USE OF DIAZEPAM, CHLORPROMAZINE AND ALIMEMAZINE IN BEHAVIOR MANAGEMENT OF HYSTERICAL AND ANXOIUS...
22
USE OF DIAZEPAM, CHLORPROMAZINE AND ALIMEMAZINE IN BEHAVIOR MANAGEMENT OF HYSTERICAL AND ANXOIUS PEDIATRIC PATIENTS. Valdemoro, C (*)., Rojo-Moreno,J (**)., Catala, M(***). Zaragoza, A(****) School of Medicine and Dentistry. Valencia. Spain (*) Pediatric Dentist, Psychiatrist, Associate Professor of Operative Dentistry. (**) Professor of Psychiatry and Professor in charge of Psychology for Dentists. (***) Professor of Pediatric Dentistry. (****)Associate Professor of Pediatric Dentistry. Address: e-mail: [email protected] ; [email protected] ABSTRACT 1
Transcript of USE OF DIAZEPAM, CHLORPROMAZINE AND ALIMEMAZINE IN BEHAVIOR MANAGEMENT OF HYSTERICAL AND ANXOIUS...

USE OF DIAZEPAM, CHLORPROMAZINE AND ALIMEMAZINE IN
BEHAVIOR MANAGEMENT OF HYSTERICAL AND ANXOIUS PEDIATRIC
PATIENTS.
Valdemoro, C (*)., Rojo-Moreno,J (**)., Catala, M(***).Zaragoza, A(****)
School of Medicine and Dentistry. Valencia. Spain
(*) Pediatric Dentist, Psychiatrist, Associate Professorof Operative Dentistry.(**) Professor of Psychiatry and Professor in charge ofPsychology for Dentists.(***) Professor of Pediatric Dentistry.(****)Associate Professor of Pediatric Dentistry.
Address: e-mail: [email protected] ; [email protected]
ABSTRACT
1

To know the response of psychopharmacological drugs in the
behavior management of pediatric dental patients, a sample of 41
children is used and a questionnaire of 20 variables is applied.
The sample is previously divided into two groups: “Anxious Group”
(AG) and “Hysterical Group” (HG). The AG is treated with Diazepam,
while the HG is treated with Alimemazine (children ten years old
or less) or Chlorpromazine (children over ten). The positive
response obtained with these psychopharmacological drugs stands
out in the management of behavior. The seven behaviors which,
basically, characterize the HG are: 1.- “Refusing to Open Mouth”,
2.- “Taking hand to mouth when about to be intervened”, 4.-
“Screaming”, 5.- “Making violent gestures to move the dentist’s
hand away”, 6.- “Kicking”, 7.- “Sitting on the dentist’s chair
with problems”. The discriminating analysis confirms that with
these seven behaviors both groups are clearly distinguishable on
the first visit. Premedicated children with hysterical behavior
respond worse to Anesthesia, Aperture, and to the Rubber Dam than
premedicated children with anxious behavior.
KEY WORDS: BEHAVIOR MANAGEMENT. CHILDREN. PEDIATRIC DENTISTRY.
QUESTIONNAIRES. PSYCHOACTIVE DRUGS. DIAZEPAM. CHLORPROMAZINE.
ALIMEMAZINE.
2

INTRODUCTION.
The purpose of our research has had two aims: firstly , to
evaluate the use of psychopharmacological drugs in controlling the
behavior of children attending a pediatric dental clinic, and to
compare the results depending on the drug used. Secondly, to
determine if using a behavior scale can help us differentiate
between anxious and hysterical behavior.
The first step was to look at the clinical diagnosis to
differentiate between two clinical syndromes:
1.- Symptoms of anxiety, which will, consequently, manifest in
anxious behaviors. 2.- Hysterical symptoms (also called
“Functional”), which result, consequently, in Hysterical
behaviors. The first group (Anxious) includes manifestations such
as “being tense”, “crying”, “hyperventilation”, etc. The second
group (Hysterical) includes behaviors which were already
designated by Krestchmer1 as “Hypobulic”, meaning, children that:
“show uncontrolled excitement”, “have a fleeting reaction”, “hold
on desperately to mother” or “squirm in the dentist’s chair” .
These Hysterical conducts often give rise to disorderly behaviors
such as fleeting (hysterical fleeting), as well as crouching down
on the floor or in a corner. Hypobulic behaviors can be modified
on certain occasions with in situ resources such as “voices of
command” or the hand-over-mouth technique. The next step was to
evaluate the change in behavior at the dental clinic, after
administering the psychopharmacological drugs, and to ascertain
which are the behaviors that characterize the anxious and
hysterical groups respectively. For this purpose the following
Material and Method were used.
3

