. Relationship between daily dose frequency
and adherence to antihypertensive pharmacotherapy: evidence from a meta-analysis.
Clin Ther. 2002;24:302–16. [PubMed
69. Hoagland AC, et al. AMJ Clin Oncol, 1983; 6:239
70. Spagnoli A, Ostino G, Borga AD, et al. Drug compliance and unreported drugs in the
elderly. J Am Geriatr Soc. 1989;37:619–24. [PubMed
71. Shaw E, Anderson JG, Maloney M, et al. Factors associated with noncompliance of patients
taking antihypertensive medications. Hosp Pharm. 1995;30:201–3.
72. Buck D, Jacoby A, Baker GA, et al. Factors influencing compliance with antiepileptic drug
regimes. Seizure. 1997;6:87–93. [PubMed]
73. Dusing R, Weisser B, Mengden T, et al. Changes in antihypertensive therapy-the role of
adverse effects and compliance. Blood Press. 1998;7:313–5. [PubMed]
74. Hungin AP, Rubin G, O’Flanagan H. Factors influencing compliance in long-term proton
pump inhibitor therapy in general practice. Br J Gen Pract. 1999;49:463–4. [PMC free
article] [PubMed]
75. Kiortsis DN, Giral P, Bruckert E, et al. Factors associated with low compliance with lipid-
lowering drugs in hyperlipidemic patients. J Clin Pharm Ther. 2000;25:445–51
76. Linden M, Gothe H, Dittmann RW, et al. Early termination of antidepressant drug
treatment. J Clin Psychopharmacol. 2000;20:523–30. [PubMed]
77. Dietrich AJ, Oxman TE, Burns MR, et al. Application of a depression management office
system in community practice: a demonstration. J Am Board Fam Pract. 2003;16:107–14;
78. Grant RW, Devita NG, Singer DE, et al. Polypharmacy and medication adherence in
patients with type 2 diabetes. Diabetes Care. 2003;26:1408–12. [PubMed]
79. Loffler W, Kilian R, Toumi M, et al. Schizophrenic patients’ subjective reasons for
compliance and noncompliance with neuroleptic treatment. Pharmacopsychiatry.
2003;36:105–12 .
80. Helene Levens Lipton;”Elderly patients and their pills: The role of compliance in safe and
effective drug use”. Pride Institute Journal of long Term Home Health Care 8,no.1
(winter1989):26-31
81. Kaplan RC, Bhalodkar NC, Brown EJ, Jr, et al. Race, ethnicity, and sociocultural
characteristics predict noncompliance with lipid-lowering medications. Prev Med.
2004;39:1249–55. [PubMed]
82. O’Donoghue MN. Compliance with antibiotics. Cutis. 2004;73(Suppl 5):30–2. [PubMed

REVIEW ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 157
83. Christensen DB. Drug-taking compliance: a review and synthesis. Health Serv Res.
1978;13:171–87. [PMC free article
84. NorrelSE,et al. Am J Hosp Pharm 1984; 41: 1183
85. Ballard DB. Am j Health-System Pharm 1996; 53 1962
86. Chizzola PR, Mansur AJ, da Luz PL, et al. Compliance with pharmacological treatment in
outpatients from a Brazilian cardiology referral center. Sao Paulo Med J. 1996;114:1259–
64. [PubMed]
87. Nikolaus T, Kruse W, Bach M, et al. Elderly patients’ problems with medication. An in-
hospital and follow-up study. Eur J Clin Pharmacol. 1996;49:255–9. [PubMed]
88. Koop CE.Proc Symp Natl Pharm Council 1984;1.
89. National Council On Patient Information and Education (NCPIE) “Advancing Precription
Medicine Compliance: New Paradigms, New Practices”. December 1994
90. Maronda RF, et al.Med Care;1989; 27: 1159
91. Drug related visits to the emergency department:”how big is the problem?” patel &peter,
pharmacotherapy,22(7):915-923,2002
92. Einarson TR. Ann Pharmacother 1993; 27: 832
93. Col N,et al.Arch Intern Med 1990; 150: 841
94. Strandberg LR.Am Health Care Assoc J 1984; 10 (7) :20
95. Vogel M. Pharmacy Today 1997; 3: 8.
96. Bowerman DL, et al. J Forensic Sci 1978; 23: 522.
97. Rovelli M, et al.Transplant Proc 1989; 21: 833 Bond WS, Hussar DA. Detection methods
and strategies for improving medication compliance. Am J Hosp Pharm. 1991;48:1978–
88. [PubMed]
98. Journal of the American pharmaceutical association 41 (2): 192-199,2001
99. "Patient Compliance with statins".Bandolier. 2004
100. R. Brian, Haynes, et al, “How to detect & manage low patient compliance in chronic
illness”, Geriatrics 355 (1980) : 91-97.
101. Cohn, DL, et al. Ibid 407.
102. Rudd P, et al. Clin Pharmacol Ther 1989; 46: 169.
103. Pullar T, et al. Ibid 163.
104. Morisky--de, green lw, levine dw. concurrent and predictive validity of a self-reported
measure of medication, adherence. medical care 1986;24:67-74
105. Rudd P, et al. Clin Pharmacol Ther 1990; 48: 676
106. Kossoy AF, et al. J Allergy Clin Immunol 1989; 84: 60.
107. Haynes RB, Montague P, Oliver T, et al. Interventions for helping patients to follow
prescriptions for medications. Cochrane Database tr
108. De Geest S, Borgermans L, Gemoets H, et al. Incidence, determinants, and consequences
of subclinical noncompliance with immunosuppressive therapy in renal transplant
recipients. Transplantation. 1995;59:340–7. [PubMed]
109. McLane CG, Zyzanski SJ, Flocke SA. Factors associated with medication noncompliance
in rural elderly hypertensive patients. Am J Hypertens. 1995;8:206–9. [PubMed]
110. Lorenc L, Branthwaite A. Are older adults less compliant with prescribed medication
than younger adults? Br J Clin Psychol. 1993;32:485–92. [PubMed]
111. Sirey JA, Bruce ML, Alexopoulos GS, et al. Stigma as a barrier to recovery: Perceived
stigma and patient-rated severity of illness as predictors of antidepressant drug
adherence. Psychiatr Serv. 2001;52:1615–20. [PubMed

REVIEW ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 158
112. Wild MR, Engleman HM, Douglas NJ, et al. Can psychological factors help us to determine
adherence to CPAP? A prospective study. Eur Respir J. 2004;24:461–5. [PubMed
113. Svartad BL. NARD J 1986; Feb: 75.
114. Rosestock IM. Milkbank Mem Fund Q 1966; 55(Jul): 94.
115. Becker MH, et al. Med Care 1977; 15(Suppl 5): 27
116. Barnes L, Moss-Morris R, Kaufusi M. Illness beliefs and adherence in diabetes mellitus: a
comparison between Tongan and European patients. N Z Med J. 2004;117:U743.
[PubMed
117. Bosley CM, Fosbury JA, Cochrane GM. The psychological factors associated with poor
compliance with treatment in asthma. Eur Respir J. 1995;8:899–904. [PubMed
118. Apter AJ, Boston RC, George M. Modifiable barriers to adherence to inhaled steroids
among adults with asthma: it’s not just black and white. J Allergy Clin Immunol.
2003;111:1219–26. [PubMed]
119. Sloan JP, Sloan MC. An assessment of default and non-compliance in tuberculosis control
in Pakistan. Trans R Soc Trop Med Hyg. 1981;75:717–8. [PubMed
120. Stromberg A, Brostrom A, Dahlstrom U, et al. Factors influencing patient compliance
with therapeutic regimens in chronic heart failure: A critical incident technique analysis.
Heart Lung. 1999;28:334–41. [PubMed]
121. Moore PJ, Sickel AE, Malat J, et al. Psychosocial factors in medical and psychological
treatment avoidance: the role of the doctor-patient relationship. J Health Psychol.
2004;9:421–33. [PubMed]
122. Gonzalez J, Williams JW, Jr, Noel PH, et al. Adherence to mental health treatment in a
primary care clinic. J Am Board Fam Pract. 2005;18:87–96. [PubMed
123. Lawson VL, Lyne PA, Harvey JN, et al. Understanding why people with type 1 diabetes
do not attend for specialist advice: a qualitative analysis of the views of people with
insulin-dependent diabetes who do not attend diabetes clinic. J Health Psychol.
2005;10:409–23. [PubMed]
124. Benarde MA, Mayerson EW. JAMA 1978; 239: 1413.
125. . Geiseler PJ, Nellson KE, Cripsen RG. Am Rev Respir Dis 1987; 135:3.2-8
126. Porter AMW. Br Med J 1969; 1: 218
127. Guidelines ror prescribers: By American Pharmaceutical Association/American Society
of Internal Medicine (March 1976)
128. Vasnik JJ, Aliotta SL, DeLor B. Medication adherence: factors influencing compliance with
prescribed medication plans. Case Manager. 2005;16:47–51. [PubMed
129. Butterworth JR, Banfield LM, Iqbal TH, et al. Factors relating to compliance with a
gluten-free diet in patients with coeliac disease: comparison of white Caucasian and
South Asian patients. Clin Nutr. 2004;23:1127–34. [PubMed
130. Dowse R, Ehlers M. Medicine labels incorporating pictograms: do they influence
understanding and adherence? Patient Educ Couns. 2005;58:63–70. [
131. PubMed Rubin RR. Adherence to pharmacologic therapy in patients with type 2 diabetes
mellitus. Am J Med. 2005;118:27s–34s. [PubMed
132. Lim TO, Ngah BA. The Mentakab hypertension study project. Part II – why do
hypertensives drop out of treatment? Singapore Med J. 1991;32:249–51. [PubMed
133. Haynes RB, Taylor DW, Sackett DL, et al. Can simple clinical measurements detect
patient noncompliance? Hypertension. 1980;2:757–64. [PubMed]

REVIEW ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 159
134. Norman SA, Marconi KM, Schezel GW, et al. Beliefs, social normative influences, and
compliance with antihypertensive medication. Am J Prev Med. 1985;1:10–7. [PubMed]
135. Olubodun JOB, Falase AO, Cole TO. Drug compliance in hypertensive Nigerians with and
without heart failure. Int J Cardiol. 1990;27:229–34. [PubMed
136. Milas NC, Nowalk MP, Akpele L, et al. Factors associated with adherence to the dietary
protein intervention in the Modification of Diet in Renal Disease Study. J Am Diet Assoc.
1995;95:1295–300. [PubMed]
137. Thomas LK, Sargent RG, Michels PC, et al. Identification of the factors associated with
compliance to therapeutic diets in older adults with end stage renal disease. J Ren Nutr.
2001;11:80–9. [PubMed]
138. Gannon K. Drug Topics 1990;134(July 9): 13
139. McKenney JM, et al. Circulation 1973; 48: 1104
140. Monson R, et al. Arch Intern Med 1981; 141: 1441.
141. Cable GL, et al. Contemp Pharm Pract 1982; 5: 38.
142. Tebbi CK. Treatment compliance in childhood and adolescence. Cancer. 1993;71:3441–
9. [PubMed
143. Williams MV, et al. JAMA 1995; 274: 1677
144. Remington IX Edn. Clinical Pharmacology, Chapter115; Pg.1966-76.
145. Dunbar JM, Agros WS. Comprehensive Handbook of Behavioral Medicine, vol 3. In
Ferguson JM, Taylor CB, eds. New York: Spectrum, 1980, p 328
146. Eraker SA, et al. Ann Intern Med 1984; 100: 258.
147. Giuffrida A, Torgerson. Should we pay, BMJ.1997 (sept 20) 315 (7110) 703-707
148. AID-Incentives. Public Health Rep. 1994 (July-Aug) 109 (4): 548-554
149. Spikmans FJ, Brug J, Doven MM, et al. Why do diabetic patients not attend appointments
with their dietitian? J Hum Nutr Diet. 2003;16:151–8. [PubMed]
150. Siegal B, Greenstein SJ. Compliance and noncompliance in kidney transplant patients:
cues for transplant coordinators. Transpl Coord. 1999;9:104–8.
151. Neal RD, Hussain-Gambles M, Allgar VL, et al. Reasons for and consequences of missed
appointments in general practice in the UK: questionnaire survey and prospective review
of medical records. BMC Fam Pract. 2005;6:47. [PMC free article] [PubMed]
152. Chuah SY. Factors associated with poor patient compliance with antituberculosis
therapy in Northwest Perak, Malaysia. Tubercle. 1991;72:261–4. [PubMed]
153. Smith DL, Am Pharm 1989;NS29(2):42
154. Alpert PL Munaiff SS et al, A Prospective study of tuberculosis and Human
immunodeficiency Virus Infection: Clinical manifestations and factors associated with
survival, Clin. Inf. Dis. 1997; 24; 661-668
155. Alwood K, Kernly J,Moore-Rice k, et al; Effectiveness of Supervised, Intermittent therapy
for Tuberculosis in HIV-Infected Patients, AIDS 1994; 8: 1103-8

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012. Page 160
INTERESTING LESIONS OF BONE MARROW WITH SPECIAL REFERENCE
TO METASTASIS.
Dr. I. Sreelakshmi, Dr. P. Sunethri, Dr. B. Bheeshma, Dr. V. Geetha, Dr. P. Jijiya bai, Dr. O. Shravan
Kumar, Dr. M. Anjani Devi, Dr. K. Ramakrishna Reddy.
1. Assistant Professor, Department of Pathology. Gandhi Medical College, Hyderabad.
2. Assistant Professor, Department of Pathology. Gandhi Medical College, Hyderabad.
3. Associate Professor, Department of Pathology. Gandhi Medical College, Hyderabad.
4. Assistant Professor, Department of Pathology. Gandhi Medical College, Hyderabad.
5. Professor & Head of Department, Department of Pathology. Gandhi Medical College, Hyderabad.
6. Professor, Department of Pathology. Gandhi Medical College, Hyderabad.
7. Post Graduate, Department of Pathology. Gandhi Medical College, Hyderabad.
8. Post Graduate, Department of Pathology. Gandhi Medical College, Hyderabad.
CORRESPONDING AUTHOR:
Dr. I. Sreelakshmi,
Gandhi Medical College,
Musheerabad, Secunderabad, AP,
Email id- [email protected],
Ph- 0091 09346371707.
ABSTRACT:
BACKGROUND: Bone marrow examination is a commonly used diagnostic modality in the
evaluation of hemato-oncological disorders and in patients with malignancies of visceral organs
to detect metastasis. This study reviews clinical, hematological and pathological data of
interesting cases with bone marrow involvement. Out of 490 bone marrow aspirations
performed during a period of 4 years, 5 cases show metastatic carcinomatous deposits which
included adenocarcinomas(3), squamous cell carcinoma(1) and neuroendocrine tumour(1),
Non-Hodgkins lymphomas(2), storage disorder(2), granulomatous lesions(1), gelatinous
transformation(1). Fever, generalized weakness, loss of appetite and loss of weight were the
main symptoms. Anemia and pancytopenia were the main hematological findings. Dry tap was a
significant finding in bone marrow aspiration in cases of metastatic cancers.
KEYWORDS : Bone Marrow Biopsy, Dry tap, Metastasis Cancer.
INTRODUCTION: Bone marrow examination is used commonly in evaluation of myeloid or
lymphoid haematological malignancies, suspected storage disorders, plasma cell neoplasms, to
detect infections & reactive changes, metastasis in patients with cancer of visceral organs &
staging of tumors. Most common tumors that metastasize to bone in adults are prostrate, breast
& lung cancer and in children neuroblastoma, rhabdomyosarcoma, Ewing’s sarcoma &
Retinoblastoma.
Infiltration of marrow is suspected in unexplained haematological abnormalities, fever
of unknown origin, failure to thrive in infants, bone pains & pathologic fractures, hot spots in
PET CT and hypercalcemia, increased alkaline phosphatase.
We studied clinical, hematological, pathological data of interesting cases with bone
marrow involvement.
MATERIALS AND METHODS: A total of 490 bone marrow aspirations performed between
2008- 2011 were analyzed. A total of 19 bone marrow aspirations, followed by biopsy were
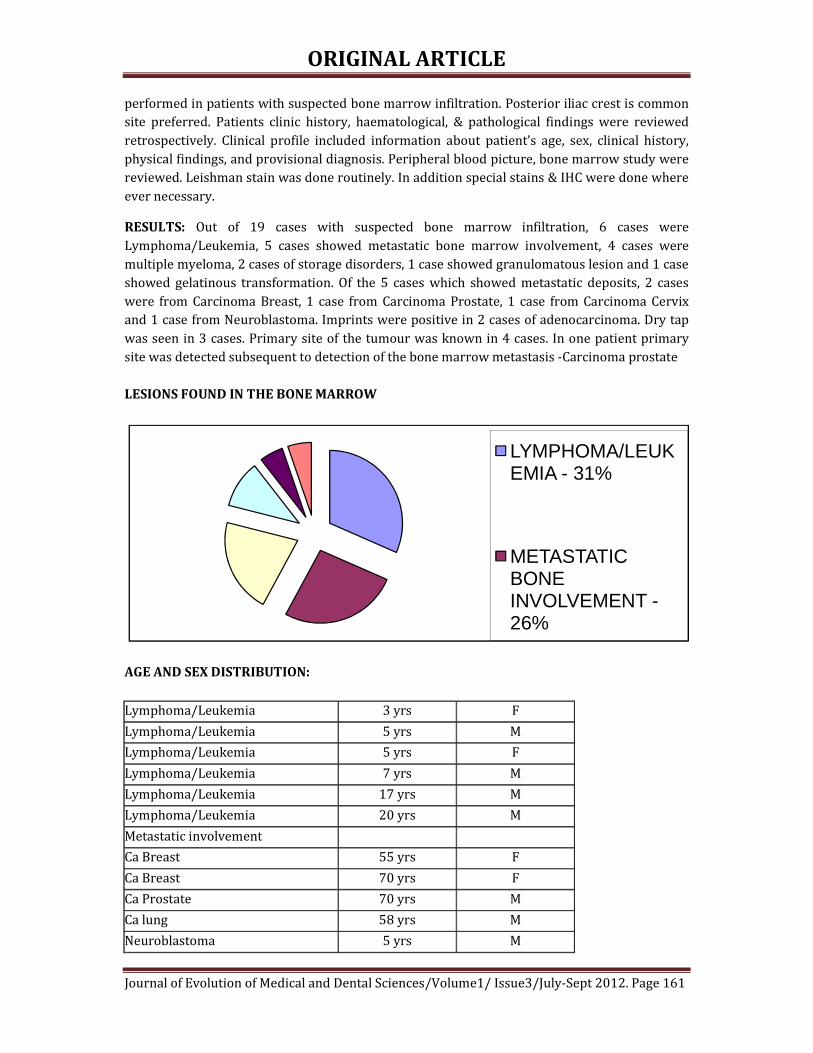
ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012. Page 161
performed in patients with suspected bone marrow infiltration. Posterior iliac crest is common
site preferred. Patients clinic history, haematological, & pathological findings were reviewed
retrospectively. Clinical profile included information about patient’s age, sex, clinical history,
physical findings, and provisional diagnosis. Peripheral blood picture, bone marrow study were
reviewed. Leishman stain was done routinely. In addition special stains & IHC were done where
ever necessary.
RESULTS: Out of 19 cases with suspected bone marrow infiltration, 6 cases were
Lymphoma/Leukemia, 5 cases showed metastatic bone marrow involvement, 4 cases were
multiple myeloma, 2 cases of storage disorders, 1 case showed granulomatous lesion and 1 case
showed gelatinous transformation. Of the 5 cases which showed metastatic deposits, 2 cases
were from Carcinoma Breast, 1 case from Carcinoma Prostate, 1 case from Carcinoma Cervix
and 1 case from Neuroblastoma. Imprints were positive in 2 cases of adenocarcinoma. Dry tap
was seen in 3 cases. Primary site of the tumour was known in 4 cases. In one patient primary
site was detected subsequent to detection of the bone marrow metastasis -Carcinoma prostate
LESIONS FOUND IN THE BONE MARROW
AGE AND SEX DISTRIBUTION:
Lymphoma/Leukemia 3 yrs F
Lymphoma/Leukemia 5 yrs M
Lymphoma/Leukemia 5 yrs F
Lymphoma/Leukemia 7 yrs M
Lymphoma/Leukemia 17 yrs M
Lymphoma/Leukemia 20 yrs M
Metastatic involvement
Ca Breast 55 yrs F
Ca Breast 70 yrs F
Ca Prostate 70 yrs M
Ca lung 58 yrs M
Neuroblastoma 5 yrs M
LYMPHOMA/LEUKEMIA - 31%
METASTATIC BONE INVOLVEMENT -26%

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012. Page 162
Multiple Myeloma 62 yrs M
Multiple Myeloma 64 yrs M
Multiple Myeloma 68 yrs M
Multiple Myeloma 57 yrs M
Storage disorders 3 yrs M
Storage disorders 9 m F
Granulamtous lesions 35 yrs M
Gelatinous transformation 40 yrs M
CLINICAL DETAILS
SYMPTOMS
Generalized weakness
NO. OF CASES
19
% OF CASES
100%
Loss of weight & loss of appetite 16 84%
Bone pain 10 52%
Fever 9 47%
Low back pain 8 42%
Organomegaly 7 36%
Lymphadenopathy 6 31%
HEMATOLOGICAL PROFILE
PERIPHERAL SMEAR FINDING
Anaemia
NO. OF CASES
19
% OF CASES
100%
Thrombocytopenia 12 63%
Pancytopenia 8 42%
Leucopenia 7 36%
Leucoerythroblastic picture 6 31%
Dry tap 3 15%
Rouleaux formation 3 15%

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012. Page 163
IMPRINT – LYMPHOMA ALCIAN-PAS POSITIVITY ON IMPRINTS
BMB: METASTATIC DEPOSITS FROM PROSTATE IHC-ER-POSITIVE IN BREAST METS TO BONE
MARROW
ROULEAUX FORMATION - MULTIPLE MYELOMA IMPRINTS OF BM- MULTIPLE MYLOMA

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012. Page 164
EPITHELOID CELLS – GRANULOMA GELATINOUS TRANSFORMATION OF BM
DISCUSSION : Bone marrow examination is very useful in the evaluation of hemato-oncological
disorders. Common findings in the peripheral blood - leucoerythroblastic blood picture,
Pancytopenia, rouleaux formation. Bone marrow aspirates and trephine biopsies are sensitive
techniques for detecting bone marrow pathology. Trephine biopsy is more sensitive than bone
marrow aspiration and sensitivity is increased by performing bilateral biopsies or by obtaining
a single large biopsy.
In adolescent individuals who were eventually diagnosed with Lymphoma/leukemia,
they initially showed pancytopenia with occasional atypical cells in the peripheral smear. Dry
tap was seen in both the cases. Imprint smears from bone marrow biopsy showed that the
marrow was packed with blasts.
Renal failure, low back pain and male predominance was common in all the cases of
multiple myeloma. All the four cases showed elevated levels of serum creatinine.
Marrow infiltration may be focal or diffuse. Reticulin and collagen fibrosis are commonly
present in bone marrow with metastasis. Fibrosis is more in case of greater degree of marrow
infiltration. Marked fibrosis is most common in carcinoma of breast, stomach, prostate, lung.
Marked fibrosis causes pancytopenia, chemotherapeutic drugs causes haemotoxicity, all these
carries bad prognosis. The two primary sites whose identification is most important because of
their sensitivity to hormonal therapy are breast and prostate. The presence of bone marrow
metastasis is helpful in detecting hormonal receptor status when it was not done on primary
tumour.
In children spleenic aspirate is supplementary to bone marrow aspiration in
identification of storage disorders. Neuroblastoma metastasis to bone marrow is very rare in
children less than one year age.
CONCLUSION: Bone marrow aspiration and trephine biopsy are effective and cheap methods of
evaluating various pathological lesions, more useful especially in visceral tumours
metastasizing to bone marrow. Bone marrow examination is indicated when there is significant
probability of identifying lesion which would affect the treatment of primary lesion. Bone
marrow examination itself sometimes gives clue to primary pathology. Imaging techniques like
radionucleide bone scan MRI, CT are usually less effective when compared to bone marrow
examination.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012. Page 165
REFERENCES:
1. Singh G, Krause JR, Breit feld V (1977) Bone marrow examination for metastatic tumor,
Cancer 40:2317-2321.
2. Finkelstein JZ, Ekert H, ISSACSH, Higgins G (1970) Bone marrow metastases in children
with solid tumors. Amj Dis child 119:49-52.
3. Moid F, Depalma L (2005) comparison of relative value of bone marrow aspirater and
bone marrow trephine biopsies in the diagnosis of solid tumors metastasis and
Hodgkins Lymphoma. Institutional experience and literature review Arch Pathol Lab
Med 129:497-501.
4. Gangadeep Kaur, Metastatic bone marrow tumors: study of nine cases and review of the
literature J Blood Disorder Transfus 2011, 2:3.
5. Saadettin Kilickap, Bone marrow metastasis of solid tumors: Clinicopathological
evaluation of 73 cases: Turkish journal of cancer.
6. Atac B, Lawrence C, Goldberg SN, metastatic tumor: the complementary role of the
marrow aspinate and biopsy. Amj Med SCi, 1991; 302:211-213.
7. Nanda A, Basus, Marwaha N. Bone marrow trephine biopsy as an adjunct to
bonemarrow aspiration. J Assoc physicians India, 2002:50:893-895.
8. Bearden JD, Ratkin GA, Coltman CA Comparison of the diagnostic value of bone marrow
biopsy and bone marrow aspiration in neoplastic disease. J clin pathol. 1974:27:738-
740.
9. Bone marrow pathology, fourth edition B.J. Bain, D.M. Clark and B.S. Wilkins (c) 2010
Barbara.j. Bain, David M. Clark, Bridget S. Wilkins ISBN:978-1-405-16825-0.
10. Jonsson U, Rundles RW (1951) tumor metastases in bone marrow: Blood 6:16-25.
11. Papac RJ (1994) bone marrow metastases-A review cancer 74:2403-2413.
12. Savage RA. Hoffman GC, Shakar K (1978) Diagnostic problems involved in detection of
metastatic neoplasms by bone marrow aspinate compared with needle biopsy Amj Clin
Pathol 70:623-627.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 166
CORRELATION BETWEEN BIOFILM FORMATION OF UROPATHOGENIC
ESCHERICHIA COLI AND ITS ANTIBIOTIC RESISTANCE PATTERN. Dr. SarojGolia, Dr. Vivek Hittinahalli, Dr. Sujatha K Karjigi, Dr. K. Mallika Reddy.
1. Professor & HOD, Department of Microbiology, Dr. B.R. Ambedkar Medical College. 2. Associate Professor, Department of Microbiology, Dr. B.R. Ambedkar Medical College.
3. Post Graduate, Department of Microbiology, Dr. B.R. Ambedkar Medical College. 4. Post Graduate, Department of Microbiology, Dr. B.R. Ambedkar Medical College.
CORRESPONDING AUTHOR:
Dr. Vivek Hittinahalli, Dr B R Ambedkar Medical College, Kadugondanhalli, Bangalore-45, Email id- [email protected], Ph- 0091 07760984581. ABSTRACT
BACKGROUND: Microorganisms growing in multilayered cell clusters embedded in a matrix of extracellular polysaccharide (slime) which facilitates the adherence of these microorganisms to biomedical surfaces and protect them from host immune system and antimicrobial therapy. There are various methods to detect biofilm production like Tissue Culture Plate (TCP) ,Tube method (TM) ,Modified Congo Red Agar Method (MCRA),bio luminescent assay ,piezoelectric sensors and fluorescent microscopic examination. OBJECTIVES : This study was conducted to compare three methods for the detection of biofilms and compare with antibiotic sensitivity pattern, in uropathogenic Escherichia coli. METHOD: This study was carried out at the Department of Microbiology Dr. B. R. Ambedkar Medical College from Dec 2011 to June 2012. Total number of 107 clinical Escherichia coli isolates were randomly selected from all age groups were subjected to biofilm detection methods and their antibiotic resistance pattern was compared. Isolates were identified by standard phenotypic methods. Biofilm detection was tested by TCP, TM and MCRA methods . Antibiotic susceptibility test of uropathogenic E coli was performed using Kirby –Bauer disc diffusion method according to CLSI guidelines.
RESULTS: From the total of 107 clinical isolate 74 (69.1 %) isolates showed biofilm formation by all the TCP, TM, CRP methods. Biofilm forming isolates from catheter associated UTI showed drug resistance to more than 6 drugs. Only 2(13.3%) isolates from Asymptomatic UTI showed biofilm by TM & MCRA methods & were sensitive all drugs. Biofilm forming isolates from symptomatic UTI showed mixed drug resistance pattern.
CONCLUSION: We conclude from our study that biofilm formation is more common in catheterized patients. TCP method is more quantitative and reliable method for the detection of biofilm forming micro-organisms as compared to TM and MCRA methods. So TCP method can be recommended for screening of biofilm as virulence marker in drug resistant E coli isolates. KEY WORDS: Escherichia coli, Biofilm, Drug Resistance, Congo Red Agar, Tissue Culture Plate

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 167
INTRODUCTION: E coli accounts for 70 to 95% of urinary tract infections1,13 Bacteria follow ascending route of infections in 90% of urinary tract infections. These are primarily derived from fecal flora of the host, but haematogenic infections do occur. Virulence factors like adhesins, toxins , lipo polysaccharides , iron acquisition , presence of capsule, or serum resistance , determine the uropathogenicity of E.coli strains. Adhesion to epithelial cells of urogenital bacteria is generally accepted as being essential for Uropathogenic bacteria because otherwise the bacteria would be washed out rapidly. In 100% E.coli isolates from pyelonephritis patients & 17% E.coli isolates from Asymptomatic bacteriuria, pap (pili associated pyelonephritis ) was a significant virulence factor. Uropathogenic E.coli (UPEC) can also express a fimbrial adhensins like AFA I , AFA III , which are encoded by gene clusters.
UPEC can invade and colonise the bladder epithelium establishing a urinary tract reservoir allowing an explanation of recurrent UTI that does not necessarily involve reinfection via the Gastrointestinal tract.1,10
Biofilm is an aggregate of micro-organism in which the cells are irreversibly attached to substratum or to each other. They are embedded in a matrix of extra cellular polymeric substances (EPS) in which they have produced and exhibit an altered phonotype with respect to growth rate and gene transcription2,3
Availability of key nutrients, chemotaxis towards surface, motility of bacteria, surface adhesins and presence of surface bacteria are some factors which influences biofilm formation.4 The bacteria enclosed within the biofilm are extremely resistant to treatment. This may be because the drug concentration obtained may be insufficient in certain areas of the film. The bacteria located at the base of the biofilm are metabolically inactive and are thus resistant to certain antibiotics and possess active antibiotic degradation mechanism that contribute to avoid the accumulation of an effective drug concentration.19
So in this study we screened 107 non Repetitive Clinical urinary Isolates of E.coli received in Department of Microbiology Dr. B.R. Ambedkar Medical college by conventional microbiological methods& were subjected to various methods of detections of biofilm production .These include Tissue Culture Plate (TCP)method,5 Tube method(TM) 6,Modified Congo Red Agar method(MCRA) 7.
The samples received by patients were also divided into three groups namely catheter associated infection, Asymptomatic bacteriuria and Symptomatic bacteriuria. The antibiotic susceptibility test was carried out by Kirby Bauer Disc diffusion Technique on Mueller Hinton agar. OBJECTIVE: Evaluation of different detection methods of biofilm formation of uropathogenic E.coli and their drug susceptibility pattern. MATERIALS AND METHODS:
PLACE AND DURATION OF THE STUDY: The prospective study was conducted at the Department of Microbiology, Dr. B.R. Ambedkar Medical College from Dec 2011 to June 2012 . INCLUSION CRITERIA: Pure growth of Escherichia coli isolates were randomly selected from all age groups.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 168
E coli isolated from significant bacteriuria, in urine samples of catheterized patients, antenatal cases ,UTI complicated by urinary obstruction, antibiotic therapy, recurrent infections, chronic prostatitis were selected. EXCLUSION CRITERIA; Insignificant bacteriuria, mixed growth & any other organism showing significant growth .
SELECTION OF THE ISOLATES : Total number of 107 urine E coli isolates were subjected to biofilms detection methods. The urine samples of patients were divided into three groups namely – Catheter associated infections, Symptomatic bacteriuria, and Asymptomatic bacteriuria.
The organisms were identified by conventional microbiological methods. The antibiotic susceptibility test was carried out by Kirby Bauer Disc diffusion method
using reference strain of positive biofilm producer E.coli ATCC-25922. Statistical method used was linear correlation. TISSUE CULTURE PLATE METHOD5,8:
The organisms isolated from fresh agar plates were inoculated in Brain Heart Infusion(BHI) with 2% sucrose incubated for 24hrs at 37O c in stationary conditions. Broth was diluted 1:100 with fresh medium. Individual wells of sterile polystyrene 96 well flat bottom culture plate well were filled with 200ul aliquots of diluted cultures. Only medium served as control to check sterility and nonspecific binding of media.9
The TCP were incubated for 24hrs at 370 c. After incubation contents of each well was gently removed by taping the plates. The wells were washed four times with 0.2ml of phosphate buffer saline (PBS pH 7.2) to remove free floating planktonic bacteria. Biofilms formed by adherent ‘sessile’ organisms in plate were fixed with sodium acetate (2%) and stained with crystal violet (0.1%w/v) for one minute. Excess stain was rinsed off by thorough washing with deionized water and plates were kept for drying. Adherent E.coli cells usually formed biofilm on all side wells and were uniformly stained with crystal violet. Optical Density (OD) of stained adherent bacteria was determined with a micro ELISA auto reader (model 680, Bio rad) at wavelength of 570 nm (OD 570nm). These OD values were considered as index of bacteria adhering to surface and forming biofilms.8
Experiment was performed in triplicate and repeated three times, the data was then averaged and standard deviation was calculated. To compensate for background absorbance, OD readings from sterile medium, fixation and dye were averaged and subtracted from all test values. The mean OD value obtained from media control well was deducted from all test values. Classification of Bacteria Adherence:
We classified based on OD values obtained for individual strains of E.coli, but moderate biofilm forming isolates are taken as biofilm forming isolates.
Mean OD value Adherence Biofilm formation
< 0.120 Non Non/weak
0.120-0.240 Moderate Moderate
0.240 Strong High

