
Untitled - MOSC medical college
1020
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Untitled - MOSC medical college


Essentials of
MedicalPharmacology


Essentials of
MedicalPharmacology
Seventh Edition
KD TRIPATHI MDEx-Director-Professor and Head of PharmacologyMaulana Azad Medical College and associated
LN and GB Pant HospitalsNew Delhi, India
JAYPEE BROTHERS MEDICAL PUBLISHERS (P) LTDNew Delhi • London • Philadelphia • Panama
®

Website: www.jaypeebrothers.comWebsite: www.jaypeedigital.com
© 2013, KD Tripathi
Managing Editor: M. Tripathi
Inquiries for bulk sales may be solicited at: [email protected]
All rights reserved. No part of this publication should be reproduced, stored in a retrieval system, or transmitted in any form or by anymeans: electronic, mechanical, photocopying, recording, or otherwise, without the prior written permission of the author and thepublisher.
This book has been published in good faith that the material provided by author is original. Every effort is made to ensure accuracy ofmaterial, but the publisher, printer and author will not be held responsible for any inadvertent error(s). In case of any dispute, all legalmatters to be settled under Delhi jurisdiction only.
Essentials of Medical Pharmacology
First Edition: 1985Second Edition: 1988Third Edition: 1994Fourth Edition: 1999, Updated Reprint: 2001Fifth Edition: 2003Sixth Edition: 2008Seventh Edition: 2013
ISBN: 978-93-5025-937-5
Printed at Ajanta Offset
Jaypee Brothers Medical Publishers (P) Ltd
Jaypee Brothers Medical Publishers (P) Ltd4838/24, Ansari Road, DaryaganjNew Delhi 110 002, IndiaPhone: +91-11-43574357Fax: +91-11-43574314Email: [email protected]
J.P. Medical Ltd.,83 Victoria Street LondonSW1H 0HW (UK)Phone: +44-2031708910Fax: +02-03-0086180Email: [email protected]
Overseas Offices
Headquarters
Jaypee-Highlights Medical Publishers Inc.City of Knowledge, Bld. 237, ClaytonPanama City, PanamaPhone: +507-301-0496Fax: +507-301-0499Email: [email protected]
®
Jaypee Brothers Medical Publishers (P) LtdShorakhute, KathmanduNepalPhone: +00977-9841528578Email: [email protected]
Jaypee Medical Inc.The Bourse111 South Independence Mall EastSuite 835, Philadelphia, PA 19106, USAPhone: + 267-519-9789Email: [email protected]
Jaypee Brothers Medical Publishers (P) Ltd17/1-B Babar Road, Block-B, ShaymaliMohammadpur, Dhaka-1207BangladeshMobile: +08801912003485Email: [email protected]

Medical pharmacology is a unique synthesis of basic pharmacology with clinical pharmacology andpharmacotherapeutics. The subject is highly dynamic. Developments are occurring both in definingmolecular targets for drug action and finding targeted drugs, as well as in accruing credible evidenceregarding the impact of different treatment modalities on therapeutic outcomes. These efforts havebegun to crystallize into evidence based medicine and clear cut therapeutic guidelines. The presentedition endeavours to amalgamate the developments with the core content of the subject.
While the primary theme of the book outlined in the preface to the first edition is maintained,the successive editions have become more descriptive and more comprehensive. In preparing thisedition, all chapters have been revisited and extensively updated. Latest therapeutic guidelines fromauthoritative sources like WHO, British National Formulary, National Formulary of India, as wellas from eminent professional bodies have been incorporated, especially in areas like hypertension,dyslipidaemias, acute coronary syndromes, surgical prophylaxis, tuberculosis (including MDR-TB),MAC-infection, leprosy, HIV-AIDS, malaria, kala-azar, etc. Recent innovations have been highlighted,notably in antidiabetic drugs, psychopharmacological agents, antiplatelet drugs, treatment ofinflammatory bowel disease, drugs affecting renin-angiotensin system, anticoagulants, antiviral (includinganti-HIV) drugs, targeted anticancer drugs, etc.
New drugs released in India have been included. Infrequently used drugs and those not availablein India are presented briefly in extract type. Important points are summarized in boxes. Use ofdistinctive headings in a hierarchical order makes the text highly systematic. Representative tradenames of drugs with available dosage forms are mentioned. Due emphasis is given to diseasesprevalent in India and similar tropical countries, alongwith their current drug therapy.
The most important objective of medical pharmacology is to train medical students in therapeuticdecision making according to specific clinical problems in individual patients. A new feature ‘problemdirected study’ has been included at the end of majority of chapters to give an exercise in therapeuticdecision making for a realistic clinical scenario. The solutions provided in Appendix-1 explain howrational decisions could be arrived at.
I thank students and other readers of this text for their valuable feedback and suggestions. Allcredit for existence of this book, especially the present edition, goes to Mr. Jitendar Pal Vij, theuntiring Group Chairman and Mr. Ankit Vij (Managing Director) of M/s Jaypee Brothers. Meticuloustypesetting by Ms. Sunita Katla and proof reading by Ms. Geeta Srivastava deserves special mention.Credit for improving the illustrations goes to Mr. Manoj Pahuja. The cooperation and editorialmanagement of my wife is acknowledged.
New Delhi KD TripathiMay 2013
Preface

Pharmacology is both a basic and an applied science. It forms the backbone of rational therapeutics.Whereas the medical student and the prescribing physician are primarily concerned with the appliedaspects, correct and skilful application of drugs is impossible without a proper understanding oftheir basic pharmacology. Medical pharmacology, therefore, must include both fundamental back-ground and clinical pharmacological information. Objective and quantitative data on the use of drugsin man, i.e., relationship between plasma concentration and intensity of therapeutic/toxic actions,plasma half lives, relative efficacy of different medications and incidence of adverse effects etc.,are being obtained with the aim of optimising drug therapy. The concepts regarding mechanismof action of drugs are changing. In addition, new drugs are being introduced in different countriesat an explosive pace. A plethora of information thus appears to be important. However, trying toimpart all this to a medical student would be counter-productive.
One of the important aims of this book is to delineate the essential information about drugs.The opening sentence in each chapter defines the class of drugs considered. A ‘prototype’ approachhas been followed by describing the representative drug of a class followed by features by whichindividual members differ from it. Leading trade names have been included. Clinically relevantdrug interactions have been mentioned. Clear-cut guidelines on selection of drugs and their clinicalstatus have been outlined on the basis of current information. Original, simple and self-explanatoryillustrations, tables and flow charts have been used with impunity. Selected chemical structures aredepicted. Recent developments have been incorporated. However, discretion has been used in includingonly few of the multitude of new drugs not yet available in India. This is based on their likelihoodof being marketed soon. The information and views have been arranged in an orderly sequenceof distinct statements.
I hope this manageable volume book would serve to dispel awe towards pharmacology fromthe minds of medical students and provide a concise and uptodate information source for prescriberswho wish to remain informed of the current concepts and developments concerning drugs.
My sincere thanks are due to my colleagues for their valuable comments and suggestions.
New Delhi KD Tripathi1st Jan., 1985
Extract fromPreface to the First Edition

Section 1General Pharmacological Principles
1. Introduction, Routes of Drug Administration 1
2. Pharmacokinetics: Membrane Transport, Absorption and Distribution of Drugs 10
3. Pharmacokinetics: Metabolism and Excretion of Drugs, Kinetics of Elimination 22
4. Pharmacodynamics: Mechanism of Drug Action; Receptor Pharmacology 37
5. Aspects of Pharmacotherapy, Clinical Pharmacology and Drug Development 61
6. Adverse Drug Effects 82
Section 2Drugs Acting on Autonomic Nervous System
7a. Autonomic Nervous System: General Considerations 92
7b. Cholinergic System and Drugs 99
8. Anticholinergic Drugs and Drugs Acting on Autonomic Ganglia 113
9. Adrenergic System and Drugs 124
10. Antiadrenergic Drugs (Adrenergic Receptor Antagonists) andDrugs for Glaucoma 140
Section 3Autacoids and Related Drugs
11. Histamine and Antihistaminics 159
12. 5-Hydroxytryptamine, its Antagonists and Drug Therapy of Migraine 170
13. Prostaglandins, Leukotrienes (Eicosanoids) and Platelet Activating Factor 181
14. Nonsteroidal Antiinflammatory Drugs and Antipyretic-Analgesics 192
15. Antirheumatoid and Antigout Drugs 210
Contents

Section 4Respiratory System Drugs
16. Drugs for Cough and Bronchial Asthma 218
Section 5Hormones and Related Drugs
17a. Introduction 234
17b. Anterior Pituitary Hormones 236
18. Thyroid Hormone and Thyroid Inhibitors 245
19. Insulin, Oral Hypoglycaemic Drugs and Glucagon 258
20. Corticosteroids 282
21. Androgens and Drugs for Erectile Dysfunction 296
22. Estrogens, Progestins and Contraceptives 306
23. Oxytocin and Other Drugs Acting on Uterus 329
24. Drugs Affecting Calcium Balance 335
Section 6Drugs Acting on Peripheral (Somatic)
Nervous System25. Skeletal Muscle Relaxants 347
26. Local Anaesthetics 360
Section 7Drugs Acting on Central Nervous System
27. General Anaesthetics 372
28. Ethyl and Methyl Alcohols 388
29. Sedative-Hypnotics 397
30. Antiepileptic Drugs 411
31. Antiparkinsonian Drugs 425
32. Drugs Used in Mental Illness: Antipsychotic and Antimanic Drugs 435
33. Drugs Used in Mental Illness: Antidepressant and Antianxiety Drugs 454
34. Opioid Analgesics and Antagonists 469
35. CNS Stimulants and Cognition Enhancers 486
viii CONTENTS

Section 8Cardiovascular Drugs
36a. Cardiac Electrophysiological Considerations 492
36b. Drugs Affecting Renin-Angiotensin System and Plasma Kinins 495
37. Cardiac Glycosides and Drugs for Heart Failure 512
38. Antiarrhythmic Drugs 526
39. Antianginal and Other Anti-ischaemic Drugs 539
40. Antihypertensive Drugs 558
Section 9Drugs Acting on Kidney
41a. Relevant Physiology of Urine Formation 575
41b. Diuretics 579
42. Antidiuretics 593
Section 10Drugs Affecting Blood and Blood Formation
43. Haematinics and Erythropoietin 599
44. Drugs Affecting Coagulation, Bleeding and Thrombosis 613
45. Hypolipidaemic Drugs and Plasma Expanders 634
Section 11Gastrointestinal Drugs
46. Drugs for Peptic Ulcer and Gastroesophageal Reflux Disease 647
47. Antiemetic, Prokinetic and Digestant Drugs 661
48. Drugs for Constipation and Diarrhoea 672
Section 12Antimicrobial Drugs
49. Antimicrobial Drugs: General Considerations 688
50. Sulfonamides, Cotrimoxazole and Quinolones 704
51. Beta-Lactam Antibiotics 716
ixCONTENTS

52. Tetracyclines and Chloramphenicol (Broad-Spectrum Antibiotics) 733
53. Aminoglycoside Antibiotics 743
54. Macrolide, Lincosamide, Glycopeptide and Other Antibacterial Antibiotics;Urinary Antiseptics 752
55. Antitubercular Drugs 765
56. Antileprotic Drugs 780
57. Antifungal Drugs 787
58. Antiviral Drugs 798
59. Antimalarial Drugs 816
60. Antiamoebic and Other Antiprotozoal Drugs 836
61. Anthelmintic Drugs 849
Section 13Chemotherapy of Neoplastic Diseases
62. Anticancer Drugs 857
Section 14Miscellaneous Drugs
63. Immunosuppressant Drugs 878
64. Drugs Acting on Skin and Mucous Membranes 886
65. Antiseptics, Disinfectants and Ectoparasiticides 897
66. Chelating Agents 905
67. Vitamins 909
68. Vaccines and Sera 919
69. Drug Interactions 928
Appendices
Appendix 1: Solution to Problem Directed Study 935
Appendix 2: List of Essential Medicines 957
Appendix 3: Prescribing in Pregnancy 962
Appendix 4: Drugs in Breastfeeding 965
Appendix 5: Drugs and Fixed Dose Combinations Banned in India$
(updated till Dec. 2012) 969
Selected References for Further Reading 971
Index 975
x CONTENTS

Ang-I/II/III Angiotensin I/II/IIIAA Amino acid
ABC ATP-binding cassette (transporter)ABLC Amphotericin B lipid complex
AB AntibodyAC Adenylyl cyclase
ACE Angiotensin II converting enzymeACh Acetylcholine
AChE AcetylcholinesteraseACS Acute coronary syndromesACT Artemisinin-based combination therapy
ACTH Adrenocorticotropic hormoneAD Alzheimer’s disease
ADCC Antibody-dependent cellular cytotoxicityADE Adverse drug eventADH Antidiuretic hormone
ADHD Attention deficit hyperactivity disorderADP Adenosine diphosphateAdr Adrenaline
ADR Adverse drug reactionADS Anti diphtheritic serumAES Atrial extrasystole
AF Atrial fibrillationAFl Atrial flutterAG Antigen
AGS Antigasgangrene serumAHG Antihaemophilic globulin
AI Aromatase inhibitorAIDS Acquired immunodeficiency syndrome
AIP Aldosterone induced proteinALA AlanineALS Amyotrophic lateral sclerosisAm Amikacin
AMA Antimicrobial agentAMB Amphotericin B
amp AmpouleAMP Adenosine mono phosphate
AMPA -Aminohydroxy methylisoxazolepropionic acid
ANC Acid neutralizing capacityANP Atrial natriuretic peptideANS Autonomic nervous system
ANUG Acute necrotizing ulcerative gingivitisAP Action potential
AP-1 Activator protein-1APC Antigen presenting cellAPD Action potential durationaPTT Activated partial thromboplastin time
AQ AmodiaquineAR Androgen receptor
ARB Angiotensin receptor blockerARC AIDS related complexARS Anti rabies serumARV Antiretrovirus
AS Artesunate5-ASA 5-Amino salicyclic acid
Asc LH Ascending limb of Loop of HenleAT-III Antithrombin IIIATG Antithymocyte globulinATP Adenosine triphosphate
ATPase Adenosine triphosphataseATPIII Adult treatment panel III
ATS Antitetanic serumAUC Area under the plasma concentration-time
curveA-V AtrioventricularAVP Arginine vasopressinAZT Zidovudine
BAL British anti lewisiteBAN British approved name
BB Borderline leprosyBBB Blood-brain barrierBCG Bacillus Calmette Guérin
BCNU Bischloroethyl nitrosourea (Carmustine)BCRP Breast cancer resistance protein
BD Twice daily-ARK adrenergic receptor kinase
BHC Benzene hexachlorideBHP Benign hypertrophy of prostate
BI Bacillary indexBL Borderline lepromatous leprosy
BMD Bone mineral densityBMR Basal metabolic rateBNP Brain nartriuretic peptideBOL 2-Bromolysergic acid diethylamide
BP Blood pressureBPN BisphosphonateBSA Body surface area
BT Borderline tuberculoid leprosyBuChE Butyryl cholinesterase
BW Body weightBZD Benzodiazepine
C-10 DecamethoniumCA Catecholamine
List of Abbreviations

CAB Combined androgen blockadeCaBP Calcium binding proteinCAD Coronary artery diseaseCAM Calmodulin
cAMP 3', 5' Cyclic adenosine monophosphatecap Capsule
CAR Conditioned avoidance responseCAse Carbonic anhydraseCAT Computerized axial tomographyCBF Cerebral blood flowCBG Cortisol binding globulinCBS Colloidal bismuth subcitrateCCB Calcium channel blocker
CCNU Chloroethyl cyclohexyl nitrosourea(lomustine)
CCR5 Chemokine coreceptor 5CD Collecting duct/Cluster of differentiation
CDC Complement dependent cytotoxicityCFTR Cystic fibrosis transport regulatorcGMP 3', 5' Cyclic guanosine monophosphateCGRP Calcitonin gene related peptide
CH CholesterolChE CholinesteraseCHE Cholesterol esterChy Chylomicron
Chy. rem. Chylomicron remnantsCHF Congestive heart failure
CI Cardiac indexCINV Chemotherapy induced nausea and vomiting
CL ClearanceCLcr Creatinine clearance
Cm CapreomycinCMI Cell mediated immunity
CMV CytomegalovirusCNS Central nervous systemc.o. Cardiac output
CoEn-A Coenzyme-ACOMT Catechol-O-methyl transferase
COX Cyclooxygenasec.p.s. Cycles per secondCPS Complex partial seizuresCPZ ChlorpromazineCQ Chloroquine
CRABP Cellular retinoic acid binding proteinCRBP Cellular retinol binding protein
CrD Crohn’s diseaseCREB Cyclic AMP response element binding protein
CRF Corticotropin releasing factorCS Cycloserine
CSF Cerebrospinal fluidCTL Cytotoxic T-lymphocytesCTZ Chemoreceptor trigger zoneCV Cardiovascular
CVP Central venous pressureCVS Cardiovascular system
CWD Cell wall deficientCYP450 Cytochrome P450
DA DopamineDA-B12 Deoxyadenosyl cobalamin
DAD Delayed after-depolarizationDAG Diacyl glycerolDAM Diacetyl monoxime
DAMP Diphenyl acetoxy-N-methyl piperidinemethiodide
DAT Dopamine transporterdDAVP Desmopressin
DDS Diamino diphenyl sulfone (Dapsone)DDT Dichloro diphenyl trichloroethaneDEC Diethyl carbamazine citrateDHA DihydroartemisininDHE Dihydroergotamine
DHFA Dihydro folic acidDHFRase Dihydrofolate reductase
DHP DihydropyridineDHT Dihydrotestosterone
DI Diabetes insipidusDIT Diiodotyrosine
dl DecilitreDLE Disseminated lupus erythematosus
DMA Dimethoxy amphetamineDMARD Disease modifying antirheumatic drug
DMCM Dimethoxyethyl-carbomethoxy--carboline DMPA Depot medroxyprogesterone acetateDMPP Dimethyl phenyl piperazinium
DMT Dimethyl tryptamine/Divalent metal transporterDNA Deoxyribose nucleic acidDOC Deoxycholate
DOCA Desoxy corticosterone acetateDOM Dimethoxymethyl amphetaminedopa Dihydroxyphenyl alanine
DOPAC 3, 4, Dihydroxyphenyl acetic acidDOSS Dioctyl sulfosuccinateDOTS Directly observed treatment short course
DPD Dihydropyrimidine dehydrogenaseDPP-4 Dipeptidyl peptidase-4
DPT Diphtheria-pertussis-tetanus triple antigenDRC Dose-response curveDRI Direct renin inhibitorDST Drug sensitivity testing (for TB)
DT Distal tubuleDT-DA Diphtheria-tetanus double antigen
d-TC d-TubocurarineDTIC DacarbazineDTPA Diethylene triamine pentaacetic acidDVT Deep vein thrombosisDYN Dynorphin
E EthambutolEACA Epsilon amino caproic acid
EAD Early after-depolarizatione.c.f. Extracellular fluidECG ElectrocardiogramECT Electroconvulsive therapy
ED Erectile dysfunction
xii ABBREVIATIONS

EDRF Endothelium dependent relaxing factorEDTA Ethylene diamine tetraacetic acid
EEG ElectroencephalogramEGF Epidermal growth factor
ELAM-1 Endothelial leukocyte adhesion molecule-1-END -Endorphin
ENS Enteric nervous systemENT Extraneuronal amine transporter
EPAC cAMP regulated guanine nucleotideexchange factors
EPEC Enteropathogenic E. coliEPO ErythropoietinEPP End plate potential
EPSP Excitatory postsynaptic potentialER Estrogen receptor
ERP Effective refractory periodES Extrasystole
ESR Erythrocyte sedimentation rateETEC Enterotoxigenic E. coli
Eto Ethionamide
FA Folic acidFAD Flavin adenine dinucleotide5-FC 5-FlucytosineFDC Fixed dose combinationFDT Fixed duration therapy (of leprosy)
FEV1 Forced expiratory volume in 1 secondFFA Free fatty acid
FKBP FK 506 (tacrolimus) binding proteinFLAP Five-lipoxygenase activating proteinFMN Favin mononucleotide
FP FerroportinFQ Fluoroquinolone
FRase Folate reductaseFSH Follicle stimulating hormone
5-FU 5-Fluorouracil
G GeneticGABA Gamma amino butyric acid
GAT GABA-transporterGC Guanylyl cyclase
GCP Good clinical practiceG-CSF Granulocyte colony stimulating factor
GDP Guanosine diphosphateGERD Gastroesophageal reflux disease
g.f. Glomerular filtrationg.f.r. Glomerular filtration rateGH Growth hormone
GHRH Growth hormone releasing hormoneGHRIH Growth hormone release inhibitory hormone
GIP Gastric inhibitory peptide/Glucose-dependent insulinotropic polypeptide
g.i.t. Gastrointestinal tractGITS Gastrointestinal therapeutic system
Glc GlucocorticoidGLP Glucagon-like peptide
GLUT Glucose transporter
GM-CSF Granulocyte macrophage colonystimulating factor
GnRH Gonadotropin releasing hormoneGPCR G-protein coupled receptor
G-6-PD Glucose-6-phosphate dehydrogenaseGPI Globus pallidus interna
GST Glutathione-S-transferaseGTCS Generalised tonic-clonic seizures
GTN Glyceryl trinitrateGTP Guanosine triphosphate
H Isoniazid (Isonicotinic acid hydrazide)HAART Highly active antiretroviral therapy
Hb HaemoglobinHBV Hepatitis B virusHCG Human chorionic gonadotropin
HDCV Human diploid cell vaccineHDL High density lipoprotein
5-HIAA 5-Hydroxyindole acetic acidHES Hydroxyethyl starch
HETE Hydroxyeicosa tetraenoic acidHIV Human immunodeficiency virus
HLA Human leucocyte antigenHMG-CoA Hydroxymethyl glutaryl coenzyme A
HMW High molecular weightHPA axis Hypothalamo-pituitary-adrenal axis
HPETE Hydroperoxy eicosatetraenoic acidhr Hour
HR Heart rateHRIG Human rabies immuneglobulinHRT Hormone replacement therapy5-HT 5-Hydroxytryptamine
5-HTP 5-HydroxytryptophanHVA Homovanillic acid
I Indeterminate leprosyIAP Islet amyloid polypeptideIBD Inflammatory bowel diseaseIBS Irritable bowel syndrome
ICAM-1 Intracellular adhesion molecule-1ICSH Interstitial cell stimulating hormone
i.d. Intradermal (injection)IDL Intermediate density lipoproteinIFN Interferon
IG ImmuneglobulinIGF Insulin-like growth factor
IL InterleukinILEU Isoleucine
i.m. IntramuscularINH Isonicotinic acid hydrazideINR International normalized ratioi.o.t. Intraocular tension
IP3 Inositol trisphosphateIP4 Inositol tetrakisphosphate
IPSP Inhibitory postsynaptic potentialIPV Inactivated poliomyelitis vaccine
xiiiABBREVIATIONS

IRS Insulin response substrateISA Intrinsic sympathomimetic activityISH Isolated systolic hypertension
IU International unitIUCD Intrauterine contraceptive device
i.v. Intravenous
JAK Janus-kinase
Km KanamycinKTZ Ketoconazole
LA Local anaestheticLCAT Lecithin cholesterol acyl transferase
LC3-KAT Long chain 3-ketoacyl-CoA-thiolaseLDL Low density lipoproteinLES Lower esophageal sphincter
leu-ENK Leucine enkephalinLH Luteinizing hormoneliq LiquidLL Lepromatous leprosy
LMW Low molecular weightLOX LipoxygenaseLSD Lysergic acid diethylamide
LT LeukotrieneLVF Left ventricular failure
MAbs Monoclonal antibodiesMAC Minimal alveolar concentrationMAC Mycobacterium avium complexMAO Monoamine oxidaseMAP Muscle action potential
MAPKinase Mitogen activated protein kinasemax Maximum
MBC Minimum bactericidal concentrationMBL Multibacillary leprosyMCI Mild cognitive impairmentMDI Manic depressive illness
MDMA Methylene dioxy methamphetamineMDR Multidrug resistantMDT Multidrug therapy (of leprosy)
met-ENK Methionine enkephalinmEq milliequivalent
methyl B12 Methyl cobalaminMf MicrofilariaeMF Multifactorial
MHC Major histocompatibility complexMHT Methylene dioxy methamphetamine
MI Myocardial infarctionMIC Minimal inhibitory concentrationMIF Migration inhibitory factormin MinimumMIT Monoiodo tyrosine
MLCK Myosin light chain kinaseMMF Mycophenolate mofetil6-MP 6-Mercaptopurine
MPPT Methylprednisolone pulse therapyMPTP 4-methyl-4-phenyltetrahydro pyridine
MQ MefloquineMRP2 Multidrug resistance associated protein-2MRSA Methicillin resistant Staphylococcus aureus
MSH Melanocyte stimulating hormoneMT Methyl transferase
mTOR Mammalian target of rapamycinMtx MethotrexatemV millivolt
MW Molecular weight
NA NoradrenalineNADP Nicotinamide adenine dinucleotide phosphate
NADPH Reduced nicotinamide adenine dinucleotidephosphate
NAG N-acetyl glucosamineNAM N-acetyl muramic acid
NANC Nonadrenergic noncholinergicNAPA N-acetyl procainamide
NAPQI N-acetyl-p-benzoquinoneimineNaSSA Noradrenergic and specific serotonergic
antidepressantNAT N-acetyl transferase
NCEP National cholesterol education programmeNEE Norethindrone enanthateNET Norepinephrine transporter
NFAT Nuclear factor of activated T-cellNFB Nuclear factor B
NIS Na+ (sodium)-iodide symporterNLEP National leprosy eradication programme
NMDA N-methyl-D-aspartatenNOS Neural nitric oxide synthase
NNRTI Nonnucleoside reverse transcriptaseinhibitor
NPY Neuropeptide-YNR Nicotinic receptor
N-REM Non rapid eye movement (sleep)NRTI Nucleoside reverse transcriptase inhibitor
NSAID Nonsteroidal antiinflammatory drugNSTEMI Non ST-segment elevation myocardial
infarctionNTS Nucleus tractus solitarius
NVBDCP National vector borne diseases controlprogramme
NYHA New York Heart Association
OAT Organic anion transporterOATP Organic anion transporting polypeptide
OC Oral contraceptiveOCD Obsessive-compulsive disorderOCT Organic cation transporter
OD Once dailyOPG OsteoprotegerinOPV Oral poliomyelitis vaccineORS Oral rehydration salt (solution)ORT Oral rehydration therapy
PABA Paraamino benzoic acidPAE Post antibiotic effect
xiv ABBREVIATIONS

PAF Platelet activating factorPAI-1 Plasminogen activator inhibitor-1
2-PAM PralidoximePAN Primary afferent neuronePAS Paraamino salicylic acidPBI Protein bound iodine
PBPs Penicillin binding proteinsPBL Paucibacillary leprosyPCA Patient controlled anaesthesia
PCEV Purified chick embryo cell vaccine (rabies)PCI Percutaneous coronary intervention
PCPA Parachloro phenylalaninePD Parkinsons’s disease
PDE PhosphodiesterasePE Pulmonary embolism
PEMA Phenylethyl malonamidePEP Postexposure prophylaxis
PF Purkinje fibrePFOR Pyruvate: ferredoxin oxidoreductase
PG ProstaglandinPGI2 ProstacyclinPgp P-glycoprotein
PI Protease inhibitorPIG Phosphatidyl inositol glycanPIP2 Phosphatidyl inositol-4,5-bisphosphatePKA Protein kinase: cAMP dependentPKC Protein kinase CPLA Phospholipase APLC Phospholipase C
Pl. ph. Platelet phospholipidpMDI pressurized multidose inhaler
PnG Penicillin GPOMC Pro-opio melanocortinPONV Postoperative nausea and vomiting
PP Partial pressurePPA Phenyl propanolamine
PPAR Paroxysome proliferator-activatedreceptor
PPH Post partum haemorrhagePPI Proton pump inhibitor
ppm Part per millionPPNG Penicillinase producing N. gonorrhoeae
PRA Plasma renin activityPRF Prolactin releasing factor
PRIH Prolactin release inhibitory hormonePSVT Paroxysmal supra-ventricular tachycardia
PT Proximal tubulePTCA Percutaneous transluminal coronary
angioplastyPTH Parathyroid hormone
PTMA Phenyl trimethyl ammoniumPTP Post-tetanic potentiation
PTSD Post-traumatic stress disorderPTZ Pentylenetetrazol
PUV A Psoralen-Ultraviolet APVP Poly vinyl pyrrolidone
PVRV Purified verocell rabies vaccine
QID Four times a day
R Rifampin (Rifampicin)RANK Receptor for activation of nuclear factor B
RANKL RANK ligandRAS Renin-angiotensin systemRBC Red blood cellsRBP Retinol binding protein
RC Respiratory centreRE Reticuloendothelial
REM Rapid eye movement (sleep)RGS Regulator of G-protein synthesisRIG Rabies immuneglobulin
RIMA Reversible inhibitor of MAO-ArINN Recommended international
nonproprietary nameRMP Resting membrane potentialRNA Ribonucleic acid
RNTCP Revised National Tuberculosis ControlProgramme
RP Refractory periodRTF Resistance transfer factor
RTKs Receptor tyrosine kinasesRXR Retinoid X receptorRyR Ryanodine receptor
S StreptomycinSA Sinoauricular (node)
SABE Subacute bacterial endocarditiss.c. Subcutaneous
SCC Short course chemotherapy (of tuberculosis)SCh Succinylcholine
SCID Severe combined immunodeficiency diseaseSERCA Sarcoplasmic-endoplasmic reticular calcium
ATPaseSERDs Selective estrogen receptor down regulatorsSERM Selective estrogen receptor modulatorSERT Serotonin transporterSGA Second generation antihistaminic
SGLT Sodium-glucose transporterSHBG Sex hormone binding globulin
SIADH Syndrome of inappropriate ADH secretions.l. Sublingual
SLC Solute carrierSLE Systemic lupus erythematosus
SMON Subacute myelo-optic neuropathySNP Single nucleotide polymorphism
SN-PC Substantia nigra-pars compactaSN-PR Substantia nigra-pars reticularis
SNRI Serotonin and noradrenaline reuptakeinhibitor
s.o.s. as requiredS/P Sulfonamide + pyrimethamine
SPF Sun protection factorSPS Simple partial seizures
SPRM Selective progesterone receptor modulatorSR Sustained release
xvABBREVIATIONS

SRS-A Slow reacting substance of anaphylaxisSSG Sodium stibogluconateSSI Surgical site infection
SSRIs Selective serotonin reuptake inhibitorsSTAT Signal transducer and activator of
transcriptionSTEMI ST-segment elevation myocardial infarction
StK StreptokinaseSU Sulfonylurea
SULT SulfotransferaseSUR Sulfonyl urea receptorsusp Suspension
SWD Shift work disorderSWS Slow wave sleep
syr Syrup
t½ Half lifeT3 TriiodothyronineT4 Thyroxine
tab TabletTAB Typhoid, paratyphoid A and B vaccine
TB Tubercle bacilliTBG Thyroxine binding globulinTCII Transcobalamin II
TCAs Tricyclic antidepressantsTCID50 Tissue culture infectious dose 50%
TDM Therapeutic drug monitoringTDS Three times a day
Tf TransferrinTG Triglyceride
6-TG 6-ThioguanineTGF- Transforming growth factor
THC TetrahydrocannabinolTHFA Tetrahydro folic acid
Thz ThiacetazoneThio TEPA Triethylene thiophosphoramide
THR ThreonineTIAs Transient ischaemic attacks
TNF- Tumour necrosis factor TOD Target organ damageTOF Train of fourt-PA Tissue plasminogen activator
TPMT Thiopurine methyl transferaset.p.r. Total peripheral resistance
TR Thyroid hormone receptorTRE Thyroid hormone response elementTRH Thyrotropin releasing hormoneTSH Thyroid stimulating hormone
TT Tuberculoid leprosyTTS Transdermal therapeutic systemTX Thromboxane
U UnitUA Unstable angina
UDP Uridine diphosphateUFH Unfractionated heparin
UGDP University group diabetic programmeUGT UDP-glucuronosyl transferase
USAN United States adopted nameUT Urea transporter
UTI Urinary tract infection
v VoltV Volume of distribution
VAL ValineVDR Vit D receptorVES Ventricular extrasystole
VF Ventricular fibrillationVIP Vasoactive intestinal peptideVit Vitamin
VKOR Vitamin K epoxide reductaseVL Visceral leishmaniasis
VLDL Very low density lipoproteinVMA Vanillyl mandelic acid
VMAT Vesicular monoamine transporterVRE Vancomycin resistant enterococci
VRSA Vancomycin resistant Staphylococcus aureusVRUT Vasopressin regulated urea transporter
VT Ventricular tachycardiavWF von Willebrand factor
WBC White blood cellsWCVs Water channel containing vesiclesWHO World Health OrganizationWPW Wolff-Parkinson-White syndrome
XDR-TB Extensively drug resistant-TB
Z PyrazinamideZollinger-Ellison (syndrome)ZE (syndrome)
xvi ABBREVIATIONS

Introduction, Routes ofDrug Administration
ChapterChapterChapterChapterChapter 11111
SECTION 1
GENERAL PHARMACOLOGICAL PRINCIPLES
INTRODUCTION
PharmacologyPharmacology is the science of drugs (Greek:Pharmacon—drug; logos—discourse in). In abroad sense, it deals with interaction of exo-genously administered chemical molecules withliving systems, or any single chemical substancewhich can produce a biological response is a‘drug’. It encompasses all aspects of knowledgeabout drugs, but most importantly those that arerelevant to effective and safe use for medicinalpurposes.
For thousands of years most drugs were crudenatural products of unknown composition andlimited efficacy. Only the overt effects of thesesubstances on the body were rather impreciselyknown, but how the same were produced wasentirely unknown. Pharmacology as an experi-mental science was ushered by Rudolf Buchheimwho founded the first institute of pharmacologyin 1847 in Germany. In the later part of the 19thcentury, Oswald Schmiedeberg, regarded as the‘father of pharmacology’, together with his manydisciples like J Langley, T Frazer, P Ehrlich, AJClark, JJ Abel propounded some of the fundamen-tal concepts in pharmacology. Since then drugshave been purified, chemically characterized and
a vast variety of highly potent and selective newdrugs have been developed. The mechanism ofaction including molecular target of many drugshas been elucidated. This has been possible dueto prolific growth of pharmacology which formsthe backbone of rational therapeutics.
The two main divisions of pharmacology arepharmacodynamics and pharmacokinetics.
Pharmacodynamics (Greek: dynamis—power)—What the drug does to the body.This includes physiological and biochemicaleffects of drugs and their mechanism of actionat organ system/subcellular/macromolecularlevels, e.g.—Adrenaline → interaction with adre-noceptors → G-protein mediated stimulation ofcell membrane bound adenylyl cyclase → increa-sed intracellular cyclic 3´,5´AMP → cardiac stimu-lation, hepatic glycogenolysis and hyperglycaemia,etc.
Pharmacokinetics (Greek: Kinesis—move-ment)—What the body does to the drug.This refers to movement of the drug in and altera-tion of the drug by the body; includes absorption,distribution, binding/localization/storage, bio-transformation and excretion of the drug, e.g.paracetamol is rapidly and almost completelyabsorbed orally attaining peak blood levels at

2S
EC
TIO
N1
GENERAL PHARMACOLOGY
30–60 min; 25% bound to plasma proteins, widelyand almost uniformly distributed in the body(volume of distribution ~ 1L/kg); extensivelymetabolized in the liver, primarily by glucuronideand sulfate conjugation into inactive metaboliteswhich are excreted in urine; has a plasma halflife (t½) of 2–3 hours and a clearance value of5 ml/kg/min.
Drug (French: Drogue—a dry herb) It is thesingle active chemical entity present in a medicinethat is used for diagnosis, prevention, treatment/cure of a disease. This disease oriented definitionof drug does not include contraceptives or useof drugs for improvement of health. The WHO(1966) has given a more comprehensivedefinition—“Drug is any substance or productthat is used or is intended to be used to modifyor explore physiological systems or pathologicalstates for the benefit of the recipient.”
The term ‘drugs’ is being also used to meanaddictive/abused/illicit substances. However, thisrestricted and derogatory sense usage is unfor-tunate degradation of a time honoured term, and‘drug’ should refer to a substance that has sometherapeutic/diagnostic application.Some other important aspects of pharmacologyare:
Pharmacotherapeutics It is the applicationof pharmacological information together withknowledge of the disease for its prevention,mitigation or cure. Selection of the most appro-priate drug, dosage and duration of treatmenttaking into account the specific features of apatient are a part of pharmacotherapeutics.
Clinical pharmacology It is the scientificstudy of drugs (both old and new) in man. Itincludes pharmacodynamic and pharmacokineticinvestigation in healthy volunteers and in patients;evaluation of efficacy and safety of drugs andcomparative trials with other forms of treatment;surveillance of patterns of drug use, adverseeffects, etc.
The aim of clinical pharmacology is togenerate data for optimum use of drugs and thepractice of ‘evidence based medicine’.
Chemotherapy It is the treatment of systemicinfection/malignancy with specific drugs that haveselective toxicity for the infecting organism/malignant cell with no/minimal effects on the hostcells.
Drugs in general, can thus be divided into:
Pharmacodynamic agents These are designedto have pharmacodynamic effects in the recipient.
Chemotherapeutic agents These are designedto inhibit/kill invading parasite/malignant cell andhave no/minimal pharmacodynamic effects in therecipient.
Pharmacy It is the art and science of compoun-ding and dispensing drugs or preparing suitabledosage forms for administration of drugs to manor animals. It includes collection, identification,purification, isolation, synthesis, standardizationand quality control of medicinal substances. Thelarge scale manufacture of drugs is called Phar-maceutics. It is primarily a technological science.
Toxicology It is the study of poisonous effectof drugs and other chemicals (household, environ-mental pollutant, industrial, agricultural, homi-cidal) with emphasis on detection, prevention andtreatment of poisonings. It also includes the studyof adverse effects of drugs, since the samesubstance can be a drug or a poison, dependingon the dose.
DRUG NOMENCLATURE
A drug generally has three categories of names:
(a) Chemical name It describes the substancechemically, e.g. 1-(Isopropylamino)-3-(1-napht-hyloxy) propan-2-ol for propranolol. This iscumbersome and not suitable for use inprescribing. A code name, e.g. RO 15-1788 (laternamed flumazenil) may be assigned by themanufacturer for convenience and simplicitybefore an approved name is coined.
(b) Non-proprietary name It is the name accep-ted by a competent scientific body/authority, e.g.the United States Adopted Name (USAN) by the

3C
HA
PTE
R1
INTRODUCTION, ROUTES OF DRUG ADMINISTRATION
USAN council. Similarly, there is the BritishApproved name (BAN) of a drug. The non-proprietary names of newer drugs are kept uniformby an agreement to use the RecommendedInternational Nonproprietary Name (rINN) in allmember countries of the WHO. The BAN of olderdrugs as well has now been modified to becommensurate with rINN. However, many olderdrugs still have more than one non-proprietarynames, e.g. ‘meperidine’ and ‘pethidine’ or‘lidocaine’ and ‘lignocaine’ for the same drugs.Until the drug is included in a pharmacopoeia, thenonproprietary name may also be called theapproved name. After its appearance in the officialpublication, it becomes the official name.
In common parlance, the term generic nameis used in place of nonproprietary name. Etymolo-gically this is incorrect: ‘generic’ should be appliedto the chemical or pharmacological group (orgenus) of the compound, e.g. phenothiazines,tricyclic antidepressants, aminoglycoside antibio-tics, etc. However, this misnomer is widelyaccepted and used even in official parlance.
(c) Proprietary (Brand) name It is the nameassigned by the manufacturer(s) and is his propertyor trade mark. One drug may have multiple pro-prietary names, e.g. ALTOL, ATCARDIL, ATECOR,ATEN, BETACARD, LONOL, TENOLOL, TENORMIN foratenolol from different manufacturers. Brandnames are designed to be catchy, short, easy toremember and often suggestive, e.g. LOPRESORsuggesting drug for lowering blood pressure. Brandnames generally differ in different countries, e.g.timolol maleate eye drops are marketed as TIMOPTICin USA but as GLUCOMOL in India. Even thesame manufacturer may market the same drugunder different brand names in different countries.In addition, combined formulations have their ownmultiple brand names. This is responsible for muchconfusion in drug nomenclature.
There are many arguments for using thenonproprietary name in prescribing: uniformity,convenience, economy and better comprehension(propranolol, sotalol, timolol, pindolol,metoprolol, acebutolol, atenolol are all β blockers,but their brand names have no such similarity).
However, when it is important to ensureconsistency of the product in terms of qualityand bioavailability, etc. and especially whenofficial control over quality of manufacturedproducts is not rigorous, it is better to prescribeby the dependable brand name.
DRUG COMPENDIA
These are compilations of information on drugsin the form of monographs; without going intothe theoretical concepts, mechanisms of actionand other aspects which help in understandingthe subject. Pharmacopoeias and Formularies arebroughtout by the Government in a country, holdlegal status and are called official compendia.In addition, some non-official compendia arepublished by professional bodies, which aresupplementary and dependable sources ofinformation about drugs.
Pharmacopoeias They contain description ofchemical structure, molecular weight, physical andchemical characteristics, solubility, identificationand assay methods, standards of purity, storageconditions and dosage forms of officially approveddrugs in a country. They are useful to drugmanufacturers and regulatory authorities, but notto doctors, most of whom never see apharmacopoeia. Examples are Indian (IP), British(BP), European (Eur P), United States (USP)pharmacopoeias.
Formularies Generally produced in easilycarried booklet form, they list indications, dose,dosage forms, contraindications, precautions,adverse effects and storage of selected drugs thatare available for medicinal use in a country. Drugsare categorized by their therapeutic class. Somerational fixed-dose drug combinations areincluded. A brief commentary on the drug classand clinical conditions in which they are usedgenerally preceeds specifics of individual drugs.Brief guidelines for treatment of selectedconditions are provided. While British NationalFormulary (BNF) also lists brand nameswith costs, the National Formulary of India (NFI)does not include these. Most formularies have

4S
EC
TIO
N1
GENERAL PHARMACOLOGY
informative appendices as well. Formularies canbe considerably helpful to prescribers.
Martindale: The Complete Drug Reference(Extrapharmacopoeia) Published every 2–3years by the Royal Pharmaceutical Society of GreatBritain, this non-official compendium is anexhaustive and updated compilation of unbiasedinformation on medicines used/registered all overthe world. It includes new launches and containspharmaceutical, pharmacological as well astherapeutic information on drugs, which can serveas a reliable reference book.
Physicians Desk Reference (PDR) and Drug:Facts and Comparisons (both from USA), etc.are other useful non-official compendia.
ESSENTIAL MEDICINES (DRUGS)CONCEPT
The WHO has defined Essential Medicines(drugs) as “those that satisfy the priority healthcareneeds of the population. They are selected withdue regard to public health relevance, evidenceon efficacy and safety, and comparative costeffectiveness. Essential medicines are intendedto be available within the context of functioninghealth systems at all times and in adequateamounts, in appropriate dosage forms, withassured quality and adequate information, and ata price the individual and the community canafford.
It has been realized that only a handful ofmedicines out of the multitude available can meetthe health care needs of majority of the peoplein any country, and that many well tested andcheaper medicines are equally (or more)efficacious and safe as their newer more expensivecongeners. For optimum utilization of resources,governments (especially in developing countries)should concentrate on these medicines byidentifying them as Essential medicines. TheWHO has laid down criteria to guide selectionof an essential medicine.(a) Adequate data on its efficacy and safety should be availablefrom clinical studies.
(b) It should be available in a form in which quality, includingbioavailability, and stability on storage can be assured.(c) Its choice should depend upon pattern of prevalentdiseases; availability of facilities and trained personnel;financial resources; genetic, demographic and environmentalfactors.(d) In case of two or more similar medicines, choice shouldbe made on the basis of their relative efficacy, safety, quality,price and availability. Cost-benefit ratio should be a majorconsideration.(e) Choice may also be influenced by comparative pharma-cokinetic properties and local facilities for manufacture andstorage.(f) Most essential medicines should be single compounds.Fixed ratio combination products should be included onlywhen dosage of each ingradient meets the requirements ofa defined population group, and when the combination hasa proven advantage in therapeutic effect, safety, adherenceor in decreasing the emergence of drug resistance.(g) Selection of essential medicines should be a continuousprocess which should take into account the changing prioritiesfor public health action, epidemiological conditions as wellas availability of better medicines/formulations and progressin pharmacological knowledge.(h) Recently, it has been emphasized to select essentialmedicines based on rationally developed treatment guidelines.
To guide the member countries, the WHObrought out its first Model List of Essential Drugsalong with their dosage forms and strengths in1977 which could be adopted after suitablemodifications according to local needs. This hasbeen revised from time to time and the currentis the 17th list (2011). India produced its NationalEssential Drugs List in 1996 and has revisedit in 2011 with the title “National List of EssentialMedicines”. This includes 348 medicines whichare considered to be adequate to meet the priorityhealthcare needs of the general population of thecountry. An alphabetical compilation of the WHOas well as National essential medicines is presentedas Appendix-2.
Adoption of the essential medicines list forprocurement and supply of medicines, especiallyin the public sector healthcare system, has resultedin improved availability of medicines, cost savingand more rational use of drugs.
Prescription and non-prescription drugsAs per drug rules, majority of drugs includingall antibiotics must be sold in retail only againsta prescription issued to a patient by a registeredmedical practitioner. These are called ‘prescription

5C
HA
PTE
R1
INTRODUCTION, ROUTES OF DRUG ADMINISTRATION
drugs’, and in India they have been placed inthe schedule H of the Drugs and Cosmetic Rules(1945) as amended from time to time. However,few drugs like simple analgesics (paracetamolaspirin), antacids, laxatives (senna, lactulose),vitamins, ferrous salts, etc. are considered relativelyharmless, and can be procured without aprescription. These are ‘non-prescription’ or ‘over-the-counter’ (OTC) drugs; can be sold even bygrocery stores.Orphan Drugs These are drugs or biological productsfor diagnosis/treatment/ prevention of a rare disease orcondition, or a more common disease (endemic only inresource poor countries) for which there is no reasonableexpectation that the cost of developing and marketing it willbe recovered from the sales of that drug. The list includessodium nitrite, fomepizole, liposomal amphotericin B,miltefosine, rifabutin, succimer, somatropin, digoxin immuneFab (digoxin antibody), liothyronine (T3) and many more.Though these drugs may be life saving for some patients,they are commercially difficult to obtain as a medicinalproduct. Governments in developed countries offer tax benefitsand other incentives to pharmaceutical companies fordeveloping and marketing orphan drugs (e.g. Orphan DrugAct in USA).
ROUTES OF DRUG ADMINISTRATIONMost drugs can be administered by a variety ofroutes. The choice of appropriate route in a givensituation depends both on drug as well as patientrelated factors. Mostly common sense consi-derations, feasibility and convenience dictate theroute to be used.
Routes can be broadly divided into those for(a) Local action and (b) Systemic action.
LOCAL ROUTES
These routes can only be used for localized lesionsat accessible sites and for drugs whose systemicabsorption from these sites is minimal or absent.Thus, high concentrations are attained at thedesired site without exposing the rest of the body.Systemic side effects or toxicity are consequentlyabsent or minimal. For drugs (in suitable dosageforms) that are absorbed from these sites/routes,the same can serve as systemic route of adminis-tration, e.g. glyceryl trinitrate (GTN) applied onthe skin as ointment or transdermal patch. Thelocal routes are:1. Topical This refers to external applicationof the drug to the surface for localized action. Itis often more convenient as well as encouragingto the patient. Drugs can be efficiently deliveredto the localized lesions on skin, oropharyngeal/nasal mucosa, eyes, ear canal, anal canal or vaginain the form of lotion, ointment, cream, powder,rinse, paints, drops, spray, lozengens, suppositoriesor pesseries. Nonabsorbable drugs given orally foraction on g.i. mucosa (sucralfate, vancomycin),inhalation of drugs for action on bronchi(salbutamol, cromolyn sodium) and irrigatingsolutions/jellys (povidone iodine, lidocaine)applied to urethra are other forms of topicalmedication.2. Deeper tissues Certain deep areas can beapproached by using a syringe and needle, butthe drug should be in such a form that systemicabsorption is slow, e.g. intra-articular injection(hydrocortisone acetate in knee joint), infiltrationaround a nerve or intrathecal injection (lidocaine),retrobulbar injection (hydrocortisone acetatebehind the eyeball).3. Arterial supply Close intra-arterial injec-tion is used for contrast media in angiography;anticancer drugs can be infused in femoral orbrachial artery to localise the effect for limbmalignancies.
SYSTEMIC ROUTES
The drug administered through systemic routesis intended to be absorbed into the blood stream
Factors governing choice of route
1. Physical and chemical properties of the drug (solid/liquid/gas; solubility, stability, pH, irritancy).
2. Site of desired action—localized and approach-able or generalized and not approachable.
3. Rate and extent of absorption of the drug fromdifferent routes.
4. Effect of digestive juices and first pass metabolismon the drug.
5. Rapidity with which the response is desired (routinetreatment or emergency).
6. Accuracy of dosage required (i.v. and inhalationalcan provide fine tuning).
7. Condition of the patient (unconscious, vomiting).

6S
EC
TIO
N1
GENERAL PHARMACOLOGY
and distributed all over, including the site of action,through circulation (see Fig. 1.1).
1. OralOral ingestion is the oldest and commonest modeof drug administration. It is safer, more convenient,does not need assistance, noninvasive, oftenpainless, the medicament need not be sterile andso is cheaper. Both solid dosage forms (powders,tablets, capsules, spansules, dragees, mouldedtablets, gastrointestinal therapeutic systems—GITs) and liquid dosage forms (elixirs, syrups,emulsions, mixtures) can be given orally.
inconvenient and embarrassing; absorption isslower, irregular and often unpredictable, thoughdiazepam solution and paracetamol suppositoryare rapidly and dependably absorbed from therectum in children. Drug absorbed into externalhaemorrhoidal veins (about 50%) bypasses liver,but not that absorbed into internal haemorrhoidalveins. Rectal inflammation can result from irritantdrugs. Diazepam, indomethacin, paracetamol,ergotamine and few other drugs are some timesgiven rectally.
4. CutaneousHighly lipid soluble drugs can be applied overthe skin for slow and prolonged absorption. Theliver is also bypassed. The drug can be incorpo-rated in an ointment and applied over specifiedarea of skin. Absorption of the drug can beenhanced by rubbing the preparation, by usingan oily base and by an occlusive dressing.
Transdermal therapeutic systems (TTS)These are devices in the form of adhesive patchesof various shapes and sizes (5–20 cm2) whichdeliver the contained drug at a constant rate intosystemic circulation via the stratum corneum (Fig.1.2). The drug (in solution or bound to a polymer)is held in a reservoir between an occlusive backingfilm and a rate controlling micropore membrane,the under surface of which is smeared with anadhesive impregnated with priming dose of thedrug. The adhesive layer is protected by anotherfilm that is to be peeled off just before applica-tion. The drug is delivered at the skin surfaceby diffusion for percutaneous absorption intocirculation. The micropore membrane is such thatrate of drug delivery to skin surface is less thanthe slowest rate of absorption from the skin. Thisoffsets any variation in the rate of absorptionaccording to the properties of different sites. Assuch, the drug is delivered at a constant andpredictable rate irrespective of site of application.Usually chest, abdomen, upper arm, lower back,buttock or mastoid region are utilized.
Transdermal patches of GTN, fentanyl,nicotine and estradiol are available in India, while
Limitations of oral route of administration
• Action of drugs is slower and thus not suitable foremergencies.
• Unpalatable drugs (chloramphenicol) are difficult toadminister; drug may be filled in capsules tocircumvent this.
• May cause nausea and vomiting (emetine).• Cannot be used for uncooperative/unconscious/
vomiting patient.• Absorption of drugs may be variable and erratic;
certain drugs are not absorbed (streptomycin).• Others are destroyed by digestive juices (penicillin G,
insulin) or in liver (GTN, testosterone, lidocaine).
2. Sublingual (s.l.) or buccalThe tablet or pellet containing the drug is placedunder the tongue or crushed in the mouth andspread over the buccal mucosa. Only lipid solubleand non-irritating drugs can be so administered.Absorption is relatively rapid—action can be pro-duced in minutes. Though it is somewhat incon-venient, one can spit the drug after the desiredeffect has been obtained. The chief advantageis that liver is bypassed and drugs with high firstpass metabolism can be absorbed directly intosystemic circulation. Drugs given sublinguallyare—GTN, buprenorphine, desamino-oxytocin.
3. RectalCertain irritant and unpleasant drugs can be putinto rectum as suppositories or retention enemafor systemic effect. This route can also beused when the patient is having recurrent vomitingor is unconscious. However, it is rather

7C
HA
PTE
R1
INTRODUCTION, ROUTES OF DRUG ADMINISTRATION
Fig. 1.1: Vascular pathway of drugs absorbed from various systemic routes of administration and sitesof first pass metabolismNote: Total drug absorbed orally is subjected to first pass metabolism in intestinal wall and liver, whileapproximately half of that absorbed from rectum passes through liver. Drug entering from any systemicroute is exposed to first pass metabolism in lungs, but its extent is minor for most drugs.

8S
EC
TIO
N1
GENERAL PHARMACOLOGY
drugs like insulin, as well as to bypass the blood-brain barrier.
7. Parenteral(Par—beyond, enteral—intestinal)Conventionally, parenteral refers to administrationby injection which takes the drug directly intothe tissue fluid or blood without having to crossthe enteral mucosa. The limitations of oraladministration are circumvented.
Drug action is faster and surer (valuable inemergencies). Gastric irritation and vomiting arenot provoked. Parenteral routes can be employedeven in unconscious, uncooperative or vomitingpatient. There are no chances of interference byfood or digestive juices. Liver is bypassed.
Disadvantages of parenteral routes are—thepreparation has to be sterilized and is costlier,the technique is invasive and painful, assistanceof another person is mostly needed (though selfinjection is possible, e.g. insulin by diabetics),there are chances of local tissue injury and, ingeneral, parenteral route is more risky than oral.The important parenteral routes are:
(i) Subcutaneous (s.c.) The drug is depositedin the loose subcutaneous tissue which is richlysupplied by nerves (irritant drugs cannot beinjected) but is less vascular (absorption is slowerthan intramuscular). Only small volumes can beinjected s.c. Self-injection is possible because deeppenetration is not needed. This route should beavoided in shock patients who are vasocons-tricted—absorption will be delayed. Repository(depot) preparations that are aqueous suspensionscan be injected for prolonged action. Some specialforms of this route are:
(a) Dermojet In this method needle is not used;a high velocity jet of drug solution is projectedfrom a microfine orifice using a gun like imple-ment. The solution passes through the superficiallayers and gets deposited in the subcutaneoustissue. It is essentially painless and suited for massinoculations.
(b) Pellet implantation The drug in the formof a solid pellet is introduced with a trochar and
Fig. 1.2: Illustration of a transdermal drug delivery system
those of isosorbide dinitrate, hyoscine, andclonidine are marketed elsewhere. For differentdrugs, TTS have been designed to last for1–3 days. Though more expensive, they providesmooth plasma concentrations of the drug withoutfluctuations; minimize interindividual variations(drug is subjected to little first pass metabolism)and side effects. They are also more convenient—many patients prefer transdermal patches to oraltablets of the same drug; patient compliance isbetter. Local irritation and erythema occurs insome, but is generally mild; can be minimizedby changing the site of application each time byrotation. Discontinuation has been necessary in2–7% cases.
5. InhalationVolatile liquids and gases are given by inhalationfor systemic action, e.g. general anaesthetics.Absorption takes place from the vast surface ofalveoli—action is very rapid. When administra-tion is discontinued the drug diffuses back andis rapidly eliminated in expired air. Thus, control-led administration is possible with moment tomoment adjustment. Irritant vapours (ether) causeinflammation of respiratory tract and increasesecretion.
6. NasalThe mucous membrane of the nose can readilyabsorb many drugs; digestive juices and liver arebypassed. However, only certain drugs like GnRHagonists and desmopressin applied as a spray ornebulized solution have been used by this route.This route is being tried for some other peptide

9C
HA
PTE
R1
INTRODUCTION, ROUTES OF DRUG ADMINISTRATION
cannula. This provides sustained release of thedrug over weeks and months, e.g. DOCA,testosterone.
(c) Sialistic (nonbiodegradable) and bio-degradable implants Crystalline drug ispacked in tubes or capsules made of suitablematerials and implanted under the skin. Slow anduniform leaching of the drug occurs over monthsproviding constant blood levels. The nonbio-degradable implant has to be removed later onbut not the biodegradable one. This has been triedfor hormones and contraceptives (e.g. NORPLANT).
(ii) Intramuscular (i.m.) The drug is injectedin one of the large skeletal muscles—deltoid,triceps, gluteus maximus, rectus femoris, etc.Muscle is less richly supplied with sensory nerves(mild irritants can be injected) and is morevascular (absorption of drugs in aqueous solutionis faster). It is less painful, but self injection isoften impracticable because deep penetration isneeded. Depot preparations (oily solutions,aqueous suspensions) can be injected by this route.Intramuscular injections should be avoided inanticoagulant treated patients, because it canproduce local haematoma.
(iii) Intravenous (i.v.) The drug is injectedas a bolus (Greek: bolos–lump) or infused slowlyover hours in one of the superficial veins. The
drug reaches directly into the blood stream andeffects are produced immediately (great value inemergency). The intima of veins is insensitiveand drug gets diluted with blood, therefore, evenhighly irritant drugs can be injected i.v., but hazardsare—thrombophlebitis of the injected vein andnecrosis of adjoining tissues if extravasation occurs.These complications can be minimized by dilutingthe drug or injecting it into a running i.v. line.Only aqueous solutions (not suspensions, becausedrug particles can cause embolism) are to beinjected i.v. and there are no depot preparationsfor this route. Chances of causing air embolismis another risk. The dose of the drug requiredis smallest (bioavailability is 100%) and even largevolumes can be infused. One big advantage withthis route is—in case response is accurately measur-able (e.g. BP) and the drug short acting (e.g.sodium nitroprusside), titration of the dose withthe response is possible. However, this is the mostrisky route—vital organs like heart, brain, etc.get exposed to high concentrations of the drug.
(iv) Intradermal injection The drug isinjected into the skin raising a bleb (e.g. BCGvaccine, sensitivity testing) or scarring/multiplepuncture of the epidermis through a drop of thedrug is done. This route is employed for specificpurposes only.
PROBLEM DIRECTED STUDY
1.1. A 5-year-old child is brought to the hospital with the complaint of fever, cough, breathlessnessand chest pain. On examination he is found to be dull, but irritable with fast pulse (116/min),rapid breathing (RR 50/min) and indrawing of lower chest during inspiration, wheezing, crepitationsand mild dehydration. Body temperature is 40°C (104°F). The paediatrician makes a provisionaldiagnosis of acute pneumonia and orders relevant haematological as well as bacteriological investig-ations. He decides to institute antibiotic therapy.(a) In case he selects an antibiotic which can be given orally as well as by i.m. or i.v. injection,which route of administration will be most appropriate in this case?(b) Should the paediatrician administer the antibiotic straight away or should he wait for thelaboratory reports?(see Appendix-1 for solution)

Pharmacokinetics: MembraneTransport, Absorption andDistribution of Drugs
ChapterChapterChapterChapterChapter 22222
Pharmacokinetics is the quantitative study of drugmovement in, through and out of the body. Theoverall scheme of pharmacokinetic processes isdepicted in Fig. 2.1. The intensity of responseis related to concentration of the drug at the siteof action, which in turn is dependent on itspharmacokinetic properties. Pharmacokineticconsiderations, therefore, determine the route(s)of administration, dose, latency of onset, timeof peak action, duration of action and frequencyof administration of a drug.
All pharmacokinetic processes involve trans-port of the drug across biological membranes.
Biological membrane This is a bilayer (about100 Å thick) of phospholipid and cholesterolmolecules, the polar groups (glyceryl phosphateattached to ethanolamine/choline or hydroxyl
group of cholesterol) of these are oriented at thetwo surfaces and the nonpolar hydrocarbon chainsare embedded in the matrix to form a continuoussheet. This imparts high electrical resistanceand relative impermeability to the membrane.Extrinsic and intrinsic protein molecules areadsorbed on the lipid bilayer (Fig. 2.2). Glyco-proteins or glycolipids are formed on the surfaceby attachment to polymeric sugars, aminosugarsor sialic acids. The specific lipid and proteincomposition of different membranes differsaccording to the cell or the organelle type. Theproteins are able to freely float through themembrane: associate and organize or vice versa.Some of the intrinsic ones, which extend throughthe full thickness of the membrane, surround fineaqueous pores. Paracellular spaces or channelsalso exist between certain epithelial/endothelial
Fig. 2.1: Schematic depiction of pharmacokinetic processes

11C
HA
PTE
R2
MEMBRANE TRANSPORT, ABSORPTION AND DISTRIBUTION OF DRUGS
cells. Other adsorbed proteins have enzymatic,carrier, receptor or signal transduction properties.Lipid molecules also are capable of lateral move-ment. Thus, biological membranes are highlydynamic structures.
Drugs are transported across the membranes by:(a) Passive diffusion and filtration(b) Specialized transport
Passive diffusionThe drug diffuses across the membrane in thedirection of its concentration gradient, themembrane playing no active role in the process.This is the most important mechanism for majorityof drugs; drugs are foreign substances(xenobiotics), and specialized mechanisms aredeveloped by the body primarily for normalmetabolites.
Lipid soluble drugs diffuse by dissolving inthe lipoidal matrix of the membrane (Fig. 2.3),the rate of transport being proportional to thelipid : water partition coefficient of the drug. Amore lipid-soluble drug attains higher concentra-tion in the membrane and diffuses quickly. Also,greater the difference in the concentration of thedrug on the two sides of the membrane, fasteris its diffusion.
Influence of pH Most drugs are weak electro-lytes, i.e. their ionization is pH dependent (contraststrong electrolytes that are nearly completely
ionized at acidic as well as alkaline pH). Theionization of a weak acid HA is given by theequation:
[A¯ ]pH = pKa + log —–— ...(1)
[HA]
pKa is the negative logarithm of acidic disso-ciation constant of the weak electrolyte. If theconcentration of ionized drug [A¯ ] is equal toconcentration of unionized drug [HA], then
[A¯ ]—–— = 1[HA]
since log 1 is 0, under this conditionpH = pKa ...(2)
Thus, pKa is numerically equal to the pH at whichthe drug is 50% ionized.If pH is increased by 1 scale, then—
log [A¯ ]/[HA] = 1 or [A¯ ]/[HA] = 10
Similarly, if pH is reduced by 1 scale, then—[A¯ ]/[HA] = 1/10
Thus, weakly acidic drugs, which form saltswith cations, e.g. sod. phenobarbitone, sod.sulfadiazine, pot. penicillin-V, etc. ionize more at
Fig. 2.2: Illustration of the organisation of biologicalmembrane
Fig. 2.3: Illustration of passive diffusion and filtrationacross the lipoidal biological membrane with aqueouspores

12S
EC
TIO
N1
GENERAL PHARMACOLOGY
alkaline pH and 1 scale change in pH causes 10fold change in ionization.
Weakly basic drugs, which form salts withanions, e.g. atropine sulfate, ephedrine HCl,chloroquine phosphate, etc. conversely ionizemore at acidic pH. Ions being lipid insoluble,do not diffuse and a pH difference across amembrane can cause differential distribution ofweakly acidic and weakly basic drugs on the twosides (Fig. 2.4).
Lipid-soluble nonelectrolytes (e.g. ethanol,diethyl-ether) readily cross biological membranesand their transport is pH independent.
FiltrationFiltration is passage of drugs through aqueouspores in the membrane or through paracellularspaces. This can be accelerated if hydrodynamicflow of the solvent is occurring under hydrostaticor osmotic pressure gradient, e.g. across mostcapillaries including glomeruli. Lipid-insolubledrugs cross biological membranes by filtrationif their molecular size is smaller than the diameterof the pores (Fig. 2.3). Majority of cells (intestinalmucosa, RBC, etc.) have very small pores (4 Å)and drugs with MW > 100 or 200 are not ableto penetrate. However, capillaries (except thosein brain) have large paracellular spaces (40 Å)and most drugs (even albumin) can filter throughthese (Fig. 2.8). As such, diffusion of drugs acrosscapillaries is dependent on rate of blood flowthrough them rather than on lipid solubility ofthe drug or pH of the medium.
Specialized transportThis can be carrier mediated or by pinocytosis.
Carrier transportAll cell membranes express a host of transmem-brane proteins which serve as carriers ortransporters for physiologically important ions,nutrients, metabolites, transmitters, etc. across themembrane. At some sites, certain transporters alsotranslocate xenobiotics, including drugs and theirmetabolites. In contrast to channels, which openfor a finite time and allow passage of specificions, transporters combine transiently with theirsubstrate (ion or organic compound)—undergoa conformational change carrying the substrateto the other side of the membrane where thesubstrate dissociates and the transporter returnsback to its original state (Fig. 2.5). Carriertransport is specific for the substrate (or the typeof substrate, e.g. an organic anion), saturable,competitively inhibited by analogues which utilizethe same transporter, and is much slower than
Fig. 2.4: Influence of pH difference on two sides of abiological membrane on the steady-state distribution ofa weakly acidic drug with pKa = 6
Implications of this consideration are:(a) Acidic drugs, e.g. aspirin (pKa 3.5) are largelyunionized at acid gastric pH and are absorbedfrom stomach, while bases, e.g. atropine (pKa10) are largely ionized and are absorbed onlywhen they reach the intestines.(b) The unionized form of acidic drugs whichcrosses the surface membrane of gastric mucosalcell, reverts to the ionized form within the cell(pH 7.0) and then only slowly passes to theextracellular fluid. This is called ion trapping,i.e. a weak electrolyte crossing a membrane toencounter a pH from which it is not able to escapeeasily. This may contribute to gastric mucosalcell damage caused by aspirin.(c) Basic drugs attain higher concentrationintracellularly (pH 7.0 vs 7.4 of plasma).(d) Acidic drugs are ionized more in alkalineurine—do not back diffuse in the kidney tubulesand are excreted faster. Accordingly, basic drugsare excreted faster if urine is acidified.

13C
HA
PTE
R2
MEMBRANE TRANSPORT, ABSORPTION AND DISTRIBUTION OF DRUGS
Fig. 2.5: Illustration of different types of carrier mediated transport across biological membraneABC—ATP-binding cassettee transporter; SLC—Solute carrier transporter; M—MembraneA. Facilitated diffusion: the carrier (SLC) binds and moves the poorly diffusible substrate along its concentration
gradient (high to low) and does not require energyB. Primary active transport: the carrier (ABC) derives energy directly by hydrolysing ATP and moves the substrate
against its concentration gradient (low to high)C. Symport: the carrier moves the substrate ‘A’ against its concentration gradient by utilizing energy from downhill
movement of another substrate ‘B’ in the same directionD. Antiport: the carrier moves the substrate ‘A’ against its concentration gradient and is energized by the downhill
movement of another substrate ‘B’ in the opposite direction
the flux through channels. Depending onrequirement of energy, carrier transport is of twotypes:a. Facilitated diffusion The transporter,belonging to the super-family of solute carrier(SLC) transporters, operates passively withoutneeding energy and translocates the substrate inthe direction of its electrochemical gradient, i.e.from higher to lower concentration (Fig. 2.5A).It mearly facilitates permeation of a poorlydiffusible substrate, e.g. the entry of glucose intomuscle and fat cells by the glucose transporterGLUT 4.b. Active transport It requires energy, isinhibited by metabolic poisons, and transports thesolute against its electrochemical gradient (low
to high), resulting in selective accumulation ofthe substance on one side of the membrane. Drugsrelated to normal metabolites can utilize thetransport processes meant for these, e.g. levodopaand methyl dopa are actively absorbed from thegut by the aromatic amino acid transporter. Inaddition, the body has developed some relativelynonselective transporters, like P-glycoprotein(P-gp), to deal with xenobiotics. Active transportcan be primary or secondary depending on thesource of the driving force.i. Primary active transport Energy isobtained directly by the hydrolysis of ATP (Fig.2.5B). The transporters belong to the superfamilyof ATP binding cassettee (ABC) transporterswhose intracellular loops have ATPase activity.

14S
EC
TIO
N1
GENERAL PHARMACOLOGY
They mediate only efflux of the solute from thecytoplasm, either to extracellular fluid or into anintracellular organelli (endoplasmic reticulum,mitochondria, etc.)
Encoded by the multidrug resistance 1 (MDR1) gene,P-gp is the most well known primary active transporterexpressed in the intestinal mucosa, renal tubules, bilecanaliculi, choroidal epithelium, astrocyte foot processesaround brain capillaries (the blood-brain barrier), testicularand placental microvessels, which pumps out many drugs/metabolites and thus limits their intestinal absorption,penetration into brain, testes and foetal tissues as well aspromotes biliary and renal elimination. Many xenobioticswhich induce or inhibit P-gp also have a similar effect onthe drug metabolizing isoenzyme CYP3A4, indicating theirsynergistic role in detoxification of xenobiotics.
Other primary active transporters of pharmacologicalsignificance are multidrug resistance associated protein 2(MRP 2) and breast cancer resistance protein (BCRP).ii. Secondary active transport In this typeof active transport effected by another set of SLCtransporters, the energy to pump one solute isderived from the downhill movement of anothersolute (mostly Na+). When the concentrationgradients are such that both the solutes move inthe same direction (Fig. 2.5C), it is called symportor cotransport, but when they move in oppositedirections (Fig. 2.5D), it is termed antiport orexchange transport. Metabolic energy (fromhydrolysis of ATP) is spent in maintaining hightransmembrane electrochemical gradient of thesecond solute (generally Na+). The SLCtransporters mediate both uptake and efflux ofdrugs and metabolites.
The organic anion transporting polypeptide (OATP) andorganic cation transporter (OCT), highly expressed in livercanaliculi and renal tubules, are secondary active transportersimportant in the metabolism and excretion of drugs andmetabolites (especially glucuronides). The Na+,Cl– dependentneurotransmitter transporters for norepinephrine, serotoninand dopamine (NET, SERT and DAT) are active SLCtransporters that are targets for action of drugs like tricyclicantidepressants, selective serotonin reuptake inhibitors(SSRIs), cocaine, etc. Similarly, the Vesicular monoaminetransporter (VMAT-2) of adrenergic and serotonergic storagevesicles transports catecholamines and 5-HT into the vesiclesby exchanging with H+ions, and is inhibited by reserpine.The absorption of glucose in intestines and renal tubulesis through secondary active transport by sodium-glucosetransporters (SGLT1 and SGLT2).
As indicated earlier, carrier transport (bothfacilitated diffusion and active transport) is
saturable and follows the Michaelis-Mentenkinetics. The maximal rate of transport isdependent on the density of the transporter ina particular membrane, and its rate constant (Km),i.e. the substrate concentration at which rate oftransport is half maximal, is governed by itsaffinity for the substrate. Genetic polymorphismcan alter both the density and affinity of thetransporter protein for different substrates and thusaffect the pharmacokinetics of drugs. Moreover,tissue specific drug distribution can occur dueto the presence of specific transporters in certaincells.
Pinocytosis It is the process of transport across the cell inparticulate form by formation of vesicles. This is applicable toproteins and other big molecules, and contributes little totransport of most drugs, barring few like vit B12 which is absorbedfrom the gut after binding to intrinsic factor (a protein).
ABSORPTION
Absorption is movement of the drug from its siteof administration into the circulation. Not onlythe fraction of the administered dose that getsabsorbed, but also the rate of absorption isimportant. Except when given i.v., the drug hasto cross biological membranes; absorption isgoverned by the above described principles. Otherfactors affecting absorption are:
Aqueous solubility Drugs given in solid formmust dissolve in the aqueous biophase before theyare absorbed. For poorly water soluble drugs(aspirin, griseofulvin) rate of dissolution governsrate of absorption. Ketoconazole dissolves at lowpH: gastric acid is needed for its absorption.Obviously, a drug given as watery solution isabsorbed faster than when the same is given insolid form or as oily solution.
Concentration Passive diffusion depends onconcentration gradient; drug given as concentratedsolution is absorbed faster than from dilutesolution.
Area of absorbing surface Larger is thesurface area, faster is the absorption.

15C
HA
PTE
R2
MEMBRANE TRANSPORT, ABSORPTION AND DISTRIBUTION OF DRUGS
Vascularity of the absorbing surface Bloodcirculation removes the drug from the site ofabsorption and maintains the concentrationgradient across the absorbing surface. Increasedblood flow hastens drug absorption just as windhastens drying of clothes.
Route of administration This affects drugabsorption, because each route has its ownpeculiarities.
OralThe effective barrier to orally administered drugsis the epithelial lining of the gastrointestinal tract,which is lipoidal. Nonionized lipid soluble drugs,e.g. ethanol are readily absorbed from stomachas well as intestine at rates proportional to theirlipid : water partition coefficient. Acidic drugs,e.g. salicylates, barbiturates, etc. are predominantlyunionized in the acid gastric juice and are absorbedfrom stomach, while basic drugs, e.g. morphine,quinine, etc. are largely ionized and are absorbedonly on reaching the duodenum. However, evenfor acidic drugs absorption from stomach isslower, because the mucosa is thick, covered withmucus and the surface area is small. Absorbingsurface area is much larger in the small intestinedue to villi. Thus, faster gastric emptyingaccelerates drug absorption in general. Dissolutionis a surface phenomenon, therefore, particle sizeof the drug in solid dosage form governs rateof dissolution and in turn rate of absorption.
Presence of food dilutes the drug and retardsabsorption. Further, certain drugs form poorlyabsorbed complexes with food constituents, e.g.tetracyclines with calcium present in milk;moreover food delays gastric emptying. Thus,most drugs are absorbed better if taken in emptystomach. However, there are some exceptions,e.g. fatty food greatly enhances lumefantrineabsorption. Highly ionized drugs, e.g. gentamicin,neostigmine are poorly absorbed when givenorally.
Certain drugs are degraded in the gastrointes-tinal tract, e.g. penicillin G by acid, insulin bypeptidases, and are ineffective orally. Entericcoated tablets (having acid resistant coating) and
sustained release preparations (drug particlescoated with slowly dissolving material) can beused to overcome acid lability, gastric irritancyand brief duration of action.
The oral absorption of certain drugs is lowbecause a fraction of the absorbed drug is extru-ded back into the intestinal lumen by the effluxtransporter P-gp located in the gut epithelium.The low oral bioavailability of digoxin and cyclo-sporine is partly accounted by this mechanism.Inhibitors of P-gp like quinidine, verapamil,erythromycin, etc. enhance, while P-gp inducerslike rifampin and phenobarbitone reduce the oralbioavailability of these drugs.
Absorption of a drug can be affected by otherconcurrently ingested drugs. This may be a luminaleffect: formation of insoluble complexes, e.g.tetracyclines and iron preparations with calciumsalts and antacids, phenytoin with sucralfate. Suchinteraction can be minimized by administering thetwo drugs at 2–3 hr intervals. Alteration of gut floraby antibiotics may disrupt the enterohepatic cyclingof oral contraceptives and digoxin. Drugs can alsoalter absorption by gut wall effects: altering motility(anticholinergics, tricyclic antidepressants, opioids,metoclopramide) or causing mucosal damage(neomycin, methotrexate, vinblastine).
Subcutaneous and IntramuscularBy these routes the drug is deposited directly inthe vicinity of the capillaries. Lipid soluble drugspass readily across the whole surface of thecapillary endothelium. Capillaries having largeparacellular spaces do not obstruct absorption ofeven large lipid insoluble molecules or ions (Fig.2.8A). Very large molecules are absorbed throughlymphatics. Thus, many drugs not absorbed orallyare absorbed parenterally. Absorption from s.c. siteis slower than that from i.m. site, but both aregenerally faster and more consistent/ predictablethan oral absorption. Application of heat andmuscular exercise accelerate drug absorption byincreasing blood flow, while vasoconstrictors, e.g.adrenaline injected with the drug (local anaesthetic)retard absorption. Incorporation of hyaluronidasefacilitates drug absorption from s.c. injection by

16S
EC
TIO
N1
GENERAL PHARMACOLOGY
promoting spread. Many depot preparations, e.g.benzathine penicillin, protamine zinc insulin, depotprogestins, etc. can be given by these routes.
Topical sites (skin, cornea, mucousmembranes)Systemic absorption after topical applicationdepends primarily on lipid solubility of drugs.However, only few drugs significantly penetrateintact skin. Hyoscine, fentanyl, GTN, nicotine,testosterone, and estradiol (see p. 8) have beenused in this manner. Corticosteroids applied overextensive areas can produce systemic effects andpituitary-adrenal suppression. Absorption can bepromoted by rubbing the drug incorporated inan olegenous base or by use of occlusive dressingwhich increases hydration of the skin. Organo-phosphate insecticides coming in contact with skincan produce systemic toxicity. Abraded surfacesreadily absorb drugs, e.g. tannic acid applied overburnt skin has produced hepatic necrosis.
Cornea is permeable to lipid soluble, unioni-zed physostigmine but not to highly ionizedneostigmine. Drugs applied as eye drops may getabsorbed through the nasolacrimal duct, e.g.timolol eye drops may produce bradycardia andprecipitate asthma. Mucous membranes of mouth,rectum, vagina absorb lipophilic drugs: estrogencream applied vaginally has produced gynaeco-mastia in the male partner.
BIOAVAILABILITY
Bioavailability refers to the rate and extent ofabsorption of a drug from a dosage form asdetermined by its concentration-time curve inblood or by its excretion in urine (Fig. 2.6). Itis a measure of the fraction (F ) of administereddose of a drug that reaches the systemic circulationin the unchanged form. Bioavailability of druginjected i.v. is 100%, but is frequently lower afteroral ingestion because—(a) the drug may be incompletely absorbed.(b) the absorbed drug may undergo first passmetabolism in the intestinal wall/liver or beexcreted in bile.
Fig. 2.6: Plasma concentration-time curves depictingbioavailability differences between three preparations ofa drug containing the same amountNote that formulation B is more slowly absorbed than A,and though ultimately both are absorbed to the sameextent (area under the curve same), B may not producetherapeutic effect; C is absorbed to a lesser extent—lower bioavailability
Incomplete bioavailability after s.c. or i.m.injection is less common, but may occur due tolocal binding of the drug.
Bioequivalence Oral formulations of a drugfrom different manufacturers or different batchesfrom the same manufacturer may have the sameamount of the drug (chemically equivalent) butmay not yield the same blood levels—biologicallyinequivalent. Two preparations of a drug areconsidered bioequivalent when the rate and extentof bioavailability of the active drug from themis not significantly different under suitable testconditions.
Before a drug administered orally in soliddosage form can be absorbed, it must break intoindividual particles of the active drug (disinte-gration). Tablets and capsules contain a numberof other materials—diluents, stabilizing agents,binders, lubricants, etc. The nature of these aswell as details of the manufacture process, e.g.force used in compressing the tablet, may affectdisintegration. The released drug must thendissolve in the aqueous gastrointestinal contents.The rate of dissolution is governed by the inherentsolubility, particle size, crystal form and other

17C
HA
PTE
R2
MEMBRANE TRANSPORT, ABSORPTION AND DISTRIBUTION OF DRUGS
physical properties of the drug. Differences inbioavailability may arise due to variations indisintegration and dissolution rates.
Differences in bioavailability are seen mostlywith poorly soluble and slowly absorbed drugs.Reduction in particle size increases the rate ofabsorption of aspirin (microfine tablets). Theamount of griseofulvin and spironolactone in thetablet can be reduced to half if the drug particleis microfined. There is no need to reduce theparticle size of freely water soluble drugs, e.g.paracetamol.
Bioavailability variation assumes practicalsignificance for drugs with low safety margin(digoxin) or where dosage needs precise control(oral hypoglycaemics, oral anticoagulants). It mayalso be responsible for success or failure of anantimicrobial regimen.
However, in the case of a large number ofdrugs bioavailability differences are negligible andthe risks of changing from branded to genericproduct or to another brand of the same drughave often been exaggerated.
DISTRIBUTION
Once a drug has gained access to the blood stream,it gets distributed to other tissues that initiallyhad no drug, concentration gradient being in thedirection of plasma to tissues. The extent andpattern of distribution of a drug depends on its:• lipid solubility• ionization at physiological pH (a function of
its pKa)• extent of binding to plasma and tissue proteins• presence of tissue-specific transporters• differences in regional blood flow.
Movement of drug proceeds until an equilibriumis established between unbound drug in the plasmaand the tissue fluids. Subsequently, there is aparallel decline in both due to elimination.
Apparent volume of distribution (V) Presumingthat the body behaves as a single homogeneouscompartment with volume V into which the druggets immediately and uniformly distributed
dose administered i.v. V = ————————— ...(3)
plasma concentration
Since in the example shown in Fig. 2.7, the drugdoes not actually distribute into 20 L of bodywater, with the exclusion of the rest of it, thisis only an apparent volume of distribution whichcan be defined as “the volume that wouldaccommodate all the drug in the body, if theconcentration throughout was the same as inplasma”. Thus, it describes the amount of drugpresent in the body as a multiple of that containedin a unit volume of plasma. Considered togetherwith drug clearance, this is a very usefulpharmacokinetic concept.
Lipid-insoluble drugs do not enter cells—V approximates extracellular fluid volume, e.g.streptomycin, gentamicin 0.25 L/kg.
Distribution is not only a matter of dilution,but also binding and sequestration. Drugsextensively bound to plasma proteins are largelyrestricted to the vascular compartment and havelow values, e.g. diclofenac and warfarin (99%bound) V = 0.15 L/kg.
A large value of V indicates that larger quantityof drug is present in extravascular tissue. Drugssequestrated in other tissues may have, V muchmore than total body water or even body mass,
Fig. 2.7: Illustration of the concept of apparent volumeof distribution (V).In this example, 1000 mg of drug injected i.v. producessteady-state plasma concentration of 50 mg/L, apparentvolume of distribution is 20 L

18S
EC
TIO
N1
GENERAL PHARMACOLOGY
e.g. digoxin 6 L/kg, propranolol 4 L/kg, morphine3.5 L/kg, because most of the drug is presentin other tissues, and plasma concentration is low.Therefore, in case of poisoning, drugs with largevolumes of distribution are not easily removedby haemodialysis.
Pathological states, e.g. congestive heartfailure, uraemia, cirrhosis of liver, etc. can alterthe V of many drugs by altering distribution ofbody water, permeability of membranes, bindingproteins or by accumulation of metabolites thatdisplace the drug from binding sites.
More precise multiple compartment modelsfor drug distribution have been worked out, butthe single compartment model, described above,is simple and fairly accurate for many drugs.
Redistribution Highly lipid-soluble drugs getinitially distributed to organs with high blood flow,i.e. brain, heart, kidney, etc. Later, less vascularbut more bulky tissues (muscle, fat) take up thedrug—plasma concentration falls and the drugis withdrawn from the highly perfused sites. Ifthe site of action of the drug was in one of thehighly perfused organs, redistribution results intermination of drug action. Greater the lipidsolubility of the drug, faster is its redistribution.
Fig. 2.8: Passage of drugs across capillariesA. Usual capillary with large paracellular spaces through which even large lipid-insoluble
molecules diffuseB. Capillary constituting blood brain or blood-CSF barrier. Tight junctions between
capillary endothelial cells and investment of glial processes or choroidal epitheliumdo not allow passage of non lipid-soluble molecules/ions
Anaesthetic action of thiopentone sod. injectedi.v. is terminated in few minutes due toredistribution. A relatively short hypnotic actionlasting 6–8 hours is exerted by oral diazepamor nitrazepam due to redistribution despite theirelimination t ½ of > 30 hr. However, when thesame drug is given repeatedly or continuouslyover long periods, the low perfusion high capacitysites get progressively filled up and the drugbecomes longer acting.
Penetration into brain and CSF Thecapillary endothelial cells in brain have tightjunctions and lack large paracellular spaces.Further, an investment of neural tissue (Fig. 2.8B)covers the capillaries. Together they constitutethe so called blood-brain barrier (BBB). A similarblood-CSF barrier is located in the choroidplexus: capillaries are lined by choroidal
Factors governing volume of drug distribution
• Lipid: water partition coefficient of the drug• pKa value of the drug• Degree of plasma protein binding• Affinity for different tissues• Fat: lean body mass ratio, which can vary
with age, sex, obesity, etc.• Diseases like CHF, uremia, cirrhosis

19C
HA
PTE
R2
MEMBRANE TRANSPORT, ABSORPTION AND DISTRIBUTION OF DRUGS
epithelium having tight junctions. Both thesebarriers are lipoidal and limit the entry of nonlipid-soluble drugs, e.g. streptomycin, neostigmine, etc.Only lipid-soluble drugs, therefore, are able topenetrate and have action on the central nervoussystem. In addition, efflux transporters likeP-gp and anion transporter (OATP) present inbrain and choroidal vessels extrude many drugsthat enter brain by other processes and serve toaugment the protective barrier against potentiallyharmful xenobiotics. Dopamine does not enterbrain but its precursor levodopa does; as such,the latter is used in parkinsonism. Inflammationof meninges or brain increases permeability ofthese barriers. It has been proposed that somedrugs accumulate in the brain by utilizing thetransporters for endogenous substances.
There is also an enzymatic BBB: Monoamineoxidase (MAO), cholinesterase and some otherenzymes are present in the capillary walls or inthe cells lining them. They do not allowcatecholamines, 5-HT, acetylcholine, etc. to enterbrain in the active form.
The BBB is deficient at the CTZ in the medullaoblongata (even lipid-insoluble drugs are emetic)and at certain periventricular sites—(anteriorhypothalamus). Exit of drugs from the CSF andbrain, however, is not dependent on lipid-solubilityand is rather unrestricted. Bulk flow of CSF(alongwith the drug dissolved in it) occurs throughthe arachnoid villi. Further, nonspecific organicanion and cation transport processes (similar tothose in renal tubule) operate at the choroid plexus.
Passage across placenta Placental membra-nes are lipoidal and allow free passage of lipo-philic drugs, while restricting hydrophilic drugs.The placental efflux P-gp and other transporterslike BCRP, MRP3 also serve to limit foetalexposure to maternally administered drugs.Placenta is a site for drug metabolism as well,which may lower/modify exposure of the foetusto the administered drug. However, restrictedamounts of nonlipid-soluble drugs, when presentin high concentration or for long periods inmaternal circulation, gain access to the foetus.
Some influx transporters also operate at theplacenta. Thus, it is an incomplete barrier andalmost any drug taken by the mother can affectthe foetus or the newborn (drug taken just beforedelivery, e.g. morphine).
Plasma protein bindingMost drugs possess physicochemical affinity forplasma proteins and get reversibly bound to these.Acidic drugs generally bind to plasma albumin andbasic drugs to α1 acid glycoprotein. Binding toalbumin is quantitatively more important. Extentof binding depends on the individual compound;no generalization for a pharmacological orchemical class can be made (even small chemicalchange can markedly alter protein binding), forexample the binding percentage of some benzo-diazepines is:
Flurazepam 10% Alprazolam 70%Lorazepam 90% Diazepam 99%
Increasing concentrations of the drug can pro-gressively saturate the binding sites: fractionalbinding may be lower when large amounts of thedrug are given. The generally expressed percen-tage binding refers to the usual therapeutic plasmaconcentrations of a drug. The clinically significantimplications of plasma protein binding are:(i) Highly plasma protein bound drugs are largelyrestricted to the vascular compartment becauseprotein bound drug does not cross membranes(except through large paracellular spaces, such
Drugs highly bound to plasma protein
To albumin To α1-acidglycoprotein
Barbiturates β-blockersBenzodiazepines BupivacaineNSAIDs LidocaineValproic acid DisopyramidePhenytoin ImipraminePenicillins MethadoneSulfonamides PrazosinTetracyclines QuinidineTolbutamide VerapamilWarfarin

20S
EC
TIO
N1
GENERAL PHARMACOLOGY
as in capillaries). They tend to have smallervolumes of distribution.
(ii) The bound fraction is not available for action.However, it is in equilibrium with the free drugin plasma and dissociates when the concentrationof the latter is reduced due to elimination. Plasmaprotein binding thus tantamounts to temporarystorage of the drug.
(iii) High degree of protein binding generallymakes the drug long acting, because bound fractionis not available for metabolism or excretion, unlessit is actively extracted by liver or by kidney tubules.Glomerular filtration does not reduce theconcentration of the free form in the efferentvessels, because water is also filtered. Activetubular secretion, however, removes the drugwithout the attendant solvent → concentration offree drug falls → bound drug dissociates and iseliminated resulting in a higher renal clearancevalue of the drug than the total renal blood flow(see Fig. 3.3). The same is true of active transportof highly extracted drugs in liver. Plasma proteinbinding in this situation acts as a carrier mechanismand hastens drug elimination, e.g. excretion ofpenicillin (elimination t½ is 30 min); metabolismof lidocaine. Highly protein bound drugs are notremoved by haemodialysis and need specialtechniques for treatment of poisoning.
(iv) The generally expressed plasma concentra-tions of the drug refer to bound as well as freedrug. Degree of protein binding should be taken
into account while relating these to concentrationsof the drug that are active in vitro, e.g. MIC ofan antimicrobial.
(v) One drug can bind to many sites on thealbumin molecule. Conversely, more than one drugcan bind to the same site. This can give rise todisplacement interactions among drugs bound tothe same site(s). The drug bound with higheraffinity will displace that bound with lower affinity.If just 1% of a drug that is 99% bound is displaced,the concentration of free form will be doubled.This, however, is often transient because thedisplaced drug will diffuse into the tissues as wellas get metabolized or excreted: the new steady-state free drug concentration is only marginallyhigher unless the displacement extends to tissuebinding or there is concurrent inhibition ofmetabolism and/or excretion. The overall impactof many displacement interactions is minimal;clinical significance being attained only in caseof highly bound drugs with limited volume ofdistribution (many acidic drugs bound to albumin)and where interaction is more complex. Moreover,two highly bound drugs do not necessarily displaceeach other—their binding sites may not overlap,e.g. probenecid and indomethacin are highlybound to albumin but do not displace each other.Similarly, acidic drugs do not generally displacebasic drugs and vice versa. Some clinicallyimportant displacement interactions are:• Aspirin displaces sulfonylureas.• Indomethacin, phenytoin displace warfarin.
Drugs concentrated in tissues
Skeletal muscle, heart — digoxin, emetine (bound to muscle proteins).Liver — chloroquine, tetracyclines, emetine, digoxin.Kidney — digoxin, chloroquine, emetine.Thyroid — iodine.Brain — chlorpromazine, acetazolamide, isoniazid.Retina — chloroquine (bound to nucleoproteins).Iris — ephedrine, atropine (bound to melanin).Bone and teeth — tetracyclines, heavy metals (bound to mucopolysaccharides of
connective tissue), bisphosphonates (bound to hydroxyapatite)Adipose tissue — thiopentone, ether, minocycline, phenoxybenzamine, DDT
dissolve in neutral fat due to high lipid-solubility; remainstored due to poor blood supply of fat.

21C
HA
PTE
R2
MEMBRANE TRANSPORT, ABSORPTION AND DISTRIBUTION OF DRUGS
• Sulfonamides and vit K displace bilirubin(kernicterus in neonates).
• Aspirin displaces methotrexate.
(vi) In hypoalbuminemia, binding may be redu-ced and high concentrations of free drug maybe attained, e.g. phenytoin and furosemide. Otherdiseases may also alter drug binding, e.g.phenytoin and pethidine binding is reduced inuraemia; propranolol binding is increased inpregnant women and in patients with inflammatorydisease (acute phase reactant α1 acid-glycoproteinincreases).
Tissue storage Drugs may also accumulatein specific organs by active transport or get boundto specific tissue constituents (see box).
Drugs sequestrated in various tissues areunequally distributed, tend to have larger volumeof distribution and longer duration of action. Somemay exert local toxicity due to high concentration,e.g. tetracyclines on bone and teeth, chloroquineon retina, streptomycin on vestibular apparatus,emetine on heart and skeletal muscle. Drugs mayalso selectively bind to specific intracellularorganelle, e.g. tetracycline to mitochondria,chloroquine to nuclei.
PROBLEM DIRECTED STUDY
2.1 A 60-year-old woman complained of weakness, lethargy and easy fatigability. Investigationshowed that she had iron deficiency anaemia (Hb. 8 g/dl). She was prescribed cap. ferrous fumarate300 mg twice daily. She returned after one month with no improvement in symptoms. Her Hb.level was unchanged. On enquiry she revealed that she felt epigastric distress after taking theiron capsules, and had started taking antacid tablets along with the capsules.(a) What could be the possible reason for her failure to respond to the oral iron medication?
2.2 A 50-year-old type-2 diabetes mellitus patient was maintained on tab. glibenclamide(a sulfonylurea) 5 mg twice daily. He developed toothache for which he took tab. aspirin650 mg 6 hourly. After taking aspirin he experienced anxiety, sweating, palpitation, weakness,ataxia, and was behaving abnormally. These symptoms subsided when he was given a glass ofglucose solution.(a) Waht could be the explanation for his symptoms?(b) Which alternative analgesic should have been taken?(see Appendix-1 for solutions)

Pharmacokinetics: Metabolismand Excretion of Drugs, Kineticsof Elimination
ChapterChapterChapterChapterChapter 33333
BIOTRANSFORMATION(Metabolism)
Biotransformation means chemical alteration ofthe drug in the body. It is needed to rendernonpolar (lipid-soluble) compounds polar (lipid-insoluble) so that they are not reabsorbed in therenal tubules and are excreted. Most hydrophilicdrugs, e.g. streptomycin, neostigmine, pancuro-nium, etc. are little biotransformed and are largelyexcreted unchanged. Mechanisms which meta-bolize drugs (essentially foreign substances) havedeveloped to protect the body from ingestedtoxins.
The primary site for drug metabolism is liver;others are—kidney, intestine, lungs and plasma.Biotransformation of drugs may lead to thefollowing.
(i) Inactivation Most drugs and their activemetabolites are rendered inactive or less active,e.g. ibuprofen, paracetamol, lidocaine, chloramp-henicol, propranolol and its active metabolite4-hydroxypropranolol.
(ii) Active metabolite from an active drugMany drugs have been found to be partiallyconverted to one or more active metabolite; theeffects observed are the sumtotal of that due tothe parent drug and its active metabolite(s) (seebox).
(iii) Activation of inactive drug Few drugs areinactive as such and need conversion in the bodyto one or more active metabolites. Such a drugis called a prodrug (see box). The prodrug mayoffer advantages over the active form in beingmore stable, having better bioavailability or otherdesirable pharmacokinetic properties or less sideeffects and toxicity. Some prodrugs are activatedselectively at the site of action.
Biotransformation reactions can be classifiedinto:
(a) Nonsynthetic/Phase I/Functionalization reac-tions: a functional group is generated or exposed—metabolite may be active or inactive.
(b) Synthetic/Conjugation/ Phase II reactions: anendogenous radical is conjugated to the drug—metabolite is mostly inactive; except few drugs,e.g. glucuronide conjugate of morphine and sulfateconjugate of minoxidil are active.
Nonsynthetic reactions
(i) Oxidation This reaction involves additionof oxygen/negatively charged radical or removalof hydrogen/positively charged radical. Oxidationsare the most important drug metabolizing reac-tions. Various oxidation reactions are:
hydroxylation; oxygenation at C, N or S atoms;N or O-dealkylation, oxidative deamination,etc.
In many cases the initial insertion of oxygenatom into the drug molecule produces short livedhighly reactive quinone/epoxide/superoxide
Active drug Active metabolite
Chloral hydrate — TrichloroethanolMorphine — Morphine-6-glucuronideCefotaxime — Desacetyl cefotaximeAllopurinol — AlloxanthineProcainamide — N-acetyl procainamidePrimidone — Phenobarbitone,
phenylethylmalonamideDiazepam — Desmethyl-diazepam,
oxazepamDigitoxin — DigoxinImipramine — DesipramineAmitriptyline — NortriptylineCodeine — MorphineSpironolactone — CanrenoneLosartan — E 3174

23C
HA
PTE
R3
METABOLISM AND EXCRETION OF DRUGS, KINETICS OF ELIMINATION
intermediates which then convert to more stablecompounds.
Oxidative reactions are mostly carried out bya group of monooxygenases in the liver, whichin the final step involve a cytochrome P-450haemoprotein, NADPH, cytochrome P-450reductase and molecular O2. More than 100cytochrome P-450 isoenzymes differing in theiraffinity for various substrates (drugs), have beenidentified.Depending upon the extent of amino acid sequence homology,the cytochrome P-450 (CYP) isoenzymes are grouped intofamilies designated by numerals (1, 2, 3.....), each havingseveral sub-families designated by capital letters (A, B, C.....),while individual isoenzymes are again alloted numerals (1, 2,3....). In human beings, only a few members of three isoenzymefamilies (CYP 1, 2 and 3) carryout metabolism of most of thedrugs, and many drugs such as tolbutamide, barbiturates,nifedipine are substrates for more than one isoform. The CYPisoenzymes important in man are:
CYP3A4/5 Carryout biotransformation of largest number(nearly 50%) of drugs. In addition to liver, these isoforms areexpressed in intestine (responsible for first pass metabolismat this site) and kidney as well. Inhibition of this isoenzymeby erythromycin, clarithromycin, ketoconazole, itraconazoleis responsible for the important drug interaction withterfenadine, astemizole and cisapride (see p. 166) which areits substrates. Losartan, nifedipine hydrocortisone, mifepris-tone, simvastatin, ritonavir, carbamazepine and cyclosporineare also metabolized by CYP3A4/5. Verapamil, diltiazem,ritonavir and a constituent of grape fruit juice are otherimportant inhibitors, while rifampicin, barbiturates and otheranticonvulsants are the important inducers.
CYP2D6 This is the next most important CYP isoform whichmetabolizes nearly 20% drugs including tricyclic antidepres-sants, selective serotonin reuptake inhibitors, many neuro-leptics, antiarrhythmics, β-blockers and opiates. Inhibition ofthis enzyme by quinidine results in failure of conversion ofcodeine to morphine → analgesic effect of codeine is lost.Human subjects can be grouped into ‘extensive’ or ‘poor’metabolizers of metoprolol and debrisoquin. The poormetabolizers have an altered CYP2D6 enzyme and exhibit lowcapacity to hydroxylate many drugs.
CYP2C8/9 Important in the biotransformation of >15commonly used drugs including phenytoin, carbamazepine,warfarin which are narrow safety margin drugs, as well asibuprofen, tolbutamide, repaglinide, celecoxib and losartan.
CYP2C19 Metabolizes > 12 frequently used drugs includingomeprazole, lansoprazole, phenytoin, diazepam, propranolol.
Rifampicin and carbamazepine are potent inducers of theCYP2C subfamily, while omeprazole is an inhibitor.
CYP1A1/2 Though this subfamily participates in the meta-bolism of only few drugs like theophylline, caffeine, paraceta-mol, carbamazepine, it is more important for activation ofprocarcinogens. Apart from rifampicin and carbamazepine,polycyclic hydrocarbons, cigarette smoke and charbroiled meatare its potent inducers.
CYP2E1 It catalyses oxidation of alcohol, holothane, andformation of minor metabolites of few drugs, notably thehepatotoxic N-acetyl benzoquinoneimine from paracetamol;chronic alcoholism induces this isoenzyme.
The relative amount of different cytochrome P-450s differsamong species and among individuals of the same species.These differences largely account for the marked interspeciesand interindividual differences in rate of metabolism of drugs.
Barbiturates, phenothiazines, imipramine,propranolol, ibuprofen, paracetamol, steroids,phenytoin, benzodiazepines, theophylline andmany other drugs are oxidized in this way. Fewdrugs like cimetidine, ranitidine, clozapine areoxidized at their N, P or S atoms by a groupof flavin-monooxygenases that are also locatedat hepatic endoplasmic reticulum, but are distinctfrom CYP enzymes. They are not susceptible toinduction or inhibition by other drugs, and thusare not involved in drug interactions. Some otherdrugs, e.g. adrenaline, alcohol, mercaptopurineare oxidized by mitochondrial or cytoplasmicenzymes.
(ii) Reduction This reaction is the converse ofoxidation and involves cytochrome P-450 enzymesworking in the opposite direction. Alcohols,aldehydes, quinones are reduced. Drugs
Prodrug Active form
Levodopa — DopamineEnalapril — Enalaprilata-Methyldopa — a-methylnorepinephrineDipivefrine — EpinephrineSulindac — Sulfide metaboliteProguanil — CycloguanilPrednisone — PrednisoloneBacampicillin — AmpicillinSulfasalazine — 5-Aminosalicylic acidCyclophos- — Aldophosphamide,phamide phosphoramide mustard,
acroleinFluorouracil — Fluorouridine
monophosphateMercaptopurine — Methylmercaptopurine
ribonucleotideAcyclovir — Acyclovir triphosphate

24S
EC
TIO
N1
GENERAL PHARMACOLOGY
primarily reduced are chloralhydrate, chloramp-henicol, halothane, warfarin.
(iii) Hydrolysis This is cleavage of drug mole-cule by taking up a molecule of water.
esteraseEster + H2O Acid + Alcohol
Similarly, amides and polypeptides are hydrolysedby amidases and peptidases. In addition, thereare epoxide hydrolases which detoxify epoxidemetabolites of some drugs generated by CYPoxygenases. Hydrolysis occurs in liver, intestines,plasma and other tissues. Examples of hydrolyseddrugs are choline esters, procaine, lidocaine,procainamide, aspirin, carbamazepine-epoxide,pethidine, oxytocin.
(iv) Cyclization This is formation of ring struc-ture from a straight chain compound, e.g. proguanil.
(v) Decyclization This is opening up of ringstructure of the cyclic drug molecule, e.g. barbi-turates, phenytoin. This is generally a minorpathway.
Synthetic reactionsThese involve conjugation of the drug or itsphase I metabolite with an endogenous substrate,usually derived from carbohydrate or amino acid,to form a polar highly ionized organic acid, whichis easily excreted in urine or bile. Conjugationreactions have high energy requirement.(i) Glucuronide conjugation This is the mostimportant synthetic reaction carriedout by a groupof UDP-glucuronosyl transferases (UGTs).Compounds with a hydroxyl or carboxylic acidgroup are easily conjugated with glucuronic acidwhich is derived from glucose. Examples are—chloramphenicol, aspirin, paracetamol, diazepam,lorazepam, morphine, metronidazole. Not onlydrugs but endogenous substrates like bilirubin,steroidal hormones and thyroxine utilize thispathway. Glucuronidation increases the molecularweight of the drug which favours its excretionin bile. Drug glucuronides excreted in bile canbe hydrolysed by bacteria in the gut—the liberateddrug is reabsorbed and undergoes the same fate.
This enterohepatic cycling (see Fig. 3.2) of thedrug prolongs its action, e.g. phenolphthalein, oralcontraceptives.(ii) Acetylation Compounds having amino orhydrazine residues are conjugated with the helpof acetyl coenzyme-A, e.g. sulfonamides, isonia-zid, PAS, dapsone, hydralazine, clonazepam,procainamide. Multiple genes control the N-acetyltransferases (NATs), and rate of acetylation showsgenetic polymorphism (slow and fast acetylators).(iii) Methylation The amines and phenols canbe methylated by methyl transferases (MT);methionine and cysteine acting as methyl donors,e.g. adrenaline, histamine, nicotinic acid,methyldopa, captopril, mercaptopurine.(iv) Sulfate conjugation The phenolic com-pounds and steroids are sulfated by sulfotrans-ferases (SULTs), e.g. chloramphenicol, methyl-dopa, adrenal and sex steroids.
(v) Glycine conjugation Salicylates, nicotinicacid and other drugs having carboxylic acid groupare conjugated with glycine, but this is not a majorpathway of metabolism.(vi) Glutathione conjugation This is carriedout by glutathione-S-transferase (GST) forminga mercapturate. It is normally a minor pathway.However, it serves to inactivate highly reactivequinone or epoxide intermediates formed duringmetabolism of certain drugs, e.g. paracetamol.When large amount of such intermediates areformed (in poisoning or after enzyme induction),glutathione supply falls short—toxic adducts areformed with tissue constituents → tissue damage.
(vii) Ribonucleoside/nucleotide synthesisThis pathway is important for the activation ofmany purine and pyrimidine antimetabolites usedin cancer chemotherapy.
Most drugs are metabolized by many path-ways, simultaneously or sequentially as illustratedin Fig. 3.1. Rates of reaction by different pathwaysoften vary considerably. A variety of metabolities(some more, some less) of a drug may beproduced. Stereoisomers of a drug may bemetabolized differently and at different rates, e.g.
→→→→→

25C
HA
PTE
R3
METABOLISM AND EXCRETION OF DRUGS, KINETICS OF ELIMINATION
The nonmicrosomal enzymes are not inducible butmany show genetic polymorphism (acetyl trans-ferase, pseudocholinesterase).
Both microsomal and nonmicrosomal enzy-mes are deficient in the newborn, especiallypremature, making them more susceptible to manydrugs, e.g. chloramphenicol, opioids. This deficitis made up in the first few months, more quicklyin case of oxidation and other phase I reactionsthan in case of glucuronide and other conjugationswhich take 3 or more months.
The amount and kind of drug metabolizingenzymes is controlled genetically and is alsoaltered by environmental factors. Thus, markedinterspecies and interindividual differences areseen, e.g. cats are deficient in UGTs while dogsare deficient in NATs. Upto 6-fold difference inthe rate of metabolism of a drug among normalhuman adults may be observed. This is one ofthe major causes of individual variation in drugresponse.
Hofmann elimination This refers to inactiva-tion of the drug in the body fluids by spontaneousmolecular rearrangement without the agency ofany enzyme, e.g. atracurium.
INHIBITION OF DRUG METABOLISMOne drug can competitively inhibit the metabolismof another if it utilizes the same enzyme orcofactors. However, such interactions are not ascommon as one would expect, because oftendifferent drugs are substrates for differentCY P-450 isoenzymes. It is thus important toknow the CYP isoenzyme(s) that carry out themetabolism of a particular drug. A drug may inhibitone isoenzyme while being itself a substrate ofanother isoenzyme, e.g. quinidine is metabolizedmainly by CYP3A4 but inhibits CYP2D6. Alsomost drugs, at therapeutic concentrations, aremetabolized by non-saturation kinetics, i.e. theenzyme is present in excess. Clinically significantinhibition of drug metabolism occurs in case ofdrugs having affinity for the same isoenzyme,specially if they are metabolized by saturationkinetics or if kinetics changes from first order
Fig. 3.1: Simultaneous and/or sequential metabolismof a drug by phase I and phase II reactions
S-warfarin rapidly undergoes ring oxidation, whileR-warfarin is slowly degraded by sidechainreduction.
Only a few drugs are metabolized by enzymesof intermediary metabolism, e.g. alcohol by dehy-drogenase, allopurinol by xanthine oxidase,succinylcholine and procaine by plasma cholines-terase, adrenaline by monoamine oxidase. Majorityof drugs are acted on by relatively nonspecificenzymes which are directed to types of moleculesrather than to specific drugs. The same enzyme canmetabolize many drugs. The drug metabolisingenzymes are divided into two types:
Microsomal enzymes These are located onsmooth endoplasmic reticulum (a system ofmicrotubules inside the cell), primarily in liver,also in kidney, intestinal mucosa and lungs. Themonooxygenases, cytochrome P450, UGTs,epoxide hydrolases, etc. are microsomal enzymes.
They catalyse most of the oxidations, reduc-tions, hydrolysis and glucuronide conjugation.Microsomal enzymes are inducible by drugs, dietand other agencies.
Nonmicrosomal enzymes These are presentin the cytoplasm and mitochondria of hepatic cellsas well as in other tissues including plasma. Theesterases, amidases, some flavoprotein oxidasesand most conjugases are nonmicrosomal.Reactions catalysed are:
Some oxidations and reductions, many hydro-lytic reactions and all conjugations exceptglucuronidation.

26S
EC
TIO
N1
GENERAL PHARMACOLOGY
to zero order over the therapeutic range (capacitylimited metabolism). Obviously, inhibition of drugmetabolism occurs in a dose related manner andcan precipitate toxicity of the object drug (whosemetabolism has been inhibited).
Because enzyme inhibition occurs by directeffect on the enzyme, it has a fast time course(within hours) compared to enzyme induction (seebelow).
Metabolism of drugs with high hepaticextraction is dependent on liver blood flow(blood flow limited metabolism). Propranololreduces rate of lidocaine metabolism by decreasinghepatic blood flow. Some other drugs whose rateof metabolism is limited by hepatic blood floware morphine, propranolol, verapamil and imipra-mine.
MICROSOMAL ENZYME INDUCTION
Many drugs, insecticides and carcinogens interactwith DNA and increase the synthesis ofmicrosomal enzyme protein, especially cytoch-rome P-450 and UGTs As a result rate of meta-bolism of inducing drug itself and/or other drugsis increased.
Different inducers are relatively selective forcertain cytochrome P-450 isoenzyme families, e.g.:• Anticonvulsants (phenobarbitone, phenytoin,
carbamazepine), rifampin, glucocorticoidsinduce CYP3A isoenzymes.
• Phenobarbitone also induces CYP2B1 andrifampin also induces CYP2D6.
• Isoniazid and chronic alcohol consumptioninduce CYP2E1.
• Polycyclic hydrocarbons like 3-methylcholan-threne and benzopyrene found in cigarettesmoke, charcoalbroiled meat, omeprazole andindustrial pollutants induce CYP1A iso-enzymes.
• Other important enzyme inducers are:phenylbutazone, griseofulvin, DDT.
Since different CYP isoenzymes are involved inthe metabolism of different drugs, every inducerincreases biotransformation of certain drugs butnot that of others. However, phenobarbitone likeinducers of CYP3A and CYP2D6 affect themetabolism of a large number of drugs, becausethese isoenzymes act on many drugs. On the otherhand induction by polycyclic hydrocarbons islimited to few drugs (like theophylline, phena-cetin) because CYP1A isoenzyme metabolizesonly few drugs.
Induction involves microsomal enzymes inliver as well as other organs and increases therate of metabolism by 2–4 fold. Induction takes4–14 days to reach its peak and is maintainedtill the inducing agent is being given. Thereafterthe enzymes return to their original value over1–3 weeks.
Consequences of microsomalenzyme induction1. Decreased intensity and/or duration of actionof drugs that are inactivated by metabolism,e.g. failure of contraception with oral contra-ceptives.2. Increased intensity of action of drugs that areactivated by metabolism. Acute paracetamol toxi-city is due to one of its metabolites—toxicityoccurs at lower doses in patients receiving enzymeinducers.3. Tolerance—if the drug induces its ownmetabolism (autoinduction), e.g. carbamazepine,rifampin.4. Some endogenous substrates (steroids, bili-rubin) are also metabolized faster.5. Precipitation of acute intermittent porphyria:enzyme induction increases porphyrin synthesis
Drugs that inhibit drug metabolizing enzymes
Allopurinol AmiodaroneOmeprazole PropoxypheneErythromycin IsoniazidClarithromycin CimetidineChloramphenicol QuinidineKetoconazole DisulfiramItraconazole DiltiazemMetronidazole VerapamilCiprofloxacin MAO inhibitorsSulfonamides Ritonavir (and otherFluoxetine (and HIV proteaseother SSRIs) inhibitors)

27C
HA
PTE
R3
METABOLISM AND EXCRETION OF DRUGS, KINETICS OF ELIMINATION
by derepressing δ-aminolevulenic acid synthe-tase.6. Intermittent use of an inducer may interferewith adjustment of dose of another drug pres-cribed on regular basis, e.g. oral anticoagulants,oral hypoglycaemics, antiepileptics, antihyperten-sives.7. Interference with chronic toxicity testing inanimals.
Drugs whose metabolism is significantlyaffected by enzyme induction are—phenytoin,warfarin, tolbutamide, imipramine, oral contra-ceptives, chloramphenicol, doxycycline, theo-phylline, griseofulvin, phenylbutazone.
Possible uses of enzyme induction1. Congenital nonhaemolytic jaundice: It is dueto deficient glucuronidation of bilirubin; pheno-barbitone hastens clearance of jaundice.2. Cushing’s syndrome: phenytoin may reducethe manifestations by enhancing degradation ofadrenal steroids which are produced in excess.3. Chronic poisonings: by faster metabolism ofthe accumulated poisonous substance.4. Liver disease.
FIRST PASS (PRESYSTEMIC)METABOLISM
This refers to metabolism of a drug during itspassage from the site of absorption into the sys-temic circulation. All orally administered drugsare exposed to drug metabolizing enzymes in theintestinal wall and liver (where they first reachthrough the portal vein). Presystemic metabolism
in the gut and liver can be avoided by adminis-tering the drug through sublingual, transdermalor parenteral routes. However, limited presystemicmetabolism can occur in the skin (transdermallyadministered drug) and in lungs (for drug reachingvenous blood through any route). The extent offirst pass metabolism differs for different drugs(Table 3.1) and is an important determinant oforal bioavailability.
Attributes of drugs with high first passmetabolism:(a) Oral dose is considerably higher than sub-lingual or parenteral dose.(b) There is marked individual variation in theoral dose due to differences in the extent of firstpass metabolism.(c) Oral bioavailability is apparently increased inpatients with severe liver disease.(d) Oral bioavailability of a drug is increased ifanother drug competing with it in first passmetabolism is given concurrently, e.g. chlorpro-mazine and propranolol.
EXCRETIONExcretion is the passage out of systemicallyabsorbed drug. Drugs and their metabolites areexcreted in:
1. Urine Through the kidney. It is the mostimportant channel of excretion for majority ofdrugs (see below).
2. Faeces Apart from the unabsorbed frac-tion, most of the drug present in faeces is derivedfrom bile. Liver actively transports into bile orga-nic acids (especially drug glucuronides by OATP
TABLE 3.1 Extent of first pass metabolism of some important drugs
Low Intermediate Highnot given orally high oral dose
Phenobarbitone Aspirin Isoprenaline PropranololPhenylbutazone Quinidine Lidocaine AlprenololTolbutamide Desipramine Hydrocortisone VerapamilTheophylline Nortriptyline Testosterone SalbutamolPindolol Chlorpromazine Glyceryl trinitrateIsosorbide Pentazocine Morphinemononitrate Metoprolol Pethidine
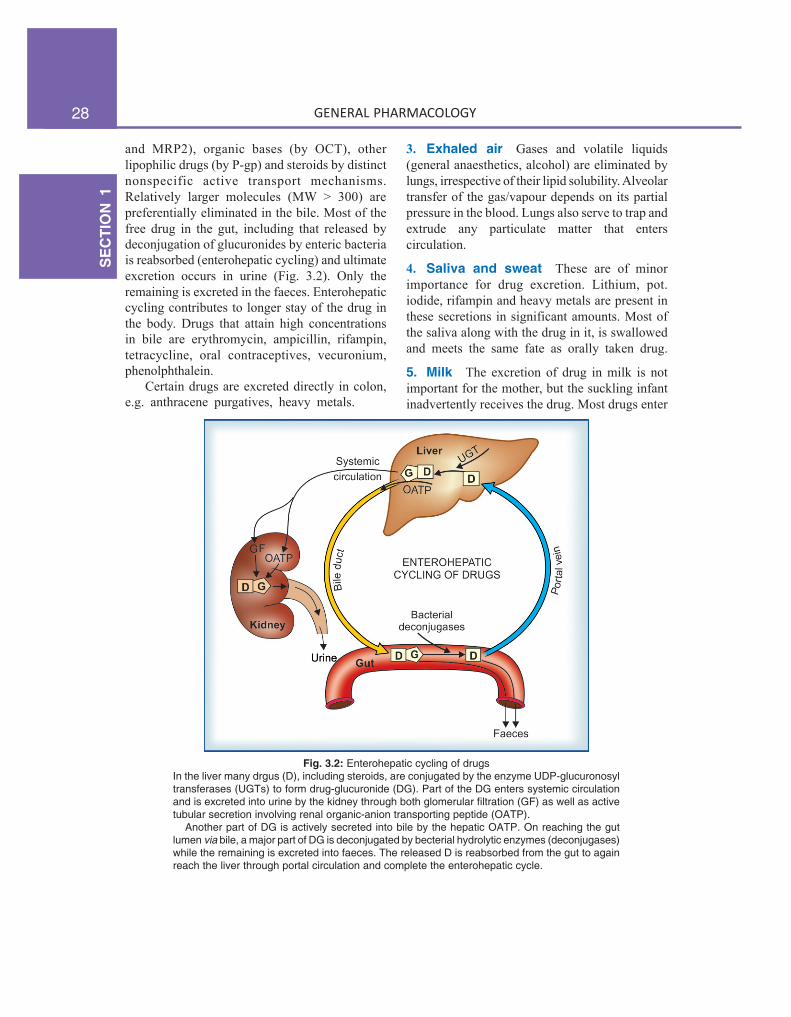
28S
EC
TIO
N1
GENERAL PHARMACOLOGY
and MRP2), organic bases (by OCT), otherlipophilic drugs (by P-gp) and steroids by distinctnonspecific active transport mechanisms.Relatively larger molecules (MW > 300) arepreferentially eliminated in the bile. Most of thefree drug in the gut, including that released bydeconjugation of glucuronides by enteric bacteriais reabsorbed (enterohepatic cycling) and ultimateexcretion occurs in urine (Fig. 3.2). Only theremaining is excreted in the faeces. Enterohepaticcycling contributes to longer stay of the drug inthe body. Drugs that attain high concentrationsin bile are erythromycin, ampicillin, rifampin,tetracycline, oral contraceptives, vecuronium,phenolphthalein.
Certain drugs are excreted directly in colon,e.g. anthracene purgatives, heavy metals.
3. Exhaled air Gases and volatile liquids(general anaesthetics, alcohol) are eliminated bylungs, irrespective of their lipid solubility. Alveolartransfer of the gas/vapour depends on its partialpressure in the blood. Lungs also serve to trap andextrude any particulate matter that enterscirculation.
4. Saliva and sweat These are of minorimportance for drug excretion. Lithium, pot.iodide, rifampin and heavy metals are present inthese secretions in significant amounts. Most ofthe saliva along with the drug in it, is swallowedand meets the same fate as orally taken drug.
5. Milk The excretion of drug in milk is notimportant for the mother, but the suckling infantinadvertently receives the drug. Most drugs enter
Fig. 3.2: Enterohepatic cycling of drugsIn the liver many drgus (D), including steroids, are conjugated by the enzyme UDP-glucuronosyltransferases (UGTs) to form drug-glucuronide (DG). Part of the DG enters systemic circulationand is excreted into urine by the kidney through both glomerular filtration (GF) as well as activetubular secretion involving renal organic-anion transporting peptide (OATP).
Another part of DG is actively secreted into bile by the hepatic OATP. On reaching the gutlumen via bile, a major part of DG is deconjugated by becterial hydrolytic enzymes (deconjugases)while the remaining is excreted into faeces. The released D is reabsorbed from the gut to againreach the liver through portal circulation and complete the enterohepatic cycle.

29C
HA
PTE
R3
METABOLISM AND EXCRETION OF DRUGS, KINETICS OF ELIMINATION
breast milk by passive diffusion. As such, morelipid soluble and less protein bound drugs crossbetter. Milk has a lower pH (7.0) than plasma,basic drugs are somewhat more concentrated init. However, the total amount of drug reachingthe infant through breast feeding is generally smalland majority of drugs can be given to lactatingmothers without ill effects on the infant. Never-theless, it is advisable to administer any drug toa lactating woman only when essential. Drugsthat are safe, as well as those contraindicatedduring breast feeding or need special caution aregiven in Appendix-4 at the end of the book.
RENAL EXCRETION
The kidney is responsible for excreting all watersoluble substances. The amount of drug or itsmetabolites ultimately present in urine is the sumtotal of glomerular filtration, tubular reabsorptionand tubular secretion (Fig. 3.3).Net renal (Glomerular filtration + tubular
=excretion secretion) – tubular reabsorption
Glomerular filtration Glomerular capillarieshave pores larger than usual; all nonprotein bounddrug (whether lipid-soluble or insoluble) presentedto the glomerulus is filtered. Thus, glomerularfiltration of a drug depends on its plasma proteinbinding and renal blood flow. Glomerular filtrationrate (g.f.r.), normally ~ 120 ml/min, declines pro-gressively after the age of 50, and is low in renalfailure.
Tubular reabsorption This occurs by passivediffusion and depends on lipid solubility andionization of the drug at the existing urinary pH.Lipid-soluble drugs filtered at the glomerulus backdiffuse in the tubules because 99% of glomerularfiltrate is reabsorbed, but nonlipid-soluble andhighly ionized drugs are unable to do so. Thus,rate of excretion of such drugs, e.g. aminogly-coside antibiotics, quaternary ammoniumcompounds parallels g.f.r. (or creatinineclearance). Changes in urinary pH affect tubularreabsorption of drugs that are partially ionized—• Weak bases ionize more and are less reabsor-
bed in acidic urine.• Weak acids ionize more and are less reabsor-
bed in alkaline urine.
This principle is utilized for facilitating elimina-tion of the drug in poisoning, i.e. urine is alkali-nized in barbiturate and salicylate poisoning.Though elimination of weak bases (morphine,amphetamine) can be enhanced by acidifyingurine, this is not practiced clinically, becauseacidosis can induce rhabdomyolysis, cardiotoxi-city and actually worsen outcome. The effect ofchanges in urinary pH on drug excretion is greatestfor those having pKa values between 5 to 8,because only in their case pH dependent passivereabsorption is significant.
Tubular secretion This is the active transferof organic acids and bases by two separate classesof relatively nonspecific transporters (OAT andOCT) which operate in the proximal tubules. Inaddition, efflux transporters P-gp and MRP2 arelocated in the luminal membrane of proximaltubular cells. If renal clearance of a drug is greater
Fig. 3.3: Schematic depiction of glomerular filtration,tubular reabsorption and tubular secretion of drugsFD—free drug; BD—bound drug; UD—unionized drug;ID—ionized drug; Dx—actively secreted organic acid (orbase) drug

30S
EC
TIO
N1
GENERAL PHARMACOLOGY
than 120 mL/min (g.f.r.), additional tubularsecretion can be assumed to be occurring.
Active transport of the drug across tubulesreduces concentration of its free form in the tubu-lar vessels and promotes dissociation of proteinbound drug, which then becomes available forsecretion (Fig. 3.3). Thus, protein binding, whichis a hinderance for glomerular filtration of thedrug, is not so (may even be facilitatory) toexcretion by tubular secretion.
(a) Organic acid transport (through OATP)operates for penicillin, probenecid, uric acid,salicylates, indomethacin, sulfinpyrazone, nitro-furantoin, methotrexate, drug glucuronides andsulfates, etc.
(b) Organic base transport (through OCT)operates for thiazides, amiloride, triamterene,furosemide, quinine, procainamide, choline,cimetidine, etc.
Inherently both transport processes are bi-directional, i.e. they can transport their substratesfrom blood to tubular fluid and vice versa. How-ever, for drugs and their metabolites (exogenoussubstances) secretion into the tubular lumenpredominates, whereas an endogenous substratelike uric acid is predominantly reabsorbed.
Drugs utilizing the same active transport com-pete with each other. Probenecid is an organicacid which has high affinity for the tubular OATP.It blocks the active transport of both penicillinand uric acid, but whereas the net excretion ofthe former is decreased, that of the latter isincreased. This is because penicillin is primarilysecreted while uric acid is primarily reabsorbed.Many drug interactions occur due to competitionfor tubular secretion, e.g.(i) Salicylates block uricosuric action of probene-cid and sulfinpyrazone and decrease tubularsecretion of methotrexate.(ii) Probenecid decreases the concentration ofnitrofurantoin in urine, increases the duration ofaction of penicillin/ampicillin and impairssecretion of methotrexate.(iii) Sulfinpyrazone inhibits excretion of tolbuta-mide.
(iv) Quinidine decreases renal and biliary clearanceof digoxin by inhibiting efflux carrier P-gp.
Tubular transport mechanisms are not welldeveloped at birth. As a result, duration of actionof many drugs, e.g. penicillin, cephalosporins,aspirin is longer in neonates. These systems matureduring infancy. Renal function again progressivelydeclines after the age of 50 years; renal clearanceof most drugs is substantially lower in the elderly(>75 yr).
KINETICS OF ELIMINATIONThe knowledge of kinetics of elimination of adrug provides the basis for, as well as servesto devise rational dosage regimens and to modifythem according to individual needs. There arethree fundamental pharmacokinetic parameters,viz. bioavailability (F), volume of distribution (V)and clearance (CL) which must be understood.The first two have already been considered.
Drug elimination is the sumtotal of metabolicinactivation and excretion. As depicted in Fig.2.1, drug is eliminated only from the centralcompartment (blood) which is in equilibrium withperipheral compartments including the site ofaction. Depending upon the ability of the bodyto eliminate a drug, a certain fraction of the centralcompartment may be considered to be totally‘cleared’ of that drug in a given period of timeto account for elimination over that period.
Clearance (CL) The clearance of a drug isthe theoretical volume of plasma from which thedrug is completely removed in unit time (analogycreatinine clearance; Fig. 3.4). It can be calculatedas
CL = Rate of elimination/C ...(1)where C is the plasma concentration.
For majority of drugs the processes involvedin elimination are not saturated over the clinicallyobtained concentrations, they follow:
First order kinetics The rate of elimination isdirectly proportional to the drug concentration,CL remains constant; or a constant fraction of

31C
HA
PTE
R3
METABOLISM AND EXCRETION OF DRUGS, KINETICS OF ELIMINATION
the drug present in the body is eliminated in unittime. This applies to majority of drugs whichdo not saturate the elimination processes (trans-porters, enzymes, blood flow, etc.) over thetherapeutic concentration range. However, ifthe dose is high enough, elimination pathwaysof all drugs will get saturated.
Few drugs normally saturate eliminating mec-hanisms and are handled by—
Zero order kinetics The rate of eliminationremains constant irrespective of drug concen-tration, CL decreases with increase in concen-tration; or a constant amount of the drug iseliminated in unit time, e.g. ethyl alcohol. Thisis also called capacity limited elimination orMichaelis-Menten elimination.
The elimination of some drugs approachessaturation over the therapeutic range, kineticschanges from first order to zero order at higherdoses. As a result plasma concentration increasesdisproportionately with increase in dose (see Fig.3.6), as occurs in case of phenytoin, tolbutamide,theophylline, warfarin.
Plasma half-life The Plasma half-life (t½) ofa drug is the time taken for its plasma concen-tration to be reduced to half of its original value.
Taking the simplest case of a drug which hasrapid one compartment distribution and first order
elimination, and is given i.v. a semilog plasmaconcentration-time plot as shown in Fig. 3.5 isobtained. The plot has two slopes.• initial rapidly declining (α) phase—due to
distribution.• later less declined (β) phase—due to elimina-
tion.At least two half-lives (distribution t½ andelimination t½) can be calculated from the twoslopes. The elimination half life derived from theβ slope is simply called the ‘half life’ of the drug.Most drugs infact have multicompartment distribution andmultiexponential decay of plasma concentration-time plot.Half-lives calculated from the terminal slopes (when plasmaconcentrations are very low) are exceptionally long, probablydue to release of the drug from slow equilibrating tissues,enterohepatic circulation, etc. Only the t½ calculated over thesteady-state plasma concentration range is clinically relevant.It is this t½ which is commonly mentioned.
Mathematically, elimination t½ is
ln2t½ = —— ...(2) k
Where ln2 is the natural logarithm of 2 (or 0.693)and k is the elimination rate constant of the drug,i.e. the fraction of the total amount of drug inthe body which is removed per unit time. For
Fig. 3.4: Illustration of the concept of drug clearance. Afraction of the drug molecules present in plasma areremoved on each passage through the organs ofelimination. In the case shown, it requires 50 mL of plasmato account for the amount of drug being eliminated everyminute: clearance is 50 mL/min
Fig. 3.5: Semilog plasma concentration-time plot of adrug eliminated by first order kinetics after intravenousinjection

32S
EC
TIO
N1
GENERAL PHARMACOLOGY
example, if 2 g of the drug is present in the bodyand 0.1 g is eliminated every hour, then
k = 0.1/2 = 0.05 or 5% per hour.It is calculated as:
CLk = —– ...(3)
V V
therefore t½ = 0.693 × —— ...(4)CL
As such, half-life is a derived parameter fromtwo variables V and CL both of which may changeindependently. It, therefore, is not an exact indexof drug elimination. Nevertheless, it is a simpleand useful guide to the sojourn of the drug inthe body, i.e. after
1 t½–50% drug is eliminated.2 t½–75% (50 + 25) drug is eliminated.3 t½ – 87.5% (50 + 25 + 12.5) drug is eliminated.4 t½–93.75% (50 + 25 + 12.5 + 6.25) drug
is eliminated.Thus, nearly complete drug elimination occurs in4–5 half lives.For drugs eliminated by—First order kinetics—t½ remains constant becauseV and CL do not change with dose.Zero order kinetics—t½ increases with dosebecause CL progressively decreases as dose isincreased.
of the drug has been worked out and its CL isknown, the dose rate needed to achieve the targetCpss can be determined—
dose rate = target Cpss × CL ...(6)
After oral administration, often only a fraction(F) of the dose reaches systemic circulation inthe active form. In such a case—
target Cpss × CLdose rate = ———————— ...(7)
FThe dose rate-Cpss relationship is linear only incase of drugs eliminated by first order kinetics.For drugs (e.g. phenytoin) which follow MichaelisMenten kinetics, elimination changes from firstorder to zero order kinetics over the therapeuticrange. Increase in their dose beyond saturationlevels causes an increase in Cpss which is outof proportion to the change in dose rate (Fig.3.6). In their case:
(Vmax) (C)Rate of drug elimination = ———— ...(8)
Km + Cwhere C is the plasma concentration of the drug,Vmax is the maximum rate of drug elimination,and Km is the plasma concentration at whichelimination rate is half maximal.
Half life of some representative drugs
Aspirin 4 hr Digoxin 40 hrPenicillin-G 30 min Digitoxin 7 daysDoxycycline 20 hr Phenobarbitone 90 hr
Repeated drug administration
When a drug is repeated at relatively short inter-vals, it accumulates in the body until eliminationbalances input and a steady state plasma concen-tration (Cpss) is attained—
dose rateCpss = ————— ...(5)
CLFrom this equation it is implied that doubling thedose rate would double the average Cpss and soon. Further, if the therapeutic plasma concentration
Fig. 3.6: Relationship between dose rate and averagesteady-state plasma concentration of drugs eliminatedby first order and Michaelis Menten (zero order) kinetics

33C
HA
PTE
R3
METABOLISM AND EXCRETION OF DRUGS, KINETICS OF ELIMINATION
Plateau principle
When constant dose of a drug is repeated beforethe expiry of 4 t½, it would achieve higher peakconcentration, because some remnant of theprevious dose will be present in the body. Thiscontinues with every dose until progressivelyincreasing rate of elimination (which increaseswith increase in concentration) balances theamount administered over the dose interval.Subsequently plasma concentration plateaus andfluctuates about an average steady-state level. Thisis known as the plateau principle of drug accu-mulation. Steady-state is reached in 4–5 half livesunless dose interval is very much longer thant½ (Fig. 3.7).
The amplitude of fluctuations in plasmaconcentration at steady-state depends on the doseinterval relative to the t½, i.e. the differencebetween the maximum and minimum levels isless if smaller doses are repeated more frequently(dose rate remaining constant). Dose intervals aregene-rally a compromise between what amplitudeof fluctuations is clinically tolerated (loss ofefficacy at troughs and side effects at peaks) andwhat frequency of dosing is convenient. However,if the dose rate is changed, a new average Cpssis attained over the next 4–5 half lives. Whenthe drug is administered orally (absorption takes
some time), average Cpss is approximately 1/3of the way between the minimal and maximallevels in a dose interval.
Target level strategy For drugs whose effectsare not easily quantifiable and safety margin isnot big, e.g. anticonvulsants, antidepressants,lithium, antiarrhythmics, theophylline, some anti-microbials, etc. or those given to prevent an event,it is best to aim at achieving a certain plasmaconcentration which has been defined to be inthe therapeutic range; such data are now availablefor most drugs of this type.
Drugs with short t½ (upto 2–3 hr) adminis-tered at conventional intervals (6–12 hr) achievethe target levels only intermittently and fluctua-tions in plasma concentration are marked. In caseof many drugs (penicillin, ampicillin, chloramp-henicol, erythromycin, propranolol) this howeveris therapeutically acceptable.
For drugs with longer t½ a dose that issufficient to attain the target concentration aftersingle administration, if repeated will accumulateaccording to plateau principle and produce toxicitylater on. On the other hand, if the dosing is suchas to attain target level at steady state, thetherapeutic effect will be delayed by about 4 halflives (this may be clinically unacceptable). Suchdrugs are often administered by initial loadingand subsequent maintenance doses.
Loading dose This is a single or few quicklyrepeated doses given in the beginning to attain targetconcentration rapidly. It may be calculated as—
target Cp × VLoading dose = —————— ...(9)
FThus, loading dose is governed only by V and notby CL or t½.
Maintenance dose This dose is one that is tobe repeated at specified intervals after theattainment of target Cpss so as to maintain the sameby balancing elimination. The maintenance doserate is computed by equation (7) and is governedby CL (or t½) of the drug. If facilities formeasurement of drug concentration are available,
Fig. 3.7: Plateau principle of drug accumulation onrepeated oral dosing.Note. The area of the two shaded portions is equal

34S
EC
TIO
N1
GENERAL PHARMACOLOGY
attainment of target level in a patient can be verifiedsubsequently and dose rate adjusted if required.
Such two phase dosing provides rapid thera-peutic effect with long term safety; frequentlyapplied to digoxin, chloroquine, long-actingsulfonamides, doxycycline, amiodarone, etc.However, if there is no urgency, maintenance dosescan be given from the beginning. The conceptof loading and maintenance dose is valid alsofor short t½ drugs and i.v. administration in criticallyill patients, e.g. lidocaine (t½ 1.5 hr) used forcardiac arrhythmias is given as an i.v. bolus dosefollowed by slow i.v. infusion or intermittentfractional dosing.
Monitoring of plasma concentration ofdrugs It is clear from the above considerationsthat the Cpss of a drug attained in a given patientdepends on its F, V and CL in that patient. Becauseeach of these parameters varies considerablyamong individuals, the actual Cpss in a patientmay be 1/3 to 3 times that calculated on the basisof population data. Measurement of plasma drugconcentration can give an estimate of thepharmacokinetic variables in that patient and themagnitude of deviation from the ‘average patient’,so that appropriate adjustments in the dosageregimen can be made.
In case of drugs obeying first order kinetics:Previous dose rate × Target CpssRevised = —————————————— ...(10)
dose rate Measured Cpss
Therapeutic drug monitoring (TDM) is particularlyuseful in the following situations:1. Drugs with low safety margin, e.g. —digoxin,
anticonvulsants, antiarrhythmics, theophylline,aminoglycoside antibiotics, lithium, tricyclicantidepressants.
2. If individual variations are large, e.g.—anti-depressants, lithium.
3. Potentially toxic drugs used in the presence ofrenal failure, e.g. —aminoglycoside antibiotics,vancomycin.
4. In case of poisoning.5. In case of failure of response without any
apparent reason, e.g. —antimicrobials.
6. To check patient compliance, e.g. —psycho-pharmacological agents.
Selection of the correct interval between drug administrationand drawing of blood sample for TDM is critical, and dependson the purpose of TDM as well as the nature of thedrug.a. When the purpose is dose adjustment: In case of drugs
which need to act continuously (relatively long-actingdrugs), it is prudent to measure the trough steady-stateblood levels, i.e. just prior to the next dose, becausethis is governed by both V and CL. On the other hand,for short-acting drugs which achieve therapeutic levelsonly intermittently (e.g. ampicillin, gentamicin), samplingis done in the immediate post-absorptive phase (usuallyafter 1–2 hours of oral/i.m. dosing) to reflect the peaklevels.
b. In case of poisoning: Blood for drug level estimationshould be taken at the earliest to confirm the poisoningand to gauge its seriousness. It should then be repeatedat intervals to monitor the progress.
c. For checking compliance to medication: Even randomblood sampling can be informative.
Monitoring of plasma concentration is of novalue for1. Drugs whose response is easily measurable,
e.g.— antihypertensives, hypoglycaemics,diuretics, oral anticoagulants, general anaes-thetics.
2. Drugs activated in the body, e.g.—levodopa.3. ‘Hit and run drugs’ (whose effect lasts much
longer than the drug itself), e.g.—reserpine,guanethidine, MAO inhibitors, omeprazole.
4. Drugs with irreversible action, e.g.—organo-phosphate anticholinesterases, phenoxybenza-mine.
PROLONGATION OF DRUG ACTIONIt is sometimes advantageous to modify a drugin such a way that it acts for a longer period.By doing so:(i) Frequency of administration is reduced—moreconvenient.(ii) Improved patient compliance—a singlemorning dose is less likely to be forgotten/omittedthan a 6 or 8 hourly regimen; a monthly orquarterly administered contraceptive over one thathas to be taken daily.

35C
HA
PTE
R3
METABOLISM AND EXCRETION OF DRUGS, KINETICS OF ELIMINATION
(iii) Large fluctuations in plasma concentrationare avoided—side effects related to high peakplasma level just after a dose (e.g. nifedipine)would be minimized; better round-the-clockcontrol of blood sugar, etc.(iv) Drug effect could be maintained overnightwithout disturbing sleep, e.g. antiasthmatics,anticonvulsants, etc.
However, all drugs do not need to be madelong acting, e.g. those used for brief therapeuticeffect (sleep-inducing hypnotic, headache remedy)or those with inherently long duration of action(doxycycline, omeprazole, digoxin, amlodipine).Drugs with t½ < 4 hr are suitable for controlledrelease formulations, while there is no need ofsuch formulations for drugs with t½ >12 hr.Methods utilized for prolonging drug action aresummarised below. Some of these have alreadybeen described.
1. By prolonging absorption from site ofadministration(a) Oral Sustained release tablets, spansulecapsules, etc.; drug particles are coated with resins,plastic materials or other substances whichtemporally disperse release of the active ingredientin the g.i.t. Another technique (controlled releasetablet/capsule; Fig. 3.8) utilizes a semipermeablemembrane to control the release of drug fromthe dosage form. Such preparations prolong theaction by 4 to 8 hours and no more, because
in that time drug particles reach the colon. Also,the drug release pattern and consequently theattained blood levels of the drug may be morevariable than the regular tablet of the same drug.(b) Parenteral The s.c. and i.m. injection ofdrug in insoluble form (benzathine penicillin, lenteinsulin) or as oily solution (depot progestins);pellet implantation, sialistic and biodegradableimplants can provide for its absorption over acouple of days to several months or even years.Inclusion of a vasoconstrictor with the drug alsodelays absorption (adrenaline with local anaes-thetics).(c) Transdermal drug delivery systems Thedrug impregnated in adhesive patches, strips oras ointment applied on skin is utilized in somecases to prolong drug action, e.g. GTN (seep. 8).
2. By increasing plasma protein bindingDrug congeners have been prepared which arehighly bound to plasma protein and are slowlyreleased in the free active form, e.g. sulfadoxine.3. By retarding rate of metabolism Smallchemical modification can markedly affect therate of metabolism without affecting the biologi-cal action, e.g. addition of ethinyl group toestradiol makes it longer acting and suitable foruse as oral contraceptive. Inhibition of specificenzyme by one drug can prolong the action ofanother drug, e.g. allopurinol inhibits thedegradation of 6-mercaptopurine, ritonavir booststhe levels of indinavir, cilastatin protects imipenemfrom degradation in kidney.
4. By retarding renal excretion The tubularsecretion of drug being an active process, canbe suppressed by a competing substance, e.g.probenecid prolongs duration of action ofpenicillin and ampicillin.
Targeted drug delivery devices
Some new devices have been invented (and manyare under development) to localise and prolongthe delivery of the contained drug to a specifictarget organ. The ones already in use are:
Fig. 3.8: Pattern of drug release from oral controlledrelease tablet/capsule; 30% of the dose outside thesemipermeable membrane is released immediately, while70% of the dose is released slowly through the membraneover the next 4–8 hours

36S
EC
TIO
N1
GENERAL PHARMACOLOGY
1. Liposomes These are unilamellar orbilamellar nano-vesicles (60–80 nM) producedby sonication of lecithin or other biodegradablephospholipids. Since liposomes injected i.v. areselectively taken up by reticuloendothelial cells,especially liver and spleen, and some malignantcells, the drug incorporated in them gets selectivelydelivered to these cells. Liposomal amphotericinB is being used in Kala azar and some seriouscases of systemic mycosis. Antibody tagging ofliposomes is being tried as a means to target otherspecific tissues.
2. Drug releasing implants The implant iscoated with the drug using special techniques andthen placed in the target organ to provideprolonged delivery of minute quantities of thedrug by slow release. Progestin impregnatedintrauterine contraceptive device (IUCD) affordsprotection for upto 5 years. It is also being triedfor other gynaecological problems. Antithromboticdrug coated stents (devices placed in thethrombosed coronary artery after balloonangioplasty to keep it patent) are in use to preventrestenosis and failure of angioplasty.
PROBLEM DIRECTED STUDY
3.1 A 30-year-old mother of 2 children weighing 60 kg was taking combined oral contraceptivepill containing levonorgestrel 0.15 mg + ethinylestradiol 30 μg per day cyclically (3 weeks treatment—1 week gap). She developed fever with cough and was diagnosed as a case of pulmonary tuberculosisafter sputum smear examination. She was put on isoniazid (300 mg) + rifampin (600 mg) +pyrazinamide (1.5 g) + ethambutol (1.0 g) daily for 2 months, followed by isoniazid (600 mg)+ rifampin (600 mg) thrice weekly. In the 3rd month she failed to have the usual withdrawalbleeding during the gap period of contraceptive cycle. After 10 days her urinary pregnancy testwas found to be positive.(a) What could be the reason for failure of the oral contraceptive?(b) What precaution could have prevented the unwanted pregnancy?
3.2 A 20-year-old patient weighing 60 kg has to be prescribed an antiepileptic drug (availableas 200 and 400 mg tablets) for generalized tonic-clonic seizures. The pharmacokinetic parametersand therapeutic plasma concentration of the selected drug are:
Target steady-state plasma concentration (Cpss) – 6 mg/LOral bioavailability (F) – 70%Volume of distribution (V) – 1.4 L/kgClearance (CL) – 80 ml/hr/kgPlasma half life (t½) – 15 hours
What should be the loading dose and the daily maintenance dose of the drug for this patient?(see Appendix-1 for solutions)

Pharmacodynamics:Mechanism of Drug Action;Receptor Pharmacology
ChapterChapterChapterChapterChapter 44444
Pharmacodynamics is the study of drug effects.It starts with describing what the drugs do, andgoes on to explain how they do it. Thus, it attemptsto elucidate the complete action-effect sequenceand the dose-effect relationship. Modification ofthe action of one drug by another drug is alsoan aspect of pharmacodynamics.
PRINCIPLES OF DRUG ACTION
Drugs (except those gene based) do not impartnew functions to any system, organ or cell; theyonly alter the pace of ongoing activity. However,this alone can have profound medicinal as wellas toxicological impact. The basic types of drugaction can be broadly classed as:
1. Stimulation It refers to selective enhancement of thelevel of activity of specialized cells, e.g. adrenaline stimulatesheart, pilocarpine stimulates salivary glands. However,excessive stimulation is often followed by depression of thatfunction, e.g. high dose of picrotoxin, a central nervous system(CNS) stimulant, produces convulsions followed by comaand respiratory depression.
2. Depression It means selective diminution of activityof specialized cells, e.g. barbiturates depress CNS, quinidinedepresses heart, omeprazole depresses gastric acid secretion.Certain drugs stimulate one type of cells but depress theother, e.g. acetylcholine stimulates intestinal smooth musclebut depresses SA node in heart. Thus, most drugs cannotbe simply classed as stimulants or depressants.
3. Irritation This connotes a nonselective, often noxiouseffect and is particularly applied to less specialized cells(epithelium, connective tissue). Strong irritation results ininflammation, corrosion, necrosis and morphological damage.This may result in diminution or loss of function.
4. Replacement This refers to the use of naturalmetabolites, hormones or their congeners in deficiency states,e.g. levodopa in parkinsonism, insulin in diabetes mellitus,iron in anaemia.
5. Cytotoxic action Selective cytotoxic action oninvading parasites or cancer cells, attenuating them withoutsignificantly affecting the host cells is utilized for cure/
palliation of infections and neoplasms, e.g. penicillin, chloro-quine, zidovudine, cyclophosphamide, etc.
MECHANISM OF DRUG ACTIONOnly a handful of drugs act by virtue of theirsimple physical or chemical property; examplesare:• Bulk laxatives (ispaghula)—physical mass• Dimethicone, petroleum jelly—physical form,
opacity• Paraamino benzoic acid—absorption of UV
rays• Activated charcoal—adsorptive property• Mannitol, mag. sulfate—osmotic activity• 131I and other radioisotopes—radioactivity• Antacids—neutralization of gastric HCl• Pot. permanganate—oxidizing property• Chelating agents (EDTA, dimercaprol)—che-
lation of heavy metals.• Cholestyramine—sequestration of bile acids
and cholesterol in the gut• Mesna—Scavenging of vasicotoxic reactive
metabolites of cyclophosphamideMajority of drugs produce their effects by
interacting with a discrete target biomolecule, whichusually is a protein. Such mechanism confersselectivity of action to the drug. Functional proteinsthat are targets of drug action can be groupedinto four major categories, viz. enzymes, ionchannels, transporters and receptors (see Fig. 4.1).However, a few drugs do act on other proteins(e.g. colchicine, vinca alkaloids, taxanes bind tothe structural protein tubulin) or on nucleic acids(alkylating agents).
I. ENZYMES
Almost all biological reactions are carried outunder catalytic influence of enzymes; hence,

38S
EC
TIO
N1
GENERAL PHARMACOLOGY
often optimally set. Thus, stimulation of enzymesby drugs, that are truly foreign substances, isunusual. Enzyme stimulation is relevant to somenatural metabolites only, e.g. pyridoxine acts asa cofactor and increases decarboxylase activity.Several enzymes are stimulated through receptorsand second messengers, e.g. adrenaline stimulateshepatic glycogen phosphorylase through b recep-tors and cyclic AMP. Stimulation of an enzymeincreases its affinity for the substrate so that rateconstant (kM) of the reaction is lowered (Fig.4.2).
Fig. 4.1: Four major types of biomacromoleculartargets of drug action.
(A) Enzyme; (B) Transmembrane ion channel;(C) Membrane bound transporter; (D) Receptor (see textfor description)
enzymes are a very important target of drug action.Drugs can either increase or decrease the rateof enzymatically mediated reactions. However,in physiological systems enzyme activities are
Fig. 4.2: Effect of enzyme induction, stimulation andinhibition on kinetics of enzyme reaction
Vmax—Maximum velocity of reaction; Vmax (s) ofstimulated enzyme; Vmax (i)—in presence of non-competitive inhibitor; kM—rate constant of the reaction;kM (s)—of stimulated enzyme; kM (i)—in presence ofcompetitive inhibitorNote: Enzyme induction and noncompetitive inhibition donot change the affinity of the enzyme (kM is unaltered),whereas enzyme stimulation and competitive inhibitionrespectively decrease and increase the kM.
Apparent increase in enzyme activity can alsooccur by enzyme induction, i.e. synthesis of moreenzyme protein. This cannot be called stimulationbecause the kM does not change. Many drugsinduce microsomal enzymes (see p. 26).
Enzyme inhibitionSome chemicals (heavy metal salts, strong acidsand alkalies, formaldehyde, phenol, etc.) denatureproteins and inhibit all enzymes nonselectively.They have limited medicinal value restricted toexternal application only. However, selective

39C
HA
PTE
R4
MECHANISM OF DRUG ACTION; RECEPTOR PHARMACOLOGY
inhibition of a particular enzyme is a commonmode of drug action. Such inhibition is eithercompetitive or noncompetitive.
(i) Competitive (equilibrium type) The drugbeing structurally similar competes with thenormal substrate for the catalytic binding site ofthe enzyme so that the product is not formedor a nonfunctional product is formed (Fig. 4.1A),and a new equilibrium is achieved in the presenceof the drug. Such inhibitors increase the kM butthe Vmax remains unchanged (Fig. 4.2), i.e. higherconcentration of the substrate is required toachieve ½ maximal reaction velocity, but ifsubstrate concentration is sufficiently increased,it can displace the inhibitor and the same maximalreaction velocity can be attained. Examples aregiven in the box above.
A nonequilibrium type of enzyme inhibitioncan also occur with drugs which react with thesame catalytic site of the enzyme but either formstrong covalent bonds or have such high affinityfor the enzyme that the normal substrate is notable to displace the inhibitor, e.g.• Organophosphates react covalently with the
esteretic site of the enzyme cholinesterase.• Methotrexate has 50,000 times higher affinity
for dihydrofolate reductase than the normalsubstrate DHFA.
In these situations, kM is increased and Vmaxis reduced.
(ii) Noncompetitive The inhibitor reacts withan adjacent site and not with the catalytic site,but alters the enzyme in such a way that it loses
its catalytic property. Thus, kM is unchanged butVmax is reduced. Examples are given in the box.
Enzyme Endogenous substrate Competitive inhibitor
• Cholinesterase Acetylcholine Physostigmine, Neostigmine
• Monoamine-oxidase A (MAO-A) Catecholamines Moclobemide
• Dopa decarboxylase Levodopa Carbidopa, Benserazide
• Xanthine oxidase Hypoxanthine Allopurinol
• Angiotensin converting enzyme (ACE) Angiotensin-1 Captopril
• 5α-Reductase Testosterone Finasteride
• Aromatase Testosterone, Androstenedione Letrozole, Anastrozole
• Bacterial folate synthase Para-amino benzoic acid (PABA) Sulfadiazine
II. ION CHANNELS
Proteins which act as ion selective channels par-ticipate in transmembrane signaling and regulateintracellular ionic composition. This makes thema common target of drug action (Fig. 4.1B). Drugscan affect ion channels, some of which actuallyare receptors, because they are operated byspecific signal molecules either directly and arecalled ligand gated channels (e.g. nicotinicreceptor, see Fig. 4.4) or through G-proteins andare termed G-protein regulated channels (e.g.cardiac β1 adrenergic receptor activated Ca2+
channel, see Table 4.1). Drugs can also act onvoltage operated and stretch sensitive channelsby directly binding to the channel and affectingion movement through it, e.g. local anaestheticswhich obstruct voltage sensitive Na+ channels(see Ch. 26). In addition, certain drugs modulateopening and closing of the channels, e.g.:
Noncompetitive Enzymeinhibitor
Acetazolamide — Carbonic anhydraseAspirin, indomethacin — CyclooxygenaseDisulfiram — Aldehyde
dehydrogenaseOmeprazole — H+ K+ ATPaseDigoxin — Na+ K+ ATPaseTheophylline — PhosphodiesterasePropylthiouracil — Peroxidase in thyroidLovastatin — HMG-CoA reductaseSildenafil — Phosphodiesterase-5

40S
EC
TIO
N1
GENERAL PHARMACOLOGY
• Quinidine blocks myocardial Na+ channels.• Dofetilide and amiodarone block myocardial
delayed rectifier K+ channel.• Nifedipine blocks L-type of voltage sensitive
Ca2+ channel.• Nicorandil opens ATP-sensitive K+ channels.• Sulfonylurea hypoglycaemics inhibit pan-
creatic ATP-sensitive K+ channels.• Amiloride inhibits renal epithelial Na+
channels.• Phenytoin modulates (prolongs the inactivated
state of) voltage sensitive neuronal Na+
channel.• Ethosuximide inhibits T-type of Ca2+ channels
in thalamic neurones
III. TRANSPORTERSSeveral substrates are translocated across mem-branes by binding to specific transporters (carriers)which either facilitate diffusion in the directionof the concentration gradient or pump themetabolite/ion against the concentration gradientusing metabolic energy (see p. 12–14; Fig. 2.5).Many drugs produce their action by directlyinteracting with the solute carrier (SLC) classof transporter proteins to inhibit the ongoingphysiological transport of the metabolite/ion (Fig.4.1C). Examples are:• Desipramine and cocaine block neuronal
reuptake of noradrenaline by interacting withnorepinephrine transporter (NET).
• Fluoxetine (and other SSRIs) inhibit neuronalreuptake of 5-HT by interacting with serotonintransporter (SERT).
• Amphetamines selectively block dopaminereuptake in brain neurons by dopaminetransporter (DAT).
• Reserpine blocks the vesicular reuptake ofnoradrenaline and 5-HT by the vesicularmono-amine transporter (VMAT-2).
• Hemicholinium blocks choline uptake intocholinergic neurones and depletes acetyl-choline.
• The anticonvulsant tiagabine acts by inhibi-ting reuptake of GABA into brain neuronesby GABA transporter GAT1.
• Furosemide inhibits the Na+K+2Cl¯ cotrans-porter in the ascending limb of loop of Henle.
• Hydrochlorothiazide inhibits the Na+Cl¯symporter in the early distal tubule.
• Probenecid inhibits active transport of organicacids (uric acid, penicillin) in renal tubulesby interacting with organic anion transporter(OAT).
IV. RECEPTORS
The largest number of drugs do not bind directlyto the effectors, viz. enzymes, channels, transpor-ters, structural proteins, template biomolecules,etc. but act through specific regulatory macro-molecules which control the above listed effectors.These regulatory macromolecules or the sites onthem which bind and interact with the drug arecalled ‘receptors’.
Receptor: It is defined as a macromolecule orbinding site located on the surface or inside theeffector cell that serves to recognize the signalmolecule/drug and initiate the response to it, butitself has no other function.
Though, in a broad sense all types of target biomole-cules, including the effectors (enzymes, channels, transporters,etc.) with which a drug can bind to produce its action havebeen denoted as ‘receptors’ by some authors, such designationtends to steal the specific meaning of this important term.If so applied, xanthine oxidase would be the ‘receptor’ forallopurinol, L-type Ca2+ channel would be the ‘receptor’ fornifedipine, serotonin transporter (SERT) would be the‘receptor’ for fluoxetine; a connotation not in consonencewith the general understanding of the term ‘receptor’. It istherefore better to reserve the term ‘receptor’ for purelyregulatory macromolecules which combine with and mediatethe action of signal molecules including drugs.
The following terms are used in describingdrug-receptor interaction:Agonist An agent which activates a receptorto produce an effect similar to that of thephysiological signal molecule.Inverse agonist An agent which activates areceptor to produce an effect in the oppositedirection to that of the agonist.Antagonist An agent which prevents the actionof an agonist on a receptor or the subsequentresponse, but does not have any effect of its own.

41C
HA
PTE
R4
MECHANISM OF DRUG ACTION; RECEPTOR PHARMACOLOGY
Partial agonist An agent which activates areceptor to produce submaximal effect butantagonizes the action of a full agonist.Ligand (Latin: ligare—to bind) Any moleculewhich attaches selectively to particular receptorsor sites. The term only indicates affinity or abilityto bind without regard to functional change: agonistsand competitive antagonists are both ligands ofthe same receptor.
The overall scheme of drug action throughreceptors is depicted in Fig. 4.1D.
Basic evidences for drug action through receptors(i) Many drugs exhibit structural specificity of action, i.e.specific chemical configuration is associated with a particularaction, e.g. isopropyl substitution on the ethylamine side chainof sympathetic drugs produces compounds with markedcardiac and bronchial activity—most b adrenergic agonistsand antagonists have this substitution. A 3 carbon internitrogenseparation in the side chain of phenothiazines results inantidopaminergic-antipsychotic compounds, whereas 2 carbonseparation produces anticholinergic-antihistaminic com-pounds. Further, chiral drugs show stereospecificity in action,e.g. levo noradrenaline is 10 times more potent than dextronoradrenaline; d-propranolol is about 100 times less potent inblocking β receptors than the l-isomer, but both are equipotentlocal anaesthetics.
Thus, the cell must have some mechanism to recognizea particular chemical configuration and three dimensionalstructure.
(iii) It was calculated by Clark that adrenaline andacetylcholine produce their maximal effect on frog’s heartby occupying only 1/6000th of the cardiac cell surface—thus, special regions of reactivity to such drugs must bepresent on the cell.
Receptor occupation theoryAfter studying quantitative aspects of drug action,Clark (1937) propounded a theory of drug actionbased on occupation of receptors by specific drugsand that the pace of a cellular function can bealtered by interaction of these receptors with drugswhich, in fact, are small molecular ligands. Heperceived the interaction between the twomolecular species, viz. drug (D ) and receptor (R)to be governed by the law of mass action, andthe effect (E) to be a direct function of the drug-receptor complex (DR) formed:
Subsequently, it has been realized that occupationof the receptor is essential but not itself sufficientto elicit a response; the agonist must also be ableto activate (induce a conformational change in)the receptor. The ability to bind with the receptordesignated as affinity, and the capacity to inducea functional change in the receptor designatedas intrinsic activity (IA) or efficacy are independentproperties. Competitive antagonists occupy thereceptor but do not activate it. Moreover, certaindrugs are partial agonists which occupy andsubmaximally activate the receptor. An all or noneaction is not a must at the receptor. A theoreticalquantity(S) denoting strength of stimulus impartedto the cell was interposed in the Clark’s equation:
Depending on the agonist, DR could generatea stronger or weaker S, probably as a functionof the conformational change brought about bythe agonist in the receptor. Accordingly:
Agonists have both affinity and maximal intrin-sic activity (IA = 1), e.g. adrenaline, histamine,morphine.
(ii) Competitive antagonism is seen between specific agonistsand antagonists. Langley in 1878 was so impressed by themutual antagonism among two alkaloids pilocarpine andatropine that he proposed that both reacted with the same‘receptive substance’ on the cell. Ehrlich (1900) observedquantitative neutralization between toxins and antitoxins anddesignated ‘receptor’ to be the anchoring group of theprotoplasmic molecule for the administered compound.

42S
EC
TIO
N1
GENERAL PHARMACOLOGY
Competitive antagonists have affinity but nointrinsic activity (IA = 0), e.g. propranolol, atro-pine, chlorpheniramine, naloxone.
Partial agonists have affinity and submaximalintrinsic activity (IA between 0 and 1), e.g.dichloroisoproterenol (on β adrenergic receptor),pentazocine (on μ opioid receptor).
Inverse agonists have affinity but intrinsic acti-vity with a minus sign (IA between 0 and –1),e.g. DMCM (on benzodiazepine receptor),chlorpheniramine (on H1 histamine receptor).
It has also been demonstrated that many fullagonists can produce maximal response even whileoccupying <1% of the available receptors. A largereceptor reserve exists in their case, or a numberof spare receptors are present.
The two-state receptor model
An attractive alternative model for explaining theaction of agonists, antagonists, partial agonistsand inverse agonists has been proposed.
The receptor is believed to exist in two inter-changeable states: Ra (active) and Ri (inactive)which are in equilibrium. In the case of majorityof receptors, the Ri state is favoured at equili-brium—no/very weak signal is generated in theabsence of the agonist—the receptor exhibits noconstitutive activation (Fig. 4.3I). The agonist (A)binds preferentially to the Ra conformation andshifts the equilibrium → Ra predominates anda response is generated (Fig. 4.3II) dependingon the concentration of A. The competitiveantagonist (B) binds to Ra and Ri with equalaffinity → the equilibrium is not altered → noresponse is generated (Fig. 4.3 III), and whenthe agonist is applied fewer Ra are available tobind it—response to agonist is decreased. If anagonist has only slightly greater affinity for Rathan for Ri, the equilibrium is only modestlyshifted towards Ra (Fig. 4.3 IV) even at saturatingconcentrations → a submaximal response isproduced and the drug is called a partial agonist(C). The inverse agonist (D) has high affinityfor the Ri state (Fig. 4.3V), therefore it can producean opposite response, provided the resting
Fig. 4.3: Illustration of the two-state receptor model(see text for explanation)
equilibrium was in favour of the Ra state. Certainion channel receptors such as benzodiazepinereceptor and some G-protein coupled receptorslike histamine H2, angiotensin AT1, adrenergic β1
and cannabinoid receptors exhibit constitutiveactivation, i.e. an appreciable intensity signal isgenerated even in the basal state (no agonistpresent). In their case the inverse agonist stabilizesthe receptor in the inactive conformation resultingin an opposite response. Only few inverse agonistsare known at present.
This model provides an explanation for thephenomenon of positive cooperativity often seenwith neurotransmitters, and is supported by studiesof conformational mutants of the receptor withaltered equilibrium. However, receptors are nowknown to be capable of adopting not just two,but multiple active and inactive conformationsfavoured by different ligands.

43C
HA
PTE
R4
MECHANISM OF DRUG ACTION; RECEPTOR PHARMACOLOGY
Nature of receptors
Receptors are regulatory macromolecules, mostlyproteins, though nucleic acids may also serve asreceptors. Hundreds of receptor proteins have beenisolated, purified, cloned and their primary aminoacid (AA) sequence has been worked out.Molecular cloning has also helped in obtainingthe receptor protein in larger quantity to studyits structure and properties, and in subclassifyingreceptors. The cell surface receptors with theircoupling and effector proteins are considered tobe floating in a sea of membrane lipids; thefolding, orientation and topography of the systembeing determined by interactions between thelipophilic and hydrophilic domains of the peptidechains with solvent molecules (water on one sideand lipids on the other). Nonpolar portions ofthe AA chain tend to bury within the membrane,while polar groups tend to come out in the aqueousmedium. In such a delicately balanced system,it is not difficult to visualize that a small molecularligand binding to one site in the receptor moleculecould be capable of tripping the balance (byaltering distribution of charges, etc.) and bringingabout conformational changes at distant sites. Eachof the four major families of receptors (describedlater) have a well defined common structural motif,while the individual receptors differ in the detailsof amino acid sequencing, length of intra/extracellular loops, etc. Majority of receptormolecules are made up of several non-identicalsubunits (heteropolymeric), and agonist bindinghas been shown to bring about changes in theirquaternary structure or relative alignment of thesubunits, e.g. on activation the subunits of nicotinicreceptor move apart opening a centrally locatedcation channel.
Many drugs act upon physiological receptorswhich mediate responses to transmitters, hormo-nes, autacoids and other endogenous signalmolecules; examples are cholinergic, adrenergic,histaminergic, steroid, leukotriene, insulin andother such receptors. In addition, now some trulydrug receptors have been described for whichthere are no known physiological ligands, e.g.
benzodiazepine receptor, sulfonylurea receptor.Receptors for which no endogenous mediator orligand is known have been called ‘Orphanreceptors’.
Receptor subtypes
The delineation of multiple types and subtypesof receptors for signal molecules has played animportant role in the development of a numberof targeted and more selective drugs. Even atan early stage of evolution of receptorpharmacology, it was observed that actions ofacetylcholine could be grouped into ‘muscarinic’and ‘nicotinic’ depending upon whether they weremimicked by the then known alkaloids muscarineor nicotine. Accordingly, they were said to bemediated by two types of cholinergic receptors,viz. muscarinic (M) or nicotinic (N); a conceptstrengthened by the finding that muscarinic actionswere blocked by atropine, while nicotinic actionswere blocked by curare. In a landmark study,Ahlquist (1948) divided adrenergic receptors into‘α’ and ‘β’ on the basis of two distinct rankorderof potencies of adrenergic agonists. Thesereceptors have now been further subdivided (M1,M2 ….M5), (NM, NN) (α1, α2) (β1, β2, β3). Multiplesubtypes of receptors for practically alltransmitters, autacoids, hormones, etc. are nowknown and have paved the way for introductionof numerous clinically superior drugs. In manycases, receptor classification has provided soundexplanation for differences observed in the actionsof closely related drugs.
The following criteria have been utilized in classifyingreceptors:a. Pharmacological criteria Classification is based on
relative potencies of selective agonists and antagonists.This is the classical and oldest approach with directclinical bearing; was used in delineating M and Ncholinergic, α and β adrenergic, H1 and H2 histaminergicreceptors, etc.
b. Tissue distribution The relative organ/tissue distri-bution is the basis for designating the subtype, e.g. thecardiac β adrenergic receptors as β1, while bronchialas β2. This division was confirmed by selective agonistsand antagonists as well as by molecular cloning.
c. Ligand binding Measurement of specific binding ofhigh affinity radio-labelled ligand to cellular fragments

44S
EC
TIO
N1
GENERAL PHARMACOLOGY
(usually membranes) in vitro, and its displacement byvarious selective agonists/antagonists is used to delineatereceptor subtypes. Multiple 5-HT receptors weredistinguished by this approach. Autoradiography hashelped in mapping distribution of receptor subtypes inthe brain and other organs.
d. Transducer pathway Receptor subtypes may bedistinguished by the mechanism through which theiractivation is linked to the response, e.g. M cholinergicreceptor acts through G-proteins, while N cholinergicreceptor gates influx of Na+ ions; α adrenergic receptoracts via IP3-DAG pathway and by decreasing cAMP,while β adrenergic receptor increases cAMP; GABAA
receptor is a ligand gated Cl– channel, while GABAB
receptor increases K+ conductance through a G-protein.e. Molecular cloning The receptor protein is cloned and
its detailed amino acid sequence as well as threedimentional structure is worked out. Subtypes aredesignated on the basis of sequence homology. Thisapproach has in the recent years resulted in a floodof receptor subtypes and several isoforms (which donot differ in ligand selectivity) of each subtype. Thefunctional significance of many of these subtypes/isoforms is dubious. Even receptors without knownligands (orphan receptors) have been described.Application of so many approaches has thrown
up several detailed, confusing and often conflictingclassifications of receptors. However, a consensusreceptor classification is now decided on acontinuing basis by an expert group of theInternational Union of Pharmacological Sciences(IUPHAR).
Silent receptors These are sites which bind specificdrugs but no pharmacological response is elicited. They arebetter called drug acceptors or sites of loss, e.g. plasmaproteins which have binding sites for many drugs. To avoidconfusion, the term receptor should be restricted to thoseregulatory binding sites which are capable of generating aresponse.
ACTION-EFFECT SEQUENCE‘Drug action’ and ‘drug effect’ are often looselyused interchangeably, but are not synonymous.Drug action It is the initial combination of thedrug with its receptor resulting in a conforma-tional change in the latter (in case of agonists),or prevention of conformational change throughexclusion of the agonist (in case of antagonists).Drug effect It is the ultimate change in biolo-gical function brought about as a consequence
of drug action, through a series of intermediatesteps (transducer).
Receptors subserve two essential functions,viz, recognition of the specific ligand moleculeand transduction of the signal into a response.Accordingly, the receptor molecule has a ligandbinding domain (spatially and energetically suitablefor binding the specific ligand) and an effectordomain (Fig. 4.4) which undergoes a functionalconformational change. These domains havenow actually been identified in some receptors.The perturbation in the receptor molecule isvariously translated into the response. The sequen-tial relationship between drug action, transducerand drug effect can be seen in Fig. 4.1D and 4.6.
TRANSDUCER MECHANISMS
Considerable progress has been made in theunderstanding of transducer mechanisms whichin most instances have been found to be highlycomplex multistep processes that provide foramplification and integration of concurrentlyreceived extra- and intra-cellular signals at eachstep. Because only a handful of transducer path-ways are shared by a large number of receptors,the cell is able to generate an integrated responsereflecting the sum total of diverse signal input.The transducer mechanisms can be grouped into5 major categories. Receptors falling in onecategory also possess considerable structuralhomology, and belong to one super-family ofreceptors.
1. G-protein coupled receptors (GPCRs)
These are a large family of cell membranereceptors which are linked to the effector (enzyme/channel/carrier protein) through one or more GTP-activated proteins (G-proteins) for responseeffectuation. All such receptors have a commonpattern of structural organization (Fig. 4.5). Themolecule has 7 α-helical membrane spanninghydrophobic amino acid (AA) segments whichrun into 3 extracellular and 3 intracellular loops.The agonist binding site is located somewherebetween the helices on the extracellular face, while

45C
HA
PTE
R4
MECHANISM OF DRUG ACTION; RECEPTOR PHARMACOLOGY
Fig. 4.4: Diagrammatic representation of receptor mediated operation of membrane ion channel.In case of nicotinic cholinergic receptor, the molecule (8 nm in diameter) is composed of 5 subunits (2α +β + γ + δ)enclosing a transmembrane ion channel within the α subunit. Normally the channel is closed (A). When two moleculesof acetylcholine bind to the two α subunits (B), all subunits move apart opening the central pore to 0.7 nm, enough toallow passage of partially hydrated Na+ ions. Anions are blocked from passage through the channel by positivecharges lining it.In other cases, K+, Ca2+ or Cl¯ ions move through the channel depending on its ion selectivity.
another recognition site formed by cytosolic seg-ments binds the coupling G-protein. The G-proteins float in the membrane with their exposeddomain lying in the cytosol, and are heterotri-meric in composition (α, β and γ subunits). Inthe inactive state GDP is bound to the α subunitat the exposed domain; activation through thereceptor leads to displacement of GDP by GTP.The activated α-subunit carrying GTP dissociatesfrom the other two subunits and either activatesor inhibits the effector. The βγ diamer has alsobeen shown to activate receptor-operated K+
channels, to inhibit voltage gated Ca2+ channelsand to promote GPCR desensitization at higherrates of activation.
A number of G proteins distinguished by theirα subunits have been described. The importantones with their action on the effector are:
Gs : Adenylyl cyclase activation, Ca2+
channel opening
Fig. 4.5: Diagrammatic representation of G-proteincoupled receptor molecule
The receptor consists of 7 membrane spanning helicalsegments of hydrophobic amino acids. The interveningsegments connecting the helices form 3 loops on eitherside of the membrane. The amino terminus of the chainlies on the extracellular face, while the carboxy terminusis on the cytosolic side. The approximate location of theagonist and G-protein binding sites is indicated

46S
EC
TIO
N1
GENERAL PHARMACOLOGY
Gi : Adenylyl cyclase inhibition, K+
channel openingGo : Ca2+ channel inhibitionGq : Phospholipase C activation
A limited number of G-proteins are sharedbetween different receptors and one receptor canutilize more than one G-protein (agonistpleotropy), e.g. the following couplers have beenassociated with different receptors.
Receptor CouplerMuscarinic M2 Gi, GoMuscarinic M1, M3 GqDopamine D2 Gi, Goβ-adrenergic Gsα1-adrenergic Gqα2-adrenergic Gi, GoGABAB Gi, GoSerotonin 5-HT1 Gi, GoSerotonin 5-HT2 GqProstanoid Gs, Gi, Gq
In addition, Gs is the coupler for histamine H2,
serotonin 5HT4-7, glucagon, thyrotropin (TSH) andmany other hormones, while Gi is utilized byopioid, cannabinoid and some other receptors.Moreover, a receptor can utilize different bio-chemical pathways in different tissues.
The α-subunit has GTPase activity: the bound GTPis slowly hydrolysed to GDP: the α-subunit thendissociates from the effector to rejoin its othersubunits, but not before the effector has beenactivated/inhibited for several seconds and thesignal has been greatly amplified. The rate of GTPhydrolysis by the α subunit and thus the period forwhich it remins activated is regulated by anotherprotein called ‘regulator of G protein signaling’(RGS). The onset time of response through thistype of receptors is also in seconds.
There are three major effector pathways (Table4.1) through which GPCRs function.
(a) Adenylyl cyclase: cAMP pathwayActivation of AC results in intracellular accumu-lation of second messenger cAMP (Fig. 4.6) whichfunctions mainly through cAMP-dependentprotein kinase (PKA). The PKA phosphorylates
and alters the function of many enzymes, ionchannels, transporters, transcription factors andstructural proteins to manifest as increasedcontractility/impulse generation (heart), relaxation(smooth muscle), glycogenolysis, lipolysis,inhibition of secretion/mediator release,modulation of junctional transmission, hormonesynthesis, etc. In addition, cAMP directly opensa specific type of membrane Ca2+ channel calledcyclic nucleotide gated channel (CNG) in theheart, brain and kidney. The other mediators ofcellular actions of cAMP are: cAMP responseelement binding protein (CREB) which is atranscription factor, cAMP regulated guaninenucleotide exchange factors called EPACs andcertain transporters. Responses opposite to theabove are produced when AC is inhibited throughinhibitory Gi-protein.
The action of cAMP is terminated intra-cellularly by phosphodiesterases (PDEs) whichhydrolyse it to 5-AMP. Some isoforms of PDE(PDE3, PDE4) are selective for cAMP, while PDE5
is selective for cGMP.
(b) Phospholipase C: IP3-DAG pathwayActivation of phospholipase Cβ (PLcβ) by theactivated GTP carrying α subunit of Gq hydrolysesthe membrane phospholipid phosphatidyl inositol4,5-bisphosphate (PIP2) to generate the secondmessengers inositol 1,4,5-trisphosphate (IP3) anddiacylglycerol (DAG). The IP3 being water solublediffuses to the cytosol and mobilizes Ca2+ fromendoplasmic reticular depots (Fig. 4.7). Thelipophilic DAG remains within the membrane,but recruits protein kinase C (PKc) and activatesit with the help of Ca2+. The activated PKc phos-phorylates many intracellular proteins (dependingon the type of effector cell) and mediates variousphysiological responses. So that it can servesignaling functions, the cytosolic concentrationof Ca2+ is kept very low (~ 100 nM) by specificpumps located at the plasma membrane and atthe endoplasmic reticulum. Triggered by IP3, thereleased Ca2+ (third messenger in this setting) actsas a highly versatile regulator acting throughcalmodulin (CAM), PKc and other effectors—

47C
HA
PTE
R4
MECHANISM OF DRUG ACTION; RECEPTOR PHARMACOLOGY
Fig. 4.6: The action-effect sequence of two G-protein coupled (β adrenergic and muscarinic M2) receptoractivation in myocardial cell
Adrenaline (Adr) binds to β-adrenergic receptor (β-R) on the cell surface inducing a conformational change whichpermits interaction of the G-protein binding site with the stimulatory G-protein (Gs). The activated α subunit of Gs nowbinds GTP (in place of GDP), and dissociates from the βγ diamer as well as the receptor. The Gsα carrying boundGTP associates with and activates the enzyme adenylyl cyclase (AC) located on the cytosolic side of the membrane:ATP is hydrolysed to cAMP which then phosphorylates and thus activates cAMP dependent protein kinase (PKA). ThePKA in turn phosphorylates many functional proteins including troponin and phospholamban, so that they interact withCa2+, respectively resulting in increased force of contraction and faster relaxation. Calcium is made available by entryfrom outside (direct activation of myocardial membrane Ca2+ channels by Gsα and through their phosphorylation byPKA) as well as from intracellular stores.
One of the other proteins phosphorylated by cAMP is phosphorylase kinase which then activates the enzymephosphorylase resulting in breakdown of glycogen to be utilized as energy source for increased contractility.
Action of acetylcholine (ACh) on muscarinic M2 receptor (M2-R), also located in the myocardial membrane,similarly activates an inhibitory G-protein (Gi). The GTP carrying active Giα subunit inhibits AC, and opposes itsactivation by Gsα. The βγ diamer of Gi activates membrane K+ channels causing hyperpolarization which depressesimpulse generation.
mediates/modulates contraction, secretion/trans-mitter release, eicosanoid synthesis, neuronalexcitability, intracellular movements, membranefunction, metabolism, cell proliferation, etc. LikeAC, the PLcβ can also be inhibited throughinhibitory G-protein when directionally oppositeresponses would be expected.
Intracellular Ca2+ release has been found to occur in waves(Ca2+ mediated Ca2+ release from successive pools facilitatedby inositol 1, 3, 4, 5-tetrakisphosphate—IP4) and exhibitsa variety of agonist and concentration dependent oscillatorypatterns. The activation of different effectors may dependon the amplitude and pattern of these oscillations. Thus,the same intracellular messenger can trigger differentresponses depending on the nature and strength of theextracellular signal.

48S
EC
TIO
N1
GENERAL PHARMACOLOGY
TABLE 4.1 Major functional pathways of G-protein coupled receptor transduction
Adenylyl cyclase: cAMP Phospholipase Channel regulationIP3-DAG
↑ ↓ Ca2+↑ Ca2+↓ K+↑
Adrenergic-β Adrenergic-α2 Adrenergic-α1 Adrenergic-β1 Dopamine-D2 Adrenergic-α2
Histamine-H2 Muscarinic-M2 Histamine-H1 (Heart, GABAB Muscarinic-M2
Dopamine-D1 Dopamine-D2 Muscarinic-M1, M3 Sk.muscle) Opioid-κ Dopamine-D2Glucagon 5-HT1 5-HT2 Adenosine-A1 5-HT1A
FSH & LH GABAB Vasopressin-Oxytocin Somatostatin GABAB
ACTH Opioid-μ, δ Bradykinin-B2 Opioid-μ, δTSH Angiotensin-AT1 Angiotensin-AT1 Adenosine-A1
Prostaglandin-EP2 Prostaglandin-EP3 Prostaglandin-FP, EP1, EP3
Prostacyclin-IP Somatostatin Thromboxane-TPAdenosine-A2 Adenosine-A1 Leukotriene BLT, cys LT
Cholecystokinin-GastrinPAF
Fig. 4.7: The important steps of phospholipase cβ(PLcβ) pathway of response effectuation (in smooth muscle)The agonist, e.g. histamine binds to its H1 receptor (H1 R) and activates the G-protein Gq. Its α subunit binds GTP inplace of GDP, dissociates from the receptor as well as from βγ diamer to activate membrane bound PLcβ thathydrolyses phosphatidyl inositol 4, 5-bisphosphate (PIP2), a membrane bound phospholipid. The products inositol1, 4, 5-trisphosphate (IP3) and diacylglycerol (DAG) act as second messengers. The primary action of IP3 is facilitationof Ca2+ mobilization from intracellular organellar pools, while DAG in conjunction with Ca2+ activates protein kinase C(PKc) which phosphorylates and alters the activity of a number of functional and structural proteins. Cytosolic Ca2+ isa veritable messenger: combines with calmodulin (CAM) to activate myosin light chain kinase (MLCK) inducingcontraction, and another important regulator calcium-calmodulin protein kinase (CCPK). Several other effectors areregulated by Ca2+ in a CAM dependent or independent manner. Cytosolic Ca2+ is recycled by uptake into the endoplasmicreticulum as well as effluxed by membrane Ca2+ pump.

49C
HA
PTE
R4
MECHANISM OF DRUG ACTION; RECEPTOR PHARMACOLOGY
(c) Channel regulation The activated G-proteins (Gs, Gi, Go) can also open or inhibitionic channels specific for Ca2+ and K+, withoutthe intervention of any second messenger likecAMP or IP3, and bring about hyperpolarization/depolarization/changes in intracellular Ca2+. TheGs opens Ca2+ channels in myocardium andskeletal muscles, while Gi and Go open K+
channels in heart and smooth muscle as well asinhibit neuronal Ca2+ channels. Direct channelregulation is mostly the function of the βγ diamerof the dissociated G protein. Physiologicalresponses like changes in inotropy, chronotropy,transmitter release, neuronal activity and smoothmuscle relaxation follow. Receptors found toregulate ionic channels through G-proteins arelisted in Table 4.1.
2. Ion channel receptorThese cell surface receptors, also called ligandgated ion channels, enclose ion selective channels(for Na+, K+, Ca2+ or Cl¯) within their molecules.Agonist binding opens the channel (Fig. 4.4)and causes depolarization/hyperpolarization/changes in cytosolic ionic composition, dependingon the ion that flows through. The nicotiniccholinergic, GABAA, glycine (inhibitory AA),excitatory AA-glutamate (kainate, NMDA andAMPA) and 5HT3 receptors fall in this category.The receptor is usually a pentameric protein; all subunits, inaddition to large intra- and extracellular segments, generallyhave four membrane spanning helical domains. The subunitsare mostly arranged round the channel like a rosette and the αsubunits usually bear the agonist binding sites.
Certain receptor-operated (or ligand-gated) ion channelsalso have secondary ligands which bind to an allosteric site andmodulate the gating of the channel by the primary ligand, e.g.the benzodiazepine receptor modulates GABAA gated Cl¯channel.Thus, in these receptors the agonist directlyoperates ion channels, without the interventionof any coupling protein or second messenger. Theonset and offset of responses through this classof receptors is the fastest (in milliseconds).
3. Transmembrane enzyme-linked receptors
This class of receptors are utilized primarily bypeptide hormones, and are made up of a large
extracellular ligand binding domain connectedthrough a single transmembrane helical peptidechain to an intracellular subunit having enzymaticproperty. The enzyme at the cytosolic side isgenerally a protein kinase, but can also be guanylylcyclase in few cases. The commonest proteinkinases are the ones which phosphorylate tyrosineresidues on the substrate proteins and are called‘receptor tyrosine kinases’ (RTKs), see Fig. 4.8.Examples are—insulin, epidermal growth factor(EGF), nerve growth factor (NGF) and many othergrowth factor receptors. However, the transfor-ming growth factor (TGF) receptor and fewothers are serine/threonine kinases—whichphosphorylate serine/threonine residues of thetarget proteins.
In the unliganded monomeric state, the kinaseremains inactive. Hormone binding inducesdimerization of receptor molecules, brings aboutconformation changes which activate the kinaseto autophosphorylate tyrosine residues on eachother, increasing their affinity for binding substrateproteins which have SH2 domains. These are thenphosphorylated and released to carry forward thecascade of phosphorylations leading to theresponse.
Fig. 4.8: Model of receptor tyrosine kinase, an enzyme-linked receptor:On binding the peptide hormone to the extracellulardomains, the monomeric receptors move laterally in themembrane and form diamers. Dimerization activatestyrosine-kinase (RTK) activity of the intracellular domainsso that they phosphorylate tyrosine (t) residues on eachother, as well as on several SH2 domain substrate proteins(SH2-Pr). The phosphorylated substrate proteins thenperform downstream signaling function.

50S
EC
TIO
N1
GENERAL PHARMACOLOGY
A large number of intracellular signalingproteins have SH2 domains. Thus, by controllingphosphorylation of key enzymes, ion channels,transporters, etc. the RTKs are able to regulatediverse cellular functions including metabolicreactions, cell growth and differentiation. One ofthe SH2 domain enzymes is phospholipase cγ(PLcγ) which is activated by certain RTKs, andwhich, like PLcβ, generates IP3 and DAG assecond messengers for response effectuation.
The transmembrane enzyme-linked receptorstransduce responses in a matter of few minutesto few hours.
Another feature of this class of receptors isthat their dimerization also promotes receptorinternalization, degradation in lysosomes anddown regulation if activation is fast enough.
In place of protein kinase the enzyme canalso be guanylyl cyclase (GC), as in the case
of atrial natriuretic peptide (ANP). Agonistactivation of the receptor generates cGMP in thecytosol as a second messenger, which in turnactivates cGMP-dependent protein kinase (PKG)and modulates cellular activity.
4. Transmembrane JAK-STAT bindingreceptors
These receptors differ from RTKs in not havingany intrinsic catalytic domain. Agonist induceddimerization alters the intracellular domainconformation to increase its affinity for a cytosolictyrosine protein kinase JAK (Janus Kinase). Onbinding, JAK gets activated and phosphorylatestyrosine residues of the receptor, which now bindanother free moving protein STAT (signaltransducer and activator of transcription). Thisis also phosphorylated by JAK. Pairs of phos-phorylated STAT dimerize and translocate to thenucleus to regulate gene transcription resultingin a biological response. Many cytokines, growthhormone, prolactin, interferons, etc. act throughthis type of receptor.
5. Receptors regulating gene expression(Transcription factors, Nuclear receptors)
In contrast to the above 3 classes of receptors,these are intracellular (cytoplasmic or nuclear)soluble proteins which respond to lipid solublechemical messengers that penetrate the cell (Fig.4.10). The receptor protein (specific for eachhormone/regulator) is inherently capable ofbinding to specific genes, but its attached proteinsHSP-90 and may be some others prevent it fromadopting the configuration needed for binding toDNA. When the hormone binds near the carboxyterminus of the receptor, the restricting proteins(HSP-90, etc.) are released, the receptor dimeri-zes and the DNA binding regulatory segmentlocated in the middle of the molecule folds intothe requisite configuration. The liganded receptordiamer moves to the nucleus and binds other co-activator/co-repressor proteins which have amodulatory influence on its capacity to alter genefunction. The whole complex then attaches to
Fig. 4.9: Model of transmembrane JAK-STAT bindingreceptor.
The intracellular domain of these receptors lacksintrinsic protein kinase activity. Cytokines/hormonesbinding to the extracellular domain induce receptor dimer-ization which activates the intracellular domain to bind freemoving JAK (Janus Kinase) molecules. The activated JAKphosphorylate tyrosine residues on the receptor which thenbinds another protein STAT (signal transducer andactivator of transcription). Tyrosine residues of STAT alsoget phosphorylated by JAK. The phosphorylated STATdimerize, dissociate from the receptor and move to thenucleus to regulate transcription of target genes.

51C
HA
PTE
R4
MECHANISM OF DRUG ACTION; RECEPTOR PHARMACOLOGY
Fig. 4.10: Operational scheme of intracellular (glucocorticoid) receptorThe glucocorticoid (G) penetrates the cell membrane and binds to the glucocorticoid receptor (GR) protein thatnormally resides in the cytoplasm in association with heat shock protein 90 (HSP90) + other proteins. The GR has asteroid binding domain near the carboxy terminus and a mid region DNA binding domain joined by a ‘hinge region’.The DNA binding domain has two ‘zinc fingers’, each made up of a loop of amino acids with chelated zinc ion. Bindingof the steroid to GR dissociates the complexed proteins (HSP90, etc) removing their inhibitory influence on it. Adimerization region that overlaps the steroid binding domain is exposed, promoting dimerization of the occupiedreceptor. The steroid bound receptor diamer translocates to the nucleus, binds coactivator/corepressor proteins andinteracts with specific DNA sequences called ‘glucocorticoid responsive elements’ (GREs) within the regulatory regionof appropriate genes. The expression of these genes is consequently altered resulting in promotion (or suppression)of their transcription. The specific mRNA thus produced is directed to the ribosome where the message is translatedinto a specific pattern of protein synthesis, which inturn modifies cell function.

52S
EC
TIO
N1
GENERAL PHARMACOLOGY
specific DNA sequences (hormone responseelements) of the target genes and facilitates orrepresses their expression so that specific mRNAis synthesized/repressed on the template of thegene. This mRNA moves to the ribosomes anddirects synthesis of specific proteins whichregulate activity of the target cells.
All steroidal hormones (glucocorticoids,mineralocorticoids, androgens, estrogens, progeste-rone), thyroxine, vit D and vit A function in thismanner. Different steroidal hormones affectdifferent target cells and produce different effectsbecause each one binds to its own receptor anddirects a unique pattern of synthesis of specificproteins. The specificity as to which hormonewill be bound is provided by the hormone bindingdomain, while that as to which gene will be activatedor repressed is a function of the DNA binding/N-terminus domain. Different ligands of the samenuclear receptor have been found to induce ligand-specific conformations of the receptor so thatdifferent combinations of co-activators and co-repressors may be bound in different target tissues,e.g. selective estrogen receptor modulators(SERMs). Chimeric receptors have also beenproduced which respond to one hormone, butproduce the effects of the other hormone.
This transduction mechanism is the slowestin its time course of action (takes hours) becauseadequate quantity of the effector protein will haveto be produced before the response occurs. Theeffects also generally out last the signal (hormone),because majority of the generated effector proteinshave slow turnover, and persist in the body evenafter the hormone has been eliminated.
Regulation of receptorsReceptors exist in a dynamic state; their densityand efficacy to elicit the response is subject toregulation by the level of on-going activity,feedback from their own signal output and otherphysiopathological influences, e.g. estrogensincrease the density of oxytocin receptors on themyometrium. The sensitivity of uterus to con-tractile action of oxytocin increases progressivelyduring the third trimester of pregnancy, especially
near term. In tonically active systems, prolongeddeprivation of the agonist (by denervation orcontinued use of an antagonist or a drug whichreduces input) results in supersensitivity of thereceptor as well as the effector system to the agonist.This has clinical relevance in clonidine/CNSdepressant/opioid withdrawal syndromes, suddendiscontinuation of propranolol in angina pectoris,etc. The mechanisms involved may be unmaskingof receptors or their proliferation (up regulation)or accentuation of signal amplification by thetransducer.
Conversely, continued/intense receptor stimu-lation causes desensitization or refractoriness: thereceptor becomes less efficient in transducingresponse to the agonist. This can be easilydemonstrated experimentally (Fig. 4.11); clinicalexamples are bronchial asthma patients treatedcontinuously with β adrenergic agonists andparkinsonian patients treated with high doses oflevodopa gradually become less reponsive. Thechanges may be brought about by:
(i) Masking or internalization of the receptor (itbecomes inaccessible to the agonist) or impaired
Fig. 4.11: Illustration of the phenomenon ofdesensitization
Contractile responses of frog’s rectus abdominis muscleto acetylcholine. Note that shortly after exposure to ahigh (100 fold) dose of the agonist, the response ismarkedly attenuated, but is regained if sufficient time isallowed to elapse.

53C
HA
PTE
R4
MECHANISM OF DRUG ACTION; RECEPTOR PHARMACOLOGY
coupling of the transducer to the receptor. In thiscase refractoriness develops as well as fadesquickly.In the case of β adrenergic receptor, it has been found thatagonist binding promotes phosphorylation of its serineresidues near the intracellular carboxy terminus by an enzymeβ adrenergic receptor kinase (βARK), allowing it to binda protein called β-arrestin which hinders its interaction withGs → receptor transduction is impaired. When the β-agonistis removed, the serine residues are dephosphorylated andreceptor mediated activation of Gs is restored.
(ii) Decreased synthesis/increased destruction ofthe receptor (down regulation): refractoriness deve-lops over weeks or months and recedes slowly.Receptor down regulation is particularly exhibitedby the tyrosine kinase receptors. Similarly, thetransducer and effector proteins are also up ordown regulated.
Some times response to all agonists whichact through different receptors but produce thesame overt effect (e.g. histamine and acetylcholineboth contract intestinal smooth muscle) is decreasedby exposure to any one of these agonists (hetero-logous desensitization), showing that mechanismsof response effectuation have become less efficient.However, often desensitization is limited to agonistsof the same receptor that is being repeatedlyactivated (homologous desensitization).Both homologous and heterologous desensitization has beenobserved in the case of GPCRs. The BARK-β arrestin mecha-nism described above produces homologous desensitization.The GPCRs transduce many responses by activating PKA
and PKC. These kinases phosphorylate many GPCRs rathernonselectively (at a site different from that of BARK) andhinder their interaction with G-proteins, resulting inheterologous desensitization.
Functions of receptorsThese can be summarized as:(a) To propagate regulatory signals from outsideto inside the effector cell when the molecularspecies carrying the signal cannot itself penetratethe cell membrane.(b) To amplify the signal.(c) To integrate various extracellular and intra-cellular regulatory signals.(d) To adapt to short term and long term changesin the regulatory melieu and maintain homeo-stasis.
Nonreceptor-mediated drug actionThis refers to drugs which do not act by bindingto specific regulatory macromolecules. Drug actionby purely physical or chemical means, interactionswith small molecules or ions (antacids, chelatingagents, cholestyramine, etc.), as well as directinteraction with enzymes, ionic channels andtransporters has already been described. In addition,there are drugs like alkylating agents which reactcovalently with several critical biomolecules,especially nucleic acids, and have cytotoxicproperty useful in the treatment of cancer. Anotherimportant class of drugs are the antimetabolites(purine/pyrimidine analogues) which lead toproduction of nonfunctional or dysfunctionalcellular components that exert antineoplastic,antiviral and immunosuppressant activity.
DOSE-RESPONSE RELATIONSHIP
When a drug is administered systemically, thedose-response relationship has two components:dose-plasma concentration relationship andplasma concentration-response relationship. Theformer is determined by pharmacokineticconsiderations and ordinarily, descriptions of dose-response relationship refer to the latter, whichcan be more easily studied in vitro.
Generally, the intensity of response increaseswith increase in dose (or more precisely concen-tration at the receptor) and the dose-response curveis a rectangular hyperbola (Fig. 4.12). This isbecause drug-receptor interaction obeys law ofmass action, accordingly—
Emax × [D]E = —————— ...(3)
KD + [D]
Where E is the observed effect at a dose [D] ofthe drug, Emax is the maximal response, KD is thedissociation constant of the drug-receptor complex,which is equal to the dose of the drug at whichhalf maximal response is produced. If the dose isplotted on a logarithmic scale, the curve becomessigmoid and a linear relationship between log ofdose and the response is seen in the intermediate(30–70% response) zone, as can be predicted from

54S
EC
TIO
N1
GENERAL PHARMACOLOGY
Fig. 4.12: Dose-response and log dose-response curves
equation (3). This is not peculiar to drugs. In factall stimuli are graded biologically by the fractionalchange in stimulus intensity, e.g. 1 kg and 2 kgweights held in two hands can be easilydifferentiated, but not 10 kg and 11 kg weights.Though the absolute difference in both casesremains 1kg, there is a 100% fractional change inthe former case but only 10% change in the lattercase. In other words, response is proportional toan exponential function (log) of the dose.Other advantages of plotting log dose-responsecurves (DRC) are:
(i) A wide range of drug doses can be easilydisplayed on a graph.
(ii) Comparison between agonists and study ofantagonists becomes easier.
The log dose-response curve (DRC) can becharacterized by its shape (slope and maxima)and position on the dose axis.
Drug potency and efficacyThe position of DRC on the dose axis is theindex of drug potency which refers to the amountof drug needed to produce a certain response.A DRC positioned rightward indicates lowerpotency (Fig. 4.13). Relative potency is often moremeaningful than absolute potency, and is generallydefined by comparing the dose (concentration)of the two agonists at which they elicit halfmaximal response (EC50). Thus, if 10 mg of
morphine = 100 mg of pethidine as analgesic,morphine is 10 times more potent than pethidine.However, a higher potency, in itself, does notconfer clinical superiority unless the potency fortherapeutic effect is selectively increased overpotency for adverse effect. Drug potency is clearlya factor in choosing the dose of a drug.
The upper limit of DRC is the index of drugefficacy and refers to the maximal response thatcan be elicited by the drug, e.g. morphine pro-duces a degree of analgesia not obtainable withany dose of aspirin—morphine is more effica-cious than aspirin. Efficacy is a more decisivefactor in the choice of a drug.
Often the terms ‘drug potency’ and ‘drugefficacy’ are used interchangeably, but theseare not synonymous and refer to differentcharacteristics of the drug. The two can varyindependently:(a) Aspirin is less potent as well as less effica-cious analgesic than morphine.(b) Pethidine is less potent but equally efficaciousanalgesic as morphine.
Fig. 4.13: Illustration of drug potency and drug efficacy.Dose-response curve of four drugs producing the samequalitative effectNote:Drug B is less potent but equally efficacious as drug A.Drug C is less potent and less efficacious than drug A.Drug D is more potent than drugs A, B, & C, but less effica-cious than drugs A & B, and equally efficacious as drug C.

55C
HA
PTE
R4
MECHANISM OF DRUG ACTION; RECEPTOR PHARMACOLOGY
(c) Furosemide is less potent but more efficaciousdiuretic than metolazone.(d) Diazepam is more potent but less efficaciousCNS depressant than pentobarbitone.
Depending on the type of drug, both higherefficacy (as in the case of furosemide conferingutility for mobilizing edema fluid and in renalfailure) or lower efficacy (as in the case ofdiazepam confering safety in over-dose) couldbe clinically advantageous.
The slope of the DRC is also important. Asteep slope indicates that a moderate increase indose will markedly increase the response (doseneeds individualization), while a flat one impliesthat little increase in response will occur overa wide dose range (standard doses can be givento most patients). Hydralazine has a steep, whilehydrochlorothiazide has a flat DRC of anti-hypertensive effect (Fig. 4.14).
expressed in terms of (a) degree of benefit/reliefafforded by the drug (in the recommended doserange) or (b) the success rate in achieving a definedtherapeutic end point. For example, the degreeof relief in parkinsonian symptoms afforded bylevodopa-carbidopa is much greater than thatpossible with trihexyphenidyl: the former hashigher therapeutic efficacy than the latter. A drugwhich makes a higher percentage of epilepticpatients totally seizure free than another drug,is the more therapeutically effective antiepileptic.
Drug selectivity
Drugs seldom produce just one action: the DRCsfor different effects of a drug may be different.The extent of separation of DRCs of a drug fordifferent effects is a measure of its selectivity,e.g. the DRCs for bronchodilatation and cardiacstimulation (Fig. 4.15) are quite similar in caseof isoprenaline, but far apart in case of salbuta-mol—the latter is a more selective bronchodilatordrug.
The gap between the therapeutic effect DRCand the adverse effect DRC defines the safetymargin or the therapeutic index of a drug. Inexperimental animals, therapeutic index is oftencalculated as:
Fig. 4.14: Steep and flat dose-response curves illustratedby antihypertensive effect of hydralazine and hydrochloro-thiazide
Therapeutic efficacyThe ‘therapeutic efficacy’ or ‘clinicaleffectiveness’ is a composite attribute of a drugdifferent from the foregoing pharmacologicaldescription of ‘potency’ and ‘efficacy’. It dependsnot only on the relative potency and efficacy ofthe drug, but on many pharmacokinetic andpathophysiological variables as well. It is often
Fig. 4.15: Illustration of drug selectivityLog dose-response curves of salbutamol for broncho-dilatation (A) and cardiac stimulation (D)Log dose-response curves of isoprenaline for broncho-dilatation (B) and cardiac stimulation (C)

56S
EC
TIO
N1
GENERAL PHARMACOLOGY
median lethal doseTherapeutic index = —————————–
median effective dose
LD50 or ——–
ED50
where: Median effective dose (ED50) is the dosewhich produces the specified effect in 50%individuals and median lethal dose (LD50) is thedose which kills 50% of the recipients.
But this is irrelevant in the clinical set up wherethe therapeutic range, also called the ‘therapeuticwindow’ is bounded by the dose which producesminimal therapeutic effect and the dose whichproduces maximal acceptable adverse effect (Fig.4.16). Because of individual variability, theeffective dose for some subjects may be toxicfor others; defining the therapeutic range for manydrugs is a challenging task. A drug may be capableof inducing a higher therapeutic response (havehigher efficacy) but development of intolerableadverse effects may preclude use of higher doses,e.g. prednisolone in bronchial asthma.
Risk-benefit ratio This term is very frequentlyused, and conveys a judgement on the estimatedharm (adverse effects, cost, inconvenience) vsexpected advantages (relief of symptoms, cure,reduction of complications/mortality, improvementin quality of life). A drug should be prescribed
only when the benefits outweigh the risks. However,risk-benefit ratio can hardly ever be accuratelymeasured for each instance of drug use, because‘risk’ is the probability of harm; and harm hasto be qualified by its nature, quantum, time-course(transient to life-long) as well as the value thatthe patient attaches to it. None of these can beprecisely ascertained beforehand in an individualpatient. As such, the physician has to rely ondata from use of drugs in large populations(pharmacoepidemiology) and his own experienceof the drug and the patient.
Drug specificitySpecificity of a drug refers to the range of actionsproduced by it. Certain drugs produce just oneor a limited number of actions, while others havewidespread effects on many organs of the body.Specificity is governed by:
(a) whether a drug acts on a single receptor/target or on many targets, and
(b) how widely the target is distributed in thebody.
Omeprazole (and other proton pump inhibitors)is an example of a highly selective drug. Thesingular perceptible action in therapeutic dosesis inhibition of gastric acid secretion, becauseit acts only on one target molecule H+K+ ATPase(proton pump) which is localized to the gastricparietal cells. An example of a drug acting onmultiple targets is chlorpromazine which hasantagonistic action on dopamine D2, α-adrenergic,muscarinic cholinergic, histamine H1 and some5-HT receptors. It also has Na+ channel blockingaction. As a result, it produces a wide range ofactions. Another case is dexamethasone whichis an agonist only of glucocorticoid receptor, butproduces effects involving many organs andtissues, because the glucocorticoid receptor isexpressed by practically every cell of the body.Drugs with all grades of specificity are available.
COMBINED EFFECT OF DRUGSWhen two or more drugs are given simultaneouslyor in quick succession, they may be either indiffe-rent to each other or exhibit synergism or
Fig. 4.16: Illustrative dose-response curves for thera-peutic effect and adverse effect of the same drug

57C
HA
PTE
R4
MECHANISM OF DRUG ACTION; RECEPTOR PHARMACOLOGY
antagonism. The interaction may take place atpharmacokinetic level (see Ch. 2 and 3) or atpharmacodynamic level.
SYNERGISM(Greek: Syn—together; ergon—work)
When the action of one drug is facilitated orincreased by the other, they are said to be syner-gistic. In a synergistic pair, both the drugs canhave action in the same direction or given aloneone may be inactive but still enhance the actionof the other when given together. Synergism canbe:
(a) Additive The effect of the two drugs is inthe same direction and simply adds up:effect of drugs A + B = effect of drug A +
effect of drug B
Fig. 4.17: Log dose-response curves of a drug ‘A’depicting additive synergism (in purple) and potentiation(Supra-additive synergism) in blue.A: An agonist drug.B: Another agonist in a fixed submaximal dose
producing 40% response.C: A potentiating drug which itself has no agonistic
activity.
Additive drug combinations
Aspirin + paracetamol as analgesic/antipyretic
Nitrous oxide + halothane as generalanaesthetic
Amlodipine + atenolol as antihypertensiveGlibenclamide + metformin as hypoglycaemicEphedrine + theophylline as bronchodilator
Supraadditive drug combinations
Drug pair Basis of potentiation
Acetylcholine + Inhibition of breakphysostigmine down
Levodopa + carbidopa/ Inhibition of peripheralbenserazide metabolism
Adrenaline + cocaine/ Inhibition ofdesipramine neuronal uptake
Sulfamethoxazole + Sequential blockadetrimethoprim
Antihypertensives Tackling two contributory(enalapril+ factorshydrochlorothiazide)
Tyramine + MAO Increasing releaseableinhibitors CA store
Side effects of the components of an additivepair may be different—do not add up. Thus, thecombination is better tolerated than higher doseof one component.
(b) Supraadditive (potentiation) The effect ofcombination is greater than the individual effectsof the components:effect of drug A + B > effect of drug A +
effect of drug B
This is always the case when one component givenalone produces no effect, but enhances the effectof the other (potentiation). Examples are givenin the box. Additive synergism and potentiationare depicted diagrammatically in Fig. 4.17.
ANTAGONISMWhen one drug decreases or abolishes the actionof another, they are said to be antagonistic:
effect of drugs A + B < effect of drug A + effect of drug B
Usually in an antagonistic pair one drug is inactiveas such but decreases the effect of the other.Depending on the mechanism involved, anta-gonism may be:
(a) Physical antagonism
Based on the physical property of the drugs, e.g.

58S
EC
TIO
N1
GENERAL PHARMACOLOGY
charcoal adsorbs alkaloids and can prevent theirabsorption—used in alkaloidal poisonings.
(b) Chemical antagonism
The two drugs react chemically and form aninactive product, e.g.• KMnO4 oxidizes alkaloids—used for gastric
lavage in poisoning.• Tannins + alkaloids—insoluble alkaloidal
tannate is formed.• Chelating agents (BAL, Cal. disod. edetate)
complex toxic metals (As, Pb).• Nitrites form methaemoglobin which reacts
with cyanide radical.
Drugs may react when mixed in the same syringeor infusion bottle:• Thiopentone sod. + succinylcholine chloride• Penicillin-G sod. + succinylcholine chloride• Heparin + penicillin/tetracyclines/streptomycin/
hydrocortisone
(c) Physiological/functional antagonism
The two drugs act on different receptors or bydifferent mechanisms, but have opposite overteffects on the same physiological function, i.e.have pharmacological effects in opposite direction,e.g.• Histamine and adrenaline on bronchial muscles
and BP.• Hydrochlorothiazide and triamterene on
urinary K+ excretion.• Glucagon and insulin on blood sugar level.
(d) Receptor antagonism
One drug (antagonist) blocks the receptor actionof the other (agonist). This is a very importantmechanism of drug action, because physiologicalsignal molecules act through their receptors,blockade of which can produce specific and oftenprofound pharmacological effects. Receptorantagonists are selective (relatively), i.e. ananticholinergic will oppose contraction ofintestinal smooth muscle induced by cholinergicagonists, but not that induced by histamine or5-HT (they act through a different set of receptors).
Fig. 4.18: Illustration of sites of action of agonists andantagonists (A), and the action of full agonist (B), partialagonist (C), competitive antagonist (D) and noncom-petitive antagonist (E) on the receptor
Receptor antagonism can be competitive ornoncompetitive.
Competitive antagonism (equilibrium type)The antagonist is chemically similar to the agonist,competes with it (Fig. 4.18 A, D) and binds tothe same site to the exclusion of the agonistmolecules. Because the antagonist has affinity butno intrinsic activity (see p. 42), no response isproduced and the log DRC of the agonist is shifted

59C
HA
PTE
R4
MECHANISM OF DRUG ACTION; RECEPTOR PHARMACOLOGY
Fig. 4.19: Dose-response curves showing competitive (a) and noncompetitive (b) antagonismA—agonist, B—competitive antagonist, C—noncompetitive antagonist
Competitive (equilibrium type) Noncompetitive
1. Antagonist binds with the same receptor as the agonist Binds to another site of receptor2. Antagonist resembles chemically with the agonist Does not resemble3. Parallel rightward shift of agonist DRC Flattening of agonist DRC4. The same maximal response can be Maximal response is suppressed
attained by increasing dose of agonist (unsurmountable antagonism)(surmountable antagonism)
5. Intensity of response depends on the concen- Maximal response depends only ontration of both agonist and antagonist the concentration of antagonist
6. Examples: ACh—Atropine Diazepam—BicucullineMorphine—Naloxone
to the right. Since antagonist binding is reversibleand depends on the relative concentration of theagonist and antagonist molecules, higher concen-tration of the agonist progressively overcomesthe block—a parallel shift of the agonist DRCwith no suppression of maximal response isobtained (Fig. 4.19a). The extent of shift isdependent on the affinity and concentration ofthe antagonist.
A partial agonist (Fig. 4.18 C), having affinityfor the same receptor, also competes with andantagonizes a full agonist, while producing asubmaximal response of its own.
Noncompetitive antagonism The antagonist ischemically unrelated to the agonist, binds to adifferent allosteric site altering the receptor in
such a way that it is unable to combine with theagonist (Fig. 4.18E), or is unable to transduce theresponse, so that the downstream chain of eventsare uncoupled. This is also called allostericantagonism. Because the agonist and the anta-gonist are combining with different sites, there isno competition between them—even high agonistconcentration is unable to reverse the blockcompletely. Increasing concentrations of theantagonist progressively flatten the agonist DRC(Fig. 4.19b). Noncompetitive antagonists have beenproduced experimentally, but are not in clinical use.
Nonequilibrium antagonism Certain antago-nists bind to the receptor with strong (covalent)bonds or dissociate from it slowly (due to veryhigh affinity) so that agonist molecules are unable

60S
EC
TIO
N1
GENERAL PHARMACOLOGY
to reduce receptor occupancy of the antagonistmolecules—law of mass action cannot apply—an irreversible or nonequilibrium antagonism isproduced. The agonist DRC is shifted to the rightand the maximal response is lowered (if sparereceptors are few). Since in this situation theagonist molecules are not able to competewith the antagonist molecules and flattening of
agonist DRC is a feature of noncompetitiveantagonism; nonequilibrium antagonism hasalso been called ‘a type of noncompetitiveantagonism’. Phenoxybenzamine is a non-equilibrium antagonist of adrenaline at the αadrenergic receptors.
Features of competitive and noncompetitiveantagonism are compared on previous page.
PROBLEM DIRECTED STUDY
4.1 A patient being treated with methotrexate (Mtx) developed oral ulceration, megaloblasticanaemia and other toxic symptoms. Given that (i) Mtx acts by inhibiting the enzyme dihydrofolatereductase (DHFRase) which generates the essential coenzyme tetrahydrofolic acid (THFA) fromdihydrofolic acid (DHFA) needed for one carbon transfer reactions, (ii) Mtx binds to the catalyticsite of DHFRase with an affinity 50,000 times greater than the natural substrate DHFA, and that(iii) two forms of folate viz. folic acid and folinic acid (N5 formyl THFA) are available for therapeuticuse:(a) Which type of enzyme inhibition will be produced by Mtx?(b) Which form of folate should be used to treat Mtx toxicity?(see Appendix-1 for solution)

Aspects of Pharmacotherapy,Clinical Pharmacology andDrug Development
ChapterChapterChapterChapterChapter 55555
Pharmaco- (drug) therapy is dynamic and an everevolving science. It requires understanding of thedrug, the disease, the patient and the milieu inwhich it is undertaken. As such, in addition toknowledge of drug action, mechanisms andpharmacokinetics, several aspects like drugdosage, sources of variability in drug response,pharmacogenetics, influence of disease on drugaction, etc. are important for otimum drug therapy.
DRUG DOSAGE
‘Dose’ is the appropriate amount of a drugneeded to produce a certain degree of responsein a given patient. Accordingly, dose of a drughas to be qualified in terms of the chosen response,e.g. the analgesic dose of aspirin for headacheis 0.3–0.6 g, its antiplatelet dose is 60–150 mg/day, while its antiinflammatory dose forrheumatoid arthritis is 3–5 g per day. Similarlythere could be a prophylactic dose, a therapeuticdose or a toxic dose of the same drug.
The dose of a drug is governed by its inherentpotency, i.e. the concentration at which it shouldbe present at the target site, and its pharmaco-kinetic characteristics. The recommended dosesare based on population data and cater to an‘average’ patient. However, individual patientsmay not be ‘average’ in respect to a number ofpharmacokinetic and pharmacodynamic para-meters, emphasizing the need for individualizingdrug dose. The strategies adopted for differenttypes of drugs and conditions are:
1. Standard dose The same dose is appro-priate for most patients—individual variations areminor or the drug has a wide safety margin sothat a large enough dose can be given to coverthem, e.g. oral contraceptives, penicillin,chloroquine, mebendazole, hydrochlorothiazide.
2. Regulated dose The drug modifies afinely regulated body function which can be easilymeasured. The dosage is accurately adjusted byrepeated measurement of the affected physiolo-gical parameter, e.g. antihypertensives, hypogly-caemics, anticoagulants, diuretics, generalanaesthetics. In their case, measurement of plasmadrug concentration is not needed.
3. Target level dose (see p. 33) The responseis not easily measurable but has been demon-strated to be obtained at a certain range of drugconcentration in plasma. An empirical dose aimedat attaining the target level is given in thebeginning and adjustments are made later by actualmonitoring of plasma concentrations. Whenfacilities for drug level monitoring are notavailable, crude adjustments are made by obser-ving the patient at relatively long intervals, e.g.antidepressants, antiepileptics, digoxin, lithium,theophylline.
4. Titrated dose The dose needed to producemaximal therapeutic effect cannot be givenbecause of intolerable adverse effects. Optimaldose is arrived at by titrating it with an acceptablelevel of adverse effect. Low initial dose andupward titration (in most non-critical situations)or high initial dose and downward titration(in critical situations) can be practised. Oftena compromise between submaximal therapeuticeffect but tolerable side effects can bestruck, e.g. anticancer drugs, corticosteroids,levodopa.
Fixed dose combinations (FDCs) of drugsA large number of pharmaceutical preparationscontain two or more drugs in a fixed dose ratio.Advantages offered by these are:

62S
EC
TIO
N1
GENERAL PHARMACOLOGY
1. Convenience and better patient compliance—when all the components present in the FDCare actually needed by the patient and theiramounts are appropriate. It may also be costsaving compared to both/all the componentsadministered separately.
2. Certain drug combinations are synergistic, e.g.sulfamethoxazole + trimethoprim; levodopa+ carbidopa/benserazide; combination oralcontraceptives, isoniazid + rifampin.
3. The therapeutic effect of two componentsbeing same may add up while the side effectsbeing different may not. For this thecomponents of the FDC should act by differentmechanisms, e.g. amlodipine + atenolol asantihypertensive.
4. The side effect of one component may becounteracted by the other, e.g. a thiazide +a potassium sparing diuretic. However, theamount of the latter may not be sufficientin all cases.
5. Combined formulation ensures that a singledrug will not be administered. This isimportant in the treatment of tuberculosis,HIV-AIDS and falciparum malaria.
Before prescribing a combination, the physicianmust consider whether any of the ingredientsis unnecessary; if it is, the combination shouldnot be prescribed. It can never be justified that adrug is given to a patient who does not need it inorder to provide him another one that he needs.
There are many inbuilt disadvantages ofFDCs:1. The patient may not actually need all the drugs
present in a combination: he is subjected toadditional side effects and expense (often dueto ignorance of the physician about the exactcomposition of the combined formulations).
2. The dose of most drugs needs to be adjustedand individualised. When a combined formu-lation is used, this cannot be done withoutaltering the dose of the other component(s).However, few combinations are available atmore than one dose ratios, e.g. levodopa(100 mg) + Carbidopa (10 mg or 25 mg),
amoxicillin (250 mg or 500 mg) + clavulanicacid (125 mg).
3. The time course of action of the componentsmay be different: administering them at thesame intervals may be inappropriate.
4. Altered renal or hepatic function of the patientmay differently affect the pharmacokinetics ofthe components.
5. Adverse effect, when it occurs, cannot be easilyascribed to the particular drug causing it.
6. Contraindication to one component (allergy,other conditions) contraindicates the wholeproduct.
7. Confusion of therapeutic aims and false senseof superiority of two drugs over one is fostered,specially in case of antimicrobials whosecombinations should be avoided. Corticoste-roids should never be combined with anyother drug meant for internal use. Drug combi-nations that are banned in India are listed inAppendix-5.
Thus, only a handful of FDCs are rational andjustified, while far too many are produced andvigorously promoted by the pharmaceuticalindustry. In fact, the latest WHO essentialmedicines list incorporates only 23 FDCs, andthe NLEM (2011) of India has only 12 FDCs (seeAppendix-2).
FACTORS MODIFYING DRUG ACTIONVariation in response to the same dose of a drugbetween different patients and even in the samepatient on different occasions is a rule rather thanexception. One or more of the following cate-gories of differences among individuals areresponsible for the variations in drug response:(1) Individuals differ in pharmacokinetic hand-ling of drugs: attain varying plasma/target siteconcentration of the drug. This is more markedfor drugs disposed by metabolism (e.g.propranolol) than for drugs excreted unchanged(e.g. atenolol).(2) Variations in number or state of receptors,coupling proteins or other components of responseeffectuation.

63C
HA
PTE
R5
PHARMACOTHERAPY, CLINICAL PHARMACOLOGY AND DRUG DEVELOPMENT
(3) Variations in neurogenic/hormonal tone orconcentrations of specific constituents, e.g.atropine tachycardia depends on vagal tone,propranolol bradycardia depends on sympathetictone, captopril hypotension depends on body Na+
status.A multitude of host and external factors
influence drug response. They fall in twocategories viz genetic and nongenetic includingall environmental, circumstantial and personalvariables. Though individual variation cannot betotally accounted for by these factors, theirunderstanding can guide the choice of appropriatedrug and dose for an individual patient. However,final adjustments have to be made by observingthe response in a given patient on a given occasion.
The factors modify drug action either:(a) Quantitatively The plasma concentrationand/or the action of the drug is increased ordecreased. Most of the factors introduce this typeof change and can be dealt with by adjustment ofdrug dosage.(b) Qualitatively The type of response isaltered, e.g. drug allergy or idiosyncrasy. This isless common but often precludes further use ofthat drug in the affected patient.
The various factors are discussed below—
1. Body size It influences the concentrationof the drug attained at the site of action. Theaverage adult dose refers to individuals of mediumbuilt. For exceptionally obese or lean individualsand for children dose may be calculated on bodyweight (BW) basis:
BW (kg)Individual dose = ———— × average adult dose
70It has been argued that body surface area (BSA)provides a more accurate basis for dose calcula-tion, because total body water, extracellular fluidvolume and metabolic activity are better paral-leled by BSA.
BSA (m2)Individual dose = ———— × average adult dose
1.7
The BSA of an individual can be calculated fromDubois formula:
BSA (m2) =BW (kg)0.425 × Height (cm)0.725 × 0.007184
or obtained from chart-form or slide-rule nomo-grams based on BW and height.
However, dose recommendations in terms ofBSA are available only for anticancer and ahandful of other drugs: for the rest BW has beenused as the index. Thus, prescribing on BSA basissuffers from lack of data base, is morecumbersome and has not thrived, except in fewcases.
2. Age The dose of a drug for children is oftencalculated from the adult dose
AgeChild dose = ———— × adult dose ... (Young’s Age + 12 formula) AgeChild dose = –—— × adult dose ... (Dilling’s
20 formula)It can also be calculated (more accurately) onBW or BSA basis (see above), and for manydrugs, manufacturers give dosage recommenda-tions on mg/kg basis. Average figures for childrenare given below.
Ideal BSA % ofAge BW (Kg) (m2) Adult dose
Newborn 3.2 0.23 12.51 month 4.0 0.26 153 months 5.5 0.32 186 months 7.5 0.4 221 year 10 0.47 253 years 14 0.62 335 years 18 0.73 407 years 23 0.88 5012 years 37 1.25 75
However, infants and children are not smalladults. They have important physiological diffe-rences from adults. The newborn has low g.f.r.and tubular transport is immature. As such, thet½ of drugs excreted by glomerular filtration(gentamicin) and tubular secretion (penicillin) isprolonged by 3 to 5 times. Glomerular filtrationreaches adult rates by 5 month of age and tubular

64S
EC
TIO
N1
GENERAL PHARMACOLOGY
secretion takes about 7 months to mature.Similarly, hepatic drug metabolizing system isinadequate in newborns —chloramphenicol canproduce gray baby syndrome. Blood-brain barrieris more permeable—drugs attain higher concen-tration in the CNS (accumulation of unconjugatedbilirubin causes kernicterus). These defects areexaggerated in the premature infant. Drugabsorption may also be altered in infants becauseof lower gastric acidity and slower intestinaltransit. Transdermal absorption however, is fasterbecause their skin is thin and more permeable.Rectal absorption is fast and more predictablein infants and young children; diazepam solutionis given rectally to control febrile seizures inchildren < 5 years. Therefore, infant doses mustbe learned as such and not derived from anyformula.
After the first year of life, drug metabolismis often faster than in adults, e.g. theophylline,phenytoin, carbamazepine t½ is shorter in children.Also, higher per kg dose is needed for drugs whichare primarily excreted unchanged by kidney, e.g.daily dose of digoxin is about 8–12 µg/kgcompared to adult dose of 3–5 µg/kg.
Solid dosage forms and metered dose inhalersare difficult to administer to young children.
Children are growing and are susceptible tospecial adverse effects of drugs, e.g. suppressionof growth can occur with corticosteroids; andro-gens may promote early fusion of epiphysis resul-ting in stunting of stature; tetracyclines getdeposited in growing teeth and discolour/deformthem. Dystonic reactions to phenothiazines aremore common in children.
Elderly In the elderly, renal function progres-sively declines (intact nephron loss) so that g.f.r.is ~ 75% at 50 years and ~ 50% at 75 yearsage compared to young adults. Drug doses haveto be reduced, e.g. daily dose of streptomycinis 0.75 g after 50 years and 0.5 g after 70 yearsof age compared to 1 g for young adults. Thereis also a reduction in the hepatic microsomal drugmetabolizing activity and liver blood flow: oralbioavailability of drugs with high hepatic extrac-tion is generally increased, but the overall effects
on drug metabolism are not uniform. Due to lowerrenal as well as metabolic clearance, the elderlyare prone to develop cumulative toxicity whilereceiving prolonged medication. Other affectedaspects of drug handling are:• slower absorption due to reduced gut motility
as well as blood flow to intestines,• lesser plasma protein binding due to lower
plasma albumin,• increased or decreased volume of distribution
of lipophilic and hydrophilic drugs respectively.
Aged are relatively intolerant to digitalis. Theresponsiveness of β adrenergic receptors to bothagonists and antagonists is reduced in the elderlyand sensitivity to other drugs also may be altered.Due to prostatism in elderly males, even mildanticholinergic activity of the drug can accen-tuate bladder voiding difficulty. Elderly are alsolikely to be on multiple drug therapy for hyper-tension, ischaemic heart disease, diabetes, arthri-tis, etc. which increases many fold the chancesof drug interactions. They are more prone to deve-lop postural instability, giddiness and mental con-fusion. In general, the incidence of adverse drugreactions is much higher in the elderly.
3. Sex Females have smaller body size andrequire doses that are on the lower side of therange. Subjective effects of drugs may differ infemales because of their mental makeup.Maintenance treatment of heart failure withdigoxin is reported to be associated with highermortality among women than among men. A num-ber of antihypertensives (clonidine, methyldopa,β-blockers, diuretics) have potential to interferewith sexual function in males but not in females.Gynaecomastia is a side effect (of ketoconazole,metoclopramide, chlorpromazine, digitalis) thatcan occur only in men. Ketoconazole causes lossof libido in men but not in women. Obviouslyandrogens are unacceptable to women andestrogens to men. In women consideration mustalso be given to menstruation, pregnancy andlactation.
Drugs given during pregnancy can affect thefoetus (see Ch. 6 and Appendix-3). There are

65C
HA
PTE
R5
PHARMACOTHERAPY, CLINICAL PHARMACOLOGY AND DRUG DEVELOPMENT
marked and progressive physiological changesduring pregnancy, especially in the third trimester,which can alter drug disposition.
(i) Gastrointestinal motility is reduced → dela-yed absorption of orally administered drug.
(ii) Plasma and extracellular fluid volumeexpands—volume of drug distribution mayincrease.
(iii) While plasma albumin level falls, that of α1acid glycoprotein increases—the unboundfraction of acidic drugs increases but that ofbasic drugs decreases.
(iv) Renal blood flow increases markedly—polardrugs are eliminated faster.
(v) Hepatic microsomal enzymes undergoinduction—many drugs are metabolizedfaster.
Thus, the overall effect on drug dispositionis complex and often difficult to predict.
4. Species and race There are many examp-les of differences in responsiveness to drugsamong different species; rabbits are resistant toatropine, rats and mice are resistant to digitalisand rat is more sensitive to curare than cat. Thesedifferences are important while extrapolatingresults from experimental animals to man.
Among human beings some racial differenceshave been observed, e.g. blacks require higherand mongols require lower concentrations ofatropine and ephedrine to dilate their pupil. β-blockers are less effective as antihypertensive inAfro-Caribbeans. Indians tolerate thiacetazonebetter than whites. Considering the widespreaduse of chloramphenicol in India and Hong Kong,relatively few cases of aplastic anaemia have beenreported compared to its incidence in the west.Similarly, quiniodochlor related cases of subacutemyelooptic neuropathy (SMON) occurred inepidemic proportion in Japan, but there is noconfirmed report of its occurrence in India despiteextensive use.
5. Genetics The dose of a drug to producethe same effect may vary by 4–6 fold amongdifferent individuals. All key determinants of drugresponse, viz. transporters, metabolizing enzymes,
ion channels, receptors with their couplers andeffectors are controlled genetically. Hence, a greatdeal of individual variability can be traced tothe genetic composition of the subject.
Pharmacogenetics The study of genetic basisfor variability in drug response is called‘Pharmacogenetics’. It deals with geneticinfluences on drug action as well as on drughandling by the body. As the genomic technologyhas advanced and the human genome project hasbeen undertaken, gene libraries and huge databases (like ‘pharmacogenetics and pharmaco-genomics knowledge base’, ‘Human genomevariation database’, etc.) have been created aimingat improving precision in drug therapy.
Pharmacogenomics is the use of geneticinformation to guide the choice of drug and doseon an individual basis. It intends to identifyindividuals who are either more likely or lesslikely to respond to a drug, as well as those whorequire altered dose of certain drugs. Attempt ismade to define the genetic basis of an individual’sprofile of drug response and to predict the besttreatment option for him/her. So far, this has beenapplied largely to patients with known geneticabnormalities, but the goal is ‘personalizedmedicine’ on a wide scale. However, a largeproportion of genetic variability still remainsunaccounted for.
A continuous variation with bell-shapedGaussian frequency distribution is seen in the caseof most drugs. In addition, there are some specificgenetic defects which lead to discontinuousvariation in drug responses, e.g.—
1. Atypical pseudocholinesterase results inprolonged succinylcholine apnoea.
2. G-6PD deficiency is responsible for haemo-lysis with primaquine and other oxidizingdrugs. This X-linked monogenic trait is morecommon in the Mediterranean, African andSoutheast Asian races. The haemolysis islargely dose related. Several variants of theG-6PD gene occur in the populationresulting in differing severity of haemolysistriggered by different oxidizing drugs.

66S
EC
TIO
N1
GENERAL PHARMACOLOGY
Haemolysis is severe in homozygousdeficient individuals of certain genotypes.Important drugs reported to cause haemo-lysis in G-6PD deficient subjects are listedin the box.
also are substrates of CYP2D6, deficientpatients are more likely to experience theirtoxicity. Codeine fails to produce analgesiain CYP2D6 deficient, because this enzymegenerates morphine from codeine.
11. Malignant hyperthermia after halothane isdue to abnormal Ca2+ release channel(ryanodine receptor) in the sarcoplasmicreticulum of skeletal muscles.
12. Inability to hydroxylate phenytoin results intoxicity at usual doses.
13. Resistance to coumarin anticoagulants isdue to an abnormal enzyme VKOR (thatregenerates the reduced form of vit. K) whichhas low affinity for the coumarins.
14. Attack of angle closure glaucoma is precipi-tated by mydriatics in individuals withnarrow iridocorneal angle.
Genetic variability in drug response could bedue to single gene mutation or polygenic.Genotype to phenotype predictability is muchbetter in monogenic phenotypic traits such asG-6PD, CYP2D6, TPMT, etc., than for multigenictraits, which are clinically less significant. Majorityof gene polymorphisms are due to substitutionof a single base pair by another. When foundin the population at a frequency of >1%, theseare called ‘Single neucleotide polymorphisms’(SNPs). Gene polymorphisms are often encoun-tered at different frequencies among differentethnic/geographical groups.
Despite accumulation of considerable phar-macogenomic data and the fact that genotypingof the individual needs to be done only once,its practical application in routine patient careis at present limited due to prerequirement ofmultiple drug specific genotypic screening. Simplespot tests for some, e.g. G-6 PD deficiency arecurrently in use.
6. Route of administration Route ofadministration governs the speed and intensityof drug response (see Ch. 1). Parenteral adminis-tration is often resorted to for more rapid, morepronounced and more predictable drug action.A drug may have entirely different uses throughdifferent routes, e.g. magnesium sulfate given
Drugs with potential* to cause haemolysisin G-6PD deficient individuals
Primaquine Nalidixic acidChloroquine FluoroquinolonesQuinine/ Quinidine ChloramphenicolProguanil NitrofurantoinPyrimethamine FurazolidoneDapsone MethyldopaSulfonamides HydralazineCotrimoxazole ProcainamideSulfasalazine ProbenecidThiazide diuretics ColchicineAspirin Methylene blue* Drugs carrying higher risk are italicized.
3. The low activity CYP2C9 variants meta-bolize warfarin at a slow rate and are athigher risk of bleeding.
4. Thiopurine methyl transferase (TPMT)deficiency increases risk of severe bonemarrow toxicity of 6-mercaptopurine andazathioprine.
5. Irinotecan induced neutropenia anddiarrhoea is more in patients with UGT1A1*28 allele of glucuronyl transferase.
6. Severe 5-fluorouracil toxicity occurs inpatients with dihydropyrimidine dehydro-genase (DPD) deficiency.
7. Over expression of P-gp results in tumourresistance to many cancer chemotherapeuticdrugs, because it pumps out the drug fromthe tumour cells.
8. Polymorphism of N-acetyl transferase 2(NAT2) gene results in rapid and slowacetylator status. Isoniazid neuropathy,procainamide and hydralazine induced lupusoccurs mainly in slow acetylators.
9. Acute intermittent porphyria—precipitatedby barbiturates is due to genetic defect inrepression of porphyrin synthesis.
10. CYP2D6 abnormality causes poor meto-prolol/debrisoquin metabolizer status. Sinceseveral antidepressants and antipsychotics

67C
HA
PTE
R5
PHARMACOTHERAPY, CLINICAL PHARMACOLOGY AND DRUG DEVELOPMENT
orally causes purgation, applied on sprainedjoints—decreases swelling, while intravenouslyit produces CNS depression and hypotension.
7. Environmental factors and time ofadministration Several environmental factorsaffect drug responses. Exposure to insecticides,carcinogens, tobacco smoke and consumption ofcharcoal broiled meat are well known to inducedrug metabolism. Type of diet and temporalrelation between drug ingestion and meals canalter drug absorption, e.g. food interferes withabsorption of ampicillin, but a fatty meal enhancesabsorption of griseofulvin and lumefantrine.Subjective effects of a drug may be markedlyinfluenced by the setup in which it is taken.Hypnotics taken at night and in quiet, familiarsurroundings may work more easily. It has beenshown that corticosteroids taken as a singlemorning dose cause less pituitary-adrenalsuppression.
8. Psychological factor Efficacy of a drugcan be affected by patient’s beliefs, attitudes andexpectations. This is particularly applicable tocentrally acting drugs, e.g. a nervous and anxiouspatient requires more general anaesthetic; alcoholgenerally impairs performance but if punishment(which induces anxiety) is introduced, it mayactually improve performance by relieving anxiety.
Placebo This is an inert substance which isgiven in the garb of a medicine. It works bypsychodynamic rather than pharmacodynamicmeans and often produces responses equivalentto the active drug. Some individuals are moresuggestible and easily respond to a placebo: andare called ‘placebo reactors’. Placebos are usedin two situations:1. As a control device in clinical trial of drugs
(dummy medication).2. To treat a patient who, in the opinion of the
physician, does not require an active drug.Placebo is a Latin word meaning ‘I shall please’.A patient responds to the whole therapeutic setting;placebo-effect largely depends on the physician-patient relationship.
Placebos do induce physiological responses,e.g. they can release endorphins in brain—caus-ing analgesia. Naloxone, an opioid antagonist,blocks placebo analgesia. When an active drugis administered, it produces effects both due toits pharmacodynamic action as well as thepsychodynamic effect of the act of medication.Placebo effects can thus supplement pharmaco-logical effects of active medicines. However,placebo effects are highly variable even in thesame individual, e.g. a placebo may induce sleepon the first night, but not subsequently. Thus,it has a very limited role in practical therapeutics.Substances commonly used as placebo are lac-tose tablets/capsules and distilled water injection.Nocebo It is the converse of placebo, and refers to negativepsychodynamic effect evoked by the pessimistic attitude ofthe patient, or by loss of faith in the medication and/orthe physician. Nocebo effect can oppose the therapeutic effectof active medication.
9. Pathological states Not only drugs modifydisease processes, several diseases can influencedrug disposition and drug action:
Gastrointestinal (g.i.) diseases Certain g.i.diseases can alter absorption of orally administereddrugs. The changes are complex and drugabsorption can increase or decrease, e.g. in coeliacdisease absorption of amoxicillin is decreased butthat of cephalexin and cotrimoxazole is increased.Thus, malabsorption syndrome does notnecessarily reduce absorption of all drugs. Gastricstasis occurring during migraine attack retardsthe absorption of ingested drugs. Achlorhydriadecreases aspirin absorption by favouring itsionization. NSAIDs can aggravate peptic ulcerdisease.
Liver disease Liver disease (especiallycirrhosis) can influence drug disposition in severalways:• Bioavailability of drugs having high first pass
metabolism (see Ch. 3) is increased due toloss of hepatocellular function and portocavalshunting.
• Serum albumin is reduced—protein bindingof acidic drugs (diclofenac, warfarin, etc.) is

68S
EC
TIO
N1
GENERAL PHARMACOLOGY
reduced and more drug is present in the freeform.
• Metabolism and elimination of some drugs(morphine, lidocaine, propranolol) isdecreased—their dose should be reduced.Alternative drugs that do not depend on hepaticmetabolism for elimination and/or have shortert½ should be preferred, e.g. oxazepam orlorazepam in place of diazepam; atenolol asβ-blocker.
• Prodrugs needing hepatic metabolism foractivation, e.g. bacampicillin are less effectiveand should be avoided.The changes are complex and there is no
simple test (like creatinine clearance for renaldisease) to guide the extent of alteration in drugdisposition; kinetics of different drugs is affectedto different extents.
Not only disposition, but action as well ofcertain drugs may be altered in liver disease, e.g.• The sensitivity of brain to depressant action
of morphine and barbiturates is markedlyincreased in cirrhotics—normal doses can pro-duce coma.
• Brisk diuresis can precipitate mental changesin patients with impending hepatic encep-halopathy, because diuretics cause hypo-kalemic alkalosis which favours conversionof NH+
4 to NH3. Ammonia enters brain easilyand causes mental derangement.
• Oral anticoagulants can markedly increaseprothrombin time, because clotting factors arealready low.
• Fluid retaining action of phenylbutazone (alsoother NSAIDs) and lactic acidosis due tometformin are accentuated.
Hepatotoxic drugs should be avoided in liverdisease.
Kidney disease It markedly affects pharmaco-kinetics of many drugs as well as alters the effectsof some drugs.
Clearance of drugs that are primarily excretedunchanged (aminoglycosides, digoxin, phenobar-bitone) is reduced parallel to decrease in creatinineclearance (CLcr). Loading dose of such a drug
is not altered (unless edema is present), butmaintenance doses should be reduced or doseinterval prolonged proportionately. A roughguideline is given in the box:
CLcr (patient) Dose rate to bereduced to
50–70 ml/min 70%30–50 ml/min 50%10–30 ml/min 30% 5–10 ml/min 20%
Dose rate of drugs only partly excretedunchanged in urine also needs reduction, but tolesser extents. If the t½ of the drug is prolonged,attainment of steady-state plasma concentrationwith maintenance doses is delayed proportionately.
Plasma proteins, especially albumin, are oftenlow or altered in structure in patients with renaldisease—binding of acidic drugs is reduced, butthat of basic drugs is not much affected.
The permeability of blood-brain barrier isincreased in renal failure; opiates, barbiturates,phenothiazines, benzodiazepines, etc. producemore CNS depression. Pethidine should beavoided because its metabolite nor-pethidinecan accumulate on repeated dosing and causeseizures. The target organ sensitivity may alsobe increased. Antihypertensive drugs producemore postural hypotension in patients with renalinsufficiency.
Certain drugs worsen the existing clinicalcondition in renal failure, e.g.• Tetracyclines have an anti-anabolic effect and
accentuate uraemia.• NSAIDs cause more fluid retention.
Antimicrobials needing dose reductionin renal failure
Even in mild failure Only in severe failure
Aminoglycosides CotrimoxazoleCephalexin CarbenicillinEthambutol CefotaximeVancomycin NorfloxacinAmphotericin B CiprofloxacinAcyclovir Metronidazole

69C
HA
PTE
R5
PHARMACOTHERAPY, CLINICAL PHARMACOLOGY AND DRUG DEVELOPMENT
digoxin is roughly proportional to thyroid function,but this only partially accounts for the observedchanges in sensitivity.
Other examples of modification of drug responseby pathological states are:• Antipyretics lower body temperature only when
it is raised (fever).• Thiazides induce more marked diuresis in
edematous patients.• Myocardial infarction patients are more prone
to adrenaline and digitalis induced cardiacarrhythmias.
• Myasthenics are very sensitive to curare, andin them weakness is aggravated by quinine.
• Schizophrenics tolerate large doses of pheno-thiazines.
• Head injury patients are prone to go intorespiratory failure with normal doses ofmorphine.
• Atropine, imipramine, furosemide can causeurinary retention in individuals with prostatichypertrophy.
• Hypnotics given to a patient in severe painmay cause mental confusion and delirium.
• Cotrimoxazole produces a higher incidence ofadverse reactions in AIDS patients.
10. Other drugs Drugs can modify theresponse to each other by pharmacokinetic orpharmacodynamic interaction between them.Many ways in which drugs can interact havealready been considered (see Ch. 2, 3, 4), anda comprehensive account of clinically importantdrug interactions is presented in Ch. 69.
11. Cumulation Any drug will cumulate in thebody if rate of administration is more than therate of elimination. However, slowly eliminateddrugs are particularly liable to cause cumulativetoxicity, e.g. prolonged use of chloroquine causesretinal damage.• Full loading dose of digoxin should not be
given if patient has received it within the pastweek.
• A course of emetine should not be repeatedwithin 6 weeks.
• Potentially nephrotoxic drugs, e.g. amino-glycosides, tetracyclines (except doxycycline),sulfonamides (crystalluria), vancomycin,nitrofurantoin, cyclosporine, amphotericin Bshould be avoided.
Thiazide diuretics tend to reduce g.f.r. They areineffective in renal failure and can worsen urae-mia; furosemide should be used. Potassium sparingdiuretics are contraindicated; can cause hyper-kalemia → cardiac depression. Repeated dosesof pethidine are likely to cause muscle twitchingand seizures due to accumulation of its excitatorymetabolite norpethidine.
Urinary antiseptics like nalidixic acid, nitro-furantoin and methenamine mandelate fail toachieve high concentration in urine and are likelyto produce systemic toxicity.
Congestive heart failure It can alter drugkinetics by—
(i) Decreasing drug absorption from g.i.t.due to mucosal edema and splanchnic vaso-constriction. A definite reduction in procaina-mide and hydrochlorothiazide absorption hasbeen documented.
(ii) Modifying volume of distribution which canincrease for some drugs due to expansion ofextracellular fluid volume or decrease forothers as a result of decreased tissue per-fusion—loading doses of drugs like lidocaineand procainamide should be lowered.
(iii) Retarding drug elimination as a result ofdecreased perfusion and congestion of liver,reduced glomerular filtration rate andincreased tubular reabsorption; dosingrate of drugs may need reduction, as forlidocaine, procainamide, theophylline.
(iv) The decompensated heart is more sensitiveto digitalis.
Thyroid disease The hypothyroid patients aremore sensitive to digoxin, morphine and CNSdepressants. Hyperthyroid patients are relativelyresistant to inotropic action but more prone toarrhythmic action of digoxin. The clearance of

70S
EC
TIO
N1
GENERAL PHARMACOLOGY
12. Tolerance It refers to the requirement ofhigher dose of a drug to produce a given response.Loss of therapeutic efficacy (e.g. of sulfonylureasin type 2 diabetes, or of β2 agonists in bronchialasthma), which is a form of tolerance, is oftencalled ‘refractoriness’. Tolerance is a widelyoccurring adaptive biological phenomenon. Drugtolerance may be:
Natural The species/individual is inherently lesssensitive to the drug, e.g. rabbits are tolerant toatropine; black races are tolerant to mydriatics.Certain individuals in any population are hypo-responders to certain drugs, e.g. to β adrenergicblockers or to alcohol.
Acquired This occurs by repeated use of adrug in an individual who was initially responsive.Body is capable of developing tolerance to mostdrugs, but the phenomenon is very easilyrecognized in the case of CNS depressants. Anuninterrupted presence of the drug in the bodyfavours development of tolerance. However,significant tolerance does not develop to atropine,digoxin, cocaine, sodium nitroprusside, etc.Tolerance need not develop equally to all actionsof a drug, consequently therapeutic index of adrug may increase or decrease with prolongeduse, e.g.:• Tolerance develops to the sedative action of
chlorpromazine but not to its antipsychoticaction.
• Tolerance occurs to the sedative action ofphenobarbitone but not as much to its anti-epileptic action.
• Tolerance occurs to analgesic and euphoricaction of morphine, but not as much to itsconstipating and miotic actions.
Cross tolerance It is the development of tole-rance to pharmacologically related drugs, e.g.alcoholics are relatively tolerant to barbituratesand general anaesthetics. Closer the two drugsare, more complete is the cross tolerance betweenthem, e.g.—There is partial cross tolerance between morphineand barbiturates but complete cross tolerancebetween morphine and pethidine.
Mechanisms of tolerance The mechanismsresponsible for development of tolerance areincompletely understood. However, tolerance maybe:
(i) Pharmacokinetic/drug disposition tole-rance—the effective concentration of thedrug at the site of action is decreased, mostlydue to enhancement of drug elimination onchronic use, e.g. barbiturates and carbama-zepine induce thier own metabolism, whilerenal excretion of amphetamine is accele-rated after regular intake.
(ii) Pharmacodynamic/cellular tolerance—drugaction is lessened; cells of the target organbecome less responsive, e.g. morphine,barbiturates, nitrates. This may be due todesensitization/down regulation of receptors(see p. 52, 53), or weakening of responseeffectuation.
Tachyphylaxis (Tachy-fast, phylaxis-protection)It refers to rapid development of tolerance whendoses of a drug repeated in quick succession resultin marked reduction in response. This is usuallyseen with indirectly acting drugs, such asephedrine, tyramine, nicotine. These drugs act byreleasing catecholamines in the body, synthesisof which is unable to match the rate of release:stores get depleted. Other mechanisms like slowdissociation of the drug from its receptor, desensi-tization/internalization or down regulation ofreceptor, etc. (see p. 52, 53) and/or compensatoryhomeostatic adaptation.
Drug resistance It refers to tolerance ofmicroorganisms to inhibitory action of anti-microbials, e.g. Staphylococci to penicillin (seeCh. 49).
RATIONAL USE OF MEDICINES
It is widely assumed that use of drugs by qualifieddoctors of modern medicine would be rational.However, in reality, irrationality abounds in almostevery aspect of drug use. Medically inappropriate,ineffective and economically inefficient use ofdrugs occurs all over the world, more so in thedeveloping countries. As per the WHO — ‘rational

71C
HA
PTE
R5
PHARMACOTHERAPY, CLINICAL PHARMACOLOGY AND DRUG DEVELOPMENT
use of medicines requires that the patients receivemedication appropriate to their clinical needs indoses that meet their own individual requirementsfor an adequate period of time, and at the lowestcost to them and to their community’.
Rational use of medicines addresses every stepin the supply-use chain of drugs, i.e. selection,procurement, storage, prescribing, dispensing,monitoring and feedback. However, only rationalprescribing and related aspects are dealt here.
Rational prescribing
Rational prescribing is not just the choice of acorrect drug for a disease, or mere matching ofdrugs with diseases, but also the appropriatenessof the whole therapeutic set up along with followup of the outcome. The criteria to evaluate rationalprescribing are:• Appropriate indication: the reason to prescribe
the medicine is based on sound medicalconsiderations.
• Appropriate drug in efficacy, tolerability, safety,and suitability for the patient.
• Appropriate dose, route and duration accordingto specific features of the patient.
• Appropriate patient: no contraindications exist;drug acceptable to the patient; likelihood ofadverse effect is minimal and less than theexpected benefit.
• Correct dispensing with appropriate infor-mation/instruction to the patient.
• Adequate monitoring of patient’s adherenceto medication, as well as of anticipated bene-ficial and untoward effects of the medication.
There is no doubt that knowledge of the prescriberabout drugs and disease is the most importantdeterminant of his/her prescribing pattern, but ithas been demonstrated time and again that simplyimproving knowledge has failed to promoterational drug use. A variety of other factorsinfluence prescribing as summarized in the box.
Irrationalities in prescribing It is helpfulto know the commonly encountered irrationalitiesin prescribing so that a conscious effort is madeto avoid them.
Factors influencing prescribing
• Knowledge of the prescriber.• Role models: one tends to follow prescribing
practices of one’s teachers or senior/popularphysicians.
• Patient load: heavy load tends to foster routinizedsymptom based prescribing.
• Attitude to afford prompt symptomatic relief at allcost.
• Imprecise diagnosis: medication is given to coverall possible causes of the illness.
• Drug promotion and unrealistic claims bymanufacturers.
• Unethical inducements (gifts, dinner parties,conference delegation, etc.).
• Patient’s demands: many patients are not satisfiedunless medication is prescribed; misconceptions,unrealistic expectations, ‘pill for every ill’ belief.
• Use of drug when none is needed; e.g. anti-biotics for viral fevers and nonspecific diar-rhoeas.
• Compulsive coprescription of vitamins/tonics.• Use of drugs not related to the diagnosis, e.g.
chloroquine/ciprofloxacin for any fever, protonpump inhibitors for any abdominal symptom.
• Selection of wrong drug, e.g. tetracycline/ciprofloxacin for pharyngitis, β blocker asantihypertensive for asthmatic patient.
• Prescribing ineffective/doubtful efficacydrugs, e.g. serratiopeptidase for injuries/swellings, antioxidants, cough mixtures,memory enhancers, etc.
• Incorrect route of administration: injectionwhen the drug can be given orally.
• Incorrect dose: either underdosing or over-dosing; especially occurs in children.
• Incorrect duration of treatment, e.g. prolongedpostsurgical use of antibiotics or stoppage ofantibiotics as soon as relief is obtained, suchas in tuberculosis.
• Unnecessary use of drug combinations, e.g.ciprofloxacin + tinidazole for diarrhoea, ampi-cillin + cloxacillin for staphylococcal infection,ibuprofen + paracetamol as analgesic.
• Unnecessary use of expensive medicines whencheaper drugs are equally effective; craze forlatest drugs, e.g. routine use of newerantibiotics.

72S
EC
TIO
N1
GENERAL PHARMACOLOGY
• Unsafe use of drugs, e.g. corticosteroids forfever, anabolic steroids in children, use ofsingle antitubercular drug.
• Polypharmacy without regard to druginteractions: each prescription on an averagehas 3–4 drugs, some may have as many as10–12 drugs, of which many are combinations.
Irrational prescribing has a number of adverseconsequences for the patient as well as thecommunity. The important ones are:
Process of rational prescribing
• Establish a diagnosis (at least provisional).• Define therapeutic problem(s), e.g. pain, infection,
etc.• Define therapeutic goals to be achieved, e.g.
symptom relief, cure, prevention of complications,etc.
• Select the class of drug capable of achieving eachgoal.
• Identify the drug (from the class selected) basedon:
EfficacySafety For the particular patientSuitabilityCost
• Decide the route, dose, duration of treatment,considering patient’s condition.
• Provide proper information and instructions aboutthe medication.
• Monitor adherence to the medication (compliance).• Monitor the extent to which therapeutic goal is
achieved, e.g. BP lowering, peptic ulcer healing,etc.
• Modify therapy if needed.• Monitor any adverse drug events that occur, and
modify therapy if needed.
⎫⎬⎭Impact of irrational prescribing
• Delay/inability in affording relief/cure of disease.• More adverse drug effects.• Prolongation of hospitalization; loss of man days.• Increased morbidity and mortality.• Emergence of microbial resistance.• Financial loss to the patient/community.• Loss of patient’s confidence in the doctor.• Lowering of health standards of patients/community.• Perpetuation of public health problem.
Rational prescribing is a stepwise process ofscientifically analyzing the therapeutic set up basedon relevant inputs about the patient as well as thedrug, and then taking appropriate decisions. It doesnot end with handing over the prescription to thepatient, but extends to subsequent monitoring,periodic evaluations and modifications as andwhen needed, till the therapeutic goals areachieved. The important steps are summarized inthe box.
Information/instructions to the patientRational prescribing also includes giving relevantand adequate information to the patient about thedrug(s) and disease, as well as necessaryinstructions to be followed.
Effects of the drug Which symptoms willdisappear and when (e.g. antidepressant will takeweeks to act); whether disease will be cured ornot (e.g. diabetes, parkinsonism can only beameliorated, but not cured), what happens if thedrug is not taken as advised (e.g. tuberculosiswill worsen and may prove fatal).
Side effects There is considerable debate asto how much the patient should be told aboutthe side effects. Detailed descriptions may havea suggestive effect or may scare the patient anddissuade him from taking the drug, while notinforming tantamounts to negligence, and the sideeffect, when it occurs, may upset the uninformedpatient. Communicating the common side effectswithout discouraging the patient is a skill to bedeveloped.
Instructions How and when to take the drug(special dosage forms like inhalers, transdermalpatches, etc. may need demonstration); how longto take the drug; when to come back to the doctor;instructions about diet and exercise if needed;what laboratory tests are needed, e.g. prothrombintime with oral anticoagulants, leucocyte count withanticancer drugs.
Precautions/warnings What precautions totake; what not to do, e.g. driving (with con-ventional antihistaminics) or drinking (withmetronidazole), or standing still (after sublingual

73C
HA
PTE
R5
PHARMACOTHERAPY, CLINICAL PHARMACOLOGY AND DRUG DEVELOPMENT
glyceryl trinitrate); risk of allergy or any seriousreaction, etc.
In the end it should be ensured that theinstructions have been properly understood bythe patient. Rational prescribing, thus, is acomprehensive process.
EXPIRY DATE OF PHARMACEUTICALSIt is a legal requirement that all pharmaceutical productsmust carry the date of manufacture and date of expiry ontheir label. The period between the two dates is called the‘life period’ or ‘shelf-life’ of the drug. Under specified storageconditions, the product is expected to remain stable (retain>95% potency) during this period. In India, the scheduleP (Rule 96) of Drugs and Cosmetics Act (1940) specifiesthe life period (mostly 1–5 years) of drugs and the conditionsof storage. The expiry of other medicines has to be specifiedby the manufacturer, but cannot exceed 5 years, unlesspermitted by the licencing authority on the basis of satisfactorystability proof.
The shelf-life of a medicine is determined by real timestability studies or by extrapolation from accelerateddegradation studies. The expiry date does not mean that themedicine has actually been found to lose potency or becometoxic after it, but simply that quality of the medicine isnot assured beyond the expiry date, and the manufactureris not liable if any harm arises from the use of the product.Infact, studies have shown that majority of solid oral dosageforms (tablets/capsules, etc.) stored under ordinary conditionsin unopened containers remained stable for 1–5 years (someeven up to 25 years) after the expiry date. Liquid formulations(oral and parenteral) are less stable. Suspensions clump byfreezing. Injectable solutions may develop precipitates,become cloudy or discoloured by prolonged storage.Adrenaline injection (in ampoules) has been found to losepotency few months after the expiry date of 1 year (it getsoxidized).
There is hardly any report of toxicity of expiredmedicines. The degradation product of only one drug(tetracycline) has caused toxicity in man. Outdated tetracyclinecapsules produced renal tubular damage resembling Fanconisyndrome in the early 1960s. The capsules have now beenreformulated to minimize degradation.
Loss of potency beyond the ‘life period’ of the formulationdepends on the drug as well as the storage conditions. Highhumidity and temperature accelerate degradation of manydrugs. Though, majority of medicines, especially solid oraldosage forms, remain safe and active years after the statedexpiry date, their use cannot be legally allowed beyond thisdate.
EVIDENCE-BASED MEDICINE
Extensive scientific investigation of drugs in manand introduction of numerous new drugs over the
past few decades is gradually transforming thepractice of medicine from ‘experience based’wherein clinical decisions are made based on theexperience (or rather impression) of the physicianto ‘evidence-based’ wherein the same are guidedby scientifically credible evidence from welldesigned clinical studies. Evidence-based medi-cine is the process of systematically finding,evaluating and using contemporary researchfindings as the basis of clinical decisions. Resultsof well designed multicentric interventional trialsare forming the basis of constantly evolvingguidelines for disease management. Today’sphysician has to be skilled in the new techniquesof searching and evaluating the literature onefficacy, safety and appropriateness of a particulartherapeutic measure (drug). Therapeutic evaluationof a drug includes:• Quantitation of benefit afforded by it.• The best way (dosage, duration, patient
selection, etc.) to use it.• How it compares with other available drugs.• Surveillance of adverse effects produced by
it.Clinical studies are basically of the following threetypes:a. Clinical trialsb. Cohort studiesc. Case control studies
Clinical trialIt is a prospective ethically designed investigationin human subjects to objectively discover/verify/compare the results of two or more therapeuticmeasures (drugs). Clinical trials are designed toanswer one or more precisely framed questionsabout the value of treating equivalent groups ofpatients by two or more modalities (drugs, dosageregimens, other interventions). Depending on theobjective of the study, clinical trial may beconducted in healthy volunteers or in volunteerpatients. Healthy volunteers may be used todetermine pharmacokinetic characteristics,tolerability, safety and for certain type of drugs(e.g. hypoglycaemic, hypnotic, diuretic) evenefficacy. For majority of drugs (e.g. antiepileptic,

74S
EC
TIO
N1
GENERAL PHARMACOLOGY
antipsychotic, antiinflammatory, antitubercular,etc.) therapeutic efficacy can only be assessedin patients.
Ethical considerations All clinical trials mustbe conducted only after scrutiny and approvalby an independent ethics committee as per the‘Good Clinical Practice’ (GCP) guidelines. InIndia, the ICMR (2006) has brought out ‘Ethicalguidelines, for biomedical research on humanparticipants: A proper written Informed consentof the patient/trial subject must be obtained. Theethics committee has to ensure that the study doesnot breach the ethical principles of:Autonomy: Freedom, dignity and confidentialityof the subject; right to choose whether or notto participate in the trial or to continue with it.Beneficence: Motive to do good to the subjectand/or the society at large.Non-maleficence: Not to do harm or put theparticipant at undue risk/disadvantage.Justice: Observence of fairness, honesty andimpartiality in obtaining, analysing and communi-cating the data.
Controlled trial The inclusion of a propercomparator (control) group in clinical trials iscrucial. The control group, which should be assimilar to the test group as possible, receives eithera placebo (if ethically permissible) or the existingstandard treatment (active control). Separate testand control groups may run simultaneously(parallel group design), or all the subjects maybe treated by the two options one after the other(cross over design) so that the same subjects serveas their own controls. Individual variation inresponse is thus avoided and sample size maybe reduced. In the cross over design, some patientsare treated first by drug ‘A’ followed by drug‘B’, while in others the order is reversed. Thisnullifies the effect (if any) of order of treatment.However, there may still be ‘carry over’ effects.This design is applicable only to certain chronicdiseases which remain stable over long periods.
When one drug is compared to another drugor to a placebo, the dosage regimen (dose,frequency, duration) of the drug is decided in
advance. The trial results are applicable only tothis chosen regimen. No conclusions can be drawnabout a higher or lower dose. To determine themost appropriate dose, separate dose-rangingstudies (trials) have to be performed.
It is well known that both the participantsand the investigators of the trial are susceptibleto conscious as well as unconscious bias in favourof or against the test drug. The greatest challengein the conduct of clinical trial is the eliminationof bias. The credibility of the trial depends onthe measures that are taken to minimize bias. Thetwo basic strategies for minimizing bias are‘randomization’ and concealment or ‘blinding’.
Randomization The subjects are allocated toeither group using a preselected random numbertable or computer programme so that any subjecthas equal chance of being assigned to the testor the control group. Discretion (and likely bias)of the investigator/subject in treatment allocationis thus avoided. If considered necessary, stratifiedrandomization according to age/sex/diseaseseverity/other patient variable may be adopted.
Blinding (masking) This refers to concealmentof the nature of treatment (test or control) fromthe subject (single blind) or both the subject aswell as the investigator (double blind). For thispurpose the two medications have to appearsimilar in looks, number, weight, taste, etc. andare to be supplied in unlabelled packets markedfor each patient. In double blind, the key/codeto treatment allocation is kept by a third ‘datamanagement’ party who is not involved in treatingor recording observations. The code is brokenat the completion of the trial and the results areanalysed according to prespecified statisticalmethod. However, all clinical trials need not beblinded. Those in which the nature of treatmentis not concealed are called ‘open’ trials.
Randomized controlled double blind trial isthe most credible method of obtaining evidenceof efficacy, safety or comparative value oftreatments.
Inclusion/exclusion criteria The characteristicsof the subject/patient (age, sex, disease/symptom,

75C
HA
PTE
R5
PHARMACOTHERAPY, CLINICAL PHARMACOLOGY AND DRUG DEVELOPMENT
severity and/or duration of illness, coexistant andpast diseases, concurrent/preceeding drug therapy,etc.) who are to be recruited in the trial or excludedfrom it must be decided in advance. The trialresults are applicable only to the populationspecified by these criteria.
End point The primary and secondary (if any)end points (cure, degree of improvement, symptomrelief, surrogate marker, avoidance of compli-cation, curtailment of hospitalization, survival,quality of life, etc.) of the trial must be specifiedin advance. The results are analysed in relationto the specified end points.
Higher efficacy may not always be the aimof a clinical trial. A trial may be designed toprove ‘non inferiority’ (of the new drug) to theexisting treatment, and possibly afford advantagesin terms of tolerability, safety, convenience, costor applicability to special patient subgroup(s).
Sample size: Both financial and ethical consi-derations demand that the number of subjects inthe trial be the minimum needed for a valid result.The minimum number of subjects for obtaininga decisive conclusion (test better than control/control better than test/no difference between thetwo) must be calculated statistically beforehand.Because the trial is conducted on a sample ofthe whole patient population, there is always achance that the sample was not representativeof the population. Thus, the results cannot beabsolutely conclusive.Two types of errors are possible:
Type I (α) error: a difference is found between the twogroups while none exists. Its possibility is called ‘significance’of the result, e.g. if test drug is found to be better thancontrol at a significance level of 0.05, it means that thereis 5% chance that this is not real.
Type II (β) error: no difference is found while it reallyexists. The probability of failing to detect an actual differenceis expressed by the ‘power’ of the trial. A power of 0.9means that there is 10% chance of missing a real difference.
The sample size of the trial depends on the desiredlevel of significance and power. The other input needed forcalculation of sample size is the magnitude of differencebetween the two groups that is expected or is consideredclinically significant, e.g. a 10% reduction in pain intensitymay not be considered clinically significant, while a 10%
reduction in mortality may be worthwhile. Larger samplesize is required to detect smaller difference. Also, higherthe significance and power level desired, greater is the numberof subjects. The variability of response in terms of the primaryend point also affects the sample size. Responses that showgreater individual variation need larger number of subjectsto achieve the desired significance and power levels.
Many large scale trials are subjected to interim analysisfrom time to time as the trial progresses by an independentcommittee which can order an early termination if a decisiveresult (positive or negative) is obtained; because it wouldbe unethical to subject some of the remaining patients toa treatment (test or control) which has been found inferior.
Multicentric trial Many large trials areconducted at more than one centre by as manyteams of investigators, sometimes spread overseveral countries. The advantages are:• Larger number of patients can be recruited
in a shorter period of time.• Results are applicable to a wider population
base which may cover several countries/ethnicgroups.
• Regulatory requirements of several countriesmay be satisfied.
• Credibility of the trial is enhanced.The phase III trials are generally multicentric.
Sequential trial
This design attempts to detect a significant result as soonas it is achieved, minimizing the number of subjects. Thetrial is conducted on matched pairs of subjects and is scoredas ‘A’ treatment better than ‘B’ or ‘B’ better than ‘A’ orno difference. This is plotted continuously as the trial pro-ceeds till the boundries of predetermined level of significantsuperiority/inferiority/no difference are touched. The trial isthen terminated. This design is applicable only to certaintypes of drugs and diseases for which clinical end pointsare achieved quickly and paired comparisons are possible.Moreover, it may not always be practicable to recruit matchingpairs of trial subjects.
Meta-analysisThis is an exercise in which data from severalsimilarly conducted randomized controlled clinicaltrials with the same drug (or class of drugs)examining the same clinical end point(s) is pooledto bring out the overall balance of evidence byenlarging the number of test and control subjectsand increasing the significance and power of theconclusions. Because individual trials are often

76S
EC
TIO
N1
GENERAL PHARMACOLOGY
conducted on relatively smaller number of patients,some may fail to detect a significant difference,while others may find it. Discordant results arepublished which confuse the medical practitioner.There are many criticisms of meta-analysis, suchas:a. bias in the selection of trials for analysis
(selection bias);b. unintentional exclusion of negative results
which are less likely to be published(publication bias);
c. nonuniformity of the trials in details ofmethodology and conduct.
Nevertheless, meta-analysis is a useful tool toarrive at conclusions that may influence medicalpractice. For example, meta-analysis of trials hasstrongly supported the use of β-adrenergicblockers in heart failure and use of statins to reducerisk of coronary artery disease.To be reliable, the meta-analysis should observe the following:• Comprehensive search of the literature to identify all
eligible trials.• Use objective criteria in selecting the trials for inclusion.• Include only randomized trials of assured quality.• Employ proper statistical methods in pooling and treating
the data from individual trials.Meta-analysis are now frequently published oncontemporary therapeutic issues.
Cohort studyThis is a type of observational study in whichno intervention for the sake of the study is done.‘Cohort’ is a group of individuals having somecommon feature. In the context of drug research,the common feature is that all study subjects havetaken a particular drug. Occurrence of events(beneficial or adverse) in users and nonusers ofthe drug is compared, i.e. prescription event moni-toring. It can be a prospective or a retrospectivestudy. In the prospective design, all patients whoreceive the study drug are followed up fortherapeutic outcomes or adverse effects. Amatching group of patients who have not receivedthe drug is identified and followed up to serveas control. Cohort studies are primarily used todiscover uncommon adverse effects that may bemissed during formal therapeutic trials which
involve fewer patients and often exclude certaintype of patients who may be susceptible to thatadverse effect. Its value for defining therapeuticoutcomes is less credible. The limitations of cohortstudies are that controls included may not beappropriate, and relatively long period of followup is needed.
In the retrospective cohort study, healthrecords of a population are scrutinized forexposure to the study drug and the subsequentbeneficial/adverse events. Its value is question-able because many events may have been missedin the records and several unknown factors mayhave contributed to the findings. However, it mayserve as pointer, or to arouse suspicion.
Case control studyThis type of observational study is used mainlyto reveal association of a suspected rare adverseevent with the use of a particular drug. Casesof the suspected adverse event (e.g. agranulo-cytosis) are collected from hospital records ordisease registries, etc. A matched control groupsimilar in other respects but not having the adverseevent is selected. Drug histories of both groupsare traced backwards to compare exposure to theindicted drug (e.g. phenylbutazone) amongpatients with the adverse event to those withoutit. The suspicion is strengthened if high associationis found. Though case control studies can beperformed rather quickly because the number ofpatients analysed is small compared to the cohortdesign, they do not prove causality. Also, thecausative drug and the adverse event have to besuspected first to plan the study, whereas cohortstudy can reveal unsuspected adverse events.Variable accuracy of retrospective records, nonrandomly selected control group, chances of biasand a variety of unknown factors make the casecontrol study a weak instrument for affordingconvincing evidence.
Grading strength of evidence
The strength of evidence from the conclusionsof various kinds of trials, studies and reports has

77C
HA
PTE
R5
PHARMACOTHERAPY, CLINICAL PHARMACOLOGY AND DRUG DEVELOPMENT
been graded from strong to weak as presentedin the box.
NEW DRUG DEVELOPMENT
In this era of bewildering new drug introductionand rapid attrition of older drugs, the doctor needsto have an overall idea of the manner in whichnew drugs are developed and marketed. Drugdevelopment now is a highly complex, tedious,competitive, costly and commercially riskyprocess. From the synthesis/identification of themolecule to marketing, a new drug takes at least10 years and costs 500–1000 million US$. Assuch, invention and development of new drugsis now possible only in the set up of big pharma-ceutical houses that alone have the resources,infrastructure and dedicated teams of scientiststo carry out the multiple specialized stages ofthe process. Though the pharmaceutical industryis often regarded cunning, greedy, unscrupulousand deceptive, there is no denying that it isresponsible for most of the progress in therapeuticsas well as pharmacological knowledge of today.
The major steps/stages in the developmentof a new drug are given in the box.
Approaches to drug discovery/inventionExploration of natural sources Plants are the oldest sourceof medicines. Clues about these have been obtained fromtraditional systems of medicine prevalent in various partsof the world; Opium (morphine), Ephedra (ephedrine),Cinchona (quinine), curare (tubocurarine), belladonna(atropine), Quinghaosu (artemisinin) are the outstandingexamples. Though animal parts have been used as cures
since early times, it was physiological experiments performedin the 19th and early 20th century that led to introductionof some animal products into medicine, e.g. adrenaline,thyroxine, insulin, liver extract, antisera, etc. Few minerals(iron/calcium salts, etc.) are the other natural medicinalsubstances. The discovery of penicillin (1941) opened theflood-gates of a vast source—microorganisms—of a new kindof drugs (antibiotics). The use of microbes for productionof vaccines is older than their use to produce antibiotics.
Though few drugs are now produced from plants, animalsor microbes, these sources of medicines are by no meansexhausted. However, they mostly serve as lead compounds.
Random or targeted chemical synthesis Syntheticchemistry made its debut in the 19th century and is nowthe largest source of medicines. Randomly synthesizedcompounds can be tested for a variety of pharmacologicalactivities. Though some useful drugs (barbiturates,chlorpromazine) have been produced serendipitously by thisapproach, it has very low probability of hitting at the rightactivity in the right compound; rarely employed now.
Lead optimization A more practical approach is tosynthesize chemical congeners of natural products/syntheticcompounds with known pharmacological activity in the hopeof producing more selective/superior drugs. Many families
Grades of strength of evidence
Grade I Systematic reviews/Meta-analysis Most reliable, may form the basis ofclinical decisions
Grade II Well powered randomized Reliable, but may be supported orcontrolled trial/more than one trials refuted by similar studies
Grade III Open label trials/pilot studies/ Less reliable, need more rigorous testing,observational (cohort and case-control) may indicate further investigationstudies (prospective or retrospective)
Grade IV Case reports/anecdotal reports/ Least reliable; may serve as pointersclinical experience to initiate formal studies
Stages in new drug development
• Synthesis/isolation of the compound: (1–2 years)• Preclinical studies: screening, evaluation,
pharmacokinetic and short-term toxicity testing inanimals: (2–4 years)
• Scrutiny and grant of permission for clinical trials:(3–6 months)
• Pharmaceutical formulation, standardization ofchemical/biological/immuno-assay of the compound:
(0.5–1 year)• Clinical studies: phase I, phase II, phase III trials;
long-term animal toxicity testing: (3–10 years)• Review and grant of marketing permission:
(0.5–2 years)• Postmarketing surveillance: (phase IV studies)

78S
EC
TIO
N1
GENERAL PHARMACOLOGY
of clinically useful drugs have been fathered by a ‘leadcompound’. Often only ‘me too’ drugs are produced, butsometimes breakthroughs are achieved, e.g. thiazide diureticsfrom acetazolamide, tricyclic antidepressants from pheno-thiazines.
Study of several congeners of the lead compound candelineate molecular features responsible for a particularproperty. Application of this structure-activity relationshipinformation has proven useful on many occasions, e.g.selective β2 agonists (salbutamol) and β blockers (propranolol,etc.) have been produced by modifying the structure ofisoprenaline, H2 blockers by modifying the side chain ofhistamine, ethinyl-estradiol by introducing a substitution thatresists metabolic degradation, mesoprostol (more stable) byesterifying PGE1.
More commonly now, as described later in the rationalapproach, identification of the target biomolecule is thestarting point for new drug invention. A lead compoundcapable of interacting with the target is searched by applyingdiverse approaches described above and below. The affinityand selectivity of the lead compound for the target isdetermined. It is then chemically modified to optimise theseparameters as well as pharmacokinetic, pharmaceutical,toxicological and other characteristics. More suitablecandidate drug(s) may thus emerge for further development.
Single enantiomers Many drugs are chiral compounds.Because pharmacological activity depends on threedimensional interaction of drug molecules with their targetbiomolecules, the enantiomers (R and S forms or d and lisomers) of chiral drugs differ in biological activity, metabolicdegradation, etc. Often only one of the enantiomers is active.Single enantiomer drug could be superior to its racemate,because the additional enantiomer may not only be a ‘silentpassenger’ but contribute to side effects, toxicity (dextro-dopais more toxic than levo-dopa), load on metabolism or evenantagonize the active enantiomer. Regulatory authorities inmany countries, led by US-FDA, have mandated separateinvestigation of the enantiomers in case the new drug is a chiralmolecule. Approval is withheld unless the pure enantiomersare shown to be no better than the racemate. Several drugs,originally introduced as racemates, have now been madeavailable as single enantiomer preparations as well (see box).
Rational approach This depends on sound physiological,biochemical, pathological knowledge and identification ofspecific target for drug action, such as H+K+ATPase for gastricacid suppression or glycoprotein IIa/IIIb receptor for plateletfunction inhibition.The drug is aimed at mitigating thederangement caused by the disease, e.g. levodopa was tried inparkinsonism based on the finding that the condition resultedfrom deficiency of dopamine in the striatum. The purine,pyrimidine, folate antimetabolites were introduced in cancerchemotherapy after elucidation of key role of these metabolitesin cell proliferation. Because virus directed reverse trans-criptase is unique to retroviruses, its inhibitors have beendeveloped as anti-HIV drugs. This approach is very attractivebut requires a lot of basic research.
Drugs marketed as single enantiomers
Enantiomer Advantage claimed
(S) atenolol half dose, better tolerated(S) metoprolol half dose(S) amlodipine half dose, less peripheral
edema(S) omeprazole better oral bioavailability
(esomeprazole)(S) pantoprazole more potent(R) salbutamol more active, (S) may
antagonize (R)(S) citalopram lower dose, less side
(escitalopram) effects(S) naproxen less burden on kidney (but
inversion occurs in vivo)cisatracurium 4× more potent, less
histamine releaselevofloxacin more active, slower eliminationlevocetirizine (R) half dose, only (R) form activedesloratadine half dose
Molecular modelling Advances in protein chemistry andcomputer aided elucidation of three dimensional structureof key receptors, enzymes, etc. has permitted designing oftargeted compounds, e.g. designing of selective COX-2inhibitors was prompted by the comparative configurationof COX-1 and COX-2 isoenzyme molecules. Study of drugbinding to mutated receptors and elucidation of configurationof drug-receptor complexes is now guiding production ofimproved drugs. Attempts are being made to produce indivi-dualized drugs according to pharmacogenomic suitability.
Combinatorial chemistry Chemical groups are combinedin a random manner to yield innumerable compounds andsubjected to high-throughput screening on cells, geneticallyengineered microbes, receptors, enzymes, etc. in roboticallycontrolled automated assay systems. Computerized analysisis used to identify the so called ‘hits.’ These compoundsare then subjected to conventional tests. This new approachhas vast potentials, but failure rates are high.
Biotechnology Several drugs are now being produced byrecombinant DNA technology, e.g. human growth hormone,human insulin, interferon, etc. Some monoclonal and chimeralantibodies have been introduced as drugs.
New molecules, especially antibiotics, regulatorypeptides, growth factors, cytokines, etc. produced bybiotechnological methods can be evaluated as putative drugs.Other experimental approaches in new drug developmentare antisense oligonucleotides and gene therapy.
Preclinical studiesAfter synthesizing/identifying a prospectivecompound, it is tested on animals to expose thewhole pharmacological profile. Experiments are

79C
HA
PTE
R5
PHARMACOTHERAPY, CLINICAL PHARMACOLOGY AND DRUG DEVELOPMENT
generally performed on a rodent (mouse, rat,guinea pig, hamster, rabbit) and then on a largeranimal (cat, dog, monkey). As the evaluationprogresses unfavourable compounds get rejectedat each step, so that only a few out of thousandsreach the stage when administration to man isconsidered.The following types of tests are performed.
1. Screening tests These are simple and rapidlyperformed tests to indicate presence or absence of aparticular pharmacodynamic activity that is sought for,e.g. analgesic or hypoglycaemic activity.
2. Tests on isolated organs, bacterial cultures, etc.These also are preliminary tests to detect specific activity,such as antihistaminic, antisecretory, vasodilator, anti-bacterial, etc.
3. Tests on animal models of human disease Suchas kindled seizures in rats, spontaneously (genetically)hypertensive rats, experimental tuberculosis in mouse,alloxan induced diabetes in rat or dog, etc.
4. Confirmatory tests and analogous activitiesCompounds found active are taken up for detailed studyby more elaborate tests which confirm and characterizethe activity. Other related activities, e.g. antipyretic andanti-inflammatory activity in an analgesic are tested.
5. Systemic pharmacology Irrespective of the primaryaction of the drug, its effects on major organ systemssuch as nervous, cardiovascular, respiratory, renal, g.i.tare worked out. Mechanism of action, includingadditional mechanisms, e.g. α adrenergic blockade,calcium channel blockade, nitro-vasodilatation, etc. in aβ adrenergic blocker antihypertensive, are elucidated.
6. Quantitative tests The dose-response relationship,maximal effect and comparative potency/efficacy withexisting drugs is ascertained.
7. Pharmacokinetics The absorption, tissue distribution,metabolism, excretion, volume of distribution and half-life of the drug are quantified.
8. Toxicity testsThe aim is to determine safety of the compound in at least 2animal species, mostly mouse/rat and dog by oral and parenteralroutes.
Acute toxicity: Single escalating doses are given to smallgroups of animals that are observed for overt effects andmortality for 1–3 days. The dose which kills 50% animals(LD50) is calculated. Organ toxicity is examined byhistopathology on all animals.
Subacute toxicity: Repeated doses are given for 2–12 weeksdepending on the duration of intended treatment in man.Doses are selected on the basis of ED50 and LD50. Animalsare examined for overt effects, food intake, body weight,haematology, etc. and organ toxicity.
Chronic toxicity: The drug is given for 6–12 months andeffects are studied as in subacute toxicity. This is generallyundertaken concurrently with early clinical trials.
Reproduction and teratogenicity: Effects on spermatogenesis,ovulation, fertility and developing foetus are studied.
Mutagenicity: Ability of the drug to induce genetic damageis assessed in bacteria (Ames test), mammalian cell culturesand in intact rodents.
Carcinogenicity: Drug is given for long-term, even the wholelife of the animal and they are watched for developmentof tumours.
Standardised procedures under ‘Good LaboratoryPractices’ (GLP) have been laid down for the conduct ofanimal experiments, especially toxicity testing.
Clinical trials
When a compound deserving trial in man isidentified by animal studies, the regulatoryauthorities are approached who on satisfactionissue an ‘investigational new drug’ (IND) licence.The drug is formulated into a suitable dosageform and clinical trials are conducted in a logicalphased manner. To minimize any risk, initiallyfew subjects receive the drug under closesupervision. Later, larger numbers are treatedwith only relevant monitoring. Standards for thedesign, ethics, conduct, monitoring, auditing,recording and analyzing data and reporting ofclinical trials have been laid down in the formof ‘Good Clinical Practice’ (GCP) guidelines byan International Conference on Harmonization(ICH). National agencies in most countries,including ICMR in India, have also framed ethicalguidelines for clinical trials. Adherence to theseprovides assurance that the data and reportedresults are credible and accurate, and that therights, integrity and confidentiality of trial subjectsare protected as enunciated in the HelsinkiDeclaration of the World Medical Association.The requirements and regulations for the conductof clinical trials on a new drug in India havebeen laid down in the schedule Y of the Drugsand Cosmetics Rules.
The clinical studies are conventionally dividedinto 4 phases.
Phase I: Human pharmacology and safetyThe first human administration of the drug iscarried out by qualified clinical pharmacologists/trained physicians in a setting where all vitalfunctions are monitored and emergency/

80S
EC
TIO
N1
GENERAL PHARMACOLOGY
resuscitative facilities are available. Subjects(mostly healthy volunteers, sometimes patients)are exposed to the drug one by one (total 20–80 subjects), starting with the lowest estimateddose and increasing stepwise to achieve theeffective dose. The emphasis is on safety,tolerability, and to detect any potentially dangerouseffects on vital functions, such as precipitous fall/rise in bloof pressure or heart rate, arrhythmias,bronchospasm, seizures, kidney/liver damage, etc.Unpleasant side effects are noted and an attemptis made to observe the pharmacodynamic effectsin man. The human pharmacokinetic parametersof the drug are measured for the first time. Noblinding is done: the study is open label.
Phase 0: Microdosing study
This is a new strategy being developed to reduce the costand time of the drug development process. The rate of rejectionof candidate drugs at various stages of clinical developmenthas progressively increased recently, discouraging pharma-ceutical companies to venture into the risky business of newdrug invention. This has alarmed the FDA (USA) and theEuropean Medicines Agency to encourage novel cost-cuttingapproaches in drug development. One such tool is themicrodosing human study undertaken before phase-1 trial,and is also called phase ‘0’ study.
Many candidate drugs fail during clinical trials due tosub-optimal human pharmacokinetics. Very low doses,generally about 1/100th of the estimated human dose, ora maximum of 100 μg total dose of candidate drug, areadministered to healthy volunteers and pharmacokinetics isworked out using highly sophisticated instrumentation, suchas Accelerator mass spectrometry (AMS) with radiolabelleddrug, or LC-Tandem mass spectrometry (LC-MS-MS) tomeasure ultra low drug levels. These subpharmacologicaldoses are not expected to produce any therapeutic or toxiceffects, but yield human pharmacokinetic information. Thesestudies may obviate the need for animal pharmacokineticstudies and can be undertaken before extensive animal toxicitytests. Thus, elaborate animal studies and costly phase 1 humantrials could be avoided for candidate drugs which wouldhave later failed due to unsuitable human pharmacokinetics.Moreover, the pharmacokinetic 0 phase data could be usefulin more precise selection of doses for phase 1 study.
The major objection against phase ‘0’ study is that themicrodose pharmacokinetics may be quite different from thatat pharmacological doses, since body may handle suchdivergent doses in different ways. The phase 0 studies havenot yet been technically fully developed or adequatelyevaluated. They are neither established nor mandatory.However, they are promising, and most regulatory authoritiesare willing to allow and consider them.
Phase II: Therapeutic exploration anddose rangingThis is conducted by physicians who are trainedas clinical investigators, and involve 100–500patients selected according to specific inclusionand exclusion criteria. The primary aim is establish-ment of therapeutic efficacy, dose range and ceilingeffect in a controlled setting. Tolerability andpharmacokinetics are studied as extension of phaseI. The study is mostly controlled and randomized,and may be blinded or open label. It is generallycarried out at 2–4 centres. The candidate drugmay get dropped at this stage if the desired levelof clinical efficacy is not obtained.
Phase III: Therapeutic confirmation/comparison
Generally these are randomized double blindcomparative trials conducted on a larger patientpopulation (500–3000) by several physicians(usually specialists in treating the target disease)at many centres. The aim is to establish the valueof the drug in relation to existing therapy. Safetyand tolerability are assessed on a wider scale,while pharmacokinetic studies may be conductedon some of the participants to enlarge the populationbase of pharmacokinetic data. Indications arefinalized and guidelines for therapeutic use areformulated. A ‘new drug application’ (NDA) issubmitted to the licencing authority, who ifconvinced give marketing permission.
Phase IV: Postmarketing surveillance/studies
After the drug has been marketed for generaluse, practicing physicians are identified throughwhom data are collected on a structured proformaabout the efficacy, acceptability and adverse effectsof the drug (similar to prescription eventmonitoring). Patients treated in the normal courseform the study population: numbers therefore aremuch larger. Uncommon/idiosyncratic adverseeffects, or those that occur only after long-termuse and unsuspected drug interactions are detectedat this stage. Patterns of drug utilization and

81C
HA
PTE
R5
PHARMACOTHERAPY, CLINICAL PHARMACOLOGY AND DRUG DEVELOPMENT
additional indications may emerge from thesurveillance data.
Further therapeutic trials involving specialgroups like children, elderly, pregnant/lactatingwomen, patients with renal/hepatic disease, etc.(which are generally excluded during clinical
PROBLEM DIRECTED STUDY
5.1 A 65-year-old male hepatic cirrhosis patient was admitted to the hospital for treatment ofgross ascites. He was administered inj. furosemide 40 mg i.m. three times a day to excrete theascitic fluid. He responded with brisk diuresis, but on the 3rd day he was found to be talkingirrelevant, was weak and partly disoriented. He had a fainting episode on getting up from thebed. His serum K+ was 2.8 mEq/L (low) and blood pH was 7.6 (raised).(a) What is the likely cause of his condition on the 3rd day?(b) What should be the principles of management of this complication?(see Appendix-1 for solution)
trials) may be undertaken at this stage. Modifiedrelease dosage forms, additional routes ofadministration, fixed dose drug combinations, etc.may be explored.
As such, most drugs continue their develop-ment even after marketing.

Adverse Drug EffectsChapterChapterChapterChapterChapter 66666
Adverse effect is ‘any undesirable or unintendedconsequence of drug administration’. It is a broadterm, includes all kinds of noxious effect—trivial,serious or even fatal.
For the purposes of detecting and quantifyingonly those adverse effects of a drug which areof some import and occur in ordinary therapeuticsetting, the term adverse drug reaction (ADR)has been defined as ‘any noxious change whichis suspected to be due to a drug, occurs at dosesnormally used in man, requires treatment ordecrease in dose or indicates caution in the futureuse of the same drug’. This definition excludestrivial or expected side effects and poisoningsor overdose.
Another term ‘adverse drug event’ (ADE) has been usedto mean ‘any untoward medical occurrence that may presentduring treatment with a medicine, but which does notnecessarily have a causal relationship with the treatment’.The idea is to record all adverse events first, and look forcausality only while analyzing pooled data.
All drugs are capable of producing adverseeffects, and whenever a drug is given a risk istaken. The magnitude of risk has to be consideredalong with the magnitude of expected therapeuticbenefit in deciding whether to use or not to usea particular drug in a given patient, e.g. evenrisk of bone marrow depression may be justifiedin treating cancer, while mild drowsiness causedby an antihistaminic in treating common cold maybe unacceptable.
Adverse effects may develop promptly or onlyafter prolonged medication or even after stoppageof the drug. Adverse effects are not rare; anincidence of 10–25% has been documented indifferent clinical settings. They are more commonwith multiple drug therapy and in the elderly.Adverse effects have been classified in many ways.One may divide them into:
Predictable (Type A or Augmented) reactions(mechanism based adverse reactions) Theseare based on the pharmacological properties ofthe drug, which means that they are augmented,but qualitatively normal response to the drug;include side effects, toxic effects and consequencesof drug withdrawal. They are more common, doserelated and mostly preventable and reversible.
Unpredictable (Type B or Bizarre) reactionsThese are based on peculiarities of the patientand not on drug’s known actions; include allergyand idiosyncrasy. They are less common, oftennon-dose related, generally more serious andrequire withdrawal of the drug. Some of thesereactions can be predicted and prevented if theirgenetic basis is known and suitable test to charac-terize the individual’s phenotype is performed.
Severity of adverse drug reactions has beengraded as:Minor: No therapy, antidote or prolongation ofhospitalization is required.Moderate: Requires change in drug therapy,specific treatment or prolongs hospital stay byatleast one day.Severe: Potentially life-threatening, causes perma-nent damage or requires intensive medical treat-ment.Lethal: Directly or indirectly contributes to deathof the patient.
PharmacovigilancePharmacovigilance has been defined by the WHO(2002) as the ‘science and activities relating tothe detection, assessment, understanding andprevention of adverse effects or any other drugrelated problems.’ The information generated by

83C
HA
PTE
R6
ADVERSE DRUG EFFECTS
pharmacovigilance is useful in educating doctorsabout ADRs and in the official regulation of druguse. Its main purpose is to reduce the risk ofdrug-related harm to the patient. It has animportant role in the rational use of medicines,as it provides the basis for assessing safety ofmedicines.
The activities involved in pharmacovigilanceare:a. Postmarketing surveillance and other methods
of ADR monitoring such as voluntary reportingby doctors (e.g. yellow card system of UK),prescription event monitoring, computerizedmedical record linkage and other cohort/casecontrol studies as well as anecdotal case reportsby doctors.
Voluntary reporting depends on the initiativeand willingness of the health professionals. Itis minimal in India, while even in the developedcountries only ~10% ADRs are reportedvoluntarily. Generally, immediately occurringreactions and those that are dramatic arereported. Though even rare reactions can bedetected by this method, it does not provideincidence of the reaction.
b. Dissemination of ADR data through ‘drugalerts’, ‘medical letters,’ advisories sent todoctors by pharmaceuticals and regulatoryagencies (such as FDA in USA, committeeon safety of medicines in UK).
c. Changes in the labelling of medicines indicatingrestrictions in use or statuary warnings,precautions, or even withdrawal of the drug,by the regulatory decision making authority.Pharmacovigilance centres have been set up in most
countries. The Uppsala Monitoring Centre (Sweden) is theinternational collaborating centre. In India, the Central DrugsStandard Control Organization (CDSCO) is coordinating thepharmacovigilance programme, under which peripheral,regional and zonal monitoring centres have been set up alongwith a National Pharmacovigilance advisory committee. Thepharmacovigilance centres collect, communicate anddisseminate ADR data by linking with hospitals as well aspractitioners and are also expected to provide expertise forassessing causality and severity of ADRs by using standardalgorithms and rating scales like the ‘Naranjo algorithm’(causalilty assessment) and modified Hartwig scale (severitygrading).
Causality assessmentWhen a patient undergoing drug therapy experiences an adverseevent, it may be due to the drug, or the disease or some othercauses. Most of the time, a clear-cut ‘yes/no’ cause and effectrelationship between a drug and the adverse event cannot bepronounced. Causality is assessed on the basis of:• Temporal relationship: How the time-sequence of the
event is related to drug administration.• Previous knowledge: Whether the drug is known to
produce the event in earlier recipients with a certain degreeof consistency.
• Dechallenge: Whether the event subsided on stoppingthe drug.
• Rechallenge: Whether the event reappeared when thedrug was administered again after a gap during whichthe event had subsided. Many times rechallenge isunethical/dangerous, and is not done.Assessed on the basis of the above criteria, causality
has been graded as:1. Definite: Causality is proven.2. Probable: Though not proven, drug is the likely cause
of the event.3. Possible: Drug as well as other causes could be responsible
for the event.4. Doubtful: Drug unlikely to be the cause, but cannot be
ruled out.
Prevention of adverse effects to drugsAdverse drug effects can be minimized but notaltogether eliminated by observing the followingpractices:1. Avoid all inappropriate use of drugs in the
context of patient’s clinical condition.2. Use appropriate dose, route and frequency of
drug administration based on patient’s specificvariables.
3. Elicit and take into consideration previoushistory of drug reactions.
4. Elicit history of allergic diseases and exercisecaution (drug allergy is more common inpatients with allergic diseases).
5. Rule out possibility of drug interactions whenmore than one drug is prescribed.
6. Adopt correct drug administration technique(e.g. intravenous injection of vancomycin mustbe slow).
7. Carry out appropriate laboratory monitoring(e.g. prothrombin time with warfarin, serumdrug levels with lithium).

84S
EC
TIO
N1
GENERAL PHARMACOLOGY
Adverse drug effects may be categorized into:
1. Side effects
These are unwanted but often unavoidable phar-macodynamic effects that occur at therapeuticdoses. Generally, they are not serious, can bepredicted from the pharmacological profile of adrug and are known to occur in a given percentageof drug recipients. Reduction in dose, usuallyameliorates the symptoms.
A side effect may be based on the same actionas the therapeutic effect, e.g. atropine is used inpreanaesthetic medication for its antisecretoryaction. The same action produces dryness of mouthas a side effect. Glyceryl trinitrate relieves anginapectoris by dilating peripheral vasculature whichis also responsible for postural hypotension andthrobbing headache.
The side effect may also be based on adifferent facet of action, e.g. promethazineproduces sedation which is unrelated to itsantiallergic action; estrogens cause nausea whichis unrelated to their antiovulatory action.
An effect may be therapeutic in one contextbut side effect in another context, e.g. codeineused for cough produces constipation as a sideeffect, but the latter is its therapeutic effect intraveller’s diarrhoea; depression of A-V conduc-tion is the desired effect of digoxin in atrialfibrillation, but the same may be undesirable whenit is used for CHF.
Many drugs have been developed from obser-vation of side effects, e.g. early sulfonamides usedas antibacterial were found to produce hypogly-caemia and acidosis as side effects which directedresearch resulting in the development of hypo-glycaemic sulfonylureas and carbonic anhydraseinhibitor—acetazolamide.
2. Secondary effectsThese are indirect consequences of a primaryaction of the drug, e.g. suppression of bacterialflora by tetracyclines paves the way for superin-fections; corticosteroids weaken host defencemechanisms so that latent tuberculosis getsactivated.
3. Toxic effects
These are the result of excessive pharmacologicalaction of the drug due to overdosage or prolon-ged use. Overdosage may be absolute (acciden-tal, homicidal, suicidal) or relative (i.e. usual doseof gentamicin in presence of renal failure). Themanifestations are predictable and dose related.They result from functional alteration (high doseof atropine causing delirium) or drug induced tis-sue damage (hepatic necrosis from paracetamoloverdosage). The CNS, CVS, kidney, liver, lung,skin and blood forming organs are most com-monly involved in drug toxicity.
Toxicity may result from extension of thetherapeutic effect itself, e.g. coma by barbiturates,complete A-V block by digoxin, bleeding dueto heparin.
Another action of the drug can also beresponsible for toxicity, e.g.—• Morphine (analgesic) causes respiratory failure
in overdosage.• Imipramine (antidepressant) overdose causes
cardiac arrhythmia.• Streptomycin (antitubercular) causes vestibular
damage on prolonged use.
Poisoning In a broad sense, poisoning impliesharmful effects of a chemical on a biological system.It may result from large doses of drugs because‘it is the dose which distinguishes a drug froma poison’. Poison is a ‘substance which endangerslife by severely affecting one or more vitalfunctions’. Not only drugs but other householdand industrial chemicals, insecticides, etc. arefrequently involved in poisonings. Specificantidotes such as receptor antagonists, chelatingagents or specific antibodies are available for fewpoisons. General supportive and symptomatictreatment is all that can be done for others, andthis is also important for poisons which have aselective antagonist.The general detoxification and supportivemeasures are:1. Resuscitation and maintenance of vitalfunctionsa. Ensure patent airway, adequate ventilation,

85C
HA
PTE
R6
ADVERSE DRUG EFFECTS
give artificial respiration/100% oxygeninhalation as needed.
b. Maintain blood pressure and heart beat byfluid and crystalloid infusion, pressor agents,cardiac stimulants, pacing, defibrillation, etc,as needed.
c. Maintain body temperature.d. Maintain blood sugar level by dextrose
infusion, especially in patients with alteredsensorium.
2. Termination of exposure (decontami-nation) by removing the patient to fresh air (forinhaled poisons), washing the skin and eyes (forpoisons entering from the surface), induction ofemesis with syrup ipecac or gastric lavage (foringested poisons). Emesis should not be attemptedin comatose or haemodynamically unstablepatient, as well as for kerosene poisoning dueto risk of aspiration into lungs. These proceduresare also contraindicated in corrosive and CNSstimulant poisoning. Emesis/gastric lavage is notrecommended if the patient presents > 2 hoursafter ingesting the poison; if the poison/its doseingested are known to be non life-threatening,or if the patient has vomited after consuming thepoison.3. Prevention of absorption of ingestedpoisons A suspension of 20–40 g (1g/kg) ofactivated charcoal, which has large surfacearea and can adsorb many chemicals, shouldbe administered in 200 ml of water. However,strong acids and alkalies, metallic salts, iodine,cyanide, caustics, alcohol, hydrocarbons and otherorganic solvents are not adsorbed by charcoal.Charcoal should not be administered if there isparalytic ileus or intestinal obstruction or whenthe patient reports > 2 hours after ingesting thepoison.4. Hastening elimination of the poison by indu-cing diuresis (furosemide, mannitol) or alteringurinary pH (alkalinization for acidic drugs, e.g.barbiturates, aspirin). However, excretion of manypoisons is not enhanced by forced diuresis andthis procedure is generally not employed now.Haemodialysis and haemoperfusion (passage of
blood through a column of charcoal or adsorbantresin) are more efficacious procedures.
4. Intolerance
It is the appearance of characteristic toxic effectsof a drug in an individual at therapeutic doses.It is the converse of tolerance and indicates alow threshold of the individual to the action ofa drug. These are individuals who fall on theextreme left side of the Gaussian frequencydistribution curve for sensitivity to the drug.Examples are:• A single dose of triflupromazine induces
muscular dystonias in some individuals,specially children.
• Only few doses of carbamazepine may causeataxia in some people.
• One tablet of chloroquine may cause vomitingand abdominal pain in an occasional patient.
5. Idiosyncrasy
It is genetically determined abnormal reactivityto a chemical. The drug interacts with some uniquefeature of the individual, not found in majorityof subjects, and produces the uncharacteristicreaction. As such, the type of reaction is restrictedto individuals with a particular genotype (see p.65). In addition, certain bizarre drug effects dueto peculiarities of an individual (for which nodefinite genotype has been described) are includedamong idiosyncratic reactions, e.g.:• Barbiturates cause excitement and mental
confusion in some individuals.• Quinine/quinidine cause cramps, diarrhoea,
purpura, asthma and vascular collapse in somepatients.
• Chloramphenicol produces nondose-relatedserious aplastic anaemia in rare individuals.
6. Drug allergy
It is an immunologically mediated reactionproducing stereotype symptoms which are unre-lated to the pharmacodynamic profile of the drug,generally occur even with much smaller dosesand have a different time course of onset and

86S
EC
TIO
N1
GENERAL PHARMACOLOGY
duration. This is also called drug hypersensitivity;but does not refer to increased response whichis called supersensitivity. The target organsprimarily affected in drug allergy are skin, airways,blood vessels, blood and gastrointestinal tract.
Allergic reactions occur only in a smallproportion of the population exposed to the drugand cannot be produced in other individuals atany dose. Prior sensitization is needed and a latentperiod of at least 1–2 weeks is required afterthe first exposure. The drug or its metabolite actsas antigen (AG) or more commonly hapten(incomplete antigen: drugs have small moleculeswhich become antigenic only after binding withan endogenous protein) and induce productionof antibody (AB)/sensitized lymphocytes. Pre-sence of AB to a drug is not necessarily followedby allergy to it. Chemically related drugs oftenshow cross sensitivity. One drug can producedifferent types of allergic reactions in differentindividuals, while widely different drugs canproduce the same reaction. The course of drugallergy is variable; an individual previouslysensitive to a drug may subsequently tolerate itwithout a reaction and vice versa.
prostaglandins, PAF, etc. resulting in urticaria,itching, angioedema, bronchospasm, rhinitis oranaphylactic shock. Anaphylaxis is usuallyheralded by paresthesia, flushing, swelling of lips,generalized itching, wheezing, palpitationfollowed by syncope. The manifestations occurquickly after challenge and are called immediatehypersensitivity. Antihistaminic drugs are bene-ficial in some of these reactions.
Type-II (cytolytic) reactions Drug + compo-nent of a specific tissue cell act as AG. Theresulting antibodies (IgG, IgM) bind to the targetcells; on reexposure AG: AB reaction takes placeon the surface of these cells, complement is acti-vated and cytolysis occurs, e.g. thrombocytopenia,agranulocytosis, aplastic anaemia, haemolysis,organ damage (liver, kidney, muscle), systemiclupus erythematosus.
Type-III (retarded, Arthus) reactions These aremediated by circulating antibodies (predominan-tly IgG, mopping AB). AG: AB complexes bindcomplement and precipitate on vascular endo-thelium giving rise to a destructive inflammatoryresponse. Manifestations are rashes, serum sick-ness (fever, arthralgia, lymphadenopathy), poly-arteritis nodosa, Stevens-Johnson syndrome(erythema multiforme, arthritis, nephritis, myo-carditis, mental symptoms). The reaction usuallysubsides in 1–2 weeks.
B. Cell mediated
Type-IV (delayed hypersensitivity) reactionsThese are mediated through production ofsensitized T-lymphocytes carrying receptors forthe AG. On contact with the AG these T cellsproduce lymphokines which attract granulocytesand generate an inflammatory response, e.g.contact dermatitis, some rashes, fever, photo-sensitization. The reaction generally takes > 12hours to develop.
Treatment of drug allergyThe offending drug must be immediately stopped.Most mild reactions (like skin rashes) subside
Cardinal features of drug allergy
• Manifestations unrelated to the pharmacodynamicactions of the drug.
• Manifestations similar to food/protein allergy, allergicdiseases.
• Severity of reaction poorly correlated with dose of thedrug; even small dose may trigger severe reaction.
• Occur only in few recipients, cannot be producedin other individuals.
• Prior sensitization (known/unknown) is needed.• Positive dechallenge (on withdrawal of drug) and
rechallenge (even with small dose).
Mechanism and types of allergic reactions
A. Humoral
Type-I (anaphylactic) reactions Reaginic anti-bodies (IgE) are produced which get fixed to themast cells. On exposure to the drug, AG: ABreaction takes place on the mast cell surface (seeFig. 11.2) releasing mediators like histamine,5-HT, leukotrienes (especially LT-C4 and D4),

87C
HA
PTE
R6
ADVERSE DRUG EFFECTS
by themselves and donot require specifictreatment. Antihistamines (H1) are beneficial insome type I reactions (urticaria, rhinitis, swellingof lips, etc.) and some skin rashes (see p. 167).In case of anaphylactic shock or angioedema oflarynx the resuscitation council of UK hasrecommended the following measures:• Put the patient in reclining position, admini-
ster oxygen at high flow rate and performcardiopulmonary resuscitation if required.
• Inject adrenaline 0.5 mg (0.5 ml of 1 in 1000solution for adult, 0.3 ml for child 6-12 yearsand 0.15 ml for child upto 6 years) i.m.; repeatevery 5–10 min in case patient does notimprove or improvement is transient. This isthe only life saving measure. Adrenaline shouldnot be injected i.v. (can itself be fatal) unlessshock is immediately life threatening. Ifadrenaline is to be injected i.v., it should bediluted to 1:10,000 or 1:100,000 and infusedslowly with constant monitoring.
• Administer a H1 antihistaminic (chlorpheni-ramine 10–20 mg) i.m./slow i.v. It may haveadjuvant value.
• Intravenous glucocorticoid (hydrocortisonesod. succinate 200 mg) should be added insevere/recurrent cases. It acts slowly, but isspecially valuable for prolonged reactions andin asthmatics. It may be followed by oralprednisolone for 3 days.
Adrenaline followed by a short course ofglucocorticoids is indicated for bronchospasmattending drug hypersensitivity. Glucocorticoidsare the only drug effective in type II, type III andtype IV reactions.
Skin tests (intradermal, patch) or intranasaltests may forewarn in case of Type I hypersen-sitivity, but not in case of other types. However,
these tests are not entirely reliable—false positiveand false negative results are not rare.
7. Photosensitivity
It is a cutaneous reaction resulting from druginduced sensitization of the skin to UV radiation.The reactions are of two types:
(a) Phototoxic Drug or its metabolite accumu-lates in the skin, absorbs light and undergoes aphotochemical reaction followed by a photobio-logical reaction resulting in local tissue damage(sunburn-like), i.e. erythema, edema, blisteringwhich have fast onset and shorter duration afterexposure ends. This is followed by hyperpigmen-tation and desquamation. The lesions may be moresevere with larger doses of the drug. The shorterwave lengths (290–320 nm, UV-B) are respon-sible. Drugs involved in acute phototoxic reactionsare tetracyclines (especially demeclocycline) andtar products. Drugs causing chronic and low gradesensitization are nalidixic acid, fluoroquinolones,dapsone, sulfonamides, phenothiazines, thiazides,amiodarone. This type of reaction is more commonthan photoallergic reaction.
(b) Photoallergic Drug or its metabolite inducesa cell mediated immune response which onexposure to light of longer wave lengths (320–400nm, UV-A) produces a papular or eczematouscontact dermatitis like picture that may persist longafter exposure. Rarely antibodies mediate photo-allergy and the reaction takes the form of immediateflare, itching and wheal on exposure to sun. Evensmall doses may trigger the reaction and lesions mayextend beyond the exposed area. Drugs involvedare sulfonamides, sulfonylureas, griseofulvin,chloroquine, chlorpromazine, carbamazepine.
8. Drug dependenceDrugs capable of altering mood and feelings areliable to repetitive use to derive euphoria,recreation, withdrawal from reality, socialadjustment, etc. Drug dependence is a state inwhich use of drugs for personal satisfaction isaccorded a higher priority than other basic needs,often in the face of known risks to health.
Drugs frequently causing allergic reactions
Penicillins SalicylatesCephalosporins CarbamazepineSulfonamides AllopurinolTetracyclines ACE inhibitorsQuinolones MethyldopaAntitubercular drugs HydralazinePhenothiazines Local anaesthetics

88S
EC
TIO
N1
GENERAL PHARMACOLOGY
There is a lot of confusion in terminologyand definitions; the following may serve todescribe different aspects of the problem.
Psychological dependence It is said to havedeveloped when the individual believes thatoptimal state of wellbeing is achieved only throughthe actions of the drug. The subject feelsemotionally distressed if the drug is not taken.It may start as liking for the drug effects andmay progress to compulsive drug use in someindividuals who then lose control over the useof the drug. The intensity of psychologicaldependence may vary from desire to craving.Obviously, certain degree of psychologicaldependence accompanies all patterns of selfmedication.
Reinforcement is the ability of the drug toproduce effects that the user enjoys and whichmake him/her wish to take it again or to inducedrug seeking behaviour. Certain drugs (opioids,cocaine) are strong reinforcers, while others(benzodiazepines) are weak reinforcers. Faster thedrug acts, more reinforcing it is. Thus, inhaleddrugs and those injected i.v. are highly reinforcing—produce an intense ‘high’ in dependent individuals.
Physical dependence It is an altered physio-logical state produced by repeated administrationof a drug which necessitates the continuedpresence of the drug to maintain physiologicalequilibrium. Discontinuation of the drug resultsin a characteristic withdrawal (abstinence) syn-drome. Since the essence of the process isadaptation of the nervous system to functionnormally in the presence of the drug, it has beencalled ‘neuroadaptation’.
Drugs producing physical dependence are—opioids, barbiturates and other depressants inc-luding alcohol and benzodiazepines. Stimulantdrugs, e.g. amphetamines, cocaine produce littleor no physical dependence.
Drug abuse Refers to use of a drug by self-medication in a manner and amount that deviatesfrom the approved medical and social patternsin a given culture at a given time. The term conveys
social disapproval of the manner and purpose ofdrug use. For regulatory agencies, drug abuserefers to any use of an ilicit drug.
The two major patterns of drug abuse are:a. Continuous use: The drug is taken regularly,
the subject wishes to continuously remain underthe influence of the drug, e.g. opioids, alcohol,sedatives.
b. Occasional use: The drug is taken off andon to obtain pleasure or high, recreation (asin rave parties) or enhancement of sexualexperience, e.g. cocaine, amphetamines, psy-chedelics, binge drinking (alcohol), cannabis,solvents (inhalation), etc.
Drug addiction It is a pattern of compulsivedrug use characterized by overwhelminginvolvement with the use of a drug. Procuringthe drug and using it takes precedence overother activities. Even after withdrawal most addictstend to relapse. Physical dependence, though astrong impetus for continued drug use, is not anessential feature of addiction. Amphetamines,cocaine, cannabis, LSD are drugs which produceaddiction but little/no physical dependence. Onthe other hand, drugs like nalorphine producephysical dependence without imparting addictionin the sense that there is little drug seekingbehaviour.
Drug habituation It denotes less intensiveinvolvement with the drug, so that its withdrawalproduces only mild discomfort. Consumption oftea, coffee, tobacco, social drinking are regardedhabituating, physical dependence is absent.
Basically, habituation and addiction implydifferent degrees of psychological dependence andit may be difficult to draw a clearcut line ofdistinction between the two. Therefore, it is betterto avoid using these terms in describing drugdependence and related conditions.
9. Drug withdrawal reactionsApart from drugs that are usually recognised asproducing dependence, sudden interruption oftherapy with certain other drugs also results inadverse consequences, mostly in the form of

89C
HA
PTE
R6
ADVERSE DRUG EFFECTS
worsening of the clinical condition for which thedrug was being used, e.g.:
(i) Acute adrenal insufficiency may be precipi-tated by abrupt cessation of corticosteroidtherapy.
(ii) Severe hypertension, restlessness andsympathetic overactivity may occur shortlyafter discontinuing clonidine.
(iii) Worsening of angina pectoris, precipitationof myocardial infarction may result fromstoppage of β blockers.
(iv) Frequency of seizures may increase onsudden withdrawal of an antiepileptic.
These manifestations are also due to adaptivechanges and can be minimized by gradual with-drawal.
10. Teratogenicity
It refers to the capacity of a drug to cause foetalabnormalities when administered to the pregnantmother. The placenta does not constitute a strictbarrier, and any drug can cross it to a greateror lesser extent. The embryo is one of the mostdynamic biological systems and in contrast toadults, drug effects are often irreversible. Thethalidomide disaster (1958–61) resulting inthousands of babies born with phocomelia (seal
like limbs) and other defects focused attentiononto this type of adverse effect.
Drugs can affect the foetus at 3 stages—(i) Fertilization and implantation—conception
to 17 days—failure of pregnancy which oftengoes unnoticed.
(ii) Organogenesis—18 to 55 days of gesta-tion—most vulnerable period, deformitiesare produced.
(iii) Growth and development—56 days onwards— developmental and functional abnorma-lities can occur, e.g. ACE inhibitors can causehypoplasia of organs, especially of lungs andkidneys; NSAIDs may induce prematureclosure of ductus arteriosus; androgens andprogestins cause masculanization of femalefoetus, antithyroid drugs and lithium causefoetal goiter.
The type of malformation depends on the drugas well as the stage at which exposure to theteratogen occurred. Foetal exposure depends onthe blood level and duration for which the drugremains in maternal circulation. The teratogenicpotential of a drug is to be considered againstthe background of congenital abnormalitiesoccurring spontaneously, which is ~ 2% of allpregnancies. Majority of implicated drugs are low
Human teratogenic drugs
Drug Abnormality
Thalidomide phocomelia, multiple defects of internal organsAnticancer drugs cleft palate, hydrocephalus, multiple defects, foetal death(methotrexate)Androgens virilization; limb, esophageal, cardiac defectsProgestins virilization of female foetusStilboestrol vaginal carcinoma in teenage female offspringTetracyclines discoloured and deformed teeth, retarded bone growthWarfarin depressed nose; eye and hand defects, growth retardationPhenytoin hypoplastic phalanges, cleft lip/palate, microcephalyPhenobarbitone various malformationsCarbamazepine neural tube defects, assorted abnormalitiesValproate sod. spina bifida and other neural tube defects, heart and limb
abnormalitiesAlcohol low IQ baby, growth retardation, foetal alcohol syndromeACE inhibitors hypoplasia of organs, growth retardation, foetal loss Lithium foetal goiter, cardiac and other abnormalitiesAntithyroid drugs foetal goiter and hypothyroidismIndomethacin/aspirin premature closure of ductus arteriosusIsotretinoin craniofacial, heart and CNS defects, hydrocephalus

90S
EC
TIO
N1
GENERAL PHARMACOLOGY
Risk category of drugs during pregnancy*
Category Examples
A Adequate studies in pregnant women have failed Inj. Mag. sulfate,No risk to demonstrate a risk to the foetus thyroxine
B Adequate human studies are lacking, but animal studies Penicillin V,No evidence have failed to demonstrate a risk to the foetus amoxicillin,
of risk or cefactor,in humans Adequate studies in pregnant women have failed to erythromycin,
demonstrate a risk to the foetus, but animal studies have paracetamol,shown an adverse effect on the foetus lidocaine
C No adequate studies in pregnant women, and animal studies Morphine,Risk are lacking or have shown an adverse effect on foetus, codeine,
cannot be but potential benefit may warrant use of the drug in pregnant atropine,ruled old women despite potential risk corticosteroids,
adrenaline,thiopentone,bupivacaine
D There is evidence of human foetal risk, but the potential Aspirin,Benefit may benefits from use of the drug may be acceptable despite phenytoin,out weigh the potential risk carbamazepine,potential valproate,
risk lorazepam,methotrexate
X Studies in animals or humans have demonstrated foetal Estrogens,Contra- abnormalities, and potential risk clearly outweighs isotretinoin,
indicated possible benefit ergometrinethalidomide
* As per US-FDA.
grade teratogens, i.e. increase the incidence ofmalformations only slightly, which may be verydifficult to detect, confirm or refute. Nevertheless,some drugs have been clearly associated withcausing foetal abnormalities in human beings.These are listed in the box. However, only fewmothers out of all those who receive these drugsduring the vulnerable period will get a deformedbaby, but the exact risk posed by a drug is difficultto estimate.
The US-FDA has graded the documentationof risk for causing birth defects into five categories(see box).
It is, therefore, wise to avoid all drugs duringpregnancy unless compelling reasons exist for theiruse regardless of the assigned pregnancy category,or presumed safety (also see Appendix-3).
Frequency of spontaneous as well as druginduced malformations, especially neural tubedefects, may be reduced by folate therapy duringpregnancy.
11. Mutagenicity and Carcinogenicity
It refers to capacity of a drug to cause geneticdefects and cancer respectively. Usually oxidationof the drug results in the production of reactiveintermediates which affect genes and may causestructural changes in the chromosomes. Covalentinteraction with DNA can modify it to inducemutations, which may manifest as heritable defectsin the next generation. If the modified DNAsequences code for factors that regulate cellproliferation/growth, i.e. are protooncogenes, or for

91C
HA
PTE
R6
ADVERSE DRUG EFFECTS
PROBLEM DIRECTED STUDY
proteins that inhibit transcription of protoon-cogenes, a tumour (cancer) may be produced. Evenwithout interacting directly with DNA, certainchemicals can promote malignant change ingenetically damaged cells, resulting in carcino-genesis. Chemical carcinogenesis generally takesseveral (10–40) years to develop. Drugs implicatedin these adverse effects are—anticancer drugs,radioisotopes, estrogens, tobacco. Generally, drugswhich show mutagenic or carcinogenic potentialare not approved for marketing/are withdrawn,unless they are useful in life-threatening conditions.
12. Drug induced diseases
These are also called iatrogenic (physician indu-ced) diseases, and are functional disturbances(disease) caused by drugs which persist even afterthe offending drug has been withdrawn and largelyeliminated, e.g.:
Peptic ulcer by salicylates and corticosteroids.Parkinsonism by phenothiazines and otherantipsychotics.Hepatitis by isoniazid.DLE by hydralazine.
6.1 A 40-year-man weighing 60 kg suffering from chronic cough with expectoration and feverwas diagnosed to have cavitary pulmonary tuberculosis. He was put on the standard 1st lineantitubercular regimen consisting of isoniazid (H) + rifampin (R) + pyrazinamide (Z) + ethambutol(E). His condition improved, but in the 4th week he developed jaundice with enlarged tenderliver and rise in serum bilirubin as well as serum transaminase levels. He was suspected to havedeveloped antitubercular drug induced hepatitis.(a) Should his antitubercular treatment be stopped or continued?(b) How would you proceed to confirm and identify the causative drug, and then select thealternative regimen?(see Appendix-1 for solution)

Autonomic Nervous System:General Considerations
SECTION 2
DRUGS ACTING ON AUTONOMIC
NERVOUS SYSTEM
ORGANIZATION AND FUNCTION
The autonomic nervous system (ANS) functionslargely below the level of consciousness andcontrols visceral functions. The major differen-ces between the somatic and autonomic nervoussystems are given in Table II.1.
Like the somatic nervous system, the ANSconsists of afferents, centre and efferents.
Autonomic afferents Most visceral nervesare mixed nerves and carry nonmyelinatedvisceral afferent fibres as well. The cell bodiesof these afferent fibres are located in the dorsalroot ganglion of spinal nerves and in the sensoryganglia (e.g. nodose ganglion of vagus) of cranialnerves. They mediate visceral pain as well ascardiovascular, respiratory and other visceralreflexes.
Central autonomic connections There areno exclusively autonomic areas in the CNS;considerable intermixing and integration ofsomatic and autonomic innervation occurs. Thehighest seat regulating autonomic functions isin the hypothalamus—posterior and lateral nucleiare primarily sympathetic while anterior andmedial nuclei are primarily parasympathetic.Many autonomic centres (pupillary, vagal, res-piratory, etc.) are located in the mid-brain andthe medulla in relation to the cranial nerves. Thelateral column in the thoracic spinal cordcontains cells which give rise to the sympatheticoutflow.
Autonomic efferents The motor limb of theANS is anatomically divided into sympatheticand parasympathetic. Many organs receive bothsympathetic and parasympathetic innervation and
TABLE II.1 Differences between somatic and autonomic nervous system
Somatic Autonomic
1. Organ supplied Skeletal muscles All other organs
2. Distal most synapse Within CNS Outside CNS (in ganglia)
3. Nerve fibres Myelinated Pregang.—myelinatedPostgang.—non-myelinated
4. Peripheral plexus formation Absent Present
5. Primary efferent transmitter Acetylcholine Acetylcholine, Noradrenaline
6. Effect of nerve section on Paralysis and atrophy Activity maintained, no atrophyorgan supplied
Chapter 7a

93SEC
TION
2ANS: GENERAL CONSIDERATIONS
the two subdivisions are functionally antagonisticin majority of these. The level of activity ofinnervated organ at a given moment is the alge-braic sum of sympathetic and parasympathetictone. However, refractory period of atrial fibresis decreased by sympathetic as well as parasym-pathetic influences. Most blood vessels, spleen,sweat glands and hair follicles receive only sym-pathetic, while ciliary muscle, bronchial smoothmuscle, gastric and pancreatic glands receiveonly parasympathetic innervation. Thus, the twodivisions of ANS are not merely check-and-balance physiological antagonists of each other.
Enteric nervous system
The enteric plexus of nerves receives inputs fromboth sympathetic and parasympathetic divisionsof ANS, but in addition functions independently
to integrate bowel movements as well as regulatesecretion and absorption (see Fig. 47.2). As such,it has also been labelled as a distinct ‘entericnervous system’.
The general layout of ANS is depicted inFig. II.1 and the important differences betweenits two subdivisions are given in Table II.2.
NEUROHUMORAL TRANSMISSION
Neurohumoral transmission implies that nervestransmit their message across synapses andneuroeffector junctions by the release of humoral(chemical) messengers.
Junctional transmission was thought to beelectrical (it does occur in some lower animalsand probably in certain areas of mammalianbrain) but observations at the turn of last centuryprompted Elliott (1905) to suggest that
Fig. II.1: The general outlay of efferent autonomic nervous system. The transmitter released and theprimary postjunctional receptor subtype is shown at each synapse/neuroeffector junction
ACh= Acetylcholine, NA= Noradrenaline, N = Nicotinic, M = Muscarinic, = adrenergic, = adrenergic
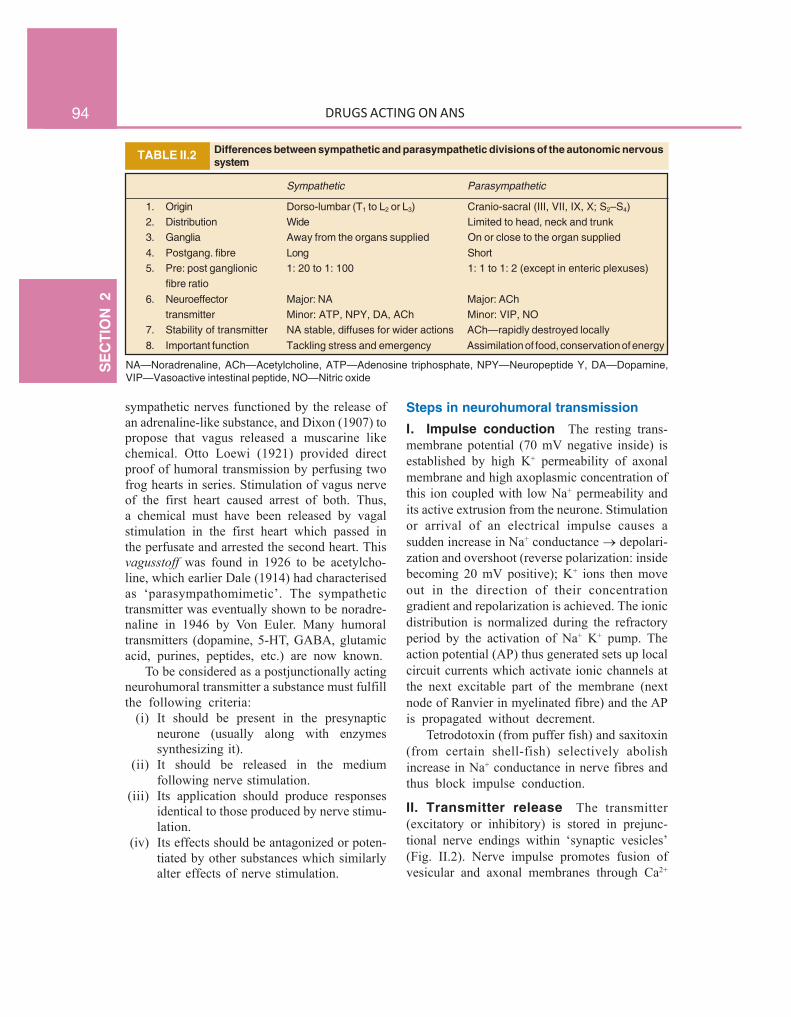
94S
EC
TIO
N2
DRUGS ACTING ON ANS
TABLE II.2 Differences between sympathetic and parasympathetic divisions of the autonomic nervoussystem
Sympathetic Parasympathetic
1. Origin Dorso-lumbar (T1 to L2 or L3) Cranio-sacral (III, VII, IX, X; S2–S4)2. Distribution Wide Limited to head, neck and trunk3. Ganglia Away from the organs supplied On or close to the organ supplied4. Postgang. fibre Long Short5. Pre: post ganglionic 1: 20 to 1: 100 1: 1 to 1: 2 (except in enteric plexuses)
fibre ratio6. Neuroeffector Major: NA Major: ACh
transmitter Minor: ATP, NPY, DA, ACh Minor: VIP, NO7. Stability of transmitter NA stable, diffuses for wider actions ACh—rapidly destroyed locally8. Important function Tackling stress and emergency Assimilation of food, conservation of energy
NA—Noradrenaline, ACh—Acetylcholine, ATP—Adenosine triphosphate, NPY—Neuropeptide Y, DA—Dopamine,VIP—Vasoactive intestinal peptide, NO—Nitric oxide
sympathetic nerves functioned by the release ofan adrenaline-like substance, and Dixon (1907) topropose that vagus released a muscarine likechemical. Otto Loewi (1921) provided directproof of humoral transmission by perfusing twofrog hearts in series. Stimulation of vagus nerveof the first heart caused arrest of both. Thus,a chemical must have been released by vagalstimulation in the first heart which passed inthe perfusate and arrested the second heart. Thisvagusstoff was found in 1926 to be acetylcho-line, which earlier Dale (1914) had characterisedas ‘parasympathomimetic’. The sympathetictransmitter was eventually shown to be noradre-naline in 1946 by Von Euler. Many humoraltransmitters (dopamine, 5-HT, GABA, glutamicacid, purines, peptides, etc.) are now known.
To be considered as a postjunctionally actingneurohumoral transmitter a substance must fulfillthe following criteria:
(i) It should be present in the presynapticneurone (usually along with enzymessynthesizing it).
(ii) It should be released in the mediumfollowing nerve stimulation.
(iii) Its application should produce responsesidentical to those produced by nerve stimu-lation.
(iv) Its effects should be antagonized or poten-tiated by other substances which similarlyalter effects of nerve stimulation.
Steps in neurohumoral transmissionI. Impulse conduction The resting trans-membrane potential (70 mV negative inside) isestablished by high K+ permeability of axonalmembrane and high axoplasmic concentration ofthis ion coupled with low Na+ permeability andits active extrusion from the neurone. Stimulationor arrival of an electrical impulse causes asudden increase in Na+ conductance depolari-zation and overshoot (reverse polarization: insidebecoming 20 mV positive); K+ ions then moveout in the direction of their concentrationgradient and repolarization is achieved. The ionicdistribution is normalized during the refractoryperiod by the activation of Na+ K+ pump. Theaction potential (AP) thus generated sets up localcircuit currents which activate ionic channels atthe next excitable part of the membrane (nextnode of Ranvier in myelinated fibre) and the APis propagated without decrement.
Tetrodotoxin (from puffer fish) and saxitoxin(from certain shell-fish) selectively abolishincrease in Na+ conductance in nerve fibres andthus block impulse conduction.
II. Transmitter release The transmitter(excitatory or inhibitory) is stored in prejunc-tional nerve endings within ‘synaptic vesicles’(Fig. II.2). Nerve impulse promotes fusion ofvesicular and axonal membranes through Ca2+

95SEC
TION
2ANS: GENERAL CONSIDERATIONS
Fig. II.2: Diagrammatic representation of steps in excitatory and inhibitory neurohumoral transmission:EPSP = Excitatory postsynaptic potential; IPSP = Inhibitory postsynaptic potential
entry which fluidizes membranes. All contents ofthe vesicle (transmitter, enzymes and otherproteins) are extruded (exocytosis) in thejunctional cleft.A number of proteins like synaptotagmin, synaptobrevin,neurexin, syntaxin and synaptophysin located on the vesicularand axonal membranes have been found to participate in thedocking and fusion of the synaptic vesicles with the axonalmembrane resulting in exocytosis. These proteins can be targetsof drug action to modify junctional transmission.
While majority of the neurotransmitters are preformed,kept stored in synaptic vesicles and released on activationby exocytosis as outlined above, some mediators likeNO, prostaglandins, endocannabinoids are synthesized ondemand and reach their target by diffusion or by activetransport.
The release process can be modulated by thetransmitter itself and by other agents throughactivation of specific receptors located on theprejunctional membrane, e.g. noradrenaline (NA)release is inhibited by NA (2 receptor), dopa-mine, adenosine, prostaglandins and enkephalinswhile isoprenaline (2 receptor) and angiotensin(AT1 receptor) increase NA release. Similarly,
2 and muscarinic agonists inhibit acetylcholine(ACh) release at autonomic neuroeffector sites(but not in ganglia and skeletal muscles).
III. Transmitter action on postjunctionalmembrane The released transmitter com-bines with specific receptors on the post-junctional membrane and depending on its natureinduces an excitatory postsynaptic potential(EPSP) or an inhibitory postsynaptic potential(IPSP).
EPSP Increase in permeability to cations Na+ or Ca2+ influx (through fast or slow channels)causes depolarization followed by K+ efflux.These ionic movements are passive as the flowis down the concentration gradients.
IPSP Increase in permeability to anions, sothat Cl¯ ions move in (axonal Cl¯ concentrationis lower than its extracellular concentration) andtend to hyperpolarize the membrane an IPSPis generated. Stabilization of the membrane orhyperpolarization can also result from selective

96S
EC
TIO
N2
DRUGS ACTING ON ANS
Fig. II.3: Mechanisms of termination of transmitter actionA. Parasympathetic neurone: The primary transmitter acetylcholine (ACh) is rapidly hydrolysed by a specific enzymeacetylcholinesterase (AChE) located strategically on the synaptic membrane. A common co-transmitter is vasoactiveintestinal peptide (VIP), which on release diffuses slowly to be degraded by peptidases at distant sites. It may act on thesame as well as neighbouring effectors.B. Sympathetic neurone: The primary transmitter noradrenaline (NA) is largely taken back into the neurone by membrane-bound norepinephrine transporter (NET) and recycled. A minor fraction diffuses away. One of the cotransmitters isneuropeptide Y (NPY), which on release meets the same fate as VIP.C. Gabaergic neurone: The amino acid transmitter gamma-aminobutyric acid (GABA) released into the synaptic cleftis partly taken up into the neurone by GABA transporter (GAT), as well as into neighbouring glial cells. Some of itdissipates by diffusion.

97SEC
TION
2ANS: GENERAL CONSIDERATIONS
Fig. II.4: CotransmissionThe cotransmitter is stored in the prejunctional nerveterminal alongwith the primary transmitter, but in separatevesicles (in some cases in the same vesicle itself). Nerveimpulse releases both the transmitters concurrently. Actingon its own receptors, the cotransmitter modifies responsi-veness of the effector to the primary transmitter or subs-titutes for it. Cotransmitter may also act on prejunctionalreceptors and modulate release of the transmitters
increase in permeability to K+ ions, which moveout carrying +ive charges.
In addition, a trophic influence on junctionalmorphology and functional status is exerted bythe background basal release of the transmitter.
IV. Postjunctional activity A suprathresholdEPSP generates a propagated postjunctional APwhich results in nerve impulse (in neurone),contraction (in muscle) or secretion (in gland).An IPSP stabilizes the postjunctional membraneand resists depolarizing stimuli.
V. Termination of transmitter action Thevarious mechanisms of termination of transmitteraction are depicted in Fig. II.3. Following itscombination with the receptor, the transmitteris either locally degraded (e.g. ACh) or is partlytaken back into the prejunctional neurone byactive reuptake and partly diffuses away (e.g.NA). Specific carrier proteins like norepinep-hrine transporter (NET), dopamine transporter(DAT), serotonin transporter (SERT) are expres-sed on the axonal membrane for this purpose.The rate of termination of transmitter actiongoverns the rate at which responses can betransmitted across a junction (1 to 1000/sec).
Aminoacid transmitters (glutamate, GABA)are also partly taken up by active transport intoneuronal and neighbouring glial cells, but noactive reuptake of peptide neurotransmitters (VIP,NPY, enkephalins, etc.) occurs. They diffuseaway and are broken down by peptidases at distantsites.
CotransmissionIt has now become apparent that the classical‘one neurone—one transmitter’ model is an oversimplification. Most peripheral and centralneurones on stimulation have been shown torelease more than one active substance. In theANS, besides the primary transmitters ACh andNA, neurones have been found to elaboratepurines (ATP, adenosine), peptides (vasoactiveintestinal peptide or VIP, neuropeptide-Y or NPY,substance P, enkephalins, somatostatin, etc.),nitric oxide (NO) and prostaglandins as co-
transmitters. In most autonomic cholinergicneurones VIP is associated with ACh, while ATPis associated with both ACh and NA. Thetransmitter at some parasympathetic sites is NO,and these are called nitrergic nerves. Vascularadrenergic nerves contain NPY which causeslong lasting vasoconstriction. The cotransmitteris stored in the same neurone but in distinctsynaptic vesicles or locations (Fig. II.4).However, ATP is stored with NA in the samevesicle. On being released by nerve impulse thecontransmitter may serve to regulate thepresynaptic release of the primary transmitterand/or postsynaptic sensitivity to it (neuro-modulator role). The cotransmitter may alsoserve as an alternative transmitter in its own rightand/or exert a trophic influence on the synapticstructures.
Nonadrenergic, noncholinergic (NANC)transmission has been demonstrated in theautonomic innervation of the gut, vas deferens,

98S
EC
TIO
N2
DRUGS ACTING ON ANS
urinary tract, salivary glands and certain bloodvessels, where nerve stimulation is able to evokelimited responses even in the presence of totaladrenergic and cholinergic blockade. Forexample, it has been shown that stimulation ofsympathetic nerve to guinea pig vas deferenselicits a biphasic contractile response, the initialshort-lasting phase of which is mediated by ATP(through P2 receptors) and the second longerlasting phase by NA (through 1 receptors).
The time-course of action of the primarytransmitter and the cotransmitter is usually
different. The cotransmitter VIP of parasympa-thetic neurones produces a slow and long-lastingresponse, while another one (NO) has anintermediate time-course of action between VIPand ACh (fast acting). Similarly, in sympatheticneurones, the cotransmitter NPY is slower actingand ATP faster acting than NA. Moreover,cotransmitters like NO, VIP, NPY diffuse to awider area, and can affect receptors at somedistance from the site of release.
Many anomalous findings have been explainedby the revelation of cotransmission.

Cholinergic System and DrugsChapter 7b
CHOLINERGIC TRANSMISSION
Acetylcholine (ACh) is a major neurohumoraltransmitter at autonomic, somatic as well as centralsites. These sites are listed in Table 7.1
Synthesis, storage and destruction of AChThe cholinergic neuronal mechanisms are sum-marized in Fig. 7.1.
Acetylcholine is synthesized locally in the cho-linergic nerve endings by the following pathway—
ATP + Acetate + CoEn-A
Acetate activating reaction
Acetyl CoEn-A
CHOLINECholine acetyl transferase
ACETYLCHOLINE + CoEn-A
CH3 O | || Cl¯
CH3—N+—CH2—CH2—O—C—CH3 |C H 3
ACETYLCHOLINE CHLORIDE
Choline is actively taken up by the axonalmembrane by a Na+: choline cotransporter andacetylated with the help of ATP and coenzyme-A by the enzyme choline acetyl transferase presentin the axoplasm. Hemicholinium (HC3) blockscholine uptake (the rate limiting step in AChsynthesis) and depletes ACh. Most of the AChis stored in ionic solution within small synapticvesicles, but some free ACh is also present inthe cytoplasm of cholinergic terminals. Activetransport of ACh into synaptic vesicles is effectedby another carrier which is blocked by vesamicol.
Release of ACh from nerve terminals occursin small quanta—amount contained in individualvesicles is extruded by exocytosis. In response
to a nerve AP synchronous release of multiplequanta triggers postjunctional events.
Two toxins interfere with cholinergic trans-mission by affecting release: botulinum toxin inhi-bits release, while black widow spider toxininduces massive release and depletion.
Botulinum toxinBotulinum toxin A and B are highly potent exotoxins producedby Clostridium botulinum that are responsible for ‘botulism’(a type of food poisoning). These neurotoxic proteins causelong-lasting loss of cholinergic transmission by interactingwith axonal proteins involved in exocytotic release of ACh.Localized injection of minute quantity of botulinum toxinA (BOTOX) or its haemagglutinin complex (DYSPORT) canbe used in the treatment of a number of spastic and otherneurological conditions due to overactivity of cholinergicnerves, like blepharospasm, spastic cerebral palsy, strabismus,spasmodic torticollis, nystagmus, hemifacial spasm, poststroke spasticity, spasmodic dysphonia, axillary hyperhydrosis,etc. It is increasing being employed as beauty treatment byremoval of age-related facial wrinkles. However, its incorrectinjection or overdose can be dangerous; ptosis, diplopia, facialswelling, dry mouth, dysphagia, dysarthria, muscular weaknessand even respiratory paralysis has occurred.
Cholinesterase Immediately after release, AChis hydrolyzed by the enzyme cholinesterase andcholine is recycled. A specific (Acetylcholines-terase—AChE or true cholinesterase) and anonspecific (Butyrylcholinesterase—BuChE orpseudocholinesterase) type of enzyme occurs inthe body; important differences between these twotypes of the enzyme are given in Table 7.2. WhileAChE is strategically located at all cholinergicsites and serves to inactivate ACh instantaneously,BuChE present in plasma and elsewhere probablyserves to metabolize ingested esters.
Acetylcholine
Cholinesterase
Choline + Acetate

100S
EC
TIO
N2
DRUGS ACTING ON ANS
TABLE 7.1 Sites of cholinergic transmission and type of receptor involved
Site Type of receptor Selective agonist Selective antagonist
1. a. All postganglionic parasymp.b. Few postganglionic symp. (sweat Muscarinic Muscarine Atropine
glands, some blood vessels)
2. a. Ganglia (both symp. andparasymp). Nicotinic (NN) DMPP* Hexamethonium
b. Adrenal medulla
3. Skeletal muscles Nicotinic (NM) PTMA** d-tubocurarine
4. CNS (cortex, basal ganglia, spinal Muscarinic Muscarine/ Atropinecord and other sites) Oxotremorine
Nicotinic Carbachol d-tubocurarine
* DMPP—Dimethyl phenyl piperazinium** PTMA—Phenyl trimethyl ammonium
Fig. 7.1: Cholinergic neuronal mechanismsMinus sign indicates inhibition while bold blue arrowindicates active transportCh—Choline, ACh—Acetylcholine, ChAT—Cholineacetyl transferase, AChE—Acetylcholinesterase, Anti-ChE—Anticholinesterase, M—Muscarinic receptor, N—Nicotinic receptor, HC3—Hemicholinium, BoT—Botulinum toxin, Vsa—Vesamicol, Na+ChT—Na+–CholineCotransporter.
CholinoceptorsTwo classes of receptors for ACh are recognised—muscarinic and nicotinic; the former is a
G protein coupled receptor, while the latter isa ligand gated cation channel.
Muscarinic These receptors are selectivelystimulated by muscarine and blocked by atropine.They are located primarily on autonomic effectorcells in heart, blood vessels, eye, smooth musclesand glands of gastrointestinal, respiratory andurinary tracts, sweat glands, etc. and in the CNS.Subsidiary muscarinic receptors are also presentin autonomic ganglia where they appear to playa modulatory role by inducing a long-lasting lateEPSP.Muscarinic autoreceptors are present prejunctionally on post-ganglionic cholinergic nerve endings: their activation inhibitsfurther ACh release. Similar ones have been demonstrated onadrenergic terminals: their activation inhibits NA release (maycontribute to vasodilator action of injected ACh). All bloodvessels have muscarinic receptors (though most of them lackcholinergic innervation) located on endothelial cells whoseactivation releases EDRF (nitric oxide) which diffuses to thesmooth muscle to cause relaxation.
Subtypes of muscarinic receptor By pharma-cological as well as molecular cloning techniques,muscarinic receptors have been divided into 5subtypes M1, M2, M3, M4 and M5. The first 3 arethe major subtypes (Table 7.3) that are present oneffector cells as well as on prejunctional nerveendings, and are expressed both in peripheralorgans as well as in the CNS. The M4 and M5
receptors are present mainly on nerve endings incertain areas of the brain and regulate the releaseof other neurotransmitters. Functionally, M1, M3

101C
HA
PTE
R 7
CHOLINERGIC SYSTEM AND DRUGS
TABLE 7.2 Differences between the two types of cholinesterases
Acetylcholinesterase (True) Butyrylcholinesterase (Pseudo)
1. Distribution All cholinergic sites, RBC, Plasma, liver, intestine, white mattergray matter
2. HydrolysisACh Very fast (in µs) SlowMethacholine Slower than ACh Not hydrolysedBenzoylcholine Not hydrolysed HydrolysedButyrylcholine Not hydrolysed Hydrolysed
3. Inhibition More sensitive to physostigmine More sensitive to organophosphates
4. Function Termination of ACh action Hydrolysis of ingested esters
TABLE 7.3 Characteristics of important subtypes of muscarinic receptor
M1 M2 M3
1. Location Autonomic Depolarization SA node: Hyperpolarization, Visceral smooth muscle:and ganglia: (late EPSP) rate of impulse generation contractionfunction Gastric Hist. release, AV node: velocity of conduction Iris: constriction of pupilsubserved glands: acid secretion Atrium: shortening of APD, Ciliary muscle: contraction
CNS: Learning, contractility Exocrine glands: secretionmemory, Ventricle: contractility (slight) Vascular endothelium:motor functions (receptors sparse) release of NO
Cholinergic nerve endings: vasodilatation ACh release
CNS: tremor, analgesiaVisceral smooth muscle:
contraction
2. Nature Gq-protein coupled Gi/Go-protein coupled Gq-protein coupled
3. Transducer IP3/DAG— cytosolic Ca2+, K+ channel opening, IP3/DAG— cytosolic Ca2+
mechanism PLA2—PG synthesis cAMP PLA2—PG synthesis
4. Agonists* MCN-343A, Oxotremorine Methacholine Bethanechol
5. Antagonists* Pirenzepine, Telenzepine Methoctramine, Solifenacin,Tripitramine Darifenacin
*Relatively selective— ACh activates and atropine blocks all 3 subtypes of muscarinic receptors.— The CNS contains all subtypes of muscarinic receptors, but M1 appear to predominate.— Most smooth muscles and glands have both M2 and M3 subtypes; M3 predominates.
and M5 fall in one class while M2 and M4 fall inanother class. Muscarinic agonists have shown littlesubtype selectivity, but some relatively selectiveantagonists have been produced (pirenzepine forM1, tripitramine for M2 and darifenacin for M3).Most organs have more than one subtype, butusually one subtype predominates in a given tissue.M1: The M1 is primarily a neuronal receptor locatedon ganglion cells and central neurones, especially
in cortex, hippocampus and corpus striatum. It playsa major role in mediating gastric secretion,relaxation of lower esophageal sphincter (LES)caused by vagal stimulation, and in learning,memory, motor functions, etc.M2: Cardiac muscarinic receptors are predomi-nantly M2 and mediate vagal bradycardia.Autoreceptors on cholinergic nerve endings are alsoof M2 subtype. Smooth muscles express some M2

102S
EC
TIO
N2
DRUGS ACTING ON ANS
TABLE 7.4 Characteristics of subtypes of nicotinic receptor
NM NN
1. Location and function Neuromuscular junction: Autonomic ganglia: depolarizationsubserved depolarization of muscle end plate —postganglionic impulse
—contraction of skeletal muscle Adrenal medulla: catecholamine releaseCNS: site specific excitation or inhibition
2. Nature Has intrinsic ion channel, pentamer Has intrinsic ion channel, pentamerof 2 or and subunits, each of only or , subunits, each subunitsubunit has 4 TM segments has 4 TM segments
3. Transducer mechanism Opening of cation (Na+, K+) channels Opening of cation (Na+, K+, Ca2+) channels
4. Agonists PTMA, Nicotine DMPP, Nicotine
5. Antagonists Tubocurarine, -Bungarotoxin Hexamethonium, Trimethaphan
receptors as well which, like M3, mediatecontraction.M3: Visceral smooth muscle contraction andglandular secretions are elicited through M3receptors, which also mediate vasodilatationthrough EDRF release. Together the M2 and M3receptors mediate most of the well-recognizedmuscarinic actions including contraction of LES.The muscarinic receptors are G-protein coupled receptorshaving the characteristic 7 membrane traversing amino acidsequences. The M1 and M3 (also M5) subtypes function throughGq protein and activate membrane bound phospholipase C(PLc)—generating inositol trisphosphate (IP3) and diacyl-glycerol (DAG) which in turn release Ca2+ intracellularly—cause depolarization, glandular secretion, raise smooth muscletone and release NO (from endothelium). They also activatephospholipase A2 resulting in enhanced synthesis and releaseof prostaglandins and leucotrienes in certain tissues. The M2(and M4) receptor opens K+ channels (through subunits ofregulatory protein Gi) and inhibits adenylyl cyclase (through subunit of Gi) resulting in hyperpolarization, reducedpacemaker activity, slowing of conduction and decreased forceof contraction in the heart. The M4 receptor has been implicatedin facilitation/inhibition of transmitter release in certain areasof the brain, while M5 has been found to facilitate dopaminerelease and mediate reward behaviour.
Nicotinic These receptors are selectively acti-vated by nicotine and blocked by tubocurarineor hexamethonium. They are rosette-like penta-meric structures (see Fig. 4.4) which enclose aligand gated cation channel: their activation causesopening of the channel and rapid flow of cationsresulting in depolarization and an action potential.On the basis of location and selective agonists
and antagonists two subtypes NM and NN(previously labelled N1 and N2) are recognized(Table 7.4).NM: These are present at skeletal muscle endplate:are selectively stimulated by phenyl trimethylammonium (PTMA) and blocked by tubocurarine.They mediate skeletal muscle contraction.NN: These are present on ganglionic cells (sym-pathetic as well as parasympathetic), adrenalmedullary cells (embryologically derived from thesame site as ganglionic cells) and in spinal cord andcertain areas of brain. They are selectively stimu-lated by dimethyl phenyl piperazinium (DMPP),blocked by hexamethonium, and constitute theprimary pathway of transmission in ganglia.
CHOLINERGIC DRUGS(Cholinomimetic, Parasympathomimetic)
These are drugs which produce actions similarto that of ACh, either by directly interacting withcholinergic receptors (cholinergic agonists) or byincreasing availability of ACh at these sites(anticholinesterases).
CHOLINERGIC AGONISTSCholine esters AlkaloidsAcetylcholine MuscarineMethacholine PilocarpineCarbachol ArecolineBethanechol

103C
HA
PTE
R 7
CHOLINERGIC SYSTEM AND DRUGS
ACTIONS (of ACh as prototype)
Depending on the type of receptor throughwhich it is mediated, the peripheral actions ofACh are classified as muscarinic or nicotinic. Thecentral actions are not so classifiable and aredescribed separately.
A. Muscarinic actions
1. Heart ACh hyperpolarizes the SA nodalcells and decreases their rate of diastolic depolari-zation. As a result, rate of impulse generationis reduced—bradycardia or even cardiac arrestmay occur.
At the A-V node and His-Purkinje fibresrefractory period (RP) is increased and conductionis slowed: P-R interval increases and partial tocomplete A-V block may be produced. The forceof atrial contraction is markedly reduced and RPof atrial fibres is abbreviated. Due to nonuniformvagal innervation, the intensity of effect on RPand conduction of different atrial fibres varies—inducing inhomogeneity and predisposing to atrialfibrillation or flutter.
Ventricular contractility is also decreased butthe effect is not marked. The cardiac muscarinicreceptors are of the M2 subtype.
2. Blood vessels All blood vessels are dila-ted, though only few (skin of face, neck, salivaryglands) receive cholinergic innervation. Fall inBP and flushing, especially in the blush areaoccurs. Muscarinic (M3) receptors are present onvascular endothelial cells: vasodilatation isprimarily mediated through the release of anendothelium dependent relaxing factor (EDRF)which is nitric oxide (NO). The PLc-IP3/DAGpathway activates endothelial NO synthase throughthe Ca+-Calmodulin mechanism. When theendothelium is damaged by disease, ACh candiffuse to the vascular smooth muscle and causevasoconstriction via M3 receptors located on theirplasma membrane.
Stimulation of cholinergic nerves to the peniscauses erection by releasing NO and dilatingcavernosal vessels through M3 receptors. However,this response is minimal with injected cholino-mimetic drugs.
3. Smooth muscle Smooth muscle in mostorgans is contracted (mainly through M3 recep-tors). Tone and peristalsis in the gastrointestinaltract is increased and sphincters relax abdominalcramps and evacuation of bowel.
Peristalsis in ureter is increased. The detrusormuscle contracts while the bladder trigone andsphincter relaxes voiding of bladder.
Bronchial muscles constrict, asthmatics arehighly sensitive bronchospasm, dyspnoea,precipitation of an attack of bronchial asthma.
4. Glands Secretion from all parasympathe-tically innervated glands is increased via M3 andsome M2 receptors: sweating, salivation, lacri-mation, increased tracheobronchial and gastricsecretion. The effect on pancreatic and intestinalglands is not marked. Secretion of milk and bileis not affected.
5. Eye Contraction of circular muscle of iris miosis.Contraction of ciliary muscle spasm of accom-modation, increased outflow facility, reduction inintraocular tension (especially in glaucomatouspatients).
B. Nicotinic actions
1. Autonomic ganglia Both sympathetic andparasympathetic ganglia are stimulated. This effectis manifested at higher doses. High dose of AChgiven after atropine causes tachycardia and risein BP due to stimulation of sympathetic gangliaand release of catecholamines.
2. Skeletal muscles Iontophoretic applica-tion of ACh to muscle endplate causes contractionof the fibre. Intraarterial injection of high dosecan cause twitching and fasciculations, but i.v.injection is generally without any effect (due torapid hydrolysis of ACh).
C. CNS actionsACh injected i.v. does not penetrate blood-brainbarrier and no central effects are seen. However,direct injection into the brain produces arousalresponse followed by depression. Cholinergic

104S
EC
TIO
N2
DRUGS ACTING ON ANS
drugs which enter brain produce complexbehavioral and neurological effects.
The important features of other choline estersare summarized in Table 7.5.
Interactions Anticholinesterases potentiate AChmarkedly, methacholine to less extent and haveonly additive action with carbachol or bethane-chol, depending upon the role of ChE in the ter-mination of action of the particular choline ester.Atropine and its congeners competitively anta-gonize muscarinic actions.Adrenaline is a physiological antagonist.Uses Choline esters are rarely, if ever, clinicallyused. ACh is not used because of evanescent andnonselective action. Methacholine was occasio-nally used to terminate paroxysmal supraventriculartachycardia but is obsolete now.Bethanechol has been used in postoperative/postpartum nonobstructive urinary retention,neurogenic bladder to promote urination. It canafford symptomatic relief in congenital megacolonand gastroesophageal reflux, but is rarely usedfor these. Side effects are prominent: belching,colic, involuntary urination/defecation, flushing,sweating, fall in BP, bronchospasm.Dose: 10–40 mg oral, 2.5–5 mg s.c.;UROTONIN, BETHACOL 25 mg tab.
CHOLINOMIMETIC ALKALOIDS
Pilocarpine It is obtained from the leaves ofPilocarpus microphyllus and other species. It hasprominent muscarinic actions and also stimulatesganglia—mainly through ganglionic muscarinicreceptors.
Pilocarpine causes marked sweating, saliva-tion and increase in other secretions. The cardio-
vascular effects are complex. Small doses generallycause fall in BP (muscarinic), but higher doseselicit rise in BP and tachycardia which is probablydue to ganglionic stimulation (through ganglionicmuscarinic receptors). Applied to the eye, itpenetrates cornea and promptly causes miosis,ciliary muscle contraction and fall in intraoculartension lasting 4–8 hours.
Pilocarpine is used only in the eye as 0.5–4% drops. It is a third-line drug in open angleglaucoma. An initial stinging sensation in the eyeand painful spasm of accommodation are frequentside effects. Other uses as a miotic are—tocounteract mydriatics after they have been usedfor testing refraction and to prevent/breakadhesions of iris with lens or cornea by alternatingit with mydriatics.
Though it can be used as a sialogogue, nooral preparation is available.PILOCAR 1%, 2%, 4% eye drops, CARPINE 0.5% eyedrops,PILODROPS 2% eyedrops.Muscarine It occurs in poisonous mushrooms Amanitamuscaria and Inocybe species and has only muscarinic actions.It is not used therapeutically but is of toxicological importance.Mushroom poisoning Depending on the toxic principlepresent in the particular species, at least 3 types of mushroompoisoning is known.Muscarine type (Early mushroom poisoning) due toInocybe and related species. Symptoms characteristic ofmuscarinic actions appear within an hour of eating themushroom, and are promptly reversed by atropine.Hallucinogenic type It is due to muscimol and other isoxazolecompounds which are present in A. muscaria and relatedmushrooms in much larger quantities than is muscarine. Thesecompounds activate amino acid receptors, and block muscarinicreceptors in the brain; have hallucinogenic property. Manifesta-tions of poisoning are primarily central. There is no specifictreatment and atropine is contraindicated. Another hallucino-genic mushroom is Psilocybe mexicana whose active principlepsilocybine is a tryptaminergic (5-HT related) compound.
TABLE 7.5 Properties of choline esters
Choline ester Hydrolysis by Actions SelectiveACh E BuChE Musc. Nico. action on
Acetylcholine ++ + + + Non selectiveMethacholine + – + ± CVSCarbachol – – + ++ g.i.t., bladderBethanechol – – + – g.i.t., bladder

105C
HA
PTE
R 7
CHOLINERGIC SYSTEM AND DRUGS
Phalloidin type (Late mushroom poisoning) It is due topeptide toxins found in A. phalloides, Galerina and relatedspecies. These inhibit RNA and protein synthesis. Thesymptoms start after many hours and are due to damage to thegastrointestinal mucosa, liver and kidney. Treatment consistsof supportive measures. Thioctic acid may have some antidotaleffect.Arecoline It is found in betel nut Areca catechu and hasmuscarinic as well as nicotinic actions, including those onskeletal muscle endplate. It also has prominent CNS effect:has been tried in dementia as an enhancer of cognitivefunctions, but not found useful—has no therapeutic use.
ANTICHOLINESTERASES
Anticholinesterases (anti-ChEs) are agents whichinhibit ChE, protect ACh from hydrolysis—pro-duce cholinergic effects in vivo and potentiateACh both in vivo and in vitro. Some anti ChEshave additional direct action on nicotinic cholino-ceptors.
ReversibleCarbamates AcridinePhysostigmine (Eserine) TacrineNeostigminePyridostigmineEdrophoniumRivastigmine, DonepezilGalantamine
IrreversibleOrganophosphates CarbamatesDyflos (DFP) Carbaryl* (SEVIN)Echothiophate Propoxur* (BAYGON)Malathion*Diazinon* (TIK-20)Tabun£, Sarin£, Soman£
CHEMISTRY
Anti-ChEs are either esters of carbamic acid orderivatives of phosphoric acid.The generic formula of carbamates and organo-phosphates is shown below:
In carbamates R1 may have a nonpolar tertiaryamino N, e.g. in physostigmine, rendering thecompound lipid soluble. In others, e.g. neostig-mine, R1 has a quaternary N+—rendering it lipidinsoluble. All organophosphates are highly lipidsoluble except echothiophate which is watersoluble.
MECHANISM OF ACTION
The anti-ChEs react with the enzyme essentiallyin the same way as ACh. The carbamates andphosphates respectively carbamylate and phos-phorylate the esteratic site of the enzyme.The mammalian AChE has been cloned and details of itsstructure as well as mode of interaction with ACh and variousanti-ChEs has been worked out.
The active region of AChE forms a gorge which containsan anionic site (near glutamate 334) and an esteratic siteformed by serine 203, and histidine 447 (Fig. 7.2A). Hydrolysisof ACh involves electrostatic attraction of positively chargedN+ of ACh to the anionic site (Fig. 7.2B) and nucleophilicattack by serine-OH which is activated by the adjacent histidineleading to acetylation of serine (Fig. 7.2C). The acetylatedenzyme reacts with water to produce acetic acid and choline(Fig. 7.2D).
Whereas the acetylated enzyme reacts withwater extremely rapidly and the esteratic site isfreed in a fraction of a millisecond, the carbamy-lated enzyme (reversible inhibitors) reacts slowly(Fig. 7.2E, F) and the phosphorylated enzyme(irreversible inhibitors) reacts extremely slowlyor not at all (Fig. 7.2G). It is noteworthy thatedrophonium and tacrine attach only to the anionicsite and do not form covalent bonds with theenzyme, while organophosphates attach only tothe esteratic site forming covalent bonds. Reactiva-tion of edrophonium-inhibited enzyme occurs in< 10 min, and does not involve hydrolysis ofthe inhibitor, but only its diffusion—action is brief.The half-life of reactivation of carbamylatedenzyme (about 30 min) is less than that of synthesisof fresh enzyme protein, while that of phosphory-lated enzyme (in days) is more than the regene-ration time. The phosphorylated enzyme may alsoundergo ‘aging’ by the loss of one of the alkylgroups and become totally resistant to hydrolysis.Thus, apparently reversible and irreversible
*Insecticides£Nerve gases forchemical warfare

106S
EC
TIO
N2
DRUGS ACTING ON ANS
Fig. 7.2: Schematic representation of reaction of acetylcholine (A–D), or carbamate anticholinesterase (E, F), ororganophosphate anticholinesterase (G) with cholinesterase enzyme; and reactivation of phosphorylated enzyme byoxime (G, H). Ser—Serine; His—Histidine; Glu—Glutamic acid.

107C
HA
PTE
R 7
CHOLINERGIC SYSTEM AND DRUGS
enzyme inhibition is obtained, though the basicpattern of inhibitor-enzyme interaction remainsthe same.
PHARMACOLOGICAL ACTIONS
The actions of anti-ChEs are due to amplificationof endogenous ACh. As such they are qualitativelysimilar to those of directly acting cholinoceptorstimulants. However, relative intensity of actionon muscarinic, ganglionic, skeletal muscle andCNS sites varies among the different agents.
Lipid-soluble agents (physostigmine and orga-nophosphates) have more marked muscarinic andCNS effects; stimulate ganglia but action onskeletal muscles is less prominent.
Lipid-insoluble agents (neostigmine and otherquaternary ammonium compounds) produce moremarked effect on the skeletal muscles (direct actionon muscle endplate cholinoceptors as well),stimulate ganglia, but muscarinic effects are lessprominent. They do not penetrate CNS and haveno central effects.
Ganglia Local hydrolysis of ACh is lessimportant in ganglia: inactivation occurs partlyby diffusion and hydrolysis in plasma. Anti-ChEsstimulate ganglia primarily through muscarinicreceptors present there. High doses cause persis-tent depolarization of the ganglionic nicotinicreceptors and blockade of transmission.
CVS Cardiovascular effects are complex. Where-as muscarinic action would produce bradycardiaand hypotension, ganglionic stimulation would tendto increase heart rate and BP. Action on medullarycentres (stimulation followed by depression) furthercomplicates the picture, so does ganglionic blockadewith high doses. Thus, the overall effects are oftenunpredictable and depend on the agent and itsdose.
Skeletal muscles After treatment with anti-ChEs, the ACh released by a single nerve impulseis not immediately destroyed—rebinds to the samereceptor, diffuses to act on neighbouring receptorsand activates prejunctional fibres repetitivefiring twitching and fasciculations. Force of
contraction in partially curarized and myasthenicmuscles is increased. Higher doses cause persistentdepolarization of endplates resulting in blockadeof neuromuscular transmission weakness andparalysis. Direct action of neostigmine and itscongeners at the muscle endplates results inaugmentation of these features.
CNS Lipophilic anti-ChEs which penetrate intobrain produce a generalized alerting response.Cognitive function may be improved in Alzheimer’sdisease. However, higher doses produce excite-ment, mental confusion, disorientation, tremorsand convulsions followed by coma.
Other effects These result from stimulationof smooth muscles and glands of the gastrointes-tinal, respiratory, urinary tracts and in the eyeas described for ACh.
PHARMACOKINETICS
Physostigmine It is rapidly absorbed from g.i.t.and parenteral sites. Applied to the eye, itpenetrates cornea freely. It crosses blood-brainbarrier and is disposed after hydrolysis by ChE.Neostigmine and congeners These are poorlyabsorbed orally; oral dose is 20–30 times higherthan parenteral dose. They do not effectivelypenetrate cornea or cross blood-brain barrier. Theyare partially hydrolysed and partially excretedunchanged in urine.Organophosphates These are absorbed fromall sites including intact skin and lungs. Theyare hydrolyzed as well as oxidized in the bodyand little is excreted unchanged.
INDIVIDUAL COMPOUNDS
The important features of physostigmine andneostigmine are presented in Table 7.6.Physostigmine eye drops are usually preparedfreshly by ophthalmology departments.BI-MIOTIC 0.25% eye drops with 2% pilocarpine nitrate.
Neostigmine PROSTIGMIN, MYOSTIGMIN,TILSTIGMIN 15 mg tab, 0.5 mg/ml in 1 ml and 5 ml inj.