MATERIAL AND METHOD.
Our sample was made up of 41 children that required dental
treatment. After the first visit we decided that it would be
beneficial to administer psychopharmacological drugs to control
the child’s behavior in the spirit of Ryder2 and Musselman’s3
recommendations.
Two judges, both of them pediatric dentists determined the use of
psychopharmacological drugs according to the clinical
characteristics of the patients (either anxious or hysterical). In
the first visit, the “group” diagnosis was made.
Children presenting, at least, the following three behaviors were
considered, a priori, to be Anxious: 1- Being tense, 2- Having
legs up or muscles contracted, 3- Crying.
Children that present at least two of the following behaviors are
considered, a priori, to be Hysterical: 1- Refusing to sit on the
dentist’s chair, 2- Kicking, 3- Violently moving the doctor’s hand
away, 4- Taking hand to mouth.
The diagnosis of the Anxious or Hysterical child was carried out
by two judges at the same time. One acted as the main judge and
the other acted as assistant judge but did not intervene directly
with the child. The assistant judge carried out the diagnosis
according to what had been observed. Only when both diagnoses
matched , leaving no room for doubt, was the child included in
the study. If there were any discrepancies whatsoever, the child
was rejected.
We have based ourselves on a series of operative characteristics
when making our “diagnosis” since we have sought to establish
two clearly differentiated groups: one where the behaviors were
4

predominantly of the anxious type, and the other group where at
least two behaviors were clearly of the hysterical type.
In all of these cases the Behavior Questionnaire (shown in detail
in Table 1) was performed on their first visit to the clinic. It
was a questionnaire designed by us, in which the selection of the
different variables (or items) was carried out based on our
experience in the field of pediatric dentistry, and according to
the “Rational Selection” method ( worked out among experts acting
as judges). This required joint work between three professional
pediatric dentists (one of which is also a psychiatrist), a
psychiatrist and a psychologist. In this questionnaire, 12
behaviors are evaluated: “Being frightened by the instruments”,
“sitting on the dentist’s chair with problems”, “opening mouth”,
“taking hand to mouth”, “moving head away”, “speaking and
conversing with the pediatric dentist”, “screaming”, “crying”,
“moving the dentist’s hand away”, “kicking”, “having legs up”,
“being tense”.
As indicated on Table 1, this questionnaire is graded from 0 to 2,
depending on how strongly the behavior is manifested.
Therefore, on the first visit, the pediatric dentist carries out
the following courses of action:
1.- Evaluating the dental lesions which have motivated the visit.
2.- Marking with a cross each item on the Scale of Behavior, thus
evaluating the child’s behavior in the dental clinic.
3.- Diagnosing the child as “Anxious” or “Hysterical”, depending
on his/her behavior.
4.- Prescribing the necessary psychopharmacological drug, which
the child will take on his/her next visit. The children considered
5
Anxious (n=25) were treated on their second visit with one dose of
Diazepam (5-15 milligrams), one hour before the dental treatment.
The children considered Hysterical (n=16) were treated with the
Neuroleptic Alimemazine if they are 10 years old or younger, in a
dosage of 1mg/kg of weight, two hours before treatment; if they
are over 10 years old they will be given one 25 mg dose of
Chlorpromazine two hours before treatment.
The procedures, possible discomforts or risks, as well as possible
benefits were explained fully to the human subjects (and/or their
parents), and their informed consent was obtained prior to the
investigation.
On the second visit, -already premedicated-, (in which the dentist
now acts therapeutically within the child’s mouth), the Behavior
Scale is marked again, and the following variables are also
evaluated: 1.- The behavior when given anesthesia, 2.- Reactions
to the rubber dam, 3.- Reactions to cavity opening, 4.- Behavior
during Drilling, and 5.- Effects of premedication (Table 1).
In performing the statistical study, besides the variables of the
conduct scale, groups have been differentiated according to age
and sex. The statistical analysis of the results has been
performed with the aid of the statistical package SPSS (for
Windows, 6.1). Basically, the “t” of “student” has been used when
making multiple comparisons, with the Bonferroni modification;
when having to use non-parametrical samples, the Chi-Square Test
has been used. Last of all, a Discriminating Analysis (Fisher) was
applied to the 41 children before and after premedication.
A standard significance level of 0.05 has been applied.
6
RESULTS.
a/ Descriptive and according to sex.
In the Global Behavior Scale, there is a clear and significant
difference when we compare the global score obtained by the sample
on the first visit, to the score obtained on the second visit,
once the children have been premedicated (Table 2). The
distribution of the sample according to gender were: boys n=19-
46.3%. Girls,n=22- 53.7%. The distribution is quite homogeneous.
On the first visit, there were no significant improvements in
behavior in relation to the gender variable nor, once
premedicated, on the second visit. There are no significant
differences in relation to the age distribution between the sexes.
b/ Comparison according to Age.
Within the range of 3-14 years of age, the relationship between
age and effect of the premedication in children was evaluated,
taking into account 4 possibilities: 1.- Awake and calm (16 cases,
average = 8.62 years old), 2.- Relaxed and responding to orders
(19 cases, average = 7.95 years old), 3.- Awake but confused (5
cases, average = 4.2 years old), 4.- Sleeping and “disconnected”
(1 case, age 5).
Multiple comparisons have been performed between the different
groups, and the only significant differences obtained were
statistical (when looking at the Age variable): in relation to the
group “Awake but confused”, the youngest children were the most
affected by the medication (p<0.01), and belong to this group.
7