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 169
Table no 1; Detection of biofilm formation by mean OD values
Negative OD <0.120
Strong positive OD > 0.240
Fig 1 Detection of biofilm formation by mean OD values.
TUBE METHOD : A quantitative assessment of biofilm formation was determined as previously described by Christensen et al BHI with2% sucrose was inoculated with loopful of microorganisms from overnight culture plates incubated for 24hrs at 37 c. Tubes were decanted and washed with PBS and dried tubes were stained with crystal violet 0.1%. Excess stain was removed and tubes were washed with deionized water Tubes were then dried inverted position and observed for biofilm formation.
Biofilm formation was considered positive when visible film lined the wall and bottom of the tube ring formation at the liquid interface was not indicative of biofilm formation, and interpreted as positive (tube 1) as negative(tube2) . Experiments were performed in triplicate and repeated three times.8 but moderate biofilm forming isolates are taken as biofilm forming isolates
Figure 2 . Tube 1 showing strong biofilm formation. Tube 2 negative for biofilm
production.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 170
MODIFIED CONGO RED AGAR METHOD (CRA): Freeman et al15 had described an alternative method of screening biofilm formation by E coli isolates. In this study we use modified Congo red agar for biofilm formation. In vitro slime production ability on the published Congo red agar by Freeman et al (1989) in diffuse black pigment in the agar with growth of black pigmented colonies but pigmentation decreased with time. In the present study the modified Congo red agar (MCRA) was optimized to get strong black pigmentation at 48hrs incubation and then for 2-4 days room temperature. Black colored colonies with dry crystalline consistency interpreted- as positive biofilm producing strains. Red coloured colonies- interpreted as negative for biofilm production
Table 2; composition of Congo red agar.
fig 3 Congo red agar plate showing biofilm formation a) dry crystalline colonies-positive
for biofilm, b)red colored colonies-negative for biofilm
Antibiotic susceptibility test of biofilm producing bacteria was done on Mueller Hinton agar using the following antibiotic discs12:
Norfloxacin, Nitrofurantoin, Ceftizoxime,ceftazidime, Amoxyclavulanic acid, Cotrimoxazole, Ampicillin ,Amikacin Imipenem,Tetracycline.
All the antibiotic disc were obtained from the Himedia. E coli ATCC 25922 were used as positive control and susceptibility testing was performed by using the Kirby Bauer Disc Diffusion Technique according CLSI guidelines.
RESULTS: Among 107 patients 65 were males and 42 were females. From the total of 107 clinical isolates 74( 69.1 %) isolates showed biofilm formation by all the TCP,TM,CRP methods. Among 67 catheter associated UTI ,60 (89.5%)isolates produced biofilm by all the three methods .
Composition /Litter Congo Red Agar Modified Congo red agar
Congo red 0.8g 0.4g
Sucrose 36g -
Glucose - 10g
BHAI 52g -
BAB-2 - 40g
Water 100ml 1000ml
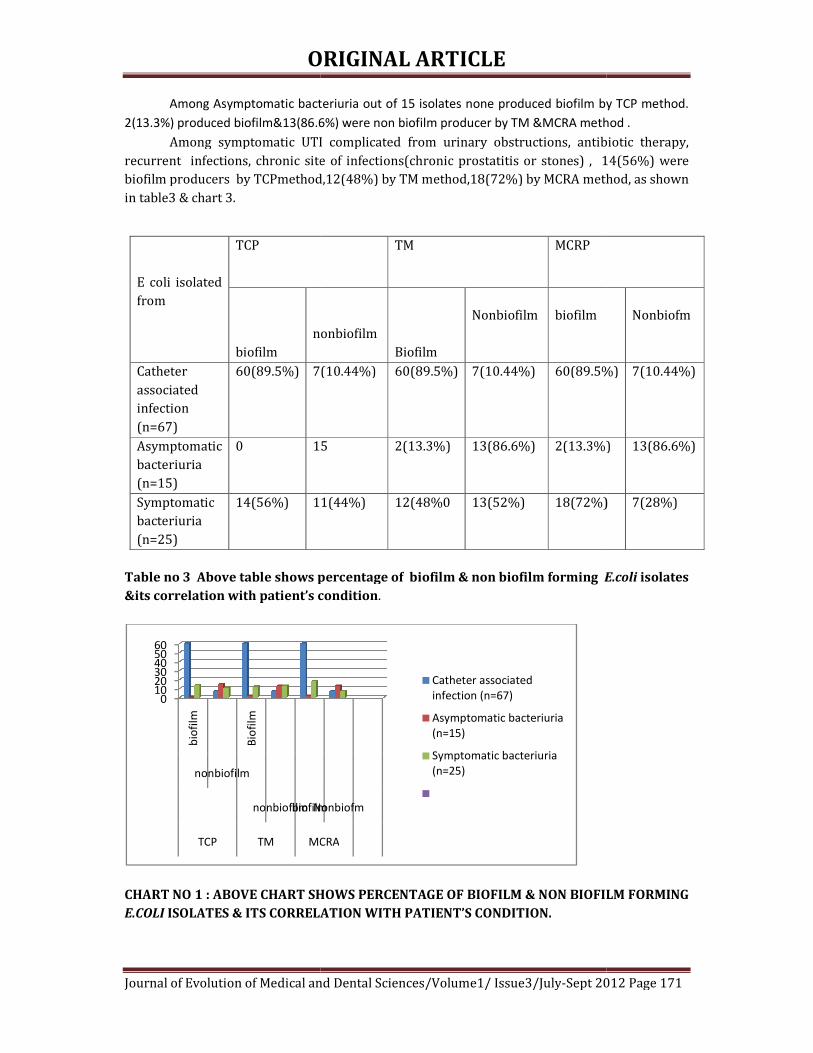
ORIGINAL
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/
Among Asymptomatic bacteriuria out of 15 isolates none produced biofilm by TCP method.
2(13.3%) produced biofilm&13(86.6%) were non biofilm producer by TM &MCRA meth
Among symptomatic UTI complicated from urinary obstructions, antibiotic therapy, recurrent infections, chronic site of infections(chronic prostatitis or stones) , 14(56%) were biofilm producers by TCPmethod,12(48%) by TM method,18(72%) by MCRA metin table3 & chart 3.
Table no 3 Above table shows percentage of
&its correlation with patient’s condition
CHART NO 1 : ABOVE CHART SHOWS PERCENTAGE OF BIOFILM & NON BIOFILM FORMING
E.COLI ISOLATES & ITS CORRELATION WITH PATIENT’S CONDITION.
0102030405060
bio
film
Bio
film
nonbiofilm
nonbiofilmbiofilmNonbiofm
TCP TM MCRA
E coli isolated from
TCP
biofilm
nonbiofilm
Catheter associated infection (n=67)
60(89.5%) 7(10.44%)
Asymptomatic bacteriuria (n=15)
0 15
Symptomatic bacteriuria (n=25)
14(56%) 11(44%)
ORIGINAL ARTICLE
of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012
Among Asymptomatic bacteriuria out of 15 isolates none produced biofilm by TCP method.
2(13.3%) produced biofilm&13(86.6%) were non biofilm producer by TM &MCRA meth
Among symptomatic UTI complicated from urinary obstructions, antibiotic therapy, infections, chronic site of infections(chronic prostatitis or stones) , 14(56%) were
biofilm producers by TCPmethod,12(48%) by TM method,18(72%) by MCRA method, as shown
Table no 3 Above table shows percentage of biofilm & non biofilm forming E.coli
with patient’s condition.
CHART NO 1 : ABOVE CHART SHOWS PERCENTAGE OF BIOFILM & NON BIOFILM FORMING
ISOLATES & ITS CORRELATION WITH PATIENT’S CONDITION.
biofilmNonbiofm
MCRA
Catheter associated
infection (n=67)
Asymptomatic bacteriuria
(n=15)
Symptomatic bacteriuria
(n=25)
TM MCRP
nonbiofilm
Biofilm
Nonbiofilm
biofilm
7(10.44%) 60(89.5%) 7(10.44%) 60(89.5%)
15 2(13.3%) 13(86.6%) 2(13.3%)
11(44%) 12(48%0 13(52%) 18(72%)
Sept 2012 Page 171
Among Asymptomatic bacteriuria out of 15 isolates none produced biofilm by TCP method.
2(13.3%) produced biofilm&13(86.6%) were non biofilm producer by TM &MCRA method .
Among symptomatic UTI complicated from urinary obstructions, antibiotic therapy, infections, chronic site of infections(chronic prostatitis or stones) , 14(56%) were
hod, as shown
E.coli isolates
CHART NO 1 : ABOVE CHART SHOWS PERCENTAGE OF BIOFILM & NON BIOFILM FORMING
Nonbiofm
60(89.5%) 7(10.44%)
2(13.3%) 13(86.6%)
18(72%) 7(28%)

ORIGINAL
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/
Table 4 & chart 4 shows resistance percentage of each antibiotic. These biofilm producingisolates were compared with drug resistance pattern as shown table 5&chart 3. Out of 74 biofilm producing isolates ,60 were catheter associated UTI &14 were from symptomatic UTI. 70( 94.5%) by TCP, 68( 91.5%) by TM method,& 71(87.6%) by MCRA method showedresistance to more than 6 drugs. E coli
drugs. Isolates from symptomatic UTI showed mixed drug resistance pattern.
Antibiotic used
Ampicillin(amp)
Cotrimoxozole
Amoxyclav
Amikacin
Ceftizoxime
Ceftazidme
Norflox
Nitrofurantoin
Tetracycline
Imipenem
Table -4 Resistance percentage
Chart 2 Resistance percentage of each antibiotic drug to E coli isolates.
TCP
Resistance to more than 6 drugs
70(94.5%)
Resistance to 5 to 6 drugs
4(5.4%)
Sensitive to all 0
Total 74
Table 5 The above table shows the relation between biofilm formation and antimicrobial
resistance pattern.
020406080
100120
0
90 82 7558
74
ORIGINAL ARTICLE
of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012
Table 4 & chart 4 shows resistance percentage of each antibiotic. These biofilm producingisolates were compared with drug resistance pattern as shown table 5&chart 3. Out of 74 biofilm producing isolates ,60 were catheter associated UTI &14 were from symptomatic UTI. 70( 94.5%) by TCP, 68( 91.5%) by TM method,& 71(87.6%) by MCRA method showed
. E coli isolates from asymptomatic UTI showed sensitive to all drugs. Isolates from symptomatic UTI showed mixed drug resistance pattern.
Number of isolates showed
resistant’s (%) n=107
90(84%)
82(76.6%)
75(70%)
58(54.2%)
74(69.1%)
79(73.8%)
81(75.7%)
78(72.9%)
74(69.8%)
30(28.3%)
4 Resistance percentage of each antibiotic drug to E coli isolates
Chart 2 Resistance percentage of each antibiotic drug to E coli isolates.
TM CRM
70(94.5%) 68(91.8%) 71(87.6%)
4(5.4%) 6(8.1%) 6(7.4%)
0 3(4.9%)
74 80
Table 5 The above table shows the relation between biofilm formation and antimicrobial
74 79 81 78 74
30
107
Sept 2012 Page 172
Table 4 & chart 4 shows resistance percentage of each antibiotic. These biofilm producing isolates were compared with drug resistance pattern as shown table 5&chart 3. Out of 74 biofilm producing isolates ,60 were catheter associated UTI &14 were from symptomatic UTI. 70( 94.5%) by TCP, 68( 91.5%) by TM method,& 71(87.6%) by MCRA method showed drug
isolates from asymptomatic UTI showed sensitive to all
Table 5 The above table shows the relation between biofilm formation and antimicrobial

ORIGINAL
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/
Chart 3The relation between biofilm formation and antimicrobial resistance pattern
Antibiotics
Catheter associated infection N=60
Ampicillin(amp) 60
Cotrimoxozole 60
Amoxyclav 58
Amikacin 50
Ceftizoxime 60
Ceftazidme 60
Norflox 60
Nitrofurantoin 60
Tetracycline 60
Imipenem 24
Table 5 The above table shows correlation between antibiotic resistance pattern with
patient’s condition & biofilm formation. (N=number of biofilm positive isolates).
Chart 4 The above chart shows correlation between patient’s condition ,biofilm
formation & antibiotic resistance pattern. N=number of biofilm positive isolates.
DISCUSSION: Bacterial adhesion has long been considered as virulence factor contributing to infection associated with catheter and other including medical devices.There are two possible explanations for the ability of materials . The first and the bacterial production of polysaccharide slime, the second one is the presence of adhesins for the host matrix proteins that are absorbed on to the biomedical surface.15
There are various methods for biofilm detection
0
Resistance to more than 6 drugs
Resistance to 5 to 6 drugs
Sensitive to all
Total
CRM
ORIGINAL ARTICLE
of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012
Chart 3The relation between biofilm formation and antimicrobial resistance pattern
Catheter associated infection
Symptomatic bacteriuria N=14
Non biofilm Forming Isolates N =33.
14 16
14 8
12 5
8 0
14 0
14 5
14 7
14 4
14 0
6 0
Table 5 The above table shows correlation between antibiotic resistance pattern with
patient’s condition & biofilm formation. (N=number of biofilm positive isolates).
shows correlation between patient’s condition ,biofilm
formation & antibiotic resistance pattern. N=number of biofilm positive isolates.
Bacterial adhesion has long been considered as virulence factor contributing to catheter and other including medical devices.13
There are two possible explanations for the ability of E coli species to colonies artificial materials . The first and the bacterial production of polysaccharide slime, the second one is the
sins for the host matrix proteins that are absorbed on to the biomedical
There are various methods for biofilm detection5,6,7.
20 40 60 80 100
CRM TM TCP
Sept 2012 Page 173
Chart 3The relation between biofilm formation and antimicrobial resistance pattern
Table 5 The above table shows correlation between antibiotic resistance pattern with
patient’s condition & biofilm formation. (N=number of biofilm positive isolates). shows correlation between patient’s condition ,biofilm
formation & antibiotic resistance pattern. N=number of biofilm positive isolates.
Bacterial adhesion has long been considered as virulence factor contributing to
species to colonies artificial materials . The first and the bacterial production of polysaccharide slime, the second one is the
sins for the host matrix proteins that are absorbed on to the biomedical

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 174
In this study we evaluated 107 isolates from urine samples by three screening methods for their ability to form biofilms .
In our study we found that the majority of biofilm producing bacteria was form catheterised patients (89.5%) similarly , Donlan 2,3 reported in his study the association of biofilm producing bacteria with urinary catheters. In our study we performed TCP and TM by addition of 2% sucrose to BHI broth. Sugar supplementations is essential for biofilm formation 8.This was reported by studies conducted by Mathur T et all.
In modified TCP method extended incubation for 24hrs could lead to a better discrimination between moderate and non- biofilm producing isolates17. This was also observed in our study.
Biofilm exhibits more resistance to broad Spectrum antibiotics20. This supports that biofilm adds to the virulence profile of microorganism’s biofilm production. 16 The Tube method correlates well with TCP test for strong biofilm production but it was difficult to discriminate between weak and biofilm negative isolates due to the variability is observed results by different observers so in agreement with previous report Tube test cannot be recommended as a general screening test to identify biofilm producing isolates.18
CONCLUSION: By this study we conclude that biofilm forming microorganisms show resistance to many drugs. TM method showed 74 isolates as biofilm formers ,TCP method also showed 74 isolates as biofilm formers but MRCA showed 80 isolates as biofilm formers .Only 74 isolates that showed biofilm formation correlated with patients condition and antibiotic resistance pattern ,by this 6 isolates were false positive by MRCA method .TCP and TM method are more reliable for detection of biofilm formation ,when correlated with patient’s clinical condition and drug resistance pattern of biofilm forming isolates TM method is more subjective ,differs with different observers, so TCP method is more reliable and accurate among all , as CRA method showed false positive. Our study concludes TCP method is better method for screening of biofilm formation as virulence marker in drug resistant E coli isolates. REFERENCES:
Book. 1)Topley And Wilsos 10th edition, bact vol 2;p1379-1380. Journals. 2)Donlan RM(2001).Biofilms and device associated infections.Emerg.infect Dis 7:277-281. 3)DonlanRM,costerton w.Biofilms:survival mechanisms of clinically relevant Microorganisms,clin Microbiol Rev 2002;15(2);167-93. 4)Thomas D,Day F.Biofilmformation by plant associated bacteria.Ann Rev Microbiol2007;61:401-22. 5)Christensen GD,simpsonWA Younger JAet al.Adherance of coagulase negative staphylococci to plastic tissue cultures ;a qualitative model for the adherence of staphylococci to medical devices J Clin Microbiol 1995;22:996 -1006. 6) Christensen GD,simpsonWA.Bisno AL, BeacheyEH Adherance of slime producing strains of staphylococcus epidermidis to smooth surfaces.InfectImmune 1982;37:318 -26. 7) Freeman DJ, Falkiner FR and Keane CT (1989). New method for detecting slime production by coagulase negative staphylococci. Journal of Clinical Pathology., 42 (8): 872-874. 8)T Mathure et al ijmm aug 19 2011, ip;27.7.49.6

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 175
9)Quantification of biofilm in microtiter plates: Overview of testing conditions and practical recommendations for assessment of biofilm production by staphylococci Stepanović, S., Vuković, D., Hola, V., Bonaventura, G.D., Djukić, S., Ćirković, I., Ruzicka, F.APMIS. 2007; 115(8): 891-899[Pubmed] 10) Stickler DJ (2005) Urinary catheters: ideal sites for the development of biofilm communities. 11)Stickler DJ, Young R, Jones G, Sabubba NA, and Morris NS (2003) Why are Foley catheters so vulnerable to www.sgm.ac.uk/pubs/micro_today/pdf/020505.pdf. Microbiology Today, Feb: 22-25.. 12) Makie & McCartney practical medical microbiology, 14th ed., Churchill Livingstone In., New York 131-149. 13)Madbhusharma, Aparna,Sarita, DOI:10.4103/0377-4929,48960. 14) Montanaro L, Arciola CR, Borsetti E, Brigotti M, and Baldassarri L (1998) A polymerase chain reaction (PCR) method for the identification of collagen adhesin gene (cna) in Staphylococcus-induced prosthesis infections. New Microbiol 21: 359–363. 15)Montanaro L, Arciola CR, Borsetti E, Brigotti M, and Baldassarri L (1998) A polymerase chain reaction (PCR) method for the identification of collagen adhesin gene (cna) in Staphylococcus-induced prosthesis infections. New Microbiol 21: 359–363. 16) Salwa S. Seif El-Din et al Journal of American Science, 2011;7(1) 17) Ludwicka A, Switalski LM, Lundin A, Pulverer G, Wadstrom T. Bioluminescent assays for measurement of bacterial attachment to polyethylene. J Microbiol Methods1985;4:169-77 18) Christensen GD, Simpson WA, Bisno AL, Beachey EH. Adherence of slime-producing strains of Staphylococcus epidermidis to smooth surfaces. Infect Immun1982;37:318-26 19)Anderson GG.Palermo JJ,Roth R,Heuser J, Hultgren SJ.Intracellular bacterial Biofilm- like pods in urinary tract infection.science 2003;301:105-7. 20)Suman E,J Jose,S Varghese,MS Kotian aug 19 2011,IP;27.7.49.6

CASE REPORT
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012. Page 176
RETROPERITONEAL HYDATD CYST: A RARE PRESENTATION
Dr. Siddesh. Basavaraj. Sirwar, Dr. Amrutha. Swati. Indupalli, Dr. Subhanulla P.
1. Professor, Department of Microbiology. Khajabanda Nawaz Institute of Medical Sciences, Gulbarga. 2. Associate Professor, Department of Community Medicine, Khajabanda Nawaz Institute of Medical Sciences. 3. Professor, Department of Surgery, Khajabanda Nawaz Institute of Medical Sciences, Gulbarga.
CORRESPONDING AUTHOR:
Dr. Siddesh. Basavaraj. Sirwar, Mathru Nilaya, Plot No: 11, Siddeshwara Colony, Old Jewargi Road, Gulbarga -02, Karnataka, Email id- [email protected], Ph- 0091 09448320166 / 09902536576. ABSTRACT: Primary retro peritoneal hydatid cyst is extremely rare and only occasional case reports have appeared since first reported this entity in 1958. We report this rare case from KBN Hospital Gulbarga Karnataka diagnosis confirmed post operatively. Mass approached through greater sac which revealed a single cavity in retroperitonium containing enormous number of typical cyst of 2-5cms diameter occupying sub hepatic, epigastria, umbilical and left lumbar regions extending to pelvis. It was never expected that such enormous 2970 cysts would be recovered. Hence, suspicion and ruling out hydatid cyst in every case of retroperitoneal cystic swelling especially in endemic areas, and a careful search for hydatid cysts in other uncommon sites should be cogitated. KEY WORDS: Hydatid Cyst, Retro Peritoneum. INTRODUCTION: Hydatid disease is a parasitic infestation by a tapeworm of the genus Echinococcus. Hydatid cysts are a manifestation of infection at the larval stage of Echinococcus granulosus. Human echinococcosis is a zoonotic infection transmitted by dogs in livestock raising areas.
Developing countries with poor hygiene, where sheep and cattle are raised are high-risk areas of acquiring this disease. Hydatid disease (Echinococcus granulosus) is endemic in the Middle East as well as other parts of the world, Africa, South America, New Zealand, Australia, Turkey and Southern Europe including India1-3, Foci of hydatid disease also exists in India where the highest prevalence is reported in Andhra Pradesh and Tamil Nadu than in other parts of the country4.
Echinococcus granulosus causes cystic echinococcosis in humans. This relatively benign parasitic disease is characterized by slowly growing cysts most commonly in the liver(accounting for 50-70% of cases), followed by the lungs(20-30%), and less frequently the spleen, kidneys, heart, bones, central nervous system, and other organs5.
The annual incidence of hydatid disease has been reported to be 18 to 20 cases per 100.000 inhabitants6. Retroperitoneal localization of hydatid cyst is unusual7 here we are reporting a case of primary retroperitoneal hydatid cyst with unusual number which is a very rare presentation.
CASE REPORT: A female aged 35 year presented with history of abdominal discomfort and distension of 1 year duration, loss of appetite, fever on and off for 3 months. On examination patient looked pallor. There was no jaundice, no edema, vital signs were, pulse 76/min, blood

CASE REPORT
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012. Page 177
pressure was 110/70 mmHg and mild fever (990F). Chest auscultation revealed normal breath sounds and heart sounds. On Local Examination of abdomen there was diffuse distension confined to upper abdomen, left flank and lower pelvis. Very soft, non tender mass felt more like fluid but no shifting dullness. Borders were indistinct.
INVESTIGATIONS: Hemoglobin-9.5gm%, Hypochromic, normocytic anemia, blood cell count 11.500/mm3, Eosinophil count 550/mm3, erythrocyte sedimentation rate 35 mm/h. The chest and abdominal ultra sound showed normal liver, spleen, kidneys and multiple cystic lesions in the peritoneal cavity occupying upper abdomen, left flank and parts of pelvis. Explorative laparotomy was done through upper midline incision Fig -1 .Liver, spleen, kidneys and peritoneum showed no cysts. Lesion appeared to be more posterior. Mass approached through greater sac which revealed a single cavity in retroperitonium containing enormous number of typical cyst of 2-5cms diameter occupying sub hepatic, epigastria, umbilical and left lumbar regions extending to pelvis . A total of 2970 cysts were delivered Fig-2. Examination of contents of cysts in laboratory revealed numerous hooklets, scolices, many pus cells. Histopathological examination also confirmed the diagnosis. ELISA test was positive for both Ig.M, and Ig.G Echinococcus. DISCUSSION: Hydatid disease in human is one of the oldest diseases known to mankind. Hydatid cysts in humans and animals have been known since Roman times, but, as was true for the other tapeworms, the relationship between the larval cyst and the adult worm was not suspected until the eighteenth century. E. granulosus was described as a separate species in 1850, and its life cycle was worked out with feeding experiments in 18638. Echinococcus granulosus, which commonly has a sheep–dog cycle, but which may also infect goats, cattle, swine, and camels, is the most likely to infect human beings. Human echinococcosis occurs primarily in sheep rearing areas. Dogs ingest cysts in the offal of dead sheep and pass eggs in their feces. Humans acquire the eggs from a dog's fur or from contaminated food or water. The adult worm lives in the proximal small bowel of the definitive host, attached by hooklets to the mucosa. Eggs are released into the host’s intestine and excreted in the feces. Humans may become intermediate hosts through contact with a definitive host (usually a domesticated dog) or ingestion of contaminated water or vegetables. The ovum loses its protective layer as it is digested in the duodenum. Once the parasitic embryo passes through the intestinal wall to reach the portal venous system or lymphatic system, the liver acts as the first line of defense and is therefore the most frequently involved organ. Secondary involvement due to hematogenous dissemination may be seen in almost any anatomic location9. Cysts holding 2 or more liters of fluid and larvae can grow for years in the liver, lungs, brain, or other organs and exert enough mechanical pressure to cause grave or fatal consequences8. The vast majority of abdominal and pelvic cysts are considered to be secondary to prior hepatic involvement following spontaneous rupture or surgical inoculation. Isolated primary retroperitoneal location is exceptional. Haemotagenous or lymphatic spread could account for a solitary retroperitoneal lesion10,11. Dow12 waddle13 had favored air borne transmission and direct implantation of the embryo in the bronchial mucosa, which is another possible mode of entry. This raises the possibility of an embryo of the parasite entering a venule after penetrating the bronchial mucosa and reaching the left side of the heart to involve other sites and thus bypassing the lung. But this remains largely theoretical and needs to be proved14. Preoperative diagnosis is difficult to make unless circumlinear calcification is seen in the plain x-ray of the abdomen. The diagnosis was missed

CASE REPORT
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012. Page 178
clinically as it was provisionally diagnosed retroperitoneal or peritoneal mass. However after ultra sound examination and during surgery, the possibility of hydatid cyst was considered but it was never expected that such enormous cysts would be recovered. Necessary precautions were taken during the excision and marsupialisation of the entire huge cyst cavity and washed with scolicidal (hypertonic saline) solutions. The rupture will result in anaphylactic shock or systemic metastasis. So the treatment of choice is surgical and complete removal of the cyst is the gold standard but its feasibility is related to the location of the cyst. Hence, one must have a high index of suspicion and rule out hydatid cyst in every case of retroperitonel cystic swelling especially in endemic areas. A careful search for hydatid cysts in other organs of abdomen including liver should be made because secondary retroperitoneal hydatids may out number primary retroperitoneal Hydatids.
FIGURES
Figure1: showing the surgical approach by Explorative laprotomy through upper midline incision to the cyst.
Figure2: Showing unusual number of isolated retro peritoneum Hydatid Cyst.

CASE REPORT
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012. Page 179
REFERENCES:
1. Goel MC, Agarwal MR, Misra A.: Percutaneous drainage of renal hydatid cyst: early results and follow-up.:Br J Urol: 1995; 75: 724—8.
2. Altinors N, Senveli E, Donmez T, Bavbek M, Kars Z, Sanli M.; Management of problematic intracranial hydatid cysts;. Infection 1995; 23: 283—7.
3. Brown RA, Millar AIW, Steiner Z, Krige JEJ, Burkimsher D, Cywes S.; Hydarid cyst of the pancreas: a case report in a child. Eur J Pediatr Surg; 1995; 5:121—4.
4. Reddy CRRM. Epidemiology of hydatid disease in Kurnool.Ind; J Med Res; 1968; 56:1205-20. 5. Kammerer WS, Schantz PM.; Echinococcal disease. Infect DisClin North Am 1993; 7:605-18. 6. Özdemir N., Akal M., Kutlay H., Yavuzer Ș. Chest Wall Echinoccocosis. Chest, 1994, 105 :
1277-9. 7. Hatipog Lu A. R, Coșkun Í, Karakaya K, Íbiș C. Retroperitoneal Localization of Hydatid Cyst
Disease. Hepato-Gastroenterology, 2001, 48 : 1037-9 8. Patterson, K David, “ Echnicoccosis (Hydatidosis)” The Cambridge World History of Human
Disease. Ed. Kenneth F.Kiple. Cambridge University Press 1993. Cambridge Histories Online. Cambridge University Press 11 September 2012 DOI: 10.1017/CHOL9780521332866.105.
9. Pedrosa I, Saiz A, Arrazola L, Ferreiros J, Pedrosa CS. “Hydatid disease: radiologic and pathologic features and complications.” RadioGraphics 2000;20:795-817
10. Elton C., Lewis M., Jourdan M. H. Unusual site of hydatid disease. Lancet, 1999, 355 : 2132. 11. Balık I. A. A.,Celebi F., Bașog˘LU M, Oren,D, Yıldırgan.I, Atmanalp.S.S.: Intra-abdominal
extrahepatic echinococcosis. Surg Today, 2001,31:881-4. 12. Dow HR Hydatid disease it’s pathology, diagnosis and treatment 1st edition, 1928, 304-315 13. Waddle.N; pulmonary hydatid disease. Aust.N.Z.J Surg, 1950,19:273-78. 14. SekarNN, Madhavan KK, Yadav RV, Katariya RN: Primary retroperitoneal hydatid cyst (A
report of three cases & review of the literature): J. Post grad Med.1982: 28:112-48.

REVIEW ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 180
EPIDEMIOLOGY, PREVENTION & CONTROL OF RABIES IN INDIA-
A REVIEW STUDY. Dr. Pranab Jyoti Bhuyan.
1. Assistant Director (Public Health) Department of Health, National Centre for Disease Control, Coonoor
branch, Coonoor.
CORRESPONDING AUTHOR:
Dr. P.J. Bhuyan,
NCDC, Coonoor branch.
Coonoor-643101.
The Nilgiris, Tamil Nadu,
Email id- [email protected],
Ph- 0091 09442181442.
ABSTRACT: Rabies is a zoonotic disease and its magnitude of problem is underestimated due to
lack of surveillance. In spite of hundred percent fatality, the optimistic view is that it is totally
and absolutely preventable with the aid of effective post-exposure prophylaxis. It is prevalent
mainly in the developing countries like Africa and Asia. Wild carnivorous animals act as
reservoir and domestic/peridomestic warm blooded animals transmit the virus to the human
population. It is popularly known as “Hydrophobia” in human and children are at particularly
risk. More than 3.3 billion people live in regions where rabies is enzootic. Dog bite is the
principal mode of infection in India and lower limb is the most common site of injury. Ineffective
surveillance, shortage of TCV and Immunoglobulin manufacturer and its high cost, peoples
ignorance of first aid measures after bite and the importance of compliance of PEP, uncontrolled
street dog population etc. are the key issues which should be addressed to tackle this problem.
KEYWORDS: Tissue culture vaccine (TCV), Ministry of Health (MOH), Nervous tissue vaccine
(NTV), Post exposure prophylaxis (PEP), Upper limb (U.limb) and Lower limb (L.limb).
INTRODUCTION: This is an infectious disease, also known as hydrophobia caused by Lyssa
virus type I, characterized by acute and profound dysfunction of CNS, nearly always terminating
in the death of the host. All warm blooded mammals are susceptible particularly carnivorous
such as dogs, cats, jackals and wolves and transmitted to man by bites or licks of rabid animals1.
Due to complete absence of any successful medical treatment for clinical rabies and the horrific
nature of the disease, most rabies victims die at home rather than being admitted to a hospital
in abysmal conditions. These circumstances add to the notorious lack of surveillance data
underestimating the health implications of rabies lead many high ranking decision makers in
public health and animal health to perceive rabies as a rare disease of human resulting from a
bite of an uneconomically important animal (dog). Therefore, rabies usually falls between two
stools and is not dealt with appropriately either by MOH or M.O. Agriculture 2.
INDIA: It is endemic in every state of India except Andaman Nicobar Island & Lakshadeep 3.
Some clinico-epidemiological studies are available in India which recorded the types of animal
bite, sites of injury, mode of transmission, usage of PEP etc. NTV has been banned since 2004
due to its life threatening complication and the current cell culture vaccine is quite safe and
effective.

REVIEW ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 181
1. MAGNITUDE OF PROBLEM, TREND AND TYPES OF ANIMALS BITE: B.K.Kathuria 4
reported cases of animal rabies from different states of India during the period of 1949-67.
Though the reporting was not regular and uniform, he summarized some important data. In
1967, majority cases of animal rabies were reported from West Bengal (59.89%) whereas 57%
dogs, 38% cattle, followed by Punjab (14.7%) whereas 22% dogs, 55% cattle. The types of the
laboratory positive cases were- dogs (59.72%), Horse & donkey (14.58%), cattle (13.19%),
buffalo (8.33%), Cat (2%), camel (1.38%) and mongoose (0.69%).
The figure 1 has shown the hydrophobia cases as reported from different states from
1956 to 1969-(including nil reporting and under reporting). The peak of the curve signifies that
most of the state reported during that period which indicates lack of reporting in non-peak
period. Admitted cases of rabies from 41 teaching hospitals of India were 247(1965) and
252(1966) 5.
Sarma S.M et.al6 studied rabies in animal with laboratory diagnostic done. The
endemicity of rabid dog was apparent from 78 rabid dog detected out of 83 rabid animals
during the period of July 1982 to June 1983. An increase of rabies in dog was observed from
October 1983 to may 1984 subsequent to detection of rabies in jackals.
Rasina S.K et.al 7 found that 83.7% cases were bitten by dog among which 21.8% was pet dog,
followed by monkey (8.2%) and cat (8.2%).
Acc. to WHO 8, India officially reported 30,000 human rabies deaths (an estimated figure
which remained constant since 1990) and it accounts to 60% of global report of 50,000 deaths
annually. Due to lack of any surveillance and proper reporting there is no report on current
situation of rabies in India. Hence, at the behest of WHO & GOI, APCRI, a registered society was
entrusted this task of doing a National Rabies survey in 2003. The burden and clinico-
epidemiological profiles are clear as per findings of APCRI/WHO study on rabies in India, the
incidence of animal bite is 1.7% with frequency 1 per sec and out of 17 million people only 3
million receive PEP. Incidentally, rabies positivity was reported very rarely in rats, rabbits and
bandicoots, total dog population 28 million; annual man day lost for animal bite 38 million.
The biting animal mainly responsible for human rabies death was dog (96.2%) of which
majority strays (75.2%) followed by pet (11.1%), wild (3.5%); cat accounted for 1.7% of deaths.
The status of biting animal was unknown (46.4%) or killed (28.5%) or dead (23%) and
surprisingly in 2.1% cases it was reported as alive by surviving household members. This might
be that either the people were observing the wrong animal or had forgotten trivial bite by a
rabid animal in the past.
Ichhpujani R.L et al9found that dog bites caused maximum morbidity (92%), followed by
monkey (3.2%), cat (1.8%), fox (0.4%) etc. Most bites were unprovoked (64.3%) by stray
animals (64.7%). Analysis of 192 cases of rabies, from two centres, revealed that dog bites
caused maximum mortality (96.9%).
2. AGE & SEX DISTRIBUTION: Rao Bhanu L.N, Kalaselvan 10studied that main victims were
adults-83.80% and predominantly males (84.42%) affected. Rasina S.K. et.al 7found that the
commonest age group was 6-25 yrs(82.4%). According to WHO & GOI, APCRI survey in 2003 8,
235 Deaths Were investigated at household level by a medical team. Majority of human rabies
were adults (64.7%), men (71.1%) and were from poor income levels (87.6%). Ichhpujani R.L et
al 9 in the study, 72.4% victims were males and 47.5% were children in age group of 2-18 years.
Nearly 40% were children below 15 years of age group and 78.6% were males indicating that it
is an exposure related disease.

REVIEW ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 182
3. TYPES OF INJURY: (Fig:2) Rao Bhanu L.N, Kalaselvan 10 found type bites i.e Class III -59.81%,
II-37.7%. RasinaS.K et.al 7studied the common categories of bite were-class II (54.4%) followed
by class I (31.3%) and class III (14.3%). The 78.9% cases completed PEP and the common sites
of bite were U.limb (40.1%) followed by L.limb (36.7%). In the study of WHO & GOI, APCRI
(2003)8, the commonest sites of injury were - lower limb (56.2%) followed by upper limb
(20.9%), hands (17%) and then the head and face (11.5%). Ichhpujani R.L et al (2008)9 found
that 63% had category III exposure as per WHO classification.
4. TREATMENT AFTER BITES: After bite, some people have the practice of washing the wound
with soap-45.6% but other harmful practices are not uncommon like application of chilly
powder (29%), oil (24.5%), turmeric powder (10.9%) etc7. WHO & GOI, APCRI (2003) 8, 39.5%
had wound clean and 47.9% received ARV and even those who had received it mostly had
incomplete/irregular/delayed treatment. The use of RIG was very low (2.1%). In 85% cases,
IP < 6 months; mean IP was lowest (42days) in bites on head & face and highest (107 & 108
days) in those on upper limb (excluding hands) and lower limbs. About 45.3% of victims had
resorted to indigenous treatment like-magico religious followed by herbal therapy, red chili
powder. Ichhpujani R.L et al 9 studied that before coming to ARCs 58.5% people had washed the
wound with water/soap or water alone. Some of the bite victims (10.8%) also applied chillies,
salt, turmeric powder, lime, snuff powder, paste of leaves, acid, ash given by Peer
Baba(magician) etc.
5. RABIES CONTROL IN DOG: A WHO expert consultation meeting on Rabies has identified
mass immunization as single most effective tool for dog rabies control whereas dog culling
alone is ineffective 11. Studies have shown that, in general, 80-90% of the dog population is
accessible for vaccination, thus confirming that the concept of controlling rabies through mass
vaccination is a sound one 12. It has also been recommended the use of oral vaccine as a
complimentary measure in dog in addition to i.m or s.c route. In the light of this oral rabies
vaccine strain, ORA-DPC would offer a major opportunity for rabies control. Better part with
ORA-DPC is that the strain elicits seroconversion too unlike other attenuated rabies vaccine
strains, could be a good indicator to monitor the vaccinated animal in the field as always regd.
by WHO 13. In the majority of industrialized countries, human rabies is under control, mainly
due to oral vaccination of wild animal, mandatory parenteral vaccination of domestic animal
and easy access to modern cell culture vaccine, immunoglobulin for PEP, whereas these are in
short supply & their high cost often prevent their use by those most in need for those product.
In India, Animal Welfare Board of India (AWBI) had successfully implemented Animal Birth
Control (ABC) Programmes among stray dogs in various places including Chennai 14.
6. CONCLUSION: Rabies is a hidden but neglected public health problem in India which affects
mostly the people of lower socio-economic group. Being a zoonotic disease, it cannot be
eradicated but elimination or control is possible with primary health care approach like-
availability of post-exposure prophylaxis, refreshment of recent guideline of PEP, re-exposure
and drop-out management to physicians & medical students; evaluation of technical feasibility
at peripheral level of intradermal route before implementation. Transmission chain will be
broken if herd of at least 75-80% of dog population is immunized on a sustained basis. Recently,
IDSP has introduced its surveillance in the reporting format.

REVIEW ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 183
*Fig 1. shows the cases of hydrophobia as reported from different states of India.
Fig-2: shows frequency of Class III bites. Source: Rao Bhanu L.N, Barman S (2000-01 &
2001-02).
REFERENCE:
1. Park K. Rabies- Park’s Textbook of Preventive and Social Medicine 2007; 19: 226-34.
2. WHO Bulletin “Human & animal rabies” Dec , 2008.
3. Seghal and Bhatia R (1985) rabies: Current Status and proposed control programme in India,
NICD, 22 Shamnath Marg, Delhi-54.
4. Kathuria B.K. Studies on rabies-its epizootology and diagnosis. Journal of Comm. Disease
1970; 2: 1-4.
5. Prakash S. Rabies in and around Delhi. J.C.Disease 1970; 2,69-75.
6. Sarma S.M, Sarmah S.B, Saxena SN. Surveillance of Rabies in animals in north India.
J.Com.Disease 1986; 18(1):9-12.
Cases of hydrophobia in diff. states.
0
200
400
600
800
1000
1200
56 57 58 59 60 61 62 63 64 65 66 67 68
Years
No
s. o
f ca
ses.
Frequency of ClassIII bites.
0
500
1000
1500
2000
2500
3000
3500
4000
1995 96 97 98 99 2000April
Years.
Fre
qu
ency
.
Total animal bite cases.
Adult-ClassIII bite.
Child-ClassIII bite.

REVIEW ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 184
7. Rasnia S.K, Bhalla S, Khanekar J, Pathi S, Matta S, Singh S. Post exposure management of
animal bite attending a P.H.C of Delhi, J. Com. Disease 2004; 36(3),195-198.
8. APCRI, Assessing burden of rabies in India: WHO National Multicentric Rabies Survey, 2003
9. Ichhpujani R.L, Chhabra M, Mittal V, Singh J, Bharadwaj M, Bhattacharya D, Pattanik SK,
Balakrishnan N et al. –Epidemiology of Animal bites and Rabies cases in India-A Multicentric
study. J.Commun.Dis. 40(1) 2008:27-36.)
10. Rao Bhanu L.N, Kalaselvan J. Epidemiology of Rabies-16 years study at PIIC-Annual Report,
2000-02, 57-60.
11. WHO Techn. Report Series,1973,No 52315.WHO Expert Consultation on Rabies: first report.
Geneva, WHO Technical Report Series, No. 931.
12. The work of WHO. 1986-87,176.
13. Bhubaneswari A, Kilari S, Visser N, Goovarerts D. Oral rabies vaccine, ORA-DPC: Dose
finding studies confirms vaccine efficacy in challenge experiments. APRICON Souvenir, 2009,
17-18.
14. The Hindu, September, 2010, 3. WHO Expert Consultation on Rabies: first report. Geneva,
WHO Technical Report Series, No. 931.