108S
EC
TIO
N2
DRUGS ACTING ON ANS
TABLE 7.6 Comparative features of physostigmine and neostigmine
Physostigmine Neostigmine
1. Source Natural alkaloid from SyntheticPhysostigma venenosum(Calabar bean)
2. Chemistry Tertiary amine derivative Quaternary ammonium compound3. Oral absorption Good Poor4. CNS actions Present Absent5. Applied to eye Penetrates cornea Poor penetration6. Direct action on NM cholinoceptors Absent Present7. Prominent effect on Autonomic effectors Skeletal muscles8. Important use Miotic (glaucoma) Myasthenia gravis9. Dose 0.5–1 mg oral/parenteral 0.5–2.5 mg i.m./s.c.
0.1–1.0% eye drops 15–30 mg orally10. Duration of action Systemic 4–6 hrs 3–4 hrs.
In eye 6 to 24 hrs
Pyridostigmine Resembles neostigmine in allrespects but is dose to dose less potent and longeracting, less frequent dosing is required inmyasthenia gravis.DISTINON, MYESTIN 60 mg tab; 1–3 tab TDS.Ambenonium is another longacting congener used inmyasthenia.Edrophonium Resembles neostigmine in action, has a briefduration (10–30 min), suitable only as a diagnostic agent formyasthenia gravis.Dose: 2–10 mg i.v.Tacrine It is a lipophilic acridine compound which interactswith ChE in a manner analogous to edrophonium. It crossesblood-brain barrier and has a longer duration of action. Byincreasing brain ACh levels it was found to produce somesymptomatic improvement in Alzheimer’s disease, but has goneinto disuse due to hepatotoxicity (see Ch. 35).
Rivastigmine This lipophilic relatively cere-broselective ChE inhibitor has been introduced forAlzheimer’s disease (AD), see Ch. 35.Donepezil Another centrally acting anti-AChEthat has produced cognitive and behavioralimprovement in AD. It is long-acting and suitablefor once daily administration (see Ch. 35).Galantamine This natural alkaloid inhibitor ofcerebral AChE has in addition weak agonisticaction on nicotinic receptors. It is being used toafford symptomatic relief in AD (see Ch. 35).Dyflos It is Diisopropyl-fluoro-phosphate (DFP), a verypotent and long-acting anti-ChE. It is now obsolete as a miotic.Echothiophate It is an organophosphate with quaternarystructure. It is water soluble; and was used as a long acting miotic.
Precautions Anti-ChEs are contraindicated insick sinus, A-V conduction defects and hypo-tensive states. They are to be used cautiously inpeptic ulcer, asthma, COPD and seizure patients.
USES
1. As miotic(a) In glaucoma: Miotics increase the tone ofciliary muscle (attached to scleral spur) andsphincter pupillae which pull on and somehowimprove alignment of the trabeculae so thatoutflow facility is increased i.o.t. falls in openangle glaucoma.
Pilocarpine is the preferred miotic. The actionis rapid and short lasting (4–6 hr); 6–8 hourlyinstillation is required and even then i.o.t. mayfluctuate inbetween. Diminution of vision,especially in dim light (due to constricted pupil),spasm of accommodation and brow pain arefrequent side effects. Systemic effects—nausea,diarrhoea, sweating and bronchospasm may occurwith higher concentration eye drops.
Physostigmine (0.1%) is used only to sup-plement pilocarpine. Miotics are now 3rd choicedrugs, used only as add on therapy in advancedcases. However, they are effective in aphakicglaucoma. Pilocarpine (along with other drugs)is used in angle closure glaucoma as well.(b) To reverse the effect of mydriatics afterrefraction testing.

109C
HA
PTE
R 7
CHOLINERGIC SYSTEM AND DRUGS
(c) To prevent formation of adhesions betweeniris and lens or iris and cornea, and even to breakthose which have formed due to iritis, cornealulcer, etc.—a miotic is alternated with a mydriatic.
2. Myasthenia gravisMyasthenia gravis is an autoimmune disorderaffecting about 1 in 10,000 population, due todevelopment of antibodies directed to the nicotinicreceptors (NR) at the muscle endplate reductionin number of free NM cholinoceptors to 1/3 ofnormal or less (Fig. 7.3) and structural damageto the neuromuscular junction. This results inweakness and easy fatigability on repeated activity,with recovery after rest. The eyelid, externalocular, facial and pharyngeal muscles are generallyinvolved first. Later, limb and respiratory musclesget affected. Neostigmine and its congenersimprove muscle contraction by allowing AChreleased from prejunctional endings to accumulateand act on the receptors over a larger area, aswell as by directly depolarizing the endplate.
Treatment is usually started with neostigmine15 mg orally 6 hourly; dose and frequency isthen adjusted to obtain optimum relief fromweakness. However, the dosage requirement mayfluctuate from time to time and there are oftenunpredictable periods of remission and exacer-bation. Pyridostigmine is an alternative whichneeds less frequent dosing. If intolerablemuscarinic side effects are produced, atropine canbe added to block them. These drugs have noeffect on the basic disorder which often progresses;ultimately it may not be possible to restore musclestrength adequately with anti-ChEs alone.
Corticosteroids afford considerable improve-ment in such cases by their immunosuppressantaction. They inhibit production of NR-antibodiesand may increase synthesis of NRs. However,their long term use has problems of its own (seeCh. 20). Prednisolone 30–60 mg/day inducesremission in about 80% of the advanced cases;10 mg daily or on alternate days can be usedfor maintenance therapy. Other immunosuppres-sants have also been used with benefit in advan-ced cases. Both azathioprine and cyclosporinealso inhibit NR-antibody synthesis by affectingT-cells, but response to the former is slow inonset (takes upto 1 year), while that to the latteris relatively quick (in 1–2 months).
Removal of antibodies by plasmapheresis(plasma exchange) is another therapeuticapproach. Dramatic but short lived improvementcan often be achieved by it in myasthenic crisis.
Thymectomy is effective in a majority of thecases. It produces gradual improvement and evencomplete remission has been obtained. Thymusmay contain modified muscle cells with NRs ontheir surface, which may be the source of theantigen for production of anti-NR antibodies inmyasthenic patients.
Myasthenic crisis is characterized by acuteweakness of respiratory muscles. It is managedby tracheal intubation and mechanical ventilation.Generally, i.v. methylprednisolone pulse therapyis given while anti-ChEs are withheld for 2–3days followed by their gradual reintroduction.
Fig. 7.3: Neuromuscular junction of myasthenic muscleIn myasthenia gravis the population of nicotinic receptors(NR) available at muscle endplate for binding acetyl-choline (ACh) is markedly reduced due to their obliterationby nicotinic receptor antibodies (NR-Ab). Acetylcholines-terase (AChE) molecules located strategically at themuscle endplate rapidly hydrolyse ACh. Anticholines-terases inhibit AChE, allowing the same ACh moleculesto repeatedly interact with the available NRs; frequencyof ACh-NR interaction is increased

110S
EC
TIO
N2
DRUGS ACTING ON ANS
Most patients can be weaned off the ventilatorin 1–3 weeks. Plasmapheresis hastens recovery.
Overtreatment with anti-ChEs If the dose ofthe antiChE is not adjusted according to the fluc-tuating requirement, relative overdose may occurfrom time-to-time. Overdose also producesweakness by causing persistent depolarization ofmuscle endplate, and is called cholinergicweakness. Late cases with high anti-ChE doserequirements often alternately experience myast-henic and cholinergic weakness and these mayassume crisis proportions.
The two types of weakness require oppositetreatments. They can be differentiated by edropho-nium test—
improvementmyasthenic crisisInjectedrophonium(2 mg. i.v.) no improvement or
worseningcholinergic crisis
Diagnostic tests for myasthenia gravis(a) Ameliorative test: Initially edrophonium2 mg is injected i.v. as a test dose. If nothinguntoward happens, the remaining 8 mg is injectedafter 30–60 sec. Reversal of weakness and short-lasting improvement in the strength of affectedmuscles occurs only in myasthenia gravis and notin other muscular dystrophies.
In case edrophonium is not available, the testcan be performed with 1.5 mg i.v. neostigmine.Atropine pretreatment may be given to block themuscarinic effects of neostigmine.(b) Provocative test: myasthenics are highly sensitive tod-tubocurarine; 0.5 mg i.v. causes marked weakness in thembut is ineffective in non-myasthenics. This test is hazardous:facilities for positive pressure respiration must be at handbefore performing it. This test is better not performed.(c) Demonstration of anti-NR antibodies in plasma or musclebiopsy specimen is a more reliable test.
3. Postoperative paralytic ileus/urinaryretention This may be relieved by 0.5–1 mgs.c. neostigmine, provided no organic obstructionis present.
4. Postoperative decurarization Neostig-mine 0.5–2.0 mg (30–50 g/kg) i.v., preceded
by atropine or glycopyrrolate 10 g/kg to blockmuscarinic effects, rapidly reverses muscle paralysisinduced by competitive neuromuscular blockers.5. Cobra bite Cobra venom has a curare likeneurotoxin. Though specific antivenom serum isthe primary treatment, neostigmine + atropineprevent respiratory paralysis.6. Belladonna poisoning Physostigmine 0.5–2 mg i.v.repeated as required is the specific antidote for poisoningwith belladonna or other anticholinergics. It penetrates blood-brain barrier and antagonizes both central and peripheralactions. However, physostigmine often itself induceshypotension, arrhythmias and undesirable central effects. Itis therefore employed only as a last resort. Neostigmine doesnot block the central effect, but is less risky.
7. Other drug overdosages Tricyclic antidepressants,phenothiazines and many antihistaminics have additionalanticholinergic property. Overdose symptoms and comaproduced by these drugs are partly antagonized byphysostigmine. However, it may worsen the fall in BP andarrhythmias; use therefore is risky. Physostigmine also appearsto have a modest nonspecific arousal effect in CNS depressionproduced by diazepam or general anaesthetics, but use forthis purpose is rarely warranted.
8. Alzheimer’s disease Characterized byprogressive dementia, AD is a neurodegenerativedisorder, primarily affecting cholinergic neuronesin the brain. Various measures to augment choli-nergic transmission in the brain have beentried. The relatively cerebroselective anti-ChEs,rivastigmine, donepezil and galantamine are nowcommonly used. For details see Ch. 35.
ANTICHOLINESTERASE POISONINGAnticholinesterases are easily available andextensively used as agricultural and householdinsecticides; accidental as well as suicidal andhomicidal poisoning is common.
Local muscarinic manifestations at the siteof exposure (skin, eye, g.i.t.) occur immediatelyand are followed by complex systemic effectsdue to muscarinic, nicotinic and central actions.They are—• Irritation of eye, lacrimation, salivation, swea-
ting, copious tracheo-bronchial secretions,miosis, blurring of vision, bronchospasm,breathlessness, colic, involuntary defecationand urination.

111C
HA
PTE
R 7
CHOLINERGIC SYSTEM AND DRUGS
• Fall in BP, bradycardia or tachycardia, cardiacarrhythmias, vascular collapse.
• Muscular fasciculations, weakness, respiratoryparalysis (central as well as peripheral).
• Irritability, disorientation, unsteadiness, tremor,ataxia, convulsions, coma and death.
• Death is generally due to respiratory failure.
Treatment1. Termination of further exposure to the poison—
fresh air, wash the skin and mucous membraneswith soap and water, gastric lavage accordingto need.
2. Maintain patent airway, positive pressurerespiration if it is failing.
3. Supportive measures—maintain BP, hydration,control of convulsions with judicious use ofdiazepam.
4. Specific antidotes—(a) Atropine It is highly effective in counter-acting the muscarinic symptoms, but higher dosesare required to antagonize the central effects. Itdoes not reverse peripheral muscular paralysiswhich is a nicotinic action. All cases of anti-ChE(carbamate or organophosphate) poisoning mustbe promptly given atropine 2 mg i.v. repeatedevery 10 min till dryness of mouth or other signsof atropinization appear (upto 200 mg has beenadministered in a day). Continued treatment withmaintenance doses may be required for 1–2 weeks.(b) Cholinesterase reactivators Oximes areused to restore neuromuscular transmission onlyin case of organophosphate anti-ChE poisoning.The phosphorylated ChE reacts very slowly ornot at all with water. However, if more reactiveOH groups in the form of oximes (generic formulaR–CH = N–OH) are provided, reactivation occursmore than a million times faster (see Fig. 7.2Gand H).
Pralidoxime (2-PAM) has a positively chargedquaternary nitrogen: attaches to the anionic siteof the enzyme which remains unoccupied in thepresence of organophosphate inhibitors. Its oximeend reacts with the phosphorus atom attached to
the esteratic site: the oxime-phosphonate soformed diffuses away leaving the reactivated ChE.Pralidoxime is ineffective as an antidote tocarbamate anti-ChEs (physostigmine, neostigmine,carbaryl, propoxur) in which case the anionic siteof the enzyme is not free to provide attachmentto it. It is rather contraindicated in carbamatepoisoning, because not only it does not reactivatecarbamylated enzyme, it has weak anti-ChEactivity of its own.
Pralidoxime (NEOPAM, PAM-A INJ. 500 mg/20 mlinfusion, LYPHE 1 g/vial for inj.) is injected i.v. slowlyin a dose of 1–2 g (children 20–40 mg/kg).Another regimen is 30 mg/kg i.v. loading dose,followed by 8–10 mg/kg/hour continuous infusiontill recovery. Pralidoxime causes more markedreactivation of skeletal muscle ChE than atautonomic sites and not at all in the CNS (doesnot penetrate into brain). Treatment should bestarted as early as possible (within few hours),before the phosphorylated enzyme has undergone‘aging’ and become resistant to hydrolysis. Dosesmay be repeated according to need (max. 12 gin first 24 hrs. Lower doses according to symptomsare continued 1–2 weeks). The use of oximesin organophosphate poisoning is secondary to thatof atropine. Moreover, the clinical benefit of oximetherapy is highly variable depending upon thecompound involved (different organophosphates‘age’ at different rates), the amount of poisonthat has entered the body, time lapse before therapyis started and dose of the oxime.
Other oximes are obidoxime (more potent than pralidoxime)and diacetyl-monoxime (DAM), which is lipophilic.
Chronic organophosphate poisoning Repeatedexposure to certain fluorine containing and triarylorganophosphates results in polyneuritis and demyelinationafter a latent period of days to weeks. Sensory disturbancesoccur first followed by muscle weakness, tendernessand depressed tendon reflexes—lower motor neuroneparalysis. In the second phase, spasticity and uppermotor neurone paralysis gradually supervenes. Recovery maytake years. The mechanism of this toxicity is not known,but it is not due to inhibition of ChE; there is no specifictreatment.

112S
EC
TIO
N2
DRUGS ACTING ON ANS
PROBLEM DIRECTED STUDY
7.1 A man aged 45 years presented with gradual onset complaints of double vision, droopingeyelids, difficulty in chewing food and weakness of limbs which is accentuated by exercise. Thesymptoms fluctuate in intensity over time. A provisional diagnosis of myasthenia gravis is made.(a) Can a pharmacological test be performed to confirm/refute the diagnosis?(b) In case the diagnosis is confirmed, can this disease be cured by medication?(c) Is there a surgical solution for this illness?(see Appendix-1 for solution)

Anticholinergic Drugs andDrugs Acting on AutonomicGanglia
ChapterChapterChapterChapterChapter 88888
ANTICHOLINERGIC DRUGS(Muscarinic receptor antagonists,
Atropinic, Parasympatholytic)
Conventionally, the term ‘anticholinergic drugs’is restricted to those which block actions of AChon autonomic effectors and in the CNS exertedthrough muscarinic receptors. Though nicotinicreceptor antagonists also block certain actions ofACh, they are generally referred to as ‘ganglionblockers’ and ‘neuromuscular blockers’.
Atropine, the prototype drug of this class, ishighly selective for muscarinic receptors, but someof its synthetic substitutes do possess significantnicotinic blocking property in addition. Theselective action of atropine can easily be demon-strated on a piece of guinea pig ileum whereACh induced contractions are blocked withoutaffecting those evoked by histamine, 5-HT or otherspasmogens. The selectivity is, however, lost atvery high doses. All anticholinergics are compe-titive antagonists.
CLASSIFICATION
1. Natural alkaloids Atropine, Hyoscine(Scopolamine).
2. Semisynthetic derivatives Homatropine,Atropine methonitrate, Hyoscine butylbromide, Ipratropium bromide, Tiotropiumbromide.
3. Synthetic compounds(a) Mydriatics: Cyclopentolate, Tropicamide.(b) Antisecretory-antispasmodics:
(i) Quaternary compounds: Propantheline,Oxyphenonium, Clidinium, Pipenzolatemethyl bromide, Isopropamide, Glycopyr-rolate.
(ii) Tertiary amines: Dicyclomine, Valetha-mate, Pirenzepine.
(c)Vasicoselective: Oxybutynin, Flavoxate,Tolterodine.
(d)Antiparkinsonian: Trihexyphenidyl (Benzhe-xol), Procyclidine, Biperiden.
In addition, many other classes of drugs, i.e.tricyclic antidepressants, phenothiazines, anti-histamines and disopyramide possess significantantimuscarinic actions.
The natural alkaloids are found in plants ofthe solanaceae family. The levo-isomers are muchmore active than the dextroisomers. Atropine isracemic while scopolamine is l-hyoscine.
PHARMACOLOGICAL ACTIONS(Atropine as prototype)
The actions of atropine can be largely predictedfrom knowledge of parasympathetic responses.Prominent effects are seen in organs whichnormally receive strong parasympathetic tone.Atropine blocks all subtypes of muscarinicreceptors.
1. CNS Atropine has an overall CNS stimu-lant action. However, these effects are not appre-ciable at low doses which produce only peripheraleffects because of restricted entry into the brain.Hyoscine produces central effects (depressant)even at low doses.• Atropine stimulates many medullary centres
—vagal, respiratory, vasomotor.• It depresses vestibular excitation and has
antimotion sickness property. The site of thisaction is not clear—probably there is acholinergic link in the vestibular pathway, orit may be exerted at the cortical level.
• By blocking the relative cholinergic over-activity in basal ganglia, it suppresses tremorand rigidity of parkinsonism.

114S
EC
TIO
N2
DRUGS ACTING ON ANS
• High doses cause cortical excitation, restless-ness, disorientation, hallucinations and deliriumfollowed by respiratory depression and coma.
Majority of the central actions are due to blockade ofmuscarinic receptors in the brain, but some actions may havea different basis.
2. CVSHeart The most prominent effect of atropineis tachycardia. It is due to blockade of M2
receptors on the SA node through which vagaltone decreases HR. Higher the existing vagaltone— more marked is the tachycardia (maximumin young adults, less in children and elderly). Oni.m./s.c. injection transient initial bradycardia oftenoccurs. Earlier believed to be due to stimulationof vagal centre, it is now thought to be causedby blockade of muscarinic autoreceptors (M1) onvagal nerve endings, thereby augmenting AChrelease. This is suggested by the finding thatselective M1 antagonist pirenzepine is equipotentto atropine in causing bradycardia. Moreover,atropine substitutes which do not cross blood-brain barrier also produce initial bradycardia.Atropine abbreviates refractory period of A-Vnode and facilitates A-V conduction, especiallyif it has been depressed by high vagal tone.P-R interval is shortened.
BP Since cholinergic impulses are not involvedin the maintenance of vascular tone, atropine doesnot have any consistent or marked effect on BP.Tachycardia and vasomotor centre stimulation tendto raise BP, while histamine release and directvasodilator action (at high doses) tend to lowerBP.
Atropine blocks vasodepressor action of choli-nergic agonists.
3. Eye The autonomic control of iris musclesand the action of mydriatics as well as mioticsis illustrated in Fig. 8.1. Topical instillation ofatropine causes mydriasis, abolition of light reflexand cycloplegia lasting 7–10 days. This resultsin photophobia and blurring of near vision.The ciliary muscles recover somewhat earlier thansphincter pupillae. The intraocular tension tendsto rise, especially in narrow angle glaucoma.
Fig. 8.1: Autonomic control of pupil (A); and site ofaction of mydriatics (B) and miotics (C)
However, conventional systemic doses of atropineproduce minor ocular effects.
4. Smooth muscles All visceral smoothmuscles that receive parasympathetic motorinnervation are relaxed by atropine (M3 blockade).Tone and amplitude of contractions ofstomach and intestine are reduced; the passageof chyme is slowed—constipation may occur,spasm may be relieved. However, peristalsis isonly incompletely suppressed because it is

115C
HA
PTE
R8
ANTICHOLINERGIC DRUGS AND DRUGS ACTING ON AUTONOMIC GANGLIA
primarily regulated by local reflexes in the entericplexus, and other neurotransmitters (5-HT,enkephalin, etc.) are involved. Enhanced motilitydue to injected cholinergic drugs is morecompletely antagonised than that due to vagalstimulation, because intramural neurones whichare activated by vagus utilize a number ofnoncholinergic transmitters as well.
Atropine causes bronchodilatation andreduces airway resistance, especially in COPD andasthma patients. Inflammatory mediators likehistamine, PGs, leucotrienes and kinins whichparticipate in asthma increase vagal activity inaddition to their direct stimulant action on bronchialmuscle and glands. Atropine attenuates their actionby antagonizing the reflex vagal component.
Atropine has relaxant action on ureter andurinary bladder; urinary retention can occur inolder males with prostatic hypertrophy. However,this relaxant action can be beneficial for increasingbladder capacity and controlling detrusorhyperreflexia in neurogenic bladder/enuresis.Relaxation of biliary tract is less marked and effecton uterus is minimal.
5. Glands Atropine markedly decreases sweat,salivary, tracheobronchial and lacrimal secretion(M3 blockade). Skin and eyes become dry, talkingand swallowing may be difficult.
Atropine decreases secretion of acid, pepsinand mucus in the stomach, but the primary actionis on volume of secretion so that pH of gastriccontents may not be elevated unless diluted byfood. Since bicarbonate secretion is also reduced,rise in pH of fasting gastric juice is only modest.Relatively higher doses are needed and atropineis less efficacious than H2 blockers in reducingacid secretion. Intestinal and pancreatic secretionsare not significantly reduced. Bile production isnot under cholinergic control, so not affected.
6. Body temperature Rise in body tempera-ture occurs at higher doses. It is due to bothinhibition of sweating as well as stimulation oftemperature regulating centre in the hypothala-mus. Children are highly susceptible to atropinefever.
7. Local anaesthetic Atropine has a mildanaesthetic action on the cornea.
Atropine has been found to enhance ACh (also NA) releasefrom certain postganglionic parasympathetic and sympatheticnerve endings, and thus produce paradoxical responses. Thisis due to blockade of release inhibitory muscarinic autorecep-tors present on these nerve terminals.
The sensitivity of different organs and tissues toatropine varies and can be graded as—
Saliva, sweat, bronchial secretion > eye, bron-chial muscle, heart > smooth muscle ofintestine, bladder > gastric glands and smoothmuscle.
The above differences probably reflect the relative dependenceof the function on cholinergic tone vis a vis other influences,and variation in synaptic gaps in different organs. The patternof relative activity is nearly the same for other atropinesubstitutes except pirenzepine which inhibits gastric secretionat doses that have little effect on other secretions, heart andeye. This is probably because atropine equally blocks M1,M2 and M3 receptors whereas pirenzepine is a selective M1
antagonist.Atropine more effectively blocks responses
to exogenously administered cholinergic drugsthan those to parasympathetic nerve activity. Thismay be due to release of ACh very close to thereceptors by nerves and involvement of cotrans-mitters (see p. 97).
Hyoscine This natural anticholinergic alkaloiddiffers from atropine in many respects, these aretabulated in Table 8.1.
PHARMACOKINETICSAtropine and hyoscine are rapidly absorbed fromg.i.t. Applied to eyes they freely penetrate cornea.Passage across blood-brain barrier is somewhatrestricted. About 50% of atropine is metabolizedin liver and rest is excreted unchanged in urine.It has a t½ of 3–4 hours. Hyoscine is morecompletely metabolized and has better blood-brainbarrier penetration.Atropine sulfate: 0.6–2 mg i.m., i.v. (children 10 µg/kg), 1–2%topically in eye. ATROPINE SULPHATE: 0.6 mg/ml inj., 1%eye drop/ointment; ATROSULPH 1% eye drop, 5% eye oint.Hyoscine hydrobromide: 0.3–0.5 mg oral, i.m.; also astransdermal patch.Combinations of atropine with analgesics and antipyretics arebanned in India.

116S
EC
TIO
N2
DRUGS ACTING ON ANS
TABLE 8.1 Comparative features of atropine and hyoscine
Atropine Hyoscine
1. Chief source Atropa belladonna, Datura stramonium Hyoscyamys niger
2. Alkaloidal ester Tropine (base) Scopine (base)of tropic acid with
3. CNS effect Excitatory Depressant (amnesia, fatigue,low dose Excitation (mild) drowsiness, N-REM sleep)high dose Excitation (strong) Excitation
4. Anticholinergic property More potent on heart, bronchial More potent on eye andmuscle and intestines secretory glands
5. Duration of action Longer Shorter
6. Anti-motion sickness + + + + +
ATROPINE SUBSTITUTES
Many semisynthetic derivatives of belladonnaalkaloids and a large number of synthetic com-pounds have been introduced with the aim ofproducing more selective action on certainfunctions. Most of these differ only marginallyfrom the natural alkaloids, but some recent onesappear promising.
Quaternary compounds
These have certain common features—• Incomplete oral absorption.• Poor penetration in brain and eye; central and
ocular effects are not seen after parenteral/oral administration.
• Elimination is generally slower; majority arelonger acting than atropine.
• Have higher nicotinic blocking property. Someganglionic blockade may occur at clinical doses→ postural hypotension, impotence areadditional side effects.
• At high doses some degree of neuromuscularblockade may also occur.
Drugs in this category are—
1. Hyoscine butyl bromide 20–40 mg oral,i.m., s.c., i.v.; less potent and longer acting thanatropine; used for esophageal and gastrointestinalspastic conditions.BUSCOPAN 10 mg tab., 20 mg/ml amp.
2. Atropine methonitrate 2.5–10 mg oral,i.m.; for abdominal colics and hyperacidity.MYDRINDON 1 mg (adult), 0.1 mg (child) tab; inSPASMOLYSIN 0.32 mg tab;
3. Ipratropium bromide 40–80 µg byinhalation; it acts selectively on bronchial musclewithout altering volume or consistency ofrespiratory secretions. Another desirable feature isthat in contrast to atropine, it does not depress muco-ciliary clearance by bronchial epithelium. It hasa gradual onset and late peak (at 40–60 min) ofbronchodilator effect in comparison to inhaledsympathomimetics. Thus, it is more suitable forregular prophylactic use rather than for rapidsymptomatic relief during an attack. Action lasts4–6 hours. It acts on receptors located mainly inthe larger central airways (contrast sympathomi-metics whose primary site of action is peripheralbronchioles, see Fig. 16.2). The parasympathetictone is the major reversible factor in chronicobstructive pulmonary disease (COPD). Therefore,ipratropium is more effective in COPD than inbronchial asthma. Transient local side effects likedryness of mouth, scratching sensation in trachea,cough, bad taste and nervousness are reported in20–30% patients, but systemic effects are rarebecause of poor absorption from the lungs and g.i.t.(major fraction of any inhaled drug is swallowed).IPRAVENT 20 µg and 40 µg/puff metered dose inhaler, 2 puffs3–4 times daily; 250 µg/ml respirator soln., 0.4–2 ml nebulizedin conjunction with a β2 agonist 2–4 times daily.

117C
HA
PTE
R8
ANTICHOLINERGIC DRUGS AND DRUGS ACTING ON AUTONOMIC GANGLIA
Also used to control rhinorrhoea in perennial rhinitis andcommon cold; IPRANASE-AQ 0.084% nasal spray (42 µg peractuation), 1–2 sprays in each nostril 3–4 times a day.
4. Tiotropium bromide A newer congener ofipratropium bromide which binds very tightly tobronchial M1/M3 muscarinic receptors producinglong lasting bronchodilatation. Binding to M2
receptors is less tight confering relative M1/M3
selectivity (less likely to enhance ACh release fromvagal nerve endings in lungs due to M2 receptorblockade). Like ipratropium, it is not absorbed fromrespiratory and g.i. mucosa and has exhibited highbronchial selectivity of action.TIOVA 18 μg rotacaps; 1 rotacap by inhalation OD.
5. Propantheline 15–30 mg oral; it was apopular anticholinergic drug used for peptic ulcerand gastritis. It has some ganglion blocking activityas well and is claimed to reduce gastric secretionat doses which produce only mild side effects.Gastric emptying is delayed and action lasts for6–8 hours. Use has declined due to availabilityof H2 blockers and proton pump inhibitors.PROBANTHINE 15 mg tab.
6. Oxyphenonium 5–10 mg (children 3–5 mg)oral; similar to propantheline, recommended forpeptic ulcer and gastrointestinal hypermotility.ANTRENYL 5, 10 mg tab.
7. Clidinium 2.5–5 mg oral; This antisecretory-antispasmodic has been used in combination withbenzodiazepines for nervous dyspepsia, gastritis,irritable bowel syndrome, colic, peptic ulcer, etc.In SPASRIL, ARWIN 2.5 mg tab with chlordiazepoxide 5 mg.NORMAXIN, CIBIS 2.5 mg with dicyclomine 10 mg andchlordiazepoxide 5 mg.
8. Pipenzolate methyl bromide 5–10 mg(children 2–3 mg) oral; It has been promotedespecially for flatulent dyspepsia, infantile colicsand abdominal cramps.In PIPEN 4 mg + dimethylpolysiloxane 40 mg/ml drops.
9. Isopropamide 5 mg oral; indicated inhyperacidity, nervous dyspepsia, irritable boweland other gastrointestinal problems, speciallywhen associated with emotional/mental disorders.In STELABID, GASTABID 5 mg tab. with trifluoperazine 1 mg.
10.Glycopyrrolate 0.1–0.3 mg i.m. (5–10μg/kg), potent and rapidly acting antimuscarinic
lacking central effects. Almost exclusively usedfor preanaesthetic medication and duringanaesthesia. GLYCO-P 0.2 mg/ml amp., 1 mg in 5 mlvial, PYROLATE 0.2 mg/ml, 1 ml amp, 10 ml vial.
Tertiary amines1. Dicyclomine 20 mg oral/i.m., children5–10 mg; has direct smooth muscle relaxantaction in addition to weak anticholinergic. It exertsantispasmodic action at doses which produce fewatropinic side effects. However, infants haveexhibited atropinic toxicity symptoms and it isnot recommended below 6 months of age. It alsohas antiemetic property: has been used in morn-ing sickness and motion sickness. Dysmenorrhoeaand irritable bowel are other indications.CYCLOSPAS-D, 20 mg with dimethicone 40 mg tab;CYCLOPAM INJ. 10 mg/ml in 2 ml, 10 ml, 30 ml amp/vial,also 20 mg tab with paracetamol 500 mg; in COLIMEX,COLIRID 20 mg with paracetamol 500 mg tab, 10 mg/ml dropswith dimethicone.
2. Valethamate: The primary indication of thisanticholinergic-smooth muscle relaxant is to hastendilatation of cervix when the same is delayedduring labour, and as visceral antispasmodic,urinary, biliary, intestinal colic.Dose: 8 mg i.m., 10 mg oral repeated as required.VALAMATE 8 mg in 1 ml inj, EPIDOSIN 8 mg inj., 10mg tab.
3. Pirenzepine 100–150 mg/day oral; it selectively blocksM1 muscarinic receptors (see p. 101) and inhibits gastricsecretion without producing typical atropinic side effects(these are due to blockade of M2 and M3 receptors). Themore likely site of action of pirenzepine in stomach is intramu-ral plexuses and ganglionic cells rather than the parietal cellsthemselves. It is nearly equally effective as cimetidine inrelieving peptic ulcer pain and promoting ulcer healing, buthas been overshadowed by H2 blockers and proton pumpinhibitors.
Vasicoselective drugs1. Oxybutynin This newer antimuscarinic hashigh affinity for receptors in urinary bladder andsalivary glands alongwith additional smoothmuscle relaxant and local anaesthetic properties.It is relatively selective for M1/M3 subtypeswith less action on the M2 subtype. Because ofvasicoselective action, it is used for detrusorinstability resulting in urinary frequency and urge

118S
EC
TIO
N2
DRUGS ACTING ON ANS
incontinence. Beneficial effects have beendemonstrated in post-prostatectomy vasical spasm,neurogenic bladder, spina bifida and nocturnalenuresis. Anticholinergic side effects are commonafter oral dosing, but intravasical instillationincreases bladder capacity with few side effects.Oxybutynin is metabolized by CYP3A4; its doseshould be reduced in patients being treated withinhibitors of this isoenzyme.Dose: 5 mg BD/TDS oral; children above 5 yr 2.5 mg BD.OXYBUTIN, CYSTRAN, OXYSPAS 2.5 mg and 5 mg tabs.
2. Tolterodine: This relatively M3 selectivemuscarinic antagonist has preferential action onurinary bladder; less likely to cause dryness ofmouth and other anticholinergic side effects. Itis indicated in overactive bladder with urinaryfrequency and urgency. Since it is metabolizedby CYP3A4, dose should be halved in patientsreceiving CYP3A4 inhibitors (erythromycin,ketoconazole, etc.)Dose: 1–2 mg BD or 2–4 mg OD of sustained release tab. oral.ROLITEN, TOLTER 1, 2 mg tabs, TORQ 2, 4 mg SR tab.
3. Flavoxate has properties similar to oxybuty-nin and is indicated in urinary frequency, urgencyand dysuria associated with lower urinary tractinfection.URISPAS, FLAVATE, FLAVOSPAS 200 mg tab, 1 tabTDS.Darifenacin and Solifenacin are other relatively M3
subtype selective antimuscarinics useful in bladderdisorders.
Drotaverine It is a novel non-anticholinergicsmooth muscle antispasmodic which acts byinhibiting phosphodiesterase-4 (PDE-4) selectivefor smooth muscle. Elevation of intracellularcAMP/cGMP attends smooth muscle relaxation.Changes in membrane ionic fluxes and membranepotential have also been shown. It has been usedorally as well as parenterally in intestinal, biliaryand renal colics, irritable bowel syndrome, uterinespasms, etc. without anticholinergic side effects.Adverse effects reported are headache, dizziness,constipation and flushing. Fall in BP can occuron i.v. injection.Dose: 40–80 mg TDS; DROTIN, DOTARIN, DOVERIN 40,80 mg tabs, 40 mg/2 ml inj.
Mydriatics
Atropine is a potent mydriatic but its slow andlong-lasting action is undesirable for refrac-tion testing. Though the pupil dilates in 30–40min, cycloplegia takes 1–3 hours, and the subjectis visually handicapped for about a week. Thesubstitutes attempt to overcome these difficulties.
1. Homatropine It is 10 times less potent thanatropine. Instilled in the eye, it acts in 45–60 min,mydriasis lasts 1–3 days while accommodationrecovers in 1–2 days. It often produces unsatisfac-tory cycloplegia in children who have high ciliarymuscle tone.HOMATROPINE EYE, HOMIDE 1%, 2% eye drops.
2. Cyclopentolate It is potent and rapidlyacting; mydriasis and cycloplegia occur in 30–60 min and last about a day. It is preferred forcycloplegic refraction, but children may showtransient behavioural abnormalities due toabsorption of the drug after passage into thenasolacrimal duct. It is also used in iritis anduveitis.CYCLOMID EYE 0.5%, 1%; CYCLOGYL, CYCLOPENT1% eye drops.
3. Tropicamide It has the quickest (20–40min) and briefest (3–6 hours) action, but is arelatively unreliable cycloplegic. However, it issatisfactory for refraction testing in adults andas a short acting mydriatic for fundoscopy. Themydriatic action can be augmented by combiningwith phenylephrine.OPTIMIDE, TROPICAMET, TROMIDE 0.5%, 1.0% eyedrops. TROPAC-P, TROPICAMET PLUS 0.8% withphenylephrine 5% eye drops.
Antiparkinsonian drugs (see Ch. 31)
USES
I. As antisecretory1. Preanaesthetic medication When irritantgeneral anaesthetics (ether) were used, prioradministration of anticholinergics (atropine,hyoscine, glycopyrrolate) was imperative to checkincreased salivary and tracheobronchial secretions.However, with current use of nonirritating

119C
HA
PTE
R8
ANTICHOLINERGIC DRUGS AND DRUGS ACTING ON AUTONOMIC GANGLIA
anaesthetics (halothane, etc.) the requirement hasdecreased, though atropine may still be employedbecause halothane sensitizes the heart to NAmediated ventricular arrhythmias which arespecially prone to occur during vagal slow-ing. Atropinic drugs also prevent laryngospasm,not by an action on laryngeal muscles, which areskeletal muscles, but by reducing respiratorysecretions that reflexly predispose to laryngo-spasm. Vasovagal attack during anaesthesia canalso be prevented.
2. Peptic ulcer Atropinic drugs decrease gastric secretion(fasting and neurogenic phase, but little effect on gastricphase) and afford symptomatic relief in peptic ulcer,though effective doses always produce side effects. They havenow been superseded by H2 blockers/proton pump inhibitors.
3. Pulmonary embolism These drugs benefitby reducing pulmonary secretions evoked reflexlyby embolism.
4. To check excessive sweating or salivation, e.g.in parkinsonism.
II. As antispasmodic1. Intestinal and renal colic, abdominal cramps:
symptomatic relief is afforded if there is nomechanical obstruction. However, parenteralopioids and NSAIDs provide greater pain reliefin renal colic than atropine. Atropine is lesseffective in biliary colic and is not able tocompletely counteract biliary spasm due toopiates (nitrates are more effective).
2. Nervous, functional and drug induced diarrhoeamay be controlled to some extent, butanticholinergics are not useful in infectivediarrhoea.
3. Spastic constipation, irritable bowel syndrome:modest symptomatic relief may be afforded.
4. Pylorospasm, gastric hypermotility, gastritis,nervous dyspepsia may be partially suppressed.
5. To relieve urinary frequency and urgency, enu-resis in children. Oxybutynin, tolterodine andflavoxate have demonstrated good efficacy, butdry mouth and other anticholinergic effects aredose limiting.
6. Dysmenorrhoea: These drugs are not veryeffective; NSAIDs are superior.
III. Bronchial asthma, asthmaticbronchitis, COPD
Reflex vagal activity is an important factor incausing bronchoconstriction and increased secretionin chronic bronchitis and COPD, but to a lesserextent in bronchial asthma. Orally administeredatropinic drugs are bronchodilators, but lesseffective than adrenergic drugs; not clinically used.They dry up secretion in the respiratory tract,may lead to its inspissation and plugging ofbronchioles resulting in alveolar collapse andpredisposition to infection. The mucociliaryclearance is also impaired. Inhaled ipratropiumbromide has been found to be specially effectivein asthmatic bronchitis and COPD, though lessso in bronchial asthma. Given by aerosol, it neitherdecreases respiratory secretions nor impairsmucociliary clearance, and there are few systemicside effects. Thus, it has a place in the managementof COPD. Its time course of action makes it moresuitable for regular prophylactic use rather thanfor control of acute attacks. The additive broncho-dilator action with adrenergic drugs is utilizedto afford relief in acute exacerbation of asthma/COPD by administering a combination of nebulizedipratropium and β2 agonist through a mask.
Tiotropium bromide is an equally effective andlonger acting alternative to ipratropium bromide.
IV. As mydriatic and cycloplegic(i) Diagnostic For testing error of refraction,both mydriasis and cycloplegia are needed.Tropicamide having briefer action has now largelyreplaced homatropine for this purpose. Thesedrugs do not cause sufficient cycloplegia inchildren: more potent agents like atropine orhyoscine have to be used. Atropine ointment (1%)applied 24 hours and 2 hours before is oftenpreferred for children below 5 years. Cyclopen-tolate drops are an alternative.
To facilitate fundoscopy only mydriasis isneeded; a short acting antimuscarinic may be used,

120S
EC
TIO
N2
DRUGS ACTING ON ANS
but phenylephrine is preferred, especially in theelderly, for fear of precipitating or aggravatingglaucoma. A combination of phenylephrine +tropicamide drops is frequently used.
(ii) Therapeutic Because of its long lastingmydriatic-cycloplegic and local anodyne (painrelieving) action on cornea, atropine is veryvaluable in the treatment of iritis, iridocyclitis,choroiditis, keratitis and corneal ulcer. It givesrest to the intraocular muscles and cuts down theirpainful spasm. Atropinic drugs alternated witha miotic prevent adhesions between iris and lensor iris and cornea and may even break them ifalready formed.
V. As cardiac vagolyticAtropine is useful in counteracting sinusbradycardia and partial heart block in selectedpatients where increased vagal tone is responsible,e.g. in some cases of myocardial infarction andin digitalis toxicity. However, cardiac arrhythmiasor ischaemia may be precipitated in some cases.
VI. For central action1. Parkinsonism (see Ch. 31) Centralanticholinergics are less effective than levodopa;They are used in mild cases, in drug inducedextrapyramidal syndromes and as adjuvant tolevodopa.
2. Motion sickness Hyoscine is the mosteffective drug for motion sickness. It is particularlyvaluable in highly susceptible individuals and forvigorous motions. The drug should be givenprophylactically (0.2 mg oral), because admi-nistration after symptoms have setin is lesseffective; action lasts 4–6 hours. A transdermalpreparation applied behind the pinna 4 hoursbefore journey has been shown to protect for 3days. Side effects with low oral doses andtransdermal medication are few, but dry mouthand sedation can occur: driving is risky.Dicyclomine is another anticholinergic used formotion sickness. These drugs are not effectivein other types of vomiting.
3. Hyoscine was used to produce sedation and amnesiaduring labour (twilight sleep) and to control maniacal states.It had earned a reputation as a ‘lie detector’ during worldwar II: its amnesic and depressant action was believed toput the subject ‘off guard’ in the face of sustained interrogationand sleep deprivation, so that he came out with the truth.
VII. To antagonise muscarinic effects ofdrugs and poisons
Atropine is the specific antidote for anti ChE andearly mushroom poisoning (see Ch. 7). Atropineor glycopyrrolate is also given to block muscarinicactions of neostigmine used for myasthenia gravis,decurarization or cobra envenomation.
SIDE EFFECTS AND TOXICITY
Side effects are quite common with the use ofatropine and its congeners; are due to facets ofits action other than for which it is being used.They cause inconvenience but are rarely serious.
Belladonna poisoning may occur due to drugoverdose or consumption of seeds and berries ofbelladonna/datura plant. Children are highlysusceptible. Manifestations are due to exaggeratedpharmacological actions.Dry mouth, difficulty in swallowing and talking.Dry, flushed and hot skin (especially over faceand neck), fever, difficulty in micturition, dec-reased bowel sounds. A scarlet rash may appear.Dilated pupil, photophobia, blurring of near vision,palpitation.Excitement, psychotic behaviour, ataxia, delirium,dreadful visual hallucinations.Hypotension, weak and rapid pulse, cardiovas-cular collapse with respiratory depression. Con-vulsions and coma occur only in severe poisoning.
Diagnosis Methacholine 5 mg or neostigmine1 mg s.c. fails to induce typical muscariniceffects.
Treatment If poison has been ingested, gastriclavage should be done with tannic acid (KMnO4
is ineffective in oxidizing atropine). The patientshould be kept in a dark quiet room. Cold spon-ging or ice bags are applied to reduce bodytemperature. Physostigmine 1–3 mg s.c. or i.v.antagonises both central and peripheral effects,

121C
HA
PTE
R8
ANTICHOLINERGIC DRUGS AND DRUGS ACTING ON AUTONOMIC GANGLIA
but has been found to produce hypotension andarrhythmias in some cases. As such, its utilityis controversial. Neostigmine does not antagonisethe central effects.
Other general measures (maintenance of bloodvolume, assisted respiration, diazepam to controlconvulsions) should be taken as appropriate.
Contraindications Atropinic drugs are absolu-tely contraindicated in individuals with a narrowiridocorneal angle—may precipitate acute con-gestive glaucoma. However, marked rise inintraocular tension is rare in patients with wideangle glaucoma.
Caution is advocated in elderly males withprostatic hypertrophy—urinary retention can occur.
Interactions1. Absorption of most drugs is slowed because
atropine delays gastric emptying. This resultsin slower absorption and greater peripheraldegradation of levodopa—less of it reachesthe brain. This does not occur when a peripheraldecarboxylase inhibitor is combined.
On the other hand, extent of digoxin andtetracycline absorption may be increased dueto longer transit time in the g.i.t.
2. Antacids interfere with absorption of anti-cholinergics.
3. Antihistaminics, tricyclic antidepressants,phenothiazines, disopyramide, pethidine haveanticholinergic property—additive side effectsoccur with atropinic drugs.
4. MAO inhibitors interfere with metabolism ofanticholinergic antiparkinsonian drugs —delirium may occur.
DRUGS ACTING ON AUTONOMICGANGLIA
Acetylcholine is the primary excitatory neuro-transmitter in both sympathetic and parasym-pathetic ganglia. Drugs which inhibit synthesis(hemicholinium) or release (botulinum toxin,procaine) of ACh can interfere with ganglionictransmission, but drugs which act on cholinergicreceptors in the ganglia are more selective.
In addition to the dominant nicotinic NN
receptors, which mediate the primary rapiddepolarization of ganglionic cells, there aresubsidiary muscarinic M1, M2, adrenergic, dopa-minergic, amino acid and peptidergic receptorswhich bring about secondary, slowly developingbut longer lasting changes in membrane potential,both positive and negative, that modulate theprimary response. Separate catecholamine (NA,DA) and amino acid transmitter containing cellsare present in ganglia, but peptides are releasedfrom the preganglionic cholinergic terminalsthemselves. Thus, autonomic ganglion is notmerely a one transmitter—one cell junction, buta complex system capable of local adjustmentsin the level of excitability.
Drugs can either stimulate or block the ganglia.
GANGLIONIC STIMULANTS
Selective nicotinic Nonselective/agonists muscarinic agonists
Nicotine (small dose) AcetylcholineLobeline CarbacholDimethyl phenyl Pilocarpinepiperazinium (DMPP) AnticholinesterasesTetramethyl ammonium MCN 343-A(TMA)Varenicline
Nicotine
It is the principal alkaloid in tobacco (Nicotianatabacum); acts as an agonist on both NN and NM
subtypes of nicotinic cholinergic receptors (NRs).Sympathetic as well as parasympathetic gangliaare stimulated, but larger doses cause persistentdepolarization and ganglionic blockade. Nicotineis important in the context of smoking and tobaccochewing; its only clinical indication is short-termnicotine replacement in tobacco abstinent subjects.There is no therapeutic application of ganglionicstimulants, because no useful purpose can beserved by stimulating both sympathetic andparasympathetic ganglia concurrently.

122S
EC
TIO
N2
DRUGS ACTING ON ANS
Treatment of smoking cessation/quitingtobacco chewingMajority of smokers (and tobacco chewers) wishto quit smoking/chewing, but fail to do so becauseof nicotine dependence. The most importantmeasure to help smokers quit is counselling andmotivation. This may be supplemented by phar-macotherapy. The goals of such pharmacotherapyare:• To reduce the craving for the satisfying
(reward) effects of nicotine.• To suppress the physical withdrawal symptoms
of nicotine.
The drugs currently utilized for the above goalsare:• Nicotine replacement• Partial agonists of α4β2 NRs (Varenicline)• Antidepressants (Bupropion)
Nicotine transdermal This patch formulationof nicotine is applied once daily on the hip/abdomen/chest/upper arm as an aid to smokingcessation. It ameliorates the symptoms of nicotinewithdrawal, but only partially suppresses thecraving, because the intermittent peak nicotineblood levels that occur during smoking are notreproduced by the patch.
NICOTINELL-TTS 10, 20, 30 cm2 patches releasing 7, 14,21 mg nicotine per 24 hr respectively. in those smoking> 20 cigarettes every day-start with 30 cm2 patch, shift tosmaller patches every 5–8 days, treat for 3–4 weeks (max.12 weeks).
Nicotine chewing gum Developed as analternative to nicotine transdermal, thisformulation is found more satisfying by somedependent subjects. The number of gum pieceschewed daily can be adjusted according to theneed felt.NULIFE 1, 2, 4 mg chewing gum; for those smoking >20cigarettes/day—start with 4 mg gum chewed and retainedin mouth for 30 min when urge to smoke is felt. After afew days change over to 2 mg gum and then to 1 mg gum.Not more than 15 pieces to be used in a day. Treatmentcan be started at lower doses for less heavy smokers.A nasal spray delivering 0.5 mg per activation, and an inhalerwith nicotine cartridge are also available in some countries.
Side effects of nicotine replacement therapy areheadache, dyspepsia, abdominal cramps, loosemotions, insomnia, flu-like symptoms and localirritation. Vasospastic angina may be precipitated.Cardiac arrhythmias and ischaemic heart diseaseare the contraindications.
Varenicline This α4β2 subtype NR selectivepartial agonist has been marketed as oral tabletsin many countries (UK, USA, Europe, etc) tohelp smoking cessation. Recent evidence hasshown that the reward (reinforcing) action ofnicotine is exerted through the α4β2 subtype ofneuronal NRs which are mainly localized innucleus accumbens and other mesolimbic areas.Activation of these NRs by nicotine induces DArelease which produces feelings of satisfaction/reward and has reinforcing effect. Sincevarenicline is a partial agonist at these receptors,it provides some level of nicotine substitution,but blocks the reward effect of smoking. Clinicallyit has been found to reduce craving as well asnicotine withdrawal symptoms in those who stopsmoking. Abstinence rates at one year of cessationare comparable to those of nicotine replacementand of bupropion. However, varenicline is notentirely safe. Side effects noted are mood changes,irrational behaviour, appetite and taste distur-bances, sleep disorder and agitation. Warning hasbeen issued that it may promote suicidal thoughts.
Dose: Initially 0.5 mg OD, gradually increase upto 1 mgBD according to need, for not more than 12 weeks; thentaper off.
Bupropion This atypical antidepressant inhibitsreuptake of DA and NA, and has been marketedas a sustained release tablet specifically forsmoking cessation. Clinical efficacy has been ratedequivalent to nicotine replacement, and it hasproduced fewer side effects (see Ch. 33).
GANGLION BLOCKING AGENTS
A. Competitive blockersQuaternary ammonium compounds
Hexamethonium, Pentolinium

123C
HA
PTE
R8
ANTICHOLINERGIC DRUGS AND DRUGS ACTING ON AUTONOMIC GANGLIA
Amines (secondary/tertiary)Mecamylamine, Pempidine
Monosulfonium compoundTrimethaphan camforsulfonate
B. Persistent depolarising blockersNicotine (large dose)Anticholinesterases (large dose)
The competitive ganglion blockers were used inthe 1950s for hypertension and peptic ulcer,but have been totally replaced now because theyproduce a number of intolerable side effects (seeTable 8.2). In fact, these side effects help in
understanding the relative roles of sympatheticand parasympathetic divisions in regulating thevarious organ functions.Trimethaphan It is an ultrashort acting ganglion blocker;has been occasionally infused i.v. to produce controlledhypotension and in hypertensive emergency due to aorticdissection.Mecamylamine Either alone or in combination with nico-tine patch, it has been tried for smoking cessation. It appearsto block the reward effect of nicotine and improve abstinencerate compared to placebo. Constipation occurred in manysubjects, and it is not an approved drug.
There is at present no clinical relevance ofganglion blockers.
TABLE 8.2 Relative autonomic tone and effects of ganglionic blockade on organ function
Organ Dominant tone Effect of ganglionic blockade (Side effect)
1. Heart Para-symp. Tachycardia (palpitation)
2. Blood vessels Symp. Vasodilatation, abolition of reflexes (postural andexercise hypotension, syncope)
3. Iris Para-symp. Mydriasis (photophobia)
4. Ciliary muscle Para-symp. Cycloplegia (blurring of near vision)
5. Intestines Para-symp. Decreased motility (distension, constipation)
6. Bladder Para-symp. Decreased tone (difficulty in micturition)
7. Male sexual function Para-symp. Inhibition of erectionSymp. Inhibition of ejaculation
(impotence)
8. Salivary glands Para-symp. Inhibition of salivation (dryness of mouth, difficultyin swallowing and talking)
9. Sweat glands Symp. (cholinergic) Inhibition of sweating (anhydrosis)
⎫⎬⎭
PROBLEM DIRECTED STUDY
8.1 An elderly male aged 74 years was brought to the hospital since he had not passed urinefor the past 24 hours and had severe pain in lower abdomen. On examination there was a bulgein the pubic region due to full urinary bladder. On catheterization, he passed 1.5L urine andthe pain was relieved.
He gave the history of having difficulty in passing urine, poor stream, frequent urge to urinateand post-void dribbling for the last 3 years. Over the past few days he had been experiencingepisodes of vertigo for which he was prescribed a medicine that he was taking for 2 days. Examinationof the prescription revealed that he was taking tab. Dimenhydrinate 50 mg 3 times daily.(a) Could there be any relationship between the anti-vertigo medication and the episode of acuteurinary retention?(see Appendix-1 for solution)

Adrenergic System and DrugsChapterChapterChapterChapterChapter 99999
ADRENERGIC TRANSMISSION
Adrenergic (more precisely ‘Noradrenergic’)transmission is restricted to the sympatheticdivision of the ANS. There are three closelyrelated endogenous catecholamines (CAs).Noradrenaline (NA) It acts as transmitter atpostganglionic sympathetic sites (except sweatglands, hair follicles and some vasodilator fibres)and in certain areas of brain.Adrenaline (Adr) It is secreted by adrenalmedulla and may have a transmitter role inthe brain.Dopamine (DA) It is a major transmitter inbasal ganglia, limbic system, CTZ, anteriorpituitary, etc. and in a limited manner in theperiphery.
1. Synthesis of CAs Catecholamines aresynthesized from the amino acid phenylalanineas depicted in Fig. 9.1. Tyrosine hydroxylaseis a specific and the rate limiting enzyme. Itsinhibition by α-methyl-p-tyrosine results indepletion of CAs. This inhibitor can be used inpheochromocytoma before surgery and ininoperable cases. All other enzymes of CAsynthesis are rather nonspecific and can act onclosely related substrates, e.g. dopa decarboxy-lase can form 5-HT from 5-hydroxytryptophanand α methyl DA from α methyl dopa. Synthesisof NA occurs in all adrenergic neurones, whilethat of Adr occurs only in the adrenal medullarycells. It requires high concentration of gluco-corticoids reaching through the intraadrenal portalcirculation for induction of the methylatingenzyme.
2. Storage of CAs NA is stored in synapticvesicles or ‘granules’ within the adrenergic nerveterminal (Fig. 9.4). The vesicular membrane
actively takes up DA from the cytoplasm andthe final step of synthesis of NA takes placeinside the vesicle which contains dopamine β-hydroxylase. NA is then stored as a complex withATP (in a ratio of 4 : 1) which is adsorbed ona protein chromogranin. In the adrenal medullathe NA thus formed within the chromaffin granulesdiffuses out into the cytoplasm, is methylatedand Adr so formed is again taken up by a separateset of granules. The cytoplasmic pool of CAs iskept low by the enzyme monoamine oxidase(MAO) present on the outer surface of mito-chondria.
3. Release of CAs The nerve impulse coupledrelease of CA takes place by exocytosis (see p.95) and all the vesicular contents (NA or Adr,ATP, dopamine β hydroxylase, chromogranin) are
Fig. 9.1: Steps in the synthesis of catecholamines

125C
HA
PTE
R9
ADRENERGIC SYSTEM AND DRUGS
poured out. In case of vesicles which in additioncontain peptides like enkephalin or neuropeptideY (NPY), these cotransmitters are simultaneouslyreleased. The release is modulated by presynapticreceptors, of which α2 inhibitory control isdominant.
The autoreceptors of other cotransmitters (Y2 of NPYand P1 of ATP) also inhibit transmitter release. In addition,numerous heteroreceptors are expressed on the adrenergicneurone which either inhibit (dopaminergic, serotonergic,muscarinic and PGE2) or enhance (β2 adrenergic, angiotensinAT1 and nicotinic) NA release.
Indirectly acting sympathomimetic amines(tyramine, etc.) also induce release of NA, butthey do so by displacing NA from the nerve endingbinding sites and by exchange diffusion utilizingnorepinephrine transporter (NET) the carrier ofuptake-1 (see below). This process is notexocytotic and does not require Ca2+.
4. Uptake of CAs There is a very efficientmechanism by which NA released from the nerveterminal is recaptured. This occurs in 2 steps—
Axonal uptake An active amine pump (NET)is present at the neuronal membrane whichtransports NA by a Na+ coupled mechanism. Ittakes up NA at a higher rate than Adr and hadbeen labelled uptake-1. The indirectly actingsympathomimetic amines like tyramine, but notisoprenaline, also utilize this pump for enteringthe neurone. This uptake is the most importantmechanism for terminating the postjunctionalaction of NA. From 75% to 90% of releasedNA is retaken back into the neurone. This pumpis inhibited by cocaine, desipramine and few otherdrugs.
Vesicular uptake The membrane ofintracellular vesicles has another amine pump the‘vesicular monoamine transporter’ (VMAT-2),which transports CA from the cytoplasm to theinterior of the storage vesicle. The VMAT-2transports monoamines by exchanging with H+
ions. The vesicular NA is constantly leaking outinto the axoplasm and is recaptured by thismechanism. This carrier also takes up DA formedin the axoplasm for further synthesis to NA. Thus,it is very important in maintaining the NA content
of the neurone. This uptake is inhibited byreserpine, resulting in depletion of CAs.
Extraneuronal uptake of CAs (uptake-2) iscarried out by extraneuronal amine transporter(ENT or OCT3) and other organic cation trans-porters OCT1 and OCT2 into cells of other tissues.In contrast to NET this uptake transports Adrat a higher rate than NA, is not Na+ dependentand is not inhibited by cocaine, but inhibited bycorticosterone. It may capture circulating Adr, butis quantitatively minor and not of physiologicalor pharmacological importance.
5. Metabolism of CAs The pathways ofmetabolism of CAs are depicted in Fig. 9.2. Partof the NA leaking out from vesicles into cytoplasmas well as that taken up by axonal transport isfirst attacked by MAO, while that which diffusesinto circulation is first acted upon by catechol-o-methyl transferase (COMT) in liver and othertissues. In both cases, the alternative enzyme cansubsequently act to produce vanillylmandelicacid (VMA). Other intermediate step enzymesinvolved are aldehyde reductase (AR), aldehydedehydrogenase (AD) and alcohol dehydrogenase(ADH). The major metabolites excreted in urineare VMA and 3-methoxy-4-hydroxy phenyl glycol(a reduced product) along with some metaneph-rine, normetanephrine and 3,4 dihydroxy man-delic acid. These metabolites are mostly conjuga-ted with glucuronic acid or sulfate before excre-tion in urine. Only 25–50 µg of NA and 2–5µg of Adr are excreted in the free form in 24hours. However, metabolism does not play animportant role in terminating the action ofneuronally released CAs.6. Adrenergic receptors Adrenergic recep-tors are membrane bound G-protein coupledreceptors which function primarily by increasingor decreasing the intracellular production ofsecond messengers cAMP or IP3/DAG. In somecases the activated G-protein itself operates K+
or Ca2+ channels, or increases prostaglandinproduction.
Ahlquist (1948), on the basis of two distinctrank order of potencies of adrenergic agonists

126S
EC
TIO
N2
DRUGS ACTING ON ANS
Fig. 9.2: Metabolism of catecholaminesMAO—Monoamine oxidase; COMT—Catechol-O-methyl transferase; AR—Aldehyde reductase;AD—Aldehyde dehydrogenase; ADH—Alcohol dehydrogenase; DOMA—3,4 dihydroxy mandelicacid; MOPEG—3-methoxy, 4-hydroxy phenyl glycol; VMA—vanillyl mandelic acid.
Fig. 9.3: Dose-response curves of 3 catecholamines adrenaline (Adr), noradrenaline (NA) and isoprenaline(Iso) on isolated aortic strip and isolated bronchial smooth muscle illustrating two distinct rank orders of potenciesrespectively for α and β adrenergic receptors
(Fig. 9.3), classified adrenergic receptors into twotypes α and β. This classification was confirmedlater by the discovery of selective α and βadrenergic antagonists. Important features of αand β receptors are given in Table 9.1.
On the basis of relative organ specificity ofselective agonists and antagonists the β receptorswere further subdivided into β1 and β2 subtypes.Later, β3 (atypical β) receptors were describedwhich are more sensitive to NA than to Adr, and

127C
HA
PTE
R9
ADRENERGIC SYSTEM AND DRUGS
TABLE 9.1 Differences between ααααα and βββββ adrenergic receptors
α β
1. Rank order of potency of agonists *Adr > NA > Iso Iso > Adr > NA
2. Antagonist Phenoxybenzamine Propranolol
3. Coupling protein Gq/Gi/Go Gs
4. Effector pathway IP3/DAG↑, cAMP ↓, K+ channel ↑ cAMP↑, Ca2+ channel ↑
* Though inherently NA is equipotent to Adr on α receptors, in test systems with intact neuronal reuptake, it appearsless potent due to faster reuptake.
TABLE 9.2 Differences between βββββ1, βββββ2 and βββββ3 receptors
β1 β2 β3
1. Location Heart, Bronchi, blood Adipose tissueJG cells in kidney vessels, uterus, liver,
g.i.t., urinary tract, eye
2. Selective agonist Dobutamine Salbutamol, terbutalin BRL 37344
3. Selective antagonist Metoprolol, ICI 118551 CGP 20712A (also β1)Atenolol α-methyl propranolol ICI 118551 (also β2)
4 Relative potency NA < Adr NA << Adr NA > Adrof NA and Adr
TABLE 9.3 Differences between ααααα1 and ααααα2 receptors
α1 α2
Location Postjunctional on effector Prejunctional on nerve ending (α2A),organs also postjunctional in brain, pancreatic
β cells and extrajunctional incertain blood vessels, platelets
Function subserved GU Smooth muscle–contraction Inhibition of transmitter releaseVasoconstriction VasoconstrictionGland—secretion Decreased central sympathetic flowGut—relaxation Decreased insulin releaseLiver—glycogenolysis Platelet aggregationHeart—arrhythmia
Selective agonist Phenylephrine, Methoxamine Clonidine
Selective antagonist Prazosin Yohimbine, Rauwolscine
Coupling protein Gq Gi/Go
Effector pathway IP3/DAG ↑ cAMP ↓Phospholipase A2 ↑—PG release K+ channel ↑
Ca2+ channel ↓ or ↑IP3/DAG ↑
GU: Genitourinary

128S
EC
TIO
N2
DRUGS ACTING ON ANS
have very low affinity for the standardβ blockers. These are located on adipocytes,mediate lipolysis and induce thermogenesis.Selective β3 agonists have the potential to be usedas antiobesity drugs.
In the mid 1970s the α receptors were demon-strated to be present prejunctionally as well. Todifferentiate these release inhibitory prejunctionalα receptors, a subdivision into α1 and α2 wassuggested. However, the present classification intoα1 and α2 is based on pharmacological criteria(selectivity of agonists and antagonists) and not
on anatomical location. Molecular cloning hasfurther identified 3 subtypes of α1 (α1A, α1B, α1D)and 3 subtypes of α2 (α2A, α2B, α2C) receptors.
Though tissue distribution of subtypes of α1 and α2
receptors has been mapped, there is lot of overlap. Sufficientlysubtype selective agonists or antagonists have also not yetbeen developed to pharmacologically exploit the molecularheterogeneity of subtypes of α1 and α2 receptors.
The adrenergic neuronal mechanisms andaction of drugs which modify them are depicted inFig. 9.4. A summary of drugs acting throughadrenergic neuronal mechanisms is presented inTable 9.4
Fig. 9.4: Schematic representation of adrenergic neurotransmission and its modification by drugsTYR—tyrosine; α M-p-Tyr—α methyl-p-tyrosine; α M-Dopa—α methyl dopa; MAO—monoamine oxidase;MAOI—monoamine oxidase inhibitor; COMT—catechol-o-methyl transferase; NMN—nor-metanephrine;VMA—vanillyl mandelic acid; NET—Norepinephrine transporter; VMAT-2—Vesicular monoamine transporter;DOMA—3,4 dihydroxy mandelic acid; MOPEG—3-Methoxy,4-hydroxy phenyl glycol.

129C
HA
PTE
R9
ADRENERGIC SYSTEM AND DRUGS
TABLE 9.4 Summary of drug action through modification of adrenergic transmission
Step/site Action Drug Response
1. Synthesis of NA Inhibition α-methyl-p-tyrosine Depletion of NAUtilisation of α-methyl dopa Replacement of NA bysame synthetic a-methyl NA (falsepathway transmitter)
2. Axonal uptake Blockade Cocaine, desipramine, Potentiation of NAguanethidine, ephedrine (endo-and exogenous),
inhibition of tyramine
3. Vesicular uptake Blockade Reserpine Depletion of NA(degraded by MAO)
4. Nerve impulse Inhibition Guanethidine, Loss of transmissioncoupled release bretyliumof NA
5. Vesicular NA Displacement Guanethidine Initially sympathomimetic,depletion of NA later
6. Membrane NA pool Exchange diffusion Tyramine, ephedrine Indirect sympathomimetic
7. Metabolism MAO-inhibition Nialamide, Potentiation of NA (slight),tranylcypromine —of tyramine (marked)
MAO-A inhibition Moclobemide Potentiation of NA andtyramine (slight)
MAO-B inhibition Selegiline Potentiation of DA in brainCOMT inhibition Tolcapone, entacapone Potentiation of NA and DA (slight)
8. Receptors Mimicking Phenylephrine α1 sympathomimeticClonidine α2–inhibition of NA release,
↓ sympathetic outflowIsoprenaline β1 + β2 —sympathomimeticDobutamine β1—sympathomimetic:
cardiac stimulationSalbutamol β2—sympathomimetic:
bronchodilatationBlockade Phenoxybenzamine α1 + α2—blockade
Prazosin α1—blockadeYohimbine α2—blockadePropranolol β1 + β2—blockadeMetoprolol β1—blockade
ADRENERGIC DRUGS(Sympathomimetics)
These are drugs with actions similar to that ofAdr or of sympathetic stimulation.
Direct sympathomimetics They act directlyas agonists on α and/or β adrenoceptors—Adr,NA, isoprenaline (Iso), phenylephrine, metho-xamine, xylometazoline, salbutamol and manyothers.
Indirect sympathomimetics They act on adre-nergic neurone to release NA, which then actson the adrenoceptors—tyramine, amphetamine.
Mixed action sympathomimetics They actdirectly as well as indirectly—ephedrine,dopamine, mephentermine.
ACTIONSThe peripheral actions of Adr in most tissues

130S
EC
TIO
N2
DRUGS ACTING ON ANS
TABLE 9.5 Adrenergic responses mediated through ααααα and βββββ receptors
α actions β actions
1. Constriction of arterioles and veins → rise Dilatation of arterioles and veins → fall in BP (β2)inBP (α1 + α2)
2. Heart—little action, arrhythmia at high Cardiac stimulation (β1), ↑ rate, force and conductiondose (α1) velocity
3. — Bronchodilatation (β2)
4. Contraction of radial muscles of iris → No effect on iris, slight relaxation of ciliary muscle,mydriasis (α1), decreased aqueous secretion Enhanced aqueous secretion
5. Intestinal relaxation, contraction of sphincters Intestinal relaxation (β2)
6. Bladder trigone—contraction (α1) Detrusor—relaxation (β2)
7. Uterus—contraction (α1) Relaxation (β2)
8. Splenic capsule—contraction (α1) Relaxation (β2) (slight)
9. Neuromuscular transmission facilitated, Active state—prolonged in fast contracting muscle,↑ ACh release abbreviated in slow contracting muscle; tremors (β2)
10. Insulin secretion inhibited (α2) (dominant) Augmented insulin (mild) and glucagon secretion (β2)
11. Liver—glycogenolysis (α in some species) Liver—glycogenolysis (β2) → hyperglycaemiaMuscle—glycogenolysis (β2) → hyperlactacidaemiaFat—lipolysis (β1 + β2 + β3) → increased blood FFA,calorigenesis
12. — Renin release from kidney (β1)
13. Male sex organs—ejaculation (α1) —
14. Salivary gland—K+ and water secretion (α1) Ptylin secretion
15. — ADH secretion from posterior pituitary (β1)
16. Nictitating membrane—contraction (in animals) —
have been clearly differentiated into those mediatedby α or β receptors depending on the predominantreceptor type present in a given tissue. These aretabulated in Table 9.5. The receptor subtype,wherever defined, has been mentioned in paren-thesis. The actions of a particular sympathomimeticamine depend on its relative activity at differenttypes of adrenergic receptors.Adr : α1 + α2 + β1 + β2 and weak β3 actionNA : α1 + α2 + β1 + β3 but no β2 actionIso : β1 + β2 + β3 but no α action
Important actions of Adr, NA and isoprenalineare compared in Table 9.6.
The overall actions are—1. Heart Adr increases heart rate by increa-sing the slope of slow diastolic depolarization
of cells in the SA node. It also activates latentpacemakers in A-V node and Purkinje fibres;arrhythmias can occur with high doses that raiseBP markedly. Raised BP reflexly depresses theSA node and unmasks the latent pacemakers.Certain anaesthetics (chloroform, halothane)sensitize the heart to arrhythmic action of Adr.Idioventricular rate is increased in patients withcomplete heart block.
Force of cardiac contraction is increased.Development of tension as well as relaxation areaccelerated. Thus, systole is shortened more thandiastole. Cardiac output and oxygen consumptionof the heart are markedly enhanced.
Conduction velocity through A-V node, bun-dle of His, atrial and ventricular fibres is increased;partial A-V block may be overcome. Refractory

131C
HA
PTE
R9
ADRENERGIC SYSTEM AND DRUGS
TABLE 9.6 Comparative effects of intravenous infusionof adrenaline, noradrenaline and isoprenaline
Adr NA Iso
1. Heart rate ↑ ↓ ↑↑2. Cardiac output ↑↑ – ↑↑3. BP—Systolic ↑↑ ↑↑ ↑
Diastolic ↓↑ ↑↑ ↓↓ Mean ↑ ↑↑ ↓
4. Blood flowSkin and mm ↓ ↓ –Sk. muscle ↑↑ –, ↓ ↑Kidney ↓ ↓ –Liver ↑↑ – ↑Coronary ↑ ↑ ↑
5. Bronchial muscle ↓↓ – ↓↓6. Intestinal muscle ↓↓ ↓ ↓7. Blood sugar ↑↑ –, ↑ ↑
period (RP) of all types of cardiac cells is reduced.All cardiac actions are predominantly β1 receptormediated.
When BP rises markedly, reflex bradycardiaoccurs due to stimulation of vagus— this is theusual response seen when NA is injected i.v.
2. Blood vessels Both vasoconstriction (α)and vasodilatation (β2) can occur depending onthe drug, its dose and vascular bed. Constrictionpredominates in cutaneous, mucous membraneand renal beds. Vasoconstriction occurs throughboth α1 and α2 receptors. However, location ofα2 (extrajunctional) receptors is such that theyare activated only by circulating CAs, whereasα1 (junctional) receptors primarily mediateresponses to neuronally released NA. Dilatationpredominates in skeletal muscles, liver and coro-naries. The direct effect on cerebral vessels isnot prominent—blood flow through this bed paral-lels change in BP.
The action is most marked on arterioles andprecapillary sphincters; larger arteries and veinsare affected at higher doses.
3. BP The effect depends on the amine, itsdose and rate of administration.• NA causes rise in systolic, diastolic and mean
BP; it does not cause vasodilatation (no
β2 action), peripheral resistance increasesconsistently due to α action.
• Isoprenaline causes rise in systolic but markedfall in diastolic BP (β1—cardiac stimulation,β2— vasodilatation). The mean BP generallyfalls.
• Adr given by slow i.v. infusion or s.c. injectioncauses rise in systolic but fall in diastolic BP;peripheral resistance decreases because vas-cular β2 receptors are more sensitive than α receptors. Mean BP generally rises. Pulsepressure is increased.
• Rapid i.v. injection of Adr (in animals)produces a marked increase in both systolicas well as diastolic BP (at high concentrationα response predominates and vasoconstric-tion occurs even in skeletal muscles). The BPreturns to normal within a few minutes anda secondary fall in mean BP follows. Themechanism is—rapid uptake and dissipationof Adr → concentration around the receptoris reduced → low concentrations are not ableto act on α receptors but continue to act onβ2 receptors.
When an α blocker has been given, only fall inBP is seen—vasomotor reversal of Dale.
4. Respiration Adr and isoprenaline, but notNA are potent bronchodilators (β2). This action

132S
EC
TIO
N2
DRUGS ACTING ON ANS
is more marked when the bronchi are constricted.Adr given by aerosol additionally decongestsbronchial mucosa by α action. Adr can directlystimulate respiratory centre (RC) but this actionis seldom manifest at clinically used doses. Rapidi.v. injection (in animals) causes transient apnoeadue to reflex inhibition of RC. Toxic doses ofAdr cause pulmonary edema by shifting bloodfrom systemic to pulmonary circuit.5. Eye Mydriasis occurs due to contractionof radial muscles of iris (α1), but this is mini-mal after topical application, because Adr pene-trates cornea poorly. The intraocular tension tendsto fall, especially in wide angle glaucoma.
Adr has complex effects on aqueous humordynamics (see p. 154).
10. Skeletal muscle Neuromuscular transmis-sion is facilitated. In contrast to action onautonomic nerve endings, α receptor activationon motor nerve endings augments ACh release,probably because it is of the α1 subtype. Thedirect effect on muscle fibres is exerted throughβ2 receptors and differs according to the type offibre. The active state is abbreviated and lesstension is developed in the slow contracting redfibres. There is incomplete fusion of individualresponses. This along with enhanced firing ofmuscle spindles is responsible for the tremorsproduced by β2 agonists. The action on rapidlycontracting white fibres is to prolong the activestate and increase the tension developed.11. CNS Adr, in clinically used doses, does notproduce any marked CNS effects because of poorpenetration in brain, but restlessness, apprehen-sion and tremor may occur. Activation of α2
receptors in the brainstem (by selective α2
agonists) results in decreased sympathetic outflow→ fall in BP and bradycardia.12. Metabolic Adr causes glycogenolysis →hyperglycaemia, hyperlactacidaemia (β2); lipoly-sis → rise in plasma free fatty acid (FFA) andcalorigenesis (β2 + β3). These are due to directaction on liver, muscle and adipose tissue cells.In addition metabolic effects result from reductionof insulin (α2) and augmentation of glucagon (β2)secretion.
Transient hyperkalaemia followed by hypo-kalaemia occurs due to initial release of K+ fromliver, and later its enhanced uptake into skeletalmuscles as well as in liver.
Biochemical mediation of adrenergic responses
β actions The β actions are mediated through cAMP (seeFig. 4.6). Adr activates membrane bound enzyme adenylylcyclase through a regulatory protein Gs → ATP is brokendown to cAMP at the inner face. This in turn phosphorylatesa number of intracellular cAMP-dependent protein kinasesand initiates a series of reactions:(i) In liver and muscle, glycogen phosphorylase is activatedcausing glycogenolysis while glycogen synthase is inhibited.Both actions result in hyperglycaemia and hyperlactacidemia.Neoglucogenesis in liver adds to the response.
K+ is first released from liver → hyperkalaemia; followedby more prolonged hypokalaemia due to K+ uptake in muscleand later in liver itself.
Action of adrenaline on aqueous humor dynamics
Receptor Agonist action
α1 : Vasoconstriction of ciliary vessels →reduced aqueous formation
α2 : Reduced secretory activity of ciliaryepithelium
?α : Augmentation of uveo-scleral outflowβ2 : Enhanced secretory activity of ciliary
epitheliumFacilitation of trabecular outflow
Overall, aqueous formation is reduced and outflowis facilitated.
6. GIT In isolated preparations of gut, rela-xation occurs through activation of both α andβ receptors. In intact animals and man peristalsisis reduced and sphincters are constricted, but theeffects are brief and of no clinical import.7. Bladder Detrusor is relaxed (β) and trigoneis constricted (α): both actions tend to hindermicturition.8. Uterus Adr can both contract and relaxuterine muscle, respectively through α and βreceptors. The overall effect varies with species,hormonal and gestational status. Human uterusis relaxed by Adr at term of pregnancy, but atother times, its concentrations are enhanced.9. Splenic capsule Contracts (α) and moreRBCs are poured in circulation. This action is notevident in man.

133C
HA
PTE
R9
ADRENERGIC SYSTEM AND DRUGS
(ii) In adipose tissue, triglyceride lipase is activated →increased plasma free fatty acids. Increased O2 consumptionand heat production result primarily by action on brownadipose tissue, which has predominant β3 receptors.(iii) In heart, proteins like troponin and phospholamban arephosphorylated. The former results in increased interactionwith Ca2+ at the myofilaments → increased force of contrac-tion; the latter causes sequestration of Ca2+ by sarcoplasmicreticulum → more rapid relaxation. The activated proteinGs, in addition, interacts directly with the Ca2+ channelsin the membrane promoting influx of Ca2+ which reinforcesthe positive inotropic action exerted through cAMP.(iv) In the gut and bronchial muscle, relaxation (accom-panied with hyperpolarization) is induced, but the intermediatesteps have not been clearly delineated.(v) In pancreatic islets activation of β2 receptors on α cellsincreases glucagon secretion, and that on β cells increasesinsulin secretion, both by raising intracellular cAMP. However,augmentation of insulin secretion is weak.
α actions The mediation of α actions is varied and lesswell defined.(i) In smooth muscles (including vascular) that are contractedthrough α1 receptors, the activated Gq-protein increases IP3/DAG production → mobilization of Ca2+ from intracellularorganelle → activation of calmodulin dependent myosin lightchain kinase → phosphorylation of myosin → contraction.The vasoconstrictor α2 receptors probably enhance Ca2+ influxwithout utilizing IP3.(ii) The prejunctional α2 receptor appears to inhibit neuronalCa2+ channels and also limit the intracellular availability ofCa2+ by decreasing cAMP production. Transmitter (NA) releaseis consequently diminished. Hyperpolarization throughactivation of G-protein gated K+ channels may also occur.(iii) In the gut, α2 receptor activation hyperpolarizes thecholinergic neurone → decreased release of ACh → reducedtone; whereas α1 receptors located directly on the smooth musclecell increase K+ efflux indirectly (by activating Ca2+ dependentK+ channels) leading to hyperpolarization → relaxation.(iv) In pancreatic β cells, stimulation of α2 receptors reducesthe formation of cAMP → decreased insulin release.
Administration and preparationsCAs are absorbed from the intestine but are rapidlydegraded by MAO and COMT present in theintestinal wall and liver. They are thus orallyinactive.1. Adrenaline (Epinephrine) For systemicaction, 0.2–0.5 mg s.c., i.m., action lasts ½ to2 hrs. ADRENALINE 1 mg/ml inj; ADRENA 4 mg (ofAdr. bitartrate=2mg Adr. base)/2 ml inj.
As local vasoconstrictor, 1 in 200,000 to 1in 100,000 added to lidocaine;
in XYLOCAINE with ADRENALINE: lidocaine 21.3mg + adrenaline 0.005 mg/ml inj; 30 ml vial.
2. Noradrenaline (Norepinephrine, levarterenol)2–4 µg/min i.v. infusion; local tissue necrosisoccurs if the solution extravasates; do not mixwith NaHCO3 in the same bottle (rapid oxidationoccurs); action starts declining within 5 min ofdiscontinuing infusion. It is rarely used now asa pressor agent. ADRENOR, NORAD, VASCUE, NOR-DRIN 2 mg (base)/2 ml amp.
3. Isoprenaline (Isoproterenol) 20 mg sublin-gual, 1–2 mg i.m., 5–10 µg/min i.v. infusion;action lasts 1–3 hrs. It is occasionally used tomaintain idioventricular rate till pacemaker isimplanted. For bronchial asthma, it has beensuperseded by selective β2 agonists.ISOPRIN, ISOSOL 4 mg/2 ml inj, NEOEPININE 20 mgsublingual tablets.
Adverse effects and contraindications• Transient restlessness, headache, palpitation,
anxiety, tremor and pallor may occur after s.c./i.m. injection of Adr.
• Marked rise in BP leading to cerebral haemor-rhage, ventricular tachycardia/fibrillation,angina, myocardial infarction are the hazards oflarge doses or inadvertant i.v. injection of Adr.
• Adr is contraindicated in hypertensive, hyper-thyroid and angina patients.
• Adr should not be given during anaesthesiawith halothane (risk of arrhythmias) and topatients receiving β blockers (marked rise inBP can occur due to unopposed α action).
THERAPEUTIC CLASSIFICATION OFADRENERGIC DRUGS
I. Pressor agentsNoradrenaline PhenylephrineEphedrine MethoxamineDopamine Mephentermine
II. Cardiac stimulantsAdrenaline DobutamineIsoprenaline
III. BronchodilatorsIsoprenaline SalmeterolSalbutamol Formoterol(Albuterol) BambuterolTerbutaline

134S
EC
TIO
N2
DRUGS ACTING ON ANS
IV. Nasal decongestantsPhenylephrine NaphazolineXylometazoline PseudoephedrineOxymetazoline Phenyl propanolamine
V. CNS stimulantsAmphetamine MethamphetamineDexamphetamine
VI. AnorecticsFenfluramine SibutramineDexfenfluramine
VII. Uterine relaxant and vasodilatorsRitodrine SalbutamolIsoxsuprine Terbutaline
Salient features of important adrenergic drugs aredescribed below.
Dopamine (DA) It is a dopaminergic (D1 andD2) as well as adrenergic α and β1 (but not β2) agonist. The D1 receptors in renal and mesentericblood vessels are the most sensitive: i.v. infusionof low dose of DA dilates these vessels (by raisingintracellular cAMP). This increases g.f.r. Inaddition DA exerts natriuretic effect by D1receptors on proximal tubular cells. Moderatelyhigh doses produce a positive inotropic (direct β1
and D1 action + that due to NA release), but littlechronotropic effect on heart. Vasoconstriction (α1
action) occurs only when large doses are infused.At doses normally employed, it raises cardiacoutput and systolic BP with little effect on diastolicBP. It has practically no effect on nonvascular αand β receptors; does not penetrate blood-brainbarrier—no CNS effects.
Dopamine is used in patients of cardiogenicor septic shock and severe CHF wherein it increa-ses BP and urine outflow. It is administered byi.v. infusion (0.2–1 mg/min) which is regulatedby monitoring BP and rate of urine formation.DOPAMINE, INTROPIN, DOPACARD 200 mg in 5 ml amp.
Dobutamine A derivative of DA, but not aD1 or D2 receptor agonist. Though it acts on bothα and β adrenergic receptors, the only prominentaction of clinically employed doses (2–8 µg/kg/min i.v. infusion) is increased force of cardiac
contraction and output, without significant changein heart rate, peripheral resistance and BP. Assuch, it is considered to be a relatively selectiveβ1 agonist. It is used as an inotropic agent inpump failure accompanying myocardial infarction,cardiac surgery, and for short term managementof severe congestive heart failure. It is lessarrhythmogenic than Adr.CRDIJECT 50 mg/4 ml and 250 mg per 20 ml amp,DOBUTREX, DOBUSTAT 250 mg vial.
Ephedrine It is an alkaloid obtained fromEphedra vulgaris. Mainly acts indirectly but hassome direct action as well on α and β receptors.Repeated injections produce tachyphylaxis,primarily because the neuronal pool of NAavailable for displacement is small. It is resistantto MAO, therefore, effective orally. It is about100 times less potent than Adr, but longer acting(4–6 hours). Ephedrine crosses to brain and causesstimulation, but central: peripheral activity ratiois lower than that of amphetamine.
Ephedrine can be used for a variety ofpurposes, but it lacks selectivity, and efficacy islow. Use is now restricted to that in mild chronicbronchial asthma and for hypotension duringspinal anaesthesia; occasionally for posturalhypotension; 15–60 mg TDS.EPHEDRINE HCl 15, 30 mg tab; SULFIDRIN 50 mg in1 ml inj, in ENDRINE 0.75% nasal drops.
Amphetamines These are synthetic compoundshaving a pharmacological profile similar toephedrine; orally active with relatively longduration (4–6 hours). They exert potent CNSstimulant and weaker peripheral cardiovascularactions. Maximal selectivity is exhibited bydextroamphetamine and methamphetamine, whichin the usual doses produce few peripheral effects.
The central actions of amphetamines arelargely mediated by release of NA from adrenergicneurones in the brain. This occurs mainly byexchange diffusion and reverse transport involvingtransporters like NET, DAT and VMAT2 asdepicted in Fig. 9.5. However, the effects onlocomotor activity, perception and the psychoticphenomena seen at high doses are probably due

135C
HA
PTE
R9
ADRENERGIC SYSTEM AND DRUGS
Fig. 9.5: Illustration of the mechanisms ofnoradrenaline release by amphetamine.
Amphetamine (Amph) enters the adrenergic neurone byutilizing the neuronal norepinephrine transporter (NET)or dopamine transporter (DAT)-(1), and then the storagevesicles through vesicular monoamine transporter(VMAT2). It then displaces the stored noradrenaline (NA)into the neuronal cytoplasm, most of which is releasedinto the synaptic cleft by exchange diffusion-(2) withextracellular Amph., or by reverse transport-(3), bothutilizing NET. Note that this release is not exocytotic anddoes not require Ca2+
.
to DA and 5-HT release by processes similar tothat for NA release. In addition, amphetamineinhibits neuronal reuptake of DA.
The central effects include alertness, increa-sed concentration and attention span, euphoria,talkativeness, increased work capacity. Fatigue isallayed. Athletic performance is improved tempo-rarily followed by deterioration. It is one of thedrugs included in the ‘dope test’ for athletes. Thereticular activating system is stimulated resultingin wakefulness and postponement of sleep depri-vation induced physical disability. But this is short-lived and may be accompanied by anxiety,restlessness, tremor, dysphoria and agitation. Usebefore examinations to keep awake can be counterproductive and needs to be condemned.
Amphetamines stimulate respiratory centre,specially if it has been depressed. Hunger issuppressed as a result of inhibition of hypo-
thalamic feeding centre. They also have weakanticonvulsant, analgesic and antiemetic actions:potentiate antiepileptics, analgesics and antimotion-sickness drugs. Peripheral effects onheart and BP are not significant at the usual doses(which cause only slight rise in BP), but toneof vesical sphincter is definitely increased.
Amphetamines are drugs of abuse and arecapable of producing marked psychological butlittle or no physical dependence. Amphetamineabusers are generally teenagers seeking thrill orkick which is obtained on rapid i.v. injection.High doses produce euphoria, restlessness,insomnia, aggression, panic, marked excitementwhich may progress to mental confusion, delirium,hallucinations and an acute psychotic state. Peri-pheral component of toxicity includes rise in BP,palpitation, arrhythmias, vomiting, abdominalcramps and vascular collapse. Death is usuallypreceded by convulsions and coma.
Repeated use is more likely to produce longlasting behavioural abnormalities; psychosis maybe precipitated.
Tolerance to central actions and toxic effectsof amphetamine develops, and is both pharma-cokinetic as well as pharmacodynamic. Starva-tion due to suppression of appetite produces acidicurine; amphetamine is ionized more at acidic pHand is excreted more rapidly.
Treatment of amphetamine toxicity includesadministration of chlorpromazine which controlsboth central as well as peripheral α adrenergiceffects.Amphetamine: 5–15 mg oral; Dexamphetamine: 5–10 mg(children 2.5–5 mg) oral.Methamphetamine: 5–10 mg oral.
Phenylephrine It is a selective α1 agonist, hasnegligible β action. It raises BP by causing vaso-constriction. Because it has little cardiac action,reflex bradycardia is prominent. Topically it isused as a nasal decongestant and in the eye forproducing mydriasis when cycloplegia is notrequired. Phenylephrine tends to reduce intraoculartension by constricting ciliary body bloodvessels. It is also a frequent constituent of orallyadministered nasal decongestant preparations.

136S
EC
TIO
N2
DRUGS ACTING ON ANS
Central effects are not seen with usual clinicaldoses.Dose: 2–5 mg i.m., 0.1–0.5 mg slow i.v. inj, 30–60 μg/min i.v. infusion; 5–10 mg oral; 0.25–0.5% nasal instillation;5–10% topically in eye;FRENIN 10 mg in 1 ml inj; DECOLD PLUS 5 mg withparacetamol 400 mg + chlorpheniramine 2 mg + caffeine15 mg tab., SINAREST 10 mg with chlorpheniramine2 mg, paracetamol 500 mg, caffeine 30 mg tab, FENOX0.25% with nephazoline 0.025% nasal drops, DROSYN 10%eye drops, in DROSYN-T, TROPAC-P 5% with tropicamide0.8% eye drops.
Methoxamine Another selective α1 agonistwith no β actions (has weak β blockingaction). Resembles phenylephrine very closely.Occasionally used as a pressor agent.Dose: 10–20 mg i.m.; 3–5 mg slow i.v. inj.VASOXINE 20 mg/ml inj.
Mephentermine It produces both cardiac sti-mulation and vasoconstriction by directly acti-vating α and β adrenergic receptors as well asby releasing NA. Cardiac output, systolic anddiastolic BP are increased. The direct positivechronotropic effect on heart is generally counterbalanced by vagal stimulation due to rise in meanBP.
Mephentermine is not a substrate for eitherMAO or COMT. Therefore it is active orally withlonger duration of action (2–6 hr). It crossesblood-brain barrier to some extent—may produceexcitatory effects at higher doses. It is used toprevent and treat hypotension due to spinalanaesthesia and surgical procedures, shock inmyocardial infarction and other hypotensive states.Dose: 10–20 mg oral/i.m., also by slow i.v. infusion.MEPHENTINE 10 mg tab, 15 mg in 1 ml amp, 30 mg/ml in10 ml vial.
SELECTIVE β2 STIMULANTS
These include, salbutamol, terbutaline, salmete-rol, formoterol and ritodrine. They cause broncho-dilatation, vasodilatation and uterine relaxation,without producing significant cardiac stimulation.β2 selectivity is only relative. Salbutamol hasβ2:β1 action ratio of about 10. They are primarilyused in bronchial asthma (for description seeCh. 16). Other uses are:
• As uterine relaxant to delay premature labour.Ritodrine is the preferred drug (see Ch. 23);
• In hyperkalaemic familial periodic paralysis—β2 agonists benefit by enhancing K+ uptakeinto muscles, thereby lowering plasma K+ levels.The most important side effect is muscle
tremor; tachycardia and arrhythmias are less likely.
Isoxsuprine It is an orally effective long-actingβ receptor stimulant which has direct smoothmuscle relaxant property as well. It has been usedas uterine relaxant for threatened abortion anddysmenorrhoea, but efficacy is poor. Beneficialeffects in peripheral and cerebral vascular diseasesare disappointing.Side effects: nausea, tachycardia, flushing,hypotension, dizziness, tremor.Dose: 5–10 mg oral, i.m. 4–6 hourly,DUVADILAN 10 mg tab, 40 mg SR cap, 10 mg/2 ml inj.
NASAL DECONGESTANTSThese are α agonists which on topical applica-tion as dilute solution (0.05–0.1%) produce localvasoconstriction. The imidazoline compounds—naphazoline, xylometazoline and oxymetazolineare relatively selective α2 agonist (like clonidine).They have a longer duration of action (12 hours)than ephedrine. After-congestion is claimed to beless than that with ephedrine or phenylephrine.They may cause initial stinging sensation(specially naphazoline). Regular use of theseagents for long periods should be avoided becausemucosal ciliary function is impaired: atrophicrhinitis and anosmia can occur due to persistentvasoconstriction. They can be absorbed from thenose and produce systemic effects, mainly CNSdepression and rise in BP. These drugs shouldbe used cautiously in hypertensives and in thosereceiving MAO inhibitors.Xylometazoline: 0.05–0.1% topical in nose; OTRIVIN 0.05%(pediatric), 0.1% (adult) nasal drops and nasal spray.Oxymetazoline: 0.025–0.05% topical in nose; NASIVION,SINAREST 0.025% (pediatric), 0.05% nasal drops.Naphazoline: 0.1% topical in nose; PRIVINE 0.1% nasaldrops.
Pseudophedrine A stereoisomer of ephedrine;causes vasoconstriction, especially in mucosae and

137C
HA
PTE
R9
ADRENERGIC SYSTEM AND DRUGS
skin, but has fewer CNS and cardiac effect andis a poor bronchodilator (little β2 agonisticactivity). It has been used orally as a decongestantof upper respiratory tract, nose and eustachiantubes. Combined with antihistaminics, mucolytics,antitussives and analgesics, it is believed to affordsymptomatic relief in common cold, allergicrhinitis, blocked eustachian tubes and upperrespiratory tract infections. However, no selectiveaction on these vascular beds has beendemonstrated; rise in BP can occur, especiallyin hypertensives.Dose: 30–60 mg TDS.SUDAFED 60 mg tab, 30 mg/5 ml syrup; in SINAREST 60mg with chlorpheniramine 2 mg + caffeine 30 mg +paracetamol 500 mg tab; in CHESTON 30 mg withchlorpheniramine 2 mg + bromhexine 4 mg per tab/5 ml syr;in ACTICOLD 60 mg with chlorpheniramine 4 mg +paracetamol 500 mg tab; in CODYLEX 60 mg withchlorpheniramine 4 mg + ibuprofen 400 mg tab.
Phenylpropanolamine (PPA) Being chemically andpharmacologically similar to ephedrine, PPA causesvasoconstriction and has some amphetamine like CNS effects,including suppression of hunger. It was included in a largenumber of oral cold/decongestant combination remedies, andin USA it was used as an appetite suppressant as well.
Following reports and case control studies associating PPAuse with haemorrhagic stroke and concerns regarding itspotential to precipitate behavioural/psychiatric disturbances,many countries, led by USA, prohibited the sale of PPAcontaining medicines decades back. However, oral decon-gestant formulations containing relatively lower amounts ofPPA (25–50 mg) continued to be available over-the-counterin India till recently. All such preparations have now beenbanned since March 2011*.
ANORECTIC AGENTS
Though amphetamines suppress appetite, their useas anorectic agents is precluded by thier adversecentral effects. A number of related drugs havebeen developed which inhibit feeding centre (likeamphetamine) but have little/no CNS stimulantaction or abuse liability. All of them act byreleasing (reverse transport) or by inhibiting thereuptake of NA/DA or 5-HT, enhancingmonoaminergic transmission in the brain.Accordingly they may be grouped into:
Noradrenergic agents: Phentermine, phenylpropanolamine(PPA), diethylpropion, mazindol.
Serotonergic agents: Fenfluramine, dexfenfluramine.
Noradrenergic/serotonergic agent: Sibutramine.
The noradrenergic agents activate hypothalamicadrenergic/dopaminergic receptors, have residualstimulatory effects; interfere with sleep andprimarily affect the appetite centre. On the otherhand, serotonergic agents have mild sedatingproperty and primarily affect the satiety centre.
Fenfluramine and dexfenfluramine reduce food seekingbehaviour by enhancing serotonergic transmission in thehypothalamus.
They were extensively used by slimming centres, thoughtolerance to the anorectic action develops in 2-3 months. Inthe late 1990s ecocardiographic abnormalities, valvular defects,pulmonary hypertension and sudden deaths were related tothe use of a combined preparation of fenfluramine + phenter-mine. The US-FDA recommended discontinuation offenfluramine, dexfenfluramine and their combinations. Mostother countries, including India followed.
Sibutramine and R-Sibutramine Introduced subsequently,these drugs inhibit both NA and 5-HT reuptake in thehypothalamus, suppress appetite in a manner similar tofenfluramine, and probably increase thermogenesis byactivating adrenergic β3 mechanism in adipose tissue. Thesedrugs caused weight loss in obese people and were routinelyused by slimming centres. Several side effects were noted;serious adverse reactions, including cardiovascular eventsand death were reported to the US-FDA and drug committeesin Europe leading to ban on their use. After its own assessment,India has also banned these drugs from March 2011.
THERAPEUTIC USES
1. Vascular uses(i) Hypotensive states (shock, spinal anaes-thesia, hypotensive drugs) One of the pressoragents can be used along with volume replacementfor neurogenic and haemorrhagic shock; also asan expedient measure to maintain cerebral circu-lation for other varieties of shock. They shouldnot be used in secondary shock when reflex vaso-constriction is already marked. Use in cardiogenicshock is tricky, because attempts to raise BP mayalso increase cardiac work. Slow i.v. infusion ofdopamine/dobutamine is more appropriate in thissituation. Dopamine increases cardiac contactilitywithout causing significant tachycardia. It also* The ban order is presently under court stay.

138S
EC
TIO
N2
DRUGS ACTING ON ANS
improves renal blood flow and may help to raiseB.P. Dobutamine has relatively more selectiveinotropic effect. Use of NA is practically obsolete.Adr 0.5 mg injected promptly i.m. is the drugof choice in anaphylactic shock (see p. 87). Itnot only raises BP, but counteracts bronchospasm/laryngeal edema that may accompany. Becauseof the rapidity and profile of action Adr is theonly life saving measure. Oral ephedrine has beenused to treat postural hypotension due toautonomic neuropathy, which may be age related,idiopathic or secondary to diabetes, etc. However,no pressor agent is entirely satisfactory becauseit cannot mimic selective NA release that occursonly on standing. Elastic stockings and use offludrocortisone to expand plasma volume are morehelpful.
(ii) Along with local anaesthetics Adr 1 in200,000 to 1 in 100,000 for infiltration, nerveblock and spinal anaesthesia. Duration ofanaesthesia is prolonged and systemic toxicity oflocal anaesthetic is reduced. Local bleeding isminimised (see Ch. 26).
(iii) Control of local bleeding From skin andmucous membranes, e.g. epistaxis : compressesof Adr 1 in 10,000, phenylephrine/ephedrine 1%soaked in cotton can control arteriolar andcapillary bleeding. NA 8 mg in 100–200 ml salineput in stomach through a tube can control bleedingfrom gastric erosions and stress ulcers.
(iv) Nasal decongestant In colds, rhinitis,sinusitis, blocked nose or eustachian tube—oneof the α-agonists is used as nasal drops. Shrinkageof mucosa provides relief, but after-congestion,atrophy of mucosa on prolonged use are still aproblem. The imidazolines should be used in lowerconcentrations in infants and young children,because they are more sensitive to central effectsof these drugs. Nasal decongestants should beused very cautiously in hypertensive patients andin elderly males.
Pseudoephedrine and phenylephrine have beenused orally as decongestants, but effective doseswill constrict other blood vessels as well and cause
rise in BP. However, oral vasoconstrictors do notproduce after-congestion.
(v) Peripheral vascular diseases like Buerger’s disease,Raynaud’s phenomena, diabetic vascular insufficiency,gangrene, frost bite, ischaemic ulcers, night leg cramps,cerebral vascular inadequacy : vasodilators includingisoxsuprine have been used, but are far from satisfactory inmost cases, because often the capacity of the affected vesselsto dilate is severely limited, and ischaemia itself is a potentvasodilator.
2. Cardiac uses(i) Cardiac arrest (drowning, electrocution,Stokes-Adams syndrome and other causes) Adrmay be used to stimulate the heart; i.v. adminis-tration is justified in this setting with externalcardiac massage.
(ii) Partial or complete A-V block Isoprenalinemay be used as temporary measure to maintainsufficient ventricular rate.
(iii) Congestive heart failure (CHF) Adrenergicinotropic drugs are not useful in the routinetreatment of CHF. However, controlled short termi.v. infusion of DA/dobutamine can tide over acutecardiac decompensation during myocardialinfarction, cardiac surgery and in resistant CHF.
3. Bronchial asthma and COPD Adrenergicdrugs, especially β2 stimulants are the primarydrugs forrelief of reversible airway obstruction(see Ch. 16).
4. Allergic disorders Adr is a physiologicalantagonist of histamine which is an importantmediator of many acute hypersensitivity reactions.It affords quick relief in urticaria, angioedema;is life saving in laryngeal edema and anaphylaxis.It is ineffective in delayed, retarded and other typesof allergies, because histamine is not involved.
5. Mydriatic Phenylephrine is used to facili-tate fundus examination; cycloplegia is notrequired. It tends to reduce intraocular tensionin wide angle glaucoma. The ester prodrug ofAdr dipivefrine is an adjuvant drug for open angleglaucoma (see p. 154).

139C
HA
PTE
R9
ADRENERGIC SYSTEM AND DRUGS
6. Central uses(i) Attention deficit hyperkinetic disorder (ADHD): alsocalled minimal brain dysfunction, is usually detected inchildhood and the sufferer is considered a ‘hyperkinetic child’,(see Ch. 35 also). Amphetamines have an apparentlyparadoxical effect to calm down hyperkinetic children. Thisdisorder is recognized as a mild grade of mental retardationor a reduction in the ability to concentrate, i.e. the span oftime for which attention can be focused on a subject is abbre-viated. Amphetamines by increasing attention span improvebehaviour and performance in studies; tolerance to this effectdoes not develop. However, growth retardation may occurdue to reduction in appetite. The risk-benefit ratio of suchtherapy often disfavours use of amphetamine.
(ii) Narcolepsy Narcolepsy is sleep occurring in fits andis adequately controlled by amphetamines. Development oftolerance, abuse and behavioural abnormalities are thecalculated risks of such therapy. Modafinil, a newerpsychostimulant with less dependence inducing potential,is being preferred now (see Ch. 35). Imipramine-like drugsare also useful in some patients, and are safer.
(iii) Epilepsy Amphetamines are occasionally used asadjuvants and to counteract sedation caused by antiepileptics.
(iv) Parkinsonism Amphetamines improve mood andreduce rigidity (slightly) but do not benefit tremor. Theyare occasionally used as adjuvants in parkinsonism.
(v) Obesity The anorectic drugs can help the obese totolerate a reducing diet for short periods, but do not improvethe long-term outlook. Their use may be considered in severeobesity, but not for cosmetic reasons or for figure improve-ment. In the absence of dietary restriction none of themhas any significant weight reducing effect, and lifestylemodification is required. Currently there is no approvedsympathomimetic anorectic drug.
The newer approaches being developed for control ofobesity are:
Orlistat An inhibitor of gastric and pancreatic lipase; itinterferes with digestion and absorption of dietary triglycerides.Absorption of cholesterol and fat soluble vitamins is alsoimpaired. It has facilitated weight loss in clinical trials. Fluidmotions, steatorrhoea, abdominal pain, nausea, flatulence andvitamin deficiency are the side effects.Dose: 120 mg with meals 3 times a day.OBELIT, ORIDUCE, ZEROFAT 120 mg tab.
Olestra is a sucrose polyester which can be used as a cookingmedium in place of fat but is neither digested nor absorbed.Its acceptability is inconsistent.
Leptin (the endogenous slimming peptide) analogues,neuropeptide Y antagonists and β3
adrenergic agonists areunder investigation as antiobesity drugs.
Rimonabant This selective cannabinoid (CB-1) receptorantagonist was used briefly as appetite reducing drug, butsoon serious adverse reaction reports appeared and it wasbanned in Europe and USA. India followed suit in Dec.2009.
7. Nocturnal enuresis in children and urinaryincontinence Amphetamine affords benefit both byits central action as well as by increasing tone of vesicalsphincter.
8. Uterine relaxant Isoxsuprine has beenused in threatened abortion and dysmenorrhoea,but efficacy is doubtful. Selective β2 stimulants,especially ritodrine, infused i.v. has been success-fully used to postpone labour but maternalmorbidity and mortality may be increased dueto its cardiac and metabolic actions and incidentsof pulmonary edema (see Ch. 23).
9. Insulin hypoglycaemia Adr may be usedas an expedient measure, but glucose should begiven as soon as possible.
PROBLEM DIRECTED STUDY
9.1 A lady aged 55 years presented for eye checkup. She has been having visual difficulty overthe past few months, and lately she had started noticing ‘halos’ around the lights. She alsohas dull chronic ache in the forehead region. Tonometry revealed her intraocular pressure (i.o.p.)to be 22 and 24 mm Hg respectively in the left and right eye.(a) Which mydriatic will be suitable for dilating her pupil for fundus examination and why?(see Appendix-1 for solution)

These are drugs which antagonize the receptoraction of adrenaline and related drugs. They arecompetitive antagonists at α or β or both α andβ adrenergic receptors and differ in importantways from the “adrenergic neurone blockingagents”, which act by interfering with the releaseof adrenergic transmitter on nerve stimulation.These differences are given in Table 10.1.
ααααα ADRENERGIC BLOCKING DRUGSThese drugs inhibit adrenergic responses media-ted through the α adrenergic receptors withoutaffecting those mediated through β receptors.
CLASSIFICATION
I. Nonequilibrium type(i) β-Haloalkylamines—Phenoxybenzamine.
II. Equilibrium type (competitive)
A. Nonselective(i) Ergot alkaloids—Ergotamine, Ergotoxine
(ii) Hydrogenated ergot alkaloids—Dihydro-ergotamine (DHE), Dihydroergotoxine
(iii) Imidazoline—Phentolamine(iv) Miscellaneous–Chlorpromazine
B. α1 selective—Prazosin, Terazosin, Doxazosin, Alfuzosin, Tamsulosin
C. α2 selective—Yohimbine
GENERAL EFFECTS OF α BLOCKERS
1. Blockade of vasoconstrictor α1 (also α2) recep-tors reduces peripheral resistance and causespooling of blood in capacitance vessels → venousreturn and cardiac output are reduced → fall inBP. Postural reflex is interfered with → markedhypotension occurs on standing → dizziness and
syncope. Hypovolemia accentuates the hypoten-sion. The α blockers abolish the pressor action ofAdr (injected i.v. in animals), which then producesonly fall in BP due to β2 mediated vasodilatation.This was first demonstrated by Sir HH Dale (1913)and is called vasomotor reversal of Dale. Pressorand other actions of selective α agonists (phenyl-ephrine) are suppressed.2. Reflex tachycardia occurs due to fall in meanarterial pressure and increased release of NA dueto blockade of presynaptic α2 receptors.3. Nasal stuffiness and miosis result fromblockade of α receptors in nasal blood vesselsand in radial muscles of iris respectively.4. Intestinal motility is increased due to partialinhibition of relaxant sympathetic influences—loose motion may occur.5. Hypotension produced by α blockers canreduce renal blood flow → g.f.r. is reducedand more complete reabsorption of Na+ and wateroccurs in the tubules → Na+ retention andexpansion of blood volume. This is accentuatedby reflex increase in renin release mediatedthrough β1 receptors.6. Tone of smooth muscle in bladder trigone,sphincter and prostate is reduced by blockadeof α1 receptors (mostly of the α1A subtype)→ urine flow in patients with benign hypertrophyof prostate (BHP) is improved.7. Contractions of vas deferens and relatedorgans which result in ejaculation are coordina-ted through α receptors—α blockers can inhibitejaculation; this may manifest as impotence.
The α blockers have no effect on adrenergiccardiac stimulation, bronchodilatation, vaso-dilatation and most of the metabolic changes,because these are mediated predominantly throughβ receptors.
Antiadrenergic Drugs(Adrenergic Receptor Antagonists)and Drugs for Glaucoma
ChapterChapterChapterChapterChapter 1010101010

141C
HA
PTE
R10
ANTIADRENERGIC DRUGS AND DRUGS FOR GLAUCOMA
TABLE 10.1 Differences between antiadrenergic and adrenergic neurone blocking drugs
Antiadrenergic drugs Adrenergic neurone blocking drugs
1. Locus of action Adrenergic receptors on Adrenergic neuronal membrane oreffector cells or neurones contents
2. Effects of adrenergic Blocked (less completely) Blocked (more completely)nerve stimulation
3. Effect of injected Adr Blocked Not blocked (may be potentiated)4. Type of effects blocked Either α or β (except Labetalol Sympathetic function decreased
by a single drug and its congeners) irrespective of the receptor type5. Examples α—Phentolamine Reserpine, Guanethidine,
β—Propranolol Bretylium, α-methyl-p-tyrosine
Apart from these common effects, most ofwhich manifest as side effects, many α blockershave some additional actions. The pharmacolo-gical profile of an α blocker is mainly governedby its central effects and by the relative activityon α1 and α2 receptor subtypes. Only the distinctivefeatures of individual α blockers are describedbelow.
Phenoxybenzamine It cyclizes sponta-neously in the body giving rise to a highly reactiveethyleniminium intermediate which reacts with αadrenoceptors and other biomolecules by formingstrong covalent bonds. The α blockade is ofnonequilibrium (irreversible) type and developsgradually (even after i.v. injection) and lasts for3–4 days till fresh receptors are synthesized.
Partial blockade of 5-HT, histaminergic andcholinergic receptors, but not β adrenergicreceptors, can be demonstrated at higher doses.
The fall in BP caused by phenoxybenzamineis mainly postural because venodilatation is moreprominent than arteriolar dilatation. In recumbentsubjects cardiac output and blood flow to manyorgans is increased due to reduction in peripheralresistance and increased venous return. It tends toshift blood from pulmonary to systemic circuitbecause of differential action on the two vascularbeds. It also tends to shift fluid from extravascularto vascular compartment. Phenoxybenzamine islipid soluble, penetrates brain and can produceCNS stimulation, nausea and vomiting on rapidi.v. injection. However, oral doses producedepression, tiredness and lethargy. Major side
effects are postural hypotension, palpitation, nasalblockage, miosis, inhibition of ejaculation.
Pharmacokinetics Oral absorption of phenoxybenzamineis erratic and incomplete; i.m. and s.c. injections are verypainful—should not be given. Though most of theadministered dose is excreted in urine in 24 hours, smallamounts that have covalently reacted remain in tissues forlong periods. Chronic administration leads to accumu-lation in adipose tissue.Dose: 20–60 mg/day oral; 1 mg/kg by slow i.v. infusionover 1 hour; used primarily in pheochromocytoma, occasio-nally in secondary shock and peripheral vascular disease.FENOXENE 10 mg cap, 50 mg/ml inj. BIOPHENOX 50mg in 1 ml inj.
Natural and hydrogenated ergot alkaloids (see Ch.12 and Ch. 21) Ergot alkaloids are the adrenergic antagonistswith which Dale demonstrated the vasomotor reversalphenomenon. The amino acid alkaloids ergotamine andergotoxine are partial agonists and antagonists at α adrenergic,serotonergic and dopaminergic receptors.The amine alkaloid ergometrine has no α blocking activity.
The natural ergot alkaloids produce long lastingvasoconstriction which predominates over their α blockingaction—peripheral vascular insufficiency and gangrene of toesand fingers occurs in ergotism. Ergotoxine is a more potentα blocker and less potent vasoconstrictor than ergotamine.Hydrogenation reduces vasoconstrictor and increases αblocking activity.
The α blockade produced by ergot alkaloids is low gradeand clinically not useful. Their principal use is in migraine(see Ch. 12). Dihydroergotoxine has been used as a cognitionenhancer (see Ch. 35).
Phentolamine This is a rapidly acting α blockerwith short duration of action (in minutes). It equallyblocks α1 and α2 receptors—NA release is increasedand venodilatation predominates over arteriolardilatation. It is used as a quick and shortacting α blocker for diagnosis and intraoperative

142S
EC
TIO
N2
DRUGS ACTING ON ANS
management of pheochromocytoma and for controlof hypertension due to clonidine withdrawal, cheesereaction, etc. It is the most suitable α blockerfor local infiltration to counteract vasoconstrictiondue to extravasated NA/DA during their i.v. infusion.Dose: 5 mg i.v. repeated as required;REGITINE, FENTANOR 10 mg/ml inj.
Prazosin It is first of the highly selective α1
blockers having α1 : α2 selectivity ratio 1000:1.All subtypes of α1 receptor (α1A, α1B, α1D) areblocked equally. It blocks sympatheticallymediated vasoconstriction and produces fall inBP which is attended by only mild tachycardia;NA release is not increased due to absence ofα2 blockade.
Prazosin dilates arterioles more than veins.Postural hypotension is less marked, occursespecially in the beginning, which may causedizziness and fainting as ‘first dose effect’. Thiscan be minimized by starting with a low doseand taking it at bedtime. Subsequently tolerancedevelops to this side effect. Other α blocking sideeffects (miosis, nasal stuffiness, inhibition ofejaculation) are also milder. For the above reasons,prazosin (also other α1 blockers) has largelyreplaced phenoxybenzamine. Prazosin, in addition,inhibits phosphodiesterase which degrades cAMP.Rise in smooth muscle cAMP could contributeto its vasodilator action.
Prazosin is effective orally (bioavailability~60%), highly bound to plasma proteins (mainlyto α1 acid glycoprotein), metabolized in liver andexcreted primarily in bile. Its plasma t½ is 2–3 hours; effect of a single dose lasts for 6–8 hours.
Prazosin is primarily used as an antihyper-tensive (see Ch. 40). Other uses are—Raynaud’sdisease and benign hypertrophy of prostate (BHP).Prazosin blocks α1 receptors in bladder trigoneand prostatic smooth muscle, thereby improvesurine flow, reduces residual urine in bladder.PRAZOPRES 0.5, 1.0 and 2.0 mg tabs. Start with 0.5–1 mg atbedtime; usual dose 1–4 mg BD or TDS.MINIPRESS XL: Prazosin GITS (gastrointestinal therapeuticsystem) 2.5 mg and 5 mg tablets; 1 tab OD.
Terazosin It is chemically and pharmacologi-cally similar to prazosin; differences are higher
bioavailability (90%) and longer plasma t½ (~12hr); a single daily dose lowers BP over 24 hrs.Terazosin is more popular for use in BHP dueto single daily dose and a probable apoptosispromoting effect on prostate. This is unrelatedto α1 receptor blockade, but may retard theprogression of prostatic hypertrophy.HYTRIN, TERALFA, OLYSTER 1, 2, 5 mg tab; usualmaintenance dose 2–10 mg OD.
Doxazosin Another long acting (t½ 18 hr) con-gener of prazosin with pharmacological profile,similar to terazosin, including the apoptosispromoting effect on prostate. It is used in hyper-tension and BHP.Dose: 1 mg OD initially, increase upto 8 mg BD;DOXACARD, DURACARD, DOXAPRESS 1, 2, 4 mg tabs.
Alfuzosin This short acting (t½ 3–5 hours)congener of prazosin has been specificallydeveloped for symptomatic treatment of BHP,despite the fact that it is nonselective for α1A,α1B and α1D subtypes. It is not approved as anantihypertensive. The metabolism of alfuzosin isinhibited by CYP34A inhibitors. Concurrenttreatment with erythromycin, ketoconazole,ritonavir etc. is to be avoided.Dose: 2.5 mg BD-QID or 10 mg as extended release (ER)tablet.ALFUSIN, ALFOO 10 mg ER tab.
Tamsulosin This relatively uroselective α1A/α1D blocker (α1A : α1B affinity 7–38 fold) hasbeen found as effective as terazosin in improvingBHP symptoms, because α1A subtype predominatein the bladder base and prostate. However, it lacksthe prostatic apoptosis promoting property ofterazosin and doxazosin. Tamsulosin does not causesignificant changes in BP or HR at doses whichrelieve urinary symptoms, and it is not used asan antihypertensive. No increase in adversecardiovascular events has been noted. Posturalhypotension is infrequent, dizziness and retrogradeejaculation are the only significant side effects.Problem of floppy iris has been encountered duringcataract surgery. Its plasma t½ is 6–9 hrs, but themodified release (MR) cap needs only once dailydosing. It may be a better tolerated α1 blockerfor BHP in patients who continue to suffer posturalhypotension with terazosin/doxazosin.

143C
HA
PTE
R10
ANTIADRENERGIC DRUGS AND DRUGS FOR GLAUCOMA
CONTIFLO–OD 0.4 mg Cap, URIMAX, DYNAPRES 0.2,0.4 mg MR cap; 1 cap (max 2) in the morning with meals. Nodose titration is needed in most patients.
Yohimbine An alkaloid from the West African plantYohimbehe. It is a relatively selective α2 blocker withshort duration of action. Also blocks 5-HT receptors. Heartrate and BP are generally elevated due to increased centralsympathetic outflow as well as enhanced peripheral NArelease. Other CNS effects include excitation, tremor, ADHrelease (antidiuresis), nausea and vomiting. It may causecongestion in genitals and has been considered to be anaphrodisiac. This effect is only psychological, but canovercome psychogenic impotence in some patients.
There are no valid indications for clinical use of yohimbine.
Chlorpromazine and some other neuroleptics have significantα adrenergic blocking activity—cause fall in BP, nasalstuffiness and inhibition of ejaculation as side effect.
USES OF α BLOCKERS
1. Pheochromocytoma It is a tumour of adre-nal medullary cells. Excess CAs are secreted whichcan cause intermittent or persistent hypertension.Estimation of urinary CA metabolites (VMA,normetanephrine) is diagnostic. In addition,pharmacological tests can be performed.
Phentolamine test Inject phentolamine 5 mg i.v.over 1 min in recumbent subject. A fall in BP> 35 mm Hg systolic and/or > 25 mm Hg diastolicis indicative of pheochromocytoma. However, itis not very reliable, both false positive and falsenegative results are possible.
Provocative tests have been performed by injectinghistamine, methacholine or glucagon—which provoke releaseof CAs and cause marked rise in BP if pheochromocytomais present. These tests are dangerous; phentolamine mustbe available to counteract excessive rise in BP.
Therapeutic Phenoxybenzamine can be used asdefinitive therapy for inoperable and malignantpheochromocytoma. Prazosin is an alternative.When surgical removal of the tumour is contemp-lated, it is desirable to give phenoxybenzamineorally for 1–2 weeks preoperatively and infuseit i.v. during surgery. The rationale is:(i) Due to excess circulating CAs blood volumeis low (they shift fluid from vascular to extra-vascular compartment). Treatment with α blockernormalizes blood volume and distribution of bodywater.
(ii) Handling of the tumour during surgery maycause outpouring of CAs in blood → marked risein BP. This is prevented by phenoxybenzaminegiven pre and intraoperatively. Alternatively, phen-tolamine drip can be instituted during the operation.(iii) Removal of the tumour is often attended bymarked fall in BP as blood vessels dilate andthe blood volume is low. This does not happenif volume has been restored before hand withthe aid of an α blocker.2. Hypertension α blockers other than thoseselective for α1 (prazosin-like) have been a failurein the management of essential hypertension,because vasodilatation is compensated by cardiacstimulation. Moreover, postural hypotension,impotence, nasal blockage and other side effectsproduced by nonselective α blockers are unaccep-table. However, phentolamine/phenoxybenzamineare of great value in controlling episodes of risein BP during clonidine withdrawal and cheesereaction in patients on MAO inhibitors.3. Benign hypertrophy of prostate (BHP) Theurinary obstruction caused by BHP has a staticcomponent due to increased size of prostate anda dynamic component due to increased tone ofbladder neck/prostate smooth muscle. Two classesof drugs are available:• α1
adrenergic blockers (prazosin like): decreasetone of prostatic/bladder neck muscles.
• 5-α reductase inhibitor (finasteride): arrestgrowth/reduce size of prostate (see Ch. 21).
Since activation of α1 adrenoceptors in bladdertrigone, prostate and prostatic urethra increasessmooth muscle tone, their blockade relaxes thesestructures, reducing dynamic obstruction, increa-sing urinary flow rate and causing more completeemptying of bladder in many patients of BHP.
Voiding symptoms (hesitancy, narrowing ofstream, dribbling and increased residual urine)are relieved better than irritative symptoms likeurgency, frequency and nocturia. The α1
blockersafford faster (within 2 weeks) and greatersymptomatic relief than finasteride which primarilyaffects static component of obstruction and hasa delayed onset taking nearly six months forclinical improvement. The α1
blockers do not affectprostate size, but are more commonly used.

144S
EC
TIO
N2
DRUGS ACTING ON ANS
However, effects last only till the drug is given.Even with continued therapy, benefit may declineafter few years due to disease progression. Theymay be used concurrently with finasteride.
Terazosin, doxazosin, alfuzosin and tamsulosinare the peferred α1
blockers because of once dailydosing. There is some evidence that terazosin anddoxazosin promote apoptosis in prostate.Tamsulosin appears to cause fewer vascular sideeffects because of relative α1A
/α1D selectivity.
4. Secondary shock Shock due to blood or fluid lossis accompanied by reflex vasoconstriction. If volume replace-ment fails to reverse this (extremities remain pale and cold,pulse pressure does not improve), therapy with an α blocker(phenoxybenzamine i.v.) can help by:(i) Counteracting vasoconstriction.(ii) Shifting blood from pulmonary to systemic circuit.(iii) Returning fluid from extravascular to the vascularcompartment so that cardiac output improves.5. Peripheral vascular diseases α blockers do increaseskin and to some extent muscle blood flow in normal individuals,but these drugs are largely disappointing in peripheral vasculardiseases when obstruction is organic (Buerger’s disease).However, when vasoconstriction is a prominent feature(Raynaud’s phenomenon, acrocyanosis), good symptomaticrelief is afforded by prazosin or phenoxybenzamine.6. Congestive heart failure (CHF) The vasodilatoraction of prazosin can afford symptomatic relief in selectedpatients of CHF in the short-term, but long-term prognosisis not improved.7. Papaverine/Phentolamine Induced Penile Erection(PIPE) therapy for impotence In patients unable to achieveerection, injection of papaverine (3–20 mg) with or withoutphentolamine (0.5–1 mg) in the corpus cavernosum has beenfound to produce penile tumescence to permit intercourse.However, the procedure requires skill and training. Priapismoccurs in 2–15% cases, which if not promptly treated leadsto permanent damage. This is reversed by aspirating bloodfrom the corpus cavernosum or by injecting phenylephrinelocally. Repeated injections can cause penile fibrosis. Othercomplications are—local haematoma, infection, paresthesiaand penile deviation. This therapy should therefore be reservedfor selected situations with proper facilities.
βββββ ADRENERGIC BLOCKING DRUGSThese drugs inhibit adrenergic responses media-ted through the β receptors.
The dichloro derivative of isoprenaline was the first com-pound found in 1958 to block adrenergic responses whichcould not be blocked till then by the available adrenergicantagonists. However, it was not suitable for clinical use.Propranolol introduced in 1963 was a therapeutic break-through. Since then, drugs in this class have proliferatedand diversified.
All β blockers are competitive antagonists.Propranolol blocks β1 and β2 receptors, but hasweak activity on β3 subtype. It is also an inverseagonist: reduces resting heart rate as well. Someβ blockers like metoprolol, atenolol, etc.preferentially block β1 receptors, while few othershave additional α1 receptor blocking and/orvasodilator properties.
CLASSIFICATION
Nonselective (β1 and β2)a. Without intrinsic sympathomimetic activity
Propranolol, Sotalol, Timolol.b. With intrinsic sympathomimetic activity
Pindololc. With additional α blocking property
Labetalol, Carvedilol
Cardioselective (β1)Metoprolol, Atenolol, Acebutolol, Bisoprolol,Esmolol, Betaxolol, Celiprolol, Nebivolol
The pharmacology of propranolol is describedas prototype.
Another system classifies β blockers into 3 generations.
First generation Second generation Third generation(older, nonselective) (β1 selective) (with additional α blocking
and/or vasodilator property)
Propranolol Metoprolol LabetalolTimolol Atenolol CarvedilolSotalol Acebutolol CeliprololPindolol Bisoprolol Nebivolol
Esmolol Betaxolol

145C
HA
PTE
R10
ANTIADRENERGIC DRUGS AND DRUGS FOR GLAUCOMA
PHARMACOLOGICAL ACTIONS
1. CVS(a) Heart Propranolol decreases heart rate,force of contraction (at relatively higher doses)and cardiac output (c.o.). It prolongs systole byretarding conduction so that synergy of contractionof ventricular fibres is disturbed. The effects ona normal resting subject are mild, but becomeprominent under sympathetic overactivity(exercise, emotion). Ventricular dimensions aredecreased in normal subjects, but dilatation canoccur in those with reduced reserve—CHF maybe precipitated or aggravated.
Cardiac work and oxygen consumption arereduced as the product of heart rate and aorticpressure decreases. Total coronary flow is reduced(blockade of dilator β receptors), but this is largelyrestricted to the subepicardial region, whileperfusion of the subendocardial area (which isthe site of ischaemia in angina patients) is notaffected. The overall effect in angina patients isimprovement of O2 supply/demand status; exercisetolerance is increased.
Propranolol abbreviates refractory period ofmyocardial fibres and decreases automaticity—rate of diastolic depolarization in ectopic foci isreduced, specially if it had been augmented byadrenergic stimuli. The A-V conduction is delayed.At high doses a direct depressant and membranestabilizing (quinidine like) action is exerted, butthis contributes little to the antiarrhythmic effectat usual doses. Propranolol blocks cardiacstimulant action of adrenergic drugs but not thatof digoxin, methylxanthines or glucagon.
(b) Blood vessels Propranolol blocks vaso-dilatation and fall in BP evoked by isoprenalineand enhances the rise in BP caused by Adr. Thereis re-reversal of vasomotor reversal that is seenafter a blockade. Propranolol has no direct effecton blood vessels and there is little acute changein BP. On prolonged administration BP graduallyfalls in hypertensive subjects but not in normo-tensives. Total peripheral resistance (t.p.r.) isincreased initially (due to blockade of β mediatedvasodilatation) and c.o. is reduced, so that there
is little change in BP. With continued treatment,resistance vessels gradually adapt to chronicallyreduced c.o. and t.p.r. decreases—both systolicand diastolic BP fall. This is considered to bethe most likely explanation of the antihypertensiveaction. Other mechanisms that may contribute are:(i) Reduced NA release from sympathetic termi-nals due to blockade of β receptor mediatedfacilitation of the release process.(ii) Decreased renin release from kidney (β1
mediated): Propranolol causes a more marked fallin BP in hypertensives who have high or normalplasma renin levels and such patients respondat relatively lower doses than those with low plasmarenin. However, pindolol does not decrease plasmarenin activity but is an effective antihypertensive.(iii) Central action reducing sympathetic out-flow. However, β blockers which penetrate brainpoorly are also effective antihypertensives.
2. Respiratory tract Propranolol increasesbronchial resistance by blocking dilator β2
receptors. The effect is hardly discernible innormal individuals because sympathetic broncho-dilator tone is minimal. In asthmatics, however,the condition is consistently worsened and a severeattack may be precipitated.
3. CNS No overt central effects are producedby propranolol. However, subtle behaviouralchanges, forgetfulness, increased dreaming andnightmares have been reported with long-term useof relatively high doses.
Propranolol suppresses anxiety in short-termstressful situations, but this is due to peripheralrather than a specific central action (see p. 467).
4. Local anaesthetic Propranolol is as potenta local anaesthetic as lidocaine, but is not clinicallyused for this purpose because it causes irritationat the injected site.
5. Metabolic Propranolol blocks adrenergicallyinduced lipolysis and consequent increase inplasma free fatty acid levels. Plasma triglyceridelevel and LDL/HDL ratio is increased duringpropranolol therapy. It also inhibits glycogenolysisin heart, skeletal muscles and in liver

146S
EC
TIO
N2
DRUGS ACTING ON ANS
(inconsistently), which occurs due to Adr releaseduring hypoglycaemia—recovery from insulinaction is delayed. Though there is no effect onnormal blood sugar level, prolonged propranololtherapy may reduce carbohydrate tolerance bydecreasing insulin release.
6. Skeletal muscle Propranolol inhibitsadrenergically provoked tremor. This is aperipheral action exerted directly on the musclefibres (through β2 receptors). It tends to reduceexercise capacity by attenuating β2 mediatedincrease in blood flow to the exercising muscles,as well as by limiting glycogenolysis and lipolysiswhich provide fuel to working muscles.
7. Eye Instillation of propranolol and someother β blockers reduces secretion of aqueoushumor, i.o.t. is lowered. There is no consistenteffect on pupil size or accommodation.
8. Uterus Relaxation of uterus in response toisoprenaline and selective β2 agonists is blockedby propranolol. However, normal uterine activityis not significantly affected.
PHARMACOKINETICS
Propranolol is well absorbed after oral adminis-tration, but has low bioavailability due to highfirst pass metabolism in liver. Oral: parenteral doseratio of up to 40:1 has been found. Interindividualvariation in the extent of first pass metabolismis marked—equieffective oral doses vary consi-derably. Propranolol is lipophilic and penetratesinto brain easily.
Metabolism of propranolol is dependent onhepatic blood flow. Chronic use of propranololitself decreases hepatic blood flow: its own oralbioavailability is increased and its t½ is prolonged(by about 30%) on repeated administration.Bioavailability of propranolol is higher when itis taken with meals because food decreases itsfirst pass metabolism. Higher bioavailability andprolongation of t½ is noted with high doses aswell, because metabolism of propranolol issaturable.
A number of metabolites of propranolol havebeen found, of which the hydroxylated producthas β blocking activity. The metabolites areexcreted in urine, mostly as glucuronides. Morethan 90% of propranolol is bound to plasmaproteins.Dose: Oral—10 mg BD to 160 mg QID (average 40–160 mg/day). Start with a low dose and gradually increase according toneed; i.v.—2 to 5 mg injected over 10 min with constant moni-toring. It is not injected s.c. or i.m. because of irritant property.INDERAL, CIPLAR 10, 40, 80 mg tab, 1 mg/ml inj.,BETABLOC 10, 40 mg tab.
INTERACTIONS
1. Additive depression of sinus node and A-Vconduction with digitalis and verapamil — cardiacarrest can occur. However, propranolol has beensafely used with nifedipine.2. Propranolol delays recovery from hypogly-caemia due to insulin and oral antidiabetics.Warning signs of hypoglycaemia mediated throughsympathetic stimulation (tachycardia, tremor) aresuppressed. In some cases BP rises due tounopposed α action of released Adr.3. Phenylephrine, ephedrine and other α agonistspresent in cold remedies can cause marked risein BP due to blockade of sympathetic vasodila-tation.4. Indomethacin and other NSAIDs attenuate theantihypertensive action of β blockers.5. Cimetidine inhibits propranolol metabolism.However, the dose range of propranolol is wide,and this may not be clinically significant.6. Propranolol retards lidocaine metabolism byreducing hepatic blood flow.7. Propranolol increases bioavailability ofchlorpromazine by decreasing its first passmetabolism.
ADVERSE EFFECTS ANDCONTRAINDICATIONS
1. Propranolol can accentuate myocardialinsufficiency and can precipitate CHF/edema byblocking sympathetic support to the heart,especially during cardiovascular stress. However,when compensation has been restored, careful

147C
HA
PTE
R10
ANTIADRENERGIC DRUGS AND DRUGS FOR GLAUCOMA
addition of certain β1 blockers is now establishedtherapy to prolong survival.2. Bradycardia: resting HR may be reduced to60/min or less. Patients of sick sinus are moreprone to severe bradycardia.3. Propranolol worsens chronic obstructive lungdisease, can precipitate life-threatening attack ofbronchial asthma: contraindicated in asthmatics.4. Propranolol exacerbates variant (vasospastic)angina due to unopposed α mediated coronaryconstriction. In some patients, even classical anginamay be worsened if ventricular dilatation andasynergy of contraction occurs—specially with highdoses.5. Carbohydrate tolerance may be impaired inprediabetics.6. Plasma lipid profile is altered on long termuse: total triglycerides and LDL-cholesterol tendto increase while HDL-cholesterol falls. This mayenhance risk of coronary artery disease. Cardio-selective β blockers and those with intrinsic sym-pathomimetic activity have little/no deleteriouseffect on blood lipids.7. Withdrawal of propranolol after chronic useshould be gradual, otherwise rebound hyper-tension, worsening of angina and even suddendeath can occur. This is due to supersensitivityof β receptors occurring as a result of long-termreduction in agonist stimulation.8. Propranolol is contraindicated in partial andcomplete heart block: arrest may occur.9. Tiredness and reduced exercise capacity: dueto blunting of β2 mediated increase in blood flowto the exercising muscles as well as attenuationof glycogenolysis and lipolysis.10. Cold hands and feet, worsening of peripheralvascular disease are noticed due to blockade ofvasodilator β2 receptors.11. Side effects not overtly due to β blockadeare—g.i.t. upset, lack of drive, nightmares, forget-fulness, rarely hallucinations. Male patients morefrequently complain of sexual distress.
OTHER β BLOCKERS
A number of β blockers have been developedhaving some special features. Their comparative
properties are presented in Table 10.2. Theassociated properties alongwith their significancecan be summarized as:Cardioselectivity (in metoprolol, atenolol, acebu-tolol, bisoprolol, nebivolol).These drugs are more potent in blocking cardiac(β1) than bronchial (β2) receptors. However,selectivity is only relative and is lost at high doses.Their features are:1. Lower propensity to cause bronchoconstric-tion, but even these drugs should usually beavoided in asthmatics and COPD patients.However, a coexisting cardiac condition maywarrant their use, which may be initiated at lowdose and under supervision.2. Less interference with carbohydrate meta-bolism and less inhibition of glycogenolysis duringhypoglycaemia—safer in diabetics.However, tachycardia in response to hypoglycae-mia is blocked.3. Lower incidence of cold hands and feet, lesschances of precipitating Raynaud’s phenomenon.4. No/less deleterious effect on blood lipidprofile.5. Ineffective in suppressing essential tremor (itoccurs through β2 action on muscle fibres).6. Less liable to impair exercise capacity.
Partial agonistic (intrinsic sympathomimetic)action (in pindolol, celiprolol, acebutolol).These drugs themselves activate β1 and/or β2
receptors submaximally. The benefits of thisproperty are controversial.1. Bradycardia and depression of contractilityat rest are not prominent, but exercise tachycardiais blocked; may be preferred in those prone tosevere bradycardia (elderly patients; sick sinus)or with low cardiac reserve.2. Withdrawal is less likely to exacerbate hyper-tension or angina; continued agonistic action onβ receptors (of the drug itself) prevents develop-ment of supersensitivity.3. Plasma lipid profile is not/less worsened.4. Not effective in migraine prophylaxis—theydilate cerebral vessels.5. Not suitable for secondary prophylaxis of MI.

148S
EC
TIO
N2
DRUGS ACTING ON ANS
TABLE 10.2 Comparative properties of βββββ blockers
Potency Partial Membrane Lipid Daily Oral First Major Plasmaβ–BLOCKER (on β1) agonistic stabilizing solubility dose (mg) bioavailability pass route of t½(hours)
action action (%) metabolism elimination
NONSELECTIVE
1. Propranolol 1 – ++ +++ 40–480 ~30 Yes Hep.* 3–5
2. Sotalol 1/3 – – ± 160–480 ~60 No Ren.!+Hep. 6–12
3. Timolol 6 – – ++ 10–40 50–75 Partial Ren.+Hep. 4–5
4. Pindolol 6 +++ ± + 10–30 90 No Ren.+Hep. 3–4
CARDIOSELECTIVE
1. Metoprolol 1 – ± ++ 100–400 40–50 Yes Hep. 3–6
2. Atenolol 1 – – – 25–100 50–60 No Ren. 6–9
3. Acebutolol 1/3 + + ± 400–1200 40–60 Yes Hep.+Ren. 3–4
4. Bisoprolol 6 – – – 2.5–10 80 No Hep.+Ren. 9–12
α + β BLOCKER1. Labetalol 1/3 + + ± 300–600 ~30 Yes Hep. 4–6
*Hep—Hepatic metabolism; !Ren.—Renal excretion
Membrane stabilizing activity (in propranolol,oxprenolol, acebutolol). This activity is claimedto contribute to the antiarrhythmic action, butappears to be significant only at high doses.
Lipid insolubility (atenolol, celiprolol,bisoprolol, sotalol)1. They are less likely to produce sleep distur-bances and nightmares.2. They are incompletely absorbed orally, butdo not undergo first pass metabolism and are primarily excreted unchanged in urine: are longeracting (t½ 6–20 hours) and tend to be effectivein a narrow dose range. In contrast, the lipidsoluble agents are primarily metabolized in liverand have shorter t½ (2–6 hours).
Salient features of important β blockers aregiven below.
1. Sotalol Nonselective β blocker with lowlipid solubility. It has additional cardiac rectifierK+ channel blocking and class III antiarrhythmicproperty.SOTAGARD 40, 80 mg tab.
2. Timolol It is the β blocker preferred fortopical use in eye for glaucoma (see p. 153).
Orally it is a potent β blocker—has been usedin hypertension, angina and prophylaxis of myo-cardial infarction.Betaxolol, Levobunolol, Cartiolol and Metipranolol areβ blockers employed exclusively for topical application tothe eye (see p. 154).
3. Pindolol A potent β blocker with prominentintrinsic sympathomimetic activity. It has beenused primarily as antihypertensive: may beadvantageous in patients who develop markedbradycardia with propranolol. Chances of reboundhypertension on withdrawal are also less. Theeffective dose range is rather narrow.PINADOL 5 mg tab, VISKEN 10, 15 mg tab.
4. Metoprolol It is the prototype of cardio-selective (β1) blockers; nearly 50 times higherdose is needed to block isoprenaline inducedvasodilatation. Some measure of inverseagonistic activity on β1 receptors has also beendemonstrated. It is less likely to worsen asthma,but is not entirely safe. It may be preferred indiabetics receiving insulin or oral hypoglycae-mics. Patients who complain of cold hands andfeet while on propranolol do better on metoprolol.
First pass metabolism of metoprolol is lessmarked than propranolol, but 90% or more is

149C
HA
PTE
R10
ANTIADRENERGIC DRUGS AND DRUGS FOR GLAUCOMA
ultimately hydroxylated by CYP2D6 beforeexcretion. There are slow and fast hydroxylatorsof metoprolol (CYP2D6 alleles); the former mayrequire a lower dose.
Side effects of metoprolol are milder. It isgenerally given orally for hypertension, anginaand CHF, but i.v. injection (5–15 mg) has beenused in myocardial infarction provided brady-cardia is absent.BETALOC 25, 50, 100 mg tab, 5 mg/ml inj. LOPRESOR,METOLAR 50, 100 mg tab.
S(–) Metoprolol is the active enantiomer, nowavailable as a single enantiomer product. It isto be used at half the dose as the racemate.Dose: 12.5–50 mg OD–BD.METPURE-XL 12.5, 25, 50 mg extended release tabs.
5. Atenolol A relatively selective β1 blockerhaving low lipid solubility. It is incompletelyabsorbed orally, but first pass metabolism is notsignificant. Because of longer duration of action,once daily dose is often sufficient. Side effectsrelated to CNS action are less likely. Nodeleterious effects on lipid profile have been noted.Effective dose for most individuals falls in anarrow range. It is one of the most commonlyused β blockers for hypertension and angina.BETACARD, ATEN, TENORMIN 25, 50, 100 mg tab.
S(–) Atenolol This pure active enantiomer iseffective at half the dose and may be bettertolerated.Dose: 12.5–50 mg OD;ATPURE, ADBETA 12.5, 25, 50 mg tabs.
6. Acebutolol Another cardioselective agentwith significant partial agonistic and membranestabilizing properties. Effect on resting heart rateis less. The side effect profile is like that ofmetoprolol. Acebutolol is rapidly metabolized toan active metabolite diacetolol which is primarilyexcreted by kidney and has a longer t½ (8–12hours). As such, a single daily dose is sufficientin many patients.SECTRAL 200, 400 mg tab., 10 mg/2 ml amp. Intravenousdose for arrhythmias 20–40 mg.
7. Bisoprolol A cardioselective β blockerlacking intrinsic sympathomimetic activity;
suitable for once daily administration in angina,hypertension and CHF.CONCOR, CORBIS 5 mg tab; ½ to 2 tab OD.
8. Esmolol It is an ultrashort acting β1 blockerdevoid of partial agonistic or membrane stabili-zing actions. It is inactivated by esterases in blood;plasma t½ is < 10 min; action disappears 15–20 min after terminating i.v. infusion—degree ofβ blockade can be titrated by regulating the rateof infusion. Rapid onset, short lasting fall in BPattends i.v. infusion of esmolol.
A loading dose of 0.5 mg/kg is given followedby 0.05–0.2 mg/kg/min infusion. It has been usedto terminate supraventricular tachycardia, episo-dic atrial fibrillation or flutter, arrhythmia duringanaesthesia, to reduce HR and BP during andafter cardiac surgery, and in early treatment ofmyocardial infarction.MINIBLOCK 100 mg/10 ml, 250 mg/10 ml inj.
9. Celiprolol It is a selective β1 blocker havingadditional weak β2 agonistic activity which reducesvascular resistance and holds promise of safetyin asthmatics. Nonadrenoceptor mediatedvasodilatation (due to NO production) adds toits antihypertensive action.Dose: 200–600 mg OD; CELIPRES 100, 200 mg tab.
10. Nebivolol This highly selective β1 blockeralso acts as a NO donor, produces vasodilatationand has the potential to improve endothelialfunction, which may delay atherosclerosis.Absence of deleterious effect on plasma lipidsand on carbohydrate metabolism is anotheradvantage. In contrast to older β blockers, hypo-tensive response to nebivolol has a rapid onset.It has been used in hypertension and CHF.Dose: 5 mg (elderly 2.5 mg) OD;NEBICARD 2.5, 5 mg tabs, NODON 5 mg tab.
USES1. Hypertension β blockers are relatively mildantihypertensives. All agents, irrespective of asso-ciated properties, are nearly equally effective.They are one of the first choice drugs becauseof good patient acceptability and cardioprotectivepotential (see Ch. 40).

150S
EC
TIO
N2
DRUGS ACTING ON ANS
2. Angina pectoris All β blockers benefit anginaof effort. Taken on a regular schedule they dec-rease frequency of attacks and increase exercisetolerance. High doses, however, may worsen anginain some patients by increasing ventricular size andreducing coronary flow. β blockers are not suitablefor variant (vasospastic) angina (see Ch. 39).
3. Cardiac arrhythmias β blockers (mainlypropranolol) suppress extrasystoles and tachy-cardias, especially those mediated adrenergically(during anaesthesia, digitalis induced)—may beused i.v. for this purpose. Propranolol controlsventricular rate in atrial fibrillation and flutter,but only occasionally restores sinus rhythm.Esmolol is an alternative drug for paroxysmalsupraventricular tachycardia (see Ch. 38).
4. Myocardial infarction (MI) In relation toMI, β blockers have been used for two purposes:(a) Secondary prophylaxis of MI: There is nowfirm evidence of benefit. Long-term use afterrecovery from MI has been found to decreasesubsequent mortality by 20%. They may act by:
(i) Preventing reinfarction(ii) Preventing sudden ventricular fibrillation at
the subsequent attack of MI.High risk patients (those who had large infarcts)should be put on β blockers (if there are nohaemodynamic contraindications) for at least2 years. β blockers with partial agonistic actionare less suitable for this purpose.(b) Myocardial salvage during evolution of MI:Administered i.v. within 4–6 hours of an attackfollowed by continued oral therapy. β blockers—
(i) May limit infarct size by reducing O2 con-sumption—marginal tissue which is partiallyischaemic may survive.
(ii) May prevent arrhythmias including ventri-cular fibrillation.
However, β blockers can be given to only thosepatients not in shock or cardiac failure and whohave heart rate > 50/min with not higher thanfirst degree heart block (P-R interval < 0.24 sec).In megatrials such therapy has been found toreduce mortality by 20–25%.
5. Congestive heart failure Although βblockers can acutely worsen heart failure, severalstudies have reported beneficial haemodynamiceffects of certain β blockers including metoprolol,bisoprolol, nebivolol, carvedilol over long-termin selected patients with dilated cardiomyopathy.Introduced gradually and maintained for long term,these drugs retard the progression of CHF andprolong life. The benefit may result fromantagonism of deleterious effects of sympatheticoveractivity (invoked reflexly by heart failure) onmyocardium. Overactivation of cardiac β1
receptors has been found to exert toxic effects onthe heart by accelerating myocyte apoptosis andpromoting functionally unfavourable remodeling.One of the above named β1 blockers, usedappropriately along with other measures, is nowestablished as standard therapy for most mild tomoderate CHF patients. However, they shouldnot be given to patients with marked fluid retentionand to those requiring i.v. vasodilators or i.v.inotropic drugs (see Ch. 37).
6. Dissecting aortic aneurysm β blockershelp by reducing cardiac contractile force andaortic pulsation. Nitroprusside infusion is oftenadded.
7. Pheochromocytoma β blockers may beused to control tachycardia and arrhythmia, butshould never be administered unless an α blockerhas been given before, otherwise dangerous risein BP can occur. They suppress cardiomyopathycaused by excess CAs.
8. Thyrotoxicosis Propranolol rapidly controlsthe sympathetic symptoms (palpitation, nervous-ness, tremor, fixed stare, severe myopathy andsweating) without significantly affecting thyroidstatus. It also inhibits peripheral conversion ofT4 to T3 and is highly valuable during thyroidstorm. Major use, however, is preoperatively andwhile awaiting response to antithyroid drugs/radioactive iodine.
9. Migraine Propranolol is the most effectivedrug for chronic prophylaxis of migraine (seep. 179).

151C
HA
PTE
R10
ANTIADRENERGIC DRUGS AND DRUGS FOR GLAUCOMA
10. Anxiety Propranolol exerts an apparentantianxiety effect, especially under conditionswhich provoke nervousness and panic, e.g.examination, unaccustomed public appearance,etc. This is probably due to blockade of peripheralmanifestations of anxiety (palpitation, tremor)which have a reinforcing effect. Propranolol islargely ineffective in anxiety neurosis, but maybenefit the somatic symptoms.
11. Essential tremor Nonselective β1+β2
blockers have now an established place in treatingessential tremor. However, they do not benefitparkinsonian tremor.12. Glaucoma Ocular β blockers are widelyused for chronic simple (wide angle) glaucoma;also used as adjuvant in angle closure glaucoma(see later in this Ch.).
13. Hypertrophic obstructive cardiomyopathyThe subaortic region is hypertrophic. Forcefulcontraction of this region under sympatheticstimulation (exercise, emotion) increases outflowresistance which has incapacitating haemodynamicconsequence. β blockers improve c.o. in thesepatients during exercise by reducing leftventricular outflow obstruction, though they havelittle effect while at rest.
ααααα + βββββ ADRENERGIC BLOCKERS
Labetalol It is the first adrenergic antagonistcapable of blocking both α and β receptors. Thereare 4 diastereomers of labetalol, each of whichhas a distinct profile of action on subtypes ofα and β receptors. The commercial preparationhas equal parts of each diastereomer and displaysβ1 + β2 + α1 blocking as well as weak β2 agonisticactivity. The β blocking potency is about 1/3 thatof propranolol, while α blocking potency is about1/10 of phentolamine.
Labetalol is 5 times more potent in blockingβ than α receptors. As such, effects of a low doseresemble those of propranolol alone while athigh dose they are like a combination of propranololand prazosin. Fall in BP (both systolic and diastolic)is due to α1 and β1 blockade as well as β2 agonism
(vasodilatation). Relatively high doses reduce bothc.o. and t.p.r. Heart rate is unchanged or slightlydecreased. In contrast to propranolol, limb bloodflow increases with labetalol. It has also beenshown to inhibit NA uptake by adrenergic nerveendings.
Labetalol is orally effective but undergoesconsiderable first pass metabolism.
It is a moderately potent hypotensive and isespecially useful in pheochromocytoma andclonidine withdrawal; can also be used in essentialhypertension.
Most important side effect is postural hypo-tension, but this is significant only in somepatients. Failure of ejaculation and other sideeffects of α and β blockers can also occur, butplasma lipid levels are not altered. Rashes andliver damage have been reported.Dose: Start with 50 mg BD, increase to 100–200 mg TDSoral. In hypertensive emergencies 20–40 mg i.v. every 10min till desired response is obtained.NORMADATE 50, 100, 200 mg tab, LABESOL, LABETA50 mg tab, 20 mg 4 ml amp.
Carvedilol It is a β1 + β2 + α1 adrenoceptorblocker; produces vasodilatation due to α1
blockade as well as calcium channel blockade,and has antioxidant property. It has been usedin hypertension and is the β blocker especiallyemployed as cardioprotective in CHF. Oralbioavailability of carvedilol is 30%. It is primarilymetabolized and has a t½ of 6–8 hrs.CHF: Start with 3.125 mg BD for 2 weeks, if well toleratedgradually increase to max. of 25 mg BD.Hypertension/angina: 6.25 mg BD initially, titrate to max.of 25 mg BD.CARVIL, CARLOC, CARVAS 3.125, 6.25, 12.5, 25 mg tabs;ORICAR 12.5, 25 mg tabs.
DRUGS FOR GLAUCOMAGlaucoma is a group of diseases characterizedby a progressive form of optic nerve damage.This is generally but not necessarily associatedwith raised (> 21 mmHg) intraocular tension (i.o.t),but the etiology is unknown and there are manyrisk factors. The chief therapeutic measure is tolower i.o.t., either by reducing secretion of aqueous

152S
EC
TIO
N2
DRUGS ACTING ON ANS
humor or by promoting its drainage. Loweringof i.o.t. retards progression of optic nerve damageeven in normal/low i.o.t. glaucoma.The site offormation and pathway of drainage of aqueoushumor as well as sites of action of antiglaucomadrugs is illustrated in Fig. 10.1. Major amountof aqueous (~90%) drains through the trabecularroute, while ~10% fluid passes into the connectivetissue spaces within the ciliary muscle—then viasuprachoroid into episcleral vessels (uveoscleraloutflow). Glaucoma is seen in two principal clinicalforms:
A. Open angle (wide angle, chronicsimple) glaucoma
It is probably a genetically predisposed degene-rative disease affecting patency of the trabecularmeshwork which is gradually lost past middleage. The i.o.t. rises insidiously and progressively.Ocular hypotensive drugs are used on a long termbasis and constitute the definitive treatment inmajority of cases. The mode of ocular hypotensiveaction of topical antiglaucoma drugs issummarized in Table 10.3.
Fig. 10.1: Illustration of aqueous humor dynamics and the sites of action of ocularhypotensive drugs
(1) Site of action of miotics in angle closure glaucoma: contraction of sphincter pupillaeremoves pupillary block and reverses obliteration of iridocorneal angle(2) Site of action of miotics in open angle glaucoma: contraction of ciliary muscle pulls onscleral spur and improves trabecular patency(3) Site of action of (a) β blockers (b) α1 agonists (c) α2 agonists (d) carbonic anhydraseinhibitors: all reduce aqueous secretion by ciliary body(4) Site of action of prostaglandins and adrenaline (α agonist action): increase uveoscleraloutflow by altering permeability and/or pressure gradients(5) Site of action of adrenaline (β2 agonist action): possibly increases aqueous conductivityof trabecular filtering cells

153C
HA
PTE
R10
ANTIADRENERGIC DRUGS AND DRUGS FOR GLAUCOMA
1. βββββ Adrenergic blockersTopical β blockers have been the first line drugstill recently, but PG F2α analogues are the preferreddrugs now. In contrast to miotics, the β blockersdonot affect pupil size, tone of ciliary muscleor outflow facility, but lower i.o.t. by reducingaqueous formation. This probably results fromdown regulation of adenylylcyclase due to β2receptor blockade in the ciliary epithelium (seeFig. 10.2) and a secondary effect due to reductionin ocular blood flow. They are as effective asmiotics and produce less ocular side effects.Ocular β blockers are lipophilic with high ocularcapture (to reduce systemic effects) and have no/weak local anaesthetic activity (to avoid cornealhypoesthesia and damage).
Ocular side effects of β blockers These aregenerally mild and infrequent—stinging, rednessand dryness of eye, corneal hypoesthesia, allergicblepharoconjunctivitis and blurred vision.
Systemic adverse effects These are the majorlimitations in the use of ocular β blockers, andoccur due to absorption through nasolacrimal duct.Life-threatening bronchospasm has been reportedin asthmatic and COPD patients. Bradycardia,accentuation of heart block and CHF are likely,especially in the elderly. In fact all adverse effectsand contraindications of systemic β blockertherapy (see p. 147) apply to ocular β blockersas well. Systemic adverse effects can be minimizedby applying mild pressure on the inner canthusof the eye for about 5 min. after instilling theeyedrop to prevent entry of the drug into naso-lacrimal duct from where it is mainly absorbed.
Timolol It is the prototype of ocular β blockers;is nonselective (β1 + β2) and has no localanaesthetic or intrinsic sympathomimetic activity.The ocular hypotensive action (20–35% fall ini.o.t.) becomes evident within 1 hour and lastsfor ~12 hours. After chronic dosing, the actionis smooth and well sustained. Some effect on i.o.t.persists for 1–2 weeks following discontinuation.This feature, in contrast to pilocarpine drops, givesa high level of clinical safety, i.e. 1 or 2 misseddoses will not affect i.o.t. control. However, ~30%cases of open angle glaucoma fail to achieve thedesired level of i.o.t. with timolol alone, and mayneed additional medication.GLUCOMOL, OCUPRES, IOTIM, LOPRES 0.25% and 0.5%eye drops; start with 0.25% drops BD, change to 0.5% dropsin case of inadequate response. TIMOLAST 0.5% asgelforming eyedrop for OD use.
Betaxolol It is β1 selective blocker offeringthe advantage of less bronchopulmonary andprobably less cardiac, central and metabolic side
Fig. 10.2: Location of α1, α2 and β2 adrenergic receptorsand of carbonic anhydrase enzyme (molecules which aretargets of drug action for reducing aqueous formation) inthe processes of the ciliary bodyα1 adrenoceptors constrict ciliary vessels and reduceaqueous production: are activated by adrenaline.α2 adrenoceptors located on ciliary epithelium reduceaqueous secretion: are activated by adrenaline/apraclonidine/brimonidine.β2 adrenoceptors located on ciliary epithelium enhanceaqueous secretion via increased cAMP. Their blockadeby timolol/betaxolol reduces secretion.Carbonic anhydrase present within ciliary epithelial cellsgenerates HCO3̄ ion which is secreted into aqueoushumor. Acetazolamide/dorzolamide inhibit it and reduceaqueous secretion.
Advantages of topical βββββ blockers over miotics
• No change in pupil size: no diminution of visionin dim light and in patients with cataract
• No induced myopia which is especially troublesomein young patients
• No headache/brow pain due to persistent spasmof iris and ciliary muscles
• No fluctuations in i.o.t. as occur with pilocarpinedrops
• Convenient twice/once daily application sufficient

154S
EC
TIO
N2
DRUGS ACTING ON ANS
effects. In addition, it appears to exert a protectiveeffect on retinal neurones independent of i.o.t.lowering, by blocking some Ca2+ channels andreducing Na+/Ca2+ influx. This action is moreprominent in betaxolol than in timolol. However,betaxolol is less efficacious in lowering i.o.t. thantimolol, because ocular β receptors are predomi-nantly of the β2 subtype. Transient stinging andburning in the eye is more common with it. Mostophthalmologists prefer to start with betaxololand change over to timolol (or a similar drug)only if i.o.t. control is insufficient or there is localintolerance to betaxolol.OPTIPRESS, IOBET, OCUBETA 0.5% eye drops; 1 drop ineach eye BD.
Levobunolol It has been introduced as a oncedaily alternative to timolol. The ocular andsystemic effects are very similar to timolol exceptfor longer duration of action.BETAGAN 0.5% ophthalmic soln., 1 drop OD.
Carteolol and Metipranolol are the other ocular β blockers.
2. ααααα Adrenergic agonists
Dipivefrine It is a prodrug of Adr; penetratescornea and is hydrolysed by the esterases presentthere into Adr, which itself has poor cornealpenetration and causes ocular smarting, reactivehyperemia. The released Adr (from dipivefrine)lowers i.o.t. by augmenting uveoscleral outflow,β2 receptor mediated increase in hydraulicconductivity of trabecular filtering cells, as wellas by reducing aqueous formation (α1 + α2receptor mediated). Though better tolerated andlonger acting than Adr, dipivefrine still producessignificant ocular burning and other side effects.It is infrequently used for add on therapy.PROPINE 0.1% eye drop; 1 drop in each eye BD.
Apraclonidine It is a polar clonidine congenerwhich does not cross blood-brain barrier, butapplied topically (0.5–1%) it lowers i.o.t. by ~25%.It decreases aqueous production by primary α2 andsubsidiary α1 action in the ciliary body. Itching,lid dermatitis, follicular conjunctivitis, mydriasis,eyelid retraction, dryness of mouth and nose arecommon side effects. Its use is restricted to short
term control of spikes of i.o.t. after lasertrabeculoplasty or iridotomy.ALFADROPS DS 1% eyedrops.
Brimonidine This clonidine congener is moreα2 selective and more lipophilic than apraclonidine.It lowers i.o.t. by 20–27% by reducing aqueousproduction and by increasing uveoscleral flow.Peak effect on i.o.t. occurs after 2 hours. Allergicconjunctivitis and other ocular side effects aresimilar to but less frequent than with apraclonidine.Because of weaker α1 action, side effects likemydriasis, eyelid retraction, conjunctival blanchingfollowed by hyperemia are less prominent, but drymouth, sedation and a small fall in BP have beennoted.
Brimonidine is indicated both for short-term(prophylaxis of i.o.t. spikes post laser/post surgery)as well as long-term use in glaucoma. It is generallyused for add on therapy only.ALPHAGAN-P, BRIMODIN-P 0.15% eyedrops, IOBRIM0.2% eyedrops; 1 drop in each eye TDS.
3. Prostaglandin analoguesLow concentration of PGF2α was found to loweri.o.t without inducing ocular inflammation. It actsby increasing uveoscleral outflow, possibly byincreasing permeability of tissues in ciliary muscleor by an action on episcleral vessels. An effect ontrabecular outflow has also been demonstrated, butis less marked. Ciliary body COX-2 has been found
TABLE 10.3 Mode of action of ocular hypo-tensive drugs
Drug/class Aqueous Trabecular Uveoscleralsecretion outflow outflow
1. β-blockers ↓ – –(Timolol)
2. Adrenaline/ ↓ ↑ ↑Dipivefrine
3. Brimonidine/ ↓ – ↑apraclonidine
4. Prostaglandins – ↑ ↑(Latanoprost)
5. Miotics – ↑ –(Pilocarpine)
6. Carbonic ↓ – –anhydraseinhibitors

155C
HA
PTE
R10
ANTIADRENERGIC DRUGS AND DRUGS FOR GLAUCOMA
to be down regulated in wide angle glaucomaindicating a physiological role of PGs in aqueoushumor dynamics.
Latanoprost Instilled in the eye, this PGF2αderivative has shown efficacy similar to timolol(i.o.t. reduction by 25–35%) and the effect is wellsustained over long-term. It reduces i.o.t. in normalpressure glaucoma also. Though ocular irritationand pain are relatively frequent, no systemic sideeffects are reported. Blurring of vision, increasediris pigmentation, thickening and darkening ofeyelashes have occurred in some cases. Macularedema can develop during treatment with anyPGF2α analogue, especially in aphakic patients; awatch should be kept to detect it early.
Because of good efficacy, once daily appli-cation and absence of systemic complications, PGanalogues have become the first choice drugs foropen angle glaucoma. High cost is a disadvantage.LACOMA, XALATAN, LATOPROST, 0.005% eyedrops, onedrop in each eye OD in the evening; LACOMA-T LAPROSTPLUS, LATOCHECK-T eyedrops with timolol 0.5% eyedrops.(To be stored in cold)
Travoprost Another selective FP-prostanoidreceptor agonist which lowers i.o.t. mainly byincreasing uveoscleral outflow and a minor effecton trabecular outflow. The effect starts within2 hours, peaks at 12 hours and lasts for 24 hoursor more. The i.o.t. lowering efficacy and sideeffects are comparable to latanoprost. Somepatients not responding well with one may respondto the other.TRAVATAN 0.004% eyedrops. One drop in each eye in theevening; refrigeration of the eyedrop is not required;TRAVACOM 0.004% with timolol 0.5% eyedrop.
Bimatoprost A synthetic prostamide derivativefound to be equally or more effective than latano-prost in lowering i.o.t. Ocular side effects are alsosimilar, but some patients may tolerate it better.LUMIGAN, CAREPROST 0.3% eyedrops; one drop in eacheye OD in the evening. The eyedrop need not be stored inrefrigerator.
4. Carbonic anhydrase inhibitorsAcetazolamide (see Ch. 41) Oral treatmentwith acetazolamide (0.25 g 6–12 hourly) reducesaqueous formation by limiting generation of
bicarbonate ion in the ciliary epithelium. It is usedto supplement ocular hypotensive drugs for shortterm indications like angle closure, before and afterocular surgery/laser therapy. Systemic sideeffects—paresthesia, anorexia, hypokalaemia,acidosis, malaise and depression restrict long-termuse to few cases in which target i.o.t. is notachieved even by concurrent use of 2–3 topicaldrugs.
Dorzolamide (2% eyedrops BD-TDS) It is atopically useful carbonic anhydrase inhibitordeveloped to circumvent systemic side effects ofacetazolamide. It lowers i.o.t. by ~20%; somewhatless efficacious than timolol. Ocular stinging,burning, itching, corneal edema and bitter tasteare the usual side effects. Systemic adverse effectsare also possible. Dorzolamide is used only asadd on drug to topical β blockers/PG analogues,or when these drugs are contraindicated.DORTAS, DORZOX 2% eyedrops.
Brinzolamide is another ocular carbonic anhydrase inhibitor.
5. Miotics: Till the 1970s topical pilocarpineand/or antiChEs were the standard antiglaucomadrugs (see Ch. 7). However, because of severaldrawbacks (see box on p. 153), they are nowused only as the last option. In open angleglaucoma, they lower i.o.t. by increasing ciliarymuscle tone thereby improving patency oftrabeculae.
The current approach to treatment of openangle glaucoma can be summarized as—startmonotherapy with latanoprost or a topical βblocker; if target i.o.t. is not attained, either changeover to the alternative drug or use both the aboveconcurrently. Brimonidine/dorzolamide (occa-sionally dipivefrine) are used only when thereare contraindications to PG analogues and/or βblockers, or to supplement their action. Topicalmiotics and oral acetazolamide are added onlyas the last resort.
B. Angle closure (narrow angle, acutecongestive) glaucoma
It occurs in individuals with a narrow iridocornealangle and shallow anterior chamber. The i.o.t.

156S
EC
TIO
N2
DRUGS ACTING ON ANS
remains normal until an attack is precipitated,usually by mydriasis (Fig. 10.3A,B). The i.o.t.rises rapidly to very high values (40–60 mmHg).It is an emergent condition with marked congestionof eyes and severe headache. Failure to loweri.o.t. quickly may result in loss of sight.
Vigorous therapy employing various measures toreduce i.o.t. is instituted.1. Hypertonic mannitol (20%) 1.5–2 g/kg or
glycerol (10%): infused i.v. decongest the eyeby osmotic action. A retention enema of 50%glycerine is also some times used.
2. Acetazolamide: 0.5 g i.v. followed by oral twicedaily is started concurrently.
3. Miotic: Once the i.o.t. starts falling due to theabove i.v. therapy, pilocarpine 1–4% is instilledevery 10 min initially and then at longerintervals. Contraction of sphincter pupillaechanges the direction of forces in the iris to
Fig. 10.3: Development of angle closure glaucoma andits reversal by miotic
A. Mydriasis occurs in an eye with narrow iridocornealangle and iris makes contact with lens blocking passageof aqueous from posterior to anterior chamber.B. Pressure builds up behind the iris which bulgesforward and closes the iridocorneal angle thus blockingaqueous outflow.C. Miotic makes the iris thin and pulls it away from thelens removing the pupillary block and restoring aqueousdrainage
PROBLEM DIRECTED STUDY
10.1 A 70-year-male presented with the complaints of weak stream of urine, sense of incompletebladder voiding, urinary frequency and nocturia. After physical examination and ultrasound, hewas diagnosed to have developed benign prostatic hypertrophy and was prescribed:Tab. Terazosin 5 mg, one tab daily at bed time.He took the medicine as advised and went off to sleep. At night, when he got up to pass urine,he felt giddy and fainted. On being laid flat on the bed, he regained consciousness within 2minutes. Later, he was gradually propped up on the bed to the sitting position and then gotup slowly and walked without any problem.(a) What is the rationale of prescribing terazosin to this patient?(b) What is the likely explanation for the fainting attack?(c) What precautions could have avoided the fainting episode?
10.2 A lady aged 55 years was brought at night to the hospital emergency with severe breathlessnessand wheezing. Chest auscultation revealed marked bronchoconstriction. She was managed with100% O2 inhalation and nebulized salbutamol + ipratropium bromide. The asthmatic attack wascontrolled in about 6 hours. Next day, history taking revealed that she was having mild episodicasthma off and on, but never had such a severe attack. Day before she had visited an ophthalmologistfor visual difficulty and frontal headache. The intraocular pressure was measured to be 24 and25 mmHg in right and left eye respectively. She was prescribed:Timolol 0.5% eyedrops in each eye twice a day.(a) What is the most likely explanation for the precipitation of severe attack of asthma?(b) How could such a complication be avoided?(see Appendix-1 for solutions)

157C
HA
PTE
R10
ANTIADRENERGIC DRUGS AND DRUGS FOR GLAUCOMA
lessen its contact with the lens and spreadsthe iris mass centrally → pupillary block isremoved and iridocorneal angle is freed (Fig.10.3C). However, when i.o.t. is very high, theiris muscle fails to respond to miotics; tensionshould be reduced by other measures beforemiotics can act.
4. Topical β blocker: Timolol 0.5% is instilled12 hourly in addition.
5. Apraclonidine (1%)/latanoprost 0.005%instillation may be added.
Drugs are used only to terminate the attack ofangle closure glaucoma. Definitive treatment issurgical or laser iridotomy. Few cases, who havechronic narrow angle glaucoma, may be treatedwith a miotic/other ocular hypotensive drug forlong periods, but often surgery/laser therapy isultimately required.

SECTION 3
AUTACOIDS AND RELATED DRUGS
Autacoid This term is derived from Greek:autos—self, akos—healing substance or remedy.
These are diverse substances produced by awide variety of cells in the body, having intensebiological activity, but generally act locally (e.g.within inflammatory pockets) at the site ofsynthesis and release.
They have also been called ‘local hormones’.However, they differ from ‘hormones’ in twoimportant ways—hormones are produced byspecific cells, and are transported through circu-lation to act on distant target tissues.
Autacoids are involved in a number of phy-siological and pathological processes (especiallyreaction to injury and immunological insult). Someautacoids, in addition, serve as transmitters or
modulators in the nervous system, but their roleat many sites is not precisely known. A numberof useful drugs act by modifying their action ormetabolism. The classical autacoids are—Amine autacoids Histamine, 5-Hydroxytryp-tamine (Serotonin)Lipid derived autacoids Prostaglandins,Leukotrienes, Platelet activating factorPeptide autacoids Plasma kinins (Bradykinin,Kallidin), Angiotensin
In addition, cytokines (interleukins, TNFα,GM-CSF, etc.) and several peptides likegastrin, somatostatin, vasoactive intestinalpeptide and many others may be considered asautacoids.

Histamine and AntihistaminicsChapterChapterChapterChapterChapter 1111111111
HISTAMINE
Histamine, meaning ‘tissue amine’ (histos—tissue)is almost ubiquitously present in animal tissuesand in certain plants, e.g. stinging nettle. Itspharmacology was studied in detail by Dale inthe beginning of the 20th century when closeparallelism was noted between its actions andthe manifestations of certain allergic reactions.It was implicated as a mediator of hypersensitivityphenomena and tissue injury reactions. It is nowknown to play important physiological roles.
Histamine is present mostly within storagegranules of mast cells. Tissues rich in histamineare skin, gastric and intestinal mucosa, lungs, liverand placenta. Nonmast cell histamine occurs inbrain, epidermis, gastric mucosa and growingregions. Turnover of mast cell histamine is slow,while that of nonmast cell histamine is fast.Histamine is also present in blood, most bodysecretions, venoms and pathological fluids.
Synthesis, storage and destructionHistamine is β imidazolylethylamine. It issynthesized locally from the amino acid histidineand degraded rapidly by oxidation and methylation(Fig. 11.1). In mast cells, histamine (positivelycharged) is held by an acidic protein and heparin(negatively charged) within intracellular granules.When the granules are extruded by exocytosis,Na+ ions in e.c.f. exchange with histamine torelease it free (Fig. 11.2). Increase in intracellularcAMP (caused by β adrenergic agonists andmethylxanthines) inhibits histamine release.Histamine is inactive orally because liver degradesall histamine that is absorbed from the intestines.
Histamine receptors Four types of histami-nergic receptors have now been clearly delineatedand cloned. Analogous to adrenergic α and βreceptors, histaminergic receptors were classified
by Asch and Schild (1966) into H1 and H2 : thoseblocked by then available antihistamines werelabelled H1. Sir James Black (1972) developedthe first H2 blocker burimamide and confirmedthis classification. A third H3 receptor, whichserves primarily as an autoreceptor controllinghistamine release from neurones in brain wasidentified in 1983. Though some selective H3
agonists and antagonists have been produced, nonehas found any clinical application. Features ofthese 3 types of histaminergic receptor arecompared in Table 11.1.Molecular cloning has revealed yet another (H4) receptorin 2001. It has considerable homology with H3 receptor andbinds many H3 ligands. 4-Methyl histamine, earlier consideredto be a specific H2 agonist, has shown greater affinity andselectivity for the H4 receptor, and is now labelled a H4
agonist. However, the H4 receptor is pharmacologically lessdistinct. Eosinophils, mast cells and basophils are the primarycells expressing H4 receptors. Activation of H4 receptorsenhances chemotaxis of these cells. The H4 receptor maybe playing a role in allergic inflammation: H4 antagonistsare being explored as potential drugs for allergic inflammatoryconditions like rhinitis and asthma. Intestines and brain arethe other sites where H4 receptors have been located.
PHARMACOLOGICAL ACTIONS
1. Blood vessels Histamine causes markeddilatation of smaller blood vessels, including arte-rioles, capillaries and venules. On s.c. injection
Fig. 11.1: Synthesis and degradation of histamineMAO-Monoamine oxidase

160S
EC
TIO
N3
AUTACOIDS AND RELATED DRUGS
TAB
LE 1
1.1
Dis
tinct
ive
feat
ures
of t
hree
type
s of
his
tam
iner
gic
rece
ptor
s
H1
H
2
H
3
1.S
elec
tive
agon
ists
2-M
ethy
l his
tam
ine
(8:1
)D
imap
rit (
1:20
00)
(R)
α-M
ethy
l his
tam
ine
(rel
ativ
e se
lect
ivity
H1:
H2)
2-P
yrid
ylet
hyla
min
e(30
:1)
Impr
omid
ine
(1:1
0,00
0)(H
1: H
3 1:
3000
)2-
Thi
azol
yl e
thyl
amin
e (9
0: 1
)lm
etit
2.S
elec
tive
anta
goni
sts
Mep
yram
ine
(600
0:1)
Cim
etid
ine
(1: 5
00)
Thi
oper
amid
e (H
1: H
3 1
: 23
000)
(rel
ativ
e se
lect
ivity
H1:
H2)
Chl
orph
enira
min
e (1
5000
:1)
Ran
itidi
ne (
l :
>50
0)Im
prom
idin
e (H
2 a
goni
st)
Tipr
olis
ant
3.R
ecep
tor
type
Gq-
prot
ein
coup
led
Gs-
prot
ein
coup
led
Gi/G
o-pr
otei
n co
uple
d
4.E
ffect
or p
athw
ayP
IP2
hydr
olys
is →
IP
3/D
AG
:A
deny
lyl c
ycla
se a
ctiv
atio
n —
a)R
estr
ictin
g C
a2+ in
flux
Rel
ease
of C
a2+ f
rom
intr
acel
lula
r st
ores
;cA
MP
↑—
phos
phor
ylat
ion
ofb)
K+ c
hann
el a
ctiv
atio
nP
rote
in k
inas
e-C
act
ivat
ion
spec
ific
prot
eins
c)cA
MP
↓N
O r
elea
se→
cGM
P
5.D
istr
ibut
ion
in b
ody:
a)S
moo
th m
uscl
e (in
test
ine,
airw
ay,
a)G
astr
ic g
land
s—ac
id s
ecre
tion
a)B
rain
(pr
esyn
aptic
ally
)—in
hibi
tion
actio
ns m
edia
ted
uter
us)—
cont
ract
ion
b)B
lood
ves
sels
(sm
ooth
of h
ista
min
e re
leas
e—se
datio
nb)
Blo
od v
esse
lsm
uscl
e)—
dila
tatio
nb)
Lung
, sp
leen
, sk
in,
gast
ric
muc
osa
—i)
End
othe
lium
: R
elea
se o
f N
O a
nd,
c)H
eart
decr
ease
his
tam
ine
rele
ase
PG
I 2—
vaso
dila
tatio
n.A
tria
: +iv
e ch
rono
trop
yc)
Ileum
—in
hibi
tion
of A
Ch
wid
enin
g of
gap
junc
tions
—V
entr
icle
s: +
ive
inot
ropy
rele
ase
from
mye
nter
ic in
crea
sed
capi
llary
per
mea
bilit
yd)
Ute
rus
(rat
)—re
laxa
tion
plex
us n
euro
nes
ii) S
moo
th m
uscl
e of
larg
ere)
Bra
in—
trans
mitt
erd)
Cer
tain
blo
od v
esse
ls—
inhi
bit N
A
vess
els—
vaso
cons
tric
tion.
rele
ase—
vaso
dila
tatio
nc)
Affe
rent
ner
ve e
ndin
gs—
stim
ulat
ion
d)G
angl
ioni
c ce
ll—st
imul
atio
n.e)
Adr
enal
med
ulla
—re
leas
e of
CA
s.f)
Bra
in—
trans
mitt
er.
PIP
2—P
hosp
hatid
yl in
osito
l bis
phos
phat
e; IP
3—In
osito
l tris
phos
phat
e; D
AG
—D
iacy
lgly
cero
ls;
ED
RF
— E
ndot
heliu
m d
epen
dent
rel
axin
g fa
ctor
; NO
—N
itric
oxi
de; P
GI 2
—P
rost
acyc
lin;
CA
s—C
atec
hola
min
es; c
AM
P —
Cyc
lic 3
', 5'
ade
nosi
ne m
onop
hosp
hate
; AC
h—A
cety
lcho
line

161C
HA
PTE
R11
HISTAMINE AND ANTIHISTAMINICS
Like many other autacoids and ACh, vasodi-latation caused by histamine is partly (H1 compo-nent) indirect, mediated through ‘endotheliumdependent relaxing factor’ (EDRF), i.e. NO; thereceptor being located on the endothelial cells.H2 receptors mediating vasodilatation are locateddirectly on the vascular smooth muscle.
Larger arteries and veins are constricted byhistamine: mediated by H1 receptor on vascularsmooth muscle. Histamine also causes increasedcapillary permeability due to separation ofendothelial cells → exudation of plasma. Thisis primarily a H1 response.Injected intradermally, it elicits the triple responseconsisting of:
Red spot: due to intense capillary dilatation.Wheal: due to exudation of fluid from
capillaries and venules.Flare: i.e. redness in the surrounding area
due to arteriolar dilatationmediated by axon reflex.
2. Heart Direct effects of histamine on in situheart are not prominent, but the isolated heart,especially of guinea pig, is stimulated—rate aswell as force of contraction is increased. Theseare primarily H2 responses but a H1 mediatednegative dromotropic (slowing of A-V conduction)effect has also been demonstrated.
3. Visceral smooth muscle Histaminecauses bronchoconstriction; guinea pigs andpatients of asthma are highly sensitive. Large dosescause abdominal cramps and colic by increasingintestinal contractions. Guineapig uterus iscontracted while that or rat is relaxed; humanuterus is not much affected as are most othervisceral smooth muscles.
Smooth muscle contraction is a H1 response.In few instances H2 mediated relaxation is alsoseen, e.g. bronchial muscle of sheep, humanbronchi after H1 blockade.
4. Glands Histamine causes marked increasein gastric secretion—primarily of acid but alsoof pepsin (see Ch. 46). This is a direct actionexerted on parietal cells through H2 receptors and
Fig. 11.2: Mechanism of antigen-antibody reactioninduced release of histamine from mast cell.
In sensitized atopic individual, specific reaginic (IgE)antibody is produced and gets bound to Fc epsilonreceptor I (FcεRI) on the surface of mast cells. Onchallenge, the antigen bridges IgE molecules resultingin transmembrane activation of a tyrosine-protein kinase(t-Pr-K) which phosphorylates and activates phospho-lipaseCγ. Phosphatidyl inositol bisphosphate (PIP2) ishydrolysed and inositol trisphosphate (IP3) is generatedwhich triggers intracellular release of Ca2+. The Ca2+ ionsinduce fusion of granule membrane with plasma mem-brane of the mast cell resulting in exocytotic release ofgranule contents. In the granule, positively chargedhistamine (Hist+) is held complexed with negativelycharged protein (Prot–) and heparin (Hep–) molecules.Cationic exchange with extracellular Na+ (and Ca2+) setshistamine free to act on the target cells.
flushing, especially in the blush area, heat,increased heart rate and cardiac output, with littleor no fall in BP are produced. Rapid i.v. injectioncauses fall in BP which has an early short lastingH1 and a slow but more persistent H2 component.With low doses only the H1 component is manifestsince H1 receptors have higher affinity. Fall inBP due to large doses is completely blocked onlyby a combination of H1 and H2 antagonists.Dilatation of cranial vessels causes pulsatileheadache.

162S
EC
TIO
N3
AUTACOIDS AND RELATED DRUGS
is mediated by increased cAMP generation, whichin turn activates the membrane proton pump (H+
K+ ATPase).Histamine can increase other secretions also,
but the effect is hardly discernable.
5. Sensory nerve endings Itching occurswhen histamine is injected i.v. or intracutaneously.Higher concentrations injected more deeply causepain. These are reflections of the capacity ofhistamine to stimulate nerve endings.
6. Autonomic ganglia and adrenalmedulla These are stimulated and release ofAdr occurs, which can cause a secondary risein BP.
7. CNS Histamine does not penetrate blood-brain barrier—no central effects are seen on i.v.injection. However, intracerebroventricular admi-nistration produces rise in BP, cardiac stimulation,behavioural arousal, hypothermia, vomiting andADH release. These effects are mediated throughboth H1 and H2 receptors.
PATHOPHYSIOLOGICAL ROLES
1. Gastric secretion Histamine has dominantphysiological role in mediating secretion ofHCl in the stomach (see Fig. 46.1). Nonmast cellhistamine occurs in gastric mucosa, possibly incells called ‘histaminocytes’ situated close to theparietal cells. This histamine has high turnoverrate. It is released locally under the influenceof all stimuli that evoke gastric secretion (feeding,vagal stimulation, cholinergic drugs and gastrin)and activates the proton pump (H+K+ ATPase)through H2 receptors.
H2 blockers not only suppress acid secretioninduced by histamine but also markedly diminishthat in response to ACh and gastrin. By a mutuallysynergistic interaction the three secretagoguesamplify responses to each other with histamineplaying the dominant role. As such, antimuscarinicdrugs dampen the response to histamine andgastrin also. All three secretagogues activatethe same proton pump (H+K+ATPase) in the
parietal cell membrane, but through their ownreceptors.
2. Allergic phenomena Mediation of hyper-sensitivity reactions was the first role ascribedto histamine. It is an important, but only one ofthe mediators of such phenomena. Released frommast cells following AG : AB reaction on theirsurface (involving IgE type of reaginic antibodies;Fig. 11.2) in immediate type of hypersensitivityreactions, histamine is causative in urticaria,angioedema, bronchoconstriction and anaphylacticshock. The H1 antagonists are effective incontrolling these manifestations to a considerableextent, except asthma and to a lesser extentanaphylactic fall in BP in which leukotrienes(especially LTD4) and PAF appear to be moreimportant. Histamine is not involved in delayedor retarded type of allergic reactions.
3. As transmitter Histamine is believed tobe the afferent transmitter which initiates the sen-sation of itch and pain at sensory nerve endings.
Nonmast cell histamine occurs in brain, espe-cially hypothalamus and midbrain. It is involvedin maintaining wakefulness; H1 antihistaminicsowe their sedative action to blockade of this func-tion. In the brain H1 agonism suppresses appetite.This may explain the appetite promoting actionof certain H1 antagonists. Histamine also appearsto participate as a transmitter regulating bodytemperature, cardiovascular function, thirst, andpossibly other functions, mainly through H2
(postsynaptic receptors) and H3 (presynapticautoreceptors).
4. Inflammation Histamine is a mediator ofvasodilatation and other changes that occur duringinflammation. It promotes adhesion of leukocytesto vascular endothelium by expressing adhesionmolecule P-selectin on endothelial cell surface,sequestrating leukocytes at the inflammatory site.It may also regulate microcirculation accordingto local needs.5. Tissue growth and repair Because growing andregenerating tissues contain high concentrations of histamine,it has been suggested to play an essential role in the processof growth and repair.

163C
HA
PTE
R11
HISTAMINE AND ANTIHISTAMINICS
6. Headache Histamine has been implicated in certainvascular headaches, but there is no conclusive evidence.
USES
Histamine has no therapeutic use. In the past it has beenused to test acid secreting capacity of stomach, bronchialhyperreactivity in asthmatics, and for diagnosis of pheo-chromocytoma, but these pharmacological tests are risky andobsolete now.
Betahistine It is an orally active, somewhatH1 selective histamine analogue, which is usedto control vertigo in patients of Meniéré’s disease:possibly acts by causing vasodilatation in theinternal ear. It is contraindicated in asthmaticsand ulcer patients.VERTIN 8 mg tab., 1/2 to 1 tab. QID.
HISTAMINE RELEASERS
A variety of mechanical, chemical and immunological stimuliare capable of releasing histamine from mast cells.1. Tissue damage: trauma, stings and venoms, proteolyticenzymes, phospholipase A.2. Antigen: antibody reaction involving IgE antibodies.3. Polymers like dextran, polyvinyl pyrrolidone (PVP).4. Some basic drugs—tubocurarine, morphine, atropine,pentamidine, polymyxin B, vancomycin and even someantihistaminics directly release histamine without animmunological reaction.5. Surface acting agents like Tween 80, compound 48/80etc. The primary action of these substances is release ofhistamine from mast cells, therefore they are called ‘histamineliberators’. They produce an ‘anaphylactoid’ reaction—itchingand burning sensation, flushing, urticaria, fall in BP,tachycardia, headache, colic and asthma. Most of thesesymptoms are controlled by a H1 antihistaminic, better stillif H2 blocker is given together.
H1 ANTAGONISTS(Conventional antihistaminics)
These drugs competitively antagonize actions ofhistamine at the H1 receptors. Recent evidenceindicates that histamine H1 receptor exhibits somedegree of constitutive activity, and the H1
antagonists are also inverse agonists. The firstcompounds of this type were introduced in thelate 1930s and have subsequently proliferated intoan unnecessary motley of drugs. Nevertheless,they are frequently used for a variety of purposes.More commonly employed now are the less
sedating/nonsedating second generation H1
antihistamines added after 1980. Seemingly, H1
antihistaminics have diverse chemical structures,but majority have a substituted ethylamine sidechain. They are classified and listed in Table 11.2.
PHARMACOLOGICAL ACTIONS
Qualitatively all H1 antihistaminics have similaractions, but there are quantitative differences,especially in the sedative property.
1. Antagonism of histamine They effec-tively block histamine induced bronchocons-triction, contraction of intestinal and other smoothmuscle and triple response—especially wheal,flare and itch. Fall in BP produced by low dosesof histamine is blocked, but additional H2
antagonists are required for complete blockadeof that caused by higher doses. Pretreatment withthese drugs protects animals from death due toi.v. injection of large doses of histamine. Releaseof Adr from adrenal medulla in response tohistamine is abolished. Constriction of larger bloodvessel by histamine is also antagonized. Actionof histamine on gastric secretion is singularly notaffected by these drugs. Cyproheptadine hadadditional 5-HT2 receptor blocking activity (seep. 174).
2. Antiallergic action Many manifestationsof immediate hypersensitivity (type I reactions)are suppressed. Urticaria, itching and angioedemaare well controlled. Anaphylactic fall in BP isonly partially prevented. Asthma in man ispractically unaffected, though anaphylacticbronchoconstriction in guinea pig is largelyprevented. This tissue and species dependenceof response probably reflects extent ofinvolvement of histamine in the reaction. It isnow well established that leukotrienes (C4 andD4) and PAF are more important mediators forhuman asthma.
3. CNS The older antihistamines producevariable degree of CNS depression. This appearsto depend on the compound’s ability to penetrate

164S
EC
TIO
N3
AUTACOIDS AND RELATED DRUGS
TABLE 11.2 Clinical classification, doses and preparations of H1 antihistaminics
Drug Dose and route Preparations
I. HIGHLY SEDATIVE
Diphenhydramine 25–50 mg oral BENADRYL 25, 50 mg cap., 12.5 mg/5ml syr.
Dimenhydrinate 25–50 mg oral, DRAMAMINE 16 mg/5 ml syr, 50 mg tab
Promethazine 25–50 mg oral, PHENERGAN 10, 25 mg tab., 5 mg/ml elixer,i.m. (1 mg/kg) 25 mg/ml inj
Hydroxyzine 25–50 mg oral, ATARAX 10, 25 mg tab., 10 mg/5 ml syr, 6 mg/mli.m. drops, 25 mg/ml inj.
II. MODERATELY SEDATIVE
Pheniramine 20–50 mg oral, AVIL 25 mg, 50 mg tab, 15 mg/5 ml syr,i.m. 22.5 mg/ml inj.
Cyproheptadine 4 mg oral PRACTIN, CIPLACTIN 4 mg tab., 2 mg/5ml syrup,
Meclozine (Meclizine) 25–50 mg oral In DILIGAN 12.5 mg + niacin 50 mg tabIn PREGNIDOXIN 25 mg + Caffeine 20 mg tab
Cinnarizine 25–50 mg oral STUGERON, VERTIGON 25 and 75 mg tab.
III. MILD SEDATIVE
Chlorpheniramine 2–4 mg (0.1 mg/kg) PIRITON, CADISTIN 4 mg tab,oral, i.m.
Dexchlorpheniramine 2 mg oral POLARAMINE 2 mg tab, 0.5 mg/ 5 ml syr
Triprolidine 2.5–5 mg oral ACTIDIL 2.5 mg tab., ACTIFED 2.5 mg withpseudoephedrine 60 mg tab.
Clemastine 1–2 mg oral TAVEGYL 1 mg tab., 0.5 mg/5 ml syr
IV. SECOND GENERATION ANTIHISTAMINICS
Fexofenadine 120–180 mg oral ALLEGRA, ALTIVA, FEXO 120, 180 mg tab
Loratadine 10 mg oral LORFAST, LORIDIN, LORMEG, 10 mg tab,1 mg/ml susp.
Desloratadine 5 mg oral DESLOR, LORDAY, NEOLORIDIN 5 mg tab
Cetirizine 10 mg oral ALERID, CETZINE, ZIRTIN, SIZON 10 mg tab,5 mg/5 ml syr.
Levocetirizine 5–10 mg oral LEVOSIZ, LEVORID, TECZINE 5, 10 mg tabLEVOCET 5 mg tab, 2.5mg/5 ml syr.
Azelastine 4 mg oral AZEP NASAL SPRAY 0.14 mg0.28 mg intranasal per puff nasal spray
Mizolastine 10 mg oral ELINA 10 mg tab
Ebastine 10 mg oral EBAST 10 mg tab
Rupatadine 10 mg oral RUPAHIST 10 mg tab
Terfenadine and astemizole are the earliest second generation H1 antihistamines that are now banned. Cyclizine,buclizine, dimethindine, mebhydroline are conventional antihistamines that have become unavailable.

165C
HA
PTE
R11
HISTAMINE AND ANTIHISTAMINICS
the blood-brain barrier and its affinity for thecentral (compared to peripheral) H1 receptors.Individual susceptibility to different agents variesconsiderably. The same drug and dose mayincapacitate some subjects, while others mayremain alert. An overall grading of the sedativeproperty of H1 antihistaminics is presented in Table11.2. Some individuals also experience stimulanteffects like restlessness and insomnia. Excitementand convulsions are frequently seen at toxic doses.The second generation antihistaminics are prac-tically nonsedating.
Certain (see below) H1 antihistamines areeffective in preventing motion sickness. It is notclear whether this is due to antagonism ofhistamine in the brain or reflects antimuscarinicproperty of these drugs. Promethazine alsocontrols vomiting of pregnancy and other causes.
Promethazine and few other antihistaminicsreduce tremor, rigidity and sialorrhoea of parkin-sonism. Anticholinergic and sedative propertiesunderlie the benefit.
Some older antihistamines, especiallycyproheptadine, have appetite stimulating effect.
Some H1 antihistamines are also effectiveantitussives (see Ch. 16).
4. Anticholinergic action Many H1 blockersin addition antagonize muscarinic actions of ACh.The anticholinergic action can be graded as:
High Low Minimal/Absent
Promethazine Chlorpheniramine FexofenadineDiphenhydramine Hydroxyzine AstemizoleDimenhydrinate Triprolidine LoratadinePheniramine Cyproheptadine Cetirizine
Mizolastine
If used concurrently with atropine or its substitutes,phenothiazines, tricyclic antidepressants or diso-pyramide, the anticholinergic action adds up.
5. Local anaesthetic Some drugs like pheni-ramine, promethazine, diphenhydramine havestrong while others have weak membranestabilizing property. However, they are not usedclinically as local anaesthetic because they causeirritation when injected s.c.
Membrane stabilizing activity also confersantiarrhythmic property to these compounds.
6. BP Most antihistaminics cause a fall in BPon i.v. injection (direct smooth muscle relaxationor α adrenergic blockade as in promethazine).However, this is not evident on oral administration.
PHARMACOKINETICS
The conventional H1 antihistaminics are wellabsorbed from oral and parenteral routes,metabolized in the liver and excreted in urine.They are widely distributed in the body and enterbrain. The newer compounds penetrate brainpoorly accounting for their low/absent sedatingaction. Duration of action of most agents is4–6 hours, except meclozine, chlorpheniramine,mesolastine, loratadine, cetirizine and fexo-fenadine which act for 12–24 hours or more.
SIDE EFFECTS AND TOXICITY
Side effects of first generation H1 antihistaminicsare frequent, but generally mild. Individuals showmarked differences in susceptibility to side effectswith different drugs. Some tolerance to side effectsdevelops on repeated use.
Sedation, diminished alertness and concen-tration, light headedness, motor incoordination,fatigue and tendency to fall asleep are the mostcommon. Objective testing shows impairment ofpsychomotor performance. Patients should becautioned not to operate motor vehicles ormachinery requiring constant attention. Alcoholsynergises in producing these effects as do otherCNS depressants. Few individuals become restless,nervous and are unable to sleep. Second generationcompounds are largely free of CNS effects.
Regular use of conventional antihistamines isnot advisable in children, because the CNSdepressant property may interfere with learningand academic tasks.Dryness of mouth, alteration of bowel movement,urinary hesitancy and blurring of vision can beascribed to anticholinergic property.Epigastric distress and headache may be felt.Local application can cause contact dermatitis.

166S
EC
TIO
N3
AUTACOIDS AND RELATED DRUGS
Some drugs like hydroxyzine, cyclizine andfexofenadine are teratogenic in animals; but thereis no evidence of excess malformations in humans.Caution is nevertheless to be exercised inprescribing an antihistaminic during pregnancy.
Acute overdose produces central excitation,tremors, hallucinations, muscular incordination,convulsions, flushing, hypotension, fever and someother features of belladonna poisoning. Death isdue to respiratory and cardiovascular failure.
SECOND GENERATION ANTIHISTAMINICS
The second generation antihistaminics (SGAs)may be defined as those H1 receptor blockersmarketed after 1980 which have one or more ofthe following properties:• Absence of CNS depressant property.• Higher H1 selectivitiy: no anticholinergic side
effects.• Additional antiallergic mechanisms apart from
histamine blockade: some also inhibit latephase allergic reaction by acting on leukotrienesor by antiplatelet activating factor effect.As per an international consensus group of experts, no
compound developed so far merits labelling as ‘third generationantihistaminic’.
These newer drugs have the advantage of notimpairing psychomotor performance (driving etc.need not be contraindicated), produce nosubjective effects, no sleepiness, do not potentiatealcohol or benzodiazepines. Some patients docomplain of sedation, but incidence is similar tothat with placebo. However, they have a narrowspectrum of therapeutic usefulness which is limitedby the extent of involvement of histamine (actingthrough H1 receptors) in the disease state. Theirprincipal indications are:
(i) Allergic rhinitis and conjunctivitis, hay fever,pollinosis—control sneezing, runny but notblocked nose, and red, watering, itchy eyes.
(ii) Urticaria, dermographism, atopic eczema.(iii) Acute allergic reactions to drugs and foods.
They have poor antipruritic, antiemetic andantitussive actions.
Fexofenadine It is the active metabolite ofterfenadine, the first nonsedating SGA that was
withdrawn because of several deaths due topolymorphic ventricular tachycarida (Torsades depointes) occurring with its higher doses or whenit was coadministered with CYP3A4 inhibitors(erythromycin, clarithromycin, ketoconazole,itraconazole, etc.). This toxicity is based onblockade of delayed rectifier K+ channels in theheart at higher concentrations. Astemizole isanother SGA banned for the same reason.Fexofenadine has a low propensity to blockdelayed rectifier K+ channels, does not prolongQTc interval. Since it is minimally metabolized,no interaction with CYP3A4 inhibitors have beenreported. It is largely free of arrhythmogenicpotential, but some cases of ventricular arrhythmiain patients with preexisting long QT interval havebeen reported. Thus, it is not entirely safe inpatients with long QT, bradycardia or hypo-kalemia.
Fexofenadine does not cross blood-brainbarrier—does not produce sedation or impairpsychomotor performance and is free of atropinicside effects. It is rapidly absorbed, excretedunchanged in urine and bile, has plasma t½11–16 hours and duration of action 24 hours.Dose: For allergic rhinitis 120 mg OD; for urticaria and otherskin allergies 180 mg OD.
Loratadine Another long-acting selective peri-pheral H1 antagonist which lacks CNS depressanteffects and is fast acting. It is partly metabolizedby CYP3A4 to an active metabolite with a longert½ of 17 hr, but has not produced cardiacarrhythmia in overdose, though seizures arereported. No interaction with macrolides orantifungals has been noted. Good efficacy hasbeen reported in urticaria and atopic dermatitis.
Desloratadine It is the major active metaboliteof loratadine effective at half the dose. Non-interference with psychomotor performance andcardiac safety are documented.
Cetirizine It is a metabolite of hydroxyzinewith marked affinity for peripheral H1 receptors;penetrates brain poorly, but mild sedation andsubjective somnolence is experienced by manyrecipients. It is not metabolized; does not prolong

167C
HA
PTE
R11
HISTAMINE AND ANTIHISTAMINICS
cardiac action potential or produce arrhythmiaswhen given with erythromycin/ketoconazole.
Cetirizine in addition inhibits release of hista-mine and of cytotoxic mediators from plateletsas well as eosinophil chemotaxis during the secon-dary phase of the allergic response. Thus, it maybenefit allergic disorders by other actions as well.It attains high and longer lasting concentrationin skin, which may be responsible for superiorefficacy in urticaria/atopic dermatitis, as well asfor once daily dosing despite elimination t½ of7–10 hr. It is indicated in upper respiratoryallergies, pollinosis, urticaria and atopic dermatitis;also used as adjuvant in seasonal asthma.
Levocetirizine is the active R(–) enantiomerof cetirizine. It is effective at half the dose andappears to produce less sedation and other sideeffects.
Azelastine This newer H1 blocker has goodtopical activity; in addition it inhibits histaminerelease and inflammatory reaction triggered byLTs and PAF. After intranasal application it hasbeen shown to down regulate intracellularadhesion molecule-1 (ICAM-1) expression onnasal mucosa. Its t½ is 24 hr, but action lastslonger due to active metabolite. Its metabolismis inhibited by CYP 3A4 inhibitors. Given bynasal spray for seasonal and perennial allergicrhinitis it provides quick symptomatic relief lasting12 hr. Stinging in the nose and altered tasteperception are the local side effects. Somesomnolence has been reported on nasal applicationand a tendency to weight gain noted after oraluse.
Mizolastine This nonsedating antihistaminic iseffective in allergic rhinitis and urticaria by singledaily dosing despite a t½ of 8–10 hr and no activemetabolite.
Ebastine Another newer SGA that rapidly getsconverted to the active metabolite carbastinehaving a t½ of 10–16 hr. It is nonsedating andactive in nasal and skin allergies. Animal studieshave found it to prolong Q-Tc interval whichmakes it liable to arrhythmogenic potential and
CYP3A4 interaction, but actual reports are stillfew.
Rupatadine This recently introduced antihis-taminic has additional PAF antagonistic property,and is indicated in allergic rhinitis.
USES
The uses of H1 antihistaminics are based on theirability to block certain effects of histamine relea-sed endogeneously, as well as on sedative andanticholinergic properties.
1. Allergic disorders Antihistaminics do notsuppress AG: AB reaction, but block the effectsof released histamine—are only palliative. Theyeffectively control certain immediate type ofallergies, e.g. itching, urticaria, seasonal hay fever,allergic conjunctivitis and angioedema of lips,eyelids, etc. However, their action is slow—Adralone is life-saving in laryngeal angioedema,though intravenously administered antihistaminicmay have adjuvant value. Similarly, they cannotbe relied upon in anaphylactic shock and havea secondary place to Adr. Benefits are less markedin perennial vasomotor rhinitis, atopic dermatitisand chronic urticarias; combination with an H2
antagonist succeeds in some cases of chronicurticaria not responding to H1 antagonist alone.The antihistaminics are ineffective in bronchialasthma: reasons may be—
(i) Leukotrienes (C4, D4) and PAF are moreimportant mediators than histamine.
(ii) Concentration of antihistamines attained atthe site may not be sufficient to block highconcentration of histamine released locallyin the bronchi.
Certain newer compounds like cetirizine haveadjuvant role in seasonal asthma.
Antihistaminics are also ineffective in othertypes of humoral and cell mediated allergies becausehistamine is not involved. They do suppress urticariaand swellings in serum sickness, but have no effecton other components of the syndrome.
Type I hypersensitivity reactions to drugs(except asthma and anaphylaxis) are suppressed.Some skin rashes also respond.

168S
EC
TIO
N3
AUTACOIDS AND RELATED DRUGS
2. Other conditions involving histamineAntihistaminics block symptoms produced byhistamine liberators; afford symptomatic relief ininsect bite and ivy poisoning. Abnormal dermo-graphism is suppressed. They have prophylacticvalue in blood/saline infusion induced rigor.3. Pruritides Many conventional antihistamineshave antipruritic action independent of H1
antagonism. Though relief is often incomplete,older antihistaminics chlorpheniramine, diphen-hydramine, cyproheptadine remain the first choicedrugs for idiopathic pruritus.4. Common cold Antihistaminics do not affectthe course of the illness but may affordsymptomatic relief by anticholinergic (reducerhinorrhoea) and sedative actions. The newernonsedating antihistamines are less effective inthis respect.5. Motion sickness Promethazine, diphenhy-dramine, dimenhydrinate and meclozine haveprophylactic value in milder types of motionsickness; should be taken one hour before startingjourney. Promethazine can also be used in morn-ing sickness, drug induced and postoperativevomiting, radiation sickness.
An ‘off label’ (unapproved) use of cyprohep-tadine is often made in anorectic/convalescentpatients for improving appetite. Such use inunderweight children is inappropriate, because itsCNS depressant action can affect learning.6. Vertigo Cinnarizine is the H1 antihistaminehaving additional anticholinergic, anti-5-HT,sedative and vasodilator properties which has beenwidely used in vertigo. It modulates Ca2+ fluxesand attenuates vasoconstrictor action of manyendogenous mediators.
Cinnarizine inhibits vestibular sensory nucleiin the inner ear, suppresses postrotatory labyrin-thine reflexes, possibly by reducing stimulatedinflux of Ca2+ from endolymph into the vestibularsensory cells. Beneficial effects have been reportedin Méniére’s disease and other types of vertigo.Side effects are sedation and mild g.i. upset.
Dimenhydrinate is another effective antivertigoantihistaminic.
DRUGS FOR VERTIGO
The therapy of vertigo occurring in Méniére’s disease andother conditions is imperfect. A variety of approaches havebeen tried and have met with only partial success.
1. Labyrinthine suppressants They suppress end-organ receptors or inhibit central cholinergic pathway (investibular nuclei).
(a) Antihistaminics (with anticholinergic action)—cinnari-zine, dimenhydrinate, diphenhydramine, promethazine.
(b) Anticholinergics—atropine, hyoscine.(c) Antiemetic phenothiazines—prochlorperazine, thie-
thylperazine.2. Vasodilators They improve blood flow to labyrinthand brainstem—betahistine, codergocrine, nicotinic acid.3. Diuretics They decrease labyrinthine fluid pressure—acetazolamide, thiazides, furosemide.4. Anxiolytics, antidepressants These drugs appearto modify the sensation of vertigo—diazepam, amitriptyline.5. Corticosteroids They suppress intralabyrinthineedema due to viral infection or other causes.
Parenteral prochlorperazine is the most effective drug forcontrolling violent vertigo and vomiting.
7. Preanaesthetic medication Promethazinehas been used for its anticholinergic and sedativeproperties.
8. Cough Antihistaminics like chlorphenira-mine, diphenhydramine and promethazine areconstituents of many popular cough remedies.They have no selective cough suppressant action,but may afford symptomatic relief by sedativeand anticholinergic property (see Ch. 16).
9. Parkinsonism Promethazine and some othersafford mild symptomatic relief in early cases—based on anticholinergic and sedative property.
10. Acute muscle dystonia Caused by anti-dopaminergic-antipsychotic drugs is promptlyrelieved by parenteral promethazine, diphenhy-dramine or hydroxyzine. This is again based oncentral anticholinergic action of the drugs.11. As sedative, hypnotic, anxiolytic Antihista-mines with CNS depressant action have been usedas sedative and to induce sleep, especially inchildren. However, promethazine has producedserious respiratory depression in young children;few deaths are on record; it is not indicated inchildren aged 2 years or less. For promotingsleep, antihistaminics are not as dependable as

169C
HA
PTE
R11
HISTAMINE AND ANTIHISTAMINICS
PROBLEM DIRECTED STUDY
11.1 A taxi driver aged 30 years presented with sudden onset running and itchy nose, boutsof sneezing, partial nasal blockage, redness and watering from the eyes, but no fever, bodyacheor malaise. He gave history of similar episodes occurring off and on during the spring season.A diagnosis of seasonal allergic rhinitis was made and the doctor decided to prescribe antiallergicmedication.(a) Which antiallergic medicine would be suitable for this patient? Which antiallergic drugs shouldbe avoided?(see Appendix-1 for solution)
benzodiazepines. Hydroxyzine has been used inanxiety associated with autonomic manifestations.(Combinations of antihistaminics with antidiarrhoeals orbronchodilators, or those containing more than oneantihistaminic are banned in India.)
H2 antagonist The first H2 blocker Burimamidewas developed by Black in 1972. Metiamide wasthe next, but both were not found suitable for
clinical use. Cimetidine was introduced in 1977 andgained wide usage. Ranitidine, famotidine,roxatidine, and many others have been addedsubsequently. They are primarily used in pepticulcer, gastroesophageal reflux and other gastrichypersecretory states. They are described in Ch. 46.
H3 antagonist Though some selective H3 antagonists havebeen produced, they have not found any clinical utility.

5-Hydroxytryptamine, itsAntagonists and Drug Therapyof Migraine
ChapterChapterChapterChapterChapter 1212121212
5-HYDROXYTRYPTAMINE(5-HT, Serotonin)
Serotonin was the name given to the vasocons-trictor substance which appeared in the serumwhen blood clotted and Enteramine to the smoothmuscle contracting substance present in entero-chromaffin cells of gut mucosa. In the early 1950sboth were shown to be 5-hydroxytryptamine(5-HT). About 90% of body’s content of 5-HTis localized in the intestines; most of the restis in platelets and brain. It is also found in waspand scorpion sting, and is widely distributed ininvertebrates and plants (banana, pear, pineapple,tomato, stinging nettle, cowhage).
SYNTHESIS, STORAGE ANDDESTRUCTION
5-HT is β-aminoethyl-5-hydroxyindole. It is syn-thesized from the amino acid tryptophan anddegraded primarily by MAO and to a small extentby a dehydrogenase (Fig. 12.1).
There is close parallelism between CAs and5-HT. The decarboxylase is non-specific, acts onDOPA as well as 5-hydroxytryptophan (5-HTP)
to produce DA and 5-HT respectively. Like NA,5-HT is actively taken up by an amine pumpserotonin transporter (SERT), a Na+ dependentcarrier, which operates at the membrane ofplatelets (therefore, 5-HT does not circulate infree form in plasma) and serotonergic nerveendings. This pump is inhibited by selectiveserotonin reuptake inhibitors (SSRIs) and tricyclicantidepressants (TCAs). Platelets do not synthesize5-HT but acquire it by uptake during passagethrough intestinal blood vessels. Again like CAs,5-HT is stored within storage vesicles, and itsuptake at the vesicular membrane by vesicularmonoamine transporter (VMAT-2) is inhibited byreserpine, which causes depletion of CAs as wellas 5-HT. The degrading enzyme MAO is alsocommon for both. The isoenzyme MAO-Apreferentially metabolizes 5-HT.
SEROTONERGIC (5-HT) RECEPTORS
Gaddum and Picarelli (1957) classified 5-HTreceptors into musculotropic (D type) and neuro-tropic (M type) on the basis of thier blockadeby Dibenzyline (phenoxybenzamine) andMorphine. The classical 5-HT antagonists methyser-gide and cyproheptadine blocked D type receptors.Subsequently 5-HT receptors were differentiatedby their high or low affinity for [3H] 5-HT inradioligand binding studies. The present systemof classifying 5-HT receptors is based on molecularcharacterization and cloning of the receptor cDNAs.Some subtypes of 5-HT receptors have specifictissue distribution, but certain tissues express morethan one subtype.
Four families of 5-HT receptors (5-HT1, 5-HT2, 5-HT3, 5-HT4-7) comprising of 14 receptorsubtypes have so far been recognized. However,only some of these have been functionallycorrelated. Selective agonists/antagonists have
Fig. 12.1: Synthesis and degradation of5-hydroxytryptamine (5-HT)

171C
HA
PTE
R12
5-HT, ITS ANTAGONISTS AND DRUG THERAPY OF MIGRAINE
been defined only for these subtypes. Knowledgeof subtypes of 5-HT receptors has assumedimportance because some newly developedtherapeutically useful drugs can only be describedin terms of 5-HT receptor subtype selectiveagonists or antagonists.
All 5-HT receptors (except 5-HT3) are G pro-tein coupled receptors which function throughdecreasing (5-HT1) or increasing (5-HT4, 5-HT6,5-HT7) cAMP production or by generating IP3/DAG (5-HT2) as second messengers. The 5-HT3
is a ligand gated cation (Na+,K+) channel whichon activation elicits fast depolarization.
5-HT1 Receptors Five subtypes (5-HT1A, B, D, E, F) havebeen identified. The 5-HT1C receptor is now designated 5HT2c.All subtypes of 5-HT1 receptor couple with Gi/Go proteinand inhibit adenylyl cyclase; 5-HT1A in addition activatesK+ channels (resulting in hyperpolarization) and inhibits Ca2+
channels. These receptors function primarily as autoreceptorsin brain—inhibit firing of 5-HT neurones or release of5-HT from nerve endings.
The most important location of 5-HT1A receptor is somato-dendritic synapses in raphe nuclei of brain stem; their activationserves to reduce firing of raphe neurones. Hippocampus isanother important site. The antianxiety drug buspirone actsas a partial agonist of 5-HT1A receptor. The 5-HT1D receptorhas been shown to regulate dopaminergic tone in substantianigra–basal ganglia, and 5-HT1D/1B (the same receptor is5-HT1D in humans and 5-HT1B in rat) to cause constrictionof cranial blood vessels. The antimigraine drug sumatriptanis a selective 5-HT1D/1B agonist. Other functions subservedby 5-HT1D receptors are inhibition of 5-HT release fromforebrain serotonergic neurones, NA release from sympatheticnerve endings and that of inflammatory neuropeptides fromnerve endings in cranial blood vessels.
5-HT2 Receptors There are 3 subtypes of 5-HT2 receptor;all are coupled to Gq protein→activate phospholipase C andfunction through generation of IP3/DAG. 5-HT2A receptor alsoinhibits K+ channels resulting is slow depolarization ofneurones. α-methyl 5-HT is a selective agonist for all 3subtypes.
5-HT2A is the most widely expressed postjunctional5-HT receptor (designated earlier as D type) located onvascular and visceral smooth muscle, platelets and cerebralneurones especially prefrontal cortex. It mediates most ofthe direct actions of 5-HT like vasoconstriction, intestinal,uterine and bronchial contraction, platelet aggregation andactivation of cerebral neurones. Ketanserin is a 5-HT2
antagonist more selective for 5-HT2A.Contraction of rat gastric fundus is mediated by
5-HT2B receptor.5-HT2C receptor is located on vascular endothelium—
elicits vasodilatation through EDRF release. Choroid plexus
expresses large number of 5-HT2C receptors which mayregulate CSF formation..
5-HT3 Receptor This is the neuronal 5-HT receptor whichrapidly depolarizes nerve endings by opening the cationchannel located within it and corresponds to the originalM type receptor. It mediates the indirect and reflex effectsof 5-HT at:(i) Somatic and autonomic nerve endings → pain, itch,coronary chemoreflex (bradycardia, fall in BP due towithdrawal of sympathetic tone, respiratory stimulation orapnoea elicited by stimulation of receptors in the coronarybed), other visceral reflexes.(ii) Nerve endings in myenteric plexus → augmentation ofperistalsis, emetic reflex.(iii) Area postrema and nucleus tractus solitarious in brain-stem → nausea, vomiting.
Ondansetron is a selective 5-HT3 antagonist whichinhibits vomiting by blocking these receptors in the brainstemas well as in gut wall. 2-Methyl 5-HT is a selective 5-HT3
agonist.
5-HT4–7 Receptors The 5-HT4 receptor couples to Gsprotein, activates adenylyl cyclase and has been demons-trated in the mucosa, plexuses and smooth muscle of thegut → probably involved in augmenting intestinal secretionand peristalsis. It is also located in brain, especially hippocam-pus and the colliculi where it causes slow depolarizationby decreasing K+ conductance.
Cisapride and renzapride are selective 5-HT4 agonists.The recently cloned 5-HT5, 5-HT6 and 5-HT7 receptors
are closely related to the 5-HT4 receptor. These are mainlylocated in specific brain areas, but their functional role isnot known. An interesting finding is that clozapine (atypicalantipsychotic) has high affinity for 5-HT6 and 5-HT7 receptorsin addition to being a 5-HT2A/2C antagonist.
ACTIONS
5-HT is a potent depolarizer of nerve endings.It thus exerts direct as well as reflex and indirecteffects. Tachyphylaxis is common with repeateddoses of 5-HT. The overall effects therefore areoften variable.
1. CVS Arteries are constricted (by directaction on vascular smooth muscle) as well asdilated (through EDRF release) by 5-HT,depending on the vascular bed and the basal tone.In addition, 5-HT releases Adr from adrenalmedulla, affects ganglionic transmission andevokes cardiovascular reflexes. The net effect iscomplex. Larger arteries and veins are charac-teristically constricted. In the microcirculation5-HT dilates arterioles and constricts venules:

172S
EC
TIO
N3
AUTACOIDS AND RELATED DRUGS
Salient features of important 5-HT receptor subtypes
5-HT1 : Autoreceptors; inhibit serotonergic neural activity in brain.5-HT1A—present in raphe nuclei and hippocampus; buspirone (antianxiety) may act through thesereceptors.5-HT1D/1B—Constricts cranial blood vessels and inhibits release of inflammatory neuropeptides inthem; sumatriptan (antimigraine) acts through these receptors.
5-HT2A : Previously D type receptor; most important postjunctional receptor mediating direct actions of5-HT like vascular and visceral smooth muscle contraction, platelet aggregation, neuronal activationin brain; ketanserin blocks these receptors.
5-HT3 : Previously M type receptor; depolarizes neurones by gating cation channels; elicits reflex effectsof 5-HT—emesis, gut peristalsis, bradycardia, transient hypotension, apnoea, pain, itch; ondansetron(antiemetic) acts by blocking these receptors.
5-HT4 : Mediate intestinal secretion, augmentation of peristalsis. Renzapride (prokinetic) is a selective5-HT4 agonist.
capillary pressure rises and fluid escapes. Thedirect action to increase capillary permeabilityis feeble.
Isolated heart is stimulated by 5-HT: bothdirectly and by release of NA from nerve endings.In intact animals, bradycardia is mostly seen dueto activation of coronary chemoreflex (BezoldJarisch reflex) through action on vagal afferentnerve endings in the coronary bed, evokingbradycardia, hypotension and apnoea.BP: a triphasic response is classically seen oni.v. injection of 5-HT in animals.• Early sharp fall in BP—due to coronary
chemoreflex.• Brief rise in BP—due to vasoconstriction and
increased cardiac output.• Prolonged fall in BP—due to arteriolar
dilatation and extravasation of fluid.However, 5-HT is not involved in the physio-logical regulation of BP.
2. Visceral smooth muscles 5-HT is apotent stimulator of g.i.t., both by direct actionas well as through enteric plexuses. Several subtypesof 5-HT recep-tors are present in the gut (Seebox). Peristalsis is increased and diarrhoea canoccur (also due to increased secretion).
It constricts bronchi, but is less potent thanhistamine. Action on other smooth muscles in manare feeble and inconsistent.
3. Glands 5-HT inhibits gastric secretion(both acid and pepsin), but increases mucus
5-HT receptor function in the gut
5-HT2A : intestinal smooth muscle—contraction.
5-HT3 : fast depolarization of enteric plexusneurones; release of 5-HT from entero-chromaffin cells.
5-HT4 : lower esophageal sphincter—contraction;enteric plexus—ACh release—enhancedperistalsis; intestinal mucosa—secretion.
5-HT1 : slow depolarization of enteric plexusneurones.
production. It thus has ulcer protective property.Effect on other glandular secretions is notsignificant.
4. Nerve endings and adrenal medullaAfferent nerve endings are activated causingtingling and pricking sensation, as well as pain.Depolarization of visceral afferents elicitsrespiratory and cardiovascular reflexes, nauseaand vomiting. 5-HT is less potent than histaminein releasing CAs from adrenal medulla.
5. Respiration A brief stimulation of respi-ration (mostly reflex from bronchial afferents) andhyperventilation are the usual response, but largedoses can cause transient apnoea through coronarychemoreflex.
6. Platelets By acting on 5-HT2A receptors5-HT causes changes in shape of platelets, butis a weak aggregator. However, it does not inducethe release reaction.

173C
HA
PTE
R12
5-HT, ITS ANTAGONISTS AND DRUG THERAPY OF MIGRAINE
7. CNS Injected i.v., 5-HT does not producecentral effects because of poor entry across blood-brain barrier. However, it serves as a transmitter,primarily inhibitory. Direct injection in the brainproduces sleepiness, changes in body tempera-ture, hunger and a variety of behavioural effects.
PATHOPHYSIOLOGICAL ROLES
1. Neurotransmitter 5-HT is a confirmed neu-rotransmitter in the brain; brain 5-HT has a fastturnover rate. Cells containing 5-HT are presentin the raphe nuclei of brainstem, substantia nigraand few other sites—send axons rostrally (tolimbic system, cortex and neostriatum) as wellas caudally to spinal cord. 5-HT appears to beinvolved in sleep, temperature regulation, thought,cognitive function, behaviour and mood, appetite,vomiting and pain perception. Some serotonergicneurones are present in intestines also.
Experimental evidence from pharmacologicalmanipulation of 5-HT metabolism, genetic models(like knock out mice), as well as therapeutic effectof selective serotonin reuptake inhibitors (SSRIs)and TCAs etc. strongly suggest a role of 5-HTin the pathogenesis of anxiety, depression,aggression and other behavioral disorders inhumans.
2. Precursor of melatonin 5-HT is theprecursor of melatonin in pineal gland. It isbelieved to regulate the biological clock and main-tain circadian rhythm.
3. Neuroendocrine function The hypothalamicneurones that control release of anterior pituitaryhormones are probably regulated by serotonergicmechanism.
4. Nausea and vomiting Especially thatevoked by cytotoxic drugs or radiotherapy ismediated by release of 5-HT and its action on5-HT3 receptors in the gut, area postrema andnucleus tractus solitarious.
5. Migraine 5-HT is said to initiate the vaso-constrictor phase of migraine and to participatein neurogenic inflammation of the affected blood
vessels. Methysergide (5-HT antagonist) is aneffective prophylactic and sumatriptan (5-HT1B/1D
agonist) can control an attack. However, therole of 5-HT in this condition is not preciselyknown.6. Haemostasis Platelets release 5-HT duringaggregation at the site of injury to blood vessel.Acting in concert with collagen and other media-tors, this 5-HT accelerates platelet aggregationand clot formation. Thus, it serves to amplifythe response. Its contractile action appears topromote retraction of the injured vessel. Both theabove actions contribute to haemostasis.7. Raynaud’s phenomenon Release of 5-HTfrom platelets may trigger acute vasospastic episo-des of larger arteries involved in Raynaud’sphenomena. Ketanserin has prophylactic value.8. Variant angina Along with thromboxane A2,5-HT released from platelets has been implicatedin causing coronary spasm and variant angina.However, the inefficacy of anti 5-HT drugs inthis condition points to the involvement of othermediators.9. Hypertension Increased responsiveness to5-HT as well as its reduced uptake and clearanceby platelets has been demonstrated in hypertensivepatients. Ketanserin has antihypertensive property.5-HT has been held responsible for preeclampticrise in BP.10. Intestinal motility Enterochromaffin cellsand 5-HT containing neurones may regulateperistalsis and local reflexes in the gut. This systemappears to be activated by intestinal distensionand vagal efferent activity.11. Carcinoid syndrome The carcinoidtumours produce massive quantities of 5-HT.Bowel hypermotility and bronchoconstriction incarcinoid is due to 5-HT but flushing andhypotension are probably due to other mediators.Pellagra may occur due to diversion of tryptophanfor synthesizing 5-HT.Use Due to widespread and variable actions,5-HT has no therapeutic use.

174S
EC
TIO
N3
AUTACOIDS AND RELATED DRUGS
DRUGS AFFECTING 5-HT SYSTEM
1. 5-HT precursor Tryptophan increases brain 5-HT andproduces behavioural effects because tryptophan hydroxylasein brain is not saturated by the amount of tryptophan availablephysiologically.
2. Synthesis inhibitor p-Chlorophenylalanine (PCPA)selectively inhibits tryptophan hydroxylase (rate limiting step)and reduces 5-HT level in tissues. It is not used clinicallydue to high toxicity.
3. Uptake inhibitor Tricyclic antidepressants inhibit5-HT uptake along with that of NA. The selective serotoninreuptake inhibitors (SSRI) like fluoxetine, sertraline, etc.inhibit only 5-HT reuptake and have antidepressant-antianxiety property.
4. Storage inhibitor Reserpine blocks 5-HT (as well asNA) uptake into storage vesicles by inhibiting VMAT-2, andcauses depletion of all monoamines. Fenfluramine selectivelyreleases 5-HT by promoting its reverse transport at serotonergicnerve endings in the brain, followed by its prolonged depletion,and has anorectic property.
5. Degradation inhibitor Nonselective MAO inhibitor(tranylcypromine) and selective MAO-A inhibitor (chlorgy-line) increase 5-HT content by preventing its degradation.
6. Neuronal degeneration 5, 6 dihydroxytryptamineselectively destroys 5-HT neurones.
7. 5-HT receptor agonists A diverse range of compoundsproducing a variety of actions have been found to activateone or more subtypes of 5-HT receptors. Notable amongthese are:(i) D-Lysergic acid diethyl amide (LSD)—Synthesizedas an ergot derivative LSD was found to be an extremelypotent hallucinogen. It is a nonselective 5-HT agonist—activates many subtypes of 5-HT receptors including 5-HT1A
on raphe cell bodies, 5-HT2A/2C (probably responsible for thehallucinogenic effect) and 5-HT5-7 in specific brain areas.However, it antagonizes 5-HT2A receptors in the ileum.A number of other hallucinogens also interact with brain5-HT receptors.(ii) Azapirones like buspirone, gepirone and ipsapirone area novel class of antianxiety drugs which do not producesedation. They act as partial agonists of 5-HT1A receptorsin the brain.(iii) Sumatriptan and other triptans are selective 5-HT1D/1B
agonists, constrict cerebral blood vessels and have emergedas the most effective treatment of acute migraine attacks.(iv) Cisapride This prokinetic drug which increases gastro-intestinal motility is a selective 5-HT4 agonist. Renzaprideis still more selective for 5-HT4 receptors.
8. 5-HT receptor antagonists A variety of drugs blockserotonergic receptors; many are nonselective, but some newerones are highly subtype selective.
5-HT ANTAGONISTS
The ability to antagonize at least some actionsof 5-HT is found in many classes of drugs, e.g.ergot derivatives (ergotamine, LSD, 2-bromo LSD,methysergide), adrenergic α blockers (phenoxy-benzamine), antihistaminics (cyproheptadine,cinnarizine), chlorpromazine, morphine, etc., butthese are nonselective and interact with severalother receptors as well. Many are partial agonistsor antagonize certain actions of 5-HT but mimicothers. The salient features of drugs which havebeen used clinically as 5-HT antagonists and somenewly developed selective antagonists aredescribed below:
1. Cyproheptadine It primarily blocks5-HT2A receptors and has additional H1 antihista-minic, anticholinergic and sedative properties (seeCh. 11). Like other antihistaminics, it has beenused in allergies and is a good antipruritic, butthe anti 5-HT action has no role in these condi-tions. It increases appetite and has been used inchildren and poor eaters to promote weight gain.The H1 antihistaminic action and an action ongrowth hormone secretion has been suggested toaccount for this.
The anti 5-HT activity of cyproheptadine hasbeen utilized in controlling intestinal manifes-tations of carcinoid and postgastrectomy dump-ing syndromes as well as in antagonizing priapism/orgasmic delay caused by 5-HT uptake inhibitorslike fluoxetine and trazodone.
Side effects drowsiness, dry mouth, confusion,ataxia, weight gain.
2. Methysergide It is chemically related to ergotalkaloids; antagonizes action of 5-HT on smooth musclesincluding that of blood vessels, without producing other ergotlike effects: does not interact with α adrenergic or dopaminereceptors. Methysergide is a potent 5-HT2A/2C antagonist withsome tissue specific agonistic actions as well; but is nonselec-tive—acts on 5-HT1 receptors also. It has been used formigraine prophylaxis, carcinoid and postgastrectomy dumpingsyndrome. Prolonged use has caused abdominal, pulmonaryand endocardial fibrosis, because of which it has gone intodisrepute.3. Ketanserin It has selective 5-HT2 receptor blockingproperty with negligible action on 5-HT1, 5-HT3 and 5 HT4

175C
HA
PTE
R12
5-HT, ITS ANTAGONISTS AND DRUG THERAPY OF MIGRAINE
receptors and no partial agonistic activity. Among 5-HT2
receptors, blockade of 5-HT2A is stronger than 5-HT2C
blockade. 5-HT induced vasoconstriction, platelet aggregationand contraction of airway smooth muscle are antagonized.It has additional weak α1, H1 and dopaminergic blockingactivities.
Ketanserin is an effective antihypertensive, but α1
adrenergic blockade appears to be causative rather than 5-HT2A blockade.
Trials of Ketanserin in vasospastic conditions have shownsymptomatic improvement only in Raynaud’s disease.Ritanserin is a relatively more 5-HT2A selective congenerof ketanserin.
4. Clozapine In addition to being a dopami-nergic antagonist (weaker than the typicalneuroleptics), this atypical antipsychotic is a5-HT2A/2C blocker (see Ch. 32). Clozapine mayalso exert inverse agonist activity at cerebral5-HT2A/2C receptors which may account for itsefficacy in resistant cases of schizophrenia.
5. Risperidone This atypical antipsychotic isa combined 5-HT2A + dopamine D2 antagonist,similar to clozapine. Like the latter, it especiallyameliorates negative symptoms of schizophrenia,but produces extrapyramidal side effects at onlyslightly higher doses.
Other atypical antipsychotics like olanzapineand quetiapine are also combined 5-HT and DAantagonists, but interact with other neuro-transmitter receptors as well.
6. Ondansetron It is the prototype of the newclass of selective 5-HT3 antagonists that haveshown remarkable efficacy in controlling nauseaand vomiting following administration of highlyemetic anticancer drugs and radiotherapy. It isdescribed in Ch. 47.Granisetron and Tropisetron are the other selective 5-HT3
antagonists.
ERGOT ALKALOIDSErgot is a fungus Claviceps purpurea which growson rye, millet and some other grains. The grainis replaced by a purple, hard, curved body called‘sclerotium’. Epidemics of ergot poisoning(ergotism), due to consumption of contaminatedgrains, have been recorded from the beginningof history. It still occurs in epidemic and sporadic
forms. Dry gangrene of hands and feet whichbecome black (as if burnt) is the most prominentfeature. Miscarriages occur in women and cattle.A convulsive type is also described.
Ergot had been used by midwives to quickenlabour since the middle ages. This use receivedmedical sanction in the 19th century, but itsdangers were recognized by the beginning of the20th century and then it was advocated only afterdelivery. Dale and Barger (1906 onwards) isolatedthe ergot alkaloids and studied their pharmacology.Ergometrine was isolated in 1935.
Ergot contains a host of pharmacologicallyactive substances—alkaloids, LSD, histamine,ACh, tyramine and other amines, sterols, etc.
Natural ergot alkaloids These are tetracyclicindole containing compounds which may be con-sidered as derivatives of lysergic acid. They aredivided into—
(a) Amine alkaloid Ergometrine (Ergonovine):which is oxytocic
(b) Amino acid alkaloids Ergotamine,Ergotoxine (mixture of ergocristine +ergocornine + ergocryptine): they arevasoconstrictor and α adrenergic blocker/partial agonist.
Other semisynthetic derivatives
(a)Dihydroergotamine (DHE), Dihydroergotoxine(Codergocrine): are antiadrenergic, cerebro-active.
(b)2-Bromo-α-ergocryptine (Bromocriptine): is adopaminergic D2 agonist (see Ch. 17).
(c)Methysergide: it is mainly anti 5-HT.The ergot alkaloid related compounds have
diverse pharmacological properties. They act asagonists, partial agonists and antagonists on certainsubtypes of a adrenergic, serotonergic and dopa-minergic receptors in a tissue specific manner.
ActionsErgotamine It acts as a partial agonist andantagonist at α adrenergic and all subtypes of5-HT1 and 5-HT2 receptors, but does not interactwith 5-HT3 or dopamine receptors: produces

176S
EC
TIO
N3
AUTACOIDS AND RELATED DRUGS
sustained vasoconstriction, visceral smooth musclecontraction, vasomotor centre depression andantagonizes the action of NA and 5-HT on smoothmuscles. The overall effect of oral/rectal dosesof ergotamine on BP is insignificant. It is a potentemetic (through CTZ and vomiting centre) andmoderately potent oxytocic. At high doses CNSstimulation and paresthesias may be experienced.On chronic exposure (ergot poisoning) vaso-constriction is accompanied by damage tocapillary endothelium—thrombosis, vascular stasisand gangrene.
Dihydroergotamine (DHE) Hydrogenation ofergotamine reduces serotonergic and α-adrener-gic agonistic actions, but enhances α-receptorblocking property. Consequently DHE is a lesspotent vasoconstrictor; primarily constricts capa-citance vessels and causes less intimal damage.It is a weaker emetic and oxytocic, but has someantidopaminergic action as well.
Dihydroergotoxine (Codergocrine) Thishydrogenated mixture of ergotoxine group ofalkaloids is a more potent α blocker and a veryweak vasoconstrictor. In the brain, a variety ofpartial agonistic/antagonistic actions on 5-HTreceptors, metabolic and vascular effects andenhancement of ACh release in cerebral cortexhave been demonstrated. It has been advocatedfor treatment of dementia (see Ch. 35).
Bromocriptine The 2 bromo derivative of ergo-cryptine is a relatively selective dopamine D2agonist on pituitary lactotropes (inhibits prolactinrelease), in striatum (antiparkinsonian) and in CTZ(emetic—but less than ergotamine). In certainbrain areas weak antidopaminergic action has alsobeen shown. It has very weak anti 5-HT or αblocking actions and is not an oxytocic.
Ergometrine (Ergonovine) This amine ergotalkaloid has very weak agonistic and practicallyno antagonistic action on α adrenergic receptors:vasoconstriction is not significant. Partial agonisticaction on 5-HT receptors has been demonstratedin uterus, placental and umbilical blood vesselsand in certain brain areas. It is a moderately potent
5-HT2 antagonist in g.i. smooth muscle and aweak dopaminergic agonist on the pituitarylactotropes as well as CTZ; emetic potential islow. The most prominent action is contractionof myometrium; used exclusively in obstetrics (seeCh. 23).
Pharmacokinetics Oral bioavailability ofamino acid ergot alkaloids and their hydrogenatedderivatives is poor (< 1%) due to slow andincomplete absorption as well as high firstpassmetabolism. Bioavailability is better after sub-lingual and rectal administration, but still oftenerratic. They are metabolized in liver and excretedprimarily in bile. Ergotamine is sequestrated intissues—produces longer lasting actions comparedto its plasma t½ of 2 hours. Ergot alkaloidseffectively cross blood-brain barrier.
Adverse effects Nausea, vomiting, abdominalpain, muscle cramps, weakness, paresthesias,coronary and other vascular spasm, chest pain(due to coronary vasoconstriction) are the frequentside effects. These drugs are contraindicated inpresence of sepsis, ischaemic heart disease, peri-pheral vascular disease, hypertension, pregnancy,liver and kidney disease.Preparations and doseErgotamine: For migraine 1–3 mg oral/sublingual, repeatas required (max 6 mg in a day); rarely 0.25–0.5 mg i.m.or s.c.; ERGOTAMINE 1 mg tab, 0.5 mg/ml inj.Dihydroergotamine: For migraine 2–6 mg oral (max 10 mg/day), 0.5–1 mg i.m., s.c. repeat hourly (max 3 mg);DIHYDERGOT, DHE 1 mg tab, MIGRANIL 1 mg/ml inj.Also used for postural hypotension, herpes zoster, mumps.Dihydroergotoxine (codergocrine) For dementia 1–1.5 mgoral or sublingual, 0.15–0.6 mg i.m., HYDERGINE 1.5 mgtab, CERELOID 1 mg tab.
DRUG THERAPY OF MIGRAINE
Migraine is a mysterious disorder characterized by pulsatingheadache, usually restricted to one side, which comes inattacks lasting 4–48 hours and is often associated with nausea,vomiting, sensitivity to light and sound, flashes of light,vertigo, loose motions and other symptoms. Two major typesare—migraine with aura (classical migraine) in whichheadache is preceded by visual or other neurological symptoms,and migraine without aura (common migraine). Pulsatiledilatation of certain large cranial vessels is the immediatecause of pain. The pathogenic mechanisms are not well

177C
HA
PTE
R12
5-HT, ITS ANTAGONISTS AND DRUG THERAPY OF MIGRAINE
understood. The Vascular theory holds that initialvasoconstriction or shunting of blood through carotid arterio-venous anastomoses produces cerebral ischaemia and startsthe attack. The Neurogenic theory considers it to be a spreadingdepression of cortical electrical activity followed by vascularphenomena. Some triggering event appears to produceneurogenic inflammation of the affected blood vessel wallwhich is amplified by retrograde transmission in the afferentnerves and release of mediators like 5-HT, neurokinin,substance P, calcitonin gene related peptide (CGRP), nitricoxide, etc.
Changes in blood/urinary levels of 5-HT and itsmetabolites during migraine attack, its precipitation by5-HT releasers and efficacy of drugs having actions in theserotonergic system to prevent/abort/terminate migraineattacks suggests a pivotal role of 5-HT in this disorder.
Drug therapy of migraine has to be individua-lized: severity and frequency of attacks andresponse of individual patients to drugs usedearlier determine the choice. The strategy mostlyadopted is summarized in the box.
Mild migraine Cases having fewer than oneattack per month of throbbing but tolerableheadache lasting upto 8 hours which does notincapacitate the individual may be classified asmild migraine.(i) Simple analgesics like paracetamol (0.5–1 g) or aspirin (300–600 mg) taken at the firstindication of an attack and repeated 4–6 hourlyabort and suppress most mild attacks.(ii) Nonsteroidal antiinflammatory drugs(NSAIDs) and their combinations Drugs likeibuprofen (400–800 mg 8 hourly), naproxen (500mg followed by 250 mg 8 hourly), diclofenac(50 mg 8 hourly), mephenamic acid (500 mg 8
hourly), indomethacin (50 mg 6–8 hourly) eitheralone or combined with paracetamol/codeine/diazepam or another sedative/diphenhydramine oranother antihistaminic/caffeine are found moresatisfactory by some patients. These drugs aremore effective in migraine without aura, butcertain patients of migraine with aura also preferthem over specific antimigraine drugs (triptans/ergot alkaloids). Drugs are taken only till the attackpasses off. Taken in the prodromal stage theycan also abort an attack, but long-term treatmenton a regular schedule to ward off migraine attacksis not advised.(iii) Antiemetics Gastric stasis occurs duringmigraine which delays absorption of oral drugs.Metoclopramide (10 mg oral/i.m.) is frequentlyused: relieves nausea, vomiting and gastric stasis.When the patient has already vomited, it is betterto give the antiemetic by injection. Domperidone(10–20 mg oral) and prochlorperazine (10–25 mgoral/i.m.) are also effective. Diphenhydramine orpromethazine exert sedative as well as antiemeticaction.
Moderate migraine Migraine may be labelledas moderate when the throbbing headache is moreintense, lasts for 6–24 hours, nausea/vomiting andother features are more prominent and the patientis functionally impaired. One or more attacksoccur per month.
Simple analgesics are usually not effective,but stronger NSAIDs or their combinations men-tioned above are beneficial in many cases. Theremaining are treated with a specific antimigrainedrug, i.e. a triptan or an ergot preparation.Antiemetics are almost regularly needed.Prophylactic therapy is advised only when attacksare more frequent than 2–3 per month.
Severe migraine These patients suffer 2–3or more attacks per month of severe throbbingheadache lasting 12–48 hours, often accompaniedby vertigo, vomiting and other symptoms; thesubject is grossly incapacitated during the attack.
Analgesics/NSAIDs and their combinationsusually donot afford adequate relief—specificdrugs have to be prescribed along with antiemetics.
Drug therapy of migraine
Severity Drug therapy
Mild : Simple analgesics/NSAIDs or theircombinations (± antiemetic)
Moderate : NSAIDs combinations/a triptan/ergotalkaloids (+ antiemetic)
Severe : a Triptan/ergot alkaloids (+ antiemetic)+ Prophylaxis• Propranolol/other β blockers• Amitriptyline/other tricyclic antidepres-
sants• Flunarizine/other Ca2+ channel blockers• Valproate/topiramate

178S
EC
TIO
N3
AUTACOIDS AND RELATED DRUGS
Prophylactic regimens lasting 6 months or moreare recommended.
SPECIFIC ANTIMIGRAINE DRUGS
Ergotamine It is the most effective ergotalkaloid for migraine. Given early in attack, reliefis often dramatic and lower doses suffice, butwhen pain has become severe—larger doses areneeded and control may be achieved only afterfew hours. Oral/sublingual route is preferred, 1mg is given at half hour intervals till relief isobtained or a total of 6 mg is given. Parenteraladministration, though rapid in action is morehazardous.
Ergotamine acts by constricting the dilatedcranial vessels and/or by specific constriction ofcarotid A-V shunt channels. Ergotamine and DHEhave also been shown to reduce neurogenic inflam-mation and leakage of plasma in duramater thatoccurs due to retrograde stimulation of perivas-cular afferent nerves. These actions appear to bemediated through partial agonism at 5-HT1D/1B
receptors in and around cranial vessels.Dihydroergotamine (DHE) It is nearly aseffective as ergotamine and preferred forparenteral administration because injected DHEis less hazardous.
Current status Because of erratic oralabsorption, frequent side effects, especially nauseaand vomiting, and availability of triptans, ergotpreparations are rarely used now, except forconsiderations of cost or when triptans fail. Ergotalkaloids have no prophylactic value: regular useis not justified—may itself produce a dullbackground headache and an attack may beprecipitated on discontinuation. Caffeine 100 mgtaken with ergotamine enhances its absorptionfrom oral and rectal routes and adds to the cranialvasoconstricting action. Many combination pre-parations are available.MIGRIL: Ergotamine 2 mg, caffeine 100 mg, cyclizine50 mg tab.VASOGRAIN: Ergotamine 1 mg, caffeine 100 mg,paracetamol 250 mg, prochlorperazine 2.5 mg tab.
Selective 5-HT1D/1B agonists (Triptans)
This novel class of antimigraine drugs selectivelyactivate 5-HT1D/1B receptors, and are called‘triptans’. Currently, they are the first line drugs forpatients who fail to respond to analgesics. Ergotalkaloids are now required only in few cases.Because these drugs have been designed to act onthe same subtype of 5-HT receptor, pharmaco-dynamic differences among them are minor, butthere are significant pharmacokinetic differences.All others have higher oral bioavailability than theprototype drug sumatriptan. Fewer headacherecurrences in an attack are reported with nara-triptan and frovatriptan due to their longer t½, butthey may be slower in affording initial pain relief.
Sumatriptan It is the first selective 5-HT1D/1B
receptor agonist; activates other subtypes of5-HT1 receptors only at very high concentrations,and does not interact with 5-HT2, 5-HT3, 5-HT4-7,α or β adrenergic, dopaminergic, cholinergic orGABA receptors. Administered at the onset ofan attack of migraine, sumatriptan is as effectiveand better tolerated than ergotamine. About3/4 patients obtain complete/significant reliefwithin 2–3 hours. However, recurrence ofheadache within 24 hr has been noted in20–40% patients, probably due to short t½ ofsumatriptan. A distinct advantage is that it tendsto suppress nausea and vomiting of migraine, whileergotamine accentuates these symptoms.
The antimigraine activity of sumatriptan hasbeen ascribed to 5-HT1D/1B receptor mediatedconstriction of dilated cranial blood vessels,especially the arterio-venous shunts in the carotidartery, which express 5-HT1D/1B receptors.Dilatation of these shunt vessels during migraineattack is believed to divert blood flow away frombrain parenchyma. Consistent with the fact that5-HT1D/1B receptors are presynaptic autoreceptors,sumatriptan can reduce 5-HT release at theseblood vessels. Alternatively or in addition, it mayinhibit inflammatory neuropeptide release aroundthe affected vessels as well as extravasation ofplasma proteins across dural vessels. Likeergotamine, the triptans have been found to

179C
HA
PTE
R12
5-HT, ITS ANTAGONISTS AND DRUG THERAPY OF MIGRAINE
suppress neurogenic inflammation of cranialvessels. The use of sumatriptan (or other triptans)should be restricted to treatment of acute attacksof moderate to severe migraine not respondingto analgesics or their combinations.
Pharmacokinetics: Sumatriptan is absorbedrapidly and completely after s.c. injection. Oralbioavailability averages only 15%. Absorption isfaster after intranasal spray, but bioavailabilityremains almost the same. It is rapidly metabolizedby MAO-A isoenzyme and metabolites areexcreted in urine; elimination t½ is ~2 hours.
Side effects: to sumatriptan are usually mild.Tightness in head and chest, feeling of heat andother paresthesias in limbs, dizziness, weaknessare short lasting, but dose related side effects.These are more common after s.c. injection, whichis painful. Slight rise in BP occurs, but has littleclinical relevance, because sumatriptan is not adrug for regular use. Bradycardia, coronaryvasospasm and risk of myocardial infarctionare the serious, but infrequent adverse effects.Few sudden deaths have been ascribed tosumatriptan. Seizures and hypersensitivityreactions are rare.
Contraindications: Ischaemic heart disease,hypertension, epilepsy, hepatic or renal impairmentand pregnancy are the contraindications. Patientsshould be cautioned not to drive.
Sumatriptan and ergotamine should not beadministered within 24 hours of each other.Interaction with 5-HT reuptake inhibitors, MAOinhibitors and lithium has been reported.Dose: 50–100 mg oral at the onset of migraine attack, maybe repeated once within 24 hours if required. Those not
responding to the first dose should not be given the seconddose. It is the only triptan available for parenteral use; 6mg s.c. may be given to patients who cannot take the drugorally or in whom the pain develops very rapidly. Afterinjection, it acts in 10–20 min and is more consistentlyeffective. Alternatively, for rapid action and in patients whovomit out the oral tablet, 25 mg nasal spray can be used.It may be repeated once after 2 hours. A bitter taste maybe felt after the nasal spray.MIGRATAN, 50, 100 mg tabs, SUMINAT 25, 50, 100 mgtab, 25 mg nasal spray, 6 mg/0.5 ml inj. SUMITREX 25,50, 100 mg tab, 6 mg/0.5 ml inj.
Rizatriptan: This congener of sumatriptan ismore potent, has higher oral bioavailability withslightly faster onset of action.Dose: 5-10 mg; repeat once after 2 hr (if required).RIZACT, RIZATAN 5, 10 mg tab.Naratriptan, Zolmitriptan, Almotriptan, Frovatriptan andEletriptan are other triptans used in some countries.Features of some triptans are compared in thebox.
PROPHYLAXIS OF MIGRAINE
Regular medication to reduce the frequencyand/or severity of attacks is recommended formoderate-to-severe migraine when 2–3 or moreattacks occur per month. Diverse classes of drugsare used but none is effective in all cases, andnone abolishes the attacks totally. It may be prudentto discontinue pophylaxis every 6 months to checkwhether its continuation is needed or not. It isimportant to avoid the precipitating factor(s).
(i) β-Adrenergic blockers Propranolol is themost commonly used drug: reduces frequency aswell as severity of attacks in upto 70% patients.Effect is generally seen in 4 weeks and is sustainedduring prolonged therapy. The starting dose is40 mg BD, which may be increased upto
Comparative features of triptans
Suma. Frova. Riza. Nara. Zolmi.
1. Oral bioavailability (%) 15 25 45 70 402. Tmax* (hr) 1.5–2 2–4 1–1.5 2–3 1.5–23. Plasma t½ (hr) ~2 26 2–3 6 2–34. Oral dose
Initial (mg) 50–100 2.5 5–10 2.5 2.5Max. in 24 hr (mg) 200 5–7.5 20 5 10
* Tmax: Time to peak plasma concentration after oral dosing.

180S
EC
TIO
N3
AUTACOIDS AND RELATED DRUGS
160 mg BD if required. The mechanism of actionis not clear; that it is due to β adrenergic blockadehas been questioned. Other nonselective (timolol)and β1 selective (metoprolol, atenolol) agents arealso effective, but pindolol and others havingintrinsic sympathomimetic action are not useful.
(ii) Tricyclic antidepressants Many tricycliccompounds of which amitriptyline (25–50 mg atbed time) has been most extensively tried, reducemigraine attacks. It is effective in many patientsbut produces more side effects than propranolol.It is not known whether its 5-HT (and othermonoamine) uptake blocking property is causallyrelated to the prophylactic effect. The antimigraineeffect is independent of antidepressant property,but this class of drugs are better suited for patientswho also suffer from depression.
(iii) Calcium channel blockers Verapamil wasfound to reduce migraine attacks, but was judgedinferior to propranolol. Flunarizine is a relativelyweak Ca2+ channel blocker that also inhibits Na+
channels. It is claimed to be as effective aspropranolol, but convincing proof is lacking.Frequency of attacks is often reduced, but effect
on intensity and duration of attacks is less welldocumented. It is claimed to be a cerebro-selectiveCa2+ channel blocker; may benefit migraine byreducing intracellular Ca2+ overload due to brainhypoxia and other causes. Side effects are sedation,constipation, dry mouth, hypotension, flushing,weight gain and rarely extrapyramidal symptoms.Dose: Flunarizine 10–20 mg OD, children 5 mg OD,NOMIGRAIN, FLUNARIN 5 mg, 10 mg caps/tab.
(iv)Anticonvulsants Valproic acid (400–1200mg/day) and gabapentin (300–1200 mg/day) havesome prophylactic effect in migraine. The newerdrug topiramate has recently been approved formigrain prophylaxis. A 50% reduction in thenumber of attacks in half of the patients was notedin 2 randomized trials. Start with topiramate 25mg OD and gradually increase to 50 mg OD orBD. Efficacy of anticonvulsants in migraine islower than that of β blockers. They are indicatedin patients refractory to other drugs or whenpropranolol is contraindicated.
(v) 5-HT antagonists The prophylactic effect ofmethysergide and cyproheptadine is less impressive than βblockers. They are seldom used now for migraine.

Prostaglandins, Leukotrienes(Eicosanoids) and PlateletActivating Factor
ChapterChapterChapterChapterChapter 1313131313
PROSTAGLANDINS AND LEUKOTRIENES(Eicosanoids)
Prostaglandins (PGs) and Leukotrienes (LTs) arebiologically active derivatives of 20 carbon atompolyunsaturated essential fatty acids that arereleased from cell membrane phospholipids. Theyare the major lipid derived autacoids.
In the 1930s human semen was found to contract isolateduterine and other smooth muscle strips and to cause fallin BP in animals. The active principle was termed ‘prostag-landin’, thinking that it was derived from prostate. Onlyin the 1960s it was shown to be a mixture of closely relatedcompounds, the chemical structures were elucidated andwidespread distribution was revealed. In 1970s it becameclear that aspirin like drugs act by inhibiting PG synthesis,and that in addition to the classical PGs (Es and Fs), throm-boxane (TX), prostacyclin (PGI) and leukotrienes (LTs) wereof great biological importance. Bergstrom, Samuelsson andVane got the Nobel prize in 1982 for their work on PGsand LTs. Over the past 40 years they have been among themost intensely investigated substances.
CHEMISTRY, BIOSYNTHESIS ANDDEGRADATION
Chemically, PGs may be considered to be deri-vatives of prostanoic acid, though prostanoic aciddoes not naturally occur in the body. It has afive membered ring and two side chains projectingin opposite directions at right angle to the planeof the ring. There are many series of PGs andthromboxanes (TXs) designated A, B, C....I,depending on the ring structure and thesubstituents on it. Each series has members withsubscript 1, 2, 3 indicating the number of doublebonds in the side chains.
Leukotrienes are so named because they werefirst obtained from leukocytes (leuko) and have3 conjugated double bonds (triene). They havealso been similarly designated A, B, C.....F andgiven subscripts 1, 2, 3, 4.
In the body PGs, TXs and LTs are all derivedfrom eicosa (referring to 20 C atoms) tri/tetra/penta enoic acids. Therefore, they can be collec-tively called eicosanoids. In human tissues, thefatty acid released from membrane lipids in largestquantity is 5,8,11,14 eicosa tetraenoic acid(arachidonic acid). During PG, TX andprostacyclin synthesis, 2 of the 4 double bondsof arachidonic acid get saturated in the processof cyclization, leaving 2 double bonds in the sidechain. Thus, subscript 2 PGs are the mostimportant in man, e.g. PGE2, PGF2α, PGI2, TXA2.No cyclization or reduction of double bondsoccurs during LT synthesis—the LTs of biologicalimportance are LTB4, LTC4, LTD4.
Eicosanoids are the most universally distri-buted autacoids in the body. Practically every celland tissue is capable of synthesizing one or moretypes of PGs or LTs. The pathways of biosynthesisof eicosanoids are summarized in Fig. 13.1.
There are no preformed stores of PGs andLTs. They are synthesized locally and the rateof synthesis is governed by the rate of releaseof arachidonic acid from membrane lipids inresponse to appropriate stimuli. These stimuliactivate hydrolases, including phospholipase A,probably through increased intracellular Ca2+.
The cyclooxygenase (COX) pathway generateseicosanoids with a ring structure (PGs, TXs,prostacyclin) while lipoxygenase (LOX) producesopen chain compounds (LTs). All tissues haveCOX—can form cyclic endoperoxides PGG2 and

182S
EC
TIO
N3
AUTACOIDS AND RELATED DRUGS
Fig. 13.1: Biosynthesis of prostaglandins (PG) and leukotrienes (LT). Less active metabolites are shown in italicsTX—Thromboxane, PGI—Prostacyclin; HPETE—Hydroperoxy eicosatetraenoic acid (Hydroperoxy arachidonic acid);HETE—Hydroxyeicosatetraenoic acid (Hydroxy arachidonic acid); SRS-A—Slow reacting substance of anaphylaxis
PGH2 which are unstable compounds. Furthercourse in a particular tissue depends on the typeof isomerases or other enzymes present in it. PGE2
and PGF2α are the primary prostaglandins (namebased on the separation procedure: PGEpartitioned into Ether while PGF into phosphate[Fosfat in Swedish] buffer; α in PGF2α refersto orientation of OH group on the ring). PGsA, B and C are not found in the body: they areartifacts formed during extraction procedures.Lung and spleen can synthesize the whole rangeof COX products. Platelets primarily synthesizeTXA2 which is—chemically unstable, sponta-neously changes to TXB2. Endothelium mainlygenerates prostacyclin (PGI2) which is alsochemically unstable and rapidly converts to6-keto PGF1α.
Cyclooxygenase is known to exist in twoisoforms COX-1 and COX-2. While both isoformscatalyse the same reactions, COX-1 is a constitutiveenzyme in most cells—it is synthesized and is activein the basal state; the level of COX-1 activity isnot much changed once the cell is fully grown. On
the other hand, COX-2 normally present ininsignificant amounts, is inducible by cytokines,growth factors and other stimuli during theinflammatory response. It is believed thateicosanoids produced by COX-1 participate inphysiological (house keeping) functions such assecretion of mucus for protection of gastric mucosa,haemostasis and maintenance of renal function,while those produced by COX-2 lead to inflam-matory and other pathological changes. However,certain sites in kidney, brain and the foetusconstitutively express COX-2 which may playphysiological role.
A splice variant of COX-1 (designated COX-3) has beenfound in the dog brain. This isoenzyme is inhibited byparacetamol and is implicated in the genesis of fever, butthe exact role in humans is not known.
Lipoxygenase pathway appears to operatemainly in the lung, WBC and platelets. Its mostimportant products are the LTs, (generated by 5-LOX) particularly LTB4 (potent chemotactic) andLTC4, LTD4 which together constitute the ‘slowreacting substance of anaphylaxis’ (SRS-A) des-cribed in 1938 to be released during anaphylaxis.

183C
HA
PTE
R13
PROSTAGLANDINS, LEUKOTRIENES AND PLATELET ACTIVATING FACTOR
A membrane associated transfer protein calledFLAP (five lipoxygenase activating protein) carrysarachidonic acid to 5-LOX, and is essential forthe synthesis of LTs. Platelets have only 12-LOX.HPETEs produced by LOX can also be converted tohepoxilins, trioxilins and lipoxins. A third enzymatic pathwayinvolving cytochrome P450 can metabolize arachidonic acidinto 19- and 20-HETEs and epoxyeicosatrienoic acids. Freeradicals can attack arachidonic acid to produce isoprostanesnonenzymatically. Brain cells couple arachidonic acid withethanolamine to produce anandamide and a few other relatedeicosanoids which are now recognized to be the endogenouscannabinoid receptor ligands, and produce cannabis likeeffects. Like the other eicosanoids, they are synthesized onlywhen needed at the site of action.
Inhibition of synthesis Synthesis of COXproducts can be inhibited by nonsteroidalantiinflammatory drugs (NSAIDs). Aspirin acety-lates COX at a serine residue and causesirreversible inhibition while other NSAIDs arecompetitive and reversible inhibitors. MostNSAIDs are nonselective COX-1 and COX-2inhibitors, but some later ones like celecoxib,etoricoxib are selective for COX-2.
The sensitivity of COX in different tissuesto inhibition by these drugs varies; selective inhibi-tion of formation of certain products may bepossible at lower doses. NSAIDs do not inhibitthe production of LTs: this may even be increasedsince all the arachidonic acid becomes availableto the LOX pathway.
Zileuton inhibits LOX and decreases the production ofLTs. It was used briefly in asthma, but has been withdrawn.
Glucocorticosteroids inhibit the release ofarachidonic acid from membrane lipids (bystimulating production of proteins called annexinswhich inhibit phospholipase A2)—indirectlyreduce production of all eicosanoids—PGs, TXsand LTs. Moreover, they inhibit the induction ofCOX-2 by cytokines at the site of inflammation.
Degradation Biotransformation of arachido-nates occurs rapidly in most tissues, but fastestin the lungs. Most PGs, TXA2 and prostacyclinhave plasma t½ of a few seconds to a few minutes.First a specific carrier mediated uptake into cellsoccurs, the side chains are then oxidized anddouble bonds are reduced in a stepwise manner
to yield inactive metabolites. Metabolites areexcreted in urine. PGI2 is catabolized mainly inthe kidney.
ACTIONS AND PATHOPHYSIOLOGICALROLES
Prostaglandins, thromboxanes andprostacyclinThe cyclic eicosanoids produce a wide varietyof actions depending upon the particular PG (orTX or PGI), species on which tested, tissue,hormonal status and other factors. PGs differ intheir potency to produce a given action anddifferent PGs sometimes have opposite effects.Even the same PG may have opposite effects underdifferent circumstances. The actions of PGs andTXA2 are summarized in Table 13.1. Sincevirtually all cells and tissues are capable of formingone or more PGs, these autacoids have beenimplicated as mediators or modulators of a numberof physiological processes and pathological states.
1. CVS PGE2 and PGF2α cause vasodilatationin most, but not all, vascular beds. In isolatedpreparations, they are more potent vasodilatorsthan ACh or histamine. PGF2α constricts manylarger veins including pulmonary vein and artery.Fall in BP occurs when PGE2 is injected i.v.,but PGF2α has little effect on BP.• PGI2 is uniformly vasodilatory and is more
potent hypotensive than PGE2.• TXA2 consistently produces vasoconstriction.• PG endoperoxides (G2 and H2) are inherently
vasoconstrictor, but often produce vasodila-tation or a biphasic response due to rapidconversion to other PGs, especially PGI2 inthe blood vessels themselves.
• PGE2 and F2α stimulate heart by weak directbut more prominent reflex action due to fallin BP. The cardiac output increases.
Role(i) PGs do not circulate in blood and have
no role in regulating systemic vascularresistance. However, PGI2 generated in the

184S
EC
TIO
N3
AUTACOIDS AND RELATED DRUGS
vascular endothelium, mainly by COX-2,appears to be involved in the regulation oflocal vascular tone as a dilator.
(ii) PGE2 is continuously produced locally in theductus arteriosus by COX-2 during foetallife—keeps it patent; at birth its synthesisstops and closure occurs. Aspirin andindomethacin induce closure when it fails tooccur spontaneously. These PGs may alsobe important in maintaining placental bloodflow.
(iii) PGs, generated mainly by COX-2, along withLTs and other autacoids may mediatevasodilatation and exudation at the site ofinflammation.
2. Platelets TXA2, which can be producedlocally by platelets, is a potent inducer of aggre-gation and release reaction. The endoperoxidesPGG2 and PGH2 are also proaggregatory. On theother hand PGI2 (generated by vascular endothe-lium) is a potent inhibitor of platelet aggregation.PGD2 has antiaggregatory action, but much lesspotent than PGI2. PGE2 has dose dependent andinconsistent effects.
Role TXA2 produced by platelets and PGI2
produced by vascular endothelium probablyconstitute a mutually antagonistic system:preventing aggregation of platelets while in circu-lation and inducing aggregation on injury, whenplugging and thrombosis are needed.
Aspirin interferes with haemostasis by inhibi-ting platelet aggregation. TXA2 produced byplatelet COX-1 plays an important role inamplifying aggregation. Before it is deacetylatedin liver, aspirin acetylates COX-1 in platelets whilethey are in portal circulation. Further, plateletsare unable to regenerate fresh COX-1 (lacknucleus: do not synthesize protein), while vesselwall is able to do so (fresh enzyme is synthesizedwithin hours). Thus, in low doses, aspirinselectively inhibits TXA2 production and hasantithrombotic effect lasting > 3 days.
3. Uterus PGE2 and PGF2α uniformly contracthuman uterus, in vivo, both pregnant as well as
nonpregnant. The sensitivity is higher during preg-nancy and there is progressive modest increasewith the advance of pregnancy. However, evenduring early stages, uterus is quite sensitive toPGs though not to oxytocin. PGs increase basaltone as well as amplitude of uterine contractions.
When tested in vitro, PGF2α consistentlyproduces contraction while PGE2 relaxes non-pregnant but contracts pregnant human uterinestrips.At term, PGs soften the cervix at low doses andmake it more compliant.
Role(i) Foetal tissues produce PGs. At term PGF2α
has been detected in maternal blood. It ispostulated that PGs mediate initiation andprogression of labour. Aspirin has beenfound to delay the initiation of labour andalso prolong its duration.
(ii) Because PGs are present in high concen-tration in semen and can be rapidly absorbedwhen lodged in the vagina at coitus, it isbelieved that they so coordinate movementsof the female genital tract that transport ofsperms and fertilization is facilitated.
(iii) Dysmenorrhoea in many women is asso-ciated with increased PG synthesis by theendometrium. This apparently inducesuncoordinated uterine contractions whichcompress blood vessels → uterine ischae-mia → pain. Aspirin group of drugs arehighly effective in relieving dysmenorrhoeain most women.
4. Bronchial muscle PGF2α, PGD2 andTXA2 are potent bronchoconstrictors (more potentthan histamine) while PGE2 is a powerful broncho-dilator. PGI2 produces mild dilatation. Asthmaticsare more sensitive to constrictor as well as dilatoreffects of PGs. PGE2 and PGI2 also inhibithistamine release and are effective by aerosol.However, these antiasthmatic effects of PGE2 andPGI2 cannot be exploited clinically because theyproduce irritation of the respiratory tract and havea brief action.

185C
HA
PTE
R13
PROSTAGLANDINS, LEUKOTRIENES AND PLATELET ACTIVATING FACTOR
TAB
LE 1
3.1
A s
umm
ary
of th
e ac
tions
of m
ajor
pro
stag
land
ins,
pro
stac
yclin
and
thro
mbo
xane
Org
anP
rost
agla
ndin
E2
(PG
E2)
Pro
stag
land
in F
2α (
PG
F 2α)
Pro
stac
yclin
(P
GI 2)
Thro
mbo
xane
A2
(TX
A2)
1.B
lood
Vas
odila
tatio
n, ↓
BP
Vas
odila
tatio
n (m
ostly
), l
arge
rV
asod
ilata
tion
(mar
ked
and
Vas
ocon
stric
tion
vess
els
vein
s co
nstr
ict,
little
effe
ct o
n B
Pw
ides
prea
d),
↓ ↓
BP
2.H
eart
Wea
k in
otro
pic,
ref
lex
Wea
k in
otro
pic
——
card
iac
stim
ulat
ion
3.P
late
lets
Var
iabl
e ef
fect
—A
ntia
ggre
gato
ryA
ggre
gatio
n a
ndre
leas
e re
actio
n
4.U
teru
sC
ontra
ctio
n (in
viv
o),
rela
xes
Con
trac
tion
(in v
ivo
and
in v
itro)
,—
—no
ngra
vid
hum
an u
teru
s in
softe
ning
of
cerv
ixvi
tro,
softe
ning
of
cerv
ix
5.B
ronc
hiD
ilata
tion,
Inh
ibit
hist
amin
eC
onst
rictio
nD
ilata
tion
(mild
), i
nhib
itC
onst
rictio
nre
leas
ehi
stam
ine
rele
ase
6.S
tom
ach
↓ ac
id s
ecre
tion,
—↓
acid
sec
retio
n (w
eak)
,—
↑ m
ucus
pro
duct
ion
muc
osal
vas
odila
tatio
n
7.In
test
ine
Con
trac
ts l
ongi
tudi
nal
& r
elax
esS
pasm
ogen
ic,
↑ flu
id &
ele
ctro
lyte
Wea
k sp
asm
ogen
ic,
inhi
bit
Wea
k sp
asm
ogen
icci
rcul
ar m
uscl
es,
↑ pe
rista
lsis
,se
cret
ion
(wea
k)to
xin-
indu
ced
fluid
sec
retio
n↑
Cl¯
& w
ater
sec
retio
n
8.K
idne
yN
atriu
resi
s, ↓
Cl¯
reab
sorp
-—
Nat
riure
sis,
vas
odila
tatio
n,V
asoc
onst
rictio
ntio
n, i
nhib
it A
DH
act
ion,
reni
n re
leas
eva
sodi
lata
tion,
ren
in r
elea
se
9.C
NS
Pyr
ogen
ic,
varie
ty o
f ef
fect
son
i.c
.v.
inj.
10.
Rel
ease
↑ o
r ↓
↑
or ↓
of N
A
11.
Affe
rent
Sen
sitiz
e to
nox
ious
stim
uli
—S
ame
as P
GE
2—
nerv
es→
ten
dern
ess
12.
End
ocrin
eR
elea
se o
f an
t. pi
tuita
ryR
elea
se o
f go
nado
trop
ins
&—
—sy
stem
horm
ones
, st
eroi
ds,
insu
lin;
prol
actin
, lu
teol
ysis
(in
ani
mal
s)TS
H-li
ke a
ctio
n
13.
Met
abol
ism
Ant
ilipo
lytic
, in
sulin
lik
e ac
tion,
——
—m
obili
zatio
n of
bon
e C
a2+

186S
EC
TIO
N3
AUTACOIDS AND RELATED DRUGS
Role Asthma may be due to an imbalance bet-ween constrictor PGs (F2α, PGD2, TXA2) and LTson one hand and dilator ones (PGE2, PGI2) onthe other. In few individuals aspirin-like drugsconsistently induce asthma, possibly by divertingarachidonic acid to produce excess LTC4 and D4.This sensitivity is not shared by selective COX-2 inhibitors, indicating that suppression of COX-1 at the pulmonary site is responsible for thereaction. In allergic human asthma, LTs play amore important role, and COX inhibitors arewithout any effect in most patients.
5. GIT (i) In isolated preparations, the longi-tudinal muscle of gut is contracted by PGE2 andPGF2α while the circular muscle is eithercontracted (usually by PGF2α) or relaxed (usuallyby PGE2). Propulsive activity is enhanced in man,especially by PGE2 → colic and watery diarrhoeaare important side effects. PGE2 acts directly onthe intestinal mucosa and increases water,electrolyte and mucus secretion. PGI2 does notproduce diarrhoea and infact opposes PGE2 andtoxin induced fluid movement.
Role PGs may be involved in mediating toxininduced increased fluid movement in secretorydiarrhoeas. In certain diarrhoeas, aspirin can reducestool volume, but is not uniformly effective. PGsappear to play a role in the growth of colonicpolyps and cancer. Association of lower incidenceof colon cancer with regular intake of aspirinis now established. NSAIDs afford relief in familialcolonic polyposis by reducing polyp formation.
(ii) PGE2 markedly reduces acid secretion in thestomach. Volume of juice and pepsin content arealso decreased. It inhibits fasting as well as stimu-lated secretion (by feeding, histamine, gastrin).Release of gastrin is suppressed (see Fig. 46.1).The gastric pH may rise upto 7.0. PGI2 alsoinhibits gastric secretion, but is less potent.Secretion of mucus and HCO3̄ by gastric mucosalepithelial cells as well as mucosal blood floware increased. Thus, PGs are antiulcerogenic.
Role PGs (especially PGI2) appear to beinvolved in the regulation of gastric mucosal blood
flow. They may be functioning as natural ulcerprotectives by enhancing gastric mucus and HCO3̄production, as well as by improving mucosalcirculation and health. The ulcerogenic action ofNSAIDs may be due to loss of this protectiveinfluence.
Normally, gastric mucosal PGs are produced by COX-1.Selective COX-2 inhibitors are less ulcerogenic. However,COX-2 gets induced during ulcer healing, and COX-2inhibitors have the potential to delay healing.
6. Kidney PGE2 and PGI2 increase water, Na+
and K+ excretion and have a diuretic effect. PGE2has been shown to have a furosemide-likeinhibitory effect on Cl¯ reabsorption as well. Theycause renal vasodilatation and inhibit tubularreabsorption. PGE2 antagonizes ADH action, andthis adds to the diuretic effect. In contrast, TXA2
causes renal vasoconstriction. PGI2, PGE2 andPGD2 evoke release of renin.
Role(i) PGE2 and PGI2 produced mainly by COX-2
in the kidney appear to function as intrarenalregulators of blood flow as well as tubularreabsorption in kidney. Accordingly, theNSAIDs, including selective COX-2 inhi-bitors, tend to retain salt and water. Thediuretic action of furosemide is blunted byindomethacin—indicating a facilitatory roleof PGs by increasing renal blood flow and/or augmenting inhibition of tubularreabsorption.
(ii) Renin release in response to sympatheticstimulation and other influences may befacilitated by PGs.
(iii) Bartter’s syndrome, characterized by decrea-sed sensitivity to angiotensin II is associatedwith increased PG production; many of themanifestations are improved by prolongeduse of NSAIDs.
7. CNS PGs injected i.v. penetrate brainpoorly, so that central actions are not prominent.However, injected intracerebroventricularly PGE2
produces a variety of effects—sedation, rigidity,behavioral changes and marked rise in bodytemperature. PGI2 also induces fever, but TXA2
is not pyrogenic.

187C
HA
PTE
R13
PROSTAGLANDINS, LEUKOTRIENES AND PLATELET ACTIVATING FACTOR
Role(i) PGE2 may mediate pyrogen induced fever
and malaise. Aspirin and other inhibitors ofPG synthesis are antipyretic. Pyrogens,including cytokines released during bacterialinfection, trigger synthesis of PGE2 in thehypothalamus, which resets the thermostatto cause fever. COX-2 is the majorisoenzyme involved; selective COX-2 inhi-bitors are equally efficacious antipyretics. Arole of COX-3 has also been proposed.
(ii) PGs may be functioning as neuromodulatorsin the brain by regulating neuronal excita-bility. A role in pain perception, sleep andsome other functions has been suggested.
8. ANS Depending on the PG, species andtissue, both inhibition as well as augmentationof NA release from adrenergic nerve endings hasbeen observed.
Role PGs may modulate sympathetic neuro-transmission in the periphery.
9. Peripheral nerves PGs (especially E2 andI2) sensitize afferent nerve endings to pain inducingchemical and mechanical stimuli (Fig. 13.2). Theyirritate mucous membranes and produce longlasting dull pain on intradermal injection.
Role PGs appear to serve as algesic agentsduring inflammation. They cause tenderness andamplify the action of other algesics. Inhibitionof PG synthesis is a major antiinflammatorymechanism. Aspirin injected locally decreases painproduced by injection of bradykinin at the samesite.
10. Eye: PGF2α induces ocular inflammation andlowers i.o.t by enhancing uveoscleral andtrabecular outflow. Non irritating congeners likelatanoprost are now first line drugs in wide angleglaucoma.
Role Locally produced PGs appear to facilitateaqueous humor drainage. The finding thatCOX-2 expression in the ciliary body is deficientin wide angle glaucoma patients supports thiscotention.11. Endocrine system PGE2 facilitates therelease of anterior pituitary hormones—growthhormone, prolactin, ACTH, FSH and LH as wellas that of insulin and adrenal steroids. It has aTSH-like effect on the thyroid.
PGF2α causes luteolysis and terminates earlypregnancy in many mammals, but this effect isnot significant in humans. Though PGs canterminate early pregnancy in women, this is notassociated with fall in progesterone levels.
12. Metabolism PGEs are antilipolytic, exertan insulin like effect on carbohydrate metabolismand mobilize Ca2+ from bone. They may mediatehypercalcaemia due to bony metastasis.
LeukotrienesThe straight chain lipoxygenase products ofarachidonic acid are produced by a more limitednumber of tissues (LTB4 mainly by neutrophils;LTC4 and LTD4—the cysteinyl LTs—mainly bymacrophages), but probably they are pathophy-siologically as important as PGs.
1. CVS and blood LTC4 and LTD4 injectedi.v. evoke a brief rise in BP followed by a moreprolonged fall. The fall in BP is not due tovasodilatation because no relaxant action has been
Fig. 13.2: Sensitization of nociceptors (pain receptors)to mediators of pain by prostaglandins at the inflammatorysite. Subs. P—Substance P; CGRP—Calcitonin generelated peptide

188S
EC
TIO
N3
AUTACOIDS AND RELATED DRUGS
seen on blood vessels. It is probably a result ofcoronary constriction induced decrease in cardiacoutput and reduction in circulating volume dueto increased capillary permeability. These LTsmarkedly increase capillary permeability and aremore potent than histamine in causing local edemaformation. LTB4 is highly chemotactic forneutrophils and monocytes; this property is sharedby HETE but not by other LTs. Migration ofneutrophils through capillaries and their clumpingat sites of inflammation in tissues is also promotedby LTB4. The cysteinyl LTs (C4, D4) arechemotactic for eosinophils.
Role LTs are important mediators of inflam-mation. They are produced (along with PGs)locally at the site of injury. While LTC4 and D4
cause exudation of plasma, LTB4 attracts theinflammatory cells which reinforce the reaction.5-HPETE and 5-HETE may facilitate local releaseof histamine from mast cells.
2. Smooth muscle LTC4 and D4 contractmost smooth muscles. They are potent broncho-constrictors and induce spastic contraction of g.i.t.at low concentrations.
They also increase mucus secretion in theairways.
Role The cysteinyl LTs (C4 and D4) are the mostimportant mediators of human allergic asthma.They are released along with PGs and otherautacoids during AG: AB reaction in the lungs.In comparison to other mediators, they are morepotent and are metabolized slowly in the lungs,exert a long lasting action. LTs may also beresponsible for abdominal colics during systemicanaphylaxis.
3. Afferent nerves Like PGE2 and I2, theLTB4 also sensitizes afferents carrying painimpulses—contributes to pain and tenderness ofinflammation.
PROSTANOID RECEPTORS
PGs, TX and prostacyclin act on their own specificreceptors located on cell membrane. Five families
of prostanoid receptors have been designated, eachafter the natural PG for which it has the greatestaffinity. This has been supported by receptorcloning. All prostanoid receptors are G-proteincoupled receptors which can be functionallycategorized into ‘excitatory’ or ‘contractile’ and‘inhibitory’ or ‘relaxant’ groups.
The contractile group (EP1, FP, TP) coupleprimarily with Gq protein and activate PLCβ togenerate IP3 and DAG. These second messengersrelease Ca2+ intracellularly resulting in excitatoryresponses like smooth muscle contraction, plateletaggregation, etc. The relaxant group (DP1, EP2,EP4 and IP) couple with Gs protein—activateadenylyl cyclase to generate intracellular secondmessenger cAMP. Smooth muscle relaxation,inhibition of platelet aggregation, etc. are producedthrough cAMP dependent protein kinase (PKA).The major characteristics of subtypes of prostanoidreceptors are:DP This receptor has strongest affinity for PGD2, but PGE2
can also activate it. Two subtypes DP1 and DP2 have beenidentified, but both have limited distribution in the body; DP1
is a relaxant receptor which dilates certain blood vessels andinhibits platelet aggregation. The DP2 receptor couples withGi protein and inhibits cAMP generation.EP This receptor is characterized by highest affinity forPGE2; enprostil is a selective agonist. Four subtypes havebeen recognized:
EP1 is a contactile receptor—contracts visceral smoothmuscle, but is less abundant in the body.EP2 and EP4 are relaxant in nature, act by increasing cAMPin smooth muscle, but the same second messenger enhancesCl¯ and water secretion by the intestinal mucosa. While EP2
is present in few organs, EP4 has wide distribution.EP3 is inhibitory, decreases cAMP generation by couplingwith Gi protein. The antilipolytic action of PGE2 is exertedby opposing cAMP generation in adipose tissue.Distribution of PGE3 receptor in the body is wide.
FP This contactile receptor is highly expressed in the femalegenital tract, and is present in many other organs. It exhibitsstrong affinity for PGF2α; fluprostenol is a selective agonist.IP This relaxant receptor is defined by highest affinity forPGI2, but PGE2 also acts on it; cicaprost is a selective agonist.It is expressed in heart, lungs, kidney, platelet (antiaggregatory),etc., but the highest density is in the vasculature.TP Characterized by high affinity for TxA2, this contractilereceptor is abundant in platelets (aggregatory), cardiovascularsystem, immune cells and many other organs. PGH2 can alsoactivate TP. Apart from IP3/DAG—Ca2+—PKc pathway, itutilizes other kinases as well to exert certain biological effects.

189C
HA
PTE
R13
PROSTAGLANDINS, LEUKOTRIENES AND PLATELET ACTIVATING FACTOR
LEUKOTRIENE RECEPTORSSeparate receptors for LTB4 (BLT1 and BLT2)and for the cysteinyl LTs (LTC4, LTD4) have beendefined. Two subtypes, cysLT1 and cysLT2 of thecysteinyl LT receptor have been cloned. All LTreceptors couple with Gq protein and functionthrough the IP3/DAG transducer mechanism. TheBLT receptors are chemotactic and primarilyexpressed in leucocytes and spleen. BLT1 receptorhas high, while BLT2 receptor has lower affinityfor LTB4. The cysLT1 receptor is mainly expressedin bronchial and intestinal muscle and has higheraffinity for LTD4 than for LTC4. The primarylocation of cysLT2 receptor is leucocytes andspleen, and it shows no preference for LTD4 overLTC4. The cysLT1 receptor antagonists, viz.Montelukast, Zafirlukast, etc. are now valuabledrugs for bronchial asthma (see Ch. 16).
USES
Clinical application of PGs and their analoguesis rather restricted because of limited availability,short lasting action, cost and frequent side effects.However, their use in glaucoma and in obstetricsis now common place. Their indications are:
1. Abortion During the first trimester, termi-nation of pregnancy by transcervical suction isthe procedure of choice. Intravaginal PGE2 pes-sary inserted 3 hours before attempting dilatationcan minimise trauma to the cervix by reducingresistance to dilatation.
Medical termination of pregnancy of upto 7weeks has been achieved with high success rateby administering mifepristone (antiprogestin) 600mg orally 2 days before a single oral dose ofmisoprostol 400 μg. It is now a valuable alternativeto suction-evacuation. Uterine contractions areprovoked and the conceptus is expelled withinthe next few hours. Intravaginal misoprostol isnow favoured by many as it produces fewer sideeffects. Sublingual route is also advocated by someexperts. Ectopic pregnancy should be ruled outbeforehand and complete expulsion should beconfirmed afterwards. Uterine cramps, vaginalbleeding, nausea, vomiting and diarrhoea are thecommon side effects. Methotrexate administered
along with misoprostol is also highly successfulfor inducing abortion in the first few weeks ofpregnancy.
PGs have a place in midterm abortion, missedabortion and molar gestation, though delayed anderratic action and incomplete abortion are aproblem. The initial enthusiasm has given wayto more considered use. PGs convert the oxytocinresistant midterm uterus to oxytocin responsiveone: a single extraamniotic injection (PGE2)followed by i.v. infusion of oxytocin or intraamnio-tic (PGF2α) with hypertonic solution produces2nd trimester abortion in a high percentage withoutundue side effects. Pretreatment with mifepristoneimproves the efficacy of PGE as abortifacient.2. Induction/augmentation of labour PGs donot offer any advantage over oxytocin for induc-tion of labour at term. They are less reliable andshow wider individual variation in action. PGE2
and PGF2α (rarely) have been used in place ofoxytocin in toxaemic and renal failure patients,because PGs do not cause fluid retention thatis possible with oxytocin. PGE2 may also be usedto augment labour, if it is slow, in primipara.Intravaginal route is preferred now: side effectscare milder; extra/intra amniotic route isinfrequently used.3. Cervical priming (ripening) Appliedintravaginally or in the cervical canal, low dosesof PGE2 which do not affect uterine motility makethe cervix soft and compliant. This procedure hasyielded good results in cases with unfavourablecervix. If needed labour may be induced 12 hourslater with oxytocin: chances of failure are reduced.4. Postpartum haemorrhage (PPH)Carboprost (15-methyl PGF2α) injected i.m. is analternative drug for control of PPH due to uterineatony, especially in patients unresponsive toergometrine and oxytocin.PGE2 (Dinoprostone) PROSTIN-E2 for induction/augmen-tation of labour, midterm abortion.
Vaginal gel (1 mg or 2 mg in 2.5 ml) 1 mg inserted intoposterior fornix, followed by 1–2 mg after 6 hour if required.Vaginal tab (3 mg) 3 mg inserted into posterior fornix,followed by another 3 mg if labour does not start within6 hour.

190S
EC
TIO
N3
AUTACOIDS AND RELATED DRUGS
Extraamniotic solution (10 mg/ml in 0.5 ml amp.)infrequently used.Intravenous solution (1 mg/ml in 0.75 ml amp., 10 mg/mlin 0.5 ml amp) i.v. route is rarely used due to more sideeffects.Oral tablet PRIMIPROST 0.5 mg tab, one tab. hourly tillinduction, max 1.5 mg per hr; rarely used.Cervical gel CERVIPRIME (0.5 mg in 2.5 ml prefilledsyringe) 0.5 mg inserted into cervical canal for preinductioncervical softening and dilatation in patients with poorBishop’s score.
Gemeprost CERVAGEM 1 mg vaginal pessary: for softeningof cervix in first trimester—1 mg 3 hr before attemptingdilatation; for 2nd trimester abortion/molar gestation—1 mgevery 3 hours, max. 5 doses.
PGF2α (Dinoprost) PROSTIN F2 ALPHA intraamnioticinjection 5 mg/ml in 4 ml amp. for midterm abortion/inductionof labour (rarely used).
15-methyl PGF2α (Carboprost) PROSTODIN 0.25 mg in1 ml amp; 0.25 mg i.m. every 30–120 min for PPH, midtermabortion, missed abortion.
T-PILL + MISO Mifepristone 200 mg tab (3 tabs) +misoprostol 200 mg (2 tabs); mifepristone 3 tab orally followed2 days later by misoprostol 2 tab orally, for termination ofpregnancy of upto 49 days.
5. Peptic ulcer Stable analogue of PGE1
(misoprostol) is occasionally used for healingpeptic ulcer, especially in patients who needcontinued NSAID therapy or who continue tosmoke (see Ch. 46).6. Glaucoma Topical PGF2α analogues likelatanoprost, travoprost, bimatoprost that are FPreceptor agonists are the first choice drugs in wideangle glaucoma (see p. 155).7. To maintain patency of ductus arteriosusin neonates with congenital heart defects, tillsurgery is undertaken. PGE1 (Alprostadil) is used;apnoea occurs in few cases.PROSTIN VR, BIOGLANDIN 0.5 mg in 1 ml amp; diluteand infuse i.v.
8. To avoid platelet damage PGI2 (Epopros-tenol) can be used to prevent platelet aggregationand damage during haemodialysis or cardiopul-monary bypass. It also improves harvest ofplatelets for transfusion.
Few cases of primary pulmonary hypertensionhave been successfully maintained on epopros-tenol infusion.FLOLAN 0.5 mg vial for reconstitution.
The other suggested uses of PGs are:1. Peripheral vascular diseases PGI2 (or PGE1) infusedi.v. can relieve rest pain and promote healing of ischaemiculcers in severe cases of intermittent claudication and inRaynaud’s disease.2. Impotence Alprostadil (PGE1) injected into the peniscauses erection lasting 1–2 hours. However, oral sildenafil/tadalafil is now preferred for erectile dysfunction.
SIDE EFFECTSSide effects are common in the use of PGs, buttheir intensity varies with the PG, the dose andthe route. These are: nausea, vomiting, waterydiarrhoea, uterine cramps, unduly forcefuluterine contractions, vaginal bleeding, flushing,shivering, fever, malaise, fall in BP, tachycardia,chest pain.
PLATELET ACTIVATING FACTOR (PAF)Like eicosanoids, platelet activating factor (PAF)is a cell membrane derived polar lipid with intensebiological activity. Discovered in 1970s PAF isactive at subnanomolar concentration and is nowrecognized to be an important signal molecule.PAF is acetyl-glyceryl ether-phosphoryl choline.The ether-linked alkyl chain in human PAF ismostly 16 or 18 C long.
Synthesis and degradation PAF is synthesized fromprecursor phospholipids present in cell membrane by thefollowing reactions:
PAF-acetylPhospholipase A2 transferase
MembraneAcyl-glycero- Lyso PAF PAFphosphocholine
Fatty acid Acetyl CoA CoA
The second step is rate limiting. Antigen-antibody reactionand a variety of mediators stimulate PAF synthesis in a Ca2+
dependent manner on demand: there are no preformed storesof PAF. In contrast to eicosanoids, the types of cells whichsynthesize PAF is quite limited—mainly WBC, platelets,vascular endothelium and kidney cells.
PAF is degraded in the following manner:
PAF acetyl- Acyl-hydrolase transferase
PAF Lyso PAF Acyl glycero-phosphocholine
(gets incorporatedAcetate Fatty acid in the membrane)

191C
HA
PTE
R13
PROSTAGLANDINS, LEUKOTRIENES AND PLATELET ACTIVATING FACTOR
Actions PAF has potent actions on many tissues/organs.
Platelets Aggregation and release reaction; alsoreleases TXA2; i.v. injection of PAF results in intravascularthrombosis.
WBC PAF is a potent chemotactic for neutrophils, eosino-phils and monocytes. It stimulates neutrophils to aggregate,to stick to vascular endothelium and migrate across it tothe site of infection. It also prompts release of lysosomalenzymes and LTs as well as generation of superoxide radicalby the polymorphs. The chemotactic action may be mediatedthrough release of LTB4. It induces degranulation ofeosinophils.
Blood vessels Vasodilatation mediated by release of EDRFoccurs → fall in BP on i.v. injection. Decreased coronaryblood flow has been observed on intracoronary injection,probably due to formation of platelet aggregates and releaseof TXA2.
PAF is the most potent agent known to increase vascularpermeability. Wheal and flare occur at the site of intradermalinjection.
Injected into the renal artery PAF reduces renal bloodflow and Na+ excretion by direct vasoconstrictor action, butthis is partly counteracted by local PG release.
Visceral smooth muscle Contraction occurs by directaction as well as through release of LTC4, TXA2 and PGs.Aerosolized PAF is a potent bronchoconstrictor. In addition,it produces mucosal edema, secretion and a delayed andlong-lasting bronchial hyper-responsiveness. It also stimulatesintestinal and uterine smooth muscle.
Stomach PAF is highly ulcerogenic: erosions and mucosalbleeding occur shortly after i.v. injection of PAF. The gastricsmooth muscle contracts.
Mechanism of action Membrane bound specificPAF receptors have been identified. The PAF receptor isa G-protein coupled receptor which exerts most of the actionsby coupling with Gq protein and generating intracellularmessengers IP3/DAG → Ca2+ release. It can also inhibitadenylyl cyclase by coupling with Gi protein.
As mentioned above, many actions of PAF are mediated/augmented by PGs, TXA2 and LTs which may be consideredits extracellular messengers. PAF also acts intracellularly,especially in the endothelial cells; rise in PAF concentrationwithin the endothelial cells is associated with exposure ofneutrophil binding sites on their surface. Similarly, itsproaggregatory action involves unmasking of fibrinogenbinding sites on the surface of platelets.
PAF antagonists A number of natural and synthetic PAFreceptor antagonists have been investigated. Important amongthese are ginkgolide B (from a Chinese plant), and somestructural analogues of PAF. The PAF antagonists have manyfoldtherapeutic potentials like treatment of stroke, intermittentclaudication, sepsis, myocardial infarction, shock, g.i.ulceration, asthma and as contraceptive. Some of them havebeen tried clinically but none has been found worth marketing.Alprazolam and triazolam antagonize some actions of PAF.
Pathophysiological roles PAF has been implicated inmany pathological states and some physiological processesby mediating cell-to-cell interaction. These are:1. Inflammation: Generated by leukocytes at the site ofinflammation PAF appears to participate in the causationof vasodilatation, exudation, cellular infiltration and hyper-algesia.2. Bronchial asthma: Along with LTC4 and LTD4, PAFappears to play a major role by causing bronchoconstriction,mucosal edema, recruiting eosinophils and provokingsecretions. It is unique in producing prolonged airway hyper-reactivity, so typical of bronchial asthma patient.3. Anaphylactic (and other) shock conditions: areassociated with high circulating PAF levels.4. Haemostasis and thrombosis: PAF may participateby promoting platelet aggregation.5. Rupture of mature graafian follicle and implantation:Early embryos which produce PAF have greater chance ofimplanting. However, PAF is not essential for reproduction.6. Ischaemic states of brain, heart and g.i.t., including g.i.ulceration.
PROBLEM DIRECTED STUDY
13.1 A full term primigravida presented with labour pains. On examination the BP was 110/70mm Hg and she was not anaemic. The presentation was vertex, head was engaged, foetal heartsound was normal, there was no cephalopelvic disproportion, no placenta previa, membraneswere intact and uterine contractions were adequate. The labour was allowed to progress underobservation. After 8 hours the cervix was still firm and not adequately dilated.(a) Can some medicaion be used to soften the cervix, help its ripening and facilitate delivery?
If so, which drug and route of administration should be used?(b) Given the above findings, is there any contraindication to the use of such medication?(see Appendix-1 for solution)

Nonsteroidal AntiinflammatoryDrugs and Antipyretic-Analgesics
ChapterChapterChapterChapterChapter 1414141414
All drugs grouped in this class have analgesic,antipyretic and antiinflammatory actions indifferent measures. In contrast to morphine theydo not depress CNS, do not produce physicaldependence, have no abuse liability and are weakeranalgesics (except for inflammatory pain). Theyare also called nonnarcotic, nonopioid or aspirin-like analgesics. They act primarily on peripheralpain mechanisms, but also in the CNS to raisepain threshold. They are more commonlyemployed and many are over-the-counter drugs.
Willow bark (Salix alba) had been used for manycenturies. Salicylic acid was prepared by hydrolysis of thebitter glycoside obtained from this plant. Sodium salicylatewas used for fever and pain in 1875; its great success ledto the introduction of acetylsalicylic acid (aspirin) in 1899.Phenacetin and antipyrine were also produced at that time.The next major advance was the development ofphenylbutazone in 1949 having antiinflammatory activityalmost comparable to corticosteroids. The term NonsteroidalAntiinflammatory Drug (NSAID) was coined to designatesuch drugs. Indomethacin was introduced in 1963. A hostof compounds heralded by the propionic acid derivativeibuprofen have been added since then and cyclooxygenase(COX) inhibition is recognised to be their most importantmechanism of action. Subsequently some selective COX-2inhibitors (celecoxib, etc.) have been added.
The antipyretic-analgesics are chemicallydiverse, but most are organic acids.
CLASSIFICATION
A. Nonselective COX inhibitors (traditionalNSAIDs)1. Salicylates: Aspirin.2. Propionic acid derivatives: Ibuprofen,
Naproxen, Ketoprofen, Flurbiprofen.3. Fenamate: Mephenamic acid.4. Enolic acid derivatives: Piroxicam,
Tenoxicam.5. Acetic acid derivatives: Ketorolac,
Indomethacin, Nabumetone.
6. Pyrazolone derivatives: Phenylbutazone,Oxyphenbutazone.
B. Preferential COX-2 inhibitorsNimesulide, Diclofenac, Aceclofenac,Meloxicam, Etodolac.
C. Selective COX-2 inhibitorsCelecoxib, Etoricoxib, Parecoxib.
D. Analgesic-antipyretics with poorantiinflammatory action1. Paraaminophenol derivative: Paracetamol
(Acetaminophen).2. Pyrazolone derivatives: Metamizol (Dipy-
rone), Propiphenazone.3. Benzoxazocine derivative: Nefopam.
NSAIDs and prostaglandin (PG)synthesis inhibitionIn 1971 Vane and coworkers made the landmarkobservation that aspirin and some NSAIDsblocked PG generation. This is now consideredto be the major mechanism of action of NSAIDs.Prostaglandins, prostacyclin (PG I2) and throm-boxane A2 (TXA2) are produced from arachidonicacid by the enzyme cyclooxygenase (see p. 182)which exists in a constitutive (COX-1) and aninducible (COX-2) isoforms; the former servesphysiological ‘house keeping’ functions, while thelatter, normally present in minute quantities, isinduced by cytokines and other signal moleculesat the site of inflammation → generation of PGslocally which mediate many of the inflammatorychanges. However, COX-2 is constitutively presentat some sites in brain, in juxtaglomerular cellsand in the foetus; it may serve physiological roleat these sites. Most NSAIDs inhibit COX-1 andCOX-2 nonselectively, but now some selectiveCOX-2 inhibitors have been produced. Features

193C
HA
PTE
R14
NSAIDs AND ANTIPYRETIC-ANALGESICS
of nonselective COX-1/COX-2 inhibitors(traditional NSAIDs) and selective COX-2inhibitors are compared in Table 14.1
Aspirin inhibits COX irreversibly by acety-lating one of its serine residues; return of COXactivity depends on synthesis of fresh enzyme.
also). However, fever can occur through non-PGmediated mechanisms as well.
Beneficial actions due to PG synthesis inhibition
• Analgesia: prevention of pain nerve endingsensitization
• Antipyresis• Antiinflammatory• Antithrombotic• Closure of ductus arteriosus in newborn
Other NSAIDs are competitive and reversibleinhibitors of COX; return of activity depends ontheir dissociation from the enzyme which in turnis governed by the pharmacokinetic characteris-tics of the compound.Analgesia PGs induce hyperalgesia (see p. 187)by affecting the transducing property of freenerve endings so that stimuli that normally donot elicit pain are able to do so. NSAIDs donot affect the tenderness induced by directapplication of PGs, but block the pain sensitizingmechanism induced by bradykinin, TNFα,interleukins (ILs) and other algesic substancesprimarily by inhibiting COX-2. This constitutesthe peripheral component of the analgesic actionof NSAIDs. They are, therefore, more effectiveagainst inflammation associated pain.
Lately the central component of analgesicaction of NSAIDs has also been shown to involveinhibition of PG synthesis in the spinal dorsalhorn neurones as well as in brain.
Antipyresis NSAIDs reduce body temperaturein fever, but do not cause hypothermia in normo-thermic individuals. Fever during infection andtissue injury is produced through the generationof pyrogens including, ILs, TNFα, interferonswhich induce PGE2 production in hypothalamus—raise its temperature set point. NSAIDs block theaction of pyrogens but not that of PGE2 injectedinto the hypothalamus. The isoform present atthis site appears to be COX-2 (possibly COX-3
Shared toxicities due to PG synthesis inhibition
• Gastric mucosal damage• Bleeding: inhibition of platelet function• Limitation of renal blood flow : Na+ and water
retention• Delay/prolongation of labour• Asthma and anaphylactoid reactions in
susceptible individuals
Antiinflammatory The most important mecha-nism of antiinflammatory action of NSAIDs isconsidered to be inhibition of COX-2 mediatedenhanced PG synthesis at the site of injury.However, there is some evidence that inhibitionof the constitutive COX-1 also contributes tosuppression of inflammation, especially in theinitial stages. The antiinflammatory potency ofdifferent compounds roughly corresponds withtheir potency to inhibit COX. However, nime-sulide is a potent antiinflammatory but relativelyweak COX inhibitor. PGs are only one of themediators of inflammation; inhibition of COXdoes not depress the production of other media-tors like LTs, PAF, cytokines, etc. Inflammationis the result of concerted participation of a largenumber of vasoactive, chemotactic and prolifera-tive factors at different stages, and there are manytargets for antiinflammatory action.
Activated endothelial cells express adhesionmolecules (ELAM-1, ICAM-1) on their surfaceand play a key role in directing circulating leuco-cytes to the site of inflammation (chemotaxis).Similarly, inflammatory cells express selectins andintegrins. Certain NSAIDs may act by additionalmechanisms including inhibition of expression/activity of some of these molecules and generationof superoxide/other free radicals. Growth factorslike GM-CSF, IL-6 as well as lymphocytetransformation factors and TNFα may also beaffected. Stabilization of leucocyte lysosomalmembrane and antagonism of certain actions ofkinins may be contributing to NSAID action.
Dysmenorrhoea Involvement of PGs in dysme-norrhoea has been clearly demonstrated: level of

194S
EC
TIO
N3
AUTACOIDS AND RELATED DRUGS
PGs in menstrual flow, endometrial biopsy andthat of PGF2α metabolite in circulation are raisedin dysmenorrhoeic women. Intermittent ischae-mia of the myometrium is probably responsiblefor menstrual cramps. NSAIDs lower uterine PGlevels—afford excellent relief in 60–70% andpartial relief in the remaining. Ancillary symp-toms of headache, muscle ache and nausea arealso relieved. Excess flow may be normalized.
Antiplatelet aggregatory NSAIDs inhibit syn-thesis of both proaggregatory (TXA2) and anti-aggregatory (PGI2) prostanoids, but effect onplatelet TXA2 (COX-1 generated) predominates→ therapeutic doses of most NSAIDs inhibitplatelet aggregation: bleeding time is prolonged.Aspirin is highly active; acetylates platelet COXirreversibly in the portal circulation before it isdeacetylated by first pass metabolism in liver.Small doses are therefore able to exert anti-thrombotic effect for several days. Risk of surgicaland anticoagulant associated bleeding is enhanced.
Ductus arteriosus closure During foetal circu-lation ductus arteriosus is kept patent by localelaboration of PGE2 by COX-2. Unknownmechanisms switch off this synthesis at birth andthe ductus closes. When this fails to occur, smalldoses of indomethacin or aspirin bring aboutclosure in majority of cases within a few hoursby inhibiting PG production. Administration ofNSAIDs in late pregnancy has been found to
promote premature closure of ductus in somecases. Risk of post-partum haemorrhage isincreased. Prescribing of NSAIDs near termshould be avoided.
Parturition Sudden spurt of PG synthesis byuterus occurs just before labour begins. This isbelieved to trigger labour as well as facilitateits progression. Accordingly, NSAIDs have thepotential to delay and retard labour. However,labour can occur in the absence of PGs.
Gastric mucosal damage Gastric pain,mucosal erosion/ulceration and blood loss areproduced by all NSAIDs to varying extents:relative gastric toxicity is a major considerationin the choice of NSAIDs. Inhibition of COX-1mediated synthesis of gastroprotective PGs (PGE2,PGI2) is clearly involved, though local actioninducing back diffusion of H+ ions in gastricmucosa also plays a role. Deficiency of PGsreduces mucus and HCO3̄ secrection, tends toenhance acid secretion and may promote mucosalischaemia. Thus, NSAIDs enhance aggressivefactors and contain defensive factors in gastricmucosa—are ulcerogenic. Paracetamol, a veryweak inhibitor of COX is practically free of gastrictoxicity and selective COX-2 inhibitors arerelatively safer. Stable PG analogues (misoprostol)administered concurrently with NSAIDscounteract their gastric toxicity.
Renal effects Conditions leading to hypovo-laemia, decreased renal perfusion and Na+ lossinduce renal PG synthesis which brings aboutintrarenal adjustments by promoting vasodila-tation, inhibiting tubular Cl¯ reabsorption (Na+
and water accompany) and opposing ADH action.NSAIDs produce renal effects by at least3 mechanisms:• COX-1 dependent impairment of renal blood
flow and reduction of g.f.r. → can worsen renalinsufficiency.
• Juxtaglomerular COX-2 (probably COX-1also) dependent Na+ and water retention.
• Ability to cause papillary necrosis on habitualintake.
TABLE14.1
Features of nonselective COX inhibi-tors and selective COX-2 inhibitors
Action COX-1/COX-2 COX-2inhibitors inhibitors
1. Analgesic + +
2. Antipyretic + +
3. Antiinflammatory + +
4. Antiplatelet aggregatory + –
5. Gastric mucosal damage + –
6. Renal salt/water retention + +
7. Delay/prolongation of labour + +
8. Ductus arteriosus closure + ?
9. Aspirin sensitive asthmaprecipitation + –

195C
HA
PTE
R14
NSAIDs AND ANTIPYRETIC-ANALGESICS
Renal effects of NSAIDs are not marked in normalindividuals, but become significant in those withCHF, hypovolaemia, hepatic cirrhosis, renaldisease and in patients receiving diuretics orantihypertensives. In them Na+ retention andedema can occur; diuretic and antihypertensivedrug effects are blunted.
Involvement of PG synthesis inhibition inanalgesic nephropathy is uncertain.Analgesic nephropathy occurs after years of heavy ingestionof analgesics. Such individuals probably have some personalitydefect. Regular use of combinations of NSAIDs and chronic/repeated urinary tract infections increase the risk of analgesicnephropathy. Pathological lesions are papillary necrosis, tubularatrophy followed by renal fibrosis. Urine concentrating abilityis lost and the kidneys shrink. Because phenacetin was firstimplicated, it went into disrepute, though other analgesics arealso liable to produce similar effects.
Anaphylactoid reactions Aspirin precipitatesasthma, angioneurotic swellings, urticaria orrhinitis in certain susceptible individuals. Thesesubjects react similarly to chemically diverseNSAIDs, ruling out immunological basis for thereaction. Inhibition of COX with consequentdiversion of arachidonic acid to LTs and otherproducts of lipoxygenase pathway may beinvolved, but there is no proof.
SALICYLATES
Aspirin (prototype)Aspirin is acetylsalicylic acid. It is rapidlyconverted in the body to salicylic acid which isresponsible for most of the actions. Other actionsare the result of acetylation of certain macromole-cules including COX. It is one of the oldest anal-gesic-antiinflammatory drugs and is still frequentlyused.
PHARMACOLOGICAL ACTIONS
1. Analgesic, antipyretic, antiinflam-matory actions Aspirin is a weaker analgesic(has lower maximal efficacy) than morphine type
drugs: aspirin 600 mg ~ codeine 60 mg. However,it effectively relieves inflammatory, tissue injuryrelated, connective tissue and integumental pain,but is relatively ineffective in severe visceral andischaemic pain. The analgesic action is mainlydue to obtunding of peripheral pain receptors andprevention of PG-mediated sensitization of nerveendings. A central subcortical action raisingthreshold to pain perception also contributes, butthe morphine-like action on psychic processingor reaction component of the pain is missing.No sedation, subjective effects, tolerance orphysical dependence is produced.
Aspirin resets the hypothalamic thermostat andrapidly reduces fever by promoting heat loss(sweating, cutaneous vasodilatation), but does notdecrease heat production.
Antiinflammatory action is exerted at highdoses (3–6 g/day or 100 mg/kg/ day). Signs ofinflammation like pain, tenderness, swelling,vasodilatation and leucocyte infiltration are sup-pressed. In addition to COX inhibition, quenchingof free radicals may contribute to its antiinflam-matory action.
2. Metabolic effects These are significantonly at antiinflammatory doses. Cellular meta-bolism is increased, especially in skeletal muscles,due to uncoupling of oxidative phosphorylation→ increased heat production. There is increasedutilization of glucose → blood sugar may dec-rease (especially in diabetics) and liver glycogenis depleted. However, hyperglycaemia often occursat toxic doses: this is due to central sympatheticstimulation → release of Adr and corticosteroids.Chronic use of large doses cause negative N2
balance by increased conversion of protein tocarbohydrate. Plasma free fatty acid andcholesterol levels are reduced.
3. Respiration The effects are dose depen-dent. At antiinflammatory doses, respiration isstimulated by peripheral (increased CO2 produc-tion) as well as central (increased sensitivity ofrespiratory centre to CO2) actions. Hyperventila-tion is prominent in salicylate poisoning. Furtherrise in salicylate level causes respiratorydepression; death is due to respiratory failure.

196S
EC
TIO
N3
AUTACOIDS AND RELATED DRUGS
4. Acid-base and electrolyte balance Usualanalgesic doses (0.3–1.0 g) have practicallyno effect. Antiinflammatory doses producesignificant changes in the acid-base and electrolytecomposition of body fluids. Initially, respiratorystimulation predominates and tends to wash outCO2 despite increased production → respiratoryalkalosis, which is compensated by increased renalexcretion of HCO3̄ (with accompanying Na+, K+
and water). Most adults treated with 4–5 g/dayof aspirin stay in a state of compensatedrespiratory alkalosis.
Still higher doses cause respiratory depres-sion with CO2 retention, while excess CO2 pro-duction continues → respiratory acidosis. To thisare added dissociated salicylic acid as well asmetabolic acids (lactic, pyruvic, acetoacetic) whichare produced in excess + metabolically derivedsulfuric and phosphoric acid which are retaineddue to depression of renal function. All thesecombine to cause uncompensated metabolicacidosis since plasma HCO3¯ is already low. Mostchildren manifest this phase during salicylatepoisoning; while in adults it is seen in late stagesof poisoning only.
Dehydration occurs in poisoning due to increa-sed water loss in urine (to accompany Na+, K+
and HCO3̄ ) increased sweating and hyperventi-lation.
5. CVS Aspirin has no direct effect on heartor blood vessels in therapeutic doses. Larger dosesincrease cardiac output to meet the increasedperipheral O2 demand, and cause direct vaso-dilatation. Toxic doses depress vasomotor centre:BP may fall. Because of increased cardiac workas well as Na+ and water retention, CHF may beprecipitated in patients with low cardiac reserve.
6. GIT Aspirin and released salicylic acid irri-tate gastric mucosa → cause epigastric distress,nausea and vomiting. It also stimulates CTZ:vomiting that occurs at higher doses has a centralcomponent as well.
Aspirin (pKa 3.5) remains unionized anddiffusible in the acid gastric juice, but on enteringthe mucosal cell (pH 7.1) it ionizes and becomes
indiffusible. This ‘ion trapping’ in the gastricmucosal cell enhances gastric toxicity. Further,aspirin particle coming in contact with gastricmucosa promotes local back diffusion of acid →focal necrosis of mucosal cells and capillaries→ acute ulcers, erosive gastritis, congestion andmicroscopic haemorrhages. The occult blood lossin stools is increased by even a single tablet ofaspirin. Blood loss averages 5 ml/day at anti-inflammatory doses. Haematemesis occursoccasionally: may be an idiosyncratic reaction.
Soluble aspirin tablets containing calcium car-bonate + citric acid and other buffered prepa-rations are less liable to cause gastric irritation,but incidence of ulceration and bleeding is notsignificantly lowered.
7. Urate excretion Dose-related effect isseen:
< 2 g/day—urate retention and antagonism ofall other uricosuric drugs.2–5 g/day—variable effects, often no change.> 5 g/day—increased urate excretion.
Aspirin is not suitable for use in chronic gout.
8. Blood Aspirin, even in small doses, irrever-sibly inhibits TXA2 synthesis by platelets. Thus,it interferes with platelet aggregation and blee-ding time is prolonged to nearly twice the normalvalue. This effect lasts for about a week (turnovertime of platelets).
Long-term intake of large dose decreases syn-thesis of clotting factors in liver and predisposesto bleeding. This can be prevented by prophylacticvit K therapy.
PHARMACOKINETICSAspirin is absorbed from the stomach and smallintestines. Its poor water solubility is the limitingfactor in absorption: microfining the drug-particlesand inclusion of an alkali (solubility is more athigher pH) enhances absorption. However, higherpH also favours ionization, thus decreasing thediffusible form.
Aspirin is rapidly deacetylated in the gutwall, liver, plasma and other tissues to releasesalicylic acid which is the major circulating

197C
HA
PTE
R14
NSAIDs AND ANTIPYRETIC-ANALGESICS
and active form. It is ~80% bound to plasmaproteins and has a volume of distribution ~0.17L/kg. Entry into brain is slow, but aspirin freelycrosses placenta. Both aspirin and salicylic acidare conjugated in liver with glycine to formsalicyluric acid (major pathway). They are alsoconjugated with glucuronic acid. Few other minormetabolites are also produced. The metabolitesare excreted by glomerular filtration and tubularsecretion. Normally, only 1/10th is excreted asfree salicylic acid, but this can be increased byalkalinization.
The plasma t½ of aspirin as such is 15–20min, but taken together with that of releasedsalicylic acid, it is 3–5 hours. However, metabolicprocesses get saturated over the therapeutic range;t½ of antiinflammatory doses may be 8–12 hourswhile that during poisoning may be as high as30 hours. Thus, elimination is dose dependent.
ADVERSE EFFECTS
(a) Side effects that occur at analgesic dose(0.3–1.5 g/day) are nausea, vomiting, epigastricdistress, increased occult blood loss in stools. Themost important adverse effect of aspirin is gastricmucosal damage and peptic ulceration.
(b) Hypersensitivity and idiosyncrasy Thoughinfrequent, these can be serious. Reactions includerashes, fixed drug eruption, urticaria, rhinorrhoea,angioedema, asthma and anaphylactoid reaction.Profuse gastric bleeding occurs in rare instances.
(c) Antiinflammatory doses (3–5 g/day)produce the syndrome called salicylism—dizzi-ness, tinnitus, vertigo, reversible impairment ofhearing and vision, excitement and mental con-fusion, hyperventilation and electrolyte imbalance.The dose has to be titrated to one which is justbelow that producing these symptoms; tinnitusis a good guide.
Aspirin therapy in children with rheumatoidarthritis has been found to raise serum transami-nases, indicating liver damage. Most cases areasymptomatic but it is potentially dangerous. Anassociation has been noted between salicylate
therapy and ‘Reye’s syndrome’, a rare form ofhepatic encephalopathy seen in children havingviral (varicella, influenza) infection.
In adults also, long-term therapy with highdose aspirin can cause insidious onset hepaticinjury. Salt and water retention occurs in a doserelated manner.
(d) Acute salicylate poisoning It is more com-mon in children. Fatal dose in adults is estimatedto be 15–30 g, but is considerably lower in chil-dren. Serious toxicity is seen at serum salicylatelevels > 50 mg/dl. Manifestations are:
Vomiting, dehydration, electrolyte imbalance,acidotic breathing, hyper/hypoglycaemia,petechial haemorrhages, restlessness, delirium,hallucinations, hyperpyrexia, convulsions,coma and death due to respiratory failure +cardiovascular collapse.
Treatment is symptomatic and supportive. Mostimportant is external cooling and i.v. fluid withNa+, K+, HCO3̄ and glucose: according to needdetermined by repeated monitoring. Gastric lavageto remove unabsorbed drug; alkaline diuresis orhaemodialysis to remove absorbed drug is indicatedin severe cases. Blood transfusion and vit K shouldbe given if bleeding occurs.
Precautions and contraindications• Aspirin is contraindicated in patients who are
sensitive to it and in peptic ulcer, bleedingtendencies, in children suffering from chickenpox or influenza. Due to risk of Reye’ssyndrome pediatric formulations of aspirin areprohibited in India and the UK.
• Cautious use in chronic liver disease: casesof hepatic necrosis have been reported.
• It should be avoided in diabetics, in those withlow cardiac reserve or frank CHF and injuvenile rheumatoid arthritis.
• Aspirin should be stopped 1 week beforeelective surgery.
• Given chronically during pregnancy it may beresponsible for low birth weight babies.Delayed or prolonged labour, greater

198S
EC
TIO
N3
AUTACOIDS AND RELATED DRUGS
postpartum blood loss and premature closureof ductus arteriosus are possible if aspirin istaken at or near term.
• It should be avoided by breastfeeding mothers.• Avoid high doses in G-6PD deficient
individuals—haemolysis can occur.
Interactions1. Aspirin displaces warfarin, naproxen, sulfonyl-ureas, phenytoin and methotrexate from bindingsites on plasma proteins: toxicity of these drugsmay occur. Its antiplatelet action increases therisk of bleeding in patients on oral anticoagu-lants.2. Aspirin at analgesic doses inhibits tubularsecretion of uric acid and antagonizes uricosuricaction of probenecid. Tubular secretion of metho-trexate is also interfered.3. Aspirin blunts diuretic action of furosemideand thiazides and reduces K+ conserving actionof spironolactone. Competition between canrenone(active metabolite of spironolactone) and aspirinfor active transport in proximal tubules has beendemonstrated.4. Aspirin reduces protein bound iodine levelsby displacement of thyroxine; but hypothyroidismdoes not occur.
USES
1. As analgesic For headache (including mildmigraine), backache, myalgia, joint pain, pulledmuscle, toothache, neuralgias and dysmenorrhoea;
it is effective in low doses (0.3–0.6 g 6–8 hourly).Analgesic effect is maximal at ~ 1000 mg (singledose).
2. As antipyretic Aspirin is effective in feverof any origin; dose is same as for analgesia.However, paracetamol, being safer, is generallypreferred. Antipyretics are not useful in fever dueto heat stroke; only external cooling lowers bodytemperature.
3. Acute rheumatic fever Aspirin is the firstdrug to be used in all cases; other drugs are addedor substituted only when it fails or in severe cases(corticosteroids act faster). In a dose of 4–5 gor 75–100 mg/kg/day (in divided portions produ-cing steady state serum salicylate concentration15–30 mg/dl) it brings about marked symptomaticrelief in 1–3 days. Dose reduction may be startedafter 4–7 days and maintenance doses (50 mg/kg/day) are continued for 2–3 weeks or till signsof active disease (raised ESR) persist. Withdrawalshould be gradual over the next 2 weeks.
Granulomatous lesions, nodules, cardiaccomplications, valvular defects, chorea andduration of disease are not altered by salicylatetherapy.
4. Rheumatoid arthritis Aspirin in a dose of3–5 g/day is effective in most cases; producesrelief of pain, swelling and morning stiffness, butprogress of the disease process is not affected.Since large doses of aspirin are poorly toleratedfor long periods it is rarely used now; otherNSAIDs are preferred.
Adverse effects of NSAIDs
GastrointestinalNausea, anorexia, gastric irritation, erosions, pepticulceration, gastric bleeding/perforation, esophagitis
RenalNa+ and water retention, chronic renal failure,nephropathy, papillary necrosis (rare)
CVSRise in BP, risk of myocardial infarction (especiallywith COX-2 inhibitors)
HepaticRaised transaminases, hepatic failure (rare)
CNSHeadache, mental confusion, vertigo, behaviouraldisturbances, seizure precipitation
HaematologicalBleeding, thrombocytopenia, haemolytic anaemia,agranulocytosisOthersAsthma exacerbation, rhinitis, nasal polyposis, skinrashes, pruritus, angioedema

199C
HA
PTE
R14
NSAIDs AND ANTIPYRETIC-ANALGESICS
5. Osteoarthritis It affords symptomatic reliefonly; may be used on ‘as and when required’basis, but paracetamol is the first choice analgesicfor most cases.
6. Postmyocardial infarction and poststrokepatients By inhibiting platelet aggregationaspirin lowers the incidence of reinfarction. TXA2
synthesis in platelets is inhibited at low doses. Ithas been argued that high doses can reverse thebeneficial effects by concurrently inhibiting PGI2
(antiaggregatory and vasodilatory) synthesis invessel wall. Large studies have demonstrated thataspirin 60–100 mg/day reduces the incidence ofmyocardial infarction (MI): it is now routinelyprescribed to post-infarct patients. Someauthorities recommend it for primary prophylaxisas well, but the risk of bleeding has to be weighedagainst the possible benefit. ‘New onset’ or‘sudden worsening’ angina is associated with highinfarction rate. This can be reduced to half by100–150 mg aspirin per day for 12 weeks.
Aspirin reduces ‘transient ischaemic attacks’and lowers incidence of stroke in such patients.But the risk of stroke in post-MI patients is notreduced.
7. Other less well established uses of aspirin are:(a) Pregnancy-induced hypertension and pre-eclampsia:imbalance between TXA2 and PGI2 is believed to be involved:aspirin 80–100 mg/day benefits many cases by selectivelysuppressing TXA2 production.(b) Patent ductus arteriosus: aspirin can bring about closureand avoid surgery.
(c) Familial colonic polyposis: aspirin and other NSAIDssuppress polyp formation and afford symptomatic relief inthis rare disorder.(d) Prevention of colon cancer: incidence of colon canceramong regular aspirin users is much lower. Colonic tumoursexpress large quantities of COX-2. However, the rofecoxibtrial (APPROVE) was prematurely terminated and the drugwithdrawn due to increased incidence of cardiovascularevents. The Adenoma Prevention with Celecoxib (APC) trialhas also been terminated due to 2.5 fold increase in riskof major fatal/nonfatal cardiovascular events.(e) To prevent flushing attending nicotinic acid ingestion,which is due to PGD2 release in the skin.
ASPIRIN 350 mg tab, COLSPRIN 100, 325 mg tabs,ECOSPRIN 75, 150, 325 mg tabs, DISPRIN 350 mg tab (withcal. carbonate 105 mg + citric acid 35 mg), LOPRIN 75, 162.5mg tabs.An injectable preparation has also been made available;BIOSPIRIN: Lysine acetylsalicylate 900 mg + glycine 100 mg/vial for dissolving in 5 ml water and i.v. injection.
Other salicylates (salicylamide, benorylate, diflunisal) are notin use.
PROPIONIC ACID DERIVATIVESIbuprofen was the first member of this class tobe introduced in 1969 as a better tolerated alter-native to aspirin. Many others have followed. Allhave similar pharmacodynamic properties butdiffer considerably in potency and to some extentin duration of action (Table 14.2).
Drug interactions with NSAIDs
Pharmacodynamic
Diuretics : ↓ diuresisβ blocker : ↓ antihypertensive effectACE inhibitors : ↓ antihypertensive effectAnticoagulants : ↑ risk of g.i. bleedSulfonylureas : ↑ risk of hypoglycaemiaAlcohol : ↑ risk of g.i. bleedCyclosporine : ↑ nephrotoxicityCorticosteroids : ↑ risk of g.i. bleedSelective serotoninreuptake inhibitors : ↑ risk of g.i. bleed
Pharmacokinetic
Oral anticoagulants MetabolismSulfonylureas inhibited;Phenytoin competitionValproate for plasma protein binding
Digoxin ↓ RenalLithium excretion ofAminoglycosides interacting drugMethotrexate
Comorbid conditions aggravated by NSAIDs
• Peptic ulcer• Hypertension• Congestive heart failure• Renal insufficiency• Hemostatic disorders

200S
EC
TIO
N3
AUTACOIDS AND RELATED DRUGS
TABLE 14.2 Dosage and preparations of propionic acid derivatives
Drug Plasma t½ Dosage Preparations
1. Ibuprofen 2-4 hr 400–600 mg BRUFEN, EMFLAM, IBUSYNTH 200, 400, 600 mg(5–10 mg/kg) TDS tab, IBUGESIC also 100 mg/5 ml susp.
2. Naproxen 12–16 hr 250 mg BD– NAPROSYN, NAXID, ARTAGEN, XENOBIDTDS 250 mg tab., NAPROSYN also 500 mg tab.
3. Ketoprofen 2–3 hr 50–100 mg KETOFEN 50, 100 mg tab; OSTOFEN 50 mg cap.BD–TDS RHOFENID 100 mg tab, 200 mg SR tab;
100 mg/2 ml amp.
4. Flurbiprofen 4–6 hr 50 mg BD–QID ARFLUR 50, 100 mg tab, 200 mg SR tab,FLUROFEN 100 mg tab.
The analgesic, antipyretic and antiinflam-matory efficacy is rated somewhat lower than highdose of aspirin. All members inhibit PG synthesis,naproxen being the most potent; but their in vitropotency to inhibit COX does not closely parallelin vivo antiinflammatory potency. Inhibition ofplatelet aggregation is short-lasting with ibuprofen,but longer lasting with naproxen.
Adverse effects Ibuprofen and all its congenersare better tolerated than aspirin. Side effects aremilder and their incidence is lower.Gastric discomfort, nausea and vomiting, thoughless than aspirin or indomethacin, are still themost common side effects. Gastric erosion andoccult blood loss are rare.CNS side effects include headache, dizziness,blurring of vision, tinnitus and depression.Rashes, itching and other hypersensitivity phe-nomena are infrequent. However, these drugsprecipitate aspirin-induced asthma.Fluid retention is less marked.They are not to be prescribed to pregnant womenand should be avoided in peptic ulcer patient.Pharmacokinetics and interactions All arewell absorbed orally, highly bound to plasmaproteins (90–99%), but displacement interactionsare not clinically significant—dose of oral anti-coagulants and oral hypoglycaemics need not bealtered. Because they inhibit platelet function, usewith anticoagulants should, nevertheless, beavoided. Similar to other NSAIDs, they are likelyto decrease diuretic and antihypertensive action ofthiazides, furosemide and β blockers.
All propionic acid derivatives enter brain,synovial fluid and cross placenta. They are largelymetabolized in liver by hydroxylation and glucu-ronide conjugation and excreted in urine as wellas bile.
Uses1. Ibuprofen is used as a simple analgesic andantipyretic in the same way as low dose of aspirin.It is particularly effective in dysmenorrhoea inwhich the action is clearly due to PG synthesisinhibition. It is available as an ‘over-the-counter’drug.2. Ibuprofen and its congeners are widely usedin rheumatoid arthritis, osteoarthritis and othermusculoskeletal disorders, especially where painis more prominent than inflammation.3. They are indicated in soft tissue injuries,fractures, vasectomy, tooth extraction, postpartumand postoperatively: suppress swelling and inflam-mation.Ibuprofen It has been rated as the safesttraditional NSAID by the spontaneous adversedrug reaction reporting system in U.K. Ibuprofen(400 mg) has been found equally or more efficaciousthan a combination of aspirin (650 mg) + codeine(60 mg) in relieving dental surgery pain, but isa weaker antiinflammatory; not suitable for acutegout and other similar conditions.
Concurrent treatment with ibuprofen has been foundto prevent irreversible COX inhibition by low dose aspirinby reversibly occupying the active serine residue ofCOX-1 and protecting it from irreversible acetylation byaspirin. Thus, the antiplatelet action of ibuprofen is short

201C
HA
PTE
R14
NSAIDs AND ANTIPYRETIC-ANALGESICS
lasting and it antagonizes the antiplatelet and cardioprotectiveeffect of low dose aspirin.
Naproxen The antiinflammatory activity isstronger and it is particularly potent in inhibitingleucocyte migration—may be more valuable inacute gout: dose 750 mg stat followed by 250mg 8 hourly till attack subsides. It is also recom-mended for rheumatoid arthritis and ankylosingspondylitis. Because of longer t½ regular use caneffectively suppress platelet function. Naproxencarries lower thrombotic risk than diclofenac,etoricoxib, etc. Dose should be reduced in theelderly.
Naproxen is marketed as active single S(–) enantiomerpreparation, which poses less renal burden. However, someR(+) enantiomer is formed in vivo due to inversion.
Ketoprofen An additional action to stabilizelysosomes and inhibit LOX has been demons-trated with ketoprofen; though antiinflammatoryefficacy is similar to ibuprofen, and side effectsare more.
Flurbiprofen more effective than ibuprofen,but gastric side effects are also more. It is usedas an ocular antiinflammatory as well.OCUFLUR, FLUR, FLURBIN, 0.03% eyedrops, 1 drop 6hourly.
Choice among different propionic acid derivativesis difficult; naproxen is probably more efficaciousand better tolerated in antiinflammatory doses.It is longer acting and has the advantage of twicedaily dosing. However, individuals vary in theirpreference for different members.
FENAMATE (Anthranilic acid derivative)
Mephenamic acid An analgesic, antipyreticand weaker antiinflammatory drug, which inhi-bits synthesis of PGs as well as antagonises someof their actions. Mephenamic acid exerts peri-pheral as well as central analgesic action.
Adverse effects Diarrhoea is the most impor-tant dose-related side effect. Epigastric distressis complained, but gut bleeding is not significant.Skin rashes, dizzines and other CNS manifesta-tions have occurred. Haemolytic anaemia is a rarebut serious complication.
Pharmacokinetics Oral absorption is slow butalmost complete. It is highly bound to plasmaproteins—displacement interactions can occur;partly metabolized and excreted in urine as wellas bile. Plasma t½ is 2–4 hours.
Uses Mephenamic acid is indicated primarilyas analgesic in muscle, joint and soft tissue painwhere strong antiinflammatory action is notneeded. It is quite effective in dysmenorrhoea.It may be useful in some cases of rheumatoidand osteoarthritis but has no distinct advantage.Dose: 250–500 mg TDS; MEDOL 250, 500 mg cap; MEFTAL250, 500 mg tab, 100 mg/5 ml susp.PONSTAN 125, 250, 500 mg tab, 50 mg/ml syrp.
ENOLIC ACID DERIVATIVES (Oxicams)
Piroxicam It is a long-acting potent NSAIDwith antiinflammatory potency similar to indo-methacin and good analgesic-antipyretic action.It is a nonselective, reversible inhibitor of COX;lowers PG concentration in synovial fluid andinhibits platelet aggregation—prolonging bleedingtime. In addition, it decreases the production ofIgM rheumatoid factor and leucocyte chemotaxis.Thus, it can inhibit inflammation in diverseways.
Pharmacokinetics It is rapidly and completelyabsorbed: 99% plasma protein bound; largelymetabolized in liver by hydroxylation and glucu-ronide conjugation; excreted in urine and bile;enterohepatic cycling occurs. Plasma t½ is long—nearly 2 days. Steady-state concentrations areachieved in a week. Single daily administrationis sufficient.
Adverse effects The g.i. side effects are morethan ibuprofen, but it is better tolerated and lessulcerogenic than indomethacin; causes less faecalblood loss than aspirin. Rashes and pruritus areseen in < 1% patients, but serious skin reactionsare possible. Edema and reversible azotaemia havebeen observed.
Uses Due to slow onset of action piroxicamis suitable for use as long-term antiinflam-matory drug in rheumatoid and osteo-arthritis,

202S
EC
TIO
N3
AUTACOIDS AND RELATED DRUGS
ankylosing spondylitis, etc., but is not a first choicedrug for any condition because of relatively highertoxicity. It has also been used for acute gout,musculoskeletal injuries and in dentistry.Dose: 20 mg BD for two days followed by 20 mg OD:DOLONEX, PIROX 10, 20 mg cap, 20 mg dispersible tab,20 mg/ml inj in 1 and 2 ml amps; PIRICAM 10, 20 mgcap.
Tenoxicam A congener of piroxicam withsimilar properties and uses.TOBITIL 20 mg tab; dose 20 mg OD.
ACETIC ACID DERIVATIVES
Ketorolac This arylacetic acid NSAID haspotent analgesic but modest antiinflammatoryactivity. In postoperative pain it has equalled theefficacy of morphine, but does not interact withopioid receptors and is free of opioid side effects.Like other NSAIDs, it inhibits PG synthesis andrelieves pain primarily by a peripheral mechanism.In short-lasting pain, it has compared favourablywith aspirin.
Ketorolac is rapidly absorbed after oral andi.m. administration. It is highly plasma proteinbound and 60% excreted unchanged in urine.Major metabolic pathway is glucuronidation;plasma t½ is 5–7 hours.
Adverse effects Nausea, abdominal pain, dys-pepsia, ulceration, loose stools, drowsiness,headache, dizziness, nervousness, pruritus, painat injection site, rise in serum transaminase andfluid retention have been noted.
Ketorolac has been used concurrently withmorphine to keep its dose low. However, it shouldnot be given to patients on anticoagulants.
Use Ketorolac is frequently used in postopera-tive, dental and acute musculoskeletal pain: 15–30 mg i.m. or i.v. every 4–6 hours (max. 90 mg/day). It may also be used for renal colic, migraineand pain due to bony metastasis.
Orally it is used in a dose of 10–20 mg 6hourly for short-term management of moderatepain. Ketorolac has been rated superior to aspirin(650 mg), paracetamol (600 mg) and equivalentto ibuprofen (400 mg). Continuous use for more
than 5 days is not recommended. It should notbe used for preanaesthetic medication or forobstetric analgesia. Topical ketorolac is quitepopular for noninfective ocular conditions.KETOROL, ZOROVON, KETANOV, TOROLAC 10 mg tab,30 mg in 1 ml amp.KETLUR, ACULAR 0.5% eye drops; 1–2 drops 2–4 times aday for noninfective ocular inflammatory conditions.
Indomethacin This indole acetic acidderivative is a potent antiinflammatory drug withprompt antipyretic action. Indomethacin relievesonly inflammatory or tissue injury related pain.It is a highly potent inhibitor of PG synthesisand suppresses neutrophil motility. In toxic dosesit uncouples oxidative phosphorylation (likeaspirin).
Pharmacokinetics Indomethacin is well absor-bed orally, rectal absorption is slow but depen-dable. It is 90% bound to plasma proteins, partlymetabolized in liver to inactive products andexcreted by kidney. Plasma t½ is 2–5 hours.
Adverse effects A high incidence (up to 50%)of gastrointestinal and CNS side effects is pro-duced.Gastric irritation, nausea, anorexia, gastricbleeding and diarrhoea are prominent.Frontal headache (very common), dizziness,ataxia, mental confusion, hallucination, depres-sion and psychosis can occur.Leukopenia, rashes and other hypersensitivityreactions are also reported.Increased risk of bleeding due to decreased plateletaggregability.It is contraindicated in machinery operators,drivers, psychiatric patients, epileptics, kidneydisease, pregnant women and in children.Dose: 25–50 mg BD-QID. Those not tolerating the drug orallymay be given nightly suppository.IDICIN, INDOCAP 25 mg cap, 75 mg SR cap, ARTICID 25,50 mg cap, INDOFLAM 25, 75 mg caps, 1% eye drop.RECTICIN 50 mg suppository.
Uses Because of prominent adverse effects,indomethacin is used as a reserve drug inconditions requiring potent antiinflammatoryaction like ankylosing spondylitis, acute exacer-bations of destructive arthropathies, psoriatic

203C
HA
PTE
R14
NSAIDs AND ANTIPYRETIC-ANALGESICS
arthritis and acute gout or rheumatoid arthritisthat are not responding to better tolerated NSAIDs.
Malignancy associated fever refractory toother antipyretics may respond to indomethacin.It has been the most common drug used formedical closure of patent ductus arteriosus: three12 hourly i.v. injections of 0.1–0.2 mg/kg achieveclosure in majority of cases.
Bartter’s syndrome responds dramatically, asit does to other PG synthesis inhibitors.
Nabumetone It is a prodrug—generates anactive metabolite (6-MNA) which inhibits bothCOX-1 and COX-2. It possesses analgesic, anti-pyretic and antiinflammatory activities; effectivein the treatment of rheumatoid and osteo-arthritisas well as in soft tissue injury. Nabumetone hascaused a lower incidence of gastric erosions, ulcersand bleeding, probably because the active COXinhibitor is produced in the tissues after absorption.However, abdominal cramps and diarrhoea canoccur, and there is no data on its relative sideeffect prevalence compared to other NSAIDs. Theplasma t½ is 24 hours.NABUFLAM 500 mg tab; 1 tab OD.
PYRAZOLONESAntipyrine (phenazone) and amidopyrine (aminopyrine)were introduced in 1884 as antipyretic and analgesic. Theiruse was associated with high incidence of agranulocytosis:are banned globally. Phenylbutazone was introduced in 1949and soon its active metabolite oxyphenbutazone was alsomarketed. These two are potent antiinflammatory drugs, inhibitCOX, but have slow onset, weak analgesic and antipyreticaction. Their gastric toxicity is high; edema due to Na+ andwater retention is frequent and CNS side effects, hypersen-sitivity reactions, hypothyroidism are reported. They have goneout of use due to residual risk of bone marrow depression andother toxicity. Two other pyrazolones available in India—meta-mizol and propiphenazone are primarily used as analgesic andantipyretic.
Metamizol (Dipyrone) In contrast to phenyl-butazone, this derivative of amidopyrine is apotent and promptly acting analgesic andantipyretic but poor antiinflammatory and noturicosuric. It can be given orally, i.m. as well asi.v, but gastric irritation, pain at injection siteoccurs. Occasionally, i.v. injection producesprecipitous fall in BP.
Few cases of agranulocytosis were reportedand metamizol is banned in the USA and someEuropean countries. However, it has beenextensively used in India and other Europeancountries. Adverse reaction data collected overfour decades shows that risk of serious toxicitywith this drug is lower than with aspirin ormany other NSAIDs. However, its fixed dosecombination with antispasmodics is banned inIndia.Dose: 0.5–1.5 g oral/i.m./i.v.; ANALGIN 0.5 g tab; NOVALGIN,BARALGAN 0.5 g tab, 0.5 g/ml in 2 ml and 5 ml amps;ULTRAGIN 0.5 g/ml inj in 2 ml amp and 30 ml vial.
Propiphenazone Another pyrazolone, similarin properties to metamizol; claimed to be bettertolerated. Agranulocytosis has not been reported.Dose: 300–600 mg TDS; marketed only in combination inseveral ‘over-the-counter’, preparations—in SARIDON,ANAFEBRIN: propiphenazone 150 mg + paracetamol 250 mgtab.DART: propiphenazone 150 mg + paracetamol 300 mg +caffeine 50 mg tab.
PREFERENTIAL COX-2 INHIBITORS
Nimesulide This NSAID is a relatively weakinhibitor of PG synthesis and moderately COX-2 selective. Antiinflammatory action may beexerted by other mechanisms as well, e.g. reducedgeneration of superoxide by neutrophils, inhibitionof PAF synthesis and TNFa release, free radicalscavanging, inhibition of metalloproteinase acti-vity in cartilage. The analgesic, antipyretic andantiinflammatory activity of nimesulide has beenrated comparable to other NSAIDs. It has beenused primarily for short-lasting painful inflam-matory conditions like sports injuries, sinusitisand other ear-nose-throat disorders, dental surgery,bursitis, low backache, dysmenorrhoea,postoperative pain, osteoarthritis and for fever.
Nimesulide is almost completely absorbedorally, 99% plasma protein bound, extensivelymetabolized and excreted mainly in urine witha t½ of 2–5 hours.
Adverse effects of nimesulide are gastrointes-tinal (epigastralgia, heart burn, nausea, loosemotions), dermatological (rash, pruritus) and

204S
EC
TIO
N3
AUTACOIDS AND RELATED DRUGS
central (somnolence, dizziness). Gastric tolera-bility of nimesulide is better, though ulcercomplications are as prevalent as with otherNSAIDs. Instances of fulminant hepatic failurehave been associated with nimesulide and it hasbeen withdrawn in Spain, Ireland, Singapore andTurkey; use in children is banned in Portugal, Israeland now in India as well. A Finish committee forproprietary medicinal products has concluded thathepatic reactions to nimesulide are similar to otherNSAIDs. Considering that it has not been marketedin many countries like the UK, USA, Australia,Canada, the overall safety of this drug, especiallyin children, has been questioned. However, mostasthmatics and those who develop bronchospasmor intolerance to aspirin and other NSAIDs donot cross react with nimesulide. Its specificusefulness appears to be only in such patients.Dose: 100 mg BD; NIMULID, NIMEGESIC, NIMODOL100 mg tab, 50 mg/5 ml susp.
Diclofenac sodium An analgesic-antipyretic-antiinflammatory drug, similar in efficacy tonaproxen. It inhibits PG synthesis and is some-what COX-2 selective. The antiplatelet action isnot appreciable due to sparing of COX-1. It alsodoes not block the cordioprotective effect of lowdose aspirin. Neutrophil chemotaxis and super-oxide production at the inflammatory site arereduced.
It is well absorbed orally, 99% protein bound,metabolized and excreted both in urine and bile.The plasma t½ is ~2 hours. However, it has goodtissue penetrability and concentration in synovialfluid is maintained for 3 times longer period thanin plasma, exerting extended therapeutic actionin joints.
Adverse effects of diclofenac are generally mild:epigastric pain, nausea, headache, dizziness,rashes. Gastric ulceration and bleeding are lesscommon. Some comparative trials have found itsgastric toxicity to be similar to celecoxib andetoricoxib. Like many NSAIDs, diclofenac canincrease the risk of heart attack and stroke.Reversible elevation of serum amino-transferaseshas been reported more commonly; kidney damageis rare.
Diclofenac is among the most extensivelyused NSAID; employed in rheumatoid andosteoarthritis, bursitis, ankylosing spondylitis,toothache, dysmenorrhoea, renal colic, post-traumatic and postoperative inflammatoryconditions—affords quick relief of pain andwound edema.Dose: 50 mg TDS, then BD oral, 75 mg deep i.m. VOVERAN,DICLONAC, MOVONAC 50 mg enteric coated tab, 100mg S.R. tab, 25 mg/ml in 3 ml amp. for i.m. inj. DICLOMAX25, 50 mg tab, 75 mg/3 ml inj.Diclofenac potassium: VOLTAFLAM 25, 50 mg tab, ULTRA-K 50 mg tab; VOVERAN 1% topical gel.DICLONAC, VOVERAN OPHTHA 0.1% eye drops.
Aceclofenac A moderately COX-2 selectivecongener of diclofenac having similar properties.Enhancement of glycosaminoglycan synthesis mayconfer chondroprotective property to aceclofenac.Dose: 100 mg BD; ACECLO, DOLOKIND 100 mg tab, 200mg SR tab.
Meloxicam This newer congener of piroxicamhas a COX-2/COX-1 selectivity ratio of about 10.Since measurable inhibition of platelet TXA2
production (a COX-1 function) occurs at thera-peutic doses of meloxicam, it has been labelled‘preferential COX-2 inhibitor’. Efficacy ofmeloxicam in osteo- and rheumatoid arthritis iscomparable to piroxicam. Plasma t½ is 15–20 hourspermiting single daily dose. In short-term studies,gastric changes with the lower dose (7.5 mg/day)were found to be similar to placebo, but at thehigher dose (15 mg/day) they were intermediatebetween placebo and piroxicam. Gastric sideeffects of meloxicam are milder, but ulcer compli-cations (bleeding, perforation) have been reportedon long-term use. There is no convincing evidencethat meloxicam is safer than other NSAIDs.Dose: 7.5–15 mg OD; MELFLAM, MEL-OD, MUVIK, M-CAM 7.5 mg, 15 mg tabs.
Etodolac This newer indole-acetic acid NSAIDis moderately COX-2 selective with propertiessimilar to diclofenac. At lower doses, gastrictolerance is better than older NSAIDs. It ismetabolized by hydroxylation and glucuronideconjugation, and excreted in urine with a t½ of7 hours. Postoperative analgesia with etodolaclasts for 6–8 hours. Side effects are abdominal

205C
HA
PTE
R14
NSAIDs AND ANTIPYRETIC-ANALGESICS
pain, rashes and dizziness. It is approved for usein osteo- and rheumatoid arthritis as well as inacute musculoskeletal pain.Dose: 200–400 mg BD–TDS; ETOVA 200, 300, 400 mg tabs.
SELECTIVE COX-2 INHIBITORS (Coxibs)
Because of the theoretical advantage of inhibitingCOX-2 without affecting COX-1 function, somehighly selective COX-2 inhibitors have beenintroduced over the past 2 decades. They causeless gastric mucosal damage; occurrence of pepticulcer and ulcer bleeds is clearly lower than withtraditional NSAIDs. They do not depress TXA2
production by platelets (COX-1 dependent); donot inhibit platelet aggregation or prolong bleedingtime, but reduce PGI2 production by vascularendothelium.
Currently, 3 selective COX-2 inhibitors (alsocalled coxibs) Celecoxib, Etoricoxib and
Parecoxib are available in India. Rofecoxib andValdecoxib were withdrawn within few years ofmarketing for increasing cardiovascular (CV) risk.Lumiracoxib marketed only in Europe has beensuspended due to hepatotoxicity.
It has been concluded that selective COX-2inhibitors should be used only in patients at highrisk of peptic ulcer, perforation or bleeds. Ifselected, they should be administered in the lowestdose for the shortest period of time. Moreover,they should be avoided in patients with historyof ischaemic heart disease/hypertension/cardiacfailure/cerebrovascular disease, who are pre-disposed to CV events. Combination of low-doseaspirin with COX-2 inhibitors for reducingcardiovascular risk increases gastroduodenalinjury, and is not advised.
Concerns, other than cardiovascular, have alsobeen expressed about selective COX-2 inhibitors.
Selective COX-2 inhibitors and cardiovascular risk
COX-2 inhibitors reduce endothelial PGI2 productionwithout affecting platelet TXA2 synthesis. This appearsto exert prothrombotic influence and enhance CV risk.• VIGOR (VIOXX gastrointestinal outcomes research)
study in over 8000 patients found 4-fold higherincidence of myocardial infarction (MI) in rofecoxib(VIOXX) recipients compared to those on naproxen.
• APPROVE (adenomatous polyp prevention onVIOXX) a placebo controlled trial among subjectswith history of colorectal adenomas was stoppedprematurely at 3 years because it confirmed higherrisk of heart attack and stroke: rofecoxib waswithdrawn globally in 2004.
• A metaanalysis of 18 trials with rofecoxib formusculoskeletal disorders has also inferred thatit increases incidence of MI.
• Valdecoxib increased occurrence of MI in patientsundergoing coronary bypass surgery. There werereports of severe skin reactions as well. It waswithdrawn in 2005.
• Though CLASS (celecoxib long-term safety study)did not find any increase in CV events, the APC(adenoma prevention with celecoxib) trial has beenterminated prematurely due to 2.5 fold higher riskof the same.
• There is no clear evidence as yet that etoricoxibalso increases CV risk.
• A joint committee in USA (2005) has concludedthat enough evidence to withdraw all selective COX-2 inhibitors is lacking, but that their labelling shouldinclude a warning of CV risk.
Other concerns with selective COX-2 inhibitors
• COX-1 generated PGs may also play a role ininflammation: COX-2 inhibitors may not have asbroad range of efficacy as traditional NSAIDs.
• Ulcer injury and H. pylori induce COX-2 in gastricmucosa, which may contribute to gastroprotectivePG synthesis; COX-2 inhibition may delay ulcerhealing. Moreover, part of gastric mucosal COX-2 activity may be constitutive.
• Juxtaglomerular COX-2 is constitutive; its inhibitioncan cause salt and water retention; pedal edema,precipitation of CHF and rise in BP can occur withall coxibs.
Celecoxib The COX-2 selectivity of celecoxibis modest and similar to that of diclofenac. Itexerts antiinflammatory, analgesic and antipyreticactions with low ulcerogenic potential.Comparative trials in rheumatoid arthritis havefound it to be as effective as naproxen ordiclofenac, without affecting COX-1 activity ingastroduodenal mucosa. Platelet aggregation inresponse to collagen exposure remained intact incelecoxib recipients and serum TXB2 levels werenot reduced. Though tolerability of celecoxib isbetter than traditional NSAIDs, still abdominalpain, dyspepsia and mild diarrhoea are thecommon side effects. Rashes, edema and a smallrise in BP have also been noted.

206S
EC
TIO
N3
AUTACOIDS AND RELATED DRUGS
Celecoxib is slowly absorbed, 97% plasmaprotein bound and metabolized primarily byCYP2C9 with a t½ of ~10 hours. It is approvedfor use in osteo- and rheumatoid arthritis in adose of 100–200 mg BD.CELACT, REVIBRA, COLCIBRA 100, 200 mg caps.
Etoricoxib This newer COX-2 inhibitor hasthe highest COX-2 selectivity. It is suitable foronce-a-day treatment of osteo/rheumatoid/acutegouty arthritis, ankylosing spondylitis, dysmenor-rhoea, acute dental surgery pain and similarconditions, without affecting platelet function ordamaging gastric mucosa. The t½ is ~ 24 hours.The rate of thrombotic cardiovascular events withetoricoxib use has been found similar to that withdiclofenac. However, it should be considered asa treatment option only as per conditions statedabove for all COX-2 inhibitors (see p. 205). Sideeffects are dyspepsia, abdominal pain, pedaledema, rise in BP, dry mouth, aphthous ulcers,taste disturbance and paresthesias.Dose: 60–120 mg OD; ETOSHINE, TOROCOXIA, ETOXIB,NUCOXIA 60, 90, 120 mg tabs.
Parecoxib It is a prodrug of valdecoxibsuitable for injection, and to be used in post-operative or similar short-term pain, with efficacysimilar to ketorolac. It shares the same risk ofserious cutaneous reactions as valdecoxib. Cautionis needed in its use; it should be stopped at thefirst appearance of a rash.Dose: 40 mg oral/i.m./i.v., repeated after 6–12 hours.REVALDO, VALTO-P 40 mg/vial inj, PAROXIB 40 mg tab.
PARA-AMINO PHENOL DERIVATIVES
Phenacetin introduced in 1887 was extensivelyused as analgesic-antipyretic, but is now bannedbecause it was implicated in analgesic abusenephropathy.
Paracetamol (acetaminophen) the deethylatedactive metabolite of phenacetin, was also
introduced in the last century but has come intocommon use only since 1950.
Actions The central analgesic action of para-cetamol is like aspirin, i.e. it raises pain threshold,but has weak peripheral antiinflammatory compo-nent. Analgesic action of aspirin and paracetamolis additive. Paracetamol is a good and promptlyacting antipyretic.
Paracetamol has negligible antiinflammatoryaction. It is a poor inhibitor of PG synthesis inperipheral tissues, but more active on COX inthe brain. One explanation offered for thediscrepancy between its analgesic-antipyretic andantiinflammatory actions is its inability to inhibitCOX in the presence of peroxides which aregenerated at sites of inflammation, but are notpresent in the brain. The ability of paracetamolto inhibit COX-3 (an isoenzyme so far locatedin dog brain) could also account for its analgesic-antipyretic action.
In contrast to aspirin, paracetamol does notstimulate respiration or affect acid-base balance;does not increase cellular metabolism. It has noeffect on CVS. Gastric irritation is insignificant—mucosal erosion and bleeding occur rarely onlyin overdose. It does not affect platelet functionor clotting factors and is not uricosuric.
Pharmacokinetics Paracetamol is well absor-bed orally, only about 1/4th is protein bound inplasma and it is uniformly distributed in the body.Metabolism occurs mainly by conjugation withglucuronic acid and sulfate: conjugates areexcreted rapidly in urine. Plasma t½ is 2–3 hours.Effects after an oral dose last for 3–5 hours.
Adverse effects In isolated antipyretic dosesparacetamol is safe and well tolerated. Nauseaand rashes occur occasionally, leukopenia is rare.
Acute paracetamol poisoning It occursespecially in small children who have low hepaticglucuronide conjugating ability. If a large dose(> 150 mg/kg or > 10 g in an adult) is taken,serious toxicity can occur. Fatality is commonwith > 250 mg/kg.

207C
HA
PTE
R14
NSAIDs AND ANTIPYRETIC-ANALGESICS
Early manifestations are just nausea, vomi-ting, abdominal pain and liver tenderness withno impairment of consciousness. After 12–18hours centrilobular hepatic necrosis occurs whichmay be accompanied by renal tubular necrosisand hypoglycaemia that may progress to coma.Jaundice starts after 2 days. Further coursedepends on the dose taken. Fulminating hepaticfailure and death are likely if the plasma levelsare above the line joining 200 µg/ml at 4 hoursand 30 µg/ml at 15 hours. If the levels are lower—recovery with supportive treatment is the rule.
Mechanism of toxicity N-acetyl-p-benzoqui-noneimine (NAPQI) is a highly reactive arylatingminor metabolite of paracetamol which isdetoxified by conjugation with glutathione. Whena very large dose of paracetamol is taken,glucuronidation capacity is saturated, more of theminor metabolite is formed—hepatic glutathioneis depleted and this metabolite binds covalentlyto proteins in liver cells (and renal tubules) causingnecrosis. Toxicity thus shows a threshold effectmanifesting only when glutathione is depleted toa critical point.
In chronic alcoholics even 5–6 g taken in oneday can result in hepatotoxicity becausealcoholism induces CYP2E1 that metabolisesparacetamol to NAPQI.
Paracetamol is not recommended in prematureinfants (< 2 kg) for fear of hepatotoxicity.Note: Exercising abundant caution, because paracetamol isan over-the-counter drug, the US-FDA (2009) hasrecommended to reduce the amount of this drug in any singledosage form (tab./cap.) to 650 mg (in place of 1000 mgearlier limit), and the total daily dose for an adult to 2600mg (in place of 4000 mg earlier). The Drugs Controller Generalof India (DCGI) has rcently (2011) issued guidelines to limitthe amount of paracetamol per dosage form (single tab./cap.) to 325 mg.
Treatment If the patient is brought early, vomi-ting should be induced or gastric lavage done.Activated charcoal is given orally or through thetube to prevent further absorption. Other sup-portive measures, as needed, should be taken.Specific: N-acetylcysteine (MUCOMIX, ANTIFEN 200mg/ml inj in 2, 5 ml amps) 150 mg/kg should be infused
i.v. over 15 min, followed by the same dose i.v.over the next 20 hours. Alternatively, 75 mg/kgmay be given orally every 4–6 hours for2–3 days. It replenishes the glutathione storesof liver and prevents binding of the toxicmetabolite to other cellular constituents.
Ingestion-treatment interval is critical; earlierthe better. It is practically ineffective if started16 hours or more after paracetamol ingestion.
Uses Paracetamol is one of the most commonlyused ‘over-the-counter’ analgesic for headache,mild migraine, musculoskeletal pain, dysmenor-rhoea, etc. but is relatively ineffective wheninflammation is prominent as in rheumatoidarthritis. Paracetamol is recommended as firstchoice analgesic for osteoarthritis by manyprofessional bodies. It is one of the best drugsto be used as antipyretic, especially in children(no risk of Reye’s syndrome).
Dose to dose it is equally efficacious as aspirinfor noninflammatory conditions. It is much saferthan aspirin in terms of gastric irritation, ulcerationand bleeding (can be given to ulcer patients),does not prolong bleeding time. Hypersensitivityreactions are rare; no metabolic effects or acid-base disturbances; can be used in all age groups(infants to elderly), pregnant/lactating women, inpresence of other disease states and in patientsin whom aspirin is contraindicated. It does nothave significant drug interactions. Thus, it maybe preferred over aspirin for most minor conditions.Dose: 325–650 mg (children 10–15 mg/kg) 3–5 times a day.CROCIN 0.5, 1.0 g tabs; METACIN, PARACIN 500 mg tab,125 mg/5 ml syrup, 150 mg/ml paed. drops, ULTRAGIN,PYRIGESIC, CALPOL 500 mg tab, 125 mg/5 ml syrup,NEOMOL, FEVASTIN, FEBRINIL 300 mg/2 ml inj., CROCINPAIN RELIEF: 650 mg + Caffeine 50 mg tab.JUNIMOL-RDS 80, 170, 250 mg suppository (for children),PARACETAMOL RECTAL SUPPOSITORY 80, 170 mg.The DCGI has allowed to manufacturers a period of 3 years tolimit the total amount of paracetamol per tab./cap. (single drugor combined formulation) to 325 mg.
BENZOXAZOCINE DERIVATIVE
Nefopam It is a nonopioid analgesic which does not inhibitPG synthesis but relieves traumatic, postoperative and short-lasting musculoskeletal pain. It may be used if pain ispersistent and is not adequately relieved by other analgesics.