c/ Anxious versus Hysterical.
The average score for the anxious group in the first visit was
9.04 (s.d:2.42) and for the hysterical group it was 20.00
(s.d:4.23)
When comparing Anxious to Hysterical children on the first visit,
there are significant differences (Table 3) in seven
manifestations of behavior: a/ “Opening Mouth” b/ “Taking hand to
mouth” c/ “Moving head away when about to be intervened”, d/
“Screaming”, e/ “Making violent gestures to move the dentist’s
hand away” f/ “Kicking” and g/ “Sitting on the dentist’s chair
with problems”. Children with Hysterical behaviors are graded
higher than Anxious children. Therefore, these are the 7 behaviors
that characterize Hysterical children on their first visit.
d/ In relation to the second visit, once the children have been
premedicated:
After premedication, the improvement in behavior management of
both, Children with an Anxious Behavior (CAB) and Children with
a Hysterical Behavior (CHB ), is significant: on the second visit.
(table 2).There was, as well, an interest in knowing which
behaviors improved most comparing both groups. The result shows
that CHB continue to “Move head away when about to be
intervened”, more than the Anxious Group (p< 0.02); “Scream” (p<
0.01), more than the Anxious Group; Last of all, two new behaviors
appear: “Being frightened by the instruments” more than the
Anxious Group (p< 0.01) and “Being tense” more than the Anxious
Group (p< 0.01); fundamentally, this difference is due to the fact
that Anxious children show a spectacular improvement after
premedication.
8

The smallest children were the most “confused” after premedication
(the average was 4.2 years of age). However, the effect of being
“confused” had no relationship with the psychopharmacological drug
used. In other words, children taking Alimemazine were no more
confused than those taking Diazepam (Chi-Square/Yates).
Another aspect that was evaluated, after the premedication, was
how the children reacted to receiving the Anesthesia, placement of
the Rubber Dam, and during the Aperture and Drilling procedures
(Table 4). Children diagnosed as CHB have a worse response to
Anesthesia, Aperture and to the Rubber Dam. There are no
significant differences in relation to Drilling when comparing
Anxious and Hysterical children.
In order to summarize, and with the results obtained up to now,
the group of Hysterical children would be defined by 7 behaviors:
1.- “Refusing to open mouth”, 2.- “Taking hand to mouth”, 3.-
“Moving head away when about to be intervened”, 4.- “Screaming”,
5.- “Making violent gestures to move the dentist’s hand away”, 6.-
“Kicking”, 7.- “Sitting on the dentist’s chair with difficult
behavior.”
The Anxious Group, on the other hand, scores very low in these
behaviors. The average score for each behavior (taking, as before,
0 as the minimum value and 2 as maximum) never reaches 1 in the
Anxious Group, while it is always greater than 1 in the Hysterical
Group.
Both groups (Anxious and Hysterical) “Are frightened by the
instruments”, “Are tense”, “Have legs up or muscles contracted”,
“Cry” and “Speak little and barely establish communication with
the pediatric dentist”. In these behaviors common to both groups,
9