ORIGINAL CASE SERIES STUDY
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 185
BENEFICIARIES VIEW POINT AND FACTORS INFLUENCING INDUCED
ABORTIONS IN A RURAL COMMUNITY OF WEST BENGAL. Dr. Debabrata Mallik. Dr. Ranadeb Biswas, Dr. S. Kole, Dr. Manob Dhar, Madhulina Mallik.
1. Assistant Professor, Department of Community Medicine, Bankura Sammilani Medical College. 2. Professor & Head, Department of Community Medicine, AIIH & PH, Kolkata.
3. Assistant Professor, Department of Community Medicine, Bankura Sammilani Medical College.
4. Medical Officer, Department of Community Medicine, AIIH & PH, Kolkata.
CORRESPONDING AUTHOR,
Dr. Debabrata Mallik,
1483, R N Tagore Road.
Dum Dum, Kol-77.
E-mail: [email protected],
Ph: 09433657571.
ABSTRACT:
BACKGROUND: Study of induced abortion in India by considering the complete birth history of
women is lacking. Induced abortion is associated with high mortality and morbidity in India.
OBJECTIVES: The objectives of the study were to find out the Induced abortions ratio and to
identify certain characteristics like perception, health care seeking behavior and the
motivational factors for such an act. METHODS: An exploratory type of investigation (a
retrospective case series study) was carried out among 46 acceptors of induced abortion in a
rural community of west Bengal, between September, 11 to February 12. RESULTS: The ratio of
induced abortions was 20.62 per year per 1000 women of reproductive age group. 89% belongs
to Hindu and 93% of them were married. Unplanned pregnancy (43.47%) and financial problem
(21.73 %) were the main reasons for acceptance of induced abortions. About 71 % of induced
abortions were carried out by qualified person in hospital set up. CONCLUSION: Eventually
induced abortions are increasing universally and several traditional methods are also found to
be life threatening. So exploration of induced abortions is important aspect and explores the
point for entry of further research.
KEY WORDS: Abortion, motivation, unplanned pregnancy, unqualified persons.
INTRODUCTION: Although abortion services in India were liberalized more than three decades
ago, access to safe services remains limited for the vast majority of women. The results
highlights that a host of factors, notably lack of awareness of the legality of abortion services;
limited access to safe services; poor quality of services; and gender roles and norms, lead
women to seek services from untrained providers. In the Indian context, where the preference
for sons is particularly strong, the practice of second trimester sex-selective abortions is
becoming widespread, and thereby also placing women at risk of undergoing unsafe abortion1.
The introduction of new technologies and legislation is expected to make safe abortion services
more accessible. However, the challenge remains in effectively implementing these measures.
An overwhelming proportion of induced abortions (6.7 million annually as per indirect
estimate1) take place in unauthorized centers, which provide abortion services of varying
degrees of safety2. At the same time, in recent years significant changes in the abortion scenario
have been taking place in the country, which have had wide ramifications. Official figures report
that about 0.6 million induced abortions take place annually inIndia2.27 Given that only

ORIGINAL CASE SERIES STUDY
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 186
approximately 10%of abortions are conducted by qualified providers in approved
institutions,28 and that abortions taking place at registered facilities are grossly under-
reported,1, this represents only a fraction of the total number of induced abortions taking place
in the country. Indirect estimates for the year 1991, using parameters arrived at on the basis of
small-scale study conducted in 1966, project the number of induced abortions annually at 6.7
million3.All the Countries in the World underestimate this abortion is much more than
spontaneous due to medical reasons, victims of sex behaviors, rape etc4.Despite the fact that, in
India these induced abortion is legalized under certain condition & facilities but evidently the
quantum of induced abortion are not matching with the such records of the Governments &
private organizations because widespread of unqualified & untrained practitioners are very
much prevalent in rural & urban society5.Among all these contraceptive failure is a unique
example of falsification & gateway of criminal abortion by the unqualified & untrained
personnel & maiming the lives of the victims due to lack of protocol of maintenance of asepsis. .
The hidden cost of contraception–such as shame, command, resistance from seniors & loss of
social prestige are the prime concern in a country where the number of children count the
prosperity of rural couple by acquiring human manpower6. Scientific advancement made these
treatment behaviors as gender specific to avoid much more harassment of life events of a girl
child. In view of ever increasing priority, quantity, context & coverage of RCH services across the
country but this induced abortion is quite paradoxical7. Needless to say that the mortality
declines of newborn & early child hood are spectacular & reduction of maternal death also
convincingly decline. Therefore to safeguard the health of the mothers & newborn it is
imperative to focus couples own perceptions & compulsions & there by appropriate modalities
for reversal of the trends should also be looked into8.
MATERIALS AND METHODS: It was an exploratory type of investigation for seeking
information regarding induced abortions to acquire certain characteristics. The study was
conducted at Diarrah village with a population of 2230 (2011 census), under Singur block at the
district of Hooghly, West Bengal. Ethical consideration was undertaken from the All India
Institute of Hygiene & public Health. The duration of the study was six months from Sep 11 –
Feb 12. Last five years records of the acceptors of induced abortions were verified from the
Singur BPHC after obtaining informed written consent from the BMOH. From the records a
check list of Diarrah village was prepared which include address of the acceptors of induced
abortions. Similar type of check list was also prepared from the Two Quack practitioners’ after
obtaining informed written consent assuming full confidentiality. Total 53 acceptor’s addresses
were framed for obtaining information. After the questionnaire was finalized, informed written
consent was taken from the Formal Leaders (Gram Panchayat) of the Community. Then the
entire clients were interviewed with the predesigned open ended questionnaire after obtaining
the written consent with assured full confidentiality. Out of 53 acceptors of induced abortion 7
were absent so the total study subjects were 46.
RESULTS: It was noted that total number of population of the study village was 2230 (2011
census) of which total number of women of reproductive age groups (15-45) were 446 (20% of
total population). The study revealed that total number of induced abortion during last 5 years
was 46.And the average induced abortion per year was 46/5=9.2. So the inducedabortion rate
per year per 1000 of women of Reproductive age group was 9.2 #1000/446 =20.62.From the
study it was noted that majority of study subjects 54.3 %( 25) belongs to younger age groups i.e.

ORIGINAL CASE SERIES STUDY
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 187
15-24 yrs. About 89.1% (41) belongs to Hindu community. 97.4% (43) acceptors of induced
abortion were married. About 67%respondent’s percapita incomes were bellow or equal to
Rs.350. Regarding literacy status only 15 % were illiterate rest of the accepters were literate.
Out of 43 married clients about 88% (38) were getting married before the age of 18 years &
majority (95.34%) gave birth within 2 years of marriage. About 80% acceptors birth spacing
was less than 2 years. It was noted from the study that about83% (36) have 2-3 children but a
considerable 16% have 4-5 children. Majority of the abortion was done 73% (34) within 2-3
month of age of the foetus. Regarding their contraceptive practice 44% (19) did not practice any
methods of contraception while rest of the acceptors practices other methods of contraception.
On enquired about the reason of such an act it was noted that 43% (20) induced abortion was
unwanted pregnancy followed by financial ground 20% & contraceptive failure 19%
respectively. Most the abortion were conducted 71% by the qualified doctors at health center.
But only 28% were conducted by the unqualified personals at their chambers. On enquired
about the reasons of their preference of act for the unqualified persons about 43% (20) replied
that maintained confidentiality was their prime concern. Other important reasons were less
harassment which constitutes about 21%. Besides those monitory problems, less time required
resistance from seniors were others reasons of less priority.
DISCUSSION: The retrospective qualitative survey was include both married and unmarried
women and the data was collected both the Govt. Hospital and untrained practitioners so the
induced abortion ratio was to some extent high.Similar findings were found in NFHS survey for
induced abortion (1998-99)9&DLHS survey (iii) GOI. (2007-08).10The study explore that
women’s age, unplanned and unwanted pregnancy, less acceptance of contraceptive methods,
financial reasons number of living children’swere the major determinants of induced abortion.
Similar findings was also found in a rural community of Maharastra (A cohort
study).11&Tamilnadu (Rabindran &Balasubramanian,2004)12The study explore that maintained
confidentiality, less harassment and less time requirement were another determinants for
accepting abortion of untrained personnel.
CONCLUSION: Traditional practitioners & untrained or ill-trained M.B.B.S practitioners, widely
perform abortion in the rural community. The complications at their hands are frequent & often
serious. Assurances of keeping secrecy attract the ignorant rural people to them. Contraceptive
acceptance is far from the requirement & sterilization acceptance is far from the requirement
acceptance is poor & often late. Repeated & early child birth, inadequate spacing, high parity
along with financial & other relevant problems need availability of M.T.P side by side with
contraceptives & sterilization in the years ahead. Rural people need awareness about the
problem of population expansion, the needs & benefits of contraceptive & sterilization & the
dangers of illegal abortions. Simultaneous publicity about M.T.P services needs to be promoted.
A comprehensive guideline thus evolved from this abortion may be replicated in several socio
economic classes & regions. Instead of indiscriminant intervention, a logical solution locally
derived agreed upon & sharing that benefit will definitely be rewarding. Last of course not the
least, that the exploration of induced abortion is important as it opens some important aspect &
explore the point of entry for further research.
ACKNOWLEDGEMENTS: We are grateful to the Director of AIIH&PH, Kolkata whose support
and guidance has been critical for conduction of the study. We are also indebted toMr.Madan

ORIGINAL CASE SERIES STUDY
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 188
Das and Mr.SukantaPandit for providing us necessary help in conducting the study. We also
extend our gratitude to the staffs of Singur BPHC and the community people through which
information were collected.
Table-1: Socio demographic characteristics of the Acceptors of Induced abortion (n=46)
Table: 2 Obstetric pattern of the Study subjects.
Socio demographic character Number Percentage
Age in years
15-24
25-34
35-44
Religion
Hindu
Muslim
Marital status
Married
unmarried
Per capita income
<350
=
>350
=
Literacy status
Primary
Secondary
Higher Secondary
Graduation
Illiterates
25
18
3
41
5
43
3
31
15
19
10
8
2
7
54.3
39.1
6.5
89.1
10.9
97.4
6.6
67.4
32.6
41.4
21.7
17.4
4.3
15.2

ORIGINAL CASE SERIES STUDY
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 189
Variables numbers percentages
Age at marriage(n=43)
<18 yrs.
First child birth <2 yrs.
Spacing <2yrs
<3yrs
No of living children 2-3
4-5
Month of abortion
1-1/2
2
2-1/2
3
>3
Contraceptive acceptance. (n=43)
Safe periods
Condom
Cup-T
OC
Nil
Sterilization
38
41
34
9
36
7
8
11
14
9
4
5
6
7
4
19
2
88.37
95.34
79.06
20.94
83.72
16.28
17.4
23.9
30.4
19.6
8.7
11.6
13.9
16.3
9.3
44.2
4.6
Table: 3 Reasons for acceptance of induced abortions.
Variables Numbers percentages #
Reasons
Financial/for well being
Unplanned pregnancy
Forced by husband
Contraceptive failure
10
20
4
9
21.7
43.4
8.7
19.5

ORIGINAL CASE SERIES STUDY
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 190
# --- Multiple responses possible
REFERENCES:
Unmarried
Performers
Qualified personals
Unqualified personals
Place of abortion.
Hospitals
Chambers of unqualified
personnel’s
Reasons for acceptance
By Unqualified personals
Maintained confidentiality
Less harassment
Monitory problems
Less time required
To avoid so many test &
Conditions by the Govt.
setup.
Resistance from seniors
To take Govt. facilities
3
33
13
33
13
20
10
4
5
3
4
6.5
71.7
28.3
71.7
28.3
43.4
21.7
8.7
10.9
6.5
8.7

ORIGINAL CASE SERIES STUDY
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 191
1. Chhabra, R. and S.C. Nuna. 1994. Abortion inIndia: An Overview. New Delhi:
VeeremdraPrinters.
2. Government of India (GOI). 2002. The MedicalTermination of Pregnancy (Amendment) Bill
(BillNo. XXXV).
3. Mallik, R. 2002. India -Recent Developments Affecting Women’s Reproductive Rights. Centre
for Health and Gender Equity (CHANGE).
4. Ministry of Health and Family Welfare (MOHFW).2003. Notification, Medical Termination of
Pregnancy Rules.http://mohfw.nic.in/MTP%20Rules.htm
5. Ministry of Health and Family Welfare (MOHFW).2000. National Population Policy, 2000. New
Delhi: Government of India.
6. Oomman, N. and B.R. Ganatra. 2002. Sexselection: The systematic elimination of
girls.Reproductive Health Matters, 10(19): 184-88.
7. Government of India (GOI). 2003. The Pre-NatalDiagnostic Techniques (Regulation and
Prevention of Misuse) Amendment Act (Act. No. 14).
8. Coyaji, K. 2002. Medical Abortion. Paper
9.M.Barsharani.Correlates of Spontaneous and Induced Abortion in India: An Investigation using
a Nationwide Large Scale Survey Data.
http://paa2011.princeton.edu/download.aspx?submissionId=111333.
10. PallikadavnathS,William Stones R. opportunites and choices programme working paper;
21;2005.
11. www.biomedcentral.com/1471-2458/12/543.
12.Rabindran TKS&Balasubramanian P, Yes to No Abortion.2004; 12: 88-99

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 192
THE MICROBIOLOGICAL PROFILE OF VENTILATOR ASSOCIATED
PNEUMONIA. Dr. Poonam C. Sharma, Dr. S. S. Raut, Dr. S. R. More, Dr. V. S. Rathod, Dr. V. M. Gujar.
1. Post Graduate Student, Department of Microbiology, Dr. Shankar Rao Chavan Government Medical College &
Sri Guru Gobind Singhji Memorial Hospital, Nanded. 2. Professor & Head of Department, Department of Microbiology, Dr. Shankar Rao Chavan Government
Medical College & Sri Guru Gobind Singhji Memorial Hospital, Nanded.
3. Associate Professor, Department of Microbiology, Dr. Shankar Rao Chavan Government Medical College &
Sri Guru Gobind Singhji Memorial Hospital, Nanded.
4. Assistant Professor, Department of Microbiology, Dr. Shankar Rao Chavan Government Medical College &
Sri Guru Gobind Singhji Memorial Hospital, Nanded.
5. Assistant Professor, Department of Microbiology, Dr. Shankar Rao Chavan Government Medical College &
Sri Guru Gobind Singhji Memorial Hospital, Nanded.
CORRESPONDING AUTHOR,
Dr. Poonam Chanderlal Sharma,
501, Abhilasha Mahal Co. Op. Hsg. Scty,
Opp. Bhatia Hospital, Ulhasnagar Dist.
Thane, Maharashtra- 421005
E-mail: [email protected],
Ph: 08888096033.
ABSTRACT: BACKGROUND- Nosocomial infections (NI) are responsible for increased
morbidity and mortality in hospitalized patients. Hospital acquired pneumonia is the
second most common nosocomial infection. AIM : To isolate and identify the organisms
causing Ventilator associated pneumonia and to know their resistance pattern. METHOD :
We conducted the study in the Intensive Care Unit of our Hospital over a period of one
year. All patients on mechanical ventilation for more than 48 hours were included in this
study. The pathogens were identified based on the standard bacteriological procedures
including Gram's stain, colony morphology on Blood agar, MacConkey agar and SDA and
biochemical reactions. FINDINGS- 50 out of 128 samples were culture positive, the
incidence being 39.06%. Out of 50 cases, 33(45.2%) were males & 17(30.9%) were
females. 50% of the cases ventilated for respiratory cause developed VAP while only
20.8% of the cases ventilated for non-respiratory cause developed VAP. Out of 50 cases,
20(40%) were early onset VAP cases, while 30(60%) were late onset VAP cases.
CONCLUSION : P. aeruginosa was the predominant organism isolated followed by E.coli
with maximum sensitivity to Imipenem.
KEYWORDS: Ventilator associated pneumonia, Pseudomonas aeruginosa, Imipenem.
INTRODUCTION: Ventilator associated pneumonia(VAP) is defined as pneumonia occurring
after 48 hours of endotracheal intubation and initiation of mechanical ventilation. VAP is
categorized as early onset VAP which occurs within four days of endotracheal intubation
whereas late onset VAP occurs after four days of endotracheal intubation. Early onset
VAP is caused by Str. pneumoniae, H. influenza, Moraxella catarrhalis, MSSA, etc. While
Late onset VAP is caused by P. aeruginosa, Acinetobacter, Enterobacter species, MRSA,
etc. VAP is frequently polymicrobial and Gram negative bacilli are the predominant
organisms isolated.[3]
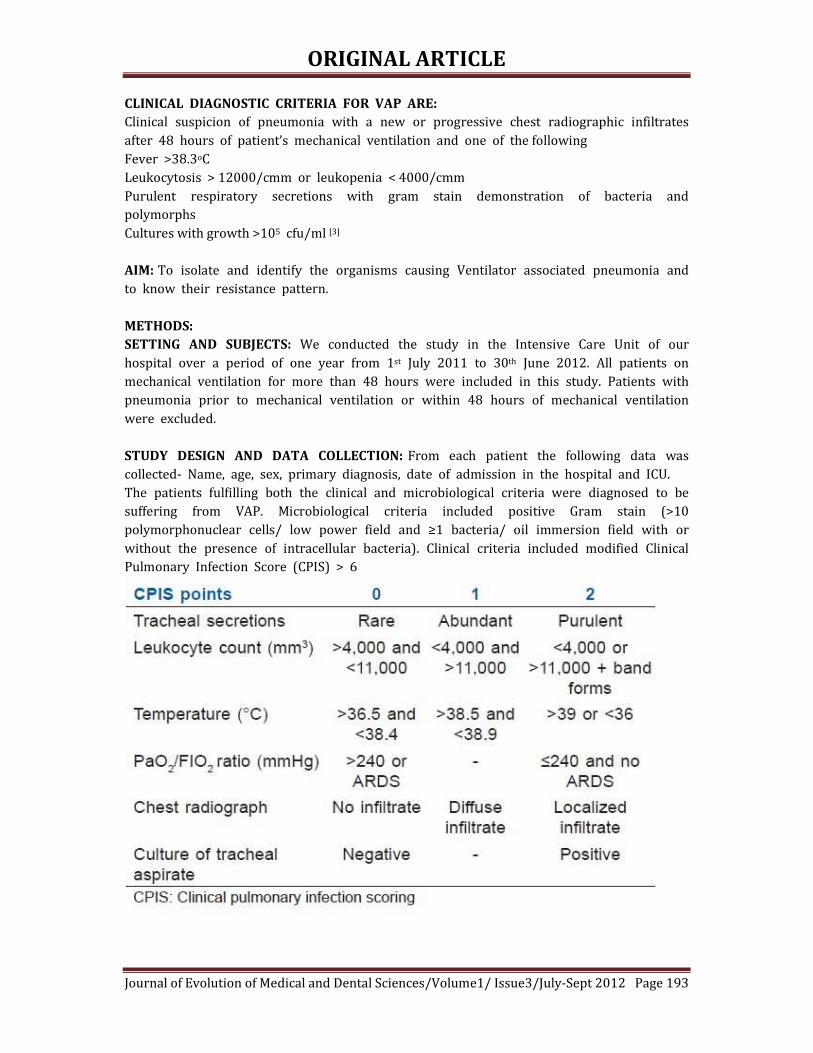
ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 193
CLINICAL DIAGNOSTIC CRITERIA FOR VAP ARE:
Clinical suspicion of pneumonia with a new or progressive chest radiographic infiltrates
after 48 hours of patient’s mechanical ventilation and one of the following
Fever >38.3oC
Leukocytosis > 12000/cmm or leukopenia < 4000/cmm
Purulent respiratory secretions with gram stain demonstration of bacteria and
polymorphs
Cultures with growth >105 cfu/ml [3]
AIM: To isolate and identify the organisms causing Ventilator associated pneumonia and
to know their resistance pattern.
METHODS:
SETTING AND SUBJECTS: We conducted the study in the Intensive Care Unit of our
hospital over a period of one year from 1st July 2011 to 30th June 2012. All patients on
mechanical ventilation for more than 48 hours were included in this study. Patients with
pneumonia prior to mechanical ventilation or within 48 hours of mechanical ventilation
were excluded.
STUDY DESIGN AND DATA COLLECTION: From each patient the following data was
collected- Name, age, sex, primary diagnosis, date of admission in the hospital and ICU.
The patients fulfilling both the clinical and microbiological criteria were diagnosed to be
suffering from VAP. Microbiological criteria included positive Gram stain (>10
polymorphonuclear cells/ low power field and ≥1 bacteria/ oil immersion field with or
without the presence of intracellular bacteria). Clinical criteria included modified Clinical
Pulmonary Infection Score (CPIS) > 6

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 194
IDENIFICATION OF VAP PATHOGENS: The pathogens were identified based on the
standard bacteriological procedures including-
- Gram’s stain
- Colony morphology on Blood agar , MacConkey agar and SDA
- Biochemical reactions. [10]
FINDINGS
INCIDENCE: 50 out of 128 samples were culture positive, the incidence being 39.06%
Characterisics of the patients-
Incidence in males and females- Table I
Incidence differences due to various causes of ventilation- Table II
Incidence due to early onset and late onset pneumonia- Table III
DISCUSSION: The incidence of VAP in our study was 39.06% which was similar to a
study conducted by Shalini et. al.(35.78%) and Rakshit et. al.[4][8] In males incidence of
VAP was 45.2% and that in females was 30.9% which was similar to the study
conducted by Gadani et. al.[11] 40% of cases were early onset VAP and 60% were late
onset VAP which tallies to other studies conducted by Chastre et. al. and Kollef et. al.[5][6]
Incidence in patients ventilated for respiratory cause was 50% and that due to non-
respiratory cause was 20.83%, which co-relates to the study conducted by Akash Deep et.
al.[7] Pseudomonas was the predominant organism in our study (31.48%) similar to that
conducted by Joseph et. al. (21.3%) and Gadani et. al. (43.24%)[9][11]
CONCLUSION: Pseudomonas aeruginosa was the predominant micro organism isolated
with maximum resistance to Tobramycin. E. coli was the second most common micro
organism with maximum resistance to Ampicillin. While both were 100% sensitive to
Imipenem. Microbiologial surveillance facilitates the monitoring of changes of dominant
micro- organisms and antibiotic susceptibilities helping in the decision of empirical
treatment regimes and as a result, selecting the right antibiotics.
ACKNOWLEDGEMENTS : Staff of Microbiology Department and Medicine Department,
Study patients.
FUNDING: None
TABLE I:
Gender No. of VAP
cases
No. of cases in
whom VAP
absent
Total no. of
cases
Male 33 (45.2%) 40 (54.8%) 73 (100%)
Female 17 (30.9%) 38 (69.1%) 55 (100%)
Χ2 =2.69
P value > 0.1 (not significant)

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 195
TABLE II
Cause of
ventilation
No. of VAP
cases
No. of cases in
whom VAP
absent
Total no. of
cases
Respiratory cause 40 (50%) 40 (50%) 80 (100%)
Non respiratory
cause
10 (20.8%) 38 (79.2%) 48 (100%)
Χ2 =10.72
P value <0.01 (highly significant)
TABLE III
Duration of ventilation No. of VAP cases Total no. of cases
Early onset 20 (40%) 50 (100%)
Late onset 30 (60%) 50 (100%)
Χ2 =4
P value < 0.05 (significant)
FIGURE 1 Causative Agents-
31.48%
16.67%14.81%
12.96%
9.26%
3.70%1.85% 1.85%1.85%1.85%
3.70%
0.00%
5.00%
10.00%
15.00%
20.00%
25.00%
30.00%
35.00%

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 196
FIGURE 2
Resistance Pattern of P. aeruginosa-
FIGURE 3
Resistance Pattern of E. coli
CONFLICT OF INTEREST: None
48%
33%
26%22%
5%
0%0%
10%
20%
30%
40%
50%
60%
95%
67%
50% 50%
20%
0%0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Ampicillin Cefazolin Tobramycin Amikacin Gentamicin Imipenem

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 197
REFERENCES:
1) Steven M. Koenig and Jonathon D. Truwit Ventilator-Associated Pneumonia:
Diagnosis, Treatment, and Prevention. PubMed Central Clin Microbiol Rev. October 2006;
19(4): 637–657.
2 ) Bailey & Scott’s Diagnostic Microbiology Eleventh Edition, Mosby Inc. Betty A. Forbes,
Daniel F. Sahm, Alice S. Weissfeld ISBN 0-323-01678-2
3) Girish L. Dandagi Nosocomial pneumonia in critically ill patients Lung India Jul-Sep
2010; 27(3)
4) Rakshit P, Nagar V S, Deshpande A K Incidence, clinical outcome, and risk stratification
of ventilator-associated pneumonia- a prospective cohort study. Indian J Crit Care Med
2005 9(4): 211-216
5) Chastre J and Fagon J Y Ventilator associated pneumonia. Am J Respir Crit Care Med
2002 165: 867-903.
6) Kollef M H Ventilator-associated pneumonia. A multivariate analysis. JAMA 1993; 270:
1965-1970.
7) Akash Deep, R. Ghildiyal, S. Kandian and N. Shinkre Clinical and Microbiological Profile
of Nosocomial infection in the PICU. Indian Pediatrics 2004 41: 1238-1246
8) Shalini S, Kranthi K, Gopalkrishna Bhat K Microbiological profile of infections in ICU. J
of Clinical and Diagnostic Research 2010 4: 3109-3112
9) Noyal Mariya Joseph, Sujatha Sistla, Tarun Kumar Dutta, Ashok Shankar Badhe,
Subhash Chandra Parija. Incidence and risk factors of VAP. J Infect Dev Ctries 2009
3(10): 771-777
10) Mackie & McCartney Practical Medical Microbiology. J. G. Collee, A. G. Fraser, B. P.
Marmion, A. Simmons. Churchill Livingstone, Fourteenth Edition, ISBN 0 443 049068
11) Gadani H, Vyas A, Kar A K. A study of ventilator-associated pneumonia: Incidence,
outcome, risk factors and measures to be taken for prevention. Indian J Anaesth 2010;
54:535-40.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 198
BACTERIOLOGICAL PROFILE OF CELL PHONES OF HEALTHCARE
WORKERS AT TERTIARY CARE HOSPITAL. Dr. Chinjal A. Panchal, Dr. Mitesh N. Kamothi, Dr. Sanjay J. Mehta,
1. Post Graduate Student, Department of Microbiology, C.U. Shah Medical College & Hospital, Surendranagar. 2. Assistant Professor, Department of Microbiology, C.U. Shah Medical College & Hospital, Surendranagar.
3. Professor & Head, Department of Microbiology, C.U. Shah Medical College & Hospital, Surendranagar.
CORRESPONDING AUTHOR,
Dr. Chinjal Arvindbhai Panchal, C. U. Shah Medical College and Hospital, Surendranagar – 363001, E-mail: [email protected], Ph: 09898576504.
ABSTRACT: BACKGROUND AND OBJECTIVES: Cell phones are increasingly used by healthcare
workers. They can harbour potential bacterial pathogens and can become an exogenous source
of nosocomial infections. Aim of this study was to identify microbial colonisation and their
antimicrobial sensitivity; from cell phones used by healthcare workers.
MATERIALS AND METHODS: A total of 100 samples were collected from cell phones of
clinical and para-clinical staff and non-medical personnel. Specimens were collected and
subjected to culture and sensitivity as per the standard guidelines.
RESULTS: Bacterial species were isolated from 65 (65%) out of total 100 samples. Coagulase
Negative Staphylococcus (42) was the most commonly isolated organism. Isolates included
Methicillin resistant Staphylococcus aureus (10), Methicillin sensitive Staphylococcus aureus
(3), Bacillusspp(15), Pseudomonas spp(4),Moraxella spp(2), E. coli (1), Klebsiella spp (1) and
Acinetobacterspp (1).
CONCLUSION: The carriage rate of bacterial isolates was higher in the clinical staff (92%)
in comparison to para-clinical staff (56%) and non-medical personnel (20%). Cell phones
may serve as potential source of nosocomial infections.
KEYWORDS: Bacterial pathogens, Multidrug resistance, Healthcare workers, Nosocomial
infections
INTRODUCTION: The global system for mobile telecommunication (GSM) was established in
1982 in Europe with a view of providing and improving communication network. Cell phones
have become one of the most indispensable accessories of professional and social
life.1Today,India has 500million Cell phone users. Cell phones increase the speed of
communication and contact within health care institutions, making health care delivery more
efficient; hence, Cell phones are increasingly used by healthcare workers.2Cell phones are
frequently used in hospital wards, casualty, laboratories, ICUs and operation theatres.3However,
Cell phones which are seldom cleaned and often touched during or after the examination of
patients without hand washing, can harbour various potential pathogens and become an
exogenous source of nosocomial infections for hospitalized patients.4Nosocomial infections are
important problem in all hospitals. These infections are increasing day-by-day and can affect
rate of mortality and morbidity. In this study, Cell phones of non-medical personnel were also
included as it represents an environment of community. Therefore bacterial isolates from Cell

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 199
phones of HCWs may vary in numbers and antibiotic sensitivity, to that found on Cell phones of
non-medical personnel.5
MATERIALS AND METHODS: The study was conducted at the Department of Microbiology, C.
U. Shah Medical College and Hospital, Surendranagar, Gujarat fromAugust 2011 to March 2012.
1) COLLECTION OF SAMPLES: Total of 100 Cell phones of healthcare workers of clinical and
para-clinical staff and non-medical personnel were randomly selected for the study.Sterile
swabs moistened with peptone water were used to collect specimens from the front, sides and
back of the Cell phones.
2) PROCESSING OF SAMPLES: Swabs taken from Cell phones were inoculated on nutrient agar,
blood agar and MacConkey agar. The culture plates were incubated at 37⁰C for 24 hours.
Isolation and identification of bacterial species were done as per standard guidelines.
Antimicrobial susceptibility testing, including detection of Methicillin Resistant Staphylococcus
aureus (MRSA) and Extended Spectrum ß-Lactamase (ESBL) was performed for potential
pathogenic isolates by disc diffusion method as per the Clinical and Laboratory Standards
Institute (CLSI) guidelines.6
RESULTS: Out of 100 Cell phones, bacterial growth was obtained in 65 (65%) Cell phones;
which includes 46 from clinicalstaff,14 from para-clinical staff and 5 from non-medical
personnel; as shown inChart-1. The carriage rate was 92% in clinical staff, 56% in para-clinical
staff and 20% from non-medical personnel.
Out of 65 Cell phones which yielded bacterial growth, 51 (78.46%) had single bacterial
isolate and 14 (21.54%) had two bacterial isolates making total of 79 isolates.
Out of total 79 isolates, 42 were Coagulase Negative Staphylococci (CONS), 15 were
Bacillusspp, 13 were S. aureus and 4 were Pseudomonas spp. Various organisms isolated
from clinical, para-clinical and non-medical personnel are shown in Table-1.
Out of 13 S. aureus, 10 and 42 CONS,21were Methicillin resistant, as shown inChart-2.AllE. coli
(1), Klebsiella spp(1), Pseudomonasspp(4) and Acinetobacterspp (1)isolates were multidrug
resistant as shown in Table – 2.
Chart – 1Growth obtained from Cell phones.
50
25 25
46
14
5
0
10
20
30
40
50
60
Clinical Para- clinical Non medical
Total
Growh obtained

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 200
Table – 1 Distribution of bacterial isolates
Organism Clinical Para - clinical Non medical Total
CONS 29 (69.04%)
11 (26.19%)
2 (4.76%)
42
Bacillus sp. 10 (66.67%)
1 (6.66%)
4 (26.67%)
15
S. aureus 10 (76.92%)
3 (23.08%)
0 13
Pseudomonas sp.
4 (100%)
0 0 4
Moraxella sp. 2 (100%)
0 0 2
Acinetobacter sp.
1 (100%)
0 0 1
Klebsiella sp. 1 (100%)
0 0 1
E. coli 1 (100%)
0 0 1
Total 58
(73.42%)
15
(18.99%)
6
(7.59%)
79
Chart – 2 Methicillin resistance among Staphylococcus species
Table - 2Percentage incidence of antibiotic sensitivity of bacterial isolates
Organism Total AS BA CH RC TE GM CX CF
CONS 42
38 (90.48%)
23 (54.76%)
33 (78.57%)
28 (66.67%)
30 (71.42%)
32 (76.19%)
21 (50%)
16 (38.09%)
S. aureus 13 11 (84.62%)
5 (38.46%)
5 (38.46%)
7 (53.85%)
7 (53.85%)
9 (69.23%)
3 (23.08%)
3 (23.08%)
Pseudomonas
spp
4 2 (50%)
1 (25%)
1 (25%)
1 (25%)
- 3 (75%)
1 (25%)
-
Moraxella
spp
2 1 (50%)
1 (50%)
1 (50%)
1 (50%)
- 1 (50%)
- -
Klebsiella spp 1 1 (100%)
- 1 (100%)
1 (100%)
- 1 (100%)
- -
E. coli 1 1 (100%)
1 (100%)
1 (100%)
1 (100%)
- 1 (100%)
- -
Acinetobacter
spp
1 1 (100%)
- - 1 (100%)
1 (100%)
1 (100%)
- -
13
42
10
21
0
10
20
30
40
50
S.aureus CONS
Nu
mb
er
of
org
an
ism
s
Organisms
Total
Methicillin Resistant

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 201
AS – Ampicillin/ Sulbactum,CH – Chloramphenicol,TE – Tetracycline,CX –Cefoxitn,
BA – Cotrimoxazole,RC – Ciprofloxacin,GM – Gentamycin,CF - Ceftiaxone
DISCUSSION: The study shows that bacterialpathogensarepresent oncellphones. The carriage
rate of bacterial isolates was 65 %, which was higher in clinical (92%) staff than in para-
clinical (56%) staff and non- medical personnels (20%). Similar pattern was observed by
Arora U. et al 2. Table-3 shows carriage ratesof bacterial isolates oncellphones reported by
various authors.Bacterial isolates from cellphones of HCWs were varying in their numbers and
antibioticsensitivity, to that found on cellphones of non-medical personnels.
Coagulase NegativeStaphylococci(CONS)were found to be the most common colonizing organisms in the present study. Similar pattern have been reported by different authors as shown inTable-4. Many bacterial pathogens isolated from cellphones of healthcare workers were also multidrug
resistant. 21(50%) Coagulase NegativeStaphylococciand 10 (76.92%)S. aureuswere methicillin
resistant.All E. coli, Klebsiella spp, PseudomonassppandAcinetobactersppwerealsomultidrug
resistant.
Table –3 Comparison of carriage rate with other studies
Study Organisms
isolated
Clinical Para -
clinical
Non-
medical
Kabir O. et al – 2009 (1) 62.00% 15.30% - 66.45% Arora U. et al - 2009(2) 40.62% 44.78% 37.77% - Jayachandra T. et al - 2011(3) 84.30% - - - Jayalakshmi J. et al - 2008(7) 91.67% 90.40% 93.30% - Bhat S.- 2011(8) 98.50% - - - Datta P. – 2009 (9) 59.60% - - 10.00% Present study 65.00% 92.00% 56.00% 20.00%
Table – 4 Comparison of CONS carriage rate with other studies
Study CONS
Kabir O. et al – 2009 (1) 42.70% Arora U. et al – 2009 (2) 27.55% Jayalakshmi J. et al-2008 (7) 47.16% Bhat S. et al-2011 (8) 21.78% Fatma U. et al – 2009 (10) 58.96% Present study 53.16%
CONCLUSION: The overall carriage rate of Cell phones was found to be 65% in the present
study. It was higher in the clinical staff (92%) as compared to para-clinical staff (50%) and non-
medical personnel 20 (20%). Cell phones harboured potential pathogens, which included
multidrug resistant strains.
Restriction of Cell phones seems impractical, prevention of nosocomial pathogens is important,
use of antibacterial agents to clean Cell phones and strict adherence to infection control
measures like hand washing and good hygienic practice can reduce the risk of spread of
nosocomial pathogens.3,9