208S
EC
TIO
N3
AUTACOIDS AND RELATED DRUGS
Nefopam produces anticholinergic (dry mouth, urinaryretention, blurred vision) and sympathomimetic (tachycardia,nervousness) side effects, and nausea is often dose limiting.It is contraindicated in epileptics.Dose: 30–60 mg TDS oral, 20 mg i.m. 6 hourly.NEFOMAX 30 mg tab, 20 mg in 1 ml amp.
Topical NSAIDsMany NSAIDs have been marketed in topicalformulations (mostly as gels) for application overpainful muscles or joints. These preparations arebeing used for osteoarthritis, sprains, sportsinjuries, tenosinovitis, backache, spondylitis andother forms of soft tissue rheumatism. It ispresumed that the drug would penetrate to thesubjacent tissues attaining high concentrations inthe affected muscles/joints, while maintaining lowblood levels. Consequently the g.i. and othersystemic adverse effects would be minimised andfirst pass hepatic metabolism would also beavoided.
While there is no doubt about their safety,doubt has been raised about their actual efficacyover and above a strong placebo effect of localapplication, massaging and that due to presenceof counter irritants like menthol, methyl salicylate,etc. in most of them. Often they are used inaddition to oral NSAID medication; and guidelinesof several professional bodies recommend theiruse in mild-to-moderate osteoarthritis of knee andhand as initial or adjunctive therapy.
Measurement of drug concentration attainedin tissues underlying the site of application, aswell as concurrent blood levels has shownthat systemic absorption from topical NSAIDpreparations is slow taking ~10 times longer timeto attain peak concentration compared to oraldosing. Highest blood levels remain below 15%of the same dose given orally. This is consistentwith their lack of systemic toxicity. Localconcentrations are high upto a depth of 4–6 mm,i.e. in dermis, but at 25 mm depth in muscles,the concentration is low and nearly the same asin blood. Marked variation has been noted in theconcentration attained in muscles and jointsdepending on the type of formulation, depth and
distance from site of application as well as amongdifferent individuals. Reports on the clinicalefficacy of topical NSAIDs are also variable.Better responses have generally been obtainedin short lasting musculoskeletal pain. Clinical trialsin osteoarthritis of knee have generally ratedtopical formulations of NSAIDs, notably thoseof diclofenac and ketoprofen to be superior toplacebo. Though overall efficacy of topicalNSAIDs in musculoskeletal pain is low, it appearsto be clinically valuable.
PreparationsDiclofenac 1% gel : VOLINI GEL, RELAXYL GEL,
DICLONAC GELIbuprofen 10% gel : RIBUFEN GELNaproxen 10% gel : NAPROSYN GELKetoprofen 2.5% gel : RHOFENID GELFlurbiprofen 5% gel : FROBEN GELNimesulide 1% gel : NIMULID TRANS GEL,
ZOLANDIN GEL,NIMEGESIC-T-GEL
Piroxicam 0.5% gel : DOLONEX GEL, MOVON GEL,PIROX GEL, MINICAM GEL
Choice of nonsteroidal antiinflammatorydrugEfficacy differences among different NSAIDs areminor, but they have their own spectrum of adverseeffects. They differ quantitatively among them-selves in producing different side effects and thereare large inter-individual differences. At presentNSAIDs are a bewildering array of stronglypromoted drugs. No single drug is superior toall others for every patient. Choice of drug isinescapably empirical.
The cause and nature of pain (mild, moderateor severe; acute or chronic; ratio of pain: inflam-mation) along with consideration of risk factorsin the given patient (age, concurrent disease anddrug therapy, history of allergy) govern selectionof the analgesic. Also to be considered are thepast experience of the patient, acceptability andindividual preference. Patients differ in theiranalgesic response to different NSAIDs. If oneNSAID is unsatisfactory in a patient, it does notmean that other NSAIDs will also be unsatis-factory. Some subjects ‘feel better’ on a particulardrug, but not on a closely related one. It is in this

209C
HA
PTE
R14
NSAIDs AND ANTIPYRETIC-ANALGESICS
context that availability of such a wide range ofNSAIDs may be welcome. Some guidelines are:
1. Mild-to-moderate pain with little inflam-mation: paracetamol or low-dose ibuprofen.
2. Postoperative or similar acute but short-lasting pain: ketorolac, a propionic acidderivative, diclofenac or nimesulide.
3. Acute musculoskeletal, osteoarthritic, injuryassociated pain: paracetamol, a propionicacid derivative or diclofenac.
4. Exacerbation of rheumatoid arthritis, anky-losing spondylitis, acute gout, acuterheumatic fever: naproxen, piroxicam,indomethacin, high dose aspirin.
5. Gastric intolerance to traditional NSAIDs orpredisposed patients: a selective COX-2inhibitor or paracetamol. Arthritis patientswho are dependent on NSAIDs and havedeveloped peptic ulcer must receive con-current proton pump inhibitor as gastropro-tective.
6. Patients with history of asthma or anaphy-lactoid reaction to aspirin/other NSAIDs:nimesulide, COX-2 inhibitor.
7. Patients with hypertension or other risk factorfor heart attack/stroke: avoid selectiveCOX-2 inhibitor; a propionic acid derivativeor aspirin may be used at the lowest dose forthe shortest period.
8. Paediatric patients: only paracetamol,aspirin, ibuprofen and naproxen have beenadequately evaluated in children — shouldbe preferred in them. Due to risk of Reye’ssyndrome, aspirin should be avoided.
9. Elderly patients: use lower dose of the chosenNSAID.
10. Fast acting drug formulation is suitable forfever, headache and other short lasting pain,while longer acting drugs/sustained releaseformulations are appropriate for chronicarthritic pain.
11. Pregnancy: paracetamol is the safest; low-dose aspirin is probably the second best.
12. Hypertensive, diabetic, ischaemic heartdisease, epileptic and other patients receivinglong-term regular medication: possibility ofdrug interaction with NSAIDs should beconsidered.
Analgesic combinationsCombination of aspirin and paracetamol is additive(not supra-additive) and a ceiling analgesic effectis obtained when the total amount of aspirin +paracetamol is ~ 1000 mg. The same is true ofcombinations of paracetamol with other NSAIDslike ibuprofen, diclofenac, etc. There is noconvincing evidence that such combinations aresuperior to single agents, either in efficacy orin safety. If at all used, such combinations shouldbe limited to short periods.
Combination of codeine (an opioid analgesic)with aspirin or paracetamol is also additive, butin this case combination provides additionalanalgesia beyond the ceiling effect of aspirin/paracetamol. However, this is true only when eachis given in full dose which will produce opioidside effects as well. The mechanisms of pain reliefby these two classes of drugs are different. Suchcombination should be considered only for painrefractory to single agent.To obviate inadvertent misuse and chance of producingdependence, the fixed dose combinations of analgesics withhypnotics/sedatives/anxiolytics is banned in India.
PROBLEM DIRECTED STUDY
14.1 A 65-year-old lady presented with pain in both knees, more on the left side. The pain isworsened by walking or standing for some time. X-ray of knee shows narrowing of joint space,mild effusion and osteophytic projections. A diagnosis of osteoarthritis of knee is made. She gavehistory of suffering a heart attack one year back which was treated by angioplasty and a stentwas placed. She regularly takes aspirin 75 mg daily for prophylaxis of further myocardial infarction.(a) Which analgesic/NSAID will be suitable for relieving her knee pain?(b) Which analgesic/NSAIDs should not be prescribed for her?(c) Whether any locally applied medication can be helpful in relieving her knee pain?(see Appendix-1 for solution)

Antirheumatoid andAntigout Drugs
ChapterChapterChapterChapterChapter 1515151515
ANTIRHEUMATOID DRUGS
These are drugs which (except corticosteroids),can suppress the rheumatoid process, bring abouta remission and retard disease progression, butdo not have nonspecific antiinflammatory oranalgesic action. They are used in rheumatoidarthritis (RA) in addition to NSAIDs and are alsoreferred to as disease modifying antirheumaticdrugs (DMARDs) or slow acting antirheumaticdrugs (SAARDs). The onset of benefit withDMARDs takes a few months of regular treatmentand relapses occur a few months after cessationof therapy. Recently, some biological agents(antibodies and other proteins) have been addedfor resistant cases.
Rheumatoid arthritis (RA) is an autoimmunedisease in which there is joint inflammation,synovial proliferation and destruction of articularcartilage. Immune complexes composed of IgMactivate complement and release cytokines(mainly TNFα and IL-1) which are chemotacticfor neutrophils. These inflammatory cells secretelysosomal enzymes which damage cartilage anderode bone, while PGs produced in the processcause vasodilatation and pain. RA is a chronicprogressive, crippling disorder with a waxing andwaning course. NSAIDs are the first line drugsand afford symptomatic relief in pain,swelling, morning stiffness, immobility, but donot arrest the disease process.The goals of drug therapy in RA are:• Ameliorate pain, swelling and joint stiffness• Prevent articular cartilage damage and bony
erosions• Prevent deformity and preserve joint function.Though mild/early cases are still mostly treatedwith NSAIDs only, the current recommendationis to add DMARDs as soon as the diagnosis ofRA is confirmed. However, use of DMARDs in
early/mild RA should be weighed against theirpotential adverse effects, which may be serious.More than one DMARD may be used con-currently; advanced cases may require 2 or 3 drugstogether, because all DMARDs tend to loseeffectiveness with time.
CLASSIFICATION
I. Disease modifying antirheumatic drugs(DMARDs)
A. Nonbiological drugs
1. Immunosuppressants: Methotrexate,Azathioprine, Cyclosporine
2. Sulfasalazine3. Chloroquine or Hydroxychloroquine4. Leflunomide
B. Biological agents
1. TNFα inhibitors: Etanercept, Infliximab,Adalimumab
2. IL-1 antagonist: Anakinra
II. Adjuvant drugs
Corticosteroids: Prednisolone and others(Gold and penicillamine are obsolete DMARDs.)
Nonbiological drugs
1. Immunosuppressants (see Ch. 63)
Methotrexate (Mtx) This dihydrofolate reductaseinhibitor has prominent immunosuppressant andantiinflammatory property. Beneficial effects inRA are probably related to inhibition of cytokineproduction, chemotaxis and cell-mediated immunereaction. Induction of oral low-dose (7.5–15 mg)weekly Mtx regimen has improved acceptabilityof this drug in RA. Onset of symptom relief isrelatively rapid (4–6 weeks), therefore preferred

211C
HA
PTE
R15
ANTIRHEUMATOID AND ANTIGOUT DRUGS
for initial treatment. Mtx is now the DMARDof first choice and the standard treatment for mostpatients, including cases of juvenile RA. Responseis more predictable and sustained over long-term.Combination regimens of 2 or 3 DMARDs includeMtx.
Oral bioavailability of Mtx is variable andmay be affected by food. Its excretion is hinderedin renal disease: not recommended for suchpatients. Probenecid and aspirin increase Mtxlevels and toxicity. Trimethoprim can add toinhibition of dihydrofolate reductase and depressbone marrow. Oral ulceration and g.i. upset arethe major side effects of low dose Mtx regimen.With prolonged therapy, dose dependent progres-sive liver damage leading to cirrhosis occurs insome patients (this is not seen with short coursesused in cancer). Incidence of chest infection isincreased. Mtx is contraindicated in pregnancy,breast-feeding, liver disease, active infection,leucopenia and peptic ulcer.NEOTREXATE, BIOTREXATE 2.5 mg tab.
Azathioprine This purine synthase inhibitor actsafter getting converted to 6-mercaptopurine bythe enzyme thiopurine methyl transferase (TPMT).It is a potent suppressant of cell-mediatedimmunity; appears to selectively affect differentia-tion and function of T-cells and natural killer cells.It also suppresses inflammation. However, remis-sion is induced in smaller percentage of RApatients and it is less commonly used. Given alongwith corticosteroids, it has a steroid sparing effect,for which it is primarily used now, especially incases with systemic manifestations. It is notcombined with Mtx.Dose: 50–150 mg/day; IMURAN 50 mg tab.
Other immunosuppressants like cyclosporine, chlorambucil,cyclophosphamide are rarely used in RA; are reserved forcases not responding to other DMARDs.
2. Sulfasalazine (see Ch. 48)
It is a compound of sulfapyridine and 5-aminosalicylic acid (5-ASA); exerts antiinflammatoryactivity in the bowel and is useful in ulcerativecolitis. In addition, it suppresses the disease in
significant number of RA patients. The mecha-nism of action is not known. Sulfapyridine splitoff in the colon by bacterial action and absorbedsystemically appears to be the active moiety(contrast ulcerative colitis, in which 5-ASA actinglocally in the colon is the active component).Generation of superoxide radicals and cytokineelaboration by inflammatory cells may besuppressed. Efficacy of sulfasalazine in RA ismodest and side effects may be unpleasant;neutropenia/thrombocytopenia occurs in about10% patients and hepatitis is possible. It is usedas a second line drug for milder cases or iscombined wih Mtx.Dose: 1–3 g/day in 2–3 divided doses.SALAZOPYRIN, SAZO-EN 0.5 g tab.
3. Chloroquine and hydroxychloroquine(see Ch. 59)
These are antimalarial drugs found to induceremission in upto 50% patients of RA, but take3–6 months. Their advantage is relatively lowtoxicity, but efficacy is also low; bony erosionsare not prevented. Their mechanism of action isnot known, however, they have been found toreduce monocyte IL–I, consequently inhibitingB lymphocytes. Antigen processing may be inter-fered with. Lysosomal stabilization and free radicalscavenging are the other proposed mechanisms.
For RA, these drugs have to be given forlong periods: accumulate in tissues (especiallymelanin containing tissue) and produce toxicity,most disturbing of which is retinal damage andcorneal opacity. This is less common andreversible in case of hydroxychloroquine, whichis preferred over chloroquine. Other adverseeffects are rashes, graying of hair, irritable bowelsyndrome, myopathy and neuropathy.
Chloroquine/hydroxychloroquine are emplo-yed in milder nonerosive disease, especially whenonly one or a few joints are involved, or theyare combined with Mtx/sulfasalazine.Chloroquine 150 mg (base) per day.Hydroxychloroquine 400 mg/day for 4–6 weeks, followedby 200 mg/day for maintenance.ZHQUINE, ZYQ 200 mg tab.

212S
EC
TIO
N3
AUTACOIDS AND RELATED DRUGS
4. LeflunomideThis immunomodulator inhibits proliferation ofstimulated lymphocytes in patients with active RA.Arthritic symptoms are suppressed and radio-logical progression of disease is retarded. Inclinical trials its efficacy has been ratedcomparable to Mtx and onset of benefit is asfast (4 weeks).
Leflunomide is rapidly converted in the bodyto an active metabolite which inhibits dihydro-orotate dehydrogenase and pyrimidine synthesisin actively dividing cells. Antibody productionby B-cells may be depressed. The active meta-bolite has a long t½ of 2–3 weeks; leflunomide,therefore, is given in a loading dose of 100 mgdaily for 3 days followed by 20 mg OD.
Adverse effects of leflunomide are diarrhoea,headache, nausea, rashes, loss of hair, thrombo-cytopenia, leucopenia, increased chances ofchest infection and raised hepatic transaminases.It is not to be used in children and pregnant/lactating women. Leflunomide is an alternativeto Mtx or can be added to it, but the combinationis more hepatotoxic. Combination with sulfa-salazine improves benefit.LEFRA 10 mg, 20 mg tabs.
Gold Injected i.m. as gold sodium thiomalate, gold is theoldest drug capable of arresting progression of RA. Becauseof high toxicity (hypertension, dermatitis, stomatitis, kidney/liver/bone marrow damage) it has gone out of use. Auranofinthe orally active gold compound is less effective and lesstoxic (causes diarrhoea, abdominal cramps etc.), but has beenreplaced now by better drugs.
d-Penicillamine It is a copper chelating agent (see Ch.66), with a gold like action in RA. Toxicity is also similarand it is no longer used in this disease.
Biological agentsRecently, several recombinant proteins/mono-clonal antibodies that bind and inhibit cytokines,especially TNFα or IL-1 have been produced andfound to afford substantial benefit in autoimmunediseases like RA, inflammatory bowel diseases,psoriasis, scleroderma, etc. All of them produceprominent adverse effects, are expensive, and areused only as reserve drugs for severe refractorydisease.
TNFααααα inhibitors
Because TNFα plays a key role in the inflam-matory cascade of RA by activating membranebound receptors (TNFR1 and TNFR2) on thesurface of T-cells, macrophages, etc., exogenouslyadministered soluble TNF-receptor protein orantibody can neutralize it and interrupt thereaction. TNF inhibitors mainly suppressmacrophage and T-cell function; inflammatorychanges in the joint regress and new erosionsare slowed. Quicker response than nonbiologicDMARDs has been obtained. Though effectiveas monotherapy, they are generally added to Mtxwhen response to the latter is not adequate orin rapidly progressing cases. Susceptibility toopportunistic infections, including tuberculosis andpneumocystis pneumonia is increased.
Etanercept: It is a recombinant fusion proteinof TNF-receptor and Fc portion of human IgG1;administered by s.c. injection 50 mg weekly. Pain,redness, itching and swelling occur at injectionsite and chest infections may be increased, butimmunogenicity is not a clinical problem.Dose: 25–50 mg s.c. once or twice weekly;ENBREL, ENBROL 25 mg in 0.5 ml, 50 mg in 1 ml inj.
Infliximab: It is a chimeral monoclonal antibody which bindsand neutralizes TNFα; 3–5 mg/kg is infused i.v. every4–8 weeks. An acute reaction comprising of fever, chills,urticaria, bronchospasm, rarely anaphylaxis may follow theinfusion. Susceptibility to respiratory infections is increasedand worsening of CHF has been noted. It is usually combinedwith Mtx which improves the response and decreases antibodyformation against infliximab.
Adalimumab: This recombinant monoclonal anti-TNFantibody is administered s.c. 40 mg every 2 weeks. Injectionsite reaction and respiratory infections are the common adverseeffects. Combination with Mtx is advised to improve theresponse and decrease antibody formation.
IL-1 antagonist
Anakinra: It is a recombinant human IL-1 receptor antagonist.Though clinically less effective than TNF inhibitors, it hasbeen used in cases who have failed on one or more DMARDs.Dose: 100 mg s.c. daily.Local reaction and chest infections are the main adverseeffects.
Abatacept which inhibits T-cell activation, and Rituximaba monoclonal antibody that destroys and depletes B-cells,are other newer biologicals being used in refractory RA.

213C
HA
PTE
R15
ANTIRHEUMATOID AND ANTIGOUT DRUGS
8. Corticosteroids (see Ch. 20)
Glucocorticoids have potent immunosuppressantand antiinflammatory activity: can be inductedalmost at any stage in RA along with first orsecond line drugs, if potent antiinflammatoryaction is required while continuing the NSAID± DMARD. Symptomatic releif is prompt andmarked but they do not arrest the rheumatoidprocess, though joint destruction may be slowedand bony erosions delayed.
Long-term use of corticosteroids carriesserious disadvantages. Therefore,• either low doses (5–10 mg prednisolone or
equivalent) are used to supplement NSAIDs(once used in this manner, it is difficult towithdraw the steroid—exacerbation is mostlyprecipitated and the patient becomes steroiddependent)
• or high doses are employed over short periodsin cases with severe systemic manifestations(organ-threatening disease, vasculitis) while thepatient awaits response from a remissioninducing drug.In cases with single or a few joint involvement
with severe symptoms, intraarticular injection ofa soluble glucocorticoid affords relief for severalweeks; joint damage may be slowed. Thisprocedure should not be repeated before 4–6months.
DRUGS USED IN GOUT
Gout It is a metabolic disorder characterizedby hyperuricaemia (normal plasma urate 2–6 mg/dl). Uric acid, a product of purine metabolism,has low water solubility, especially at low pH.When blood levels are high, it precipitates anddeposits in joints, kidney and subcutaneous tissue(tophy).
Secondary hyperuricaemia occurs in:
(a) Leukaemias, lymphomas, polycythaemia—especially when treated with chemotherapy orradiation: due to enhanced nucleic acid meta-bolism and uric acid production.
(b) Drug induced—thiazides, furosemide, pyra-zinamide, ethambutol, levodopa reduce uric acidexcretion by kidney.
Drugs used in gout are:For acute gout
NSAIDsColchicine
CorticosteroidsFor chronic gout/hyperuricaemiaUricosurics Synthesis inhibitorsProbenecid AllopurinolSulfinpyrazone Febuxostat
ACUTE GOUTAcute gout manifests as sudden onset of severeinflammation in a small joint (commonest ismetatarso-phalangeal joint of great toe) due toprecipitation of urate crystals in the joint space.The joint becomes red, swollen and extremelypainful: requires immediate treatment.
1. NSAIDsOne of the strong antiinflammatory drugs, e.g.naproxen, piroxicam, diclofenac, indomethacinor etoricoxib is given in relatively high andquickly repeated doses. They are quite effectivein terminating the attack, but may take 12–24hours, i.e. response is somewhat slower than withcolchicine, but they are generally better tolerated;majority of patients prefer them over colchicine.Their strong antiinflammatory (not uricosuric)action is responsible for the benefit. Naproxenand piroxicam specifically inhibit chemotacticmigration of leucocytes into the inflamed joint.After the attack is over, they may be continuedat lower doses for 3–4 weeks while drugs tocontrol hyperuricaemia take effect. They are notrecommended for long term management due torisk of toxicity.
The NSAIDs have also substituted colchicinefor covering up the period of initiation of therapy(6–8 weeks) with allopurinol or uricosurics inchronic gout.

214S
EC
TIO
N3
AUTACOIDS AND RELATED DRUGS
2. ColchicineIt is an alkaloid from Colchicum autumnale whichwas used in gout since 1763. The pure alkaloidwas isolated in 1820.
Colchicine is neither analgesic nor anti-inflammatory, but it specifically suppresses goutyinflammation. It does not inhibit the synthesisor promote the excretion of uric acid. Thus, ithas no effect on blood uric acid levels.
An acute attack of gout is started by theprecipitation of urate crystals in the synovial fluid.On being engulfed by the synovial cells, theyrelease mediators and start an inflammatoryresponse. Chemotactic factors are produced →granulocyte migration into the joint; they phago-cytose urate crystals and release a glycoproteinwhich aggravates the inflammation by:
(i) Increasing lactic acid production frominflammatory cells → local pH is reduced→ more urate crystals are precipitated inthe affected joint.
(ii) Releasing lysosomal enzymes which causejoint destruction.
Colchicine does not affect phagocytosis of uratecrystals, but inhibits release of chemotactic factorsand of the glycoprotein, thus suppressing thesubsequent events. By binding to fibrillar proteintubulin, it inhibits granulocyte migration into theinflamed joint and thus interrupts the vicious cycle.Other actions of colchicine are:
(a) Antimitotic: causes metaphase arrest bybinding to microtubules of mitotic spindle.It was tried for cancer chemotherapy butabandoned due to toxicity. It is used toproduce polyploidy in plants.
(b) Increases gut motility through neural mecha-nisms.
Pharmacokinetics Colchicine is rapidly absor-bed orally, partly metabolized in liver and excretedin bile—undergoes enterohepatic circulation;ultimate disposal occurs in urine and faeces overmany days. Binding of colchicine to intracellulartubulin contributes to its large volume ofdistribution and slow elimination. Inhibitors ofCYP3A4 retard colchicine metabolism andenhance its toxicity.
Toxicity is high and dose related.Nausea, vomiting, watery or bloody diarrhoea andabdominal cramps occur as dose limiting adverseeffects. Accumulation of the drug in intestine andinhibition of mitosis in its rapid turnover mucosais responsible for the toxicity. In overdose, colchi-cine produces kidney damage, CNS depression,intestinal bleeding; death is due to muscularparalysis and respiratory failure.Chronic therapy with colchicine is not recom-mended because it causes aplastic anaemia,agranulocytosis, myopathy and loss of hair.
Use
(a) Treatment of acute gout Colchicine is thefastest acting drug to control an acute attack ofgout; 0.5 mg 1–3 hourly with a total of 3 dosesin a day; maximum 6.0 mg in a course spread over3–4 days. Control of attack is usually achievedin 4–12 hours. A second course should not bestarted before 3–7 days. The response is dramatic,so much so that it may be considered diagnostic.However, because of higher toxicity, it is used onlywhen NSAIDs are ineffective or cannot be used.Maintenance doses (0.5–1 mg/day) may be givenfor 4–8 weeks in which time control of hyper-uricaemia is achieved with other drugs.
(b) Prophylaxis Colchicine 0.5–1 mg/day canprevent further attacks of acute gout, but NSAIDsare generally preferred.
Taken at the first symptom of an attack, smalldoses (0.5–1.5 mg) of colchicine abort it.ZYCOLCHIN, GOUTNIL 0.5 mg tab.
3. CorticosteroidsIntraarticular injection of a soluble steroidsuppresses symptoms of acute gout. Crystallinepreparations should not be used. It is indicatedin refractory cases and those not toleratingNSAIDs/colchicine.
Systemic steroids are rarely needed. They arehighly effective and produce nearly as rapid aresponse as colchicine, but are reserved forpatients with renal failure/history of peptic ulcer

215C
HA
PTE
R15
ANTIRHEUMATOID AND ANTIGOUT DRUGS
bleed in whom NSAIDs are contraindicated orfor cases not responding to or not toleratingNSAIDs. Prednisolone 40–60 mg may be givenin one day, followed by tapering doses over fewweeks.
CHRONIC GOUT
When pain and stiffness persist in a joint betweenattacks, gout has become chronic. Other cardinalfeatures are hyperuricaemia, tophi (chalk-likestones under the skin in pinna, eyelids, nose,around joints and other places) and urate stonesin the kidney. In majority of patients, hyper-uricaemia is due to undersecretion of uric acid,while in few it is due to over production. Chronicgouty arthritis may cause progressive disabilityand permanent deformities.
A. URICOSURIC DRUGS
1. ProbenecidIt is a highly lipid-soluble organic acid developedin 1951 to inhibit renal tubular secretion ofpenicillin so that its duration of action could beprolonged. It competitively blocks active transportof organic acids by OATP at all sites; that inrenal tubules being the most prominent. Thistransport is bidirectional: net effect depends onwhether secretion or reabsorption of the particularorganic acid is quantitatively more important, e.g.:(a) Penicillin is predominantly secreted by theproximal tubules, its reabsorption is minimal. Neteffect of probenecid is inhibition of penicillinexcretion; more sustained blood levels areachieved.(b) Uric acid is largely reabsorbed by activetransport, while less of it is secreted; only 1/10thof the filtered load is excreted in urine. The majortransporter involved is URAT-1, a member of theOATP family. Probenecid, therefore, promotes uricacid excretion and lowers its blood level.
Probenecid does not have any other signi-ficant pharmacological action; it is neitheranalgesic nor antiinflammatory.
Interactions
1. In addition to penicillins, probenecid inhibitsthe urinary excretion of cephalosporins, sulfona-mides, Mtx and indomethacin.2. It inhibits biliary excretion of rifampicin.Pyrazinamide and ethambutol may interfere withuricosuric action of probenecid.3. Probenecid inhibits tubular secretion ofnitrofurantoin which may not attain antibacterialconcentration in urine.4. Salicylates block uricosuric action of pro-benecid.
Pharmacokinetics Probenecid is completelyabsorbed orally; 90% plasma protein bound: partlyconjugated in liver and excreted by the kidney;plasma t½ is 6–8 hours.
Adverse effects Probenecid is generally welltolerated.Dispepsia is the most common side effect (upto25% incidence with high doses). It should beused cautiously in peptic ulcer patients. Rashesand other hypersensitivity phenomena are rare.Toxic doses cause convulsions and respiratoryfailure.
Uses
1. Chronic gout and hyperuricaemia: Probenecidis a second line/adjuvant drug to allopurinol.Started at 0.25 g BD and increased to 0.5 g BD,it gradually lowers blood urate level; arthritis,tophi and other lesions may take months to resolve.Colchicine/NSAID cover is advised during theinitial 1–2 months to avoid precipitation of acutegout.
Probenecid and other uricosurics are ineffec-tive in the presence of renal insufficiency (serumcreatinine > 2 mg/dl). Plenty of fluids should begiven with probenecid to avoid urate crystalli-zation in urinary tract.
2. Probenecid is also used to prolong penicillinor ampicillin action by enhancing and sustainingtheir blood levels, e.g. in gonorrhoea, SABE.

216S
EC
TIO
N3
AUTACOIDS AND RELATED DRUGS
3. Probenecid is given along with cidofovir, a drug forCMV retinitis in AIDS patients, to prevent its nephrotoxicity.
BENEMID, BENCID 0.5 g tab.
2. Sulfinpyrazone
It is a pyrazolone derivative, related to phenylbutazone, havinguricosuric action, but is neither analgesic nor anti-inflammatory.It inhibits tubular reabsorption of uric acid, but smaller dosescan decrease urate excretion as do small doses of probenecid.Though equally efficacious as probenecid, sulfinpyrazone hasgone into disuse because of more gastric irritation and otherside effects. It has been withdrawn in USA. Sulfinpyrazoneinhibits platelet aggregation as well.
Benzbromarone is another uricosuric drug with restricteduse due to hepatotoxicity.
B. URIC ACID SYNTHESIS INHIBITORS
AllopurinolThis hypoxanthine analogue was synthesized as apurine antimetabolite for cancer chemotherapy.However, it had no antineoplastic activity but wasa substrate as well as inhibitor of xanthine oxidase,the enzyme responsible for uric acid synthesis(Fig. 15.1).
Allopurinol itself is a short-acting (t½ 2 hrs)competitive inhibitor of xanthine oxidase, but itsmajor metabolite alloxanthine (oxypurine) is along-acting (t½ 24 hrs) and noncompetitiveinhibitor—primarily responsible for uric acid
synthesis inhibition in vivo. At high concentrations,allopurinol also becomes noncompetitive inhibitor.During allopurinol administration, plasma concen-tration of uric acid is reduced and that of hypoxan-thine and xanthine is somewhat increased. In placeof uric acid alone, all 3 oxipurines are excretedin urine. Since xanthine and hypoxanthine aremore soluble, have a higher renal clearance thanthat of uric acid and each has its individual solu-bility, precipitation and crystallization in tissuesand urine does not occur.
Because of raised levels of xanthine and hypo-xanthine, some feedback inhibition of de novopurine synthesis and reutilization of metabolicallyderived purine also occurs.Pharmacokinetics About 80% of orally admi-nistered allopurinol is absorbed. It is not boundto plasma proteins; metabolized largely to allo-xanthine. During chronic medication, it inhibitsits own metabolism and about 1/3rd is excretedunchanged, the rest as alloxanthine.
Interactions(a) Allopurinol inhibits the degradation of6-mercaptopurine and azathioprine: their dosesshould be reduced to 1/3rd, but not that ofthioguanine, because it follows a differentmetabolic path (S-methylation).
Fig. 15.1: Uric acid synthesis and the action of allopurinol

217C
HA
PTE
R15
ANTIRHEUMATOID AND ANTIGOUT DRUGS
(b) Probenecid given with allopurinol has complexinteraction; while probenecid shortens t½ ofalloxanthine, allopurinol prolongs t½ ofprobenecid.(c) Allopurinol can potentiate warfarin andtheophylline by inhibiting their metabolism.(d) A higher incidence of skin rashes has beenreported when ampicillin is given to patients onallopurinol.Adverse effects These are uncommon.Hypersensitivity reaction consisting of rashes,fever, malaise and muscle pain is the mostfrequent. It subsides on stopping the drug. Renalimpairment increases the incidence of rashes andother reactions to allopurinol.Stevens-Johnson syndrome is a rare but seriousrisk.Gastric irritation, headache, nausea and dizzinessare infrequent; do not need withdrawal.Liver damage is rare.Precautions and contraindications Liberalfluid intake is advocated during allopurinoltherapy. It is contraindicated in hypersensitivepatients, during pregnancy and lactation.It should be cautiously used in the elderly, childrenand in patients with kidney or liver disease.
Uses Allopurinol is the first choice drug inchronic gout. It can be used in both over producersand under excretors of uric acid, particularly moresevere cases, with tophi or nephropathy.Uricosurics are infrequently used in India; theyare less effective when g.f.r. is low and areinappropriate in stone formers. The two classesof drugs can also be used together when the bodyload of urate is large.
With long-term allopurinol therapy, tophigradually disappear and nephropathy is halted,even reversed.
Secondary hyperuricaemia due to cancer chemo-therapy/radiation/thiazides or other drugs: can becontrolled by allopurinol. It can even be usedprophylactically in these situations.
To potentiate 6-mercaptopurine or azathioprinein cancer chemotherapy and immunosuppressanttherapy.
Dose: Start with 100 mg OD, gradually increase as neededto 300 mg/day; maximum 600 mg/day.ZYLORIC 100, 300 mg tabs., ZYLOPRIM, CIPLORIC 100mg cap.
Caution Allopurinol as well as uricosuricsshould not be started during acute attack of gout.During the initial 1–2 months of treatment withthese drugs, attacks of acute gout are morecommon—probably due to fluctuating plasmaurate levels favouring intermittent solubilizationand recrystallization in joints; cover with NSAIDs/colchicine should be provided.Kala-azar Allopurinol inhibits Leishmania by altering itspurine metabolism. It was tried as adjuvant to sodiumstibogluconate, but abandoned due to poor efficacy.
FebuxostatIt is a recently introduced nonpurine xanthineoxidase inhibitor, equally or more effective thanallopurinol in lowering blood uric acid level inpatients with hyperuricaemia and gout. It is rapidlyabsorbed orally, highly plasma protein bound,oxidized as well as glucuronide conjugated inthe liver and excreted by kidney; the plasma t½is ~ 6 hours.
The most important adverse effect is liverdamage; liver function needs to be monitoredduring febuxostat therapy. Diarrhoea, nausea andheadache are the usual side effects. By inhibitingxanthine oxidase, it has the potential to interactwith mercaptopurine, azathioprine and theophyl-line; should not be given to patients receiving thesedrugs.
Febuxostat is an alternative drug for treatingsymptomatic gout only in patients intolerant toallopurinol, or in those with some contraindica-tions. It is not indicated in malignancy associatedhyperuricaemia. Like other drugs used to treathyperuricaemia, NSAID/colchicine cover shouldbe provided for 1–2 months while initiatingfebuxostat therapy.Dose: 40–80 mg OD.FABULAS, FABUSTAT, ZURIG 40,80,120 mg tabs.
Rasburicase It is a new recombinant xanthine oxidaseenzyme that oxidizes uric acid to soluble and easily excretedallantoin. It is indicated only for preventing chemotherapyassociated hyperuricaemia when massive lysis of leukaemicor solid tumor mass is induced by cytotoxic drugs in children.

Drugs for Cough andBronchial Asthma
ChapterChapterChapterChapterChapter 1616161616
SECTION 4
RESPIRATORY SYSTEM DRUGS
DRUGS FOR COUGH
Cough is a protective reflex, its purpose beingexpulsion of respiratory secretions or foreign parti-cles from air passages. It occurs due to stimulationof mechano- or chemoreceptors in throat,respiratory passages or stretch receptors in thelungs. Cough may be useful or useless. Useless(nonproductive) cough should be suppressed.Useful (productive) cough serves to drain theairway, its suppression is not desirable, may evenbe harmful, except if the amount of expectorationachieved is small compared to the effort ofcontinuous coughing. Apart from specific remedies(antibiotics, etc. see box), cough may be treatedas a symptom (nonspecific therapy) with:
1. Pharyngeal demulcents Lozenges, coughdrops, linctuses containing syrup, glycerine,liquorice.
2. Expectorants (Mucokinetics)(a) Bronchial secretion enhancers: Sodium or
Potassium citrate, Potassium iodide, Guai-phenesin (Glyceryl guaiacolate), balsum ofTolu, Vasaka, Ammonium chloride.
(b) Mucolytics: Bromhexine, Ambroxol, Acetylcysteine, Carbocisteine
3. Antitussives (Cough centre suppressants)(a) Opioids: Codeine, Ethylmorphine,
Pholcodeine.(b) Nonopioids: Noscapine, Dextromethorphan,
Chlophedianol.(c) Antihistamines: Chlorpheniramine, Diphen-
hydramine, Promethazine.(d) Peripherally acting: Prenoxdiazine.
4. Adjuvant antitussivesBronchodilators: Salbutamol, Terbutalin.
DEMULCENTS AND EXPECTORANTS
Pharyngeal demulcents sooth the throat and reduceafferent impulses from the inflamed/irritatedpharyngeal mucosa, thus provide symptomaticrelief in dry cough arising from throat.
Expectorants (Mucokinetics) are drugsbelieved to increase bronchial secretion or reduceits viscosity, facilitating its removal by coughing.
Sodium and potassium citrate are consideredto increase bronchial secretion by salt action.Potassium iodide is secreted by bronchial glandsand can irritate the airway mucosa. Prolongeduse can affect thyroid function and produce iodism.It is not used now. Guaiphenesin, vasaka, tolubalsum are plant products which are supposed

219C
HA
PTE
R16
DRUGS FOR COUGH AND BRONCHIAL ASTHMA
to enhance bronchial secretion and mucociliaryfunction while being secreted by tracheobronchialglands. Ammonium salts are nauseating—reflexlyincrease respiratory secretions. A variety of expec-torant formulations containing an assortment ofthe above ingredients, often in combination withantitussives/antihistaminics are marketed andbriskly promoted, but objective evidence of effi-cacy of these is non-conclusive. The US-FDAhas stopped marketing of all expectorants, exceptguaiphenesin. Steam inhalation and proper hydra-tion may be more helpful in clearing airwaymucus.
MucolyticsBromhexine A derivative of the alkaloid vasi-cine obtained from Adhatoda vasica (Vasaka),is a potent mucolytic and mucokinetic, capableof inducing thin copious bronchial secretion. Itdepolymerises mucopolysaccharides directly aswell as by liberating lysosomal enzymes—networkof fibres in tenacious sputum is broken. It isparticularly useful if mucus plugs are present.Side effects are rhinorrhoea and lacrimation,nausea, gastric irritation, hypersensitivity.Dose: adults 8 mg TDS, children 1–5 years 4 mg BD, 5–10years 4 mg TDS.BROMHEXINE 8 mg tablet, 4 mg/5 ml elixir.
Ambroxol A metabolite of bromhexine havingsimilar mucolytic action, uses and side effects.
Dose: 15–30 mg TDS.AMBRIL, AMBROLITE, AMBRODIL, MUCOLITE 30mg tab, 30 mg/5 ml liquid, 7.5 mg/ml drops.
Acetylcysteine It opens disulfide bonds in mucoproteinspresent in sputum—makes it less viscid, but has to beadministered directly into the respiratory tract.MUCOMIX 200 mg/ml inj in 1,2,5 ml amps; injectablesolution may be nebulized/instilled through trachiostomy tube.
Carbocisteine It liquefies viscid sputum in thesame way as acetylcysteine and is administeredorally (250–750 mg TDS). Some patients ofchronic bronchitis have been shown to benefit.It may break gastric mucosal barrier; iscontraindicated in peptic ulcer patients. Sideeffects are gastric discomfort and rashes.MUCODYNE 375 mg cap, 250 mg/5 ml syr.It is available in combination with amoxicillin or cephalexinfor treatment of bronchitis, bronchiectasis, sinusitis, etc.CARBOMOX: Carbocisteine 150 mg + amoxicillin 250 or500 mg caps. CARBICEF: Carbocisteine 150 mg + cephalexin250 or 500 mg caps.
ANTITUSSIVESThese are drugs that act in the CNS to raise thethreshold of cough centre or act peripherally inthe respiratory tract to reduce tussal impulses,or both these actions. Because they aim to controlrather than eliminate cough, antitussives shouldbe used only for dry nonproductive cough or ifcough is unduly tiring, disturbs sleep or ishazardous (hernia, piles, cardiac disease, ocularsurgery).
Specific treatment approaches to cough
Etiology of cough Treatment approach
• Upper/lower respiratory tract infection Appropriate antibiotics• Smoking/chronic bronchitis/bronchiectasis Cessation of smoking/avoidance of pollutants,
steam inhalation, postural drainage• Pulmonary tuberculosis Antitubercular drugs• Asthmatic cough Inhaled β2 agonists/corticosteroids/ipratropium• Cough in pulmonary eosinophilia Diethyl carbamazine citrate, inhaled corticosteroids• Postnasal drip due to sinusitis Antibiotic, nasal decongestant, H1 antihistaminic• Postnasal drip due to allergic/perennial Avoidance of precipitating factor(s), corticosteroid
rhinitis nasal spray, H1 antihistaminic• Gastroesophageal reflux Bed head elevation, light dinner, diet modification,
H2 blocker, proton pump inhibitor, mosapride• ACE inhibitor associated cough Substitute ACE inhibitor by losartan, NSAIDs
may reduce cough• Post-viral cough No specific treatment, subsides by itself.

220S
EC
TIO
N4
RESPIRATORY SYSTEM DRUGS
OpioidsCodeine (see Ch. 34) An opium alkaloid, quali-tatively similar to and less potent than morphine,but is more selective for cough centre. Codeineis regarded as the standard antitussive; suppressescough for about 6 hours. The antitussive actionis blocked by naloxone indicating that it is exertedthrough opioid receptors in the brain. Abuseliability is low, but present; constipation is thechief drawback. At higher doses respiratorydepression and drowsiness can occur, especiallyin children. Driving may be impaired. Likemorphine, it is contraindicated in asthmatics andin patients with diminished respiratory reserve;should be avoided in children.Dose: 10–30 mg; children 2–6 years 2.5–5 mg, 6–12 years5–10 mg, frequently used as syrup codeine phos. 4–8 ml.CODINE 15 mg tab, 15 mg/5 ml linctus.
Ethylmorphine It is closely related to codeinewhich is methylmorphine, and has antitussive,respiratory depressant properties like it, but isbelieved to be less constipating.Dose: 10–30 mg TDS; DIONINDON 16 mg tab.
Pholcodeine It has practically no analgesic or addictingproperty, but is similar in efficacy as antitussive to codeineand is longer acting—acts for 12 hours; dose: 10–15 mg.
NonopioidsNoscapine (Narcotine) An opium alkaloid ofthe benzoisoquinoline series (see Ch. 34). It depres-ses cough but has no narcotic, analgesic or depen-dence inducing properties. It is nearly equipotentantitussive as codeine, especially useful inspasmodic cough. Headache and nausea occuroccasionally as side effect. It can release histamineand produce bronchoconstriction in asthmatics.Dose: 15–30 mg, children 2–6 years 7.5 mg, 6–12 years 15 mg.COSCOPIN 7 mg/5 ml syrup, COSCOTABS 25 mg tab.
Dextromethorphan A synthetic central NMDA(N-methyl D-aspartate) receptor antagonist; thed-isomer has antitussive action while l-isomer isanalgesic. Dextromethorphan does not depressmucociliary function of the airway mucosa andis practically devoid of constipating action.Though considered nonaddicting, some drugabusers indulge in it. The antitussive action of
dextromethorphan has been rated equivalent tocodeine, but some clinical studies have found itto be no better than placebo.Side effect: Dizziness, nausea, drowsiness; at highdoses hallucinations and ataxia may occur.Dose: 10–20 mg, children 2–6 years 2.5–5 mg, 6–12 years5–10 mg. It is a common ingredient of many proprietary coughformulations (see antitussive combinations below).
Chlophedianol It is a centrally acting anti-tussive with slow onset and longer duration ofaction.Side effect: Dryness of mouth, vertigo, irritability.Dose: 20–40 mg; DETIGON, TUSSIGON 20 mg/5 ml linctuswith Ammon. chloride 50 mg and menthol 0.25 mg.
AntihistaminesMany H1 antihistamines have been conventionallyadded to antitussive/expectorant formulations (seebelow). They afford relief in cough due to theirsedative and anticholinergic actions, but lackselectivity for the cough centre. They have noexpectorant property, may even reduce secretionsby anticholinergic action. They have been speciallypromoted for cough in respiratory allergic states,though their lack of efficacy in asthma islegendary.
Chlorpheniramine (2–5 mg), Diphenhydra-mine (15–25 mg) and Promethazine (15–25 mg;PHENERGAN 5 mg/5 ml elixir) are commonly used.Second generation antihistamines like fexofena-dine, loratadine, etc. are ineffective.
Peripherally acting antitussivesPrenoxdiazine In contrast to other antitussives,it acts peripherally; desensitizes the pulmonarystretch receptors and reduces tussal impulsesoriginating in the lungs. It is indicated incough of bronchial origin. Efficacy, however, isnot impressive. Though an old drug developedin Hungary, it has been introduced recently inIndia.Dose: 100–200 mg TDS-QID; PRENOXID 100, 200 mg tab.
Bronchodilators Bronchospasm can induce oraggravate cough. Stimulation of pulmonaryreceptors can trigger both cough and broncho-constriction, especially in individuals with

221C
HA
PTE
R16
DRUGS FOR COUGH AND BRONCHIAL ASTHMA
bronchial hyperreactivity. Bronchodilators relievecough in such individuals and improve theeffectiveness of cough in clearing secretions byincreasing surface velocity of airflow during theact of coughing. They should be used onlywhen an element of bronchoconstriction ispresent and not routinely. Their fixed dosecombinations with antitussives are not satisfactorybecause of differences in time course of actionof the components and liability for indiscriminateuse.Fixed dose combinations of a centrally acting antitussivewith a bronchodilator or with an antihistaminic having highatropinic activity have been banned in India, but many arestill marketed.Aeromatic chest rub is widely advertized as a coughremedy. Though it has been shown to reduce experimentallyinduced cough in healthy volunteers, there is no evidenceof benefit in pathological cough.
SOME ANTITUSSIVE-EXPECTORANTCOMBINATIONS
ASTHALIN EXPECTORANT: Salbutamol 2 mg, guaiphe-nesin 100 mg per 10 ml syr; dose 10–20 ml.ASCORIL-C: Codeine 10 mg, chlorpheniramine 4 mg per5 ml syr.AXALIN: Ambroxol 15 mg, guaiphenesin 50 mg, salbutamol1 mg, menthol 1 mg per 5 ml syr.BRONCHOSOLVIN: Guaiphenesin 100 mg, terbutalin 2.5mg, bromhexine 8 mg per 10 ml susp.CADICOFF, GRILINCTUS: Dextromethorphan 5 mg,chlorpheniramine 2.5 mg, guaiphenesin 50 mg, Amm. chloride60 mg per 5 ml syr.BENADRYL COUGH FORMULA: Diphenhydramine 14 mg,amm. chlor. 138 mg, sod. citrate 57 mg, menthol 1.1 mgper 5 ml syrup; dose 5–10 ml, children 2.5–5 ml.BRO-ZEDEX: Bromhexine 8 mg, guaiphenesin 100 mg,terbutaline 2.5 mg, menthol 5 mg per 10 ml syrup; dose10 ml.CADISTIN EXPECTORANT: Chlorpheniramine 2 mg,glyceryl guaiacolate 80 mg, amm. chlor. 100 mg, sod. citrate44 mg, menthol 0.8 mg, terpin hydrate 4 mg, tolu balsum6 mg, Vasaka syrup 0.13 ml per 5 ml syrup; dose 10 ml.CHERICOF: Dextromethorphan 10 mg, chlorpheniramine 2mg, phenylpropanolamine 12.5 mg per 5 ml liq.CLISTIN: Carbinoxamine 4 mg, amm. chlor. 240 mg, sod.citrate 240 mg per 10 ml syrup.COREX: Chlorpheniramine 4 mg, codeine phos. 10 mg,menthol 0.1 mg per 5 ml syrup; dose 5 ml, children 1.25–2.5 ml.
COSCOPIN LINCTUS: Noscapine 7 mg, chlorpheniramine2 mg, citric acid 29 mg, sod. citrate 3 mg, amm. chlor.28 mg, per 5 ml syrup; dose 10–20 ml.COSOME: Dextromethorphan 10 mg, phenylpropanolamine25 mg, chlorpheniramine 4 mg per 10 ml syr; dose 10 ml.GRILINCTUS: Dextromethorphan 5 mg, chlorpheniramine 2.5mg, guaiphenesin 50 mg, ammon. chlor. 60 mg/5 ml syr; dose5–10 ml.GRILINCTUS SOFTCAPS: Dextromethorphan 10 mg,chlorpheniramine 2 mg, phenylpropanolamine 12.5 mgsoftcaps.SOLVIN EXPECTORANT: Bromhexine 4 mg, pseudoephe-drine 30 mg tablet and in 10 ml liquid; dose 1 tablet/5ml liquid.TOSSEX: Codeine phos 10 mg, chlorpheniramine 4 mg.menthol 1.5 mg, sod. citrate 75 mg per 5 ml liquid; dose5 ml.VENTORLIN EXPECTORANT: Salbutamol 2 mg, guaiphe-nesin 100 mg per 10 ml syrup; dose 10 ml, children 2.5–7.5 ml.ZEET LINCTUS: Dextromethorphan 10 mg, guaiphenesin50 mg, phenylpropanolamine 25 mg per 5 ml syr; dose 5 ml.
DRUGS FOR BRONCHIAL ASTHMABronchial asthma is characterised by hyperres-ponsiveness of tracheobronchial smooth muscleto a variety of stimuli, resulting in narrowing ofair tubes, often accompanied by increased secre-tion, mucosal edema and mucus plugging.Symptoms include dyspnoea, wheezing, cough andmay be limitation of activity.
Asthma is now recognized to be a primarilyinflammatory condition: inflammation underlyinghyperreactivity. An allergic basis can be demon-strated in many adult, and higher percentage ofpediatric patients. In others, a variety of triggerfactors (infection, irritants, pollution, exercise,exposure to cold air, psychogenic) may beinvolved:Extrinsic asthma: It is mostly episodic, less proneto status asthmaticus.Intrinsic asthma: It tends to be perennial, statusasthmaticus is more common.
Mast cells (present in lungs) and inflammatorycells recruited as a result of the initial reactionproduce a multitude of mediators by the followingprocesses:• Release of mediators stored in granules
(immediate): histamine, protease enzymes,TNFα.

222S
EC
TIO
N4
RESPIRATORY SYSTEM DRUGS
• Release of phospholipids from cell membranefollowed by mediator synthesis (withinminutes): PGs, LTs, PAF.
• Activation of genes followed by proteinsynthesis (over hours): Interleukins, TNFα.These mediators together constrict bronchial
smooth muscle, cause mucosal edema, hyperemiaand produce viscid secretions, all resulting inreversible airway obstruction. The inflammationperpetuates itself by cell-to-cell communicationand recruitment of more and more inflammatorycells. Bronchial smooth muscle hypertrophy,increase in the population of mucus secreting cellsand blood vessels occurs over time and damageto bronchial epithelium accentuates the hyper-reactivity. Vagal discharge to bronchial muscleis enhanced reflexly. Airway remodelingprogressively worsens the disease.Chronic obstructive pulmonary disease (COPD) is alsoan inflammatory disease of the lungs characterized byprogressive emphysema (alveolar destruction) and bronchiolarfibrosis in variable proportions. Loss of bronchiolar elasticityleads to closure of smaller air tubes during expiration. Theairway obstruction is accentuated during exercise causingshortness of breath. The expiratory airflow limitation doesnot fluctuate markedly over long periods of time, but thereare exacerbations precipitated by respiratory infections,pollutants, etc. It is clearly related to smoking and charac-teristically starts after the age of 40. Quiting smoking reducesthe rate of decline in lung function. Bronchodilators preventclosure of peripheral air tubes during expiration and affordsymptomatic relief in COPD patients, but improvement inforced expiratory volume in 1st second (FEV1) followinginhalation of a shortacting β2 agonist is generally <15%.An increasing part of airway obstruction is irreversible.
APPROACHES TO TREATMENT
1. Prevention of AG:AB reaction—avoidanceof antigen, hyposensitization—possible in ext-rinsic asthma and if antigen can be identified.
2. Neutralization of IgE (reaginic antibody)—Omalizumab.
3. Suppression of inflammation and bronchialhyperreactivity—corticosteroids.
4. Prevention of release of mediators—mastcell stabilizers.
5. Antagonism of released mediators—leuko-triene antagonists, antihistamines, PAFantagonists.
6. Blockade of constrictor neurotransmitter—anticholinergics.
7. Mimicking dilator neurotransmitter—sympa-thomimetics.
8. Directly acting bronchodilators—methylxan-thines.
CLASSIFICATION
I. BronchodilatorsA. β2 Sympathomimetics: Salbutamol, Terbutaline,
Bambuterol, Salmeterol, Formoterol,Ephedrine.
B. Methylxanthines: Theophylline (anhydrous),Aminophylline, Choline theophyllinate,Hydroxyethyl theophylline, Theophyllineethanolate of piperazine, Doxophylline.
C. Anticholinergics: Ipratropium bromide,Tiotropium bromide.
II. Leukotriene antagonistsMontelukast, Zafirlukast.
III. Mast cell stabilizersSodium cromoglycate, Ketotifen.
IV. CorticosteroidsA. Systemic: Hydrocortisone, Prednisolone and
others.B. Inhalational: Beclomethasone dipropionate,
Budesonide, Fluticasone propionate, Fluniso-lide, Ciclesonide.
V. Anti-IgE antibodyOmalizumab
SYMPATHOMIMETICS (see Ch. 9)
Adrenergic drugs cause bronchodilatation throughβ2 receptor stimulation → increased cAMP forma-tion in bronchial muscle cell → relaxation. Inaddition, increased cAMP in mast cells and otherinflammatory cells decreases mediator release.Since β2 receptors on inflammatory cellsdesensitize quickly, the contribution of this actionto the beneficial effect of β2 agonists in asthmawhere airway inflammmation is chronic, isuncertain, and at best minimal. Adrenergic drugsare the mainstay of treatment of reversible airway

223C
HA
PTE
R16
DRUGS FOR COUGH AND BRONCHIAL ASTHMA
obstruction, but should be used cautiously inhypertensives, ischaemic heart disease patients andin those receiving digitalis. They are the mosteffective and fastest acting bronchodilators wheninhaled.
Though adrenaline (β1+β2+α receptor agonist)and isoprenaline (β1+β2 agonist) are effectivebronchodilators, it is the selective β2 agonists thatare now used in asthma to minimize cardiac sideeffects.
Salbutamol (Albuterol) A highly selective β2
agonist; cardiac side effects are less prominent.Selectivity is further increased by inhaling thedrug. Inhaled salbutamol delivered mostly frompressurized metered dose inhaler (pMDI) producesbronchodilatation within 5 min and the actionlasts for 2–4 hours. It is, therefore, used to abortand terminate attacks of asthma, but is not suitablefor round-the-clock prophylaxis. Muscle tremorsare the dose related side effect. Palpitation,restlessness, nervousness, throat irritation andankle edema can also occur. Hypokalaemia is apossible complication. Salbutamol undergoespresystemic metabolism in the gut wall, oralbioavailability is 50%. Oral salbutamol acts for4–6 hours, is longer acting and safer than isopre-naline, but not superior in bronchodilator efficacy.
Because of more frequent side effects, oralβ2 agonist therapy is reserved for patients whocannot correctly use inhalers or as alternative/adjuvant drugs in severe asthma.Dose: 2–4 mg oral, 0.25–0.5 mg i.m./s.c., 100–200 µg byinhalation.ASTHALIN 2, 4 mg tab., 8 mg SR tab., 2 mg/5 ml syrup, 100µg metered dose inhaler; 5 mg/ml respirator soln., 200 µg rotacaps; CROYSAL 0.5 mg/ml inj, SALOL 2.5 mg/3 ml inj;VENTORLIN 2 mg/5 ml syr, 4 mg, 8 mg CR caps;DERIHALER 100 μg metered dose inhaler.
Single enantiomer preparation of R(–) salbutamol has alsobeen marketed, because it is the active β2 agonist and morepotent bronchodilator which may produce fewer side effectsthan the racemate.
Terbutaline It is similar to salbutamol inproperties and use.Dose: 5 mg oral, 0.25 mg s.c., 250 µg by inhalation.TERBUTALINE, BRICAREX 2.5, 5 mg tab., 3 mg/5 mlsyrup, 0.5 mg/ml inj; MISTHALER 250 µg/metered dose,
10 mg/ml nebulizing soln.; BRICANYL 0.5 mg/ml inj, 2.5mg, 5 mg tabs, 1.5 mg/5 ml syr.
Inhaled salbutamol and terbutaline are cur-rently the most popular drugs for quick reversalor bronchospasm, but should not be used on anyregular schedule. Regular use does not reducebronchial hyperreactivity: may even worsen it.This may be responsible for the diminishedresponsiveness seen after long-term use of thesedrugs. Regular use also down regulates bronchialβ2 receptors. It is advised that patients requiringregular medication should be treated with inhaledsteroids, with or without inhaled long actingβ2 agonists (e.g. salmeterol), while short actingβ2 agonist inhalers should be restricted to sympto-matic relief of wheezing.
Bambuterol This biscarbamate ester prodrugof terbutaline is slowly hydrolysed in plasma andlungs by pseudocholinesterase to release the activedrug over 24 hours. Reversible inhibition ofpseudocholinesterase occurs in a dose dependentmanner. It is indicated in nocturnal and chronicasthma as a single evening dose of 10–20 mg oral.BAMBUDIL 10 mg, 20 mg tabs, 5 mg/5 ml oral soln;BETADAY 10, 20 mg tabs.
Salmeterol It is the first long acting selectiveβ2 agonist with a slow onset of action; used byinhalation on a twice daily schedule for main-tenance therapy and for nocturnal asthma, butnot for acute symptoms. It is more β2 selectivethan salbutamol, as well as more lipophilic whichprobably accounts for its longer duration of action.Concern of asthma worsening due to regular useof inhaled β2 agonists applies to salmeterol also.Recent epidemiological studies indicate thatrisk of life-threatening asthma attacks may beincreasd by regular use of long acting β2 agonists.Concurrent inhaled steroid appears to limit thisrisk. Excess mortality among asthmatics treatedcontinuously with long acting β2 agonist inhala-tions has been reported. However, clinical studieshave shown sustained improvement in asthmasymptoms and lung function in majority ofpatients. Concurrent use of inhaled salmeterol withinhaled glucocorticoid produces effects equivalentto double dose of the corticoid alone. It is

224S
EC
TIO
N4
RESPIRATORY SYSTEM DRUGS
advocated that long-acting β2 agonists shouldbe used only in combination with an inhaledsteroid; combined formulations are available.
COPD: Long-acting β2 agonists are superior toshort-acting ones, and equivalent to inhaledanticholinergics in COPD. They reduce breathless-ness by preventing expiratory closure of peripheralairways and abolishing the reversible componentof airway obstruction.SALMETER, SEROBID 25 µg per metered dose inhaler;2 puffs BD; severe cases 4 puffs BD; also SEROBIDROTACAPS 50 µg; 1–2 caps BD by inhalation.SEROFLO—100/250/500 ROTACAPS: Salmeterol 50 µg +fluticasone 100 µg/250 µg/500 µg per rotacapSEROFLO—125/250 INHALERS, COMBITIDE INHALER:Salmeterol 25 µg + fluticasone 125 µg/250 µg per puff.
Formoterol Another long-acting selective β2
agonist which acts for 12 hrs when inhaled. Incomparison to salmeterol, it has a faster onsetof action. It is used on a regular morning-eveningschedule for round-the-clock bronchodilatation.Dose: 12–24 µg by inhalation twice daily.FORATEC 12 µg rotacaps.Ephedrine This oral sympathomimetic has α + β1 + β2
actions; causes mild slowly developing bronchodilatationlasting for 3–5 hours. It is a constituent of older combinationformulations and is used for mild to moderate chronic asthma.Because of low efficacy and frequent side effects, it is notpreferred now.
METHYL XANTHINES
Theophylline and its compounds have beenextensively used in asthma, but are not consideredfirst line drugs any more. They are used moreoften in COPD. Theophylline is one of the threenaturally occurring methylated xanthine alkaloidscaffeine, theophylline and theobromine. Thechemical relation between the three is depictedbelow:
They are consumed as beverages. The sourcesand average alkaloid contents of the beverages,as they are usually prepared are given below.
Source Alkaloid content in beverage
1. Thea sinensis Caffeine 50 mg in an average(Tea leaves) Theophylline 1 mg cup of tea
2. Coffea arabica Caffeine 75 mg in an average(Coffee seeds) cup of coffee
3. Theobroma cacao Theobromine 200 mg in an average(Cocoa, chocolate) Caffeine 4 mg cup of cocoa
4. Cola acuminata Caffeine 30 mg in 200 ml bottle(Guru nuts) of cola drink
All three alkaloids have qualitatively similaractions, but there are marked quantitative (Table16.1) and pharmacokinetic differences.
TABLE 16.1 Comparative pharmacologicalactions of caffeine and theophylline
ACTION CAFF. THEO.
1. CNS—stimulation (low dose) +++ ++ —toxicity ++ +++
2. Heart—stimulation ++ +++3. Blood vessel—relaxation + ++4. Bronchi—dilatation + +++5. Kidney—diuresis + ++6. Sk. muscle—increased contractility +++ ++7. Gastric mucosa—irritation + ++8. Phosphodiesterase inhibition ++ +++9. Adenosine antagonism ++ +++
CAFF—Caffeine; THEO—TheophyllineTheobromine is of no therapeutic importance.
Pharmacological actions1. CNS Caffeine and theophylline are CNSstimulants, primarily affect the higher centres.Caffeine 150–250 mg produces a sense of well-being, alertness, beats boredom, allays fatigue,thinking becomes clearer even when dullness hastended to prevail after a sustained intellectualeffort. It tends to improve performance andincrease motor activity. Caffeine is more activethan theophylline in producing these effects.Higher doses cause nervousness, restlessness,panic, insomnia and excitement. Still higher dosesproduce tremors, delirium and convulsions.

225C
HA
PTE
R16
DRUGS FOR COUGH AND BRONCHIAL ASTHMA
Theophylline has greater propensity to producethese adverse effects at higher doses and isdefinitely more toxic than caffeine.
These alkaloids also stimulate medullaryvagal, respiratory and vasomotor centres. Vomitingat high doses is due to both gastric irritation andCTZ stimulation.
2. CVS Methylxanthines directly stimulate theheart and increase force of myocardial contrac-tions. They tend to increase heart rate by cardiacaction, but decrease it by causing vagal stimu-lation—net effect is variable. Tachycardia is morecommon with theophylline, but caffeine generallylowers heart rate. Cardiac output and cardiac workare increased. At high doses cardiac arrhythmiasmay be produced.While consumption of > 9 cups of coffee per day has beenfound to be associated with increased incidence of arrhy-thmias, moderate ingestion of caffeine (upto 500 mg/day)does not increase frequency or severity of cardiac arrhythmiaseven in patients with ischaemic heart disease or preexistingventricular extrasystoles.
Methylxanthines, especially theophylline,dilate systemic blood vessels, including corona-ries, by direct action: peripheral resistance is redu-ced. However, cranial vessels are constricted,especially by caffeine; this is one of the basisof its use in migraine.Effect on BP is variable and unpredictable—• Vasomotor centre and direct cardiac stimu-
lation—tends to raise BP.• Vagal stimulation and direct vasodilatation—
tends to lower BP.Usually a rise in systolic and fall in diastolicBP is observed.
3. Smooth muscles All smooth muscles arerelaxed, most prominent effect is exerted onbronchi, especially in asthmatics. Theophyllineis more potent than caffeine. Slow and sustaineddose-related bronchodilatation is produced, butthe effect is much less marked compared to inhaledβ2 agonists. Vital capacity is increased. Biliaryspasm is relieved, but effect on intestines andurinary tract is negligible.
4. Kidney Methylxanthines are mild diuretics;act by inhibiting tubular reabsorption of Na+ and
water as well as increased renal blood flow andg.f.r. Theophylline is more potent, but action isbrief.5. Skeletal muscles Caffeine enhancescontractile power of skeletal muscles. At highconcentrations it increases release of Ca2+ fromsarcoplasmic reticulum by direct action. At lowdoses, twitch response to nerve stimulation isaugmented, while at toxic doses contracture isproduced.
In addition, caffeine facilitates neuromusculartransmission by increasing ACh release. Its centralaction relieves fatigue and increases muscularwork. Enhanced diaphragmatic contractility notedwith theophylline in the therapeutic concentrationrange probably contributes to its beneficial effectsin dyspnoea and COPD.6. Stomach Methylxanthines enhance secretionof acid and pepsin in stomach, even on parenteralinjection. They are also gastric irritants—theo-phylline more than caffeine.7. Metabolism Caffeine and to a smaller extenttheophylline increase BMR: plasma free fattyacid levels are raised. Release of endogenouscatecholamines appears to be partly responsiblefor these effects.8. Mast cells and inflammatory cells Theo-phylline decreases release of histamine and othermediators from mast cells and activated inflam-matory cells. This may contribute to its thera-peutic effect in bronchial asthma.
Mechanism of action Three distinct cellularactions of methylxanthines have been defined—(a) Release of Ca2+ from sarcoplasmic reticulum,especially in skeletal and cardiac muscle.(b) Inhibition of phosphodiesterase (PDE) whichdegrades cyclic nucleotides intracellularly.ATP adenylylcyclase cAMP phosphodiesterase 5-AMPor or or
GTP guanylylcyclase cGMP INHIBITED BY 5-GMPTHEOPHYLLINE
The concentration of cyclic nucleotides isincreased. Bronchodilatation, cardiac stimulationand vasodilatation occur when cAMP level risesin the concerned cells.

226S
EC
TIO
N4
RESPIRATORY SYSTEM DRUGS
Several isoenzymes of the PDE superfamily exist indifferent tissues. Theophylline is a subtype nonselectiveand weak PDE inhibitor, but PDE4 inhibition is mainlyresponsible for bronchodilatation. However, someselective PDE4 inhibitors like Cilomilast and Roflumilasthave been disappointing clinically in efficacy as well asside effects.(c) Blockade of adenosine receptors: adenosineacts as a local mediator in CNS, CVS and otherorgans—contracts smooth muscles, especiallybronchial; dilates cerebral blood vessels, depres-ses cardiac pacemaker and inhibits gastric secre-tion. Methylxanthines produce opposite effects.
Action (a) is exerted only at concentrationsmuch higher than therapeutic plasma concentra-tions of caffeine and theophylline (ranging from5–20 µg/ml). Action (b) and action (c) are exertedat concentrations in the therapeutic range and appearto contribute to bronchodilatation. Raised cAMPlevels in inflammatory cells may attenuate mediatorrelease and promote eosinophil apoptosis addingto the therapeutic effect of theophylline in asthma.Adenosine A1 receptor antagonism is consideredresponsible for cardiac arrhythmias and seizuresoccurring in theophylline toxicity.
Recent evidence suggests that low concentations oftheophylline ehnace histone deacetylation in airway inflam-matory cells, suppressing proinflammatory gene transcription.Thus, even sub-bronchodilator doses of theophylline may exertsome beneficial effect in asthma.(Pharmacokinetics, adverse effects and uses of caffeine aredescribed in Ch. 35)
Theophylline
Pharmacokinetics Theophylline is well absor-bed orally; rectal absorption from suppositoriesis erratic. It is distributed in all tissues—crossesplacenta and is secreted in milk, (V 0.5 l/kg),50% plasma protein bound and extensivelymetabolized in liver by demethylation andoxidation primarily by CYP1A2. Only 10% isexcreted unchanged in urine. Its elimination ratevaries considerably with age. At therapeuticconcentrations, the t½ in adults is 7–12 hours.Children eliminate it much faster (t½ 3–5 hours)and elderly more slowly. In premature infants alsothe t½ is prolonged (24–36 hours). There aremarked interindividual variations in plasmaconcentrations attained with the same dose.
Theophylline metabolizing enzymes aresaturable, t½ is prolonged with higher doses (toas much as 60 hours) as kinetics changes fromfirst to zero order. Plasma concentrations, there-fore, increase disproportionately with dose.
Factors which need dose reduction are— age> 60 yr (× 0.6), CHF (× 0.6), pneumonia (× 0.4),liver failure (× 0.2–0.4).
Adverse effects Theophylline has a narrowmargin of safety. Dose-dependent toxicity startsfrom the upper part of therapeutic concentrationrange (Fig. 16.1). Adverse effects are primarilyreferable to the g.i.t., CNS and CVS. Headache,nervousness and nausea are early symptoms.Children are more liable to develop CNS toxicity.
Fig. 16.1: Relationship between efficacy and toxicity oftheophylline with its plasma concentration. The depictedconcentration ranges are approximate
The irritant property of theophylline is reflec-ted in gastric pain (with oral), rectal inflammation(with suppositories) and pain at site of i.m. injec-tion. Rapid i.v. injection causes precordial pain,syncope and even sudden death—due to markedfall in BP, ventricular arrhythmias or asystole.
Interactions
1. Agents which enhance theophylline metabo-lism primarily by inducing CYP1A2 lower itsplasma level: dose has to be increased by thefactor given in parenthesis.Smoking (1.6), phenytoin (1.5), rifampicin (1.5),phenobarbitone (1.2), charcoal broiled meat meal(1.3).

227C
HA
PTE
R16
DRUGS FOR COUGH AND BRONCHIAL ASTHMA
2. Drugs which inhibit theophylline metabolismand increase its plasma level are—erythromycin,ciprofloxacin, cimetidine, oral contraceptives,allopurinol; dose should be reduced to 2/3.3. Theophylline enhances the effects of—furose-mide, sympathomimetics, digitalis, oral anticoagu-lants, hypoglycaemics.4. Theophylline decreases the effects of—pheny-toin, lithium.5. Aminophylline injection should not be mixedin the same infusion bottle/syringe with—ascor-bic acid, chlorpromazine, promethazine, morphine,pethidine, phenytoin, phenobarbitone, insulin,penicillin G, tetracyclines, erythromycin.
Preparations and dose
(i) Theophylline (Anhydrous) Poorly water soluble,cannot be injected. 100–300 mg TDS (15 mg/kg/day)THEOLONG 100, 200 mg SR cap., DURALYN-CR 400mg continuous release cap, UNICONTIN 400 mg, 600 mgCR tabs, THEOBID 200 mg, 300 mg SR tabs.Only sustained release (SR) tab./caps. are used, because fastrelease tabs. produce high peak and low trough plasmaconcentrations.
Because solubility of theophylline is low, a number of solublecomplexes and salts have been prepared, particularly forparenteral use.
(ii) Aminophylline (Theophylline-ethylenediamine; 85%theophylline) water soluble, can be injected i.v. but noti.m. or s.c.—highly irritating. 250–500 mg oral or slow i.v.injection; children 7.5 mg/kg i.v.; AMINOPHYLLINE 100mg tab, 250 mg/10 ml inj.
(iii) Hydroxyethyl theophylline (Etophylline, 80%theophylline) water soluble; can be injected i.v. and i.m.(but not s.c.), less irritating; 250 mg oral/i.m./i.v.;DERIPHYLLIN 100 mg tab., 300 mg SR tab., 220 mg/2 ml inj.
(iv) Choline theophyllinate (Oxtriphylline; 64%theophylline) 250–500 mg oral, CHOLIPHYLLINE 125 mgcap., 125 mg/5 ml elixir.
(v) Theophylline ethanolate of piperazine 250–500 mgoral or i.v.; CADIPHYLLATE 80 mg/5 ml elixir,ETOPHYLATE 125 mg/5 ml syrup.
Doxophylline A long-acting oral methylxanthine that isclaimed not to interfere with sleep or stimulate gastricsecretion.Dose: 400 mg OD or BD, children 12 mg/kg/day; OXYPUR400 mg tab, DOXORIL 400 mg tab, 100 mg/5 ml syr.
The double salts/derivatives of theophylline areclaimed to be less gastric irritant and betterabsorbed. However, anhydrous theophylline iscompletely absorbed and gastric irritancy of thesalts is the same in terms of theophylline content.
Uses
1. Bronchial asthma and COPD: Theophyllinebenefits by causing bronchodilatation as well asby decreasing release of inflammatory mediators,promoting eosinophil apoptosis, improvedmucociliary clearance, stimulation of respiratorydrive and by augmenting diaphragmatic contrac-tility. However, because of narrow margin of safetyand limited efficacy, its use has declined. Sustainedrelease theophylline can be used in mild-to-moderately severe asthma, as a 3rd line oralternative/adjuvant drug, especially in patientswith nocturnal asthma. It is more useful in COPD;is often added to other drugs.
Use of intravenous aminophylline in statusasthmaticus is outmoded.
2. Apnoea in premature infant: Theophyllinereduces the frequency and duration of episodesof apnoea that occur in some preterm infants inthe first few weeks of life. Closely monitoredoral or i.v. treatment is employed for 1–3 weeks.Caffeine is equally effective.
ANTICHOLINERGICS (see Ch. 8)
Atropinic drugs cause bronchodilatation byblocking M3 receptor mediated cholinergicconstrictor tone; act primarily in the larger airways(Fig. 16.2) which receive vagal innervation.However, some recent evidence points to presenceof M3 receptors on peripheral bronchiolar musclesas well, though they are not vagally innervated.
Ipratropium bromide is a short acting (duration4–6 hours) inhaled anticholinergic bronchodilator,while tiotropium bromide is long acting (duration24 hours). Both are less efficacious than inhaledβ2 sympathomimetics in bronchial asthma.However, patients of asthmatic bronchitis, COPDand psychogenic asthma respond better to

228S
EC
TIO
N4
RESPIRATORY SYSTEM DRUGS
anticholinergics. They are the bronchodilators ofchoice in COPD. Reflex cholinergic tone appearsto be the major reversible component of airwayobstruction in COPD. Tiotropium is rated moreeffective than ipratropium in COPD; more suitablefor severe cases (FEV1<50% of predicted). Nodecline in its clinical efficacy has been noted overa period of 4 years. The inhaled anticholinergicsproduce slower response than inhaled β2
sympathomimetics and are better suited for regularprophylactic use (ipratropium 2–4 puffs 6 hourlyor tiotropium 1 rotacap OD) than for quick reliefof breathlessness. Combination of inhaledipratropium with β2 agonist produces more markedand longer lasting bronchodilatation; since theireffects are additive. This can be utilized in severeasthma or COPD. Nebulized ipratropium mixedwith salbutamol is employed in refractory asthma.Combined formulations are available.
Salbutamol + IpratropiumDUOLIN INHALER, 100 μg + 20 μg per metered doseCOMBIMIST INHALERDUOLIN ROTACAP: 200 μg + 40 μg per rotacapDUOLIN RESPULES, 2.5 mg + 500 μg in 2.5 ml solutionCOMBIMIST RESPULES
LEUKOTRIENE ANTAGONISTS
Since it was realized that cystenyl leukotrienes(LT-C4/D4) are important mediators of bron-chial asthma, efforts were made to developtheir antagonists and synthesis inhibitors. TwocysLT1 receptor antagonists montelukast andzafirlukast are available.
Montelukast and Zafirlukast Both havesimilar actions and clinical utility. They competi-tively antagonize cysLT1 receptor mediatedbronchoconstriction, airway mucus secretion,increased vascular permeability and recruitmentof eosinophils. Bronchodilatation, reduced sputumeosinophil count, suppression of bronchialinflammation, mucus and hyperreactivity are notedin asthma patients. Parameters of lung functionshow variable improvement. Some studies havefound that certain patients are ‘responders’ whileothers are ‘nonresponders’ to anti-LT therapy. Thismay reflect differing extent of involvement ofLTs as asthma mediators.
Montelukast and zafirlukast are indicated forprophylactic therapy of mild-to-moderate asthmaas alternatives to inhaled glucocorticoids. Thoughefficacy is low, they may obviate need for inhaledsteroids, and may be more acceptable in children.In severe asthma, they have additive effect withinhaled steroids, may permit reduction in steroiddose and need for rescue β2 agonist inhalations,but the additive effect of long-acting β2 agonistsis greater. They are not to be used for terminatingasthma episodes. cysLT1 antagonists are modestlyeffective in aspirin-induced asthma and exerciseinduced asthma, but are of no value in COPD.
Both montelukast and zafirlukast are very safedrugs; produce few side effects like headacheand rashes. Eosinophilia and neuropathy areinfrequent. Few cases of Churg-Strauss syndrome(vasculitis with eosinophilia) have been reported.
They are well absorbed orally, highly plasmaprotein bound and metabolized by CYP2C9(montelukast by CYP3A4 as well). The plasma t½of montelukast is 3–6 hours, while that of zafirlukastis 8–12 hours.
Fig. 16.2: Primary sites of bronchodilator action of inhaledadrenergic β2 agonists and inhaled anticholinergics.Salbutamol mainly relaxes bronchiolar smooth muscle;Ipratropium blocks bronchoconstriction mainly in thelarger airways

229C
HA
PTE
R16
DRUGS FOR COUGH AND BRONCHIAL ASTHMA
Montelukast: 10 mg OD; children 2–5 yr 4 mg OD,6–14 yr 5 mg OD; in the evening.EMLUKAST, MONTAIR, VENTAIR 4 mg, 5 mg, 10 mgtabsZafirlukast: 20 mg BD; children 5–11 yr 10 mg BD;ZUVAIR 10 mg, 20 mg tabs.
Zileuton It is a 5-LOX inhibitor, blocks LTC4/D4 as wellas LTB4 synthesis. It therefore has the potential to preventall LT induced responses including those exerted by activationof cysLT1 receptor. However, clinical efficacy in asthma issimilar to montelukast. The duration of action of zileutonis short and it has hepatotoxic potential. These limitationshave restricted its use.
MAST CELL STABILIZERS
Sodium cromoglycate (Cromolyn sod.)
It is a synthetic chromone derivative which inhibitsdegranulation of mast cells (as well as other inflammatorycells) by trigger stimuli. Release of mediators of asthma likehistamine, LTs, PAF, interleukins, etc. is restricted. The basisof this effect is not well understood, but may involve a delayedCl¯ channel in the membrane of these cells. Chemotaxisof inflammatory cells is inhibited. Long-term treatmentdecreases the cellular inflammatory response; bronchialhyperreactivity is reduced to variable extents. Bronchospasminduced by allergens, irritants, cold air and exercise maybe attenuated. It is also not a bronchodilator and does notantagonize constrictor action of histamine, ACh, LTs, etc.Therefore, it is ineffective if given during an asthmatic attack.
Pharmacokinetics Sod. cromoglycate is not absorbedorally. It is administered as an aerosol through metered doseinhaler delivering 1 mg per dose: 2 puffs 4 times a day.Only a small fraction of the inhaled drug is absorbed syste-mically; this is rapidly excreted unchanged in urine and bile.
Uses
1. Bronchial asthma: Sod. cromoglycate is a long-termprophylactic in mild-to-moderate asthma. Decrease in thefrequency and severity of attacks is more likely in extrinsic(atopic) and exercise-induced asthma, especially in youngerpatients. Therapeutic benefit (when it occurs) develops slowlyover 2–4 weeks and lasts 1–2 weeks after discontinuing.However, it is less effective than inhaled steroids and isseldom used now.2. Allergic rhinitis: Cromoglycate is not a nasal decon-gestant, but regular 4 times daily use as a nasal spray producessome symptomatic improvement in many patients after4–6 weeks. The need for nasal decongestants may be reduced.3. Allergic conjunctivitis: Regular use as eye drops isbeneficial in some chronic cases.
FINTAL inhaler: 1 mg and CROMAL 5 mg/puff metereddose inhaler; 2 puffs 4 times daily.FINTAL nasal spray: 2% CROMAL AQ 2.8 mg/dose; 2squeezes in each nostril QID.
FINTAL eye drops: 2% CROMAL 2% and 4% eye drops;1 drop in each eye QID.
Adverse effects Because of poor aqueous solubility,absorption of cromoglycate is negligible; systemic toxicityis minimal. Bronchospasm, throat irritation and cough occursin some patients, especially with fine powder inhalation.Rarely nasal congestion, headache, dizziness, arthralgia andrashes have been reported.
Ketotifen It is an antihistaminic (H1) with some cromo-glycate like action; stimulation of immunogenic andinflammatory cells (mast cells, macrophages, eosinophils,lymphocytes, neutrophils) and mediator release are reduced.It is not a bronchodilator; produces sedation.
After prolonged use, modest symptomatic relief mayoccur in some patients of bronchial asthma, atopic dermatitis,perennial rhinitis, conjunctivitis, urticaria and food allergy.Thus, it may be tried in patients with multiple allergicdisorders.
Adverse effects Generally well tolerated. Sedation anddry mouth are common. Other side effects are dizziness,nausea, weight gain.Dose: 1–2 mg BD; children 0.5 mg BD.ASTHAFEN, 1 mg tab, 1 mg/5 ml syrup; KETOVENT1 mg tab, KETORID 0.25% eye drops.
CORTICOSTEROIDSGlucocorticoids are not bronchodilators. Theybenefit by reducing bronchial hyperreactivity,mucosal edema and by suppressing inflammatoryresponse to AG:AB reaction or other triggerstimuli. Their mechanism of action is detailedin Ch. 20.
The realization that asthma is primarily aninflammatory disorder which, if not controlled,accentuates with time, and the availability ofinhaled steroids that produce few adverse effectshas led to early introduction and more extensiveuse of glucocorticoids in asthma. Corticosteroidsafford more complete and sustained symptomaticrelief than bronchodilators or cromoglycate;improve airflow, reduce asthma exacerbations andmay influence airway remodeling, retardingdisease progression. They also increase airwaysmooth muscle responsiveness to β2 agonists andreverse refractoriness to these drugs. Inhaledcorticosteroids have thus markedly changed theoutlook on asthma therapy. However, long-termsystemic steroid therapy has its own adverseeffects which may be worse than asthma itself.

230S
EC
TIO
N4
RESPIRATORY SYSTEM DRUGS
SYSTEMIC STEROID THERAPY
Systemic steroid therapy is resorted to in asthmaunder the following two situations:(i) Severe chronic asthma: not controlled bybronchodilators and inhaled steroids, or when thereare frequent recurrences of increasing severity;start with prednisolone 20–60 mg (or equivalent)daily; attempt dose reduction after 1–2 weeks ofgood control and finally try shifting the patientonto an inhaled steroid. Only few patients requirelong term oral steroids—in them dose should bekept at minimum.In patients requiring long-term glucocorticoid therapy,alternative treatment with immunosuppressants likemethotrexate (low dose) or cyclosporine has been tried.
(ii) Status asthmaticus/acute asthma exacer-bation: Asthma attack not responding to intensivebronchodilator therapy: start with high dose ofa rapidly acting i.v. glucocorticoid which gene-rally acts in 6–24 hours—shift to oral therapyfor 5–7 days and then discontinue abruptly ortaper rapidly.
COPD A short course (1–3 week) of oralglucocorticoid may benefit some patients of COPDduring an exacerbation.
INHALED STEROIDSThese are glucocorticoids with high topical andlow systemic activity (due to poor absorption and/or marked first pass metabolism). Beclomethasonedipropionate, Budesonide and Fluticasone havesimilar properties. Ciclesonide is a later addition.Because airway inflammation is present in earlymild disease as well, and bronchial remodelingstarts developing from the beginning, it has beenadvocated that inhaled steroids should be the ‘stepone’ for all asthma patients. However, currentlyinhaled steroids are not considered necessary forpatients with mild and episodic asthma. They areindicated in all cases of persistent asthma wheninhaled β2 agonists are required almost daily orthe disease is not only episodic. Start with 100–200 µg BD, titrate dose upward every 3–5 days;max. 400 µg QID, beyond which no further benefitgenerally occurs.
Inhaled steroids suppress bronchial inflam-mation, increase peak expiratory flow rate, reduceneed for rescue β2-agonist inhalations and preventepisodes of acute asthma. However, they haveno role during an acute attack or in statusasthmaticus. Peak effect is seen after 4–7 daysof instituting inhaled steroids and benefit persistsfor a few weeks after discontinuation. They canbe started in patients who in the past have requiredoral steroids as well as in those with no suchhistory. Patients who are to be switched over fromoral steroid should receive inhaled steroid inaddition for 1–2 weeks before oral steroid istapered, otherwise steroid withdrawal maymanifest (precipitation of asthma, muscular pain,lassitude, depression, hypotension). This confirmslack of systemic activity of inhaled steroids (atdoses < 600 µg/day). Long-term experience hasshown that efficacy of inhaled steroids ismaintained and reinstitution of oral steroids isseldom needed. Short courses of oral steroids maybe added during periods of exacerbation. Somepatients who remain well controlled for longperiods can even stop inhaled steroids withoutworsening of asthma.
COPD: The airway inflammation in COPD isnot very responsive to corticosteroids. As such,only high dose inhaled steroids are beneficial inadvanced COPD with frequent exacerbations;should not be used in early/mild cases. Thereis no proof that they slow disease progression.
Adverse effects Hoarseness of voice, dysphonia,sore throat, asymptomatic or symptomaticoropharyngeal candidiasis are the most commonside effects. These can be minimized by the useof a spacer, gargling after every dose (to washoff the drug deposited on oral and pharyngealmucosa) and prevented as well as treated bytopical nystatin/clotrimazole. There is no evidenceof mucosal damage or increased incidence of chestinfections, even on prolonged use.
Systemic effects of long-term inhaled gluco-corticoids are clinically relevant only at doses> 600 µg/day. The significant ones are—moodchanges, osteoporosis, growth retardation in

231C
HA
PTE
R16
DRUGS FOR COUGH AND BRONCHIAL ASTHMA
children, bruising, petechiae, hyperglycaemia andpituitary-adrenal suppression; several reports ofadrenal crisis have appeared, especially inchildren, during stress (of an infection, etc).
Inhaled steroids are safe during pregnancy.
Beclomethasone dipropionateBECLATE INHALER 50 µg, 100 µg, 200 µg per metereddose, 200 doses inhaler, BECORIDE 50, 100, 250 µg perpuff inhaler.BECLATE ROTACAPS (with rotahaler) 100, 200, 400 µgpowder per cap.AEROCORT INHALER 50 µg/metered aerosol dose withsalbutamol 100 µg.AEROCORT ROTACAPS 100 µg with salbutamol 200 µgrotacaps (with rotahaler).
Intranasal spray (50 µg in each nostril BD–TDS)is effective in perennial rhinitis.
Budesonide A nonhalogenated glucocorticoidwith high topical: systemic activity ratio (greaterfirst pass metabolism than beclomethasone). Smallfraction that is absorbed is rapidly metabolized;less systemic effects, may be preferred in moresevere cases.Dose: 200–400 µg BD–QID by inhalation in asthma; 200–400 µg/day by intranasal spray for allergic rhinitis.PULMICORT 100, 200, 400 µg/metered dose inhaler,BUDECORT 100 µg/metered dose inhalation.FORACORT: Formoterol 6 µg + Budesonide 100 µg/200µg rotacaps.RHINOCORT 50 µg per metered dose nasal spray;BUDENASE AQ 100 µg metered dose aqueous nasal spray;for prophylaxis and treatment of seasonal and perennialallergic or vasomotor rhinitis, nasal polyposis; initially 2puffs in each nostril every morning, maintenance 1 puff ineach nostril in the morning.
Nasal irritation, sneezing, crusting, itching of throat anddryness may occur, especially in the beginning. Contraindi-cated in presence of infection or nasal ulcers.
Fluticasone propionate This inhaled gluco-corticoid has high potency (about double ofbeclomethasone); longer duration and negligibleoral bioavailability. The dose swallowed afterinhalation has little propensity to producesystemic effects. At high doses, systemic effectsmay be due to absorption from the lungs. Theinhalational dose is 100–250 µg BD (max 1000µg/day). May be preferred in patients requiringhigher doses.
FLOHALE INHALER 25 µg, 50 µg, 125 µg per actuation.FLOHALE ROTACAPS 50 µg, 100 µg, 250 µg rotacaps.FLOMIST 50 µg per actuation nasal spray.
Flunisolide This topical steroid is available forprophylaxis and treatment of seasonal andperennial rhinitis.SYNTARIS 25 µg per actuation nasal spray; one spray in eachnostril 2–3 times daily.
Ciclesonide This inhalational steroid utilizesa novel approach to improve topical: systemicactivity ratio. It is a prodrug that is cleaved byesterases in the bronchial epithelium to releasethe active moiety. Though it is absorbed fromthe lungs, oral bioavailability is <1%. In thecirculation it is extensively bound to plasmaproteins, further minimizing exposure of tissuecells to the free and active drug.Dose: 80–160 μg by inhalation OD, preferably in the evening.CICLEZ 80 μg and 160 μg per metered dose inhaler withHFA propellant.
ANTI-IgE ANTIBODY
Omalizumab It is a humanized monoclonal antibodyagainst IgE. Administered s.c., it neutralizes free IgE incirculation without activating mast cells and otherinflammatory cells. On antigen challenge, little IgE is availablebound to the mast cell surface receptors (FcεR1) to triggermediator release (see Fig. 11.2) and cause bronchoconstriction.In severe extrinsic asthma, omalizumab has been found toreduce exacerbations and steroid requirement. No benefithas been noted in nonallergic asthma. It is very expensive;use is reserved for resistant asthma patients with positiveskin tests or raised IgE levels who require frequent hospi-talization. It is being tried in other allergic diseases as well.
INHALED ASTHMA MEDICATION
Four classes of antiasthma drugs, viz. β2 agonists, anti-cholinergics, cromoglycate and glucocorticoids are availablefor inhalational use. They are aimed at delivering the drugto the site of action so that lower dose is needed and systemicside effects are minimized. Faster action of bronchodilatorscan be achieved compared to oral administration. Most asthmapatients are now maintained on inhaled medication only.Aerosols are of two types:
(i) use drug in solution: pressurized metered dose inhaler(pMDI), nebulizers.
(ii) use drug as dry powder: spinhaler, rotahalerPressurized metered dose inhalers use chlorofluorocarbon
(banned now for their effect on ozone layer) or hydro-fluroalkane (HFA) propellants and deliver a specified doseof the drug in spray form per actuation. Device actuation

232S
EC
TIO
N4
RESPIRATORY SYSTEM DRUGS
has to be properly coordinated with deep inspiration,which many patients are unable to learn. A large volume‘spacer’ (chamber interposed between the inhaler andthe patient’s mouth) can be used to improve drug deliveryby obviating the need for precise coordination. Moreover,larger particles settle on the walls of the spacer reducingthe fraction that deposits in the throat and is laterswallowed. Local complications (candidiasis with inhaledsteroids) as well as systemic exposure are reduced. Jetnebulizers produce a mist of the drug solution generatedby pressurized air or oxygen which can be inhaled througha mouth piece, face mask or in a tent. Ultrasonicnebulizers use electrically vibrated crystals; pressurizedair/oxygen is not needed. Metered dose inhalers areconvenient hand-held devices which can be carried along,while nebulizers are used at patient’s bed side. Nebulizersare preferred for severe episodes of asthma as well asfor children and elderly. More than one drug can benebulized simultaneously.
Dry powder inhalers are also portable devices in whichthe capsule (rotacap) containing the drug is punctured/cutacross and the powder is aerosolized by the inspiratory airflow of the patient. It requires high velocity inspiration whichchildren, elderly and the very sick may not be capable of.The dry powder is also more likely to irritate the air passage—producing cough and bronchoconstriction.
Efficacy of aerosolized drug depends on the particlesize: 1–5 µm diameter particles deposit on the bronchiolesand effectively deliver the drug. Larger particles settle onthe oropharynx, while very fine particles do not settle any-where and are exhaled out. On an average only ~10% ofthe inhaled drug reaches the site of action. A considerablefraction is swallowed. Therefore, to minimize systemic action,the drug should have low oral bioavailability. Spacer devicesimprove inhaled to swallowed drug ratio. Slow and deepinbreathing after device actuation and holding the breathafter inhalation also enhances efficacy of the inhaler. Greaterproportion of smaller particles in a relatively narrow bandwidth of 1-2 μM can be generated using the newer HFApropellant based pMDIs. This improves delivary of the drugto the smaller bronchioles. However, systemic absorptionfrom the peripheral lungs is also more.
CHOICE OF TREATMENTThe severity of asthma symptoms ranges fromtransient respiratory difficulty to incapacitatingbreathlessness and characteristically fluctuatesover time. A stepwise guideline to the treatmentof asthma as per needs of the patient has beenrecommended. After the asthma is under controlfor 3–6 months, an attempt to reduce medicationshould be made in stepwise manner.
1. Mild episodic asthma (symptoms less thanonce daily, normal in between attacks): Inhaled
short-acting β2 agonist at onset of each episode.Since asthma is intermittent, it does not requirecontinuous prophylactic therapy (Step-1).
2. Seasonal asthma Start regular low-doseinhaled steroid (200–400 μg/day) or cromoglycate3–4 weeks before anticipated seasonal attacks andcontinue till 3–4 weeks after the season is over.Treat individual episodes with inhaled short-actingβ2 agonist.
3. Mild chronic (persistent) asthma withoccasional exacerbations (symptoms once dailyor so, subnormal ventilatory performance).Regular low-dose (100–500 μg/day) inhaledsteroid (Step-2). Alternatively, inhaled cromogly-cate or oral theophylline, but these are lesseffective. Episode treatment with inhaled short-acting β2 agonist.
4. Moderate asthma with frequent exa-cerbations (attacks affect activity, occur> 1 per day or mild baseline symptoms) Increasingdoses of inhaled steroid (up to 800 µg/day) +inhaled long-acting β2 agonist (Step-3). In viewof the potential risk of prolonged treatment withlong-acting β2 agonists, attempt should be madeto discontinue it after maintaining asthma controlover few months. Leukotriene antagonists maybe tried in place of long-acting β2 agonists, buttheir additive effect is less marked. Sustainedrelease theophylline may be used as alternativeadditional drug to long-acting β2 agonists,especially in nocturnal asthma.
5. Severe asthma (continuous symptoms;activity limitation; frequent exacerbations/hospitalization) Regular high dose inhaled steroid(800–2000 µg/day) through a large volumespacer device + inhaled long-acting β2 agonist(salmeterol) twice daily. Additional treatment withone or more of the following (Step-4):
Leukotriene antagonist/sustained release oraltheophylline/oral β2 agonist/inhaled ipratropiumbromide.
Rescue treatment with short-acting inhaled β2
agonist.

233C
HA
PTE
R16
DRUGS FOR COUGH AND BRONCHIAL ASTHMA
In patients not adequately controlled or thoseneeding frequent emergency care—institute oralsteroid therapy (Step-5). Efficacy of oral steroidsis proven, but should be the last resort. Attemptto withdraw it should be made periodically. TheBritish guidelines recommend continuing highdose inhaled steroids along with oral steroids.
6. Status asthmaticus/Refractory asthmaAny patient of asthma has the potential to developacute severe asthma which may be life-threatening.Upper respiratory tract infection is the mostcommon precipitant.
(i) Hydrocortisone hemisuccinate 100 mg (orequivalent dose of another glucocorticoid)i.v. stat, followed by 100–200 mg 4–8 hourlyinfusion; may take upto 6 hours to act.
(ii) Nebulized salbutamol (2.5–5 mg) + ipratro-pium bromide (0.5 mg) intermittentinhalations driven by O2.
(iii) High flow humidified oxygen inhalation.(iv) Salbutamol/terbutaline 0.4 mg i.m./s.c. may
be added, since inhaled drug may not reachsmaller bronchi due to severe narrowing/plugging with secretions.
(v) Intubation and mechanical ventilation, ifneeded.
(vi) Treat chest infection with intensive anti-biotic therapy.
(vii) Correct dehydration and acidosis with saline+ sod. bicarbonate/lactate infusion.
Aminophylline 250–500 mg diluted in 20–50 ml glucose(5%) solution injected i.v. over 20–30 min had been routinelyused, but recent evidence shows that it does not affordadditional benefit; may even produce more adverse effects;use is restricted to resistant cases.
Some antiasthma combinationsBRONKOPLUS: Salbutamol 2 mg, anhydrous theophylline100 mg tab., also per 5 ml syrup.BRONKOTUS: Bromhexine 8 mg, salbutamol 2 mg tab.,also syrup—bromhexine 4 mg, salbutamol 2 mg per 5 ml.TERPHYLIN: Terbutaline 2.5 mg, etophylline 100 mg tab,and per 10 ml syr.THEO ASTHALIN: Salbutamol 2 mg, theophylline anhydrous100 mg tab, and per 10 ml syr.THEO ASTHALIN-SR: Salbutamol 4 mg, theophylline 300mg SR tab.THEO BRIC: Terbutaline 2.5 mg, theophylline 100 mg tab.THEOBRIC SR: Terbutaline 5 mg, theophylline 300 mg SRtab.DURASALYN-CR: Salbutamol 4 mg, theophylline 200 mgCR cap.
PROBLEM DIRECTED STUDY
16.1 A 60-year-old male patient of moderately severe chronic obstructive pulmonary disease(COPD) with FEV1 45% of predicted, who has quit smoking for the last 5 years, and is maintainedon—Ipratropium br. 20 μg/puff metered dose inhaler, 2 puffs 3 times a day, and Theophylline400 mg SR tab. twice a day, developed sore throat and fever. He was prescribed—Tab Erythromycin 250 mg, one tab 4 times a day for 5 daysTab Paracetamol 500 mg 3 times a day till fever persists.After 3 days he presented with pain in epigastrium, restlessness, irritability, inability to sleep,palpitation, tremor of fingers and hand, and had vomited twice. His fever had subsided andthroat was better.(a) What could be the reason for his recent illness?(b) Could this illness be prevented, if so, how?(see Appendix-1 for solution)

Introduction
SECTION 5
HORMONES AND RELATED DRUGS
Hormone (Greek hormaein—to stir up) is a sub-stance of intense biological activity that isproduced by specific cells in the body and istransported through circulation to act on its targetcells.
Hormones regulate body functions to bringabout a programmed pattern of life events andmaintain homeostasis in the face of markedlyvariable external/internal environment.
1. Pituitary
(a) Anterior Growth hormone (GH), Prolactin(Prl),Adrenocorticotropic hormone (ACTH, Corti-cotropin),Thyroid stimulating hormone (TSH, Thyro-tropin),Gonadotropins—Follicle stimulating hormone(FSH) and Luteinizing hormone (LH).
(b) Posterior—Oxytocin,Antidiuretic hormone (ADH, Vasopressin).
2. Thyroid Thyroxine (T4), Triiodothyronine(T3), Calcitonin.
3. Parathyroid Parathormone (PTH).4. Pancreas (Islets of Langerhans) Insulin,
Glucagon.5. Adrenals(a) Cortex Glucocorticoids (hydrocortisone)
Mineralocorticoids (aldosterone)Sex steroids (dehydroepiandro-sterone)
(b) Medulla Adrenaline, Noradrenaline6. Gonads Androgens (testosterone)
Estrogens (estradiol)Progestins (progesterone)
In addition, hypothalamus, which is a part of theCNS and not a gland, produces many releasing
Body function Major regulatorhormone(s)
1. Availability of fuel : Insulin, Glucagon,Growth hormone
2. Metabolic rate : Triiodothyronine, Thyroxine
3. Somatic growth : Growth hormone,Insulin-like growth factors
4. Sex and : Gonadotropins, Androgens,reproduction Estrogens, Progestins
5. Circulating : Aldosterone,volume Antidiuretic hormone
6. Adaptation to : Glucocorticoids,stress Adrenaline
7. Calcium balance : Parathormone, Calcitonin,Vitamin D
Hormones are secreted by the endocrine orductless glands. These are:
Chapter 17a

235S
EC
TION
5HORMONES AND RELATED DRUGS
1. At cell membrane receptorsa. Through alteration Adrenaline, Glucagon,
of intracellular TSH, FSH, LH,cAMP concentra- PTH, Calcitonin,tion alteration of ACTH, someprotein kinase A hypothalamicregulation of cell releasing hormones,function: Ca2+ acting Vasopressin (V2)as third messengerin some situations.
b. Through IP3/DAG Vasopressin (V1),generation: release Oxytocinof intracellular Ca2+
and protein kinase Cactivation.
c. Direct transmembrane Insulin,activation of tyrosine Growth hormoneprotein kinase Prolactinphosphorylationcascade regulationof various enzymes.
2. At cytoplasmic receptorsPenetrating cell Steroidal hormones:membrane, hormone Glucocorticoidscombines with a Mineralocorticoidcytoplasmic receptor Androgens exposes its DNA Estrogensbinding domain Progestins;migrates to nucleus Calcitrioland binds to specificgenes DNA media-ted mRNA synthesis synthesis offunctional proteins.
3. At nuclear receptorThe hormone pene- Thyroid hormones:trates the nucleus Thyroxine,combines with its Triiodothyroninereceptor altersDNA- RNA mediatedprotein synthesis.
and inhibitory hormones which control thesecretion of anterior pituitary hormones. Someimportant ones of these are given in the box.
Placenta also secretes many hormones:Chorionic gonadotropin ProlactinEstrogens ProgesteronePlacental lactogen Chorionic
thyrotropin
The natural hormones and in many casestheir synthetic analogues which may be moresuitable therapeutically, are used as drugs forsubstitution therapy as well as for pharma-cotherapy. In addition, hormone antagonists andsynthesis/release inhibitors are of therapeuticimportance.
Sites and mechanisms of hormone actionThe hormones act on their specific receptorslocated on or within their target cells. Receptoractivation by the hormones is translated intoresponse in a variety of ways.
Hypothalamic Chemicalhormone/factor nature
1. Thyrotropin releasing Tripeptidehormone (TRH)
2. Corticotropin releasing Peptidehormone (CRH) (41 AAs)
3. Gonadotropin releasing Decapeptidehormone (GnRH,LH-RH/FSH-RH),Gonadorelin
4. Prolactin release inhibi- Dopaminetory hormone (PRIH)
5. Growth hormone Peptidereleasing hormone (40, 44 AAs)(GHRH)
6. Somatostatin (Growth Peptide (14 AA)hormone releaseinhibitory hormone)

Anterior Pituitary HormonesChapter 17b
Anterior pituitary (adenohypophysis), the masterendocrine gland, elaborates a number of importantregulatory hormones. All of these are peptide innature and act at extracellular receptors locatedon their target cells. Their secretion is controlledby the hypothalamus through releasing andrelease-inhibitory hormones that are transportedvia hypothalamohypophyseal portal system, andis subjected to feedback inhibition by thehormones of their target glands. Each anteriorpituitary hormone is produced by a separate groupof cells, which according to their stainingcharacteristic are either acidophilic or basophilic.
The acidophils are either somatotropes GH;or lactotropes Prolactin.
The basophils are gonadotropes FSH andLH; thyrotropes TSH; and corticotrope-lipo-tropes ACTH. The latter in addition to ACTHalso produce two melanocyte stimulatinghormones (MSHs) and two lipotropins, but theseare probably not important in man.
GROWTH HORMONE (GH)
It is a 191 amino acid, single chain peptide ofMW 22000.
Physiological functions GH promotes growthof bones and all other organs by inducing hyper-plasia. In general, there is a proportionate increasein the size and mass of all parts, but in the absenceof gonadotropins, sexual maturation does not takeplace. The growth of brain and eye is independentof GH. It promotes retention of nitrogen, calciumand other tissue constituents: more protoplasm isformed. The positive nitrogen balance results fromincreased uptake of amino acids by tissues andtheir synthesis into proteins. GH promotes utili-zation of fat and spares carbohydrates: uptake ofglucose by muscles is reduced while its outputfrom liver is enhanced; fat is broken down.
GH acts on cell surface JAK-STAT binding protein kinasereceptors (see p. 50) which are present on practically allcells. Binding of one GH molecule to the extracellular domainof a GH-receptor diamer results in the formation of a ternarycomplex which undergoes a conformational change andactivates the intracellular domain to associate with cytoplasmicJAK-STAT tyrosine-protein kinase resulting in metaboliceffects as well as regulation of gene expression.
Fig. 17.1: Action of growth hormone (GH) andregulation of its secretion
GHRH—Growth hormone releasing hormone; IGF-1:Insulin like growth factor-1; Stimulation (——); Inhibition(- - - -)

237C
HA
PTE
R 17
ANTERIOR PITUITARY HORMONES
The growth promoting, nitrogen retaining andcertain metabolic actions of GH are exertedindirectly through the elaboration of peptidescalled Somatomedins or Insulin-like growth factors(mainly IGF-1, also IGF-2) which are extracellularmediators of GH response (Fig. 17.1). Liver isthe major source of circulating IGF-1, while IGF-1 produced by other target cells acts locally ina paracrine manner. Like insulin, IGF-1 promoteslipogenesis and glucose uptake by muscles. TheIGF-1 receptor also is structurally and functionallyanalogous to the insulin receptor (see p. 261).
GH acts directly as well to induce lipolysisin adipose tissue, gluconeogenesis and glyco-genolysis in liver and decreased glucose utilizationby muscles. These effects are opposite to thoseof IGF-1 and insulin. As such, GH accentuatesthe metabolic derangement in diabetes.Regulation of secretion The hypothalamus producesGH releasing (GHRH) as well as release inhibitory(somatostatin) hormones. Both are peptides. Somatostatinis also produced by D cells of islets of Langerhans in thepancreas and by few other tissues. Receptors for GHRHand somatostatin are G protein coupled receptors (GPCRs)which enhance or inhibit GH secretion by increasing ordecreasing cAMP formation respectively in pituitarysomatotropes. Somatostatin has also been shown to inhibitCa2+ channels and open K+ channels.
Stimuli that cause GH release are—fasting, hypo-glycaemia, exercise, stress and i.v. infusion of arginine. GHsecretion is inhibited by rise in plasma free fatty acid levelsand by high doses of glucocorticoids. Dopaminergic agentscause a brief increase in GH release in normal subjects butparadoxically depress it in acromegalics. IGF-1 causesfeedback inhibition of GH secretion. Short-loop feedbackinhibition of secretion by GH itself has also been described.
Pathological involvements Excess production of GH isresponsible for gigantism in childhood and acromegaly inadults. Hyposecretion of GH in children results in pituitarydwarfism. Adult GH deficiency is rare, but when it occurs, itresults in low muscle and bone mass, lethargy, decreased workcapacity, hyperlipidaemia and increased cardiovascular risk.
Preparations and use The primary indication for GHis pituitary dwarfism—0.03–0.06 mg/kg daily in the eveningor on alternate days, upto the age of 20 years or more. HumanGH produced by recombinant DNA technique (rhGH)somatropin (191AA) is available for clinical use. Somatropincauses IGF-1 to appear in plasma after a delay of severalhours. IGF-1 then remains detectable for upto 48 hours. Earlydiagnosis and institution of GH therapy restores stature tonear normal. rhGH can also be used in Turner’s syndromeand in children with renal failure.
Somatropin has been tried in children with constitutionalshort stature (only if epiphyses are open) with encouragingresults. Commercial interests are promoting it for acceleratinggrowth in children without GH deficiency, but medical, ethical,cost-benefit and social objections have been raised.
In adult GH deficient patients, rHGH 150–300 g/days.c. adjusted later according to response increases lean bodymass, decreases body fat, improves energy and mentationand may reudce excess morbidity and mortality, but statureis unaffected. Benefits of rHGH therapy in GH deficientadults are now well recognized. Unlimited availability ofrecombinant GH has provided opportunity for its trial incatabolic states like severe burns, bedridden patients, chronicrenal failure, osteoporosis, etc. It is now approved for AIDS-related wasting: higher dose (0.05–0.1 mg/kg/day) is needed.However, it should not be given to postoperative, trauma,cancer and other critically ill patients. Somatropin is alsobeing promoted for ageing, but benefits are uncertain. Itsabuse by athletes is banned, and it is one of the drugs includedin ‘dope testing’.Somatropin: NORDITROPIN 5, 10, 15 mg inj, HUMATROPE6 mg, 12 mg cartridges, 1.33 and 5.33 mg vials.
Adverse effects Somatropin has low immunogenicity;allergic reactions or resistance to treatment are not a problem.Pain at injection site, lipodystrophy, glucose intolerance,hypothyroidism (due to unmasking of TSH deficiency), saltand water retention, hand stiffness, myalgia, headache arethe possible adverse effects. Rise in intracranial tension occursin few cases.
GH InhibitorsSomatostatinThis 14 amino acid peptide inhibits the secretion of GH,prolactin, and TSH by pituitary; insulin and glucagon bypancreas, and of almost all gastrointestinal secretions includingthat of gastrin and HCl. The g.i. action produces steator-rhoea, diarrhoea, hypochlorhydria, dyspepsia and nausea asside effect. Somatostatin constricts splanchnic, hepatic andrenal blood vessels. The decreased g.i. mucosal blood flowcan be utilized for controlling bleeding esophageal varicesand bleeding peptic ulcer, but octreotide is preffered nowdue to longer duration of action. Its antisecretory action isbeneficial in pancreatic, biliary or intestinal fistulae; canalso be used to reduce complications after pancreatic surgery.It also has adjuvant value in diabetic ketoacidosis (byinhibiting glucagon and GH secretion).
Use of somatostatin in acromegaly is limited by its shortduration of action (t½ 2–3 min), lack of specificity forinhibiting only GH secretion and GH rebound ondiscontinuation. Surgical removal of pituitary adenomas isthe preferred treatment modality, but somatostatin analoguesare being increasingly used.
Dose: (for upper g.i.bleeding) 250 µg slow i.v. injection over3 min followed by 3 mg i.v. infusion over 12 hours.

238S
EC
TIO
N5
HORMONES AND RELATED DRUGS
STILMEN, SOMATOSAN, SOMASTAT 250 µg and 3 mgamps.
Octreotide This synthetic octapeptide surrogateof somatostatin is 40 times more potent insuppressing GH secretion and longer acting (t½~90 min), but only a weak inhibitor of insulinsecretion. It is preferred over somatostatin foracromegaly and secretory diarrhoeas associatedwith carcinoid, AIDS, cancer chemotherapy ordiabetes. Control of diarrhoea is due to sup-pression of hormones which enhance intestinalmucosal secretion.Dose: Initially 50–100 µg s.c. twice daily, increased upto 200µg TDS; for acromegaly maintain with 10-30 mg i.m. ofmicrosphere formulation every 4 weeks.
Adverse effects are abdominal pain, nausea,steatorrhoea, diarrhoea, and gall stones (due tobiliary stasis).
Octreotide injected i.v. (100 µg followed by25–50 µg/hr) reduces hepatic blood flow and helpsstop esophageal variceal bleeding.SANDOSTATIN, OCTRIDE 50 µg, 100 µg in 1 ml amps.SANDOSTATIN LAR (microsphere formulation) 20 mg/5 mlinj.Lanreotide Another long-acting analogue of somatostatin,very similar in actions and specificity to octreotide, which oni.m. injection acts for 10–15 days. It is indicated forpharmacotherapy of acromegaly.Pegvisomant This polyethylene glycol complexed mutantGH binds to the GH receptor but does not trigger signaltransduction: acts as a GH antagonist. It is approved fortreatment of acromegaly due to small pituitary adenomas.
PROLACTIN
It is a 199 amino acid, single chain peptide ofMW 23000; quite similar chemically to GH. Itwas originally described as the hormone whichcauses secretion of milk from crop glands ofpigeon and later found to be of considerableimportance in human beings as well.
Physiological function Prolactin is theprimary stimulus which in conjunction withestrogens, progesterone and several otherhormones, causes growth and development ofbreast during pregnancy. It promotes proliferationof ductal as well as acinar cells in the breastand induces synthesis of milk proteins and lactose.
After parturition, prolactin induces milk secretion,since the inhibitory influence of high estrogenand progesterone levels is withdrawn.
Prolactin suppresses hypothalamo-pituitary-gonadal axis by inhibiting GnRH release. Continuedhigh level of prolactin during breastfeeding isresponsible for lactational amenorrhoea, inhibitionof ovulation and infertility for several monthspostpartum. Prolactin may affect immune responsethrough action on T-lymphocytes.A specific prolactin receptor is expressed on the surface oftarget cells, which is structurally and functionally analogousto GH receptor: action is exerted by transmembrane activationof JAK—cytoplasmic tyrosine protein kinases and STAT.Placental lactogen and GH also bind to prolactin receptorand exert similar effects, but prolactin does not bind to GHreceptor.
Regulation of secretion Prolactin is under predominantinhibitory control of hypothalamus through PRIH which isdopamine that acts on pituitary lactotrope D2 receptor.Dopaminergic agonists (DA, bromocriptine, cabergoline)decrease plasma prolactin levels, while dopaminergic antago-nists (chlorpromazine, haloperidol, metoclopramide) and DAdepleter (reserpine) cause hyperprolactinemia.
Though TRH, prolactin releasing peptide and VIP canstimulate prolactin secretion, no specific prolactin releasingfactor has been identified. Endogenous opioid peptides mayalso be involved in regulating prolactin secretion, but nofeedback regulation by any peripheral hormone is known.Prolactin levels in blood are low in childhood, increase ingirls at puberty and are higher in adult females than in males.A progressive increase occurs during pregnancy, peaking atterm. Subsequently, high prolactin secretion is maintainedby suckling: it falls if breast feeding is discontinued. Stress,exertion and hypoglycaemia also stimulate prolactin release.
Physio-pathological involvement Hyperpro-lactinaemia is responsible for the galactorrhoea–amenorrhoea–infertility syndrome in women. Inmales it causes loss of libido and depressedfertility. The causes of hyperprolactinaemia are:
(i) Disorders of hypothalamus removing theinhibitory control over pituitary.
(ii) Antidopaminergic and DA depleting drugs—these are a frequent cause now.
(iii) Prolactin secreting tumours—these may bemicroprolactinomas or macroprolactinomas.
(iv) Hypothyroidism with high TRH levels—alsoincreases prolactin secretion.
Use There are no clinical indications for prolactin.

239C
HA
PTE
R 17
ANTERIOR PITUITARY HORMONES
Prolactin inhibitors
BromocriptineThis synthetic ergot derivative 2-bromo--ergocryptine is a potent dopamine agonist; mostof its actions are based on this property. It hasgreater action on D2 receptors, while at certaindopamine sites in the brain it acts as a partialagonist or antagonist of D1 receptor. It is alsoa weak adrenergic blocker but not an oxytocic.
Actions
1. Decreases prolactin release from pituitary byactivating dopaminergic receptors on lactotropecells: is a strong antigalactopoietic.
2. Increases GH release in normal individuals,but decreases the same from pituitary tumoursthat cause acromegaly.
3. Has levodopa like actions in CNS—anti-parkinsonian and behavioral effects.
4. Produces nausea and vomiting by stimulatingdopaminergic receptors in the CTZ.
5. Hypotension—due to central suppression ofpostural reflexes and weak peripheral aadrenergic blockade.
6. Decreases gastrointestinal motility.
Pharmacokinetics Only 1/3 of an oral doseof bromocriptine is absorbed; bioavailability isfurther lowered by high first pass metabolism inliver. Even then, it has higher oral: parenteralactivity ratio than ergotamine. Metabolites areexcreted mainly in bile. Its plasma t½ is 3–6 hours.PROCTINAL, PARLODEL, SICRIPTIN, BROMOGEN 1.25mg, 2.5 mg tabs.
Uses Bromocriptine should always be startedat a low dose, 1.25 mg BD and then graduallyincreased till response occurs otherwise sideeffects become limiting.
1. Hyperprolactinemia due to microprolactino-mas causing galactorrhoea, amenorrhoea andinfertility in women; gynaecomastia, impotenceand sterility in men. Bromocriptine andcabergoline are the first line drug for most cases.Relatively lower doses (bromocriptine 2.5–10mg/day or cabergoline 0.25–1.0 mg twice weekly)are effective. Response occurs in a few weeks
and serum prolactin levels fall to the normal range;many women conceive. Bromocriptine should bestopped when pregnancy occurs, though noteratogenic effect is reported. Most (60–75%)tumours show regression during therapy andneurological symptoms (visual field defects, etc.)due to pressure on optic chiasma ease. However,response is maintained only till the drug is given—recurrences occur in many, but not all patients.
2. Acromegaly due to small pituitary tumoursand inoperable cases. Relatively higher doses arerequired (5–20 mg/day) and it is less effectivethan octreotide/lanreotide. Oral administration andlower cost are the advantages..
3. Parkinsonism Bromocriptine, if used alone,is effective only at high doses (20–80 mg/day)which produce marked side effects. However,response is similar to that of levodopa. It is nowrecommended in low dose only, as an adjunctto levodopa in patients not adequately benefitedand in those showing marked ‘on-off’ effect.4. Diabetes mellitus (DM) A new use of bromocriptinebased on its dopamine D2 agonistic action in thehypothalamus has been found in type 2 DM, and it hasbeen approved by US-FDA as an adjunctive drug.
5. Hepatic coma: Bromocriptine may cause arousal.
6. Bromocriptine suppresses lactation and breast engor-gement in case of neonatal death, but is not recommendeddue to unfavourable risk: benefit ratio.
Side effects: Side effects are frequent and doserelated.Early: Nausea, vomiting, constipation, nasal block-age. Postural hypotension may be marked atinitiation of therapy—syncope may occur ifstarting dose is high. Hypotension is more likelyin patients taking antihypertensives.Late: Behavioral alterations, mental confusion,hallucinations, psychosis—are more prominentthan with levodopa.Abnormal movements, livedo reticularis.
CabergolineIt is a newer D2 agonist; more potent; more D2selective and longer acting (t½ > 60 hours) than

240S
EC
TIO
N5
HORMONES AND RELATED DRUGS
bromocriptine; needs to be given only twiceweekly. Incidence of nausea and vomiting is alsolower; some patients not tolerating or not respon-ding to bromocriptine have been successfullytreated with cabergoline. It is preferred fortreatment of hyperprolactinemia and acromegaly.Some patients who achieve total regression ofprolactinoma and normalization of prolactin levelscan stop cabergoline without recurrence.Dose: Start with 0.25 mg twice weekly; if needed increaseafter every 4–8 weeks to max. of 1 mg twice weekly.CABERLIN 0.5 mg tab, CAMFORTE 0.5, 1 mg tabs.
GONADOTROPINS (Gns)
The anterior pituitary secretes two Gns viz. FSHand LH. Both are glycoproteins containing23–28% sugar and consist of two peptide chains.The -chain (92AA) is common between FSHand LH, but their -chains are different: FSH(111 AA), LH (121 AA). Paradoxically the MWof FSH (~33KD) is greater than that of LH (~30KD), because of the sugar moieties.
Physiological functions FSH and LH actin concert to promote gametogenesis and secretionof gonadal hormones.
FSH In the female it induces follicular growth,development of ovum and secretion of estrogens.In the male it supports spermatogenesis and hasa trophic influence on seminiferous tubules.Ovarian and testicular atrophy occurs in theabsence of FSH.
LH It induces preovulatory swelling of the ripegraafian follicle and triggers ovulation followedby luteinization of the ruptured follicle and sustainscorpus luteum till the next menstrual cycle. Itis also probably responsible for atresia of theremaining follicles. Progesterone secretion occursonly under the influence of LH. In the male LHstimulates testosterone secretion by the interstitialcells and is designated interstitial cell stimulatinghormone (ICSH).
Distinct LH and FSH receptors are expressed onthe target cells. Both are G protein coupled receptors whichon activation increase cAMP production. This in turnstimulates gametogenesis and conversion of cholesterol to
pregnenolone—the first step in progesterone, testosterone andestrogen synthesis. In the testes FSH receptor is expressedon seminiferous (Sertoli) cells while LH receptor is expressedon interstitial (Leydig) cells. In the ovaries FSH receptorsare present only on granulosa cells, while LH receptors arewidely distributed on interstitial cells, theca cells, preovulatorygranulosa cells and luteal cells.
Regulation of secretion A single releasing factor(decapeptide designated GnRH) is produced by the hypo-thalamus which stimulates synthesis and release of both FSHand LH from pituitary. It is, therefore, also referred to asFSH/LH-RH or simply LHRH or gonadorelin. It has beendifficult to explain how hypothalamus achieves a divergentpattern of FSH and LH secretion in menstruating womenthrough a single releasing hormone. Since GnRH is secretedin pulses and the frequency as well as amplitude of thepulses differs during follicular (high frequency, low amplitude)and luteal (lower frequency, higher amplitude) phases, it isconsidered that frequency and amplitude of GnRH pulsesdetermines whether FSH or LH or both will be secreted,as well as the amount of each. Further, the feedback regulationof FSH and LH may be different. In general, feedbackinhibition of LH is more marked than that of FSH. In femalesestradiol and progesterone inhibit both FSH and LH secretionmainly through hypothalamus, but also by direct action onpituitary. However, the marked and sustained preovulatoryrise in estrogen level paradoxically stimulates LH and FSHsecretion. In addition there are other regulatory substances,e.g. Inhibin—a peptide from ovaries and testes, selectivelyinhibits FSH release, but not LH release. Dopamine inhibitsonly LH release. Testosterone is weaker than estrogens ininhibiting Gn secretion, but has effect on both FSH andLH. GnRH acts on gonadotropes through a G-protein coupledreceptor which acts by increasing intracellular Ca2+ throughPIP2 hydrolysis.
The Gn secretion increases at puberty and is higherin women than in men. In men, the levels of FSH and LHremain practically constant (LH > FSH) while in menstrua-ting women they fluctuate cyclically. During the follicularphase, moderate levels of FSH and low levels of LH prevail.There is a midcycle surge of both, but more of LH, justbefore ovulation, followed by progressive fall during the lutealphase. Gn levels are high in menopausal women due to lossof feedback inhibition by sex steroids and inhibin.
Pathological involvement Disturbances of Gn secretionfrom pituitary may be responsible for delayed puberty orprecocious puberty both in girls and boys.
Inadequate Gn secretion results in amenorrhoea andsterility in women; oligozoospermia, impotence and inferti-lity in men. Excess production of Gn in adult women causespolycystic ovaries.
Preparations
All earlier gonadotropin preparations were administered byi.m. route. The newer more purified preparations can be

241C
HA
PTE
R 17
ANTERIOR PITUITARY HORMONES
given s.c. They are partly metabolized, but mainly excretedunchanged in urine: t½ 2–6 hours.1. Menotropins (FSH + LH): is a preparation obtainedfrom urine of menopausal women:PREGNORM, PERGONAL, GYNOGEN 75/150; 75 IU FSH+ 75 IU LH activity per amp, also 150 IU FSH + 150 IULH per amp.
2. Urofollitropin or Menotropin (pure FSH): METRODIN,FOLGEST, FOLICULIN, PUREGON 75 IU and 150 IU peramp. This preparation has been preferred over the combinedFSH + LH preparation for induction of ovulation in womenwith polycystic ovarian disease: these patients have elevatedLH/FSH ratio; use of FSH alone is considered advantageous.It is also claimed to improve chances of obtaining goodquality ova for in vitro fertilization.
3. Human chorionic gonadotropin (HCG): is derived fromurine of pregnant women.CORION, PROFASI, PUBERGEN 1000 IU, 2000 IU, 5000 IU,10,000 IU, all as dry powder with separate solvent for injection.The foetal placenta secretes HCG which is absorbed inmaternal circulation and maintains corpus luteum ofpregnancy. It is a glycoprotein with 33% sugar and 237amino acids in two chains, MW 38000. It is excreted inurine by the mother from which it is commercially obtained.HCG binds to LH receptor with equal avidity; action ofHCG is indistinguishable from that of LH.
Recombinant human FSH (rFSH: Follitropin and follitropin) and recombinant human LH (rLH: Lutropin) as well asrecombinant HCG (rHCG: Choriogonadotropin ) havebecome available. These are more purified and have vertuallyreplaced the urine derived preparations in the developedcountries. They are more expensive.
Recombinant human LH (rhLH) is marketed asLUVERIS 75 IU inj.; indications and use is similar to HCG.
Uses1. Amenorrhoea and infertility When it is dueto deficient production of Gns by pituitary. Gnsare generally tried when attempts to induceovulation with clomiphene have failed or whennonovulation is due to polycystic ovaries. Theprocedure is to give 1 injection of menotropins(75 IU FSH + 75 IU LH or 75 IU pure FSH))i.m. daily for 10 days followed the next day by10,000 IU of HCG. Ovulation occurs within thenext 24–48 hours in upto 75% cases and thewoman may conceive. However, rates of abortionand multiple pregnancy are high, but not ofteratogenesis.
To improve predictability of time ofovulation (controlled ovarian hyperstimulation)most experts now concurrently suppress
endogenous FSH/LH secretion either bycontinuous pretreatment with a superactive GnRHagonist or by a GnRH antagonist.
2. Hypogonadotrophic hypogonadism inmales manifesting as delayed puberty or defectivespermatogenesis oligozoospermia, malesterility. Generally, sexual maturation is inducedby androgens and therapy with HCG is startedwhen fertility is desired. Start with 1000–4000IU of HCG i.m. 2–3 times a week (to stimulatetestosterone secretion), add FSH 75 IU + LH75 IU after 3–4 months (to stimulate spermato-genesis) and reduce dose of HCG; continuetreatment for 6–12 months for optimumresults, which nevertheless are not alwaysimpressive.3. Cryptorchidism Since undescended testescan cause infertility and predispose to testicularcancer, medical/surgical treatment is imperative.Descent of testes can be induced by androgenswhose production is stimulated by LH. Treatmentwith HCG can be tried at the earliest after theage of 1 year, preferably before 2 years if thereis no anatomical obstruction; 1000–2000 IU isgiven i.m. 2–3 times a week till the testes descend.If 2–6 week treatment does not induce descent,surgery should be performed.
4. To aid in vitro fertilization Menotropins(FSH + LH or pure FSH) have been used toinduce simultaneous maturation of several ovaand to precisely time ovulation so as to facilitatetheir harvesting for in vitro fertilization.
Adverse effects and precautions
Ovarian hyperstimulation—polycystic ovary, painin lower abdomen and even ovarian bleeding andshock can occur in females.Precocious puberty is a risk when given tochildren.Allergic reactions have occurred and skin testsare advised. Hormone dependent malignancies(prostate, breast) must be excluded.Other side effects are edema, headache, moodchanges.

242S
EC
TIO
N5
HORMONES AND RELATED DRUGS
GONADOTROPIN RELEASING HORMONE (GnRH):GONADORELIN
Synthetic GnRH injected i.v. (100 µg) induces prompt releaseof LH and FSH followed by elevation of gonadal steroidlevels. It has a short plasma t½ (4–8 min) due to rapidenzymatic degradation; has been used for testing pituitary-gonadal axis in male as well as female hypogonadism.
Since only pulsatile exposure to GnRH induces FSH/LHsecretion, while continuous exposure desensitizes pituitarygonadotropes resulting in loss of Gn release, therapy withGnRH or its analogues is not useful in the treatment ofhypogonadism.
Superactive / long-acting GnRH agonistsMany analogues of GnRH, e.g. Goserelin, Leuprolide,Nafarelin, Triptorelin, have been developed which are 15-150times more potent than natural GnRH and longer acting(t½ 2–6 hours) because of high affinity for GnRH receptorand resistance to enzymatic hydrolysis. Because physiologicalrelease of GnRH is in pulses, whereas these agonists actcontinuously; they only initially increase Gn secretion. After1–2 weeks they cause desensitization and down regulationof GnRH receptors inhibition of FSH and LH secretion suppression of gonadal function. Spermatogenesis orovulation cease and testosterone or estradiol levels fall tocastration levels. Recovery occurs within 2 months of stoppingtreatment.
The superactive GnRH agonists are used as nasal sprayor injected s.c. Long-acting preparations for once a months.c. injection have been produced (triptorelin, goserelin depot).The resulting reversible pharmacological oophorectomy/orchidectomy is being used in precocious puberty, prostaticcarcinoma, endometriosis, premenopausal breast cancer,uterine leiomyoma, polycystic ovarian disease and to assistinduced ovulation. They also have potential to be used ascontraceptive for both males and females.
Nafarelin This long-acting GnRH agonist is150 times more potent than native GnRH. It isused as intranasal spray from which bioavailabilityis only 4–5%.NASAREL 2 mg/ml soln for nasal spray; 200 µg per actuation.Down regulation of pituitary GnRH receptorsoccurs in10 days but peak inhibition of Gn releaseoccurs at one month. It is broken down in thebody to shorter peptide segments; plasma t½ is2–3 hours. Uses are:Assisted reproduction: Endogenous LH surgeneeds to be suppressed when controlled ovarianhyperstimulation is attempted by exogenous FSHand LH injection, so that precisely timed matureoocytes can be harvested. This is achieved by400 g BD intranasal nafarelin, reduced to200 g BD when menstrual bleeding occurs.
Uterine fibroids: Nafarelin 200 g BD intranasalfor 3–6 months can reduce the size of leiomyomaand afford symptomatic relief.Endometriosis: 200 µg in alternate nostril BDfor upto 6 months. As effective as danazol, butsecond course cannot be given due to risk ofosteoporosis.Central precocious puberty: 800 µg BD by nasalspray; breast and genital development is arrestedin girls and boys. The effect is reversible; pubertalchanges resume when therapy is discontinued.Adverse effects: Hot flashes, loss of libido,vaginal dryness, osteoporosis, emotional lability.Goserelin Another long-acting GnRH agonistavailable as a depot s.c./i.m. injection to be usedboth for endogenous Gn suppression beforeovulation induction, as well as for endometriosis,carcinoma prostate, etc. To achieve pituitarydesensitization before ovulation induction withexogenous Gns: 3.6 mg of the depot injectionis given once in the anterior abdominal wall1–3 weeks earlier.
For endometriosis and carcinoma prostate 3.6mg is injected in the same way every 4 weeksor 10.8 mg is injected every 3 months. Anandrogen antagonist (bicalutamide) is givenconcurrently for 3–4 weeks when goserelin is usedfor carcinoma prostate.ZOLADEX 3.6 mg prefilled syringe, ZOLDEX L-A 10.8mg vial depot injection.
Triptorelin: This long acting GnRH agonist isformulated as a regular release daily s.c. injectionfor short term indications, such as femaleinfertility, and as a depot i.m. monthly injectionfor long-term Gn suppression in the treatmentof carcinoma prostate, endometriosis, precociouspuberty and uterine leiomyoma. For prostatecancer, it is combined with an androgen antagonistflutamide or bicalutamide to prevent the initialflare up of the tumour that occurs due to increasein Gn secretion for the first 1–2 weeks.
Continuous treatment with any GnRH agonistis not advised beyond 6 months due to risk ofosteoporosis and other complications.

243C
HA
PTE
R 17
ANTERIOR PITUITARY HORMONES
Fibroids, endometriosis, carcinoma prostate: 3.75–7.5 mgi.m. every 4 weeks.Precocious puberty: 50 g/kg i.m. of depot inj. every 4 weeks.Assisted reproduction: 0.1 mg s.c. daily for 10 days from2nd day of cycle.DECAPEPTYL DAILY 0.1 mg inj., DECAPEPTYL DEPOT3.75 mg inj.
Leuprolide This long acting GnRH agonist isinjected s.c./i.m. daily or as a depot injection oncea month for palliation of carcinoma prostatealongwith an androgen antagonist, as well as forother conditions needing long term Gn suppression.LUPRIDE 1 mg inj., 3.75 mg depot inj., PROGTASE 1 mg/mlinj.
GnRH antagonists Some more extensively substitutedGnRH analogues act as GnRH receptor antagonists. Theyinhibit Gn secretion without causing initial stimulation. Theearly GnRH antagonists had the limitation of producingreactions due to histamine release. Later agents like ganirelixand cetrorelix have low histamine releasing potential andare being clinically used as s.c. inj. in specialized centresfor inhibiting LH surges during controlled ovarian stimulationin women undergoing in vitro fertilization. Their advantagesover long-acting GnRH agonists include:• They produce quick Gn suppression by competitive
antagonism, need to be started only from 6th day ofovarian hyperstimulation.
• They carry a lower risk of ovarian hyperstimulationsyndrome.
• They achieve more complete suppression of endogenousGn secretion.
However, pregnancy rates are similar or may even be lower.
THYROID STIMULATING HORMONE(TSH, THYROTROPIN)
It is a 210 amino acid, two chain glycoprotein(22% sugar), MW 30000.
Physiological function TSH stimulatesthyroid to synthesize and secrete thyroxine (T4)and triiodothyronine (T3). Its actions are:• Induces hyperplasia and hypertrophy of thyroid
follicles and increases blood supply to thegland.
• Promotes trapping of iodide into thyroid byincreasing Na+: Iodide symporter (NIS).
• Promotes organification of trapped iodine andits incorporation into T3 and T4 by increasingperoxidase activity.
• Enhances endocytotic uptake of thyroid colloid
by the follicular cells and proteolysis of thyro-globulin to release more of T3 and T4. Thisaction starts within minutes of TSHadministration.
The TSH receptor present on thyroid cells is a GPCR whichutilizes the adenylyl cyclase-cAMP transducer mechanism(by coupling to Gs protein) to produce its effects. In humanthyroid cells high concentration of TSH also inducesPIP2 hydrolysis by the linking of TSH receptor to Gq protein.The resulting increase in cytosolic Ca2+ and protein kinase Cactivation may also mediate TSH action, particularlygeneration of H2O2 needed for oxidation of iodide andiodination of tyrosil residues.
Regulation of secretion Synthesis and release of TSHby pituitary is controlled by hypothalamus primarily throughTRH, while somatostatin inhibits TSH secretion. Dopaminealso reduces TSH production induced by TRH. The TRHreceptor on pituitary thyrotrope cells is a GPCR which islinked to Gq protein and activates PLC–IP3/DAG–cytosolicCa2+ pathway to enhance TSH synthesis and release. Thenegative feedback for inhibiting TSH secretion is providedby the thyroid hormones which act primarily at the levelof the pituitary, but also in the hypothalamus. T3 has beenshown to reduce TRH receptors on the thyrotropes.
Pathological involvement Only few cases of hypo-or hyperthyroidism are due to inappropriate TSH secretion.In majority of cases of myxoedema TSH levels are markedlyelevated because of deficient feedback inhibition. Graves’disease is due to an immunoglobulin of the IgG class whichattaches to the thyroid cells and stimulates them in the sameway as TSH. Consequently, TSH levels are low. Contraryto earlier belief, TSH is not responsible for exophthalmosseen in Graves’ disease because TSH levels are low.
Use Thyrotropin has no therapeutic use. Thyroxine is thedrug of choice even when hypothyroidism is due to TSHdeficiency. The diagnostic application is to differentiatemyxoedema due to pituitary dysfunction from primary thyroiddisease.
ADRENOCORTICOTROPIC HORMONE(ACTH, CORTICOTROPIN)
It is a 39 amino acid single chain peptide, MW4500, derived from a larger peptide pro-opiomelanocortin (MW 30,000) which also gives riseto endorphins, two lipotropins and two MSHs.
Physiological function ACTH promotessteroidogenesis in adrenal cortex by stimulatingcAMP formation in cortical cells (through specificcell surface GPCRs) rapidly increases the

244S
EC
TIO
N5
HORMONES AND RELATED DRUGS
availability of cholesterol for conversion topregnenolone which is the rate limiting step inthe production of gluco, mineralo and weaklyandrogenic steroids. Induction of steroidogenicenzymes occurs after a delay resulting in 2nd phaseACTH action. The stores of adrenal steroids arevery limited and rate of synthesis primarilygoverns the rate of release. ACTH also exertstrophic influence on adrenal cortex (again throughcAMP): high doses cause hypertrophy and hyper-plasia. Lack of ACTH results in adrenal atrophy.However, zona glomerulosa is little affectedbecause angiotensin II also exerts trophic influenceon this layer and sustains aldosterone secretion.Regulation of secretion Hypothalamus regulatesACTH release from pituitary through corticotropin-releasinghormone (CRH). The CRH receptor on corticotropes is alsoa GPCR which increases ACTH synthesis as well as releaseby raising cytosolic cAMP. Secretion of ACTH has a circadianrhythm. Peak plasma levels occur in the early morning,decrease during day and are lowest at midnight.Corticosteroids exert inhibitory feedback influence on ACTHproduction by acting directly on the pituitary as well asindirectly through hypothalamus.
A variety of stressful stimuli, e.g. trauma, surgery, severepain, anxiety, fear, blood loss, exposure to cold, etc. generateneural impulses which converge on median eminence to causeelaboration of CRH. The feedback inhibition appears tobe overpowered during stress—rise in ACTH secretioncontinues despite high plasma level of cortisol induced by it.Arginine vasopressin (AVP) enhances the action of CRH oncorticotropes and augments ACTH release. AVP release andaugmentation of ACTH action appears to be important duringstress.
Pathological involvement Excess production of ACTHfrom basophil pituitary tumours is responsible for some casesof Cushing’s syndrome. Hypocorticism occurs in pituitaryinsufficiency due to low ACTH production. Iatrogenicsuppression of ACTH secretion and pituitary adrenal axisis the most common form of abnormality encounteredcurrently due to the use of pharmacological doses ofglucocorticoids in nonendocrine diseases.
Use ACTH is used primarily for the diagnosis of disordersof pituitary adrenal axis. Injected i.v. 25 IU causes increasein plasma cortisol if the adrenals are functional. Direct assayof plasma ACTH level is now preferred.
For therapeutic purposes, ACTH does not offer anyadvantage over corticosteroids and is more inconvenient,expensive as well as less predictable.

Thyroid Hormones andThyroid Inhibitors
ChapterChapterChapterChapterChapter 1818181818
THYROID HORMONE
The thyroid gland secretes 3 hormones—thyro-xine (T4), triiodothyronine (T3) and calcitonin.The former two are produced by thyroid follicles,have similar biological activity and the term‘thyroid hormone’ is restricted to these only.Calcitonin produced by interfollicular ‘C’ cellsis chemically and biologically entirely different.It is considered along with parathormone, (Ch.24) with which it regulates calcium metabolism.
The physiological significance of thyroid gland wasrecognized only after Graves and Basedow (1835, 1840)associated the clinical features of the ‘Graves’ disease’ withswelling of thyroid gland and Gull (1874) correlated myxo-edema with its atrophy. Kendall (1915) obtained crystallinethyroxine and postulated its chemical formula which wasconfirmed in 1926. Thyroxine was the first hormone to besynthesized in the laboratory. Since, T4 could not accountfor all the biological activity of thyroid extract, search wasmade and more potent T3 was discovered in 1952.
CHEMISTRY AND SYNTHESIS
Both T4 and T3 are iodine containing derivativesof thyronine which is a condensation productof two molecules of the amino acid tyrosine.Thyroxine; is 3, 5, 3´, 5´–tetraiodothyronine whileT3 is 3, 5, 3´ triiodothyronine.
The thyroid hormones are synthesized andstored in the thyroid follicles as part of thyroglo-bulin molecule—which is a glycoprotein synthe-sized by thyroid cells, MW 660 KDa, contains10% sugar. The synthesis, storage and releaseof T4 and T3 is summarized in Fig. 18.1 andinvolves the following processes.
1. Iodide uptake The total body content ofI2, obtained from food and water, is 30–50 mg,out of which about 1/5 is present in the thyroid.Concentration of iodide in blood is low(0.2–0.4 µg/dl) but thyroid cells have an active
transport process Na+:: iodide symporter (NIS)to concentrate this anion; this trapping is stimu-lated by TSH to exceed a gradient of more than100 fold by inducing and activating NIS. TheI2 content of thyroid gland somehow regulatesthe uptake mechanism: meagre store activatingand large store inhibiting it. The iodide concen-trating mechanism is not peculiar to thyroid. Skin,salivary glands, gastric mucosa, intestine, mam-mary glands and placenta also possess it, butuptake in these organs is not stimulated by TSH.
2. Oxidation and iodination Iodide trappedby follicular cells is carried across the apical mem-brane by another transporter termed ‘pendrin’ andoxidized by the membrane bound thyroidperoxidase enzyme to iodinium (I+) ions orhypoiodous acid (HOI) or enzyme-linked hypo-iodate (E-OI) with the help of H2O2. These formsof iodine combine avidly with tyrosil residuesof thyroglobulin, apparently without anyenzymatic intervention, to form monoiodotyrosine(MIT) and diiodotyrosine (DIT) while theseresidues are still attached to the thyroglobulinchains.3. Coupling Pairs of iodinated tyrosil residuescouple together (Fig. 18.2) to form T3 and T4.
Normally much more T4 than T3 is formed,but during I2 deficiency relatively more MIT isavailable and a greater proportion of T3 is formed.Thus, more active hormone is generated withlesser amount of I2.
Coupling is an oxidative reaction and iscatalysed by the same thyroid peroxidase.Thyroglobulin is the most efficient protein,compared to other similar proteins, in supportingcoupling by providing favourable spatial configu-ration to facilitate the reaction. Oxidation of iodideand coupling are both stimulated by TSH.

246S
EC
TIO
N5
HORMONES AND RELATED DRUGS
Fig. 18.1: Synthesis, storage and secretion of thyroid hormoneTG—Thyroglobulin; MIT—Monoiodotyrosine; DIT—Diiodotyrosine; T3—Triiodothyronine; T4—Thyroxine(Tetraiodothyronine); HOI—Hypoiodous acid; EOI—Enzyme linked hypoiodate; NIS—Na+-iodidesymporter; Thyroid-stimulating hormone (TSH) activates steps 1, 2, 3, 4, and 5; Ionic inhibitors blockstep 1; Excess iodide interferes with steps 1, 2, 3 and 5 with primary action on step 3 and 5; Propylthiouracilinhibits steps 2 and 6; Carbimazole inhibits step 2 only
Fig. 18.2: Coupling of monoiodotyrosine (MIT) and diiodotyrosine (DIT)to produce triiodothyronine (T3)

247C
HA
PTE
R 18
THYROID HORMONES AND THYROID INHIBITORS
4. Storage and release Thyroglobulincontaining iodinated tyrosil and thyronil residuesis transported to the interior of the follicles andremains stored as thyroid colloid till it is takenback into the cells by endocytosis and brokendown by lysosomal proteases. The T4 and T3 soreleased is secreted into circulation while MITand DIT residues are deiodinated and the iodidereleased is reutilized. The uptake of colloid andproteolysis are stimulated by TSH: the quiscentgland has follicles distended with colloid and cellsare flat or cubical, while the TSH stimulated glandhas columnar cells and colloid virtually disappears.Normal human thyroid secretes 60–90 µg of T4
and 10–30 µg of T3 daily.
5. Peripheral conversion of T4 to T3 Peripheraltissues, especially liver and kidney, convert T4
to T3. About 1/3 of T4 secreted by thyroid under-goes this change and most of the T3 in plasmais derived from liver. Target tissues take up T3
from circulation for their metabolic need, exceptbrain and pituitary which take up T4 and convertit to T3 within their own cells. Almost equal amountsof 3, 5, 3´ triiodothyronine (normal T3 : active)and 3, 3´, 5´ triiodothyronine (reverse T3 or rT3:inactive) are produced in the periphery. The T4
to T3 conversion is carried out by the enzymeiodothyronine deiodinase which exists in 3 forms(D1, D2, D3). These forms differ in their organand cellular localization as well as product formed.Whereas type 2 deiodinase (D2) generates T3 andD3 generates rT3, the D1 form generates bothT3 and rT3. The antithyroid drug propylthiouracil(but not carbimazole) inhibits Type1 deiodinaseand the antiarrhythmic amiodarone inhibits bothD1 and D2 forms. Propranolol (high dose) andglucocorticoids also inhibit peripheral conversionof T4 to T3 (except in brain and in pituitary).
TRANSPORT, METABOLISM ANDEXCRETION
Thyroid hormones are avidly bound to plasmaproteins—only 0.03–0.08% of T4 and 0.2–0.5%of T3 are in the free form. Almost all proteinbound iodine (PBI) in plasma is thyroid hormone,
of which 90–95% is T4 and the rest T3. Bindingoccurs to 3 plasma proteins in the followingdecreasing order of affinity for T4:
(i) Thyroxine binding globulin (TBG)(ii) Thyroxine binding prealbumin (trans-
thyretin)(iii) Albumin
The normal concentration of PBI is 4–10 µg/dl; only 0.1–0.2 µg/dl of this is T3, rest is T4.During pregnancy thyroxine binding globulin isincreased—PBI levels are elevated, but there isno effect on thyroid status because theconcentration of free hormone remains unaltered.
Only the free hormone is available for actionas well as for metabolism and excretion. Meta-bolic inactivation of T4 and T3 occurs by deiodi-nation and glucuronide/sulfate conjugation of thehormones as well as that of their deiodinatedproducts. Liver is the primary site (also salivaryglands and kidneys). The conjugates are excretedin bile, of which a significant fraction is deconju-gated in intestines and reabsorbed (enterohepaticcirculation) to be finally excreted in urine.
Plasma t½ of T4 is 6–7 days, while that ofT3 is 1–2 days. The half-lives are shortened inhyperthyroidism and prolonged in hypothyroidismdue respectively to faster and slower metabolism.
REGULATION OF SECRETION
The secretion of hormones from the thyroid iscontrolled by anterior pituitary by the elaborationof thyrotropin, while TSH secretion itself isregulated by TRH produced in hypothalamus (seep. 243). Somatostatin elaborated by hypothalamusinhibits not only GH and prolactin, but also TSHsecretion from pituitary. The relation betweenthyroid, anterior pituitary and hypothalamus isdepicted in Fig. 18.3. The negative feedback bythe thyroid hormones is exercised directly on thepituitary as well as through hypothalamus. Theaction of TRH on pituitary and that of TSH onthyroid cells is mediated by enhanced cAMPsynthesis. High concentration of TSH also actsvia IP3/DAG–increased intracellular Ca2+ pathwayin the thyroid cells.

248S
EC
TIO
N5
HORMONES AND RELATED DRUGS
ACTIONS
The actions of T4 and T3 are qualitatively similarand are nicely depicted in the features of hypoand hyperthyroidism. They affect the function ofpractically every body cell.
1. Growth and development T4 and T3 areessential for normal growth and development. Themost remarkable action is metamorphosis oftadpole to frog: the tail is used-up to build lungs,limbs and other organs. The action cannot bebroadly labelled as catabolic or anabolic. It isexerted through a critical control of proteinsynthesis in the translation of the genetic code.Congenital deficiency of T4 and T3 resulting incretinism emphasizes their importance. Themilestones of development are delayed andpractically every organ and tissue of the bodysuffers. The greatest sufferer, however, is the ner-vous system. Retardation and nervous deficit isa consequence of paucity of axonal and dendriticramification, synapse formation and impairedmyelination. In adult hypothyroidism also, intel-ligence is impaired and movements are slow.
2. Intermediary metabolism Thyroidhormones have marked effect on lipid, carbo-hydrate and protein metabolism.
Lipid T4 and T3 indirectly enhance lipolysis bypotentiating the action of catecholamines and otherlipolytic hormones, probably by suppressing aphosphodiesterase → increased cAMP. As a resultplasma free fatty acid levels are elevated.Lipogenesis is also stimulated. All phases ofcholesterol metabolism are accelerated, but itsconversion to bile acids dominates. Thus,hyperthyroidism is characterized by hypocholes-terolemia. LDL levels in blood are reduced.
Carbohydrate Carbohydrate metabolism is alsostimulated. Though utilization of sugar by tissuesis increased (mainly secondary to increased BMR),glycogenolysis and gluconeogenesis in liver aswell as faster absorption of glucose from intestinesmore than compensate it → hyperglycaemia anddiabetic-like state with insulin resistance occurin hyperthyroidism.
Protein Synthesis of certain proteins is increa-sed, but the overall effect of T3 is catabolic—increased amounts of protein being used as energysource. Prolonged action results in negativenitrogen balance and tissue wasting. Weight lossis a feature of hyperthyroidism. T3, T4 in lowconcentrations inhibit mucoprotein synthesiswhich so characteristically accumulates inmyxoedema.
3. Calorigenesis T3 and T4 increase BMRby stimulation of cellular metabolism and resettingof the energystat. This is important for maintainingbody temperature. However, metabolic rate inbrain, gonads, uterus, spleen and lymph nodesis not significantly affected. The mechanism ofcalorigenesis was believed to be uncoupling ofoxidative phosphorylation: excess energy beingreleased as heat. However, this occurs only atvery high doses and is not involved in mediatingthe physiological actions of T3, T4. Dinitrophenoluncouples oxidative phosphorylation, but has nothyroid-like activity.
4. CVS T3 and T4 cause a hyperdynamic stateof circulation which is partly secondary toincreased peripheral demand and partly due todirect cardiac actions. Heart rate, contractility and
Fig. 18.3: Regulation of thyroid functionTSH—Thyroid stimulating hormone; TRH—Thyrotropinreleasing hormone; T3—Triiodothyronine; T4—Thyroxine;SST—Somatostatin

249C
HA
PTE
R 18
THYROID HORMONES AND THYROID INHIBITORS
output are increased resulting in a fast, boundingpulse. T3 and T4 stimulate heart by direct actionon contractile elements (increasing the myosinfraction having greater Ca2+ ATPase activity) andprobably by up regulation of β adrenergic recep-tors. Atrial fibrillation and other irregularities arecommon in hyperthyroidism. Thyroid hormonescan also precipitate CHF and angina. BP, speciallysystolic, is often raised. Myocardial O2
consumption can be markedly reduced byinduction of hypothyroidism.
5. Nervous system T3, T4 have profoundfunctional effect on CNS. Mental retardation isthe hallmark of cretinism; sluggishness and otherbehavioral features are seen in myxoedema.Hyperthyroid individuals are anxious, nervous,excitable, exhibit tremors and hyperreflexia.
6. Skeletal muscle Muscles are flabby andweak in myxoedema, while thyrotoxicosis produ-ces increased muscle tone, tremor and weaknessdue to myopathy.
7. GIT Propulsive activity of gut is increasedby T3/T4. Hypothyroid patients are often consti-pated, while diarrhoea is common in hyperthy-roidism.
8. Kidney T3 and T4 do not cause diuresisin euthyroid individuals, but the rate of urine flowis often increased when myxoedematous patientsare treated with it.
9. Haemopoiesis Hypothyroid patients suf-fer from some degree of anaemia which is res-tored only by T4 treatment. Thus, T4 appears tobe facilitatory to erythropoiesis.
10. Reproduction Thyroid has an indirecteffect on reproduction. Fertility is impaired inhypothyroidism and women suffer from oligo-menorrhoea. Normal thyroid function is requiredfor maintenance of pregnancy and lactation.
Mechanism of actionBoth T3 and T4 penetrate cells by active transportand produce majority of their actions by combiningwith a nuclear thyroid hormone receptor (TR)
which belongs to the steroid and retinoidsuperfamily of intracellular receptors.Two TR isoform families (TRα and TRβ) have been identified.Both bind T3 and function in similar manner, but their tissuedistribution differs, which may account for quantitativedifferences in the sensitivity of different tissues to T3.
In contrast to the steroid receptor, the TRresides in the nucleus even in the unligandedinactive state. It is bound to the ‘thyroid hormoneresponse element’ (TRE) in the enhancer regionof the target genes along with corepressors (Fig.18.4). This keeps gene transcription suppressed.When T3 binds to the ligand-binding domain ofTR, it heterodimerizes with retinoid X receptor(RXR) and undergoes a conformation changereleasing the corepressor and binding thecoactivator. This induces gene transcription →production of specific mRNA and a specificpattern of protein synthesis → various metabolicand anatomic effects. The expression of certaingenes is repressed by T3. In their case, theunliganded TR allows gene transcription, whilebinding of T3 to TR halts the process.
Many of the effects, e.g. tachycardia, arrhy-thmias, raised BP, tremor, hyperglycaemia aremediated, at least partly, by sensitization ofadrenergic receptors to catecholamines. Inductionof adenylyl cyclase, proliferation of β adreno-ceptors and a better coupling between these twohas been demonstrated.
Apart from the nuclear T3 receptor, other sites of thyroidhormone action have been described. It acts on cell membraneto enhance amino acid and glucose entry and on mitochondriato increase oxygen consumption. At these sites T4 appearsto be equipotent to T3, while at the nuclear receptor T4 hasmuch lower affinity, and even when bound to the TR, T4
does not promote gene transcription.
Relation between T4 and T3
• Thyroid secretes more T4 than T3, but in iodinedeficient state this difference is reduced.
• T4 is the major circulating hormone becauseit is 15 times more tightly bound to plasmaproteins.
• T3 is 5 times more potent than T4 and actsfaster. Peak effect of T3 comes in 1–2 dayswhile that of T4 takes 6–8 days.

250S
EC
TIO
N5
HORMONES AND RELATED DRUGS
Fig. 18.4: Mechanism of action of thyroid hormone on nuclear thyroid hormone receptor (TR).T3—Triiodothyronine; T4—Thyroxine; TRE—Thyroid hormone response element; RXR—Retinoid Xreceptor; mRNA—Messenger ribonucleic acid; 5’DI—5’Deiodinase (See text for explanation)
• T3 is more avidly bound to the nuclear receptorthan T4
and the T4-receptor complex is unableto activate/derepress gene transcription.
• About 1/3 of T4 is converted to T3 in the thyroidcells, liver and kidney by type 1 deiodinase(D1) and released into circulation. In addition,T3 is generated within the target cells (skeletalmuscle, heart, brain, pituitary) by another type(D2) of deiodinase.
Thus, it may be cocluded that T3 is the activehormone, while T4 is mainly a transport form;functions as a prohormone of T3. However, itmay directly produce some nongenomic actions.
Preparations
l-thyroxine sod.: ELTROXIN 25 μg, 50 μg, 100 μg tabs,ROXIN 100 µg tab, THYRONORM 12.5 μg, 25 μg, 50μg, 62.5 μg, 75 μg, 88 μg, 100 μg, 112 μg, 125 μg, 137μg, 150 μg tabs, THYROX 25 µg, 50 µg, 75 µg, 100 µgtabs. An injectable preparation for i.v. use is available elsewhere.
Triiodothyronine (Liothyronine) is not freely available in India.It is occasionally used i.v. along with l-thyroxine inmyxoedema coma.Clinically, l-thyroxine is preferred for all indi-cations over liothyronine because of moresustained and uniform action as well as lowerrisk of cardiac arrhythmias.
Pharmacokinetics and interactions
Oral bioavailability of l-thyroxine is ~ 75%, butsevere hypothyroidism can reduce oral absorp-tion. It should be administered in empty stomachto avoid interference by food. Sucralfate, iron,calcium and proton pump inhibitors also reducel-thyroxine absorption. CYP3A4 inducers likerifampin, phenytoin and carbamazepine acceleratemetabolism of T4; dose of l-thyroxine may needenhancement.

251C
HA
PTE
R 18
THYROID HORMONES AND THYROID INHIBITORS
USES
The most important use of thyroid hormone isfor replacement therapy in deficiency states:
1. Cretinism It is due to failure of thyroiddevelopment or a defect in hormone synthesis(sporadic cretinism) or due to extreme iodinedeficiency (endemic cretinism). It is usuallydetected during infancy or childhood; butscreening of neonates is the best preventivestrategy. Treatment with thyroxine (8–12 µg/kg)daily should be started as early as possible,because mental retardation that has already ensuedis only partially reversible. Response is dramatic:physical growth and development are restored andfurther mental retardation is prevented.
2. Adult hypothyroidism (Myxoedema)This is one of the commonest endocrine disorderswhich develops as a consequence of autoimmunethyroiditis or thyroidectomy; It may accompanysimple goiter if iodine deficiency is severe.Antibodies against thyroid peroxidase orthyroglobulin are responsible for majority of casesof adult hypothyroidism. Important drugs that cancause hypothyroidism are 131I, iodides, lithium andamiodarone. Treatment with T4 is most gratifying.It is often wise to start with a low dose—50 µgof l-thyroxine daily and increase every 2–3 weeksto an optimum of 100–200 µg/day (adjusted byclinical response and serum TSH levels). Furtherdose adjustments are made at 4–6 week intervalsneeded for reaching steady-state. Individualiza-tion of proper dose is critical, aiming atnormalization of serum TSH levels. Increase indose is mostly needed during pregnancy.
Subclinical hypothyroidism characterized byeuthyroid status and normal free serum thyroxine(FT4) level (> 9 pmol/L) but raised TSH level(>10 mU/L) should be treated with T4. For TSHlevel between 6–10 mU/L, replacement therapyis optional. It is preferable if patient has othercardiovascular risk factors.3. Myxoedema coma It is an emergency;characterized by progressive mental deteriorationdue to acute hypothyroidism: carries significantmortality. Rapid thyroid replacement is crucial.
Though liothyronine (T3) acts faster, its use isattended by higher risk of cardiac arrhythmias,angina, etc. Drug of choice is l-thyroxine (T4)200–500 μg i.v. followed by 100 μg i.v. OD tilloral therapy can be instituted. Some authoritiesrecommend adding low dose i.v. T3 10 μg8 hourly in younger patients with no arrhythmiaor ischaemia. Alternatively oral T4 500 μg loadingdose followed by 100–300 μg daily may be used,but in severe hypothyroidism, oral absorption isdelayed and inconsistent.
Other essential measures needed are—warming the patient, i.v. corticosteroids to coverattendant adrenal insufficiency, ventilatory andcardiovascular support, correction of hypo-natraemia and hypoglycaemia.4. Nontoxic goiter It may be endemic or spo-radic. Endemic is due to iodine deficiency whichmay be accentuated by factors present in water(excess calcium), food or milk (goitrin, thiocya-nates). A defect in hormone synthesis may beresponsible for sporadic cases. In both types,deficient production of thyroid hormone leads toexcess TSH → thyroid enlarges, more efficienttrapping of iodide occurs and probably greaterproportion of T3 is synthesized → enough hormoneto meet peripheral demands is produced so thatthe patient is clinically euthyroid. Thus, treatmentwith T4 is in fact replacement therapy in thiscondition as well, despite no overt hypothyroi-dism. Full maintenance doses must be given. Mostcases of recent diffuse enlargement of thyroidregress. Long-standing goiter with degenerativeand fibrotic changes and nodular goiter regresslittle or not at all. Thyroxine therapy may bewithdrawn after a year or so in some cases ifadequate iodine intake is ensured. Others needlife-long therapy.Endemic goiter and cretinism due to iodine deficiency inpregnant mother is preventable by ensuring daily ingestionof 150–200 µg of iodine. This is best achieved by iodizingedible salt by adding iodate (preferred over iodide). In Indiaiodization of table salt (100 µg iodine/g salt) is requiredunder the National Programme, but recently mandatoryiodization rule has been withdrawn.
5. Thyroid nodule Certain benign functioningnodules regress when TSH is suppressed by

252S
EC
TIO
N5
HORMONES AND RELATED DRUGS
T4 therapy. Nonfunctional nodules and those non-responsive to TSH (that are associated with lowTSH levels) do not respond and should not betreated with levothyroxine. T4 therapy should bestopped if the nodule does not decrease in sizewithin 6 months, and when it stops regressingafter the initial response.
6. Papillary carcinoma of thyroid Thistype of cancer is often responsive to TSH. Innonresectable cases, full doses of T4 suppressendogenous TSH production and may inducetemporary regression.
7. Empirical uses T4 has been sometimes used in thefollowing conditions without any rationale; response isunpredictable.
Refractory anaemias.Mental depressionMenstrual disorders, infertility not corrected by usualtreatment.Chronic/non-healing ulcers.Obstinate constipation.
Thyroxine is not to be used for obesity and as a hypo-cholesterolemic agent.
THYROID INHIBITORSThese are drugs used to lower the functionalcapacity of the hyperactive thyroid gland.
Thyrotoxicosis is due to excessive secretionof thyroid hormones. The two main causes areGraves’ disease and toxic nodular goiter. Graves’disease is an autoimmune disorder: IgG class ofantibodies to the TSH receptor are detected inblood. They bind to and stimulate thyroid cells,and produce other TSH like effects. Due to feed-back inhibition, TSH levels are low. The accom-panying exophthalmos is due to autoimmuneinflammation of periorbital tissues.
Toxic nodular goiter, which produces thyroidhormone independent of TSH, mostly superveneson old nontoxic goiters. It is more common inthe elderly; ocular changes are generally absent.
CLASSIFICATION
1. Inhibit hormone synthesis (Antithyroiddrugs)Propylthiouracil, Methimazole, Carbimazole.
2. Inhibit iodide trapping (Ionic inhibitors)Thiocyanates (–SCN), Perchlorates (–ClO4),Nitrates (–NO3).
3. Inhibit hormone releaseIodine, Iodides of Na and K, Organic iodide.
4. Destroy thyroid tissueRadioactive iodine (131I, 125I, 123I).
Compounds in groups 1 and 2 may be collec-tively called goitrogens because, if given in excess,they cause enlargement of thyroid by feedbackrelease of TSH.In addition, certain drugs used in high doses for prolongedperiods cause hypothyroidism/goiter as a side effect:• Lithium: inhibits thyroid hormone release.• Amiodarone: inhibits peripheral conversion of T4 to T3;
also interferes with thyroid hormone action.• Sulfonamides, paraaminosalicylic acid: inhibit thyro-
globulin iodination and coupling reaction.• Phenobarbitone, phenytoin, carbamazepine, rifampin:
induce metabolic degradation of T4/T3.
Goitrin—found in plants (cabbage, turnip, mustard, etc.),is the cause of goiter in cattle who feed on these plants.May contribute to endemic goiter in certain iodine deficientregions.
ANTITHYROID DRUGS (Thioamides)
By convention, only the hormone synthesisinhibitors are called antithyroid drugs, thoughthis term has also been applied to all thyroidinhibitors.
Thiourea derivatives were found to produce goiterand hypothyroidism in rats in the 1940s. Open chaincompounds were found to be toxic. Subsequently, methyland propyl thiouracil and thioimidazole derivativesmethimazole and carbimazole were found to be safe andeffective.
Antithyroid drugs bind to the thyroidperoxidase and prevent oxidation of iodide/iodotyrosyl residues, thereby;
(i) Inhibit iodination of tyrosine residues inthyroglobulin
(ii) Inhibit coupling of iodotyrosine residues toform T3 and T4.
Action (ii) has been observed at lowerconcentration of antithyroid drugs than action (i).Thyroid colloid is depleted over time and bloodlevels of T3/T4 are progressively lowered.

253C
HA
PTE
R 18
THYROID HORMONES AND THYROID INHIBITORS
TABLE 18.1 Differences between propylthiouracil and carbimazole
Propylthiouracil Carbimazole
1. Dose to dose less potent About 5 × more potent2. Highly plasma protein bound Less bound3. Less transferred across placenta and in milk Larger amounts cross to foetus and in milk4. Plasma t½ 1–2 hours 6–10 hours5. Single dose acts for 4–8 hours 12–24 hours6. No active metabolite Produces active metabolite—methimazole7. Multiple (2–3) daily doses needed Mostly single daily dose8. Inhibits peripheral conversion of T4 to T3 Does not inhibit T4 to T3 conversion
Thioamides do not interfere with trapping ofiodide and do not modify the action of T3 andT4 on peripheral tissues or on pituitary. Goiteris not the result of potentiation of TSH actionon thyroid, but is due to increased TSH releaseas a consequence of reduction in feedbackinhibition. No goiter occurs if antithyroid drugsare given to hypophysectomised animals or if T4
is given along with them. Antithyroid drugs donot affect release of T3 and T4—their effects arenot apparent till thyroid is depleted of its hormonecontent.
Propylthiouracil also inhibits peripheralconversion of T4 to T3 by D1 type of 5’DI, butnot by D2 type. This may partly contribute toits antithyroid effects. Methimazole andcarbimazole do not have this action (Table 18.1)and may even antagonize that of propylthiouracil.
Pharmacokinetics All antithyroid drugs arequickly absorbed orally, widely distributed in thebody, enter milk and cross placenta; are meta-bolized in liver and excreted in urine primarilyas metabolites. All are concentrated in thyroid:intrathyroid t½ is longer: effect of a single doselasts longer than would be expected from theplasma t½. Carbimazole acts largely by gettingconverted to methimazole in the body and is longeracting than propythiouracil.
Adverse effects Hypothyroidism and goitercan occur due to overtreatment, but is reversibleon stopping the drug. It is indicated by enlarge-
ment of thyroid, and is due to excess TSHproduction. Goiter does not develop withappropriate doses which restore T4 concentrationto normal so that feedback TSH inhibition ismaintained.Important side effects are: g.i. intolerance, skinrashes and joint pain.Loss or graying of hair, loss of taste, fever andliver damage are infrequent.A rare but serious adverse effect is agranulocytosis(1 in 500 to 1000 cases); It is mostly reversible.There is partial cross reactivity between propyl-thiouracil and carbimazole.
Preparations and dose
Propylthiouracil: 50–150 mg TDS followed by 25–50 mgBD–TDS for maintenance. PTU 50 mg tab.Methimazole: 5–10 mg TDS initially, maintenance dose5–15 mg daily in 1–2 divided doses.Carbimazole: 5–15 mg TDS initially, maintenance dose2.5–10 mg daily in 1–2 divided doses, NEO MERCAZOLE,THYROZOLE, ANTITHYROX 5 mg tab.
Carbimazole is more commonly used in India.Propylthiouracil (600–900 mg/day) may be prefer-red in thyroid storm for its inhibitory action onperipheral conversion of T4 to more active T3.It is also used in patients developing adverseeffects with carbimazole.Use Antithyroid drugs control thyrotoxicosis inboth Graves’ disease and toxic nodular goiter.Clinical improvement starts after 1–2 weeks ormore (depending on hormone content of thyroidgland). Iodide loaded patients (who have received

254S
EC
TIO
N5
HORMONES AND RELATED DRUGS
iodide containing contrast media/cough mixtures,amiodarone) are less responsive. Maintenancedoses are titrated on the basis of clinical statusof the patient. The following strategies areadopted.(i) As definitive therapy (a) Remission mayoccur in upto half of the patients of Graves’ diseaseafter 1–2 years of treatment: the drug can then bewithdrawn. If symptoms recur—treatment isreinstituted. This is preferred in young patients witha short history of Graves’ disease and a small goiter.(b) Remissions are rare in toxic nodular goiter:surgery (or 131I) is preferred. However, in frailelderly patient with multinodular goiter who maybe less responsive to 131I, permanent maintenancetherapy with antithyroid drugs can be employed.
(ii) Preoperatively Surgery in thyrotoxic patientsis risky. Young patients with florid hyperthyroidismand substantial goiter are rendered euthyroid withcarbimazole before performing subtotal thyroidec-tomy.
(iii) Along with 131I Initial control with antithy-roid drug—1 to 2 weeks gap—radioiodine dosing—resume antithyroid drug after 5–7 days and gra-dually withdraw over 3 months as the responseto 131I develops. This approach is preferred inolder patients who are to be treated with 131I,but require prompt control of severe hyperthyroi-dism. This will also prevent initial hyperthyroidismfollowing 131I due to release of stored T4.Advantages of antithyroid drugs over surgery/131Iare:
(a) No surgical risk, scar or chances of injury toparathyroid glands or recurrent laryngealnerve.
(b) Hypothyroidism, if induced, is reversible.(c) Can be used even in children and young
adults.Disadvantages are:
(a) Prolonged (often life-long) treatment isneeded because relapse rate is high.
(b) Not practicable in uncooperative/unintelli-gent patient.
(c) Drug toxicity.
Thyroidectomy and 131I are contraindicated duringpregnancy. With antithyroid drugs risk of foetalhypothyroidism and goiter is there. However, lowdoses of propylthiouracil are preferred: its greaterprotein binding allows less transfer to the foetus.For the same reason it is to be preferred in thenursing mother. However, methimazole has alsonow been found to be safe during pregnancy.
Propylthiouracil is used in thyroid storm aswell (see p. 256).
IONIC INHIBITORS
Certain monovalent anions inhibit iodide trapping by NISinto the thyroid probably because of similar hydrated ionicsize—T4/T3 cannot be synthesized. Perchlorate is 10 timesmore potent than thiocyanate in blocking NIS, while nitrateis very weak.They are toxic and not clinically used now.Thiocyanates: can cause liver, kidney, bone marrow and braintoxicity.Perchlorates: produce rashes, fever, aplastic anaemia,agranulocytosis.
IODINE AND IODIDES
Though iodine is a constituent of thyroidhormones, it is the fastest acting thyroid inhibitor.In Grave’s disease the gland, if enlarged, shrinks,becomes firm and less vascular. The thyroid statusstarts returning to normal at a rate commensuratewith complete stoppage of hormone release fromthe gland. The thyroid gland involutes and colloidis restored. The response to iodine and iodidesis identical, because elemental iodine is reducedto iodide in the intestines. With daily adminis-tration, peak effects are seen in 10–15 days, afterwhich ‘thyroid escape’ occurs and thyrotoxicosismay return with greater vengeance. Worseningof hyperthyroidism especially occurs inmultinodular goiter.
All facets of thyroid function seem to be affec-ted, but the most important action is inhibitionof hormone release—‘thyroid constipation’. Endo-cytosis of colloid and proteolysis of thyroglobulincomes to a halt. The mechanism of action is notclear. Excess iodide inhibits its own transport intothyroid cells by interfering with expression ofNIS on the cell membrane. In addition, it

255C
HA
PTE
R 18
THYROID HORMONES AND THYROID INHIBITORS
attenuates TSH and cAMP induced thyroidstimulation. Excess iodide rapidly and brieflyinterferes with iodination of tyrosil and thyronilresidues of thyroglobulin (probably by alteringredox potential of thyroid cells) resulting inreduced T3/T4 synthesis (Wolff-Chaikoff effect).However, within a few days, the gland ‘escapes’from this effect and hormone synthesis resumes.
Preparations and dose Lugol’s solution (5% iodinein 10% Pot. iodide solution): LUGOL’S SOLUTION,COLLOID IODINE 10%: 5–10 drops/day. COLLOSOL8 mg iodine/5 ml liq.Iodide (Sod./Pot.) 100–300 mg/day (therapeutic), 5–10 mg/day (prophylactic) for endemic goiter.
Uses1. Preoperative preparation for thyroidectomyin Graves’ disease: Iodine is generally given for10 days just preceding surgery. The aim is tomake the gland firm, less vascular and easier tooperate on. Though iodide itself will lower thethyroid status, it cannot be relied upon to attaineuthyroidism which is done by use of carbimazolebefore starting iodide. Propranolol may be givenadditionally for rapid control of symptoms.
2. Thyroid storm Lugol’s iodine (6–10 drops)or iodine containing radiocontrast media (iopanoicacid/ipodate) orally are used to stop any furtherrelease of T3/T4 from the thyroid and to decreaseT4 to T3 conversion.
3. Prophylaxis of endemic goiter It isgenerally used as “iodized salt”(see p. 251).
4. Antiseptic As tincture iodine, povidoneiodine, etc. see Ch. 65.
Adverse effects1. Acute reaction It occurs only in individualssensitive to iodine, and can be triggered evenby a minute quantity. Manifestations are swellingof lips, eyelids, angioedema of larynx (may bedangerous), fever, joint pain, petechial haemor-rhages, thrombocytopenia, lymphadenopathy.Further exposure to iodine should be stoppedimmediately.
2. Chronic overdose (iodism) Inflammationof mucous membranes, salivation, rhinorrhoea,sneezing, lacrimation, swelling of eyelids, burn-ing sensation in mouth, headache, rashes, g.i.symptoms, etc. The symptoms regress on stop-ping iodide ingestion.Long-term use of high doses can cause hypo-thyroidism and goiter.
Iodide may cause flaring of acne in adoles-cents. Given to pregnant or nursing mothers, itmay be responsible for foetal/infantile goiter andhypothyroidism. Thyrotoxicosis may be aggra-vated in multinodular goiter.
RADIOACTIVE IODINE
The stable isotope of iodine is 127I. Its radioactiveisotope of medicinal importance is:
131I: physical half-life 8 days.The chemical behaviour of 131I is similar to thestable isotope.131I emits X-rays as well as β particles. The formerare useful in tracer studies, because they traversethe tissues and can be monitored by a counter,while the latter are utilized for their destructiveeffect on thyroid cells. 131I is concentrated bythyroid, incorporated in colloid—emits radiationfrom within the follicles. The β particles penetrateonly 0.5–2 mm of tissue. The thyroid follicularcells are affected from within, undergo pyknosisand necrosis followed by fibrosis when asufficiently large dose has been administered,without damage to neighbouring tissues. Withcarefully selected doses, it is possible to achievepartial ablation of thyroid.
Radioactive iodine is administered as sodiumsalt of 131I dissolved in water and taken orally.Diagnostic 25–100 µ curie is given; countingor scanning is done at intervals. No damage tothyroid cells occurs at this dose.
Therapeutic The most common indication ishyperthyroidism due to Graves’ disease or toxicnodular goiter. The average therapeutic dose is3–6 m curie—calculated on the basis of previoustracer studies and thyroid size. Higher doses aregenerally required for toxic multinodular goiter

256S
EC
TIO
N5
HORMONES AND RELATED DRUGS
than for Graves’ disease. The response is slow—starts after 2 weeks and gradually increases,reaching peak at 3 months or so. Thyroid statusis evaluated after 3 months, and a repeat dose,if needed, is given. About 20–40% patients requireone or more repeat doses.
Advantages
1. Treatment with 131I is simple, convenientlygiven on outpatient basis and inexpensive.
2. No surgical risk, scar or injury to parathyroidglands/recurrent laryngeal nerves.
3. Once hyperthyroidism is controlled, cure ispermanent.
Disadvantages
1. Hypothyroidism: About 5–10% patients ofGraves’ disease treated with 131I become hypo-thyroid every year (upto 50% or more patientsmay ultimately require supplemental thyroxinetreatment). This probably reflects the naturalhistory of Graves’ disease, because only fewpatients of toxic nodular goiter treated with131I develop hypothyroidism. Moreover,eventual hypothyroidism is a complication ofsubtotal thyroidectomy/prolonged carbimazoletherapy as well.
2. Long latent period of response.3. Contraindicated during pregnancy—foetal
thyroid will also be destroyed resulting incretinism, other abnormalities if given duringfirst trimester.
4. Not suitable for young patients: they aremore likely to develop hypothyroidism laterand would then require life-long T4 treatment.Genetic damage/cancer is also feared, thoughthere is no evidence for it.
131I is the treatment of choice after 25 years ofage and if CHF, angina or any other contra-indication to surgery is present.
Metastatic carcinoma of thyroid (especiallypapillary or those cases of follicular carcinomawhich concentrate iodine), 131I may be used aspalliative therapy after thyroidectomy. Much
higher doses are required and prior stimulationwith TSH is recommended.
β ADRENERGIC BLOCKERS
Propranolol (and other nonselective β blockers)have emerged as an important form of therapyto rapidly alleviate manifestations of thyrotoxi-cosis that are due to sympathetic overactivity, viz.palpitation, tremor, nervousness, severe myopathy,sweating. They have little effect on thyroidfunction and the hypermetabolic state. They areused in hyperthyroidism in the followingsituations.(i) While awaiting response to propylthiouracil/carbimazole or 131I.(ii) Along with iodide for preoperative prepara-tion before subtotal thyroidectomy.(iii) Thyroid storm (thyrotoxic crisis): This isan emergency due to decompensated hyper-thyroidism. Vigorous treatment with the followingis indicated:• Nonselective β blockers (e.g. propranolol) are
the most valuable measure. They afforddramatic symptomatic relief. In addition, theyreduce peripheral conversion of T4 to T3.Propranolol 1–2 mg slow i.v. may be followedby 40–80 mg oral every 6 hours .
• Propylthiouracil 200–300 mg oral 6 hourly:reduces hormone synthesis as well as peripheralT4 to T3 conversion.
• Iopanoic acid (0.5–1 g OD oral) or ipodateare iodine containing radiocontrast media. Theyare potent inhibitors of thyroid hormone releasefrom thyroid, as well as of peripheral T4 toT3 conversion.
• Corticosteroids (hydrocortisone 100 mg i.v. 8hourly followed by oral prednisolone): helpto tide over crisis, cover any adrenal insuffi-ciency and inhibit conversion of T4 to T3 inperiphery.
• Diltiazem 60–120 mg BD oral may be addedif tachycardia is not controlled by propranololalone, or when it is contraindicated.
• Rehydration, anxiolytics, external cooling andappropriate antibiotics are the other measures.

257C
HA
PTE
R 18
THYROID HORMONES AND THYROID INHIBITORS
PROBLEM DIRECTED STUDY
18.1 A 20-year girl was diagnosed as a case of recent onset Graves’ disease with mild diffusepulsatile thyroid enlargement. She was treated with tab. Carbimazole 5 mg 2 tab 3 times a day.Her symptoms started subsiding after 2 weeks and were fully controlled after 3 months. Thethyroid swelling also subsided and she was maintained on a dose of carbimazole 5 mg twicedaily. After one year she noticed that the neck swelling was reappearing and her body weightincreased by 2 kg in the last one month, but without recurrence of her earlier symptoms. Sherather felt dull, sleepy and depressed. The serum TSH was 12 μU/ml and free thyroxine (FT4)was 9 pmol/L.(a) Why was the initial response to carbimazole delayed? Could any additional medicine be givento her initially to afford more rapid symptomatic relief?(b) What was the cause of reappearance of the neck swelling and her condition after 1 year?What measures need to be taken at this stage?(see Appendix-1 for solution)

Insulin, Oral HypoglycaemicDrugs and Glucagon
ChapterChapterChapterChapterChapter 1919191919
Diabetes mellitus (DM) It is a metabolic dis-order characterized by hyperglycaemia, glycosuria,hyperlipidaemia, negative nitrogen balance andsometimes ketonaemia. A widespread pathologicalchange is thickening of capillary basementmembrane, increase in vessel wall matrix andcellular proliferation resulting in vascular comp-lications like lumen narrowing, early atheroscle-rosis, sclerosis of glomerular capillaries, retino-pathy, neuropathy and peripheral vascularinsufficiency.
Enhanced nonenzymatic glycosylation of tissue proteinsdue to persistent exposure to high glucose concentrationsand the accumulation of larger quantities of sorbitol (a reducedproduct of glucose) in tissues are believed to be causativein the pathological changes of diabetes. The concentrationof glycosylated haemoglobin (HbA1c) is taken as an indexof protein glycosylation: it reflects the state of glycaemiaover the preceding 2–3 months.
Two major types of diabetes mellitus are:
Type I Insulin-dependent diabetes mellitus(IDDM)/juvenile onset diabetes mellitus:There is β cell destruction in pancreatic islets;majority of cases are autoimmune (type 1A)antibodies that destroy β cells are detectable inblood, but some are idiopathic (type 1B)—noβ cell antibody is found. In all type 1 cases
circulating insulin levels are low or very low,and patients are more prone to ketosis. This typeis less common and has a low degree of geneticpredisposition.
Type II Noninsulin-dependent diabetes mellitus(NIDDM)/maturity onset diabetes mellitus:There is no loss or moderate reduction in β cellmass; insulin in circulation is low, normal or evenhigh, no anti-β-cell antibody is demonstrable; hasa high degree of genetic predisposition; generallyhas a late onset (past middle age). Over 90%cases of diabetes are type 2 DM. Causes maybe:• Abnormality in gluco-receptor of β cells so
that they respond at higher glucose concen-tration or relative β cell deficiency. In eitherway, insulin secretion is impaired; may progressto β cell failure.
• Reduced sensitivity of peripheral tissues toinsulin: reduction in number of insulin recep-tors, ‘down regulation’ of insulin receptors.Many hypertensives are hyperinsulinaemic, butnormoglycaemic; and have associated dyslipi-daemia, hyperuricaemia, abdominal obesity(metabolic syndrome). Thus, there is relativeinsulin resistance, particularly at the level of
Approaches to drug therapy in type 2 DM
Improve insulin availability Overcome insulin resistance
Exogenous insulin BiguanidesSulfonylureas ThiazolidinedionesMeglitinide/phenylalanine analogues α glucosidase inhibitorsDipeptidyl peptidase-4 inhibitors (DPP-4Is)
Major limitations (except for DPP-4Is) Major limitations
Hypoglycaemic episodes Inability to achieve normoglycaemia by themselvesWeight gain in many patients, especially moderate-to-severe casesConcern about premature atherosclerosis
due to hyperinsulinaemia

259C
HA
PTE
R 19
INSULIN, ORAL HYPOGLYCAEMIC DRUGS AND GLUCAGON
liver, muscle and fat. Hyperinsulinaemia perse has been implicated in causing angiopathy.
• Excess of hyperglycaemic hormones (glucagon,etc.)/obesity: cause relative insulin defi-ciency—the β cells lag behind.
Other rare forms of DM are those due to specific geneticdefects (type-3) like ‘maturity onset diabetes of young’(MODY), other endocrine disorders, pancreatectomy and‘gestational diabetes mellitus’ (GDM, type-4).
INSULINInsulin was discovered in 1921 by Banting andBest who demonstrated the hypoglycaemic actionof an extract of pancreas prepared after degene-ration of the exocrine part due to ligation ofpancreatic duct. It was first obtained in purecrystalline form in 1926 and the chemical structurewas fully worked out in 1956 by Sanger.
Insulin is a two chain polypeptide having 51amino acids and MW about 6000. The A-chainhas 21 while B-chain has 30 amino acids. Thereare minor differences between human, pork andbeef insulins:
Thus, pork insulin is more homologous to humaninsulin than is beef insulin. The A and B chainsare held together by two disulfide bonds.
Insulin is synthesized in the β cells ofpancreatic islets as a single chain peptidePreproinsulin (110 AA) from which 24 AAs arefirst removed to produce Proinsulin (Fig. 19.1).The connecting or ‘C’ peptide (35 AA) is splitoff by proteolysis in Golgi apparatus; both insulinand C peptide are stored in granules within thecell. The C peptide is secreted in the blood alongwith insulin.
Assay Insulin is bioassayed by measuring blood sugardepression in rabbits (1 U reduces blood glucose of a fastingrabbit to 45 mg/dl) or by its potency to induce hypoglycaemicconvulsions in mice. 1 mg of the International Standard ofinsulin = 28 units. With the availability of pure preparations,it can now be assayed chemically and quantity expressedby weight. Plasma insulin can be measured by radio-immunoassay or enzyme immunoassay.
Regulation of insulin secretionUnder basal condition ~1U insulin is secretedper hour by human pancreas. Much larger quantityis secreted after every meal. Secretion of insulinfrom β cells is regulated by chemical, hormonaland neural mechanisms.
Chemical The β cells have a glucose sensingmechanism dependent on entry of glucose intoβ cells (through the aegis of a glucose transporterGLUT1) and its phosphorylation by glucokinase.Glucose entry and metabolism leads to activationof the glucosensor which indirectly inhibits theATP-sensitive K+ channel (K+
ATP) resulting inpartial depolarization of the β cells (see Fig. 19.6).This increases intracellular Ca2+ availability (dueto increased influx, decreased efflux and releasefrom intracellular stores) → exocytotic releaseof insulin storing granules. Other nutrients thatcan evoke insulin release are—amino acids, fattyacids and ketone bodies, but glucose is theprincipal regulator and it stimulates synthesis ofinsulin as well. Glucose induces a brief pulseof insulin output within 2 min (first phase)followed by a delayed but more sustained secondphase of insulin release.
Fig. 19.1: Human proinsulin; simplified structure depictingthe main features. The connecting peptide, having 35amino acids, is split off leaving insulin molecule with twochains joined by two disulfide bridges
Species A-chain B-chain
8th AA 10th AA 30th AAHuman THR ILEU THRPork THR ILEU ALABeef ALA VAL ALA

260S
EC
TIO
N5
HORMONES AND RELATED DRUGS
Glucose and other nutrients are more effective in invokinginsulin release when given orally than i.v. They generatechemical signals ‘incretins’ from the gut which act on βcells in the pancreas to cause anticipatory release of insulin.The incretins involved are glucagon-like peptide-1 (GLP-1), glucose-dependent insulinotropic polypeptide (GIP),vasoactive intestinal peptide (VIP), pancreozymin-cholecys-tokinin, etc.; but different incretin may mediate signal fromdifferent nutrient. Glucagon and some of these peptides enhanceinsulin release by increasing cAMP formation in the β cells.
Hormonal A number of hormones, e.g. growthhormone, corticosteroids, thyroxine modify insu-lin release in response to glucose. PGE has beenshown to inhibit insulin release. More importantare the intra-islet paracrine interactions betweenthe hormones produced by different types of isletcells. The β cells constitute the core of the isletsand are the most abundant cell type. The α cells,comprising 25% of the islet cell mass, surroundthe core and secrete glucagon. The δ cells(5–10%) elaborating somatostatin are interspersedbetween the α cells. There are some PP (pancreaticpolypeptide containing) cells as well.• Somatostatin inhibits release of both insulin
and glucagon.• Glucagon evokes release of insulin as well as
somatostatin.• Insulin inhibits glucagon secretion. Amylin,
another β cell polypeptide released with insulin,inhibits glucagon secretion through a centralsite of action in the brain.
The three hormones released from closely situa-ted cells influence each other’s secretion andappear to provide fine tuning of their output inresponse to metabolic needs (Fig. 19.2).
Neural The islets are richly supplied by sympa-thetic and vagal nerves.• Adrenergic α2 receptor activation decreases
insulin release (predominant) by inhibiting βcell adenylyl cyclase.
• Adrenergic β2 stimulation increases insulinrelease (less prominent) by stimulating β celladenylyl cyclase.
• Cholinergic—muscarinic activation by ACh orvagal stimulation causes insulin secretionthrough IP3/DAG-increased intracellular Ca2+
in the β cells.
These neural influences appear to governboth basal as well as evoked insulin secretion,because the respective blocking agents have effectsopposite to that mentioned above. The primarycentral site of regulation of insulin secretion isin the hypothalamus: stimulation of ventrolateralnuclei evokes insulin release, whereas stimulationof ventromedial nuclei has the opposite effect.
ACTIONS OF INSULIN
The overall effects of insulin are to dispose mealderived glucose, amino acids, fatty acids andfavour storage of fuel. It is a major anabolichormone: promotes synthesis of gylcogen, lipidsand protein. The actions of insulin and the resultsof its deficiency can be summarized as:
1. Insulin facilitates glucose transport across cellmembrane; skeletal muscle and fat are highlysensitive. The availability of glucose intracellu-larly is the limiting factor for its utilization inthese and some other tissues. However, glucoseentry in liver, brain, RBC, WBC and renal medullarycells is largely independent of insulin. Ketoacidosisinterferes with glucose utilization by brain andcontributes to diabetic coma. Muscular activityinduces glucose entry in muscle cells without theneed for insulin. As such, exercise has insulinsparing effect.
The intracellular pool of vesicles containingglucose transporter glycoproteins GLUT4 (insulinactivated) and GLUT1 is in dynamic equilibrium
Fig. 19.2: Paracrine modulation of hormone secretionwithin the pancreatic islets of Langerhans

261C
HA
PTE
R 19
INSULIN, ORAL HYPOGLYCAEMIC DRUGS AND GLUCAGON
with the GLUT vesicles inserted into the mem-brane. This equilibrium is regulated by insulinto favour translocation to the membrane.Moreover, on a long-term basis, synthesis ofGLUT4 is upregulated by insulin.
2. The first step in intracellular utilization ofglucose is its phosphorylation to form glucose-6-phosphate. This is enhanced by insulin throughincreased production of glucokinase. Insulinfacilitates glycogen synthesis from glucose in liver,muscle and fat by stimulating the enzyme glycogensynthase. It also inhibits glycogen degradingenzyme phosphorylase → decreased glyco-genolysis in liver.
3. Insulin inhibits gluconeogenesis (from pro-tein, FFA and glycerol) in liver by gene mediateddecreased synthesis of phosphoenol pyruvatecarboxykinase. In insulin deficiency, proteins andamino acids are funneled from peripheral tissuesto liver where these substances are converted tocarbohydrate and urea. Thus, in diabetes thereis underutilization and over production of glucose→ hyperglycaemia → glycosuria.
4. Insulin inhibits lipolysis in adipose tissueand favours triglyceride synthesis. In diabetesincreased amount of fat is broken down due tounchecked action of lipolytic hormones (gluca-gon, Adr, thyroxine, etc.) → increased FFA andglycerol in blood → taken up by liver to produceacetyl-CoA. Normally acetyl-CoA is resynthesizedto fatty acids and triglycerides, but this processis reduced in diabetics and acetyl CoA is divertedto produce ketone bodies (acetone, acetoacetate,β-hydroxy-butyrate). The ketone bodies are relea-
sed in blood—partly used up by muscle and heartas energy source, but when their capacity isexceeded, ketonaemia and ketonuria result.5. Insulin enhances transcription of vascularendothelial lipoprotein lipase and thus increasesclearance of VLDL and chylomicrons.6. Insulin facilitates AA entry and their synthesisinto proteins, as well as inhibits protein breakdownin muscle and most other cells. Insulin deficiencyleads to protein breakdown → AAs are released inblood → taken up by liver and converted to pyruvate,glucose and urea. The excess urea produced isexcreted in urine resulting in negative nitrogenbalance. Thus, catabolism takes the upper hand overanabolism in the diabetic state.
Most of the above metabolic actions of insulinare exerted within seconds or minutes and arecalled the rapid actions. Others involving DNAmediated synthesis of glucose transporter andsome enzymes of amino acid metabolism havea latency of few hours—the intermediate actions.In addition insulin exerts major long-term effectson multiplication and differentiation of many typesof cells.Mechanism of action Insulin acts on specific receptorslocated on the cell membrane of practically every cell, but theirdensity depends on the cell type: liver and fat cells are very rich.The insulin receptor is a receptor tyrosine kinase (RTK) whichis heterotetrameric glycoprotein consisting of 2 extracellularα and 2 transmembrane β subunits linked together by disulfidebonds. It is oriented across the cell membrane as a heterodimer(Fig. 19.3). The α subunits carry insulin binding sites, whilethe β subunits have tyrosine protein kinase activity.
Binding of insulin to α subunits induces aggregationand internalization of the receptor along with the bound insulinmolecules. This activates tyrosine kinase activity of the βsubunits → pairs of β subunits phosphorylate tyrosine residues
Actions of insulin producing hypoglycaemia
Liver Muscle Adipose tissue
▲ Increases glucose uptake ▲ Increases glucose uptake ▲ Increases glucose uptake andand glycogen synthesis and utilization storage as fat and glycogen
▲ Inhibits glycogenolysis ▲ Inhibits proteolysis and ▲ Inhibits lipolysis andand glucose output release of amino acids, release of FFA + glycerol
▲ Inhibits gluconeogenesis pyruvate, lactate into blood which form substratefrom protein, pyruvate, FFA which form the substrate for for gluconeogenesisand glycerol gluconeogenesis in liver in liver

262S
EC
TIO
N5
HORMONES AND RELATED DRUGS
on each other → expose the catalytic site to phosphorylatetyrosine residues of Insulin Receptor Substrate proteins (IRS1,IRS2, etc). In turn, a cascade of phosphorylation anddephosphorylation reactions is set into motion which amplifiesthe signal and results in stimulation or inhibition of enzymesinvolved in the rapid metabolic actions of insulin.
Certain second messengers like phosphatidyl inositoltrisphosphate (PIP3) which are generated through activationof a specific PI3-kinase also mediate the action of insulin onmetabolic enzymes.
Insulin stimulates glucose transport across cell membraneby ATP dependent translocation of glucose transporter GLUT4to the plasma membrane. The second messenger PIP3 and certaintyrosine phosphorylated guanine nucleotide exchange proteinsplay crucial roles in the insulin sensitive translocation of GLUT4from cytosol to the plasma membrane, especially in skeletalmuscle and adipose tissue. Over a period of time insulin alsopromotes expression of the genes directing synthesis of GLUT4.Genes for a large number of enzymes and carriers are regulatedby insulin through Ras/Raf and MAP-Kinase as well as throughthe phosphorylation cascade. Long-term effects of insulin are
exerted by generation of transcription factors promotingproliferation and differentiation of specific cells.
The internalized receptor-insulin complex is eitherdegraded intracellularly or returned back to the surface fromwhere the insulin is released extracellularly. The relativepreponderance of these two processes differs among differenttissues: maximum degradation occurs in liver, least in vascularendothelium.
Fate of insulin Insulin is distributed only extra-cellularly. It is a peptide; gets degraded in theg.i.t. if given orally. Injected insulin or that releasedfrom pancreas is metabolized primarily in liverand to a smaller extent in kidney and muscles.Nearly half of the insulin entering portal veinfrom pancreas is inactivated in the first passagethrough liver. Thus, normally liver is exposed toa much higher concentration (4–8 fold) of insulinthan are other tissues. As noted above, degradation
Fig. 19.3: A model of insulin receptor and mediation of its metabolic and cellular actions.T—Tyrosine residue; GLUT4—Insulin dependent glucose transporter; IRS—Insulin receptor substrate proteins;PIP3—Phosphatidyl inositol trisphosphate; MAP kinase—Mitogen-activated protein kinase; T-PrK—Tyrosine proteinkinase; Ras—Regulator of cell division and differentiation (protooncogene product).

263C
HA
PTE
R 19
INSULIN, ORAL HYPOGLYCAEMIC DRUGS AND GLUCAGON
TABLE 19.1 Types of insulin preparations and insulin analogues
Type Appearance Onset Peak Duration Can be mixed(hr) (hr) (hr) with
Rapid actingInsulin lispro Clear 0.2–0.3 1–1.5 3–5 Regular, NPHInsulin aspart Clear 0.2–0.3 1–1.5 3–5 Regular, NPHInsulin glulisine Clear 0.2–0.4 1–2 3–5 Regular, NPH
Short actingRegular (soluble) insulin Clear 0.5–1 2–3 6–8 All preparations
(except insulinglargine/detemir)
Intermediate actingInsulin zinc suspension or Lente* Cloudy 1–2 8–10 20–24 RegularNeutral protamine hagedorn Cloudy 1–2 8–10 20–24 Regular(NPH) or isophane insulin
Long acting
Insulin glargine Clear 2–4 — 24 NoneInsulin detemir Clear 1–4 — 20–24 None
* Lente insulin is a 7:3 mixture of ultralente (crystalline) and semilente (amorphous) insulin zinc suspension.Ultralente (long-acting) and semilente (short-acting) are not separately marketed. The older protamine zinc insulinis also not marketed.
of insulin after receptor mediated internalizationoccurs to variable extents in most target cells.During biotransformation the disulfide bonds arereduced—A and B chains are separated. Theseare further broken down to the constituent aminoacids. The plasma t½ is 5–9 min.
Preparations of insulinThe older commercial preparations were producedfrom beef and pork pancreas. They contained ~1%(10,000 ppm) of other proteins (proinsulin, otherpolypeptides, pancreatic proteins, insulin deriva-tives, etc.) which were potentially antigenic. Theyare no longer produced and have been totallyreplaced by highly purified pork/beef insulins/recombinant human insulins/insulin analogues.
Highly purified insulin preparations
In the 1970s improved purification techniques likegel filtration and ion-exchange chromatographywere applied to produce ‘single peak’ and‘monocomponent (MC)’ insulins which contain<10 ppm proinsulin. The MC insulins are morestable and cause less insulin resistance or injectionsite lipodystrophy. The immunogenicity of pork
MC insulin is similar to that of recombinant humaninsulin.
Types of insulin preparationsRegular (soluble) insulin It is a bufferedneutral pH solution of unmodified insulin stabili-zed by a small amount of zinc. At the concentrationof the injectable solution, the insulin moleculesself aggregate to form hexamers around zinc ions.After s.c. injection, insulin monomers are releasedgradually by dilution, so that absorption occursslowly. Peak action is produced only after2–3 hours and action continues upto 6–8 hours.The absorption pattern is also affected by dose;higher doses act longer. When injected s.c. justbefore a meal, this pattern often creates a mismatchbetween need and availability of insulin to resultin early postprandial hyperglycaemia and latepostprandial hypoglycaemia. It is generallyinjected ½-1 hour before a meal. Regular insulininjected s.c. is also not suitable for providing alow constant basal level of action in the interdiges-tive period. The slow onset of action is not appli-cable to i.v. injection, because insulin hexamerdissociates rapidly to produce prompt action.

264S
EC
TIO
N5
HORMONES AND RELATED DRUGS
To overcome the above problems, some long-acting ‘modified’ or ‘retard’ preparations of insulinwere soon developed. Recently, both rapidly actingas well as peakless and long-acting insulin analogueshave become available.
For obtaining retard preparations, insulin isrendered insoluble either by complexing it withprotamine (a small molecular basic protein) orby precipitating it with excess zinc and increasingthe particle size.
Lente insulin (Insulin-zinc suspension): Twotypes of insulin-zinc suspensions have beenproduced. The one with large particles iscrystalline and practically insoluble in water(ultralente). It is long-acting. The other has smallerparticles and is amorphous (semilente), is short-acting. Their 7:3 ratio mixture is called ‘Lenteinsulin’ and is intermediate-acting.
Isophane (Neutral Protamine Hagedorn orNPH) insulin: Protamine is added in a quantityjust sufficient to complex all insulin molecules;neither of the two is present in free form andpH is neutral. On s.c. injection, the complexdissociates slowly to yield an intermediate durationof action. It is mostly combined with regularinsulin (70:30 or 50:50) and injected s.c. twicedaily before breakfast and before dinner (split-mixed regimen).1. Highly purified (monocomponent) pork regular insulin:
ACTRAPID MC, RAPIDICA 40 U/ml inj.2. Highly purified (MC) pork lente insulin: LENTARD,
MONOTARD MC, LENTINSULIN-HPI, ZINULIN 40U/ml
3. Highly purified (MC) pork isophane (NPH) insulin:INSULATARD 40 U/ml inj.
4. Mixture of highly purified pork regular insulin (30%)and isophane insulin (70%): RAPIMIX, MIXTARD40 U/ml inj.
Human insulins In the 1980s, the human insu-lins (having the same amino acid sequence ashuman insulin) were produced by recombinantDNA technology in Escherichia coli—‘proinsulinrecombinant bacterial’ (prb) and in yeast—‘precursor yeast recombinant’ (pyr), or by‘enzymatic modification of porcine insulin’ (emp).1. HUMAN ACTRAPID: Human regular insulin; 40 U/
ml, 100 U/ml, ACTRAPID HM PENFIL 100 U/ml pen
inj., WOSULIN-R 40 U/ml inj vial and 100 U/ml peninjector cartridge.
2. HUMAN MONOTRAD, HUMINSULIN-L: Human lenteinsulin; 40 U/ml, 100 U/ml.
3. HUMAN INSULATARD, HUMINSULIN-N: Humanisophane insulin 40 U/ml. WOSULIN-N 40 U/ml inj.vial and 100 U/ml pen injector cartridge.
4. HUMAN ACTRAPHANE, HUMINSULIN 30/70,HUMAN MIXTARD: Human soluble insulin (30%) andisophane insulin (70%), 40 U/ml. and 100 U/ml vials.WOSULIN 30/70: 40 U/ml vial and 100 U/ml cartridge.
5. ACTRAPHANE HM PENFIL: Human soluble insulin30% + isophane insulin 70% 100 U/ml pen injector.
6. INSUMAN 50/50: Human soluble insulin 50% +isophane insulin 50% 40 U/ml inj; HUMINSULIN 50:50,HUMAN MIXTARD 50; WOSULIN 50/50 40 U/ml vial,100 U/ml cartridge.
In the USA pork and beef insulins are no longermanufactured, but they are still available in U.K.,India and some European countries. In Britain now> 90% diabetics who use insulin are taking humaninsulins or insulin analogues. In India also humaninsulins and analogues are commonly used, exceptfor considerations of cost. Human insulin is morewater soluble as well as hydrophobic than porcineor bovine insulin. It has a slightly more rapid s.c.absorption, earlier and more defined peak andslightly shorter duration of action. Human insulinis also modified similarly to produce isophane(NPH) and lente preparations. Lente human insulinis no longer prepared in the USA.The allegation that human insulin produces morehypoglycaemic unawareness has not been substantiated.However, after prolonged treatment, irrespective of the typeof insulin, many diabetics develop relative hypoglycaemicunawareness/change in hypoglycaemic symptoms, because ofautonomic neuropathy, changes in perception/attitude andother factors.
Clinical superiority of human insulin over pork MC insulinhas not been demonstrated. Though new patients may be startedon human insulins, the only indication for transfer from purifiedpork to human insulin is allergy to pork insulin. It is unwise totransfer stabilized patients from one to another species insulinwithout good reason.
Insulin analoguesUsing recombinant DNA technology, analoguesof insulin have been produced with modifiedpharmacokinetics on s.c. injection, but similarpharmacodynamic effects. Greater stability andconsistency are the other advantages.

265C
HA
PTE
R 19
INSULIN, ORAL HYPOGLYCAEMIC DRUGS AND GLUCAGON
Insulin lispro: Produced by reversing proline andlysine at the carboxy terminus B 28 and B 29positions, it forms very weak hexamers thatdissociate rapidly after s.c. injection resulting ina quick and more defined peak as well as shorterduration of action. Unlike regular insulin, it needsto be injected immediately before or even afterthe meal, so that dose can be altered accordingto the quantity of food consumed. A better controlof meal-time glycaemia and a lower incidenceof late post-prandial hypoglycaemia have beenobtained. Using a regimen of 2–3 daily meal-time insulin lispro injections, a slightly greaterreduction in HbA1c compared to regular insulinhas been reported. Fewer hypoglycaemic episodesoccurred.HUMALOG 100 U/ml, 3 ml cartridge, 10 ml vial.
Insulin aspart: The proline at B 28 of humaninsulin is replaced by aspartic acid. This changereduces the tendency for self-aggregation, and atime-action profile similar to insulin lispro isobtained. It more closely mimics the physiologicalinsulin release pattern after a meal, with the sameadvantages as above.NOVOLOG, NOVORAPID 100 U/ml inj; Biphasic insulinaspart - NOVO MIX 30 FEXPEN injector.
Insulin glulisine: Another rapidly acting insulin analoguewith lysine replacing asparagine at B 23 and glutamic acidreplacing lysine at B 29. Properties and advantages are similarto insulin lispro. It has been particularly used for continuoussubcutaneous insulin infusion (CSII) by a pump.
Insulin glargine: This long-acting biosyntheticinsulin has 2 additional arginine residues at thecarboxy terminus of B chain and glycine replacesasparagine at A 21. It remains soluble at pH4of the formulation, but precipitates at neutral pHencountered on s.c. injection. A depot is createdfrom which monomeric insulin dissociates slowlyto enter the circulation. Onset of action is delayed,but relatively low blood levels of insulin aremaintained for upto 24 hours. A smooth ‘peakless’effect is obtained. Thus, it is suitable for oncedaily injection to provide background insulinaction. Fasting and interdigestive blood glucoselevels are effectively lowered irrespective of timeof the day when injected or the site of s.c.
injection. It is mostly injected at bed time. Lowerincidence of night-time hypoglycaemic episodescompared to isophane insulin has been reported.However, it does not control meal-time glycaemia,for which a rapid acting insulin or an oralhypoglycaemic is used concurrently. Because ofacidic pH, it cannot be mixed with any otherinsulin preparation; must be injected separately.LANTUS OPTISET 100 U/ml in 5 ml vial and 3 ml prefilledpen injector.
Insulin detemir Myristoyl (a fatty acid) radical is attachedto the amino group of lysine at B29 of insulin chain. Asa result, it binds to albumin after s.c. injection from whichthe free form becomes available slowly. A pattern of insulinaction almost similar to that of insulin glargine is obtained,but twice daily dosing may be needed.
REACTIONS TO INSULIN
1. Hypoglycaemia This is the most frequentand potentially the most serious reaction. It iscommonly seen in patients of ‘labile’ diabetesin whom insulin requirement fluctuates unpredic-tably. Hypoglycaemia can occur in any diabeticfollowing inadvertent injection of large dose, bymissing a meal after injection or by performingvigorous exercise. The symptoms can be dividedinto those due to counter-regulatory sympatheticstimulation—sweating, anxiety, palpitation,tremor; and those due to deprivation of the brainof its essential nutrient glucose (neuroglucopenicsymptoms)—dizziness, headache, behaviouralchanges, visual disturbances, hunger, fatigue,weakness, muscular incoordination and sometimesfall in BP. Generally, the reflex sympatheticsymptoms occur before the neuroglucopenic, butthe warning symptoms of hypoglycaemia differfrom patient to patient and also depend on therate of fall in blood glucose level. After long-term treatment about 30% patients lose adrenergicsymptoms. Diabetic neuropathy can abolish theautonomic symptoms. Hypoglycaemic unaware-ness tends to develop in patients who experiencefrequent episodes of hypoglycaemia.
Finally, when blood glucose falls further (to< 40 mg/dl) mental confusion, abnormalbehaviour, seizures and coma occur. Irreversible

266S
EC
TIO
N5
HORMONES AND RELATED DRUGS
neurological deficits are the sequelae of prolongedhypoglycaemia.
Treatment Glucose must be given orally or i.v.(for severe cases)—reverses the symptoms rapidly.Glucagon 0.5–1 mg i.v. or Adr 0.2 mg s.c. (lessdesirable) may be given as an expedient measurein patients who are not able to take sugar orallyand injectable glucose is not available.
2. Local reactions Swelling, erythema and stingingsometimes occur at the injected site, especially in the begin-ning. Lipodystrophy of the subcutaneous fat around theinjection site may occur if the same site is injected repeatedly.This is rare with the newer preparations.
3. Allergy This is due to contaminating proteins, andis very rare with human/highly purified insulins.Urticaria, angioedema and anaphylaxis are the manifestations.
4. Edema Some patients develop short-lived dependentedema (due to Na+ retention) when insulin therapy is started.
Drug interactions
1. β adrenergic blockers prolong hypoglycaemiaby inhibiting compensatory mechanisms opera-ting through β2 receptors (β1 selective blockersare less liable). Warning signs of hypoglycaemialike palpitation, tremor and anxiety are masked.Rise in BP can occur due to unopposed α actionof released Adr.2. Thiazides, furosemide, corticosteroids,oral contraceptives, salbutamol, nifedipine tendto raise blood sugar and reduce effectiveness ofinsulin.3. Acute ingestion of alcohol can precipitatehypoglycaemia by depleting hepatic glycogen.4. Lithium, high dose aspirin and theophyllinemay also accentuate hypoglycaemia by enhancinginsulin secretion and peripheral glucose utilization.
USES OF INSULIN
Diabetes mellitus The purpose of therapy indiabetes mellitus is to restore metabolism tonormal, avoid symptoms due to hyperglycaemiaand glucosuria, prevent short-term complications(infection, ketoacidosis, etc.) and long-term seque-lae (cardiovascular, retinal, neurological, renal,etc.)
Insulin is effective in all forms of diabetesmellitus and is a must for type 1 cases, as wellas for post pancreatectomy diabetes andgestational diabetes. Many type 2 cases can becontrolled by diet, reduction in body weight andappropriate exercise supplemented, if required,by oral hypoglycaemics. Insulin is needed by suchpatients when:• Not controlled by diet and exercise or when
these are not practicable.• Primary or secondary failure of oral hypo-
glycaemics or when these drugs are nottolerated.
• Under weight patients.• Temporarily to tide over infections, trauma,
surgery, pregnancy. In the perioperative periodand during labour, monitored i.v. insulininfusion is preferable.
• Any complication of diabetes, e.g. ketoacidosis,nonketotic hyperosmolar coma, gangrene ofextremities.
When instituted, insulin therapy has to be tailoredaccording to the requirement and convenience ofeach patient. A tentative regimen is instituted andthe insulin requirement is assessed by testing urineor blood glucose levels (glucose oxidase basedspot tests and glucometers are available). Mosttype 1 patients require 0.4–0.8 U/kg/day. In type2 patients, insulin dose varies (0.2–1.6 U/kg/day)with the severity of diabetes and body weight:obese patients require proportionately higher dosesdue to relative insulin resistance.
Any satisfactory insulin regimen should providebasal control by inhibiting hepatic glucose output,lipolysis and protein breakdown, as well as supplyextra amount to meet postprandial needs fordisposal of absorbed glucose and amino acids.A single daily injection of any long/intermediate/short-acting insulin or a mixture of these cannotfulfil both these requirements. Either multiple(2-4) injections daily of long and short actinginsulins or a single injection daily of long-actinginsulin supplemented by oral hypoglycaemics formeal time glycaemia is used. A frequently selectedregimen utilizes mixture of regular with lente/

267C
HA
PTE
R 19
INSULIN, ORAL HYPOGLYCAEMIC DRUGS AND GLUCAGON
isophane insulin. The total daily dose of a 30:70or 50:50 mixture of regular and NPH insulin isusually split into two (split-mixed regimen) andinjected s.c. before breakfast and before dinner.Several variables, viz. site and depth of s.c.injection, posture, regional muscular activity,injected volume and type of insulin can alter therate of absorption of s.c. injected insulin, so thatthe anticipated time-course of insulin action maynot be obtained each time. The advantage is thatonly two daily injections are required, but thepost-lunch glycaemia may not be adequatelycovered (see Fig. 19.4 A), and late postprandialhypoglycaemia may occur.
A more intensive regimen termed the ‘basal-bolus regimen’ that is now advised needs 3–4daily injections (see Fig. 19.4B). A long-actinginsulin (glargine) is injected once daily eitherbefore breakfast or before bed-time for basalcoverage along with 2–3 meal-time injections ofa rapid acting preparation (insulin lispro or aspart).Such intensive regimens more completely meetthe objective of achieving round-the-clockeuglycaemia, but are more demanding andexpensive. The large multicentric Diabetes Controland Complications Trial (DCCT) among type 1patients has established that intensive insulintherapy markedly reduces the occurrence ofprimary diabetic retinopathy, neuropathy,nephropathy and slows progression of thesecomplications in those who already have them,in comparison to conventional regimens whichattain only intermittent euglycaemia. Thus, therisk of microvascular disease appears to be relatedto the glycaemia control. The ‘UK prospectivediabetes study’ (UK PDS, 1998) has extendedthese observations to type 2 DM patients as well.Since the basis of pathological changes in bothtype 1 and type 2 DM is accumulation ofglycosylated proteins and sorbitol in tissues asa result of exposure to high glucose concentrations,tight glycaemia control can delay end-organdamage in all diabetic subjects.
However, regimens attempting near normo-glycaemia are associated with higher incidence
Fig. 19.4: Diagrammatic depiction of pattern of insulinaction obtained with two commonly employed insulinregimens.Arrow indicates subcutaneous insulin injection.I. Ana—Insulin analogue (rapid acting); I. Glar—Insulinglargine; R.I—Regular insulin; NPH—Neutral protamineHagedorn (isophane) insulin
of severe hypoglycaemic episodes. Moreover,injected insulin fails to reproduce the normalpattern of increased insulin secretion in responseto each meal, and liver is exposed to the sameconcentration of insulin as other tissues, whilenormally it receives much higher concentrationthrough portal circulation. As such, the overalldesirability and practicability of intensive insulintherapy has to be determined in individual patients.Intensive insulin therapy is best avoided in youngchildren (risk of hypoglycaemic brain damage)and in the elderly (more prone to hypoglycaemiaand its serious consequences).
Diabetic ketoacidosis (Diabetic coma)Ketoacidosis of different grades generally occursin insulin dependent diabetics. It is infrequentin type 2 DM. The most common precipitatingcause is infection; others are trauma, stroke,pancreatitis, stressful conditions and inadequatedoses of insulin.

268S
EC
TIO
N5
HORMONES AND RELATED DRUGS
The development of cardinal features of diabeticketoacidosis is outlined in Fig. 19.5. Patients maypresent with varying severity. Typically they aredehydrated, hyperventilating and have impairedconsciousness. The principles of treatment remainthe same, irrespective of severity, only the vigourwith which therapy is instituted is varied.
1. Insulin Regular insulin is used to rapidlycorrect the metabolic abnormalities. A bolus doseof 0.1–0.2 U/kg i.v. is followed by 0.1 U/kg/hrinfusion; the rate is doubled if no significant fallin blood glucose occurs in 2 hr. Fall in bloodglucose level by 10% per hour can be consideredadequate response.
Usually, within 4–6 hours blood glucosereaches 300 mg/dl. Then the rate of infusion isreduced to 2–3 U/hr. This is maintained till thepatient becomes fully conscious and routinetherapy with s.c. insulin is instituted.
2. Intravenous fluids It is vital to correct dehy-dration. Normal saline is infused i.v., initially atthe rate of 1 L/hr, reducing progressively to 0.5
L/4 hours depending on the volume status. OnceBP and heart rate have stabilized and adequaterenal perfusion is assured change over to ½Nsaline. After the blood sugar has reached 300mg/dl, 5% glucose in ½N saline is the most appro-priate fluid because blood glucose falls beforeketones are fully cleared from the circulation. Alsoglucose is needed to restore the depleted hepaticglycogen.
3. KCl Though upto 400 mEq of K+ may belost in urine during ketoacidosis, serum K+ isusually normal due to exchange with intracellularstores. When insulin therapy is instituted ketosissubsides and K+ is driven back intracellularly—dangerous hypokalemia can occur. After 4 hoursit is appropriate to add 10–20 mEq/hr KCl tothe i.v. fluid. Further rate of infusion is guidedby serum K+ measurements and ECG.
4. Sodium bicarbonate It is not routinelyneeded. Acidosis subsides as ketosis is controlled.However, if arterial blood pH is < 7.1, acidosisis not corrected spontaneously or hyperventilation
Fig. 19.5: Schematic depiction of the development of diabetic ketoacidosis due to insulin lack.Symptoms produced are shown within boxes

269C
HA
PTE
R 19
INSULIN, ORAL HYPOGLYCAEMIC DRUGS AND GLUCAGON
is exhausting, 50 mEq of sod. bicarbonate is addedto the i.v. fluid. Bicarbonate infusion is continuedslowly till blood pH rises above 7.2.
5. Phosphate When serum PO4 is in the low-normal range, 5–10 m mol/hr of sod./pot. phos-phate infusion is advocated. However, routine useof PO4 in all cases is still controversial.
6. Antibiotics and other supportive measuresand treatment of precipitating cause must beinstituted simultaneously.
Hyperosmolar (nonketotic hypergly-caemic) coma This usually occurs in elderlytype 2 patients. Its cause is obscure, but appearsto be precipitated by the same factors as keto-acidosis, especially those resulting in dehydration.Uncontrolled glycosuria of DM produces diure-sis resulting in dehydration and haemoconcen-tration over several days → urine output is finallyreduced and glucose accumulates in blood rapidlyto > 800 mg/dl, plasma osmolarity is > 350 mOsm/L → coma, and death can occur if not vigorouslytreated.
The general principles of treatment are thesame as for ketoacidotic coma, except that fasterfluid replacement is to be instituted and alkaliis usually not required. These patients are proneto thrombosis (due to hyperviscosity and sluggishcirculation), prophylactic heparin therapy isrecommended.
Despite intensive therapy, mortality inhyperosmolar coma remains high. Treatment ofprecipitating factor and associated illness is vital.
Insulin resistanceInsulin resistance refers to suboptimal responseof body tissues, especially liver, skeletal muscleand fat to physiological amounts of insulin. Asalready stated, relative insulin resistance is integralto type 2 DM. Advanced age, obesity andsedentary life-style promote insulin resistance.
Insulin sensitivity has been found to declinewith age. Glucose entry into muscle and liverin response to insulin is deficient in individualswith large stores of body fat. Bigger adipocytes
have fewer insulin receptors. However, in mosttype 2 diabetics the transducer mechanism linkinginsulin receptor to the response appears to befaulty, rather than the receptor itself. Exerciseincreases insulin sensitivity and lack of itcontributes to insulin resistance.
Pregnancy and oral contraceptives often inducerelatively low grade and reversible insulin resis-tance. Other rare causes are—acromegaly,Cushing’s syndrome, pheochromocytoma, lipo-atrophic diabetes mellitus. Hypertension is oftenaccompanied with relative insulin resistance aspart of metabolic syndrome.
Acute insulin resistance This form of insulinresistance develops rapidly and is usually a shortterm problem. Causes are—(a) Infection, trauma, surgery, emotional stressinduce release of corticosteroids and otherhyperglycaemic hormones which oppose insulinaction.(b) Ketoacidosis—ketone bodies and FFA inhibitglucose uptake by brain and muscle. Also insulinbinding may increase resulting in insulinresistance.
Treatment is to overcome the precipitatingcause and to give high doses of regular insulin.The insulin requirement comes back to normalonce the condition has been controlled.
Treatment is to overcome the precipitatingcause and to give high doses of regular insulin.The insulin requirement comes back to normalonce the condition has been controlled.
Newer insulin delivery devices A number of innova-tions have been made to improve ease and accuracy of insulinadministration as well as to achieve tight glycaemia control.These are:
1. Insulin syringes Prefilled disposible syringes containspecific types or mixtures of regular and modified insulins.
2. Pen devices Fountain pen like: use insulin cartridgesfor s.c. injection through a needle. Preset amounts(in 2 U increments) are propelled by pushing a plunger;convenient in carrying and injecting.
3. Inhaled insulin An inhaled human insulin preparationwas marketed in Europe and the USA, but withdrawn dueto risk of pulmonary fibrosis and other complications. The

270S
EC
TIO
N5
HORMONES AND RELATED DRUGS
fine powder delivered through a nebulizer controlled meal-time glycaemia, but was not suitable for round-the-clockbasal effect. Attempts are being made to overcome theshortcomings.
4. Insulin pumps Portable infusion devices connectedto a subcutaneously placed cannula—provide ‘continuoussubcutaneous insulin infusion’ (CSII). Only regular insulinor a fast acting insulin analogue is used. The pump canbe programmed to deliver insulin at a low basal rate (approx.1 U/hr) and premeal boluses (4–15 times the basal rate)to control post-prandial glycaemia. Though, theoretically moreappealing, no definite advantage of CSII over multidose s.c.injection has been demonstrated. Moreover, cost, strictadherence to diet, exercise, care of the device and cannula,risk of pump failure, site infection, are too demanding onthe patient. The CSII may be appropriate for selected type2 DM cases only.
5. Implantable pumps Consist of an electromechanicalmechanism which regulates insulin delivery from a percu-taneously refillable reservoir. Mechanical pumps, propellantdriven and osmotic pumps have been utilized.
6. Other routes of insulin delivery Intraperitoneal, oral(by complexing insulin into liposomes or coating it withimpermeable polymer) and rectal routes are being tried. Thesehave the advantage of providing higher concentrations inthe portal circulation, which is more physiological.
ORAL HYPOGLYCAEMIC DRUGS
These drugs lower blood glucose levels and areeffective orally. The chief draw back of insulinis—it must be given by injection. Orally activedrugs have always been saught.
The early sulfonamides tested in 1940s produced hypo-glycaemia as side effect. Taking this lead, the first clinicallyacceptable sulfonylurea tolbutamide was introduced in 1957.Others followed soon after. In the 1970s many so called‘second generation’ sulfonylureas were developed which are20–100 times more potent. Clinically useful biguanidephenformin was produced parallel to sulfonylureas in 1957.Newer approaches have constantly been explored andhave lately yielded thiazolidinediones, meglitinide analogues,α-glucosidase inhibitors and the latest are dipeptidylpeptidase-4 (DPP-4) inhibitors.
CLASSIFICATIONA. Enhance Insulin secretion1. Sulfonylureas (KATP Channel blockers)
First generation: TolbutamideSecond generation: Glibenclamide (Glyburide),Glipizide, Gliclazide, Glimepiride
2. Meglitinide/phenylalanine analoguesRepaglinide, Nateglinide
3. Glucagon-like peptide-1 (GLP-1) receptoragonists (Injectable drugs)Exenatide, Liraglutide
4. Dipeptidyl peptidase-4 (DPP-4) inhibitorsSitagliptin, Vildagliptin, Saxagliptin, Alogliptin,Linagliptin
B. Overcome Insulin resistance1. Biguanide (AMPK activator)
Metformin2. Thiazolidinediones (PPARγ activator)
PioglitazoneC. Miscellaneous antidiabetic drugs1. α-Glucosidase inhibitors
Acarbose, Miglitol, Voglibose2. Amylin analogue
Pramlintide3. Dopamine-D2 receptor agonist
Bromocriptin4. Sodium-glucose cotransport-2 (SGLT-2)
inhibitorDapagliflozin
Sulfonylureas (KATP Channel blockers)
The generic formula of sulfonylureas (SUs) is—
All SUs have similar pharmacological profile, theirsole significant action being lowering of bloodglucose level in normal subjects and in type 2diabetics, but not in type 1 diabetics. Being morepotent and clinically superior, only the secondgeneration SUs are employed now. All firstgeneration compounds have been discontinuedexcept tolbutamide which is infrequently used.Mechanism of action Sulfonylureas provokea brisk release of insulin from pancreas, themechanism of which is detailed in Fig. 19.6. Therate of insulin secretion at any glucose concen-tration is increased, i.e. insulin release is provokedeven at low-glucose concentration riskingproduction of severe and unpredictable hypo-glycaemia. In type 2 DM the kinetics of insulinrelease in response to glucose or meals is delayed

271C
HA
PTE
R 19
INSULIN, ORAL HYPOGLYCAEMIC DRUGS AND GLUCAGON
and subdued. The SUs primarily augment the 2ndphase insulin secretion with little effect on the1st phase. That they do not cause hypoglycaemiain pancreatectomised animals and in type1 diabetics (presence of at least 30% functionalβ cells is essential for their action), confirms theirindirect action through pancreas.
A minor action reducing glucagon secretion,probably by increasing insulin and somatostatinrelease has been demonstrated. Hepaticdegradation of insulin is also slowed.Extrapancreatic action After few months ofadministration, the insulinaemic action of SUsdeclines, probably due to down regulation ofsulfonylurea receptors (SUR1) on β cells, butimprovement in glucose tolerance is maintained.In this phase, they sensitize the target tissues(especially liver) to the action of insulin. Thisis due to increase in number of insulin receptorsand/or a postreceptor action—improving trans-lation of receptor activation. It is hypothesizedthat long-term improvement in carbohydratetolerance leads to overall lowering of circulatinginsulin concentration which reverses the downregulation of insulin receptors. An apparentincrease in their number occurs. A directextrapancreatic action of SUs to increase insulinreceptors on target cells and to inhibit gluco-neogenesis in liver has been proposed, but appearsto have little clinical relevance.Pharmacokinetics All SUs are well absorbedorally, and are 90% or more bound to plasmaproteins: have low volumes of distribution(0.2–0.4 L/kg). They are primarily metabolized—may produce active metabolite. The metabolites(active/inactive) are excreted in urine. As such,they should be used cautiously in patients withliver or kidney dysfunction.
The distinctive features of different SUs aregiven in Table 19.2.
Interactions
Drugs that enhance SU action (mayprecipitate hypoglycaemia) are—(a) Displace from protein binding: Phenylbuta-zone, sulfinpyrazone, salicylates, sulfonamides.
(b) Inhibit metabolism/excretion: Cimetidineketoconazole, sulfonamides, warfarin, chloram-phenicol, acute alcohol intake (also synergisesby causing hypoglycaemia).(c) Synergise with or prolong pharmacodynamicaction: Salicylates, propranolol (cardioselectiveβ1 blockers are less liable), sympatholyticantihypertensives, lithium, theophylline, alcohol(by inhibiting gluconeogenesis).
Drugs that decrease SU action (vitiatediabetes control) are—(a) Induce metabolism: Phenobarbitone, pheny-toin, rifampicin, chronic alcoholism.(b) Opposite action/suppress insulin release:Corticosteroids, thiazides, furosemide, oralcontraceptives.
Adverse effects Incidence of adverse effectsis quite low (3–7%).
1. Hypoglycaemia It is the commonest prob-lem, may occasionally be severe and rarely fatal.It is more common in elderly, liver and kidneydisease patients and when potentiating drugs areadded. Tolbutamide carries lowest risk due to itslow potency and short duration of action.Treatment of hypoglycaemic episode is to giveglucose, may be for a few days because hypogly-caemia may recur.
2. Nonspecific side effects Majority ofdiabetics started on SUs tend to gain 1–3 kgweight. This may be a consequence of theirinsulinaemic action. Nausea, vomiting, flatulence,diarrhoea or constipation, headache and pares-thesias are generally mild and infrequent.
3. Hypersensitivity Rashes, photosensitivity,purpura, transient leukopenia, rarely agranulo-cytosis.
Flushing and a disulfiram-like reaction afteralcohol is reported to occur in some individualstaking SUs.
Tolbutamide reduces iodide uptake by thyroidbut hypothyroidism does not occur.
Safety of SUs during pregnancy is notestablished. Change over to insulin is advised.

272S
EC
TIO
N5
HORMONES AND RELATED DRUGS
TAB
LE 1
9.2
Impo
rtan
t fea
ture
s of
ora
l hyp
ogly
caem
ics
Dru
gP
repa
ratio
nsP
lasm
aD
urat
ion
Cle
aran
ceD
aily
No.
of
Rem
arks
t½ (
hr)
of a
ctio
nro
ute*
dose
dose
s pe
r(h
r)da
y
SU
LFO
NY
LUR
EA
S1.
Tolb
utam
ide
RA
STI
NO
N,
66–
8L
0.5–
3 g
2–3
Wea
ker,
shor
ter
actin
g, fl
exib
le d
osag
e, s
afer
in0.
5 g
tab.
elde
rly a
nd in
thos
e pr
one
to h
ypog
lyca
emia
.2.
Glib
encl
amid
eD
AO
NIL
,2–
424
L2.
5–15
mg
1–2
Pot
ent b
ut s
low
act
ing,
hig
her
inci
denc
e of
(Gly
burid
e)E
UG
LUC
ON
, BE
TAN
AS
Ehy
pogl
ycae
mia
, sin
gle
daily
dos
e de
spite
sho
rt t½
2.5,
5 m
g ta
b.du
e to
act
ive
met
abol
ite a
nd s
eque
stra
tion
in β
cel
ls.
3.G
lipiz
ide
GLY
NA
SE
, GLI
DE
3–5
12L
5–20
mg
1–2
Fast
and
sho
rter
actin
g, h
ighe
r da
ily d
ose
to b
eM
INID
IAB
5 m
g ta
bde
vide
d, h
ypog
lyca
emia
and
wei
ght g
ain
less
like
ly,
pref
erab
le in
eld
erly
.4.
Glic
lazi
deD
IAM
ICR
ON
80
mg
tab.
8–20
12–2
4L
40–2
40 m
g1–
2H
as a
ntip
late
let a
ctio
n, g
ener
ates
onl
y in
activ
eD
IAZI
DE
20,
80
mg
tab
met
abol
ite, d
aily
dos
e >
80m
g to
be
divi
ded.
GLI
ZID
30,
40,
80
mg
tab
5.G
limep
iride
AM
AR
YL,
GLY
PR
IDE
5–7
24L
1–6
mg
1–2
Long
act
ing,
onl
y in
activ
e m
etab
olite
. Stro
nger
ext
ra-
GLI
ME
R 1
, 2 m
g ta
bpa
ncre
atic
act
ion.
Low
er in
cide
nce
of h
ypog
lyca
emia
.
ME
GLI
TIN
IDE
/ P
HE
NY
LALA
NIN
E A
NA
LOG
UE
S
1.R
epag
linid
eE
UR
EP
A, R
AP
LIN
< 1
3–5
L1–
8 m
g3–
4G
iven
½ h
r be
fore
eac
h m
eal f
or li
miti
ng p
.p.
RE
GA
N 0
.5, 1
, 2 m
g ta
bhy
perg
lyca
emia
.2.
Nat
eglin
ide
GLI
NA
TE, N
ATE
LID
E1.
52–
4L
180–
480
3–4
Stim
ulat
es 1
st p
hase
insu
lin s
ecre
tion,
less
like
ly60
,120
mg
tab
mg
to c
ause
del
ayed
hyp
ogly
caem
ia.
DP
P-4
INH
IBIT
OR
S
1.S
itagl
iptin
JAN
UV
IA 1
00 m
g ta
b.~1
224
K10
0 m
g1
Non
-cov
alen
t bin
ding
to D
PP
-4; e
xcre
ted
unch
ange
d in
urin
e. L
ow ri
sk o
f hyp
ogly
caem
ia. B
ody
wei
ght n
eutra
l.2.
Vild
aglip
tinG
ALV
US
, JA
LRA
,2–
412
–24
L,K
50–1
00 m
g1–
2C
oval
ent
bind
ing
to D
PP
-4;
Met
abol
ized
in
liver
.ZO
ME
LIS
50
mg
cap
Hep
atot
oxic
ity r
epor
ted.
BIG
UA
NID
E
1.M
etfo
rmin
GLY
CIP
HA
GE
,G
LYC
OM
ET
1.5–
36–
8K
0.5–
2.5
g1–
2N
o hy
pogl
ycae
mia
. Not
met
abol
ized
. Lac
tic a
cido
sis
0.5,
0.8
5 g
tab,
0.5
gra
re, o
nly
in k
idne
y di
seas
e.an
d 1.
0 g
SR
tabs
THIA
ZOLI
DIN
ED
ION
E
1.P
iogl
itazo
neP
ION
OR
M, P
IOR
ES
T,3–
524
L15
–45
mg
1M
ay im
prov
e lip
id p
rofil
e. R
ever
ses
insu
lin r
esis
-P
IOZO
NE
15,
30
mg
tab
tanc
e. N
o hy
pogl
ycae
mia
, C/I
in li
ver a
nd h
eart
dise
ase.
*L—
Met
abol
ized
in li
ver;
K—
Exc
rete
d un
chan
ged
by k
idne
y; p
.p.—
post
pran
dial

273C
HA
PTE
R 19
INSULIN, ORAL HYPOGLYCAEMIC DRUGS AND GLUCAGON
Sulfonylureas are secreted in milk: should notbe given to nursing mothers.Chlorpropamide is one of the first SUs which has beendiscontinued because of long duration of action (> 2 days)and frequent hypoglycaemia. It was also prone to causedilutional hyponatraemia (by sensitizing kidney to ADHaction), cholestatic jaundice and alcohol flush.
Meglitinide / D-phenylalanine analogues(KATP Channel blockers)
These are KATP channel blockers with a quickand short lasting insulinemic action.
Repaglinide This meglitinide analogue oralhypoglycaemic is designed to normalise meal-time glucose excursions. Though not a sulfonyl-urea, it acts in an analogous manner by bindingto SUR → closure of ATP dependent K+ channels→ depolarisation → insulin release (see Fig. 19.6).
Repaglinide is quickly absorbed and rapidlymetabolized. It induces fast onset short-lastinginsulin release. Because of this characteristic itspattern of use is different from that of SUs. Itis administered before each major meal to controlpostprandial hyperglycaemia; the dose should beomitted if a meal is missed. Because of shortlasting action it may have a lower risk of serioushypoglycaemia. Side effects are mild headache,dyspepsia, arthralgia and weight gain.
Repaglinide is indicated only in selectedtype 2 diabetics who suffer pronounced postprandial hyperglycaemia, or to supplementmetformin/long-acting insulin. It should beavoided in liver disease.
Nateglinide It is a D-phenylalanine derivativewhich principally stimulates the 1st phase insulinsecretion by closing β cell KATP channels resultingin faster onset and shorter lasting hypoglycaemiathan repaglinide. Ingested 10 min before meal,it limits postprandial hyperglycaemia in type 2diabetics without producing late phase hypo-glycaemia. There is little effect on fasting bloodglucose level. Episodes of hypoglycaemia are lessfrequent than with SUs. Side effects are dizziness,nausea, flu like symptoms and joint pain. It is
used in type 2 DM along with other antidiabetics,to control postprandial rise in blood glucose.
Glucagon-like peptide-1 (GLP-1) receptoragonists
GLP-1 is an important incretin released from thegut in response to ingested glucose. It inducesinsulin release from pancreatic β cells, inhibitsglucagon release from α cells, slows gastricemptying and suppresses appetite by activatingspecific GLP-1 receptors, which are cell surfaceGPCRs (see Fig. 19.6) expressed on β and αcells, central and peripheral neurones, gastro-intestinal mucosa, etc. Characteristically GLP-1induces insulin release only at high glucoseconcentration. The incretin system appears topromote β cell health as well. Failure of incretinshas been implicated in the pathogenesis of β celldysfunction of type 2 DM, particularly progressionof the disease. GLP-1 based therapy appears tobe the most effective measure for preserving βcell function in type 2 DM.
GLP-1 itself is not suitable for clinical usebecause of rapid degradation by the enzymedipeptidyl peptidase-4 (DPP-4) which is expressedon the luminal membrane of capillary endothelialcells, kidney, liver gut mucosa and immune cells.Another incretin glucose-dependent insulinotropicpeptide (GIP) also induces insulin release, but inhuman beings GLP-1 is the more important incre-tin and GIP has poor action in type 2 diabetics.The GIP receptor is distinct from GLP-1 receptor,but mediates mostly similar responses. Some morestable analogues of GLP-1 have been producedfor clinical use in type-2 DM.
Exenatide It is a synthetic DPP-4 resistant analogue whichactivates GLP-1 receptors (Fig. 19.6) and produces the sameresponses. Being a peptide, it is inactive orally. After s.c.injection its plasma t½ is ~ 3 hours and duration of action6–10 hours. It is marketed in USA, UK, Europe for usemainly as add-on drug to metformin/SU or a combinationof these or pioglitazone in poorly controlled type 2 diabetics.Benefits noted are lowering of postprandial as well as fastingblood glucose, HbA1c and body weight. The most importantside effect is nausea and vomiting occurring in ~ 50%recipients, but tolerance develops later.

274S
EC
TIO
N5
HORMONES AND RELATED DRUGS
Fig. 19.6: Mechanism of action of insulin secretagoguesThe sulfonylureas (SU) and meglitinide analogues (Megli) block the sulfonylurea receptor (SUR1) which constitutes asubunit of the inwardly rectifying ATP-sensitive K+ channel (KATP) in the membrane of pancreatic β cells. The inwardflow of K+ ions is thereby restricted, intracellular K+ concentration falls and the membrane is partially depolarizedaugmenting Ca2+ channel opening as well as release of Ca2+ from intracellular stores. The Ca2+ ions promote fusionof insulin containing intracellular granules with the plasma membrane and exocytotic release of insulin.
Incretins such as glucagon-like peptide 1 (GLP1) and glucose-dependent insulinotropic polypeptide (GIP) actupon their own G-protein coupled receptors on the β cell membrane to activate adenylyl cyclase and generate cAMP,which also promotes exocytosis of insulin. Exenatide (Exe) and liraglutide (Lira) are GLP1 receptor agonists—producethe same response as GLP1. The incretins GLP1 and GIP are rapidly inactivated by the capillary endothelial enzymedipeptidyl peptidase-4 (DPP-4). Their action is enhanced by DPP-4 inhibitors sitagliptin (sita) and vildagliptin (vilda).The DPP-4 inhibitors thus markedly accentuate the insulin response to ingested glucose/meal and attenuate post-prandial glycaemia.
Liraglutide This recently developed long-acting GLP-1agonist is closely related to the native peptide but its tightbinding to plasma proteins extends t½ to > 12 hours andduration of action to > 24 hours. Injected s.c. once daily,alone or added to oral metformin ± SU or pioglitazone, ithas achieved improved glycaemic control in type 2 diabetics.Nausea and diarrhoea are the frequent side effects, butdecrease in incidence over time. Use of liraglutide is attendedby weight loss, and it is being evaluated as an antiobesitydrug even for nondiabetics.
Hypoglycaemia is rare with exenatide/liraglutide mono-therapy, but can occur when combined with SUs/metformin.
Dipeptidyl peptidase-4 (DPP-4) inhibitors
Realizing the key role of the enzyme DPP-4 inrapid degradation of endogenous GLP-1, orallyactive inhibitors of this enzyme have beendeveloped as indirectly acting insulin secreta-gogues. In the past few years, DPP-4 inhibitors
have emerged as important adjunctive drugs intype 2 DM.
Sitagliptin This is the first DPP-4 inhibitorintroduced in USA in 2006 and now availableworld wide. It is a competitive and selectiveDPP-4 inhibitor which potentiates the action ofGLP-1 (Fig. 19.6) and GIP, boosts post prandialinsulin release, decreases glucagon secretion andlowers meal-time as well as fasting blood glucosein type 2 diabetics. No effect on gastric emptyingand appetite have been noted. It is body weightneutral and carries low risk of hypoglycaemiaunless combined with SUs or insulin. The HbA1c
lowering caused by sitagliptin is equivalent tothat with metformin. Further lowering of HbA1c
occurs when it is added to pioglitazone/SUs/insulin

275C
HA
PTE
R 19
INSULIN, ORAL HYPOGLYCAEMIC DRUGS AND GLUCAGON
with or without metformin. However, sitagliptinmonotherapy is recommended only whenmetformin cannot be used. Most professionalguidelines recommend DPP-4 inhibitors primarilyas adjuvant drugs in type 2 diabetics not wellcontrolled by metformin/SUs/pioglitazone orinsulin. Though clinical efficacy of all DPP-4inhibitors is comparable, one metaanalysis hasfound sitagliptin to cause greater reduction offasting blood glucose than vildagliptin.
Sitagliptin is well absorbed orally, is littlemetabolized and is largely excreted unchangedin urine with a t½ averaging 12 hours. Dosereduction is needed in renal impairment, but notin liver disease. Sitagliptin is well tolerated, sideeffects are nausea, loose stools, headache, rashes,allergic reactions and edema. Nasopharyngitis andcough occurs in some patients, which has beenascribed to prevention of substance P degradation.Pancreatitis is rare.
Vildagliptin This is the second DPP-4 inhibitoravailable in Europe and India which binds to theenzyme covalently. The complex dissociates veryslowly resulting in persistent DPP-4 inhibitioneven after the free drug has been cleared fromcirculation. This explains the longer duration ofaction (12–24 hours) despite short plasma t½(2–4 hours). The major route of elemination isby hepatic metabolism; only 20–25% is excretedunchanged in urine. Dose reduction is neededin moderately severe liver and kidney disease.No significant drug interactions have beenreported. Vildagliptin is less selective thansitagliptin for DPP-4; causes some inhibition ofDPP-8, DPP-9 as well, but the clinical significanceof this feature is not known. The tolerability ofvildagliptin is similar to that of sitagliptin, buthepatotoxicity has been reported. Vildagliptin mayrequire twice daily dosing; though single dailydose suffices in most cases when combined withanother hypoglycaemic.
Saxagliptin It has been available in USA since2009, and is recently marketed in India. Likevildagliptin, it binds covalently with DPP-4 andacts for 24 hours despite a plasma t½ of 2–4
hours. It is metabolized by CYP3A4 and generatesan active metabolite that has a t½ of 3–7 hours.Drug interactions with CYP3A4 inhibitors arepossible.Dose: 5 mg OD; reduce by half in moderately severe renalfailure, but not in liver disease.ONGLYZA 2.5, 5 mg tabs
Alogliptin is marketed in Japan and Linagliptin has beenrecently approved in USA.
Biguanide (AMPK activator)
Two biguanide antidiabetics, phenformin andmetformin were introduced in the 1950s. Becauseof higher risk of lactic acidosis, phenformin waswithdrawn and has been banned in India since2003.
H — N — C — N — C — N — CH3
| || | || | H NH H NH CH3
METFORMIN
Metformin It differs markedly from SUs:causes little or no hypoglycaemia in nondiabeticsubjects, and even in diabetics, episodes ofhypoglycaemia are rare. It does not stimulatepancreatic β cells. Metformin is reported toimprove lipid profile as well in type 2 diabetics.
Mechanism of action Biguanides do notcause insulin release, but presence of insulin isessential for their action. Metformin is not effectivein pancreatectomized animals and in type 1diabetics. Though the details are not clear, recentstudies have recognized activation of AMP-dependent protein kinase (AMPK) to play a crucialrole in mediating the actions of metformin, thekey features of which are:1. Suppresses hepatic gluconeogenesis and
glucose output from liver. This is the majoraction responsible for lowering of bloodglucose in diabetics.
2. Enhances insulin-mediated glucose uptake anddisposal in skeletal muscle and fat. Insulinresistance exhibited by type-2 diabetics is thusovercome. This translates into—• glycogen storage in skeletal muscle

276S
EC
TIO
N5
HORMONES AND RELATED DRUGS
• reduced lipogenesis in adipose tissue andenhanced fatty acid oxidation.
3. Interferes with mitochondrial respiratory chainand promotes peripheral glucose utilizationthrough anaerobic glycolysis.
AMPK activation by metformin appears to bean indirect consequence of interference withcellular respiration and lowering of intracellularATP and other energy sources.Metformin also retards intestinal absorptionof glucose, other hexoses, amino acids andVit B12.
Pharmacokinetics The important features ofmetformin pharmacokinetics are given in Table19.2. Clearance of metformin approximates g.f.r.It accumulates in renal failure and increases therisk of lactic acidosis.
Adverse effects Side effects with metforminare frequent, but generally not serious. Abdominalpain, anorexia, bloating, nausea, metallic taste,mild diarrhoea and tiredness are the usualcomplaints, which tend to subside with time.Metformin does not cause hypoglycaemia exceptin overdose.Lactic acidosis Small increase in blood lactate occurs withmetformin, but lactic acidosis is rare (<1 per 10,000 patientyears) because it is poorly concentrated in hepatic cells.Alcohol ingestion can precipitate lactic acidosis.
Vit B12 deficiency due to interference with its absorptioncan occur with high dose of metformin.
In addition to general restrictions for use oforal hypoglycaemics (see below), metformin iscontraindicated in hypotensive states, heart failure,severe respiratory, hepatic and renal disease, aswell as in alcoholics because of increased riskof lactic acidosis.
Drugs like cimetidine, furosemide maycompete with metformin excretion and enhanceits toxicity.
Uses Metformin is now established as a firstchoice drug for all type 2 DM patients, exceptwhen not tolerated or contraindicated.
Advantages of metformin are:• nonhypoglycaemic
• weight loss promoting• has potential to prevent macrovascular as well
as microvascular complications of diabetes• no acceleration of β cell exhaustion/ failure
in type 2 DM.• antihyperglycaemic efficacy (HbA1c reduction
by 0.8–1.2%) equivalent to other oral drugs.• can be combined with any other oral or
injectable antidiabetic, if one drug is notadequate.The limiting feature is g.i. intolerance,
especially at higher doses, but lack of serioustoxicity is well established by decades of use.Infertility: Metformin has been found to improve ovulationand fertility in some infertile women with polycystic ovary.This benefit is observed irrespective of the glycaemic statusof the woman. It may be due to mitigation of insulin resistanceand lowering of circulating insulin levels.
Thiazolidinedione (PPARγ agonist)
Pioglitazone Only one thiazolidinedionePioglitazone is currently available. Rosiglitazone,the other member, is banned in India since 2010and has been withdrawn in Europe due tounacceptable increase in risk of myocardialinfarction, CHF, stroke and death. This class oforal antidiabetic drugs are selective agonists forthe nuclear peroxisome proliferator-activatedreceptor γ (PPARγ) which is expressed mainlyin fat cells, but also in muscle and some othercells. It enhances the transcription of severalinsulin responsive genes. Glitazones tend toreverse insulin resistance by enhancing GLUT4expression and translocation. Entry of glucoseinto muscle and fat is improved. Hepatic gluconeo-genesis is also suppressed. Activation of genesregulating fatty acid metabolism and lipogenesisin adipose tissue contributes to the insulinsensitizing action. Lipolysis and plasma fatty acidlevels are reduced. Adipocyte turnover anddifferentiation is accelerated by glitazones. Thus,fatty tissue is a major site of their action. Themagnitude of blood glucose reduction is somewhatless than SUs and metformin. Improved glycae-mic control results in lowering of circulatingHbA1C and insulin levels in type 2 DM patients.

277C
HA
PTE
R 19
INSULIN, ORAL HYPOGLYCAEMIC DRUGS AND GLUCAGON
Pioglitazone, in addition, lowers serum trigly-ceride level and raises HDL level without muchchange in LDL level, probably because it actson PPARα as well to induce expression of reversecholesterol transporter and some apoproteins.
Pioglitazone is well tolerated; adverseeffects are plasma volume expansion, edema,weight gain, headache, myalgia and mild anaemia.Monotherapy with glitazones is not associatedwith hypoglycaemic episodes. Few cases ofhepatic dysfunction have been reported; CHF maybe precipitated or worsened. Monitoring of liverfunction is advised. It is contraindicated in liverdisease and in CHF. Glitazones increase the riskof fractures, especially in elderly women.
Pioglitazone is metabolized by both CYP2C8and CYP3A4. Failure of oral contraception mayoccur during pioglitazone therapy. Ketoconazoleinhibits and rifampin induces metabolism ofpioglitazone.
Pioglitazone is indicated in type 2 DM, butnot in type 1 DM. It reduces blood glucose andHbA1c (by 0.5–1.2%) without increasing circula-ting insulin. About 25% patients may not respond(nonresponders), probably due to low baselineinsulin levels. It should be stopped if HbA1c
reduction is < 0.5% at 6 months. Pioglitazoneis primarily used to supplement SUs/metforminand in case of insulin resistance. However, it isnot likely to be effective when β cell failure hasset in, which may be the cause of loss of efficacyto a combination of SUs + metformin. It mayalso be used as monotherapy (along with dietand exercise) in mild cases.
Several reports describe greater fluid retention,weight gain and precipitation of CHF aftercombined use of glitazones with insulin. Expertsadvise avoiding such combination. Pioglitazoneshould not be used during pregnancy. The DiabetesPrevention Programme (2005) has shown thatglitazones have the potential to delay progressionof prediabetics to overt type 2 DM. They mayhelp to conserve β cell function in diabetics.
ααααα Glucosidase inhibitorsAcarbose It is a complex oligosaccharide whichreversibly inhibits α-glucosidases, the final
enzymes for the digestion of carbohydrates inthe brush border of small intestine mucosa. Itslows down and decreases digestion and absorptionof polysaccharides (starch, etc.) and sucrose. Inaddition, GLP-1 release is promoted which maycontribute to the effect. Postprandial glycaemiais reduced without significant increase in insulinlevels. Regular use lowers HbA1c modestly (by0.4–0.8%), but change in body weight and lipidlevels is minimal. The stop-NIDDM trial (2002)has shown that long-term acarbose treatment inprediabetics reduces occurrence of type 2 DMas well as hypertension and cardiac disease. Indiabetics, it reduces cardiovascular events.
Acarbose is a mild antihyperglycaemic andnot a hypoglycaemic; may be used as an adjuvantto diet (with or without metformin/SU) in obesediabetics. Dose 50–100 mg TDS is taken at thebeginning of each major meal. Only a smallfraction of the dose is absorbed. Flatulence,abdominal discomfort and loose stool areproduced in about 50% patients due tofermentation of unabsorbed carbohydrates. Patientacceptability of α-glucosidase inhibitors is poordue to uncomfortable g.i. symptoms. Hepatictransaminases may rise, but liver damage is rare.GLUCOBAY 50, 100 mg tabs, ASUCROSE, GLUCAR 50mg tabs.
Miglitol It has a smaller molecule than acarbose,and it is a stronger inhibitor of sucrase. Potencyfor other α-glucosidases is equivalent to acarbose.Absorption of miglitol is substantial, but variable.The absorbed drug is excreted by the kidney. Nosystemic toxicity is known.Dose: 25–100 mg TDS at beginning of each meal.MIGTOR, DIAMIG, ELITOX 25, 50 mg tabs.
Voglibose Has properties, use and side effectssimilar to that of acarbose.Dose: 200–300 mg TDS just before meals.VOGLITOR, VOLIX, VOLIBO 0.2, 0.3 g tabs.
Amylin analogueAmylin, also called ‘islet amyloid polypeptide’ (IAP), isproduced by pancreatic β cells and acts in the brain to reduceglucagon secretion from α cells, delay gastric emptying, retardglucose absorption and promote satiety.

278S
EC
TIO
N5
HORMONES AND RELATED DRUGS
Pramlintide It is a synthetic amylin analogue which ons.c. injection before meal attenuates postprandial glycaemiaand exerts a centrally mediated anorectic action. The durationof action is 2–3 hours. It has been used as an adjuvantto meal time insulin injection to suppress the glycaemic peakin both type 1 and type 2 diabetics. Reduction in body weightis an additional benefit.
Dopamine D2 agonistBromocriptine Recently (2009) a quick release oralformulation of bromocriptine has been approved by US-FDAfor adjunctive treatment of type 2 DM. Taken early in themorning it is thought to act on the hypothalamic dopaminergiccontrol of the circadian rhythm of hormone (GH, prolactin,ACTH, etc.) release and reset it to reduce insulin resistance.Bromocriptin can be taken alone to supplement diet+exerciseor added to metformin or SU or both. Started at 0.8 mgOD and increased upto 4.8 mg OD (as needed) it has beenshown to marginally improve glycaemic control and lowerHbA1c by upto 0.5%.
Sodium-glucose co-transport-2 (SGLT-2) inhibitorPractically all the glucose filtered at the glomerulus isreabsorbed in the proximal tubules. The major transporterwhich accomplishes this is SGLT-2, whose inhibition inducesglucosuria and lowers blood glucose in type 2 DM, as wellas causes weight loss.
Dapagliflozin This SGLT-2 inhibitor has been recentlytested in type 2 DM patients. After single daily dose itproduces round-the-clock glucosuria and lowers blood glucoselevels. The concerns which appear inbuilt due to itsmechanism of action are—glycosuria which can predisposeto urinary and genital infections, electrolyte imbalance andincreased urinary frequency. Tolerability and safety of thisdrug is yet to be established.
Status of oral hypoglycaemics indiabetes mellitusAfter 8 years of prospective study involving largenumber of patients, the University Group Diabe-tes Programme (UGDP) of USA (1970) presentedfindings that cardiovascular mortality was higherin patients treated with biguanides and SUs thanin those treated with diet and exercise alone orwith insulin. A decline in their use followed.Subsequent studies both refuted and supportedthese conclusions.
The controversy has been settled by the UKPDS trial which found that both SUs andmetformin did not increase cardiovascularmortality over > 10 years observation period.
Related to degree of glycaemia control, bothinsulin and SUs reduced microvascular complica-tions (retinopathy, neuropathy, nephropathy) intype 2 DM, but did not have significant effecton macrovascular complications (coronary arterydisease, stroke, etc). Metformin, however, couldreduce macrovascular complications as well; itdecreased risk of death and other diabetes relatedendpoints in overweight patients. This may berelated to the fact that both SUs and exogenousinsulin improve glycaemic control by increasinginsulin supply rather than by reducing insulinresistance, while metformin can lower insulinresistance which is a pathogenic factor in type 2DM. All oral hypoglycaemics do however controlsymptoms that are due to hyperglycaemia andglycosuria, and are much more convenient thaninsulin.
Oral hypoglycaemics are indicated only intype 2 diabetes, in addition to diet and exercise.They are most effective in patients with—1. Age above 40 years at onset of disease.2. Obesity at the time of presentation.3. Duration of disease < 5 years when starting
treatment.4. Fasting blood sugar < 200 mg/dl.5. Insulin requirement < 40 U/day.6. No ketoacidosis or a history of it, or any other
complication.
The Diabetes Prevention Programme (2002)has established that in middle aged, obese predia-betics metformin prevented progression to type2 DM, but not in older nonobese prediabetics.Glitazones also appear to have prophylacticpotential. Long-term acarbose therapy as well candelay type 2 DM.
Oral hypoglycaemics should be used to sup-plement dietary management and not to replaceit. In view of the prophylactic and outcomebenefits, current recommendation is to institutemetformin therapy right at the diagnosis of type2 DM, along with dietary and other lifestylemeasures, without waiting to see if the latter aloneare sufficient. Metformin may delay progressionof diabetic severity by favourably affecting β cell

279C
HA
PTE
R 19
INSULIN, ORAL HYPOGLYCAEMIC DRUGS AND GLUCAGON
health and retarding β cell failure. It is especiallyvaluable for obese patients; may also aid weightreduction. Further, it has the potential to reducethe risk of myocardial infarction and stroke. Thus,unless contraindicated/not tolerated, metformin isprescribed to all type 2 diabetics, despite itsinferior patient acceptability due to g.i. side effects.
Many type 2 DM patients do not attain desiredlevel of glycaemia control and HbA1c reduction(to < 7%) with metformin alone, and a seconddrug is needed. SUs are the most commonlyselected 2nd drug. They have good patientacceptability, convenient dosing and high efficacy,but can cause weight gain and hypoglycaemia.There is some evidence that SUs given over long-term (2–10 years) expedite β cell apoptosis andfailure. Receptor desensitization may also be acause, and SUs tend to lose efficacy in few years(5–10% per year failure rate). There is nodifference in the clinical efficacy of different 2ndgeneration SUs. However, this does not indicatethat choice among them is irrelevant. Differencesamong them are mainly in dose, onset and durationof action which govern flexibility of regimens.Some specific features of various SUs are givenin Table 19.2. If a particular SU proves inadequatein a given patient, another one may still work.
Patients with near normal fasting bloodglucose but prominent post-prandial hypergly-caemia, or those experiencing late postmealhypoglycaemia may do better with a premealmeglitinide/phenyl alanine analogue.
Pioglitazone is usually the 3rd choice drug;may be added to metformin or a combinationof metformin + SU. Though it reduces insulinresistance, tends to preserve β cell function anddoes not cause hypoglycaemia, it is infrequentlyselected for monotherapy. Its major limitationsare—tendency to fluid retention, weight gain,increased risk of heart failure and fractures, needto monitor liver function and inefficacy in asignificant number of patients.
Acarbose-like drugs are mild antihypergly-caemics, mostly used as supplementary drugs toa combination hypoglycaemic regimen. They aredisliked by many patients because of bloating,indigestion and other abdominal symptoms.
The latest hypoglycaemics gaining popularityare the DPP-4 inhibitors. Their favourable featuresare:• Insulin release is glucose dependent; therefore
not likely to induce hypoglycaemia.• Suppress glucagon release, thus lowering
fasting blood glucose as well.• Improve β cell health and retard progression
of β cell failure.• Body weight neutral.• Mostly single daily dose, well tolerated with
few side effects, no serious toxicity, no druginteractions, except with saxagliptin.
However, they are new drugs and have notwithstood the test of time yet. Their impact oncardiovascular mortality and other outcomes isyet to be measured. As such, most professionalguidelines place them as second line/add onantidiabetic drugs. They are especially valuablefor patients having body weight problem and thoseexperiencing frequent episodes of hypoglycaemia.
Upto 50% patients of type 2 DM initiallytreated with oral hypoglycaemics ultimately needinsulin. Moreover, when a diabetic on oralhypoglycaemics presents with infection, severetrauma or stress, pregnancy, ketoacidosis or anyother complication, or has to be operated upon—switchover to insulin (see Flow chart in Fig. 19.7).Metformin and/or SUs or DPP-4 inhibitors canalso be combined with insulin, particularly whena single daily injection of long-acting (e.g.glargine) insulin is used to provide basal control.The oral drug given before meals serves to checkpostprandial glycaemia.
Epalrestat Sorbitol is a minor metabolite of glucosegenerated by the enzyme aldose reductase. In diabetics, excesssorbitol is produced and gets deposited in nerves and othertissues. This is involved in the pathogenesis of diabeticneuropathy and other complications. Epalrestat is an aldosereductase inhibitor developed in Japan which has been foundto delay sorbitol accumulation in sciatic nerve/other tissuesof diabetics imparting potential to delay progression ofdiabetic neuropathy. In trials it has caused modestimprovement in nerve conduction, neuropathic pain and othersymptoms. However, magnitude of benefit and safety areyet to be defined. Nausea, vomiting and elevation of liverenzymes are the adverse effects.Dose: 50 mg TDS before meals; ALRISTA 50 mg tab.

280S
EC
TIO
N5
HORMONES AND RELATED DRUGS
GLUCAGONA hyperglycaemic principle was demonstrated to be presentin the pancreatic islets just two years after the discoveryof insulin in 1921. It was named ‘glucagon’. Glucagon isa single chain polypeptide containing 29 amino acids, MW3500. It is secreted by the α cells of the islets of Langerhansand commercially produced now by recombinant DNAtechnology.
Regulation of Secretion Like insulin, glucagon is alsoderived by cleavage of a larger peptide prohormone. Itssecretion is regulated by glucose levels, other nutrients,paracrine hormones and nervous system. Glucose has oppositeeffects on insulin and glucagon release, i.e. high glucoselevel inhibits glucagon secretion. The incretin GLP-1, FFAand ketone bodies also inhibit glucagon release. Amino acids,however, induce both insulin and glucagon secretion. Insulin,amylin and somatostatin, elaborated by the neighbouring βand δ cells, inhibit glucagon secretion. Sympatheticstimulation consistently and parasympathetic stimulationunder certain conditions evokes glucagon release.
Actions Glucagon is hyperglycaemic; most of its actionsare opposite to that of insulin. Glucagon causes hyperglycaemiaprimarily by enhancing glycogenolysis and gluconeogenesisin liver; suppression of glucose utilization in muscle and fatcontributes modestly. Glucagon is considered to be the hormoneof fuel mobilization. Its secretion is increased during fasting,and is largely responsible for the high fasting blood glucoselevels in type 2 diabetics. It plays an essential role in thedevelopment of diabetic ketoacidosis. Increased secretion ofglucagon has been shown to attend all forms of severe tissueinjury.
Glucagon increases the force and rate of cardiac contractionand this is not antagonized by β blockers. It has a relaxantaction on the gut and inhibits gastric acid production.
Mechanism of action Glucagon, through its own receptorand coupling Gs protein activates adenylyl cyclase andincreases cAMP in liver, fat cells, heart and other tissues;most of its actions are mediated through this cyclic nucleotide.
Glucagon is inactive orally; that released from pancreasis broken down in liver, kidney, plasma and other tissues.Its t½ is 3–6 min.
Fig. 19.7: Simplified flow chart of management approaches in diabetes mellitus.Met—Metformin; SU—Sulfonylurea; Megli—Meglitinide/d-phenylalanine analogue; DPP-4i—Dipeptidyl peptidase-4inhibitor; α Gli—α Glucosidase inhibitor; Pio—PioglitazoneNote: A meglitinide drug is indicated only in patients with predominant postprandial hyperglycaemia.
An α glucosidase inhibitor can be additional add on drug.

281C
HA
PTE
R 19
INSULIN, ORAL HYPOGLYCAEMIC DRUGS AND GLUCAGON
Uses
1. Hypoglycaemia due to insulin or oral hypoglycaemics;use of glucagon is; only an expedient measure for theemergency, and must be followed by oral glucose/sugar givenrepeatedly till the blood glucose level stabilizes. It may notwork if hepatic glycogen is already depleted.Dose: 0.5–1.0 mg i.v. or i.m.GLUCAGON 1 mg inj.
2. Cardiogenic shock to stimulate the heart in βadrenergic blocker treated patients. However, action is notvery marked.
3. To facilitate radiographic examination of upper/lowerg.i. tract by relaxing stomach and intestines.
Other hyperglycaemicsDiazoxide Chemically related to thiazides, it inhibits insulinrelease from β cells and causes hyperglycaemia lasting4–8 hours. Its action on ATP sensitive K+ channels ofβ cells is opposite to that of SUs. Other actions which maycontribute to hyperglycaemia are decreased peripheralutilization of glucose and release of catecholamines. It hasbeen used to prevent hypoglycaemia in insulinomas. Otheractions are vasodilatation, fall in BP and antidiuresis.Somatostatin It causes hyperglycaemia primarily byinhibiting insulin release.Streptozocin It is obtained from Streptomyces achromo-genes. Causes selective damage to insulin secretingβ cells. It has been used to produce experimental diabetesin animals and to treat insulin secreting tumours of pancreas.
PROBLEM DIRECTED STUDY
19.1 During routine medical checkup a 50-year male office executive with sedentary lifestylewas diagnosed to have developed type 2 diabetes mellitus. His fasting and post-meal blood glucosewas 130 mg/dl and 190 mg/dl respectively, HbA1C was 7.8%, BP was 130/82 mm Hg and bodymass index was 27 kg/m2. He was asymptomatic and investigations revealed no end organ damage.He was advised suitable diet, exercise and other lifestyle modifications.(a) Should he be prescribed an antidiabetic medication as well? If so, which drug/combinationof drugs should be selected, and why?(see Appendix-1 for solution)

CorticosteroidsChapterChapterChapterChapterChapter 2020202020
The adrenal cortex secretes steroidal hormoneswhich have glucocorticoid, mineralocorticoid andweakly androgenic activities. Conventionally, theterm ‘corticosteroid’ or ‘corticoid’ includes naturalgluco- and mineralo-corticoids and their syntheticanalogues.
By the middle of 19th century it was demonstrated thatadrenal glands were essential for life. Later it was appreciatedthat the cortex was more important than the medulla. A numberof steroidal active principles were isolated and their structureswere elucidated by Kendall and his coworkers in the 1930s.However, the gate to their great therapeutic potential wasopened by Hench (1949) who obtained striking improvementin rheumatoid arthritis by using cortisone. The Nobel Prizewas awarded the very next year to Kendall, Reichstein andHench.
BIOSYNTHESISThe corticoids (both gluco and mineralo) are 21carbon compounds having a cyclopentanoper-hydro-phenanthrene (steroid) nucleus. They aresynthesized in the adrenal cortical cells fromcholesterol. A simplified version of the biosyn-thetic pathways is presented in Fig. 20.1. Adrenal
steroidogenesis takes place under the influenceof ACTH which makes more cholesterol availablefor conversion to pregnenolone and induces steroi-dogenic enzymes. Since adrenal cortical cells storeonly minute quantities of the hormones, rate ofrelease is governed by the rate of biosynthesis.The circulating corticosteroids inhibit ACTHrelease from pituitary as well as CRH productionfrom hypothalamus (see Ch. 17) and thus providenegative feed back regulation of the hypothalamo-pituitary-adrenal (HPA) axis.
The normal rate of secretion of the two principalcorticoids in man is—
Hydrocortisone—10–20 mg daily (nearly half ofthis in the few morning hours).
Aldosterone — 0.125 mg daily.
ACTIONS
The corticoids have widespread actions. Theymaintain fluid-electrolyte, cardiovascular and
Fig. 20.1: Simplified depiction of the pathways of adrenal steroid hormone biosynthesis

283C
HA
PTE
R 20
CORTICOSTEROIDS
Fig. 20.2: Hypothalamo-pituitary-adrenal (HPA) axis; regulation of corticosteroid production andresponse to stress which overrides the negative feedback regulation of ACTH release
energy substrate homeostasis and functional statusof skeletal muscles and nervous system. Theyprepare the body to withstand effects of all kindsof noxious stimuli and stress. The involvementof hypothalamo-pituitary-adrenal axis in stressresponse is depicted in Fig. 20.2.
Corticoids have some direct and somepermissive actions. By permissive action is meantthat while they do not themselves produce aneffect, their presence facilitates other hormonesto exert that action, e.g. they do not have anyeffect on BP but the pressor action of Adr ismarkedly blunted in their absence. Actions ofcorticoids are divided into:
Glucocorticoid Effects on carbohydrate, proteinand fat metabolism, and other actions that areinseparably linked to these.
Mineralocorticoid Effects on Na+, K+ and fluidbalance.
Marked dissociation between these two typesof actions is seen among natural as well as syntheticcorticoids. Accordingly, compounds are labelledas ‘glucocorticoid’ or ‘mineralocorticoid’.
Mineralocorticoid actionsThe principal mineralocorticoid action is enhan-cement of Na+ reabsorption in the distal convo-luted tubule in kidney. There is an associatedincrease in K+ and H+ excretion. Its deficiencyresults in decreased maximal tubular reabsorptivecapacity for Na+; kidney is not able to retain Na+
even in the Na+ deficient state → Na+ isprogressively lost: kidneys absorb water withoutthe attendant Na+ (to maintain e.c.f. volume which

284S
EC
TIO
N5
HORMONES AND RELATED DRUGS
nevertheless decreases) → dilutional hyponatrae-mia → excess water enters cells → cellularhydration: decreased blood volume and raisedhaematocrit. Hyperkalaemia and acidosis accom-pany. These distortions of fluid and electrolytebalance progress and contribute to the circulatorycollapse. As such, these actions make adrenalcortex essential for survival.
Similar action on cation transport is exertedin other tissues as well. The action of aldosteroneis exerted by gene mediated increased transcrip-tion of m-RNA in renal tubular cells which directssynthesis of proteins (aldosterone-inducedproteins—AIP). The Na+K+ ATPase of tubularbasolateral membrane responsible for generatinggradients for movement of cations in these cellsis the major AIP (see Fig. 41.3). Synthesis ofβ subunit of amiloride sensitive Na+ channel isalso induced. Because of the time taken to induceprotein synthesis, aldosterone action has a latencyof 1–2 hours. In addition, aldosterone rapidlyinduces phosphorylation and activation ofamiloride sensitive Na+ channel.
The main adverse effect of excessive mine-ralocorticoid action is fluid retention and hyper-tension. The natural and some of the syntheticglucocorticoids have significant mineralocorticoidactivity responsible for side effects like edema,progressive rise in BP, hypokalemia and alkalosis.The diuretic induced hypokalemia is aggravatedby mineralocorticoid excess.
Aldosterone has been shown to promote CHFassociated myocardial fibrosis and progressionof the disease (see Ch. 37).
Glucocorticoid actions
1. Carbohydrate and protein metabolismGlucocorticoids promote glycogen deposition inliver (they are assayed on the basis of this action)by inducing hepatic glycogen synthase andpromoting gluconeogenesis. They inhibit glucoseutilization by peripheral tissues. This along withincreased glucose release from liver results inhyperglycaemia, resistance to insulin and adiabetes-like state. They also cause proteinbreakdown and amino acid mobilization from
peripheral tissues. This is responsible for sideeffects like muscle wasting, lympholysis, loss ofosteoid from bone and thinning of skin. The aminoacids so mobilized funnel into liver → used upin gluconeogenesis, excess urea is produced →negative nitrogen balance. Glucocorticoids arethus catabolic. Their function appears to be aimedat maintaining blood glucose levels duringstarvation—so that brain continues to get itsnutrient. When food is withheld from anadrenalectomized animal—liver glycogen israpidly depleted and hypoglycaemia occurs.Glucocorticoids also increase uric acid excretion.
2. Fat metabolism The action of glucocor-ticoids on fat metabolism is primarily permissivein nature. They promote lipolysis due to glucagon,growth hormone, Adr and thyroxine. cAMPinduced breakdown of triglycerides is enhanced.Fat depots in different areas of the body responddifferently—redistribution of body fat occurs.Subcutaneous tissue over extremities loses fatwhich is deposited over face, neck and shoulderproducing ‘moon face’, ‘fish mouth’ and ‘buffalohump’. Explanation offered is—becauseperipheral adipocytes are less sensitive to insulinand more sensitive to corticosteroid-facilitatedlipolytic action of GH and Adr, break down offat predominates, whereas truncal adipocytesrespond mainly to raised insulin levels causedby glucocorticoid induced hyperglycaemia.
Difference in the sensitivity of adipocytes at different locationsto glucocorticoids is believed to arise from different levelsof expression of the isoenzyme 11β-hydroxysteroid dehydroge-nase type 1 (11β HSD1) which generates active hydrocortisonefrom inactive cortisone in the target tissues. Greater expressionof 11βHSD1 in peripheral adipocytes than in truncaladipocytes would direct glucocorticoid-facilitated lipolysisto the subcutaneous fat in the limbs.
11βHSD1Cortisone Hydrocortisone
11βHSD2
On the other hand, high expression of the type 2 isoenzyme(11βHSD2) in the kidney tubule (also colon and salivarygland) which express mineralocorticoid receptor (MR) isbelieved to account for only weak mineralocorticoid activityof hydrocortisone whose inherent potency on MR is similarto that of aldosterone. As shown above, 11βHSD2 catalysesthe reverse reaction inactivating hydrocortisone.

285C
HA
PTE
R 20
CORTICOSTEROIDS
3. Calcium metabolism Glucocorticoidsinhibit intestinal absorption and enhance renalexcretion of Ca2+. Loss of osteoid (decreasedformation and increased resorption) indirectlyresults in loss of Ca2+ from bone, producingnegative calcium balance. Spongy bones(vertebrae, ribs, pelvis, etc.) are more sensitive.
4. Water excretion The effect on waterexcretion is independent of action on Na+
transport; hydrocortisone and other glucocorti-coids, but not aldosterone, maintain normal g.f.r.In adrenal insufficiency, the capacity to excretea water load is markedly reduced—such patientsare prone to water intoxication from i.v. infusions.
Glucocorticoids also enhance secretory acti-vity of renal tubules.
5. CVS Glucocorticoids restrict capillary per-meability, maintain tone of arterioles and myo-cardial contractility. Applied topically, they causecutaneous vasoconstriction. They have a permis-sive role for the pressor action of Adr andangiotensin. They also play a permissive role indevelopment of hypertension—should be usedcautiously in hypertensives.
Adrenal insufficiency is attended by low car-diac output, arteriolar dilatation, poor vasocons-trictor response to Adr (repeated doses of Adrcause destructive changes in blood vessels) andincreased permeability of capillaries. Thesechanges along with hypovolemia (due to lack ofmineralocorticoid) are responsible for cardio-vascular collapse.
6. Skeletal muscles Optimum level ofcorticosteroids is needed for normal muscularactivity. Weakness occurs in both hypo- andhypercorticism, but the causes are different.Hypocorticism: diminished work capacity andweakness are primarily due to hypodynamiccirculation.Hypercorticism: excess mineralocorticoid action→ hypokalaemia → weakness;Excess glucocorticoid action → muscle wastingand myopathy → weakness.
7. CNS Mild euphoria is quite common withpharmacological doses of glucocorticoids. This
is a direct effect on brain, independent of reliefof disease symptoms, and sometimes progressesto cause increased motor activity, insomnia, hypo-mania or depression. On the other hand, patientsof Addison’s disease suffer from apathy,depression and occasionally psychosis.
Glucocorticoids also maintain the level ofsensory perception and normal level of excita-bility of neurones. High doses lower seizurethreshold. Use in epileptics requires caution. Thisaction is independent of electrolyte changes inthe brain and is not shared by aldosterone.
8. Stomach Secretion of gastric acid and pep-sin is increased—may aggravate peptic ulcer.
9. Lymphoid tissue and blood cellsGlucocorticoids enhance the rate of destructionof lymphoid cells (T cells are more sensitive thanB cells); but in man the effect on normal lymphoidtissue is modest. However, a marked lytic responseis shown by malignant lymphatic cells. This isthe basis of their use in lymphomas.
Glucocorticoids increase the number of RBCs,platelets and neutrophils in circulation. Theydecrease lymphocytes, eosinophils and basophils.This is not due to destruction of the concernedcells, but due to their sequestration in tissues.Blood counts come back to normal after 24 hours.
10. Inflammatory responses Irrespective ofthe type of injury or insult, the attending inflamma-tory response is suppressed by glucocorticoids.This is the basis of most of their clinical uses.The action is nonspecific and covers all compo-nents and stages of inflammation. This includesattenuation of—increased capillary permeability,local exudation, cellular infiltration, phagocyticactivity and late responses like capillary prolife-ration, collagen deposition, fibroblastic activityand ultimately scar formation. This action isdirect and can be restricted to a site by localadministration. The cardinal signs of inflam-mation—redness, heat, swelling and pain aresuppressed.
Glucocorticoids interfere at several stepsin the inflammatory response (see cellular

286S
EC
TIO
N5
HORMONES AND RELATED DRUGS
mechanism below), but the most important overallmechanism appears to be limitation of recruitmentof inflammatory cells at the local site andproduction of proinflammatory mediators likePGs, LTs, PAF through indirect inhibition ofphospholipase A2.
Corticoids are only palliative; do not removethe cause of inflammation; the underlying diseasecontinues to progress while manifestations aredampened. They favour spread of infections becausecapacity of defensive cells to kill microorganismsis impaired. They also interfere with healing andscar formation: peptic ulcer may perforate asymp-tomatically. Indiscriminate use of corticoids ishazardous.
11. Immunological and allergic responsesGlucocorticoids impair immunological compe-tence. They suppress all types of hypersensitizationand allergic phenomena. At high concentrationsand in vitro they have been shown to interfere
with practically every step of the immunologicalresponse, but at therapeutic doses in vivo thereis no impairment of antibody production or comp-lement function. The clinical effect appears tobe due to suppression of recruitment of leukocytesat the site of contact with antigen and ofinflammatory response to the immunological injury.
Glucocorticoids cause greater suppression ofCMI in which T cells are primarily involved, e.g.delayed hypersensitivity and graft rejection. Thisis the basis of their use in autoimmune diseasesand organ transplantation (see Ch. 63). Factorsinvolved may be inhibition of IL-1 release frommacrophages; inhibition of IL-2 formation andaction → T cell proliferation is not stimulated;suppression of natural killer cells, etc.
The broad action seems to be interruption ofcommunication between cells involved in theimmune process by interfering with productionof or action of lymphokines.
Gene mediated cellular actions of glucocorticoids
Mechanism Action
• Translocation of glucose transporters from plasma • ↓ glucose uptake and utilization in peripheralmembrane to deeper sites. tissues.
• Induction of hepatic gluconeogenetic enzymes. • ↑ production of glucose from amino acids.• Induction of hepatic glycogen synthase. • Deposition of glycogen in hepatocytes.• Site specific changes in sensitivity of adipocytes • Altered distribution of body fat.
to GH, Adr, insulin.• ↑ expression of vascular adrenergic and AT1 receptor. • Enhanced reactivity to vasopressor substances.• ↓ expression of POMC gene in pituitary corticotropes • ↓ production of ACTH.
Antiinflammatory and Immunosuppressant actions
• Induction of annexins in macrophages, • Annexins inhibit phospholipase A2 → decreasedendothelium and fibroblasts. production of PGs, LTs & PAF.
• Negative regulation of COX-2 • ↓ inducible PG production.• Negative regulation of genes for cytokines in • ↓ production of IL-1, IL-2, IL-3, IL-6, TNFα,
macrophages, endothelial cells and lymphocytes. GM-CSF, γ interferon → fibroblast proliferationand T-lymphocyte function are suppressed,chemotaxis interfered.
• ↓ production of acute phase reactants from • Complement function is interfered.macrophages and endothelial cells
• ↓ production of ELAM-1 and ICAM-1 in • Adhesion and localization of leukocytes is interfered.endothelial cells.
• ↓ expression of transcription factors • ↓ histone acetylationAP-1, NF-κB • ↓ MAP kinase
• ↓ production of collagenase and stromolysin • Prevention of tissue destruction
POMC—Proopiomelanocortin; IL—Interleukin; TNFα—Tumour necrosis factor α; GM-CSF—Granulocyte macrophagecolony stimulating factor; ELAM-1—Endothelial leukocyte adhesion molecule-1; ICAM-1—Intracellular adhesionmolecule-1; AP-1–Activator protein-1; NF-κB–Nuclear factor κB; MAP kinase–Mitogen activated protein kinase.

287C
HA
PTE
R 20
CORTICOSTEROIDS
Mechanism of action at cellular levelCorticosteroids penetrate cells and bind to a highaffinity cytoplasmic receptor protein → a struc-tural change occurs in the steroid receptor comp-lex that allows its migration into the nucleus andbinding to glucocorticoid response elements(GRE) on the chromatin → transcription ofspecific m-RNA → regulation of protein synthesis(see Fig. 4.10). This process takes at least 30–60 min : effects of corticosteroid are notimmediate, and once the appropriate proteins aresynthesized—effects persist much longer than thesteroid itself. In many tissues, the overall effectis catabolic, i.e. inhibition of protein synthesis.This may be a consequence of steroid directedsynthesis of an inhibitory protein.
The glucocorticoid receptor (GR) is verywidely distributed (in practically all cells). It hasbeen cloned and its structure determined. It ismade up of ~ 800 amino acids.Several coactivators and corepressors modulate the interactionof liganded GR with the GREs, altering the intensity ofresponse.Because the GR largely maintains uniformity throughout thebody, tissue specificity is not exhibited by differentglucocorticoids, and all members produce the sameconstellation of effects.The functional scheme of GR is presented in Fig.4.10. Direct evidence of gene expression mediatedaction has been obtained for actions listed in thebox (see p. 286).
Some actions of corticoids are exerted morerapidly (like inhibition of ACTH release frompituitary). These may be mediated by a cellmembrane receptor or a different mechanism notinvolving protein synthesis.
PHARMACOKINETICSAll natural and synthetic corticoids, except DOCAare absorbed and are effective by the oral route.Absorption into systemic circulation occurs fromtopical sites of application as well, but the extentvaries depending on the compound, site, area ofapplication and use of occlusive dressing. Watersoluble esters, e.g. hydrocortisone hemisuccinate,dexamethasone sod. phosphate can be given i.v.
or i.m., act rapidly and achieve high concentra-tions in tissue fluids. Insoluble esters, e.g. hydro-cortisone acetate, triamcinolone acetonide cannotbe injected i.v., but are slowly absorbed fromi.m. site and produce more prolonged effects.
Hydrocortisone undergoes high first pass meta-bolism, has low oral: parenteral activity ratio. Oralbioavailability of synthetic corticoids is high.
Hydrocortisone is 90% bound to plasmaprotein, mostly to a specific cortisol-bindingglobulin (CBG; transcortin) as well as to albumin.Transcortin concentration is increased duringpregnancy and by oral contraceptives—corticoidlevels in blood are increased but hypercorticismdoes not occur, because free cortisol levels arenormal.
The corticosteroids are metabolized primarilyby hepatic microsomal enzymes. Pathways are—
(i) Reduction of 4, 5 double bond and hydroxy-lation of 3-keto group.
(ii) Reduction of 20-keto to 20-hydroxy form.(iii) Oxidative cleavage of 20C side chain (only
in case of compounds having a 17-hydroxylgroup) to yield 17-ketosteroids.
These metabolites are further conjugated withglucuronic acid or sulfate and are excreted inurine.
The plasma t½ of hydrocortisone is 1.5 hours.However, the biological t½ is longer because ofaction through intracellular receptors and regu-lation of protein synthesis—effects that persistlong after the steroid is removed from plasma.
The synthetic derivatives are more resistantto metabolism and are longer acting.
Phenobarbitone and phenytoin induce meta-bolism of hydrocortisone, prednisolone and dexa-methasone, etc. to decrease their therapeutic effect.
CHEMISTRY AND RELATIVE ACTIVITYOF CORTICOIDS
Fig. 20.3 depicts the chemical structure of desoxy-corticosterone in blue line. It is a selective mineralo-corticoid. Chemical modifications that result inclinically useful compounds are also indicated.Fluorination at position 9 or 6 has resulted in

288S
EC
TIO
N5
HORMONES AND RELATED DRUGS
Fig. 20.3: Chemical structure of corticosteroids. The structure in blue is desoxycorticosterone.Important substitutions which yield other useful compounds are shown in red
+ OH at 11 — Corticosterone+ OH at 11 + OH at 17 — Hydrocortisone(if O at 11) + OH at 17 — Cortisone+ OH at 11 + OH at 17 + Δ 1, 2 — Prednisolone+ OH at 11 + OH at 17 + Δ 1, 2 + F at 9 + OH at 16 — Triamcinolone+ OH at 11 + OH at 17 + Δ 1, 2 + F at 9 + CH3 α at 16 — Dexamethasone+ OH at 11 + OH at 17 + Δ 1, 2 + F at 9 + CH3 β at 16 — BetamethasoneHydrocortisone + F at 9 — FludrocortisoneCorticosterone + CHO at 18 — Aldosterone
highly potent compounds. Synthetic steroids havelargely replaced the natural compounds intherapeutic use, because they are potent, longeracting, more selective for either glucocorticoidor mineralocorticoid action and have high oralactivity.
DISTINCTIVE FEATURES
The relative potency and activity of differentnatural and synthetic corticosteroids employedsystemically is compared in Table 20.1.
1. Hydrocortisone (cortisol) Acts rapidlybut has short duration of action. In addition toprimary glucocorticoid, it has significant minera-locorticoid activity as well. Used for:Replacement therapy—20 mg morning + 10 mgafternoon orally.Shock, status asthmaticus, acute adrenal insuf-ficiency—100 mg i.v. bolus + 100 mg 8 hourlyi.v. infusion.Topically (see Ch. 64) and as suspension forenema in ulcerative colitis (see Ch. 48).
LYCORTIN-S, EFCORLIN SOLUBLE 100 mg/2 ml inj. (ashemisuccinate for i.v. inj.) WYCORT, EFCORLIN 25 mg/mlinj (as acetate for i.m./intraarticular inj.). PRIMACORT 100,200, 400 mg/vial inj.
2. Prednisolone It is 4 times more potentthan hydrocortisone, also more selective gluco-corticoid, but fluid retention does occur with highdoses. Has intermediate duration of action: causesless pituitary-adrenal suppression when a singlemorning dose or alternate day treatment is given.Used for allergic, inflammatory, autoimmunediseases and in malignancies: 5–60 mg/day oral,10–40 mg i.m., intraarticular; also topically.DELTACORTRIL, HOSTACORTIN-H, 5, 10 mg tab, 20 mg/ml (as acetate) for i.m., intraarticular inj., WYSOLONE,NUCORT, 5, 10, 20, 30, 40 mg tabs.
3. Methylprednisolone Slightly more potentand more selective than prednisolone: 4–32 mg/day oral. Methylprednisolone acetate has beenused as a retention enema in ulcerative colitis.
Pulse therapy with high dose methylpredni-solone (1 g infused i.v. every 6–8 weeks) hasbeen tried in nonresponsive active rheumatoid

289C
HA
PTE
R 20
CORTICOSTEROIDS
TABLE 20.1 Relative activity of systemic corticosteroids
Compound Gluco Mineralo Equiv. dose(antiinflammatory)
Short acting 1. Hydrocortisone 1 1 20 mg(Biological (cortisol)t½ < 12 hr)
Intermediate 2. Prednisolone 4 0.8 5 mgacting 3. Methyl- 5 0.5 4 mg(Biological prednisolonet½ 12–36 hr) 4. Triamcinolone 5 0 4 mg
5. Deflazacort 3–4 0 6 mg
Long acting 6. Dexamethasone 25 0 0.75 mg(Biological 7. Betamethasone 25 0 0.75 mgt½ > 36 hr)
Equiv. saltretaining dose
8. Desoxycortico- 0 100 2.5 mgsterone acetate (DOCA) (sublingual)
9. Fludrocortisone 10 150 0.2 mg10. Aldosterone 0.3 3000 not used clinically
GLU
CO
CO
RTI
CO
IDS
MIN
ER
ALO
-C
OR
TIC
OID
S
arthritis, renal transplant, pemphigus, etc. withgood results and minimal suppression of pituitary-adrenal axis.SOLU-MEDROL Methylprednisolone (as sod. succinate)4 mg tab; 40 mg, 125 mg, 0.5 g (8 ml) and 1.0 g (16ml) inj, for i.m. or slow i.v. inj, DEESOLONE 4, 16 mgtabs, 0.5 g and 1.0 g. inj.
The initial effect of methylprednisolone pulse therapy (MPPT)is probably due to its antiinflammatory action, while longterm benefit may be due to temporary switching off of theimmunodamaging processes as a consequence of lymphopeniaand decreased Ig synthesis.
4. Triamcinolone Slightly more potent thanprednisolone but highly selective glucocorticoid:4–32 mg/day oral, 5–40 mg i.m., intraarticularinjection. Also used topically.KENACORT, TRICORT 1, 4, 8 mg tab., 10 mg/ml, 40 mg/ml(as acetonide) for i.m., intraarticular inj., LEDERCORT 4 mg tab.
5. Dexamethasone Very potent and highlyselective glucocorticoid. It is also long-acting,causes marked pituitary-adrenal suppression, butfluid retention and hypertension are not a problem.
It is used for inflammatory and allergic condi-tions 0.5–5 mg/day oral. For shock, cerebraledema, etc. 4–20 mg/day i.v. infusion or i.m.injection is preferred. It can also be used topically.
DECADRON, DEXONA 0.5 mg tab, 4 mg/ml (as sod.phosphate) for i.v., i.m. inj., 0.5 mg/ml oral drops;WYMESONE, DECDAN 0.5 mg tab, 4 mg/ml inj.
6. Betamethasone Similar to dexamethasone,0.5–5 mg/ day oral, 4–20 mg i.m., i.v. injectionor infusion, also topical.BETNESOL, BETACORTRIL, CELESTONE 0.5 mg, 1 mgtab, 4 mg/ml (as sod. phosphate) for i.v., i.m. inj., 0.5 mg/mloral drops. BETNELAN 0.5 mg, 1 mg tabs.
Dexamethasone or betamethasone are prefer-red in cerebral edema and other states in whichfluid retention must be avoided.
7. Deflazacort The glucocorticoid potency ofthis newer steroid is somewhat less than ofprednisolone, but it lacks mineralocorticoidactivity. It is claimed to produce fewer adverseeffects, but that may be due to its lower potency.In some trials it caused lesser growth retardationin children; has been particularly recommendedfor pediatric patients. It is used mainly forinflammatory and immunological disorders.Dose: 60–120 mg/day initially, 6–18 mg/day for maintenance;children 0.25–1.5 mg/kg daily or on alternate days.DEFGLU 6, 30 mg tabs, DEFLAR, DEFZA, DFZ 1, 6, 30 mgtabs.

290S
EC
TIO
N5
HORMONES AND RELATED DRUGS
8. Desoxycorticosterone acetate (DOCA) It has onlymineralocorticoid activity. Used occasionally for replacementtherapy in Addison’s disease: 2–5 mg sublingual,10–20 mg i.m. once or twice weekly.In DOCABOLIN 10 mg/ml inj (along with nandrolone).
9. Fludrocortisone A potent mineralocorti-coid having some glucocorticoid activity as well,orally active, used for:Replacement therapy in Addison’s disease 50–200 µg daily.Congenital adrenal hyperplasia in patients with salt wasting50–200 µg/day.Idiopathic postural hypotension 100–200 µg/day.FLORICORT 100 µg tab.
10. Aldosterone It is the most potent mineralocorticoid.Not used clinically because of low oral bioavailability anddifficulties in regulating doses.
In addition a number of topically activeglucocorticoids have been developed.
Beclomethasone dipropionate budesonide,fluticasone, etc. are used by inhalation in asthma,as spray in nasal allergy, as well as for skin andmucous membrane lesions (see Ch. 16).
Fluocinolone acetonide, fluocortolone, clo-betasol propionate and esters of betamethasone,dexamethasone, triamcinolone are described inCh. 64.
USES
A. Replacement therapy1. Acute adrenal insufficiency It is an emer-gency. Hydrocortisone or dexamethasone aregiven i.v., first as a bolus injection and then asinfusion, along with isotonic saline and glucosesolution. The amount of fluid infused i.v. is guidedby monitoring central venous pressure, becausethese patients have reduced capacity to excretewater load. Short-term i.v. infusion of avasopressor (dopamine) may be needed. The causeof adrenal insufficiency should be treated.
2. Chronic adrenal insufficiency (Addison’sdisease) Hydrocortisone given orally is themost commonly used drug along with adequatesalt and water allowance. Some patients whocontinue to excrete excess Na+ need additionalmineralocorticoid: fludrocortisone is added.
3. Congenital adrenal hyperplasia (Adreno-genital syndrome) It is a familial disorder dueto genetic deficiency of steroidogenic enzymes,mostly 21-hydroxylase. As a result the synthesisof hydrocortisone and aldosterone suffers. Thereis compensatory increase in ACTH secretion—adrenals hypertrophy; enzyme deficiency beingonly partial in most cases, normal amounts ofgluco- and mineralocorticoids are produced alongwith excessive amounts of weak androgens →virilization and/or precocious sexual development.If the deficiency is severe, salt wasting also occurs.
Treatment is to give hydrocortisone 0.6 mg/kg daily in divided doses round the clock tomaintain feed back suppression of pituitary. Ifsalt wasting persists—fludrocortisone 50–200 µg/day may be added.
B. Pharmacotherapy(for nonendocrine diseases)
Systemic as well as topical corticosteroids haveone of the widest spectrum of medicinal uses fortheir antiinflammatory and immunosuppressiveproperties. Corticosteroids are powerful drugs.They have the potential to cause dramaticimprovement in many severe diseases as well asproduce equally dramatic adverse effects if notproperly used. The use in nonendocrine diseasesis empirical and palliative, but may be life saving.The following general principles must beobserved.(a) A single dose (even excessive) is not harmful:can be used to tide over mortal crisis, even whenbenefit is not certain.(b) Short courses (even high dose) are not likelyto be harmful in the absence of contraindications;starting doses can be high in severe illness.(c) Long-term use is potentially hazardous: keepthe duration of treatment and dose to minimum,which is found by trial and error; even partialrelief may have to be tolerated.(d) Initial dose depends on severity of the disease;start with a high dose in severe illness—reducegradually after symptoms subside, while in mildcases start with the lowest dose and titrate upwards

291C
HA
PTE
R 20
CORTICOSTEROIDS
to find the correct dose. The dose should bereassessed from time-to-time.(e) No abrupt withdrawal after a corticoid hasbeen given for > 2 to 3 weeks: may precipitateadrenal insufficiency.(f) Infection, severe trauma, surgery or any stressduring corticoid therapy—increase the dose.(g) Use local therapy (cutaneous, inhaled, intra-nasal, etc) wherever possible.
1. Arthritides(i) Rheumatoid arthritis: Corticosteroids areindicated only in severe cases as adjuvants toNSAIDs when distress and disability persistsdespite other measures, or to suppress exacer-bations, or when there are systemic manifestations(see Ch. 15).(ii) Osteoarthritis: It is treated with analgesicsand NSAIDs; systemic use of corticoids is rare.Intraarticular injection of a steroid may be usedto control an acute exacerbation. Injections maybe repeated 2–3 times a year, but have the potentialto cause joint destruction.(iii) Rheumatic fever: Corticoids are used onlyin severe cases with carditis and CHF with theaim of rapid suppression of symptoms, becausethey act faster than aspirin, or in patients notresponding to aspirin. Aspirin is given in additionand is continued after corticoids have beenwithdrawn.(iv) Gout: Corticoids (short course) should onlybe used in acute gouty arthritis when NSAIDshave failed to afford relief and colchicine is nottolerated. Intraarticular injection of a solubleglucocorticoid is preferable to systemic therapy(see p. 214).
Though they are uricosuric—use in chronicgout is not recommended.
2. Collagen diseases Most cases of systemiclupus erythematosus, polyarteritis nodosa, derma-tomyositis, nephrotic syndrome, glomerulo-nephritis and related diseases need corticosteroidtherapy. They may be life saving in these diseases.Therapy is generally started with high doses whichare tapered to maintenance dose when remissionoccurs. Later other immunosuppressants may beadded or substituted.
3. Severe allergic reactions Corticoids maybe used for short periods in anaphylaxis, angioneu-rotic edema, urticaria and serum sickness.However, even i.v. injection of a glucocorticoidtakes 1–2 hours to act and is not a substitutefor Adr (which acts immediately) in anaphylacticshock and angioedema of larynx. Topical use ismade in allergic conjunctivitis and rhinitis.
4. Autoimmune diseases Autoimmunehaemolytic anaemia, idiopathic thrombocytopenicpurpura, active chronic hepatitis respond tocorticoids. Prednisolone 1–2 mg/kg/day is giventill remission, followed by gradual withdrawal orlow-dose maintenance depending on the response.Remission may also be induced in severe casesof myasthenia gravis, in which their use isadjunctive to neostigmine. Patients requiring longterm maintenance therapy are better shifted toother immunosuppressants.
5. Bronchial asthma Early institution ofinhaled glucocorticoid therapy is now recom-mended in most cases needing inhaled β2 agonistsalmost daily (see Ch. 16). Systemic corticosteroidsare used only for:• Status asthmaticus: give i.v. glucocorticoid;
withdraw when emergency is over.• Actue asthma exacerbation: short-course of
high dose oral corticoid, followed by gradualwithdrawal.
• Severe chronic asthma not controlled byinhaled steroids and bronchodilators: add lowdose prednisolone daily or on alternate days.
6. Other lung diseases Corticosteroidsbenefit aspiration pneumonia and pulmonaryedema from drowning. Given during latepregnancy, corticoids accelerate lung maturationand surfactant production in the foetal lung andprevent respiratory distress syndrome at birth. Twodoses of betamethasone 12 mg i.m. at 24 hourinterval may be administered to the mother ifpremature delivery is contemplated.
7. Infective diseases Administered undereffective chemotherapeutic cover, corticosteroidsare indicated only in serious infective diseases

292S
EC
TIO
N5
HORMONES AND RELATED DRUGS
to tideover crisis or to prevent complications. Theyare indicated in conditions like severe forms oftuberculosis (miliary, meningeal, renal, etc.),severe lepra reaction, certain forms of bacterialmeningitis and Pneumocystis carinii pneumoniawith hypoxia in AIDS patients.
8. Eye diseases Corticoids are used in a largenumber of inflammatory ocular diseases—mayprevent blindness. Topical instillation as eyedrops or ointment is effective in diseases of theanterior chamber—allergic conjunctivitis, iritis,iridocyclitis, keratitis, etc. Ordinarily, steroidsshould not be used in infective conditions. Butif inflammation is severe, they may be appliedin conjunction with an effective antibiotic.Steroids are contraindicated in herpes simplexkeratitis and in ocular injuries. Posterior segmentafflictions like retinitis, optic neuritis, uveitisrequire systemic steroid therapy. Retrobulbarinjection is occasionally given to avoid systemicside effects.
9. Skin diseases (see Ch. 64) Topicalcorticosteroids are widely employed and are highlyeffective in many eczematous skin diseases.Systemic therapy is needed (may be life-saving)in pemphigus vulgaris, exfoliative dermatitis,Stevens-Johnson syndrome and other severeafflictions.
10. Intestinal diseases Ulcerative colitis,Crohn’s disease, coeliac disease are inflammatorybowel diseases with exacerbations and remissions.Corticoids are indicated during acute phases—may be used orally or as retention enema (forcolonic involvement). They are particularlyvaluable for patients with systemic manifestions,and are given in addition to sulfasalazine/mesalazine + other measures (see Ch. 48). Somespecialists advocate small maintenance doses toprevent relapses.
11. Cerebral edema due to tumours, tubercularmeningitis, etc., responds to corticoids. Dexa-orbetamethasone are preferred because they donothave Na+ retaining activity. Their value in trauma-
tic and poststroke cerebral edema is questionable.Large doses given i.v. soon after spinal injurymay reduce the resulting neurological sequelae.
A short course (2–4 weeks) of oralprednisolone can hasten recovery from Bell’s palsyand acute exacerbation of multiple sclerosis. Inthe latter, methyl prednisolone 1 g i.v. daily for2–3 days may be given in the beginning.
Neurocysticercosis: When albendazole/prazi-quantel is used to kill cysticerci lodged in thebrain, prednisolone 40 mg/day or equivalent isgiven for 2–4 weeks to suppress the reaction tothe dying larvae.
12. Malignancies Corticoids are an essentialcomponent of combined chemotherapy of acutelymphatic leukaemia, Hodgkin’s and otherlymphomas, because of their marked lympholyticaction in these conditions. They have a secondaryplace in hormone responsive breast carcinoma—act probably by causing HPA suppression so asto reduce production of adrenal androgens whichare converted to estrogens in the body (see Ch.62).
Corticoids also afford symptomatic relief inother advanced malignancies by improvingappetite and controlling secondary hypercalcae-mia. For hypercalcaemia, however, bisphos-phonates are more effective and have supersededcorticosteroids.13. Organ transplantation and skin allograftHigh dose corticoids are given along with otherimmunosuppressants to prevent the rejectionreaction. Low maintenance doses are generallycontinued over long term + maintenance dosesof companion drugs. (see Ch. 63).14. Septic shock High-dose corticosteroidtherapy for septic shock has been abandoned,because it worsens the outcome. However, manysuch patients have relative adrenal insufficiency.Recent studies have documented beneficial effectsof low-dose (hydrocortisone 100 mg 8 hourly i.v.infusion for 5–7 days) therapy in patients whoare adrenal deficient and do not respondadequately to fluid replacement and vasopressors.

293C
HA
PTE
R 20
CORTICOSTEROIDS
15. Thyroid storm Many patients in thyroidstorm have concomitant adrenal insufficiency.Moreover, corticosteroids reduce peripheral T4
to T3 conversion. Hydrocortisone 100 mg i.v. 8hourly may improve outcome.16. To test pituitary-adrenal axis functionDexamethasone suppresses pituitary-adrenal axisat doses which do not contribute to steroidmetabolites in urine. Responsiveness of the axiscan be tested by measuring daily urinary steroidmetabolite excretion after dosing withdexamethasone.
ADVERSE EFFECTS
These are extension of the pharmacological actionwhich become prominent with prolonged therapy,and are a great limitation to the use of corticoidsin chronic diseases.
A. Mineralocorticoid Sodium and waterretention, edema, hypokalaemic alkalosis and aprogressive rise in BP. These are now rare dueto availability of highly selective glucocorticoids.
Gradual rise in BP occurs due to excessglucocorticoid action as well.
B. Glucocorticoid1. Cushing’s habitus: characteristic appearance
with rounded face, narrow mouth, supra-clavicular hump, obesity of trunk withrelatively thin limbs.
2. Fragile skin, purple striae—typically onthighs and lower abdomen, easy bruising,telangiectasis, hirsutism. Cutaneous atrophylocalized to the site occurs with topicalapplication as well.
3. Hyperglycaemia, may be glycosuria, preci-pitation of diabetes.
4. Muscular weakness: proximal (shoulder,arm, pelvis, thigh) muscles are primarilyaffected. Myopathy occurs occasionally,warrants withdrawal of the corticoids.
5. Susceptibility to infection: this is nonspeci-fic for all types of pathogenic organisms.Latent tuberculosis may flare; opportunisticinfections with low grade pathogens(Candida, etc.) set in.
6. Delayed healing: of wounds and surgicalincisions.
7. Peptic ulceration: risk is doubled; bleedingand silent perforation of ulcers may occur.Dyspeptic symptoms are frequent with highdose therapy.
8. Osteoporosis: especially involving vertebraeand other flat spongy bones. Compressionfractures of vertebrae and spontaneous frac-ture of long bones can occur, especially inthe elderly. Radiological evidence of osteo-porosis is an indication for withdrawal ofcorticoid therapy. Corticosteroid inducedosteoporosis can be prevented/arrested bycalcium supplements + vit D, and byestrogen/raloxifene or androgen replacementtherapy in females and males respectively.However, bisphosphonates are the mosteffective drugs in this regard.
Avascular necrosis of head of femur,humerous, or knee joint is an occasionalabrupt onset complication of high dosecorticosteroid therapy.
9. Posterior subcapsular cataract may developafter several years of use, especially inchildren.
10. Glaucoma: may develop in susceptibleindividuals after prolonged topical therapy.
11. Growth retardation: in children occurs evenwith small doses if given for long periods.Large doses do inhibit GH secretion, butgrowth retardation may, in addition, be adirect cellular effect of corticoids. Recombi-nant GH given concurrently can preventgrowth retardation, but risk/benefit of suchuse is not known.
12. Foetal abnormalities: Cleft palate and otherdefects are produced in animals, but havenot been encountered on clinical use inpregnant women. The risk of abortion, still-birth or neonatal death is not increased, butintrauterine growth retardation can occurafter prolonged therapy, and neurological/behavioral disturbances in the offspring arefeared. Prednisolone appears safer than dexa/beta methasone, because it is metabolizedby placenta, reducing foetal exposure. There

294S
EC
TIO
N5
HORMONES AND RELATED DRUGS
is no evidence of foetal growth retardationoccurring after short term use in the mother.
Prolonged corticosteroid therapy duringpregnancy increases the risk of gestationaldiabetes, pregnancy induced hypertensionand preeclampsia.
13. Psychiatric disturbances: mild euphoriafrequently accompanies high dose steroidtreatment. This may rarely progress to manicpsychosis. Nervousness, decreased sleep andmood changes occur in some patients.Rarely a depressive illness may be inducedafter long-term use.
14. Suppression of hypothalamo-pituitary-adre-nal (HPA) axis: occurs depending both ondose and duration of therapy. In time,adrenal cortex atrophies and stoppage ofexogenous steroid precipitates withdrawalsyndrome consisting of malaise, fever,anorexia, nausea, postural hypotension,electrolyte imbalance, weakness, pain inmuscles and joints and reactivation of thedisease for which they were used. Subjectedto stress, these patients may go into acuteadrenal insufficiency leading to cardiovas-cular collapse.
Any patient who has received > 20–25 mg/day hydrocortisone, or ≥ 5 mg prednisolone/dayor equivalent for longer than 2–3 weeks shouldbe put on a scheme of gradual withdrawal: 20mg hydrocortisone/ day reduction every week andthen still smaller fractions once this level has beenachieved. Such patients may need protection witha corticosteroid (oral or i.v.) if a stressful situationdevelops up to one year after withdrawal.Administration of ACTH during withdrawal doesnot hasten recovery because it has been foundthat adrenals recover earlier than pituitary andhypothalamus.
If a patient on steroid therapy develops aninfection—the steroid should not be discontinueddespite its propensity to weaken host defence anddelay healing. Rather, the dose may have to beincreased to meet the stress of infection. Surgeryis such a patient should be covered by intra-
operative and postoperative i.v. hydrocortisonetill the condition stabilizes, followed by oralprednisolone.Measures that minimise HPA axis suppression are:(a) Use shorter acting steroids (hydrocortisone,
prednisolone) at the lowest possible dose.(b) Use steroids for the shortest period of time
possible.(c) Give the entire daily dose at one time in the
morning.(d) Switch to alternate-day therapy if possible.
It has been found that moderate dose of a short acting steroid(e.g. prednisolone) given at 48 hr interval did not causeHPA suppression, whereas the same total amount given in4 divided 12 hourly doses produced marked HPA suppression.Alternate-day therapy also resulted in less immunologicalsuppression—lower risk of infection. The longer actingsteroids (dexamethasone, etc.) are not suitable for alternate-day therapy. Only problem with alternate-day therapy is thatmany steroid dependent patients are incapacitated on the‘off day’.
(e) If appropriate, use local (dermal, inhaled, ocu-lar, nasal, rectal, intrasynovial) preparationsof a steroid with poor systemic availability(beclomethasone, triamcinolone acetonide,fluticasone, etc.)
CONTRAINDICATIONS
The following diseases are aggravated by corti-costeroids. Since corticosteroids may have to beused as a life-saving measure, all of these arerelative contraindications in the presence of whichthese drugs are to be employed only undercompelling circumstances and with dueprecautions.
1. Peptic ulcer2. Diabetes mellitus3. Hypertension4. Viral and fungal infections5. Tuberculosis and other infections6. Osteoporosis7. Herpes simplex keratitis8. Psychosis9. Epilepsy
10. CHF11. Renal failure

295C
HA
PTE
R 20
CORTICOSTEROIDS
Combination of any other drug with cortico-steroids in fixed dose formulation for internal useis banned.Metyrapone Inhibits 11-β hydroxylase in adrenal cortexand prevents synthesis of hydrocortisone so that its bloodlevel falls → increased ACTH release → increased synthesis,release and excretion of 11-desoxycortisol in urine. Thus,it is used to test the responsiveness of pituitary and its ACTHproducing capacity.
Aminoglutethimide, trilostane and high doses of the anti-fungal drug Ketoconazole also inhibit steroidogenic
enzymes—can be used to treat Cushing’s disease when surgeryor other measures are not an option. Ketoconazole reducesgonadal steroid synthesis as well.
Glucocorticoid antagonist The antiprogestin mifepri-stone (see p. 319–20) acts as a glucocorticoid receptorantagonist as well. In Cushing’s syndrome, it can suppress themanifestations of corticosteroid excess, but blockade of feedbackACTH inhibition leads to oversecretion of ACTH → morehydrocortisone is produced, which tends to annul the GRblocking action of mifepristone. It is indicated only forinoperable cases of adrenal carcinoma and in patients withectopic ACTH secretion.
PROBLEM DIRECTED STUDY
20.1 A 35-year female patient of inflammatory bowel disease was treated with prednisolone40 mg/day and mesalazine 800 mg TDS. After 4 weeks, the symptoms subsided and prednisolonedose was tapered at the rate of 10 mg every 2 weeks. When she was taking 10 mg prednisolone/day, she met with a road-side accident and suffered compound fracture of both bones of theright leg. Internal fixation of the fracture and suturing of wounds under general anaesthesiais planned.(a) Whether any additional measure needs to be taken during surgery in view of her corticosteroidtherapy?(b) Does the prednisolone therapy need discontinuation or any alteration in the postoperativeperiod? Give reasons.
(see Appendix-1 for solution)

Androgens and Drugs forErectile Dysfunction
ChapterChapterChapterChapterChapter 2121212121
ANDROGENS(Male Sex Hormones)
These are substances which cause developmentof secondary sex characters in the castrated male.That testes are responsible for the male charactersis known since prehistoric times. Its endocrinefunction was established by Berthold in 1849.Testosterone was isolated as the testicularhormone, its structure was worked out and it wassynthetically prepared by the year 1935.
Natural androgens Testes of adult male pro-duce 5–12 mg of testosterone daily, a part ofwhich is converted in extraglandular tissues tothe more active dihydrotestosterone (DHT); bythe enzyme steroid 5 α-reductase; cholesterol isthe starting material and the same pathwaydepicted in Fig. 20.1 is utilized. Adrenal cortexproduces small quantities of dehydroepiandro-sterone and androstenedione which are called‘weak androgens’ (potency 1/20 to 1/30), but areinfact inactive as such and derive their weakactivity from partial conversion to testosteronein peripheral tissues. Adrenals themselves do not
produce significant quantity of testosterone. Inwomen ovary produces small quantity of testo-sterone; this together with that derived indirectlyfrom adrenals amounts to 0.25–0.5 mg/day.
Androsterone It is a metabolite of testosteronewhich is excreted in urine. It has 1/10 the activityof testosterone.
Synthetic androgens Methyltestosterone andfluoxymesterone are 17-alkyl substituted deriva-tives of testosterone which are orally activebecause of resistance to first pass metabolism,but have submaximal androgenic efficacy andpotential to cause cholestatic jaundice. Otherorally active compounds are testosteroneundecanoate which is administered as oily solutionto be absorbed through lymphatics bypassing theliver, and mesterolone. A number of lipid-solubleesters of testosterone have been produced, suitablefor injection in oily vehicle, from which they areabsorbed slowly and exert prolonged action afterdeesterification in the body.
Regulation of secretion
Testosterone is secreted by the interstitial (Leydig)cells of the testes under the influence of pulsatilesecretion of LH from pituitary. FSH is mainlyresponsible for promotion of spermatogenesis intubular (Sertoli) cells. The mediator of feedbackrelationship with pituitary is uncertain. Whilerelatively high concentration of testosteroneinhibits LH secretion and in time causes atrophyof interstitial cells, it has only weak inhibitoryaction on FSH secretion. Estrogens are morepotent inhibitors of Gn secretion even in males,and it is believed that the small amount of estradiolproduced by testes as well as that resulting fromconversion of testosterone to estradiol in liverand fat plays a role in feedback inhibition. Inhibin,

297C
HA
PTE
R 21
ANDROGENS AND DRUGS FOR ERECTILE DYSFUNCTION
ACTIONS
1. Sex organs and secondary sexcharacters (Androgenic) Testosterone isresponsible for all the changes that occur in aboy at puberty:Growth of genitals—penis, scrotum, seminalvesicles, prostate.Growth of hair—pubic, axillary, beard, moust-ache, body hair and male pattern of its distribution.Thickening of skin which becomes greasy dueto proliferation and increased activity of seba-ceous glands—especially on the face. The ductoften gets blocked and infection occurs resultingin acne. Subcutaneous fat is lost and veins lookprominent.Larynx grows and voice deepens.Behavioral effects are—increased physical vigour,aggressiveness, penile erections. Male libidoappears to be activated by testosterone directly,and probably to a greater extent by estradiolproduced from testosterone.Testosterone is also important for the intrauterinedevelopment of the male phenotype. Relativelylarge amounts of testosterone are produced bythe foetal testes during the first half of intrauterinelife.
2. Testes Moderately large doses cause testi-cular atrophy by inhibiting Gn secretion frompituitary. Still larger doses have a direct sustain-ing effect and atrophy is less marked. Testoste-rone is needed for normal spermatogenesis andmaturation of spermatozoa. High concentrationof testosterone is attained locally in the spermato-genic tubules by diffusion from the neighbouringLeydig cells and stimulates spermatogenesis.
3. Skeleton and skeletal muscles(Anabolic) Testosterone is responsible for thepubertal spurt of growth in boys and to a smallerextent in girls. There is rapid bone growth, bothin thickness as well as in length. After puberty,the epiphyses fuse and linear growth comes toa halt. Estradiol produced from testosterone, andnot testosterone itself, is responsible for fusionof epiphyses in boys as well as in girls. Moreover,
Fig. 21.1: Regulation and production of sex steroids inthe male.
In liver and many target cells 5α-reductase enzymeconverts testosterone to the more potent androgendihydrotestosterone (DHT) which combines more avidlywith the androgen receptor (AR). The aromatase enzymein testes, liver and adipose tissue converts sometestosterone into estradiol which exerts certain actionsin male target cells by combining with estrogen receptor(ER) and is probably important for feedback inhibition ofgonadotropins (LH/FSH) as well as that of gonadotropinreleasing hormone (GnRH) from hypothalamus.
(a protein) produced by Sertoli cells, has strongFSH inhibitory action and may be mediating thefeedback inhibition. Testosterone and estradiol acton hypothalamus to reduce GnRH as well as actdirectly on pituitary. The plasma level oftestosterone in adult males ranges from 0.3 to1 µg/dl. In women, small amounts of testosteroneare produced by corpus luteum and adrenal cortex;blood levels remain low (20–60 ng/dl).

298S
EC
TIO
N5
HORMONES AND RELATED DRUGS
estradiol largely mediates the effect of testosteroneon bone mineralization. Testosterone also promotesmuscle building, especially if aided by exercise.There is accretion of nitrogen, minerals (Na, K,Ca, P, S) and water—body weight increases rapidly,more protoplasm is built. Appetite is improvedand a sense of well being prevails. Testosteronegiven to patients prone to salt and water retentionmay develop edema.
4. Erythropoiesis Testosterone accelerateserythropoiesis by increasing erythropoietin pro-duction and probably direct action on haemesynthesis. Men have higher hematocrit than women.
Mechanism of actionTestosterone can largely be regarded as the circu-lating prohormone. In most target cells, the4–5 double bond is reduced producing dihydro-testosterone—which binds more avidly with thecytoplasmic androgen receptor (AR), and thiscomplex is more active than testosterone-receptorcomplex in combining with DNA. No subtypesof AR are known; both genital and nongenital(muscle, bone) cells express the same AR. Aftercombining with androgen response elements ofthe target genes, DNA transcription is enhanced/repressed with the help of coactivators orcorepressors, which may be tissue specific. Theeffects are expressed through modification ofprotein synthesis.
The 5α-reductase enzyme exists in two isoforms: 5α-reductase-1and 5α-reductase-2. The genital skin of both sexes and urogenital
tract of male contains 5α- reductase-2 which is more sensitiveto inhibition by finasteride. Genetic deficiency of this isoenzymecauses male pseudohermaphroditism because of inability ofmale genitalia to produce the active hormone dihydro-testosterone from circulating testosterone. 5α-reductase-1has a wider distribution in the body including nongenitalskin and liver; and is inhibited by finasteride to a lesserextent.
Testosterone itself appears to be the activehormone at certain sites, such as—• foetal genital rudiments• hypothalamus/pituitary site involved in feed
back regulation• erythropoietic cells• spermatogenic cells in testes.
PHARMACOKINETICS
Testosterone is inactive orally due to high firstpass metabolism in liver. The duration of actionafter i.m. injection is also very short. Therefore,slowly absorbed esters of testosterone are usedby this route—are hydrolysed to the active freeform. Testosterone in circulation is 98% boundto sex hormone binding globulin (SHBG) andto albumin. The SHBG bound testosterone isunavailable for action due to tight binding.
The major metabolic products of testosteroneare androsterone and etiocholanolone which areexcreted in urine, mostly as conjugates withglucuronic acid and sulfate. Small quantities ofestradiol are also produced from testosteroneby aromatization of A ring in extraglandular tissues(liver, fat, hypothalamus). Plasma t½ oftestosterone is 10–20 min.
Testosterone Dihydrotestosterone
Pituitary: LH inhibition • External genitalia (scrotum, penis, male urethra)Testes: Spermatogenesis formation in foetus and maturation during pubertyInternal genitalia (epididymis, • Pubertal changes, sexual maturity, male behaviourvas deferens, seminal vesicle) • Prostate growth; hypertrophy in elderlydevelopment in foetus • Hair follicles: growth during puberty,
Erythropoiesisscalp hair loss in adults
Bone and skeletal muscle: increase in mass and strength
Principal androgen for different target tissue actions

299C
HA
PTE
R 21
ANDROGENS AND DRUGS FOR ERECTILE DYSFUNCTION
Methyltestosterone and fluoxymesterone aremetabolized slowly and have a longer durationof action, but are weaker androgens. Estrogensare not produced from fluoxymesterone anddihydrotestosterone.
Preparations and Dose1. Testosterone (free): 25 mg i.m. daily to twice weekly;AQUAVIRON 25 mg in 1 ml inj.2. Testosterone propionate: 25–50 mg i.m. daily to twiceweekly: TESTOVIRON, PARENDREN, TESTANON 25, 50mg/ml inj.3. TESTOVIRON DEPOT 100: testo. propionate 25 mg+ testo. enanthate 100 mg in 1 ml amp; 1 ml i.m. weekly.4. TESTOVIRON DEPOT 250: testo. propionate 250 mg+ testo. enanthate 250 mg in 1 ml amp; i.m. every 2–4weeks.5. SUSTANON ‘100’: testo. propionate 20 mg + testo.phenyl propionate 40 mg + testo. isocaproate 40 mg in 1ml amp; 1 ml i.m. every 2–3 weeks.6. SUSTANON ‘250’: testo. propionate 30 mg + testo.phenylpropionate 60 mg + testo. isocaproate 60 mg + testo.decanoate 100 mg in 1 ml amp; 1 ml i.m. every 3–4 weeks.7. NUVIR, ANDRIOL; Testosterone undecanoate 40 mgcap, 1–3 cap daily for male hypogonadism, osteoporosis.8. Mesterolone: Causes less feedback inhibition of Gn secre-tion and spermatogenesis, and has been promoted for treatmentof male infertility PROVIRONUM, RESTORE, MESTILON25 mg tab; 1–3 tab daily for androgen deficiency, oligozoo-spermia and male infertility.
Transdermal androgen Recently delivery ofandrogen across skin has been achieved bydeveloping suitable solvents and absorptionfacilitators. By cutaneous delivery, testosterone/dihydrotestosterone circumvent hepatic first passmetabolism; uniform blood levels are producedround the clock. A gel formulation has beenmarketed for once daily application which hasbecome the preferred method of androgenreplacement for hypogonadism and impotence.ANDRACTIM: Dihydrotestosterone 25 mg/g gel (100 g tube);5–10 g gel to be applied over nonscrotal skin once daily.
Fixed dose combinations of testosterone with yohimbine,strychnine and vitamins are banned in India.
SIDE EFFECTS
1. Virilization, excess body hair and menstrualirregularities in women. Many effects, e.g. voicechange may be permanent after prolonged therapy.2. Acne: in males and females.
3. Frequent, sustained and often painful erec-tions in males in the beginning of therapy; subsidespontaneously after sometime.4. Oligozoospermia can occur with moderatedoses given for a few weeks to men with normaltestosterone levels. Prolonged use may producetesticular atrophy.5. Precocious puberty, premature sexualbehaviour, and stunting of stature due to earlyclosure of epiphysis—if testosterone is givencontinuously to young boys for increasing stature.6. Salt retention and edema: especially whenlarge doses are used in patients with heart orkidney disease. It is rare with the doses used forhypogonadism.7. Cholestatic jaundice: occurs with methyltes-tosterone and other 17-alkyl substituted derivatives(fluoxymesterone and some anabolic steroids likeoxymetholone, stanozolol) in a dose dependentmanner, but not with parenterally used esters oftestosterone. For this reason, the latter are prefer-red. However, jaundice is reversible ondiscontinuation.8. Hepatic carcinoma: incidence is higher inpatients who have received long-term methyl-testosterone or other oral androgens.9. Gynaecomastia: may occur, especially inchildren and in patients with liver disease. Thisis due to peripheral conversion of testosteroneto estrogens. Dihydrotestosterone does not causegynaecomastia because it is not converted toestradiol.10. Lowering of HDL and rise in LDL levels,especially with 17α-alkylated analogues.
Contraindications Androgens are contraindi-cated in carcinoma of prostate and male breast,liver and kidney disease and during pregnancy(masculinization of female foetus). They shouldnot be given to men aged >65 years, and to thosewith coronary artery disease or CHF. Androgentherapy can worsen sleep apnoea, migraine andepilepsy.
USES
1. Testicular failure It may be primary—inchildren, resulting in delayed puberty. Treatment

300S
EC
TIO
N5
HORMONES AND RELATED DRUGS
with parenteral testosterone esters or transdermaltestosterone/dihydrotestosterone in courses of4–6 months at a time is highly satisfactory.Secondary testicular failure occurring later in lifemanifests mainly as loss of libido, muscle massand energy, feminization, mild anaemia and impo-tence. These are corrected gradually over monthsby androgen treatment. However, impotence dueto psychological and other factors, and nottestosterone deficiency, does not respond.
2. Hypopituitarism Hypogonadism is one ofthe features of hypopituitarism. Androgens areadded at the time of puberty to other hormonalreplacement.
3. AIDS related muscle wasting Testosteronetherapy has been shown to improve weakness andmuscle wasting in AIDS patients with lowtestosterone levels.
4. Hereditary angioneurotic edema This isa genetic disorder. The attacks can be preventedby 17α-alkylated androgens (methyltestosterone,stanozolol, danazol) but not by testosterone. Thesedrugs act by increasing synthesis of complement(C1) esterase inhibitor.5. Ageing Because testosterone levels decline in old age,it has been administered to elderly males to improve bonemineralization and muscle mass. However, safety of suchtherapy in terms of metabolic, cardiovascular and prostaticcomplications is not known.
Occasionally small amount of androgen is added topostmenopausal hormone replacement.
6. Idiopathic male infertility Since high intratesticularlevel of testosterone is essential for spermatogenesis, it ispresumed that exogenous androgens will stimulatespermatogenesis or improve sperm maturation in epididymis.On the other hand, androgens can adversely affectspermatogenesis by suppressing Gn secretion. Sincemesterolone causes less feedback inhibition of Gn (probablydue to restricted entry into brain) it is believed that moderatedoses will predominantly stimulate testis directly.
A recent metaanalysis of 11 clinical trials has foundthat oral androgens (mesterolone and testosteroneundecanoate) had no effect on sperm count or sperm motilityas well as on subsequent pregnancy rate when given to oligo-astheno-spermic subfertile men. As such, use of theseandrogens for improving male fertility is unjustified.
ANABOLIC STEROIDS
These are synthetic androgens with supposedlyhigher anabolic and lower androgenic activity.Drugs are Nandrolone, Oxymetholone, Stanozololand Methandienone.
The anabolic : androgenic activity ratio isdetermined by injecting the drug in castrated ratsand measuring the increase in weight of levatorani muscles to that of ventral prostate. Theanabolic : androgenic ratio of testosterone isconsidered as 1; The anabolic selectivity of thesesteroids is modest with ratios between 1 to 3in the rat model, and probably still lower in man.The anabolic effects are similar to that of testo-sterone and are mediated through the samereceptor as the androgenic effects. For all practicalpurposes, they are androgens.
Preparations and dose
1. Methandienone: 2–5 mg OD–BD oral; children 0.04mg/kg/day, 25 mg i.m. weekly; ANABOLEX 2, 5 mg tab,2 mg/ml drops, 25 mg/ml inj.2. Nandrolone phenyl propionate: 10–50 mg; children10 mg; i.m. once or twice weekly; DURABOLIN 10, 25 mg/ml inj.3. Nandrolone decanoate: 25–100 mg i.m. every 3 weeks,DECADURABOLIN, 25, 100 mg/ml inj.4. Oxymetholone: 5–10 mg, children 0.1 mg/kg, OD;ADROYD 5 mg tab.5. Stanozolol: 2–6 mg/day, MENABOL, NEURABOL,TANZOL 2 mg tab.Combination of anabolic steroids with any other drug isbanned in India.
Side effects Anabolic steroids were developedwith the idea of avoiding the virilizing side effectsof androgens while retaining the anabolic effects.But the same adverse effect profile applies tothese compounds.The 17-alkyl substituted compounds oxymetho-lone, stanozolol, can produce jaundice and worsenlipid profile.Contraindications are same as for testosterone.
Uses
1. Catabolic states Acute illness, severetrauma, major surgery, etc. are attended by

301C
HA
PTE
R 21
ANDROGENS AND DRUGS FOR ERECTILE DYSFUNCTION
negative N balance. Anabolic steroids can reduceN2 loss over short periods, but long-term benefitsare questionable. They may cause a transientresponse in the elderly, under-nourished ordebilitated individuals, but controlled studies havefailed to demonstrate a difference in the totalweight gained. However, short-term use may bemade during convalescence for the sense ofwellbeing and improvement in appetite causedby such treatment.2. Osteoporosis In elderly males and that occurring dueto prolonged immobilization may respond to anabolic steroids,but bisphosphonates are more effective and are the preferreddrugs.
3. Suboptimal growth in boys Use is controversial;somatropin is a better option. Brief spurts in linear growthcan be induced by anabolic steroids, but this probably doesnot make a difference in the final stature, except inhypogonadism. Use for more than 6 months is not recom-mended—premature closure of epiphyses and shortening ofultimate stature may result.
4. Hypoplastic, haemolytic and malignancy associatedanaemia Majority of properly selected patients respondto anabolic steroids/androgens by an increase in RBCcount and Hb%. However, erythropoietin therapy is moreeffective.
5. To enhance physical ability in athletes Whenadministered during the period of training androgens/anabolicsteroids can increase the strength of exercised muscles.However, effects are mostly short-lived and the magnitudeof improvement in performance is uncertain except in women.This is considered illegal and anabolic steroids are includedin the list of ‘dope test’ performed on athletes beforecompetitive games.
IMPEDED ANDROGENS/ANTIANDROGENSSuperactive GnRH agonists are the most potent inhibitorsof gonadal function. Administered over a few days, theymarkedly inhibit LH and FSH release, resulting in loss ofandrogen secretion (see Ch. 17).Ketoconazole at high doses inhibits steroidogenic CYP 450enzymes: testosterone as well as adrenal steroid productionis interfered. Plasma protein binding of testosterone is alsoreduced. However, toxicity of high doses precludes its useto suppress androgens.Cimetidine and spironolactone have weak antiandrogenicaction which manifests as side effects. Progesterone has weakandrogen receptor blocking action.
Drugs that have been clinically used to modifyandrogen action are:
Danazol It is an orally active ethisteronederivative having weak androgenic, anabolic andprogestational activities. Though labelled as animpeded/attenuated androgen, because it binds tothe AR and induces some androgen-specific mRNAproduction, the most prominent action issuppression of Gn secretion from pituitary in bothmen and women → inhibition of testicular/ovarianfunction. In addition, it suppresses gonadalfunction directly by inhibiting steroidogenicenzymes. In women endometrial atrophy occursover few a weeks and amenorrhoea may supervene.Danazol is metabolized with a t½ of 12–18 hours.Dose: 200–600 mg/day; DANAZOL, LADOGAL,DANOGEN, GONABLOK 50, 100, 200 mg cap.
Uses are:1. Endometriosis Danazol causes impro-vement in ~75% cases by inhibiting ovarianfunction. Relief of dysmenorrhoea is prompt. Pain,dyspareunia and excessive bleeding regress slowly.Estrogen-progestin combination contraceptive isthe first line drug. Non-responsive cases are treatedby a high dose progestin alone. Danazol isinfrequently used now because of androgenic sideeffects and risk of liver damage.2. Menorrhagia Danazol reduces menstrualblood loss. Usually complete amenorrhoea doesnot occur with 200 mg/day. It is a second linedrug to an oral progestin.3. Fibrocystic breast disease (chronic cysticmastitis): 3–6 months danazol treatment causesimprovement with decrease in pain, nodularityand engorgement in ~ 75% cases.4. Hereditary angioneurotic edema Danazolis a 17α alkylated steroid: has prophylactic effectin this condition by inducing complement (C1)esterase inhibitor (see above).Side effects are frequent and dose related.Complete amenorrhoea occurs with higher doses.Androgenic side effects are acne, hirsutism,decreased breast size, deepening of voice, edemaand weight gain. Loss of libido in men, hot flashesin women and night sweats, muscle cramps, g.i.upset, elivation of hepatic enzymes are the otherproblems.

302S
EC
TIO
N5
HORMONES AND RELATED DRUGS
Cyproterone acetate This relatively weak AR antagonistis chemically related to progesterone. In contrast to flutamidewhich increases LH release by blocking feedback inhibition,cyproterone inhibits LH release by its progestational activity.Lowering of serum testosterone (consequent to LH inhibition)supplements the direct antiandrogenic action of cyproterone.
Given to boys in relatively higher doses, it preventspubertal changes, while in adult men libido and androgenicanabolism are suppressed. Its clinical indications are—precocious puberty in boys, inappropriate sexual behaviour inmen, acne and hirsutism in women (usually in combinationwith an estrogen). Its efficacy in metastatic prostate carcinomais inferior to other forms of androgen deprivation.Hepatotoxicity limits its use.Dose: 2 mg OD; GINETTE-35, DINAC-35; cyproteroneacetate 2 mg + ethinyl estradiol 35 μg tab.
Flutamide A nonsteroidal AR antagonist withno other hormonal activity. Its active metabolite2-hydroxyflutamide competitively blocks andro-gen action on accessory sex organs as well ason pituitary. Thus, it increases LH secretion byblocking feedback inhibition. Plasma testosteronelevels increase in males which partially overcomethe direct antiandrogenic action. This limits utilityof monotherapy with antiandrogens in carcinomaprostate. They are now used only in conjunctionwith a GnRH agonist (to suppress LH andtestosterone secretion) or after castration to blockthe residual action of adrenal androgens ascombined androgen blockade (CAB) therapy ofmetastatic carcinoma prostate (also see p. 872).It is preferably started 3 days before the GnRHagonist to block the initial flare up that may occurdue to excess release of LH and testosterone inthe beginning (before GnRH receptors aredesensitized). However, long-term benefit of CABover GnRH agonist alone is not established. Alongwith oral contraceptives it has been tried in femalehirsutism, but its hepatotoxic potential may notjustify such use. Though gynaecomastia and breasttenderness occur frequently, libido and potencyare largely preserved during flutamide treatment.Reports of liver damage have restricted its use.Dose: 250 mg TDSPROSTAMID, FLUTIDE, CYTOMID 250 mg tab.
Bicalutamide This more potent and longeracting (t½ 6 days) congener of flutamide is suitablefor once daily administration in metastatic carci-noma of prostate as a component of CAB therapy.
When used along with a GnRH agonist orcastration, 50 mg OD affords marked relief in bonepain and other symptoms due to the metastasis. Sideeffects are hot flashes, chills, edema and loosestools, but it is better tolerated and less hepatotoxicthan flutamide. Elevation of hepatic transaminaseabove twice normal is a signal for stopping thedrug.BIPROSTA, CALUTIDE, TABI 50 mg tab.
5 α-REDUCTASE INHIBITOR
Finasteride A competitive inhibitor of theenzyme 5 α-reductase which converts testosteroneinto more active DHT responsible for androgenaction in many tissues including the prostate glandand hair follicles. It is relatively selective for 5α-reductase type 2 isoenzyme which predominatesin male urogenital tract. Circulating and prostaticDHT concentration are lowered, but plasma LHand testosterone levels remain unchanged becausetestosterone itself mediates feedback pituitary LHinhibition.
Treatment with finasteride has resulted indecreased prostate size and increased peak urinaryflow rate in ~50% patients with symptomaticbenign hypertrophy of prostate (BHP). The bene-ficial effects are typically delayed needing ~6months for maximum symptomatic relief. Patientswith large prostate (volume > 40 ml) obtain greaterrelief than those with smaller gland. Upto 20%reduction in prostate size may be obtained.
Withdrawal of the drug results in regrowth ofprostate, but with continued therapy benefit ismaintained for 3 years or more. The relief ofobstructive symptoms, however, is less markedcompared to surgery and adrenergic α1 blockers(see p. 143). It primarily reduces the static compo-nent of obstruction, while α1 blockers overcomethe dynamic component. Concurrent treatment withboth produces greater symptomatic relief.
Finasteride has also been found effective inmale pattern baldness, though hair follicles haveprimarily type 1 enzyme. In such subjects itpromotes hair growth and prevents further hairloss. Observable response takes 3 or more monthstherapy and benefit is reversed within 1 year of

303C
HA
PTE
R 21
ANDROGENS AND DRUGS FOR ERECTILE DYSFUNCTION
treatment cessation. However, 20–30% cases donot improve.
Finasteride is effective orally, extensivelymetabolized in liver—metabolites are excreted inurine and faeces; plasma t½ 4–8 hours (elderly6–15 hours). It is well tolerated by most patients;side effects are decreased libido, impotence anddecreased volume of ejaculate (each in 3–4%patients). Gynaecomastia, skin rashes, swellingof lips are rare.Dose for BHP 5 mg OD, review after 6 months;for male pattern baldness 1 mg/day.FINCAR, FINAST, FINARA 5 mg tab; FINPECIA, ASTIFINE1 mg tab.
Dutasteride This newer congener of finasterideinhibits both type 1 and type 2 5α-reductaseand reduces DHT levels. It is metabolized byCYP3A4 and is very long-acting (t½ is ~ 9 weeks).It is approved for use in BHP and can benefitmale pattern baldness. In clinical trias, bothfinasteride and dutasteride have been found toreduce the risk of developing carcinoma prostateby upto 25%. Interactions with CYP3A4 inducersand inhibitors are possible.Dose: 0.5 mg OD; DUPROST, DURIZE 0.5 mg tab.
DRUGS FOR ERECTILE DYSFUNCTION
Erectile dysfunction (ED) refers to the inabilityof men to attain and maintain an erect penis withsufficient rigidity to allow sexual intercourse. Itoccurs mainly past middle-age and is commonafter the age of 65 years. A variety of vascular,neurogenic, hormonal, pharmacologic or psycho-genic causes may underlie the disorder.
Sexual arousal increases blood flow to thepenis and relaxes the cavernosal sinusoids so thatthey fill up with blood, making the penis rigid,elongated and erect. Nitric oxide (NO) releasedfrom parasympathetic nonadrenergic noncholi-nergic (NANC) nerves and vascular endotheliumis the major transmitter causing relaxation ofsmooth muscle in corpus cavernosum and theblood vessels supplying it; ACh and PGs alsoplay a role. A variety of mechanical/prostheticdevices and surgery have been used for ED, butdrug therapy has made a big impact recently.
1. AndrogensHypogonadism is an infrequent cause of ED.Parenteral testosterone esters or transdermaltestosterone therapy is effective only whenandrogen deficiency is proven to be responsiblefor the loss of libido and ED.
2. Phosphodiesterase-5 (PDE-5) inhibitorsThis class of drugs have become the first linetherapy for ED.
Nitric oxide causes smooth muscle relaxationby generating cGMP intracellularly which thenpromotes dephosphorylation of myosin light chainkinase (MLCK) so that myosin fails to interactwith actin (see Fig. 39.3). Inhibition ofPDE-5, the cGMP degrading isoenzyme incavernosal and vascular smooth muscle, resultsin accumulation of cGMP and marked potentiationof NO action. Sildenafil, Tadalafil and vardenafilare selective PDE-5 inhibitors found effective ina majority of patients with ED.
cGMP PDE-5
5-GMPInhibited bysildenafil
Sildenafil It is an orally active drug, marketedin the USA in 1998 and 2 years later in India,for treatment of ED. It became an instant hit,and evoked worldwide response. Sildenafil actsby selectively inhibiting PDE-5 and enhancingNO action in corpus cavernosum. Peniletumescence during sexual arousal is improved,but it has no such effect in the absence of sexualactivity. It does not cause priapism in mostrecipients.
Oral bioavailability of sildenafil is ~40%, peakblood levels are attained in 1–2 hr; it is metabolizedlargely by CYP3A4 and an active metabolite isproduced; t½ in men <65 years averages 4 hours.It is recommended in a dose of 50 mg (for men> 65 years 25 mg), if not effective then 100 mg1 hour before intercourse. Duration and degreeof penile erection is increased in 74–82% menwith ED including diabetic neuropathy cases. Over

304S
EC
TIO
N5
HORMONES AND RELATED DRUGS
20 controlled trials have confirmed its efficacy.However, sildenafil is ineffective in men who havelost libido or when ED is due to cord injury ordamaged nervi eregantis.
Adverse effects Side effects are mainly dueto PDE-5 inhibition related vasodilatation—headache, nasal congestion, dizziness, facialflushing and fall in BP, loose motions. Relaxationof lower esophageal sphincter may cause gastricreflux and dyspepsia. Sildenafil, in addition,weakly inhibits the isoenzyme PDE-6 which isinvolved in photoreceptor transduction in theretina. As such, impairment of colour vision,especially blue-green discrimination, occurs insome recipients. Few cases of sudden loss of visiondue to nonarteritic ischaemic optic neuropathy(NAION) among users of PDE-5 inhibitors havebeen reported.
Sildenafil markedly potentiates the vasodilatoraction of nitrates; precipitous fall in BP; MI canoccur. After >6 million prescriptions dispensedin USA, the FDA received reports of 130 deathsrelated to sildenafil use by the year 2002. Mostdeaths occurred in patients with known riskfactors, drug interactions or contraindications, andwere timed either during or within 4–5 hours ofsex. Sildenafil is contraindicated in patients ofcoronary heart disease and those taking nitrates.Though sildenafil remains effective for <8 hours,it is advised that nitrates be avoided for 24 hours.Caution is advised in presence of liver or kidneydisease, peptic ulcer, bleeding disorders. Inhibitorsof CYP3A4 like erythromycin, ketoconazole,verapamil, cimetidine potentiate its action. Cautionis required also in patients of leukaemia, sicklecell anaemia or myeloma which predispose topriapism.
Sildenafil is erroneously perceived as anaphrodisiac. Men even without ED are going forit to enhance sexual satisfaction/pleasure.PENEGRA, CAVERTA, EDEGRA 25, 50, 100 mg tabs.
Pulmonary arterial hypertension (PAH) SinceNO is an important regulator of pulmonaryvascular resistance, PDE-5 inhibitiors lowerpulmonary arterial pressure. Sildenafil is more
selective for pulmonary circulation than vardenafil,and has been shown to improve arterial oxyge-nation in pulmonary hypertension. It significantlyincreases exercise capacity. Sildenafil 20 mg TDShas now become the drug of choice for PAH.
Tadalafil It is a more potent and longer actingcongener of sildenafil; t½ 18 hours and durationof action 24–36 hours. Peak plasma levels areattained between 30–120 min; time to onset ofaction may be longer. Side effects, risks,contraindications and drug interactions are similarto sildenafil. In addition, back pain is reported,which has been ascribed to some degree ofPDE II inhibition by tadalafil. Because of itslonger lasting action, nitrates are contraindicatedfor upto 3 days after tadalafil. Due to its loweraffinity for PDE-6, visual disturbances occur lessfrequently.Dose: 10 mg at least 30 min before intercourse (max.20 mg)MEGALIS, TADARICH, TADALIS 10, 20 mg tabs,MANFORCE 10 mg tab.
Vardenafil Another congener of sildenafil with similartime-course of action; peak levels in 30–120 min and t½4–5 hours. Side effects, contraindications and interactionsare also the same. It prolongs Q-T interval; should be avoidedin hyperkalaemia and in patients with long Q-T or thosereceiving class IA and class III antiarrhythmics.Dose: 10 mg (elderly 5 mg), max 20 mg.
3. Papaverine/Phentolamine induced penileerection (PIPE) therapyInjection of papaverine (3–20 mg) with or without phento-lamine (0.5–1 mg) in the corpus cavernosum produces peniletumescence to permit intercourse. However, the procedurerequires skill and training. Priapism occurs in 2–15% cases,which if not promptly treated leads to permanent damage. Thisis reversed by aspirating blood from the corpus cavernosumor by injecting phenylephrine locally. Repeated injections cancause penile fibrosis. Other complications are—local haema-toma, infection, paresthesia and penile deviation. In view ofthe availability of PDE-5 inhibitors, it is rarely used now; onlyin cases not responding to sildenafil and alprostadil.
4. Prostaglandin E1
Alprostadil (PGE1) injected directly into the corpus cavernosumusing a fine needle produces erection lasting 1–2 hours topermit intercourse. Alprostadil injections are less painful thanpapaverine, but local tenderness may occur. Penile fibrosis andpriapism are rare. It is now the most commonly used drug inpatients not responding to PDE-5 inhibitors, such as neurogenicand psychogenic ED.

305C
HA
PTE
R 21
ANDROGENS AND DRUGS FOR ERECTILE DYSFUNCTION
A transurethral pellet termed ‘medicated urethralsystem for erection’ (MUSE) has been developed
which avoids intracavernosal injection, but is lesseffective and may cause urethral burning.
PROBLEM DIRECTED STUDY
21.1 A 65-year-old man presented with severe pain in the left shoulder region. The pain hasprogressively increased over the last 4 weeks, is not relieved by analgesics or NSAIDs and isworsened by pressure or movement. He also has increasing micturition difficulty for the last6 months. Shoulder X-ray showed osteolytic lesion in the head of humerus. Rectal examinationwas consistent with prostate cancer which was confirmed by needle biopsy and raised serumPSA level (30 ng/ml). He refused orchidectomy and was prescribed injection triptorelin 3.75 mgi.m. to be repeated after one week and then every 4 weeks. After 1 week of 1st injection, hereported increased bone pain and greater bladder voiding difficulty. The serum PSA level was34 ng/ml.(a) What is the cause of the increase in bone pain and urinary obstructive symptoms? Is thechoice of the drug incorrect?(b) Could this flaring of symptoms be avoided; if so how?(c) Can any other drug be given to relieve the bone pain?(see Appendix-1 for solution)

Estrogens, Progestins andContraceptives
ChapterChapterChapterChapterChapter 2222222222
ESTROGENS(Female Sex Hormones)
These are substances which can induce estrus inspayed (ovariectomized) animals.
It was established in the year 1900 that ovariescontrol female reproductive function through ahormonal mechanism. Allen and Doisy (1923)found that an alcoholic extract of ovaries wascapable of producing estrus and devised a simplebioassay method. The active principle estradiolwas obtained in pure form in 1929 and soon itschemical structure was worked out.
males also from aromatization of testosterone inthe testes and extraglandular tissues. In mare, largequantity of equilin is produced which has 1/5estrogenic potency of estradiol.
Synthetic estrogens Natural estrogens areinactive orally and have a short duration of actiondue to rapid metabolism in liver. To overcomethis, synthetic compounds have been produced:
Steroidal Ethinylestradiol, Mestranol,Tibolone.
Nonsteroidal Diethylstilbestrol (stilbestrol)Hexestrol, Dienestrol
The nonsteroidal compounds assume a transconfiguration as depicted below and stericallyresemble natural estrogens.
Natural estrogens Estradiol is the major estro-gen secreted by the ovary. It is synthesized inthe graafian follicle, corpus luteum and placentafrom cholesterol. Steps depicted on the right handside in Fig. 20.1 are carried out. Further stepsare shown below.
Estradiol is rapidly oxidized in liver to estronewhich is hydroxylated to form estriol. All threeare active and circulate in blood, but estradiolis the most potent estrogen. Small quantity(2–20 µg/day) of estradiol is derived in human
Regulation of secretion The daily secretionof estrogens in menstruating women varies from10–100 µg depending on the phase of the cycle.Its secretion starts from the graafian follicle underthe influence of FSH and the blood level risesgradually during the follicular phase. Due to themodest preovulatory FSH surge, estrogens furtherrise transiently. After ovulation, corpus luteumcontinues to secrete estrogens till about twodays before menstruation. Estrogens exercisefeedback inhibition of FSH (also of LH at higher

307C
HA
PTE
R 22
ESTROGENS, PROGESTINS AND CONTRACEPTIVES
concentrations) by direct action on pituitary aswell as through hypothalamus (see p. 240).
During pregnancy, placenta secretes largequantities of estrogens, (mainly estrone and estriol)reaching a peak of upto 30 mg/day at term. Theirlevel declines sharply after delivery. In thepostmenopausal women, daily production ofestrogen has been estimated as 2–10 µg—derivedprimarily by extraglandular aromatization ofadrenal androgens.
ACTIONS
1. Sex organs The estrogens bring aboutpubertal changes in the female including growthof uterus, fallopian tubes and vagina. Vaginalepithelium gets thickened, stratified and corni-fied. They are responsible for the proliferationof endometrium in the preovulatory phase, andit is only in concert with estrogens that proges-terone brings about secretory changes.
In the absence of progesterone (anovulatorycycles) withdrawal of estrogens alone producesmenstruation. If modest doses of estrogen aregiven continuously without added progesterone—menstruation is delayed but breakthroughbleeding occurs at irregular intervals. However,the normal event which triggers menstruation isprogesterone withdrawal. The progesterone with-drawal bleeding cannot be suppressed even byhigh doses of estrogens.
Estrogens augment rhythmic contractions ofthe fallopian tubes and uterus, and induce a wateryalkaline secretion from the cervix. This is favou-rable to sperm penetration. They also sensitizethe uterus to oxytocin. Deficiency of estrogensis responsible for atrophic changes in the femalereproductive tract that occur after menopause.
2. Secondary sex characters Estrogensproduced at puberty cause growth of breasts—proliferation of ducts and stroma, accumulationof fat. The pubic and axillary hair appear, femininebody contours and behaviour are influenced.
Acne is common in girls at puberty as it isin boys—probably due to small amount of andro-gens produced simultaneously. Administration of
estrogens to suppress pituitary-gonadal axis causesregression of acne.
3. Metabolic effects Estrogens are anabolic,similar to but weaker than testosterone. There-fore, small amount of androgen may be contri-buting to the pubertal growth spurt even in girls,as estrogens do in boys. Continued action ofestrogen promotes fusion of epiphyses both ingirls and boys.
Estrogen is important in maintaining bonemass primarily by retarding bone resorption.Osteoclast pit formation is inhibited and thereis increased expression of bone matrix proteinssuch as osteonectin, osteocalcin, collagen andalkaline phosphatase. It promotes positive calciumbalance, partly by inducing renal hydroxylaseenzyme which generates the active form ofVit D3.
Both osteoblasts and osteoclasts express estrogen receptors(ERs). The major action of estrogens is to reduce maturationand activity of osteoclasts by modifying regulatory cytokinesignals from osteoblasts (see Ch. 24 for bone remodelingmechanisms). Estrogens enhance elaboration of OPG fromosteoblasts which binds RANKL and prevents activation ofosteoclast-precursors from fusing and maturing into osteoclasts.The direct action on osteoclasts is to accelerate their apoptosis.
Pharmacological doses of estrogens can causemild salt and water retention—edema occurs inpredisposed patients, but it can be treated withdiuretics. BP may rise after prolonged use.Combination contraceptives containing higherdoses of estrogens and progestins impair glucosetolerance. Normal blood sugar is not affected butdiabetes may be precipitated or its control vitiated.However, amounts used for HRT and low dosecontraception do not affect carbohydrate meta-bolism.
Estrogens decrease plasma LDL cholesterolwhile HDL and triglyceride levels are raised. Theraised HDL : LDL ratio is probably responsiblefor rarity of atherosclerosis in premenopausalwomen. However, blood coagulability is increa-sed due to induction of synthesis of clotting factors(factors II, VII, IX and X). Fibrinolytic activityin plasma also tends to increase due to loweringof plasminogen-activator inhibitor-1 (PAI-1).

308S
EC
TIO
N5
HORMONES AND RELATED DRUGS
Estrogens induce nitric oxide synthase andPGI2 production in vascular endothelium. Theincreased availability of NO and PGI2 couldpromote vasodilatation. They increase lithogeni-city of bile by increasing cholesterol secretionand reducing bile salt secretion. Plasma levelsof sex hormone binding globulin (SHBG),thyroxine binding globulin (TBG) and cortisolbinding globulin (CBG) are elevated—but withoutany change in hormonal status.
Mechanism of actionEstrogens bind to specific nuclear receptors intarget cells and produce effects by regulatingprotein synthesis. Estrogen receptors (ERs) havebeen demonstrated in female sex organs, breast,pituitary, liver, bone, blood vessels, heart, CNSand in certain hormone responsive breastcarcinoma cells. The ER is analogous to othersteroid receptors: agonist binding to the ligandbinding domain brings about receptor dimerizationand interaction with ‘estrogen response elements’(EREs) of target genes. Gene transcription ispromoted through certain coactivator proteins.On binding an estrogen antagonist the receptorassumes a different conformation and interactswith other corepressor proteins inhibiting genetranscription.
Two distinct ERs designated ERα and ERβhave been identified, cloned and structurallycharacterized. Most tissues express both subtypes,but ERα predominates in uterus, vagina, breast,bone, hypothalamus and blood vessels, while ERβpredominates in prostate gland of males andovaries in females. Estradiol binds to both ERαand ERβ with equal affinity, but certain ligandshave differing affinities. More importantly ERαand ERβ may have a different pattern ofinteraction with coactivators and corepressors.
Few nongenomic rapid actions of estrogensin certain tissues mediated through the same ERsbut located on the cell membrane have also beenobserved.
PHARMACOKINETICS
Estrogens are well absorbed orally and trans-dermally, but natural estrogens are inactive by
the oral route due to rapid metabolism in liver.Estradiol esters injected i.m. are slowly absorbedand exert prolonged action. Natural estrogens incirculation are largely plasma protein bound—to SHBG as well as to albumin.
Estradiol is converted to estrone and vice versain liver. Estriol is derived from estrone. All threeare conjugated with glucuronic acid and sulfate—excreted in urine and bile. Considerable entero-hepatic circulation occurs due to deconjugationin intestines and reabsorption—ultimate disposaloccurs mostly in urine.
Ethinylestradiol is metabolized very slowly(t½ 12–24 hours). It is orally active and morepotent.
Preparations and dose
All estrogen preparations have similar action. Their equivalentparenteral doses are—Estradiol 0.1 mg = Ethinylestradiol 0.1 mg = Mestranol 0.15mg = Conjugated estrogens 10 mg = Estriol succinate 16mg = Diethylstilbestrol 10 mg.
The oral potencies differ from the above due to differingextents of first pass metabolism. Estradiol is inactive orally,conjugated estrogens and estriol succinate undergo partialpresystemic metabolism, while in case of ethinylestradiol,mestranol and diethylstilbestrol the oral and parenteral dosesare practically the same.
The preferred route of administration of estrogens isoral. Intramuscular injection is resorted to only when largedoses have to be given, especially for carcinoma prostate.1. Estradiol benzoate/cypionate/enanthate/valarate: 2.5–10mg i.m.; OVOCYCLIN-P 5 mg inj, PROGYNON DEPOT10 mg/ml inj.2. Conjugated estrogens: 0.625–1.25 mg/day oral;PREMARIN 0.625 mg, 1.25 mg tab, 25 mg inj (fordysfunctional uterine bleeding).3. Ethinylestradiol: for menopausal syndrome 0.02–0.2 mg/day oral; LYNORAL 0.01, 0.05, 1.0 mg tab, PROGYNON-C 0.02 mg tab.4. Mestranol: acts by getting converted to ethinylestradiolby demethylation in the liver: 0.1–0.2 mg/day oral; inOVULEN 0.1 mg tab, with ethynodiol diacetate 1 mg.5. Estriol succinate: 4–8 mg/day initially, maintenance dosein menopause 1–2 mg/day oral: EVALON 1, 2 mg tab, 1mg/g cream for vaginal application in atrophic vaginitis 1–3 times daily.6. Fosfestrol tetrasodium: initially 600–1200 mg slow i.v.inj for 5 days, maintenance 120–240 mg/day oral or 300mg 1–3 times a week i.v. HONVAN 120 mg tab, 60 mg/ml inj 5 ml amp.7. Dienestrol: 0.01% topically in vagina: DIENESTROL0.01% vaginal cream.

309C
HA
PTE
R 22
ESTROGENS, PROGESTINS AND CONTRACEPTIVES
Transdermal estradiol A transdermal patch(Estradiol-TTS) is available in 3 sizes, viz. 5,10 and 20 cm2 delivering 0.025 mg, 0.05 mgand 0.1 mg respectively in 24 hr for 3–4 days.The usual dose in menopause is 0.05 mg/daywhich produces plasma estradiol levels seen inpremenopausal women in the early or midfollicular phase. Cyclic therapy (3 weeks on, 1week off) with estradiol-TTS is advised with anoral progestin added for the last 10–12 days.Beneficial effects of estradiol-TTS on menopausalsymptoms, bone density, vaginal epithelium andplasma Gn levels are comparable to those of oraltherapy, but improvement is serum lipid profileis less marked.
Systemic side effects of estradiol-TTS are thesame as with oral estrogens, but are milder. Oraltherapy delivers high dose of the hormone to theliver and increases synthesis of several proteins.Estradiol-TTS avoids high hepatic delivery:consequently plasma levels of TBG, CBG, angio-tensinogen and clotting factors are not elevated—risk of thromboembolic phenomena may not beincreased.
ESTRADERM-MX: Estradiol 25, 50 or 100 µg per 24 hrtransdermal patches; apply to nonhairy skin below waist,replace every 3–4 days using a different site; add an oralprogestin for last 10–12 days every month.
Recently a combined estradiol 50 µg + norethisteroneacetate 0.25 mg patch has become available in some countries(ESTRAGEST-TTS). Two weeks of estraderm-TTS followedby 2 weeks estragest-TTS with patches changed twice weeklyis used for total transdermal HRT.
A gel formulation of estradiol for application over skinis also available. OESTRAGEL, E2 GEL 3 mg/5 g in80 g tube, SANDRENA 1 mg/g gel; apply over the armsand spread to cover a large area once daily for HRT.
ADVERSE EFFECTS
Most of the adverse effects of estrogens aredescribed with HRT and with oral contraceptives(see p. 325).In addition, dose dependent adverse effects notedwhen use is made for other indications are—1. Suppression of libido, gynaecomastia andfeminization when given to males.2. Fusion of epiphyses and reduction of adultstature when given to children.
3. In postmenopausal women, estrogens canincrease the risk of irregular bleeding andendometrial carcinoma (5–15 fold). A progestingiven concurrently blocks the risk.4. Estrogens can accelerate the growth of existingbreast cancer, but low-dose estrogen only HRTdoes not appear to increase the risk of developingnew breast cancer (see p. 311).5. Long-term estrogen therapy doubles theincidence of gallstones. Benign hepatomas aremore common in women taking estrogens in theirteens and twenties.6. Migraine, epilepsy and endometriosis may beworsened by estrogens.7. Stilbestrol given to pregnant women, especially duringfirst trimester (as test of pregnancy or otherwise)—increasedthe incidence of vaginal and cervical carcinoma in the femaleoffspring in childhood or early adulthood. Other genitalabnormalities are possible in the female as well as maleoffspring. Estrogens are contraindicated during pregnancy.
USES
Currently, the two most common uses of estrogensare as contraceptives and for hormone replace-ment therapy in postmenopausal women, but thereare some other indications as well.
1. Hormone replacement therapy (HRT)Due to cessation of ovarian function at meno-pause women suffer a number of physical,psychological and emotional consequences.Medical problems related to menopause are:• Vasomotor disturbances Hot flushes, chilly sensation,
inappropriate sweating, faintness, paresthesias, aches andpains.
• Urogenital atrophy Change in vaginal cytology and pH,vaginal dryness, vulval shrinkage, dyspareunia, vaginitis,itching, urinary urgency, predisposition to urinary tractinfection.
• Osteoporosis Loss of osteoid as well as calcium →thinning and weakening of bone → minimal traumafractures especially of femur, hip, radius, vertebrae.
• Dermatological changes Thinning, drying and loss ofelasticity of skin, wrinkles, thin and listless hairs.
• Psychological/Cognitive disturbances Irritability, depres-sed mood, loss of libido and self confidence, anxietyand dementia.
• Increased risk of cardiovascular diseases Coronary arterydisease, myocardial infarction, stroke.

310S
EC
TIO
N5
HORMONES AND RELATED DRUGS
The vasomotor symptoms tend to subside over a few years,but the other changes progress continuously.
Estrogen ±progestin HRT or ‘menopausalhormone therapy’ (MHT) is highly efficaciousin suppressing the perimenopausal syndrome ofvasomotor instability, psychological disturbancesas well as in preventing atrophic changes andosteoporosis. However, several recent findingshave emphasized a number of risks and limitationsof long-term HRT, so that the whole outlook haschanged.
The dose of estrogen used in HRT is sub-stantially lower than that for contraception.Typically conjugated estrogens are used at 0.625mg/day dose (equivalent to ethinylestradiol 10μg) either cyclically (3 weeks treatment 1 weekgap) or continuously, but there is a trend nowto use lower doses (0.3–0.45 mg/day). A progestin(medroxy progesterone acetate/norethisterone2.5 mg daily) is added for the last 10–12 dayseach month. Though the progestin may attenuatethe metabolic and cardiovascular benefits ofestrogen, it is needed to block the increased riskof dysfunctional uterine bleeding and endometrialcarcinoma due to continuous estrogenicstimulation of endometrium. Estrogen alone isused in hysterectomised women and when aprogestin is not tolerated or is contraindicated.Transdermal estradiol (with oral or transdermalprogestin) appears to have certain advantages (seeabove) and is preferred by some.
The benefits and risks of HRT are consideredbelow:a. Menopausal symptoms and atrophic changes Thevasomotor symptoms respond promptly and almostcompletely. They are the primary indication for using HRTwhich also improves general physical, mental and sexualwell being. HRT should be discontinued once the vasomotorsymptoms abate. Estrogens also arrest genital and dermalatrophic changes; vulval and urinary problems resolve. Vaginalapplication of estrogen is effective in relieving local symptomsand should be preferred when this is the only aim of HRT.b. Osteoporosis and fractures HRT restores Ca2+
balance; further bone loss is prevented and the excess fracturerisk is nullified. When used for this purpose, HRT shouldbe initiated before significant bone loss has occurred, becausereversal of osteoporosis is none or slight. Calcium +vit D supplements and exercise aid the beneficial effect ofHRT. However, accelerated bone loss starts again on cessationof HRT. The ‘Women’s health, osteoporosis, progestin-
estrogen’ trial (2002) has shown that even lower doses ofconjugated estrogens (0.3, 0.45 mg/day) increased bonemineral density in postmenopausal women, though 0.625mg/day was more effective.
Not withstanding the above, appreciation of the otherrisks of HRT (see below) has dislodged estrogen from itsprime position in the treatment of osteoporosis.Bisphosphonates are more effective and the drugs of choice.If prevention and treatment of osteoporosis is the goal, HRTis not the best option, and is not recommended beyond 5years of use.c. Cardiovascular events Since hypertension and cardio-vascular disease are rare in premenopausal women, andestrogens improve HDL : LDL ratio, retard atherogenesis,reduce arterial impedance, increase NO and PGI2 productionand prevent hyperinsulinaemia, it was believed that estrogentherapy in postmenopausal women will have a protectivecardiovascular influence. This was supported by early reportsrelying mainly on retrospective/epidemiological studies andthose using surrogate markers to indicate that HRT inotherwise healthy women reduced risk of coronary arterydisease (CAD), myocardial infarction (MI) and stroke. Thislead to the extensive use of HRT; a segment of doctorscontended that menopausal women should take HRT for therest of their lives.
In the past decade many large scale placebo controlledrandomized interventional trials and cohort studies haveyielded opposite results. The ‘Heart and estrogen/progestinreplacement study’ (HERS and HERS II) conducted in olderwomen with preexisting cardiovascular disease found thatHRT triples the risk of venous thromboembolism, increasesrisk of MI in the 1st year and affords no secondary prophylaxisof CAD in the long-term. The larger ‘women’s health initiative’(WHI) study conducted in over 16000 younger women withoutCAD found 24% increase in CAD, 40% increase in strokeand doubling of venous thromboembolism with the use ofcombined HRT. The study was terminated prematurely in2002. The increased risk of MI was attributed to the progestincomponent, since women who took estrogen alone had noincrease in the incidence of MI. Reexamination of the datahas revealed ~30% reduction in incidence of MI amongwomen who took HRT within 10 years of menopause. Assuch, a few years of HRT just after menopause may beprotective. The committee on safety of medicines (CSM)of UK has estimated that ~20 out of 1000 women aged60–69 years and not using HRT develop venousthromboembolism over 5 years; 4 extra cases occur in thosetaking estrogen alone, while 9 extra cases occur in thosetaking combined HRT. Thus, progestin use adds to the risk.d. Cognitive function and dementia: Contrary to earlierbelief, the ‘women’s health initiative memory study’ (WHIMS)conducted among older women (65–79 years) has failed todetect any protection against cognitive decline by eitherestrogen alone or combined HRT. There was in fact a slightglobal deterioration. Surprisingly, the incidence of dementia(Alzheimer’s) was doubled.e. Cancer: That estrogens enhance the growth of breastcancer has been well recognized. However, it was contended

311C
HA
PTE
R 22
ESTROGENS, PROGESTINS AND CONTRACEPTIVES
that small replacement doses of estrogens will not inducenew cancer. This appears to be supported by the estrogenalone arm of WHI study in hysterectomized women, as theoccurrence of breast cancer was actually lower (butinsignificantly). However, in the combined HRT group, asignificantly higher incidence of cancer breast occurred,indicating that medroxyprogesterone was the culprit. Theprospective observational cohort ‘Million women study’(MWS) in the UK found a marginally higher incidence ofbreast cancer with estrogen alone, but a clearly higher onewith estrogen + progestin. Some other studies have alsoimplicated the progestin, and the CSM of UK has drawnsimilar conclusions. Thus, the protective effect of progestinon endometrial cancer appears to be counter balanced bythe procarcinogenic effect on the breast.
Estrogen is well known to induce endometrial hyperplasiaand its continuous use unopposed by progestin results inirregular uterine bleeding. In the long-term it predisposesto endometrial carcinoma. The MWS has supported thiscontention. The standard practice is to give combined HRTto women with an intact uterus. However, a CochraneDatabase Review has concluded that lower dose unopposedestrogen does not increase endometrial carcinoma risk; maybe used in women with intact uterus when a progestin iscontraindicated.
A small protective effect of combined HRT on colorectalcarcinoma has been detected by the WHI study, but thisneeds to be confirmed.f. Gallstone, migraine: Estrogens slightly increase therisk of developing gallstones, while progestins may triggermigraine.
Tibolone It is a 19-norsteroid developed speci-fically to be used for HRT. It is converted into3 metabolites which exert estrogenic, progesta-tional and weak androgenic actions in specific
tissues. In a dose of 2.5 mg daily, it suppressesmenopausal symptoms and lowers the raised Gnlevels. No endometrial stimulation has been noted.Urogenital atrophy, psychological symptoms,libido and osteoporosis are improved similar toother forms of HRT. Contraindications are thesame as for conventional HRT, but long termbenefits and risks are not defined.
Weight gain, increased facial hair andoccasional vaginal spotting may be noted.LIVIAL 2.5 mg tab, one tab daily without interruption; institutetherapy only after the women has been menopausal for atleast12 months.
2. Senile vaginitis Estrogens change vaginalcytology to the premenopausal pattern and areeffective in preventing as well as treating atrophicvaginitis that occurs in elderly women. Oraltherapy can be given but more commonly a topicalpreparation is used; an antibacterial may becombined. Estrogens help in overcoming infectionand relieve symptoms of Kraurosis vulvae.
3. Delayed puberty in girls It may be dueto ovarian agenesis (Turner’s syndrome) orhypopituitarism. In both, pubertal changes arebrought about by estrogen treatment, except therapid gain in height for which growth hormoneand/or a small dose of androgen may be added.Usually cyclic treatment is given; some preferto start with a lower dose and gradually attainthe full replacement dose.
Current conclusions regarding HRT
1. The main indication of HRT is vasomotor and other symptoms in the perimenopausal period. It should beused at the smallest effective dose and for the shortest duration.
2. Young women with premature menopause clearly deserve HRT.3. Hysterectomized women should receive estrogen alone, while those with intact uterus be given estrogen +
progestin.4. Perimenopausal women should be given cyclic HRT rather than continuous HRT.5. HRT is not the best option to prevent osteoporosis and fractures.6. HRT affords protection against coronary artery disease only in early postmenopausal women. Combined
HRT at conventional dose may even increase the risk of venous thromboembolism, MI and stroke in elderlywomen.
7. HRT does not protect against cognitive decline; may increase the risk of dementia.8. Combined HRT increases the risk of breast cancer, gallstones and migraine.9. Transdermal HRT may have certain advantages over oral HRT.
10. The need for HRT should be assessed in individual women, and not prescribed routinely.