there are no differences of statistical significance between the
groups (t Student).
e/ Applying the Discriminating Function to the results obtained
with the 41 children of our study, we obtained two Function
Values: -4.16406 (Anxious Group), and +6.50635 (Hysterical Group).
The sign + or -, which has no quantitative value, indicates that
these two groups are clearly differentiated.
Looking at the behaviors which fundamentally discriminate both
groups, two constant behaviors appear: 1.- The Hysterical group
“makes violent gestures to move the dentist’s hand away”. (This
variable absolutely discriminates the Hysterical Group).
2.- The Anxious Group, as well as the Hysterical, reach the
maximum score in the behavior: “Being Tense”. (This variable is non-
discriminating).
The next stage consists of finding out the discriminating value of
the ten remaining behaviors. The coefficients of these ten
behaviors are shown on Table 5 (ordered from highest to lowest
“weighting”).
Fundamentally, the 6 behaviors that discriminate both groups are:
1- “Taking hand to mouth”, 2- “Moving head away when about to be
intervened”, 3- “Kicking”, 4- “Screaming”, 5- “Opening mouth”, and
6- “Sitting on the dentist’s chair with problems”. Due to the (+)
sign of these coefficients, the Hysterical Group is the one
fundamentally defined by these behaviors.
Therefore, these 6 behaviors, together with “Making violent
gestures to move the dentist’s hand away” define the Hysterical
Group, confirming the results obtained with the “t” of “student”.
10
The next step consists of applying this Discriminating Function to
the results obtained on the second visit. After premedication, the
value of the Function in the Anxious Group is -1,17859 and, in the
Hysterical Group, it is +1,84155. Hence, the values are very
similar. The children have improved their behavior approximating
normality and both groups are barely distinguishable.
DISCUSSION
The results clearly show the effectiveness of tranquilizers in
Children with Anxious Behaviors (CAB), and neuroleptic medication
in Children with Hysterical Behaviors (CHB). In addition, the
Questionnaire efficiently discriminates the CHB from the CAB.
Klein´s 4 recommendation of treating the children in the afternoon
was always followed.
It is true that the use of sedative substances has been practiced
frequently, 2-5-6-7-8 often combining several of these substances 9-10-11-
12-13 .These two substances (Tranquilizers and Neuroleptics) have
been chosen for comparison because psychiatric science has shown
how a response is more favorable against anxious conduct and
states when providing tranquilizers; the same occurs in Hysterical
behaviors with neuroleptics as indicated by Rojo-Sierra 14 . In
addition, the use of Benzodiazepines has been highly recommended
in the treatment of anxious behaviors, just like Neuroleptics have
been highly recommended in the control of impulsive behaviors in
children as stated by Espiegel15 and Popper16. Neuroleptics have
11

been used as well for sedation and control of nausea/vomiting in
children undergoing dental treatment .17-18-19
No significant differences in behavior were found related to sex
during the first visit, nor in the response to sedative
substances; this disagrees with what Udin,20 found when observing
that girls are more manageable than boys. However, other authors,
like ourselves, find no such differences 21-22.
In relation to the age variable, when multiple comparisons were
made among different groups, the only significant result was found
when this variable was contrasted to the item “awake but
confused”, with a total of five cases in which the average was 4.2
years of age. This was independent of the psychopharmacological
drug used, and it occurred on the smallest children. Although the
youngest children were the ones “confused” after premedication,
their behavior continued to improve in manageability in the same
way as the other age groups, even though their state of
consciousness had decreased. Despite the fact that many research
papers show that behavior management is more difficult with
smaller children 23-24 , in our case, once psychopharmacological
drugs are used, the behaviors of all children are equally
manageable, regardless of age.
On the other hand, different investigations have shown positive
results of Diazepam in behavior management with non-cooperative
children 25-2-11 , but have not made a distinction between hysterical
and anxious behaviors. The results of these studies cannot be
contrasted to our own, since this distinction was made from the
beginning in our study.
12