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 202
ACKNOWLEDGMENT: We are sincerely thankful to the Dean, Dr. H. H. Agravat and
Superintendent Dr. K.G. Patel of C.U. Shah Medical College& Hospital for their permission to
carry out this study.
REFERENCES:
1) Kabir O, Audu D, Olabisi O, Akitoye O. The potential roleof mobile phones in spread of
bacterial infections.JinfectDevCtries2009; 3(8):628-32.
2) Arora U, Pushpa D, Chadha A, Malhotra S. Cell phones amodernstayhouse for bacterial
pathogens. JK Science2009;11(3):127-9.
3) Jayachandra T, LakshmiprasannaT, Venkateswar A. Astudy on isolation and
identificationofbacteria causing nosocomial infections on mobile phones of health care
workers. CalicutMedical Journal 2011; 9(1):1-6.
4) SrikanthP, Rajaram E,Sudharsanam S, Lakshmanan A, UmamaheswariS, Kalyani J. The
mobile phone in a tropical setting – emerging threat for infection control. Sri
Ramachandra Journal of Medicine 2009;2(2):18-20
5) Chawla K, Mukhopadhayay C, Gurung B, Bhate P, Bairy I. Bacterial ‘Cell’ Phones: Do
cell phones carry potential pathogens?Online J Health AlliedScs.2009; 8(1):8-12.
6) Clinical and Laboratory Standards Institute. Performance standard for antimicrobial
susceptibility testing;20thinformational supplementM100-S20,Vol 30 No 1. Clinical and
Laboratory Standards Institute, Wayne,PA, USA; 2010.
7) Jayalakshmi J, Appalaraju B, Usha. Cell phonesas reservoirs of nosocomial pathogens. J
AssocPhy India 2008;56:388-9.
8) Bhat S, Hegde S, Salian S. Potential of mobile phones to serve as a reservoir in spread of
nosocomial pathogens. Online JHealth AlliedScs. 2011;10(2):14-20.
9) Datta P, Rani H,ChanderJ, Gupta V. Bacterial Contamination of Mobile Phones of
HealthCare Workers. Ind J Med Microbiol 2009; 27(3):279-81.
10) Ulger F, Esen S, Dilek A, Yanik K, Gunaydin M, Leblebicioglu H. Are we aware how
contaminated our mobile phones with nosocomial pathogens?Annals of Microbiology
and Antimicrobials2009,8:7.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 203
STUDY OF HEMATOLOGICAL PARAMETERS AMONG NEONATES
ADMITTED WITH NEONATAL JAUNDICE. Dr. Amar Shah, Dr. C. K Shah, Dr. Venu Shah.
1. Assistant Professor, Department of Pathology, Pramukhswami Medical College, Karamsad, Anand, Gujrat.
2. Professor, Department of Pathology, Smt. NHL Medical College, Ahmedabad.
3. Assistant Professor, Department of Community Medicine, GCS Medical College, Ahmedabad.
CORRESPONDING AUTHOR,
Dr. Amar Shah,
Pramukhswami Medical College,
Karamsad, Anand, Gujarat,
E-mail: [email protected], Ph: 09909927725.
ABSTRACT: INTRODUCTION: Jaundice is most common problem faced by neonates in the first
week of life. Although physiological jaundice is more frequent as compared to pathological
jaundice it is very important to differentiate between the two as pathological jaundice may lead
to kernicterus and subsequently brain damage. There are various modalities of investigations
e.g. Serum bilirubin, Direct and indirect coomb’s test, Blood group, G-6PD deficiency,
reticulocyte count by which we can reach at diagnosis. Treatment is also dependent upon the
amount of serum bilirubin and various other laboratory investigations. Thus laboratory workup
is very important for diagnosis and prevention of neonatal hyperbilirubinemia in newborn.
With this background present study was conducted to study the clinico- pathological profile
among infants with neonatal hyperbilirubinemia. METHODOLOGY: A prospective study was
carried out for the duration of 1 year in one of the teaching hospitals. RESULTS: Altogether 63
babies were enrolled in the study. Male babies out numbered the female (58.7% vs.
41.3%).Mean age of the study population was 2.97 days with standard deviation of 1.2 days.
Percentage of Pre-term babies was 30.1. Neonates having low birth weight were 17(26.9%).
Physiological jaundice constituted (40)62% cases of Neonatal hyperbilirubinemia. ABO
incompatibility was the commonest cause of pathological jaundice followed by septicemia.
Statistically significant rise in the serum bilirubin was noted in pathological jaundice as
compared to physiological jaundice. C-reactive protein (CRP) was found to be positive in all the
cases of septicemia. Direct and indirect Coomb’s test was positive in all the cases with Rh
incompatibility. CONCLUSION: Neonatal hyperbilirubinemia is associated with various other
clinical morbidities. Causes of hyperbilirubinemia should be investigated comprehensively. ABO
and Rh typing should be done along with Coombs Test, reticulocyte count and G6PD screening.
KEY WORDS: neonates, hyperbilirubinemia, hematological parameters.
INTRODUCTION: Neonatal hyperbilirubinemia is a very common condition in newborn
sometimes leading to kernicterus causing brain damage. There are various conditions, both
physiological and pathological leading to hyperbilirubinemia in newborn. Neonatal
hyperbilirubinemia, defined as a total serum bilirubin level above 5 mg per dL (86 µmol per L),
is a frequently encountered problem in developed as well as developing countries. Although up
to 60 percent of term newborns have clinical jaundice in the first week of life, few have
significant underlying disease.1 It is very important for pathologists and pediatricians to
differentiate the physiological and pathological causes of hyperbilirubinemia. Treatment is

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 204
dependent upon the amount of serum bilirubin and various other laboratory investigations. So
there is very important role of the pathologist in this condition to classify the neonatal
hyperbilirubinemia.
The most common cause of neonatal hyperbilirubinemia in India is physiological
jaundice. Various other conditions in decreasing order are preterm infant, blood group
incompatibility, Neonatal septicemia, G-6PD deficiency, cephalhematoma, drug induced, RBC
membrane disorders and many others.
Though the history and clinical presentation of the newborn plays a major role, the
laboratory plays an important role in diagnosing the cause of hemolysis in is also helpful in
diagnosing antenatally by amniocentesis and other recent available modality thereby
preventing the hemolytic sequel in newborn. There are various modalities of investigations e.g.
Direct and indirect coomb’s test, Blood group, G-6PD deficiency, reticulocyte count by which we
can reach at diagnosis. Thus laboratory workup is very important for diagnosis and prevention
of neonatal hyperbilirubinemia in newborn. With this background present study was conducted
to study the laboratory profile among infants with neonatal hyperbilirubinemia admitted to the
hospital.
OBJECTIVES:
1. To study different causes of neonatal hyperbilirubinemia
2. To study laboratory profile of neonatal hyperbilirubunemia
MATERIAL AND METHODS: A prospective cross sectional study on neonatal
hyperbilirubinemia was conducted at one of the teaching institutes of Ahmedabad. Infants
admitted with significant neonatal jaundice in first week of life are included in the study.
Significant Jaundice was defined as total serum bilirubin exceeding 15mg/dl or even between 5
mg/dl and 15 mg/dl within 24 hour of birth or the same persisting beyond one week of life.
Total 63 such cases of newborn were admitted during the study period of August 2007 to
October2008.Written informed consent were taken from the guardian of neonates. Detailed
history of baby and mother was taken. Following investigations were done in all cases.
BLOOD GROUP (ABO/RH) OF MOTHER, FATHER AND BABY: The blood grouping was done
by using known antisera with slide and tube methods
SERUM BILIRUBIN ESTIMATION OF BABY: It has been done on auto analyzer by Diazo
method of Pearlman and lee.
COMPLETE BLOOD COUNT WITH PERIPHERAL SMEAR EXAMINATION: It included
haemoglobin, total count, different count, band cells, peripheral smear examination and
reticulocyte count.
DIRECT AND INDIRECT COOMB’S TEST OF BABY AND MOTHER RESPECTIVELY
RETICULOCYTE COUNT: Reticulocytes count has been done by stain –Briliant cresyl blue.
TEST FOR G-6-PD DEFICIENCY: Test for G-6-PD deficiency has been carried out by using SPAN
Diagnostic Reagent Kit from the red cell hemolysate.
C-REACTIVE PROTEIN OF BABY: has been carried out by Latex agglutination method
Data was entered and analyzed by using appropriate statistical software. t test was used as a
test of significance to find out the probability value.
RESULTS AND OBSERVATION: The present study includes 63 cases of newborn admitted in
one of the tertiary care institutes. Various laboratory investigations of neonatal jaundice were

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 205
carried out. Out of 63 neonates, almost two thirds (63.5%) were 2 to 3 days old. Mean age of the
neonates was 2.97 days with standard deviation of 1.2 days. 37(58.7%) were male while
26(41.3%) were females. Percentage of Pre-term babies was 30.1. Neonates having low birth
weight were 17(26.9%). (Table 1) Physiological jaundice constituted (40) 62% cases of
Neonatal hyperbilirubinemia. ABO incompatibility was the commonest cause of pathological
jaundice and Septicemia is second commonest cause of pathological jaundice. (Table 2) Among
half of the cases (33, 52.4%) range of serum total bilirubun was found between 15 and 19.9
mg/dl. 5(7.9%) were having the serum total bilirubin more than 25 mg/dl.(Figure 1)
Hemoglobin level was lowest (12.1 gm %) in Rh incompatibility. Highest level of serum bilirubin
was found in Rh Incompatibility whereas highest level of reticulocytes was noted in G-6PD
Deficiency. Pre-term and low birth weight babies were having higher levels of serum total
bilirubin but the difference was not significant (P>0.05) (Table 3) The rise in serum bilirubin
level was found to be more in pathological jaundice as compare to physiological jaundice.
Difference was significant statistically with p value of <0.05. (Table 4) Direct Coomb’s test and
Indirect Coomb’s test were found to be positive in all case in Rh incompatibility while they were
positive in 77% of cases in ABO incompatibility. (Table 5) In cases of septicemia CRP was found
to be positive in 100% of cases. CRP was found to be positive in a few cases of ABO
incompatibility (22.2%) and physiological jaundice (5%). (Table 6)
DISCUSSION: Study included 63 cases of Neonatal hyperbilirubinemia cases. Mean age of the
neonates was 2.97 ±1.2 days. Among them 37(58.7%) were male while 26(41.3%) were
females. In the study of Choudhury Habibur Rasul2 male-to-female ratio among the neonatal
jaundice cases was 1.3:1 and mean age at the appearance of jaundice was 4.5±2.3days. Neonatal
hyperbilirubinemia was more common in male babies as compared to female babies in two
different studies done by Mantani et al 3(62% vs. 38%) and Sharma et al 4(1.3:1)
In present study, percentage of Pre-term (<37 weeks) babies was 30.1 and neonates
having low birth weight (<2.5 kg) were 17(26.9%). In the study of Nepal D et al5 LBW babies
constituted 19.2%. Where as in the study of Choudhury Habibur Rasul2 42% patients with
neonatal jaundice had low birth weight and 37% were preterm.
In our study out of 63, 40(62%) cases were diagnosed as having physiological jaundice
by while others were having ABO incompatibility (15%), Rh incompatibility(8%),
septicemia(12%) and G-6 PD deficiency(3%). In the study of Nepal D et al5 they noted that
clinical sepsis as defined by WHO criteria was found in 86.3% of babies. Nearly 1/3rd (32.9%)
babies were ABO incompatible and 4.1% babies were Rh incompatible. Choudhury Habibur
Rasul et al2 mentioned that Physiological jaundice was most common and was diagnosed in
114(26.7%) cases. In their study Prematurity (20.9%) and sepsis (17.6%) were also
major causes of jaundice. C. N. Onyearugha6 concluded in their study that septicaemia followed
by prematurity were the leading aetiological factors of neonatal jaundice. Joshi et al7 reported
that in Septicemia, ABO incompatibility, Rh incompatibility were observed in 36.36%, 31.8%,
4.54% cases of neonatal jaundice respectively.G-6 PD deficiency was there in 3 percent of cases
in present study. Singhal et al reported almost similar finding (G-6 PD deficiency in 5% of cases)
in their study.8
In present study mean Hb level was 14.2+/- 1.7 gm/dl with range of 10-18gm/dl.
Similar findings were noted in the study carried out by Joshi et al7. The findings of their study
showed Mean Hb level of 13.87+/- 3.59gm/dl with a range of 8– 19.4 gm/dl.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 206
In any infant, 24 hours old any jaundice is considered pathologic and requires evaluation. This
evaluation should minimally include a serum bilirubin and workup for hemolytic disease.
Guidelines for therapy depend upon the serum concentration of bilirubin and the patient’s age.
Also serum bilirubin is most important investigation to judge severity and management of
patient. In present study serum bilirubin was highest in ABO incompatibility and Rh
Incompatibility. Among half of the cases (52.4%) range of serum total bilirubun was found
between 15 and 19.9 mg/dl. Same results were observed in the study of Nepal D et al5. They
mentioned that maximum number (67.1%) of infants' peak serum bilirubin fell in the range of
15-19.9 mg/dl.
DCT and ICT were positive in 100% cases of Rh incompatibility while in ABO
incompatibility they were found to be positive in 77% of cases. The reason for this difference
may have been that “A” and “B” antigens are weaker antigens and the distance between a/b
antigen sites on the fetal red cells as compared to adult red cells is more. In all cases of
septicemia CRP was positive in present study. It is an acute phase reactant; is synthesized by the
liver and it becomes positive after any inflammation. It is a very reliable indicator.
To conclude, most of the cases were having idiopathic jaundice although septicemia and
ABO-Rh incompatibility were not exceptional. Peak serum bilirubin levels were found to be
more among the pathological jaundice. Also prematurity and low birth weight were having
higher levels of s. bilirubin. Special care must be given to them in order to avoid future
complications of hyperbilirubinemia
ACKNOWLEDGEMENT: We are thankful to parents/guardians of all the neonates for their
cooperation while carrying out the study.
TABLE-1 Demographic profile of Neonatal Hyperbilirubinemia cases
Variables No. Percentage
Age (in Days)
1 5 7.9
2 19 30.2
3 21 33.3
4 13 20.6
5 2 3.2
6 2 3.2
7 1 1.6
Sex
Female 26 41.3
Male 37 58.7
Gestational Age
Pre-Term 19 30.1
Term 44 69.9
Birth weight
Normal 46 73.1
LBW 17 26.9
TABLE-2 Etiology wise distribution of Neonatal Hyperbilirubinemia
Etiology No. Of Cases Percentage
Physiological Jaundice 40 62
Suspected ABO Incompatibility 09 15

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 207
Septicemia 08 12
Rh Incompatibility 04 08
G-6PD deficiency 02 03
Total 63 100
TABLE-3 Mean level of Hemoglobin, Serum bilirubin and Reticulocyte count in Neonatal
hyperbilirubinemia
Etiology Mean Hb
(gm %)
Mean serum
Bilirubin level
(mg/dl)
Mean
Reticulocyte
count (%)
Physiological
Jaundice 14.8 15.5 2.53
ABO
Incompatibility 14.2 19.6 3.77
Rh Incompatibility 12.1 18 5.5
Septicemia 12.6 20.2 4.6
G-6PD deficiency 13.7 19.2 6
TABLE-4 Mean Serum bilirubin value: physiological Vs Pathological Neonatal Jaundice
Neonatal Jaundice Mean Level of S. Bilirubin(mg/dl) t- value P value
Physiological(n=40) 15.4± 2.8
4.6 <0.05 Pathological(n=23) 19.5± 4.1
TABLE-5 Result of Coomb’s test in Rh and ABO incompatibility
DCT ICT
+ve -ve Total +ve -ve Total
Rh
incompatibility
4 (100%) 0 4 4 (100%) 0 4
ABO
incompatibility
7(77%) 2(23%) 9 7(77%) 2(23%) 9
TABLE-6 Result of C - reactive protein in Neonatal Septicemia
Etiology CRP positive
n(%)
Total No. of Cases
Septicemia 08 (100) 08
Physiological
Jaundice
02(5) 40
ABO
Incompatibility
02(22.2) 09
Rh Incompatibility 00(00) 04
G-6PD deficiency 00(00) 02

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 208
Figure: 1 Level of serum total bilirubin (mg/dl) among the neonatal jaundice cases
REFERENCES:
1. American Academy of Pediatrics. Report of the committee on infectious disease
(Redbook).Elk Grove Village III: AAP, 24th Ed.1997, p5054.
2. Choudhury Habibur Rasul, Md Abul Hasan, Farhana Yasmin. Outcome of Neonatal
Hyperbilirubinemia in a Tertiary Care Hospital in Bangladesh Malaysian J Med Sci. Apr-
Jun 2010; 17(2): 40-44
3. Mantani M, Patel A, Renge R, Kulkarni H. Prognostic value of direct bilirubin in Neonatal
Hyperbilirubinemia. Indian J Pediatr 2007; 79: 819-22.
4. Sharma P, Chhangani NP, Meena KR, Jora R, Sharma N, Gupta BD. Brainstem Evoked
Response Audiometry (BAER) in neonates with hyperbilirubinemia. Indian J Pediatr
2006; 73: 413-16.
5. Nepal D, Banstola D, Dhakal AK ,Mishra U, Mahaseth C Clinico-Laboratory Profile and
Immediate Outcomes of Hyperbilirubinemic Babies Admitted in Kanti Children
Hospital Journal of Nepal Paediatric Society; January-June, 2010/Vol 30/Issue 1
6. C. N. Onyearugha, B. N. Onyire and H. A. A. Ugboma. Neonatal jaundice: Prevalence and
associated factors as seen in Federal Medical Centre Abakaliki, Southeast Nigeria.
Journal of Clinical Medicine and Research Vol. 3(3) pp. 40-45, March 2011
7. Joshi BD, Singh R, Mahato D and Prasad R. Clinico-Laboratory Profile of Neonatal
Hyper-bilirubinemia in Term Babies at B.P. Koirala Institute of Health Sciences
(BPKIHS), Dharan, Nepal. Journal of Nepal Health Research Council Vol. 2 No. 2 October
2004
8. Singhal PK, Singh M, Paul VK, Deorari AK, Ghorpade MG. Spectrum of neonatal
hyperbilirubinemia: An analysis of 454 cases. Indian Pediatr 1992; 29: 319-325.
27.0
52.4
12.77.9
0.0
10.0
20.0
30.0
40.0
50.0
60.0
<15 15-19.9 20-24.9 >25
Per
cent
age
Levels of serum total bilirubin (mg/dl )

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 209
ESBL DETECTION: PREVALENCE & COMPARISON WITH NEW CRITERIA Dr. Ashwini Manhas, Dr. Prerna Aggarwal, Dr. Manju Bala, Dr. Satish Gupte.
1. Assistant Professor, Department of Microbiology, Giansagar Medical College, Patiala (Punjab).
2. Associate Professor, Department of Microbiology, Giansagar Medical College, Patiala (Punjab).
3. Assistant Professor, Department of Microbiology, Giansagar Medical College, Patiala (Punjab).
4. Professor, Department of Microbiology, Giansagar Medical College, Patiala (Punjab).
CORRESPONDING AUTHOR
Dr. Ashwini Manhas
Giansagar Medical College,Ramnagar,
Rajpura,Dist. Patiala (Punjab) Pin code-140601
E-mail: [email protected],
Ph: 09888473208.
ABSTRACT: AIM: To study the prevalence of ESBL producing organisms in our area both by
phenotypic method and latest CLSI breakpoints. Effect of change in break points on predicting
ESBL was also studied. MATERIAL & METHODS: Successive clinical isolates were tested by
phenotypic assay and zone diameters compared by Kirby Bauer’s disc diffusion method.
RESULTS: Total 231 clinical isolates were studied of which 81.8% were ESBL producers.
Cefotaxime had high sensitivity (97.91%), specificity (97.43%) and positive predictive value
(99.47%). Cefpodoxime had strikingly 100% specificity and positive predictive value but a very
poor negative predictive value. Aztreonam had a very high sensitivity (99.4%) and negative
predictive value (97.61%) CONCLUSION: Cefotaxime was found to be the most appropriate
antibiotic when used as single agent.
KEYWORDS: ESBL, Double Disc Synergy Test, Drug Resistance
INTRODUCTION: Since their first description more than twenty years ago, pathogens
producing extended-spectrum β- lactamases (ESBLs) have become an increasing cause of
clinical concern for several reasons1-3. First, systemic infections due to ESBL-producing
Enterobacteriaceae are associated with adverse clinical outcomes. Second, initially restricted to
certain, these enzymes have spread globally and their prevalence varies geographically. Third,
primarily characterized in limited bacteria such as Escherichia coli and Klebsiella spp., ESBLs
have been spreading and reaching other genera, principally Enterobacter and Proteus spp.
Finally, besides the growing species diversity, ESBL phenotypes have become more complex
due to the production of multiple enzymes including inhibitor-resistant ESBL variants, plasmid-
borne AmpC, production of ESBLs in AmpC - producing bacteria, production of ESBLs in KPC-
producing bacteria, enzyme hyperproduction and porin loss1-4.
A strong relationship exists between third-generation cephalosporin use and acquisition
of an ESBL producing strain5. Other antibiotic classes associated with infections due to ESBL-
producing organisms include quinolones, trimethoprim-sulphamethoxazole, aminoglycosides
and metronidazole.6 In some centers from India as many as 86 percent of Klebsiellae have been
found to be ESBL producers7.
Despite Clinical and Laboratory Standard Institute’s (CLSI) recommendations 6,8 that
clinical microbiology laboratories perform specialized tests for detection of ESBLs, many of
them make no effort to detect ESBL production or are ineffective at doing so. In India there is no
regulation regarding performance and reporting of ESBL isolates from various hospitals and

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 210
clinical laboratories. Many laboratories lack sufficient expertise to identify and report ESBLs.
There is a need for simple yet effective methodologies which can be routinely used for
monitoring the prevalence of ESBL producing organisms.
The most common method of testing for extended spectrum β-lactamases (ESBLs) is
screening for reduced susceptibility to cefpodoxime/ cefotaxime/ ceftriaxone/ ceftazidime/
aztreonam followed by phenotypic confirmatory testing by demonstrating a synergistic effect
between an indicator cephalosporin and a β-lactamase inhibitor i.e., clavulanic acid 9,10. The
sensitivity of screening for ESBLs can vary depending on the type of antimicrobial agent
tested.11, 12 According to Clinical Laboratory Standards Institute (CLSI) M100-S13 guidelines,10
use of more than one of the five indicator cephalosporins suggested for screening improves the
sensitivity of ESBL detection. Some studies have reported that if it should be necessary to rely
on a single screening antibiotic, cefpodoxime or ceftazidime is the recommended antibiotic for
ESBL detection in Klebsiella spp.11, 12 Phenotypic methods are easier to perform as compared to
genotypic and at the same time they are indicative of gene expression. If criteria for ESBL
detection could be incorporated in routine susceptibility testing the detection and
interpretation would become simpler.
So a study was planned to estimate the prevalence of ESBL producing organisms in our
area both by phenotypic method and latest CLSI breakpoints. The isolates studied belonged to
family Enterobacteriacae.
MATERIALS & METHODS: The study was conducted in Giansagar Medical College and Hospital
which is a 600 bedded tertiary care hospital. A prospective study on successive clinical isolates
of family enterobacteriacae was undertaken. All isolates were screened for ESBL production by
Kirby- Bauer’s disc diffusion method demonstrating reduced susceptibility to cefpodoxime (30
μg), cefotaxime (30μg), ceftazidime (30 μg), and aztreonam (30 μg). Cut-off zone sizes as an
indicator of potential ESBL producer for K. pneumoniae, K. oxytoca & E. coli were ≤ 27 mm for
cefotaxime, ≤ 22 mm for ceftazidime, ≤ 27 mm for aztreonam and ≤17 mm for cefpodoxime. For
P. mirabilis the zone size cut offs were cefotaxime ≤ 27 mm, ceftazidime ≤ 22 mm, aztreonam ≤
27 mm and cefpodoxime ≤ 22 mm. Escherichia coli ATCC 25922 & Klebsiella pneumoniae ATCC
700603 (ESBL positive) were used as quality control for ESBL detection.
Phenotypic confirmatory test was performed for confirmation. The combined disk
method was used to confirm the presence of ESBL on all the isolates of enterobacteriacae family
by placing a disk of ceftazidime (30 μg) and ceftazidime (30 μg)/ clavulanic acid (10 μg) besides
cefotaxime (30 μg) and cefotaxime (30 μg)/ clavulanic acid (10 μg) on a Mueller-Hinton agar
plate as recommended by CLSI. A ≥ 5 mm increase in zone diameter for either antimicrobial
agent tested in combination with clavulanic acid vs its zone when tested alone was considered
ESBL producer. CLSI has reviewed the interpretation criteria as shown in Table 2.18 If new
interpretation criteria are being used then the screening test need not be performed. Penicillins,
cephalosporins and aztreonam should be reported as found on susceptibility testing without
altering susceptibility status as recommended earlier.
RESULTS: Altogether 231 clinical isolates were studied. The most prevalent isolate was E. coli
(78.3%) followed by Klebsiella spp.(12.1%), Proteus mirabilis (4.3%), Citrobacter spp. (2.1%) &
others (Table 1). Overall ESBL producers were 81.8% and ESBL non producers were 18.2%.
Outpatient clinics contributed to 65 isolates of total 231 isolates. Amongst them the prevalence
of ESBLs was 75.38% (49/65). From inpatients 166 isolates were obtained amongst which the
prevalence of ESBLs was 84.34% (140/166) (Table 3).
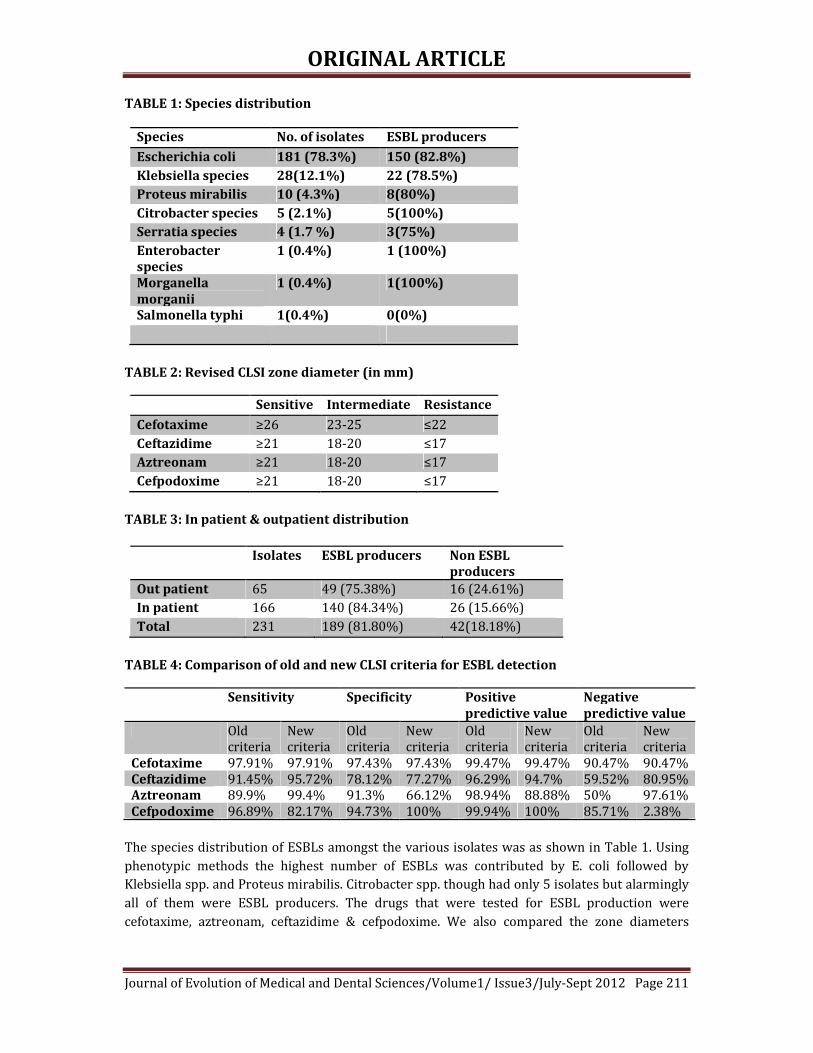
ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 211
TABLE 1: Species distribution
Species No. of isolates ESBL producers
Escherichia coli 181 (78.3%) 150 (82.8%)
Klebsiella species 28(12.1%) 22 (78.5%)
Proteus mirabilis 10 (4.3%) 8(80%)
Citrobacter species 5 (2.1%) 5(100%)
Serratia species 4 (1.7 %) 3(75%)
Enterobacter
species
1 (0.4%) 1 (100%)
Morganella
morganii
1 (0.4%) 1(100%)
Salmonella typhi 1(0.4%) 0(0%)
TABLE 2: Revised CLSI zone diameter (in mm)
Sensitive Intermediate Resistance
Cefotaxime ≥26 23-25 ≤22
Ceftazidime ≥21 18-20 ≤17
Aztreonam ≥21 18-20 ≤17
Cefpodoxime ≥21 18-20 ≤17
TABLE 3: In patient & outpatient distribution
Isolates ESBL producers Non ESBL
producers
Out patient 65 49 (75.38%) 16 (24.61%)
In patient 166 140 (84.34%) 26 (15.66%)
Total 231 189 (81.80%) 42(18.18%)
TABLE 4: Comparison of old and new CLSI criteria for ESBL detection
Sensitivity Specificity Positive
predictive value
Negative
predictive value
Old
criteria
New
criteria
Old
criteria
New
criteria
Old
criteria
New
criteria
Old
criteria
New
criteria
Cefotaxime 97.91% 97.91% 97.43% 97.43% 99.47% 99.47% 90.47% 90.47%
Ceftazidime 91.45% 95.72% 78.12% 77.27% 96.29% 94.7% 59.52% 80.95%
Aztreonam 89.9% 99.4% 91.3% 66.12% 98.94% 88.88% 50% 97.61%
Cefpodoxime 96.89% 82.17% 94.73% 100% 99.94% 100% 85.71% 2.38%
The species distribution of ESBLs amongst the various isolates was as shown in Table 1. Using
phenotypic methods the highest number of ESBLs was contributed by E. coli followed by
Klebsiella spp. and Proteus mirabilis. Citrobacter spp. though had only 5 isolates but alarmingly
all of them were ESBL producers. The drugs that were tested for ESBL production were
cefotaxime, aztreonam, ceftazidime & cefpodoxime. We also compared the zone diameters

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 212
according to old and current CLSI criteria to see if a single drug was better predictor of ESBL
activity when used in the absence of ESBL phenotypic assay.
The effect of change in CLSI criteria on predicting ESBL production is shown in Table 4.
For cefotaxime the sensitivity, specificity, positive predictive value and negative predictive
value was 97.91%, 97.43%, 99.47% & 90.47% respectively. Upon testing with ceftazidime the
sensitivity was 95.72% and positive predictive value was 94.7%. A fall in specificity (77.27%)
and negative predictive value (80.95%) was observed. With ceftazidime 182 isolates were
confirmed ESBL producers, 25 were ESBL non producers and 24 were doubtful. Out of these
isolates 17 were later found to be non ESBL producers and 7 were ESBL producers. With
aztreonam 187 isolates were confirmed ESBL producers, 21 were non ESBL producers and 23
were doubtful. Of these 23, 21 isolates were found to be non ESBL producers but 2 were ESBL
producers. Aztreonam showed improved sensitivity (99.4%) and negative predictive value
(97.61%) but reduced specificity (66.12%) and positive predictive value (88.88%). For
cefpodoxime the current criteria resulted in 100% specificity and positive predictive value but a
poorer sensitivity (82.17%) and negative predictive value (2.38%).
DISCUSSION: ESBL producing bacteria have become quite prevalent in Indian hospitals and
community. Different studies from India have quoted variable ESBL detection rates. According
to multicentric SMART study conducted in Asia Pacific region during the year 2007 ESBL rates
in India for E. coli, Klebsiella pneumoniae, and Klebsiella oxytoca were 79.0%, 69.4%, and
100%, respectively13. Another study found ESBL producing E. coli increase from 40 per cent in
2002 to 61 per cent in 2009, with a significant (P<0.05) rise in resistance to cefotaxime (75 to
97%). This study also found the resistance directly related to high antibiotic usage.14 A study
from central India reports the incidence of 69% and 41% ESBL producing isolates of E. coli and
Klebsiella pneumoniae respectively.15 Another study from Vellore in South India found 50.29 %
of inpatients and 45.86 % of outpatients harboring ESBL producers.16 A study from
Northwestern India found ESBL production as 23.83% in E. coli strains and 8.69% in Klebsiella
strains17. We observed that 81.8% of clinical isolates were ESBL producers. From outpatient
clinics the reporting of ESBL producers was 75.38% whereas from inpatient clinics it was
84.34%.
Though ESBLs are prevalent in our hospitals and community they are not specifically
reported by Microbiology labs. For certain reasons there is also a wide variability in prevalence
reporting of ESBLs. The possible factors could be different geographical locations, variable
proficiency levels of microbiology trained technical staff, different antibiotic cut offs being used,
different guidelines being followed (as they differ between different infectious diseases unions
throughout the world) and different techniques being used for ESBL detection.
In developing countries like India it is desirable to incorporate both ESBL detection and
antimicrobial susceptibility testing. Different drugs have been used to detect ESBLs but no
single antibiotic has been perfect at ruling -in or -out an ESBL producer. CLSI has recently
changed the breakpoints of for aztreonam, cefotaxime and ceftazidime for routine testing.
Criteria for cefotaxime to be used for ESBL detection have remained unchanged. With
high sensitivity, specificity and positive predictive value it remains the best drug for ESBL
detection. Ceftazidime has remained almost equally sensitive and specific as old criteria with
improvement in negative predictive value from 59.52% to 80.95% with almost sustained
sensitivity, specificity and positive predictive value. Aztreonam had shown improved sensitivity

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 213
from 89.9% to 99.4% but reduction in specificity from 91.3% to 66.12%. Its positive predictive
value drops from 98.94% to 88.88% with significant increase in negative predictive value to
97.61%. Therefore, to improve the interpretation aztreonam remains additional preferred agent
besides cefotaxime. Cefpodoxime has shown reduced sensitivity from 96.89% to 82.17% with
sustained improvement in specificity and positive predictive value to 100%. The most striking
observation was a very poor negative predictive value. This will result in need to perform
additional confirmatory tests if used as single agent.
Overall we found that cefotaxime was the single most appropriate antibiotic for
predicting ESBL production. Cefpodoxime can be considered a good agent due to high specificity
and positive predictive value. However, it has a very poor negative predictive value. Therefore,
no single agent can be recommended for predicting ESBL production.
CLSI has so far not given any specific criteria with the use of above mentioned four
antibiotics for detecting ESBLs while performing routine susceptibility testing. At the same time
it recommends that with the current criteria antibiotics should be reported as observed on
susceptibility testing. Earlier it recommended the reporting of all drugs as resistant when it was
observed as resistant to any one drug of the four. These guidelines are based on PK/PD analysis.
More clinical studies are needed to support the current recommendation which is based
on PK/PD measurements of the above mentioned drugs. Therapeutic failure or success of
antibiotic therapy when one drug is sensitive and other resistant in vitro needs to be studied in
parallel with clinical outcome of cases.
To conclude, cefotaxime was found to be the most appropriate drug when used as single
agent with both old as well as current criteria. Adding Aztreonam to the interpretation
improves the detection of ESBL. The current criteria definitely reduce the need for ESBL
screening test due to increased sensitivity and negative predictive value with at least three out
of four antibiotics. However, the need for using more than one drug for predicting ESBL activity
continues to be there as before.
ACKNOWLEDGEMENT: “We are thankful to the Management & Principal, Giansagar Medical
College, Patiala for approving and facilitating the study.”
REFERENCE:
1. Kim YK, Pai H, Lee HJ, Park SE, Choi EH, Kim J, Kim JH, Kim EC. Bloodstream infections by
extended-spectrum beta-lactamase-producing Escherichia coli and Klebsiella
pneumoniae in children: epidemiology and clinical outcome. Antimicrob Agents
Chemother 2002;46 : 1481- 1491.
2. Schwaber MJ, Navon-Venezia JS, Kaye KS, Ben-Ami R, Schwartz D, Carmeli Y. Clinical and
economic impact of bacteremia with extended-spectrum-{beta}-lactamase-producing
Enterobacteriaceae. Antimicrob Agents Chemother 2006; 50: 1257-1262.
3. Perez F, Endimiani A, Hujer KM, Bonomo RA. The continuing challenge of ESBLs. Curr
Opin Pharmacol 2007; 7: 459-469.
4. Tsakris A, Poulou A, Themeli-Digalaki K, Voulgari E, Pittaras T, Sofianou D, Pournaras S,
Petropoulou D. Use of boronic acid disk tests to detect extended spectrum beta-