312S
EC
TIO
N5
HORMONES AND RELATED DRUGS
4. Dysmenorrhoea While PG synthesis inhibitors arethe first line drugs, cyclic estrogen therapy (with addedprogestin to ensure withdrawal bleeding) benefits by inhibitingovulation (anovular cycles are painless) and decreasingprostaglandin synthesis in endometrium; but this should bereserved for severe cases.5. Acne It occurs at puberty due to increased androgensecretion in both boys and girls. Estrogens benefit bysuppressing ovarian production of androgen by inhibitingGn release from pituitary. Cyclic treatment (with addedprogestin) is quite effective. Use of estrogen in boys is outof question. Even in girls, topical therapy with antimicrobials,tretinoin and other drugs is preferred (see Ch. 64).6. Dysfunctional uterine bleeding A progestin givencyclically is the rational and effective therapy. Estrogens haveadjuvant value.7. Carcinoma prostate Estrogens are palliative; producerelief in primary as well as metastatic carcinoma prostateby suppressing androgen production (through pituitary).GnRH agonists with or without androgen antagonist arepreferred.
ANTIESTROGENS AND SELECTIVEESTROGEN RECEPTOR MODULATORS(SERMs)
Two nonsteroidal compounds clomiphene citrateand tamoxifen citrate previously grouped asestrogen antagonists have been in use since 1970s,but their differing antagonistic and agonisticactions depending on species, target organ andhormonal background could not be explained. Therecent discovery of two estrogen receptors (ERαand ERβ) and that ligand binding could changetheir configuration in multiple ways allowing inter-action with different coactivators and corepres-sors in a tissue specific manner has paved theway for development of compounds with uniqueprofile of agonistic and antagonistic actionsin different tissues. These drugs have beendesignated ‘selective estrogen receptormodulators’ (SERMs), and two new compoundsRaloxifene and Toremifene are in clinical use. Ithas been demonstrated that the conformation ofER after binding tamoxifen or raloxifene isdifferent from that after binding estradiol.
Antiestrogens
Clomiphene citrate It binds to both ERα andERβ and acts as a pure estrogen antagonist in
all human tissues, but the racemate displays weakagonistic action in rats. It induces Gn secretionin women by blocking estrogenic feedbackinhibition of pituitary. The amount of LH/FSHreleased at each secretory pulse is increased. Inresponse, the ovaries enlarge and ovulation occursif the ovaries are responsive to Gn. Antagonismof peripheral actions of estrogen results in hotflushes. Endometrium and cervical mucus maybe modified.
The chief use of clomiphene is for infertilitydue to failure of ovulation: 50 mg once dailyfor 5 days starting from 5th day of cycle.Treatment is given monthly. Conception occursin many women who previously were amenor-rhoeic or had anovular cycles. If 1–2 monthstreatment does not result in conception—the dailydose may be doubled for 2–3 cycles. No morethan 6 treatment cycles should be tried. Theantiestrogenic effect of clomiphene on developingfollicle, endometrium or cervical mucus can becounterproductive. Luteal phase dysfunction hasalso been blamed for therapeutic failures. Additionof menotropins or chorionic gonadotropin on thelast 2 days of the course improves the successrate.
Clomiphene is well absorbed orally, gets depo-sited in adipose tissue and has long t½ of ~6days. It is largely metabolized and excreted inbile.
Adverse effects Polycystic ovaries, multiplepregnancy, hot flushes, gastric upset, vertigo,allergic dermatitis. Risk of ovarian tumour maybe increased.
Other uses To aid in vitro fertilization Clomi-phene given with Gns causes synchronous matu-ration of several ova—improves their harvestingfor in vitro fertilization.
Oligozoospermia: In men also clomiphene inc-reases Gn secretion → promotes spermatogenesisand testosterone secretion. For male infertility—25 mg daily given for 24 days in a month with6 days rest for upto 6 months has been recom-mended. However, success rates are low.

313C
HA
PTE
R 22
ESTROGENS, PROGESTINS AND CONTRACEPTIVES
CLOMID, FERTOMID. CLOFERT, CLOME 25, 50, 100 mgtab.
Fulvestrant It is the first member of a distinct class of ERligands called ‘selective estrogen receptor down-regulators’(SERDs) or ‘pure estrogen antagonists’ that has beenintroduced for the treatment of metastatic ER positive breastcancer in postmenopausal women which has stoppedresponding to tamoxifen. In contrast to tamoxifen, it inhibitsER dimerization so that ER interaction with DNA is preventedand receptor degradation is enhanced. The ER is thus downregulated resulting in more complete suppression of ERresponsive gene function. This feature along with its higheraffinity for the ER probably accounts for its efficacy intamoxifen resistant cases.
Fulvestrant is administered as (250 mg) monthly i.m.injections in the buttock. It is slowly absorbed and has anelimination t½ of more than a month.
Selective estrogen receptor modulators(SERMs)
These are drugs which exert estrogenic as wellas antiestrogenic actions in a tissue selectivemanner.
Tamoxifen citrate Though chemically relatedto clomiphene, it has complex actions; acts aspotent estrogen antagonist in breast carcinomacells, blood vessels and at some peripheral sites,but as partial agonist in uterus, bone, liver andpituitary. Inhibition of human breast cancer cellsand hot flushes reflect antiestrogenic action, whilethe weak estrogen agonistic action manifests asstimulation of endometrial proliferation, loweringof Gn and prolactin levels in postmenopausalwomen as well as improvement in their bonedensity.
A decrease in total and LDL cholesterolwithout any change in HDL and triglyceride levelreflects estrogenic action. Similar to estrogen HRT,it increases the risk of deep vein thrombosis by2–3 times.
Till recently tamoxifen has been the standardhormonal treatment of breast cancer in both pre-and post-menopausal women, but aromataseinhibitors have now gained prominence. In earlycases tamoxifen is given as postmastectomyadjuvant therapy, while in advanced cases, it isa constituent of palliative treatment. Responserates are high in ER-positive breast carcinomas,but some ER-negative tumours also respond
suggesting additional nonhormonal mechanism ofaction. Tamoxifen is the only drug approved forprimary as well as metastatic breast carcinomain premenopausal women. It is also effective insurgically treated cancer of male breast.
Based on large epidemiological studies whichhave shown 45% reduction in the incidence ofER-positive breast cancer, tamoxifen has beenapproved for primary prophylaxis of breast cancerin high-risk women. Recurrence rate in ipsilateralas well as contralateral breasts is reduced bytamoxifen, but benefits of prophylactic therapybeyond 5 years are not proven; outcomes mayeven be worse. Adjuvant therapy of breast carcinomawith tamoxifen when used in postmenopausalwomen is now generally replaced after 2 yearsby an aromatase inhibitor, while in premenopausalwomen, tamoxifen itself is continued till 5 yearspostmastectomy.
Improvement in bone mass due to anti-resorptive effect, and in lipid profile are the otherbenefits of tamoxifen therapy. However, endo-metrial thickening occurs and risk of endometrialcarcinoma is increased 2–3 fold due to estrogenicaction.
Tamoxifen is effective orally; has a biphasicplasma t½ (10 hours and 7 days) and a longduration of action. Some metabolites of tamoxifenare more potent antiestrogens. The drug is excretedprimarily in bile.Dose 20 mg/day in 1 or 2 doses, max. 40 mg/day;TAMOXIFEN, MAMOFEN, TAMODEX 10, 20 mg tabs.
Male infertility: May be used as alternative toclomiphene.
Side effects Hot flushes, vomiting, vaginalbleeding, vaginal discharge, menstrual irregula-rities are the side effects. Increased risk of venousthromboembolism is due to estrogenic action onclotting mechanism.Dermatitis, anorexia, depression, mild leucopeniaand ocular changes are infrequent.Tamoxifen is much less toxic than other anticancerdrugs.Toremifene It is a newer congener of tamoxifen with similaractions, but is a weaker ER agonist. Uses and adverse effectsare also similar.

314S
EC
TIO
N5
HORMONES AND RELATED DRUGS
Raloxifene This SERM has a different patternof action than tamoxifen. It is an estrogen partialagonist in bone and cardiovascular system, butan antagonist in endometrium and breast. It hashigh affinity for both ERα and ERβ, and hasa distinct DNA target the ‘raloxifene responseelement’ (RRE).
Several long-term multicentric studies haveshown that raloxifene prevents bone loss inpostmenopausal women; bone mineral density(BMD) may even increase by 0.9–3.4% over yearsin different bones, particularly the lumbarvertebrae. However, accelerated bone loss occurswhen raloxifene is stopped. The risk of vertebralfracture is reduced to half, but not that of longbones. Reloxifene is less efficacious thanbisphosphonates in preventing fractures.
In postmenopausal women raloxifene reducesLDL cholesterol, probably by upregulating hepaticLDL receptors. In contrast to estrogen HRT thereis no increase in HDL and triglyceride levels. Followup studies have shown that raloxifene reduces therisk of breast cancer by 65%, though the protectionwas confined to ER-positive breast cancer.
Raloxifene does not stimulate endometrialproliferation and there is no increase in the riskof endometrial carcinoma. No relief of menopausalvasomotor symptoms occurs; rather hot flushesmay be induced in some women.
Raloxifene is absorbed orally but has lowbioavailability due to extensive first pass glucuro-nidation. The t½ is 28 hours and major routeof excretion is faeces.
Side effects Hot flushes, leg cramps are gene-rally mild; vaginal bleeding is occasional. Theonly serious concern is 3-fold increase in riskof deep vein thrombosis and pulmonary embolism.However, similar risk attends estrogen HRT.
Use Raloxifene is a second line drug forprevention and treatment of osteoporosis inpostmenopausal women; Ca2+ and vit Dsupplements enhance the benefit. According toBritish guidelines, raloxifene is not recommendedfor primary prophylaxis of osteoporotic fracturesin postmenopausal women, but is an alternativeoption for secondary prevention and treatment
of vertebral fractures, i.e. in those who havealready suffered a fracture. It has no use in men.Dose: 60 mg/day;BONMAX, RALOTAB, ESSERM 60 mg tab.
AROMATASE INHIBITORS
Aromatization of ‘A’ ring of testosterone andandrostenedione is the final and key step in theproduction of estrogens (estradiol/estrone) in thebody. In addition to the circulating hormone,locally produced estrogens appear to play animportant role in the development of breast cancer.Though some aromatase inhibitors (AIs) wereproduced in the past, three recent ‘third generation’AIs Letrozole, Anastrozole and Exemestane havedemonstrated clinical superiority and are widelyused now in the treatment of breast cancer.
Properties of AIs are compared with that oftamoxifen in Table 22.1.
Letrozole It is an orally active nonsteroidal(type 2) compound that reversibly inhibitsaromatization all over the body, including thatwithin the breast cancer cells, resulting in nearlytotal estrogen deprivation. Proliferation of estrogendependent breast carcinoma cells is suppressedto a greater extent than with tamoxifen. Letrozoleis rapidly absorbed with 100% oral bioavailability,large volume of distribution, slow metabolism anda t½ of ~40 hours. Randomized clinical trialshave established its utility in:(a) Early breast cancer: Letrozole is a first linedrug for adjuvant therapy after mastectomy inER+ive postmenopausal women. Extendedadjuvant therapy with letrozole beyond thestandard 5 year tamoxifen treatment continues toafford protection, whereas continuation oftamoxifen is not useful. Replacement of tamoxifenby an AI is now recommended after 2 years(sequential therapy). Survival is prolonged inpatients who have positive axillary lymph nodes.(b) Advanced breast cancer: Current guidelinesrecommend letrozole as first line therapy becauseof longer time to disease progression and higherresponse rate obtained with it compared totamoxifen. It is also effective as second linetreatment when tamoxifen has failed.

315C
HA
PTE
R 22
ESTROGENS, PROGESTINS AND CONTRACEPTIVES
TABLE 22.1 Comparative properties of tamoxifen (SERM) and letrozole/anastrozole (AIs)
Tamoxifen Letrozole/Anastrozole
1. Estrogen antagonist in breast and blood vessels, 1. Inhibits production of estrogens in all tissues.but agonist in uterus, bone, liver and pituitary. Nearly total estrogen deprivation.
2. Can be used for breast Ca. in premenopausal 2. Not to be used in premenopausal women.women as well.
3. Less effective in delaying recurrence when 3. More effective in delaying recurrence of early stageused as adjuvant therapy after surgery. breast Ca. (adjuvant therapy)
4. Prophylactic use for breast Ca. recurrence 4. Continues to exert prophylactic effect beyond 5 years.limited to 5 years.
5. Less delay in disease progression and lower 5. Greater delay in disease progression and greatersurvival advantage in advanced/metastatic survival advantage in palliative treatment of advanced/breast Ca. than AIs. metastatic breast Ca.
6. Not effective in failure cases. 6. Effective in tamoxifen failure cases of advancedbreast Ca.
7. Causes endometrial hyperplasia, predisposes to 7. No endometrial hyperplasia/cancer predisposition.endometrial carcinoma
8. No bone losss, no increase in fractures or 8. Accelerates bone loss, predisposes to fractures,arthritic symptoms arthritic symptoms.
9. Increases risk of venous thromboembolism 9. No increase in thromboembolic risk10. Improves lipid profile; small lowering of LDL Ch. 10. No effect on lipid profile.
SERM—Selective estrogen receptor modulate; AIs—aromatase inhibitors; Ca.—Carcinoma; LDL Ch—Low densitylipoprotein cholesterol
Adverse effects Hot flushes, nausea, diarrhoea,dyspepsia and thinning of hair are the side effects.Joint pain is common and bone loss may beaccelerated. However, there is no endometrialhyperplasia or increased risk of endometrialcarcinoma. Risk of venous thromboembolism isalso not increased, and there is no deteriorationof lipid profile.Dose: 2.5 mg OD oral.LETOVAL, LETROZ, FEMARA, ONCOLET 2.5 mg tab.
Though contraindicated in premenopausal women, letrozolewas clandestinely promoted and tested as an ovulationinducing fertility drug. Use of letrozole for inducing ovulationin infertile women has been banned in India since Oct. 2011.
Anastrozole Another nonsteroidal and reversi-ble (Type 2) AI, more potent than letrozole andsuitable for single daily dosing. It accumulatesin the body to produce peak effect after 7–10days. Anastrozole is useful as adjuvant therapyin early ER+ive breast cancer as well as forpalliation of advanced cases in postmenopausalwomen. In early cases, tumor recurrence time wasfound to be longer than with tamoxifen. Risk ofnew tumor appearing in the contralateral breast
was also lower with anastrozole. A longer timeto disease progression compared to tamoxifen hasbeen obtained in advanced ER+ive breast cancer.Many tamoxifen resistant cases responded withincreased survival. Like letrozole, it is also a firstline drug for early as well as advanced breastcarcinoma in postmenopausal women. Side effectsare hot flushes, vaginal dryness, vaginal bleeding,nausea, diarrhoea, thinning of hair. Arthralgia andacceleration of osteoporosis are prominent.However, it does not predispose to endometrialcarcinoma or to venous thromboembolism.Dose: 1 mg OD.ALTRAZ, ARMOTRAZ, ANABREZ 1 mg tab.
Exemestane: This steroidal and irreversible (Type 1)inhibitor of aromatase acts like a suicide substrate by covalentbinding to the enzyme. As a result >90% suppression ofestradiol production is obtained. However, it has weakandrogenic activity similar to androstenedione. Exemestanehas been found beneficial in early breast cancer by reducingthe risk of disease progression when it was substituted fortamoxifen as adjuvant therapy. In advanced breast cancer,longer survival, increased time to disease progression andfewer treatment failures have been obtained with exemestane.It is administered orally and is well tolerated. Adverse effectsare similar to other AIs.

316S
EC
TIO
N5
HORMONES AND RELATED DRUGS
PROGESTINS
These are substances which convert the estrogenprimed proliferative endometrium to secretoryand maintain pregnancy in animals spayed afterconception (Progestin = favouring pregnancy).
At the turn of the last century it becameapparent that ovaries secrete two hormones, andthat corpus luteum was essential for maintenanceof pregnancy. Progesterone was isolated in1929, but its full therapeutic potential has beenexploited only after the 1950s when a large numberof orally active synthetic progestins weredeveloped.
Natural progestin Progesterone, a 21 carbonsteroid, is the natural progestin and is derivedfrom cholesterol (see Fig. 20.1). It is secretedby the corpus luteum (10–20 mg/day) in the laterhalf of menstrual cycle under the influence ofLH. Its production declines a few days beforethe next menstrual flow. If the ovum gets fertilizedand implants—the blastocyst immediately startsproducing chorionic gonadotropin which isabsorbed into maternal circulation and sustainsthe corpus luteum in early pregnancy. Placentastarts secreting lots of estrogens and progesteronefrom 2nd trimester till term. Men produce 1–5 mg progesterone per day from adrenals andtestes; its role if any, in males is not known.
Synthetic progestins A number of syntheticprogestins with high oral activity have beenproduced. These are either progesterone deri-vatives (21 C) or 19-nortestosterone derivatives,also called ‘estranes’ (18 C).
The progesterone derivatives are almost pureprogestins, have weaker antiovulatory action and
are used primarily as adjuvants to estrogens forHRT in postmenopausal women, threatenedabortion, endometriosis, etc. for selective proges-tational effect. The older 19-nortestosteronederivatives developed in the 1950-60s haveadditional weak estrogenic, androgenic, anabolicand potent antiovulatory action: are used primarilyin combined contraceptive pills. Estranes with a13-ethyl substitution are called ‘gonanes’, e.g.norgestrel. Gonanes are more potent (especiallythe levoisomers, e.g. levonorgestrel) and havereduced androgenic activity.
In the 1980-90s a number of other gonanecompounds were introduced, of which desogestrelhas been marketed in India. Desogestrel andnorgestimate are prodrugs. In addition to beingvery potent progestins they have strongantiovulatory action (gestodene inhibits ovulationat as low as 40 µg/day dose), and little or noandrogenic property. Therefore, they do notantagonise the beneficial action of estrogens onlipid profile and are preferable in women withhyperandrogenemia. High antiovulatory potencyallows reduction of ethinylestradiol dose whenthese are combined in oral contraceptives.
The newer 19-norprogesterone derivativenomegestrol has weak antiandrogenic property, isless antiovulatory, but has strong antiestrogeniceffect on endometrium. Adverse effects on lipidprofile and glucose tolerance appear to be lacking.
PROGESTERONE DERIVATIVES
Medroxyprogesterone acetateMegestrol acetateDydrogesteroneHydroxyprogesterone caproate
Newer compoundNomegestrol acetate
19-NORTESTOSTERONE DERIVATIVES
Older compounds Newer compounds
Norethindrone (Gonanes)(Norethisterone) Desogestrel
Lynestrenol Norgestimate(Ethinylestrenol) Gestodene
AllylestrenolLevonorgestrel (Gonane)

317C
HA
PTE
R 22
ESTROGENS, PROGESTINS AND CONTRACEPTIVES
ACTIONS
The main function of progesterone is preparationof the uterus for nidation and maintenance ofpregnancy. The latter is due to prevention ofendometrial shedding, decreased uterine motilityand inhibition of immunological rejection of thefoetus: progesterone depresses T-cell function andcell-mediated immunity (CMI).
1. Uterus Progesterone brings about secretorychanges in the estrogen primed endometrium:hyperemia, tortuocity of glands and increasedsecretion occurs while epithelial proliferation ishalted. It is lack of progestational support whichcauses mucosal shedding during menstruation.
Continued action of progesterone (whenpregnancy occurs) brings about decidual changesin endometrium—stroma enlarges and becomesspongy, glands atrophy, and sensitivity ofmyometrium to oxytocin is decreased.
2. Cervix Progesterone converts the waterycervical secretion induced by estrogens to viscid,scanty and cellular secretion which is hostile tosperm penetration.
3. Vagina Progesterone induces pregnancy likechanges in the vaginal mucosa: leukocyteinfiltration of cornified epithelium occurs.
4. Breast Progesterone causes proliferation ofacini in the mammary glands. Cyclic epithelialproliferation and turnover occurs during lutealphase, but continuous exposure to progesteroneduring pregnancy halts mitotic activity andstabilizes mammary cells. Acting in concert withestrogens, it prepares breast for lactation.Withdrawal of these hormones after deliverycauses release of prolactin from pituitary and milksecretion starts.5. CNS High circulating concentration of pro-gesterone (during pregnancy) appears to have asedative effect. It can also affect mood.6. Body temperature A slight (0.5oC) rise inbody temperature by resetting the hypothalamicthermostat and increasing heat production isinduced. This is responsible for the higher bodytemperature seen during the luteal phase.
7. Respiration Progestins in relatively higherdoses stimulate respiration, as occurs duringpregnancy.8. Metabolism Prolonged use of oral contra-ceptives impairs glucose tolerance in somewomen. This has been ascribed to the progesta-tional component. Progestins, especially those withandrogenic activity (19-nortestosterone deriva-tives) tend to raise LDL and lower HDLcholesterol levels. This may reduce the beneficialeffect of estrogen used concurrently for HRT orin contraceptives. Micronized oral progesteroneformulation (referred to as ‘natural progesterone’)has been shown not to counteract the beneficialeffect of estrogen on LDL and HDL cholesterol.9. Pituitary Progesterone is a weak inhibitorof Gn secretion from pituitary. It exerts negativefeedback primarily at the level of hypothalamicpulse generator—reducing the frequency of GnRHpulses. However, the amount of LH at each pulsemay increase. Administration of progestin duringfollicular phase suppresses the preovulatory LHsurge and prevents ovulation. It synergises withestrogen for this action. The gonanes markedlysuppress GnRH and are potent antiovulatorydrugs.
Mechanism of actionUnlike other steroid receptors, the progesteronereceptor (PR) has a limited distribution in thebody: confined mostly to the female genital tract,breast, CNS and pituitary. The PR is normallypresent in the nucleus of target cells. Analogousto ER, upon hormone binding the PR undergoesdimerization, attaches to progesterone responseelement (PRE) of target genes and regulatestranscription through coactivators. The anti-progestins also bind to PR, but the conformationassumed is different from agonist bound receptorand opposite effects are produced by interactionwith corepressors.
The PR exists in a short (PR-A) and a longer (PR-B)isoforms. The two have differing activities, but because theligand binding domain of both is identical, all agonists andantagonists display similar binding properties for them. Tissueselective modulation of PR has not yet been possible, as has

318S
EC
TIO
N5
HORMONES AND RELATED DRUGS
been in the case of ER. Progesterone also acts on cell membranereceptors in certain tissues and produces rapid effects, likeCa2+ release from spermatozoa and oocyte maturation, but theirphysiological significance is not clear.
Estrogens have been shown to increase PRdensity, whereas progesterone represses ER andenhances local degradation of estradiol.
PHARMACOKINETICS
Progesterone, unless specially formulated, isinactive orally because of high first-pass meta-bolism in liver. It is mostly injected i.m. in oilysolution. Even after an i.m. dose it is rapidlycleared from plasma, has a short t½ (5–7 min).Nearly complete degradation occurs in the liver—major product is pregnanediol which is excretedin urine as glucuronide and sulfate conjugates.However, effects of progesterone last longer thanthe hormone itself.
A micronized formulation of progesteronehas been developed for oral administration.Microfine particles of the drug are suspended inoil and dispensed in gelatin capsules. Absorptionoccurs through lymphatics bypassing liver. Thoughbioavailability is low, effective concentrations areattained in the body.
Most of the synthetic progestins are orallyactive and are metabolized slowly; have plasmat½ ranging from 8–24 hours.
Preparations and dose
1. Progesterone: 10–100 mg i.m. (as oily solution) OD;PROGEST, PROLUTON, GESTONE 50 mg/ml inj., 1 and2 ml amp; 100–400 mg OD oral: NATUROGEST,DURAGEST, OGEST 100, 200, 400 mg caps containingmicronized oily suspension.2. Hydroxyprogesterone caproate: 250–500 mg i.m. at2–14 days intervals; PROLUTON DEPOT, MAINTANE INJ,PROCAPRIN 250 mg/ml in 1 and 2 ml amp.3. Medroxyprogesterone acetate: 5–20 mg OD–BD oral,50–150 mg i.m. at 1–3 month interval; FARLUTAL 2.5,5, 10 mg tab., PROVERA, MEPRATE, MODUS 2.5, 10mg tab, DEPOT-PROVERA 150 mg in 1 ml inj. (as contra-ceptive). Has weak androgenic and antiestrogenic property.4. Dydrogesterone: 5–10 mg OD/TDS oral; DUPHASTON5 mg tab. It has poor antiovulatory action: may be preferredwhen contraceptive effect is not required.5. Norethindrone (Norethisterone): 5–10 mg OD–BD oral;PRIMOLUT-N, STYPTIN, REGESTRONE, NORGEST 5 mgtab; REGESTRONE HRT, NORETA HRT 1 mg tab (for
HRT); NORISTERAT 200 mg/ml inj (as enanthate) forcontraception 1 ml i.m every 2 months; has androgenic, anabolicand antiestrogenic activity.6. Lynestrenol (Ethinylestrenol): 5–10 mg OD oral;ORGAMETRIL 5 mg tab. Has additional androgenic, anabolicand estrogenic activity.7. Allylestrenol: 10–40 mg/day; GESTANIN, FETUGARD,MAINTANE 5 mg tab. Has been especially used for threatened/habitual abortion, PROFAR 25 mg tab.8. Levonorgestrel: 0.1–0.5 mg/day; DUOLUTON-L,OVRAL 0.25 mg+ ethinylestradiol 0.05 mg tab. Hasandrogenic, anabolic and antiestrogenic property.9. Desogestrel 150 µg + ethinylestradiol 30 µg (NOVELON)tab, 1 tab OD 3 week on 1 week off cyclic therapy.(Other preparations are given with oral contraceptives).
ADVERSE EFFECTS
• Breast engorgement, headache, rise in bodytemperature, edema, esophageal reflux, acneand mood swings may occur with higher doses.
• Irregular bleeding or amenorrhoea can occurif a progestin is given continuously.
• The 19-nortestosterone derivatives lowerplasma HDL levels—may promote atheroge-nesis, but progesterone and its derivatives haveno such effect.
• Long-term use of progestin in HRT mayincrease the risk of breast cancer.
• Blood sugar may rise and diabetes may beprecipitated by long-term use of potent agentslike levonorgestrel.
• Intramuscular injection of progesterone ispainful.
• Given in early pregnancy, progestins can causemasculinization of female foetus and othercongenital abnormalities.
Use of a progestin for diagnosis of pregnancyis contraindicated.
USES
1. As contraceptive Most common use (seelater).
2. Hormone replacement therapy (HRT)In nonhysterectomised postmenopausal womenestrogen therapy is supplemented with a progestinfor 10–12 days each month to counteractthe risk of inducing endometrial carcinoma.

319C
HA
PTE
R 22
ESTROGENS, PROGESTINS AND CONTRACEPTIVES
A progesterone derivative lacking androgenicactivity is preferred.
3. Dysfunctional uterine bleeding It is oftenassociated with anovular cycles. Continuedestrogenic action on endometrium (causinghyperplasia) without progesterone induction andwithdrawal resulting in incomplete sloughing leadsto irregular, often profuse bleeding. A progestinin relatively large doses (medroxyprogesteroneacetate/norethindrone 10–20 mg/day or equi-valent) promptly stops bleeding and keeps it inabeyance as long as given. Subsequently cyclictreatment at lower doses regularizes and norma-lizes menstrual flow. A progestin with inherentestrogenic action is preferred; often supplementaldose of estrogen is combined, or a combinationoral contraceptive pill is given cyclically for3–6 months.
4. Endometriosis This condition results frompresence of endometrium at ectopic sites.Manifestations are dysmenorrhoea, painful pelvicswellings and infertility. Continuous administrationof progestin induces an anovulatory, hypo-estrogenic state by suppressing Gn release. Thedirect action on endometrium prevents bleedingin the ectopic sites by suppressing menstruation.Treatment for a few months causes atrophy andregression of the ectopic masses. Therapy canbe withdrawn in many cases after 6 months withoutreactivation. Fertility returns in some patients.Progestin treatment of endometriosis is cheap andgenerally well tolerated, but not all cases respondand recurrences are frequent. Initial progestintherapy is often replaced by cyclic tratment withan estrogen-progestin contraceptive pill given for3–6 months. GnRH agonist and danazol arealternatives used in nonresponsive cases.Aromatase inhibitors are being tried in resistantcases.
5. Premenstrual syndrome/tension Somewomen develop headache, irritability, fluidretention, distention and breast tenderness a fewdays preceding menstruation. When depressionpredominates, it has been labelled ‘premenstrualdysphoric disorder’. Fluoxetine and other SSRIs
given daily on symptom days dampen irritabilityand mood changes in majority of women. If severe,premenstrual syndrome requires suppression ofovulation by combined estrogen-progesteronetreatment given cyclically. Relatively higher doseof progestin is generally used. Progestins areadded to estrogen when it is used for severe dys-menorrhoea.
6. Threatened/habitual abortion In most suchpatients there is no progesterone deficiency;administration of excess hormone is of no benefit.Progestin therapy may be considered in thosepatients who have established deficiency.However, progestins are briskly promoted andalmost routinely prescribed in India. There is somerecent evidence of its efficacy in preventingpremature delivery in high risk pregnancy. If suchuse is made—a pure progestin without estrogenicor androgenic activity should be employed.
7. Endometrial carcinoma Progestins are pal-liative in about 50% cases of advanced/ metastaticendometrial carcinoma. High doses are needed.
ANTIPROGESTIN
Mifepristone It is a 19-norsteroid with potentantiprogestational and significant antigluco-corticoid, antiandrogenic activity.
Given during the follicular phase, its antipro-gestin action results in attenuation of the midcycleGn surge from pituitary → slowing of folliculardevelopment and delay/failure of ovulation. Ifgiven during the luteal phase, it prevents secretorychanges by blocking progesterone action on theendometrium. Later in the cycle, it blocksprogesterone support to the endometrium,unrestrains PG release from it—this stimulatesuterine contractions. Mifepristone also sensitizesthe myometrium to PGs and induces menstruation.If implantation has occurred, it blocksdecidualization, so that conceptus is dislodged,HCG production falls, secondary luteolysisoccurs–endogenous progesterone secretion decrea-ses and cervix is softened. All these effects leadto abortion.

320S
EC
TIO
N5
HORMONES AND RELATED DRUGS
Mifepristone is a partial agonist and com-petitive antagonist at both A and B forms of PR.In the absence of progesterone (during anovulatorycycles or after menopause) it exerts weakprogestational activity—induces predecidualchanges. Therefore, it is now regarded as‘progesterone receptor modulator’ rather than‘pure antagonist.’ The weak agonistic action isnot manifest in the presence of progesterone.
The antiglucocorticoid action of usual dosesis also not manifest in normal individuals becauseblockade of the negative feedback at hypothalamic-pituitary level elicits ACTH release → plasmacortisol rises and overcomes the direct antigluco-corticoid action. Amelioration of Cushing’ssymptoms has been obtained with large doses(see p. 295).
Pharmacokinetics Mifepristone is active orally,but bioavailability is only 25%. It is largelymetabolized in liver by CYP 3A4 and excretedin bile; some enterohepatic circulation occurs; t½20–36 hr.
Interaction with CYP 3A4 inhibitors (erythro-mycin, ketoconazole) and inducers (rifampin,anticonvulsants) has been reported.
Uses
1. Termination of pregnancy of up to 7weeks: 600 mg as single oral dose causes completeabortion in 60–85% cases. To improve the successrate, current recommendation is to follow it up48 hours later by a single 400 mg oral dose ofmisoprostol. This achieves >90% success rate andis the accepted nonsurgical method of early firsttrimester abortion. In place of oral misoprostol,a 1 mg gemeprost pessary can be inserted intra-vaginally. Mifepristone administered within 10days of a missed period results in an apparentlate heavy period (with dislodged blastocyst) inupto 90% cases.
This procedure is generally safe, but prolongedbleeding and failed abortion are the problemsin some cases. Anorexia, nausea, tiredness,abdominal discomfort, uterine cramps, loosemotions are the other side effects.
2. Cervical ripening 24–30 hours beforeattempting surgical abortion or induction of labour,mifepristone 600 mg results in softening of cervix;the procedure is facilitated.
3. Postcoital contraceptive Mifepristone 600mg given within 72 hr of intercourse interfereswith implantation and is a highly effective methodof emergency contraception. The subsequentmenstrual cycle, however, is disturbed.
4. Once-a-month contraceptive A single 200 mg doseof mifepristone given 2 days after midcycle each monthprevents conception on most occasions. Administeringmifepristone in late luteal phase to dislodge the embryo (ifpresent) and to ensure menstruation irrespective of concep-tion, has also been tried. These alternative methods ofcontraception, though attractive, may prolong/disrupt the nextmenstrual cycle, and thus cannot be used continuously. Thereis little experience and little justification to use these methodson regular basis.
5. Induction of labour By blocking the relaxant actionof progesterone on uterus of late pregnancy, mifepristonecan promote labour. It may be tried in cases with intrauterinefoetal death and to deliver abnormal foetuses.
6. Cushing’s syndrome Mifepristone has palliative effectdue to glucocorticoid receptor blocking property. May beused for inoperable cases.Other proposed uses are—in endometriosis, uterine fibroid,certain breast cancers and in meningioma.
MIFEGEST, MIFEPRIN 200 mg tab.T-PILL + MISO: Mifepristone 200 mg (3 tabs) + Misoprostol200 μg (2 tabs); for medical termination of pregnancy ofupto 49 days: take 3 tablets of T-PILL on day 1, followedon day 3 by 2 tablets of MISO.
Ulipristal It is a recently approved ‘selectiveprogesterone receptor modulator’ (SPRM) for useas emergency contraceptive. It inhibits ovulationby suppressing LH surge as well as by directeffect on follicular rupture. In addition, its actionon endometrium can interfere with implantation.In clinical trials the efficacy of ulipristal (30 mg)as emergency contraceptive has been rated equalto that of levonorgestrel (1.5 mg) when takenwithin 72 hours of unprotected intercourse, andto extend for 2 more days. Thus, it may havean advantage, if the woman misses to take thedrug within 3 days.
Headache, nausea, vomiting, abdominal painand menstrual delay are the side effects, as they

321C
HA
PTE
R 22
ESTROGENS, PROGESTINS AND CONTRACEPTIVES
are with levonorgestrel. Few cases of ovariancysts are reported.
The antiglucocorticoid activity of ulipristal isweaker than that of mifepristone.
Onapristone (a pure progesterone antagonist) and Gestinone(more efficacious in endometriosis) are the otherantiprogestins.
HORMONALCONTRACEPTIVES
These are hormonal preparations used forreversible suppression of fertility. Because of ouralarming population trends, antifertility drugs arethe need of the day. In developing countriesparticularly, the mortality rate has declined andbirth rate has increased due to urbanization. Inthe earlier part of 20th century, methods ofcontraception used (condoms, diaphragms, sper-micidal creams, foam tablets, etc.) were intimatelyrelated to sexual intercourse, therefore, despisedby most couples. These also have higher failurerate. Rock and Pincus (1955) announced the suc-cessful use of an oral progestin for contraception,separating fertility control from coitus.
It was soon discovered that addition of a smallquantity of an estrogen enhanced their efficacy;combined pills have become the most popularmethod of contraception, particularly because thehormone content of the pills has been reduced,minimizing the potential harm and affording otherhealth benefits.
FEMALE CONTRACEPTION
Over 100 million women worldwide are currentlyusing hormonal contraceptives. With these drugs,fertility can be suppressed at will, for as longas desired, with almost 100% confidence andcomplete return of fertility on discontinuation.The efficacy, convenience, low cost and overallsafety of oral contraceptives (OCs) has allowedwomen to decide whether and when they wantto become pregnant and to plan their activities.A variety of oral and parenteral preparations arenow available offering individual choices.
TYPES OF METHODSOral1. Combined pill It contains an estrogen anda progestin in fixed dose for all the days of atreatment cycle (monophasic). With accumulatedexperience, it has been possible to reduce theamount of estrogen and progestin in the ‘secondgeneration’ OC pills without compromisingefficacy, but reducing side effects andcomplications. ‘Third generation’pills containingnewer progestins like desogestrel with improvedprofile of action have been introduced in the1990s. Ethinylestradiol 30 µg daily is consideredthreshold but can be reduced to 20 µg/day if aprogestin with potent antiovulatory action isincluded. The progestin is a 19-nortestosteronebecause these have potent antiovulatory action.Used alone the ovulation inhibitory dose (per day)of the currently used progestins is estimated tobe—levonorgestrel 60 µg, desogestrel 60 µg,norgestimate 200 µg, gestodene 40 µg, but theamount in the pill is 2–3 times higher to attain100% certainty. While both estrogens andprogestins synergise to inhibit ovulation, theprogestin ensures prompt bleeding at the end ofa cycle and blocks the risk of developingendometrial carcinoma due to the estrogen. Onetablet is taken daily for 21 days, starting on the5th day of menstruation. The next course is startedafter a gap of 7 days in which bleeding occurs.Thus, a cycle of 28 days is maintained. Calendarpacks of pills are available (Table 22.2). Thisis the most popular and most efficacious method.2. Phased pill Triphasic regimens have beenintroduced to permit reduction in total steroiddose without compromising efficacy by mimickingthe normal hormonal pattern in a menstrual cycle.The estrogen dose is kept constant (or varied slightlybetween 30–40 µg), while the amount of progestinis low in the first phase and progressively higherin the second and third phases.
Phasic pills are particularly recommended forwomen over 35 years of age and for those withno withdrawal bleeding or breakthrough bleedingwhile on monophasic pill, or when other riskfactors are present.

322S
EC
TIO
N5
HORMONES AND RELATED DRUGS
TABLE 22.2 Oral contraceptive preparations
PROGESTIN ESTROGEN TRADE NAME
COMBINED PILLS1. Norgestrel 0.3 mg Ethinylestradiol 30 μg MALA–D (21 tabs + 7
ferrous sulfate 60 mg tabs.)2. Norgestrel 0.5 mg Ethinylestradiol 50 µg OVRAL-G 20 tabs.3. Levonorgestrel 0.25 mg Ethinylestradiol 50 µg OVRAL, DUOLUTON-L 21 tabs.4. Levonorgestrel 0.15 mg Ethinylestradiol 30 µg OVRAL-L, OVIPAUZ 21 tabs.5. Levonorgestrel 0.1 mg Ethinylestradiol 20 µg LOETTE, OVILOW, COMBEE
21 tabs6. Desogestrel 0.15 mg Ethinylestradiol 30 µg NOVELON 21 tabs.7. Desogestrel 0.15 mg Ethinylestradiol 20 µg FEMILON 21 tabs.
PHASED PILL1. Levonorgestrel 50–75 Ethinylestradiol 30–40 TRIQUILAR (6 + 5 + 10
–125 µg –30 µg tablets)2. Norethindrone 0.5–0.75 Ethinylestradiol 35–35 ORTHONOVUM 7/7/7
–1.0 mg –35 µg (7+7+7 tabs)
POSTCOITAL PILL1. Levonorgestrel 0.25 mg Ethinylestradiol 50 µg OVRAL, DUOLUTON-L
(2+2 tabs)2. Levonorgestrel 0.75 mg -Nil- — NORLEVO, ECEE2 (1+1 tab)
1.5 mg -Nil- — iPILL, NOFEAR-72, OH GOD (1 tab)MINI PILLS1. Norethindrone 0.35 mg -Nil- — MICRONOR*, NOR-QD*2. Norgestrel 75 µg -Nil- — OVRETTE*
*Not marketed in India.
3. Progestin-only pill (Minipill) It has beendevised to eliminate the estrogen, because manyof the long-term risks have been ascribed to thiscomponent. A low-dose progestin-only pill is analternative for women in whom an estrogen iscontraindicated. It is taken daily continuouslywithout any gap. The menstrual cycle tends tobecome irregular and ovulation occurs in 20–30%women, but other mechanisms contribute to thecontraceptive action. The efficacy is lower (96–98%) compared to 98–99.9% with combined pill.Pregnancy should be suspected if amenorrhoeaof more than 2 months occurs. This method isless popular.
4. Emergency (postcoital) pill These are foruse in a woman not taking any contraceptive whohad a sexual intercourse risking unwantedpregnancy. The most commonly used and standardregimen is—
• Levonorgestrel 0.75 mg two doses 12 hoursapart, or 1.5 mg single dose taken as soonas possible, but before 72 hours of unprotectedintercourse.
Trials conducted globally by a WHO taskforce on postovulatory methods of fertilitycontrol have found this regimen to be 2–3 timesmore effective and better tolerated than theearlier ‘Yuzpe method’ which used levonor-gestrel 0.5 mg + ethinylestradiol 0.1 mg, twodoses at 12 hour interval within 72 hours ofexposure. Incidence of nausea and vomitingis ~6% in the progestin only regimen comparedto 20–50% with the estrogen+progestinregimen. Headache and other side effects arealso milder. However, the next period may bedelayed or disrupted with either regimen.
Recently (2010) a SPRM ulipristal has beenapproved for emergency contraception.

323C
HA
PTE
R 22
ESTROGENS, PROGESTINS AND CONTRACEPTIVES
• Ulipristal 30 mg single dose as soon aspossible, but within 120 hours of intercourse.
It is an equally effective (failure rate1–3% compared to levonorgestrel 2–4%) andequally well tolerated alternative method nowavailable with an extended window ofprotective action (see p. 320).
Another antiprogestin that has been used,particularly in Europe and China, with highsuccess rate and few side effects is—
• Mifepristone 600 mg single dose taken within72 hours of intercourse.Emergency postcoital contraception should be
reserved for unexpected or accidental exposure(rape, condom rupture) only, because allemergency regimens have higher failure rate andside effects than regular low-dose combined pill.
InjectableThese have been developed to obviate the needfor daily ingestion of pills. They are given i.m.as oily solution; are highly effective; over 50million women have used them so far. Their majorlimitations are:(a) Animal data has indicated carcinogenicpotential, but there is no proof from human studiesdespite >30 years of experience. No increase inoverall risk of cervical, ovarian or hepatic cancerhas been noted by a WHO sponsored study.Breast cancer risk may be slightly increased inyounger women (< 35 yr). The logistics ofadministration and supervision for mass use areconsidered inadequate in developing countriesand use–effectiveness in field conditions is low.In India approval has been granted for use onlyunder close supervision, but not on mass scaleunder the National Programme.(b) Menstrual irregularities, excessive bleeding oramenorrhoea are very common; incidence ofamenorrhoea increases with increasing durationof use. Return of fertility may take 6–30 monthsafter discontinuation; permanent sterility mayoccur in some women. Weight gain and headacheoccur in >5% subjects. Bone mineral density maydecrease after 2–3 years of use (especially withDMPA) due to low estrogen levels caused by
Gn suppression. This may also producemenopause-like symptoms (hot flushes, vaginaldryness, reduced libido).Only the long-acting progestin only injectionsare in use now. They are injected once in2–3 months depending on the steroid and its dose.Two compounds have been marketed:
(a) Depot medroxyprogesterone acetate(DMPA) 150 mg at 3-month intervals. Afteri.m. injection peak blood levels are reachedin 3 weeks and decline with a t½ of ~ 50 days.DEPOT-PROVERA 150 mg in 1 ml vial for deep i.m.injection during first 5 days of menstrual cycle. Repeatevery 3 months.
(b) Norethindrone (Norethisterone) enanthate(NEE) 200 mg at 2-month intervals.NORISTERAT 200 mg in 1 ml vial for deep i.m.injection during first 5 days of menstrual cycle. Repeatevery 2 months.
The most important drawback is completedisruption of menstrual bleeding pattern or totalamenorrhoea (more common with DMPA). It isnot suitable for adolescent girls and lactatingmothers. Use of DMPA is generally restricted towomen who are unlikely to use other contra-ceptives effectively. NEE is shorter acting andfailure rates have been higher than with DMPA.All fixed dose combination injectable preparations of syntheticestrogens and progestins are not allowed in India anddiscontinued in most countries.
Implants These are drug delivery systems implanted underthe skin, from which the steroid is released slowly over aperiod of 1–5 years. They consist of either—(a) Biodegradable polymeric matrices—do not need to beremoved on expiry.(b) Non-biodegradable rubber membranes—have to beremoved on expiry.NORPLANT: A set of 6 capsules each containing 36 mglevonorgestrel (total 216 mg) for subcutaneous implantationis available in some countries, but has been discontinuedin the USA. Works for up to 5 years.
A progesterone impregnated intrauterine insert(PROGESTASERT) has been introduced in some countries.It contains 52 mg of levonorgestrel which primarily actslocally on endometrium. The device remians effectivefor 5 years, but efficacy is rated lower.
MECHANISM OF ACTION
Hormonal contraceptives interfere with fertilityin many ways; the relative importance depends

324S
EC
TIO
N5
HORMONES AND RELATED DRUGS
on the type of method. This is summarized inTable 22.3.1. Inhibition of Gn release from pituitary byreinforcement of normal feedback inhibition. Theprogestin reduces frequency of LH secretorypulses (an optimum pulse frequency is requiredfor tiggering ovulation) while the estrogenprimarily reduces FSH secretion. Both synergiseto inhibit midcycle LH surge. When the combi-ned pill is taken both FSH and LH are reducedand the midcycle surge is abolished. As a result,follicles fail to develop and fail to rupture—ovulation does not occur.
The minipill and progestin only injectable regi-men also attenuate LH surge but less consis-tently—ovulation may occur irregularly in ~ 1/3cycles. Postcoital pill when taken before ovulationcan dampen LH surge and inhibit ovulation insome cases. However, pregnancy is still preventedby direct actions on the genital tract.2. Thick cervical mucus secretion hostile tosperm penetration is evoked by progestin action.As such, this mechanism can operate with allmethods except postcoital pill.3. Even if ovulation and fertilization occur, theblastocyst may fail to implant because endomet-rium is either hyperproliferative or hypersecre-tory or atrophic and in any case out of phase
with fertilization—not suitable for nidation. Thisaction appears to be the most important in caseof minipills and postcoital pill.4. Uterine and tubal contractions may bemodified to disfavour fertilization. This actionis uncertain but probably contributes to theefficacy of minipills and postcoital pill.5. The postcoital pill may dislodge a justimplanted blastocyst or may interfere withfertilization/implantation.
Practical considerations1. Discontinuation of all OCs results in full returnof fertility within 1–2 months. There may evenbe a rebound increase in fertility—chances ofmultiple pregnancy are more if conception occurswithin 2–3 cycles. With injectable preparations,return of fertility is delayed. The cycles takeseveral months to normalize or may not do soat all. They are to be used only if the risk ofpermanent infertility is acceptable.2. If a woman on combined pills misses to takea tablet, she should be advised to take two tabletsthe next day and continue as usual. If more than2 tablets are missed, then the course should beinterrupted, an alternative method of contracep-tion used and next course started on the 5th dayof bleeding.
TABLE 22.3 Effects of different forms of hormonal contraception
Oral pills Injections
Combined Minipill Postcoital ProgestinE + P only P only P only
1. FSH inhibition ++ – – +
2. LH inhibition +++ + + +++
3. Antiovulatory effect +++ + +,– ++
4. Hostile cervical mucus +++ +++ – +++
5. Endometrium Hyper- Out of Unfavourable Atrophicsecretory phase
6. Failure rate 0.1–0.3 2–3 2–4% < 0.5(pregnancy/100 women years)
7. Contraceptive efficacy ++++ +++ ++ ++++
E—Estrogen; P—Progestin

325C
HA
PTE
R 22
ESTROGENS, PROGESTINS AND CONTRACEPTIVES
3. If pregnancy occurs during use of hormonalcontraceptives—it should be terminated bysuction-aspiration, because the risk of malforma-tions, genital carcinoma in female offspring andundescended testes in male offspring is increased.4. While for most women a pill containing30 µg ethinylestradiol is sufficient, the obese mayrequire a pill containing 50 µg, and only 20 µgmay be appropriate/sufficient for those withcardiovascular risk factor, as well as for thoseabove 40 yr age.5. If breakthrough bleeding occurs—switchover to a pill containing higher estrogen dose.6. In women with contraindications for estrogen(see below), a progestin only contraceptive maybe used.
ADVERSE EFFECTS
Since contraceptives are used in otherwise healthyand young women, adverse effects, especiallylong-term consequences assume great significance.The adverse effects are dose dependent; most ofthe past data with high-dose preparations cannotbe directly extrapolated to the present-day low-dose preparations which carry relatively minorrisk. The following applies primarily to combinedoral pill which has been most extensively used.
A. Nonserious side effects These arefrequent, especially in the first 1–3 cycles, andthen disappear gradually.1. Nausea and vomiting: similar to morningsickness of pregnancy.2. Headache is generally mild; migraine may beprecipitated or worsened.3. Breakthrough bleeding or spotting: especiallywith progestin only preparations. Rarely bleedingfails to occur during the gap period. Prolongedamenorrhoea or cycle disruption occurs in fewwomen taking injectables or minipill.4. Breast discomfort.
B. Side effects that appear later1. Weight gain, acne and increased body hairmay be noted due to androgenic action of older19-nortestosterone progestins. The newer ones likedesogestrel are relatively free of this effect.
2. Chloasma: pigmentation of cheeks, nose andforehead, similar to that occurring in pregnancy.3. Pruritus vulvae is infrequent.4. Carbohydrate intolerance and precipitation ofdiabetes in few subjects taking high dosepreparations; but this is unlikely with the presentpills. Many large studies have found no linkbetween OC use and development of diabetes.5. Mood swings, abdominal distention areoccasional; especially reported with progesteroneonly contraceptives.
C. Serious complications1. Leg vein thrombosis and pulmonaryembolism: The older preparations increased theincidence of venous thromboembolism, but thisis found to be only marginal with the newerreduced steroid content pills. Those who developsuch complication, generally do it in the 1st yearof use. However, even low-dose pills posesignificant risk in women >35 years of age,diabetics, hypertensives and in those who smoke.The excess risk normalizes shortly after stoppingthe OC.2. Coronary and cerebral thrombosis resultingin myocardial infarction or stroke: A 2 to 6-foldincrease in risk was estimated earlier, but recentstudies have found no increased incidence withthe low dose pills in the absence of other riskfactors.
The estrogen component of OC has beenmainly held responsible for venous thromboembo-lism, while both estrogen and progestin have beenblamed for the arterial phenomena. Themechanisms involved may be:• Increase in blood clotting factors (coagulabi-
lity is enhanced).• Decreased antithrombin III.• Decreased plasminogen activator in endo-
thelium.• Increased platelet aggregation.3. Rise in BP: occurred in 5–10% women takingthe earlier pills. This again is less frequent andsmaller in magnitude with the low-dose pills oftoday. If the BP rises, best is to stop OCs—BPnormalizes in the next 3–6 months. Boththe estrogen and progestin components are

326S
EC
TIO
N5
HORMONES AND RELATED DRUGS
responsible for this effect, probably by increasingplasma angiotensinogen level and renin activitywhich induces salt and water retention.4. Estrogen tends to raise plasma HDL/LDL ratio(beneficial), but the progestin nullifies this benefit.Lipid profile is not significantly altered by lowdose OCs, except that triglyceride level may risemarginally which poses no excess risk.5. Genital carcinoma: an increased incidence ofvaginal, cervical, and breast cancers was fearedon the basis of animal data, but extensiveepidemiological data over the past 30 years hasrepeatedly shown that oral as well as injectedcontraceptives do not increase the occurrence ofthese cancers in the general population. However,risk is increased in predisposed individuals.Growth of already existing hormone dependenttumour may be hastened.
Epidemiological data has recorded minorincrease in breast cancer incidence among currentOC users, but not among past users. Since breastcancer is rare in young women, this finding isconsidered inconsequential.
A protective effect against endometrial carci-noma has been shown for the progestincomponent. Prolonged suppression of gonado-tropic stimulation of ovary may account for thelower incidence of ovarian malignancy noted incontraceptive users.6. Benign hepatomas: which may rupture or turnmalignant; incidence of this rare tumour appearsto be slightly higher in OC users.7. Gallstones: Estrogens increase biliary choles-terol excretion; incidence of gallstones is slightlyhigher in women who are taking OCs, or afterlong-term use.
ContraindicationsThe combined oral contraceptive pill is absolu-tely contraindicated in:1. Thromboembolic, coronary and cerebrovas-cular disease or a history of it.2. Moderate-to-severe hypertension; hyperlipi-daemia.3. Active liver disease, hepatoma or h/o jaun-dice during past pregnancy.
4. Suspected/overt malignancy of genitals/breast.5. Prophyria.6. Impending major surgery—to avoid excessrisk of postoperative thromboembolism.
Relative contraindications (requiring avoidance/cautious use under supervision)
1. Diabetes: control may be vitiated.2. Obesity3. Smoking4. Undiagnosed vaginal bleeding5. Uterine leiomyoma: may enlarge with estro-
genic preparations; progestin only pills canbe used.
6. Mentally ill7. Age above 35 years8. Mild hypertension9. Migraine
10. Gallbladder disease
Interactions Contraceptive failure may occurif the following drugs are used concurrently:(a) Enzyme inducers: phenytoin, phenobarbitone,primidone, carbamazepine, rifampin, ritonavir.Metabolism of estrogenic as well as progestationalcomponent is increased.(b) Suppression of intestinal microflora: tetracyc-lines, ampicillin, etc. Deconjugation of estrogensexcreted in bile fails to occur → their entero-hepatic circulation is interrupted → blood levelsfall.
With both types of interacting drugs, it is wiseto switch over to a preparation containing 50 µgof ethinylestradiol or to use alternative methodof contraception. Rifampin is usually taken fora long time and is such a potent enzyme inducerthat alternative contraception should be advised.
Other health benefits Apart from benefitsdue to prevention of unwanted pregnancy andthe risks during delivery, use of oralcontraceptives affords certain other beneficialeffects as a bonus:• Lower risk of developing endometrial and
ovarian carcinoma; probably colorectal canceras well.

327C
HA
PTE
R 22
ESTROGENS, PROGESTINS AND CONTRACEPTIVES
• Reduced menstrual blood loss and associatedanaemia; cycles if irregular become regular;premenstrual tension, dysmenorrhoea andmenorrhagia are ameliorated.
• Endometriosis and pelvic inflammatory diseaseare improved.
• Reduced incidence as well as symptomatic reliefof fibrocystic breast disease and ovarian cysts.
Ormeloxifene (Centchroman) It is a non-steroidal SERM developed at CDRI India as anoral contraceptive. It has predominant estrogenantagonistic action in uterus and breast with littleaction on vaginal epithelium and cervical mucus.Endometrial proliferation is suppressed by downregulation of endometrial ER. Contraceptive actionis probably due to utero-embyonic asynchronyand failure of implantation. Pituitary, ovarian andother endocrine functions remain practicallyunaffected. Menstrual cycle is not disrupted, butin some women it may be lengthened irregularly.Excessive bleeding attending anovulatory cycles(that generally occurs near menopause) isdiminished; ormeloxifene is approved for use indysfunctional uterine bleeding.
The plasma t½ of ormeloxifene is long(~1 week). It prevents conception as long as takenwith return of fertility few months after stoppage.Failure rate is considered acceptable, but it hasfailed to gain popularity for widespread use. Sideeffects are nausea, headache, fluid retention,weight gain, rise in BP and prolongation ofmenstrual cycles.Dose: For contraception—30 mg twice a week for 12 weeksfollowed by once a week.For dysfunctional uterine bleeding—60 mg twice a weekfor 12 weeks, then once a week for 12 weeks.CENTRON 30 mg tab, SAHELI 60 mg tab.
MALE CONTRACEPTIVEThe only way to suppress male fertility by drugsis to inhibit spermatogenesis. Though consider-able effort has been made in this direction andeffective drugs have been found, no satisfactory/acceptable solution is yet tangible. Reasons are—
1. Complete suppression of spermatogenesis isrelatively difficult without affecting other tissues:millions of spermatozoa are released at eachejaculation vs a single ovum per month in women.
2. Spermatogenesis takes 64 days. A drug whicheven completely inhibited spermatogenesis willtake a long latent period to produce infertility.Accordingly, return of fertility will be slow.
3. Gonadotropin suppression inhibits testos-terone secretion as well, resulting in loss of libidoand impotence: unacceptable to all men and tomost spouses.
4. Risk of adverse effects.
5. Most importantly—men don’t get pregnant:few would be ready to bear the contingency ofregular medication so that their sexual partnersdo not become pregnant.
Drugs and approaches tried are—
1. Antiandrogens Depress spermatogenesis, but raiseGns; cause unacceptable loss of libido.
2. Estrogens and progestins Act by suppressing Gns—cause unacceptable feminization.
3. Androgens They inhibit Gns but have poor efficacy.Even combination with progestin is not reliable.
4. Superactive Gn RH analogues They inhibit Gn releaseby continuous action; inhibit testosterone secretion as well;produce impotence, loss of libido.
5. Cytotoxic drugs Cadmium, nitrofurans and indolessuppress spermatogenesis, but are toxic.
6. Gossypol It is a nonsteroidal compound, obtained fromcotton seed; has been studied in China. It is effective orally—causes suppression of spermatogenesis and reduces spermmotility—infertility develops after a couple of months. Fertilityis restored several months after discontinuation. However,about 10% men remain oligozoospermic. During treatmentserum LH and testosterone levels do not change: libido andpotency are not affected. The mechanism of action isuncertain; probably involves direct toxicity on seminiferousepithelium.
Most important adverse effect is hypokalaemia (due to renalloss of K+) with its attendant muscular weakness (evenparalysis). Other side effects are—edema, diarrhoea,breathlessness and neuritis.

328S
EC
TIO
N5
HORMONES AND RELATED DRUGS
PROBLEM DIRECTED STUDY
22.1 A 55-year-old postmenopausal woman developed a cancerous lump in the left breast forwhich radical mastectomy was performed. The tumour was ER positive and only one of the excisedaxillary lymph nodes had metastasis. She was put on adjuvant therapy with tamoxifen 20 mgper day. On her checkup visit one year later, she was found to be asymptomatic with no signof local recurrence or lymph node enlargement, but ultrasound examination of the uterus revealedthickening of endometrium.(a) What could be the cause and implication of the increase in endometrial thickness?(b) Should the same adjuvant therapy continue, or should it be stopped altogether, or be replacedby another drug? Give reasons.
22.2 A 28-year-old mother with a 9 month baby wants to space out her next child and consultsyou for taking oral contraceptive.(a) What questions will you ask, what physical examination will you perform and what investigationswill you order before advising her whether she should take oral contraceptive or not, as wellas for selecting the contraceptive preparation most suitable for her?(see Appendix-1 for solutions)

Oxytocin and Other DrugsActing on Uterus
ChapterChapterChapterChapterChapter 2323232323
Drugs acting on uterus can primarily affect theendometrium or the myometrium. The mostimportant drugs affecting endometrium areestrogens, progestins and their antagonists.Myometrium receives both sympathetic andparasympathetic innervation: autonomic drugs canaffect its motility. However, directly acting drugsare more important and have more selective action.The responsiveness of myometrium to drugs ismarkedly affected by the hormonal and gestationalstatus.
UTERINE STIMULANTS(Oxytocics, Abortifacients)
These drugs increase uterine motility, especiallyat term.1. Posterior pituitary hormone Oxytocin,
Desamino oxytocin2. Ergot alkaloids Ergometrine (Ergonovine),
Methylergometrine3. Prostaglandins PGE2, PGF2α, 15-methyl
PGF2α, Misoprostol4. Miscellaneous Ethacridine, Quinine.
OXYTOCIN
Oxytocin is a nonapeptide secreted by the posteriorpituitary along with vasopressin (ADH). Pituitaryextract was first used in labour in 1909.Controversy as to whether the antidiuretic anduterine stimulating activities were due to onesubstance or two separate substances was finallyresolved by du Vigneaud in 1953 when heseparated Oxytocin and Vasopressin, determinedtheir chemical structure and synthesized them.Both are nonapeptides which differ at positions3 and 8.
Both oxytocin and ADH are synthesized withinthe nerve cell bodies in supraoptic and paraven-
tricular nuclei of hypothalamus; are transporteddown the axon and stored in the nerve endingswithin the neurohypophysis. They are stored inseparate neurones as complexes with their specificbinding proteins (neurophysins) to form granules.Both are released by stimuli appropriate foroxytocin, i.e. coitus, parturition, suckling; or forADH, i.e. hypertonic saline infusion, water depri-vation, haemorrhage, etc., or nonspecific, i.e. painand apprehension. However, the proportion ofoxytocin to ADH can vary depending upon thenature of the stimulus.
ACTIONS
1. Uterus Oxytocin increases the force andfrequency of uterine contractions. With low doses,full relaxation occurs inbetween contractions;basal tone increases only with high doses.Increased contractility is due to hightened elec-trical activity of the myometrial cell membrane—burst discharges are initiated and accentuated.Estrogens sensitize the uterus to oxytocin; increaseoxytocin receptors. Nonpregnant uterus and thatduring early pregnancy is rather resistant tooxytocin; sensitivity increases progressively in thethird trimester; there is a sharp increase near termand quick fall during puerperium. Progestinsdecrease the sensitivity, but this effect is notmarked in vivo.
At term the increased contractility is restrictedto the fundus and body; lower segment is notcontracted; may even be relaxed.
Mechanism of action Action of oxytocin onmyometrium is independent of innervation. Thereare specific G-protein coupled oxytocin receptorswhich mediate the response mainly by depo-larization of muscle fibres and influx of Ca2+ ions

330S
EC
TIO
N5
HORMONES AND RELATED DRUGS
as well as through phosphoinositide hydrolysisand IP3 mediated intracellular release of Ca2+ ions.The number of oxytocin receptors increasesmarkedly during later part of pregnancy. Oxytocinincreases PG synthesis and release by theendometrium which may contribute to thecontractile response. Distinct subtypes of oxytocinreceptors have been shown on the myometriumand the endometrium.
2. Breast Oxytocin contracts the myoepi-thelium of mammary alveoli and forces milk intothe bigger milk sinusoids—‘milk ejection reflex’(milk letdown in cattle) is initiated by sucklingso that it may be easily sucked by the infant.Oxytocin has been used in milch cattle to facilitatemilking.
3. CVS Conventional doses used in obstetricshave no effect on BP, but higher doses causevasodilatation → brief fall in BP, reflextachycardia and flushing. This action is mostmarked in chicken and is used for bioassay ofoxytocin. The umbilical vessels are markedlyconstricted; oxytocin may help in their closureat birth.
4. Kidney Oxytocin in high doses exertsADH-like action—urine output is decreased:pulmonary edema can occur if large amounts ofi.v. fluids and oxytocin are infused together.Conventional doses are without any effect.
Physiological role1. Labour Oxytocin is released during labourand the uterus is highly sensitive to it at thistime. However, it does not appear to be obligatoryfor initiating parturition—delivery occurs evenin hypophysectomized animals and humans,though labour may be prolonged in its absence.A facilitatory role is more plausible. PGs andPAF are complementary to oxytocin.
2. Milk ejection reflex Suckling inducesoxytocin release from pituitary which contractsthe myoepithelial cells. These cells in breast aremore sensitive than myometrium to oxytocin. Milk
ejection reflex is absent in the hypophysectomizedanimal.
3. Neurotransmission Oxytocin appears tofunction as a peptide neurotransmitter ofoxytocinergic neurones in the hypothalamus andbrainstem to regulate autonomic outflow.
PHARMACOKINETICS
Being a peptide, oxytocin is inactive orally andis generally administered by i.m. or i.v. routes,rarely by intranasal spray. It is rapidly degradedin liver and kidney; plasma t½ 6–12 min, andis still shortened at term. Pregnant uterus andplacenta elaborate a specific aminopeptidasecalled oxytocinase—which can be detected inmaternal plasma.
Unitage and preparations 1 IU of oxytocin = 2 µgof pure hormone. Commercially available oxytocin is producedsynthetically.OXYTOCIN, SYNTOCINON 2 IU/2 ml and 5 IU/ml inj.,PITOCIN 5 IU/0.5 ml inj.
USE
1. Induction of labour Labour needs to beinduced in case of postmaturity or prematurelyin toxaemia of pregnancy, diabetic mother, erythro-blastosis, ruptured membranes or placentalinsufficiency. For this purpose oxytocin is givenby slow i.v. infusion: 5 IU is diluted in 500 mlof glucose or saline solution (10 milli IU/ml)—infusion is started at a low rate and progressivelyaccelerated according to response (0.2–2.0 ml/min). Before starting infusion, confirm that:• presentation is correct• foetal lungs are adequately mature• there is no cephalopelvic disproportion• no placenta previa• no foetal distress and• no uterine scar (due to previous surgery).Uterine contractions are then closely monitored:the drug is discontinued when they are strongenough. Usually a total of 2–4 IU is needed.
2. Uterine inertia When uterine contrac-tions are feeble and labour is not progressing

331C
HA
PTE
R 23
OXYTOCIN AND OTHER DRUGS ACTING ON UTERUS
satisfactorily—oxytocin can be infused i.v. (asdescribed above) to augment contractions. Itshould not be used to hasten normally progressinglabour. Before deciding to use an oxytocic forstrengthening uterine contractions, all theconditions as setout above (for induction of labour)must be fulfilled. Too strong contraction can becatestrophic: use should only be made in selectedcases and by experienced people.
Oxytocin is the drug of choice and is preferredover ergometrine/PGs for the above two purposes:(a) Because of its short t½ and slow i.v. infusion,intensity of action can be controlled and actioncan be quickly terminated.(b) Low concentrations allow normal relaxationinbetween contractions—foetal oxygenation doesnot suffer.(c) Lower segment is not contracted: foetaldescent is not compromised.(d) Uterine contractions are consistentlyaugmented.3. Postpartum haemorrhage, Caesareansection Oxytocin 5 IU may be injected i.m.or by i.v. infusion for an immediate response,especially in hypertensive women in whomergometrine is contraindicated. It acts by forcefullycontracting the uterine muscle which compressesthe blood vessels passing through its mesh workto arrest haemorrhage from the inner surfaceexposed by placental separation.4. Breast engorgement It may occur due toinefficient milk ejection reflex. Oxytocin is effec-tive only in such cases; an intranasal spray maybe given few minutes before suckling. It doesnot increase milk production.5. Oxytocin challenge test It is performed to determineuteroplacental adequacy in high risk pregnancies. Oxytocinis infused i.v. at very low concentrations till uterinecontractions are elicited every 3–4 mins. A marked increasein foetal heart rate indicates uteroplacental inadequacy. Thetest is risky and is rarely performed.
Adverse effects(i) Injudicious use of oxytocin during labour canproduce too strong uterine contractions forcing
the presenting part through incompletely dilatedbirth canal, causing maternal and foetal soft tissueinjury, rupture of uterus, foetal asphyxia and death.(ii) Water intoxication: This occurs due to ADHlike action of large doses given along with i.v.fluids, especially in toxaemia of pregnancy andrenal insufficiency. It is a serious (may be fatal)complication.Desamino-oxytocin It has been developed as a buccalformulation; action is similar to injected oxytocin, but lessconsistent. Its indications are:Induction of labour: 50 IU buccal tablet repeated every 30min, max 10 tabs.Uterine inertia: 25 IU every 30 min.Promotion of uterine involution 25–50 IU 5 times daily for7 days.Breast engorgement 25–50 IU just before breast feeding.BUCTOCIN 50 IU tab
Carbetocin It is a long-acting analogue of oxytocin thathas been introduced recently for prevention of uterine atonyafter caesarean section and to control PPH.
ERGOMETRINE, METHYLERGOMETRINE
The pharmacology of ergot alkaloids is describedin Ch. 12. Only the amine ergot alkaloid ergo-metrine (ergonovine) and its derivative methyl-ergometrine are used in obstetrics. Both havesimilar pharmacological property.1. Uterus They increase force, frequency andduration of uterine contractions. At low doses,contractions are phasic with normal relaxation inbetween, but only moderate increase in dose raisesthe basal tone, contracture occurs with high doses.Gravid uterus is more sensitive, especially at termand in early puerperium. Their stimulant actioninvolves the lower segment also. The uterotonicaction is believed to result from partial agonisticaction on 5-HT2 and α adrenergic receptors.2. CVS Ergometrine and methylergometrineare much weaker vasoconstrictors than ergotamineand have low propensity to cause endothelialdamage. Though they can raise BP, this is notsignificant at doses used in obstetrics.3. CNS No overt effects occur at usual doses.However, high doses produce complex actions—partial agonistic/antagonistic interaction with

332S
EC
TIO
N5
HORMONES AND RELATED DRUGS
adrenergic, serotonergic and dopaminergic recep-tors in the brain have been shown.
4. GIT High doses can increase peristalsis.
Methylergometrine is 1½ times more potent thanergometrine on the uterus, but other actions areless marked. It has thus replaced ergometrine atmany obstetric units.
Pharmacokinetics In contrast to the amino acidergot alkaloids, ergometrine and methylergomet-rine are rapidly and nearly completely absorbedfrom the oral route. The onset of uterine actionis: Oral—15 min; i.m.—5 min; i.v.—almost imme-diate.
They are partly metabolized in liver andexcreted in urine. Plasma t½ is 1–2 hours.Effects of a single dose last 3–4 hours.
Adverse effects Ergometrine and methylergo-metrine are less toxic than ergotamine. Whencorrectly used in obstetrics—hardly any compli-cations arise. Nausea, vomiting and rise in BPoccur occasionally. They can decrease milksecretion if higher doses are used for many dayspostpartum; this is due to inhibition of prolactinrelease (dopaminergic action).Ergometrine should be avoided in—(i) patients with vascular disease, hypertension,toxaemia.(ii) presence of sepsis—may cause gangrene.(iii) liver and kidney disease.They are contraindicated during pregnancy andbefore 3rd stage of labour.
Use1. The primary indication for ergometrine/methylergometrine is to control and preventpostpartum haemorrhage (PPH): 0.2–0.3 mg i.m.at delivery of anterior shoulder reduces bloodloss attending delivery and prevents PPH.However, routine use in all cases is not justified—only in those expected to bleed more, e.g. grandmultipara, uterine inertia. Multiple pregnancyshould be excluded before injecting.
If PPH is occurring—0.5 mg i.v. is recom-mended. A combination of 0.5 mg ergometrine
with oxytocin 5 IU i.m./i.v. may be used in severebleeding.These drugs produce sustained tonic uterinecontraction: perforating uterine arteries arecompressed by the myometrial meshwork—bleeding stops.2. After caesarean section/instrumental delivery—to prevent uterine atony.3. To ensure normal involution: A firm and activeuterus involutes rapidly. To ensure this: 0.125mg of ergometrine or methylergometrine has beengiven TDS orally for 7 days. However, routineuse in all cases is not justified because normalinvolution is not hastened. Multipara and othersin whom slow involution is apprehended, thesedrugs may be given prophylactically.4. Diagnosis of variant angina: A small dose of ergometrineinjected i.v. during coronary angiography causes promptconstriction of reactive segments of coronary artery that areresponsible for variant angina.ERGOMETRINE 0.25, 0.5 mg tab, 0.5 mg/ml inj.Methylergometrine: METHERGIN, METHERONE,ERGOMET 0.125 mg tab, 0.2 mg/ml inj.
PROSTAGLANDINS
PGE2, PGF2α and 15-methyl PGF2α are potentuterine stimulants, especially in the later part ofpregnancy and cause ripening of cervix. Theiractions and use in obstetrics is described inCh. 13. Since misoprostol (a PG analogue usedfor peptic ulcer) produces less side effects, it isbeing used for obstetric indications as well.
Ethacridine Available as 50 mg/50 ml solution(EMCREDIL, VECREDIL) for extra-amniotic infusion:150 ml (containing 150 mg) is injected slowly for medicaltermination of pregnancy in the 2nd trimester. This is analternative method used occasionally.
UTERINE RELAXANTS(Tocolytics)
These are drugs which decrease uterine motility.They have been used to delay or postpone labour,arrest threatened abortion and in dysmenorrhoea.Prevention of premature labour in those at higherrisk due to past history has been attempted byadministration of high dose progesterone in the

333C
HA
PTE
R 23
OXYTOCIN AND OTHER DRUGS ACTING ON UTERUS
later half of pregnancy, with some success.Suppression of premature labour may be neededto allow the foetus to mature, to allow time forinitiating glucocorticoid therapy for foetal lungmaturation or to transfer the mother in labour toa centre with proper facilities. However, no clearlysatisfactory drug is available since none of themhas been shown to improve foetal outcome. Anattempt to delay premature labour is likely tosucceed only if cervical dilatation is < 4 cm and‘taking up’ of lower segment is minimal. Measuresto delay labour should not be undertaken ifmembranes have ruptured, antepartumhaemorrhage is occurring, in severe toxaemia ofpregnancy, intrauterine infection or foetal death.
1. Adrenergic agonists (see Ch. 9)Ritodrine, the β2 selective agonist having moreprominent uterine relaxant action is approved tosuppress premature labour and to delay deliveryin case of some exigency or acute foetal distress.For dependable action it is started as 50 µg/mini.v. infusion, the rate is increased every 10 mintill uterine contractions cease or maternal HR risesto 120/min. Contractions are kept suppressed bycontinuing i.v. infusion or by 10 mg i.m. 4–6hourly followed by 10 mg oral 4–6 hourly.However, treatment beyond 48 hours is notrecommended, since risk to mother increases andbenefit is uncertain. Delivery can be postponed inabout 70% cases by few hours to few weeks.However, cardiovascular (hypotension, tachycar-dia, arrhythmia, pulmonary edema) and metabolic(hyperglycaemia, hyperinsulinaemia, hypo-kalaemia) complications and anxiety, restlessness,headache occur frequently. Use of ritodrine toarrest labour has been found to increase maternalmorbidity. Foetal pulmonary edema can develop;volume of i.v. infusion should be kept to aminimum to avoid fluid overload. The neonatemay develop hypoglycaemia and ileus. It shouldnot be used if mother is diabetic, having heartdisease, or receiving β blockers or steroids.Ritodrine has been discontinued in the USA, but is stillavailable in UK and India.
YUTOPAR, RITROD 10 mg/ml inj (5 ml amp), 10 mg tab.RITODINE 10 mg tab, 10 mg in 1 ml inj.
Salbutamol and terbutaline can be used asalternatives to ritodrine. Isoxsuprine oral/i.m. hasbeen used to stop threatened abortion, but efficacyis uncertain.
2. Calcium channel blockers Becauseinflux of Ca2+ ions plays an important role inuterine contractions, Ca2+ channel blockers (seeCh. 39) reduce the tone of myometrium andoppose contractions. These drugs, especiallynifedipine, which has prominent smooth musclerelaxant action, can postpone labour if used earlyenough. Efficacy comparable to β2 adrenergicagonists has been demonstrated and side effectsare fewer. Oral nifedipine 10 mg repeated onceor twice after 20–30 min, followed by 10 mg6 hourly has been used. Tachycardia andhypotension are prominent at doses whichsuppress uterine contractions. Reduced placentalperfusion causing foetal hypoxia is apprehended.However, fewer babies delivered after nifedipineneeded intensive care.
3. Oxytocin antagonist Atosiban is a peptide analogueof oxytocin that acts as antagonist at the oxytocin receptors.In clinical trials, it has been found to suppress prematureuterine contractions and postpone preterm delivery with fewercardiovascular and metabolic complications than β2 adrenergicagonists. In Europe and UK it is available for inhibitionof labour between 24–33 weeks of gestation, and may offerbetter benefit: risk ratio than other tocolytics. However, itis not yet approved in USA and India.
4. Magnesium sulfate Infused i.v. it is a first line drugfor prevention and treatment of seizures in preeclampsia andeclampsia. It also acts as a tocolytic by competing with Ca2+
ions for entry into myometrium through both voltage sensitiveas well as ligand gated Ca2+ channels. However, its use todelay premature labour is risky, may increase perinatalmortality and is not recommended now.5. Miscellaneous drugs Ethyl alcohol, nitrates, proges-terone, general anaesthetics and indomethacin (PG synthesisinhibitors) are the other drugs, which can depress uterinecontractions. However, their effect is not dependable andthey are not used clinically as tocolytics.
Halothane is an efficacious uterine relaxant that has beenused as the anaesthetic when external or internal version isattempted.

334S
EC
TIO
N5
HORMONES AND RELATED DRUGS
PROBLEM DIRECTED STUDY
23.1 A full term primigravida aged 26 years is brought to the hospital with the complaint ofhaving labour pains for the past 24 hours without making much progress. Two hours ago shehad passed meconium stained liquor. The lady is in distress, mildly dehydrated and looks exhausted.The presentation is vertex and head is engaged, but cervix is incompletely dilated and uterinecontractions are relatively weak. Foetal tachycardia is noted with irregularity during contractions.(a) What course of action is appropriate?(b) Can she be administered a uterine stimulant to strengthen the contractions? If yes, whichdrug should be given and how? If no, then why?(see Appendix-1 for solution)

Drugs Affecting Calcium BalanceChapterChapterChapterChapterChapter 2424242424
CALCIUM
After C, O, H and N, calcium is the most abun-dant body constituent, making up about 2% ofbody weight, or 1–1.5 kg in an adult. Over 99%of this is stored in bones, the rest being distributedin plasma and all tissues and cells. Calcium servesimportant physiological roles.
Physiological roles1. Calcium controls excitability of nerves andmuscles and regulates permeability of cell mem-branes. It also maintains integrity of cellmembranes and regulates cell adhesion.2. Ca2+ ions are essential for excitation-contrac-tion coupling in all types of muscle and excitation-secretion coupling in exocrine and endocrineglands, release of transmitters from nerve endingand other release reactions.3. Ca2+ is an intracellular messenger forhormones, autacoids and transmitters.4. Ca2+ controles impulse generation in heart;determines level of automaticity and A-Vconduction.5. Ca2+ is essential for coagulation of blood.6. Calcium serves structural function in boneand teeth.
Plasma calcium level It is precisely regulatedby 3 hormones almost exclusively devoted to thisfunction, viz. parathormone (PTH), calcitonin andcalcitriol (active form of vit D). These regulatorscontrol its intestinal absorption, exchange withbone and renal excretion as summarized in Fig.24.1. In addition, several other hormones, meta-bolites and drugs influence calcium homeostasis(see box).
Normal plasma calcium is 9–11 mg/dl. Of thisabout 40% is bound to plasma proteins—chiefly
Influences affecting bone turnover
↑ Resorption ↓ Resorption
Corticosteroids Androgens/EstrogensParathormone CalcitoninThyroxine (excess) Growth hormoneHypervitaminosis D BisphosphonatesProstaglandin E2 FluorideInterleukin 1 & 6 Gallium nitrateAlcoholism MithramycinLoop diuretics Thiazide diuretics
to albumin; 10% is complexed with citrate, phos-phate and carbonate in an undissociable form;the remaining (about 50%) is ionized and physio-logically important. For example, in hypoalbu-minemia, total plasma calcium may be low butthe concentration of Ca2+ ion is usually normal.Acidosis favours and alkalosis disfavours ioniza-tion of calcium. As such, hyperventilation (byraising plasma pH) precipitates tetany andlaryngospasm in calcium deficiency by reducingionization.Calcium turnover Major fraction of calcium in the boneis stored as crystalline hydroxyapatite deposited on the organicbone matrix osteoid, while a small labile pool is in dynamicequilibrium with plasma. Even the fully laid down partsof the bone undergo constant remodeling by way of twoclosely coupled but directionally opposite processes ofresorption and new bone formation (Fig. 24.2). Millions oftiny remodeling units are working on the surface of bonetrabeculae and Haversian canals to dig micropits byosteoclastic activity and then repair by osteoblastic activityin which first collagen and other proteins (osteoid) aredeposited followed by mineralization; the full cycle taking4–6 months. Diet, exercise, several hormones and drugsregulate the number and efficiency of bone remodeling unitsat any given time. Remodeling deficits accumulate over life-time to account for age related bone loss, the pace of whichcan be retarded or accelerated by modulating the above listedinfluences. Estrogen lack after menopause mainly causes lossof trabecular bone, particularly affecting vertebrae, wrist bonesand femoral neck. Minimal trauma/compression fractures aremost common at these sites.

336S
EC
TIO
N5
HORMONES AND RELATED DRUGS
Fig. 24.1: Regulation of plasma level of calcium.————→ stimulation, - - - - - - → Inhibition; Bold arrow indicates—major action.
PTH—Parathormone; 25-OHD3—Calcifediol; 1,25 (OH)2D3—Calcitriol.
Absorption and excretion Calcium is absor-bed by facilitated diffusion from the entire smallintestine as well as from duodenum by a carrier-mediated active transport under the influenceof vit D. Phytates, phosphates, oxalates andtetracyclines complex with Ca2+ in an insolubleform in the intestines and interfere with itsabsorption. Glucocorticoids and phenytoin alsoreduce calcium absorption.
Ionized calcium is totally filtered at the glome-rulus and most of it is reabsorbed in the tubules.Vit D and PTH increase, while calcitonin decreasestubular reabsorption of Ca2+. About 300 mg ofendogenous calcium is excreted daily: half in urineand half in faeces. To maintain calcium balance,the same amount has to be absorbed in the smallintestine from the diet. Because normally only 1/3rdof ingested calcium is absorbed, the dietaryallowance for calcium is 0.8–1.5 g per day. However,fractional calcium absorption is greater in presenceof calcium deficiency and low dietary calcium.
Thiazide diuretics impede calcium excretionby facilitating tubular reabsorption.
Preparations1. Calcium carbonate (40% Ca): It is an insoluble, tastelessand nonirritating salt. Reacts with gastric HCl to form chloride,and can be used as antacid. It is the most common saltpresent in calcium supplements, but gastric acid is requiredfor converting it into the absorbable form. Calcium availabilityfrom it is poor in patients taking proton pump inhibitors(PPIs), H2 blockers, and in elderly.2. Calcium citrate (as tetrahydrate, 21% Ca2+): Slightlysoluble in water, but dissolves well in presence of HCl. Itis nonirritating and is used in supplements; absorption inpatients taking PPIs/H2 blockers and elderly is satisfactory.3. Calcium gluconate (9% Ca): is available as 0.5 g and1 g tablets and 10% injection (5 ml amp.). It is nonirritatingto g.i.t. and the vascular endothelium. A sense of warmthis produced on i.v. injection: extravasation should be guarded.It is the preferred injectable salt.4. Calcium lactate: (13% Ca) is given orally, nonirritatingand well tolerated.5. Calcium dibasic phosphate (23% Ca): is insoluble,reacts with HCl to form soluble chloride in the stomach.It is bland; used orally as antacid and to supplement calcium.Availability of calcium from it is reduced by PPIs and H2
blockers.6. Calcium chloride (27% Ca): It is freely soluble in water,but highly irritating to gastric mucosa and tissues; thereforenot used.
Side effects Calcium supplements areusually well tolerated; only g.i. side effects like

337C
HA
PTE
R 24
DRUGS AFFECTING CALCIUM BALANCE
constipation, bloating and excess gas (especiallywith cal. carbonate) have been reported.Some combined formulationsCALCINOL-RB: Cal. carb 0.375 g, Cal. Phos 75 mg + vitD3 250 IU tab.MILICAL: Cal. citrate 1 g + vit D3 200 IU tab.CALCIBONE: Cal. citrate 1 g + vit D3 200 IU tab and susp.CALSHINE: Cal. citrate 0.5 g + vit D3 500 IU tab.CALCIUM-SANDOZ: Cal. gluco-bionate 137.5 mg/ml inj.10 ml amp., also tabs containing cal. carbonate 650 mg.KALZANA: Cal. dibasic phos 430 mg + Vit C and D3 200IU tab, also syrup: Cal. gluconate 300 mg, Cal. lactobionate1.1 g, Cal. phos. 75 mg per 5 ml, containing Vit A, C,niacinamide and D3 200 IU.OSTOCALCIUM: Cal. phos 380 mg + Vit D3 400 IU tab,also syrup: Cal. phos 240 mg per 5 ml containing Vit D3200 IU and B12.SHELCAL: Cal. carb. 625 mg (eq 250 mg elemental cal),Vit D3 125 IU tab and per 5 ml syr.MACALVIT: Cal. carb. 1.25 g, cholecalciferol 250 IU tab;Cal. gluconate 1.18 g, Cal. lactobionate 260 mg + Vit D3
100 IU per 5 ml syr.CALCIMAX: Cal. carb. (150 mg cal), dibasic cal. phos.(23.3 mg cal) with magnesium, zinc and vit D3 200 IUtab.; also syrup cal. carb. (150 mg cal) with magnesium,zinc and vit D3 200 IU per 5 ml syrup.
Use1. Tetany For immediate treatment of severecases 10–20 ml of Cal. gluconate (elementalcalcium 90–180 mg) is injected i.v. over 10 min,followed by slow i.v. infusion. A total of 0.45-0.9 g calcium (50 to 100 ml of cal. gluconatesolution) over 6 hours is needed for completelyreversing the muscle spasms. Supportive treatmentwith i.v. fluids and oxygen inhalation may berequired. Long-term oral treatment to provide 1–1.5 g of calcium daily is instituted along withvit. D. Milder cases need oral therapy only.2. As dietary supplement especially in growingchildren, pregnant, lactating and menopausalwomen. The dietary allowance recommended byNational Institute of Health (1994) is—• Children 1–10 yr : 0.8–1.2 g• Young adult 11–24 yr, pregnant
and lactating women : 1.2–1.5 g• Men 25–65 yr, women 25–50 yr
and 51–65 yr if taking HRT : 1.0 g• Women 51–65 yr not taking HRT,
every one > 65 yr : 1.5 gCalcium supplement can reduce bone loss in
predisposed women as well as men. It is often
given to fracture patients, but if diet is adequatethis does not accelerate healing.3. Osteoporosis In the prevention and treat-ment of osteoporosis with alendronate/HRT/raloxifene, it is important to ensure that calciumdeficiency does not occur. Calcium + vit D3 haveadjuvant role to these drugs in prevention andtreatment of osteoporosis.
However, the efficacy of calcium ± vit Dsupplements alone in increasing bone mass orpreventing fractures among menopausal women/elderly men is controversial. It does not appear toreduce fracture risk in otherwise healthy subjectstaking adequate diet. In the recently concluded7 year prospective WHI study involving >36000postmenopausal women (51–79 years), the overallrisk of fractures was the same in the calcium(1 g/day) + vit D (400 IU/day) group as in theplacebo group, though the bone mineral densityat the hip was 1% higher in the treated group.Certain subgroups of osteoporotic subjects maybenefit from calcium supplements, but the benefitappears to be marginal and limited to corticalbone loss only. On the other hand, a metaanalysishas shown that subjects receiving calciumsupplements had a 27% higher incidence of MI.Thus, calcium supplements should be given onlyto subjects taking diet low in calcium.4. Empirically, Cal. gluconate i.v. has been usedin dermatoses, paresthesias, weakness and othervague complaints. Any benefit is probably psy-chological due to warmth and other subjectiveeffects produced by the injection.5. As antacid (see Ch. 46).
PARATHYROID HORMONE(Parathormone)
Vassale and Generali (1900) were the first to perform selectiveparathyroidectomy (without removing thyroids) and foundthat it produced tetany and death. MacCallum and Voegtlinin 1909 established this to be due to decrease in plasmacalcium levels; parathormone (PTH) was isolated in 1925.
PTH is a single chain 84 amino acid poly-peptide, MW 9500. It is synthesized as prepro-PTH, the excess amino acids are split off in twosteps and it is then stored in intracellular vesicles.Secretion of PTH is regulated by plasma Ca2+

338S
EC
TIO
N5
HORMONES AND RELATED DRUGS
concentration through a calcium-sensing receptor(CaSR), that is a G-protein coupled receptor onthe surface of parathyroid cells. There is no trophichormone for it. Fall in plasma Ca2+ induces PTHrelease and rise inhibits secretion by decreasingcAMP in the parathyroid cells. Agents that increasecAMP cause PTH release, but direct activationof protein kinase C by fall in Ca2+ concentrationis more important physiologically. Prolongedhypocalcaemia causes hypertrophy andhyperplasia of parathyroids, while sustainedhypercalcaemia has the opposite effect. Changesin phosphate concentration in plasma affect PTHsecretion indirectly by altering Ca2+ concentration.The active form of vit. D calcitriol inhibitsexpression of PTH gene in parathyroid cellsreducing PTH production. PTH is rapidlydegraded in liver and kidney; its plasma t½ is2–5 min.
Actions
PTH increases plasma calcium levels by:
1. Bone PTH promptly increases resorption ofcalcium from bone. This is the most prominentaction of PTH—exerted by increasing the numberof bone remodeling units and activating osteo-clasts when high concentrations are presentcontinuously. Since bone resorption is followedby new bone deposition, this is also promotedby PTH: increased bone formation occurs whenPTH is given intermittently and in low doses.
2. Kidney PTH increases calcium reabsorptionin the distal tubule and provides moment tomoment regulation of calcium excretion. It alsopromotes phosphate excretion which tends tosupplement the hypercalcaemic effect. However,grossly increased plasma calcium level occurringin hyperparathyroidism overrides the direct actionon tubules and calcium excretion in urine isactually increased. The converse occurs inhypoparathyroidism.
3. Intestines PTH has no direct effect oncalcium absorption but increases it indirectly byenhancing the formation of calcitriol (active form
of vit D) in the kidney by activating 1α-hydroxylase. Calcitriol then promotes intestinalabsorption of calcium.
4. PTH decreases calcium levels in milk, salivaand ocular lens. This may be responsible fordevelopment of cataract in hypoparathyroidism.
Mechanism of action The PTH receptor isa G protein coupled receptor which on activationincreases cAMP formation and intracellular Ca2+
in target cells. In bone, the target cell is the osteo-blast because PTH receptors are not expressedon the surface of osteoclasts. Acting on theosteoblast, PTH induces a factor ‘Receptor foractivation of nuclear factor-κB-ligand’ (RANKL)which diffuses and combines with RANK onosteoclast precursors and transforms them intoosteoclasts as well as activates osteoclasts (Fig.24.2). In addition, birth rate of bone remodelingunits into which osteoclasts are recruited isenhanced. Formation of the remodeling pit isfollowed by osteoblastic deposition of new boneinto it. PTH enhances proliferation anddifferentiation of preosteoblasts and depositionof osteoid as well. Bone resorption predominateswhen high concentrations of PTH are presentcontinuously, but intermittent exposure to lowconcentrations has the opposite effect.
Hypoparathyroidism Manifestations are:Low plasma calcium levels, tetany, convulsions, laryngospasm,paresthesias, cataract and psychiatric changes. Pseudohypo-parathyroidism occurs due to reduced sensitivity of targetcells to PTH caused by a mutant G protein that couplesPTH receptor activation to cAMP generation in target cells.Hyperparathyroidism It is mostly due to parathyroidtumour. It produces—Hypercalcaemia, decalcification of bone—deformities andfractures (osteitis fibrosa generalisata), metastatic calcification,renal stones, muscle weakness, constipation and anorexia.
Treatment is surgical removal of the parathyroid tumour.When this is not possible—low calcium, high phosphate dietwith plenty of fluids is advised.
Cinacalcet It activates the Ca2+ sensing receptor (CaSR) inthe parathyroids and blocks PTH secretion. It is indicated insecondary hyperparathyroidism due to renal disease and inparathyroid tumour.
Use PTH is not used in hypoparathyroidism because plasmacalcium can be elevated and kept in the normal range more

339C
HA
PTE
R 24
DRUGS AFFECTING CALCIUM BALANCE
Fig. 24.2: Hormonal regulation of bone remodeling unitThe monocyte osteoclast precursor cells in the marrow near the bony surface are activated to proliferate and fuse toform multinucleated osteoclasts. The osteoclast-precursors express a ‘receptor for activation of nuclear factor-κ B’(RANK) on their surface. The osteoblasts on activation release a protein RANK-ligand (RANKL). When RANKL isbound to RANK on the surface of osteoclast-precursors they are transformed into mature osteoclasts and developbone lysing ruffled surface. A bone resorption pit is dug out by secretion of acid and proteolytic acid hydrolases.
Osteoblasts produce another protein osteoprotegerin (OPG) as well, which can bind RANKL and prevent it fromcombining with RANK to activate osteoclasts. Thus, osteoblasts by producing RANKL and OPG regulate boneresorption.
After formation of the remodeling pit, preosteoblasts from bone marrow stem cells proliferate, migrate to the baseof the pit, transform into mature osteoblasts and laydown new osteoid, which is later mineralized.
Parathormone (PTH) acts on PTH-receptor located on the osteoblast membrane and induces RANKL production—indirectly activating osteoclast differentiation and function. Subsequently PTH promotes new bone formation as well.
Calcitriol also induces RANKL in osteoblasts to indirectly activate osteoclasts. Similarly, it promotes laying ofosteoid as well as bone mineralization.
Calcitonin directly inhibits osteoclast function and probably enhances osteoblastic new bone formation.
conveniently by vit D therapy. PTH has to be givenparenterally, while vit D can be given orally. Vit D is cheap.However, recombinant human PTH (1–84 amino acid) hasbeen produced and is being clinically evaluated for use inhypoparathyroidism.
Teriparatide This recombinant preparation of 1–34 residuesof amino terminal of human PTH has been recently introducedfor the treatment of severe osteoporosis. It duplicates allthe actions of long (1–84) PTH. Injected s.c. 20 μg oncedaily, it acts only for 2–3 hours, and has been found toincrease bone mineral density in osteoporotic women. Theeffect was faster and more marked than that produced byestrogens and bisphosphonates (BPNs). Teriparatide is theonly agent which stimulates bone formation, whereas theother two only check bone resorption. In clinical trials itwas found to be equally or more effective than estrogensand BPNs in reducing risk of vertebral as well as non-vertebralfractures in osteoporotic women as well as men. After s.c.injection its plasma t½ is 1 hr; given once daily only
intermittent action is produced and the bone forming actionpredominates over bone resorbing action. High cost and needfor daily s.c. injections are the limitations. Its use may bejustified in severely osteoporotic women, those who havealready suffered osteoporotic fractures or have multiple riskfactors for fracture. Treatment beyond 2 years is notrecommended. Side effects include dizziness and legcramps. Pagets disease and hypercalcaemia are the contraindi-cations.
Diagnostic use To differentiate pseudo from true hypopara-thyroidism: teriparatide is given i.v.: if plasma calcium levelfails to rise, then it is pseudohypoparathyroidism.
CALCITONIN
Calcitonin is the hypocalcaemic hormone dis-covered by Copp in 1962. It is a 32 amino acidsingle chain polypeptide (MW 3600) produced

340S
EC
TIO
N5
HORMONES AND RELATED DRUGS
by parafollicular ‘C’ cells of thyroid gland.Parathyroids, thymus and cells of medullarycarcinoma of thyroid also contain calcitonin.
Synthesis and secretion of calcitonin is regu-lated by plasma Ca2+ concentration itself: rise inplasma Ca2+ increases, while fall in plasma Ca2+
decreases calcitonin release. However, circulatinglevel of calcitonin is low and its physiologicalrole in regulating plasma Ca2+ appears to be minor.The plasma t½ of calcitonin is 10 min, but itsaction lasts for several hours.
Actions
The actions of calcitonin are generally oppositeto that of PTH. It inhibits bone resorption bydirect action on osteoclasts—decreasing theirruffled surface which forms contact with theresorptive pit. Whether it also promotes calciumdeposition by osteoblasts is not certain. Thehypocalcaemic action of calcitonin lasts ~8 hours.
Calcitonin inhibits proximal tubularreabsorption of calcium and phosphate by directaction on the kidney. However, hypocalcaemiaoverrides the direct action by decreasing the totalcalcium filtered at the glomerulus—urinary Ca2+
is actually reduced.The actions of calcitonin are mediated through
a G-protein coupled calcitonin receptor (CTR)and increase in cAMP formation, but its targetcells are different from that of PTH.Preparation and unitage Synthetic salmon calcitoninis used clinically, because it is more potent and longer actingdue to slower metabolism. Human calcitonin has also beenproduced.1 IU = 4 µg of the standard preparation.CALSYNAR, ZYCALCIT: Synthetic salmon calcitonin 100IU/ml amp. for i.m. or s.c. injection.Nausea, flushing and tingling of fingers is frequent aftercalcitonin injection. Bad taste, flu-like symptoms, allergicreactions and joint pain are the other adverse effects.
Uses1. Hypercalcaemic states Hyperparathyroidism, hyper-vitaminosis D, osteolytic bony metastasis and hypercalcaemiaof malignancy; 4–8 IU/kg i.m. 6–12 hourly only for 2 days.It acts rapidly within 4 hours, the response peaks at 48 hoursand then refractoriness develops. It also relieves bone pain.
For emergency treatment of hypercalcaemia 5–10IU/kg may be diluted in 500 ml saline and infused i.v. over6 hours. Calcitonin is a relatively weak hypocalcaemic drug.
Therefore, used only to supplement BPNs initially, becauseBPNs take 24–48 hours to act.2. Postmenopausal osteoporosis Though i.m. or s.c.calcitonin can be used, a nasal spray formulation delivering200 IU per actuation is employed. MIACALCIN NASALSPRAY, OSTOSPRAY 2200 IU metered dose vial,CALCINASE 200 IU per actuation nasal spray. One sprayin alternate nostril daily has been shown to increase bonemineral density in menopausal women and to reduce vertebral,but not nonvertebral, fractures. It is less effective than BPNs/HRT. Calcitonin is indicated only when other drugs cannotbe given and in women who are menopausal for at least5 years with definite evidence of osteoporosis. Though nauseaand flushing are less with nasal spray, rhinitis, epistaxis,nasal ulceration and headache are produced frequently.
3. Paget’s disease 100 IU i.m./s.c. daily or on alternatedays produces improvement for few months. Later, resistanceusually develops due to production of antibodies.Bisphosphonates are preferred; calcitonin may be used asadjuvant or 2nd line drug.
4. Diagnosis of medullary carcinoma of thyroid Detectionof high blood level of calcitonin is diagnostic of this tumour,which arises from the calcitonin producing parafollicular cellsof thyroid.
VITAMIN D
Vitamin D is the collective name given toantirachitic substances synthesized in the bodyand found in foods activated by UV radiation.D3 : cholecalciferol — synthesized in the skin
under the influence of UV rays.D2 : calciferol—present in irradiated food—
yeasts, fungi, bread, milk.D1 : mixture of antirachitic substances found in
food—only of historic interest.In 1919 it was established that rickets was due to deficiencyof a dietary factor as well as lack of exposure to sunlight.McCollum (1922) showed that this fat soluble dietary factorwas different from vit A and its structure was determinedin 1935. The interrelation between calciferol andcholecalciferol and their activation in the body has beenfully understood only in the 1970s.
Activation of vit D It takes place in thefollowing manner—Ergosterol differs from 7-dehydrocholesterol inhaving an extra double bond between C22–23and a methyl group at C24. In man vit D2 andD3 are equally active and calcitriol (active formof D3) is more important physiologically; 25-OHD3 is released in blood from the liver and binds

341C
HA
PTE
R 24
DRUGS AFFECTING CALCIUM BALANCE
7-DEHYDROCHOLESTEROL ERGOSTEROL(Synthesized in skin) (yeast, bread, milk)
UV Light
CHOLECALCIFEROL (Vit D3) CALCIFEROL (Vit D2)
Liver microsomes
CALCIFEDIOL (25-OH-D3) 25-OH-D2
Kidney mitochondria
CALCITRIOL (1,25 (OH)2D3) 1,25 (OH)2D2
ACTIVE FORMS
loosely to a specific vit D binding globulin. Thefinal 1α-hydroxylation in kidney is rate limitingand is controlled by many factors. This step isactivated or induced by calcium/vit D deficiencyas well as by PTH, estrogens and prolactin, whilecalcitriol inhibits it in a feedback manner.
Thus, vit D should be considered a hormonebecause:(a) It is synthesized in the body (skin); underideal conditions it is not required in the diet.(b) It is transported by blood, activated and thenacts on specific receptors in the target tissues.(c) Feedback regulation of vit D activationoccurs by plasma Ca2+ level and by the activeform of vit D itself.
Actions
1. Calcitriol enhances absorption of calcium andphosphate from intestine. This is brought aboutby increasing the synthesis of calcium channelsand a carrier protein for Ca2+ called ‘calciumbinding protein’ (Ca BP) or Calbindin. The actionof calcitriol is analogous to that of steroidhormones. It binds to a cytoplasmic vitamin Dreceptor (VDR) → translocate to the nucleus →increase synthesis of specific mRNA → regulationof protein synthesis. Another line of evidencesuggests that activation of VDR promotesendocytotic capture of calcium, its transportacross the duodenal mucosal cell and finally itsactive extrusion through the serosal membrane.At least part of vit D action is quick (withinminutes) and, therefore, appears to be exerted
by mechanisms not involving gene regulation.2. Calcitriol enhances resorption of calcium andphosphate from bone by promoting recruitmentand differentiation of osteoclast precursors in thebone remodeling units, but mature osteoclasts lackVDR. Like PTH, calcitriol induces RANKL inosteoblasts which may then activate theosteoclasts. Osteoblastic cells express VDR andrespond to calcitriol by laying down osteoid, butit mainly appears to help bone mineralizationindirectly by maintaining normal plasma calciumand phosphate concentration. Its action is indepen-dent of but facilitated by PTH.3. Calcitriol enhances tubular reabsorption ofcalcium and phosphate in the kidney, but theaction is less marked than that of PTH. However,in hypervitaminosis D, influence of hypercal-caemia overrides the direct action and morecalcium is excreted in urine.4. Other actions Actions of calcitriol on immu-nological cells, lymphokine production, prolifera-tion and differentiation of epidermal and certainmalignant cells, neuronal and skeletal musclefunction have also been demonstrated.
Vit D deficiency Plasma calcium and phos-phate tend to fall due to inadequate intestinalabsorption. As a consequence, PTH is secreted→ calcium is mobilized from bone in order torestore plasma Ca2+. The bone fails to mineralizenormally in the newly laid area, becomes soft→ rickets in children and osteomalacia in adults.However, in contrast to osteoporosis, the organicmatrix (osteoid) is normal in these conditions.

342S
EC
TIO
N5
HORMONES AND RELATED DRUGS
Hypervitaminosis D It may occur due to chronic ingestionof large doses (~50,000 IU/day) or due to increased sensi-tivity of tissues to vit D. Manifestations are due to elevatedplasma calcium and its ectopic deposition. These are:hypercalcaemia, weakness, fatigue, vomiting, diarrhoea,sluggishness, polyuria, albuminuria, ectopic Ca2+ deposition(in soft tissues, blood vessels, parenchymal organs), renalstones or nephrocalcinosis, hypertension, growth retardationin children. Even coma has been reported.Treatment: consists of withholding the vitamin, low calciumdiet, plenty of fluids and corticosteroids. Recovery may beincomplete in many cases.
Pharmacokinetics
Vit D is well absorbed from the intestines in thepresence of bile salts, mainly through lymphatics.Absorption of the D3 form is somewhat betterthan that of D2. Malabsorption and steatorrhoeainterfere with its absorption.
In the circulation, it is bound to a specificα globulin and is stored in the body, mostly inadipose tissues, for many months. It is hydroxy-lated in the liver to active and inactive metabolites.The t½ of different forms varies from 1–18 days:25-OHD3, having the longest t½ , constitutes theprimary circulating form. Calcitriol is clearedrapidly.Metabolites of vit D are excreted mainly in bile.
Unitage and preparations1 µg of cholecalciferol = 40 IU of vit D.The daily requirement varies, depending on exposure tosunlight. It is estimated that if no vit D3 is synthesizedin the body, a dietary allowance of 400 IU/day will preventdeficiency symptoms. However, higher amounts (upto 1000IU/day) are also recommended. The forms in which vit Dis supplied are—1. Calciferol (Ergocalciferol, vit D2) As solution in oil,filled in gelatin capsules 25,000 and 50,000 IU caps.2. Cholecalciferol (vit D3) As granules for oral ingestionand oily solution for i.m. injection.ARACHITOL 300,000 IU (7.5 mg) and 600,000 IU (15 mg)per ml inj.CALCIROL, CALCIBEST SACHET 60,000 IU in 1 ggranules—suspended in milk/water and taken at 3–4 weeksintervals, and then every 2–6 months.3. Calcitriol 0.25–1 µg orally daily or on alternate days;CALTROL, ROLSICAL, ROCALTROL 0.25 µg cap. CALCI-BEST 1 μg in 1 ml aqueous inj; 0.5–1 μg i.v. on alternatedays.Hypercalcaemia is the main adverse effect; must be watchedfor and therapy promptly stopped if plasma Ca2+ rises.
4. Alfacalcidol It is 1 α-OHD3—a prodrug that is rapidlyhydroxylated in the liver to 1,25 (OH)2 D3 or calcitriol.Therefore, it does not require hydroxylation at position 1 whichis the limiting step in the generation of active form of vit D,and which takes place in the kidney. As such, it is effectivein renal bone disease, vit D dependent rickets, vit D resistantrickets, hypoparathyroidism, etc. i.e. indications for whichcalcitriol is needed. It is also being used in osteoporosis.
Alfacalcidol is orally active and clinically equally effectiveon long term basis to calcitriol. Its metabolic activation in liverdoes not pose a problem even in severe liver disease.Dose: 1–2 µg/day, children < 20 kg 0.5 µg/day. Repeatedserum calcium measurements are essential for regulation ofmaintenance dose. Hypercalcaemia should be watched forand therapy promptly interrupted for few days when itdevelops.ONE ALPHA, ALPHA D3, ALPHADOL 0.25 and 1 µg caps,ALFACAL 0.25, 0.5 µg caps.5. Dihydrotachysterol A synthetic analogue of vit D2 thatis much less active in antirachitic tests, but directly mobilizescalcium from bone after 25-hydroxylation in liver, and doesnot require PTH dependent activation in the kidney. It isparticularly useful in hypoparathyroidism and renal bonedisease.Dose: 0.25–0.5 mg/day.Combination preparations of vit D are listed on p. 337 and inTable 67.2.
Use
1. Prophylaxis (400 IU/day) and treatment(3000–4000 IU/day) of nutritional vit Ddeficiency This is given to prevent and treatrickets in children and osteomalacia in adults.Alternatively 300,000–600,000 IU can be givenorally or i.m. once in 2–6 months. Prophylactictreatment may be given in obstructive jaundice,steatorrhoea and other conditions whichpredispose to vit D deficiency.
2. Metabolic rickets These are a group ofconditions in which tissues do not respond tonormal doses of vit D.(a) Vit D resistant rickets: X-linked hereditarydisease in which vit D metabolism is normal butcalcium and phosphate metabolism is deranged.Administration of phosphate with high dose ofcalcitriol or alfacalcidol is beneficial.(b) Vit D dependent rickets: Another geneticdisorder due to deficiency of renal hydroxylatingmechanism which converts 25-OHD3 into calci-triol. Administration of calcitriol or alfacalcidolis effective in normal doses.

343C
HA
PTE
R 24
DRUGS AFFECTING CALCIUM BALANCE
(c) Renal rickets: Conversion of 25-OHD3 intocalcitriol does not occur due to chronic renaldisease. Calcitriol/alfacalcidol or dihydrotachys-terol are needed in usual doses.
3. Senile or postmenopausal osteoporosisAge-related decrease in calcium absorption fromgut has been noted. Vit D3 + calcium have beenshown to improve calcium balance in osteoporoticfemales and elderly males. However, benefit interms of improved bone mass or reduced fracturerisk is controversial or marginal (see p. 337). Butthis does not apply to active therapy with calcitriol/alfacalcidol for patients with established osteo-porosis, treated with BPNs, etc. because calcitriolsuppresses parathyroids and reduces boneremodeling. Vit D deficiency results in secondaryhyperparathyroidism which contributes toosteoporosis. Calcitriol therapy carries the riskof hypercalcaemia, calcium stones and metastaticcalcification which should be watched for.
4. Hypoparathyroidism Dihydrotachysterol orcalcitriol/alfacalcidol are more effective than vit,D2 or D3, because they act quickly and directlywithout requiring hydroxylation in kidney whichneeds PTH. Alternatively, conventionalpreparations of vit D3 may be given in high doses(25000-100,000 IU/day).
5. Fanconi syndrome Vit D can raise thelowered phosphate levels that occur in thiscondition.
6. A nonhypercalcaemic analogue of vit DCalcipotriol (DAIVONEX 0.005% oint) is usedlocally in plaque type psoriasis, and has yieldedgood results (see Ch. 64). Systemically it hasbeen tried in skin cancer and immunologicaldisorders.
Interactions1. Cholestyramine and chronic use of liquidparaffine can reduce vit D absorption.2. Phenytoin and phenobarbitone reduce theresponsiveness of target tissues to calcitriol; theirprolonged use (for epilepsy) can cause rickets/osteomalacia. It was believed earlier that these
drugs enhance degradation of vit D. However,now it has been shown that plasma level ofcalcitriol is normal, but its effect on intestine andbone is diminished.
BISPHOSPHONATES
Bisphosphonates (BPNs) are analogues of pyro-phosphate: carbon atom replacing oxygen inthe P-O-P skeleton. They inhibit bone resorptionand have recently attracted considerable attentionbecause of their ability to prevent osteoporosisin addition to their usefulness in metabolic bonediseases and hypercalcaemia. They are the mosteffective antiresorptive drugs. Chronologically andaccording to potency, the BPNs can be groupedinto 3 generations (see box). The first generationcompounds have simpler side chains, are the leastpotent and seldom used now. The second andthird generation compounds have an amino ornitrogenous ring substitution in the side chain,are more potent, have higher efficacy and additionalmode of action.
O OH OHO || | || OH
P — C — PNaO | ONa
CH2 — CH2 — NH2
O R1 OHO || | || OH
P — C — PNaO | ONa
R2
Bisphosphonate
Pamidronate
Bisphosphonate Relative potency
First generation BPNs
Etidronate 1*Tiludronate 10Second generation BPNsPamidronate 100Alendronate 100–500*Ibandronate 500–1000Third generation BPNsRisedronate 1000Zoledronate 5000
* Not marketed in India

344S
EC
TIO
N5
HORMONES AND RELATED DRUGS
The mechanism of action of BPNs is not fullyunderstood, but two facets of action have beendelineated:(a) BPNs have strong affinity for calciumphosphate and have selective action in calcifiedtissue. The two main components of bone areprotein matrix and the solid mineral phase(hydroxyapatite). On the surface of resorptive pitsthe mineral phase is solubilized in the clear acidiczone created at the ruffled border of osteoclasts,followed by resorption of protein matrix in thisarea by acid hydrolases secreted from osteoclasts.BPNs localise in the acidic zone under theosteoclasts due to their high affinity for Ca2+ ions.When Ca2+ ions are released from the bone surfacedue to high acidity, the BPNs are also releasedand are internalized into osteoclasts byendocytosis. This results in:• Accelerated apoptosis of osteoclasts reducing
their number.• Disruption of cytoskeleton and ruffled border
of osteoclasts.In addition, BPNs appear to affect osteoclastprecursors and inhibit their differentiation bysuppressing IL-6.(b) It has been shown now that BPNs, especiallythe second and third generation potent amino-derivatives like alendronate, zoledronate, haveimportant metabolic effects in the mevalonatepathway for isoprenoid lipid synthesis. Theyinhibit prenylation of certain GTP-binding proteinsinvolved in cytoskeletal organization, membraneruffling and vesicle movement. The net result isinactivation of osteoclasts, impaired vesicle fusionand enhanced apoptosis. Interference withmevalonate pathway may also impart antitumoraction on bony metastasis.
All oral BPNs are poorly absorbed, and producegastric irritation, esophagitis as the major sideeffect. They are contraindicated in gastroesophagealreflux, peptic ulcer and renal impairment.
The BPNs are useful in conditions characteri-zed by enhanced bone turnover.
1. Osteoporosis The second and thirdgeneration BPNs (e.g. alendronate, risedronate)
are effective in preventing and treating post-menopausal osteoporosis in women as well asage related, idiopathic and steroid-inducedosteoporosis in both men and women. Alendronateis equally or more effective than HRT or raloxifenein conserving bone mineral density and hasreduced the risk of vertebral as well as hip fractureby 47–56%.
Estrogens prevent vertebral but not otherfractures. BPNs are more effective than calcitoninand continue to afford protection for at least 5years of continuous use. Thus, they are the firstchoice drugs now for osteoporosis. Since the t½of alendronate in bone is ~ 10 years, treatmentbeyond 5 years is considered unnecessary.
2. Paget’s disease This disease due to abnor-mal osteoclast function producing disordered boneremodeling and honeycomb-like bone architectureis benefited by BPNs. They arrest osteolyticlesions, reduce bone pain and improve secondarysymptoms. Long-lasting remissions may beinduced. Alendronate, risedronate, pamidronateand zoledronate are used now. They are moreconvenient, more effective and cheaper thancalcitonin. Combined use of BPNs and calcitoninfurther increases efficacy. Treatment with BPNsshould not exceed 6 months; but courses maybe repeated after a gap.
3. Hypercalcaemia of malignancy Severehypercalcaemia, a common complication ofmalignancy, is a medical emergency with alteredconsciousness. Pamidronate (60–90 mg i.v. over2–4 hours) or zoledronate (4 mg i.v. over 15 min)are the most effective drugs, but take 24–48 hoursto act. They may be supplemented by i.m.calcitonin 6–12 hourly for 2 days to achieve rapidaction. Vigorous i.v. hydration is instituted first.After volume repletion, furosemide is added toenhance Ca2+ excretion and to prevent volumeoverload. This is followed by BPN infusion. Thistherapy reduces serum calcium within few hoursand corrects the attending dehydration. Oral BPNsare not useful. Corticosteroids also lower plasmaCa2+, but are slow to act, take 1–2 weeks.

345C
HA
PTE
R 24
DRUGS AFFECTING CALCIUM BALANCE
4. Osteolytic bone metastasis Parenteralpamidronate/zoledronate arrests osteolytic lesionsand reduces bone pain.
Etidronate This is the first BPN to be used clinically,employed in hypercalcaemia and Paget’s disease. However,it also interferes with bone mineralization: continuous therapyproduces osteomalacia. Therefore, it has been largely replacedby zoledronate for hypercalcaemia and alendronate/risedronatefor Paget’s disease. Etidronate is administered both orallyand i.v., but is not preferred now.Dose: 5–7.5 mg/kg/day.DRONATE-OS 200 mg tab, 300 mg inj.
Pamidronate A second generation potent BPNwhich is administered only by i.v. infusion in adose of 60–90 mg over 2–4 hours weekly ormonthly depending on the condition. It is usedin Paget’s disease, hypercalcaemia of malignancyand in bony metastasis. Adverse effects arethrombophlebitis of injected vein, bone pain, feverand leukopenia. A flu-like reaction may occurinitially due to cytokine release.AREDIA 15, 30, 60 mg inj; AREDRONET 30, 90 mg inj.BONAPAM 30, 60, 90 mg inj.
Alendronate This potent orally effectivesecond generation amino-BPN is used primarilyfor prevention and treatment of osteoporosis bothin women and men, as well as for Paget’s disease.It is to be taken on empty stomach in the morningwith a full glass of water and patient is instructednot to lie down or take food for at least 30 min.These measures are needed to prevent contactof the drug with esophageal mucosa which resultsin esophagitis. Calcium, iron, antacids, mineralwater, tea, coffee, fruit juice interfere withalendronate absorption. NSAIDs accentuategastric irritation caused by alendronate. Otheradverse effects are gastric erosion, retrosternalpain, flatulence, headache, bodyache and initialfall in serum Ca2+ level.Dose: 5–10 mg OD; or 35–70 mg weekly; weekly treatment isas effective, more convenient and better tolerated.OSTEOPHOS, DENFOS 5, 10, 35, 70 mg tab. RESTOFOS,DRONAL 10, 70 mg tab.
Oral bioavailability of alendronate is ~1%.Up to 50% of the drug entering the body issequestrated in bone while the rest is excreted
unchanged mainly by the kidney. The terminalelimination t½ of alendronate has been measuredas 10.5 years.
Risedronate It is an oral 3rd generation BPN,more potent than alendronate, but equallyefficacious. Oral bioavailability of 1% and otherfeatures are similar to alendronate. It is indicatedin the treatment of osteoporosis and Paget’sdisease.Dose: 35 mg/week oral in the morning with a full glassof water.RISOFO 5, 35, 70 mg tabs. GEMFOS, ACTONEL 35 mgtab.
Zoledronate This parenteral highly potent 3rdgeneration BPN is indicated for hypercalcaemia,bony metastasis, osteolytic lesions, and Paget’sdisease. Osteoclastic activity is markedlysuppressed and an additional antitumor effect maybe exerted by interference with mevalonatepathway. Proliferation of bony metastasis ofprostate/breast cancer and multiple myeloma cellsmay be arrested. For hypercalcaemia, it is moreeffective, faster acting than pamidronate andtherefore the drug of choice now. Anotheradvantage is that it can be infused over 15 min(because of less venous irritation), whereaspamidronate needs 2–4 hours. Flu-like symptomsdue to cytokine release attend the i.v. infusion.Nausea, vomiting, bodyache, dizziness are alsocommon. Renal toxicity has been encountered.Osteonecrosis of the jaw is a rare complicationof i.v. high dose BPN therapy.
Zoledronate 4 mg infused i.v. once every 12months has been used for osteoporosis inpostmenopausal women who do not tolerate oralalendronate/risedronate.Dose: 4 mg diluted in 100 ml saline/glucose solution andinfused i.v. over 15 min; may be repeated after 7 days andthen at 3–4 week intervals.ZOBONE, ZOLDRIA, ZOLTERO 4 mg/vial inj.
Other drugs for hypercalcaemia
1. Gallium nitrate: It is a potent inhibitor of bone resorption;acts by depressing ATP-dependent proton pump at the ruffledmembrane of osteoclasts. Indicated in resistant cases of hyper-calcaemia, it is given by continuous i.v. infusion daily for 5days. It is nephrotoxic and only a reserve drug.

346S
EC
TIO
N5
HORMONES AND RELATED DRUGS
2. Glucocorticoids: High doses of prednisolone (and others)enhance calcium excretion, decrease calcium absorption andhave adjuvant role in hypercalcaemia due to lymphoma,myeloma, leukaemia, carcinoma breast, etc.
Other drugs for osteoporosis1. Strontium ranelate: It suppresses bone resorption as wellas stimulates bone formation, and has been introduced as
a reserve drug for elderly women >75 years age who havealready suffered osteoporotic fracture and are unable to tolerateBPNs.2. Denosumab: It is a human monoclonal antibody whichinhibits osteoclast differentiation and function as well aspromotes their apoptosis. It is a treatment option forpostmenopausal osteoporosis when no other drug isappropriate.

Skeletal Muscle RelaxantsChapterChapterChapterChapterChapter 2525252525
SECTION 6
DRUGS ACTING ON PERIPHERAL (SOMATIC)NERVOUS SYSTEM
Skeletal muscle relaxants are drugs that actperipherally at neuromuscular junction/musclefibre itself or centrally in the cerebrospinal axisto reduce muscle tone and/or cause paralysis.The neuromuscular blocking agents are used pri-marily in conjunction with general anaestheticsto provide muscle relaxation for surgery, whilecentrally acting muscle relaxants are used mainlyfor painful muscle spasms and spastic neuro-logical conditions.
PERIPHERALLY ACTING MUSCLERELAXANTS
I. Neuromuscular blocking agents
A. Nondepolarizing (Competitive) blockers1. Long acting: d-Tubocurarine, Pancuronium,
Doxacurium, Pipecuronium2. Intermediate acting: Vecuronium,
Atracurium, Cisatracurium, Rocuronium,Rapacuronium
3. Short acting: Mivacurium
B. Depolarizing blockersSuccinylcholine (SCh., Suxamethonium),Decamethonium (C-10)
II. Directly acting agents
Dantrolene sodiumQuinine
Note: 1. Decamethonium is not used clinically.2. Aminoglycoside, tetracycline, polypeptide anti-
biotics interfere with neuromuscular transmission at highdoses, but are not employed as muscle relaxants.
NEUROMUSCULAR BLOCKINGAGENTS
Curare It is the generic name for certain plant extracts usedby south American tribals as arrow poison for game hunting.The animals got paralysed even if not killed by the arrow.Natural sources of curare are Strychnos toxifera, Chondro-dendron tomentosum and related plants. Muscle paralysingactive principles of these are tubocurarine, toxiferins, etc.
Tubocurarine was first clinically used in 1930s; manysynthetic compounds including Succinylcholine wereintroduced subsequently. Search has continued forneuromuscular blockers to provide greater cardiovascularstability during surgery and for drugs with differing onsetand duration of action to suit specific requirements. The latestadditions are doxacurium, pipecuronium, rocuronium,mivacurium, rapacuronium and cisatracurium.
MECHANISM OF ACTION
The site of action of both competitive anddepolarizing blockers is the end plate of skeletalmuscle fibres.
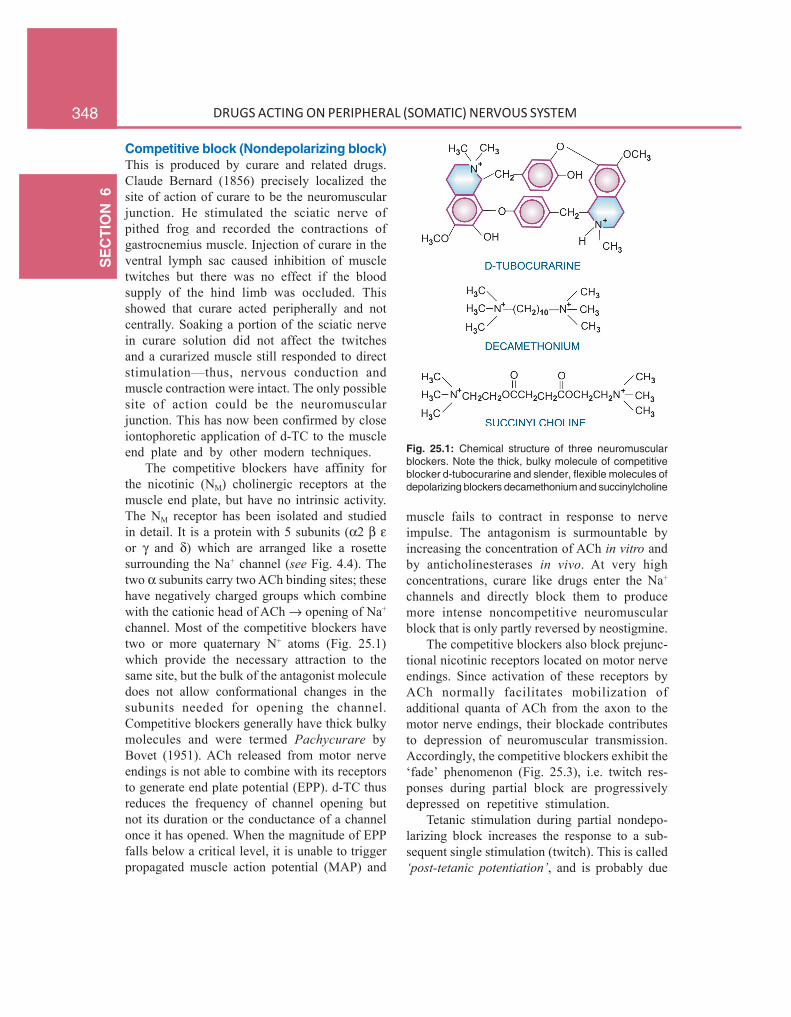
348S
EC
TIO
N6
DRUGS ACTING ON PERIPHERAL (SOMATIC) NERVOUS SYSTEM
Competitive block (Nondepolarizing block)This is produced by curare and related drugs.Claude Bernard (1856) precisely localized thesite of action of curare to be the neuromuscularjunction. He stimulated the sciatic nerve ofpithed frog and recorded the contractions ofgastrocnemius muscle. Injection of curare in theventral lymph sac caused inhibition of muscletwitches but there was no effect if the bloodsupply of the hind limb was occluded. Thisshowed that curare acted peripherally and notcentrally. Soaking a portion of the sciatic nervein curare solution did not affect the twitchesand a curarized muscle still responded to directstimulation—thus, nervous conduction andmuscle contraction were intact. The only possiblesite of action could be the neuromuscularjunction. This has now been confirmed by closeiontophoretic application of d-TC to the muscleend plate and by other modern techniques.
The competitive blockers have affinity forthe nicotinic (NM) cholinergic receptors at themuscle end plate, but have no intrinsic activity.The NM receptor has been isolated and studiedin detail. It is a protein with 5 subunits (α2 β εor γ and δ) which are arranged like a rosettesurrounding the Na+ channel (see Fig. 4.4). Thetwo α subunits carry two ACh binding sites; thesehave negatively charged groups which combinewith the cationic head of ACh → opening of Na+
channel. Most of the competitive blockers havetwo or more quaternary N+ atoms (Fig. 25.1)which provide the necessary attraction to thesame site, but the bulk of the antagonist moleculedoes not allow conformational changes in thesubunits needed for opening the channel.Competitive blockers generally have thick bulkymolecules and were termed Pachycurare byBovet (1951). ACh released from motor nerveendings is not able to combine with its receptorsto generate end plate potential (EPP). d-TC thusreduces the frequency of channel opening butnot its duration or the conductance of a channelonce it has opened. When the magnitude of EPPfalls below a critical level, it is unable to triggerpropagated muscle action potential (MAP) and
muscle fails to contract in response to nerveimpulse. The antagonism is surmountable byincreasing the concentration of ACh in vitro andby anticholinesterases in vivo. At very highconcentrations, curare like drugs enter the Na+
channels and directly block them to producemore intense noncompetitive neuromuscularblock that is only partly reversed by neostigmine.
The competitive blockers also block prejunc-tional nicotinic receptors located on motor nerveendings. Since activation of these receptors byACh normally facilitates mobilization ofadditional quanta of ACh from the axon to themotor nerve endings, their blockade contributesto depression of neuromuscular transmission.Accordingly, the competitive blockers exhibit the‘fade’ phenomenon (Fig. 25.3), i.e. twitch res-ponses during partial block are progressivelydepressed on repetitive stimulation.
Tetanic stimulation during partial nondepo-larizing block increases the response to a sub-sequent single stimulation (twitch). This is called‘post-tetanic potentiation’, and is probably due
Fig. 25.1: Chemical structure of three neuromuscularblockers. Note the thick, bulky molecule of competitiveblocker d-tubocurarine and slender, flexible molecules ofdepolarizing blockers decamethonium and succinylcholine

349C
HA
PTER25
SKELETAL MUSCLE RELAXANTS
to a transient increase in prejunctional AChmobilization following tetanic stimulation.
Depolarizing block Decamethonium and SChhave affinity as well as submaximal intrinsicactivity at the NM cholinoceptors. They depola-rize muscle end plates by opening Na+ channels(just as ACh does) and initially produce twitch-ing and fasciculations. Because in the focallyinnervated mammalian muscle, stimulation istransient; longer lasting depolarization of muscleend plate produces repetitive excitation of thefibre. In the multiplely innervated contracturemuscle (rectus abdominis of frog) stimulationis prolonged resulting in sustained contraction.These drugs do not dissociate rapidly from thereceptor and are not hydrolysed by AChE. Theyinduce prolonged partial depolarization of theregion around muscle end plate → Na+ channelsget inactivated (because transmembrane potentialdrops to about –50 mV) → ACh released frommotor nerve endings is unable to generatepropagated MAP → flaccid paralysis inmammals. In other words a zone of inexcitabilityis created around the end plate preventingactivation of the muscle fibre. In birds, the areaof depolarization is more extensive and spasticparalysis occurs.
Depolarizing blockers also have 2 quaternaryN+ atoms, but the molecule is long, slender andflexible—termed Leptocurare by Bovet. Thefeatures of classical depolarizing block differmarkedly from that of nondepolarizing block (seeFig. 25.2 and Table 25.1).
However, in many species, e.g. dog, rabbit,rat, monkey, in slow contracting soleus muscleof cat, and under certain conditions in man thedepolarizing agents injected in high doses orinfused continuously produce dual mechanismneuromuscular blockade which can be dividedinto two phases:
Phase I block It is rapid in onset, results frompersistent depolarization of muscle end plate andhas features of classical depolarization blockade.This depolarization declines shortly afterwardsand repolarization occurs gradually despite
continued presence of the drug at the receptor,but neuromuscular transmission is not restoredand phase II block supervenes.
Phase II block It is slow in onset and resultsfrom desensitization of the receptor to ACh. It,therefore, superficially resembles block produ-ced by d-TC. The muscle membrane is nearlyrepolarized, recovery is slow, contraction is notsustained during tetanic stimulation (‘fade’occurs) and the block is partially reversed byanticholinesterases.
In man and fast contracting muscle (tibialisanterior) of cat, normally only phase I block isseen. Phase II block may be seen in manwhen SCh is injected in high dose or infused
Fig. 25.2: Illustration of characteristics of competitive (A)and depolarizing (B) neuromuscular blockade in sciaticnerve-gastrocnemius muscle of catA. Tubocurarine (d-TC) produces progressive decreasein twitch tension; tetanic stimulation (TET) produces poorlysustained contracture, which is followed by post-tetanicpotentiation (PTP); Neostigmine (Neo) restores the twitchcontractions.B. Succinylcholine (SCh) produces initial augmentationof twitches followed by progressive block; tetanus is wellsustained, but there is no PTP; block is not reversed (ratherworsened) by neostigmine.

350S
EC
TIO
N6
DRUGS ACTING ON PERIPHERAL (SOMATIC) NERVOUS SYSTEM
TABLE 25.1 Features of competitive and typical depolarizing block
Competitive block Depolarizing (phase I)(d-TC) block (SCh)
1. Paralysis in man Flaccid Fasciculations → flaccid2. Paralysis in chick Flaccid Spastic3. Effect on isolated No contraction, Contraction
frog’s rectus muscle antagonism of ACh4. Species sensitivity Rat > rabbit > cat Cat > rabbit > rat5. Human neonates More sensitive Relatively resistant6. Tetanic stimulation Poorly sustained contraction Well sustained contraction
during partial block7. Neostigmine Antagonises block No effect8. Post tetanic potentiation Present Absent9. Ether anaesthesia Synergistic No effect
10. Order of paralysis Fingers, eyes → limbs → neck, Neck, limbs → face, jaw, eyes,face → trunk → respiratory pharynx → trunk → respiratory
11. Effect of lowering Reduces block Intensifies blocktemperature
12. Effect of cathodal Lessens block Enhances blockcurrent to end plate
continuously, particularly, if fluorinated anaes-thetics have been used. SCh readily producesphase II block in patients with atypical ordeficient pseudocholinesterase.
ACTIONS
1. Skeletal muscles Intravenous injectionof nondepolarizing blockers rapidly producesmuscle weakness followed by flaccid paralysis.Small fast response muscles (fingers, extraocular)are affected first; paralysis spreads to hands,feet—arm, leg, neck, face—trunk—intercostalmuscles—finally diaphragm: respiration stops.The rate of attainment of peak effect and theduration for which it is maintained depends on thedrug (Table 25.2), its dose, anaesthetic used,haemodynamic, renal and hepatic status of thepatient and several other factors. Recovery occursin the reverse sequence; diaphragmatic contrac-tions resume first. In general, the more potentnondepolarizing blockers have a longer onset ofaction.
Depolarizing blockers typically produce fas-ciculations lasting a few seconds before indu-cing flaccid paralysis, but fasciculations are not
prominent in well-anaesthetized patients. Thoughthe sequence in which muscles are involved issomewhat different from the competitiveblockers (Table 25.1), the action of SCh developswith such rapidity that this is not appreciated.Apnoea generally occurs within 45–90 sec, butlasts only 2–5 min; recovery is rapid.
Clinical monitoring of neuromuscular blockIn anaesthetic practice neuromuscular block (especially duringrecovery) is monitored by recording contractile responses ofthumb muscles to transcutaneous ulnar nerve stimulation.Since single twitch responses have to be interpreted incomparison to twitches before the blocker, and are not reliable,several other protocols are used. One such method is ‘train-of-four’ (TOF) protocol. Four supramaximal electrical stimuliare applied in 2S (2Hz) and contractions of thumb muscle arerecorded (Fig. 25.3A). The TOF-ratio is obtained by dividingthe strength of 4th contraction by that of the 1st. In theuntreated subject all the 4 contractions remain equal andTOF-ratio is 1.0.
During partial competitive block (as during onset andrecovery or reversal) the degree of block corresponds to thedecrease in TOF-ratio, because competitive blockers exhibit‘fade’ phenomenon. As the muscles recover, the TOF-ratioimproves and becomes 1.0 at complete recovery.
On the other hand, classical or phase-I depolarizing blockdoes not exhibit fade; the TOF-ratio remains 1.0, though allthe 4 twitches are depressed equally depending on the degreeof block. Fade is again seen when phase II or desensitization

351C
HA
PTER25
SKELETAL MUSCLE RELAXANTS
Fig. 25.3: Clinical assessment of neuromuscular block.(A) Train-of-four (TOF) protocol: Contractile responses ofadductor pollicis muscle to transcutaneous ulnar nervestimulation with train-of-four protocol of impulses duringrecovery of neuromuscular block. TOF-R—Train of four ratio(strength of 4th contraction divided by that of the 1st).(B) Double-burst stimulation (DBS3, 2): Evoked responsesto burst of three 0.2 ms pulses at 50 Hz followed 750 mslater by a second burst of two similar pulses. Note ‘fade’in the second burst after nondepolarizing block.
block occurs with prolonged use of a depolarizing agent andTOF-ratio is depressed as in the case of competitive block.However, SCh generally requires no monitoring.
Rather than measuring each contraction and calculatingTOF ratio, in practice, it is easier to simply observe thedisappearance (during onset) or reappearance (duringrecovery) of the successive twitches. Reappearance of 2ndtwitch (T2) corresponds to ~10% recovery (~90% residualblock) and that of 4th twitch (T4) to ~25% recovery.
Because fade is more prominent during sustainedstimulation, an alternate method is ‘tetanic stimulation’protocol, in which 0.2 ms pulses are applied at 50–100 Hzfor 4–5 seconds and presence or absence of fade is noted(see fade in Fig. 25.2A).
Many anaesthesiologists prefer to use the less painfulvariant of tetanic stimulation, viz ‘double-burst stimulation’
(DBS). A burst of three 0.2 ms pulses at 50 Hz is followedafter a gap of 750 ms by a second burst of 2 or 3 similarpulses (Fig. 25.3B). The strength of response during the 2ndburst relative to the first is a measure of the recovery fromblock.
Measurement of ‘post-tetanic count (PTC)’ is anotherclinically used method.
2. Autonomic ganglia Because the choliner-gic receptors in autonomic ganglia are nicotinic(though of a different subclass NN), competitiveneuromuscular blockers produce some degreeof ganglionic blockade; d-TC has the maximumpropensity in this regard, while the newer drugs(vecuronium, etc.) are practically devoid of it.SCh may cause ganglionic stimulation by itsagonistic action on nicotinic receptors.
3. Histamine release d-TC releases histaminefrom mast cells. This does not involve immunesystem and is due to the bulky cationic natureof the molecule. Histamine release contributesto the hypotension produced by d-TC. Flushing,bronchospasm and increased respiratorysecretions are other effects. Intradermal injectionof d-TC produces a wheal similar to that producedby injecting histamine. Histamine releasing poten-tial of other neuromuscular blockers is gradedin Table 25.2.
Heparin may also be simultaneously releasedfrom mast cells.
4. C.V.S.d-Tubocurarine produces significant fall in BP.This is due to—
(a) ganglionic blockade(b) histamine release and(c) reduced venous return—a result of paralysis
of limb and respiratory muscles.Heart rate may increase due to vagal ganglionicblockade. Pancuronium and vecuronium also tendto cause tachycardia. All newer nondepolarizingdrugs have negligible effects on BP and HR.
Cardiovascular effects of SCh are variable.Generally bradycardia occurs initially due toactivation of vagal ganglia followed by tachy-cardia and rise in BP due to stimulation ofsympathetic ganglia. BP occasionally falls onaccount of its muscarinic action causing

352S
EC
TIO
N6
DRUGS ACTING ON PERIPHERAL (SOMATIC) NERVOUS SYSTEM
TABLE 25.2 Comparative properties of neuromuscular blocking drugs
Drug Dose£ Onset* Duration@ Hist. Gang. Vagal(mg/kg) (min) (min) release block block
LONG ACTING1. d–Tubocurarine 0.2–0.4 4–6 30–60 +++ ++ ±
2. Pancuronium 0.04–0.1 4–6 60–120 ± ± +
3. Doxacurium 0.03–0.08 4–8 60–120 + – –
4. Pipecuronium 0.05–0.08 2–4 50–100 ± – –
INTERMEDIATE ACTING5. Vecuronium 0.08–0.1 2–4 30–60 ± – ±
6. Atracurium 0.3–0.6 2–4 20–40 + – –
7. Cisatracurium 0.15–0.2 3–6 20–40 – – –
8. Rocuronium 0.6–0.9 1–2 25–40 – – ±
SHORT ACTING9. Mivacurium 0.15–0.2 2–4 15–30 + – –
10. Succinylcholine 0.5–0.8 1–1.5 5–8 ++ St. St.
£ Initial paralysing dose for opioid/nitrous oxide + oxygen anaesthesia. In patients anaesthetised with ether/halothane/isoflurane, the dose may be 1/3–1/2 of the figure given.
* Time to maximal block after i.v. injection.@ Duration of surgical grade relaxation after usual clinical doses; time to 95% recovery of muscle twitch is
nearly double of the figure given (especially for long-acting drugs). Duration is dose dependent as well.St.—Stimulation
vasodilatation. Prolonged administration of SChhas caused cardiac arrhythmias and even arrestin patients with burns, soft tissue injury andtetanus. Efflux of intracellular K+ occurs in theseconditions which is augmented by prolongeddepolarization of skeletal muscles.
5. G.I.T. The ganglion blocking activity ofcompetitive blockers may enhance postoperativeparalytic ileus after abdominal operations.
6. C.N.S. All neuromuscular blockers arequaternary compounds—do not cross blood-brainbarrier. Thus, on i.v. administration no centraleffects follow. However, d-TC applied to braincortex or injected in the cerebral ventriclesproduces strychnine like effects.
PHARMACOKINETICSAll neuromuscular blockers are polar quaternarycompounds—not absorbed orally, do not crosscell membranes, have low volumes of distri-
bution and do not penetrate placental or blood-brain barrier. They are practically always giveni.v., though i.m. administration is possible.Muscles with higher blood flow receive moredrug and are affected earlier. Redistribution tonon-muscular tissues plays a significant role inthe termination of surgical grade musclerelaxation, but residual block may persist fora longer time depending on the elimination t½.The duration of action of competitive blockersis directly dependent on the elimination t½.Drugs that are primarily metabolized in theplasma/liver, e.g. vecuronium, atracurium,cisatracurium, rocuronium, and especiallymivacurium have relatively shorter t½ andduration of action (20–40 min), while thoselargely excreted by the kidney, e.g. pancuronium,d-Tc, doxacurium and pipecuronium have longert½ and duration of action (>60 min). Withrepeated administration redistribution sites arefilled up and duration of action is prolonged.

353C
HA
PTER25
SKELETAL MUSCLE RELAXANTS
The unchanged drug is excreted in urine as wellas in bile.
SCh is rapidly hydrolysed by plasma pseudo-cholinesterase to succinylmonocholine and thensuccinic acid + choline (action lasts 5–8 min).Some patients have genetically determinedabnormality (low affinity for SCh) or deficiencyof pseudocholinesterase. In subjects who arehomozygous for the abnormal enzyme (1 in> 3000 population), SCh causes prolonged phaseII blockade resulting in muscle paralysis andapnoea lasting 4–6 hours, because SCh is a poorsubstrate for the more specific AChE found atthe motor end plate. However, duration ofparalysis is increased only by 2–3 times insubjects who are heterozygous for the abnormalenzyme (1 in ~ 50), or have only relativedeficiency. The prolonged apnoea can be tidedover only by mechanical ventilation.
NOTES ON INDIVIDUAL COMPOUNDS1. d-Tubocurarine Because of its prominent histaminereleasing, ganglion blocking and cardiovascular actions aswell as long duration of paralysis needing pharmacologicalreversal, d-TC is not used now.
2. Succinylcholine Despite its propensity tocause muscle fasciculations and soreness,changes in BP and HR, arrhythmias, histaminerelease and K+ efflux from muscles causinghyperkalaemia and its complications, SCh is themost commonly used muscle relaxant for passingtracheal tube. It induces rapid, complete andpredictable paralysis with spontaneous recoveryin ~5 min. Excellent intubating condition viz.relaxed jaw, vocal cords apart and immobile withno diaphragmatic movements, is obtained within1–1.5 min. Occasionally SCh is used bycontinuous i.v. infusion for producing controlledmuscle relaxation of longer duration. It shouldbe avoided in younger children unless absolutelynecessary, because risk of hyperkalaemia andcardiac arrhythmia is higher. Risk of regurgita-tion and aspiration of gastric contents isincreased by SCh in GERD patients and in theobese, especially if stomach is full.MIDARINE, SCOLINE, MYORELEX, ENTUBATE 50 mg/mlinj, 2 ml amp.
3. Pancuronium A synthetic steroidal com-pound, ~5 times more potent and longer actingthan d-TC; provides good cardiovascular stability(little ganglionic blockade), seldom inducesflushing, bronchospasm or cardiac arrhythmiasbecause of lower histamine releasing potential.Rapid i.v. injection may cause rise in BP andtachycardia due to vagal blockade and NA release.It is primarily eliminated by renal excretion.Because of longer duration of action, needingreversal, its use is now restricted to prolongedoperations, especially neurosurgery.PAVULON, PANURON, NEOCURON 2 mg/ml in 2 ml amp.
4. Doxacurium A bisquaternary muscle relaxant havingthe least rapid onset and the longest action: suitable for longduration surgeries. It is primarily eliminated by kidney, thoughhepatic metabolism also occurs. Cardiovascular changes areless marked.
5. Pipecuronium Another muscle relaxantwith a slow onset and long duration of action;steroidal in nature; recommended for prolongedsurgeries. It exerts little cardiovascular action,though transient hypotension and bradycardia canoccur. Elimination occurs through both kidneyand liver.ARDUAN 4 mg/2 ml inj.
6. Vecuronium A close congener of pancu-ronium with a shorter duration of action due torapid distribution and metabolism. It is excretedmainly in bile, recovery is generally sponta-neous, but may need neostigmine reversal.Cardiovascular stability is still better due to lackof histamine releasing and ganglionic action;tachycardia sometimes occurs. Currently, it isthe most commonly used muscle relaxant forroutine surgery and in intensive care units.NORCURON 4 mg amp, dissolve in 1 ml solvent supplied.NEOVEC 4 mg amp, 10 mg vial.
7. Atracurium A bisquaternary competitiveblocker, 4 times less potent than pancuroniumand shorter acting: reversal is mostly notrequired. The unique feature of atracurium isinactivation in plasma by spontaneous non-enzymatic degradation (Hofmann elimination) inaddition to that by cholinesterases. Consequentlyits duration of action is not altered in patients

354S
EC
TIO
N6
DRUGS ACTING ON PERIPHERAL (SOMATIC) NERVOUS SYSTEM
with hepatic/renal insufficiency or hypodynamiccirculation. It is the preferred muscle relaxantfor liver/kidney disease patients as well as forneonates and the elderly. Hypotension may occurdue to dose dependent histamine release.TRACRIUM 10 mg/ml inj in 2 ml vial.
8. Cisatracurium This R-Cis, R-Cis enantiomer ofatracurium is nearly 4 times more potent, slower in onset,but similar in duration of action. Like atracurium it undergoesHofmann elimination, but in contrast it is not hydrolysed byplasma cholinesterase. Most importantly, it does not provokehistamine release.
Side effects are fewer.
9. Rocuronium A newer nondepolarizingblocker with a rapid onset and intermediateduration of action which can be used as alternativeto SCh for tracheal intubation without thedisadvantages of depolarizing block and cardio-vascular changes. The same drug also serves asmaintenance muscle relaxant, seldom needingreversal. The onset of action is dose-dependent;intubating conditions are attained in 90 sec with0.6 mg/kg, but within 60 sec at 1.0 mg/kg. Withinlimits, the duration of paralysis is also dose-dependent. This neuromuscular blocker isgaining popularity for its versatility and moreprecisely timed onset and duration of action.Infused i.v. (0.3–0.6 mg/kg/hour), it is also beingused to facilitate mechanical ventilation inintensive care units. Though little metabolized,it is eliminated mainly in bile. Mild vagolyticaction increases HR somewhat.ROCUNIUM, CUROMID 50 mg/5 ml, 100 mg/10 ml vials.
10. Mivacurium It is the shortest acting competitiveblocker; does not need reversal. Dose and speed of injectionrelated transient cutaneous flushing can occur due tohistamine release. Fall in BP is possible, but change in HRis minimal. It is metabolized rapidly by plasma cholinesterases.Prolonged paralysis can occur in pseudocholinesterasedeficiency, but this can be reversed by neostigmine (unlikeparalysis due to SCh).
INTERACTIONS
1. Thiopentone sod and SCh solutions shouldnot be mixed in the same syringe—react chemi-cally.2. General anaesthetics potentiate competi-tive blockers; ether in particular, followed by
fluorinated hydrocarbons. Isofluorane, desfluraneand sevoflurane potentiate to a greater extentthan halothane. Nitrous oxide potentiates theleast. Ketamine also intensifies nondepolarizingblock. Fluorinated anaesthetics predispose tophase II blockade by SCh. Malignant hyper-thermia produced by halothane and isofluranein rare (genetically predisposed) individuals ismore common in patients receiving SCh as well.3. Anticholinesterases reverse the action ofcompetitive blockers. Neostigmine 0.5–2 mg(30–50 μg/kg) i.v. is almost routinely used afterpancuronium and other long/intermediate actingblockers to hasten recovery at the end ofoperation. Though neostigmine also reversesganglionic blockade to some extent, hypotensionand bronchospasm can occur due to muscarinicaction of neostigmine; this can be prevented byprior atropinization (atropine or glycopyrrolate5–10 μg/kg i.v.). Pretreatment with H1 antihista-mines reduces hypotension due to d-TC andothers which release histamine.4. Antibiotics Aminoglycoside antibioticsreduce ACh release from prejunctional nerveendings by competing with Ca2+. They interferewith mobilization of ACh containing vesiclesfrom a central location to near the terminalmembrane, and have a weak stabilizing actionon the postjunctional membrane. In clinicallyused doses, they do not by themselves producemuscle relaxation, but potentiate competitiveblockers. The dose of competitive blocker shouldbe reduced in patients receiving high doses ofthese antibiotics. Application of streptomycinpowder locally at the end of bowel surgery hascaused prolonged apnoea if a competitive blockerhad been used during the operation. Tetracyclines(by chelating Ca2+), polypeptide antibiotics,clindamycin and lincomycin also synergise withcompetitive blockers.5. Calcium channel blockers Verapamil andothers potentiate both competitive and depola-rizing neuromuscular blockers.6. Diuretics may produce hypokalemia whichenhances competitive block.

355C
HA
PTER25
SKELETAL MUSCLE RELAXANTS
7. Diazepam, propranolol and quinidineintensify competitive block, while high dose ofcorticosteroids reduces it.
Sugamadex This is a novel reversing agent developed forterminating the action of nondepolarizing muscle relaxantsrocuronium and vecuronium. Sugamadex is a modifiedγ-cyclodextrin with high affinity for rocuronium andvecuronium; encapsulates one molecule of the blocker withinits molecule forming an inactive chelate which is excreted inurine with a t½ of ~ 2 hours. As the plasma concentrationof free rocuronium falls, it rapidly dissociates from the Nmreceptor and neuromuscular transmission is restored. Thus,the mechanism of reversal by sugamadex is entirely differentfrom that of the currently used reversing agents neostigmineand edrophonium. Sugamadex 2–4 mg/kg i.v. reversesrocuronium block within 3 min. in majority of patients. Itsside effects are mild precordial pain, nausea, alteration of tasteand rarely allergy. No cardiovascular effects have been noted.
TOXICITY
1. Respiratory paralysis and prolonged apnoeais the most important problem.
2. Flushing is common with d-TC (due tohistamine release), can occasionally occurwith atracurium and mivacurium, rare withothers.
3. Fall in BP and cardiovascular collapse canoccur, especially in hypovolemic patients.This is less likely with the newer drugs.Muscle relaxants should be used with greatcaution in patients with severe hepatic andrenal disease.
4. Cardiac arrhythmias and even arrest haveoccurred, especially with SCh, particularly indigitalized patients. SCh releases K+ frommuscles. Intubating dose generally raisesserum K+ by 0.5 mEq/L, but dangeroushyperkalemia can occur, especially in patientswith extensive burns and soft tissue injuries.
5. Precipitation of asthma by histamine releasingneuromuscular blockers.
6. Postoperative muscle soreness and myalgiamay be complained after SCh.
7. Malignant hyperthermia can be triggered bySCh in patients anaesthetized with fluorinatedanaesthetics.
USES
1. The most important use of neuromuscularblockers is as adjuvants to general anaesthesia;adequate muscle relaxation can be achieved atlighter planes. Many surgical procedures areperformed more safely and rapidly by employ-ing muscle relaxants. Muscle relaxants alsoreduce reflex muscle contraction in the regionundergoing surgery, and assist maintenance ofcontrolled ventilation during anaesthesia. Theyare particularly helpful in abdominal and thoracicsurgery, intubation and endoscopies, orthopedicmanipulations, etc.
Choice of the neuromuscular blockerdepends on the nature and duration of theprocedure, pharmacokinetics of the blocker andcardiovascular stability that it provides.Vecuronium and rocuronium are the mostfrequently selected nondepolarizing blockers.
SCh is employed for brief procedures, e.g.endotracheal intubation, laryngoscopy, broncho-scopy, esophagoscopy, reduction of fractures,dislocations, and to treat laryngospasm. Forocular surgery competitive blockers arepreferred, because they paralyse extraocularmuscles at doses which have little effect onlarger muscles. Other factors which should beconsidered in selecting the relaxant are—onsetof action, duration of blockade required, cardio-vascular effects of the drug as well as patient’shepatic, renal and haemodynamic status.
Advantages of newer neuromuscular blockers overthe older ones
• No or minimal ganglionic, cardiac or vascular effects.• No or minimal histamine release.• Many are short acting: easy reversal.• Some are rapid acting: provide alternative to SCh
without the attendant complications.
2. Assisted ventilation: Critically ill patients inintensive care units often need ventilatorysupport. This can be facilitated by continuousinfusion of subanaesthetic doses of a competitiveneuromuscular blocker which reduces the chestwall resistance to inflation. Vecuronium is most

356S
EC
TIO
N6
DRUGS ACTING ON PERIPHERAL (SOMATIC) NERVOUS SYSTEM
commonly used, but after prolonged infusion itcan cause blockade lasting 1–3 days due toaccumulation of an active metabolite and/ordevelopment of neuropathy.3. Convulsions and trauma from electrocon-vulsive therapy can be avoided by the use ofmuscle relaxants without decreasing the thera-peutic benefit. SCh is most commonly used forthis purpose. The short acting competitiveblocker mivacurium is an alternative.4. Severe cases of tetanus and status epilep-ticus, who are not controlled by diazepam orother drugs, may be paralysed by a neuromus-cular blocker (repeated doses of a competitiveblocker) and maintained on intermittent positivepressure respiration till the disease subsides.
DIRECTLY ACTING MUSCLE RELAXANTS
Dantrolene This muscle relaxant is chemicallyand pharmacologically entirely different fromneuromuscular blockers; effect superficiallyresembles that of centrally acting musclerelaxants. Neuromuscular transmission or MAPare not affected, but muscle contraction isuncoupled from depolarization of the membrane.Dantrolene acts on the RyR1 (RyanodineReceptor) calcium channels in the sarcoplasmicreticulum of skeletal muscles and prevents Ca2+
induced Ca2+ release through these channels.Intracellular release of Ca2+ needed forexcitation-contraction coupling is interferedwith. Fast contracting ‘twitch’ muscles areaffected more than slow contracting ‘antigravity’muscles. Since Ca2+ channels in the sarcoplasmicreticulum of cardiac and smooth muscles areof a different subtype (RyR2), these musclesare affected little by dantrolene.
Dantrolene is slowly but adequately absorbedfrom the g.i.t. It penetrates brain and producessome sedation, but has no selective effect onpolysynaptic reflexes responsible for spasticity.It is metabolized in liver and excreted by kidneywith a t½ of 8–12 hours.
Used orally dantrolene (25–100 mg QID)reduces spasticity in upper motor neuronedisorders, hemiplegia, paraplegia, cerebral palsy
and multiple sclerosis. However, it also reducesvoluntary power; the resulting weakness consi-derably neutralizes the benefit and limits use tobedridden patients.
Used i.v. (1 mg/kg repeated as required) itis the drug of choice for malignant hyperthermiawhich is due to persistent release of Ca2+ fromsarcoplasmic reticulum (induced by fluorinatedanaesthetics and SCh in genetically susceptibleindividuals with abnormal RyR1, see p. 379).Reversal has also been obtained in neurolepticmalignant syndrome, though this reaction has adifferent pathogenesis.
Adverse effects Muscular weakness is thedose limiting side effect. Sedation, malaise, lightheadedness and other central effects occur, butare less pronounced than with centrally actingmuscle relaxants. Troublesome diarrhoea isanother problem. Long term use causes dosedependent serious liver toxicity in 0.1–0.5%patients. This has restricted its use in chronicdisorders.
Quinine (see Ch. 59) It increases refractoryperiod and decreases excitability of motor endplates. Thus, responses to repetitive nervestimulation are reduced. It decreases muscletone in myotonia congenita. Taken at bed time(200–300 mg) it may abolish nocturnal legcramps in some patients.
CENTRALLY ACTING MUSCLERELAXANTS
These are drugs which reduce skeletal muscletone by a selective action in the cerebrospinalaxis, without altering consciousness. They selec-tively depress spinal and supraspinal polysynap-tic reflexes involved in the regulation of muscletone without significantly affecting monosynap-tically mediated stretch reflex. Polysynapticpathways in the ascending reticular formationwhich are involved in the maintenance of wake-fullness are also depressed, though to a lesserextent. All centrally acting muscle relaxants dohave some sedative property. They have no effect

357C
HA
PTER25
SKELETAL MUSCLE RELAXANTS
on neuromuscular transmission and on musclefibres, but reduce decerebrate rigidity, uppermotor neurone spasticity and hyperreflexia.
The prominent differences between peri-pherally and centrally acting muscle relaxantsare listed in Table 25.3.
CLASSIFICATION
(i) Mephenesin Mephenesin,congeners Carisoprodol,
Chlorzoxazone,Chlormezanone,Methocarbamol.
(ii) Benzodiazepines Diazepam and others.(iii) GABA mimetic Baclofen,
Thiocolchicoside(iv) Central α2 agonist Tizanidine1. Mephenesin It was the first drug found to cause musclerelaxation in animals without producing unconsciousness andwas called internuncial neurone blocking agent because itsprimary site of action is the spinal internuncial neurone whichmodulates reflexes maintaining muscle tone. It is not usedclinically because orally it causes marked gastric irritation,and injected i.v., it causes thrombophlebitis, haemolysis andfall in BP. It has been included in counterirritant ointments(MEDICREME, RELAXYL) where its irritant rather than musclerelaxant property could be affording relief.
2. Carisoprodol It has a favourable musclerelaxant: sedative activity ratio with weak anal-gesic, antipyretic and anticholinergic properties.It is used in musculoskeletal disorders associatedwith muscle spasm.CARISOMA 350 mg tab; one tab. TDS-QID, SOMAFLAM175 mg + ibuprofen 400 mg tab.
3. Chlorzoxazone It is pharmacologicallysimilar to mephenesin, but has a longer durationof action and is better tolerated orally.FLEXON-MR 250 mg + ibuprofen 400 mg + paracetamol325 mg tab; ULTRAZOX 250 mg + diclofenac 50 mg +paracetamol 325 mg tab; MOBIZOX 500 mg + diclofenac50 mg + paracetamol 500 mg tab; PARAFON: 250 mg +paracetamol 300 mg tab, 1–2 tab TDS.
4. Chlormezanone It has antianxiety andhypnotic actions as well, and has been used fortension states associated with increased muscletone.DOLOBAK 100 mg + paracetamol 450 mg tab, 1–2 tab TDS.
5. Methocarbamol It is less sedative andlonger acting than mephenesin. Orally it has beenused in reflex muscle spasms and chronic neuro-logical diseases. It can be injected i.v. withoutproducing thrombophlebitis and haemolysis—used for orthopedic procedures and tetanus.ROBINAX 0.5 g tab, 1 TDS: 100 mg/ml inj. for i.v. or i.m.use. ROBIFLAM 750 mg + ibuprofen 200 mg tab; NEUROMOL-MR 400 mg + paracetamol 500 mg tab.
Clinical efficacy of none of the above drugsas muscle relaxant is well established. Gastricirritation and sedation are the most importantside effects.6. Diazepam (see Ch. 29) It is the prototypeof benzodiazepines (BZDs) which act in the brainon specific receptors enhancing GABAergictransmission. Muscle tone is reduced by supra-spinal rather than spinal action; muscle relaxant:sedative activity ratio is low. No gastric irritationoccurs and it is very well tolerated, though
TABLE 25.3 Comparative features of centrally and peripherally acting muscle relaxants
Centrally acting Peripherally acting
1. Decrease muscle tone without reducing Cause muscle paralysis, voluntary movementsvoluntary power lost
2. Selectively inhibit polysynaptic reflexes in CNS Block neuromuscular transmission
3. Cause some CNS depression No effect on CNS
4. Given orally, sometimes parenterally Practically always given i.v.
5. Used in chronic spastic conditions, Used for short-term purposesacute muscle spasms, tetanus (surgical operations)

358S
EC
TIO
N6
DRUGS ACTING ON PERIPHERAL (SOMATIC) NERVOUS SYSTEM
sedation limits the dose which can be used forreducing muscle tone. It is particularly valuablein spinal injuries and tetanus. Combined withanalgesics, it is popular for rheumatic disordersassociated with muscle spasm.Dose: 5 mg TDS orally, 10–40 mg i.v. (in tetanus).
7. Baclofen This analogue of the inhibitorytransmitter GABA acts as a selective GABAB
receptor agonist. The GABA receptors have beendivided into:
GABAA receptor Intrinsic ion channel receptorwhich increases Cl¯ conductance; blocked bybicuculline; facilitated by BZDs.
GABAB receptor G-protein coupled receptor;hyperpolarizes neurones by increasing K+
conductance and altering Ca2+ flux; bicucullineinsensitive, but blocked by saclofen.
Baclofen does not affect Cl¯ conductanceand its actions are not antagonized by bicuculline.
The primary site of action of baclofen isconsidered to be in the spinal cord where itdepresses both polysynaptic and monosynapticreflexes. As such, it does produce muscleweakness, but is less sedative than diazepam.Spasticity in many neurological disorders likemultiple sclerosis, amyotropic lateral sclerosis(ALS), spinal injuries and flexor spasms isreduced, and baclofen is the preferred drug forsymptomatic relief. However, it is relativelyineffective in stroke, cerebral palsy, rheumaticand traumatic muscle spasms and parkinsonism.
Baclofen is well absorbed orally and isprimarily excreted unchanged in urine with a t½of 3–4 hours.
Side effects are drowsiness, mental confusion,weakness and ataxia; serum transaminases mayrise. Sudden withdrawal after chronic use maycause hallucinations, tachycardia and seizures.Dose: 10 mg BD to 25 mg TDS.LIORESAL, LIOFEN 10 mg, 25 mg tab.
8. Thiocolchicoside Chemically related tocolchicine, this muscle relaxant is believed toact as a GABA mimetic and glycinergic drug.Combined with NSAIDs, it is being used for
painful muscle spasms, such as torticolis, sprains,backache, etc. Side effects are gastric upset andphotosensitivity reactionsDose: 4 mg TDS-QID;NUCOXIA-MR: Thiocolchicoside 4 mg + etoricoxib 60 mg tabs.
9. Tizanidine This clonidine congener is acentral α2 adrenergic agonist—inhibits releaseof excitatory amino acids in the spinal inter-neurones. It may facilitate the inhibitorytransmitter glycine as well. Polysynaptic reflexesare inhibited resulting in decreased muscle toneand frequency of muscle spasms without reducingmuscle strength. Efficacy similar to baclofen ordiazepam has been noted in multiple sclerosis,spinal injury and stroke, with fewer side effects.
Tizanidine is absorbed orally, undergoes firstpass metabolism and is excreted by the kidney;t½ 2–3 hours. It is indicated in spasticity dueto neurological disorders and in painful musclespasms of spinal origin. Side effects are dry-mouth, drowsiness, night-time insomnia andhallucinations. Dose-dependent elevation of liverenzymes occurs. Though no consistent effect onBP has been observed, it should be avoided inpatients receiving antihypertensives, especiallyclonidine.Dose: 2 mg TDS; max 24 mg/day.SIRDALUD 2, 4, 6 mg tab, TIZAN 2, 4 mg tab; BRUFEN-MR, TIZAFEN 2 mg + ibuprofen 400 mg tab; TIZANAC 2mg + diclofenac 50 mg tab, PROXIVON-MR 2 mg +nimesulide 100 mg cap.
Uses of centrally acting muscle relaxants
1. Acute muscle spasms Overstretching ofa muscle, sprain, tearing of ligaments andtendons, dislocation, fibrositis, bursitis,rheumatic disorders, etc. cause painful spasmof muscles. The mephenesin-like and BZDmuscle relaxants, combined with analgesics, arecommonly used, but efficacy is not impressive.
2. Torticollis, lumbago, backache, neuralgiasThese are other conditions in which painfulspasm of certain muscles is a prominent feature;respond in the same way as acute muscle spasms.
3. Anxiety and tension Increased tone ofmuscles often attends these states. Diazepam group

359C
HA
PTER25
SKELETAL MUSCLE RELAXANTS
of drugs and chlormezanone benefit by theirantianxiety as well as muscle relaxant actions.4. Spastic neurological diseases Impairmentof descending pathways in the cerebrospinal axisand withdrawal of inhibitory influence over thestretch reflex causes chronic increase in muscletone or spasticity. Hemiplegia, paraplegia, spinalinjuries, multiple sclerosis, ALS and cerebral palsyfall in this category. These conditions are benefitedby baclofen, diazepam, tizanidine and dantrolenebut not by mephenesin group of drugs. However,therapy of these disorders is far from satisfactory.
5. Tetanus Most commonly diazepam is infu-sed i.v. and the dose is titrated by the response.Methocarbamol is an alternative.
6. Electroconvulsive therapy Diazepam dec-reases the intensity of convulsions resulting fromECT, without diminishing its therapeutic effect.Often SCh is used in addition for total sup-pression of the muscular component of ECT.
7. Orthopedic manipulations These proce-dures may be performed under the influence ofdiazepam or methocarbamol given i.v.
PROBLEM DIRECTED STUDY
25.1 A 30-year lady brought to the hospital emergency with 40% burn injury has to be operatedunder general anaesthesia.(a) Which muscle relaxant should be preferred for tracheal intubation and a brief surgicalprocedure in this patient? Give reasons.(see Appendix-1 for solution)

Local AnaestheticsChapterChapterChapterChapterChapter 2626262626
Local anaesthetics (LAs) are drugs which upontopical application or local injection cause rever-sible loss of sensory perception, especially ofpain, in a restricted area of the body. They blockgeneration and conduction of nerve impulse atany part of the neurone with which they come incontact, without causing any structural damage.Thus, not only sensory but also motor impulsesare interrupted when a LA is applied to a mixednerve, resulting in muscular paralysis and lossof autonomic control as well.
Important differences between general andlocal anaesthesia are tabulated in Table 26.1.
CLASSIFICATION
Injectable anaesthetic
Low potency, short durationProcaineChloroprocaine
Intermediate potency and durationLidocaine (Lignocaine)Prilocaine
High potency, long durationTetracaine (Amethocaine)BupivacaineRopivacaineDibucaine (Cinchocaine)
Surface anaesthetic
Soluble InsolubleCocaine BenzocaineLidocaine ButylaminobenzoateTetracaine (Butamben)Benoxinate Oxethazaine
Mepivacaine, Etidocaine, Articaine, Dyclonine, Proparacaineare other local anaesthetics, occasionally used in somecountries.
Some other drugs, e.g. propranolol, chlorpromazine, H1
antihistaminics, quinine have significant LA activity, but arenot used for this purpose because of local irritancy or otherprominent systemic activity. Local anaesthesia can beproduced by cooling as well, e.g. application of ice, CO2
snow, ethylchloride spray.
CHEMISTRY
The clinically useful LAs are weak bases withamphiphilic property. A hydrophilic secondary
TABLE 26.1 Comparative features of general and local anaesthesia
General Localanaesthesia anaesthesia
1. Site of action CNS Peripheral nerves
2. Area of body involved Whole body Restricted area
3. Consciousness Lost Unaltered
4. Care of vital functions Essential Usually not needed
5. Physiological trespass High Low
6. Poor health patient Risky Safer
7. Use in non-cooperative patient Possible Not possible
8. Major surgery Preferred Cannot be used
9. Minor surgery Not preferred Preferred

361C
HA
PTER26
LOCAL ANAESTHETICS
or tertiary amine on one side and a lipophilicaromatic residue on the other are joined by analkyl chain through an ester or amide linkage.
Ester-linked LAs Cocaine, procaine, chloro-procaine, tetracaine, benzocaine.
Amide-linked LAs Lidocaine, bupivacaine,dibucaine, prilocaine, ropivacaine.
Features of amide LAs(compared to ester LAs)
• Produce more intense and longer lasting anaesthesia• Bind to α1 acid glycoprotein in plasma• Not hydrolysed by plasma esterases• Rarely cause hypersensitivity reactions; no
cross sensitivity with ester LAs
Because of their short duration, less intenseanalgesia and higher risk of hypersensitivity, theester-linked LAs are rarely used for infiltrationor nerve block, but are still used topically onmucous membranes.
MECHANISM OF ACTION
The LAs block nerve conduction by decreasingthe entry of Na+ ions during upstroke of actionpotential (AP). As the concentration of the LAis increased, the rate of rise of AP and maximumdepolarization decreases (Fig. 26.1) causingslowing of conduction. Finally, local depolari-zation fails to reach the threshold potential andconduction block ensues.
The LAs interact with a receptor situatedwithin the voltage sensitive Na+ channel and raisethe threshold of channel opening: Na+ permea-
Fig. 26.1: Effect of progressively increasing concentrations(b,c,d) of a local anaesthetic on the generation of an actionpotential in a nerve fibre, (a) Untreated nerve fibre
bility fails to increase in response to an impulseor stimulus. Impulse conduction is interruptedwhen the Na+ channels over a critical length ofthe fibre (2–3 nodes of Ranvier in case ofmyelinated fibres) are blocked. The details areexplained in Fig. 26.2. At physiological pH, theLA molecule is partly ionized. The equilibriumbetween the unionized base form (B) and theionized cationic form (BH+) depends on the pKaof the LA.
Potency of a LA generally corresponds tothe lipid solubility of its base form (B), becauseit is this form which penetrates the axon.However, the predominant active species is thecationic form of the LA which is able to approachits receptor only when the channel is open at theinner face, and it binds more avidly to theactivated and inactivated states of the channel,than to the resting state. Binding of the LAprolongs the inactivated state. The channel takeslonger to recover → refractory period of thefibre is increased. A resting nerve is ratherresistant to blockade. Blockade develops rapidlywhen the nerve is stimulated repeatedly. Thedegree of blockade is frequency dependent:greater blockade occurs at higher frequency ofstimulation. Moreover, exposure to higherconcentration of Ca2+ reduces inactivation of Na+

362S
EC
TIO
N6
DRUGS ACTING ON PERIPHERAL (SOMATIC) NERVOUS SYSTEM
Fig. 26.2: A model of the axonal Na+channel depicting the site and mechanism of action of local anaesthetics.The Na+ channel has an activation gate (make or ‘m’ gate) near its extracellular mouth and an inactivation gate( halt or ‘h’ gate) at the intracellular mouth. In the resting state the activation gate is closed. Threshold depolarizationof the membrane opens the activation gate allowing Na+ ions to flow in along the concentration gradient. Withina few msec, the inactivation gate closes and ion flow ceases. The channel recovers to the resting state ina time-dependent manner.
The local anaesthetic (LA) receptor is located within the channel in its intracellular half. The LA traversesthe membrane in its unionized lipophilic form (B), reionizes in the axoplasm and approaches the LA receptorthrough the intracellular mouth of the channel. It is the cationic form (BH+) of the LA which primarily bindsto the receptor. The receptor has higher affinity, or is more accessible to the LA in the activated as well asinactivated states compared to the resting state. Binding of LA to its receptor stabilizes the channel in theinactivated state and thus reduces the probability of channel opening.
The neuronal Na+ channel is a 300 KD glycoprotein composed of a large (α) and two small (β1, β2) subunits.The α subunit encloses the Na+ selective pore within its 4 homologous domains (I to IV), each domain has6 membrane spanning helical segments (S1 to S6) connected alternately by intracellular and extracellular loops.The wall of the pore is formed by all four S5-S6 segments, while the short nonhelical loops connecting S5-S6 on the extracellular surface fold into the pore and serve as the activation gate. Voltage sensors locatedin the S4 segments move vertically on depolarization and open the activation gate by allosteric conformationalchange. A few msec later, the short intracellular loop connecting domains III and IV folds into the inner mouthof the pore inactivating the channel. The LA receptor is located in the S6 segment of domain IV. Channel activationeither transforms the LA receptor to a higher affinity conformation or exposes it on the wall of the pore, andthis persists during the subsequent inactivation phase.
channels and lessens the degree of block.Blockade of conduction by LA is not due tohyperpolarization; in fact, resting membranepotential is unaltered because K+ channels areblocked only at higher concentrations of LA.
The onset time of blockade is related prima-rily to the pKa of the LA. Those with lower pKa(7.6–7.8), e.g. lidocaine, mepivacaine are fastacting, because 30–40% LA is in the undisso-ciated base form at pH 7.4 and it is this formwhich penetrates the axon. Procaine, tetracaine,bupivacaine have higher pKa (8.1–8.9), only 15%
or less is unionized at pH 7.4; these are slowacting. Chloroprocaine is an exception, havingrapid onset despite high pKa (9.1).
LOCAL ACTIONS
The clinically used LAs have no/minimal localirritant action and block sensory nerve endings,nerve trunks, neuromuscular junction, ganglio-nic synapse and receptors (non-selectively), i.e.those structures which function through increa-sed Na+ permeability. They also reduce release

363C
HA
PTER26
LOCAL ANAESTHETICS
of acetylcholine from motor nerve endings.Injected around a mixed nerve they causeanaesthesia of skin and paralysis of the voluntarymuscle supplied by that nerve.
Sensory and motor fibres are inherentlyequally sensitive, but some LAs do exhibitunequal ability to block them, e.g. bupivacaineproduces sensory block at much lowerconcentration than that needed for motor block.The sensitivity to LA is determined by diameterof the fibres as well as by fibre type. Diameterremaining the same, myelinated nerves areblocked earlier than nonmyelinated. In general,smaller fibres are more sensitive than largerfibres. Fibres differ in the critical length of theaxon that must be exposed to the LA for effectiveblockade. Smaller fibres tend to have shortercritical lengths, because in them voltage changespropagate passively for shorter distances. Also,more slender axons have shorter internodaldistances and LAs easily enter the axon at thenodes of Ranvier. The density of Na+ channel ismuch higher at these nodes. Moreover, frequencydependence of blockade makes smaller sensoryfibres more vulnerable since they generate highfrequency longer lasting action potentials thanthe motor fibres. Thus, fibre diameter itself maynot govern sensitivity to LA.
Autonomic fibres are generally more suscep-tible than somatic fibres. Among the somaticafferents order of blockade is: pain—temper-ature sense—touch—deep pressure sense. Sincepain is generally carried by smaller diameterfibres than those carrying other sensations ormotor impulses, pain in the first modality to beaffected. Applied to the tongue, bitter taste islost first followed by sweet and sour, and saltytaste last of all.
In general, fibres that are more susceptibleto LA are the first to be blocked and the lastto recover. Also, location of the fibre within anerve trunk determines the latency, duration andoften the depth of local anaesthesia. Nervesheaths restrict diffusion of the LA into the nervetrunk so that fibres in the outer layers are blockedearlier than the inner or core fibres. As a result,
the more proximal areas supplied by a nerve areaffected earlier because axons supplying themare located more peripherally in the nerve thanthose supplying distal areas. The differentialarrangement of various types of sensory andmotor fibres in a mixed nerve may partly accountfor the differential blockade. Motor fibres areusually present circumferentially; may beblocked earlier than the sensory fibres in thecore of the nerve.
The LA often fails to afford adequate paincontrol in inflamed tissues (like infected tooth).The likely reasons are:a. Inflammation lowers pH of the tissue—
greater fraction of the LA is in the ionizedform hindering diffusion into the axolemma.
b. Blood flow to the inflamed area isincreased—the LA is removed more rapidlyfrom the site.
c. Effectiveness of Adr injected with the LA isreduced at the inflamed site.
d. Inflammatory products may oppose LAaction.Addition of a vasoconstrictor, e.g. adrenaline
(1:50,000 to 1:200,000):• Prolongs duration of action of LAs by
decreasing their rate of removal from thelocal site into the circulation: contact timeof the LA with the nerve fibre is prolonged.
• Enhances the intensity of nerve block.• Reduces systemic toxicity of LAs: rate of
absorption is reduced and metabolism keepsthe plasma concentration lower.
• Provides a more bloodless field for surgery.• Increases the chances of subsequent local
tissue edema and necrosis as well as delayswound healing by reducing oxygen supply andenhancing oxygen consumption in the affectedarea.
• May raise BP and promote arrhythmia insusceptible individuals.
SYSTEMIC ACTIONS
Any LA injected or applied locally is ultimatelyabsorbed and can produce systemic effects

364S
EC
TIO
N6
DRUGS ACTING ON PERIPHERAL (SOMATIC) NERVOUS SYSTEM
depending on the concentration attained in theplasma and tissues.
C.N.S.
All LAs are capable of producing a sequence ofstimulation followed by depression. Cocaine isa powerful CNS stimulant causing in sequenceeuphoria—excitement—mental confusion—restlessness—tremor and twitching of muscles—convulsions—unconsciousness—respiratorydepression—death, in a dose-dependent manner.
Procaine and other synthetic LAs are muchless potent in this regard. At safe clinical doses,they produce little apparent CNS effects. Higherdose or accidental i.v. injection produces CNSstimulation followed by depression.
The early neurological symptoms of overdosewith lidocaine and other clinically used LAsare—circumoral numbness, abnormal sensationin the tongue, dizziness, blurred vision, tinnitusfollowed by drowsiness, dysphoria and lethargy.Still higher doses produce excitation, restlessness,agitation, muscle twitching, seizures and finallyunconsciousness.
The basic action of all LAs is neuronal inhibi-tion; the apparent stimulation seen initially isdue to inhibition of inhibitory neurones. At highdoses, all neurones are inhibited and flatteningof waves in the EEG is seen.
C.V.S.
Heart LAs are cardiac depressants, but nosignificant effects are observed at conventionaldoses. At high doses (2–3 times the dosesproducing CNS effects) or on inadvertent i.v.injection, they decrease automaticity, excitability,contractility, conductivity and prolong effectiverefractory period (ERP). They have a quinidine-like antiarrhythmic action. Procaine is not usedas antiarrhythmic because of short duration ofaction and propensity to produce CNS effects,but its amide derivative procainamide is a classIA antiarrhythmic (see Ch. 38). Electro-physiological properties of heart may bemarkedly altered at high plasma concentrations
of LAs : QTc interval is prolonged and LAs canthemselves induce cardiac arrhythmias.Bupivacaine is relatively more cardiotoxic andhas produced ventricular tachycardia or fibril-lation. Lidocaine has little effect on contractilityand conductivity; it abbreviates ERP and hasminimal proarrhythmic potential. It is used as anantiarrhythmic (see Ch. 38).
Blood vessels LAs tend to produce fall inBP. This is primarily due to sympathetic blockade,but high concentrations, as obtained locally atthe site of injection, do cause direct relaxationof arteriolar smooth muscle. Bupivacaine is morevasodilatory than lidocaine, while prilocaine isthe least vasodilatory. Toxic doses of LAsproduce cardiovascular collapse. Cocaine hassympathomimetic property; increases sympa-thetic tone, causes local vasoconstriction,marked rise in BP and tachycardia.
Procaine and related drugs have weak anticholinergic,antihistaminic, ganglion blocking, neuromuscular blocking andsmooth muscle relaxant properties, but these are clinicallyinsignificant.
PHARMACOKINETICSBecause LAs act near their site of administration,pharmacokinetic characteristics are not importantdeterminants of their efficacy, but markedlyinfluence their systemic effects and toxicity.
Soluble surface anaesthetics (lidocaine, tetra-caine) are rapidly absorbed from mucousmembranes and abraded areas, but absorption fromintact skin is minimal. Procaine does notsignificantly penetrate mucous membranes. Rateof absorption depends on the blood flow to thearea of application or injection. The absorbed LAbeing lipophilic is widely distributed; rapidlyenters highly perfused brain, heart, liver, andkidney, followed by muscle and other viscera.
Procaine is negligibly bound to plasma pro-teins, but amide LAs are bound to plasma α1 acidglycoprotein. LAs are rapidly but temporarilybound to tissues, especially nerves, at the site ofinjection. Ester-linked LAs (procaine, etc.) arerapidly hydrolysed by plasma pseudocholin-esterase and the remaining by esterases in the

365C
HA
PTER26
LOCAL ANAESTHETICS
liver. Amide-linked LAs (lidocaine, etc.) aredegraded only in the liver microsomes bydealkylation and hydrolysis. Metabolism oflidocaine is hepatic blood-flow dependent. Themaximal safe dose of LAs is lower in patientswith hepatic disease and in the elderly who havedecreased liver function.
After oral ingestion both procaine andlidocaine have high first pass metabolism in theliver. Thus, they are not active orally for anti-arrhythmic purposes.
ADVERSE EFFECTS
Systemic toxicity on rapid i.v. injection is relatedto the intrinsic anaesthetic potency of the LA.However, toxicity after topical application orregional injection is influenced by the relativerates of absorption and metabolism. Those rapidlyabsorbed but slowly metabolized are more toxic.(1) CNS effects are light-headedness, dizziness,auditory and visual disturbances, mental confu-sion, disorientation, shivering, twitchings, invo-luntary movements, finally convulsions andrespiratory arrest. This can be prevented andtreated by diazepam.(2) Cardiovascular toxicity of LAs is manifestedas bradycardia, hypotension, cardiac arrhythmiasand vascular collapse.(3) Injection of LAs may be painful, but localtissue toxicity of LAs is low. However, woundhealing may be sometimes delayed. Addition ofvasoconstrictors enhances the local tissuedamage; rarely necrosis results. Vasoconstrictorsshould not be added for ring block of hands,feet, fingers, toes, penis and in pinna. Bupivacainehas the highest local tissue irritancy.(4) Hypersensitivity reactions like rashes, angio-edema, dermatitis, contact sensitization, asthmaand rarely anaphylaxis occur. These are morecommon with ester-linked LAs, but rare withlidocaine or its congeners. Cross reactivity isfrequent among ester compounds, but not withamide-linked LAs.
Often methylparaben added as preservativein certain LA solutions is responsible for theallergic reaction.
Precautions and interactions1. Before injecting the LA, aspirate lightly toavoid intravascular injection.2. Inject the LA slowly and take care not toexceed the maximum safe dose, especially inchildren.3. Propranolol (probably other β blockers also)may reduce metabolism of lidocaine and otheramide LAs by reducing hepatic blood flow.4. Vasoconstrictor (adrenaline) containing LAshould be avoided for patients with ischaemicheart disease, cardiac arrhythmia, thyrotoxicosis,uncontrolled hypertension, and those receivingβ blockers (rise in BP can occur due tounopposed α action) or tricyclic antidepressants(uptake blockade and potentiation of Adr).
INDIVIDUAL COMPOUNDS
Important properties of local anaesthetics arecompared in Table 26.2.Cocaine It is a natural alkaloid from leaves of Erythroxyloncoca, a south American plant growing on the foothills of theAndes. The natives of Peru and Bolivia habitually chewthese leaves. Cocaine is a good surface anaesthetic and israpidly absorbed from buccal mucous membrane. It was firstused for ocular anaesthesia in 1884. Cocaine should never beinjected; it is a protoplasmic poison and causes tissue necrosis.Cocaine produces prominent CNS stimulation with markedeffect on mood and behaviour. It induces a sense of wellbeing,delays fatigue and increases power of endurance. Insusceptible individuals it produces a state referred to as‘high’ leadting to strong psychological but little physicaldependence. Cocaine is unique among drugs of abuse in notproducing significant tolerance on repeated use; sometimesreverse tolerance is seen (behavioural effects are experiencedat lower doses).
Cocaine also stimulates vagal centre→bradycardia;vasomotor centre→rise in BP; vomiting centre→nausea andvomiting; temperature regulating centre→pyrexia (also due toincreased heat production as a result of enhanced muscularactivity).
In the periphery, it blocks uptake of NA and Adr intoadrenergic nerve endings, (see Fig. 9.4) resulting in higherconcentration of the transmitter around the receptors→sympathomimetic effect, potentiation of directly actingsympathomimetics and suppression of indirectly actingsympathomimetics. Local vasoconstriction, tachycardia, risein BP and mydriasis are the manifestations of its sympatho-mimetic action.

366S
EC
TIO
N6
DRUGS ACTING ON PERIPHERAL (SOMATIC) NERVOUS SYSTEM
TABLE 26.2 Comparative properties of important local anaesthetics
Potency Concn. Safe max* Metabolism inused dose (inj.) Onset Duration of
surface injection toxic of plasma liver nerve block Total (mg) (mg/kg) action (min.)
Cocaine 1 1 1 – not injected fast – + –
Procaine 1/10 1/2 1/6 1–2% 400 (6) slow + + 30–60
Lidocaine 1 2 1/6 0.5–2% 300 (4.5) fast – + 60–120
Tetracaine 4 10 2 0.25–0.5% 80 (1.2) slow + + 180–480
Bupivacaine – 10 2 0.25–0.5% 100 (1.5) interm. – + 120–360
Dibucaine 6 15 3 0.25–0.5% 50 slow – + 180–600
* Without adrenaline; addition of adrenaline may increase safe limit by upto 40%
The only indication for cocaine is in ocular anaesthesia.However, it causes constriction of conjunctival vessels,clouding and rarely sloughing of cornea (due to drying andlocal tissue toxicity). Its use, therefore, is not warranted.
Procaine It is the first synthetic local anaesthetic introducedin 1905. Its popularity declined after the introduction oflidocaine, and it is not used now. It is not a surface anaesthetic.
Procaine forms poorly soluble salt with benzyl penicillin;procaine penicillin injected i.m. acts for 24 hours due toslow absorption from the site of injection.
Lidocaine (Lignocaine) Introduced in 1948,it is currently the most widely used LA. It is aversatile LA, good both for surface applicationas well as injection and is available in a varietyof forms. Injected around a nerve it blocks con-duction within 3 min, whereas procaine may take15 min; also anaesthesia is more intense andlonger lasting. Vasodilatation occurs in theinjected area. It is used for surface application,infiltration, nerve block, epidural, spinal andintravenous regional block anaesthesia. Crosssensitivity with ester LAs is not seen. In con-trast to other LAs, early central effects oflidocaine are depressant, i.e. drowsiness, mentalclouding, dysphoria, altered taste and tinnitus.Overdose causes muscle twitching, convulsions,cardiac arrhythmias, fall in BP, coma andrespiratory arrest like other LAs. Lidocaine is apopular antiarrhythmic (see Ch. 38)XYLOCAINE, GESICAIN 4% topical solution, 2% jelly, 2%viscous, 5% ointment, 1% and 2% injection (with or withoutadrenaline), 5% heavy (for spinal anaesthesia); 100 mg/mlspray (10 mg per actuation).
A transdermal patch of lidocaine has been produced forapplication over the affected skin for relief of burning pain dueto postherpetic neuralgia.
Prilocaine It is similar to lidocaine but does not causevasodilatation at the site of infiltration and has lower CNStoxicity due to larger volume of distribution. One of itsmetabolites has potential to cause methaemoglobinaemia. Ithas been used mainly for infiltration, nerve block andintravenous regional anaesthesia.
Eutectic lidocaine/prilocaine This is aunique preparation which can anaesthetise intactskin after surface application. Eutectic mixturerefers to lowering of melting point of two solidswhen they are mixed. This happens when lidocaineand prilocaine are mixed in equal proportion at25°C. The resulting oil is emulsified into waterto form a cream that is applied under occlusivedressing for 1 hr before i.v. cannulation, splitskin graft harvesting and other superficialprocedures. Anaesthesia up to a depth of 5 mmlasts for 1–2 hr after removal. It has been usedas an alternative to lidocaine infiltration.PRILOX 5% cream.
Tetracaine (Amethocaine) A highly lipid-soluble PABA ester, more potent and more toxicdue to slow hydrolysis by plasma pseudocho-linesterase. It is both surface and conductionblock anaesthetic, but its use is restricted totopical application to the eye, nose, throat,tracheobronchial tree and rarely for spinal orcaudal anaesthesia of long duration. Though it isslow acting, absorption from tracheobronchial

367C
HA
PTER26
LOCAL ANAESTHETICS
spray is very fast and blood concentrationsapproach those attained after i.v. injection.ANETHANE powder for solution, 1% ointment.
Bupivacaine A potent and long-acting amide-linked LA: used for infiltration, nerve block, epi-dural and spinal anaesthesia of long duration. A0.25–0.5% solution injected epidurally produ-ces adequate analgesia without significant motorblockade. As a result, it has become very popularin obstetrics (mother can actively cooperate invaginal delivery) and for postoperative pain reliefby continuous epidural infusion. It has high lipid-solubility; distributes more in tissues than inblood after spinal/epidural injection. Therefore,it is less likely to reach the foetus (when usedduring labour) to produce neonatal depression.Bupivacaine is more prone to prolong QTcinterval and induce ventricular tachycardia orcardiac depression—should not be used forintravenous regional analgesia. Epidural anaes-thesia with 0.75% bupivacaine during labour hascaused few fatalities due to cardiac arrest; useof this concentration is contraindicated.MARCAIN 0.5%, 1% (hyperbaric for spinal anaesthesia).SENSORCAINE 0.25%, 0.5% inj, 0.5% heavy inj.The S(–) enantiomer Levobupivacaine is equally potent butless cardiotoxic and less prone to cause seizures (afterinadvertant intravascular injection) than racemic bupivacaine.It has been introduced in some countries as a singleenantiomer preparation.
Ropivacaine A newer bupivacaine congener, equally longacting but less cardiotoxic. It blocks Aδ and C fibres (involvedin pain transmission) more completely than Aβ fibres whichcontrol motor function. Though equieffective concentrationsof ropivacaine are higher than those of bupivacaine, a greaterdegree of separation between sensory and motor block hasbeen obtained with epidural ropivacaine. Continuous epiduralropivacaine is being used for relief of postoperative andlabour pain. It can also be employed for nerve blocks. Recently,it has been approved for use in India.
Dibucaine (Cinchocaine) It is the most potent, most toxicand longest acting LA. It is used as a surface anaesthetic onless delicate mucous membranes (anal canal). Use for spinalanaesthesia of long duration has declined after the availabilityof bupivacaine.NUPERCAINE 0.5% inj., NUPERCAINAL 1% ointment, inOTOGESIC 1% ear drops.
Benoxinate It is a good surface anaestheticfor the eye; has little irritancy. A 0.4% solution
rapidly produces corneal anaesthesia sufficientfor tonometry without causing mydriasis orcorneal damage.BENDZON 0.4% eyedrops.
Benzocaine and Butylaminobenzoate(Butamben) Because of very low aqueoussolubility, these LAs are not significantlyabsorbed from mucous membranes or abradedskin. They produce long-lasting anaesthesiawithout systemic toxicity. They are used aslozenges for stomatitis, sore throat; as dustingpowder/ointment on wounds/ulcerated surfacesand as suppository for anorectal lesions. Bothare PABA derivative—can antagonize sulfona-mides locally.PROCTOSEDYL-M: Butylaminobenzoate 1% oint withframycetin and hydrocortisone acetate: for piles.PROCTOQUINOL 5% ointment of benzocaine. ZOKEN 20%gel.
Oxethazaine A potent topical anaesthetic, unique inionizing to a very small extent even at low pH values. It is,therefore, effective in anaesthetising gastric mucosa despiteacidity of the medium. Swallowed along with antacids it affordssymptomatic relief in gastritis, drug induced gastric irritation,gastroesophageal reflux and heartburn of pregnancy. Dosesexceeding 100 mg/day may produce dizziness and drowsiness.MUCAINE 0.2% in alumina gel + magnesium hydroxidesuspension; 5–10 ml orally.TRICAINE-MPS: Oxethazaine 10 mg with methyl polysiloxane125 mg, alum. hydroxide gel 300 mg, mag. hydroxide 150 mgper 5 ml gel.
USES AND TECHNIQUES OF LOCALANAESTHESIA
1. Surface anaesthesia It is produced bytopical application of a surface anaesthetic tomucous membranes and abraded skin. Only thesuperficial layer is anaesthetised and there is noloss of motor function. Onset and durationdepends on the site, the drug, its concentrationand form, e.g. lidocaine (10%) sprayed in thethroat acts in 2–5 min and produces anaesthesiafor 30–45 min. Addition of Adr does not affectduration of topical anaesthesia, but phenylephrinecan cause mucosal vasoconstriction and prolongtopical anaesthesia. Absorption of solubleLAs from mucous membranes is rapid; bloodconcentrations of lidocaine and tetracaine

368S
EC
TIO
N6
DRUGS ACTING ON PERIPHERAL (SOMATIC) NERVOUS SYSTEM
sprayed in throat/tracheobronchial tree approachthose attained on i.v. injection—toxicity canoccur. Except for eutectic lidocaine/prilocaine,no other LA is capable of anaesthetizing intactskin. The sites and purposes for which surfaceanaesthesia is used are given in Table 26.3.
2. Infiltration anaesthesia Dilute solutionof LA is infiltrated under the skin in the area ofoperation—blocks sensory nerve endings. Onsetof action is almost immediate and duration isshorter than that after nerve block, e.g. lidocaine30–60 min, bupivacaine 90–180 min. Infiltrationis used for minor operations, e.g. incisions,excisions, hydrocele, herniorrhaphy, etc. whenthe area to be anaesthetised is small. Relativelylarger amount of LA is required compared to thearea anaesthetized, but motor function is notaffected.
3. Conduction block The LA is injectedaround nerve trunks so that the area distal toinjection is anaesthetised and paralysed. Choiceof the LA and its concentration is mainly dictatedby the required duration of action; lidocaine
(1–2%) with intermediate duration of action ismost commonly used, but for longer lastinganaesthesia bupivacaine may be selected.
(a) Field block It is produced by injecting theLA subcutaneously in a manner that all nervescoming to a particular field are blocked—as isdone for herniorrhaphy, appendicectomy, dentalprocedures, scalp stitching, operations on fore-arms and legs, etc. Larger area beginning 2–3 cmdistal to the line of injection can be anaesthetisedwith lesser drug compared to infiltration. Thesame concentration of LA as for infiltration isused for field block.
(b) Nerve block It is produced by injectingthe LA around the appropriate nerve trunks orplexuses. The area of resulting anaesthesia isstill larger compared to the amount of drug used.Muscles supplied by the injected nerve/plexusare paralysed. The latency of anaesthesia dependson the drug and the area to be covered bydiffusion, e.g. lidocaine anaesthetises intercostalnerves within 3 min, but brachial plexus blockmay take 15 min. For plexus block a ‘flooding’
TABLE 26.3 Sites and uses of surface anaesthesia
Site Drugs Form Purpose
1. Eye Tetracaine 1–2% ointment, drops tonometry, surgeryBenoxinate 0.4% drops tonometry
2. Nose, ear Lidocaine 2–4% drops painful lesions, polypsTetracaine 1–2%
3. Mouth, throat Benzocaine lozenges stomatitis, sore throatLidocaine 2% rinse solution painful ulcers
4. Pharynx, larynx, Lidocaine 4–10% spray tonsillectomy, endotrachealtrachea, bronchi Tetracaine 1–2% intubation, endoscopies
5. Esophagus, Oxethazaine 0.2% suspension gastritis, esophagitis,stomach heartburn
6. Abraded skin Tetracaine 1% cream, ointment, ulcers, burns,Benzocaine 1–2% dusting powder itching dermatosesButamben 1–2%
7. Intact skin Eutectic lidocaine/ cream under i.v. cannulation,prilocaine 5% occlusion skin surgery
8. Urethra Lidocaine 2% jelly for dilatation, catheterisation
9. Anal canal, Lidocaine 4% ointment, cream, fissure, painful piles,rectum Dibucaine 1% suppository surgery,
Benzocaine 5% proctoscopy

369C
HA
PTER26
LOCAL ANAESTHETICS
technique is used and larger volumes are needed.Nerve block lasts longer than field block orinfiltration anaesthesia. Frequently performednerve blocks are—lingual, intercostal, ulnar,sciatic, femoral, brachial plexus, trigeminal,facial, phrenic, etc.—used for tooth extraction,operations on eye, limbs, abdominal wall, fracturesetting, trauma to ribs, neuralgias, persistenthiccup, etc.The primary purpose of nerve block anaesthesia is to abolishpain and other sensations. The accompanying motor paralysismay be advantageous by providing muscle relaxation duringsurgery, as well as disadvantageous if it interferes withbreathing, ability to walk after the operation, or participation ofthe patient in labour or produces postural hypotension.
4. Spinal anaesthesia The LA is injectedin the subarachnoid space between L2–3 orL3–4 i.e. below the lower end of spinal cord.The primary site of action is the nerve roots inthe cauda equina rather than the spinal cord.Lower abdomen and hind limbs are anaesthetisedand paralysed. The level of anaesthesia dependson the volume and speed of injection, specificgravity of drug solution and posture of the patient.The drug solution could be hyperbaric (in 10%glucose) or isobaric with CSF.
Nerve roots rapidly take up and retain the LA,therefore, its concentration in CSF falls quicklyafter injection. The level of anaesthesia does notchange with change of posture (becomes fixed)after 10 min. Also, higher segments are exposedto progressively lower concentrations of the LA.Since autonomic preganglionic fibres are moresensitive and somatic motor fibres less sensitivethan somatic sensory fibres, the level ofsympathetic block is about 2 segments higher andthe level of motor paralysis about 2 segmentslower than the level of cutaneous analgesia.
The duration of spinal anaesthesia dependson the drug used and its concentration. Additionof 0.2–0.4 mg of adrenaline to the LA prolongsspinal anaesthesia by about 1/3rd when measuredby the time taken for the level of sensory blockto recede to L1. Adr may be enhancing spinalanaesthesia by reducing spinal cord blood flowor by its own analgesic effect exerted through
spinal α2 adrenoceptors (intrathecal clonidine,an α2 agonist, produces spinal analgesia by itself).
Women during late pregnancy require lessdrug for spinal anaesthesia, because inferior venacava compression leads to engorgement of thevertebral system and a decrease in the capacityof subarachnoid space.
Spinal anaesthesia is used for operations onthe lower limbs, pelvis, lower abdomen, e.g. pros-tatectomy, fracture setting, obstetric procedures,caesarean section, etc. Choice of the LA forspinal anaesthesia primarily depends on the natureand duration of the operative procedure. The LAsemployed with their doses and duration ofanaesthesia are given in Table 26.4.Advantages of spinal anaesthesia over generalanaesthesia are:
(i) It is safer.(ii) Produces good analgesia and muscle rela-
xation without loss of consciousness.(iii) Cardiac, pulmonary, renal disease and
diabetes pose less problem.
Complications of spinal anaesthesia
1. Respiratory paralysis with proper care, thisis rare; intercostal muscles may be paralysed,but diaphragm (supplied by phrenic nerve)maintains breathing. Hypotension and ischaemiaof respiratory centre is more frequently thecause of respiratory failure than diffusion of theanaesthetic to higher centres. Due to paralysisof external abdominal and intercostal muscles,coughing and expectoration becomes lesseffective. This may lead to pulmonary complica-tions.
TABLE 26.4 Drugs used for spinal anaesthesiaand their duration of action
Drug Concentration Volume Total Duration(%) (ml) dose of action
(mg) (min)
Lidocaine 1.5–5 1–2 25–100 60–90
Bupivacaine 0.5–0.75 2–3 10–25 90–150
Tetracaine 0.25–0.5 1–3 5–15 90–180

370S
EC
TIO
N6
DRUGS ACTING ON PERIPHERAL (SOMATIC) NERVOUS SYSTEM
2. Hypotension It is due to blockade ofsympathetic vasoconstrictor outflow to bloodvessels; venous pooling and decreased return tothe heart contributes more to the fall in BP thanarteriolar dilatation. Paralysis of skeletalmuscles of lower limb is another factor reducingvenous return. Decreased sympathetic flow toheart and low venous return produce bradycardia.Raising the foot end overcomes the hypotensionby promoting venous drainage. Sympatho-mimetics, especially those with prominentconstrictor effect on veins (ephedrine, mephen-termine) effectively prevent and counteracthypotension.
3. Headache is due to seepage of CSF; canbe minimised by using smaller bore needle.
4. Cauda equina syndrome is a rareneurological complication resulting in prolongedloss of control over bladder and bowelsphincters. It may be due to traumatic damage tonerve roots or chronic arachnoiditis caused byinadvertent introduction of the antiseptic orparticulate matter in the subarachnoid space.
5. Septic meningitis This may occur due toinfection introduced during lumbar puncture.Actual incidence is very low in majority ofhospitals.
6. Nausea and vomiting after abdominaloperations is due to reflexes triggered by tractionon abdominal viscera. Premedication with opioidanalgesics prevents it.
5. Epidural anaesthesia The spinal duralspace is filled with semiliquid fat through whichnerve roots travel. The LA injected in this space—acts primarily on nerve roots (in the epidural aswell as subarachnoid spaces to which it diffuses)and small amount permeates through interverte-bral foramina to produce multiple paravertebralblocks. Epidural anaesthesia can be divided into3 categories depending on the site of injection.(i) Thoracic Injection is made in the midtho-racic region. The epidural space in this region isrelatively narrow, smaller volume of drug is
needed and a wide segmental band of analgesiainvolving the middle and lower thoracic derma-tomes is produced. It is used generally for painrelief following thoracic/upper abdominalsurgery. Specially designed catheters areavailable which can be placed for repeatedinjections or continuous infusion of the LA toachieve epidural analgesia lasting few days.(ii) Lumbar Relatively large volume of drug isneeded because epidural space is wide. It produ-ces anaesthesia of lower abdomen, pelvis andhind limbs. Use of lumbar epidural anaesthesiais similar to that of spinal anaesthesia.(iii) Caudal Injection is given in the sacralcanal through the sacral hiatus—producesanaesthesia of pelvic and perineal region. It isused mostly for vaginal delivery, anorectal andgenitourinary operations.
Lidocaine (1–2%) and bupivacaine (0.25–0.5%) are popular drugs for epidural anaesthesia.Onset is slower and duration of anaesthesia islonger with bupivacaine and action of both thedrugs is prolonged by addition of adrenaline.Technically epidural anaesthesia is more difficultthan spinal anaesthesia and relatively largervolumes of drug are needed. Consequently,blood concentrations of the LA are higher.Cardiovascular complications are similar to thatafter spinal anaesthesia, but headache andneurological complications are less likely,because intrathecal space is not entered. Spreadof the LA in the epidural space is governed bythe volume injected: larger volume anaesthetizesmore extensive area. Zone of differential sympa-thetic blockade is not evident after epidural
Contraindications to spinal anaesthesia
• Hypotension and hypovolemia.
• Uncooperative or mentally ill patients.
• Infants and children—control of level is difficult.
• Bleeding diathesis.
• Raised intracranial pressure.
• Vertebral abnormalities e.g. kyphosis, lordosis, etc.
• Sepsis at injection site.

371C
HA
PTER26
LOCAL ANAESTHETICS
injection but motor paralysis is 4–5 segmentscaudal, especially with lower concentrations ofthe drug. Greatest separation between sensoryand motor block is obtained by use of 0.25%bupivacaine. This is especially valuable forobstetric purposes (mother can participate inlabour without feeling pain) and for postopera-tive pain relief.6. Intravenous regional anaesthesia (Intravascularinfiltration anaesthesia) It consists of injection of LA ina vein of a tourniquet occluded limb such that the drugdiffuses retrograde from the peripheral vascular bed tononvascular tissues including nerve endings. The limb is firstelevated to ensure venous drainage by gravity and thentightly wrapped in an elastic bandage for maximal
exsanguination. Tourniquet is then applied proximally andinflated to above arterial BP. Elastic bandage is now removedand 20–40 ml of 0.5% lidocaine is injected i.v. under pressuredistal to the tourniquet. Regional analgesia is produced within2–5 min and lasts till 5–10 min after deflating the tourniquetwhich is kept inflated for not more than 15–60 min to avoidischaemic injury. Deflation in < 15 min may allow toxic amountsof the LA to enter systemic circulation. The safety of theprocedure depends on the rapid uptake of LA by peripheraltissues; only 1/4 of the injected drug enters systemic circu-lation when the tourniquet is released. Bradycardia can occur.
It is mainly used for the upper limb and for orthopedicprocedures. Obstructing the blood supply of lower limb ismore difficult and larger volume of anaesthetic is needed.Therefore, it is rarely used for lower limb, except the foot.Bupivacaine should not be employed because of its highercardiotoxicity.
PROBLEM DIRECTED STUDY
26.1 A healthy full-term primigravida aged 26 years who has gone into labour presents fordelivery. There is no cephalopelvic disproportion or any other contraindication to normal vaginaldelivery. However, she demands relief of pain associated with labour and delivery.(a) Can some form of regional anaesthesia be used to relieve her pain? If so, which typeof regional anaesthesia with which drug would be most suitable for her?(see Appendix-1 for solution)

General AnaestheticsChapterChapterChapterChapterChapter 2727272727
SECTION 7
DRUGS ACTING ON CENTRAL
NERVOUS SYSTEM
General anaesthetics (GAs) are drugs whichproduce reversible loss of all sensation andconsciousness. The cardinal features of generalanaesthesia are:• Loss of all sensation, especially pain• Sleep (unconsciousness) and amnesia• Immobility and muscle relaxation• Abolition of somatic and autonomic reflexes.
In the modern practice of balanced anaesthesia,these modalities are achieved by using combi-nation of inhaled and i.v. drugs, each drug for aspecific purpose. Anaesthesia has developed asa highly specialized science in itself.
History Before the middle of 19th century a number ofagents like alcohol, opium, cannabis, or even concussion andasphyxia were used to obtund surgical pain, but operationswere horrible ordeals. Horace Wells, a dentist, picked up theidea of using nitrous oxide (N2O) from a demonstration oflaughing gas in 1844. However, he often failed to relievedental pain completely and the use of N2O had to wait tillother advances were made. Morton, a dentist and medicalstudent at Boston, after experimenting on animals, gave ademonstration of ether anaesthesia in 1846, and it soonbecame very popular. Chloroform was used by Simpson inBritain for obstetrical purpose in 1847, and despite its toxicpotential, it became a very popular surgical anaesthetic.Cyclopropane was introduced in 1929, but the new generationof anaesthetics was heralded by halothane in 1956. The firsti.v. anaesthetic thiopentone was introduced in 1935.
MECHANISM OF GENERALANAESTHESIA
The mechanism of action of GAs is not preciselyknown. A wide variety of chemical agents pro-duce general anaesthesia. Therefore, GA actionhad been related to some common physicoche-mical property of the drugs. Mayer and Overton(1901) pointed out a direct parallelism betweenlipid/water partition coefficient of the GAs andtheir anaesthetic potency.
Minimal alveolar concentration (MAC) isthe lowest concentration of the anaesthetic inpulmonary alveoli needed to produce immobilityin response to a painful stimulus (surgicalincision) in 50% individuals. It is accepted as avalid measure of potency of inhalational GAs,because it remains fairly constant for most youngadults. The MAC of all inhalational anaestheticsdeclines progressively as age advances beyond50 years.
The MAC of a number of GAs showsexcellent correlation with their oil/gas partitioncoefficient. However, this only reflects capacityof the anaesthetic to enter into CNS and attainsufficient concentration in the neuronalmembrane, but not the mechanism by which

373C
HA
PTER27
GENERAL ANAESTHETICS
anaesthesia is produced. The ‘unitary hypothesis’that some single common molecular mechanism(l ike membrane expansion/per turbat ion/fluidization) is responsible for the action of allinhalational anaesthetics has now been replacedby the ‘agent specific theory’ according to whichdifferent GAs produce anaesthesia by differentmechanisms.
Recent evidence favours a direct interactionof the GA molecules with hydrophobic domainsof membrane proteins or the lipid-proteininterface.
Not only different anaesthetics appear to actby different molecular mechanisms, they alsomay exhibit stereospecific effects, and thatvarious components of the anaesthetic state mayinvolve action at discrete loci in the cerebro-spinal axis. The principal locus of causation ofunconsciousness appears to be in the thalamusor reticular activating system, amnesia may resultfrom action in cerebral cortex and hippocampus,while spinal cord is the likely seat of immobilityon surgical stimulation.
Recent findings show that ligand gated ionchannels (but not voltage sensitive ion channels)are the major targets of anaesthetic action. TheGABAA receptor gated Cl¯ channel is the mostimportant of these. Many inhalational anaes-thetics, barbiturates, benzodiazepines and propo-fol potentiate the action of inhibitory transmitterGABA to open Cl¯ channels. Each of the aboveanaesthetics appears to interact with its ownspecific binding site on the GABAA receptor-Cl¯ channel complex, but none binds to theGABA binding site as such; though some inhaledanaesthetics and barbiturates (but not benzodia-zepines) can directly activate Cl¯ channels.Action of glycine (another inhibitory transmitterwhich also activates Cl¯ channels) in the spinalcord and medulla is augmented by barbiturates,propofol and many inhalational anaesthetics. Thisaction may block responsiveness to painfulstimuli resulting in immobility of the anaestheticstate. Certain fluorinated anaesthetics andbarbiturates, in addition, inhibit the neuronalcation channel gated by nicotinic cholinergic
receptor which may mediate analgesia andamnesia.
On the other hand, N2O and ketamine do notaffect GABA or glycine gated Cl¯ channels.Rather they selectively inhibit the excitatoryNMDA type of glutamate receptor. This receptorgates mainly Ca2+ selective cation channels inthe neurones, inhibition of which appears to bethe primary mechanism of anaesthetic action ofketamine as well as N2O. The volatile anaes-thetics have little action on this receptor.
Neuronal hyperpolarization caused by GAshas been ascribed to activation of a specific typeof K+ channels called ‘two-pore domain’channels. This may cause inhibition of presy-naptic transmitter release as well as postsynapticactivation. Inhibition of transmitter release frompresynaptic neurones has also been related tointeraction with certain critical synaptic proteins.Thus, different facets of anaesthetic action mayhave distinct neuronal basis, as opposed to theearlier belief of a global neuronal depression.
Unlike local anaesthetics which act primarilyby blocking axonal conduction, the GAs appearto act by depressing synaptic transmission.
STAGES OF ANAESTHESIA
GAs cause an irregularly descending depressionof the CNS, i.e. the higher functions are lostfirst and progressively lower areas of the brainare involved, but in the spinal cord lowersegments are affected somewhat earlier than thehigher segments. The vital centres located in themedulla are paralysed the last as the depth ofanaesthesia increases. Guedel (1920) describedfour stages with ether anaesthesia, dividing theIII stage into 4 planes. These clear-cut stagesare not seen now-a-days with the use of fasteracting GAs, premedication and employment ofmany drugs together. The precise sequence ofevents differs somewhat with anaesthetics otherthan ether. However, ether continues to be usedin resource poor remote areas, and descriptionof these stages still serves to define the effectsof light and deep anaesthesia. Important featuresof different stages are depicted in Fig. 27.1.

374S
EC
TIO
N7
DRUGS ACTING ON CENTRAL NERVOUS SYSTEM
Fig. 27.1: Physiological changes during stages of general anaesthesia (with ether)
I. Stage of analgesia Starts from beginning ofanaesthetic inhalation and lasts upto the loss of conscious-ness. Pain is progressively abolished. Patient remainsconscious, can hear and see, and feels a dream like state;amnesia develops by the end of this stage. Reflexes andrespiration remain normal.
Though some minor operations can be carried out duringthis stage, it is rather difficult to maintain—use is limited toshort procedures.
II. Stage of delirium From loss of consciousness tobeginning of regular respiration. Apparent excitement isseen—patient may shout, struggle and hold his breath;muscle tone increases, jaws are tightly closed, breathing isjerky; vomiting, involuntary micturition or defecation mayoccur. Heart rate and BP may rise and pupils dilate due tosympathetic stimulation.
No stimulus should be applied or operative procedurecarried out during this stage. This stage is inconspicuous inmodern anaesthesia.
III. Surgical anaesthesia Extends from onset of regularrespiration to cessation of spontaneous breathing. This hasbeen divided into 4 planes which may be distinguished as:Plane 1 Roving eyeballs. This plane ends when eyes
become fixed.Plane 2 Loss of corneal and laryngeal reflexes.
Plane 3 Pupil starts dilating and light reflex is lost.Plane 4 Intercostal paralysis, shallow abdominal
respiration, dilated pupil.As anaesthesia passes to deeper planes, progressively—
muscle tone decreases, BP falls, HR increases with weak pulse,respiration decreases in depth and later in frequency also.Thoracic respiration lags behind abdominal respiration.IV. Medullary paralysis Cessation of breathing to failureof circulation and death. Pupil is widely dilated, muscles are totallyflabby, pulse is thready or imperceptible and BP is very low.
Many of the above indices of anaesthesia havebeen robbed by the use of atropine (pupillary,heart rate), morphine (respiration, pupillary),muscle relaxants (muscle tone, respiration, eyemovements, reflexes), etc. and the modernanaesthetist has to depend on several otherobservations to gauge the depth of anaesthesia.• If eyelash reflex is present and patient is
making swallowing movements—stage II hasnot been reached.
• Loss of response to painful stimulus (e.g.pressure on the upper nasal border of orbit)— stage III has been reached.

375C
HA
PTER27
GENERAL ANAESTHETICS
• Incision of the skin causes reflex increasein respiration, BP rise or other effects;insertion of endotracheal tube is resisted andinduces coughing, vomiting, laryngospasm;tears appear in eye; passive inflation of lungsis resisted—anaesthesia is light.
• Fall in BP, cardiac and respiratory depressionare signs of deep anaesthesia.In the present day practice, anaesthesia is
generally kept light; adequate analgesia, amnesiaand muscle relaxation are produced by the useof intravenous drugs. Premedication with CNSdepressants and opioids or their concurrent uselowers MAC of the inhaled anaesthetic. Whena combination of two inhalational anaesthetics(e.g. N2O + isoflurane) is used, their MACs areadditive: lower concentration of each is required,e.g. 0.5 MAC of N2O (53%) and 0.5 MAC ofisoflurane (0.6%) produce CNS depressionequivalent to 1 MAC of isoflurane alone. Thedose-response relationship of inhaled anaes-thetics is very steep; just 30% higher concen-tration (1.3 MAC) immobilizes 95% subjects.Concentrations of inhalational anaestheticsexceeding 1.5 MAC are rarely used, and 2–3MAC is often lethal. Anaesthetized subjectsgenerally wake up when anaesthetic concen-tration falls to 0.4 MAC.
PHARMACOKINETICS OFINHALATIONAL ANAESTHETICS
Inhalational anaesthetics are gases or vapours thatdiffuse rapidly across pulmonary alveoli andtissue barriers. The depth of anaesthesia dependson the potency of the agent (MAC is an index ofpotency) and its partial pressure (PP) in the brain,while induction and recovery depend on the rateof change of PP in the brain. Transfer of theanaesthetic between lung and brain depends on aseries of tension gradients which may besummarized as—
Alveoli Blood BrainFactors affecting the PP of anaesthetic attainedin the brain are—
1. PP of anaesthetic in the inspired gasThis is proportional to its concentration in theinspired gas mixture. Higher the inspired tensionmore anaesthetic will be transferred to the blood.Thus, induction can be hastened by administeringthe GA at high concentration in the beginning.2. Pulmonary ventilation It governs deliveryof the GA to the alveoli. Hyperventilation willbring in more anaesthetic per minute and respi-ratory depression will have the opposite effect.Influence of minute volume on the rate ofinduction is greatest in the case of agents whichhave high blood solubility because their PP inblood takes a long time to approach the PP inalveoli. However, it does not affect the terminaldepth of anaesthesia attained at any givenconcentration of a GA.3. Alveolar exchange The GAs diffuse freelyacross alveoli, but if alveolar ventilation andperfusion are mismatched (as occurs in emphy-sema and other lung diseases) the attainment ofequilibrium between alveoli and blood isdelayed: well perfused alveoli may not be wellventilated—blood draining these alveoli carriesless anaesthetic and dilutes the blood comingfrom well ventilated alveoli. Induction andrecovery both are slowed.
4. Solubility of anaesthetic in blood Thisis the most important property determininginduction and recovery. Large amount of ananaesthetic that is highly soluble in blood (ether)must dissolve before its PP is raised. The riseas well as fall of PP in blood and consequentlyinduction as well as recovery are slow. Drugswith low blood solubility, e.g. N2O, sevoflurane,desflurane induce quickly.
Blood: gas partition coefficient (λ) given bythe ratio of the concentration of the anaestheticin blood to that in the gas phase at equilibriumis the index of solubility of the GA in blood.
5. Solubility of anaesthetic in tissuesRelative solubility of the anaesthetic in bloodand tissue determines its concentration in thattissue at equilibrium. Most of the GAs are

376S
EC
TIO
N7
DRUGS ACTING ON CENTRAL NERVOUS SYSTEM
equally soluble in lean tissues as in blood, butmore soluble in fatty tissue. Anaesthetics withhigher lipid solubility (halothane) continue toenter adipose tissue for hours and also leave itslowly. The concentration of these agents ismuch higher in white matter than in grey matter.
6. Cerebral blood flow Brain is a highly per-fused organ; as such GAs are quickly deliveredto it. This can be hastened by CO2 inhalationwhich causes cerebral vasodilatation—inductionand recovery are accelerated. Carbon dioxidestimulates respiration and this also speeds upthe transport.
Elimination When anaesthetic inhalation isdiscontinued, gradients are reversed and thechannel of absorption (pulmonary epithelium)becomes the channel of elimination. All inhaledanaesthetics are eliminated mainly through lungs.The same factors which govern induction alsogovern recovery. Anaesthetics, in general,continue to enter and persist for long periods inadipose tissue because of their high lipid solu-bility and low blood flow to fatty tissues.Muscles occupy an intermediate positionbetween brain and adipose tissue. Most GAs areeliminated unchanged. Metabolism is significantonly for halothane which is >20% metabolizedin liver. Others are practically not metabolized.Recovery may be delayed after prolongedanaesthesia, especially in case of more lipid-soluble anaesthetics (halothane, isoflurane),because large quantities of the anaesthetic haveentered the muscle and fat, from which it isreleased slowly into blood.
Second gas effect and diffusion hypoxiaIn the initial part of induction, diffusion gradientfrom alveoli to blood is high and larger quantityof anaesthetic is entering blood. If the inhaledconcentration of anaesthetic is high, substantialloss of alveolar gas volume will occur and thegas mixture will be sucked in, independent ofventilatory exchange—gas flow will be higherthan tidal volume. This is significant only withN2O, since it is given at 70–80% concentration;though it has low solubility in blood, about
1 litre/min of N2O enters blood in the first fewminutes. As such, gas flow is 1 litre/min higherthan minute volume. If another potentanaesthetic, e.g. halothane (1–2%) is being givenat the same time, it also will be delivered toblood at a rate 1 litre/min higher than minutevolume and induction will be faster. This is called‘second gas effect’.
The reverse occurs when N2O is discontinuedafter prolonged anaesthesia; N2O having lowblood solubility rapidly diffuses into alveoli anddilutes the alveolar air, and PP of oxygen inalveoli is reduced. The resulting hypoxia, calleddiffusion hypoxia, is not of much consequenceif cardiopulmonary reserve is normal, but maybe dangerous if it is low. Diffusion hypoxia canbe prevented by continuing 100% O2 inhalationfor a few minutes after discontinuing N2O,instead of straight away switching over to air.Diffusion hypoxia is not significant with otheranaesthetics, because they are administered atlow concentrations (0.2–4%) and cannot dilutealveolar air by more than 1–2% in any case.
TECHNIQUES OF INHALATION OF ANAESTHETICS
Different techniques are used according to facility available,agent used, condition of the patient, type and duration ofoperation.
1. Open drop method Liquid anaesthetic is poured overa mask with gauze and its vapour is inhaled with air. A lot ofanaesthetic vapour escapes in the surroundings and theconcentration of anaesthetic breathed by the patient cannotbe determined. It is wasteful—can be used only for a cheapanaesthetic. However, it is simple and requires no specialapparatus. Use now is limited to peripheral areas. Either is theonly agent administered by this method, especially in children.
2. Through anaesthetic machines Use is made of gascylinders, specialized graduated vaporisers, flow meters,unidirectional valves, corrugated rubber tubing and reservoirbag.
The gases are delivered to the patient through a tightlyfitting face mask or endotracheal tube. Administration of theanaesthetic can be more precisely controlled and in manysituations its concentration estimated. Respiration can becontrolled and assisted by the anaesthetist.(a) Open system The exhaled gases are allowed to escapethrough a valve and fresh anaesthetic mixture is drawn ineach time. No rebreathing is allowed—flow rates are high—more drug is consumed. However, predetermined O2 andanaesthetic concentration can be accurately delivered.

377C
HA
PTER27
GENERAL ANAESTHETICS
(b) Closed system The patient rebreaths the exhaled gasmixture after it has circulated through sodalime which absorbsCO2. Only as much O2 and anaesthetic as have been taken up bythe patient are added to the circuit. Flow rates are low. This isespecially useful for expensive and explosive agents (littleanaesthetic escapes in the surrounding air). Halothane, isoflurane,desflurane can be used through closed system. However, controlof inhaled anaesthetic concentration is imprecise.(c) Semiclosed system Partial rebreathing is allowedthrough a partially closed valve. Conditions are intermediatewith moderate flow rates.
Properties of an ideal anaestheticA. For the patient It should be pleasant, non-irritating, should not cause nausea or vomiting.Induction and recovery should be fast with noafter effects.B. For the surgeon It should provide adequateanalgesia, immobility and muscle relaxation.It should be noninflammable and nonexplosiveso that cautery may be used.
C. For the anaesthetist Its administrationshould be easy, controllable and versatile.• Margin of safety should be wide—no fall in
BP.
• Heart, liver and other organs should not beaffected.
• It should be potent so that low concentrationsare needed and oxygenation of the patient doesnot suffer.
• Rapid adjustments in depth of anaesthesiashould be possible.
• It should be cheap, stable and easily stored.• It should not react with rubber tubing or soda
lime.
The important physical and anaesthetic proper-ties of inhalational anaesthetics are presentedin Table 27.1.
CLASSIFICATION
Inhalational
Gas Volatile liquidsNitrous oxide Ether
HalothaneIsofluraneDesfluraneSevoflurane
TABLE 27.1 Physical and anaesthetic properties of inhalational anaesthetics
Anaesthetic Boiling Inflamma- Irritancy Oil: Gas Blood: Gas MAC Induction Musclepoint (°C) bility (odour) partition partition (%) relaxation
coefficient* coefficient*
1. Ether 35 Infl. + +++ 65 12.1 1.9 Slow V. goodExplo. (Pungent)
2. Halothane 50 Noninfl. – 224 2.3 0.75 Interm. Fair(Pleasant)
3. Isoflurane 48 Noninfl. ± 99 1.4 1.2 Interm. Good(Unpleasant)
4. Desflurane 24 Noninfl. + 19 0.42 6.0 Fast Good(Unpleasant)
5. Sevoflurane 59 Noninfl. – 50 0.68 2.0 Fast Good(Pleasant)
6. Nitrous oxide Gas Noninfl. – 1.4 0.47 105 Fast Poor
*At 37°C; Oil: gas and blood: gas partition coefficients are measures of solubility of the anaesthetic in lipid and bloodrespectively.MAC—Minimal alveolar concentration; Infl.—Inflammable; Explo.—Explosive; Interm.—Intermediate

378S
EC
TIO
N7
DRUGS ACTING ON CENTRAL NERVOUS SYSTEM
Intravenous
Fast acting drugs Slower acting drugsThiopentone sod. BenzodiazepinesMethohexitone sod. DiazepamPropofol LorazepamEtomidate Midazolam
Dissociative anaesthesiaKetamine
Opioid analgesiaFentanyl
Cyclopropane, trichloroethylene, methoxyflurane andenflurane are no longer used.
INHALATIONAL ANAESTHETICS1. Nitrous oxide (N2O) It is a colourless,odourless, heavier than air, noninflammable gassupplied under pressure in steel cylinders. It isnonirritating, but low potency anaesthetic;unconsciousness cannot be produced in allindividuals without concomitant hypoxia; MACis 105% implying that even pure N2O cannotproduce adequate anaesthesia at 1 atmospherepressure. Patients maintained on 70% N2O +30% O2 along with muscle relaxants often recallthe events during anaesthesia, but some loseawareness completely.
Nitrous oxide is a good analgesic; even 20%produces analgesia equivalent to that producedby conventional doses of morphine. Musclerelaxation is minimal. Neuromuscular blockersare mostly required. Onset of N2O action is quickand smooth (but thiopentone is often used forinduction), recovery is rapid, because of its lowblood solubility. Second gas effect and diffusionhypoxia occur with N2O only. Post-anaestheticnausea is not marked. It tends to increasesympathetic tone which counteracts weak directdepressant action on heart and circulation.
Nitrous oxide is generally used as a carrierand adjuvant to other anaesthetics. A mixture of70% N2O + 25–30% O2 + 0.2–2% anotherpotent anaesthetic is employed for most surgicalprocedures. In this way concentration of theother anaesthetic can be reduced to 1/3 for thesame level of anaesthesia. Because N2O has little
effect on respiration, heart and BP: breathingand circulation are better maintained with themixture than with the potent anaesthetic givenalone in full doses. However, N2O can expandpneumothorax and other abnormal air pockets inthe body. It increases cerebral blood flow andtends to elevate intracranial pressure.
As the sole agent, N2O (50%) has been usedwith O2 for dental and obstetric analgesia. It isnontoxic to liver, kidney and brain. However,prolonged N2O anaesthesia has the potential todepress bone marrow and cause peripheralneuropathy. Metabolism of N2O does not occur;it is quickly removed from the body by lungs. Itis cheap and commonly used.2. Ether (Diethyl ether) It is a highly volatileliquid, produces irritating vapours which areinflammable and explosive.
(C2H5 — O — C2H5)
Ether is a potent anaesthetic, produces goodanalgesia and marked muscle relaxation byreducing ACh output from motor nerve endings.The dose of competitive neuromuscular blockersshould be reduced to about 1/3.
It is highly soluble in blood. Induction isprolonged and unpleasant with struggling, breath-holding, salivation and marked respiratorysecretions (atropine must be given as premedi-cation to prevent the patient from drowning inhis own secretions). Recovery is slow; post-anaesthetic nausea, vomiting and retching aremarked.
Respiration and BP are generally well main-tained because of reflex stimulation and highsympathetic tone. It does not sensitize the heartto Adr, and is not hepatotoxic.
Ether is not used now in developed countriesbecause of its unpleasant and inflammableproperties. However, it is still used in developingcountries, particularly in peripheral areas becauseit is—cheap, can be given by open drop method(though congestion of eye, soreness of tracheaand ether burns on face can occur) without theneed for any equipment, and is relatively safeeven in inexperienced hands.

379C
HA
PTER27
GENERAL ANAESTHETICS
3. Halothane (FLUOTHANE) It is a volatileliquid with sweet odour, nonirritant and nonin-flammable. Solubility in blood is intermediate—induction is reasonably quick and pleasant.
It is a potent anaesthetic—precise controlof administered concentration is essential. Forinduction 2–4% and for maintenance 0.5–1% isdelivered by the use of a special vaporizer. It isnot a good analgesic or muscle relaxant, but itpotentiates competitive neuromuscular blockers.
Halothane causes direct depression of myo-cardial contractility by reducing intracellularCa2+ concentration. Moreover, sympatheticactivity fails to increase reflexly. Cardiac outputis reduced with deepening anaesthesia. BP startsfalling early and parallels the depth. A 20–30mm Hg drop in BP is common. Many vascularbeds dilate but total peripheral resistance is notsignificantly reduced. Heart rate is reduced byvagal stimulation, direct depression of SA nodalautomaticity and absence of baroreceptoractivation even when BP falls. It tends tosensitize the heart to the arrhythmogenic actionof Adr. The electrophysiological effects are con-ducive to reentry—tachyarrhythmias occuroccasionally.
Halothane causes relatively greater depressionof respiration; breathing is shallow and rapid—PP of CO2 in blood rises if respiration is notassisted. Cerebral blood flow increases.Ventilatory support with added oxygen is fre-quently required. It tends to accentuate perfusion-ventilation mismatch in the lungs by causingvasodilatation in hypoxic alveoli.
Pharyngeal and laryngeal reflexes are aboli-shed early and coughing is suppressed whilebronchi dilate. As such, halothane is preferredfor asthmatics. It inhibits intestinal and uterinecontractions. This property is utilized forfacilitating external or internal version duringlate pregnancy. However, its use during labour
can prolong delivery and increase postpartalblood loss.
Urine formation is decreased during halo-thane anaesthesia—primarily due to low g.f.r. asa result of fall in BP.
Hepatitis occurs in rare susceptible individuals(1 in 35000 to 1 in 10,000) especially after repea-ted use and in those with familial predisposition.A metabolite of halothane is probably involved—causes chemical or immunological injury.
A genetically determined reaction malignanthyperthermia occurs rarely. Many susceptiblesubjects have an abnormal RyR1 (Ryanodinereceptor) calcium channel at the sarcoplasmicreticulum of skeletal muscles. This channel istriggered by halothane to release massive amountsof Ca2+ intracellularly causing persistent musclecontraction and increased heat production.Succinylcholine accentuates the condition (see Ch.25). Rapid external cooling, bicarbonate infusion,100% O2 inhalation and i.v. dantrolene (see p. 356)are used to treat malignant hyperthermia.
About 20% of halothane that enters blood ismetabolized in the liver, the rest is exhaled out.Elimination may continue for 24–48 hours afterprolonged administration due to accumulationin fatty and other tissues. Recovery from halo-thane anaesthesia is smooth and reasonablyquick; shivering may occur but nausea andvomiting are rare. Psychomotor performance andmental ability remain depressed for several hoursafter regaining consciousness.
Halothane is a popular anaesthetic indeveloping countries, because it is relativelycheap and nonirritant, noninflammable, pleasantwith relatively rapid action. It is particularlysuitable for use in children, both for inductionas well as maintenance. In adults, it is mainlyused as a maintenance anaesthetic after i.v.induction. Halothane toxicity is less frequent inchildren. However, in affluent countries it hasbeen largely replaced by the newer agents whichare costlier. Its deficiencies in terms of pooranalgesia and muscle relaxation are compensatedby concomitant use of N2O or opioids andneuromuscular blockers.
HALOTHANE

380S
EC
TIO
N7
DRUGS ACTING ON CENTRAL NERVOUS SYSTEM
4. Isoflurane (SOFANE, FORANE, ISORANE) Thisfluorinated anaesthetic introduced in 1981 iscurrently the routinely used anaesthetic all over.It has totally replaced its earlier introducedisomer enflurane. Isoflurane is somewhat lesspotent and less soluble in blood as well as in fatthan halothane, but equally volatile. Comparedto halothane, it produces relatively rapidinduction and recovery, and is administeredthrough a special vaporizer; 1.5–3% inducesanaesthesia in 7–10 min, and 1–2% is used formaintenance.
Magnitude of fall in BP is similar to halothane,but unlike halothane, this is primarily due tovasodilatation, while cardiac output is wellmaintained. Heart rate is increased. Thesecardiovascular effects probably result fromstimulation of β adrenergic receptors, but it doesnot sensitize the heart to adrenergic arrhythmias.Isoflurane dilates coronaries. Though notencountered clinically, possibility of ‘coronarysteal’ has been apprehended in coronary arterydisease patients on theoretical grounds.Respiratory depression is prominent and assis-tance is usually needed to avoid hypercarbia.Secretions are slightly increased.Uterine and skeletal muscle relaxation is similarto halothane. Potentiation of neuromuscularblockers is greater than that with halothane.Metabolism of isoflurane is negligible. Renaland hepatic toxicity has not been encountered.Postanaesthetic nausea and vomiting is low.Pupils do not dilate and light reflex is not losteven at deeper levels.Though mildly pungent, isoflurane has manyadvantages, i.e. better adjustment of depth ofanaesthesia and low toxicity. It is a goodmaintenance anaesthetic, but not preferred forinduction because of ether like odour which isnot liked by conscious patients, especially
children. In contrast to enflurane, it does notprovoke seizures and is particularly suitable forneurosurgery.
5. Desflurane It is a newer all fluorinatedcongener of isoflurane which has gainedpopularity as an anaesthetic for out patientsurgery. Though it is highly volatile, a thermo-statically heated special vapourizer is used todeliver a precise concentration of puredesflurane vapour in the carrier gas (N2O + O2)mixture. Its distinctive properties are lower lipidsolubility as well as very low solubility in bloodand tissues, because of which induction andrecovery are very fast. Depth of anaesthesiachanges rapidly with change in inhaled concen-tration giving the anaesthetist better control.Postanaesthetic cognitive and motor impairmentis shortlived, so that patient can be discharged afew hours after surgery.
Desflurane is 5 times less potent thanisoflurane; higher concentration has to be usedfor induction which irritates air passage and mayinduce coughing, breath-holding and laryngo-spasm. A somewhat pungent odour makes itunsuitable for induction. Rapid induction some-times causes brief sympathetic stimulation andtachycardia which may be risky in those withcardiovascular disease. Degree of respiratorydepression, muscle relaxation, vasodilatation andfall in BP are similar to isoflurane. Cardiaccontractility and coronary blood flow aremaintained. Lack of seizure provoking potentialarrhythmogenicity and absence of liver as wellas kidney toxicity are also similar to isoflurane.It is rapidly exhaled unchanged. As such,desflurane can serve as a good alternative toisoflurane for routine surgery as well, especiallyprolonged operations. If closed circuit is used,soda lime should be fresh and well hydrated.
ISOFLURANE
DESFLURANE

381C
HA
PTER27
GENERAL ANAESTHETICS
6. Sevoflurane (SEVORANE) This new poly-fluorinated anaesthetic has properties inter-mediate between isoflurane and desflurane.Solubility in blood and tissues as well as potencyare less than isoflurane but more than desflurane.
Induction and emergence from anaesthesia arefast so that rapid changes in depth can beachieved. Absence of pungency makes it pleasantand administrable through a face mask. Unlikedesflurane, it poses no problem in induction andis frequently selected for this purpose.Acceptability is good even by pediatric patients.Recovery is smooth; orientation, cognitive andmotor functions are regained almost as quicklyas with desflurane. Sevoflurane is suitable bothfor outpatient as well as inpatient surgery,induction as well as maintenance, but its highcost and need for high-flow open or semiclosedsystem makes it very expensive to use. In India,only high-end hospitals are using it.
Sevoflurane does not cause sympatheticstimulation and airway irritation even during rapidinduction. Fall in BP is due to vasodilatation aswell as modest cardiac depression. Respiratorydepression, and absence of seizure or arrhythmiaprecipitating propensity are similar to isoflurane.About 3% of absorbed sevoflurane is meta-bolized, but the amount of fluoride liberated issafe for kidney and liver. However, it reacts withsodalime—not recommended for use in fullyclosed circuit.
INTRAVENOUS ANAESTHETICS
FAST ACTING DRUGS
These are drugs which on i.v. injection produceloss of consciousness in one arm-brain circu-lation time (~11 sec). They are generally usedfor induction because of rapidity of onset ofaction. Anaesthesia is then usually maintainedby an inhalational agent. They also serve to
reduce the amount of maintenance anaesthetic.Supplemented with analgesics and musclerelaxants, they can also be used as the soleanaesthetic.
1. Thiopentone sod. It is an ultrashortacting thiobarbiturate, highly soluble in wateryielding a very alkaline solution, which must beprepared freshly before injection. Extravasationof the solution or inadvertent intraarterialinjection produces intense pain; necrosis andgangrene can occur.
Injected i.v. (3–5 mg/kg) as a 2.5% solution,it produces unconsciousness in 15–20 sec. Itsundissociated form has high lipid solubility—enters brain almost instantaneously. Initial distri-bution depends on organ blood flow—brain getslarge amounts. However, as other less vasculartissues (muscle, fat) gradually take up the drug,blood concentration falls and it back diffusesfrom the brain: consciousness is regained in 6–10 min (t½ of distribution phase is 3 min).
On repeated injection, the extracerebral sitesare gradually filled up—lower doses produceanaesthesia which lasts longer. Its ultimatedisposal occurs mainly by hepatic metabolism(elimination t½ is 8–12 hr), but this is irrelevantfor termination of action of a single dose.Residual CNS depression may persist for > 12hr. The patient should not be allowed to leavethe hospital without an attendant before this time.
Thiopentone is a poor analgesic. Painfulprocedures should not be carried out under itsinfluence unless an opioid or N2O has been given;otherwise, the patient may struggle, shout andshow reflex changes in BP and respiration.
It is a weak muscle relaxant; does not irritateair passages. Respiratory depression with indu-cing doses of thiopentone is generally markedbut transient. With large doses it can be severe.BP falls immediately after injection mainly dueto vasodilatation, but recovers rapidly.Cardiovascular collapse may occur if hypovole-mia, shock or sepsis are present. Reflextachycardia occurs, but thiopentone does notsensitize the heart to Adr, arrhythmias are rare.
SEVOFLURANE

382S
EC
TIO
N7
DRUGS ACTING ON CENTRAL NERVOUS SYSTEM
TABLE 27.2 Effects of intravenous anaesthetics on vital functions
Anaesthetic drug HR BP Resp. CBF
1. Thiopentone ↑ ↑ ↓ ↓ ↓ ↓ ↓ ↓ ↓
2. Propofol –, ↓ ↓ ↓ ↓ ↓ ↓ ↓ ↓ ↓ ↓
3. Etomidate – ↓ ↓ ↓ ↓ ↓
4. Diazepan –, ↑ ↓ ↓ ↓ ↓ ↓
5. Ketamine ↑ ↑ ↑ ↑ ↓, – ↑ ↑ ↑
6. Fentanyl ↓ ↓ ↓ ↓ ↓ ↓
HR—Heart rate; BP—Systemic arterial blood pressure; Resp.—Respiratory drive;CBF—Cerebral blood flow. (Changes in intracranial pressure parallel CBF).
Cerebral blood flow is reduced, both due tofall in BP as well as constriction of cerebralvessels. However, cerebral oxygenation does notsuffer, because there is greater decrease incerebral O2 consumption and cerebral perfusionis maintained. A comparative summary of effectsof i.v. anaesthetics is presented in Table 27.2.
Thiopentone is a commonly used inducingagent. It can be employed as the sole anaestheticfor short operations that are not painful.
Adverse effects Laryngospasm occurs gene-rally when respiratory secretions or other irri-tants are present, or when intubation is attemptedwhile anaesthesia is light. This can be preventedby atropine premedication and administration ofsuccinylcholine immediately after thiopentone.Succinylcholine and thiopentone react chemi-cally—should not be mixed in the same syringe.
Shivering and delirium may occur duringrecovery. Pain in the postoperative period islikely to induce restlessness; adequate analgesiashould be provided. Postanaesthetic nausea andvomiting are uncommon.
It can precipitate acute intermittent porphyriain susceptible individuals, therefore contra-indicated.
Other uses Occasionally used for rapidcontrol of convulsions.Gradual i.v. infusion of subanaesthetic dosescan be used to facilitate verbal communicationwith psychiatric patients and for ‘narcoanalysis’of criminals; acts by knocking off guarding.
PENTOTHAL, INTRAVAL SODIUM 0.5, 1 g powder for makingfresh injectable solution.
2. Methohexitone sod. It is similar to thiopentone, 3times more potent, has a quicker and briefer (5–8 min) action.Excitement during induction and recovery is more common.It is more rapidly metabolized (t½ 4 hr) than thiopentone:patient may be roadworthy more quickly.
3. Propofol Currently, propofol has super-seded thiopentone as an i.v. anaesthetic, both forinduction as well as maintenance. It is an oilyliquid employed as a 1% emulsion. Unconscious-ness after propofol injection occurs in 15–45sec and lasts 5–10 min. Propofol distributesrapidly (distribution t½ 2–4 min). Eliminationt½ (100 min) is much shorter than that ofthiopentone due to rapid metabolism.
Intermittent injection or continuous infusionof propofol is frequently used for total i.v.anaesthesia when supplemented by fentanyl.It lacks airway irritancy and is not likely toinduce bronchospasm: preferred in asthmatics.It is particularly suited for outpatient surgery,because residual impairment is less marked andshorter-lasting. Incidence of postoperative nauseaand vomiting is low; patient acceptability is verygood. Excitatory effects and involuntarymovements are noted in few patients. Inductionapnoea lasting ~1 min is common. Fall in BPdue primarily to vasodilatation with less markedcardiac depression occurs consistently, and isoccasionally severe, but short lasting. Baroreflexis suppressed; heart rate remains unchanged ormay decrease. Maintenance anaesthesia with

383C
HA
PTER27
GENERAL ANAESTHETICS
propofol produces dose-dependent respiratorydepression which is more marked than withthiopentone. Effect of cerebral blood flow andO2 consumption is similar to thiopentone. Painduring injection is frequent; can be minimizedby combining with lidocaine.Dose: 2 mg/kg bolus i.v. for induction; 100–200 μg/kg/min formaintenance.PROPOVAN 10 mg/ml and 20 mg/ml in 10, 20 ml vials.In subanaesthetic doses (25–50 μg/kg/min) it isthe drug of choice for sedating intubated patientsin intensive care units. However, it is notapproved for such use in children; prolongedsedation with higher doses has caused severemetabolic acidosis, lipaemia and heart failureeven in adults.
4. Etomidate It is another induction anaesthetic (0.2–0.5mg/kg) which has a briefer duration of action (4–8 min) thanthiopentone; produces little cardiovascular and respiratorydepression, but motor restlessness and rigidity is moreprominent as are pain on injection or nausea and vomiting onrecovery. It is a poor analgesic and has not found muchfavour.
SLOWER ACTING DRUGS
1. Benzodiazepines (BZDs) In addition topreanaesthetic medication, BZDs are nowfrequently used for inducing, maintaining andsupplementing anaesthesia as well as for‘conscious sedation’. Relatively large doses(diazepam 0.2–0.3 mg/kg or equivalent) injectedi.v. produce sedation, amnesia and then uncon-sciousness in 5–10 min. If no other anaestheticor opioid is given, the patient becomes respon-sive in 1 hr or so due to redistribution of thedrug (distribution t½ of diazepam is 15 min),but amnesia persists for 2–3 hr and sedation for6 hr or more. Recovery is further delayed iflarger doses are given. BZDs are pooranalgesics : an opioid or N2O is usually added ifthe procedure is painful.
By themselves, BZDs donot markedly dep-ress respiration, cardiac contractility or BP, butwhen opioids are also given these functions areconsiderably compromised. BZDs decreasemuscle tone by central action, but requireneuromuscular blocking drugs for muscle
relaxation of surgical grade. They do not provokepostoperative nausea or vomiting. Involuntarymovements are not stimulated.
BZDs are now the preferred drugs for endo-scopies, cardiac catheterization, angiographies,conscious sedation during local/regional anaes-thesia, fracture setting, ECT, etc. They are afrequent component of balanced anaesthesiaemploying several drugs. The anaesthetic actionof BZDs can be rapidly reversed by flumazenil0.5–2 mg i.v.
Diazepam 0.2–0.5 mg/kg by slow undilutedinjection in a running i.v. drip: this techniquereduces the burning sensation in the vein andincidence of thrombophlebitis.VALIUM, CALMPOSE 10 mg/2 ml inj.
Lorazepam Three times more potent, sloweracting and less irritating than diazepam. Itdistributes more gradually—awakening may bedelayed. Amnesia is more profound.Dose: 2–4 mg (0.04 mg/kg) i.v. CALMESE 4 mg/2 ml inj.
Midazolam This BZD is water soluble, non-irritating to veins, faster and shorter acting(t½ 2 hours) and 3 times more potent thandiazepam. Fall in BP is somewhat greater thanwith diazepam. It is being preferred overdiazepam for anaesthetic use: 1–2.5 mg i.v.followed by 1/4th supplemental doses. Also usedfor sedation of intubated and mechanically venti-lated patients and in other critical care anaes-thesia as 0.02–0.1 mg/kg/hr continuous i.v.infusion.FULSED, MEZOLAM, SHORTAL 1 mg/ml, 5 mg/ml inj.
2. Ketamine This unique anaesthetic ispharmacologically related to the hallucinogenphencyclidine. It induces a so called‘dissociative anaesthesia’ characterized byprofound analgesia, immobility, amnesia withlight sleep. The patient appears to be conscious,i.e. opens his eyes, makes swallowingmovements and his muscles are stift, but he isunable to process sensory stimuli and does notreeact to them. Thus, the patient appears to bedissociated from his body and surroundings. Theprimary site of action is in the cortex and

384S
EC
TIO
N7
DRUGS ACTING ON CENTRAL NERVOUS SYSTEM
subcortical areas; not in the reticular activatingsystem, which is the site of action of barbiturates.
Respiration is not depressed, bronchi dilate,airway reflexes are maintained, muscle toneincreases. Non-purposive limb movements occur.Heart rate, cardiac output and BP are elevateddue to sympathetic stimulation. A dose of 1–2(average 1.5) mg/kg i.v. or 3–5 mg/kg i.m.produces the above effects within a minute, andrecovery starts after 10–15 min, but patientremains amnesic for 1–2 hr. Emergence deli-rium, hallucinations and involuntary movementsoccur in upto 50% patients during recovery; butthe injection is not painful. Children tolerate thedrug better. Ketamine is rapidly metabolized inthe liver and has an elimination t½ of 2–4 hr.
Ketamine has been used for operations onthe head and neck, in patients who have bled, inasthmatics (relieves bronchospasm), in those whodo not want to lose consciousness and for shortoperations. It is good for repeated use; parti-cularly suitable for burn dressing. Combined withdiazepam, it has found use in angiographies,cardiac catheterization and trauma surgery. It maybe dangerous for hypertensives, in ischaemicheart disease (increases cardiac work), incongestive heart failure and in those with raisedintracranial pressure (ketamine increases cere-bral blood flow and O2 consumption), but is goodfor hypovolemic patients.KETMIN, KETAMAX, ANEKET 50 mg/ml in 2 ml amp,10 ml vial.
Clandestinely mixed in drinks, ketamine has beenmisused as rape drug.
3. Fentanyl This highly lipophilic, short acting(30–50 min) potent opioid analgesic related topethidine (see Ch. 34) is generally given i.v. atthe beginning of painful surgical procedures.Reflex effects of painful stimuli are abolished.It is frequently used to supplement anaestheticsin balanced anaesthesia. This permits use oflower anaesthetic concentrations with betterhaemodynamic stability. Combined with BZDs,it can obviate the need for inhaled anaestheticsfor diagnostic, endoscopic, angiographic and
other minor procedures in poor risk patients, aswell as for burn dressing. Anaesthetic awarenesswith dreadful recall is a risk.
After i.v. fentanyl (2–4 µg/kg) the patientremains drowsy but conscious and his co-operation can be commanded. Respiratorydepression is marked, but predictable; the patientmay be encouraged to breathe and assistancemay be provided. Tone of chest muscles andmasseters may increase with rapid fentanylinjection: a muscle relaxant is then required tofacilitate mechanical ventilation. Heart ratedecreases, because fentanyl stimulates vagus. Fallin BP is slight and heart is not sensitized to Adr.Cerebral blood flow and O2 consumption areslightly decreased. Supplemental doses offentanyl are needed every 30 min or so, butrecovery is prolonged after repeated doses.
Nausea, vomiting and itching often occursduring recovery. The opioid antagonist naloxonecan be used to counteract persisting respiratorydepression and mental clouding. Fentanyl is alsoemployed as adjunct to spinal and nerve blockanaesthesia, and to relieve postoperative pain.TROFENTYL, FENDOP, FENT 50 µg/ml in 2 ml amp, 10 ml vial.
Alfentanil, Sufentanil and remifentanil are still shorter actinganalogues which can be used in place of fentanyl.
4. Dexmedetomidine Activation of central α2 adrener-gic receptors has been known to cause sedation and analgesia.Clonidine (a selective α2 agonist antihypertensive) givenbefore surgery reduces anaesthetic requirement. Dexmedeto-midine is a centrally active selective α2A agonist that has beenintroduced for sedating critically ill/ventilated patients inintensive care units. It is also being used as an adjunct toanaesthesia.Analgesia and sedation are produced with littlerespiratory depression, amnesia or anaesthesia. Sympatheticresponse to stress and noxious stimulus is blunted. It isadministered by i.v. infusion. Side effects are similar to thosewith clonidine, viz. hypotension, bradycardia and dry mouth.It has been recently approved for use in India as well.
CONSCIOUS SEDATION
‘Conscious sedation’ is a monitored state of alteredconsciousness that can be employed (supplemented withlocal/regional anaesthesia), to carryout diagnostic/shorttherapeutic/dental procedures in apprehensive subjects ormedically compromised patients, in place of generalanaesthesia. It allows the operative procedure to be performedwith minimal physiologic and psychologic stress. In conscious

385C
HA
PTER27
GENERAL ANAESTHETICS
sedation, drugs are used to produce a state of CNSdepression (but not unconsciousness), sufficient towithstand the trespass of the procedure, while maintainingcommunication with the patient, who at the same timeresponds to commands and is able to maintain a patentairway. The difference between conscious sedation andanaesthesia is one of degree. The protective airway andother reflexes are not lost, making it safer. Drugs usedfor conscious sedation are:
1. Diazepam It is injected i.v. in small (1–2 mg)repeated doses or by slow infusion until the desired levelof sedation is produced indicated by relaxation,indifference, slurring of speech, ptosis, etc. Furtherinjection is stopped, after which this state lasts for about1 hour and psychomotor impairment persists for 6–24hours; an escort is needed to take the patient back tohome. Flumazenil can be used to reverse the sedation,but repeated doses are needed.
Midazolam (i.v.) is a shorter acting alternative to diazepam.Oral diazepam administered 1 hr before is also used with thelimitation that level of sedation cannot be titrated. The patientremains sedated (not roadworthy) for several hours.
2. Propofol Because of brief action, it has to beadministered as continuous i.v. infusion throughout theprocedure by using a regulated infusion pump. Advantageis that level of sedation can be altered during the procedureand recovery is relatively quick, permitting early dischargeof the patient.
3. Nitrous oxide The patient is made to breathe 100%oxygen through a nose piece or hood and N2O is added in10% increments (to a maximum of 50%, rarely 70%) till thedesired level of sedation assessed by constant verbal contactis obtained. This is maintained till the procedure is performed.Thereafter, N2O is switched off, but 100% O2 is continuedfor next 5 min. The patient is generally roadworthy in30–60 min.
4. Fentanyl Injected i.v. (1–2 μg/kg every 15–30 min), itcan be used alone or in combination with midazolam/propofol.
COMPLICATIONS OF GENERALANAESTHESIA
A. During anaesthesia1. Respiratory depression and hypercarbia.2. Salivation, respiratory secretions. This is less
problematic now as nonirritant anaestheticsare mostly used.
3. Cardiac arrhythmias, asystole.4. Fall in BP.5. Aspiration of gastric contents: acid pneumo-
nitis.6. Laryngospasm and asphyxia.
7. Awareness: dreadful perception and recall ofevents during surgery. This may occur dueto use of light anaesthesia + analgesics andmuscle relaxants.
8. Delirium, convulsions and other excitatoryeffects are generally seen with i.v. anaes-thetics; especially if phenothiazines orhyoscine have been given in premedication.These are suppressed by opioids.
9. Fire and explosion. This is rare now due touse of non-inflammable anaesthetics.
B. After anaesthesia1. Nausea and vomiting.2. Persisting sedation: impaired psychomotor
function.3. Pneumonia, atelectasis.4. Organ toxicities: liver, kidney damage.5. Nerve palsies—due to faulty positioning.6. Emergence delirium.7. Cognitive defects: prolonged excess cognitive
decline has been observed in some patients,especially the elderly, who have undergonegeneral anaesthesia, particularly of longduration.
DRUG INTERACTIONS
1. Patients on antihypertensives given generalanaesthetics—BP may fall markedly.
2. Neuroleptics, opioids, clonidine and mono-amine oxidase inhibitors potentiate anaes-thetics.
3. Halothane sensitizes the heart to Adr.4. If a patient on corticosteroids is to be
anaesthetized, give 100 mg hydrocortisoneintraoperatively because anaesthesia is astressful state—can precipitate adrenalinsufficiency and cardiovascular collapse.
5. Insulin need of a diabetic is increased duringGA: switch over to plain insulin even if thepatient is on oral hypoglycaemics.
PREANAESTHETIC MEDICATIONPreanaesthetic medication refers to the use ofdrugs before anaesthesia to make it morepleasant and safe. The aims are:

386S
EC
TIO
N7
DRUGS ACTING ON CENTRAL NERVOUS SYSTEM
1. Relief of anxiety and apprehension preopera-tively and to facilitate smooth induction.
2. Amnesia for pre- and postoperative events.3. Supplement analgesic action of anaesthetics
and potentiate them so that less anaestheticis needed.
4. Decrease secretions and vagal stimulation thatmay be caused by the anaesthetic.
5. Antiemetic effect extending to the postope-rative period.
6. Decrease acidity and volume of gastric juiceso that it is less damaging if aspirated.
Different drugs achieve different purposes. Oneor more drugs may be used in a patient depen-ding on the needs.
1. Sedative-antianxiety drugs Benzodiaze-pines like diazepam (5–10 mg oral) or lorazepam(2 mg oral or 0.05 mg/kg i.m. 1 hour before)have become popular drugs for preanaestheticmedication because they produce tranquility andsmoothen induction; there is loss of recall ofperioperative events (especially with lorazepam)with little respiratory depression or accentuationof postoperative vomiting. They counteract CNStoxicity of local anaesthetics and are being usedalong with pethidine/fentanyl for a variety ofminor surgical and endoscopic procedures.
Midazolam is a good amnesic with potentand shorter lasting action; it is also better suitedfor i.v. injection, due to water solubility.
Promethazine (50 mg i.m.) is an antihistaminicwith sedative, antiemetic and anticholinergicproperties. It causes little respiratory depression.
2. Opioids Morphine (10 mg) or pethidine (50–100 mg),i.m. allay anxiety and apprehension of the operation, producepre- and postoperative analgesia, smoothen induction, reducethe dose of anaesthetic required and supplement pooranalgesics (thiopentone, halothane) or weak anaesthetics(N2O). Postoperative restlessness is also reduced.
Disadvantages They depress respiration, interfere withpupillary signs of anaesthesia, may cause fall in BPduring anaesthesia, can precipitate asthma and tend todelay recovery. Other disadvantages are lack of amnesia,flushing, delayed gastric emptying and biliary spasm. Somepatients experience dysphoria. Morphine particularlycontributes to postoperative constipation, vomiting and
urinary retention. Tachycardia sometimes occurs whenpethidine has been used.
Use of opioids is now mostly restricted tothose having preoperative pain. When indicated,fentanyl is mostly injected i.v. just beforeinduction.
3. Anticholinergics (see Ch. 8) Atropine orhyoscine (0.6 mg or 10–20 μg/kg i.m./i.v.) orglycopyrrolate (0.2–0.3 mg or 5–10 μg/kg i.m./i.v.) have been used, primarily to reduce salivaryand bronchial secretions. This need is infrequentnow due to use of non-irritant anaesthetics.However, they must be given beforehand whenether is used. The main aim of their use now isto prevent vagal bradycardia and hypotension(which occur reflexly due to certain surgicalprocedures), and prophylaxis of laryngospasmwhich is precipitated by respiratory secretions.
Hyoscine, in addition, produces amnesia andantiemetic effect, but tends to delay recovery.Some patients get disoriented; emergence deli-rium is more common. Moreover, antibrady-cardiac effect of hyoscine is less marked.Therefore, it is infrequently selected for useduring anaesthesia.
Glycopyrrolate is twice as potent and longeracting quaternary antimuscarinic which does notproduce central effects. Antisecretory action ismore marked than atropine, while tachycardia isless marked, especially after i.m. injection. It actsrapidly when given i.v. and is the preferredantimuscarinic in anaesthetic practice.
Action Atropine Glycopyrrolate
1. Antisecretory ++ +++2. Tachycardia +++ ++3. CNS effects + _
4. Bronchodilatation ++ ++
Antimuscarinics facilitate assisted ventilationby reducing airway resistance, but tend toincrease the anatomic dead space. They dilatepupils, abolish the pupillary signs and increasechances of gastric reflux by decreasing tone oflower esophageal sphincter (LES). They shouldnot be used in febrile patients. Dryness of mouth

387C
HA
PTER27
GENERAL ANAESTHETICS
in the pre- and postoperative period may bedistressing. As such, they are now mostly usedi.v. intraoperatively when need arises.
4. Neuroleptics Chlorpromazine (25 mg), triflupro-mazine (10 mg) or haloperidol (2–4 mg) i.m. areinfrequently used in premedication. They allay anxiety,smoothen induction and have antiemetic action. However,they potentiate respiratory depression and hypotensioncaused by the anaesthetics and delay recovery.
Involuntary movements and muscle dystonias can occur,especially in children.
5. H2 blockers/proton pump inhibitorsPatients undergoing prolonged operations,caesarian section and obese patients are atincreased risk of gastric regurgitation and aspirationpneumonia. Ranitidine (150 mg)/famotidine (20 mg)or omeprazole (20 mg)/pantoprazole (40 mg) givennight before and in the morning benefit by raisingpH of gastric juice and may also reduce its volumeand thus chances of regurgitation. The chances ofreflux and damage to lungs on aspiration is minimal
if volume of gastric juice is <25 ml and pH is >3.5.Prevention of stress ulcers is another advantage.They are now routinely used before prolongedsurgery.6. Antiemetics Metoclopramide 10–20 mgi.m. preoperatively is effective in reducing post-operative vomiting. By enhancing gastric emp-tying and tone of LES, it reduces the chances ofreflux and its aspiration. Extrapyramidal effectsand motor restlessness can occur. Combined useof metoclopramide and H2 blockers is moreeffective.Domperidone is nearly as effective and doesnot produce extrapyramidal side effects.Ondansetron (4–8 mg i.v.) the selective 5-HT3
blocker has been found highly effective inreducing the incidence of post-anaestheticnausea and vomiting (see Ch. 47). It is practicallydevoid of side effects and has become theantiemetic of choice in anaesthetic practice.

Ethyl and Methyl AlcoholsChapterChapterChapterChapterChapter 2828282828
ETHYL ALCOHOL (Ethanol)
Alcohols are hydroxy derivatives of aliphatichydrocarbons. When unqualified, ‘alcohol’ refersto ethyl alcohol or ethanol. Pharmacology ofalcohol is important for its presence in beverages(which have been used since recorded history),alcoholism and for alcohol intoxication, ratherthan as a medicinal substance.Alcohol is manufactured by fermentation ofsugars:
ZymaseC6H12O6 2CO2 + 2C2H5OH
(in yeast)
Fermentation proceeds till alcohol contentreaches ~ 15%. Then the reaction is inhibitedby alcohol itself. Starchy cereals, e.g. barley,when soaked produce malt:
Convertase STARCH MALTOSE
which can then be fermented by yeast to producealcohol. The major source of commercial alcoholis mollases, a byproduct of sugar industry.
ALCOHOLIC BEVERAGES
There are a large variety of alcoholic beverages.
A. Malted liquors Obtained by fermentation of germi-nating cereals; are undistilled—alcohol content is low(3–6%) e.g. Beers, Stout. Now strong beers (upto 10%) arealso available.
B. Wines Produced by fermentation of natural sugars aspresent in grapes and other fruits. These are also undistilled.
Light wines Claret, Cider; alcohol content 9–12%, cannotexceed 15%.
Fortified wines Port, Sherry (alcohol 16–22%): distilledbeverages are added from outside.
Effervescent wines Champagne (12–16% alcohol): bottledbefore fermentation is complete.Wines are called ‘dry’ when all sugar present has beenfermented and ‘sweet’ when some is left.
C. Spirits These are distilled after fermentation; e.g. Rum,Gin, Whiskey, Brandy, Vodka, etc. Though the alcohol contentof these can vary from 40–55%, in India (and almostinternationally) for all licenced brands it is standardized to42.8% v/v or 37% w/w.
The taste, flavour and value of alcoholic beveragesdepends not only on alcohol content but on the presenceof higher ethers, higher alcohols, aldehydes, esters, polymers,and volatile oils; many of these are formed during ‘maturation’of the beverage.
Other forms of alcohol
1. Absolute alcohol 99% w/w ethanol (dehydratedalcohol).2. Rectified spirit 90% w/w ethyl alcohol produced fromfermented mollases, by distillation.3. Proof spirit It is an old term. If whiskey is poured ongun powder and ignited and it explodes, then it was labelledto be of ‘proof strength’. If water is mixed to it, gun powderwill not ignite. 100% proof spirit is 49.29% w/w or 57.1%v/v alcohol.4. Methylated spirit (industrial) Also called ‘denaturedspirit’ is produced by adding 5 parts of wood naphtha (methylalcohol) to 95 parts of rectified spirit so as to render it unfitfor drinking. It is tinted blue by methylene blue dye fordistinction. It can be applied on the skin for antiseptic, cleaningand astringent purposes.
PHARMACOLOGICAL ACTIONS
1. Local actions Ethanol is a mildrubefacient and counterirritant when rubbed onthe skin. By evaporation it produces cooling.Applied to delicate skin (scrotum) or mucousmembranes it produces irritation and burningsensation. Concentrated alcohol (spirit) shouldnot be applied in the mouth, nose, etc. Injecteds.c. it causes intense pain, inflammation andnecrosis followed by fibrosis. Injected arounda nerve it produces permanent damage.
Applied to the surface, alcohol is anastringent—precipitates surface proteins andhardens the skin. By precipitating bacterialproteins it acts as an antiseptic. The antiseptic

389C
HA
PTER28
ETHYL AND METHYL ALCOHOLS
action increases with concentration from 20 to70%, remains constant from 70 to 90% anddecreases above that. That 100% ethanol is moredehydrating but poorer antiseptic than 90%ethanol, shows that antibacterial action is notdue to dehydration of bacterial protoplasm.Alcohol does not kill bacterial spores.
2. CNS Alcohol is a neuronal depressant.Since the highest areas are most easily derangedand these are primarily inhibitory—apparent exci-tation and euphoria are experienced at lowerplasma concentrations (30–60 mg/dl). Hesita-tion, caution, self-criticism and restraint are lostfirst. Mood and feelings are altered; anxiety maybe allayed. With increasing concentration (80–150 mg/dl) mental clouding, disorganization ofthought, impairment of attention, memory andother faculties, alteration of gait and perceptionand drowsiness supervene. At 150–200 mg/dlthe person is sloppy, ataxic and drunk, ‘black-outs’ occur; 200–300 mg/dl result in stupor andabove this unconsciousness prevails, medullarycentres are paralysed and death may occur.Though, alcohol can produce anaesthesia, marginof safety is narrow.
Any measurable concentration of alcohol pro-duces a measurable slowing of reflexes: drivingis dangerous. Performance is impaired, fine dis-crimination and precise movements are oblitera-ted; errors increase, except if fear of punishmentand anxiety of failure has already impaired it.Under such situation performance may beimproved by allaying of anxiety and fear.
At any given blood alcohol level, centraleffects are more marked when the concentrationis rising than when it is falling. This is consi-dered to be a manifestation of acute tolerance.
Alcohol can induce sleep but is not adependable hypnotic. Some individuals reportpoor quality of sleep and repeated or earlymorning awakening. Sleep architecture may be
disorganized and sleep apnoea aggravated.‘Hangover’ (headache, dry mouth, laziness,disturbed mood, impaired performance) mayoccur the next morning. Alcohol raises painthreshold and also alters reaction to it, but isnot a dependable analgesic—severe pain canprecipitate confusion and convulsions. Duringthe time alcohol is acting on brain, it exertsanticonvulsant action, but this is followed bylowering of threshold: seizures may be precipi-tated in epileptics. Chronic alcohol abuse damagesbrain neurones, causes shrinkage of brain.
The cortex and the reticular activating systemare most sensitive to alcohol; other areas getdepressed as concentration rises.Mechanism of action Alcohol was believed to produceCNS depression by a generalized membrane action alteringthe state of membrane lipids. However, lately specific effecton multiple receptor operated and voltage gated ion channels/other critical proteins has been demonstrated at concen-trations attained during moderate drinking. Thus, severalneurohumoral systems are concurrently affected producinga complex pattern of action quite different from that producedby other depressants like barbiturates and benzodiazepines,which predominantly facilitate GABAA receptor mediated Cl¯channel opening. Alcohol has been shown to enhance GABArelease at GABAA sites in the brain. It also inhibits NMDAand kainate type of excitatory amino acid receptors (operatingthrough cation channels). Action of 5-HT on 5-HT3 inhibitoryautoreceptor (having an intrinsic ion channel) is augmented.Some studies suggest that cerebral nicotinic cholinergic recep-tor (operating through Na+ channel) may also be one of thetargets of alcohol action. Ethanol can indirectly reduceneurotransmitter release by inhibiting voltage sensitiveneuronal Ca2+ channels. It also activates specific type of K+
channels in certain brain areas. Release and turnover of DAin brain is enhanced through β endorphin release in nucleusaccumbens and an opioid receptor dependent mechanism.This is probably important in the pleasurable reinforcingeffects of alcohol and in the genesis of alcohol dependence.Activity of membrane bound enzymes like Na+ K+ ATPaseand adenylyl cyclase is also altered. The activity andtranslocation of channel/enzyme proteins in the membranecould be affected by alcohol through protein kinase C (PKC)and protein kinase A (PKA) mediated alteration in the stateof their phosphorylation.
Alcohol : conscious anaesthesia death.
Ether : conscious anaesthesia death.

390S
EC
TIO
N7
DRUGS ACTING ON CENTRAL NERVOUS SYSTEM
3. CVS The effects are dependent on dose.Small doses: produce only cutaneous (especiallyon the face) and gastric vasodilatation. Skin iswarm and flushed and there may be conjunctivalinjection; BP is not affected.Moderate doses: cause tachycardia and a mildrise in BP due to increased muscular activityand sympathetic stimulation.Large doses: cause direct myocardial as wellas vasomotor centre depression and there is fallin BP.
Epidemiological studies have confirmed thatchronic alcoholism contributes to hypertensionand can lead to cardiomyopathy. Atrial fibrilla-tion and other cardiac arrhythmias may occurdue to conduction defects and Q-T prolongation.
4. Blood Regular intake of small to moderateamounts of alcohol (1–2 drinks) has been foundto raise HDL-cholesterol levels and decreaseLDL oxidation. This may be responsible for the15–35% lower incidence of coronary arterydisease in such individuals. Risk reduction isgreatest in high risk subjects and protection islost if > 3 drinks are consumed daily. However,it is considered inapproptiate to advisenondrinkers to start drinking on this account,since other adverse consequences may more thannullify this benefit. Mild anaemia is commonin chronic alcoholics. Megaloblastic anaemiaoccurring in chronic alcoholism is due tointerference with folate metabolism.
5. Body temperature Alcohol is reputed tocombat cold. It does produce a sense of warmthdue to cutaneous and gastric vasodilatation, butheat loss is actually increased in cold surroun-dings. High doses depress temperature regula-ting centre.
6. Respiration Brandy or whiskey are reputedas respiratory stimulants in collapse. They irritatebuccal and pharyngeal mucosa which may tran-siently stimulate respiration reflexly. However,it is better not to depend on this, because thedirect action of alcohol on respiratory centreis only a depressant one.
7. GIT Alcoholic beverages have variableeffect on gastric secretion depending on thebeverage itself and whether the individual likesit. However, dilute alcohol (optimum 10%) putin the stomach by Ryle’s tube is a strongstimulant of gastric secretion (especially ofacid). It acts directly as well as reflexly. Higherconcentrations (above 20%) inhibit gastricsecretion, cause vomiting, mucosal congestionand gastritis. Alcoholism is an important causeof chronic gastritis. Lower esophageal sphincter(LES) tone is reduced by alcohol. Drinking mayaccentuate gastric reflux. Bowel movements maybe altered in either direction. Acute pancreatitisis a complication of heavy drinking.8. Liver Neither brief alcohol intoxicationnor chronic intake of small-to-moderate amountscause significant liver damage, provided adequatenutrition is maintained. However, it does mobi-lize peripheral fat and increases fat synthesisin liver in a dose-dependent manner. Proteinsmay also accumulate in liver because theirsecretion is decreased. Chronic alcoholismexposes liver to oxidative stress and causescellular necrosis followed by fibrosis.Acetaldehyde produced during metabolism ofalcohol appears to damage the hepatocytes andinduce inflammation, especially on chronicingestion of large amounts. Increased lipidperoxidation and glutathione depletion occurs.These combined with vitamin and othernutritional deficiencies may be responsible forthe so called alcoholic cirrhosis.
Regular alcohol intake induces microsomalenzymes.9. Skeletal muscle Alcohol produces littledirect effect. Fatigue is allayed by small doses,but muscle work is increased or decreaseddepending on the predominating central effect.Weakness and myopathy occurs in chronicalcoholism.10. Kidney Diuresis is often noticed afteralcohol intake. This is due to water ingested alongwith drinks as well as alcohol induced inhibitionof ADH secretion. It does not impair renalfunction.

391C
HA
PTER28
ETHYL AND METHYL ALCOHOLS
11. Sex Alcohol is reputed as an aphrodisiac.Aggressive sexual behaviour is due to loss ofrestraint and inhibition. However, performanceof the sexual act is often impaired. Chronicalcoholism can produce impotence, testicularatrophy, gynaecomastia and infertility in bothmen and women.
12. Endocrine effects Moderate amounts ofalcohol increase Adr release which can causehyperglycaemia and other sympathetic effects.However, acute intoxication is often associatedwith hypoglycaemia and depletion of hepaticglycogen, because gluconeogenesis is inhibited.Glucagon, thus fails to reverse it and glucosemust be given to counteract hypoglycaemia.
13. Uterine contractions are suppressed atmoderate blood levels.
PHARMACOKINETICS
Rate of alcohol absorption from the stomachis dependent on its concentration, presence offood, and other factors, but is generally quiteslow. Absorption from intestines is very fast;peak levels are attained after ~30 min. Thus,gastric emptying determines rate of absorption.Limited first pass metabolism occurs in stomachand liver. Absorption of alcohol from skin ofadults is minimal but may be significant in infantsgiven alcohol sponges.
Alcohol gets distributed widely in the body(vol of distribution 0.7 L/kg), crosses bloodbrain barrier efficiently: concentration in brainis very near blood concentration. It also crossesplacenta freely. Alcohol is oxidized in liver tothe extent of 98%. Even with high doses, notmore than 10% escapes metabolism.
Alcohol AldehydeEthyl Acetaldehyde Acetate CO2+alcohol dehydro- dehydro- H2O
genase genase
In addition to alcohol dehydrogenase, smallamounts of alcohol are oxidized by hepaticmicrosomal enzymes (mainly CYP2E1) as well.Metabolism of alcohol follows zero orderkinetics, i.e. a constant amount (8–12 ml of
absolute alcohol/ hour) is degraded in unit time,irrespective of blood concentration. Thus, rateof consuming drinks governs whether a personwill get drunk.
Excretion of alcohol occurs through kidneyand lungs, but neither is quantitatively significant.Concentration in exhaled air is about 0.05% ofblood concentration: this is utilized for medico-legal determination of drunken state. The subjectblows in a balloon and alcohol is measured byportable breath analyser.
INTERACTIONS
1. Alcohol synergises with anxiolytics, anti-depressants, antihistaminics, hypnotics,opioids → marked CNS depression withmotor impairment can occur: Chances ofaccidents increase.
2. Individuals taking a sulfonylurea, cefope-razone, or metronidazole have experiencedbizarre, somewhat disulfiram-like reactionswhen they consume alcohol. This reactionoccurs only in some individuals and its basisis unclear. It passes off with time as alcoholis metabolized. Only reassurance andsupportive treatment is needed.
3. Acute alcohol ingestion inhibits, while chronicintake induces CYP enzymes (especiallyCYP2E1). Formation of toxic metabolite ofparacetamol (NAPQI) is increased in chronicalcoholics (see p. 207). Safe dose limit ofparacetamol is lower in them. Metabolism oftolbutamide, phenytoin and some other drugsis similarly affected by acute and chronicalcohol intake.
4. Hypoglycaemic action of insulin and sul-fonylureas is enhanced by alcohol ingestion.
5. Aspirin and other NSAIDs cause more gastricbleeding when taken with alcohol.
Food value
Alcohol requires no digestion and is metabo-lized rapidly. It is an energy yielding substrate:7 Cal/g, but these cannot be stored. However,it spares carbohydrates and fats as energy source,so that regular intake can contribute to obesity.

392S
EC
TIO
N7
DRUGS ACTING ON CENTRAL NERVOUS SYSTEM
Alcohol does not supply body building and otheressential constituents of food. Those whoconsume substantial part of their caloric intakeas alcohol, often suffer from nutritionaldeficiencies. Thus, alcohol is an imperfect andexpensive food.
CONTRAINDICATIONS
Alcohol is seldom prescribed medically. How-ever, it is rampently consumed. Intake of alcoholshould be avoided by—1. Peptic ulcer, hyperacidity and gastroesopha-
geal reflux patients (alcohol increases gastricsecretion and relaxes LES).
2. Epileptics: seizures may be precipitated.3. Severe liver disease patients.4. Unstable personalities: they are likely to abuse
it and become excessive drinkers.5. Pregnant women: Even moderate drinking
during pregnancy can produce foetal alcoholsyndrome resulting in intrauterine and post-natal growth retardation, low IQ, micro-cephaly, cranio-facial and other abnormalities,and immunological impairment→increasedsusceptibility to infections. Heavy drinkingduring pregnancy, in addition, increases theincidence of miscarriage, stillbirths and lowbirth-weight babies.
Guidelines for safe drinking Physicians areoften asked to advise on safe ways of drinking.Various official agencies, physician organizationsand alcoholism experts have putforth guidelinesin this regard, but they are not uniform. Thefollowing may be concluded:• On an average 1–2 drinks per day is usually
safe.• Not more than 3 drinks on any one occasion.• Consumption of >3 drinks per day is associa-
ted with documented adverse health effects.• Do not drive or engage in hazardous activities
after drinking.• Do not drink if an interacting drug has been
taken.• Subjects with any contraindication should not
drink.
• Safe limits are somewhat lower for womenthan for men, because metabolism of alcoholis slower and its bioavailability higher (dueto less first pass metabolism in stomach) inwomen than in men.
[Note: 1 drink = 50 ml of spirits = 150 ml ofwines = 400 ml of beer; all have roughly 16 galcohol, which taken in empty stomach producesa peak alcohol blood level of ~ 30 mg/dl in anadult male of average built.]
TOXICITY
A. Side effects of moderate drinking Nausea,vomiting, flushing, hangover, traffic accidents.
B. Acute alcoholic intoxication Unawareness,unresponsiveness, stupor, hypotension, gastritis,hypoglycaemia, respiratory depression, collapse,coma and death.
Treatment: Gastric lavage is helpful only whenthe patient is brought soon after ingestingalcohol, which is rare. Since most patients aredisoriented or comatose, the first priority is tomaintain patent airway and prevent aspiration ofvomitus. Tracheal intubation and positivepressure respiration may be needed if it ismarkedly depressed. Analeptics should not begiven. They may precipitate convulsions. Mostpatients will recover with supportive treatment,maintenance of fluid and electrolyte balance andcorrection of hypoglycaemia by glucose infusiontill alcohol is metabolized. Thiamine (100 mgin 500 ml glucose solution infused i.v.) shouldbe added. Recovery can be hastened by haemo-dialysis. Insulin + fructose drip has been foundto accelerate alcohol metabolism. However, itsclinical impact is not remarkable.
C. Chronic alcoholism On chronic intake,tolerance develops to subjective and behavioraleffects of alcohol, but is generally of a lowdegree. It is both pharmacokinetic (reduced rateof absorption due to gastritis and faster meta-bolism due to enzyme induction) and cellulartolerance. Psychic dependence often occurs evenwith moderate drinking; depends a lot on

393C
HA
PTER28
ETHYL AND METHYL ALCOHOLS
individual’s likings and attitudes. It is manifestedin alcohol-seeking behaviour, and the prioritythat the subject accords to obtaining and consu-ming alcohol over other needs, or the extentto which he will go for maintaining alcoholintake.
Recent studies have confirmed that a genetic basis contributesto progression from social drinking to alcoholism in about50% individuals. Alcoholism is often a familial trait. Somedifferences in sensitivity of various neuronal systems toalcohol among ‘predisposed’ and ‘not predisposed’individuals have been demonstrated.
There is no single explanation for why people drink.Diverse feelings and behaviours are provoked by alcohol indifferent individuals and in the same individual on differentoccasions. Alcohol can make people happy as well as sad,curtious as well as mean, talkative as well as silent, friendlyas well as hostile. All this cannot be explained on the basisof pharmacological actions of alcohol alone. Attitudes, beliefs,peer groups, social setting and learned experiences all havea bearing. Alcohol is said to produce good mood, sense ofwellbeing, self confidence, sociability, etc. But these infactare learned behaviours. In some societies, alcoholic beverageshave become an acceptable form of extending courtesy andof entertainment. Drinking is often related to ‘celebration’ and‘high living’. There is ‘wine snobbery’ in high social groups.
To some, excess drinking provides the excitement of risktaking. People often boast of their capacity to drink. To theyoung, drinking may be a symbol of rebellion against theoppressive older generation and rejection of the values ofthe establishment. ‘Binge drinking’ is a specific behaviouralpattern of bouts of excessive drinking. Alcohol is often anexcuse for bad behaviour. Society’s view that intoxicatedperson is unaware of his actions (therefore not responsible)makes intoxication an attractive state, because there isincreased freedom of what one can say or do after drinking.Thus, there are a variety of motivations for drinking.
Physical dependence occurs only on heavy andround-the-clock drinking (if alcohol is presentin the body continuously). Heavy drinking isoften associated with nutritional deficiencies,because food is neglected and malabsorptionmay occur. In addition to impaired mental andphysical performance, neurological afflictionsare common—polyneuritis, pellagra, tremors,seizures, loss of brain mass, Wernicke’s encep-halopathy, Korsakoff’s psychosis and megalo-blastic anaemia. Alcoholic cirrhosis of liver,hypertension, cardiomyopathy, CHF, arrhythmias,stroke, acute pancreatitis, impotence, gynae-comastia, infertility and skeletal myopathy are
other complications. Incidence of oropharyngeal,esophageal and hepatic malignancy and respi-ratory infections is high; immune function isdepressed.
Withdrawal syndrome When a physicallydependent subject stops drinking, withdrawalsyndrome appears within a day. Its severitydepends on the duration and quantity of alcoholconsumed by the subject. It consists of anxiety,sweating, techycardia, tremor, impairment ofsleep, confusion, hallucinations, deliriumtremens, convulsions and collapse.
Treatment Psychological and medical suppor-tive measures are needed during withdrawal.Many CNS depressants like barbiturates, pheno-thiazines, chloral hydrate have been used as sub-stitution therapy in the past (to suppress with-drawal syndrome) but benzodiazepines (chordia-zepoxide, diazepam) are the preferred drugs now.These have a long duration of action and canbe gradually withdrawn later.
Naltrexone: Several studies have demonstratedinvolvement of opioid system in the pleasurablereinforcing effects of alcohol through dopaminemediated reward function. The post-addict treatedwith the long-acting opioid antagonist naltrexone(see Ch. 34) does not experience the samepleasurable effect on taking alcohol; reinforce-ment is weakened. Trials have shown that it helpsprevent relapse of alcoholism. It reduced alcoholcraving, number of drinking days and chancesof resumed heavy drinking. Naltrexone isapproved for use as adjuvant in comprehensivetreatment programmes for alcohol dependentsubjects and is being used in India at mostdeaddiction centres, after the individual hasundergone withdrawal and is motivated.
Acamprosate It is a weak NMDA-receptor antagonist withmodest GABAA receptor agonistic activity that is being usedin USA, UK and Europe for maintenance therapy of alcoholabstinence. In conjunction with social and motivationaltherapy, it has been found to reduce relapse of the drinkingbehaviour. The efficacy of acamprosate in this regard is ratedcomparable to naltrexone. It should be started soon afterwithdrawing alcohol and then given continuously at a dose

394S
EC
TIO
N7
DRUGS ACTING ON CENTRAL NERVOUS SYSTEM
of 666 mg 2–3 times a day. Loose motion is a common sideeffect. Others are nausea, abdominal pain and itching.
The 5-HT3 antagonist ondansetron and the antiepileptictopiramate have also shown some promise in treatingalcoholism.
CLINICAL USES
Medicinal uses of ethanol are primarilyrestricted to external application and as a vehiclefor liquid preparations used internally.1. As antiseptic (see Ch. 65).2. Rubefacient and counterirritant for sprains,
joint pains, etc. Spirit is generally used asvehicle for other ingredients.
3. Rubbed into the skin to prevent bedsores. Itshould not be applied on already formedsores. Astringent action of alcohol is utilizedin antiperspirant and aftershave lotions.
4. Alcoholic sponges to reduce body tempera-ture in fever. However, cold water/ice maybe better.
5. Intractable neuralgias (trigeminal and others),severe cancer pain. Injection of alcohol roundthe nerve causes permanent loss of trans-mission.
6. To ward off cold. Alcohol in the form ofwhiskey or brandy may benefit by causingvasodilatation of blanched mucosae; butfurther exposure after taking alcohol may bedeleterious because alcohol increases heatloss due to cutaneous vasodilatation.
7. As appetite stimulant and carminative:30–50 ml of 7–10% alcohol may be takenas beverages or tinctures (of ginger/cardemom, etc.) before meal.
8. Reflex stimulation in fainting/hysteria: 1 dropin nose.
9. To treat methanol poisoning (see below).
Aldehyde dehydrogenase inhibitorDisulfiram It inhibits the enzyme aldehydedehydrogenase (Fig. 28.1) probably after conver-sion into active metabolites. When alcohol isingested after taking disulfiram, the concentrationof acetaldehyde in tissues and blood rises anda number of highly distressing symptoms(aldehyde syndrome) are produced promptly.
These are—flushing, burning sensation, throbbingheadache, perspiration, uneasiness, tightness inchest, dizziness, vomiting, visual disturbances,mental confusion, postural fainting andcirculatory collapse. Duration of the syndrome(1–4 hours) depends on the amount of alcoholconsumed. Because of risk of severe reaction,disulfiram is to be used with great caution, onlyin well-motivated subjects.
Disulfiram aversion therapy is indicated inabstinent subjects who sincerely desire to leavethe habit. After making sure that the subject hasnot taken alcohol in the past 12 hours, disufiramis given at a dose of 500 mg/day for one weekfollowed by 250 mg daily. Sensitization to alcoholdevelops after 2–3 hours of first dose, reachesits peak at ~12 hours and lasts for 7–14 daysafter stopping it, because inhibition of aldehydedehydrogenase with disulfiram is irreversible:synthesis of fresh enzyme is required for returnof activity. The subject’s resolve not to drinkis reinforced by the distressing symptoms thatoccur if he drinks a little bit. The subject shouldbe cautioned to avoid alcohol altogether.Disulfiram should not be used in patients whoare physically dependent on alcohol.
Side effects of disulfiram (as such) are infre-quent, include rashes, metallic taste, nervous-ness, malaise and abdominal upset. It inhibitsa number of other enzymes as well includingalcohol dehydrogenase, dopamine β hydroxylaseand several cytochrome P450 isoenzymes. Thus,it prolongs t½ of many drugs.ESPERAL, ANTADICT, DEADICT 250 mg tab. (internationallymarketed as ANTABUSE)
METHYL ALCOHOL(Methanol, Wood alcohol)
Methyl alcohol is added to industrial rectifiedspirit to render it unfit for drinking. It is onlyof toxicological importance. Mixing ofmethylated spirit with alcoholic beverages bybootlegers or its inadvertent ingestion resultsin methanol poisoning.
Methanol is metabolized to formaldehyde andformic acid by alcohol and aldehyde dehydro-

395C
HA
PTER28
ETHYL AND METHYL ALCOHOLS
genases respectively (Fig. 28.1), but the rate is1/7th that of ethanol. Like ethanol, metabolismof methanol also follows zero order kineticsand t½ of 20–60 hours has been measured.
Methanol also is a CNS depressant, but lessinebriating than ethanol. Toxic effects ofmethanol are largely due to formic acid, sinceits further metabolism is slow and folatedependent. A blood level of >50 mg/dl methanolis associated with severe poisoning. Even 15 mlof methanol has caused blindness and 30 ml hascaused death; fatal dose is regarded to be75–100 ml.
Manifestations of methanol poisoning arevomiting, headache, epigastric pain, uneasiness,drunkenness, disorientation, tachypnoea,dyspnoea, bradycardia and hypotension. Deliriumand seizures may occur and the patient maysuddenly pass into coma. Acidosis is prominentand entirely due to production of formic acid.The specific toxicity of formic acid is retinaldamage. Blurring of vision, congestion of opticdisc followed by blindness always precede deathwhich is due to respiratory failure.
Treatment1. Keep the patient in a quiet, dark room; protect
the eyes from light.
2. Gastric lavage with sod. bicarbonate if thepatient is brought within 2 hours of ingestingmethanol. Supportive measures to maintainventilation and BP should be instituted.
3. Combat acidosis by i.v. Sod. bicarbonate infu-sion. This is the most important measure;prevents retinal damage and other symptoms;large quantities may be needed.
4. Pot. chloride infusion is needed only whenhypokalemia occurs due to alkali therapy.
5. Ethanol is preferentially metabolized byalcohol dehydrogenase over methanol. At aconcentration of 100 mg/dl in blood itsaturates alcohol dehydrogenase and retardsmethanol metabolism. This helps by reducingthe rate of generation of formaldehyde andformic acid. Ethanol (10% in water) isadministered through a nasogastric tube;loading dose of 0.7 ml/kg is followed by 0.15ml/kg/hour. Because pharmacokinetics ofalcohol changes over time and no i.v.formulation is available, maintenance of afixed concentration is difficult. Alcohol bloodlevel needs to be repeatedly measured.Moreover, the enzyme saturating concentra-tion of ethanol itself produces intoxicationand can cause hypoglycaemia. Use of ethanolfor this purpose is tricky. Treatment has tobe continued for several days because thesojourn of methanol in body is long.
6. Haemodialysis: clears methanol as well asformate and hastens recovery.
7. Fomepizole (4-methylpyrazole) is a specificinhibitor of alcohol dehydrogenase and thedrug of choice for methanol poisoning byretarding its metabolism. A loading dose of15 mg/kg i.v. followed by 10 mg/kg every12 hours till serum methanol falls below20 mg/dl, has been found effective and safe.It has several advantages over ethanol, viz.longer t½ and lack of inebriating action, butis not available commercially in India.
8. Folate therapy: Calcium leucovorin 50 mginjected 6 hourly has been shown to reduceblood formate levels by enhancing its oxi-dation. This is a promising adjuvant approach.
Fig. 28.1: Shared metabolic pathway of ethyl andmethyl alcohols

396S
EC
TIO
N7
DRUGS ACTING ON CENTRAL NERVOUS SYSTEM
PROBLEM DIRECTED STUDY
28.1 A school boy aged 16 years developed tonic-clonic epilepsy and was maintained oncarbamazepine 200 mg 3 times a day. He was seizure free for the last one year, but reportedback one afternoon with the complaint of recurrence of two seizure episodes since morning.On questioning, he revealed that last evening he attended a party with his friends and consumed4 drinks of whiskey, and was awake till late night. This was the first time that he had takenan alcoholic drink.(a) Could the recurrence of seizures be related to the intake of alcohol previous night? Ifso, what could be the mechanism?(b) Does his antiepileptic therapy need any change or adjustment of doses due to this recurrenceof seizures. What further advise will you give to this patient?(see Appendix-1 for solution)
Ethylene glycol poisoning Ethylene glycol poisoning hasoccurred sporadically, especially among children. It is anindustrial solvent, coolant and antifreeze. Ethylene glycol isoxidized in the body by alcohol dehydrogenase to glyco-aldehyde and then to glycolic acid—glyoxylic acid—oxalic acidin steps. Ethylene glycol itself can cause intoxication similar to
ethanol, but generation of metabolites results in acidosis,cardiopulmonary complications and renal tubular necrosis.
Fomepizole used in the same manner as for methanolpoisoning is the drug of choice. It is approved by US-FDA forthis indication and has ‘orphan drug status’. Ethanol isemployed as an alternative.

Sedative-HypnoticsChapterChapterChapterChapterChapter 2929292929
Sedative A drug that subdues excitement andcalms the subject without inducing sleep, thoughdrowsiness may be produced. Sedation refers todecreased responsiveness to any level ofstimulation; is associated with some decreasein motor activity and ideation.
Hypnotic A drug that induces and/or maintainssleep, similar to normal arousable sleep. Thisis not to be confused with ‘hypnosis’ meaninga trans-like state in which the subject becomespassive and highly suggestible.
The sedatives and hypnotics are more or lessglobal CNS depressants with somewhat diffe-ring time-action and dose-action relationships.Those with quicker onset, shorter duration andsteeper dose-response curves are preferred ashypnotics while more slowly acting drugs withflatter dose-response curves are employed assedatives. However, there is considerableoverlap; a hypnotic at lower dose may act assedative. Thus, sedation—hypnosis—generalanaesthesia may be regarded as increasing gradesof CNS depression. Hypnotics given in highdoses can produce general anaesthesia. However,benzodiazepines (BZDs) cannot be considerednonselective or global CNS depressants likebarbiturates and others.
Treatment of insomnia is the most importantuse of this class of drugs.
Alcohol and opium have been the oldest hypnotics andcontinue to be used for this purpose as self-medication bypeople. Bromides introduced in 1857 are now obsolete, soare chloral hydrate (1869) and paraldehyde (1882). Fischerand von Mering introduced barbitone in 1903 andphenobarbitone in 1912. Barbiturates reigned supreme till 1960swhen benzodiazepines started eroding their position and havenow totally replaced them. In the mean time, a number ofother sedative-hypnotics (glutethimide, methyprilon,methaqualone) were introduced but none was significantlydifferent from barbiturates; all are redundant now. Some non-BZD hypnotics have become available over the past two
decades, and a novel melatonin receptor agonist ramelteonhas been introduced.
SleepThe duration and pattern of sleep varies considerably amongindividuals. Age has an important effect on quantity anddepth of sleep. It has been recognized that sleep is anarchitectured cyclic process (Fig. 29.1). The different phasesof sleep and their characteristics are—Stage 0 (awake) From lying down to falling asleep andoccasional nocturnal awakenings; constitutes 1–2% of sleeptime. EEG shows α activity when eyes are closed and βactivity when eyes are open. Eye movements are irregularor slowly rolling.Stage 1 (dozing) α activity is interspersed with θ waves.Eye movements are reduced but there may be bursts of rolling.Neck muscles relax. Occupies 3–6% of sleep time.Stage 2 (unequivocal sleep) θ waves with interspersedspindles, K complexes can be evoked on sensory stimulation;little eye movement; subjects are easily arousable. Thiscomprises 40–50% of sleep time.Stage 3 (deep sleep transition) EEG shows θ, δ and spindleactivity, K complexes can be evoked with strong stimuli only.Eye movements are few; subjects are not easily arousable;comprises 5–8% of sleep time.
Stage 4 (cerebral sleep) δ activity predominates in EEG,K complexes cannot be evoked. Eyes are practically fixed;subjects are difficult to arouse. Night terror may occur at thistime. It comprises 10–20% of sleep time.
During stage 2, 3 and 4 heart rate, BP and respiration aresteady and muscles are relaxed. Stages 3 and 4 together arecalled slow wave sleep (SWS).
REM sleep (paradoxical sleep) EEG has waves of allfrequency, K complexes cannot be elicited. There are marked,irregular and darting eye movements; dreams and nightmares
The EEG waves have been divided into—α: high amplitude, 8–14 c.p.s. (cycles per second)β: low amplitude, 15–35 c.p.s.θ: low amplitude, 4–7 c.p.s.δ: high amplitude, 0.5–3 c.p.s.
K complex: deep negative wave followed by positive waveand a few spindles.

398S
EC
TIO
N7
DRUGS ACTING ON CENTRAL NERVOUS SYSTEM
Fig. 29.1: A normal sleep cycle
occur, which may be recalled if the subject is aroused. Heartrate and BP fluctuate; respiration is irregular. Muscles arefully relaxed, but irregular body movements occur occasionally.Erection occurs in males. About 20–30% of sleep time is spentin REM.
Normally stages 0 to 4 and REM occur in successionover a period of 80–100 min. Then stages 1–4–REM arerepeated cyclically.
CLASSIFICATION
1. BarbituratesLong acting Short acting Ultra-short
actingPhenobarbitone Butobarbitone Thiopentone
Pentobarbitone Methohexitone
2. Benzodiazepines
Hypnotic Antianxiety AnticonvulsantDiazepam Diazepam DiazepamFlurazepam Chlordiazepoxide LorazepamNitrazepam Oxazepam ClonazepamAlprazolam Lorazepam ClobazamTemazepam AlprazolamTriazolam
3. Newer nonbenzodiazepine hypnoticsZopiclone Zolpidem Zaleplon
Chloral hydrate, Triclophos, Paraldehyde, Glutethimide,Methyprylon, Methaqualone and Meprobamate are historicalsedative-hypnotics no longer used. They are described in earliereditions of this book.
In addition some antihistaminics (promethazine,diphenhydramine), some neuroleptic/antidepressants(chlorpromazine, amitriptyline), some anticholinergic (hyoscine)and opioids (morphine, pethidine) have significant sedativeaction, but are not reliable for treatment of insomnia.
BARBITURATES
Barbiturates have been popular hypnotics andsedatives of the last century upto 1960s, but arenot used now to promote sleep or to calm patients.However, they are described first because theyare the prototype of CNS depressants.
Barbiturates are substituted derivatives of barbituric acid(malonyl urea). Barbituric acid as such is not a hypnotic butcompounds with alkyl or aryl substitution on C5 are.Replacement of O with S at C2 yields thiobarbiturates whichare more lipid-soluble and more potent. Barbiturates havevariable lipid solubility, the more soluble ones are more potentand shorter acting. They are insoluble in water but their sodiumsalts dissolve yielding highly alkaline solution.
PHARMACOLOGICAL ACTIONS
Barbiturates are general depressants for allexcitable cells, the CNS is most sensitive wherethe effect is almost global, but certain areas aremore susceptible.
1. CNS Barbiturates produce dose-dependenteffects:
sedation → sleep → anaesthesia → coma.

399C
HA
PTER29
SEDATIVE-HYPNOTICS
Hypnotic dose shortens the time taken to fallasleep and increases sleep duration. The sleepis arousable, but the subject may feel confusedand unsteady if waken early. Night awakeningsare reduced. REM and stage 3, 4 sleep aredecreased; REM-NREM sleep cycle is disrupted.The effects on sleep become progressively lessmarked if the drug is taken every nightconsecutively. A rebound increase in REM sleepand nightmares is often noted when the drug isdiscontinued after a few nights of use and it takesseveral nights for normal pattern to be restored(Fig. 29.2). Hangover (dizziness, distortions ofmood, irritability and lethargy) may occur in themorning after a nightly dose.
Higher dose of a barbiturate induces apredominance of slow, high voltage EEG activity.Progressive burst suppression occurs if dose isincreased further. Barbiturates depress all areasof the CNS, but reticular activating system isthe most sensitive; its depression is primarilyresponsible for inability to maintain wakefulness.
Mechanism of action Barbiturates appear toact primarily at the GABA : BZD receptor–Cl¯
channel complex (see Fig. 29.3) and potentiateGABAergic inhibition by increasing the lifetimeof Cl¯ channel opening induced by GABA(contrast BZDs which enhance frequency of Cl¯
channel opening). They do not bind to the BZDreceptor, but bind to another site on the samemacromolecular complex to exert the GABA-facilitatory action. The barbiturate site appearsto be located on α or β subunit, because presenceof only these subunits is sufficient for theirresponse. Presence of γ subunit is not necessaryas is the case with BZDs. They also enhanceBZD binding to its receptor. At high concentra-tions, barbiturates directly increase Cl¯ conduc-tance (GABA-mimetic action; contrast BZDswhich have only GABA-facilitatory action) andinhibit Ca2+ dependent release of neurotrans-mitters. In addition they depress glutamateinduced neuronal depolarization through AMPA
Sedative dose (smaller dose of a longer actingbarbiturate) given at daytime can producedrowsiness, reduction in anxiety and excitability.However, they do not have selective antianxietyaction. Barbiturates can impair learning, short-term memory and judgement. They have noanalgesic action; small doses may even causehyperalgesia. Euphoria may be experienced byaddicts.
Barbiturates have anticonvulsant property.The 5-phenyl substituted compounds (pheno-barbitone) have higher anticonvulsant : sedativeratio, i.e. they have specific anticonvulsant actionindependent of general CNS depression.
Fig. 29.2: Effect of hypnotic use for 6 consecutivenights on the ratio of REM / Non-REM sleep duration

400S
EC
TIO
N7
DRUGS ACTING ON CENTRAL NERVOUS SYSTEM
receptors (a type of excitatory amino acid recep-tors). At very high concentrations, barbituratesdepress voltage sensitive Na+ and K+ channelsas well. A dose-dependent effect on multipleneuronal targets appears to confer the ability toproduce any grade of CNS depression.
2. Other systems
Respiration is depressed by relatively higher doses.Neurogenic, hypercapneic and hypoxic drives to respiratorycentre are depressed in succession. Barbiturates donot haveselective antitussive action.
CVS Hypnotic doses of barbiturates produce a slightdecrease in BP and heart rate. Toxic doses produce markedfall in BP due to vasomotor centre depression, ganglionicblockade and direct decrease in cardiac contractility. Reflextachycardia can occur, though pressor reflexes are depressed.However, the dose producing cardiac arrest is about 3 timeslarger than that causing respiratory failure.
Skeletal muscle Hypnotic doses have little effect butanaesthetic doses reduce muscle contraction by action onneuromuscular junction.
Smooth muscles Tone and motility of bowel is decreasedslightly by hypnotic doses; more profoundly duringintoxication. Action on bronchial, ureteric, vesical and uterinemuscles is not significant.
Kidney Barbiturates tend to reduce urine flow by decreasingBP and increasing ADH release. Oliguria attends barbiturateintoxication.
PHARMACOKINETICS
Barbiturates are well absorbed from the g.i. tract. They arewidely distributed in the body. The rate of entry into CNSis dependent on lipid solubility. Highly-lipid solublethiopentone has practically instantaneous entry, while lesslipid-soluble ones (pentobarbitone) take longer; pheno-barbitone enters very slowly. Plasma protein binding varieswith the compound, e.g. thiopentone 75%, phenobarbitone20%. Barbiturates cross placenta and are secreted in milk;can produce effects on the foetus and suckling infant.
Three processes are involved in termination of actionof barbiturates: the relative importance of each varies withthe compound.
(a) Redistribution It is important in the case of highly lipid-soluble thiopentone. After i.v. injection, consciousness isregained in 6–10 min due to redistribution (see Ch. 2) whilethe ultimate disposal occurs by metabolism (t½ of eliminationphase is 9 hours).
(b) Metabolism Drugs with intermediate lipid-solubility(short-acting barbiturates) are primarily metabolized in liver
by oxidation, dealkylation and conjugation. Their plasma t½ranges from 12–40 hours.
(c) Excretion Barbiturates with low lipid-solubility (long-acting agents) are significantly excreted unchanged in urine.The t½ of phenobarbitone is 80–120 hours. Alkalinization ofurine increases ionization and excretion. This is mostsignificant in the case of long-acting agents.
Barbiturates induce several hepatic micro-somal enzymes and increase the rate of theirown metabolism as well as that of many otherdrugs.
USES
Except for phenobarbitone in epilepsy (Ch. 30)and thiopentone in anaesthesia (Ch. 27) no otherbarbiturate is used now. As hypnotic andanxiolytic they have been superseded by BZDs.They are occasionally employed as adjuvants inpsychosomatic disorders.Phenobarbitone 30–60 mg oral OD–TDS; 100–200 mg i.m./i.v.GARDENAL 30, 60 mg tab, 20 mg/5 ml syr; LUMINAL 30 mgtab; PHENOBARBITONE SOD 200 mg /ml inj.
ADVERSE EFFECTS
Side effects Hangover was common after the use ofbarbiturates as hypnotic. On repeated use they accumulatein the body—produce tolerance and dependence. Mentalconfusion, impaired performance and traffic accidents mayoccur (also see Ch. 30).
Idiosyncrasy In an occasional patient barbiturates produceexcitement. This is more common in the elderly.Precipitation of porphyria in susceptible individuals is anotheridiosyncratic reaction.
Hypersensitivity Rashes, swelling of eyelids, lips, etc.—more common in atopic individuals.
Tolerance and dependence Both cellular andpharmacokinetic (due to enzyme induction) tolerance developson repeated use. However, fatal dose is not markedly increa-sed: addicts may present with acute barbiturate intoxication.There is partial cross tolerance with other CNS depressants.
Psychological as well as physical dependence occurs andbarbiturates have considerable abuse liability. This is one ofthe major disadvantages. Withdrawal symptoms are—excitement, hallucinations, delirium, convulsions; deaths haveoccurred.
Acute barbiturate poisoning Mostly suicidal, sometimesaccidental. It is infrequently encountered now due toinavailability of barbiturates. However, the principles oftreatment apply to any CNS depressant poisoning.

401C
HA
PTER29
SEDATIVE-HYPNOTICS
Manifestations are due to excessive CNS depression—patient is flabby and comatose with shallow and failingrespiration, fall in BP and cardiovascular collapse, renal shutdown, pulmonary complications, bullous eruptions.
Lethal dose depends on lipid solubility. It is 2–3 g forthe more lipid-soluble agents (short-acting barbiturates) and5–10 g for less lipid-soluble phenobarbitone.
Treatment
1. Gastric lavage; leave a suspension of activated charcoalin the stomach to prevent absorption of the drug fromintestines.2. Supportive measures: such as, patent airway, assistedrespiration, oxygen, maintenance of blood volume by fluidinfusion and use of vasopressors—dopamine may bepreferred for its renal vasodilating action.3. Alkaline diuresis: with sodium bicarbonate 1 mEq/kg i.v.with or without mannitol is helpful only in the case of long-acting barbiturates which are eliminated primarily by renalexcretion.4. Haemodialysis and haemoperfusion (through a columnof activated charcoal or other adsorbants) is highly effectivein removing long-acting as well as short-acting barbiturates.
There is no specific antidote for barbiturates. In the past,analeptics like metrazol, bemegride, etc. have been used inan attempt to awaken the patient. This is dangerous, mayprecipitate convulsions while the patient is still comatose—mortality is increased. The emphasis now is on keeping thepatient alive till the poison has been eliminated.
Interactions1. Barbiturates induce several CYP iso-enzymes, including glucuronyl transferase, andincrease the metabolism of many drugs andreduce their effectiveness—warfarin, steroids(including contraceptives), tolbutamide,griseofulvin, chloramphenicol, theophylline.2. Additive action with other CNS depressants—alcohol, antihistamines, opioids, etc.3. Sodium valproate increases plasma concen-tration of phenobarbitone.4. Phenobarbitone competitively inhibits as wellas induces phenytoin and imipramine meta-bolism: complex interaction.5. Phenobarbitone decreases absorption ofgriseofulvin from the g.i.t.
BENZODIAZEPINES (BZDs)
Chlordiazepoxide and diazepam were introducedaround 1960 as antianxiety drugs. Since then this
class has proliferated and has replaced barbitu-rates as hypnotic and sedative as well, because—1. BZDs produce a lower degree of neuronaldepression than barbiturates. They have a hightherapeutic index. Ingestion of even 20 hypnoticdoses does not usually endanger life—there isno loss of consciousness (though amnesiaoccurs) and patient can be aroused; respirationis mostly not so depressed as to need assistance.
2. Hypnotic doses do not affect respiration orcardiovascular functions. Higher doses producemild respiratory depression and hypotensionwhich is problematic only in patients withrespiratory insufficiency or cardiac/haemo-dynamic abnormality.3. BZDs have practically no action on otherbody systems. Only on i.v. injection the BP falls(may be marked in an occasional patient) andcardiac contractility decreases. Fall in BP incase of diazepam and lorazepam is due toreduction in cardiac output while that due tomidazolam is due to decrease in peripheralresistance. The coronary arteries dilate on i.v.injection of diazepam.4. BZDs cause less distortion of sleep architec-ture; rebound phenomena on discontinuation ofregular use are less marked.5. BZDs do not alter disposition of other drugsby microsomal enzyme induction.6. They have lower abuse liability: tolerance ismild, psychological and physical dependence,drug seeking and withdrawal syndrome are lessmarked.7. A specific BZD antagonist flumazenil is avai-lable which can be used in case of poisoning.

402S
EC
TIO
N7
DRUGS ACTING ON CENTRAL NERVOUS SYSTEM
CNS actions The overall action of all BZDsis qualitatively similar, but there are prominentdifferences in selectivity for different facets ofaction, and in their time-course of action.Different members are used for differentpurposes. In contrast to barbiturates, they arenot general depressants, but exert relativelyselective anxiolytic, hypnotic, muscle relaxantand anticonvulsant effects in different measures.Even when apparently anaesthetic dose ofdiazepam is administered i.v., some degree ofawareness is maintained, though because ofanterograde amnesia (interference with establi-shment of memory trace) the patient does notclearly recollect the events on recovery.
Antianxiety: Some BZDs exert relativelyselective antianxiety action (see Ch. 33) whichis probably not dependent on their sedativeproperty. With chronic administration relief ofanxiety is maintained, but drowsiness wanes offdue to development of tolerance.
Sleep: While there are significant differencesamong different BZDs, in general, they hastenonset of sleep, reduce intermittent awakeningand increase total sleep time (specially in thosewho have a short sleep span). Time spent in stage2 is increased while that in stage 3 and 4 isdecreased. They tend to shorten REM phase, butmore REM cycles may occur, so that effect ontotal REM sleep is less marked than with barbitu-rates. Nitrazepam has been shown to actuallyincrease REM sleep. Night terrors and bodymovements during sleep are reduced and stageshifts to stage 1 and 0 are lessened. Mostsubjects wake up with a feeling of refreshingsleep. Some degree of tolerance develops to thesleep promoting action of BZDs after repeatednightly use.
Muscle relaxant: BZDs produce centrallymediated skeletal muscle relaxation withoutimpairing voluntary activity (see Ch. 25).Clonazepam and diazepam have more markedmuscle relaxant property. Very high dosesdepress neuromuscular transmission.
Anticonvulsant: Clonazepam, diazepam, nitra-zepam, lorazepam and flurazepam have moreprominent anticonvulsant activity than otherBZDs. Diazepan and lorazepam are highlyeffective for short-term use in status-epilepticus,but their utility in long-term treatment ofepilepsy is limited by development of toleranceto the anticonvulsant action.
Given i.v., diazepam (but not others) causesanalgesia. In contrast to barbiturates, BZDs donot produce hyperalgesia.
Other actions Diazepam decreases nocturnalgastric secretion and prevents stress ulcers.BZDs do not significantly affect bowelmovement.
Short-lasting coronary dilatation is producedby i.v. diazepam.
Site and mechanism of actionBenzodiazepines act preferentially on midbrainascending reticular formation (which maintainswakefulness) and on limbic system (thought andmental functions). Muscle relaxation is producedby a primary medullary site of action and ataxiais due to action on cerebellum.
BZDs act by enhancing presynaptic/post-synaptic inhibition through a specific BZDreceptor which is an integral part of the GABAA
receptor–Cl¯ channel complex. The subunits ofthis complex form a pentameric transmembraneanion channel (Fig. 29.3) gated by the primaryligand (GABA), and modulated by secondaryligands which include BZDs. Only the α and βsubunits are required for GABA action, and mostlikely the binding site for GABA is located onthe β subunit, while the α/γ subunit interfacecarrys the BZD binding site. The modulatoryBZD receptor increases the frequency of Cl¯
channel opening induced by submaximalconcentrations of GABA. The BZDs alsoenhance GABA binding to GABAA receptor.The GABAA antagonist bicuculline antagonizesBZD action in a noncompetitive manner. It isnoteworthy that the BZDs do not themselvesincrease Cl¯ conductance; have only GABA

403C
HA
PTER29
SEDATIVE-HYPNOTICS
Fig. 29.3: Schematic depiction of GABAA-benzodiazepine receptor-chloride channel complex The chloride channel is gated by the primary ligand GABA acting on GABAA receptor located on the β subunit. Thebenzodiazepine (BZD) receptor located on the interface of α and γ subunits modulates GABAA receptor in either direction:agonists like diazepam facilitate, while inverse agonists like DMCM hinder GABA mediated Cl¯ channel opening, andBZD antagonist flumazenil blocks the action of both. The barbiturate receptor, located either on α or β subunit alsofacilitates GABA and is capable of opening Cl¯ channel directly as well. Bicuculline blocks GABAA receptor, whilepicrotoxin blocks the Cl¯ channel directly
facilitatory but no GABA mimetic action. Thisprobably explains the lower ceiling CNS depres-sant effect of BZDs.
The BZD receptor exhibits a considerabledegree of constitutive activation. As such, it iscapable of fine tuning GABA action in eitherdirection. While the BZD-agonists enhanceGABA induced hyperpolarization (due to influxof Cl¯ ions), and decrease firing rate ofneurones, other compounds called BZD-inverseagonists like dimethoxyethyl-carbomethoxy-β-carboline (DMCM) inhibit GABA action and areconvulsants. The competitive BZD-antagonistflumazenil blocks the sedative action of BZDsas well as the convulsant action of DMCM.The GABAA-BZD receptor-Cl– channel complex is composedof five α, β, γ, and in some cases δ, ε, θ or π subunits aswell. Several isoforms of α, β and γ subunits have been cloned.
The subunit composition of the complex differs at differentsites, i.e. there are multiple subtypes of BZD receptor. The(α12 β2 2 γ2) pentamer appears to be the most commonlyexpressed BZD receptor isoform.
Based on studies conducted in genetically mutated mice,it has been suggested that BZD receptor isoforms containingthe α1 subunit are involved in mediating sedative, hypnotic,and amnesic actions of BZDs, while those containing α2
subunits mediate anxiolytic and muscle relaxant actions.Diazepam has similar affinity for BZD receptor containingdifferent (α1 or α2, or α3 or α5) subunits, and has broadspectrum action. Receptor inhomogeneity may provide anexplanation for the pharmacological diversity of other BZDs.The newer non-BZD hypnotics zaleplon, Zolpidem, etc. havehigh affinity for α1 subunit isoform of BZD receptor and exertselective hypnotic-amnesic effect, but have little antiseizureor muscle relaxant property.
At high concentrations BZDs also potentiate the depres-sant action of adenosine by blocking its uptake. Certainactions of BZDs are countered by the adenosine antagonisttheophylline. Thus, BZDs could be acting through othermechanisms as well.

404S
EC
TIO
N7
DRUGS ACTING ON CENTRAL NERVOUS SYSTEM
Drugs affecting GABAA-receptor gated chloride channel
• GABA : Endogenous agonist at GABAA receptor → promotes Cl– influx
• Muscimol : Agonist at GABAA site
• Bicuculline : Competitive antagonist at GABAA receptor
• Picrotoxin : Blocks Cl¯ channel noncompetitively; acts on picrotoxin sensitive site
• Barbiturates : Agonist at an allosteric site; prolong GABA action; and open Cl¯ channel
• Alcohol, : Open Cl¯ channel directly; allosteric facilitation of GABAInhalational
anaesthetics,Propofol
• Benzodiazepines : Agonist at an allosteric BZD site → facilitate GABA action
• β-Carboline : Inverse agonist at BZD site → impede GABA action(DMCM)
• Flumazenil : Competitive antagonist at BZD site
PHARMACOKINETICS
There are marked pharmacokinetic differencesamong BZDs because they differ in lipid-solubility by > 50 fold. These differences areimportant factors governing their choice fordifferent uses. Oral absorption of some is rapidwhile that of others is slow. Absorption fromi.m. sites is irregular except for lorazepam.Plasma protein binding also varies markedly(flurazepam 10% to diazepam 99%). BZDs arewidely distributed in the body. The more lipidsoluble members enter brain rapidly and havea two phase plasma concentration decay curve;first due to distribution to other tissues and laterdue to elimination. A relatively short durationof action is obtained with single dose of a drugthat is rapidly redistributed, even though it mayhave a long elimination t½. Using the eliminationt½ alone to predict duration of action may bemisleading. However, elimination t½ determinesduration of action in case of drugs whoseelimination is by far the dominant feature orwhen the drug is given repeatedly.
Benzodiazepines are metabolized in livermainly by CYP3A4 and CYP2C19 to dealkylatedand hydroxylated metabolites, some of whichmay be active. The biological effect half-life ofthese drugs may be much longer than the plasmat½ of the administered compound. The phase I
metabolites and certain BZDs themselves areconjugated with glucuronic acid. Some BZDs(e.g. diazepam) undergo enterohepatic circu-lation. BZDs and their phase I metabolites areexcreted in urine as glucuronide conjugates.BZDs cross placenta and are secreted in milk.
Drugs with a long t½ or those which generateactive metabolites cumulate on nightly use; theiraction may then extend into the next day. Somefeatures of BZDs used as hypnotic are given inTable 29.1.BZDs may be categorized according to theirpharmacokinetic profile into:
I. Slow elimination of parent drug or activemetabolite
Flurazepam Produces an active metabolitewhich has a long t½. Residual effects are likelynext morning; cumulation occurs on dailyingestion peaking after 3–5 days. It is suitablefor patients who have frequent nocturnal awaken-ings and in whom some day time sedation isacceptable.NINDRAL, FLURAZ 15 mg cap.
II. Relatively slow elimination but markedredistribution
Diazepam It is the oldest and all purposeBZD, used as anxiolytic, hypnotic, muscle

405C
HA
PTER29
SEDATIVE-HYPNOTICS
TABLE 29.1 Some pharmacokinetic and clinical features of benzodiazepines used as hypnotics
Drug t½ (hr)* Redistribution$ Hypnotic Clinical indicationsdose (mg)
I. LONG ACTINGFlurazepam 50–100 – 15–30 Chronic insomnia, short-term insomniaDiazepam 30–60 + 5–10 with anxiety; Frequent nocturnal awakening;Nitrazepam 30 ± 5–10 Night before operation
II. SHORT ACTINGAlprazolam 12 + 0.25–0.5 Individuals who react unfavourably toTemazepam 8–12 + 10–20 unfamiliar surroundings or unusual timingsTriazolam 2–3 ± 0.125–0.25 of sleep. Sleep onset difficulties.
* t½ of elimination phase, including that of active metabolite$ + indicates that redistribution contributes to termination of action of single dose
relaxant, premedicant, anaesthetic and foremergency control of seizures due to its broadspectrum activity. It generates active metabolites(desmethyl-diazepam, oxazepam). On occasionaluse it is free of residual effects. With regularuse accumulation occurs and prolonged anxio-lytic effect may be obtained. It is less likelyto cause rebound insomnia on discontinuationof chronic use. Withdrawal phenomena are mild.VALIUM 2, 5, 10 mg tab., 10 mg/2 ml inj., CALMPOSE 2.5, 5, 10mg tab, 2 mg/5 ml syr, 10 mg/2 ml inj, PLACIDOX 2, 5, 10 mg tab,10 mg/2 ml inj.
Nitrazepam Dose to dose equipotent asdiazepam. Accumulation and residual effects canbe avoided only if ingestion is occasional. Goodfor patients with frequent nocturnal awakenings,when some day time sedation is acceptable.SEDAMON, HYPNOTEX, NITRAVET 5 mg tab., 5, 10 mg cap.
III. Relatively rapid elimination andmarked redistribution
Alprazolam The primary indication of thispotent and intermediate acting BZD is anxietydisorder (see Ch. 33), but it is also beingemployed as night-time hypnotic with fewresidual effects the next day. Discontinuationafter regular use has produced relatively markedwithdrawal phenomena.Temazepam It is an intermediate acting BZD. Absorptionis slow in case of tablet but fast when used in soft gelatincapsule. Good for sleep onset difficulty, free of residual effects.
Accumulation can occur on daily ingestion. Does not produceactive metabolites.
IV. Ultrarapid elimination
Triazolam Very potent, peak effect occurs in < 1 hour;good for sleep induction but poor for maintaining it. Patientmay wake up early in the morning and feel anxious. This maybe a withdrawal phenomenon. Rebound insomnia may occurwhen it is discontinued after a few nights of use. It doesnot accumulate on repeated nightly use and no residual effectsare noted in the morning. However, higher doses can altersleep architecture, produce anterograde amnesia and anxietythe following day. Some cases of paranoia and otherpsychiatric disturbances have been noted. For this reason,it has been withdrawn from U.K., but is employed in othercountries for elderly patients, shift workers, travellers, etc.
Midazolam Extremely rapid absorption—peak in 20 min.It can cause problems in the elderly (ataxia, blackouts); moreliable for abuse. Therefore, it is not available now for oraluse as a hypnotic. It is mainly used as an i.m. premedicantor an i.v. anaesthetic (see p. 383).
ADVERSE EFFECTS
Benzodiazepines are relatively safe drugs. Sideeffects of hypnotic doses are dizziness, vertigo,ataxia, disorientation, amnesia, prolongation ofreaction time—impairment of psychomotorskills (should not drive). Hangover is lesscommon, but may be noted if larger doses areused, especially of longer acting drugs.Weakness, blurring of vision, dry mouth andurinary incontinence are sometimes complained.Older individuals are more susceptible to

406S
EC
TIO
N7
DRUGS ACTING ON CENTRAL NERVOUS SYSTEM
psychomotor side effects. Like any hypnotic,BZDs can aggravate sleep apnoea.
Paradoxical stimulation, irritability and swea-ting may occur in an occasional patient,especially with flurazepam. Some patients expe-rience increase in nightmares and behaviouralalterations, especially with flurazepam andnitrazepam.
Tolerance to the sedative effects developsgradually, but there is little tendency to increasethe dose. Cross tolerance to alcohol and otherCNS depressants occurs.
The dependence producing liability of BZDsis low. They are weak reinforcers (lesspleasurable) and seldom abused alone. Drugabusers find them rather bland and prefer otherCNS depressants. Withdrawal syndrome isgenerally mild; may be more intense in case ofultrarapid elimination drugs. Anxiety, insomnia,restlessness, malaise, loss of appetite, baddreams is all that occurs in most cases. Agitation,panic reaction, tremors and delirium areoccasional; convulsions are rare. Drug seekingbehaviour is not prominent.
An earlier report of increased birth defectson use of diazepam during pregnancy has beendisputed. Administration during labour may causeflaccidity and respiratory depression in theneonate.
INTERACTIONS
BZDs synergise with alcohol and other CNSdepressants leading to excessive impairment.Concurrent use with sod. valproate has provokedpsychotic symptoms.
Drug interactions due to displacement fromprotein binding or microsomal enzyme induc-tion are not significant.
Since CYP 3A4 isoenzyme plays importantrole in metabolism of several BZDs, their actioncan be prolonged by CYP 3A4 inhibitors likeketoconazole, erythromycin and others. Cimeti-dine, isoniazid and oral contraceptives also retardBZD metabolism.
NON-BENZODIAZEPINE HYPNOTICS
This lately developed group of hypnotics arechemically different from BZDs, but act asagonists on a specific subset of BZD receptors.Their action is competitively antagonized by theBZD antagonist flumazenil, which can be usedto treat their overdose toxicity. The non-BZDhypnotics act selectively on α1 subunit contain-ing BZD receptors and produce hypnotic-amnesic action with only weak antianxiety,muscle relaxant and anticonvulsant effects. Theyhave lower abuse potential than hypnotic BZDs.Given their shorter duration of action, they arebeing preferred over BZDs for the treatment ofinsomnia.
Zopiclone This is the first of the non-BZDhypnotics, which acts as an agonist at a subtypeof BZD receptor involved in the hypnotic action.The effect on sleep resemble those of BZDs,but it does not alter REM sleep and tends toprolong stages 3 and 4. It is reported not todisturb sleep architecture, but some degree ofnext morning impairment can occur. Zopiclonehas been used to wean off insomniacs takingregular BZD medication. Its t½ is 5–6 hours.
Zopiclone is indicated for short term (< 2weeks) treatment of insomnia. Side effects aremetallic or bitter after-taste, impaired judgementand alertness, psychological disturbances, drymouth and milder dependence. Safety in overdoseis similar to BZDs.ZOPITRAN, ZOPICON, ZOLIUM, 7.5 mg tab, one tab at bedtimefor not more than 2–4 weeks (elderly 3.75 mg).
Eszopiclone The active (S) enantiomer of zopiclone hasrecently been approved. It produces little tolerance andphysical dependence, and is considered suitable for treatmentof short-term as well as chronic insomnia.
Zolpidem This structurally non-BZD, butselective BZD receptor agonist has pronouncedhypnotic effect. Sleep latency is shortened, sleepduration is prolonged in insomniacs, but anti-convulsant, muscle relaxant and antianxietyeffects are not evident. Its advantages are: relativelack of effect on sleep stages (REM suppressionis slight); minimal residual day time sedation

407C
HA
PTER29
SEDATIVE-HYPNOTICS
or fading of hypnotic action on repeated nightlyuse; no/little rebound insomnia on discontin-uation; near absence of tolerance and low abusepotential combined with safety in overdose likeBZDs.
Zolpidem is nearly completely metabolizedin liver (t½ 2 hr), and has short duration ofaction. It is indicated for short-term (1–2 weeks)use in sleep onset insomnia as well as forintermittent awakenings. Because the plasma t½is short, next day sedation is minimal, butmorning sedation or prolongation of reaction-time can occur if it is taken late at night. Sideeffects are few. Even large doses do notmarkedly depress respiration. Currently, it is oneof the most commonly prescribed hypnotics.Dose: 5–10 mg (max 20 mg) at bedtime; ½ dose in elderly andliver disease patients.NITREST, ZOLDEM, DEM 5, 10 mg tabs.
Zaleplon This is the shortest acting of thenewer non-BZD hypnotics that selectively act ona subset of BZD receptors containing the α1
subunit which appear to mediate the hypnoticaction. It is rapidly absorbed; oral bioavailabilityis ~30% due to first pass metabolism; is rapidlycleared by hepatic metabolism with a t½ of1 hour. No active metabolite is produced. As suchit is effective only in sleep-onset insomnia; doesnot prolong total sleep time or reduce the numberof awakenings. Because of brevity of action, itcan be taken late at night (> 4 hour before wakingtime) without causing morning sedation.Surprisingly, despite very short action, no day-time anxiety or rebound insomnia has beenobserved, and hypnotic effect does not fade onnightly use. However, its use should be limitedto 1–2 weeks. The hypnotic efficacy of zaleplonis rated similar to zolpidem. Like the latter, effecton sleep stages and REM sleep are less than thatof BZDs. Tolerance and dependence is unusual.Dose: 5–10 mg (max 20 mg) at bed time.ZAPLON, ZALEP, ZASO 5, 10 mg tabs.
USES
Currently, BZDs are one of the most frequentlyprescribed drugs. They have also been combined
with many other categories of drugs with a viewto improve efficacy by relieving attendantanxiety.
1. As hypnotic A hypnotic should not becasually prescribed for every case of insomnia.Understanding the pattern and cause of insomniain the specific patient is important, and use ofa variety of other measures can avoid unnecessaryhypnotic medication. When indicated, BZDs orthe newer non-BZDs like zolpidem, zaleplon arethe hypnotic of choice. A wide range of compoundshave been developed to suit specific require-ments. Some important points are outlined below:• A hypnotic may be used to shorten sleep
latency, to reduce nocturnal awakenings, orto provide anxiolytic effect the next day wheninsomnia is accompanied with marked elementof anxiety.
• In the use of hypnotics, consideration mustbe given to onset and duration of action ofthe drug. The most suitable pharmacokineticprofile drug should be chosen for a given case.
• Next morning impairment is largely relatedto the dose and pharmacokinetic profile ofthe drug. The next day effects are either dueto prolonged sedation (longer acting drugs)or rebound anxiety (shorter acting drugs).
• Any hypnotic (probably except zolpidem-likedrugs) becomes ineffective after regular usefor a few days; may actually be harmful.
• Though effect of the drug on EEG stages ofsleep, including REM sleep, could be physio-logically relevant, most important is thesubject’s own assessment of having sleptrestfully and waking up feeling fresh with noimpairment the following day. The subjectiveimpression that quality of sleep was poor isthe major criterion of insomnia. This probablycorrelates more closely with effect of thehypnotic on the cyclic alternating pattern(CAP) of sleep.
• Insomnia arises under a variety of circum-stances. It could be a long-term (months-years), short-term (weeks) or transient (a dayor two, mostly situational) problem.

408S
EC
TIO
N7
DRUGS ACTING ON CENTRAL NERVOUS SYSTEM
Chronic insomnia (> 3 weeks) Uncertaintyexists about the use of hypnotics in this situa-tion. The patient may have a personality disor-der, but often there is no specific stress factor.He may have used hypnotics for long periodsor may be alcoholic or have some somaticdisease, e.g. gastroesophageal reflux, pain,COPD, etc. which interfere with sleep. Measureslike aerobic exercise, training at mentalrelaxation, avoiding anxiety about past/futureperformance while in bed, attempting sleep whensleepiness is maximum, avoiding napping at day-time, maintaining regular sleep-wake timings andother sleep-hygiene measures, coffee/alcoholrestriction, treatment of concurrent somaticillness, psychotherapy and controlled sleepcurtailment may succeed. Good nightly sleepimproves the quality of day-time wakefulness.Patients of obstructive sleep apnoea have poorsleep and feel sleepy during the day. All hyp-notics aggravate sleep apnoea and are contraindi-cated.
Intermittent use of a hypnotic, say once every3 days, may be tried. Risk of tolerance and abuseare maximum among chronic insomniacs. Aslowly eliminated drug is preferable becauserebound insomnia and withdrawal symptoms areleast marked with such drugs.
Short-term insomnia (3–21 days) Emotionalproblem (occupational stress, bereavement)and physical illness are the usual causes. Patientmay have induction difficulty or may be wakingup early. Cautious use of low doses of anappropriate drug for the type of sleep disturbancemay be made. Generally a hypnotic, free ofresidual effects should be selected, but whenanxiety is a dominant feature, a BZD whoseaction extends into the next day may be better.Short acting drugs are preferable in the elderly.Intermittent hypnotic use should be limited to2–3 weeks.
Transient insomnia (1–3 days) Due toalterations in the circumstances of sleep, e.g.unusual noise, on an overnight train, new place,unusual pattern of work, shift workers, inter-
continental travel–jetlag, etc. A rapidly elimi-nated hypnotic or one with marked distributionis to be preferred to avoid residual effects thenext morning. However, night before surgery—a long acting drug is better.
2. Other uses(a) As anxiolytic and for day-time sedation (see
Ch. 33).(b) As anticonvulsant, especially emergency
control of status epilepticus, febrile convul-sions, tetanus, etc. (see Ch. 30).
(c) As centrally acting muscle relaxant (see Ch.25).
(d) For preanaesthetic medication, i.v. anaes-thesia and conscious sedation (see Ch. 27).
(e) Before ECT, electrical cardioversion ofarrhythmias, cardiac catheterization, endo-scopies, in obstetrics and many minorprocedures—diazepam i.v. has gained popu-larity because of its calming-amnesic-analgesic and muscle relaxant properties andrelative safety.
(f) Alcohol withdrawal in dependent subjects.(g) Along with analgesics, NSAIDs, spasmo-
lytics, antiulcer and as adjuvants to treat‘gas’ or nonspecific dyspeptic symptoms.
Fixed dose combinations of sedative/hypnotic/anxiolytic drugswith analgesic-antipyretics has been banned in India.
BENZODIAZEPINE ANTAGONIST
Flumazenil It is a BZD analogue which haslittle intrinsic activity (practically no effect onnormal subjects), but competes with BZDagonists as well as inverse agonists for the BZDreceptor and reverses their depressant orstimulant effects respectively.
Flumazenil abolishes the hypnogenic,psychomotor, cognitive and EEG effects ofBZDs. At higher doses it has some week BZDagonist-like as well as inverse agonist-likeactivity in animal models, but these are of noclinical significance.
Flumazenil is absorbed orally; oral bioavai-lability is ~16%, but it is not used orally. Oni.v. injection, action of flumazenil starts in

409C
HA
PTER29
SEDATIVE-HYPNOTICS
seconds and lasts for 1–2 hr; elimination t½ is1 hr, due to rapid metabolism.
Uses
1. To reverse BZD anaesthesia Patientsanaesthetized/sedated with a BZD wakeup, getoriented and regain motor control within 1 minof an i.v. injection of 0.3–1 mg of flumazenil.Resedation generally occurs within 1 hour (morewith diazepam than with midazolam): supple-mental doses of flumazenil may be given. Thismay allow early discharge of patients after diag-nostic procedures and facilitates postanaestheticmanagement.
2. BZD overdose Majority of patients ofBZD overdose require only supportive measureslike patent airway, maintenance of BP, cardiacand renal function (by fluid transfusion, etc.). Inaddition, flumazenil 0.2 mg/min may be injectedi.v. till the patient regains consciousness.Practically all patients intoxicated with a BZDalone respond within 5 min. However, reversalof respiratory depression is incomplete. Fluma-zenil blocks the hypnotic effect of zolpidem-likenon-BZDs as well. In mixed CNS depressantpoisoning, whatever sedation is not abolished by5 mg of flumazenil should be taken to be dueto a non-BZD/non-Zolpidem-like depressant. Itthus helps in differential diagnosis of suchpatients.
Adverse effects Flumazenil is safe and welltolerated.Agitation, discomfort, tearfulness, anxiety, cold-ness and withdrawal seizures are the occasionalside effects.Melatonin It is the principal hormone of the pineal glandwhich is secreted at night and has been found to play an
important role in entraining (synchronizing) the sleep-wakefulness cycle with the circadian rhythm. Two subtypesof melatonin receptor MT1 and MT2 have been identified inthe brain. Both are GPCRs and are believed to carry out thefunction of facilitating sleep onset and fixing its timing inrelation to the circadian clock. Though high doses (80 mg)of melatonin administered orally can induce sleep, low doses(2–10 mg) do not depress the CNS, but probably increasethe propensity of falling asleep. Started before the flight ithas been shown to reduce jet-lag symptoms and to hastenreentrainment with day-night cycle of the new place inintercontinental travellers. Beneficial effects in shift workersand in individuals with delayed sleep phase syndrome havealso been reported. Elderly insomniacs have reportedsubjective improvement in sleep quality. However, melatoninis not a dependable hypnotic; has little effect on latency andduration of sleep, especially in non-elderly insomniacs. A meta-analysis has concluded that it is no more effective thanplacebo in the short-term for sleep disorders. Though it doesnot have the disadvantages of conventional hypnotics, itslong-term safety is not known. Use may therefore be restrictedto treatment of jet-lag, shift workers and elderly insomniacs.
Since melatonin secretion declines with age, it has beenargued that melatonin supplementation might retard ageing.Though there is no proof of benefit, melatonin (2–5 mg/day)is being consumed as a health food in USA and some othercountries. It has also been tried in cluster headache. In Indiait is marketed as a remedy for disturbed biorhythms and sleepdisorders.MELOSET 3 mg tab, ZYTONIN, ETERNEX melatonin 3 mg +pyridoxine 10 mg tab; one tab at evening daily.Ramelteon It is a MT1 as well as MT2 melatonin receptoragonist introduced in USA and now approved in India as well,as a new class of hypnotic for sleep onset insomnia, that doesnot produce the usual BZD-like side effects. Administered in adose of 8 mg ½ hour before going to bed, it is shown to hastensleep onset as well as increase sleep duration, without causingnext morning sedation or impairment.
In clinical trial on chronic insomnia patients, continuousnightly treatment with ramelteon maintained its effect to shortensleep latency and was found to be free of rebound phenomenaon stoppage. No dependence producing potential has beennoted so far. It is rapidly absorbed orally, undergoes extensivefirst pass metabolism in liver, so that bioavailability is low andelimination t½ is 1–3 hours.
Ramelteon appears to be a promizing novel hypnotic,provided its efficacy is established.ROZEREM 8 mg tab: 1 tab 1/2 hour before going to bed.

410S
EC
TIO
N7
DRUGS ACTING ON CENTRAL NERVOUS SYSTEM
PROBLEM DIRECTED STUDY
29.1 A 70-year-old man consults his family physician for the problem of failing to fall asleepoccasionally (3–4 times in a month) for the past few months. He usually sleeps well andhas a 6–7 hour sleep duration. However, on certain nights he keeps lying in bed for 2–3hours before getting sleep. Such episodes are unpredictable, and he cannot relate them toany disturbance, anxiety, worry or physical illness. He has tried relaxing, getting up and walkingaround or reading, but nothing helps. As a result, next day he feels lethargic, impaired, unableto concentrate and has poor creativity. He requests a sleeping pill that he can take after failingto fall asleep.(a) Can he be prescribed a hypnotic for occasional use? If so, which drug would be suitablefor late night intake without next morning sedation?(see Appendix-1 for solution)

Antiepileptic DrugsChapterChapterChapterChapterChapter 3030303030
Epilepsies These are a group of disorders ofthe CNS characterized by paroxysmal cerebraldysrhythmia, manifesting as brief episodes(seizures) of loss or disturbance of conscious-ness, with or without characteristic bodymovements (convulsions), sensory or psychiatricphenomena. These episodes are unpredictable andtheir frequency is highly variable. Epilepsy hasa focal origin in the brain, manifestations dependon the site of the focus, regions into which thedischarges spread and postictal depression ofthese regions. Recognised from the dawn ofhistory as ‘disease of lightening’, it was correctlydescribed by JH Jackson little over a centuryago. Epilepsies have been classified variously;major types are described below.
I. Generalised seizures
1. Generalised tonic-clonic seizures (GTCS, major epi-lepsy, grand mal): commonest, lasts 1–2 min.The usual sequence is aura—cry—unconsciousness—tonicspasm of all body muscles—clonic jerking followed byprolonged sleep and depression of all CNS functions.2. Absence seizures (minor epilepsy, petit mal): prevalentin children, lasts about 1/2 min.Momentary loss of consciousness, patient apparently freezesand stares in one direction, no muscular component or littlebilateral jerking. EEG shows characteristic 3 cycles per secondspike and wave pattern.3. Atonic seizures (Akinetic epilepsy): Unconsciousnesswith relaxation of all muscles due to excessive inhibitorydischarges. Patient may fall.4. Myoclonic seizures Shock-like momentary contractionof muscles of a limb or the whole body.5. Infantile spasms (Hypsarrhythmia) Seen in infants.Probably not a form of epilepsy. Intermittent muscle spasmand progressive mental deterioration. Diffuse changes in theinterseizure EEG are noted.
II. Partial seizures
1. Simple partial seizures (SPS, cortical focal epilepsy):lasts 1/2–1 min. Often secondary. Convulsions are confined
to a group of muscles or localized sensory disturbancedepending on the area of cortex involved in the seizure,without loss of consciousness.2. Complex partial seizures (CPS, temporal lobe epilepsy,psychomotor): attacks of bizarre and confused behaviour andpurposeless movements, emotional changes lasting 1–2 minalong with impairment of consciousness. An aura oftenprecedes. The seizure focus is located in the temporal lobe.
3. Simple partial or complex partial seizures secondarilygeneralized The partial seizure occurs first and evolves intogeneralized tonic-clonic seizures with loss of consciousness.
Most of the cases of epilepsy are primary(idiopathic), some may be secondary to trauma/surgery on the head, intracranial tumour,tuberculoma, cysticercosis, cerebral ischaemia,etc. Treatment is symptomatic and the samewhether epilepsy is primary or secondary.Experimental models These models for testing antiepi-leptic drugs have also shed light on the etiopathogenesisof epilepsy.
1. Maximal electroshock seizures Brief high intensityshock is applied to the head of a rodent (just as in ECT):produces tonic flexion—tonic extension—clonic convulsions.The tonic phase (especially extensor) is selectively abolishedby drugs effective in GTCS. Activity in this model representsaction on spread of seizure discharge.2. Pentylenetetrazol (PTZ) clonic seizures Injection ofPTZ in rats or mice produces clonic convulsions which areprevented by drugs effective in myoclonic and absenceseizures. Activity in this model represents action on seizurefocus itself.3. Chronic focal seizures Produced by application ofalumina cream on the motor cortex of monkey.4. Kindled seizures Brief bursts of weak electrical impul-ses are applied to the brain (especially amygdala) intermittentlyover days. After-discharges increase progressively and tonic-clonic seizures are produced after 10–15 shocks. With timespontaneous seizures set in, usually after >100 shocks. Thisindicates that seizures have a self perpetuating and reinforcingeffect: more neuronal circuits are facilitated and recruited inthe seizure process. Kindling is probably involved in thegenesis of clinical epilepsy.

412S
EC
TIO
N7
DRUGS ACTING ON CENTRAL NERVOUS SYSTEM
CLASSIFICATION
1. Barbiturate Phenobarbitone2. Deoxybarbiturate Primidone3. Hydantoin Phenytoin
Fosphenytoin4. Iminostilbene Carbamazepine
Oxcarbazepine5. Succinimide Ethosuximide6. Aliphatic carboxylic Valproic acid
acid (sodiumvalproate)Divalproex
7. Benzodiazepines ClonazepamDiazepamLorazepamClobazam
8. Phenyltriazine Lamotrigine9. Cyclic GABA Gabapentin
analogues Pregabalin10. Newer drugs Topiramate
ZonisamideLevetiracetamVigabatrinTiagabineLacosamide
Felbamate, rufinamide and few other newer antiseizure drugshave been introduced in some countries as second line/add-ondrugs for refractory partial seizures.
Chemistry Most of the older anticonvulsantshave close structural similarity. This is depicted inFig. 30.1. However, benzodiazepines, carbamaze-pine, valproic acid and the newer drugs are chemi-cally diverse. Presence of a phenyl substitutionconfers activity against tonic-clonic seizures.
Phenobarbitone (see Ch. 29)Phenobarbitone was the first efficacious anti-epileptic introduced in 1912. The mechanismof CNS depressant action of barbiturates isdescribed on p. 399. The same may apply toanticonvulsant action. Enhancement of GABAA
receptor mediated synaptic inhibition appears tobe most important mechanism. However, pheno-barbitone has specific anticonvulsant activitywhich is not entirely dependent on general CNSdepression. Quantitative differences in the
different facets of action (GABA-facilitatory,GABA-mimetic, antiglutamate, Ca2+ entryreduction) have been noted for phenobarbitonecompared to hypnotic barbiturates. The higheranticonvulsant: hypnotic ratio of phenobarbitonemay be due to its minimal effect on Ca2+ channelsand glutamate release compared to hypnotic bar-biturates. With continued use of phenobarbitonesedation wanes off but not anticonvulsant action.It has a wide spectrum of anticonvulsantproperty—raises seizure threshold as well aslimits spread and suppresses kindled seizures.
Phenobarbitone has slow oral absorption anda long plasma t½ (80–120 hours), is metabo-lized in liver as well as excreted unchanged bykidney. Steady-state concentrations are reachedafter 2–3 weeks, and a single daily dose canbe used for maintenance.
The major drawback of phenobarbitone as anantiepileptic is its sedative action. Long termadministration (as needed in epilepsy) mayproduce additional side effects like—behavioralabnormalities, diminution of intelligence, impair-ment of learning and memory, hyperactivity inchildren, mental confusion in older people.
Rashes, megaloblastic anaemia and osteo-malacia (similar to that with phenytoin) occurin some patients on prolonged use.
Fig. 30.1: Chemical structures of classicalanticonvulsant drugs

413C
HA
PTER30
ANTIEPILEPTIC DRUGS
Uses Phenobarbitone is one of the cheapestand least toxic antiepileptics.It has broad spectrum efficacy in generalizedtonic-clonic (GTC), simple partial (SP) andcomplex partial (CP) seizures in a dose of 60 mg1–3 times a day in adults; in children (3–5 mg/kg/day); However, it has become less popularthan carbamazepine, phenytoin or valproatebecause of its dulling and behavioural side effects.
Status epilepticus: Phenobarbitone sod. may beinjected i.m. or i.v. but response is slow todevelop.It is not effective in absence seizures.GARDENAL 30, 60 mg tabs, 20 mg/5 ml syr; LUMINAL30 mg tab, PHENOBARBITONE SODIUM 200 mg/ml inj.
Primidone A deoxybarbiturate, converted byliver to phenobarbitone and phenylethyl malona-mide (PEMA). Its antiepileptic activity is mainlydue to these active metabolites because t½ ofprimidone (6–14 hr) is less than that of its activemetabolites. About 1/3 primidone is excretedunchanged by kidney. Dose to dose primidoneis less potent, but antiepileptic efficacy is similarto phenobarbitone. It is infrequently used nowin GTCS and partial epilepsy, mainly as anadjuvant to phenytoin or carbamazepine.
Adverse effects are similar to phenobarbi-tone. In addition, anaemia, leukopenia, psychoticreaction and lymph node enlargement occurrarely.Dose: 250–500 mg BD, children 10–20 mg/kg/day.MYSOLINE 250 mg tab.
Phenytoin (Diphenylhydantoin)It was synthesized in 1908 as a barbiturate ana-logue, but shelved due to poor sedative property.Its anticonvulsant activity was specifically testedin 1938 in the newly developed electroshockseizure model and since then it is a majorantiepileptic drug.
Phenytoin is not a CNS depressant; somesedation occurs at therapeutic doses, but thisdoes not increase further with dose; rather toxicdoses produce excitement and muscular rigidity.The most outstanding action is abolition of tonicphase of maximal electroshock seizures, with
no effect on or prolongation of clonic phase.It limits spread of seizure activity. Threshold forPTZ convulsions is not raised. Tonic-clonicepilepsy is suppressed but paroxysmal focal EEGdischarge and ‘aura’ persist.
Mechanism of action Phenytoin has astabilizing influence on neuronal membrane—prevents repetitive detonation of normal braincells during ‘depolarization shift’ that occursin epileptic patients and consists of a synchro-nous and unusually large depolarization overwhich action potentials are superimposed. Thisis achieved by prolonging the inactivated stateof voltage sensitive neuronal Na+ channel (Fig.30.2) that governs the refractory period of theneurone. As a result high frequency dischargesare inhibited with little effect on normal lowfrequency discharges which allow Na+ channelsto recover even when their inactivation is pro-longed. This effect has been noted at therapeuticconcentration of phenytoin, while other effectslike reduction in Ca2+ influx, inhibition of gluta-mate and facilitation of GABA responses havebeen demonstrated at higher/toxic concentra-tions. Intracellular accumulation of Na+ thatoccurs during repetitive firing is prevented.
Therapeutic concentrations have no effect onresting membrane potential: normal synaptictransmission is not impaired. Phenytoin, incontrast to phenobarbitone and valproate, doesnot interfere with kindling. Its ability to selec-tively inhibit high frequency firing confersefficacy in trigeminal neuralgia and cardiacarrhythmias as well.
Pharmacokinetics Absorption of phenytoinby oral route is slow, mainly because of its pooraqueous solubility. Bioavailability of differentmarket preparations may differ. It is widelydistributed in the body and is 80–90% boundto plasma proteins.
Phenytoin is metabolized in liver by hydroxy-lation involving CYP2C9 and 2C19 as well asby glucuronide conjugation. The kinetics ofmetabolism is capacity limited; changes fromfirst order to zero order over the therapeutic

414S
EC
TIO
N7
DRUGS ACTING ON CENTRAL NERVOUS SYSTEM
Fig. 30.2: Major mechanisms of anticonvulsant actionm: Activation gate; h: Inactivation gate; GABA-T: GABA transaminase;
SSA: Succinic semialdehyde; GAT-1: GABA transporter
range. As a result small increments in doseproduce disproportionately high plasma concen-trations. The t½ (12–24 hours at therapeuticlevels), progressively increases (upto 60 hr)when plasma concentration rises above 10 µg/ml because metabolizing enzymes get saturated.Monitoring of plasma concentration is veryhelpful in tailoring dosage. Only 5% unchangedphenytoin is excreted in urine.
Adverse effects After prolonged usenumerous side effects are produced attherapeutic plasma concentration; others occuras a manifestation of toxicity due to overdose.
At therapeutic levels• Gum hypertrophy: Commonest (20% inci-
dence), more in younger patients. It is dueto overgrowth of gingival collagen fibres. This
can be minimized by maintaining oral hygiene.• Hirsutism, coarsening of facial features
(troublesome in young girls), acne.• Hypersensitivity reactions are—rashes, DLE,
lymphadenopathy; neutropenia is rare butrequires discontinuation of therapy.
• Megaloblastic anaemia: Phenytoin decreasesfolate absorption and increases its excretion.
• Osteomalacia: Phenytoin interferes withmetabolic activation of vit D and with calciumabsorption/metabolism.
• It can inhibit insulin release and cause hyper-glycaemia.
• Used during pregnancy, phenytoin canproduce ‘foetal hydantoin syndrome’(hypoplastic phalanges, cleft palate, hare lip,microcephaly), which is probably caused byits areneoxide metabolite.

415C
HA
PTER30
ANTIEPILEPTIC DRUGS
At high plasma levels (dose related toxicity)(a) Cerebellar and vestibular manifestations:
ataxia, vertigo, diplopia, nystagmus are themost characteristic features.
(b) Drowsiness, behavioral alterations, mentalconfusion, hallucinations, disorientationand rigidity.
(c) Epigastric pain, nausea and vomiting. Thesecan be minimised by taking the drug withmeals.
(d) Intravenous injection can cause local vascu-lar injury → intimal damage and thrombosisof the vein → edema and discolouration ofthe injected limb. Rate of injection shouldnot exceed 50 mg/min. Tissue necrosisoccurs if the solution extravasates.
(e) Fall in BP and cardiac arrhythmias occuronly on i.v. injection which, therefore, mustbe given under continuous ECG monitoring.
Interactions Phenytoin is a potent inducer ofCYP2C8/9, CYP3A4/5 and some other CYPs.It competitively inhibits CYP2C9/19.• Phenobarbitone competitively inhibits
phenytoin metabolism, while by enzymeinduction both enhance each other’s degra-dation—unpredictable overall interaction.
• Carbamazepine and phenytoin induce eachother’s metabolism.
• Valproate displaces protein bound phenytoinand decreases its metabolism: plasma levelof unbound phenytoin increases.
• Chloramphenicol, isoniazid, cimetidine andwarfarin inhibit phenytoin metabolism—canprecipitate its toxicity.
• Phenytoin competitively inhibits warfarinmetabolism.
• Phenytoin induces microsomal enzymes andincreases degradation of steroids (failure oforal contraceptives), doxycycline, theo-phylline.
• A number of acidic drugs displace it fromprotein binding sites. However, rise is freephenytoin level enhances its clearance. Thus,concentration of free form does not changemuch.
• Sucralfate binds phenytoin in g.i. tract anddecreases its absorption.
Uses Phenytoin is a first line antiepilepticdrug, but less commonly used now because sideeffects are frequent and marginal overdosecauses steep rise in plasma concentration,producing neurotoxicity. Indications are:1. Generalized tonic-clonic, simple and comp-lex partial seizures. It is ineffective in absenceseizures.Dose: 100 mg BD, maximum 400 mg/day; Children5–8 mg/kg/day.2. Status epilepticus: occasionally used by slowi.v. injection (fosphenytoin has replaced it).3. Trigeminal neuralgia: second choice drug tocarbamazepine.DILANTIN 25 mg, 100 mg cap., 100 mg/4 ml oral suspension,100 mg/2 ml inj; EPSOLIN 100 mg tab, 100 mg/2 ml inj; EPTOIN50, 100 mg tab, 25 mg/ml syr; FENTOIN-ER 100 mg extendedrelease cap.
Fosphenytoin This water soluble prodrug ofphenytoin has been introduced to overcome thedifficulties in i.v. administration of phenytoin,which it has replaced for use in statusepilepticus. In the body, it is rapidly convertedto phenytoin; its doses are expressed asphenytoin equivalents (PE). On i.v. injection itis less damaging to the intima; only minorvascular complications are produced and it canbe injected at a faster rate (150 mg/min), butlike phenytoin sod., it requires ECG monitoring.While phenytoin cannot be injected in a dripof glucose solution (because it gets precipitated),fosphenytoin can be injected with both salineand glucose.FOSOLIN 50 mg/ml in 2 ml, 10 ml inj.
CarbamazepineChemically related to imipramine, it was intro-duced in the 1960s for trigeminal neuralgia. Nowit is a first line antiepileptic drug. Its pharma-cological actions resemble phenytoin, butimportant differences have been noted in experi-mental studies. Carbamazepine modifies maximalelectroshock seizures as well as raises thresholdto PTZ and electroshock convulsions. It also

416S
EC
TIO
N7
DRUGS ACTING ON CENTRAL NERVOUS SYSTEM
inhibits kindling. Though its action on Na+
channels (prolongation of inactivated state) issimilar to phenytoin, the profile of action onneuronal systems in brain is different.
Carbamazepine exerts a lithium-like thera-peutic effect in mania and bipolar mood dis-order. It also has antidiuretic action, probablyby enhancing ADH action on renal tubules.
Pharmacokinetics Oral absorption of carba-mazepine is slow and variable because of poorwater solubility. It is 75% bound to plasmaproteins and metabolized in liver by oxidationto an active metabolite (10-11 epoxy carba-mazepine) as well as by hydroxylation andconjugation to inactive ones. It is a substrateas well as inducer of CYP3A4 and CYP2C9.Initially its plasma t½ is 20–40 hours but,decreases to 10–20 hr on chronic medicationdue to autoinduction of metabolism.
Adverse effects Carbamazepine producesdose-related neurotoxicity—sedation, dizziness,vertigo, diplopia and ataxia. Vomiting, diarrhoea,worsening of seizures are also seen with higherdoses. Acute intoxication causes coma, convul-sions and cardiovascular collapse.Hypersensitivity reactions are rashes, photosen-sitivity, hepatitis, lupus like syndrome, rarelyagranulocytosis and aplastic anaemia. Somedegree of leucopenia due to hypersensitivity ismore common.Water retention and hyponatremia can occur inthe elderly because it enhances ADH action.Increased incidence of minor foetal malforma-tions has been reported. Its combination withvalproate doubles teratogenic frequency.
Interactions Carbamazepine is an enzymeinducer; can reduce efficacy of haloperidol, oralcontraceptives, lamotrigine, valproate and topira-mate. Metabolism of carbamazepine is inducedby phenobarbitone, phenytoin, and vice versa.Erythromycin, fluoxetine, isoniazid inhibitmetabolism of carbamazepine.
Uses Carbamazepine is the most effectivedrug for CPS and also the most commonly useddrug for GTCS and SPS.
Trigeminal and related neuralgias: Carba-mazepine is the drug of choice. These neuralgiasare characterized by attacks of high intensityelectric shock-like or stabbing pain set off byeven trivial stimulation of certain trigger zonesin the mouth or on the face. Drugs benefit byinterrupting temporal summation of afferentimpulses (by a selective action on high frequencynerve impulses). Carbamazepine is not an anal-gesic, but has a specific action (almostdiagnostic) in these neuralgias. About 60%patients respond well. Phenytoin, lamotrigineand baclofen are less efficacious alternatives.Gabapentin can be tried in nonresponders.
Carbamazepine is not useful in diabetic,traumatic and other forms of neuropathic pain.Manic depressive illness and acute mania: asan alternative to lithium (see Ch. 32).Dose: 200–400 mg TDS; Children 15–30 mg/kg/day.TEGRETOL, MAZETOL 100, 200, 400 mg tab, 100 mg/5 mlsyr; CARBATOL 100, 200, 400 mg tab.MAZETOL SR, TEGRITAL CR 200, 400 mg sustained release/continuous release tabs. to avoid high peaks and low troughsin plasma concentration. These are the preferred formulations.
Oxcarbazepine This newer congener ofcarbamazepine is rapidly converted to an activemetabolite that is only glucuronide conjugatedbut not oxidized. Toxic effects due to the epoxidemetabolite are avoided. Drug interactions andautoinduction of own metabolism are lessmarked, because it is a weak enzyme inducer.Risk of hepatotoxicity is estimated to be lowerthan carbamazepine; but that of hyponatraemiais more. Indications are the same as forcarbamazepine, but it may be better tolerated.Dose to dose it is 1½ times less potent.OXETOL, OXCARB, OXEP 150, 300, 600 mg tabs.
EthosuximideThe most prominent action of ethosuximide isantagonism of PTZ induced clonic seizures atdoses which produce no other discernable action.It raises seizure threshold but does not modifymaximal electroshock seizures or inhibit kind-ling. Clinically it is effective only in absenceseizures.