As Glasrud 26 and Klingherg 23 , among other authors, have pointed
out, it is important to avoid traumatic dental experiences among
children to prevent, as well, the fear of dentists that adults so
often have. The use of tranquilizers and neuroleptics can help in
this task. If types of behavior are differentiated, tranquilizers
and neuroleptics will be more effective in controlling, when
necessary, anxious and hysterical behaviors respectively. In this
line of thinking, we believe that it is possible that
neuroleptics can control anxious behavior. Nevertheless
Benzodiazepines are recommended in the treatment of anxiety due
to their efficacy, speed of effect and easy management. On the
other hand, although the effects of benzodiazepines on
hysterical behavior has not been studied in our research, we have
observed how it can partially sedate hysterical children even
though it does not control the impulsiveness of hysterical
behaviors. The use of neuroleptics has enabled us to deal with
these children without having to use other kinds of physical
restraints.
Conclusions .
1. The use of diazepam has been very positive in the management
of anxious behaviors in pediatric patients. The use of
neuroleptics (Alimemazine and Chlorpromazine) in children with
hysterical behaviors has been equally positive.
2. Seven different behaviors have been identified in hysterical
children.
13

3. Premedicated children with hysterical behavior respond worse to
Anesthesia, Aperture, and to the Rubber Dam than premedicated
children with anxious behavior.. However, they show no more
difficulties than anxious children in behavior management when
obturation is being performed
4. At an operative level, our Behavior Questionnaire is very
useful for identifying hysterical behaviors in children visiting
pediatric dental clinics.
14