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 214
lactamases in clinical isolates of KPC carbapenemase-possessing Enterobacteriaceae. J
Clin Microbiol 2009; 47: 3420- 3426
5. Lautenbach E, Patel JB, Bilker WB, Edelstein PH, Fishman NO. Extended-spectrum beta-
lactamase-producing Escherichia coli and Klebsiella pneumoniae: risk factors for
infection and impact of resistance on outcomes. Clin Infect Dis 2001; 32: 1162-71.
6. Paterson DA, Bonomo RA. Extended-spectrum b-lactamases: a clinical update. Clin
Microbiol Rev 2005; 18: 657-86.
7. Jain A, Mondal R. Prevalence & antimicrobial resistance pattern of extended spectrum
beta-lactamase producing Klebsiella spp. isolated from cases of neonatal septicemia.
Indian J Med Res 2007; 125: 699-700.
8. Clinical and Laboratory Standards Institute. Performance standards for antimicrobial
susceptibility testing. 13th Informational Supplement. Wayne, Pennsylvania. CLSI
Document M100-S13: 2003.
9. Sturenburg E, Mack D. Extended spectrum beta-lactamases: implications for the clinical
microbiology laboratory, therapy, and infection control. J infect 2003; 47 : 273 -95.
10. Clinical and Laboratory Standards Institute. Performance standards for antimicrobial
susceptibility testing; 16th Informational Supplement; Wayne, Pennsylvania. CLSI
Document M100-S16; 2006.
11. MacKenzie FM, Miller CA, Gould IM. Comparison of screening methods for TEM- and
SHV-derived extended spectrum beta-lactamase detection. Clin Microbiol Infect 2002; 8:
715-24.
12. Ho PL, Tsang DN, Ho M, Yuen KY. Comparison of screening methods for detection of
extended spectrum beta-lactamases and their prevalence among Escherichia coli and
Klebsiella species in Hong Kong. APIMS 2000; 108: 237-40.
13. Hawser SP, Bouchillon SK, Hoban DJ, Badal RE, Hsueh PR, Paterson DL, et al. Emergence
of high levels of extended-spectrum-ß-lactamase-producing gram-negative bacilli in the
Asia-Pacific region: data from the Study for Monitoring Antimicrobial Resistance Trends
(SMART) program, 2007. Antimicrob Agents Chemother. 2009; 53: 3280–4
14. Datta S, Wattal C, Goel N, Oberoi JO, Raveendran R and Prasad KJ. A ten year analysis of
multi-drug resistant blood stream infections caused by Escherichia coli & Klebsiella
pneumoniae in a tertiary care hospital. Indian J Med Res. 2012 June; 135(6): 907–912
15. Pathak A, Marothi Y, Kekre V, Mahadik K, Macaden R, Lundborg CS. High prevalence of
extended-spectrum β-lactamase-producing pathogens: results of a surveillance study in
two hospitals in Ujjain, India. Infect Drug Resist. 2012;5:65-73
16. Sankar S, Narayanan H, Kuppanan S, Nandagopal B. Frequency of extended-spectrum β-
lactamase (ESBL)-producing Gram-negative bacilli in a 200-bed multi-specialty hospital
in Vellore district, Tamil Nadu, India. Infection. 2012 Aug;40(4):425-9
17. Sood S, Gupta R. Antibiotic resistance pattern of community acquired uropathogens at a
tertiary care hospital in jaipur, rajasthan. Indian J Community Med. 2012 Jan;37(1):39-
44
18. Clinical and Laboratory Standards Institute. Performance standards for antimicrobial
susceptibility testing; 21st Informational Supplement; Wayne, Pennsylvania. CLSI
Document M100-S21; 2011.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 215
PREDICTION OF OUTCOME OF PATIENTS WITH PERFORATION
PERITONITIS ON THE BASIS OF APACHE-II SCORING SYSTEM Dr. S. K. Katiyar, Dr. S. K. Gahlot.
1. Assistant Professor, Department of Surgery, Rama Medical College Hospital & Research Centre, Kanpur.
2. Assistant Professor, Department of Anesthesiology, Major S.D. Singh Memorial Medical College & Hospital,
Farrukhabad.
CORRESPONDING AUTHOR
Dr. S. K. Katiyar
M.S., FIAGES,
675, Singhpur Kanpur-208017,
E-mail: [email protected],
Ph: 09415044878
ABSTRACT: Peritonitis is the inflammation of the peritoneum and is most commonly due to
localized or generalized infection. It is most common surgical emergency in India. Most common
causes in India are perforated gastric /duodenal ulcer. Any type of peritonitis can be very
serious and life threatening if not evaluated and treated properly. Prognosis in peritonitis is
decisively influenced by the health status of the patients at beginning of treatment. Accurate
prediction of the outcome of the disease can initially be made on the basis of the prognostic
scoring systems, currently several scoring systems are employed.
The APACHE prognostic scoring system for measuring severity of illness in critically ill
patients was developed in 1981 by William A Knaus1. APACHE - II introduced in 1985 was a
simplified modification of original APACHE. APACHE - II was further refined to APACHE - III in
1991. It is important for surgeons to develop at least a rudimentary knowledge of scoring
system for perforation peritonitis, as it will play an increasing role to explain the prognosis of
the disease. Aims & objectives of study are to predict the outcome of the patients with
perforation peritonitis on the basis of APACHE - III scoring system. This study was conducted on
72 patients, admitted to emergency ward of Rama Medical college hospital & Research centre,
Mandhana Kanpur, who were diagnosed as cases of perforation peritonitis from January 2009 –
January 2011. All the patients were evaluated according to APACHE - III scoring system within
24 hours of admission. All the patients admitted in emergency ward initially examined clinically
then required investigations were done. Total APACHE III score range for (0-299). Patients with
lower scores have more favourable prognosis than patients with higher scores. Thus it was
concluded from this study that patients with low scores have favourable outcome as compared
to patients with high scores.
KEYWORDS: Peritonitis, APACHE, Prognosis, Outcome.
INTRODUCTION: Peritonitis is the inflammation of the peritoneum and is most commonly due
to localized or generalized infection. Currently Peritonitis is organized into three divisions
based upon the source and nature of microbial contamination.
1. Primary peritonitis is diffuse bacterial infection without loss of integrity of GI tract, and
is most commonly caused by Streptococcus pneumonia.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 216
2. Secondary peritonitis occurs due to acute peritoneal inflammation resulting from GI
tract perforation , infected pancreatic necrosis, perforations of other infected viscera e.g.
hepatic abscess or pyometra and penetrating abdominal injuries.
3. Tertiary peritonitis develops following treatment failure of secondary peritonitis.
Peritonitis is most common surgical emergency in India. Most common causes in India are
perforated gastric /duodenal ulcer followed by appendicitis, GIT perforation due to blunt
trauma, typhoid fever and tuberculosis.
Signs and symptoms of peritonitis are-
1. Severe pain in abdomen and worsened by movement
2. Abdominal distention
3. Board like rigidity
4. Fever and chills
5. Nausea and vomiting
6. Inability to pass flatus & faeces
7. Low BP
8. Limited urine output
Any type of peritonitis can be very serious and life threatening if not evaluated and treated
properly.
Prognosis in peritonitis is decisively influenced by the health status of the patients at
beginning of treatment accurate prediction of the outcome of the disease can initially be made
on the basis of the prognostic scoring systems, currently several scoring systems are employed.
The APACHE prognostic scoring system for measuring severity of illness in critically ill
patients was developed in 1981 by William A Knaus1, Statistical detail on the predictive power
of APACHE was published in 1983, which showed that by using estimated equation to forecast
death rates for independent data, APACHE allowed accurate estimates of death rates for groups
of patients.
APACHE - II introduced in 1985 was a simplified modification of original APACHE. The
APACHE - II scores consisted of three parts –
1. 12 acute physiological variables (0-60) points
2. Age (0-6) points
3. Chronic health status (0-5) points
The probability of death can be calculated from the individual APACHE - II total scores (0-71)
points. APACHE - II scores has received far more attention in the literature than any other
prognostic model. APACHE - II was further refined to APACHE - III in 1991, Five new variables –
1. Blood urea nitrogen
2. Urine output
3. Serum bilirubin,
4. Serum albumin
5. Glucose
It is important for surgeons to develop at least a rudimentary knowledge of scoring
system for perforation peritonitis, as it will play an increasing role to explain the prognosis of
the disease.
Aims & objectives of study are to predict the outcome of the patients with perforation
peritonitis on the basis of APACHE - III scoring system.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 217
MATERIAL AND METHODS: This study was conducted on 72 patients, admitted to emergency
ward of Rama Medical college hospital & Research centre, Mandhana Kanpur, who were
diagnosed as cases of perforation peritonitis from January 2009 –January 2011. All the patients
were evaluated according to APACHE - III scoring system within 24 hours of admission.
All the patients admitted in emergency ward initially examined clinically then required
investigations were done.
• Plain x-ray abdomen
1. Erect view
2. Supine view
• USG whole abdomen
• Aspiration of peritoneal fluid
The following acute physiological parameters of APACHE III scoring system were assessed and
recorded at the time of admission-
1. Pulse rate
2. Respiratory rate
3. Mean arterial pressure (mm of Hg)
4. Temperature ( 0C)
5. Urine out put ( 24 hr ).
6. Hematocrit (%)
7. White blood cell count
8. Serum sodium (mmol./L)
9. Serum creatinine (mg/dl)
10. Serum albumin (g/dl)
11. Serum bilirubin (mg/dl)
12. Blood urea nitrogen (mg/dl)
13. Blood sugar (mg/dl)
14. Arterial pH
15. Oxygenation (PaO2 in mm of Hg with FiO2 <0.05)
16. Glasgow coma score
These values were scored in accordance to the APACHE III chart scoring for abnormally
high or low range. Zero score represents a normal value. These parameters represent Acute
physiology Score.
(A) Acute Physiology score (0-252)
1. Pulse rate 0 – 17
2. Mean B.P. 0 – 23
3. Temperature 0 – 20
4. Respiratory rate 0 – 18
5. PaO2 /AaDO2 0 - 15 / 0 - 14
6. Hematocrit 0 - 3
7. WBC 0 - 19
8. Creatinine 0 - 10
9. Urine output 0 - 15
10. BUN 0 - 12
11. Sodium 0 - 4

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 218
12. Albumin 0 - 11
13. Bilirubin 0 - 16
14. Glucose 0 - 9
15. pH 0 - 12
16. GCS 0 – 48
(B) Age points (0-24)
1 < 44 0
1 45 – 59 5
1 60 - 64 11
1 65 – 69 13
1 70 – 74 16
1 75 – 84 17
1 > 85 24
(C) Chronic health points (0-23)
1. None 0
2. Cirrhosis 4
3. Immunosupression 10
4. Leukemia/multiple myeloma 10
5. Metastatic cancer 11
6. Lymphoma 13
7. Hepatic failure 16
8. AIDS 23
APACHE III Score = (A) + (B) +(C)
= 252 +24 + 23
= 299
Total APACHE III score range for (0-299)
RESULTS:
TABLE –I
CAUSES OF PERFORATION PERITONITIS ( n = 72)
SI.
No.
Cause
Patients
Male
Female
1. Gastric / Duodenal
40 55% 35 87.5% 5 12.5%
2. Small bowel
Perforation
15 20.8% 9 60%
6 40%
3. Colon perforation 2 2.7% 1 50%
1 50%
4. Appendicular
Perforation
3 4.1% 2 66%
1 33%
5. Gall bladder
Perforation
2 2.7% 0 0% 2 100%
6. Blunt abdominal
Trauma
8 11% 6 75%
2 2.5%
7. Stab injury
Abdomen
1 1.3% 1 100%
0 0%

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 219
8. Firearm injury
Abdomen
1 1.3% 1 100% 0 0%
TABLE – II
DISTRIBUTION OF PATIENTS WITH POST OPERATIVE COMPLICATION ACCORDING TO
APACHE - III SCORE
SI. No.
APACHE III
Score
No.of
Cases
Wound
Infection
Septicemia Burst
Abdomen
Fecal
fistula
1.
0 - 30 35 9 1 3 0
2.
31 – 60 25 6 2 5 2
3.
> 60 12 3 5 3 0
TABLE – III
DISTRIBUTION OF PATIENTS WITH OUTCOME ACCORDING TO APACHE – III SCORE
SI.
No.
APACHE
III score
No. of
patients
Survived Expired LAMA Observed
Mortality
1.
0 – 30 35 33 1 1 2.8%
2.
31 – 60 25 22 2 1 8%
3.
>60 12 7 5 0 41.6%
TABLE – IV
COMPARISON OF OBSERVED AND PREDICTED MORTALITY
SI.
No.
APACHE
III score
No. of patients Expired Mortality
Observed
predicted
1. 0 - 30
35 1 2.8% 7.5%
2. 31 – 60 25 2 8%
25.2%
3. > 60 12 5 41.6%
42.6%
DISCUSSION: Perforation peritonitis is a frequently encountered surgical emergency in tropical
countries like India. In majority of cases presentation to hospital is late with well established
generalized peritonitis with purulent / faecal contamination and varying degree of septicemia.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 220
Clinical presentation of patients varied according to site of perforation. Abdominal distension
was found in 84% along with vomiting in 50% and constipation in 60% cases. 15% patients
were in shock at the time of admission. Only 64% patients had evidence of pneumoperitoneum
on chest X- ray done in erect posture.
The most elaborate study on APACHE III prognostic system and the risk prediction has
been conducted by knaus et al 2, where they prospectively collected data on 17,440 medical /
surgical ICU patients and found that a 5 points increase in APACHE III score ( range 0 – 299 ) is
independently associated with a statistically significant increase in the relative risk of hospital
death. We categorised patients into 3 groups according to APACHE – III score of 30 points each
and found an increase in the mortality risk as the scores increased from < 30 to > 60.
Perforations of proximal gastrointestinal tract are more common than of distal gastrointestinal
tract as has been noted in earlier studies from India70 , which is in sharp contrast to studies
form developed countries like United States71 and Japan72
Rajender Singh Jhobta et al3 in their study concluded that most common cause of
perforation was perforated dupdenal ulcer (57%) followed by appendicitis (11%) and blunt
trauma (9.1%). These findings are similar to present study in which most common cause of
perforation was gastric / duodenal ulcer (55%), blunt trauma (8%) and appendicitis (3%). A
study done by Mathkere LR et al4 also showed perforation of peptic ulcer was most common
cause of peritonitis (64%). Not only the site but the etiological factors also show a wide
geographical variation. Khanna et al5 from Varanasi studied 204 consecutive patients of
gastrointestinal perforation and found that over half (100 cases ) were due to typhoid. Duodenal
ulcer (58), appendicitis (9), amoebiasis (8) and tuberculosis (4). These figures show the
importance of infection and infestation in third word. At the other end of spectrum, Noon et al6
from Texas studied 430 patients of gastrointestinal perforations and found 2010 cases to be due
to penetrating trauma. This shows the importance of trauma in developed countries.
The mean length of hospital stay was 13 days. For survivors mean length of stay was
17.8 days as comparable to 18 days in the study by Bohnen et al7. The study by Adesunkanmi et
al8 showed an incidence of postoperative complications of 42.4% similar to present study with
an incidence of 54% patients having higher APACHE – III score had higher incidence of
postoperative complications. In this series, the major cause of postoperative morbidity were
wound infection (25%), wound dehiscence (15.2%), septicemia (11%) and faceal fistula (2.7%)
as compared to series by Rajender Singh Jhobta et al9 in their study wound infection rate was
(25%), wound dehiscence (9%) and septicemia (18%). Markgrof R et al51 done a
showed that hospital morality rate was higher than predicted for APACHE III
score > 60 is 41.6% as compared to predicted mortality rate of 42.5%.
CONCLUSION: All the patients were evaluated according to APACHE –III scoring system within
24 hours of admission. Age is a significant factor contributing to survival. Majority of survivors
belong to age group 20- 60 yrs. In this series, male patients were 55 (76%) and female patients
were 17 (23%). Mortality was higher in females (23.5%) as compared to male (7.2%). Most
common cause of perforation peritonitis was gastric / duodenal perforations (55%) followed by
small bowel perforations (20%), blunt abdominal trauma (11%), appendicular perforation
(4%), colon perforation (2.7%), gall bladder perforation (2.7%), stab injury abdomen (1.3%)
and firearm injury abdomen (1.3%). Most of the patients (72%) were managed with primary
repair of perforations. Mean duration of hospital stay is 13 days. Major causes of postoperative
complications were wound infection (25%), wound dehiscence (15%), septicemia (8%) and

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 221
faecal fistula (2.7%). Patients with lower scores have more favourable prognosis than patients
with higher score. Observed mortality rate was 41.6% in the group with APACHE –III score of
>60, which was comparable to predicted mortality of 42.6%.
Thus it was concluded from this study that patients with low scores have favourable
outcome as compared to patients with high scores. And APACHE III score, as measured before
the treatment of perforation peritonitis, correlates significantly with the outcome of disease
with respect to both morbidity and mortality.
REFERENCES:
I. W.A. Knaus. APACHEs The development of a quality assurance system based on
prognosis: Milestones and personal reflections. Arch Surg 137 (2002), pp. 37 –
41.
II. Kanus W.A., Wagner D.P: Individual patients decision. Chaper 6, Crit Care Med.
17 : S204 – 209.
III. Rajender Singh Jhobta, Ashok Kumar Attri, Robin Kaushik, Rajeev Sharma and
Anupam Jhobta : Spectrum of perforation peritonitis in India – review of 504
consecutive cases. World Journal of Emergency Surgery 2006, 1 : 26.
IV. Mathikere Lingaish Ramachandra, Beellary Jagadesh, Sathees BC Chandra :
Clinical study and management of secondary peritonitis due to perforated hollow
viscous. Arc Med Sci. 2007 ; 3, 1: 61-68.
V. Khanna AK, Mishra MK : Typhoid perforation of the gut. Postgraduate Medical
Journal 1984, 60 : 523.
VI. Noon GP, Beall AC, Jorden GL : clinical eveluation of peritoneal irrigation with
antibiotic solution. Surgery 1967, 67 : 73.
VII. Bohnen JM, Mustard RA, Oxhalm SE, Schouten BD: APACHE II score and
abdominal sepsis. Arch Surg. 1988; 123 : 225 - 229.
VIII. Adesunkanmi ARK, Badmus TA, Fadiora FO, Agbakwuru EK: Generalised
peritonitis secondary to typhoid ileal perforation : Assessment of senerity using
modified APACHE II score. Indian J Surg 2005; 67 : 29 – 33.
IX. MR Capoor, D Nair, MS Chintamani, J Khanna, P Aggarwal, D Bhatnagar : Role of
enteric fever in Ileal perforations: An overstated problem in tropics ? Indian J
Med Microbiol 2008 ; 26 : 54 - 57.
X. A. Horiuchi, y. Watanable, T. Doi, K. Sato, S. Yukumi, M. Yashida, Y. Yamamoto, H.
Sugishita, K. Kawachi : Evaluation of prognostic factors and scoring in colonic
perforation. World J Gastroenterol 2007; 13(23): 3228 – 3231.
XI. A.Y. Ukewenya, Ilyasu Muhammad and P.T. Nmadu: Assessing severity of
intraabdominal infections ; the value of APACHE II scoring system. Nigerian
Journal of Surgical Research, Vol 8, No. 1-2, 2006, pp. 24-29.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 222
ALTERATIONS OF SERUM ENZYMES IN PROTEIN ENERGY
MALNUTRITION Dr. A. K. Tadas, Dr. A. N. Jadhao, Dr. S. A. Tadas.
1. Associate Professor, Department of Biochemistry, Government Medical College, Nagpur. 2. Junior Resident, Department of Biochemistry, Government Medical College, Nagpur.
3. Assistant Professor, Department of Physiology, Government Medical College, Nagpur.
CORRESPONDING AUTHOR,
Dr. A.K. Tadas,
437 A, Hanuman Nagar,
Nagpur – 440009,
E-mail: [email protected],
Ph: 09423100663.
ABSTRACT: OBJECTIVES: To study the correlation of serum enzymes (alkaline phosphatase,
aspartate aminotransferase, alanine aminotransferase, amylase) abnormalities in protein
energy malnutrition and to assess their clinical significance. MATERIAL AND METHOD: 30
cases of PEM admitted to the pediatric wards of Government Medical College and Hospital,
Nagpur were studied from 5 Jan 2011 to 15 August 2011. 30 age and sex matched controls were
selected from children of normal weight for age attending OPD or wards. All the clinical details,
along with the relevant clinical history were noted. Venous blood sample was collected for
estimation of alkaline phosphatase, aspartate aminotransferase, alanine aminotransferase, and
amylase. RESULTS AND OBSERVATIONS: Patients with PEM had reduced serum alkaline
phosphatase. Amylase was found to be reduced in kwashiorkor while it remained unchanged in
marasmus. Increase in aspartate aminotransferase, alanine aminotransferase was found in PEM.
Serum amylase in kwashiorkor is lower than marasmus. DISCUSSION: In patients with PEM, we
found higher levels of AST and ALT ,as there is increased tissue breakdown in PEM to
metabolise the amino acids released by protein catabolism, the process of transamination is
enhanced leading to increased activity of related enzymes AST and ALT. Reduced serum
Alkaline phosphatase may be due to impairment of protein synthesis. Many of these
alternations of enzymes may be due to metabolic readjustment resulting from protein
deficiency.
KEY WORDS: Protein Energy Malnutrition, Enzymes, Alanine Aminotransferase, Aspartate
aminotransferase,Alkaline phosphatase,Amylase.
INTRODUCTION: The World Bank estimates that after Bangladesh, India is ranked 2nd in
number of children suffering from malnutrition (in 1998), where 47% of the children exhibit a
degree of malnutrition. The prevalence of underweight children in India is among the highest in
the world, and is nearly double that of Sub-Saharan Africa with dire consequences for mobility,
mortality, productivity and economic growth1. The UN estimates that 2.1 million Indian children
die before reaching the age of 5 every year – four every minute – mostly from preventable
illnesses such as diarrhoea, typhoid, malaria, measles and pneumonia. Every day, 1,000 Indian
children die because of diarrhoea alone1. According to the 1991 census of India, it has around
150 million children, constituting 17.5% of India's population, who are below the age of 6 years.
Enzymes being proteins, disturbances in their functions and levels in the body are
expected to occur in PEM of any severity 2. Our aim is to determine if any biochemical

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 223
parameters could be helpful in early diagnosis of PEM and to understand the correlation of
abnormalities of serum enzymes (alkaline phosphatase, aspartate aminotransferase, alanine
aminotransferase, amylase) in protein energy malnutrition and to assess their clinical
significance.
METHODS: The study was carried out in 60 children of six months to five years of age of both
sexes. Group A includes 30 children suffering from various grades of PEM were selected as
experimental group and excludes hepatobiliary and other disease by history, physical
examination and investigations i.e. serum bilirubin and ultrasonography of abdomen.. Group B
includes 30 age and sex matched healthy children. The exclusion criteria for group A was
children suffering from any systemic disease other than PEM, but minor association like
diarrhoea, cough and cold was included in the study .Protocol of study had been accepted by
the Ethical Committee. After taking the informed consent from the mothers and guardians they
were asked a pre-coded questionnaire to collect data related to the study.
By aseptic precautions 5 ml of blood was drawn from patient’s dorsal hand or wrist vein
and collect with a smaller gauge needle (22g or 23g) .Serum was separated immediately by
centrifugation at 3000 rpm for 10 min. Estimation of enzyme was carried out immediately
METHODS: Enzymes were estimated by kinetic method.
ALKALINE PHOSPHATASE BY KIT METHOD8
PRINCIPLE: Alkaline phosphatase cleaves p-nitrophenyl phosphate (p-Npp) into p-nitrophenol
and phosphate. p-nitrophenol is a yellow colour compound in alkaline medium and absorbs
light at 405nm.The rate of increase in absorbance at 405 nm is proportional to alkaline
phosphatase activity in specimen.
p-nitrophenyl phosphate � p-nitrophenol + phosphate
ASPARTATE AMINOTRANSFERASE(AST) BY KIT METHOD9
PRINCIPLE:- L-Asparate + α-ketoglutarate AST Oxaloacetate + L-Glutamate
Oxaloacetate + NADH + H+ MDH L-Malate + NAD+
This conversion of NADH to NAD+ is proportional to the concentration of AST in serum and is
measured at 340 nm, as rate of decrease in absorbance.
ALANINE AMINOTRANSFERASE(ALT) BY KIT METHOD10
PRINCIPLE:-SGPT catalses the transfer of amino group from L-alanine to 2-oxoglutarate with
the formation of pyruvate and L-glutarate.The pyruvate so formed is allowed to react with
NADH to produce L-lactate.The rate of this reactioin is monitored by an indicator reaction
coupled with LDH(lactate dehydrogenase) in the presence of NADH.The oxidation of NADH in
this reaction is measured as a decrease in the absorbance of NADH at340nm,which is
proportional to SGPT activity
L-alanine + 2-oxoglutarate ALT pyruvate + L-glutamate
Pyruvate + NADH LDH L-actetate + NADH
AMYLASE BY KIT METHOD11
PRINCIPLE: Amylase test involves use of a chromogenic substrate Gal G2 –α CNP (2-chloro -4-
nitrophenyl linked with galactosylmaltosid).The direct action of amylase with this substrate
results in the release of more than 90% of 2-chloro -4-nitrophenol, which can be monitored by

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 224
kinectic assay at 405 nm.The increase in absorbance is directly proportional to the amylase
activity in sample.
Gal G2 –α CNP α- amylase CNP + Gal G2
STATISTICAL ANALYSIS
� Data was analysed using primer software..
� The values were quoted in the form of mean ± standard deviation.
Statistical analysis of the result was done by unpaired student “t”-test.
� The p value (p< 0.05) was used to find the significance.
RESULTS: In our study, the mean values of transaminases (ALT&AST) levels were significantly
increased in PEM than in controls ( table I).
Table I .Comparision of ALP, AST and ALT Between group A (PEM) and Group B (Control)
Enzyme (units) Group A PEM ( N =30 )
.Mean ± SD
Group B CONTROL ( N =30 )
.Mean ± SD
P value
ALP (IU/L)
6.77*** ± 0.23 12.82 ± 0.27
<0.001
AST(IU/L)
73.43*** ± 2.73 31.83 ± 1.16
<0.001
ALT(IU/L)
82.96*** ± 2.11 29.43 ± 0.90
<0.001
The mean values of Alkaline phosphatase leve(ALP) was significantly higher in PEM than
controls shown in table I.
Table II. Comparison of serum amylase between group A (Kwashiorkor) and Group B
(Control)
Kwashiorkor
Enzyme (units) PEM ( N =17) CONTROL ( N =17 ) P value
AMYLASE (U/L) 47.64*** ± 10.97 80.17 ± 9.04 <0.001
The mean values of serum amylase was significantly higher in kwashiorkor than controls ( table
II).
Table III. Comparision of serum amylase between group A (marasmus) and Group B
(Control)
Marasmus
Enzyme (units) PEM ( N =13) CONTROL ( N =13 ) P value
AMYLASE (U/L) 79.30**± 7.66 81± 6.97 >0.05
The mean value of serum amylase was significantly higher in marasmus than controls ( table
III).

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 225
DISCUSSION: In our study, serum AST and ALT levels in PEM were significantly higher than that
of controls. Similar findings were reported by Kumari R et al 2 that the mean serum values of
aspartate aminotransferase, alanine aminotransferase in patients with PEM were significantly
higher than the controls. Similerly our findings also mimics with study conducted by McLean
AEM 3 in his study he showed that the activity of alanine aminotransferase in serum was
increased, and that greater the value greater was the mortality. Our finding also resembles with
Rao A et al 4 in their study, the aminotransferase elevated. Our study also coinside with
Karmacharya K et al5 .It is suggested that the moderate rise in aminotransferases found in
PEM is not due to damage to the liver. There is increased metabolism of amino acids released
from increased tissue breakdown. Thus process of transamination is enhanced leading to
increased activity of ALT and AST 13.
Serum alkaline phosphatase level in PEM was significantly lowered than controls.
Similar findings were reported by Karmacharya K5,Singh R.S et al7 and Schwartz R6 In PEM,
lowering of serum values of ALP could be explained on the basis of generalized protein
deficiency leading to impaired synthesis. Failure of bone growth may also contribute to the
lowering ALP value14.
Serum amylase in kwashiorkor was lower than marasmus.The low levels of amylase in
serum are accompanied by a reduced output of pancreatic enzymes into the gut, as pancreas is
the first organ to get damaged leading to degeneration and atrophy12.
CONCLUSION: The present study shows that any type of PEM can be associated with alteration
in levels of serum enzymes. Many of these abnormalities are probably due to metabolic
readjustment resulting from PEM. The ultimate practical objective of the enzyme studies which
have been described is to help in the management of PEM, as it is often supposed that this is a
practical problem for which new scientific knowledge is not needed.
Above mentioned view is a superficial. We are faced with the possibility that 'marginal
malnutrition' in childhood may cause a permanent impairment, and yet we cannot recognize or
define this 'marginal malnutrition' with any precision. But this can be done with the enzyme
studies described above.
REFERENCES:
I. 1."World Bank Report". Source: The World Bank (2009).
http://web.worldbank.org/WBSITE/EXTERNAL/COUNTRIES/SOUTHASIAEXT/
0,,contentMDK:20916955~pagePK:146736~piPK:146830~theSitePK:223547,0
0.html. Retrieved 2009-03-13. "World Bank Report on Malnutrition in India"
II. Kumari R., Rao Y.N., Talukdar B. et.al., Serum Enzyme Abnormalities in Protein
Energy Malnutrition, Indian Pedtr 1993;30:469-473.
III. McLean AEM. Heptic Failure in Malnutrition. Lancet 1962,2; 1292-1294.
IV. Rao A., Cherian A., Onuora C.U. Suvarnabai P.C. Serum Amonitransferases and r-
glutamyl transferase in Protein Energy Malnutrition. Trop Geogr Med. 1985,
37:11-14.
V. Karmacharya K, Islam MN, Role of Serum Alanine Aminotransferase Aspartate
Aminotransferase and Alkaline Phosphatase in Early Detection of Protein Energy

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 226
VI. Malnutrition, J. Nepal Paediatr. Soc. Vol 27, No. 2.
VII. Schwartz R. Alkaline Phosphatase Activity in Kwashiorkor, Journal Clin Path
1956, 9:333
VIII. Singh R.S, Agrawal S.P. & Dikshit S.K., Serum Enzymes in Nutritional Muscular
Wasting. Ind J. Pedtr. 1972, 39:299: 383-388.
IX. 8.Autozyme new alkaline phosphatase enzymatic, manufactured by Accurex
Biomedical private limited, Thane, India. Kit.
X. 9.Autozyme new aspartate aminotransferase enzymatic, manufactured by
Accurex Biomedical private limited, Thane, India. Kit.
XI. Autozyme alanine aminotransferase enzymatic, manufactured by Accurex
Biomedical private limited, Thane, India. Kit.
XII. Autozyme infinite amylase enzymatic, manufactured by Accurex Biomedical
private limited, Thane, India. Kit.

CASE REPORT
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 227
CLEAR CELL MYOEPITHELIAL CARCINOMA OF OROPHARYNX : A CASE
REPORT Dr. Adil S. A. K, Dr. G. Nataraju, Dr. Ravi Kumar T.
1. Assistant Professor, Department of Pathology, Mysore Medical College & Research Institute, Mysore.
2. Professor, Department of Pathology, Mysore Medical College & Research Institute, Mysore.
3. Post Graduate Student, Department of Pathology, Mysore Medical College & Research Institute, Mysore.
CORRESPONDING AUTHOR
Dr. S.A.K. Adil,
# 259, 5th Main,
Bannimantap, ‘C’ Layout, Mysore, E-mail: [email protected], Ph: 09019691259.
ABSTRACT: Myoepitheliomas are rare neoplasms. We present a case of clear cell myoepithelial
carcinoma arising from submucosal minor salivary glands of oropharynx.The significance of this
lesion is that it is a recent entity1,2 and it shares morphological similarities with many
neoplasms that pose a challenge in the diagnosis.
It has to be distinguished from benign myoepitheliomas and neoplasms with
predominantly clear cells like mucoepidermoid carcinoma, clear cell carcinoma, acinic cell
carcinoma, metastatic renal cell carcinoma etc. Imaging studies were unremarkable and
immunohistochemistry was crucial for the diagnosis.
KEYWORDS: Myoepithelial Carcinoma- clear cell variant, minor salivary gland, Oropharynx.
INTRODUCTION: Primary myoepithelial tumors in oral cavity are rare neoplasms.1 Clinically,
they commonly present as painless mass.
Clear cell myoepithelial carcinoma is very rare and it is recently considered as a separate
tumour entity2.Awareness of this lesion is important as the differential diagnosis of this lesion
can be extensive. These neoplasms diagnostically require evidence of myoepithelial
differentiation.
In this report, we present a rare case of clear cell myoepithelial carcinoma arising from
minor salivary glands in oropharynx.
CASE HISTORY: A 75-year-old male, presented with difficulty in swallowing not associated
with pain since one month. No history of known malignant diseases was present. Clinical
examination revealed a proliferative growth of 4x3 cm in the oropharynx on the posterior
pharyngeal wall.X-ray chest and ultrasonographic study of abdomen was found to be normal.
PATHOLOGICAL FINDINGS: Grossly, the specimen consisted of an irregular brown bit of tissue
measuring 1x0.5 cms. Cut section was grey white. The entire tissue was taken for processing.
Microscopically the sections showed a neoplasm comprising of monomorphic population of
clear cells arranged in solid nodules separated by fibrous septa. These cells contain abundant
amount of cytoplasm and bland nucleus, which was central to eccentrically placed.Occasional
cells showed granular eosinophilic cytoplasm.The neoplasm showed invasion into the adjacent
stroma.Necrosis was not evident and mitotic figures were rare. Immunohistochemical studies

CASE REPORT
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 228
confirmed the nature of the tumor. The cells showed immunopositivity for cytokeratins, p63, S-
100 and caldesmon.
DISCUSSION: Myoepithelial carcinoma has been recently recognised as a separate tumour
entity1,2.. Clear cell variant of myoepithelial carcinoma is comparatively much rarer than other
variants and only few cases have been reported in literature.
It has a wide age distribution ranging from 14-86yrs1 and is usually encountered in the
parotid gland, nasopharynx, paranasal sinus, nasal cavity and breast. Clinically, they usually
present as painless mass.
The neoplasm exhibits a wide spectrum of cytomorphologic features and the tumour
cells often are spindled, stellate, epithelioid, plasmacytoid (hyaline), or, occasionally, vacuolated
With signet ring like appearance.1,5.
Clear cell tumours are a challenge to diagnosis as variety of lesions have similar
morphological features. Myoepithelial carcinoma can be distinguished from benign
myoepithelial tumours by invasion of the neoplasm into the adjacent stroma1, which was
evident in our case.
The neoplasm showed monomorphic population of clear cells similar to clear cell-rich
salivary gland tumors which include mucoepidermoid carcinoma, pleomorphic adenoma, acinic
cell carcinoma, clear cell carcinoma.
Mucoepidermoid carcinoma consists of mucin containing cells, squamous cells, and
intermediate cells. Pleomorphic adenoma is identified by the distinct chondro/fibromyxoid
stroma and acinic cell carcinoma and clear cell carcinoma stain negatively for myoepithelial
markers.
Imaging studies were undertaken to exclude any renal mass.
Immunohistochemistry plays a critical role in the diagnosis of this tumour.
Cytokeratin expression indicated the epithelial nature of this neoplasm and the
myoepithelial markers p63, caldesmon and S-100 which were positive in our case,confirmed the
diagnosis as myopithelial carcinoma.
Literature search reveals the therapy options for this lesion are conservative excision
with a margin of uninvolved tissue or radiation and chemotherapy which also has resulted in a
significant shrinkage of the tumour.5, 6, 7.
CONCLUSION: Clear cell myoepithelial carcinoma can share morphological features with
various clear cell entities and pathologists should be aware of this lesion.
New immunohistochemical markers for myoepithelial cells which are crucial for
accurate diagnoses of this neoplasm are p63, and caldesmon along with S-100.