417C
HA
PTER30
ANTIEPILEPTIC DRUGS
The primary action appears to be exerted onthalamocortical system which is involved in thegeneration of absence seizures. The EEG inabsence seizures shows characteristic bilaterallysynchronous 3 Hz spike and wave rhythmgenerated by reciprocal activation and oscillationof impulses between thalamus and neocortexthrough reverberatory synaptic connections.Thalamic neurones exhibit prominent ‘T’(transient) current which is low threshold Ca2+
current (due to inward flow of Ca2+ through T typeCa2+ channels) that acts as the pacemaker andamplifies repetitive spikes. Ethosuximideselectively suppresses T current without affectingother types of Ca2+ or Na+ currents. It also doesnot potentiate GABA at therapeutic concentra-tions. This correlates well with its selectiveaction in absence seizures.
Ethosuximide is rather slowly but completely absorbed,not protein bound, evenly distributed in body, and largelymetabolized in liver by hydroxylation and glucuronidation,and excreted in urine—about ¼th in the unchanged form.Plasma t½ averages 48 hours in adults and 32 hours in children.
Adverse effects Dose-related side effects are gastro-intestinal intolerance, tiredness, mood changes, agitation,headache, drowsiness and inability to concentrate.Hypersensitivity reactions like rashes, DLE and blooddyscrasias are rare. No liver or kidney damage.
Use The only indication for ethosuximide is absence seizures;in that also it has been superseded by valproate.Dose: 20–30 mg/kg/day; ZARONTIN 250 mg/5 ml syr.
Valproic acid (Sodium valproate)It is a branched chain aliphatic carboxylic acidwith a broad spectrum anticonvulsant action. Itis more potent in blocking PTZ seizures thanin modifying maximal electroshock. Establish-ment of chronic experimental seizure foci andkindling are also prevented. Remarkably, atanticonvulsant doses, valproate produces littlesedation or other central effects. Likewise, itis effective in partial seizures and GTCS as wellas absence seizures.Valproate appears to act by multiple mecha-nisms:(i) A phenytoin-like frequency-dependentprolongation of Na+ channel inactivation.
(ii) Weak attenuation of Ca2+ mediated ‘T’ current(ethosuximide like).(iii) Augmentation of release of inhibitory trans-mitter GABA by inhibiting its degradation (byGABA-transaminase) as well as probably byincreasing its synthesis from glutamic acid.However, responses to exogenously appliedGABA are not altered.
Pharmacokinetics Oral absorption of valproicacid is good. It is 90% bound to plasmaproteins; completely metabolized in liver byoxidation mainly by CYP2C9 and 2C19 (somemetabolites are active) and glucuronide conjuga-tion, and then excreted in urine. Plasma t½ is10–15 hours; but anticonvulsant effects arelonger lasting.
Adverse effects The toxicity of valproate isrelatively low.Anorexia, vomiting, loose motions and heart burnare common but mild. Drowsiness, ataxia andtremor are dose-related side effects. However,cognitive and behavioral effects are not pro-minent.Alopecia, curling of hair, weight gain andincreased bleeding tendency have been observed.Rashes and thrombocytopenia are infrequenthypersensitivity phenomena.Asymptomatic rise in serum transaminase isoften noted; monitoring of liver function isadvised.A rare but serious adverse effect is fulminant hepatitis; occursonly in children (especially below 3 yr). Those with hepaticdisease or who receive other anticonvulsant or hepatotoxicdrug are at greater risk. Pancreatitis is also reported. Long-term use of valproate in young girls has been associated withhigher incidence of polycystic ovarian disease and menstrualirregularities.Used during pregnancy, it has produced spinabifida and other neural tube defects in theoffspring; should be avoided.Dose: Adults—start with 200 mg TDS, maximum 800 mg TDS;children—15–30 mg/kg/day.VALPARIN CHRONO 200, 300, 500 mg tabs, 200 mg/5 mlsyr; ENCORATE 200, 300, 500 mg regular and controlledrelease tabs, 200 mg/5 ml syr, 100 mg/ml inj.
Uses Valproic acid is the drug of choice forabsence seizures.

418S
EC
TIO
N7
DRUGS ACTING ON CENTRAL NERVOUS SYSTEM
It is an alternative/adjuvant drug for GTCS, SPSand CPS.Myoclonic and atonic seizures—control is oftenincomplete, but valproate is the drug of choice.Mania and bipolar illness: as alternative tolithium. It has also been used for panic attacks.Valproate has some prophylatic efficacy inmigraine.
Interactions• Valproate increases plasma levels of phenob-
arbitone and lamotrigine by inhibiting theirmetabolism.
• It displaces phenytoin from protein bindingsite and decreases its metabolism → pheny-toin toxicity.
• Valproate inhibits hydrolysis of active epoxidemetabolite of carbamazepine.
• Concurrent administration of clonazepam andvalproate is contraindicated because absencestatus may be precipitated.
• Foetal abnormalities are more common ifvalproate and carbamazepine are given con-currently.
Divalproex (Semisodium valproate) It is thecoordination compound of valproic acid withsodium valproate (1:1). Oral absorption is slower,but bioavailability is the same. Gastric tolerancemay be better.DIPROEX, VALANCE, 125, 250, 500 mg tabs; DEPAKOTE250, 500 mg tabs.
ClonazepamIt is a benzodiazepine with prominent anticon-vulsant properties: blocks PTZ seizures at doseswhich produce mild sedation. Efficacy inmodifying maximal electroshock seizures is low.Though in experimental models of chronicepilepsy it inhibits spread rather than the focusitself, it is singularly ineffective in GTCS.Production of generalized seizures by kindlingis suppressed, but local after-discharges persist.
Benzodiazepines potentiate GABA inducedCl– influx to produce sedation and the samemechanism has been held responsible for theanticonvulsant property, but the sites of action
in the brain may be different. At large doses,high frequency discharges are inhibited akin tophenytoin.
Pharmacokinetics Oral absorption of clonazepam is good.It is 85% bound to plasma proteins, completely metabolizedin liver and excreted in urine; t½ averages 24 hours. It doesnot produce any active metabolite.
Adverse effects The most important side effect ofclonazepam is sedation and dullness. This can be minimizedby starting at low dose; some tolerance develops with chronictherapy. Lack of concentration, irritability, temper and otherbehavioral abnormalities may occur in children. Motordisturbances and ataxia are dose-related adverse effects.Salivation and increased respiratory secretions may becomplained of.
Uses Clonazepam has been primarily employed in absenceseizures. It is also useful as an adjuvant in myoclonic andakinetic epilepsy and may afford some benefit in infantilespasms. However, its value is limited by development oftolerance to the therapeutic effect within six months or so.It has also been used to suppress acute mania.Dose: adults 0.5–5 mg TDS, children 0.02–0.2 mg/kg/day.LONAZEP, CLONAPAX, RIVOTRIL 0.5, 1.0, 2.0 mg tab.
Clobazam It is a 1,5 benzodiazepine (diazepamand others are 1,4 benzodiazepines) introducedfirst as anxiolytic and later found to possess use-ful antiepileptic efficacy in partial, secondarilygeneralized tonic-clonic as well as absence andatonic seizures, including some refractory cases.Sedation and psychomotor retardation are lessprominent, but side effect profile is similar toother BZDs. It appears to act by facilitatingGABA action.
Oral bioavailability of clobazam is ~90% andelimination t½ 18 hrs, but an active metaboliteis produced which has longer t½ (>35 hr). Itis generally used as adjuvant to other anti-epileptic drugs like phenytoin, carbamazepine orvalproate in refractory epilepsy.Dose: start with 10–20 mg at bedtime, can be increased upto 60mg/day; FRISIUM, LOBAZAM, CLOZAM, 5, 10, 20 mg cap.
Diazepam (see Ch. 29)
It has anticonvulsant activity in a variety ofmodels but is not used for long term therapyof epilepsy because of prominent sedative actionand rapid development of tolerance to the anti-epileptic effect. However, it is a first line drug

419C
HA
PTER30
ANTIEPILEPTIC DRUGS
for emergency control of convulsions, e.g. statusepilepticus, tetanus, eclampsia, convulsant drugpoisoning, etc.
For this purpose 0.2–0.5 mg/kg slow i.v.injection is followed by small repeated dosesas required; maximum 100 mg/day. Thrombo-phlebitis of injected vein is not uncommon.Marked fall in BP and respiratory depressioncan occur; resuscitative measures should be athand before the drug is injected.
Rectal instillation of diazepam is now thepreferred therapy for febrile convulsions inchildren.
Lorazepam 0.1 mg/kg injected i.v. at a ratenot exceeding 2 mg/min is better suited thandiazepam in status epilepticus or for emergencycontrol of convulsions of other etiology, becauseof lesser local thrombophlebitic complicationsand more sustained action than that of diazepamwhich is rapidly redistributed.
Lamotrigine A new anticonvulsant havingcarbamazepine-like action profile: modifiesmaximal electroshock and decreases electricallyevoked as well as photic after-discharge dura-tion. Prolongation of Na+ channel inactivationand suppression of high frequency firing has beendemonstrated. In addition, it may directly blockvoltage sensitive Na+ channels, thus stabilizingthe presynaptic membrane and preventing releaseof excitatory neurotransmitters, mainlyglutamate and aspartate. This may account forits broader-spectrum of antiseizure efficacy.However, it does not antagonize PTZ seizuresor block NMDA type of glutamate receptors.
Lamotrigine is a broad-spectrum antiepi-leptic. Initially found useful as add-on therapyin refractory cases of partial seizures and GTCS,it has now been shown effective as monotherapyas well. Absence and myoclonic or akinetic epi-lepsy cases have also been successfully treated.Reduction in seizure frequency or completecontrol is obtained as frequently as withcarbamazepine.
Lamotrigine is well absorbed orally andmetabolized completely in liver. Its t½ is 24 hr,
but is reduced to ~16 hr in patients receivingphenytoin, carbamazepine or phenobarbitone. Onthe contrary valproate inhibits glucuronidation oflamotrigine and doubles its blood level, but val-proate levels are lowered by lamotrigine. Reducethe dose of lamotrigine to half in patients takingvalproate. However, metabolism of other anticon-vulsants and oral contraceptives is not altered.
Side effects are sleepiness, dizziness, dip-lopia, ataxia and vomiting. In some comparativetrials lamotrigine has been found to be bettertolerated than carbamazepine or phenytoin.Negative effect on cognitive function is notreported. Rash may be a severe reaction,particularly in children, requiring withdrawal.Dose: 50 mg/day initially, increase upto 300 mg/day as needed;not to be used in children.LAMETEC, LAMITOR, LAMIDUS 25, 50, 100 mg tabs.
Gabapentin This lipophilic GABA derivativecrosses to the brain and enhances GABA release,but does not act as agonist at GABAA receptor.It modifies maximal electroshock as well asinhibits PTZ induced clonic seizures.
Gabapentin and its newer congener pregabalinexert a specific analgesic effect in neuropathicpain. Recently they have been found to modulatea subset of neuronal voltage sensitive Ca2+
channels which contain α2δ-1 subunits. It ispostulated that decreased entry of Ca2+ into thepresynaptic neurone through these channelscould reduce glutamate release, loweringneuronal excitability. However, whether α2δ-1Ca2+ channel modulation or the GABA enhancingaction is responsible for the anticonvulsant/analgesic effect of gabapentin and pregabalin,is not known.
Added to a first line drug, gabapentin reducesseizure frequency in refractory partial seizureswith or without generalization. Though gabapentinmonotherapy as well has been found effectivein SPS and CPS, it is mostly employed as add-on drug. Gabapentin is considered to be a firstline drug for neuralgic pain due to diabeticneuropathy and postherpetic neuralgia. It hassome prophylactic effect in migraine and is analternative drug for phobic states.

420S
EC
TIO
N7
DRUGS ACTING ON CENTRAL NERVOUS SYSTEM
Gabapentin is well absorbed orally and excretedunchanged in urine with a t½ of 6 hrs. No druginteractions have been noted, and no change in doseof primary antiepileptic drug is required whengabapentin is added. Side effects are mild sedation,tiredness, dizziness and unsteadiness.Dose: Start with 300 mg OD, increase to 300–600 mg TDS asrequired; NEURONTIN 300 mg, 400 mg cap, GABANTIN,GABAPIN 100, 300, 400 mg cap.
Pregabalin This newer congener of gabapentinhas similar pharmacodynamic, pharmacokineticproperties and clinical indications in seizuredisorders. It has been particularly used for neuro-pathic pain, such as diabetic neuropathy, posther-petic neuralgia, complex regional pain syndrome(CRPS) and certain other types of chronic pain.Sedative side effects are claimed to be lessprominent, but poor concentration, rashes andallergic reactions have been complained.Dose: 75–150 mg BD, max 600 mg/dayPREGABA, NEUGABA, TRUEGABA 75, 150 mg caps.
Topiramate This weak carbonic anhydraseinhibitor has broad spectrum anticonvulsant activityin maximal electroshock, PTZ induced clonicseizures and in kindling model. It appears to actby multiple mechanisms, viz phenytoin likeprolongation of Na+ channel inactivation, GABApotentiation by a postsynaptic effect, antagonismof certain glutamate receptors and neuronalhyperpolarization through certain K+ channels.
Topiramate is indicated as monotherapy aswell as for supplementing primary antiepilepticdrug in refractory SPS, CPS and GTCS. Promisingresults have been obtained in myoclonic epilepsy.Topiramate is readily absorbed orally and mainlyexcreted unchanged in urine with an average t½of 24 hours. Adverse effects are impairment ofattention, sedation, ataxia, word finding difficulties,poor memory, weight loss, paresthesias and renalstones.
Recently, topiramate has been approved forprophylaxis of migraine; may be used when βblockers/other prophylactics are contraindicatedor are not effective.Dose: Initially 25 mg OD, increase weekly upto 100–200 mg BDas required.TOPEX, EPITOP, TOPAMATE, NEXTOP 25, 50, 100 mg tabs.
Zonisamide Another newer anticonvulsantwith weak carbonic anhydrase inhibitory actionthat modifies maximal electroshock seizures andinhibits kindled seizures, but does not antagonizePTZ. Prolongation of Na+ channel inactivationresulting in suppression of repetitive neuronalfiring has been observed. It has also been foundto suppress T-type of Ca2+ currents in certainneurones.
Zonisamide is well absorbed orally and mainlyexcreted unchanged in urine with a t½ of > 60hours. A small fraction is oxidized and conjugatedwith glucuronic acid. It is indicated as add-on drugin refractory partial seizures. Side effects aresomnolence, dizziness, headache, irritability andanorexia. Metabolic acidosis and renal stones canoccur. Zonisamide is to be avoided in patientssensitive to sulfonamides.Dose: 25–100 mg BD. Not to be given to children.ZONISEP, ZONICARE, ZONIT 50, 100 mg cap.
Levetiracetam A unique anticonvulsant whichsuppresses kindled seizures, but is ineffectiveagainst maximal electroshock or PTZ. Clinicalefficacy has been demonstrated both as adjuvantmedication as well as monotherapy in refractorypartial seizures with or without generalization.The mechanism of action is not known. Noneof the major anticonvulsant mechanisms appearto be applicable. However, it may modify synapticrelease of glutamate/GABA by binding to a specificsynaptic protein labelled ‘SV2A’. This may or maynot account for the antiepileptic property.
Levetiracetam is completely absorbed orally,partly hydrolysed, but mainly excreted unchangedin urine with a t½ of 6–8 hours. It is neitheroxidized by CYP enzymes nor induces or inhibitsthem. As such, it is free of drug interactions. Fewside effects like sleepiness, dizziness, weaknessand rarely behavioural changes are reported.Driving may be impaired. Because of goodtolerability, levetiracetam is being increasinglyused in CPS, GTCS and myoclonic epilepsy,mainly as add-on drug. It is not approved for usein children below 4 years.Dose: 0.5 g BD, increase upto 1.0 g BD (max 3 g/day), children 4-15 year 10–30 mg/kg/day.LEVOREXA, TORLEVA, LEVTAM 0.25, 0.5, 1.0 g tabs.

421C
HA
PTER30
ANTIEPILEPTIC DRUGS
Tiagabine This newer anticonvulsant potentiates GABAmediated neuronal inhibition by depressing GABA transporterGAT-1 which removes synaptically released GABA intoneurones and glial cells. Maximal electroshock and kindledseizures are suppressed. Currently it is approved only foradd-on therapy of partial seizures with or without secondarygeneralization, when not adequately controlled by standardantiepileptic drugs alone. Side effects are mild sedation,nervousness, asthenia, amnesia and abdominal pain.
Vigabatrin (γγγγγ vinyl GABA) It is an inhibitor of GABA-transaminase, the enzyme which degrades GABA.Anticonvulsant action may be due to increase in synapticGABA concentration. It is effective in many patients withrefractory epilepsy, especially CPS with or withoutgeneralization. It is approved only for adjuvant medication.
Visual field contraction and production of behaviouralchanges, depression or psychosis has restricted its use toonly as a reserve drug.
Lacosamide This recently approved (in 2010 in India)antiseizure drug is indicated in adults only for add-on therapyof partial seizures with or without generalization. It acts byenhancing Na+ channel inactivation and suppressing repetitivefiring of neurones. Lacosamide is metabolized by CYP2C19 andexcreted in urine. No alteration in dose of companion anti-epileptic drug is needed, because it neither induces nor inhibitsdrug metabolizing enzymes. Adverse effects are ataxia, vertigo,diplopia, tremour, depression and cardiac arrhythmia.Dose: Initially 50 mg BD, increase upto 200 mg BD.
TREATMENT OF EPILEPSIESAntiepileptic drugs suppress seizures, but do notcure the disorder; the disease may fadeout though
after years of successful control. The aim ofdrugs is to control and totally prevent all seizureactivity at an acceptable level of side effects.With the currently available drugs, this can beachieved in about half of the patients. Another20–30% attain partial control, while the restremain refractory. The cause of epilepsy shouldbe searched in the patient; if found and treatable,an attempt to remove it should be made. Somegeneral principles of symptomatic treatment withantiepileptic drugs are:
(i) Choice of drug (Table 30.1) and dose isaccording to the seizure type(s) and need of theindividual patient.
(ii) Initiate treatment early, because each seizureepisode increases the propensity to furtherattacks, probably by a process akin to kindling.Start with a single drug, preferably at low dose—gradually increase dose till full control ofseizures or side effects appear. If full controlis not obtained at maximum tolerated dose ofone drug, substitute another drug. Use combina-tions when all reasonable monotherapy fails.Combining drugs with different mechanisms ofaction, such as those which prolong Na+ channelinactivation with those facilitating GABA appearsmore appropriate. Pharmacokinetic interactions
TABLE 30.1 Choice of antiseizure drugs
Type of seizure First choice drugs Second choice drugs Alternative/Add-on drugs
1. Generalised tonic-clonic/ Carbamazepine, Valproate, Lamotrigine, Gabapentin,simple partial with or Phenytoin Phenobarbitone Topiramate, Primidone,without generalization Levetiracetam
2. Complex partial with or Carbamazepine, Gabapentin, Clobazam, Zonisamide,without generalization Valproate, Lamotrigine, Topiramate
Phenytoin Levetiracetam
3. Absence Valproate Ethosuximide, Clobazam,Lamotrigine Clonazepam
4. Myoclonic Valproate Lamotrigine, Levetiracetam,Topiramate Clonazepam
5. Atonic Valproate Clonazepam, LamotrigineClobazam
6. Febrile seizures Diazepam (rectal) — —
7. Status epilepticus Lorazepam (i.v.), Fosphenytoin (i.v.) Gen. anaestheticsDiazepam (i.v.) Phenobarbitone (i.v., i.m.)

422S
EC
TIO
N7
DRUGS ACTING ON CENTRAL NERVOUS SYSTEM
among anticonvulsants are common; doseadjustment guided by therapeutic drug moni-toring is warranted.
(iii) A single tonic-clonic seizure in a subjectwith no predisposing factor for development ofepilepsy (history of head injury, family historyof epilepsy, neurological abnormality, abnormalEEG or brain scan) may not merit initiation ofantiepileptic therapy.
(iv) Therapy should be as simple as possible.A seizure diary should be maintained.
(v) All drug withdrawals should be gradual(except in case of toxicity. Abrupt stoppage oftherapy without introducing another effectivedrug can precipitate status epilepticus. Prolon-ged therapy (may be life-long, or at least 3 yearsafter the last seizure) is needed. Stoppage oftherapy may be attempted in selected cases.Features favourable to withdrawal are:• childhood epilepsy,• absence of family history,• primary generalized tonic-clonic epilepsy,• recent onset at start of treatment,• absence of cerebral disorder and normal inter-
seizure EEG.Even with these features recurrence rates of12–40% have been reported.(vi) Dose regulation may be facilitated bymonitoring of steadystate plasma drug levels.Monitoring is useful because:
(a) Therapeutic range of concentrations hasbeen defined for many older drugs.
(b) There is marked individual variation in theplasma concentration attained with the samedaily dose.
(c) Compliance among epileptic patients isoften poor.
Plasma levels given in Table 30.2 are to serveas rough guides:
(vii) When women on antiepileptic therapy con-ceive, antiepileptic drugs should not be stopped.Though, most antiseizure drugs increase theincidence of birth defects, discontinuation oftherapy carries a high risk of status epilepticus.Fits occurring during pregnancy themselvesincrease birth defects and may cause mentalretardation in the offspring (anoxia occurs duringseizures). An attempt to reduce the dose of drugsshould be cautiously made. It may be advisableto substitute valproate.
Prophylactic folic acid supplementation in2nd and 3rd trimester along with vit. K in thelast month of pregnancy is recommended,particularly in women receiving antiepilepticdrugs to minimise neural tube defects andbleeding disorder respectively in the neonate.
(viii) Individual seizure episodes do not requireany treatment. During an attack of tonic-clonicseizures, the first priority is to prevent injury dueto fall or biting. The patient should be put in prone
TABLE 30.2 Plasma half life, therapeutic and toxic plasma concentrationrange of some important antiepileptic drugs
Drug Half Plasma concentration (µg/ml)life (hr)
Therapeutic Toxic
Phenobarbitone 80–120 10–30 > 30 mild> 60 severe
Phenytoin 12–36 10–20 > 20 mild> 35 severe
Carbamazepine 10–40 5–10 > 12
Ethosuximide 30–50 50–100* >200
Valproate 10–15 40–100* –
Clonazepam 20–40 0.01–0.1* –
* Poorly correlated with response.

423C
HA
PTER30
ANTIEPILEPTIC DRUGS
or lateral position and a gag should be placedbetween the teeth. The head should be turned andpatency of airway ensured. The attack usuallypasses off in 2–3 min, but the patient may not beroadworthy for a couple of hours.
1. Generalised tonic-clonic and simplepartial seizures In large comparative trials,considering both efficacy and toxicity, carbama-zepine and phenytoin have scored highest,phenobarbitone was intermediate, while primi-done was lowest among the older drugs.Carbamazepine was the best in partial seizures,while valproate was equally effective insecondarily GTCS. Valproate is a good secondline drug but should be used cautiously in youngchildren for fear of hepatic toxicity. Carbama-zepine is preferred in young girls because ofcosmetic side effects of phenytoin.
Lamotrigine, gabapentin and topiramate haveemerged as good alternatives. Levetiracetam isanother close contender. Clonazepam is a short-term alternative. Newer drugs are mostly usedas add-on therapy in cases with incomplete/poorresponse. They are being increasingly used formonotherapy as well, either to initiate therapyor as alternative medication, particularly whendrug interactions are to be avoided. The newerdrugs generally are less sedating and producefewer side effects. However, experience with themis less extensive and comparative trials are few.
Complete control can be obtained in upto90% patients with generalized seizures, but inonly 50% or less patients with partial seizures.
Phenobarbitone, phenytoin, valproate andcarbamazepine have been used to treat early post-head injury seizures. Phenobarbitone andphenytoin are often prescribed empirically forprophylaxis of late-onset (8 days to 2 yrs later)post-traumatic epilepsy, but risk/benefit ratio ofsuch use is not clear. Decision has to be takenon individual basis.
2. Complex partial seizures This type ofepilepsy is difficult to control completely;relapses are more common on withdrawal.Carbamazepine is the preferred drug, but
phenytoin or valproate may have to be added toit. The newer drugs levetiracetam, lamotrigine,gabapentin, topiramate or zonisamide may beadded in refractory cases.
3. Absence seizures Ethosuximide and val-proate are equally efficacious, but the latter ismore commonly used because it would alsoprevent kindling and emergence of GTCS.Valproate is clearly superior in mixed absenceand GTCS, which is more common than pureabsence seizures. Lamotrigine has emerged asa good alternative. Clonazepam is a second linedrug limited by its sedative property and deve-lopment of tolerance. Clobazam is an alternativewith promise of more sustained response.4. Myoclonic and atonic seizures Valproateis the preferred drug and lamotrigine is aneffective alternative. Topiramate may be addedin case of poor response. Levetiracetam isgenerally added in nonresponsive cases.5. Febrile convulsions Some children, espe-cially under 5 years age, develop convulsionsduring fever. Seizures may recur every time withfever and few may become chronic epileptics.Every attempt should be made to see that theydo not develop fever, but when they do,temperature should not be allowed to rise byusing paracetamol and external cooling.
The best treatment of febrile convulsions isrectal diazepam 0.5 mg/kg given at the onsetof convulsions. The i.v. preparation can be usedwhere the rectal formulation is not available.A rectal solution (5 mg in 2.5 ml) in tubes isavailable in the UK and some other countries.Seizures generally stop in 5 min; if not, anotherdose may be given. The drug is repeated 12hourly for 4 doses. If fever is prolonged a gapof 24–48 hr is given before starting next seriesof doses.
In recurrent cases or those at particular riskof developing epilepsy—intermittent prophylaxiswith diazepam (oral or rectal) started at the onsetof fever is recommended. Chronic prophylaxiswith phenobarbitone advocated earlier has beenabandoned, because of poor efficacy andbehavioural side effects.

424S
EC
TIO
N7
DRUGS ACTING ON CENTRAL NERVOUS SYSTEM
6. Infantile spasms (hypsarrhythmia)Therapy is unsatisfactory, antiepileptic drugs aregenerally useless. Corticosteroids affordsymptomatic relief. Valproate and clonazepamhave adjuvant value. Vigabatrin has some efficacy.
7. Status epilepticus When seizure activityoccurs for >30 min, or two or more seizuresoccur without recovery of consciousness, thecondition is called status epilepticus. Recurrenttonic-clonic convulsions without recovery ofconsciousness in between is an emergency; fitshave to be controlled as quickly as possible toprevent death and permanent brain damage.• Lorazepam 4 mg (0.1 mg/kg in children)
injected i.v. at the rate of 2 mg/min, repeatedonce after 10 min if required, is the first choicedrug now. It is effective in 75–90% casesand produces a more sustained anticonvulsanteffect (lasting 6–12 hours) than diazepam,because of lower lipid solubility and slowerredistribution. Moreover, thrombophlebitis ofinjected vein is less likely with lorazepam.
• Diazepam 10 mg (0.2–0.3 mg/kg) injectedi.v. at 2 mg/min, repeated once after 10 minif required, has been the standard therapy tillrecently. However, its anticonvulsant effectstarts fading after 20 min, and manysupplemental doses may be required. It is alsomore damaging to the injected vein.
• Fosphenytoin 100–150 mg/min i.v. infusion toa maximum of 1000 mg (15–20 mg/kg) undercontinuous ECG monitoring is a slower actingdrug which should be given if the seizures recuror fail to respond 20 min after onset, despitelorazepam/diazepam. It may also be employedto continue anticonvulsant cover after theseizures have been controlled by the BZD.
• Phenytoin sod. It should be used only whenfosphenytoin is not available, because it canbe injected only at the rate of 25–50 mg/min and causes more marked local vascularcomplications.
• Phenobarbitone sod. 50–100 mg/min i.v.injection to a maximum of 10 mg/kg is anotherslower acting drug which can be used asalternative to fosphenytoin. It is also employedto maintain seizure free state over short termbefore definitive oral therapy is instituted.
• Refractory cases who fail to respond tolorazepam and fosphenytoin within 40 minof seizure onset may be treated with i.v.midazolam/propofol/thiopentone anaesthesia,with or without curarization and full intensivecare.
• General measures, including maintenance ofairway (intubation if required), oxygenation,fluid and electrolyte balance, BP, normalcardiac rhythm, euglycaemia and care of theunconscious must be taken.
PROBLEM DIRECTED STUDY
30.1 A young lady aged 25 years comes for consultation along with her husband for havingsuffered two episodes of fits lasting 2–3 min each over the past one week. Just before eachfit, she experienced flickering in her right arm. Description of the fit given by the husbandcorresponds to generalized tonic-clonic seizures. She gave the history of having met a caraccident about one year back in which she received head injury. There is no family historyof epilepsy. General physical and neurological examination revealed no abnormality.Investigations, including EEG and MRI scan of the brain, were ordered.(a) What instructions should be given to the husband regarding care to be taken, if and when,the next fit occurs?(b) Should antiepileptic drug/drugs be started right away, or therapy be delayed till findingsof the investigations become available or till more fits occur?(c) In case antiseizure therapy has to be started right away, should a single drug or a combinationof drugs be given? Which drug(s) would be the most appropriate for this patient?(see Appendix-1 for solution)

Antiparkinsonian DrugsChapterChapterChapterChapterChapter 3131313131
These are drugs that have a therapeutic effectin parkinsonism.
Parkinsonism It is an extrapyramidal motordisorder characterized by rigidity, tremor andhypokinesia with secondary manifestations likedefective posture and gait, mask-like face andsialorrhoea; dementia may accompany. If untrea-ted the symptoms progress over several yearsto end-stage disease in which the patient is rigid,unable to move, unable to breathe properly;succumbs mostly to chest infections/embolism.Parkinson’s disease (PD) is a progressive degenerativedisorder, mostly affecting older people, first described byJames Parkinson in 1817. Majority of the cases are idiopathic,some are arteriosclerotic while postencephalitic are now rare.Wilson’s disease (hepatolenticular degeneration) due tochronic copper poisoning, is a rare cause.
The most consistent lesion in PD is degeneration ofneurones in the substantia nigra pars compacta (SN-PC) andthe nigrostriatal (dopaminergic) tract. This results in deficiencyof dopamine (DA) in the striatum which controls muscle toneand coordinates movements. An imbalance betweendopaminergic (inhibitory) and cholinergic (excitatory) systemin the striatum occurs giving rise to the motor defect. Thoughthe cholinergic system is not primarily affected, its sup-pression (by anticholinergics) tends to restore balance.
The cause of selective degeneration of nigrostriatalneurones is not precisely known, but appears to bemultifactorial. Oxidation of DA by MAO-B and aldehydedehydrogenase generates hydroxyl free radicals (•OH) in thepresence of ferrous iron (basal ganglia are rich in iron).Normally these free radicals are quenched by glutathione andother protective mechanisms. Age-related and/or otherwiseacquired defect in protective mechanism allows the freeradicals to damage lipid membranes and DNA resulting inneuronal degeneration. Genetic predisposition may contributeto the high vulnerability of substantia nigra neurones.
Ageing induces defects in mitochondrial electrontransport chain. Environmental toxins and/or genetic factorsmay accentuate these defects in specific areas. A synthetictoxin N-methyl-4-phenyl tetrahydropyridine (MPTP), whichoccurred as a contaminant of some illicit drugs, producesnigrostriatal degeneration and manifestations similar to PDby impairing energy metabolism in dopaminergic neurones.It has been proposed that MPTP-like chemicals may be present
in the environment, small quantities of which accelerate agerelated or otherwise predisposed neuronal degeneration ofparkinsonism, but there is no proof.
Excess of the excitatory transmitter glutamate can cause‘excitotoxic’ neuronal death by inducing Ca2+ overload throughNMDA receptors.
Drug-induced temporary parkinsonism due to neuro-leptics, metoclopramide (dopaminergic blockers) is now fairlycommon, while that due to reserpine (DA depleter) is historical.
Belladonna alkaloids had been empirically usedin PD. A breakthrough was made in 1967 whenlevodopa was found to produce dramaticimprovement. Its use was based on sound scien-tific investigations made in the preceding 10years that:• DA is present in the brain;• it (along with other monoamines) is depleted
by reserpine;• reserpine induced motor defect is reversed
by DOPA (the precursor of DA);• striatum of patients dying of PD was deficient
in DA.Thus, parkinsonism was characterized as a DAdeficiency state and levodopa was used to makegood this deficiency, because DA itself does notcross the blood-brain barrier. In the subsequentyears, a number of levodopa potentiators and DAagonists have been developed as adjuvants/alternatives.
CLASSIFICATION
I. Drugs affecting brain dopaminergicsystem(a) Dopamine precursor : Levodopa (l-dopa)(b) Peripheral decarboxylase inhibitors :
Carbidopa, Benserazide.(c) Dopaminergic agonists: Bromocriptine,
Ropinirole, Pramipexole(d) MAO-B inhibitor: Selegiline, Rasagiline(e) COMT inhibitors: Entacapone, Tolcapone

426S
EC
TIO
N7
DRUGS ACTING ON CENTRAL NERVOUS SYSTEM
(f) Glutamate (NMDA receptor) antagonist(Dopamine facilitator): Amantadine.
II. Drugs affecting brain cholinergicsystem(a) Central anticholinergics: Trihexyphe-
nidyl (Benzhexol), Procyclidine,Biperiden.
(b) Antihistaminics : Orphenadrine,Promethazine.
LEVODOPA
Levodopa has a specific salutary effect in PD:efficacy exceeding that of any other drug usedalone. It is inactive by itself, but is the immediateprecursor of the transmitter DA. More than 95%of an oral dose is decarboxylated in theperipheral tissues (mainly gut and liver). DA thusformed is further metabolized, and the remainingacts on heart, blood vessels, other peripheralorgans and on CTZ (though located in the brain,i.e. floor of IV ventricle, it is not bound by blood-brain barrier). About 1–2% of administeredlevodopa crosses to the brain, is taken up bythe surviving dopaminergic neurones, convertedto DA which is stored and released as a trans-mitter. Brains of parkinsonian patients treatedwith levodopa till death had higher DA levelsthan those not so treated. Further, those patientswho had responded well had higher DA levelsthan those who had responded poorly.
ACTIONS
1. CNS Levodopa hardly produces any effectin normal individuals or in patients with otherneurological diseases. Marked symptomaticimprovement occurs in parkinsonian patients.Hypokinesia and rigidity resolve first, latertremor as well. Secondary symptoms of posture,gait, handwriting, speech, facial expression,mood, self care and interest in life are graduallynormalized. Therapeutic benefit is nearlycomplete in early disease, but declines as thedisease advances.
The effect of levodopa on behaviour has beendescribed as a ‘general alerting response’. In
some patients this progresses to excitement—frank psychosis may occur. Embarrassinglydisproportionate increase in sexual activity hasalso been noted. Dementia, if present, does notimprove; rather it predisposes to emergence ofpsychiatric symptoms.
Levodopa has been used to produce a non-specific ‘awakening’ effect in hepatic coma.Two subtypes of DA receptors (D1, D2) were originallydescribed. Three more (D3, D4, D5) have now been identifiedand cloned. All are G protein coupled receptors and aregrouped into two families:D1 like (D1, D5) Are excitatory: act by increasing cAMPformation and PIP2 hydrolysis thereby mobilizing intracellularCa2+ and activating protein kinase C through IP3 and DAG.D2 like (D2, D3, D4) Are inhibitory: act by inhibitingadenylyl cyclase/opening K+ channels/depressing voltagesensitive Ca2+ channels.
The various subtypes of DA receptors are differentiallyexpressed in different areas of the brain, and appear to playdistinct roles. Both D1 and D2 receptors are present in thestriatum and are involved in the therapeutic response tolevodopa. They respectively regulate the activity of twopathways having opposite effects on the thalamic input to themotor cortex (Fig. 31.1). Thus, stimulation of excitatory D1 aswell as inhibitory D2 receptors in the striatum achieves thesame net effect of smoothening movements and reducing muscletone.
Dopamine receptor in SN-PC and in pituitary is also ofD2 type. The D3 receptors predominate in nucleus accumbansand hypothalamus, but are sparse in caudate and putamen,while D4 and D5 are mostly distributed in neocortex, midbrain,medulla and hippocampus.
2. CVS The peripherally formed DA cancause tachycardia by acting on β adrenergicreceptors. Though DA can stimulate vascularadrenergic receptors as well, rise in BP is notseen. Instead, postural hypotension is quitecommon. This may be a central action. ExcessDA and NA formed in the brain decrease sym-pathetic outflow; also DA formed in autonomicganglia can impede ganglionic transmission.
Gradual tolerance develops to both cardiac stimulant andhypotensive actions.
3. CTZ Dopaminergic receptors are present inthis area and DA acts as an excitatory transmitter.The DA formed peripherally gains access to theCTZ without hindrance—elicits nausea andvomiting. Tolerance develops gradually to thisaction.

427C
HA
PTER31
ANTIPARKINSONIAN DRUGS
Fig. 31.1: Simplified scheme of side loop circuits in the basal ganglia that provide modulatory input to the motor cortex.The striatal GABAergic neurones receive side-loop excitatory glutamatergic (Glu) input from the motor cortex andmodulatory dopaminergic (DA) projections from the substantia nigra pars compacta (SN-PC). There are also balancingcholinergic (ACh) interneurones. The striatal neurones express both excitatory D1 and inhibitory D2 receptors. Theoutput from the striatum to substantia nigra pars reticulata (SN-PR) and internal globus pallidus (GP-I) follows a directand an indirect pathway. The direct pathway modulated by DI receptors releases inhibitory transmitter GABA, while thedominant indirect pathway modulated by D2 receptors has two inhibitory (GABAergic) relays and an excitatory(glutamatergic) terminal. Due to this arrangement, dopaminergic action in the striatum exerts inhibitory influence on SN-PR and GP-I via both the pathways. The output neurones from SN-PR and GP-I feedback on the motor cortex throughthe thalamus using an inhibitory GABAergic link and an excitatory glutamatergic terminal. The basal ganglia modulatoryloop serves to smoothen output to the spinal motor neurone and reduce basal tone.
The degenerative lesion (in SN-PC) of Parkinson’s disease (PD) decreases dopaminergic input to the striatum,producing an imbalance between DA and ACh, resulting in hypokinesia, rigidity and tremor.
4. Endocrine DA acts on pituitary mammo-tropes to inhibit prolactin release and on soma-totropes to increase GH release. Though pro-lactin levels in blood fall during levodopa therapy,increased GH levels are not noted in parkinso-nian patients. Probably the mechanisms regula-ting GH secretion are altered in these patients.
PHARMACOKINETICSLevodopa is rapidly absorbed from the smallintestines by utilizing the active transport processmeant for aromatic amino acids. Bioavailabilityof levodopa is affected by:(i) Gastric emptying: if slow, levodopa isexposed to degrading enzymes present in gut wall

428S
EC
TIO
N7
DRUGS ACTING ON CENTRAL NERVOUS SYSTEM
Fig. 31.2: Metabolic pathways of levodopa in the periphery and the brain.3-OMD—3-O-methyldopa; COMT—Catechol-O-methyl transferase; MAO—monoamine oxidase; 3-MT—3-methoxytyramine; DOPAC—3,4 dihydroxy phenylacetic acid; HVA—Homovanillic acid (3-methoxy-4-hydroxy phenylacetic acid), DDC—Dopa decarboxylase
and liver for a longer time—less is availableto penetrate blood-brain barrier.(ii) Amino acids present in food compete forthe same carrier for absorption: blood levels arelower when taken with meals.
Levodopa undergoes high first pass meta-bolism in g.i. mucosa and liver. The peripheraland central pathway of metabolism of levodopais depicted in Fig. 31.2.
About 1% of administered levodopa that entersbrain, aided by amino acid carrier mediated activetransport across brain capillaries, also undergoesthe same transformation. The plasma t½ oflevodopa is 1–2 hours. Pyridoxal is a cofactorfor the enzyme dopa-decarboxylase. Themetabolites are excreted in urine mostly afterconjugation.
ADVERSE EFFECTS
Side effects of levodopa therapy are frequentand often troublesome. Most are dose-relatedand limit the dose that can be administered, butare usually reversible. Some are prominent inthe beginning of therapy while others appear late.
At the initiation of therapy These sideeffects can be minimized by starting with a lowdose.1. Nausea and vomiting It occurs in almostevery patient. Tolerance gradually develops andthen the dose can be progressively increased.2. Postural hypotension It occurs in about1/3 of patients, but is mostly asymptomatic; somepatients experience dizziness, few have faintingattacks. It is more common in patients receivingantihypertensives. Tolerance develops withcontinued treatment and BP normalizes.3. Cardiac
arrhythmias4. Exacerbation
of angina
5. Alteration in taste sensation
After prolonged therapy1. Abnormal movements (dyskinesias) Facialtics, grimacing, tongue thrusting, choreoathetoidmovements of limbs start appearing after afew months of use of levodopa at optimum
Due to β adrenergic actionof peripherally formed DA;more in patients with pre-existing heart disease.
⎫⎬⎭

429C
HA
PTER31
ANTIPARKINSONIAN DRUGS
therapeutic dose. These dyskinesias worsen withtime and practically all patients get involved afterfew years. Their intensity corresponds withlevodopa levels. No tolerance develops tothis adverse effect, but dose reduction decreasesseverity. Abnormal movements may become asdisabling as the original disease itself, and arethe most important dose-limiting side effects.
2. Behavioural effects Range from mildanxiety, nightmares, etc. to severe depression,mania, hallucinations, mental confusion or frankpsychosis. Excessive DA action in the limbicsystem is probably responsible (antidopaminergicdrugs are antipsychotic). Levodopa is contra-indicated in patients with psychotic illness.
3. Fluctuation in motor performance After2–5 years of therapy, the level of control ofparkinsonian symptomatology starts showingfluctuation. ‘End of dose’ deterioration (wearingoff) which is initially gradual, develops into rapid‘switches’ or ‘on-off’ effect. With time ‘all ornone’ response develops, i.e. the patient isalternately well and disabled. Abnormalmovements may jeopardise even the ‘on’ phase.This is probably a reflection of progression ofthe disorder. With progressive degeneration ofDA neurones the ability to regulate storage andrelease of DA may be largely lost: DA is thensynthesized in the striatum on a moment-to-moment basis resulting in rapid and unpredic-table fluctuations in motor control. Dosefractionation and more frequent administrationtends to diminish these fluctuations for a time.
Cautious use of levodopa is needed in theelderly; patients with ischaemic heart disease;cerebrovascular, psychiatric, hepatic and renaldisease; peptic ulcer; glaucoma and gout.Dose: Start with 0.25 g BD after meals, gradually increase tilladequate response is obtained. Usual dose is 2–3 g/day.LEVOPA, BIDOPAL 0.5 g tab.
Interactions1. Pyridoxine: Abolishes the therapeutic effectof levodopa (not combined with carbidopa) byenhancing its peripheral decarboxylation so thatless of it remains available to cross to the brain.
2. Phenothiazines, butyrophenones, metoclo-pramide reverse the therapeutic effect oflevodopa by blocking DA receptors. Theantidopaminergic domperidone blocks levodopainduced nausea and vomiting without abolishingits antiparkinsonian effect, because domperidonedoes not cross blood-brain barrier, but reachesCTZ. Reserpine abolishes levodopa action bypreventing entry of DA into synaptic vesicles.3. Nonselective MAO inhibitors: prevent degra-dation of DA and NA that is synthesized inexcess from the administered levodopa atperipheral sites. This may cause hypertensivecrisis.4. Antihypertensive drugs: postural hypotensioncaused by levodopa is accentuated in patientsreceiving antihypertensive drugs; reduce theirdose if levodopa is started.5. Atropine, and antiparkinsonian anticho-linergic drugs have additive therapeutic actionwith low doses of levodopa, but retard itsabsorption—more time is available for peripheraldegradation—efficacy of levodopa may bereduced.
PERIPHERAL DECARBOXYLASEINHIBITORS
Carbidopa and benserazide are extracerebraldopa decarboxylase inhibitors; they do notpenetrate blood-brain barrier and do not inhibitconversion of levodopa to DA in the brain.Administered along with levodopa, they increaseits t½ in the periphery and make more of itavailable to cross blood-brain barrier and reachits site of action.
Benefits of the combination are—1. The plasma t½ of levodopa is prolonged and
its dose is reduced to approximately 1/4th.2. Systemic concentration of DA is reduced,
nausea and vomiting are not prominent—therapeutic doses of levodopa can be attainedquickly.
3. Cardiac complications are minimized.4. Pyridoxine reversal of levodopa effect does
not occur.

430S
EC
TIO
N7
DRUGS ACTING ON CENTRAL NERVOUS SYSTEM
5. ‘On-off’ effect is minimized since cerebralDA levels are more sustained.
6. Degree of improvement may be higher; somepatients, not responding adequately tolevodopa alone, also improve.
Problems not resolved or accentuated are—
1. Involuntary movements2. Behavioural abnormalities
3. Excessive day time sleepiness in somepatients.
4. Postural hypotension.
Currently, levodopa is practically always usedalong with a decarboxylase inhibitor, except inpatients who develop marked involuntarymovements with the combination.
Combination of levodopa with carbidopa hasbeen given the name ‘Co-careldopa’.
Preparations and dose
Carbidopa Levodopa (per tab/cap)
TIDOMET-LS, SYNDOPA-110, 10 mg + 100 mgSINEMET, DUODOPA-110 10 mg + 100 mgTIDOMET PLUS, SYNDOPA PLUS 25 mg + 100 mgTIDOMET FORTE, SYNDOPA-275 25 mg + 250 mgBENSPAR, MADOPAR: Benserazide 25 mg + levodopa100 mg cap.
Usual daily maintenance dose of levodopa is 0.4–0.8 g alongwith 75–100 mg carbidopa or 100–200 mg benserazide, givenin 3–4 divided doses. Therapy is started at a low dose andsuitable preparations are chosen according to the needs ofindividual patients, increasing the dose as required.
DOPAMINERGIC AGONISTSThe DA agonists can act on striatal DA receptorseven in advanced patients who have largely lostthe capacity to synthesize, store and release DAfrom levodopa. Moreover, they are longer acting,can exert subtype selective activation of DAreceptors involved in parkinsonism and not sharethe concern expressed about levodopa ofcontributing to dopaminergic neuronal damageby oxidative metabolism.
Bromocriptine (see Ch. 17) It is an ergotderivative which acts as potent agonist on D2,
but as partial agonist or antagonist on D1receptors. Improvement in parkinsonian symp-toms occurs within ½–1 hr of an oral dose ofbromocriptine and lasts for 6–10 hours. If usedalone, doses needed in parkinsonism are high,expensive and often produce intolerable sideeffects, especially vomiting, hallucinations,hypotension, nasal stuffiness, conjunctivalinjection. Marked fall in BP with the ‘first dose’has occurred in some patients, especially thoseon antihypertensive medication.
Bromocriptine has been largely replaced bythe newer DA agonists ropinirole and prami-pexole. However, it can be used in late casesas a supplement to levodopa to improve controland smoothen ‘on off’ fluctuations.Dose: Initially 1.25 mg once at night, increase as needed upto5 mg TDS.PROCTINAL, SICRIPTIN, PARLODEL, 1.25, 2.5 mg tabs,ENCRIPT 2.5, 5 mg tabs.
Ropinirole and Pramipexole These are twononergoline, selective D2/D3 receptor agonistswith negligible affinity for D1 and nondopa-minergic receptors. Pramipexole has relativelygreater affinity for D3 receptors. The therapeuticeffect as supplementary drugs to levodopa inadvanced cases of PD as well as side effect profileis similar to bromocriptine, but they are bettertolerated with fewer g.i. symptoms. Consequentlydose titration for maximum improvement canbe achieved in 1–2 weeks, while the same maytake several months with bromocriptine.
Ropinirole and pramipexole are nowfrequently used as monotherapy for early PDas well. Trials have found them to afford symp-tom relief comparable to levodopa. Fewer casestreated with ropinirole needed supplementallevodopa than those treated with bromocriptine.The Parkinson Study Group and other multi-centric trials have noted lower incidence of dys-kinesias and motor fluctuations among patientstreated with these drugs than those treated withlevodopa. There is some indirect evidence thatuse of ropinirole/pramipexole in place oflevodopa-carbidopa may be associated withslower rate of neuronal degeneration. Such
⎫⎬⎭
may even be morepronounced andappear earlier.

431C
HA
PTER31
ANTIPARKINSONIAN DRUGS
encouraging findings indicate that the newer DAagonists are effective alternatives to levodopaand may afford longer symptom-free life to PDpatients.
Ropinirole is rapidly absorbed orally, 40%plasma protein bound, extensively metabolized,mainly by hepatic CYP1A2, to inactive meta-bolites, and eliminated with a terminal t½ of6 hrs. It is thus longer acting than levodopa,useful in the management of motor fluctuationsand reducing frequency of on-off effect.
Side-effects are nausea, dizziness, halluci-nations, and postural hypotension. Episodes ofday time sleep have been noted with ropiniroleas well as pramipexole. The higher incidenceof hallucinations and sleepiness may disfavourtheir use in the elderly. Patients should beadvised not to drive if they suffer this side effect.
Ropinirole is FDA approved for use in‘restless leg syndrome’.
Ropinirole: Starting dose is 0.25 mg TDS, titrated to amaximum of 4–8 mg TDS. Early cases generally require1–2 mg TDS.ROPITOR, ROPARK, ROPEWAY 0.25, 0.5, 1.0, 2.0 mg tabs.Also 1,2,4 and 8 mg ER tabs are approved.
Pramipexole: It is twice as potent as ropinirole, butcomparable in efficacy and tolerability. Starting dose 0.125mg TDS, titrate to 0.5–1.5 mg TDS.PRAMIPEX 0.5 mg tab; PARPEX 0.5, 1.0, 1.5 mg tabs,PRAMIROL 0.125, 0.25, 0.5, 1.0, 1.5 mg tabs.
Restless legs syndrome (RLS): It is a peculiar sensory-motor disorder affecting the legs during periods of relaxation,especially sleep. The affected subject feels an irresistable urgeto constantly move the legs, usually associated with tingling,itching, discomfort, aching or cramps. The symptoms abateby walking and do not appear during activity. The disordermay be mild and go unnoticed. In some cases, symptomsare severe and disrupt sleep, resulting in day-time sleepiness.The disorder may be primary (idiopathic) or secondary to irondeficiency anaemia, folate or other vitamin deficiencies,varicose veins, peripheral neuropathy (diabetic/uraemic,etc.), or be associated with pregnancy. A genetic basis andmild dopaminergic hypofunction in the brain have beenimplicated.
The nonergot dopaminergic agonists are the most effectivedrugs. Relatively low doses: ropinirole (0.25–1.0 mg) orpramipexole (0.125–0.5 mg) taken 2–3 hours before bed-timeeach day afford dramatic relief in many cases. Other drugs usedare benzodiazepines, gabapentin or pregabalin, but these aremostly reserved for nonresponsive cases.
MAO-B INHIBITORSelegiline (Deprenyl) It is a selective andirreversible MAO-B inhibitor. Two isoenzymeforms of MAO, termed MAO-A and MAO-B arerecognized; both are present in peripheraladrenergic structures and intestinal mucosa,while the latter predominates in the brain andblood platelets. Unlike nonselective MAOinhibitors, selegiline in low doses (10 mg/day)does not interfere with peripheral metabolismof dietary amines; Accumulation of CAs andhypertensive reaction does not develop, whileintracerebral degradation of DA is retarded (Fig.31.2). This is responsible for the therapeuticeffect in parkinsonism. Higher doses can producehypertensive interactions with levodopa andindirectly acting sympathomimetic amines.
Selegiline alone has mild antiparkinsonianaction in early cases. Administered with levo-dopa, it prolongs levodopa action, attenuatesmotor fluctuations and decreases ‘wearing off’effect. As an adjuvant to levodopa, it is beneficialin 50–70% patients and permits 20–30%reduction in levodopa dose. However, advancedcases with ‘on-off’ effect are not improved andthe peak dose levodopa side effects such asdyskinesias, mental confusion or hallucinationsmay be worsened. Moreover, clinical benefitsderived from selegiline are short lived (6–26months).
Based on the hypothesis that oxidation ofDA and/or environmental toxins (MPTP-like) inthe striatum by MAO to free radicals was causa-tive in parkinsonism, it was proposed that earlytherapy with selegiline might delay progressionof the disorder. However, no difference in thecourse of the disease has been detected onfollow up of selegiline treated patients in largemulticentric studies. Nevertheless, there is somerecent data supporting a neuroprotective effectof rasagiline, another MAO-B inhibitor, inparkinsonism.
Adverse effects Postural hypotension, nausea,confusion, accentuation of levodopa inducedinvoluntary movements and psychosis. Selegiline

432S
EC
TIO
N7
DRUGS ACTING ON CENTRAL NERVOUS SYSTEM
is partly metabolized by liver into amphetaminewhich sometimes causes insomnia and agitation.Selegiline is contraindicated in patients withconvulsive disorders.Selegiline interacts with pethidine possibly byfavouring its metabolism to norpethidine whichcauses excitement, rigidity, hyperthermia,respiratory depression. It may also interact withtricyclic antidepressants and selective serotoninreuptake inhibitors.ELDEPRYL 5, 10 mg tab; SELERIN, SELGIN 5 mg tab;Dose: 5 mg with breakfast and with lunch, either alone (in earlycases) or with levodopa/carbidopa. Reduce by 1/4th levodopadose after 2–3 days of adding selegiline.
Rasagiline Another newer selective MAO-Binhibitor with selegiline-like therapeutic effectin parkinsonism. However, it is 5 times morepotent, longer acting and not metabolized toamphetamine. It is therefore given once a dayin the morning, and does not produce excitatoryside effects.Dose: 1 mg OD in the morning.RELGIN, RASALECT 0.5, 1.0 mg tabs, RASIPAR 1 mg tab.
COMT INHIBITORS
Two selective, potent and reversible COMTinhibitors Entacapone and Tolcapone have beenintroduced as adjuvants to levodopa-carbidopafor advanced PD. When peripheral decarbox-ylation of levodopa is blocked by carbidopa/benserazide, it is mainly metabolized by COMTto 3-O-methyldopa (see Fig. 31.2). Blockade ofthis pathway by entacapone/tolcapone prolongsthe t½ of levodopa and allows a larger fractionof administered dose to cross to brain. SinceCOMT plays a role in the degradation of DAin brain as well, COMT inhibitors could preserveDA formed in the striatum and supplement theperipheral effect (Fig. 31.2). However, entaca-pone acts only in the periphery (probablybecause of short duration of action ~2 hr). Fortolcapone also, the central action is lessimportant.
Both entacapone and tolcapone enhance andprolong the therapeutic effect of levodopa-carbidopa in advanced and fluctuating PD. They
may be used to smoothen ‘wearing off’, increase‘on’ time, decrease ‘off’ time, improve activitiesof daily living and allow levodopa dose to bereduced. They are not indicated in early PD cases.Entacapone: 200 mg with each dose of levodopa-carbidopa,max. 1600 mg/day.ADCAPON 100 mg tab, COMTAN 200 mg tab.Tolcapone: 100–200 mg BD or TDS.
Worsening of levodopa adverse effects suchas nausea, vomiting, dyskinesia, postural hypo-tension, hallucinations, etc. occurs often whena COMT inhibitor is added. However, this canbe minimised by adjustment of levodopa dose.Other prominent side effect is diarrhoea in 10–18% patients (less with entacapone) and yellow-orange discolouration of urine.
Because of reports of acute fatal hepatitis andrhabdomyolysis, tolcapone has been suspended in Europeand Canada, while in USA its use is allowed only in thosenot responding to entacapone. Entacapone is not hepatotoxic.
GLUTAMATE (NMDA receptor)ANTAGONIST (Dopamine facilitator)
Amantadine Developed as an antiviral drugfor prophylaxis of influenza A2, it was foundserendipitiously to benefit parkinsonism. It actsrapidly but has lower efficacy than levodopa,which is equivalent to or higher than anti-cholinergics. About 2/3rd patients derive somebenefit. However, tolerance develops overmonths and the efficacy is gradually lost.Amantadine promotes presynaptic synthesis andrelease of DA in the brain and has anticholinergicproperty. These were believed to explain all itsbeneficial effect in parkinsonism. However, anantagonistic action on NMDA type of glutamatereceptors, through which the striatal dopaminer-gic system exerts its influence is now consideredto be more important.
Amantadine can be used in milder cases, orin short courses to supplement levodopa foradvanced cases. In the latter situation, it servesto suppress motor fluctuations and abnormalmovements. Fixed dose of 100 mg BD is used(not titrated according to response). The effectof a single dose lasts 8–12 hours;AMANTREL, COMANTREL 100 mg tab.

433C
HA
PTER31
ANTIPARKINSONIAN DRUGS
Side effects These are generally not serious:insomnia, restlessness, confusion, nightmares,anticholinergic effects and rarely hallucinations.A characteristic side effect due to local releaseof CAs resulting in postcapillary vasoconstric-tion is livedo reticularis (bluish discolouration)and edema of ankles.Side effects are accentuated when it is combinedwith anticholinergics.
CENTRAL ANTICHOLINERGICS
These are drugs having a higher central : peri-pheral anticholinergic action ratio than atropine,but the pharmacological profile is similar to it.In addition, certain H1 antihistaminics havesignificant central anticholinergic property.There is little to choose clinically among thesedrugs, though individual preferences vary.
They act by reducing the unbalanced choli-nergic activity in the striatum of parkinsonianpatients. All anticholinergics produce 10–25%improvement in parkinsonian symptoms lasting4–8 hours after a single dose. Generally, tremoris benefited more than rigidity; hypokinesia isaffected the least. Sialorrhoea is controlled bytheir peripheral action. The overall efficacy ismuch lower than levodopa. However, they arecheap and produce less side effects thanlevodopa. They may be used alone in mild casesor when levodopa is contraindicated. In others,they can be combined with levodopa in an attemptto lower levodopa dose.
Anticholinergics are the only drugs effectivein drug (phenothiazine) induced parkinsonism.
The side effect profile is similar to atropine.Impairment of memory, organic confusionalstates and blurred vision are more common inthe elderly. Urinary retention is possible inelderly males. The antihistaminics are lessefficacious than anticholinergics, but are bettertolerated by older patients. Their sedative actionalso helps. Orphenadrine has mild euphoriantaction.
Trihexyphenidyl It is the most commonlyused drug. Start with the lowest dose in 2–3
divided portions per day and gradually increasetill side effects are tolerated.1. Trihexyphenidyl (benzhexol): 2–10 mg/day; PACITANE,
PARBENZ 2 mg tab.2. Procyclidine: 5–20 mg/day; KEMADRIN 2.5, 5 mg tab.3. Biperiden: 2–10 mg/day oral, i.m. or i.v.: DYSKINON 2 mg
tab., 5 mg/ml inj.4. Orphenadrine: 100–300 mg/day; DISIPAL, ORPHIPAL 50
mg tab.5. Promethazine: 25–75 mg/day; PHENERGAN 10, 25 mg tab.
Some general points1. None of the above drugs alter the basic patho-logy of PD—the disease continues to progress.Drugs only provide symptomatic relief and givemost patients an additional 3–6 years of happierand productive life.
Considering that oxidative metabolism of DAgenerates free radicals which may rather hastendegeneration of nigrostriatal neurones, it hasbeen argued that levodopa therapy might acce-lerate progression of PD. There is no proof yetfor such a happening, and controlled prospectivestudies have not detected any difference in theprogression of disease due to levodopa therapy.However, appearance of dyskinesias is relatedto dose and duration of levodopa therapy. Thus,it may be prudent to delay use of levodopa andbegin with anticholinergics/amantadine/selegilineor newer direct DA agonists in early/mild/younger patients.2. Initially, when disease is mild, only anticholi-nergics or selegiline may be sufficient. However,anticholinergics are often not tolerated by elderlypatients, especially males. Monotherapy withnewer DA agonists ropinirole or pramipexoleis being increasingly employed for early cases,especially in younger patients, because of fewermotor complications. However, psychoticsymptoms and sudden onset sleep has to bewatched for. Selegiline may also be combinedwith levodopa during the deterioration phase oftherapy to overcome ‘wearing off’ effect.3. Combination of levodopa with a decarboxy-lase inhibitor is the standard therapy, and hasreplaced levodopa alone. Slow and carefulinitiation over 2–3 months, increasing the dose

434S
EC
TIO
N7
DRUGS ACTING ON CENTRAL NERVOUS SYSTEM
as tolerance to early side effects develops andthen maintenance at this level with frequentevaluation gives the best results. Full benefit lastsfor about 2–3 years, then starts declining.4. Subsequently the duration of benefit from alevodopa dose progressively shortens—end ofdose ‘wearing off’ effect is seen. Dyskinesiasappear, mostly coinciding with the peak of levodopaaction after each dose. Relief of parkinsoniansymptoms gets linked to the production of dyski-nesias. Still later (4–8 years) the ‘on-off’ phenomenaand marked dyskinesias may become so prominentthat the patient is as incapacitated with the drugas without it. However, withdrawal of levodopaor dopamine agonists, particularly when higherdoses have been employed, may precipitate markedrigidity hampering even respiratory excursions,hyperthermia, mental deterioration and a stateresembling the ‘neuroleptic malignant syndrome’.5. Combination of levodopa with decarboxylaseinhibitor increases efficacy and reduces earlybut not late complications.
6. Levodopa alone is now used only in thosepatients who develop intolerable dyskinesias witha levodopa-decarboxylase inhibitor combination.
7. Amantadine may be used with levodopa forbrief periods during exacerbations.
8. The direct DA agonists, especially ropinirole/pramipexole, are commonly used to supplementlevodopa in late cases to smoothen ‘on off’phenomenon, to reduce levodopa dose andpossibly limit dyskinesias.
9. In advanced cases, the COMT inhibitorentacapone may be added to levodopa-carbidopato prolong its action and subdue ‘on off’fluctuation. It can be given to patients receivingselegiline or DA agonists as well.
10. ‘Drug holiday’ (withdrawal of levodopa for4–21 days) to reestablish striatal sensitivity toDA by increasing dopaminergic receptorpopulation is no longer practiced.
PROBLEM DIRECTED STUDY
31.1 A 70-year-old man has been under treatment for Parkinson’s disease for the last 5 years.He is currently receiving Tab. levodopa 100 mg + carbidopa 25 mg two tablets in the morning,afternoon and night. He now suffers stiffness, shaking and difficulty in getting up from bedin the morning. These symptoms decrease about ½ hour after taking the medicine, but againstart worsening by noon. He notices one-sided twitching of facial muscles which is more frequent1–2 hour after each dose of levodopa-carbidopa.(a) Should his levodopa-carbidopa medication be stopped/replaced by another drug or thedose be increased further? Alternatively, can another drug be added to his ongoing medication?If so, should levodopa-carbidopa dose be changed or left unaltered?(see Appendix-1 for solution)

Drugs Used in Mental Illness:Antipsychotic and Antimanic Drugs
ChapterChapterChapterChapterChapter 3232323232
The psychopharmacological agents or psycho-tropic drugs are those having primary effectson psyche (mental processes) and are used fortreatment of psychiatric disorders.
During the past 60 years psychiatric treat-ment has witnessed major changes due to adventof drugs which can have specific salutary effectin mental illnesses. The trend has turned fromcustodial care towards restoring the individualpatient to his place in the community. All thatcould be done before 1952 was to dope andquieten agitated and violent patients. The intro-duction of chlorpromazine (CPZ) in that yearhas transformed the lives of schizophrenics; mostcan now be rehabilitated to productive life.Reserpine was discovered soon after. Though itis a powerful pharmacological tool to studymonoaminergic systems in brain and periphery,its clinical use in psychiatry lasted only fewyears. Next came the tricyclic and MAO inhibitorantidepressants in 1957–58 and covered anothergroup of psychiatric patients. Many novel andatypical antipsychotics, selective serotonin reup-take inhibitors (SSRIs) and other antidepressantshave been introduced since the 1980s. Meproba-mate (1954) aroused the hope that anxiety couldbe tackled without producing marked sedation.This goal has been realised more completely bythe development of Chlordiazepoxide (1957)and other benzodiazepines in the 1960s.Buspirone is a significant later addition.
Little attention was paid to Cade’s report in1949 that Lithium could be used for excitementand mania: its effective use started in the 1960sand now it has a unique place in psychiatry.Interestingly some antiepileptics like carbamaze-pine, valproate and lamotrigine as well as someatypical antipsychotics, etc. have shown promisein mania and bipolar disorders.
Psychiatric diagnostic categories are often imprecise. Thecriteria adopted overlap in individual patients. Nevertheless,broad divisions have to be made, primarily on the basis ofpredominant manifestations, to guide the use of drugs. It isimportant to make an attempt to characterise the primaryabnormality, because specific drugs are now available for mostcategories. Principal types are:Psychoses These are severe psychiatric illness with seriousdistortion of thought, behaviour, capacity to recognise realityand of perception (delusions and hallucinations). There isinexplicable misperception and misevaluation; the patient isunable to meet the ordinary demands of life.(a) Acute and chronic organic brain syndromes (cognitivedisorders) Such as delirium and dementia with psychoticfeatures; some toxic or pathological basis can often bedefined. Prominent features are confusion, disorientation,defective memory, disorganized thought and behaviour.(b) Functional disorders No underlying cause can be defi-ned; memory and orientation are mostly retained but emotion,thought, reasoning and behaviour are seriously altered.(i) Schizophrenia (split mind), i.e. splitting of perception andinterpretation from reality—hallucinations, inability to thinkcoherently.(ii) Paranoid states with marked persecutory or other kindsof fixed delusions (false beliefs) and loss of insight into theabnormality.
(iii) Mood (affective) disorders The primary symptom ischange in mood state; may manifest as:
Mania—elation or irritable mood, reduced sleep,hyperactivity, uncontrollable thought and speech, may beassociated with reckless or violent behaviour, or
Depression—sadness, loss of interest and pleasure,worthlessness, guilt, physical and mental slowing,melancholia, self-destructive ideation.
A common form of mood disorder is bipolar disorderwith cyclically alternating manic and depressive phases. Therelapsing mood disorder may also be unipolar (mania ordepression) with waxing and waning course.
Neuroses These are less serious; ability to comprehendreality is not lost, though the patient may undergo extremesuffering. Depending on the predominant feature, it may belabelled as:(a) Anxiety An unpleasant emotional state associated withuneasiness, worry, tension and concern for the future.(b) Phobic states Fear of the unknown or of some specificobjects, person or situations.

436S
EC
TIO
N7
DRUGS ACTING ON CENTRAL NERVOUS SYSTEM
(c) Obsessive-compulsive disorder Limited abnormalityof thought or behaviour; recurrent intrusive thoughts or ritual-like behaviours which the patient realizes are abnormal or stupid,but is not able to overcome even on voluntary effort. Theobsessions generate considerable anxiety and distress.(d) Reactive depression due to physical illness, loss, blowto self-esteem or bereavement, but is excessive or dispro-portionate.(e) Post-traumatic stress disorder Varied symptoms fol-lowing distressing experiences like war, riots, earthquakes, etc.(f) Hysterical Dramatic symptoms resembling seriousphysical illness, but situational, and always in the presenceof others; the patient does not feign but actually undergoesthe symptoms, though the basis is only psychic and notphysical.
Pathophysiology of mental illness is not clear,though some ideas have been formed, e.g. dopa-minergic overactivity in the limbic system maybe involved in schizophrenia and mania, whilemonoaminergic (NA, 5-HT) deficit may underliedepression. Treatment is empirical, symptomoriented and not disease specific. However, itis highly effective in many situations. Dependingon the primary use, the psychotropic drugs maybe grouped into:1. Antipsychotic (neuroleptic, ataractic,major tranquillizer) useful in all types offunctional psychosis, especially schizophrenia.(The term ‘Neuroleptic’ is applied to chlorpromazine/haloperidol-like conventional antipsychotic drugs which have potent D2receptor blocking activity and produce psychic indifference,emotional quietening with extrapyramidal symptoms, butwithout causing ataxia or cognitive impairment.)
2. Antimanic (mood stabiliser) used to controlmania and to break into cyclic affective disorders.3. Antidepressants used for minor as well asmajor depressive illness, phobic states,obsessive-compulsive behaviour, and certainanxiety disorders.4. Antianxiety (anxiolytic-sedative, minor tran-quillizer) used for anxiety and phobic states.5. Psychotomimetic (psychedelic, psycho-dysleptic, hallucinogen). They are seldom usedtherapeutically, but produce psychosis-like states.Majority of them are drugs of abuse, e.g. cannabis,LSD.Tranquillizer It is an old term meaning “a drug whichreduces mental tension and produces calmness without
inducing sleep or depressing mental faculties.” This term wasused to describe the effects of reserpine or chlorpromazine.However, it has been interpreted differently by different people;some extend it to cover both chlorpromazine-like andantianxiety drugs, others feel that it should be restricted tothe antianxiety drugs only. Their division into major and minortranquillizers is not justified, because the ‘minor tranquillizers’(diazepam-like drugs) are not less important drugs: they aremore frequently prescribed and carry higher abuse liabilitythan the ‘major tranquillizers’ (chlorpromazine-like drugs). Theterm tranquillizer is, therefore, best avoided.
ANTIPSYCHOTIC DRUGS(Neuroleptics)
These are drugs having a salutary therapeuticeffect in psychoses.
CLASSIFICATION
1. PhenothiazinesAliphatic side chain: Chlorpromazine
TriflupromazinePiperidine side chain: ThioridazinePiperazine side chain: Trifluoperazine
Fluphenazine2. Butyrophenones Haloperidol
TrifluperidolPenfluridol
3. Thioxanthenes Flupenthixol4. Other heterocyclics Pimozide, Loxapine5. Atypical antipsychotics
Clozapine AripiprazoleRisperidone ZiprasidoneOlanzapine AmisulpirideQuetiapine Zotepine

437C
HA
PTER32
ANTIPSYCHOTIC AND ANTIMANIC DRUGS
Many more drugs have been marketed in othercountries but do not deserve special mention.Pharmacology of chlorpromazine (CPZ) isdescribed as prototype; others only as they differfrom it. Their comparative features are presentedin Table 32.1.
PHARMACOLOGICAL ACTIONS
1. CNS Effects differ in normal andpsychotic individuals.
In normal individuals CPZ produces indiffe-rence to surroundings, paucity of thought, psycho-motor slowing, emotional quietening, reductionin initiative and tendency to go off to sleep fromwhich the subject is easily arousable. Spontaneousmovements are minimized but slurring of speech,ataxia or motor incoordination does not occur.This has been referred to as the ‘neurolepticsyndrome’ and is quite different from the sedativeaction of barbiturates and other similar drugs.Accordingly the typical antipsychotics which exertCPZ-like action, have potent dopamine D2receptor blocking property and produceextrapyramidal motor side effects. They are alsocalled ‘Neuroleptic drugs’. The effects areperceived as ‘neutral’ or ‘unpleasant’ by mostnormal individuals.
In a psychotic CPZ reduces irrational beha-viour, agitation and aggressiveness and controlspsychotic symptomatology. Disturbed thoughtand behaviour are gradually normalized, anxietyis relieved. Hyperactivity, hallucinations anddelusions are suppressed.
All phenothiazines, thioxanthenes and buty-rophenones have the same antipsychotic efficacy,but potency differs in terms of equieffectivedoses. The aliphatic and piperidine side chainphenothiazines (CPZ, triflupromazine, thiorida-zine) have low potency, produce more sedationand cause greater potentiation of hypnotics,opioids, etc. The sedative effect is producedpromptly, while antipsychotic effect takes weeksto develop. Moreover, tolerance develops to thesedative but not to the antipsychotic effect. Thus,the two appear to be independent actions.
Performance and intelligence are relativelyunaffected, but vigilance is impaired. Extrapyra-midal motor disturbances (see adverse effects)are intimately linked to the antipsychotic effect,but are more prominent in the high potency com-pounds and least in thioridazine, clozapine andother atypical antipsychotics. A predominanceof lower frequency waves occurs in the EEGand arousal response is dampened. However, noconsistent effect on sleep architecture has beennoted. The disturbed sleep pattern in a psychoticis normalized.
Chlorpromazine lowers seizure threshold andcan precipitate fits in untreated epileptics. Thepiperazine side chain compounds have a lowerpropensity for this action. Temperature controlis knocked off at relatively higher dosesrendering the individual poikilothermic. Bodytemperature falls if surroundings are cold. Themedullary respiratory and other vital centres arenot affected, except at very high doses. It is verydifficult to produce coma with overdose of thesedrugs. Neuroleptics, except thioridazine, havepotent antiemetic action exerted through theCTZ. However, they are ineffective in motionsickness.
In animals, neuroleptics selectively inhibit ‘conditionedavoidance response’ (CAR) without blocking the uncon-ditioned response to a noxious stimulus. This action hasshown good correlation with the antipsychotic potency ofdifferent compounds. However, these two effects (CAR inanimals and antipsychotic effect in humans) may be basedon different facets of action. In animals, a state of rigidity andimmobility (catalepsy) is produced which resembles thebradykinesia seen clinically.
Mechanism of action All antipsychotics(except clozapine-like atypical ones) have potentdopamine D2 receptor blocking action.Antipsychotic potency has shown goodcorrelation with their capacity to bind to D2receptor. Phenothiazines and thioxanthenes alsoblock D1, D3 and D4 receptors, but there isno correlation of such blockade with their anti-psychotic potency. Blockade of dopaminergicprojections to the temporal and prefrontal areasconstituting the ‘limbic system’ and inmesocortical areas is probably responsible forthe antipsychotic action. This contention is

438S
EC
TIO
N7
DRUGS ACTING ON CENTRAL NERVOUS SYSTEM
strengthened by the observation that drugs whichincrease DA activity (amphetamines, levodopa,bromocriptine) induce or exacerbate schizo-phrenia. A ‘dopamine theory of schizophrenia’has been propounded envisaging DA overactivityin limbic area to be responsible for the disorder.Accordingly, blockade of DA overactivity inlimbic area produces the antipsychotic effect,while that in basal ganglia produces theparkinsonian adverse effects. The delayed onsetof these effects may be explained by initialadaptive increase in the firing of DA neuronesand DA turnover, which gradually subsides anda state of persistent inactivation supervenes asthe drug is continued, corresponding to theemergence of the therapeutic effect as well asthe extrapyramidal side effects.
However, DA overactivity in the limbic areais not the only abnormality in schizophrenia.Other monoaminergic (5-HT) as well as amino-acid (glutamate) neurotransmitter systems mayalso be affected. Moreover, DA activity inprefrontal cortex is actually diminished inschizophrenia. Only the positive symptoms(hallucinations, aggression, etc.) appear to beclosely linked to DA overactivity in mesolimbicareas, but not the negative symptoms (apathy,cognitive deficit, withdrawal, etc). Not with-standing the above, reduction of dopaminergicneurotransmission is the major mechanism ofantipsychotic action.
The DA hypothesis fails to explain the anti-psychotic activity of clozapine and other atypicalantipsychotics which have weak D2 blockingaction. However, they have significant 5-HT2 andα1 adrenergic blocking action, and some arerelatively selective for D4 receptors. Thus, anti-psychotic property may depend on a specificprofile of action of the drugs on several neuro-transmitter receptors. Positron emission tomo-graphy (PET) studies of D2 and other receptoroccupancy in brains of antipsychotic drug treatedpatients have strengthened this concept.
Dopaminergic blockade in pituitary lacto-tropes causes hyperprolactinemia, while that inCTZ is responsible for the antiemetic action.
2. ANS Neuroleptics have varying degrees ofα adrenergic blocking activity which may begraded as:
CPZ = triflupromazine = thioridazine > cloza-pine > fluphenazine > haloperidol > trifluo-perazine > pimozide, i.e. more potentcompounds have lesser α blocking activity.
Anticholinergic property of neuroleptics is weakand may be graded as:
thioridazine > CPZ > triflupromazine> trifluoperazine = haloperidol.
The phenothiazines have weak H1-antihistaminicand anti-5-HT actions as well.
3. Local anaesthetic Chlorpromazine is aspotent a local anaesthetic as procaine. However,it is not used for this purpose because of itsirritant action. Other antipsychotic drugs haveweaker/no membrane stabilizing action.
4. CVS Neuroleptics produce hypotension (pri-marily postural) by a central as well as periphe-ral action on sympathetic tone. The hypotensiveaction is more marked after parenteral adminis-tration and roughly parallels the α adrenergicblocking potency. Hypotension is not prominentin psychotic patients, but is accentuated by hypo-volemia. Partial tolerance to hypotensive actiondevelops after chronic use. Reflex tachycardiaaccompanies hypotension.
High doses of CPZ directly depress the heartand produce ECG changes (Q-T prolongation andsuppression of T wave). CPZ exerts someantiarrhythmic action, probably due to membranestabilization. Arrhythmia may occur in overdose,especially with thioridazine.
5. Skeletal muscle Neuroleptics have nodirect effect on muscle fibres or neuromusculartransmission. However, they reduce certain typesof spasticity: the site of action being in the basalganglia or medulla oblongata. Spinal reflexes arenot affected.
6. Endocrine Neuroleptics consistently inc-rease prolactin release by blocking the inhibitoryaction of DA on pituitary lactotropes. This mayresult in galactorrhoea and gynaecomastia.

439C
HA
PTER32
ANTIPSYCHOTIC AND ANTIMANIC DRUGS
They reduce gonadotropin secretion, butamenorrhoea and infertility occur only occa-sionally. ACTH release in response to stress isdiminished. As a result corticosteroid levels failto increase under such circumstances. Releaseof GH is also reduced but this is not sufficientto cause growth retardation in children or to bebeneficial in acromegaly. Decreased release ofADH may result in an increase in urine volume.A direct action on kidney tubules may add toit, but Na+ excretion is not affected.
Though in general, antipsychotic drugs do notaffect blood sugar level, CPZ and few othershave the potential to impair glucose toleranceor aggravate diabetes, as well as elevate serumtriglycerides. This is often associated with weightgain, which may be a causative factor along withaccentuation of insulin resistance.
Tolerance and dependenceTolerance to the sedative and hypotensive actionsdevelops within days or weeks, but maintenancedoses for therapeutic effect in most psychoticsremain fairly unchanged over years, despiteincreased DA turnover in the brain. The anti-psychotic, extrapyramidal and other actions basedon DA antagonism do not display tolerance.
Neuroleptics are hedonically (pertaining topleasure) bland drugs, lack reinforcing effect sothat chronic recipients do not exhibit drugseeking behaviour. Physical dependence isprobably absent, though some manifestations ondiscontinuation have been considered withdrawalphenomena.
PHARMACOKINETICS
Oral absorption of CPZ is somewhat unpredic-table and bioavailability is low. More consistenteffects are produced after i.m. or i.v. administra-tion. It is highly bound to plasma as well as tissueproteins; brain concentration is higher thanplasma concentration. Volume of distribution,therefore, is large (20 L/kg). It is metabolizedin liver, mainly by CYP 2D6 into a number ofmetabolites.
The acute effects of a single dose of CPZgenerally last for 6–8 hours. The eliminationt½ is variable, but mostly is in the range of 18–30 hours. The drug cumulates on repeatedadministration, and it is possible to give the totalmaintenance dose once a day. Some metabolitesare probably active. The intensity of antipsy-chotic action is poorly correlated with plasmaconcentration. Nevertheless, therapeutic effectmay be seen at 30–200 ng/ml. The metabolitesare excreted in urine and bile for months afterdiscontinuing the drug.
The broad features of pharmacokinetics ofother neuroleptics are similar.
DISTINCTIVE FEATURES OFNEUROLEPTICS
Antipsychotic drugs differ in potency and in theirpropensity to produce different effects. This issummarized in a comparative manner in Table32.1.
1. Triflupromazine An aliphatic side chainphenothiazine, somewhat more potent than CPZ.Used mainly as antiemetic; it frequently producesacute muscle dystonias in children; especiallywhen injected.
2. Thioridazine A low potency phenothiazinehaving marked central anticholinergic action.Incidence of extrapyramidal side effects is verylow. Cardiac arrhythmias and interference withmale sexual function are more common. Riskof eye damage limits long-term use.
3. Trifluoperazine, fluphenazine These arehigh potency piperazine side chain phenothia-zines. They have minimum autonomic actions.Hypotension, sedation and lowering of seizurethreshold are not significant. They are less likelyto impair glucose tolerance, cause jaundice andhypersensitivity reactions. However, extrapyra-midal side effects are marked.
Fluphenazine decanoate can be given as adepot i.m. injection every 2–4 weeks inuncooperative psychotics.ANATENSOL DECANOATE, PROLINATE 25 mg/ml inj.

440S
EC
TIO
N7
DRUGS ACTING ON CENTRAL NERVOUS SYSTEM
TAB
LE 3
2.1
Com
para
tive
prop
ertie
s an
d pr
epar
atio
ns o
f ant
ipsy
chot
ic d
rugs
Dru
gA
ntip
sych
otic
Rel
ativ
e ac
tivity
Pre
para
tions
dose
(mg/
day)
Ext
rapy
ram
idal
Sed
ativ
eH
ypot
ensi
veA
ntie
met
ic
1.C
hlor
prom
azin
e10
0–80
0+
+++
++
++
+C
HLO
RP
RO
MA
ZIN
E, L
AR
GA
CTI
L 10
, 25,
50,
100
mg
tab.
5 m
g/5
ml (
pedi
atric
) & 2
5 m
g/5
ml (
adul
t) S
yr.,
50 m
g/2
ml i
nj.
2.Tr
iflup
rom
azin
e50
–200
++±
+++
++
+++
SIQ
UIL
10
mg
tab;
10
mg/
ml i
nj.
3.Th
iorid
azin
e10
0–40
0+
+++
+++
±M
ELL
ER
IL 2
5, 1
00 m
g ta
b, T
HIO
RIL
10,
25,
50,
100
mg
tab.
4.Tr
ifluo
pera
zine
2–20
+++
++
+++
TRIN
ICA
LM 1
, 5 m
g ta
b, N
EO
CA
LM 5
, 10
mg
tab
5.Fl
uphe
nazi
ne1–
10++
++
+++
+A
NA
TEN
SO
L 1
mg
tab,
0.5
mg/
ml e
lixir.
6.H
alop
erid
ol2–
20++
++
+++
+S
ER
EN
AC
E 1
.5, 5
, 10,
20
mg
tab;
2 m
g/m
l liq
, 5 m
g/m
lin
j., S
EN
OR
M 1
.5, 5
, 10
mg
tab,
5 m
g/m
l inj
.,H
ALO
PID
OL
2, 5
, 10,
20
mg
tab,
2 m
g/m
l liq
, 10
mg/
ml d
rops
7.Tr
iflup
erid
ol1–
8++
++
+++
+TR
IPE
RID
OL
0.5
mg
tab,
2.5
mg/
ml i
nj.
8.Fl
upen
thix
ol3–
15++
++
++
FLU
AN
XO
L 0.
5, 1
, 3 m
g ta
b; F
LUA
NX
OL
DE
PO
T20
mg/
ml i
n 1
and
2 m
l am
p.
9.P
imoz
ide
2–6
+++
++
+O
RA
P, N
EU
RA
P, P
IMO
DA
C 2
, 4 m
g ta
b.
10.
Loxa
pine
20–5
0+
++
++
+LO
XA
PA
C 1
0, 2
5, 5
0 m
g ca
ps, 2
5 m
g/ 5
ml l
iqui
d
11.
Clo
zapi
ne10
0–30
0–
+++
+++
–LO
ZAP
IN, S
IZO
PIN
, SK
IZO
RIL
25,
100
mg
tabs
12.
Ris
perid
one
2–8
++
++
++
–R
ES
PID
ON
, SIZ
OD
ON
, RIS
PE
RD
AL
1, 2
, 3, 4
mg
tabs
.
13.
Ola
nzap
ine
2.5–
20+
++
+–
OLA
CE
, OLA
ND
US
2.5
, 5, 7
.5, 1
0 m
g ta
bs, O
LZA
P 5
, 10
mg
tab
14.
Que
tiapi
ne50
–400
±++
++
+–
QU
EL,
SO
CA
LM, S
ER
OQ
UIN
25,
100
, 200
mg
tabs
15.
Arip
ipra
zole
5–30
±±
±–
AR
IPR
A, A
RIL
AN
, BIL
IEF
10, 1
5 m
g ta
bs;
AR
IVE
10,
15,
20,
30
mg
tabs
.
16.
Zipr
asid
one
40–1
60+
++
–A
ZON
A, Z
IPS
YD
ON
20,
40,
80
mg
tabs
.

441C
HA
PTER32
ANTIPSYCHOTIC AND ANTIMANIC DRUGS
4. Haloperidol It is a potent antipsychoticwith pharmacological profile resembling that ofpiperazine substituted phenothiazines. It producesfew autonomic effects, is less epileptogenic,does not cause weight gain, jaundice is rare.It is the preferred drug for acute schizophrenia,Huntington’s disease and Gilles de la Tourette’ssyndrome. It is metabolised by CYP3A4 and2D6 both. Elimination t½ averages 24 hours.5. Trifluperidol It is similar to but slightlymore potent than haloperidol.6. Penfluridol An exceptionally long actingneuroleptic, recommended for chronic schizo-phrenia, affective withdrawal and social mal-adjustment.Dose: 20–60 mg oral (max 120 mg) once weekly; SEMAP,FLUMAP, PENFLUR 20 mg tab.
7. Flupenthixol This thioxanthine is lesssedating than CPZ; indicated in schizophrenia andother psychoses, particularly in withdrawn andapathetic patients, but not in those with psycho-motor agitation or mania. Infrequently used now.8. Pimozide It is a selective DA antagonistwith little α adrenergic or cholinergic blockingactivity. Because of long duration of action(several days; elimination t½ 48–60 hours) aftera single oral dose, it is considered good formaintenance therapy but not when psychomotoragitation is prominent. Incidence of dystonicreactions is low, but it tends to prolong myo-cardial APD and carries risk of arrhythmias. Ithas been particularly used in Gilles de la Tourett’ssyndrome and in ticks.9. Loxapine A dibenzoxazepine having CPZlike DA blocking and antipsychotic activity. Theactions are quick and short lasting (t½ 8 hr).No clear cut advantage over other antipsychoticshas emerged.
ATYPICAL (Second generation)ANTIPSYCHOTICS
These are newer (second generation) antipsy-chotics that have weak D2 blocking but potent5-HT2 antagonistic activity. Extrapyramidal sideeffects are minimal, and they tend to improvethe impaired cognitive function in psychotics.
1. Clozapine It is the first atypical anti-psychotic; pharmacologically distinct from CPZand related drugs in that it has only weak D2blocking action, produces few/no extrapyramidalsymptoms; tardive dyskinesia is rare andprolactin level does not rise. Both positive andnegative symptoms of schizophrenia areimproved and clozapine is the most effectivedrug in refractory schizophrenia, i.e. patients notresponding to typical neuroleptics may respondto it. The differing pharmacological profile maybe due to its relative selectivity for D4 receptors(which are sparse in basal ganglia) and additional5-HT2 as well as α adrenergic blockade. It isquite sedating, moderately potent anticholinergic,but paradoxically induces hypersalivation.Significant H1 blocking property is present.
Clozapine is metabolized by CYP1A2,CYP2C19 and CYP3A4 into active and inactivemetabolites with an average t½ of 12 hours. Itsmajor limitation is higher incidence of agranu-locytosis (0.8%) and other blood dyscrasias:weekly monitoring of leucocyte count is required.Metabolic complication like weight gain,hyperlipidemia and precipitation of diabetes isanother major limilation. High dose can induceseizures even in nonepileptics. Other side effectsare sedation, unstable BP, tachycardia and urinaryincontinence. Few cases of myocarditis have beenreported which start like flu but may progressto death.
Clozapine is used as a reserve drug inrefractory schizophrenia.2. Risperidone Another compound whoseantipsychotic activity has been ascribed to acombination of D2 + 5-HT2 receptor blockade.In addition it has high affinity for α1, α2 andH1 receptors: blockade of these may contributeto efficacy as well as side effects like posturalhypotension. However, BP can rise if it is usedwith a SSRI. Risperidone is more potent D2blocker than clozapine; extrapyramidal sideeffects are less only at low doses (<6 mg/day).Prolactin levels rise disproportionately duringrisperidone therapy, but it is less epileptogenicthan clozapine, though frequently causesagitation. Weight gain and incidence of new-onset

442S
EC
TIO
N7
DRUGS ACTING ON CENTRAL NERVOUS SYSTEM
diabetes is less than with clozapine. Caution hasbeen issued about increased risk of stroke inthe elderly.
3. Olanzapine This atypical antipsychotic;resembles clozapine in blocking multiplemonoaminergic (D2, 5-HT2, α1, α2) as well asmuscarinic and H1 receptors. Both positive andnegative symptoms of schizophrenia tend tobenefit. A broader spectrum of efficacy coveringschizo-affective disorders has been demon-strated, and it is approved for use in mania.
Olanzapine is a potent antimuscarinic, pro-duces dry mouth and constipation. Weaker D2blockade results in few extrapyramidal sideeffects and little rise in prolactin levels, but ismore epileptogenic than high potency pheno-thiazines. It causes weight gain and carries ahigher risk of impairing glucose tolerance orworsening diabetes as well as elevating serumtriglyceride. These metabolic complications havediscouraged its use. Incidence of stroke may beincreased in the elderly. Agranulocytosis has notbeen reported with olanzapine. It is metabolizedby CYP1A2 and glucuronyl transferase. The t½is 24–30 hours.
4. Quetiapine This new short-acting (t½ 6 hours)atypical antipsychotic requires twice daily dosing.It blocks 5-HT1A, 5-HT2, D2, α1, α2 and H1
receptors in the brain, but D2 blocking activityis low: extrapyramidal and hyperprolactinaemicside effects are minimal. However, it is quitesedating (sleepiness is a common side effect),and major portion of daily dose is given at night.Postural hypotension can occur, especially duringdose titration. Urinary retention/incontinence arereported in few patients. Weight gain and risein blood sugar are moderate, and it causes somedegree of QTc prolongation, risking arrhythmiaonly at high doses. Quetiapine has not been foundto benefit negative symptoms of schizophrenia,but there is evidence of efficacy in acute maniaas well as in bipolar depression, because of whichit is frequently selected for maintenance therapy.It is metabolized mainly by CYP3A4; can interactwith macrolides, antifungals, anticonvulsants, etc.
5. Aripiprazole This atypical antipsychotic isunique in being a partial agonist at D2 and5-HT1A receptor, but antagonist at 5-HT2 receptor.The high affinity but low intrinsic activity ofaripiprazole for D2 receptor impedes dopami-nergic transmission by occupying a large fractionof D2 receptors but activating them minimally.It is not sedating, may even cause insomnia.Extrapyramidal side effects, hyperprolactinaemiaand hypotension are not significant. Littletendency to weight gain and rise in bloodsugar has been noted. A moderate prolongationof Q-Tc interval occurs at higher doses. Frequentside effects are nausea, dyspepsia, constipationand light-headedness, but not antimuscariniceffects.
Aripiprazole is quite long-acting (t½ ~ 3days); dose adjustments should be done after2 weeks treatment. It is metabolized by CYP3A4as well as CYP2D6; dose needs to be halvedin patients receiving ketoconazole or quinidine,and doubled in those taking carbamazepine.Aripiprazole is indicated in schizophrenia as wellas mania and bipolar illness. Efficacy iscomparable to haloperidol.
6. Ziprasidone Another atypical antipsychoticwith combined D2 + 5-HT2A/2C + H1 + α1
blocking activity. Antagonistic action at 5-HT1D
+ agonistic activity at 5-HT1A receptors alongwith moderately potent inhibition of 5-HT andNA reuptake indicates some anxiolytic andantidepressant property as well. Like otheratypical antipsychotics, ziprasidone has lowpropensity to cause extrapyramidal side effectsor hyperprolactinaemia. It is mildly sedating,causes modest hypotension and little weight gainor blood sugar elevation. Nausea and vomitingare the common side effects but it lacksantimuscarinic effects. More importantly, a dose-related prolongation of Q-T interval occursimparting potential to induce serious cardiacarrhythmias, especially in the presence ofpredisposing factors/drugs.
The t½ of ziprasidone is ~8 hours; needstwice daily dosing. In comparative trials, its

443C
HA
PTER32
ANTIPSYCHOTIC AND ANTIMANIC DRUGS
efficacy in schizophrenia has been rated equiva-lent to haloperidol. It is also indicated in mania.
7. Amisulpiride This congener of Sulpiride(typical antipsychotic) is categorized with theatypical antipsychotics because it produces fewextrapyramidal side effects and improves manynegative symptoms of schizophrenia as well.However, it retains high affinity for D2 (and D3)receptors and has low-affinity for 5-HT2
receptors. Hyperpolactinemia occurs similar totypical neuroleptics. Antidepressant property hasalso been noted. Amisulpiride is not a sedative.Rather, insomnia, anxiety and agitation arecommon side effects. Risk of weight gain andmetabolic complications is lower, but Q-Tprolongation has been noted, especially inpredisposed elderly patients. Amisulpiride isabsorbed orally and mainly excreted unchangedin urine with a t½ of 12 hours.Dose: 50–300 mg/day in 2 doses for schizophrenia withpredominant negative symptoms. Also for acute psychosis200–400 mg BD.SULPITAC, AMIPRIDE, ZONAPRIDE 50, 100, 200 mg tabs.
8. Zotepine Another atypical antipsychoticwith dopamine D2+D1, 5-HT2, α1 adrenergic andhistamine H1 receptor blocking activities. It alsoinhibits NA reuptake. Like other drugs of theclass, it benefits both positive and negativesymptoms of schizophrenia, but is rated lesseffective than clozapine. Extrapyramidal sideeffects are less prominent than with typicalneuroleptics, but more than clozapine. Hyperpro-lactinemia is noted. Zotepine lowers seizurethreshold and incidence of seizures is increasedat high doses. Weight gain, hyperglycaemia anddyslipidemia are likely as with clozapine.Common side effects are weakness, headache,and postural hypotension.
Absorption after oral ingestion is good butfirst pass metabolism is extensive. The elimina-tion t½ is 14 hours. Zotepine is available in Indiafor use in schizophrenia, but does not offer anyspecific advantage. It has been discontinued inthe U.K.Dose: Initially 25 mg TDS; increase upto 100 mg TDS.ZOLEPTIL, NIPOLEPT 25, 50 mg tabs.
ADVERSE EFFECTS
Antipsychotics are very safe drugs in single orinfrequent doses: deaths from overdose arealmost unknown. However, side effects arecommon and often limit their use.
I. Based on pharmacological actions(dose related)
1. CNS Drowsiness, lethargy, mental con-fusion; more with low potency typical anti-psychotics and some atypical ones like quetiapineand clozapine. Tolerance to sedative effect maydevelop. Other side effects are increased appetiteand weight gain (not with haloperidol); aggra-vation of seizures in epileptics; even nonepi-leptics may develop seizures with high dosesof some antipsychotics like clozapine andoccasionally olanzapine. However high potency,phenothiazines, risperidone, quetiapine aripipra-zole and ziprasidone have little effect on seizurethreshold.2. CVS Postural hypotension, palpitation, inhi-bition of ejaculation (especially with thiorida-zine) are due to α adrenergic blockade; morecommon with low potency phenothiazines.Q-T prolongation and cardiac arrhythmias are arisk of overdose with thioridazine, pimozide andziprasidone. Excess cardiovascular mortality hasbeen attributed to antipsychotic drug therapy.3. Anticholinergic Dry mouth, blurring ofvision, constipation, urinary hesitancy in elderlymales (thioridazine has the highest propensity);absent in high potency agents. Dry mouth andconstipation is common with olanzapine. Somelike clozapine induce hypersalivation despiteanticholinergic property, probably due to centralaction.4. Endocrine Hyperprolactinemia (due to D2blockade) is common with typical neurolepticsand risperidone. This can lower Gn levels, butamenorrhoea, infertility, galactorrhoea andgynaecomastia occur infrequently after pro-longed treatment. The atypical antipsychotics,except risperidone, do not appreciably raiseprolactin levels.

444S
EC
TIO
N7
DRUGS ACTING ON CENTRAL NERVOUS SYSTEM
5. Metabolic effects Elevation of bloodsugar and triglyceride levels as a consequenceof chronic therapy with certain antipsychotics isa major concern now. Low potency pheno-thiazines (CPZ, thioridazine) and some atypicalantipsychotics, particularly olanzapine andclozapine have high risk of precipitating diabetesor worsening it. High potency drugs like triflu-perazine, fluphenazine, haloperidol and atypicalantipsychotics like risperidone, aripiprazole andziprasidone have low/no risk. The mechanism ofthis effect is not clear; may be due to weightgain and/or accentuation of insulin resistance.
Raised triglyceride level is another conse-quence of insulin resistance. Cardiovascularmortality among schizophrenics is higher;increased use of atypical antipsychotics may bea contributory factor.
6. Extrapyramidal disturbances These arethe major dose-limiting side effects; moreprominent with high potency drugs likefluphenazine, haloperidol, pimozide, etc., leastwith thioridazine, clozapine, and all other atypicalantipsychotics, except higher dose ofrisperidone. The extrapyramidal effects may becategorized into:
(a) Parkinsonism with typical manifesta-tions—rigidity, tremor, hypokinesia, mask likefacies, shuffling gait; appears between 1–4 weeksof therapy and persists unless dose is reduced.If that is not possible, one of the anticholinergicantiparkinsonian drugs may be given concurren-tly. Changing the antipsychotic, especially to anatypical agent, may help. Though quite effective,routine combination of the anticholinergic fromthe start of therapy in all cases is not justified,because they tend to worsen memory and impairintellect, in addition to dry mouth and urinaryretention. Amantadine is an alternative. Levodopais not effective since D2 receptors are blocked.
A rare form of extrapyramidal side effectis perioral tremors ‘rabbit syndrome’ thatgenerally occurs after a few years of therapy.It often responds to central anticholinergic drugs.
(b) Acute muscular dystonias Bizarre musclespasms, mostly involving linguo-facial muscles—grimacing, tongue thrusting, torticollis, lockedjaw; occurs within a few hours of a single doseor at the most in the first week of therapy. Itis more common in children below 10 yearsand in girls, particularly after parenteral adminis-tration; overall incidence is 2%. It lasts for oneto few hours and then resolves spontaneously.One of the central anticholinergics, prometha-zine or hydroxyzine injected i.m. clears thereaction within 10–15 min.
(c) Akathisia Restlessness, feeling of discom-fort, apparent agitation manifested as a compel-ling desire to move about, but without anxiety,is seen in some patients between 1–8 weeks oftherapy: upto 20% incidence. It may be mistakenfor exacerbation of psychosis. The mechanismof this complication is not understood; nospecific antidote is available. A central anti-cholinergic may reduce the intensity in somecases; but a benzodiazepine like clonazepam ordiazepam is the first choice treatment of themotor restlessness. Propranolol is moreeffective; may be given to non-responsive cases.Most patients respond to reduction in dose ofthe neuroleptic or changeover to an atypicalantipsychotic like quetiapine.
(d) Malignant neuroleptic syndrome Itoccurs rarely with high doses of potent agents.The patient develops marked rigidity, immobility,tremor, hyperthermia, semiconsciousness,fluctuating BP and heart rate; myoglobin may bepresent in blood. The syndrome lasts 5–10 daysafter drug withdrawal and may be fatal. Theneuroleptic must be stopped promptly andsymptomatic treatment instituted. Though,antidopaminergic action of the neuroleptic maybe involved in the causation of this syndrome;anticholinergics are of no help. Intravenousdantrolene may benefit. Bromocriptine in largedoses has been found useful.
(e) Tardive dyskinesia It occurs late intherapy, sometimes even after withdrawal of the

445C
HA
PTER32
ANTIPSYCHOTIC AND ANTIMANIC DRUGS
neuroleptic: manifests as purposeless involun-tary facial and limb movements like constantchewing, pouting, puffing of cheeks, lip licking,choreoathetoid movements. It is more commonin elderly women, and is a manifestation ofprogressive neuronal degeneration along withsupersensitivity to DA. It is accentuated byanticholinergics and temporarily suppressed byhigh doses of the neuroleptic (this should notbe tried except in exceptional circumstances).An incidence of 10–20% has been reported afterlong term treatment. This reaction is uncommonwith clozapine and all other atypical anti-psychotics. The dyskinesia may subside monthsor years after withdrawal of therapy, or may belifelong. There is no satisfactory solution of theproblem.
7. Miscellaneous Weight gain often occursdue to long-term antipsychotic therapy, sugar andlipids may tend to rise. Blue pigmentation ofexposed skin, corneal and lenticular opacities,retinal degeneration (more with thioridazine)occur rarely after long-term use of high dosesof phenothiazines.
II. Hypersensitivity reactions These arenot dose related.1. Cholestatic jaundice with portal infiltra-tion; 2–4% incidence; occurs between 2–4 weeksof starting therapy. It calls for withdrawal of thedrug; resolves slowly. More common with lowpotency phenothiazines; rare with haloperidol.2. Skin rashes, urticaria, contact dermatitis,photosensitivity (more with CPZ).3. Agranulocytosis is rare; more common withclozapine.4. Myocarditis Few cases have occurred withclozapine.
INTERACTIONS
1. Neuroleptics potentiate all CNS depressants—hypnotics, anxiolytics, alcohol, opioids andantihistaminics. Overdose symptoms may occur.2. Neuroleptics block the actions of levodopaand direct DA agonists in parkinsonism.
3. Antihypertensive action of clonidine andmethyldopa is reduced, probably due to centralα2 adrenergic blockade.4. Phenothiazines and others are poor enzymeinducers—no significant pharmacokinetic inter-actions occur. Enzyme inducers (barbiturates,anticonvulsants) can reduce blood levels ofneuroleptics.
USES1. PsychosesSchizophrenia The antipsychotics are used pri-marily in functional psychoses. They have anindefinable but definite therapeutic effect in allforms of schizophrenia: produce a wide rangeof symptom relief. They control positive symp-toms (hallucinations, delusions, disorganizedthought, restlessness, insomnia, anxiety, fighting,aggression) better than negative symptoms(apathy, loss of insight and volition, affectiveflattening, poverty of speech, social withdrawal).They also tend to restore affective and motordisturbances and help upto 90% patients to leada near normal life in the society. However,intellect and cognition are little benefited. Somepatients do not respond, and virtually noneresponds completely. They are only symptomatictreatment, do not remove the cause of illness;long-term (even life-long) treatment may berequired. Judgement, memory and orientation areonly marginally improved. Patients with recentonset of illness and acute exacerbations respondbetter. The goal of therapy is to relieve symp-toms and functionally rehabilitate the patient.
Choice of drug is largely empirical, guidedby the presenting symptoms (it is the targetsymptoms which respond rather than the illnessas a whole), associated features and mood state,and on the type of side effect that is moreacceptable in a particular patient. Individualpatients differ in their response to differentantipsychotics; there is no way to predict whichpatient will respond better to which drug. Thefollowing may help drug selection:• Agitated, combative and violent—haloperidol,
quetiapine, CPZ, thioridazine.

446S
EC
TIO
N7
DRUGS ACTING ON CENTRAL NERVOUS SYSTEM
• Withdrawn and apathetic—trifluoperazine,fluphenazine, aripiprazole, ziprasidone.
• Patient with mainly negative symptoms andresistant cases—clozapine is the mosteffective; alternatives are olanzapine, risperi-done, aripiprazole, ziprasidone.
• Patient with mood elevation, hypomania—haloperidol, fluphenazine, quetiapine,olanzapine.
• If extrapyramidal side effects must be avoided—thioridazine, clozapine or any other atypicalantipsychotic.
• Elderly patients who are more prone to seda-tion, mental confusion and hypotension—ahigh potency phenothiazine, haloperidol oraripiprazole.Currently, the newer atypical antipsychotics
are more commonly prescribed. Though, thereis no convincing evidence of higher efficacy,they produce fewer side effects and neurologicalcomplications. Moreover, they may improve thenegative symptoms as well. They are preferablefor long-term use in chronic schizophrenia dueto lower risk of tardive dyskinesia. Of the older,typical neuroleptics, the high potency agents arepreferred over the low potency ones.
Mania Antipsychotics are required in highdoses for rapid control of acute mania, and maniapatients tolerate them very well. CPZ orhaloperidol may be given i.m.—act in 1–3 days.Lithium or valproate may be started simul-taneously or after the acute phase. Such combina-tion therapy is more effective. The antipsychoticmay be continued for months or may be withdrawngradually after 1–3 weeks when lithium has takeneffect. Now, oral therapy with one of the atypicalantipsychotics olanzapine/risperidone/aripi-prazole/quetiapine is mostly used to avoidextrapyramidal side effects, especially for casesnot requiring urgent control.
Organic brain syndromes Antipsychoticdrugs have limited efficacy in dementia anddelirium associated with psychotic features. Theymay be used in low doses on a short-term basis.One of the potent drugs is preferred to avoid
mental confusion, hypotension and precipitationof seizures. Moreover, low potency drugs (CPZ,thioridazine) have significant antimuscarinicproperty which may worsen delirium anddementia. Haloperidol, risperidone, ripiprazoleor ziprasidone are mostly selected.
General comments The dose of antipsychoticdrugs has to be individualized by titration withthe symptoms and kept at minimum. In chronicschizophrenia maximal therapeutic effect is seenafter 2–4 months therapy. However, injectedneuroleptics control aggressive symptoms ofacute schizophrenia over hours or a few days.Combination of two or more antipsychotics isnot advantageous. However, a patient onmaintenance therapy with a nonsedative drug maybe given additional CPZ or haloperidol by i.m.injection to control exacerbations or violentbehaviour.
In a depressed psychotic, a tricyclic/SSRIantidepressant may be combined with relativelylower dose of an antipsychotic. One of theatypical agents is mostly used because they areeffective in bipolar disorder. Quetiapine is thepreferred drug, because it is effective as mono-therapy as well. Benzodiazepines may be addedfor brief periods in the beginning.
Low dose maintenance or intermittent regi-mens of antipsychotics have been tried in relap-sing cases. Depot injections, e.g. fluphenazine/haloperidol decanoate given at 2–4 week inter-vals are preferable in many cases.
2. Anxiety Antipsychotics have antianxietyaction but should not be used for simple anxietybecause of psychomotor slowing, emotionalblunting, autonomic and extrapyramidal sideeffects. Benzodiazepines are preferable. However,low dose of quetiapine, risperidone or olanzepinehave been found useful as adjuvants to SSRIs ingeneralized anxiety disorder. Patients having apsychotic basis for anxiety may be treated witha neuroleptic.
3. As antiemetic The typical neurolepticsare potent antiemetics. They control a wide rangeof drug and disease induced vomiting at doses

447C
HA
PTER32
ANTIPSYCHOTIC AND ANTIMANIC DRUGS
much lower than those needed in psychosis.However, they should not be given unless thecause of vomiting has been identified. Thougheffective in morning sickness, they shouldnot be used for this condition. They areineffective in motion sickness: probably becausedopaminergic pathway through the CTZ is notinvolved. With the availability of 5-HT3 antago-nists and other antiemetics, use of neurolepticsfor control of vomiting has declined.
4. Other uses(a) To potentiate hypnotics, analgesics and
anaesthetics: such use is rarely justifiednow.
(b) Intractable hiccough may respond toparenteral CPZ.
(c) Tetanus CPZ is an alternative drug torelieve skeletal muscle spasm.
(d) Alcoholic hallucinosis, Huntington’sdisease and Gilles de la Tourette’ssyndrome are rare indications.
ANTIMANIC AND MOOD STABILIZINGDRUGS (Drugs for bipolar disorder)
LITHIUM CARBONATE
Lithium is a small monovalent cation. In 1949,it was found to be sedative in animals and toexert beneficial effects in manic patients.
In the 1960s and 1970s the importance ofmaintaining a narrow range of serum lithiumconcentration was realized and unequivocalevidence of its clinical efficacy was obtained.Lithium is a drug of its own kind to suppressmania and to exert a prophylactic effect in bipolar(manic depressive) disorder at doses which haveno overt CNS effects. Lithium is established asthe standard antimanic and mood stabilizing drug.Over the past 2 decades, several anticonvulsantsand atypical antipsychotics have emerged asalternatives to lithium with comparable efficacy.
Actions and mechanism
1. CNS Lithium has practically no acuteeffects in normal individuals as well as in bipolar
patients. It is neither sedative nor euphorient;but on prolonged administration, it acts as a moodstabiliser in bipolar disorder. Given to patientsin acute mania, it gradually suppresses theepisode taking 1–2 weeks; continued treatmentprevents cyclic mood changes. The markedlyreduced sleep time of manic patients isnormalized.
The mechanism of antimanic and moodstabilizing action of lithium is not known.However, the following mechanisms have beenproposed:(a) Li+ partly replaces body Na+ and is nearlyequally distributed inside and outside the cells(contrast Na+ and K+ which are unequallydistributed); this may affect ionic fluxes acrossbrain cells or modify the property of cellularmembranes. However, relative to Na+ and K+
concentration, the concentration of Li+
associated with therapeutic effect is very low.(b) Lithium decreases the presynaptic release ofNA and DA in the brain of treated animalswithout affecting 5-HT release. This may correctany imbalance in the turnover of brain mono-amines.(c) The above hypothesis cannot explain why Li+
has no effect on people not suffering from mania.An attractive hypothesis has been put forwardbased on the finding that lithium in therapeuticconcentration range inhibits hydrolysis ofinositol-1-phosphate by inositol monophos-phatase. As a result, the supply of free inositolfor regeneration of membrane phosphatidyl-inositides, which are the source of IP3 and DAG,is reduced (Fig. 32.1). The hyperactive neuronesinvolved in the manic state may be preferentiallyaffected, because supply of inositol fromextracellular sources is meagre. Thus, lithiummay ignore normally operating receptors, but‘search out’ and selectively, though indirectly,dampen signal transduction in the overactivereceptors functioning through phosphatidylinositol hydrolysis. In support of this hypothesis,it has been recently demonstrated that valproate,which has Li+ like effect in mania andbipolar disorder, also reduces intraneuronal

448S
EC
TIO
N7
DRUGS ACTING ON CENTRAL NERVOUS SYSTEM
Fig. 32.1: Proposed mechanism of antimanic action of lithiumPIP—Phosphatidyl inositol phosphate; PIP2—Phosphatidyl inositol bisphosphate;IP3—Inositol trisphosphate; IP—Inositol-1-phosphate; PLc—Phospholipase C;DAG—Diacylglycerol; PKc—Protein Kinase C; Gq—Coupling Gq protein;R—Neurotransmitter receptor
concentration of inositol in human brain byinhibiting de novo inositol synthesis.
Several other mechanisms involving elementsof neuronal signalling like PKc, glutamate,arachidonate, etc. have also been proposed toexplain lithium action.
2. Other actions Lithium inhibits the actionof ADH on distal tubules in the kidney and causesa diabetes insipidus like state.An insulin-like action on glucose metabolismis exerted.Leukocyte count is increased by lithium therapy.Lithium inhibits release of thyroid hormonesresulting in feedback stimulation of thyroidthrough pituitary. Majority of Li+ treated patientsremain in a state of compensated euthyroidism,but few get decompensated and becomeclinically hypothyroid.
Pharmacokinetics and control of therapyLithium is slowly but well absorbed orally andis neither protein bound nor metabolized. It first
distributes in extracellular water, then graduallyenters cells and penetrates into brain, ultimatelyattaining a rather uniform distribution in totalbody water. The CSF concentration of Li+ is abouthalf of plasma concentration. Apparent volumeof distribution at steady-state averages 0.8 L/kg.
Lithium is handled by the kidney in muchthe same way as Na+. Nearly 80% of the filteredLi+ is reabsorbed in the proximal convolutedtubule. When Na+ is restricted, a larger fractionof filtered Na+ is reabsorbed, so is Li+. Aftera single dose of Li+, its urinary excretion is rapidfor 10–12 hours, followed by a much slowerphase lasting several days. The t½ of the latterphase is 16–30 hours. Renal clearance of lithiumis 1/5 of creatinine clearance. On repeatedmedication, steady-state plasma concentration isachieved in 5–7 days. Levels are higher in olderpatients and in those with renal insufficiency.
There is marked individual variation in therate of lithium excretion. Thus, with the samedaily dose, different individuals attain widelydifferent plasma concentrations. However, in any

449C
HA
PTER32
ANTIPSYCHOTIC AND ANTIMANIC DRUGS
individual the clearance remains fairly constantover time. Since the margin of safety is narrow,monitoring of serum lithium concentration isessential for optimising therapy. Serum lithiumlevel is measured 12 hours after the last doseto reflect the steady-state concentration;0.5–0.8 mEq/L is considered optimum for main-tenance therapy in bipolar disorder, while0.8–1.1 mEq/L is required for episodes of acutemania. Toxicity symptoms occur frequently whenserum levels exceed 1.5 mEq/L.
Peaks in plasma lithium level over and abovethe steady-state level occur after every dose.Divided daily dosing in 2–3 portions or SR tabletis needed to avoid high peaks, but this causesmore polyuria. Lithium is excreted in sweat andsaliva as well, and secreted in breast milk.Mothers on lithium should not breastfeed.
Adverse effects Side effects are common,but are mostly tolerable. Toxicity occurs at levelsonly marginally higher than therapeutic levels.1. Nausea, vomiting and mild diarrhoea occurinitially, can be minimized by starting at lowerdoses.2. Thirst and polyuria are experienced by most,some fluid retention may occur initially, butclears later.3. Fine tremors are noted even at therapeuticconcentrations.4. CNS toxicity manifests as plasma concen-tration rises producing coarse tremors, giddiness,ataxia, motor incoordination, nystagmus, mentalconfusion, slurred speech, hyper-reflexia.Overdose symptoms are regularly seen at plasmaconcentration above 2 mEq/L. In acute intoxi-cation these symptoms progress to muscletwitchings, drowsiness, delirium, coma andconvulsions. Vomiting, severe diarrhoea,albuminuria, hypotension and cardiac arrhythmiasare the other features.
Treatment It is symptomatic. There is nospecific antidote. Osmotic diuretics and sod.bicarbonate infusion promote Li+ excretion.Haemodialysis is indicated if serum levelsare > 4 mEq/L.
5. On long-term use, some patients developrenal diabetes insipidus. Most patients gain somebody weight. Goiter has been reported in about4%. This is due to interference with release ofthyroid hormone → fall in circulating T3, T4
levels → TSH secretion from pituitary →enlargement and stimulation of thyroid. Enoughhormone is usually produced due to feedbackstimulation so that patients remain euthyroid.However, few become hypothyroid. Lithiuminduced goiter and hypothyroidism does notwarrant discontinuation of therapy; can be easilymanaged by thyroid hormone supplementation.6. Lithium is contraindicated during pregnancy:foetal goiter and other congenital abnormalities,especially cardiac, can occur; the newborn isoften hypotonic.7. At therapeutic levels, Li+ can cause reductionof T-wave amplitude. At higher levels, SA nodeand A-V conduction may be depressed, butarrhythmias are infrequent. Lithium is contra-indicated in sick sinus syndrome.
Lithium can cause dermatitis and worsenacne.
Interactions1. Diuretics (thiazide, furosemide) by causingNa+ loss promote proximal tubular reabsorptionof Na+ as well as Li+ → plasma levels of lithiumrise. Potassium sparing diuretics cause milderLi+ retention.2. Tetracyclines, NSAIDs and ACE inhibitorscan also cause lithium retention.3. Lithium reduces pressor response to NA.4. Lithium tends to enhance insulin/sulfonylureainduced hypoglycaemia.5. Succinylcholine and pancuronium have pro-duced prolonged paralysis in lithium treatedpatients.6. Neuroleptics, including haloperidol, havebeen frequently used along with lithium withoutproblem. However, sometimes, the combinationof haloperidol and lithium produces markedtremor and rigidity. The neuroleptic actionappears to be potentiated by lithium.

450S
EC
TIO
N7
DRUGS ACTING ON CENTRAL NERVOUS SYSTEM
UseLithium is used as its carbonate salt becausethis is less hygroscopic and less gastric irritantthan LiCl. It is converted into chloride in thestomach. Lithium citrate is used in syrupformulations.LICAB, LITHOSUN 300 mg tab, 400 mg SR tab.It is generally started at 600 mg/day and gradually increasedto yield therapeutic plasma levels; mostly 600–1200 mg/dayis required.
1. Acute mania (inappropriate cheerfullnessor irritability, motor restlessness, high energylevel, nonstop talking, flight of ideas, little needfor sleep and progressive loss of contact withreality; sometimes violent behaviour). Thoughlithium is effective in controlling acute mania,response is slow and control of plasma levelsis difficult during the acute phase. Mostpsychiatrists now prefer to use an atypicalantipsychotic orally or by i.m. injection, withor without a potent BZD like clonazepam/lorazepam, and start lithium after the episodeis under control. Maintenance lithium therapyis generally given for 6–12 months to preventrecurrences.2. Prophylaxis in bipolar disorder Lithiumhas proven efficacy in bipolar disorder: isgradually introduced and maintained at plasmaconcentration between 0.5–0.8 mEq/L. Suchtreatment lengthens the interval between cyclesof mood swings: episodes of mania as well asdepression are attenuated, if not totallyprevented. Bipolar disorder is the most commonand definite indication of lithium. Risks andbenefits of prolonged lithium therapy are to beweighed in individual cases. This depends on thetype of bipolar disorder, i.e. Type I (maniaepisodes only or both manic and depressivephases), Type II (cycles of hypomania alternatingwith major depression) or unipolar depression;cycle length and comorbid conditions, con-current medications, etc. Patients have beenmaintained on lithium therapy for over a decade.Most cases relapse when lithium is discontinued.Withdrawal, when attempted should be gradualover months.
Recurrent unipolar depression also respondsto lithium therapy. Combination of antidepressant+ lithium is often used initially, and lithium aloneis continued in the maintenance phase.3. Lithium is being sporadically used in manyother recurrent neuropsychiatric illness, clusterheadache and as adjuvant to antidepressants inresistant nonbipolar major depression.4. Cancer chemotherapy induced leukopenia and agranu-locytosis: Lithium may hasten the recovery of leukocyte count.5. Inappropriate ADH secretion syndrome: Lithium tendsto counteract water retention, but is not dependable.
ALTERNATIVES TO LITHIUM
Approximately 30% patients of mania and bipolardisorder (especially rapidly cycling cases) showincomplete or poor response to lithium. Many donot tolerate it, or are at special risk of toxicity.In the last two decades, several anticonvulsantsand atypical antipsychotics have been extensivelyevaluated as alternatives to lithium. Strongevidence of efficacy of some of these in differentphases of the disorder now exists. In view of thelimitations and problems in the use of lithium,use of valproate and some atypical antipsychoticshas overtaken that of lithium.1. Sodium valproate A reduction in manicrelapses is noted when valproate is used inbipolar disorder. It is now a first line treatmentof acute mania in which high dose valproate actsfaster than lithium and is an alternative toantipsychotic ± benzodiazepine. It can be usefulin those not responding to lithium or nottolerating it. Patients with rapid cycling patternmay particularly benefit from valproate therapy.A combination of lithium and valproate maysucceed in cases resistant to monotherapy witheither drug. Valproate has a favourable toler-ability profile, and now its use as prophylacticin bipolar disorder has exceeded that of lithium.Combination of valproate with an atypicalantipsychotic has high efficacy in acute mania.Divalproex, a compound of valproate, is morecommonly used due to better gastric tolerance.Dosage guidelines are the same as for epilepsy.

451C
HA
PTER32
ANTIPSYCHOTIC AND ANTIMANIC DRUGS
2. Carbamazepine Soon after its introduc-tion as antiepileptic, carbamazepine (CBZ) wasfound to prolong remission in bipolar disorder.Its efficacy in mania and bipolar disorder hasnow been confirmed. However, it is less popularthan valproate as an alternative to lithium.Carbamazepine is less effective than lithium orvalproate in acute mania. Moreover, acute maniarequires rapidly acting drug, while effective dosesof carbamazepine have to be gradually built up.Initiation of therapy with high doses needed forefficacy produce neurotoxicity and are poorlytolerated. Compared to lithium and valproate,efficacy of carbamazepine for long-termprophylaxis of bipolar disorder and suicides isless well established. Nevertheless, it is avaluable alternative/adjunct to lithium. The doseand effective plasma concentration range is thesame as for treatment of epilepsy.3. Lamotrigine There is now strong evidenceof efficacy of this newer anticonvulsant forprophylaxis of depression in bipolar disorder.Lamotrigine is not effective for treatment as wellas prevention of mania. It is now extensively usedin the maintenance therapy of type II bipolardisorder, because in this condition risk of inducingmania is minimal. Lamotrigine can be combinedwith lithium to improve its efficacy. Thetolerability profile of lamotrigine is favourable.
4. Atypical antipsychotics Lately, severalstudies have testified to the efficacy of atypicalantipsychotics in acute mania. Olanzapine,risperidone, aripiprazole, quetiapine, with orwithout a BZD, are now the first line drugs forcontrol of acute mania, except cases requiringurgent parenteral therapy, for which the olderneuroleptics are still the most effective.Aripiprazole has recently emerged as thefavoured drug for treatment of mania in bipolar Idisorder, both as monotherapy as well as adjuvantto lithium or valproate. Maintenance therapy witharipiprazole prevents mania, but not depressiveepisodes. Lack of metabolic effects, favours itslong-term use.
Olanzapine is also approved for maintenancetherapy of bipolar disorder. Though both manic
and depressive phases are suppressed, it is notconsidered suitable for long-term therapy dueto higher risk of weight gain, hyperglycaemia,etc. Strong evidence of efficacy of quetiapinehas emerged in bipolar depression. Combinationof an atypical antipsychotic with valproate orlithium has demonstrated high efficacy in acutephases as well as for maintenance therapy ofbipolar disorder.
HALLUCINOGENS(Psychotomimetics, Psychedelics,Psychodysleptics, Psychotogens)
These are drugs which alter mood, behaviour,thought and perception in a manner similar tothat seen in psychosis. Many natural productshaving hallucinogenic property have beendiscovered and used by man since prehistorictimes. A number of synthetic compounds havealso been produced. The important ones arebriefly described below.
INDOLE AMINES1. Lysergic acid diethylamide (LSD)Synthesized by Hofmann (1938) who wasworking on chemistry of ergot alkaloids, andhimself experienced its hallucinogenic effect.It is the most potent psychedelic, 25–50 µgproduces all the effects. In addition to the mentaleffects, it produces pronounced centralsympathetic stimulation. Its action appears toinvolve serotonergic neuronal systems in brain.2. Lysergic acid amide A close relative of LSD but10 times less potent; found in morning glory (Ipomoea violace)seeds.3. Psilocybin Found in a Mexican mushroom Psilocybemexicana; it has been used by Red Indian tribals duringreligious rituals.4. Harmine It is present in a vine Banisteriopsis caapi,found in the Amazon region. The Brazilian natives have usedit as a snuff.
5. Bufotenin Isolated from skin of a toad (Bufo marinus).It is also found in ‘Cohaba Snuff’ and in the mushroomAmanita muscaria.
The above are all Indolealkylamines related chemically to5-HT. A number of other synthetic derivatives likeDimethyltryptamine (DMT) are also hallucinogenic.

452S
EC
TIO
N7
DRUGS ACTING ON CENTRAL NERVOUS SYSTEM
PHENYLALKYL AMINES
Mescaline From Mexican ‘Peyote cactus’ Lophophorawilliamsi. It is a low potency hallucinogen used by nativesduring rituals. It is a phenylalkylamine but does not havemarked sympathomimetic effects.Ecstasy Methylene dioxy methamphetamine (MDMA, ortenamphetamine) is an amphetamine-like synthetic compoundwith stimulant and hallucinogenic properties, that has beenabused as a recreational and euphoriant drug, especially bycollege students under the name ‘Ecstasy’. Fear ofneurotoxicity has reduced its popularity.Yaba This is a combination of methamphetamine withanother stimulant methylhexanamine or caffeine. Popular asa ‘street drug’ in Thailand and Myanmar, it has spread tomany countries including India, as a ‘party drug’ among theyouth. Users claim it to be an aphrodisiac and produces a‘high’. The risk of neurotoxicity is similar to amphetamine.
Other synthetic phenylalkylamines with hallucinogenicproperty are—Dimethoxymethyl amphetamine (DOM) andMethylene dioxyamphetamine (MDA). High doses and repeateduse of amphetamine can also cause psychosis.
ARYLCYCLOHEXYL AMINES
Phencyclidine It is an anticholinergic, which activates σreceptors in brain causing disorientation, distortion of bodyimage, hallucinations and an anaesthetic like state. Ketamineis a closely related compound with lower hallucinogenicpotential and is used in anaesthesia. Mixed with drinks,ketamine has been abused as a ‘rape drug’, because of itsfast and strong depressant-amnesic action.
CANNABINOIDS9ΔΔΔΔΔ Tetrahydrocannabinol (9ΔΔΔΔΔ THC) It is theactive principle of Cannabis indica (Marijuana),which has been the most popular recreational andritualistic intoxicant used for millennia. Its usehas spread worldwide. The following are thevarious forms in which it is used.Bhang the dried leaves—is generally taken byoral route after grinding and making a paste. Itacts slowly.Ganja the dried female inflorescence—ismore potent and is smoked: effects are producedalmost instantaneously.Charas is the dried resinous extract from theflowering tops and leaves—most potent and isusually smoked along with tobacco; also called‘hashish’.
Cannabis is the drug of abuse having thelowest acute toxicity. Even habitual use is not
clearly associated with neurotoxicity or damageto any organ system. Though, personality andpsychiatric problems are more common amongcannabis users, it is not definite whether suchtraits led to cannabis use or cannabis causedthem. Young abusers may exhibit ‘amotivationalsyndrome’, i.e. loss of interest in work or self-improvement activities.
Considerable insight has been obtained recently incannabinoid pharmacology. Since 1990 two cannabinoidreceptors CB1 (in CNS) and CB2 (in peripheral tissues) havebeen identified and cloned. A host of endogenous ligandsfor the cannabinoid receptors have also been isolated.Anandamide, the ethanolamide of arachidonic acid is theprincipal endocannabinoid synthesized in the brain. Thephysiological function subserved by central and peripheralcannabinoid system is not clearly known. Endocannabinoidsare released by macrophages during haemorrhagic shock andcause fall in BP. However, all actions of cannabis are notmimicked by anandamide.
Cannabis produces potent analgesic, antiemetic, anti-inflammatory and many other pharmacological actions. Thecrude herb, its active constituents and some syntheticanalogues have been tried in a variety of conditions and manypotential clinical applications are proposed.• To ameliorate muscle spasm and pain in multiple sclerosis,
and certain dystonias.• Cancer chemotherapy induced vomiting. The synthetic
cannabinoids nabilone and dronabinol (9Δ THC) arelicenced for this use.
• As a neuronal protective after head injury and cerebralischaemia.
• To relieve anxiety and migraine.• To reduce i.o.t. in glaucoma.• As appetite stimulant.• As bronchodilator in asthma.
However, the hallucinogenic and psychomotor effects area limitation; nonhallucinogenic congeners are beinginvestigated.
The hallucinogens, particularly marijuana,produce a dream-like state with disorientation,loss of contact with reality, field of vision mayappear to sway and objects distorted like imagesin a curved mirror, faces may appear grotesque.On closing the eyes an unending series ofcolourful, very realistic and fantastic images appearto surge; time sense is altered, music appearstangible. Ability to concentrate is impaired, onecan read but does not know what he is reading;however, ataxia is not prominent. Many subjectsfeel relaxed and supremely happy, may laughuncontrollably (experience a ‘high’) or may

453C
HA
PTER32
ANTIPSYCHOTIC AND ANTIMANIC DRUGS
become sad and weep. With higher doses—panicreactions and sinking sensation are common.
Some degree of tolerance occurs, butreverse tolerance is not unusual.
Psychological dependence on hallucinogensmay be mild (occasional trips) to marked
(compulsive abuse), but physical dependencedoes not occur. All are drugs of abuse.
Hallucinogens have been rarely used inpsychiatry to facilitate conversation and foropening up the inner self in case of withdrawnpatients.
PROBLEM DIRECTED STUDY
32.1 A 25-year-male was diagnosed as a case of schizophrenia on the basis of disturbed thinkingprocess, inappropriate talking and behaviour, restlessness, bursts of temper, anxiety, poor self-care, disturbed sleep, delusional beliefs and occasional auditory hallucinations. He was treatedwith tab. haloperidol 5 mg once daily at bed time. The dose was increased to 7.5 mg dailyin the 2nd week and to 10 mg daily in the 3rd week. His symptoms gradually subsided andhe appeared more calm and organized. However, in the 5th week his family members reportedthat his restlessness has reappeared, he keeps pacing around in the room, but is not aggressiveor combative. On questioning the patient admited an uncontrollable urge to move aroundand that he feels uncomfortable in remaining still. He is not worried or anxious, but hasdifficulty in falling asleep.(a) What could be the reason for the motor restlessness? Should the dose of haloperidolbe increased or decreased, or should it be changed to another antipsychotic drug?(b) Should any other drug be given to relieve the condition?(see Appendix-1 for solution)

Drugs Used in Mental Illness:Antidepressant and AntianxietyDrugs
ChapterChapterChapterChapterChapter 3333333333
Major depression and mania are two extremesof affective disorders which refer to a patho-logical change in mood state. Major depressionis characterized by symptoms like sad mood,loss of interest and pleasure, low energy,worthlessness, guilt, psychomotor retardation oragitation, change in appetite and/or sleep,melancholia, suicidal thoughts, etc. It may bea unipolar or a bipolar disorder in which cyclesof mood swings from mania to depression occurover time. The mood change may have apsychotic basis with delusional thinking oroccur in isolation and induce anxiety. On theother hand, pathological anxiety may lead todepression. Anxiety and depression are theleading psychiatric disorders now.
ANTIDEPRESSANTS
These are drugs which can elevate mood indepressive illness. Practically all antidepressantsaffect monoaminergic transmission in the brainin one way or the other, and many of them haveother associated properties. Over the past threedecades, a large number of antidepressants withan assortment of effects on reuptake/metabolismof biogenic amines, and on pre/post-junctionalaminergic/cholinergic receptors have becomeavailable so that a cogent classification isdifficult. The following working classificationmay be adopted.
CLASSIFICATION
I. Reversible inhibitors of MAO-A (RIMAs)Moclobemide, Clorgyline
II. Tricyclic antidepressants (TCAs)A. NA + 5-HT reuptake inhibitors
Imipramine, Amitriptyline,
Trimipramine, Doxepin, Dothiepin,Clomipramine
B. Predominantly NA reuptake inhibitorsDesipramine, Nortriptyline, Amoxapine,Reboxetine
III. Selective serotonin reuptake inhibitors(SSRIs)Fluoxetine, Fluvoxamine, Paroxetine,Sertraline, Citalopram, Escitalopram,Dapoxetine
IV. Serotonin and noradrenaline reuptakeinhibitors (SNRIs)Venlafaxine, Duloxetine
V. Atypical antidepressantsTrazodone, Mianserin, Mirtazapine,Bupropion, Tianeptine, Amineptine,Atomoxetine
Many other drugs like Protriptyline, Maprotiline, Nafazodone,etc. are marketed in other countries.
MAO INHIBITORS
MAO is a mitochondrial enzyme involved in the oxidativedeamination of biogenic amines (Adr, NA, DA, 5-HT). Twoisoenzyme forms of MAO have been identified.
MAO-A: Preferentially deaminates 5-HT and NA, andis inhibited by clorgyline, moclobemide.
MAO-B: Preferentially deaminates phenylethylamine andis inhibited by selegiline.
Dopamine is degraded equally by both isoenzymes.Their distribution also differs. Peripheral adrenergic nerve
endings, intestinal mucosa and human placenta containpredominantly MAO-A, while MAO-B predominates in certainareas (mainly serotonergic) of brain and in platelets. Livercontains both isoenzymes.
Two hydrazine drugs—isoniazid and iproniazid wereused for tuberculosis in 1951; the latter was especially foundto cause disproportionate elevation of mood. Its capacity toinhibit degradation of biogenic amines was soon discoveredand was believed to be responsible for the mood elevatingaction. Its less hepatotoxic congeners like phenelzine and

455C
HA
PTER33
ANTIDEPRESSANT AND ANTIANXIETY DRUGS
isocarboxazid and some nonhydrazine MAO inhibitors(related to amphetamine) like tranylcypromine were used asantidepressants in the 1960s. They inhibited MAO irreversiblyand were nonselective for the two isoforms. Because of hightoxicity and interactions with foods and other drugs, theyhave become obsolete.
The selective MAO-A inhibitors possess antidepressantproperty. Selegiline selectively inhibits MAO-B at lower doses(5–10 mg/day), but these are not effective in depression. Itis metabolized to amphetamine and at higher doses it becomesnonselective MAO inhibitor—exhibits antidepressant andexcitant properties.
Nonselective MAO Inhibitors
The nonselective MAO inhibitors elevate the mood ofdepressed patients; in some cases it may progress tohypomania and mania. Excitement and hypomania may beproduced even in nondepressed individuals.
The active metabolites of nonselective MAO inhibitorsinactivate the enzyme irreversibly. The drugs themselves stayin the body for relatively short periods, but their effects last for2–3 weeks after discontinuation: they are ‘hit and run’ drugs.Return of MAO activity depends on synthesis of fresh enzyme;tissue monoamine levels remain elevated long after the drughas been largely eliminated.
Interactions These drugs inhibit a number of other enzymesas well, and interact with many food constituents and drugs.(i) Cheese reaction Certain varieties of cheese, beer,wines, pickled meat and fish, yeast extract contain largequantities of tyramine, dopa, etc. In MAO inhibited patientsthese indirectly acting sympathomimetic amines escapedegradation in the intestinal wall and liver → reaching intosystemic circulation they displace and release large amountsof NA from transmitter loaded adrenergic nerve endings →hypertensive crisis, cerebrovascular accidents. When sucha reaction occurs, it can be treated by i.v. injection of a rapidlyacting α blocker, e.g. phentolamine. Prazosin or chlorpromazineare alternatives.
(ii) Cold and cough remedies They contain ephedrineor other sympathomimetics—hypertensive reaction can occur.
(iii) Reserpine, guanethidine, tricyclic antidepressantsExcitement, rise in BP and body temperature can occur whenthese drugs are given to a patient on MAO inhibitors. Thisis due to their initial NA releasing or uptake blocking action.
(iv) Levodopa Excitement and hypertension occur due toincrease in biological t½ of DA and NA that are producedfrom levodopa.
(v) Antiparkinsonian anticholinergics Hallucinations andsymptoms similar to those of atropine poisoning occur.
(vi) Barbiturates, alcohol, opioids, antihistamines Actionof these drugs is intensified and prolonged. Respiration mayfail.
(vii) Pethidine High fever, sweating, excitation, delirium,convulsions and severe respiratory depression have occurred.The most accepted explanation is—MAO inhibitors retard hydrolysis of pethidine but not itsdemethylation. Thus, excess of norpethidine (normally a minormetabolite—see p. 475) is produced which has excitatoryactions.
Reversible inhibitors of MAO-A (RIMAs)Moclobemide It is a reversible and selectiveMAO-A inhibitor with short duration of action;full MAO activity is restored within 1–2 daysof stopping the drug. Because of competitiveenzyme inhibition, tyramine is able to displaceit from the enzyme, so that potentiation ofpressor response to ingested amines is minor,and dietary restrictions are not required. Clinicaltrials have shown moclobemide to be anefficacious antidepressant, comparable to TCAs,except in severe cases. It lacks the anticho-linergic, sedative, cognitive, psychomotor andcardiovascular adverse effects of typical TCAsand is safer in overdose. This makes it a parti-cularly good option in elderly patients and inthose with heart disease.Dose: 150 mg BD–TDS (max 600 mg/day)RIMAREX, TRIMA 150, 300 mg tabs.
Adverse effects are nausea, dizziness,headache, insomnia, rarely excitement and liverdamage. Chances of interaction with other drugsand alcohol are remote, but caution is advisedwhile coprescribing pethidine, SSRIs and TCAs.
Moclobemide has emerged as a well toleratedalternative to TCAs for mild to moderate depres-sion and for social phobia.
TRICYCLIC ANTIDEPRESSANTS (TCAs)
Imipramine, an analogue of CPZ was foundduring clinical trials (1958) to selectivelybenefit depressed but not agitated psychotics.In contrast to CPZ, it inhibited NA and 5-HT

456S
EC
TIO
N7
DRUGS ACTING ON CENTRAL NERVOUS SYSTEM
reuptake into neurones. A large number of con-geners were soon added and are called tricyclicantidepressants (TCAs).
These older compounds, in addition to uptakeblockade have direct effects on adrenergic,cholinergic and histaminergic receptors, and arereferred to as ‘first generation antidepressants,’a group which also includes MAOIs.
The subsequently produced second genera-tion antidepressants have more selective actionon amine uptake; are either Selective serotoninreuptake inhibitors (SSRIs), or Serotonin andnoradrenaline reuptake inhibitors (SNRIs), withno direct action on cholinergic/adrenergic/histaminergic receptors, or have some atypicalfeatures. They have a limited spectrum of actionresulting in fewer side effects.
PHARMACOLOGICAL ACTIONS
The most prominent action of TCAs is theirability to inhibit norepinephrine transporter(NET) and serotonin transporter (SERT) locatedat neuronal/platelet membrane at low andtherapeutically attained concentrations.
The TCAs inhibit monoamine reuptake andinteract with a variety of receptors viz. musca-rinic, α adrenergic, histamine H1, 5-HT1, 5-HT2
and occasionally dopamine D2. However, rela-tive potencies at these sites differ amongdifferent compounds. The actions of imipramineare described as prototype.
1. CNS Effects differ in normal individuals andin the depressed.In normal individuals It induces a peculiarclumsy feeling, tiredness, light-headedness,sleepiness, difficulty in concentrating andthinking, unsteady gait. These effects tend toprovoke anxiety. There is no mood elevation oreuphoria; effects are rather unpleasant and maybecome more so on repeated administration.In depressed patients Little acute effects areproduced, except sedation (in the case of drugswhich have sedative property). After 2–3 weeksof continuous treatment, the mood is graduallyelevated, patients become more communicative
and start taking interest in self and surroundings.Thus, TCAs are not euphorients but only anti-depressants. In depressed patients who havepreponderance of REM sleep, this phase issuppressed and awakenings during night arereduced. The EEG effects of low doses aresimilar to hypnotics but high doses causedesynchronization. Sedative property variesamong different compounds (see Table 33.1).The more sedative ones are suitable fordepressed patients showing anxiety and agitation.The less sedative or stimulant ones are betterfor withdrawn and retarded patients.
The TCAs lower seizure threshold and pro-duce convulsions in overdose. Clomipramine andbupropion have the highest seizure precipitatingpotential. Amitriptyline and imipramine depressrespiration in overdose only.
Mechanism of action The TCAs and relateddrugs inhibit NET and SERT which mediate activereuptake of biogenic amines NA and 5-HT intotheir respective neurones and thus potentiatethem. They, however, differ markedly in theirselectivity and potency for different amines (seeclassification above).
Most of the compounds do not inhibit DAuptake, except bupropion. Moreover, ampheta-mine and cocaine (which are not antidepressantsbut CNS stimulants) are strong inhibitors of DAuptake. However, it has been proposed that TCAsindirectly facilitate dopaminergic transmissionin forebrain that may add to the mood elevatingaction.
Reuptake inhibition results in increased con-centration of the amines in the synaptic cleftin both CNS and periphery. Tentative conclusionsdrawn are:• Inhibition of DA uptake correlates with stimu-
lant action; but is not primarily involved inantidepressant action.
• Inhibition of NA and 5-HT uptake is asso-ciated with antidepressant action.
Certain findings indicate that uptake blockadeis not directly responsible for the antidepressantaction, e.g.

457C
HA
PTER33
ANTIDEPRESSANT AND ANTIANXIETY DRUGS
• Uptake blockade occurs quickly but anti-depressant action develops after weeks
• Mianserin is antidepressant but has no uptakeblocking action.
Initially the presynaptic α2 and 5-HT1
autoreceptors are activated by the increasedamount of NA/5-HT in the synaptic cleftresulting in decreased firing of locus coeruleus(noradrenergic) and raphe (serotonergic) neu-rones. After, long-term administration, antidep-ressants desensitise the presynaptic α2, 5-HT1A,5-HT1D autoreceptors and induce other adaptivechanges in the number and sensitivity of pre andpost synaptic NA and/or 5-HT receptors as wellas in amine turnover of brain, the net effect ofwhich is enhanced nor-adrenergic and seroto-nergic transmission. Thus, uptake blockadeappears to initiate a series of time-dependentchanges that culminate in antidepressant effect.
None of the TCAs, except amoxapine, blockDA receptors or possess antipsychotic activity.
2. ANS Most TCAs are potent anticholiner-gics—cause dry mouth, blurring of vision,constipation and urinary hesitancy as side effect.The anticholinergic potency is graded in Table33.1.
They potentiate exogenous and endogenousNA by blocking uptake, but also have weak α1
adrenergic blocking action. Some, e.g. amitripty-line, doxepin, trimipramine have slight H1
antihistaminic action as well.
3. CVS Effects on cardiovascular function areprominent, occur at therapeutic concentrationsand may be dangerous in overdose.Tachycardia: due to anticholinergic and NApotentiating actions.Postural hypotension: due to inhibition ofcardiovascular reflexes and α1 blockade.ECG changes and cardiac arrhythmias: T wavesuppression or inversion is the most consistentchange. Arrhythmias occur in overdose mainlydue to interference with intraventricularconduction. The NA potentiating + ACh blockingactions along with direct myocardial depressioncompound the proarrhythmic potential. Older
patients are more susceptible. The SSRIs, SNRIsand atypical antidepressants are safer in thisregard.
Tolerance and dependenceTolerance to the anticholinergic and hypotensiveeffects of imipramine-like drugs develops gra-dually, but antidepressant action is sustained.
Psychological dependence on these drugsis rare, because their acute effects are notpleasant.
There is some evidence of physical depen-dence occurring when high doses are used forlong periods—malaise, chills, muscle pain mayoccur on discontinuation and have been consi-dered withdrawal phenomena. Gradual withdrawalis recommended, but antidepressants do not carryabuse potential.
PHARMACOKINETICSThe oral absorption of TCAs is good, thoughoften slow. They are highly bound to plasma andtissue proteins, therefore have large volumes ofdistribution (~20 L/kg). They are extensivelymetabolized in liver; the major route forimipramine and amitriptyline is demethylationwhereby active metabolites—desipramine andnortriptyline respectively are formed. Both thesemetabolites predominantly block NA reuptake.Few other TCAs also produce active metabolites.Inactivation occurs by oxidation and glucuronideconjugation. Various CYP isoenzymes likeCYP2D6, CYP3A4, CYP1A2 and othersmetabolise tricylic and related antidepressants.Metabolites are excreted in urine over 1–2weeks. The plasma t½ of amitriptyline,imipramine and doxepin range between 16–24hours. The t½ is longer for some of their activemetabolites. Because of relatively long t½s, oncedaily dosing (at bed time) is practicable in themaintenance phase.
An unusual therapeutic window phenomenonhas been observed, i.e. optimal antidepressanteffect is exerted at a narrow band of plasmaconcentrations (between 50–200 ng/ml ofimipramine, amitriptyline, nortriptyline). Both

458S
EC
TIO
N7
DRUGS ACTING ON CENTRAL NERVOUS SYSTEM
TAB
LE 3
3.1
Com
para
tive
prop
ertie
s an
d pr
epar
atio
ns o
f tric
yclic
and
rela
ted
antid
epre
ssan
ts
Dru
gS
edat
ion
Ant
i-mus
carin
icH
ypot
ensi
onC
ardi
acS
eizu
reD
aily
Pre
para
tions
arrh
ythm
iapr
ecip
itatio
n d
ose
(mg)
Tric
yclic
ant
idep
ress
ants
(TC
As)
1.Im
ipra
min
e+
++
++
+++
++
50–2
00D
EP
SO
NIL
, AN
TID
EP
25
mg
tab,
75
mg
SR
cap
.2.
Am
itrip
tylin
e++
+++
+++
+++
++
+50
–200
AM
LIN
E, S
AR
OTE
NA
, TR
YP
TOM
ER
, 10,
25,
75
mg
tabs
.3.
Trim
ipra
min
e++
+++
++
+++
++
+50
–150
SU
RM
ON
TIL
10, 2
5 m
g ta
b.4.
Dox
epin
+++
++
++
+++
++
50–1
50S
PE
CTR
A, D
OX
IN, D
OX
ETA
R 1
0, 2
5, 7
5 m
g ta
b/ca
p.5.
Clo
mip
ram
ine
++
+++
++
+++
+++
50–1
50C
LOFR
AN
IL, 1
0, 2
5, 5
0 m
g ta
b, 7
5 m
g S
R ta
b.C
LON
IL, A
NA
FRA
NIL
10,
25
mg
tab.
6.D
othi
epin
++
++
++
++
++
50–1
50P
RO
THIA
DE
N, D
OTH
IN 2
5, 7
5 m
g ta
b.(D
osul
pin)
7.N
ortri
ptyl
ine
++
++
++
+50
–150
SE
NS
IVA
L, P
RIM
OX
25
mg
tab.
8.A
mox
apin
e+
++
++
++
+10
0–30
0D
EM
OLO
X 5
0, 1
00 m
g ta
b.S
elec
tive
sero
toni
n re
upta
ke in
hibi
tors
(SS
RIs
)1.
Fluo
xetin
e±
——
—±
20–4
0FL
UD
AC
20
mg
cap,
20
mg/
5 m
l sus
p.FL
UN
IL 1
0, 2
0 m
g ca
ps;
FLU
PA
R, P
RO
DA
C 2
0 m
g ca
p.2.
Fluv
oxam
ine
±—
——
—50
–200
FLU
VO
XIN
50,
100
mg
tab.
3.P
arox
etin
e±
±—
——
20–5
0X
ET
10, 2
0, 3
0, 4
0 m
g ta
bs.
4.S
ertra
line
±—
——
—50
–150
SE
RE
NA
TA, S
ER
LIN
, SE
RTI
L 50
, 100
mg
tabs
.5.
Cita
lopr
am—
——
——
20–4
0C
ELI
CA
10,
20,
40
mg
tabs
.6.
Esc
italo
pram
——
——
—10
–20
ES
DE
P, F
ELI
Z-S
5, 1
0, 2
0 m
g ta
bs.
Ser
oton
in a
nd n
orad
rena
line
reup
take
inhi
bito
rs (S
NR
Is)
1.V
enla
faxi
ne—
——
±—
75–1
50V
EN
LOR
25,
37.
5, 7
5 m
g ta
bs,
VE
NIZ
-XR
37.
5, 7
5, 1
50 m
g E
R c
aps.
2.D
ulox
etin
e—
——
——
30-8
0D
ELO
K, D
ULA
NE
, DU
ZAC
, 20,
30,
40
mg
caps
.A
typi
cal a
ntid
epre
ssan
ts1.
Traz
odon
e++
+—
±±
—50
–200
TRA
ZOD
AC
25,
50
mg
tab,
TRA
ZON
IL, T
RA
ZALO
N 2
5, 5
0, 1
00 m
g ta
bs.
2.M
ians
erin
++
++
++
++
30–1
00TE
TRA
DE
P 1
0, 2
0, 3
0 m
g ta
b, S
ER
IDA
C 1
0, 3
0 m
g ta
b.3.
Bup
ropi
on–,
-—
——
+++
150–
300
SM
OQ
UIT
150
mg
tab.
4.M
irtaz
apin
e++
+—
±—
—15
–45
MIR
T 15
, 30,
45
mg
tabs
, MIR
TAZ
15, 3
0 m
g ta
b.

459C
HA
PTER33
ANTIDEPRESSANT AND ANTIANXIETY DRUGS
below and above this range, beneficial effectsare suboptimal.
Wide variation in the plasma concentrationattained by different individuals given the samedose has been noted. Thus, doses need to beindividualized and titrated with the response, butplasma concentrations are not a reliable guidefor adjusting the dose of TCAs.
ADVERSE EFFECTSSide effects are common with TCAs becauseof which SSRIs, SNRIs and atypical anti-depressants have become the first line drugs.
1. Anticholinergic: dry mouth, bad taste,constipation, epigastric distress, urinaryretention (especially in males with enlargedprostate), blurred vision, palpitation.
2. Sedation, mental confusion and weakness,especially with amitriptyline and moresedative congeners.
3. Increased appetite and weight gain is notedwith most TCAs and trazodone, but not withSSRIs, SNRIs and bupropion.
4. Some patients receiving any antidepressantmay abruptly ‘switch over’ to a dysphoric-agitated state or to mania. Most likely,these are cases of bipolar depression, theother pole being unmasked by theantidepressant. Patients receiving higherdoses, especially of TCAs, are at greaterrisk than those receiving lower doses andSSRIs or bupropion.
5. Sweating (despite antimuscarinic action)and fine tremors are relatively common.
6. Seizure threshold is lowered—fits may beprecipitated, especially in children.Bupropion, clomipramine, amoxapine havegreater propensity, while desipramine,SSRIs and SNRIs are safer in this regard.
7. Postural hypotension, especially in olderpatients. It is less severe with desipramine-like drugs and insignificant with SSRIs/SNRIs.
8. Sexual distress: especially delay orinterference with erection, ejaculation andoccasionally with orgasm.
9. Cardiac arrhythmias, especially in patientswith ischaemic heart disease. Arrhythmiasmay be responsible for sudden death in thesepatients. Amitriptyline and dosulpin areparticularly dangerous in overdose; higherincidence of arrhythmia is reported withthem.
10. Rashes and jaundice due to hypersensitivityare rare. Mianserin is more hepatotoxic.
Acute poisoning Poisoning with TCAs isfrequent; usually self-attempted by the depressedpatients, and may endanger life. Manifestationsare:Excitement, delirium and other anticholinergicsymptoms as seen in atropine poisoning, fol-lowed by muscle spasms, convulsions and coma.Respiration is depressed, body temperature mayfall, BP is low, tachycardia is prominent. ECGchanges and ventricular arrhythmias are common.Treatment is primarily supportive with gastriclavage, respiratory assistance, fluid infusion,maintenance of BP and body temperature. Aci-dosis must be corrected by bicarbonate infusion.
Diazepam may be injected i.v. to controlconvulsions and delirium. Most important is thetreatment of cardiac arrhythmias, for which propra-nolol/lidocaine may be used. The class IA andIC antiarrhythmics and digoxin themselves depresscardiac conduction; are therefore contraindicated.
INTERACTIONS1. TCAs potentiate directly acting sympathomi-
metic amines (present in cold/asthmaremedies). Adrenaline containing localanaesthetic should be avoided. However, TCAsattenuate the action of indirect sympathomi-metics (ephedrine, tyramine).
2. TCAs abolish the antihypertensive actionof guanethidine and clonidine by preventingtheir transport into adrenergic neurones.
3. TCAs potentiate CNS depressants, includingalcohol and antihistaminics.
4. Phenytoin, phenylbutazone, aspirin andCPZ can displace TCAs from protein bindingsites and cause transient overdose symptoms.

460S
EC
TIO
N7
DRUGS ACTING ON CENTRAL NERVOUS SYSTEM
5. Phenobarbitone competitively inhibits aswell as induces imipramine metabolism.Carbamazepine and other enzyme inducersenhance metabolism of TCAs.
6. SSRIs inhibit metabolism of several drugs(see later) including TCAs—dangerous toxi-city can occur if the two are given concur-rently.
7. By their anticholinergic property, TCAs delaygastric emptying and retard their own as wellas other drug’s absorption. However, digoxinand tetracyclines may be more completelyabsorbed. When used together, the anticho-linergic action of neuroleptics and TCAs mayadd up.
8. MAO inhibitors—dangerous hypertensivecrisis with excitement and hallucinations hasoccurred when given with TCAs.
Amoxapine This tetracyclic compound isunusual in that it blocks dopamine D2 receptorsin addition to inhibiting NA reuptake. It ischemically related to the antipsychotic drugloxapine and has mixed antidepressant +neuroleptic properties—offers advantage forpatients with psychotic depression. Risk ofextrapyramidal side effects is also there. Seizures(including status epilepticus) occur in its overdose.
Reboxetine This is a newer selective NAreuptake blocker with weak effect on 5-HTreuptake. Antimuscarinic and sedative actions areminimal. It appears to produce fewer side effectsand may be safer in overdose than the older TCAs.Usual side effects are insomnia, palpitation, drymouth, constipation, sexual distress and urinarysymptoms.Dose: 4 mg BD or 8 mg OD.NAREBOX 4, 8 mg tab.
SELECTIVE SEROTONIN REUPTAKEINHIBITORS (SSRIs)
The major limitations of TCAs (first generationantidepressants) are:• Frequent anticholinergic, cardiovascular and
neurological side effects.• Relatively low safety margin. They are
hazardous in overdose; fatalities are common.
• Lag time of 2–4 weeks before antidepressantaction manifests.
• Significant number of patients respondincompletely and some do not respond.
To overcome these shortcomings, a large numberof newer (second generation) antidepressantshave been developed since 1980s. The mostsignificant of these are the SSRIs and SNRIswhich selectively inhibit membrane associatedSERT or both SERT and NET. Though, somepatients may not respond even to these drugs,the efficacy of second generation antidepressantsis rated higher than older TCAs and RIMAs.Some patients not responding to one type ofdrug may respond to another type. Moreimportantly the newer drugs have improvedtolerability, both in therapeutic dose as well asin overdose. It has been claimed that certaindrugs (bupropion, venlafaxine, mirtazapine) havefaster onset of antidepressant action, but thishas not been unequivocally established.
The relative safety and better acceptabilityof SSRIs has made them 1st line drugs in depres-sion and allowed their extensive use in anxiety,phobias, OCD and related disorders. The SSRIsproduce little or no sedation, do not interferewith cognitive and psychomotor function orproduce anticholinergic side effects. They aredevoid of α adrenergic blocking action—posturalhypotension does not occur, making themsuitable for elderly patients. They have practi-cally no seizure precipitating propensity and donot inhibit cardiac conduction—overdosearrhythmias are not a problem. Prominent sideeffects are gastrointestinal; all SSRIs frequentlyproduce nausea (due to 5-HT3 receptorstimulation), but tolerance develops over time.Loose motions are due to 5-HT uptake blockadein the gut and activation of 5-HT receptors onenteric plexus neurones. Weight gain is not aproblem with SSRIs, but they more commonlyinterfere with ejaculation or orgasm. A new cons-tellation of mild side effects, viz. nervousness,restlessness, insomnia, anorexia, dyskinesia andheadache is associated with them, but patientacceptability is good. Increased incidence of

461C
HA
PTER33
ANTIDEPRESSANT AND ANTIANXIETY DRUGS
epistaxis and ecchymosis has been reported,probably due to impairment of platelet function.Gastric blood loss due to NSAIDs may beincreased by SSRIs.
The SSRIs inhibit drug metabolizing iso-enzymes CYP2D6 and CYP3A4: elevate plasmalevels of TCAs, haloperidol, clozapine, terfena-dine, astemizole, warfarin, β blockers, someBZDs and carbamazepine. ‘Serotonin syndrome’manifesting as agitation, restlessness, rigidity,hyperthermia, delirium, sweating, twitchingsfollowed by convulsions can be precipitated whenany serotonergic drug (e.g. MAOIs, tramadol,pethidine) is taken by a patient receiving SSRIs.Some degree of tolerance to antidepressantaction of SSRIs has been noted in few patientsafter months of use. Discontinuation reactionconsisting of paresthesias, bodyache, bowelupset, agitation and sleep disturbances occursin some patients. However, risk of switchingover to hypomania during treatment is less withSSRIs than with TCAs.
Some authorities now consider SSRIs to bemore effective antidepressants than TCAs.However, some patients not responding to SSRIsmay respond to TCAs. The converse is also true,and there is no way to predict which patient willrespond to which drug. Because of freedom frompsychomotor and cognitive impairment, SSRIsare preferred for prophylaxis of recurrentdepression (should be combined with lithium/valproate). Metaanalysis of comparative trials hasshown no significant difference in efficacyamong individual SSRIs, but there are pharma-cokinetic differences and incidence of particularside effects differs somewhat.
Fluoxetine A bicyclic compound, is the firstSSRI to be introduced, and the longest acting.Its plasma t½ is 2 days and that of its activedemethylated metabolite is 7–10 days. It hasbeen approved for use in children 7 years orolder for depression and OCD on the basis ofsimilar efficacy and side effect profile as inadults, but should be given to children only whenpsychotherapy fails. Agitation and dermatological
reactions are more frequent than other SSRIs.Because of slower onset of antidepressant effect,it is considered less suitable for patients needingrapid effect, but is more appropriate for poorlycompliant patients. Its stimulant effect couldworsen patients showing agitation.
Fluvoxamine It is a shorter-acting SSRI witha t½ of 18 hours and no active metabolite, whichhas been specifically recommended for genera-lized anxiety disorder and OCD, rather than fordepression. Relatively more nausea, dyspepsia,flatulence, nervousness and discontinuationreactions have been reported with fluvoxamine.
Paroxetine Another short acting SSRI (t½ 20hours) which does not produce active metabolite.A higher incidence of g.i. side effects, sexualdistress, agitation and discontinuation reactionthan with other SSRIs has been noted.
Sertraline This SSRI has gained popularity,because in clinical trials fewer patients stoppedsertraline due to side effects. Efficacy in juveniledepression has been demonstrated, and it isrecommended for anxiety and post-traumaticstress disorder (PTSD) as well. Drug interactionsdue to inhibition of CYP isoenzymes are lesslikely to occur with this SSRI. Its plasma t½is 26 hours and it produces a still longer-lastingactive metabolite.
Citalopram This SSRI shares with sertralinea lower propensity to cause drug interactions.Its t½ is 33 hours and no active metabolite isknown. However, few deaths due to overdoseof citalopram are on record, because of whichit is to be avoided in patients likely to attemptsuicide. Citalopram is the preferred SSRI formood disorders in premenstrual syndrome.
Escitalopram It is the active S(+) enantiomerof citalopram, effective at half the dose, withsimilar properties. Side effects are milder andsafety is improved.
Dapoxetine A SSRI which has been developedand is being promoted for delaying prematureejaculation, a property common to many SSRIs

462S
EC
TIO
N7
DRUGS ACTING ON CENTRAL NERVOUS SYSTEM
and some TCAs. Dapoxetine acts rapidly and canbe taken 1 hour before sexual intercourse.Combined with behavioural therapies, it has beenfound to help many sufferers. Side effects arenausea, vomiting, loose motions, headache,dizziness and occasionally insomnia.Dose: 60 mg taken 1 hour before intercourse; older patients30 mg.SUSTINEX, DURALAST, KUTUB 30 mg, 60 mg tabs.
Other uses of SSRIs The SSRIs are now1st choice drugs for OCD, panic disorder, socialphobia, eating disorders, premenstrual dysphoricdisorder and PTSD. They are also beingincreasingly used for anxiety disorders, bodydysmorphic disorder, compulsive buying, klepto-mania and premature ejaculation. Elevation ofmood and increased work capacity has beenreported in postmyocardial infarction and otherchronic somatic illness patients. Thus, SSRIs arebeing used to improve outlook on life and tofeel good, even in apparently nondepressedpatients. Wisdom of such use though isquestionable.
SEROTONIN AND NORADRENALINEREUPTAKE INHIBITORS (SNRIs)
1. Venlafaxine A novel antidepressantreferred to as SNRI, because it inhibits uptakeof both NA and 5-HT but, in contrast to olderTCAs, does not interact with cholinergic,adrenergic or histaminergic receptors or havesedative property. Trials have shown it to be aseffective antidepressant as TCAs and may workin some resistant cases. A faster onset of actionis claimed. Mood changes and hot flushes inmenopausal syndrome, some anxiety and eatingdisorders are also benefited by venlafaxine. Itdoes not produce the usual side effects of TCAs;tends to raise rather than depress BP and is saferin overdose. Prominent side effects are nausea,sweating, anxiety, dizziness, impotence andwithdrawal reactions on discontinuation.
2. Duloxetine A newer SNRI similar to venla-faxine. It is neither sedative, nor anticholinergic,nor antihistaminic, nor α blocker. Side effects,
including g.i. and sexual problems are milder, butsome agitation, insomnia and rise in BP can occur.Antidepressant efficacy is comparable to TCAs.Duloxetine is also indicated in panic attacks,diabetic neuropathic pain, fibromyalgia and stressurinary incontinence in women (because itincreases urethral tone).
ATYPICAL ANTIDEPRESSANTS1. Trazodone It is the first atypical anti-depressant; less efficiently blocks 5-HT uptakeand has prominent α adrenergic and weak 5-HT2
antagonistic actions. The latter may contributeto its antidepressant effect, which neverthelessis modest. It is sedative but not anticholinergic,causes bradycardia rather than tachycardia, doesnot interfere with intracardiac conduction—lessprone to cause arrhythmia and better suited forthe elderly. Nausea is felt, especially in thebeginning. Mild anxiolytic effect has been notedand it has benefited cases of OCD. Inappropriate,prolonged and painful penile erection (priapism)occurs in few recipients resulting in impotencein a fraction of these. The α1 adrenergic blockingproperty has been held responsible for this effectas well as for postural hypotension. In general,trazodone is infrequently used now in depression.2. Mianserin It is unique in not inhibitingeither NA or 5-HT uptake; but blocks presynapticα2 receptors thereby increasing release andturnover of NA in brain which may be respon-sible for the antidepressant effect. Antagonisticaction at 5-HT2, 5-HT1c as well as H1 receptorshas also been shown. It is a sedative—relievesassociated anxiety and suppresses panic attacks.While anticholinergic and cardiac side effectsare less prominent, it has caused seizures in over-dose. However, overdose fatality is low. Reportsof blood dyscrasias and liver dysfunction haverestricted its use.
3. Mirtazapine This antidepressant acts bya novel mechanism, viz. blocks α2 auto- (on NAneurones) and hetero- (on 5-HT neurones)receptors enhancing both NA and 5-HT release.The augmented NA further increases firing of

463C
HA
PTER33
ANTIDEPRESSANT AND ANTIANXIETY DRUGS
serotonergic raphe neurones via α1 receptors.Selective enhancement of antidepressive 5-HT1
receptor action is achieved by concurrentblockade of 5-HT2 and 5-HT3 receptors whichare held responsible for some of the adverseeffects of high serotonergic tone. Accordingly,it has been labelled as “noradrenergic andspecific serotonergic antidepressant” (NaSSA).It is a H1 blocker and quite sedative, but notanticholinergic or antidopaminergic. Efficacy inmild as well as severe depression is reportedto be comparable to TCAs, and given once dailyat bed time, it is particularly suitable for thosewith insomnia. Increased appetite and weight gainis frequent. Sexual dysfunction is not a problemwith mirtazapine.
4. Bupropion This inhibitor of DA and NAuptake has excitant rather than sedative property.It is metabolized into an amphetamine likecompound which can cause presynaptic releaseof DA and NA. A sustained-release formulationis marketed as an aid to smoking cessation. Inclinical trials it has been found to yield highersmoking abstinence and quitting rates thanplacebo and equivalent to nicotine replacement.Bupropion may be acting by augmenting thedopaminergic reward function. Better results areobtained when it is combined with nicotine patch.The nicotine withdrawal symptoms were lesssevere in bupropion recipients. However, long-term efficacy is not known, and it can causeinsomnia, agitation, dry mouth and nausea, butnot sexual side effects. Seizures occur in overdose and in predisposed patients due to loweringof seizure threshold. The dose of 150 mg BDshould not be exceeded. It is contraindicated ineating disorders and in bipolar illness. Bupropionis infrequently used to treat depression; may beadded to a SSRI.5. Tianeptine This antidepressant is reportedto increase rather than inhibit 5-HT uptake, andis neither sedative nor stimulant. It has shownefficacy in anxiodepressive states, particularlywith psychosomatic symptoms, as well as inendogenous depression. Side effects are dry
mouth, epigastric pain, flatulence, drowsiness/insomnia, tremor and bodyache.Dose: 12.5 mg BD–TDS; STABLON 12.5 mg tab.
6. Amineptine Like tianeptine it enhances5-HT uptake, and has antidepressant property. Itproduces anticholinergic side effects includingtachycardia, confusion and delirium. Posturalhypotension, conduction disturbances andarrhythmias can occur, especially in patients withheart disease.Dose: 100 mg BD at breakfast and lunch.SURVECTOR 100 mg tab.
7. Atomoxetine It is unrelated to tricyclic antidepressants,but is a selective NA reuptake inhibitor. It is approved onlyfor treatment of attention deficit hyperactivity disorder(ADHD), and is described in Ch. 35.
USES
1. Endogenous (major) depression: The aimis to relieve symptoms of depression and restorenormal social behaviour. The tricyclic and relatedantidepressants are of proven value. Responsetakes at least 2–3 weeks to appear, full benefitstake still longer. Choice of a particular drug foran individual patient depends on the secondaryproperties (sedative, anticholinergic, hypotensive,cardiotoxic, seizure precipitating, etc.) asdescribed above. The SSRIs are currently usedas first choice for their better tolerability, safetyand may be higher efficacy as well. The SNRIsand newer atypical agents also offer someadvantages. The only antidepressants clearly shownto be effective in juvenile depression are fluoxetineand sertraline. The TCAs are mostly used asalternatives in non-responsive cases or in thosenot tolerating the second generation antidepres-sants. Substituting a drug with a different patternof aminergic action often succeedes in non-responsive cases. However, few patients fail anyantidepressant. Moclobemide is a well toleratedoption for mild to moderate depression, especiallysuited for elderly and cardiac patients. However,antidepressants are not the answer to every grief,loss, set back and other sad events that are partof life, but the less toxic and more patient-friendlySSRIs/SNRIs/atypical antidepressants are nowmore readily prescribed for depressive illness.

464S
EC
TIO
N7
DRUGS ACTING ON CENTRAL NERVOUS SYSTEM
After a depressive episode has beencontrolled, continued treatment at maintenancedoses (about 100 mg imipramine/day or equi-valent) for months is recommended to preventrelapse. Discontinuation of the antidepressantmay be attempted after 6–12 months. Long-termtherapy may be needed in patients who tend torelapse. ECT may be given in the severelydepressed, especially initially while the effectof antidepressants is developing, because noantidepressant has been clearly demonstrated toact fast enough to prevent suicide. The TCAsor SSRIs must be combined with lithium/valproate/lamotrigine for bipolar depression, andnot used alone due to risk of switching overto mania.
Combination of one of the SSRIs with anatypical antipsychotic (such as olanzapine,aripiprazole or quetiapine) is also accepted asa treatment option for bipolar depression.
2. Obsessive-compulsive and phobic states:The SSRIs, particularly fluoxamine, are the drugsof choice due to better patient acceptability.TCAs, especially clomipramine, are highlyeffective in OCD and panic disorders: more than25% improvement occurs in OCD rating scaleand panic attacks are reduced in >75% patients.SSRIs and TCAs also reduce compulsive eatingin bulimia, and help patients with bodydysmorphic disorder, compulsive buying andkleptomania, though these habits may notcompletely die.
3. Anxiety disorders: Antidepressants,especially SSRIs, exert a delayed but sustainedbeneficial effect in many patients of generalizedanxiety disorder; may be used along with a shortcourse of BZDs to cover exacerbations. SSRIshave also proven helpful in phobic disorders,sustained treatment of panic attacks and in post-traumatic stress disorder.
4. Neuropathic pain: Amitriptyline and otherTCAs afford considerable relief in diabetic andsome other types of chronic pain. Amitriptylinereduces intensity of post-herpetic neuralgia in
~50% patients. The SSRIs are less effective inthese conditions. Duloxetine, a SNRI, is nowa first line drug for diabetic neuropathy, fibro-myalgia, etc. Other drugs useful in neuropathicpain are pregabalin or gabapentin. Combinationof duloxetine + pregabalin may work ifmonotherapy is not satisfactory.
5. Attention deficit-hyperactivity disorder(ADHD) in children: TCAs with less depressantproperties like imipramine, nortriptyline andamoxapine are now first line drugs in this dis-order, comparable in efficacy to amphetamine-like drugs, with the advantage of less fluctuatingaction and fewer behavioural side effects.Atomoxetine is a NA reuptake inhibitor unrelatedto both TCAs as well as amphetamine, whichis used specifically in ADHD.6. Premature ejaculation: It refers to repeatedoccurrences of ejaculation before or shortly afterpenetration, or with minimal sexual stimulation.It is a very common sexual complaint, whichis often interpreted as sexual weakness; can causeconsiderable distress and dissatisfaction in thepatient as well as in his partner. Sometimes thesubject has unreasonable expectations about theoptimal/desirable length of intercourse.
Most SSRIs and some TCAs, especiallyclomipramine have the common property ofdelaying and in some cases inhibiting ejaculation(this itself can cause sexual distress). Theprimary treatment of premature ejaculation iscounselling and behavioural therapy, but this canbe supplemented by drugs. Dapoxetine is a SSRIwhich has been specifically introduced for thispurpose. It acts rapidly; 60 mg taken 1 hourbefore intercourse has helped many subjects.Clomipramine 10–25 mg three times a day isa slow acting drug which needs to be takenregularly for maximum benefit. For on demanduse, 25 mg may be taken 6 hours before sex.7. Enuresis: In children above 5 years, imipra-mine 25 mg at bedtime is effective, but bedwetting may again start when the drug is stopped.Eldery subjects with bed wetting have alsobenefited.

465C
HA
PTER33
ANTIDEPRESSANT AND ANTIANXIETY DRUGS
8. Migraine: Amitriptyline has some prophy-lactic value, especially in patients with mixedheadaches.9. Pruritus: Some tricyclics have antipruriticaction. Topical doxepin has been used to relieveitching in atopic dermatitis, lichen simplex, etc.NOCTADERM 5% cream.
ANTIANXIETY DRUGSAnxiety It is an emotional state, unpleasantin nature, associated with uneasiness, discomfortand concern or fear about some defined orundefined future threat. Some degree of anxietyis a part of normal life. Treatment is neededwhen it is disproportionate to the situation andexcessive. Some psychotics and depressedpatients also exhibit pathological anxiety.
Cardiac neurosis (unfounded fear of heart disease—palpitation, functional precordial pain); g.i. neurosis (fixationon bowel movement, distention, eructation, reflux, acidity);social anxiety (fear of being observed and evaluated byothers); obsessive-compulsive disorder (OCD), post-traumaticstress disorder and various forms of phobias are some specifictypes of anxiety disorders.
Antianxiety drugs These are an ill-definedgroup of drugs, mostly mild CNS depressants,which are aimed to control the symptoms ofanxiety, produce a restful state of mind withoutinterfering with normal mental or physicalfunctions. The anxiolytic-sedative drugs differmarkedly from antipsychotics, and more closelyresemble sedative-hypnotics. They:1. Have no therapeutic effect to control thought
disorder of schizophrenia.2. Do not produce extrapyramidal side effects.3. Have anticonvulsant property.4. Produce physical dependence and carry abuse
liability.5. Do not selectively block conditioned avoi-
dance response in animals.
CLASSIFICATION
1. Benzodiazepines DiazepamChlordiazepoxideOxazepamLorazepam, Alprazolam
2. Azapirones Buspirone, Gepirone,Ispapirone
3. Sedative Hydroxyzineantihistaminic
4. β blocker Propranolol
In addition to the above drugs, antidepres-sants, especially the SSRIs and SNRIs areeffective in OCD, phobias, panic and many typesof severe generalized anxiety disorders.
BENZODIAZEPINES
The pharmacology of benzodiazepines (BZDs)as a class is described in Ch. 29.
Some members have a slow and prolongedaction, relieve anxiety at low doses withoutproducing significant CNS depression. They havea selective taming effect on aggressive animalsand suppress induced aggression. They alsosuppress the performance impairing effect ofpunishment. In contrast to barbiturates, they aremore selective for the limbic system and haveproven clinically better in both quality andquantity of improvement in anxiety and stress-related symptoms.
At antianxiety doses, cardiovascular andrespiratory depression is minor.
Because anxiety is a common complaint andis a part of most physical and mental illness,and because the BZDs—• have little effect on other body systems• have lower dependence producing liability
than barbiturates and other sedatives;withdrawal syndrome is milder and delayeddue to their long half lives
• are relatively safe even in gross overdosage,they are presently one of the widely used classof drugs. Potent BZDs like lorazepam andclonazepam injected i.m. have adjuvant role inthe management of acutely psychotic and manicpatients.
BZDs act primarily by facilitating inhibitoryGABAergic transmission, but other additionalmechanisms of action have been suggested.Higher doses induce sleep and impair perfor-mance.

466S
EC
TIO
N7
DRUGS ACTING ON CENTRAL NERVOUS SYSTEM
Adverse effects of BZDs noted in theiruse as hypnotics are described in Ch. 29. Sideeffects that occur in their use to relieve anxietyare—sedation, light-headedness, psychomotorand cognitive impairment, confusional state(especially in the elderly), increased appetite andweight gain, alterations in sexual function.Rashes are uncommon. Some women fail toovulate while on regular use of BZDs. The majorconstraint in their long-term use for anxiety dis-orders is their potential to impair mentalfunctions and to produce dependence.
Differences between individual BZDs recom-mended for anxiety are primarily pharmaco-kinetic: choice of one over the other is largelyempirical.
1. Chlordiazepoxide It was the first BZDto be used clinically. Oral absorption is slow.A smooth long lasting effect is produced. It ispreferred in chronic anxiety states. Chlordiaze-poxide is often combined with other drugs inpsychosomatic disorders, and has been the com-monest BZD used to cover alcohol withdrawal.Its t½ is 6–12 hours, but active metabolites areproduced which extend the duration of action.Its anticonvulsant action is weak.Daily dose: 25–100 mg; LIBRIUM 10, 25 mg tabs;EQUILIBRIUM 10 mg tab.
2. Diazepam It is quickly absorbed; producesa brief initial phase of strong action followedby prolonged milder effect due to a two phaseplasma concentration decay curve (distributivephase t½ 1 hr, elimination phase t½ 20–30hours). The biological effect t½ is still longerdue to production of active metabolites. It ispreferred in acute panic states and anxietyassociated with organic disease.Daily dose: 5–30 mg; VALIUM, PLACIDOX 2, 5, 10 mg tabs;CALMPOSE 5, 10 mg tab, 2 mg/5 ml Syr.
3. Oxazepam It is slowly absorbed; beingrelatively polar, its penetration in brain is alsoslow. The plasma t½ is about 10 hours. It ismetabolized only by glucuronide conjugation,therefore no active metabolite is produced.
Duration of action is relatively shorter makingit preferable for the elderly and in those withliver disease. It has been used mainly in shortlasting anxiety states.Daily dose: 30–60 mg in 2–3 divided portions;SEREPAX 15, 30 mg tab.
4. Lorazepam Has slow oral absorption.Being less lipid-soluble than diazepam, its rateof entry in brain is slower. The plasma t½ isshorter (10–20 hours); no active metabolite isproduced, since it is directly conjugated withglucuronic acid, and is suitable for older patients.However, it is quite sedative and capable ofproducing marked amnesia when injected i.v.Injection site complications are minor.Therefore, it is the only BZD recommended fori.m. use. It has been preferred for short lastinganxiety states, panic, OCD and tension syn-dromes, as well as for psychosomatic diseasesand for i.v. use in status epilepticus.Daily dose: 1–6 mg; LARPOSE, ATIVAN 1, 2 mg tab.CALMESE 1, 2 mg tabs, 4 mg/2 ml inj.
5. Alprazolam A high potency anxiolyticBZD which in addition has some mood eleva-ting action in mild depression. As such, it isparticularly useful in anxiety associated withdepression. Good response has been obtainedin panic disorders with severe anxiety andautonomic symptoms. Its plasma t½ is about 12hours, but an active metabolite is produced.Alprazolam is also used as hypnotic. Whenadministered daily as anxiolytic, some patientsexperience anxiety in between doses, which maybe obviated by employing sustained releasetablet. Withdrawal symptoms may be moremarked on discontinuation than with other BZDs.Dose: 0.25–1.0 mg TDS; upto 6 mg/day in panic disorder;ALPRAX 0.25, 0.5, 1.0 mg tabs., 0.5, 1.0, 1.5 mg SR tabs;ALZOLAM 0.25, 0.5, 1.0 mg tabs; 1.5 mg SR tab,ALPROCONTIN 0.5, 1.0, 1.5 mg CR tabs. RESTYL 0.25, 0.5,1.0 mg tabs, RESTYL-SR 0.5, 1.0, 1.5 mg SR tabs.
OTHER ANTIANXIETY DRUGS
Buspirone It is the first azapirone, a new classof antianxiety drugs, distinctly different fromBZDs. Buspirone:

467C
HA
PTER33
ANTIDEPRESSANT AND ANTIANXIETY DRUGS
• Does not produce significant sedation orcognitive/functional impairment.
• Does not interact with BZD receptor ormodify GABAergic transmission.
• Does not produce tolerance or physical depen-dence.
• Does not suppress BZD or barbiturate with-drawal syndrome.
• Has no muscle relaxant or anticonvulsantactivity.Buspirone relieves mild-to-moderate genera-
lized anxiety, but is ineffective in severe cases,in those showing panic reaction and in OCD.The therapeutic effect develops slowly;maximum benefit may be delayed up to 2 weeks.The mechanism of anxiolytic action is not clearlyknown, but may be dependent on its selectivepartial agonistic action on 5-HT1A receptors. Bystimulating presynaptic 5-HT1A autoreceptors, itreduces the activity of dorsal raphe serotonergicneurones. Antagonistic action at certainpostsynaptic 5-HT1A receptors has also beendemonstrated. After chronic treatment, adaptivereduction in cortical 5-HT2 receptors may occur.Buspirone has weak dopamine D2 blockingaction but no antipsychotic or extrapyramidaleffects. A mild mood elevating action has beennoted occasionally, which may be due tofacilitation of central noradrenergic system.
Buspirone is rapidly absorbed; undergoesextensive first pass metabolism; (bioavailability<5%), one metabolite is active and excretionoccurs both in urine and faeces; t½ is 2–3.5hrs. Side effects are minor: dizziness, nausea,headache, light-headedness, rarely excitement.It may cause rise in BP in patients on MAOinhibitors, but does not potentiate CNS depres-sants. Though most patients on buspirone remainalert, those operating machinery/motor vehiclesshould be cautioned.Dose: 5–15 mg OD–TDS:ANXIPAR, BUSPIN, BUSCALM 5, 10 mg tab.
Hydroxyzine An H1 antihistaminic with sedative, antiemetic,antimuscarinic and spasmolytic properties. It is claimed tohave selective anxiolytic action, but the accompanyingsedation is quite marked. Hydroxyzine may be used in reactiveanxiety or that associated with marked autonomic symptoms.
Due to antihistaminic and sedative property, it is useful inpruritus and urticaria.Daily dose 50–200 mg;ATARAX 10, 25 mg tab, 10 mg/5 ml syr, 25 mg/2 ml inj.
βββββ Blockers (see Ch. 10)Many symptoms of anxiety (palpitation, rise inBP, shaking, tremor, gastrointestinal hurrying,etc.) are due to sympathetic overactivity, andthese symptoms reinforce anxiety. Propranololand other nonselective β blockers help anxiouspatients troubled by these symptoms, by cuttingthe vicious cycle and provide symptomatic relief.They do not affect the psychological symptomssuch as worry, tension and fear, but are valuablein acutely stressful situations (examination fear,unaccustomed public appearance, etc.). They maybe used for performance/situational anxiety oras adjuvant to BZDs. The role of β blockersin anxiety disorders is quite limited.
TREATMENT OF ANXIETY
Anxiety is a universal phenomenon, and toexperience it in appropriate circumstances is thenormal response. It may serve to enhance vigi-lance and drive. However, if anxiety symptomsare frequent and persist in a severe form, theyare a cause of distress/suffering and markedlyimpair performance. Anxiety should be treatedwith drugs only when excessive and disablingin its own right.
The established drugs are BZDs which actquickly, while buspirone and SSRIs/SNRIs actonly after chronic treatment. The BZDs shouldbe used in the smallest possible dose. The dosehas to be found out for each patient by titrationwith symptoms of anxiety. Acute anxiety statesgenerally respond better than chronic anxiety.The drug should be withdrawn as soon as it isno longer required. However, when large doseshave been used for longer periods, withdrawalshould be gradual. Long-term use of BZDs isof questionable merit due to cognitive impair-ment and risk of dependence.
The usual practice is to give 1/2 to 2/3 ofthe daily dose at bed time to ensure good nightly

468S
EC
TIO
N7
DRUGS ACTING ON CENTRAL NERVOUS SYSTEM
rest; the remaining is divided in 2–3 doses givenat day time. Though the t½ of BZDs used inanxiety are longer, divided day time doses orSR tab. are required to avoid high peaks.
Buspirone is a nonsedating alternative toBZDs for chronic treatment of less severe formsof generalized anxiety. The SSRIs and SNRIs arenow extensively used in most forms of chronicanxiety disorders, but are not good for acuteanxiety. They produce a delayed but oftengratifying response and can be combined withBZDs. The SSRIs are now drugs of choice forsocial anxiety, OCD, eating disorders and PTSDin which BZDs, though effective, carry abusepotential on long-term use.
Panic attacks are initially treated with arapidly acting BZD (e.g. diazepam, alprazolam),
but BZDs are not suitable for long-term therapy.SSRIs and duloxetine are the drugs of choicefor sustained treatment, which in the initial fewweeks may be supplemented by continuing theBZD. Valproate is an alternative to SSRIs. Phobicdisorders are mostly treated by a SSRI, such asparoxetine, fluvoxamine or sertraline. In situa-tional phobias, propranolol may be added as andwhen required. Gabapentin has been used asalternative to SSRI.
Patients with hypertension, peptic ulcer,ulcerative colitis, irritable bowel syndrome,gastroesophageal reflux, thyrotoxicosis, anginapectoris are often given low doses of BZD inaddition to specific therapy, though anxiety maynot be a prominent manifestation.Fixed dose combination of tranquillizers with vitamins has beenbanned.
PROBLEM DIRECTED STUDY
33.1 A businessman aged 35 years suffered loss and his employees left. He became verydepressed and stopped taking interest in the business. Gradually he stopped going out andwithdrew socially. He felt guilty, worthless and tired all the time, lost interest in pleasureand sex, stopped eating properly and had disturbed sleep. When he showed no sign of recoveryeven after 3 months, the family members consulted a doctor, who diagnosed him to be acase of major depression and prescribed—
Tab Sertraline 50 mg twice a day, and a multivitamin.The family members brought him back after one week and complained that there was noimprovement. On questioning the patient revealed that he felt more restless, had nausea,pain in upper abdomen, headache and no desire to eat.(a) What could be the reason for no improvement in the depressive symptoms? Is the choiceof drug inappropriate? Does the medication needs to be changed, dose increased or decreased?Should another drug be added at this stage?(see Appendix-1 for solution)

Opioid Analgesics andAntagonists
ChapterChapterChapterChapterChapter 3434343434
Algesia (pain) is an ill-defined, unpleasantbodily sensation, usually evoked by an externalor internal noxious stimulus.
Analgesic A drug that selectively relieves painby acting in the CNS or on peripheral painmechanisms, without significantly altering con-sciousness.
Pain is a warning signal, primarily protectivein nature, but causes discomfort and suffering;may even be unbearable and incapacitating. It isthe most important symptom that brings thepatient to the physician. Excessive pain mayproduce other effects—sinking sensation, appre-hension, sweating, nausea, palpitation, rise or fallin BP, tachypnoea. Analgesics relieve pain as asymptom, without affecting its cause. They areused when the noxious stimulus (evoking thepain) cannot be removed or as adjuvants to moreetiological approach to pain. Analgesics aredivided into two groups, viz.A. Opioid/narcotic/morphine-like analgesics.B. Nonopioid/non-narcotic/aspirin-like/antipy-
retic or antiinflammatory analgesics (descri-bed in Ch. 14).
OPIOID ANALGESICS
Opium A dark brown, resinous material obtai-ned from poppy (Papaver somniferum) capsule.It contains two types of alkaloids.
Phenanthrene derivativesMorphine (10% in opium)Codeine (0.5% in opium)Thebaine (0.2% in opium), (Nonanalgesic)
Benzoisoquinoline derivativesPapaverine (1%)
NonanalgesicNoscapine (6%)
Opium has been known from the earliest times. It is mentionedin the Eber’s papyrus (1500 BC), in the writings ofTheophrastus (300 BC) and Galen (2nd century AD). Opiumeating became a social custom in China in the 18th century.Serturner, a pharmacist, isolated the active principle of opiumin 1806 and named it ‘morphine’ after the Greek god of dreamsMorpheus. In the last century a large number of semisyntheticand synthetic compounds have been developed with mor-phine-like, antagonistic and mixed agonistic-antagonisticproperties.
Compounds that are derived from opium or are chemicallyrelated to morphine are called ‘opiates’, while all those havingmorphine-like action, irrespective of chemical nature, are called‘opioids’. Accordingly, pethidine, endorphins, etc. are opioids,but not opiates.
MORPHINE
Morphine is the principal alkaloid in opium andis widely used till today. Therefore, it is descri-bed as prototype.
PHARMACOLOGICAL ACTIONS
1. CNS Morphine has site specific depressantand stimulant actions in the CNS by interactingprimarily with the μ opioid receptor (for whichit has the highest affinity), as a full agonist. Thedepressant actions are:
(a) Analgesia Morphine is a strong analgesic.Though dull, poorly localized visceral pain is
⎫⎬⎭

470S
EC
TIO
N7
DRUGS ACTING ON CENTRAL NERVOUS SYSTEM
relieved better than sharply defined somatic pain;higher doses can mitigate even severe pain;degree of analgesia increasing with dose. Noci-ceptive pain arising from stimulation ofperipheral pain receptors is relieved better thanneuretic pain (such as trigeminal neuralgia)produced by inflammation of or damage to neuralstructures. The associated reactions to intensepain (apprehension, fear, autonomic effects) arealso dampened. Suppression of pain perceptionis selective, without affecting other sensationsor producing proportionate generalized CNSdepression (contrast general anaesthetics).
Perception of pain and the emotionalcomponent (anxiety, fear, suffering, distress)induced by it are both altered so that pain isno longer as unpleasant or distressing, i.e. thepatient tolerates pain better. The analgesic actionof morphine has both spinal and supraspinalcomponents. Intrathecal injection of morphinehas been shown to cause segmental analgesiawithout affecting other modalities. It acts in thesubstantia gelatinosa of dorsal horn to inhibitrelease of excitatory transmitters (e.g. substanceP) from primary afferents carrying painimpulses. The action appears to be exertedthrough interneurones which are involved in the‘gating’ of pain impulses. Release of glutamatefrom primary pain afferents in the spinal cordand its postsynaptic action on dorsal hornneurones is inhibited by morphine. Action atsupraspinal sites in medulla, periaqueductal graymatter, limbic and cortical areas may alterprocessing and interpretation of pain impulses.It also sends inhibitory impulses throughdescending pathways to the spinal cord. Severalaminergic (5-HT, NA), GABAergic and otherneuronal systems appear to be involved in theaction of morphine. Simultaneous action atspinal and supraspinal sites greatly amplifies theanalgesia.
A peripheral action of opioids on small primary afferentterminals in skin or deeper structures, attenuating theirsensitization following tissue injury has also beendemonstrated. This may play a role in the analgesic actionof morphine in conditions like burns and trauma.
(b) Sedation which is different from thatproduced by hypnotics is seen. Drowsiness andindifference to surroundings as well as to ownbody occurs without motor incoordination, ataxiaor apparent excitement (contrast alcohol).Higher doses progressively induce sleep and thencoma. Morphine has no anticonvulsant action,rather, fits may be precipitated.
(c) Mood and subjective effects These areprominent. Morphine has a calming effect; thereis loss of apprehension, feeling of detachment,lack of initiative, limbs feel heavy and bodywarm, mental clouding and inability toconcentrate occurs. In the absence of pain orapprehension, these are generally appreciated asunpleasant by normal people. However, patientsin pain or anxiety, and especially addicts, perceiveit as pleasurable floating sensation: refer it as‘high’. Rapid i.v. injection by addicts gives thema ‘kick’ or ‘rush’ which is intensely pleasurable—akin to orgasm. Thus, one has to learn to perceivethe euphoric effect of morphine.
The pleasurable and reinforcing effects of µ opioid agonists(morphine-like) appear to involve a separate set of neuronalmechanisms than those involved in analgesia and sedation.The euphoric effects are most likely mediated by DA release innucleus accumbance, whereas κ agonists (nalorphine like)inhibit DA release and produce aversion. The μ opioid receptorsappear to inhibit the inhibitory GABAergic neurones, therebyfacilitating DA release in nucleus accumbens. Inhibition of NArelease in locus ceruleus by opioids is implicated in their actionto allay apprehension and fear.
(d) Respiratory centre Morphine depressesrespiratory centre in a dose dependent manner;rate and tidal volume are both decreased.However, analgesic dose in an otherwise healthyindividual produces no cognizable respiratorydepression, but it may be marked in the presenceof other sedatives, cardiopulmonary/liver/kidneydisease, etc. Death in morphine poisoning is dueto respiratory failure. Neurogenic, hypercapnoeicand later hypoxic drives to the respiratory centreare suppressed in succession. In addition, thereis indifference to breathing: apnoeic patient maybreath if commanded.
(e) Cough centre It is depressed by morphine,and is more sensitive than respiratory centre.

471C
HA
PTER34
OPIOID ANALGESICS AND ANTAGONISTS
(f) Temperature regulating centre It isdepressed; hypothermia occurs in cold sur-roundings.
(g) Vasomotor centre It is depressed at higherdoses and contributes to the fall in BP.
Morphine stimulates:
(a) CTZ Nausea and vomiting occur as sideeffects, especially if stomach is full and thepatient stands or moves about. Thus, morphineappears to sensitize the CTZ to vestibular andother impulses. Larger doses depress vomitingcentre directly: emetics should not be tried inmorphine poisoning.
(b) Edinger Westphal nucleus of III nerveis stimulated producing miosis. No miosis occurson topical application of morphine to the eye,since this is a central action. Morphine producesthis effect by inhibiting the GABAergic inter-neurone which tonically inhibits the Edinger-Westphal nucleus. Mydriasis occurs in somespecies like cats. Another ocular effect is adecrease in intraocular tension.
(c) Vagal centre It is stimulated→ bradycardiais the usual response to morphine.
(d) Certain cortical areas and hippocampalcells are stimulated. Muscular rigidity andimmobility is consistently manifested at highdoses (especially on i.v. injection). Thisresembles catalepsy seen in rats and mice.Morphine lowers seizure threshold. Convulsionsmay occur in morphine poisoning. The procon-vulsant action has been ascribed to inhibitionof GABA release by hippocampal interneurones.Morphine causes excitation instead of sedationin an occasional individual. Species like cat, lion,horse, sheep and cow are uniformly excited andshow hyperthermia.
2. Neuro-endocrine Hypothalamic acti-vation by afferent collaterals is dampened.Hypothalamic influence on pituitary is reduced.As a result FSH, LH, ACTH levels are lowered,while prolactin and GH levels are raised (these
are under predominant inhibitory control). Thesex hormone and cortisol levels are lowered.Some degree of tolerance may develop to thiseffect, but heavy abusers often suffer loss oflibido, impotence, menstrual irregularities andinfertility. Clinical hypocorticism is unusual.Morphine can release ADH and reduce urinevolume.
3. CVS Morphine causes vasodilatation dueto:(a) histamine release.(b) depression of vasomotor centre.(c) direct action decreasing tone of bloodvessels.
There is a shift of blood from pulmonaryto systemic circuit due to greater vasodilatationin the latter. Therapeutic doses cause littlechange in the BP of recumbent normovolaemicpatient. Postural hypotension and fainting dooccur due to venodilatation and impairment ofvascular reflexes. Morphine has little directeffect on heart; rate generally decreases due tostimulation of vagal centre, but may increasereflexly if the BP falls. Cardiac work is consis-tently reduced due to decrease in peripheralresistance, imparting anti-ischaemic property tomorphine. Intracranial tension tends to rise asa consequence of CO2 retention leading tocerebral vasodilatation.
4. GIT The enteric plexus neurones and g.i.mucosa are rich in opioid receptors. Morphineexerts marked effect on g.i. motility as well ason fluid dynamics across g.i. mucosa.Constipation is a prominent feature of morphineaction. Several factors contribute:(a) Action directly on intestines and in the CNSincreases tone and segmentation but decreasespropulsive movements. Tone of duodenum andcolon may be increased to the level of spasm.(b) Spasm of pyloric, ileocaecal and analsphincters.(c) Decrease in all gastrointestinal secretions dueto reduction in movement of water and electro-lytes from mucosa to the lumen. This is mainlya peripheral action through opioid receptors on

472S
EC
TIO
N7
DRUGS ACTING ON CENTRAL NERVOUS SYSTEM
enteric plexus neurones, but also a central action.Absorption of fluid is increased due to stasis.(d) Central action causing inattention todefecation reflex.No tolerance develops to this action: addictsremain chronically constipated.
5. Other smooth muscles
(a) Biliary tract Morphine causes spasm ofsphincter of Oddi → intrabiliary pressure isincreased several fold → may cause biliary colic.This action is only partly counteracted byatropine but more completely by opioidantagonist naloxone and direct smooth musclerelaxants like nitrates.
(b) Urinary bladder Tone of both detrusor andsphincter muscle is increased → urinary urgencyand difficulty in micturition. Contractions ofureter are also increased.
(c) Uterus The action is clinically insigni-ficant, may slightly prolong labour.
(d) Bronchi Morphine releases histamine (dueto its bulky basic molecule; the mechanism isnonimmunological), which can cause broncho-constriction. This is of no consequence in normalindividuals, but can be dangerous in asthmatics.
6. ANS Morphine causes mild hyperglycae-mia due to central sympathetic stimulation. Ithas weak anticholinesterase action.
PHARMACOKINETICS
The oral absorption of morphine is unreliablebecause of high and variable first pass meta-bolism; oral bioavailability is 1/6th to 1/4th ofparenterally administered drug. About 30% isbound to plasma proteins. Distribution is wide;concentration in liver, spleen and kidney is higherthan that in plasma. Only a small fraction entersbrain rather slowly. Morphine freely crossesplacenta and can affect the foetus more than themother. It is primarily metabolized in liver byglucuronide conjugation. Morphine-6-glucuro-nide is an active metabolite (more potent than
morphine on μ opioid receptors), which accu-mulates during chronic dosing and contributesto analgesia, despite its restricted passageacross blood-brain barrier. Another metabolitemorphine-3-glucuronide has neuroexcitatoryproperty. Plasma t½ of morphine averages2–3 hours. Effect of a parenteral dose lasts4–6 hours. Elimination is almost complete in24 hours and morphine is noncumulative.However, small amounts persist in the body dueto enterohepatic circulation.
ADVERSE EFFECTS
1. Side effects Sedation, mental clouding,lethargy and other subjective effects which mayeven be dysphoric in some subjects; vomitingis occasional in recumbent patient; constipationis common and distressing. Respiratorydepression, blurring of vision, urinary retention(especially in elderly male) are other sideeffects. BP may fall, especially in hypovolaemicpatient and if he/she walks about.
2. Idiosyncrasy and allergy Allergicreactions manifesting as urticaria, swelling of lipsoccur infrequently. Anaphylactoid reaction is rare.A local reaction at injection site and generalizeditching may occur due to histamine release.
3. Apnoea of the newborn This may occurwhen morphine is given to the mother duringlabour. The blood-brain barrier of the foetus isundeveloped, morphine attains higher concen-tration in foetal brain than in that of mother.Naloxone 10 µg/kg injected in the umbilical cordis the treatment of choice.
4. Acute morphine poisoning It may beaccidental, suicidal or seen in drug abusers. Inthe nontolerant adult, 50 mg of morphine i.m.produces serious toxicity. The human lethal doseis estimated to be about 250 mg. Manifestationsare extensions of the pharmacological action.
Stupor or coma, flaccidity, shallow andoccasional breathing, cyanosis, pinpoint pupil,fall in BP and shock; convulsions may be seenin few, pulmonary edema occurs at terminalstages, death is due to respiratory failure.

473C
HA
PTER34
OPIOID ANALGESICS AND ANTAGONISTS
Treatment: consists of respiratory support (posi-tive pressure respiration also opposes pulmonaryedema formation) and maintenance of BP (i.v.fluids, vasoconstrictors). Gastric lavage should bedone with pot. permanganate to remove unabsorbeddrug. Lavage is indicated even when morphine hasbeen injected. Being a basic drug it is partitionedto the acid gastric juice, ionizes there and doesnot diffuse back into blood.
Specific antidote: Naloxone 0.4–0.8 mg i.v.repeated every 2–3 min till respiration picks up,is the specific antagonist of choice because itacts rapidly, does not have any agonistic actionand does not per se depress respiration (seep. 483). Due to short duration of action, naloxoneshould be repeated every 1–4 hours, accordingto the response.
5. Tolerance and dependence High degreeof tolerance can be developed to morphine andrelated opioids if the drug is used repeatedly.It is partly pharmacokinetic (enhanced rate ofmetabolism), but mainly pharmacodynamic(cellular tolerance). Tolerance is exhibited tomost actions, but not to constipating and mioticactions. Addicts tolerate morphine in grams:lethal dose is markedly increased. Patients inintense pain are relatively tolerant to depressanteffects. Cross tolerance among opioids is of highdegree. Morphine tolerant subjects are partiallycross tolerant to other CNS depressants as well.
Morphine produces pronounced psycholo-gical and physical dependence, its abuse liabilityis rated high. Recently the NMDA antagonistsand nitric oxide synthase inhibitors have beenfound to block morphine tolerance and depen-dence in animals. Thus, the analgesic action ofmorphine can be dissociated from tolerance anddependence which contribute to its abuse.Concern about abuse has been a major limitationin the use of morphine, but appropriate medicaluse of morphine seldom progresses to depen-dence and abuse. Morphine abuse is higheramong medical and paramedical personnelbecause they have easier access to the drug.
Earlier, morphine addicts tended to be from themiddle age group, but now younger individualsare also opting for it. Opium eating has beenprevalent among natives in the orient.
Withdrawal of morphine is associated withmarked drug-seeking behaviour. Physical mani-festations of abstinence are—lacrimation,sweating, yawning, anxiety, fear, restlessness,gooseflesh, mydriasis, tremor, insomnia,abdominal colic, diarrhoea, dehydration, rise inBP, palpitation and rapid weight loss. Deliriumand convulsions are not a characteristic feature(contrast barbiturates) and are seen onlyoccasionally. Cardiovascular collapse and fatalityare rare if supportive measures are instituted.
Opioid antagonists (naloxone, nalorphine)precipitate acute withdrawal syndrome in thedependent subject. In the more severely depen-dent, even 0.2 mg of naloxone can precipitatemarked withdrawal.
Treatment: consists of withdrawal of mor-phine and substitution with oral methadone(long-acting, orally effective) followed bygradual withdrawal of methadone. However,relapse rate among postaddicts is high. Long-term methadone maintenance and othertechniques using agonist-antagonistic drugs arealso employed.
PRECAUTIONS ANDCONTRAINDICATIONS
Morphine is a drug of emergency, but due carehas to be taken in its use.1. Infants and the elderly are more susceptibleto the respiratory depressant action of morphine.2. It is dangerous in patients with respiratoryinsufficiency (emphysema, pulmonary fibrosis,cor pulmonale); sudden deaths have occurred.Morphine accentuates sleep apnoea; hypoxicbrain damage can occur.3. Bronchial asthma: Morphine can precipitatean attack by its histamine releasing action. A highpotency opioid with lower histamie releasingpotential (e.g. fentanyl) should be used, ifunavoidable, in an asthmatic.

474S
EC
TIO
N7
DRUGS ACTING ON CENTRAL NERVOUS SYSTEM
4. Head injury: morphine is contraindicated inpatients with head injury. Reasons are—• By retaining CO2, it increases intracranial
tension which will add to that caused by headinjury itself.
• Even therapeutic doses can cause markedrespiratory depression in these patients.
• Vomiting, miosis and altered mentation pro-duced by morphine interfere with assessmentof progress in head injury cases.
5. Hypotensive states and hypovolaemia exag-gerate fall in BP due to morphine.6. Undiagnosed acute abdominal pain: morphinecan aggravate certain conditions, e.g. diverti-culitis, biliary colic, pancreatitis. Inflamedappendix may rupture. Morphine can be givenafter the diagnosis is established. Pentazocine,buprenorphine are less likely to aggravate biliaryspasm.7. Elderly male: chances of urinary retentionare high.8. Hypothyroidism, liver and kidney diseasepatients are more sensitive to morphine.9. Unstable personalities: are liable to continuewith its use and become addicted.
InteractionsPhenothiazines, tricyclic antidepressants, MAOinhibitors, amphetamine and neostigmine poten-tiate morphine and other opioids, either by retar-ding its metabolism or by a pharmacodynamicinteraction at the level of central neurotrans-mitters.Morphine retards absorption of many orallyadministered drugs by delaying gastric emptying.Dose: 10–50 mg oral, 10–15 mg i.m. or s.c. or 2–6 mg i.v.; 2–3 mgepidural/intrathecal; children 0.1–0.2 mg/kg. i.m. or s.c.MORPHINE SULPHATE 10 mg/ml inj; MORCONTIN 10, 30, 60,100 mg continuous release tabs; 30–100 mg BD; RILIMORF 10,20 mg tabs, 60 mg SR tab.
CLASSIFICATION OF OPIOIDS
1. Natural opium alkaloids: Morphine, Codeine
2. Semisynthetic opiates: Diacetylmorphine(Heroin), Pholcodeine, Ethylmorphine.
Many others like—Hydromorphone, Oxymorphone, Hydro-codone, Oxycodone are not used in India.
3. Synthetic opioids: Pethidine (Meperidine),Fentanyl, Methadone, Dextropropoxyphene,Tramadol.Many others like—Levorphanol, Dextromoramide, Dipipanone,Alfentanil, Sufentanil, Remifentanil are not available in India.
1. Codeine It is methyl-morphine, occursnaturally in opium, and is partly converted inthe body to morphine. It is less potent thanmorphine (1/10th as analgesic), also less effica-cious; is a partial agonist at μ opioid receptorwith a low ceiling effect. The degree of analgesiais comparable to aspirin (60 mg codeine ~ 600mg aspirin); can relieve mild to moderate painonly.
However, codeine is more selective coughsuppressant (1/3rd as potent as morphine);subanalgesic doses (10–30 mg) suppress cough(see p. 220). Codeine has very low affinity foropioid receptors. The analgesic action has beenascribed to morphine generated by its demethy-lation by CYP2D6. Codeine fails to produceanalgesia in subjects with polymorphic CYP2D6who cannot demethylate codeine. However,receptors involved in the antitussive actionappear to be distinct, because they bind codeineas well as morphine.
Codeine has good activity by the oral route(oral: parenteral ratio 1:2). A single oral doseacts for 4–6 hours. Constipation is a prominentside effect when it is used as analgesic. Codeinehas been used to control diarrhoea (see Ch. 48).Other side effects are milder. The abuse liabilityis low. Though codeine phosphate is watersoluble and can be injected, parenteral pre-paration is not available.2. Pholcodeine, Ethylmorphine They have codeinelike properties and have been used mainly as antitussive (seep. 220); claimed to be less constipating.
3. Heroin (Diamorphine, Diacetylmorphine) It is about 3times more potent than morphine; more lipid soluble, thereforeenters the brain more rapidly, but duration of action is similar.It is considered to be more euphorient (especially on i.v.injection) and highly addicting. Because of its high potency,it has been favoured in illicit drug trafficking. The sedative,

475C
HA
PTER34
OPIOID ANALGESICS AND ANTAGONISTS
emetic and hypotensive actions are said to be less prominent.However, it has no outstanding therapeutic advantage overmorphine and has been banned in most countries except U.K.
4. Pethidine (Meperidine)Pethidine was synthesized as an atropinesubstitute in 1939, and has some actions likeit. Though chemically unrelated to morphine, itinteracts with μ opioid receptors and its actionsare blocked by naloxone. Important differencesin comparison to morphine are:1. Dose to dose 1/10th in analgesic potency;however, analgesic efficacy approaches near tomorphine and is greater than codeine.2. After i.m. injection, the onset of action ismore rapid but duration is shorter (2–3 hours).3. It does not effectively suppress cough.4. Spasmodic action on smooth muscles is lessmarked—miosis, constipation and urinaryretention are less prominent.
Pethidine is believed to induce less biliary spasm thanmorphine; traditionally preferred in cholecystitis/biliary colic.However, there is no objective evidence to support this belief.One study* in patients undergoing cholecystectomy foundpethidine to raise common bile duct pressure 14% more thanequianalgesic dose of morphine.
5. It is equally sedative and euphoriant, hassimilar abuse potential. The degree of respiratorydepression seen at equianalgesic doses isequivalent to that with morphine.6. Tachycardia (due to antimuscarinic action)occurs instead of bradycardia.7. It causes less histamine release and is saferin asthmatics.8. It has local anaesthetic action: corneal anaes-thesia is seen after systemic doses.9. It is well absorbed, oral: parenteral activityratio is higher (1/3 to 1/2). Pethidine is nearlycompletely metabolized in liver. The plasma t½of pethidine is 2–3 hours. Acidification of urineincreases excretion of unchanged pethidine.
Side effects These are similar to morphineexcept those mentioned above. Some atropiniceffects (dry mouth, blurred vision, tachycardia)may be noted in addition.
Overdose of pethidine produces many excita-tory effects—tremors, mydriasis, hyperreflexia,delirium, myoclonus and convulsions. This is dueto accumulation of norpethidine which hasexcitant effects. Renal failure patients givenrepeated doses of pethidine are prone toexperience similar effects.
Nonselective MAO inhibitors interfere withhydrolysis but not with demethylation ofpethidine—norpethidine is produced in excessand excitement occurs. Pethidine injected inpatients receiving a selective serotonin reuptakeinhibitor (SSRI) may produce the ‘serotoninsyndrome’ (see p. 461) by enhancing 5-HTrelease.
Tolerance and physical dependence developslowly with pethidine. Probably due to its shorterduration of action, body functions get time torecover. For the same reason withdrawalsyndrome develops more rapidly. Autonomicdisturbances are less marked during pethidinewithdrawal, than after morphine withdrawal.
Use Pethidine is primarily used as an analgesic(substitute of morphine) and in preanaestheticmedication, but not for cough or diarrhoea. Ithas also been used to control shivering duringrecovery from anaesthesia or that attending i.v.infusions. Conventional antihistaminics, NSAIDsand corticosteroids augment this effect ofpethidine. Potential adverse effects due toaccumulation of norpethidine limit its utility inpatients who require repeated dosing. It is thepreferred opioid analgesic during labour, becauseat equianalgesic doses neonatal respiratorydepression is less marked, but still significant.
Hydrolysis Meperidinic acid Conjugated(major metabolite) with glucuronic
Pethidine acid and excre-Demethylation Norpethidine ted in urine
(minor metabolite)
⎫⎬⎭
* See Lee F and Cundiff D; Arch Intern. Med. 158, (1998), 2399.

476S
EC
TIO
N7
DRUGS ACTING ON CENTRAL NERVOUS SYSTEM
Dose: 50–100 mg i.m., s.c. (may cause irritation, local fibrosis onrepeated injection). It is occasionally given orally or i.v.PETHIDINE HCL 100 mg/2 ml inj; 50, 100 mg tab.
5. Fentanyl A pethidine congener, 80–100times more potent than morphine, both inanalgesia and respiratory depression. In analgesicdoses it produces few cardiovascular effects.Cardiac contractility and heart rate are onlymarginally reduced, and it has less propensity torelease histamine. Because of high lipid solubility,it enters brain rapidly and produces peak analgesiain 5 min after i.v. injection. The duration of actionis short: starts wearing off after 30–40 min dueto redistribution, while elimination t½ is ~4 hr.In the injectable form it is almost exclusivelyused in anaesthesia (see p. 384). Transdermalfentanyl has become available for use in cancer/terminal illness or other types of chronic painfor patients requiring opioid analgesia. Buccaluse is possible, but not oral.DUROGESIC transdermal patch delivering 12 μg/hr, 25 µg/hr,50 µg/hr, 75 µg/hr or 100 µg per hour; the patch is changedevery 3 days.
6. Methadone A synthetic opioid, chemicallydissimilar but pharmacologically very similar tomorphine. It has analgesic, respiratory depres-sant, emetic, antitussive, constipating and biliaryactions similar to morphine.
The most important feature of methadone ishigh oral: parenteral activity ratio (1 : 2) andits firm binding to tissue proteins. In single dosesit is only slightly more potent than morphineand has comparable duration of action (4–6hours on i.m. injection), but it cumulates intissues on repeated administration—duration ofaction is progressively lengthened due to gradualrelease from these sites; plasma t½ on chronicuse is 24–36 hours. Plasma protein binding is90% and it is metabolized in liver, primarily bydemethylation and cyclization. Metabolites areexcreted in urine. Rifampin and phenytoin cancause withdrawal symptoms to appear inmethadone dependent subjects by inducing itsmetabolism.
Because of slow and persistent nature ofaction, sedative and subjective effects are less
intense. It is probably incapable of giving a ‘kick’.The abuse potential is rated lower than morphine.Tolerance develops more slowly, probably dueto progressive filling of tissue stores.Withdrawal syndrome is of gradual onset, taking1–2 days after discontinuation, is prolonged andless severe.
Methadone has been used primarily as sub-stitution therapy for opioid dependence: 1 mgof oral methadone can be substituted for 4 mgof morphine, 2 mg of heroin and 20 mg ofpethidine. Another technique is methadonemaintenance therapy in opioid addicts—sufficient dose of methadone (10–40 mg/day)is given orally over long term to produce highdegree of tolerance so that pleasurable effectsof i.v. doses of morphine or heroin are notperceived and the subject gives up the habit.
Methadone can also be used as an analgesicfor the same conditions as morphine; dose 2.5–10 mg oral or i.m. but not s.c. It is occasionallyemployed as antitussive.METHADONE 5mg/ml and 10mg/ml syr; 5, 10, 20, 40 mg tabs(for maintenance therapy of opioid dependence).PHYSEPTONE 10 mg inj, 2 mg/5 ml linctus.
7. Dextropropoxyphene It is chemicallyrelated to methadone but is quite similar inanalgesic action and in side effects to codeine,except that it is a poor antitussive, probably lessconstipating, and nearly half as potent as codeine,with a lower oral: parenteral activity ratio. It ismetabolized in liver; t½ is variable (4–12 hours).Delirium and convulsions have occurred inoverdose. The demethylated metabolite ofpropoxyphene has a longer t½ (>24 hours),accumulates on repeated dosing and iscardiotoxic. The abuse liability is similar to orlower than codeine.
Dextropropoxyphene (60–120 mg) is usedas a mild oral analgesic. It is marketed only incombination with paracetamol ± other drugs; butthe contribution of dextropropoxyphene to theanalgesic effect of the combination is ques-tionable. The cardiac toxicity of its demethylatedmetabolite and seizures are dangerous inoverdose. The toxicity is only partly antagonized

477C
HA
PTER34
OPIOID ANALGESICS AND ANTAGONISTS
by naloxone. Because of reported fatalities andno clear advantage of the combinations overparacetamol alone, such preparations have beenwithdrawn in the UK and Europe, a warning hasbeen put on the labels in the US, but they arequite popular in India, probably due to theperceived addictive potential of codeine.PARVODEX 60 mg cap: PARVON, PROXYVON, WALAGESIC:dextropropoxyphene 65 mg + paracetamol 400 mg cap;WYGESIC, SUDHINOL 65 mg + paracetamol 650 mg cap.
8. Tramadol This centrally acting analgesicis an atypical opioid which relieves pain byopioid as well as additional mechanisms. Itsaffinity for µ opioid receptor is low, while thatfor κ and δ is very low. Unlike other opioids,it inhibits reuptake of NA and 5-HT, increases5-HT release, and thus activates monoaminergicspinal inhibition of pain. Its analgesic action isonly partially reversed by the opioid antagonistnaloxone.
Injected i.v. 100 mg tramadol is equianalgesicto 10 mg i.m. morphine. Oral bioavailability oftramadol is good (oral: parenteral dose ratio is1.4). The t½ is 5–6 hours and effects last for4–6 hrs. Tramadol causes less respiratorydepression, sedation, constipation, urinaryretention and rise in intrabiliary pressure thanmorphine. It is well tolerated; side effects aredizziness, nausea, sleepiness, dry mouth, sweatingand lowering of seizure threshold. Haemo-dynamic effects are minimal. Tramadol shouldnot be given to patients taking SSRI therapybecause of risk of ‘serotonin syndrome’ (seep. 461).
Tramadol is indicated for mild-to-moderateshort-lasting pain due to diagnostic procedures,injury, surgery, etc, as well as for chronic painincluding cancer pain, but is not effective insevere pain. Little tendency to dose escalationby chronic users is seen and abuse potential islow.Dose: 50–100 mg oral/i.m./slow i.v. infusion (children 1–2 mg/kg) 4–6 hourly.CONTRAMAL, DOMADOL, TRAMAZAC 50 mg cap, 100mg SR tab; 50 mg/ml inj in 1 and 2 ml amps.
USES (Of morphine and its congeners)
1. As analgesic Opioid analgesics are indi-cated in severe pain of any type. However, theyonly provide symptomatic relief withoutaffecting the cause. Pain may be valuable fordiagnosis; should not be relieved by a potentanalgesic unless proper assessment of the patienthas been done. Indiscriminate use of opioids canbe hazardous. On the other hand, inadequate doseor reluctance to use an opioid for a patient indistress is equally deplorable.
Morphine (or one of its parenteral congeners)is indicated especially in traumatic, visceral,ischaemic (myocardial infarction), postoperative,burn, cancer pain, renal colic and the like. It shouldbe given promptly in myocardial infarction toallay apprehension and reflex sympatheticstimulation. Opioids, especially pethidine, havebeen extensively used for obstetric analgesia, butone must be prepared to deal with the foetal andmaternal complications.
Adequate use of morphine (even i.v.) is indi-cated in an emergency. It may prevent neuro-genic shock and other autonomic effects ofexcruciating pain such as that of crush injuries.Patients in severe pain require higher doses ofopioids and tolerate them without manifestingtoxicity. There is considerable individual varia-bility in the response to opioids. They shouldnot be restricted in case of pain of terminalillness (cancer pain), but for other chronicconditions, due consideration must be given totheir addicting liabilities. Neuropathic painresponds less predictably to opioid analgesics,while pregabalin, amitriptyline, duloxetine arethe major drugs for such pain.
Epidural (2–3 mg) or intrathecal (0.2 mg) injection ofmorphine produces segmental analgesia lasting ~12 hourwithout affecting other sensory, motor or autonomic modalities.It is being used for surgical analgesia in abdominal, lowerlimb and pelvic operations as well as for labour, postoperative,cancer and other intractable pain. Respiratory depressionoccurs after a delay due to ascent of the opioid through thesubarachnoid space to the respiratory centre. Use of fentanylin place of morphine produces faster analgesia and reducesthe risk of respiratory depression because of greater uptakeof fentanyl by nerves at the site of injection.

478S
EC
TIO
N7
DRUGS ACTING ON CENTRAL NERVOUS SYSTEM
Patient controlled analgesia (PCA) is an attractivetechnique of postoperative pain control in which the patienthimself regulates the rate of i.v. fentanyl infusion accordingto intensity of pain felt.
Transdermal fentanyl is a suitable option forchronic cancer and other terminal illness pain.The patch produces analgesia after ~12 hr, butthen blood levels of fentanyl and intensity ofanalgesia remain fairly uniform if the patch ischanged every 3 days. For severe chronic paincontinuous opioid analgesia with a long-actingpreparation works better than a short-actingopioid given intermittently. Rescue short-actingopioid is to be added to the continuous analgesiafor ‘breakthrough pain’.
For milder pain, e.g. toothache, headache,arthralgia, etc., aspirin-like analgesics arepreferred. When they are not effective—codeine/dextropropoxyphene may be used orally, eitheralone or in combination with aspirin-like drug. Thecombination enhances the ceiling analgesia. Formajority of painful conditions, especially moresevere and longerlasting pain, a NSAID may becombined with the opioid. This helps to enhanceanalgesia while keeping the opioid dose low.
2. Preanaesthetic medication Morphine andpethidine are used in few selected patients (seep. 386).
3. Balanced anaesthesia and surgical anal-gesia Fentanyl, morphine, pethidine, alfentanilor sufentanil are an important component ofanaesthetic techniques (see p. 384).
4. Relief of anxiety and apprehensionEspecially in myocardial infarction, internalbleeding (haematemesis, threatened abortion, etc.)morphine or pethidine have been employed. Theymay prevent worsening of the condition bysuppressing reflex overactivity. However, theyshould not be used as anxiolytics or to inducesleep.
5. Acute left ventricular failure (cardiacasthma) Morphine injected i.v. affords dramaticrelief by—
(a) Reducing preload on heart due to vaso-dilatation and peripheral pooling of blood.
(b) Tending to shift blood from pulmonary tosystemic circuit; relieves pulmonary con-gestion and edema.
(c) Allays air hunger and dyspnoea by depres-sing respiratory centre.
(d) Cuts down sympathetic stimulation bycalming the patient, thereby reduces cardiacwork.
Morphine is also indicated to relieve pulmonaryedema due to infarction of lung, but not dueto irritant gases. It is contraindicated in bronchialasthma.6. Cough Codeine or its substitutes arewidely used for suppressing dry, irritating cough(see Ch. 16).7. Diarrhoea The constipating action ofcodeine has been used to check diarrhoea andto increase the consistency of stools in colo-stomy. Loperamide and diphenoxylate aresynthetic opioids used exclusively as anti-diarrhoeals. The risk and benefits of their useare detailed in Ch. 48.
OPIOID RECEPTORS
Morphine and other opioids exert their actionsby interacting with specific receptors presenton neurones in the CNS and in peripheral tissues.Chemical modification of morphine structure hasyielded a number of compounds which have acomplex pattern of morphine-like and otheragonistic and antagonistic actions that cannot beexplained on the basis of a single opioidreceptor. Radioligand binding studies divided theopioid receptors into three types (µ, κ, δ); whichhave been cloned, mapped and studied withmodern techniques. Each has a specificpharmacological profile and pattern of anato-mical distribution in the brain, spinal cord andperipheral tissues (mainly gut, blood vessels,heart, lungs and immune cells). Subtypes of µand κ receptor have been identified. The proposedfunctional role of the 3 types of opioid receptorsis listed in Table 34.1.
Opioid ligands can interact with differentopioid receptors as agonists, partial agonists or

479C
HA
PTER34
OPIOID ANALGESICS AND ANTAGONISTS
TABLE 34.1 Actions ascribed to different types of opioid receptors
µ (mu) κ (kappa) δ (delta)
Analgesia Analgesia (spinal κ1) Analgesia (spinal + affective
(supraspinal µ1 + spinal µ
2) (supraspinal-κ
3) component of supraspinal)
Respiratory depression (µ2) Respiratory depression (lower ceiling) Respiratory depression
Sedation Dysphoria, psychotomimetic Affective behaviourEuphoria Miosis (lower ceiling) Reinforcing actionsMiosis Sedation Reduced g.i. motilityMuscular rigidity Physical dependence (nalorphine type) ProconvulsantReduced g.i. motility (µ
2) Reduced g.i. motility
Physical dependence (morphine type)
competitive antagonists. The overall pattern ofeffect of a particular agent depends not only onthe nature of its interaction with different opioidreceptors, but also on its relative affinity forthese, e.g. morphine is an agonist on µ, κ andδ receptors, but its affinity for µ receptors ismuch higher than that for the other two. Theeffects, therefore, are primarily the result of µreceptor activation.
The nature and intensity of action of complexaction opioids and antagonists are summarizedin Table 34.2.µ receptor The µ receptor is characterizedby its high affinity for morphine. It is the majorreceptor mediating actions of morphine and its
congeners. Endogenous ligands for µ receptor—peptides called Endomorphins 1 and 2, haveonly recently been found in mammalian brain.They produce biological effects ascribed to µreceptor. Other opioid peptides viz. β-endorphin,enkephalins and dynorphins bind to µ receptorwith lower affinity. β-funaltrexamine is arelatively selective but irreversible µ antagonist.High density of µ receptors has been detectedin periaqueductal gray, thalamus, nucleus tractussolitarious, nucleus ambiguus and area postrema.Two subtypes of µ receptor have been proposed:µ1: Has higher affinity for morphine, mediates supraspinal
analgesia and is selectively blocked by naloxonazine.µ2: Has lower affinity for morphine, mediates spinal analgesia,
respiratory depression and constipating action.
TABLE 34.2 Nature of interaction of opioid ligands with the three major types of opioid receptors, alongwith equivalent analgesic doses
Ligand µ (mu) κ (kappa) δ (delta) Analgesic*dose (mg)
1. Morphine Ago. (St) Ago. (W) Ago. (W) 10
2. Nalorphine Anta. (St) Ago. (M) — —
3. Pentazocine P.Ago., Anta. (W) Ago. (M) — 30–60
4. Butorphanol P.Ago (W) Ago. (St) — 1–3
5. Buprenorphine P.Ago Anta. (M) — 0.3–0.4
6. Naloxone Anta. (St) Anta. (M) Anta. (W) —
7. Naltrexone Anta. (St) Anta. (St) Anta. (W) —
8. Met/Leu enkephalin Ago. (M) — Ago. (St) —
9. β-Endorphin Ago. (St) — Ago. (St) —
10. Dynorphin A, B Ago. (W) Ago. (St) Ago. (W) —
* Equivalent single parenteral analgesic dose.Ago—Agonist; Anta.—AntagonistP. Ago—Partial agonist: have lower efficacy, though affinity (potency) may be high.St—Strong action; M—Moderate action; W—Weak action (low affinity).

480S
EC
TIO
N7
DRUGS ACTING ON CENTRAL NERVOUS SYSTEM
κκκκκ receptor This receptor is defined by its highaffinity for ketocyclazocine and dynorphin A;the latter is considered to be its endogenousligand. Norbinaltorphimine is a selective κantagonist. Two subtypes of κ receptor κ1 andκ3 are functionally important. Analgesia causedby κ agonists is primarily spinal (through κ1
receptor). However, κ3 receptors mediate lowerceiling supraspinal analgesia. Other κ actions arelisted in Table 34.1.
δδδδδ receptor This receptor has high affinityfor leu/met enkephalins which are its endogenousligands. The δ mediated analgesia is again mainlyspinal (δ receptors are present in dorsal hornof spinal cord). The limbic areas are rich in δreceptors, suggesting role of these receptors inthe affective component of supraspinal analgesia,reinforcing actions and dependence. Theproconvulsant action is more prominent inδ agonists. Myenteric plexus neurones expresshigh density of δ receptors, which mediatereduced g.i. motility. Naltrindole is a selectiveδ antagonist.
It thus appears that μ and δ receptorresponses are quite similar, but those exertedthrough κ receptor are distinct. In certain areasκ actions are antagonistic to μ actions.The σ (sigma) receptor is no longer considered an opioidreceptor, because it is neither activated by morphine nor blockedby naloxone. However, certain opioids, e.g. pentazocine,butorphanol and many unrelated compounds (including thehallucinogens phencyclidine) bind to σ receptors. Certainnaloxone insensitive effects of pentazocine like drugs, e.g.dysphoria, psychotomimetic action, tachycardia, mydriasis arebelieved to be mediated by σ receptors.
Opioid receptor transducer mechanisms All3 types of opioid receptors (µ, κ, δ) have beencloned; all are GPCRs located mostly onprejunctional neurones. They generally exerciseinhibitory modulation by decreasing release ofthe junctional transmitter (Fig. 34.1). As such,various monoaminergic (NA, DA, 5-HT), GABA,glutamate (NMDA/AMPA) pathways areintricately involved in opioid actions.
Opioid receptor activation reduces intra-cellular cAMP formation and opens K+ channels
(mainly through µ and δ receptors) or suppressesvoltage gated N type Ca2+ channels (mainly κreceptor). These actions result in neuronalhyperpolarization and reduced availability ofintracellular Ca2+ → decreased neurotransmitterrelease by cerebral, spinal, and myentericneurones (e.g. glutamate from primary noci-ceptive afferents). However, other mechanismsand second messengers may also be involved,particularly in the long-term.
COMPLEX ACTION OPIOIDS ANDOPIOID ANTAGONISTS
1. Agonist-antagonists (κ analgesics)Nalorphine, Pentazocine, Butorphanol
2. Partial/weak µ agonist + κ antagonistBuprenorphine
3. Pure antagonistsNaloxone, Naltrexone, Nalmefene
Clinically, the agonist-antagonist (agonist at oneopioid receptor, antagonist at another) andpartial/weak agonist (low intrinsic activity)opioids are analgesics of limited efficacyequivalent to low doses of morphine. They causelow ceiling respiratory depression and have lowerabuse potential. However, in only few situationsthey have proven to be advantageous over thefull μ receptor agonists. Their clinical utility israther limited.1. Nalorphine It is N-allyl-normorphine; was thefirst opioid antagonist introduced in 1951 which could reversemorphine action. Later it was found to have agonistic actionon κ receptor as well, producing lower ceiling analgesia. Itis not used clinically because of dysphoric and psychotomimeticeffects.
2. Pentazocine It is the first agonist-anta-gonist to be used as an analgesic. It has weakμ antagonistic and more marked κ agonisticactions. The profile of action is similar tomorphine; important differences are:(a) Analgesia caused by pentazocine is primarilyspinal (κ1) and has a different character than thatcaused by morphine. Parenterally 30 mgpentazocine = 10 mg morphine; but ceiling effect

481C
HA
PTER34
OPIOID ANALGESICS AND ANTAGONISTS
Fig. 34.1: Opioid receptor transducer mechanismsAC-Adenylyl cyclase; Gi-coupling protein; cAMP-Cyclic AMP
is lower, i.e. at higher doses proportionateincrease in analgesia does not occur.(b) Sedation and respiratory depression is 1/3to 1/2 of morphine at lower doses, and has alower ceiling, does not increase much beyond60 mg dose.(c) Tachycardia and rise in BP are produced athigher doses due to sympathetic stimulation. Thismay increase cardiac work; better avoided incoronary ischaemia and myocardial infarction.(d) Biliary spasm and constipation are lesssevere.(e) Vomiting is less frequent. Other side effectsare sweating and lightheadedness.(f) Subjective effects are pleasurable (morphine-like) at lower doses: recognised by post-addictsas an opiate. However, as dose is increased, thesebecome unpleasant (nalorphine-like at > 60 mgi.m.) and psychotomimetic effects (κ, σmediated) appear.
Tolerance, psychological and physical depen-dence to pentazocine develops on repeated use.Withdrawal syndrome has features of bothmorphine and nalorphine abstinence, but ismilder in intensity. ‘Drug seeking’ occurs. Abuseliability is rated lower than morphine.
Injected in morphine dependent subjects, itprecipitates withdrawal. The μ receptor anta-gonistic action is 1/5th as potent as nalorphinewhich is not enough to be useful in morphinepoisoning. In pentazocine dependent subjects,naloxone precipitates withdrawal, but at higherdoses.
Pharmacokinetics and use Pentazocine iseffective orally, though considerable first passmetabolism occurs; oral: parenteral ratio is 1 : 3.
It is oxidized and glucuronide conjugated inliver and excreted in urine. Plasma t½ is 3–4hours, duration of action of a single dose is4–6 hours.

482S
EC
TIO
N7
DRUGS ACTING ON CENTRAL NERVOUS SYSTEM
Oral dose: 50–100 mg, efficacy like codeine.Parenteral dose: 30–60 mg i.m., s.c., may cause local fibrosison repeated injection due to irritant property.FORTWIN 25 mg tab., 30 mg/ml inj., FORTSTAR, SUSEVIN 30mg/ml inj; FORTAGESIC pentazocine 15 mg+paracetamol 500mg tab.
Pentazocine is indicated for postoperativeand moderately severe pain in burns, trauma,fracture, cancer, etc. Though abuse liability islow, frequent side effects and potential for dys-phoric/psychotomimetic effect limits its utilityin chronic (cancer) pain.
3. Butorphanol It is a κ analgesic, similarto but more potent than pentazocine (butorphanol2 mg = pentazocine 30 mg). Likewise, analgesiaand respiratory depression have a lower ceilingthan morphine. Sedation, nausea, cardiacstimulation and other side effects are similarto pentazocine, but subjective effects are lessdysphoric. Psychotomimetic effects are notprominent (it is a weaker σ agonist at higherdoses). BP is not increased.
Postaddicts recognize butorphanol as abarbiturate rather than opiate and mostly dislikeit. However, it produces physical dependence;withdrawal can be precipitated by high dose ofnaloxone, but the syndrome is mild. The abusepotential of butorphanol is low. The most out-standing feature is that butorphanol can neithersubstitute for, nor antagonize morphine. Thisshows its very weak interaction with µ receptors.
It has been used in a dose of 1–4 mg i.m.or i.v. for postoperative and other short-lasting(e.g. renal colic) painful conditions, but shouldbe avoided in patients with cardiac ischaemia.The t½ and duration of action is similar tomorphine.BUTRUM 1 mg/ml, 2 mg/ml inj.
4. Buprenorphine It is a synthetic thebainecongener, highly lipid-soluble µ analgesic thatis 25 times more potent than morphine but withlower intrinsic activity and ceiling effect. Theonset of action is slower and duration longer.After a single dose, analgesia lasts for 6–8 hours;but with repeated dosing, duration of action
increases to ~24 hours due to accumulation intissues. Certain other effects last still longer.
Sedation, vomiting, miosis, subjective andcardiovascular effects are similar to morphine,but constipation is less marked. Postural hypo-tension is prominent. Respiratory depression(and analgesia) exhibit ceiling effect. It substi-tutes for morphine at low levels of morphinedependence, but precipitates withdrawal in highlymorphine dependent subjects, reflecting its partialagonistic action at µ receptors. Antagonisticaction on κ receptor has also been detected.
Lower degree of tolerance and physical aswell as psychological dependence develops withbuprenorphine on chronic use. Its withdrawalsyndrome resembles that of morphine, but isdelayed for several days, is milder and longerlasting. ‘Drug seeking’ is present. Abuse liabilityis rated lower than morphine.
Naloxone (high dose) can prevent buprenor-phine effect, but does not reverse it when givenafterwards; does not precipitate buprenorphinewithdrawal; probably because of more tightbinding of buprenorphine to opioid receptors.
Buprenorphine has good efficacy by sublin-gual route, is highly plasma protein boundand remains in tissues for several days; terminalt½ is 40 hours. It is mostly excreted unchangedin bile and finds its way out of the body in faeces.Dose: 0.3–0.6 mg i.m., s.c. or slow i.v., also sublingual 0.2–0.4mg 6–8 hourly.NORPHIN, TIDIGESIC 0.3 mg/ml inj. 1 and 2 ml amps. 0.2mg sublingual tab; BUPRIGESIC, PENTOREL 0.3 mg/ml injin 1, 2 ml amp.
Use: Buprenorphine is indicated for long-lastingpainful conditions requiring an opioid analgesic,e.g. cancer pain. It has also been recommendedfor premedication, postoperative pain, in myo-cardial infarction and in the treatment ofmorphine dependence.
Buprenorphine is not suitable for use duringlabour, because if respiratory depression occursin the neonate, it cannot be effectively reversedby naloxone.Nalbuphine, Meptazinol and Dezocine are other agonist-antagonist opioids introduced in some countries.

483C
HA
PTER34
OPIOID ANALGESICS AND ANTAGONISTS
PURE OPIOID ANTAGONISTS
1. Naloxone It is N-alylnor-oxymorphone anda competitive antagonist on all types of opioidreceptors. However, it blocks µ receptors at muchlower doses than those needed to block κ or δreceptors. It is devoid of any kind of agonisticactivity even at high doses (20 times µ blockingdose). No subjective or autonomic effects areproduced in individuals who have not received anopioid. No physical/psychological dependence orabstinence syndrome has been observed.
Injected intravenously (0.4–0.8 mg) it promp-tly antagonizes all actions of morphine: anal-gesia is gone, respiration is not only normalizedbut stimulated—probably due to sudden sensiti-zation of respiratory centre to the retained CO2,or it may be a manifestation of acute withdrawal;pupils dilate. However, sedation is lesscompletely reversed.
At 4–10 mg dose it also antagonizes theagonistic actions of nalorphine, pentazocine,etc., but the dysphoric and psychotomimeticeffects of some of them are incompletelysuppressed. The naloxone insensitive componentis believed to be mediated through σ receptors.
Actions of buprenorphine are prevented butnot effectively reversed by naloxone, becauseit fails to displace buprenorphine that has alreadybound to the opioid receptors.
Naloxone 0.4 mg i.v. precipitates morphinewithdrawal in dependent subjects: the syndromelasts for 2–3 hours; 5 mg or more is requiredto precipitate nalorphine and pentazocine with-drawal.
Naloxone also blocks the actions of endo-genous opioid peptides (see below). Thesepeptides have been implicated in a variety ofphysiological functions; it is surprising thatnaloxone does not produce hyperalgesia or othereffects in normal individuals. However, it hasbeen found to render those individuals moresusceptible to pain who normally have hightolerance. It blocks placebo, acupuncture andstress-induced analgesia, showing involvementof endogenous opioid peptides in these
responses. Naloxone partly antagonizes respira-tory depression produced by certain nonopioids,e.g. N2O, diazepam as well.
Naloxone is inactive orally because of highfirst pass metabolism in liver. Injected i.v. it actsin 2–3 min. The primary pathway of metabolismis glucuronidation. Plasma t½ is 1 hour in adultsand 3 hours in newborns.
Adverse effects of naloxone are uncommon;may include rise in BP and pulmonary edema.NARCOTAN 0.4 mg in 1 ml (adult) and 0.04 mg in2 ml (infant) amps; NALOX, NEX 0.4 mg inj.
Use Naloxone is the drug of choice formorphine poisoning (0.4–0.8 mg i.v. every 2–3 min: max 10 mg) and for reversing neonatalasphyxia due to opioid use during labour(10 μg/kg in the cord). It is also used to treatoverdose with other opioids and agonist-antagonists (except buprenorphine).Other possible clinical applications of naloxone are:• To reverse respiratory depression due to intraoperative
use of opioids: 0.1–0.2 mg i.v. (this dose usually preservesanalgesia in the postoperative period).
• It has also been tried as an adjunct to intraspinal opioidanalgesia: reverses respiratory depression withoutabolishing pain relief.
• Diagnosis of opioid dependence—precipitates withdrawalin dependent subjects.
• It also partially reverses alcohol intoxication.• Naloxone has been found to elevate BP in endotoxic or
hypovolaemic shock, stroke and spinal injury. In theseconditions injection of morphine worsens cardiovascularstatus. Opioid peptides are believed to be involved inthe pathogenesis. However, the value of naloxonecompared to conventional therapy is uncertain.
2. Naltrexone It is chemically related to nalo-xone and is another pure opioid antagonist, thatis devoid of subjective and other agonistic effects,but very high doses have caused unpleasantfeelings in some individuals. It is more potentthan naloxone. Naltrexone differs from naloxonein being orally active and having a long durationof action (1–2 days) which makes it suitablefor ‘opioid blockade’ therapy of postaddicts: 50mg/day is given orally so that if the subject takeshis/her usual shot of the opioid, no subjectiveeffects are produced and the craving subsides.Alcohol craving is also reduced by naltrexone,

484S
EC
TIO
N7
DRUGS ACTING ON CENTRAL NERVOUS SYSTEM
and it is approved for prevention of relapse ofheavy drinking (see p. 393). Nausea is a commonside effect; another is headache. High doses cancause hepatotoxicity.NALTIMA 50 mg tab.
3. Nalmefene This pure opioid antagonist lacks hepa-totoxicity of naltrexone, has higher oral bioavailability andis longer acting.
Methyl naltrexone This derivative of naltrexone does notpenetrate the blood-brain barrier, but effectively blocksperipheral action of μ opioids. It is being used to reverseconstipation in cancer patients receiving chronic opioidanalgesia and in those taking methadone maintenancetherapy.
ENDOGENOUS OPIOID PEPTIDES
In the mid 1970s, with herculean efforts, anumber of peptides having morphine-like actionswere isolated from mammalian brain, pituitary,spinal cord and g.i.t. These peptides are activein very small amounts, their actions are blockedby naloxone, and they bind with high affinity tothe opioid receptors. There are 3 distinct familiesof opioid peptides. Each is derived from aspecific large precursor polypeptide.
1. Endorphins β-endorphin (β-END) having31 amino acids is the most important of theendorphins. It is derived from Pro-opio-melanocortin (POMC) which also gives rise toγ-MSH, ACTH and two lipotropins. β-END isprimarily µ agonist, but also has δ action.
2. Enkephalins Methionine-enkephalin(met-ENK) and leucine-enkephalin (leu-ENK)are the most important. Both are pentapeptides.The large precursor peptide proenkephalin has4 met-ENK and 1 leu-ENK residues. The twoENKs have a slightly different spectrum ofactivity; while met-ENK has equal affinity forµ and δ sites, leu-ENK prefers δ receptors.
3. Dynorphins Dynorphin A and B (DYN-A, DYN-B) are 8–17 amino acid peptides derivedfrom prodynorphin which contains 3 leu-ENKresidues also. DYNs are more potent on κreceptors, but also activate µ and δ receptors.
Distribution of the 3 families of peptides is summarizedbelow:1. POMC – Arcuate nucleus which sends pro-
(limited jections to limbic areas anddistribution) medulla.
– Anterior pituitary (modulateshormone release).
– Pancreatic islets (modulates insulin,glucagon release).
2. Proenkephalin – Pain areas in spinal cord, trigeminal(wide nucleus, periaqueductal greydistribution) matter.
– Affective areas in limbic system,locus coeruleus and cortex.
– Medulla (autonomic functions).– Median eminence of hypothalamus
(neuro-endocrine control).– Adrenal medulla, gastric and
intestinal glands.3. Prodynorphin – Wide distribution roughly parallel
to proenkephalin, but in distinctneurones of the same area.
Receptor selectivity of the 3 major opioid peptide familiesmay be graded as:
Opioid peptide Relative receptor selectivityβ-Endorphin μ > δ >> κEnkephalin (Met/Leu) δ ≥ μ >> κDynorphin A,B κ >> μ = δ
The opioid peptides constitute an endogenousopioid system which normally modulates painperception, mood, hedonic (pertaining topleasure) and motor behaviour, emesis, pituitaryhormone release and g.i.t. motility, etc.
β-END injected directly into the brain is20–40 times more potent analgesic thanmorphine. Its primary localization in hypothala-mus and pituitary and its long t½ prompts thatit has a neurohormone function which modulatesthe release of other hormones. β-END decreasesLH, FSH release and increases GH, prolactinrelease. Naloxone has opposite effects on thelevels of these hormones—suggesting that thesystem is constitutively active.
The wide distribution of ENKs and DYNs alongwith their short t½ suggests that they functionas neuromodulator or neurotransmitter. Theyappear to regulate pain responsiveness at spinaland supraspinal levels. Naloxone blocks placebo,acupuncture and stress-induced analgesia,suggesting the involvement of opioid peptides in

485C
HA
PTER34
OPIOID ANALGESICS AND ANTAGONISTS
these responses. Opioid peptides also appear toparticipate in regulation of affective behaviourand autonomic function.
A novel opioid peptide Nociceptin/orphanin FQ (N/OFQ)has been isolated from mammalian brain. It is localized in cortex,hippocampus, spinal cord and certain sensory sites; is believedto play a role in stress response, reward and reinforcing actions,learning and memory. The N/OFQ receptor, is now calledNociceptin opioid peptide (NOP) receptor. At certain sites,N/OFQ can act as an ‘antiopioid’ through the NOP receptor. In
the pain control mechanisms, N/OFQ appears to play bothopioid-like as well as antagonistic roles, depending on the siteand the basal state of pain.
Morphine and other opioids act as exogenousagonists on some of the receptors for thesepeptides. This has given an explanation for theexistence of specific receptors in the body forexogenous substances like morphine. Morphineitself has now been detected in mammalian brain.
PROBLEM DIRECTED STUDY
34.1 A boy aged 14 years is brought to the hospital emergency with crush injury of bothlower legs. An eye witness who brought the boy told that a bus had run over his legs about20 min. ago. The legs were crushed but he had not bled much. He also told that initiallythe boy was shrieking in pain, but had fainted on way to the hospital. Preliminary examinationreveals that the patient is in a semiconscious state, looks pale, the pulse is fast, low volumeand collapsing. Both legs have sustained multiple fractures, the skin and soft tissues havelacerated from which blood is oozing, but there is no active bleeding. There is no apparenthead injury.(a) Should any medicine be administered immediately, before even completing a thoroughphysical examination? If so, which drug, by what route, and why?(see Appendix-1 for solution)

CNS Stimulants andCognition Enhancers
ChapterChapterChapterChapterChapter 3535353535
CNS STIMULANTS
These are drugs whose primary action is tostimulate the CNS globally or to improvespecific brain functions.
The CNS stimulants mostly produce ageneralized action which may, at high doses,result in convulsions. Given below is a workingclassification based primarily on the clinical use,because clearcut differences do not exist.
CLASSIFICATION
1. Convulsants Strychnine, Picrotoxin,Bicuculline, Pentylenetetrazol (PTZ).
2. Analeptics Doxapram3. Psychostimulants Amphetamines,
Methylphenidate, Atomoxetine, Modafinil,Armodafinil, Pemoline, Cocaine, Caffeine.
Many other drugs are capable of causing CNSstimulation as side effect or at high doses.
I. CONVULSANTS
1. Strychnine It is an alkaloid from the seeds of Strychnosnux-vomica, and a potent convulsant. The convulsions arereflex, tonic-clonic and symmetrical. It has been labelled as aspinal convulsant because the dose producing convulsions isthe same in spinal animals as in intact animals; actually itstimulates the whole cerebrospinal axis.
Strychnine acts by blocking post-synaptic inhibitionproduced by the inhibitory transmitter glycine. One of the sitesthat has been clearly demonstrated is the Renshaw cell-motoneurone junction in the spinal cord through whichinhibition of antagonistic muscles is achieved. Due to loss ofsynaptic inhibition, any nerve impulse becomes generalized,resulting in apparent excitation and convulsions.
There are no valid uses of strychnine now. Accidentalpoisonings, especially in children, do occur. Treatment ofpoisoning is similar to that of status epilepticus (see Ch. 30).
2. Picrotoxin Obtained from ‘fish berries’ of EastIndies Anamirta cocculus. It is a potent convulsant—convulsions are clonic, spontaneous and asymmetrical. Theconvulsions are accompanied by vomiting, respiratory and
vasomotor stimulation. Though regarded as a medullarystimulant, it has little selectivity in site of action.
Picrotoxin acts by blocking presynaptic inhibition mediatedthrough GABA. However, it is not a competitive antagonist;does not act on GABA receptor itself, but on a distinct site andprevents Cl¯ channel opening (see p. 403). Diazepam, whichfacilitates GABAergic transmission, is the drug of choice forpicrotoxin poisoning. Picrotoxin has no therapeutic indicationnow.
3. Bicuculline This synthetic convulsant has picrotoxin-like actions. It is a competitive GABAA receptor (intrinsic Cl¯
channel receptor) antagonist, while GABAB receptor (G-proteincoupled receptor) is insensitive to it. It is only a research tool.
4. Pentylenetetrazol (PTZ, Metrazol, Leptazol) It isa powerful CNS stimulant, believed to be acting by directdepolarization of central neurones. However, it has also beenshown to interfere with GABAergic inhibition—may be actingin a manner analogous to picrotoxin.
Low doses cause excitation, larger doses produceconvulsions which are similar in pattern to those caused bypicrotoxin. Antagonism of PTZ induced convulsions is anestablished method of testing anticonvulsant drugs inlaboratory animals (see Ch. 30).
II. ANALEPTICS (Respiratory stimulants)
These are drugs which stimulate respiration and can haveresuscitative value in coma or fainting. They do stimulaterespiration in subconvulsive doses, but margin of safety isnarrow; the patient may get convulsions while still in coma.Mechanical support to respiration and other measures toimprove circulation are more effective and safe.
The role of analeptics in therapeutics is very limited.Situations in which they may be employed are:(a) As an expedient measure in hypnotic drug poisoning untill
mechanical ventilation is instituted.(b) Suffocation on drowning, acute respiratory insufficiency.(c) Apnoea in premature infant.(d) Failure to ventilate spontaneously after general anaesthesia.However, the overall utility of analeptics is dubious.
Doxapram It acts by promoting excitation of centralneurones. At low doses it is more selective for the respiratorycentre than other analeptics. Respiration is stimulated throughcarotid and aortic body chemoreceptors as well. Falling BP rises.Continuous i.v. infusion of doxapram may abolish episodes ofapnoea in premature infant not responding to theophylline.Other uses: see above.

487C
HA
PTER35
CNS STIMULANTS AND COGNITION ENHANCERS
Dose: 40–80 mg i.m. or i.v.; 0.5–2 mg/kg/hr i.v. infusion.CAROPRAM 20 mg/ml in 5 ml amp.
Reflex stimulation Smelling ammonia or a drop of alcohol in thenose may be enough for hysterical fainting; analeptics shouldnot be used.
III. PSYCHOSTIMULANTS
These drugs have predominant cortical action;their psychic effects are more prominent thanthose on medullary vital centres.
1. Amphetamines These are central sympa-thomimetics. Compared to amphetamine, highercentral: peripheral activity ratio is exhibited bydextroamphetamine and methamphetamine. Theystimulate mental rather than motor activity;convulsive doses are much higher. Their phar-macology and uses are described in Ch. 9.
2. Methylphenidate It is chemically andpharmacologically similar to amphetamine. Bothact primarily by releasing NA and DA in the brain.Both produce increase in mental activity at doseswhich have little action on other central and peri-pheral functions. However, it is a CNS stimulant,and high doses can produce convulsions.Methylphenidate is considered superior toamphetamine for attention deficit hyperkineticdisorder (ADHD) because it causes lessertachycardia and growth retardation. Behaviourand learning ability are improved in 3 out of4 treated children. It can also be used forconcentration and attention defect in adults, andfor narcolepsy, but should not be employed totreat depression, dementia, obesity or to keepawake.
Methylphenidate is well absorbed orally,metabolized and excreted in urine, plasma t½is 4–6 hours, but central effect lasts much longer.Twice daily dosing (morning and afternoon) isenough.Side effects are anorexia, insomnia, growthretardation, abdominal discomfort and bowelupset.Dose: Adults 5–10 mg BD; children 0.25 mg/kg/day initially,increased up to 1 mg/kg/day if needed.RETALIN 5, 10, 20, 30 mg tab.
3. Atomoxetine This is a selective NA reup-take inhibitor, unrelated to amphetamine as wellas to imipramine, which does not enhance DArelease in the brain, and is neither a CNS stimulantnor an antidepressant. However, it has been foundto improve attention span and behaviour in ADHD.It is indicated in children >6 years and in adultswith concentration and attention problems.
Atomoxetine is absorbed orally, hydroxylatedby CYP2D6 and excreted in urine, mainly asglucuronide. While majority of individuals areextensive metabolizers (EM), few are poor meta-bolizers (PM) due to polymorphism of CYP2D6.Inhibitors of CYP2D6 like fluoxetine, paroxe-tine, quinidine increase concentration andtoxicity of atomoxetine. It should not be givenwith MAO inhibitors and is contraindicated inglaucoma.Dose: 0.5 mg/kg/day in the morning, may be increased upto1.2 mg/kg/day and split into morning and afternoon doses.Adults 40 mg OD, max 100 mg/day.ATTENTROL 10, 18, 25, 40 mg caps AXEPTA 18, 25 mg caps.
Atomoxetine is relatively well tolerated, doesnot produce agitation, seizures, dependene orarrhythmias. Common side effect is dyspepsia,anorexia and other abdominal symptoms. Othersare sleep disturbances, mood swings, emotionallability, rarely suicidal thoughts and hepatotoxicity.Growth retardation is possible in children.
4. Modafinil This newer psychostimulant ispopular with night-shift (call centre) workers andother professionals who want to improve alert-ness and keep awake. It is claimed to increaseattention span and improve accuracy that has beencompromized by fatigue and sleepiness. Although,modafinil has been shown to inhibit NA and DAuptake as well as alter junctional concentrationof glutamate and GABA, its actual mechanism ofaction is not known. The approved indications areday-time sleepiness due to narcolepsy, sleep-apnoea syndrome and shift-work disorder (SWD).It has also been found to reduce euphoriaproduced by cocaine and to suppress cocainewithdrawal symptoms; is being evaluated as a drugto prevent relapse of cocaine dependence.

488S
EC
TIO
N7
DRUGS ACTING ON CENTRAL NERVOUS SYSTEM
The most common side effects are insomniaand headache. Others are nausea, dyspepsia,dizziness, confusion, amnesia, personality dis-orders, tremors and hypertension. Dependenceis a possibility on long-term use.
Modafinil is absorbed within 2–4 hours oforal administration, and is eliminated with a t½of 15 hours.Dose: 100–200 mg morning and afternoon for day-timesleepiness due to narcolepsy or sleep-apnoea syndrome; or200 mg 1 hour before starting night-shift work.MODALERT, PROVAKE 100, 200 mg tabs.
Armodafinil A congener of modafinil which has beenrecently approved for improving wakefulness in patients withobstructive sleep apnoea (OSA), SWD and narcolepsy.
5. Pemoline Though chemically unrelated, pemoline hasCNS stimulant actions similar to those of methylphenidate.Sympathomimetic and CVS actions are insignificant. Pemolinehas been used in ADHD, narcolepsy and excessive day-timesleepiness, with benefits and side effects similar tomethylphenidate. However, because of slow onset of actionand hepatotoxicity, it has been discontinued in USA, and isnot available in India.
6. Cocaine (see Ch. 26)7. Caffeine Out of the three naturally occur-ring methylxanthines, only caffeine is used asa CNS stimulant. Its pharmacological actions aredescribed in Ch. 16 along with those oftheophylline.Pharmacokinetics Caffeine has poor watersolubility; is rapidly but irregularly absorbedafter oral administration. It is < 50% bound toplasma proteins, distributed all over the body,and nearly completely metabolized in liver bydemethylation and oxidation. Metabolites areexcreted in urine; plasma t½ is 3–6 hours inadults.
Adverse effects Toxic effects of caffeine areextensions of its pharmacological actions.Caffeine poisoning is rare, and it is less toxicthan theophylline.Gastric irritation, nausea and vomiting may occuras side effects.Excitatory and motor effects such as nervous-ness, insomnia, agitation, muscular twitching,rigidity, rise in body temperature, delirium andconvulsions are produced at toxic doses.
Tachycardia, occasionally extrasystoles occur athigh doses.Caffeine is to be avoided in peptic ulcer patients.It is not contraindicated in gout because it isnot converted in the body to uric acid. Moderatecoffee drinking does not contribute to develop-ment of hypertension.
Uses1. In analgesic mixture: caffeine benefits head-ache probably by allaying fatigue and boredom.It has no analgesic action of its own.2. Migraine: Caffeine is used in combinationwith ergotamine for treatment of migraine attack.It appears to benefit by augmenting constrictionof cranial vessels and by enhancing absorptionof ergotamine from the g.i.t.3. Apnoea in premature infants: as alternativeto theophylline (see Ch. 16).Caffeine is available only in combined formulations withergotamine or analgesics in tablets.CAFERGOT: Caffeine 100 mg + ergotamine 1 mg tab.MICROPYRIN: Caffeine 20 mg + aspirin 350 mg tab.
Tonics containing caffeine are banned in India.
COGNITION ENHANCERS(Cerebroactive drugs)
These are a heterogenous group of drugsdeveloped for use in dementia and other cerebraldisorders. They do elicit pharmacologicaleffects, but widely different mechanisms ofaction are claimed. Therapeutic benefits arelimited, and at the best, short-lasting.
Dementia Refers to acquired global impairment of intellect,memory and personality (cognitive functions) in the absenceof gross clouding of consciousness or motor involvement.Memory, capacity to solve problems of day to day living,performance of learned motor skills, social skills and controlof emotions are primarily affected.
Alzheimer’s disease (AD) A progressive neurodegene-rative disorder which affects older individuals and is the mostcommon cause of dementia. It may progress to a totallyvegitative state. Atrophy of cortical and subcortical areas isassociated with deposition of β-amyloid protein in the formof extracellular senile (amyloid) plaques and formation ofintracellular neurofibrillary tangles. These abnormal proteinsaccumulate mostly due to reduced clearance, but in some cases,due to overproduction, and cause neuronal damage. There

489C
HA
PTER35
CNS STIMULANTS AND COGNITION ENHANCERS
is marked cholinergic deficiency in the brain, though otherneurotransmitter systems, especially glutamate and neuro-peptide, are also affected.
The indications of cognition enhancers include:1. Alzheimer’s disease (AD) and multi-infarct
dementia (MID).2. Mild cognitive impairment (MCI) or
‘common symptoms’ of the elderly; dizzinessand episodic memory lapses.
3. Mental retardation in children, learningdefects, attention deficit disorder.
4. Transient ischaemic attacks (TIAs), cerebro-vascular accidents, stroke.
5. Organic psychosyndromes and sequelae ofhead injury, ECT, brain surgery.
Apart from some cholinergic activators andglutamate antagonist introduced lately, the abovetherapeutic field is barren and commerciallyhighly profitable. A variety of drugs have beenbriskly promoted by manufacturers and wishfullyprescribed by physicians. The mechanism bywhich they are believed to act are:1. Increasing global/regional cerebral blood flow
(CBF)2. Direct support of neuronal metabolism.3. Enhancement of neurotransmission.4. Improvement of descrete cerebral functions,
e.g. memory.All cerebroactive drugs are tested for their vaso-dilator activity. The basic assumption has beenthat improvement in cerebral circulation is pos-sible, real and therapeutically useful. However,precise measurements have shown that in manycases such claims are merely expectations. Instroke a global vasodilator effect may even beharmful by worsening cerebral edema andinducing ‘steal’ phenomenon, i.e. diversion ofblood flow to non-ischaemic areas to thedetriment of ischaemic area. Cerebral blood flowis reduced in AD, but this is probably a conse-quence of loss of neurones and not its cause.
The cerebroactive drugs may be grouped into:a. Cholinergic activators:
Tacrine, Rivastigmine, Donepezil,Galantamine
b. Glutamate (NMDA) antagonist:Memantine
c. Miscellaneous cerebroactive drugs:Piracetam, Pyritinol (Pyrithioxine), Dihydro-ergotoxine (Codergocrine), Citicoline,Piribedil, Ginkgo biloba.
1. Cholinergic activators Since brain AChlevels are markedly reduced and cholinergicneurotransmission is the major sufferer in AD,various approaches to augment brain ACh havebeen tried. Precursor loading with choline orlecithin have failed because there is no shortageof these substrates in the brain. Cholinergicagonists (arecoline, bethanechol, oxotremorine)and conventional anticholinesterases (anti-ChEs)like physostigmine produce symptom improve-ment, but at the cost of marked peripheral sideeffects. Over the past two decades 4 cerebro-selective antiChEs have been introduced and 3are widely used in AD.Tacrine It is the first centrally acting anti-ChE to beintroduced for AD. In clinical trials tacrine produced significantimprovement in memory, attention, praxis, reason andlanguage. However, it does not alter the course of underlyingdisease process. Frequent side effects and hepatotoxicity haverestricted its use.
Rivastigmine This carbamate derivative ofphysostigmine inhibits both AChE and BuChE,but is more selective for the G1 isoform of AChEthat predominates in certain areas of the brain.Rivastigmine is highly lipid-soluble—entersbrain easily. Greater augmentation of cholinergictransmission in brain is obtained with mildperipheral effect. The carbamyl residue intro-duced by rivastigmine into AChE moleculedissociates slowly resulting in inhibition ofcerebral AChE for upto 10 hours despite the2 hr plasma t½ of the drug.
In clinical trials an average of 3.8 pointimprovement in Alzheimer’s Disease AssessmentScale (ADAS-cog) has been obtained comparedto placebo. Other symptoms like apathy, delu-sions, hallucinations and agitation also improve,but to a lesser extent. Disease progression isbriefly slowed or is not affected. Peripheral cho-linergic side effects are mild. It has not producedliver damage. Rivastigmine is indicated in mild-to-moderate cases of AD, but not in advanceddisease.

490S
EC
TIO
N7
DRUGS ACTING ON CENTRAL NERVOUS SYSTEM
Dose: Initially 1.5 mg BD, increase every 2 weeks by 1.5 mg/dayupto 6 mg/BD.EXELON, RIVAMER 1.5, 3, 4.5, 6.0 mg caps.
Donepezil This cerebroselective and reversibleanti-AChE produces measurable improvement inseveral cognitive as well as non-cognitive(activities of daily living) scores in AD, whichis maintained at least upto 2 years. The benefitis ascribed to elevation of ACh level in thecortex, especially in the surviving neurones thatproject from basal forebrain to cerebral cortexand hippocampus. Therapeutic doses produceonly weak peripheral AChE inhibition:cholinergic side effects are mild. Because oflong t½ (~70 hr), donepezil is administered oncedaily at bed time; a distinct advantage overrivastigmine and galantamine which need twicedaily dosing. Moreover, it can be used even inrelatively severe case of AD. Donepezil isgenerally well tolerated and is not hepatotoxic.Dose: 5 mg OD HS (max 10 mg OD);DONECEPT, DOPEZIL, DORENT 5, 10 mg tabs.Oral dispersible tablets of donepezil have also been approvedfor the benefit of patients who have problem in swallowing theregular tablet.
Galantamine It is a natural alkaloid whichselectively inhibits cerebral AChE and has somedirect agonistic action on nicotinic receptors aswell. Galantamine has produced cognitive andbehavioural benefits in AD which are compa-rable to rivastigmine and donepezil. It is welltolerated, but needs twice daily dosing.Dose: 4 mg BD (max 12 mg BD)GALAMER 4, 8, 12 mg tabs.
There is now firm evidence that rivastigmine,donepezil and galantamine afford similar, butmodest symptomatic benefit in AD. Cognitivedecline is slowed or halted for a short time,but not prevented. Their side effects, mostly g.i.smptoms, muscle pain and weird dreams, are alsocomparable among the three. There is now someevidence to support their use in MCI and non-Alzheimer dementia as well.2. Memantine This new NMDA receptorantagonist, related to amantadine (that is alsoa NMDA antagonist), has been found to slowthe functional decline in moderate-to-severe AD,
but benefit in milder disease are unclear. Itappears to block excitotoxicity of the transmitterglutamate in a noncompetitive and use-dependentmanner. Beneficial effects have also been notedin parkinsonism.
Memantine is better tolerated than anti-AChEs used in AD. Side effects are constipation,tiredness, headache, dizziness, and drowsiness.It is indicated in moderate-to-severe AD, eitherto replace anti-AChEs or to supplement them.Memantine can be used for other types ofdementia as well.Dose: Initially 5 mg OD, increase gradually upto 10 mg BD;stop if no clinical benefit in 6 months.ADMENTA, MENTADEM 5, 10 mg tabs, ALMANTIN5 mg tab.
3. Piracetam This cyclic GABA derivative has no GABA-like activity and has been called ‘nootropic’ meaning a drugthat selectively improves efficiency of higher telencephalicintegrative activities.
Piracetam is not a vasodilator, does not affect total/regionalCBF, but may reduce blood viscosity. In India and some othercountries it has been promoted for cognitive impairment anddementia in the elderly as well as for mental retardation inchildren for over 30 years. However, a Cochrane Databasereview (2004) has concluded that published data does notsupport such use. Some later studies have demonstrated aneuroprotective effect of piracetam during coronary bypasssurgery, and that it may benefit cognitive disorders ofcerebrovascular and traumatic origin. In the UK, it is approvedfor adjunctive treatment of cortical myoclonus, but is notrecommended for children. It is not approved in the USA.
Side effects are minor: gastric discomfort, nervousness,excitement, insomnia, dizziness and skin rash.Dose: 0.8–1 g TDS oral; children 20 mg/kg BD–TDS;1–3 g i.m. 6 hourly in stroke/head injury.NORMABRAIN, NEUROCETAM, NOOTROPIL 400, 800 mgcap, 500 mg/5 ml syr., 300 mg/ml inj.
4. Pyritinol (Pyrithioxine) Pyritinol consists of twopyridoxine molecules joined through a disulfide bridge, buthas no vit B6 activity. It is claimed to activate cerebralmetabolism by selectively increasing glucose transport acrossblood-brain barrier and improving regional blood flow inischaemic brain areas. It has been promoted for:• Sequelae of cerebrovascular accidents, head injury,
prolonged anaesthesia.• Infants and children with developmental disorders of CNS,
delayed milestones.• Concentration and memory defects, senility, organic brain
syndromes.However, therapeutic benefit, if any, is uncertain.ENCEPHABOL 100, 200 mg tab. 100 mg/5 ml suspension; 200mg dry powder with 2 ml solvent for i.v. infusion.

491C
HA
PTER35
CNS STIMULANTS AND COGNITION ENHANCERS
Dose: 100–200 mg TDS, children 50–100 mg TDS orally; 200–400 mg every 4–6 hours (max. 1 g/day) has been giveni.v. for recovery from cerebral hypoxia due to cardiac arrest,anaesthesia, brain operations and stroke.Side effects: Only mild g.i. upset was noted initially. Laterskin rashes, itching and taste disturbances (attributable tothe disulfide moiety) have been reported. It has beenwithdrawn in some countries.5. Dihydroergotoxine (Codergocrine): It is a semi-synthetic ergot alkaloid having α adrenergic blockingproperty; claimed to increase cerebral blood flow selectively.It is believed to act by protecting altered brain metabolism.In a dose of 1.0–1.5 mg TDS oral/sublingual or 0.3 mg i.m.OD, it has been recommended for MCI and dementia, buttherapeutic valve is not established.HYDERGINE 1 mg tab, 0.3 mg/ml inj. CERELOID 1 mg tab.Side effects: flushing, headache, nasal congestion, posturalhypotension, g.i. disturbances and rashes.6. Piribedil: It is a dopaminergic agonist claimed toimprove memory, concentration, vigilance, giddiness andtinnitus in the elderly due to circulatory insufficiency, butbenefit is unsubstantiated. Minor efficacy in parkinsonismhas also been reported. Side effects are mild g.i. complaints.Dose: 50 mg OD, BD; TRIVASTAL LA 50 mg tab.7. Citicoline It is a compound derived from choline andcytidine, that is involved in biosynthesis of lecithin. Citicoline
is believed to improve cerebral function by increasing bloodflow to the brain and enhancing cerebral metabolism. Somestudies have demonstrated short-term improvement in memoryand behaviour in cerebrovascular disorders, but there is littleevidence of clear-cut benefit. In the absence of effectivemedicines and under promotional pressure, citicoline is beingcommonly prescribed for impaired brain function due toischaemic stroke, parkinsonism, head injury, etc.Dose: 0.5–1 g/day i.m. or i.v. inj, 200–600 mg/day oral in divideddoses.CITILIN, CITINOVA 500 mg tab, 500 mg/2 ml inj, STROLIN 500mg tab.8. Ginkgo biloba The dried extract of this Chinese plantcontains a mixture of ginkgoflavon glycosides (e.g. ginkgolideB) which have PAF antagonistic action. Since PAF has beenimplicated in cerebral thrombosis and infarcts, it is professedthat G. biloba will prevent cerebral impairment in cerebrovascularinsufficiency. It has been promoted for a variety of cognitiveand behavioural disorders in the elderly, but a Cochranemetaanalysis (2007) concluded that G. biloba produced slightoverall improvement in cognitive performance. However, mosttrials were small and results were inconsistant.
Side effects are mild upper g.i.t. symptoms, and increasedrisk of bleeding.Dose: 40–80 mg TDS for a minimum period of 4 weeks;GINKOCER, BILOVAS, GINKOBA 40 mg tab.
PROBLEM DIRECTED STUDY
35.1 A 75-year-old man was brought with a history of progressive functional decline, somuch so that he now needs to be looked-after all the time. He misplaces his daily need articles,forgets what he said few minutes ago, is unable to perform simple calculations, mixes upwhat happened today and what happened yesterday, has poor control of emotions, but vision,hearing and other sensations are well preserved, and there is no gross ataxia. He was diagnosedto be having moderately advanced Alzheimer’s disease and was prescribed Tab Donepezil 5mg at bed time daily. After one week, his son reported that while his mental and functionalstate is unchanged, he has developed pain in abdomen, muscle ache, loud eructations, loosemotion and is refusing to take the medicine.(a) What could be the reason for no improvement in the mental and functional state of thepatient? Are the new symptoms due to the medication? Should the drug be stopped, changedor another one added at this stage? What alternative drug could be used?(see Appendix-1 for solution)

Cardiac ElectrophysiologicalConsiderations
SECTION 8
CARDIOVASCULAR DRUGS
Drugs having their major action on heart or bloodvessels, or those used primarily for cardio-vascular disorders are designated cardiovasculardrugs. They can act directly on the cardiovas-cular structures or through autonomic/centralnervous system, kidney, autacoids or hormoneswhich regulate cardiovascular function.
CARDIAC ELECTROPHYSIOLOGY
The properties which are especially importantfor understanding drug action on heart are:1. Impulse generation Electrophysiologi-cally, two types of myocardial fibres can bedistinguished (Fig. VIII.1).(a) Nonautomatic fibres These are the ordinaryworking myocardial fibres; cannot generate an
impulse of their own. During diastole, the restingmembrane potential remains stable (approxima-tely 90 mv negative inside). When stimulated,they depolarize very rapidly (fast 0 phase) withconsiderable overshoot (+ 30 mv) rapid returnto near isoelectric level (phase-1) maintenanceof membrane potential at this level for a consi-derable period (phase-2, plateau phase) duringwhich Ca2+ ions flow in and bring about con-traction relatively rapid repolarization (phase-3) during which membrane Na+K+ pump getsactivated and tends to restore ionic distributionto the resting pattern. Resting membrane potential,once attained, does not decay (stable phase-4).
(b) Automatic fibres These are present in thesinoatrial (SA) and atrioventricular (A-V) nodes,and in the His-Purkinje system, i.e. especializedconducting tissue. In addition, patches of auto-matic tissue are present in the interatrial septum,A-V ring and around openings of the great veins.The most characteristic feature of these fibresis phase-4 or slow diastolic depolarization, i.e.after repolarizing to the maximum value, themembrane potential decays spontaneously. Whenit reaches a critical threshold value—suddendepolarization occurs automatically. Thus, theyare capable of generating their own impulse. Therate of impulse generation by a particular fibredepends on the value of maximal diastolicpotential, the slope of phase-4 depolarization andthe value of threshold potential.
Fig. VIII.1: Transmembrane potential of automatic (red)and nonautomatic (purple) myocardial fibres recordedthrough intracellular electrodes
Chapter 36a

493SEC
TION
8CARDIAC ELECTROPHYSIOLOGY
Normally, the SA node has the steepest phase-4 depolarization, undergoes self-excitation andpropagates the impulse to rest of the heart. Inother words, it acts as the pacemaker. Otherautomatic fibres which are also undergoingphase-4 depolarization, but at a slower rate,receive the propagated impulse before reachingthreshold value and remain as latent pacemakers.
Two types of action potential (AP) arepossible. These are depicted in Fig. VIII.2. Theircharacteristics are given in Table VIII.1.
The slow channel AP is characterised by:(a) Initiation at a higher threshold (less negative
level).(b) Slower depolarization during 0 phase.(c) Less overshoot, low amplitude.(d) Very slow propagation, decremental conduc-
tion and a low safety factor for conduction.
(e) Can arise and propagate in fibres too depola-rized to support fast channel responses.
Slow channel AP in SA node, A-V node, etc. hasa shorter duration and phases 1–3 are not clearlydemarkated. Slow channel AP can occur inPurkinje fibres (PF) also, but this has a muchlonger duration with a prominent plateau phase.
2. Conduction The rate of conduction througha fibre is a function of its membrane responsive-ness, which is defined by rate of rise of AP (dv/dt) as a function of membrane potential at whichactivation occurs (Fig. VIII.3); a more completelypolarized membrane depolarizes faster becausemore Na+ channels have recovered (voltage-dependent reactivation). This type of relationshipis seen in atrial, ventricular and Purkinje fibres(fast channel fibres which depolarize by Na+
current), but not in SA and A-V nodal cells whichremain refractory for some time even afterattainment of maximal resting potential (Ca2+
channel reactivation is time-dependent).The Na+ channels get progressively inactivated as the
resting membrane potential (RMP) drops over the –80 to–60 mV range. Consequently, less negative the RMP at whichactivation occurs, fewer are the Na+ channels available foractivation—slope of ‘0’ phase depolarization, AP amplitudeand conduction velocity are reduced.
A drug which reduces the slope of 0 phase(at any given resting membrane potential) willshift the membrane responsiveness curve to theright and impede conduction. The reverse occurswith a drug that shifts the curve to the left.Membrane responsiveness curve can also bealtered by disease.
Fig. VIII.2: (A) Fast channel action potential (AP) in aPurkinje fibre, (B) Slow channel action potential in a SAnode fibre
TABLE VIII.1 Characteristics of fast channel and slow channel action potentials
Fast channel AP Slow channel AP
1. Sites of occurrence Atria, ventricles, SA and A-V nodes, round A-VPurkinje fibres ring, coronary sinus opening
2. Predominant ion moving in 0 phase Na+ Ca2+
3. Activation-inactivation kinetics Fast Slow4. Channel reactivation Voltage-dependent Time-dependent5. Activation potential (threshold voltage) –60 to –70 mv –45 to –55 mv6. Conduction velocity 0.5–5 m/sec 0.01–0.1 m/sec7. ERP–APD* relationship ERP < APD ERP > APD8. Selective channel blocker Tetrodotoxin, Verapamil,
Local anaesthetics Diltiazem, Mn2+
*ERP—Effective refractory period; APD—Action potential duration.

494S
EC
TIO
N8
CARDIOVASCULAR DRUGS
Small cells at the upper margin of A-V nodehave very low conduction velocity (20 mm/sec).Normally Purkinje fibres (PFs) have the highestconduction velocity (4000 mm/sec) except neartheir junction with the ventricular fibres ‘gateregion’, or if they change over from fast channelto slow channel response.
3. Excitability This property of a fibre isdefined by the strength of stimulus required to
VIII.3: Membrane responsiveness curve of a myocardialfibre showing the relationship between membrane polari-zation and dv/dt of 0 phase. Note the depressant action ofquinidine
elicit a response or to produce an AP. Hyper-polarization decreases excitability while smallreductions in resting membrane potential inc-rease excitability by respectively increasing anddecreasing the gap between it and the thresholdpotential. Thus, in fast channel fibres excitabilityis generally super-normal during the end ofphase-3. However, when the resting membranepotential is reduced to a value below the thre-shold potential, the fibre becomes inexcitable.
4. Refractory period Pharmacologically, theeffective refractory period (ERP) which is theminimum interval between two propagating APs,is the most important. It is closely related tothe AP duration (APD). An AP can be evokedin fast channel fibres even before completerepolarization, because Na+ channels recover ina voltage-dependent manner above the thresholdpotential. As such ERP/APD is <1. By contrast,the Ca2+ channels recover in a time-dependentmanner progressively after the fibre has fullyrepolarized. Thus, in slow channel fibres ERP/APD is > 1. Most antiarrhythmic drugs increaseERP/APD ratio.
Autonomic influences on cardiacelectrophysiology and contractilityIt would be profitable to recapitulate theinfluence of sympathetic and parasympatheticstimulation on variables of cardiac function,because many cardiovascular drugs have indirect/secondary autonomic effects (Table VIII.2).
TABLE VIII.2 Autonomic influences on cardiac electrophysiology and contractility
Parameter Effect of stimulation
Parasympathetic (ACh) Sympathetic (Adr)
1. AutomaticitySA node Bradycardia TachycardiaEctopic ventricular — Enhanced
2. Refractory periodAtria Shortened (inhomogeneous) ShortenedConducting tissue Prolonged Shortened
3. Conductivity Decreased Enhanced
4. Contractility Decreased (little effect on ventricle) Increased

Drugs Affecting Renin-Angiotensin System andPlasma Kinins
Chapter 36b
RENIN-ANGIOTENSIN SYSTEM
Angiotensin-II (Ang II) is an octapeptide generatedin the plasma from a precursor plasma 2 globulin,which is involved in electrolyte, blood volumeand pressure homeostasis. Pressor action of kidneyextracts was known since the turn of the 19thcentury. The active material was termed ‘Renin’.In the 1940s renin was shown to be an enzymewhich acted indirectly by producing a pressorprinciple from plasma protein. Subsequently, itbecame clear that the product of renin action wasan inactive decapeptide angiotensin-I (Ang I)which was converted to the active octapeptideAng II by an angiotensin converting enzyme(ACE). The renin-angiotensin system (RAS) has
attracted considerable attention over the past 30years, particularly after the development of ACEinhibitor captopril.
Circulating renin-angiotensin system Thegeneration and metabolism of Ang II in circulationis depicted in Fig. 36.1. Normally, the amountof renin in plasma acts as the limiting factor forAng II generation. The plasma t½ of renin is15 min. The biological potency of Ang I is only1/100 that of Ang II, but it is rapidly convertedinto the latter by ACE which is a dipeptidylcarboxypeptidase, an ectoenzyme locatedprimarily on the luminal surface of vascularendothelial cells (especially in lungs). CirculatingAng II also has a very short t½ (1 min). The
Fig. 36.1: Physiological regulation of electrolyte balance, plasma volumeand blood pressure by the renin-angiotensin system

496S
EC
TIO
N8
CARDIOVASCULAR DRUGS
first degradation product produced by the actionof an aminopeptidase is the heptapeptide termedAngiotensin-III (Ang III). It is 2–10 times lesspotent than Ang II, except in stimulatingaldosterone secretion, in which it is equipotent.Ang III is again attacked by another amino-peptidase, and the resulting hexapeptide (3-8) iscalled Ang IV which has very different central(and some peripheral) actions elicited through aspecific AT4 receptor. Both Ang III and Ang IVare broken into inactive fragments by nonspecificpeptidases termed angiotensinases.
Tissue (local) renin-angiotensin systems
Extrinsic local RAS Apart from Ang II generatedin circulation as described above, blood vesselscapture circulating angiotensinogen and renin toproduce Ang II at the surface of their wall. ThisAng II diffuses to act locally on the angiotensinreceptors producing localized responses.
Intrinsic local RAS Many tissues, especiallyheart, blood vessels, brain, kidneys, adrenals possessthe capacity to synthesize all components of RASwithin their cells. They generate Ang II and IIIintracellularly as per physiological need andpathological status. These signal molecules areinstrumental in regulating organ function, cellgrowth (hypertrophy), cell death (apoptosis),remodeling and fibrosis.
The local RAS operate in several organs inaddition to the liver and kidney dependentcirculating RAS.
Prorenin and (Pro) renin receptor (PRR) Reninis synthesized in juxtaglomerular (JG) cells ofkidney and in tissues expressing local RAS asa larger peptide pre-prorenin. In response toappropriate stimuli both prorenin and renin aresecreted; the former in much larger quantities.The concentration of prorenin in circulation is5–10 fold higher than that of renin. Till recently,prorenin was considered to be only the inactiveprecursor of renin, but now it is recognized tobe active in its own right.
Prorenin is activated both enzymatically andnon-enzymatically (see Fig. 36.2). The enzymatic
activation is carried out by proteases likeproconvertase-1/Cathepsin B, which cleave offthe hindering ‘propeptide’ to produce renin withexposed catalytic domain. This activation isirreversible. Nonenzymatic and reversibleactivation occurs by binding of prorenin to anothercell surface protein called (Pro) renin receptor(PRR), because it binds renin as well. The PRRis richly expressed in heart, blood vessels, kidney,brain, eye and liver. Binding of prorenin to PRRbrings about a conformational change, the‘propeptide’ segment unfolds and the catalyticdomain is exposed. When renin binds to PRR,its catalytic activity is augmented several fold.however, prorenin/renin can dissociate from PRRto return to their original state. Nonenzymaticactivation of prorenin plays a major role in localRAS, where prorenin exerts effects via Ang IIdependent and Ang II independent pathways (Fig.36.3).
(a) Ang II dependent pathway: Activation ofprorenin/renin generates Ang I which is convertedto Ang II by ACE. Ang II acts on AT receptorson the tissue cells to produce effects on cellgrowth, inflammation, apoptosis, etc.
(b) Ang II independent pathway: Binding ofprorenin/renin to PRR on cell surface directlytriggers intracellular signalling via activation ofMAP kinase, plasminogen activator-inhibitor-1(PAI-1), JAK-STAT pathway, transcription factors,protooncogenes, etc. to regulate cell growth,collagen deposition, fibrosis and apoptosis.Overactivity of RAS via such signalling
Fig. 36.2: Activation of prorenin and augmentation ofrenin in the tissue (local) renin-angiotensin system.PRR—(Pro) renin receptor

497C
HA
PTE
R36
DRUGS AFFECTING RENIN-ANGIOTENSIN SYSTEM AND PLASMA KININS
abundantly contributes to pathological changesand end-organ damage in many conditions likehypertensive vascular/ventricular hypertrophy,post-infarction myocardial fibrosis andremodeling, congestive heart failure, nephropathy,retinopathy, etc. The ratio of circulating proreninto renin is markedly elevated in diabetes, whichmay be causative in nephropathy and retinopathy.
Alternative (ACE-independent) pathway ofAng II productionIn addition to the primary pathway described above, smallquantities of Ang I and Ang II can be produced from angio-tensinogen by the action of other proteases like cathepsin.Moreover, chymase can convert (although at a much slowerrate) Ang I to Ang II, particularly in heart and kidney.
Other angiotensin peptidesIn addition to Ang II and Ang III some other biologicallyactive angiotensin peptides are produced in small quantitieswhose physio-pathological role is not well understood.
Angiotensin IV (Ang IV) It is a hexapeptide (Ang 3-8)produced by removal of arginine from aminoterminal ofAng III by an aminopeptidase. Ang IV inhibits an insulinregulated aminopeptidase (IRAP) which is considered to beits specific receptor and is labelled AT4 receptor. Bindingof Ang IV to IRAP prevents degradation of neuropeptides
involved in cognitive function and memory in animals. ThusAng IV improves memory. Some vascular, renal and otherperipheral effects of Ang IV have also been described.
Angiotensin (1-7) This heptapeptide can be produced fromAng I or Ang II by the action of another carboxy-peptidaselabelled ACE 2. In animals, Ang (1-7) produces effects whichare in general opposite to those of Ang II, including NO-dependent vasodilatation, antithrombotic, anti-ischaemic andantiproliferative effects by binding to a protooncogenereceptor. The clinically used ACE inhibitors do not inhibitACE 2. Rather, when these drugs are given levels of Ang(1-7) are increased due to diversion of Ang I from ACEand inhibition of degradation of Ang (1-7).
Attempts are being made to therapeutically exploit theAng II related peptides.
ACTIONS
1. CVS The most prominent action of Ang IIis vasoconstriction—produced directly as well asby enhancing Adr/NA release from adrenalmedulla/adrenergic nerve endings and by increa-sing central sympathetic outflow. In addition, itinhibits reuptake of NA and augments respon-siveness of vascular smooth muscle to it. Vaso-constriction involves arterioles and venules andoccurs in all vascular beds. However, it is lessmarked in cerebral, skeletal muscle, pulmonaryand coronary vessels. Ang II induced vasoconstric-tion promotes movement of fluid from vascularto extravascular compartment. Ang II injected i.v.is much more potent than NA as a pressor agent.No tachyphylaxis is seen in the pressor actionof Ang II; rather long-term infusion of lowconcentration of Ang II produces progressive andsustained rise in BP by its renal effects promotingsalt and water reabsorption, as well as byenhancing endothelin generation.
Ang II increases force of myocardialcontraction by promoting Ca2+ influx. Though,it can increase heart rate by enhancing sympatheticactivity, reflex bradycardia predominates in theintact animal. Cardiac output is often reducedand cardiac work is increased (due to rise in peri-pheral resistance). In contrast to NA, Ang II doesnot activate latent pacemakers. As such, it haslittle arrhythmogenic propensity.
Ang II acting on a chronic basis induces hyper-trophy, hyperplasia and increased intercellular
Fig. 36.3: (Pro) renin receptor (PRR) mediated action oftissue prorenin/renin through angiotensin II (Ang II)dependent and Ang II independent pathways.PAI-1—Plasminogen activator inhibitor-1;Trans. F—Transcription factors

498S
EC
TIO
N8
CARDIOVASCULAR DRUGS
matrix production in the myocardium and vascularsmooth muscle by direct cellular effects involvingexpression of proto-oncogenes and transcriptionof several growth factors. Indirectly, volumeoverload and increased t.p.r. caused by Ang IIcontributes to the hypertrophy and remodeling(abnormal redistribution of muscle mass) in heartand blood vessels. Long standing hypertensionincreases vessel wall as well as intimal thicknessand causes ventricular hypertrophy. Fibrosis anddilatation of infarcted area with hypertrophy ofthe noninfarcted ventricular wall is seen aftermyocardial infarction. Progressive cardiac myo-cyte death and fibrotic transformation occursin CHF. These changes are important risk factorsfor cardiovascular morbidity and mortality.ACE inhibitor therapy retards/reverses many ofthese changes imparting a pivotal role toAng II in vascular and ventricular hypertrophy,apoptosis and remodeling. As described above,the local RAS and prorenin-PRR systems arecrucial in these responses.2. Smooth muscles Ang II contracts manyvisceral smooth muscles in vitro, but invivo effects are insignificant.3. Adrenal cortex Ang II and Ang III aretrophic to the zona glomerulosa of adrenal cortex.They enhance synthesis and release of aldosteronewhich acts on distal tubule in kidney to promoteNa+ reabsorption and K+/H+ excretion. Theseeffects are exerted at concentrations lower thanthose required to cause vasoconstriction.4. Kidney In addition to exerting indirecteffect on kidney through aldosterone, Ang II pro-motes Na+/H+ exchange in proximal tubule increased Na+, Cl¯ and HCO3
¯ reabsorption.Further, Ang II reduces renal blood flow and GFR,and produces intrarenal haemodynamic effectswhich normally result in Na+ and water retention.However, an opposite effect has been observedin cirrhotics and renovascular disease patients inwhom it increases GFR by stongly constrictingglomerular efferent vessels.5. CNS It has been noted that systemicallyadministered Ang II can gain access to certain
periventricular areas of the brain to inducedrinking behaviour and ADH release—both ofwhich would be conducive to plasma volumeexpansion. Ang II also increases centralsympathetic outflow, which contributes to thepressor response. Brain has its own tissue RASand generates Ang II locally as well.6. Peripheral sympathetic structuresAng II enhances sympathetic activity by peripheralaction as well. It releases Adr from adrenalmedulla, stimulates autonomic ganglia andincreases the output of NA from adrenergic nerveendings.Angiotensin receptors and transducermechanisms Specific Ang II receptors areexpressed on the surface of target cells. Two sub-types (AT1 and AT2) have been differentiatedpharmacologically: Losartan is a selective AT1
antagonist, while PD 123177 is a selective AT2
antagonist. Both subtypes are GPCRs. However,all major effects of Ang II are mediated by AT1
receptor. Ang III also activates AT1 and AT2
receptors, but is a much weaker agonist at mostsites, except on adrenal cortex causing aldosteronerelease.
The AT2 receptor is abundantly expressed in foetaltissues. In adults, it has been demonstrated in vascularendothelium, adrenal medulla, kidney and some brain areas.The functional role of AT2 receptor is not well delineated, butis generally opposite to that of AT1 receptor. Activation of AT2
receptor causes NO-dependent vasodilatation, promotesapoptosis, myocardial fibrosis, inhibits cell proliferation andmay lower BP.
Other angiotensin peptides like Ang IV and Ang(1-7) act on their own (AT4 and Mas respectively) receptors.
The AT1 GPCR utilizes different transducermechanisms in different tissues. By coupling withGq protein the phospholipaseC–IP3/DAG–intracellular Ca2+ release mechanism underliesvascular and visceral smooth muscle contractionby activating myosin light chain kinase (MLCK).In addition, membrane Ca2+ channels are activated.Enhanced Ca2+ movement also induces aldosteronesynthesis/release, cardiac inotropy, depolarizationof adrenal medullary/autonomic ganglionic cellresulting in CA release/ sympathetic discharge.DAG activates protein kinase C (PKC) which

499C
HA
PTE
R36
DRUGS AFFECTING RENIN-ANGIOTENSIN SYSTEM AND PLASMA KININS
phosphorylates several intracellular proteins andaugments the above responses as well as participatesin promotion of cell growth. In liver and kidney,Ang II inhibits adenylyl cyclase by AT1 coupledto Gi protein. The intrarenal homeostatic actioninvolves phospholipase A2 activation and PG/LTproduction.
In many tissues, especially myocardium, vas-cular smooth muscle and fibroblasts, AT1 receptoralso mediates long-term effects of Ang II on cellgrowth. Ang II activates MAP kinase, TAK2tyrosine protein kinase, PKC and utilizes the JAK-STAT pathway which together enhance expressionof proto-oncogenes, transcription factors andgrowth factors. As a result, cell growth is promo-ted and more intercellular matrix is synthesized.
PATHOPHYSIOLOGICAL ROLES1. Mineralocorticoid secretion There is nodoubt that Ang II (also Ang III) is the physiologicalstimulus for aldosterone secretion from adrenalcortex. It also exerts trophic influence on theglomerulosa cells so that effects are augmentedunder conditions which persistently raise Ang IIlevels.
2. Electrolyte, blood volume and pressurehomeostasis The RAS plays an important rolein maintaining electrolyte composition and volumeof extracellular fluid (see Fig. 36.1). Changes thatlower blood volume or blood pressure, or decreaseNa+ content induce renin release by threemechanisms.
(i) Intrarenal baroreceptor pathway: Bydecreasing tension in the afferent glomerulararterioles, it operates partly through increa-sed production of prostaglandins (PGs) andpartly via stretch sensitive ion channels.
(ii) Macula densa pathway: Low Na+ and Cl¯
concentration in the tubular fluid sensed bymacula densa cells triggers this pathway. Ithas been found that COX-2 and neuronalnitric oxide synthase (nNOS) are induced inmacula densa cells by Na+ depletion release of PGE2
and PGI2 is enhanced bothdue to increased amount of COX-2 as well
as its activation by NO. The locally releasedPGs act on juxtaglomerular cells to promoterenin secretion.
(iii) adrenoceptor pathway: Baroreceptor andother reflexes which increase sympatheticimpulses to JG cells activate 1 adrenoceptorsexpressed on their surface increased intra-cellular cAMP triggers renin release.
Increased renin is translated into increased plasmaAng II which produces acute rise in BP byvasoconstriction, and more long-lasting effects bydirectly as well as indirectly increasing Na+ andwater reabsorption in the kidney. Rise in BP inturn inhibits renin release : the long-loop nega-tive feedback mechanism. It has been shown thatAng II can be formed within the kidney and exertsimportant local regulatory effects. A short-loopnegative feedback mechanism operates within thekidney : activation of AT1 receptors on JG cellsinhibits renin release directly. Long-term stabili-zation of BP despite varying salt and water intakeappears to be achieved through these mechanisms.
The mechanisms of regulation of renin releasehave important pharmacological implications:• ACE inhibitors and AT1 antagonists enhance
renin release by interfering with both theshort-loop and long-loop negative feedbackmechanisms.
• Vasodilators and diuretics stimulate reninrelease by lowering BP.
• Loop diuretics increase renin production byreducing entry of Na+ and Cl¯ into macula densacells.
• Central sympatholytics and blockers dec-rease renin release by interfering with the adrenoceptor pathway.
• NSAIDs, including selective COX-2 inhibitors,and nNOS inhibitors decrease renin releaseby inhibiting PG production cause Na+ andwater retention.
3. Development of hypertension The RASis directly involved in renovascular hypertension:plasma renin activity (PRA) is raised in mostpatients. In essential hypertension also it appearsto have a permissive role, though PRA may be

500S
EC
TIO
N8
CARDIOVASCULAR DRUGS
either raised or low. Since ACE inhibitors consis-tently lower BP in hypertensives, the involvementof this system appears to be more widespread.A positive correlation between circulating angio-tensinogen levels and essential hypertension hasalso been found. Several evidences point tocausation of pregnancy-induced hypertension(preeclampsia) by production of autoantibodieswhich activate AT1 receptor. The role of Ang IIin hypertrophy/remodeling of heart and bloodvessels is now well recognized (see above).4. Secondary hyperaldosteronism The RASis instrumental in the development of secondaryhyperaldosteronism.5. CNS Ang II can be formed locally in thebrain and may function as transmitter or modulator.Regulation of thirst, hormone release and sym-pathetic outflow may be the responses mediated.Ang II is not available commercially, and not used clinically.
Inhibition of renin-angiotensin systemThis can be achieved by:1. Sympathetic blockers ( blockers, adrenergic
neurone blockers, central sympatholytics)—decrease renin release.
2. Direct renin inhibitors (DRIs): block reninaction—interfere with generation of Ang I fromangiotensinogen (rate limiting step).
3. Angiotensin converting enzyme (ACE)inhibitors—prevent generation of the activeprinciple Ang II.
4. Angiotensin receptor blockers (ARBs)—antagonise the action of Ang II on targetcells.
5. Aldosterone antagonists—block mineralocor-ticoid receptors.
ANGIOTENSIN CONVERTINGENZYME INHIBITORS
Teprotide was the first ACE inhibitor to be synthesizedtaking a lead from the bradykinin potentiating factor(BPF) found in pit viper venom and the finding that thekininase II was also ACE. Teprotide, a nonapeptide inhibitedgeneration of Ang II from Ang I and lowered BP. However,it had limitations of parenteral administration and briefduration of action.
Captopril, an orally active dipeptide analoguewas introduced in 1977 and quickly gained wideusage. A multitude of ACE inhibitors have sincebeen added, of which—captopril, enalapril,lisinopril, benazepril, ramipril, fosinopril,quinapril, trandolapril, imidapril and perindoprilare available in India. Many others are marketedelsewhere.The pharmacology of captopril isdescribed as prototype, since most of its effectsare class effects common to all ACE inhibitors.
CaptoprilIt is a sulfhydryl containing dipeptide surrogateof proline which abolishes the pressor action ofAng I but not that of Ang II: does not blockAT1 or AT2 receptors.
ACE is a relatively nonspecific enzyme; splitsoff a dipeptidyl segment from several peptidesincluding bradykinin, substance P, a natural stemcell regulating peptide, etc. in addition toAng I. As such, captopril increases plasma kininlevels and potentiates the hypotensive action ofexogenously administered bradykinin. Pretreat-ment with B2 kinin receptor antagonist has shownthat kinins do contribute to the acute vasodepressoraction of ACE inhibitors, but they appear to havelittle role in the long-term hypotensive effect,probably because, firstly kinins play only a minorrole, if at all, in BP regulation, and, secondlyanother enzyme ‘Kininase I’ (which also degradesbradykinin) is not inhibited by captopril.Nevertheless, elevated kinins (and PGs whosesynthesis is enhanced by kinins) may be respon-sible for cough and angioedema induced byACE inhibitors in susceptible individuals. ACEinhibitors interfere with degradation of substanceP also. Rise in the level of stem cell regulatorpeptide caused by ACE inhibitors could, in part,be responsible for their cardioprotective effectin CHF.
Captopril lowers BP, but in the short-term,magnitude of response is dependent on Na+ statusand the level of RAS activity. In normotensiveNa+ replete individuals, the fall in BP attendinginitial few doses of ACE inhibitors is modest.

501C
HA
PTE
R36
DRUGS AFFECTING RENIN-ANGIOTENSIN SYSTEM AND PLASMA KININS
This is more marked when Na+ has been depletedby dietary restriction or diuretics, because reninlevel is high. In CHF also, the renin level is raisedand antihypertensive doses of captopril causemarked fall in BP initially. ACE inhibitor therapyin these situations has to be initiated at muchlower doses. A greater fall in BP occurs in reno-vascular, accelerated and malignant hypertensionas well. In essential hypertension it has been foundthat RAS is overactive in 20%, normal in 60%and hypoactive in the rest. Thus, it contributesto maintenance of vascular tone in over 80% casesand its inhibition results in lowering of BP.Treatment with ACE inhibitors causes feed backincrease in renin release resulting in over-production of Ang I. Since its conversion toAng II is blocked, Ang I is diverted to producemore Ang (1-7) which has vasodilator property,and could contribute to the BP lowering actionof ACE inhibitors. While the initial fall in BPis dependent on renin and Ang II levels, in thelong-term no correlation has been observed bet-ween plasma renin activity (PRA) and magnitudeof fall in BP due to captopril.
Captopril induced hypotension is a result ofdecrease in total peripheral resistance. Thearterioles dilate and compliance of larger arteriesis increased. Both systolic and diastolic BP fall.It has no effect on cardiac output. Cardiovascularreflexes are not interfered with and there is littledilatation of capacitance vessels. As such, posturalhypotension is not a problem. Reflex sympatheticstimulation does not occur despite vasodilatation,
and ACE inhibitors can be safely used in patientswith ischaemic heart disease. The renal bloodflow is not compromized even when BP fallssubstantially. This is due to greater dilatation ofrenal vessels (Ang II markedly constricts them).Cerebral and coronary blood flow are also notcompromized.
Reflex (postural) changes in plasma aldoste-rone are abolished and basal levels are somewhatdecreased as a consequence of loss of its regulationby Ang II. However, physiologically sufficientmineralocorticoid is still secreted under theinfluence of ACTH and plasma K+. Levels ofplasma renin and Ang I are increased as acompensatory measure, but the physiologicalsignificance of this appears to be minor (mostactions are exerted through generation of Ang II).
Pharmacokinetics About 70% of orally admi-nistered captopril is absorbed. Presence offood in stomach reduces its bioavailability.Penetration in brain is poor. It is partly metabolizedand partly excreted unchanged in urine. Theplasma t½ is ~2 hours, but actions last for6–12 hours.
Adverse effects The adverse effect profileof all ACE inhibitors is similar. Captopril is welltolerated by most patients, especially if daily doseis kept below 150 mg.• Hypotension: an initial sharp fall in BP occurs
especially in diuretic treated and CHF patients;persistent hypotension may be troublesome inMI patients.
TABLE 36.1 Comparative features of some ACE inhibitors
Captopril Enalapril Lisinopril Fosinopril Perindopril Ramipril
1. Chemical nature Sulfhydryl Carboxyl Carboxyl Phosphinate Carboxyl Carboxyl
2. Activity status Active Prodrug Active Prodrug Prodrug Prodrug
3. Bioavailability 70% 50% 25% 30% 30–50% 60%(as active form)
4. Time to peak action 1 hr 4–6 hr 6–8 hr 3–5 hr 6 hr 3–6 hr
5. Elimination t½* 2 hr 11 hr 12 hr 12 hr 25–30 hr 8–48 hr
6. Mode of excretion Renal Renal Renal Renal/hepatic Renal Renal
7. Duration of action 6–12 hr 24 hr > 24 hr 24 hr > 24 hr >24 hr
8. Daily dose (mg) 25–150 2.5–40 5–40 10–40 2–8 1.25–10
* t½ including that of active metabolite

502S
EC
TIO
N8
CARDIOVASCULAR DRUGS
• Hyperkalaemia: more likely in patients withimpaired renal function and in those takingK+ sparing diuretics, NSAIDs or blockers.In others significant rise in plasma K+ is rare.
• Cough: a persistent brassy cough occurs in4–16% patients within 1–8 weeks, often requi-res discontinuation of the drug—subsides4–6 days thereafter. It is not dose related andappears to be caused by inhibition ofbradykinin/substance P breakdown in the lungsof susceptible individuals.
• Rashes, urticaria: occur in 1–4% recipients;but do not usually warrant drug discontinuation.
• Angioedema: resulting in swelling of lips,mouth, nose, larynx may develop within hoursto few days in 0.06–0.5% patients; may causeairway obstruction. This can be treated withAdr, antihistaminics and corticosteroidsaccording to need.
• Dysgeusia: reversible loss or alteration of tastesensation due to captopril occurs in fewpatients. A still lower incidence with other ACEinhibitors has been noted.
• Foetopathic: foetal growth retardation, hypo-plasia of organs and foetal death may occurif ACE inhibitors are given during later halfof pregnancy. A recent report indicates2.7-fold higher malformation rate in foetusesexposed to ACE inhibitors in the first trimester.ACE inhibitors must be stopped when thewoman conceives.
• Headache, dizziness, nausea and bowel upset:each reported in 1–4% patients.
• Granulocytopenia and proteinuria: arerare, but warrant withdrawal. Renal diseasepredisposes to these adverse effects. However,ACE inhibitors retard diabetic nephropathy,reduce attendant proteinuria, and are renopro-tective.
• Acute renal failure: is precipitated byACE inhibitors in patients with bilateral renalartery stenosis due to dilatation of efferentarterioles and fall in glomerular filtrationpressure. ACE inhibitors are contraindicatedin such patients.
Interactions• Diuretics synergise with the hypotensive action
of ACE inhibitors by depleting Na+ and raisingrenin levels. In diuretic treated patients, thestarting dose of ACE inhibitors should be low.
• Indomethacin (and other NSAIDs) attenuatethe hypotensive action by retaining salt andwater. Incidents of renal failure have beenreported when a NSAID was given to patients(especially elderly) receiving ACE inhibitor +diuretic.
• Hyperkalaemia can occur if K+ supplements/K+ sparing diuretics are given with captopril.
• Antacids reduce bioavailability of captopril.• ACE inhibitors reduce Li+ clearance and
predispose to its toxicity.
Dose: 25 mg BD, increased gradually upto 50 mg TDSaccording to response. In patients on diuretics and in CHFpatients it is wise to start with 6.25 mg BD to avoid markedfall in BP initially. Tablets should be taken 1 hr before or2 hr after a meal.
Captopril has become less popular due to need for twice/thrice daily dosing and possibly higher incidence of side effectscompared to other ACE inhibitors.ANGIOPRIL 25 mg tab, ACETEN, CAPOTRIL 12.5, 25 mgtab.
OTHER ACE INHIBITORS
All ACE inhibitors have the same pharmacologicalactions, therapeutic uses and spectrum of adverseeffects, drug interactions and contraindications.Differences among them are primarily pharma-cokinetic, reflected in time course of action. Nosingle drug is superior to others.
Enalapril This is the second ACE inhibitor tobe introduced. It is a prodrug, deesterified inthe liver to enalaprilat (a tripeptide analogue),which is not used as such orally because of poorabsorption, but is marketed as injectablepreparation in some countries. Enalapril has thesame pharmacological, therapeutic and adverseeffect profile as captopril, but may offer certainadvantages:1. More potent, effective dose 5–20 mg OD or
BD.2. Its absorption is not affected by food.

503C
HA
PTE
R36
DRUGS AFFECTING RENIN-ANGIOTENSIN SYSTEM AND PLASMA KININS
3. Onset of action is slower (due to need forconversion to active metabolite), less liableto cause abrupt first dose hypotension.
4. Has a longer duration of action: most hyper-tensives can be treated with single daily dose.
5. Rashes and loss of taste are probably lessfrequent.
ENAPRIL, ENVAS, ENAM 2.5, 5, 10, 20 mg tab.
Lisinopril It is the lysine derivative of enala-prilat; does not require hydrolysis to becomeactive ACE inhibitor. Its oral absorption is slow(making first dose hypotension less likely) andincomplete, but unaffected by food. The durationof action is considerably longer, permitting singledaily dose and ensuring uniform hypotensiveaction round the clock. A reduction in venousreturn, cardiac contractility and cardiac outputhas been noted after few weeks of lisinopril use.LINVAS, LISTRIL, LIPRIL 2.5, 5, 10 mg tab, LISORIL 2.5,5, 10, 20 mg tab.
Perindopril Another long-acting ACE inhibitorwith a slow onset of action: less chance of firstdose hypotension. Though 66–95% of orallyadministered perindopril is absorbed, only about20% is converted to the active metabolite perindo-prilat. Extensive metabolism to other inactiveproducts occurs. Efficacy and tolerance ofperindopril are similar to other ACE inhibitors.COVERSYL 2, 4 mg tab.
Fosinopril This ACE inhibitor is unique inbeing a phosphinate compound that is glucuronideconjugated and eliminated both by liver andkidney. The t½ is not altered by renal impairmentand the dose remains the same. However, likemost others, it is a prodrug suitable for once dailyadministration. First dose hypotension is morelikely.Dose: Initially 10 mg (elderly 5 mg) OD; maximum40 mg/day.FOSINACE, FOVAS 10, 20 mg tabs.
Ramipril The distinctive feature of this long-acting ACE inhibitor is its extensive tissue distri-bution. Greater inhibition of local RAS has beenclaimed. However, whether this confers anytherapeutic advantage is not known. The plasma
t½ of its active metabolite ramiprilat is 8–18 hours,but terminel t½ is longer due to slow release oftissue bound drug.CARDACE, RAMIRIL, CORPRIL, R.PRIL 1.25, 2.5, 5 mgcaps.
Quinapril A prodrug carboxyl ACE inhibitor thatis rapidly and completely converted in the liverto the active form Quinaprilat. Like ramiprilat,it is highly bound to the tissue ACE and exhibitsa biphasic plasma t½ of 2 hours and 24 hours.Elimination occurs in urine and bile in a ratioof 2:1.Dose: 10–40 mg/dayACCUPRIL-H: Quinapril 20 mg + hydrochlorothiazide 12.5mg tab.
Trandolapril It is a carboxyl prodrug thatis 40–60% bioavailable in the active form.Absorption is delayed but not decreased by food.The peak effect occurs at 4–6 hours. It is partlymetabolized and eliminated both in urine and faeces.The plasma t½ of active metabolite is biphasic10–24 hours, suitable for once daily dosing.Dose: 2–4 mg (max 8 mg) OD; ZETPRIL 1, 2 mg tabs.
Imidapril The oral bioavailability of this long-acting prodrug ACE inhibitor is 40%, which isreduced by taking the drug with meals. The peakeffect occurs at 6–8 hours and plasma t½ is >24hours.Dose: Initially 5 mg OD taken 1 hour before food; usualmaintenance dose 10 mg OD.TANATRIL 5, 10 mg tabs.
Benazepril Another nonsulfhydryl prodrugACE inhibitor; has a bioavailability of 37% andis excreted by kidney with a t½ of 10–12 hr.Dose: 10 mg initially, max 20–40 mg/day;BENACE 5, 10, 20 mg tab.
USES
1. Hypertension The ACE inhibitors are firstline drugs in all grades of hypertension, but theangiotensin receptor blockers (ARBs) have nowsurpassed them in popularity. About 50% patientsof essential hypertension respond to monotherapywith ACE inhibitors and majority of the rest totheir combination with diuretics or blockers.

504S
EC
TIO
N8
CARDIOVASCULAR DRUGS
The hypotensive effect of lower doses developsgradually over 2–3 weeks. They offer thefollowing advantages:• Free of postural hypotension, electrolyte
disturbances, feeling of weakness and CNSeffects.
• Safety in asthmatics, diabetics and peripheralvascular disease patients.
• Long-term ACE inhibitor therapy has thepotential to reduce incidence of type 2 diabetesin high risk subjects.
• Secondary hyperaldosteronism and K+ loss dueto diuretics is prevented.
• Renal blood flow is well maintained.• Left ventricular hypertrophy and increased
wall-to-lumen ratio of blood vessels that occursin hypertensive patients is reversed.
• No hyperuricaemia, no deleterious effect onplasma lipid profile.
• No rebound hypertension on withdrawal.• Minimum worsening of quality of life
parameters like general wellbeing, work perfor-mance, sleep, sexual performance, etc.
Large multicentric trials have confirmed that ACEinhibitors reduce cardiovascular morbidity andincrease life expectancy of hypertensive patients.It appears that by their specific effect onmyocardial and vascular cell growth/remodeling,they have greater protective potential than otherclasses of antihypertensive drugs.
ACE inhibitors are highly effective and firstchoice drugs in renovascular and resistanthypertension. They are particularly suitable fordiabetic hypertensives in whom they reducecardiovascular complications more than otherantihypertensive drugs, probably by improvingendothelial function.
2. CHF ACE inhibitors cause both arteriolarand venodilatation in CHF patients; reduce after-load as well as preload. Haemodynamic measure-ments in severe CHF patients have shownreduction in right atrial pressure, pulmonaryarterial pressure, pulmonary capillary wedgepressure, systemic vascular resistance, systolicwall stress and systemic BP. Though they have
no direct myocardial action, stroke volume andcardiac output are increased, while heart rate isreduced. Diuresis occurs initially and theaccumulated salt and water are lost due toimproved renal perfusion and abolition ofmineralocorticoid mediated Na+ retention. Car-diac work as measured by heart rate × pressureproduct is reduced; thereby, exercise capacity ofCHF patients is enhanced. Beneficial effects arewell sustained with chronic therapy and the NYHAfunctional class of most patients is improved.
Robust multicentric trials have shown thatACE inhibitors retard the progression of leftventricular systolic dysfunction and prolongsurvival of CHF patients of all grades (I to IV).Mortalility is reduced by ~ 20% in symptomaticCHF patients. Unless contraindicated, ACE inhi-bitors are now advocated by several professionalbodies, including American Heart Association andAmerican College of Cardiology, as first line drugsin all patients with symptomatic as well asasymptomatic left ventricular inadequacy. Adiuretic, blocker with or without digitalis maybe added according to need. ACE inhibitors reduceepisodes of decompensation, myocardial infarctionand sudden death. In addition to improvedhaemodynamics, long-term benefits of ACEinhibitors accrue from withdrawal of Ang IImediated ventricular hypertrophy, remodeling,accelerated myocyte apoptosis and fibrosis.Indirect benefits occur due to reduction insympathetic activation and aldosterone levels.The Assessment of Treatment with Lisinopril and Survival(ATLAS) trial on 3164 heart failure patients (NYHA class IIto IV) has shown that high dose lisinopril (32.5–35 mg/day)given for 39–58 months was more effective in reducing allcause mortality, hospitalization for heart failure and risk ofMI than lower dose (2.5–5 mg/day). To afford maximumprotection against progression of heart failure, the dose of ACEinhibitors needs to be titrated to nearly the upper limit ofrecommended dose range, as shown in other mega trials likeGISSI-3, SOLVD, AIRE, etc. as well. ACE inhibitors areeffective in reducing development of ventricular dysfunction,heart failure and related mortality in post-MI patients also(SAVE, TRACE, AIRE trials).
3. Myocardial infarction (MI) Several mega-trials have established that oral ACE inhibitorsadministered while MI is evolving (within 24 hr

505C
HA
PTE
R36
DRUGS AFFECTING RENIN-ANGIOTENSIN SYSTEM AND PLASMA KININS
of an attack) and continued for 6 weeks reduceearly as well as long-term mortality, irrespectiveof presence or absence of systolic dysfunction,provided hypotension is avoided. In high riskpatients and those with latent or overt ventriculardysfunction (CHF) extension of therapy conti-nues to afford survival benefit over years. Inunstable angina/non-ST segment elevation MI(NSTEMI), long-term ACE inhibitor therapyreduces recurrent MI and need for coronaryangioplasty (SAVE and SOLVD trials), thoughno benefit was apparent in the short-term (ISIS-4 study). Current evidence shows that if thereare no contraindications, all MI patients standto gain from ACE inhibitor therapy, thoughmagnitude of benefit is greatest in those havingassociated hypertension and/or diabetes.
4. Prophylaxis in high cardiovascular risksubjects The results of Heart OutcomesPrevention Evaluation (HOPE) study in 9297post-MI and other high risk subjects, but havingno left ventricular dysfunction or heart failurehave shown that ramipril reduced cardiac deathand MI or stroke by 22% over a period of 4.5years. Risk of developing heart failure or diabeteswas also reduced. These results have beenconfirmed by the EUROPA trial and appear tohold true even for patients who have undergonecoronary revascularization (APRES trial). Thus,ACE inhibitors are protective in high cardiovas-cular risk subjects even when there is no associatedhypertension or left ventricular dysfunction.Protective effect is exerted both on myocardiumas well as vasculature; may involve improvedendothelial function, and is independent ofhypotensive action.
5. Diabetic nephropathy Prolonged ACEinhibitor therapy has been found to prevent ordelay end-stage renal disease in type I as wellas type II diabetics. Albuminuria (an index ofglomerulopathy) remains stable in those treatedwith ACE inhibitor, but aggravates in untreateddiabetics. Treated patients have higher creatinineclearance, require less dialysis and have longerlife expectancy. Benefits appear to be due to
haemodynamic (systemic and intrarenal) as wellas abnormal mesangial cell growth attenuatingeffects of ACE inhibitors. They reduce intraglo-merular pressure and hyperfiltration. ACEinhibitors arrest/partly reverse any degree ofalbuminuria, but benefits in type 2 diabetics arerather limited once macroalbuminuria has set in.The RAS seems to accentuate micro- andmacrovascular complications in diabetics, andACE inhibitors have specific organ protectiveeffect by attenuating the same. All patients withdiabetic nephropathy, whether hypertensive ornormotensive, deserve ACE inhibitor therapy.Deterioration of retinopathy in diabetics alsoappears to be retarded by ACE inhibitors.
Nondiabetic nephropathy There is evidencenow that chronic renal failure due to nondiabeticcauses may also be improved by ACE inhibitors.These drugs reduce proteinuria by decreasingpressure gradient across glomerular capillaries aswell as by altering membrane permeability. Thisretards disease progression. Among hypertensivenephropathy patients the incidence of doublingof serum creatinine or end stage renal failure issignificantly lower in those treated with ACEinhibitors than those treated with other anti-hypertensive drugs.
6. Scleroderma crisis The marked rise inBP and deterioration of renal function in sclero-derma crisis is mediated by Ang II. ACE inhibitorsproduce dramatic improvement and are life savingin this condition.
Captopril test This test has been devised to obviate the needfor renal angiography for diagnosis of renovascular hyper-tension. The basis of the test is—acute blockade of Ang IIformation by captopril results in a reactive increase in PRAwhich is much higher in renovascular compared to essentialhypertension. However, this test is only of adjunctive value.
ANGIOTENSIN ANTAGONISTS(Angiotensin receptor blockers or ARBs)Over the past 2 decades, several nonpeptideorally active AT1 receptor blockers (ARBs) havebeen developed as alternatives to ACE inhibitors.These include losartan, candesartan, valsartan,

506S
EC
TIO
N8
CARDIOVASCULAR DRUGS
telmisartan, olmesartan and irbesartan. Selectiveantagonists of AT2 receptors as well as combinedAT1 + AT2 antagonists have also been produced,but are not used clinically.
Losartan It is a competitive antagonist andinverse agonist, 10,000 times more selective forAT1 than for AT2 receptor; does not block anyother receptor or ion channel, except thromboxaneA2 receptor (has some platelet antiaggregatoryproperty). All overt actions of Ang II, viz. vaso-constriction, central and peripheral sympatheticstimulation, release of aldosterone and Adr fromadrenals, renal actions promoting salt and waterreabsorption, central actions like thirst, vasopressinrelease and growth-promoting actions on heartand blood vessels are blocked. No inhibition ofACE has been noted.
Pharmacologically, ARBs differ from ACEinhibitors in the following ways:• They do not interfere with degradation of
bradykinin and other ACE substrates: norise in level or potentiation of bradykinin,substance P occurs. Consequently, ACEinhibitor related cough is rare.
• They result in more complete inhibition of AT1
receptor activation, because responses toAng II generated via alternative pathways andconsequent AT1 receptor activation (whichremain intact with ACE inhibitors) are alsoblocked.
• They result in indirect AT2 receptor activation.Due to blockade of AT1 receptor mediatedfeedback inhibition—more Ang II is producedwhich acts on AT2 receptors that remainunblocked. ACE inhibitors result in attenuationof both AT1 and AT2 receptor activation.
• ARBs cause little increase in the level of Ang(1-7) which is raised by ACE inhibitors, sinceAng (1-7) is partly degraded by ACE.The impact of these differences on clinical
efficacy and therapeutic value of the two classesof RAS inhibitors is not known.
Losartan causes fall in BP in hypertensivepatients which lasts for 24 hours, while HRremains unchanged and cardiovascular reflexes
are not interfered. No significant effect on plasmalipid profile, carbohydrate tolerance, insulinsensitivity has been noted. A mild probenecid-like uricosuric action is produced.
Pharmacokinetics Oral absorption of losartanis not affected by food, but bioavailability is only33% due to first pass metabolism. It is partiallycarboxylated in liver to an active metabolite(E3174) which is a 10–30 times more potentnoncompetitive AT1 receptor antagonist. After oralingestion peak plasma levels are attained at 1hr for losartan and at 3–4 hours for E3174. Bothcompounds are 98% plasma protein bound, donot enter brain and are excreted by the kidney.The plasma t½ of losartan is 2 hr, but that ofE3174 is 6–9 hr. No dose adjustment is requiredin renal insufficiency, but dose should be reducedin presence of hepatic dysfunction.
Adverse effects Losartan is well tolerated; hasside effect profile similar to placebo. Like ACEinhibitors it can cause hypotension and hyper-kalemia, but first dose hypotension is uncommon.Though, a few reports of dry cough have appeared,losartan is considered to be free of cough anddysgeusia inducing potential. Patients with ahistory of ACE inhibitor related cough have takenlosartan without recurrence. Angioedema isreported in fewer cases. Headache, dizziness,weakness and upper g.i. side effects are mild andoccasional. However, losartan has fetopathicpotential like ACE inhibitors—not to beadministered during pregnancy.Dose: 50 mg OD, rarely BD; in liver disease or volumedepleted patients 25 mg OD; addition of hydrochlorothiazide12.5–25 mg enhances its effectiveness.LOSACAR, TOZAAR, ALSARTAN 25, 50 mg tabs.
Candesartan It has the highest affinity forthe AT1 receptor and produces largely unsurmoun-table antagonism, probably due to slowdissociation from the receptors or receptordesensitization. Elimination occurs by both hepaticmetabolism and renal excretion with a t½ of 8-12 hours: action lasts 24 hours.Dose: 8 mg OD (max 8 mg BD), liver/kidney impairment4 mg OD.

507C
HA
PTE
R36
DRUGS AFFECTING RENIN-ANGIOTENSIN SYSTEM AND PLASMA KININS
CANDESAR 4, 8, 10 mg tab., CANDILONG, CANDESTAN4, 8 mg tabs.
Irbesartan The oral bioavailability of this ARBis relatively high. It is partly metabolized andexcreted mainly in bile. The t½ is ~12 hours.Dose: 150–300 mg OD.IROVEL, IRBEST 150, 300 mg tabs.
Valsartan The AT1 receptor affinity of valsartanis similar to that of losartan. Its oral bioavailabilityaverages 23% and food interferes with itsabsorption. Elimination occurs mainly by the liverin unchanged form with a t½ of 6–9 hours; actionlasts 24 hours.Dose: 80–160 mg OD 1 hour before meal (initial dose inliver disease 40 mg).DIOVAN, STARVAL, VALZAAR 40, 80, 160 mg tabs.
Olmesartan Another potent ARB with highaffinity for AT1 receptor. It is available as an esterprodrug which is completely hydrolysed duringabsorption from the gut. It is eliminated in urine aswell as in bile with a t½ of ~12 hours. No doseadjustment is needed in liver or kidney disease,unless it is severe.Dose: 20–40 mg OD; OLMAT 20, 40 mg tabs.
Telmisartan The AT1 receptor blocking actionof telmisartan is similar to losartan, but it does notproduce any active metabolite. After an oral dose,peak action occurs in 3 hours and action lasts > 24hours. It is largely excreted unchanged in bile; dosereduction is needed in liver disease.Dose: 20–80 mg OD.TELMA, TELSAR, TELVAS 20, 40, 80 mg tabs.
Uses of ARBsThe ARBs have the same overall range of clinicalutility as ACE inhibitors, but the suitability/efficacy of one over the other is not clearlydefined; may depend on the condition beingtreated and/or specific features of the patient. Thevalue of combined use of ACE inhibitors andARBs versus monotherapy is also still unsettled.
Hypertension Losartan and other ARBs arenow first line drugs, comparable in efficacy anddesirable features to ACE inhibitors, with theadvantage of not inducing cough and a lowerincidence of angioedema, rashes and dysgeusia.
As such, they are more commonly prescribed nowthan ACE inhibitors, though superiority of oneover the other is not established. Like ACEinhibitors, the maximum antihypertensive effectis reached in 2–4 weeks and ventricular/vascularhypertrophy/remodeling is arrested/reversedsimilarly.The Losartan intervention for endpoint reduction inhypertension (LIFE, 2002) study has found losartan to bemore effective than -blockers in reducing stroke among> 9000 hypertensive patients with left ventricular hypertrophy,and is approved for stroke prevention. In cirrhotics, losartanhas been found to control portal hypertension.
CHF The ARBs afford clear-cut symptomaticrelief as well as survival benefit in CHF. However,their relative value compared to ACE inhibitors,especially in long-term morbidity and mortalityreduction, is still uncertain.A number of large randomized endpoint trials like Evaluationof losartan in the elderly (ELITE, 1997), ELITE-II (2000),OPTIMAAL (2002), Valsartan in acute MI (VALIANT, 2003)have produced inconsistent results. Some find ACE inhibitorsmore effective, others find ARBs more effective, while stillothers find them equieffective. For CHF, the current consensusis to use ACE inhibitors as the first choice drugs and to reserveARBs for those who fail to respond well or who developcough/angioedema/other intolerance to ACE inhibitors.
Myocardial infarction The evidence so farindicates that utility of ARBs in MI, includinglong-term survival, is comparable to ACEinhibitors. However, the latter are generally usedfirst, since there is greater experience with them.
Diabetic nephropathy Several studies haveconfirmed that ARBs are renoprotective in type 2diabetes mellitus, independent of BP lowering.The magnitude of benefit is comparable to ACEinhibitors, but because of better tolerability profile,many consider ARBs to be the first choice now.
Combination of ACE inhibitors with ARBsThere are theoretical reasons to combine an ACEinhibitor with an ARB to obtain more completesuppression of RAS and achieve added cardio-protection in CHF or renoprotection in diabeticnephropathy. These are:• Ang II is generated in several tissues (especially heart
and kidney) by non-ACE mechanisms, whose effect canbe blocked by ARBs.

508S
EC
TIO
N8
CARDIOVASCULAR DRUGS
• ACE inhibitors produce bradykinin and Ang (1-7) relatedvasodilatation and other effects that are not producedby ARBs.
• ARBs cause compensatory increase in Ang II productionthat can be checked by ACE inhibitors.
• ARBs enhance unblocked AT2 receptor mediated effectsthat can be prevented by concurrent ACE inhibition.Additional haemodynamic and symptomatic
improvement over short-term has been obtainedin CHF with addition of an ARB to exhistingACE inhibitor therapy. However, several largerandomized trials including Randomized eva-luation of strategies for left ventricular dysfunction(RESOLVD, 1999), Valsartan heart failure trial(VAL-He FT, 2001), CHARM-additive trial(2003), VALIANT (2003) trial, OngoingTelmisartan alone and in combination withramipril global endpoint trial (ON TARGET,2008) of combinations of ARBs and ACEinhibitors Vs their monotherapy in affordingmortality and other endpoint benefits in CHF haveyielded discordant results. Thus, it is not yetclarified whether long-term use of ARB + ACEinhibitor combination is advisable or not.
In non-diabetic renal disease, the Combinationtreatment of ARB and ACE inhibitor randomizedtrial (COOPERATE, 2003) has concluded thatARB + ACE inhibitor combination therapy retardsprogression of non-diabetic renal disease to agreater extent compared with their monotherapy.
DIRECT RENIN INHIBITOR
AliskirenDirect renin inhibitors (DRIs) are the latest classof RAS inhibitory drugs, of which only onemember Aliskiren has become available for thetreatment of cardiovascular and renal diseases inwhich ACE inhibitors and ARBs are currentlyused. Aliskiren is a nonpeptide which bindsselectively to the catalytic site of renin and compe-titively blocks the access of angiotensinogen tothis site Ang I is not produced and the chainof RAS is interrupted. While the concentrationof renin in plasma is increased by feed back,the plasma renin activity (PRA) is decreased.Ang I and Ang II levels fall.
Aliskiren causes fall in BP which is moremarked in the Na+ depleted subjects with highbasal PRA. Similar to ACE inhibitors, plasmaaldosterone levels are lowered accompanied bymild natriuresis and a tendency to K+ retention.The antihypertensive efficacy of aliskiren isequivalent to that of ACE inhibitors or ARBs.Combination of these drugs with aliskirenproduces greater fall in BP, at least in the shortterm. This may be due to blockade of rise inPRA caused by ACE inhibitors/ARBs. The patternof haemodynamic effect of aliskiren resemblesACE inhibitors; postural hypotension is not aproblem.
Trials so far have shown that aliskiren canreduce hypertensive left ventricular hypertrophyand benefit CHF patients, but its value comparedto ACE inhibitors/ARBs as monotherapy and asadditional drug remains to be determined.Aliskiren has renoprotective effect as well inhypertension and diabetes mellitus. Its long-termbenefits and comparative position in relation toACE inhibitors/ARBs is being evaluated.
At present, aliskiren is recommended as analternative antihypertensive drug (for those whodo not respond/do not tolerate 1st line drugs)and in combination with others for greater BPlowering.
Pharmacokinetics Aliskiren is administeredorally, but bioavailability is very low due to activeextrusion of absorbed drug by P-glycoprotein. Thedrug is mainly eliminated in faeces; small amountin urine. The plasma t½ is > 24 hours, and itsBP lowering effect persists for days after regularintake.
Adverse effects Aliskiren produces few andmild side effects—mainly dyspepsia, abdominalpain, loose motions, headache and dizziness. Acutehypotension, hyperkalaemia, cough, angioedemaand rashes are much less frequent than with ACEinhibitors. Aliskiren is contraindicated duringpregnancy.Dose: 150–300 mg OD; RASILEZ 150 mg tab;RASILEZ-HC: along with hydrochlorothiazide.

509C
HA
PTE
R36
DRUGS AFFECTING RENIN-ANGIOTENSIN SYSTEM AND PLASMA KININS
PLASMA KININS(Bradykinin and Kallidin)
Plasma kinins are polypeptides split off from aplasma globulin Kininogen by the action ofspecific enzymes Kallikreins. The two importantplasma kinins, Kallidin (decapeptide) and Brady-kinin (nonapeptide) were discovered around 1950by two independent lines of investigation intothe hypotensive activity of urine and certain snakevenoms. These and other biological fluids werefound to act indirectly: they contained enzymeswhich generated active substances in the plasma.
Kinins are generated by proteolytic reactionstriggered by tissue injury, inflammation, allergicreaction, etc., and play important mediator roles.
Generation and metabolism Kininogens are 2
globulins present in plasma which also contains inactivekininogenase prekallikrein.
Prekallikrein is activated by Hageman factor (factor XII)which itself is activated by tissue injury and contact withsurfaces having negative charge, e.g. collagen, basementmembrane, bacterial liposaccharides, urate crystals, etc.Plasmin facilitates contact activation of Hageman factor(Fig. 36.4). Kinins are also generated by trypsin, proteolyticenzymes in snake and wasp venoms and by kallikrein presentin kidney, pancreas and other tissues. Bradykinin is generatedfrom high molecular weight (HMW) kininogen by the actionof plasma kallikrein, because HMW-kininogen does not crossthe capillaries. On the other hand, kallidin can be produced
from both low molecular weight (LMW) kininogen as wellas HMW-kininogen by the action of tissue kallikreins.Bradykinin can also be generated from kallidin on the removalof lysine residue by an aminopeptidase.
Plasma and tissues also contain kininogenase inhibitoryfactors of which complement (C1) esterase inhibitor is themost important. Moreover, kallikreins are normally presentin their inactive forms. Thus, physiologically only smallamounts of kinins are generated in plasma and tissues.
Kinins are very rapidly degraded, primarily in lungs,but also in other tissues and have a t½ of < 1 min. Theprincipal degrading enzyme is Kininase II, also known as‘angiotensin-II converting enzyme’ (ACE) which splits off2 amino acids from the carboxyterminal of the peptide chain.Another carboxypeptidase Kininase I removes only one aminoacid (arginine) producing selective B1 receptor agonisticmetabolites (desArg bradykinin and desArg kallidin) whichare further degraded by other peptidases.
ACTIONS
Bradykinin and kallidin have similar actions.
1. CVS Kinins are more potent vasodilatorsthan ACh and histamine. The dilatation is media-ted through endothelial NO and PGI2 generation,and involves mainly the arterioles. Larger arteries,most veins and vessels with damaged endothe-lium are constricted through direct action on thesmooth muscle. In addition, they can releasehistamine and other mediators from mast cells.Injected i.v. kinins cause flushing, throbbing
Fig. 36.4: Generation and degradation of plasma kininsHMW—High molecular weight; LMW—Low molecular weight

510S
EC
TIO
N8
CARDIOVASCULAR DRUGS
headache and fall in BP. They markedly increasecapillary permeability due to separation ofendothelial cells exudation and inflammationoccurs if they are injected in a tissue. Intradermalinjection produces wheal and flare (similar tohistamine).
Kinins have no direct action on heart; reflexstimulation occurs due to fall in BP.
2. Smooth muscle Kinin-induced contractionof intestine is slow (bradys—slow, kinein—tomove). They cause marked bronchoconstrictionin guineapigs and in asthmatic patients. Actionon other smooth muscles is not prominent, somemay be relaxed also.
3. Neurones Kinins strongly stimulate nerveendings that transmit pain and produce a burningsensation. Applied to blister base/injected intra-peritoneally or in the brachial artery, bradykininproduces intense, transient pain and has been usedin analgesic testing.
Kinins release CAs from adrenal medulla.Injected directly in brain they produce a varietyof effects including enhanced sympatheticdischarge. They increase permeability of theblood-brain barrier.
4. Kidney Kinins increase renal blood flowas well as facilitate salt and water excretion byaction on tubules. The diuretic effect of furose-mide is reduced by kinin B2 receptor antagonists,indicating participation of locally generated kininsin this response.
Kinin receptors Existance of two types of kinin receptors(B1, B2) has been established. Bradykinin and Kallidin areselective agonists of B2 receptors, while their des-Argmetabolites generated by the action of kininase I are selectiveagonists of B1 receptor. Most of the kinin actions in noninfla-med tissues are mediated by B2 receptors which areconstitutively present on:
(i) Visceral smooth muscle—contraction of intestine,uterus, airway.
(ii) Vascular endothelium—NO release, vasodilatation,increased permeability.
(iii) Sensory nerves—acute pain.
The B2 receptor is a GPCR coupled to Gq and Gi proteinswhich utilizes the phospholipaseC—IP3/DAG—intracellularCa2+ mobilization transducer mechanism. Endothelial NO
synthase (eNOS) is activated causing vasodilatation. Certainresponses to kinins, e.g. bronchoconstriction and renal vaso-dilatation are attenuated by pretreatment with PG synthesisinhibitors (aspirin). Kinin induced acute pain involves B2
receptors. Aspirin injected i.p. before bradykinin throughthe same cannula blocks its algesic action. These responsesare mediated by phospholipase A activation—release ofarachidonic acid and generation of PGs.The activated Gqprotein also mediates production of NFB and triggeringof MAP kinase pathway leading to generation of pro-inflammatory mediators.
The B1 receptor is located on the smooth muscle oflarge arteries and veins—mediates contraction of these vessels,but is expressed minimally in normal tissues. Inflammationinduces synthesis of B1 receptors, which colocalize withkininase I enzyme, so that the B1 agonistic des-Arg kininsare produced locally. Activated B1 receptor also transducesthrough Gq and Gi proteins and produces similar responses,especially enhanced PG synthesis, leukocyte recruitment,activation of inducible NOS (iNOS) and chronic pain ininflammed tissues.
PATHOPHYSIOLOGICAL ROLES
1. Mediation of inflammation Kinins produce all thesigns of inflammation—redness, exudation, pain andleukocyte mobilization. Tissue injury can cause local kininproduction which then sets in motion the above defensiveand reparative processes. Activation of B1 receptors on macro-phages induces production of IL-1, TNF- and otherinflammatory mediators.
Kinins appear to play important role in allergicinflammation manifesting as angioedema, rhinitis and asthma.2. Mediation of pain By directly stimulating nerveendings and by increasing PG production, kinins appear toserve as mediators of pain. The B2 antagonists block acutepain produced by bradykinin, but induced B1 receptors appearto mediate pain of chronic inflammation.3. Functional hyperemia (in glands during secretion)and regulation of microcirculation—especially in kidney maybe occurring through local kinin production.4. Production of kinins is integrated with clotting,fibrinolysin and complement systems. Kallikreins may haveroles in these systems which are independent of kininproduction.5. Kinins appear to play no significant role in the regulationof normal BP. However, they may serve to oppose overactiveRAS and exert antiproliferative influence on cardiac andvascular muscle in hypertensive states.
Potentiation of endogenous bradykinin appears to partlyaccount for the cardioprotective effect of ACE inhibitors.Recent evidence indicates that ischaemic preconditioningwhich limits tissue damage during myocardial infarctioninvolves kinins.6. Kinins cause closure of ductus arteriosus, dilatation offoetal pulmonary artery and constriction of umbilical vessels.

511C
HA
PTE
R36
DRUGS AFFECTING RENIN-ANGIOTENSIN SYSTEM AND PLASMA KININS
Thus, they may be involved in adjusting from foetal toneonatal circulation.7. Kinins play a major role in the development of angioedema.They also appear to be involved in shock, rhinitis, asthma,ACE inhibitor induced cough, carcinoid, postgastrectomydumping syndrome, fluid secretion in diarrhoea, acutepancreatitis and certain immunological reactions.
Because of evanescent and unpleasant actions, kininshave no clinical use.
Bradykinin antagonistsAfter characterization of B1 and B2 kinin receptors,several peptide and nonpeptide kinin antagonists
have been produced. The synthetic peptide HOE140 (icatibant) is a selective B2 antagonist,resistant to kinin degrading enzymes and havinglonger t½. The compound FR 173657 and someothers are orally active nonpeptide B2 antagoniststhat have helped in defining the pathophysiologicalroles of kinins and have undergone limited trialsas analgesic, antiinflammatory drugs and in pan-creatitis, head injury, etc. Icatibant has beenrecently approved in Europe for symptomatictreatment of hereditary angioedema.
PROBLEM DIRECTED STUDY
36.1 A 65-year-male was diagnosed to be suffering from congestive heart failure (CHF). He hadpitting edema of feet, dyspnoea and cough on mild exertion, fatigue, engorged neck veins, softenlargement of liver, pulmonary congestion and mild cardiac dilatation. The pulse was 100/min,respiration 20/min and BP 130/86 mm of Hg. He was prescribed—Tab furosemide 40 mg once daily in the morningTab captopril 25 mg twice daily, morning and evening.After 2 hours of taking the medicines, he started passing increased quantity of urine and inthe next few hours he gradually started feeling weakness, nausea, sweating and fainted whilewalking to the toilet. The pulse was recorded as 110/min and BP 80/40 mm Hg.(a) What could be the cause of sudden onset symptoms and the marked fall in BP?(b) Is the choice of drugs incorrect?(c) How could such adverse event be prevented?(d) What immediate management is required?(see Appendix-1 for solution)

Cardiac Glycosides andDrugs for Heart Failure
ChapterChapterChapterChapterChapter 3737373737
CARDIAC GLYCOSIDES
These are glycosidic drugs having cardiac inotro-pic property. They increase myocardial contrac-tility and output in a hypodynamic heart withouta proportionate increase in O2 consumption. Thus,efficiency of failing heart is increased. In contrast,‘cardiac stimulants’ (Adr, theophylline) increaseO2 consumption rather disproportionately and tendto decrease myocardial efficiency.William Withering, a Birmingham physician, learnt that adecoction containing ‘foxglove’ (Digitalis) with other herbals,prepared by an old lady, relieved dropsy. He tried extract offoxglove alone and found it to be remarkably effective in somecases. He published his classic monograph ‘An account of theFoxglove and some of its medicinal uses: with practical remarkson dropsy and other diseases’ in 1785 and ascribed thebeneficial effect to an action on the kidney. Cushney andMackenzie, in the beginning of 20th century, established itsaction on the heart and its use in congestive heart failure (CHF).
Cardiac glycosides are found in several plantsand in toad skin (Bufotoxin). Digitalis lanatais the source of Digoxin, the only glycoside thatis currently in use. Others like Digitoxin (fromDigitalis purpurea) and Ouabain (from Strophanthus gratus), etc. are no longer clinically usedor marketed.
By convention the term, ‘Digitalis’ has come tomean ‘a cardiac glycoside’.
Chemistry
The cardiac glycosides consist of an aglycone (genin) to whichare attached one or more sugar (glucose or digitoxose) moieties.
The aglycone consists of a cyclopentanoperhydro-phenanthrene (steroid) ring to which is attached a 5 or 6membered unsaturated lactone ring.
PHARMACOLOGICAL ACTIONS
All digitalis glycosides have qualitatively similaraction. Digoxin is described as prototype.
1. Heart Digitalis has direct effects on myo-cardial contractility and electrophysiological pro-perties. In addition, it has vagomimetic action,reflex effects due to alteration in haemodynamicsand direct CNS effects altering sympatheticactivity.
Force of contraction Digitalis causes a dosedependent increase in force of contraction ofheart—a positive inotropic action. This isespecially seen in the failing heart which isexquisitely sensitive. There is increased velocityof tension development and higher peak tensioncan be generated. Systole is shortened, diastoleis prolonged. When a normal heart is subjectedto increased impedance to outflow, it generatesincreased tension so that stroke volume ismaintained upto considerably higher values ofimpedance (Fig. 37.1), while the failing heart isnot able to do so and the stroke volume progres-sively decreases. The digitalized failing heartregains some of its capacity to contract moreforcefully when subjected to increased resistanceto ejection. There is more complete emptying offailing and dilated ventricles—cardiac output isincreased and end-diastolic volume is reduced.However, therapeutic doses of digoxin do notincrease resting tension (tone) in myocardialfibres.
Rate Heart rate is decreased by digitalis.Bradycardia is more marked in CHF patients
DIGOXIN

513C
HA
PTE
R37
CARDIAC GLYCOSIDES AND DRUGS FOR HEART FAILURE
because improved circulation (due to positiveinotropic action) restores the diminished vagaltone and abolishes sympathetic overactivity. Inaddition, digitalis slows the heart by vagal andextravagal actions.Vagal tone is increased reflexly by sensitizationof baroreceptors, as well as by stimulation ofvagal centre.Extravagal A direct depressant action on SAand A-V nodes. This component of bradycardiais not reversed by atropine.
Electrophysiological properties The electro-physiological effects of digitalis on different typesof cardiac fibres differ quantitatively and quali-tatively. The Purkinje fibres, automatic andconducting tissues are more sensitive. In additionto direct effects, the indirect autonomic influencesare important in the in situ heart.(a) Action potential (AP ): The effects are illus-trated diagrammatically in Fig. 37.2.• The resting membrane potential (RMP) is
progressively decreased (to less negativevalues) with increasing doses. Excitability isenhanced at low doses but depressed at toxicdoses because Na+ channels are inactivated.
• The rate of 0 phase depolarization is reducedresulting in slowing of conduction. This actionis most marked in A-V node and bundle ofHis.
• The slope of phase-4 depolarization is increasedin the PFs—ectopic automaticity is enhanced—
latent pacemakers become overt at high dosesproducing extrasystoles. High doses of digitalisproduce coupled beats by another mechanism:the RMP shows oscillations during phase-4;when their magnitude is sufficient enough,delayed after-depolarizations result (see Fig.38.1). The SA and A-V node automaticity isreduced at therapeutic concentrations by vagalaction which hyperpolarizes these cells andreduces their phase-4 slope. Toxic dosesmarkedly reduce RMP of SA nodal cells bydirect action and stop impulse generation.
• The action potential duration (APD) is reduced(primarily at phase-2) and amplitude of APis diminished.
(b) Effective refractory period (ERP):
decreased byvagal action
Atriumincreased bydirect action
A-V node andbundle of His
Ventricle—ERP is abbreviated by direct action.
Fig. 37.1: Relationship between peripheral resistance andstroke output in normal and failing heart, and the actionof digitalis on failing heart
Fig. 37.2: Effect of digitalis on Purkinje fibre actionpotential
Vagal action normallypredominates, causesinhomogeneity; allowsthe atria to respond at ahigher rate and in anasynchronous manner.
⎫⎬⎭
Increased by direct, vagomimeticand antiadrenergic actions; themaximum rate at which impulsescan be transmitted is reduced.
⎫⎬⎭

514S
EC
TIO
N8
CARDIOVASCULAR DRUGS
(c) Conduction: A-V conduction is demonstrablyslowed by therapeutic doses. At high doses,intraventricular conduction in PFs is alsodepressed by uncoupling of gap junctions.(d) ECG : Therapeutic doses of digitalis producechanges in the ECG. These are accentuated athigh doses—may also produce arrhythmias.• Decreased amplitude or inversion of T wave.• Increased P-R interval (due to slowing of
A-V conduction), A-V block at toxic doses.• Shortening of Q-T interval (reflecting shor-
tening of systole).• Depression of ST segment (at high doses—
due to interference with repolarization).
Mechanism of action Digitalis increasesforce of cardiac contraction by a direct actionindependent of innervation. It selectively bindsto extracellular face of the membrane associatedNa+K+ ATPase of myocardial fibres and inhibitisthis enzyme (Fig. 37.3). Inhibition of this cationpump results in progressive accumulation of
Na+ intracellularly. This indirectly results inintracellular Ca2+ accumulation.
During depolarization Ca2+ ions enter the celldriven by the steep Ca2+ gradient (>1 mM extra-cellular to < 100 nM cytosolic during diastole)through voltage sensitive L type Ca2+ channels.This triggers release of larger amount of Ca2+
stored in sarcoplasmic reticulum (SR) throughRyanodine calcium channel 2 (RYR2) → cytosolicCa2+ increases transiently to about 500 nM(calcium transients) → triggers contraction byactivating troponin C on myofibrils. Thesarcoplasmic-endoplasmic reticular Cal. ATPase2 (SERCA2) is then activated which pumps Ca2+
back into the SR. A fraction (equal to that whichentered from outside during depolarization) isextruded mainly by 3Na+/1Ca2+ exchange trans-porter (NCX-antiporter) and to a lesser extentby sarcolemmal Ca2+ pump (Ca2+ ATPase). Duringphase 3 of AP, membrane Na+K+ATPase moves3 intracellular Na+ ions for 2 extracellular
Fig. 37.3: Mechanism of positive inotropic action of cardiac glycosides. SR—Sarcoplasmicreticulum; TnC—Troponin C; NCX—Na+-Ca2+ exchanger; RyR2—Ryanodine receptor calciumchannel 2; PL—Phospholamban; SERCA2—Sarcoplasmic-endoplasmic reticulum calciumATPase 2.

515C
HA
PTE
R37
CARDIAC GLYCOSIDES AND DRUGS FOR HEART FAILURE
K+ ions. The slight (1–1.5 mM) increase incytosolic Na+ over normal (8–10 mM) due topartial inhibition of Na+K+ATPase by digitalisreduces transmembrane gradient of Na+ whichdrives the extrusion of Ca2+. The excess Ca2+
remaining in cytosol is taken up into SR whichprogressively get loaded with more Ca2+ →subsequent calcium transients are augmented.
The relationship of cytosolic [Na+] and [Ca2+] is suchthat a small percentage increase in Na+ concentration leadsto a large percentage increase in Ca2+ concentration. Moreover,raised cytosolic Ca2+ induces greater entry of Ca2+ throughvoltage sensitive Ca2+ channels during the plateau phase.It has been shown that 1 mM rise in cytosolic [Na+] resultsin 20–30% increase in the tension developed by ventricularfibres.
Binding of glycoside to Na+K+ATPase is slow.Moreover, after Na+K+ATPase inhibition, Ca2+
loading occurs gradually. As such, inotropic effectof digitalis takes hours to develop, even afteri.v. administration.
Inhibition of Na+K+ ATPase is clearly invol-ved in the toxic actions of digitalis. At high doses,there is depletion of intracellular K+; and digitalistoxicity is partially reversed by infusing K+,because K+ decreases binding of glycoside toNa+K+ ATPase. Excessive Ca2+ loading of SRresults in spontaneous cycles of Ca2+ release anduptake producing oscillatory after-depolarizationsand after-contractions. Since both therapeutic andtoxic effects of digitalis are due to myocardialCa2+ loading, these are inseparable and therapeuticindex is low.
2. Blood vessels Digitalis has mild directvasoconstrictor action—peripheral resistance isincreased in normal individuals. However, in CHFpatients this is more than compensated by theindirect effect of improvement in circulation, i.e.reflex sympathetic overactivity is withdrawn anda net decrease in peripheral resistance occurs.
Digitalis has no prominent effect on BP:systolic BP may increase and diastolic may fallin CHF patients—pulse pressure increases. Hyper-tension is no contraindication to the use ofdigitalis.
Therapeutic doses of digitalis have nosignificant effect on coronary circulation—
coronary insufficiency is no contraindication toits use.
3. Kidney Diuresis occurs promptly in CHFpatients, secondary to improvement in circulationand renal perfusion. The retained salt and wateris gradually excreted. No diuresis occurs in normalindividuals or in patients with edema due to othercauses.
4. CNS Digitalis has little apparent CNS effectin therapeutic dose. Higher doses cause CTZactivation → nausea and vomiting. Still higherdoses produce hyperapnoea, central sympatheticstimulation, mental confusion, disorientation andvisual disturbances.
PHARMACOKINETICS
The pharmacokinetic features of digoxin are listedin Table 37.1.
Bioavailability of digoxin tablets fromdifferent manufacturers may differ. Presence offood in stomach delays absorption of digoxin.The volume of distribution of digoxin is large(6–8 L/Kg). It is concentrated in the heart (~20times than plasma), skeletal muscle, liver andkidney.
Digoxin is primarily excreted unchanged bythe kidney: mainly by glomerular filtration; rate
TABLE 37.1 Pharmacokinetic features of digoxin
DIGOXIN
1. Oral absorption 60–80%2. Plasma protein binding 25%3. Time course of action*
–Onset 15–30 min–Peak 2–5 hr–Duration 2–6 days
4. Plasma t½ 40 hr5. Therapeutic concn. 0.5–1.4 ng/ml6. Toxic concn. > 2 ng/ml7. Daily maintenance dose 0.125–0.5 mg8. Daily elimination** 35%9. Route of elimination Renal
(predominant) excretion10. Route of administration Oral, i.v.
* Of full digitalizing dose given i.v.; ** fraction of totalamount present in the body.

516S
EC
TIO
N8
CARDIOVASCULAR DRUGS
of excretion is altered parallel to creatinineclearance. Its t½ is prolonged in elderly patientsand in those with renal insufficiency: dose hasto be reduced.
Digoxin is a cumulative drug. Whenmaintenance doses are given from the beginning,steady state levels and full therapeutic effect areattained after 4 × t½, i.e. 6–7 days.Digoxin is the only cardiac glycoside availablewidely and used clinically now.Digoxin: DIGOXIN 0.25 mg tab., 0.05 mg/ml pediatricelixir, 0.5 mg/2 ml inj. LANOXIN 0.25 mg tab,CARDIOXIN, DIXIN 0.25 mg tab, 0.5 mg/2 ml inj.
ADVERSE EFFECTS
Toxicity of digitalis is high, margin of safety islow (therapeutic index 1.5–3). Higher cardiacmortality has been reported among patients withsteady-state plasma digoxin levels > 1.1 ng/mlbut still within the therapeutic range duringmaintenance therapy. About 25% patients deve-lop one or other toxic symptom. The manifes-tations are:
Extracardiac Anorexia, nausea, vomiting andabdominal pain are usually reported first: are dueto gastric irritation, mesenteric vasoconstrictionand CTZ stimulation. Fatigue, malaise, headache,mental confusion, restlessness, hyperapnoea,disorientation, psychosis and visual disturbancesare the other complaints. Skin rashes andgynaecomastia are rare.
Cardiac Almost every type of arrhythmia canbe produced by digitalis: pulsus bigeminus, nodaland ventricular extrasystoles, ventriculartachycardia and terminally ventricular fibrillation.Partial to complete A-V block may be the solecardiac toxicity, or it may accompany otherarrhythmias. Severe bradycardia, atrial extra-systoles, AF or AFl have also been noted. In about2/3 patients showing toxicity, extracardiacsymptoms precede cardiac; in the rest seriouscardiac arrhythmias are the first manifestation.
Treatment Further doses of digoxins must bestopped at the earliest sign of toxicity; nothingmore needs to be done in many patients, especiallyif the manifestations are only extracardiac.
(a) For tachyarrhythmias When caused bychronic use of digitalis and diuretics (both induceK+ depletion)—infuse KCl 20 m.mol/hour (max.100 m. mol) i.v. or give orally in milder cases.High extracellular K+ decreases binding of theglycosides to Na+K+ATPase by favouring aconformation of the enzyme that has lower affinityfor the glycoside, and K+ tends to antagonizedigitalis induced enhanced automaticity. Whentoxicity is due to acute ingestion of large dosesof digoxin, plasma K+ may be high; it shouldnot be given from outside. In any case, it isdesirable to measure serum K+ to guide KCltherapy. K+ is contraindicated if higher degreeof A-V block is present, because completeA-V block and ventricular asystole may beprecipitated.
(b) For ventricular arrhythmias Lidocaine i.v.repeated as required is the drug of choice. Itsuppresses the excessive automaticity, but doesnot accentuate A-V block. Quinidine, procaina-mide and propafenone are contraindicated.
(c) For supraventricular arrhythmiasPropranolol may be given i.v. or orally dependingon the urgency.
(d) For A-V block and bradycardia Atropine0.6–1.2 mg i.m. may help; otherwise cardiacpacing is recommended.
Cardioversion by DC shock is contraindicated becausesevere conduction defects may be unmasked in the digitalisintoxicated heart. Attempts to enhance the elimination ofdigoxin by diuretics or haemodialysis are not very effective.
Digoxin antibody Developed for measuring plasmaconcentration of digoxin by radioimmunoassay, it has beenfound effective in treating toxicity as well. Digoxin specificantibody crossreacts with digitoxin also. The Fab fragmenthas been marketed in Europe as DIGIBIND (38 mg vial).It is nonimmunogenic because it lacks the Fc fragment. Givenby i.v. infusion it has markedly improved the survival ofseriously digitalis intoxicated patients. The digoxin-Fabcomplex is rapidly excreted by kidney.
PRECAUTIONS AND CONTRAINDICATIONS
(a) Hypokalemia: enhances digitalis toxicity.(b) Elderly, renal or severe hepatic disease: patients aremore susceptible to digoxin toxicity.

517C
HA
PTE
R37
CARDIAC GLYCOSIDES AND DRUGS FOR HEART FAILURE
(c) Myocardial ischaemia: severe arrhythmias are morelikely.(d) Thyrotoxicosis: patients are more prone to developdigitalis arrhythmias.(e) Myxoedema: these patients eliminate digoxin moreslowly; cumulative toxicity can occur.(f) Ventricular tachycardia: digitalis is contraindicatedbecause it may precipitate ventricular fibrillation.(g) Partial A-V block: may be converted to completeA-V block by digoxin.(h) Acute myocarditis: Diphtheria, acute rheumatic carditis,toxic carditis—inotropic response to digitalis is poor, moreprone to arrhythmias.(i) Wolff-Parkinson-White syndrome: Digitalis is con-traindicated because it decreases the ERP of bypass tractin 1/3 patients. In them rapid atrial impulses may be trans-mitted to ventricles → VF may occur. Digitalis can increasethe chances of reentry by slowing conduction in the normalA-V bundle and accelerating it in the aberrant pathway.
INTERACTIONS
1. Diuretics: cause hypokalemia which increases the riskof digitalis arrhythmias; potassium supplements should begiven prophylactically.2. Calcium: synergises with digitalis → precipitates toxicity.3. Quinidine: reduces binding of digoxin to tissue proteinsas well as its renal and biliary clearance by inhibiting effluxtransporter P-glycoprotein → plasma concentration of digoxinis doubled → toxicity can occur. Verapamil, diltiazem,captopril, propafenone and amiodarone also increase plasmaconcentration of digoxin to variable extents.4. Adrenergic drugs: can induce arrhythmias in digitalizedpatients; both increase ectopic automaticity.5. Digoxin absorption may be reduced by metoclopramide,sucralfate, antacids, neomycin, sulfasalazine. Absorption ofdigoxin is increased by atropinic drugs, including tricyclicantidepressants.6. Propranolol, verapamil, diltiazem and disopyramide:may additively depress A-V conduction and oppose positiveinotropic action.7. Succinylcholine: can induce arrhythmias in digitalizedpatients.
USES
The two main indications of digitalis are CHFand control of ventricular rate in atrial fibrilla-tion/flutter.
1. Congestive heart failureCHF occurs when cardiac output is insufficientto meet the demands of tissue perfusion or does
so by elevating filling pressure. Heart failure mayprimarily be due to systolic dysfunction ordiastolic dysfunction.
Systolic dysfunction The ventricles are dilatedand unable to develop sufficient wall tension toeject adequate quantity of blood. This occurs inischaemic heart disease, valvular incompetence,dilated cardiomyopathy, myocarditis, tachyarrhy-thmias (mostly atrial fibrillation).
Diastolic dysfunction The ventricular wall isthickened and unable to relax properly duringdiastole; ventricular filling is impaired becauseof which output is low. It occurs in sustainedhypertension, aortic stenosis, congenital heartdisease, A-V shunts, hypertrophic cardiomyopathy.
However, most patients, especially long-standing CHF, have both systolic and diastolicdysfunction. Cardiac glycosides afford only symp-tomatic relief, primarily in systolic dysfunction.Best results are obtained when myocardium isnot primarily deranged, e.g. in hypertension,valvular defects or CHF due to rapid heart ratein atrial fibrillation. Poor response and moretoxicity is likely when the myocardium has beendamaged by ischaemia, inflammation ordegenerative changes and in thiamine deficiency,as well as in high output failure (in anaemia).Cardiac glycosides are incapable of reversing the pathologicalchanges of CHF or even arresting their progress. Associatedwith hypertrophy, cardiac muscle undergoes remodeling whichmay involve changes in various functional proteins suchas myosin, creatine kinase, Na+K+ATPase, matrix components,etc. as a result of altered myocyte gene function. Cardiacglycosides do not affect remodeling.
Because of lower inotropic state, the failingheart is able to pump much less blood at thenormal filling pressure (Fig. 37.4), more bloodremains in the ventricles at the end of systole.The venous return is added to it and Frank-Starlingcompensation is utilized to increase fillingpressure: the heart may be able to achieve therequired stroke volume, but at a filling pressurewhich produces congestive symptoms (venousengorgement, edema, enlargement of liver,pulmonary congestion → dyspnoea, renalcongestion → oliguria).