TABLE 1 Behavior Questionnaire used in all the cases of our sample, once on the first visit at the same time the group diagnose was made, and the second time on the next visit, during which the dentist applies therapeutic treatment to the premedicated child. The variables “Response to Anesthesia”, “Response to Rubber Dam”, “Behavior during Cavity Opening”, “Behavior during Drilling”, as well as the variable “Effect of premedication”, are only evaluatedon the second visit with the children already premedicated.
BEHAVIORS: 0 points 1 point 2 points
1.- Being frightened by the instruments.
NO AVERAGE YES
2.- Sitting on the dentist’s chair with problems.
NO AVERAGE YES
3.- Opening mouth. YES AVERAGE NO4.- Being tense. NO AVERAGE YES5.- Having legs up or muscles contracted.
NO AVERAGE YES
6.- Making violent movements trying to move the doctor’s handaway.
NO AVERAGE YES
7.- Moving head away when about to be intervened.
NO AVERAGE YES
8.- Taking hand to mouth. NO AVERAGE YES9.- Kicking. NO AVERAGE YES10.- Crying. NO AVERAGE YES11.- Screaming. NO AVERAGE YES12.- Speaking, establishing communication with dentist.
YES AVERAGE NO
-------------------------------------------------
-----------
----------------------
-----------
13.- Response to Anesthesia. Good Average Bad 14.- Response to the Rubber Dam. Good Average Bad 15.- Response to cavity opening. Good Average Bad 16.- Response to drilling. Good Average Bad 17.- EFFECT OF PREMEDICATION -Awake but confused.-Sleeping and “disconnected”.
15
-Relaxed but responding to orders.
DIAGNOSIS ANXIOUS HYSTERICAL
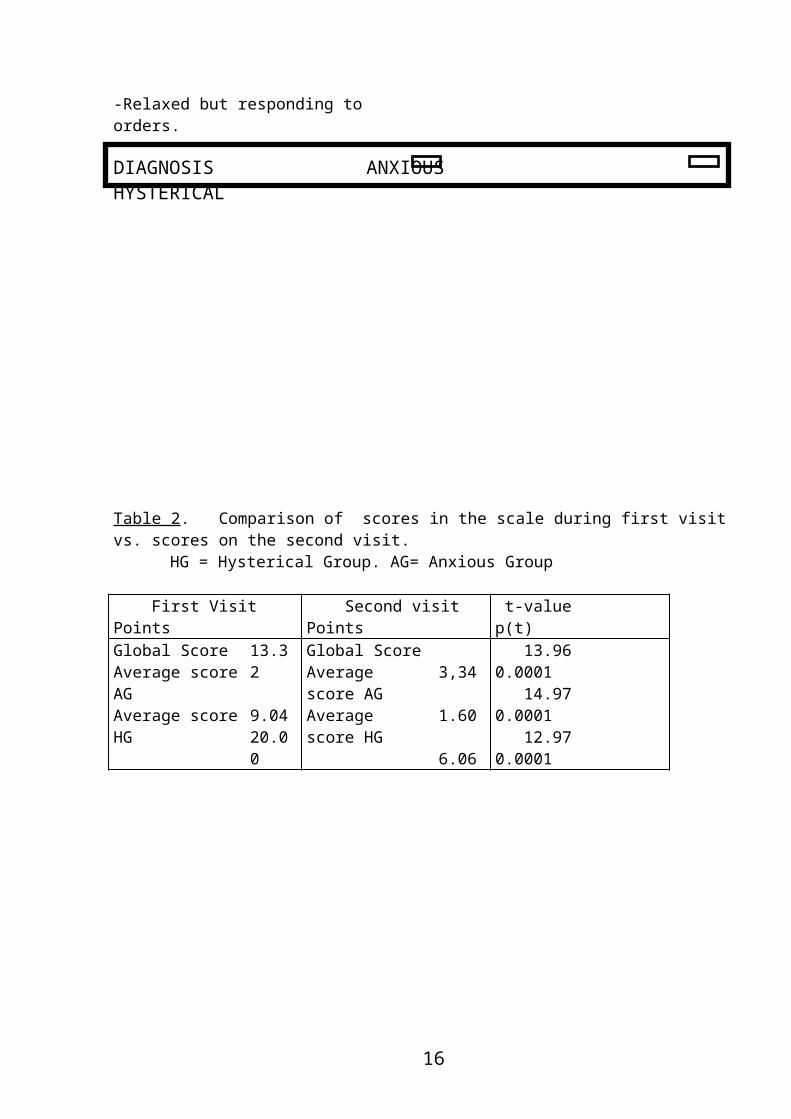
Table 2. Comparison of scores in the scale during first visit vs. scores on the second visit.
HG = Hysterical Group. AG= Anxious Group
First Visit Points
Second visit Points
t-value p(t)
Global Score Average scoreAGAverage scoreHG
13.32 9.0420.00
Global ScoreAverage score AGAverage score HG
3,34 1.60 6.06
13.96 0.0001 14.97 0.0001 12.97 0.0001
16

Table 3. Comparison between groups. Anxious (A) vs. Hysterical (H). Behaviors which differentiate Anxious andHysterical children on the first visit.
BEHAVIORS SIGNIFICANCE OBSERVATIONS Opening mouth pt= 0.0001 “H” children
do not open mouth.
Taking hand to mouth.
pt= 0.0001 “H” take hand to mouth.
Moving head away when about to be intervened.
pt= 0.0001 “H” move head away.
Screaming. pt= 0.01 “H” scream more.
Making violent movements trying to move doctor’s hand away.
pt= 0.0001 “H” move doctor’s hand away.
kicking. pt= 0.0001 “H” kick. Sitting on the dentist’s chair with problems.
pt= 0.002 “H” do not siton dentist’s chair.
17