CASE REPORT
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 229
fig1 Malignant cells with clear cytoplasm
and bland nucleus(H & E,X 40)
Fig 3- Tumor cells showing cytoplasmic
positivity for cytokeratin
immunostain(X 20)
5- Tumor cells showing cytoplasmic
positivity for caldesmon immunostain(X
10)
Fig 2- Malignant cells infiltrating into
stroma(H & E,X 20)
Fig 4- Tumor cells showing nuclear
positivity for p63 immunostain(X 20)
6- Tumor cells showing variable nuclear
and cytoplasmic light intensity stain in
myoepithelial cells for S- 100 (X 40)
REFERENCES:
I. Barnes L, Eveson J. W, Reichart P, and Sidransky D. World Health Organization
Classification of Tumours. Pathology and Genetics of Head and Neck Tumours,
IARC Press, Lyon, France, 2005.p242-243
II. Wang B,Brandwein M, Gordon R, Robinson R, Urken M, Zarbo R J. Primary
Salivary Clear Cell Tumors-A Diagnostic Approach. Arch Pathol Lab Med. 2002;

CASE REPORT
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 230
Vol126 (6):676-685
III. Savera A T, Sloman A, Huvos A G, Klimstra D S. Myoepithelial carcinoma of the
salivary glands: a clinicopathologic study of 25 cases. Am J Surg Pathol. 2000; vol
24(6):761-74.
IV. Fletcher.C.D.M. Diagnostic pathology of tumors, 2ndedition, Vol.1, London;
Churchill Livingstone, 2000.p250-251
V. Rosai.J.Rosai and Ackerman's Surgical Pathology.9thedition.Vol 1
India;Elsevier, 2011.p888-89
VI. Ren J,Liu Z,Liu X,Li Y,Zhang X , Li Z,Yang Y,Yang Y,Chen Y,Jiang S Primary
myoepithelial carcinoma of palate. World J Surg Oncol.2011; 9:104
doi10.1186/1477-7819-9-104.
VII. Mills S.E,Carter.D,Greenson.K.J,Oberman.A.H, Reutar.V,Stoler.M.H.Sternbergs
Diagnostic Surgical Pathology.Vol 2.U.S.A.Lippincott Williams &Wilkins.2004.pp 943-944.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 231
A COMMUNITY BASED STUDY ON INFANT AND YOUNG FEEDING
PRACTICES IN A RURAL AREA OF KARNATAKA. Dr. Sharvanan Udayar E. Dr. Angadi M. M, Dr. Rekha Udgiri, Dr. Santosh Patil D.
1. Assistant Professor, Department of Community Medicine, PES Institute of Medical Science and Research,
Kuppam. 2. Professor & HOD, Department of Community Medicine, BLDEU’s Shri B. M. Patil Medical College, Bijapur.
3. Professor, Department of Community Medicine, Shri. B. M. Patil Medical College, Bijapur.
4. Assistant Professor, Department of Community Medicine, Shri B. M. Patil Medical College, Bijapur.
CORRESPONDING AUTHOR:
Dr. Sharvanan. E,
PES Institute of Medical Science and Research,
Kuppam, Chittoor Dist, Andhra Pradesh-517425,
E-mail: [email protected],
Ph: 09618292770/08095515455.
ABSTRACT: BACKGROUND: Adequate nutrition during infancy and early childhood is critical
to the development of children’s full human potential. OBJECTIVE: The main objective was to
assess the Infant and Young Child Feeding (IYCF) practices and associated socio demographic
variables among children aged less than two years in rural areas METHODS: A community
based, cross sectional descriptive study was done during Sept 09-Aug 2010 which is the rural
field practice area of Shri. B. M. Patil Medical College SBMPMC. The data was computed and
analyzed using SPSS statistical package (version 13.0). RESULTS: During the study period 264
mothers of infants and young children interviewed with the questionnaire and 159 out of 264
had received prelacteal feeds (males 64 % and females56.3 %). Illiterate mothers (69.7%)
practiced more prelacteal feeding than the literate mothers (54.6%). 36% received exclusive
breast feeding for a period six months. Majority of the illiterate mothers were practicing early
(31.4%) and delayed weaning (32.5%).Poor socioeconomic status, illiteracy, birth spacing and
cultural beliefs had significant effect on infant and young children feeding practices.
CONCLUSIONS: The study re-emphasized the need for conducting continued infant and child
feeding intervention programmes especially for the mother during antenatal and postnatal
checkups.
KEY WORDS: Exclusive breast feeding, Weaning, Infant and Young children.
INTRODUCTION: Adequate nutrition during infancy and early childhood is critical to the
development of children’s full human potential. Poor Infant and Young Child Feeding (IYCF)
practices, coupled with high rates of infectious diseases, are the proximate causes of
malnutrition during the first two years of life. The second half of an infant’s first year is an
especially vulnerable time, when breast milk alone is no longer sufficient to meet his or her
nutritional requirements and complementary feeding should start1. Of the 19 million infants in
the developing world who have low birth weight (< 2,500 grams), 8.3 million are in India. This
means that approximately 43 per cent of all the world’s infants who are born with a low birth
weight are born in India. Malnutrition is an underlying cause in up to 50 per cent of all under-
five deaths. About 55 million, or one-third, of the world’s underweight children under age five
live in India.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 232
Children need complementary foods in addition to breast milk from the age of six
months. In India, common problems include the provision of poor quality complementary foods,
insufficient amounts of complementary foods, insufficient breastfeeding, detrimental feeding
practices, and contamination of complementary food and feeding utensils. In addition, if
complementary foods are given too early or too frequently, they displace breast milk, which is of
higher nutritional value than other foods. Various social, economic and cultural factors in rural
areas will also influence the IYCF practices2.
The timely introduction of complementary feeding can prevent almost 6% of under-five
mortality. It was estimated that, if 90% of infants are covered with a package of intervention to
protect, promote, and support the optimal IYCF practices, almost one-fifth of overall under-five
mortality can be averted. The World Health Organization (WHO) and other various
international agencies recommended exclusive breastfeeding for the first six months of life with
early initiation and continuation of breastfeeding for two years or more together with
nutritionally-adequate, safe, age-appropriate complementary feeding starting at six months3.
With this background, the present study was undertaken to assess the IYCF practices and
associated socio demographic variables among children aged less than two years in rural areas
of Bijapur, District, Karnataka.
METHODS: A community-based, cross-sectional descriptive study was conducted in Shivanagi
during Sept 09-Aug 2010 which is the rural field practice area of Shri B.M.Patil Medical College,
situated 27km away from Bijapur and has population of 7060.4A house to house survey was
done and mothers with children aged less than two years were included in the study. Those who
were not permanent residents and not willing to participate were excluded and Modified
B.G.Prasad socioeconomic classification5 was used classifying socioeconomic status.
ETHICS: The Institutional Ethics Committee of the Shri B.M.Patil Medical College approved the
study.
STATISTICS: Analysis was done using the SPSS software (version 13.0), Simple proportions
were calculated for each IYCF practice. The differences in the feeding practices and
sociodemographic variables if any were noted using chi-square test.
RESULTS: In the present study 264 infants and young children up to 2 years were studied of
whom 136 were males and 128 were females.159 out of 264 had received prelacteal feeds
(males 64 % and females 56.3%).Illiterate mothers (69.7%) practiced more prelacteal feeding
than the literate mothers (54.6%) and the observed difference according to education of the
mother was not statistically significant in our study (p=0.015). 53.3% of nuclear families
were giving more prelacteal than three generation (62%) and joint family (63%) (Table1).
However the difference in type of family and prelacteal practices was not
statistically significant in our study (p=0.38). The study also found that the practice of prelacteal
feeding was more prevalent in lower socioeconomic group than in higher class and this
difference was found to be statistically significant(P<0.001).
Only 36% received exclusive breast feeding for a period six months and less than half of
the infants and young children belonged to Hindu and Muslim families received exclusive breast
feeding, literate mothers (41.9%) were more aware about it as compared to illiterate
mothers(26.3%).Statistically significant difference was observed according to socioeconomic

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 233
status and exclusive breastfeeding (p<0.001).Similarly with the birth interval (p=0.07) (Table
2).
With respect to weaning, majority of the illiterate mothers were practicing early
(31.4%) and delayed weaning (32.5%).Only literate mothers (56.9%) initiated it at the age of 6
months as per the WHO guidelines5. Poor socioeconomic status (p=0.001) and birth interval
(p=0.002) also had an effect on initiation of weaning.
DISCUSSION: In our study more than half of the infants and young children had received
prelacteal feeds and it was high in children with illiterate mothers belonging to poor
socioeconomic status and most important reason for this was family customs and relatives
advice. Similar findings were observed in a study by Devang raval6 (2001) in which 61.9% of
infants had received prelacteal feeds. According to NFHS-3 report7 (2005-2006) 57% newborns
received prelacteal feeds (57.3% male and 57% female) and 67.5% of the illiterate mothers
gave prelacteal feeds. Saurav et al8(2003) also reported similar findings.
Exclusive breastfeeding by mothers as derived from our study is much lower than the
values reported by Devang raval6, Chatterjee Saurav et al8 and however this when compared to
study by Vyas Shaili et al 9 in rural areas of Uttarakhand was much higher. This may be because
of the low literacy levels and customs and many of the mothers gave reasons as insufficient
breast milk and could not able to feed during illness.
Majority of the mothers practiced early and delayed weaning and this trend observed
higher among illiterate mothers. The findings from the present study clearly highlights the
importance of educating the women on infant and child feeding practices and the knowledge
may be imparted even at the school or college level. The Government of India recommends that
children should be exclusively breastfed for the first six months of life (that is, they should be
given only breast milk with no other liquids or food). There are many reasons for
recommending exclusive breastfeeding for the first six months. First, breast milk is nutritionally
superior to other liquids and solid foods. Second, when a child consumes other liquids and solid
foods, the intake of breast milk is reduced, which in turn decreases the mother’s supply of milk.
Third, feeding young infants liquids and solid foods increases their exposure to pathogens,
putting them at greater risk of contracting diarrhoeal disease. There is also need for conducting
infant and child feeding intervention programmes especially for the mother during antenatal
and postnatal checkups.
Practices such as early or delayed inititation of weaning should be discouraged and
women organizations need to be associated for active dissemination of information on infant
and child feeding practices to educationally deprived women.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 234
Table 1: Distribution of Prelacteal feed practices in infants and young children (n=264).
Parameters
Prelacteal
feed given n=159
percent (60.3%)
Prelacteal
feed not given
n=105 percent
(30.7%)
Chi
square
Gender
Male136 (51.8)
Female128 (48.2)
87 (64.0)
72 (56.3)
49(36.0)
56(43.7)
Chi
sq.:1.61
p=0.2
Religion
Hindu 236 (89.7)
Muslim28 (10.3)
147(62.3)
12(43.0)
89(37.7)
16(57.0)
Chi
sq.:3.99
p=0.04
Education
of Mother
Illiterate99 (37.5)
Literate165 (62.5)
57(69.7)
82(54.6)
42(30.3)
83(45.4)
Chi sq.:
1.6
p>0.5
Type of Family
Nuclear 62 (23.5)
3gene 105 (40.0)
Joint 97 (36.5)
33(53.0)
65(62.0)
61(63.0)
29(47.0)
40(38.0)
36(37.0)
Chi sq.:
1.68
p=0.43
Socio
Economical class
Class I 7 (2.90)
Class II 7 (2.9)
Class III 66 (25.10)
Class IV 89 (33.75)
Class V 95 (35.40)
2(28.6)
6(85.8)
23(34.9)
63(70.8)
65(68.4)
5(71.4)
1(14.2)
43(65.1)
26.(29.2)
30(31.6)
Chi
sq: 24.64
p<0.001

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 235
Table 2: Distribution of exclusivebreastfeeding practices in infants and young
children (n=264).
Parameters
EBF given
n=95 percent
(36.0%)
EBF not given
n=169 percent
(64.0%)
Chi square
Gender
Male136 (51.8)
Female128 (48.2)
40(29.4)
55(42.3)
96(70.6)
73(57.7)
Chi sq.:5.4
p=0.02
Religion
Hindu 236 (89.7)
Muslim28 (10.3)
87(36.9)
8(28.6)
149(63.1)
20(71.4)
Chi sq.:0.68
p=0.38
Education
of Mother
Illiterate99 (37.5)
Literate165 (62.5)
29(26.3)
66(41.9)
70(73.7)
99(58.1)
Chi sq.: 3.06
P=0.07
Type of Family
Nuclear 62 (23.5)
3gene 105 (40.0)
Joint 97 (36.5)
24(38.7)
32(30.5)
39(40.2)
38(61.3)
73(69.5)
58(59.8)
Chi sq.: 2.33
p=0.31
Socio
Economical class
Class I 7 (2.90)
Class II 7 (2.9)
Class III 66 (25.10)
Class IV 89 (33.75)
Class V 95 (35.40)
2(28.5)
5(71.4)
38 (57.6)
23 (25.9)
29(30.6)
5(71.5)
2(28.6)
28(42.4)
66(74.1)
66(69.4)
Chi sq: 19.9
p<0.001
Birth interval
<1yr 45 (17.3)
1-2 yr 143(54.3)
>3yrs 76(28.4)
28(62.2)
51(35.7)
34(44.8)
17(37.8)
92(64.3)
42(55.2)
Chi sq: 10.0
p=0.007

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 236
REFERENCES:
I. Improving Complementary Feeding Practices: A Review of Evidence from South Asia .
Evidence review series march 2008; Available from
http://www.intrahealth.org/~intrahea/files/media/maternal-neonatal-and-childrens-
healthfamily-planning/ER_Brief_CF%202.pdf.
II. Cooperative for Assistance and Relief Everywhere(CARE). Infant and Young Child
Feeding Practices. Collecting and Using Data: A Step-by-Step Guide.2010.Available from
http://windowofopp.files.wordpress.com/2010/12/final-iycf-guide-iycf-practices.pdf.
III. Apurba S, Dipta KM, Tanmay KP, Asit BS, Nirmal KM, Akhil BB. Infant and Young Child
feeding Practices in Bankura District, West Bengal, India. J Health Popul Nutr
2010Jun;28(3):294-299.
IV. Govt.of India (2001).Census of India 2001, Provisional Population Totals, Paper-1 of
2001.
V. Insurance worker volume XLVII, No.12, Dec 2008 and Insurance worker volume XLVIII
No. 10, Oct 2009.
VI. World Health Organization (WHO). Maternal, newborn, child and adolescent health:
Indicators for assessing infant and young child feeding practices – part I: definition;
2008.
Availablefromhttp://www.who.int/maternaments/9789241596664/en/l_child_adolesc
ent/docu.Accessed latest on 28-08-2012.
VII. Devang R, Jankar DV, Singh MP. A study of breast feeding practices among infants
living in slums of Bhavnagar city, Gujarat, India. healthline Jul-Dec 2011; 2(2):73-82.
VIII. National Family Health Survey 2005-2006 (NFHS-3). Mumbai: International Institute of
Population Sciences.Available from: http://www.nfhsindia.org.
IX. Chatterjee Saurav , Saha Sandhita: A study on KP of mothers regarding infant feeding
and nutritional status of Under 5 children attending immunization clinic of Medical
college 2008.Avalable from http://www.ispub.com/journal/the-internet-journal-of-
nutrition-and-wellness/archives.html.Accessed latest on 29-08-2012.
X. Vyas S, Sharma P, Kandpal S D, Semwal J, Srivastava A, Nautiyal V. A community based
study on breastfeeding practices in a rural area of Uttarakhand. National J Commuity
Med Apr-jun2012;3(2):283-287.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 237
ATHEROGENIC INDEX OF PLASMA IN MYOCARDIAL INFARCTION IN
RURAL POPULATION OF MARATHWADA REGION
Dr. Ganesh D Ghuge, Dr. Rahul Zine.
1. Associate Professor, Department of Biochemistry, Rural Medical College, Loni, Ahmednagar, Maharashtra.
2. Assistant Professor, Department of Biochemistry, Indian Institute of Medical Sciences and Research, Jalna,
Maharashtra.
CORRESPONDING AUTHOR
Dr. Ganesh D Ghuge, Associate Professor, Department of Biochemistry,
Rural Medical College, Loni, Taluka- Rahata,
District- Ahmednagar, Maharashtra 413736.
E-mail: [email protected],
Ph: 91-9850694964, 91-7588846300.
ABSTRACT: BACKGROUND: Extensive research work by mankind over several decades has
concluded that cure as well as the treatment of CAD is very difficult hence attention towards
prevention of such ischemic events is of utmost importance. METHODS: The present study was
conducted with an aim to study the Atherogenic Index and various lipid levels of plasma in
Acute Myocardial Infarction (AMI) and to compare lipid profile and Atherogenic Index of plasma
in the patients of Myocardial Infarction with healthy controls. RESULTS: A total of 150acute
Myocardial Infarction (AMI) patients for the study were selected from the Medicine Ward, ICU,
and OPD. Normal healthy person of matched number, age and sex of the study group were used
as control. Serum cholesterol, TGVLDLc, LDLc and AIP were significantly higher in AMI patients
as compared. CONCLUSION: Atherogenic Index of plasma is very useful research tool to assess
the effect of risk factors pertaining cardiovascular diseases.
KEYWORDS: Atherogenic index, lipid profile, myocardial infarction, triglycerides.
INTRODUCTION: Coronary Artery diseases (CAD) are the most frequent cause of death in
developing country like India (1). Extensive research work by mankind over several decades
has concluded that cure as well as the treatment of CAD is very difficult hence attention towards
prevention of such ischemic events is of utmost importance. The famous Framingham study
firmly established cholesterol as an important risk factor for CAD and now we have a clear
perception of the inter-relationship between serum lipids, Atherosclerosis & Ischemic Heart
Disease (IHD) (2). Therefore research laboratories have made conflicting claims to the helpful
serum lipid level predictor for detecting and managing IHD with emphasis on the measurement
of levels of serum cholesterol, lipoproteins and Triglycerides. The Atherogenic index of plasma
defined as log (TG / HDLc) has recently been proposed as a marker of plasma atherogenicity
(3). It is increased in people at higher risk of CAD .Tan et al used the AIP, calculated as log (TG /
HDLc) with TG and HDLc expressed in molar concentration(4). Value of AIP corresponds closely
to those of esterification rate in apo-B-lipoprotein – depleted plasma and to lipoprotein particle
size. AIP reflects the delicate metabolic interactions within the whole lipoprotein complex (3).
The present study was conducted with an aim to study the Atherogenic Index and various lipid
levels of plasma in Acute Myocardial Infarction (AMI) and to compare lipid Profile and
Atherogenic Index of plasma in the patients of Myocardial Infarction with healthy controls.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 238
MATERIALS AND METHODS: The present study was conducted in Department of
Biochemistry, S R T R Medical College Ambejogai, Maharashtra, India. A total of 150 Acute
Myocardial Infarction (AMI) patients for the study were selected from the Medicine Ward, ICU,
and OPD. Normal healthy person of matched number, age and sex of the study group were used
as control.
COLLECTION OF SAMPLE: The fasting blood sample was obtained in plain bulb from the study
group and control group from antecubital vein with all aseptic precaution.
ESTIMATION OF LIPID PROFILE: The blood samples collected from the study and control
group were estimated for lipid profile by a routine biochemical Kits methods using ERBA Chem
5+ Semi-automated machine. Estimation of Serum Cholesterol was done by (Enzymatic)
Dynamic extended stability CHOD – PAP method, End point with Lipid clearing agent. Serum
HDL cholesterol was estimated by Phosphotungstic Acid Method, End Point. Estimation of
Serum Triglyceride was done by Dynamic extended stability End point with Lipid clearing agent,
Trinder Method. VLDLc and LDLc are calculated parameters and they calculated using
Friedwald’s Formula, TG/5 where TG is less than 400 mg/dl, LDLc was calculated as : TC -
(HDLc + VLDLc) these two are calculated parameters. AIP calculated as log (TG/HDLc) when
expressed in molar concentration. Conversion factor for Cholesterol –mg% X 0.026 = mmol/lt.
Conversion factor for Triglyceride - mg% X 0.0113 = mmol/lt (Glycerol phosphate oxidase).
RESULT: As shown in table 1 Serum cholesterol, TG, VLDLc, LDLc and AIP were significantly
higher in AMI patients as compared to controls while HDLc was significantly lower in AMI
patients as compared to controls.
DISCUSSION: The coronary atherosclerosis is the major cause of IHD, which is chief single cause
of death both in developed and developing countries. Early diagnosis of coronary
atherosclerosis can reduce the mortality and morbidity. There are several biochemical ratios
indicating the risk of atherosclerosis. Gaziano et al reported that the ratio of triglyceride to
HDLc was a strong predictor of MI (5). As the search for the risk factor responsible for the CAD
goes on many ratio of the lipid have been described as better predictor of CAD. These ratios are
total cholesterol / HDLc, LDLc / HDLc and HDLc2 / HDLc3. Result of the Lipid Research Clinics
Prevalence Study showed that the ratio of Total Cholesterol / HDLc was better predictor of CAD
(6). Tan et al found AIP to be a suitable and statically reliable for evaluating the atherogenicity
index (4). Although an independent, inverse relationship between HDLc and cardiovascular risk
has been demonstrated beyond any doubt. TG has also been proposed to be a major
determinate of cholesterol esterification / Transfer and HDL remodeling in human plasma (7).
Fraction etherification rate of cholesterol and ratio of TG / HDLc are powerful predictor of
positive finding on coronary angiography (8) .The plasma parameter of log ( TG / HDLc ) as an
atherogenic index has correlation with lipoprotein particle size and esterification rate in apo B –
lipoprotein depleted plasma ( FER HDL ) (5). There is a high significant association between
FER HDL and AIP, suggesting that AIP reflects the delicate metabolic interaction with in the
whole lipoprotein complex (9). AIP provides information about the atherogenicity of plasma.
Application of AIP to data from earlier trials may offer new insights. The authors, Tan et al
should be complimented for evaluating this Atherogenic Index to test it’s significance and
statistical reliability in a large study with 1669 Diabetic patients (10). Nwagha and Ikekpeazy
also reported AI of plasma as an useful predictor of cardiovascular risk among postmenopausal
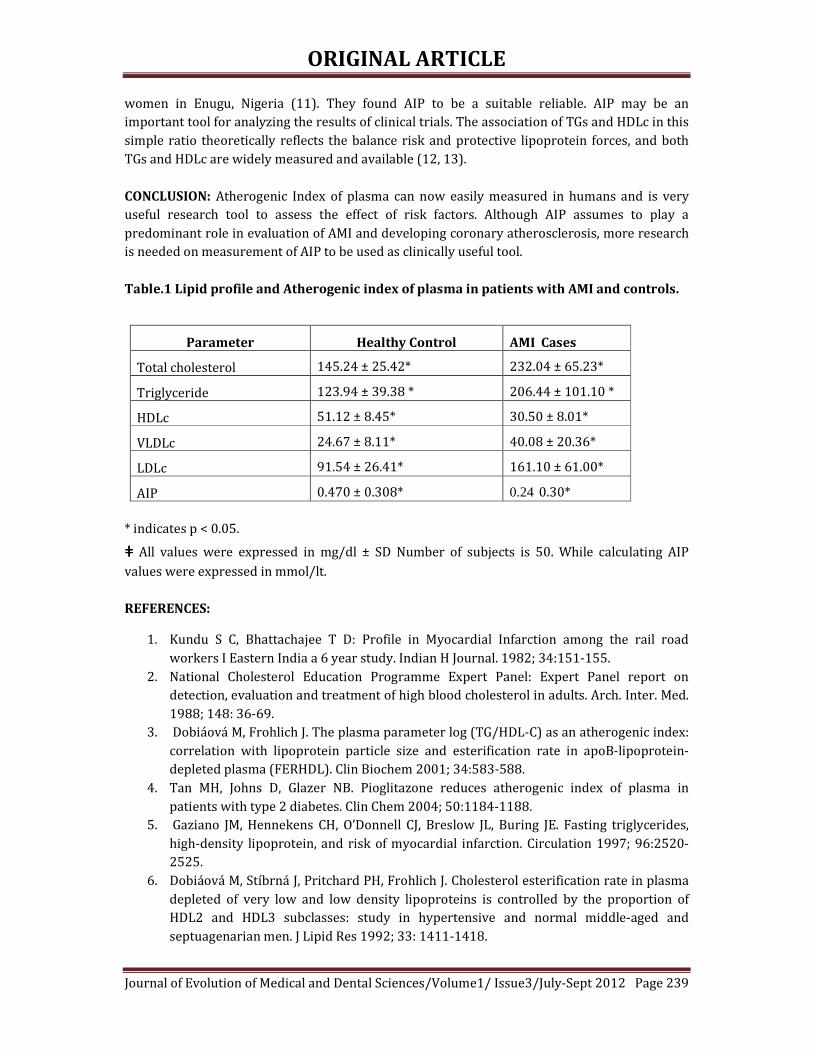
ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 239
women in Enugu, Nigeria (11). They found AIP to be a suitable reliable. AIP may be an
important tool for analyzing the results of clinical trials. The association of TGs and HDLc in this
simple ratio theoretically reflects the balance risk and protective lipoprotein forces, and both
TGs and HDLc are widely measured and available (12, 13).
CONCLUSION: Atherogenic Index of plasma can now easily measured in humans and is very
useful research tool to assess the effect of risk factors. Although AIP assumes to play a
predominant role in evaluation of AMI and developing coronary atherosclerosis, more research
is needed on measurement of AIP to be used as clinically useful tool.
Table.1 Lipid profile and Atherogenic index of plasma in patients with AMI and controls.
Parameter Healthy Control AMI Cases
Total cholesterol 145.24 ± 25.42* 232.04 ± 65.23*
Triglyceride 123.94 ± 39.38 * 206.44 ± 101.10 *
HDLc 51.12 ± 8.45* 30.50 ± 8.01*
VLDLc 24.67 ± 8.11* 40.08 ± 20.36*
LDLc 91.54 ± 26.41* 161.10 ± 61.00*
AIP 0.470 ± 0.308* 0.24 0.30*
* indicates p < 0.05.
ƢƢƢƢ All values were expressed in mg/dl ± SD Number of subjects is 50. While calculating AIP
values were expressed in mmol/lt.
REFERENCES:
1. Kundu S C, Bhattachajee T D: Profile in Myocardial Infarction among the rail road
workers I Eastern India a 6 year study. Indian H Journal. 1982; 34:151-155.
2. National Cholesterol Education Programme Expert Panel: Expert Panel report on
detection, evaluation and treatment of high blood cholesterol in adults. Arch. Inter. Med.
1988; 148: 36-69.
3. Dobiáová M, Frohlich J. The plasma parameter log (TG/HDL-C) as an atherogenic index:
correlation with lipoprotein particle size and esterification rate in apoB-lipoprotein-
depleted plasma (FERHDL). Clin Biochem 2001; 34:583-588.
4. Tan MH, Johns D, Glazer NB. Pioglitazone reduces atherogenic index of plasma in
patients with type 2 diabetes. Clin Chem 2004; 50:1184-1188.
5. Gaziano JM, Hennekens CH, O’Donnell CJ, Breslow JL, Buring JE. Fasting triglycerides,
high-density lipoprotein, and risk of myocardial infarction. Circulation 1997; 96:2520-
2525.
6. Dobiáová M, Stíbrná J, Pritchard PH, Frohlich J. Cholesterol esterification rate in plasma
depleted of very low and low density lipoproteins is controlled by the proportion of
HDL2 and HDL3 subclasses: study in hypertensive and normal middle-aged and
septuagenarian men. J Lipid Res 1992; 33: 1411-1418.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 240
7. Frohlich J, Dobiáová M. Fractional esterification rate of cholesterol and ratio of
triglycerides to HDL-cholesterol are powerful predictors of positive findings on
coronary angiography. Clin Chem 2003; 49:1873-1880.
8. Dobiáová M, Ralová K, Rauchová H, Vohnout B, Ptáková K, Frohlich J. Atherogenic
lipoprotein profile in families with and without history of early myocardial infarction;
fractional esterification rate of cholesterol in plasma depleted of apoB lipoproteins
(FERHDL) and logarithmically transformed ratio of triglycerides to HDL-cholesterol.
Physiol Res 2001; 50: 1-8.
9. Dobiáová M. Atherogenic Index of Plasma [Log (Triglycerides/HDL-Cholesterol)]:
Theoretical and Practical Implications. Clin. Chem 2004; 50: 1113-1115.
10. Lehto S, Ronnemaa T, Pyorala K, Laakso M. Cardiovascular risk factors clustering with
endogenous hyperinsulinaemia predict death from coronary heart disease in patients
with type II diabetes. Diabetologia 2000; 43:148-155.
11. Nwagha UI, Ikekpeazy EJ. Atherogenic index of plasma as useful predictor of
cardiovascular risk among postmenopausal women in Enugu, Nigeria. Afr. Health Sci
2010; 10(3):248-252.
12. Hokanson JE, Austin MA. Plasma triglyceride level is a risk factor to cardiovascular
disease independent of high-density lipoprotein cholesterol level: a meta-analysis of
population based prospective studies. J Cardiovasc Risk 1996; 3:213-219.
13. Guérin M, Le Goff W, Lassel TS, Van Tol A, Steiner G, Chapman MJ. Proatherogenic role of
elevated CE transfer from HDL to VLDL1 and dense LDL in type 2 diabetes. Arterioscler
Thromb Vasc Biol 2001; 21:282-289.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 241
SPECIES DISTRIBUTION AND ANTIFUNGAL SUSCEPTIBILITY PROFILE
OF CANDIDA SPECIES ISOLATED FROM BLOOD STREAM INFECTIONS Sachin C. Deorukhkar, Dr. Santosh Saini.
1. Assistant Professor and PhD Student, Department of Microbiology, Rural Medical College, Loni,
Ahmednagar, Maharashtra.
2. Professor and Head, and PhD guide, Department of Microbiology, Rural Medical College, Maharashtra.
CORRESPONDING AUTHOR
Sachin C Deorukhkar,
Assistant Professor, Department of Microbiology,
Rural Medical College, Loni, Taluka- Rahata,
District- Ahmednagar, Maharashtra 413736.
E-mail: [email protected],
Ph: 91-9545181908, 91-9850775564.
ABSTRACT: BACKGROUND: Candidemia remains as one of the major cause of morbidity and
mortality in health care setting. Over the last two decades, the proportion of blood stream
infection (BSI) due to non-albicans Candida (NAC) species has increased. Several NAC spp. are
inherently resistant to commonly used antifungal drugs. The increased isolation rates of NAC
spp. and a gradual shift in the antifungal susceptibility profile underlines the need of early and
accurate diagnosis of infecting Candida spp. along with antifungal susceptibility testing for
selecting the most appropriate antifungal agent for therapy. AIM: The Aim of the present study
was to investigate the distribution pattern of Candida spp. isolated from candidemia patients
and evaluate its antifungal susceptibility pattern. SETTING AND DESIGN: The present study
was conducted in the department of Microbiology for a period of six years (January 2006 to
December 2011) which included, 194 Candida spp. isolated from the cases of candidemia.
MATERIALS AND METHODS: Candida isolates were speciated by conventional techniques and
HiCandida identification kit. Antifungal susceptibility test was performed using two disc
diffusion methods. Clinical details and risk factors were recorded and analyzed. RESULTS AND
CONCLUSIONS: Isolation of NAC spp. was significantly higher than Candida albicans. The most
important risk factor associated with candidemia was intensive care unit stay, followed by
diabetes and HIV infection. Azole resistance was more in NAC species as compared to C.
albicans. The early and accurate diagnosis of infecting Candida spp. along with antifungal
susceptibility testing plays a pivotal role in preventing morbidity and mortality associated with
Candida BSI. Disc diffusion technique for antifungal susceptibility using glucose methylene blue
Mueller- Hinton (GM-MH) agar was found to be simple, cost effective and sufficiently accurate
for the routine testing of antifungal susceptibility of Candida spp. in resource constrained
microbiology laboratories.
KEY WORDS: Candidemia, Candida albicans, NAC species, antifungal resistance
INTRODUCTION: Candida blood stream infection (BSI) has become a major problem in tertiary
care hospital worldwide 1. Despite some improvement in fungal BSI diagnosis during recent
years, diagnosis of candidemia remains difficult 2. Candidemia has been associated with many
risk factors like long- term hospitalization, antibiotic therapy, use of intravascular catheters, and
underlying diseases like diabetes and malignancy. Although Candida albicans continues to be

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 242
the most common cause of Candidal BSI, the epidemiology of species causing candidemia is
changing. Recent longitudinal studies have detected an increase proportion of BSI by non-
albicans Candida (NAC) species 3, 4.
Importantly many NAC spp. have decreased susceptibility to antifungal agents.
Specifically C. krusei and C. glabrata demonstrate decreased susceptibility to fluconazole 5. The
changing epidemiology of Candida BSI has generated concern about the emergence of azole
drug resistance and its clinical relevance.
Clinicians now depend on identification of Candida to the species level in order to
optimize the selection of antifungal agents allowing them to provide the best possible patient
care 6. Therefore there is a need for continuous surveillance to monitor trends in incidence,
species distribution and antifungal drug susceptibility profiles of Candida BSI.
The Clinical and Laboratory Standards Institute (CLSI) (previously National Committee
for Clinical Laboratory Standards (NCCLS)) after collaborative efforts with various laboratories
has recommended an in-vitro standardized macro broth dilution antifungal susceptibility
testing technique for yeasts 7. CLSI has recommended alternative techniques like ATB fungus,
API, Vitek and disc diffusion to address issues in different laboratories. These methodologies
give reproducible results.8 Disc diffusion procedure appears to be generally acceptable as a
simple, in house standardized procedure for antifungal susceptibility of yeasts 9.
The present study was carried out in a rural tertiary care hospital with an aim to
determine the distribution of Candida spp. isolated from the cases of candidemia and to
compare the efficacy of yeast nitrogen base with glucose (YNBG) media and glucose methylene
blue Mueller- Hinton (GM-MH) agar for the antifungal susceptibility testing of Candida isolates.
MATERIALS AND METHODS: The present study is part of a PhD thesis and was approved by
the Institutional Ethics Committee (Registration No.FN.32/2010). A total 194 Candida spp.
isolated from the blood of patients was included in the study.
The culture was considered true candidemia only when Candida spp. was isolated from
at least two blood culture samples or from a clinically significant single blood culture sample
among hospitalized patients 10. Patient's demographic features such as age, sex, ward, date of
admission, underlying illness, various associated risk factors like presence of urinary catheter,
respiratory ventilation, central line insertion, duration of antibiotic therapy and antifungal
prophylaxis if any, were recorded and analyzed.
SPECIES IDENTIFICATION: Speciation of Candida isolates was done by conventional
techniques and colony colour on Chrom agar 11 Hicandida identification kit (Himedia
Laboratories Pvt. Ltd Mumbai, India) was used for the identification of isolates which could not
be identified by conventional techniques.
ANTIFUNGAL AGENTS: The antifungal agents used were amphotericin B (10 µg), fluconazole
(25 µg), and itraconazole (10µg). Antifungal discs were procured from Himedia Laboratories
Pvt. Ltd Mumbai, India.
ANTIFUNGAL SUSCEPTIBILITY TESTS:
Antifungal susceptibility tests were performed using 2 disc diffusion methods.
1. Yeast Nitrogen base with glucose (YNBG) media.
2. Glucose methylene blue Mueller- Hinton (GM-MH) agar.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 243
ANTIFUNGAL SUSCEPTIBITY TESTING USING YNBG MEDIA:9 YNBG media was prepared
using yeast nitrogen base 10g and glucose 10g, dissolved in 100ml of distilled water and filter
sterilized. Susceptibility test against azoles was performed with addition of 1.5% L-asparagine
to YNBG media. YNBG media mixed with 2% sterile Difco agar (Difco, USA) was poured into 9cm
diameter Petri dishes. Inoculum size of 106 Candida cells/ml was inoculated in one half with the
control strain (C. kefyr Y/16). The cell density was spectrophotometrically adjusted to 0.5
McFarland standard. Inoculation was done by swabbing from the edge of the plate to the centre
using a sterile swab. Discs were placed in the centre of the control and test organism with the
help of sterile forceps. After incubation of the plate at 370C for 48 hours the diameter of
inhibition was read.
The result of the disc diffusion method was interpreted according to the following
criteria: test strain was considered sensitive when the zone diameter was ≥ 80% of the zone
diameter of control strain; intermediate when the zone diameter was < 80% but there was
visible zone of the inhibition; resistant, when there was no zone of inhibition.
2. BY USING GM-MH AGAR: Mueller-Hinton (MH) agar was solidified after addition of 2%
glucose and 0.5ug of methylene blue. Inoculum was prepared by picking five distinct colonies of
approximately 1mm from 24 hours old culture grown on Sabouraud's dextrose agar (SDA).
Colonies were suspended in 5ml of sterile 0.85% saline. This suspension was vortexed to adjust
the turbidity yielding 1x106-5x106 cells/ml and streaked on the entire surface of GM-MH agar.
The antifungal disc was placed 24mm apart from each other. The plates were incubated at 37oC
for 24 hours. If insufficient growth was observed after 24 hours the plates were read after 48
hours. Zone diameters were interpreted as per the approved CLSI /NCCLS (M44-A) guidelines 12. The quality control test was performed by using C. parapsilosis (ATCC 22019), C. krusei
(ATCC 6258), and C. albicans (ATCC 90028).
RESULTS: Between January 2006 to December 2011, out of 4984 blood culture samples
processed in Department of Microbiology, Candida spp. were isolated from the blood culture of
194 patients. Male predominance was noted in our study (n=126/194) 64.9%. Candidemia was
common in more than 50 years age group in males (n=58/126) 46.03%, whereas in females it
was with 0-10 years age group (n=22/68) 32.35% (Figure.1). The most important risk factor
associated with candidemia was ICU stay (49\194) 25.25%, followed by diabetes (40\194)
20.61% and HIV infection (38\194) 19.58% (Figure.2). In this study predominant isolates were
NAC spp. C. albicans was isolated from 78 (40.2%) cases. Among the NAC species, C. tropicalis, C.
glabrata and C. krusei were the major isolates. (Figure.3). All 194 isolates recovered were tested
for antifungal susceptibility by using YNGB medium and GM-MH agar. Their pattern of
resistance is summarized in Table 1. NAC spp. showed more resistance to antifungal agents as
compared to C. albicans.
DISCUSSION: In the last twenty years, various factors like the AIDS epidemic, increase in the
number immunosuppressive therapy recipients and the use of long term antibiotic therapy
have altered the epidemiology of invasive mycoses in general and of candidemia in particular.
Candida spp. is the fourth most common pathogens isolated from the blood of hospitalized
patients13. More recently, NAC spp. has been recovered with increasing frequency. Linked with
this is a recent increase in treatment failure of these infections to standard antifungal therapy,
largely due to the emergence of drug resistance in fungi.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 244
In our study the Candida spp. were isolated from 3.9% of total blood cultures processed
in the Department of Microbiology. Lot of variation in the prevalence and incidence of
candidemia have been reported from India. Kumar et al14 from South India reported an
incidence rate of 5.7% for candidemia among children with onco-haematological malignancies.
Verma et al 15 reported an incidence rate of 1.61% whereas, Xess et al 16 found a prevalence rate
of 6% for candidemia. A study by Sahni et al 17 from Maulana Azad Medical College, New Delhi,
found an incidence rate of 6.9% for Candida spp.
The age and sex distribution of the patients in our study correlates with the observation
of other researchers like Verma et al 15 and Hajjeh et al 18. The importance of risk factors analysis
cannot be over emphasized for infection like candidemia so that preventive measures and
prophylactic therapy can be initiated for patients at risk. Many studies have established
independent risk factors for candidemia on the basis of multivariate analyses. The ICU stay
followed by diabetes and HIV infection was the major risk factors responsible for candidemia in
our study. This was also an observation of other researchers like, Shivaprakasha et al 10, Verma
et al 15and Sandven et al 19. This might be because of severely ill and immunocompromised
patients being cared for in the unit with most of them being on life support systems. Wenzel and
Gennings 20 and Shorr et al 21 have tried to develop risk assessment strategies and calculate
“Candida scores” to predict the true risk of disease in patients admitted in ICU. Candida risk
scores may help clinician to rule out candidemia and to identify the patients at high risk of
developing Candida BSI in the hospital stay. Al- Attas et al 22 have reported high Candida spp.
colonization in diabetic patients compared to control subjects. Isolates colonizing diabetic
patients have also been found to show a greater degree of resistance to antifungal agents than
strains isolated from control subjects.
Our study also underlines the importance of HIV infection as factor contributing to
candidemia. In the United State the proportion of candidemia cases varied from 10% to 15% 23.
The contribution of HIV infection as a predisposing risk factor for candidemia is further
emphasized by a report from Italy, where Candida spp. was the third most common cause of
blood stream infections in HIV patients 24. From India Chowta et al 25 also reported HIV as one of
the major predisposing risk for candidemia. The duration of hospital stay, antibiotic prophylaxis
and treatment, level of immunosuppression, presence of other opportunistic infection and other
clinical types of candidiasis increases the risk of candidemia in HIV infected patients.
The emergence of new species Candida as potential pathogens is a reflection of the
changing scenario in medicine since 1960s. More than 17 species of Candida have been
implicated in human infections till date. However, the list of new species continues to grow. The
use of automated identification system in addition to conventional methods and increase in the
number of HIV infected patients can explain this fact. The incidence of BSI caused by NAC spp.
was higher than C. albicans at our hospital. Among the NAC spp., C. tropicalis followed by C.
glabrata and C. krusei predominately caused BSI. A number of international surveillance
programs like ARTEMIS Antifungal Surveillance Study conducted in 127 health-care centres in
39 countries have documented increased prevalence of NAC species like C. tropicalis and C.
parapsilosis 26.
Epidemiological studies from India reports C. tropicalis as aetiological agent in as many as
67-90% cases of candidemia. Shivprakasha et al 10 found C. tropicalis to be the most common
isolate from candidemia patients. Other workers have also documented the similar observation 16. The increased use of fluconazole has been determined to be the major reason for
predominance of C. tropicalis over C. albicans.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 245
C. glabrata has emerged as an important opportunistic pathogen worldwide. It is the
second most common yeast isolated as part of normal flora and its role as a pathogen has only
been recognized in the past few decades. Trick et al 27reported a considerable increase in the
incidence in the rate of isolation of C. glabrata from BSI patients. There is concern over an
increase in azole resistance among strains of C. glabrata.
With the increased incidence of candidemia and the growing number of antifungal
agents, laboratory aids to guide in the selection of antifungal therapy have gained greater
attention. The standardized broth micro dilution method is expensive, laborious and
cumbersome for use in clinical microbiology laboratories. Recently, a disc diffusion method has
been approved by CLSI for antifungal susceptibility testing of yeast.
In the present study we performed disc diffusion method for antifungal susceptibility
testing of Candida isolates. In our study Fluconazole resistance was noted in 19.07% of Candida
isolates, 11.9% showed resistance to itraconazole and 4.63% of Candida isolates showed
resistance to amphotericin B. In India, there is lack of multicentric studies regarding antifungal
susceptibility pattern. Goel et al 28 and Capoor et al 29 reported less incidence of resistance to
fluconazole. On the other hand, workers like Kumar et al 14, Kothari et al 30 and Gupta et al 31
reported high incidence of resistance to fluconazole.
The resistance to fluconazole is of great concern because it is the most common azole
used for treatment of disseminated candidiasis including candidemia. It is available in both
intravenous and oral formulation with high bioavailability and is more cost effective than other
antifungal agents. Although Amphotericin B is effective against most strains of Candida species,
it is not the first choice for the treatment of candidemia because of nephrotoxicity associated
with it. Itraconazole is used for treatment of mucosal candidiasis 32. Studies regarding its role in
treatment of candidemia are less. In a study by Kothari et al 30 24% of Candida isolates were
resistant to itraconazole.
In the present investigation, resistance to antifungal agents was observed more in NAC
spp. as compared to C. albicans. Fluconazole resistance was high in C. tropicalis and C. glabrata.
Itraconazole resistance was more in C. tropicalis. Amphotericin B resistance was higher in C.
glabrata isolates. Other researchers have also documented high antifungal resistance among
NAC spp as compared to C. albicans 1, 3.
We have compared the efficacy of YNBG medium and GM-MH agar for the antifungal
susceptibility testing of Candida isolate. Trailing phenomena around the zone margin were
infrequent and minimal on the GM-MH agar. Zone edges with this method were frequently
definite and clear, facilitating the measurement of zone sizes and minimizing subjectivity in
zone size measurements. The occurrence of the macrocolonies near the center of the clear zone
was also less with this method. The methylene blue in this medium stained the Candida colony
facilitating the identification. Our study showed that there is less variation in the result of GM-
MH agar and YNBG medium. Therefore GM-MH agar can be recommended as simple, cost
effective and sufficiently accurate medium for the routine testing of antifungal susceptibility of
Candida spp.
To conclude, the spectrum of Candida BSI has shifted dramatically from C. albicans to
NAC spp. Hence, it is essential that an early and accurate diagnosis be made of infecting species
of Candida, since each species varies markedly in susceptibility to the currently used antifungal
drugs. It is imperative that antifungal susceptibility testing be carried out routinely in the
laboratory. This will aid the clinician in timely institution of the appropriate and accurate