518S
EC
TIO
N8
CARDIOVASCULAR DRUGS
Fig. 37.4: Relationship between filling pressure andcardiac output in normal and failing heart. Digitalis tendsto shift the curve towards normal
Digitalis induced enhancement of contractilityincreases ventricular ejection and shifts the curverelating stroke output to filling pressure towardsnormal, so that adequate output may be obtainedat a filling pressure that does not produce conges-tive symptoms. Improved tissue perfusion resultsin withdrawal of sympathetic overactivity → heartrate and central venous pressure (CVP) are loweredtowards normal. Compensatory mechanisms retain-ing Na+ and water are inactivated, diuresis occursand edema is cleared. Liver regresses, pulmonarycongestion is reduced → dyspnoea abates, cyanosisdisappears. Low output symptoms like decreasedcapacity for muscular work are mitigated.
A dilated ventricle automatically becomesinefficient according to Laplace equation.
Wall tension = Intraventricular pressure ×ventricular radius
i.e. to generate the same ejection pressure a dilatedventricle has to develop higher wall tension. Byreducing end diastolic volume (due to betteremptying), digitalis restores efficiency oftranslation of cardiac work into cardiac output.That is why O2 consumption does not increaseproportionately.
Dosage In mild to moderate heart failure, digoxin therapyis now initiated with the estimated maintenance doses (0.125–0.25 mg/day) without any loading dose. Full response takes5–7 days to develop when steady-state is reached. In caseof inadequate response, the dose is increased to 0.375 and0.5 mg/day at weekly intervals. Reduction in heart rate andrelief of heart failure symptoms are the best guide to dosing.
If an early response is required, a loading dose of0.75–1.25 mg spread over 24–48 hours may be given in thebeginning, but requires close monitoring. Intravenous digoxinis seldom required now for CHF. When imperative 0.25 mgmay be injected slowly with continuous ECG, BP and CVPmonitoring.
There is some recent evidence that maintenance therapywith sub-maximal inotropic doses (producing steady-stagedigoxin levels < 1 ng/ml) may benefit by counteractingneurohumoral activation of CHF, without risk of toxicity.
Current status of digitalis Before the intro-duction of high ceiling diuretics, ACE inhibitorsand β blockers, digitalis was considered anindispensible part of anti-CHF treatment. It is notso now. Many mild-to-moderate cases aremanaged without digitalis. Now ACE inhibitors/ARBs, β adrenergic blockers and diuretics arethe standared treatment. However, digitalis is stillthe most effective drug capable of relievingsymptoms of CHF and restoring cardiaccompensation, especially in patients with dilatedheart and low ejection fraction. All patients whoremain symptomatic even while receiving ACEinhibitor/ARB, β blocker and diuretic should betreated with digitalis. Uncertainty exists in thearea of maintenance therapy, i.e. after decom-pensation has been corrected in patients with sinusrhythm and not having atrial fibrillation (AF).Two large trials—Randomized assessment of digoxin oninhibition of angiotensin converting enzyme (RADIANCE,1993) and Prospective randomized study of ventricular failureand efficacy of digoxin (PROVED, 1993) on CHF patientsin sinus rhythm showed that discontinuation of digitalisresulted in reduced exercise capacity and haemodynamicdeterioration in a significant number of cases despitecontinued use of diuretic with or without ACE inhibitor.However, digitalis could be withdrawn without haemodynamicdeterioration in 60% (not receiving ACE inhibitor) and in72% (receiving ACE inhibitor) patients.
Thus, if stable clinical state has been main-tained for 2–3 months, withdrawal of digitalismay be attempted. Early reinstitution of digitalisis recommended if cardiac status declines.

519C
HA
PTE
R37
CARDIAC GLYCOSIDES AND DRUGS FOR HEART FAILURE
Continued digitalis therapy is the best course inCHF patients with atrial fibrillation who needventricular rate control.
Large studies including those by DigoxinInvestigation Group (DIG) have found no evidencethat digitalis decreases overall mortality in CHFpatients, though episodes of decompensation andheart failure deaths are reduced. The two majorlimitations in the use of cardiac glycosides arelow margin of safety and lack of effect on neuro-humoral contributors to pathogenesis of CHF.
2. Cardiac arrhythmiasAtrial fibrillation (AF) Digitalis is used forcontrolling ventricular rate in AF, whetherassociated with CHF or not. However, it isincapable of curing AF, i.e. does not revert itto sinus rhythm, even perpetuates it.
Digitalis reduces ventricular rate in AF bydecreasing the number of impulses that are ableto pass down the A-V node and bundle of His.(a) It increases ERP of A-V node by direct,vagomimetic and antiadrenergic actions: theminimum interval between consecutive impulsesthat can successfully traverse the conducting tissueis increased.(b) Because of the relatively long ERP of A-Vnode, many of the atrial impulses (~500/min)falling in the relative refractory period getextinguished by decremental conduction. Theseconcealed impulses, nevertheless, leave the uppermargin of A-V node refractory for a further period.Digoxin increases the number of concealedimpulses and indirectly prolongs the intervalbetween any two impulses that are successfullyconducted to the ventricle.
When digoxin is given in AF, averageventricular rate decreases in a dose-dependentmanner and pulse deficit is abolished. It isparticularly effective in controlling ventricular rateat rest, but has less effect during exercise. Thus,it is preferred in sedentary patients. For physicallyactive patients, β blockers/verapamil/diltiazemprovide better rate control. If a single drug failsto decrease the heart rate to the desired level,
one out of propranolol/verapamil/diltiazem maybe combined with digoxin.
Atrial flutter (AFI) The atrial rate is 200–350/min (less than that in AF), but atrial contractionsare regular and synchronous. A variable degreeof A-V block, depending on the mean ERP ofA-V node, is naturally established. Digitalisenhances this A-V block, reduces ventricular rateand prevents sudden shift of A-V block to a lowerdegree. Ventricular rate control in AFl is generallyan interim measure before it is abolished bycardioversion/radiofrequency ablation/anti-arrhythmic drugs, or when definitive therapy isnot possible. For rate control, a β blocker/verapamil/diltiazem are mostly used. Digoxin isemployed in patients with CHF, or as an addondrug in case of inadequate rate control with βblocker, etc. Digitalis may convert AFl to AFby reducing atrial ERP and making it inhomo-geneous. This is a welcome response becausecontrol of ventricular rate is easier in AF (gradedresponse occurs) than in AFl (A-V block shiftsin steps).
Paroxysmal supraventricular tachycardia(PSVT) It is a common arrhythmia with arate 150–200/min and 1 : 1 A-V conduction. Itis mostly due to reentry involving the SA orA-V node. A parenteral glycoside may be injectedi.v.—increases vagal tone and depresses the paththrough the SA/A-V node, or the ectopic focus,and terminates the arrhythmia (success in 1/3cases). Adenosine and verapamil are moreeffective, less toxic and act faster. Digitalis is nowreserved for preventing recurrences in selectedcases.
TREATMENT OF CHF
There are two distinct goals of drug therapy inCHF:
(a) Relief of congestive/low output symptomsand restoration of cardiac performance. Thiscan be achieved by:Inotropic drugs—Digoxin, dobutamine/dopamine, amrinone/milrinone

520S
EC
TIO
N8
CARDIOVASCULAR DRUGS
Diuretics—Furosemide, thiazidesRAS inhibitors—ACE inhibitors/ARBsVasodilators—hydralazine, nitrate,
nitroprussideβ blocker—Metoprolol, bisoprolol,
carvedilol, Nebivolol(b) Arrest/reversal of disease progression and
prolongation of survival, possible with:ACE inhibitors/ ARBs, β blockersAldosterone antagonist—Spironolactone,
eplerenoneImportant nonpharmacological measures are restand salt restriction.
Rest reduces peripheral needs, but should be advisedonly till compensation is restored, beyond that it may lowermyocardial reserve and be counterproductive. Salt restrictionlimits edema formation and is advised in all grades of CHF.The underlying cause of CHF, if treatable like hypertension,myocardial ischaemia, valvular defects, A-V shunts,arrhythmias, thyrotoxicosis, anaemia, should be corrected.
Till 1980 drugs available for CHF (digitalis and diuretics)addressed only the consequences of CHF, but not its genesis.As such, these drugs while affording symptomatic relief,did not modify the course of CHF. Drugs developed thereafter(ACE inhibitors/ARBs, β adrenergic blockers, aldosteroneantagonists, etc.) impact the neurohumoral perpetrators ofCHF, myocardial apoptosis, fibrosis, matrix abnormalities,etc. in addition to haemodynamic effects, and have becomethe primary therapeutic modality.
The pathophysiological mechanisms thatperpetuate heart failure and contribute to diseaseprogression, along with site of drug action aredepicted in Fig. 37.5. The current pattern of useof drugs in various stages of heart failure issummarized in Fig. 37.6.
DiureticsAlmost all cases of symptomatic CHF are treatedwith a diuretic. High ceiling diuretics (furosemide,bumetanide) are the diuretics of choice formobilizing edema fluid; later they may becontinued in low doses. In advanced CHF afterchronic use, resistance may develop to even highceiling diuretics. Addition of a thiazide/metolazone/spironolactone to furosemide mayovercome the resistance. Thiazide alone has verylimited role in CHF. Diuretics:(a) Decrease preload and improve ventricularefficiency by reducing circulating volume.(b) Remove peripheral edema and pulmonarycongestion.
Intravenous furosemide promptly increasessystemic venous capacitance and produces rapidsymptomatic relief in acute left ventricular failure.It has, in conjunction with vasodilators, virtually
Fig. 37.5: The vicious cycle in CHF: compensatory mechanisms evoked in response to reduced cardiac outputthemselves perpetuate failure and contribute to remodeling responsible for disease progression. The parameterwhich is improved by different therapeutic measures is indicated

521C
HA
PTE
R37
CARDIAC GLYCOSIDES AND DRUGS FOR HEART FAILURE
Fig. 37.6: Current pattern of clinical use of various classes of drugs in different stages of heart failure (HF)LVD—Left ventricular dysfunction; ACE—Angiotensin converting enzyme; ARB—Angiotensin receptor blocker
obviated the need for i.v. digitalization. Further,most mild cases can be maintained symptom freeon diuretics without recourse to chronic digitalistherapy. However, diuretics have no role inasymptomatic left ventricular dysfunction, andbrisk diuresis can worsen some cases whosecardiac output is critically dependent uponvolume overload. They do not influence thedisease process in CHF, though they maydramatically improve symptoms. Despite decadesof experience, no prognostic benefit has beendemonstrated for diuretics. On the other hand,they may cause activation of RAS (if hypovolemiaoccurs) which has adverse cardiovascularconsequences. Chronic diuretic therapy tends tocause hypokalaemia, alkalosis and carbohydrateintolerance. Current opinion is to treat mild heartfailure with ACE inhibitors/ARBs ± β blockersonly, because they afford survival benefit, whilediuretics may be added intermittently for symptomrelief. Chronic diuretic therapy should be reservedfor relatively advanced cases with tendency tofluid retention when diuretic is stopped. Doseshould be titrated to the lowest that will check
fluid retention, but not cause volume depletionto activate RAS.
Renin-angiotensin system (RAS) inhibitorsSince RAS activation is pivotal to developmentof symptoms and disease progression in CHF, theACE inhibitors and ARBs are the sheet anchorof drug therapy in CHF (see p. 504 and 507).They afford symptomatic as well as diseasemodifying benefits in CHF by causing vasodila-tation, retarding/preventing ventricular hyper-trophy, myocardial cell apoptosis, fibrosisintercellular matrix changes and remodeling. Inaddition to decreasing Ang II production, ACEinhibitors raise the level of kinins which stimulategeneration of cardioprotective NO and PGs.Symptomatic and prognostic benefits of ACEinhibitors/ARBs have been established in mild tosevere (NYHA class I to IV) CHF as well as insubjects with asymptomatic systolic dysfunction.They are thus recommended for all grades of CHF,unless contraindicated, or if renal functiondeteriorates by their use (mainly in those withdecresed renal blood flow/renal artery stenosis).

522S
EC
TIO
N8
CARDIOVASCULAR DRUGS
ACE inhibitor therapy is generally started atlow doses which are gradually increased to obtainmaximum benefit or to near the highest recom-mended doses.
VasodilatorsVasodilators were first used i.v. to treat acute heartfailure that occurs in advanced cases or followingMI, and serve to tide over crisis. Their use byoral route has been extended to long-term therapyof chronic CHF, but vasodilators other than ACEinhibitors/ARBs have only limited utility.Vasodilators with differing profiles of arteriolarand venodilator action are available (see box).
(i) Preload reduction: Nitrates cause poolingof blood in systemic capacitance vessels to reduceventricular end-diastolic pressure and volume.With reduction in size of ventricles, effectivenessof myocardial fibre shortening in causing ejectionof blood during systole improves (Laplacerelationship). Controlled i.v. infusion of glyceryltrinitrate affords rapid relief in acute left ventri-cular failure, particularly that due to myocardialischaemia/infarction. It is indicated when thecentral venous pressure (CVP) is raised and indilated cardiomyopathy. However, lowering ofpreload (by vasodilators + strong diuretics) beyonda limit may reduce output of a failing heart whoseperformance is dependent upon elevated fillingpressure. Occurrence of nitrate tolerance limitstheir utility in routine treatment of CHF.(ii) Afterload reduction Hydralazine dilatesresistance vessels and reduces aortic impedanceso that even weaker ventricular contraction is ableto pump more blood; systolic wall stress isreduced. It is effective in forward failure whencardiac index (CI = min output/body surface area)is low (< 2.5 L/min/m2) without a marked increasein CVP (< 18 mm Hg). Marked tachycardia,worsening of myocardial ischaemia and fluidretention limit long-term use of hydralazinemonotherapy.
Minoxidil is a more potent arteriolar dilator, but hasfound little use in heart failure; so has nicorandil a morespecific pot. channel opener. Trials of the three prototypecalcium channel blockers verapamil, diltiazem and nifedipine
in systolic dysfunction have been disappointing, even negativewith occasional worsening of symptoms and increase inmortality. This may be due to reflex sympathetic activation(nifedipine) or negative inotropic property (verapamil,diltiazem). Verapamil, however, is useful in diastolicdysfunction due to hypertrophic cardiomyopathy. Trials withlong-acting and more vasoselective dihydropyridines(felodipine, amlodipine) have also not been encouraging.
(iii) Pre- and after load reduction Sod. nitro-prusside is a high efficacy i.v. dilator with equalaction on the two types of vessels. It acts byboth the above mechanisms, i.e. reducesventricular filling pressure as well as systemicvascular resistance. Cardiac output and renal bloodflow are increased. The action is very fast andbrief. Titrated i.v. infusion of nitroprusside isemployed in conjunction with a loop diuretic +i.v. inotropic drug to tideover crisis in severelydecompensated patients. For symptomatictreatment of acute heart failure, choice of i.v.vasodilator (glyceryl trinitrate or hydralazine ornitroprusside) depends on the primary haemo-dynamic abnormality in individual patients.
In the long term oral therapy, survival benefithas been obtained only with a combination ofhydralazine + isosorbide dinitrate, but the ACEinhibitors and ARBs are clearly superior in thisregard. Hydralazine causes more marked renal
Venodilators Route(primarily ↓↓↓↓↓ preload) (for CHF)
Glyceryl trinitrate s.l./i.v.Isosorbide dinitrate s.l./oral
Arteriolar dilators(primarily ↓↓↓↓↓ afterload)
Pot. channel openersHydralazine oral/i.v.Minoxidil i.v.Nicorandil _
Cal. channel blockers _
Mixed dilators(↓↓↓↓↓ pre- and afterload)
ACE inhibitors oralARBs (AT1 receptor antagonists) oralα1 blocker (Prazosin) —PDE 3 inhibitors
Amrinone, Milrinone i.v.Nitroprusside sod. i.v.

523C
HA
PTE
R37
CARDIAC GLYCOSIDES AND DRUGS FOR HEART FAILURE
vasodilatation. Along with isosorbide dinitrate itmay be selected for patients with renal insuffi-ciency, low renal blood flow or renal arterystenosis, who cannot tolerate ACE inhibitors orARBs. Hydralazine alone or a nitrate alone havenot proven useful in the treatment of chronic heartfailure. However, when combined they supplementeach other and nitrate tolerance is attenuated byhydralazine. Severe CHF patients alreadyreceiving ACE inhibitors + digoxin + diuretic haveobtained extra benefit from addition of hydra-lazine with or without a nitrate.
For reasons not known, the α1 blocker prazosin hasnot been able to afford prognostic benefit.
βββββ-Adrenergic blockersExtensive studies over the past 30 years haveestablished the utility of β1 blockers (mainlymetoprolol, bisoprolol, nebivolol) and thenonselective β + selective α1 blocker carvedilolin mild to moderate CHF treated with ACEinhibitor ± diuretic, digitalis.
A large number of randomized trials including Metoprololin dilated cardiomyopathy trial (1993), US carvedilol trial(1996), MERIT-HF trial (1999), CIBIS-II trial (1999),CAPRICORN trial (2001), COPERNICUS trial (2002) havedemonstrated subjective, objective, prognostic and mortalitybenefits of the above named β blockers over and above thatafforded by ACE inhibitors + diuretic ± digitalis.
Though the immediate hemodynamic actionof β blockers is to depress cardiac contractilityand ejection fraction, these parameters graduallyimprove over weeks. After a couple of monthsejection fraction is generally higher than baseline,and slow upward titration of dose further improvescardiac performance. The hemodynamic benefitis maintained over long-term and hospitalization/mortality due to worsening cardiac failure, as wellas all cause mortality is reduced. The benefitsappear to be due to antagonism of ventricularwall stress enhancing, apoptosis promoting andpathological remodeling effects of excesssympathetic activity (occurring reflexly) in CHF,as well as due to prevention of sinister arrhythmias.Incidence of sudden cardiac death as well as thatdue to worsening CHF is decreased. β blockerslower plasma markers of activation of sympathetic,renin-angiotensin systems and endothelin-1.
However, β blocker therapy in CHF requirescaution, proper patient selection and observanceof several guidelines:• Greatest utility of β blockers has been
shown in mild to moderate (NYHA class II,III) cases of dilated cardiomyopathy withsystolic dysfunction in which they arenow routinely coprescribed unless contraindi-cated.
• Encouraging results (upto 35% decrease inmortality) have been obtained in class IV casesas well, but use in severe failure could be riskyand needs constant monitoring.
• There is no place for β blockers in decompen-sated patients. β blockers should be stoppedduring an episode of acute heart failure andrecommenced at lower doses followed byuptitration after compensation is retored.Conventional therapy should be continuedalong with them.
• Starting dose should be very low—then titratedupward as tolerated to the target level(carvedilol 50 mg/day, bisoprolol 10 mg/day,metoprolol 200 mg/day) or near it, formaximum protection.
• In few patients any attempt to introduce aβ blocker results in worsening of heartfailure. β blockers should not be used in suchpatients.
• A long-acting preparation (e.g. sustained releasemetoprolol) or 2–3 times daily dosing toproduce round-the-clock β blockade should beselected.
• There is no evidence of benefit in asymptomaticleft ventricular dysfunction.
Aldosterone antagonist(Spironolactone, Eplerenone)
Over the past 2 decades it has been realized thatrise in plasma aldosterone in CHF, in additionto its well known Na+ and water retaining action,is an important contributor to disease progressionby direct and indirect effects:(a) Expansion of e.c.f. volume → increasedcardiac preload.

524S
EC
TIO
N8
CARDIOVASCULAR DRUGS
(b) Fibroblast proliferation and fibrotic changein myocardium → worsening systolic dysfunctionand pathological remodeling.(c) Hypokalemia and hypomagnesemia →increased risk of ventricular arrhythmias andsudden cardiac death.(d) Enhancement of cardiotoxic and remodelingeffect of sympathetic overactivity.
The aldosterone antagonist spironolactone isa weak diuretic (see Ch. 41), but can benefit CHFby antagonizing the above effects of aldosterone.
In addition to several small studies, a large Randomisedaldactone evaluation study (RALES, 1999) conducted on1663 NYHA class III and IV patients having left ventricularejection fraction < 35% has confirmed the additional survivalbenefit (30%) of spironolactone when added to conventionaltherapy with ACE inhibitors + other drugs. A subsequenttrial (EPHESUS, 2003) using another aldosterone antagonisteplerenone in post acute MI heart failure has furthersubstantiated the mortality and anti-remodeling benefit overand above that of ACE inhibitors ± β blockers.
Though ACE inhibitors themselves loweraldosterone levels, this effect is incomplete andshort lasting. Current evidence suggests thefollowing regarding spironolactone/eplerenonetherapy in CHF:• It is indicated as add-on therapy to ACE
inhibitors + other drugs in moderate-to-severeCHF.
• It can retard disease progression, reduceepisodes of decompensation and death due toheart failure as well as sudden cardiac deaths,over and above the protection afforded by ACEinhibitors/ARBs ± β blockers.
• Only low doses (12.5–25 mg/day) of spiro-nolactone should be used to avoid hyper-kalaemia; particularly because of concurrentACE inhibitor/ARB therapy.
• It may help restoration of diuretic responseto furosemide when refractoriness hasdeveloped.The onset of benefit of aldosterone/antagonist
in CHF is slow. It is contraindicated in renalinsufficiency because of risk of hyperkalemia—requires serum K+ monitoring. Gynaecomastiaoccurs in a number of male patients treated withspironolactone. This can be avoided by usingeplerenone. Aldosterone antagonists are a
significant additional therapeutic measure inmoderate-severe CHF with prognostic benefits.
Sympathomimetic inotropic drugs(see Ch. 9)
Drugs with β adrenergic and dopaminergic D1agonistic actions have positive inotropic and (atlow doses) vasodilator properties which may beutilized to combat emergency pump failure.
Dobutamine (2–8 μg/kg/min) a relativelyselective β1 agonist with prominent inotropicaction is the preferred drug for i.v. infusion inacute heart failure accompanying myocardialinfarction (MI), cardiac surgery as well as to tideover crisis in advanced decompensated CHF.
Dopamine (3–10 μg/kg/min by i.v. infusion)has been used in cardiogenic shock due to MIand other causes. While dobutamine does not raise(may lower) systemic vascular resistance and ispreferred in heart failure, dopamine tends toincrease afterload, especially at higher rates ofinfusion (>5 μg/kg/min) and has limited utilityin patients who are not in shock. Low rates ofdopamine infusion (~2 μg/kg/min) cause selectiverenal vasodilatation (D1 agonistic action) whichimproves renal perfusion and g.f.r. This can restorediuretic response to i.v. furosemide in refractoryCHF.
These drugs afford additional haemodynamicsupport over and above vasodilators, digitalis anddiuretics, but benefits are short-lasting. Due todevelopment of tolerance and cardiotoxic potentialwhen used regularly, these drugs have no rolein the long-term management of CHF.
Phosphodiesterase 3 inhibitorsTheophylline is a phosphodiesterase inhibitor that is non-selective for different isoforms of this enzyme which degradesintracellular cAMP and cGMP. Intravenous aminophyllinehad been used in past for acute left ventricular failure withlimited benefits, but unacceptable toxicity.
Inamrinone (amrinone) It is chemically and pharmacolo-gically distinct from digitalis and catecholamines. Thisbipyridine derivative is a selective phosphodiesterase 3(PDE3) inhibitor. The PDE3 isoenzyme is specific forintracellular degradation of cAMP in heart, blood vessels

525C
HA
PTE
R37
CARDIAC GLYCOSIDES AND DRUGS FOR HEART FAILURE
and bronchial smooth muscles. Amrinone increases myocardialcAMP and transmembrane influx of Ca2+. It does not inhibitNa+K+ATPase, and its action is independent of tissuecatecholamines as well as adrenergic receptors.
The two most important actions of amrinone are positiveinotropy and direct vasodilatation: has been called an‘inodilator’. Both preload and afterload on the heart is reduced.Compared to dobutamine, proportionately greater decreasein systemic vascular resistance is noted.
In CHF patients i.v. amrinone action starts in 5 minand lasts 2–3 hours; elimination t½ is 2–4 hours. It increasescardiac index, left ventricular ejection fraction and decreasesperipheral vascular resistance, CVP, left ventricular enddiastolic volume and pressure accompanied by mildtachycardia and slight fall in BP.
Adverse effects Thrombocytopenia is the most prominentand dose related side effect, but is mostly transient andasymptomatic.Nausea, diarrhoea, abdominal pain, liver damage, fever andarrhythmias are the other adverse effects.
Use Though amrinone is active orally, its oral use in main-tenance therapy of CHF has been abandoned, because efficacywas lost and mortality was increased in comparison to placebo.
It is indicated only for short-term i.v. use in severe andrefractory CHF, as an additional drug to conventional therapywith digitalis, diuretics and vasodilators.Dose: 0.5 mg/kg bolus injection followed by 5–10 µg/kg/min i.v. infusion (max. 10 mg/kg in 24 hours). AMICOR,CARDIOTONE 5 mg/ml (as lactate) 20 ml amp.
Milrinone Related to inamrinone, it has similaraction but is more selective for PDE3, and isat least 10 times more potent. It is shorter-actingwith a t½ of 40–80 min.
Thrombocytopenia is not significant. In longterm prospective trials, increased mortality hasbeen reported with oral milrinone also. Milrinoneis preferred over amrinone and should be restrictedto short-term use only.Dose: 50 µg/kg i.v. bolus followed by 0.4–1.0 µg/kg/mininfusion.PRIMACOR IV 10 mg/10 ml inj.
Nesiritide This recombinant brain natriuretic peptide(BNP) has been approved for i.v. use to relieve dyspnoeaand other symptoms in refractory CHF. It enhances salt andwater excretion and is a potent vasodilator with profile ofaction similar to i.v. glyceryl trinitrate; reduces ventricularfilling pressure. Additional haemodynamic and symptomaticimprovement can be obtained for short-periods, but no long-term benefits are evident in CHF.
Tolvaptan This is an orally active nonpeptide vasopressinV2 receptor antagonist introduced recently for the correction ofwater retention and hyponatremia occurring in ‘syndrome ofinappropriate ADH secretion’ (SIADH) as well as in advancedCHF. In clinical trials on CHF patients with hyponatremia,tolvaptan has afforded short-term improvement by increasingwater excretion, restoring serum Na+ and relieving dyspnoea.However, no long-term benefits have been noted.
PROBLEM DIRECTED STUDY
37.1 A 72-year-old man presents with swelling over ankle and feet, also noticeable over facein the morning, shortness of breath and palpitation on walking ~100 m, weakness, fatigue andcough at night. The pulse is 110/min, BP 114/78 mm Hg, there is pitting edema over feet, liveris enlarged 2 cm below costal margin, neck veins are filled upto 3 cm above clavicle, crepitationsare heard at the base of lungs, apex beat is in the 6th intercostal space and heart sounds aremuffled. Chest X-ray and echocardiography show enlarged cardiac shadow and an ejection fractionof 28%. A diagnosis of moderate grade congestive heart failure due to dilated cardiomyopathyis made. The doctor prescribed bed rest, salt restriction and:
Tab enalapril 5 mg twice a dayTab furosemide 40 mg in the morning
(a) Can the patient be prescribed any other drug to hasten relief of symptoms? If so, whichdrug and in what dosage?(b) Should the dose of enalapril be changed over time or should it be withdrawn, if so when?(c) Should a β adrenergic blocking drug be added to the treatment regimen concurrently?(see Appendix-1 for solution)

Antiarrhythmic DrugsChapterChapterChapterChapterChapter 3838383838
These are drugs used to prevent or treat irregula-rities of cardiac rhythm.
Nearly 3 out of 4 patients of acute myocardialinfarction (MI) and about half of those given ageneral anaesthetic exhibit at least someirregularity of cardiac rhythm. Arrhythmias arethe most important cause of sudden cardiac death.However, only few arrhythmias need to be treatedwith antiarrhythmic drugs.
Abnormal automaticity or impaired conduc-tion or both underlie cardiac arrhythmias. Thegeneration and propagation of cardiac impulseand properties of excitability and refractorinessare described on p. 492 to 494. Ischaemia,electrolyte and pH imbalance, mechanical injury,stretching (due to heart failure), neurogenic anddrug influences, including antiarrhythmic drugsthemselves, can cause arrhythmias by alteringelectrophysiological properties of cardiac fibres.
Important mechanisms of cardiac arrhythmias are:A. Enhanced/ectopic pacemaker activity The slopeof phase-4 depolarization may be increased pathologicallyin the automatic fibres or such activity may appear in ordinary
fibres. Ectopic impulse may also result from current of injury.Myocardial cells damaged by ischaemia become partiallydepolarized: a current may flow between these and normallypolarized fibres (injury current) and initiate an impulse.B. After-depolarizations These are secondary depola-rizations accompanying a normal or premature action potential(AP), Fig. 38.1.
Early after-depolarization (EAD) Repolarization duringphase-3 is interrupted and membrane potential oscillates. If theamplitude of oscillations is sufficiently large, neighbouringtissue is activated and a series of impulses are propagated.EADs are frequently associated with long Q-T interval due toslow repolarization and markedly prolonged APs. They resultfrom depression of delayed rectifier K+ current.
Delayed after-depolarization (DAD) After attaining restingmembrane potential (RMP) a secondary deflection occurswhich may reach threshold potential and initiate a singlepremature AP. This generally results from Ca2+ overload(digitalis toxicity, ischaemia-reperfusion).
Because an AP is needed to trigger after-depolarizations,arrhythmias based on these have been called triggeredarrhythmias.
C. Reentry Due primarily to abnormality of conduction,an impulse may recirculate in the heart and cause repetitiveactivation without the need for any new impulse to begenerated. These are called reentrant arrhythmias.
Fig. 38.1: Action potential in a nonautomatic ventricular fibre (in red) followed by early or delayed after-depolarizations.

527C
HA
PTE
R38
ANTIARRHYTHMIC DRUGS
(i) Circus movement reentry It occurs in an anatomicallydefined circuit. A premature impulse, temporarily blockedin one direction by refractory tissue, makes a one-way transitaround an obstacle (natural orifices in the heart, A-V nodalregion) or through an abnormal tract, finds the original spotin an advanced state of recovery and reexcites it, settingup recurrent activation of adjacent myocardium (Fig. 38.2).This type of reentry is often responsible for PSVT, atrialflutter and atrioventricular reciprocal rhythm in WPW.
Reentry occurring in an anatomically fixed circuit canbe permanently cured by radiofrequency catheter ablationof the defined pathway.
(ii) Functional reentry In this type of reentry there is nofixed ‘obstacle’ or ‘pathway’. Rather, a functional obstacle(core of the circuit) and unidirectional conduction pathway iscreated by a premature impulse which travels through electro-physiologically inhomogeneous myocardium. On encounteringrefractory tissue in one direction, the wavefront travels throughpartially recovered fibres—gets markedly slowed and can setup small reentry circuits which may constantly shift location.Functional reentry may be responsible for ventricular extra-systoles, polymorphic ventricular tachycardia, atrial/ventricularfibrillation.
(iii) Fractionation of impulse When atrial ERP is brief andinhomogeneous (under vagal overactivity), an impulse generatedearly in diastole gets conducted irregularly over the atrium,i.e. it moves rapidly through fibres with short ERP (whichhave completely recovered) slowly through fibres with longerERP (partially recovered) and not at all through those stillrefractory. Thus, asynchronous activation of atrial fibres occurs→ atrial fibrillation (AF). This arrhythmia must be initiatedby a premature depolarization, but is self sustaining, becausepassage of an irregular impulse leaves a more irregular refractorytrace and perpetuates the inhomogeneity of ERPs.
The important cardiac arrhythmias are:1. Extrasystoles (ES) are premature ectopic
beats due to abnormal automaticity or after-depolarization arising from an ectopic focusin the atrium (AES), A-V node (nodal ES)or ventricle (VES). The QRS complex in VESis broader and abnormal in shape.
2. Paroxysmal supraventricular tachycardia(PSVT) is sudden onset episodes of atrialtachycardia (rate 150–200/min) with 1:1atrioventricular conduction: mostly due tocircus movement type of reentry occurringwithin or around the A-V node or using anaccessory pathway between atria and ventricle(Wolff-Parkinson-White syndrome or WPW).
3. Atrial flutter (AFI) Atria beat at a rate of 200–350/min and there is a physiological 2:1 to4:1 or higher A-V block (because A-V nodecannot transmit impulses faster than 200/min).This is mostly due to a stable re-entrant circuitin the right atrium, but some cases may bedue to rapid discharge of an atrial focus.
4. Atrial fibrillation (AF) Atrial fibres are activa-ted asynchronously at a rate of 350–550/min(due to electrophysiological inhomogeneity ofatrial fibres), associated with grossly irregularand often fast (100–160/min) ventricularresponse. Atria remain dilated and quiver likea bag of worms.
5. Ventricular tachycardia (VT) is a run of 4or more consecutive ventricular extrasystoles.It may be a sustained or nonsustainedarrhythmia, and is due either to discharges froman ectopic focus, after-depolarizations or singlesite (monomorphic) or multiple site(polymorphic) reentry circuits.
Fig. 38.2: Diagrammatic depiction of circus movementreentry in atrium
For reentry to occur, the path length of the circuit shouldbe greater than the wave length (ERP × conduction velocity)of the impulse. Slow conduction in the reentrant circuit maybe caused by:(a) Partial depolarization of the membrane—decreased slopeof phase 0 depolarization, i.e. depressed fast channel response.(b) Cells changing over from fast channel to slow channeldepolarization which conducts extremely slowly. When a fibreis depolarized to a RMP of about –60 mv, the Na+ (fast)channels are inactivated, but the fibre can still develop Ca2+
(slow) channel response.Reentry can be abolished both by marked slowing of
conduction (converting unidirectional block to bidirectionalblock) as well as by acceleration of impulse (retrogradeimpulse reaches so early as to meet refractory tissue).

528S
EC
TIO
N8
CARDIOVASCULAR DRUGS
6. Torsades de pointes (French: twisting ofpoints) is a life-threatening form of polymor-phic ventricular tachycardia with rapidasynchronous complexes and an undulatingbaseline on ECG. It is generally associated withlong Q-T interval.
7. Ventricular fibrillation (VF) is grosslyirregular, rapid and fractionated activation ofventricles resulting in incoordinated contractionof its fibres with loss of pumping function.It is fatal unless reverted within 2–5 min;is the most common cause of sudden cardiacdeath.
8. Atrio-ventricular (A-V) block is due todepression of impulse conduction through theA-V node and bundle of His, mostly due tovagal influence or ischaemia.First degree A-V block: Slowed conductionresulting in prolonged P-R interval.Second degree A-V block: Some supra-ventricular complexes are not conducted: dropbeats.Third degree A-V block: No supraventricularcomplexes are conducted; ventricle generatesits own impulse; complete heart block.
Proarrhythmic potential of antiarrhythmic drugsMost antiarrhythmics can themselves be the cause of seriousarrhythmias, especially during long-term prophylactic use.Two multicentric trials ‘Cardiac Arrhythmia Suppression TrialI and II’ (CAST I, II, 1991, 1992) showed that post-MIpatients randomized to receive on a long-term basis encainide,flecainide, moricizine had higher incidence of sudden death,though initially the same drugs had suppressed VES in thesepatients. It is possible that during transient episodes ofischaemia, the intraventricular conduction slowing action ofthese drugs gets markedly accentuated resulting in VT andVF. Similar increased mortality has been reported by the“Mortality in the survival with D-sotalol (SWORD) trial.It is therefore not prudent to try and suppress all extrasystoles/arrhythmias, especially those not causing symptoms, withchronic prophylactic antiarrhythmic therapy. Only the βblockers and amiodarone have been found to decrease cardiacmortality in the long term.
CLASSIFICATIONAntiarrhythmic drugs act by blocking myocardialNa+, K+ or Ca2+ channels. Some have additionalor even primary autonomic effects. Classification
of antiarrhythmic drugs has been difficult, becausemany drugs have more than one action. VaughanWilliams and Singh (1969) proposed a 4 classsystem which takes into account the primaryelectrophysiological action of a drug that mayserve to indicate the type of clinical effects andtherapeutic utility. However, different drugs withina class have their own specific set of properties.
A simplified clinical classification of anti-arrhythmic drugs is given at the end of the chapter.
CLASS I
The primary action of drugs in this class is tolimit the conductance of Na+ (and K+) across cellmembrane—a local anaesthetic action. They alsoreduce rate of phase-4 depolarization in automaticcells.
SUBCLASS IA
The subclass IA containing the oldest anti-arrhythmic drugs quinidine and procainamide areopen state Na+ channel blockers which alsomoderately delay channel recovery (channelrecovery time τrecovery 1–10s), suppress A-Vconduction and prolong refractoriness. The Na+
channel blockade is greater at higher frequency(premature depolarization is affected more). Theseactions serve to extinguish ectopic pacemakersthat are often responsible for triggered arrhythmiasand abolish reentry by converting unidirectionalblock into bidirectional block.
Drugs that prolong Q-T interval(have potential to precipitate Torsades de pointes)
1. Antiarrhythmics : Quinidine, procainamide,disopyramide, propafenone,amiodarone
2. Antimalarials : Quinine, mefloquine,artemisinin, halofantrine
3. Antibacterials : Sparfloxacin, moxifloxacin
4. Antihistaminics : Terfenadine, astemizole, ebastine
5. Antidepressants: Amitryptyline and other tricyclics
6. Antipsychotics : Thioridazine, pimozide,aripiprazole, ziprasidone
7. Prokinetic : Cisapride

529C
HA
PTE
R38
ANTIARRHYTHMIC DRUGS
Antiarrhythmic drugs
Class Actions Drugs
I. Membrane stabilizing agents(Na+ channel blockers)A. Moderately decrease dv/dt of 0 phase Quinidine, Procainamide, DisopyramideB. Little decrease in dv/dt of 0 phase Lidocaine, MexiletineC. Marked decrease in dv/dt of 0 phase Propafenone, Flecainide
II. Antiadrenergic agents (β blockers) Propranolol, Esmolol, Sotalol (also class III)
III. Agents widening AP Amiodarone, Dronedarone(prolong repolarization and ERP) Dofetilide, Ibutilide
IV. Calcium channel blockers Verapamil, Diltiazem
Note: Class IA agents also have Class III property; Propranolol has Class I action as well; sotalol has bothClass II and Class III actions.
In addition1. For PSVT : Adenosine, Digoxin2. For A-V block : Sympathomimetics—Isoprenaline, etc.
Anticholinergics—Atropine.3. Digitalis is used in AF, AFl and PSVT to control ventricular rate.
QuinidineIt is the dextro isomer of the antimalarial alkaloid quininefound in cinchona bark. In addition to Na+ channel blockade,quinidine has cardiac antivagal action which augmentsprolongation of atrial ERP and minimizes RP disparityof atrial fibres. A-V node ERP is increased by directaction of quinidine, but decreased by its antivagal action;overall effect is inconsistent. Quinidine depresses myocardialcontractility; failure may be precipitated in damagedhearts.
ECG: Quinidine increases P-R and Q-T intervals and tendsto broaden QRS complex. Changes in the shape of T wavemay be seen reflecting effect on repolarization.
Mechanism of action: Quinidine blocks myocardial Na+
channels in the open state—reduces automaticity and maximalrate of 0 phase depolarization in a frequency dependentmanner. Prolongation of APD is due to K+ channel block,while lengthening of ERP is caused by its moderate effecton recovery of Na+ and K+ channels. At high concentrationsit also inhibits L type Ca2+ channels. Quinidine decreasesthe availability of Na+ channels as well as delays theirreactivation.
The other actions of quinidine are fall in BP (due toweak α adrenergic blockade and direct cardiac depression),decreased skeletal muscle contractility, augmented uterinecontractions, vomiting, diarrhoea and neurological effectslike ringing in ears, vertigo, deafness, visual disturbancesand mental changes (Cinchonism). Like its levo isomer, ithas antimalarial action, and has been used as a parenteralalternative to quinine for falciparum malaria. The importantdrug interactions of quinidine are:
• Rise in blood levels and toxicity of digoxin due todisplacement from tissue binding and inhibition of P-glycoprotein mediated renal and biliary clearance ofdigoxin.
• Marked fall in BP in patients receiving vasodilators.• Risk of torsades de pointes is increased by hypokalaemia
caused by diuretics.• Synergistic cardiac depression with β-blockers,
verapamil, K+ salts.• Quinidine inhibits CYP2D6: prolongs t½ of propafenone
and inhibits conversion of codeine to morphine.
Use: Though quinidine is effective in many atrial andventricular arrhythmias, it is seldom used now, because ofrisk of adverse effects, including that of torsades de pointes,sudden cardiac arrest or VF; idiosyncratic angioedema,vascular collapse, thrombocytopenia, etc. In a dose of100–200 mg TDS quinidine may rarely be used to maintainsinus rhythm after termination of AF or AFI.QUINIDINE SULPHATE 200 mg tab; QUININGA 300 mgtab, 600 mg/2 ml inj; NATCARDINE 100 mg tab.
ProcainamideIt is orally active amide derivative of the localanaesthetic procaine, with cardiac electrophysio-logical actions almost identical to those ofquinidine, viz. slowing of 0 phase depolarizationand impulse conduction, prolongation of APD,ERP, QRS complex and Q-T interval. Significantdifferences between the two are:

530S
EC
TIO
N8
CARDIOVASCULAR DRUGS
• It is less effective in suppressing ectopicautomaticity.
• It causes less marked depression of contractilityand A-V conduction.
• Antivagal action is absent.• It is not an α blocker: causes less fall in BP;
at high doses, fall in BP is due to ganglionicblockade.
Pharmacokinetics Oral bioavailability of procainamide isabout 75%, peak plasma concentration occurs in 1 hour. It ismetabolized in liver, primarily by acetylation to N-acetyl-procainamide (NAPA) which has no Na+ channel blockingproperty but blocks K+ channels and prolongs repolarization:APD is lengthened. There are fast and slow acetylators ofprocainamide (as there are for isoniazid). Plasma t½ is relativelyshort (3–4 hours).
Dose: For abolition of arrhythmia—0.5–1 g oral or i.m.followed by 0.25–0.5 g every 2 hours; or 500 mg i.v. loadingdose (25 mg/min injection) followed by 2 mg/kg/hour.Maintenance dose—0.5 g every 4–6 hours.PRONESTYL 250 mg tab., 1 g/10 ml inj.
Adverse effects Gastrointestinal tolerance of procainamideis better than quinidine, but nausea and vomiting do occur.CNS: weakness, mental confusion and hallucinations are notedat higher doses.Flushing and hypotension are seen on rapid i.v. injection.Cardiac toxicity, ability to cause torsades de pointes aresimilar to quinidine.Hypersensitivity reactions are rashes, fever, angioedema.Agranulocytosis and aplastic anaemia is rare.Long-term high dose procainamide therapy can cause systemiclupus erythematosus (SLE), especially in slow acetylators.
Use Procainamide (i.v.) is occasionally used to terminatemonomorphic VT and some supraventricular arrhythmias.Many WPW reciprocal VTs respond and it has been usedto prevent recurrences of VF. However, procainamide is notsuitable for prolonged oral therapy because of poor efficacyand high risk of lupus.
DisopyramideIt is a quinidine like Class IA drug that hasprominent cardiac depressant and anticholinergicactions, but no α adrenergic blocking property.Disopyramide usually has no effect on sinus ratebecause of opposing direct depressant andantivagal actions. Prolongation of P-R intervaland QRS broadening are less marked.Pharmacokinetics Bioavailability of oral disopyramide isabout 80%. It is partly metabolized in liver by dealkylation,nearly half is excreted unchanged in urine; plasma t½ is
6–8 hrs. The t½ is increased in patients of MI and in renalinsufficiency.
Dose: 100–150 mg 6–8 hourly oral.NORPACE 100, 150 mg cap, REGUBEAT 100 mg tab.
Adverse effects Disopyramide causes less g.i. effects.Anticholinergic side effects are the most prominent: drymouth, constipation, urinary retention (especially in elderlymales) and blurred vision.Depression of cardiac contractility is more prominent. Cardiacdecompensation and hypotension may occur in patients withdamaged hearts because it also increases peripheral resistance,so that cardiac output may be markedly decreased.Contraindications are—sick sinus, cardiac failure and prostatehypertrophy.
Use The primary indication of disopyramideis as a second line drug for prevention of recur-rences of ventricular arrhythmia. It may also beused for maintenance therapy after cardioversionof AF or AFl.
SUBCLASS IB
These drugs block Na+ channels more in theinactivated than in the open state, but do not delaychannel recovery (channel recovery time < 1S).They do not depress A-V conduction or prolong(may even shorten) APD, ERP and Q-T.
Lidocaine (Lignocaine)It is the most commonly used local anaesthetic(see Ch. 26). In addition, it is a popular anti-arrhythmic in intensive care units.
The most prominent cardiac action oflidocaine is suppression of automaticity in ectopicfoci. Enhanced phase-4 depolarization in partiallydepolarized or stretched PFs, and after-depolari-zations are antagonized, but SA node automaticityis not depressed.
The rate of 0 phase depolarization and conduc-tion velocity in A-V bundle or ventricles is notdecreased. Lidocaine decreases APD in PF andventricular muscle, but has practically no effecton APD and ERP of atrial fibres. Atrial reentryis not affected. However, it can suppress reentrantventricular arrhythmias either by abolishing one-way block or by producing two way block.
Lidocaine is a blocker of inactivated Na+
channels more than that of open state. As such,

531C
HA
PTE
R38
ANTIARRHYTHMIC DRUGS
it is relatively selective for partially depolarizedcells and those with longer APD (whose Na+
channels remain inactivated for longer period).While normal ventricular and conducting fibresare minimally affected, depolarized/damagedfibres are significantly depressed. Brevity of atrialAP and lack of lidocaine effect on channelrecovery might explain its inefficacy in atrialarrhythmias.
Lidocaine has minimal effect on normal ECG;QT interval may decrease. It causes littledepression of cardiac contractility or arterial BP.There are no significant autonomic actions: allcardiac effects are direct actions.
Pharmacokinetics Lidocaine is inactive orallydue to high first pass metabolism in liver. Actionof an i.v. bolus lasts only 10–20 min because ofrapid redistribution. It is hydrolysed, deethylatedand conjugated; metabolites are excreted in urine.Metabolism of lidocaine is hepatic blood flowdependent.
The t½ of early distribution phase is 8 minwhile that of later elimination phase is nearly2 hours. Its t½ is prolonged in CHF, becauseof decrease in volume of distribution and hepaticblood flow.Dose and preparations Lidocaine is given only by i.v.route: 50–100 mg bolus followed by 20–40 mg every 10–20 min or 1–3 mg/min infusion.XYLOCARD, GESICARD 20 mg/ml inj. (5, 50 ml vials).These preparations for cardiac use contain no preservative.The local anaesthetic preparations should not be used for thispurpose.
Propranolol prolongs t½ of lidocaine by reducinghepatic blood flow. Cimetidine also increasesplasma levels of lidocaine.
Adverse effects The main toxicity is dose rela-ted neurological effects:Drowsiness, nausea, paresthesias, blurred vision,disorientation, nystagmus, twitchings and fits.Lidocaine has practically no proarrhythmicpotential and is the least cardiotoxic anti-arrhythmic. Only excessive doses cause cardiacdepression and hypotension.
Use Lidocaine is safe if given by slow i.v.injection; is used to suppress VT and preventVF. It is ineffective in atrial arrhythmias. Becauseof rapidly developing and titratable action it isa good drug in the emergency setting, e.g.arrhythmias following acute MI or during cardiacsurgery. In acute MI, i.v. infusion of lidocainecan prevent VF, but a metaanalysis has shownthat it fails to improve survival; may even increaseshort term mortality. Therefore, lidocaine is nolonger administered prophylactically to all MIpatients, but may be used in selected cases, andto treat ventricular arrhythmias when they occur.
Efficacy of lidocaine in chronic ventriculararrhythmia is poor, but it suppresses VT due todigitalis toxicity, for which it is used becauseit does not worsen A-V block.
Mexiletine
It is a local anaesthetic and an orally active antiarrhythmic;chemically and pharmacologically similar to lidocaine.Automaticity in PF is reduced both by decreasingphase-4 slope and by increasing threshold voltage. By reducingthe rate of 0 phase depolarization in ischaemic PF it mayconvert one-way block to two-way block.
Mexiletine is almost completely absorbed orally, 90%metabolized in liver and excreted in urine; plasma t½9–12 hours.
Bradycardia, hypotension and accentuation of A-V blockmay attend i.v. injection of mexiletine.Neurological side effects—tremor, nausea and vomiting arecommon; dizziness, confusion, blurred vision, ataxia can occur.
Dose: 100–250 mg i.v. over 10 min., 1 mg/min infusion.Oral: 150–200 mg TDS with meals.MEXITIL 50, 150 mg caps, 250 mg/10 ml. inj.
Use Parenteral mexiletine may be used in post-infarctionsinister ventricular arrhythmias as alternative to lidocaine.Oral use to chronically suppress VES/VT is of questionablemerit.
SUBCLASS IC
These are the most potent Na+ channel blockerswith more prominent action on open state andthe longest recovery times (> 10S). They mar-kedly delay conduction, prolong P-R interval,broaden QRS complex, but have variable effecton APD. Drugs of this subclass have high

532S
EC
TIO
N8
CARDIOVASCULAR DRUGS
proarrhythmic potential when administeredchronically; sudden deaths have occurred.
Propafenone By blocking Na+ channelspropafenone considerably depresses impulsetransmission and has profound effect on His-Purkinje as well as accessory pathway conduction.Anterograde as well as retrograde conduction inthe bypass tract of WPW syndrome is retarded.Propafenone prolongs APD and has β adrenergicblocking property—can precipitate CHF andbronchospasm. Sino-atrial block has occurredoccasionally.
Propafenone is absorbed orally and undergoesvariable first pass metabolism; there beingextensive or poor metabolizers because the majormetabolic isoenzyme CYP2D6 is deficient in poormetabolizers. CYP2D6 inhibitors like fluoxetineincrease its bioavailability and plasma concen-tration. Bioavailability and t½ differs considerablyamong individuals. Some metabolites are active.Side effects are nausea, vomiting, bitter taste,constipation and blurred vision. As mentionedabove, it can worsen CHF, asthma and increasethe risk of sudden death.
Propafenone is used for prophylaxis andtreatment of ventricular arrhythmias, reentranttachycardias involving AV node/accessorypathway and to maintain sinus rhythm in AF.However, it can occasionally increase ventricularrate in AFl by slowing atrial rate and allowing1:1 A-V transmission. Some reentrant VTs mayalso be worsened.Dose: 150 mg BD–300 mg TDS;RHYTHMONORM 150 mg tab.Flecainide It is the prototype class IC antiarrhythmic whichmarkedly delays Na+ channel recovery. In contrast topropafenone, flecainide has no consistent effect on APD andno β adrenergic blocking property. It suppresses VES, VT,WPW tachycardia and prevents recurrences of AF and PSVT.But in the CAST study it was found to increase mortalityin patients recovering from MI; can itself provoke arrhythmiasduring chronic therapy. It is reserved for resistant cases ofparoxysmal AF and for life-threatening sustained VT inpatients not having associated CHF.
CLASS IIThe primary action of class II drugs is to sup-press adrenergically mediated ectopic activity.
Propranolol (see Ch. 10) It is the mostcommonly selected β blocker for treatment andprevention of cardiac arrhythmias; has somequinidine like direct membrane stabilizing actionat high doses. However, in the clinically useddose range—antiarrhythmic action is exertedprimarily because of cardiac adrenergic block-ade. In a normal resting individual propranololhas only mild depressant action on SA nodeautomaticity, but marked decrease in the slopeof phase-4 depolarization and automaticity occursin SA node, PF and other ectopic foci when thesame has been increased under adrenergicinfluence. The other most important action is toprolong the ERP of A-V node (an antiadrenergicaction). This impedes A-V conduction so that noparadoxical tachycardia can occur when atrial rateis reduced in AF or AFl.
Slow channel responses and after-depolari-zations that have been induced by catecholamines(CAs) are suppressed. Reentrant arrhythmias thatinvolve A-V node (many PSVTs) or that aredependent on slow channel/depressed fast channelresponse may be abolished by its marked depressantaction on these modalities.
The most prominent ECG change is prolon-gation of PR interval. Depression of cardiaccontractility and BP are mild.
Administration For rapid action, propranolol may beinjected i.v. 1 mg/min (max. 5 mg) under close monitoring.The usual oral antiarrhythmic dose is 40–80 mg 2–4 times aday.
Use Propranolol is very useful in treatinginappropriate sinus tachycardia. Atrial and nodalESs, especially those provoked by emotion orexercise are suppressed by propranolol, but needto be treated only when symptomatic anddisturbing. Propranolol is less effective thanadenosine and verapamil for termination of PSVT(success rate ~ 60%), but can be used to preventrecurrences.
Propranolol rarely abolishes AF or AFl, butis used to control ventricular rate. It is highlyeffective in sympathetically mediated arrhythmiasseen in pheochromocytoma and during anaesthesia

533C
HA
PTE
R38
ANTIARRHYTHMIC DRUGS
with halothane. Digitalis induced tachyarrhythmiasmay be suppressed.
Non-sustained VT may be treated with a βblocker (propranolol, esmolol), but its efficacyin terminating sustained VT is low. However,propranolol may prevent recurrences of VT andits antiischaemic action may be protective.Prophylactic treatment with β blockers reducesmortality in post-MI patients. Propranolol oresmolol injected i.v. may terminate torsades depointes. Along with a class IA or IC drug, it maybe used for WPW reciprocal rhythms.
Sotalol (see p. 148) It is a nonselective β blockerhaving prominent Class III action of prolongingrepolarization by blocking cardiac inward rectifierK+ channels. It is not a Na+ channel blocker—does not depress conduction in fast response tissue,but delays A-V conduction and prolongs its ERP.Sotalol is effective in polymorphic VT, some WPWarrhythmias and for maintaining sinus rhythm inAF/AFl. Due to prolongation of APD and Q-T,risk of dose-dependent torsades de pointes is themajor limitation. It is contraindicated in patientswith long Q-T interval.
Esmolol (see p. 149) This quick and shortacting β1 blocker administered i.v. is very usefulfor emergency control of ventricular rate inAF/AFl. It can terminate supraventricular tachy-cardia, and is mainly used for arrhythmias asso-ciated with anaesthesia where rapidly developingβ adrenergic blockade is desired.MINIBLOCK 100 mg/10 ml, 250 mg/10 ml inj.; 0.5 mg/kg in1 min followed by 0.05–0.2 mg/kg/min i.v. infusion.
CLASS III
The characteristic action of this class is prolon-gation of repolarization (phase-3); AP is widenedand ERP is increased. The tissue remainsrefractory even after full repolarization: reentrantarrhythmias are terminated.
AmiodaroneThis unusual iodine containing highly lipophiliclong-acting antiarrhythmic drug exerts multipleactions:
• Prolongs APD and Q-T interval attributableto block of myocardial delayed rectifier K+
channels. This also appears to reduce non-uniformity of refractoriness among differentfibres.
• Preferentially blocks inactivated Na+ channels(like lidocaine) with relatively rapid rate ofchannel recovery: more effective in depressingconduction in cells that are partially depolarizedor have longer APD.
• Partially inhibits myocardial Ca2+ channels, hasnoncompetitive β adrenergic blocking propertyand alters thyroid function. Thus amiodaroneis a multichannel blocker with some additionalactivities.
Conduction is slowed and ectopic automaticityis markedly depressed, but that of SA node isonly slightly affected. Effect of oral doses oncardiac contractility and BP are minimal, but i.v.injection frequently causes myocardial depressionand hypotension.
Despite prolongation of APD, the arrhythmia (torsadesde pointes) provoking potential of amiodarone is low, probablybecause it does not exhibit ‘reverse use-dependence’ of APDprolongation or because of its multiple antiarrhythmicmechanisms. The prolongation of APD by other class IIIdrugs is more marked at slower rates of activation(encouraging EAD) than at higher rates (reverse use-dependence), while with amiodarone it is independent ofrate of activation.
Pharmacokinetics Amiodarone is incompletelyand slowly absorbed from the g.i.t. On daily oralingestion the action develops over several days,even weeks. However, on i.v. injection, actiondevelops rapidly. It accumulates in muscle andfat from which it is slowly released and thenmetabolized in liver mainly by CYP3A4. Onemetabolite is active. The duration of action isexceptionally long; t½ 3–8 weeks.Dose: Amiodarone is mainly used orally 400–600 mg/dayfor few weeks, followed by 100–200 mg OD for maintenancetherapy. 100–300 mg (5 mg/kg) slow i.v. injection over30–60 min.CORDARONE, ALDARONE, EURYTHMIC 100, 200 mgtabs, 150 mg/3 ml inj.
Use Amiodarone is effective in a wide rangeof ventricular and supraventricular arrhythmiasincluding PSVT, nodal and ventricular tachycardia,

534S
EC
TIO
N8
CARDIOVASCULAR DRUGS
AF, AFl, etc. Resistant VT and recurrent VF arethe most important indications. It is also usedto maintain sinus rhythm in AF when other drugshave failed. Rapid termination of ventricular (VTand VF) and supraventricular arrhythmias can beobtained by i.v. injection. WPW tachyarrhythmiais terminated by suppression of both normal andaberrant pathways.
Long duration of action makes amiodaronesuitable for chronic prophylactic therapy. Apartfrom propranolol, it is the only antiarrhythmicdrug which in the long term has been found toreduce sudden cardiac death. Because of highand broad spectrum efficacy and relatively lowproarrhythmic potential, amiodarone is acommonly used antiarrhythmic, despite its organtoxicity.
Adverse effects These are dose-related andincrease with duration of therapy. Fall in BP,bradycardia and myocardial depression occurson i.v. injection and after drug cumulation.Nausea, gastrointestinal upset may attend oralmedication, especially during the loading phase.Photosensitization and sun burn like skinpigmentation occurs in about 10% patients.Corneal microdeposits are common with long-term use, may cause headlight dazzle, but arereversible on discontinuation.Pulmonary alveolitis and fibrosis is the mostserious toxicity of prolonged use, but is rare ifdaily dose is kept below 200 mg.Peripheral neuropathy generally manifests asweakness of shoulder and pelvic muscles. Liverdamage is rare. Amiodarone interferes with thyroidfunction in many ways including inhibition ofperipheral conversion of T4 to T3 and interactionwith thyroid hormone receptor. Goiter,hypothyroidism and rarely hyperthyroidism maydevelop on chronic use.
Interactions Amiodarone can increase digoxinand warfarin levels by reducing their renal clea-rance. Additive A-V block can occur in patientsreceiving β blockers or calcium channel blockers.Inducers and inhibitors of CYP3A4 respectivelydecrease and increase amiodarone levels.
Dronedarone This is a recently introducednoniodinated congener of amiodarone, less toxic,but also less effective class III antiarrhythmic.Clinical utility of dronedarone is limited tosupraventricular arrhythmias; primary indicationbeing maintenance of sinus rhythm in haemo-dynamically stable patients of paroxysmal/non-permanent AF, and to control ventricular rateduring AF/AFl.
In clinical trials, recurrence time for AF wasincreased by 2–3 times in dronedarone recipients.Like amiodarone, dronedarone is a multichannelblocker, inhibits delayed rectifier and other typesof cardiac K+ channels, inward Na+ channel andL-type Ca2+ channel. The noncompetitive βadrenergic blocking activity is more markedcompared to amiodarone, but it does not interferewith thyroid function. It increases myocardialAPD, ERP and slows A-V conduction.
Dronedarone is less lipophilic and is meta-bolized by CYP3A4 and CYP2D6; inhibitors ofthese isoenzymes (Ketoconazole, erythromycin,metoprolol, etc.) markedly increase its bloodlevels. The elimination t½ is 24 hours. Side effectsare mainly gastrointestinal disturbances, brady-cardia, weakness, cough and dermatologicalreactions. Though it prolongs Q-T interval, riskof torsades de pointes is very low. Hypothyroidism,pulmonary fibrosis and peripheral neuropathy doesnot occur. Dronedarone is contraindicated inmoderate-to-severe CHF, 2nd/3rd degree A-Vblock and in permanent AF.Dose: 400 mg BD oral; MULTAQ 400 mg tab.Note: On the basis of two clinical trials PALLAS and ATHENA,the US-FDA in Dec 2011 issued a safety alert that dronedaroneshould not be used in AF patients who cannot and will not beconverted to sinus rhythm (permanent AF), because it doublesthe rate of stroke, heart failure and cardiovascular death insuch patients. If during dronedarone therapy the patient is foundto have AF, he should either be cardioverted or dronedaroneshould be stopped. A recent meta-analysis has also notedunfavourable cardiovascular and mortality outcomes withdronedarone, especially in patients with cardiovascular riskfactors.
Dofetilide This newer antiarrhythmic prolongs APD andERP by selectively blocking rapid component of delayedrectifier K+ current without affecting other channels orreceptors; has no autonomic or peripheral actions. It istherefore labelled as pure class III antiarrhythmic.

535C
HA
PTE
R38
ANTIARRHYTHMIC DRUGS
Oral dofetilide can convert AF or AFl to sinus rhythm in~30% cases, but is more effective in maintaining sinus rhythmin converted patients—its primary indication. Significantly,chronic therapy with dofetilide in patients with high risk ofsudden cardiac death/post MI cases has not increased mortality,despite provoking torsades de pointes in some recipients. It ismainly excreted unchanged in urine and produces few sideeffects.
Ibutilide is another new class III antiarrhythmic used i.v.for pharmacological conversion of AFl and AF to sinus rhythm.Efficacy is higher in recent onset AF/AFl and in AFl comparedto AF. Induction of Torsades de pointes is a risk.
CLASS IV
The primary action of this class of drugs is toinhibit Ca2+ mediated slow channel inward current.
VerapamilOf the many Ca2+ channel blockers, verapamilhas the most prominent cardiac electrophysio-logical action (Table 38.1). It blocks L type Ca2+
channels and delays their recovery. Its anti-arrhythmic aspects are described here, while otheraspects are covered in Ch. 39 and 40.
The basic action of verapamil is to depressCa2+ mediated depolarization. This suppressesautomaticity and reentry dependent on slowchannel response. Phase-4 depolarization in SAnode is reduced resulting in bradycardia. Reflexsympathetic stimulation due to vasodilatationpartly counteracts the direct bradycardia producingaction. Delayed after-depolarizations in PFs aredampened.
The most consistent action of verapamil isprolongation of A-V nodal ERP. As a result
A-V conduction is markedly slowed (P-R intervalincreases) and reentry involving A-V node isterminated. Intraventricular conduction, however,is not affected. Verapamil has negative inotropicaction due to interference with Ca2+ mediatedexcitation-contraction coupling in myocardium.
Uses and precautions
1. PSVT—Verapamil can terminate attacks ofPSVT; 5 mg i.v. over 2–3 min is effective in~ 80% cases. However, i.v. verapamil carries therisk of marked bradycardia, A-V block, cardiacarrest and hypotension. It should not be used ifPSVT is accompanied with hypotension or CHF.For preventing recurrences of PSVT, verapamil60 to 120 mg TDS may be given orally.2. To control ventricular rate in AF or AFl;Verapamil causes a dose dependent (40–120 mgTDS oral) reduction in ventricular rate in AF andAFl, and is a first line drug for this purpose. In caseof inadequate response, digoxin may be added to it.Verapamil can also be injected i.v. for emergencycontrol of ventricular rate in AF and AFl.
Reentrant supraventricular and nodalarrhythmias are susceptible to verapamil, but itis contraindicated in broad QRS complex WPWtachycardia in which it may abbreviate the ERPof bypass tract. A class IA (procainamide) orIC (propafenone) drug which prolongs ERP ofbypass tract and depresses conduction is to becombined with verapamil so as to concurrentlydepress A-V conduction.
Verapamil has poor efficacy in ventriculararrhythmias. In contrast to β blockers, verapamil
TABLE 38.1 Electrophysiological actions of calcium channel blockers
Verapamil Diltiazem Nifedipine
1. SA node automaticity ↓ ↓,– —2. Ventricular automaticity ↓,– — —3. ERP : atrial — — —
: A-V nodal ↑↑ ↑ ↑↓: ventricular — — —: bypass tract ↑↓ ↑↓ —
4. ECG : R-R interval ↑ ↑↓ ↓P-R interval ↑ ↑ —
↑ : increase; ↓ : decrease; —: no change

536S
EC
TIO
N8
CARDIOVASCULAR DRUGS
prophylaxis does not reduce mortality in post-MI patients. In some patients of VT, i.v. injectionof verapamil has precipitated VF: thereforecontraindicated. It is also not recommended fordigitalis toxicity, because additive A-V block mayoccur. It is contraindicated in partial heart blockand sick sinus.CALAPTIN 40, 80 mg tab; 120, 240 mg SR tab, 5 mg/2 mlinj.
Diltiazem The direct cardiac actions of diltiazemare similar to those of verapamil. However,bradycardia and depression of cardiac contractilityare less marked. It is an alternative to verapamilfor termination as well as prophylaxis of PSVT.
For rapid control of ventricular rate in AFor AFl, i.v. diltiazem is preferred over verapamil,because it can be more easily titrated to the targetheart rate, causes less hypotension or myocardialdepression and can be used even in the presenceof mild-to-moderate CHF.DILZEM 30, 60, 90 mg tabs, 25 mg/5 ml inj.
Drugs for PSVTAn attack of PSVT can be terminated by reflexvagal stimulation through Valsalva maneuver,splashing ice cold water on face, hyperflexion(head between knees), etc. Alternatively, or if itdoes not work, the drug of choice is adenosine(i.v.). Other alternatives are i.v. injection ofverapamil/di l t iazem/esmolol . To preventrecurrences, oral therapy with verapamil, diltiazemor propranolol alone or combined with digoxinmay be prescribed.
AdenosineAdministered by rapid i.v. injection (over 1–3sec) either as the free base (6–12 mg) or as ATP(10–20 mg), adenosine terminates within 30 sec.more than 90% episodes of PSVT involving theA-V node. It activates ACh sensitive K+ channelsand causes membrane hyperpolarization throughinteraction with A1 type of adenosine GPCRson SA node (pacemaker depression → brady-cardia), A-V node (prolongation of ERP →slowing of conduction) and atrium (shorteningof AP, reduced excita-bility). It indirectly reduces
Ca2+ current in A-V node. Depression of thereentrant circuit through A-V node is responsiblefor termination of majority of PSVTs. Adrener-gically induced DADs in ventricle are alsosuppressed. Coronary dilatation occurs transiently.ADENOJECT, ADENOCOR 3 mg adenosine (base) per ml in2 ml and 10 ml amp.
Adenosine has a very short t½ in blood (~10sec) due to uptake into RBCs and endothelialcells where it is converted to 5-AMP and inosine.Almost complete elimination occurs in a singlepassage through coronary circulation. Injected ATPis rapidly converted to adenosine. Dipyridamolepotentiates its action by inhibiting uptake, whiletheophylline/ caffeine antagonize its action byblocking adenosine receptors. Higher doses maybe required in heavy tea/coffee drinkers. Patientson carbamazepine are at greater risk of developingheart block. Advantages of adenosine for termina-tion of PSVT are:• Efficacy equivalent to or better than verapamil.• Action lasts < 1 min; adverse effects (even
cardiac arrest, if it occurs) are transient.• No haemodynamic deterioration; can be given
to patients with hypotension, CHF or thosereceiving β blockers. Verapamil is contra-indicated in these situations.
• Safe in wide QRS tachycardia (verapamil isunsafe).
• Effective in patients not responding toverapamil.However, adenosine produces transient
dyspnoea, chest pain, fall in BP and flushing in30–60% patients; ventricular standstill for fewsec or VF occurs in some patients. Bronchospasmmay be precipitated in asthmatics; verapamil isthe drug of choice for such patients. Adenosinehas to be rapidly injected in a large vein andhas brief action. Therefore, it is not suitable forprophylaxis in recurrent cases.
Other uses of adenosine
(a) Diagnosis of tachycardias dependent on A-V node.(b) To induce brief coronary vasodilatation during certain
diagnostic/interventional procedures.(c) To produce controlled hypotension during surgery.

537C
HA
PTE
R38
ANTIARRHYTHMIC DRUGS
Clinical classification of antiarrhythmic drugs
Supraventricular Supraventricular and Ventricular arrhythmiasarrhythmias only ventricular arrhythmias only
Adenosine Amiodarone Procainamide LidocaineVerapamil β blockers Disopyramide MexiletineDiltiazem Propranolol QuinidineDronedarone Sotalol FlecainideDigoxin Esmolol Propafenone
Drugs for A-V BlockThe definitive treatment of chronic heart blockis pacing with an implanted cardiac pacemaker.Drugs are of value only for acute/transient A-Vblock and as an interim measure.
Atropine: When A-V block is due to vagaloveractivity, e.g. digitalis toxicity, some casesof MI; it can be improved by atropine 0.6–1.2mg i.m. Atropine abbreviates A-V node ERPand increases conduction velocity in bundle ofHis.
Sympathomimetics (Adr, isoprenaline): Thesedrugs may overcome partial heart block byfacilitating A-V conduction and shortening ERPof conducting tissues.
They may also be used in complete (3rddegree) heart block to maintain a sufficientidioventricular rate (by increasing automaticityof ventricular pacemakers) till external pacemakercan be implanted.
Choice and use of antiarrhythmic drugsMere detection of an arrhythmia does notnecessitate treatment.
Asymptomatic arrhythmias and those whichdo not jeopardize haemodynamics, e.g. most AESand occasional VES, first degree A-V block,bundle branch block, etc. in an otherwise normalheart, do not require antiarrhythmic treatment;reassurance is enough. If a patient is particularlydisturbed by AES, propranolol is the best option.Chronic prophylactic therapy with class I and classIV antiarrhythmics does not appear to affordsurvival benefit, except in few selected cases. Only
propranolol and to some extent amiodarone havebeen shown to reduce cardiovascular mortalityin the long-term. On the other hand, vigoroustherapy is indicated when:• Arrhythmia is life-threatening, e.g. sustained
VT, torsades de pointes, VF.• Arrhythmia is causing hypotension, breath-
lessness, activity limitation or cardiac failure.• Palpitation is marked, e.g. in PSVT, sustained
VT, AF, torsades de pointes.• When simple arrhythmia may lead to more
serious ones, e.g. after MI (warning arrhy-thmias).
In the above situations antiarrhythmics are mostlyneeded for short periods. Majority of antiarrhy-thmic drugs have narrow margin of safety. Asimple clinical classification of antiarrhythmicdrugs is presented in the box below.The selection of an antiarrhythmic in a patientdepends on:(a) ECG diagnosis(b) Possible mechanism underlying the arrhythmia(c) Mechanism of action and range of anti-arrhythmic activity of the drug(d) Pharmacokinetic profile of the drug.(e) Haemodynamic effects of the drug.The aim is to improve cardiovascular functioneither by restoring sinus rhythm, or by controllingventricular rate, or by conversion to a moredesirable pattern of electrical and mechanicalactivity.
Despite extensive investigation, choice of anantiarrhythmic is still largely empirical. A practicalguide to the choice and use of antiarrhythmicdrugs is summarized in the box on next page.

538S
EC
TIO
N8
CARDIOVASCULAR DRUGS
Choice of antiarrhythmics for cardiac arrhythmias
Arrhythmia Clinical objective Drug(s)
1. Atrial extrasystoles No drug if asymptomatic or non-disturbingSymptomatic : Suppression, symptom relief Propranolol (only if disturbing)
2. Paroxysmal supraventricular : Termination of PSVT i.v. adenosine/verapamil/diltiazem/esmololtachycardia (PSVT) : Prevention of recurrence Oral verapamil/diltiazem/propranolol/sotalol
3. Atrial fibrillation (AF) : Reversal to SR Cardioversion(for paroxysmal/persistent AF) i.v. amiodarone
: Maintenance of SR Sotalol/propafenone/amiodarone/dronedarone/disopyramide
: Ventricular rate control oral verapamil/diltiazem/propranolol +(for permanent AF/during digoxinrecurrence of AF)
: Urgent vent. rate control i.v. esmolol/verapamil/amiodarone
4. Atrial flutter (AFl) : Reversal to SR Cardioversion, radiofrequency ablation,Propafenone (after rate control withverapamil/propranolol)
: Ventricular rate control Propranolol/verapamil/diltiazem + digoxinor Amiodarone
5. Wolff-Parkinson-White : Termination Radiofrequency ablation, cardioversionsyndrome (WPW) : Maintenancetachycardia - narrow QRS Propafenone/procainamide
- wide QRS Propafenone + verapamil/propranololor Amiodarone/sotalol
6. Acute-MI arrhythmiaBradycardia : Reversal to normal rate Atropine (i.v.)—no effect—PacingVent. extrasystoles/ : Abolition to prevent i.v. Lidocaine/procainamide/amiodaronetachycardia serious arrhythmia Cardioversion (if haemodynamically unstable)
7. Chronic vent. tachycardiaNonsustained VT : Suppression Propranolol/amiodarone (oral)Sustained VT : Abolition i.v. Amiodarone + propranolol
or cardioversionor propafenone/lidocaine (i.v.)
: Maintenance therapy Amiodarone/sotalol(prevention of VF/arrest) Implantable defibrillator
8. Ventricular fibrillation (VF) : Termination Defibrillation + amiodarone (i.v.): Recurrence prevention Amiodarone (oral)/propranolol
SR—Sinus rhythm
PROBLEM DIRECTED STUDY
38.1 A sales executive aged 55 years presented with palpitation felt off-and-on, both during activity as well asat rest for the last one month or so. He also complained of tiredness and anxiety. The pulse was irregular involume and frequency with average rate 104/min, respiration 20/min, BP 130/84 mm Hg, apex beat was irregular,with an average rate 120/min. Heart sounds were irregular, but there was no murmur. The ECG showed atrialfibrillation (AF) with no sign of ischaemia. A diagnosis of persistent AF was made, and it was decided to electricallycardiovert him. He was put on warfarin sod. 5 mg twice daily for 2 days followed by 5 mg once daily and doseto be adjusted to an INR between 2–2.5. This was to be maintained for 1 month before attempting cardioversion.(a) Why the patient has been put on warfarin therapy before attempting cardioversion?(b) Can some drug be given to control and regularize his heart rate in the mean time? If so, which drug(s)?(c) If electrical cardioversion does not succeed, can some drug be given to revert him to sinus rhythm (SR)?(d) After cardioversion, can some drug(s) be given to maintain SR and prevent recurrence of AF?(see Appendix-1 for solution)

Antianginal and OtherAnti-ischaemic Drugs
ChapterChapterChapterChapterChapter 3939393939
ANTIANGINAL DRUGS
Antianginal drugs are those that prevent, abortor terminate attacks of angina pectoris.
Angina pectoris Is a pain syndrome due toinduction of an adverse oxygen supply/demandsituation in a portion of the myocardium. Twoprincipal forms are recognized:
(a) Classical angina (common form) Attacksare predictably provoked (stable angina) byexercise, emotion, eating or coitus and subsidewhen the increased energy demand is withdrawn.The underlying pathology is—severe arterio-sclerotic affliction of larger coronary arteries(conducting vessels) which run epicardially andsend perforating branches to supply the deepertissue (Fig. 39.1). The coronary obstruction is‘fixed’; blood flow fails to increase duringincreased demand despite local factors mediateddilatation of resistance vessels (Fig. 39.2) andischaemic pain is felt. Due to inadequacy ofischaemic left ventricle, the end diastolic leftventricular pressure rises from 5 to about 25 mmHg—produces subendocardial ‘crunch’ duringdiastole (blood flow to the subendocardial region
occurs only during diastole) and aggravates theischaemia in this region. Thus, a form of acutelydeveloping and rapidly reversible left ventricularfailure results which is relieved by taking restand reducing the myocardial workload.
Drugs that are useful, primarily reduce cardiacwork (directly by acting on heart or indirectlyby reducing preload hence end diastolic pressure,and afterload). They may also cause favourableredistribution of blood flow to the ischaemic areas.
(b) Variant/Prinzmetal/Vasospastic angina(uncommon form) Attacks occur at rest or duringsleep and are unpredictable. They are due to
Fig. 39.1: Diagrammatic representation of subendocardial‘crunch’ during an attack of angina
Fig. 39.2: Diagrammatic representation of coronaryartery calibre changes in classical and variant angina

540S
EC
TIO
N8
CARDIOVASCULAR DRUGS
recurrent localized (occasionally diffuse) coronaryvasospasm (Fig. 39.2) which may be superimposedon arteriosclerotic coronary artery disease.Abnormally reactive and hypertrophied segmentsin the coronary arteries have been demonstrated.Drugs are aimed at preventing and relieving thecoronary vasospasm.
Unstable angina (UA) with rapid increase induration and severity of attacks is mostly dueto rupture of an atheromatous plaque attractingplatelet deposition and progressive occlusion ofthe coronary artery; occasionally with associatedcoronary vasospasm.
Chronically reduced blood supply causes atro-phy of cardiac muscle with fibrous replacement(reduced myocardial work capacity → CHF) andmay damage conducting tissue to produce unstablecardiac rhythms. Antianginal drugs relieve cardiacischaemia but do not alter the course of coronaryartery pathology: no permanent benefit is afforded.On the other hand, aspirin, ACE inhibitors andstatins (hypocholesterolaemic) can modifycoronary artery disease and improve prognosis.
Glyceryl trinitrate, the drug unsurpassed in its ability toabort and terminate anginal attack, was introduced by Murrellin 1879. Other organic nitrates were added later, but abreakthrough was achieved in 1963 when propranolol wasused for chronic prophylaxis. The calcium channel blockershave been a major contribution of the 1970s. A numberof vasodilator and other drugs have been promoted fromtime to time, but none is as uniformly effective. Somepotassium channel openers (nicorandil), metabolic modulator(trimetazidine) and late Na+ current inhibitor (ranolazine)have been introduced lately.
CLASSIFICATION
1. Nitrates(a) Short acting: Glyceryl trinitrate (GTN,
Nitroglycerine)(b) Long acting: Isosorbide dinitrate (short
acting by sublingual route), Isosorbidemononitrate, Erythrityl tetranitrate,Pentaerythritol tetranitrate
2. β Blockers Propranolol, Metoprolol, Atenololand others.
3. Calcium channel blockers(a) Phenyl alkylamine: Verapamil
(b) Benzothiazepine: Diltiazem(c) Dihydropyridines: Nifedipine, Felodipine,
Amlodipine, Nitrendipine, Nimodipine,Lacidipine, Lercanidipine, Benidipine
4. Potassium channel opener Nicorandil5. Others Dipyridamole, Trimetazidine,
Ranolazine, Ivabradine, Oxyphedrine
Clinical classification
A. Used to abort or terminate attack GTN,Isosorbide dinitrate (sublingually).
B. Used for chronic prophylaxis All other drugs.
NITRATES (GTN as prototype)
All organic nitrates share the same action; differonly in time course. The only major action isdirect nonspecific smooth muscle relaxation.
Preload reduction The most prominent actionis exerted on vascular smooth muscle. Nitratesdilate veins more than arteries → peripheralpooling of blood → decreased venous return, i.e.preload on heart is reduced → end diastolic sizeand pressure are reduced → decreased cardiacwork according to Laplace relationship—whichdescribes the effectiveness of ventricular walltension in elevating intraventricular pressure andthe extent to which fibre shortening results insystolic ejection.
Wall tension = intraventricular pressure ×ventricular radius
Thus, reduction in ventricular radius decreasesthe tension that must be generated in the ventri-cular wall—hence decreased O2 consumption.Reduction in cardiac output (c.o.) occurs at restbut is less marked during angina due to betterventricular emptying. The decrease in end diastolicpressure abolishes the subendocardial crunch byrestoring the pressure gradient across ventricularwall due to which subendocardial perfusion occursduring diastole. It is through their action onperipheral veins that nitrates exert major beneficialeffects in classical angina.

541C
HA
PTE
R39
ANTIANGINAL AND OTHER ANTI-ISCHAEMIC DRUGS
Afterload reduction Nitrates also produce somearteriolar dilatation → slightly decrease totalperipheral resistance (t.p.r.) or afterload on heart;BP falls somewhat; systolic more than diastolic(reflex sympathetic activity tends to maintain dia-stolic BP). This action contributes to the reductionin cardiac work which is directly proportionalto aortic impedance.
With usual doses, and if the patient does notstand still (which favours pooling of blood inthe legs), tachycardia is not prominent. With largedoses and if the mean BP falls significantly, reflexsympathetic stimulation occurs → tachycardia,increased cardiac contractility → increased car-diac work → angina may be precipitated. Faintingand cold sweat occur due to cerebral ischaemia.All these can be prevented by lying down andraising the foot end.
Redistribution of coronary flow In the arterialtree, nitrates preferentially relax bigger conduc-ting (angiographically visible) coronary arteriesthan arterioles or resistance vessels. This patternof action may cause favourable redistribution ofblood flow to ischaemic areas in angina patients.Dilatation of conducting vessels all over by nitratealong with ischaemia-induced dilatation ofautoregulatory resistance vessels only in theischaemic zone increases blood flow to this area(see Fig. 39.4B), while in the non-ischaemic zones,resistance vessels maintain their tone → flow doesnot increase, or may decrease to compensate forincreased flow to ischaemic zone. In fact, nitratesdo not appreciably increase total coronary flowin angina patients.
Mechanism of relief of angina The relaxanteffect on larger coronary vessels is the principalaction of nitrates benefiting variant angina bycounteracting coronary spasm. In classical anginaundoubtedly the primary effect is to reduce cardiacwork by action on peripheral vasculature, thoughincreased blood supply to ischaemic area maycontribute. Exercise tolerance of angina patientsis improved because the same amount of exercisecauses lesser augmentation of cardiac work.
Heart and peripheral blood flow Nitrates haveno direct stimulant or depressant action on theheart. They dilate cutaneous (especially over faceand neck → flushing) and meningeal vesselscausing headache. Splanchnic and renal bloodflow decreases to compensate for vasodilatationin other areas. Nitrates tend to decongest lungsby shifting blood to systemic circulation.
Other smooth muscles Bronchi, biliary tractand esophagus are mildly relaxed. Effect onintestine, ureter, uterus is variable and insignificant.
Mechanism of action Organic nitrates arerapidly denitrated enzymatically in the smoothmuscle cell to release the reactive free radicalnitric oxide (NO) which activates cytosolicguanylyl cyclase → increased cGMP → causesdephosphorylation of myosin light chain kinase(MLCK) through a cGMP dependent proteinkinase (Fig. 39.3). Reduced availability ofphosphorylated (active) MLCK interferes withactivation of myosin → it fails to interact withactin to cause contraction. Consequently relaxationoccurs. Raised intracellular cGMP may also reduceCa2+ entry—contributing to relaxation.
Fig. 39.3: Mechanism of vascular smooth muscle relaxantaction of nitrodilators like glyceryl trinitrate and calciumchannel blockers; (- - - →) InhibitionCAM—Calmodulin; NO—Nitric oxide; MLCK—Myosinlight chain kinase; MLCK-P—Phosphorylated MLCK;GTP—Guanosine triphosphate; cGMP—Cyclic guano-sine monophosphate

542S
EC
TIO
N8
CARDIOVASCULAR DRUGS
Veins express greater amount of mitochondrial aldehydedehydrogenase, the enzyme that generates NO from GTN, thanarteries. This may account for the predominant venodilatoraction. It has been suggested that preferential dilatation ofepicardial conducting arteries over autoregulatory arteriolesis also due to differential distribution of nitrate metabolizingenzymes in these vessels.
Platelets Though platelets are poor in mitochondrial aldehydedehydrogenase, the NO generated from nitrates activatescGMP production in platelets as well, leading to a mildantiaggregatory effect. This action may be valuable in unstableangina.
Pharmacokinetics Organic nitrates are lipid-soluble: well absorbed from buccal mucosa, intes-tines and skin. Ingested orally, all except isosor-bide mononitrate undergo extensive and variablefirst pass metabolism in liver. They are rapidlydenitrated by a glutathione reductase and amitochondrial aldehyde dehydrogenase. The partlydenitrated metabolites are less active, but havelonger t½. Though nitrates have been traditionallyclassified into short-acting and long-acting, it isthe rate of absorption from the site of adminis-tration and the rate of metabolism that governthe duration of action of a particular nitrate. Forexample, GTN and isosorbide dinitrate are bothshort-acting from sublingual but longer-actingfrom oral route.
Adverse effects These are mostly due to vaso-dilatation.1. Fullness in head, throbbing headache; some
degree of tolerance develops on continued use.2. Flushing, weakness, sweating, palpitation,
dizziness and fainting; these are mitigated bylying down. Erect posture and alcoholaccentuate these symptoms.
3. Methemoglobinemia: is not significant withclinically used doses. However, in severeanaemia, this can further reduce O2 carryingcapacity of blood.
4. Rashes are rare, though relatively morecommon with pentaerythritol tetranitrate.
Tolerance Attenuation of haemodynamic andantiischaemic effect of nitrates occurs in a doseand duration of exposure dependent manner ifthey are continuously present in the body. This
tolerance weans off rapidly (within hours) whenthe body is free of the drug. Clinically, nosignificant tolerance develops on intermittent useof sublingual GTN for attacks of angina. However,it may become important when GTN is used orally,transdermally or by continuous i.v. infusion roundthe clock, as well as with the use of long actingagents, especially sustained release formulations.Cross tolerance occurs among all nitrates.Tolerance occurs more readily with higher doses.
The mechanism of nitrate tolerance is not well understood.Reduced ability to generate NO due to depletion of cellularSH radicals has been demonstrated experimentally. However,thiol replinishing agents only partially overcome nitratetolerance. This form of therapy has not met clinical success.Other changes which interfere with NO production couldbe involved. Products formed during generation of NO inhibitmitochondrial aldehyde dehydrogenase. Activation of compen-satory mechanisms including volume expansion, sympatheticand renin-angiotensin system stimulation or other humoralpathways as well as oxidative stress due to free radicalsgenerated during denitration may contribute to nitrate tolerance.
The most practical way to prevent nitratetolerance is to provide nitrate free intervalseveryday.
Dependence On organic nitrates is now wellrecognized. Sudden withdrawal after prolongedexposure has resulted in spasm of coronary andperipheral blood vessels. MI and sudden deathshave been recorded. Angina threshold is loweredduring the nitrate free interval in some patients:episodes of angina may increase. In such patientsan antianginal drug of another class should beadded. Withdrawal of nitrates should be gradual.
Interactions Sildenafil causes dangerouspotentiation of nitrate action: severe hypotension,MI and deaths are on record (see p. 304). Additivehypotension is also possible when nitrate is givento a patient receiving other vasodilators.
INDIVIDUAL DRUGS
1. Glyceryl trinitrate (GTN, Nitroglycerine)It is a volatile liquid which is adsorbed on theinert matrix of the tablet and renderednonexplosive. The tablets must be stored in atightly closed glass (not plastic) container lest

543C
HA
PTE
R39
ANTIANGINAL AND OTHER ANTI-ISCHAEMIC DRUGS
the drug should evaporate away. The sublingualroute is used when terminating an attack oraborting an imminent one is the aim. The tabletmay be crushed under the teeth and spread overbuccal mucosa. It acts within 1–2 min (peak bloodlevel in 3–6 min) because of direct absorptioninto systemic circulation (bypassing liver wherealmost 90% is metabolized).
Plasma t½ is 2 min, duration of action dependson the period it remains available for absorptionfrom buccal mucosa. When anginal pain isrelieved, the remaining part of tablet may be spitor swallowed. A sublingual spray formulation hasbeen recently marketed—acts more rapidly thansublingual tablet. Hepatic metabolizing capacitycan be overwhelmed by administering a large dose(5–15 mg) orally. Sustained release oral capsulescontaining much larger amounts of GTN can beused for chronic prophylaxis.
Nitroglycerine is readily absorbed from theskin. In the early 1970s, cutaneous applicationas ointment was found to produce haemodynamiceffects for 4–6 hours. A transdermal patch in which
the drug is incorporated into a polymer bondedto adhesive plaster (see p. 6) has been developedwhich provides steady delivery for 24 hours. Itstarts working within 60 min and has abioavailability of 70–90%. However, developmentof tolerance and dependence may jeopardise itsvalue. It is advised that the patch be taken offfor 8 hours daily. A transmucosal dosage formwhich has to be stuck to the gums under the upperlip has also been produced—acts in 5 min andreleases the drug for 4–6 hours.
Intravenous infusion of GTN provides rapid,steady, titratable plasma concentration for as longas desired. It has been successfully used forunstable angina, coronary vasospasm, LVFaccompanying MI, hypertension during cardiacsurgery, etc. Begin with 5 µg/min, adjust accordingto need. Early institution of infusion may limitthe size of infarct in MI.
2. Isosorbide dinitrate It is a solid butsimilar in properties to GTN; can be usedsublingually at the time of attack (slightly slower
TABLE 39.1 Organic nitrates available for angina pectoris
Drug Preparations Dose & route Duration of action
1. GTN (Nitroglycerine) ANGISED 0.5 mg tab 0.5 mg sublingual 10–30 minNITROLINGUAL, GTN SPRAY 0.4–0.8 mg s.l. spray 10–30 min0.4 mg per sprayANGISPAN-TR 2.5, 6.5 mg SR cap. 5–15 mg oral 4–8 hrNITROCONTIN, CORODIL 2.6,6.4 mg tabs.NITRODERM-TTS 5 or 10 mg patch One patch for 14–16 Till applied,
hr per day max 24 hr.MYOVIN, MILLISROL, NITROJECT 5–20 µg/min i.v. Till infused5 mg/ml inj
2. Isosorbide dinitrate SORBITRATE 5, 10 mg tab, 5–10 mg sublingual 20–40 minISORDIL 5 mg sublingual 10–20 mg oral 2–3 hr& 10 mg oral tab.DITRATE 5, 10 mg tab; 20, 40 mg 20–40 mg oral 6–10 hrSR tab
3. Isosorbide-5- MONOTRATE 10, 20, 40 mg tab, 20–40 mg oral 6–10 hrmononitrate 25, 50 mg SR tabs
5-MONO, MONOSORBITRATE10, 20, 40 mg tab.
4. Erythrityl-tetranitrate CARDILATE 5, 15 mg tab 15–60 mg oral 4–6 hr
5. Pentaerythritol- PERITRATE 10 mg tab 10–40 mg oral 3–5 hrtetranitrate PERITRATE-SA 80 mg SR tab 80 mg oral 8–12 hr

544S
EC
TIO
N8
CARDIOVASCULAR DRUGS
cardiac mortality. In terms of prognostic benefitchronic prophylactic therapy with CCBsis superior to long-acting nitrates in variantangina.
2. Acute coronary syndromes (ACS) Theseare characterized by rapid worsening of anginalstatus of the patient : include unstable angina(UA) and non-ST segment elevation myocardialinfarction (NSTEMI). It needs aggressive therapywith a combination of drugs intended to preventfurther coronary occlusion, increase coronary bloodflow and decrease myocardial stress (oxygendemand). Nitrates are useful by decreasingpreload (myocardial work) as well as by increasingcoronary flow (dilatation and antagonism ofcoronary spasm, if present). Initially GTN is givensublingually, but if pain persists after 3 tablets5 min apart, i.v. infusion of GTN is started. Therole of nitrates appears to be limited to reliefof pain, because no mortality benefit has beendemonstrated in large randomized clinical trialssuch as GISSI-3 (1994) and ISIS-4 (1995).Antiplatelet drugs like aspirin, clopidogrel, GPIIb/IIIa
antagonists, with or without heparin are the primary measuresin UA/NSTEMI. The β blockers are indicated in all patients(if there are no contraindications) to reduce myocardial oxygendemand. A CCB is indicated only when coronary spasmis not effectively counteracted by the nitrate. Revascularizationby thrombolytics/coronary angioplasty with stents/coronarybypass surgery is considered in high risk patients.
3. Myocardial infarction (MI) Administeredby carefully titrated i.v. infusion to avoid hypo-tension and tachycardia, GTN is frequently usedduring evolving MI with the aim of relieving chestpain, pulmonary congestion and limiting the areaof necrosis by favourably altering O2 balance inthe marginal partially ischaemic zone (a con-sequence of preload reduction). However,evidence that it decreases mortality is not robust;prognostic benefits appear marginal. Properpatient selection is important. GTN should notbe administered if:• Systolic BP is < 90 mm Hg• Heart rate is < 50 or > 100 beats/min• Right ventricular infarction is suspected
in action than GTN, peak in 5–8 min) as wellas orally for chronic prophylaxis. Presystemicmetabolism on oral administration is pronouncedand variable. The t½ is 40 min, but sustainedrelease formulation may afford protection for6–10 hours. Last dose should not be taken laterthan 6 PM to allow nitrate level to fall duringsleep at night.
3. Isosorbide mononitrate This is an activemetabolite of isosorbide dinitrate. When adminis-tered orally it undergoes little first pass meta-bolism: bioavailability is high, interindividualdifferences are minimal and it is longer acting(t½ 4–6 hr). Last dose is to be taken in theafternoon; SR tablet once a day in the morning.
4. Erythrityl tetranitrate and pentaery-thritol tetranitrate These are longer-actingnitrates used only for chronic prophylaxis.Sustained release oral preparations are nowavailable for 2–3 times a day dosing.
There has been considerable scepticism in thepast about the efficacy of orally administered long-acting nitrates. Studies with high doses have shownthat firstpass metabolism in liver can be saturatedand haemodynamic effects lasting 4–6 hours dooccur.
USES
1. Angina pectoris Nitrates are effective inclassical as well as variant angina. For abortingor terminating an attack, sublingual GTN tabletor spray, or isosorbide dinitrate is taken on ‘asand when required’ basis. GTN produces reliefwithin 3 min in 75% patients, the rest may requireanother dose or take longer (upto 9 min). Nitratesincrease exercise tolerance and postpone ECGchanges of ischaemia. Longer-acting formulations(oral, transdermal) of GTN or other nitrates areused on regular schedule for chronic prophylaxis.However, development of tolerance and depen-dence may limit the usefulness of this approach:6–8 drug free hours daily are advisable. Moreover,chronic nitrate therapy in angina does not decrease

545C
HA
PTE
R39
ANTIANGINAL AND OTHER ANTI-ISCHAEMIC DRUGS
• Hypotension caused by nitrate limits theadministration of β blockers which have morepowerful salutary effects.*
• Patient has taken sildenafil in the past 24hours.
4. CHF and acute LVF The role of vasodilatorsin CHF is described in Ch. 37. Nitrates affordrelief by venous pooling of blood (which canbe aided by sitting posture while managing acuteLVF or severe chronic CHF) → reduced venousreturn (preload) → decreased end diastolic volume→ improvement in left ventricular function byLaplace law and regression of pulmonarycongestion. Intravenous GTN is the preparationof choice for emergency use. Rate of infusionmust be guided by continuous haemodynamicmonitoring.
5. Biliary colic due to disease or morphine—responds to sublingual GTN or isosorbidedinitrate.
6. Esophageal spasm Sublingual GTNpromptly relieves pain. Nitrates taken before ameal facilitate feeding in esophageal achalasiaby reducing esophageal tone.
7. Cyanide poisoning Nitrates generate met-haemoglobin which has high affinity for cyanideradical and forms cyanomethaemoglobin.However, this may again dissociate to releasecyanide. Therefore, sodium thiosulfate is givento form Sod. thiocyanate which is poorlydissociable and is excreted in urine.
Cytochrome and other oxidative enzymes arethus protected from cyanide; even that which hascomplexed CN is reactivated. However, earlytreatment is critical. The antidotes should berepeated as required.
HaemoglobinSod. nitrite (10 ml of 3% solution i.v.)
MethaemoglobinCyanide
CyanomethaemoglobinSod. thiosulfate (50 ml of 25% solution i.v.)
Methaemoglobin + Sod. thiocyanate↓
Excreted in urineSodium nitrite is used for this purpose because it isa very weak vasodilator; large doses (>300 mg)sufficient to generate enough methaemoglobin can beinjected i.v. without producing hypotension.
βββββ BLOCKERS (see Ch. 10)
These drugs do not dilate coronaries or otherblood vessels; total coronary flow is rather reduceddue to blockade of dilator β2 receptors. However,flow to the ischaemic subendocardial region isnot reduced because of favourable redistributionand decrease in ventricular wall tension. β blockersact by reducing cardiac work and O2 consumptionas a consequence of decreased heart rate, inotropicstate and mean BP. This is marginal at rest. Moreimportantly, β blockers limit increase in cardiacwork that occurs during exercise or anxiety byantiadrenergic action on heart.
All β blockers are nearly equally effectivein decreasing frequency and severity of attacksand in increasing exercise tolerance in classicalangina, but cardioselective agents (atenolol,metoprolol) are preferred over nonselective β1
+ β2 blockers (e.g. propranolol). The latter areparticularly prone to worsen variant angina dueto unopposed α receptor mediated coronaryconstriction that may accentuate the coronaryspasm. Long term β blocker therapy clearly lowersrisk of sudden cardiac death among ischaemicheart disease patients.
In angina pectoris, β-blockers are to be takenon a regular schedule; not on ‘as and whenrequired’ basis. The dose has to be individua-lized. Abrupt discontinuation after chronic usemay precipitate severe attacks, even MI.
* American Heart Association/American College ofCardiology guidelines for the management of patientswith acute myocardial infarction. Circulation 2004, 110,588-636.

546S
EC
TIO
N8
CARDIOVASCULAR DRUGS
Voltage sensitive calcium channels
L-type T-type N-type(Long lasting current) (Transient current) (Neuronal)
1. Conductance 25 pS 8 pS 12–20 pS 2. Activation threshold High Low Medium 3. Inactivation rate Slow Fast Medium 4. Location and • Excitation-contraction • SA node—pace- • Only on neurones
function coupling in cardiac and maker activity in CNS, sympatheticsmooth muscle • ‘T’ current and and myenteric plexuses
• SA, A-V node—con- repetitive spikes —transmitter releaseductivity in thalamic and
• Endocrine cells— other neuroneshormone release • Endocrine cells—
• Neurones—transmitter hormone releaserelease • Certain arteries—
constriction 5. Blocker Nifedipine, diltiazem, Mibefradil, flunari- ω-Conotoxin
verapamil verapamil zine, ethosuximide
Unstable angina (UA)/Non-ST-elevation MI(NSTEMI) Unless contraindicated, β blockersare routinely used in UA/NSTEMI. However, theyshould be given only after starting nitrate ±calcium channel blocker to counteract coronaryvasospasm, if present (β blockers carry the riskof worsening coronary vasospasm). β blockersreduce myocardial O2 demand and affordadditional benefit by reducing risk of impendingMI/sudden cardiac death.
CALCIUM CHANNEL BLOCKERSVerapamil was developed in Germany in 1962 as a coronarydilator. It had additional cardiodepressant property, but itsmechanism of action was not known. Fleckenstein (1967)showed that it interfered with Ca2+ movement into the cell.In the subsequent years, a large number of chemically diverseCa2+ channel blockers (CCBs) with different pharmacologicalprofiles have been produced.
Three important classes of calcium channelblockers are examplified by:
Verapamil—a phenyl alkylamine, hydrophilicpapaverine congener.Nifedipine—a dihydropyridine (lipophilic).Diltiazem—a hydrophilic benzothiazepine.
The dihydropyridines (DHPs) are the most potentCa2+ channel blockers, and this subclass hasproliferated exceptionally.
Calcium channelsThree types of Ca2+ channels have been described in smoothmuscles (other excitable cells as well):(a) Voltage sensitive channel Activated when membranepotential drops to around –40 mV or lower.(b) Receptor operated channel Activated by Adr andother agonists—independent of membrane depolarization (NAcontracts even depolarized aortic smooth muscle by promotinginflux of Ca2+ through this channel and releasing Ca2+ fromsarcoplasmic reticulum).(c) Leak channel Small amounts of Ca2+ leak into theresting cell and are pumped out by Ca2+ATPase. Mechanicalstretch promotes inward movement of Ca2+, through the leakchannel or through separate stretch sensitive channel.
The voltage sensitive Ca2+ channels are heterogeneous: threemajor types have been identified (see box):
All voltage sensitive Ca2+ channels are membrane spanningfunnel shaped glycoproteins that function as ion selectivevalves. They are composed of a major α1 subunit whichencloses the ion channel and other modulatory subunits likeα2,β, γ and δ. In L-type Ca2+ channels each subunit existsin multiple isoforms which may be site specific, e.g.
Skeletal muscle L-channels are: α1s . α2/δa . β1 . γCardiac muscle L-channels are: α1ca . α2/δc . β2
Smooth muscle L-channels are: α1cb . α2/δ . β3
Even smooth muscle L-channels differ between vascular andnonvascular. Moreover, distribution may be heterogeneousin different parts of the vascular bed.
Only the voltage sensitive L-type channels are blockedby the CCBs. The 3 groups of CCBs viz. phenylalkylamines(verapamil), benzothiazepine (diltiazem) and dihydropyridines

547C
HA
PTE
R39
ANTIANGINAL AND OTHER ANTI-ISCHAEMIC DRUGS
(nifedipine) bind to their own specific binding sites on theα1 subunit; all restricting Ca2+ entry, though characteristicsof channel blockade differ. Further, different drugs may havediffering affinities for various site specific isoforms of theL-channels. This may account for the differences in actionexhibited by various CCBs. The vascular smooth musclehas a more depolarized membrane (RMP about –40 mV)than heart. This may contribute to vascular selectivity ofcertain CCBs.
PHARMACOLOGICAL ACTIONS ANDADVERSE EFFECTSThe common property of all three subclasses ofCCBs is to inhibit Ca2+ mediated slow channelcomponent of action potential (AP) in smooth/cardiac muscle cell. The two most importantactions of CCBs are:
(i) Smooth muscle (especially vascular) relaxa-tion.
(ii) Negative chronotropic, inotropic and dromo-tropic action on heart.
Smooth muscle Smooth muscles depolarizeprimarily by inward Ca2+ movement throughvoltage sensitive channel. These Ca2+ ions triggerrelease of more Ca2+ from intracellular stores andtogether bring about excitation-contractioncoupling through phosphorylation of myosin lightchain as depicted in Fig. 39.3. The CCBs causerelaxation by decreasing intracellular availabilityof Ca2+. They markedly relax arterioles but havemild effect on veins. Extravascular smooth mus-cle (bronchial, biliary, intestinal, vesical, uterine)is also relaxed.
The dihydropyridines (DHPs) have the mostmarked smooth muscle relaxant and vasodilatoraction; verapamil is somewhat weaker followedby diltiazem.Nitrendipine and few other DHPs have been shown to releaseNO from endothelium and inhibit cAMP-phosphodiesteraseresulting in raised smooth muscle cAMP. These additionalmechanisms may account for their predominant smoothmuscle relaxant action. Released endothelial NO may exertantiatherosclerotic action.
Heart In the working atrial and ventricularfibres, Ca2+ moves in during the plateau phaseof AP and releases more Ca2+ from sarcoplasmicreticulum. This Ca2+ surge causes contraction
through binding to troponin—allowing interactionof myosin with actin (see Fig. 37.3). The CCBswould thus have negative inotropic action.
The 0 phase depolarization in SA and A-Vnodes is largely Ca2+ mediated. Automaticity andconductivity of these cells appear to be dependenton the rate of recovery of the Ca2+ channel.
The L-type Ca2+ channels activate as well asinactivate at a slow rate. Consequently, Ca2+ depo-larized cells (SA and A-V nodal) have aconsiderably less steep 0 phase and longerrefractory period. The recovery process whichrestores the channel to the state from which itcan again be activated (Fig. 39.4) by membranedepolarization is delayed by verapamil anddiltiazem (resulting in depression of pacemakeractivity and conduction), but not by DHPs (theyhave no negative chronotropic/dromotropicaction). Moreover, channel blockade by verapamilis enhanced at higher rates of stimulation, thatby nifedipine is independent of frequency, whilediltiazem is intermediate. Thus, verapamil slowssinus rate and A-V conduction, but nifedipine doesnot. Effect of diltiazem on sinus node automaticityand A-V conduction is similar to that of verapamil.
Fig. 39.4: Activation–inactivation–recovery cycle ofcardiac Ca2+ channels

548S
EC
TIO
N8
CARDIOVASCULAR DRUGS
The relative potencies to block slow channelsin smooth muscle do not parallel those in theheart. The DHPs are more selective for smoothmuscle L channels. At concentrations which causevasodilatation they have negligible negativeinotropic action which is most prominent inverapamil. Diltiazem causes less depression ofcontractility than verapamil. Important differen-ces between the three representative CCBs aresummarized in Table 39.2. Their cardiac electro-physiological effects are compared in Table 38.1.
Verapamil It dilates arterioles and has someα adrenergic blocking activity—decreases t.p.r.but BP is only modestly lowered. The pronounceddirect cardiodepressant effect is partially offsetin vivo by reflex effects of peripheral vasodilata-tion. The HR generally decreases, A-V conduc-tion is slowed, but c.o. is maintained by reflexsympathetic stimulation and reduction in aorticimpedance. However, ventricular contractility maybe markedly impaired in CHF patients. Coronaryflow is increased.Dose: 40–160 mg TDS oral, 5 mg by slow i.v. injection.CALAPTIN 40, 80 mg tabs, 120, 240 mg SR tabs, 5 mg/2 mlinj. VASOPTEN 40, 80, 120 mg tab.
Adverse effects Nausea, constipation andbradycardia are more common than with other
CCBs, while flushing, headache and ankle edemaare less common. Hypotension is occasional andtachycardia (common with DHPs) is absent. Itcan accentuate conduction defects (contraindicatedin 2nd and 3rd degree A-V block) and precipitateCHF in patients with preexisting disease. Cardiacarrest has occurred on i.v. injection and whenit is given to patients with sick sinus.
Interactions Verapamil should not be givenwith β blockers—additive sinus depression,conduction defects or asystole may occur.It increases plasma digoxin level by decreasingits excretion: toxicity can develop.It should not be used along with other cardiacdepressants like quinidine and disopyramide.
Diltiazem It is somewhat less potent vasodilatorthan nifedipine and verapamil, and has modestdirect negative inotropic action, but directdepression of SA node and A-V conduction areequivalent to verapamil. Usual clinical dosesproduce consistent fall in BP with little changeor decrease in HR. Large dose or i.v. injectiondecreases t.p.r. markedly which may elicit reflexcardiac effects. Diltiazem dilates coronaries.Dose: 30–60 mg TDS–QID oral; DILZEM, 30, 60 mg tabs,90 mg SR tab; 25 mg/5 ml inj; ANGIZEM 30, 60, 90, 120,180 mg tab, DILTIME 30, 60 mg tab; 90, 120 mg SR tab.
TABLE 39.2 Comparative properties of representative calcium channel blockers
Verapamil Nifedipine Diltiazem
1. Channel blocking potency ++ +++ +2. Frequency dependence of ++ – +
channel blockade3. Channel recovery rate Much delayed No effect Delayed4. Cardiac effects (In vivo
at usual clinical doses)Heart rate ↓ ↑ ↓, –A-V conduction velocity ↓↓ – ↓↓Contractility –, ↓ ↑ ↓,↑Output –, ↓ ↑ –, ↑
5. Vascular smooth muscle ++ +++ +relaxation
6. Clinical use in Arrhythmia Angina AnginaAngina Hypertension Hypertension(Hypertension) Arrhythmia

549C
HA
PTE
R39
ANTIANGINAL AND OTHER ANTI-ISCHAEMIC DRUGS
Adverse effects Side effects are milder, butthe profile is similar to verapamil. Like verapamil,it also increases plasma digoxin level.Diltiazem should not be given to patients withpreexisting sinus, A-V nodal or myocardialdisease. Only low doses should be given to patientson β blockers.
Nifedipine It is the prototype DHP with a rapidonset and short duration of action. The overridingaction of nifedipine is arteriolar dilatation → t.p.r.decreases, BP falls. The direct depressant actionon heart requires much higher dose, but a weaknegative inotropic action can be unmasked afterβ blockade. As described above, it does notdepress SA node or A-V conduction. Reflexsympathetic stimulation of heart predominatesproducing tachycardia, increased contractility andc.o. No decrease in venous return along withlowering of afterload aids increase in c.o.Coronary flow is increased.Dose: 5–20 mg BD–TDS oral.CALCIGARD, DEPIN, NIFELAT 5, 10 mg cap, also 10 mg,20 mg S.R. (RETARD) tab; ADALAT RETARD 10, 20 mgSR tab.
Adverse effects Frequent side effects are palpi-tation, flushing, ankle edema, hypotension,headache, drowsiness and nausea. These arerelated to peaks of drug level in blood: can beminimized by low starting dose or fractionationof dose or use of retard formulation. Ankle edemais not due to fluid retention, but because of greaterdilatation of precapillary than postcapillaryvessels. Nifedipine has paradoxically increasedthe frequency of angina in some patients. Highermortality among post MI patients has been con-firmed. However, it has been safely administeredwith β blockers and digoxin.
By its relaxant effect on bladder nifedipinecan increase urine voiding difficulty in elderlymales. Gastroesophageal reflux may be worsenedby all DHPs due to relaxation of lower esophagealsphincter. It has also been reported to hamperdiabetes control by decreasing insulin release.
Other dihydropyridines (DHPs)All DHPs have pharmacodynamic profile similarto nifedipine. However, minor differences in organ
selectivity and major differences in pharmaco-kinetic characteristics exhist (Table 39.3). Theslower and longer acting ones induce less reflexsympathetic stimulation. Tachycardia, propensityto increase cardiac work, flushing, headache,dizziness are subdued. They are the favouredDHPs because of milder side effects and becauseincreased mortality among post-MI patients isreported with the regular short-acting nifedipineformulation.
Felodipine It differs from nifedipine in havinggreater vascular selectivity, larger tissue distribu-tion and longer t½. The extended release prepara-tion is suitable for once daily administration.Dose: 5–10 mg OD, max. 10 mg BD.FELOGARD, PLENDIL, RENDIL 2.5, 5, 10 mg ER tab.
Amlodipine Pharmacokinetically it is the mostdistinct DHP and the most popular. Oralabsorption is slow, but complete; peak blood leveloccurs. after 6 to 9 hr—the early vasodilator sideeffects (palpitation, flushing, headache, posturaldizziness) are largely avoided. Because of lessextensive and less variable first pass metabolism,its oral bioavailability is higher and moreconsistent. Volume of distribution and t½ areexceptionally long: diurnal fluctuation in bloodlevel is small and action extends over the nextmorning.Dose: 5–10 mg OD; AMLOPRES, AMCARD, AMLOPIN,MYODURA 2.5, 5, 10 mg tabs.
S(–)Amlodipine The single enantiomer prepa-ration is effective at half the dose and is claimedto cause less ankle edema.Dose: 2.5–5 mg OD;S-NUMLO, S-AMCARD, ASOMEX, ESAM 2.5, 5 mg tabs.
Nitrendipine A DHP with oral bioavailabilityof 10–30% and elimination t½ of 4–12 hours.It has been shown to release NO from theendothelium and inhibit cAMP phosphodiesterase.These may be the additional mechanisms ofvasodilator action. The endothelial NO may retardatherosclerosis. Ventricular contractility andA-V conduction are not depressed. Nitrendipineis indicated in hypertension and angina pectoris.Dose: 5–20 mg OD; NITREPIN, CARDIF 10, 20 mg tabs.

550S
EC
TIO
N8
CARDIOVASCULAR DRUGS
Lacidipine A highly vasoselective newer DHPsuitable for once daily administration. It is claimedto attain higher concentration in vascular smoothmuscle membrane, and is approved only for useas antihypertensive.Dose: 4 mg OD, increase to 6 mg OD if required.LACIVAS, SINOPIL 2, 4 mg tabs.
Nimodipine It is a short-acting DHP whichpenetrates blood-brain barrier very efficiently dueto high lipid solubility. As such, it is believedto selectively relax cerebral vasculature and isapproved for prevention and treatment ofneurological deficit due to cerebral vasospasmfollowing subarachnoid haemorrhage or rupturedcongenital intracranial aneurysms. Side effects areheadache, flushing, dizziness, palpitation andnausea.Dose: 30–60 mg 4–6 hourly for 3 weeks followingsubarachnoid haemorrhage; VASOTOP, NIMODIP,NIMOTIDE 30 mg tab; 10 mg/50 ml inj.
Lercanidipine Another DHP similar to nifedi-pine, but with longer duration of action. Peakplasma concentrations occur at 1.5–3 hrs; t½ is5–10 hours. It is indicated in hypertension at adose of 10–20 mg OD.LEREZ, LERKA 10, 20 mg tabs.
Benidipine A long-acting DHP that owes itslong duration of action to slow dissociation fromthe DHP receptor on the smooth muscle cell.Marketed only in India and Japan, it is indicatedin hypertension and angina pectoris.Dose: 4–8 mg OD; CARITEC 4, 8 mg tab.
PHARMACOKINETICS
The pharmacokinetic parameters of representativeCa2+ channel blockers are tabulated in Table 39.3.
All are 90–100% absorbed orally, peak occurringat 1–3 hr (except amlodipine 6–9 hr). The oralbioavailability of Ca2+ channel blockers isincomplete with marked inter- and intra-individualvariations. This is due to high first pass metabolism(modest and less variable for amlodipine). Allare highly plasma protein bound (min.: diltiazem80%, max.: felodipine 99%).
The Ca2+ channel blockers are high clearancedrugs with extensive tissue distribution. All are> 90% metabolized in liver and excreted in urine.Some metabolites are active. The elimination t½are in the range of 2–6 hr, but that of amlodipineis exceptionally long; followed by lacidipine,nitrendipine and felodipine.
On chronic use verapamil decreases its ownmetabolism—bioavailability is nearly doubled andt½ is prolonged.
USES
Calcium channel blockers can be safely givento patients with obstructive lung disease andperipheral vascular disease in whom β blockersare contraindicated. The problem of reboundworsening of angina on withdrawal after chronicuse is less marked with CCBs than with β blockers.
1. Angina pectoris All CCBs are effective inreducing frequency and severity of classical aswell as variant angina. Benefit in classical anginaappears to be primarily due to reduction in cardiacwork: mainly as a result of reduced afterload andthe BP × HR product. Though, they can increasecoronary flow in normal individuals, this isunlikely to be significant in patients with fixedarterial obstruction. Exercise tolerance isincreased.
TABLE 39.3 Pharmacokinetic characteristics of calcium channel blockers
Drug Bioavailability Vd CL Active Elimin.(L/Kg) (L/hr/Kg) metabolite t½ (hr)
1. Verapamil 15–30% 5.0 0.9 Yes 4–62. Diltiazem 40–60% 3.0 0.7 Yes 5–63. Nifedipine 30–60% 0.8 0.42 Minor 2–54. Felodipine 15–25% 10.0 1.0 None 12–185. Amlodipine 60–65% 21.0 0.42 None 35–45

551C
HA
PTE
R39
ANTIANGINAL AND OTHER ANTI-ISCHAEMIC DRUGS
Many controlled studies and metaanalysishave concluded that myocardial ischaemia maybe aggravated by short-acting DHPs. This maybe due to decreased coronary flow secondary tofall in mean arterial pressure, reflex tachycardiaand coronary steal. The direct cardiac effect ofverapamil and diltiazem to reduce O2 requirement.In addition, less marked reflex sympathetic stimu-lation makes them unlikely to aggravate ischaemia.
Trials using high dose regular short-actingnifedipine formulation have reported increasedmortality among MI patients. The sudden rushof sympathetic activity evoked by each dose ofthese preparations has been held responsible forthe deleterious effect. The slow and long-actingDHPs do not share this disadvantage. There issome evidence that verapamil and diltiazem reducereinfarction and mortality in MI patients (similarto that achieved by β blockers) with uncom-promised ventricular function.
Myocardial infarction: The concensus opinionis against use of CCBs in evolving MI as wellas to prevent further attacks, but verapamil/diltia-zem may be employed for secondary prophylaxiswhen β blockers are contraindicated.
The capacity of CCBs to prevent arterialspasm is undoubtedly responsible for thebeneficial effect in variant angina. Reduction ofcardiac O2 demand would also work in the samedirection. No significant difference in efficacyamong different CCBs has been noted in anginapectoris.
CCBs are not a first line treatment of unstableangina, but may be used as add on therapy tonitrates when coronary vasospasm is prominentand is not counteracted by nitrate alone. Antiplateletdrugs and β blockers + a nitrate are the primarydrugs which reduce infarction and mortality inUA. Use of nifedipine/DHPs in non β blockedpatients is to be avoided.
2. Hypertension All DHPs, diltiazem andverapamil are among the first line drugs forhypertension (see Ch. 40).
3. Cardiac arrhythmias Verapamil and diltia-zem are highly effective in PSVT and for control
of ventricular rate in supraventricular arrhythmias(see Ch. 38).
4. Hypertrophic cardiomyopathy The negativeinotropic action of verapamil can be salutary inthis condition.
5. Other uses Nifedipine is an alternative drugfor premature labour (see p. 333). Verapamil hasbeen used to suppress nocturnal leg cramps. TheDHPs reduce severity of Raynaud’s episodes.
DRUG COMBINATIONS IN ANGINA
Along with any of the drugs used for chronicprophylaxis of angina, sublingual short-actingnitrate is allowed on ‘as and when’ required basisto abort and terminate anginal attacks when theyoccur. In addition to the symptomatic treatmentwith antianginal drugs, therapy aimed at modifyingcourse of coronary artery disease (CAD), and atcardioprotection with antiplatelet drugs, statinsand ACE inhibitors is advised by professionalguidelines. The β blockers ward-off attacks ofangina as well as afford cardioprotection.
Of the three major classes of antianginal drugsdescribed above, generally one agent is usedinitially; choice depends on the stage and severityof disease, associated cardiac/other medicalconditions and individual acceptability of sideeffects. The antianginal efficacy and tolerabilityof long-acting nitrates (including transdermalGTN), β blockers and long-acting CCBs is similar.However, direct comparative studies have foundβ blockers to achieve greater reduction in thenumber of anginal attacks than CCBs, butobjective measurements and outcome were notdifferent. When monotherapy is unable to provideadequate relief in tolerated doses, concurrent useof 2 or 3 drugs may be required.I. β blocker + long-acting nitrate combinationis rational in classical angina because:
(a) Tachycardia due to nitrate is blocked by βblocker.
(b) The tendency of β blocker to cause ventri-cular dilatation is counteracted by nitrate.
(c) The tendency of β blocker to reduce totalcoronary flow is opposed by nitrate.

552S
EC
TIO
N8
CARDIOVASCULAR DRUGS
II. The above advantages may also be obtainedby combining a slow acting DHP (in place ofnitrate) with β blocker. The DHPs are particularlysuitable if there is an element of coronary vaso-spasm in classical angina. However, verapamilor diltiazem should not be used with β blockersince their depressant effects on SA and A-V nodemay add up.III. Nitrates primarily decrease preload, whileCCBs have a greater effect on afterload and oncoronary flow. Their concurrent use may decreasecardiac work and improve coronary perfusion toan extent not possible with either drug alone. Thiscombination may be especially valuable in severevasospastic angina, and when β blockers arecontraindicated.IV. In the more severe and resistant cases ofclassical angina, combined use of all the threeclasses is indicated. Since their primarymechanism of benefit is different, supraadditiveresults may be obtained.• Nitrates primarily decrease preload.• CCBs mainly reduce afterload + increase
coronary flow.• β blockers decrease cardiac work primarily
by direct action on heart.Verapamil/diltiazem should be avoided in suchcombinations.In randomized comparative studies, combinations have beenfound superior to monotherapy only in more severe cases,but not in mild angina. Recent evidence suggests a greaterrole of reflex vasospasm of arteriosclerotic segments ofcoronary arteries in precipitating attacks of angina. As such,coronary dilator action of DHPs/nitrates may be more relevant.
POTASSIUM CHANNEL OPENERS
Minoxidil and diazoxide are K+ channel openerswhich were used earlier in severe hypertensionand hypertensive emergencies. Novel K+ channelopeners like nicorandil, pinacidil and cromakalimhave been developed in the 1990s.
The chemical (intracellular 150 mM vs extracellular4–5 mM) and electrical (inside –90 mV) gradients for K+
across the plasma membrane are in opposite directions. Assuch, depending on the channel, this ion can move in eitherdirection. Such movement is regulated by multiple types ofK+ channels, viz:• Voltage dependent K+ channel
• ATP activated K+ channel• Ca2+ activated K+ channel• Receptor operated K+ channel• Na+ activated K+ channel• Cell volume sensitive K+ channelThese channels regulate K+ movement outward as well asinward, serve diverse functions and exhibit differentsensitivities to drugs. As such, K+ channel openers exhibitconsiderable diversity in action.
The above mentioned drugs open ATP activated K+
channels in smooth muscles. Their most prominent actionis hyperpolarization and relaxation of vascular as well asvisceral smooth muscle. The hypotensive K+ channel openerdiazoxide reduces insulin secretion, while sulfonylureaspromote insulin release by blocking K+ channels in pancreaticβ cells. Nicorandil has been introduced as an antianginaldrug in the 1990s.
Nicorandil This dual mechanism antianginaldrug activates ATP sensitive K+ channels (KATP)thereby hyperpolarizing vascular smooth muscle.The vasodilator action is partly antagonized byK+ channel blocker glibenclamide. Like nitratesit also acts as a NO donor—relaxes blood vesselsby increasing cGMP. Thus, arterial dilatation iscoupled with venodilatation. Coronary flow isincreased; dilatation of both epicardial conduc-ting vessels and deeper resistance vessels has beendemonstrated. No significant cardiac effects oncontractility and conduction have been noted.
Beneficial effects on angina frequency andexercise tolerance comparable to nitrates andCCBs have been obtained in stable as well asvasospastic angina. Nicorandil is believed to exertcardioprotective action by simulating ‘ischaemicpreconditioning’ as a result of activation of mito-chondrial KATP channels. Ischaemic precondition-ing in a phenomenon in which brief periods ofischaemia and reperfusion exert a cardioprotectiveeffect on subsequent total vascular occlusion, andinvolves opening of mito.KATP channels.
A large ‘Impact of nicorandil in angina’ (IONA, 2002)randomized trial found nicorandil to reduce acute coronaryevents in high risk stable angina patients.
Nicorandil is well absorbed orally, nearlycompletely metabolized in liver and is excretedin urine. It exhibits biphasic elimination; the initialrapid phase t½ is 1 hour and later slow phaset½ is 12 hours.
Side effects of nicorandil are flushing,palpitation, weakness, headache, dizziness, nausea

553C
HA
PTE
R39
ANTIANGINAL AND OTHER ANTI-ISCHAEMIC DRUGS
and vomiting. Large painful aphthous ulcers inthe mouth, which heal on stopping nicorandil havebeen reported. Nitrate like tolerance does notoccur with nicorandil, but it has the potential tointeract with sildenafil.Dose: 5–20 mg BD; NIKORAN, 5, 10 mg tabs, 2 mg/vial, 48mg/vial inj; KORANDIL 5, 10 mg tabs.Though nicorandil is an alternative antianginaldrug, its efficacy and long term effects are lesswell established. It has failed to acquire wideacceptance, but may be useful in resistant anginawhen combined with other drugs. Administeredi.v. during angioplasty for acute MI, it is believedto improve outcome.
OTHER ANTIANGINAL DRUGS1. Dipyridamole It is a powerful coronary dilator;increases total coronary flow by preventing uptake anddegradation of adenosine which is a local mediator involvedin autoregulation of coronary flow in response to ischaemia.It dilates resistance vessels and abolishes autoregulation, buthas no effect on larger conducting coronary vessels. Cardiacwork is not decreased because venous return is not reduced.BP is minimally altered. Accordingly, it fails to relieve anginalsymptoms or avert ECG changes.
The pharmacological success but therapeutic failure ofdipyridamole has been explained on the basis of ‘coronarysteal’ phenomenon (Fig. 39.5C). By dilating resistance vesselsin nonischaemic zone as well, it diverts the already reducedblood flow away from the ischaemic zone.
Dipyridamole inhibits platelet aggregation. Bypotentiating PGI2 and increasing cAMP in platelets, itenhances antiaggregatory influences. Though not useful asan antianginal drug, it is being employed for prophylaxis
of coronary and cerebral thrombosis in post-MI and post-stroke patients, as well as to prevent thrombosis in patientswith prosthetic heart valves (see Ch. 44).Dose: 25–100 mg TDS; PERSANTIN, CARDIWELL 25, 75,100 mg tab.
2. Trimetazidine This antianginal drug acts bynonhaemodynamic mechanisms. There is no effecton determinants of myocardial O2 consumption,such as HR and BP, both at rest as well as duringexercise, but angina frequency is reduced andexercise capacity is increased. In patients notadequately controlled by long-acting nitrate/βblocker/CCB, addition of trimetazidine furtherreduced anginal attacks and increased exerciseduration. The mechanism of action of trimetazidineis uncertain, but it may improve cellular toleranceto ischaemia by:• Inhibiting mitochondrial long chain 3-ketoacyl-CoA-
thiolase (LC3-KAT) a key enzyme in fatty acid oxidation—thereby reducing fatty acid metabolism and increasingglucose metabolism in myocardium. Ischaemic myo-cardium shifts to utilizing fatty acid as substrate, therebyincreasing requirement of O2 for the same amount ofATP generated. Since oxidation of fatty acid requiresmore O2, shift back of substrate to glucose would reduceO2 demand.Trimetazidine has been labelled as pFOX (fattyacid oxidation pathway) inhibitor.
• Limiting intracellular acidosis and Na+, Ca2+ accumulationduring ischaemia.
• Protecting against O• free radical induced membranedamage.Trimetazidine is absorbed orally, partly meta-
bolized and largely excreted unchanged in urine;t½ is 6 hr. It is generally well tolerated; side effects
Fig. 39.5: Diagrammatic representation of coronary haemodynamics. A—in classical angina, B — Selective nitrateaction on conducting vessels, which along with ischaemic dilatation of resistance vessels, increases flow to thesubendocardial region → relief of angina. C—Dipyridamole action on all resistance vessels increases blood flow tononischaemic zone to the detriment of ischaemic zone → coronary steal

554S
EC
TIO
N8
CARDIOVASCULAR DRUGS
are—gastric burning, dizziness, fatigue and musclecramps. Reversible parkinsonism has been reportedin the elderly.
Trimetazidine has also been advocated forvisual disturbances, tinnitus, Méniére’s disease,dizziness, etc., but conclusive evidence of efficacyin these conditions is lacking. For ischaemic heartdisease, it has been widely used in France, Spain,some other European countries and India, but notin the UK or USA. It is mostly an add onmedication to conventional therapy in angina andpost-MI patients.Dose: 20 mg TDS.FLAVEDON, CARVIDON, TRIVEDON 20 mg tabs, 35 mgmodified release tab.
3. Ranolazine This novel antianginal drugprimarily acts by inhibiting a late Na+ current(late INa) in the myocardium which indirectlyfacilitates Ca2+ entry through Na+/Ca2+ exchanger.Reduction in Ca2+ overload in the myocardiumduring ischaemia decreases contractility and hasa cardioprotective effect. Sparing of fatty acidoxidation during ischaemia in favour of more O2
efficient carbohydrate oxidation by inhibitingLC3KAT has also been demonstrated. This wasearlier believed to be the main mechanism ofantianginal action of ranolazine, but is nowconsidered secondary. Ranolazine has no effecton HR and BP, but prolongs exercise durationin angina patient.
The efficacy of ranolazine in decreasing frequencyof anginal attacks and in prolonging exercise durationhas been demonstrated both as monotherapy as well aswhen added to conventional drugs in multicentric randomizedtrials: MARISA (monotherapy assessment of ranolazinein stable angina, 2004), CARISA (Combination assessmentof ranolazine in stable angina, 2004), ERICA (Efficacyof ranolazine in chronic angina, 2005). In the MERLIN-TIMI36 (2007) trial on non ST-elevation acute coronarysyndrome patients, ranolazine use was associated with a lowerrate of ventricular arrhythmias. Incidence of AF was alsodecreased. However, ranolazine prolongs Q-T interval, andshould not be used along with other Q-T prolonging drugs(class I and III antiarrhythmics, and other drugs listed onp. 528).
Oral absorption of ranolazine is slow taking4–6 hours with a bioavailability of 30–50%. Itis metabolized in liver mainly by CYP3A4 andexcreted in urine, with an average t½ of 7 hours.
Side effects reported are dizziness, weakness,constipation, postural hypotension, headache anddyspepsia. It should not be given to patients takingCYP3A4 inhibitors.Dose: 0.5–1.0 g BD as SR tab; RANOZEX, RANK,CARTINEX, REVULANT, RANOLAZ 0.5 g SR tab.
4. Ivabradine This ‘pure’ heart rate loweringantianginal drug has been introduced recently asan alternative to β blockers. The only significantaction of ivabradine is blockade of cardiacpacemaker (sino-atrial) cell ‘f’ channels, whichare ‘funny’ cation channels that open during earlypart of slow diastolic (phase 4) depolarization.The resulting inward current (If) determines theslope of phase 4 depolarization. Selectiveblockade of If current by ivabradine results inheart rate reduction without any other electro-physiological or negative inotropic or negativelucitropic (slowing of myocardial relaxation)effect. Heart rate reduction decreases cardiac O2
demand and prolongation of diastole tends toimprove myocardial perfusion (O2 supply).Accordingly, in clinical trials, ivabradine has beenfound to improve exercise tolerance in stableangina and reduce angina frequency.
Ivabradine is well absorbed orally, 40% bioavailable dueto first pass metabolism; degraded by CYP3A4 and excretedin urine with a t½ of 2 hours. Apart from excess bradycardia,the most important adverse effect is visual disturbance.Extrasystoles, prolongation of P-R interval, headache, dizzinessand nausea are the other problems. It should not be used ifheart rate is <60/min, in sick sinus and in AF. Concurrent useof drugs which prolong Q-T or which inhibit CYP3A4 iscontraindicated.
Ivabradine is indicated in chronic stable anginain patients with sinus rhythm who are intolerant toβ blockers or when the latter are contraindicated. Itcan also be used in inappropriate sinus tachycardia.Dose: Initially 5 mg BD, increase if needed to 7.5 mg BD,Elderly 2.5 mg BD.IVABRAD, BRADIA 5, 7.5 mg tab.
5. Oxyphedrine This drug is claimed to improvemyocardial metabolism so that heart can sustain hypoxiabetter. Though used in angina and MI for over 3 decades,its efficacy and status in coronary artery disease is not defined.It can diminish or alter taste sensation.Dose: 8–24 mg TDS oral, 4–8 mg i.v. OD-BD; ILDAMEN8, 24 mg tab., 4 mg/2 ml inj.

555C
HA
PTE
R39
ANTIANGINAL AND OTHER ANTI-ISCHAEMIC DRUGS
DRUGS FOR PERIPHERAL VASCULARDISEASES
Peripheral vascular diseases (PVDs) are either primarilyocclusive (Buerger’s disease with intermittent claudicationof legs), or mainly vasospastic (Raynaud’s phenomenon withepisodic blanching ± cyanosis of fingers followed byhyperaemia), or both as in arteriosclerotic/diabetic vascularinsufficiency, ischaemic leg ulcers, frost bite, gangrene,cerebrovascular inadequacy, etc. Increased cardiovascular riskis associated with all PVDs. Measures that reduce cardio-vascular risk (smoking cessation, BP normalization, anti-platelet drugs, diabetes control, statins, weight management,exercise training) have solutary effect on PVDs as well. Inaddition, vasodilators and some other drugs have been used.
1. Cyclandelate It is a papaverine like general smoothmuscle relaxant which increases cutaneous, skeletal muscleand cranial blood flow in normal individuals. However,efficacy in PVDs is not different from placebo. Side effectsare flushing, palpitation and headache.Dose: 200–400 mg TDS; CYCLOSPASMOL, CYCLASYN200, 400 mg tab/cap.
2. Xanthinol nicotinate (Nicotinyl xanthinate) It isa compound of xanthine and nicotinic acid, both of whichare vasodilators. It increases blood flow in many vascularbeds and has been promoted for cerebrovascular disordersand PVDs, but therapeutic benefits are insignificant.Dose: 300–600 mg TDS oral; 300 mg by i.m. or slow i.v.injection; COMPLAMINA 150 mg tab, 500 mg retard tab,300 mg/2 ml inj.
3. Pentoxiphylline (Oxpentifylline) Ananalogue of theophylline and a weak phospho-diesterase (PDE) inhibitor, it has been shown toincrease blood flow in ischaemic areas by reducingwhole blood viscosity and by improving flexibilityof RBCs. The rheological (dealing with propertyof flow) action rather than vasodilatation is saidto be responsible for improving passage of bloodthrough microcirculation. Thus, the ‘steal’phenomenon is not likely. Oral doses do not affectheart rate, t.p.r. or BP.
Pentoxiphylline is usually well tolerated: sideeffects are nausea, vomiting, dyspepsia andbloating which can be minimized by taking thedrug after meals.Dose: 400 mg BD–TDS; TRENTAL-400, FLEXITAL 400mg SR tab, 300 mg/15 ml for slow i.v. injection.
Pentoxiphylline is mainly used in intermittent claudication(calf pain on walking) due to occlusive vascular disease(Buerger’s disease); walking distance is increased. Other
conditions claimed to be improved are: trophic leg ulcers,transient ischaemic attacks (TIAs), nonhaemorrhagic stroke,and chronic cerebrovascular insufficiency. However, overallbenefits are modest and restricted to a fraction of patients.
4. Cilostazole This is a PDE-3 inhibitor (likethe inodilator inamrinone, p.524) which increasesintracellular cAMP in platelets and vascularsmooth muscle resulting in antiaggregatory andvasodilator effects. In clinical trials it has increasedwalking distance in patients with intermittentclaudication and appears to be more effective thanpentoxiphylline. Since long-term oral milrinonetherapy for heart failure has increased cardiacmortality and has been discontinued, concern isexpressed about long-term safety of cilostazole.However, no increase in cardiovascular mortalityhas so far been observed with cilostazole, buta warning has been issued not to use cilostazolein patients with heart failure. It is also not tobe used in patients who have pain even at rest,or in those with tissue necrosis.
The most common side effect is headache.Others are palpitation, dizziness, nausea, vomiting,weakness and increase in ventricular ectopics ornonsustained VT. Cilostazole is extensivelymetabolized by CYP3A4 and CYP2C19 intoactive and inactive metabolites, together havingelimination t½ of ~ 12 hours. It should not beadministered along with inhibitors of CYP3A4and CYP2C19, which increase its toxicity.
Cilostazole is indicated for intermittent claudi-cation in patients with no rest pain or heart failure.Dose: 100 mg BD, 30 min before or 2 hour after food.PLETOZ, CILODOC, STILOZ 50, 100 mg tabs.
Comment Apart from the above drugs, βadrenergic agonists like isoxsuprine, CCBslike nifedipine and α blockers like prazosin,phenoxybenzamine have been used in PVDs.However, no vasodilator can overcome organicobstruction. Because ischaemia itself is the mostpotent vasodilator stimulus in skeletal muscle andcerebral beds, vasodilators can even divert theblood to nonischaemic areas (steal phenomenon).They obviously are more useful when vasospasmis wholely or partly involved, e.g. in Raynaud’sphenomenon. PGI2 has been employed in severecases with rest pain (p. 190).

556S
EC
TIO
N8
CARDIOVASCULAR DRUGS
DRUG THERAPY IN MYOCARDIALINFARCTION
According to severity, the acute coronarysyndromes may be graded into:• Unstable angina (UA): Vascular obstruction is incomplete,
myocardial necrosis is absent—biochemical markers ofischaemia (see p. 632) do not appear in blood, and STsegment is not elevated in ECG.
• Non ST segment elevation myocardial infarction(NSTEMI): Vascular obstruction is incomplete, but isattended by relatively smaller area of myocardial necrosis;biochemical markers appear in blood, but ST segmentis not elevated.
• ST segment elevation myocardial infarction (STEMI):Vascular obstruction is complete, larger area ofmyocardium is necrosed, biochemical markers areprominent and ST segment in ECG is elevated.
However, UA and NSTEMI may progress to STEMI.Myocardial infarction (MI) is ischaemic necrosisof a portion of the myocardium due to suddenocclusion of a branch of coronary artery. An acutethrombus at the site of atherosclerotic obstructionis the usual cause. About ¼ patients die beforetherapy can be instituted. The remaining are besttreated in specialized coronary care units withcontinuous monitoring of the haemodynamicparameters, biochemical markers and ECG to guidethe selection of drugs and dosage. Those whoreceive such facility can be greatly benefitted bydrug therapy, which according to individual needsis directed to:
1. Pain, anxiety and apprehension After painis not relieved by 3 doses of GTN given 5 minapart, an opioid analgesic (morphine/pethidine)or diazepam is administered parenterally.
2. Oxygenation By O2 inhalation and assistedrespiration, if needed.
3. Maintenance of blood volume, tissueperfusion and microcirculation Slow i.v.infusion of saline/low molecular weight dextran(avoid volume overload).
4. Correction of acidosis Acidosis occurs dueto lactic acid production; can be corrected byi.v. sod. bicarbonate infusion.
5. Prevention and treatment of arrhythmiasProphylactic i.v. infusion of a β blocker (unless
contraindicated) as soon as the MI patient is seenand its continuation orally for a few days hasbeen shown to reduce the incidence of arrhythmiasand mortality. β blockers used early in evolvingMI can reduce the infarct size (myocardialsalvage) and subsequent complications.
Tachyarrhythmias may be treated with i.v.lidocaine, procainamide or amiodarone. Routineprophylactic lidocaine infusion is not recom-mended now. Bradycardia and heart block maybe managed with atropine or electricalpacing.
6. Pump failure The objective is to increasec.o. and/or decrease filling pressure without undulyincreasing cardiac work or lowering BP. Drugsused for this purpose are:(a) Furosemide: indicated if pulmonary wedgepressure is > 20 mm Hg. It decreases cardiacpreload.(b) Vasodilators: venous or combined dilator isselected according to the monitored haemody-namic parameters. Drugs like GTN (i.v.), ornitroprusside have been mainly used.(c) Inotropic agents: dopamine or dobutamine i.v.infusion (rarely digoxin if AF present) may beneeded to augment the pumping action of heartand tide over the crisis.
7. Prevention of thrombus extension,embolism, venous thrombosis Aspirin(162–325 mg) should be given for chewing andswallowing as soon as MI is suspected (if notalready being taken on a regular basis). This iscontinued at 80–160 mg/day. Anticoagulants(heparin followed by oral anticoagulants) are usedprimarily to prevent deep vein thrombosis(increased risk due to bed rest) and pulmonary/systemic arterial embolism. Its value in checkingcoronary artery thrombus extension is uncertain.Any benefit is short-term; anticoagulants arenot prescribed on long-term basis now (seeCh. 44).
8. Thrombolysis and reperfusion Fibrinolyticagents, i.e. plasminogen activators—streptokinase/urokinase/alteplase to achieve reperfusion of

557C
HA
PTE
R39
ANTIANGINAL AND OTHER ANTI-ISCHAEMIC DRUGS
the infarcted area (see Ch. 44). Unlessthrombolysis can be started within 1–2 hours ofMI symptom onset, primary percutaneouscoronary intervention (PCI) with stenting is nowthe preferred revascularization procedure,wherever available.
9. Prevention of remodeling and subsequentCHF ACE inhibitors/ARBs are of provenefficacy and afford long-term survival benefit (seeCh. 36).
10. Prevention of future attacks(a) Platelet inhibitors—aspirin or clopidogrelgiven on long-term basis are routinely prescribed(see Ch. 44).(b) β blockers—reduce risk of reinfarction, CHFand mortality. All patients not having anycontraindication are put on a β blocker for atleast 2 years.(c) Control of hyperlipidaemia—dietary substi-tution with unsaturated fats, hypolipidemic drugsespecially statins (see Ch. 45).
PROBLEM DIRECTED STUDY
39.1 A 55-year-old man presented with complaints of tightness and discomfort over middlepart of chest felt episodically, particularly after walking briskly or climbing stairs or during sex.This is relieved within 5–10 minutes of rest. One or two episodes occur practically every day.He is a past smoker who quit smoking 5 years back when he was diagnosed to have chronicobstructive pulmonary disease (COPD), for which he regularly takes 2 inhalations of Ipratropium Br.3 times a day and 2 puffs of salbutamol inhalation whenever he feels out of breath. The pulsewas 90/min and BP 124/82 mm Hg. The resting ECG was normal, but stress test was positive.A diagnosis of exertional angina was made and he was prescribed—Tab glyceryl trinitrate0.5 mg to be put under the tongue as soon as he begins to feel the chest discomfort, as wellas before undertaking any physical exertion.(a) Should he be prescribed another drug to be taken on a regular basis to prevent episodesof angina? If so, which drugs can be given to him and which cannot be given?(b) Should additional medication be given to prevent long-term complications and improve survival?(see Appendix-1 for solution)

Antihypertensive DrugsChapterChapterChapterChapterChapter 4040404040
These are drugs used to lower BP in hypertension.Hypertension is a very common disorder,
particularly past middle age. It is not a diseasein itself, but is an important risk factor for cardio-vascular mortality and morbidity. The cutoffmanometric reading between normotensives andhypertensives is arbitrary. For practical purposes‘hypertension’ could be that level of BP at orabove which long-term antihypertensive treatmentwill reduce cardiovascular mortality. The JNC 7*(2003) and WHO-ISH@ guidelines (2003) havedefined it to be 140 mm Hg systolic and 90 mmHg diastolic, though risk appears to increase evenabove 120/80 mm Hg. Epidemiological studieshave confirmed that higher the pressure (systolicor diastolic or both) greater is the risk ofcardiovascular disease.
Majority of cases are of essential (primary)hypertension, i.e. the cause is not known. Sympa-thetic and renin-angiotensin systems (RAS) mayor may not be overactive, but they do contributeto the tone of blood vessels and c.o. in hyper-tensives, as they do in normotensives. Manyantihypertensive drugs interfere with theseregulatory systems at one level or the other.Antihypertensive drugs, by chronically loweringBP, may reset the barostat to function at a lowerlevel of BP.
Antihypertensive drug therapy has been remarkably improvedin the last 60 years. Different classes of drugs have receivedprominence with passage of time in this period. Before 1950hardly any effective and tolerated antihypertensive wasavailable. Veratrum and Sod. thiocyanate could lower BP,but were toxic and difficult to use. The ganglion blockersdeveloped in the 1950s were effective, but inconvenient.Reserpine was a breakthrough, but produced mental
depression. The therapeutic potential of hydralazine couldnot be tapped fully because of marked side effects when itwas used alone. Guanethidine introduced in 1961 was animprovement on ganglion blockers. The antihypertensives ofthe 1960–70s were methyldopa, β blockers, thiazide andhigh ceiling diuretics and clonidine. The status of β blockersand diuretics was consolidated in the 1970s and selectiveα1 blocker prazosin broke new grounds. The antihypertensivesof the 1980–90s are angiotensin II converting enzyme(ACE) inhibitors and calcium channel blockers. Angiotensinreceptor blockers (losartan, etc.) were added soon after,and the direct renin inhibitor aliskiren is the latest drug.With the development of many types of drugs, delineationof their long-term benefits and complications, andunderstanding of the principles on which to combine them,hypertension can now be controlled in most cases withminimum discomfort.
CLASSIFICATION
1. DiureticsThiazides: Hydrochlorothiazide,
Chlorthalidone, IndapamideHigh ceiling:Furosemide, etc.K+ Sparing: Spironolactone, Amiloride
2. ACE inhibitorsCaptopril, Enalapril, Lisinopril,Perindopril, Ramipril, Fosinopril, etc.
3. Angiotensin (AT1 receptor) blockersLosartan, Candesartan, Irbesartan, Valsartan,Telmisartan
4. Direct renin inhibitorAliskiren
5. Calcium channel blockersVerapamil, Diltiazem, Nifedipine, Felodipine,Amlodipine, Nitrendipine, Lacidipine, etc.
6. β Adrenergic blockersPropranolol, Metoprolol, Atenolol, etc.
* JNC 7—The seventh report of Joint National Committee (of USA) on prevention, detection, evaluation and treatment of highblood pressure.@ WHO-ISH—World Health Organization and International Society of Hypertension.

559C
HA
PTE
R40
ANTIHYPERTENSIVE DRUGS
7. β + α Adrenergic blockersLabetalol, Carvedilol
8. α Adrenergic blockersPrazosin, Terazosin, DoxazosinPhentolamine, Phenoxybenzamine
9. Central sympatholyticsClonidine, Methyldopa
10. VasodilatorsArteriolar: Hydralazine, Minoxidil,
DiazoxideArteriolar + venous: Sodium nitroprusside
Adrenergic neurone blockers (Reserpine, Guanethidine, etc.)and ganglion blockers (Pentolinium, etc.) are only of histo-rical importance, though reserpine is still marketed.
DIURETICS
Diuretics have been the standard antihyperten-sive drugs over the past 4 decades, thoughthey do not lower BP in normotensives. Theirpharmacology is described in Ch. 41.
Thiazides (hydrochlorothiazide, chlorthalidone)These are the diuretic of choice for uncomplicatedhypertension; have similar efficacy and are doseto dose equivalent. All megatrials have beencarried out with these two only. Chlorthalidoneis longer acting (~ 48 hours) than hydro-chlorothiazide (< 24 hours) and may have betterround-the-clock action. Indapamide (see later) isalso mainly used as antihypertensive, and isequally effective. There is little experience withother members of the thiazide class, and theyshould not be considered interchangeable withhydrochlorothiazide/chlorthalidone as anti-hypertensive. The proposed mechanism of anti-hypertensive action is:1. Initially, the diuresis reduces plasma and e.c.f.volume by 5–15%, and this decreases c.o.2. Subsequently, compensatory mechanismsoperate to almost regain Na+ balance and plasmavolume; c.o. is restored, but the fall in BP ismaintained by a slowly developing reduction int.p.r.3. The reduction in t.p.r. is most probably anindirect consequence of a small (~5%) persistingNa+ and volume deficit. Decrease in intracellular
Na+ concentration in the vascular smooth musclemay reduce stiffness of vessel wall, increase theircompliance and dampen responsiveness toconstrictor stimuli (NA, Ang II). Similar effectsare produced by salt restriction; antihypertensiveaction of diuretics is lost when salt intake is high.A mild slowly developing vasodilator action ofthiazides due to opening of smooth muscle K+
ATP
channels and hyperpolarization has been proposed,but does not appear to be real.
The fall in BP develops gradually over2–4 weeks. During long-term treatment with thia-zides, the heart rate and c.o. remain unaffected,while t.p.r. is reduced despite compensatoryincrease in plasma renin activity, which confirmspersisting Na+ deficit. Thiazides have no effecton capacitance vessels, sympathetic reflexes arenot impaired: postural hypotension is rare.Thiazides are mild antihypertensives, average fallin mean arterial pressure is ~10 mm Hg. Theyare effective by themselves in ~ 30% cases (mostlylow grade hypertension) but they potentiate allother antihypertensives (except DHPs) and preventdevelopment of tolerance to these drugs by notallowing expansion of plasma volume. Thus, incombination, they are useful in any grade ofhypertension. They are more effective in theelderly and maximal antihypertensive efficacy isreached at 25 mg/day dose, though higher dosesproduce greater diuresis. Their antihypertensiveaction is attenuated by NSAIDs.
High ceiling diuretics Furosemide, the pro-totype of this class, is a strong diuretic, but theantihypertensive efficacy does not parallel diureticpotency. Furosemide is a weaker antihypertensivethan thiazides: fall in BP is entirely dependenton reduction in plasma volume and c.o. Theexplanation to this paradox may lie in its briefduration of action. The natriuretic action lastingonly 4–6 hr after the conventional morning doseis followed by compensatory increase in proximaltubular reabsorption of Na+. The Na+ deficientstate in vascular smooth muscle may not bemaintained round-the-clock. The t.p.r. and vascularresponsiveness are not reduced. Moreover, the

560S
EC
TIO
N8
CARDIOVASCULAR DRUGS
high ceiling diuretics are more liable to causefluid and electrolyte imbalance, weakness andother side effects. They are indicated inhypertension only when it is complicated by:
(a) Chronic renal failure: thiazides are ineffec-tive, both as diuretic and as antihypertensive.
(b) Coexisting refractory CHF.(c) Resistance to combination regimens contain-
ing a thiazide, or marked fluid retention dueto use of potent vasodilators.
Desirable properties of thiazide diuretics asantihypertensives are:1. Once a day dosing and flat dose-response curve
permitting simple standardized regimens.2. No fluid retention, no tolerance.3. Low incidence of postural hypotension and
relative freedom from side effects, especiallyCNS, compared to sympatholytics.
4. Effective in isolated systolic hypertension(ISH).
5. Lessened risk of hip fracture in the elderlydue to hypocalciuric action of thiazides.
6. Low cost.
Current status of diuretics asantihypertensivesThe popularity of diuretics as antihypertensivehas had ups and downs. In the 1960–70s theywere almost routinely prescribed alone or incombination, to nearly all hypertensive patients.The usual dose used was hydrochlorothiazide/chlorthalidone 50 mg/day. Soon a number ofdrawbacks were highlighted:• Hypokalaemia—muscle pain, fatigue and loss
of energy.• Erectile dysfunction in males.• Carbohydrate intolerance: due to inhibition of
insulin release (probably secondary to K+
depletion which interferes with conversion ofproinsulin to insulin), precipitation of diabetes.
• Dyslipidemia: rise in total and LDL cholesteroland triglycerides with lowering of HDL. Thiscould increase atherogenic risk, but no directevidence has been obtained.
• Hyperuricaemia: by inhibiting urate excre-tion—increased incidence of gout.
• Increased incidence of sudden cardiac death:attributed to episodes of torsades de pointesand ischaemic ventricular fibrillationprecipitated by hypokalaemia.Consequently, prescribing of diuretics fell.
Over the past 25 years thiazides have been usedat lower doses (12.5–25 mg/day hydrochlorothia-zide or equivalent) alone and in combination witha K+ sparing diuretic.The multiple risk factor intervention trial (1982), the Medicalresearch council trial (1987, 1992), the systolic hypertensionin the elderly programme (SHEP, 1991) and a case controlstudy (1994) demonstrated that increased incidence of deathassociated with thiazide use in the elderly was dose-dependent,and that 25 mg/day yielded the best benefit-risk ratio.Favourable results obtained with ≤ 25 mg/day in the aboveand subsequent studies, including ALLHAT (2002) and ameta-analysis (2003) have reinstated thiazide diuretics asthe first choice antihypertensive.Findings with low dose thiazide therapy are:• Though serum K+ falls a little, significant
hypokalaemia does not occur.• Continuous ECG recording studies have failed
to document increased incidence of arrhythmiasduring low-dose thiazide therapy.
• Impairment of glucose tolerance or increasein serum cholesterol or hyperuricaemia overlong-term are minimal.
• Whereas earlier data had failed to documentreduction in the incidence of MI with thiazides,analysis of recent trials has found them toreduce fatal and nonfatal MI by 27–44%. Theincidence of stroke is reduced by 31–49%.Overall mortality and morbidity is reduced inlong-term trials.
• Though not as effective as ACE inhibitors inreversing left ventricular hypertrophy, somerecent trials in mild to moderate hypertensionhave found thiazides to reduce left ventricularmass.The JNC 7 recommends instituting low-dose
(12.5–25 mg) thiazide therapy, preferably withadded K+ sparing diuretic, as a first choicetreatment of essential hypertension, especially inthe elderly. Higher doses are neither more effectivenor safe. If the low dose (25 mg/day) fails toreduce BP to desired level, another antihyper-tensive should be added, rather than increasing

561C
HA
PTE
R40
ANTIHYPERTENSIVE DRUGS
dose of the diuretic. However, in the treatment ofsevere hypertension when potent vasodilators/sympatholytics have induced fluid retention,higher dose of thiazide or a loop diuretic may beappropriate. Not withstanding the above, there aresubsets of patients in whom other antihyper-tensives are more suitable. Some patients complainimpairment of quality of life with diuretics.
Indapamide It is a mild diuretic, chemicallyrelated to chlorthalidone; reduces BP at doseswhich cause little diuresis. Electrolyte disturban-ces and K+ loss are minimal at antihypertensivedoses. It probably has additional vasodilator actionexerted through alteration of ionic fluxes acrossvascular smooth muscle cell.
Indapamide is well absorbed orally, has anelimination t½ of 16 hr. Single daily dose (2.5mg) is enough.LORVAS, NATRILIX 2.5 mg tab, NATRILIX-SR 1.5 mg SR tabIt is well tolerated: side effects are minor g.i. symp-toms and fatigue. Hypokalaemia is infrequent.
Potassium sparing diuretics Spironolactone,eplerenone and amiloride but not triamterenethemselves lower BP slightly. However, they areused only in conjunction with a thiazide diureticto prevent K+ loss and to augment the anti-hypertensive action. Spironolactone is notfavoured because of its hormonal side effects(gynaecomastia, impotence, menstrual irregu-larities). This problem has been offset in the neweraldosterone antagonist eplerenone, and it isincreasingly used.With the recent appreciation of the role of aldosterone inpromoting hypertension related ventricular and vascularhypertrophy and renal fibrosis, it is considered that aldosteroneantagonists will attenuate these complications. As such, thereis resurgence in their use, especially in refractory hypertension.
Hyperkalemia should be watched when K+
sparing diuretics are used with ACE inhibitors/ARBs.
ANGIOTENSIN CONVERTING ENZYME(ACE) INHIBITORS
The ACE inhibitors are one of the first choicedrugs in all grades of essential as well asrenovascular hypertension (except those with
bilateral renal artery stenosis). Most patientsrequire relatively lower doses (enalapril 2.5–10mg/day or equivalent) which are well tolerated.Used alone they control hypertension in ~50%patients, and addition of a diuretic/β blockerextends efficacy to ~90%. Because of supraaddi-tive synergism, only a low dose of diuretic (12.5mg of hydrochlorothiazide, rarely 25 mg) needsto be added. The pharmacology and use of ACEinhibitors in hypertension are described in Ch.36. Of particular mention are their renal bloodflow improving action, their potential to retarddiabetic nephropathy and their capacity to regressleft ventricular/vascular hypertrophy. They are themost appropriate antihypertensives in patients withdiabetes, nephropathy (even nondiabetic), leftventricular hypertrophy, CHF, angina and postMI cases. Several large prospective studiesincluding AIRE (1993), HOPE (2000), ALLHAT(2002) have confirmed the antihypertensive andcardioprotective effects of ACE inhibitors. Theyappear to be more effective in younger (< 55year) hypertensives than in the elderly. Drypersistent cough is the most common side effectrequiring discontinuation of ACE inhibitors.
ANGIOTENSIN RECEPTOR BLOCKERS
The pharmacology of losartan and other ARBs isdescribed on p. 506. In a dose of 50 mg/daylosartan is an effective antihypertensive. Actionmanifests early and progresses to peak at 2–4weeks. Addition of 12.5 mg/day hydrochlo-rothiazide further enhances the fall in BP. Thenewer ARBs—valsartan, candesartan, irbesartanand telmisartan have been shown to be as effectiveantihypertensives as ACE inhibitors, while losartanmay be somewhat weaker than high doses of ACEinhibitors. ARBs are remarkably free of sideeffects. Because they do not increase kinin levels,the ACE inhibitor related cough is not encoun-tered. Angioedema, urticaria and taste disturbanceare also rare. Though effects of ACE inhibitors andARBs are not identical, the latter have all themetabolic and prognostic advantages of ACEinhibitors.

562S
EC
TIO
N8
CARDIOVASCULAR DRUGS
Several interventional endpoint reduction trials like LIFE(2002), VALUE (outcomes in hypertensive patients withvalsartan or amlodipine, 2004), SCOPE (study on cognitionand prognosis in the elderly; stroke prevention withcandesartan in elderly with isolated systolic hypertension,2004), JLIGHT (Japanese losartan therapy intended for globalrenal protection in hypertensive patients, 2004) have attestedto the favourable effects of ARBs on morbidity and mortalityin hypertensive patients.
As antihypertensive, use of ARBs has out-stripped that of ACE inhibitors. The value ofcombining ARBs with ACE inhibitors is discussedon p. 507.
DIRECT RENIN INHIBITORS
Aliskiren the only available member of the latest class ofRAS inhibitors which act by blocking catalytic activity ofrenin and inhibiting production of Ang I and Ang II. It isdescribed in Ch. 36. Aliskiren is an equally effectiveantihypertensive as ACE inhibitors and ARBs, but experiencewith it so far is limited. However, no remarkable featureshave emerged and presently it is a second line antihypertensivewhich may be employed when the more established ACEinhibitors or ARBs cannot be used, or to supplement them.
CALCIUM CHANNEL BLOCKERS
Calcium channel blockers (CCBs) are anotherclass of first line antihypertensive drugs. Theirpharmacology is described in Ch. 39. All3 subgroups of CCBs, viz. dihydropyridines(DHPs, e.g. amlodipine), phenylalkylamine(verapamil) and benzothiazepine (diltiazem) areequally efficacious antihypertensives. They lowerBP by decreasing peripheral resistance withoutcompromising c.o. Despite vasodilatation, fluidretention is insignificant.Ankle edema that occurs in some patients is due to increasedhydrostatic pressure across capillaries of the dependent partsas a result of reflex constriction of post capillary vesselsin these vascular beds.
The onset of antihypertensive action is quick.With the availability of long acting preparations,most agents can be administered once a day.Monotherapy with CCBs is effective in ~ 50%hypertensives; their action is independent ofpatient’s renin status, and they may improvearterial compliance. Other advantages of CCBsare:
1. Do not compromise haemodynamics: noimpairment of physical work capacity.
2. No sedation or other CNS effects; cerebralperfusion is maintained.
3. Not contraindicated in asthma, angina(especially variant) and PVD patients: maybenefit these conditions.
4. Do not impair renal perfusion.5. Do not affect male sexual function.6. No deleterious effect on plasma lipid profile,
uric acid level and electrolyte balance.7. Shown to have no/minimal effect on quality
of life.8. No adverse foetal effects; can be used during
pregnancy (but can weaken uterine contractionsduring labour).
In the past few years large amount of data from controlledtrials (HINT, TRENT, SPRINT I, II) and metaanalysis hasconsistently indicated increased mortality/reinfarction inpatients treated with standard nifedipine (or other short-actingDHP) formulations. This increase in mortality is dose-related.Worsening of unstable angina and CHF has also been noted.The CCBs do not decrease venous return. DHPs may evenincrease it and jeopardise haemodynamics in patients withdiastolic dysfunction. DHPs (especially short-acting) also tendto increase HR and c.o. by invoking reflex sympatheticstimulation. The increased mortality among coronary heartdisease patients has been attributed to repeated surges ofadrenergic discharge and marked swings of BP attendingeach dose of rapidly acting DHP. However, this risk cannotbe extrapolated to verapamil/diltiazem as broughtout byDAVIT I, II and other controlled studies, as well as to slowacting DHPs (amlodipine type) including nifedipine GITS(gastrointestinal therapeutic system).
The Systolic hypertension in Europe (Syst-EUR) trialhas shown that nitrendipine (long-acting DHP) reducescardiovascular morbidity and mortality in elderly hyper-tensives. The Hypertension optimal treatment (HOT), andSweedish trial in old patients with hypertension-2 (STOP-2) studies have also found CCBs equi-effective as diuretics/β blockers/ACE inhibitors in reducing cardiovascular/totalmortality. No excess mortality with the use of amlodipinein post MI and acute coronary syndrome patients has beennoted in the ALLHAT (2002) study. On the other hand, CCBsdo not afford survival benefit in post MI patients as β blockers,ACE inhibitors or low dose thiazides do. CCBs are alsonot as effective in suppressing left ventricular hypertrophy(a major risk factor in ischaemic heart disease) as ACEinhibitors.
The JNC 7 have considered CCBs to be lesssuitable for monotherapy in hypertensives withno other risk factors, because they appear to afford

563C
HA
PTE
R40
ANTIHYPERTENSIVE DRUGS
less prognostic benefits than thiazides, β blockersand ACE inhibitors/ARBs. However, some recentlarge trials including ASCOT-BPLA (2005) andACCOMPLISH (2008) have testified to superiorefficacy of amlodipine both as monotherapy andwhen combined with an ACE inhibitor forreducing cardiovascular events in high riskhypertensive patients. Thus, CCBs continue tobe used as one of the first line monotherapyoptions because of their high efficacy and excellenttolerability. They are preferred in the elderlyhypertensive. Also there is convincing evidenceof their stroke preventing potential (syst EUR,ALLHAT studies). The long-acting DHPs are nextto ACE inhibitors in reducing albuminuria andslowing disease progression in hypertensive/diabetic nephropathy. They are the most usefulantihypertensives in cyclosporine inducedhypertension in renal transplant recipients.
Use of rapid acting oral nifedipine for urgentBP lowering in hypertensive emergencies is outmoded. In fact, there is currently no therapeuticindication for rapid and short-acting oral DHPsin hypertension.
Other concerns in the use of CCBs as antihyper-tensive are:
(i) The negative inotropic/dromotropic actionof verapamil/diltiazem may worsen CHF andcardiac conduction defects (DHPs are lesslikely to do so).
(ii) By their smooth muscle relaxant action, theDHPs can worsen gastroesophageal reflux.
(iii) CCBs (especially DHPs) may accentuatebladder voiding difficulty in elderly males.
β-ADRENERGIC BLOCKERS
The pharmacology and mechanism of antihyper-tensive action of β blockers is described inCh. 10. They are mild antihypertensives; do notsignificantly lower BP in normotensives. Usedalone they suffice in 30–40% patients—mostlystage I cases. Additional BP lowering may beobtained when combined with other drugs.
The hypotensive response to β blockersdevelops over 1–3 weeks and is then well
sustained. Despite short and differing plasma halflives, the antihypertensive action of most βblockers is maintained over 24 hr with a singledaily dose.
All β blockers, irrespective of associated pro-perties, exert similar antihypertensive effect. Drugswith intrinsic sympathomimetic activity (ISA)cause less/no reduction of HR and c.o. but lowervascular resistance by β2 agonism. Nebivololreduces t.p.r. by generating NO. The nonselectiveβ blockers slightly reduce renal blood flow andg.f.r., but this is minimal in the β1 selectiveblockers and in those with ISA.
There are several contraindications to βblockers, including cardiac, pulmonary andperipheral vascular disease. The nonselectiveβ blockers have an unfavourable effect on lipidprofile (raise triglyceride level and LDL/HDLratio). They have also fared less well on qualityof life parameters like decreased work capacity,fatigue, loss of libido and subtle cognitive effects(forgetfulness, low drive), nightmares and increa-sed incidence of antidepressant use. Many of thesedrawbacks are minimized in the β1 selective agentsand in those which penetrate brain poorly. Patient’sacceptability of a β1 selective hydrophilic druglike atenolol is better than that of propranolol.However, some recent studies have pointed outthat atenolol monotherapy may be less effectivein preventing hypertension related stroke andcoronary artery disease.
Because of absence of postural hypotension,bowel alteration, salt and water retention; a lowincidence of side effects, and once a day regimen,β blockers retain their place among the first choicedrugs recommended by JNC 7 and WHO-ISH,especially for relatively young non-obese hyper-tensives, those prone to psychological stress orthose with ischaemic heart disease. β blockersand ACE inhibitors are the most effective drugsfor preventing sudden cardiac death in post-infarction patients. However, they are less effectivefor primary prophylaxis of MI and for preventingleft ventricular hypertrophy. All cause mortalityhas been lowered in long-term trials by β blockers.Hypertensives with stable heart failure should be

564S
EC
TIO
N8
CARDIOVASCULAR DRUGS
treated with one of the selected β blockers (meto-prolol/bisoprolol/carvedilol/nebivolol) along withan ACE inhibitor/ARB (CIBIS, 1999; MERIT-HF, 1999, COPERNICUS, 2002 studies). Barringthe above subsets of patients with compellingindications and suitability criteria, β blockers arenow less commonly selected as the initialantihypertensive. β blockers are considered lesseffective and less suitable for the older hyper-tensive. The LIFE (2002) and ALLHAT (2002)trials have found β blockers to be inferior to low-dose thiazide or ACE inhibitor/ARB (losartan)or a combination of these in preventing stroke,as well as in diabetic patients. As monotherapy,ACE inhibitors/ARBs and CCBs appear tocompromise quality of life less than β blockers.Rebound hypertension has occurred on suddendiscontinuation of β blockers; myocardialischaemia may be aggravated and angina or MImay be precipitated.
β+α ADRENERGIC BLOCKERSLabetalol (see Ch. 10). It is a combined α and β blocker;reduces t.p.r. and acts faster than pure β blockers. It has beenused i.v. for rapid BP reduction in hyperadrenergic states,cheese reaction, clonidine withdrawal, eclampsia, etc. Orallabetalol therapy is restricted to moderately severe hypertensionnot responding to a pure β blocker, because side effects ofboth α blocker and β blocker occur with it.
Carvedilol This nonselective β + weak selective α1 blockerproduces vasodilatation and has additional antioxidant/freeradical scavenging properties. Whether these ancilliaryproperties confer any superiority is not known. Carvedilolis a frequently selected drug for long-term treatment of CHF,and is approved as an antihypertensive as well. Side effectsare similar to labetalol; liver enzymes may rise in some.
α-ADRENERGIC BLOCKERS
Prazosin (see Ch. 10)This prototype selective α1 antagonist dilatesboth resistance and capacitance vessels; effect onthe former predominating. The haemodynamiceffects, viz reduction in t.p.r. and mean BPaccompanied by minor decrease in venous returnand c.o. are similar to that produced by a directacting vasodilator. However, unlike hydralazine,there is little reflex cardiac stimulation and reninrelease during long-term therapy. Tachycardia does
not compensate for the fall in BP, because releaseinhibitory α2 (presynaptic) receptors are notblocked: autoregulation of NA release remainsintact. It probably decreases central sympathetictone also.
Renal blood flow and g.f.r. are maintainedbut fluid retention may attend fall in B.P. Cardio-vascular reflexes are not appreciably impairedduring chronic therapy, but postural hypotensionand fainting may occur in the beginning—called‘first dose effect’, and with dose increments. Thisdisappears with continued therapy, but may persistin the elderly. For this reason, prazosin is alwaysstarted at low dose (0.5 mg) given at bedtimeand gradually increased with twice dailyadministration till an adequate response isproduced (max. dose 10 mg BD). An oral doseproduces peak fall in BP after 4–5 hours andthe effect lasts for nearly 12 hours, though plasmat½ is only 3 hours. This may be due to generationof active metabolites.
Other advantages of prazosin are:• Does not impair carbohydrate metabolism;
suitable for diabetics, but not if neuropathyis present, because postural hypotension isaccentuated.
• Has a small but favourable effect on lipidprofile: lowers LDL cholesterol and trigly-cerides, increases HDL.
• Affords symptomatic improvement in coexis-ting benign prostatic hypertrophy.
MINIPRESS XL: Prazosin GITS 2.5 mg, 5 mg tabs.;PRAZOPRESS 1, 2 mg tabs.
Adverse effects Prazosin is generally well tole-rated at low doses. Apart from postural hypo-tension related symptoms (particularly in thebeginning), other side effects are headache,drowsiness, dry mouth, weakness, palpitation,nasal blockade, blurred vision and rash.Ejaculation may be impaired in males: especiallywith higher doses. Fluid retention attendingprazosin monotherapy may precipitate CHF.
Use Prazosin is a moderately potent antihyper-tensive, but is not used as a first line drug becausefluid retention and tolerance gradually develops

565C
HA
PTE
R40
ANTIHYPERTENSIVE DRUGS
with monotherapy—necessitating dose increase—more side effects and risk of CHF. It may beadded to a diuretic + β blocker in those notachieving target BP.
Terazosin, Doxazosin These are long-actingcongeners of prazosin with similar properties butsuitable for once daily dosing (see p. 142). Inthe ALLHAT (2002) study doxazosin monotherapyhas doubled the incidence of CHF; but this canoccur with any α1 blocker. A higher incidenceof stroke relative to patients receiving a thiazidediuretic was also noted. Their status inhypertension is similar to that of prazosin.
Nonselective ααααα blockers (Phentolamine,Phenoxybenzamine)
The nonselective α blockers have been disappointing forroutine treatment of hypertension, because fall in t.p.r. iscompensated by increased HR and c.o. They block both α1
and α2 receptors—NA release is accentuated. They arereserved for special situations like pheochromocytoma,clonidine withdrawal, cheese reaction, etc., where circulatingCAs are responsible for the rise in BP.
CENTRAL SYMPATHOLYTICS
Clonidine It is an imidazoline derivative havingcomplex actions. Clonidine is a partial agonistwith high affinity and high intrinsic activity atα2 receptors, especially α2A subtype in brainstem.The major haemodynamic effects result fromstimulation of α2A receptors present mainlypostjunctionally in medulla (vasomotor centre).This decreases sympathetic out flow → fall inBP and bradycardia. Enhanced vagal tonecontributes to bradycardia. Plasma NA declines.Though clonidine is capable of reducing NArelease from peripheral adrenergic nerve endings(release inhibitory prejunctional α2 action), thisis not manifest at clinically used doses. Clonidineis a moderately potent antihypertensive.
Clonidine also activates Imidazoline receptors whichare distinct from α2 receptors and are present in the brainas well as periphery. Activation of medullary imidazolinereceptors also causes decreased sympathetic outflow and fallin BP.
Rapid i.v. injection of clonidine raises BP transientlydue to activation of peripheral postsynaptic vasoconstrictorα2B receptors at the high concentrations so attained. Oral
doses producing lower plasma clonidine levels cause onlyfall in BP, because clonidine has lower intrinsic activity onα2B receptors which predominate in vascular smooth muscle.Probably for the same reason clonidine exhibits the therapeuticwindow phenomenon: optimum lowering of BP occursbetween blood levels of 0.2–2.0 ng/ml. At higherconcentrations fall in BP is less marked.
On chronic administration of clonidine decrease in c.o.contributes more to the fall in BP than decrease in t.p.r.Cardiovascular reflexes are affected little. Decreasedsympathetic flow to the kidney results in reduced renin release.Plasma lipid levels are not altered.
Pharmacokinetics Clonidine is well absorbed orally; peakoccurs in 2–4 hours; 1/2 to 2/3 of an oral dose is excretedunchanged in urine, the rest as metabolites. Plasma t½ is8–12 hours. Effect of a single dose lasts for 6–24 hours.
Dose: Start with 100 µg OD or BD, max. 300 µg TDS, orallyor i.m.CATAPRES 150 µg tab, ARKAMIN 100 µg tab.
Adverse effects Side effects with clonidine are relativelycommon.• Sedation, mental depression, disturbed sleep; dryness of
mouth, nose and eyes (secretion is decreased by centralaction), constipation (antisecretory effect on the intestines).
• Impotence, salt and water retention, bradycardia.• Postural hypotension occurs, but is mostly asymptomatic.• Alarming rise in BP, in excess of pretreatment level, with
tachycardia, restlessness, anxiety, sweating, headache,nausea and vomiting occur in some patients when dosesof clonidine are missed for 1–2 days. The syndrome isvery similar to that seen in pheochromocytoma: plasmacatecholamine (CA) concentration is increased. This isdue to:(a) Sudden removal of central sympathetic inhibition
resulting in release of large quantities of stored CAs.(b) Supersensitivity of peripheral adrenergic structures
to CAs that develops due to chronic reduction ofsympathetic tone during clonidine therapy.
A combination of α blocker with a β blocker, or a potentvasodilator (nitroprusside) or clonidine itself can be usedto treat the syndrome.
Interactions Tricyclic antidepressants and chlorpromazineabolish the antihypertensive action of clonidine, probablyby blocking α receptors on which clonidine acts.
Use Clonidine was a popular antihypertensivein the late 1960s and 1970s, but frequent sideeffects, risk of withdrawal hypertension anddevelopment of tolerance have relegated it to a3rd or 4th choice drug. There is no data onprognostic benefits, if any, of clonidine. At present,it is occasionally used in combination with adiuretic.

566S
EC
TIO
N8
CARDIOVASCULAR DRUGS
Other indications
1. Opioid withdrawal: Opioid and α2 adrenergic systemsconverge on the same effectors in many systems; both activatethe Gi regulatory protein. Clonidine suppresses sympatheticoveractivity of opioid withdrawal syndrome and reducescraving to some extent.
Clonidine has also facilitated alcohol withdrawal andsmoking cessation.2. Clonidine has analgesic activity. It has been used tosubstitute morphine for intrathecal/epidural surgical andpostoperative analgesia.3. Clonidine attenuates vasomotor symptoms of menopausalsyndrome.4. Clonidine has been used to control loose motions dueto diabetic neuropathy. It may be acting by α2 receptormediated enhancement of salt absorption in gut mucosa.
Methyldopa This α-methyl analogue of dopa,the precursor of dopamine (DA) and NA is oneof the first rationally designed antihypertensives.The α methyl-NA (a selective α2 agonist) formedin the brain from methyldopa acts on central α2
receptors to decrease efferent sympathetic acti-vity. Because methyldopa decreases t.p.r. morethan HR or c.o., it may be acting on a differentpopulation of neurones in the vasomotor centrethan clonidine. In large doses, methyldopa inhibitsthe enzyme dopa decarboxylase in brain and peri-phery → reduces NA synthesis and forms thefalse transmitter methyl-NA in periphery as well.These mechanisms were considered to beresponsible for the antihypertensive effect; butit was demonstrated that neither responses tostimulation of sympathetic nerves nor their NAcontent was reduced at clinically used anti-hypertensive doses. Moreover, α methyl NA isas potent vasoconstrictor as NA. The primarycentral site of action of methyldopa has beenconfirmed.
Methyldopa is a moderate efficacy anti-hypertensive. Circulating levels of NA and renintend to fall due to reduction in sympathetic tone.Inhibition of postural reflexes is mild.Pharmacokinetics Though methyldopa is transportedactively by intestinal amino acid carrier, less than 1/3 ofan oral dose is absorbed. It is partly metabolized and partlyexcreted unchanged in urine. Antihypertensive effect developsover 4–6 hours and lasts for 12–24 hours.Dose: 0.25–0.5 g BD–QID oral.
EMDOPA, ALPHADOPA 250 mg tab.
Adverse effects Sedation, lethargy and reduced mentalcapacity are common side effects. Cognitive impairment maydevelop. Dryness of mouth, nasal stuffiness, headache, fluidretention, weight gain, impotence are the other side effects.Postural hypotension is generally mild.Positive Coomb’s test occurs in 1/6 patients, few develophaemolytic anaemia. Fever, rash, hepatitis, ‘flu’ like illness,thrombocytopenia and rarely lupus syndrome occur.Rebound hypertension on sudden withdrawal of methyldopais mild and less common.
Interactions Tricyclic antidepressants reverse its action byblocking its active transport into the adrenergic neurones.
Use Methyldopa was a widely used anti-hypertensive, especially in combination with adiuretic. However, it is infrequently used now,except to treat hypertension during pregnancywherein it has a long track record of safety, bothfor the mother as well as the foetus.
VASODILATORS
Hydralazine/Dihydralazine Introduced in the1950s, it is a directly acting arteriolar vasodilatorwith little action on venous capacitance vessels;reduces t.p.r. and causes greater decrease indiastolic than in systolic BP. Reflex compensatorymechanisms are evoked which cause tachycardia,increase in c.o. and renin release → increasedaldosterone → Na+ and water retention. Thedisproportionate cardiac stimulation appears toinvolve direct augmentation of NA release andmyocardial contractility as well. Thus, ahyperdynamic circulatory state is induced—anginamay be precipitated due to increased cardiac workas well as steal phenomenon. There is no reductionin renal blood flow despite fall in BP. However,fluid retention and edema may occur by the abovemechanism. Tolerance to the hypotensive actiondevelops unless diuretics or β blockers or bothare given together to block the compensatorymechanisms.
The mechanism of vascular smooth musclerelaxant action of hydralazine is not clearly known.Interference with Ca2+ release, opening of certainK+ channels and/or NO generation may beinvolved.

567C
HA
PTE
R40
ANTIHYPERTENSIVE DRUGS
Pharmacokinetics Hydralazine is well absorbed orally, andis subjected to first pass metabolism in liver. The chiefmetabolic pathway is acetylation which exhibits a bimodaldistribution in the population: there are slow and fastacetylators. Bioavailability is higher in slow acetylators, butthese patients are more prone to develop the lupus syndrome.
Hydralazine is completely metabolized both in liver andplasma; the metabolites are excreted in urine, t½ 1–2 hours.However, hypotensive effect lasts longer (12 hours), probablybecause of its persistence in the vessel wall.
Dose: 25–50 mg OD–TDS; NEPRESOL 25 mg tab.
Adverse effects are frequent and mainly due tovasodilatation.• Facial flushing, conjunctival injection, throbbing
headache, dizziness, palpitation, nasal stuffiness, fluidretention, edema, CHF.
• Angina and MI may be precipitated in patients withcoronary artery disease.
• Postural hypotension is not prominent because of littleaction on veins: venous return and c.o. are not reduced.
• Paresthesias, tremor, muscle cramps, rarely peripheralneuritis.
• Lupus erythematosus or rheumatoid arthritis likesymptoms develop on prolonged use of doses above100 mg/day. This is more common in women and inslow acetylators.
Use Hydralazine is now used as a second linealternative only in combination with a diureticand/or β blocker for patients not achieving targetBP with first line drugs. It is one of the preferredantihypertensives during pregnancy, especiallypreeclampsia, because of decades of safety record.Parenterally, it is occasionally employed inhypertensive emergencies. Hydralazine iscontraindicated in older patients and in those withischaemic heart disease.
The arteriolar dilator action of hydralazinecan be employed in the management of CHFparticularly in combination with isosorbidedinitrate (see p. 522).Minoxidil It is a powerful vasodilator, the pattern of actionresembling hydralazine, i.e. direct relaxation of arteriolarsmooth muscle with little effect on venous capacitance.Marked vasodilatation elicits strong compensatory reflexes:increased renin release and proximal tubular Na+ reabsorption→ marked Na+ and water retention → edema and CHF mayoccur. Reflex sympathetic activity causes palpitation andincreased c.o. To offset these, it has to be used along witha loop diuretic and a β blocker.
Minoxidil is a prodrug—converted to an active metabolite(by sulfate conjugation) which is an opener of ATP operatedK+ channels; acts by hyperpolarizing smooth muscle.
Minoxidil is indicated only rarely in severe or life-threatening hypertension.
Use in alopecia Oral minoxidil increasesgrowth of body hair. Applied topically (2% twicedaily) it promotes hair growth in male patternbaldness and alopecia areata. The response isslow (takes 2–6 months) and incomplete, but upto60% subjects derive some benefit, albeit for shortperiods. Baldness recurs when therapy isdiscontinued. The mechanism of increased hairgrowth is not known; may involve:(a) Opening of K+ channels and enhancedmicrocirculation around hair follicles.(b) Direct stimulation of resting hair follicles.(c) Alteration of androgen effect on geneticallyprogrammed hair follicles.Local irritation, itching and burning sensation arefrequent. Dermatological reaction and systemicside effects (headache, dizziness, palpitation)occur in 1–3% cases.MINTOP, GROMANE 2% scalp lotion, MULTIGAIN 2%topical solution and metered spray, MANEXIL 5% gel; applytwice a day.
Diazoxide This K+ channel opener arteriolar dilator wasused in the past for rapid reduction of BP in hypertensiveemergencies. Administered by rapid i.v. injection it can beemployed in place of nitroprusside, when regulated i.v.infusion or close monitoring is not possible.
Sodium nitroprusside It is a rapidly (withinseconds) and consistently acting vasodilator; hasbrief duration of action (2–5 min) so that vasculartone can be titrated with the rate of i.v. infusion.It relaxes both resistance and capacitance vessels:reduces t.p.r. as well as c.o. (by decreasing venousreturn). Myocardial work is reduced—ischaemiais not accentuated, as occurs with selective arte-riolar dilators (hydralazine). Little reflex tachy-cardia is produced in supine posture. Plasma reninis increased.
In patients with heart failure and ventriculardilatation, nitroprusside improves ventricularfunction and c.o. mainly by reducing aorticimpedance (afterload), but also by lowering atrialfilling pressure (preload).
Endothelial cells, RBCs (and may be othercells) split nitroprusside to generate NO which

568S
EC
TIO
N8
CARDIOVASCULAR DRUGS
relaxes vascular smooth muscle. This occurs bothenzymatically and nonenzymatically. The enzymesinvolved are different from those that produceNO from glyceryl trinitrate. Nonenzymatically itis converted to NO (and CN) by glutathione. Thismay be responsible for the different pattern ofvasodilator action compared to nitrates, as wellas for the fact that no nitrate like tolerancedevelops to nitroprusside action.
Nitroprusside has gained popularity in themanagement of hypertensive emergencies; 50 mgis added to a 500 ml bottle of saline/glucosesolution. The infusion is started at 0.02 mg/minand titrated upward with the response: 0.1–0.3mg/min is often needed. It decomposes at alkalinepH and on exposure to light: the infusion bottleshould be covered with black paper.
Nitroprusside is split to release cyanide. Thelatter is converted in liver to thiocyanate whichis excreted slowly. If larger doses are infusedfor more than 1–2 days, excess thiocyanate mayaccumulate and produce toxicity, includingpsychosis.
Side effects mainly due to vasodilatation are—palpitation, nervousness, vomiting, perspiration,pain in abdomen, weakness, disorientation, andlactic acidosis (caused by the released cyanide).
Nitroprusside has also been used to producecontrolled hypotension, in refractory CHF (seep. 522), pump failure accompanying MI and inacute mitral regurgitation.SONIDE, PRUSIDE, NIPRESS 50 mg in 5 ml inj.
ADRENERGIC NEURONE BLOCKERS
Reserpine It is an alkaloid from the roots of Rauwolfiaserpentina (sarpgandha) indigenous to India which has beenused in ‘Ayurvedic’ medicine for centuries. The pure alkaloidwas isolated in 1955 and later found to act by causing CAand 5-HT depletion. It was a popular antihypertensive ofthe late 1950s and early 1960s, but is now used only asa pharmacological tool.
Reserpine acts at the membrane of intraneuronal vesicleswhich store monoamines (NA, DA, 5-HT) and irreversiblyinhibits the vesicular monoamine transporter (VMAT2). Themonoamines are gradually depleted and degraded by MAO.The effects last long after the drug is eliminated (hit andrun drug) because tissue CA stores are restored only gradually.
Higher doses deplete CAs and 5-HT in the brain aswell; cause sedation and mental depression. Antipsychotic
effect (mild) and extrapyramidal symptoms are produced dueto DA depletion.SERPASIL 0.25 mg tab; 1 mg/ml inj.
Guanethidine It is a polar guanidine compound whichis taken up into the adrenergic nerve endings byactive amine transport, and has three important facets ofaction:(a) Displaces NA from storage granules stoichiometrically.(b) Inhibits nerve impulse coupled release of NA.(c) Engages and blocks NA uptake mechanism at the axonalmembrane.
Guanethidine has gone out of use now due to marked sideeffects.
TREATMENT OF HYPERTENSION
The aim of antihypertensive therapy is to preventmorbidity and mortality associated with persis-tently raised BP by lowering it to an acceptablelevel, with minimum inconvenience to thepatient. Both systolic and diastolic BP predictthe likelihood of target organ damage (TOD) andcomplications such as:(a) Cerebrovascular disease, transient ischaemicattacks, stroke, encephalopathy.(b) Hypertensive heart disease—left ventricularhypertrophy, CHF.(c) Coronary artery disease (CAD), angina, myo-cardial infarction, sudden cardiac death.(d) Arteriosclerotic peripheral vascular disease,retinopathy.(e) Dissecting aneurysm of aorta.(f) Glomerulopathy, renal failure.Patients who have already suffered some TODhave greater risk of further organ damage anddeath at any level of raised BP, than those withoutTOD.
The JNC 7 (2003) has reclassified BP readingsas:
Since the risk of complications depends notonly on the level of BP, but also on other riskfactors (see box) and existing TOD, these have
BP (mm Hg)BP classification Systolic Diastolic
1. Normal <120 and <80 2. Prehypertension 120–139 or 80–89 3. Hypertension Stage I 140–159 or 90–99 4. Hypertension Stage II ≥ 160 or ≥ 100

569C
HA
PTE
R40
ANTIHYPERTENSIVE DRUGS
also to be considered in deciding when to startdrug therapy, as well as in selection of drugsand in devising therapeutic regimens.
activity or exercise, weight reduction, moderationin alcohol intake, mental relaxation, etc.) shouldbe tried first and concurrently with drugs. Thelevel to which BP should be lowered is uncertain.A value of < 140 systolic and < 90 mmHg diastolicis considered adequate response, because it clearlyreduces morbidity and mortality, though riskreduction may continue upto 120/80 mm Hg interms of CAD, heart failure, stroke, etc. Whensignificant cardiovascular and/or renal damage hasalready occurred, lowering BP to normotensivelevel may not be tolerated: edema, CHF, angina,rise in blood urea and syncope may beprecipitated. Therefore, reduce BP gradually andonly to the level tolerated.
The Swedish trial in old patients with hypertension-2(STOP-2, 1999) conducted over 5 years in 6614 hypertensivesaged 70–84 years showed that conventional therapy withdiuretic and/or β blockers is as effective in reducing BPand risk of major cardiovascular events as are ACE inhibitorsor CCBs. The ALLHAT (2002) study comparing chlorthalidone,lisinopril and amlodipine has also found no difference inthe primary outcomes of death and MI. The results conveythat efficacywise there is little to choose among the 4 classesof drugs; choice of initial drug has to be guided by associatedfeatures/contraindications and acceptable side effects inindividual patients.
With the recognition of 4 groups of first choiceantihypertensive drugs viz. diuretics, ACEinhibitor/ARBs, CCBs and β blockers, as wellas their evaluation in large randomized trials, a‘stepped care’ approach (initially using a singledrug and progressively adding 1–3 more drugs,as required, from different groups), is recom-mended by most experts and therapeuticguidelines. The drug for initial therapy is selectedon the basis of compelling indications (if present),suitability criteria taking into consideration theage, life style issues, risk factors, concomitantmedical conditions, tolerability in respect of theindividual patient and cost of different drugs. Foreach class of antihypertensive drugs, certainpatients can be identified who are best suited tobe treated with it, and those in whom it shouldbe avoided (see box).
The general principles of antihypertensivetherapy enunciated in JNC7, WHO-ISH and
Cardiovascular risk factors
1. Age > 55 years (men), > 65 years (women)2. Family h/o premature CV disease3. Smoking4. Dyslipidemia (↑LDL, ↓HDL, ↑TG)5. Diabetes mellitus6. Hypertension7. Obesity (BMI ≥ 30)8. Microalbuminuria or g.f.r. < 60 ml/min
The JNC7 have also identified compellingindications (see box) which may mandate use ofspecific antihypertensive drugs even in patientswith BP values in the ‘prehypertension’ range.Moreover, presence of compelling indications maysuggest fixing a lower target BP value to beattained by drug therapy.
Compelling indications for use ofantihypertensive drugs
1. Heart failure2. High coronary artery disease (CAD) risk3. H/o MI in the past4. H/o stroke in the past5. Diabetes6. Chronic renal disease
Beneficial effects of lowering BP has beenestablished in all patients having BP above140/90 mm Hg, and even in the 120–139 (systolic)or 80–89 mm Hg (diastolic) range in those withcompelling indications or cardiovascular riskfactors; e.g. in diabetics, lowering diastolic BPto 80 mmHg was found to reduce cardiovascularevents more than reducing it upto 90 mm Hg.
Data from several large studies has shownthat effective use of antihypertensive drugs reducesoccurrence of stroke by 30–50%, heart failureby 40–50% and coronary artery disease (CAD)by ~15%.
If the cause of hypertension can be identified(hormonal, vascular abnormality, tumour, renaldisease, drugs) all efforts should be made toremove it. Nonpharmacological measures (lifestyle modification—diet, Na+ restriction, aerobic

570S
EC
TIO
N8
CARDIOVASCULAR DRUGS
Selection of first line antihypertensive drugs
Compelling indications Suitable for To be avoided in
Diuretics1. Heart failure 1. Older patients 1. Gout or family history of gout2. High CAD risk 2. Isolated systolic hypertension 2. Abnormal lipid profile3. Recurrent stroke prevention 3. Obese with volume overload 3. Pregnancy induced hypertension4. Diabetes 4. Low cost therapy
ACE inhibitors/Ang II receptor blockers1. Heart failure 1. Relatively young patients 1. Bilateral renal artery stenosis2. Post-MI 2. Patients with left ventricular or that in single kidney3. High CAD risk hypertrophy 2. Pregnancy4. Diabetes 3. Gout, PVD, dyslipidemic 3. Hyperkalaemia5. Chronic kidney disease patients 4. Preexisting dry cough6. Recurrent stroke prevention (ACE inhibitor)
βββββ Adrenergic blockers(especially applicable tononselective β blockers)
1. Stable heart failure 1. Coexisting anxiety or tachycardia 1. Asthma, COPD2. Post-MI 2. Relatively young patient 2. Bradycardia, conduction defects3. High CAD risk 3. Migraine patients 3. Decompensated heart failure
4. Low cost therapy 4. PVD5. Abnormal lipid profile
Calcium channel blockers1. Recurrent stroke prevention 1. Older with poor 1. Myocardial in-
arterial wall compliance adequacy, CHF Verapamil2. Isolated systolic hypertension 2. Conduction defects, and3. Asthma/COPD patients sick sinus diltiazem4. Raynaud’s (and other 3. Receiving β blockers
PVD) patients 4. Ischaemic heart5. Pregnant hypertensive disease; post MI cases6. Diabetics 5. Males with prostate DHPs
enlargement6. Gastroesophageal reflux
⎫⎬⎭
⎫⎬⎭
British Hypertension Society* (BHS) 2004,guidelines may be summarized as:1. Except for stage II hypertension, start with
a single most appropriate drug, which formajority of patients is a thiazide. However,an ACE inhibitor/ARB or CCB or in somecases β blocker may also be considered. Manyexperts now opine that β blockers should nolonger be regarded as first choice drugs, exceptfor patients with compelling indications orsuitability features.
2. The BHS (2004) recommended following the AB C D rule (A—ACE inhibitor/ARB; B—βblocker; C—CCB, D—diuretic). While A and(in some cases) B are preferred in youngerpatients (<55 years), C and D are preferred in theolder (> 55 years) for the step I or monotherapy.
3. Initiate therapy at low dose; if needed increasedose moderately. Thiazide dose should be12.5–25 mg/day hydrochlorothiazide orchlorthalidone.
4. If only partial response is obtained, add a drugfrom another complimentary class or changeto low dose combination (antihypertensiveaction of the components adds up, while sideeffects being different, do not).
* Williams B: British Hypertension Society. Guidelinesfor management of hypertension: report of the 4th workingparty of the British Hypertension Society. J HumHypertens. 2004; 18(3): 139-185.

571C
HA
PTE
R40
ANTIHYPERTENSIVE DRUGS
5. If no response, change to a drug from anotherclass, or low dose combination from otherclasses.
6. In case of side effect to the initially chosendrug, either substitute with drug of anotherclass or reduce dose and add a drug fromanother class.
7. Majority of stage II hypertensives are startedon a 2 drug combination; one of which usuallyis a thiazide diuretic.
With the above approach 50–70% stage Ihypertensives can be successfully treated, at leastinitially, with monodrug therapy. A simple regimenwith once or twice daily drug dosing is most likelyto be complied with. Because most stage I andsome stage II hypertension patients are asymp-tomatic, a drug which makes them symptomatic(one or the other side effect) is not likely to beaccepted for prolonged periods. Effect of the drugon quality of life measured by sense of wellbeing,energy level, mental acuity, drive, libido, sleep,life satisfaction, etc. is an important criterion indrug selection.
Combination therapy Though JNC 7, WHO-ISH and BHS guidelines emphasise on single drugtherapy, the addition of a second (and third oreven fourth) drug is also highlighted whenmonotherapy fails. In practice, a large majorityof hypertensives ultimately require 2 or moredrugs. In the HOT study 70% patients whoachieved target BP were being treated with 2drugs.
Since BP is kept up by several interrelatedfactors, an attempt to block one of them tendsto increase compensatory activity of the others.It is rational in such cases to combine drugs withdifferent mechanisms of action or different patternsof haemodynamic effects:
(a) Drugs which increase plasma renin activity—diuretics, vasodilators, CCBs, ACE inhi-bitors may be combined with drugs whichlower plasma renin activity—β blockers,clonidine, methyldopa.
(b) All sympathetic inhibitors (except β bloc-kers) and vasodilators, except CCBs, cause
fluid retention leading to tolerance. Additionof a diuretic checks fluid retention anddevelopment of tolerance.
(c) Hydralazine and DHPs cause tachycardiawhich is counteracted by β blockers, whilethe initial increase in t.p.r. caused by non-selective β blockers is counteracted by thevasodilator.
(d) ACE inhibitors/ARBs are particularly syner-gistic with diuretics; this combination is verygood for patients with associated CHF or leftventricular hypertrophy.
(e) In step 2 when two drugs are to be used, theBHS recommend combining one out of A orB with one out of C or D.
(f) Use of combined formulation improvescompliance and usually lowers cost.
(g) In the step 3 (when two drugs are inadequatein achieving target BP lowering), triple drugregimen is prescribed. Both C and D arecombined with A or B, whereby large majo-rity of patients are adequately controlled.
(h) Patients who fail to reach the goal BP despitebeing adherent to full doses of an appropriate3 drug (including a diuretic) regimen, havebeen labelled by JNC7 as ‘resistant hyper-tension’. In them even 4 drug therapy step 4may have to be given to achieve the targetBP. However, the patient must be reevaluatedand factors like non-compliance, pseudoto-lerance, need for a loop diuretic, drug inter-actions, secondary hypertension, etc. mustbe first excluded. All four first line drugs areused together, or an α1 blocker is includedwith 3 first line drugs. Eplerenone also isbeing used as the 4th drug now. Hydralazineor clonidine are rarely included.
Combinations to be avoided
1. An α or β adrenergic blocker with clonidine:apparent antagonism of clonidine action hasbeen observed.
2. Hydralazine with a DHP or prazosin; becauseof similar pattern of haemodynamic action.

572S
EC
TIO
N8
CARDIOVASCULAR DRUGS
3. Verapamil or diltiazem with β blocker, becausemarked bradycardia, A-V block can occur.
4. Methyldopa with clonidine or any two drugsof the same class.
Some antihypertensive combinations1. Amlodipine 5 mg + Lisinopril 5 mg—AMLOPRES-
L, LISTRIL-AM2. Amlodipine 5 mg + Atenolol 50 mg—AMCARD-AT,
AMLOPIN-AT, AMLOPRES-AT3. Amlodipine 5 mg + Enalapril 5 mg—AMACE,
AMTAS-E4. Atenolol 25 mg or 50 mg + chlorthalidone 12.5 mg—
TENOCLOR, TENORIC5. Enalapril 10 mg + Hydrochlorothiazide 25 mg—
ENACE-D, VASONORM-H6. Ramipril 2.5 mg + Hydrochlorothiazide 12.5 mg—
CARDACE-H7. Losartan 50 mg + Hydrochlorothiazide 12.5 mg—
LOSAR-H, TOZAAR-H, LOSACAR-H8. Lisinopril 5 mg + Hydrochlorothiazide 12.5 mg—
LISTRIL PULS, LISORIL-HT9. Losartan 50 mg + Ramipril 2.5 mg or 5 mg—TOZAAR-
R, LAPIDO-R10. Losartan 50 mg + Amlodipine 5 mg—AMCARD-LP,
AMLOPRESS-Z, LOSACAR-A11. Losartan 50 mg + Ramipril 2.5 mg + Hydrochlorothiazide
12.5 mg—LOSANORM-HR12. Irbesartan 150 mg + Hydrochlorothiazide 12.5 mg—
IROVEL-H, XARB-H.
When the BP has been well controlled for > 1year, stepwise reduction in dose and/or withdrawalof one or more components of a combinationmay be attempted to workout a minimal regimenthat will maintain the target BP. However, in mostpatients of essential hypertension, drug therapyis usually life-long.
Hypertension in pregnancy A sustained BPreading above 140/90 mm Hg during pregnancyhas implications both for the mother and thefoetus: reduction of BP clearly reduces risks. Twotypes of situations are possible:
(a) A woman with preexisting essential hyper-tension becomes pregnant.
(b) Pregnancy induced hypertension; as intoxaemia of pregnancy—preeclampsia.
Toxaemic hypertension is associated witha hyperadrenergic state, decrease in plasmavolume (despite edema) and increase in vascularresistance.
In the first category the same therapy insti-tuted before pregnancy may be continued.However, one of the ‘safer’ drugs listed belowmay be substituted if one of the ‘drugs to beavoided’ was being used.
Antihypertensives to be avoided duringpregnancy
ACE inhibitors, ARBs: Risk of foetal damage,growth retardation.Diuretics: Tend to reduce blood volume—accentuate uteroplacental perfusion deficit (oftoxaemia)—increase risk of foetal wastage,placental infarcts, miscarriage, stillbirth.Nonselective β blockers: Propranolol has beenimplicated to cause low birth weight, decreasedplacental size, neonatal bradycardia andhypoglycaemia.Sod. nitroprusside: Contraindicated in eclampsia.
Antihypertensives found safer duringpregnancyHydralazineMethyldopa (a positive Coombs’ test occurs, buthas no adverse implication).Dihydropyridine CCBs: if used, they should be
discontinued before labour as they weakenuterine contractions.
Cardioselective β blockers and those with ISA,e.g. atenolol, metoprolol, pindolol, acebutolol:may be used if no other choice.
Prazosin and clonidine—provided that posturalhypotension can be avoided.
Hypertensive emergencies and urgenciesSystolic BP > 220 or diastolic BP > 120 mm Hg with evidenceof active end organ damage is labelled ‘hypertensiveemergency’, while the same elevation of BP without overtsigns of endorgan damage is termed ‘hypertensive urgency’.Severity and rate of progress of TOD determines theseriousness of the condition.
Controlled reduction of BP over minutes (inemergencies) or hours (in urgencies) is requiredto counter threat to organ function and life in:1. Cerebrovascular accident (haemorrhage) or
head injury with high BP.2. Hypertensive encephalopathy.

573C
HA
PTE
R40
ANTIHYPERTENSIVE DRUGS
3. Hypertensive acute LVF and pulmonary edema.4. Unstable angina or MI with raised BP.5. Dissecting aortic aneurysm.6. Acute renal failure with raised BP.7. Eclampsia.8. Hypertensive episodes in pheochromocytoma,
cheese reaction or clonidine withdrawal.
Oral therapySome rapidly acting oral hypotensive drugs have been usedin hypertensive urgencies, but are now considered neithernecessary nor safe.
Nifedipine (10 mg soft geletine cap.) orally or s.l. every30 min was widely employed in urgencies. This practicehas now been abandoned because it often causes abrupt fallin BP and precipitates MI or stroke, or may be fatal. Oncethe drug is ingested, rate and degree of fall in BP cannotbe controlled, and adverse consequences outweigh anyadvantage.
Captopril (25 mg oral every 1–2 hours) was also used, butresponse is variable and it carries risk of excessivehypotension.
Clonidine (100 μg every 1–2 hours oral) acts mostly in30–60 min, but produces sedation and rebound rise in BPon stopping the drug.
Parenteral therapyParenteral (preferably i.v.) drugs with controllableaction are used both in emergencies and inurgencies (less vigorously in the latter).
However, many experts consider that in theabsence of end organ damage (urgencies), i.v.drugs are not necessary; slow reduction of BPwith oral drugs is adequate and safer.
Mean BP should be lowered by no more than25% over a period of minutes or a few hoursand then gradually to not lower than 160/100mm Hg. Drugs employed are:1. Sodium nitroprusside (see p. 567) Because
of predictable, instantaneous, titratable andbalanced arteriovenous vasodilatory actionwhich persists without tolerance till infused,nitroprusside (20–300 μg/min) is the drug ofchoice for most hypertensive emergencies.However, it is toxic in high dose and whenused for longer period. GTN may be betterchoice when there is associated MI or LVF.In aortic dissection, nitroprusside may require
concurrent esmolol infusion. Another limitationis that nitroprusside needs an infusion pumpand constant monitoring.
2. Glyceryl trinitrate (see p. 543) Given byi.v. infusion (5–20 μg/min) GTN also actswithin 2–5 min and has brief titratableaction, but is a less potent hypotensive. Itspredominant venodilator action makes itparticularly suitable for lowering BP aftercardiac surgery and in acute LVF, MI, unstableangina, but not in other conditions. Tolerancestarts developing after 18–24 hours ofcontinuous infusion.
3. Hydralazine (see p. 566) 10–20 mg i.m. or slow i.v.injection; acts in 20–30 min and keeps BP low for4–8 hours, but is less predictable, and not a first linedrug. It has been especially used in eclampsia. It causestachycardia and should be avoided in patients withmyocardial ischaemia or aortic dissection.
4. Esmolol (see p. 149) This β blocker given as0.5 mg/kg bolus followed by slow i.v. injection(50–100 μg/kg/min) acts in 1–2 min; actionlasts for 10–20 min. It is particularly usefulwhen cardiac contractility and work is to bereduced, such as in aortic dissection. Nitroprus-side is given concurrently, because the BP lower-ing action is weaker. It is a useful hypotensiveand bradycardiac drug during and after anaes-thesia. Excess bradycardia is to be guarded.
5. Phentolamine (see p. 141) This nonselectiveα1 + α2 blocker is the drug of choice for hyper-adrenergic states, e.g. hypertensive episodesin pheochromocytoma, cheese reaction orclonidine withdrawal. Injected i.v. (5–10 mg)it acts in 2 min and action lasts 5–15 min.Tachycardia and myocardial ischaemiamay complicate its use. A β blocker may beadded.
6. Labetalol Injected i.v., it is an alternativeto an α blocker + a β blocker combinationfor lowering BP in pheochromocytoma, etc.but has only weak α blocking action. It hasbeen used to lower BP in MI, unstable angina,eclampsia as well. It is also good for patientswith altered consciousness, because it does notcause sedation or increase intracranial pressure.Concomitant CHF or asthma preclude its use.

574S
EC
TIO
N8
CARDIOVASCULAR DRUGS
7. Furosemide (20–80 mg oral or i.v.) It may be givenas an adjunct with any of the above drugs if thereis volume overload (acute LVF, pulmonary edema,CHF) or cerebral edema (in encephalopathy), butshould be avoided when patient may be hypovolemicdue to pressure induced natriuresis (especially ineclampsia, pheochromocytoma).
PROBLEM DIRECTED STUDY
40.1 A 70-year-old male presented with complaint of dull headache, giddiness, weakness andoccasional breathlessness. He gave history of left sided paralytic stroke about 2 years back, fromwhich he has recovered nearly completely, but is taking Aspirin 75 mg per day. The pulse was66/min. The BP was found to range between 152–160 mm Hg systolic and 82–86 mm Hg diastolic,when measured on 3 occasions over one week. The ECG showed signs of left ventricular hypertrophy,but no ischaemia. Fundus examination revealed mild age related changes. Fasting blood sugarwas 96 mg/dl; kidney function, liver function tests and lipid profile were within normal range.(a) Should he be prescribed antihypertensive medication? If so, whether one, or more than one,antihypertensive should be prescribed concurrently, and which drug/drugs will be more suitablefor him?(see Appendix-1 for solution)
Fenoldopam (depamine agonist), nicardipine andclevidipine (parenteral DHPs), enalaprilat (aparenteral ACE inhibitor) and trimethaphan (aganglion blocker) are other drugs for hypertensiveemergencies. They are occasionally used in othercountries.

Relevant Physiology ofUrine Formation
SECTION 9
DRUGS ACTING ON KIDNEY
Urine formation starts from glomerular filtration(g.f.) in a prodigal way. Normally, about 180 Lof fluid is filtered everyday: all soluble
constituents of blood minus the plasma proteins(along with substances bound to them) and lipids,are filtered at the glomerulus. More than 99%
Fig. IX.1: Diagrammatic representation of nephron showing the four sites of solute reabsorption.The thick ascending limb of loop of Henle is impermeable to water; Glu.—Glucose; A.A.—Amino acid;Org. An.—Organic anions.
Chapter 41a

576S
EC
TIO
N9
DRUGS ACTING ON KIDNEY
of the glomerular filtrate is reabsorbed in thetubules; about 1.5 L urine is produced in 24 hours.The diuretics act primarily by inhibiting tubularreabsorption: just 1% decrease in tubular reab-sorption would more than double urine output.
The mechanisms that carryout ion movementacross tubular cells are complex and involve avariety of energy dependent transmembranepumps as well as channels in between the loosefitting cells of the proximal tubule (PT). All Na+
that enters tubular cells through the luminalmembrane is pumped out of it into the renalinterstitium at the basolateral membrane byNa+K+ATPase energised Na+-K+ antiporter (seeFigs 41.1 and 41.2). Because there is a largeintracellular to extracellular gradient for K+, itdiffuses out through K+ channels to be recircu-lated by the Na+-K+ antiporter. For simpli-fication, tubular reabsorption can be divided intofour sites (Fig. IX.1).
Site I: Proximal tubule Four mechanismsof Na+ transport have been defined in thissegment.(a) Direct entry of Na+ along a favourableelectrochemical gradient. This is electrogenic.(b) Transport of Na+ and K+ coupled to activereabsorption of glucose, amino acids, other orga-nic anions and PO4
3¯ through specific symporters.Only the glucose coupled Na+ reabsorption iselectrogenic.(c) Exchange with H+: The PT cells secrete H+
with the help of a Na+-H+ antiporter (Na+-H+
exchanger) located at the luminal membrane. Thisexchange moves Na+ from tubular fluid to insidethe cell. The secreted H+ combines with HCO3
¯
in the tubular fluid to form carbonic acid (Fig.IX.2). This H2CO3 is broken into H2O + CO2
by membrane bound brush border CAse (TypeIV enzyme), because spotaneous dissociationof H2CO3 is very slow. Both CO2 and H2Odiffuse inside the cell and recombine to formH2CO3 (intracellular soluble type II CAsecatalysed reaction) which is the source of H+.The dissociated HCO3
¯ in the cell is transported
to cortical e.c.f. by basolateral membraneNa+-HCO3
¯ symporter resulting in net reabsorp-tion of NaHCO3. Practically all HCO3
¯ isreabsorbed in PT by this mechanism, becausetubular membrane, as such, is relativelyimpermeable to HCO3
¯.(d) The disproportionately large HCO3
¯, acetate,PO4
3¯, amino acid and other anion reabsorptioncreate passive driving forces for Cl¯ to diffusethrough the paracellular pathway (in betweentubular cells), particularly in the later PT. Thistakes Na+ and water along to maintain electricalneutrality and isotonicity; reabsorption in PT isisotonic.
Major part of filtered K+ is reabsorbed inthe PT. Thus, an isotonic tubular fluid with majorchanges in composition enters the thindescending limb of loop of Henle.
Site II: Ascending limb of loop of Henle(Asc LH) The thick AscLH can be distinguishedinto two distinct portions:
(i) Medullary part lined by cuboidal cells.(ii) Cortical part lined by flattened cells.
Both portions are relatively impermeable to waterbut absorb salt actively and thus dilute the tubularfluid.
In the medullary portion a distinct luminalmembrane carrier transports ions in the stoichio-metric ratio of Na+-K+-2Cl¯ (see Fig. 41.1),and is nonelectrogenic. The Na+ that enters thecell is pumped to e.c.f. by Na+ K+ ATPase at thebasolateral membrane. In addition, a Na+-Cl¯
Fig. IX.2: The carbonic anhydrase (C.Ase) mediatedbicarbonate absorption in proximal tubule (P.T.)

577SEC
TION
9PHYSIOLOGY OF URINE FORMATION
symporter moves Cl¯ down its electrochemicalgradient into e.c.f. and carries Na+ along. As thetubular fluid traverses AscLH it progressivelybecomes hypotonic. Accumulation of NaCl inthe medullary interstitium without accompanyingwater makes it hypertonic: a corticomedullaryosmotic gradient is set up. This draws in waterfrom the descending limb of loop of Henle(this thin segment has high osmotic waterpermeability but lacks active NaCl transport) sothat the fluid that enters AscLH becomeshypertonic. A 4 times higher osmolarity ofmedullary tip (papilla) is maintained by thehairpin structure of the loop of Henle acting aspassive counter current multiplier and thearrangement of blood vessels as vasa recti withshunts that prevents washing away of the osmoticgradient by progressively reducing blood flowto the inner medulla. Because of meagre bloodsupply, renal papilla is so prone to necrosis andsuffers maximum damage when a toxic substanceis being excreted.
Site III: Cortical diluting segment of loopof Henle This segment, also impermeable towater, continues to absorb salt, but here it isthrough a Na+-Cl¯ symporter (see Fig. 41.2).Tubular fluid gets further diluted.
Site IV: Distal tubule (DT) and collectingduct (CD) In the late DT and CD, Na+ is againactively reabsorbed; the cation-anion balancebeing maintained partly by passive Cl¯ diffusionand partly by secretion of K+ and H+. Absorptionof Na+ at this site occurs through a specificamiloride sensitive Na+ channel and is controlledto a large extent by aldosterone (see Fig. 41.3).This provides fine tuning to electrolyte excretionaccording to body needs.
In common with other cells, the DT and CDcells are rich in K+; a chemical gradient existsfor its diffusion into tubular lumen which isaided by the lumen negative transepithelialpotential difference in this part of the tubule.The luminal membrane possesses an activesecretory pump for H+ which is again governedby movement of Na+ in the reverse direction.
Any diuretic acting proximal to the aldosteronesensitive ion exchange site causes an increaseddelivery of Na+ to the distal nephron—moreexchange with K+ takes place. Thus, K+ isreabsorbed in the PT and AscLH, and is secretedin the DT and CD. The net K+ loss is regulatedby variations in the secretory process anddepends on:
(i) The Na+ load delivered to distal segment(ii) Presence or absence of aldosterone
(iii) Availability of H+
(iv) Intracellular K+ storesThe characteristic feature of cells lining CD istheir responsiveness to antidiuretic hormone(ADH). If ADH is absent, the hypotonic fluidentering CD is passed as such dilute urine isproduced during water loading. If ADH levelsare high, CD cells become fully permeable towater equilibrate with hyperosmotic medulla concentrated urine is passed, as occurs duringwater deprivation or hypertonic saline infusion.
The CD and thin AscLH are the only seg-ments permeable to urea. ADH promotesinsertion of urea transporter (UT1 or VRUT) intothe luminal membrane of CD cells more ureais accumulated in the medullary interstitium,reinforcing the medullary hypertonicity duringwater deprivation.
Free water clearance It is defined as thevolume of urine excreted per unit time in excessof that required to excrete the contained soluteisoosmotically with plasma. It is positive whendilute urine is passed in the absence of ADH andnegative when concentrated urine is passed inthe presence of ADH. If isotonic urine is passed,regardless of its volume, free water clearance iszero.
Both positive and negative free water clea-rance are dependent on the production of acorticomedullary osmotic gradient; diureticsacting on medullary AscLH depress both.
Organic ion transport The PT has non-specific bidirectional active transportmechanism, separately for organic acids andorganic bases. However, the magnitude of

578S
EC
TIO
N9
DRUGS ACTING ON KIDNEY
transport in the two directions may vary fromcompound to compound, e.g. reabsorption of uricacid is generally more than its secretion, whilein case of penicillin the converse is true.Important diuretics like furosemide, thiazides andamiloride utilize this transport to approach theirsite of action from the luminal side of the tubulein the AscLH/DT/CD.
Regulation of renal function
Glomerular filtration rate (g.f.r.) is dependent on the pumpingaction of heart, the magnitude of renal blood flow and therelative dimensions of afferent and efferent glomerular vessels.Thus, systemic and intrarenal haemodynamic changes canreflect in g.f.r.
About 80% nephrons lie in outer cortex, have shortloops of Henle and low Na+ reabsorptive capacity; while 20%or so are juxtamedullary, possess long loops of Henle and arelargely responsible for creating the corticomedullary osmoticgradient. Redistribution of blood flow between these twotypes of nephrons can alter salt and water excretion. Further,haemodynamic changes within different segments of renalvasculature can alter pressure relationships which governflow of solute and water.
The renin-angiotensin-aldosterone system has a profoundbearing on distal tubular reabsorption of Na+ and secretionof K+/H+. Angiotensin II produced locally in the kidney hasdirect effects on intrarenal vascular beds as well as on saltand water reabsorption (see Ch. 36).
Sympathetic stimulation of kidney results in renin releasewhich would indirectly affect tubular transport. In addition,adrenergic drugs can directly enhance reabsorption of saltand water.
Prostaglandins (PGs) are produced locally in kidney; actas modulators of renal circulation and renin release. PGE2
inhibits the action of ADH and has direct effects on tubularreabsorption.
A natriuretic hormone produced by the atrium (atrialnatriuretic peptide: ANP) and may be other sites also hasbeen found to be important in inducing natriuresis in responseto salt and volume overload. It mediates ‘escape’ from long-term aldosterone action.
All nephrons are so arranged that the Asc LH passesclose to the early PT of the same nephron. The macula densacells are thus in close contact with afferent and efferentarterioles. This provides opportunity for feedback regulationof single unit function.
Relation to diuretic actionThe relative magnitudes of Na+ reabsorption atdifferent tubular sites are:
PT 65–70%; Asc LH 20–25%;DT 8–9%; CD 1–2%.
The maximal natriuretic response to a diureticcan give a clue to its site of action. It may appearthat diuretics acting on PT should be the mostefficacious. However, these agents are either tooweak or cause distortion of acid-base balance(CAse inhibitors). Moreover, their effect maybe obscured by compensatory increase inreabsorption further down the nephron, becausethe reserve reabsorptive capacity of dilutingsegments is considerable and can overshadowmore proximal actions.
A diuretic having primary action onmedullary Asc LH (furosemide) can producesubstantial effect because of limited capacity forsalt absorption in DT and CD. This also explainswhy agents acting on DT and CD (K+ sparingdiuretics) evoke only mild saluretic effect.Diuretics acting on cortical diluting segment(thiazides) are intermediate between these two.

DiureticsChapter 41b
Diuretics (natriuretics) are drugs which cause anet loss of Na+ and water in urine. However, Na+
balance is soon restored, even with continuingdiuretic action, by compensatory homeostaticmechanisms of the body, albeit with a certaindegree of persisting Na+ deficit and reduction inextracellular fluid volume.
Based on the diuretic action of calomel, organomercurialsgiven by injection were introduced in the 1920s and dominatedfor nearly 40 years. The CAse inhibitors were developedin the 1950s from the observation that early sulfonamidescaused acidosis and mild diuresis. The first modern orallyactive diuretic chlorothiazide was produced in 1957, andby early 1960s its congeners (thiazide diuretics) were alreadyin common use. Availability of furosemide and ethacrynicacid by mid 1960s revolutionized the pattern of diureticuse. The aldosterone antagonist and other K+ sparing diureticsspironolactone and triamterene/amiloride were developedin parallel to these.
Diuretics are among the most widely pres-cribed drugs. Application of diuretics in themanagement of hypertension has outstripped theiruse in edema. Availability of diuretics has alsohad a major impact on the understanding of renalphysiology.
CLASSIFICATION
1. High efficacy diuretics (Inhibitors of Na+-K+-2Cl¯ cotransport)
Sulphamoyl derivativesFurosemide, Bumetanide, Torasemide
2. Medium efficacy diuretics (Inhibitors ofNa+-Cl¯ symport)
(a) Benzothiadiazines (thiazides)Hydrochlorothiazide, Benzthiazide,Hydroflumethiazide, Bendroflumethiazide
(b) Thiazide like (related heterocyclics)Chlorthalidone, Metolazone, Xipamide,Indapamide, Clopamide
3. Weak or adjunctive diuretics(a) Carbonic anhydrase inhibitors
Acetazolamide(b) Potassium sparing diuretics
(i) Aldosterone antagonist:Spironolactone, Eplerenone
(ii) Inhibitors of renal epithelial Na+
channel: Triamterene, Amiloride.(c) Osmotic diuretics
Mannitol, Isosorbide, GlycerolOther high ceiling diuretics, viz. ethacrynic acid andorganomercurials (mersalyl) are only historical.
HIGH CEILING (LOOP) DIURETICS(Inhibitors of Na+-K+-2Cl¯ Cotransport)
Furosemide (Frusemide) Prototype drugThe development of this rapidly acting highlyefficacious oral diuretic was a breakthrough. Itsmaximal natriuretic effect is much greater thanthat of other classes. The diuretic response goeson increasing with increasing dose: upto 10 Lof urine may be produced in a day. It is activeeven in patients with relatively severe renal failure.The onset of action is prompt (i.v. 2–5 min., i.m.10–20 min., oral 20–40 min.) and duration short(3–6 hours).
The major site of action is the thick AscLH(therefore called loop diuretics) where furosemideinhibits Na+- K+-2Cl¯ cotransport (site II, Fig.41.1). A minor component of action on PT has alsobeen indicated. It is secreted in PT by organic aniontransport and reaches AscLH where it acts fromluminal side of the membrane. The cortico-medullary osmotic gradient is abolished andpositive as well as negative free water clearance isblocked. K+ excretion is increased mainly due tohigh Na+ load reaching DT. However, at equinatri-uretic doses, K+ loss is less than that with thiazides.

580S
EC
TIO
N9
DRUGS ACTING ON KIDNEY
Fig. 41.1: Mechanism of salt reabsorption in the thick ascending limb of loop of Henle(AscLH) cell, and site of action of furosemide on the Na+-K+-2Cl¯ cotransporter
Furosemide has weak CAse inhibitory action;increases HCO3
¯ excretion as well; urinary pHmay rise but the predominant urinary anion is Cl¯.Therefore, acidosis does not develop. The diureticaction is independent of acid-base balance of thebody and it causes little distortion of the same;mild alkalosis occurs at high doses.
In addition to its prominent tubular action,furosemide causes acute changes in renal andsystemic haemodynamics. After 5 min of i.v.injection, renal blood flow is transiently increasedand there is redistribution of blood flow fromouter to midcortical zone; g.f.r. generally remainsunaltered due to compensatory mechanismsdespite increased renal blood flow. Pressurerelationship between vascular, interstitial andtubular compartments is altered, the net result ofwhich is decreased PT reabsorption. The intrarenalhaemodynamic changes are brought about byincreased local PG synthesis.
Furosemide also sets in motion compensatorymechanisms which tend to limit its diuretic action. Interferencewith Na+ entry into maculadensa causes marked renin release.Activation of the renin-angiotensin-aldosterone system is themajor compensatory mechanism. Reflex sympathetic
stimulation of the kidney reinforces renin release. Thesemechanisms restore Na+ balance after termination of thediuretic action. Because of this phenomenon and short t½ offurosemide, its once daily administration may have lessmarked overall effect on Na+ status of the body.
Intravenous furosemide causes promptincrease in systemic venous capacitance anddecreases left ventricular filling pressure, evenbefore the saluretic response is apparent. Thisaction also appears to be PG mediated and isresponsible for the quick relief it affords in LVFand pulmonary edema.
Furosemide increases Ca2+ excretion (contrastthiazides which reduce it) as well as Mg2+
excretion by abolishing transepithelial potentialdifference in the thick AscLH which drivesreabsorption of these divalent cations. It tends toraise blood uric acid level by competing with itsproximal tubular secretion as well as by increasingreabsorption in PT which is a consequence ofreduced e.c.f. volume. The magnitude ofhyperuricaemia is lower than that with thiazides.A small rise in blood sugar level may be notedafter regular use of furosemide, but is again lessmarked compared to thiazides.

581C
HA
PTE
R41
DIURETICS
Molecular mechanism of action: A glycoproteinwith 12 membrane spanning domains has beenfound to function as the Na+-K+-2Cl¯ cotransporterin many epithelia performing secretory/absorbingfunction, including AscLH. Recently, distinctabsorptive and secretory isoforms of Na+-K+-2Cl¯
cotransporter have been isolated. The former isexclusively expressed at the luminal membraneof thick AscLH—furosemide attaches to the Cl¯
binding site of this protein to inhibit its transportfunction. The secretory form is expressed on thebasolateral membrane of most glandular andepithelial cells.
Pharmacokinetics Furosemide is rapidly absor-bed orally but bioavailability is about 60%. Insevere CHF oral bioavailability may be markedlyreduced necessitating parenteral administration.Lipid-solubility is low, and it is highly bound toplasma proteins. It is partly conjugated withglucuronic acid and mainly excreted unchangedby glomerular filtration as well as tubularsecretion. Some excretion in bile and directly inintestine also occurs. Plasma t½ averages 1–2hour but is prolonged in patients with pulmonaryedema, renal and hepatic insufficiency.
Dose Usually 20–80 mg once daily in the morning. Inrenal insufficiency, upto 200 mg 6 hourly has been given byi.m./i.v. route. In pulmonary edema 40–80 mg may be giveni.v.LASIX 40 mg tab., 20 mg/2 ml inj. LASIX HIGH DOSE 500mg tab, 250 mg/25 ml inj; (solution degrades spontaneouslyon exposure to light), SALINEX 40 mg tab, FRUSENEX 40,100 mg tab.
Bumetanide It is similar to furosemide in allrespects, but is 40 times more potent. It inducesvery rapid diuresis and is highly effective inpulmonary edema. However, the site of action,ceiling effect, renal haemodynamic changes andduration of action are similar to furosemide. Asecondary action in PT has also been demon-strated. Bumetanide may act in some cases notresponding to furosemide, and may be tolerated bypatients allergic to furosemide. Hyperuricaemia,K+ loss, glucose intolerance and ototoxicity areclaimed to be less marked, but it may rarely causemyopathy.
Bumetanide is more lipid-soluble; oralbioavailability is 80–100%. It is preferred for oraluse in severe CHF, because its bioavailability isimpaired to a lesser extent than that of furosemide.Bumetanide is extensively bound to plasmaproteins, partly metabolized and partly excretedunchanged in urine. Its accumulation in tubularfluid is less dependent on active secretion. Plasmat½ ~60 min. It gets prolonged in renal and hepaticinsufficiency.Dose: 1–5 mg oral OD in the morning, 2–4 mg i.m./i.v.,(max. 15 mg/day in renal failure).BUMET, 1 mg tab., 0.25 mg/ml inj.
Torasemide (Torsemide) Another highceiling diuretic with properties similar tofurosemide, but 3 times more potent. Oralabsorption is more rapid and more complete. Theelimination t½ (3.5 hours) and duration of action(4–8 hours) are longer. Torasemide has been usedin edema and in hypertension.Dose: 2.5–5 mg OD in hypertension; 5–20 mg/day in edema;upto 100 mg BD in renal failure.DIURETOR 10, 20 mg tabs, DYTOR, TIDE 5, 10, 20, 100mg tabs, 10 mg/2 ml inj.
Use of high ceiling diuretics1. Edema Diuretics are used irrespective ofetiology of edema—cardiac, hepatic or renal. Thehigh ceiling diuretics are preferred in CHF forrapid mobilization of edema fluid (see Ch. 37).Thiazides may be used for maintenance, but oftenprove ineffective and high ceiling drugs are calledin. For nephrotic and other forms of resistantedema, only the high ceiling diuretics are effective,and are the drugs of choice. In chronic renal failuremassive doses have to be used, but they continueto be effective while thiazides just do not produceany action. In impending acute renal failure, loopdiuretics may decrease the need for dialysis.2. Acute pulmonary edema (acute LVF,following MI): Intravenous administration offurosemide or its congeners produces promptrelief. This is due to vasodilator action thatprecedes the saluretic action. Subsequently,decrease in blood volume and venous return isresponsible for the improvement.

582S
EC
TIO
N9
DRUGS ACTING ON KIDNEY
3. Cerebral edema Though osmotic diureticsare primarily used to lower intracranial pressureby withdrawing water, furosemide may becombined to improve efficacy.4. Hypertension High ceiling diuretics areindicated in hypertension only in the presence ofrenal insufficiency, CHF, or in resistant cases andin hypertensive emergencies; otherwise thiazidesare preferred (see p. 460).5. Along with blood transfusion in severeanaemia, to prevent volume overload. Infused withhypertonic saline, it may be helpful in hypo-natraemia.6. Hypercalcaemia of malignancy Thiscondition may present as a medical emergencywith severe volume depletion. Rapid and largevolume i.v. saline infusion is the most importantmeasure. Addition of furosemide (10–20 mg/hour)to the i.v. drip after volume replacement, augmentsCa2+ excretion and prevents volume overload.Forced diuresis with saline and furosemide infusion is nolonger recommended to treat poisonings.
THIAZIDE AND RELATED DIURETICS(Inhibitors of Na+-Cl¯ symport)
Chlorothiazide was synthesized as a CAseinhibitor variant which (unlike acetazolamide)produced urine that was rich in Cl¯, and diuresisoccurred in alkalosis as well as acidosis. A largenumber of congeners were developed subsequentlyand the thiadiazine ring was replaced by otherheterocyclic rings, but the type of activityremained the same. The important features ofrepresentative thiazide and thiazide-like diureticsare presented in Table 41.1.
These are medium efficacy diuretics withprimary site of action in the cortical dilutingsegment or the early DT (Site III). Here theyinhibit Na+–Cl¯ symport at the luminal membrane.They do not affect the corticomedullary osmoticgradient indicating lack of action at the medullarythick AscLH. Positive free water clearance isreduced, because tubular fluid is not maximallydiluted (very dilute urine cannot be passed in the
absence of ADH), but negative free waterclearance (in the presence of ADH) is not affected.This strengthens the view that the site of actionis in between thick AscLH and late DT. Thesedrugs gain access to their site of action via organicacid secretory pathway in PT and then along thetubular fluid to the early DT, where they bind tospecific receptors located on the luminalmembrane. Like the Na+-K+-2Cl¯ cotransporter,the Na+-Cl¯ symporter is also a glycoprotein with12 membrane spanning domains that bindsthiazides but not furosemide or any other class ofdiuretics. It has been cloned and shown to beselectively expressed on the luminal membranein the DT. The site of action of thiazide diureticsis shown in Fig. 41.2.
Some of the thiazides and related drugshave additional CAse inhibitory action in PT;intensity of this action differs among differentcompounds (Table 41.1), but it is generally weak.However, it may confer some proximal tubularaction to the compounds, and accounts for theincrease in HCO3
¯ and PO43¯ excretion.
Under thiazide action, increased amount ofNa+ is presented to the distal nephron, more of itexchanges with K+ urinary K+ excretion isincreased in parallel to the natriuretic response.The maximal diuresis induced by differentagents falls in a narrow range; though potency(reflected in daily dose) differs markedly.Nevertheless, they are moderately efficaciousdiuretics, because nearly 90% of the glomerularfiltrate has already been reabsorbed before itreaches their site of action. Thiazides have a flatdose response curve; little additional diuresisoccurs when the dose is increased beyond 100mg of hydrochlorothiazide or equivalent. Theydo not cause significant alteration in acid-basebalance of the body.
By their action to reduce blood volume, aswell as intrarenal haemodynamic changes, theytend to reduce g.f.r. This is one reason whythiazides are not effective in patients with lowg.f.r. They decrease renal Ca2+ excretion andincrease Mg2+ excretion by a direct distal tubularaction. Thiazides cause greater reduction in urate

583C
HA
PTE
R41
DIURETICS
Fig. 41.2: Mechanism of salt reabsorption in early distal tubular cell and site ofaction of thiazide diuretics on Na+Cl¯ symporter
Chlorthalidone It is a particularly long actingcompound with a t½ 40–50 hours, usedexclusively as antihypertensive.
Metolazone In common with loop diuretics, itis able to evoke a clinically useful response evenin severe renal failure (g.f.r. ~15 ml/min), and hasmarked additive action when combined withfurosemide. An additional proximal tubular actionhas been demonstrated; PO4 reabsorption thatoccurs in PT, is inhibited. It is excreted unchangedin urine. Metolazone has been used mainly foredema (5–10 mg/day, rarely 20 mg), andoccasionally for hypertension (2.5–5 mg/day).
Xipamide It has more pronounced diureticaction similar to low doses of furosemide. Thoughoverall reduction in plasma K+ level is similar tothiazides, several instances of severe hypokalemiawith ventricular arrhythmias have been reported.It is used both as antihypertensive (10–20 mg/day) and for treatment of edema (40 mg/day, max.80 mg/day).
Indapamide It has little diuretic action in theusual doses, probably because it is highly lipid-
excretion than furosemide, but the mechanism isthe same (see p. 580).
The extrarenal actions of thiazides consist ofa slowly developing fall in BP in hypertensivesand elevation of blood sugar in some patients dueto decreased insulin release which probably is aconsequence of hypokalaemia.
Pharmacokinetics All thiazides and relateddrugs are well absorbed orally. There are noinjectable preparations of these drugs. Their actionstarts within 1 hour, but the duration varies from6–48 hours (Table 41.1). The more lipid-solubleagents have larger volumes of distribution (someare also bound in tissues), lower rates of renalclearance and are longer acting. The proteinbinding is also variable. Most of the agentsundergo little hepatic metabolism and are excretedas such. They are filtered at the glomerulus aswell as secreted in the PT by organic aniontransport. Tubular reabsorption depends on lipidsolubility: the more lipid soluble ones are highlyreabsorbed—prolonging duration of action.
The elimination t½ of hydrochlorothiazide is3–6 hours, but action persists longer (6–12 hours).

584S
EC
TIO
N9
DRUGS ACTING ON KIDNEY
TABLE 41.1 Thiazides and related diuretics
Drug Trade name Daily dose CAse Duration(Tab. strength) (mg) inhibition of action(mg) (Hr)
1. Hydrochlorothiazide AQUAZIDE, HYDRIDE 12.5–100 + 6–12THIAZIDE (12.5, 25, 50 mg)ESIDREX (50)
2. Chlorthalidone HYTHALTON (50,100) 50–100 ++ 48HYDRAZIDE, THALIZIDE (12.5, 25)
3. Metolazone XAROXOLYN (5, 10) 5–20 + 12–24DIUREM, METORAL (2.5, 5, 10)
4. Xipamide XIPAMID (20) 20–40 + 12
5. Indapamide LORVAS (2.5) 2.5–5 – 12–24
6. Clopamide BRINALDIX (20) 10–60 ± 12–18
soluble, is extensively metabolized and only smallquantity of unchanged drug is present in the tubularfluid. However, it retains antihypertensive actionand is used for that purpose only (see p. 561).
Uses1. Edema Thiazides may be used for mild-to-moderate cases. For mobilization of edema fluidmore efficacious diuretics are preferred, butthiazides may be considered for maintenancetherapy. They act best in cardiac edema; are lesseffective in hepatic or renal edema. Thiazides arepowerless in the presence of renal failure, butmetolazone may still act. Cirrhotics often developrefractoriness to thiazides due to development ofsecondary hyperaldosteronism.2. Hypertension Thiazides and related diure-tics, especially chlorthalidone are one of the firstline drugs (Ch. 40).3. Diabetes insipidus Thiazides decreasepositive free water clearance and are the onlydrugs effective in nephrogenic diabetes insipidus.However, they reduce urine volume in pituitaryorigin cases as well (see Ch. 42).4. Hypercalciuria with recurrent calcium stonesin the kidney. Thiazides act by reducing Ca2+
excretion.
Complications of high ceiling andthiazide type diuretic therapyMost of the adverse effects of these drugs arerelated to fluid and electrolyte changes caused bythem. They are remarkably safe in low doses usedover short periods. Many subtle metabolic effectshave been reported in their long-term use asantihypertensives at the relatively higher dosesused in the past (see p. 560).1. Hypokalaemia This is the most significantproblem. It is rare at low doses, but may be of graveconsequence when brisk diuresis is induced or onprolonged therapy, especially if dietary K+ intakeis low. Degree of hypokalaemia appears to berelated to the duration of action of the diuretic;longer acting drugs cause more K+ loss. The usualmanifestations are weakness, fatigue, musclecramps; cardiac arrhythmias are the seriouscomplications. Hypokalaemia is less common withstandard doses of high ceiling diuretics than withthiazides, possibly because of shorter duration ofaction of the former which permits intermittentoperation of compensatory repletion mechanisms.Hypokalaemia can be prevented and treated by:(a) High dietary K+ intake or(b) Supplements of KCl (24–72 mEq/day) or(c) Concurrent use of K+ sparing diuretics.

585C
HA
PTE
R41
DIURETICS
Measures (b) and (c) are not routinely indicated,but only when hypokalaemia has been documen-ted or in special risk situations, e.g. cirrhotics,cardiac patients—especially post MI, those recei-ving digitalis, antiarrhythmics, or tricyclicantidepressants and elderly patients. Serum K+
levels are only a rough guide to K+ depletion,because K+ is primarily an intracellular ion.Nevertheless, an attempt to maintain serum K+ ator above 3.5 mEq/L should be made.
Combined tablets of diuretics and KCl are notrecommended because:
• they generally contain insufficient quantity of K+
(8–12 mEq only).• may cause gut ulceration by releasing KCl at one spot.• K+ is retained better if given after the diuresis is over.
K+ sparing diuretics are more efficacious and moreconvenient in correcting hypokalaemia than areK+ supplements. ACE inhibitors/AT1 antagonistsgiven with thiazides tend to prevent developmentof hypokalaemia.
Alkalosis may occur with hypokalaemia,because more H+ exchanges with Na+ in DT whenless K+ is available for exchange.2. Acute saline depletion Overenthusiasticuse of diuretics, particularly high ceiling ones,may cause dehydration and marked fall in BP(especially in erect posture). Haemoconcentrationincreases risk of peripheral venous thrombosis.Serum Na+ and Cl¯ levels remain normal becauseisotonic saline is lost. It should be treated bysaline infusion.3. Dilutional hyponatraemia Occurs in CHFpatients when vigorous diuresis is induced withhigh ceiling agents, rarely with thiazides. Kidneytends to retain water, though it is unable to retainsalt due to the diuretic; e.c.f. gets diluted, hypo-natraemia occurs and edema persists despitenatriuresis. Patients feel very thirsty. Treatmentof this distortion of fluid-electrolyte balance isdifficult: withhold diuretics, restrict water intakeand give glucocorticoid which enhances excretionof water load. If hypokalaemia is present, itscorrection helps.4. GIT and CNS disturbances Nausea, vomi-ting and diarrhoea may occur with any diuretic.
Headache, giddiness, weakness, paresthesias,impotence are occasional complaints withthiazides as well as loop diuretics.5. Hearing loss Occurs rarely, only with highceiling diuretics and when these drugs are used inthe presence of renal insufficiency. Increased saltcontent of endolymph and a direct toxic action onthe hair cells in internal ear appear to be causative.
6. Allergic manifestations Rashes, photosen-sitivity occur, especially in patients hypersensitiveto sulfonamides. Blood dyscrasias are rare; anydiuretic may be causative.
7. Hyperuricaemia Long-term use of higherdose thiazides in hypertension has caused rise inblood urate level. This is uncommon now due touse of lower doses (see Ch. 40). Furosemideproduces a lower incidence of hyperuricaemia.This effect can be counteracted by allopurinol.Probenecid is better avoided, because it mayinterfere with the diuretic response, particularlyof loop diuretics.
8. Hyperglycaemia and hyperlipidemia Haveoccurred in the use of diuretics as antihypertensive(see p. 560). These metabolic changes are minimalwith low dose thiazides now recommended.
9. Hypocalcaemia may occur with high ceilingdiuretics when these are administered chronically.Thiazides, on the otherhand, tend to raise serumCa2+; may aggravate hypercalcaemia due to othercauses.
10. Magnesium depletion It may develop afterprolonged use of thiazides as well as loop diure-tics, and may increase the risk of ventriculararrhythmias, especially after MI or when patientsare digitalized. K+ sparing diuretics given con-currently minimise Mg2+ loss.
11. Thiazides have sometimes aggravated renalinsufficiency, probably by reducing g.f.r.
12. Brisk diuresis induced in cirrhotics mayprecipitate mental disturbances and hepatic coma.It may be due to hypokalaemia, alkalosis andincreased blood NH3 levels.

586S
EC
TIO
N9
DRUGS ACTING ON KIDNEY
13. Diuretics should be avoided in toxaemia ofpregnancy in which blood volume is low despiteedema. Diuretics may further compromiseplacental circulation increasing the risk ofmiscarriage, foetal death.
Interactions1. Thiazides and high ceiling diuretics poten-tiate all other antihypertensives. This interactionis intentionally employed in therapeutics.2. Hypokalaemia induced by these diuretics:
• Enhances digitalis toxicity.• Increases risk of polymorphic ventricular
tachycardia due to drugs which prolongQ-T interval (see p. 528).
• Reduces sulfonylurea action.3. High ceiling diuretics and aminoglycosideantibiotics are both ototoxic and nephrotoxic;produce additive toxicity; should be used togethercautiously.4. Cotrimoxazole given with diuretics has causedhigher incidence of thrombocytopenia.5. Indomethacin and other NSAIDs diminish theaction of high ceiling diuretics by inhibiting PGsynthesis in the kidney, through which furosemideand related drugs induce intrarenal haemodynamicchanges which secondarily affect salt output.Antihypertensive action of thiazides and furo-semide is also diminished by NSAIDs.6. Probenecid competitively inhibits tubularsecretion of furosemide and thiazides: decreasestheir action by lowering concentration in thetubular fluid, while diuretics diminish uricosuricaction of probenecid.7. Serum lithium level rises due to enhancedreabsorption of Li+ (and Na+) in PT.
Resistance to high ceiling diureticsRefractoriness (progressive edema despiteescalating diuretic therapy) is more common withthiazides, but occurs under certain circumstanceswith high ceiling diuretics as well. The causesand mechanism of such resistance include:
Cause Mechanism1. Renal insufficiency Decreased access of diuretic to
(including advanced its site of action due to low g.f.r.age) and low proximal tubular
secretion.
2. Nephrotic syndrome Binding of diuretic to urinaryprotein, other pharmacodyna-mic causes.
3. Cirrhosis of liver Abnormal pharmacodynamics;hyperaldosteronism;mechanism not clear.
4. CHF Impaired oral absorption dueto intestinal congestion,decreased renal blood flow andglomerular filtration,increased salt reabsorptionin PT.
Long-term use of loop diuretics causes distalnephron hypertrophy resistance. Addition ofmetolazone, or to some extent a thiazide, whichact on distal tubule overcome the refractorinessin many cases. Fractionation of daily dose mayprevent operation of compensatory mechanismsand restart diuresis. Bedrest also helps.
CARBONIC ANHYDRASE INHIBITORS
Carbonic anhydrase (CAse) is an enzyme whichcatalyses the reversible reaction H2O + CO2 H2CO3. Carbonic acid spontaneously ionizesH2CO3 H+ + HCO3
¯ (Fig. IX.2). Carbonicanhydrase thus functions in CO2 and HCO3
¯
transport and in H+ ion secretion. The enzyme ispresent in renal tubular cell (especially PT) gastricmucosa, exocrine pancreas, ciliary body of eye,brain and RBC. In these tissues a gross excess ofCAse is present, more than 99% inhibition isrequired to produce effects.
AcetazolamideIt is a sulfonamide derivative which noncompeti-tively but reversibly inhibits CAse (type II) in PTcells resulting in slowing of hydration of CO2 decreased availability of H+ to exchange withluminal Na+ through the Na+-H+ antiporter.Inhibition of brush border CAse (type IV) retardsdehydration of H2CO3 in the tubular fluid so thatless CO2 diffuses back into the cells. The net effectis inhibition of HCO3
¯ (and accompanying Na+)reabsorption in PT. However, the resulting alkalinediuresis is only mild (maximal fractional Na+ loss5%), because part of the Na+ (but not HCO3
¯)rejected in the PT is reabsorbed at the highcapacity AscLH.

587C
HA
PTE
R41
DIURETICS
Secretion of H+ in DT and CD is also inter-fered. Though H+ is secreted at this site by aH+-ATPase, it is generated in the cell by CAsemediated reaction. As such, this is a subsidiarysite of action of CAse inhibitors. When CAseinhibitors are given, the distal Na+ exchange takesplace only with K+ which is lost in excess. For thesame degree of natriuresis CAse inhibitors causethe most marked kaliuresis compared to otherdiuretics. The urine produced under acetazola-mide action is alkaline and rich in HCO3
¯ whichis matched by both Na+ and K+. Continued actionof acetazolamide depletes body HCO3
¯ and causesacidosis; less HCO3
¯ (on which its diuretic actiondepends) is filtered at the glomerulus lessdiuresis occurs (self-limiting diuretic action).The extrarenal actions of acetazolamide are:
(i) Lowering of intraocular tension due todecreased formation of aqueous humour(aqueous is rich in HCO3
¯).(ii) Decreased gastric HCl and pancreatic
NaHCO3 secretion: This action requires veryhigh doses—not significant at clinically useddoses.
(iii) Raised level of CO2 in brain and loweringof pH sedation and elevation of seizurethreshold.
(iv) Alteration of CO2 transport in lungs andtissues. These actions are masked by com-pensatory mechanisms.
Pharmacokinetics Acetazolamide is wellabsorbed orally and excreted unchanged in urine.Action of a single dose lasts 8–12 hours.
Uses Because of self-limiting action, produc-tion of acidosis and hypokalaemia, acetazolamideis not used as diuretic. Its current clinical usesare:
1. Glaucoma: as adjuvant to other ocularhypotensives (see Ch. 10).
2. To alkalinise urine: for urinary tract infectionor to promote excretion of certain acidicdrugs.
3. Epilepsy: as adjuvant in absence seizureswhen primary drugs are not fully effective.
4. Acute mountain sickness: for symptomaticrelief as well as prophylaxis. Benefit occursprobably due to reduced CSF formation aswell as lowering of CSF and brain pH.
5. Periodic paralysis.Dose: 250 mg OD–BD; DIAMOX, SYNOMAX 250 mg tab.IOPAR-SR 250 mg SR cap.
Adverse effects are frequent.Acidosis, hypokalaemia, drowsiness, paresthesias,fatigue, abdominal discomfort.Hypersensitivity reactions—fever, rashes.Bone marrow depression is rare but serious.It is contraindicated in liver disease: may preci-pitate hepatic coma by interfering with urinaryelimination of NH3 (due to alkaline urine).Acidosis is more likely to occur in patients ofCOPD.Methazolamide and Dichlorphenamide are the other systemicCAse inhibitors, while Dorzolamide and Brinzolamide aretopical CAse inhibitors used in glaucoma (see Ch.10).
POTASSIUM SPARING DIURETICS
Aldosterone antagonists and renal epithelial Na+
channel inhibitors indirectly conserve K+ whileinducing mild natriuresis, and are called‘potassium sparing diuretics’.
Aldosterone antagonist
SpironolactoneIt is a steroid, chemically related to the minera-locorticoid aldosterone. Aldosterone penetratesthe late DT and CD cells (Fig. 41.3) and acts bycombining with an intracellular mineralocorticoidreceptor (MR) induces the formation of‘aldosterone-induced proteins’ (AIPs). The AIPspromote Na+ reabsorption by a number ofmechanisms (legend to Fig. 41.3) and K+ secretion.Spironolactone acts from the interstitial side ofthe tubular cell, combines with MR and inhibitsthe formation of AIPs in a competitive manner. Ithas no effect on Na+ and K+ transport in theabsence of aldosterone, while under normalcircumstances, it increases Na+ and decreases K+
excretion.

588S
EC
TIO
N9
DRUGS ACTING ON KIDNEY
Fig. 41.3: Site and mechanism of action of potassium sparing diuretics on the late distal tubule/collecting duct cellAldosterone (Aldo) penetrates the cell from the interstitial side and combines with the mineralocorticoid receptor(MR). The complex translocates to the nucleus—promotes gene mediated mRNA synthesis. The mRNA then directssynthesis of aldosterone induced proteins (AIPs). The AIPs include Na+K+ ATPase and renal epithelial (amiloridesensitive) Na+ channels. More of these proteins are synthesized. The AIPs also activate these Na+ channels and,translocate them from cytosolic site to luminal membrane. They also translocate Na+K+ATPase to the basolateralmembrane. AIPs also increase ATP production by mitochondria. All these changes promote Na+ reabsorption. MoreK+ and H+ is secreted indirectly. Spironolactone binds to MR, prevents Aldo action and produces opposite effects.
Amiloride approaches the Na+ channel from the luminal side and blocks it—reducing the lumen negativetransepithelial potential difference which governs K+ and H+ secretion
Spironolactone is a mild saluretic becausemajority of Na+ has already been reabsorbedproximal to its site of action. However, itantagonises K+ loss induced by other diureticsand slightly adds to their natriuretic effect/reversesresistance to them due to secondary hyperaldo-steronism. The K+ retaining action develops over3–4 days. Spironolactone increases Ca2+ excretionby a direct action on renal tubules.
Pharmacokinetics The oral bioavailability ofspironolactone from microfine powder tablet is75%. It is highly bound to plasma proteins andcompletely metabolized in liver; converted toactive metabolites, the most important of whichis Canrenone that is responsible for 1/2–2/3 of itsaction in vivo. The t½ of spironolactone is1–2 hours, while that canrenone is ~18 hours.Some enterohepatic circulation occurs.
Dose: 25–50 mg BD–QID; max 400 mg/dayALDACTONE 25, 50, 100 mg tabs.ALDACTIDE: Spironolactone 25 mg + hydroflumethiazide 25mg tab. LACILACTONE, SPIROMIDE: Spironolactone 50 mg+ furosemide 20 mg tab, TORLACTONE Spironolactone 50 mg+ torasemide 10 mg tab.
Use Spironolactone is a weak diuretic in itsown right and is used only in combination withother more efficacious diuretics.1. To counteract K+ loss due to thiazide and loopdiuretics.2. Edema: It is more useful in cirrhotic andnephrotic edema in which aldosterone levels aregenerally high. Spironolactone is frequently addedto a thiazide/loop diuretic in the treatment of ascitisdue to cirrhosis of liver. It breaks the resistanceto thiazide diuretics that develops due to secondaryhyperaldosteronism and reestablishes the response.

589C
HA
PTE
R41
DIURETICS
Thus, it is particularly employed in refractoryedema.3. Hypertension: Used as adjuvant to thiazide toprevent hypokalaemia, it may slightly add to theirantihypertensive action. More importantly, it mayhave the potential to attenuate hypertension relatedrenal fibrosis and ventricular/vascular hypertrophy(see p. 561).4. CHF: As additional drug to conventionaltherapy in moderate to severe CHF; can retarddisease progression and lower mortality (seep. 524).
Interactions
1. Given together with K+ supplements—dangerous hyperkalaemia can occur.
2. Aspirin blocks spironolactone action byinhibiting tubular secretion of its activemetabolite canrenone.
3. More pronounced hyperkalaemia can occur inpatients receiving ACE inhibitors/ARBs.
4. Spironolactone increases plasma digoxin con-centration.
Adverse effects The side effects are drowsi-ness, ataxia, mental confusion, epigastric distressand loose motions. Spironolactone interactswith progestin and androgen receptors as well. Inaddition, it may enhance testosterone clearanceor its peripheral conversion to estradiol, producingdose and duration of treatment related hormonalside effects like gynaecomastia, erectile dys-function or loss of libido in men, and breasttenderness or menstrual irregularities in women.
Most serious is hyperkalaemia that may occur,especially if renal function is inadequate. Acidosisis a risk, particularly in cirrhotics. Peptic ulcermay be aggravated; it is contraindicated in ulcerpatients.
EplerenoneIt is a newer and more selective aldosteroneantagonist which has much lower affinity for othersteroidal receptors; therefore much less likely toproduce hormonal disturbances like gnaecomastia,impotence, menstrual irregularities, etc. This
feature makes it particularly suitable for longtermuse in the therapy of hypertension and chronicCHF. However, the risk of hyperkalaemia andg.i. side effects are like spironolactone. Other sideeffects have an incidence similar to placebo, andit has a better tolerability profile.
Eplerenone is well absorbed orally, inactivatedin liver by CYP3A4, and excreted in urine(2/3rd) as well as faeces (1/3rd). The t½ is4–6 hours. Inhibitors of CYP3A4 (clarithromycin,itraconazole, etc.) increase its blood levels, whileinducers like carbamazepine, rifampin, etc. maydecrease its efficacy.
Eplerenone is indicated specifically in mode-rate to severe CHF, post-infarction left ventriculardysfunction and hypertension. It can also be usedas alternative to spironolactone.Dose: 25–50 mg BD;EPLERAN, EPTUS, ALRISTA 25, 50 mg tabs.
Inhibitors of renal epithelial Na+ channelTriamterene and amiloride are two nonsteroidalorganic bases with identical actions. Their mostimportant effect is to decrease K+ excretion,particularly when it is high due to large K+ intakeor use of a diuretic that enhances K+ loss. This isaccompanied by a small increase in Na+ excretion.The excess urinary Na+ is matched by Cl¯ andvariable amounts of HCO3
¯ ; urine is slightlyalkalinized. The effect on urinary electrolytepattern is superficially similar to spironolactone,but their action is independent of aldosterone.Ca2+ and Mg2+ exretion is also reduced, but thereis no effect on renal haemodynamics.
Mechanism of action The luminal membraneof late DT and CD cells expresses a distinct ‘renalepithelial’ or ‘amiloride sensitive’ Na+ channelthrough which Na+ enters the cell down itselectrochemical gradient which is generated byNa+K+ ATPase operating at the basolateralmembrane (Fig. 41.3). This Na+ entry partiallydepolarizes the luminal membrane creating a–15 mV transepithelial potential difference whichpromotes secretion of K+ into the lumen throughK+ channels. Though there is no direct coupling

590S
EC
TIO
N9
DRUGS ACTING ON KIDNEY
between Na+ and K+ channels, more the deliveryof Na+ to the distal nephron—greater is its entrythrough the Na+ channel—luminal membrane isdepolarized to a greater extent—driving force forK+ secretion is augmented. As such, all diureticsacting proximally (loop diuretics, thiazides, CAseinhibitors) promote K+ secretion. Amiloride andtriamterene block the luminal Na+ channels andindirectly inhibit K+ excretion, while the net excessloss of Na+ is minor, because this is only a smallfraction of the total amount of Na+ excreted inurine.
The intercalated cells in CD possess an ATPdriven H+ pump which secretes H+ ions into thelumen. This pump is facilitated by the lumennegative potential. Amiloride, by reducing thelumen negative potential, decreases H+ ionsecretion as well and predisposes to acidosis. Thus,amiloride conserves both K+ and H+ whilemarginally increasing Na+ excretion.
Both triamterene and amiloride are used inconjunction with a thiazide type or a high ceilingdiuretic to prevent hypokalaemia and slightly aug-ment the natriuretic response. The antihypertensiveaction of thiazide is also supplemented. Risk ofhyperkalaemia is the most important adverse effectof amiloride and triamterene. These drugs shouldnot be given with K+ supplements; dangeroushyperkalaemia may develop. Hyperkalaemia isalso more likely in patients receiving ACEinhibitors/ARBs, blockers, NSAIDs and in thosewith renal impairment.Both drugs elevate plasma digoxin levels.
Triamterene It is incompletely absorbed orally,partly bound to plasma proteins, largelymetabolized in liver to an active metabolite andexcreted in urine. Plasma t½ is 4 hours, effect ofa single dose lasts 6–8 hours.
Side effects are infrequent: consist of nausea,dizziness, muscle cramps and rise in blood urea.Impaired glucose tolerance and photosensitivityare reported, but urate level is not increased.Dose: 50–100 mg daily; DITIDE, triamterene 50 mg +benzthiazide 25 mg tab;FRUSEMENE, triamterene 50 mg + furosemide 20 mg tab.
Amiloride It is 10 times more potent thantriamterene (dose 5–10 mg OD–BD). At higherdoses it also inhibits Na+ reabsorption in PT, butthis is clinically insignificant. It decreases Ca2+
and Mg2+ excretion but increases urate excretion.Thus, hypercalcaemic action of thiazides isaugmented but hyperuricaemic action is partlyannuled. A mild antihypertensive action is alsoreported.
Only ¼ of an oral dose is absorbed. It is notbound to plasma proteins and not metabolized.The t½ (20 hours) and duration of action arelonger than triamterene.BIDURET, KSPAR: Amiloride 5 mg + hydrochlorothiazide50 mg tab, LASIRIDE, amiloride 5 mg + furosemide 40 mgtab.
Usual side effects are nausea, diarrhoea andheadache.
Amiloride blocks entry of Li+ through Na+
channels in the CD cells and mitigates diabetesinsipidus induced by lithium.
Given as an aerosol it affords symptomaticimprovement in cystic fibrosis by increasingfluidity of respiratory secretions.
OSMOTIC DIURETICS
MannitolMannitol is a nonelectrolyte of low molecularweight (182) that is pharmacologically inert—can be given in large quantities sufficient to raiseosmolarity of plasma and tubular fluid. It isminimally metabolized in the body; freely filteredat the glomerulus and undergoes limitedreabsorption: therefore excellently suited to beused as osmotic diuretic. Mannitol appears to limittubular water and electrolyte reabsorption in avariety of ways:
1. Retains water isoosmotically in PT—dilutesluminal fluid which opposes NaCl reabsorp-tion.
2. Inhibits transport processes in the thickAscLH by an unknown mechanism.Quantitatively this appears to be the largestcontributor to the diuresis.

591C
HA
PTE
R41
DIURETICS
3. Expands extracellular fluid volume (becauseit does not enter cells, mannitol draws waterfrom the intracellular compartment)—increases g.f.r. and inhibits renin release.
4. Increases renal blood flow, especially to themedulla—medullary hypertonicity is redu-ced (due to washing off)—corticomedullaryosmotic gradient is dissipated—passive saltreabsorption is reduced.
Though the primary action of mannitol is toincrease urinary volume, excretion of all cations(Na+, K+, Ca2+, Mg2+) and anions (Cl¯, HCO3
¯,PO4
3¯) is also enhanced.
Administration Mannitol is not absorbed orally;has to be given i.v. as 10–20% solution. It isexcreted with a t½ of 0.5–1.5 hour.MANNITOL 10%, 20%, in 100, 350 and 500 ml vac.
Uses Mannitol is never used for the treatmentof chronic edema or as a natriuretic. Its indica-tions are:1. Increased intracranial or intraocular tension(acute congestive glaucoma, head injury, stroke,etc.): by osmotic action it encourages movementof water from brain parenchyma, CSF and aqueoushumour; 1–1.5 g/kg is infused over 1 hour as20% solution to transiently raise plasma osmo-larity. It is also used before and after ocular/brainsurgery to prevent acute rise in intraocular/intracranial pressure.
2. To maintain g.f.r. and urine flow in impen-ding acute renal failure, e.g. in shock, severetrauma, cardiac surgery, haemolytic reactions:500–1000 ml of the solution may be infused over24 hours. However, prognostic benefits inconditions other than cardiac surgery are stillunproven. If acute renal failure has already set in,kidney is incapable of forming urine even after anosmotic load; mannitol is contraindicated: it willthen expand plasma volume pulmonary edemaand heart failure may develop.3. To counteract low osmolality of plasma/e.c.f.due to rapid haemodialysis or peritoneal dialysis(dialysis disequilibrium).
Mannitol along with large volumes of saline was infusedi.v. to produce ‘forced diuresis’ in acute poisonings in thehope of enhancing excretion of the poison. However, thishas been found to be ineffective and to produce electrolyteimbalances. Not recommended now.
Mannitol is contraindicated in acute tubularnecrosis, anuria, pulmonary edema; acute leftventricular failure, CHF, cerebral haemorrhage.The most common side effect is headache. Nauseaand vomiting may occur; hypersensitivity reactionsare rare.Isosorbide and glycerol These are orally active osmoticdiuretics which may be used to reduce intraocular orintracranial tension. Intravenous glycerol can causehaemolysis.Dose: 0.5–1.5 g/kg as oral solution.
TABLE 41.2 Urinary electrolyte pattern and natriuretic efficacy of some diuretics
Urinary electrolyte excretion Max. % of filtered EfficacyDiuretic Na+ K+ Cl¯ HCO3̄ Na+ excreted
1. Furosemide ,– 25% High
2. Thiazide 8% Intermediate
3. Acetazolamide ,– 5% Mild
4. Spironolactone –, 3% Low
5. Amiloride –, 3% Low
6. Mannitol 20% High

592S
EC
TIO
N9
DRUGS ACTING ON KIDNEY
PROBLEM DIRECTED STUDY
41.1 A 50-year-old male patient of hepatic cirrhosis with ascitis and pedal edema was treatedwith tab Furosemide 80 mg twice a day, in addition to bed rest, suitable dietary advice andvitamin supplementation. He started passing larger quantity of urine and the ascitis/edema startedregressing. After a week, he was brought with incoherent talking, drowsiness, tremor and ataxia.The relatives informed that for the past 2 days he was no longer passing the increased amountof urine as at the start of medication. Serum K+ measurement found a value of 2.8 mEq/L.(a) What is the cause of the neurological symptoms and diminution of the diuretic responseto furosemide? Was the choice of the diuretic appropriate?(b) How should this patient be managed at the present stage?(see Appendix-1 for solution)

AntidiureticsChapterChapterChapterChapterChapter 4242424242
Antidiuretics (more precisely ‘anti-aquaretics’,because they inhibit water excretion withoutaffecting salt excretion) are drugs that reduce urinevolume, particularly in diabetes insipidus (DI)which is their primary indication. Drugs are:
1. Antidiuretic hormone (ADH, Vasopressin),Desmopressin, Lypressin, Terlipressin
2. Thiazide diuretics, Amiloride.3. Miscellaneous: Indomethacin,
Chlorpropamide, Carbamazepine.
ANTIDIURETIC HORMONE(Argenine Vasopressin-AVP)
It is a nonapeptide secreted by posterior pituitary(neurohypophysis) along with oxytocin (see Ch.23). It is synthesized in the hypothalamic(supraoptic and paraventricular) nerve cell bodiesas a large precursor peptide along with its bindingprotein ‘neurophysin’. Both are transported downthe axons to the nerve endings in the medianeminence and pars nervosa. Osmoreceptorspresent in hypothalamus and volume receptorspresent in left atrium, ventricles and pulmonaryveins primarily regulate the rate of ADH releasegoverned by body hydration. Osmoreceptors arealso present in the hepatic portal system whichsense ingested salt and release ADH even beforeplasma osmolarity is increased by the ingestedsalt. Impulses from baroreceptors and highercentres also impinge on the nuclei synthesizingADH and affect its release. The two mainphysiological stimuli for ADH release are risein plasma osmolarity and contraction of e.c.f.volume.
Several neurotransmitters, hormones and drugs modifyADH secretion. It is enhanced by angiotensin II, prostaglandins(PGs), histamine, neuropeptide Y and ACh. GABA and atrialnatriuretic peptide (ANP) decrease its release. Opioids haveagent-specific and dose dependent action. Low-dose morphine
inhibits ADH secretion, but high doses enhance it. Opioidpeptides are mostly inhibitory. Nicotine and imipraminestimulate, while alcohol, haloperidol, phenytoin andglucocorticoids decrease ADH release.
The human ADH is 8-arginine-vasopressin(AVP); 8-lysine-vasopressin (lypressin) is foundin swine and has been synthetically prepared.Other more potent and longer acting peptideanalogues of AVP having agonistic as well asantagonistic action have been prepared.
ADH (Vasopressin) receptorsThese are G protein coupled cell membranereceptors; two subtypes V1 and V2 have beenidentified, cloned and structurally characterized.
V1 Receptors All vasopressin receptors exceptthose on renal CD cells, AscLH cells and vascularendothelium are of the V1 type. These are furtherdivided into V1a and V1b subtypes:
V1a receptors are present on vascular smoothmuscle (including that of vasa recta in renalmedulla), uterine and other visceral smoothmuscles, interstitial cells in renal medulla, corticalCD cells, adipose tissue, brain, platelets, liver,etc. The V1b receptors are localized to the anteriorpituitary, certain areas in brain and in pancreas.
The V1 receptors function mainly through thephospholipase C–IP3/DAG pathway—release Ca2+
from intracellular stores—causing vasoconstric-tion, visceral smooth muscle contraction, glyco-genolysis, platelet aggregation, ACTH release, etc.These actions are augmented by enhanced influxof Ca2+ through Ca2+ channels as well as by DAGmediated protein kinase C activation whichphosphorylates relevant proteins. V1 receptors, inaddition, activate phospholipase A2—releasearachidonic acid resulting in generation of PGsand other eicosanoids which contribute to manyof the V1 mediated effects. Persistent V1 receptor

594S
EC
TIO
N9
DRUGS ACTING ON KIDNEY
stimulation activates protooncogenes (possiblythrough IP3/DAG pathway) resulting in growth(hypertrophy) of vascular smooth muscle and otherresponsive cells.
V2 Receptors These are located primarily onthe collecting duct (CD) principal cells in thekidney—regulate their water permeability throughcAMP production. Some V2 receptors are alsopresent on AscLH cells which activate Na+K+2Cl¯
cotransporter. Vasodilatory V2 receptors arepresent on endothelium of blood vessels.
The V2 receptors are more sensitive (respondat lower concentrations) to AVP than are V1
receptors.Selective peptide agonists and antagonists of
the subtypes of vasopressin receptors are:Selective agonist
V1a Receptor [Phe2, Ile2, Orn8] AVPV1b Receptor Deamino [D-3 {pyridyl)-Ala2] AVPV2 Receptor Desmopressin (dDAVP)
Selective antagonistV1a Receptor d(CH2)5 [Tyr (Me2)] AVPV1b Receptor dp [Tyr (me2)] AVPV2 Receptor d(CH2)5 [D-Ile2, Ile4, Ala-NH2
9] AVP
Some orally active nonpeptide V1a, V1b and V2 receptorantagonists have been produced. Tolvaptan and Mozavaptanare nonpeptide V2 selective antagonists that are now in clinicaluse.
ActionsKidney AVP acts on the collecting duct (CD)principal cells to increase their water permeability—water from the duct lumen diffuses to the interstitiumby equilibrating with the hyperosmolar renalmedulla (see Fig. IX.1). In man, maximal osmolarityof urine that can be attained is 4 times higherthan plasma. When AVP is absent, CD cells remainimpermeable to water → dilute urine (producedby the diluting segment) is passed as such. Gradedeffect occurs at lower concentrations of AVP: urinevolume closely balances fluid intake.
Mechanism of action Vasopressin is instru-mental in rapid adjustments of water excretionaccording to the state of body hydration, as wellas in dealing with conditions prevailing over long-
term. The V2 subtype of ADH receptors are presenton the basolateral membrane of principal cellsin CDs (see Fig. 42.1). Activation of these recep-tors increases cAMP formation intracellularly →activation of cAMP dependent protein kinase A→ phosphorylation of relevant proteins whichpromote exocytosis of ‘aquaporin-2’ waterchannel containing vesicles (WCVs) through theapical membrane → more aqueous channels getinserted into the apical membrane. The rate ofendocytosis and degradation of WCVs isconcurrently reduced. The water permeability ofCD cells is increased in proportion to the popu-lation of aquaporin-2 channels in the apicalmembrane at any given time. Continued V2
receptor stimulation (during chronic waterdeprivation) in addition upregulates aquaporin-2synthesis through cAMP response element of thegene encoding aquaporin-2.
Other aquaporins like aquaporin-1 (in PT) and aquaporin-3,4(on basolateral membrane of CD cells) also participate in watertransport at these sites.
To achieve maximum concentration of urine,activation of V2 receptors increases urea per-meability of terminal part of CDs in inner medullaby stimulating a vasopressin regulated ureatransporter (VRUT or UT-1)—which in turnaugments medullary hypertonicity. Recently, V2
receptor mediated actions of AVP on AscLH havealso been demonstrated which further reinforcemedullary hypertonicity by translocating toluminal membrane and activating the Na+K+2Cl¯
cotransporter in the short-term and increasing itssynthesis in the long-term.
The V1 receptors also participate in the renalresponse to AVP. Activation of V1 receptorsconstricts vasa recta to diminish blood flow toinner medulla which reduces washing off effectand helps in maintaining high osmolarity in thisregion. Thus, it contributes to antidiuresis. Onthe other hand, activation of medullary interstitialcell V1 receptors enhance PG synthesis whichattenuate cAMP generation in CD cells and opposeV2 mediated antidiuresis. V1 receptors are alsopresent on CD cells. Their stimulation activates

595C
HA
PTE
R42
ANTIDIURETICS
Fig. 42.1: Mechanisms of rapid and long-term anti-aquaretic action of vasopressin
All V2 receptor (V2R) mediated actions are exerted through the adenylyl cyclase (AC)-cyclic AMP (cAMP) pathway,while the V1a receptor (V1aR) mediated action is exerted via the phospholipase C—IP3: DAG pathway.
Rapid actions
(1) Translocation of water channel containing vesicles (WCVs) and exocytotic insertion of aquaporin 2 waterchannels into the apical membrane of principal cells of collecting ducts; the primary action responsible forantidiuresis.
(2) Inhibition of endocytotic removal of aquaporin 2 channels from the apical membrane.(3) Activation of vasopressin regulated urea transporter (VRUT) at apical membrane of collecting ducts in the
inner medulla.(4) Translocation of Na+K+2Cl¯ cotransporter to the luminal membrane of cells in thick ascending limb of loop of
Henle (AscLH).(5) Activation of Na+K+2Cl¯ cotransporter in AscLH cells.(6) V1a receptor (V1aR) mediated vasoconstriction of vasa recta
Long-term actions(7) Gene mediated increased expression of aquaporin 2 channels in collecting duct cells.(8) Gene mediated increased expression of Na+K+2Cl¯ cotransporter in AscLH cells.
PKA—cAMP dependent protein kinase.

596S
EC
TIO
N9
DRUGS ACTING ON KIDNEY
PKc which directly diminishes responsiveness ofCD cells to V2 receptors and restrains V2 mediatedwater permeability. The logic of this apparentparadox may lie in the fact that these V1 actionsare produced at much higher concentrations ofAVP, so that physiologically they may serve torestrict V2 effects only when blood levels of AVPare very high.
Lithium and demeclocycline partially antagonize AVP action(probably by limiting cAMP formation), reduce the urineconcentrating ability of the kidney, produce polyuria andpolydipsia. They have been used in patients with inappropriateADH secretion. On the other hand NSAIDs (especiallyindomethacin) augment AVP induced antidiuresis byinhibiting renal PG synthesis. Carbamazepine andchlorpropamide also potentiate AVP action on kidney.
Blood vessels AVP constricts blood vesselsthrough V1 receptors and can raise BP (hencethe name vasopressin), but much higher concen-tration is needed than for maximal antidiuresis.The cutaneous, mesenteric, skeletal muscle, fatdepot, thyroid, and coronary beds are particularlyconstricted. Though vasoconstrictor action of AVPdoes not appear to be physiologically important,some recent studies indicate that it may play arole in CHF, haemorrhage, hypotensive states, etc.Prolonged exposure to AVP causes vascularsmooth muscle hypertrophy.
The V2 receptor mediated vasodilatation canbe unmasked when AVP is administered in thepresence of a V1 antagonist. It can also bedemonstrated by the use of selective V2 agonistdesmopressin, and is due to endotheliumdependent NO production.
Other actions Most visceral smooth musclescontract. Increased peristalsis in gut (especiallylarge bowel), evacuation and expulsion of gasesmay occur.
Uterus is contracted by AVP acting on oxytocinreceptors. In the nonpregnant and early pregnancyuterus, AVP is equipotent to oxytocin. Only atterm sensitivity to oxytocin increases selectively.
CNS Exogenously administered AVP does notpenetrate blood-brain barrier. However, it is nowrecognized as a peptide neurotransmitter in many
areas of brain and spinal cord. AVP may beinvolved in regulation of temperature, systemiccirculation, ACTH release, and in learning of tasks.
AVP induces platelet aggregation and hepaticglycogenolysis. It releases coagulation factor VIIIand von Willebrand’s factor from vascular endo-thelium through V2 receptors.
Pharmacokinetics AVP is inactive orallybecause it is destroyed by trypsin. It can beadministered by any parenteral route or byintranasal application. The peptide chain of AVPis rapidly cleaved enzymatically in many organs,especially in liver and kidney; plasma t½ is short~25 min. However, the action of aqueousvasopressin lasts 3–4 hours.Aqueous vasopressin (AVP) inj: POSTACTON 10 U inj;for i.v., i.m. or s.c. administration.
VASOPRESSIN ANALOGUES
Lypressin It is 8-lysine vasopressin. Thoughsomewhat less potent than AVP, it acts on bothV1 and V2 receptors and has longer duration ofaction (4–6 hours). It is being used in place ofAVP—mostly for V1 receptor mediated actions.PETRESIN, VASOPIN 20 IU/ml inj; 10 IU i.m. or s.c. or 20IU diluted in 100–200 ml of dextrose solution and infused i.v.over 10–20 min.
Terlipressin This synthetic prodrug of vaso-pressin is specifically used for bleeding esophagealvarices; may produce less severe adverse effectsthan lypressin.Dose: 2 mg i.v., repeat 1–2 mg every 4–6 hours as needed.GLYPRESSIN 1 mg freeze dried powder with 5 ml diluent forinj, T-PRESSIN, TERLINIS 1 mg/10 ml inj.
Desmopressin (dDAVP) This syntheticpeptide is a selective V2 agonist; 12 times morepotent antidiuretic than AVP, but has negligiblevasoconstrictor activity. It is also longer actingbecause enzymatic degradation is slow; t½1–2 hours; duration of action 8–12 hours.Desmopressin is the preparation of choice forall V2 receptor related indications. The intranasalroute is preferred, though bioavailability is only10–20%. An oral formulation has been recentlymarketed with a bioavailability of 1–2%; oral dose

597C
HA
PTE
R42
ANTIDIURETICS
is 10–15 times higher than intranasal dose, butsystemic effects are produced and nasal sideeffects are avoided. Many patients find oral tabletmore convenient.Dose: Intranasal: Adults 10–40 µg/day in 2–3 divided doses,children 5–10 µg at bed time.Oral: 0.1–0.2 mg TDS.Parenteral (s.c. or i.v.) 2–4 µg/day in 2–3 divided doses.MINIRIN 100 µg/ml nasal spray (10 µg per actuation); 100µg/ml intranasal solution in 2.5 ml bottle with applicator; 0.1mg tablets; 4 µg/ml inj.
UsesA. Based on V2 actions (Desmopressin is thedrug of choice)1. Diabetes insipidus DI of pituitary origin(neurogenic) is the most important indication forvasopressin. It is ineffective in renal (nephrogenic)DI, since kidney is unresponsive to ADH. Life-long therapy is required, except in some casesof head injury or neurosurgery, where DI occurstransiently.
The dose of desmopressin is individualized bymeasuring 24 hour urine volume. Aqueousvasopressin or lypressin injection is impracticablefor long-term treatment. It can be used in transientDI and to differentiate neurogenic from nephro-genic DI—urine volume is reduced and itsosmolarity increased if DI is due to deficiency ofADH, but not when it is due to unresponsivenessof kidney to ADH. Desmopressin 2 µg i.m. is thepreparation of choice now for the same purpose.
2. Bedwetting in children and nocturia inadults Intranasal or oral desmopressin at bed-time controls primary nocturia by reducing urinevolume. Nocturnal voids are reduced to nearlyhalf and first sleep period in adults is increasedby ~2 hr. Fluid intake must be restricted 1 hrbefore and till 8 hr after the dose to avoid fluidretention. Monitor BP and body weight perio-dically to check fluid overload. Withdraw for oneweek every 3 months for reassessment.
3. Renal concentration test 5–10 U i.m. ofaqueous vasopressin or 2 µg of desmopressincauses maximum urinary concentration.
4. Haemophilia, von Willebrand’s diseaseAVP may check bleeding by releasing coagulationfactor VIII and von Willebrand’s factor.Desmopressin is the preferred preparation in adose of 0.3 µg/kg diluted in 50 ml saline andinfused i.v. over 30 min.
B. Based on V1 actions1. Bleeding esophageal varices Vasopressin/terlipressin often stop bleeding by constrictingmesenteric blood vessels and reducing blood flowthrough the liver to the varices, allowing clotformation. Terlipressin stops bleeding in ~80%and has been shown to improve survival. It hasreplaced AVP because of fewer adverse effectsand greater convenience in use. Octreotide (asomatostatin analogue) injected i.v. is analternative. However, definitive therapy of varicesremains endoscopic obliteration by sclerotherapy.
2. Before abdominal radiography AVP/lypressin hasbeen occasionally used to drive out gases from bowel.
Adverse effects Because of V2 selectivity,desmopressin produces fewer adverse effects thanvasopressin, lypressin or terlipressin. However,transient headache and flushing are frequent.
Nasal irritation, congestion, rhinitis, ulcera-tion and epistaxis can occur on local application.Systemic side effects are: belching, nausea,abdominal cramps, pallor, urge to defecate,backache in females (due to uterine contraction).Fluid retention and hyponatraemia may develop.Symptoms of hyponatremia are due to shift of waterintracellularly resulting in cerebral edema producing headache,mental confusion, lassitude, nausea, vomiting and evenseizures. Children are more susceptible.
AVP can cause bradycardia, increase cardiacafterload and precipitate angina by constrictingcoronary vessels. It is contraindicated in patientswith ischaemic heart disease, hypertension,chronic nephritis and psychogenic polydipsia.Urticaria and other allergies are possible with anypreparation.
THIAZIDES
Diuretic thiazides paradoxically exert anantidiuretic effect in DI. High ceiling diuretics

598S
EC
TIO
N9
DRUGS ACTING ON KIDNEY
are also effective but are less desirable becauseof their short and brisk action. Thiazides reduceurine volume in both pituitary origin as well asrenal DI. They are especially valuable for thelatter in which AVP is ineffective. However, theirefficacy is low; urine can never become hypertonicas can occur with AVP in neurogenic DI. Themechanism of action is not well understood,possible explanation is:
Thiazides induce a state of sustainedelectrolyte depletion so that glomerular filtrateis more completely reabsorbed iso-osmotically inPT. Further, because of reduced salt reabsorptionin the cortical diluting segment, a smaller volumeof less dilute urine is presented to the CDs andthe same is passed out. That salt restriction hasa similar effect, substantiates this mechanism ofaction. Secondly, thiazides reduce g.f.r. and thusthe fluid load on tubules.
Hydrochlorothiazide 25–50 mg TDS or equi-valent dose of a longer acting agent is commonlyused. Though less effective than AVP, it is moreconvenient and cheap even for pituitary originDI; may reduce polyuria to some extent.K+ supplements are needed.
Amiloride is the drug of choice for lithium inducednephrogenic DI (see p. 590).
Indomethacin has also been found to reduce
polyuria in renal DI to some extent by reducingrenal PG synthesis. It can be combined with athiazide ± amiloride in nephrogenic DI. OtherNSAIDs are less active.Chlorpropamide It is a long-acting sulfonylurea oralhypoglycaemic, found to reduce urine volume in DI ofpituitary origin but not in renal DI. It sensitizes the kidneyto ADH action; thus its efficacy depends on small amountsof the circulating hormone; it is not active when ADH istotally absent.
Carbamazepine It is an antiepileptic (see Ch. 30) whichreduces urine volume in DI of pituitary origin, but mechanismof action is not clear. Higher doses are needed; adverse effectsare marked; it is of little value in treatment of DI.
VASOPRESSIN ANTAGONISTSTolvaptan It is an orally active nonpeptide selective V2
receptor antagonist that has been recently introduced for thetreatment of hyponatraemia due to CHF, cirrhosis of liveror syndrome of inappropriate ADH secretion (SIADH). Itincreases free water clearance by the kidney (aquaretic) andhelps to correct the low plasma Na+ levels. In clinical trialssymptoms of worsening heart failure were improved. However,too rapid correction of hyponatraemia should not be attempted,because thrombotic complications can occur due tohaemoconcentration. The most frequent side effect is thirstand dry mouth. Others are fever, g.i. upset and hyper-glycaemia. Tolvaptan is metabolized by CYP3A4; shouldnot be given to patients receiving inhibitors of this isoenzyme.The t½ is 6–8 hours, and it is given once daily.
Mozavaptan (V2 selective antagonist) and Conivaptan(V1a+V2 antagonist) are the other vasopressin antagonists thatare in clinical use.

Haematinics andErythropoietin
ChapterChapterChapterChapterChapter 4343434343
SECTION 10
DRUGS AFFECTING BLOOD AND
BLOOD FORMATION
Haematinics These are substances required inthe formation of blood, and are used for treat-ment of anaemias.Anaemia occurs when the balance between pro-duction and destruction of RBCs is disturbed by:(a) Blood loss (acute or chronic)(b) Impaired red cell formation due to:
• Deficiency of essential factors, i.e. iron,vitamin B12, folic acid.
• Bone marrow depression (hypoplastic anae-mia), erythropoietin deficiency.
(c) Increased destruction of RBCs (haemolyticanaemia)
In this chapter essential factors required for normalformation or pigmentation of RBCs will becovered.
IRONIron has for long been considered important for the body.Lauha bhasma (calcined iron) has been used in ancient Indianmedicine. According to Greek thought Mars is the God ofstrength, and iron is dedicated to Mars: as such, iron wasused to treat weakness, which is common in anaemia. In1713 iron was shown to be present in blood. In the early19th century Blaud developed his famous ‘Blaud’s pill’consisting of ferrous sulfate and potassium carbonate foranaemia. All important aspects of iron metabolism have beenlearned in the past 60 years.
Distribution of iron in body Iron is anessential body constituent. Total body iron in anadult is 2.5–5 g (average 3.5 g). It is more inmen (50 mg/kg) than in women (38 mg/kg). Itis distributed into:
Haemoglobin (Hb) : 66%Iron stores as ferritin and : 25%haemosiderinMyoglobin (in muscles) : 3%Parenchymal iron (in enzymes, etc.) : 6%
Haemoglobin is a protoporphyrin; each moleculehaving 4 iron containing haeme residues. It has0.33% iron; thus loss of 100 ml of blood (con-taining 15 g Hb) means loss of 50 mg elementaliron. To raise the Hb level of blood by 1 g/dl—about 200 mg of iron is needed. Iron is storedonly in ferric form, in combination with a largeprotein apoferritin.
aggregatesApoferritin + Fe3+ Ferritin Haemosiderin
(not reutilized)
Ferritin can get saturated to different extents; atfull saturation it can hold 30% iron by weight.The most important storage sites are reticuloendo-thelial (RE) cells. Parenchymal iron occurs asprosthetic group in many cellular enzymes—

600S
EC
TIO
N10
DRUGS AFFECTING BLOOD AND BLOOD FORMATION
cytochromes, peroxidases, catalases, xanthineoxidase and some mitochondrial enzymes.Though, the primary reflection of iron deficiencyoccurs in blood, severe deficiency affects prac-tically every cell.
Daily requirement To make good average dailyloss, iron requirements are:
Adult male : 0.5–1 mg (13 µg/kg)Adult female : 1–2 mg (21 µg/kg)
(menstruating)Infants : 60 µg/kgChildren : 25 µg/kgPregnancy : 3–5 mg (80 µg/kg)
(last 2 trimesters)
Dietary sources of iron
Rich : Liver, egg yolk, oyster, dry beans, dryfruits, wheat germ, yeast.
Medium : Meat, chicken, fish, spinach, banana,apple.
Poor : Milk and its products, root vegetables.
Iron absorptionThe average daily diet contains 10–20 mg of iron.Its absorption occurs all over the intestine, but
majority in the upper part. Dietary iron is presenteither as haeme or as inorganic iron. Absorptionof haeme iron is better (upto 35% compared toinorganic iron which averages 5%) and occursdirectly without the aid of a carrier (Fig. 43.1).However, it is a smaller fraction of dietary iron.The major part of dietary iron is inorganic andin the ferric form. It needs to be reduced to theferrous form before absorption. Two separate irontransporters in the intestinal mucosal cells functionto effect iron absorption. At the luminal membranethe divalent metal transporter 1 (DMT1) carrysferrous iron into the mucosal cell. This along withthe iron released from haeme is transported acrossthe basolateral membrane by another irontransporter ferroportin (FP). These irontransporters are regulated according to the bodyneeds. Absorption of haeme iron is largelyindependent of other foods simultaneouslyingested, but that of inorganic iron is affectedby several factors.
Factors facilitating iron absorption
1. Acid: by favouring dissolution and reductionof ferric iron.
Fig. 43.1: Schematic depiction of intestinal absorption, transport, utilization and storage of iron (see text for description)Fe2+—Ferrous iron; Fe3+—Ferric iron; DMT1—Divalent metal transporter 1; Hb—Haemoglobin; RE cell—Reticuloendothelial cell; FP1—Ferroportin; Tf—Transferrin; TfR—Transferrin receptor

601C
HA
PTE
R43
HAEMATINICS AND ERYTHROPOIETIN
2. Reducing substances: ascorbic acid, aminoacids containing SH radical. These agentsreduce ferric iron and form absorbablecomplexes.
3. Meat: by increasing HCl secretion andproviding haeme iron.
Factors impeding iron absorption
1. Alkalies (antacids) render iron insoluble,oppose its reduction.
2. Phosphates (rich in egg yolk)3. Phytates (in maize, wheat)4. Tetracyclines5. Presence of other foods in the stomach.
In general, bioavailability of iron from cerealbased diets is low.
Mucosal block The gut has a mechanism toprevent entry of excess iron in the body. Ironreaching inside mucosal cell is either transportedto plasma or oxidised to ferric form and com-plexed with apoferritin to form ferritin (Fig. 43.1).This ferritin generally remains stored in the muco-sal cells and is lost when they are shed (lifespan2–4 days). This is called the ‘Ferritin curtain’.
The iron status of the body and erythropoieticactivity govern the balance between these twoprocesses, probably through a ‘haematopoietictranscription factor’, and thus the amount of ironthat will enter the body. A larger percentage isabsorbed during iron deficiency. When body ironis low or erythropoiesis is occurring briskly,ferritin is either not formed or dissociates soon—the released iron is transported to the blood.
Mucosal block however, can be overwhelmedby gross excess of iron.
Transport, utilization, storage andexcretionFree iron is highly toxic. As such, on enteringplasma it is immediately converted enzymaticallyto the ferric form and complexed with aglycoprotein transferrin (Tf). Iron circulates inplasma bound to Tf (two Fe3+ residues permolecule). The total plasma iron content (~3 mg)is recycled 10 times everyday (turnover of ironis 30 mg/day).
Iron is transported inside erythropoietic andother cells through attachment of transferrin tospecific membrane bound transferrin receptors(TfRs). The complex is engulfed by receptormediated endocytosis. Iron dissociates from thecomplex at the acidic pH of the intracellularvesicles; the released iron is utilized forhaemoglobin synthesis or other purposes, whileTf and TfR are returned to the cell surface tocarry fresh loads. In iron deficiency and haemo-lytic states when brisk erythropoiesis is occurring,erythropoietic cells express more TfRs, but othercells do not. Thus, the erythron becomes selecti-vely more efficient in trapping iron.
After entering the storage cells through TfRs,iron is stored in RE cells (in liver, spleen, bonemarrow), as well as in hepatocytes and myocytesas ferritin and haemosiderin. Apoferritin synthesisis regulated by iron status of the body. Whenit is low—the ‘iron regulating element’ (IRE) onmRNA is blocked—transcription of apoferritindoes not occur, while more Tf is produced. Onthe other hand, more apoferritin is synthesizedto trap iron when iron stores are rich. Plasmairon derived from destruction of old RBCs(lifespan ~120 days), from stores and fromintestinal absorption forms a common pool thatis available for erythropoiesis, to all other cellsand for restorage.
Iron is tenaciously conserved by the body;daily excretion in adult male is 0.5–1 mg, mainlyas exfoliated g.i. mucosal cells, some RBCs andin bile (all lost in faeces). Other routes aredesquamated skin, very little in urine and sweat.In menstruating women, monthly menstrual lossmay be averaged to 0.5–1 mg/day. Excess ironis required during pregnancy for expansion ofRBC mass, transfer to foetus and loss duringdelivery; totalling to about 700 mg. This is tobe met in the later 2 trimesters.
Preparations and doseOral iron
The preferred route of iron administration is oral.Dissociable ferrous salts are inexpensive, havehigh iron content and are better absorbed than
⎫⎬⎭
Bycomplexingiron

602S
EC
TIO
N10
DRUGS AFFECTING BLOOD AND BLOOD FORMATION
TABLE 43.1 Some combination preparations of iron
Trade name Iron compound Other ingredients
CONVIRON Cap Fe. sulfate (dried) 60 mg B12 15 µg, folic acid 1.5 mg, B6 1.5 mg, vit. C 75 mg
FESOVIT-SPANSULE Cap Fe. sulfate (dried) 150 mg B12 15 µg, folic acid 1 mg, nicotinamide 50 mg,B6 2 mg
FERSOLATE-CM tab Fe. sulfate (dried) 195 mg Cu sulfate 2.6 mg, Mn. sulfate 2 mg
FEFOL SPANSULE Cap Fe. sulfate 150 mg Folic acid 0.5 mg
HEMGLOB syr (15 ml) Fe. gluconate 300 mg B12 15 µg, B1 5 mg, B2 5 mg, B6 1.5 mg,niacinamide 45 mg
AUTRIN Cap Fe. fumarate 300 mg B12 15 µg, folic acid 1.5 mg
DUMASULES Cap Fe. fumarate 300 mg B12 7.5 µg, folic acid 0.75 mg, B1 5 mg,niacinamide 50 mg, vit. C 75 mg, B6 1.5 mg
HEMSYNERAL Cap Fe. fumarate 200 mg B12 15 µg, folic acid 1.5 mg
ANEMIDOX Cap Fe fumarate 360 mg Folic acid 1.5 mg, vit B12 15 μg, Cal. carb.200 mg, vit C 75 mg, vit D 400 i.u.
HEMSI syr. (5 ml) Fe. fumarate 100 mg Vit B12 5 μg, folic acid 0.5 mg, Zn 3.3 mg,Cu 0.035 mg, Mn 0.2 mg
FERRICARB Cap Carbonyl iron (100 mg iron) Folic acid 1.5 mg, vit B12 15 μg, zinc sulfate88 mg, pyridoxine 3 mg, sod. selenite 60 μg
HBFAST tab Carbonyl iron (100 mg iron) Folic acid 0.35 mg
HEMATRINE Cap Fe. succinate 100 mg B12 2.5 µg, folic acid 0.5 mg, vit. C 25 mg,niacinamide 15 mg
POLYRON tab, BIOFER tab Ferric hydroxy polymaltose Folic acid 0.35 mgPOLYFER chewable tab (Iron 100 mg)
MUMFER syr (5 ml) Ferric hydroxy polymaltose(50 mg iron)
drops (1 ml) —do—(50 mg iron)
FERROCHELATE syr (5 ml) Ferric ammon. cit. (Iron 60 mg) B12 5 µg, folic acid 1 mgdrops (1 ml) —do—(Iron 20 mg) B12 4 µg, folic acid 0.2 mg
RARICAP tab Iron cal. complex (Iron 25 mg) Folic acid 0.3 mg
PROBOFEX Cap Fe. aminoate (60 mg iron) B12 15 µg, folic acid 1.5 mg, B6 3 mg
DEXORANGE Cap, Ferric ammon. cit. 160 mg B12 7.5 µg, folic acid 0.5 mg, Zn 7.5 mgsyrup (15 ml) (as sulfate)
Combination of iron with strychnine, arsenic and yohimbine and all fixed dose combination of haemoglobin in anyform are banned in India.

603C
HA
PTE
R43
HAEMATINICS AND ERYTHROPOIETIN
ferric salts, especially at higher doses. Gastricirritation and constipation (the most important sideeffects of oral iron) are related to the total quantityof elemental iron administered. If viewed in termsof iron content, nearly all preparations have thesame degree of gastric tolerance, the limits ofwhich are fairly well defined in individual patients.Some simple oral preparations are:1. Ferrous sulfate: (hydrated salt 20% iron, driedsalt 32% iron) is the cheapest; may be preferredon this account. It often leaves a metallic tastein mouth; FERSOLATE 200 mg tab.2. Ferrous gluconate (12% iron): FERRONICUM300 mg tab, 400 mg/15 ml elixer.3. Ferrous fumarate (33% iron): is less watersoluble than ferrous sulfate and tasteless;NORI-A 200 mg tab.4. Colloidal ferric hydroxide (50% iron):FERRI DROPS 50 mg/ml drops.5. Carbonyl iron: It is high purity metallic ironin very fine powder form (particle size < 5 μM),prepared by decomposition of iron pentacarbonyl,a highly toxic compound. It is claimed to beabsorbed from intestines over a long time, andgastric tolerance may be better. However,bioavailability is about 3/4th that of ferrous sulfate.
Other forms of iron present in oral formu-lations are:
Ferrous succinate (35% iron)Iron choline citrateIron calcium complex (5% iron)Ferric ammonium citrate (20% iron)Ferrous aminoate (10% iron)Ferric glycerophosphateFerric hydroxy polymaltose
These are claimed to be better absorbed and/orproduce less bowel upset, but this is primarilydue to lower iron content. They are generallymore expensive.
A number of oral formulations containing oneof the iron compounds along with one to manyvitamins, yeast, amino acids and other mineralsare widely marketed and promoted. Some of theseare listed in Table 43.1, but should be consideredirrational.
A Technical Advisory Board (India) has recommendedthat B complex vitamins and zinc should not be includedin iron and folic acid containing haematinic preparations.
Ferric hydroxy polymaltose has been marketed by manypharmaceuticals and vigorously promoted for its high ironcontent, no metallic taste, good g.i. tolerability and directabsorption from the intestines. Because the complex releaseslittle free iron in the gut lumen—g.i. irritation is minimal.However, the high bioavailability observed in rats has notbeen found in humans and reports of its poor efficacy intreating iron deficiency anaemia have appeared. Its therapeuticefficacy is questionable.
The elemental iron content and not the quantityof iron compound per dose unit should be takeninto consideration. Sustained release preparationsare more expensive and not rational because mostof the iron is absorbed in the upper intestine,while these preparations release part of their ironcontent lower down. Bioavailability of iron fromsuch preparations, though claimed to be good,is actually variable. Liquid formulations may stainteeth: should be put on the back of tongue andswallowed. In general, they are less satisfactory.
A total of 200 mg elemental iron (infants andchildren 3–5 mg/kg) given daily in 3 divided dosesproduces the maximal haemopoietic response.Prophylactic dose is 30 mg iron daily. Absorptionis much better when iron preparations are takenin empty stomach. However, side effects are alsomore; some prefer giving larger amounts aftermeals, while others like to give smaller dosesin between meals.
Adverse effects of oral iron These arecommon at therapeutic doses and are related toelemental iron content. Individuals differ insusceptibility. Side effects are:Epigastric pain, heartburn, nausea, vomiting,bloating, staining of teeth, metallic taste, colic,etc. Tolerance to oral iron can be improved byinitiating therapy at low dose and graduallyescalating to the optimum dose.Constipation is more common (believed to bedue to astringent action of iron) than diarrhoea(thought to reflect irritant action). However, thesemay be caused by alteration of intestinal floraas well.

604S
EC
TIO
N10
DRUGS AFFECTING BLOOD AND BLOOD FORMATION
Parenteral ironIron therapy by injection is indicated onlywhen:1. Oral iron is not tolerated: bowel upset is too
much.2. Failure to absorb oral iron: malabsorption;
inflammatory bowel disease. Chronic inflam-mation (rheumatoid arthritis) decreases ironabsorption, as well as the rate at which ironcan be utilized.
3. Non-compliance to oral iron.4. In presence of severe deficiency with chronic
bleeding.5. Along with erythropoietin: oral ion may not
be absorbed at sufficient rate to meet thedemands of induced rapid erythropoiesis.
Parenteral iron therapy needs calculation of thetotal iron requirement of the patient for whichseveral formulae have been devised. A simpleone is:
Iron requirement (mg) = 4.4 × body weight (kg) × Hb deficit (g/dl)
This formula includes iron needed for replenish-ment of stores. The rate of response with parenteraliron is not faster than with optimal doses givenorally, except probably in the first 2–3 weekswhen dose of oral iron is being built up. However,iron stores can be replenished in a shorter timeby parenteral therapy, because after correctionof anaemia, a smaller fraction of ingested ironis absorbed.
The ionized salts of iron used orally cannotbe injected because they have strong proteinprecipitating action and free iron in plasma ishighly toxic. Four organically complexedformulations of iron are currently available inIndia; two of these Iron-dextran and Iron-sorbitol-citric acid have been in use for over 50 years,while two relatively new ones Ferrous sucroseand Ferric carboxymaltose have been added inthe past few years. The newer formulations areless risky and have improved ease of adminis-tration. Few other formulations are marketedelsewhere.
Iron-dextran It is a high molecular weightcolloidal solution containing 50 mg elemental iron/ml; is the only preparation that can be injectedi.m. as well as i.v. By i.m. route it is absorbedthrough lymphatics, circulates without binding totransferrin and is engulfed by RE cells whereiron dissociates and is made available to theerythron for haeme synthesis. In the injectedmuscle 10–30% of the dose remains locally boundand becomes unavailable for utilization for severalweeks. Thus, 25% extra needs to be added tothe calculated dose. Iron-dextran is not excretedin urine or in bile. Because dextran is antigenic,anaphylactic reactions are more common than withthe newer preparations.IMFERON, FERRI INJ: iron dextran 100 mg in 2 ml for i.m./i.v. injection.
Intramuscular: Injection is given deeply in thegluteal region using Z track technique (to avoidstaining of the skin). Iron dextran can be injected2 ml daily, or on alternate days, or 5 ml eachside on the same day (local pain lasting weeksmay occur with the higher dose).
Intravenous: After a test dose of 0.5 ml iron-dextran injected i.v. over 5–10 min, 2 ml canbe injected per day taking 10 min for the injection.Alternatively, the total calculated dose is dilutedin 500 ml of glucose/saline solution and infusedi.v. over 6–8 hours under constant observation.Injection should be terminated if the patientcomplains of giddiness, paresthesias or tightnessin the chest.
Adverse effectsLocal Pain at site of i.m. injection, pigmentationof skin, sterile abscess—especially in old anddebilitated patient.
Systemic Fever, headache, joint pains, flushing,palpitation, chest pain, dyspnoea, lymph nodeenlargement.An anaphylactoid reaction resulting in vascularcollapse and death occurs rarely.Iron-sorbitol-citric acid It is a low molecular weight complexwhich can be injected only i.m., from where absorption occursdirectly into circulation and not through lymphatics. No local

605C
HA
PTE
R43
HAEMATINICS AND ERYTHROPOIETIN
binding in muscle occurs, but about 30% of the dose is excretedin urine; the calculated total dose has to be increasedaccordingly. Patient may be alarmed because the urine turnsbrown after some time. Iron-sorbitol-citric acid binds totransferrin in plasma and may saturate it if present in largequantity. That is why it is not suitable for i.v. injection orinfusion, as the remaining free iron is highly toxic. Even withthe recommended i.m. dose, incidence of immediate reaction,including ventricular tachycardia, A-V block, other irregu-larities, hypotension, flushing is higher. It is contraindicatedin patients with kidney disease. This formulation is notfavoured now.Dose: 75 mg i.m. (max 100 mg) daily or on alternate days.FERIMAX: iron-sorbitol-citric acid 75 mg, folic acid 0.75mg, hydroxocobalamin 75 μg in 1.5 ml amp.
Ferrous-sucrose This newer formulation is ahigh molecular weight complex of iron hydroxidewith sucrose, that on i.v. injection is taken upby RE cells, where iron dissociates and is utilized.It is safer than the older formulations and a doseof 100 mg (max 200 mg) can be injected i.v.taking 5 min, once daily to once weekly till thetotal calculated dose (including that to replenishstores) is administered. However, total dose i.v.infusion is not possible. The solution is highlyalkaline ruling out i.m./s.c. injection.
The incidence of hypersensitivity reaction isvery low. Though, some consider a test dose to beunnecessary, the British guidelines recommend itbefore the first dose. Other side effects are alsomilder. This preparation is particularly indicatedfor anaemia in kidney disease patients, but reportsof kidney damage are on record. Oral iron shouldnot be given concurrently and till 5 days after thelast injection.UNIFERON, ICOR, MICROFER: ferrous sucrose 50 mg in2.5 ml and 100 mg in 5 ml amp. for i.v. inj.
Ferric carboxymaltose It is the latestformulation of iron in which a ferric hydroxidecore is stabilized by a carbohydrate shell. Themacromolecule is rapidly taken up by the RE cells,primarily in bone marrow (upto 80%), as well asin liver and spleen. Iron is released and deliveredsubsequently to the target cells. It is administeredeither as daily 100 mg i.v. injection, or upto 1000mg is diluted with 100 ml saline (not glucosesolution) and infused i.v. taking 15 min or more.Infusion may be repeated after a week. It should
not be injected i.m. In clinical trials, it has causeda rapid increase in haemoglobin level in anaemiapatients and replenished stores. The incidence ofacute reaction is very low. Pain at injection site,and rashes have occurred, but anaphylaxis is rare.Headache, nausea, abdominal pain are generallymild. Hypotension, flushing and chest pain areinfrequent. Due to lack of safety data, it is notrecommended for children <14 years.ENCICARB INJ: Ferric carboxymaltose 50 mg/ml in 2 mland 10 ml vials.
Use1. Iron deficiency anaemia It is the mostimportant indication for medicinal iron. Irondeficiency is the commonest cause of anaemia,especially in developing countries where a sizablepercentage of population is anaemic. The RBC aremicrocytic and hypochromic due to deficient Hbsynthesis. Other metabolic manifestations are seenwhen iron deficiency is severe. Apart fromnutritional deficiency, chronic bleeding from g.i.tract (ulcers, inflammatory bowel disease, hook-worm infestation) is a common cause. Irondeficiency also accompanies repeated attacks ofmalaria and chronic inflammatory diseases. Thecause of iron deficiency should be identified andtreated. Iron should be normally administeredorally; parenteral therapy is to be reservedfor special circumstances. A rise in Hb level by0.5–1 g/dl per week is an optimum response to irontherapy. It is faster in the beginning and whenanaemia is severe. Later, the rate of increase in Hb%declines. However, therapy should be continuedtill normal Hb level is attained (generally takes1–3 months depending on the severity) and 2–3months or more thereafter to replenish the stores.
Prophylaxis: The amount of iron available fromaverage diet and the absorptive processes in theintestine place a ceiling on iron absorption of ~3mg/day. Thus, iron balance is precarious in mostmenstruating women. Later half of pregnancy andinfancy are periods when iron deficiency willdevelop unless medicinal iron is supplemented.In these situations as well as others (chronic

606S
EC
TIO
N10
DRUGS AFFECTING BLOOD AND BLOOD FORMATION
illness, menorrhagia, after acute blood loss, etc.)prophylactic use of iron is indicated.
2. Megaloblastic anaemia When briskhaemopoiesis is induced by vit B12 or folatetherapy, iron deficiency may be unmasked. Theiron status of these patients should be evaluatedand iron given accordingly.
ACUTE IRON POISONING
It occurs mostly in infants and children: 10–20iron tablets or equivalent of the liquid prepara-tion (> 60 mg/kg iron) may cause serious toxicityin them. It is very rare in adults.
Manifestations are vomiting, abdominal pain,haematemesis, diarrhoea, lethargy, cyanosis,dehydration, acidosis, convulsions; finally shock,cardiovascular collapse and death. In few casesdeath occurs early (within 6 hours), but is typicallydelayed to 12– 36 hours, with apparent improve-ment in the intervening period. The pathologicallesion is haemorrhage and inflammation in thegut, hepatic necrosis and brain damage.
Treatment It should be prompt.
To prevent further absorption of iron from gut(a) Induce vomiting or perform gastric lavage
with sodium bicarbonate solution—to renderiron insoluble.
(b) Give egg yolk and milk orally: to complexiron. Activated charcoal does not adsorb iron.
To bind and remove iron already absorbed
Desferrioxamine (an iron chelating agent—seeCh. 66) is the drug of choice. It should be injectedi.m. (preferably) 0.5–1 g (50 mg/kg) repeated4–12 hourly as required, or i.v. (if shock is present)10–15 mg/kg/hour; max 75 mg/kg in a day tillserum iron falls below 300 µg/dl. Early therapywith desferrioxamine has drastically reducedmortality of iron poisoning.
Alternatively DTPA or calcium edetate (seeCh. 66) may be used if desferrioxamine is notavailable. BAL is contraindicated because its ironchelate is also toxic.
Supportive measures Fluid and electrolytebalance should be maintained and acidosiscorrected by appropriate i.v. infusion. Respirationand BP may need support. Diazepam i.v. shouldbe cautiously used to control convulsions, if theyoccur.
Miscellaneous/Adjuvant haematinics
1. Copper Haeme synthesis is interfered in copperdeficiency. However, copper is a trace metal for man andclinical deficiency is very rare. Its routine use is, therefore,not justified. However, when copper deficiency isdemonstrated, 0.5–5 mg of copper sulphate/day may be giventherapeutically; prophylactic dose is 0.1 mg/day. It is presentin some haematinic combinations (see Table 43.1).
2. Pyridoxine (see Ch. 67) Pyridoxine responsiveanaemia is a rare entity. It is due to inherent abnormalityin haeme synthesis. Sideroblastic anaemia associated withisoniazid and pyrazinamide (which interfere with pyridoxinemetabolism and action) therapy needs to be treated withpyridoxine. Some other sideroblastic anaemias show partialimprovement with large doses of pyridoxine. However, routineuse of pyridoxine in anaemia is wasteful.
3. Riboflavin (see Ch. 67) Hypoplastic anaemia occursin riboflavin deficiency which is generally a part of multipledeficiencies in protein-calorie malnutrition. In the absenceof specific deficiency, use of riboflavin in anaemia is ofno value.
MATURATION FACTORS
Deficiency of vit B12 and folic acid, which areB group vitamins, results in megaloblastic anaemiacharacterized by the presence of large red cellprecursors in bone marrow and their large andshortlived progeny in peripheral blood. Vit B12
and folic acid are therefore called maturationfactors. The basic defect is in DNA synthesis.Apart from haemopoietic, other rapidly proli-ferating tissues also suffer.
VITAMIN-B12
Cyanocobalamin and hydroxocobalamin arecomplex cobalt containing compounds present inthe diet and referred to as vit B12.Thomas Addison (1849) described cases of anaemia notresponding to iron. This was later called ‘pernicious’(incurable, deadly) anaemia and its relation with atrophyof gastric mucosa was realized. Minot and Murphy (1926)

607C
HA
PTE
R43
HAEMATINICS AND ERYTHROPOIETIN
treated such patients by including liver in diet and receivedNobel prize. Castle (1927–32) propounded the hypothesisthat there was an extrinsic factor present in diet whichcombined with an intrinsic factor produced by stomach togive rise to the haemopoietic principle. Vit B12 was isolatedin 1948 and was shown to be the extrinsic factor as wellas the haemopoietic principle, the intrinsic factor only helpedin its absorption.
Vit B12 occurs as water soluble, thermostablered crystals. It is synthesized in nature only bymicroorganisms; plants and animals acquire itfrom them.
Dietary sources Liver, kidney, sea fish, egg yolk, meat,cheese are the main vit B12 containing constituents of diet.The only vegetable source is legumes (pulses) which getit from microorganisms harboured in their root nodules.
Vit B12 is synthesized by the colonic microflora, butthis is not available for absorption in man. The commercialsource is Streptomyces griseus; as a byproduct of streptomycinindustry.
Daily requirement 1–3 µg, pregnancy andlactation 3–5 µg.
Metabolic functions Vit B12 is intricatelylinked with folate metabolism in many ways;megaloblastic anaemia occurring due to deficiencyof either is indistinguishable. In addition, vit B12
has some independent metabolic functions as well.The active coenzyme forms of B12 generated inthe body are deoxyadenosyl-cobalamin (DAB12)and methyl-cobalamin (methyl B12).
(i) Vit B12 is essential for the conversion of homo-cysteine to methionine
methyl-THFA B12 methionine
THFA methyl-B12 homocysteine
Methionine is needed as a methyl group donorin many metabolic reactions and for proteinsynthesis. This reaction is also critical in makingtetrahydrofolic acid (THFA) available for reutili-zation. In B12 deficiency THFA gets trappedin the methyl form and a number of onecarbon transfer reactions suffer (see under folicacid).
(ii) Purine and pyrimidine synthesis is affectedprimarily due to defective ‘one carbon’ transferbecause of ‘folate trap’. The most important of
these is inavailability of thymidylate for DNAproduction.
(iii) Malonic acid Succinic acidis an important step in propionic acid metabolism.It links the carbohydrate and lipid metabolisms.This reaction does not require folate and has beenconsidered to be responsible for demyelinationseen in B12 deficiency, but not in pure folatedeficiency. That myelin is lipoidal, supports thiscontention.(iv)Now it appears that interference with thereaction:
Methionine S-adenosyl methionine
may be more important in the neurological damageof B12 deficiency, because it is needed in thesynthesis of phospholipids and myelin.
(v) Vit B12 is essential for cell growth and multi-plication.
Utilization of vit B12 Vit B12 is present infood as protein conjugates and is released bycooking or by proteolysis in stomach facilitatedby gastric acid. Intrinsic factor (a glycoprotein,MW60,000) secreted by stomach forms a complexwith B12—attaches to specific receptors presenton intestinal mucosal cells and is absorbed byactive carrier mediated transport. This mechanismis essential for absorption of vit B12 ingested inphysiological amounts. However, when grossexcess is taken, a small fraction is absorbedwithout the help of intrinsic factor.
Vit B12 is transported in blood in combinationwith a specific β globulin transcobalamin II(TCII). Congenital absence of TCII or presenceof abnormal protein (TCI or TCIII, in liver andbone marrow disease) may interfere with deliveryof vit B12 to tissues. Vit B12 is especially takenup by liver cells and stored: about 2/3 to 4/5of body’s content (2–8 mg) is present in liver.
Vit B12 is not degraded in the body. It isexcreted mainly in bile (3–7 µg/day); all but0.5–1 µg of this is reabsorbed—considerableenterohepatic circulation occurs. Thus, in theabsence of intrinsic factor or when there is
DAB12
DAB12

608S
EC
TIO
N10
DRUGS AFFECTING BLOOD AND BLOOD FORMATION
malabsorption, B12 deficiency develops muchmore rapidly than when it is due to nutritionaldeficiency. It takes 3–5 years of total absenceof B12 in diet to deplete normal body stores.
Vit B12 is directly and completely absorbedafter i.m. or deep s.c. injection. Normally, onlytraces of B12 are excreted in urine, but whenpharmacological doses (> 100 µg) are given orallyor parenterally—a large part is excreted in urine,because the plasma protein binding sites get satu-rated and free vit B12 is filtered at the glomerulus.Hydroxocobalamin is more protein bound andbetter retained than cyanocobalamin.
Deficiency Vit B12 deficiency occurs due to:1. Addisonian pernicious anaemia: is an autoimmune
disorder which results in destruction of gastric parietalcells → absence of intrinsic factor in gastric juice (alongwith achlorhydria) → inability to absorb vit B12.It israre in India.
2. Other causes of gastric mucosal damage, e.g. chronicgastritis, gastric carcinoma, gastrectomy, etc.
3. Malabsorption (damaged intestinal mucosa), bowelresection, inflammatory bowel disease.
4. Consumption of vit B12 by abnormal flora in intestine(blind loop syndrome) or fish tape worm.
5. Nutritional deficiency: is a less common cause; mayoccur in strict vegetarians.
6. Increased demand: pregnancy, infancy.
Manifestations of deficiency are:(a) Megaloblastic anaemia (generally the firstmanifestation), neutrophils with hypersegmentednuclei, giant platelets.(b) Glossitis, g.i. disturbances: damage to epi-thelial structures.(c) Neurological: subacute combined degenera-tion of spinal cord; peripheral neuritis—dimi-nished vibration and position sense, paresthesias,depressed stretch reflexes; mental changes—poormemory, mood changes, hallucinations, etc. arelate effects.
Preparations, dose, administrationCyanocobalamin: 35 μg/5 ml liq.Hydroxocobalamin: 500 μg, 1000 μg inj.In India both oral and injectable vit B12 is available mostlyas combination preparation along with other vitamins, withor without iron. The leading ones are listed in Tables 43.1 and67.2. Some selected brands with their vit B12 content are:
NEUROBION FORTE (1000 μg/3 ml inj; 15 μg/tab.),OPTINEURON (1000 μg/3 ml inj.), NEUROXIN-12 (500μg/10 ml inj.), POLYBION (15 μg/cap), BECOSULES (5μg/cap), FESOVIT (15 μg/cap), AUTRIN (15 μg/cap)FERRICARB (15 μg/cap).
Because of higher protein binding and betterretention in blood, hydroxocobalamin is preferredfor parenteral administration to treat vit B12
deficiency. In Britain it has totally replacedcyanocobalamin, which is restricted to oral use.However, professionals in USA consider thathydroxocobalamin may induce antibody formationin some patients and its blood level may declineas rapidly (within 1 month) as that of cyano-cobalamin. Therefore, they use cyanocobalaminorally as well as parenterally.Prophylactic dose: 3–10 μg/day orally in thoseat risk of developing deficiency.Therapeutic dose: Oral vit B12 is not dependablefor treatment of confirmed vit B12 deficiencybecause its absorption from the intestine isunreliable. Injected vit B12 is a must whendeficiency is due to lack of intrinsic factor(pernicious anaemia, other gastric causes), sincethe absorptive mechanism is totally non-functional.Various regimens are in use. The one followedin Britain is—hydroxocobalamin 1 mg i.m./s.c.daily for 2 weeks or till neurological symptoms(when present) abate, followed by 1 mg injectedevery 2 months for maintenance. The regimenpopular in USA is—cyanocobalamin 100 μg i.m./s.c. daily for 1 week, then weekly for 1 month,and then monthly for maintenance indefinitely.Methylcobalamin (methyl B12) is the activecoenzyme form of vit B12 for synthesis ofmethionine and S-adenosylmethionine that isneeded for integrity of myelin. This preparationof vit B12 in a dose of 1.5 mg/day has beenespecially promoted for correcting theneurological defects in diabetic, alcoholic andother forms of peripheral neuropathy. However,in USA and many other countries, it is used onlyas a nutritional supplement, and not as a drug.
Methylcobalamin BIOCOBAL, DIACOBAL, METHYL-COBAL 0.5 mg tab.

609C
HA
PTE
R43
HAEMATINICS AND ERYTHROPOIETIN
Uses1. Treatment of vit B12 deficiency: vit B12 is usedas outlined above. It is wise to add 1–5 mg oforal folic acid and an iron preparation, becausereinstitution of brisk haemopoiesis may unmaskdeficiency of these factors. Response to vit B12
is dramatic—symptomatic improvement starts in2 days: appetite improves, patient feels better;mucosal lesions heal in 1–2 weeks; reticulocytecount increases; Hb% and haematocrit start risingafter 2 weeks; platelet count normalises in 10days and WBC count in 2–3 weeks. Time takenfor complete recovery of anaemia depends onthe severity of disease to start with. Neurologicalparameters improve more slowly—may takeseveral months; full recovery may not occur ifvit B12 deficiency has been severe or had persistedfor 6 months or more.2. Prophylaxis: needs to be given only when thereare definite predisposing factors for developmentof deficiency (see above).3. Mega doses of vit B12 have been used inneuropathies, psychiatric disorders, cutaneoussarcoid and as a general tonic to allay fatigue,improve growth—value is questionable.4. Tobacco amblyopia: hydroxocobalamin is ofsome benefit—it probably traps cyanide derivedfrom tobacco to form cyanocobalamin.
Adverse effects Even large doses of vit B12
are quite safe. Allergic reactions have occurredon injection, probably due to contaminants. Ana-phylactoid reactions (probably to sulfite containedin the formulation) have occurred on i.v. injection:this route should never be employed.
FOLIC ACID
It occurs as yellow crystals which are insolublein water, but its sodium salt is freely water soluble.Chemically it is Pteroyl glutamic acid (PGA)consisting of pteridine + paraaminobenzoic acid(PABA) + glutamic acid.Wills (1932–37) had found that liver extract contained a factor,other than vit B12, which could cure megaloblastic anaemia.Mitchell in 1941 isolated an antianaemia principle from
spinach and called it ‘folic acid’ (from leaf). Later the Will’sfactor was shown to be identical to folic acid.
Dietary sources Liver, green leafy vegetables (spinach),egg, meat, milk. It is synthesized by gut flora, but this islargely unavailable for absorption.
Daily requirement of an adult is < 0.1 mg butdietary allowance of 0.2 mg/day is recommen-ded. During pregnancy, lactation or any conditionof high metabolic activity, 0.8 mg/day isconsidered appropriate.
Utilization Folic acid is present in food as poly-glutamates; the additional glutamate residues aresplit off primarily in the upper intestine beforebeing absorbed. Reduction to DHFA and methy-lation also occurs at this site. It is transportedin blood mostly as methyl-THFA which is partlybound to plasma proteins. Small, physiologicalamounts of folate are absorbed by specific carrier-mediated active transport in the intestinal mucosa.Large pharmacological doses may gain entry bypassive diffusion, but only a fraction is absorbed.
Folic acid is rapidly extracted by tissues andstored in cells as polyglutamates. Liver takes upa large part and secretes methyl-THFA in bilewhich is mostly reabsorbed from intestine: entero-hepatic circulation occurs. Alcohol interferes withrelease of methyl-THFA from hepatocytes. Thetotal body store of folates is 5–10 mg. Normally,only traces are excreted, but when pharma-cological doses are given, 50–90% of the absorbeddose may be excreted in urine.
Metabolic functions Folic acid is inactive assuch and is reduced to the coenzyme form intwo steps: FA → DHFA → THFA by folatereductase (FRase) and dihydrofolate reductase(DHFRase). THFA mediates a number of onecarbon transfer reactions by carrying a methylgroup as an adduct (see under vit. B12 also).1. Conversion of homocysteine to methionine:vit B12 acts as an intermediary carrier of methylgroup (see p. 607). This is the most importantreaction which releases THFA from the methylatedform.2. Generation of thymidylate, an essentialconstituent of DNA:

610S
EC
TIO
N10
DRUGS AFFECTING BLOOD AND BLOOD FORMATION
Deoxyuridylate methylene-THFA Glycine
Thymidylate DHFA THFA Serine
DHFRase
3. Conversion of serine to glycine: needs THFAand results in the formation of methylene-THFAwhich is utilized in thymidylate synthesis.4. Purine synthesis: de novo building of purinering requires formyl-THFA and methenyl-THFA(generated from methylene-THFA) to introducecarbon atoms at position 2 and 8.5. Generation and utilization of ‘formate pool’.6. Histidine metabolism: for mediating formi-mino group transfer.Ascorbic acid protects folates in the reduced form.Other cofactors, e.g. pyridoxal, etc. are requiredfor some of the above reactions.
Deficiency Folate deficiency occurs due to:(a) Inadequate dietary intake(b) Malabsorption: especially involving upper intestine—coeliac disease, tropical sprue, regional ileitis, etc. Deficiencydevelops more rapidly as both dietary and biliary folate isnot absorbed.(c) Biliary fistula; bile containing folate for recirculationis drained.(d) Chronic alcoholism: intake of folate is generally poor.Moreover, its release from liver cells and recirculation areinterfered.(e) Increased demand: pregnancy, lactation, rapid growthperiods, haemolytic anaemia and other diseases with highcell turnover rates.(f) Drug induced: prolonged therapy with anticonvulsants(phenytoin, phenobarbitone, primidone) and oralcontraceptives—interfere with absorption and storage offolate.
Manifestations of deficiency are:(i) Megaloblastic anaemia, indistinguishable fromthat due to vit B12 deficiency. However, folatedeficiency develops more rapidly if externalsupply is cut off: body stores last 3–4 monthsonly. In malabsorptive conditions megaloblastosismay appear in weeks.(ii) Epithelial damage: glossitis, enteritis, diar-rhoea, steatorrhoea.(iii) Neural tube defects, including spina bifidain the offspring, due to maternal folate deficiency.
(iv) General debility, weight loss, sterility. How-ever, neurological symptoms do not appear inpure folate deficiency.
Preparations and doseFolic acid: FOLVITE, FOLITAB 5 mg tab;Liquid oral preparations and injectables are available onlyin combination formulation (see Tables 43-1 and 67-2).Oral therapy is adequate except when malabsorption is presentor in severely ill patient—given i.m.Dose: therapeutic 2 to 5 mg/day, prophylactic 0.5 mg/day.Folinic acid; CALCIUM LEUCOVORIN 3 mg/ml inj.FASTOVORIN 3 mg, 15 mg amps, 50 mg vial; RECOVORIN15 mg tab, 15 mg, 50 mg vial for inj.
Uses1. Megaloblastic anaemias due to:(a) Nutritional folate deficiency; manifests ear-lier than vit B12 deficiency. Oral folic acid2–5 mg/day is adequate, but in acutely ill patients,therapy may be initiated with injection of folicacid 5 mg/day. Response occurs as quickly aswith vit B12.(b) Increased demand: pregnancy, lactation,infancy, during treatment of severe iron deficiencyanaemia, haemolytic anaemias.(c) Pernicious anaemia: folate stores may be lowand deficiency may be unmasked when vit B12
induces brisk haemopoiesis. Folic acid has onlysecondary and adjuvant role in this condition.
Folic acid should never be given alone topatients with vit B12 deficiency, because haemato-logical response may occur, but neurologicaldefect may worsen due to diversion of meagreamount of vit B12 present in body to haemopoiesis.(d) Malabsorption syndromes: Tropical sprue,coeliac disease, idiopathic steatorrhoea, etc.(e) Antiepileptic therapy: Megaloblastic anaemiacan occur due to prolonged phenytoin/pheno-barbitone therapy (see Ch. 30). This is treatedby folic acid, but large doses should be avoidedas they may antagonize anticonvulsant effect.
2. Prophylaxis of folate deficiency: only whendefinite predisposing factors are present. Routinefolate supplementation (1 mg/day) is recom-mended during pregnancy to reduce the risk ofneural tube defects in the newborn.

611C
HA
PTE
R43
HAEMATINICS AND ERYTHROPOIETIN
3. Methotrexate toxicity Folinic acid (Leuco-vorin, citrovorum factor, 5-formyl-THFA) is anactive coenzyme form which does not need tobe reduced by DHFRase before it can act.Methotrexate is a DHFRase inhibitor; its toxicityis not counteracted by folic acid, but antagonizedby folinic acid (3.0 mg i.v. repeated as required).
Folinic acid is expensive and not needed forthe correction of simple folate deficiency for whichfolic acid is good enough.4. Citrovorum factor rescue In certain malig-nancies, high dose of methotrexate is injected i.v.and is followed within ½ –1 hour with 1–3 mgi.v. of folinic acid to rescue the normal cells.It is ineffective if given > 3 hours aftermethotrexate.5. To enhance anticancer efficacy of5-fluorouracil (5-FU) Folinic acid is nowroutinely infused i.v. along with 5-FU (see p. 864),because THFA is required for inhibition ofthymidylate synthase by 5-FU.
Adverse effects Oral folic acid is entirely non-toxic. Injections rarely cause sensitivity reactions.
ERYTHROPOIETIN
Erythropoietin (EPO) is a sialoglycoproteinhormone (MW 34000) produced by peritubularcells of the kidney that is essential for normalerythropoiesis. Anaemia and hypoxia are sensedby kidney cells and induce rapid secretion of EPO→ acts on erythroid marrow and:(a) Stimulates proliferation of colony formingcells of the erythroid series.(b) Induces haemoglobin formation and erythro-blast maturation.(c) Releases reticulocytes in the circulation.EPO binds to specific receptors on the surfaceof its target cells. The EPO receptor is aJAK-STAT-binding receptor that alters phosphory-lation of intracellular proteins and activatestranscription factors to regulate gene expression.It induces erythropoiesis in a dose dependentmanner, but has no effect on RBC lifespan.
The recombinant human erythropoietin(Epoetin α, β) is administered by i.v. or s.c.injection and has a plasma t½ of 6–10 hr, butaction lasts several days.
Use The primary indication for epoetin isanaemia of chronic renal failure which is dueto low levels of EPO. Only smptomatic patientswith Hb ≤ 8 g/dl should be considered for EPOtherapy. Epoetin 25–100 U/kg s.c. or i.v. 3 timesa week (max. 600 U/kg/week) raises haematocritand haemoglobin, reduces need for transfusionsand improves quality of life. It is prudent to startwith a low dose and titrate upwards to keephaematocrit between 30–36%, and Hb 10–11 g(max 12 g) per dl. Trials have found highermortality if Hb level was raised to normal (13.5g/dl). Some recent studies have indicated that dosereduction by about 30% is possible when epoetinis given s.c. compared to i.v. Exercise capacityand overall wellbeing of the patients is improved.Most patients have low iron stores; requireconcurrent parenteral/oral iron therapy for anoptimum response. Other uses are:1. Anaemia in AIDS patients treated with
zidovudine.2. Cancer chemotherapy induced anaemia.3. Preoperative increased blood production for
autologous transfusion during surgery.
Adverse effects Epoetin is nonimmunogenic.Adverse effects are related to sudden increasein haematocrit, blood viscosity and peripheral vas-cular resistance (due to correction of anaemia).These are—increased clot formation in theA-V shunts (most patients are on dialysis), hyper-tensive episodes, serious thromboembolic events,occasionally seizures. Flu like symptoms lasting2–4 hr occur in some patients.HEMAX 2000 IU/ml and 4000 IU/ml vials; EPREX 2000IU, 4000 IU and 10000 IU in 1 ml prefilled syringes; ZYROP(epoetin β) 2000 IU and 4000 IU vials.
Recently, a hyperglycosylated modified EPO Darbepoetin hasbeen introduced that has a t½ >24 hours, is longer actingand can be administered once every 2–4 weeks.

612S
EC
TIO
N10
DRUGS AFFECTING BLOOD AND BLOOD FORMATION
PROBLEM DIRECTED STUDY
43.1 A lady aged 40 years consults you for treatment of her anaemia that is not improvingwith medicine prescribed by a local doctor. She told that she is suffering from weakness, fatigueand occasional giddiness for the last 4–5 months. She went to a local doctor 2 months agowho got her blood tested, which showed Hb was 7.5 g/dl. A liquid medicine was prescribed,that she has been taking 1 tablespoonful daily without any benefit. The medicine was foundto be syrup Ferric ammonium citrate 160 mg/15 ml along with folic acid 0.5 mg and vit B12
7.5 μg. She also revealed that she suffers from heart burn, and has been taking a tablet (Rabeprazole20 mg) once daily for the last 2–3 years. Repeat blood testing showed Hb to be 7.6 g/dl, haematocritwas 27%, RBCs were microcytic-hypochromic, and other values were consistent with iron deficiencyanaemia. Her periods were normal and detailed examination showed no evidence of bleedingfrom any site.(a) What could be the reason for her failure to improve with oral iron therapy that she hasbeen taking?(b) Can she still be treated with oral iron, or does she require parenteral iron therapy? Whattreatment would be appropriate for her?(see Appendix-1 for solution)

Drugs Affecting Coagulation,Bleeding and Thrombosis
ChapterChapterChapterChapterChapter 4444444444
Haemostasis (arrest of blood loss) and bloodcoagulation involve complex interactions betweenthe injured vessel wall, platelets and coagulationfactors. A cascading series of proteolytic reactions(Fig. 44.1) is started by:(i) Contact activation of Hageman factor: intrin-sic system, in which all factors needed forcoagulation are present in plasma. This pathwayis responsible for clotting when blood is keptin a glass tube, and for amplification of thecommon pathway. This is slow and takes severalminutes to activate factor X.(ii) Tissue thromboplastin: extrinsic system, needsa tissue factor, but activates factor X in seconds.In the normal course, coagulation after injury tovessel wall occurs by this pathway.
The subsequent events are common in thetwo systems and result in polymerization offibrinogen to form fibrin strands. Blood cells aretrapped in the meshwork of fibrin strandsproducing clot.
Two in vitro tests ‘activated partial thromboplastin time’(aPTT) and ‘prothrombin time’ (PT) are employed for testingintegrity of the intrinsic, extrinsic and common pathwaysof the coagulation cascade. The results are interpreted as:
PT aPTTIntrinsic pathway Normal Prolonged
interfered (12–14S)Extrinsic pathway Prolonged Normal
interfered (26–32S)Common pathway Prolonged Prolonged
interfered
Most clotting factors are proteins present in plasmain the inactive (zymogen) form. By partialproteolysis they themselves become an activeprotease and activate the next factor. In additionto its critical role in cleaving and polymerizingfibrinogen, thrombin activates many upstreamfactors (especially f. XI, VIII and V) of the intrinsic
and common pathways—amplifying its owngeneration and continuation of clot formation. Itis also a potent activator of platelets.
On the other hand, factors like antithrombin,protein C, protein S, antithromboplastin and thefibrinolysin system tend to oppose coagulation andlyse formed clot. Thus, a check and balance systemoperates to maintain blood in a fluid state whilein circulation and allows rapid haemostasisfollowing injury.
COAGULANTSThese are substances which promote coagulation,and are indicated in haemorrhagic states.
Fresh whole blood or plasma provide all thefactors needed for coagulation and are the besttherapy for deficiency of any clotting factor; alsothey act immediately. Other drugs used to restorehaemostasis are:1. Vitamin KK1 (from plants, : Phytonadione
fat-soluble) (Phylloquinone)K3 (synthetic)
—Fat-soluble : Menadione,Acetomenaphthone
—Water-soluble : Menadione sod. bisulfite: Menadione
sod. diphosphate2. Miscellaneous
Fibrinogen (human)Antihaemophilic factorDesmopressinAdrenochrome monosemicarbazoneRutin, Ethamsylate
VITAMIN K
It is a fat-soluble dietary principle required forthe synthesis of clotting factors.

614S
EC
TIO
N10
DRUGS AFFECTING BLOOD AND BLOOD FORMATION
Fig. 44.1: The coagulation cascade. The vit. K dependent factors have been encircled,Factors inactivated by heparin (H) in red; the more important inhibited steps are highlighted by thick arrow.
a—activated form; Pl.Ph.—Platelet phospholipid; HMW—High molecular weight; TF—Tissue factor (factor III)
Dam (1929) produced bleeding disorder in chicken by feedingdeficient diet. This was later found to be due to decreasedconcentration of prothrombin in blood and that it could becured by a fat soluble fraction of hog liver. This factor wascalled Koagulations vitamin (vit K) and soon its structurewas worked out. A similar vitamin was isolated in 1939from alfalfa grass and labelled vit K1, while that from sardine(sea fish) meal was labelled K2. Synthetic compounds havebeen produced and labelled K3.
Dietary sources are—green leafy vegetables, such as cabbage,spinach; and liver, cheese, etc.
Daily requirement It is uncertain, because a variableamount of menaquinone (vit K2) produced by colonic bacteriabecomes available. Even 3–10 µg/day external source maybe sufficient. However, the total requirement of an adulthas been estimated to be 50–100 µg/day.
Action Vit K acts as a cofactor at a late stagein the synthesis by liver of coagulation proteins—prothrombin, factors VII, IX and X. The vit Kdependent change (γ carboxylation of glutamateresidues of these zymogen proteins; see Fig. 44.2)confers on them the capacity to bind Ca2+ andto get bound to phospholipid surfaces—propertiesessential for participation in the coagulationcascade.
Utilization Fat-soluble forms of vit K areabsorbed from the intestine via lymph and require
Chemistry and source Vit K has a basic naphthoquinonestructure, with or without a side chain (R) at position 3.The side chain in K1 is phytyl, in K2 prenyl, while in K3
there is no side chain.

615C
HA
PTE
R 44
DRUGS AFFECTING COAGULATION, BLEEDING AND THROMBOSIS
bile salts for absorption, while water-soluble formsare absorbed directly into portal blood. An activetransport process in the jejunum has beendemonstrated for K1, while K2 and K3 are absorbedby simple diffusion. Vit K is only temporarilyconcentrated in liver, but there are no significantstores in the body. It is metabolized in liver byside chain cleavage and glucuronide conjugation;metabolites are excreted in bile and urine.
Deficiency Deficiency of vit K occurs due toliver disease, obstructive jaundice, malabsorption,long-term antimicrobial therapy which altersintestinal flora. However, deficient diet is rarelyresponsible. The most important manifestation isbleeding tendency due to lowering of the levelsof prothrombin and other clotting factors in blood.Haematuria is usually first to occur; other commonsites of bleeding are g.i.t., nose and under theskin—ecchymoses.
Preparations
Phytonadione: VITAMIN-K, KVI, K-WIN 10 mg/ml for i.m.injection.Menadione: 0.66 mg in GYNAE CVP with vit C 75 mg,ferrous gluconate 67 mg, Cal. lactate 300 mg and citrasbioflavonoid 150 mg per cap:Acetomenaphthone: ACETOMENADIONE 5, 10 mg tab;KAPILIN 10 mg tab.Menadione sod. bisulfite: 20 mg, in CADISPER-C with vitC 100 mg, adrenochrome monosemicarbazone, 1 mg, rutin60 mg, methylhesperidin 40 mg, Cal. phosphate 100 mgper tab.STYPTOCID 10 mg with adrenochrome monosemicarbazone0.5 mg, rutin 50 mg, vit C 37.5 mg, vit D 200 i.u., Cal.phosphate 260 mg per tab.
Use The only use of vit K is in prophylaxisand treatment of bleeding due to deficiency ofclotting factors in the following situations:(a) Dietary deficiency: of vit K is very rare inadults. However, when it occurs 5–10 mg/dayoral or parenteral vit K rapidly corrects the defects.(b) Prolonged antimicrobial therapy: treat in thesame way as dietary deficiency of vit K.(c) Obstructive jaundice or malabsorption syn-dromes (sprue, regional ileitis, steatorrhoea, etc.):vit K 10 mg i.m./day, or orally along with bilesalts.
(d) Liver disease (cirrhosis, viral hepatitis): asso-ciated bleeding responds poorly to vit K. Becauseof hepatocellular damage, synthesis of clottingfactors is inadequate despite the presence of vitK. However, vit K may be of some use if itsabsorption had been affected due to lack of bilesalts.(e) Newborns: All newborns have low levels ofprothrombin and other clotting factors. Furtherdecrease occurs in the next few days. The causeis both lower capacity to synthesize clottingfactors as well as deficiency of vit K. The defectis exaggerated in the premature infant. Vit K1 mg i.m. soon after birth has been recommendedroutinely. Some prefer administering 5–10 mgi.m. to the mother 4–12 hours before delivery.Haemorrhagic disease of the newborn can beeffectively prevented/treated by such medication.
Menadione (K3) should not be used for thispurpose (see below).(f) Overdose of oral anticoagulants: This is themost important indication of vit K. Phytonadione(K1) is the preparation of choice, because it actsmost rapidly; dose depends on the severity ofhypoprothrombinaemia (measured INR) andbleeding. Unnecessary high dose is to be avoidedbecause it will render the patient unresponsiveto oral anticoagulants for several days.Severe: 10 mg i.m. followed by 5 mg 4 hourly;bleeding generally stops in 6–12 hours, but normallevels of coagulation factors are restored onlyafter 24 hr. This dose of vit K will blockanticoagulant action for 7–10 days.Moderate: 10 mg i.m. followed by 5 mg onceor twice according to response.Mild: Just omit a few doses of the anticoagulant.
(g) Prolonged high dose salicylate therapy causeshypoprothrombinemia; vit K should be givenprophylactically. If bleeding occurs—treat as fororal anticoagulants.
Adverse effects Phytonadione injected i.m. orgiven orally hardly produces any adverse effect;allergic reactions are rare. Severe anaphylactoid

616S
EC
TIO
N10
DRUGS AFFECTING BLOOD AND BLOOD FORMATION
reactions can occur on i.v. injection of emulsifiedformulation; this route should not be used.
Menadione and its water-soluble derivatives can causehaemolysis in a dose-dependent manner. Patients withG-6-PD deficiency and neonates are especially susceptible.In the newborn menadione or its salts can precipitate kernicterus:(a) by inducing haemolysis and increasing bilirubin load.(b) by competitively inhibiting glucuronidation of bilirubin.Glucuronide conjugation is, as such, inadequate in neonates.
Because of poor efficacy and higher toxicity, there islittle justification to use menadione and its water solublesalts for any indication.
Fibrinogen The fibrinogen fraction of human plasma isemployed to control bleeding in haemophilia, antihaemo-philic globulin (AHG) deficiency and acute afibrinogenemicstates; 0.5 g is infused i.v.FIBRINAL 0.5 g/bottle for i.v. infusion.
Antihaemophilic factor It is concentrated human AHGprepared from pooled human plasma. It is indicated (alongwith human fibrinogen) in haemophilia and AHG deficiency.It is highly effective in controlling bleeding episodes, butaction is short-lasting (1 to 2 days).Dose: 5–10 U/kg by i.v. infusion, repeated 6–12 hourly.FIBRINAL-H, ANTIHAEMOPHILIC FACTOR: 150 U or 200U + fibrinogen 0.5 g/bottle for i.v. infusion.
Desmopressin It releases factor VIII and von Willebrand’sfactor from vascular endothelium and checks bleeding inhaemophilia and von Willebrand’s disease (see p. 597).
Adrenochrome monosemicarbazone It is believed toreduce capillary fragility, control oozing from raw surfacesand prevent microvessel bleeding, e.g. epistaxis, haematuria,secondary haemorrhage from wounds, etc. Its efficacy isuncertain.Dose: 1–5 mg oral, i.m.STYPTOCHROME 3 mg/2 ml inj., STYPTOCID: 2 mg/2 ml inj.
Rutin It is a plant glycoside claimed to reduce capillarybleeding. It has been used in a dose of 60 mg oral BD–TDS along with vit C which is believed to facilitate itsaction. Its efficacy is uncertain.In CADISPER-C 60 mg tab.
Ethamsylate It reduces capillary bleeding when plateletsare adequate; probably exerts antihyaluronidase action orcorrects abnormalities of platelet adhesion, but does notstabilize fibrin (not an antifibrinolytic). Ethamsylate has beenused in the prevention and treatment of capillary bleedingin menorrhagia, after abortion, PPH, epistaxis, malena,hematuria and after tooth extraction, but efficacy isunsubstantiated. Side effects are nausea, rash, headache, andfall in BP (only after i.v. injection).Dose: 250–500 mg TDS oral/i.v.; ETHAMSYL, DICYNENE,HEMSYL, K. STAT 250, 500 mg tabs; 250 mg/2 ml inj.
LOCAL HAEMOSTATICS (STYPTICS)
After injury to arterioles and other smaller bloodvessels, normal haemostasis occurs successivelyby contraction of injured vessel wall (lasting fewminutes), adhesion and aggregation of plateletsto form a plug, formation of a blood clot, andfinally in due course dissolution of the clot byfibrinolysis. External bleeding is usually stoppedby manual pressure, cotton-gauze pressure packor by suturing. Control of bleeding may be aidedby local haemostatics (styptics) that are substancesused to stop bleeding from a local andapproachable site. They are particularly effectiveon oozing surfaces, e.g. tooth socket, abrasions,etc. Absorbable materials like fibrin (preparedfrom human plasma and dryed as sheet or foam),gelatin foam, oxidized cellulose (as strips whichcan be cut and placed in the wound) providea meshwork which activates the clotting mecha-nism and checks bleeding. Left in situ thesematerials are absorbed in 1–4 weeks and generallycause no foreign body reaction. Thrombin obtainedfrom bovine plasma may be applied as dry pow-der or freshly prepared solution to the bleedingsurface in haemophiliacs. Vasoconstrictors like0.1% Adr solution may be soaked in sterile cotton-gauze and packed in the bleeding tooth socketor nose in case of epistaxis to check bleedingwhen spontaneous vasoconstriction is inadequate.Astringents such as tannic acid or metallic saltsare occasionally applied for bleeding gums,bleeding piles, etc.
SCLEROSING AGENTS
These are irritants, cause inflammation, coagulationand ultimately fibrosis, when injected into haemorrhoids(piles) or varicose vein mass. They are used only for localinjection.1. Sod. tetradecyl sulfate (3% with benzyl alcohol 2%):
0.5–2 ml at each site. SETROL 2 ml inj.2. Polidocanol (3% inj): 2 ml; ASKLEROL 2 ml inj.
ANTICOAGULANTS
These are drugs used to reduce the coagulabilityof blood. They may be classified into:

617C
HA
PTE
R 44
DRUGS AFFECTING COAGULATION, BLEEDING AND THROMBOSIS
I. Used in vivoA. Parenteral anticoagulants(i) Indirect thrombin inhibitors: Heparin, Low
molecular weight heparins, Fondaparinux,Danaparoid
(ii) Direct thrombin inhibitors: Lepirudin,Bivalirudin, Argatroban
B. Oral anticoagulants(i) Coumarin derivatives: Bishydroxycoumarin
(dicumarol), Warfarin sod, Acenocoumarol(Nicoumalone), Ethylbiscoumacetate
(ii) Indandione derivative: Phenindione.(iii) Direct factor Xa inhibitors: Rivaroxaban(iv) Oral direct thrombin inhibitor: Dabigatran
etexilate
II. Used in vitroA. Heparin:
150 U to prevent clotting of 100 ml blood.B. Calcium complexing agents:
Sodium citrate: 1.65 g for 350 ml of blood; used tokeep blood in the fluid state for transfusion;ANTICOAGULANT ACID CITRATE DEXTROSESOLUTION 2.2 g/100 ml (75 ml is used for 1 unit ofblood).Sodium oxalate:10 mg for 1 ml bloodSodium edetate:2 mg for 1 ml blood
HEPARIN
McLean, a medical student, discovered in 1916 that livercontains a powerful anticoagulant. Howell and Holt (1918)named it ‘heparin’ because it was obtained from liver.However, it could be used clinically only in 1937 whensufficient degree of purification was achieved.
Chemistry and occurrence Heparin is anon-uniform mixture of straight chain mucopoly-saccharides with MW 10,000 to 20,000. It containspolymers of two sulfated disaccharide units:
D-glucosamine-L-iduronic acidD-glucosamine-D-glucuronic acid
Heparin carries strong electronegative chargesand is the strongest organic acid present in thebody. It occurs in mast cells as a much bigger
molecule (MW ~75,000) loosely bound to thegranular protein. Thus, heparin is present in alltissues containing mast cells; richest sources arelung, liver and intestinal mucosa. Commerciallyit is produced from ox lung and pig intestinalmucosa.
ACTIONS1. Anticoagulant Heparin is a powerful andinstantaneously acting anticoagulant, effective bothin vivo and in vitro. It acts indirectly by activatingplasma antithrombin III (AT III, a serine proteinaseinhibitor). The heparin-AT III complex then bindsto clotting factors of the intrinsic and commonpathways (Xa, IIa, IXa, XIa, XIIa and XIIIa) andinactivates them but not factor VIIa operative inthe extrinsic pathway. At low concentrations ofheparin, factor Xa mediated conversion ofprothrombin to thrombin is selectively affected.The anticoagulant action is exerted mainly byinhibition of factor Xa as well as thrombin (IIa)mediated conversion of fibrinogen to fibrin.
Low concentrations of heparin prolong aPTTwithout significantly prolonging PT. High con-centrations prolong both. Thus, low concentra-tions interfere selectively with the intrinsic path-way, affecting amplification and continuation ofclotting, while high concentrations affect thecommon pathway as well.Antithrombin III is itself a substrate for the protease clottingfactors; binds with the protease to form a stable complex(suicide inhibitor). However, in the absence of heparin, thetwo interact very slowly. Heparin enhances the action ofAT III in two ways:(a) Long heparin molecule provides a scaffolding for theclotting factors (mainly Xa and IIa) as well as AT III toget bound and interact with each other.(b) Heparin induces conformational change in AT III to exposeits interactive sites. A specific pentasaccharide sequence, whichis present in only some of the heparin molecules, binds toAT III with high affinity to induce the conformational changeneeded for rapid interaction with clotting factors. This hasbeen synthesized and named fondaparinux.
Inhibition of IIa requires both the mechanisms, but Xainhibition can occur by mechanism ‘b’ alone. This probablyexplains why low molecular weight heparin, which isinsufficient to provide a long scaffolding, selectively inhibitsfactor Xa.
Higher doses of heparin given for some timecause reduction in AT-III levels, probably a
⎫⎬⎭
used in blood taken forinvestigations
⎫⎬⎭
chain length and proportionof the two disaccharide unitsvaries. Some glucosamineresidues are N-acetylated.

618S
EC
TIO
N10
DRUGS AFFECTING BLOOD AND BLOOD FORMATION
compensatory phenomenon. Sudden stoppage ofconventional-dose therapy may result in reboundincrease in coagulability for few days.
2. Antiplatelet Heparin in higher doses inhi-bits platelet aggregation and prolongs bleedingtime.
3. Lipaemia clearing Injection of heparinclears turbid post-prandial lipaemic plasma byreleasing a lipoprotein lipase from the vessel walland tissues, which hydrolyses triglycerides ofchylomicra and very low density lipoproteins tofree fatty acids. These then pass into tissues andthe plasma looks clear. This action requires lowerconcentration of heparin than that needed foranticoagulation.
Facilitation of fatty acid transport may be thephysiological function of heparin; but since, itis not found in circulating blood and its storageform in tissues is much less active, this seemsonly conjectural.
PHARMACOKINETICS
Heparin is a large, highly ionized molecule; there-fore not absorbed orally. Injected i.v. it actsinstantaneously, but after s.c. injection anticoagu-lant effect develops after ~60 min. Bioavailabilityof s.c. heparin is inconsistent. Heparin does notcross blood-brain barrier or placenta (it is theanticoagulant of choice during pregnancy). It ismetabolized in liver by heparinase and fragmentsare excreted in urine.
Heparin released from mast cells is degradedby tissue macrophages—it is not a physiologi-cally circulating anticoagulant.
After i.v. injection of doses < 100 U/kg, thet½ averages 1 hr. Beyond this, dose-dependentinactivation is seen and t½ is prolonged to1–4 hrs. The t½ is longer in cirrhotics and kidneyfailure patients, and shorter in patients withpulmonary embolism.
Unitage and administration Because of variablemolecular size of unfractionated heparin (UFH), it isstandardized only by bioassay: 1 U is the amount of heparinthat will prevent 1 ml of citrated sheep plasma from clotting
for 1 hour after the addition of 0.2 ml of 1% CaCl2 solution.Heparin sod. 1 mg has 120–140 U of activity.HEPARIN SOD., BEPARINE, NUPARIN 1000 and 5000 U/ml in 5 ml vials for injection.
Heparin should not be mixed with penicillin,tetracyclines, hydrocortisone or NA in the samesyringe or infusion bottle. Heparinized blood isnot suitable for blood counts (alters the shapeof RBCs and WBCs), fragility testing and comple-ment fixation tests.Dosage Heparin is conventionally given i.v. in a bolusdose of 5,000–10,000 U (children 50–100 U/kg), followedby continuous infusion of 750–1000 U/hr. Intermittent i.v.bolus doses of UFH are no longer recommended. The rateof infusion is controlled by aPTT measurement which iskept at 50–80 sec. or 1.5–2.5 times the patient’s pretreatmentvalue. If this test is not available, whole blood clotting timeshould be measured and kept at ~2 times the normal value.
Deep s.c. injection of 10,000–20,000 U every 8–12 hrscan be given if i.v. infusion is not possible. Needle usedshould be fine and trauma should be minimum to avoidhaematoma formation. Haematomas are more common withi.m. injection—this route should not be used.
Low dose (s.c.) regimen 5000 U is injected s.c. every8–12 hours, started before surgery and continued for 7–10days or till the patient starts moving about. This regimenhas been found to prevent postoperative deep vein thrombosiswithout increasing surgical bleeding. It also does not prolongaPTT or clotting time. However, it should not be used incase of neurosurgery or when spinal anaesthesia is to begiven. The patients should not be receiving aspirin or oralanticoagulants. It is ineffective in high-risk situations, e.g.hip joint or pelvic surgery.
ADVERSE EFFECTS
1. Bleeding due to overdose is the most seriouscomplication of heparin therapy. Haematuria isgenerally the first sign. With proper monitoring,serious bleeding occurs only in 1–3% patients.2. Thrombocytopenia is another common prob-lem. Generally it is mild and transient; occursdue to aggregation of platelets. Occasionallyserious thromboembolic events result. In somepatients antibodies are formed to the heparin-platelet complex and marked depletion of plateletsoccurs—heparin should be discontinued insuch cases. Even low molecular weight (LMW)heparins are not safe in such patients.3. Transient and reversible alopecia is infrequent.Serum transaminase levels may rise.

619C
HA
PTE
R 44
DRUGS AFFECTING COAGULATION, BLEEDING AND THROMBOSIS
4. Osteoporosis may develop on long-term useof relatively high doses.5. Hypersensitivity reactions are rare; manifes-tations are urticaria, rigor, fever and anaphylaxis.Patients with allergic diathesis are more liable.
Contraindications1. Bleeding disorders, history of heparin inducedthrombocytopenia.2. Severe hypertension (risk of cerebral haemor-rhage), threatened abortion, piles, g.i. ulcers (riskof aggravated bleeding).3. Subacute bacterial endocarditis (risk ofembolism), large malignancies (risk of bleedingin the central necrosed area of the tumour),tuberculosis (risk of hemoptysis).4. Ocular and neurosurgery, lumbar puncture.5. Chronic alcoholics, cirrhosis, renal failure.6. Aspirin and other antiplatelet drugs shouldbe used very cautiously during heparin therapy.
Low molecular weight (LMW) heparinsHeparin has been fractionated into LMWforms (MW 3000–7000) by different techniques.LMW heparins have a different anticoagulantprofile; i.e. selectively inhibit factor Xa with littleeffect on IIa. They act only by inducingconformational change in AT III and not byproviding a scaffolding for interaction of AT IIIwith thrombin. As a result, LMW heparins havesmaller effect on aPTT and whole blood clottingtime than unfractionated heparin (UFH) relativeto antifactor Xa activity. Also, they have lesserantiplatelet action—less interference withhaemostasis. Thrombocytopenia is less frequent.A lower incidence of haemorrhagic complicationscompared to UFH has been reported in somestudies, but not in others. However, major bleedingmay be less frequent. They are eliminatedprimarily by renal excretion; are not to be usedin patients with renal failure. The more importantadvantages of LMW heparins are pharma-cokinetic:• Better subcutaneous bioavailability (70–90%)
compared to UFH (20–30%): Variability inresponse is minimized.
• Longer and more consistent monoexponentialt½: (4–6 hours); making possible once dailys.c. administration.
• Since aPTT/clotting times are not prolonged,laboratory monitoring is not needed; dose iscalculated on body weight basis.
• Risk of osteoporosis after long term use is muchless with LMW heparin compared with UFH.
Most studies have found LMW heparins to beequally efficacious to UFH except during cardio-pulmonary bypass surgery, in which high doseUFH is still the preferred anticoagulant, becauseLMW heparin and fondaparinux are less effectivein preventing catheter thrombosis and their effectsare not fully reversed by protamine. Indicationsof LMW heparins are:1. Prophylaxis of deep vein thrombosis andpulmonary embolism in high-risk patientsundergoing surgery; stroke or other immobilizedpatients.2. Treatment of established deep vein thrombosis.3. Unstable angina and MI: they have largelyreplaced continuous infusion of UFH.4. To maintain patency of cannulae and shuntsin dialysis patients.A number of LMW heparins have been marketed. They differin composition, pharmacokinetics and dosage.
Enoxaparin: CLEXANE 20 mg (0.2 ml) and 40 mg (0.4ml) prefilled syringes; 20–40 mg OD, s.c. (start 2 hour beforesurgery).
Reviparin: CLIVARINE 13.8 mg (eq. to 1432 anti Xa IU)in 0.25 ml prefilled syringe; 0.25 ml s.c. once daily for5-10 days.
Nadroparin: FRAXIPARINE 3075 IU (0.3 ml) and 4100IU (0.4 ml) inj., CARDIOPARIN 4000 anti Xa IU/0.4 ml,6000 anti Xa IU/0.6 ml, 100, 000 anti Xa IU/10 ml inj.
Dalteparin: 2500 IU OD for prophylaxis; 100 U/Kg 12 hourlyor 200 U/Kg 24 hourly for treatment of deep vein thrombosis.FRAGMIN 2500, 5000 IU prefilled syringes.
Parnaparin: 0.6 ml s.c. OD for unstable angina andprophylaxis of DVT; FLUXUM 3200 IU (0.3 ml), 6400 IU(0.6 ml) inj.
Ardeparin: 2500-5000 IU OD; INDEPARIN 2500 IU, 5000IU prefilled syringes.
Fondaparinux: The pentasaccharide withspecific sequence that binds to AT III with high

620S
EC
TIO
N10
DRUGS AFFECTING BLOOD AND BLOOD FORMATION
affinity to selectively inactivate factor Xa withoutbinding thrombin (factor IIa), has been recentlyproduced synthetically and given the namefondaparinux. It is being increasingly used andhas been marketed in India as well. The bio-availability of fondaparinux injected s.c. is 100%and it is longer acting (t½ 17 hours). Metabolismis minimal, and it is largely excreted unchangedby the kidney. As such, it is not to be used inrenal failure patients. Fondaparinux is less likelyto cause thrombocytopenia compared to evenLMW heparins. Risk of osteoporosis after pro-longed use is also minimal. Fondaparinux doesnot require laboratory monitoring of aPTT, andis a longer acting alternative to LMW heparinswith the above advantages.Dose: 5–10 mg s.c. once daily. FONDAPARINUX, ARIXTRA5 mg/0.4 ml, 7.5 mg/0.6 ml and 10 mg/0.8 ml prefilledsingle dose syringe.
Danaparoid is a preparation containing mainly heparansulfate which is a heparin-like substance found in manytissues, having less potent anticoagulant action than heparin.Danaparoid is obtained from pig gut mucosa, and is usedin cases with heparin induced thrombocytopenia.
DIRECT THROMBIN INHIBITORS
Unlike heparin, these recently developed anticoagulants binddirectly to thrombin and inactivate it without the need tocombine with and activate AT III.
Lepirudin This recombinant preparation of hirudin (apolypeptide anticoagulant secreted by salivary glands of leech)binds firmly to the catalytic as well as the substrate recognitionsites of thrombin and inhibits it directly. Injected i.v., itis indicated only in patients who are at risk of heparin inducedthrombocytopenia. On repeated/prolonged administration,antibodies against the lepirudin-thrombin complex maydevelop resulting in prolonged anticoagulant effect andpossibility of anaphylaxis. Its action cannot be reversed byprotamine or any other antidote.
Bivalirudin It is a smaller peptide prepared syntheticallywhich has actions and uses similar to lepirudin. However, itsaction is slowly reversible due to cleavage of its peptide bondsby thrombin itself.
Argatroban This is a synthetic nonpeptide compoundwhich binds reversibly to the catalytic site of thrombin, butnot to the substrate recognition site. As such, it produces arapid and short-lasting antithrombin action. Administered byi.v. infusion, it can be used in place of lepirudin for short-termindications in patients with heparin induced thrombocytopenia.
HEPARIN ANTAGONIST
Protamine sulfate It is a strongly basic, lowmolecular weight protein obtained from the spermof certain fish. Given i.v. it neutralises heparinweight for weight, i.e. 1 mg is needed for every100 U of heparin. For the treatment of heparininduced bleeding, due consideration must be givento the amount of heparin that may have beendegraded by the patient’s body in the mean time.However, it is needed infrequently because theaction of heparin disappears by itself in a fewhours, and whole blood transfusion is needed toreplenish the loss when bleeding occurs. Protamineis more commonly used when heparin action needsto be terminated rapidly, e.g. after cardiac orvascular surgery. Protamine does not neutralizefondaparinux, and it only partially reverses theanticoagulant effect of LMW heparins.
In the absence of heparin, protamine itselfacts as a weak anticoagulant by interacting withplatelets and fibrinogen. Being basic in natureit can release histamine in the body. Hypersensi-tivity reactions have occurred. Rapid i.v. injectioncauses flushing and breathing difficulty.PROTA, PROTAMINE SULFATE 50 mg in 5 ml inj.
ORAL ANTICOAGULANTSA haemorrhagic disease was described in cattle in 1924 whichwas due to feeding them on spoiled sweet clover hay. Thedisorder was found to be due to prothrombin deficiency andthe toxic principle was identified as bishydroxycoumarin in1939. It was cured by feeding alfalfa grass. First clinicaluse of bishydroxycoumarin was made in 1941 and manycongeners were added later. Warfarin was initially used asrat poison; demonstration of its safety led to clinical trial;it is now a commonly employed oral anticoagulant.
Action and mechanism
Warfarin and its congeners act as anticoagulantsonly in vivo, not in vitro. This is so because theyact indirectly by interfering with the synthesisof vit K dependent clotting factors in liver. Theyapparently behave as competitive antagonists ofvit K and lower the plasma levels of functionalclotting factors in a dose-dependent manner.In fact, they inhibit the enzyme vit K epoxide

621C
HA
PTE
R 44
DRUGS AFFECTING COAGULATION, BLEEDING AND THROMBOSIS
reductase (VKOR) and interfere with regenerationof the active hydroquinone form of vit K (Fig.44.2) which acts as a cofactor for the enzymeγ-glutamyl carboxylase that carries out the finalstep of γ carboxylating glutamate residues ofprothrombin and factors VII, IX and X. Thiscarboxylation is essential for the ability of theclotting factors to bind Ca2+ and to get boundto phospholipid surfaces, necessary for thecoagulation sequence to proceed.
Factor VII has the shortest plasma t½ (6 hr),its level falls first when warfarin is given, followedby factor IX (t½ 24 hr), factor X (t½ 40 hr)and prothrombin (t½ 60 hr). Though the syn-thesis of clotting factors diminishes within 2–4hours of warfarin administration, anticoagulanteffect develops gradually over the next 1–3 daysas the levels of the clotting factors already presentin plasma decline progressively. Thus, there isalways a delay between administration of thesedrugs and the anticoagulant effect. Larger initialdoses hasten the effect only slightly.
Therapeutic effect occurs when synthesis ofclotting factors is reduced by 40–50%.
Protein C, protein S (both having anticoagulant property)and osteocalcin contain glutamate residues that requirevit. K dependent γ carboxylation. These are also inhibitedby oral anticoagulants, but density of adult bone is notaffected, though new bone formation may be depressed.
The differences between different oral anticoagu-lants are primarily pharmacokinetic and in theadverse side effects produced by them. These aresummarized in Table 44.1.
Racemic Warfarin sod. It is the most popularoral anticoagulant. The commercial preparationof warfarin is a mixture of R (dextrorotatory)and S (levorotatory) enantiomers. The S form ismore potent and is metabolized relatively fasterby ring oxidation carried out by CYP2C9, whileR form is less potent and degraded by side chainreduction carried out by CYP1A and CYP3A4.
TABLE 44.1 Pharmacokinetic and adverse effect profile of oral anticoagulants
Drug t½ Duration Dose (mg) Adverse side effects(hour) of action (other than bleeding)
(days) Loading Maintenance*
1. Bishydroxycoumarin 25–100 4–7 200 for 50–100 Frequent g.i.t. disturbances(dose dependent) 2 days
2. Warfarin sod. 36–48 3–6 5–10 2–10£ Alopecia, dermatitis, diarrhoea
3. Acenocoumarol 18–24 2–3 8–12 2–8 Oral ulceration, g.i.t. distur-(Nicoumalone) bances, dermatitis, urticaria,
alopecia
4. Ethylbiscoumacetate 2 1–3 900 300–600 Alopecia, bad taste
5. Phenindione 5 1–3 200 50–100 Orange urine, rashes, fever,leukopenia, hepatitis, nephro-pathy, agranulocytosis
* Daily maintenance dose: to be adjusted by measurement of prothrombin time (INR).£ To be taken in a single dose at the same hour (usually bed time) each day.
Fig. 44.2: Mechanism of action of oral anticoagulantsNAD—Nicotinamide adenine dinucleotide; NADH—itsreduced form

622S
EC
TIO
N10
DRUGS AFFECTING BLOOD AND BLOOD FORMATION
Both are partially conjugated with glucuronic acidand undergo some enterohepatic circulation;finally excreted in urine.
Warfarin is rapidly and completely absorbedfrom intestines and is 99% plasma protein bound.It crosses placenta and is secreted in milk;however, quantity of active form is generallyinsufficient to affect the suckling infant.UNIWARFIN 1, 2, 5 mg tabs; WARF-5: 5 mg tab.
Bishydroxycoumarin (Dicumarol) It is slowlyand unpredictably absorbed orally. Its metabo-lism is dose dependent—t½ is prolonged at higherdoses. Has poor g.i. tolerance; not preferred now.DICOUMAROL 50 mg tab.
Acenocoumarol (Nicoumalone) The t½ ofacenocoumarol as such is 8 hours, but an activemetabolite is produced so that overall t½ is about24 hours. Acts more rapidly.ACITROM, 1, 2, 4 mg tabs.
Ethyl biscoumacetate It has a rapid and brief action;occasionally used to initiate therapy, but difficult to maintain.
Phenindione Apart from risk of bleeding, it produces moreserious organ toxicity; should not be used.DINDEVAN 50 mg tab.
Adverse effects Bleeding as a result of exten-sion of the desired pharmacological action is themost important problem causing ecchymosis,epistaxis, hematuria, bleeding in the g.i.t.Intracranial or other internal haemorrhages mayeven be fatal. Bleeding is more likely if therapyis not properly monitored, or when INR exceeds4, or interacting drugs/contraindications are present.Treatment: of bleeding due to oral anticoagulantsconsists of:• Withhold the anticoagulant.• Give fresh blood transfusion; this supplies
clotting factors and replenishes lost blood.Alternatively fresh frozen plasma may be usedas a source of clotting factors.
• Give vit K1 which is the specific antidote (seep. 615), but it takes 6–24 hours for the clottingfactors to be resynthesized and released inblood after vit K administration.
Adverse effects unrelated to anticoagulation aregiven in Table 44.1. Cutaneous necrosis is a rare
complication that can occur with any oralanticoagulant.Phenindione produces serious toxicity; should notbe used.Warfarin and acenocoumarol are considered tobe the most suitable and better tolerated drugs.Dose regulation The dose of oral anticoagu-lant must be individualised by repeated measure-ment of prothrombin time; the aim is to achievea therapeutic effect without unduly increasing thechances of bleeding.The optimum ratio of PT during treatment with the oralanticoagulant to the normal value (of the testing laboratory)has been defined for various indications. But this value differsdepending on whether rabbit brain or human brainthromboplastin (Tp) has been used for the test. A standardizedsystem called the International Normalized Ratio (INR) basedon the use of human brain Tp has been developed by WHOand adopted in all countries.
Recommended INR for various indications oforal anticoagulants
INR1. Prophylaxis of deep vein thrombosis
and similar indications 2–2.52. Treatment of deep vein thrombosis,
pulmonary embolism, TIAs, hip surgery 2–33. Recurrent thromboembolism, arterial
disease (MI), prosthetic heart valves 3–3.5
Factors enhancing effect of oral anticoagu-lants are:• Debility, malnutrition, malabsorption and
prolonged antibiotic therapy: the supply of vitK to liver is reduced in these conditions.
• Liver disease, chronic alcoholism: synthesisof clotting factors may be deficient.
• Hyperthyroidism: the clotting factors aredegraded faster.
• Newborns: have low levels of vit K and clottingfactors (there should be no need of these drugsin neonates anyway).
Factors decreasing effect of oral anticoagu-lants are:• Pregnancy: plasma level of clotting factors is
higher.• Nephrotic syndrome: drug bound to plasma
protein is lost in urine.