Table 4. Comparison between Anxious (A) vs. Hysterical (H), on response to the procedure of Anaesthetizing, Cavity Opening, Placement of the Rubber Dam, and Cavity Drilling, already premedicated.
Dental procedure Significance. p(t)
Observations
ANAESTHESIA p= 0.02 Children with Hysterical conducts respondworse to the procedure of Anaesthetizing,
APERTURE p= 0.04 Cavity Opening,RUBBER DAM p= 0.008 and to placement
of the Rubber Dam.
OBTURATION n.s
18
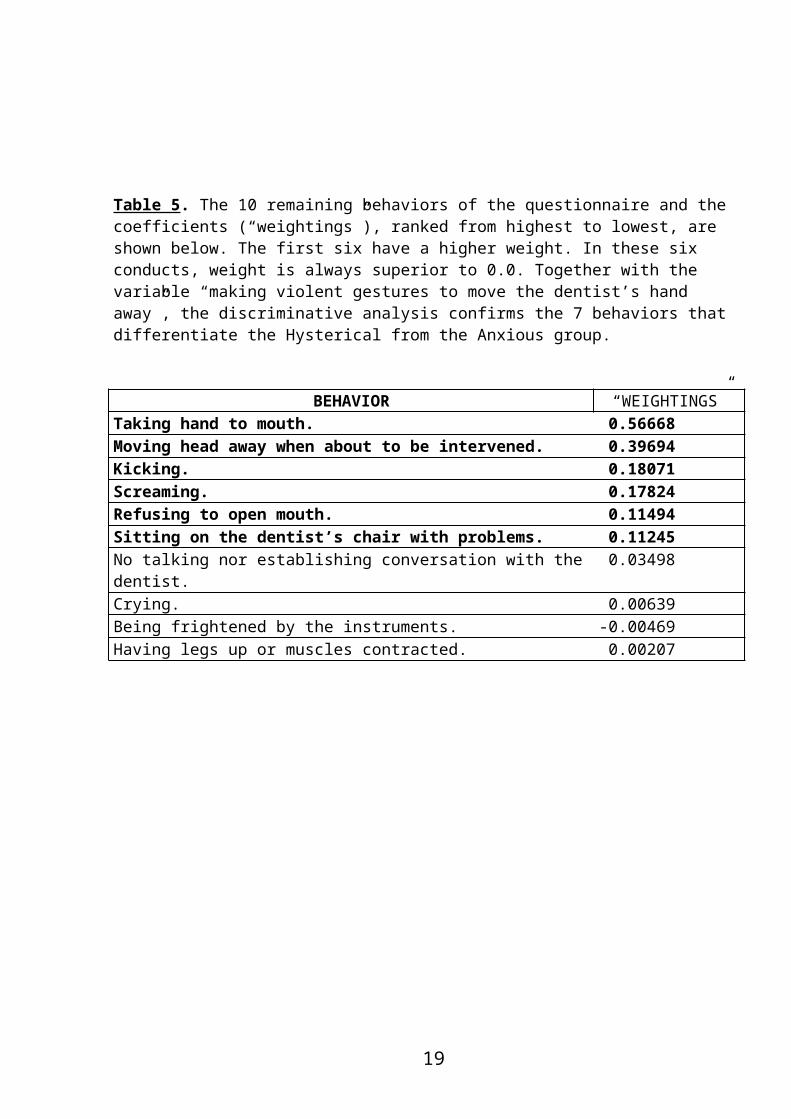
Table 5. The 10 remaining behaviors of the questionnaire and the coefficients (“weightings”), ranked from highest to lowest, are shown below. The first six have a higher weight. In these six conducts, weight is always superior to 0.0. Together with the variable “making violent gestures to move the dentist’s hand away”, the discriminative analysis confirms the 7 behaviors that differentiate the Hysterical from the Anxious group.
BEHAVIOR “WEIGHTINGS”Taking hand to mouth. 0.56668Moving head away when about to be intervened. 0.39694Kicking. 0.18071Screaming. 0.17824Refusing to open mouth. 0.11494Sitting on the dentist’s chair with problems. 0.11245No talking nor establishing conversation with thedentist.
0.03498
Crying. 0.00639Being frightened by the instruments. -0.00469Having legs up or muscles contracted. 0.00207
19
BIBLIOGRAPHY.
1. Krestchmer,E. Psicología Médica. Labor,Ed, 1954.2. Ryder,W., Wright,P.A:Dental sedation. A review. Br.Dent. 7:165:207-16,1988.
3. Musselman,R.J: considerations in behavior management of the pediatric dental patient.Helping children cope with dental treatment. Pediatric Clin. North Am. 38:1309-24,1991.
4. Klein ,A: Physical restraint, informed consent and the child patient. J.Dent. Child.121-26,1987.
5. Kraig,C., Mckee., Nazif,M.M.,Jackson,D.L., Barnhart,D.C., Close,J., Moore,P.A: Dose-responsive characteristics of Meperidine sedation in preschool children. Pediatr. Dent.12: 222-27,1990.
6. Lambert,L.A., Nazif,M.M.,Moore,P.A.,Zullo,T.G: Nonlinear dose-response characteristics of alphaprodinesedation in preschool children. Pediatr. Dent. 10 : 30-33, 1988.
7. Wilson, S.T: Chloral hydrate and its effects in multiple physiological parameters in young children: a dose-response study. Pediatr. Dent, 14 :171-77,1992.
8. Vererkamp,J.S;Van Ameronger,W,E; Hoogstraten,J; Croen,H.J: Dental treatment of fearful children, using nitrous oxide: Treatment times. J.Dent.Child,58:453-57,1991.
9. Hasty,M.F., Vann,W.F., Dilley,D.C., Anderson,J.A: Conscious sedation of pediatric dental patients: an investigation of chloral hydrate, hydroxyzine pamoate, and meperidine v.s chloral hydrate and hydroxyzine pamoate.Pediatr. Dent, 13: 10-19,1991.
10. Shapira,J., Holan,G., Guelmann,M., Cahan,S: Evaluation of the effect of nitrous oxide and hydroxyzine in controlling the behavior of the
20