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July
antifungal drug to be used and will restrict the empirical use of antifungal
commonly done today.
Figure 1. Age and sex distribution of candidemia patients.
Figure 2. Risk factors predisposing
0
20
40
60
80
100
120
140
0-10 years
11-20 years
26
5
22
6
38
15
12
8
8
86
6 4
ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012
antifungal drug to be used and will restrict the empirical use of antifungal agents, as being
sex distribution of candidemia patients.
Figure 2. Risk factors predisposing Candidemia.
21-30 years
31-40 years
41-50 years
>50 years
Total
413
20
58
126
4 9 12 15
68
Male Female
49
40
ICU stay
Diabetes
HIV infection
Urinary catheter
Ventilator
Renal failure
Central line
Neonate
Malignancy
surgery in last 3 months
Dialysis
Sept 2012 Page 246
agents, as being

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 247
Figure 3. Species distribution of Candida isolates obtained from candidemia patients.
Table 1 Comparison of antifungal resistance pattern of Candida isolates using YNBG
medium and GM-MH agar.
Isolate Total Amphotericin B Fluconazole Itraconazole
YNBG GM-MH YNBG GM-MH YNBG GM-MH
C. albicans 78 02 02 07 07 04 03
C. tropicalis 52 02 02 19 19 20 21
C. glabrata 27 05 04 08 08 05 05
C. krusei 20 - - 02 02 02 02
C. guilliermondii 10 - - 01 01 01 01
C. parapsilosis 05 - - - - - -
C. dubliniensis 02 - - - - - -
REFERENCES:
1. Tortorano AM, Biraghi E, Astolfi A, Ossi C, Tejada M, Farina C et al. European
confederation of Medical Mycology (ECMM) prospective survey of candidaemia:
report from one Italian region. J Hosp Infect 2002;51:297-304.
2. Gudlaugsson O, Gillespie S, Lee K, Vande BJ, Hu J, Messer S, et al. Attributable
mortality of nosocomial candidemia, revisited. Clin Infect Dis 2003;37:1172-
1177.
3. Almirante B, Rodriguez D, Park B J, Cuenca-Estrella, Planes AM, Almela M et al.
Epidemiology and predictors of mortality in the cases of Candida bloodstream
infection: results from population-based surveillance, Barcelona, Spain, from
78
52
27
20
105
2
C. albicans
C. tropicalis
C. glabrata
C. krusei
C. guilliermondii
C. parapsilosis
C. dubliniensis

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 248
2002 to 2003. J Clin Microbiol 2005;43:1829-1835.
4. Pfaller M, Diekema D. Role of Sentinel Surveillance of Candidemia: trends in
species distribution and antifungal susceptibility. J. Clin. Microbiol
2002;40:3551-3557.
5. Iwata K. Drug resistance in human pathogenic fungi. Eur J Epidemiol 1992;
8:407-421.
6. Horvarth L, Hospenthal D, Murray C, Dooley D. Direct isolation of Candida spp.
from blood cultures on chromogenic medium on CHROMagar Candida. J Clin
Microbiol 2003;41:2629-2632.
7. National Committee for Clinical Laboratory Standards. Reference method for
broth dilution antifungal susceptibility testing for yeasts: Proposed standard
M27-P (National committee for Clinical Laboratory Standards, Villanova, Pa)
1992;12:No.25.
8. Khan S, Singhal S, Mathur T, Upadhyay DJ, Rattan A. Antifungal susceptibility
testing method for resource constrained laboratories. Indian J Med Microbiol
2006;24:171-176.
9. Chakrabarti A, Ghosh A, Kanta A, Kumar P. In Vitro antifungal susceptibility of
Candida. Indian J Med Res 1995;102:13-19.
10. Shivaprakasha S, Radhakrishnan K, Karim P. Candida spp. other than Candida
albicans: A major cause of fungaemia in a tertiary care centre. Indian J Med
Microbiol 2007;25:405-407.
11. Sachin CD, Ruchi K, Santosh S. In vitro evaluation of proteinase, phospholipase
and haemolysin activities of Candida species isolated from clinical specimens. Int
J Med Biomed Res 2012; 1:153-157.
12. National Committee for Clinical Laboratory Standards. Methods for antifungal
disk diffusion susceptibility testing of yeasts. Approved guidelines M-44A.
Wayne, PA: NCCLS;2004.
13. Berrounae Y, Herwalat l, Pfaller. Trends in antifungal use and epidemiology of
nosocomial yeast infection in a university hospital. J Clin Microbiol 1999;37:531-
537.
14. Kumar CP, Sundarajan T, Menon T, Venkatadesikalu M. Candidiosis in children
with onco-hematological studies in Chennai, South India. Jpn J Infect Dis
2005;58:218-221.
15. Verma AK, Prasad KN, Singh M, Dixit AK, Ayyagari A. Candidaemia in patients of a
tertiary health care hospital from north India. Indian J Med Res 2003;117:122-
128.
16. Xess I, Jain N, Hasan F, Mandal P, Banerjee U. Epidemiology of candidemia in a
tertiary care centre of North India: 5-year study. Infection 2007;35:256-259.
17. Sahni V, Agarwal SK, Singh NP, Anuradha S, Sikdar S, Wadhwa A. Candidemia-An
Under-recognized nosocomial infection in Indian Hospitals. J Assoc Physicians
India 2005;53:607-611.
18. Hajjeh RA, Sofair AN, Harrison LH, Lyon GM, Arthington-Skaggs BA, Mirza SA et
al. Incidence of bloodstream infections due to Candida species and In Vitro
susceptibilities of isolates collected from 1998 to 2000 in a population-based
active surveillance program. J Clin Microbiol.2004;42:1519-1527.
19. Sandven P, Bevanger L, Digranes A, Gaustad P, Haukland HH, Steinbakk M.
Constant low rate of fungaemia in Norway, 1991 to 1996. The Norwegian Yeast
Study Group. J .Clin. Microbiol. 1998;36:3455-3459.
20. Wenzel RP, Gennings C. Bloodstream infections due to Candida species in

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 249
intensive care unit: Identifying especially high-risk patients to determine
prevention strategies. Clin Infect Dis 2005; 41:S389-S393.
21. Shorr AF, Tabak YP, Johannes RS, Sun X, Splading J, Kollef MH. Candidemia on
presentation to the hospital: Development and validation of a risk score. Crit
Care 2009 (13: 1-10.doi:10.1186/cc8110.
22. Al-Attas SA, Amro SO. Candidial colonisation, strain diversity and antifungal
susceptibility among adult diabetic patients. Ann Saudi Med 2010;30:101-108.
23. Kao AS, Brandt ME, Pruitt WR, Conn LA, Perkins BA, Stephens DS et al. The
Epidemiology of candidemia in Two United States Cities: Results of a population-
based active surveillance. Clin Infect Dis 1999;29:1164-1170.
24. Petrosilo N, Viale P, Nicastri E, Arici C, Bombana E, Caeila A, et al. Nosocomial
blood stream infections among human immunodeficiency virus infected patients:
Incidence and risk factors. Clin Infect Dis 2002;34:677-685.
25. Chowta MN, Adhikari P, Rajeev A, Shenoy AK. Study of risk factors and
prevalence of invasive candidiasis in a tertiary care hospital. Indian J Crit Care
Med 2007;11:67-73.
26. Pfaller MA, Diekema DJ, Rinaldi MG, Barnes R, Hu B, Veselov AV. Results from the
ARTEMIS DISK Global antifungal surveillance study: A 6.5-year analysis of
susceptibilities of Candida and other yeasts species to fluconazole and
voriconazole by standardized disk diffusion testing. J Clin Microbiol
2005;43:5848-5859.
27. Trick WE, Fridkin SK, Edwards JR, Hajjeh RA, Gaynes RP. Secular trends of
hospital-acquired candidemia among intensive care unit patients in the United
States during 1989-1999. Clin Infect Dis 2002;35:627-630.
28. Goel N, Ranjan PK, Agarwal R, Chaudhary U, Sanjeev N. Emergence of
nonalbicans Candida in neonatal septicemia and antifungal susceptibility:
Experience from tertiary care centre. J Lab Physicians 2009;1:53-55.
29. Capoor MR, Nair D, Deb M, Verma PK, Srivastava L, Aggarwal P. Emergence of
non-albicans Candida and antifungal resistance in a tertiary care hospital. Jpn J
Infect Dis 2005;58:344-348.
30. Kothari A, Sagar V. Epidemiology of Candida Bloodstream Infection in a Tertiary
Care Institute in India. Indian J Med Microbiol 2009;27:171-172.
31. Gupta N, Mittal N, Sood P, Kumar S, Kaur R, Mathur MD. Candidemia in neonatal
intensive care unit. Indian J Pathol Microbiol 2001;44:45-48.
32. Pappas PG, Kauffman CA, Andens D, Benjamin DK, Calandra TF, Edwards JE.
Clinical practice guidelines for the management of candidiasis: 2009 Update by
infectious diseases society of America. Clin Infect Dis 2009;48:503-535.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 250
ASSESSMENT OF UMBILICAL CORD BLOOD IRON AND TIBC LEVELS IN
NEONATES OF ANAEMIC MOTHERS Dr. Durdana Sayeed, Dr. Ghouse M Ali, Dr. Arshiya Masood Osmani, Dr. Rohini N.
Dr. MD. Siddique Ahmed Khan.
1. Assistant Professor, Department of Biochemistry, Dr. VRK Women’s Medical College & Allied Hospitals,
Hyderabad.
2. Professor and HOD, Department of Biochemistry, Dr. VRK Women’s Medical College & Allied Hospitals,
Hyderabad.
3. Assistant Professor, Department of Biochemistry, Dr. VRK Women’s Medical College & Allied Hospitals,
Hyderabad.
4. Assistant Professor, Department of Biochemistry, Dr. VRK Women’s Medical College & Allied Hospitals,
Hyderabad.
5. Associate Professor, Department of Biochemistry, Dr. VRK Women’s Medical College & Allied Hospitals,
Hyderabad.
CORRESPONDING AUTHOR
Dr. Durdana Sayeed,
H.NO-10-1-128/1/2/E,
”ALIMANOR” MASAB TANK,
Hyderabad. AP-500028,
E-mail: [email protected],
Ph: 9848502341/9866226286.
ABSTRACT: The most common cause of anaemia in pregnancy is Iron deficiency which can
affect the newborns. This study was done to compare the serum Iron & Total Iron Binding
Capacity (TIBC) levels in the 20 newborns of non–anaemic and anaemic mothers each.
Results showed that Haemoglobin % was significantly lower (P≤ 0.001) in newborns of anaemic
mothers. Serum Iron levels did not show any significant difference (P = 0.1) & TIBC levels were
significantly higher (P≤ 0.01) in newborns of anaemic mothers as compared to newborns of
non- anaemic mothers.
KEYWORDS: Umbilical Cord blood, Iron deficiency anaemia, pregnancy, Serum Iron, S. TIBC.
INTRODUCTION: Anaemia is one of the most common conditions prevalent in our country. The
most common cause of anaemia in pregnancy is Iron deficiency.
WHO defines anaemia in pregnancy when Hb % is ≤ 11 gm/dl1.
Hb % ≤ 11 gm/dl especially in late pregnancy should be considered abnormal and due to Iron
deficiency rather than due to hypovolemia of pregnancy2.
The mean Hb level in cord blood is 13.5 – 20.5 gm/dl and Hb % ≤ 14 gm/dl at birth is
considered abnormal2.
AIM: This study was done to compare the Haemoglobin, serum Iron & TIBC levels in 20
newborns of non-anaemic mothers and anaemic mothers each.
MATERIALS & METHODS: The study done by the approval of ethical committee of Dr.
VRKWMC, Teaching Hospital & Research Centre. The study group is comprised of 20 pregnant
women without anaemia and their 20 newborns (Group I). The control group included 20
pregnant women with anaemia (Hb levels < 10 gm/dl) and their 20 newborns (Group II). Cord

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 251
blood was collected from the newborns’ end of the umbilical cord within 5 minutes of the
delivery.
FOR ESTIMATION OF HAEMOGLOBIN – We followed Cyanmethaemoglobin method3.
FOR ESTIMATION OF SERUM IRON & TIBC – We followed Dipyridyl method4.
The instrument used was Spectrophotometer (Elico sl 159).
RESULTS:
TABLE I-SHOWING Hb, IRON AND TIBC LEVELS IN NEWBORNS OF NON-ANAEMIC
MOTHERS (GROUP I)
Hb in gm% S. Fe in ugm% TIBC ugm%
MEAN 14.7 107.5 256.3
S. D +/_ 0.91 30.61 114.04
S.E +/_ 0.2 6.84 25.4
TABLE II – SHOWING Hb, IRON and TIBC LEVELS IN NEW BORNS OF ANAEMIC MOTHERS
(GROUP II)
Hb in gm% S. Fe in ugm% TIBC ugm%
MEAN 12.6 99.7 301.45
S.D +/_ 0.96 34 56.31
S.E +/_ 0.22
TABLE III – COMPARISSION of Hb, IRON AND TIBC LEVELS B/W GROUPS I & II
Hb in gm% S. Fe in ugm% TIBC ugm%
t-value 6.93 0.76 1.59
p-value < 0.001 = 0.1 ≤0.01
Df 38 38 38
The stastical analysis done was done using SAS Version of software.
Newborns of anaemic mothers showed
I. Significantly lower levels of Hb(P<0.001) when compared to newborns of non anaemic
mothers.
II. Serum Iron did not show any significant difference (P = 0.1).
III. Serum TIBC levels were significantly higher (P ≤0.01) in
New borns of anaemic mothers as compared to new borns of non- anaemic mothers.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 252
DISCUSSION: In our study comparison of newborns of non-anaemic and anaemic mothers
showed
� Haemoglobin of Group I is 14.7gm% and that of Group II is 12.6gm % with p value
(<0.001).
� Serum Iron showed Group I is 107.5µgm/dl and that of Group II is 99.7 µgm/dl with p
value (=0.1).
� Serum TIBC of Group I is 256.3 µgm/dl and that of Group II is 301.45 µgm/dl with p (≤
0.01).
A significant difference in all parameters except SERUM IRON reflects the metabolic demands
created by the foetus for erythropoiesis and foetus draws its full requirement from the mother.
Iron deficiency anaemia in mother is considered as a risk factor for Iron deficiency in infancy 5,6
Chitra Upadhyaya et al7 , found that there was a significant decrease in Hb% in the new borns of
anaemic groups when compared to the newborns of nonanaemic mothers. Similarly serum iron
levels was also having a significant difference .Where as in our study there is no significant
difference in serum iron levels.
TABLE IV – COMPARISSION B/W REFERENCE STUDY & OUR STUDY
NEWBORNSOFANAEMIC
MOTHERS
Hb in gm% S.IRON(µgm/dl) TIBC(µgm/dl)
REFERENCE STUDY 14.9 108.0 288.9
OUR STUDY 14.7 107.5 256.3
NEWBORNS OF NON-
ANAEMIC MOTHERS
REFERENCE STUDY 13.1 76.7 332.8
OUR STUDY 12.6 99.7 301.45
CONCLUSION: Compared to previous study7, our study shows that serum iron does not show
any significant difference in the newborns of non-anaemic and anaemic mothers,whereas Hb &
TIBC showing significant difference.
In the socio-economic conditions of our country , people are scared of nutritional deficiency for
the newborn children. But it has been observed in our study that the newborns of anaemic
mothers have no iron deficiency inspite of being born to anaemic mothers.
LIMITATIONS OF THE STUDY:
i) Samples for study has to be collected only from those cases which are
delivered before noon, because S.iron levels show a diurnal variation-S.iron
levels decline by almost 50% from 8:00 to 14:00 hours.
ii) Sample collection from umbilical cord fails, if there is delay in drawing the
sample.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 253
ACKNOWLEDGMENT: We are extremely thankful to Dr. SARIB RASOOL KHAN – Managing
Director DR. V R K WMC, Teaching Hospital & Research Centre and Allied Hospitals, for
providing all the facilities for the research work.
Our sincere thanks to Dr. SIKANDER HUSSAIN – Professor –Dept. of Physiology for the
cooperation.
REFERENCES:
1. Saraiya.Rao.Chatterjee,Principles of Obs and Gyn forPGs , 2nd edition pg-33.
2. Williams, Obstetrics-21st Edn.
3. Harold Varley, Practical Clinical Biochemistry, 4th Edn ,pg no.585.
4. Harold Varley, Practical Clinical Biochemistry, 4th Edn. pg no. 472.
5. Kilbride, J., Baker,T.G., Parapia, L.A.,Khoury,S.A..Shuqaidef , S.W., & Jerwood, D.Anaemia
During Pregnancy as a Risk Factor for Iron Defeciency Anaemia in infancy. Int J
Epidemiol (1999) 28: 461- 468 .
6. J. Colomer, C. colomer ,D. Gutierrez, A. Jubert A. Nolosaco, J. Donat,
R.Fernandez- Delgado, F. Donat and C. Alavarez- Dardet. Anaemia During Pregnancy as
a Risk Factor for Infant Iron Deficiency. Paediatric & Perinatal Epidemiology 1990,4
(2).196 – 204.
7. Chitra Upadhyaya et al, Serum Iron, copper & Zinc status in Maternal & Cord blood, IJCB
, 2004, 48 – 52.

CASE REPORT
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 254
ENTEROCOCCAL BRAIN ABSCESS OF OTOGENIC ORIGIN: A CASE
REPORT
Dr. K. Vidyasagar, Dr. R. Ravikumar. Dr. Nupur Pruthi.
1. Non-PG Senior Resident, Department of Neuromicrobiology, NIMHANS, Hosur Road, Bangalore.
2. Professor and Head, Department of Neuromicrobiology, NIMHANS, Hosur Road, Bangalore.
3. Assistant professor, Department of Neurosurgery, NIMHANS, Hosur Road, Bangalore
CORRESPONDING AUTHOR
Dr. R. Ravikumar MD,
Professor and Head, Department of Neuromicrobiology,
NIMHANS, Hosur Road, Bangalore-560029,
E-mail: [email protected],
Ph: 09448073965.
ABSTRACT: Various aerobic and anaerobic bacteria have been reported as causative agents of
brain abscess but only a few cases of enterococcal brain abscesses have been reported. We
report a case of enterococcal brain abscess of otogenic origin in a 35 year old male who was
known case of chronic suppurative otitis media (CSOM) and cholesteotoma of the right ear. The
abscess material culture yielded an isolate which was identified as Enterococcus faecium by
standard biochemical reaction. The isolate was sensitive to penicillin, ampicillin, gentamicin,
vancomycin, ofloxacin, lincomycin, and cloxacillin.
KEY-WORDS: Brain abscess, Enterococcus faecium, Computerized tomography
INTRODUCTION: Despite the advent of modern neurosurgical techniques, new antibiotics and
new powerful imaging technologies, brain abscess remains a potentially fatal central nervous
system (CNS) infection.1-4Brain abscess is a relatively uncommon infection with an incidence of
0.3-1.3/100,000 persons per year 1. Most of these cases occur in association with the
predisposing conditions such as otitis media, sinusitis, or presence of pyogenic infections in
other parts of the body. Dental infections are associated with around 2% of the brain abscesses.2
The causative pathogens of bacterial brain abscess vary with time period, geographic
distribution, age, underlying medical and/or surgical conditions and mode of infection. A large
number of Gram positive cocci, Gram negative aerobic bacilli, anaerobes and Mycobacterium
tuberculosis have been reported as the causative agents of bacterial brain abscess.1-4The
commonest organisms causing brain abscess following an otogenic source include
Staphylococcus aureus, Streptococcus pneumoniae, H. influenzae, Escherichia.coli, Proteus and
Pseudomonas species. Very few studies have reported Enterococcus species as one of the
causative agents of brain abscesses2-4.
We report a rare case of enterococcalbrain abscess of otogenic origin in a 35 years old
male which was managed successfully with surgical drainage and antibiotics.
CASE HISTORY: A 35-year old male patient presented to the Department of Neurosurgery with
three days of headache, giddiness and vomiting. The patient was a known case of CSOM and
cholesteotoma of right ear for the past three years having ear discharge and ear pain. The
patient underwent radical mastoidectomy with excision of cholesteotoma. On third post op day

CASE REPORT
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 255
patient developed headache, vomiting and giddiness with blurring of vision with no h/o fever,
seizures or limb weakness. At time of admission patient was conscious, had no fever and neck
stiffness. Neurological examination revealed left hemi paresis with grade two power, bilateral
papilledema, nystagmus and right cerebellar dysfunction. Cardiovascular, respiratory and
abdominal examinations were found to be normal.
His white blood cell (WBC) count was 13000/mm3 with 70% neutrophils. The
erythrocyte sedimentation rate (ESR) was 10mm/hr. Biochemical parameters were within
normal limits. CT of brain showed right cerebro-pontine angle cistern enhancing lesion with
loculation of size 4.4 × 3.5 × 3.0 cm2 with mass effect on fourth ventricle. Intracranial mass or
abscess was suspected as the probable diagnosis and craniotomy was performed and excision of
right cerebro-pontine angle abscess with EVD placement was done. Abscess material was
processed in the lab. Gram stain of the smear showed plenty of pus cells and Gram positive cocci
in pairs and short chain along with Gram negativebacilli. ZN stain showed no acid fast bacilli.
Abscess material was cultured on blood agar, MacConkey agar, thioglycollate broth and
anaerobic blood agar aerobically and anaerobically. A culture was also put up in LJ medium.
Culture yielded a bacterium which was identified as Enterococcus faecium by standard
biochemical reactions)6.
LJ medium showed no growth after eight weeks of incubation. The isolate was sensitive
to penicillin, ampicillin, gentamicin, vancomycin, ofloxacin, lincomycin and cloxacillin by disc
diffusion method. Patient was treated with iv ampicillin, iv gentamicin and metronidazole iv for
3 weeks. After three weeks of antibiotic therapy he was discharged without any neurological
deficit. The patient on follow up visits was doing well with no residual neurological deficit and
marked improvement in the radiological findings on a follow-up CT scan(fig1 B&C).

CASE REPORT
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 256
DISCUSSION: There have been many advances with respect to the diagnosis and management
of brain abscess, resulting in a corresponding increase of survival rates. However its incidence is
high, approximately 5% per million people, and the number of immuno-deficient hosts having
high risk of opportunistic infections might be increasing. This disease continues to be one of the
most common neurosurgical diseases[1-5].
Regarding portal of entry, brain abscess is almost always secondary to a focus of
suppuration elsewhere in the body or may develop either by a contiguous focus of infection,
head trauma or hematogenous spread from a distant focus.1-5 Thus the predisposing factors for
the development of brain abscess include infections of the middle ear, mastoid, paranasal
sinuses, orbit, face, scalp penetrating skull injury, intracranial surgery including insertion of
ventriculo-peritoneal shunts5-6.
A previous study conducted by Malik et al.6from Mumbai showed that in 47 cases of
brain abscess, the primary focus of infection could be established in 37 cases (78.7%) and
otogenic source was the commonest in 34% cases.
Another prospective study of pattern of brain abscess reported from India7 showed
chronic suppurative otitis media to be the commonest predisposing factor in 48% of patients.
The location and number of abscesses depends upon the predisposing factors. The temporal
abscess and the cerebellum are the commonest sites following otogenic source as observed in
the present case. The list of bacteria causing brain abscesses is very large. It includes Gram
negative aerobic bacilli like Klebsiella pneumoniae, Pseudomonas aeruginosa, Escherichia coli,
Salmonella species, Proteus species, Klebsiella oxytoca, Haemophilus influenzae, Pasturella
species, Vibrio cholerae non 01; Gram positive bacteria like Staphylococcus aureus, other
Staphylococcus species, Streptococcus pneumoniae, Enterococcus species, Viridans
streptococci, other Streptococcal species. The anaerobic organisms reported are Bacteroides
species, Fusobacterium species, Peptostreptococcus and Propionibacterium species.1-4
The commonest organisms causing brain abscess following an otogenic source include
Staphylococcus aureus, Streptococcus pneumoniae, H. influenzae, Escherichia.coli, Proteus and
Pseudomonas species.1-7 Very few studies have reported Enterococcus species as one of the
causative agents of brain abscesses in India.
Kurien et al.2in 1993 reported Enterococcus faecalis as one of the causative agents of
brain abscesses in India, while studying 153 cases of brain abscesses.
In the year 2002, Park et al.4from Korea reported a case of otogenic brain abscess due to
Enterococcusfaecium.
A recent case report from India by Mohanty et al. 3 in the year 2005 reported a brain
abscess due to Enterococcus avium in a 19-year-old man with chronic otitis media since
childhood.
Enterococcus faecalis and Enterococcus faecium are responsible for most enterococcal
infections in humans, while Enterococcus gallinarum, Enterococcus avium and Enterococcus
casseliflavus are not frequently reported8.Enterococciare clearly unusual etiological agents of
brain abscess, and they account for 0.3–4% of reported cases of brain abscess9.Based on a
clinical spectrum of symptoms and findings, enterococcal brain abscess can be found in two
clinical forms postoperative and spontaneous. Postoperative brain abscess appears as a
nosocomial infection usually associated with neurosurgical procedures and shunt devices10. Our
patient had CSOM and also underwent radical mastoidectomy with excision of cholesteotoma
which was considered as risk factors for his enterococcal brain abscess. For most clinical
microbiological laboratories, the primary method of identifying Enterococcus species strains

CASE REPORT
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 257
relies on phenotypic characterization [10]. The treatment of enterococcal brain abscess includes
administration of appropriate antibiotics that have in vitro activity against the strain, and can
efficiently penetrate the cerebrospinal fluid, in addition to the elimination of the predisposing
factors if necessary10.
We would like to stress that a high index of suspicion, timely diagnostic support by CT
scan, surgical intervention and vigorous antimicrobial therapy are crucial for better outcome.
REFERENCES:
1. Lu CH, Chang WN, Lin YC, Tsai NW, Liliang PC, Su TM, et al. Bacterial brain abscess:
microbiological features, epidemiological trends, therapeutic outcomes. QJM. 2002;
95:501–09.
2. Kurien M, Job A, Mathew J, Chandy M. Otogenic intracranial abscess. Concurrent
craniotomy and mastoidectomy- Changing trends in a developing country. Arch
Otolaryngol Head Neck Surg. 1998; 124:1353–56.
3. Mohanty S, Dhawan B, Kapil A, Das BK, Pandey P, Gupta A. Brain abscess due to
Enterococcus avium. Am J Med Sci. 2005; 329:161–62.
4. Park SY, Min JH, Ryu JW, Ko YS. Enterococcal otogenic brain abscess. Korean J
Otolaryngol Head Neck Surg. 2002; 45:1188–92.
5. Sung DJ, Ealaan K, Chang YL, Kim IS, Son EIK, Kim DW, et al. Clinical features and
surgical treatment of brain abscess. J Korean Neurosurg Soc. 2007; 41:391–96.
6. Malik S, Joshi SM, Kandoth PW, Vengsarkar US. Experience with brain abscesses.
Indian Pediatr. 1994; 31:661–66.
7. Lakshmi V, Rao RR, Dinkar I. Bacteriology of brain abscess--observations on 50
cases. J Med Microbiol. 1993; 38:187–90.
8. Sood S, Malhotra M, Das BK, Kapil A. Enterococcal infections & antimicrobial
resistance. Indian J Med Res. 2008; 128: 111-21.
9. Kurup A, TeeW, Loo I, Lin R. Infection of central nervous system by motile
Enterococcus: First case report. J Clin Microbiol.2001; 39:820-22.
10. Murray BE.The life and times of the Enterococcus. ClinMicrobiol Rev.1990;3: 46-65.

CASE REPORT
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 258
MYOFIBROBLASTIC SARCOMA: A CASE REPORT Dr. Rithesh. K. B, Dr. Nandesh Shetty, Dr. Sumukh. M, Dr. Ashish Shetty. Dr. Raghavendra. P
1. Assistant Professor, Department of OMFS, A. J. Institute of Dental Sciences, Kuntikana, Mangalore.
2. Head of the Department, Department of OMFS, A. J. Institute of Dental Sciences, Kuntikana, Mangalore.
3. Post Graduate Student, Department of OMFS, A. J. Institute of Dental Sciences, Kuntikana, Mangalore.
4. Assistant Professor, Department of OMFS, A. J. Institute of Dental Sciences, Kuntikana, Mangalore.
5. Assistant Professor, Department of Pedodontics, A. J. Institute of Dental Sciences, Kuntikana, Mangalore.
CORRESPONDING AUTHOR
Dr. Sumukh. M,
Dept. of Oral & Maxillofacial Surgery,
A. J. Institute of Dental Sciences, N.H 17,
Kuntikana, Mangalore-575004,
E-mail: [email protected],
Ph: 09886809202.
ABSTRACT: Myofibroblastic Sarcoma is a rare or uncommon neoplasm characterized by
myofibroblastic proliferation. The tumour may present as single or multiple nodules of soft
tissue, bone, or internal organs. When encountered in the jaws, the lesions exhibit clinical and
radiographic features suggestive of several odontogenic and non-odontogenic neoplasms.
Myofibroblastic Sarcoma of the jaws are usually well-demarcated, but sometimes can be poorly
delineated or infiltrated that may result in misdiagnosis and mistreatment1. A painless,
enlarging mass is the most common clinical presentation, but a definitive diagnosis requires
both histopathological and immunohistochemical analyses. In this paper we are going to discuss
a case of 64 years old male with Myofibroblastic Sarcoma of left side of face. The patient
underwent excision of the lesion in toto with reconstruction of the floor of the orbit using
prolene mesh.
KEYWORDS: Myofibroblastic Sarcoma, Myofibroma, Maxilla, Alveolus, Floor of Orbit, Prolene
mesh.
INTRODUCTION: Defining neoplastic Myofibroblastic Sarcoma (MS) as a distinct entity was
controversial. With increasing case reports, it became clear that Myofibroma was a distinct
entity in soft tissue sarcomas. Even though only low-grade Myofibroma was classified as a
distinct entity in the newly published World Health Organization classification of soft tissue
tumours, intermediate- and high-grade Myofibroma cases were documented in the literature.
Some cases of MYOFIBROBLASTIC SARCOMA were easy to misdiagnose as reactive lesions
because of the common existence of myofibroblasts in reactive granuloma. In addition, the
frequent exhibition of bland cytologic features in MYOFIBROBLASTIC SARCOMA is an important
factor in persuading pathologists toward a benign diagnosis. MYOFIBROBLASTIC SARCOMA,
especially low-grade MYOFIBROBLASTIC SARCOMA, is easily confused with myofibroblasts
composing nodular fasciitis because of their morphologic similarity and the overlapping
immunophenotype.
MYOFIBROBLASTIC SARCOMA is a common mesenchymal neoplasm that occurs most
frequently in the uterus and gastrointestinal tract. The occurrence of primary
MYOFIBROBLASTIC SARCOMA in the oral soft tissues or jawbones is very unusual. 1) Only 31
cases have been reported in the literature.2) Among cases of oral soft tissue MYOFIBROBLASTIC

CASE REPORT
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 259
SARCOMA, six arose in the cheek, five in the gingiva, five in the tongue and the remainder were
located in the floor of the mouth, soft palate, hard palate, mandibular alveolar mucosa, posterior
maxillary soft tissue and maxillary sinus. Among the jawbone lesion cases, six occurred in the
mandible and four in the maxilla2.
This paper discusses an unusual case of primary MYOFIBROBLASTIC SARCOMA of the
oral cavity, which arose in the maxillary buttress and had the growth pattern of a polyp.
DESCRIPTION OF CASE: A 64-year-old Male patient visited the Department of Oral & Maxillo-
facial Surgery at A. J. Institute of Dental Sciences, Mangalore with the chief complaint of a
swelling over the left side of the face region since 2 months duration. Swelling was insidious in
onset, initially small in size and associated with pain which was mild in intensity and continuous
type. Extent
Anteriorly: Left lateral aspect of the nose.
Posteriorly: 3 cm in front of the tragus.
Superiorly: Infraorbital rim
Inferiorly: Line joining corner of the mouth to tragus of the ear on the left side.
Size: 5 cm x 4 cm.
Patient had previously visited a dentist with complaints of pain and swelling and
underwent extraction of the two upper left molars as they were mobile. After extraction
swelling rapidly increased in size to its present size. Pain was moderate type and not subsiding
with medications. Patient is hypertensive and is on medication. On examination bucco-palatal
expansion was noted in the upper left molar region and 1st premolar region. Physical
examination revealed a firm swollen region, which showed tenderness, pain at palpation.
Surface was smooth, irregular in shape with ill defined margin with normal overlying skin.
Gingival swellings extended from the left maxillary canine to the 3rd molar. However, the patient
had not experienced any symptoms. On radiographic examination an extensive radiolucent
lesion with sclerotic borders was revealed above the left maxillary canine and molar region.
Root resorption of involved teeth was observed with grade III mobility of the 2nd and 3rd molar
teeth for which patient was treated with extraction and Incision & Drainage was done for the
swelling as the swelling was believed to be a periodontal abscess. On cross-sectional view of
occlusal projection expansion of buccal and palatal cortical bone of the maxilla with partial
resorption of buccal cortical bone was observed. Skin over the swelling was normal in
appearance but stretched. Obliteration of the nasolabial fold was seen. Watery discharge was
seen from the left eye.
Provisional diagnosis was Peripheral Ossifying Fibroma, Fibrosarcoma, Osteosarcoma.
Incisional biopsy was performed under local anaesthesia with adrenaline (1:200000) and the
sample was sent to Department of oral pathology for histopathological examination.
Histopathological examination suggested the lesion to be Osteosarcoma (Chondroblastic
Variant).
Patient was admitted in our hospital and all the necessary blood investigations were
carried out along with ECG, ECHO, Chest X ray and C. T. Scan of the Head. After obtaining a
medical clearance, the patient was taken up for Tumour excision under general anesthesia.
Reconstruction of the orbital floor was done using prolene mesh which was suture using 3.0
vicryl. Intra orally suturing was done using 3.0 vicryl and skin suturing using 5.0 prolene. The
excised tumour was then sent for histopathological examination.
Furthermore, patient was advised for therapeutic radiotherapy.