623C
HA
PTE
R 44
DRUGS AFFECTING COAGULATION, BLEEDING AND THROMBOSIS
• Genetic warfarin resistance: the affinity ofwarfarin (as well as of vit K epoxide) to bindto the reductase (VKOR) enzyme, which gene-rates the active vit K hydroquinone, is low.Dose of oral anticoagulant is 4–5 times higher.
Contraindications All contraindications toheparin (see p. 619) apply to these drugs as well.Factors which enhance the effect of oralanticoagulants (see above) should also be takeninto consideration.
Oral anticoagulants should not be usedduring pregnancy. Warfarin given in early preg-nancy increases birth defects, especially skeletalabnormalities. It can produce foetal warfarinsyndrome—hypoplasia of nose, eye socket, handbones, and growth retardation. Given later inpregnancy, it can cause CNS defects, foetalhaemorrhage, foetal death and accentuatesneonatal hypoprothrombinemia.
Drug interactions A large number of drugsinteract with oral anticoagulants at pharmaco-kinetic or pharmacodynamic level, and eitherenhance or decrease their effect. These interactionsare clinically important (may be fatal if bleedingoccurs) and may involve more than onemechanism; the exact mechanism of an interactionis not always definable.
A. Enhanced anticoagulant action1. Broad-spectrum antibiotics: inhibit gut flora
and reduce vit K production.2. Newer cephalosporins (ceftriaxone, cefopera-
zone) cause hypoprothrombinaemia by thesame mechanism as warfarin —additive action.
3. Aspirin: inhibits platelet aggregation andcauses g.i. bleeding—this may be hazardousin anticoagulated patients. High doses ofsalicylates have synergistic hypoprothrom-binemic action and also displace warfarin fromprotein binding site.
4. Long acting sulfonamides, indomethacin,phenytoin and probenecid: displace warfarinfrom plasma protein binding.
5. Chloramphenicol, erythromycin, celecoxib,cimetidine, allopurinol, amiodarone andmetronidazole: inhibit warfarin metabolism.
6. Tolbutamide and phenytoin: inhibit warfarinmetabolism and vice versa.
7. Liquid paraffin (habitual use): reduces vit Kabsorption.
B. Reduced anticoagulant action1. Barbiturates (but not benzodiazepines),
carbamazepine, rifampin and griseofulvininduce the metabolism of oral anticoagulants.The dose of anticoagulant determined duringtherapy with these drugs would be higher: ifthe same is continued after withdrawing theinducer—marked hypoprothrombinemia canoccur—fatal bleeding is on record.
2. Oral contraceptives: increase blood levels ofclotting factors.
DIRECT FACTOR Xa INHIBITORS
Recently some orally active drugs have been produced whichdirectly bind to and inactivate factor Xa, instead of inhibitingits synthesis. They, therefore, act rapidly without a lag time(as in case of warfarin, etc.), and have short-lasting action.
RivaroxabanIt is an orally active direct inhibitor of activated factor Xawhich has become available for prophylaxis and treatmentof DVT. Its anticoagulant action develops rapidly within3–4 hours of ingestion and lasts for ~24 hours. It is largelymetabolized, but also excreted unchanged in urine; plasmat½ is 7–11 hours. Another advantage is that it requires nolaboratory monitoring of PT or aPTT, and is recommendedin a fixed dose of 10 mg once daily starting 6–10 hoursafter surgery for prophylaxis of venous thromboembolismfollowing total knee/hip replacement. In comparative trials,its efficacy has been found similar to a regimen of LMWheparin followed by warfarin. Rivaroxaban has also beenfound equally effective as warfarin for preventing stroke inpatients with atrial fibrillation. Side effects reported arebleeding, nausea, hypotension, tachycardia and edema.
ORAL DIRECT THROMBIN INHIBITOR
Dabigatran etexilate It is a prodrug which after oraladministration is rapidly hydrolysed to dabigatran, a directthrombin inhibitor which reversibly blocks the catalytic siteof thrombin and produces a rapid (within 2 hours)anticoagulant action. Though oral bioavailability is low, theanticoagulant effect is consistent, and no laboratory monitoringis required. The plasma t½ is 12–14 hours and durationof action 24 hours. In the UK, Canada and Europe it isapproved for prevention of venous thromboembolismfollowing hip/knee joint replacement surgery. Administeredin a dose of 110 mg (75 mg for elderly > 75 years) once

624S
EC
TIO
N10
DRUGS AFFECTING BLOOD AND BLOOD FORMATION
TABLE 44.2 Some comparative aspects of heparin and oral anticoagulants
Heparin Warfarin
1. Chemistry Mucopolysaccharide Coumarin derivative2. Source Hog lung, pig intestine Synthetic3. Route of admin. Parenteral (i.v., s.c.) Oral4. Onset of action Immediate Delayed (1–3 days)5. Duration of action 4–6 hrs 3–6 days6. Activity In vitro and in vivo In vivo only7. Mechanism Blocks action of factor X and Inhibits synthesis of clotting factors
thrombin8. Antagonist Protamine sulphate Vit K9. Variability in response Little Marked
10. Lab. control aPTT/clotting time Prothrombin time/INR(desirable) (essential)
11. Drug interactions Few and not significant Many and significant12. Use To initiate therapy For maintenance
daily, it has been found comparable to warfarin. In anotherlarge trial dabigatran etexilate 150 mg twice daily has yieldedsuperior results to warfarin for prevention of embolism andstroke in patients of atrial fibrillation. In the USA it is approvedfor this indication. Adverse effects are bleeding and lesscommonly hepatobiliary disorders.
USES OF ANTICOAGULANTS
The aim of using anticoagulants is to preventthrombus extension and embolic complicationsby reducing the rate of fibrin formation. Theydo not dissolve already formed clot, but preventrecurrences. Heparin is utilized for rapid and short-lived action, while oral anticoagulants are suitablefor maintenance therapy. Generally, the two arestarted together; heparin is discontinued after4–7 days when warfarin has taken effect.
The important features of heparin and oralanticoagulants are compared in Table 44.2.
1. Deep vein thrombosis (DVT) and pulmo-nary embolism (PE) Because venous thrombiare mainly fibrin thrombi, anticoagulants areexpected to be highly effective. The best evidenceof efficacy of anticoagulants comes from treatmentand prevention of venous thrombosis and pulmo-nary embolism. Prophylaxis is recommended forall high risk patients including bedridden, elderly,postoperative, postpartum, poststroke and legfracture patients. When deep vein thrombosis/
pulmonary embolism has occurred, immediateheparin/LMW heparin followed by warfarintherapy should be instituted. Three monthsanticoagulant therapy (continued further if riskfactor persists) has been recommended byAmerican College of Chest Physicians (2001).
Introduction of low dose s.c. heparin pro-phylaxis for patients undergoing elective surgeryhas considerably reduced the incidence of leg veinthrombosis and pulmonary embolism in thepostoperative period. It has been extended to othersituations needing prolonged immobilization. It isbased on the premise that inhibition of smallamount of activated factor X prevents furtheramplification of active products—particularlythrombin. This is the regimen of choice which doesnot need laboratory monitoring; spontaneousbleeding does not occur. LMW heparin/fonda-parinux have now practically replaced UFH, exceptin case of major surgery and in high risk cases,because action of UFH can be terminated rapidly.
Anticoagulants are of little value in chronicperipheral vascular diseases.
2. Myocardial infarction (MI) Arterial thrombiare mainly platelet thrombi; anticoagulants areof questionable value. Their use in acute MI hasdeclined. They do not alter immediate mortalityof MI. It was hoped that anticoagulants will

625C
HA
PTE
R 44
DRUGS AFFECTING COAGULATION, BLEEDING AND THROMBOSIS
prevent extension of the thrombus and ward offa recurrent attack. This has not been supportedby the collected statistics. They may benefit bypreventing mural thrombi at the site of infarctionand venous thrombi in leg veins. Thus, anti-coagulants may be given for a short period tillpatient becomes ambulatory. For secondaryprophylaxis against a subsequent attack—anticoagulants are inferior to antiplatelet drugs.
Heparin (i.v.) or preferably LMW heparin/fondaparinux s.c. once or twice daily for 2–8days followed by oral anticoagulants for 3 monthsor continuation of LMW heparin for 2–3 monthsare generally given after recanalization of coronaryartery by fibrinolytic therapy. Heparin is also usedduring coronary angioplasty and stent placement.
3. Unstable angina Short-term use of heparinhas reduced the occurrence of MI in unstableangina patients; aspirin is equally effective.Current recommendation is to use aspirin +heparin/LMW heparin followed by warfarin.
4. Rheumatic heart disease; Atrial fibrillation(AF) All atrial fibrillation patients should beprotected against thromboembolism fromfibrillating atria and the resulting stroke. For thispurpose, the effective options are warfarin/lowdose heparin/low dose aspirin. The ‘Strokeprevention in Atrial Fibrillation’ trial and ametaanalysis have shown warfarin to be moreeffective than aspirin. Current guideline is to givewarfarin to a target INR of 2–3 in AF patientswith high risk for stroke (elderly, heart failure,etc.), and to reserve aspirin for low risk patientsor for those unable to take warfarin. Anticoagu-lants are given for 3–4 weeks before and afterattempting conversion of AF to sinus rhythm.
5. Cerebrovascular disease Anticoagulantsare of little value in cerebral thrombosis. Theyhave been used with the aim of preventing clotpropagation, but all the trials conducted, includingInternational Stroke Trial (IST), have failed todemonstrate significant benefit. Neurologicalsequelae are similar whether anticoagulants areused or not. Moreover, in the initial stages it is
difficult to rule out cerebral haemorrhage (unlessCAT scan is done) in which they can be devas-tating. They may be used in cerebral embolism,because showers of emboli are often recurrentand can be prevented by anticoagulants. A latestart (after one week) anticoagulant therapy isadvocated by many in case of large embolic stroke.Oral anticoagulants may be beneficial in transientischaemic attacks (TIAs), but antiplatelet drugsare simpler to use and probably better.
6. Vascular surgery, prosthetic heart valves,retinal vessel thrombosis, extracorporealcirculation, haemodialysis Anticoagulants areindicated along with antiplatelet drugs forprevention of thromboembolism.
Heparin flushes (200 U in 2 ml) every4–8 hr are used to keep patent long-term intra-vascular cannulae/catheters.
7. Defibrination syndrome or ‘disseminatedintravascular coagulation’ occurs in abruptioplacentae and other obstetric conditions, certainmalignancies and infections. The coagulationfactors get consumed for the formation of intra-vascular microclots and blood is incoagulable.Heparin paradoxically checks bleeding in suchpatients by preserving the clotting factors.However, in some cases heparin may aggravatebleeding.
FIBRINOLYTICS (Thrombolytics)
These are drugs used to lyse thrombi/clot torecanalize occluded blood vessels (mainlycoronary artery). They are therapeutic rather thanprophylactic and work by activating the naturalfibrinolytic system (Fig. 44.3).
Haemostatic plug of platelets formed at the site ofinjury to blood vessels is reinforced by fibrin depositionto form a thrombus. Once repair is over, the fibrinolyticsystem is activated to remove the fibrin. The enzymeresponsible for digesting fibrin is a serine protease Plasmingenerated from plasminogen by tissue plasminogen activator(t-PA), which is produced primarily by vascular endothelium.Plasminogen circulates in plasma as well as remains boundto fibrin. The t-PA selectively activates fibrin-bound plasmino-gen within the thrombus, and any plasmin that leaks isinactivated by circulating antiplasmins. Fibrin bound plasmin

626S
EC
TIO
N10
DRUGS AFFECTING BLOOD AND BLOOD FORMATION
Fig. 44.3: The plasminogen-plasmin systemt-PA—Tissue plasminogen activator; rt-PA—Recombinant t-PA; PAI-1—Plasminogen activator inhibitor-1
is not inactivated by antiplasmins because of common bindingsite for both fibrin and antiplasmin.The t-PA itself isinactivated by plasminogen activator inhibitor-1 and -2(PAI-1, PAI-2).
When excessive amounts of plasminogen are activated(by administered fibrinolytics), the α2 antiplasmin is exhaustedand active plasmin persists in plasma. Plasmin is a rathernonspecific protease: degrades coagulation factors (includingfibrinogen) and some other plasma proteins as well. Thus,activation of circulating plasminogen induces a lytic statewhose major complication is haemorrhage. Even selectiveactivation of thrombus bound plasmin can cause bleedingby dissolving physiological thrombi.
In general, venous thrombi are lysed more easilyby fibrinolytics than arterial, and recent thrombirespond better. They have little effect on thrombi> 3 days old. The clinically important fibrinolyticsare:
Streptokinase Alteplase (rt-PA)Urokinase Reteplase
TenecteplaseStreptokinase (Stk) Obtained from β haemolyticStreptococci group C, it is the first fibrinolytic drug to beused clinically, but is not employed now except for conside-rations of cost. Streptokinase is inactive as such; combineswith circulating plasminogen molecules to form an activatorcomplex which then causes limited proteolysis of otherplasminogen molecules to generate the active enzyme plasmin.Stk. is non-fibrin specific, i.e. activates both circulating aswell as fibrin bound plasminogen. Therefore, it depletescirculating fibrinogen and predisposes to bleeding. Comparedto newer more fibrin-specific tissue plasminogen activators
(alteplase, etc.) it is less effective in opening occluded coronaryarteries, and causes less reduction in MI related mortality.
There are several other disadvantages as well with Stk.Antistreptococcal antibodies due to past infections inactivateconsiderable fraction of the initial dose of Stk. A loading dosetherefore is necessary. Plasma t½ is estimated to be 30–80min. Stk is antigenic—can cause hypersensitivity reactions;anaphylaxis occurs in 1–2% patients. It cannot be used secondtime due to neutralization by antibodies generated in responseto the earlier dose. Fever, hypotension and arrhythmias arereported. However, being less expensive, it is still used inresource poor areas, but not in Europe or USA.STREPTASE, (freeze dried powder in vials) 2.5 lac, 7.5lac and 15 lac IU/vial, ESKINASE, CARDIOSTREP 7.5 lac,15 lac IU/vial.For MI: 7.5–15 lac IU infused i.v. over 1 hr.For deep vein thrombosis and pulmonary embolism: 2.5 lacIU loading dose over ½–1 hr, followed by 1 lac IU/hr for24 hr.
Urokinase It is an enzyme isolated from human urine; butcommercially prepared from cultured human kidney cells.It activates plasminogen directly and has a plasma t½ of10–15 min. It is nonantigenic. Fever occurs during treatment,but hypotension and allergic phenomena are rare. Urokinaseis Indicated in patients in whom streptokinase has been givenfor an earlier episode, but is seldom used now.UROKINASE, UROPASE, 2.5 lac, 5 lac, 7.5 lac, 10 lac IUper vial inj.For MI: 2.5 lac IU i.v. over 10 min followed by 5 lac IU overnext 60 min (stop in between if full recanalization occurs) or6000 IU/min for upto 2 hr.For venous thrombosis and pulmonary embolism: 4400IU/kg over 10 min i.v. followed by 4400 IU/kg/hr for12 hr.

627C
HA
PTE
R 44
DRUGS AFFECTING COAGULATION, BLEEDING AND THROMBOSIS
Alteplase (recombinant tissue plasminogenactivator (rt-PA) Produced by recombinantDNA technology from human tissue culture, itis moderately specific for fibrin-bound plasmino-gen, so that circulating fibrinogen is lowered onlyby ~ 50%. It is rapidly cleared by liver andinactivated by plasminogen activator inhibitor-1(PAI-1). The plasma t½ is 4–8 min. Becauseof the short t½, it needs to be given by slowi.v. infusion and often requires heparin co-administration. It is nonantigenic, but nausea, mildhypotension and fever may occur. It is expensive.ACTILYSE 50 mg vial with 50 ml solvent water.For MI: (accelerated regimen) 15 mg i.v. bolus injectionfollowed by 50 mg over 30 min, then 35 mg over the next 1 hr.(total 90 min).For pulmonary embolism: 100 mg i.v. infused over 2 hr.For ischaemic stroke: 0.9 mg/kg by i.v. infusion over60 min, with 10% of the dose injected in the first minute.
Reteplase It is a modified form of rt-PA that is longeracting, but somewhat less specific for fibrin-bound plasmi-nogen. The longer duration of action enables bolus doseadministration (10 mg over 10 min repeated after 30 min).
Tenecteplase This genetically engineeredsubstitution mutant of native t-PA has higher fibrinselectivity, slower plasma clearance (longerduration of action) and resistance to inhibitionby PAI-1. It is the only fibrinolytic agent thatcan be injected i.v. as a single bolus dose over10 sec, while alteplase requires 90 min infusion.This feature makes it possible to institute fibrino-lytic therapy immediately on diagnosis of STsegment elevation myocardial infarction (STEMI),even during transport of the patient to the hospital.Several randomized multicentric trials haveassessed its efficacy in STEMI and found it tobe at least equally efficacious to alteplase. Riskof noncerebral bleeding may be lower with tenec-teplase, but cranial bleeding incidence is similar.Dose: 0.5 mg/kg single i.v. bolus injection.ELAXIM 30 mg, 50 mg per vial inj.
Uses of fibrinolytics1. Acute myocardial infarction is the chiefindication. Fibrinolytics are an alternative firstline approach to emergency percutaneous coronaryintervention (PCI) with stent placement.
Recanalization of thrombosed coronary artery hasbeen achieved in 50–90% cases. Time lag instarting the infusion is critical for reducing areaof necrosis, preserving ventricular function andreducing mortality. The benefits of i.v. throm-bolytic therapy have been established by largerandomised studies. Aspirin with or withoutheparin is generally started concurrently or soonafter thrombolysis to prevent reocclusion.
Alteplase has advantages over streptokinase,including higher thrombolytic efficacy. However,incidence of haemorrhage is not lower. Its strongerlytic effect on physiological haemostatic plugsmay compensate for the lesser systemic fibrinolyticstate.
2. Deep vein thrombosis in leg, pelvis,shoulder etc.; up to 60% patients can besuccessfully treated. Thrombolytics can decreasesubsequent pain and swelling, but the mainadvantage is preservation of venous valves andmay be a reduced risk of pulmonary embolism,though at the risk of haemorrhage. Comparableresults have been obtained with Stk, urokinaseand alteplase.
3. Pulmonary embolism Fibrinolytic therapyis indicated in large, life-threatening PE. The lungfunction may be better preserved, but reductionin mortality is not established.4. Peripheral arterial occlusion Fibrinolytics recanalise~40% limb artery occlusions, especially those treated within72 hr. However, it is indicated only when surgicalthrombectomy is not possible. Regional intraarterialfibrinolytics have been used for limb arteries with greatersuccess. Peripheral arterial thrombolysis is followed by short-term heparin and long-term aspirin therapy.
Fibrinolytics have no role in chronic peripheral vasculardiseases.
5. Stroke: Thrombolytic therapy of ischaemicstroke is controversial. Possibility of improvedneurological outcome is to be balanced with riskof intracranial haemorrhage. No net benefit wasconcluded by the ATLANTIS trial in patientstreated at 3–5 hours of stroke onset. However,alteplase is approved for use in ischaemic stroke,and current opinion strongly recommends use ofi.v. alteplase in carefully selected patients who

628S
EC
TIO
N10
DRUGS AFFECTING BLOOD AND BLOOD FORMATION
can be treated within 3 hours of onset, and inwhom intracranial haemorrhage is ruled outalong with all risk factors for bleeding (seecontraindications in box).
Evaluation All patients with STEMI arecandidates for reperfusion therapy. No consistentbenefit of fibrinolytics has been demonstrated innon-STEMI cases, while possibility of haemor-rhage is increased. Only selected cases ofNSTEMI may be treated with fibrinolytics. Bothshort-term and long-term outcome is determinedby early restoration of flow in the occluded artery,regardless of whether it is achieved by throm-bolysis or by PCI. Best results are obtained ifperfusion can be restored within the first hour(the golden hour). While the efficacy of fibrino-lytics in dissolving the thrombus diminishes withpassage of time (little benefit after 6 hours ofMI onset), reperfusion by PCI is affected to alesser extent by the time lapse. Thrombolysis maybe favoured if it can be started within 1–2 hoursof onset. After 3 hours, PCI is favoured. Moreover,PCI has the advantage of lower bleeding risk,higher grade of flow in the reperfused artery andreduction in the rate of nonfatal recurrent MIcompared to thrombolysis. As such, PCI hasyielded superior results compared to fibrinolyticsand is being preferred at centres where it canbe performed swiftly with requisite expertise.Primary PCI is the procedure of choice for patientswith contraindications to thrombolytics (see box).Fibrinolytic therapy requires careful patientselection, but often can be instituted with lessdelay, and even at centres not well equipped forPCI.
Another approach is ‘facilitated PCI’ whereinfull or reduced dose fibrinoytic therapy is followedat the earliest by PCI. The results of this approachare comparable to those of primary PCI. TheEuropean as well as American (ACC, AHA) guide-lines provide that STEMI patients should betreated with primary PCI or with fibrinolytic drugsfollowed by immediate rescue PCI, if reperfusionfails with the fibrinolytic. Aspirin and heparinare continued after thrombolysis.
ANTIFIBRINOLYTIC DRUGS
These are drugs which inhibit plasminogenactivation and dissolution of clot, and are usedto check fibrinolysis associated bleeding.
Epsilon amino-caproic acid (EACA) It isa lysine analogue which combines with the lysine-binding sites of plasminogen and plasmin so thatthe latter is not able to bind to fibrin and lyseit. It is a specific antidote for fibrinolytic agentsand has been used in many hyperplasminaemicstates associated with excessive intravascularfibrinolysis resulting in bleeding. The primaryindication is to counteract the effect of fibrinolyticdrugs and bleeding due to their use. In haemophi-liacs, it has adjunctive value for controllingbleeding due to tooth extraction, prostatectomy,trauma, etc.
In haematuria it can cause ureteric obstructionby the unlysed clots. Therefore, fibrinolysis mustbe established firmly before using it. It can causeintravascular thrombosis. Rapid i.v. injectionresults in hypotension, bradycardia and may bearrhythmias. It should be used cautiously whenrenal function is impaired. Myopathy occurs rarely.The large dose needed is a limitation, andtranexamic acid is mostly preferred.Initial priming dose is 5 g oral/i.v., followed by 1 g hourlytill bleeding stops (max. 30 g in 24 hrs).AMICAR, HEMOCID, HAMOSTAT 0.5 g tab., 1.25 g/5 mlsyr., 5 g/20 ml inj.
Tranexamic acid Like EACA, it binds to thelysine binding site on plasminogen and preventsits combination with fibrin leading to fibrinolysis.It is 7 times more potent than EACA, and is
Contraindications to thrombolytic therapy
1. H/o Intracranial haemorrhage2. H/o Ischaemic stroke in past 3 months3. H/o Head injury in past 3 months4. Intracranial tumour/vascular abnormality/
aneurysms5. Active bleeding/bleeding disorders6. Peptic ulcer, esophageal varices7. Any wound or recent fracture or tooth extraction8. H/o major surgery within 3 weeks9. Uncontrolled hypertension
10. Pregnancy

629C
HA
PTE
R 44
DRUGS AFFECTING COAGULATION, BLEEDING AND THROMBOSIS
preferred for prevention/control of excessivebleeding due to:• Fibrinolytic drugs.• Cardio-pulmonary bypass surgery.• Tonsillectomy, prostatic surgery, tooth extrac-
tion in haemophiliacs.• Menorrhagia, especially due to IUCD.• Recurrent epistaxis, hyphema due to ocular
trauma, peptic ulcer.Main side effects are nausea and diarrhoea.Thromboembolic events, disturbed colour visionand allergic reactions are infrequent. Thrombo-phlebitis of injected vein can occur.Dose: 10–15 mg/kg 2–3 times a day or 1–1.5 g TDS oral,0.5–1 g TDS by slow i.v. infusion.DUBATRAN, PAUSE, TRANAREST 500 mg tab, 500 mg/5ml inj.
ANTIPLATELET DRUGS(Antithrombotic drugs)
These are drugs which interfere with plateletfunction and are useful in the prophylaxis ofthromboembolic disorders.
Platelets express several glycoprotein (GP) integrinreceptors on their surface. Reactive proteins like collagenare exposed when there is damage to vascular endothelium,and they react respectively with platelet GPIa and GPIb
receptors. This results in platelet activation and release ofproaggregatory and vasoconstrictor mediators like TXA2, ADPand 5-HT. The platelet GPIIb/IIIa receptor undergoes a confor-mational change favouring binding of fibrinogen andvonWillebrand factor (vWF) that crosslink platelets inducingaggregation and anchorage to vessel wall/other surfaces. Thus,a ‘platelet plug’ is formed. In veins, due to sluggish bloodflow, a fibrinous tail is formed which traps RBCs ‘the redtail’. In arteries, platelet mass is the main constituent ofthe thrombus. Antiplatelet drugs are, therefore, more usefulin arterial thrombosis, while anticoagulants are more effectivein venous thrombosis.
Prostacyclin (PGI2), synthesized in the intima of bloodvessels, is a strong inhibitor of platelet aggregation. A balancebetween TXA2 released from platelets and PGI2 released fromvessel wall appears to control intravascular thrombus forma-tion. Platelets also play a role in atherogenesis.
In the above scheme, various drugs act ondifferent targets to interfere with platelet function.Therefore, given together, their actions aresynergistic. The clinically important antiplateletdrugs are:
Aspirin It acetylates and inhibits the enzymeCOX1 and TX-synthase—inactivating them irre-versibly. Because TXA2 is the major arachidonicacid product generated by platelets, and thatplatelets are exposed to aspirin in the portalcirculation before it is deacetylated during firstpass in the liver, and because platelets cannotsynthesize fresh enzyme (have no nuclei), TXA2
formation is suppressed at very low doses andtill fresh platelets are formed. Thus, aspirininduced prolongation of bleeding time lasts for5–7 days. Effect of daily doses cumulates andit has now been shown that doses as low as 40mg/day have an effect on platelet aggregation.Maximal inhibition of platelet function occurs at75–150 mg aspirin per day. However, aspirin maynot effectively inhibit platelet aggregation in somepatients.
Inhibition of COX-1 by aspirin in vessel walldecreases PGI2 synthesis as well. However, sinceintimal cells can synthesize fresh enzyme, activityreturns rapidly. It is possible that at low doses(75–150 mg/day or 300 mg twice weekly), TXA2
formation by platelets is selectively suppressed,whereas higher doses (> 900 mg/day) maydecrease both TXA2 and PGI2 production.
Aspirin inhibits the release of ADP fromplatelets and their sticking to each other, but hasno effect on platelet survival time and theiradhesion to damaged vessel wall.ASA 50 mg tab., COLSPRIN, DISPRIN CV-100: aspirin 100mg soluble tab, LOPRIN 75 mg tab, ASPICOT 80 mg tab,ECOSPRIN 75, 150 mg tab.
Other NSAIDs are reversible inhibitors of COX, produceshort-lasting inhibition of platelet function—are not clinicallyuseful.
Dipyridamole It is a vasodilator that was intro-duced for angina pectoris (see Ch. 39). It inhibits
Antiplatelet Drugs
AspirinDipyridamole
P2Y12 Receptor Blockers GPIIb/IIIa AntagonistsTiclopidine AbciximabClopidogrel EptifibatidePrasugrel Tirofiban

630S
EC
TIO
N10
DRUGS AFFECTING BLOOD AND BLOOD FORMATION
phosphodiesterase as well as blocks uptake ofadenosine to increase platelet cAMP which inturn potentiates PGI2 and interferes with aggre-gation. Levels of TXA2 or PGI2, are not altered,but platelet survival time reduced by disease isnormalized.
Dipyridamole alone has little clinically signifi-cant effect, but improves the response to warfarin,along with which it is used to decrease theincidence of thromboembolism in patients withprosthetic heart valves.
Dipyridamole has also been used to enhancethe antiplatelet action of aspirin. This combinationmay additionally lower the risk of stroke in patientswith transient ischaemic attacks (TIAs), but trialshave failed to demonstrate additional benefit inprophylaxis of MI.Dose: 150–300 mg/day. PERSANTIN 25, 100 mg tabs,THROMBONIL 75, 100 mg tabs, DYNASPRIN: dipyridamole75 mg + aspirin 60 mg e.c. tab., CARDIWELL PLUS:dipyridamole 75 mg + aspirin 40 mg tab.
Ticlopidine It is the first thienopyridine whichalters surface receptors on platelets and inhibitsADP as well as fibrinogen-induced plateletaggregation. The Gi coupled P2Y12 (also labelledP2YAC) type of purinergic receptors which mediateadenylyl cyclase inhibition due to ADP areblocked irreversibly by the active metabolite ofticlopidine. As a result, activation of platelets isinterfered. Fibrinogen binding to platelets isprevented without modification of GPIIb/IIIareceptor. There is no effect on platelet TXA2,but bleeding time is prolonged and platelet survivalin extra-corporeal circulation is increased. Becauseof different mechanism of action, it has synergisticeffect on platelets with aspirin. Their combinationis a potent platelet inhibitor.
Ticlopidine is well absorbed orally, is con-verted in liver to an active metabolite, and iseliminated with a plasma t½ of 8 hours. However,because it causes irreversible blockade of P2Y12
receptors, the effect on platelets cumulates; peakplatelet inhibition is produced after 8–10 daystherapy, and the effect lasts 5–6 days afterdiscontinuing the drug.
Ticlopidine has produced beneficial effects in strokeprevention, TIAs, intermittent claudication, unstable angina,PCI, coronary artery bypass grafts and secondary prophylaxisof MI. Combined with aspirin, it has markedly loweredincidence of restenosis after PCI and stent thrombosis.
Because of its potential for serious adversereactions, use of ticlopidine has markedly declinedin favour of clopidogrel.Side effects: Diarrhoea, vomiting, abdominal pain, headache,tinnitus, skin rash. Serious adverse effects are bleeding,neutropenia, thrombocytopenia, haemolysis and jaundice.Several fatalities have occurred.Dose: 250 mg BD with meals; effect persists severaldays after discontinuation; TYKLID, TICLOVAS, TICLOP,250 mg tab; ASTIC ticlopidine 250 mg + aspirin 100 mg tab.
Clopidogrel This newer and more potentcongener of ticlopidine has similar mechanismof action, ability to irreversibly inhibit plateletfunction and range of therapeutic efficacy, butis safer and better tolerated (CLASSICS study).The clopidogrel vs aspirin in patients at risk ofischaemic events (CAPRIE) trial has foundclopidogrel recipients to have a slightly lowerannual risk of primary ischaemic events thanaspirin recipients. Combination of clopidogrel andaspirin is synergistic in preventing ischaemicepisodes, and is utilized for checking restenosisof stented coronaries.
Like ticlopidine, clopidogrel is also a prodrug.About 50% of the ingested dose is absorbed, andonly a fraction of this is slowly activated in liverby CYP2C19, while the rest is inactivated byother enzymes. It is a slow acting drug; antiplateletaction takes about 4 hours to start and developsover days. Since CYP2C19, exhibits geneticpolymorphism, the activation of clopidogrel andconsequently its antiplatelet action shows highinterindividual variability. Some patients arenonresponsive. Omeprazole, an inhibitor ofCYP2C19, reduces metabolic activation ofclopidogrel and its antiplatelet action. However,like ticlopidine, the action of clopidogrel lasts5–7 days due to irreversible blockade of plateletP2Y12 receptors.
The most important adverse effect is bleeding.Addition of aspirin to clopidogrel has been found

631C
HA
PTE
R 44
DRUGS AFFECTING COAGULATION, BLEEDING AND THROMBOSIS
to double the incidence of serious bleeding amonghigh risk stroke patients (MATCH study).However, neutropenia, thrombocytopenia andother bone marrow toxicity is rare. Side effectsare diarrhoea, epigastric pain and rashes.Dose: 75 mg OD; CLODREL, CLOPILET, DEPLATT 75mg tab.
Prasugrel This is the latest, most potent andfaster acting P2Y12 purinergic receptor blocker,that is being increasingly used in acute coronarysyndromes (ACS) and when strong antiplateletaction is required. Like its predecessors, it is alsoa prodrug, but is more rapidly absorbed and morerapidly as well as more completely activated,resulting in faster and more consistent plateletinhibition. Though CYP2C19 is involved in acti-vation of prasugrel as well, genetic polymorphismrelated decrease in response, or interference byomeprazole treatment has not been prominent.
Because of rapid action, prasugrel is parti-cularly suitable for use in STEMI. It is thepreferred thienopyridine for ACS to cover angio-plasty with or without stent placement. TheTRITON trial compared prasugrel with clopido-grel in STEMI and NSTEMI. There was 19%greater reduction in death from cardiovascularcauses in the prasugrel group. Superior clinicaloutcomes and reduction in stent thrombosis havebeen obtained with prasugrel. Bleeding compli-cations are also more frequent and more serious.Patients with history of ischaemic stroke and TIAsare at greater risk of intracranial haemorrhage.Prasugrel is contraindicated in such patients.Dose: 10 mg OD; elderly or those <60 kg body weight5 mg OD; a loading dose of 60 mg may be given for urgentaction.PRASULET, PRASUSAFE, PRASUREL 5 mg, 10 mg tabs.
Glycoprotein (GP) IIb/IIIa receptorantagonistsGP IIb/IIIa antagonists are a newer class of potentplatelet aggregation inhibitors which act byblocking the key receptor involved in plateletaggregation. The GPIIb/IIIa is an adhesive receptor(integrin) on platelet surface for fibrinogen andvWF through which agonists like collagen,thrombin, TXA2, ADP, etc. finally induce platelet
aggregation. Thus, GP IIb/IIIa antagonists blockaggregation induced by all platelet agonists.
Abciximab It is the Fab fragment of a chimericmonoclonal antibody against GP IIb/IIIa, protein,but is relatively nonspecific and binds to someother surface proteins as well. Given along withaspirin + heparin during PCI it has markedlyreduced the incidence of restenosis, subsequentMI and death. In the ISAR-REACT2 trial additionof abciximab to clopidogrel (600 mg oral loadingdose) for PCI in high-risk ACS patients, reducedischaemic events by 25%. After a bolus dose,platelet aggregation remains inhibited for 12–24hr, while the remaining antibody is cleared fromblood with a t½ of 10–30 min.Dose: 0.25 mg/kg i.v. 10–60 min before PCI, followed by 10µg/min for 12 hr. REOPRO 2 mg/ml inj.
Abciximab is nonantigenic. The main risk ishaemorrhage, incidence of which can be reducedby carefully managing the concomitant heparintherapy. Thrombocytopenia is another compli-cation. It should not be used second time, sincerisk of thrombocytopenia increases. Constipation,ileus and arrhythmias can occur. It is expensive,but is being used in unstable angina and asadjuvant to coronary thrombolysis/PCI with stentplacement.
Eptifibatide It is a synthetic cyclic peptide thatselectively binds to platelet surface GPIIb/IIIareceptor and inhibits platelet aggregation. Thoughits plasma t½ (2.5 hours) is longer than that ofabciximab, platelet inhibition reverses in a shortertime (within 6–10 hours) because it quicklydissociates from the receptor. Infused i.v.,eptifibatide is indicated in:Unstable angina: 180 μg/kg i.v. bolus, followed by 2 μg/kg/min infusion upto 72 hours.Coronary angioplasty: 180 μg/kg i.v. bolus, immediatelybefore procedure; follow with 2 μg/kg/min for 12–24 hours.CLOTIDE, COROMAX, UNIGRILIN 20 mg/10 ml and75 mg/100 ml vials.Aspirin and heparin are generally given concurrently.Bleeding and thrombocytopenia are the majoradverse effects. Rashes and anaphylaxis are rare.
Tirofiban This is a nonpeptide but specificGPIIb/IIIa antagonist that is similar in properties

632S
EC
TIO
N10
DRUGS AFFECTING BLOOD AND BLOOD FORMATION
to eptifibatide. Its plasma t½ is 2 hours, and itdissociates rapidly from the receptors. Theindications and adverse effects are also similarto eptifibatide.Acute coronary syndromes: 0.4 μg/kg/min for 30 min followedby 0.1 μg/kg/min for upto 48 hours. If angioplasty is performed,infusion to continue till 12–24 hours thereafter.AGGRAMED, AGGRITOR, AGGRIBLOC 5 mg/100 mlinfusion.
Uses of antiplatelet drugsThe aim of using antiplatelet drugs is to preventintravascular thrombosis and embolization, withminimal risk of haemorrhage. The intensity ofantiplatelet therapy is selected according to thethrombotic influences present in a patient. Forindications like maintenance of vascularrecanalization, stent placement, vessel grafting,etc. potent inhibition of platelet function isrequired. This is now possible and is achievedby combining antiplatelet drugs which act bydifferent mechanisms.
1. Coronary artery disease On the basis oftrials in post-MI patients as well as in those withno such history, it is recommended that aspirin75–150 mg/day be given to all individuals withevidence of coronary artery disease and in thosewith risk factors for the same, but routine usein the whole population is not warranted. Primaryprevention of ischaemia with aspirin is of noproven benefit. It reduces the incidence of fatalas well as nonfatal MI, but increases the riskof cerebral haemorrhage. Clopidogrel is analternative to aspirin in symptomatic patients ofischaemia. Continued aspirin/clopidogrelprophylaxis in post-MI patients clearly preventsreinfarction and reduces mortality.
2. Acute coronary syndromes (ACSs) Thesecomprise of a range of acute cardiac ischaemicstates from unstable angina (UA) to non-STelevation myocardial infarction (NSTEMI) toSTEMI (see p. 556).
The coronary obstruction in UA and NSTEMI is partial,while that in STEMI is total. UA and NSTEMI are differentiatedon the basis of absence or presence of laboratory markers ofcardiac myocyte necrosis (myoglobin, CK, troponin I, etc.).The ischaemic status is often dynamic and the patient mayrapidly shift from one category to the next.
Soluble aspirin (325 mg oral) and a LMW heparin(s.c.) are given at presentation to all patients withACS.
Unstable angina Aspirin reduces the risk ofprogression to MI and sudden death. Clopidogrelis generally combined with aspirin, or may be usedas alternative if aspirin cannot be given. Formaximum protection the antiplatelet drugs aresupplemented with heparin followed by warfarin.The ‘Clopidogrel in unstable angina to prevent recurrent events’(CURE) trial has found that addition of clopidogrel to aspirinfurther reduced cardiovascular mortality, nonfatal MI andstroke by 20%.
NSTEMI Patients of NSTEMI who are managedwithout PCI/thrombolysis are generally put ona combination of aspirin + clopidogrel, whichis continued upto one year.
STEMI Primary PCI with or without stentplacement is the procedure of choice for allSTEMI as well as high risk NSTEMI patientswho present within 12 hours. Prasugrel + aspirinis the antiplatelet regimen most commonly selectedfor patients who are to undergo PCI. Prasugrelacts rapidly and more predictably than clopidogrel.Prasugrel is also perferred over clopidogrel indiabetics. The GPIIb/IIIa antagonists are the mostpowerful antiplatelet drugs; are combined withaspirin for high risk patients undergoing PCI.Abciximab/eptifibatide/tirofiban infused i.v. alongwith oral aspirin and s.c. heparin markedly reduceincidence of restenosis and subsequent MI aftercoronary angioplasty. The GPIIb/IIIa antagonistsare infused for a maximum of 72 hours.
Aspirin and/or clopidogrel are routinely givento ACS patients treated with thrombolysis.Coronary artery bypass surgery is also coveredby intensive antiplatelet regimen including aspirin+ GPIIb/IIIa antagonists/prasugrel.
The patency of recanalized coronary arteryor implanted vessel is improved and incidenceof reocclusion is reduced by continuing aspirin+ clopidogrel/prasugrel almost indefinitely. Dualantiplatelet therapy is recommended after stentplacement. Prasugrel is used when stent throm-bosis occurs during clopidogrel treatment.

633C
HA
PTE
R 44
DRUGS AFFECTING COAGULATION, BLEEDING AND THROMBOSIS
3. Cerebrovascular disease Antiplateletdrugs do not alter the course of stroke due tocerebral thrombosis. However, aspirin has reducedthe incidence of TIAs and of stroke in patientswith TIAs. Occurrence of stroke is also reducedin patients with persistent atrial fibrillation andin those with history of stroke in the past. Aspirinor clopidogrel is recommended in all suchindividuals. The European stroke preventionstudy-2 (ESPS) has found combination ofdipyridamole with low dose aspirin to besynergistic in secondary prevention of stroke.
4. Prosthetic heart valves and arteriovenousshunts Antiplatelet drugs, used with warfarinreduce formation of microthrombi on artificialheart valves and the incidence of embolism.Aspirin is clearly effective but increases risk of
bleeding due to warfarin. Dipyridamole does notincrease bleeding risk, but incidence of throm-boembolism is reduced when it is combinedwith an oral anticoagulant. Antiplatelet drugsalso prolong the patency of chronic arteriovenousshunts implanted for haemodialysis and of vasculargrafts.5. Venous thromboembolism Anticoagulantsare routinely used in DVT and PE. Trials haveshown antiplatelet drugs also to have a prophy-lactic effect, but their relative value in comparisonto, or in addition to anticoagulants is notestablished; they are infrequently used.6. Peripheral vascular disease Aspirin/clopidogrel may produce some improvement inintermittent claudication and reduce the incidenceof thromboembolism.
PROBLEM DIRECTED STUDY
44.1 A 35-year-old woman was on maintenance therapy with warfarin for leg vein thrombosisthat she had developed during a complicated delivery 2 months back. The dose was adjustedby repeated measurement of INR, and for the last one month it was maintained between2.4–2.8 with 4 mg taken daily at bed time. She developed a pelvic infection for which she wasadmitted to the hospital and given Inj. Ceftriaxone 1 g i.v. 8 hourly. On the 3rd day she startedbleeding per-vaginum and reported passing dark urine. The haemoglobin level fell to 9.0 g/dl,while on admission 3 days back, it was 11.0 g/dl. The INR was measured to be 5.4.(a) What could be the cause of bleeding per-vaginum, passing dark urine; fall in Hb level andrise in INR value? Could this complication be prevented?(b) How should this patient be managed?(see Appendix-1 for solution)

Hypolipidaemic Drugs andPlasma Expanders
ChapterChapterChapterChapterChapter 4545454545
HYPOLIPIDAEMIC DRUGS
These are drugs which lower the levels of lipidsand lipoproteins in blood.
The hypolipidaemic drugs have attractedconsiderable attention because of their potentialto prevent cardiovascular disease by retarding theaccelerated atherosclerosis in hyperlipidaemicindividuals.
Lipid transportLipids are carried in plasma in lipoproteins aftergetting associated with several apoproteins; plasmalipid concentrations are dependent on theconcentration of lipoproteins. The core of lipo-protein globules consists of triglycerides (TGs)or cholesteryl esters (CHEs) while the outer polarlayer has phospholipids, free cholesterol (CH) andapoproteins. The lipoproteins have been dividedinto 6 classes on the basis of their particle sizeand density. They also differ in the nature ofapoproteins, the ratio of TG and CHE, tissue oforigin and fate. These are given in Table 45.1.
Dietary lipids are absorbed in the intestine with the helpof bile acids. Chylomicrons (Chy) are formed and passedinto lacteals—reach blood stream via thoracic duct. Duringtheir passage through capillaries, the endothelium boundlipoprotein lipase hydrolyses the TGs into fatty acids whichpass into muscle cells to be utilized as energy source andin fat cells to be reconverted into TGs and stored. Theremaining part—chylomicron remnant (Chy. rem.) containingmainly CHE and little TG is engulfed by liver cells, whichhave receptors for the surface apoproteins of Chy. rem., anddigested. Free CH that is liberated is either stored in livercells after reesterification or incorporated into a differentlipoprotein and released in blood or excreted in bile as CH/bile acids.
Liver secretes very low density lipoproteins (VLDL)containing mainly TG and some CHE into blood. VLDLis acted upon by endothelial lipoprotein lipase in the sameway as on Chy and the fatty acids pass into adipose tissueand muscle; the remnant called intermediate densitylipoprotein (IDL) now contains more CHE than TG. Abouthalf of the IDL is taken back by the liver cells by attachmentto another receptor (LDL receptor), while the rest loses theremaining TGs gradually and becomes low density lipoprotein(LDL) containing only CHE. The LDL circulates in plasmafor a long time; its uptake into liver and other tissues isdependent on the need for CH. The rate of LDL uptakeis regulated by the rate of LDL receptor synthesis in aparticular tissue.
TABLE 45.1 Characteristics and function of plasma lipoproteins
Lipoprotein Diameter Lipid Source Functionclass (nm) contained of lipid
1. Chy. 100–500 TG >> CHE Diet Dietary TG transport
2. Chy. rem. 30–50 CHE >> TG Diet, Chy. Dietary CH transport
3. VLDL 40–80 TG >> CHE Liver Endogenous TG transport
4. IDL 30–35 CHE > TG VLDL Transport CHE & TG to liver,source of LDL
5. LDL 20–25 CHE IDL Transport CH to tissues and liver
6. HDL 5–10 Phospholipid, Tissues, Removal of CH from tissuesCHE cell memb.
Chy—Chylomicrons; Chy. rem.—Chylomicron remnant; VLDL—Very low density lipoprotein; IDL—Intermediatedensity lipoprotein; LDL—Low density lipoprotein; HDL—High density lipoprotein; CHE—Cholesteryl esters;TG—Triglyceride; CH—Cholesterol

635C
HA
PTE
R 45
HYPOLIPIDAEMIC DRUGS AND PLASMA EXPANDERS
TABLE 45.2 Types of primary hyperlipoproteinaemias
Type Disorder Cause Occurrence Elevated Plasma lipidsplasmalipoprotein CH TG
I Familial lipoprotein G Very rare Chylomicron ↑↑ ↑↑↑lipase deficiency
IIa Familial G Less common LDL ↑↑ Nhypercholesterolaemia
IIb Polygenic MF Commonest LDL ↑ Nhypercholesterolaemia
III Familial G Rare IDL, Chy. rem. ↑ ↑dysbetalipoproteinaemia
IV Hypertriglyceridaemia MF, G Common VLDL N ↑↑
V Familial combined G Less common VLDL, LDL ↑ ↑hyperlipidaemia
CH—Cholesterol; TG—Triglycerides; G—Genetic; MF—Multifactorial; Chy. rem.—Chylomicron remnants;VLDL—Very low density lipoprotein; IDL—Intermediate density lipoprotein; LDL—Low density lipoprotein.The genetic defect in some of the monogenic disorders is:Type I : absence of lipoprotein lipase—TG in Chy cannot be utilized.Type IIa : deficiency of LDL receptor—LDL and IDL are taken up very slowly by liver and tissues.Type III : the apoprotein in IDL and Chy. rem. (apoE) is abnormal, these particles are cleared at a lower rate.Type IV : this type of hypertriglyceridaemia is both multifactorial and monogenic, the former is more prevalent
than the latter.
The CHE of LDL is deesterified and used mainly forcell membrane formation. The CH released into blood fromdegradation of membranes is rapidly incorporated in highdensity lipoproteins (HDL), esterified with the help of anenzyme lecithin: cholesterol acyltransferase (LCAT) andtransferred back to VLDL or IDL, completing the cycle.
The excess lipoproteins in plasma are phagocytosed bymacrophages for disposal. When too much of lipoproteinshave to be degraded in this manner, CH is deposited inatheromas (in arterial walls) and xanthomas (in skin andtendons). Raised levels of VLDL, IDL and LDL (rarely Chyand Chy. rem. also) are atherogenic, while HDL may beprotective, because HDL facilitates removal of CH from tissues.
Hyperlipoproteinaemias can be:(i) Secondary: associated with diabetes, myxo-edema, nephrotic syndrome, chronic alcoholism,drugs (corticosteroids, oral contraceptives, βblockers) etc.(ii) Primary: due to:
(a) A single gene defect: is familial and called‘monogenic’ or genetic.
(b) Multiple genetic, dietary and physical acti-vity related causes: ‘polygenic’ or multi-factorial.
On the whole, LDL is the primary carrier of plasmaCHE, and VLDL that of TGs. The importantfeatures of major types of hyperlipoproteinaemiasare given in Table 45.2.
CLASSIFICATION
1. HMG-CoA reductase inhibitors (Statins):Lovastatin, Simvastatin, Pravastatin,Atorvastatin, Rosuvastatin, Pitavastatin
2. Bile acid sequestrants (Resins):Cholestyramine, Colestipol
3. Lipoprotein lipase activators (PPARαactivators, Fibrates): Clofibrate, Gemfibrozil,Bezafibrate, Fenofibrate.
4. Lipolysis and triglyceride synthesisinhibitor:Nicotinic acid.
5. Sterol absorption inhibitor:Ezetimibe.The mechanism of action and profile of lipid
lowering effect of important hypolipidaemic drugsis summarized in Table 45.3.

636S
EC
TIO
N10
DRUGS AFFECTING BLOOD AND BLOOD FORMATION
TABLE 45.3 Mechanism of action and pattern of lipid lowering effect of important hypolipidaemic drugs
Drug (daily dose) Mechanism of action Effect on lipids (%)
HMG-CoA reductase inhibitorsLovastatin (10–80 mg) ↓ CH synthesis by inhibition of rate LDL ↓ 20–55Simvastatin (5–40 mg) limiting HMG-CoA reductase HDL ↑ 5–15Atorvastatin (10–80 mg) TG ↓ 10–35Rosuvastatin (5–20 mg)
Bile acid sequestrantsCholestyramine (4–16 g) ↓ bile acid absorption, ↑ hepatic LDL ↓ 15–30Colestipol (5–30 g) conversion of CH to bile acids, HDL ↑ 3–5
↑ LDL receptors on hepatocytes TG not affected, may ↑ in some
Fibric acid derivativesGemfibrozil (1200 mg) ↑ Activity of lipoprotein lipase, LDL ↓ 5–20*Bezafibrate (600 mg) ↓ release of fatty acids from adipose HDL ↑ 10–20Fenofibrate (200 mg) tissue TG ↓ 20–50
Nicotinic acid (2–6 g) ↓ Production of VLDL, ↓ lipolysis LDL ↓ 15–25in adipocytes HDL ↑ 20–35
TG ↓ 20–50
* Gemfibrozil may ↑ LDL-CH when TG levels are high; bezafibrate and fenofibrate not likely to raise LDL-CH
HMG-CoA REDUCTASE INHIBITORS(Statins)Introduced in the 1980s, this class of compoundsare the most efficacious and best toleratedhypolipidaemic drugs. They competitively inhibitconversion of 3-Hydroxy-3-methyl glutarylcoenzyme A (HMG-CoA) to mevalonate (ratelimiting step in CH synthesis) by the enzymeHMG-CoA reductase. Therapeutic doses reduceCH synthesis by 20–50%. This results incompensatory increase in LDL receptor expres-sion on liver cells → increased receptor mediateduptake and catabolism of IDL and LDL. Overlong-term, feedback induction of HMG-CoAreductase tends to increase CH synthesis, but asteady-state is finally attained with a dose-dependent lowering of LDL-CH levels.
Different statins differ in their potency andmaximal efficacy in reducing LDL-CH. The dailydose for lowering LDL-CH by 30–35% islovastatin 40 mg, pravastatin 40 mg, simvastatin20 mg, atorvastatin 10 mg, rosuvastatin 5 mgand pitavastatin 2 mg. Moreover, at their maximumrecommended doses simvastatin (80 mg) causes45–50% reduction, while atorvastatin (80 mg) androsuvastatin (40 mg) can reduce LDL-CH by upto
55%. The ceiling effect of lovastatin andpravastatin is 30–40% LDL-CH reduction. Allstatins produce peak LDL-CH lowering after1–2 weeks therapy. Hepatic synthesis of VLDLis concurrently reduced and its removal fromplasma is enhanced.
A dose-dependent effect is seen with all statins.With lovastatin a mean reduction of LDL-CH by25% at 20 mg/day, 32% at 40 mg/day and 40%at 80 mg/day has been measured. Atorvastatinis more potent; the corresponding figures of LDL-CH reduction are 33% at 10 mg/day, 40% at 20mg/day, 45% at 40 mg/day and 50–55% at 80mg/day. A concurrent fall by 10–30% in plasmaTG level, probably due to reduction of VLDLoccurs. A modest rise in HDL-CH by 5–15% isalso noted. Simultaneous use of bile salt seques-trant augments the LDL lowering effect upto 60%and addition of nicotinic acid to this combinationmay boost the effect to 70% reduction inLDL-CH. Statins are effective in secondaryhypercholesterolaemias also. The more efficaciousstatins (simvastatin, atorvastatin, rosuvastatin)given at their higher doses effectively reduce TGs(by 25% to 35%) when they are moderately raised,but not when they are markedly raised.

637C
HA
PTE
R 45
HYPOLIPIDAEMIC DRUGS AND PLASMA EXPANDERS
Because HMG-CoA reductase activity is maxi-mum at midnight, all statins are administered atbed time to obtain maximum effectiveness.However, this is not necessary for atorvastatinand rosuvastatin, which have long plasma t½.
All statins, except rosuvastatin are meta-bolized primarily by CYP3A4. Inhibitors andinducers of this isoenzyme respectively increaseand decrease statin blood levels.
Lovastatin It is the first clinically used statin;is lipophilic and given orally in the precursorlactone form. Absorption is incomplete and firstpass metabolism is extensive. Metabolites areexcreted mainly in bile. The t½ is short (1–4hours).Dose: 10–40 mg/day (max. 80 mg).ROVACOR, AZTATIN, LOVAMEG 10, 20 mg tabs.
Simvastatin It is twice as potent as lovastatin;also more efficacious. A greater rise in HDL-CH (when low) has been noted with simvastatinthan lovastatin or pravastatin. Like lovastatin, itis lipophilic and given in the lactone precursorform. Oral absorption is better and first passmetabolism extensive; t½ is 2–3 hr.Dose: 5–20 mg/day (max. 80 mg)SIMVOTIN, SIMCARD, ZOSTA 5, 10, 20 mg tabs.
Pravastatin It is hydrophilic and given in theactive form. At low doses it is equipotent tolovastatin, but at higher dose (40 mg/day), CHlowering effect is less. It can be employed whenreduction of LDL-CH by < 25% is contemplated.An additional action of decrease in plasma fibrino-gen level has been observed. The t½ is 1–3 hours.PRAVATOR 10, 20 mg tabs.
Atorvastatin This newer and most popular statinis more potent and appears to have the highestLDL-CH lowering efficacy at maximal daily doseof 80 mg. At this dose a greater reduction inTGs is noted if the same was raised at baseline.Atorvastatin has a much longer plasma t½ of 18–24 hr than other statins, and has additionalantioxidant property.Dose: 10-40 mg/day (max. 80 mg)AZTOR, ATORVA, ATORLIP 5, 10, 20 mg tabs.
Rosuvastatin This is another newer, commonlyused and potent statin (10 mg rosuvastatin ~ 20mg atorvastatin), with a plasma t½ of 18–24 hours.Greater LDL-CH reduction can be obtained insevere hypercholesterolaemia; partly due to itslonger persistence in the plasma. In patients withraised TG levels, rosuvastatin raises HDL-CH by15–20% (greater rise than other statins).Dose: Start with 5 mg OD, increase if needed upto 20 mg/day, (max 40 mg/day)ROSUVAS, ROSYN 5, 10, 20 mg tabs.
Pitavastatin This is the latest and dose-to-dosethe most potent statin. However, no specificadvantages compared to other statins have beendemonstrated, and experience with its use islimited. A ceiling response of 40% LDL-CHreduction with the maximum recommended dailydose of 4 mg is noted. The plasma t½ is 12 hours.Use of pitavastatin in combination with gemfibrozilshould be avoided, as the latter decreases itsclearance.Dose: 1–4 mg per day; FLOVAS 1.0, 2.0 mg tabs.
Adverse effects All statins are remarkablywell tolerated; overall incidence of side effects notdiffering from placebo. Notable side effects are:
Gastrointestinal complaints and headache areusually mild. Rashes and sleep disturbances areuncommon. Rise in serum transaminase can occur,but liver damage is rare. Monitoring of liverfunction is recommended.
Muscle aches are the commonest (10%) sideeffect. Rise in CPK levels occurs infrequently.Myopathy is the only serious reaction, but is rare(< 1 per 1000). Few fatalities due to rhabdo-myolysis are on record. Myopathy is morecommon when nicotinic acid/gemfibrozil orCYP3A4 inhibitor—ketoconazole/ erythromycin/cyclosporine/HIV protease inhibitor is givenconcurrently. Gemfibrozil inhibits the hepaticuptake of statins by the organic anion transporterOATP2. Fenofibrate interferes the least with statinuptake/metabolism and should be preferred forcombining with them. A lower dose of statin isadvisable when a fibrate is given concurrently.Statins should not be given to pregnant women,since there is no data on their safety.

638S
EC
TIO
N10
DRUGS AFFECTING BLOOD AND BLOOD FORMATION
Use Statins are the first choice drugs for primaryhyperlipidaemias with raised LDL and total CHlevels, with or without raised TG levels (TypeIIa, IIb, V), as well as for secondary (diabetes,nephrotic syndrome) hypercholesterolaemia.
Efficacy of statins in reducing raised LDL-CH associated mortality and morbidity is nowwell established. Since the dose-response relation-ship of each statin is quite well documented, theinitial dose of selected statin should aim to bringdown the LDL-CH to the target level. It shouldthen be adjusted by LDL-CH measurements every3–4 weeks.
In the ‘Scandinavian Simvastatin Survival Study’ (4Sstudy, 1994), patients with history of MI (80%) or angina(20%) and raised serum CH level (> 212 mg/dl) were treatedwith simvastatin or placebo. Simvastatin reduced total CHby 25%, LDL-CH by 35%, raised HDL-CH by 8%. Overa period of 6 years coronary artery disease (CAD) mortalitywas less by 42%, overall mortality by 30% and cerebrovascularevents by 30% in the simvastatin group. Similar results havebeen obtained with other statins, e.g. the West of ScotlandCoronary Prevention Study (WOSCOPS) in men with nohistory of MI has found pravastatin to lower risk of MIby 31% and all cause mortality by 22%.
Subsequent studies like Long-term intervention withpravastatin in ischaemic disease (LIPID-1998), Airforce/Texascoronary atherosclerosis prevention study (AFCAPS/TexCAPS-1998), Cholesterol and recurrent events (CARE-1998), and trials conducted by Heart Protection StudyCollaborative Group (2002, 2004) in over 20,000 patientshave confirmed the mortality and morbidity benefits of statins,including stroke prevention.
Beneficial effects in subjects who have raisedCH levels but no evidence of CAD may relateto improved coronary artery compliance and athe-romatous plaque stabilization due to suppressionof macrophage mediated inflammation, reducingchances of plaque rupture and thrombus formation.Improvement in endothelial function due toincreased NO production and reduction in LDLoxidation are proposed as additional mechanismsby which statins may exert antiatheroscleroticaction. Recently, a reduction in venousthromboembolism has also been observed withrosuvastatin. On the basis of these results as wellas the excellent patient acceptability, the statinsare being increasingly used for primary andsecondary hypercholesterolaemia with or withoutraised TG levels. They are the first choice drugs
for dyslipidaemia in diabetics. Statin therapy iscontinued indefinitely, unless adverse effectsoccur.
BILE ACID SEQUESTRANTS (Resins)Cholestyramine and Colestipol These are basic ionexchange resins supplied in the chloride form. They are neitherdigested nor absorbed in the gut: bind bile acids in the intestineinterrupting their enterohepatic circulation. Faecal excretionof bile salts and CH (which is absorbed with the help ofbile salts) is increased. This indirectly leads to enhancedhepatic metabolism of CH to bile acids. More LDL receptorsare expressed on liver cells: clearance of plasma IDL, LDLand indirectly that of VLDL is increased.
Resins have been shown to retard atherosclerosis, butare not popular clinically because they are unpalatable,inconvenient, have to be taken in large doses, cause flatulenceand other g.i. symptoms, interfere with absorption of manydrugs and have poor patient acceptability.
LIPOPROTEIN-LIPASE ACTIVATORS(Fibrates)The fibrates (isobutyric acid derivatives) primarilyactivate lipoprotein lipase which is a key enzymein the degradation of VLDL resulting in loweringof circulating TGs. This effect is exerted throughperoxisome proliferator-activated receptor α(PPARα) that is a gene transcription regulatingreceptor expressed in liver, fat and muscles.Activation of PPARα enhances lipoprotein lipasesynthesis and fatty acid oxidation. PPARα mayalso mediate enhanced LDL receptor expressionin liver seen particularly with second generationfibrates like bezafibrate, fenofibrate. Fibratesdecrease hepatic TG synthesis as well. A peri-pheral effect reducing circulating free fatty acidshas also been shown.
Drugs in this class primarily lower TG levelsby 20–50%, generally accompanied by 10–15%decrease in LDL-CH and a 10–15% increase inHDL-CH. In some patients with hypertriglyceri-daemia LDL-CH may rise, partly because ofinability of LDL receptor to clear the excess numberof LDL particles generated by enhanced VLDLcatabolism. The increase in HDL-CH is at leastin part due to transfer of surface lipid componentsfrom catabolized VLDL to HDL, and partly dueto increased production of HDL apoproteins (apoA-I, apo A-II) by liver. Gemfibrozil also appearsto reduce VLDL secretion by liver.

639C
HA
PTE
R 45
HYPOLIPIDAEMIC DRUGS AND PLASMA EXPANDERS
LDL composition may be altered. Gemfibroziland bezafibrate have been shown to shift smalldense LDL particles (believed to be more athero-genic) to larger less dense particles.
Clofibrate It was a widely used hypolipidaemic drug, butlater evidence showed that it does not prevent atherosclerosis,therefore has gone out of use.
Gemfibrozil This fibric acid derivative effecti-vely lowers plasma TG level by enhancingbreakdown and suppressing hepatic synthesis ofTGs. Besides high efficacy in type III hyperlipo-proteinemia, gemfibrozil has shown action insubjects with raised blood CH in addition. In the‘Helsinki Heart Study’ men without known CADtreated with gemfibrozil had a 34% reduction infatal and nonfatal MI, though overall mortalitywas not affected. That these benefits extend tosecondary prevention of coronary events in menwith existing CAD and low HDL-CH, has beendemonstrated in another trial. Additional actionsto decrease the level of clotting factor VII-phos-pholipid complex and promotion of fibrinolysishave been observed, which may contribute to theantiatherosclerotic effect.
Pharmacokinetics Gemfibrozil is completelyabsorbed orally, metabolized by glucuronidationand undergoes some enterohepatic circulation. Itis excreted in urine; elimination t½ is 1–2 hr.
Adverse effects Common side effects areepigastric distress, loose motions.Skin rashes, body ache, eosinophilia, impotence,headache and blurred vision have been reported.Myopathy is uncommon. Gemfibrozil + statinincreases risk of myopathy.Incidence of gallstone is not increased as wasseen with clofibrate.
It is contraindicated during pregnancy.GEMPAR, NORMOLIP 300 mg cap. LOPID 300 mg cap, 600mg and 900 mg tabs.
Use In a dose of 600 mg BD taken before meals,gemfibrozil is a first line drug for patients withmarkedly raised TG levels, whether or not CHlevels are also raised. Episodes of acute pancrea-titis are prevented in patients with chylomicro-
naemia and severe hypertriglyceridaemia. It ismost effective in type III hyperlipoproteinaemia;also beneficial in type IV and type V disease.Patients with raised TG and low HDL-CH levels(as is the case with metabolic syndrome, type2 diabetes) are the most suitable to be treatedwith fibrates. Fibrates may also be used tosupplement statins.
Bezafibrate This second generation fibricacid derivative is an alternative to gemfibrozilin mixed hyperlipidaemias (type III, IV and V).Though it has also been indicated in hypercholes-terolaemia (type II), it is inferior to statins andresins. Bezafibrate has not shown propensity toincrease LDL-CH in hypertriglyceridaemicpatients and appears to have greater LDL-CHlowering action than gemfibrozil. Circulatingfibrinogen and glucose levels may decrease. The5 year ‘Bezafibrate Coronary AtherosclerosisIntervention Trial’ (BECAIT) in young male post-MI subjects showed an atherosclerosis slowingeffect and reduction in coronary events. TheBezafibrate Infarction Prevention (BIP) registryhas also noted reduction in coronary events insubjects with high TG and low HDL-CH levels.
Adverse effects and contraindications aresimilar to other fibrates. Main side effects areg.i. upset, myalgia, rashes. Dose reduction isneeded in elderly and in renal insufficiency. Actionof oral anticoagulants may be enhanced.
In contrast to gemfibrozil, combination ofbezafibrate with a statin has not so far been foundto increase the incidence of rhabdomyolysis.Dose: 200 mg TDS with meals.BEZALIP 200, 400 mg tab.
Fenofibrate Another 2nd generation prodrugfibric acid derivative which has greater HDL–CH raising and greater LDL-CH lowering actionthan other fibrates: may be more appropriate asan adjunctive drug in subjects with raised LDL-CH levels in addition to raised TG levels. Norise in LDL-CH has been observed in patientswith high TG levels. Its t½ is 20 hr. Adverseeffects are myalgia, hepatitis, rashes. Cholelithiasisand rhabdomyolysis are rare. Fenofibrate appears

640S
EC
TIO
N10
DRUGS AFFECTING BLOOD AND BLOOD FORMATION
to be the most suitable fibrate for combining withstatins, because statin metabolism is minimallyaffected and enhancement of statin myopathy riskis lower. Indications of fenofibrate are similarto that of gemfibrozil.Dose: 200 mg OD with meals.FENOLIP, LIPICARD 200 mg cap.
LIPOLYSIS AND TRIGLYCERIDESYNTHESIS INHIBITOR
Nicotinic Acid (Niacin)
It is a B group vitamin (see Ch. 67) which inmuch higher doses reduces plasma lipids. Thisaction is unrelated to its vitamin activity and notpresent in nicotinamide. When nicotinic acid isgiven, TGs and VLDL decrease rapidly, followedby a modest fall in LDL-CH and total CH. A20–50% reduction in plasma TGs and 15–25%reduction in CH levels has been recorded.Nicotinic acid is the most effective drug to raiseHDL-CH, probably by decreasing rate of HDLdestruction; a 20–35% increase is generallyobtained. Relatively lower dose suffices to raiseHDL–CH. It also reduces lipoprotein Lp (a), whichis considered more atherogenic.
Nicotinic acid reduces production of VLDLin liver by inhibiting TG synthesis. Indirectly theVLDL degradation products IDL and LDL arealso reduced. No direct effect on CH and bileacid metabolism has been found. It inhibits intra-cellular lipolysis in adipose tissue and increasesthe activity of lipoprotein lipase that clears TGs.
A cell surface Gi-protein coupled receptor whichnegatively regulates adipocyte adenylyl cyclase has been foundto selectively bind nicotinic acid, and has been called ‘niacinreceptor’. Nicotinic acid appears to inhibit lipolysis in adiposetissue by decreasing hormone stimulated intracellular cAMPformation through this receptor. Hepatic VLDL productionis believed to be decreased due to reduced flow of fattyacids from adipose tissue to liver.
Adverse effects The large doses needed forhypolipidaemic action are poorly tolerated. Onlyabout half of the patients are able to take thefull doses.
Nicotinic acid is a cutaneous vasodilator:marked flushing, heat and itching (especially in
the blush area) occur after every dose. This isassociated with release of PGD2 in the skin, andcan be minimized by starting with a low dosetaken with meals and gradually increasing astolerance develops. Use of sustained release (SR/ER) tablet also subdues flushing. Aspirin takenbefore niacin substantially attenuates flushing byinhibiting PG synthesis. Laropiprant is a specificantiflushing drug with no hypolipidaemic actionof its own, that has been combined with nicotinicacid to minimize flushing. An ER tablet containing1.0 g nicotinic acid and 20 mg laropiprant is usedin UK and Europe.Dyspepsia is very common; vomiting anddiarrhoea occur when full doses are given. Pepticulcer may be activated.Dryness and hyperpigmentation of skin can betroublesome. Other long-term effects are:Liver dysfunction and jaundice. Serious liverdamage is the most important risk.Hyperglycaemia, precipitation of diabetes (shouldnot be used in diabetics).Hyperuricaemia and gout, atrial arrhythmias.It is contraindicated during pregnancy and inchildren.
Interaction Postural hypotension may occur inpatients on antihypertensives when they takenicotinic acid.Risk of myopathy due to statins is increased.
Dose: Start with 100 mg TDS, gradually increase to2–4 g per day in divided doses. It should be taken justafter food to minimize flushing and itching.NIALIP, NEASYN-SR 375, 500 mg tabs.
Use Nicotinic acid is a wide spectrum hypo-lipidaemic drug. It is highly efficacious inhypertriglyceridaemia (type III, IV, V) whetherassociated with raised CH level or not. It is mostlyused to lower VLDL and raise HDL levels, andas an adjunctive drug to statins/fibrates.
Nicotinic acid is the most effective drug inreducing plasma TG levels. Its most importantindication is to control pancreatitis associated withsevere hypertriglyceridaemia, mostly in genetictype IV and type V disorders. Long-term useprevents further attacks of pancreatitis. Given over

641C
HA
PTE
R 45
HYPOLIPIDAEMIC DRUGS AND PLASMA EXPANDERS
long-term in post-MI patients, it has been foundto reduce recurrences of MI and overall mortality.However, doses above 2 g/day are poorly tolera-ted; should seldom be exceeded for maintenancepurposes. Because of potential toxicity, use ofnicotinic acid is restricted to high-risk cases only.
STEROL ABSORPTION INHIBITOR
Ezetimibe It is a novel drug that acts byinhibiting intestinal absorption of cholesterol andphytosterols. It interferes with a specific CHtransport protein NPC1L1 in the intestinal mucosaand reduces absorption of both dietary and biliaryCH. There is compensatory increase in hepaticCH synthesis, but LDL-CH level is lowered by15–20%. The enhanced CH synthesis can beblocked by statins, and the two drugs havesynergistic LDL-CH lowering effect.
Due to very poor aqueous solubility, ezetimibeis not absorbed as such. A fraction is absorbedafter getting conjugated with glucuronic acid inthe intestinal mucosa. This is secreted in bile andundergoes enterohepatic circulation to be mainlyexcreted in faeces. A plasma t½ of 22 hours hasbeen calculated.
Used alone, ezetimibe is a weak hypocholes-terolaemic drug; LDL-CH lowering beyond15–20% is not obtained by increasing the dose.Though it may be used alone in mild hypercho-lesterolaemia when a statin is contraindicated/nottolerated, its main value is to supplement statinswithout increasing their dose. The combinationof ezetimibe + low dose of a statin is as effectivein lowering LDL-CH as high dose of statin alone.Upto 60% decrease in LDL-CH level has beenobtained with a combination of simvastatin +ezetimibe. The ENHANCE trial has found thatthough addition of ezetimibe to simvastatin furtherdecreased LDL-CH, it caused little reduction incarotid artery intima : media thickness (IMT) ratio,a measure of subintimal CH deposition. Whilethis could be due to the fact that the subjectswere on long-term statin therapy and had relativelylow basal IMT ratio, the actual clinical benefitof adding ezetimibe to a statin needs confirmation.
Another study has found statin + niacin to causegreater reduction in IMT of carotid than statin+ ezetimibe.
No specific adverse effect, except reversiblehepatic dysfunction and rarely myositis has beennoted with ezetimibe.Dose: 10 mg OD; ZETICA, EZEDOC 10 mg tab.BITORVA, LIPIVAS-EZ, LIPONORM-EZ: Atorvastatin10 mg + ezetimibe 10 mg tab; SIMVAS-EZ, STARSTAT-EZ: Simvastatin 10 mg + ezetimibe 10 mg tabs.
CETP-INHIBITORSThe cholesteryl ester transfer protein (CETP) facilitatesexchange of CHEs with TGs between HDL particles andchylomicrons, VLDL, LDL, etc. It plays an important rolein the disposal of HDL-associated CH. Inhibitors of thisprotein, torcetrapib, anacetrapib, etc. markedly raise HDL-CH and lower LDL. They were presumed to haveantiatherosclerotic action. However, during a large randomizedclinical trial, torcetrapib was found to increase cardiovascularevents like angina, MI, heart failure and death. The trialand further development of the drug was stopped in 2007.Whether other CETP inhibitors will have therapeutic valueis being investigated, but appears doubtful.
Summary guidelines on the use ofhypolipidaemic drugsRaised plasma CH is a major risk factor forcoronary artery disease (CAD); higher the CHlevel, greater is the risk of CAD. Abundantdata has confirmed that lowering the level ofLDL-CH, when the same is high, results inlowering of cardiovascular mortality andmorbidity. More recent evidence (HPS, 2002;ASCOT-LLA, 2003 studies) has indicated thatprophylactic use of a statin in CAD/hypertensivepatients even with average or lower than averageCH levels lowers coronary and stroke events. Withthe availability of effective, well tolerated andsafe hypolipidaemic drugs, it has become astandard practice to prescribe statin therapy afteran acute coronary event irrespective of lipid levels.Evidence that elevated plasma TG level or lowplasma HDL-CH level poses independent highrisk of CAD and stroke is also quite strong now.
Whereas raised LDL-CH is atherogenic, ahigher HDL-CH level is either itself protectiveor indicates a low atherogenic state.

642S
EC
TIO
N10
DRUGS AFFECTING BLOOD AND BLOOD FORMATION
The US National Cholesterol EducationProgramme (NCEP) in its third report (2001)delineated the optimal levels of plasma lipids andvarious grades of hyperlipidaemias (Table 45.4)and revised the guidelines for use of hypolipi-daemic drugs (Adult Treatment Panel III orATP III).
Subsequently, the results of some largerandomized controlled trials like HPS (2002,2004), ASCOT-LLA (2003), PROVE-IT (2004)became available and necessitated further revisionof the treatment guidelines. A 2004 revision ofthe ATP III guidelines has been published (Grundyet al, 2004). These guidelines are likely to berevised soon in NCEP-ATPIV. The salient featuresof the current ATPIII guidelines are incorporatedin the following summary.
Lifestyle modification, such as low fat, lowcholesterol diet, limitation of saturated and trans-fats, regular exercise, body weight control,smoking cessation, restriction of alcohol are theprimary approach, whether drugs are used or not.
The decision to prescribe hypolipidaemicdrugs depends not only on the LDL-CH leveland the type of lipid abnormality, but also onassociated CAD risk factor(s) or existing CADor its equivalent like diabetes, peripheral/cerebralvascular disease, etc. in an individual patient (seebox).
Treatment based on LDL-CH level Therevised NCEP-ATP III guidelines are summarizedin Table 45.5. All subjects should receive statin(or statin-based combination) therapy if LDL-CHis ≥ 190 mg/dl. The dose should be titrated toachieve the goal LDL-CH level or 30–40%reduction, which-ever is lower. This degree oflipid lowering has been found to yield optimumprognostic benefit. For subjects who already haveCAD or CAD equivalent, there is no lowerthreshold LDL-CH level; all subjects shouldreceive lipid lowering drug. Though, LDL-CHvalue upto 100 mg/dl is considered optimal for
TABLE 45.4 Interpretation of plasma lipid levels*
Plasma lipid levels (mg/dl)Total CH LDL-CH HDL-CH TGs
1. Optimal/desirable < 200 < 100 > 40 (men) < 150(< 70 for CAD pts) > 50 (women)
2. Borderline high 200–239 130–159 — 150–199
3. High ≥ 240 160–189 > 60 200–499
4. Very high — ≥190 — ≥ 500
* Adopted from NCEP (2001)
1. HPS (2002, 2004): Heart protection study. Lancet (2002) 360, 7-22, and Lancet (2004) 363, 757-767.2. ASCOT-LLA (2003): Anglo-Scandinavian cardiac outcomes trial–Lipid lowering arm. Lancet (2003) 361, 1149-
1158.3. PROVE-IT (2004): Intensive versus moderate lipid lowering with statins after acute coronary syndromes. NEJM
(2004), 350, 1495-1504.4. NCEP-ATP III (2004 revision). Grundy. SM et al. Circulation (2004) 110, 227-239.
Risk factors for coronary artery disease*
• Men > 45 years, women > 55 years• Family history of MI/sudden cardiac death before 55
year (men), 65 year (women) age in first degreerelative
• Smoking• Hypertension (BP > 140/90 or use of anti-
hypertensive medication)• Diabetes mellitus£
• Low HDL-CH (< 40 mg/dl in men, < 50 mg/dl inwomen)
• High LDL-CH (≥ 160 mg/dl) or total CH ≥ 240 mg/dl• Obesity (BMI > 25 Kg/m2)†
or waist > 40″ (men),> 35″ (women)
* Adopted from the NCEP-ATP III (2001)£ Diabetes is considered equivalent to existing CAD† Not included in NCEP guideline (2001)

643C
HA
PTE
R 45
HYPOLIPIDAEMIC DRUGS AND PLASMA EXPANDERS
TABLE 45.5 LDL-CH lowering treatment guidelines*
Risk category LDL-CH goal LDL-CH (mg/dl) level for initiation of(mg/dl) Lifestyle modifications Drug therapy
1. Very high risk <70† All subjects All subjects(CAD/CAD equivalent£ + one$)
2. High risk < 100† All subjects All subjects(CAD/CAD equivalent)
3. Moderately high risk(≥ 2 CAD risk factors + < 130 ≥ 100ψ ≥ 13010 yr CAD risk° 10–20% (or < 100#) (or 100–129#)
4. Moderate risk < 130 ≥ 130ψ ≥ 160(≥ 2 CAD risk factors +10 yr CAD risk° < 10%)
5. Low risk < 160 ≥ 160ψ ≥ 190(0–1 CAD risk factor) (or 160–189#)
* Adopted from the US National Cholesterol Education Programme (NCEP); 2004 revision of adult treatmentpanel III (ATP III)
£ CAD equivalent includes—diabetes mellitus; 10 yr CAD risk > 20%; peripheral vascular disease; abdominal-aortic aneurysm; symptomatic carotid artery disease
$ One additional feature from (i) ≥ 2 CAD risk factors (ii) Single uncontrolled CAD risk factor (iii) diabetesmellitus (iv) metabolic syndrome (v) acute coronary syndrome
° As per risk assessment tables from the Framingham Heart Study† When LDL-CH is near or below the goal value, then a statin dose to lower LDL-CH by 30–40% should
be employed# Patients with a severe risk factor or multiple risk factors.ψ Any subject who has life-style related risk factor(s), such as obesity, physical inactivity, smoking, etc.
is a candidate for life-style change of the risk factor(s) regardless of the LDL-CH level.
non-CAD subjects, the goal for CAD patients hasbeen lowered to 70 mg/dl. These decisions arebased on the findings of recent studies which havecompared mortality as well as CAD and strokeprevention benefits of standard vs intensive CHlowering regimens. Metaanalysis by CholesterolTreatment Trialists collaborators and othersconclude that standard statin therapy loweringLDH-CH by 30–40% reduces cardiovascularevents by 30–35%, while intensive LDL-CHlowering by ~50% curtails cardiovascular eventsby nearly 50%. The JUPITER trial (2008)demonstrated a 44% reduction in combined end-point of stroke, MI, unstable angina andcardiovascular death by using high potencyrosuvastatin. Moreover, the criteria for gradingthe cardiovascular disease risk as ‘very high’ to‘low’ have been defined, and threshold as wellas goal LDL-CH levels have been demarcatedfor each category of risk (see Table 45.5).
The primary drugs to lower LDL-CH arestatins. Statin therapy should be commenced atthe dose estimated to attain target LDL-CHlowering. In case of inadequate response, doseshould be doubled at 6 week intervals (till maxrecommended doses are reached), or another drug(fibrate/nicotinic acid/ezetimibe) should be addedto achieve the target LDL-CH level. Intensivelipid lowering by adequate dose of statin is nowconsidered to imporove endothetial function andstabilize plaques in addition to the antiathero-sclerotic effect; all of these leading to reductionin CAD, stroke and death.
Treatment of low HDL-CH level Epidemio-logical data has shown that most patients withpremature CAD have low HDL-CH level. Thetotal CH: HDL-CH ratio has been recognized asa more important determinant of CAD risk. Whilea ratio of ≤ 3.5 is considered desirable, a ratio

644S
EC
TIO
N10
DRUGS AFFECTING BLOOD AND BLOOD FORMATION
of >4.5 is associated with higher risk. Recenttrials have shown that statin therapy reduces CADendpoints in subjects with low HDL-CH eventhough LDL-CH may be in the normal range.Most low HDL-CH subjects have metabolicsyndrome (obesity, hypertriglyceridaemia, insulinresistance/diabetes, hypertension). Therapydirected towards components of this syndromeoften helps to normalise HDL-CH. In additionto these measures, the primary approach of therapyin subjects with low HDL-CH is to reduceLDL-CH to the target level as per theirLDL-CH risk category or to achieve a total CH:HDL-CH ratio of ≤ 3.5, whichever is moreintensive. This may require reduction of total CHeven to <150 mg/dl and LDL-CH to < 100 mg/dl. None of the currently available lipid modifyingdrugs has a marked effect to raise HDL-CH, butnicotinic acid has the highest efficacy followedby fibrates. These drugs may be usefully combinedwith the statin, watching for signs of myositis.
Treatment of raised TG level: On the basisof metaanalysis of studies, the NCEP have reco-gnized elevated TGs to be an independent CAD
risk factor. Treatment strategy for hypertriglyceri-daemia depends on its cause (obesity, physicalinactivity, smoking, alcohol, high carbohydratediet, diabetes, renal failure, drugs like cortico-steroids, estrogens, high dose β blockers andgenetic disorders) and its severity. Initial treatmentis directed to achieving the target LDL-CH levelappropriate for the patient’s CAD risk category(by using a statin). This may itself lower the TGlevel. The primary TG lowering drugs are fibratesand nicotinic acid. In case of failure to reduceserum TG to < 200 mg/dl, a fibrate (preferablyfenofibrate) or nicotinic acid may be added tothe statin regimen, with extra vigilance to guardagainst the increased risk of myopathy.
PLASMA EXPANDERS
These are high molecular weight substances whichexert colloidal osmotic (oncotic) pressure, andwhen infused i.v. retain fluid in the vascularcompartment. They are used to correct hypo-volemia due to loss of plasma/blood.
Human plasma or reconstituted humanalbumin would seem to be the best. However, theformer carries risk of transmitting serum hepatitis,AIDS, etc., and the latter is expensive. Therefore,synthetic colloids are more often used. Thedesirable properties of a plasma expander aregiven in the box.
Therapeutic intervention for raised TG level
a. Plasma TG < 150 mg/dl (normal)No TG lowering needed; treat as per CH levels
b. Plasma TG 200-499 mg/dl (high)• Lifestyle modification• Treatment of cause if identified• Statin therapy to achieve the goal LDL-CH level
as per CAD risk category• Specific TG lowering drug (fibrate/nicotinic acid)
may be considered if—(i) CAD present(ii) family history of premature CAD(iii) non-HDL-CH ≥ 190 mg/dl(iv) HDL-CH < 40 mg/dl(v) genetic dysbetalipoproteinaemia (type III) or
familial combined hyperlipidaemia (type v)(vi) multiple risk factors present
c. Plasma TG > 500 mg/dl (very high)Vigorous measures to lower TG level needed sincerisk of acute pancreatitis is high• control diabetes and other causes• institute very low fat diet• reduce weight; curtail alcohol• specific TG lowering drugs strongly indicated.
Desirable properties of plasma expander
1. Should exert oncotic pressure comparable toplasma.
2. Should remain in circulation and not leak out intissues, or be too rapidly disposed.
3. Should be pharmacodynamically inert.4. Should not be pyrogenic or antigenic.5. Should not interfere with grouping and cross-
matching of blood.6. Should be stable, easily sterilizable and cheap.
Substances employed are:
Human AlbuminDextranPolygelineHetastarch

645C
HA
PTE
R 45
HYPOLIPIDAEMIC DRUGS AND PLASMA EXPANDERS
Human albumin It is obtained from pooled human plasma;100 ml of 20% human albumin solution is the osmoticequivalent of about 400 ml of fresh frozen plasma or 800 mlof whole blood. It can be used without regard to patient’sblood group and does not interfere with coagulation. Unlikewhole blood or plasma, it is free of risk of transmitting serumhepatitis because the preparation is heat treated. There is alsono risk of sensitization with repeated infusions.
The 20% solution draws and holds additional fluid fromtissues: crystalloid solutions must be infused concurrently foroptimum benefit. Apart from burns, hypovolemia, shock, etc.,it has been used in acute hypoproteinaemia, acute liver failureand dialysis. Dilution of blood using albumin and crystalloidsolutions can be used before cardiopulmonary bypass. Febrilereaction to human albumin occurs occasionally. It is expensive.
Human albumin 20%: ALBUDAC, ALBUPAN 50, 100 ml inj.,ALBUMED 5%, 20% infusion (100 ml)
Dextran It is a polysaccharide obtained from sugar beat,and is available in two forms.
Dextran-70 (MW 70,000): DEXTRAN-70, LOMODEX-70;6% solution in dextrose or saline, 540 ml vac.Dextran-40 (MW 40,000; low MW dextran): LOMODEX10% solution in dextrose or saline, 540 ml vac.
The more commonly used preparation is dextran-70. Itexpands plasma volume for nearly 24 hours, and is slowlyexcreted by glomerular filtration as well as oxidized in thebody over weeks. Some amount is deposited in RE cells.Dextran has nearly all the properties of an ideal plasmaexpander except:(a) It may interfere with blood grouping and cross-matching.(b) Though the dextran used clinically is not antigenic, its
structure is similar to other antigenic polysaccharides.Some polysaccharide reacting antibodies, if present, maycross react with dextran and trigger anaphylactic reaction.Urticaria, itching, bronchospasm, fall in BP occuroccasionally; anaphylactic shock is rare.
(c) It can interfere with coagulation and platelet function,and thus prolong bleeding time; should not be used inhypofibrinogenaemia, thrombocytopenia or in presenceof bleeding.
Dextran-40 It acts more rapidly than dextran-70. It reducesblood viscosity and prevents RBC sludging that occurs inshock by coating them and maintaining their electronegativecharge. Microcirculation may improve. However, it is rapidlyfiltered at the glomerulus: expands plasma volume for a shorterperiod, and may get highly concentrated in the tubule ifoliguria develops—tubular obstruction may occur. The totaldose should not exceed 20 ml/kg in 24 hr.
Dextrans can be stored for 10 years and are cheap. Theyare the most commonly used plasma expanders.
Polygeline (Degraded gelatin polymer) It is apolypeptide with average MW 30,000 which exerts oncoticpressure similar to albumin and is not antigenic;
hypersensitivity reactions are rare, but should be watchedfor. It does not interfere with grouping and cross-matchingof blood and remains stable for three years. It is not metabo-lized in the body; excreted slowly by the kidney. Expansionof plasma volume lasts for 12 hours. It is more expensivethan dextran. It can also be used for priming of heart-lungand dialysis machines.Hypersensitivity reactions like flushing, rigor, urticaria,wheezing and hypotension can occur.HAEMACCEL,SERACCEL 500 ml vac. (as 3.5% solutionin balanced electrolyte medium).
Hetastarch It is a complex mixture of ethoxylatedamylopectin of various molecular sizes; average MW 4.5 lac(range 10,000 to 1 million). The colloidal properties of 6%hetastarch approximate those of human albumin. Plasmavolume expands slightly in excess of the volume infused.Haemodynamic status is improved for 24 hour or more.Hetastarch is incompatible with many drugs; no injectabledrug should be added to the infusion. Blood grouping andcross matching may be vitiated.
Smaller molecules (MW < 50,000) are excreted rapidlyby kidney; 40% of infused dose appears in urine in 24 hr.Larger molecules are slowly broken down to smaller onesand eliminated with a t½ of 17 days.
Adverse effects are vomiting, mild fever, itching, chills,flu like symptoms, swelling of salivary glands. Urticaria,periorbital edema and bronchospasm are the anaphylactoidreactions.
It has also been used to improve harvesting of granu-locytes because it accelerates erythrocyte sedimentation.EXPAN 6% inj (100, 500 ml vac)
USE OF PLASMA EXPANDERSThese colloidal solutions are used primarily assubstitutes for plasma in conditions where plasmahas been lost or has moved to extravascularcompartment, e.g. in burns (acute phase only),hypovolemic and endotoxin shock, severe traumaand extensive tissue damage. They can also beused as a temporary measure in cases of wholeblood loss till the same can be arranged: but theydo not have O2 carrying capacity. Apart fromalbumin, other plasma expanders should not beused for maintenance of plasma volume inconditions like burns, where proteins leakout withfluids for several days.
Contraindications to plasma expanders are—severe anaemia, cardiac failure, pulmonary edema,liver disease, renal insufficiency.

646S
EC
TIO
N10
DRUGS AFFECTING BLOOD AND BLOOD FORMATION
PROBLEM DIRECTED STUDY
45.1 The routine medical checkup of a 50-year-old male, asymptomatic, non-smoker businessexecutive with sendentary job and no family history of premature cardiac death has yieldedthe following findings:
Body mass index—27, waist circumferance—92 cm (38”), BP—130/86 mm Hg, fasting bloodglucose—98 mg/dl, total serum cholesterol (CH) 268 mg/dl, LDL-CH 198 mg/dl, HDL-CH 38 mg/dl, serum triglyceride 160 mg/dl. Liver, kidney and thyroid function test values and ECG are withinnormal limits. There are no remarkable findings on physical examination.(a) Apart from counselling on life-style modification, does this person require any medication?(b) In case he needs medication, which drug and dose would be appropriate? What should
be the goal of drug therapy?(see Appendix-1 for solution)

Drugs for Peptic Ulcer andGastroesophageal Reflux Disease
ChapterChapterChapterChapterChapter 4646464646
SECTION 11
GASTROINTESTINAL DRUGS
PEPTIC ULCER
Peptic ulcer occurs in that part of the gastrointes-tinal tract (g.i.t.) which is exposed to gastric acidand pepsin, i.e. the stomach and duodenum. Theetiology of peptic ulcer is not clearly known.It results probably due to an imbalance betweenthe aggressive (acid, pepsin, bile and H. pylori)and the defensive (gastric mucus and bicarbonatesecretion, prostaglandins, nitric oxide, highmucosal blood flow, innate resistance of the muco-sal cells) factors. A variety of psychosomatic,humoral and vascular derangements have beenimplicated and the importance of Helico-bacter pylori infection as a contributor toulcer formation and recurrence has been reco-gnized.
In gastric ulcer, generally acid secretion isnormal or low, while deficient mucosal defence(mostly impaired mucus and bicarbonatesecretion) plays a greater role. In duodenalulcer, acid secretion is high in about half of thepatients but normal in the rest. Notwithstandingwhether production of acid is normal or high,it does contribute to ulceration as an aggressivefactor, reduction of which is the main approachto ulcer treatment. An understanding of themechanism and control of gastric acid secretion
will elucidate the targets of antisecretory drugaction.
Regulation of gastric acid secretion
The mechanisms operating at the gastric parietal cells aresummarized in Fig. 46.1. The terminal enzyme H+K+ATPase(proton pump) which secretes H+ ions in the apical canaliculiof parietal cells can be activated by histamine, ACh and gastrinacting via their own receptors located on the basolateralmembrane of these cells. Out of the three physiologicalsecretagogues, histamine, acting through H2 receptors, playsthe dominant role, because the other two, gastrin and AChact partly directly and to a greater extent indirectly by releasinghistamine from paracrine enterochromaffin-like (ECL) cellscalled “histaminocytes” located in the oxyntic glands. WhileH2 receptors activate H+K+ATPase by generating cAMP,muscarinic and gastrin/cholecystokinin (CCK2) receptorsappear to function through the phospholipase C → IP3–DAGpathway that mobilizes intracellular Ca2+. The cAMP mediatedproton pump activation also involves Ca2+. The secretomotorresponse to gastrin and cholinergic agonists is expressed fullyonly in the presence of cAMP generated by H2 activation.As such, histamine participates in the acid response to gastrinand ACh at more than one levels, and H2 antagonists suppressnot only histamine, but also ACh, pentagastrin and in factany gastric acid secretory stimulus.
Gastrin is secreted from the antrum in response to risein antral pH, food constituents and vagally mediated reflexesinvolving ganglion cells of the enteric nervous system (ENS).The postganglionic ENS neurones elicit gastrin release fromgastrin secreting ‘G’ cells by elaborating ACh as well as gastrinreleasing peptide (GRP). The dominant muscarinic receptormediating vagal responses is of the M1 subtype. Its location

648S
EC
TIO
N11
GASTROINTESTINAL DRUGS
Figure 46.1: Secretion of HCl by gastric parietal cell and its regulationC.Ase.—Carbonic anhydrase; Hist.—Histamine; ACh.—Acetylcholine; CCK2—Gastrin cholecystokinin receptor;M.—Muscarinic receptor; N—Nicotinic receptor; H2—Histamine H2 receptor; EP3—Prostaglandinreceptor; ENS—Enteric nervous system; ECL cell—Enterochromaffin-like cell; GRP—Gastrin releasing peptide;+ Stimulation; – Inhibition.
on the ganglion cells of the intramural plexuses has beenconfirmed. The parietal cell muscarinic receptor is of the M3
subtype, but the subtype of muscarinic receptor on ECL cellshas not been defined. Vagus releases ACh in close proximityto ECL cells and ‘G’ cells, but apparently at a distance fromthe parietal cells. As such, vagal effects are exerted largelyindirectly through histamine and gastrin.
Prostaglandins have been ascribed a “cytoprotective”role in the gastric mucosa by augmenting mucus andbicarbonate secretion. from gastric mucosal epithelial cells,as well as other actions. Soon after secretion, the gastric mucustransforms into an adherent gell-like film over the mucosawhich traps the secreted HCO3
¯ ions and prevents theirneutralization by creating a barrier for the H+ ions in the juice.
It also sheilds the mucosa from attack by pepsin. PGE2
produced by gastric mucosa, inhibits acid secretion byopposing cAMP generation (in parietal cells) and gastrinrelease (from antral G cells).
Peptic ulcer (especially duodenal) is achronic remitting and relapsing disease lastingseveral years. The goals of antiulcer therapy are:• Relief of pain
• Ulcer healing• Prevention of complications (bleeding, perfo-
ration)• Prevention of relapse.

649C
HA
PTER46
DRUGS FOR PEPTIC ULCER AND G.E.R.D.
Approaches for the treatment of peptic ulcer are:
1. Reduction of gastric acid secretion(a) H2 antihistamines: Cimetidine,
Ranitidine, Famotidine, Roxatidine(b) Proton pump inhibitors: Omeprazole,
Esomeprazole, Lansoprazole,Pantoprazole, Rabeprazole,Dexrabeprazole
(c) Anticholinergic drugs: Pirenzepine,Propantheline, Oxyphenonium
(d) Prostaglandin analogue: Misoprostol
2. Neutralization of gastric acid (Antacids)(a) Systemic: Sodium bicarbonate,
Sod. citrate(b) Nonsystemic: Magnesium hydroxide,
Mag. trisilicate, Aluminium hydroxidegel, Magaldrate, Calcium carbonate
3. Ulcer protectives: Sucralfate, Colloidalbismuth subcitrate (CBS)
4. Anti-H. pylori drugs: Amoxicillin,Clarithromycin, Metronidazole, Tinidazole,Tetracycline
H2 ANTAGONISTS
These are the first class of highly effective drugsfor acid-peptic disease, but have been surpassedby proton pump inhibitors (PPIs). Four H2
antagonists cimetidine, ranitidine, famotidine androxatidine are available in India; many others aremarketed elsewhere. Their interaction with H2
receptors has been found to be competitive incase of cimetidine, ranitidine and roxatidine, butcompetitive-noncompetitive in case of famoti-dine. Cimetidine was the first H2 blocker to beintroduced clinically and is described as theprototype, though other H2 blockers are morecommonly used now.
Pharmacological actions
1. H2 blockade Cimetidine and all other H2
antagonists block histamine-induced gastricsecretion, cardiac stimulation (prominent in
isolated preparations, especially in guinea pig),uterine relaxation (in rat) and bronchial relaxa-tion (H2 blockers potentiate histamine inducedbronchospasm). They attenuate fall in BP dueto histamine, especially the late phase responseseen with high doses. They are highly selective:have no effect on H1 mediated responses or onthe action of other transmitters/autacoids.
2. Gastric secretion The only significant invivo action of H2 blockers is marked inhibitionof gastric secretion. All phases (basal, psychic,neurogenic, gastric) of secretion are suppresseddose-dependently, but the basal nocturnal acidsecretion is suppressed more completely.Secretory responses to not only histamine butall other stimuli (ACh, gastrin, insulin, alcohol,food) are attenuated. This reflects the permissiverole of histamine in amplifying responses toother secretagogues. The volume, pepsin contentand intrinsic factor secretion are reduced, butthe most marked effect is on acid. However,normal vit B12 absorption is not interfered: novit B12 deficiency occurs even after prolongeduse.
The usual ulcer healing doses produce60–70% inhibition of 24 hr acid output. TheH2 blockers have antiulcerogenic effect. Gastriculceration due to stress and drugs (NSAIDs,cholinergic, histaminergic) is prevented. Theydo not have any direct effect on gastric oresophageal motility or on lower esophagealsphincter (LES) tone.
Pharmacokinetics
Cimetidine is adequately absorbed orally, thoughbioavailability is 60–80% due to first passhepatic metabolism. Absorption is not interferedby presence of food in stomach. It crossesplacenta and reaches milk, but penetration inbrain is poor because of its hydrophilic nature.About 2/3 of a dose is excreted unchanged inurine and bile, the rest as oxidized metabolites.The elimination t½ is 2–3 hr. Dose reductionis needed in renal failure.

650S
EC
TIO
N11
GASTROINTESTINAL DRUGS
Adverse effects
Cimetidine is well tolerated by most patients:adverse effects occur in < 5%. These aregenerally mild.• Headache, dizziness, bowel upset, dry mouth, rashes.• Cimetidine (but not other H2 blockers) has antiandrogenic
action (displaces dihydrotestosterone from its cytoplasmicreceptor), increases plasma prolactin and inhibits degra-dation of estradiol by liver. High doses given for longperiods have produced gynaecomastia, loss of libido,impotence and temporary decrease in sperm count.
• Transient elevation of plasma aminotransferases; buthepatotoxicity is rare.
InteractionsCimetidine inhibits several cytochrome P-450isoenzymes and reduces hepatic blood flow. Itinhibits the metabolism of many drugs so thatthey can accumulate to toxic levels, e.g. theophyl-line, phenytoin, carbamazepine, phenobarbitone,sulfonylureas, metronidazole, warfarin, imipra-mine, lidocaine, nifedipine, quinidine. Meta-bolism of propranolol and diazepam is alsoretarded, but this may not be clinically significant.
Antacids reduce absorption of all H2 blockers.When used concurrently a gap of 2 hr shouldbe allowed. Ketoconazole absorption is decreasedby H2 blockers due to reduced gastric acidity.Dose: For ulcer healing—400 mg BD or 800 mg at bed timeorally; maintenance—400 mg at bed time.For stress ulcer—50 mg/hr i.v. infusion. Rapid or higher dosei.v. injection can cause confusional state, hallucinations,convulsions, bradycardia, arrhythmias, coma or cardiac arrest.CIMETIDINE 200 mg, 400 mg, 800 mg tabs, 200 mg/2 ml inj.,LOCK-2 200 mg tab.
Ranitidine A nonimidazole (has a furan ring)H2 blocker, it has several desirable features com-pared to cimetidine:• About 5 times more potent than cimetidine.
Though its pharmacokinetic profile and t½of 2–3 hr is similar to cimetidine, a longerduration of action with greater 24 hr acidsuppression is obtained clinically because ofhigher potency.
• No antiandrogenic action, does not increaseprolactin secretion or spare estradiol fromhepatic metabolism—no effect on malesexual function or gynaecomastia.
• Lesser permeability into the brain: lowerpropensity to cause CNS effects. In fact, littleeffect outside g.i.t. has been observed.
• Less marked inhibition of hepatic metabolismof other drugs; drug interactions mostly haveno clinical relevance.
• Overall incidence of side effects is lower:headache, diarrhoea/constipation, dizzinesshave an incidence similar to placebo.
Dose: for ulcer healing 300 mg at bed time or 150 mg BD;for maintenance 150 mg at bed time. Parenteral dose—50 mgi.m. or slow i.v. inj. every 6–8 hr (rapid i.v. injection can causehypotension), 0.1–0.25 mg/kg/hr by i.v. infusion has been usedfor prophylaxis of stress ulcers. For gastrinoma 300 mg3–4 times a day.ULTAC, ZINETAC 150 mg, 300 mg tabs; HISTAC, RANITIN,ACILOC, RANTAC 150 mg, 300 mg tabs, 50 mg/2 ml inj.
Famotidine A thiazole ring containing H2
blocker which binds tightly to H2 receptors andexhibits longer duration of action despite anelimination t½ of 2.5–3.5 hr. Some inverseagonistic action on H2 receptors (in the absenceof histamine) has been demonstrated. It is5–8 times more potent than ranitidine. Antiandro-genic action is absent. Because of low affinityfor cytochrome P450 and the low dose, drugmetabolism modifying propensity is minimal.
The oral bioavailability of famotidine is40–50%, and it is excreted by the kidney, 70%in the unchanged form. Incidence of adverseeffects is low: only headache, dizziness, bowelupset, rarely disorientation and rash have beenreported. Because of the higher potency andlonger duration, it has been considered moresuitable for ZE syndrome and for prevention ofaspiration pneumonia.Dose: 40 mg at bed time or 20 mg BD (for healing); 20 mgat bed time for maintenance; upto 480 mg/day in ZE syndrome;parenteral dose 20 mg i.v. 12 hourly or 2 mg/hr i.v. infusion.
FAMTAC, FAMONITE, TOPCID 20 mg, 40 mg tabs; FAMOCID,FACID 20, 40 mg tabs, 20 mg/2 ml inj.
Roxatidine The pharmacodynamic, pharmaco-kinetic and side effect profile of roxatidine issimilar to that of ranitidine, but it is twice aspotent and longer acting. It has no antiandro-genic or cytochrome P450 inhibitory action.

651C
HA
PTER46
DRUGS FOR PEPTIC ULCER AND G.E.R.D.
Dose: 150 mg at bed time or 75 mg BD; maintenance 75 mgat bed time.ROTANE, ZORPEX 75 mg, 150 mg SR tabs.
Uses
The H2 blockers are used in conditions in whichit is profitable to suppress gastric acid secretion.Used in appropriate doses, all available agentshave similar efficacy. However, PPIs, becauseof higher efficacy and equally good tolerability,have outstripped H2 blockers.1. Duodenal ulcer H2 blockers produce rapidand marked pain relief (within 2–3 days);60–85% ulcers heal at 4 weeks and 70–95%ulcers at 8 weeks, but they are seldom used nowto heal existing ulcers.
Suppression of nocturnal secretion by singlehigh bed time dose is equally efficacious andphysiologically more sound. About ½ of thepatients relapse within 1 year of healing withH2 blockers. Maintenance therapy with bed timedose reduces the relapse rate to 15–20% peryear as long as given.
2. Gastric ulcer Healing rates obtained ingastric ulcer are somewhat lower (50–75% at8 weeks). However, doses remain the same. H2
blockers can heal NSAID associated ulcers, butare less effective than PPIs or misoprostol.3. Stress ulcers and gastritis Acutelystressful situations like hepatic coma, severeburns and trauma, prolonged surgery, prolongedintensive care, renal failure, asphyxia neona-torum, etc. are associated with gastric erosionsand bleeding. Mucosal ischaemia along with acidis causative. Intravenous infusion of H2 blockerssuccessfully prevents the gastric lesions andhaemorrhage as well as promotes healing oferosions that have occurred.4. Zollinger-Ellison syndrome It is a gastrichypersecretory state due to a rare tumour secre-ting gastrin. H2 blockers in high doses controlhyperacidity and symptoms in many patients, butPPIs are the drugs of choice. Definitive treatmentis surgical.
5. Gastroesophageal reflux disease (GERD)H2 blockers afford symptomatic relief andfacilitate healing of esophageal erosions, but areless effective than PPIs. They are indicated onlyin mild or stage-1 cases of GERD (see p. 659).6. Prophylaxis of aspiration pneumonia H2
blockers given preoperatively (preferably eveningbefore also) reduce the risk of aspiration ofacidic gastric contents during anaesthesia andsurgery.7. Other uses H2 blockers have adjuvantbeneficial action in certain cases of urticaria whodo not adequately respond to an H1 antagonistalone.
PROTON PUMP INHIBITORS (PPIs)
Omeprazole It is the prototype member ofsubstituted benzimidazoles which inhibit the finalcommon step in gastric acid secretion. The PPIshave overtaken H2 blockers for acid-pepticdisorders. The only significant pharmacologicalaction of omeprazole is dose dependent suppres-sion of gastric acid secretion; without anticholi-nergic or H2 blocking action. It is a powerfulinhibitor of gastric acid: can totally abolish HClsecretion, both resting as well as that stimulatedby food or any of the secretagogues, withoutmuch effect on pepsin, intrinsic factor, juicevolume and gastric motility.
Omeprazole is inactive at neutral pH, but atpH < 5 it rearranges to two charged cationicforms (a sulphenic acid and a sulphenamideconfigurations) that react covalently with SHgroups of the H+K+ATPase enzyme and inacti-vate it irreversibly, especially when two mole-cules of omeprazole react with one molecule ofthe enzyme. After absorption into bloodstreamand subsequent diffusion into the parietal cell, itgets concentrated in the acidic pH of thecanaliculi because the charged forms generatedthere are unable to diffuse back. Moreover, itgets tightly bound to the enzyme by covalentbonds. These features and the specific locali-zation of H+K+ATPase to the apical membrane

652S
EC
TIO
N11
GASTROINTESTINAL DRUGS
of the parietal cells confer high degree of selec-tivity of action to omeprazole. Acid secretionresumes only when new H+K+ATPase moleculesare synthesized (reactivation half time 18 hours).It also inhibits gastric mucosal carbonicanhydrase.
Pharmacokinetics All PPIs are administeredorally in enteric coated (e.c.) form to protectthem from molecular transformation in theacidic gastric juice. The e.c. tablet or granulesfilled in capsules should not be broken orcrushed before swallowing. Oral bioavailabilityof omeprazole is ~50% due to acid lability. Asthe gastric pH rises, a higher fraction (up to3/4) may be absorbed. Bioavailability of all PPIsis reduced by food; they should be taken in emptystomach, followed 1 hour later by a meal toactivate the H+K+ ATPase and make it moresusceptible to the PPI. Omeprazole is highlyplasma protein bound, rapidly metabolised inliver by CYP2C19 and CYP3A4 (plasma t½ ~1hr). The metabolites are excreted in urine. Nodose modification is required in elderly or inpatients with renal/hepatic impairment. Becauseof tight binding to its target enzyme—it can bedetected in the gastric mucosa long after itsdisappearance from plasma. As such, inhibitionof HCl secretion occurs within 1 hr, reachesmaximum at 2 hr, is still half maximal at 24 hrand lasts for 2–3 days. Since only actively acidsecreting proton pumps are inhibited, and onlyfew pumps may be active during the brief intervalthat the PPI is present (all have 1–2 hours plasmat½), antisecretory action increases on dailydosing to reach a plateau after 4 days. At steady-state all PPIs produce 80–98% suppression of24 hour acid output with conventional doses.Secretion resumes gradually over 3–5 days ofstopping the drug.
Uses
1. Peptic ulcer: Omeprazole 20 mg OD isequally or more effective than H2 blockers.Relief of pain is rapid and excellent. Fasterhealing has been demonstrated with 40 mg/day:
some duodenal ulcers heal even at 2 weeks andthe remaining (over 90%) at 4 weeks. Gastriculcer generally requires 4–8 weeks. It has causedhealing of ulcers in patients not responding toH2 blockers. Continued treatment (20 mg dailyor thrice weekly) can prevent ulcer relapse. PPIsare an integral component of anti-H. pyloritherapy. PPIs are the drugs of choice for NSAIDinduced gastric/duodenal ulcers. Healing mayoccur despite continued use of the NSAID.However, higher doses given for longer periodsare generally required. When the NSAID cannotbe stopped, it is advisable to switch over to aCOX-2 selective NSAID. Maintenance PPI treat-ment reduces recurrence of NSAID associatedulcer.2. Bleeding peptic ulcer: Acid enhances clotdissolution promoting ulcer bleed. Suppressionof gastric acid has been found to facilitate clotformation reducing blood loss and rebleed. Highdose i.v. PPI therapy (pantoprazole 40–120 mg/day or rabeprazole 40–80 mg/day) profoundlyinhibits gastric acid, and has been shown toreduce rebleeding after therapeutic endoscopy.Even in cases where the bleeding vessel couldnot be visualized, i.v. followed by oral PPIreduces recurrence of bleeding and need forsurgery.3. Stress ulcers: Intravenous pantoprazole/rabeprazole is as effective prophylactic (if notmore) for stress ulcers as i.v. H2 blockers (seep. 651).4. Gastroesophageal reflux disease(GERD): Omeprazole produces more completeround-the-clock inhibition of gastric acidresulting in rapid symptom relief and is moreeffective than H2 blockers in promoting healingof esophageal lesions. PPIs are the drugs ofchoice (see p. 659). Higher doses than for pepticulcer or twice daily administration is generallyneeded.5. Zollinger-Ellison syndrome: Omeprazoleis more effective than H2 blockers in controllinghyperacidity in Z-E syndrome. However, 60–120mg/day or more (in 2 divided doses) is often

653C
HA
PTER46
DRUGS FOR PEPTIC ULCER AND G.E.R.D.
required for healing of ulcers. Inoperable caseshave been treated for >6 years with sustainedbenefit and no adverse effects. Other gastrichypersecretory states like systemic mastocytosis,endocrine adenomas, etc. also respond well.6. Aspiration pneumonia: PPIs are an alter-native to H2 blockers for prophylaxis of aspirationpneumonia due to prolonged anaesthesia.OMIZAC, NILSEC 20 mg cap. OMEZ, OCID, OMEZOL 10, 20mg caps, PROTOLOC 20, 40 mg caps containing enteric coatedgranules. Capsules must not be opened or chewed; to be takenin the morning before meals.
Adverse effects PPIs produce minimaladverse effects. Nausea, loose stools, headache,abdominal pain, muscle and joint pain, dizzinessare complained by 3–5%. Rashes (1.5%incidence), leucopenia and hepatic dysfunctionare infrequent. On prolonged treatment atrophicgastritis has been reported occasionally.
No harmful effects of PPIs during pregnancyare known. Though manufacturers advise to avoid,PPIs have often been used for GERD duringpregnancy.
Because of marked and long-lasting acid suppression,compensatory hypergastrinemia has been observed. Thisinduces proliferation of parietal cells and gastric carcinoidtumours in rats, but not in humans. Though patients havebeen treated continuously for > 11 years without any problem,it may appear prudent to be apprehensive of prolongedachlorhydria and hypergastrinaemia; and if possible, avoidlong-term use of PPIs.
Lately, few reports of gynaecomastia and erectiledysfunction (possibly due to reduced testosterone level) onprolonged use of omeprazole have appeared. Acceleratedosteoporosis among elderly patients (possibly due to reducedcalcium absorption) has been recently associated with high-dose long-term use of PPIs for GERD.
Interactions Omeprazole inhibits oxidation ofcertain drugs: diazepam, phenytoin and warfarinlevels may be increased. It interferes with acti-vation of clopidogrel by inhibiting CYP2C19.Reduced gastric acidity decreases absorption ofketoconazole and iron salts. Clarithromycininhibits omeprazole metabolism and increasesits plasma concentration.
Esomeprazole It is the S-enantiomer ofomeprazole; claimed to have higher oralbioavailability and to produce better control of
intragastric pH than omeprazole in GERDpatients because of slower elimination and longert½. Higher healing rates of erosive esophagitisand better GERD symptom relief have beenreported in comparative trials with omeprazole.Side effect and drug interaction profile is similarto the racemic drug.Dose: 20–40 mg OD; NEXPRO, RACIPER, IZRA 20,40 mg tabs.
Lansoprazole Somewhat more potent thanomeprazole but similar in properties. Inhibitionof H+ K+ ATPase by lansoprazole is partlyreversible. It has higher oral bioavailability, fasteronset of action and slightly longer t½ thanomeprazole. Dose should be reduced in liverdisease. Side effects are similar, but drug inter-actions appear to be less significant; diazepamand phenytoin metabolism may be reduced.Ulcer healing dose: 15–30 mg OD; LANZOL, LANZAP,LEVANT, LANPRO 15, 30 mg caps.
Pantoprazole It is similar in potency andclinical efficacy to omeprazole, but is more acidstable and has higher oral bioavailability. It isalso available for i.v. administration; particularlyemployed in bleeding peptic ulcer and forprophylaxis of acute stress ulcers. Affinity forcytochrome P450 is lower than omeprazole orlansoprazole: risk of drug interactions is minimal.Dose: 40 mg OD; PANTOCID, PANTODAC 20, 40 mgenteric coated tab; PANTIUM , PANTIN 40 mg tab, 40 mg injfor i.v. use.
S-Pantoprazole It is the active single enantio-mer, twice as potent as the racemate.PANPURE, ZOSECTA 20 mg tab.
Rabeprazole This newer PPI is claimed tocause fastest acid suppression. Due to higherpKa, it is more rapidly converted to the activespecies. However, potency and efficacy aresimilar to omeprazole.Dose: 20 mg OD; ZE syndrome — 60 mg/day.RABLET, RABELOC, RABICIP, RAZO, HAPPI 10, 20 mg tab,20 mg/vial inj.
Dexrabeprazole It is the active dextro-isomerof rabeprazole; produces similar acid suppres-sion at half the dose, i.e. 10–20 mg daily.DEXPURE 5, 10 mg tabs.

654S
EC
TIO
N11
GASTROINTESTINAL DRUGS
ANTICHOLINERGICS (See Ch. 8)
Atropinic drugs reduce the volume of gastric juice withoutraising its pH unless there is food in stomach to dilute thesecreted acid. Stimulated gastric secretion is less completelyinhibited. Effective doses (for ulcer healing) of nonselectiveantimuscarinic drugs (atropine, propantheline, oxyphenonium)invariably produce intolerable side effects. Introduction of H2
blockers and PPIs has sent them into oblivion.
Pirenzepine (see p. 117) It is a selective M1 anticholinergicthat has been used in Europe for peptic ulcer. Gastric secretionis reduced by 40–50% without producing intolerable sideeffects, but side effects do occur with slight excess. It hasnot been used in India and USA.
PROSTAGLANDIN ANALOGUE
PGE2 and PGI2 are produced in the gastricmucosa and appear to serve a protective role byinhibiting acid secretion and promoting mucusas well as HCO3̄ secretion (see Ch. 13). Inaddition, PGs inhibit gastrin release, increasemucosal blood flow and probably have an ill-defined “cytoprotective” action. However, themost important appears to be their ability toreinforce the mucus layer covering gastric andduodenal mucosa which is buffered by HCO3 ¯secreted into this layer by the underlyingepithelial cells.
Natural PGs have very short t½. Misoprostol (methyl-PGE1 ester) is a longer acting synthetic PGE1 derivative whichinhibits acid output dose dependently. However, reduction in24 hour acid production is less than H2 blockers because ofshorter duration of action (~3 hr.) Ulcer healing ratescomparable to cimetidine have been obtained in 4–8 weeks,but misoprostol is poorer in relieving ulcer pain. Some patientsmay even complain of increased pain during the first week oftherapy.Dose: 200 µg QID;CYTOLOG 200 µg tab; MISOPROST 100 µg, 200 µg tabs.
Major problems in the use of misoprostol are—diarrhoea,abdominal cramps, uterine bleeding, abortion, and need formultiple daily doses. Patient acceptability is poor.
The primary indication of misoprostol is the preventionand treatment of NSAID associated gastrointestinal injuryand blood loss. However, it is seldom employed now becausePPIs are more effective, more convenient, better tolerated andcheaper.
ANTACIDS
These are basic substances which neutralizegastric acid and raise pH of gastric contents.
Peptic activity is indirectly reduced if the pHrises above 4, because pepsin is secreted as acomplex with an inhibitory terminal moiety thatdissociates below pH 5: optimum peptic activityis exerted between pH 2 to 4.
Antacids do not decrease acid production;rather, agents that raise the antral pH to > 4evoke reflex gastrin release → more acid issecreted, especially in patients with hyperacidityand duodenal ulcer; “acid rebound” occurs andgastric motility is increased.
The potency of an antacid is generallyexpressed in terms of its acid neutralizingcapacity (ANC), which is defined as number ofmEq of 1N HCl that are brought to pH 3.5 in 15min (or 60 min in some tests) by a unit dose ofthe antacid preparation. This takes into considera-tion the rate at which the antacid dissolves andreacts with HCl. This is important because asingle dose of any antacid taken in emptystomach acts for 30–60 min only, since in thistime any gastric content is passed into duodenum.Taken with meals antacids may act for at themost 2–3 hr.
Systemic Antacids
Sodium bicarbonate It is water soluble, acts instan-taneously, but the duration of action is short. It is a potentneutralizer (1 g → 12 mEq HCl), pH may rise above 7. However,it has several demerits:(a) Absorbed systemically: large doses will induce alkalosis.(b) Produces CO2 in stomach → distention, discomfort,
belching, risk of ulcer perforation.(c) Acid rebound occurs, but is usually short lasting.(d) Increases Na+ load: may worsen edema and CHF.
Use of sod. bicarbonate is restricted to casual treatmentof heartburn. It provides quick symptomatic relief. Other usesare to alkalinize urine and to treat acidosis.
Sodium citrate Properties similar to sod. bicarbonate;1 g neutralizes 10 mEq HCl; CO2 is not evolved.
Nonsystemic Antacids
These are insoluble and poorly absorbed basic compounds;react in stomach to form the corresponding chloride salt. Thechloride salt again reacts with the intestinal bicarbonate sothat HCO3
¯ is not spared for absorption—no acid-base distur-bance occurs. However, small amounts that are absorbedhave the same alkalinizing effect as NaHCO3.

655C
HA
PTER46
DRUGS FOR PEPTIC ULCER AND G.E.R.D.
Mag. hydroxide has low water solubility: its aqueoussuspension (milk of magnesia) has low concentration of OH¯
ions and thus low alkalinity. However, it reacts with HClpromptly and is an efficacious antacid (1 g → 30 mEq HCl).Rebound acidity is mild and brief.
MILK OF MAGNESIA 0.4 g/5 ml suspension: 5 ml neutralizes12 mEq acid.
Magnesium trisilicate has low solubility and reactivity;1 g can react with 10 mEq acid, but in clinical use only about1 mEq is neutralized.
About 5% of administered Mg is absorbed systemi-cally—may cause problem if renal function is inadequate. AllMg salts have a laxative action by generating osmoticallyactive MgCl2 in the stomach and through Mg2+ ion inducedcholecystokinin release. Soluble Mg salts are used as osmoticpurgatives.
Aluminium hydroxide gel It is a bland, weak and slowlyreacting antacid. On keeping it slowly polymerizes to variableextents into still less reactive forms. Thus, the ANC of apreparation gradually declines on storage. Also, the productfrom different manufacturers may have differing ANCs; usuallyit varies from 1–2.5 mEq/g. Thus, 5 ml of its suspension mayneutralize just 1 mEq HCl. As such, little worthwhile acidneutralization is obtained at conventional doses.
The Al3+ ions relax smooth muscle. Thus, it delays gastricemptying. Alum. hydrox. frequently, causes constipation dueto its smooth muscle relaxant and mucosal astringent action.
Alum. hydrox. binds phosphate in the intestine andprevents its absorption—hypophosphatemia occurs on regularuse. This may:(a) cause osteomalacia(b) be used therapeutically in hyperphosphatemia andphosphate stones.
Small amount of Al3+ that is absorbed is excreted bykidney. This is impaired in renal failure—aluminium toxicity(encephalopathy, osteoporosis) can occur.ALUDROX 0.84 g tab, 0.6 g/10 ml susp.
Magaldrate It is a hydrated complex of hydroxymagnesiumaluminate that initially reacts rapidly with acid and releasesalum. hydrox. which then reacts more slowly. The freshlyreleased alum. hydrox. is in the unpolymerized more reactiveform. Thus, magaldrate cannot be equated to a physical mixtureof mag. and alum. hydroxides. It is a good antacid with promptand sustained neutralizing action. Its ANC is estimated to be28 mEq HCl/g.STACID 400 mg tab, 400 mg/5 ml susp.; ULGEL 400 mg with20 mg simethicone per tab or 5 ml susp.
Calcium carbonate It is a potent and rapidly acting acidneutralizer (1 g → 20 mEq HCl), but ANC of commercialpreparations is less and variable due to differing particle sizeand crystal structure. Though it liberates CO2 in the stomachat a slower rate than NaHCO3, it can cause distention anddiscomfort. The Ca2+ ions are partly absorbed.
The greatest drawback of CaCO3 as an antacid is that Ca2+
ions diffuse into the gastric mucosa—increase HCl productiondirectly by parietal cells as well as by releasing gastrin. Acidrebound occurs. Mild constipation or rarely loose motionsmay be produced. The absorbed calcium can be dangerousin renal insufficiency.
Milk alkali syndrome In the past, large quantity of milkwas prescribed with CaCO3 (or NaHCO3) for peptic ulcer.Such regimen often produced a syndrome characterized byheadache, anorexia, weakness, abdominal discomfort,abnormal Ca deposits and renal stones due to concurrenthypercalcaemia and alkalosis. It is rare now.
Antacid combinations A combination oftwo or more antacids is frequently used. Thesemay be superior to any single agent on thefollowing accounts:(a) Fast (Mag. hydrox.) and slow (Alum. hydrox.)acting components yield prompt as well assustained effect.(b) Mag. salts are laxative, while alum. salts areconstipating: combination may annul each other’saction and bowel movement may be leastaffected.(c) Gastric emptying is least affected; whilealum. salts tend to delay it, mag./cal. salts tendto hasten it.(d) Dose of individual components is reduced;systemic toxicity (dependent on fractionalabsorption) is minimized.Some available antacid combinations are:ACIDIN: Mag. carb. 165 mg, dried alum. hydrox. gel 232 mg,cal. carb. 165 mg, sod. bicarb. 82 mg, with kaolin 105 mg andbelladonna herb 30 µg per tab.
ALMACARB: Dried alum. hydrox. gel 325 mg, mag. carb. 50mg, methyl polysilox. 40 mg, deglycyrrhizinated liquorice 380mg per tab.
ALLUJEL-DF: Dried alum. hydrox. gel 400 mg, mag. hydrox.400 mg, methyl polysilox. 30 mg per 10 ml susp.
DIGENE: Dried alum. hydrox. gel 300 mg, mag. alum. silicate50 mg, mag. hydrox. 25 mg, methylpolysilox. 10 mg per tab.
DIGENE GEL: Mag. hydrox. 185 mg, alum. hydrox. gel 830 mg,sod. carboxymethyl cellulose 100 mg, methylpolysilox. 25 mgper 10 ml susp.
GELUSIL: Dried alum. hydrox. gel 250 mg, mag. trisilicate 500mg per tab.
GELUSIL LIQUID: Mag. trisilicate 625 mg, alum. hydrox. gel312 mg per 5 ml susp.
MUCAINE: Alum. hydrox. 290 mg, mag. hydrox. 98 mg,oxethazaine 10 mg per 5 ml susp.

656S
EC
TIO
N11
GASTROINTESTINAL DRUGS
TRICAINE-MPS: Alum. hydrox. gel 300 mg, mag. hydrox. 150mg, oxethazaine 10 mg, simethicone 10 mg per 5 ml gel.
MAYLOX: Dried alum. hydrox. gel 225 mg, mag. hydrox. 200mg, dimethicone 50 mg per tab and 5 ml susp.
POLYCROL FORTE GEL: Mag. hydrox. 100 mg, dried alum.hydrox. gel 425 mg, methylpolysilox. 125 mg per 5 ml susp.
Drug interactions By raising gastric pH andby forming complexes, the non-absorbableantacids decrease the absorption of many drugs,especially tetracyclines, iron salts, fluoroquino-lones, ketoconazole, H2 blockers, diazepam, phe-nothiazines, indomethacin, phenytoin, isoniazid,ethambutol and nitrofurantoin. Stagger theiradministration by 2 hours. The efficacy ofnitrofurantoin is also reduced by alkalinizationof urine.Uses Antacids are no longer used for healingpeptic ulcer, because they are needed in largeand frequent doses, are inconvenient, can causeacid rebound and bowel upset, afford littlenocturnal protection and have poor patientacceptability. Antacids are now employed onlyfor intercurrent pain relief and acidity, mostlyself-prescribed by the patients as over thecounter preparations. They continue to be usedfor nonulcer dyspepsia and minor episodes ofheartburn.Gastroesophageal reflux Antacids affordfaster symptom relief than drugs which inhibitacid secretion, but do not provide sustainedbenefit. May be used off and on for acideructation and heartburn.
ULCER PROTECTIVES
Sucralfate It is a basic aluminium salt of sulfated sucrose;a drug of its own kind. Sucralfate polymerizes at pH < 4 bycross linking of molecules, assuming a sticky gel-likeconsistency. It preferentially and strongly adheres to ulcerbase, especially duodenal ulcer; has been seen endoscopicallyto remain there for ~ 6 hours. Surface proteins at ulcer baseare precipitated, together with which it acts as a physicalbarrier preventing acid, pepsin and bile from coming in contactwith the ulcer base. Dietary proteins get deposited on thiscoat, forming another layer.
Sucralfate has no acid neutralizing action, but delaysgastric emptying—its own stay in stomach is prolonged.Augmented gastric mucosal PG synthesis may supplementphysical protective action of sucralfate.
Sucralfate is minimally absorbed after oral administration.Its action is entirely local. It promotes healing of both duo-denal and gastric ulcers. Healing efficacy has been foundsimilar to cimetidine at 4 weeks, and may be superior inpatients who continue to smoke. However, sucralfate isinfrequently used now because of need for 4 large well-timeddaily doses and the availability of simpler and more effectiveH2 blockers/PPIs.
Dose: The ulcer healing dose of sucralfate is 1 g taken inempty stomach 1 hour before the 3 major meals and at bedtime for 4–8 weeks. Antacids should not be taken with sucralfatebecause its polymerization is dependent on acidic pH.ULCERFATE, SUCRACE, RECULFATE 1 g tab.
Side effects are few; constipation is reported by 2% patients.It has potential for inducing hypophosphatemia by bindingphosphate ions in the intestine. Dry mouth and nausea areinfrequent.
Other uses Bile reflux, gastritis and prophylaxis of stressulcers.
In intensive care units, acid suppressant (with i.v./intragastric H2 blocker/PPI) prophylaxis of stress ulcers isalmost routinely used now. This practice is considered tocontribute to occurrence of pneumonia due to overgrowthof bacteria in the stomach. Intragastric sucralfate provideseffective prophylaxis of stress ulcers without acid suppression,and is an alternative to i.v. H2 blocker/PPI..As a suspension in glycerol, it has been tried in stomatitis.
A topical formulation of sucralfate PEPSIGARD LIGHTGEL is available for application on burns, bedsores, diabetic/radiation ulcers, excoriated skin, etc. as a protective.
Interactions Sucralfate adsorbs many drugs and interfereswith the absorption of tetracyclines, fluoroquinolones,cimetidine, phenytoin and digoxin. Antacids given concur-rently reduce the efficacy of sucralfate.
Colloidal bismuth subcitrate (CBS; Tripotassiumdicitratobismuthate)
It is a colloidal bismuth compound; water soluble butprecipitates at pH < 5. It is not an antacid but heals 60%ulcers at 4 weeks and 80–90% at 8 weeks. The mechanism ofaction of CBS is not clear; probabilities are:• May increase gastric mucosal PGE2, mucus and HCO3
¯
production.• May precipitate mucus glycoproteins and coat the ulcer
base.• May detach and inhibit H.pylori directly.
Gastritis and nonulcer dyspepsia associated with H. pylori arealso improved by CBS. The regimen for CBS is 120 mg (asBi2O3) taken ½ hr before 3 major meals and at bedtime for 4–8weeks. Milk and antacids should not be taken concomitantly.TRYMO, DENOL 120 mg tab.
Most of the ingested CBS passes in the faeces. Small amountsabsorbed are excreted in urine. Side effects are diarrhoea,headache and dizziness. Patient acceptance of CBS is

657C
HA
PTER46
DRUGS FOR PEPTIC ULCER AND G.E.R.D.
compromised by blackening of tongue, dentures and stools;and by the inconvenience of dosing schedule. Presently, it isused occasionally as a component of triple drug anti-H. pyloriregimen.
ANTI-HELICOBACTER PYLORI DRUGS
H. pylori is a gram negative bacillus uniquelyadapted to survival in the hostile environment ofstomach. It attaches to the surface epitheliumbeneath the mucus, has high urease activity—produces ammonia which maintains a neutralmicroenvironment around the bacteria, andpromotes back diffusion of H+ ions. It has beenfound as a commensal in 20–70% normalindividuals, and is now accepted as an importantcontributor to the causation of chronic gastritis,dyspepsia, peptic ulcer, gastric lymphoma andgastric carcinoma. H. pylori infection starts witha neutrophilic gastritis lasting 7–10 days whichis usually asymptomatic. Once established,H. pylori generally persists for the life of thehost. Up to 90% patients of duodenal and gastriculcer have tested positive for H. pylori.
Eradication of H. pylori concurrently withH2 blocker/PPI therapy of peptic ulcer has beenassociated with faster ulcer healing and largelyprevents ulcer relapse. All H. pylori positiveulcer patients should receive H. pylori eradi-cation therapy. In the absence of H. pyloritesting, all cases with failed conventional ulcertherapy and relapse cases must be given thebenefit of H. pylori eradication.
Antimicrobials that are used clinically againstH. pylori are: amoxicillin, clarithromycin, tetra-
cycline and metronidazole/tinidazole. However,any single antibiotic is ineffective. Resistancedevelops rapidly, especially to metronidazole/tinidazole and clarithromycin, but amoxicillinresistance is infrequent. In tropical countries,metronidazole resistance is more common thanclarithromycin resistance. Since bismuth (CBS)is active against H. pylori and resistance doesnot develop to it, combination regimens includingbismuth may be used in case of metronidazoleand clarithromycin double resistance. Routineuse of CBS is precluded by poor patient accepta-bility. Acid suppression by PPIs/H2 blockersenhances effectiveness of anti-H. pylori anti-biotics, and optimum benefits are obtained whengastric pH is kept >5 for at least 16–18 hoursper day. This is a higher degree of round-the-clock acid suppression than is needed forduodenal ulcer healing or for reflux esophagitis.Only twice daily PPI dosing can achieve thisdegree of acid suppression. The PPIs benefit byaltering the acid environment for H. pylori aswell as by direct inhibitory effect. One of thePPIs is an integral component of all anti-H.pylori regimens along with 2 (triple drug) or3 (quadruple drug) antimicrobials.
A number of 3 drug regimens of 1 or 2 weeksare being used. One week regimens are adequatefor many patients, but 2 week regimens achievehigher (upto 96%) eradication rates, thoughcompliance is often poor due to side effects.Some commonly used 1 week and 2 weeks tripledrug regimens are given in the box.
Anti-H. pylori Regimens*
Proton pump inhibitor Amoxicillin Clarithromycin Metronidazole/Tinidazole
One week-twice dailyOmeprazole (20 mg) or 1.0 g 500 mg —Esomeprazole (20 mg) or — 250 mg 400 mg/500 mgLansoprazole (30 mg) or 1.0 g — 400 mg/500 mgPantoprazole (40 mg) orRabeprazole (20 mg)
Two weeks-twice dailyOmeprazole (20 mg) or 750 mg — 400 mg/500 mgLansoprazole (30 mg) or — 250 mg 400 mg/500 mgPantoprazole (40 mg) 750 mg 500 mg —
* Adopted from British National Formulary (BNF) Sept. 2010

658S
EC
TIO
N11
GASTROINTESTINAL DRUGS
The US-FDA approved regimen is:Lansoprazole 30 mg + Amoxicillin 1000 mg+ clarithromycin 500 mg, all given twice dailyfor 2 weeks.
This has achieved 86–92% eradication rate.Better tolerability of regimens which exclude anitroimidazole favour using amoxicillin +clarithromycin + PPI, particularly in India wheremetronidazole resistance is more prevalent.However, for the sake of simplicity and economy,the National Formulary of India (NFI, 2010)suggests a model H. pylori eradication regimenof 1 week consisting of:• Omeprazole 40 mg OD + Metronidazole 400
mg TDS + Amoxicillin 500 mg TDS.For large ulcers (> 10 mm in diameter) or thosecomplicated by bleeding/perforation, the PPIshould be continued beyond the 2 weeks-tripledrug regimen till complete healing occurs. Forpatients who have, in the near past, received anitroimidazole (for other infections) or a macro-lide antibiotic, metronidazole or clarithromycin,as the case may be, should be excluded.
Quadruple therapy with CBS 120 mg QID +tetracycline 500 mg QID + metronidazole 400mg TDS + omeprazole 20 mg BD is advocatedfor eradication failure cases.
All regimens are complex and expensive, sideeffects are frequent and compliance is poor.Higher failure rates (20–40%) of H. pylorieradication have been reported from India. Also,5 year recurrence rate of H. pylori infection ishigher. Three week treatment is being advocatedby some. Nevertheless, long-term benefits ofanti-H. pylori therapy include lowering of ulcerdisease prevalence and prevention of gastriccarcinoma/lymphoma; but benefits in nonulcerdyspepsia are equivocal.
H. pylori vaccines are under development.Some available anti-H. pylori kits (one kit to be taken dailyin 2 doses)HP-KIT, HELIBACT, OMXITIN: Omeprazole 20 mg 2 cap +Amoxicillin 750 mg 2 tab + Tinidazole 500 mg 2 tab.PYLOMOX: Lansoprazole 15 mg 2 cap + Amoxicillin 750 mg2 tab + Tinidazole 500 mg 2 tab.LANSI KIT: Lansoprazole 30 mg 1 cap + Amoxicillin 750 mg1 tab + Tinidazole 500 mg 1 tab (one kit twice a day)
PYLOKIT, HELIGO: Lansoprazole 30 mg 2 cap + Clarithromycin250 mg 2 cap + Tinidazole 500 mg 2 tab.LANPRO AC: Lansoprazole 30 mg 2 cap + Clarithromycin250 mg 2 tab + Amoxicillin 750 mg 2 tab.
GASTROESOPHAGEAL REFLUXDISEASE (GERD)
Reflux is a very common problem presenting as‘heart-burn’, acid eructation, sensation ofstomach contents coming back in the foodpipe,especially after a large meal, aggravated bystooping or lying flat. Some cases have ananatomical defect (hiatus hernia) but majorityare only functional, wherein there is relaxationof lower esophageal sphincter (LES) in theabsence of swallowing. Repeated reflux of acidgastric contents into lower 1/3rd of esophaguscauses esophagitis, erosions, ulcers, pain onswallowing, dysphagia, strictures, and increasesthe risk of esophageal carcinoma.There may alsobe extraesophageal complications.The primary barrier to reflux is the tone of LES which can bealtered by several influences:Inherent tone: of sphincteric smooth muscle.Hormonal: gastrin increases, progesterone decreases (reflux
is common in pregnancy).Neurogenic: vagus is motor to the sphincter, promotes
esophageal peristalsis.Dietary: fats, alcohol, coffee, chocolates decrease, while
protein rich foods increase LES tone.Drugs: anticholinergics, tricyclic antidepressants, Ca2+ channel
blockers, nitrates reduce LES tone.Smoking: relaxes LES.
Delayed gastric emptying and increasedintragastric pressure may overcome the LESbarrier to reflux. GERD is a wide spectrum ofconditions from occasional heartburn (majority ofcases) to persistent incapacitating reflux whichinterferes with sleep and results in esophageal,laryngotracheal and pulmonary complications.Severity of GERD may be graded as:
Stage 1: occasional heartburn (<3 episodes/week), mostly only in relation to a precipitatingfactor, mild symptoms, no esophageal lesions.
Stage 2: > 3 episodes/week of moderatelysevere symptoms, nocturnal awakening due toregurgitation, esophagitis present or absent.

659C
HA
PTER46
DRUGS FOR PEPTIC ULCER AND G.E.R.D.
Stage 3: Daily/chronic symptoms, disturbedsleep, esophagitis/erosions/stricture/extraeso-phageal symptoms like laryngitis, hoarseness, drycough, asthma. Symptoms recur soon aftertreatment stopped.
Though GERD is primarily a g.i. motilitydisorder, acidity of gastric contents is the mostimportant aggressive factor in causing symptomsand esophageal lesions. The functional abnor-mality is persistent; though short-term remis-sions do occur. Dietary and other lifestylemeasures (light early dinner, raising head end ofbed, weight reduction and avoidance ofprecipitating factors) must be taken.
Treatment of GERD is individualized accor-ding to severity and stage of the disorder.
The site and mechanism of benefit affordedby different classes of drugs in GERD isdepicted in Fig. 46.2.1. Proton pump inhibitors (PPIs) These arethe most effective drugs, both for symptomaticrelief as well as for healing of esophageal lesions.
Intragastric pH >4 maintained for ~18 hr/day isconsidered optimal for healing of esophagitis.This level of acid suppression can be consistentlyachieved only by PPIs. Therefore, PPIs are thedrugs of choice for patients with all stages ofGERD, particularly stage 2 and 3 cases. Symptomrelief is rapid and 80–90% esophageal lesionsheal in 4–8 weeks. Dose titration is neededaccording to response in individual patients. Somepatients, especially stage 2 and 3 cases, need twicedaily dosing. Prolonged (often indefinite) therapyis required in chronic cases because symptomsrecur a few days after drug stoppage. PPIs have noeffect on LES tone.2. H2 blockers They reduce acidity of gastriccontents and have no effect on LES tone. H2
blockers cause less complete acid suppressionthan PPIs, viz elevate intragastric pH to >4 forless than 8 hours in 24 hours with theconventional doses given twice daily. Adequatesymptom relief is obtained only in mild cases;healing of esophagitis may occur in 50–70%patients. H2 antagonists are indicated in stage-1cases, or as alternative to PPIs in stage 2 or 3cases. The daily dose should be divided into2–3 portions for better response.3. Antacids Their use in GERD is limited tooccasional or intercurrent relief of heartburnbecause they act within few minutes. Antacidsare no longer employed for healing ofesophagitis, which they are incapable of.4. Sodium alginate It forms a thick frothy layer whichfloats on the gastric contents like a raft may prevent contactof acid with esophageal mucosa. It has no effect on LES tone.Combination of alginate with antacids may be used in placeof antacids alone, but real benefit is marginal.REFLUX LIQUID: Sod. alginate 200 mg + alum. hydrox. gel300 mg + mag. trisilicate 125 mg/10 ml susp; REFLUX FORTEAginic acid 20 mg + sod. bicarb. 70 mg + alum. hydrox. 300mg tab; GAVISCON Alginic acid 500 mg + mag. trisilicate 25mg + alum. hydrox. gel 100 mg + sod. bicarb. 170 mg tab.
5. Prokinetic drugs Metoclopramide, cisa-pride and other prokinetic drugs may relieveregurgitation and heartburn by increasing LEStone, improving esophageal clearance andfacilitating gastric emptying, but do not affectgastric acidity or promote healing of esophagitis.
Figure 46.2: Sites and mechanisms of drug action ingastroesophageal reflux disease.
Metoclopramide increases lower esophageal sphincter(LES) tone and promotes gastric emptying. Proton pumpinhibitor (PPI) and H2 blocker (H2B) inhibit acid secretion,while antacids neutralize it. Alginate floats on gastriccontents and prevents contact of esophageal mucosa withgastric acid

660S
EC
TIO
N11
GASTROINTESTINAL DRUGS
Symptom control afforded by prokinetic drugsis much inferior to that by PPIs/H2 blockers.Their use in GERD has declined. Prokinetic
PROBLEM DIRECTED STUDY
46.1 A 45-year-old male patient presents with dyspepsia and dull epigastric pain which hasbeen worsening gradually over the last one month. The pain is partly relieved by food, butbecomes worse after 2 hours or so. Heart burn and pain which awakens him is often feltat night. Epigastric tenderness is detected on palpation. Upper gastrointestinal endoscopy revealsan ulcer measuring 12 mm X 18 mm in the 1st part of duodenum. His medical records showthat he suffered similar episode of pain about 9 months ago. No endoscopy was done, buthe was treated with omeprazole 20 mg OD for 6 weeks. Subsequently, nearly 3 months back,he suffered from loose motions and abdominal pain which was treated with a 5 day courseof metronidazole + norfloxacin. Facility for H. pylori testing is not available. There is no historyof NSAID use.(a) What would be the most appropriate treatment option for him to achieve fast symptomrelief, ulcer healing and prevention of further recurrences?(see Appendix-1 for solution)
drugs are often coprescribed with PPI/H2 blockertherapy, but whether this improves outcome isnot clear.

Antiemetic, Prokinetic andDigestant Drugs
ChapterChapterChapterChapterChapter 4747474747
Emesis Vomiting occurs due to stimulation ofthe emetic (vomiting) centre situated in the medullaoblongata. Multiple pathways can elicit vomiting(Fig. 47.1). The chemoreceptor trigger zone (CTZ)located in the area postrema and the nucleus tractussolitarius (NTS) are the most important relay areasfor afferent impulses arising in the g.i.t, throat andother viscera. The CTZ is also accessible to blood-borne drugs, mediators, hormones, toxins, etc.because it is unprotected by the blood-brain barrier.Cytotoxic drugs, radiation and other g.i. irritantsrelease 5-HT from enterochromaffin cells → actson 5-HT3 receptors present on extrinsic primaryafferent neurones (PAN) of the enteric nervoussystem (ENS). These neurones connect with vagaland spinal visceral afferents to send impulses toNTS and CTZ. Released in large quantity, 5-HTmay also spill into circulation and reach CTZ viathe vascular route. 5-HT may as well be releasedfrom platelets by inflammatory mediators.However, 5-HT is not the only mediator of suchsignals: many peptides, e.g. substance P and othermessengers are also involved.
The CTZ and NTS express a variety of recep-tors, e.g. histamine H1, dopamine D2, serotonin5-HT3, cholinergic M, neurokinin NK1 (activatedby substance P), cannabinoid CB1 and opioid µreceptors through which the emetic signals arerelayed and which could be targets of antiemeticdrug action.
The vestibular apparatus generates impulseswhen body is rotated or equilibrium is disturbedor when ototoxic drugs act. These impulses reachthe vomiting centre mainly relayed from thecerebellum and utilize muscarinic as well as H1receptors. Various unpleasant sensory stimuli suchas bad odour, ghastly sight, severe pain as well asfear, recall of an obnoxious event, anticipation ofan emetic stimulus (repeat dose of cisplatin) causenausea and vomiting through higher centres.
Nausea is accompanied by reduced gastrictone and peristalsis. In the emetic response fun-dus and body of stomach, esophageal sphincterand esophagus relax, glottis closes, whileduodenum and pyloric stomach contract in aretrograde manner. Rhythmic contractions ofdiaphragm and abdominal muscles then compressthe stomach and evacuate its contents via themouth. Conditions that inhibit gastric emptyingpredispose to vomiting.
EMETICS
These are drugs used to evoke vomiting.1. Act on CTZ : Apomorphine2. Act reflexly and on CTZ : IpecacuanhaVomiting needs to be induced only when an undesirablesubstance (poison) has been ingested. Powdered mustardsuspension or strong salts solution may be used in emergency.They act reflexly by irritating the stomach.
Apomorphine It is a semisynthetic derivative of morphine;acts as a dopaminergic agonist on the CTZ. Injected i.m./s.c.in a dose of 6 mg, it promptly (within 5 min) induces vomiting.It should not be used if respiration is depressed, because ithas inherent respiratory and CNS depressant actions. Oraluse of apomorphine is not recommended because the emeticdose is larger, slow to act and rather inconsistent in action.
Apomorphine has a therapeutic effect in parkinsonism,but is not used due to side effects.
Ipecacuanha The dried root of Cephaelis ipecacuanhacontains emetine and is used as syrup ipecac (15–30 ml inadults, 10–15 ml in children, 5 ml in infants) for inducingvomiting. It is less dependable than parenteral apomorphineand takes 15 min or more for the effect, but is safer; has beenused as a household remedy. It acts by irritating gastric mucosaas well as through CTZ.
All emetics are contraindicated in:(a) Corrosive (acid, alkali) poisoning: risk of
perforation and further injury to esophagealmucosa.
(b) CNS stimulant drug poisoning: convulsionsmay be precipitated.

662S
EC
TIO
N11
GASTROINTESTINAL DRUGS
Fig. 47.1: Major central and visceral structures involved in emesis and the neurohumoral receptors mediatingthe emetic response.NTS–Nucleus tractus solitarius; VC–Vomiting centre; CTZ—Chemoreceptor trigger zone; 5-HT3–5-HT3 receptor;H1–Histamine H1 receptor; D2–Dopamine 2 receptor; M–Muscarinic receptor; NK1–Neurokinin1 receptor;CB1–Cannabinoid 1 receptor
(c) Kerosine (petroleum) poisoning: chances ofaspiration of the liquid (due to low viscosity)and chemical pneumonia are high.
(d) Unconscious patient: may aspirate thevomitus, because laryngeal reflex is likelyto be impaired.
(e) Morphine or phenothiazine poisoning:emetics may fail to act.
ANTIEMETICSThese are drugs used to prevent or suppressvomiting.
CLASSIFICATION
1. Anticholinergics Hyoscine, Dicyclomine2. H1 antihistaminics Promethazine,
Diphenhydramine,Dimenhydrinate,Doxylamine,Meclozine (Meclizine),Cinnarizine.
3. Neuroleptics Chlorpromazine,(D2 blockers) Triflupromazine,
Prochlorperazine,Haloperidol, etc.

663C
HA
PTE
R47
ANTIEMETIC, PROKINETIC AND DIGESTANT DRUGS
4. Prokinetic drugs Metoclopramide,Domperidone,Cisapride, Mosapride,Itopride
5. 5-HT3 antagonists Ondansetron,Granisetron,Palonosetron,Ramosetron
6. NK1 receptor Aprepitant,antagonists Fosaprepitant
7. Adjuvant Dexamethasone,antiemetics Benzodiazepines,
Dronabinol, Nabilone
ANTICHOLINERGICS (See Ch. 8)
Hyoscine (0.2–0.4 mg oral, i.m.) is the mosteffective drug for motion sickness. However, ithas a brief duration of action; produces sedation,dry mouth and other anticholinergic side effects;suitable only for short brisk journies. Antiemeticaction is exerted probably by blocking conductionof nerve impulses across a cholinergic link in thepathway leading from the vestibular apparatus tothe vomiting centre and has poor efficacy invomiting of other etiologies.
A transdermal patch containing 1.5 mg of hyoscine, tobe delivered over 3 days has been developed. Applied behindthe pinna, it suppresses motion sickness while producingonly mild side effects.
Dicyclomine (10–20 mg oral) has been usedfor prophylaxis of motion sickness and formorning sickness. It has been cleared ofteratogenic potential.
H1 ANTIHISTAMINICS (See Ch. 11)Some antihistaminics are antiemetic. They areuseful mainly in motion sickness and to a lesserextent in morning sickness, postoperative andsome other forms of vomiting. Their antiemeticeffect appears to be based on anticholinergic,antihistaminic, weak antidopaminergic andsedative properties.
Promethazine, diphenhydramine, dimenhydri-nate These drugs afford protection of motionsickness for 4–6 hours, but produce sedation anddryness of mouth. By their central anticholinergic
action they block the extrapyramidal side effectsof metoclopramide while supplementing its anti-emetic action. Promethazine is a phenothiazine;has weak central antidopaminergic action as well.Their combination has been used in chemotherapyinduced nausea and vomiting (CINV).
Promethazine theoclate (AVOMINE 25 mg tab.)This salt of promethazine has been speciallypromoted as an antiemetic, but the action doesnot appear to be significantly different frompromethazine HCl.
Doxylamine It is a sedative H1 antihistaminicwith prominent anticholinergic activity. Marketedin combination with pyridoxine, it is specificallypromoted in India for ‘morning sickness’ (vomitingof early pregnancy), although such use is not madein UK and many other countries.After over 2 decades of worldwide use of a combinationproduct of doxylamine for morning sickness, some reportsof foetal malformation appeared and the product waswithdrawn in 1981. Subsequent studies have both supportedand refuted its teratogenic potential. Though the US-FDAand CSM in UK found no credible evidence of increasein birth defects, they did not rule out the possibility. Theproduct remained suspended in these countries, probably toavoid litigation, but not due to safety or efficacy concerns.Recently, the American College of Obstetricians andGynaecologists have recommended a combination ofdoxylamine + pyridoxine as first line treatment of morningsickness. However, it is still not used in U.K.Oral absorption of doxylamine is slow, and itst½ is 10 hr. The side effects are drowsiness, drymouth, vertigo and abdominal upset.Dose: 10–20 mg at bed time; if needed additional dosesmay be given in morning and afternoon.DOXINATE, GRAVIDOX, VOMNEX, NOSIC 10 mg withpyridoxine 10 mg tab.
Meclozine (meclizine) It is less sedative andlonger-acting; protects against sea sickness fornearly 24 hours.DILIGAN: meclozine 12.5 mg + nicotinic acid 50 mg tab;PREGNIDOXIN: meclozine 25 mg + caffeine 20 mg tab.
Cinnarizine It is an antivertigo drug havingantimotion sickness property. It probably actsby inhibiting influx of Ca2+ from endolymph intothe vestibular sensory cells which mediateslabyrinthine reflexes.

664S
EC
TIO
N11
GASTROINTESTINAL DRUGS
Motion sickness Antiemetics with anticholiner-gic-antihistaminic property are the first choicedrugs for motion sickness. Antidopaminergic andanti-HT3 drugs are less effective. All antimotionsickness drugs act better when taken ½–1 hourbefore commencing journey. Once sickness hasstarted, it is more difficult to control; higher doses/parenteral administration may be needed.
Morning sickness The antihistaminics aresuspected to have teratogenic potential, but thereis no conclusive proof. Nevertheless, it is betterto avoid them for morning sickness. Most casesof morning sickness can be managed by reas-surance and dietary adjustment. If an antiemetichas to be used, dicyclomine, promethazine,prochlorperazine or metoclopramide may beprescribed in low doses.
NEUROLEPTICS (see Ch. 32)
The older neuroleptics (phenothiazines, halo-peridol) are potent antiemetics; act by blockingD2 receptors in the CTZ; antagonize apomor-phine induced vomiting and have additionalantimuscarinic as well as H1 antihistaminicproperty. They have broad spectrum antiemeticaction effective in:
(a) Drug induced and postoperative nausea andvomiting (PONV).
(b) Disease induced vomiting: gastroenteritis,uraemia, liver disease, migraine, etc.
(c) Malignancy associated and cancer chemo-therapy (mildly emetogenic) inducedvomiting.
(d) Radiation sickness vomiting (less effective).(e) Morning sickness: should not be used except
in hyperemesis gravidarum.Neuroleptics are less effective in motion sickness:the vestibular pathway does not involve dopami-nergic link.
Most of these drugs produce significant degreeof sedation. Acute muscle dystonia may occurafter a single dose, especially in children andgirls. The antiemetic dose is generally much lowerthan antipsychotic doses. These agents should not
be administered until the cause of vomiting hasbeen diagnosed; otherwise specific treatment ofconditions like intestinal obstruction, appendicitis,etc. may be delayed due to symptom relief.
Prochlorperazine This D2 blocking phenothia-zine is a labyrinthine suppressant, has selectiveantivertigo and antiemetic actions. It is highlyeffective when given by injection in vertigoassociated vomiting, and to some extent in CINV.Prochlorperazine is used as an antiemetic, but notas antipsychotic. Muscle dystonia and other extra-pyramidal side effects are the most importantlimiting features.Dose: 5–10 mg BD/TDS oral, 12.5–25 mg by deep i.m.injection.STEMETIL 5 mg tabs., 12.5 mg/ml inj, 1 ml amp, VOMTIL5 mg tab.
PROKINETIC DRUGS
These are drugs which promote gastrointestinaltransit and speed gastric emptying by enhancingcoordinated propulsive motility. This excludestraditional cholinomimetics and anti-ChEs whichproduce tonic and largely uncoordinatedcontraction.
MetoclopramideMetoclopramide, a substituted benzamide, ischemically related to procainamide, but has nopharmacological similarity with it. Introduced inearly 1970s as a ‘gastric hurrying’ agent, it is acommonly used antiemetic.
Actions
GIT: Metoclopramide has more prominent effecton upper g.i.t.; increases gastric peristalsis whilerelaxing the pylorus and the first part of duodenum→ speeds gastric emptying, especially if it wasslow. This action is independent of vagalinnervation, but is stronger when vagus is intact.Lower esophageal sphincter (LES) tone isincreased and gastroesophageal reflux is opposed.It also increases intestinal peristalsis to someextent, but has no significant action on colonicmotility and gastric secretion.

665C
HA
PTE
R47
ANTIEMETIC, PROKINETIC AND DIGESTANT DRUGS
Fig. 47.2: Schematic depiction of seronergic (5-HT)regulation of peristaltic reflex, and sites of action ofprokinetic drugs.
Distention and other luminal stimuli trigger 5-HT releasefrom the enterochromaffin cells (EC) located in the entericmucosa. This stimulates intrinsic and extrinsic primaryafferent neurones (PAN) of the enteric nervous system(ENS) through peripheral variant of 5-HT1 receptor (5-HT1PR) and 5-HT3 receptor (5-HT3R). The extrinsic PANconvey impulses to the CNS via vagus and dorsal rootganglia and participate in the causation of vomiting whenstimulation is strong. Ondansetron (Ondan) acts partly byblocking activation of extrinsic PAN through 5-HT3R.
The intrinsic PAN interact with excitatory and inhibitoryinterneurones of the ENS to mediate both contraction (ofproximal gut muscles) and relaxation (of distal gut muscles)to coordinate the peristaltic reflex, respectively throughrelease of acetylcholine (ACh)/calcitonin gene relatedpeptide (CGRP) and nonadrenergic–noncholinergic (NANC)transmitter, which mainly is nitric oxide (NO). Cisapride(Cisa.) and metoclopramide (Meto.) activate the pre-junctional 5-HT4 receptors (5-HT4R) located on the terminalsof the intrinsic PAN and promote ACh/CGRP release, andthereby the contractile activity. The weak 5-HT3 blockingaction of Cisa. and Meto., in addition, reduces activity inthe inhibitory interneurone (minor action).
Domperidone (Dom) and Meto also block the action ofdopamine (DA) on prejunctional D2 receptor (D2R) whichnormally inhibits ACh release from the myenteric motorneurone, and thus augment smooth muscle contractionelicited through muscarinic M3 receptor (M3R)
CNS Metoclopramide is an effective antiemetic;acting on the CTZ, blocks apomorphine inducedvomiting. The gastrokinetic action may contri-bute to the antiemetic effect. However, it hasno chlorpromazine (CPZ) like antipsychoticproperty, though it does share the extrapyramidaland prolactin secretion augmenting action ofCPZ.
Mechanism of action: Metoclopramide actsthrough both dopaminergic and serotonergicreceptors (see Fig. 47.2)
(a) D2 antagonism Dopamine (acting throughD2 receptors) is an inhibitory transmitter in theg.i.t.— normally acts to delay gastric emptyingwhen food is present in stomach. It also appearsto cause gastric dilatation and LES relaxationattending nausea and vomiting. Metoclopramideblocks D2 receptors and has an opposite effect—
hastening gastric emptying and enhancing LEStone by augmenting ACh release. However,clinically this action is secondary to that exertedthrough 5HT4 receptors.
The central antidopaminergic (D2) action ofmetoclopramide on CTZ is clearly responsiblefor its antiemetic property. Other manifestationsof D2 blockade are antagonism of apomorphineinduced vomiting, CPZ like extrapyramidal effectsand hyperprolactinaemia.
(b) 5-HT4 agonism Metoclopramide acts in theg.i.t. to enhance ACh release from myentericmotor neurones. This results from 5-HT4 receptoractivation on primary afferent neurones (PAN)of the ENS via excitatory interneurones (Fig.47.2). The gastric hurrying and LES tonic effectsare mainly due to this action which is synergisedby bethanechol and attenuated by atropine.

666S
EC
TIO
N11
GASTROINTESTINAL DRUGS
(c) 5-HT3 antagonism At high concentrationsmetoclopramide can block 5-HT3 receptors presenton inhibitory myenteric interneurones and in NTS/CTZ. The peripheral action can augment AChrelease in the gut, but appears to be minor. Thecentral anti 5-HT3 action appears to be significantonly when large doses are used to control CINV.
Pharmacokinetics Metoclopramide is rapidlyabsorbed orally, enters brain, crosses placenta andis secreted in milk. It is partly conjugated in liverand excreted in urine within 24 hours; t½ is 3–6 hours. Orally it acts in ½–1 hr, but within 10min after i.m. and 2 min after i.v. injection. Actionlasts for 4–6 hours.
Interactions It hastens the absorption of manydrugs, e.g. aspirin, diazepam, etc. by facilitatinggastric emptying. The extent of absorption ofdigoxin is reduced by allowing less time for it.Bioavailability of cimetidine is also reduced.
By blocking DA receptors in basal ganglia, itabolishes the therapeutic effect of levodopa.
Adverse effects Metoclopramide is generallywell tolerated.Sedation, dizziness, loose stools, muscle dystonias(especially in children) are the main side effects.Long-term use can cause parkinsonism, galactor-rhoea and gynaecomastia, but it should not beused to augment lactation. No harmful effects areknown when used during pregnancy. Though theamount secreted in milk is small, but sucklinginfant may develop loose motions, dystonia,myoclonus.
Dose: 10 mg (children 0.2–0.5 mg/kg) TDS oral or i.m. ForCINV 0.3–2 mg/kg slow i.v./i.m.PERINORM, MAXERON, REGLAN, SIGMET, 10 mg tab; 5mg/5 ml syr; 10 mg/2 ml inj.; 50 mg/10 ml inj.
Uses1. Antiemetic: Metoclopramide is an effectiveand popular drug for many types of vomiting—postoperative, drug induced, disease associated(especially migraine), radiation sickness, etc, butis less effective in motion sickness. Thoughondansetron is preferred, metoclopramide conti-
nues to be used for prophylaxis and treatment ofvomiting induced by emetogenic anticancer drugs(cisplatin, etc.). A higher dose (1–2 mg/kg i.v.) isoften needed, but is effective when phenothiazinesand antihistamines do not work. Promethazine,diphenhydramine, diazepam or lorazepam injectedi.v. along with metoclopramide supplement itsantiemetic action and reduce the attending dystonicreactions. Dexamethasone i.v. also augments theefficacy of metoclopramide.
Though no teratogenic effects have beenreported, metoclopramide should be used formorning sickness only when not controlled byother measures.
2. Gastrokinetic: To accelerate gastric emptying:(a) When emergency general anaesthesia has to
be given and the patient has taken food lessthan 4 hours before.
(b) To relieve postvagotomy or diabetic gastro-paresis associated gastric stasis.
(c) To facilitate duodenal intubation.Clinical efficacy is moderate.
3. Dyspepsia and other functional g.i. dis-orders. Metoclopramide may succeed in stoppingpersistent hiccups.
4. Gastroesophageal reflux disease (GERD)Metoclopramide may benefit milder cases ofGERD, but is much less effective than PPIs/H2blockers. It does not aid healing of esophagitis,but may be used as adjuvant to acid suppressivetherapy. Any additional benefit is uncertain.
Domperidone It is a D2 receptor antagonist,chemically related to haloperidol, but pharmacolo-gically related to metoclopramide. The antiemeticand prokinetic actions have a lower ceiling. Unlikemetoclopramide, its prokinetic action is notattenuated by atropine and is based only on D2receptor blockade in upper g.i.t. Domperidonecrosses blood-brain barrier poorly. Accordingly,extrapyramidal side effects are rare, but hyperpro-lactinaemia can occur. The antiemetic action isexerted mainly through CTZ which is not protectedby blood-brain barrier. Because of poor entry intoCNS, it does not block the therapeutic effect of

667C
HA
PTE
R47
ANTIEMETIC, PROKINETIC AND DIGESTANT DRUGS
levodopa and bromocriptine in parkinsonism, butcounteracts their dose-limiting emetic action.
Domperidone is absorbed orally, but bioavaila-bility is only ~15% due to first pass metabolism.It is completely biotransformed and metabolitesare excreted in urine. Plasma t½ is 7.5 hr.
Side effects Are much less than with metoclo-pramide. Dry mouth, loose stools, headache,rashes, galactorrhoea are generally mild. Cardiacarrhythmias have developed on rapid i.v. injection.
Its indications are similar to that of metoclo-pramide, but it is a less efficacious gastrokineticand not useful against highly emetogenicchemotherapy.Dose: 10–40 mg (Children 0.3–0.6 mg/kg) TDS.DOMSTAL, DOMPERON, NORMETIC 10 mg tab, 1 mg/ml susp, MOTINORM 10 mg tab, 10 mg/ml drops.
Cisapride This benzamide derivative is a prokinetic withlittle antiemetic property, because it lacks D2 receptorantagonism. Effects of cisapride on gastric motility resemblemetoclopramide, i.e. gastric emptying is accelerated, LEStone is improved and esophageal peristalsis is augmented.It restores and facilitates motility throughout the g.i.t.,including colon (metoclopramide/domperidone do notaccelerate colonic transit). The prokinetic action is exertedmainly through 5-HT4 agonism which promotes ACh releasefrom myenteric neurones, aided by weak 5-HT3 antagonismwhich suppresses inhibitory transmission in myenteric plexus.Enteric neuronal activation via 5-HT4 receptor also promotescAMP-dependent Cl– secretion in the colon, increasing watercontent of stools. Thus, cisapride often produces loose stoolsby enhancing colonic motility and secretion. It is devoidof action on CTZ, and does not produce extrapyramidalsymptoms or hyperprolactinaemia.
Cisapride is primarily inactivated by CYP3A4 with at½ of ~ 10 hours.
Safety of cisapride was challenged by reports of seriousventricular arrhythmias and death, mainly among patientswho took CYP3A4 inhibitors like azole antifungals, macrolideantibiotics, antidepressants, HIV protease inhibitors, etc.concurrently. At high concentrations, cisapride blocks delayedrectifying K+ channels in heart—prolongs Q-Tc interval andpredisposes to torsades de pointes/ventricular fibrillation.Following such reports, cisapride was suspended frommarketing in most countries several years back, but wasavailable in India till it was banned in March 2011. In USAit is made available only for limited investigational use.
Mosapride A subsequently introduced congenerof cisapride with similar gastrokinetic and LEStonic action due to 5-HT4 agonistic (major) and
5-HT3 antagonistic (minor) action in the myentericplexus. Like cisapride, it has no clinically usefulantiemetic action and does not produceextrapyramidal or hyperprolactinaemic side effectsbecause of absence of D2 blocking property. Sideeffects are diarrhoea, abdominal pain, headache,dizziness and insomnia.
Preclinical studies showed that it may not havethe potential to prolong Q-T interval and carryrisk of arrhythmias. Therefore, it was introducedas a safe prokinetic. However, after general usesome reports of Q-T prolongation and arrhythmias,including torsades de pointes, among recipientshave appeared. Like cisapride, its plasmaconcentration is elevated by erythromycin andother CYP3A4 inhibitors increasing the risk ofQ-T prolongation. Though, it has not been banned,it may not be as safe as considered earlier.Indications of mosapride are—nonulcer dyspepsia,diabetic gastroparesis, GERD (as adjuvant to H2
blockers/PPIs), and some cases of chronicconstipation. However, efficacy is not impressive.Dose: 5 mg (elderly 2.5 mg) TDS.KINETIX 5 mg tab, MOZA, MOZASEF, MOPRIDE 2.5 mg,5 mg tabs; MOZA MPS: 5 mg + methylpolysiloxane 125 mgtab.
Itopride Another substituted benzamide producedin Japan and marketed in few countries, but notin UK or USA, as a prokinetic drug. It has D2antidopaminergic and anti-ChE (ACh potentiating)activity, but very low affinity for 5-HT4 receptor.Thus, the basis of prokinetic action may bedifferent from that of cisapride and mosapride.Animal studies showed that it lacked Q-Tprolonging potential. In healthy volunteers it wasfound unlikely to cause cardiac arrhythmias. Thismay be due to its low affinity for cardiac 5-HT4
receptors which have been implicated in theadverse cardiac effects of cisapride.
Itopride is metabolized mainly by flavinmonooxygenases and not by CYP450 iso-enzymes. Thus, unlike cisapride and mosapride,it is devoid of drug interactions with CYP3A4inhibitors (macrolides, azoles, etc.) resulting incardiac arrhythmias. As such, itopride may be asafer prokinetic drug. Side effects of itopride are

668S
EC
TIO
N11
GASTROINTESTINAL DRUGS
diarrhoea, abdominal pain, headache; galactor-rhoea and gynaecomastia occur infrequently. Noextrapyramidal effects are reported.Dose: 50 mg TDS before meals.GANATON, ITOFLUX, ITOKINE, ITOPRID 50 mg tab.
5-HT3 ANTAGONISTS
Ondansetron It is the prototype of a distinctclass of antiemetic drugs developed to controlcancer chemotherapy/radiotherapy inducedvomiting, and later found to be highly effective inPONV and disease/drug associated vomiting aswell. It blocks the depolarizing action of 5-HTexerted through 5-HT3 receptors on vagal afferentsin the g.i.t. as well as in NTS and CTZ. Cytotoxicdrugs/radiation produce nausea and vomiting bycausing cellular damage → release of mediatorsincluding 5-HT from intestinal mucosa → acti-vation of vagal afferents in the gut → emetogenicimpulses to the NTS and CTZ. Ondansetron blocksemetogenic impulses both at their peripheral originand their central relay. It does not block dopaminereceptors. Apomorphine or motion sicknessinduced vomiting is not suppressed. A weakgastrokinetic action due to 5-HT3 blockade hasbeen detected, but this is clinically insignificant.A minor 5-HT4 antagonistic action has also beenshown, but seems to have no clinical relevance.
Pharmacokinetics: Oral bioavailability of ondan-setron is 60–70% due to first pass metabolism. Itis hydroxylated by CYP1A2, 2D6 and 3A,followed by glucuronide and sulfate conjugation.No clinically significant drug interactions havebeen noted. It is eliminated in urine and faeces,mostly as metabolites; t½ is 3–5 hrs, and durationof action is 8–12 hrs (longer at higher doses).
Dose and efficacy: For cisplatin and other highly emetogenicdrugs—8 mg i.v. by slow injection over 15 min ½ hr beforechemotherapeutic infusion, followed by 2 similar doses4 hour apart. Single 24 mg i.v. dose on first day has also beenused. To prevent delayed emesis 8 mg oral is given twice aday for 3–5 days. For PONV 4–8 mg i.v. given beforeinduction is repeated 8 hourly. For less emetogenic drugs andfor radiotherapy, an oral dose of 8 mg is given 1–2 hr priorto the procedure and repeated twice 8 hrly. It is effective in
60–80% cases; similar to or better than high doses ofmetoclopramide, but does not cause dystonias or sedationlike the latter. However, many patients obtain only partialrelief, and adjuvant drugs are now mostly used along with itto improve chances of complete response.EMESET, VOMIZ, OSETRON, EMSETRON 4,8 mg tabs,2 mg/ml inj in 2 ml and 4 ml amps. ONDY, EMESET2 mg/5 ml syrup.
In patients who do not obtain optimum protectionby ondansetron alone, addition of dexamethasone,promethazine/diazepam or both dexamethasone+ NK1 antagonist aprepitant enhances antiemeticefficacy. Adjuvant drugs are more often requiredfor delayed phase vomiting that occurs on thesecond to fifth day of cisplatin therapy, in some,but not all patients.
Ondansetron alone is less effective in delayedvomiting than in acute vomiting which occurswithin 24 hours of cisplatin dose in all patients.
Other types of vomiting: Efficacy of 5-HT3
antagonists in prevention and treatment of PONVis now well established. Since this vomiting ismultifactorial in origin, many other classes of anti-emetic drugs are also protective. In comparativetrials, superiority of ondansetron in terms ofefficacy as well as lack of side effects and druginteractions has been demonstrated overmetoclopramide and phenothiazines. Administeredbefore surgery ondansetron (4–8 mg i.v.) repeatedafter 4 hours has become the first choice antiemeticat many centres.
Vomiting occurring as side effect of drugsor due to drug overdosage, g.i. disorders, uraemiaand neurological injuries is also suppressed.However, efficacy in motion sickness is poor. Dueto lack of safety data, ondansetron (also other5-HT3 antagonists) should be used duringpregnancy only when unavoidable, such as inhyperemesis gravidarum.
Side effects: Ondansetron is generally well tole-rated: the only common side effect is headacheand dizziness. Mild constipation and abdominaldiscomfort occur in few patients. Hypotension,bradycardia, chest pain and allergic reactions arereported, especially after i.v. injection.

669C
HA
PTE
R47
ANTIEMETIC, PROKINETIC AND DIGESTANT DRUGS
Granisetron It is 10 times more potent thanondansetron and probably more effective duringthe repeat cycle of chemotherapy. The weak5-HT4 blockade seen in ondansetron has not beendetected in granisetron. Its plasma t½ is longer(8–12 hrs) and it needs to be given only twice onthe day of chemotherapy. Side effect profile issimilar to ondansetron.Dose: 1–3 mg diluted in 20–50 ml saline and infused i.v. over5 min before chemotherapy, repeated after 12 hr. For lessemetogenic regimen 2 mg oral 1 hr before chemotherapy or1 mg before and 1 mg 12 hr after it. For PONV 1 mg dilutedin 5 ml and injected i.v. over 30 sec before starting anaesthesiaor 1 mg orally every 12 hours.GRANICIP, GRANISET 1 mg, 2 mg tabs; 1 mg/ml inj. (1,3 ml amps).
Palonosetron It is longest acting 5-HT3
blocker having the highest affinity for the 5-HT3
receptor. Efficacy against acute phase CINV iscomparable to ondansetron, but it is more effectivein suppressing delayed vomiting occurring between2nd to 5th days, probably because of its longerduration of action (elimination t½ is 40 hours).It is the only drug of its class approved by US-FDA for delayed CINV. Antiemetic efficacy ismaintained during repeat cycles of chemotherapy.
Palonosetron is metabolized in liver as wellas in kidney, mainly by CYP2D6, but also byCYP3A4 and CYP1A2. Side effects are headache,fatigue, dizziness, abdominal pain. AdditiveQ-T prolongation can occur when given withmoxifloxacin, erythromycin, anti-psychotics,antidepressants, etc. Rapid i.v. injection has causedblurring of vision.Dose: 250 μg by slow i.v. injection 30 min beforechemotherapy. Do not repeat before 7 days.For PONV 75 μg i.v. as a single injection just before induction.PALONOX 0.25 mg/ml inj, PALZEN 0.25 mg/50 ml inj.
Ramosetron It is a potent 5-HT3 antagonistdeveloped in Japan and marketed only in fewSoutheast Asian countries. The general propertiesare similar to ondansetron. It is used forCINV in a dose of 0.3 mg injected i.v. beforechemotherapy, and repeated once daily. For lowemetogenic chemotherapy, it can be given orallyin a dose of 0.1 mg once daily. Ramosetron 0.3mg i.v. is as effective as ondansetron 8 mg i.v.
in preventing PONV. Since it has shown potentialto normalize disturbed colonic function,ramosetron is also indicated for diarrhoea-predominant irritable bowel syndrome.NOZIA 0.1 mg tab, 0.3 mg in 2 ml amp.
NK1 RECEPTOR ANTAGONISTS
Realizing that activation of neurokinin (NK1)receptor in CTZ and NTS by substance P releaseddue to emetogenic chemotherapy and other stimuliplays a role in the causation of vomiting, selectiveantagonists of this receptor have been produced,and are being used as antiemetic.
Aprepitant It is a recently introduced selective,high affinity NK1 receptor antagonist thatblocks the emetic action of substance P, with littleeffect on 5 HT3 and D2 or other receptors.Gastrointestinal motility is not affected. Oralaprepitant (125 mg + 80 mg + 80 mg over 3days) combined with standard i.v. ondansetron+ dexamethasone regimen significantly enhancedthe antiemetic efficacy against high emetogeniccisplatin based chemotherapy. Greater additionalprotection was afforded against delayed vomitingthan against acute vomiting. It was particularlyuseful in patients undergoing multiple cycles ofchemotherapy. Adjuvant benefit of aprepitant hasalso been demonstrated in cyclophosphamidebased moderately emetogenic chemotherapy. Asingle (40 mg) oral dose of aprepitant has beenfound equally effective as ondansetron in PONVas well.
Aprepitant is well absorbed orally. It penetrates blood-brain barrier and is metabolized in liver, mainly by CYP3A4.Metabolites are eliminated via bile in faeces and in urine;t½ is 9–13 hours, but clearance is reduced with increasein dose. Inducers and inhibitors of CYP3A4 are likely tointeract with aprepitant. Dose of dexamethasone and warfarinneeds to be reduced. Aprepitant should not be given withQ-T interval prolonging drugs like cisapride.
Tolerability of aprepitant is good. Adverseeffects of combined regimen were similar to thoseproduced by ondansetron + dexamethasone with-out aprepitant. Symptoms attributed to aprepitantare weakness, fatigue, flatulence and rearely risein liver enzymes.

670S
EC
TIO
N11
GASTROINTESTINAL DRUGS
Dose: For CINV—125 mg before chemotherapy + 80 mg eachon 2nd and 3rd day (all oral) along with i.v. ondansetron +dexamethasone.For PONV—40 mg (single dose) oral before abdominal or othersurgery.APRECAP, APRESET, APRELIFE, EMPOV 125 mg (one cap)+ 80 mg (2 caps) kit.
Fosaprepitant It is a parenterally administered prodrug ofaprepitant.
ADJUVANT ANTIEMETICS
Corticosteroids (e.g. dexamethasone 8–20 mg i.v.) canpartly alleviate nausea and vomiting due to moderately emeto-genic chemotherapy, but are more often employed to augmentthe efficacy of other primary antiemetic drugs like metoclopra-mide and ondansetron against highly emetogenic regimens.Corticosteroids benefit both acute and delayed emesis. Thebasis of the effect appears to be their anti-inflammatory action.They also serve to reduce certain side effects of the primaryantiemetic.
Benzodiazepines The weak antiemetic property of BZDsis primarily based on the sedative action. Used as adjuvantto metoclopramide/ondansetron, diazepam/lorazepam (oral/i.v.) help by relieving the psychogenic component, anticipatoryvomiting and produce amnesia for the unpleasant procedure.They also suppress dystonic side effects of metoclopramide.
Cannabinoids Δ9 Tetrahydrocannabinol (Δ9 THC) is theactive principle of the hallucinogen Cannabis indica thatpossesses antiemetic activity against moderately emetogenicchemotherapy. It probably acts through the CB1 subtype ofcannabinoid receptors located on neurones in the CTZ and/or the vomiting centre itself.
Dronabinol is pure Δ9THC produced synthetically orextracted from Cannabis. In a dose of 5–10 mg/m2 BSAorally (repeated as required) it can be used as an alternativeantiemetic for moderately emetogenic chemotherapy inpatients who cannot tolerate other antiemetics or areunresponsive to them. The hallucinogenic, disorienting andother central sympathomimetic effects (described on p. 452)are produced, and some subjects may experience a ‘high’,that may lead to addiction. The CNS actions limit the use ofdronabinol to few nonresponsive patients. Its antiemetic actioncan be supplemented by dexamethasone.
Dronabinol is an appetite stimulant as well; has beenused in lower doses to improve feeding in cachectic/AIDSpatients.
Nabilone is another cannabinoid with antiemetic property.
DIGESTANTS
These are substances intended to promote digestion of food.A number of proteolytic, amylolytic and lipolytic enzymesare marketed in combination formulations and are vigorouslypromoted for dyspeptic symptoms, and as appetite stimulantsor health tonics. They are occasionally beneficial, only when
elaboration of enzymes in g.i.t. is deficient. Their routine usein tonics and appetite improving mixtures is irrational.
1. Pepsin May be used along with HCl in gastric achyliadue to atrophic gastritis, gastric carcinoma, perniciousanaemia, etc.
2. Papain It is a proteolytic enzyme obtained from rawpapaya. Its efficacy after oral ingestion is doubtful.
3. Pancreatin It is a mixture of pancreatic enzymesobtained from hog and pig pancreas. It contains amylase,trypsin and lipase, and is indicated in chronic pancreatitis orother exocrine pancreatic deficiency states. Fat and nitrogencontent of stools may be reduced and diarrhoea/steatorrhoeamay be prevented. It has to be used as enteric coated tabletsor capsules to protect the enzymes from being themselvesdigested in stomach by pepsin. Nausea, diarrhoea andhyperuricaemia are the occasional side effects.
4. Diastase and Takadiastase These are amylolyticenzymes obtained from the fungus Aspergillus oryzae. Theyhave been used in pancreatic insufficiency, but efficacy isequivocal.
PreparationsARISTOZYME: Fungal diastase 50 mg, pepsin 10 mg,simethicone 50 mg cap and per 5 ml liquid.DIGEPLEX: Diastase 62.5 mg, pepsin 20 mg per 10 ml afterdissolving the tablet in sorbitol base provided.ENTOZYME: Fungal diastase 50 mg, pepsin 10 mg per 5 mlsyr.LUPIZYME: Pepsin 125 mg, fungal diastase 18.75 mg,thiamine 2 mg, riboflavine 1 mg, pyridoxine 1.5 mg, vit B12
1 μg, nicotinamide 15 mg per cap and per 5 ml syr.PANZYNORM: Pancreatine 100 mg, bile ext. 40 mg, drystomach ext. 110 mg tab.UNIENZYME: Fungal diastase 20 mg, papain 30 mg,simethicone 50 mg, nicotinamide 25 mg, activated charcoal75 mg tab.VITAZYME: Fungal diastase 40 mg, cinnamon oil 0.25mg, caraway oil 0.5 mg, cardamom oil 0.5 mg per 10 mlliq.Enzyme preparations containing an antispasmodic or alaxative and fixed dose combinations of pancreatine orpancrelipase containing amylase, protease and lipase withany other enzyme are banned in India.
Methyl polysiloxane (Dimethyl polysiloxane,Simethicone, Dimethicone) It is a siliconepolymer, a viscous amphiphilic liquid—reducessurface tension and collapses froth, ‘antifoamingagent’. It is not absorbed from g.i.t. and is phar-macologically inert. Added to antacid, digestantand antireflux preparations (see above), it isbriskly promoted as a remedy for ‘gas’, a very

671C
HA
PTE
R47
ANTIEMETIC, PROKINETIC AND DIGESTANT DRUGS
common gastric complaint. It is also claimed tocoat and protect ulcer surface, to aid dispersionof antacids in gastric contents, and to preventgastroesophageal reflux. However clinical efficacyis equivocal.Dose: 40–120 mg 3 to 4 times a day.DIMOL 40 mg tab. (single ingredient).
GALLSTONE DISSOLVING DRUGS
Cholesterol (CH) remains dissolved in bile with the help ofbile salts (salts of cholic acid and chenodeoxycholic acidconjugated with glycine and taurine) because bile salts arehighly amphiphilic. A high CH : bile salt ratio favours crystal-lization of CH in bile; these crystals act as nidi for stoneformation. Chenodeoxycholic acid (Chenodiol) andUrsodeoxycholic acid (Ursodiol) decrease CH content of bile,enabling solubilization of CH from stone surface. These twobile acids act differently.
CHENODIOL URSODIOL1. Acts primarily by inhi- Little inhibition of hepatic
biting CH synthesis in CH synthesis.liver.Does not reduce intes- Acts primarily by inhibitingtinal CH absorption. intestinal CH absorption.
2. Raises plasma LDL-CH Does not raise plasmaby reducing LDL LDL-CH level.receptors in liver.
3. Reduces CH secretion Promptly reduces CHin bile after prolonged secretion in bile.administration.
4. Generates a more litho- Itself lowers CH saturationlytic bile acid pool. index of bile.
5. Promotes micellar Promotes solubilization bysolubilization of CH. liquid crystal formation.
Chenodiol Administered daily it has been found to partiallyor completely dissolve CH gallstones in about 40% patientsover 1/2 to 2 years. However, only 1/3 of these had completedissolution.
Diarrhoea is common.Aminotransferase level may rise, but overt liver damage occursin only 3% patients.Gastric and esophageal mucosal resistance to acid is impairedfavouring ulceration.
Ursodiol It is a hydroxy epimer of chenodiol, is moreeffective and needs to be used at lower doses. Completedissolution of CH stones has been achieved in upto 50% cases.It is also much better tolerated. Diarrhoea and hypertrans-aminaemia are infrequent, but effect on mucosal resistanceis similar to chenodiol. Calcification of some gall stones maybe induced.Dose: 450–600 mg daily in 2–3 divided doses after meals;UDCA, UDIHEP 150 mg tab.
Dissolution of gallstones is a very slow process: patientcompliance is often poor. However, medical treatment is nowpossible in selected patients:
Once treatment is discontinued after stone dissolution,recurrences are common, because bile returns to its CHsupersaturated state. Repeat courses may have to be given.Because of these problems the pros and cons of medicaltherapy must be weighed against cholecystectomy.
PROBLEM DIRECTED STUDY
47.1 A 4-year-old girl is brought to the hospital emergency. The parents are very alarmed byher condition that has developed over the past one hour, when she started making bizarre faces.The neck has become rigid and head has tilted to one side. The teeth are clinched and sheis not speaking. The eyes are staring in one direction and there are intermittent purposelessmovements of the upper limbs. The parents inform that she had vomited twice in the morningand was taken to a local doctor, who had given her an injection. The vomiting had stopped,but after about 2 hours of the injection she developed the above symptoms.(a) What is the most likely cause of her symptoms? Could it be due to the injection given toher? If so, which drug could have caused it?(b) How should this patient be treated?(see Appendix-1 for solution)
Drugs for Constipationand Diarrhoea
ChapterChapterChapterChapterChapter 4848484848
LAXATIVES(Aperients, Purgatives, Cathartics)
These are drugs that promote evacuation ofbowels. A distinction is sometimes made accordingto the intensity of action.(a) Laxative or aperient: milder action,elimination of soft but formed stools.(b) Purgative or cathartic: stronger actionresulting in more fluid evacuation.Many drugs in low doses act as laxative and inlarger doses as purgative.
CLASSIFICATION
1. Bulk formingDietary fibre: Bran, Psyllium (Plantago)Ispaghula, Methylcellulose
2. Stool softenerDocusates (DOSS), Liquid paraffin
3. Stimulant purgatives(a) Diphenylmethanes
Phenolphthalein, Bisacodyl, Sodiumpicosulfate
(b) Anthraquinones (Emodins)Senna, Cascara sagrada
(c) 5-HT4 agonistPrucalopride
(d) Fixed oilCastor oil
4. Osmotic purgativesMagnesium salts: sulfate, hydroxideSodium salts: sulfate, phosphateSod. pot. tartrateLactulose
MECHANISM OF ACTION
All purgatives increase the water content of thefaeces by:
(a) A hydrophilic or osmotic action, retainingwater and electrolytes in the intestinallumen—increase volume of colonic contentand make it easily propelled.
(b) Acting on intestinal mucosa, decrease netabsorption of water and electrolyte; intestinaltransit is enhanced indirectly by the fluidbulk.
(c) Increasing propulsive activity as primaryaction—allowing less time for absorption ofsalt and water as a secondary effect.
For some of the drugs, controversy continues asto whether they increase water content of stoolsas the primary action or it is a consequence ofincreased motility, because the amount of waterabsorbed largely depends on transit time.However, certain purgatives do increase motilitythrough an action on the myenteric plexuses.Laxatives modify the fluid dynamics of themucosal cell and may cause fluid accumulationin gut lumen by one or more of followingmechanisms:
(a) Inhibiting Na+K+ATPase of villous cells—impairing electrolyte and water absorption.
(b) Stimulating adenylyl cyclase in crypt cells—increasing water and electrolyte secretion.
(c) Enhancing PG synthesis in mucosa whichincreases secretion.
(d) Increasing NO synthesis which enhancessecretion and inhibits non-propulsivecontrations in colon.
(e) Structural injury to the absorbing intestinalmucosal cells.
BULK PURGATIVES
Dietary fibre: bran Dietary fibre consists ofunabsorbable cell wall and other constituents ofvegetable food—cellulose, lignins, gums, pectins,

673C
HA
PTE
R48DRUGS FOR CONSTIPATION AND DIARRHOEA
glycoproteins and other polysaccharides. Bran isthe residual product of flour industry whichconsists of ~40% dietary fibre. It absorbs waterin the intestines, swells, increases water contentof faeces—softens it and facilitates colonic transit.Osmotically active products may be formed inthe colon by bacterial degradation of pectins,gums, etc. which act to retain water. Dietary fibresupports bacterial growth in colon whichcontribute to the faecal mass. Certain dietary fibres(gums, lignins, pectins) bind bile acids andpromote their excretion in faeces → degradationof cholesterol in liver is enhanced → plasma LDL-cholesterol may be somewhat lowered.
Increased intake of dietary fibres is the mostappropriate method for prevention of functionalconstipation. It is the first line approach for mostpatients of simple constipation. Prolonged intakeof bran and other bulk forming agents reducesrectosigmoid intraluminal pressure and helps torelieve symptoms of irritable bowel syndrome(IBS) including pain, constipation as well asdiarrhoea. Symptoms of chronic diverticulosis mayalso be relieved. It is also useful when strainingat stools has to be avoided.
Drawbacks: Bran is generally safe, but it isunpalatable, large quantity (20–40 g/day) needsto be ingested. It has been included in somebreakfast cereals, biscuits, etc. Full effect requiresdaily intake for at least 3–4 days. It does notsoften faeces already present in colon or rectum.As such, bran is useful for prevention ofconstipation, but not for treating alreadyconstipated subjects. Flatulence may occur.
It should not be used in patients with gutulcerations, adhesions, stenosis and when faecalimpaction is a possibility.
Psyllium (Plantago) and Ispaghula Theycontain natural colloidal mucilage whichforms a gelatinous mass by absorbing water. Itis largey fermented in colon: increases bacterialmass and softens the faeces. Refined ispaghulahusk 3–8 g is freshly mixed with cold milk, fruit
juice or water and taken once or twice daily. Itacts in 1–3 days. It should not be swallowed dry(may cause esophageal impaction).Ispaghula husk (refined): ISOGEL (27 g/ 30 g), NATURECURE (49 g/100 g), FYBOGEL (3.5 g/5.4 g) powderFIBRIL (3.4 g/11 g) powder;Psyllium hydrophilic mucilloid: ISOVAC (65 g/100 g)granules.
Methylcellulose A semi-synthetic, colloidal,hydrophilic derivative of cellulose that remainslargely unfermented in colon. A dose of 4–6g/day is satisfactory in most individuals.
Generous amounts of water must be takenwith all bulk forming agents. The choice amongdifferent bulking agents is a matter of personalpreferences.
STOOL SOFTENER
Docusates (Dioctyl sodium sulfosuccinate:DOSS) It is an anionic detergent, softens thestools by net water accumulation in the lumenby an action on the intestinal mucosa. It emulsifiesthe colonic contents and increases penetration ofwater into the faeces. By a detergent action, itcan disrupt the mucosal barrier and enhanceabsorption of many nonabsorbable drugs, e.g.liquid paraffin—should not be combined with it.It is a mild laxative; especially indicated whenstraining at stools must be avoided.Dose: 100–400 mg/day; acts in 1–3 days.CELLUBRIL 100 mg cap; LAXICON 100 mg tab, DOSLAX150 mg cap.As enema 50–150 mg in 50–100 ml;LAXICON 125 mg in 50 ml enema.Cramps and abdominal pain can occur. It isbitter; liquid preparations may cause nausea.Hepatotoxicity is feared on prolonged use.Liquid paraffin It is a viscous liquid; a mixture ofpetroleum hydrocarbons, that was introduced as a laxativeat the turn of 19th century. Millions of gallons have passedthrough the intestinal pipeline since then. It is pharmaco-logically inert. Taken for 2–3 days, it softens stools andis said to lubricate hard scybali by coating them.Dose: 15–30 ml/day—oil as such or in emulsified form.
Disadvantages
(a) It is bland but very unpleasant to swallow because ofoily consistency.

674S
EC
TIO
N11
GASTROINTESTINAL DRUGS
(b) Small amount passes into the intestinal mucosa—iscarried into the lymph → may produce foreign bodygranulomas in the intestinal submucosa, mesenteric lymphnodes, liver and spleen.(c) While swallowing it may trickle into lungs—cause lipidpneumonia.(d) Carries away fat soluble vitamins with it into the stools:deficiency may occur on chronic use.(e) Leakage of the oil past anal sphincter may embarrass.(f) May interfere with healing in the anorectal region.Thus, it should be used only occasionally.
STIMULANT PURGATIVES
They are powerful purgatives: often producegriping. They irritate intestinal mucosa and thuswere thought to primarily stimulate motor activity.Though some of them do directly increase motilityby acting on myenteric plexuses, the moreimportant mechanism of action is accumulationof water and electrolytes in the lumen by alteringabsorptive and secretory activity of the mucosalcell. They inhibit Na+K+ATPase at the basolateralmembrane of villous cells—transport of Na+ andaccompanying water into the interstitium isreduced. Secretion is enhanced by activation ofcAMP in crypt cells as well as by increased PGsynthesis. The laxative action of bisacodyl andcascara is shown to be partly dependent uponincreased NO synthesis/action in the colon.
Larger doses of stimulant purgatives cancause excess purgation resulting in fluid andelectrolyte imbalance. Hypokalaemia can occuron regular intake. Routine and long-term use mustbe discouraged, because it can produce colonicatony. They can reflexly stimulate gravid uterus,therefore are contraindicated during pregnancy.Subacute or chronic intestinal obstruction isanother contraindication.
DiphenylmethanesPhenolphthalein is a litmus-like indicator whichis in use as purgative from the beginning of the20th century. It turns urine pink if alkaline.
Bisacodyl is a later addition and is more popular.They are partly absorbed and reexcreted in
bile. The enterohepatic circulation is greater incase of phenolphthalein which can produce
protracted action. Bisacodyl is activated in theintestine by deacetylation. The primary site ofaction of diphenyl methanes is in the colon wherethey irritate the mucosa, produce mild inflam-mation and increase secretion. One or two semi-formed motions occur after 6–8 hours. Optimumdoses vary considerably among individuals.Average doses are:
Phenolphthalein 60–130 mg: LAXIL 130 mg tab.To be taken at bedtime (tab. not to be chewed).
Bisacodyl 5–15 mg: DULCOLAX 5 mg tab; 10 mg(adult), 5 mg (child) suppository: CONLAX 5 mg, 10 mgsuppository, BIDLAX-5 5 mg tab.
These doses may be ineffective in some indivi-duals, but produce fluid evacuations and crampsin others. Morphological alterations in the colonicmucosa have been observed; the mucosa becomesmore leaky.
Allergic reactions—skin rashes, fixed drugeruption and Stevens-Johnson syndrome have beenreported.
Phenolphthalein has been found to produce tumours in miceand genetic damage. The US-FDA has ordered its withdrawalfrom the market.
Bisacodyl is also available as 5 mg (infant) and10 mg (adult) suppository, which acts by irritatingthe anal and rectal mucosa → reflex increase inmotility → evacuation occurs in 20–40 min. Butit can cause inflammation and mucosal damage.Sodium picosulfate: Another diphenylmethanerelated to bisacodyl. It is hydrolysed by colonicbacteria to the active form, which then acts locallyto irritate the mucosa and activate myentericneurones. Bowel movement generally occurs after6–12 hours of oral dose. Along with mag. citratesolution, it has been used to evacuate the colonfor colonoscopy and colonic surgery.Dose: 5–10 mg at bed time. Indications and side effectsare similar to bisacodyl.CREMALAX, LAXICARE 10 mg tab; PICOFIT 5 mg/5 mlsyr.
AnthraquinonesThese are plant products used in household/traditional medicine for centuries.

675C
HA
PTE
R48DRUGS FOR CONSTIPATION AND DIARRHOEA
Senna is obtained from leaves and pods ofcertain Cassia sp., while Cascara sagrada is thepowdered bark of the buck-thorn tree. These anda number of other plant purgatives containanthraquinone glycosides, also called emodins.Senna is most popularly used. The glycosides arenot active as such. Unabsorbed in the smallintestine, they are passed to the colon wherebacteria liberate the active anthrol form, whicheither acts locally or is absorbed into circulation—excreted in bile to act on small intestine. Thus,they take 6–8 hours to produce action. Takenby lactating mothers, the amount secreted in milkis sufficient to cause purgation in the sucklinginfant.
The purgative action and uses of anthraqui-nones are quite similar to those of diphenyl-methanes. Taken at bed time—a single, soft butformed evacuation generally occurs in themorning. Cramps and excessive purging occurin some individuals. The active principle of thesedrugs acts on the myenteric plexus to increaseperistalsis and decrease segmentation. They alsopromote secretion and inhibit salt and waterabsorption in the colon. Senna anthraquinone hasbeen found to stimulate PGE2 production in ratintestine. This is prevented by indomethacin andthe purgative action is reduced.
Skin rashes, fixed drug eruption are theoccasional adverse effects.
Regular use for 4–12 months causes colonicatony and mucosal pigmentation (melanosis).Sennosides (Cal. salt): GLAXENNA 11.5 mg tab;PURSENNID 18 mg tab; SOFSENA 12 mg tab.
Prucalopride It is a selective 5-HT4 receptor agonistmarketed recently in Europe, UK and Canada for the treatmentof chronic constipation in women, when other laxatives failto provide adequate relief. It activates prejunctional 5-HT4
receptors on intrinsic enteric neurones to enhance releaseof the excitatory transmitter ACh, thereby promotingpropulsive contractions in ileum and more prominently incolon. Colonic transit and stool frequency is improved inconstipation-predominant irritable bowel syndrome (IBS).
A 5-HT4 receptor partial agonist tegaserod with similaraction on colon was introduced few years back, but waswithdrawn soon after when postmarketing studies showed thatit increased the risk of edema, heart attack and stroke. Theseadverse consequences were ascribed to its interaction with
5-HT1B/1D receptors in addition to 5-HT4 receptors. Prucaloprideis shown to have low affinity for 5-HT1B/1D receptor, as well asfor cardiac K+ channels. It is therefore, believed to be free ofcardiovascular risk. No Q-T prolongation has been noted duringclinical trial. Side effects are headache, dizziness, fatigue,abdominal pain and diarrhoea; but generally subside during use.Dose: 2 mg OD, elderly start with 1 mg OD.
Lubiprostone This PG analogue (EP4 receptor agonist),developed recently, represents a new strategy in the treatmentof constipation-predominant IBS and chronic constipationby stimulating mucosal Cl¯ channels and increasing intestinalsecretion. Its comparative value is being investigated.
Castor oilIt is one of the oldest purgatives. Castor oil is a bland vegetableoil obtained from the seeds of Ricinus communis. It mainlycontains triglyceride of ricinoleic acid which is a polar long-chain fatty acid. Castor oil is hydrolysed in the ileum bylipase to ricinoleic acid and glycerol. Ricinoleic acid, beingpolar, is poorly absorbed. It was believed to irritate the mucosaand stimulate intestinal contractions. The primary action isnow shown to be decreased intestinal absorption of waterand electrolytes, and enhanced secretion by a detergent likeaction on the mucosa. Structural damage to the villous tipshas also been observed. Peristalsis is increased secondarily.Dose: 15–25 ml (adults) 5–15 ml (children) is generallytaken in the morning. Because the site of action is smallintestine, purgation occurs in 2–3 hours—motion is semifluidand often accompanied by griping.
Due to its unpalatability, frequent cramping, a ratherviolent action, possibility of dehydration and after-constipation(due to complete evacuation of colon), it is no longer afavoured purgative. Regular use is particularly to be avoided—may damage intestinal mucosa.
OSMOTIC PURGATIVESSolutes that are not absorbed in the intestine retainwater osmotically and distend the bowel—increasing peristalsis indirectly.Magnesium ions release cholecystokinin which augmentsmotility and secretion, contributing to purgative action ofMag. salts. All inorganic salts used as osmotic (saline)purgatives have similar action—differ only in dose, palata-bility and risk of systemic toxicity.• Mag. sulfate (Epsom salt): 5–15 g; bitter in taste, may
nauseate.• Mag. hydroxide (as 8% W/W suspension—milk of
magnesia) 30 ml; bland in taste, also used as antacid.• Sod. sulfate (Glauber’s salt): 10–15 g; bad in taste.• Sod. phosphate: 6–12 g, taste not unpleasant.• Sod. pot. tartrate (Rochelle salt): 8–15 g, relatively pleasant
tasting.
The salts taken in above mentioned doses, dissolved in150–200 ml of water, produce 1–2 fluid evacuations within

676S
EC
TIO
N11
GASTROINTESTINAL DRUGS
1–3 hours with mild cramping; cause nearly completeemptying of bowels. Smaller doses may have a milder laxativeaction.
Mag. salts are contraindicated in renal insufficiency, whileSod. salts should not be given to patients of CHF and otherSod. retaining states. Repeated use of saline purgatives cancause fluid and electrolyte imbalance.
Saline purgatives are not used now for thetreatment of constipation because they are incon-venient/unpleasant, produce watery stools and afterconstipation. However, they may be preferred forpreparation of bowel before surgery and colo-noscopy; in food/drug poisoning and as after-purgein the treatment of tapeworm infestation.
Lactulose It is a semisynthetic disaccharideof fructose and lactose which is neither digestednor absorbed in the small intestine—retains water.Further, it is broken down in the colon by bacteriato osmotically more active products. In a doseof 10 g BD taken with plenty of water, it producessoft formed stools in 1–3 days. Flatulence andflatus is common, cramps occur in few. Somepatients feel nauseated by its peculiar sweet taste.
In patients with hepatic encephalopathy,lactulose causes reduction of blood NH3 concen-tration by 25–50%. The breakdown products oflactulose are acidic—lower the pH of stools.Ammonia produced by bacteria in colon isconverted to ionized NH
4+ salts that are not
absorbed. For this purpose 20 g TDS or moremay be needed. Loose motions are produced atthis dose.LACSAN, MTLAC 10 g/15 ml liq. DUPHALAC, LIVO-LUK6.67 g/10 ml liq.
Other drugs used to reduce blood NH3 in hepatic comaare sod. benzoate and sod. phenyl acetate. They combine withNH3 in blood to form hippuric acid or phenyl acetic glutaminerespectively: these are rapidly excreted in urine.
CHOICE AND USE OF PURGATIVES
Laxatives are as important for their harmfulnessas they are for their value in medicine.All laxatives are contraindicated in:
(i) A patient of undiagnosed abdominal pain,colic or vomiting.
(ii) Organic (secondary) constipation due tostricture or obstruction in bowel, hypo-
thyroidism, hypercalcaemia, malignanciesand certain drugs, e.g.—opiates, sedatives,anticholinergics including antiparkinsonian,antidepressants and antihistaminics, oraliron, clonidine, verapamil and laxative abuseitself.
The primary cause should be treated in these cases.Valid indications of laxatives are:
1. Functional constipation Constipation isinfrequent production of hard stools requiringstraining to pass, or a sense of incompleteevacuation. A stool frequency of once in 2 daysto 2–3 times per day is considered normal bydifferent individuals. Constipation is a symptomrather than a disease. Various aspects of thepatient’s lifestyle may contribute:
(a) Misconception about the normal/necessaryfrequency, amount or consistency of stools.
(b) Inadequate fibre in diet, less fluid intake.(c) Lack of exercise, sedentary nature of work.(d) Irregular bowel habits, rushing out for job.
Proper assessment of the causative factor in thepatient and its correction leaves only a minorityof cases to be treated by drugs.Constipation may be spastic or atonic.
(i) Spastic constipation (irritable bowel): Thestools are hard, rounded, stone like and difficultto pass. The first choice laxative is dietary fibreor any of the bulk forming agents taken overweeks/months. Stimulant purgatives arecontraindicated.
(ii) Atonic constipation (sluggish bowel): mostlydue to advanced age, debility or laxative abuse.Non-drug measures like plenty of fluids, exercise,regular habits and reassurance should be tried.In resistant cases a bulk forming agent shouldbe prescribed. In case of poor compliance or ifthe patient is not satisfied—bisacodyl or sennamay be given once or twice a week for as shorta period as possible.
2. Bedridden patients (myocardial infarction,stroke, fractures, postoperative): bowel movementmay be sluggish and constipation can beanticipated.

677C
HA
PTE
R48DRUGS FOR CONSTIPATION AND DIARRHOEA
To prevent constipation: Give bulk forming agentson a regular schedule; docusates, lactulose andliquid paraffin are alternatives.To treat constipation: Enema (soap-water/glycerine) is preferred; bisacodyl or senna maybe used.Alvimopan It is a recently approved peripherally actingμ opioid receptor antagonist for the treatment of postoperativeileus and constipation following abdominal surgery. Alvimopanabsorption from gut and its penetration into brain is poordue to its polar nature. Administered orally before and aftersurgery, it hastened recovery of bowel function.
3. To avoid straining at stools (hernia,cardiovascular disease, eye surgery) and inperianal afflictions (piles, fissure, anal surgery)it is essential to keep the faeces soft. One shouldnot hesitate to use adequate dose of a bulk formingagent, lactulose or docusates.4. Preparation of bowel for surgery, colono-scopy, abdominal X-ray The bowel needs tobe emptied of the contents including gas. Salinepurgative, bisacodyl or senna may be used; castoroil only in exceptional circumstances.5. After certain anthelmintics (especially fortapeworm) Saline purgative or senna may be usedto flush out the worm and the anthelmintic drug.Fixed dose combinations of an anthelmintic (other thanpiperazine) with a purgative is banned in India, as are laxativeswith enzyme preparations.
6. Food/drug poisoning The idea is to driveout the unabsorbed irritant/poisonous materialfrom the intestines. Only saline purgatives aresatisfactory.
The choice of a purgative depends on thelatency of action and type of stools desired. Thisis given in Table 48.1.
Some combined preparationsAGAROL: Liquid paraffin 9.5 ml, phenolphthalein 400 mg,agar 60 mg per 30 ml emulsion.CREMAFFIN: Milk of magnesia 11.25 ml, liq. paraffin 3.75ml per 15 ml emulsion; CREMAFFIN PINK withphenolphthalein 50 mg per 15 ml.JULAX: Bisacodyl 10 mg, casanthranol 10 mg dragees.PURSENNID-IN (with DOS): Purified senna ext. (cal salt)18 mg, docusates 50 mg tab.
Purgative abuse Some individuals are obsessedwith using purgatives regularly. This may be thereflection of a psychological problem. Others usea purgative casually, obtain thorough bowelevacuation, and by the time the colon fills up fora proper motion (2–3 days) they get convincedthat they are constipated and start taking the drugregularly. Chronic use of purgatives must bediscouraged. Once the purgative habit forms, itis difficult to break. Dangers of purgative abuse are:1. Flairing of intestinal pathology, rupture of
inflamed appendix.2. Fluid and electrolyte imbalance, especially
hypokalaemia.3. Steatorrhoea, malabsorption syndrome.4. Protein losing enteropathy.5. Spastic colitis.
TREATMENT OF DIARRHOEASDiarrhoea is too frequent, often too precipitatepassage of poorly formed stools. It is definedby WHO as 3 or more loose or watery stoolsin a 24 hour period. In pathological terms, it occursdue to passage of excess water in faeces.Thismay be due to:• Decreased electrolyte and water absorption.• Increased secretion by intestinal mucosa.• Increased luminal osmotic load.• Inflammation of mucosa and exudation into
lumen.Diarrhoeal diseases constitute a major cause of morbidity
and mortality worldwide; especially in developing countries.It is more prevalent among children. The global burden ofpediatric diarrhoea is estimated to be 1.5 billion episodeswith 1.5–2.5 million deaths under 5 years of age per year.In India around 1000 children die every day due to diarrhoea.Recurrent or protracted diarrhoea is also a major cause ofprotein-calorie malnutrition in developing countries. Evenmild diarrhoea, and that in adults, is a disabling symptomand an inconvenience.
TABLE 48.1Type of stools and latency ofaction of purgatives employed inusually recommended doses
Soft, formed Semifluid Wateryfaeces stools evacuation(take 1–3 days) (take 6–8 hrs) (within 1–3 hrs)
Bulk forming Phenolphthalein Saline purgativesDocusates Bisacodyl Castor oilLiquid paraffin Sod. picosulfateLactulose Senna

678S
EC
TIO
N11
GASTROINTESTINAL DRUGS
Relevant pathophysiologyWater and electrolytes are absorbed as well assecreted in the intestine. Jejunum is freely per-meable to salt and water which are passivelyabsorbed secondary to nutrient (glucose, aminoacids, etc.) absorption. In the ileum and colonactive Na+K+ATPase mediated salt absorptionoccurs, primarily in the mature cells lining thevillous tips, water follows isoosmotically. Inaddition glucose facilitated Na+ absorption takesplace in the ileum by Na+-glucose cotransporter;one Na+ ion is transported along with eachmolecule of glucose absorbed. This mechanismremains intact even in severe diarrhoeas.
Absorption of Cl¯ and HCO3¯ is passive
(paracellular) as well as by exchange of HCO3¯
for Cl¯ (transcellular). Bicarbonate is absorbedalso by the secretion of H+ (similar to that inproximal tubule of kidney) and Na+ accompaniesit. K+ is excreted in faecal water by exchangewith Na+, as well as by secretion into mucus andin desquamated cells. The osmotic load of luminalcontents plays an important role in determiningfinal stool water volume. When nonabsorbablesolutes are present and in disaccharidase defi-ciency (which occurs during starvation), the stoolwater is increased. Inhibition of Na+K+ATPaseand structural damage to mucosal cell (by Rotavirus) causes diarrhoea by reducing absorption.
Intracellular cyclic nucleotides are importantregulators of absorptive and secretory processes(Fig. 48.1). Stimuli enhancing cAMP or cGMPcause net loss of salt and water, both by inhibitingNaCl absorption in villous cells and by promo-ting anion secretion (Na+ accompanies) in the cryptcells which are primarily secretory. Many bacterialtoxins, e.g. cholera toxin, exotoxin elaborated byEnterotoxigenic E. coli (ETEC), Staph. aureus,Salmonella, etc. activate adenylyl cyclase whichenhances secretion that reaches its peak after3–4 hours and persists until the stimulated cellsare shed in the normal turnover, i.e. 36 hoursafter a single exposure. Concurrent inhibition ofabsorption adds to the rate of salt and water loss.Prostaglandins (PGs) and intracellular Ca2+ alsostimulate the secretory process. All acute enteric
infections produce secretory diarrhoea. The heatstable toxin (ST) of ETEC, Clostridium difficileand E. histolytica cause accumulation of cGMPwhich also stimulates anion secretion (less potentthan cAMP) and inhibits Na+ absorption.
Diarrhoea associated with carcinoid (secre-ting 5-HT) and medullary carcinoma of thyroid(secreting calcitonin) is mediated by cAMP.Excess of bile acids also cause diarrhoea byactivating adenylyl cyclase.
Traditionally, hypermotility of bowel has beenascribed a crucial role in diarrhoea. However,changes in intestinal motility are now thought tobe of secondary importance and may be due tofluid accumulation in the lumen. Decreasedsegmenting activity in the intestine may promotediarrhoea by allowing less time for the absorptiveprocesses.
Principles of managementRational management of diarrhoea depends onestablishing the underlying cause and institutingspecific therapy (only if necessary), since mostdiarrhoeas are self-limiting. Majority of entero-pathogens are taken care of by motility and other
Fig. 48.1: Action of cyclic nucleotides on electrolytetransport of intestinal mucosal cells. In crypt cells cAMPplays the dominant role

679C
HA
PTE
R48DRUGS FOR CONSTIPATION AND DIARRHOEA
defence mechanisms of the gut. Therapeuticmeasures may be grouped into:
(a) Treatment of fluid depletion, shock andacidosis.
(b) Maintenance of nutrition.(c) Drug therapy.
The relative importance of each measure isgoverned by the severity and nature of diarrhoea.
REHYDRATION
In majority of cases, this is the only measureneeded. Rehydration can be done orally or i.v.
Intravenous rehydration It is needed onlywhen fluid loss is severe, i.e. > 10% body weight,(if not promptly corrected, it will lead to shockand death) or if patient is losing > 10 ml/kg/hr, or is unable to take enough oral fluids dueto weakness, stupor or vomiting. The recommen-ded composition of i.v. fluid (Dhaka fluid) is:
NaCl 85 mM = 5 gKCl 13 mM = 1 gNaHCO3 48 mM = 4 g
This provides 133 mM Na+, 13 mM K+, 98 mMCl¯ and 48 mM HCO
3¯. Ringer lactate (Na+ 130,
Cl¯ 109, K+ 4, lactate 28 mM) recommended byWHO (1991) could be used alternatively.
Volume equivalent to 10% BW should beinfused over 2–4 hours; the subsequent rate ofinfusion is matched with the rate of fluid loss. Inmost cases, oral rehydration can be instituted afterthe initial volume replacement.
Oral rehydration Advent of oral rehydrationtherapy (ORT) is considered a major advance ofrecent times. If the fluid loss is mild (5–7% BW)or moderate (7.5–10% BW) ORT can be institutedfrom the very beginning.
Rationale of ORS composition
Oral rehydration is possible if glucose is addedwith salt. It capitalizes on the intactness of glucosecoupled Na+ absorption, even when other mecha-nisms have failed or when intestinal secretion isexcessive, because the secreted fluid lacks glucose
and cannot be reabsorbed. The composition oforal rehydration salt/solution (ORS) has beendebated. The general principles are:(a) It should be isotonic or somewhat hypotonic,i.e. total osmolarity 200–310 mOsm/L (diarrhoeafluids are approximately isotonic with plasma).
(b) The molar ratio of glucose should be equalto or somewhat higher than Na+ (excess glucosewill be utilized in absorbing Na+ present in theintestinal secretions in addition to that presentin ORS itself), but not exceed 110 mM.
(c) Enough K+ (15–25 mM) and bicarbonate/citrate (8–12 mM) should be provided to makeup the losses in stool.The WHO recommended a standard formula which providedNa+ 90 mM, K+ 20 mM, Cl¯ 80 mM, citrate (base) 10 mM,glucose 110 mM and had a total osmolarity of 310 mOsm/L. Trisod. citrate was included in place of sod. bicarbonatebecause bicarbonate containing powder caked and developeda brown colour due to formation of furfural compounds withglucose: had a short shelf life.
The above formula propounded by WHO in 1984 wasbased on the composition of cholera stools in children. Whengiven to children with noncholera diarrhoea, it often producedperiorbital edema due to excess Na+ absorption. Based onthe Na+ content of ETEC stools, many paediatricians favoured60 mM Na+ and 90 mM glucose ORS.
New formula WHO-ORS In 2002 a newformula low Na+ low glucose ORS was releasedby the WHO. Over the past 20 years WHOsponsored studies were carried out in severaldeveloping countries among children and adultssuffering from diarrhoeas. It was found thatmaximum water absorption occurs from a slightlyhypotonic solution and when glucose concen-tration is between 60–110 mM. At higherconcentrations, glucose appears in the stools andtakes its osmotic penalty—stool volume isincreased. A combined analysis of studies usinglow osmolarity ORS has revealed that stoolvolume is reduced by 20% and incidence ofvomiting by 30%. It also permits faster waterabsorption, precludes risk of hypernatremia andis cheaper. The new formula ORS has provenas effective and as safe in cholera as well, butthere is some risk of hyponatremia in adults withcholera.
⎫⎬⎭
in 1 L of wateror 5% glucosesolution.

680S
EC
TIO
N11
GASTROINTESTINAL DRUGS
The WHO and UNICEF have recommendedreplacement of standard (310 mOsm/L) ORSformula by the new (245 mOsm/L).
Non-diarrhoeal uses of ORT
(a) Postsurgical, postburn and post-trauma maintenance ofhydration and nutrition (in place of i.v. infusion).(b) Heat stroke.(c) During changeover from intravenous to enteral alimen-tation.
Zinc in pediatric diarrhoea Recent studies haveshown that administration of Zinc along with lowosmolarity ORS reduces the duration and severityof acute diarrhoea episodes in children below5 years of age. Continued Zinc supplementation(20 mg/day for 6–60 months age; 10 mg/day for0–6 month age) for 10–14 days following theepisode also reduces recurrences of diarrhoea forthe next 2–3 months. Accordingly, the WHOjointly with UNICEF and USAID have recommen-ded that all children with acute diarrhoea shouldbe given Zinc supplementation along with ORSand continued for the next 10–14 days. The IndianAcademy of Pediatrics has endorsed the WHOrecommendation and the Govt. of India hasinitiated providing Zinc in addition to ORSthrough its National Rural Health Mission.
The mechanism of benefit of Zinc in diarrhoea is notknown. In vitro studies have suggested that Zinc could reducefluid secretion in the intestine by indirectly inhibiting cAMPdependent Cl¯ transport across the mucosa through an actionon the basolateral membrane K+ channels. It could alsostrengthen the immune response and help regeneration ofintestinal epithelium.
Zinc can be administered to children by dissolving Zincsulfate dispersible tablets.ULSEEL (50 mg Zn) Cap (for adults)ZIORAL 10 mg and 20 mg (Zn) dispersible tabs for infantsand children respectively.
MAINTENANCE OF NUTRITION
Contrary to traditional view, patients of diarrhoeashould not be starved. Fasting decreases brushborder disaccharidase enzymes and reducesabsorption of salt, water and nutrients; may leadto malnutrition if diarrhoea is prolonged or recurrent.Feeding during diarrhoea has been shown to increaseintestinal digestive enzymes and cell proliferationin mucosa. Simple foods like breast milk or ½strength buffalo milk, boiled potato, rice, chickensoup, banana, sago, etc. should be given as soonas the patient can eat.
New formula WHO-ORSContent Concentrations
NaCl : 2.6 g Na+ — 75 mMKCl : 1.5 g K+ — 20 mMTrisod. citrate : 2.9 g Cl¯ — 65 mMGlucose : 13.5 g Citrate — 10 mMWater : 1 L Glucose — 75 mM
Total osmolarity 245 mOsm/L
(available as ORETRAL-A, ELECTROBION, ELECTRAL21 g sachet for 1000 ml; WALYTE, RELYTE 4.2 g sachetfor 200 ml).
Potassium is an important constituent of ORS,since in most acute diarrhoeas K+ loss is substan-tial. The base (bicarbonate, citrate, lactate) isadded to correct acidosis due to alkali loss instools. It may independently promote Na+ andwater absorption. However, relying on the abilityof the kidney to restore acid-base balance, acidoticstates have been managed without an exogenousbase. Base free ORS has been found to be equallyeffective in rehydrating, but correction of acidosisis slower. Thus, there is a trend to consider baseas a nonessential constituent of ORS, but if presentit may be beneficial, especially in severe caseswith overt acidosis.
Administration of ORT Patients are encouragedto drink ORS at ½–1 hourly intervals. Initially5–7.5% BW volume equivalent is given in2–4 hours (5 ml/kg/hr in children). Thirst dueto volume depletion provides an adequate drivingforce. Subsequently it may be left to demand,but should at least cover the rate of loss in stools.In a weak child who refuses to drink ORS atthe desired rate, it can be given by intragastricdrip; restoring hydration within 6 hours shouldbe aimed.
ORT is not designed to stop diarrhoea, butto restore and maintain hydration, electrolyte andpH balance until diarrhoea ceases, mostly spon-taneously. It is the best and not a second choiceapproach to i.v. hydration.

681C
HA
PTE
R48DRUGS FOR CONSTIPATION AND DIARRHOEA
DRUG THERAPY
Drugs used in diarrhoeas may be categorised into:1. Specific antimicrobial drugs2. Probiotics3. Drugs for inflammaory bowel disease (IBD)4. Nonspecific antidiarrhoeal drugs.
1. Antimicrobials in diarrhoeaOne or more antimicrobial agent is almost routi-nely prescribed to most patients of diarrhoea.However, such drugs have a limited role in theoverall treatment of diarrhoeal diseases; thereasons are:• Bacterial pathogen is responsible for only a
fraction of cases.• Even in bacterial diarrhoea, antimicrobials alter
the course of illness only in selected cases.• Antimicrobials may prolong the carrier state.
Diarrhoea patients can be broadly placed in oneof the two categories:(a) Abundant watery diarrhoea lacking mucus orblood, usually dehydrating with frequent vomiting,but little or no fever. These are generally causedby adhesive but noninvasive enterotoxigenicbacteria such as cholera, ETEC, Salmonellaenteritidis or by rota virus and other viruses whichstimulate massive secretion by activating cAMPin intestinal mucosal cell. ORS and notantimicrobials are the main therapy.(b) Slightly loose, smaller volume stools, frequen-tly with mucus and/or blood, mild dehydration,usually attended with fever and abdominal pain,but not vomiting. These symptoms are indicationsof mucosal invasion, generally caused by entero-invasive organisms like Shigella, enteropathogenicE. coli (EPEC), Campy. jejuni, Salmonellatyphimurium, Yersinia enterocolitica, E.histolytica, Clostri. difficile. Antimicrobials areneeded in many of these.
A. Antimicrobials are of no value In diar-rhoea due to noninfective causes, such as:
(i) Irritable bowel syndrome (IBS)(ii) Coeliac disease
(iii) Pancreatic enzyme deficiency
(iv) Tropical sprue (except when there issecondary infection)
(v) Thyrotoxicosis.
Rotavirus is an important pathogen of acutediarrhoea, especially in children in developedcountries. Along with other diarrhoea causingviruses, it is not amenable to chemotherapy.
Salmonella food poisoning is generally a self-limiting disease. Antibiotics have been widelyused, but may be harmful rather than beneficial.Treated patients have been found to pass orga-nisms in stool for longer periods than untreatedpatients. However, very severe illness or that ininfants/elderly or immunocompromized patientsmay be treated with ciprofloxacin or azithromycinor i.v. ceftriaxone.
B. Antimicrobials are useful only in severedisease (but not in mild cases):
(i) Travellers’ diarrhoea: mostly due to ETEC,Campylobacter or virus: cotrimoxazole, norfloxa-cin, doxycycline reduce the duration of diarrhoeaand total fluid needed only in severe cases.
Rifaximin It is a minimally absorbed oralrifamycin (related to rifampin) active against E.coli and many other gut pathogens. It is recentlyapproved by US-FDA for the empiric treatmentof travellers’ diarrhoea caused by non-invasivestrains of E.coli. Approval has also been grantedin 33 countries for various conditions. A reviewof data from controlled trials using rifaximin 200mg TDS for 3 days has rated it to be superiorto placebo, and as effective as ciprofloxacin inreducing duration of travellers’ diarrhoea,irrespective of whether the causative pathogenwas identified or not. It has also been used indiarrhoeal phase of IBS as well as for prophylaxisbefore and after gut surgery. A higher strength(550 mg) tablet is marketed for reducing risk ofhepatic encephalopathy recurrence by suppressingNH3 forming gut bacteria.
The tolerability profile of rifaximin is similarto placebo. Side effects are flatulence, abdominalpain, defecation urgency and headache. Because

682S
EC
TIO
N11
GASTROINTESTINAL DRUGS
of poor absorption, systemic toxicity is notexpected. Clinical experience with rifaximin islimited, and efficacy for empirical treatment ofdiarrhoea is still to be convincingly establishedagainst local strains of the bacteria.RIFAGUT, TORFIX, 200 mg tab; RACFAX 200, 400 mgtabs.
(ii) EPEC: is less common, but causes Shigella-like invasive illness. Cotrimoxazole, or afluoroquinolone or colistin may be used in acutecases and in infants.
(iii) Shigella enteritis: only when associated withblood and mucus in stools may be treated withciprofloxacin or norfloxacin. Cotrimoxazole andampicillin are alternatives, but many strains areresistant to these.
(iv)Nontyphoid Salmonella enteritis is ofteninvasive; severe cases may be treated with afluoroquinolone, cotrimoxazole or ampicillin.
(v) Yersinia enterocolitica: common in colderplaces, not in tropics. Cotrimoxazole is the mostsuitable drug in severe cases; ciprofloxacin is analternative.
C. Antimicrobials are regularly useful in:
(i) Cholera: Though only fluid replacement is lifesaving, tetracyclines reduce stool volume to nearlyhalf. Cotrimoxazole is an alternative, especiallyin children. Lately, multidrug resistant cholerastrains have arisen. These can be treated withnorfloxacin/ciprofloxacin. Ampicillin and erythro-mycin are also effective.
(ii) Campylobacter jejuni: Norfloxacin andother fluoroquinolones eradicate the organismfrom the stools and control diarrhoea.Erythromycin is fairly effective and is the preferreddrug in children.
(iii) Clostridium difficile: produces antibioticassociated pseudomembranous enterocolitis.The drug of choice for this superinfection ismetronidazole, while vancomycin given orally isan alternative. The offending antibiotic must bestopped.
(iv) Diarrhoea associated with bacterial growthin blind loops/diverticulitis may be treated withtetracycline or metronidazole.(v) Amoebiasis metronidazole, diloxanide furoate,(vi) Giardiasis are effective drugs (see Ch. 60).
2. Probiotics in diarrhoeaThese are microbial cell preparations, either livecultures or lyophillised powders, that are intendedto restore and maintain healthy gut flora or haveother health benefits. Diarrhoeal illnesses andantibiotic use are associated with alteration in thepopulation, composition and balance of gutmicroflora. Recolonization of the gut by non-pathogenic, mostly lactic acid forming bacteriaand yeast is believed to help restore thisbalance. Organisms most commonly used are—Lactobacillus sp., Bifidobacterium, Streptococcusfaecalis, Enterococcus sp. and the yeastSaccharomyces boulardii, etc.
Several reviews and metaanalysis of clinicaltrials have suggested that probiotics significantlyreduce antibiotic-associated diarrhoea, acuteinfective diarrhoea and risk of traveller’s diarrhoea.They also note that most of the randomised placebocontrolled trials have been carried out in health-care setting in developed countries, while data fromcommunity based studies carried out in resource-poor countries is minimal. Several probioticstrains, either alone or in combination, have beenused in different studies, but the protective effecthas been more or less similar, though collationof data is difficult.
While probiotics appear to be useful adjunctsto conventional therapy of acute infectiousdiarrhoea, and are loudly promoted as well asfrequently prescribed, convincing evidence of theirefficacy is lacking. This prevents them from beingaccepted as a standard component of diarrhoeatherapy. Stronger evidence of efficacy has emergedagainst antibiotic-associated diarrhoea, but thereis no justification yet for routine use of probioticsalong with antibiotics. Natural curd/yogurt is anabundant source of lactic acid producingorganisms, which can serve as probiotic. For allpractical purposes, probiotics are safe. Infections
⎫⎬⎭

683C
HA
PTE
R48DRUGS FOR CONSTIPATION AND DIARRHOEA
and acidosis caused by probiotics are very rare,though caution may be prudent in immuno-compromized patients.ECONORM, STIBS: Saccharomyces boulardii 250 mg sachet.BIFILAC: Lactobacillus 50 M (million), Streptococcusfaecalis 30 M, Clostridium butyricum 2M, Bacillusmesentericus 1M per cap/sachet.BIFILIN: Lactobacillus sp, 1 billion (B) Bifidobacteriumbifidum 1B, Streptococcus thermophillus 0.25B,Saccharomyces boulardii 0.25B cap and sachet.ACTIGUT: Lactobacillus sp., Bifidobacterium sp. cap.ENTEROGERMINA: Bacillus clausii 2 billion spores/5 mloral amp.
3. Drugs for inflammatory bowel disease(IBD)
IBD is a chronic relapsing inflammatory diseaseof the ileum, colon, or both, that may be associatedwith systemic manifestations. It is idiopathic, butappears to have an important immune componenttriggered by a variety of factors. The two majortypes of IBD are ulcerative colitis (UC) andCrohn’s disease (CrD).Ulcerative colitis It involves only the colon starting fromthe anal canal. It may remain restricted to the rectum orextend proximally in a contiguous manner to variable extentupto caecum. The lesions are mucosal and may be diffuseor confluent.
Crohn’s disease In CrD lesions are patchy and transmural;may involve any part of the g.i.t. from mouth to the anus.Majority of patients have ileocaecal disease upto ascendingcolon, but in some it may be restricted to the small intestine,while in others to the colon. Because the lesions aretransmural, complications like perforation, abscess, fistula,strictures, etc. occur. CrD is less amenable to medical therapythan is UC. Though UC and CrD are distinct clinical entities,few patients have features of both and cannot be clearlycategorized into UC or CrD.
The drugs used in UC and CrD are the same,but their roles and efficacy do differ. Drugs usedin IBD can be grouped into:• 5-Amino salicylic acid (5-ASA) compounds• Corticosteroids• Immunosuppressants• TNFα inhibitors
Sulfasalazine (Salicylazosulfapyridine) Itis a compound of 5-aminosalicylic acid (5-ASA)with sulfapyridine linked through an azo bond,and has a specific therapeutic effect in IBD.
Having low solubility, it is poorly absorbed fromthe ileum. The azo bond is split by colonic bacteriato release 5-ASA and sulfapyridine. The formerexerts a local antiinflammatory effect, the mecha-nism of which is not clear. Though it inhibitsboth COX and LOX, decreased PG and LTproduction appears to play a minor role in thetherapeutic effect. Inhibition of cytokine, PAF,TNFα and nuclear transcription factor (NFκB)generation seems to be more important. Migrationof inflammatory cells into bowel wall is interferedand mucosal secretion is reduced, affordingsymptomatic relief in UC and to a lesser extentin colon-restricted CrD (releases 5-ASA only incolon). Given during active phase of the diseaseit reduces number of stools, abdominal crampsand fever, but is less effective than corticosteroids;may be employed for mild to moderate exacer-bation. A dose of 3–4 g/day induces remissionover a few weeks in many patients, but relapsesare common after stoppage. Maintenance therapywith 1.5–2 g/day has been found to postponerelapse in majority, but not all cases. The primaryvalue of sulfasalazine is in maintaining remissionin UC, but not in CrD, while corticosteroids arereserved to treat acute exacerbations.
The beneficial effect of sulfasalazine is clearlynot due to any antibacterial action (bowel floraremains largely unaffected). The sulfapyridinemoiety only serves to carry 5-ASA to the colonwithout being absorbed proximally. However, mostof the released sulfapyridine is absorbed in thecolon and is responsible for adverse effects likerashes, fever, joint pain, haemolysis and blooddyscrasias. Nausea, vomiting, headache, malaiseand anaemia are other frequent dose related sideeffects. Upto 1/3rd patients suffer intolerableadverse effects. Oligozoospermia and male infer-tility is reported. Sulfasalazine interferes with

684S
EC
TIO
N11
GASTROINTESTINAL DRUGS
folate absorbtion. Folic acid supplementationshould always be given during its use.
Sufasalazine has also been used as a diseasemodifying drug in rheumatoid arthritis. Theabsorbed sulfapyridine moiety appears to beresponsible for the therapeutic effect (see p. 211).SALAZOPYRIN, SAZO-EN 0.5 g tab.
Mesalazine (Mesalamine) These are theofficial names given to 5-ASA. Realizing that5-ASA is the active moiety in UC, but is noteffective orally because of inability to reach thelarge bowel (it is absorbed in the small intestine),it has been formulated as a delayed releasepreparation or has been coated with pH sensitiveacrylic polymer. The pattern of release over thelength of jejunum, ileum and colon differs amongthe different formulations. The coated formulation(ASACOL, MESACOL) delivers 5-ASA to the distalsmall bowel and colon. A daily dose of 2.4 g hasbeen found to improve over 50% patients of UC(upto 80% mild-to-moderate cases). Less than halfof the 5-ASA released from these preparations isabsorbed systemically, acetylated in the liver andexcreted in urine. Like sulfasalazine, the primaryuse of mesalazine is in preventing relapse of UC,though it may also be employed to treat mild-to-moderate exacerbations or as adjunct to cortico-steroid in more severe active disease. Higher doseof coated mesalazine may induce remission inmild cases of Crohn’s colitis as well, but efficacyis uncertain. It is not useful in maintainingremission in CrD.MESACOL 400 mg, 800 mg tab, 0.5 g suppository; ASACOL,TIDOCOL 400 mg tab; ETISA 500 mg sachet.
Adverse effects Coated mesalazine is muchbetter tolerated than sulfasalazine. Side effectsnoted are nausea, diarrhoea, abdominal pain andheadache, but are mild and less frequent. Seriousadverse effects are fever, itching and leucopenia.Rashes and hypersensitivity reactions are rare.Bone marrow depression and decreased spermcount has not occurred. Mesalazine has nephro-toxic potential, because 30–40% of 5-ASA isreleased in the ileum and is absorbed. It iscontraindicated in renal and hepatic impairment.
Drug interactions Coated mesalazine mayenhance the gastric toxicity of glucocorticoids andhypoglycaemic action of sulfonylureas. Interactionwith coumarins, furosemide, spironolactone,methotrexate and rifampicin are possible.
5-ASA enema Another mode of delivery of5-ASA to colon is to administer it by a retentionenema: 4 g enema once or twice daily is effectivein distal ulcerative colitis and proctitis, includingsome refractory cases.5-ASA enema is not usefulfor maintenance of remission.MESACOL ENEMA 4 g/60 ml.
Olsalazine It consists of two molecules of 5-ASA coupledtogether by azo bond. It is poorly absorbed in the ileum,the azo bond is split in the colon to provide 5-ASA locally.No separate carrier moiety is needed. Olsalazine is probablythe most reliable preparation for delivery of 5-ASA to thecolon. However, it often aggravates diarrhoea initially bydecreasing transit time through the bowels.
Balsalazide This is 5-ASA linked to4-aminobenzoyl-β-alanine as the carrier which,unlike sulfapyridine, is inert. The 5-ASA isreleased in the colon, and the carrier is poorlyabsorbed. It can be used as a safer alternativeto sulfasalazine.Dose: 1.5 g BD to 2.25 g TDS.COLOREX 750 mg cap and per 5 ml syr., INTAZIDE 750 mgtab.
Corticosteroids Prednisolone (40–60 mg/day)or equivalent are highly effective in controllingsymptoms as well as in inducing remission inboth UC and CrD. They are the drugs of choicefor moderately severe exacerbations. In responsivepatients symptomatic relief usually starts within3–7 days and remission is induced in 2–3 weeks.In more severe disease with extraintestinal mani-festations and for rapid relief therapy may beinitiated with i.v. methyl prednisolone 40–60 mg12 to 24 hourly for few days. Hydrocortisoneenema, or foam (ENTOFOAM 10%) can be used fortopical treatment of proctitis and distal ulcerativecolitis, but is less effective. Corticosteroids aregenerally used for short term, and discontinuedafter remission is induced. Mesalazine startedduring steroid therapy is continued to preventrelapses. Corticosteroids are neither effective nor

685C
HA
PTE
R48DRUGS FOR CONSTIPATION AND DIARRHOEA
suitable for maintaining remission either in UCor CrD.
A sizeable percentage of severe IBD patientseither relapse on stoppage of the steroid (steroid-dependent) or do not respond to it (steroid-resistant). Specific immunosuppressant drugs arestrongly indicated in such IBD patients, and arenow frequently prescribed. They also serve toavoid long-term steroid therapy which carrieshazards.
Immunosuppressants (see Ch. 62, 63)
Immunosuppressants have now come to play animportant role in the long-term management ofIBD, especially CrD. About 60% patients withCrD and substantial number of UC patients requireimmunosuppressive therapy. However, risks ofchronic immunosuppression must be weighed ineach patient before instituting therapy with thesedrugs. Because of long latency of response, theyare not suitable for acute flareups of the disease,but have good remission maintaining and steroid-sparing property.
Azathioprine This purine antimetabolite is themost effective and most commonly usedimmunosuppressant in IBD. 6-Mercaptopurine (into which azathioprine is converted in the body)can be used in its place. It is indicated in steroid-dependent, streroid-resistant and relatively severecases of IBD, or those who experience frequentflareups. Although, azathioprine has its ownadverse effect potential, the same is rated lowerthan that of prolonged steroid therapy. Somepatients experience higher bone marrow toxicityof azathioprine and 6-MP due to geneticabnormality of one of its metabolizing enzymesTPMT. These drugs cannot be used in suchpatients.Dose: Azathioprine 1.5–2.5 mg/kg/day, 6-MP 1–1.5 mg/kg/day for IBD.
Methotrexate This dihydrofolate reductase inhibitor withimmunosuppressant property is a 2nd line drug in IBD,especially CrD. It acts faster than azathioprine and hasremission inducing property as well. The doses effective inIBD are higher than those for rheumatoid arthritis. Weeklyparenteral therapy is needed, since absorption and efficacy
by oral route are poor in IBD. Toxicity therefore is higher.Thus, it has a limited role in severe CrD and in patientsnot responsive to or not tolerating azathioprine.
Cyclosporine This potent immunosuppressant isoccasionally used in severe UC patients who do not improvewith corticosteroid therapy. In this setting, i.v. cyclosporineusually controls symptoms in 7–10 days, and can be usedas ‘bridge’ therapy for 2–3 months till azathioprine takeseffect. Though, cyclosporine has remission maintaining effectin UC and CrD, it is not preferred for this purpose becauseof its renal toxicity and poor efficacy in IBD by the oralroute.
TNFα inhibitors
Infliximab It is chimeric anti-TNFα antibody that isindicated in severe active CrD, fistulating CrD and severeUC which has not improved with i.v. corticosteroids andimmunosuppressants, or when the latter are inappropriate.Infused i.v. every 2–8 weeks, it decreases acute flareups andhelps in fistula closure. Therapy is continued till responseis maintained. Infliximab produces substantial toxicity,including acute reactions, formation of antibodies andlowering of resistance to infections. Thus, it is only a reservedrug for selected patients with refractory disease.
Adalimumab and some other TNFα inhibitors are alsobeing used in severe and refractory IBD.
4. Nonspecific antidiarrhoeal drugsThese drugs can be grouped into:A. Absorbants and adsorbantsB. Antisecretory drugsC. Antimotility drugs
A. Absorbants These are colloidal bulk formingsubstances like ispaghula, methyl cellulose, carboxy methylcellulose which absorb water and swell. They modify theconsistency and frequency of stools and give an impressionof improvement, but do not reduce the water and electrolyteloss. They are of value in selected conditions like diarrhoeaphase of IBS, and to increase the consistency of faeces incolostomy patients. Ispaghula and other bulk forming colloidsare useful in both constipation and diarrhoea phases of IBSand reduce abdominal pain as well. Substances that do notferment in colon are preferred for diarrhoea.
Adsorbants like kaolin, pectin, attapulgite are believed toadsorb bacterial toxins in the gut and coat/protect the mucosa.They were ones very popular ingredients of diarrhoea remedies,but are now banned in India, because there is no objectiveproof of their efficacy.
B. Antisecretory drugs
Racecadotril This recently introduced prodrug israpidly converted to thiorphan, an enkephalinase

686S
EC
TIO
N11
GASTROINTESTINAL DRUGS
inhibitor. It prevents degradation of endogenousenkephalins (ENKs) which are mainly δ opioidreceptor agonists. Racecadotril decreases intes-tinal hypersecretion, without affecting motility(motility appears to be regulated through μreceptors) by lowering mucosal cAMP due toenhanced ENK action. It is indicated in the short-term treatment of acute secretory diarrhoeas. Incontrast to loperamide/diphenoxylate, it is notcontraindicated in children. The elimination t½as thiorphan is 3 hr. Side effects are nausea,vomiting, drowsiness, flatulence.Dose: 100 mg (children 1.5 mg/kg) TDS for not more than7 days.CADOTRIL, RACIGYL 100 mg cap, 15 mg sachet; REDOTIL100 mg cap. ZEDOTT, ZOMATRIL 100 mg tab, 10 mgand 30 mg sachet and dispersible tab.
Bismuth subsalicylate Taken as suspension (60 ml 6hourly) it is thought to act by decreasing PG synthesis inthe intestinal mucosa, thereby reducing Cl¯ secretion. It hassome prophylactic value in travellers’ diarrhoea (probablydue to weak antibacterial action as well), but it is ratherinconvenient to carry and take.Though quite popular in USA,it is not used in India and UK.
Anticholinergics Atropinic drugs can reduce bowel motilityand secretion, but have poor efficacy in secretory diarrhoeas.They may benefit nervous/drug (neostigmine, metoclopra-mide) induced diarrhoeas and provide some symptomaticrelief in dysenteries, diverticulitis.
Octreotide This somatostatin analogue (see p. 238) hasa long plasma t½ (90 min) as well as potent antisecretory/antimotility action on the gut. It has been used to controldiarrhoea in carcinoid and vasoactive intestinal peptide (VIP)secreting tumours, and for refractory diarrhoea in AIDSpatients, but needs to be given by s.c. injection.
Opioids In addition to their well recognized antimotilityaction, opioids reduce intestinal secretion. Loperamide hasbeen clearly shown to reduce secretion, probably throughspecific opioid receptors, but does not affect mucosal cAMPor cGMP levels.
C. Antimotility drugsThese are opioid drugs which increase small boweltone and segmenting activity, reduce propulsivemovements and diminish intestinal secretionswhile enhancing absorption. They afford onlysymptomatic relief in diarrhoea. The major actionappears to be mediated through µ opioid receptorslocated on enteric neuronal network, but direct
action on intestinal smooth muscle and secretory/absorptive epithelium has also been demonstrated.The δ receptors are believed to promote absorptionand inhibit secretion, while the μ receptorsenhance absorption and decrease propulsivemovements. Overall they increase resistance toluminal transit and allow more time for theabsorptive processes. No tolerance develops totheir constipating action.
Codeine (see p. 474) This opium alkaloid has prominentconstipating action at a dose of 60 mg TDS. The antidiarrhoealeffect is attributed primarily to its peripheral action on smallintestine and colon. It does have central effects, butdependence producing liability is low. Side effects are nausea,vomiting and dizziness. Due to its abuse potential andavailability of loperamide, codeine is seldom, if ever, usedfor diarrhoea.
Diphenoxylate (2.5 mg) + atropine (0.025 mg):LOMOTIL tab and in 5 ml liquid.Dose: 5–10 mg, followed by 2.5–5 mg 6 hourly.
It is a synthetic opioid, chemically related topethidine; used exclusively as constipating agent;action is similar to codeine. The antidiarrhoealaction is most prominent, but because it isabsorbed systemically and crosses blood-brainbarrier—CNS effects do occur. Atropine is addedin subpharmacological dose to discourage abuseby taking several tablets. Abuse liability is ratedlow, and overdose will produce disturbingatropinic side effects. It has caused respiratorydepression, paralytic ileus and toxic megacolonin children. Response is more variable in them—contraindicated below 6 years of age. Loperamidehas largely superseded it.
Loperamide It is an opiate analogue with majorperipheral µ opioid and additional weak anti-cholinergic property. As a constipating agent itis much more potent than codeine. Because ofpoor water solubility—little is absorbed from theintestines. Entry into brain is negligible—CNSeffects are rare and occur only with high doses;no abuse liability. The duration of action is longer(12 hr) than codeine and diphenoxylate.
In addition to its opiate like action on motility,loperamide also inhibits secretion. Direct

687C
HA
PTE
R48DRUGS FOR CONSTIPATION AND DIARRHOEA
interaction with calmodulin may be responsiblefor the antidiarrhoeal action. Faecal continence isimproved by enhancement of anal sphincter tone.
Adverse effects Abdominal cramps and rashesare the most common side effects. Paralytic ileus,toxic megacolon with abdominal distension is aserious complication in young children—fatali-ties have occurred, probably due to absorptionof toxins from the intestines. Loperamide iscontraindicated in children < 4 yr. However, itappears to be the most effective and most suitableof the antimotility antidiarrhoeal drugs.Dose: 4 mg followed by 2 mg after each motion (max. 10 mgin a day); 2 mg BD for chronic diarrhoea.IMODIUM, LOPESTAL, DIARLOP: 2 mg tab, cap.Liquid formulation has been withdrawn to prevent use in youngchildren.
The utility of antimotility drugs in diarrhoeais limited to noninfective diarrhoea, mildtraveller’s diarrhoea, and when diarrhoea isexhausting or idiopathic diarrhoea in AIDSpatients. Low doses may be used for chronicdiarrhoea in IBS, but higher doses must beavoided. Their use is a short-term measure only.
Antimotility drugs are contraindicated in acuteinfective diarrhoeas because they delay clearance
of the pathogen from the intestine. If invasiveorganisms (Shigella, EPEC, EH, etc.) are present,antimotility drugs can be disastrous by increasingthe risk of systemic invasion. Careful use maybe made in mild IBD when loose motions andurgency are interfering with daily activities,but antimotility drugs are contraindicated insevere disease, since they may raise intraluminalpressure.
Antimotility drugs can be used to inducedeliberate short-term constipation, e.g. after analsurgery, and to reduce the volume, fluidity andbag cleaning frequency in ileostomy/colostomypatients.NOTE: Drugs Controller General of India has banned thefollowing category of antidiarrhoeal drugs:1. Containing adsorbants like Kaolin, pectin, attapulgite,
activated charcoal, etc.2. Containing phthalylsulfathiazole, succinylsulfathiazole,
sulfaguanidine, neomycin, streptomycin, dihydrostrep-tomycin.
3. For pediatric use containing diphenoxylate, loperamide,atropine, belladonna, hyosciamine, halogenated hydroxy-quinolines.
4. Fixed dose combinations of antidiarrhoeals withelectrolytes.
5. Fixed dose combination of loperamide with furazolidone.6. Fixed dose combination of antidiarrhoeals with
antihistaminics.
PROBLEM DIRECTED STUDY
48.1 A 35-year-old man has come with complaint of acute onset diarrhoea. The stools are relativelysmall volume, liquid but not watery, frothy and are preceded by griping pain in abdomen. Foulsmelling wind, eructation and mild fever are the other complaints. He has passed 4 loose motionsin the past 8 hours and there is no appetite. He admits to have eaten spicy snacks last eveningat a road side stall. Physical examination reveals body temperature 101°F, no signs of dehydration,but diffuse abdominal tenderness. A tentative diagnosis of enteroinvasive diarrhoea is made.(a) Does this patient require rehydration therapy?(b) Should an antibiotic be prescribed? If so, which antibiotic would be appropriate?(c) Should an antimotility-antidiarrhoeal drug be coprescribed to reduce the number of stools?(d) Should any other symptomatic drug be given to him?(see Appendix-1 for solution)

Antimicrobial Drugs:General Considerations
ChapterChapterChapterChapterChapter 4949494949
SECTION 12
ANTIMICROBIAL DRUGS
Antimicrobial drugs are the greatest contributionof the 20th century to therapeutics. Their adventchanged the outlook of the physician about thepower drugs can have on diseases. They are oneof the few drugs which can cure, and not justpalliate disease. Their importance is magnifiedin the developing countries, where infectivediseases predominate. As a class, they are oneof the most frequently used as well as misuseddrugs.
Drugs in this class differ from all others inthat they are designed to inhibit/kill the infectingorganism and to have no/minimal effect on therecipient. This type of therapy is generally calledchemotherapy which has come to mean ‘treatmentof systemic infections with specific drugs thatselectively suppress the infecting microorganismwithout significantly affecting the host.’ The basisof selective microbial toxicity is the action ofthe drug on a component of the microbe (e.g.bacterial cell wall) or metabolic processes (e.g.folate synthesis) that is not found in the host,or high affinity for certain microbial biomole-cules (e.g. trimethoprim for bacterial dihydro-folate reductase). Due to analogy between themalignant cell and the pathogenic microbes,treatment of neoplastic diseases with drugs is alsocalled ‘chemotherapy’.
Antibiotics These are substances produced bymicroorganisms, which selectively suppress thegrowth of or kill other microorganisms at verylow concentrations. This definition excludesother natural substances which also inhibit micro-organisms but are produced by higher forms (e.g.antibodies) or even those produced by microbesbut are needed in high concentrations (ethanol,lactic acid, H2O2).Chemotherapeutic agent Initially this termwas restricted to synthetic compounds, but nowsince many antibiotics and their analogues havebeen synthesized, this criterion has becomeirrelevant; both synthetic and microbiologicallyproduced drugs need to be included together.It would be more meaningful to use the termAntimicrobial agent (AMA) to designatesynthetic as well as naturally obtained drugs thatattenuate microorganisms.
The history of chemotherapy may be divided into 3phases.(a) The period of empirical use: of ‘mouldy curd’ by Chineseon boils, chaulmoogra oil by the Hindus in leprosy,chenopodium by Aztecs for intestinal worms, mercury byParacelsus (16th century) for syphilis, cinchona bark (17thcentury) for fevers.
(b) Ehrlich’s phase of dyes and organometallic compounds(1890–1935): With the discovery of microbes in the later half

689C
HA
PTER49
GENERAL CONSIDERATIONS
of 19th century and that they are the cause of many diseases;Ehrlich toyed with the idea that if certain dyes couldselectively stain microbes, they could also be selectively toxicto these organisms. He tried methylene blue, trypan red, etc.He developed the arsenicals—atoxyl for sleeping sickness,arsphenamine in 1906 and neoarsphenamine in 1909 forsyphilis. He coined the term ‘chemotherapy’ because he useddrugs of known chemical structure (that of most other drugsin use at that time was not known) and showed that selectiveattenuation of infecting parasite was a practical proposition.
(c) The modern era of chemotherapy was ushered by Domagkin 1935 by demonstrating the therapeutic effect of Prontosil,a sulfonamide dye, in pyogenic infection. It was soon realizedthat the active moiety was paraamino benzene sulfonamide,and the dye part was not essential. Sulfapyridine (M & B693) was the first sulfonamide to be marketed in 1938.
The phenomenon of antibiosis was demonstrated byPasteur in 1877: growth of anthrax bacilli in urine was inhibitedby air-borne bacteria. Fleming (1929) found that a diffusiblesubstance was elaborated by Penicillium mould which coulddestroy Staphylococcus on the culture plate. He named thissubstance penicillin but could not purify it. Chain and Floreyfollowed up this observation in 1939 which culminated in theclinical use of penicillin in 1941. Because of the great potentialof this discovery in treating war wounds, commercialmanufacture of penicillin soon started.
In the 1940s, Waksman and his colleagues undertooka systematic search of Actinomycetes as source of antibioticsand discovered streptomycin in 1944. This group of soilmicrobes proved to be a treasure-house of antibiotics andsoon tetracyclines, chloramphenicol, erythromycin and manyothers followed. All three groups of scientists, Domagk,Fleming-Chain-Florey and Waksman received the Nobel Prizefor their discoveries.
In the past 50 years emphasis has shifted from searchingnew antibiotic producing organisms to developingsemisynthetic derivatives of older antibiotics with moredesirable properties or differing spectrum of activity. Fewnovel synthetic AMAs, e.g. fluoroquinolones, oxazolidinoneshave also been produced.
CLASSIFICATION
Antimicrobial drugs can be classified in manyways:
A. Chemical structure1. Sulfonamides and related drugs: Sulfa-
diazine and others, Sulfones—Dapsone(DDS), Paraaminosalicylic acid (PAS).
2. Diaminopyrimidines: Trimethoprim,Pyrimethamine.
3. Quinolones: Nalidixic acid, Norfloxacin,Ciprofloxacin, Prulifloxacin, etc.
4. β-Lactam antibiotics: Penicillins, Cepha-losporins, Monobactams, Carbapenems.
5. Tetracyclines: Oxytetracycline, Doxy-cycline, etc.
6. Nitrobenzene derivative: Chloramp-henicol.
7. Aminoglycosides: Streptomycin, Genta-micin, Amikacin, Neomycin, etc.
8. Macrolide antibiotics: Erythromycin,Clarithromycin, Azithromycin, etc.
9. Lincosamide antibiotics: Lincomycin,Clindamycin.
10. Glycopeptide antibiotics: Vancomycin,Teicoplanin.
11. Oxazolidinone: Linezolid.12. Polypeptide antibiotics: Polymyxin-B,
Colistin, Bacitracin, Tyrothricin.13. Nitrofuran derivatives: Nitrofurantoin,
Furazolidone.14. Nitroimidazoles: Metronidazole, Tinida-
zole, etc.15. Nicotinic acid derivatives: Isoniazid,
Pyrazinamide, Ethionamide.16. Polyene antibiotics: Nystatin, Amphote-
ricin-B, Hamycin.17. Azole derivatives: Miconazole, Clotrima-
zole, Ketoconazole, Fluconazole.18. Others: Rifampin, Spectinomycin, Sod.
fusidate, Cycloserine, Viomycin, Ethambu-tol, Thiacetazone, Clofazimine, Griseoful-vin.
B. Mechanism of action1. Inhibit cell wall synthesis: Penicillins,
Cephalosporins, Cycloserine, Vancomycin,Bacitracin.
2. Cause leakage from cell membranes:Polypeptides—Polymyxins, Colistin,Bacitracin. Polyenes—Amphotericin B,Nystatin, Hamycin.
3. Inhibit protein synthesis: Tetracyclines,Chloramphenicol, Erythromycin, Clinda-mycin, Linezolid.
4. Cause misreading of m-RNA code andaffect permeability: Aminoglycosides—Streptomycin, Gentamicin, etc.

690S
EC
TIO
N12
ANTIMICROBIAL DRUGS
5. Inhibit DNA gyrase: Fluoroquinolones—Ciprofloxacin and others.
6. Interfere with DNA function: Rifampin.7. Interfere with DNA synthesis: Acyclovir,
Zidovudine.8. Interfere with intermediary metabolism:
Sulfonamides, Sulfones, PAS, Trimetho-prim, Pyrimethamine, Metronidazole.
C. Type of organisms against whichprimarily active
1. Antibacterial: Penicillins, Aminoglycosi-des, Erythromycin, Fluoroquinolones, etc.
2. Antifungal: Griseofulvin, Amphotericin B,Ketoconazole, etc.
3. Antiviral: Acyclovir, Amantadine, Zido-vudine, etc.
4. Antiprotozoal: Chloroquine, Pyrimetha-mine, Metronidazole, Diloxanide, etc.
5. Anthelmintic: Mebendazole, Pyrantel, Nic-losamide, Diethyl carbamazine, etc.
D. Spectrum of activityNarrow-spectrum Broad-spectrumPenicillin G TetracyclinesStreptomycin ChloramphenicolErythromycin
The initial distinction between narrow and broad-spectrum antibiotics is no longer clearcut. Drugswith all ranges of intermediate band width, e.g.extended spectrum penicillins, newer cepha-losporins, aminoglycosides, fluoroquinolonesare now available. However, the terms ‘narrow-spectrum’ and ‘broad-spectrum’ are still applied.
E. Type of actionPrimarily bacteriostatic
Sulfonamides ErythromycinTetracyclines ClindamycinChloramphenicol Linezolid
Ethambutol
Primarily bactericidalPenicillins CephalosporinsAminoglycosides Vancomycin
Polypeptides CiprofloxacinRifampin MetronidazoleIsoniazid CotrimoxazolePyrazinamide
Some primarily static drugs may become cidalat higher concentrations (as attained in theurinary tract), e.g. erythromycin, nitrofurantoin.On the other hand, some cidal drugs, e.g.cotrimoxazole, streptomycin may only be staticunder certain circumstances.
F. Antibiotics are obtained from:Fungi
Penicillin GriseofulvinCephalosporin
BacteriaPolymyxin B TyrothricinColistin AztreonamBacitracin
ActinomycetesAminoglycosides MacrolidesTetracyclines PolyenesChloramphenicol
PROBLEMS THAT ARISE WITHTHE USE OF AMAs
1. Toxicity(a) Local irritancy: This is exerted at the siteof administration. Gastric irritation, pain andabscess formation at the site of i.m. injection,thrombophlebitis of the injected vein are thecomplications. Practically all AMAs, especiallyerythromycin, tetracyclines, certain cephalo-sporins and chloramphenicol are irritants.
(b) Systemic toxicity: Almost all AMAs pro-duce dose related and predictable organ toxi-cities. Characteristic toxicities are exhibited bydifferent AMAs.Some have a high therapeutic index—doses upto 100-fold range may be given without apparentdamage to host cells. These include penicillins,some cephalosporins and erythromycin.

691C
HA
PTER49
GENERAL CONSIDERATIONS
Others have a lower therapeutic index—doseshave to be individualized and toxicity watchedfor, e.g.:
Aminoglycosides : 8th cranial nerve andkidney toxicity.
Tetracyclines : liver and kidneydamage, antianaboliceffect.
Chloramphenicol : bone marrow depres-sion.
Still others have a very low therapeutic index—use is highly restricted to conditions where nosuitable alternative is available, e.g.:
Polymyxin B : neurological and renaltoxicity.
Vancomycin : hearing loss, kidneydamage.
Amphotericin B : kidney, bone marrowand neurological toxi-city.
2. Hypersensitivity reactionsPractically all AMAs are capable of causing hyper-sensitivity reactions. These are unpredictable andunrelated to dose. The whole range of reactionsfrom rashes to anaphylactic shock can beproduced. The more commonly involved AMAsin hypersensitivity reactions are—penicillins,cephalosporins, sulfonamides, fluoroquinolones.
3. Drug resistanceIt refers to unresponsiveness of a microorganismto an AMA, and is akin to the phenomenon oftolerance seen in higher organisms.
Natural resistance Some microbes havealways been resistant to certain AMAs. They lackthe metabolic process or the target site whichis affected by the particular drug. This isgenerally a group or species characteristic, e.g.gram-negative bacilli are normally unaffected bypenicillin G; aerobic organisms are not affectedby metronidazole; while anaerobic bacteria arenot inhibited by aminoglycoside antibiotics, orM. tuberculosis is insensitive to tetracyclines.
This type of resistance does not pose asignificant clinical problem.
Acquired resistance It is the development ofresistance by an organism (which was sensitivebefore) due to the use of an AMA over a periodof time. This can happen with any microbe andis a major clinical problem. However, develop-ment of resistance is dependent on the micro-organism as well as on the drug. Some bacteriaare notorious for rapid acquisition of resistance,e.g. staphylococci, coliforms, tubercle bacilli.Others like Strep. pyogenes and spirochetes havenot developed significant resistance to penicillindespite its widespread use for > 50 years.Gonococci quickly developed resistance tosulfonamides, but only slowly and low-graderesistance to penicillin. However, in the past 40years, highly penicillin resistant gonococciproducing penicillinase have appeared.
Resistance may be developed by mutationor gene transfer.
Mutation It is a stable and heritable geneticchange that occurs spontaneously and randomlyamong microorganisms. Any sensitive populationof a microbe contains a few mutant cells whichrequire higher concentration of the AMA forinhibition. These are selectively preserved andget a chance to proliferate when the sensitivecells are eliminated by the AMA. Thus, in timeit would appear that a sensitive strain has beenreplaced by a resistant one, e.g. when a singleantitubercular drug is used. This is called verticaltransfer of resistance; is relatively slow andusually of lower grade. Mutation and resistancemay be:
(i) Single step: A single gene mutation may confer highdegree of resistance; emerges rapidly, e.g. enterococci tostreptomycin, E. coli and Staphylococci to rifampin.
(ii) Multistep: A number of gene modifications are involved;sensitivity decreases gradually in a stepwise manner.Resistance to erythromycin, tetracyclines and chloramphenicolis developed by many organisms in this manner.
Sometimes mutational acquisition of resistance isaccompanied by decrease in virulence, e.g. certain rifampin-resistant staphylococci and low grade penicillin-resistantgonococci have decreased virulence.

692S
EC
TIO
N12
ANTIMICROBIAL DRUGS
Gene transfer (infectious resistance) Theresistance causing gene is passed from oneorganism to the other; is called horizontaltransfer of resistance. Rapid spread of resistancecan occur by this mechanism and high levelresistance to several antibiotics (multidrugresistance) can be acquired concurrently.
(i) Conjugation Sexual contact through the formation ofa bridge or sex pilus is common among gram-negative bacilliof the same or another species. This may involve chromosomalor extrachromosomal (plasmid) DNA. The gene carrying the‘resistance’ or ‘R’ factor is transferred only if another‘resistance transfer factor’ (RTF) is also present. Conjugationfrequently occurs in the colon where a large variety of gram-negative bacilli come in close contact. Even nonpathogenicorganisms may transfer R factor to pathogenic organisms,which may become widespread by contamination of food orwater. Chloramphenicol resistance of typhoid bacilli,streptomycin resistance of E. coli, penicillin resistance ofHaemophilus and gonococci and many others have beentraced to this mechanism.
(ii) Transduction It is the transfer of gene carryingresistance through the agency of a bacteriophage. The Rfactor is taken up by the phage and delivered to anotherbacterium which it infects. Many Staph. aureus strains haveacquired resistance by transduction. Certain instances ofpenicillin, erythromycin and chloramphenicol resistance havebeen found to be phage mediated.
(iii) Transformation A resistant bacterium may release theresistance carrying DNA into the medium and this may beimbibed by another sensitive organism—becomingunresponsive to the drug. This mechanism is probably notclinically significant.
Resistance once acquired by any of the abovemechanisms becomes prevalent due to theselection pressure of a widely used AMA, i.e.presence of the AMA provides opportunity forthe resistant subpopulation to thrive in prefe-rence to the sensitive population.
Resistant organisms can broadly be of thefollowing three types:
(a) Drug tolerant Loss of affinity of the targetbiomolecule of the microorganism for a parti-cular AMA, e.g. resistant Staph. aureus and E.coli develop a RNA polymerase that does notbind rifampin, certain penicillin-resistant pneu-mococcal strains have altered penicillin bindingproteins; trimethoprim-resistance results fromplasmid-mediated synthesis of a dihydrofolate
reductase that has low affinity for trimethoprim.Mutational target site modification is animportant mechanism of fluoroquinolone andmacrolide resistance. Another mechanism isacquisition of an alternative metabolic pathway,e.g. certain sulfonamide resistant bacteria switchover to utilizing preformed folic acid in placeof synthesizing it from PABA taken up from themedium.
(b) Drug destroying The resistant microbe ela-borates an enzyme which inactivates the drug,e.g.(i) β-lactamases are produced by staphylococci,Haemophilus, gonococci, etc. which inactivatepenicillin G. The β-lactamases may be presentin low quantity but strategically located peri-plasmically (as in gram-negative bacteria) so thatthe drug is inactivated soon after entry, or maybe elaborated in large quantities (by gram-positive bacteria) to diffuse into the medium anddestroy the drug before entry.(ii) Chloramphenicol acetyl transferase is acqui-red by resistant E. coli, H. influenzae andS. typhi.(iii) Many of the aminoglycoside-resistantcoliforms have been found to produce enzymeswhich adenylate/acetylate/phosphorylate specificaminoglycoside antibiotics.
(c) Drug impermeable Many hydrophilicantibiotics gain access into the bacterial cellthrough specific channels formed by proteinscalled ‘porins’, or need specific transportmechanisms. These may be lost by the resistantstrains, e.g. concentration of some aminoglyc-osides and tetracyclines in the resistant gram-negative bacterial strains has been found to bemuch lower than that in their sensitive counter-parts when both were exposed to equalconcentrations of the drugs. Similarly, the lowdegree penicillin-resistant gonococci are lesspermeable to penicillin G; chloroquine-resistantP. falciparum accumulates less chloroquine. Thebacteria may also acquire plasmid directedinducible energy dependent efflux proteins intheir cell membrane which pump out

693C
HA
PTER49
GENERAL CONSIDERATIONS
tetracyclines. Active efflux-based resistance hasbeen detected for erythromycin and fluoro-quinolones as well.
Cross resistance Acquisition of resistanceto one AMA conferring resistance to anotherAMA, to which the organism has not beenexposed, is called cross resistance. This is morecommonly seen between chemically ormechanistically related drugs, e.g. resistance toone sulfonamide means resistance to all others,and resistance to one tetracycline meansinsensitivity to all others. Such cross resistanceis often complete. However, resistance to oneaminoglycoside may not extend to another, e.g.gentamicin-resistant strains may respond toamikacin. Sometimes unrelated drugs showpartial cross resistance, e.g. between tetra-cyclines and chloramphenicol, between erythro-mycin and lincomycin.
Cross resistance may be two-way, e.g. bet-ween erythromycin and clindamycin and viceversa, or one-way, e.g. development of neomycinresistance by enterobacteriaceae makes theminsensitive to streptomycin but many strepto-mycin-resistant organisms remain susceptible toneomycin.
Prevention of drug resistance It is ofutmost clinical importance to curb developmentof drug resistance. Measures are:(a) No indiscriminate and inadequate or undulyprolonged use of AMAs should be made. Thiswould minimize the selection pressure and resis-tant strains will get less chance to preferentiallypropagate. For acute localized infections in other-wise healthy patients, symptom-determined shor-ter courses of AMAs are advocated.(b) Prefer rapidly acting and selective (narrow-spectrum) AMAs whenever possible; broad-spec-trum drugs should be used only when a specificone cannot be determined or is not suitable.(c) Use combination of AMAs whenever pro-longed therapy is undertaken, e.g. tuberculosis,SABE, HIV-AIDS.(d) Infection by organisms notorious fordeveloping resistance, e.g. Staph. aureus, E. coli,
M. tuberculosis, Proteus, etc. must be treatedintensively.
4. Superinfection (Suprainfection)This refers to the appearance of a new infectionas a result of antimicrobial therapy.
Use of most AMAs causes some alterationin the normal microbial flora of the body. Thenormal flora contributes to host defence byelaborating substances called bacteriocins whichinhibit pathogenic organisms. Further, ordinarily,the pathogen has to compete with the normalflora for nutrients, etc. to establish itself. Lackof competition may allow even a normally non-pathogenic component of the flora, which is notinhibited by the drug (e.g. Candida), to predomi-nate and invade. More complete the suppressionof body flora, greater are the chances of deve-loping superinfection. Thus, it is commonly asso-ciated with the use of broad/extended-spectrumantibiotics, such as tetracyclines, chlorampheni-col, ampicillin, newer cephalosporins; especiallywhen combinations of these are employed. Tetra-cyclines are more liable than chloramphenicoland ampicillin is more liable than amoxicillinto cause superinfection diarrhoeas because ofincomplete absorption—higher amounts reachthe lower bowel and cause greater suppressionof colonic bacteria.
Superinfections are more common when hostdefence is compromised.
Sites involved in superinfection are those thatnormally harbour commensals, i.e. oropharynx;intestinal, respiratory and genitourinary tracts;occasionally skin.
Conditions predisposing to superinfections
• Corticosteroid therapy• Leukaemias and other malignancies, especially
when treated with anticancer drugs (these drugs arealso immunosuppressants and decrease WBCcount)
• Acquired immunodeficiency syndrome (AIDS)• Agranulocytosis• Diabetes, disseminated lupus erythematosus

694S
EC
TIO
N12
ANTIMICROBIAL DRUGS
Superinfections are generally more difficultto treat. The organisms frequently involved, themanifestations and drugs for treating super-infections are:(a) Candida albicans: monilial diarrhoea,thrush, vulvovaginitis; treat with nystatin orclotrimazole.(b) Resistant staphylococci: enteritis; treat withcloxacillin or vancomycin/linezolid.(c) Clostridium difficile: pseudomembranousenterocolitis associated with the use ofclindamycin, tetracyclines, aminoglycosides,ampicillin, etc. It is more common aftercolorectal surgery. The organism produces anenterotoxin which damages gut mucosa formingplaques; metronidazole and vancomycin are thedrugs of choice.(d) Proteus: Urinary tract infection, enteritis;treat with a cephalosporin or gentamicin.(e) Pseudomonas: Urinary tract infection,enteritis; treat with carbenicillin, piperacillin,ceftazidime, cefoperazone or gentamicin.To minimize superinfections:
(i) Use specific (narrow-spectrum) AMAwhenever possible.
(ii) Do not use antimicrobials to treat trivial,self-limiting or untreatable (viral) infec-tions.
(iii) Do not unnecessarily prolong antimicrobialtherapy.
5. Nutritional deficienciesSome of the B complex group of vitamins andvit K synthesized by the intestinal flora is utilizedby man. Prolonged use of antimicrobials whichalter this flora may result in vitamin deficiencies.
Neomycin causes morphological abnorma-lities in the intestinal mucosa—steatorrhoea andmalabsorption syndrome can occur.
6. Masking of an infectionA short course of an AMA may be sufficientto treat one infection but only briefly suppressanother one contacted concurrently. The other
infection will be masked initially, only tomanifest later in a severe form. Examples are:
(i) Syphilis masked by the use of a single doseof penicillin which is sufficient to curegonorrhoea.
(ii) Tuberculosis masked by a short course ofstreptomycin given for trivial respiratoryinfection.
CHOICE OF AN ANTIMICROBIAL AGENT
After having established the need for using asystemic AMA in a patient by assessing that thecondition is due to a treatable (mostly bacterial)infection, and that it is not likely to resolve byitself or by local measures (antiseptics, drainageof pus, etc) only, one has to choose a particularAMA from the large number available. The choicedepends on the particulars of the patient, theinfecting organism and the drug.
Patient factors1. Age may affect kinetics of many AMAs,and certain AMAs produce age-related effects.Conjugation and excretion of chloramphenicolis inefficient in the newborn: larger doses pro-duce gray baby syndrome. Sulfonamidesdisplace bilirubin from protein binding sites—can cause kernicterus in the neonate because theirblood-brain barrier is more permeable. The t½of aminoglycosides is prolonged in the elderlyand they are more prone to develop VIII nervetoxicity. Tetracyclines deposit in the developingteeth and bone—discolour and weaken them—are contraindicated below the age of 6 years.
2. Renal and hepatic function Cautious useand modification of the dose of an AMA (withlow safety margin) becomes necessary when theorgan of its disposal is defective (see box).
3. Local factors The conditions prevailing atthe site of infection greatly affect the actionof AMAs.(a) Presence of pus and secretions decrease theefficacy of most AMAs, especially sulfonamidesand aminoglycosides. Drainage of the abscess

695C
HA
PTER49
GENERAL CONSIDERATIONS
(f) Penetration barriers at certain sites mayhamper the access of the AMA to the site, suchas in subacute bacterial endocarditis (SABE),endophthalmitis, prostatitis. However, trimetho-prim and fluoroquinolones attain high concen-tration in prostate due to ion trapping.
4. Drug allergy History of previous exposureto an AMA should be obtained. If an AMA hascaused allergic reaction—it has to be avoidedin that patient, e.g. drug of choice for syphilisin a patient allergic to penicillin is tetracycline.β-lactams, sulfonamides, fluoroquinolones andnitrofurantoin frequently cause allergy.
5. Impaired host defence Integrity of hostdefence plays a crucial role in overcoming aninfection. Pyogenic infections occur readily inneutropenic patients, while if cell-mediatedimmunity is impaired (e.g. AIDS), infections bylow grade pathogens and intracellular organismsabound. In an individual with normal host defence,a bacteriostatic AMA may achieve cure; whileintensive therapy with cidal drugs is imperativein those with impaired host defence (conditionsgiven on p. 693) or when the organisms areprotected by a barrier—as in SABE. Even thencomplete eradication of the organism may notoccur.
6. Pregnancy All AMAs should be avoidedin the pregnant woman because of risk to thefoetus. Penicillins, many cephalosporins anderythromycin are safe, while safety data on mostothers is not available. Therefore, manufacturerslabel ‘contraindicated during pregnancy’.Tetracyclines are clearly contraindicated. Theycarry risk of acute yellow atrophy of liver,pancreatitis and kidney damage in the mother,as well as cause teeth and bone deformities inthe offspring. Aminoglycosides can cause foetalear damage. Animal studies indicate increasedrisk to the foetus, especially with fluoro-quinolones, cotrimoxazole, chloramphenicol,sulfonamides and nitrofurantoin. Thoughmetronidazole has not been found teratogenic,its mutagenic potential warrants caution in itsuse during pregnancy.
Antimicrobials needing dose reduction/avoidance in renal failure
Reduce dose even in mild failureAminoglycosides Amphotericin BCephalosporins EthambutolVancomycin Flucytosine
Reduce dose only in moderate-severe failureMetronidazole CarbenicillinCotrimoxazole FluoroquinolonesAztreonam ClarithromycinMeropenem Imipenem
Drugs to be avoidedNalidixic acid TalampicillinNitrofurantoin Tetracyclines
(except doxycycline)
Antimicrobials in liver disease
Drugs to be avoidedErythromycin estolate TetracyclinesPyrazinamide Nalidixic acidTalampicillin Pefloxacin
Dose reduction neededChloramphenicol IsoniazidMetronidazole RifampinClindamycin
reduces the population of the causative bacteria,suppresses anaerobes by exposure to oxygen, andimproves diffusion of the antibiotic into theabscess.(b) Presence of necrotic material or foreignbody including catheters, implants and prosthesismakes eradication of infection practicallyimpossible. Bacteria adhering to foreign surfacescreate a biofilm around them and grow veryslowly, rendering them difficult to reach and lessvulnerable to the antibiotic.(c) Haematomas foster bacterial growth; tetra-cyclines, penicillins and cephalosporins getbound to the degraded haemoglobin in thehaematoma.(d) Lowering of pH at the site of infectionreduces activity of macrolide and amino-glycoside antibiotics.(e) Anaerobic environment in the centre of anabscess impairs bacterial transport processeswhich concentrate aminoglycosides in thebacterial cell, rendering them less susceptible.

696S
EC
TIO
N12
ANTIMICROBIAL DRUGS
7. Genetic factors Primaquine, nitrofurantoin,sulfonamides, chloramphenicol and fluoroquino-lones carry the risk of producing haemolysis inG-6-PD deficient patient.
Organism-related considerationsEach AMA has a specific effect on a limitednumber of microbes. Successful chemotherapymust be rational and demands a diagnosis. How-ever, most of the time, definitive bacteriologicaldiagnosis is not available before initiating treat-ment. Bacteriological testing takes time, isexpensive and appropriate samples of infectedmaterial for bacteriology may not be obtainable.Empirical therapy has to be instituted. A clinicaldiagnosis should first be made, at least tenta-tively, and the likely pathogen guessed.The following line of action may be taken:1. Clinical diagnosis itself directs choice ofthe AMA The infecting organism and itssensitivity pattern are by-and-large known, e.g.syphilis, chancroid, diphtheria, tetanus, plague,cholera, trachoma thrush, tuberculosis, lobarpneumonia, leprosy, amoebiasis, herpes simplex,etc.2. A good guess can be made from theclinical features and local experience about thetype of organism and its sensitivity, e.g.tonsillitis, otitis media, boils, vaginitis, urethritis;the most appropriate specific AMA should beprescribed and the response watched for. A Gramstained smear examination of infected materialmay help to aid the choice.3. Choice to be based on bacteriologicalexamination No guess can be made about theinfecting organism or its sensitivity, e.g. broncho-pneumonia, empyema, meningitis, osteomyelitis,urinary tract infection, wound infection, etc. Inthese situations, an AMA should be selected onthe basis of culture and sensitivity testing; butthis may not be always possible.(a) Bacteriological services are not available:empirical therapy to cover all likely organismswith a broad-spectrum drug like fluoroquinolone,
tetracycline or a combination such as gentamicin+ a cephalosporin may be used (with metronida-zole or clindamycin if anaerobes are suspected).Further therapy is modified on the basis ofclinical response; but hasty and arbitrary changesin the selection of AMA should be avoided.(b) Bacteriological services are available, buttreatment cannot be delayed: as in seriousinfections like meningitis, septicaemias, etc.,specimens for bacteriological examinationshould be collected and empirical therapy startedprovisionally as in (a). In case of inadequateresponse, the AMA should be changed later inthe light of bacteriological findings.(c) Bacteriological services are available andtreatment can be delayed for a few days: asin chronic urinary tract infection; it is betterto wait for the culture and sensitivity report; startdefinitive therapy thereafter.Bacteriological sensitivity testing This is generally doneby disk-agar diffusion method using standardized concen-trations of antibiotics based on clinically attained plasmaconcentrations of these. As such, they provide only qualitativeresults; may serve as indicators, and cannot be blindlyextrapolated to the clinical situation in every patient and forevery organism. Broth cultures with break-point concentration(concentration that demarcates between sensitive and resistantbacteria) of antibiotics probably yield more reliable results.Break-point concentrations are to be related to clinicallyattainable serum concentrations of the antibiotic.
Minimum inhibitory concentration (MIC), i.e the lowestconcentration of an antibiotic which prevents visible growthof a bacterium after 24 hours incubation in microwell cultureplates using serial dilutions of the antibiotic is moreinformative. Lately, the disk-diffusion method has been refinedto provide a quantitative estimate of the inhibitory action ofan AMA and its MIC. In this test called the Epsilometer test(E-test) a rectangular test strip impregnated with ascendingconcentrations of the AMA is placed on an inoculated agarplate and the bacterial growth is observed after a specificperiod, depending on the organism. The curved line separatingthe clear zone from the zone with bacterial growth dividesthe strip at the MIC value of concentration.
Minimum bactericidal concentration (MBC) of the anti-biotic is determined by subculturing from tubes with no visiblegrowth. If the organism is killed, no growth will occur; butif it was only inhibited in the parent culture—it will growon subculturing in antibiotic-free medium. MBC is theconcentration of the antibiotic which kills 99.9% of thebacteria. A small difference between MIC and MBC indicatesthat the antibiotic is primarily bactericidal, while a large

697C
HA
PTER49
GENERAL CONSIDERATIONS
difference indicates bacteriostatic action. MBC is not usedto guide selection of antibiotics in clinical practice.
Postantibiotic effect (PAE) After a brief exposure if theorganism is placed in antibiotic-free medium, it startsmultiplying again, but after a lag period which depends onthe antibiotic as well as the organism. This lag period in growthresumption is known as ‘postantibiotic effect’ and is the timerequired for reattainment of logarithmic growth. It is generallycalculated from the time required to attain 10 fold increasein bacterial count in the culture for antibiotic exposed andunexposed tubes. A long and dose-dependent PAE has beennoted with fluoroquinolones, aminoglycosides and rifampin.
Drug factorsWhen any one of a number of AMAs could beused to treat an infection, choice among themis based upon specific properties of these AMAs:1. Spectrum of activity: For definitive therapy,a narrow-spectrum drug which selectively affectsthe concerned organism is preferred, becauseit is generally more effective than a broad-spectrum AMA, and is less likely to disturb thenormal microbial flora. However, for empiricaltherapy, often a broad-spectrum drug has to beused to cover all likely pathogens.2. Type of activity: Many infections in patientswith normal host defence respond equally wellto bacteriostatic and bactericidal AMAs. Butseveral acute infections resolve faster with acidal than a static drug, because the cidal drugdirectly reduces the number of bacteria at thesite of infection, while the static drug onlyprevents increase in their number. Manybactericidal drugs exert prolonged postantibioticeffect so that maintenance of drug levelcontinuously above the MIC is not essential.With bacteriostatic AMAs the bacteria startmultiplying quickly when drug level falls belowthe MIC, resulting in relapse of infection.
A bactericidal antibiotic is clearly superiorto bacteriostatic one in treating patients withimpaired host defence, life-threateninginfections, infections at less accessible sites(SABE) or when carrier state is possible (e.g.typhoid).3. Sensitivity of the organism: Assessed onthe basis of MIC values (if available) andconsideration of postantibiotic effect.
4. Relative toxicity: Obviously, a less toxicantibiotic is preferred, e.g. a β-lactam over anaminoglycoside or erythromycin overclindamycin.5. Pharmacokinetic profile: For optimumaction the antibiotic has to be present at the siteof infection in sufficient concentration for anadequate length of time. This depends on theirpharmacokinetic characteristics. Most anti-biotics are given at 2 to 4 half-life intervals—thus attaining therapeutic concentrations onlyintermittently. For many organisms, amino-glycosides, fluoroquinolones and metronidazoleproduce ‘concentration-dependent inhibition’,i.e. inhibitory effect depends on the ratio of peakconcentration to the MIC. The same daily doseof gentamicin produces better action when givenas a single dose than if it is divided into2–3 portions. On the other hand, β-lactams,glycopeptides and macrolides produce ‘time-dependent inhibition’, i.e. antimicrobial actiondepends on the length of time the concentrationremains above the MIC; division of daily doseimproves the effect. However, the doses shouldbe so spaced that the surviving organisms againstart multiplying and a cidal action is exerted.
Penetration to the site of infection alsodepends on the pharmacokinetic properties ofthe drug. A drug which penetrates better andattains higher concentration at the site ofinfection is likely to be more effective. Thefluoroquinolones have excellent tissue pene-tration—attain high concentrations in softtissues, lungs, prostate, joints, etc. Ciprofloxacinand rifampin have very good intracellularpenetration. Cefuroxime, ceftriaxone, chloramp-henicol, ciprofloxacin attain high CSF concentra-tion. On the other hand, penicillins and amino-glycosides penetrate poorly into CSF unlessmeninges are inflamed. Ampicillin, cephalospo-rins and erythromycin attain high biliaryconcentration.6. Route of administration: Many AMAs canbe given orally as well as parenterally, but amino-glycosides, penicillin G, carbenicillin, manycephalosporins, vancomycin, etc. have to be

698S
EC
TIO
N12
ANTIMICROBIAL DRUGS
given by injection only. For less severeinfections, an oral antibiotic is preferable; butfor serious infections, e.g. meningitis, spreadingcellulitis, septicaemias, a parenteral antibioticwould be more reliable.7. Evidence of clinical efficacy: Relative valueof different AMAs in treating an infection isdecided on the basis of comparative clinical trials.Optimum dosage regimens and duration of treat-ment are also determined on the basis of suchtrials. Reliable clinical trial data, if available, isthe final guide for choice of the antibiotic.8. Cost: Less expensive drugs are to bepreferred.
COMBINED USE OF ANTIMICROBIALS
More than one AMA are frequently used con-currently. This should be done only with aspecific purpose and not blindly in the hope thatif one is good, two should be better and threeshould cure almost any infection. The objectivesof using antimicrobial combinations are:
1. To achieve synergism Every AMA hasa specific effect on selected microorganisms.Depending on the drug pair as well as the orga-nism involved, either synergism (supra-additiveeffect), additive action, indifference or antago-nism may be observed when two AMAs belongingto different classes are used together.
Synergism may manifest in terms of decreasein the MIC of one AMA in the presence ofanother, or the MICs of both may be lowered.If the MIC of each AMA is reduced to 25%or less, the pair is considered synergistic, 25–50% of each is considered additive and morethan 50% of each indicates antagonism. Thus,a synergistic drug sensitizes the organisms tothe action of the other member of the pair. Thismay also manifest as a more rapid lethal actionof the combination than either of the individualmembers resulting in faster cure of the infec-tion. Synergistic prolongation of postantibioticeffect has also been demonstrated for combina-tions of β-lactams with an aminoglycoside, andby addition of rifampin to a variety of antibiotics.
Every combination is unique; the same drugsmay be synergistic for one organism but anta-gonistic for another. However, general guidelinesare:(a) Two bacteriostatic agents are often additive,rarely synergistic, i.e. combination of tetra-cyclines, chloramphenicol, erythromycin, etc. Asulfonamide used with trimethoprim is a specialcase where supraadditive effect is obtainedbecause of sequential block in folate metabolismof certain bacteria (Ch. 50). The combinationoften exerts cidal action, while the individualcomponents are only static.
Another special example is the combinationof a β-lactamase inhibitor clavulanic acid orsulbactam with amoxicillin or ampicillin forβ-lactamase producing H. influenzae, N.gonorrhoeae and other organisms.
(b) Two bactericidal drugs are frequently addi-tive and sometime synergistic if the organismis sensitive to both, e.g.:• Penicillin/ampicillin + streptomycin/gentami-
cin or vancomycin + gentamicin forenterococcal SABE. Penicillins by acting onthe cell wall may enhance the penetration ofthe aminoglycoside into the bacterium.
• Carbenicillin/ticarcillin + gentamicin forPseudomonas infection, especially inneutropenic patients.
• Ceftazidime + ciprofloxacin for Pseudo-monas infected orthopedic prosthesis.
• Rifampin + isoniazid in tuberculosis.
In the above cases, the combination producesfaster cure and reduces the chances of relapseby more complete eradication of the pathogen.(c) Combination of a bactericidal with a bacterio-static drug may be synergistic or antagonisticdepending on the organism. In general:(i) If the organism is highly sensitive to the cidaldrug—response to the combination is equal tothe static drug given alone (apparent antagonism),because cidal drugs act primarily on rapidlymultiplying bacteria, while the static drug retardsmultiplication. This has been seen with penicillin

699C
HA
PTER49
GENERAL CONSIDERATIONS
+ tetracycline/chloramphenicol on pneumococciwhich are highly sensitive to penicillin.Pneumococcal meningitis treated with penicillin+ tetracycline had higher mortality than thosetreated with penicillin alone. Penicillin +erythromycin for group A Streptococci andnalidixic acid + nitrofurantoin for E. coli havealso shown antagonism.(ii) If the organism has low sensitivity to thecidal drug—synergism may be seen, e.g.:• Penicillin + sulfonamide for actinomycosis• Streptomycin + tetracycline for brucellosis• Streptomycin + chloramphenicol for K. pneu-
moniae infection• Rifampin + dapsone in leprosy.Thus, wherever possible, synergistic combina-tions may be used to treat infections that arenormally difficult to cure. Full doses ofindividual drugs are given for this purpose.
2. To reduce severity or incidence ofadverse effects This is possible only if thecombination is synergistic so that the doses canbe reduced. This is needed for AMAs with lowsafety margin, which when used alone in effectivedoses, produce unacceptable toxicity, e.g.• Streptomycin + penicillin G for SABE due
to Strep. faecalis.• Amphotericin B + rifampin or minocycline:
the latter drugs are not themselves antifungal,but enhance the action of amphotericin B.
• Amphotericin B + flucytosine: a shortercourse is needed, specially for cryptococcalmeningitis, than when amphotericin is usedalone.
Otherwise, the doses of individual drugs in asynergistic pair should generally not be reduced.
3. To prevent emergence of resistanceMutation conferring resistance to one AMA isindependent of that conferring resistance toanother. If the incidence of resistant mutants ofa bacillus infecting an individual for drug P is10–5 and for drug Q is 10–7, then only one outof 1012 bacilli will be resistant to both. Thechances of its surviving host defence and causinga relapse would be meagre.
This principle of using two or more AMAstogether is valid primarily for chronic infectionsneeding prolonged therapy; has been widelyemployed in tuberculosis, leprosy, HIV and nowadopted for H. pylori, malaria as well. It is oflittle value in most acute and short-livedinfections. However, rifampin given with cipro-floxacin prevents development of resistance tothe latter by Staph. aureus.
4. To broaden the spectrum of anti-microbial action This is needed in:
(a) Treatment of mixed infection Bronchiec-tasis, peritonitis, certain urinary tract infections,brain abscesses, diabetic foot infection, bed-sores, gynaecological infections are mostlymixed infections. Often, aerobic and anaerobicorganisms sensitive to different drugs areinvolved. Obviously two or more AMAs have tobe used to cover the pathogens. Drugs shouldbe chosen on the basis of bacteriologicaldiagnosis and sensitivity pattern (known orpresumed), and should be employed in full doses.Clindamycin or metronidazole are generallyincluded to cover anaerobes. However, it maysometimes be possible to find a single agenteffective against all the causative organisms.
(b) Initial treatment of severe infections Forempirical therapy, since bacterial diagnosis isnot known; drugs covering gram-positive andgram-negative (in certain situations anaerobesas well), e.g. penicillin + streptomycin; cepha-losporin or erythromycin + an aminoglycoside± metronidazole or clindamycin, may be giventogether. Rational combinations improve thecertainty of curing the infection in the firstattempt, but should be continued only tillbacteriological data become available. When theorganism and its sensitivity has been determined,severity of infection is in itself not an indicationfor combination therapy. Combinations shouldnot be used as a substitute for accurate diagnosis.
(c) Topically Generally, AMAs which are notused systemically, are poorly absorbed from thelocal site and cover a broad range of gram-

700S
EC
TIO
N12
ANTIMICROBIAL DRUGS
positive and gram-negative bacteria are combi-ned for topical application, e.g. bacitracin,neomycin, polymyxin B.
Disadvantages of antimicrobialcombinations1. They foster a casual rather than rational out-
look in the diagnosis of infections and choiceof AMA.
2. Increased incidence and variety of adverseeffects. Toxicity of one agent may beenhanced by another, e.g. vancomycin +tobramycin and gentamicin + cephalothinproduce exaggerated kidney failure.
3. Increased chances of superinfections.4. If inadequate doses of nonsynergistic drugs
are used—emergence of resistance may bepromoted.
5. Higher cost of therapy.
PROPHYLACTIC USE OFANTIMICROBIALS
This refers to the use of AMAs for preventingthe setting in of an infection or suppressingcontacted infection before it becomes clinicallymanifest. The latter is also called ‘preemptivetherapy’, which capitalizes on the smallpopulation of pathogen in the body before thedisease is manifest. AMAs are frequently givenprophylactically, but in a number of circum-stances this is at best wasteful if not harmful.The difference between treating an infection andpreventing it is that treatment is directed againsta specific organism infecting an individual patient(targeted therapy), while prophylaxis is oftenagainst all organisms that may cause infection.The valid as well as improper prophylactic usesmay be categorized as:
1. Prophylaxis against specific organismsThis in general is highly satisfactory and thechoice of drug is clearcut, because it is targeted.(a) Rheumatic fever: A long acting penicillin Gis the drug of choice for preventing infectionby group A streptococci which cause recurrences.
(b) Tuberculosis: Children, HIV positive andother susceptible contacts of open cases needto be protected. Isoniazid alone or with rifampinis recommended.(c) Mycobacterium avium complex (MAC):HIV/AIDS patients with low CD4 count may beprotected against MAC infection by azithro-mycin/clarithromycin.(d) HIV infection: Health care workers exposedto blood by needle stick injury are to be protectedby zidovudine + lamivudine ± indinavir. Offspringof HIV positive woman can be protected byzidovudine given to pregnant mother and thento the newborn for 6 weeks.(e) Meningococcal meningitis: during an epide-mic, especially in contacts; rifampin/ sulfadia-zine/ceftriaxone may be used.(f) Gonorrhoea/syphilis: before or immediatelyafter contact: ampicillin/ceftriaxone.(g) Recurrent genital herpes simplex: Acyclovirprophylaxis may be given when four or morerecurrences occur in a year.(h) Malaria: Travellers to endemic areas withhigh transmission rate many be covered bymefloquine or doxycycline.(i) Influenza A2 : during an epidemic, especiallyin contacts: amantadine.(j) Cholera: tetracycline prophylaxis may begiven to close contacts of a case.(k) Whooping cough: non-immunized childcontact during the incubation period: erythro-mycin can abort clinical disease.(l) Plague: Doxycycline prophylaxis isrecommended for contacts during an epidemic.(m) Pneumocystis jiroveci pneumonia: Trans-plant recipients on immunosuppressants/leukaemia or AIDS patients may be protectedby cotrimoxazole.
2. Prevention of infection in high risksituations Such use of AMAs may be validand satisfactory in certain situations, but iscontroversial in others.(a) Dental extraction, tonsillectomy, endoscopiescause damage to mucosa harbouring bacteria andinduce bacteremia. This is harmless in most

701C
HA
PTER49
GENERAL CONSIDERATIONS
subjects, but in those with valvular defects, thiscan cause endocarditis. Appropriate prophylaxiswith amoxicillin or clindamycin may be givenfew hours before to few hours after theprocedure.(b) Catheterization or instrumentation of urinarytract: prophylaxis with cotrimoxazole or norflo-xacin decreases the risk of urinary tract infection(UTI). Patients with cardiac valvular lesions maybe protected with ampicillin, gentamicin orvancomycin during catheterization.(c) To prevent recurrences of UTI in patientswith abnormalities of the tract: cotrimoxazoleor nitrofurantoin may be given on a long-termbasis since the organism mostly is E. coli.(d) Chronic obstructive lung disease, chronicbronchitis: ampicillin/doxycycline/ciprofloxacinhas been used to prevent acute exacerbations;but are of doubtful value.(e) Immunocompromized patients (receivingcorticosteroids or antineoplastic chemotherapyor immunosuppressants after organ transplan-tation, neutropenic patients): penicillin/cephalo-sporin ± an aminoglycoside or fluoroquinoloneare often used to prevent respiratory tractinfections and septicaemia, but incidence ofsuperinfections is high.
Prophylaxis of surgical site infectionSurgical site infection (SSI) includes superficialincisional infections (e.g. stitch abscess), deepincisional infection (of soft tissue) and organ/space infection. The purpose of surgical prophy-laxis is to reduce the incidence of SSI withminimal alteration of normal microbial flora ofthe host and minimal adverse effects.
For grading the need and intensity of antimicrobialprophylaxis, the operative wounds have been classified into4 categories with increasing risk of SSI (see box).
Wound infection occurs due to microbialcontamination of the surgical site. It is importantfor the surgeon to see that the wound left aftersurgery does not get infected. Use of sterileinstruments, cross-infection control measures(antiseptic/disinfectant, etc.) and good surgicaltechnique to minimise tissue damage, haematoma
and devascularization are the primary, and oftenthe only, measures needed. However, extensive,prolonged and often combined use of AMAs ismade for prophylaxis of infection after practicallyall surgeries. Such misuse is particularly rampentin developing countries, probably because ofunreliability of infection control measures. TheSSI is directly related to the number of bacteriapresent in the surgical wound at the time ofclosure. Systemic antimicrobial prophylaxisshould be employed only when there is clear riskof more than the critical number of bacteriaremaining in the wound at the time of closureand occurrence of SSI. In general, it is notrequired for clean surgery, except in patient atspecial risk. Clean surgery in otherwise healthysubjects is associated with very low risk of SSI.
Incidence of postoperative infection is higherwhen surgery had lasted 2 hours or more.Prophylaxis should be given for surgeries inwhich a prosthesis is inserted into the bone orsoft tissue. Even clean surgery needs to becovered by AMA in diabetics, corticosteroidrecipients and other immunocompromisedsubjects, infants, elderly, malnourished and whenthere is extensive tissue handling/use of electro-cautery, etc.
The selection of drug, dose, timing andduration of prophylactic medication is crucial.It is important that the antibiotic is not started
Classification of operative wounds* withincreasing risk of infection
• Clean: Elective, nontraumatic surgery, no viscera ortract (respiratory, g.i., biliary, genitourinary) entered,no infection at site, no break in technique.
• Clean-contaminated: Otherwise clean but emergencysurgery, or elective surgery with opening of any viscera/tract but minimal spillage, no contact with infectedmaterial or minor break in technique.
• Contaminated: Gross spillage from g.i. tract (gutresection), opening of infected biliary or genitourinarytract, penetrating injury < 4 hr old, grafting on chronicopen wound, major break in technique.
• Dirty: Opening of abscess or purulent site, pre-operative perforation of g.i./respiratory/genitourinarytract/penetrating injury > 4 hr old.
* based on National Research Council (NRC) criteria.

702S
EC
TIO
N12
ANTIMICROBIAL DRUGS
prematurely and is not continued beyond the timewhen bacteria have access to the surgical wound.Administration of the AMA has to be so timedthat peak blood levels occur when clot is formingin the surgical wound, and it is present through-out the procedure. Thus, most of the oral drugsare given 1 hour before incision, while i.v.administration just before/after anaesthesia bestensures effective blood levels of the AMA duringsurgery. Most AMAs do not penetrate the clotonce it is formed and is older than 3 hours. Thus,late and prolonged presence of the antibiotic incirculation serves no purpose, but can fosterresistant organisms. In case of prolonged surgery,the AMA may be repeated i.v. during theprocedure. Postoperative administration of theAMA, especially after 4 hours of wound closureis recommended only in case of contaminatedand dirty surgery, in which case it may be givenfor upto 5 days.
To be maximally effective, a relatively highdose of the AMA is selected which yields peakblood level several times higher than MIC forthe likely pathogens. The drug or combinationof drugs is selected based on the knowledge ofthe organism most commonly causing SSI in agiven procedure. Local patterns of woundinfection (e.g. prevalence of MRSA) andsensitivities of the causative organisms shouldguide the selection. The commonly employedAMAs for prophylaxis in case of clean and clean-contaminated surgeries are listed in the box.
Dirty contaminated wounds (including road sideaccidents): The antimicrobial regimens generallyadministered for 5 days in case of contaminateddirty wounds are:1. Cefazolin 1 g i.v. 8 hourly
+ vancomycin 1 g i.v. 12 hourly.2. Cefoxitin 1 g i.v. 6 hourly/ceftizoxime 1 g
i.v. 12 hourly.3. Clindamycin 0.6 g i.v. 8 hourly
+ Gentamicin 80 mg i.v. 8 hourly.4. Ampicillin 2 g i.v. 6 hourly/vancomycin 1 g
i.v. 12 hourly+ Gentamicin 80 mg i.v. 8 hourly+ Metronidazole 0.5 g i.v. 8 hourly.
5. Amoxicillin 1 g + Clavulanate 0.2 g i.v. 12hourly.All given for 5 days
3. Prevention of infection in general Thisis highly unsatisfactory in most cases and mustbe condemned. Examples are:(a) Neonates, especially after prolonged orinstrumental delivery.(b) To prevent postpartum infections in themother after normal delivery.(c) Viral upper respiratory tract infections: toprevent secondary bacterial invasion.(d) To prevent respiratory infections in uncons-cious patients or in those on respirators.
Antimicrobial prophylaxis in these situationsmay be hazardous. Infection by resistantorganisms, fungal and other superinfections canoccur, because it is not possible to prevent allinfections, at all times, in all individuals.
FAILURE OF ANTIMICROBIAL THERAPY
The success of antimicrobial therapy can be mea-sured either clinically in terms of improvementin symptoms/signs or microbiologically as eradi-cation of the infecting organism.
Commonly used antimicrobials drugs forsurgical prophylaxis
Oral (single dose given 1 hour before procedure)
1. Amoxicillin 2 g (50 mg/kg)2. Cephalexin 2 g (50 mg/kg)3. Cefadroxil 2 g (50 mg/kg)4. Clindamycin 600 mg (20 mg/kg) For patients5. Azithromycin 500 mg (15 mg/kg) allergic to6. Clarithromycin 500 mg (15 mg/kg) penicillin
Parenteral (single injection just before procedure)
1. Ampicillin 2 g (50 mg/kg) i.m./i.v.2. Cefazolin 1 g (25 mg/kg) i.v.3. Vancomycin 1 g (20 mg/kg) i.v. (in MRSA prevalent
areas and/or penicillin allergic patients).4. Clindamycin 600 mg (20 mg/kg) i.v. (for penicillin
allergic patients).5. Cefuroxime 1.5 g (30 mg/kg) i.v.
+ Metronidazole 0.5 g (10 mg/kg) i.v.6. Gentamicin 160 mg (3 mg/kg) i.v.
+ Metronidazole 0.5 g (10 mg/kg) i.v.
⎫⎬⎭
⎫⎬⎭
For gutand biliarysurgery

703C
HA
PTER49
GENERAL CONSIDERATIONS
Antimicrobials may fail to cure an infection/fever, or there may be relapses. This is rare whenantimicrobial therapy was begun, in the firstplace, on sound clinical and/or bacteriologicalbasis. When a real or apparent failure of theantimicrobial regimen occurs, the diagnosis andtherapy should be reviewed. One of the followingcauses will usually be identified.1. Improper selection of drug, dose, route orduration of treatment.2. Treatment begun too late.3. Failure to take necessary adjuvant measures,e.g. drainage of abscesses, empyema, etc.;removal of renal stones, other foreign bodies
or infected gall bladder, adjustment of properurinary pH in case of UTI; cavity closure; controlof diabetes, etc.4. Poor host defence—as in leukaemias, neutro-penia and other causes, especially if a bacterio-static AMA is used.5. Infecting organism present behind barriers,such as vegetation on heart valves (SABE), insidethe eyeball, blood brain-barrier.6. Trying to treat untreatable (viral) infectionsor other causes of fever (malignancy, collagendiseases).7. Presence of dormant or altered organisms(the persisters) which later give rise to a relapse.
PROBLEM DIRECTED STUDY
49.1 A lady aged 40 years and weighing 60 kg is to undergo elective cholecystectomy formultiple gallstones. She is asymptomatic.(a) Does she require antimicrobial prophylaxis?(b) If she does, which antimicrobial(s) should be selected? When, by what route and dose,and how long the antimicrobial(s) should be administered?(see Appendix-1 for solution)

Sulfonamides, Cotrimoxazole andQuinolones
ChapterChapterChapterChapterChapter 5050505050
SULFONAMIDES
Sulfonamides were the first antimicrobial agents(AMAs) effective against pyogenic bacterialinfections. Sulfonamido-chrysoidine (ProntosilRed) was one of the dyes included by Domagkto treat experimental streptococcal infectionin mice and found it to be highly effective.Subsequently an infant was cured of staphylo-coccal septicaemia (which was 100% fatal atthat time) by prontosil. By 1937, it became clearthat prontosil was broken down in the body torelease sulfanilamide which was the activeantibacterial agent. A large number of sulfonamideswere produced and used extensively in thesubsequent years, but because of rapid emergenceof bacterial resistance and the availability of manysafer and more effective antibiotics, their currentutility is limited, except in combination withtrimethoprim (as cotrimoxazole) or pyrimeth-amine (for malaria).
2. Intermediate acting (8–12 hr):Sulfamethoxazole
3. Long acting (~7 days): Sulfadoxine,Sulfamethopyrazine
4. Special purpose sulfonamides:Sulfacetamide sod., Mafenide, Silversulfadiazine, Sulfasalazine
ANTIBACTERIAL SPECTRUMSulfonamides are primarily bacteriostatic againstmany gram-positive and gram-negative bacteria.However, bactericidal concentrations may beattained in urine. Sensitivity patterns amongmicroorganisms have changed from time-to-timeand place-to-place. Those still sensitive are:
many Strepto. pyogenes, Haemophilusinfluenzae, H. ducreyi, Calymmatobacteriumgranulomatis, Vibrio cholerae. Only a fewStaph. aureus, gonococci, meningococci,pneumococci, Escherichia coli, and Shigellarespond, but majority are resistant.Anaerobic bacteria are not susceptible.Chlamydiae: trachoma, lymphogranuloma vene-reum, inclusion conjunctivitis, are sensitive, asare Actinomyces, Nocardia and Toxoplasma.
Mechanism of action Many bacteria syn-thesize their own folic acid (FA) of whichp-aminobenzoic acid (PABA) is a constituent, andis taken up from the medium. Woods and Fildes(1940) proposed the hypothesis that sulfona-mides, being structural analogues of PABA, inhibitbacterial folate synthase → FA is not formed anda number of essential metabolic reactions suffer.Sulfonamides competitively inhibit the union ofPABA with pteridine residue to form dihydrop-teroic acid which conjugates with glutamic acid
NOTE: Nonabsorbable sulfonamides—Phthlylsulfathiazole, Succinyl sulfathiazole, Sulfaganidine are banned in India
Chemistry All sulfonamides may be considered to be deri-vatives of sulfanilamide (p-aminobenzene sulfonamide).Individual members differ in the nature of N1 (SulfonamidoN) substitution, which governs solubility, potency andpharmacokinetic property. A free amino group in the paraposition (N4) is required for antibacterial activity.
Sulfonamides that are still of clinical interestare:1. Short acting (4–8 hr): Sulfadiazine

705C
HA
PTER50
SULFONAMIDES, COTRIMOXAZOLE AND QUINOLONES
to produce dihydrofolic acid. Also, beingchemically similar to PABA, the sulfonamide mayitself get incorporated to form an altered folatewhich is metabolically injurious.
Human cells also require FA, but they utilizepreformed FA supplied in diet and are unaffectedby sulfonamides. Evidences in favour of thismechanism of action of sulfonamides are:
(a) PABA, in small quantities, antagonizes theantibacterial action of sulfonamides.
(b) Only those microbes which synthesize theirown FA, and cannot take it from the mediumare susceptible to sulfonamides.
Pus and tissue extracts contain purines andthymidine which decrease bacterial requirementfor FA and antagonize sulfonamide action. Pusis also rich in PABA.
Resistance to sulfonamides Most bacteriaare capable of developing resistance to sulfona-mides. Prominent among these are gonococci,pneumococci, Staph. aureus, meningococci, E.coli, Shigella and some Strep. pyogenes, Strep.viridans and anaerobes. The resistant mutantseither:
(a) produce increased amounts of PABA, or(b) their folate synthase enzyme has low
affinity for sulfonamides, or(c) adopt an alternative pathway in folate
metabolism.Resistance developed in vivo is quite persistent.Sensitivity patterns have changed depending onthe extent of use. When an organism is resistantto one sulfonamide, it is resistant to them all.No cross resistance between sulfonamides andother AMAs has been noted. Development ofresistance has markedly limited the clinicalusefulness of this class of compounds.
PHARMACOKINETICS
Sulfonamides are rapidly and nearly completely absorbed fromg.i.t. Extent of plasma protein binding differs considerably(10–95%) among different members. The highly protein boundmembers are longer acting. Sulfonamides are widely distributedin the body—enter serous cavities easily. The free form ofsulfadiazine attains the same concentration in CSF as inplasma. They cross placenta freely.
The primary pathway of metabolism of sulfonamides isacetylation at N4 by nonmicrosomal acetyl transferase, primarilyin liver. There are slow and fast acetylators, but the differenceis mostly insufficient to be clinically significant. The extentof metabolism differs for different members. The acetylatedderivative is inactive, but can contribute to the adverse effects.It is generally less soluble in acidic urine than the parentdrug—may precipitate and cause crystalluria.
Sulfonamides are excreted mainly by the kidney throughglomerular filtration. Both renal tubular secretion andreabsorption occur. The more lipid-soluble members are highlyreabsorbed in the tubule, therefore are longer acting.
Sulfadiazine It is the prototype of the general purposesulfonamides that is rapidly absorbed orally and rapidlyexcreted in urine. Plasma protein binding is 50%, and it is20–40% acetylated. The acetylated derivative is less solublein urine, crystalluria is likely. It has good penetrabilityin brain and CSF—was the preferred compound for meningitis.Dose: 0.5 g QID to 2 g TDS; SULFADIAZINE 0.5 g tab.
Sulfamethoxazole It has slower oral absorption andurinary excretion resulting in intermediate duration of action;t½ in adults averages 10 hours. It is the preferred compoundfor combining with trimethoprim because the t½ of both issimilar. However, a high fraction is acetylated, which isrelatively insoluble—crystalluria can occur.Dose: 1 g BD for 2 days, then 0.5 g BD. GANTANOL 0.5 g tab.
Sulfadoxine, Sulfamethopyrazine These are ultralongacting compounds, action lasting > 1 week because of highplasma protein binding and slow renal excretion (t½ 5–9 days).They attain low plasma concentration (of free form) and arenot suitable for treatment of acute pyogenic infections, butare used in combination with pyrimethamine in the treatmentof malaria (especially chloroquine resistant P. falciparum; SeeCh. 59), Pneumocystis jiroveci pneumonia in AIDS patientsand in toxoplasmosis. Because they have caused seriouscutaneous reactions, large-scale use of the combination forprophylaxis of malaria is not recommended.
Sulfacetamide sod. It is a highly soluble compoundyielding neutral solution which is only mildly irritating to theeye in concentrations up to 30%. It is used topically for ocularinfections due to susceptible bacteria and chlamydia, includingophthalmia neonatorum caused by Ch. oculogenitalis. Itattains high concentrations in anterior segment and aqueoushumour after topical instillation. The incidence of sensitivityreactions with ocular use of sulfacetamide sod. has been low;but it must be promptly stopped when they occur.LOCULA, ALBUCID 10%, 20%, 30% eye drops, 6% eye oint.
Mafenide It is not a typical sulfonamide, because a —CH2—bridge separates the benzene ring and the amino group. Itis used only topically—inhibits a variety of gram- positiveand gram-negative bacteria. In contrast to typical sulfonamides,it is active in the presence of pus and against Pseudomonas,clostridia which are not inhibited by typical sulfonamides.It has been mainly employed for burn dressing to preventinfection, but not to treat already infected cases.

706S
EC
TIO
N12
ANTIMICROBIAL DRUGS
The biggest limitation is that mafenide produces burningsensation and severe pain when applied to raw surface. Itis rapidly absorbed from the raw surface, metabolized andexcreted in urine. Mafenide and its metabolite are carbonicanhydrase (CAse) inhibitors. Accordingly, they alkalinize urine,can cause acidosis and hyperventilation. Mafenide must notbe applied over large areas. Allergic reactions, particularlyrashes also occur.SULFAMYLON 1% cream for surface application.
Silver sulfadiazine Used topically as 1% cream, it is activeagainst a large number of bacteria and fungi, even thoseresistant to other sulfonamides, e.g. Pseudomonas. It slowlyreleases silver ions which appear to be largely responsiblefor the antimicrobial action. It is considered to be one of themost effective drugs for preventing infection of burnt surfacesand chronic ulcers and is well tolerated. However, it is notgood for treating established infection.SILVIRIN 1% cream, ARGENEX 1% cream with chlorhexidine0.2%.Local side effects are—burning sensation on application anditch.Released sulfadiazine may be absorbed systemically andproduce its own adverse effects.
Sulfasalazine (see p. 211, 683) used in ulcerative colitisand rheumatoid arthritis.
ADVERSE EFFECTS
Adverse effects to sulfonamides are relatively common. Theseare:• Nausea, vomiting and epigastric pain.• Crystalluria is dose related, but infrequent now.
Precipitation in urine can be minimized by taking plentyof fluids and by alkalinizing the urine in whichsulfonamides and their acetylated derivatives are moresoluble.
• Hypersensitivity reactions occur in 2–5% patients. Theseare mostly in the form of rashes, urticaria and drug fever.Photosensitization is reported. Stevens-Johnson syndromeand exfoliative dermatitis are serious reactions reportedwith the long-acting agents.
• Hepatitis, unrelated to dose, occurs in 0.1% patients.• Topical use of sulfonamides is not allowed, because of risk
of contact sensitization. However, ocular use is permitted.• Haemolysis can occur in G-6-PD deficient individuals with
high doses of sulfonamides. Neutropenia and other blooddyscrasias are rare.
• Kernicterus may be precipitated in the newborn, especiallypremature, whose blood-brain barrier is more permeable,by displacement of bilirubin from plasma protein bindingsites.
Interactions Sulfonamides inhibit the metabolism (possiblydisplace from protein binding also) of phenytoin, tolbutamideand warfarin—enhance their action.They displace methotrexate from binding sites and decreaseits renal excretion—toxicity can occur.
Fixed dose combinations of sulfonamides with penicillin arebanned in India.
USES
Systemic use of sulfonamides alone (notcombined with trimethoprim or pyrimethamine)is rare now. Though they can be employed forsuppressive therapy of chronic urinary tractinfection, for streptococcal pharyngitis and guminfection; such uses are outmoded.
Combined with trimethoprim (as cotrimoxa-zole) sulfamethoxazole is used for manybacterial infections, P. jiroveci and nocardiosis(see below). Along with pyrimethamine, certainsulfonamides are used for malaria (see Ch. 59)and toxoplasmosis.
Ocular sulfacetamide sod. (10–30%) is acheap alternative in trachoma/inclusion conjunc-tivitis, though additional systemic azithromycinor tetracycline therapy is required for eradicationof the disease. Topical silver sulfadiazine ormafenide are used for preventing infection onburn surfaces.
COTRIMOXAZOLE
The fixed dose combination of trimethoprimand sulfamethoxazole is called cotrimoxazole.Trimethoprim is a diaminopyrimidine related tothe antimalarial drug pyrimethamine whichselectively inhibits bacterial dihydrofolatereductase (DHFRase). Cotrimoxazole introducedin 1969 causes sequential block of folate meta-bolism as depicted in Fig. 50.1. Trimethoprim
Fig. 50.1: Sequential block in bacterial folate metabolismPABA—Para aminobenzoic acid; DHFA—Dihydrofolicacid; THFA—Tetrahydrofolic acid

707C
HA
PTER50
SULFONAMIDES, COTRIMOXAZOLE AND QUINOLONES
is >50,000 times more active against bacterialDHFRase than against the mammalian enzyme.Thus, human folate metabolism is not interferedat antibacterial concentrations of trimethoprim.Individually, both sulfonamide and trimethoprimare bacteriostatic, but the combination becomescidal against many organisms. Maximumsynergism is seen when the organism is sensitiveto both the components, but even when it ismoderately resistant to one component, theaction of the other may be enhanced.
Sulfamethoxazole was selected for combi-ning with trimethoprim because both have nearlythe same t½ (~ 10 hr). Optimal synergy in caseof most organisms is exhibited at a concentrationratio of sulfamethoxazole 20 : trimethoprim 1,the MIC of each component may be reducedby 3–6 times. This ratio is obtained in the plasmawhen the two are given in a dose ratio of5 : 1, because trimethoprim enters many tissues,has a larger volume of distribution than sulfa-methoxazole and attains lower plasma concen-tration. However, the concentration ratio in manytissues is less than 20 : 1. Trimethoprimadequately crosses blood-brain barrier andplacenta, while sulfamethoxazole has a poorerentry. Moreover, trimethoprim is more rapidlyabsorbed than sulfamethoxazole—concentrationratios may vary with time. Trimethoprim is 40%plasma protein bound, while sulfamethoxazoleis 65% bound. Trimethoprim is partly metabo-lized in liver and excreted in urine.Spectrum of action Antibacterial spectra oftrimethoprim and sulfonamides overlap consi-derably. Additional organisms covered by thecombination are—Salmonella typhi, Serratia,Klebsiella, Enterobacter, Yersinia entero-colitica, Pneumocystis jiroveci and manysulfonamide-resistant strains of Staph. aureus,Strep. pyogenes, Shigella, enteropathogenic E.coli, H.influenzae, gonococci and meningococci.Resistance Bacteria are capable of acquiringresistance to trimethoprim mostly throughplasmid mediated acquisition of a DHFRase
having lower affinity for the inhibitor. Resistanceto the combination has been slow to developcompared to either drug alone, but widespreaduse of the combination over a long period hasresulted in reduced responsiveness of over 30%originally sensitive strains.
Adverse effects All adverse effects seenwith sulfonamides can be produced by cotri-moxazole.• Nausea, vomiting, stomatitis, headache and
rashes are the usual manifestations.• Folate deficiency (megaloblastic anaemia) is
infrequent, occurs only in patients withmarginal folate levels.
• Blood dyscrasias occur rarely.Cotrimoxazole should not be given duringpregnancy. Trimethoprim being an antifolate,there is theoretical teratogenic risk. Neonatalhaemolysis and methaemoglobinaemia can occurif it is given near term.• Patients with renal disease may develop
uremia. Dose should be reduced in modera-tely severe renal impairment.
• A high incidence (upto 50%) of fever, rashand bone marrow hypoplasia has been reportedamong AIDS patients with Pneumocystisjiroveci infection when treated with high dosecotrimoxazole.
• The elderly are also at greater risk of bonemarrow toxicity from cotrimoxazole.
• Diuretics given with cotrimoxazole haveproduced a higher incidence of thrombocyto-penia.
Preparations SEPTRAN, SEPMAX, BACTRIM, CIPLIN,ORIPRIM, SUPRISTOL, FORTRIMTrimethoprim Sulfamethoxazole
80 mg + 400 mg tab: 2 BD for 2 days then 1 BD.160 mg + 800 mg tab: double strength (DS); 1 BD.20 mg + 100 mg pediatric tab.40 mg + 200 mg per 5 ml susp; infant 2.5 ml (not
to be used in newborns), children 1–5yr 5 ml, 6–12 year 10 ml (all BD).
160 mg + 800 mg per 3 ml for i.m. injection12 hourly. (CIPLIN, ORIPRIM-IM)
80 mg + 400 mg per 5 ml for i.v. injection(WK-TRIM, ORIPRIM-IV) 10–15 ml BD.

708S
EC
TIO
N12
ANTIMICROBIAL DRUGS
Cotrimazine It is a combination of trimethoprim withsulfadiazine. Its utility is similar to that of cotrimoxazole.Trimethoprim Sulfadiazine
90 mg + 410 mg: AUBRIL tab, 2 tab BD for2 days, then 1 BD.
180 mg + 820 mg: TRIGLOBE FORTE tab.
Uses
Though cotrimoxazole is still used, its popularityin the treatment of systemic infections hasdeclined. Common indications are:
1. Urinary tract infections Most acuteuncomplicated infections respond rapidly. Singledose therapy with 4 tablets of cotrimoxazole hasbeen used successfully for acute cystitis.Courses of 3–10 days have been advised forlower and upper urinary tract infections,according to associated features. Cotrimoxazoleis specially valuable for chronic or recurrentcases or in prostatitis, because trimethoprim isconcentrated in prostate.
2. Respiratory tract infections Both upperand lower respiratory tract infections, includingchronic bronchitis and facio-maxillary infec-tions, otitis media caused by gram positive cocciand H. influenzae respond well.
3. Bacterial diarrhoeas and dysentery Cotri-moxazole may be used for severe and invasiveinfections by E. coli, Shigella, nontyphoidSalmonella, and Y. enterocolitica (see p. 682).Though response rate is lower than previously,and fluoroquinolones are more commonly used,it is still a valuable alternative for empiricaltherapy of infective diarrhoea.
4. Pneumocystis jiroveci causes severepneumonia in neutropenic and AIDS patients.Cotrimoxazole has prophylactic as well astherapeutic value, but high doses are needed. OneDS tablet 4–6 times/day for 2–3 weeks may becurative, but adverse effects necessitatediscontinuation in upto 20% cases. One DS tab.daily has been used for prophylaxis and this isbetter tolerated.
5. Chancroid Cotrimoxazole (800 + 160 mg)BD for 14 days is a 3rd choice, but less expen-sive, alternative to ceftriaxone, azithromycin orciprofloxacin.
6. Typhoid Initially cotrimoxazole was an effectivealternative to chloramphenicol. However, it has becomeunreliable, and is seldom used now.
7. Cotrimoxazole is an alternative to penicillin forprotecting agranulocytosis patients and for treating respiratoryor other infections in them. Intensive parenteral cotrimoxazoletherapy has been used successfully in septicaemias, but otherdrugs are more commonly employed now.
QUINOLONES
These are synthetic antimicrobials having aquinolone structure that are active primarilyagainst gram-negative bacteria, though the newerfluorinated compounds also inhibit gram-positiveones. The first member Nalidixic acid intro-duced in mid-1960s had usefulness limited tourinary and g.i. tract infections because of lowpotency, modest blood and tissue levels,restricted spectrum and high frequency ofbacterial resistance. A breakthrough was achievedin the early 1980s by fluorination of thequinolone structure at position 6 and intro-duction of a piperazine substitution at position7 resulting in derivatives called fluoroquinoloneswith high potency, expanded spectrum, slowdevelopment of resistance, better tissue pene-tration and good tolerability.

709C
HA
PTER50
SULFONAMIDES, COTRIMOXAZOLE AND QUINOLONES
Nalidixic acidIt is active against gram-negative bacteria, espe-cially coliforms: E. coli, Proteus, Klebsiella,Enterobacter, Shigella but not Pseudomonas.It acts by inhibiting bacterial DNA gyrase andis bactericidal. Resistance to nalidixic aciddevelops rather rapidly.
Nalidixic acid is absorbed orally, highly plasma proteinbound and partly metabolized in liver: one of the metabolitesis active. It is excreted in urine with a plasma t½ ~8 hrs.Concentration of the free drug in plasma and most tissuesattained with the usual doses is nontherapeutic for systemicinfections (MIC values for most susceptible bacteria justapproach the ‘break-point’ concentration). However, highconcentration attained in urine (20–50 times that in plasma)and gut lumen is lethal to the common urinary pathogensand diarrhoea causing coliforms.
Adverse effects These are relatively infrequent, consistmostly of g.i. upset and rashes.Most important toxicity is neurological—headache,drowsiness, vertigo, visual disturbances, occasionally seizures(especially in children).Phototoxicity is rare. Individuals with G-6-PD deficiency maydevelop haemolysis.Nalidixic acid is contraindicated in infants.Dose: 0.5–1 g TDS or QID; GRAMONEG 0.5 g tab, 0.3 g/5 mlsusp, DIARLOP 0.3 g/5 ml susp.
Use
1. Nalidixic acid is primarily used as a urinaryantiseptic, generally as a second line drug inrecurrent cases or on the basis of sensitivityreports.Nitrofurantoin should not be given concurren-tly—antagonism occurs.2. It has also been employed in diarrhoea causedby Proteus, E. coli, Shigella or Salmonella, butnorfloxacin/ciproloxacin are more commonlyused now.
FLUOROQUINOLONES
These are quinolone antimicrobials having oneor more fluorine substitutions. The ‘firstgeneration’ fluoroquinolones (FQs) introducedin 1980s have one fluoro substitution. In the1990s, compounds with additional fluoro andother substitutions have been developed—furtherextending antimicrobial activity to gram-positive
cocci and anaerobes, and/or confering metabolicstability (longer t½). These are referred to as‘second generation’ FQs.
Mechanism of action The FQs inhibit theenzyme bacterial DNA gyrase (primarily activein gram negative bacteria), which nicks double-stranded DNA, introduces negative supercoils andthen reseals the nicked ends. This is necessaryto prevent excessive positive supercoiling of thestrands when they separate to permit replicationor transcription. The DNA gyrase consists oftwo A and two B subunits: The A subunit carriesout nicking of DNA, B subunit introducesnegative supercoils and then A subunit resealsthe strands. FQs bind to A subunit with highaffinity and interfere with its strand cutting andresealing function. In gram-positive bacteria themajor target of FQ action is a similar enzymetopoisomerase IV which nicks and separatesdaughter DNA strands after DNA replication.Greater affinity for topoisomerase IV mayconfer higher potency against gram-positivebacteria. The bactericidal action probably resultsfrom digestion of DNA by exonucleases whoseproduction is signalled by the damaged DNA.
In place of DNA gyrase or topoisomeraseIV, the mammalian cells possess an enzymetopoisomerase II (that also removes positivesupercoils) which has very low affinity for FQs—hence the low toxicity to host cells.
Mechanism of resistance Because of theunique mechanism of action, plasmid mediatedtransferable resistance is less likely. Resistancenoted so far is due to chromosomal mutationproducing a DNA gyrase or topoisomerase IV
First generation fluoroquinolones
Norfloxacin OfloxacinCiprofloxacin Pefloxacin
Second generation fluoroquinolones
Levofloxacin MoxifloxacinLomefloxacin GemifloxacinSparfloxacin Prulifloxacin

710S
EC
TIO
N12
ANTIMICROBIAL DRUGS
with reduced affinity for FQs, or due to reducedpermeability/increased efflux of these drugsacross bacterial membranes. In contrast tonalidixic acid which selects single step resistantmutants at high frequency, FQ-resistant mutantsare not easily selected. Therefore, resistance toFQs has been slow to develop. However,increasing resistance has been reported amongSalmonella, Pseudomonas, staphylococci,gonococci and pneumococci.
Ciprofloxacin (prototype)
It is the most potent first generation FQ activeagainst a broad range of bacteria, the mostsusceptible ones are the aerobic gram-negativebacilli, especially the Enterobacteriaceae andNeisseria. The MIC of ciprofloxacin againstthese bacteria is usually < 0.1 µg/ml, while gram-positive bacteria are inhibited at relatively higherconcentrations. The spectrum of action issummarized below:
Highly susceptibleE. coli Neisseria gonorrhoeaeK. pneumoniae N. meningitidisEnterobacter H. influenzaeSalmonella typhi H. ducreyiNontyphoid Salmonella Campylobacter jejuniShigella Yersinia enterocoliticaProteus Vibrio cholerae
Moderately susceptiblePseudomonas aeruginosa LegionellaStaph. aureus Brucella
(including few MRSA) ListeriaStaph. epidermidis Bacillus anthracisBranhamella catarrhalis Mycobact. tuberculosis
Organisms which have shown low/variablesusceptibility are: Strep. pyogenes, Strep.faecalis, Strep. pneumoniae, Mycoplasma,Chlamydia, Mycobact. kansasii, Mycobact.avium.
Notable resistant bacteria are: Bacteroidesfragilis, Clostridia, anaerobic cocci.The distinctive microbiological features of cipro-floxacin (also other FQs) are:
• Bactericidal activity and high potency: MBCsare close to MICs.
• Relatively long post-antibiotic effect on Ente-robacteriaceae, Pseudomonas and Staph.
• Low frequency of mutational resistance.• Low propensity to select plasmid type resis-
tant mutants.• Protective intestinal streptococci and anae-
robes are spared.• Active against many β-lactam and amino-
glycoside resistant bacteria.• Less active at acidic pH.
Pharmacokinetics Ciprofloxacin is rapidlyabsorbed orally, but food delays absorption, andfirst pass metabolism occurs. The pharmaco-kinetic characteristics are given in Table 50.1.Ciprofloxacin (and other FQs) have good tissuepenetrability: concentration in lung, sputum,muscle, prostate and phagocytes exceeds thatin plasma, but CSF and aqueous levels are lower.It is excreted primarily in urine, both by glo-merular filtration and tubular secretion. Urinaryand biliary concentrations are 10–50 fold higherthan plasma.
Adverse effects Ciprofloxacin has goodsafety record: side effects occur in ~10%patients, but are generally mild; withdrawal isneeded only in 1.5%.• Gastrointestinal: nausea, vomiting, bad taste,
anorexia. Because gut anaerobes are notaffected—diarrhoea is infrequent.
• CNS: dizziness, headache, restlessness,anxiety, insomnia, impairment of concen-tration and dexterity (caution while driving).Tremor and seizures are rare, occur only athigh doses or when predisposing factors arepresent: possibly reflect GABA antagonisticaction of FQs.
• Skin/hypersensitivity: rash, pruritus, photo-sensitivity, urticaria, swelling of lips, etc.Serious cutaneous reactions are rare.
• Tendinitis and tendon rupture: a few cases haveoccurred. Risk of tendon damage is higherin patients above 60 years of age and in thosereceiving corticosteroids. The FQ should bestopped at the first sign of tendinitis.

711C
HA
PTER50
SULFONAMIDES, COTRIMOXAZOLE AND QUINOLONES
TABLE 50.1 Pharmacokinetic characteristics and doses of fluoroquinolones
CIPROFL NORFL PEFL OFL LEVOFL GEMI PRULI MOXI
1. Oral bioavailability (%) 60–80 35–45 90–100 85–95 ~100 70 90 852. Plasma protein binding (%) 20–35 15 20–30 25 25 55–73 45 403. Vol. of distribution (L/kg) 3–4 2 2 1.5 1.3 — — 24. Percent metabolized 20 25 85 5–10 5 — >90 70–805. Elimination t½ (hr) 3–5 4–6 8–14 5–8 8 7 10–12 10–156. Routes of administration oral, i.v. oral oral, i.v. oral, i.v. oral, i.v. oral oral oral, i.v.7. Dose (mg) : oral 250–750 400 400 200–400 500 320 600 400
(BD) (BD) (BD) (BD) (OD) (OD) (OD) (OD): iv 100–200 — 400 200 500 — — 400
Ciprofloxacin and other FQs are contraindicatedduring pregnancy.On the basis of the finding that administered to immature pupsciprofloxacin (and other FQs) caused cartilage damage in weightbearing joints, the FQs were contraindicated in children.However, under pressing situations like Pseudomonaspneumonia in cystic fibrosis and multi-resistant typhoid,ciprofloxacin has been administered to millions of children inIndia and elsewhere. Though a few cases of joint painand swelling have been reported, cartilage damage has notoccurred. Caution, nevertheless, is needed while using FQs inchildren.
Interactions
• Plasma concentration of theophylline,caffeine and warfarin is increased byciprofloxacin (also by norfloxacin andpefloxacin) due to inhibition of metabolism:CNS toxicity can occur by concurrent useof theophylline and a FQ.
• NSAIDs may enhance the CNS toxicity ofFQs; seizures are reported.
• Antacids, sucralfate and iron salts given con-currently reduce absorption of FQs.
CIFRAN, CIPLOX, CIPROBID, QUINTOR, CIPROLET 250, 500,750 mg tab, 200 mg/100 ml i.v. infusion, 3 mg/ml eye drops.
Uses Ciprofloxacin is effective in a broadrange of infections. Because of wide-spectrumbactericidal activity, oral efficacy and goodtolerability, it is being extensively employed forempirical therapy of any infection, but shouldnot be used for minor cases or where gram-positive organisms and/or anaerobes are primarilycausative. In severe infections, therapy may be
initiated by i.v. infusion and then switched overto oral route.1. Urinary tract infections: High cure rates,even in complicated cases or those with indwellingcatheters/prostatitis, have been achieved.Comparative trials have reported higher successrates than with cotrimoxazole. Chronic Pseudo-monas infections respond less completely.2. Gonorrhoea: Initially a single 500 mg dosewas nearly 100% curative in non-PPNG as wellas PPNG infections, but cure rate has declineddue to emergence of resistance, and it is no longera first line drug; may be used if strain is sensitive.3. Chancroid: 500 mg BD for 3 days is asecond line alternative drug to ceftriaxone/azithromycin.4. Bacterial gastroenteritis: Currently, it is themost commonly used drug for empirical therapyof diarrhoea. However, it should be reserved forsevere cases due to EPEC, Shigella, Salmonellaand Campy. jejuni infection. Ciprofloxacin canreduce stool volume in cholera.5. Typhoid: Ciprofloxacin is one of the firstchoice drugs in typhoid fever since chloram-phenicol, ampicillin and cotrimoxazole havebecome unreliable due to development ofresistance. In India and elsewhere up to 95%S. typhi isolates were sensitive to ciprofloxacin.However, increasing number of nonresponsivecases are being reported. Ceftriaxone (orcefotaxime/cefoperazone) are more commonly

712S
EC
TIO
N12
ANTIMICROBIAL DRUGS
used. Ciprofloxacin given in a dose of 750 mgBD for 10 days is recommended. Patients unableto take the drug orally may be treated with 200mg. i.v. 12 hourly in the beginning. Beingbactericidal the advantages of ciprofloxacin are:• Quick defervescence: fever usually subsides
in 4–5 days but may take longer now.• Early abetment of symptoms; low incidence
of complications and relapse.• Prevention of carrier state due to cidal action,
good penetration into infected cells, highbiliary and intestinal mucosal concentration.
It can also be used to treat typhoid carriers (750mg BD for 4–8 weeks). This has been foundto achieve 92% eradication rate compared to50% by ampicillin.
(For alternative drugs see box)6. Bone, soft tissue, gynaecological andwound infections: caused by resistant Staph. andgram-negative bacteria respond to ciprofloxacin.High cure rates have been obtained in osteo-myelitis and joint infections but prolongedtreatment (6–8 weeks) with high doses (750 mgBD) is required. Used along with clindamycin/metronidazole (to cover anaerobes) it is a gooddrug for diabetic foot.7. Respiratory infections: Ciprofloxacin shouldnot be used as the primary drug becausepneumococci and streptococci have low andvariable susceptibility. However, it can treatMycoplasma, Legionella, H. influenzae, Branh.catarrhalis and some streptococcal andpneumococcal infections besides gram-negativeones. Several 2nd generation FQs have nowbecome available for the treatment ofpneumonias and chronic bronchitis.The US-FDA has approved use of ciprofloxacin for postexposure treatment of inhalational anthrax which may occurdue to bioterrorism.
8. Tuberculosis It is a second line drug whichcan be used as a component of combinationchemotherapy against multidrug resistanttuberculosis. Recently, even FQ-resistant TB(extensively drug resistant or XDR-TB) havearisen.
9. Gram-negative septicaemias: Parenteralciprofloxacin may be combined with a thirdgeneration cephalosporin or an aminoglycoside.10. Meningitis: Though penetration in CSF isnot very good, ciprofloxacin has been success-fully used in gram-negative bacterial meningitis,especially that occurring in immunocom-promised patients or those with CSF shunts.11. Prophylaxis: of infections in neutropenic/cancer and other susceptible patients.
Drugs for typhoid fever
1. Ceftriaxone (see p. 728 ): Currently, it is the mostreliable and fastest acting bactericidal drug for entericfever. Practically all S. typhi isolates, includingmultidrug resistant ones, are susceptible. However, ithas to be injected i.v. (4 g daily for 2 days followed by2 g/day till 2 days after fever subsides; children 75mg/kg/day) and is expensive. Generally 7–10 daystreatment is required. Being bactericidal, it alsoprevents relapses and carrier state. Ceftriaxone is tobe preferred over FQs in children, pregnant womenand in areas with FQ resistance.Cefoperazone and cefotaxime are the other thirdgeneration cephalosporins used in typhoid.
2. Fluoroquinolones: Ciprofloxacin (750 mg BD) ismostly used. Ofloxacin (400 mg BD), levofloxacin (500mg OD/BD) are nearly equally efficacious alternatives.
3. Chloramphenicol (see p. 741): Since majority of S.typhi strains are now chloramphenicol resistant, it hasbecome clinically unreliable. It is seldom used, only incase the local strain is known to be sensitive andclinical experience supports its use. It is administeredorally (0.5 g 6 hourly till fever subsides, then 0.25 g 6hourly for another 5–7 days).
4. Azithromycin (500 mg OD for 7 days) is a secondline alternative in multidrug resistant typhoid, and inpatients to whom the 1st line drugs cannot be given.
5. Cotrimoxazole (see p. 708): It was effective in typhoidtill plasmid mediated multidrug resistance spreadamong S. typhi. Now it is rarely used.
6. Ampicillin/amoxicillin (see p. 722): These antibioticsare no longer dependable therapy for typhoid becauseof multi-drug resistance. Response rate is low anddefervescence takes longer even in patients whorespond.
7. Combination therapy: There is no evidence thatcombination of any two or more AMAs is better thanthe single drug to which the infecting strain of S. typhiis responsive.

713C
HA
PTER50
SULFONAMIDES, COTRIMOXAZOLE AND QUINOLONES
12. Conjunctivitis: by gram-negative bacteria:topical therapy is effective.
Norfloxacin It is less potent than cipro-floxacin: MIC values for most gram-negativebacteria are 2–4 times higher. Many Pseudo-monas and gram-positive organisms are notinhibited. Moreover, it attains lower concen-tration in tissues which are non-therapeutic.Unchanged drug as well as metabolites areexcreted in urine.
Norfloxacin is primarily used for urinary andgenital tract infections. Given for 8–12 weeks,it can treat chronic UTI. It is also good forbacterial diarrhoeas, because high concentrationsare present in the gut, and anaerobic flora ofthe gut is not disturbed. Norfloxacin is notrecommended for respiratory and other systemicinfections.NORBACTIN, NORFLOX 200, 400, 800 mg tab, 3 mg/ml eyedrops; UROFLOX, NORILET 200, 400 mg tab. BACIGYL 400mg tab, 100 mg/5 ml susp.
Pefloxacin It is the methyl derivative ofnorfloxacin which is more lipid soluble,completely absorbed orally, penetrates tissuesbetter and attains higher plasma concentrations.Passage into CSF is greater than other FQs—preferred for meningeal infections. It is highlymetabolized—partly to norfloxacin whichcontributes to its activity. Pefloxacin has longert½: cumulates on repeated dosing achievingplasma concentrations twice as high as after asingle dose. Because of this it is effective inmany systemic infections as well. Dose ofpefloxacin needs to be reduced in liver disease,but not in renal insufficiency. It is less effectivein gram-positive coccal and Listeria infections.PELOX, 200, 400 mg tab, to be taken with meals; 400 mg/5 ml inj(to be diluted in 100–250 ml of glucose solution but notsaline, because it precipitates in presence of Cl¯ ions), PERTI,400 mg tab.
Ofloxacin This FQ is somewhat less activethan ciprofloxacin against gram-negative bacteria,but equally or more potent against gram-posi-tive ones and certain anaerobes. Good activityagainst Chlamydia and Mycoplasma has been
noted. It is an alternative drug for nonspecificurethritis, cervicitis and atypical pneumoniacaused by Chlamydia trachomatis. It alsoinhibits M. tuberculosis; can be used in resistantcases of TB. High activity is exhibited againstM. leprae, and it is being used in alternativemultidrug therapy regimens.
Ofloxacin is relatively lipid soluble; oralbioavailability is high, and higher plasmaconcentrations are attained. Food does notinterfere with its absorption. It is excreted largelyunchanged in urine; dose needs to be reducedin renal failure.
Ofloxacin is comparable to ciprofloxacin inthe therapy of systemic and mixed infections.It is suitable for chronic bronchitis and otherrespiratory or ENT infections. Inhibition oftheophylline metabolism is less marked.
Gonorrhoea caused by FQ sensitive strainshas been treated with a single 200 to 400 mgdose. It is also useful in chlamydia urethritisas an alternative drug.ZANOCIN, TARIVID 100, 200, 400 mg tab; 200 mg/100 ml i.v.infusion, ZENFLOX also 50 mg/5 ml susp.ZANOCIN, OFLOX, EXOCIN 0.3% eye drops.
Levofloxacin It is the active levo(s) isomerof ofloxacin having improved activity againstStrep. pneumoniae and some other gram-positiveand gram-negative bacteria. Anaerobes aremoderately susceptible. Oral bioavailability oflevofloxacin is nearly 100%; oral and i.v. dosesare similar. It is mainly excreted unchanged, anda single daily dose is sufficient because of slowerelimination and higher potency.
Theophylline, warfarin, cyclosporine andzidovudine pharmacokinetics has been found toremain unchanged during levofloxacin treatment.The primary indication of levofloxacin iscommunity acquired pneumonia and exacerbationsof chronic bronchitis in which upto 90% curerate has been obtained. High cure rates have beennoted in sinusitis, pyelonephritis, prostatitis andother UTI, as well as skin/soft tissue infections.TAVANIC, GLEVO 500 mg tab, 500 mg/100 ml inj.LOXOF, GLEVO, LEVOFLOX, LEVODAY 250, 500, 750 mg tabs,500 mg/100 ml inj; GLEVO 0.5% eye drops.

714S
EC
TIO
N12
ANTIMICROBIAL DRUGS
Lomefloxacin It is a second generation difluo-rinated quinolone, equal in activity to ciprofloxa-cin but more active against some gram-negativebacteria and chlamydia. Because of longer t½ andpersistence in tissues, it is suitable for single dailyadministration. However, due to higher incidenceof phototoxicity andQ-T prolongation, it has been withdrawn in USAand some other countries, but is available in India,though infrequently used.LOMEF-400, LOMEDON, LOMADAY 400 mg tab.LOMIBACT, LOX 0.3% eye drops.
Sparfloxacin Another second generation difluorinatedquinolone which has enhanced activity against gram-positivebacteria (especially Strep. pneumoniae, Staphylococcus,Enterococcus), Bacteroides fragilis, other anaerobes andmycobacteria. Its major indications include pneumonia, exacer-bations of chronic bronchitis, sinusitis and other ENT infections.However, it has frequently caused phototoxic reactions:recipients should be cautioned not to go out in the sun.Prolongation of QTc interval has been noted in 3% recipients.Fatal arrhythmias have occurred in patients taking other Q-T prolonging drugs concurrently. It has been discontinuedin many countries including USA, but not yet in India.Dose: 200–400 mg OD oral.TOROSPAR 200, 400 mg tab; SPARTA, SPARQUIN, SPARDAC100, 200 mg tab, ZOSPAR, SPARC, EYPAR 0.3% eye drops.
Gatifloxacin This 2nd generation FQ with higher affinityfor bacterial topoisomerase IV was frequently used for grampositive coccal (mainly respiratory and ENT) infections.However, it caused Q-T prolongation, arrhythmias,phototoxicity, and unpredictable hypoglycaemia, because ofwhich it was discontinued in most countries and has beenbanned in India since March 2011.
Moxifloxacin A long-acting 2nd generationFQ having high activity against Str. pneumoniae,other gram-positive bacteria including β-lactam/macrolide resistant ones and some anaerobes.It is the most potent FQ against M. tuberculosis.Bacterial topoisomerase IV is the major targetof action. Moxifloxacin is primarily used forpneumonias, bronchitis, sinusitis, otitis media,in which efficacy is comparable to β-lactamantibiotics. However, it is not good for urinarytract infections. It is primarily metabolized inliver; should not be given to liver disease patients.Side effects are similar to other FQs. It shouldnot be given to patients predisposed to seizuresand to those receiving proarrhythmic drugs,
because it can prolong Q-Tc interval. Photo-toxicity occurs rarely.Dose: 400 mg OD; MOXIF 400 mg tab; STAXOM 400 mg tab,400 mg/250 ml i.v. infusion.MOXICIP, MILFLOX, VIGAMOX 0.5% eye drops forconjunctivitis caused by gram-positive as well as negativebacteria.
Gemifloxacin Another broad spectrum FQ,active mainly against aerobic gram positivebacteria, especially Strep. pneumoniae, H.influenzae, Moraxella, Mycoplasma pneumo-niae, Chlamydia pneumophila, Klebsiellaincluding some multidrug resistant strains. Someanaerobes are also inhibited. It is rapidly absorbed,undergoes limited metabolism, and is excretedin urine as well as faeces, both as unchanged drugand as metabolites. Dose needs to be halved ifcreatinine clearance is <40 ml/min.
Side effects are diarrhoea, nausea, headache,dizziness and rise in serum amino-transferases.Skin rashes are more common. It can enhancewarfarin effect, and carries the risk of additiveQ-T prolongation. Gemifloxacin is indicated incommunity acquired pneumonia and for acuteexacerbations of chronic bronchitis.Dose: 320 mg OD for 5–7 days.TOPGEM, GEMBAX, GEMISTAR, GEMI 320 mg tab.
Prulifloxacin This newer 2nd generation FQis a prodrug of Ulifloxacin, a broad spectrumantibacterial active against both gram positiveas well as gram negative bacteria, including manyresistant strains. Prulifloxacin is rapidly absorbedand converted to ulifloxacin during first passmetabolism. Ulifloxacin is then excretedprimarily unchanged in urine. Prulifloxacin hasshown good efficacy in acute exacerbations ofchronic bronchitis, as well as in uncomplicatedor complicated UTI. Its side effect profile issimilar to that of ciprofloxacin. Gastrointestinaland CNS disturbances, urticaria and photo-sensitivity are reported. It is claimed not toprolong Q-T interval. Photosensitivity, blooddyscrasias and renal toxicity are rare.Dose: 600 mg OD, single dose in uncomplicated lower UTI;upto 10 days treatment for complicated UTI and bronchitis.ALPRULI, PRULIFOX, PRULIFACT 600 mg tab.

715C
HA
PTER50
SULFONAMIDES, COTRIMOXAZOLE AND QUINOLONES
PROBLEM DIRECTED STUDY
50.1 A 62-year-old lady presented with acute onset frontal headache which is worse in themorning, thick, yellowish discharge from the nose, nasal blockage and fever for the past2 days. She has been suffering from cold and cough for the last one week. The foreheadis tender on pressing, particularly in the middle. A plain X-ray of the face and head showedboth sided frontal sinusitis. Her husband informed that 3 months back she sufferred an episodeof depression, for which she is receiving Tab amitryptyline 75 mg once daily at bed timeand her mental condition is stable now. The doctor decides to start empirical therapy withmoxifloxacin 400 mg once daily for 10 days. He also prescribes paracetamol 500 mg 8 hourlyfor fever and oxymetazoline nasal drops twice daily for blocked nose.(a) Is the choice of antibiotic appropriate for her? If yes, what could be the considerationsfor selecting moxifloxacin. If no, then give reasons, and suggest the alternative antibiotic(s)that would be appropriate.(see Appendix-1 for solution)
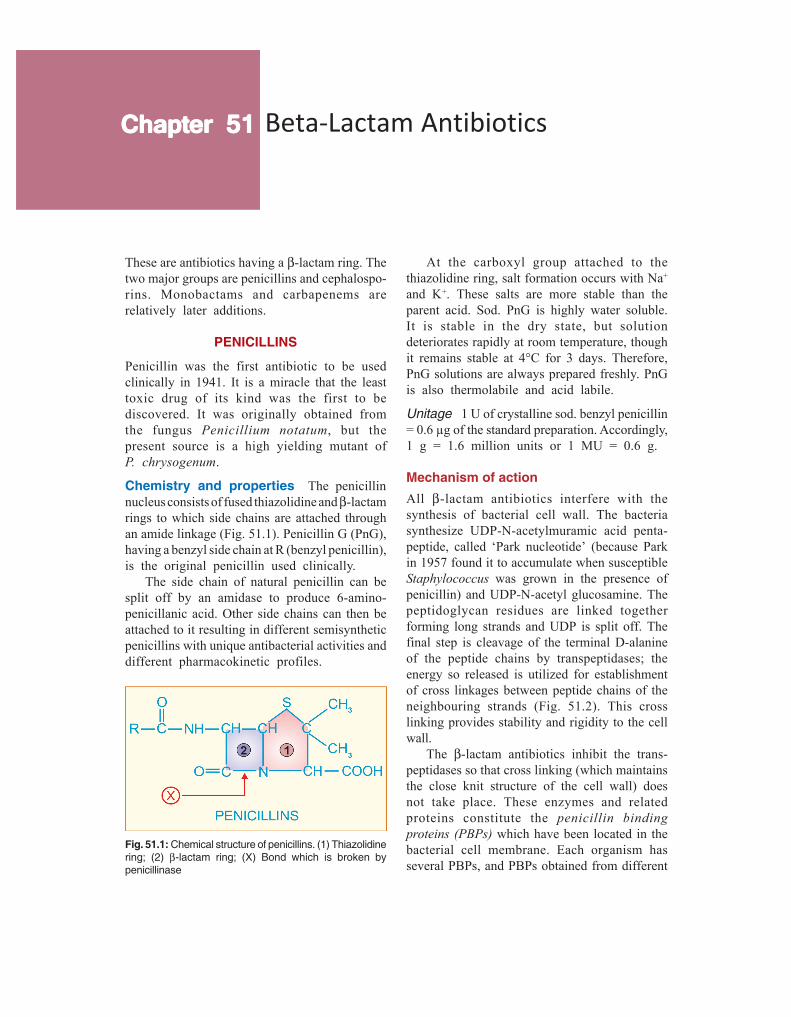
Beta-Lactam AntibioticsChapterChapterChapterChapterChapter 5151515151
These are antibiotics having a β-lactam ring. Thetwo major groups are penicillins and cephalospo-rins. Monobactams and carbapenems arerelatively later additions.
PENICILLINS
Penicillin was the first antibiotic to be usedclinically in 1941. It is a miracle that the leasttoxic drug of its kind was the first to bediscovered. It was originally obtained fromthe fungus Penicillium notatum, but thepresent source is a high yielding mutant ofP. chrysogenum.
Chemistry and properties The penicillinnucleus consists of fused thiazolidine and β-lactamrings to which side chains are attached throughan amide linkage (Fig. 51.1). Penicillin G (PnG),having a benzyl side chain at R (benzyl penicillin),is the original penicillin used clinically.
The side chain of natural penicillin can besplit off by an amidase to produce 6-amino-penicillanic acid. Other side chains can then beattached to it resulting in different semisyntheticpenicillins with unique antibacterial activities anddifferent pharmacokinetic profiles.
At the carboxyl group attached to thethiazolidine ring, salt formation occurs with Na+
and K+. These salts are more stable than theparent acid. Sod. PnG is highly water soluble.It is stable in the dry state, but solutiondeteriorates rapidly at room temperature, thoughit remains stable at 4°C for 3 days. Therefore,PnG solutions are always prepared freshly. PnGis also thermolabile and acid labile.
Unitage 1 U of crystalline sod. benzyl penicillin= 0.6 µg of the standard preparation. Accordingly,1 g = 1.6 million units or 1 MU = 0.6 g.
Mechanism of actionAll β-lactam antibiotics interfere with thesynthesis of bacterial cell wall. The bacteriasynthesize UDP-N-acetylmuramic acid penta-peptide, called ‘Park nucleotide’ (because Parkin 1957 found it to accumulate when susceptibleStaphylococcus was grown in the presence ofpenicillin) and UDP-N-acetyl glucosamine. Thepeptidoglycan residues are linked togetherforming long strands and UDP is split off. Thefinal step is cleavage of the terminal D-alanineof the peptide chains by transpeptidases; theenergy so released is utilized for establishmentof cross linkages between peptide chains of theneighbouring strands (Fig. 51.2). This crosslinking provides stability and rigidity to the cellwall.
The β-lactam antibiotics inhibit the trans-peptidases so that cross linking (which maintainsthe close knit structure of the cell wall) doesnot take place. These enzymes and relatedproteins constitute the penicillin bindingproteins (PBPs) which have been located in thebacterial cell membrane. Each organism hasseveral PBPs, and PBPs obtained from different
Fig. 51.1: Chemical structure of penicillins. (1) Thiazolidinering; (2) β-lactam ring; (X) Bond which is broken bypenicillinase

717C
HA
PTER51
BETA-LACTAM ANTIBIOTICS
Fig. 51.2: Key features of bacterial cell wall synthesisand cell wall structure, depicting the site of action ofβ-lactam antibiotics and vancomycin.A. Cross linking of peptidoglycan residues of neighbouring
strands by cleavage of terminal D-alanine (D-Ala/D)and transpeptidation with the chain of 5 glycine (Gly5)residues. The β-lactam antibiotics (β-L) block cleavageof terminal D-Ala and transpeptidation. The peptidogly-can units are synthesized within the bacterial cell andare transported across the cell membrane byattachment to a bactoprenol lipid carrier for assemblyinto strands. Vancomycin (V) binds tightly to theterminal D-Ala-D-Ala sequence and prevents itsrelease from the carrier, so that further transpeptidationcannot take place.
B. The highly cross linked peptidoglycan strands inbacterial cell wall
NAM—N-acetyl muramic acidNAG—N-acetylglucosamineL-Ala—L-alanineD-Glu—D-glutamic acidL-Lys—L-Lysine
species differ in their affinity towards differentβ-lactam antibiotics. This fact probably explainstheir differing sensitivity to the various β-lactamantibiotics.
When susceptible bacteria divide in thepresence of a β-lactam antibiotic—cell walldeficient (CWD) forms are produced. Becausethe interior of the bacterium is hyperosmotic,the CWD forms swell and burst → bacterial lysisoccurs. This is how β-lactam antibiotics exertbactericidal action. Under certain conditions andin case of certain organisms, bizarre shaped orfilamentous forms, which are incapable ofmultiplying, result. Grown in hyperosmoticmedium, globular ‘giant’ forms or protoplastsare produced. Lytic effect of these antibioticsmay also be due to derepression of somebacterial autolysins which normally functionduring cell division.
Rapid cell wall synthesis occurs when theorganisms are actively multiplying; β-lactamantibiotics are more lethal in this phase.
The peptidoglycan cell wall is unique tobacteria. No such substance is synthesized(particularly, D-alanine is not utilized) by higheranimals. This is why penicillin is practicallynontoxic to man.
In gram-positive bacteria, the cell wall isalmost entirely made of peptidoglycan, whichis >50 layers thick and extensively cross linked,so that it may be regarded as a single giant muco-peptide molecule. In gram-negative bacteria, itconsists of alternating layers of lipoprotein andpeptidoglycan (each layer 1–2 molecule thickwith little cross linking). This may be the reasonfor higher susceptibility of the gram-positivebacteria to PnG.
Blood, pus, and tissue fluids do not interferewith the antibacterial action of β-lactam anti-biotics.
PENICILLIN-G (BENZYL PENICILLIN)
Antibacterial spectrum PnG is a narrowspectrum antibiotic; activity is limited primarilyto gram-positive bacteria, few gram negativeones and anaerobes.