pediatric dental patient. Pediatr. Dent, 14 :167-70, 1992.
11. Holst,A., Schroder,U., Ek,L., Hallonsten,A., Crossner,C.L: Prediction of behavior management problems in children. Scand J.Dent.Res,96:457-65,1988.
12. Holst,A., Hallonsten,A.L., Schroder,U., Ek,L., Edlund,K:Prediction of behavior management problems in 3 year old children.Scand,J.Dent.Res.101 :110-14, 1993.
13. Houpt,M., Manetas,C., Joshi,A., Desjardins,P: Effect of chloral on nitrous oxide sedation of children .Pediatr.Dent.11 :26-29,1989.
14. Rojo-Sierra,M: Lecciones de Psiquiatría, Tomo III. Promolibro,Ed.Valencia,1983.
15. Espiegel,D: Trastornos disociativos: En “ Tratado de Psiquiatría,” 2ª Edición, Hales,R.E;Yudofsky,S.C and Talbott,J.A. The American Psychiatric Press.Edición Española,Ancora,S.A,1996.
16. Popper, Ch,W and Steingard,R.J: Trastornos de inicioen la infancia, la niñez o la adolescencia. En “Tratado de Psiquiatría”, 2ª Edición, Hales,R.E;Yudofsky,S.C and Talbott,J.A. The American Psychiatric Press.Edición Española, Ancora,S.A,1996.
17. Davis,P.J;McGowan,F.X;Landsman,I, et al: Effect of antiemetic therapy on recovery and hospital discharge time. A double-blind assessment of ondansetron, droperidol, and placebo in pediatric patients undergoing ambulatory surgery. anesthesiology. 83: 956-60, 1995.
18. Trapp,L.D:An evaluation of Droperidol for preventing nausea and vomiting after deep intravenous sedation for ambulatory dental surgery.Anesth.Prog. 36:9-12, 1989.
19. Valanne,J; Korttila,K : Effect of a small dose of droperidol on nausea,vomiting, and recovery after outpatient enflurane anesthesia. Acta Anaesthesiol.Scand. 29: 359-62, 1985.
21
20. Udin,R.D :Predictors of dental behavior of disabled children. The J. of Dedontics.12 : 250-59,1988.
21. Jonson,R and Baldwin,D: Relationship of maternal anxiety to the behavior of young children undergoing dental extraction. J.Dent.Res. 47:801-805,1968.
22. Jonson,R and Baldwin,D:Maternal anxiety and child behavior. J.Dent. Child. 36:87-92,1969.
23. Klingberg,G: Dental fear and behavior management problems in children. A study of measurement, prevalence, concomitant factors and clinical effects. Swed. Dent.J.Suppl. 103:1-78, 1995
24. Klingberg,G., Vannas-Lofqvist,L., Bjarnason,S., Noren,J.G: Dental behavior management problem in swedish children. Comm.Dent-Oral.Epid,22: 202-205,1994.
25. Flaitz, C.M., Nowak,A.J: Evaluation of sedative effects of rectally administered diazepam for the youngdental patient. Pediatr. Dent. 7 : 292-96,1985.
26. Glasrud,P.H: Dentists’characteristics and child behavior management techniques. J.of Dent. for child.:337-342, sep-oct,1984.
22