CASE REPORT
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 260
HISTO PATHOLOGICAL ASSESSMENT: Sections show a cellular spindle cell tumour arranged
in intersecting fascicles and slight swirling striform and whorl-like pattern. The tumour cells are
spindly to lump to stellate shaped showing mild pleomorphism, with vesicular nucleus some
showing conspicuous nucleolus and ill-defined pale eosinophilic cytoplasm. Focal nuclear
hyperchromasia is also seen. The stroma is myxoid at places and contains many thin walled
dilated and congested blood vessels. Large ares of hemorrhage are also seen in the studied
sections. Mitosis is low. A sparse chronic inflammatory infiltrate is also seen. Tumor tissue is
seen infiltrating the surgical resected margin.
Histological features are suggestive of low grade malignant SPINDLE CELL SARCOMA.
Immunohistochemistry for further evaluation and confirmation of histopathological changes
(CD34, S- 100 CD 99, Desmin, Actin).
IMMUNOPHENOTYPING REPORT:
SMA : Positive in some of the tumour cells.
Desmin : Negative in tumour cells.
S-100 : Negative in tumour cells.
CD99 : Negative in tumour cells.
CD34 : Negative in tumour cells.
IMPRESSION: With above features, Myofibroblastic Sarcoma has to be considered.
DISCUSSION: Myofibroblasts are modified fibroblasts, which can occur in normal tissues (e.g.
periodontal ligaments), reparative granulation tissue and reactive soft-tissue lesions. The cause
of Myofibroma is presently unknown. A number of authors have suggested that the tumors are
inherited in an autosomal dominant or alternatively in an autosomal recessive trait. However,
its low familial incidence suggests that there are probably factors other than genetics that play
an important role in the cause of this disease7.They are, however, also a principal cell type in
benign and malignant soft-tissue tumours. Myofibroblasts are spindle-shaped or stellate cells
with ovoid pale nucleus and distinct nucleolus. The cytoplasm is usually amphophilic and there
are indistinct cell borders. Ultrastructurally, myofibroblasts can be distinguished from
fibroblasts and smooth muscle cells by the findings of indentation of nucleus, presence of
peripheral or subplasmalemmal bundles of thin cytoplasmic filaments, termed stress fibres, and
a distinctive cell-stromal attachment termed fibronexus4. Myofibroblastic Sarcoma is a well
defined malignant tumour composed of myofibroblasts. It can occur at any age with slight male
predominance; the tumour size varies from 1.5 cm to 17 cm. MYOFIBROBLASTIC SARCOMA can
arise in soft tissues of various anatomic sites, including extremities, trunk (e.g. retroperitoneum,
breast and heart) and genital tract, but there is a predilection for the head and neck region. Oral
cavity (especially tongue, cheek and gingiva), nasal cavity, salivary glands and bones (e.g.
maxilla and mandible) can be affected. Grossly, most cases were described as firm, gray-white
coloured tumours with ill-defined margins. Histologically, the tumour cells show diffuse
fascicular or storiform growth pattern and they infiltrate surrounding tissues (e.g. skeletal
muscle). The cytological and ultrastructural characteristics of neoplastic cells are consistent
with myofibroblasts (described above). Increased mitotic activity of tumour cells and tumour
necrosis is associated with more aggressive behaviour of MYOFIBROBLASTIC SARCOMA5.
Tumour cells in MYOFIBROBLASTIC SARCOMA show a variable immunophenotype: actin
positive/desmin negative, actin negative/desmin positive, and actin positive/desmin positive

CASE REPORT
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 261
cases. In addition, neoplastic cells can express fibronectin, calponin, CD 34, CD 99 and CD 117,
whereas S-100 protein, epithelial markers and h-caldesmon are negative. MYOFIBROBLASTIC
SARCOMA is usually a tumour of low grade malignancy, prone to local recurrence (about 30% in
general), even after many years5. However, metastases to lungs have been also reported.
Therefore, close clinical follow-up of the patient is mandatory. Differential diagnosis of
MYOFIBROBLASTIC SARCOMA includes reactive myofibroblastic lesions, benign
myofibroblastic lesions and other Myofibroblastic Sarcomas. In these cases,
immunohistochemistry is not helpful and the differential diagnosis is based on careful
examination of the slides stained with hematoxylin-eosin. On the other hand, many
histogenetically different spindle-cell tumours can be distinguished from MYOFIBROBLASTIC
SARCOMA using immunohistochemistry. Nodular fasciitis is a rapidly growing lesion,
histologically with variable cellularity and myxoid stroma. It is less cellular and uniform than
MYOFIBROBLASTIC SARCOMA. Although mitoses can be present, the cells lack nuclear atypia,
which is usually present in MYOFIBROBLASTIC SARCOMA. Fibromatoses are composed of
uniform, collagen-producing myofibroblasts without nuclear pleomorphism. Inflammatory
myofibroblastic tumour (IMT) is histologically characterized by fasciitis-like, fascicular and
sclerosing areas with a prominent chronic inflammatory infiltrate with numerous plasma cells.
In addition, anaplastic lymphoma kinase (ALK) can be immunohistochemically detected in 30–
40% of Inflammatory myofibroblastic tumours6. The inflammatory infiltration in the presented
case of MYOFIBROBLASTIC SARCOMA was, however, due to tumour ulceration. High grade
Myofibroblastic Sarcoma is often difficult to distinguish from other high grade sarcomas. This
diagnosis should be established in those cases, where the presence of myofibroblasts is
confirmed by electronmicroscopy. Histogenetically different spindle-cell tumours can be
distinguished from MYOFIBROBLASTIC SARCOMA using immuno-histochemistry. Spindle-cell
carcinoma shows positivity for cytokeratins, fibrosarcoma is SMA negative, leiomyosarcoma has
a different microscopic appearance and shows desmin and h-caldesmon positivity. Spindle-cell
rhabdomyosarcoma shows SCMA positivity, angiosarcoma shows positivity for endothelial
markers (e.g. F VIII, CD 31 and CD 34) and malignant peripheral nerve sheath tumour shows at
least focal positivity for S-100 protein. In summary, MYOFIBROBLASTIC SARCOMA is a well-
defined myofibroblastic malignancy with predilection for head and neck region, which is prone
to local recurrency, rather than metastasing. For the diagnosis, a careful examination of
routinely stained slides is crucial. Immunohistochemistry can be useful in differential diagnosis
from some other spindle cell lesions and tumours. Electronmicroscopic examination can
support the diagnosis of MYOFIBROBLASTIC SARCOMA by proving the origin of tumour cells.
LEGENGS:
1. Frontal pre -operative photograph.
2. Birds eye view pre – operative photograph.
3. Intra oral lesion pre – operative photograph.
4. Intra operative photograph after excision of the lesion.
5. Excised lesion in toto.
6. Frontal view Post operative photograph.
7. Birds eye view Post operative photograph.
8. Histopathology Photograph.
9. C. T. Scan Pre opertive sub mento vertex view.
10. Occlual Radiograph

CASE REPORT
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 262

CASE REPORT
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sept 2012 Page 263
ACKNOWLEDGEMENTS:
Our sincere gratitude to Dr. Vinay Kumar Hegde, General Practitioner, Moodbidri, Dr. Aravind,
Consultant Pathologist, A. J. Hospital & Research Hospital, Mangalore and Department of Oral
Pathology, A. J. Institute of Dental Sciences, Mangalore.
REFERENCES:
1. Chiu-Kwan Poon and Po-Cheung Kwan. Myofibroma of the Mandible: A Case Report.
Chin J Oral Maxillofac Surg 16: 156-165, September 2005.
2. Hideki Mizutani, Iwai Tohnai, Makoto Yambe and Minoru Veda. LEIOMYOSARCOMA OF
THE MAXILLARY GINGIVA: A CASE REPORT. Nagoya J. Med. Sci. 165 - 170, 1995.
3. Nada O. Binmadi, Harold Packman, John C. Papadimitriou and Mark Scheper Oral
Inflammatory Myofibroblastic Tumor: Case Report and Review of Literature. The Open
Dentistry Journal, 2011, 5, 66-70.
4. Eyden, B. P.: The fibronexus in reactive and tumoral myofibroblasts: further
characterisation by electron microscopy. Histol. Histopathol., 16, 2001, s. 57–70.
5. Mentzel, T., Dry, S., Katenkamp, D., Fletcher, C. D.: Low-grade myofibroblastic sarcoma:
analysis of 18 cases in the spectrum of myofibroblastic 1tumors. Am. J. Surg. Pathol., 22,
1998, s. 1228–1238.
6. Li, X. Q., Hisaoka, M., Shi, D. R., Zhu, X. Z., Hashimoto, H.: Expression of anaplastic
lymphoma kinase in soft tissue tumors: an immunohistochemical and molecular study of
249 cases. Hum.1 Pathol., 35, 2004, s. 711–721.
7. Jin-Soo Kim, Sung-Eun Kim, Jae-Duk Kim. Myofibroma of the mandible: A case report.
Korean Journal of Oral and Maxillofacial Radiology 2006; 36 : 211-5.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sep 2012 Page 264
INDIRECT BONDING WITH NEW TRANSFER TRAY - LIGHT TRAY
Dr. R. Satish, Dr. T. Srinivasan, Dr. R. Suresh, Dr. Sujith sivarajan
1. Associate Professor, Department of Orthodontics, Adhiparasakthi Dental College and Hospital.
Melmaruvathur, Tamil Nadu.
2. Reader, Department of Orthodontics, Adhiparasakthi Dental College and Hospital. Melmaruvathur, Tamil
Nadu.
3. Senior lecturer, Department of Orthodontics, Adhiparasakthi Dental College and Hospital. Melmaruvathur,
Tamil Nadu.
4. Senior lecturer, Department of Orthodontics, Adhiparasakthi Dental College and Hospital. Melmaruvathur,
Tamil Nadu.
CORRESPONDING AUTHOR
Dr. R. Satish,
Adhiparasakthi Dental College and Hospital,
Melmaruvathur, Kanchipuram District,
Tamilnadu, India-603319,
E-mail: [email protected], Ph: 91 09444183900
ABSTRACT: BACKGROUND: Indirect bonding is a technique in which orthodontic brackets are
transferred from dental casts onto the dentition using a transfer tray. The aim of this paper is to
describe a simple and efficient procedure of indirect bonding. The transfer tray used here is
Light tray (Ivoclar), light polymerised resin composite special tray material, which is used to
fabricate customized trays for fixed and removable implant-restorations. This light tray has
many advantages when compared with similar trays for indirect bonding.
KEYWORDS: Indirect bonding, light tray
INTRODUCTION: Traditional bracket placement involves hand placing each bracket directly in
the mouth. Accurate direct bracket placement is very difficult for even the most experienced
orthodontist. Indirect bonding has been an exciting advancement in orthodontics. It has great
benefit to the patient as it improves patient comfort, reduces the amount of time in the dental
chair, improves the accuracy of bracket placement, and reduces treatment time. Indirect
Bonding of brackets using light-curing transfer trays,(Fig.1), has several advantages like easy
mouldable, fast and easy working, accurate adaptation, stability of shape immediately after
polymerization and excellent elastic memory. Light trays can be cured by Light curing unit for 3
minutes or exposing to direct day light for 5 minutes.
Fig .1 Light Tray.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sep 2012 Page 265
LABORATARY PROCEDURE: The indirect bonding technique starts by taking impressions of
the patient teeth. The impressions are used to make a stone model of the teeth, (Fig.2). The
brackets are secured to the stone model with water soluble glue (fevi stick,Fig.3). Use wax to
block and prevent adapting light tray in to the bracket wings and slots. Adapt the Light tray over
the brackets mounted on the patient cast from labial to lingual surface. Trim the excess tray
material with a wax knife, (Fig.4). Light cure the tray for 4 minutes, (Fig.5). Soak the working
model with the custom transfer tray in warm water for a minimum of one hour to dissolve
water soluble glue from the bracket base and release the custom tray from the model.
Fig.2. Model with markings of Bracket Position.
Fig.3 The brackets are fixed with water soluble glue.
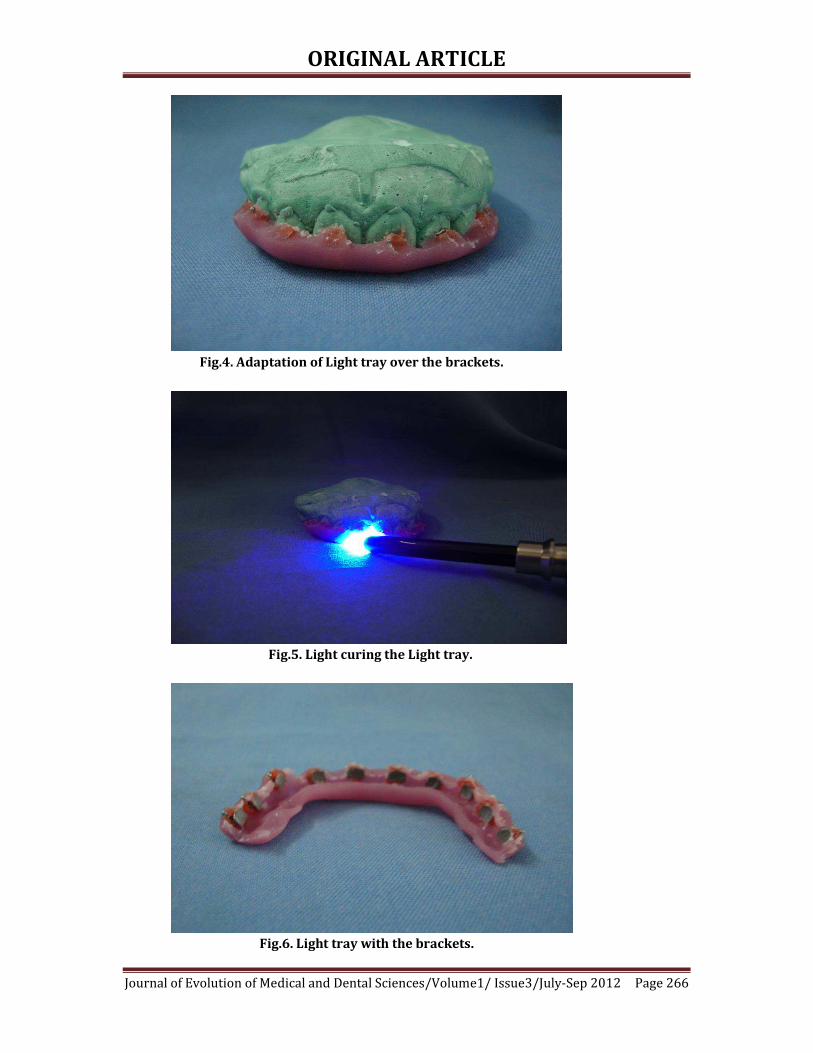
ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sep 2012 Page 266
Fig.4. Adaptation of Light tray over the brackets.
Fig.5. Light curing the Light tray.
Fig.6. Light tray with the brackets.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sep 2012 Page 267
CLINICAL APPLICATION: Apply bonding agent and light cure adhesive on the brackets in
transfer tray. Etch the teeth and apply the bonding agent. Keep a dry field. Place the tray in the
mouth and the adhesive part of the tray pressed on to the teeth with fingers. Light cure the
adhesive for 20 seconds for each bracket, (Fig.7). Remove the tray and cure all the brackets for
10 seconds. Remove any excess adhesive from the teeth surface, (Fig.8).
Fig .7. Light tray with brackets on the teeth
Fig .8. After the removal of the light tray
CONCLUSION: Indirect bonding offers many advantages combined with safety, especially the
exact positioning of brackets. One of the main problems, however, is their transfer to the mouth
with precision and sufficient adhesion. Currently, there are various transfer trays for indirect
bonding available—opaque, translucent silicone-based polymer, and thermoplastic transfer
devices. The technique described in this article serves to simplify tray fabrication. This is
accomplished by using Light tray. The Light tray is easier to adapt, stability of shape
immediately after polymerization, excellent elastic memory, easy to trim, less bulky, easy to
transfer than other types, extremely cheap and cost effective. Light tray- transfer trays offer an
accurate bracket positioning and hence it could be treated as one of the preferable methods of
bracket placement.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sep 2012 Page 268
REFERENCES:
1. Gottlieb, E.L.; Nelson, A.H.; and Vogels, D.S.III: 1996 JCO Study of Orthodontic
Diagnosis and Treatment Procedures, Part I: Results and trends. J. Clin. Orthod.
30:615-630, 1996.
2. White, L.W.: An expedited indirect bonding technique. J. Clin. Orthod. 35: 36-41,
January 2001.
3. Bishara, S.E.; Gordan, V.V.; VonWald, L; Olson, M.E.: Effect of an acidic primer on
shear bond strength of orthodontic brackets, Am. J. Orthod. and Dentofacial
Orthop. 114: 243-247, September 1998.
4. Miles PG: Indirect bonding with a flowable light-cured adhesive. J Clin Orthod
36:646, 2002
5. Sondhi A. Effective and efficient indirect bonding: The Sondhi
6. method. Semin Orthod ;13:43-57 2007

BRIEF COMMUNICATION
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sep 2012 Page 269
MODIFIED PERIODONTAL EXPLORER FOR EXPANSION SCREW
ACTIVATION
Dr. T. Srinivasan, Dr. R. Satish, Dr. R. Suresh, Dr. Sujith Sivarajan
1. Reader, Department of Orthodontics, Adhiparasakthi Dental College and Hospital. Melmaruvathur, Tamil
Nadu.
2. Associate Professor, Department of Orthodontics, Adhiparasakthi Dental College and Hospital.
Melmaruvathur, Tamil Nadu.
3. Senior lecturer, Department of Orthodontics, Adhiparasakthi Dental College and Hospital. Melmaruvathur,
Tamil Nadu.
4. Senior lecturer, Department of Orthodontics, Adhiparasakthi Dental College and Hospital. Melmaruvathur,
Tamil Nadu.
CORRESPONDING AUTHOR
Dr. T. Srinivasan,
Adhiparasakthi Dental College and Hospital,
Melmaruvathur, Kanchipuram District,
Tamilnadu, India-603319,
E-mail: [email protected], Ph: 91 09841611886.
INTRODUCTION: Accidents with expansion screw activation keys are reported in the
literature1,2. A simple method to prevent such accident is to use a modified periodontal explorer
as a key for expansion screw activation. A no.17 periodontal explorer (fig 1) is cut at its first
terminal bend (fig 2). The second section is bent more vertically to the long axis of the shaft (fig
3). This part which is tapered and stiff enough to activate the screw is tried extra orally into the
screw. It is further trimmed in such a way that only a mm of instrument can project through the
screw hole (fig 4). Now a safe key for activating the maxillary expansion screw is ready to use
(fig 5). Once the patient’s parent or guardian successfully repeat the activation procedure in
office, the instrument can be given to them for home use.

BRIEF COMMUNICATION
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sep 2012 Page 270
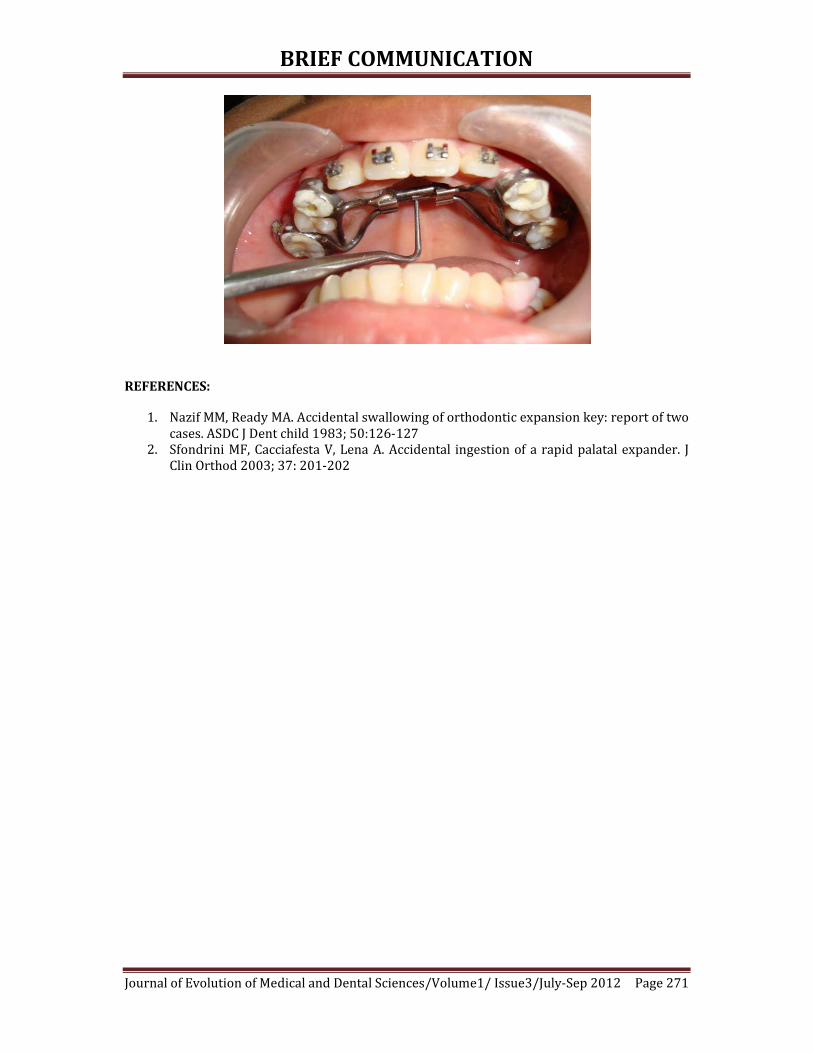
BRIEF COMMUNICATION
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sep 2012 Page 271
REFERENCES:
1. Nazif MM, Ready MA. Accidental swallowing of orthodontic expansion key: report of two
cases. ASDC J Dent child 1983; 50:126-127
2. Sfondrini MF, Cacciafesta V, Lena A. Accidental ingestion of a rapid palatal expander. J
Clin Orthod 2003; 37: 201-202

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sep 2012 Page 272
INCIDENTAL RADIOGRAPHIC FINDINGS AND THEIR RESTORATIVE
IMPLICATIONS R. Sridevi, Sai Laxman Bharadwaj B, R. Thirumalai Prabhu
1. Senior lecturer, Department of Prosthodontics, Adhiparasakthi Dental College and Hospital. Melmaruvathur,
Tamil Nadu.
2. Intern, Department of Orthodontics, Adhiparasakthi Dental College and Hospital. Melmaruvathur, Tamil
Nadu.
3. Intern, Department of Orthodontics, Adhiparasakthi Dental College and Hospital. Melmaruvathur, Tamil
Nadu.
CORRESPONDING AUTHOR
Dr. R. Sridevi,
A-11, Laxmi Apartments,
Meenambal ST, Melmaruvathur, ,
Tamilnadu, India,
E-mail: [email protected], Ph: 91 09952363999.
ABSTRACT: Radiographs are an irreplaceable diagnostic tool, especially in dealing with
dentofacial hard tissues. Guidelines like the ALARA require professionals to limit the number of
radiographs prescribed to patient, thereby minimizing radiation dose. On the other hand, for
prosthetic evaluation, a latest radiograph has the potential to uncover new findings that can
alter the treatment planning sequence or affect the outcome of the planned treatment. This
review article discusses ten such radiographs. The significant findings in each radiograph have
been highlighted and treatment protocols tailored to the same. The aim of this article is to help
the reader adopt a meticulous approach and a keen eye for detecting problems, and emphasizes
the efficacy of radiographs in patient evaluation for restorative care.
KEYWORDS: Incidental, Findings, Treatment, Interpretation
INTRODUCTION: Dental clinics here in our country are teeming with patients keeping dental
personnel on a tight schedule. Efficient practice in this scenario demands a good balance
between speed, time management and prescribing what is needed and best for the patient.
Frequently patients present for prosthetic rehabilitation with radiographs taken during
previous treatment sittings and we often avoid prescribing a new one. Considering the
possibility of incidental findings, it is wise practice to prescribe a new radiograph during
abutment evaluation. This additional measure avoids unnecessary failures and the need for
prosthetic retreatment like the removal and re-fabrication of fixed bridges which can cause
considerable damage to both tooth structure and the patients’ wallet.
All the radiographs reviewed here, presented to the Prosthodontic clinic in our
institution for rehabilitation. A thorough perusal of this article will tell us how, and bring to
light a multitude of possibilities and occurrences during diagnostic radiography; for what the
mind does not know, the eyes do not see!

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue
Radiograph 1 – RESIDUAL ROOT FRAGMENT
Fracture of a root during exodontia, particularly long,divergent ones is a common
complication 1. The edentulous area in this radiograph reveals the presence of a root fragment
following extraction of the maxillary left second premolar. This incidental finding is familiar
even with novice dental practitioners and cannot be missed. The fragment in thi
more than 5mm in length.
Current guidelines suggest that a root fragment of up to 5mm can be left in situ in a
healthy patient provided there is no evidence of apical pathology
Radiograph 2 – ADJACENT TOOTH PATHOLOGY
In endodontic practice, pulp sensibility testing of the tooth in question is corroborated
with the response of control teeth which are usually adjacent teeth. These tests are indirect and
subject to false positive and false negative readings
interpretation of radiographic findings are an invaluable adjunct to pulp sensibility testing.
In the above radiograph, exposed to evaluate 26 for crown placement, a periapical lesion was
identified in relation to 25. Clinical exami
Class I composite filling, tenderness to percussion and poor response to electric pulp testing
when compared to the contra lateral 15. Endodontic treatment of 25 prior to restoration of 26
was considered prudent to avoid patient discomfort and minimize the number of prosthetic
visits.
ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sep 2012
RESIDUAL ROOT FRAGMENT
Fig 1
Fracture of a root during exodontia, particularly long,divergent ones is a common
. The edentulous area in this radiograph reveals the presence of a root fragment
following extraction of the maxillary left second premolar. This incidental finding is familiar
even with novice dental practitioners and cannot be missed. The fragment in this radiograph is
Current guidelines suggest that a root fragment of up to 5mm can be left in situ in a
healthy patient provided there is no evidence of apical pathology2.
ADJACENT TOOTH PATHOLOGY
Fig 2
endodontic practice, pulp sensibility testing of the tooth in question is corroborated
with the response of control teeth which are usually adjacent teeth. These tests are indirect and
subject to false positive and false negative readings3. In such cases, careful evaluation and
interpretation of radiographic findings are an invaluable adjunct to pulp sensibility testing.
In the above radiograph, exposed to evaluate 26 for crown placement, a periapical lesion was
identified in relation to 25. Clinical examination was positive for the presence of an occlusal
Class I composite filling, tenderness to percussion and poor response to electric pulp testing
when compared to the contra lateral 15. Endodontic treatment of 25 prior to restoration of 26
prudent to avoid patient discomfort and minimize the number of prosthetic
2012 Page 273
Fracture of a root during exodontia, particularly long,divergent ones is a common
. The edentulous area in this radiograph reveals the presence of a root fragment
following extraction of the maxillary left second premolar. This incidental finding is familiar
s radiograph is
Current guidelines suggest that a root fragment of up to 5mm can be left in situ in a
endodontic practice, pulp sensibility testing of the tooth in question is corroborated
with the response of control teeth which are usually adjacent teeth. These tests are indirect and
careful evaluation and
interpretation of radiographic findings are an invaluable adjunct to pulp sensibility testing.
In the above radiograph, exposed to evaluate 26 for crown placement, a periapical lesion was
nation was positive for the presence of an occlusal
Class I composite filling, tenderness to percussion and poor response to electric pulp testing
when compared to the contra lateral 15. Endodontic treatment of 25 prior to restoration of 26
prudent to avoid patient discomfort and minimize the number of prosthetic

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue
Radiograph 3 – MISSED ROOTS
The root canal treated tooth approximating the maxillary right first molar in this
radiograph shows clear evidence of two
The case notes for the patient under reference reveal that this tooth was designated as
15. However, obtaining the past dental history elicits extraction of the upper second premolars
for orthodontic purposes. A maxillary firs
palatal roots, whereas a maxillary second premolar has a single root with a single canal
effect the tooth in question was a first premolar and was scheduled for orthograde retreatment.
This radiograph is significant for two other findings
1. The orientation dot has been positioned mesio
2. The restorative margin in the first premolar is at the level of the interdental bone
distally due to tipping. Adjunctive periodontal therapy is imminent to ensure healthy
placement of crown margins for long
Radiograph 4 – CORONAL SEAL
1
2
ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sep 2012
Fig 3
The root canal treated tooth approximating the maxillary right first molar in this
radiograph shows clear evidence of two root outlines (white arrows)
The case notes for the patient under reference reveal that this tooth was designated as
15. However, obtaining the past dental history elicits extraction of the upper second premolars
for orthodontic purposes. A maxillary first premolar has two canals one each in buccal and
palatal roots, whereas a maxillary second premolar has a single root with a single canal
effect the tooth in question was a first premolar and was scheduled for orthograde retreatment.
h is significant for two other findings
The orientation dot has been positioned mesio-apical instead of mesio-occlusal
The restorative margin in the first premolar is at the level of the interdental bone
distally due to tipping. Adjunctive periodontal therapy is imminent to ensure healthy
placement of crown margins for long-term success.
CORONAL SEAL
Fig 4
2012 Page 274
The root canal treated tooth approximating the maxillary right first molar in this
The case notes for the patient under reference reveal that this tooth was designated as
15. However, obtaining the past dental history elicits extraction of the upper second premolars
t premolar has two canals one each in buccal and
palatal roots, whereas a maxillary second premolar has a single root with a single canal 4. In
effect the tooth in question was a first premolar and was scheduled for orthograde retreatment.
occlusal
The restorative margin in the first premolar is at the level of the interdental bone
distally due to tipping. Adjunctive periodontal therapy is imminent to ensure healthy

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue
Hermetic apical seal for eras has been considered the gold standard for endodontic
success. Contemporary concepts stress that both the coronal and apical seal play an equal role
in determining the same. Coronal seal refers to the protection rendered
restoration (direct or indirect). If the coronal seal is not intact, leakage through the dentinal
tubules can establish reinfection within three months in the canal system leading to failure
The temporary restoration shown in the r
portion adequately. Though marginal discrepancies can be detected clinically on facial and
lingual aspects, the presence and extent of such defects in the approximal regions are detected
with relative ease and precision on radiographs during follow
in this radiograph is a victim of proximal (distal) under preparation and an over contoured
crown (arrow).The necessary adjustments have to done and the crown has to be replaced at
earliest.
Radiograph 5 – ROOT FRACTURE
This is a pretreatment radiograph for a maxillary anterior diastema closure.
Transverse root fractures can occur in the coronal, middle and apical third. Apical third
fractures are usually asymptomatic,
approach for treatment6.
Apical root fractures are by and large detected on radiographs as depicted here in tooth 22.
Prosthetic treatment planning for such teeth involves
1. Eliciting the history of trauma
2. Thorough sensibility testing for all the teeth in the segment
3. Adjuvant endodontic therapy where mandatory
4. In case these teeth are to be used as fixed partial denture abutments, it should be borne
in mind that there is an effective reduction in pericemental area available for support,
especially in a weak abutment like the lateral incisor.
ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sep 2012
Hermetic apical seal for eras has been considered the gold standard for endodontic
success. Contemporary concepts stress that both the coronal and apical seal play an equal role
in determining the same. Coronal seal refers to the protection rendered by a post endodontic
restoration (direct or indirect). If the coronal seal is not intact, leakage through the dentinal
tubules can establish reinfection within three months in the canal system leading to failure
The temporary restoration shown in the radiograph does not seal and cover the coronal
portion adequately. Though marginal discrepancies can be detected clinically on facial and
lingual aspects, the presence and extent of such defects in the approximal regions are detected
precision on radiographs during follow-up visits. Also, the restored tooth
in this radiograph is a victim of proximal (distal) under preparation and an over contoured
crown (arrow).The necessary adjustments have to done and the crown has to be replaced at
ROOT FRACTURE
Fig 5
This is a pretreatment radiograph for a maxillary anterior diastema closure.
Transverse root fractures can occur in the coronal, middle and apical third. Apical third
fractures are usually asymptomatic, exhibit no mobility and advocate a wait and watch
Apical root fractures are by and large detected on radiographs as depicted here in tooth 22.
Prosthetic treatment planning for such teeth involves
Eliciting the history of trauma
Thorough sensibility testing for all the teeth in the segment
Adjuvant endodontic therapy where mandatory
In case these teeth are to be used as fixed partial denture abutments, it should be borne
effective reduction in pericemental area available for support,
especially in a weak abutment like the lateral incisor.
2012 Page 275
Hermetic apical seal for eras has been considered the gold standard for endodontic
success. Contemporary concepts stress that both the coronal and apical seal play an equal role
by a post endodontic
restoration (direct or indirect). If the coronal seal is not intact, leakage through the dentinal
tubules can establish reinfection within three months in the canal system leading to failure 5.
adiograph does not seal and cover the coronal
portion adequately. Though marginal discrepancies can be detected clinically on facial and
lingual aspects, the presence and extent of such defects in the approximal regions are detected
up visits. Also, the restored tooth
in this radiograph is a victim of proximal (distal) under preparation and an over contoured
crown (arrow).The necessary adjustments have to done and the crown has to be replaced at the
This is a pretreatment radiograph for a maxillary anterior diastema closure.
Transverse root fractures can occur in the coronal, middle and apical third. Apical third
exhibit no mobility and advocate a wait and watch
Apical root fractures are by and large detected on radiographs as depicted here in tooth 22.
In case these teeth are to be used as fixed partial denture abutments, it should be borne
effective reduction in pericemental area available for support,

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sep 2012 Page 276
Radiograph 6 – CYSTIC LESIONS
Fig 6
Fig 7
Cystic lesions in the jaws are generally incidental findings on radiographs. The extent
and the nature of the lesion determine the prognosis. Henceforth, it is wise to subject these
lesions to histopathological examination before harping on a treatment plan for the patient.
The periapical radiograph and the ortho-pantomograph are those of two different
patients. The anterior maxillary lesion in the periapical (Fig 6) revealed a residual cyst. The
right mandibular posterior lesion in the panoramic view (Fig 7) turned out to be an odontogenic
keratocyst.
Significance – Residual cyst can expand and interfere with the fit of a prosthesis7, and
the presence of this multilocular odontogenic keratocyst presents an absolute contraindication
to implant placement or immediate replacement with fixed bridges owing to their aggressive
behavior and high recurrence rate 8. The residual cyst has to be thoroughly enucleated and
following the period of healing definitive prosthesis can be fabricated. As far as the Gorlins cyst
goes, it demands radical treatment and an extended follow up period to ensure complete
regression of the lesion before any form of definitive rehabilitation is planned.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sep 2012 Page 277
Radiograph 7 – FURCATION INVOLVEMENT
Fig 8
The pulp and the periodontium have an embryologic, anatomic and functional
interrelationship. When the two are involved in disease simultaneously it is known as an endo-
perio lesion which classically can be demonstrated by furcation involvement of an
endodontically compromised or previously root treated tooth.
The radiograph depicts a Class III furcation involvement in 36 and has the potential to be
treated by surgical periodontal therapy9, but a close examination of the radiograph reveals
1) Poor quality endodontic therapy
2) Apical overextension of gutta percha in mesial root
3) Grossly destroyed coronal tooth structure
4) Class I restorations in the adjacent teeth
Taking into account all the above factors, the consensus was to extract the tooth and replace
with a fixed partial denture with support from 35 and 37.
Radiograph 8 – POST LENGTH
Fig 9
Anterior teeth are strategically located and designed to withstand the lateral forces. Post
endodontic restoration of extensively damaged crowns warrants the use of a post for retention
of the core.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sep 2012 Page 278
In selecting posts for anterior teeth, it is vital that the post should be long enough to satisfy
clinical requirements without jeopardizing the root integrity10. The standard parameters are11,
1) The post should be 2/3rd the length of the root
2) The length of the post can also equal the coronal length of the tooth
3) The post should extend into one half the length of the root embedded in its supporting
bone.
In this patient the core in 22 is supported by a screwed post that does not extend to the
adequate depth. The bone levels are well below normal and the post stops at the level of
alveolar support. Short, stiff posts transfer forces to the unsupported root extending above the
alveolus and can cause root fracture11. It was decided to use only the central incisor 21 as a
terminal abutment to restore the edentulous area and follow up on the prognosis of the lateral
incisor.
Radiograph 9 – ANKYLOSED TOOTH
Fig 10
The patient presented for single unit restoration of root canal treated 26.
Accidental finding includes ankylosed maxillary left second premolar as evident in the absence
of a distinct periodontal ligament space, definitive pulp canals and chamber and infraoccluded
position.
Ankylosis is a pathologic fusion of the cementum or dentin of a tooth root to the alveolar
bone12. Adults, with their slower rate of replacement resorption may retain an ankylosed tooth
for many years with minimal treatment or minor cosmetic modifications13. At present, there are
no guidelines in the dental literature for the treatment of ankylosis14. The parameters that
influence treatment in this case include
1) Adult presentation and diagnosis of ankylosis
2) Mild infraocclusion
3) Considerable rotation and misplaced proximal contacts which necessitates pulp therapy
before preparation for full coverage restorations.
4) An adjacent root treated molar
Therefore, it was decided to restore the molar with a full metal coverage crown combined with a
minimal preparation onlay restoration on 25 to restore function.
CONCLUSION: A patient’s radiograph is an indicator of both past and current disease
experience. Dental professionals should aim at absorbing as much information as possible from

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sep 2012 Page 279
a given radiograph, for, this information may possess the power to reroute our original
treatment plan in lieu of the patient’s best interests.
An incidental finding is one that accompanies and does not constitute the major reason
for exposing the radiograph. Majority of these findings can be attributed to iatrogenic causes
except for pathologies like cysts and fractures. Timely identification of these errors can best
avoid irreversible damage to the dentition.
REFERENCES :
1. Peterson. Ellis. Hupp. Tucker: Ch 11 Prevention and management of surgical
complication in Contemporary oral and maxillofacial surgery, 4 ed, Pg 221-237
2. Abhay N Dhatarkar: Ch 13 in Exodontia Practice 1ed, Pg 129 – 134
3. V Gopikrishna et al; Assessment of pulp vitality – A review. International Journal of
Pediatric Dentistry 2009, Vol 19: 3-15.
4. T.R Pitt Ford, Ch 3 in Endodontics- Problem Solving In Clinical Practice, Pg 33-35
5. B A Begotka et al, The importance of coronal seal following root canal treatment.
Virginia Association Dental Journal, 1996, Oct-Dec, 73(4); 8-10
6. J.O Andreasen and F.M Andresen: Ch 12 Root fractures in Text Book and Color Atlas of
Traumatic Injuries to the teeth 4ed, pg 337-371
7. Cawson and Odell: Cysts of the jaws in Essentials of Oral Pathology and Medicine 7ed,
Pg 102-128
8. Nakamura et al: Marsupilization of Odontogenic Keratocysts – Long term follow up
analysis of the effect and changes in growth characteristics, Oral Surgery Oral Medicine
Oral Pathology Radiology Endodontology, 2002 Vol 94: 543-553.
9. Murray Arlin, Oral Health 1987 Vol 77(5): 29-34
What this article tells us?
To always consider the possibility of spotting pathologies on
routine radiography
Why is it important?
The preservation of that which remains is of utmost importance
than the meticulous replacement of that which has been lost.
How can we identify them?
A thorough knowledge combined with adequate experience
Where to learn these skills from?
Practice is the key.
It is the onus of every practitioner to keep himself up-to-date on
changing trends in treatment planning and diagnosis and apply
them on a daily basis.

ORIGINAL ARTICLE
Journal of Evolution of Medical and Dental Sciences/Volume1/ Issue3/July-Sep 2012 Page 280
10. Goodacre CJ et al: The Prosthodontic Management of Endodontically treated teeth – A
literature review II – Maintaining the apical seal, Journal of Prosthetic Dentistry 4:51,
1995
11. Stephen Cohen, Ch 21 Restoration of Endodontically treated teeth in Pathways of the
Pulp, Pg 786 – 821
12. William Biederman et al, Etiology and treatment of tooth ankylosis, American Journal of
Orthodontics, Vol 48(9): 670–684
13. Ebeleseder KA, Friehs S, et al, A study of replanted permanent teeth in different age
groups. Endod Dent Traumatol 14(6):274-8, 1998
14. Moffat MA et al , Intentional surgical repositioning of ankylosed permanent maxillary
incisor Dental Traumatology 2002; 18: 222–226
Copyright © 2022 FDOKUMEN