718S
EC
TIO
N12
ANTIMICROBIAL DRUGS
Cocci: Streptococci (except viridans, group D or enterococci)are highly sensitive, so are many pneumococci. Staph. aureus,though originally very sensitive, has acquired resistance tosuch an extent that it must be counted out of PnG spectrum.Gram negative cocci—Neisseria gonorrhoeae and N.meningitidis are susceptible to PnG, though increasing numberof gonococci have developed partial and others high degreeresistance.
Bacilli: Gram-positive bacilli—majority of B. anthracis,Corynebacterium diphtheriae, and practically all Clostridia(tetani and others), Listeria are highly sensitive, so arespirochetes (Treponema pallidum, Leptospira, and others),but Bacteroides fragilis is largely resistant.
Actinomyces israelii is only moderately sensitive.Majority of aerobic gram-negative bacilli, Mycobacteriumtuberculosis, rickettsiae, chlamydiae, protozoa, fungi andviruses are totally insensitive to PnG.
Bacterial resistance Many bacteria are inhe-rently insensitive to PnG because in them thetarget enzymes and PBPs are located deeperunder lipoprotein barrier where PnG is unableto penetrate or have low affinity for PnG. Theprimary mechanism of acquired resistance isproduction of penicillinase.
Penicillinase It is a narrow spectrum β-lacta-mase which opens the β-lactam ring and inacti-vates PnG and some closely related congeners.Majority of Staphylococci and some strains ofgonococci, B. subtilis, E. coli, H. influenzaeand few other bacteria produce penicillinase. Thegram-positive penicillinase producers elaboratelarge quantities of the enzyme which diffusesinto the surroundings and can protect otherinherently sensitive bacteria. In gram-negativebacteria, penicillinase is found in small quantity,but is strategically located inbetween thelipoprotein and peptidoglycan layers of the cellwall. Staphylococcal penicillinase is inducible,and methicillin is an important inducer; whilein gram-negative organisms, it is mostly aconstitutive enzyme.
Penicillinase has been successfully used to destroy PnG inpatient’s blood sample so that it does not interfere withbacterial growth when such blood is cultured.
Some resistant bacteria become penicillintolerant and not penicillin destroying. Theirtarget enzymes are altered to have low affinity
for penicillin, e.g. highly resistant pneumococciisolated in some areas have altered PBPs.The methicillin-resistant Staph. aureus (MRSA)have acquired a PBP which has very low affinityfor β-lactam antibiotics. Some penicillinresistant pneumococci and enterococci havealtered PBPs. The low level penicillin-resistantgonococci are less permeable to the drug, whilehigh degree resistant ones produce penicillinase,as do highly resistant H. influenzae. Both theseappear to have acquired the penicillinase plasmidby conjugation or transduction and thenpropagated it by selection.
The gram-negative bacteria have ‘porin’channels formed by specific proteins located intheir outer membrane. Permeability of variousβ-lactam antibiotics through these channelsdiffers: ampicillin and other members which areactive against gram-negative bacteria cross theporin channels much better than PnG. Somegram-negative bacteria become resistant by lossor alteration of porin channels.
Pharmacokinetics
Penicillin G is acid labile, therefore destroyed by gastricacid. As such, less than 1/3rd of an oral dose is absorbedin the active form. Absorption of sod. PnG from i.m. site israpid and complete; peak plasma level is attained in 30 min.It is distributed mainly extracellularly; reaches most bodyfluids, but penetration in serous cavities and CSF is poor.However, in the presence of inflammation (sinovitis, meningitis,etc.) adequate amounts may reach these sites. About 60%is plasma protein bound. It is little metabolized because ofrapid excretion.
The pharmacokinetics of PnG is dominated by very rapidrenal excretion; about 10% by glomerular filtration and therest by tubular secretion. The plasma t½ of PnG in healthyadult is 30 min. Neonates have slower tubular secretion—t½ of PnG is longer; but approaches adult value at 3 monthsand then is even shorter during childhood. Aged and thosewith renal failure excrete penicillin slowly. Tubular secretionof PnG can be blocked by probenecid—higher and longerlasting plasma concentrations are achieved. Probenecid alsodecreases the volume of distribution of penicillins.
Preparations and dose
1. Sod. penicillin G (crystalline penicillin) injection 0.5–5 MU i.m./i.v. 6–12 hourly. It is available as dry powder invials to be dissolved in sterile water at the time of injection.BENZYL PENICILLIN 0.5, 1 MU inj.

719C
HA
PTER51
BETA-LACTAM ANTIBIOTICS
Repository penicillin G injections These are insoluble saltsof PnG which must be given by deep i.m. (never i.v.) injection.They release PnG slowly at the site of injection, which thenmeets the same fate as soluble PnG.
1. Procaine penicillin G inj. 0.5–1 MU i.m. 12–24 hourlyas aqueous suspension. Plasma concentrations attained arelower, but are sustained for 12–24 hours; PROCAINEPENICILLIN-G 0.5, 1 MU dry powder in vial.
Fortified procaine penicillin G inj: contains 3 lac U procainepenicillin and 1 lac U sod. penicillin G to provide rapid aswell as sustained blood levels. FORTIFIED P.P. INJ 3+1 lacU vial; BISTREPEN 6+4 lac U/vial.
2. Benzathine penicillin G 0.6–2.4 MU i.m. every 2–4 weeksas aqueous suspension. It releases penicillin extremelyslowly—plasma concentrations are very low but remaineffective for prophylactic purposes for up to 4 weeks:PENIDURE-LA (long acting), LONGACILLIN, PENCOM, 0.6,1.2, 2.4 MU as dry powder in vial.
Adverse effects
Penicillin G is one of the most nontoxicantibiotics; up to 20 MU has been injected ina day without any organ toxicity.
Local irritancy and direct toxicity Pain ati.m. injection site, nausea on oral ingestion andthrombophlebitis of injected vein are dose-related expressions of irritancy.
Toxicity to the brain may be manifested asmental confusion, muscular twitchings, convul-sions and coma, when very large doses (> 20MU) are injected i.v.; especially in patients withrenal insufficiency. Bleeding has also occurredwith such high doses due to interference withplatelet function. Intrathecal injection of PnGis no longer recommended because it has causedarachnoiditis and degenerative changes in spinalcord.
Accidental i.v. injection of procaine penicillinproduces CNS stimulation, hallucinations andconvulsions due to procaine. Being insoluble,it may also cause microembolism.
Hypersensitivity These reactions are themajor problem in the use of penicillins. Anincidence of 1–10% is reported. Individuals withan allergic diathesis are more prone to developpenicillin reactions. PnG is the most common
drug implicated in drug allergy, because of whichit has practically vanished from use in generalpractice.
Frequent manifestations of penicillin allergyare—rash, itching, urticaria and fever. Wheezing,angioneurotic edema, serum sickness and exfo-liative dermatitis are less common. Anaphylaxisis rare (1 to 4 per 10,000 patients), but maybe fatal.
All forms of natural and semisynthetic peni-cillins can cause allergy, but it is more com-monly seen after parenteral than oral adminis-tration. Incidence is highest with procaine peni-cillin: procaine is itself allergenic. The courseof penicillin hypersensitivity is unpredictable,i.e. an individual who tolerated penicillin earliermay show allergy on subsequent administrationand vice versa.
There is partial cross sensitivity betweendifferent types of penicillins; an individual whohas exhibited immediate type of hypersensiti-vity—urticaria, angioedema, bronchospasm, ana-phylaxis or serum sickness with one penicillinshould not be given any other type of penicillin.However, if the earlier reaction had been onlya rash, penicillin may be given cautiously—oftenno untoward effect is seen. History of penicillinallergy must be elicited before injecting it. Ascratch test or intradermal test (with 2–10 U)may be performed first. On occasions, this itselfhas caused fatal anaphylaxis. Testing with benzyl-penicilloyl-polylysine is safer. However, anegative intradermal test does not rule outdelayed hypersensitivity. It should also berealised that presence of antibodies to penicillindoes not mean allergy to it, because practicallyeveryone who receives penicillin developsantibodies to it.
For the development of antibodies, penicillinor a product of it (mostly penicilloyl moiety—major determinant) acts as a hapten. There aremany minor determinants as well.
Topical application of penicillin is highlysensitizing (contact dermatitis and otherreactions). Therefore, all topical preparations ofpenicillin (including eye ointment) have been

720S
EC
TIO
N12
ANTIMICROBIAL DRUGS
banned, except for use in eye as freshly preparedsolution in case of gonococcal ophthalmia.
If a patient is allergic to penicillin, it is bestto use an alternative antibiotic. Hyposensitizationby the injection of increasing amounts ofpenicillin intradermally at hourly intervals maybe tried only if there is no other choice.
Superinfections These are rare with PnG because of itsnarrow spectrum; though bowel, respiratory and cutaneousmicroflora does undergo changes.
Jarisch-Herxheimer reaction Penicillin injected in asyphilitic patient (particularly secondary syphilis) may produceshivering, fever, myalgia, exacerbation of lesions, even vascularcollapse. This is due to sudden release of spirochetal lyticproducts and lasts for 12–72 hours. It does not recur anddoes not need interruption of therapy. Aspirin and sedationafford relief of symptoms.
Uses
Penicillin G is the drug of choice for infectionscaused by organisms susceptible to it, unlessthe patient is allergic to this antibiotic. However,use has declined very much due to fear of causinganaphylaxis.1. Streptococcal infections Like pharyngitis, otitis media,scarlet fever, rheumatic fever respond to ordinary doses ofPnG because Strep. pyogenes has not developed significantresistance. However, the risk of injecting PnG for this infectionis seldom taken now. For subacute bacterial endocarditis(SABE) caused by Strep. viridans or faecalis high doses(10–20 MU i.v. daily) along with gentamicin given for 2–6weeks is needed.
2. Pneumococcal infections PnG is not used now forempirical therapy of pneumococcal (lobar) pneumonia andmeningitis because many strains have become highly penicillinresistant. However, PnG 3–6 MU i.v. every 6 hours is thedrug of choice if organism is sensitive.
3. Meningococcal infections are still mostly responsive;meningitis and other infections may be treated withintravenous injection of high doses.
4. Gonorrhoea PnG has become unreliable for treatmentof gonorrhoea due to spread of resistant strains. For alternativeregimens see Table 54-1.
The treatment of ophthalmia neonatorum due to sensitiveN. gonorrhoeae consists of saline irrigation + sod. PnG 10,000–20,000 U/ml 1 drop in each eye every 1–3 hours. In severecases, give 50,000 U i.m. BD for 1 week in addition.
5. Syphilis T. pallidum has not shown anyresistance and PnG is the drug of choice. Early
and latent syphilis is treated either with dailyi.m. injection of 1.2 MU of procaine penicillinfor 10 days or with 1–3 weekly doses of 2.4MU benzathine penicillin. For late syphilis,benzathine penicillin 2.4 MU weekly for 4 weeksis recommended. Cardiovascular and neuro-syphilis requires sod. PnG 5 MU i.m. 6 hourlyfor 10–14 days followed by the above regimen.Leptospirosis: PnG 1.5 MU injected i.v. 6 hourlyfor 7 days is curative.
6. Diphtheria Antitoxin therapy is of prime importance.Procaine penicillin 1–2 MU daily for 10 days is used to preventcarrier state.
7. Tetanus and gas gangrene Antitoxin and othermeasures are more important; PnG 6–12 MU/day is used tokill the causative organism and has adjuvant value.
8. Penicillin G is the drug of choice for rare infections likeanthrax, actinomycosis, rat bite fever and those caused byListeria monocytogenes, Pasteurella multocida.
For trench mouth or acute necrotizing ulcerative gingivitis(ANUG) which is a mixed infection caused by spirochetesand fusobacteria, PnG (i.m.)/penicillin V (oral) or amoxicillinare generally combined with metronidazole.
9. Prophylactic uses(a) Rheumatic fever: Low concentrations of penicillin preventcolonization by streptococci that are indirectly responsiblefor rheumatic fever. Benzathine penicillin 1.2 MU every 4 weekstill 18 years of age or 5 years after an attack, whichever ismore.(b) Bacterial endocarditis: Dental extractions, endoscopies,catheterization, etc. cause bacteremia which in patients withvalvular defects can cause endocarditis. PnG can affordprotection, but amoxicillin is preferred now.(c) Agranulocytosis patients: Penicillin has been used aloneor in combination with streptomycin to prevent respiratoryand other acute infections, but cephalosporins + an amino-glycoside or fluoroquinolone are preferred now.
SEMISYNTHETIC PENICILLINS
Semisynthetic penicillins are produced bychemically combining specific side chains (inplace of benzyl side chain of PnG) or byincorporating specific precursors in the mouldcultures. Thus, procaine penicillin and benzathinepenicillin are salts of PnG and not semisyntheticpenicillins. The aim of producing semisyntheticpenicillins has been to overcome the short-comings of PnG, which are:
1. Poor oral efficacy.

721C
HA
PTER51
BETA-LACTAM ANTIBIOTICS
2. Susceptibility to penicillinase.3. Narrow spectrum of activity.4. Hypersensitivity reactions (this has not
been overcome in any preparation).In addition, some β-lactamase inhibitors have
been developed which themselves are not anti-bacterial, but augment the activity of penicillinsagainst β-lactamase producing organisms.
CLASSIFICATION
1. Acid-resistant alternative to penicillin GPhenoxymethyl penicillin (Penicillin V).
2. Penicillinase-resistant penicillinsMethicillin, Cloxacillin, Dicloxacillin.
3. Extended spectrum penicillins(a) Aminopenicillins: Ampicillin,
Bacampicillin, Amoxicillin.(b) Carboxypenicillins: Carbenicillin.(c) Ureidopenicillins: Piperacillin,
Mezlocillin.β-lactamase inhibitors Clavulanic acid
Sulbactam, Tazobactam
ACID-RESISTANT ALTERNATIVE TOPENICILLIN-G
Phenoxymethyl penicillin (Penicillin V)It differs from PnG only in that it is acid stable.Oral absorption is better; peak blood level isreached in 1 hour and plasma t½ is 30–60 min.
The antibacterial spectrum of penicillin Vis identical to PnG, but it is about 1/5 as activeagainst Neisseria, other gram negative bacteriaand anaerobes. It cannot be depended upon formore serious infections and is used only forstreptococcal pharyngitis, sinusitis, otitis media,prophylaxis of rheumatic fever (when an oraldrug has to be selected), less serious pneumo-coccal infections and trench mouth.Dose: 250–500 mg, infants 60 mg, children 125–250 mg; given 6hourly, (250 mg = 4 lac U). CRYSTAPEN-V, KAYPEN 125, 250mg tab, 125 mg/5 ml dry syr—for reconstitution, PENIVORAL65, 130 mg tab.
PENICILLINASE-RESISTANTPENICILLINS
These congeners have side chains that protectthe β-lactam ring from attack by staphylococcalpenicillinase. However, this also partially protectsthe bacteria from the β-lactam ring: nonpenicilli-nase producing organisms are much lesssensitive to these drugs than to PnG. Their onlyindication is infections caused by penicillinaseproducing Staphylococci, for which they are thedrugs of choice, except in areas where methicillinresistant Staph. aureus (MRSA) has becomeprevalent. These drugs are not resistant to β-lactamases produced by gram negative bacteria.
Methicillin It is highly penicillinase resistant but not acidresistant—must be injected. It is also an inducer ofpenicillinase production.
MRSA have emerged in many areas. These are insensitiveto all penicillinase-resistant penicillins and to other β-lactamsas well as to erythromycin, aminoglycosides, tetracyclines,etc. The MRSA have altered PBPs which do not bindpenicillins. The drug of choice for these organisms isvancomycin/linezolid, but ciprofloxacin can also be used.
Haematuria, albuminuria and reversible interstitialnephritis are the specific adverse effects of methicillin. It hasbeen replaced by cloxacillin.
Cloxacillin/Dicloxacillin It has an isoxazolylside chain and is highly penicillinase as well asacid resistant. Activity against PnG sensitiveorganisms is weaker, and it should not be usedas a substitute for PnG. It is more active thanmethicillin against penicillinase producing Staph,but not against MRSA.
Cloxacillin/dicloxacillin are incompletelybut dependably absorbed from oral route,especially if taken in empty stomach. It is> 90% plasma protein bound. Elimination occursprimarily by kidney, also partly by liver. Plasmat½ is about 1 hour.Dose: 0.25–0.5 g orally every 6 hours; for severe infections0.25–1 g may be injected i.m. or i.v.—higher blood levels areproduced.KLOX, BIOCLOX, 0.25, 0.5 g cap; 0.25, 0.5 g/vial inj., CLOPEN0.25, 0.5 g cap.
Oxacillin, Flucloxacillin (Floxacillin) are other isoxazolylpenicillins, similar to cloxacillin, but not marketed in India.Nafcillin is another parenteral penicillinase resistant penicillin.

722S
EC
TIO
N12
ANTIMICROBIAL DRUGS
EXTENDED SPECTRUM PENICILLINS
These semisynthetic penicillins are active againsta variety of gram-negative bacilli as well. Theycan be grouped according to their spectrum ofactivity.
1. AminopenicillinsThis group, led by ampicillin, has an aminosubstitution in the side chain. Some are prodrugsand all have quite similar antibacterial spectra.None is resistant to penicillinase or to otherβ-lactamases.
Ampicillin It is active against all organismssensitive to PnG. In addition, many gram-negativebacilli, e.g. H. influenzae, E. coli, Proteus,Salmonella Shigella and Helicobacter pyloriare inhibited. However, due to wide-spreaduse, many of these have developed resistance;usefulness of this antibiotic has decreasedconsiderably.
Ampicillin is more active than PnG forStrep. viridans, enterococci and Listeria;equally active for pneumococci, gonococci andmeningococci (penicillin-resistant strains areresistant to ampicillin as well); but less activeagainst other gram-positive cocci. Penicillinaseproducing Staph. are not affected, as are othergram-negative bacilli, such as Pseudomonas,Klebsiella, indole positive Proteus and anae-robes like Bacteroides fragilis.
Pharmacokinetics Ampicillin is not degradedby gastric acid; oral absorption is incompletebut adequate. Food interferes with absorption.It is partly excreted in bile and reabsorbed—enterohepatic circulation occurs. However,primary channel of excretion is kidney, but tubularsecretion is slower than for PnG; plasma t½ is1 hr.Dose: 0.5–2 g oral/i.m./i.v. depending on severity of infection,every 6 hours; children 50–100 mg/kg/day.AMPILIN, ROSCILLIN, BIOCILIN 250, 500 mg cap; 125, 250mg/5 ml dry syr; 100 mg/ml pediatric drops; 250, 500 mg and1.0 g per vial inj.
Uses1. Urinary tract infections: Ampicillin has beenthe drug of choice for most acute infections,but resistance has increased and fluoroquino-lones/cotrimoxazole are now more commonlyused for empirical therapy.2. Respiratory tract infections: including bron-chitis, sinusitis, otitis media, etc. are usuallytreated with ampicillin, but higher doses (50–80mg/kg/day) are generally required now.3. Meningitis: Ampicillin has been a first linedrug, but a significant number of meningococci,pneumococci and H. influenzae are nowresistant. For empirical therapy, it is now usedonly in combination with a third generationcephalosporin with or without another antibiotic.4. Gonorrhoea: It is one of the first line drugsfor oral treatment of nonpenicillinase producinggonococcal infections. A single dose of 3.5 gampicillin + 1 g probenecid (ROSCIND, DYNACIL-PRB cap) is adequate and convenient for urethritis.5. Typhoid fever: Due to emergence of resistance, it is nowrarely used, only when the organism is shown to be sensitive.Salmonella diarrhoeas should usually not be treated withantimicrobials, including ampicillin.6. Bacillary dysentery: due to Shigella often responds toampicillin, but many strains are now resistant; quinolones arepreferred.
7. Cholecystitis: Ampicillin is a good drugbecause high concentrations are attained in bile.8. Subacute bacterial endocarditis: Ampicillin2 g i.v. 6 hourly is used in place of PnG.Concurrent gentamicin is advocated.9. H. pylori: Though amoxicillin is mostly usedfor eradication of H. pylori from stomach andduodenum, ampicillin is also active.10. Septicaemias and mixed infections: Injectedampicillin may be combined with gentamicin orone of the third generation cephalosporins.11. ANUG: Ampicillin/amoxicillin are generallypreferred over penicillin V for combining withmetronidazole in treating this condition.
Adverse effects Diarrhoea is frequent afteroral administration. Ampicillin is incompletely

723C
HA
PTER51
BETA-LACTAM ANTIBIOTICS
absorbed—the unabsorbed drug irritates thelower intestines as well as causes markedalteration of bacterial flora.
It produces a high incidence (up to 10%)of rashes, especially in patients with AIDS, EBvirus infections or lymphatic leukaemia.Concurrent administration of allopurinol alsoincreases the incidence of rashes. Sometimesthe rashes may not be allergic, but toxic in nature.
Patients with a history of immediate typeof hypersensitivity to PnG should not be givenampicillin as well.
Interactions Hydrocortisone inactivates ampi-cillin if mixed in the i.v. solution.By inhibiting colonic flora, it may interfere withdeconjugation and enterohepatic cycling of oralcontraceptives → failure of oral contraception.Probenecid retards renal excretion of ampicillin.
Bacampicillin It is an ester prodrug ofampicillin which is nearly completely absorbedfrom the g.i.t.; and is largely hydrolysed duringabsorption. Thus, higher plasma levels areattained. Incidence of diarrhoea is claimed to belower, because of lesser alteration in intestinalecology.Dose: 400–800 mg BD; PENGLOBE 200, 400 mg tab.
Talampicillin, Pivampicillin, Hetacillin are other prodrugs ofampicillin.
Note: A fixed dose combination of ampicillin + cloxacillin(AMPILOX and others) containing 250 mg of each per cap orper vial for injection is vigorously promoted for postoperative,skin and soft tissue, respiratory, urinary and other infections.This combination is not synergistic since cloxacillin is not activeagainst gram-negative bacteria, while ampicillin is not activeagainst staphylococci. Since mixed staphylococcal and gram-negative bacillary infections are uncommon, for any giveninfection, one of the components is useless but adds to thecost and adverse effects. Since the amount of the drug which isactually going to act in any individual patient is halved (whenthe combination is used), efficacy is reduced and chances ofselecting resistant strains are increased. Both drugs areineffective against MRSA. Blind therapy with this combinationis irrational and harmful.
Amoxicillin It is a close congener ofampicillin (but not a prodrug); similar to it inall respects except:
• Oral absorption is better; food does notinterfere with absorption; higher and moresustained blood levels are produced.
• Incidence of diarrhoea is lower.• It is less active against Shigella and H.
influenzae.• It is more active against penicillin resistant
Strep. pneumoniae.Many physicians now prefer it over ampicillinfor bronchitis, urinary infections, SABE andgonorrhoea. It is a component of most tripledrug H. pylori eradication regimens (see p. 657).Dose: 0.25–1 g TDS oral/i.m.; or slow i.v. injection, child 25–75mg/kg/day. AMOXYLIN, NOVAMOX, SYNAMOX 250, 500 mgcap, 125 mg/5 ml dry syr. AMOXIL, MOX 250, 500 mg caps; 125mg/5 ml dry syr; 250, 500 mg/vial inj. MOXYLONG: Amoxicillin250 mg + probenecid 500 mg tab (also 500 mg + 500 mg DS tab).
2. CarboxypenicillinsCarbenicillin The special feature of this peni-cillin congener is its activity against Pseudo-monas aeruginosa and indole positive Proteuswhich are not inhibited by PnG or amino-penicillins. It is less active against Salmonella,E. coli and Enterobacter, while Klebsiella andgram-positive cocci are unaffected by it. Pseudo-monas strains less sensitive to carbenicillin havedeveloped in some areas, especially wheninadequate doses have been used.
Carbenicillin is neither penicillinase-resistantnor acid resistant. It is inactive orally and isexcreted rapidly in urine (t½ 1 hr). It is usedas sodium salt in a dose of 1–2 g i.m. or1–5 g i.v. every 4–6 hours. At the higher doses,enough Na may be administered to cause fluidretention and CHF in patients with borderlinerenal or cardiac function.
High doses have also caused bleeding byinterferring with platelet function. This appearsto result from perturbation of agonist receptorson platelet surface.CARBELIN 1 g, 5 g, per vial inj.
The indications for carbenicillin are—seriousinfections caused by Pseudomonas or Proteus,e.g. burns, urinary tract infection, septicaemia,but piperacillin is now mostly used. Carbenicillin

724S
EC
TIO
N12
ANTIMICROBIAL DRUGS
may be combined with gentamicin, but the twoshould not be mixed in the same syringe.
Carbenicillin indanyl is an orally active ester of carbenicillin,used for treatment of UTI caused by Pseudomonas andProteus.
3. UreidopenicillinsPiperacillin This antipseudomonal penicillinis about 8 times more active than carbenicillin.It has good activity against Klebsiella, manyEnterobacteriaceae and some Bacteroides. It isfrequently employed for treating serious gram-negative infections in neutropenic/immunocom-promised or burn patients. Elimination t½ is1 hr. Concurrent use of gentamicin or tobramycinis advised.Dose: 100–150 mg/kg/day in 3 divided doses (max 16 g/day)i.m. or i.v. The i.v. route is preferred when > 2 g is to be injected.PIPRAPEN 1 g, 2 g vials; PIPRACIL 2 g, 4 g vials for inj; contains2 mEq Na+ per g.
Mezlocillin Another antipseudomonas penicillin, notavailable in India.
BETA-LACTAMASE INHIBITORS
β-lactamases are a family of enzymes producedby many gram-positive and gram-negative bacteriathat inactivate β-lactam antibiotics by openingthe β-lactam ring. Different β-lactamases differin their substrate affinities. Three inhibitors ofthis enzyme clavulanic acid, sulbactam andtazobactam are available for clinical use.
Clavulanic acid Obtained from Streptomycesclavuligerus, it has a β-lactam ring but noantibacterial activity of its own. It inhibits a widevariety (class II to class V) of β-lactamases (butnot class I cephalosporinase) produced by bothgram-positive and gram-negative bacteria.
Clavulanic acid is a ‘progressive’ inhibitor:binding with β-lactamase is reversible initially,but becomes covalent later—inhibition increas-ing with time. Called a ‘suicide’ inhibitor, it getsinactivated after binding to the enzyme. Itpermeates the outer layers of the cell wall ofgram-negative bacteria and inhibits theperiplasmically located β-lactamase.
Pharmacokinetics Clavulanic acid has rapidoral absorption and a bioavailability of 60%; canalso be injected. Its elimination t½ of 1 hr andtissue distribution matches amoxicillin, withwhich it is combined (called coamoxiclav).However, it is eliminated mainly by glomerularfiltration and its excretion is not affected byprobenecid. Moreover, it is largely hydrolysedand decarboxylated before excretion, whileamoxicillin is primarily excreted unchanged bytubular secretion.
Uses Addition of clavulanic acid re-establishesthe activity of amoxicillin against β-lactamaseproducing resistant Staph. aureus (but not MRSAthat have altered PBPs), H. influenzae,N. gonorrhoeae, E. coli, Proteus, Klebsiella,Salmonella and Shigella. Though Bact. fragilisand Branhamella catarrhalis are not responsiveto amoxicillin alone, they are inhibited by thecombination. Clavulanic acid does not potentiatethe action of amoxicillin against strains that arealready sensitive to it. Coamoxiclav is indicatedfor:• Skin and soft tissue infections, intra-
abdominal and gynaecological sepsis, urinary,biliary and respiratory tract infections:especially when empiric antibiotic therapy isto be given for hospital acquired infections.
• Gonorrhoea (including PPNG) single doseamoxicillin 3 g + clavulanic acid 0.5 g +probenecid 1 g is highly curative.
AUGMENTIN, ENHANCIN, AMONATE: Amoxicillin 250 mg +clavulanic acid 125 mg tab; also 500 mg + 125 mg tab; 125 mg +31.5 mg per 5 ml dry syr; CLAVAM 250 + 125 mg tab, 500 + 125mg tab, 875 + 125 mg tab, 125 mg + 32 mg per 5 ml dry syr, 1–2tab TDS.Also AUGMENTIN, CLAVAM: Amoxicillin 1 g + clavulanic acid0.2 g vial and 0.5 g + 0.1 g vial; inject 1 vial deep i.m. or i.v. 6–8hourly for severe infections.It is more expensive than amoxicillin alone.
Adverse effects are the same as for amoxicil-lin alone; but g.i. tolerance is poorer—especiallyin children. Other adverse effects are Candidastomatitis/vaginitis and rashes. Some cases ofhepatic injury have been reported with thecombination.

725C
HA
PTER51
BETA-LACTAM ANTIBIOTICS
Sulbactam It is a semisynthetic β-lactamaseinhibitor, related chemically as well as in activityto clavulanic acid. It is also a progressiveinhibitor, highly active against class II to V butpoorly active against class I β-lactamase. Onweight basis, it is 2–3 times less potent thanclavulanic acid for most types of the enzyme,but the same level of inhibition can be obtainedat the higher concentrations achieved clinically.Sulbactam does not induce chromosomalβ-lactamases, while clavulanic acid can inducesome of them.
Oral absorption of sulbactam is inconsistent.Therefore, it is preferably given parenterally. Ithas been combined with ampicillin for useagainst β-lactamase producing resistant strains.Absorption of its complex salt with ampicillin—sultamicillin tosylate is better, which is givenorally. Indications are:• PPNG gonorrhoea; sulbactam per se also
inhibits N. gonorrhoeae.• Mixed aerobic-anaerobic infections, intra-
abdominal, gynaecological, surgical and skin/soft tissue infections, especially thoseacquired in the hospital.
SULBACIN, AMPITUM: Ampicillin 1 g + sulbactam 0.5 g pervial inj; 1–2 vial deep i.m. or i.v. injection 6–8 hourly.Sultamicillin tosylate: BETAMPORAL, SULBACIN 375 mg tab.Sulbactam has been combined with cefoperazone andceftriaxone also (see p.728).
Pain at site of injection, thrombophlebitis ofinjected vein, rash and diarrhoea are the mainadverse effects.
Tazobactam It is another β-lactamase inhi-bitor similar to sulbactam. Its pharmacokineticsmatches with piperacillin with which it has beencombined for use in severe infections likeperitonitis, pelvic/urinary/respiratory infectionscaused by β-lactamase producing bacilli.However, the combination is not active againstpiperacillin-resistant Pseudomonas, becausetazobactam (like clavulanic acid and sulbactam)does not inhibit inducible chromosomal β-lactamase produced by Enterobacteriaceae. It isalso of no help against Pseudomonas that developresistance by losing permeability to piperacillin.
Dose: 0.5 g combined with piperacillin 4 g injected i.v. over30 min 8 hourly.PYBACTUM, TAZACT, TAZOBID, ZOSYN 4 g + 0.5 g vialfor inj.Tazobactam has been combined with ceftriaxone as well (seep. 728).
CEPHALOSPORINS
These are a group of semisynthetic antibioticsderived from ‘cephalosporin-C’ obtained froma fungus Cephalosporium. They are chemicallyrelated to penicillins; the nucleus consists ofa β-lactam ring fused to a dihydrothiazine ring,(7-aminocephalosporanic acid). By addition ofdifferent side chains at position 7 of β-lactamring (altering spectrum of activity) and at position3 of dihydrothiazine ring (affecting pharmaco-kinetics), a large number of semisynthetic com-pounds have been produced. These have beenconventionally divided into 4 generations. Thisdivision has a chronological sequence ofdevelopment, but more importantly, takes intoconsideration the overall antibacterial spectrumas well as potency.
All cephalosporins are bactericidal and have thesame mechanism of action as penicillin, i.e.inhibition of bacterial cell wall synthesis.However, they bind to different proteins thanthose which bind penicillins. This may explaindifferences in spectrum, potency and lack ofcross resistance.
Acquired resistance to cephalosporins couldhave the same basis as for penicillins, i.e.:
(a) alteration in target proteins (PBPs) reducingaffinity for the antibiotic.
(b) impermeability to the antibiotic or itsefflux so that it does not reach its site ofaction.

726S
EC
TIO
N12
ANTIMICROBIAL DRUGS
First generation cephalosporins
Parenteral OralCefazolin Cephalexin
Cefadroxil
Second generation cephalosporins
Parenteral OralCefuroxime CefaclorCefoxitin* Cefuroxime axetil
Cefprozil
Third generation cephalosporins
Parenteral OralCefotaxime CefiximeCeftizoxime Cefpodoxime proxetilCeftriaxone CefdinirCeftazidime CeftibutenCefoperazone Ceftamet pivoxil
Fourth generation cephalosporins
ParenteralCefepimeCefpirome
*Not available in India
(c) elaboration of β-lactamases which destroyspecific cephalosporins (cephalospori-nases); the most common mechanism.
Though the incidence is low, resistance has beendeveloped by some organisms, even against thethird generation compounds. Individual cepha-losporins differ in their:
(a) Antibacterial spectrum and relative potencyagainst specific organisms.
(b) Susceptibility to β-lactamases elaboratedby different organisms.
(c) Pharmacokinetic properties—many have tobe injected, some are oral; majority are notmetabolized, and are excreted rapidly by thekidney; have short t½s, probenecid inhibitstheir tubular secretion.
FIRST GENERATION CEPHALOSPORINSThese were developed in the 1960s, have highactivity against gram-positive but weaker againstgram-negative bacteria.
Cefazolin It is the prototype first generationcephalosporin that is active against most PnGsensitive organisms, i.e. Streptococci (pyogenesas well as viridans), gonococci, meningococci,
C. diphtheriae, H. influenzae, clostridia andActinomyces. Activity against Klebsiella,Moraxella catarrhalis and E. coli is relativelyhigh, but it is quite susceptible to staphylococcalβ-lactamase. It can be given i.m. (less painful)as well as i.v. and has a longer t½ (2 hours)due to slower tubular secretion; attains higherconcentration in plasma and in bile. It is thepreferred parenteral first generation cephalo-sporin, especially for surgical prophylaxis.Dose: 0.5 g 8 hourly (mild cases), 1 g 6 hourly (severe cases),children 25–50 mg/kg/day i.m. or i.v.; surgical prophylaxis1.0 g 1/2 hour before surgery.REFLIN, ALCIZON, ORIZOLIN 0.25 g, 0.5 g, 1 g per vial inj.
Cephalexin It is the most commonly usedorally effective first generation cephalosporin,similar in spectrum to cefazolin, but less activeagainst penicillinase producing staphylococci andH. influenzae. Plasma protein binding is low;it attains high concentration in bile and isexcreted unchanged in urine; t½ ~60 min.Dose: 0.25–1 g 6–8 hourly (children 25–100 mg/kg/day).CEPHACILLIN 250, 500 mg cap; SPORIDEX, ALCEPHIN,CEPHAXIN 250, 500 mg cap, 125 mg/5 ml dry syr., 100 mg/mlpediatric drops.ALCEPHIN-LA: Cephalexin + probenecid (250 + 250 mg and500 + 500 mg) tabs.
Cefadroxil A close congener of cephalexin;has good tissue penetration—exerts more sus-tained action at the site of infection, because ofwhich it can be given 12 hourly despite a t½ of1 hr. It is excreted unchanged in urine; the doseneeds to be reduced only if creatinine clearanceis < 50 ml/min. The antibacterial activity ofcefadroxil and indications are similar to thoseof cephalexin.Dose: 0.5–1 g BD. DROXYL 0.5, 1 g tab, 250 mg/5 ml syr;CEFADROX 0.5 g cap, 125 mg/5 ml syr and 250 mg kid tab;KEFLOXIN 0.5 g cap, 0.25 g Distab, 125 mg/5 ml susp.
SECOND GENERATIONCEPHALOSPORINS
These were developed subsequent to the firstgeneration compounds and are more activeagainst gram-negative organisms, with somemembers active against anaerobes as well, butnone inhibits P. aeruginosa. They are weaker

727C
HA
PTER51
BETA-LACTAM ANTIBIOTICS
than the first generation compounds against grampositive bacteria. Their utility has declined infavour of the 3rd generation agents.
Cefuroxime It is resistant to gram-negativeβ-lactamases: has high activity against organismsproducing these enzymes including PPNG andampicillin-resistant H. influenzae, while retain-ing significant activity on gram-positive cocciand certain anaerobes, but not B. fragilis. It iswell tolerated by i.m. route and attains relativelyhigher CSF levels, but has been superseded by3rd generation cephalosporins in the treatmentof meningitis. It can be employed for single dosei.m. therapy of gonorrhoea due to PPNG.CEFOGEN, SUPACEF, FUROXIL 250 mg and 750 mg/vial inj;0.75–1.5 g i.m. or i.v. 8 hourly, children 30–100 mg/kg/day.For gonorrhoea 1.5 g divided at 2 sites i.m. inj + probenecid1.0 g oral single dose.
Cefuroxime axetil This ester of cefuroximeis effective orally, though absorption is incomp-lete. The activity depends on in vivo hydrolysisand release of cefuroxime.Dose: 250–500 mg BD, children half dose; CEFTUM, SPIZEF125, 250, 500 mg captab and 125 mg/5 ml susp.
Cefaclor It retains significant activity by theoral route and is more active than the firstgeneration compounds against H. influenzae,E. coli, Pr. mirabilis and some anaerobes.Dose: 0.25–1.0 g 8 hourlyKEFLOR, VERCEF, DISTACLOR 250 mg cap, 125 and 250 mgdistab, 125 mg/5 ml dry syr, 50 mg/ml ped. drops.
Cefprozil This 2nd generation cephalosporinhas good oral absorption (>90%) with augmentedactivity against Strep. pyogenes, Strep. pneumo-niae, Staph. aureus, H. influenzae, Moraxellaand Klebsiella. It is excreted by the kidney, witha t½ of 1.3 hours. The primary indications arebronchitis, ENT and skin infections.Dose: 250–500 mg BD, (child 20 mg/kg/day).ORPROZIL, ZEMETRIL 250, 500 mg tab; REFZIL 250, 500 mgtab., 125 mg/5 ml and 250 mg/5 ml syr.
THIRD GENERATION CEPHALOSPORINSThese compounds introduced in the 1980s havehighly augmented activity against gram-negativeEnterobacteriaceae; and few members inhibit
Pseudomonas as well. All are highly resistantto β-lactamases from gram-negative bacteria.However, they are less active on gram-positivecocci and anaerobes.
Cefotaxime It is the prototype of the thirdgeneration cephalosporins; exerts potent actionon aerobic gram-negative as well as some gram-positive bacteria, but is not active on anaerobes(particularly Bact. fragilis), Staph. aureus andPs. aeruginosa. Prominent indications are menin-gitis caused by gram-negative bacilli (attains rela-tively high CSF levels), life-threatening resistant/hospital-acquired infections, septicaemias andinfections in immunocompromised patients. It isan alternative to ceftriaxone for typhoid fever,and can be utilized for single dose therapy(1 g i.m. + 1 g probenecid oral) of PPNGurethritis, but is not dependable for Pseudomonasinfections.
Cefotaxime is deacetylated in the body; themetabolite exerts weaker but synergistic actionwith the parent drug. The plasma t½ of cefota-xime is 1 hr, but is longer for the deacetylatedmetabolite—permitting 12 hourly doses in manysituations. Penetration into CSF is good.Dose: 1–2 g i.m./i.v. 6–12 hourly, children 50–100mg/kg/day.OMNATAX, ORITAXIM, CLAFORAN 0.25, 0.5, 1.0 g per vialinj.
Ceftizoxime It is similar in antibacterialactivity and indications to cefotaxime, butinhibits B. fragilis also. It is not metabolized—excreted by the kidney at a slower rate; t½1.5–2 hr.Dose: 0.5–2.0 g i.m./i.v. 8 or 12 hourly.CEFIZOX, EPOCELIN 0.5 and 1 g per vial inj.
Ceftriaxone The distinguishing feature of thiscephalosporin is its longer duration of action(t½ 8 hr), permitting once, or at the most twicedaily dosing. Penetration into CSF is good andelimination occurs equally in urine and bile.
Ceftriaxone has shown high efficacy in a widerange of serious infections including bacterialmeningitis (especially in children), multiresistanttyphoid fever, complicated urinary tract infec-tions, abdominal sepsis and septicaemias.

728S
EC
TIO
N12
ANTIMICROBIAL DRUGS
A single dose of 250 mg i.m. has proven curativein gonorrhoea including PPNG, and in chancroid.
Hypoprothrombinaemia and bleeding are thespecific adverse effects. Haemolysis is reported.OFRAMAX, MONOCEF, MONOTAX 0.25, 0.5, 1.0 g per vialinj.For skin/soft tissue/urinary infections: 1–2 g i.v. or i.m./day.Meningitis: 4 g followed by 2 g i.v. (children 75–100 mg/kg)once daily for 7–10 days.Typhoid: 4 g i.v. daily × 2 days followed by 2 g/day (children 75mg/kg) till 2 days after fever subsides.To overcome resistance, it has been combined with sulbactamor tazobactam.CEFTICHEK, SUPRAXONE ceftriaxone + sulbactam 250 mg +125 mg and 1.0 g + 0.5 g vial.MONTAZ, EXTACEF-TAZO, FINECEF-T ceftriaxone 1 g +tazobactam 125 mg vial.
Ceftazidime The most prominent feature ofthis third generation cephalosporin is its highactivity against Pseudomonas aeruginosa, andthe specific indications are—febrile neutropenicpatients with haematological malignancies, burn,etc. Its activity against Enterobacteriaceae issimilar to that of cefotaxime, but it is less activeon Staph. aureus, other gram positive cocci andanaerobes like Bact. fragilis. Its plasma t½ is1.5–1.8 hr.
Neutropenia, thrombocytopenia, rise inplasma transaminases and blood urea have beenreported.Dose: 0.5–2 g i.m. or i.v. every 8 hr, children 30 mg/kg/day.Resistant typhoid 30 mg/kg/day.FORTUM, CEFAZID, ORZID 0.25, 0.5 and 1 g per vial inj.
Cefoperazone Like ceftazidime, it differsfrom other third generation compounds in havingstronger activity on Pseudomonas and weakeractivity on other organisms. It is good for S.typhi and B. fragilis also, but more susceptibleto β-lactamases. The indications are—severeurinary, biliary, respiratory, skin-soft tissueinfections, typhoid, meningitis and septicaemias.It is primarily excreted in bile; t½ is 2 hr. Ithas hypoprothrombinaemic action but does notaffect platelet function. A disulfiram-likereaction with alcohol has been reported.Dose: 1–3 g i.m./i.v. 8–12 hourly.MAGNAMYCIN 0.25 g, 1, 2 g inj; CEFOMYCIN, NEGAPLUS1 g inj.It has been combined with sulbactam.
CEFOBETA, KEFBACTUM Cefoperazone 500 mg + sulbactam500 mg vial, CEFACTUM 1 g + 1 g vial.
Cefixime It is an orally active third generationcephalosporin highly active against Enterobacte-riaceae, H. influenzae, Strep. pyogenes, and isresistant to many β-lactamases. However, it isnot active on Staph. aureus, most pneumococciand Pseudomonas. It is longer acting (t½ 3 hr)and has been used in a dose of 200–400 mg BDfor respiratory, urinary and biliary infections.Stool changes and diarrhoea are the mostprominent side effects.TOPCEF, ORFIX 100, 200 mg tab/cap, CEFSPAN 100 mg cap,100 mg/5 ml syr, TAXIM-O 100, 200 mg tab, 50 mg/5 ml inj.
Cefpodoxime proxetil It is the orally activeester prodrug of 3rd generation cephalosporincefpodoxime. In addition to being highly activeagainst Enterobacteriaceae and streptococci, itinhibits Staph. aureus. It is used mainly for respi-ratory, urinary, skin and soft tissue infections.Dose: 200 mg BD (max 800 mg/day)CEFOPROX, CEPODEM, DOXCEF 100, 200 mg tab, 50 mg/5 mland 100 mg/5 ml dry syr.
Cefdinir This orally active 3rd generationcephalosporin has good activity against many βlactamase producing organisms. Most respiratorypathogens including gram-positive cocci aresusceptible. Its indications are pneumonia, acuteexacerbations of chronic bronchitis, ENT andskin infections.Dose: 300 mg BDSEFDIN, ADCEF 300 mg cap, 125 mg/5 ml susp.
Ceftibuten Another oral 3rd generation cepha-losporin, active against gram-positive and fewgram-negative bacteria, but not Staph. aureus.It is stable to β-lactamases, and is indicated inrespiratory and ENT infections; t½ 2–3 hours.Dose: 200 mg BD or 400 mg OD.PROCADAX 400 mg cap, 90 mg/5 ml powder for oralsuspension.
Ceftamet pivoxil This ester prodrug ofceftamet, a 3rd generation cephalosporin has highactivity against gram-negative bacteria, especiallyEnterobacteriaceae and N. gonorrhoea; used inrespiratory, skin-soft tissue infections, etc.Dose: 500 mg BD–TDS.ALTAMET 250 mg tab; CEPIME-O 500 mg tab.

729C
HA
PTER51
BETA-LACTAM ANTIBIOTICS
FOURTH GENERATIONCEPHALOSPORINS
The distinctive feature of this last developedsubgroup of cephalosporins is non-susceptibilityto inducible chromosomal β lactamases in addi-tion to high potency against Enterobacteriaceaeand spectrum of activity resembling the 3rd
generation compounds.
Cefepime Developed in 1990s, this 4th gene-ration cephalosporin has antibacterial spectrumsimilar to that of 3rd generation compounds, butis highly resistant to β-lactamases, hence activeagainst many bacteria resistant to the earlierdrugs. Ps. aeruginosa and Staph. aureus are alsoinhibited but not MRSA. Due to high potencyand extended spectrum, it is effective in manyserious infections like hospital-acquiredpneumonia, febrile neutropenia, bacteraemia,septicaemia. Higher concentrations are attainedin the CSF, and it is excreted by the kidney witha t½ of 2 hours.Dose: 1–2 g i.v. 8–12 hourly. Child with febrile neutropenia50 mg/kg i.v. 8 hourly.KEFAGE, CEFICAD, CEPIME 0.5, 1.0 g inj.
Cefpirome This 4th generation cephalosporinis indicated for the treatment of serious andresistant hospital-acquired infections includingsepticaemias, lower respiratory tract infections,etc. Its zwitterion character permits better pene-tration through porin channels of gram-negativebacteria. It is resistant to many β-lactamases;inhibits type 1 β-lactamase producing Entero-bacteriaceae and it is more potent against gram-positive and some gram-negative bacteria thanthe 3rd generation compounds.Dose: 1–2 g i.m./i.v. 12 hourly;CEFROM, CEFORTH 1 g inj; BACIROM, CEFOR 0.25, 0.5, 1.0 ginj.
Adverse effectsCephalosporins are generally well tolerated, butare more toxic than penicillin.1. Pain after i.m. injection occurs with manycephalosporins, but some can be injected i.m.,while others are injected only i.v. (see individual
compounds). Thrombophlebitis of injected veincan occur.2. Diarrhoea due to alteration of gut ecologyor irritative effect is more common with orallyadministered compounds like cephalexin,cefixime and parenteral cefoperazone, which islargely excreted in bile.3. Hypersensitivity reactions are the mostimportant adverse effects of cephalosporins.Manifestations are similar to penicillin, butincidence is lower. Rashes are the most frequentmanifestation, but anaphylaxis, angioedema,asthma and urticaria have also occurred. About10% patients allergic to penicillin show crossreactivity with cephalosporins. Those with ahistory of immediate type of reactions topenicillin should better not be given a cephalo-sporin. Skin tests for sensitivity to cephalosporinsare unreliable.
A positive Coombs’ test occurs in manypatients, but haemolysis is rare.4. Nephrotoxicity Some cephalosporins havelow-grade nephrotoxicity which may be accentua-ted by preexisting renal disease, concurrentadministration of an aminoglycoside or loopdiuretic.5. Bleeding occurs with cephalosporins havinga methylthiotetrazole or similar substitution atposition 3 (cefoperazone, ceftriaxone). This isdue to hypoprothrombinaemia caused by thesame mechanism as warfarin and is morecommon in patients with cancer, intra-abdominalinfection or renal failure.6. Neutropenia and thrombocytopenia are rareadverse effects reported with ceftazidime andsome others.7. A disulfiram-like interaction with alcohol hasbeen reported with cefoperazone.
UsesCurrently cephalosporins are one of the mostcommonly used antibiotics. Among them theycover a wide range of gram-positive and gram-

730S
EC
TIO
N12
ANTIMICROBIAL DRUGS
negative bacteria including some anaerobes butnot B. fragilis, or MRSA, enterococci, myco-bacteria and chlamydia. Their indications are:
1. As alternatives to penicillins for ENT, upperrespiratory and cutaneous infections, one of thefirst generation compounds may be used.
2. Respiratory, urinary and soft tissue infectionscaused by gram-negative organisms, especiallyKlebsiella, Proteus, Enterobacter, Serratia.Cephalosporins preferred for these infectionsare cefuroxime, cefotaxime, ceftriaxone.
3. Penicillinase producing staphylococcalinfections.
4. Septicaemias caused by gram-negativeorganisms: an aminoglycoside may be combinedwith a cephalosporin.
5. Surgical prophylaxis: the first generationcephalosporins are popular drugs. Cefazolin (i.m.or i.v.) is employed for most types of surgeriesincluding those with surgical prosthesis such asartificial heart valves, artificial joints, etc.
6. Meningitis: Optimal therapy of pyogenicmeningitis requires bactericidal activity in theCSF, preferably with antibiotic concentrationsseveral times higher than the MBC for theinfecting organism. For empirical therapy beforebacterial diagnosis, i.v. cefotaxime/ceftriaxoneis generally combined with ampicillin orvancomycin or both. Ceftazidime + gentamicinis the most effective therapy for Pseudomonasmeningitis.
7. Gonorrhoea caused by penicillinase pro-ducing organisms: ceftriaxone is a first choicedrug for single dose therapy of gonorrhoea ifthe penicillinase producing status of the orga-nism is not known. Cefuroxime and cefotaximehave also been used for this purpose. Forchancroid also, a single dose is as effective aserythromycin given for 7 days.
8. Typhoid: Currently, ceftriaxone andcefoperazone injected i.v. are the fastest acting
and most reliable drugs for enteric fever. Theyare preferred over fluoroquinolones (especiallyin children) for empirical therapy, since manyS. typhi strains are resistant to chloramphenicol,ampicillin, cotrimoxazole, and FQs.
9. Mixed aerobic-anaerobic infections in cancerpatients, those undergoing colorectal surgery,obstetric complications: cefuroxime, cefaclor orone of the third generation compounds is used.
10. Hospital acquired infections, especiallyrespiratory and other infections in intensive careunits, resistant to commonly used antibiotics:cefotaxime, ceftizoxime or a fourth generationdrug may work.
11. Prophylaxis and treatment of infections inneutropenic patients: ceftazidime or another thirdgeneration compound, alone or in combinationwith an aminoglycoside.
MONOBACTAMSAztreonam It is a novel β-lactam antibioticin which the other ring is missing (hence mono-bactam), but acts by binding to specific PBPs.It inhibits gram-negative enteric bacilli and H.influenzae at very low concentrations andPseudomonas at moderate concentrations, butdoes not inhibit gram-positive cocci or faecalanaerobes. Thus, it is a β-lactam antibiotic witha spectrum resembling aminoglycosides, and isresistant to gram-negative β-lactamases. Themain indications of aztreonam are hospital-acquired infections originating from urinary,biliary, gastrointestinal and female genital tracts.
Lack of cross sensitivity with other β-lactamantibiotics except ceftazidime (which haschemical similarity to aztreonam) is the mostprominent feature of aztreonam: permiting itsuse in patients allergic to penicillins or cephalo-sporins. Rashes and rise in serum aminotrans-ferases are the notable adverse effects. It iseliminated unchanged in urine with a t½ of 1.8 hr.Dose: 0.5–2 g i.m. or i.v. 6–12 hourly.AZENAM, TREZAM 0.5, 1.0, 2.0 g/vial inj.

731C
HA
PTER51
BETA-LACTAM ANTIBIOTICS
CARBAPENEMS
Imipenem A derivative of thienamycin,imipenem is an extremely potent and broad-spectrum β-lactam antibiotic whose range ofactivity includes gram-positive cocci,Enterobacteriaceae, Ps. aeruginosa, Listeria aswell as anaerobes like Bact. fragilis and Cl.difficile. It is resistant to most β-lactamases;inhibits penicillinase producing staphylococci.Though some MRSA are inhibited, it is notreliable for treating such infections.
A limiting feature of imipenem is its rapidhydrolysis by the enzyme dehydropeptidase Ilocated on the brush border of renal tubular cells.An innovative solution to this problem is itscombination with cilastatin, a reversible inhibitorof dehydropeptidase I, which has matchedpharmacokinetics with imipenem (t½ of both is1 hr) and protects it.
Imipenem-cilastatin 0.5 g i.v. 6 hourly (max4 g/day) has proved effective in a wide rangeof serious hospital-acquired respiratory, urinary,abdominal, pelvic, skin and soft tissue infectionsincluding those in neutropenic, cancer and AIDSpatients. For Ps. aeruginosa infections, it shouldbe combined with gentamicin.
Imipenem has propensity to induce seizuresat higher doses and in predisposed patients.Diarrhoea, vomiting, skin rashes and otherhypersensitivity reactions are the side effects.IMINEM: Imipenem + cilastatin 250 mg + 250 mg and 500mg + 500 mg/vial inj.LASTINEM: Imipenem + cilastatin 125 + 125 mg, 250 + 250mg, 500 + 500 mg and 1000 mg + 1000 mg/vial inj.
Meropenem This newer carbapenem is nothydrolysed by renal peptidase; does not need tobe protected by cilastatin. Like imipenem, it isactive against both gram-positive and gram-
negative bacteria, aerobes as well as anaerobes;somewhat more potent on gram-negative aerobes,especially Ps. aeruginosa but less potent ongram-positive cocci.
Meropenem is a reserve drug for thetreatment of serious nosocomial infections likesepticaemia, febrile neutropenia, intraabdominaland pelvic infections, etc. caused bycephalosporin-resistant bacteria and diabeticfoot. For Ps. aeruginosa infections, it shouldbe combined with an aminoglycoside. Theadverse effects of meropenem are similar toimipenem, but it is less likely to cause seizures.Dose: 0.5–2.0 g (10–40 mg/kg) by slow i.v. injection8 hourly.MERONEM, MENEM, UBPENEM 0.5, 1.0 g/vial inj.
Faropenem Another carbapenem β-lactamantibiotic that is orally active against many gram-positive as well as gram-negative bacteria,including some anaerobes. Strep. pneumoniae,H. influenzae, Moraxella catarrhalis are highlysusceptible. It has been mainly used inrespiratory, ENT and genitourinary infections.Usual side effects are diarrhoea, abdominal pain,nausea and rashes.Dose: 150–300 mg oral TDS; FARONEM, FAROZET 150 mg,200 mg tab.
Doripenem Introduced recently, this carba-penem has antimicrobial activity similar tomeropenem, but is more active against someresistant Pseudomonas. Other properties,including nonsusceptibility to renal peptidase,as well as clinical indications are also similarto meropenem. Adverse effects are nausea,diarrhoea, superinfections and phlebitis of theinjected vein. Seizures are less likely.Dose: 500 mg by slow i.v. infusion over 1 hr, every 8 hours.DORIGLEN 500 mg/vial inj., SUDOPEN 250, 500 mg/vial inj.

732S
EC
TIO
N12
ANTIMICROBIAL DRUGS
PROBLEM DIRECTED STUDY
51.1 A 10-year-old boy weighing 25 kg is brought with continuous fever for the past 7 days.Initially the fever was mild, but has gradually increased and the body temp. now is 103°F.The boy also complains of abdominal pain, bloating, loose motions, loss of appetite, occasionalvomiting, weakness, malaise and cough. A local doctor had given some tablets for the past3 days, but the condition has worsened. He looks ill, mildly dehydrated with coated tongue;pulse is 70/min, abdomen is distended and tender on pressing. Liver and spleen are palpable.The total leucocyte count is 5000/cumm. Blood for culture is sent. A provisional diagnosisof typhoid (enteric) fever is made.(a) Should antibiotic therapy be started right away, or the report of blood culture awaited?(b) If treatment is to be started, which antibiotic would be the most appropriate, and why?What should be the dose and duration of antibiotic therapy?(c) Should a single antibiotic or a combination be used?(see Appendix-1 for solution)

Tetracyclines andChloramphenicol(Broad-Spectrum Antibiotics)
ChapterChapterChapterChapterChapter 5252525252
TETRACYCLINES
These are a class of antibiotics having a nucleusof four cyclic rings.
by binding to 30S ribosomes in susceptible orga-nism. Subsequent to such binding, attachmentof aminoacyl-t-RNA to the acceptor (A) site ofmRNA-ribosome complex is interferred with(Fig. 52.1). As a result, the peptide chain failsto grow.
The sensitive organisms have an energy depen-dent active transport process which concentratestetracyclines intracellularly. In gram-negativebacteria tetracyclines diffuse through porinchannels as well. The more lipid-solublemembers (doxycycline, minocycline) enter bypassive diffusion also (this is partly responsiblefor their higher potency). The carrier involvedin active transport of tetracyclines is absent inthe host cells. Moreover, protein synthesizingapparatus of host cells is less susceptible totetracyclines. These two factors are responsiblefor the selective toxicity of tetracyclines forthe microbes.
Antimicrobial spectrum When originallyintroduced, tetracyclines inhibited practically alltypes of pathogenic microorganisms except fungiand viruses; hence the name ‘broad-spectrumantibiotic’. However, promiscous and oftenindiscriminate use has gradually narrowed thefield of their usefulness.1. Cocci: All gram-positive and gram-negativecocci were originally sensitive, but now onlyfew Strep. pyogenes, Staph. aureus (includingMRSA) and enterococci respond. Responsive-ness of Strep. pneumoniae has decreasedsomewhat. Tetracyclines (especially mino-cycline) are now active against relatively fewN. gonorrhoeae and N. meningitidis.2. Most gram-positive bacilli, e.g. Clostridiaand other anaerobes, Listeria, Corynebacteria,Propionibacterium acnes, B. anthracis are
All are obtained from soil actinomycetes. The first to beintroduced was chlortetracycline in 1948 under the nameaureomycin (because of the golden yellow colour of S.aureofaciens colonies producing it). It contrasted markedlyfrom penicillin and streptomycin (the other two antibioticsavailable at that time) in being active orally and in affectinga wide range of microorganisms—hence called ‘broad-spectrum antibiotic’. Oxytetracycline soon followed; otherswere produced later, either from mutant strains orsemisynthetically. A new synthetic subclass ‘glycylcyclines’represented by Tigecycline has been added recently.
All tetracyclines are slightly bitter solidswhich are slightly water soluble, but their hydro-chlorides are more soluble. Aqueous solutionsare unstable. All have practically the sameantimicrobial activity (with minor differences).The subsequently developed members have highlipid solubility, greater potency and some otherdifferences. The tetracyclines still available inIndia for clinical use are:Tetracycline DoxycyclineOxytetracycline MinocyclineDemeclocycline
Glycylcycline: Tigecycline
Many others like Chlortetracycline, Methacycline,Rolitetracycline, Lymecycline are no longer commerciallyavailable.
Mechanism of action The tetracyclines areprimarily bacteriostatic; inhibit protein synthesis

734S
EC
TIO
N12
ANTIMICROBIAL DRUGS
Fig. 52.1: Bacterial protein synthesis and the site of action of antibiotics
The messenger RNA (mRNA) attaches to the 30S ribosome. The initiation complex of mRNA starts protein synthesisand polysome formation. The nacent peptide chain is attached to the peptidyl (P) site of the 50S ribosome. The nextamino acid (a) is transported to the acceptor (A) site of the ribosome by its specific tRNA which is complementary to thebase sequence of the next mRNA codon (C). The nascent peptide chain is transferred to the newly attached amino acidby peptide bond formation. The elongated peptide chain is shifted back from the ‘A’ to the ‘P’ site and the ribosomemoves along the mRNA to expose the next codon for amino acid attachment. Finally the process is terminated by thetermination complex and the protein is released.(1) Aminoglycosides bind to several sites at 30S and 50S subunits as well as to their interface—freeze initiation,interfere with polysome formation and cause misreading of mRNA code.(2) Tetracyclines bind to 30S ribosome and inhibit aminoacyl tRNA attachment to the ‘A’ site.(3) Chloramphenicol binds to 50S subunit—interferes with peptide bond formation and transfer of peptide chain from ‘P’ site.(4) Erythromycin and clindamycin also bind to 50S ribosome and hinder translocation of the elongated peptide chainback from ‘A’ site to ‘P’ site and the ribosome does not move along the mRNA to expose the next codon. Peptidesynthesis may be prematurely terminated.
inhibited but not Mycobacteria, except M. leprae(to minocycline) and some atypical ones.3. Sensitive gram-negative bacilli are—H. ducreyi, Calymmatobacterium granulomatis,V. cholerae, Yersinia pestis, Y. enterocolitica,Campylobacter, Helicobacter pylori, Brucella,Pasteurella multocida, F. tularensis and manyanaerobes. Some H. influenzae have becomeinsensitive.
Enterobacteriaceae are now largely resistant.Notable bacilli that are not inhibited are Pseudo-monas aeruginosa, Proteus, Klebsiella,Salmonella typhi and many Bact. fragilis. MICagainst anaerobes is relatively higher.4. Spirochetes, including T. pallidum andBorrelia are quite sensitive.
5. All rickettsiae (typhus, etc.) and chlamydiaeare highly sensitive.6. Mycoplasma and Actinomyces are mode-rately sensitive.7. Protozoa like Entamoeba histolytica andPlasmodia are inhibited at high concentrations.Resistance Resistance to tetracyclinesdevelops slowly in a graded manner. In suchbacteria, usually the tetracycline concentratingmechanism becomes less efficient or thebacteria acquire capacity to pump it out. Anothermechanism is plasmid mediated synthesis of a‘protection’ protein which protects the ribosomalbinding site from tetracycline. Elaboration oftetracycline inactivating enzymes is anunimportant mechanism of the tetracycline

735C
HA
PTER52
TETRACYCLINES AND CHLORAMPHENICOL
resistance. Due to widespread use, tetracyclineresistance has become common among gram-positive cocci, E. coli, Enterobacter and manyothers.
Incomplete cross resistance is seen amongdifferent members of the tetracycline group.Some organisms not responding to other tetra-cyclines may be inhibited by therapeuticallyattained concentrations of doxycycline andminocycline (the most potent agent).
Partial cross resistance between tetracyclinesand chloramphenicol has been noted.
PharmacokineticsThe pharmacokinetic differences between indi-vidual tetracyclines are included in Table 52.1.The older tetracyclines are incompletelyabsorbed from g.i.t.; absorption is better if takenin empty stomach. Doxycycline and minocyclineare completely absorbed irrespective of food.Tetracyclines have chelating property—forminsoluble and unabsorbable complexes withcalcium and other metals. Milk, iron prepara-tions, nonsystemic antacids and sucralfate reducetheir absorption. Administration of thesesubstances and tetracyclines should be staggered,if they cannot be avoided altogether.
Tetracyclines are widely distributed in thebody (volume of distribution > 1 L/kg). Variabledegree of protein binding is exhibited by differentmembers. They are concentrated in liver, spleenand bind to the connective tissue in bone and teeth.Intracellularly, they bind to mitochondria. Mino-cycline being highly lipid soluble accumulatesin body fat. The CSF concentration of mosttetracyclines is about 1/4 of plasma concen-tration, whether meninges are inflamed or not.
Most tetracyclines are primarily excreted inurine by glomerular filtration; dose has to bereduced in renal failure; doxycycline is anexception to this. They are partly metabolizedand significant amounts enter bile—some degreeof enterohepatic circulation occurs. They aresecreted in milk in amounts sufficient to affectthe suckling infant.
Enzyme inducers like phenobarbitone andphenytoin enhance metabolism and shorten thet½ of doxycycline.
Administration Oral capsule is the dosageform in which tetracyclines are most commonlyadministered. The capsule should be taken ½ hrbefore or 2 hr after food. Liquid oral preparationsfor pediatric use are banned in India.
Tetracyclines are not recommended by i.m.route because it is painful and absorption fromthe injection site is poor. Slow i.v. injection maybe given in severe cases, but is rarely requirednow.
A variety of topical preparations (ointment,cream, etc.) are available, but should not be used,because there is high risk of sensitization. How-ever, ocular application is not contraindicated.
Preparations
1. Oxytetracycline: TERRAMYCIN 250, 500 mg cap, 50 mg/mlin 10 ml vials inj; 3% skin oint, 1% eye/ear oint.
2. Tetracycline: ACHROMYCIN, HOSTACYCLINE,RESTECLIN 250, 500 mg cap. 3% skin oint, 1% eye/eardrops and oint.
3. Demeclocycline (Demethylchlortetracycline):LEDERMYCIN 150, 300 mg cap/tab.
4. Doxycycline: TETRADOX, DOXICIP, DOXT, NOVADOX100 mg cap.
5. Minocycline: CYANOMYCIN, CNN 50, 100 mg caps.
Adverse effects
Irritative effects Tetracyclines have irritantproperty; can cause epigastric pain, nausea,vomiting and diarrhoea on oral ingestion. Theirritative diarrhoea is to be distinguished fromthat due to superinfection. Odynophagia andesophageal ulceration has occurred by releaseof the material from capsules in the esophagusduring swallowing, especially with doxycycline.Intramuscular injection of tetracyclines isvery painful; thrombophlebitis of the injectedvein can occur, especially on repeated i.v.injection.
Organ toxicity This is dose related.1. Liver damage Fatty infiltration of liver andjaundice occurs occasionally. Oxytetracycline and

736S
EC
TIO
N12
ANTIMICROBIAL DRUGS
TABLE 52.1 Comparative features of tetracyclines
Tetracycline (T) Demeclocycline Doxycycline (Doxy)Oxytetracycline (OxyT) Minocycline (Mino)
1. Source Oxy T: S. rimosus S. aureofaciens Doxy: semisyntheticT: semisynthetic (mutant) Mino: semisynthetic
2. Potency Low Intermediate High (Doxy < Mino)
3. Intestinal absorption 60–80% 60–80% 95–100%no interference by food
4. Plasma protein Oxy T: Low High Highbinding T: Moderate
5. Elimination T: Rapid renal Partial metabolism, Doxy: Primarily excreted inOxy T: excretion slower renal excretion faeces as conjugate
Mino: Primarily metabolized,excreted in urine and bile
6. Plasma t½ 6–10 hr. 16–18 hr. 18–24 hr.
7. Dosage 250–500 mg QID 300 mg BD 200 mg initially,or TDS then 100–200 mg OD
8. Alteration of Marked Moderate Leastintestinal flora
9. Incidence of diarrhoea High Intermediate Low
10. Phototoxicity Low Highest Doxy: High
11. Specific toxicity Oxy T: less tooth More phototoxic, Doxy: Low renal toxicity.discolouration diabetes insipidus Mino: Vestibular toxicity,
less superinfections
tetracycline are safer in this regard. Tetracyclinesare risky in pregnant women; can precipitate acutehepatic necrosis which may be fatal.
2. Kidney damage It is a risk only in thepresence of existing kidney disease. All tetracyc-lines, except doxycycline, accumulate andenhance renal failure. A reversible Fanconisyndrome like condition is produced by outdatedtetracyclines. This is caused by degradedproducts—epitetracycline, anhydrotetracyclineand epianhydrotetracycline which damageproximal tubules. Exposure to acidic pH,moisture and heat favours such degradation.
3. Phototoxicity A sunburn-like or othersevere skin reaction on exposed parts is seenin some individuals. A higher incidence has beennoted with demeclocycline and doxycycline.Distortion of nails occurs occasionally.
4. Teeth and bones Tetracyclines havechelating property. Calcium-tetracycline chelategets deposited in developing teeth and bone.Given from midpregnancy to 5 months of extra-uterine life, the deciduous teeth are affected:brown discolouration, ill-formed teeth which aremore susceptible to caries. Tetracyclines givenbetween 3 months and 6 years of age affect thecrown of permanent anterior dentition. Repeatedcourses are more damaging.
Given during late pregnancy or childhood,tetracyclines can cause temporary suppressionof bone growth. The ultimate effect on statureis mostly insignificant, but deformities and reduc-tion in height are a possibility with prolonged use.5. Antianabolic effect Tetracyclines reduceprotein synthesis and have an overall cataboliceffect. They induce negative nitrogen balance andcan increase blood urea.
⎫⎬⎭

737C
HA
PTER52
TETRACYCLINES AND CHLORAMPHENICOL
6. Increased intracranial pressure is notedin some infants.
7. Diabetes insipidus Demeclocyclineantagonizes ADH action and reduces urineconcentrating ability of the kidney. It has beentried in patients with inappropriate ADHsecretion.
8. Vestibular toxicity Minocycline can causeataxia, vertigo and nystagmus, which subsidewhen the drug is discontinued.
Hypersensitivity This is infrequent with tetra-cyclines. Skin rashes, urticaria, glossitis, pruritusani and vulvae, even exfoliative dermatitis havebeen reported. Angioedema and anaphylaxis areextremely rare. Complete cross sensitization isexhibited by different tetracyclines.
Superinfection Tetracyclines are frequentlyresponsible for superinfections, because theycause more marked suppression of the residentflora.
Though mouth, skin or vagina may be invol-ved, intestinal superinfection by Candidaalbicans is most prominent (for details seep. 693); pseudomembranous enterocolitis is rarebut serious. Higher doses suppress the flora morecompletely—greater chance of superinfection:doses on the lower side of the range should beused whenever possible. The tetracycline shouldbe discontinued at the first sign of superinfectionand appropriate therapy instituted.
Doxycycline and minocycline are less liableto cause diarrhoea, because only small amountsreach the lower bowel in the active form.
Precautions1. Tetracyclines should not be used during
pregnancy, lactation and in children.2. They should be avoided in patients on
diuretics: blood urea may rise in such patients.3. They should be used cautiously in renal or
hepatic insufficiency.4. Preparations should never be used beyond
their expiry date.
5. Do not mix injectable tetracyclines withpenicillin—inactivation occurs.
6. Do not inject tetracyclines intrathecally.
Uses
Although tetracyclines are broad-spectrumantibiotics, they should be employed only forthose infections for which a more selective andless toxic AMA is not available. Clinical use oftetracyclines has very much declined due toavailability of fluoroquinolones and otherefficacious AMAs.
1. Empirical therapy Tetracyclines are oftenemployed when the nature and sensitivity of theinfecting organism cannot be reasonably guessed.However, they are not dependable for empiricaltreatment of serious/life-threatening infections.They may also be used for initial treatment ofmixed infections, although a combination ofβ-lactam and an aminoglycoside antibiotic or athird generation cephalosporin or a fluoroquino-lone are now preferred.
2. Tetracyclines are the first choice drugs:Despite development of resistance by manyorganisms, tetracyclines are still the preferreddrugs for:(a) Venereal diseases:• Chlamydial nonspecific urethritis/endo-
cervicitis: 7 day doxycycline treatment is aseffective as azithromycin single dose.
• Lymphogranuloma venereum: resolves in2–3 weeks (see Table 54.1).
• Granuloma inguinale: due to Calymm.granulomatis: a tetracycline administered for3 weeks is the most effective treatment.
(b) Atypical pneumonia: due to Mycoplasmapneumoniae: duration of illness is reduced bytetracycline therapy. Psittacosis is treated in 2weeks by tetracyclines.(c) Cholera: Tetracyclines have adjuvant valueby reducing stool volume and limiting theduration of diarrhoea.(d) Brucellosis: Tetracyclines are highly effica-cious; cause rapid symptomatic relief; therapy

738S
EC
TIO
N12
ANTIMICROBIAL DRUGS
of choice is doxycycline 200 mg/day + rifampin600 mg/day for 6 weeks. Gentamicin may becombined with doxycycline in acute cases.(e) Plague: Tetracyclines are highly effectivein both bubonic and pneumonic plague. They arepreferred for blind/mass treatment of suspectedcases during an epidemic, though streptomycinoften acts faster.(f) Relapsing fever: due to Borrelia recurrentisresponds adequately.(g) Rickettsial infections: typhus, rockymountain spotted fever, Q fever, etc. responddramatically. Chloramphenicol is an alternative.
3. Tetracyclines are second choice drugs:(a) To penicillin/ampicillin for tetanus, anthrax,actinomycosis and Listeria infections.(b) To ceftriaxone, amoxicillin or azithromycinfor gonorrhoea, especially for penicillin resistantnon-PPNG; also in patients allergic to penicillin,but response rate has decreased.(c) To ceftriaxone for syphilis in patients allergicto penicillin; early syphilis can be treated in2 weeks but late syphilis requires 1 month.(d) To penicillin for leptospirosis; doxycycline100 mg BD for 7 days is curative. Weeklydoxycycline (200 mg) has been used as pro-phylactic in subjects at risk during an epidemic.(e) To azithromycin for pneumonia due toChlamydia pneumoniae. Oral as well as topicaltetracycline has been used in trachoma.(f) To ceftriaxone/azithromycin for chancroid.(g) To streptomycin for tularemia.
4. Other situations in which tetracyclinesmay be used are:(a) Urinary tract infections: Odd cases in whichthe organism has been found sensitive.(b) Community-acquired pneumonia, when amore selective antibiotic cannot be used.(c) Amoebiasis: along with other amoebicidesfor chronic intestinal amoebiasis.(d) As adjuvant to quinine or artesunate forchloroquine-resistant P. falciparum malaria (seep. 829).(e) Acne vulgaris: prolonged therapy with lowdoses may be used in severe cases (since
Propionibacterium acnes is sensitive totetracyclines), but simpler treatments arepreferred in most cases (see Ch. 64).(f) Chronic obstructive lung disease: prophylac-tic use may reduce the frequency of exacerba-tions, but the risk : benefit ratio is controversial.
TigecyclineIt is the first member of a new class of synthetictetracycline analogues (glycyl-cyclines) whichare active against most bacteria that have deve-loped resistance to the classical tetracyclines.Thus, they have the braodest spectrum of activity.Tigecycline is a derivative of minocycline, andwas introduced in 2005.
Tigecycline is active against most gram-positive and gram-negative cocci and anaerobes,including tetracycline resistant strains of Strep.pyogenes, Strep. pneumoniae, Staph. aureus,MRSA, VRSA, Enterococcus faecalis andVRE, most Enterobacteriaceae, Acinetobacter,as well as tetracycline sensitive organismslike Rickettsia, Chlamydia, Mycoplasma,Legionella, etc. However, Pseudomonas andProteus are inherently nonresponsive totigecycline.
Tigecycline acts in the same manner astetracyclines. The lack of cross resistancebetween the two groups is mainly because thetetracycline efflux pumps acquired by manyresistant bacteria have low affinity for tigecyclineand are unable to pump it out. In other resistantbacteria, the ribosomal protection protein againsttetracycline is less active in protecting theribosomal binding site from tigecycline. Thus,the two most important mechanisms oftetracycline resistance do not operate againsttigecycline.
Tigecycline is poorly absorbed from g.i.t; theonly route of administration is by slow i.v.infusion. It is widely distributed in tissues,volume of distribution is large (>7 L/kg).Consequently, plasma concentrations are low. Itis eliminated mainly in the bile; dose adjustmentis not needed in renal insufficiency. The durationof action is long; elimination t½ is 37–67 hours.

739C
HA
PTER52
TETRACYCLINES AND CHLORAMPHENICOL
Though, tigecycline can be used in manyinfections, it is approved only for treatment ofserious and hospitalized patients of communityacquired pneumonia, complicated skin and skinstructure infections (but not diabetic foot),complicated intraabdominal infections caused byenterococci, anaerobes and Enterobacteriaceae.It is not recommended for hospital acquired/ventilator-associated chest infections, because ina comparative trial, all cause mortality was higherin tigecycline group than in the comparator groupreceiving other antibiotics. It is also not suitablefor urinary tract infection, because only lowconcentrations are attained in urine. The clinicalefficacy of tigecycline in other infective condi-tions is still to be established.
Dose: 100 mg loading dose, followed by 50 mg 12 hourly by i.v.infusion over 30–60 min, for 5–14 days.TYGACIL, TEVRAN, TIGIMAX 50 mg lyophilized powder/vial inj.
The most common side effect is nausea andoccasionally vomiting. Others are epigastricdistress, diarrhoea, skin reactions, photosen-sitiviy and injection site complications.Superinfections and other adverse effects oftetracyclines can occur with tigecycline as well.It is not recommended for children and duringpregnancy. Few cases of pancreatitis are reported.
CHLORAMPHENICOL
Chloramphenicol was initially obtained fromStreptomyces venezuelae in 1947. It was soonsynthesized chemically and the commercialproduct now is all synthetic.
It is a yellowish white crystalline solid,aqueous solution is quite stable, stands boiling,but needs protection from light. The nitro-benzene moiety of chloramphenicol is probablyresponsible for the antibacterial activity as wellas its intensely bitter taste.
Mechanism of action Chloramphenicolinhibits bacterial protein synthesis by interferingwith ‘transfer’ of the elongating peptide chainto the newly attached aminoacyl-tRNA at theribosome-mRNA complex. It specificallyattaches to the 50S ribosome near the acceptor(A) site and prevents peptide bond formationbetween the newly attached aminoacid and thenascent peptide chain (see Fig. 52.1) withoutinterfering with the aminoacyl-tRNA attachmentto the 30S ribosome (the step blocked bytetracycline).
At high doses, it can inhibit mammalianmitochondrial protein synthesis as well. Bonemarrow cells are especially susceptible.
Antimicrobial spectrum Chloramphenicolis primarily bacteriostatic, though highconcentrations have been shown to exert cidaleffect on some bacteria, e.g. H. influenzae andN. meningitidis. It is a broad-spectrumantibiotic, active against nearly the same rangeof organisms (gram-positive and negative cocciand bacilli, rickettsiae, mycoplasma) as tetra-cyclines. Notable differences between these twoare:(a) Chloramphenicol was highly active againstSalmonella including S. typhi, but resistantstrains are now rampant.(b) It is more active than tetracyclines againstH. influenzae (though some have now developedresistance), B. pertussis, Klebsiella, N.meningitidis and anaerobes including Bact.fragilis.(c) It is less active against gram-positive cocci,spirochetes, certain Enterobacteriaceae andChlamydia. Entamoeba and Plasmodia are notinhibited.
Like tetracyclines, it is ineffective againstMycobacteria, Pseudomonas, many Proteus,viruses and fungi.
Resistance Most bacteria are capable ofdeveloping resistance to chloramphenicol, whichgenerally emerges in a graded manner, aswith tetracyclines. Being orally active, broad-spectrum and relatively cheap, chloramphenicol

740S
EC
TIO
N12
ANTIMICROBIAL DRUGS
was extensively and often indiscriminately used,especially in developing countries, resulting inhigh incidence of resistance among many gram-positive and gram-negative bacteria.
In many areas, highly chloramphenicol resis-tant S. typhi have emerged due to transfer ofR factor by conjugation. Resistance among gram-negative bacteria is generally due to acquisitionof R plasmid encoded for an acetyl transferase—an enzyme which inactivates chloramphenicol.Acetyl-chloramphenicol does not bind to thebacterial ribosome. In many cases, this plasmidhas also carried resistance to ampicillin andtetracycline. Multidrug-resistant S. typhi havearisen.
Decreased permeability into the resistantbacterial cells (chloramphenicol appears to enterbacterial cell both by passive diffusion as wellas by facilitated transport) and lowered affinityof bacterial ribosome for chloramphenicol arethe other mechanisms of resistance. Partial crossresistance between chloramphenicol anderythromycin/clindamycin has been noted,because all these antibiotics bind to 50Sribosome at adjacent sites and one may hinderaccess of the other to its site of action. Somecross resistance with tetracyclines also occurs,though the latter binds to 30S ribosome.
PharmacokineticsChloramphenicol is rapidly and completelyabsorbed after oral ingestion. It is 50–60% boundto plasma proteins and very widely distributed:volume of distribution 1 L/kg. It freely penetra-tes serous cavities and blood-brain barrier: CSFconcentration is nearly equal to that of unbounddrug in plasma. It crosses placenta and is secretedin bile and milk.
Chloramphenicol is primarily conjugated withglucuronic acid in the liver and little is excretedunchanged in urine. Cirrhotics and neonates, whohave low conjugating ability, require lower doses.The metabolite is excreted mainly in urine. Plasmat½ of chloramphenicol is 3–5 hours in adults.It is increased only marginally in renal failure:dose need not be modified.
Preparations and administration
The commonest route of administration of chloramphenicolis oral—as capsules; 250–500 mg 6 hourly (max. 100 mg/kg/day), children 25–50 mg/kg/day. Significant bioavailabilitydifferences among different market preparations have beenshown. It is also available for application to eye/ear, but topicaluse at other sites is not recommended.CHLOROMYCETIN, ENTEROMYCETIN, PARAXIN, 250 mg,500 mg cap, 1% eye oint, 0.5% eye drops, 5% ear drops, 1%applicaps.
Chloramphenicol palmitate (CHLOROMYCETINPALMITATE, ENTEROMYCETIN, PARAXIN 125 mg/5 ml oralsusp) is an insoluble tasteless ester of chloramphenicol, whichis inactive as such. It is nearly completely hydrolysed in theintestine by pancreatic lipase and absorbed as freechloramphenicol, but produces lower plasma concentration.
Chloramphenicol succinate (ENTEROMYCETIN,CHLOROMYCETIN SUCCINATE, KEMICETINE 1 g/vial inj,PHENIMYCIN 0.25, 0.5, 1.0 g inj. is the soluble but inactiveester which is used in the parenteral preparations. Intramuscularinjection is painful and produces lower blood levels. It is hydro-lysed in tissues to the free active form. However, bioavailabilityeven on i.v. injection is only 70% due to renal excretion ofthe ester before hydrolysis.also VANMYCETIN 0.4% eye drops, 250 mg opticaps,LYKACETIN 1% skin cream, 10% otic solution, OCUCHLOR0.5% eye drops.
Adverse effects
1. Bone marrow depression Of all drugs,chloramphenicol is the most important cause ofaplastic anaemia, agranulocytosis, thrombocyto-penia or pancytopenia. Two forms are reco-gnized:(a) Non-dose related idiosyncratic reaction:This is rare (1 in 40,000), unpredictable, butserious, often fatal, probably has a genetic basisand is more common after repeated courses.Aplastic anaemia is the most commonmanifestation. Apparently, a longer latent periodof onset of marrow aplasia is associated withhigher mortality. Many victims, even if theysurvive, develop leukaemias later.(b) Dose and duration of therapy relatedmyelosuppression: a direct toxic effect,predictable and probably due to inhibition ofmitochondrial enzyme synthesis in theerythropoietic cells. This is often reversiblewithout long-term sequelae. Liver and kidneydisease predisposes to such toxicity.

741C
HA
PTER52
TETRACYCLINES AND CHLORAMPHENICOL
Indications of chloramphenicol are:
1. Pyogenic meningitis: Third generationcephalosporins (± vancomycin) are presently thefirst line drugs for empirical therapy of bacterialmeningitis (see Ch. 51). Chloramphenicol in adose of 50–75 mg/kg/day may be used as asecond line drug for H. influenzae andmeningococcal meningitis, especially in youngchildren and cephalosporin allergic patients,because it has excellent penetration into CSFand clinical efficacy has been demonstrated.2. Anaerobic infections caused by Bact.fragilis and others (wound infections,intraabdominal infections, pelvic abscess, andbrain abscess, etc.) respond well to chloram-phenicol. However, clindamycin or metronidazoleare mostly used for these. Chloramphenicol maybe given in addition, or as an alternative inpatients not tolerating these drugs. A penicillin/cephalosporin is generally combined since mostof these are mixed infections.3. Intraocular infections Chloramphenicolgiven systemically attains high concentration inocular fluid. It is the preferred drug forendophthalmitis caused by sensitive bacteria.4. Enteric fever: Chloramphenicol was the first antibioticand the drug of choice for typhoid fever till the 1980s whenresistant S. typhi emerged and spread globally, including mostparts of India. As a result, it became clinically unreliable; 50–80% isolates showed in vitro resistance. Many of these aremultidrug resistant—not responsive to ampicillin andcotrimoxazole as well. However, few recent reports from certainparts of India indicate return of sensitivity to chloramphenicol.Being orally active and inexpensive, it may be used only ifthe local strain is known to be sensitive and responsiveclinically. The dose is 0.5 g 6 hourly (children 50 mg/kg/day)till fever subsides, then 0.25 g 6 hourly for another 5–7 days,because bacteriological cure takes longer.
Being bacteriostatic, relapses occur in ~ 10%chloramphenicol treated patients. Also, it does not preventor cure the carrier state. Bactericidal action is required toeradicate carrier state, because in this state, host defencemechanisms do not operate against these pathogenic bacteria;as if they were commensals.
5. As second choice drug(a) to tetracyclines for brucellosis and rickettsial infections,especially in young children and pregnant women in whomtetracyclines are contraindicated.(b) to erythromycin for whooping cough.
2. Hypersensitivity reactions Rashes, fever,atrophic glossitis, angioedema are infrequent.
3. Irritative effects Nausea, vomiting, diar-rhoea, pain on injection.
4. Superinfections These are similar to tetra-cyclines, but less common.
5. Gray baby syndrome It occurred when high doses(~100 mg/kg) were given prophylactically to neonates,especially premature. The baby stopped feeding, vomited,became hypotonic and hypothermic, abdomen distended,respiration became irregular; an ashen gray cyanosisdeveloped in many, followed by cardiovascular collapse anddeath. Blood lactic acid was raised.
It occurs because of inability of the newborn to adequatelymetabolize and excrete chloramphenicol. At higherconcentration, chloramphenicol blocks electron transport in theliver, myocardium and skeletal muscle, resulting in the abovesymptoms. Chloramphenicol should be avoided in neonates,and even if given, dose should be ~ 25 mg/kg/day.
Interactions Chloramphenicol inhibits metabolism of tolbu-tamide, chlorpropamide, warfarin, cyclophosphamide andphenytoin. Toxicity can occur if dose adjustments are notdone. Phenobarbitone, phenytoin, rifampin enhance chloram-phenicol metabolism → reduce its concentration → failureof therapy may occur.
Being bacteriostatic, chloramphenicol can antagonizethe cidal action of β-lactams/aminoglycosides on certainbacteria.
UsesClinical use of chloramphenicol for systemicinfections is now highly restricted due to fearof fatal toxicity. Because of risk of serious(though rare) bone marrow aplasia:(a) Never use chloramphenicol for minor infec-tions or those of undefined etiology.(b) Do not use chloramphenicol for infectionstreatable by other safer antimicrobials.(c) Avoid repeated courses.(d) Daily dose not to exceed 2–3 g; durationof therapy to be < 2 weeks, total dose in a course< 28 g.(e) Regular blood counts (especially reticulo-cyte count) may detect dose-related bonemarrow toxicity but not the idiosyncratic type.(f) Combined formulation of chloramphenicolwith any drug meant for internal use is bannedin India.

742S
EC
TIO
N12
ANTIMICROBIAL DRUGS
6. Urinary tract infections Use of chloramphenicol isimproper when safer drugs are available. It should be usedonly when kidney substance is involved and the organismis found to be sensitive only to this drug.
7. Topically In conjunctivitis, external earinfections—chloramphenicol 0.5–5.0% is highlyeffective. Topical use on skin or other areas is notrecommended because of risk of sensitization.
PROBLEM DIRECTED STUDY
52.1 A 30-year-old mother of 2 children attends the gynaecology OPD of the District Hospitalwith the complaint of whitish watery foul smelling vaginal discharge for the past 2 months.She also suffers lower backache and feels deep pelvic pain during intercourse, which she hasirregularly, because her husband works in the city and visits her off and on. She feels weak,but there is no fever. Her periods are regular, but somewhat painful. Last menstruation was10 days back. Vaginal examination reveals mucopurulent discharge from the cervical canaland pelvic tenderness, but there is no pelvic mass or abscess. She expresses inability to getany investigations done, as she is poor and has to return to her village. A provisional diagnosisof chlamydial nonspecific endocervicitis is made, with possibility of gonococcal infection,concurrently or alone.(a) What is the most appropriate drug treatment for her?(b) Should her husband be also examined and treated?(see Appendix-1 for solution)

Aminoglycoside AntibioticsChapterChapterChapterChapterChapter 5353535353
These are a group of natural and semisyntheticantibiotics having polybasic amino groups linkedglycosidically to two or more aminosugar(streptidine, 2-deoxy streptamine, garosamine)residues.
Unlike penicillin, which was a chance disco-very, aminoglycosides are products of deliberatesearch for drugs effective against gram-negativebacteria. Streptomycin was the first member dis-covered in 1944 by Waksman and his colleagues.It assumed great importance because it wasactive against tubercle bacilli. Others wereproduced later, and now aminoglycosides are asizable family. All aminoglycosides are producedby soil actinomycetes and have many commonproperties (see box).
Systemic aminoglycosidesStreptomycin AmikacinGentamicin SisomicinKanamycin NetilmicinTobramycin Paromomycin
Topical aminoglycosidesNeomycin Framycetin
MECHANISM OF ACTION
The aminoglycosides are bactericidal antibiotics,all having the same general pattern of actionwhich may be described in two main steps:(a) Transport of the aminoglycoside through thebacterial cell wall and cytoplasmic membrane.(b) Binding to ribosomes resulting in inhibitionof protein synthesis.
Transport of aminoglycoside into thebacterial cell is a multistep process. They diffuseacross the outer coat of gram-negative bacteriathrough porin channels. Entry from the peri-plasmic space across the cytoplasmic membraneis carrier mediated which is linked to the electrontransport chain. Thus, penetration is dependentupon maintenance of a polarized membrane andon oxygen dependent active processes (energydependent phase I or EDP1 entry). Theseprocesses are inactivated under anaerobic condi-tions; anaerobes are not sensitive and facultativeanaerobes are more resistant when O2 supply isdeficient, e.g. inside big abscesses. Penetrationis also favoured by high pH; aminoglycosidesare ~20 times more active in alkaline than inacidic medium. Inhibitors of bacterial cell wall(β-lactams, vancomycin) enhance entry ofaminoglycosides and exhibit synergism.
Once inside the bacterial cell, streptomycinbinds to 30S ribosomes, but other aminoglyco-sides bind to additional sites on 50S subunit,as well as to 30S-50S interface. They freezeinitiation of protein synthesis (see Fig. 52.1),prevent polysome formation and promote theirdisaggregation to monosomes so that only oneribosome is attached to each strand of mRNA.Binding of aminoglycoside to 30S-50S juncturecauses distortion of mRNA codon recognitionresulting in misreading of the code: one or more
Common properties of aminoglycoside antibiotics
1. All are used as sulfate salts, which are highly watersoluble; solutions are stable for months.
2. They ionize in solution; are not absorbed orally;distribute only extracellularly; do not penetrate brainor CSF.
3. All are excreted unchanged in urine by glomerularfiltration.
4. All are bactericidal and more active at alkaline pH.5. They act by interfering with bacterial protein synthesis.6. All are active primarily against aerobic gram-negative
bacilli and do not inhibit anaerobes.7. There is only partial cross resistance among them.8. They have relatively narrow margin of safety.9. All exhibit ototoxicity and nephrotoxicity.

744S
EC
TIO
N12
ANTIMICROBIAL DRUGS
wrong amino acids are entered in the peptidechain and/or peptides of abnormal lengths areproduced. Different aminoglycosides causemisreading at different levels depending upontheir selective affinity for specific ribosomalproteins.
The cidal action of these drugs appears tobe based on secondary changes in the integrityof bacterial cell membrane, because otherantibiotics which inhibit protein synthesis(tetracyclines, chloramphenicol, erythromycin)are only static. After exposure to aminoglycosi-des, sensitive bacteria become more permeable;ions, amino acids and even proteins leak outfollowed by cell death. This probably results fromincorporation of the defective proteins into thecell membrane. One of the consequences ofaminoglycoside induced alteration of cellmembrane is augmentation of the carrier-mediated energy-dependent phase II (EDP2) entryof the antibiotic. This reinforces their lethalaction.
The cidal action of aminoglycosides isconcentration dependent, i.e. rate of bacterialcell killing is directly related to the ratio ofthe peak antibiotic concentration to the MICvalue. They also exert a long and concentrationdependent ‘postantibiotic effect’ (see p. 697).It has, therefore, been argued that despite theirshort t½ (2–4 hr), single injection of the totaldaily dose of aminoglycoside may be moreeffective and possibly less toxic than itsconventional division into 2–3 doses.
MECHANISM OF RESISTANCE
Resistance to aminoglycosides is acquired byone of the following mechanisms:(a) Acquisition of cell membrane bound inactiva-ting enzymes which phosphorylate/ adenylate oracetylate the antibiotic. The conjugated amino-glycosides do not bind to the target ribosomesand are incapable of enhancing active transportlike the unaltered drug. These enzymes areacquired mainly by conjugation and transfer ofplasmids. Nosocomial microbes have become
rich in such plasmids, some of which encodefor multidrug resistance. This is the mostimportant mechanism of development ofresistance to aminoglycosides. Susceptibility ofdifferent aminoglycosides to these enzymesdiffers. Thus, cross resistance was found betweengentamicin and tobramycin or netilmicin, butnot between these and streptomycin. Manynosocomial gram-negative bacilli resistant togentamicin/tobramycin respond to amikacin.(b) Mutation decreasing the affinity of ribosomalproteins that normally bind the aminoglycoside:this mechanism can confer high degreeresistance, but operates to a limited extent, e.g.E. coli that develop streptomycin resistance bysingle step mutation do not bind the antibioticon the polyribosome. Only a few other instancesare known. This type of resistance is specificfor a particular aminoglycoside.(c) Decreased efficiency of the aminoglycosidetransporting mechanism: either the pores in theouter coat become less permeable or the activetransport is interfered. This again is not fre-quently encountered in the clinical setting. Insome Pseudomonas which develop resistance,the antibiotic induced 2nd phase active transporthas been found to be deficient.
SHARED TOXICITIES
The aminoglycosides produce toxic effectswhich are common to all members, but therelative propensity differs (see Table 53.1).
TABLE 53.1 Comparative toxicity of amino-glycoside antibiotics (tentative)
Systemically used Ototoxicity Nephrotoxicityaminoglycoside vestibular cochlear
1. Streptomycin ++ ± +
2. Gentamicin ++ + ++
3. Kanamycin + ++ ++
4. Tobramycin +± + +
5. Amikacin + ++ ++
6. Sisomicin ++ + ++
7. Netilmicin ++ + ++

745C
HA
PTER53
AMINOGLYCOSIDE ANTIBIOTICS
1. Ototoxicity This is the most importantdose and duration of treatment related adverseeffect. The vestibular or the cochlear part maybe primarily affected by a particular amino-glycoside. These drugs are concentrated in thelabyrinthine fluid and are slowly removed fromit when the plasma concentration falls.Ototoxicity is greater when plasma concentrationof the drug is persistently high and above athreshold value. For gentamicin this is estimatedto be ~ 2 μg/ml; if the trough level is above thisvalue, vestibular damage becomes concentrationdependent. It is recommended that dosing ofgentamicin should be such that the measuredtrough plasma concentration is < 1 μg/ml to avoidtoxicity. The vestibular/cochlear sensory cells andhairs undergo concentration dependent destruc-tive changes. Aminoglycoside ear drops can causeototoxicity when instilled in patients withperforated eardrum; are contraindicated in them.
Cochlear damage It starts from the base andspreads to the apex; hearing loss affects the highfrequency sound first, then progressively encom-passes the lower frequencies. No regenerationof the sensory cells occurs; auditory nerve fibresdegenerate in a retrograde manner—deafness ispermanent. Older patients and those withpreexisting hearing defect are more susceptible.Initially, the cochlear toxicity is asymptomaticand can be detected only by audiometry. Tinnitusthen appears, followed by progressive hearingloss. On stopping the drug, tinnitus disappearsin 4–10 days, but frequency loss persists.
Vestibular damage Headache is usually firstto appear, followed by nausea, vomiting,dizziness, nystagmus, vertigo and ataxia. Whenthe drug is stopped at this stage, it passes intoa chronic phase lasting 6 to 10 weeks in whichthe patient is asymptomatic while in bed and hasdifficulty only during walking. Compensation byvisual and proprioceptive positioning andrecovery (often incomplete) occurs over 1–2years. Permanency of changes depends on theextent of initial damage and the age of the patient(elderly have poor recovery).
2. Nephrotoxicity It manifests as tubulardamage resulting in loss of urinary concentratingpower, low g.f.r., nitrogen retention, albuminuriaand casts. Aminoglycosides attain high concen-tration in the renal cortex (proximal tubules) andtoxicity is related to the total amount of thedrug received by the patient. However, in patientswith normal renal function, single daily dosingregimen appears to cause lesser nephrotoxicitythan the conventional thrice daily dosing. It ismore in the elderly and in those with preexistingkidney disease. Provided the drug is promptlydiscontinued renal damage caused by amino-glycosides is totally reversible. It has beenpostulated that aminoglycosides interfere withthe production of PGs in the kidney and thatthis is causally related to the reduced g.f.r. Animportant implication of aminoglycoside-induced nephrotoxicity is reduced clearance ofthe antibiotic resulting in higher and morepersistent blood levels causing enhanced oto-toxicity. Streptomycin and possibly tobramycinare less nephrotoxic than the other amino-glycosides.3. Neuromuscular blockade All aminoglycosidesreduce ACh release from the motor nerve endings. Theyinterfere with mobilization of centrally located synaptic vesiclesto fuse with the terminal membrane (probably by antagonizingCa2+) as well as decrease the sensitivity of the muscle end-plates to ACh. The effect of this action is not manifestedordinarily in the clinical use of these drugs. However, apnoeaand fatalities have occurred when streptomycin/neomycin wasput into peritoneal or pleural cavity after an operation,especially if a curare-like muscle relaxant was administeredduring surgery. Rapid absorption form the peritoneum/pleuraproduces high blood levels and adds to the residual actionof the neuromuscular blocker.
Neomycin and streptomycin have higher propensity thankanamycin, gentamicin or amikacin, while tobramycin is leastlikely to produce this effect. The neuromuscular blockproduced by aminoglycosides can be partially antagonizedby i.v. injection of a calcium salt. Neostigmine has inconsistentreversing action.
Myasthenic weakness is accentuated by these drugs.Neuromuscular blockers should be used cautiously in patientsreceiving aminoglycosides.
PRECAUTIONS AND INTERACTIONS
1. Avoid aminoglycosides during pregnancy: riskof foetal ototoxicity.

746S
EC
TIO
N12
ANTIMICROBIAL DRUGS
2. Avoid concurrent use of other nephrotoxicdrugs, e.g. NSAIDs, amphotericin B, vanco-mycin, cyclosporine and cisplatin.
3. Cautious use of other potentially ototoxicdrugs like vancomycin, minocycline andfurosemide, though clinical evidence ofpotentiated ototoxicity is meagre.
4. Cautious use in patients >60 years age andin those with kidney damage.
5. Cautious use of muscle relaxants in patientsreceiving an aminoglycoside.
6. Do not mix aminoglycoside with any drug inthe same syringe/infusion bottle.
PHARMACOKINETICS
All systemically administered aminoglycosideshave similar pharmacokinetic features. They arehighly ionized, and are neither absorbed nordestroyed in the g.i.t. However, absorption frominjection site in muscles is rapid: peak plasmalevels are attained in 30–60 minutes. They aredistributed only extracellularly, so that volumeof distribution (~0.3 L/kg) is nearly equal tothe extracellular fluid volume. Low concentra-tions are attained in serous fluids like synovial,pleural and peritoneal, but these levels may besignificant after repeated dosing. Relativelyhigher concentrations are present in endolymphand renal cortex, which are responsible forototoxicity and nephrotoxicity. Penetration inrespiratory secretions is poor. Concentrationsin CSF and aqueous humour are nontherapeuticeven in the presence of inflammation.Aminoglycosides cross placenta and can be foundin foetal blood/amniotic fluid. Their use duringpregnancy can cause hearing loss in theoffspring, and must be avoided unless absolutelyessential. The plasma protein binding ofaminoglycosides is clinically insignificant,though streptomycin is bound to some extent.
Aminoglycosides are not metabolized in thebody, and are excreted unchanged in urine.Glomerular filtration is the main channel,because tubular secretion as well as reabsorptionare negligible. The plasma t½ ranges between2–4 hours, but small amount of drug persists
longer in tissues. After chronic dosing, the drugmay be detectable in urine for 2–3 weeks. Renalclearance of aminoglycosides parallels creati-nine clearance (CLcr), and is approximately2/3 of it. The t½ is prolonged and accumulationoccurs in patients with renal insufficiency, inthe elderly and in neonates who have low g.f.r.Reduction in dose or increase in dose-intervalis essential in these situations. This should bedone according to the measured CLcr.Nomograms are available to help calculation ofCLcr, but actual measurement in the individualpatient is preferable. Generally, there is no needto reduce the daily dose till CLcr is above70 ml/min. A simple guide to dose calculationbelow this level is given in the box.
Guideline for dose adjustment of gentamicin inrenal insufficiency
CLcr (ml/min) % of daily dose
70 70% daily50 50% daily30 30% daily20–30 80% alternate day10–20 60% alternate day<10 40% alternate day
DOSING REGIMENS
Because of low safety margin, the daily doseof systemically administered aminoglycosidesmust be precisely calculated accordingly to bodyweight and level of renal function. For an averageadult with normal renal function (CLcr >70ml/min), the usual doses are:Gentamicin/tobramycin/
sisomicin/netilmicin 3–5 mg/kg/day
Streptomycin/kanamycin/amikacin 7.5–15 mg/kg/day
Considering the short t½ (2–4 hr) ofaminoglycosides the daily doses are conven-tionally divided into 3 equal parts and injectedi.m. (or i.v. slowly over 60 min) every 8 hours.However, most authorities now recommend asingle total daily dose regimen for patients withnormal renal function. This is based on theconsiderations that:
⎫⎬⎭⎫⎬⎭

747C
HA
PTER53
AMINOGLYCOSIDE ANTIBIOTICS
• Aminoglycosides exert concentration depen-dent bactericidal action and a long post-antibiotic effect, therefore higher plasmaconcentrations attained after the single dailydose will be equally or more effective thanthe divided doses.
• With the single daily dose, the plasmaconcentration will remain subthreshold forototoxicity and nephrotoxicity for a longerperiod each day allowing washout of the drugfrom the endolymph and the renal cortex.
Several comparative studies with gentamicin andfew other aminoglycosides and meta-analyses ofthese studies have validated this concept. Thesingle daily dose regimen has been found to beless nephrotoxic, but no dosing regimen appearsto be less ototoxic than another. Both regimensare equally effective. Single daily doses are alsomore convenient and cheaper (require less manpower). However, the safety of the high doseextended interval regimen in patients with renalinsufficiency and in children is not established,and is therefore avoided. It is also notrecommended when gentamicin is combined witha β-lactam antibiotic for obtaining cidal effectin bacterial endocarditis, etc.
GentamicinIt was the 3rd systemically administered amino-glycoside antibiotic to be introduced for clinicaluse, and was obtained from Micromonosporapurpurea in 1964. It quickly surpassedstreptomycin because of higher potency andbroader spectrum of activity. Currently, it is themost commonly used aminoglycoside for acuteinfections and may be considered prototype ofthe class. It is active mainly against aerobic gram-negative bacilli, including E. coli, Klebsiellapneumoniae, Enterobacter, H. influenzae,Proteus, Serratia and Pseudomonas aerugi-nosa. Many strains of Brucella, Campylobacter,Citrobacter, Fransisella and Yersinia are alsosensitive. Limited number of gram-positivebacteria are susceptible, especially Staph.aureus, Strep. faecalis and some Listeria, but
Strep. pyogenes, Strep. pneumoniae andenterococci are usually insensitive.
Gentamicin is ineffective against Mycobac-terium tuberculosis and other mycobacteria. Itis more potent (its MIC are lower) thanstreptomycin, kanamycin and amikacin, butequally potent as tobramycin, sisomicin andnetilmicin. Bacteria that acquire resistanceagainst gentamicin generally exhibit crossresistance to tobramycin and sisomicin also. Itsynergises with β-lactam antibiotics, especiallyagainst Enterococcus (endocarditis) and Pseudo-monas (meningitis).Dose: 3–5 mg/kg/day (single dose or divided in 3 doses) i.m.or in an i.v. line over 30–60 min.GARAMYCIN, GENTASPORIN, GENTICYN 20, 60, 80, 240 mgper vial inj; also 0.3% eye/ear drops, 0.1% skin cream.
Uses Gentamicin is the cheapest (other thanstreptomycin) and the first line aminoglycosideantibiotic. It is often added when a combinationantibiotic regimen is used empirically to treatserious infections by extending the spectrum ofcoverage. Because of low therapeutic index, itsuse should be restricted to serious gram-negativebacillary infections.1. Gentamicin is very valuable for preventingand treating respiratory infections in criticallyill patients; in those with impaired host defence(receiving anticancer drugs or high-dosecorticosteroids; AIDS; neutropenic), patients inresuscitation wards, with tracheostomy or onrespirators; postoperative pneumonias; patientswith implants and in intensive care units. It isoften combined with a penicillin/cephalosporinor another antibiotic in these situations.However, resistant strains have emerged in manyhospitals and nosocomial infections are lessamenable to gentamicin now. Another amino-glycoside (tobramycin, amikacin, netilmicin) isthen selected on the basis of the local sensitivitypattern, but strains resistant to gentamicin aregenerally cross resistant to tobramycin andsisomicin. Aminoglycosides should not be usedto treat community acquired pneumonias whichare mostly caused by gram-positive cocci andanaerobes.

748S
EC
TIO
N12
ANTIMICROBIAL DRUGS
Gentamicin is often added to the peritonealdialysate to prevent or treat peritonitis.2. Pseudomonas, Proteus or Klebsiella infec-tions: burns, urinary tract infection, pneumonia,lung abscesses, osteomyelitis, middle earinfection, septicaemia, etc., caused mostly bythe above bacteria are an important area of useof gentamicin. It may be combined withpiperacillin or a third generation cephalosporinfor serious infections. Topical use on infectedburns and in conjunctivitis is permissible.3. Meningitis caused by gram negative bacilli:Because this is a serious condition, drugcombinations including an aminoglycoside areoften used. The third generation cephalosporinsalone or with an aminoglycoside are favouredfor this purpose.4. Subacute bacterial endocarditis (SABE):Gentamicin (1 mg/kg 8 hourly i.m.) is generallycombined with penicillin/ampicillin/vancomycin.
Streptomycin
It is the oldest aminoglycoside antibiotic obtai-ned from Streptomyces griseus; which was usedextensively in the past, but is now practicallyrestricted to treatment of tuberculosis. It is lesspotent (MICs are higher) than many otheraminoglycosides. The antimicrobial spectrum ofstreptomycin is relatively narrow: primarilycovers aerobic gram-negative bacilli. Sensitiveorganisms are—H. ducreyi, Brucella, Yersiniapestis, Francisella tularensis, Nocardia, Calym.granulomatis, M. tuberculosis. Only few strainsof E. coli, H. influenzae, V. cholerae, Shigella,Klebsiella, enterococci and some gram-positivecocci are now inhibited, that too at higherconcentrations. All other organisms includingPseudomonas are unaffected.
Resistance Many organisms rapidly developresistance to streptomycin, either by one-stepmutation or by acquisition of plasmid which codesfor inactivating enzymes. In the intestinal andurinary tracts, resistant organisms may emergewithin 2 days of therapy. E. coli, H. influenzae,Str. pneumoniae, Str. pyogenes, Staph. aureus
have become largely resistant. If it is used alone,M. tuberculosis also become resistant.
Streptomycin dependence Certain mutants grown in thepresence of streptomycin become dependent on it. Theirgrowth is promoted rather than inhibited by the antibiotic.This occurs when the antibiotic induced misreading of thegenetic code becomes a normal feature for the organism. Thisphenomenon is probably significant only in the use ofstreptomycin for tuberculosis.
Cross resistance Only partial and oftenunidirectional cross resistance occurs betweenstreptomycin and other aminoglycosides.
Adverse effects About 1/5 patients givenstreptomycin 1 g BD i.m. experience vestibulardisturbances. Auditory disturbances are lesscommon.
Streptomycin has the lowest nephrotoxicityamong aminoglycosides; probably because it isnot concentrated in the renal cortex. Hypersen-sitivity reactions are rare; rashes, eosinophilia,fever and exfoliative dermatitis have beenreported. Anaphylaxis is very rare. Topical useis contraindicated for fear of contact sensi-tization.Superinfections are not significant. Pain at injec-tion site is common. Paraesthesias and scotomaare occasional. It is contraindicated duringpregnancy due to risk of foetal ototoxicity.AMBISTRYN-S 0.75, 1 g dry powder per vial for inj.Acute infections: 1 g (0.75 g in those above 50 yr age) i.m. ODor BD for 7–10 days.Tuberculosis: 1 g or 0.75 g i.m. OD or thrice weekly for 30–60days.
Uses
1. Tuberculosis: see Ch. 55.2. Subacute bacterial endocarditis (SABE): Streptomycin(now mostly gentamicin) is given in conjunction with penicillin/ampicillin/vancomycin for 4–6 weeks.3. Plague: It effects rapid cure (in 7–12 days); may beemployed in confirmed cases, but tetracyclines have beenmore commonly used for mass treatment of suspected casesduring an epidemic.4. Tularemia: Streptomycin is the drug of choice for thisrare disease; effects cure in 7–10 days. Tetracyclines are thealternative drugs, especially in milder cases.
In most other situations, e.g. urinary tractinfection, peritonitis, septicaemias, etc. where

749C
HA
PTER53
AMINOGLYCOSIDE ANTIBIOTICS
streptomycin was used earlier, gentamicin or oneof the newer aminoglycosides is now preferreddue to widespread resistance to streptomycin andits low potency.Oral use of streptomycin for diarrhoea is banned in India.
KanamycinObtained from S. kanamyceticus (in 1957), it was the secondsystemically used aminoglycoside to be developed afterstreptomycin. It is similar to streptomycin in all respectsincluding efficacy against M. tuberculosis and lack of activityon Pseudomonas. However, it is more toxic, both to the cochleaand to kidney. Hearing loss, which is irreversible, is morecommon than vestibular disturbance.
Because of toxicity and narrow spectrum of activity, it hasbeen largely replaced by other aminoglycosides for treatmentof gram-negative bacillary infections; may be used only ifmandated by sensitivity report of the infecting strain. It is occa-sionally used as a second line drug in resistant tuberculosis.Dose: 0.5 g i.m. BD (15 mg/kg/day); KANAMYCIN, KANCIN,KANAMAC 0.5 g, 0.75 g, 1.0 g inj.
TobramycinIt was obtained from S. tenebrarius in the1970s. The antibacterial and pharmacokineticproperties, as well as dosage are almost identicalto gentamicin, but it is 2–4 times more activeagainst Pseudomonas and Proteus, includingsome resistant to gentamicin, but majority arecross resistant. However, it is not useful forcombining with penicillin in the treatment ofenterococcal endocarditis. It should be usedonly as an alternative to gentamicin. Seriousinfections caused by Pseudomonas and Proteusare its major indications. Ototoxicity and nephro-toxicity is probably less than gentamicin.Dose: 3–5 mg/kg day in 1–3 doses.TOBACIN 20, 60, 80 mg in 2 ml inj. 0.3% eye drops.TOBRANEG 20, 40, 80 mg per 2 ml inj, TOBRABACT 0.3% eyedrops.
AmikacinIt is a semisynthetic derivative of kanamycin towhich it resembles in pharmacokinetics, doseand toxicity. The outstanding feature of amikacinis its resistance to bacterial aminoglycosideinactivating enzymes. Thus, it has the widestspectrum of activity, including many organismsresistant to other aminoglycosides. However,relatively higher doses are needed for Pseudo-monas, Proteus and Staph. infections.
The range of conditions in which amikacincan be used is the same as for gentamicin. Itis recommended as a reserve drug for empiricaltreatment of hospital acquired gram-negativebacillary infections where gentamicin/tobra-mycin resistance is high. It is effective intuberculosis, but used only for multidrugresistant infection. More hearing loss thanvestibular disturbance occurs in toxicity.Dose: 15 mg/kg/day in 1–3 doses; urinary tract infection 7.5mg/kg/day.AMICIN, MIKACIN, MIKAJECT 100 mg, 250 mg, 500 mg in 2ml inj.
SisomicinIntroduced in 1980s, it is a natural aminoglycosidefrom Micromonospora inyoensis that ischemically and pharmacokinetically similar togentamicin, but somewhat more potent onPseudomonas, a few other gram-negative bacilliand β haemolytic Streptococci. It is moderatelyactive on faecal Streptococci—can be combinedwith penicillin for SABE. However, it issusceptible to aminoglycoside inactivatingenzymes and offers no advantage in terms ofototoxicity and nephrotoxicity. It can be usedinterchangeably with gentamicin for the samepurposes in the same doses.ENSAMYCIN, SISOPTIN 50 mg, 10 mg (pediatric) per ml in 1 mlamps, 0.3% eyedrops, 0.1% cream.
NetilmicinThis semisynthetic derivative of gentamicin hasa broader spectrum of activity than gentamicin.It is relatively resistant to many aminoglycosideinactivating enzymes and thus effective againstsome gentamicin-resistant strains. It is moreactive against Klebsiella, Enterobacter andStaphylococci, but less active against Ps.aeruginosa.
Pharmacokinetic characteristics and dosageof netilmicin are similar to gentamicin. Experi-mental studies have shown it to be less ototoxicthan gentamicin and tobramycin, but clinicalevidence is inconclusive: hearing loss occurs,though fewer cases of vestibular damage havebeen reported.

750S
EC
TIO
N12
ANTIMICROBIAL DRUGS
A marginal improvement in antibacterialspectrum, clinical efficacy and possibly reducedtoxicity indicates that netilmicin could be a usefulalternative to gentamicin.Dose: 4–6 mg/kg/day in 1–3 doses; NETROMYCIN 10, 25, 50mg in 1 ml, 200 mg in 2 ml and 300 mg in 3 ml inj., NETICIN 200mg (2 ml), 300 mg (3 ml) inj.
NeomycinObtained from S. fradiae, it is a wide-spectrumaminoglycoside, active against most gram-negative bacilli and some gram-positive cocci.However, Pseudomonas and Strep. pyogenes arenot sensitive. Neomycin is highly toxic to theinternal ear (mainly auditory) and to kidney. Itis, therefore, not used systemically. Absorptionfrom the g.i.t. is minimal. Oral and topicaladministration does not ordinarily cause systemictoxicity.Dose: 0.25–1 g QID oral, 0.3–0.5% topical.NEOMYCIN SULPHATE 350, 500 mg tab, 0.3% skin oint, 0.5%skin cream, eye oint.NEBASULF: Neomycin sulph. 5 mg, bacitracin 250 U,sulfacetamide 60 mg/g oint. and powder for surface application.POLYBIOTIC CREAM: Neomycin sulph. 5 mg, polymyxin 5,000IU, gramicidin 0.25 mg/g cream.NEOSPORIN: Neomycin 3400 iu, polymyxin B 5000 iu, bacitracin400 iu/g oint and powder for surface application. NEOSPORIN-H: Neomycin 3400 iu, polymyxin B 5000 iu, hydrocortisone 10mg per g oint and per ml ear drops.
Uses
1. Topically (often in combination with poly-myxin, bacitracin, etc.) for infected wound,ulcers, burn, external ear infections, conjuncti-vitis, but like other topical antiinfectivepreparations, benefits are limited.2. Orally for:(a) Preparation of bowel before surgery:(3 doses of 1.0 g along with metronidazole0.5 g on day before surgery) may reducepostoperative infections.(b) Hepatic coma: Normally NH3 is produced by colonicbacteria. This is absorbed and converted to urea by liver.In severe hepatic failure, detoxication of NH3 does not occur,blood NH3 levels rise and produce encephalopathy. Neomy-cin, by suppressing intestinal flora, diminishes NH3 productionand lowers its blood level; clinical improvement is seen within2–3 days. However, because of toxic potential it is infrequentlyused for this purpose; Lactulose (see p. 676) is preferred.
Adverse effects Applied topically neomycinhas low sensitizing potential. However, rashesdo occur.Oral neomycin has a damaging effect on intestinal villi.Prolonged treatment can induce malabsorption syndrome withdiarrhoea and steatorrhoea. It can decrease the absorptionof digoxin and many other drugs, as well as bile acids.Due to marked suppression of gut flora, superinfection byCandida can occur.
Small amounts that are absorbed from thegut or topical sites are excreted unchanged bykidney. This may accumulate in patients withrenal insufficiency—cause further kidneydamage and ototoxicity. Neomycin is contra-indicated if renal function is impaired.Applied to serous cavities (peritoneum), it cancause apnoea due to muscle paralysing action.Neomycin containing antidiarrhoeal formulations are bannedin India.
FramycetinObtained from S. lavendulae, it is very similarto neomycin. It is too toxic for systemicadministration and is used topically on skin, eye,ear in the same manner as neomycin.SOFRAMYCIN, FRAMYGEN 1% skin cream, 0.5% eye dropsor oint.
ParomomycinChemically related to neomycin, this amino-glycoside antibiotic has pronounced activityagainst many protozoan parasites, includingE. histolytica, Giardia lamblia, Trichomonasvaginalis, Cryptosporidium and Leishmania, inaddition to many bacteria sensitive to neomycin.Like other aminoglycosides, it is not absorbedfrom the gut. An oral formulation was marketedin many countries, including India, in the 1960sfor treatment of intestinal amoebiasis andgiardiasis, but was soon discontinued whenmetronidazole gained popularity. Recently, it hasbeen reintroduced and is described in Ch. 60.For its antibacterial activity in the gut, it canbe used as an alternative to neomycin for hepaticencephalopathy. Parenterally, it is being used forvisceral leishmaniasis (see Ch. 60).Dose: Oral 500 mg TDS (25–30 mg/kg/day)PAROMYCIN, HUMATIN 250 mg cap.

751C
HA
PTER53
AMINOGLYCOSIDE ANTIBIOTICS
PROBLEM DIRECTED STUDY
53.1 A 75-year-old unconscious male patient of cerebral stroke is maintained on ventilatorin the intensive care unit of the hospital. On the 4th day he developed fever, and the totalleucocyte count rose to 14000/μL, along with signs of chest infection. A sample of bronchialaspirate is sent for bacteriological tests, and it is decided to institute empirical treatmentwith cefotaxime and gentamicin. His body weight is 60 kg and creatinine clearance is estimatedto be 50 ml/min.(a) What should be the appropriate dose and dosing regimen for gentamicin and cefotaximefor this patient?(see Appendix-1 for solution)

Macrolide, Lincosamide,Glycopeptide and OtherAntibacterial Antibiotics;Urinary Antiseptics
ChapterChapterChapterChapterChapter 5454545454
MACROLIDE ANTIBIOTICS
These are antibiotics having a macrocycliclactone ring with attached sugars. Erythromycinis the first member discovered in the 1950s,Roxithromycin, Clarithromycin and Azithro-mycin are the later additions.
ERYTHROMYCIN
It was isolated from Streptomyces erythreus in1952. Since then it has been widely employed,mainly as alternative to penicillin. Water solubi-lity of erythromycin is limited, and the solutionremains stable only when kept in cold.
Mechanism of action Erythromycin is bac-teriostatic at low but cidal (for certain bacteriaonly) at high concentrations. Cidal actiondepends on the organism concerned and its rateof multiplication. Sensitive gram-positivebacteria accumulate erythromycin intracellularlyby active transport which is responsible for theirhigh susceptibility to this antibiotic. Activity isenhanced several fold in alkaline medium,because the nonionized (penetrable) form of thedrug is favoured at higher pH.
Erythromycin acts by inhibiting bacterialprotein synthesis. It combines with 50S ribo-some subunits and interferes with ‘translocation’(see Fig. 52.1). After peptide bond formationbetween the newly attached amino acid and thenacent peptide chain at the acceptor (A) site,the elongated peptide is translocated back to thepeptidyl (P) site, making the A site available fornext aminoacyl tRNA attachment. This is preven-ted by erythromycin and the ribosome fails tomove along the mRNA to expose the next codon.As an indirect consequence, peptide chain may
be prematurely terminated: synthesis of largerproteins is especifically suppressed.
Antimicrobial spectrum It is narrow,includes mostly gram-positive and a few gram-negative bacteria, and overlaps considerably withthat of penicillin G. Erythromycin is highly activeagainst Str. pyogenes and Str. pneumoniae, N.gonorrhoeae, Clostridia, C. diphtheriae andListeria, but penicillin-resistant Staphylococciand Streptococci are now resistant to erythro-mycin also.
In addition, Campylobacter, Legionella,Branhamella catarrhalis, Gardnerella vaginalisand Mycoplasma, that are not affected bypenicillin, are highly sensitive to erythromycin.Few others, including H. ducreyi, H. influenzae,B. pertussis, Chlamydia trachomatis, Str.viridans, N. meningitidis and Rickettsiae aremoderately sensitive. Enterobacteriaceae, othergram-negative bacilli and B. fragilis are notinhibited.
Resistance All cocci readily develop resis-tance to erythromycin, mostly by acquiring thecapacity to pump it out. Resistant Enterobac-teriaceae have been found to produce an erythro-mycin esterase. Alteration in the ribosomal bind-ing site for erythromycin by a plasmid encodedmethylase enzyme is an important mechanism ofresistance in gram-positive bacteria. All the abovetypes of resistance are plasmid mediated. Changein the 50S ribosome by chromosomal mutationreducing macrolide binding affinity occurs insome gram-positive bacteria.
Bacteria that develop resistance to erythro-mycin are cross resistant to other macrolidesas well. Cross resistance with clindamycin and

753C
HA
PTER54
MACROLIDE AND OTHER ANTIBACTERIAL ANTIBIOTICS
chloramphenicol also occurs, because theribosomal binding sites for all these antibioticsare proximal to each other.
Pharmacokinetics Erythromycin base isacid labile. To protect it from gastric acid, itis given as enteric coated tablets, from whichabsorption is incomplete and food delaysabsorption by retarding gastric emptying. Its acidstable esters are better absorbed.
Erythromycin is widely distributed in thebody, enters cells and into abscesses, crossesserous membranes and placenta, but not blood-brain barrier. Therapeutic concentration isattained in the prostate. It is 70–80% plasmaprotein bound, partly metabolized and excretedprimarily in bile in the active form. Renalexcretion is minor; dose need not be altered inrenal failure. The plasma t½ is 1.5 hr, buterythromycin persists longer in tissues.
Preparations and dose
Dose: 250–500 mg 6 hourly (max. 4 g/day), children 30–60mg/kg/day.1. Erythromycin (base): ERYSAFE 250, mg tabs, EROMED333 mg tab, 125 mg/5 ml susp.2. Erythromycin stearate: blood levels produced are similarto those after erythromycin base. ERYTHROCIN 250, 500mg tab, 100 mg/5 ml susp., 100 mg/ml ped. drops. ETROCIN,ERYSTER 250 mg tab, 100 mg/5 ml dry syr.3. Erythromycin estolate (lauryl sulfate): it is relatively acidstable and better absorbed after oral administration. However,concentration of free and active drug in plasma may be thesame as after administration of erythromycin base. Certainorganisms hydrolyse it to liberate the free form intracellularlyand are more susceptible to it.ALTHROCIN 250, 500 mg tab, 125 mg kid tab, 125 mg/5 ml and250 mg/5 ml dry syr, 100 mg/ml ped. drops, E-MYCIN 100, 250mg tab, 100 mg/5 ml dry syr, EMTHROCIN 250 mg tab, 125 mg/5 ml dry syr.4. Erythromycin ethylsuccinate: well absorbed orally;ERYNATE 100 mg/5 ml dry syr, ERYTHROCIN 100 mg/mldrops, 125 mg/5 ml syr.
A 30% ointment (GERY OINTMENT) is marketed fortopical treatment of boils, carbuncles and skin infections, butefficacy is doubtful.
Adverse effects Erythromycin base is aremarkably safe drug, but side effects do occur.1. Gastrointestinal Mild-to-severe epigastricpain is experienced by many patients, especially
children, on oral ingestion. Diarrhoea isoccasional.
Erythromycin stimulates motilin (an upper gastrointestinalpeptide hormone) receptors in the g.i.t.—thereby inducesgastric contractions, hastens gastric emptying and promotesintestinal motility without significant effect on colonic motility.On the basis of this action erythromycin has been occasionallyused to afford short-term symptomatic relief in diabeticgastroparesis.However, tolerance quickly develops to thisaction (probably due to receptor down-regulation) andundesirable alteration of bacterial flora limit use oferythromycin as a prokinetic agent. Contribution of this actionto the g.i. side effects of erythromycin is not known.
2. Very high doses of erythromycin have causedreversible hearing impairment.3. Hypersensitivity Rashes and fever areinfrequent. Other allergic manifestations are rarewith erythromycin base or esters other thanestolate.
Hepatitis with cholestatic jaundice resembling viralhepatitis or extrahepatic biliary obstruction occurs with theestolate ester (rarely with ethyl succinate or stearate ester) after1–3 weeks. Incidence is higher in pregnant women. It clearson discontinuation of the drug, and is probably due tohypersensitivity to the estolate ester; erythromycin base orother esters can be given to these patients without recurrence.Though the estolate is acid stable, tasteless and betterabsorbed, it has been banned in some countries (but not inIndia).
Interaction Erythromycin inhibits hepatic oxi-dation of many drugs. The clinically significantinteractions are—rise in plasma levels of theo-phylline, carbamazepine, valproate, ergotamineand warfarin.
Several cases of Q-T prolongation, seriousventricular arrhythmias and death have beenreported due to inhibition of CYP3A4 by erythro-mycin/clarithromycin resulting in high bloodlevels of concurrently administered terfenadine/astemizole/cisapride (see p. 166 and 667).
UsesA. As an alternative to penicillin1. Streptococcal pharyngitis, tonsillitis, mastoi-
ditis and community acquired respiratoryinfections caused by pneumococci and H.influenzae respond equally well to erythro-mycin. It is an alternative drug for prophylaxis

754S
EC
TIO
N12
ANTIMICROBIAL DRUGS
of rheumatic fever and SABE. However, manybacteria resistant to penicillin are alsoresistant to erythromycin.
2. Diphtheria: For acute stage as well as forcarriers—7 day treatment is recommended.Some prefer it over penicillin. Antitoxin isthe primary treatment.
3. Tetanus: as an adjuvant to antitoxin, toxoidtherapy.
4. Syphilis and gonorrhoea: only if otheralternative drugs, including tetracyclines alsocannot be used: relapse rates are higher.
5. Leptospirosis: 250 mg 6 hourly for 7 daysin patients allergic to penicillins.
B. As a first choice drug for1. Atypical pneumonia caused by Mycoplasma
pneumoniae: rate of recovery is hastened.2. Whooping cough: a 1–2 week course of
erythromycin is the most effective treatmentfor eradicating B. pertussis from upper res-piratory tract. However, effect on the symp-toms depends on the stage of disease whentreatment is started.(a) Prophylactic: during the 10 day
incubation period—disease is prevented.(b) Catarrhal stage: which lasts for about a
week—erythromycin may abort the nextstage or reduce its duration and severity.
(c) Paroxysmal stage: lasting 2–4 weeks—no effect on the duration and severity of’croup’ despite eradication of thecausative organism.
(d) Convalescent stage: during which ‘croup’gradually resolves (4–12 weeks)—is notmodified.
Azithromycin, clarithromycin, and chloramphenicol are thealternative antimicrobials. Cough sedatives are not veryeffective. Corticosteroids may reduce the duration ofparoxysmal stage but increase the risk of superinfections andcarrier stage; they should be reserved for severe cases only.Adrenergic β2 stimulants may reduce the severity ofparoxysms, and are more useful in infants.
3. Chancroid : erythromycin 2 g/day for 7 daysis one of the first line drugs, as effectiveas single dose azithromycin or ceftriaxone(see p. 763).
C. As a second choice drug in1. Campylobacter enteritis: duration of diarrhoea and presence
of organisms in stools is reduced. However, fluoro-quinolones are superior.
2. Legionnaires’ pneumonia: 3 week erythromycin treatmentis effective, but azithromycin/ciprofloxacin are preferred.
3. Chlamydia trachomatis infection of urogenital tract:erythromycin 500 mg 6 hourly for 7 days is an effectivealternative to single dose azithromycin (see p. 763).
4. Penicillin-resistant Staphylococcal infections: its value hasreduced due to emergence of erythromycin resistance aswell. It is not effective against MRSA.
NEWER MACROLIDES
In an attempt to overcome the limitations oferythromycin like narrow spectrum, gastricintolerance, gastric acid lability, low oralbioavailability, poor tissue penetration and shorthalf-life, a number of semisynthetic macrolideshave been produced, of which roxithromycin,clarithromycin and azithromycin have beenmarketed.
Roxithromycin It is a semisynthetic longer-acting acid-stable macrolide whose antimicrobialspectrum resembles closely with that oferythromycin. It is more potent against Branh.catarrhalis, Gard. vaginalis and Legionella butless potent against B. pertussis. Good enteralabsorption and an average plasma t½ of 12 hrmaking it suitable for twice daily dosing, as wellas better gastric tolerability are its desirablefeatures.
Though its affinity for cytochrome P450 islower, drug interactions with terfenadine,cisapride and others are not ruled out. Thus, itis an alternative to erythromycin for respiratory,ENT, skin and soft tissue and genital tractinfections with similar efficacy.Dose: 150–300 mg BD 30 min before meals, children2.5–5 mg/kg BD.ROXID, ROXIBID, RULIDE 150, 300 mg tab, 50 mg kid tab,50 mg /5 ml liquid; ROXEM 50 mg kid tab, 150 mg tab.
Clarithromycin The antimicrobial spectrumof clarithromycin is similar to erythromycin; inaddition, it includes Mycobact. avium complex(MAC), other atypical mycobacteria, Mycobact.leprae and some anaerobes but not Bact. fragilis.

755C
HA
PTER54
MACROLIDE AND OTHER ANTIBACTERIAL ANTIBIOTICS
It is more active against Helicobacter pylori,Moraxella, Legionella, Mycoplasma pneumo-niae and sensitve strains of gram-positivebacteria. However, bacteria that have developedresistance to erythromycin are resistant toclarithromycin also.
Clarithromycin is more acid-stable thanerythromycin, and is rapidly absorbed; oral bio-availability is ~50% due to first pass metabolism;food delays but does not decrease absorption.It has slightly larger tissue distribution thanerythromycin and is metabolized by saturationkinetics—t½ is prolonged from 3–6 hours atlower doses to 6–9 hours at higher doses. Anactive metabolite is produced. About 1/3 of anoral dose is excreted unchanged in urine, butno dose modification is needed in liver diseaseor in mild-to-moderate kidney failure.
Clarithromycin is indicated in upper andlower respiratory tract infections, sinusitis, otitismedia, whooping cough, atypical pneumonia,skin and skin structure infections due to Strep.pyogenes and some Staph. aureus. Used as acomponent of triple drug regimen (see p. 657)it eradicates H. pylori in 1–2 weeks. It is a firstline drug in combination regimens for MACinfection in AIDS patients and a second line drugfor other atypical mycobacterial diseases as wellas leprosy.Dose: 250 mg BD for 7 days; severe cases 500 mg BD up to 14days.CLARIBID 250, 500 mg tabs, 250 mg/5 ml dry syr; CLARIMAC250, 500 mg tabs; SYNCLAR 250 mg tab, 125 mg/5 ml dry syr.
Side effects of clarithromycin are similarto those of erythromycin, but gastric toleranceis better. High doses can cause reversible hearingloss. Few cases of pseudomembranous entero-colitis, hepatic dysfunction or rhabdomyolysisare reported. Its safety in pregnancy and lactationis not known. It inhibits CYP3A4, and the druginteraction potential is similar to erythromycin.
Azithromycin This azalide congener oferythromycin has an expanded spectrum, impro-ved pharmacokinetics, better tolerability anddrug interaction profiles. It is more active than
other macrolides against H. influenzae, but lessactive against gram-positive cocci. High activityis exerted on respiratory pathogens—Myco-plasma, Chlamydia pneumoniae, Legionella,Moraxella and on others like Campylobacter.Ch. trachomatis, H. ducreyi, Calymm. granu-lomatis, N. gonorrhoeae. However, it is notactive against erythromycin-resistant bacteria.Penicillinase producing Staph. aureus areinhibited but not MRSA. Good activity is notedagainst MAC.
The remarkable pharmacokinetic propertiesare acid-stability, rapid oral absorption (fromempty stomach), larger tissue distribution andintracellular penetration. Concentration in mosttissues exceeds that in plasma. Particularly highconcentrations are attained inside macrophagesand fibroblasts; volume of distribution is ~30L/kg. Slow release from the intracellular sitescontributes to its long terminal t½ of >50 hr.It is largely excreted unchanged in bile, renalexcretion is ~ 10%.
Because of higher efficacy, better gastrictolerance and convenient once a day dosing,azithromycin is now preferred over erythromycinas first choice drug for infections such as:(a) Legionnaires’ pneumonia: 500 mg OD oral/i.v. for 2 weeks. Erythromycin or a FQ are thealternatives.(b) Chlamydia trachomatis: nonspecific ure-thritis and genital infections in both men andwomen —1 g single dose is curative, while 3weekly doses are required for lymphogranulomavenereum (see p. 763). It is also the drug of choicefor chlamydial pneumonia and is being preferredover tetracycline for trachoma in the eye.(c). Donovanosis caused by Calymmatobac-terium granulomatis: 500 mg OD for 7 daysor 1.0 g weekly for 4 weeks is as effective asdoxycycline.(d) Chancroid and PPNG urethritis: single1.0 g dose is highly curative (see p. 763).
The other indications of azithromycin arepharyngitis, tonsillitis, sinusitis, otitis media,pneumonias, acute exacerbations of chronic

756S
EC
TIO
N12
ANTIMICROBIAL DRUGS
bronchitis, streptococcal and some staphylococcalskin and soft tissue infections. In combinationwith at least one other drug it is effective inthe prophylaxis and treatment of MAC in AIDSpatients. Other potential uses are in multidrugresistant typhoid fever in patients allergic tocephalosporins; and in toxoplasmosis.Dose: 500 mg once daily 1 hour before or 2 hours after food(food decreases bioavailability); (children above 6 month—10mg/kg/day) for 3 days is sufficient for most infections.AZITHRAL 250, 500 mg cap and 250 mg per 5 ml dry syr;AZIWOK 250 mg cap, 100 mg kid tab, 100 mg/5 ml and 200 mg/5 ml susp. AZIWIN 100, 250, 500 mg tab, 200 mg/5 ml liq. AlsoAZITHRAL 500 mg inj.
Side effects are mild gastric upset, abdominalpain (less than erythromycin), headache anddizziness. Azithromycin has been found not toaffect hepatic CYP3A4 enzyme. Interaction withtheophylline, carbamazepine, warfarin, terfena-dine and cisapride is not likely, but caution maybe exercised.
Spiramycin This macrolide antibiotic, though availablefor more than a decade, has been employed only sporadically.It resembles erythromycin in spectrum of activity andproperties. Distinctively, it has been found to limit risk oftransplacental transmission of Toxoplasma gondii infection.Its specific utility is for toxoplasmosis and recurrent abortionin pregnant women; 3 week courses of 3 MU 2–3 times aday are repeated after 2 week gaps till delivery. Otherindications are similar to erythromycin, for which 6 MU/dayis given for 5 days. Side effects are gastric irritation, nausea,diarrhoea and rashes.ROVAMYCIN 1.5 MU, 3 MU tabs, 0.375 MU/ 5 ml susp.
LINCOSAMIDE ANTIBIOTICS
ClindamycinThis potent lincosamide antibiotic is similar inmechanism of action (inhibits protein synthesisby binding to 50S ribosome) and spectrum ofactivity to erythromycin with which it exhibitspartial cross resistance. Modification of theribosomal binding site by the constitutivemethylase enzyme confirs resistance to both, butnot the inducible enzyme. Antibiotic efflux isnot an important mechanism of clindamycinresistance. Clindamycin inhibits most gram-positive cocci (including most species ofstreptococci, penicillinase producing Staph., but
not MRSA), C. diphtheriae, Nocardia, Actino-myces, Toxoplasma and has slow action onPlasmodia. However, the distinctive feature isits high activity against a variety of anaerobes,especially Bact. fragilis. Aerobic gram-negativebacilli, spirochetes, Chlamydia, Mycoplasma andRickettsia are not affected.
Oral absorption of clindamycin is good. Itpenetrates into most skeletal and soft tissues,but not in brain and CSF; accumulates in neutrophilsand macrophages. It is largely metabolized andmetabolites are excreted in urine and bile. Thet½ is 3 hr.
Side effects are rashes, urticaria, abdominalpain, but the major problem is diarrhoea andpseudomembranous enterocolitis due to Clostri-dium difficile superinfection which is potentiallyfatal. The drug should be promptly stopped andoral metronidazole (alternatively vancomycin)given to treat it. Thrombophlebitis of the injectedvein can occur on i.v. administration.
Because of the potential toxicity, use of clin-damycin is restricted to anaerobic and mixedinfections, especially those involving Bact.fragilis causing abdominal, pelvic and lungabscesses. It is a first line drug for theseconditions, and is generally combined with anaminoglycoside or a cephalosporin. Metroni-dazole and chloramphenicol are the alternativesto clindamycin for covering the anaerobes. Skinand soft tissue infections in patients allergic topenicillins can be treated with clindamycin.Anaerobic streptococcal and Cl. perfringensinfections, especially those involving bone andjoints respond well. It has also been employedfor prophylaxis of endocarditis in penicillin aller-gic patients with valvular defects who undergodental surgery, as well as to prevent surgical siteinfection in colorectal/pelvic surgery.
In AIDS patients, it has been combined withpyrimethamine for toxoplasmosis and with pri-maquine for Pneumocystis jiroveci pneumonia.It is an alternative to doxycycline for supple-menting quinine/artesunate in treating multidrugresistant falciparum malaria. Topically it is usedfor infected acne vulgaris.

757C
HA
PTER54
MACROLIDE AND OTHER ANTIBACTERIAL ANTIBIOTICS
Clindamycin, erythromycin and chloramphe-nicol can exhibit mutual antagonism, probablybecause their ribosomal binding sites are proximal;binding of one hinders access of the other toits target site. Clindamycin slightly potentiatesneuromuscular blockers.Dose: 150–300 mg (children 3–6 mg/kg) QID oral; 200–600 mgi.v. 8 hourly; DALCAP 150 mg cap; CLINCIN 150, 300 mg cap;DALCIN, DALCINEX 150, 300 mg cap, 300 mg/2 ml and 600 mg/4 ml inj. ACNESOL, CLINDAC-A 1% topical solution and gel.
Lincomycin
It is the forerunner of clindamycin; has similar antibacterialand toxic properties, but is less potent and produces a higherincidence of diarrhoea and colitis—deaths have occurred.Thus, it has been largely replaced by clindamycin. It isabsorbed orally and excreted mainly in bile; plasma t½ 5 hrs.Dose: 500 mg TDS-QID oral; 600 mg i.m. or by i.v. infusion6–12 hrly.LINCOCIN 500 mg cap, 600 mg/2 ml inj; LYNX 250, 500 mgcap, 125 mg/5 ml syr, 300 mg/ml inj in 1, 2 ml amp.
GLYCOPEPTIDE ANTIBIOTICS
VancomycinIt is a glycopeptide antibiotic discovered in 1956as a penicillin substitute which assumed specialsignificance due to efficacy against MRSA,Strep. viridans, Enterococcus and Cl. difficile.Bactericidal action is exerted on gram-positivecocci, Neisseria, Clostridia and diphtheroids.However, in hospitals where it has beenextensively used for surgical prophylaxis, etc.,vancomycin-resistant Staph. aureus (VRSA) andvancomycin-resistant Enterococcus (VRE) haveemerged. These nosocomial bacteria are resistantto methicillin and most other antibiotics as well.Gram-negative bacilli are inherently non-respon-sive to vancomycin.
Vancomycin acts by inhibiting bacterial cellwall synthesis. It binds to the terminal dipeptide‘D-ala-D-ala’ sequence of peptidoglycan units—prevents its release from the bactoprenol lipidcarrier so that assembly of the units at the cellmembrane and their cross linking to form thecell wall cannot take place (see Fig. 51.2).Enterococcal resistance to vancomycin is dueto a plasmid mediated alteration of the dipeptidetarget site, reducing its affinity for vancomycin.
Vancomycin is not absorbed orally. After i.v.administration, it is widely distributed, penetratesserous cavities, inflamed meninges and isexcreted mainly unchanged by glomerular filtra-tion with a t½ of 6 hours. Dose reduction isneeded in renal insufficiency.
Toxicity: Systemic toxicity of vancomycin ishigh. It can cause plasma concentration-depen-dent nerve deafness which may be permanent.Kidney damage is also dose-related. Other oto-and nephrotoxic drugs like aminoglycosides mustbe very carefully administered when vancomycinis being used. Skin allergy and fall in BP duringi.v. injection can occur. Vancomycin has thepotential to release histamine by direct actionon mast cells. Rapid i.v. injection has causedchills, fever, urticaria and intense flushing—called ‘Red man syndrome’.
Uses: Given orally (125–500 mg 6 hourly), itis the second choice drug to metronidazole forantibiotic associated pseudomembranous entero-colitis caused by C. difficile. Staphylococcalenterocolitis is another indication of oralvancomycin.
Systemic use (500 mg 6 hourly or 1 g 12hourly infused i.v. over 1 hr) is restricted toserious MRSA infections for which it is the mosteffective drug, and as a penicillin substitute (inallergic patients) for enterococcal endocarditisalong with gentamicin. It is an alternative drugfor serious skin, soft tissue and skeletal infectionsin which gram-positive bacteria are mostlycausative. For empirical therapy of bacterialmeningitis, i.v. vancomycin is usually combinedwith i.v. ceftriaxone/cefotaxime. It is also usedin dialysis patients and those undergoing cancerchemotherapy. Penicillin-resistant pneumococcalinfections and infection caused by diphtheroidsrespond very well to vancomycin.
Vancomycin is the preferred surgical pro-phylactic in MRSA prevalent areas and inpenicillin allergic patients.VANCOCIN-CP, VANCOGEN, VANCORID-CP 500 mg/vial inj;VANCOLED 0.5, 1.0 g inj. VANCOMYCIN 500 mg tab, VANLID250 mg cap, 500 mg/vial inj.

758S
EC
TIO
N12
ANTIMICROBIAL DRUGS
TeicoplaninThis newer glycopeptide antibiotic is a mixtureof 6 similar compounds, active against gram-positive bacteria only. The mechanism of actionand spectrum of activity is similar to vanco-mycin. Notable features are:• It is more active than vancomycin against
enterococci, and equally active against MRSA.• Some VRE but not VRSA are susceptible to
teicoplanin.• It can be injected i.m. as well; is largely
excreted unchanged by kidney; dose needs tobe reduced in renal insufficiency; has a verylong t½ (3–4 days).
• Toxicity is less than vancomycin; adverseeffects are rashes, fever, granulocytopenia andoccasionally hearing loss. Reactions due tohistamine release are rare (1 in 2500).
Teicoplanin is indicated in enterococcal endo-carditis (along with gentamicin); MRSA andpenicillin resistant streptococcal infections,osteomyelitis and as alternative to vancomycinfor surgical prophylaxis, etc.Dose: 400 mg first day—then 200 mg daily i.v. or i.m.; severeinfection 400 mg × 3 doses 12 hourly—then 400 mg daily.TARGOCID, TECOPLAN, TECOCIN 200, 400 mg per vial inj.for reconstitution.
OXAZOLIDINONE
LinezolidThis is the first member of a new class ofsynthetic AMAs ‘Oxazolidinones’ useful in thetreatment of resistant gram-positive coccal(aerobic and anaerobic) and bacillary infections.It is active against MRSA and some VRSA, VRE,penicillin-resistant Strep. pyogenes, Strep.viridans and Strep. pneumoniae, M. tuber-culosis, Corynebacterium, Listeria, Clostridiaand Bact. fragilis. It is primarily bacteriostatic,but can exert cidal action against some strepto-cocci, pneumococci and B. fragilis. Gram-negative bacteria are not affected.
Linezolid inhibits bacterial protein synthesisby acting at an early step and a site different fromthat of other AMAs. It binds to the 23S fraction
(P site) of the 50S ribosome and interferes withformation of the ternary N-formylmethionine-tRNA (tRNAfMet) -70S initiation complex. Bindingof linezolid distorts the tRNA binding siteoverlapping both 50S and 30S ribosomal subunitsand stops protein synthesis before it starts. Assuch, there is no cross resistance with any otherclass of AMAs. Linezolid resistance due tomutation of 23S ribosomal RNA has been detectedamong enterococci.
Linezolid is rapidly and completely absorbedorally, partly metabolized nonenzymatically andexcreted in urine. Plasma t½ is 5 hrs. Dosemodification has not been necessary in renalinsufficiency.
Linezolid given orally or i.v. is used foruncomplicated and complicated skin and softtissue infections, community and hospital-acquired pneumonias, bacteraemias and otherdrug-resistant gram-positive infections with83–94% cure rates. However, in order to preventemergence of resistance to this valuable drug,use should be restricted to serious hospital-acquired pneumonias, febrile neutropenia, woundinfections and others caused by multidrug-resistant gram-positive bacteria such as VRE,vancomycin resistant-MRSA, multi-resistant S.pneumoniae, etc. Being bacteriostatic, it is notsuitable for treatment of enterococcal endo-carditis.Dose: 600 mg BD, oral/ i.v.; LIZOLID 600 mg tab; LINOX,LINOSPAN 600 mg tab, 600 mg/300 ml i.v. infusion.
Side effects to linezolid have been few;mostly mild abdominal pain, nausea, taste distur-bance and diarrhoea. Occasionally, rash, pruritus,headache, oral/vaginal candidiasis have beenreported. Neutropenia, anaemia and thrombocyto-penia are infrequent and mostly associated withprolonged use. Optic neuropathy has occurredafter linezolid is given for >4 weeks. Becauselinezolid is a MAO inhibitor, interactions withadrenergic/serotonergic drugs (SSRIs, etc.) andexcess dietary tyramine are expected. Nocytochrome P450 enzyme related interactionsseem likely.

759C
HA
PTER54
MACROLIDE AND OTHER ANTIBACTERIAL ANTIBIOTICS
MISCELLANEOUS ANTIBIOTICS
Spectinomycin It is a chemically distinct (aminocyclitol),narrow spectrum, bacteriostatic antibiotic which inhibits alimited number of gram-negative bacteria, notably Neisseriagonorrhoeae. It acts by binding to 30S ribosome andinhibiting bacterial protein synthesis, but the action is distinctfrom that of aminoglycosides. The single approved indicationof spectinomycin is treatment of drug resistant gonorrhoea,or when the first line drugs (β-lactams/macrolides, etc.) cannot be used due to allergy or other contraindication.Dose: 2.0 g i.m. single dose; for less responsive cases 4.0 g (2.0g at 2 sites).MYSPEC, TROBICIN 2.0 g/vial inj.The single dose is well tolerated; chills, fever and urticariaare occasional side effects. Repeated doses may causeanaemia, renal and hepatic impairment.
Quinupristin/Dalfopristin It is a combination of twosemisynthetic pristinamycin antibiotics which together exertsynergistic inhibition of bacterial protein synthesis. It is activeagainst most gram-positive cocci including MRSA, someVRSA and some VRE; as well as certain Neisseria, Legionellaand Chlamydia pneumoniae. The combination is bactericidalagainst strepto and staphylococci but bacteriostatic againstE. faecium.
It is being used for serious nosocomial MRSA, VRE andother resistant gram-positive infections.
Mupirocin This topically used antibiotic obtained from aspecies of Pseudomonas is active mainly against gram-positivebacteria, including Strep. pyogenes (penicillin sensitive/resistant), Staph aureus. MRSA, etc. It inhibits bacterialprotein synthesis by blocking the production of t-RNA forisoleucin. As such, no cross resistance with any otherantibiotic is seen. Though primarily bacteriostatic, highconcentrations applied topically may be bactericidal. It isindicated in furunculosis, folliculitis, impetigo, infected insectbites and small wounds. Local itching, irritation and rednessmay occur.BACTROBAN, MUPIN, T-BACT 2% oint. for topicalapplication thrice daily.
Fusidic acid It is a narrow spectrum steroidal antibiotic,blocks bacterial protein synthesis. It is active againstpenicillinase producing Staphylococci and few other gram-positive bacteria. It is used only topically for boils, folliculitis,sycosis barbae and other cutaneous infections.FUCIDIN-L, FUCIBACT, FUSIDERM; 2% oint. and cream.
POLYPEPTIDE ANTIBIOTICS
These are low molecular weight cationic polypeptideantibiotics. All are powerful bactericidal agents, but not usedsystemically due to toxicity. All are produced by bacteria.Clinically used ones are:
Polymyxin BColistinBacitracin
Polymyxin B and Colistin Polymyxin and colistin wereobtained in the late 1940s from Bacillus polymyxa and B.colistinus respectively. They are active against gram-negativebacteria only; all except Proteus, Serratia and Neisseria areinhibited. Both have very similar range of activity, but colistinis more potent on Pseudomonas, Salmonella and Shigella.
Mechanism of action They are rapidly acting bactericidalagents; have a detergent-like action on the cell membrane.They have high affinity for phospholipids: the peptidemolecules (or their aggregates) orient between the phospho-lipid and protein films in gram-negative bacterial cell membranecausing membrane distortion or pseudopore formation. Asa result ions, amino acids, etc. leak out. Sensitive bacteriatake up more of the antibiotic. They may also inactivate thebacterial endotoxin.
They exhibit synergism with many other AMAs byimproving their penetration into the bacterial cell.
Resistance Resistance to these antibiotics has never beena problem. There is no cross resistance with any other AMA.
Adverse effects Little or no absorption occurs from oralroute or even from denuded skin (burn, ulcers). Appliedtopically, they are safe—no systemic effect or sensitizationoccurs. A rash is rare.• Given orally, side effects are limited to the g.i.t.—occasional
nausea, vomiting, diarrhoea.• Systemic toxicity of these drugs (when injected) is high:
flushing and paresthesias (due to liberation of histaminefrom mast cells), marked kidney damage, neurologicaldisturbances, neuromuscular blockade.
Preparation and dose
Polymyxin B: (1 mg = 10,000 U)NEOSPORIN POWDER: 5000 U with neomycin sulf. 3400 U andbacitracin 400 U per g.NEOSPORIN EYE DROPS: 5000 U with neomycin sulf. 1700 Uand gramicidin 0.25 mg per ml.NEOSPORIN-H EAR DROPS: 10,000 U with neomycin sulf. 3400U and hydrocortisone 10 mg per ml.
Colistin sulfate: 25–100 mg TDS oralWALAMYCIN 12.5 mg (25000 i.u.) per 5 ml dry syr, COLISTOP12.5 mg/5 ml and 25 mg/5 ml dry syr.
Uses
(a) Topically Usually in combination with other antimicro-bials for skin infections, burns, otitis externa, conjunctivitis,corneal ulcer—caused by gram-negative bacteria includingPseudomonas.
(b) Orally Gram-negative bacillary (E. coli, Salmonella,Shigella) diarrhoeas, especially in infants and children;Pseudomonas superinfection enteritis.
Bacitracin It is one of the earliest discovered antibioticsfrom a strain of Bacillus subtilis. In contrast to polymyxin,

760S
EC
TIO
N12
ANTIMICROBIAL DRUGS
it is active mainly against gram-positive organisms (both cocciand bacilli). Neisseria, H. influenzae and few other bacteriaare also affected.
It acts by inhibiting cell wall synthesis at a step earlierthan that inhibited by penicillin. Subsequently, it increasesthe efflux of ions by binding to cell membrane. It is bactericidal.
Bacitracin is not absorbed orally. It is not given parenterallybecause of high toxicity, especially to the kidney. Use isrestricted to topical application for infected wounds, ulcers,eye infections—generally in combination with neomycin,polymyxin, etc.NEBASULF Bacitracin 250 U + neomycin 5 mg + sulfacetamide60 mg/g powder, skin oint, eye oint; in NEOSPORIN 400 U/gpowder (1 U = 26 µg).It does not penetrate intact skin, therefore, is of little valuein furunculosis, boils, carbuncles, etc.
URINARY ANTISEPTICS
Some orally administered AMAs attain antibac-terial concentration only in urine, with little orno systemic antibacterial effect. Like many otherdrugs, they are concentrated in the kidney tubules,and are useful mainly in lower urinary tractinfection. They have been called urinaryantiseptics because this may be considered asa form of local therapy. Nitrofurantoin andmethenamine are two such agents; infrequentlyused now. Nalidixic acid (see p. 709) can alsobe considered to be a urinary antiseptic.
Nitrofurantoin
It is primarily bacteriostatic, but may be cidal at higherconcentrations and in acidic urine. Its activity is enhancedat lower pH. Many gram-negative bacteria were susceptible,but due to development of resistance, activity is now restrictedlargely to E. coli. Resistance to nitrofurantoin does notdevelop during continued therapy. No cross resistance withany other AMA is known, though it antagonizes thebactericidal action of nalidixic acid. Susceptible bacteriaenzymatically reduce nitrofurantoin to generate reactiveintermediates which damage DNA.
Pharmacokinetics Nitrofurantoin is well absorbed orally;rapidly metabolized in liver and other tissues; less than halfis excreted unchanged in urine; plasma t½ is 30–60 min.Antibacterial concentrations are not attained in blood ortissues. Probenecid inhibits its tubular secretion and reducesthe concentration attained in urine—may interfere with itsurinary antiseptic action. Renal excretion is reduced inazotaemic patients; effective concentrations may not bereached in the urine, while toxicity increases. As such, it iscontraindicated in renal failure; also during pregnancy andin neonates.
Adverse effects Commonest is gastrointestinal intole-rance—nausea, epigastric pain and diarrhoea.
An acute reaction with chills, fever and leucopenia occursoccasionally.
Peripheral neuritis and other neurological effects arereported with long-term use. Haemolytic anaemia is rare, exceptin G-6-PD deficiency. Liver damage and a pulmonary reactionwith fibrosis on chronic use are infrequent events.
Urine of patients taking nitrofurantoin turns dark brownon exposure to air.
Use The only indication for nitrofurantoin is uncomplicatedlower urinary tract infection not associated with prostatitis,but it is infrequently used now. Acute infections due toE. coli can be treated with 50–100 mg TDS (5–7 mg/kg/day)given for 5–10 days. These doses should not be used for> 2 weeks at a time. Suppressive long-term treatment has beensuccessful with 50 mg BD or 100 mg at bed time. This dosecan also be employed for prophylaxis of urinary tract infectionfollowing catheterization or instrumentation of the lowerurinary tract and in women with recurrent cystitis.FURADANTIN 50, 100 mg tab, URINIF 100 mg tab..NEPHROGESIC: Nitrofurantoin 50 mg + phenazopyridine 100mg tab.
Methenamine (Hexamine)
It is hexamethylene-tetramine, which is inactive as such;decomposes slowly in acidic urine to release formaldehydewhich inhibits all bacteria. This drug exerts no antimicrobialactivity in blood and tissues, including kidney parenchyma.Acidic urine is essential for its action; urinary pH must bekept below 5.5 by administering an organic acid which isexcreted as such, e.g. mandelic acid or hippuric acid or ascorbicacid.
Methenamine is administered in enteric coated tabletsto protect it from decomposing in gastric juice. Mandelicacid, given as methenamine mandelate, is excreted in urine→lowers urinary pH and promotes decomposition ofmethenamine. Lower urinary pH itself disfavours growth ofurinary pathogens.MANDELAMINE : Methenamine mandelate 0.5 g, 1 g tab: 1 gTDS or QID with fluid restriction (daily urine volume between1–1.5 L) to ensure adequate concentration of formaldehyde inurine.It is not an effective drug for acute urinary tract infectionsor for catheterization prophylaxis. Its use is restricted tochronic, resistant type of urinary tract infections, not involvingkidney substance. Resistance to formaldehyde does not occur,but methenamine is rarely used now.
Adverse effects Gastritis can occur due to release offormaldehyde in stomach—patient compliance is poor dueto this. Chemical cystitis and haematuria may develop withhigh doses given for long periods. CNS symptoms areproduced occasionally.

761C
HA
PTER54
MACROLIDE AND OTHER ANTIBACTERIAL ANTIBIOTICS
URINARY ANALGESIC
Phenazopyridine It is an orange dye which exertsanalgesic action in the urinary tract and affords symptomaticrelief of burning sensation, dysuria and urgency due tocystitis. It does not have antibacterial property. Side effectsare nausea and epigastric pain.Dose: 200–400 mg TDS: PYRIDIUM 200 mg tab.
TREATMENT OF URINARY TRACTINFECTIONS
The general principles of use of AMAs forurinary tract infections (UTIs) remain the sameas for any other infection. Some specific consi-derations are highlighted below.
Most UTIs are caused by gram-negativebacteria, especially coliforms. Majority of acuteinfections involve a single organism (commonestis E. coli); chronic and recurrent infections maybe mixed infections. Acute infections are largelyself limiting; high urine flow rates with frequentbladder voiding may suffice. Many single doseantimicrobial treatments have been successfullytried, but a three day regimen is consideredoptimal for lower UTIs. Upper UTIs requiremore aggressive and longer treatment. In anycase, treatment for more than 2 weeks is seldomwarranted.
Bacteriological investigations are veryimportant to direct the choice of drug. Though,treatment may not wait till report comes, urinesample must be collected for bacteriology beforecommencing therapy. Most AMAs attain highconcentration in urine, smaller than usual dosesmay be effective in lower UTIs, becauseantibacterial action in urine is sufficient, mucosatakes care of itself. In upper UTI (pyelonephritis)antimicrobial activity in kidney tissue is needed.Therefore, doses are similar to those for anysystemic infection.
The least toxic and cheaper AMA should beused, just long enough to eradicate the pathogen.It is advisable to select a drug which does notdisrupt normal gut and perineal flora. If recur-rences are frequent, chronic suppressive treat-ment with cotrimoxazole, nitrofurantoin, methe-namine, cephalexin or norfloxacin may be given.
The status of AMAs (other than urinary anti-septics) in urinary tract infections is summarizedbelow:1. Sulfonamides Dependability in acute UTIshas decreased; they are not used now as singledrug. May occasionally be employed for suppres-sive and prophylactic therapy.
2. Cotrimoxazole (see p. 708) Thoughresponse rate and use have declined, it may beemployed empirically in acute UTI withoutbacteriological data, because majority of urinarypathogens, including Chlamydia trachomatis,are covered by cotrimoxazole. Given once dailyat bed time cotrimoxazole 480 mg is often usedfor prophylaxis of recurrent cystitis in women,as well as in catheterized patients. It should notbe used to treat UTI during pregnancy.
3. Quinolones (see p. 711) The first generationFQs, especially norfloxacin and ciprofloxacin arehighly effective and currently the most populardrugs, because of potent action against gram-negative bacilli and low cost. Nalidixic acid isseldom employed. However, to preserve theirefficacy, use should be restricted. FQs areparticularly valuable in complicated cases, those
Antimicrobial regimens for acute UTI(all given orally for 3–5 days)*
1. Norfloxacin 400 mg 12 hourly 2. Ciprofloxacin 250–500 mg 12 hourly3. Ofloxacin 200–400 mg 12 hourly 4. Cotrimoxazole 960 mg 12 hourly 5. Cephalexin 250–500 mg 6 hourly 6. Cefpodoxime proxetil 200 mg 12 hourly 7. Amoxicillin + clavulanic acid (500 + 125 mg)
8 hourly 8. Nitrofurantoin 50 mg 8 hourly or 100 mg 12
hourly × 5–7 days
* For upper UTI (pyelonephritis), the same drugs may begiven for 2–3 weeks. Nitrofurantoin is not suitable forpyelonephritis.
The commonly used antimicrobial regimensfor empirical therapy of uncomplicated acute UTIare given in the box.

762S
EC
TIO
N12
ANTIMICROBIAL DRUGS
with prostatitis or indwelling catheters and forbacteria resistant to cotrimoxazole/ampicillin.Norfloxacin given for upto 12 weeks mayachieve cure in chronic UTI. The FQs shouldnot be given to pregnant women.
4. Ampicillin/Amoxicillin (see p. 722) Fre-quently used in the past as first choice drug forinitial treatment of acute infections withoutbacteriological data, but higher failure andrelapse rates have made them unreliable forempirical therapy. Many E. coli strains are nowampicillin-resistant. Amoxicillin + clavulanicacid is more frequently employed. Parenteralcoamoxiclav is often combined with gentamicinfor initial treatment of acute pyelonephritis.5. Cloxacillin Use is restricted to penicillinase producingstaphylococcal infection, which is uncommon in urinarytract.
6. Piperacillin/Carbenicillin Only in serious Pseudomonasinfection in patients with indwelling catheters or chronicurinary obstructin (prostatic hypertrophy, calculi), and inhospitalized patients on the basis of in vitro sensitivity.
7. Cephalosporins Use is increasing, espe-cially in women with nosocomial Klebsiella andProteus infections. They should normally beemployed only on the basis of sensitivity report,but empirical use for community acquired infec-tion is also common. Some guidelines recom-mend them as one of the option for empiricaltreatment of acute lower UTI. Cephalexin givenonce daily is an alternative drug for prophylaxisof recurrent cystitis, especially in women likelyto get pregnant.
8. Gentamicin (see p. 747) Very effectiveagainst most urinary pathogens including Pseudo-monas. However, because of narrow margin ofsafety and need for parenteral administration, itis generally used only on the basis of in vitrobacteriological sensitivity testing. In acute pyelo-nephritis gentamicin + parenteral amoxicillin-clavulanate, may be initiated empirically beforebacteriological report becomes available. Thenewer aminoglycosides may be needed forhospital-acquired infections.9. Chloramphenicol Though effective in many cases, useshould be restricted (for fear of toxicity) to pyelonephritis
in cases where the causative bacteria is sensitive only tothis antibiotic.
10. Tetracyclines They are seldom effective now, becausemost urinary pathogens have become resistant. Though broadspectrum, they are used only on the basis of sensitivity reportand in Ch. trachomatis cystitis.
Urinary pH in relation to use of AMAsCertain AMAs act better in acidic urine, whileothers in alkaline urine (see Box). However,specific intervention to produce urine of desiredreaction (by administering acidifying oralkalinizing agents) is seldom required (exceptfor methenamine), because most drugs used inUTI attain high concentration in urine and minorchanges in urinary pH do not affect clinicaloutcome. In case of inadequate response or incomplicated cases, measurement of urinary pHand appropriate corrective measure may help.
Favourable urinary pH for antimicrobial action
Acidic Alkaline pH immaterial
Nitrofurantoin Cotrimoxazole ChloramphenicolMethenamine Aminoglycosides AmpicillinTetracyclines (Gentamicin, etc.)Cloxacillin Cephalosporins
Fluoroquinolones
In certain urease positive Proteus (they spliturea present in urine into NH3) infections it isimpossible to acidify urine. In such cases,acidification should not be attempted and drugswhich act better at higher pH should be used.
Urinary infection in patients withrenal impairmentThis is relatively difficult to treat because mostAMAs attain lower urinary concentration.Methenamine mandelate, tetracyclines (exceptdoxycycline) and certain cephalosporins arecontraindicated.
Nitrofurantoin, nalidixic acid and amino-glycosides are better avoided. Every effort mustbe made to cure the infection, because if itpersists, kidneys may be further damaged.Bacteriological testing and followup cultures are

763C
HA
PTER54
MACROLIDE AND OTHER ANTIBACTERIAL ANTIBIOTICS
TAB
LE 5
4.1
Reg
imen
s fo
r the
trea
tmen
t of s
exua
lly tr
ansm
itted
dis
ease
s
⎫ ⎬ ⎭
DIS
EA
SE
/CA
US
AT
IVE
TR
EA
TM
EN
TO
RG
AN
ISM
1st
Cho
ice
Alte
rnat
ives
1.G
onor
rhoe
aA
mox
icill
in 3
g o
ral,
or
+
Pro
bene
cid
Cef
ixim
e 40
0 m
g on
ce o
ral,
orN
onpe
nici
llina
seA
mpi
cilli
n 3.
5 g
oral
1 g
ora
l sin
gle
dose
Dox
ycyc
line
100
mg
BD
× 7
day
s or
al,
orpr
oduc
ing
(Non
PP
NG
)E
ryth
rom
ycin
500
mg
QID
× 5
day
s or
al,
or
Pen
icill
inas
eC
eftri
axon
e 25
0 m
g i.m
. or
+
Pro
bene
cid
Cip
roflo
xaci
n 25
0–50
0 m
g or
al o
nce
orpr
oduc
ing
(PP
NG
)C
efur
oxim
e 1.
5 g
i.m o
r
1 g
ora
l sin
gle
dose
Oflo
xaci
n 20
0–40
0 m
g or
al o
nce
Azi
thro
myc
in 1
.0 g
ora
lsi
ngle
dos
e
2.S
yphi
lisE
arly
(P
rimar
y, S
econ
dary
Ben
zath
ine
Pen
. 2.
4 M
U i.
m.,
1–3
wee
kly
inj.,
or
Dox
ycyc
line
100
mg
BD
ora
l × 1
5 da
ys,
oran
d La
tent
<1
yr)
Pro
c. P
en.G
1.2
MU
i.m
. × 1
0 da
ysC
eftri
axon
e 1
g i.m
. ×
7 da
ys,
orE
ryth
rom
ycin
500
mg
QID
ora
l × 1
5 da
ys
Late
(>1
yr)
Ben
zath
ine
Pen
. 2.
4 M
U i.
m.
wee
kly
× 4
wee
ks,
orD
oxyc
yclin
e or
Ery
thro
myc
in f
or 3
0 da
ys,
orP
roc.
Pen
.G 1
.2 M
U i.
m. ×
20
days
Cef
triax
one
1 g
i.m./i
.v.
× 15
day
s.
3.C
hlam
ydia
tra
chom
atis
Azi
thro
myc
in 1
g o
ral
sing
le d
ose
orE
ryth
rom
ycin
500
mg
QID
ora
l × 7
day
sN
onsp
ecifi
cur
ethr
itis/
endo
cerv
iciti
sD
oxyc
yclin
e 10
0 m
g B
D o
ral ×
7 d
ays
Oflo
xaci
n 40
0 m
g B
D o
ral X
7 d
ays
Lym
phog
ranu
lom
aA
zith
rom
ycin
1.0
g o
ral w
eekl
y ×
3 w
eeks
or
Ery
thro
myc
in 5
00 m
g Q
ID o
ral ×
3 w
eeks
vene
reum
Dox
ycyc
line
100
mg
BD
ora
l × 3
wee
ks(a
spira
te f
luct
uant
lym
ph n
ode)
4.G
ranu
lom
a in
guin
ale/
Tetra
cycl
ine
500
mg
QID
ora
l × 3
wee
ks o
rE
ryth
rom
ycin
500
mg
QID
ora
l × 3
wee
ksD
onov
anos
isD
oxyc
yclin
e 10
0 m
g B
D o
ral ×
3 w
eeks
or
(Cal
ymm
.gra
nulo
mat
is)
Azi
thro
myc
in 5
00 m
g O
D o
ral ×
7 d
ays
or1.
0 w
eekl
y or
al ×
4 w
eeks
5.C
hanc
roid
Cef
tria
xone
0.2
5 g
i.m.
sing
le d
ose
orC
ipro
floxa
cin
500
mg
BD
ora
l ×
3 da
ys o
r(H
. du
crey
i)A
zith
rom
ycin
1.0
g o
ral
sing
le d
ose
orD
oxyc
yclin
e 10
0 m
g B
D o
ral
× 7
days
or
Ery
thro
myc
in 0
.5 g
QID
ora
l ×
7 da
ysC
otrim
oxaz
ole
960
mg
BD
ora
l ×
14 d
ays
6.G
enita
l H
erpe
s si
mpl
exF
irst
epis
ode
Acy
clov
ir 20
0 m
g 5
times
a d
ay/4
00 m
g T
DS
ora
l ×
10 d
ays
orD
oes
not
prev
ent
Val
acyc
lovi
r 0.
5–1.
0 g
BD
ora
l ×
10 d
ays
orre
curr
ence
sF
amci
clov
ir 25
0 m
g T
DS
ora
l ×
5 da
ys(A
cycl
ovir
5% o
int
loca
lly 6
tim
es a
day
× 1
0 da
ys m
ay a
fford
rel
ief
in m
ild c
ases
)R
ecur
rent
epi
sode
The
abo
ve d
rugs
are
giv
en f
or 3
–5 d
ays
(Top
ical
acy
clov
ir is
ine
ffect
ive)
Sup
pres
sive
tre
atm
ent
Acy
clov
ir 40
0 m
g B
D o
ral
× 6–
12 m
onth
s or
Val
acyc
lovi
r 50
0 m
g O
D o
ral
× 6–
12 m
onth
s or
Fam
cicl
ovir
250
mg
BD
ora
l ×
6–12
mon
ths
7.T
richo
mon
asM
etro
nida
zole
2 g
sin
gle
dose
or
400
mg
TDS
× 7
day
s,C
lotri
maz
ole
100
mg
intra
vagi
nal
vagi
nitis
or T
inid
azol
e 2
g si
ngle
dos
e or
600
mg
OD
× 7
day
sev
ery
nigh
t ×
6 to
12
days
(trea
t th
e m
ale
partn
er a
lso
if re
curr
ent)
⎫ ⎬ ⎭ ⎫ ⎬ ⎭

764S
EC
TIO
N12
ANTIMICROBIAL DRUGS
a must to select the appropriate drug and toensure eradication of the pathogen. Potassiumsalts and acidifying agents are contraindicated.
Prophylaxis for urinary tract infectionThis may be given when:(a) Women of child bearing age have recurrentcystitis.(b) Catheterization or instrumentation inflictingtrauma to the lining of the urinary tract isperformed; bacteremia frequently occurs andinjured lining is especially susceptible.(c) Indwelling catheters are placed.(d) Uncorrectable abnormalities of the urinarytract are present.
(e) Inoperable prostate enlargement or otherchronic obstruction causes urinary stasis.The most frequently used drugs for prophylaxisof lower UTI are:• Cotrimoxazole 480 mg*• Nitrofurantoin 100 mg*• Norfloxacin 400 mg*• Cephalexin 250 mg** All drugs are given once daily at bed time.
TREATMENT OF SEXUALLYTRANSMITTED DISEASES (STDs)
The effectiveness of various AMAs in treatingdifferent STDs is described with the individualdrugs. The preferred drugs and regimens forimportant STDs are summarized in Table 54.1.
PROBLEM DIRECTED STUDY
54.1 A 35-year-old woman came to the OPD with complaints of urinary urgency, pain andburning during urination, suprapubic discomfort and low-grade fluctuating fever for the past2 days. She had 3–4 similar episodes over the last year, for which she took treatment froma local doctor. She is married, has 3 children and her last menstrual period was 10 daysback. She is neither using nor is willing to use a contraceptive. Physical examination revealstenderness in the suprapubic region and body temperature 100.4°F. A diagnosis of acute cystitisis made and she is advised to get urine culture and blood tests done.(a) Should empirical antimicrobial treatment be started after urine sample has been taken
for testing? If so, which drug(s) would be appropriate?(b) Can any drug be given to rapidly relieve urinary symptoms?(c) Should long-term prophylactic drug be prescribed in her case? If so, which drug would
be suitable for her?(see Appendix-1 for solution)

Antitubercular DrugsChapterChapterChapterChapterChapter 5555555555
Tuberculosis is a chronic granulomatous diseaseand a major health problem in developing coun-tries. About 1/3rd of the world’s population isinfected with Mycobact. tuberculosis. As perWHO statistics for 2010, there were 9.4 millionactive TB cases globally, to which India was thehighest contributor with 2.3 million cases. Indiahas the dubious distinction of being the highestTB burden country for the past many years; andwhere about 1000 people die from TB everyday. In 2012, the Government of India hasdeclared TB to be a notifiable disease, so thatany doctor who treats a TB patient, has to notifyit to the Govt. In India, control and treatmentof TB is covered under a National programmewhich provides free treatment to all TB cases.The Revised National Tuberculosis ControlProgramme (RNTCP) was launched in 1997, andits treatment guidelines have been further revisedin 2010.
A new dimension got added in the 1980s dueto spread of HIV with high prevalence of tuber-culosis and Mycobact. avium complex (MAC)infection among these patients. India has a largeload of HIV infected subjects, and these patientsare especially vulnerable to severe forms of tuber-cular/MAC infection. While lately, the increasein TB case rate associated with HIV infectionhas been halted in the USA, no such trend isapparent in India; out of all fresh TB cases, 1.2%are coinfected with HIV. Emergence of ‘multidrugresistant’ (MDR) TB which now accounts for 15%of previously treated, and 3% of new TB casesworldwide, is threatening the whole future ofcurrent antitubercular chemotherapy.
Remarkable progress has been made in thelast 65 years since the introduction of Streptomy-cin in 1947 for the treatment of tuberculosis.Its full therapeutic potential could be utilized only
after 1952 when isoniazid was produced toaccompany it. The discovery of ethambutol in1961, rifampin in 1962, and redefinition of therole of pyrazinamide has changed the strategiesin the chemotherapy of tuberculosis. Since 1970efficacy of short course (6–9 months) anddomiciliary regimens has been demonstrated andclear-cut treatment guidelines have been formu-lated.
Fluoroquinolones, newer macrolides andsome rifampin congeners are the recent additionsto the antimycobacterial drugs, while some novelcompounds are under advanced stage of develop-ment.
According to their clinical utility the anti-TBdrugs can be divided into:
First line: These drugs have high antitubercularefficacy as well as low toxicity; are usedroutinely.
Second line: These drugs have either lowantitubercular efficacy or higher toxicity or both;and are used as reserve drugs.
First line drugs
1. Isoniazid (H) 4. Ethambutol (E)2. Rifampin (R) 5. Streptomycin (S)3. Pyrazinamide (Z)
Second line drugs
• Ethionamide (Eto) Fluoroquinolones• Prothionamide (Pto) • Ofloxacin (Ofx)• Cycloserine (Cs) • Levofloxacin (Lvx/Lfx)• Terizidone (Trd) • Moxifloxacin (Mfx)• Para-aminosalicylic • Ciprofloxacin (Cfx)
acid (PAS) Injectable drugs• Rifabutin • Kanamycin (Km)• Thiacetazone (Thz) • Amikacin (Am)
• Capreomycin (Cm)

766S
EC
TIO
N12
ANTIMICROBIAL DRUGS
Alternative grouping of antitubercular drugs*
Group I First line oral anti-TB drugs Isoniazid (INH), Rifampin, Pyrazinamide, Ethambutol
Group II Injectable anti-TB drugs Streptomycin, Kanamycin, Amikacin, Capreomycin
Group III Fluoroquinolones Ofloxacin, Levofloxacin, Moxifloxacin, Ciprofloxacin
Group IV Second line oral anti-TB drugs Ethionamide, Prothionamide, Cycloserine, Terizidone,Para-aminosalicylic acid
Group V Drugs with unclear efficacy£ Thiacetazone, Clarithromycin, Clofazimine, Linezolid,Amoxicillin/clavulanate, Imipenem/cilastatin
* Adopted from: Treatment of Tuberculosis Guidelines; WHO, Fourth edition (2010) and Revised National TuberculosisControl Programme (RNTCP), DOTS-Plus Guidelines 2010.£ Not recommended by WHO for routine use in MDR-TB patients.
Group I: are the most potent and best tolerated oral drugs used routinely.Group II: are potent and bactericidal, but injectable drugs.Group III: includes fluoroquinolones (FQs) which are well tolerated bactericidal oral drugs; all patients with
drug resistant TB should receive one FQ.Group IV: are less effective, bacteriostatic/more toxic oral drugs for resistant TB.Group V: are drugs with uncertain efficacy; not recommended for MDR-TB; may be used in extensively resistant
TB (XDR-TB).
An alternative grouping of antitubercular drugsreflecting hierarchy in efficacy/priority in usehas also been done (see box).
Isoniazid (Isonicotinic acid hydrazide, H)Isoniazid is an excellent antituber-cular drug, and an essentialcomponent of all antitubercularregimens, unless the patient is notable to tolerate it or bacilli areresistant. It is primarily tuber-culocidal. Fast multiplying organisms are rapidlykilled, but quiescent ones are only inhibited. Itacts on extracellular as well as on intracellularTB (bacilli present within macrophages), and isequally active in acidic or alkaline medium. Itis one of the cheapest antitubercular drugs.However, most nontubercular mycobacteria arenot inhibited by INH.
The primary mechanism of action of INHis inhibition of synthesis of mycolic acids whichare unique fatty acid components of myco-bacterial cell wall. This may explain the highselectivity of INH for mycobacteria (it is notactive against any other microorganism). Thelipid content of mycobacteria exposed to INHis reduced. Two gene products labelled ‘InhA’
and ‘KasA’, which function in mycolic acidsynthesis are the targets of INH action. INHenters sensitive mycobacteria which convert itby a catalase-peroxidase enzyme into a reactivemetabolite. This then forms adduct with NADthat inhibits InhA and KasA. The reactive INHmetabolite forms adduct with NADP as wellwhich inhibits mycobacterial DHFRase resultingin interruption of DNA synthesis.
About 1 in 106 tubercle bacilli is inherentlyresistant to clinically attained INH concentra-tions. If INH is given alone, such bacilliproliferate selectively and after 2–3 months(sometimes even earlier) an apparently resistantinfection emerges. The most common mecha-nism which confers high level INH resistanceis by mutation of the catalase-peroxidase (KatG)gene so that the bacilli do not generate thereactive metabolite of INH. However, bacilli thatlose catalase activity also appear to become lessvirulent; many physicians like to continue INHeven when bacilli are apparently resistant to itin vitro. INH resistance may also involvemutation in the inhA or kasA genes. Resistancebased on efflux of INH from the bacterial cellis also possible. Other resistant TB bacilli losethe active INH concentrating process.

767C
HA
PTER55
ANTITUBERCULAR DRUGS
The incidence of primary INH resistancevaries widely among different populations,depending on the extent of use and misuse ofINH in that area. According to WHO, the globalweighted mean of any INH resistance (excludingMDR) among new TB patients is 7.4%. In Indiaresistance to INH alone or in combination withother anti-TB drugs is estimated to be 18%.Combined with other drugs, INH has good resis-tance preventing action. No cross resistance withother antitubercular drugs occurs.
Pharmacokinetics INH is completely absorbedorally and penetrates all body tissues, tubercularcavities, placenta and meninges. It is extensivelymetabolized in liver; most important pathwaybeing N-acetylation by NAT2. The acetylatedmetabolite is excreted in urine. The rate of INHacetylation shows genetic variation. There areeither:
Fast acetylators(30–40% of Indians) t½ of INH 1 hr.
Slow acetylators(60–70% of Indians) t½ of INH 3 hr.
The proportion of fast and slow acetylatorsdiffers in different parts of the world. However,acetylator status does not matter if INH is takendaily, but biweekly regimens are less effectivein fast acetylators. Isoniazid induced peripheralneuritis is more common in slow acetylators.A hepatotoxic minor metabolite is produced byCYP2E1 from acetylhydrazine.
Interactions Aluminium hydroxide inhibitsINH absorption.INH retards phenytoin, carbamazepine, diazepam,theophylline and warfarin metabolism byinhibiting CYP2C19 and CYP3A4, and may raisetheir blood levels. Since rifampin is an enzymeinducer, its concurrent use counteracts theinhibitory effect of INH. However, the net effecton metabolism of many drugs is unpredictable.PAS inhibits INH metabolism and prolongsits t½.Dose of all first line drugs is given in Table55.1.
Adverse effects INH is well tolerated by mostpatients. Peripheral neuritis and a variety ofneurological manifestations (paresthesias, numb-ness, mental disturbances, rarely convulsions)are the most important dose-dependent toxiceffects. These are due to interference withproduction of the active coenzyme pyridoxalphosphate from pyridoxine, and its increasedexcretion in urine (see Ch. 67). Pyridoxine givenprophylactically (10 mg/day) prevents theneurotoxicity even with higher doses. Prophylacticpyridoxine must be given to diabetics, chronicalcoholics, malnourished, pregnant, lactating andHIV infected patients, but routine use is notmandatory. INH neurotoxicity is treated bypyridoxine 100 mg/day.
Hepatitis, a major adverse effect of INH, israre in children, but more common in olderpeople and in alcoholics (chronic alcoholisminduces CYP2E1 which generates the hepato-toxic metabolite). INH hepatotoxicity is due todose-related damage to liver cells, but isreversible on stopping the drug.
Other side effects are lethargy, rashes, fever,acne and arthralgia.ISONEX 100, 300 mg tabs, ISOKIN 100 mg tab, 100 mg per 5 mlliq.
Rifampin (Rifampicin, R)It is a semisynthetic derivative of rifamycin Bobtained from Streptomyces mediterranei.Rifampin is bactericidal to M. tuberculosis andmany other gram-positive and gram-negativebacteria like Staph. aureus, N. meningitidis, H.influenzae, E. coli, Klebsiella, Pseudomonas,Proteus and Legionella. Against TB bacilli, itis as efficacious as INH and better than all otherdrugs. The bactericidal action covers allsubpopulations of TB bacilli, but acts best onslowly or intermittently dividing ones (spurters).M. leprae is highly sensitive, while MAC andsome other mycobacteria, but not M. fortuitum,are moderately susceptible. Both extra- andintracellular organisms are affected. It has goodsterilizing and resistance preventing actions.

768S
EC
TIO
N12
ANTIMICROBIAL DRUGS
Rifampin interrupts RNA synthesis by bindingto β subunit of mycobacterial DNA-dependentRNA polymerase (encoded by rpoB gene andblocking its polymerizing function. The basis ofselective toxicity is that mammalian RNApolymerase does not avidly bind rifampin.
Mycobacteria and other organisms developresistance to rifampin rather rapidly. However,the incidence of resistant bacilli is less than10–7 and it is quite unusual for a patient to haveprimary rifampin resistant tubercular infection.In India it is estimated to be 2%. Rifampinresistance is nearly always due to mutation inthe rpoB gene reducing its affinity for the drug.No cross resistance with any other antituberculardrug, except rifampin congeners, has been noted.
Pharmacokinetics It is well absorbed orally,(bioavailability is ~ 70%), but food decreasesabsorption; rifampin is to be taken in emptystomach. It is widely distributed in the body:penetrates intracellularly, enters tubercularcavities, caseous masses and placenta. Though itcrosses meninges, it is largely pumped out fromCNS by P-glycoprotein. It is metabolized in liverto an active deacetylated metabolite which isexcreted mainly in bile, some in urine also.Rifampin and its desacetyl derivative undergoenterohepatic circulation. The t½ of rifampin isvariable (2–5 hours).
Interactions Rifampin is a microsomalenzyme inducer—increases several CYP450isoenzymes, including CYP3A4, CYP2D6,CYP1A2 and CYP2C subfamily. It thus enhancesits own metabolism (area under the plasmaconcentration-time curve is reduced by ~35%)as well as that of many drugs including warfarin,oral contraceptives, corticosteroids, sulfonyl-ureas, steroids, HIV protease inhibitors, non-nucleoside reverse transcriptase inhibitors(NNRTIs), theophylline, metoprolol, fluconazole,ketoconazole, clarithromycin, phenytoin, etc.Contraceptive failures have occurred. It isadvisable to switch over to an oral contraceptivecontaining higher dose (50 µg) of estrogen oruse alternative method of contraception.
Adverse effects The incidence of adverseeffects is similar to INH.
Hepatitis, a major adverse effect, generallyoccurs in patients with preexisting liver diseaseand is dose-related; infrequent with < 600 mg/day dose. Development of jaundice requiresdiscontinuation of the drug—then it is reversible.Minor reactions, usually not requiring drug with-drawal and more common with intermittentregimens, are:• Cutaneous syndrome: flushing, pruritus +
rash (especially on face and scalp), rednessand watering of eyes.
• Flu syndrome: with chills, fever, headache,malaise and bone pain.
• Abdominal syndrome: nausea, vomiting,abdominal cramps with or without diarrhoea.
Urine and secretions may become orange-red—but this is harmless.Other serious but rare reactions are:• Respiratory syndrome: breathlessness which may be
associated with shock and collapse.• Purpura, haemolysis, shock and renal failure.
Other uses of rifampin
1. Leprosy (see Ch. 56)2. Prophylaxis of Meningococcal and H.
influenzae meningitis and carrier state.3. Second/third choice drug for MRSA,
diphtheroids and Legionella infections.4. Combination of doxycycline and rifampin is
the first line therapy of brucellosis.RCIN 150, 300, 450, 600 mg caps, 100 mg/5 ml susp.RIMACTANE, RIMPIN 150, 300, 450 mg caps, 100 mg/5 ml syr.;RIFAMYCIN 450 mg cap, ZUCOX 300, 450, 600 mg tabs; to betaken 1 hour before or 2 hour after meals.
Pyrazinamide (Z)Chemically similar to INH, pyrazinamide (Z) wasdeveloped parallel to it in 1952. It is weaklytuberculocidal and more active in acidic medium.It is more lethal to intracellularly located bacilliand to those at sites showing an inflammatoryresponse (pH is acidic at both these locations).It is highly effective during the first 2 monthsof therapy when inflammatory changes are

769C
HA
PTER55
ANTITUBERCULAR DRUGS
present. By killing the residual intracellularbacilli it has good ‘sterilizing’ activity. Itsinclusion has enabled duration of treatment tobe shortened and risk of relapse to be reduced.The mechanism of action of Z is not wellestablished, but like INH it is also convertedinside the mycobacterial cell into an activemetabolite pyrazinoic acid by an enzyme(pyrazinamidase) encoded by the pncA gene. Thismetabolite gets accumulated in acidic mediumand probably inhibits mycolic acid synthesis, butby interacting with a different fatty acid synthase.Pyrazinoic acid also appears to disruptmycobacterial cell membrane and its transportfunction. Resistance to Z develops rapidly if itis used alone, and is mostly due to mutationin the pncA gene.
Pyrazinamide is absorbed orally, widelydistributed, has good penetration in CSF, becauseof which it is highly useful in meningeal TB;extensively metabolized in liver and excreted inurine; plasma t½ is 6–10 hours.
Hepatotoxicity is the most important dose-related adverse effect, but it appears to be lesscommon in the Indian population than in westerncountries. Daily dose is now limited to 25–30mg/kg which produces only a low incidence ofhepatotoxicity. It is contraindicated in patientswith liver disease. Safety during pregnancy isuncertain (see p. 776).
Hyperuricaemia is common and is due toinhibition of uric acid secretion in kidney: goutcan occur.
Other adverse effects are abdominal distress,arthralgia, flushing, rashes, fever and loss ofdiabetes control: repeated blood glucosemonitoring is warranted in diabetics.PYZINA 0.5, 0.75, 1.0 g tabs, 0.3 g kid tab; PZA-CIBA 0.5, 0.75 gtabs, 250 mg/5 ml syr; RIZAP 0.75, 1.0 g tabs.
Ethambutol (E)Ethambutol is selectively tuberculostatic and isactive against MAC as well as some othermycobacteria, but not other types of bacteria.Fast multiplying bacilli are more susceptible.Added to the triple drug regimen of RHZ it has
been found to hasten the rate of sputum conversionand to prevent development of resistance, thelatter being the primary purpose of using it.
The mechanism of action of E is not fullyunderstood, but it has been found to inhibitarabinosyl transferases (encoded by embABgenes) involved in arabinogalactan synthesisthereby interfering with mycolic acid incor-poration in mycobacterial cell wall. Resistanceto E develops slowly and is most commonlyassociated with mutation in embB gene, reducingthe affinity of the target enzyme for E. No crossresistance with any other antitubercular drug hasbeen noted.
About 3/4 of an oral dose of E is absorbed.It is distributed widely, but penetrates meningesincompletely and is temporarily stored in RBCs.Less than ½ of E is metabolized. It is excretedin urine by glomerular filtration and tubularsecretion; plasma t½ is ~4 hrs. Caution isrequired in its use in patients with renal disease.
Patient acceptability of E is very good andside effects are few. Loss of visual acuity/colourvision, field defects due to optic neuritis is themost important dose and duration of therapydependent toxicity. Patients should be instructedto stop the drug at the first indication of visualimpairment. Because young children may beunable to report early visual impairment, it wascontraindicated, but is now allowed with dueprecaution. With early recognition and stoppageof the drug, visual toxicity is largely reversible.It is contraindicated in patients with optic neuri-tis. Ethambutol produces few other symptoms:nausea, rashes, fever, rarely peripheral neuritis.Hyperuricemia is due to interference with urateexcretion. It is safe during pregnancy. Ethambutolis used in MAC infection as well.MYCOBUTOL, MYAMBUTOL, COMBUTOL 0.2, 0.4, 0.6, 0.8,1.0 g tabs.
Streptomycin (S)The pharmacology of streptomycin is describedin Ch. 53. It was the first clinically usefulantitubercular drug. It is tuberculocidal, but lesseffective than INH or rifampin; acts only onextracellular bacilli (because of poor penetration

770S
EC
TIO
N12
ANTIMICROBIAL DRUGS
into cells). Thus, other drugs and host defencemechanisms are needed to eradicate the disease.It penetrates tubercular cavities, but does not crossto the CSF, and has poor action in acidic medium.
Resistance developed rapidly when strepto-mycin was used alone in tuberculosis—mostpatients had a relapse. Recent studies indicateworldwide increase in resistance to S. In caseof S-resistant infection, it must be stopped atthe earliest because of risk of S-dependence,in which case the infection flourishes when thedrug is continued. Most nontubercular myco-bacteria are unaffected by S.
Because of need for i.m. injections and lowermargin of safety (ototoxicity and nephrotoxicity,especially in the elderly and in those withimpaired renal function) S is used only as analternative to or in addition to other 1st line anti-TB drugs. Use is restricted to a maximum of2 months. It is thus also labelled as a‘supplemental’ 1st line drug.
SECOND LINE ANTI-TB DRUGS
These are less effective and/or less well toleratedanti-TB drugs that are used only in case the bacilliare resistant to one or more 1st line drugs orwhen these are not tolerated/are contraindicated.
1. Kanamycin (Km), Amikacin (Am)These are tuberculocidal aminoglycoside antibiotics (describedin Ch. 53), very similar in antitubercular activity, pharmacokineticproperties and types of adverse effects to S. Many S resistantand MDR strains of M.tuberculosis remain sensitive to them.One of these is mostly included in the regimen for MDR-TBduring the intensive phase. The RNTCP standardized regimenfor MDR-TB includes Km (probably because it is less expensivethan Am), but in many countries Am is preferred, because it isconsidered less toxic. Cross resistance between Km and Am isvery common. Both Km and Am produce less vestibular toxicitythan hearing loss, but are equally nephrotoxic. Patients shouldbe instructed to report vertigo and tinnitus. Audiometry andmonitoring of renal function is recommended.Dose: 0.75–1.0 g/day (10–15 mg/kg/day) i.m.
2. Capreomycin (Cm)It is a cyclic peptide antibiotic, chemically very different fromaminoglycosides, but with similar mycobactericidal activity,ototoxicity and nephrotoxicity. In addition, Cm often causeseosinophilia, rashes, fever and injection site pain. It has to be
injected i.m. and is used only as alternative toaminoglycoside antibiotics. Many M.tuberculosis isolatesresistant to S and Am, as well as MDR-TB remain susceptibleto Cm.Dose: 0.75–1.0 g/day i.m.KAPOCIN 0.5 g, 0.75 g, 1.0 g inj, CAPREOTEC 1.0 inj.
3. Fluoroquinolones (FQs)Fluoroquinolones (FQs) like ofloxacin (Ofx),levofloxacin (Lfx), ciprofloxacin (Cfx) andmoxifloxacin (Mfx) are relatively new potent oralbactericidal drugs for TB, that have gainedprominence as well tolerated alternatives to 1stline anti-TB drugs. They are active against MAC,M. fortuitum and some other atypical mycobac-teria as well. Mfx is the most active FQ againstM.tuberculosis, while Lvx is more active than Ofxand Cfx. On the other hand, Cfx is more activethan Lfx against atypical mycobacteria. The FQspenetrate cells and kill mycobacteria lodgedinside macrophages as well. Though Cfx wasinitially used in TB, it is not favoured now becauseof its extensive use in other bacterial infectionsand chances of resistance.
The primary indication of FQs is for treatmentof drug resistant TB. They have also been tried in1st line regimens for new cases. Substitution of Ewith Mfx to accompany RHZ in the four drugregimen has been found to enhance the rate ofbacillary killing and cause faster sputumconversion. In contrast Cfx, Ofx and Lfx did notenhance the sterilizing ability of R and H, and wereno better than E. Thus, addition of Mfx to RHZregimen holds the possibility of reducing theduration of treatments of TB from 6 months withRHZE used currently. However, experience withMfx in the treatment of TB is still limited, and itis not routinely used.
FQs are a key component of all regimens forMDR-TB, except when bacilli are found to beresistance to them. The RNTCP have included Ofx/Lfx in the standardized regimen for MDR-TB. Ifused alone, mycobacterial resistance to Ofx, Lfxand Cfx develops rapidly by mutation of DNAgyrase gene. Interestingly, experimental dataindicates that resistance against Mfx is slow to

771C
HA
PTER55
ANTITUBERCULAR DRUGS
develop.Dose: Ofloxacin 800 mg OD
Levofloxacin 750 mg OD For > 45 kgMoxifloxacin 400 mg OD body weight
4. Ethionamide (Eto)It is an antitubercular drug of moderate efficacy, introduced in1956, which acts on both extra- and intracellular bacilli. Fewatypical mycobacteria including MAC are also susceptible.Chemically it resembles INH, but contains sulfur. The mecha-nism of action is also similar to INH: it is converted bymycobacteria into an active intermediate which interferes withmycolic acid synthesis. Resistance to Eto mosly results frommutation of the gene that encodes for the Eto activating enzyme.Eto is nearly completely absorbed orally, distributed all overand crosses into CSF. It is completely metabolized in liver andhas a short t½ of 2–3 hours.
Tolerability of Eto is poor; frequent adverse effects are—anorexia, nausea, vomiting, salivation, metallic taste, epigastricdiscomfort, sulfurous belching and hepatitis. It also causesaches and pains, peripheral neuritis, behavioural changes,rashes, impotence, menstrual disturbances and goiter onprolonged use. To improve tolerance, dosing may initiatedat 250 mg/day, and increased every 5–6 days to reach 750mg/day (10–15 mg/kg/day). Pyridoxine (100 mg/day) canmitigate the neurological adverse effects.
Ethionamide is used only for drug-resistant TB. It is acomponent of the RNTCP standardized regimen for MDR-TBand an optional drug for inclusion into the treatment regimen ofMAC infection in AIDS patients. It is also a reserve drug forleprosy.ETHIDE, MYOBID, ETHIOKOX 250 mg tab.
5. Prothionamide (Pto)A close congener of Eto, to which it resembles in antimyco-bacterial property, mechanism of action, pharmacokinetics andadverse effects. Clinically it is cosidered interchangeable withEto for use in MDR-TB, MAC infection, etc.PROTHICID, PETHIDE 250 mg tab.
6. Cycloserine (Cs)This antibiotic obtained from S.orchidaceus is an analogue ofD-alanine. Accordingly, it inhibits bacterial cell well synthesisby inactivating the enzymes which racemize L-alanine and linktwo D-alanine residues. Cs is tuberculostatic; in additioninhibits MAC as well as some other gram-positive bacteria,E.coli and Chlamydia. Resistance to Cs develops slowly; nocross resistance with any other anti-TB drugs occurs.
Oral absorption of Cs is good; it diffuses all over the body;CSF concentration is equal to that in plasma. About 1/3 of adose is metabolized; the rest is excreted unchanged in urine;plasma t½ is 9 hours. Adverse effects of Cs are primarilyneurological; about half of the recipients experience neuro-psychiatric symptoms, viz. sleepiness, headache, tremor, slurringof speech, altered behaviour, depression or frank psychosis.Seizures are infrequent. Pyridoxine 100 mg/day can reduceneurotoxicity and prevent convulsions. Fall in BP has
been noted. Cs is contraindicated in patients with a historyof mental illness or seizures. Cycloserine is used only forresistant TB, especially MDR cases. It is included in thestandardized regimen used by RNTCP for MDR-TB.Dose: Start with 250 mg BD, increase if tolerated to750 mg/day for patients with body weight >45 kg.CYCLORINE, COXERIN, MYSER 250 mg cap.
7. TerizidoneIt contains 2 molecules of cycloserine and has antibacterialproperties as well as mechanism of action similar to it; butis believed to be less neurotoxic; reported incidence of adverseeffects is lower. It is used as a substitute of Cs, especiallyin genitourinary TB, because it attains higher and longerlasting concentration in urine. Dosage are similar to Cs;500–750 mg/day.TERICOX 250 mg cap.
8. Para-amino salicylic acid (PAS)Introduced in 1946, PAS is related to sulfonamides and actsprobably by the same mechanism, i.e. inhibition of folatesynthase. It is not active against other bacteria, and thisselectivity may be due to difference in the affinity for folatesynthase of M.tuberculosis compared to that of other bacteria.However, other mechanisms of action are also possible.
PAS is tuberculostatic and one of the least active drugs:does not add to the efficacy of more active drugs that are givenwith it; only delays development of resistance—probably bydirectly inhibiting episomal resistance transfer. Resistance toPAS is slow to develop. It is used as the sodium salt (largedoses that are needed may cause Na+ overload) or calcium salt(better gastric tolerance is claimed).
PAS is absorbed completely by the oral route anddistributed all over except in CSF. About 50% PAS is acetylated;competes with acetylation of INH and prolongs its t½. It isexcreted rapidly by glomerular filtration and tubular secretion;t½ is short, ~1 hour.
Patient acceptability of PAS is poor because of frequentanorexia, nausea and epigastric pain. Other adverse effects arerashes, fever, malaise, hypokalaemia, goiter, liver dysfunctionand rarely blood dyscrasias.
PAS is used only in resistant TB. The RNTCP includes it inthe standardized regimen for MDR-TB only when one of thetuberculocidal drugs (Km, Ofx, Z, Eto) or both the static drugs(E, Cs) cannot be used.Dose: 10–12 g (200 mg/kg) per day in divided doses;SODIUM-PAS 0.5 g tab, 80 g/100 g granules.
9. Thiacetazone (Thz)Its efficacy in TB is now considered uncertain, and it is notindicated, even as a reserve drug, in MDR-TB.
10. RifabutinIt is related to rifampin in structure and mechanism of action,but is less active against M.tuberculosis, and more activeagainst MAC. Majority of M.tuberculosis isolates resistantto R are cross resistant to rifabutin. Thus, it is not an optionfor treatment of MDR-TB. The only place of rifabutin
⎫⎬⎭

772S
EC
TIO
N12
ANTIMICROBIAL DRUGS
in the treatment of TB is as a substitute for R to minimisedrug interactions due to strong enzyme inducing propertyof R. Rifabutin is a much weaker inducer of CYP enzymesthan R. This is especially needed in HIV coinfectedpatients of TB who receive a protease inhibitor (PI)and/or a non-nucleoside reverse transcriptase inhibitor(NNRTI) whose metabolism is markedly induced by Rrendering them ineffective.
The primary indication of rifabutin is for prophylaxis andtreatment of MAC infection in HIV-AIDS patients. Forprophylaxis of MAC, rifabutin alone 300 mg/day is analternative to azithromycin/clarithromycin, while for treatmentof MAC infection, it is combined with 2–3 other anti-MACdrugs. Gastrointestinal intolerance, rashes, granulocytopenia,myalgia and uveitis have been reported with rifabutin.Reactions similar to those caused by R can also occur. Oralbioavailability of rifabutin is low (~20%), but t½ is much longer(>30 hours).Dose: 300 mg (5 mg/kg) OD oral; RIBUTIN 150 mg tab.
Some antitubercular combinationsRIFATER: Rifampin 120 mg, isoniazid 80 mg, pyrazinamide 250mg tab.R-CINEX: Rifampin 600 mg, isoniazid 300 mg tab; R-CINEX-Z:Rifampin 225 mg, isoniazid 150 mg, pyrazinamide 750 mg tab.RIMACTAZID, RIFADIN-INH, Rifampin 450 mg, isoniazid 300mg tab.MYCONEX 600 and 800; Isoniazid 300 mg, ethambutol 600 mgor 800 mg tab, COMBUNEX Isoniazid 300 mg, ethambutol 800mg tab.ARZIDE, ISORIFAM: Rifampin 450 mg, isoniazid 300 mg cap.BI-TEBEN, ISOZONE, UNITHIBEN: Isoniazid 75 mg, thiace-tazone 37.5 mg tab, ISOZONE FORTE—double strength.INAPAS: sod PAS 834 mg, isoniazid 25 mg tab; sod PAS 3.34 g+ isoniazid 100 mg per measure granules.INABUTOL: Isoniazid 150 mg, ethambutol 400 mg tab;INABUTOL FORTE—double strength.ISOKIN–300: Isoniazid 300 mg, vit B6 10 mg tab.IPCAZIDE: Isoniazid 100 mg, vit B6 5 mg per 5 ml liq.
Antitubercular combipacks (packs of 1 day’s dose)AKT-4: R 450 mg 1 cap + Z 750 mg 2 tab +
E 800 mg H 300 mg 1 tab.AKT-3: R 450 mg 1 cap + E 800 mg H 300 mg
1 tab.CX-5: R 450 mg 1 cap + Z 750 mg 2 tab + E 800
mg H 300 mg pyridoxine 10 mg 1 tab.RIFACOM-Z and: R 450 mg H 300 mg 1 tab. + Z 750 mgRIMACTAZIDE-Z 2 tab.RIFACOM-EZ: R 450 mg H 300 mg 1 tab. + Z 750 mg
2 tab + E 800 mg 1 tab.Fixed dose combination of antitubercular drugs with vitamins(except INH + Vit B6) are banned in India.
TREATMENT OF TUBERCULOSISThe therapy of tuberculosis has undergoneremarkable changes.
The ‘conventional’ 12–18 month treatment hasbeen replaced by more effective and less toxic6 month (short course) treatment which also yieldshigher completion rates. This has been possibledue to better understanding of the biology oftubercular infection and the differential propertiesof the antitubercular drugs.Biology of tubercular infection M. tuberculosis isan aerobic organism. In unfavourable conditions it growsonly intermittently or remains dormant for prolongedperiods. Several subpopulations of bacilli, each with adistinctive metabolic state, could exist in an infectedpatient, e.g.:(a) Rapidly growing with high bacillary load as in thewall of a cavitary lesion where oxygen tension is high andpH is neutral. These bacilli are highly susceptible to H andto a lesser extent to R, E and S.(b) Slow growing located intracellularly (inside macro-phages) and at inflamed sites where pH is low. They areparticularly vulnerable to Z, while H, R and E are less active,and S is inactive.(c) Spurters found mostly within caseous material whereoxygen tension is low but pH is neutral: the bacilli growintermittently with occasional spurts of active metabolism. R ismost active on this subpopulation.
(d) Dormant some bacilli remain totally inactive forprolonged periods. No antitubercular drug is significantly activeagainst them.
However, there is continuous shifting of bacilli betweenthese subpopulations.
The goals of antitubercular chemotherapy are:
(a) Kill dividing bacilli Drugs with earlybactericidal action rapidly reduce bacillary loadin the patient and achieve quick sputum negativityso that the patient is non-contagious to the com-munity: transmission of TB is interrupted. Thisalso affords quick symptom relief.
(b) Kill persisting bacilli To effect cure andprevent relapse. This depends on sterilizingcapacity of the drug.
(c) Prevent emergence of resistance So thatthe bacilli remain susceptible to the drugs.
The relative activity of the first line drugs inachieving these goals differs, e.g. H and R arethe most potent bactericidal drugs active againstall populations of TB bacilli, while Z acts beston intracellular bacilli and those at inflamed

773C
HA
PTER55
ANTITUBERCULAR DRUGS
sites. It thus has very good sterilizing activity.On the other hand S is active only against rapidlymultiplying extracellular bacilli. E is bacterio-static—mainly serves to prevent resistance andmay hasten sputum conversion.
Drug combinations are selected to maximisethe above actions together with considerationsof cost, convenience and feasibility. The generalprinciples of antitubercular chemotherapy are:• Use of any single drug in tuberculosis results
in the emergence of resistant organisms andrelapse in almost 3/4th patients. A combina-tion of two or more drugs must be used. Therationale is: the incidence of resistant bacillito most drugs ranges from 10–8 to 10–6.Because an average patient of pulmonarytuberculosis harbours 108 to 1010 bacilli, thenumber of organisms that will not respond toa single drug is high and cannot be dealt bythe host defence. During protracted treatment,these bacilli multiply and become dominantin 3–4 months. Because insensitivity to onedrug is independent of that to another, i.e.incidence of H resistance among bacilliresistant to R will be 10–6 and vice versa; onlyfew bacilli will be resistant to both; thesecan be handled by host defence. By thesame rationality, massive infection (>1010
organisms) has to be treated by at least 3 drugs;and a single drug is sufficient for prophylaxis,because the number of bacilli is small.
• Isoniazid and R are the most efficacious drugs;their combination is definitely synergistic—duration of therapy is shortened from > 12months to 9 months. Addition of Z for theinitial 2 months further reduces duration oftreatment to 6 months.
• A single daily dose of all first line anti-tubercular drugs is preferred. The ‘directlyobserved treatment short course’ (DOTS) wasrecommended by the WHO in 1995.
• Response is fast in the first few weeks asthe fast dividing bacilli are eliminated rapidly.Symptomatic relief is evident within 2–4weeks. The rate of bacteriological, radio-logical and clinical improvement declines
subsequently as the slow multiplying orga-nisms respond gradually. Bacteriological curetakes much longer. The adequacy of anyregimen is decided by observing sputumconversion rates and 2–5 year relapse ratesafter completion of treatment.
Conventional regimens These consist of H + Tzn or Ewith or without S (for initial 2 months) and require 12–18months therapy. Failure rates are high, compliance is poor—therefore not used now.
SHORT COURSE CHEMOTHERAPY
After several years of trial, the WHO introduced6–8 month multidrug ‘short course’ regimensin 1995 under the DOTS programme. An expertgroup framed clearcut treatment guidelines in1997 for different categories of TB patients,who were grouped according to site and severityof disease, sputum smear positivity/negativity andhistory of previous treatment (new case/previously treated case) into 4 categories:Category I: New case of sputum smear positive or severepulmonary TB, or severe forms of extrapulmonary TB(meningitis, etc.).Category II: Defaulted, irregularly treated and relapse cases.Category III: New sputum smear negative pulmonary TB andless severe forms of extrapulmonary TB (glandular/skin TB,etc.).Category IV: Chronic cases who remained or again becamesputum smear positive after receiving fully supervisedcategory II treatment.The dose of all first line drugs was standardizedon body weight basis, applicable to both adultsand children. These guidelines were implementedby India and other WHO member countries,making major progress in global TB control. The‘stop TB strategy’ of WHO was launched in 2006and the spread of MDR-TB was taken intoaccount. On the basis of experience gained, newguideline with revised categorization of patientshas been brought out in 2010. According to these,the category III has been merged with categoryI, and patients of TB are now classified onlyas “New cases’ or ‘Previously treated’ patients,and drug resistant including MDR-TB. Therecommended doses of first line drugs are givenin Table 55.1 and the treatment regimens aresummarized in Table 55.2.

774S
EC
TIO
N12
ANTIMICROBIAL DRUGS
TABLE 55.1 Recommended doses of antitubercular drugs@
Daily dose 3 times per week dose
DRUG mg/kg maximum mg/kg daily maximum
Isoniazid (H) 5 (4–6) 300 mg 10 (8–12) 900 mg
Rifampin (R) 10 (8–12) 600 mg 10 (8–12) 600 mg
Pyrazinamide (Z) 25 (20–30) - 35 (30–40) -
Ethambutol (E) 15 (15–20) - 30 (25–35) -
Streptomycin (S)* 15 (12–18) - 15 (12–18) 1000 mg
* Patients over 60 years age—10 mg/kg or 500–750 mg/day (i.m.).@ Adopted from Treatment of Tuberculosis: Guidelines, 4th edition (2010), WHO, Geneva.
TABLE 55.2 Categorywise treatment regimens for tuberculosis (adopted from WHO guidelines 2010)*
Category Intensive phase Continuation phase Duration Comment(months)
I 2$ HRZE daily 4$ HR daily 6$ OptimalNew patient
2 HRZE daily 4 HR thrice weekly 6 Acceptable if DOT ensured
2 HRZE thrice 4 HR thrice weekly 6 Acceptable if DOT ensured,weekly and no HIV coinfection or
its risk
IIPreviously treated 2 HRZES daily 5 HRE daily 8 For patient with low/mediumpatients pending + risk of MDR-TBDST result 1 HRZE daily (failure, default, etc.)
Empirical£ Empirical 18–24 For patient with high risk of(standardized) (standardized) or MDR-TB (failure, 2nd default,MDR-regimen MDR-regimen till DST contact of MDR-TB, etc.)
result
DST—Drug sensitivity testing; DOT—Directly observed therapyH, R, Z, E, S—Standard codes for isoniazid, rifampin, pyrazinamide, ethambutol and streptomycin, respectively.$—The neumerals indicate duration of a phase/total duration in months.£—Empirical (Standardized) MDR regimen is country specific depending upon local data and situation (Indianregimen on p.776)
*Treatment of tuberculosis: Guidelines, 4th edition (2010), WHO, Geneva.
All regimens have an initial intensive phasewith 4–5 drugs lasting 2–3 months aimed torapidly kill the bacilli, bringing about sputumconversion and afford fast symptomatic relief.This is followed by a continuation phase with2–3 drugs lasting 4–5 months during which theremaining bacilli are eliminated so that relapsedoes not occur.
New patient (Category I)Initial treatment with 4 drugs (HRZE) including3 bactericidal drugs reduces the risk of selectingresistant bacilli, especially in the face of increa-sing primary H resistance which is now 7–18%among new cases. After the intensive phase whenfew bacilli are left, only 2 highly effective cidaldrugs in the continuation phase are enough toeffect cure. Extension of intensive phase beyond

775C
HA
PTER55
ANTITUBERCULAR DRUGS
2 months (suggested earlier for patients whoremain sputum positive at 2 months) is notrecommended now. However, in such cases, someauthorities recommend 9 month treatmentinstead of 6 months.
The frequency of dosing during the intensivephase or the continuation phase or both can bedaily or thrice weekly (Table 55.2). Daily treat-ment during both phases is considered optimal,because it may help to prevent acquisition ofresistance even in patients who start with primaryH resistance. However, keeping in view theconstraints in organizing daily supervision ofdrug administration, and to reduce drug costs,thrice weekly therapy is acceptable in the conti-nuation phase, provided each dose is supervised.If constraints are still pressing, even the intensivephase could be thrice weekly, but then HIVcoinfection or possibility of contacting it duringtherapy is to be ruled out. In areas with highlevel of primary H resistance, WHO suggestsinclusion of E (along with H and R) in thecontinuation phase.
Previously treated patients (Category II)Smear positive TB patients who in the past havebeen exposed to anti-TB drugs, but did notcomplete the course or took inadequate/irregularmedication, or relapsed after responding, orfailed to respond run a higher risk of harbouringdrug resistant (DR) bacilli.As per WHO data 13% of globally notified TB patients in2007 were retreatment cases. In 2010 India notified a totalof about 1.52 million TB patients out of which about0.29 million (~ 19%) were retreatment cases (RNTCP data).
The bacilli may be resistant to one or more1st line drugs. It is crucial to identify MDR cases,because in them continuing treatment with Ist
line drugs alone is not only ineffective, but alsoamplifies drug resistance. It is important toculture the bacilli in each of the retreatmentcases and determine drug sensitivity, which willhelp in identifying MDR cases and in devisingthe most appropriate drug therapy for that patient.Drug sensitivity testing (DST) is still mostlydone by conventional methods which take atleast4–6 weeks. However, rapid DSTs are now
available at few places which take <10 days, butare expensive and not routinely done. Most ofthe time the DST results are not available beforestarting treatment. The recommended strategy insuch situation is outlined in Table 55.2.
The option of thrice weekly drug therapy isnot available for retreatment cases, because alltypes of DR-TB must receive daily treatment.The risk of MDR-TB should be assessed in eachcase taking help of the local surveillance data.In general defaulting, interrupted treatment andrelapse patients have lower risk of MDR-TBcompared to failure cases, especially those whofail after receiving R for 6 months, or thosewho interrupt treatment more than once or havecontacted infection from a MDR-TB case.
If the risk of MDR-TB in a particular patientis assessed as low or medium, a regimencontaining 1st line drugs is prescribed. In theintensive phase HRZES (5 drugs) are given dailyfor 2 months and HRZE (4 drugs) for anothermonth. This is followed by the continuation phaseof 3 drugs (HRE) for the next 5 months. This8 month empirical regimen should not beaugmented by an injectable 2nd line drug or aFQ, because this may compromise efficacy ofthese drugs which are crucial for treatment ofMDR-TB. The treatment regimen should bemodified as and when result of DST becomesavailable. Outcome of all regimens should bemonitored by clinical assessment as well as bysputum smear and culture examination.
Retreatment patients whose MDR-TB risk isassessed as high should be started on anempirical/standardized MDR-TB regimen whichis formulated by each country according to itslocal surveillance data and other factors. Thesepatients are treated as presumed MDR cases tillDST results become available. The definitiveregimen is decided thereafter.
Multidrug-resistant (MDR) TBMDR-TB is defined as resistance to both H andR, and may be any number of other (1st line)drug(s). MDR-TB has a more rapid course withworse outcomes. Its treatment requires complex

776S
EC
TIO
N12
ANTIMICROBIAL DRUGS
multiple 2nd line drug regimens which are longer,more expensive and more toxic. In India MDR-TB accounts for 2.8% of all new TB cases and12–17% of retreatment cases in different states.These figures are close to the global average inci-dence. As per WHO, India has the highest numberof MDR-TB cases in South-East Asia. The generalprinciples of treatment of MDR-TB are:• The regimen should have at least 4 drugs
certain to be effective. Often 5–6 drugs areincluded, since efficacy of some may beuncertain.
• Reliance about efficacy may be placed onsurvey of similar patients who have beentreated, DST results (applicable to H, R, Km,Am, Cm, FQs), and the anti-TB drugs usedpreviously in that individual.
• Avoid combining cross resistance drugs, e.g.two FQs, Km with Am or Eto with Pto, orCs with terizidone.
• Include drugs from group I to group IV(alternative classification) in a hierarchialorder. Group I drugs (except H and R) canbe included, add one injectable drug (groupII), One FQ (group III) and one or two groupIV drugs.
The RNTCP initiated the DOTS-plus programmein the year 2000 to cover the diagnosis andtreatment of MDR-TB. It has updated its strategyand brought up the revised DOTS-Plus guidelinesin 2010, so that they are in consonance withthe current WHO guidelines. According to theDOTS-Plus guidelines a case of R resistanceis also treated as MDR-TB. The RNTCP hasdevised a ‘standardized’ treatment regimen (alsocalled category IV regimen), of 6 drugs intensivephase lasting 6–9 months and 4 drugscontinuation phase of 18 months (see box), whichis used in all confirmed or suspect MDR-TBcases, unless DST results or other specifics(intolerance, etc.) of an individual casenecessitate use of an ‘individualized regimen’,which is constructed taking into account theseindividual specific features.
The minimal 6 month intensive phase isextended by 1 month each time till a maximum
of 9 months, if the sputum culture put up atthe end of 4th, 5th and 6th month respectivelyare positive. PAS is substituted in place of anyone of the cidal drugs (Km, Ofx, Z or Eto) ortwo of the static drugs (E, Cs) when these arenot tolerated. Pyridoxine 100 mg/day is givento all patients during the whole course of therapyto prevent neurotoxicity of the anti-TB drugs.This standardized regimen used under DOTS-Plus has been found to be highly successful, withfailure rate of 6% among category-2MDR cases(patients who had failed 1st line treatment) and2% among category-1MDR cases (contacts ofMDR-TB).
Extensively drug-resistant TB These areMDR-TB cases that are also resistant to FQsas well as one of the injectable 2nd line drugsand may be any number of other drugs. Thebacilli thus are resistant to at least 4 mosteffective cidal drugs, viz. H,R,FQ and one ofKm/Am/Cm.
In USA 3% of MDR-TB cases have been found to be XDR.The exact incidence of XDR-TB in India is not known, but withexpanding laboratory facilities to conduct sensitivity tests for2nd line drugs more XDR-TB cases are likely to be confirmed.The MDR-TB treatment failure cases (between 2–6%) may bepresumed to be XDR.
The XDR-TB is very difficult to treat, hasa rapid course and high mortality. However, toprevent further amplification of resistance, thestandardized MDR regimen (category IV treat-ment) must be immediately stopped when XDR-
Standardized RNTCP regimen for MDR-TB*
Intensive phase Continuation phase(6–9 months) (18 months)
1. Kanamycin (Km) 1. Ofloxacin or2. Ofloxacin (Ofx) or Levofloxacin
Levofloxacin (Lfx) 2. Ethionamide3. Ethionamide (Eto) 3. Cycloserine4. Cycloserine (Cs) 4. Ethambutol5. Pyrazinamide (Z)6. Ethambutol (E)
+ Pyridoxine 100 mg/day
* Revised National Tuberculosis Control Programme:DOTS-Plus Guidelines (2010); Central TB Division,Directorate General of Health Services, Ministry of Health& Family Welfare, New Delhi.

777C
HA
PTER55
ANTITUBERCULAR DRUGS
TB is detected or suspected. An expert panel maydecide on instituting category V treatment,including the group V drugs (alternativeclassification, see p. 766), which have uncertainefficacy and are expensive. Some new drugs likePA-824 and TMC-207 are also being evaluated.
Tuberculosis in pregnant women TheWHO and British Thoracic Society consider H,R, E and Z to be safe to the foetus andrecommend the standard 6 month (2HRZE +4HR) regimen for pregnant women with TB.S is contraindicated because it is ototoxic tothe foetus. However, Z is not recommended inthe USA (due to lack of adequate teratogenicitydata). In India, it is advised to avoid Z, and totreat pregnant TB patients with 2 HRE + 7HR(total 9 months). Treatment of TB should notbe withheld or delayed because of pregnancy.All pregnant women being treated with INHshould receive pyridoxine 10–25 mg/day.
Treatment of breastfeeding women Allanti-TB drugs are compatible with breastfeeding;full course should be given to the mother, butthe baby should be watched (See Appendix-4).The infant should receive BCG vaccination and6 month isoniazid preventive treatment afterruling out active TB.
Management of patients with adverse drugreactions to antitubercular drugs Minorside effects are to be managed symptomaticallywithout altering medication; e.g. nausea, ano-rexia—give the drugs with small meals; drowsi-ness—give drugs before bed time; flu syndromedue to intermittent dosing of R—change to dailydosing of R; Z induced arthralgia can be treatedby analgesic-NSAIDs; peripheral neuritis due toH can be mitigated by pyridoxine. If more severereactions like skin rashes, itching develop, alldrugs should be stopped promptly. Afterresolution of the reaction, the drugs are to bereintroduced one at a time by challenging withsmall doses and increasing every 3 days. Whenthe offendng drug is identified, it should bestopped and the regimen reconstituted. However,R should never be reintroduced in case of severe
reaction such as haemolysis, thrombocytopeniaor renal failure. Ethambutol should bediscontinued at the first sign of optic neuritis.
Hepatotoxicity is the most common problemwith antitubercular drugs. Any one or more ofH, R and Z could be causative and the reactionoccurs more frequently when, as per standardprotocol, combination of these drugs is used.In case hepatitis develops, all drugs should bestopped and the reaction allowed to subside. IfTB is severe nonhepatotoxic drugs S + E + OneFQ should be started while the reaction clears.Subsequently, drugs are restarted one at a time.Generally, R is resumed first followed 7 dayslater by H. If hepatitis recurs, the last added drugis stopped permanently and the regimen isreconstructed. In case both R and H aretolerated—do not restart Z but prolong therapywith R and H to 9 months. If R is the culprit,HES may be given for 2 months followed byHE for 10 months. If H is implicated, REZ maybe given for 9 months. If both R and H cannotbe given, the S, E, FQ regimen should beadministered for 18–24 months.
Chemoprophylaxis The purpose is to preventprogression of latent tubercular infection to activedisease. This is indicated only in :(a) Contacts of open cases who show recentMantoux conversion.(b) Children with positive Mantoux and a TBpatient in the family.(c) Neonate of tubercular mother.(d) Patients of leukaemia, diabetes, silicosis, orthose who are HIV positive but are not anergic,or are on corticosteroid therapy who show apositive Mantoux.(e) Patients with old inactive disease who areassessed to have received inadequate therapy.
The standard drug for chemoprophylaxis of TBis H 300 mg (10 mg/kg in children) daily for 6months. This is as effective in HIV patients as inthose with normal immune function. Because ofspread of INH resistance, a combination of H (5mg/kg) and R (10 mg/kg, maximum 600 mg) dailygiven for 3 months is preferred in some areas. The

778S
EC
TIO
N12
ANTIMICROBIAL DRUGS
CDC (USA) recommends 4 months R prophylaxisin case H cannot be used.
Several regimens, including one with E + Z± one FQ, have been suggested for subjectsexposed to MDR-TB. However, there is noconsensus about the most appropriate drug(s)or duration of prophylaxis that should be used.The RNTCP therefore recommend that MDR-TB contacts should be watched without givingany prophylactic medication, and treatedpromptly if they develop active disease.
Role of corticosteroids Corticosteroidsshould not be ordinarily used in tubercularpatients. However, they may be used underadequate chemotherapeutic cover:(a) In seriously ill patients (miliary or severepulmonary TB) to buy time for drugs to act.(b) When hypersensitivity reactions occur toantitubercular drugs.(c) In meningeal/renal/pericardial TB or pleuraleffusion—to reduce exudation, prevent itsorganisation and strictures, etc.(d) In AIDS patients with severe manifestationsof tuberculosis.
Corticosteroids are contraindicated in intestinaltuberculosis because silent perforation can occur.
Corticosteroids, if given, should be graduallywithdrawn when the general condition of thepatient improves.
Tuberculosis in AIDS patients The associa-tion of HIV and TB infection is a seriousproblem. HIV positive cases have a higherincidence of extrapulmonary, more severe, morelethal and more infectious TB. HIV infectionis the strongest risk factor for unmasking latentTB. Moreover, adverse reactions to anti-TB drugsare more common in HIV patients. It is estimatedthat 2.4 million Indians are currently living withHIV. Recent countrywide data shows that 5% ofTB patients in India are HIV positive.
On the other hand, institution of ‘highly activeantiretroviral therapy’ (HAART) and improvementin CD4 cell count of the subject markedly reducesthe incidence of TB among HIV-AIDS patients.When CD4 count is <150 cells/µL, extrapulmonaryand dual TB is more commonly encountered.
In case of M. tuberculosis infection, drugsused are the same as in non-HIV cases, and atleast 4 drugs are used. Initial intensive phasetherapy with daily HRZE for 2 months is startedimmediately on the diagnosis of TB, and isfollowed by a continuation phase of HR for4–7 months (total 6–9 months). Thrice weeklyregimen should not be used, because it isassociated with 2–3 times higher rate of relapseand failure among HIV positive patients, and riskof acquiring resistance to R is increasedcompared to daily treatment. Some expertsrecommend prolonging the continuation phasewith HR from 4 months to 7 months or to give3 drugs (HRE) for 4 months in the continuationphase. Pyridoxine 25–50 mg/day is routinelygiven along with H to counteract its neurologicalside effects, which are more likely in AIDSpatients. All HIV positive TB patients should alsoreceive cotrimoxazole preventive therapy at leastthroughout the anti-TB regimen. This has beenfound to reduce mortality, probably by preventingPneumocystis jirovecii and other infections.
Consideration also has to be given to possibledrug interactions between anti-TB and anti-retroviral (ARV) drugs. Rifampin, a potentinducer of CYP isoenzymes, markedly enhancesthe metabolism of protease inhibitors (PIs, viz.indinavir, nelfinavir, ritonavir) and of NNRTIs,viz. nevirapine, efavirenz (to a lesser extent)making them ineffective. In patients receivingthese drugs, rifabutin (a less potent enzymeinducer) given for 9–12 months may besubstituted for rifampin. The metabolism ofnucleoside reverse transcriptase inhibitors(NRTIs, zidovudine, etc.) is not induced byrifampin, and no dose adjustment is needed. Analternative regimen of 3 NRTIs (zidovudine +lamivudine + abacavir) has been advocated forpatients who are to be treated by rifampin. If2 NRTI + NNRTI is to be used, efavirenz shouldbe selected as the NNRTI because its metabolismis induced to a lesser extent.
MDR-TB in HIV-AIDS patients should betreated in the same way as that in non-HIVinfected patient for a total of 18–24 months.

779C
HA
PTER55
ANTITUBERCULAR DRUGS
Mycobacterium avium complex (MAC)infectionMAC is an opportunistic pathogen which causesdisseminated and multifocal disease in immuno-compromized (HIV-AIDS) patients. The diseasedevelops when cell mediated immunity ismarkedly depressed, i.e. when CD4 count dropsto <50 cells/μL, HIV-RNA load is high and otheropportunistic infections (P. jirovecii, etc.) arealso present. The newer macrolide antibioticsare particularly active drugs against MAC.Clarithromycin and azithromycin have weak activity againstM.tuberculosis but are the most active drugs against MAC,M. fortuitum, M. kansasii and M. marinum. Clarithromycin haslower MICs against these mycobacteria than azithromycin, butthe latter may be equally efficacious due to its higher tissueand intracellular levels as well as longer stay in the body.
Therapy of MAC infection Eradication ofMAC has not been achieved by any drug orregimen. Therapy is directed to suppress thedisease and afford symptomatic relief untillimmune status of the patient improves byHAART. A favoured regimen consists of 3 or4 drug intensive phase followed by 2 drug main-tenance phase as outlined in the box. The benefitof adding a FQ as the 4th drug is not clear.
The duration of intensive phase is dependenton the response, viz. till CD4 count rises > 100cells/μL and symptomatic relief is obtained, whichmay take 2–6 months. The maintenance therapyis continued till a minimum of 12 months, or thepatient becomes asymptomatic for MAC infection
PROBLEM DIRECTED STUDY
55.1 A 45-year-old male factory worker weighing 60 kg reports to the hospital with coughand expectoration, mild chest pain, weakness and fatigue for the last one month. In additionhe has developed low grade fever for the last one week. He gives history of having sufferedfrom TB of the lung one year back for which he took treatment from the hospital and becameall right in 2 months. He stopped taking the medicines after another 1 month, though hewas told by the doctor to continue treatment. The sputum was found to be positive for AFBand X-ray chest showed a 5 cm cavitary lesion in the right middle lobe and fibrotic changesin the upper lobe. He was diagnosed to be a defaulted patient of pulmonary TB.(a) Should any specific laboratory test be ordered in this case; if so, should the treatmentstart immediately or after the report is available?(b) What should be the regimen of antitubercular drugs for this patient? Can he be treatedwith a thrice weekly dosing regimen?(see Appendix-1 for solution)
and CD4 count stays > 100 cell/μL for at least 6months. All patients must simultaneously receiveHAART for the HIV infection. Despite therapy,mortality remains high.
Prophylaxis of MAC infectionThis is aimed at protecting the AIDS patient fromdeveloping active MAC disease during the periodCD4 count remains below 50 cell/μL. A singledrug is used—azithromycin 1200 mg/week orclarithromycin 500 mg twice a day are thepreferred drugs. Rifabutin 300 mg/day is usedif either of these drugs cannot be given. Thisis continued till the simultaneously institutedHAART achieves complete suppression of HIVreplication, CD4 count rises above 100 cell/μLand stays there for at least 3 months.
Regimen for treatment of MAC infection
Intensive phase1. Clarithromycin 500 mg twice daily or
Azithromycin 500 mg once daily2. Ethambutol 1000 mg (15 mg/kg) per day3. Rifabutin 300 mg per day
+Ciprofloxacin 500 mg twice daily orLevofloxacin 500 mg once daily orMoxifloxacin 400 mg once daily
Maintenance phase*1. Clarithromycin/Azithromycin2. Ethambutol/Rifabutin/One fluoroquinolone
* Doses in the maitenance phase are the same asin intensive phase

Antileprotic DrugsChapterChapterChapterChapterChapter 5656565656
Leprosy, caused by Mycobacterium leprae, hasbeen considered incurable since ages and bearsa social stigma. Due to availability of effectiveantileprotic drugs now, it is entirely curable, butdeformities/defects already incurred may notreverse.
Chaulmoogra oil with weak antileprotic property was usedin Indian medicine for centuries. Shortly after thedemonstration of antibacterial property of sulfonamides,congeners were tested and dapsone, the parent sulfone, wasfound to be an active antileprotic. Demonstration of itsefficacy in experimental tuberculosis and leprosy led to clinicaltrials in the 1940s, and since then it is the sheet-anchor oftreatment of leprosy. Few other sulfones were added, but nonecould excel dapsone. Clofazimine was inducted in the early1960s as a useful adjunct, and soon rifampin, developed forTB, was found to be a rapidly acting cidal drug for M.lepraeas well. Lately good antileprotic activity has been detectedin some fluoroquinolones, macrolides and minocycline.
CLASSIFICATION
1. Sulfone Dapsone (DDS)2. Phenazine derivative Clofazimine3. Antitubercular drugs Rifampin,
Ethionamide4. Other antibiotics Ofloxacin,
Moxifloxacin,Minocycline,Clarithromycin
Dapsone (DDS)It is diamino diphenyl sulfone (DDS), thesimplest, oldest, cheapest, most active and mostcommonly used member of its class. All othersulfones have become obsolete.
Activity and mechanism Dapsone is che-mically related to sulfonamides and has the samemechanism of action, i.e. inhibition of PABAincorporation into folic acid by folate synthase.The antibacterial action of dapsone is antagonizedby PABA. It is leprostatic at very low concentra-tions, while growth of many other bacteriasensitive to sulfonamides is arrested at relativelyhigher concentrations. Specificity for M. lepraemay be due to difference in the affinity of itsfolate synthase. Doses of dapsone needed fortreatment of acute pyogenic bacterial infectionsare too toxic, so not used.
Dapsone-resistance among M. leprae, firstnoted in 1964, has spread and has necessitatedthe use of multidrug therapy (MDT). Whendapsone resistance is encountered in an untreatedpatient, it is called ‘primary’, and indicates thatthe infection was contacted from a patientharbouring resistant bacilli. Resistance whichdevelops during monotherapy in an individualpatient with dapsone is called ‘secondary’.Theincidence of primary dapsone resistance reportedfrom different parts of the world, from time-to-time, has been variable; whereas secondarydapsone resistance occurred in upto 20% patientstreated with monotherapy. The mechanism ofsecondary resistance appears to be the same asfor M. tuberculosis, i.e. selective propagationof resistant bacilli over time. Dapsone resistantM. leprae have mutated folate synthase whichhas lower affinity for dapsone. However, the peakserum concentration of dapsone after 100 mg/day dose exceeds MIC for M. leprae by nearly500 times; it continues to be active against lowto moderately resistant bacilli, and the risk ofrelapse due to dapsone resistance is reportedto be 2–3%. In addition to resistance, there isthe problem of ‘persisters’, that are drug

781C
HA
PTER56
ANTILEPROTIC DRUGS
sensitive bacilli which become dormant, hide insome tissues and are not affected by any drug.They may stage a comeback after the drug iswithdrawn.
Dapsone is active against certain protozoaas well. Combined with pyrimethamine, it is analternative to sulfadoxine-pyrimethamine forP. falciparum and Toxoplasma gondii infections,as well as for the fungus Pneumocystis jirovecii.Antiinflammatory property has been detected indapsone.
Pharmacokinetics Dapsone is completelyabsorbed after oral administration and is widelydistributed in the body, though penetration in CSFis poor. It is 70% plasma protein bound, but moreimportantly it is concentrated in skin (especiallylepromatous skin), muscle, liver and kidney.
Dapsone is acetylated as well as glucuronideand sulfate conjugated in liver. Metabolites areexcreted in bile and reabsorbed from intestine,so that ultimate excretion occurs mostly in urine.The plasma t½ of dapsone is variable, thoughoften > 24 hrs. The drug is cumulative due toretention in tissues and enterohepatic circulation.Elimination takes 1–2 weeks or longer.DAPSONE 25, 50, 100 mg tab.
Adverse effects Dapsone is generally welltolerated at doses 100 mg/day or less.Mild haemolytic anaemia is common. It is a dose-related toxicity—reflects oxidising property ofthe drug. Patients with G-6-PD deficiency aremore susceptible; doses > 50 mg/day producehaemolysis in such subjects.Gastric intolerance—nausea and anorexia arefrequent in the beginning, decrease later.Other side effects are methaemoglobinaemia,headache, paresthesias, mental symptoms anddrug fever.Cutaneous reactions include allergic rashes,fixed drug eruption, hypermelanosis, photo-toxicity and rarely exfoliative dermatitis.Hepatitis and agranulocytosis are rare complica-tions.
Sulfone syndrome It is the reaction whichdevelops 4–6 weeks after starting dapsone
treatment: consists of fever, malaise, lymph nodeenlargement, desquamation of skin, jaundice andanaemia. It is generally seen in malnourishedpatients, and has become more frequent after theintroduction of MDT. Some or all of the abovesymptoms may occur. Its treatment consists ofstopping dapsone and instituting corticosteroidtherapy along with supportive measures.
Contraindications Dapsone should not be usedin patients with severe anaemia (Hb < 7 g/dl),G-6-PD deficiency and in those showing hyper-sensitivity reactions.
Other use In combination with pyrimethamine,dapsone can be used for chloroquine-resistantmalaria, toxoplasmosis and P. jirovecii infection.
Clofazimine (Clo)It is a dye with leprostatic and antiinflammatoryproperties. The putative mechanisms of anti-leprotic action of clofazimine are:• Interference with template function of DNA
in M.leprae• Alteration of membrane stucture and its
transport function.• Disruption of mitochondrial electron trans-
port chain.When used alone, the clinical response to
clofazimine is slower than that to dapsone, andresistance develops in 1–3 years. Dapsone-resistant M. leprae respond to clofazimine, butapparently after a lag period of about 2 months.
Clofazimine is orally active (40–70% absor-bed). It accumulates in macrophages and getsdeposited in many tissues including subcuta-neous fat, as needle-shaped crystals. However,entry in CSF is poor. The t½ is 70 days so thatintermittent therapy is possible.CLOFOZINE, HANSEPRAN 50, 100 mg cap.
Clofazimine is used as a component ofmultidrug therapy (MDT) of leprosy. Becauseof its antiinflammatory property, it is valuablein lepra reaction.
Occasionally, it is used as a component ofMDT for MAC infection.

782S
EC
TIO
N12
ANTIMICROBIAL DRUGS
Adverse effects In the doses employed forMDT, clofazimine is well tolerated.
Skin The major disadvantage is reddish-blackdiscolouration of skin, especially on exposedparts. Discolouration of hair and body secretionsmay also occur. Dryness of skin and itching isoften troublesome. Acneform eruptions andphototoxicity have been noted. Conjunctivalpigmentation may create cosmetic problem.
GI symptoms Nausea, anorexia, abdominalpain, weight loss and enteritis with intermittentloose stools can occur, particularly when higherdoses are used to control lepra reaction. Theearly syndrome is a reflection of irritant effectof the drug—subsides with dose adjustment andby taking the drug with meals. A late syndromeoccurring after few months of therapy—is dueto deposition of clofazimine crystals in theintestinal submucosa.
Clofazimine is to be avoided during earlypregnancy and in patients with liver or kidneydamage.
Rifampin (R)This important tuberculocidal drug is also themost potent cidal drug for M.leprae; rapidlyrenders leprosy patients noncontagious. Upto99.99% M.leprae are killed in 3–7 days by 600mg/day dose. Clinical effects of rifampin arevery rapid; nasal symptoms in lepromatousleprosy subside within 2–3 weeks and skinlesions start regressing by 2 months. However,nerve damage already incurred is little benefited.Moreover, it is not satisfactory if used alone;some bacilli persist even after prolongedtreatment and resistance develops. Rifampin hasbeen included in the MDT of leprosy wherebyit shortens the duration of treatment, and noresistance develops. Persistence of dormantrifampin-sensitive bacilli, even after prolongedtherapy has also been noted. However, relapsecaused by such bacilli can be treated with thesame MDT. Rifampin remains effective inleprosy even if given once a month. The 600mg monthly dose used in MDT is practically
nontoxic and does not cause enzyme inductionto affect metabolism of other drugs. However,it should not be given to patients with hepaticor renal dysfunction, as well as during ‘erythemanodosum leprosum’ (ENL) and ‘reversalreaction’ in leprosy patients, because it canrelease large quantities of mycobacterialantigens by inducing rapid bacillary killing.
Ethionamide This antitubercular drug has significantantileprotic activity, but is poorly tolerated and causeshepatotoxicity in ~ 10% patients. It has been used as analternative to clofazimine, but other substitutes are preferred.Ethionamide 250 mg/day may be used only when absolutelynecessary.
OfloxacinMany fluoroquinolones like ofloxacin, pefloxa-cin, moxifloxacin, sparfloxacin are highly activeagainst M.leprae, but ciprofloxacin has pooractivity. Clinically, ofloxacin has been used tothe largest extent. As a component of MDT, ithas been found to hasten the bacteriological andclinical response. It is cidal to M.leprae, andin one study, over 99.9% bacilli were found tobe killed by 22 daily doses of ofloxacinmonotherapy. However, it is not yet included inthe standard treatment protocols, but can be usedin alternative regimens in case rifampin cannotbe used, or to shorten the duration of treatmentand reduce chances of drug resistance. Its safetyduring long-term use is not well documented.Dose: 400 mg/day.
Moxifloxacin is the most potent fluoro-quinolone against M. leprae. Recently, it hasbeen tried in some combination regimens withgood clinical and bacteriological results.
MinocyclineBecause of high lipophilicity, this tetracyclinepenetrates into M.leprae and is active againstthem. A dose of 100 mg/day produces peak bloodlevels that exceed MIC against M. leprae by10–20 times. Its antileprotic activity is lessmarked than that of rifampin, but greater thanthat of clarithromycin. In one trial minocycline100 mg daily monotherapy rendered all 8 patientsof lepromatous leprosy negative for M. leprae

783C
HA
PTER56
ANTILEPROTIC DRUGS
after 8 weeks. A good clinical response in termsof relief of lepromatous symptoms has also beenreported. Vertigo is the only serious complica-tion of its long-term use. It is being tried inalternative MDT regimens.
ClarithromycinIt is the only macrolide antibiotic with significantactivity against M. leprae. However, it is lessbactericidal than rifampin. Monotherapy withclarithromycin 500 mg daily caused 99.9%bacterial killing in 8 weeks. Rapid clinicalimprovement also occurred in lepromatouspatients. A synergistic action with minocyclinehas been demonstrated. It is being included inalternative MDT regimens.
TREATMENT OF LEPROSY
Leprosy is a chronic granulomatous infectioncaused by Mycobacterium leprae; primarilyaffecting skin, mucous membranes and nerves.It is more prevalent among the lowest socio-economic strata. Many patients exploit it forbegging and do not come forward for treatment.In India, the National Leprosy Control Programmewas launched in 1955, and was changed toNational Leprosy Eradication Programme (NLEP)in 1982. Following the initiative under WHOAction Programme for Elimination of Leprosy,India introduced multidrug therapy (MDT) forleprosy through NLEP in 1982 and achievedelimination of leprosy as a public health problem(prevalence rate < 1 case per 10,000 population)in Dec. 2005, though some states still had >1case per 10,000.*
Though the burden of leprosy has fallendrastically after introduction of MDT, bothglobally and in India, WHO data (2010) showthat 65% of all new leprosy cases worldoverare from India. Brazil and Indonesia are the othermajor contributors.
Leprosy manifests in several clinical forms.The most widely used classification of leprosy
is that of Ridley and Jopling (1966) who dividedleprosy into Lepromatous (LL), Borderlinelepromatous (BL), Borderline (BB), Borderlinetuberculoid (BT), and Tuberculoid (TT). Theimportant features of the two polar types aregiven in the box:
Tuberculoid leprosy Lepromatous leprosy
Anaesthetic patch Diffuse skin and mucousmembrane infiltration,nodules
Cell mediated immunity CMI is absent(CMI) is normalLepromin test—positive Lepromin test—negativeBacilli rarely found in Skin and mucous mem-biopsies brane lesions teeming
with bacilliProlonged remissions Progresses to anaesthesiawith periodic of distal parts, atrophy,exacerbations ulceration, absorption of
digits, etc.
For operational purposes WHO divided leprosyinto:1. Paucibacillary leprosy (PBL) Patient has
few bacilli and is noninfectious. It includedthe TT and BT types.
2. Multibacillary leprosy (MBL) Patient haslarge bacillary load and is infectious. Itincluded the LL, BL and BB types.To further simplify the classification so that
it may be applied at the field level, WHOreclassified leprosy in 1998 into:• Single lesion paucibacillary leprosy (SL PB):
With a solitary cutaneous lesion.• Paucibacillary leprosy (PB): With 2–5 skin
lesions. Both SLPB and PB cases are skinsmear negative for M.leprae.
• Multibacillary leprosy (MB): With > 6 skinlesions, as well as all smear positive cases.
The classification being followed by NLEP since2009 is given in the box (see p. 884).
Conventionally, all forms of leprosy had beentreated with dapsone alone (monotherapy: MT)100–200 mg daily, 5 days a week; duration oftreatment depending on the type: TT–4 to 5 years,LL–8 to 12 years or lifelong. With this mono-therapy symptomatic relief occurred in fewmonths, but bacteriological cure was delayed or
* India achieves National elimination of leprosy. Ind. J. Leprosy2006; 78(1): 101.

784S
EC
TIO
N12
ANTIMICROBIAL DRUGS
NLEP (2009) Classification of Leprosy
Paucibacillary (PB) Multibacillary (MB)
• 1-5 skin lesions • 6 or more skin lesions• No nerve/only one nerve involvement, • > 1 nerve involved irrespective of
+ 1–5 skin lesions. number of skin lesions• Skin smear negative at all sites • Skin smear positive at any one site
did not occur. Emergence of dapsone resistancesince 1964 threatened the efficacy of monotherapyand upto 20% patients relapsed. Even primarydapsone resistance was increasingly encountered.Monotherapy is no longer given.
Multidrug therapy (MDT) of leprosyTo deal with dapsone resistant strains ofM. leprae and to shorten the duration of treat-ment (as well as to eliminate microbial persis-ters, i.e. dormant forms, if possible), multidrugtherapy with rifampin, dapsone and clofaziminewas introduced by the WHO in 1981. This wasimplemented under the NLEP in 1982. The MDTis the regimen of choice for all cases of leprosy.Its advantages are:• Effective in cases with primary dapsone resis-
tance.• Prevents emergence of dapsone resistance.• Affords quick symptom relief and renders
MBL cases noncontagious within few days.• Reduces total duration of therapy.
Initially under standard MDT, the PBL caseswere treated with dapsone + rifampin for 6months, while the MBL cases were treated withdapsone + rifampin + clofazimine for a minimumof 2 years or till disease inactivity/skin smearnegativity was achieved. The MBL cases werekept under surveillance without treatment for thenext 5 years.
A WHO expert group (1994) reviewed the data collectedover the past 12 years as well as results of clinical trials,and made observations which are summarized below:• MDT had been highly successful, both in MBL and PBL.
The estimated cases of leprosy fell from 10–12 million to2.7 million.
• Relapse rate after MDT had been very low (0.77%) inMBL and 1.07% in PBL over a period of 9 years.
• The efficacy, safety and acceptability of MDT had beenexcellent.
• Some reports, mostly from India, had found that foruniformly satisfactory response, treatment of PBL had tobe extended beyond the mandatory 6 months (mostly to12 months). However, no difference in the relapse rate wasfound among 12000 Indian patients treated with MDT eitherfor 6 months or for 1 year. As such, the WHO expert grouprecommended continuation of 6 months MDT for PBL.
• No resistance to rifampin developed with MDT. Nearlyall M. leprae isolated from relapse cases remained fullysensitive to rifampin. No resistance to clofazimine hadbeen reported. New cases of drug resistance were notreported after application of MDT. Retreatment of relapsecases with the same MDT had been successful, and wasrecommended.
• Drug toxicity had not been a major problem with MDT.• Prevalence of lepra reaction had not increased due to
use of MDT.• No specific association of leprosy with HIV infection had
been found. Leprosy in HIV-positive cases is to be treatedin the same manner as in others.
Due to operational reasons, NLEP in Indiaexperimented with ‘fixed duration therapy of 24months’ (FDT-24) for MBL cases withoutextending for smear negativity to be achieved(if needed), and found that relapse rates weresimilar to that with the standard protocol. Asa result, FDT-24 was introduced by NLEP inselected areas for MBL cases in 1990. The WHOexpert group (1994) recommended FDT-24 forall MBL cases whether disease inactivity or skinsmear negativity was attained or not. The6 months FDT continues for PBL cases.
MBL Encouraged by the very low relapse rateswith 2 yrs FDT-24 and keeping in view operationalconstraints, studies were undertaken under theaegis of WHO to compare short-duration12 months (FDT-12) with standard 24 monthsFDT-24. In the field situation the two were foundto yield similar relapse rates over 3–5 yr follow

785C
HA
PTER56
ANTILEPROTIC DRUGS
up. Accordingly, a WHO expert committee onleprosy (1997) recommended shortening of MDTto 12 months. This was implemented globallyincluding India.* The currently used MDT(FDT-12) is given in the box:
Multidrug therapy (MDT) of leprosy
Multibacillary Paucibacillary
Rifampin 600 mg once a 600 mg once amonth supervised month supervised
Dapsone 100 mg daily self 100 mg daily selfadministered administered
Clofazimine 300 mg once a month —supervised and50 mg daily selfadministered
Duration 12 months 6 months
Doses to be reduced suitably for children.
Blister packs of tablets for 28 day treatment are made availablefree of cost to all MBL cases, and 12 such blister packs have tobe consumed by each MBL patient. Separate blister packs aregiven to PBL cases and 6 packs are to be taken by each patient.
A few studies, (mostly institutional) haveshown that despite 2 yr MDT, some patients conti-\nue to harbour viable M. leprae (persisters).Relapse rates are higher in the later years offollow up and in the subgroup of patients withlarge bacillary load, i.e. bacillary index (BI)> 4+. Thus, the length of MDT could depend onthe aim of therapy, resources, and feasibility offollow up.
The primary purpose of mass programmes(WHO Action Programme for the Eliminationof Leprosy, or NLEP-India) is to render patientsnon-contagious so as to cut down transmission.For this, 1 yr FDT may be considered adequate.Even if some patients relapse later, they can betreated by reinstituting MDT (dormant bacilliremain sensitive to the same drugs). This is morecost-effective than treating all patients with alonger MDT to prevent a few relapses. Moreover,case reports and prolonged follow ups show thatsome patients relapse upto 15 years after beingcured of MBL by extended-MDT till smear nega-tivity. Thus, few relapses cannot be prevented
irrespective of the duration of regimen or thedrugs used in the regimen, probably reflectinginvincibility of the ‘persister’ bacilli.
On the other hand, in private or institutionalcare, the aim is cure of every individual patient.For this extended treatment is required tilldisease inactivity or skin smear negativity isachieved. Upto 4 years may be needed for this,particularly in highly bacillated patients (BI> 4+). In the USA more intensive (daily) andlonger lasting (3–10 years) regimens are used.
PBL For PBL, 6 month 2 drug therapy has nowbeen used for > 25 yrs with very encouragingresults. Field studies from various parts of theworld suggest that this is adequate, provided thatthe patient is kept on follow up for thesubsequent 1–2 years. However, institutionalstudies have found larger proportion of patientsto have active disease after 6 month FDT. Somereports indicate that proportion of patientsstaying active can be reduced by 12 month MDT.Independent leprologists prefer to extend therapyof PBL for 12 months or longer till diseaseinactivity is achieved.
It may be concluded that, where feasible,treatment till cure of individual patient shouldbe ensured both in MBL and in PBL, while inmass programmes FDT-12 may be the morepractical approach to cover every leprosy patient.
* Short Course Treatment of Leprosy: present status; ICMRBulletin 2002; 32(2): 13–19.
Highlights of multidrug therapy (MDT) of leprosy*
• Worldover the case load of leprosy was ~ 12 millionbefore introduction of MDT, whereas only 0.228million new cases were detected during 2010.
• Globally 14.2 million patients of leprosy have beencured with very few relapses by MDT between1985–2005, out of which 10.8 million cases werefrom India.
• In 1981 India recorded a total of 3.95 million leprosycases. With institution of MDT in 1982, it has fallento 0.127 million new cases detected during 2010-11.
• India achieved elimination of leprosy as a publichealth problem (prevalence rate < 1 case per 10,000population) in Dec. 2005, by the use of MDT.
• The prevalence of leprosy in India was 57.6 casesper 10,000 population in 1981. It has fallen to 0.69cases per 10,000 in 2010.
* The figures are based on WHO and NLEP data

786S
EC
TIO
N12
ANTIMICROBIAL DRUGS
Alternative regimens Many alternative regi-mens incorporating newer antileprotic drugs havebeen investigated. However, these are used onlyin case of rifampin-resistance or when it isimpossible/inadvisable to employ the standardMDT regimen. Some of these are:• Intermittent ROM: Rifampin 600 mg + ofloxacin 400 mg
+ minocycline 100 mg are given once a month for 3–6month for PBL and for 12 or 24 month for MBL cases,without any drug in between.
• Single dose ROM: A single dose of rifampin + ofloxacin+ minocycline was given for single lesion PBL, but thishas been discontinued.
• Cloflazimine 50 mg + any two of ofloxacin 400 mg/minocycline100 mg/clarithromycin 500 mg daily for 6 month, followedby clofazimine 50 mg + any one of ofloxacin 400 mg/minocycline 100 mg daily for additional 18 months.
• Four drug regimen of rifampin 600 mg + sparfloxacin 200mg + clarithromycin 500 mg + minocycline 100 mg dailyfor 12 weeks has yielded equivalent clinical improvementin MBL cases to standard 12 month MDT.
• In case of refusal to accept clofazimine: ofloxacin 400 mgor minocycline 100 mg daily can be substituted for it inthe standard MDT. Use of ethionamide as a substituteis not recommended.
• Intermitent RMMx: Moxifloxacin 400 mg + minocycline200 mg + rifampin 600 mg is administered once a month:6 doses given for PBL and 12 doses given for MBL caseshave produced rapid and marked clinical response.
Reactions in leprosyLepra reaction This occurs in LL, usuallycoincides with institution of chemotherapy and/or intercurrent infection. It is a JarishHerxheimer (Arthus) type of reaction due torelease of antigens from the killed bacilli, andmay be mild, severe or life-threatening, i.e.erythema nodosum leprosum (ENL).
Lepra reaction is of abrupt onset; existinglesions enlarge, become red, swollen and painful;several new lesions may appear. Malaise, feverand other constitutional symptoms generallyaccompany and may be marked.
Temporary discontinuation of dapsone isrecommended only in severe cases. Clofazimine(200 mg daily) is effective in controlling thereaction (except the severe one), probablybecause of its antiinflammatory property. Forsevere reaction, prednisolone 40–60 mg/day isstarted immediately and continued till thereaction subsides. The dose is then tapered over2–3 months.Thalidomide is an anxiolytic, antiemetic drug withantiinflammatory, cytokine (TNFα, ILs, interferon) modulatoryproperty. It can be used in ENL as an alternative toprednisolone. Thalidomide was introduced in 1958 for morningsickness and was found to be highly teratogenic (see p. 89),and withdrawn in 1961. It has been reintroduced for ENL aswell as a variety of other conditions in which cytokines playan important role. It is also indicated in multiple myeloma.Dose: For ENL 100–300 mg OD at bed time.THAANGIO, THALODA 50, 100 mg cap.
Other drugs used are—analgesics, antipyre-tics, antibiotics, etc. according to symptoms andneed. Chloroquine also suppresses lepra reaction.Reversal reaction This is seen in TT and BLcases, and is a manifestation of delayed hyper-sensitivity to M. leprae antigens. Cutaneousulceration, multiple nerve involvement withswollen, painful and tender nerves, occursuddenly even after completion of therapy. It istreated with clofazimine or corticosteroids inthe same way as ENL, but thalidomide isineffective.
PROBLEM DIRECTED STUDY
56.1 A 50-year-old male attends the hospital OPD with multiple, diffusely raised nodulesover the face and arms for the past 1 month. The skin over the lesions is reddish and glossy.Sensation over face and arms is diminished and the ulnar nerve is thickened. He informsthat 6 years back he had suffered from similar lesions and had taken regular medication forthe same for one year and was declared cured. The treatment records revealed that he wasgiven the standard multidrug therapy with rifampin, clofazimine and dapsone and had successfullycompleted the one year course. The skin smear is positive for M. leprae.(a) What could be the cause of relapse of leprosy in this case? What treatment should beprescribed?(see Appendix-1 for solution)

Antifungal DrugsChapterChapterChapterChapterChapter 5757575757
These are drugs used for superficial and deep(systemic) fungal infections.
A disquietening trend after 1950s is the risingprevalence of more sinister type of fungalinfections which are, to a large extent, iatrogenic.Fungal infections are mostly associated with theuse of broad-spectrum antibiotics, cortico-steroids, anticancer/immunosuppressant drugs,dentures, indwelling catheters and implants, andemergence of AIDS. As a result of breakdownof host defence mechanisms by the above agents,saprophytic fungi easily invade living tissue.
Many topical antifungals have been availablesince the antiseptic era. Two important antibio-tics viz. amphotericin B—to deal with systemicmycosis, and griseofulvin—to supplement attackon dermatophytes were introduced around 1960.Antifungal property of flucytosine was noted in1970, but it could serve only as a companiondrug to amphotericin. The development ofimidazoles in the mid 1970s and triazoles in1980s has been an advancement. Terbinafine isa novel antifungal. A group of potent semisyn-thetic antifungal antibiotics, the Echinocandinsare the latest addition.
CLASSIFICATION
1. AntibioticsA. Polyenes: Amphotericin B (AMB),
Nystatin, HamycinB. Echinocandins:Caspofungin, Micafungin,
AnidulafunginC. Heterocyclic benzofuran: Griseofulvin
2. Antimetabolite Flucytosine (5-FC)3. Azoles
A. ImidazolesTopical: Clotrimazole, Econazole,
Miconazole, OxiconazoleSystemic: Ketoconazole
B. Triazoles: Fluconazole,(systemic) Itraconazole,
Voriconazole,Posaconazole
4. Allylamine Terbinafine5. Other topical agentsTolnaftate, Undecylenic acid, Benzoic acid,Quiniodochlor, Ciclopirox olamine, Butenafine,Sod. thiosulfate.
POLYENE ANTIBIOTICS
The name polyene is derived from their highlydouble-bonded structure. Amphotericin B isdescribed as the prototype.
Amphotericin B (AMB)It is obtained from Streptomyces nodosus.
Chemistry and mechanism of action Thepolyenes possess a macrocyclic ring, one sideof which has several conjugated double bondsand is highly lipophilic, while the other side ishydrophilic with many OH groups. A polaraminosugar and a carboxylic acid group arepresent at one end in some. They are all insolublein water and unstable in aqueous medium.
The polyenes have high affinity forergosterol present in fungal cell membrane. Theycombine with it, get inserted into the membraneand several polyene molecules together orientthemselves in such a way as to form a‘micropore’. The hydrophilic side forms theinterior of the pore through which ions, aminoacids and other water-soluble substances moveout. The micropore is stabilized by membranesterols which fill up the spaces between the AMBmolecules on the lipophilic side—constitutingthe outer surface of the pore. Thus, cellpermeability is markedly increased.

788S
EC
TIO
N12
ANTIMICROBIAL DRUGS
Cholesterol, present in host cell membranes,closely resembles ergosterol; the polyenes bindto it as well, though with lesser affinity. Thus,the selectivity of action of polyenes is low, andAMB is one of the most toxic systemically usedantibiotics, though it is the least toxic polyene.Bacteria do not have sterols and are unaffectedby polyenes.
It has been found that AMB enhancesimmunity in animals, and this action may aidimmunocompromised individuals in handlingfungal infection.
Antifungal spectrum AMB is active againsta wide range of yeasts and fungi—Candidaalbicans, Histoplasma capsulatum, Crypto-coccus neoformans, Blastomyces dermatitidis,Coccidioides immitis, Torulopsis, Rhodotorula,Aspergillus, Sporothrix, etc. Dermatophytes areinhibited in vitro, but concentrations of AMBattained in infected skin are low and ineffective.It is fungicidal at high and static at lowconcentrations.
Resistance to AMB during therapy has beenrarely noted among Candida in a selected groupof leucopenic cancer patients, but it is not aproblem in the clinical use of the drug.
AMB is also active on various species ofLeishmania, a protozoa.
Pharmacokinetics AMB is not absorbedorally; it can be given orally for intestinal candi-diasis without systemic toxicity. Administeredi.v. as a suspension made with the help ofdeoxycholate (DOC), it gets widely distributedin the body, but penetration in CSF is poor. Itbinds to sterols in tissues and to lipoproteinsin plasma and stays in the body for long periods.The terminal elimination t½ is 15 days. About60% of AMB is metabolized in the liver.Excretion occurs slowly both in urine and bile,but urinary concentration of active drug is low.
Administration and dose Amphotericin B can beadministered orally (50–100 mg QID) for intestinal moniliasis;also topically for vaginitis, otomycosis, etc.:FUNGIZONE OTIC 3% ear drops.
Conventional formulation of AMB (C-AMB) For systemicmycosis, C-AMB is available as dry powder along withdeoxycholate (DOC) for extemporaneous dispersion before use:FUNGIZONE INTRAVENOUS, MYCOL 50 mg vial.It is first suspended in 10 ml water and then diluted to 500ml with glucose solution (saline makes the suspension coarse,should be avoided). Initially 1 mg test dose is injected i.v. over20 minutes. If no serious reaction follows, 0.3 mg/kg is infusedover 4–8 hours. Daily dose may be gradually increased to 0.7mg/kg depending on tolerance of the patient. The total doseof AMB for majority of cases is 3–4 g given over 2–3 months.
Intrathecal injection of 0.5 mg twice weekly has beengiven in fungal meningitis.Liposomal amphotericin B (L-AMB) It has been producedto improve tolerability of i.v. infusion of AMB, reduce itstoxicity and achieve targeted delivery. It consists of 10% AMBincorporated in uniform sized (60–80 nM) unilamellarliposomes made up of lecithin and other biodegradablephospholipids.The special features of this preparation are:• It produce milder acute reaction on i.v. infusion.• It can be used in patients not tolerating infusion of
conventional AMB formulation.• It has lower nephrotoxicity.• It causes minimal anaemia.• It delivers AMB particularly to reticuloendothelial cells
in liver and spleen—especially valuable for kala azar andin immunocompromised patients.The liposomal-AMB produces equivalent blood levels,
has similar clinical efficacy with less acute reaction and renaltoxicity than conventional preparaton. It thus appears moresatisfactory, can be infused at higher rates (3–5 mg/kg/day),but is many times costlier than conventional AMB. L-AMBis specifically indicated for empirical therapy in febrileneutropenic patients not responding to antibacterialantibiotics, critically ill deep mycosis cases and in kala azar.FUNGISOME (liposomal AMB) 10 mg, 25 mg, 50 mg per vialinj., AMPHOLIP 10 mg/2 ml, 50 mg/10 ml, 100 mg/20 ml inj.
Another formulation amphotericin B colloidal dispersion(ABCD) containing 50% each of AMB and cholesteryl sulfatehas been produced, but is not superior.
Adverse effects The toxicity of AMB is high.(a) Acute reaction This occurs with each infu-sion and consists of chills, fever, aches and painall over, nausea, vomiting and dyspnoea lastingfor 2–5 hour, probably due to release of cyto-kines (IL, TNFα). When the reaction is severe—the dose should be increased gradually. Usuallythe intensity of reaction decreases with continuedmedication. Injection of hydrocortisone 0.6 mg/kg with the infusion may reduce the intensityof reaction.Thrombophlebitis of the injected vein can occur.

789C
HA
PTER57
ANTIFUNGAL DRUGS
(b) Long-term toxicity Nephrotoxicity is themost important. It occurs fairly uniformly andis dose-related. Manifestations are—azotemia,reduced g.f.r., acidosis, hypokalaemia andinability to concentrate urine. It reverses slowlyand often incompletely after stoppage of therapy.Anaemia: Most patients develop slowly progress-ing anaemia which is due to bone marrowdepression. It is largely reversible.CNS toxicity: occurs only on intrathecalinjection—headache, vomiting, nerve palsies, etc.
Uses Amphotericin B can be applied topicallyfor oral, vaginal and cutaneous candidiasis andotomycosis.
It is the most effective drug for various typesof systemic mycoses and is the gold standardof antifungal therapy. However, because of highertoxicity of AMB, the azole antifungals are nowpreferred in conditions where their efficacyapproaches that of AMB (see Table 57-1).
Febrile neutropenia: Empirical use of i.v. AMBis often made in neutropenic patients whose feveris not responding to i.v. bactericidal antibiotics.
Leishmaniasis: AMB is the most effective drugfor resistant cases of kala azar and muco-cutaneous leishmaniasis (see Ch. 60).
Interactions Flucytosine has supra-additiveaction with AMB in the case of fungi sensitiveto both (AMB increases the penetration of 5-FC into the fungus).Aminoglycosides, vancomycin, cyclosporine andother nephrotoxic drugs enhance the renalimpairment caused by AMB.
NystatinObtained from S. noursei, it is similar to AMBin antifungal action and other properties.However, because of higher systemic toxicity,it is used only locally in superficial candidiasis.MYCOSTATIN 5 lakh U tab, 1 lakh U vaginal tab, 1 lakh U/goint, NYSTIN EYE 1 lakh U/g ophthalmic oint.
Given orally, it is not absorbed; can be used formonilial diarrhoea (due to superinfection orotherwise), 5 lac U TDS (1 mg = 2000 U).Nausea and bad taste in mouth are the only sideeffects.
TABLE 57.1 Choice of drugs for systemic mycoses
Disease Drugs
1st Choice 2nd Choice
1. Candidiasisoral / vaginal / cutaneous FLU / NYS / CLO ITRdeep / invasive AMB / VORI FLU / CAS / POSA
2. Cryptococcosis AMB ± 5-FC FLU
3. Histoplasmosis ITR / AMB FLU
4. Coccidioidomycosis AMB / FLU ITR / KTZ
5. Blastomycosis ITR / AMB KTZ / FLU
6. Sporotrichosis (disseminated) AMB ITR
7. Paracoccidioidomycosis ITR AMB
8. Aspergillosis VORI / AMB ITR / CAS / POSA
9. Mucormycosis AMB POSA
10. Chromomycosis ITR TER / POSA
AMB—Amphotericin B; 5-FC—Flucytosine; KTZ—Ketoconazole; FLU—Fluconazole;ITR—Itraconazole; NYS—Nystatin; CLO—Clotrimazole; VORI—Voriconazole;CAS—Caspofungin; POSA—Posaconazole;TER—Terbinafine

790S
EC
TIO
N12
ANTIMICROBIAL DRUGS
Nystatin is effective (but less than azoles)in monilial vaginitis—1 lac U tab inserted twicedaily. For oral thrush, the vaginal tab may becrushed and suspended in glycerine for applicationin mouth. Corticosteroid aerosols (e.g. beclomet-hasone) can cause oral candidiasis: nystatin iseffective in preventing as well as treating it.
Similarly, it is used for corneal, conjunctivaland cutaneous candidiasis in the form of anointment. No irritation or other side effect isordinarily seen.
Candidal resistance to nystatin is not a clinicalproblem. It is ineffective in dermatophytosis.
Hamycin It was isolated from S. pimprina and developedby Hindustan Antibiotics at Pimpri. It is similar to nystatin,but more water soluble. A fraction of the orally administereddose is absorbed, but cannot be relied upon for the treatmentof systemic mycosis: use is restricted to topical applicationfor oral thrush, cutaneous candidiasis, monilial andtrichomonas vaginitis and otomycosis by Aspergillus.HAMYCIN, 5 lakh U/g oint, 2 lakh U/ ml susp for topical use,4 lakh U vaginal ovules.
ECHINOCANDINS
These are a new class of potent semisyntheticantifungal antibiotics with a complex cycliclipopeptide structure, which stand out due to theirlow toxicity compared to AMB.
CaspofunginIt is the first and the prototype member of the class,active mainly against Candida and Aspergillus.Strains of candida that have become resistant toazoles are susceptible to caspofungin. Themechanism of action is different from otherantifungals, viz. it inhibits the synthesis ofβ-1, 3-glucan, which is a unique component ofthe fungal cell wall. Cross linking between chitin(a fibrillar polysaccharide) and β-1, 3-glucan givestoughness to the fungal cell wall. Weakening ofthe cell wall by caspofungin leads to osmoticsusceptibility of fungal cell, which then succumbs.
Caspofungin is not absorbed orally; has to beinfused i.v. It is distributed into tissues, but doesnot enter CSF. Metabolism is extensive and
metabolites are excreted in urine as well as faeceswith a plasma t½ of 10 hours. Caspofungin isapproved for use in deep and invasive candidiasis,esophageal candidiasis and salvage therapy ofnonresponsive invasive aspergillosis. Because ofgood tolerability, it is now increasingly used inneutropenic immunocompromised patients whosefever is not responding to antibacterial antibiotics.Dose: 70 mg loading dose infused i.v. over 1 hour, followedby 50 mg i.v. daily.CANCIDAS 70 mg in 10 ml and 50 mg in 10 ml inj.
An acute febrile reaction some times attendsthe i.v. infusion of caspofungin, as does phlebitisof the injected vein. Rash, vomiting, dyspnoea,hypokalemia and joint pain may occur. However,organ toxicity has not been noted.
Micafungin and Anidulafungin are the otherechinocandins with similar properties.
HETEROCYCLIC BENZOFURAN
GriseofulvinIt was one of the early antibiotics extracted from Penicilliumgriseofulvum. However, because of lack of antibacterialactivity, little attention was paid to it: clinical utility indermatophytosis was demonstrated only around 1960.
Griseofulvin is fungistatic for most dermato-phytes, including Epidermophyton, Trichophy-ton, Microsporum, etc., but not against Candidaand other fungi causing deep mycosis. Bacteriaare also insensitive. Dermatophytes activelyconcentrate it: this feature probably accounts forits selective toxicity. Resistance can be inducedin vitro and this is associated with loss ofconcentrating ability. However, emergence ofresistance during clinical use is rare.
Griseofulvin interferes with mitosis—multi-nucleated and stunted fungal hyphae are producedunder its action. It also causes abnormal meta-phase configurations. However, unlike the typicalmitotic inhibitors (colchicine, vinca alkaloids),it does not cause metaphase arrest; rather thedaughter nuclei fail to move apart or move onlya short distance. It does not inhibit polymerizationof tubulin (microtubular protein which pulls thechromosomes apart), but binds to polymerizedmicrotubules and interferes with their function.

791C
HA
PTER57
ANTIFUNGAL DRUGS
Pharmacokinetics The absorption of griseofulvin from g.i.t.is somewhat irregular because of its very low water solubility.Absorption is improved by taking it with fats and bymicrofining the drug particles; now ultramicrofine particlepreparations from which absorption is still better are available.
Griseofulvin gets deposited in keratin forming cells ofskin, hair and nails. It is especially concentrated and retainedin tinea infected cells.
Griseofulvin is largely metabolized, primarily bymethylation, and excreted in urine. Plasma t½ is 24 hrs, butit persists for weeks in skin and keratin.
Adverse effects Toxicity of griseofulvin is low and usuallynot serious. Headache is the commonest complaint, followedby g.i.t. disturbances. CNS symptoms and peripheral neuritisare occasional.Rashes, photoallergy may warrant discontinuation.Gynaecomastia is reported.Transient leukopenia and albuminuria (without renal damage)are infrequent.
Use Griseofulvin is used orally only for derma-tophytosis. On getting deposited in the skinthrough circulation, it prevents fungal invasionof keratin. Because it is fungistatic and not cidal,the newly formed keratin is not invaded by thefungus, but the fungus persists in already infectedkeratin, till it is shed off. Thus, the duration oftreatment is dependent upon the site of infection,thickness of infected keratin and its turnoverrate. It is ineffective topically. Systemic azolesand terbinafine are equally or more efficacious,and are preferred now.Dose: 125–250 mg QID with meals; duration depends on thesite of infection (turnover rate of keratin).
Scalp 4 weeksPalm, soles 6 to 8 weeksFinger nails 6 to 8 monthsToe nails 10 to 12 months
Majority of localized tinea infections are treatedwith topical agents. Griseofulvin should bereserved for cases with nail, or large body surfaceinvolvement and tinea capitis. It is effective inathletes foot, but not in pityriasis versicolor.GRISOVIN-FP, WALAVIN, GRISORAL 250 mg tab.
Interactions Griseofulvin induces CYP450enzymes and hastens warfarin metabolism.Efficacy of oral contraceptives may be lost.Phenobarbitone reduces the oral absorption andinduces the metabolism of griseofulvin—failureof therapy may occur.Griseofulvin can cause intolerance to alcohol.
ANTIMETABOLITE
Flucytosine (5-FC)It is a pyrimidine antimetabolite which is inactive assuch. After uptake into fungal cells, it is converted into5-fluorouracil and then to 5-fluorodeoxyuridylic acid whichis an inhibitor of thymidylate synthesis. Thymidylic acid isa component of DNA. The fungal selectivity of 5-FC dependson the fact that mammalian cells (except some marrow cells)have low capacity to convert 5-FC into 5-fluorouracil, whichis a potent anticancer drug.
5-FC is a narrow spectrum fungistatic, active againstCryptococcus neoformans, Torula, Chromoblastomyces; anda few strains of Candida. Other fungi and bacteria are insensitive.Adverse effects Toxicity of 5-FC is lower than that of AMB;consists of dose-dependent bone marrow depression andgastrointestinal disturbances, particularly enteritis and diarrhoea.Liver dysfunction is mild and reversible.Use Flucytosine is not employed as the sole therapy exceptoccasionally in chromoblastomycosis. Rapid development ofresistance limits its utility in deep mycosis. In cryptococcosis(both meningeal and nonmeningeal) its synergistic action withAMB is utilized to reduce the total dose of the more toxiclatter drug. Therapy with 5-FC is generally limited to first 2weeks of AMB regimen to avoid its bone marrow toxicity.
IMIDAZOLES AND TRIAZOLES
These are presently the most extensively usedantifungal drugs.
Four imidazoles are entirely topical, whileketoconazole is used both orally and topically.Two triazoles fluconazole and itraconazole havelargely replaced ketoconazole for systemicmycosis because of greater efficacy, longer t½,as well as fewer side effects. Some newertriazoles have been added.
The imidazoles and triazoles have broad-spectrum antifungal activity covering dermato-phytes, Candida, other fungi involved in deepmycosis (except mucor), Nocardia andLeishmania.
The mechanism of action of imidazoles andtriazoles is the same. They inhibit the fungalcytochrome P450 enzyme ‘lanosterol 14-demethylase’ and thus impair ergosterolsynthesis leading to a cascade of membraneabnormalities in the fungus. The lower hosttoxicity of triazoles compared to imidazoles hascorrelated with their lower affinity formammalian CYP450 enzymes and lesserpropensity to inhibit mammalian sterol synthesis.

792S
EC
TIO
N12
ANTIMICROBIAL DRUGS
Development of fungal resistance to azoleshas been noted among Candida infectingadvanced AIDS patients, but has not so far posedsignificant clinical problem in immunocompetentpatients, except fluconazole resistance amongCandida causing esophageal and other deepcandidasis. Many of fluconazole-resistantCandida respond to itraconazole or to vorico-nazole. Mutation of the gene encoding for fungal14-demethylase enzyme underlies azoleresistance.
Clotrimazole It is effective in the topicaltreatment of tinea infections like ringworm:60–100% cure rates are reported with 2–4weeks application on a twice daily schedule.Athletes’ foot, otomycosis and oral/cutaneous/vaginal candidiasis have responded in >80%cases. It is particularly favoured for vaginitisbecause of a long lasting residual effect afteronce daily application. A 7 day course isgenerally used. For oropharyngeal candidiasis 10mg troche of clotrimazole is allowed to dissolvein the mouth 3–4 times a day, or the lotion/gel is applied/swirled in the mouth for as longas possible. It is also effective in skin infectionscaused by Corynebacteria, but like most topicalantifungals, has poor efficacy in tinea capitis(scalp) and tinea unguium (nails).
Clotrimazole is well tolerated by mostpatients. Local irritation with stinging andburning sensation occurs in some. No systemictoxicity is seen after topical use.SURFAZ, CLODERM 1% lotion, cream, powder; 100 mg vaginaltab. CANDID 1% cream, mouth paint, powder.
Econazole It is similar to clotrimazole;penetrates superficial layers of the skin and ishighly effective in dermatophytosis, otomycosis,oral thrush, but is somewhat inferior toclotrimazole in vaginitis. No adverse effects,except local irritation in few is reported.ECONAZOLE 1% oint, 150 mg vaginal tab; ECODERM 1%cream.
Miconazole It is a highly efficacious (>90%cure rate) drug for tinea, pityriasis versicolor,otomycosis, cutaneous and vulvovaginal candi-diasis. Because of its good penetrating power,
it has been found effective, though partially, evenin onychomycosis; single application on skinacts for a few days.
Irritation after cutaneous application isinfrequent. No systemic adverse effects are seen.However, a higher incidence of vaginal irritationis reported in comparison to clotrimazole; evenpelvic cramps have been experienced.DAKTARIN 2% gel, 2% powder and solution;GYNODAKTARIN 2% vaginal gel; ZOLE 2% oint, lotion,dusting powder and spray, 1% ear drops, 100 mg vaginal ovules.
Oxiconazole Another newer topical imidazoleantifungal effective in tinea and other derma-tophytic infection, as well as vaginal candidiasis.Local irritation can occur in some patients.OXIZON, ZODERM: oxiconazole 1% with benzoicacid 0.25% cream/lotion; apply topically once or twice daily.
Ketoconazole (KTZ)It is the first orally effective broad-spectrumantifungal drug, useful in both dermatophytosisand deep mycosis. The oral absorption of KTZis facilitated by gastric acidity because it is moresoluble at lower pH. Hepatic metabolism isextensive; metabolites are excreted in urine andfaeces. Elimination of KTZ is dose dependent:t½ varies from 1½ to 6 hours. Penetration inCSF is poor; therefore not effective in fungalmeningitis. However, therapeutic concentrationsare attained in the skin and vaginal fluid.
In spite of relatively short t½, a single dailydose is satisfactory in less severe cases. Theusual dose is 200 mg OD or BD.FUNGICIDE, NIZRAL, FUNAZOLE, KETOVATE 200 mg tab.FUNGINOC 2% oint, 2% shampoo (for dandruff), KETOVATE2% cream. NIZRAL 2% cream, 2% lotion; DANRUF 2%shampoo, HYPHORAL 2% lotion.
Adverse effects Ketoconazole is much lesstoxic than AMB, but more side effects occurthan with itraconazole or fluconazole, that havelargely replaced it for systemic use.The most common side effects are nausea and vomiting; canbe reduced by giving the drug with meals. Others are—lossof appetite, headache, paresthesia, rashes and hair loss.
The most important draw back of KTZ is its hormonaleffects. It decreases androgen production from testes, anddisplaces testosterone from protein binding sites.

793C
HA
PTER57
ANTIFUNGAL DRUGS
Gynaecomastia, loss of hair and libido, and oligozoospermiamay occur when the drug is used for a few weeks. Menstrualirregularities occur in some women due to suppression ofestradiol synthesis.A dose-dependent decrease in serum hydrocortisone due tosynthesis inhibition has also been noted, but without anyclinical manifestations in normal individuals.Mild and asymptomatic elevation of serum transaminases occursin ~5% patients, but serious hepatotoxicity is infrequent.It is contraindicated in pregnant and nursing women.
Interactions Ketoconazole (and most azoles)interact with several drugs. Due considerationmust be given when they are coprescribed withother drugs.
H2 blockers, proton pump inhibitors andantacids decrease oral absorption of KTZ byreducing gastric acidity.
Rifampin, phenobarbitone, carbamazepine andphenytoin induce KTZ metabolism and reduceits efficacy.
Ketoconazole inhibits CYP450 enzymes,especially CYP3A4, CYP2C9; CYP2C19 andraises the blood levels of several drugs including:
Phenytoin DigoxinCarbamazepine OmeprazoleDiazepam CyclosporineHaloperidol Nifedipine and other DHPsWarfarin HIV protease inhibitorsSulfonylureas Statins
The dangerous interaction with terfenadine, astemizole andcisapride resulting in polymorphic ventricular tachycardia dueto excessive rise in plasma levels of these drugs has resultedin their withdrawal (see p. 166).
Use Orally administered KTZ is effective indermatophytosis because it is concentrated inthe stratum corneum. It is an alternative to griseo-fulvin, but use is restricted due to potentialadverse effects. Used as a lotion or shampoo,KTZ is quite effective in seborrhoea of scalpand dandruff.
Though effective in monilial vaginitis, oraltherapy (for 5–7 days) with KTZ is reserved forrecurrent cases or those not responding to topicalagents.
Systemic mycosis: Administered orally, KTZ is effective inseveral types of systemic mycosis, but triazoles, being moreactive with fewer side effects, have largely replaced it forthese indications.
KTZ is occasionally used in dermal leishmaniasis and in kalaazar.High-dose KTZ has been used in Cushing’s syndrome todecrease corticosteroid production.
Fluconazole It is a water-soluble triazolehaving a wider range of activity than KTZ;indications include cryptococcal meningitis,systemic and mucosal candidiasis in both normaland immunocompromised patients, coccidioidalmeningitis and some tinea infections.
Fluconazole is 94% absorbed; oral bioavai-lability is not affected by food or gastric pH.It is primarily excreted unchanged in urine witha t½ of 25–30 hr. Fungicidal concentrations areachieved in nails, vagina and saliva; penetrationinto brain and CSF is good. Dose reduction isneeded in renal impairment.
Adverse effects Fluconazole produces fewerside effects: mostly nausea, vomiting, abdominalpain, rash and headache. Incidence and severityof these side effects increases with dose andduration of therapy.Selectivity for fungal cytochrome P450 is higher;unlike KTZ, it does not inhibit steroid synthesisin man: antiandrogenic and other endocrine sideeffects have not occurred.Elevation of hepatic transaminase has been notedin AIDS patients.It is not recommended in pregnant and lactatingmothers.
Interactions Though it affects hepatic drugmetabolism to a lesser extent than KTZ,increased plasma levels of phenytoin, astemizole,cisapride, cyclosporine, warfarin, zidovudine andsulfonylureas have been observed. A few casesof ventricular tachycardia have been reportedwhen fluconazole was given with cisapride. Thesame caution as with KTZ or itraconazole needsto be applied in coadministering other drugs.Proton pump inhibitors and H2 blockers do notaffect its absorption.
Use Fluconazole can be administered orallyas well as i.v. (in severe infections).

794S
EC
TIO
N12
ANTIMICROBIAL DRUGS
A single 150 mg oral dose can cure vaginalcandidiasis with few relapses.
Oral fluconazole (100 mg/day for 2 weeks)is highly effective in oropharyngeal candidiasis,but is reserved for cases not responding to topicalantifungals. Fluconazole (100 mg/day) for2–3 weeks is the first line treatment for candidaesophagitis.
Most tinea infections and cutaneous candi-diasis can be treated with 150 mg weeklyfluconazole for 4 weeks.
For disseminated candidiasis, cryptococcal/coccidioidal meningitis and other systemicfungal infections the dose is 200–400 mg/dayfor 4–12 weeks or longer. It is the preferreddrug for fungal meningitis, because of good CSFpenetration. Long-term oral fluconazole main-tenance therapy after initial treatment with i.v.fluconazole/AMB is used in AIDS patients withfungal meningitis.
An eye drop is useful in fungal keratitis.Fluconazole is ineffective in aspergillosis and
mucormycosis, and inferior to itraconazole forhistoplasmosis, blastomycosis and sporo-trichosis, as well as in tinea unguim.SYSCAN, ZOCON, FORCAN, FLUZON 50, 100, 150, 200 mgcaps, 200 mg/100 ml i.v. infusion.SYSCAN 0.3% eye drops.
Itraconazole This orally active triazole anti-fungal has a broader spectrum of activity than
KTZ or fluconazole; includes some moulds likeAspergillus. Some fluconazole resistant Candidaare susceptible. It is fungistatic, but effective inimmunocompromised patients. Steroid hormonesynthesis inhibition is absent in itraconazole, andserious hepatotoxicity is rare.
Oral absorption of itraconazole is variable.It is enhanced by food and gastric acid.Itraconazole is highly protein bound, has a largevolume of distribution (10 L/Kg), accumulatesin vaginal mucosa, skin and nails, but penetrationinto CSF is poor. It is largely metabolized in liverby CYP3A4; an active metabolite is producedwhich is excreted in faeces; t½ varies from30–64 hours.
Itraconazole is well tolerated in doses below200 mg/day. Gastric intolerance is significant at> 400 mg/day. Dizziness, pruritus, headache andhypokalaemia are the other common side effects.Unsteadiness and impotence are infrequent.Plasma transaminase may rise transiently.However, antiandrogenic and other hormonaladverse effects are not seen. Impaired leftventricular function has been worsened in somepatients.
Drug interactions Oral absorption of itracona-zole is reduced by antacids, H2 blockers andproton pump inhibitors.
TABLE 57.2 Properties of drugs used for systemic mycoses
Characteristic AMB Caspo 5-FC KTZ FLU ITR VORI
Antifungal spectrum Broad Narrow Narrow Broad Broad Broad Broad
Absorbed orally No No Yes Yes Yes Yes Yes
Administered i.v. Yes Yes Yes No Yes Yes Yes
Resistance (in vivo) No No Yes Limited Limited No No
Nephrotoxicity Yes No No No No No No
Anaemia Yes No Mild No No No No
Leucopenia No No Yes No No No No
Gastrointestinal upset Yes Mild Yes Mild Mild Moderate Mild
Overall toxicity High Low Medium Medium Low Low Low
AMB—AmphotericinB; 5-FC—Flucytosine; KTZ—Ketoconazole; FLU—Fluconazole; ITR—ItraconazoleCaspo—Caspofungin, VORI—Voriconazole

795C
HA
PTER57
ANTIFUNGAL DRUGS
Rifampin, phenobarbitone, phenytoin andcarbamazepine induce itraconazole metabolismand reduce its efficacy.On the other hand, clarithromycin and HIVprotease inhibitors reduce the metabolism ofitraconazole and raise its blood levels.Itraconazole inhibits CYP3A4; drug interactionprofile is similar to KTZ; ventricular arrhythmiashave occurred with terfenadine, astemizole, cisap-ride and class III antiarrhythmics. Phenytoin,digoxin, sulfonylureas, statins, dihydropyridines,protease inhibitors, warfarin and cyclosporinelevels are also increased.
Uses Itraconazole is the preferred azoleantifungal for most systemic mycosis (see Table57.1) that are not associated with meningitis.It is superior to fluconazole for histoplasmosis,blastomycosis, sporotrichosis and is the drug ofchoice for the rare fungal infections—paracocci-dioidomycosis and chromomycosis. It alsoaffords some relief in aspergillosis. A dose of200 mg OD/BD with meals is used for 3 monthsor more.Vaginal candidiasis: 200 mg OD oral for 3 daysis as effective as intravaginal clotrimazole.Dermatophytosis: 100–200 mg OD for 7–15days: more effective than griseofulvin, but lesseffective than fluconazole.Onychomycosis: 200 mg/day for 3 months. Anintermittent pulse regimen of 200 mg BD for1 week each month for 3 months is equallyeffective. Relapses have occurred after itracona-zole therapy, though it remains in the nail forfew months after completion of the course.SPORANOX, CANDITRAL, CANDISTAT, ITASPOR,FLUCOVER 100 mg cap. ITASPOR 100 mg cap, 200 mg/20 mlvial.Important features of drugs used for systemicmycosis are compared in Table 57.2.
Voriconazole It is a second generation broad-spectrum triazole introduced lately for difficultto treat fungal infections like invasive aspergil-losis, disseminated infections caused by flucona-zole resistant Candida, Fusarium infections, andfebrile neutropenia not responding to antibac-terial therapy. Serious cases are first treated i.v.
followed by oral voriconazole. It is completelyabsorbed orally, except when taken with a fattymeal, widely distributed into tissues andmetabolized extensively by CYP2C19, CYP3A4,CYP2C9. Metabolites are excreted in urine. Thet½ is 6 hours. It also inhibits CYP isoenzymesand the drug interaction profile is similar to KTZ.Rashes, visual disturbances, QTc prolongationand an acute reaction on i.v. injection are thesignificant adverse effects.Dose: 200 mg oral BD taken 1 hour before or 1 hour after meal.Begin i.v. infusion with 6 mg/kg 12 hourly infused over 2 hourstwice followed by 3–4 mg/kg 12 hourly.VFEND 50, 200 mg tabs, 40 mg/ml oral suspension; 200 mg/vialinj. , FUNGIVOR 200 mg tab.
Posaconazole This recently introduced broad-spectrum triazole has more potent antifungalactivity and is the only azole which has shownefficacy in mucormycosis. It is indicated forsalvage therapy of this difficult to treat fungalinfection. Because of its high cost and limitedexperience, it is reserved for nonresponsivecases of aspergillosis and invasive candidiasis.Favourable results have been reported in febrileneutropenia and as a prophylactic in immuno-suppressed patients. It has also been used asalternative to itraconazole for chromomycosis.
Side effects to posaconazole are common,but mostly limited to nausea, abdominal pain,loose motions, headache, dizziness and drowsi-ness. Anaemia, neutropenia, cardiac arrhythmiasand visual disturbances are rare. Administered asan oral suspension, absorption of posaconazoleis improved by low pH and fatty food. It is partlymetabolized by CYP2C19 and glucuronidation,but excreted mostly unchanged in faeces. The t½is > 24 hours. It can increase levels of drugsmetabolized by CYP3A4.Dose: 200 mg QID or 400 mg BD with meals.NOXAFIL 200 mg/5 ml susp.
ALLYLAMINE
TerbinafineThis orally and topically active drug againstdermatophytes and Candida belongs to anew allylamine class of antifungals. In contrastto azoles which are primarily fungistatic,

796S
EC
TIO
N12
ANTIMICROBIAL DRUGS
terbinafine is fungicidal. It acts as a non-competitive inhibitor of ‘squalene epoxidase’,an early step enzyme in ergosterol biosynthesisby fungi. Accumulation of squalene within fungalcells appears to be responsible for the fungicidalaction. The mammalian enzyme is inhibited onlyby 1000-fold higher concentration of terbinafine.
Approximately 75% of oral terbinafine isabsorbed, but only 5% or less from unbrokenskin. First pass metabolism reduces oralbioavailability to < 50%. It is widely distributedin tissues, strongly plasma protein bound andhas high affinity for keratin. Therefore, it isconcentrated in sebum, stratum corneum of skinand into nail plates. Inactivation occurs bymetabolism and it is excreted mainly in urine,but about 20% in faeces as well. Eliminationt½ after single dose is 11–16 hours, but isprolonged to 10 days after repeated dosing.
Oral terbinafine is usually well tolerated.Side effects are gastric upset, rashes, tastedisturbance. Some cases of hepatic dysfunction,haematological disorder and severe cutaneousreaction are reported. Enzyme inducers lower,and enzyme inhibitors raise its steady-stateplasma levels. Terbinafine does not inhibitCYP450.
Topical terbinafine can cause erythema,itching, dryness, irritation, urticaria and rashes.
Use Terbinafine applied topically as 1% creamtwice daily is indicated in localized tinea pedis/cruris/corporis and pityriasis versicolor; 2–4weeks treatment is required according to the site,yielding high efficacy. Oral treatment with 250mg OD is reserved for onychomycosis, tineacapitis and wide spread lesions. Duration oftreatment varies from 3–6 months or moredepending on the site. Efficacy in nail infectionis ~80%, which is higher than griseofulvin anditraconazole.
Terbinafine is less effective against cuta-neous and mucosal candidiasis: 2–4 weeks oraltherapy may be used as an alternative tofluconazole.LAMISIL, SEBIFIN, DASKIL 250 mg tab, 1% topical cream.EXIFINE 125, 250 mg tabs, 1% cream; TERBIDERM 1% cream.
OTHER TOPICAL ANTIFUNGALS
All these drugs are used for dermatophytosis.
1. Tolnaftate It is an effective drug for tineacruris and tinea corporis, and most cases respondin 1–3 weeks. Because of poor penetrability, itis less effective in tinea pedis and otherhyperkeratinized lesions. For the same reason,it is ineffective in tinea capitis (involving scalp)and tinea unguium (involving nails).
Symptomatic relief occurs early, but ifapplications are discontinued before the fungusbearing tissue is shed—relapses are common.Resistance does not occur. Salicylic acid canaid tolnaftate by keratolytic action.
Tolnaftate causes little irritation, but isinferior in efficacy to imidazoles. It is noteffective in candidiasis or other types ofsuperficial mycosis.TINADERM, TINAVATE 1% lotion, TOLNADERM 1%cream.
2. Ciclopirox olamine It is a newer drugeffective in tinea infections, pityriasis versicolorand dermal candidiasis. High cure rates arereported. It penetrates superficial layers andreaches hair roots but systemic absorption isnegligible. Local tolerance without irritation isgood. Sensitization occurs occasionally. Formu-lated as nail lacquer, it has been used inonychomycosis. Vaginal candidiasis can betreated by 1% ciclopirox vaginal cream.BATRAFEN 1% cream, 1% topical solution, 1% vaginal cream,OLAMIN 1% cream.
3. Undecylenic acid It is fungistatic usedtopically, generally in combination with its zincsalt. It is inferior to the drugs described above;cure rates are low even after prolonged treatment.However, it is still used for tinea pedis, nappyrash and tinea cruris. Irritation and sensitizationare infrequent.TINEAFAX: Zinc undecenoate 8%, zinc naphthenate 8%,mesulphen 8%, methyl salicylate 2.5%, terpineol 2.5% oint.
4. Benzoic acid It has antifungal and anti-bacterial property in slightly acidic medium.Fungistatic action is weaker than tolnaftate;

797C
HA
PTER57
ANTIFUNGAL DRUGS
eradication of the fungus needs prolongedapplication till infected keratin is totally shed.
On hyperkeratotic lesions, it is used incombination with salicylic acid (as Whitfield’sointment: benzoic acid 5%, salicylic acid 3%).The latter, by its keratolytic action, helps toremove the infected tissue and promotes thepenetration of benzoic acid into the lesion.Irritation and burning sensation are experiencedby many patients.RINGCUTTER ointment.
5. Butenafine It is a benzylamine congenerof terbinafine with the same mechanism of action.However, it is used only topically in dermato-phytosis. Efficacy in tinea cruris/corporis/pedisis similar to that of topical terbinafine.BUTOP, FINTOP 1% cream; apply locally once or twice daily.
6. Quiniodochlor By the oral route, it isused as a luminal amoebicide (Ch. 60). It alsohas weak antifungal and antibacterial activity. Byexternal application, it has been used fordermatophytosis, mycosis barbae, seborrhoeicdermatitis, infected eczema, furunculosis andpityriasis versicolor.
Quiniodochlor is also used in vaginal creamsfor monilial and trichomonas vaginitis.VIOFORM 3% cream; DERMOQUINOL 4%, 8% cream.
7. Sodium thiosulfate It is a weak fungis-tatic, active against Malassezia furfur. A 20%solution applied twice daily for 3–4 weeks iseffective in pityriasis versicolor. However, normalpigmentation of the skin takes longer to return.It is not useful in other superficial mycosis.in KARPIN LOTION 20%.
PROBLEM DIRECTED STUDY
57.1 A 50-year-old woman presents with complaints of constant pain in the retrosternalregion for the past 2 weeks. The pain is markedly aggravated during swallowing. The conditionhas progressively worsened, and now even drinking water hurts. There is difficulty in swallowingas well. She informs that she is a diabetic and takes Tab. Glibenclamide 5 mg twice a dayfor the past two years, but has not checked her blood glucose for the last few months. Endoscopyreveals diffuse streaks of creamy yellow mucosal plaques and a few erosions in the esophagus.Scrapings from the plaque are sent for microbiological examination. Fasting blood glucoseis found to be 180 mg/dl. She is diagnosed as a case of esophageal candidiasis with poorlycontrolled diabetes mellitus.(a) What drug/drugs should be prescribed to treat her esophageal condition? What shouldbe the duration of therapy?(b) What are the aspects to be considered in view of the fact that the patient is a poorlycontrolled diabetic taking a sulfonylurea medication?(see Appendix-1 for solution)

Antiviral DrugsChapterChapterChapterChapterChapter 5858585858
Viruses are the ultimate expression of parasitism.They not only take nutrition from the host cell butalso direct its metabolic machinery to synthesizenew virus particles. Viral chemotherapy, thereforewas considered impossible, as it would requireinterference with cellular metabolism in the host.However, in the past 50 years virus directedenzymes have been identified in the infected celland some viruses have few enzymes of their ownwhich may have higher affinities for someantimetabolites or inhibitors than the regularcellular enzymes. In addition, drugs have beendeveloped which target virus specific steps likecell penetration, uncoating, reverse transcription,virus assembly or maturation, etc. Anotherstumbling block is that in majority of acuteinfections viral replication is already at its peakwhen symptoms appear. To be effective, therefore,therapy has to be started in the incubation period,i.e. has to be prophylactic or preemptive.
CLASSIFICATION
1. Anti-Herpes virusIdoxuridine, Trifluridine, Acyclovir,Valacyclovir, Famciclovir, Ganciclovir,Valganciclovir, Cidofovir, Foscarnet,Fomivirsen
2. Anti-Influenza virusAmantadine, Rimantadine, Oseltamivir,Zanamivir
3. Anti-Hepatitis virus/Nonselective antiviraldrugsPrimarily for hepatitis B: Lamivudine,Adefovir dipivoxil, TenofovirPrimarily for hepatitis C: Ribavirin,Interferon α
4. Anti-Retrovirus(a) Nucleoside reverse transcriptase
inhibitors (NRTIs): Zidovudine (AZT),
Didanosine, Stavudine,Lamivudine, Abacavir, Emtricitabine,Tenofovir (Nt RTI)
(b) Nonnucleoside reverse transcriptaseinhibitors (NNRTIs): Nevirapine, Efavi-renz, Delavirdine
(c) Protease inhibitors: Ritonavir,Atazanavir, Indinavir, Nelfinavir,Saquinavir, Amprenavir, Lopinavir
(d) Entry (Fusion) inhibitor: Enfuvirtide(e) CCR5 receptor inhibitor: Maraviroc(f) Integrase inhibitor: Raltegravir
ANTI-HERPES VIRUS DRUGS
These are drugs active against the Herpes groupof DNA viruses which include Herpes simplexvirus-1 (HSV-1), Herpes simplex virus-2(HSV2), Varicella-Zoster virus (VZV), Epstein-Barr virus (EBV), and Cytomegalovirus (CMV).Idoxuridine It is 5-iodo-2-deoxyuridine (IUDR), which actsas a thymidine analogue. It was the first pyrimidineantimetabolite to be used as antiviral drug. It competes withthymidine, gets incorporated in DNA so that faulty DNA isformed which breaks down easily. It is effective only againstDNA viruses and clinical utility is limited to topical treatmentof Herpes simplex keratitis. Because of low virus selectivity,higher local toxicity and rapid development of viral resistance,use of idoxuridine is restricted to superficial dendritic keratitiswhen rapid action is required. Idoxuridine eye drops act fasterthan acyclovir eye ointment, which is more effective whenthere is stromal involvement of the cornea. Ocular irritationoccurs with idoxuridine eye drops.Dose: 0.1% eye drops to be instilled hourly, then 2 hourlyand 4 hourly; apply 0.1% eye ointment at night.IDURIN, TOXIL 0.1% eye drops and eye oint.
Trifluridine It is a fluorinated nucleoside which acts in thesame way as idoxuridine, and inhibits HSV-1, HSV-2, CMVand related viruses. However, virus selectivity is low and DNAsynthesis in host cells is also affected. In India trifluridineeye drop is approved for use in H. simplex keratitis. Higherefficacy than idoxuridine eye drops is reported. Ocular irritationand lid edema can occur.

799C
HA
PTER58
ANTIVIRAL DRUGS
AcyclovirThis deoxiguanosine analogue antiviral drugrequires a virus specific enzyme for conversionto the active metabolite that inhibits DNAsynthesis and viral replication.
AcyclovirHerpes virus specific thymidine kinase
Acyclovir monophosphate Cellular kinases
Inhibits herpes virus DNApolymerase competitively
Acyclovirtriphosphate Gets incorporated in viral DNA
and stops lengthening of DNAstrand. The terminated DNAinhibits DNA-polymeraseirreversibly.
Acyclovir is preferentially taken up by the virusinfected cells. Because of selective generationof the active inhibitor in the virus infected celland its greater inhibitory effect on viral DNAsynthesis, acyclovir has low toxicity for hostcells: a several hundred-fold chemotherapeuticindex has been noted.
Acyclovir is active only against herpes groupof viruses; HSV-1 is most sensitive followed byHSV-2 > VZV=EBV, while CMV is practicallynot affected. HSV and VZV have been found todevelop resistance to acyclovir during therapy;the former primarily due to mutants deficientin thymidine kinase activity and the latterprimarily by change in specificity of virusdirected enzyme so that its affinity for acycloviris decreased.
Pharmacokinetics Only about 20% of an oraldose of acyclovir is absorbed. It is little plasmaprotein bound and is widely distributed attainingCSF concentration that is 50% of plasma con-centration. After topical application, it penetratescornea well. Acyclovir is primarily excretedunchanged in urine, both by glomerular filtrationand tubular secretion; plasma t½ is 2–3 hours.Renal impairment necessitates dose reduction.ZOVIRAX 200 mg tab, 250 mg/vial for i.v. inj; CYCLOVIR 200mg tab, 5% skin cream; HERPEX 200 mg tab, 3% eye oint, 5%
skin cream; OCUVIR 200, 400, 800 mg tab, 3% eye oint, ACIVIR-DT 200, 400, 800 mg tab. ACIVIR EYE 3% oint.
Use Acyclovir is effective in patients withnormal as well as deficient immune status.
1. Genital Herpes simplex Generally causedby type-2 virus; can be treated by topical, oralor parenteral acyclovir depending on stage andseverity of disease.
Primary disease: Topical treatment has lowefficacy; 5% ointment is applied locally 6 timesa day for 10 days. This is useful only if startedearly and in mild cases. Late and more severecases should receive oral therapy (1 g/day in 5divided doses or 400 mg TDS for 10 days) inaddition to local therapy. Both local and oraltherapies afford symptomatic relief and rapidhealing of lesions, but do not prevent recurrences.
Recurrent disease: Topical therapy is totallyineffective. Response to oral treatment is slowand incomplete; severe cases may be treatedparenterally—5 mg/kg i.v. infused over 1 hr,repeated 8 hourly for 10 days. Suppressive oraltherapy with 400 mg BD has been shown toprevent recurrences as long as given. It isrecommended to stop treatment after 1 yr andascertain whether the patient is still havingrecurrences; if so restart treatment. After prolon-ged therapy frequency of recurrences is reduced.Continuous acyclovir prophylaxis is generallyadvocated in patients with > 8 recurrences peryear. However, suppressive therapy reduces, butdoes not toally prevent, disease transmission tosexual partner.
2. Mucocutaneous H. simplex It is a type-1virus disease, remains localized to lips and gums;does not usually require specific treatment, butacyclovir skin cream may provide some relief.Spreading lesions may be treated with 10 dayoral acyclovir. Prophylactic oral therapy mayprevent sun exposure related recurrences. Thedisease often gets disseminated in immuno-compromised individuals and may be treated withoral or i.v. acyclovir (15 mg/kg/day) for 7 days,but recurrences are not prevented.

800S
EC
TIO
N12
ANTIMICROBIAL DRUGS
3. H. simplex encephalitis (type-1 virus):Acyclovir 10 to 20 mg/kg/8 hr i.v. for >10 daysis the drug of choice. Treatment is effective onlyif started early: delay precludes salutary effecton mortality and neurological complications.
4. H. simplex (type I) keratitis: Acyclovir isequally effective as idoxuridine in superficialdendritic corneal ulcer, and may be better fordeep stromal infections because of good cornealpenetration. Though acyclovir eye ointment actsslower than idoxuridine eye drops, blindness canbe prevented. The eye ointment should be applied5 times daily till 3 days after healing.
5. Herpes zoster: The varicella-zoster virus isless susceptible to acyclovir. As such, higherdoses are needed and it should be used only inimmunodeficient individuals or in severe cases:10 mg/kg/8 hr i.v. for 7 days. Oral therapy with800 mg 5 times daily is beneficial only if startedearly. It affords symptomatic relief and fasterhealing of lesions. Postherpetic neuralgia is notprevented, though its duration may be shortened.Acyclovir skin cream may be applied on herpeticulcers.
6. Chickenpox: in patients with immunodefi-ciency and in neonates only calls for specifictherapy. Acyclovir (15 mg/kg/day i.v. × 7 days)is the drug of choice: reduces fever, eruptions,hastens healing and prevents visceral complica-tions.
Oral acyclovir 400 mg 4 times a day for7 days given during the incubation period mayabort chickenpox in susceptible contacts.
Adverse effectsTopical: Stinging and burning sensation after eachapplication.Oral: The drug is well tolerated; headache, nausea,malaise and some CNS effects are reported.Intravenous: Rashes, sweating, emesis and fallin BP occur only in few patients.Dose-dependent decrease in g.f.r. is the mostimportant toxicity; occurs especially in thosewith kidney disease; normalises on disconti-nuation of the drug.
Reversible neurological manifestations (tremors,lethargy, disorientation, hallucinations, con-vulsions and coma) have been ascribed to higherdoses.No teratogenic potential has been noted.
Valacyclovir It is an ester prodrug ofacyclovir with improved oral bioavailability(55–70%) due to active transport by peptidetransporters in the intestine. During passagethrough intestine and liver, it is completelyconverted to acyclovir in the first passage byesterases. Thus, higher plasma levels of acyclovirare obtained improving clinical efficacy incertain conditions; e.g. it is the drug of choicein herpes zoster. Valaciclovir is excreted in urineas acyclovir with a t½ of 3 hours.Dose: For genital herpes simplex—first episode 0.5–1.0 g BD ×10 days; recurrent episode 0.5 g BD × 3 days; suppressivetreatment 0.5 g OD × 6–12 months.For orolabial herpes 2 g BD × 1 day; in immunocompromisedpatient 1 g BD × 5 days.For herpes zoster 1 g TDS × 7 days.VALCIVIR 0.5 g, 1.0 g tabs.
Famciclovir It is an ester prodrug of aguanine nucleoside analogue penciclovir, whichhas good oral bioavailability and prolonged intra-cellular t½ of the active triphosphate metabolite.Like acyclovir, it needs viral thymidine kinasefor generation of the active DNA polymeraseinhibitor. Famciclovir inhibits H. simplex, H.zoster but not acyclovir-resistant strains. Someactivity against hepatitis B virus (HBV) has beennoted. It is used as an alternative to acyclovirfor genital or orolabial herpes and herpes zoster.Early treatment of herpes zoster reduces theduration of post herpetic neuralgia, but not itsincidence.Dose: Genital herpes (1st episode) 250 mg TDS × 5 days;recurrent cases 250 mg BD for up to 1 year. Herpes zoster andorolabial herpes 500 mg TDS for 7–10 days.FAMTREX 250, 500 mg tabs.Famciclovir is a less active alternative tolamivudine in chronic hepatitis B, but not inresistant cases. Side effects are headache, nausea,loose motions, itching, rashes and mentalconfusion.Penciclovir, the active metabolite of famciclovir is available fori.v. use in some countries.

801C
HA
PTER58
ANTIVIRAL DRUGS
Ganciclovir It is an analogue of acyclovir which is activeagainst all herpes viruses including H. simplex, H. zoster, EBVand CMV against which it is most active. Ganciclovir is alsoactivated intracellularly by virus specific thymidine kinase andits triphosphate nucleotide preferentially inhibits viral DNApolymerase. This active metabolite attains much higherconcentration inside CMV infected cells. The precursor cellsin bone marrow are also quite sensitive to ganciclovir, andthis may account for its bone marrow toxicity. Due to poororal absorption, bioavailability of ganciclovir is low (<10%).Valganciclovir, the valyl prodrug, has ~ 8 times higher bio-availability, and is preferred, where available. Ganciclovir andits active metabolite are mostly excreted unchanged in urine.The plasma t½ of ganciclovir is 2–4 hrs, but that of itstriphosphate inside CMV infected cells is > 24 hrs. Thesefactors account for its high activity against CMV infections.CMV can develop ganciclovir resistance by mutation of viralphosphokinase and/or viral DNA polymerase.
Systemic toxicity of ganciclovir is high (bone marrowdepression, rash, fever, vomiting, neuropsychiatric distur-bances). Therefore, use is restricted to prophylaxis andtreatment of severe CMV infections (pneumonia/colitis/retinitis) in immunocompromised (AIDS, transplant recipient)patients. Treatment may be initiated with i.v. infusion ofganciclovir 10 mg/kg/day which can prevent blindness in AIDSpatients with CMV retinitis. Oral valganciclovir has replacedi.v. ganciclovir for long-term therapy. After control of retinitis,oral suppressant therapy is indicated.Dose: Prophylaxis and treatment of CMV infections inimmunocompromised patients: 5 mg/kg twice daily for 1–3weeks, followed by 5 mg/kg once daily.GANGUARD 250, 500 mg tabs.
Cidofovir It is a monophosphate nucleotide analogue ofcytidine which inhibits most DNA viruses including HSV, CMV,pox and adenoviruses. Many HSV resistant to acyclovir andmany CMV resistant to ganciclovir are susceptible. Becauseit is a monophosphate, it does not require viral phosphokinaseand is converted to the active diphosphate by cellularenzymes. Cidofovir diphosphate does not preferentiallyaccumulate in virus infected cells, but remains intracellularlyfor long periods to inhibit viral DNA polymerase, as well asacts as its alternative substrate. Weekly therapy is, therefore,possible despite short plasma t½ (2–3 hours) of cidofoviritself. CMV develops cidofovir resistance by mutation of itsDNA polymerase.
Very little cidofovir is absorbed orally. It is administeredby infusion with pre and post dose oral probenecid whichinhibits its tubular secretion and improves its availability forentering into cells, as well as reduces nephrotoxicity. Cidofovir5 mg/kg i.v. weekly and then every 15 dyas is used for CMVretinitis in AIDS patients, particularly those who have failedganciclovir therapy. It can also be used for acyclovir-resistantmucocutaneous herpes simplex in immunosuppressed patients.It can be applied topically on anogenital warts. The primarytoxicity of cidofovir is dose related kidney damage. Gastricdisturbances, constitutional symptoms, hypersensitivityreactions, neutropenia and uveitis are the other adverse effects.
Foscarnet It is a simple straight chain phosphonateunrelated to any nucleic acid precursor which inhibits viralDNA polymerase and reverse transcriptase. It is active againstH. simplex (including strains resistant to acyclovir), CMV(including ganciclovir-resistant ones), other herpes groupviruses and HIV. Viral resistance to foscarnet is minimal.However, viral selectivity of foscarnet is low. Oral absorptionis poor. Its t½ is 4–8 hours, and it is not metabolised.
Toxicity of foscarnet is high: damages kidney— producesa renal diabetes like condition, acute renal failure can alsooccur. Anaemia, phlebitis, tremor, convulsions and otherneurological as well as constitutional symptoms due tohypocalcaemia are frequent. Administered by i.v. infusion,foscarnet has been used for:1. CMV retinitis and other CMV infections in AIDS patients;efficacy is similar to ganciclovir, includes resistant cases, butproduces more adverse effects.2. Acyclovir-resistant mucocutaneous H. simplex type 2 andvaricella-zoster infections in AIDS patients.
When used to treat associated CMV/H. simplex/VZVinfection in AIDS patient, it decreases HIV viral titre, andmay improve outcome in patients receiving highly activeantiretroviral therapy (HAART).
Fomivirsen It is an antisense oligonucleotide which bindsto the mRNA of CMV and interferes with transcription ofearly peptides in viral replication. CMV that has becomeresistant to ganciclovir, cidofovir and foscarnet is inhibitedby fomivirsen. For CMV retinitis it has been injected weekly-to-monthly into the vitreous humor. Ocular complications arecommon and it has been discontinued in USA.
ANTI-INFLUENZA VIRUS DRUGS
AmantadineChemically, it is a unique tricyclic amineunrelated to any nucleic acid precursor, butinhibits replication of influenza A virus (amyxovirus). The antiviral activity of amantadineis strain specific; influenza B is not affected.Moreover, H5N1 (avian influenza/bird flu) andH1N1 (swine flu) strains of influenza A areresistant in most areas. It appears to act at anearly step (possibly uncoating) as well as at alate step (viral assembly) in viral replication. Aprotein designated ‘M2’ which acts as an ionchannel has been identified as one of its targetsof action. Resistance to amantadine develops bymutation causing amino acid substitutions in theM2 protein. Amantadine is well absorbed orallyand excreted unchanged in urine over 2–3 days(t½ 16 hr).

802S
EC
TIO
N12
ANTIMICROBIAL DRUGS
Adverse effects Generally well tolerated;nausea, anorexia, insomnia, dizziness, nightmares,lack of mental concentration, rarely hallucinationshave been reported. Ankle edema occurs due tolocal vasoconstriction.
Uses
1. Prophylaxis of influenza A2 during anepidemic or seasonal influenza, especially in highrisk patients. Influenza season and epidemicsgenerally last ~ 2 months, and only this periodneeds to be covered by prophylaxis. Only whenthe epidemic causing strain of virus is known tobe sensitive to amantadine, should prophylacticuse be considered. For seasonal prophylaxissuccess rate is variable, but often substantial.Amantadine does not interfere with antibodyresponse to influenza vaccination; both may begiven together. If the vaccine is given, amantadinecan be stopped after 2 weeks. However, amanta-dine is no longer recommended in UK, either forprophylaxis or for treatment of influenza.2. Treatment of influenzal (A2) illness: a modesttherapeutic effect (reduction in fever, conges-tion, cough and quicker recovery) occurs if thedrug is given immediately after the symptomsappear. A 5 day treatment is advised.3. Parkinsonism (see Ch. 31)Dose: 100 mg BD, elderly—half dose, children 5 mg/kg/day;100 mg OD may be used for prophylaxis.AMANTREL, NEAMAN 100 mg tab.
Contraindications: epilepsy and other CNSdisease; gastric ulcer, pregnancy.
Rimantadine This methyl derivative of amanta-dine is more potent, longer acting (t½ 30 hours)and better tolerated than the parent drug.Incidence of side effects is lower. Oral bioavai-lability of rimantadine is higher and it is largelymetabolized by hydroxylation followed byglucuronide conjugation. The metabolites areexcreted in urine. Dose and clinical applicationin influenza A is similar to amantadine and itis being preferred over the latter. However,amantadine resistant virus is resistant torimantadine as well.
Dose: 100 mg BD; elderly and renal insufficiency patients 100OD; children 5 mg/kg/day.FLUMADINE 100 mg tab.
Oseltamivir This newer anti-influenza virusdrug is a sialic acid analogue with broad spectrumactivity covering influenza A (amantadine sensi-tive as well as resistant), H5N1 (bird flu), nH1N1(swine flu) strains and influenza B. It is an esterprodrug that is rapidly and nearly completelyhydrolysed during absorption in intestine and byliver to the active form oseltamivir carboxylatewith an oral bioavailability of ~ 80%. The activemetabolite is not further metabolized and isexcreted by the kidney with a t½ of 6–10 hours.It acts by inhibiting influenza virus neuraminidaseenzyme which is needed for release of progenyvirions from the infected cell. Spread of the virusin the body is thus checked. Resistance candevelop by mutation of the viral neuraminidaseenzyme. In many areas oseltamivir-resistantH1N1 (seasonal influenza) and H5N1 have beenencountered, though swine flu (nH1N1) is stillmostly sensitive. Some oseltamivir-resistantstrains remain susceptible to zanamivir and viceversa.
Oseltamivir is indicated both for prophylaxisas well as treatment of influenza A, swine flu,bird flu and influenza B. Started at the onset ofsymptoms, it is the most effective drug; reducesthe severity, duration and complications of theillness. Prophylactic use for 5–10 days preventsillness in contacts of influenza patients.Dose: therapeutic 75 mg oral BD for 5 days; prophylactic75 mg OD.TAMIFLU, ANTIFLU 75 mg cap, 12 mg/ml susp., FLUVIR75 mg cap.
Side effects are nausea and abdominal paindue to gastric irritation (reduced by taking thedrug with food), headache, weakness, sadness,diarrhoea, cough and insomnia. Skin reactionshave been reported.
Zanamivir Another influenza A (includingamantadine-resistant, nH1N1, H5N1 strains) andinfluenza B virus neuraminidase inhibitor thatis administered by inhalation as a powder dueto very low oral bioavailability. Small amount

803C
HA
PTER58
ANTIVIRAL DRUGS
that is absorbed after inhalation is excreted bythe kidney with a t½ of 2–5 hours. Themechanism of action, clinical utility and efficacyof zanamivir are similar to that of oseltamivir.Some variant strains resistant to oseltamivirremain sensitive to zanamivir and vice versa.It can be used as an alternative to oseltamivir,and is equally effective in reducing severity,duration and complications of the disease.Prophylactic use may be made for 7–10 daysin household contacts.Dose: 10 mg through breath actuated inhaler, BD × 5 daysfor treatment, and OD for prophylaxis.RELENZA 5 mg/actuation powder inhaler.
The inhaled powder can induce bronchospasmin some individuals. This may be severe in asth-matics; contraindicated in them. Headache,dizziness, nausea and rashes are mild andinfrequent side effects.
ANTI-HEPATITIS VIRUS/NONSELECTIVEANTIVIRAL DRUGS
Several antiviral drugs are relatively virus non-selective and inhibit viruses belonging todifferent classes; even cover both DNA and RNAviruses. While hepatitis B virus (HBV) is a DNAvirus which, like retroviruses, can integrate intohost chromosomal DNA to establish permanentinfection, the hepatitis C virus (HCV) is a RNAvirus, which does not integrate into chromo-somal DNA, does not establish noncurableinfection, but frequently causes chronic hepatitis.
Lamivudine, a nucleoside analogue, is activeagainst HVB as well as HIV, and is describedwith antiretroviral drugs on p. 807–08.
Adefovir dipivoxil Adefovir is a mono-phosphate analogue of AMP which is activeagainst HBV and some other DNA as well asRNA viruses, but is used only for hepatitis causedby HBV. Esterases in the intestine and liverrelease the active drug during absorption to attainoral bioavailability of ~60% in terms of adefovir,which is then distributed in whole body water.On entering cells, adefovir is phosphorylated tothe diphosphate which has high affinity for HBV
DNA polymerase compared to host cell DNApolymerase. This enzyme is inhibited andadefovir itself gets incorporated in the viral DNAresulting in termination of the DNA chain.Adefovir is primarily excreted by the kidney.While its plasma t½ is 7 hours, intracellulart½ of the diphosphate is upto 18 hours.
Adefovir is indicated in chronic hepatitis B,including lamivudine-resistant cases and thosehaving concurrent HIV infection. There isno cross resistance between adefovir andlamivudine. Clinical, biochemical (liver functiontests), histological, serological and virologicalresponse occurs in nearly 50% patients within1 year. More cases respond with continuedtreatment. The optimum duration of treatmentis uncertain. Ocurrence of adefovir resistanceis infrequent.Dose: 10 mg/day; ADESERA, ADFOVIR 10 mg tab.
At 10 mg/day dose adefovir is well tolerated.Side effects are sore throat, headache, weakness,abdominal pain and flu syndrome. Nephrotoxicityoccurs at higher doses and in those withpreexisting renal insufficiency. Lactic acidosisis a risk in patients receiving anti-HIV drugs.
Tenofovir It is a monophosphate nucleotiderelated to AMP, which is active against HBV aswell as HIV. Due to very low oral absorption,it is used as the disoproxil ester prodrug, whichnot only improves bioavailability, but also intra-cellular passage of the active form. Tenofovirreleased from hydrolysis of the prodrug isdiphosphorylated by cellular kinases into tenofovirdiphosphate which preferentially inhibits HBV-DNA polymerase and HIV-reverse transcriptase.Affinity for host DNA-polymerase is very low.It also gets incorporated in the viral DNA to causechain termination.
Tenofovir disoproxil is incompletely, butadequately absorbed after oral intake, and islargery excreted by the kidney with a plasmat½ of ~ 16 hours. It produces few side effects,which are mostly limited to the g.i. tract: nausea,flatulence, abdominal discomfort, loose motionsand headache. Remarkably, renal toxicity is quiterare, though slight increase in serum creatinineoccurs. Drug interactions are also not significant.

804S
EC
TIO
N12
ANTIMICROBIAL DRUGS
Administered in a dose of 300 mg daily,tenofovir disoproxil has produced good clinicaland virological response in chronic hepatitis B.In a comparative study, higher percentage ofpatients responded within one year of use thanwith adefovir. A response rate of > 90% has beenreported among HBe antigen negative patients.Tenofovir-resistance has not developed duringtreatment of chronic hepatitis B, and it is effectivein lamivudine-resistant cases. Due to its highefficacy, good tolerability and low risk ofresistance, tenofovir is being preferred for HBVinfection, especially lamivudine resistant cases.TENTIDE, TENOF 300 mg tab; 1 tab OD.
Ribavirin This purine nucleoside analogue hasbroad-spectrum antiviral activity, including thatagainst influenza A and B, respiratory syncytialvirus and many other DNA and double strandedRNA viruses. Its mono- and triphosphate deriva-tives generated intracellularly inhibit GTP andviral RNA synthesis and have other sites of actionas well. Viral resistance to ribavirin is rare.
Oral bioavailability of ribavirin is ~50%. Itis partly metabolized and eliminated in a multi-exponential manner; accumulates in the body ondaily dosing and persists months after disconti-nuation; long term t½ is > 10 days.
Administered orally or i.v. ribavirin has beenused in severe influenza A/B and measles inimmunosuppressed patients as well as for herpesvirus infections, acute hepatitis, but is not a firstline drug for any of these. The most commontherapeutic use of oral ribavirin is in chronichepatitis C. Though ribavirin monotherapy mayproduce a response, it is incomplete. As percurrent recommendation, the first line treatmentof chronic hepatitis C is oral ribavirin combinedwith injected peginterferon for 6–12 months.Recurrent cases are treated in the same way.Nebulized ribavirin is used for respiratory syncy-tial virus bronchiolitis in infants and children,particularly those with congenital heart disease,prematurity or other high risk conditions. It hasalso shown efficacy in some rare viral infections.Dose: 200 mg QID; 400 mg TDS for body weight > 75 kg(children 15 mg/kg/day).VIRAZIDE, RIBAVIN 100, 200 mg caps, 50 mg/5 ml syr.
Prominent toxic effects are anaemia, bonemarrow depression, haemolysis, CNS and g.i.symptoms. It is also teratogenic. The aerosol cancause irritation of mucosae and bronchospasm.
Interferon αααααInterferons (IFNs)are low molecular weightglycoprotein cytokines produced by host cellsin response to viral infections, TNFα, IL-1 andsome other inducers. They have nonspecificantiviral as well as other complex effects onimmunity and cell proliferation. Interferons bindto specific cell surface receptors and affect viralreplication at multiple steps, viz. viralpenetration, synthesis of viral mRNA, assemblyof viral particles and their release, but the mostwidespread effect is direct or indirectsuppression of viral protein synthesis, i.e.inhibition of translation. Interferon receptors areJAK-STAT tyrosine protein kinase receptorswhich on activation phosphorylate cellularproteins. These then migrate to the nucleus andinduce transcription of ‘interferon-induced-proteins’ which exert antiviral effects.
Interferons inhibit many RNA and DNAviruses, but they are host specific: those producedby another species have poor activity in man.Three types of human IFNs (α, β and γ) are knownto have antiviral activity. Only IFNα2A and IFNα2B
produced by recombinant technology are availableand are clinically used. Both are nonglycosylatedlow MW proteins administered by i.m. or s.c.injection. Their pegylated forms are meant fors.c. injection at weekly intervals. Plasma levelsof pegIFNα2A are sustained twice longer thanthose of pegIFNα2B.
After i.m./s.c. injection, interferon is distri-buted to tissues. It is degraded mainly in liver andkidney, and remains detectable in plasma for24 hours. However, cellular effects are longerlasting because the interferon induced proteinspersist, so that IFN is generally administered thriceweekly. Complexed with polyethylene glycol(peginterferon), it is absorbed more slowly—exerts more sustained effects, permiting weeklyadministration and improving clinical efficacy.

805C
HA
PTER58
ANTIVIRAL DRUGS
PegIFN has replaced IFN, except for conside-ration of cost.ALFERON: Interferon α2A 3MU/vial inj, ZAVINEX 3MU, 5MUvials for inj.REALFA-2B, SHANFERON, VIRAFERON: Interferon α2B 3MU,5MU vials for inj.
Uses
1. Chronic hepatitis B: IFNα2Α 2.5−5 ΜU/m2
or IFNα2Β 5−10 ΜU given 3 times per weekfor 4–6 months causes disappearance of HBV-DNA from plasma and improvement in liverfunction tests/histology in nearly half of thepatients. High doses (10 MU) injected thriceweekly for 6 months often produce prolongedremission, but relapses do occur. The pegIFNs180 μg s.c. once weekly for 24−48 weeksproduce better and more sustained responses.2. Chronic hepatitis C: IFNα2Β 3ΜU 3 timesweekly for 6–12 months has produced remissionin 50–70% patients. Viral RNA becomesundetectable and liver function tests return tonormal. Histology improves if response issustained. However, relapses occur in majorityof patients. PegIFNs 180 μg/week are moreeffective and induce longer lasting remissions.Combination with oral ribavirin increases numberof responders, and decreases chances of relapse.Combination therapy with IFN/pegIFN +ribavirin is particularly indicated in patients whodo not respond to IFN alone.3. AIDS-related Kaposi’s sarcoma: IFN is usedto treat AIDS related Kaposi’s sarcoma, but notto treat HIV as such. However, interferon accen-tuates haematological toxicity of zidovudine.4. Condyloma acuminata: caused by papillomavirus is usually treated with topical podophyllin.Intralesional interferon injection may be usedin refractory cases.5. H. simplex, H. zoster and CMV: For theseinfections in immunocompromised patients,interferon is inferior to acyclovir/ganciclovir. Itmay be used as second line/adjuvant drug.6. Interferons are also used in chronic myeloidleukaemia, follicular lymphoma, cutaneous T-celllymphoma and multiple myeloma.
Interferon is not effective orally. Clinicalutility of s.c. or i.m. injected interferon is limitedby substantial adverse effects.
Adverse effects
• Flu-like symptoms—fatigue, aches and pains,malaise, fever, dizziness, anorexia, nausea,taste and visual disturbances develop fewhours after each injection, but become milderlater.
• Neurotoxicity—numbness, neuropathy, alteredbehaviour, mental depression, tremor, sleepi-ness, rarely convulsions.
• Myelosuppression: dose dependent neutro-penia, thrombocytopenia.
• Thyroid dysfunction (hypo as well as hyper).• Hypotension, transient arrhythmias, alopecia
and liver dysfunction.
ANTI-RETROVIRUS DRUGS
These are drugs active against human immuno-deficiency virus (HIV) which is a retrovirus. Theyare useful in prolonging and improving the qualityof life and postponing complications of acquiredimmunodeficiency syndrome (AIDS) or AIDS-related complex (ARC), but do not cure theinfection. The clinical efficacy of antiretrovirusdrugs is monitored primarily by plasma HIV-RNAassays and CD4 lymphocyte count carried outat regular intervals.HIV is a single stranded RNA retrovirus which uniquely carriesout reverse transcription of proviral DNA from viral RNA(normally RNA is transcripted from DNA) with the help ofa viral RNA-dependent DNA polymerase (reverse trans-criptase). The primary cell type attacked by HIV is the CD4+helper T-lymphocyte, but later macrophages and some othercell types may also be infected. When population of CD4cells declines markedly (<200 cells/μL), cell mediated immunity(CMI) is lost and opportunistic infections abound, to whichthe victim ultimately succumbs, unless treated. Because theHIV genome integrates with the host DNA, eradication ofthe virus from the body of the victim appears impossible atpresent.
Over the past 30 years, a number of virusspecific targets have been identified and drugsfor these developed. We now have drugs whicheffectively suppress HIV replication and restore

806S
EC
TIO
N12
ANTIMICROBIAL DRUGS
CMI for variable periods of time. The twoestablished targets for anti-HIV attack are:(a) HIV reverse transcriptase: Which transcriptsHIV-RNA into proviral DNA.(b) HIV protease: Which cleaves the large virusdirected polyprotein into functional viralproteins.
In addition, some newer targets being exploitedare:• Fusion of viral envelope with plasma
membrane of CD4 cells through which HIV-RNA enters the cell.
• Chemokine coreceptor (CCR5) on host cellswhich provide anchorage for the surfaceproteins of the virus.
• HIV-integrase: Viral enzyme which integratesthe proviral DNA into host DNA.
The first anti-retrovirus (ARV) drug zidovudinewas made available for use in 1987. Over thepast 25 years a large number of drugs belongingto 3 classes viz. Nucleoside or Non-nucleosidereverse transcriptase inhibitors (NRTIs andNNRTIs) and HIV-protease inhibitors (PIs) havebeen produced and extensively used. Recentlyfew drugs for the newer targets have also becomeavailable for use in patients who have failedseveral regimens employing the 3 major groupsof drugs, and have viral multiplication despiteoptimized background therapy.
The aim of anti-HIV therapy is to causemaximal suppression of viral replication for themaximal period of time that is possible. For this,ARV drugs are always used in combination ofat least 3 drugs and regimens have to be changedover time due to development of resistance. Lifelong therapy is required.
Over the past 35 years, HIV infection has emerged as amajor global health problem. Though, with the use of effectiveantiretroviral therapy (ART) the prevalence is declining in thepresent century, WHO estimate in 2009 showed that 33.3 millionpeople world wide were living with HIV, and HIV/AIDS killed1.8 million people in 2010, most of them in subsaharan Africa.India is a relatively low HIV prevalence country, but it has the3rd largest number of people living with HIV, which was 2.4million in 2009, concentrated mostly among female sex workers,injection drug abusers, transgenders, etc. India launched itsNational AIDS Control Programme (NACP) in 1992, but theprevalence and annual death rate has declined steadily only
after 2004 when the National AIDS Control Organization (NACO)rolled-out free combination ART to eligible registered patients.Currently ~ 5 lac patients are alive on ART*, and new infectionshave declined by > 50% during the last decade, which in a largemeasure, is due to effective use of combination ART.
Nucleoside reverse transcriptaseinhibitors (NRTIs)
Zidovudine It is a thymidine analogue (azido-thymidine, AZT), the prototype NRTI. Afterphosphorylation in the host cell—zidovudinetriphosphate selectively inhibits viral reversetranscriptase in preference to cellular DNApolymerase.
Single-stranded viral RNAVirus directed reverse transcriptase(inhibited by zidovudine triphosphate)
Double-stranded proviral DNAOn the template of single-stranded RNA genomeof HIV, a double-stranded DNA copy is producedby viral reverse transcriptase. This proviral DNAtranslocates to the nucleus and is integrated withchromosomal DNA of the host cell (by viralintegrase enzyme) which then starts transcribingviral genomic RNA as well as viral mRNA. Underthe direction of viral mRNA, viral regulatory andstructural proteins are produced in the form ofa polyprotein. Finally, viral particles areassembled and matured after fractionation of thepolyprotein by viral protease. Zidovudine thusprevents infection of new cells by HIV, but hasno effect on proviral DNA that has alreadyintegrated into the host chromosome. It iseffective only against retroviruses. Zidovudineitself gets incorporated into the proviral DNAand terminates chain elongation. Resistance toAZT occurs by point mutations which alterreverse transcriptase enzyme. In the past, whenAZT was used alone, >50% patients becamenonresponsive to AZT within 1–2 years therapydue to growth of resistant mutants.
Pharmacokinetics The oral absorption of AZTis rapid, but bioavailability is ~65%. It is quickly
* NACO Annual report 2011-12 [http/www.nacoonline.org]

807C
HA
PTER58
ANTIVIRAL DRUGS
cleared by hepatic glucuronidation (t½ 1 hr);15–20% of the unchanged drug along with themetabolite is excreted in urine. Plasma proteinbinding is 30% and CSF level is ~50% of thatin plasma. It crosses placenta and is found in milk.Dose Adults 300 mg BD; Children 180 mg/m2 (max 200 mg)6–8 hourly.RETROVIR, ZIDOVIR 100 mg cap, 300 mg tab, 50 mg/5 ml syrVIRO-Z, ZIDOMAX, ZYDOWIN 100 mg cap, 300 mg tab. (to betaken with plenty of water).
Adverse effects Toxicity is mainly due topartial inhibition of cellular mitochondrial DNApolymerase γ which has higher affinity forzidovudine triphosphate than chromosomal DNApolymerase. Anaemia and neutropenia are themost important and dose-related adverse effects.Nausea, anorexia, abdominal pain, headache,insomnia and myalgia are common at the startof therapy, but diminish later.Myopathy, pigmentation of nails, lactic acidosis,hepatomegaly, convulsions and encephalopathyare infrequent.
Interactions Paracetamol increases AZT toxi-city, probably by competing for glucuronidation.Azole antifungals also inhibit AZT metabolism.Other nephrotoxic and myelosuppressive drugsand probenecid enhance toxicity. Stavudine andzidovudine exhibit mutual antagonism bycompeting for the same activation pathway.
Use Zidovudine is used in HIV infected patientsonly in combination with at least 2 other ARVdrugs. It is one of the two optional NRTIs usedby NACO for its first line triple drug ARVregimen. Its efficacy as monotherapy in AIDS wasconfirmed in the past. HIV-RNA titer is reducedto undetectable levels and CD4 count increasesprogressively. Immune status is improved andopportunistic infections become less common.There is a sense of well-being and patients gainweight. AZT also reduces neurological manifesta-tions of AIDS and new Kaposi’s lesions do notappear. Mortality among AIDS patients is reduced.However, beneficial effects are limited from afew months to a couple of years after whichprogressively non-responsiveness develops.
AZT, along with two other ARV drugs is thestandard choice for post-exposure prophylaxisof HIV, as well as for mother to offspringtransmission (see p. 814-15).
Didanosine (ddI) It is a purine nucleosideanalogue which after intracellular conversion todidanosine triphosphate competes with ATP forincorporation into viral DNA, inhibits HIVreverse transcriptase and terminates proviralDNA. Antiretroviral activity of didanosine isequivalent to AZT. Mutational resistance deve-lops, but only few AZT resistant mutants are non-responsive to didanosine also. Its use hasdeclined due to higher toxicity than other NRTIs.Dose: 400 mg/day (for > 60 kg BW), 250 mg/day (< 50 kg BW)1 hour before or 2 hour after meals.DINEX EC, DDRETRO, VIROSINE DR 250 mg, 400 mg tabs.
Oral absorption of didanosine is somewhat erratic due to acidlability. It is metabolized as well as excreted unchanged; t½1 to 1.5 hr. In contrast to AZT, it does not cause myelo-suppression. The major dose-related toxicity is peripheral(stocking and glove) neuropathy, which may be irreversible,and rarely acute pancreatitis. Diarrhoea, abdominal pain, drymouth and nausea are the side effects.
Stavudine (d4T) It is also a thymidine ana-logue which acts in the same way as AZT. Byutilizing the same thymidine kinase for activation,AZT antagonises the effect of stavudine and thetwo should not be used together. It should alsonot be combined with didanosine, because bothcause peripheral neuropathy. Resistance tostavudine develops as for other NRTIs.
It is well absorbed orally and rapidly meta-bolized (t½ 1.5 hr). The anti-HIV efficacy ofstavudine is comparable to AZT, and it is usedin combination regimens. Frequent peripheralneuropathy, lipodystrophy, lactic acidosis, andrarely pancreatitis are the serious adverse effectswhich have restricted its use. However foroperational and cost considerations, stavudineis one of the optional components of first lineregimen used by NACO.Dose: 30 mg BD irrespective of body weight (WHO and NACOguidelines 2007)STAG, STAVIR, VIROSTAV 30, 40 mg caps.
Lamivudine (3TC) This deoxycytidineanalogue is phosphorylated intracellularly and

808S
EC
TIO
N12
ANTIMICROBIAL DRUGS
inhibits HIV reverse transcriptase as well as HBVDNA polymerase. Its incorporation into DNAresults in chain termination. Most human DNApolymerases are not affected and systemic toxi-city of 3TC is low. Point mutation in HIV-reversetranscriptase and HBV-DNA polymerase givesrise to rapid lamivudine resistance. However,certain lamivudine-resistant mutants becomeslow growing and have lower virulence. Somecross-resistance with didanosine has been notedamong HIV.
Oral bioavailability of 3TC is high and plasmat½ longer (6–8 hours). Intracellular t½ is stilllonger (> 12 hr). It is mainly excreted unchangedin urine.
Lamivudine is used in combination with otheranti-HIV drugs, and appears to be as effectiveas AZT. It synergises with most other NRTIs forHIV, and is an essential component of all firstline triple drug NACO regimens for AIDS. Itis also a first line drug for chronic hepatitisB. HBV-DNA titre is markedly reduced andbiochemical as well as histological indices ofliver function improve. However, viral titres riseagain after discontinuation. Even with continuedmedication HBV viraemia tends to return after1–4 years due to emergence of resistant mutants.Dose: For chronic hepatitis B—100 mg ODFor HIV infection— 150 mg BD, or 300 mg OD.LAMIVIR 150 mg tab, 150 mg/ 5 ml soln; LAMIVIR-HBV 100mg tab; HEPTAVIR, LAMIDAC, LAMUVID, VIROLAM 100,150 mg tabs;
Lamivudine is generally well tolerated andhas low toxicity, because of which it is accordedhigh priority in use. Side effects are few—headache, fatigue, rashes nausea, anorexia,abdominal pain. Pancreatitis and neuropathy arerare. Hematological toxicity does not occur.Abacavir (ABC) This guanosine analogue isa clinically potent ARV drug that acts afterintracellular conversion to carbovir triphosphate,which gets incorporated in proviral DNA andterminates chain elongation. Rapid reduction inplasma HIV-RNA count and rapid rise in CD4cell count has been noted when abacavir wasgiven to AIDS patients. Resistance to ABCdevelops slowly, and it exhibits little crossresistance with other NRTIs. Its oral bioavaila-
bility is 80% and it is mainly eliminated bymetabolism. The plasma t½ is 1–1.5 hour, butintracellular t½ of the active metabolite is >12hours. Hypersensitivity reactions such as rashes,fever, abdominal pain, bowel, upset, flu-likerespiratory and constitutional symptoms, whichoccur in 2–5% adult patients, are the majorproblems. Abacavir must be promptly stoppedwhen the reaction occurs, because fatalities haveoccurred when patients developing the reactionwere given further doses of ABC. A genetic basisand massive release of TNFα have been relatedto this reaction. Abacavir should never be givenagain to a patient who has developed this reaction.Other side effects are not serious. Lypodystrophyis least likely. Avoidance of alcohol is advised.Combination regimens including abacavir arefrequently used.Dose: 300 mg BD or 600 mg OD.ABAVIR, ABAMUNE 300 mg tab.
Tenofovir This is the only nucleotide (notnucleoside) analogue that is a relatively neweraddition to the clinically used anti-HIV drugs.It is also active against HBV, and its pharma-cology is described on p. 803. Tenofovir wasinitially used only in previously treated patients,but because of good tolerability profile, it isnow being included in first line regimens as well.Tenofovir containing regimens have been foundat least as effective and less toxic as other firstline regimens. NACO includes tenofovir in itsfirst line 3 drug regimen as an alternative wheneither zidovudine or nevirapine/efavirenz cannotbe used due to toxicity/contraindication.
Non-nucleoside reverse transcriptaseinhibitors (NNRTIs)
Nevirapine (NVP) and Efavirenz (EFV)These are nucleoside unrelated compounds whichdirectly inhibit HIV reverse transcriptase withoutthe need for intracellular phosphorylation. Theirlocus of action on the enzyme is also different,and they are non-competitive inhibitors. Theyare more potent than AZT on HIV-1, but do notinhibit HIV-2. Accordingly, they are not indicatedin infections caused by HIV-2. If used alone,viral resistance to NNRTIs develops rapidly by

809C
HA
PTER58
ANTIVIRAL DRUGS
point mutation of the enzyme; they should alwaysbe combined with 2 other effective drugs. Cross-resistance between NVP and EFV is common,but not with NRTIs or PIs. A patient failing anyNNRTI regimen should not be treated withanother NNRTI.
NVP is well absorbed orally; is extensivelymetabolized, mainly by CYP3A4 and to a lesserextent by CYP2B6, with a t½ of ~ 30 hours. Oralabsorption of EFV is ~ 50%, but the t½ is longer(48 hours). It is completely metabolized, mainlyby CYP2B6 and a smaller fraction by CYP3A4.Both are enzyme inducers, and cause auto-induction of their own metabolism. However, EFVinhibits CYP3A4 as well. Nevirapine is startedat a lower dose (200 mg/day); the dose is doubledafter 2 weeks when its blood levels go down dueto autoinduction. Such dose escalation is notrequired for EFV. Rifampin induces NVPmetabolism and makes it ineffective, but has littleeffect on EFV levels. If a patient being treatedwith NVP develops TB and is put on rifampin,NVP should be replaced by EFV.
The NNRTIs are indicated in combinationregimens for HIV. Either NVP or EFV is includedin the first line triple drug regimen used byNACO. These drugs have also succeeded inreducing HIV-RNA levels when an earlier regimen(not including an NNRTI) has failed.
Nevirapine (NVP)Dose: Initially 200 mg/day, to be increased after 2 weeks to200 mg twice daily (because autoinduction reduces levels).NEVIMUNE, NEVIVIR, NEVIPAN, NEVIRETRO 200 mg tab.Rashes are the commonest adverse effect,followed by nausea and headache. Occasionallyskin reactions are severe. Fever and rise intransaminases occurs dose dependently. NVP ispotentially hepatotoxic. In patients developingNVP toxicity, it should be replaced by EFV whichhas low hepatotoxicity. NVP should not be usedin patients with hepatic dysfunction.
Efavirenz (EFV) Its side effects are headache,rashes, dizziness, insomnia and a variety ofneuropsychiatric symptoms. However, thesesymptoms decrease over time and discontinu-
ation rate (due to adverse effect) is low. EFVis contraindicated in pregnancy and in womenlikely to get pregnant, since it is teratogenic.Because of its longer plasma t½, occasionalmissed doses of EFV are less damaging.Dose: 600 mg OD on empty stomach.EFFERVEN, VIRANZ, EVIRENZ 200 mg cap, 600 mg tab.
Retroviral protease inhibitors (PIs)An aspartic protease enzyme encoded by HIVis involved in the production of structural proteinsand enzymes (including reverse transcriptase andintegrase) of the virus from the large viralpolyprotein synthesized in the infected cell. Thepolyprotein is broken into various functionalcomponents by this protease enzyme. It acts ata late step in HIV replication, i.e. maturation ofthe new virus particles when the RNA genomeacquires the core proteins and enzymes. Sixprotease inhibitors—Atazanavir (ATV), Indinavir(IDV), Nelfinavir (NFV), Saquinavir (SQV),Ritonavir (RTV) and Lopinavir (in combinationwith ritonavir LPV/r) have been marketed in Indiafor use against HIV. They bind to the active siteof protease molecule, interfere with its cleavingfunction, and are more effective viral inhibitorsthan AZT. Because they act at a late step of viralcycle, they are effective in both newly as wellas chronically infected cells. Under theirinfluence, HIV-infected cells produce immaturenoninfectious viral progeny—hence preventfurther rounds of infection.
Oral bioavailability of PIs is variable (IDVand RTV ~65%, NFV >20%, SQV 15%) and theirplasma t½ ranges from 2–8 hours. All areextensively metabolized mainly by CYP3A4,except NFV which is mainly a substrate ofCYP2C19. All PIs (especially ritonavir andlopinavir) are potent inhibitors of CYP3A4, whilesome other CYP isoenzymes are induced.The PIs interact with many drugs. Nelfinavir,lopinavir and ritonavir induce their own meta-bolism.
In the past monotherapy with one of thesedrugs in previously AZT treated patients reducedHIV viral levels, increased CD4 cell count and

810S
EC
TIO
N12
ANTIMICROBIAL DRUGS
improved the clinical condition. However, viralresistance developed against the PIs over monthsdue to selection of resistant mutants in astepwise manner. Combination of NRTIs with PIshas been found more effective than either druggiven alone, and triple therapy is more effectivethan double therapy. Current recommendationsare to use a PI in combination with either twoNRTIs or one NRTI + one NNRTI. However, PIsare avoided in 1st line regimens, because theiruse in initial regimens markedly restricts secondline regimen options. Most guidelines, includingthat of NACO, reserve them for failure cases.
Because different PIs inhibit as well as inducespecific CYP isoenzymes to different extents,drug interactions with them are common andoften unpredictable. Manufacturer’s packageinserts should be consulted while coprescribingany other drug. Specifically, metabolism of PIsis induced by rifampin and other enzyme inducersrendering them ineffective. Another problem intheir use is the large tablet load. In case ofdifferent PIs, 6–18 tablets are to be taken daily,some on empty stomach, but others with meals;and this has to go on for months and years.Therefore, patient acceptability and complianceare often low. One of the strategies adopted toreduce the dose of ATV, IDV, LPV and SQV isto combine them with a low and subtherapeuticdose (100 mg) of ritonavir. By reducing first passmetabolism, ritonavir increases the bioavailabilityand by slowing systemic metabolism decreasesclearance of the companion PI. This ‘boosted PIregimen’ permits reduction in the number/frequency of tablets to be taken each day.Lopinavir is marketed only in combination withritonavir. Nelfinavir is not to be combined withritonavir because it is metabolized mainly byCYP2C19 that is not inhibited.
The most prominent adverse effects of PIsare gastrointestinal intolerance, asthenia,headache, dizziness, limb and facial tingling,numbness and rashes. Of particular concern arelipodystrophy (abdominal obesity, buffalo humpwith wasting of limbs and face), dyslipidaemia(raised triglycerides and cholesterol) which may
necessitate hypolipidaemic drugs, and insulinresistance. Diabetes may be exacerbated. Indinavircrystalises in urine and increases risk of urinarycalculi.
Atazanavir (ATV) This PI is administered withlight meal which improves absorption, while acidsuppressant drugs decrease its absorption. ATVis primarily metabolized by CYP3A4, which isalso moderately inhibited by it. Bioavailabilityand efficacy of ATV is improved by combiningwith RTV. The t½ is 6–8 hours. Dyslipidaemiaand other metabolic complications are minimalwith ATV, but jaundice occurs in some patientswithout liver damage due to inhibition of hepaticglucuronyl transferase.Dose: 300 mg OD with ritonavir 100 mg taken at meal time.ATAZOR 100, 150, 200, 300 mg caps.
Indinavir (IDV) It is to be taken on emptystomach; g.i. intolerance is common; excessfluids must be consumed to avoid nephrolithiasis.Hyperbilirubinaemia occurs. It is less frequentlyused now.Dose: 800 mg TDS (BD if taken with 100 mg RTV).INDIVAN, INDIVIR, VIRODIN 400 mg cap.
Nelfinavir (NFV) It is to be taken with meals,since food increases absorption, but bioavai-lability is erratic. NFV is mainly metabolizedby CYP2C19. Often produces diarrhoea andflatulence; clinical efficacy may be somewhatlower than other PIs; less popular now.Dose: 750 mg TDS; NELFIN, NELVIR, NEIVEX 250 mg tab.
Ritonavir (RTV) It is a potent PI; also a potentCYP3A4 inhibitor. Drug interactions, nausea,diarrhoea, paresthesias, fatigue and lipidabnormalities are prominent. Though RTV (600mg twice daily) can be used as an antiretroviraldrug, it is more commonly employed in a lowdose (100 mg BD) to boost other PIs like LPV,ATV, SQV, IND, but not NFV.RITOMUNE, RITOMAX 100 mg cap; RITOVIR 250 mg tab.
Saquinavir (SQV) Two types of formulations(hard gel and soft gel capsules) with differing,but low oral bioavailability have been produced.The tablet load is large and side effects are

811C
HA
PTER58
ANTIVIRAL DRUGS
frequent; photosensitivity can occur. Importantly,it is a weak inhibitor of CYP3A4.Dose: 1200 mg TDS on full stomach; 1000 mg BD (with RTV 100mg).SAQUIN 200 mg tab.
Lopinavir It is available only in combinationwith RTV to improve bioavailability, though itis itself a CYP3A4 inhibitor. Diarrhoea, abdo-minal pain, nausea and dyslipidaemias are morecommon. Its dose needs to be increased by1/3rd if either NVP or EFV is used concurrently.Dose: 400 mg (with ritonavir 100 mg) BD with food.RITOMAX-L: V-LETRA: lopinavir 133.3 mg + ritonavir 33.3 mgcap.
Entry (fusion) inhibitorEnfuvirtide This HIV-derived synthetic peptide acts bybinding to HIV-1 envelope transmembrane glycoprotein (gp41)which is involved in fusion of viral and cellular membranes.Fusion of the two membrances is thus prevented and entryof the virus into the cell is blocked. It is not active againstHIV-2. No cross resistance with other classes of ARV drugsoccurs. Administered s.c. twice daily, it is used as add ondrug to an optimized regimen in selected patients who havefailed many earlier regimens and for whom there is no othertreatment option. The injections are painful and cause localnodules/cysts. The cost and inconvenience are prohibitive.
CCR5 receptor inhibitorMaraviroc The globular glycoprotein gp120 of the HIVenvelope anchors to the CD4 site of host cell by binding to acell membrane receptor, which mostly is the CCR5 chemokinereceptor (most HIV are CCR5-tropic). Maraviroc is a novel anti-HIV drug which targets the host cell CCR5 receptor and blocksit. Attachment of the virus and subsequent entry of viral genomeinto the cell is thus interfered. It has no effect on HIV strainsthat are CXCR4 receptor tropic (CXCR4 is an alternativechemokine receptor which also can bind gp 120), or dual CCR5/CXCR4 tropic.
Added to optimized background therapy in patients whohave already been treated with several regimens and who haveCCR5-tropic HIV infection, maraviroc has resulted in markedreduction in HIV-RNA load, and improvement in CD4 count. Itis active orally and there is no cross resistance with any otherARV drug. However, CCR5-tropism must be proven beforeusing it.
Though a number of side effects are reported, tolerabilityin general is satisfactory. Since it blocks one of the humanchemokine receptor, there is concern about impaired immunesurveillance and increased risk of infection/malignancy.
Integrase inhibitorRaltegravir The HIV-proviral DNA transcripted in thecytoplasm of host cell translocates to the nucleus along withan integrase enzyme. The HIV-integrase nicks host chromosomal
DNA and integrates the proviral DNA with it. Raltegravir is anorally active drug that blocks this step by inhibiting theintegrase enzyme. It is active against both HIV-1 and HIV-2.Because of its unique mechanism of action, there is no crossresistance between it and any other ARV drug. Addition ofraltegravir to optimized background therapy in repeatedly treatedpatients caused disappearance of HIV-RNA from circulation ina higher percentage of cases and improved the CD4 cell count.It has also shown good efficacy in untreated patients as acomponent of initial triple drug regimen along with two NRTIs.Side effects are nonspecific; myopathy is a potential toxicity. Itis otherwise well tolerated. However, raltegravir is a new drug;efficacy and safety need to be established.
Some antiretroviral combinations
1. Lamivudine 150 mg + Zidovudine 300 mg tab (1 tab BD);COMBIVIR, CYTOCOM, DUOVIR, LAMUZID tab.
2. Lamivudine 150 mg + Stavudine 30 mg or 40 mg tab (1tab BD); LAMIVIR-S, LAMOSTAD, VIROLIS tab.
3. Lamivudine 150 mg + Zidovudine 300 mg + Nevirapine200 mg tab (1 tab BD); DUOVIR-N, CYTOCOM-N,NEXIVIR-Z.
4. Lamivudine 150 mg + Stavudine 30 mg or 40 mg +Nevirapine 200 mg tab (1 tab BD); LAMOSTAD-N,TROMUNE, VIROLANS.
5. Lamivudine 150 mg + Zidovudine 300 mg 2 tab andEfavirenz 600 mg 1 tab kit; CYTOCOM-E kit.
HIV TREATMENT PRINCIPLES ANDGUIDELINES
The treatment of HIV infection and its compli-cations is complex, prolonged, needs expertise,strong motivation and commitment of the patient,resources and is expensive. Antiretroviral therapy(ART) is only 25 years old, and is still evolving.Initially, anti-HIV drugs were used singly one afterthe other as each failed in a patient due toemergence of resistance. Understanding thebiology of HIV infection and availability ofseveral potent drugs belonging to different classeshas mandated ‘highly active antiretroviral therapy’(HAART) with combination of 3 or more drugswhenever indicated. Monotherapy is contra-indicated.
It has been realized that even with HAART, which rapidlykills > 99% virions, a small number survive within the restingCD4 lymphocytes and invariably give rise to relapse whentreatment is discontinued despite complete absence ofdetectable viraemia and normal CD4 cell count for years.Relapses occur even if the same ART is continued afterdisappearance of viraemia and immune reconstitution. This isbecause HIV-reverse transcriptase is highly copying error prone,

812S
EC
TIO
N12
ANTIMICROBIAL DRUGS
implying that viral replication produces changes at some basepairs (and codons) with high frequency—rate of mutation ishigh. Some mutations confer resistance to one or the otherantiretroviral drugs. The resistant mutants are selected by anti-HIV therapy and in time an apparently sensitive population isreplaced by resistant virions. As the disease progresses in theindividual (and several anti-HIV drugs are used) the HIVpopulation becomes genetically complex and diverse withrespect to susceptibility to drugs. Each failing regimen limitsfuture treatment options. Even primary drug resistance (i.e. inuntreated patients) is being detected in 5–20% HIV patients.In developed countries, drug resistance studies are beingrecommended before initiating ART.
Since none of the currently available regi-mens can eradicate HIV from the body of thepatient, the goal of therapy is to maximally anddurably inhibit viral replication so that the patientcan attain and maintain effective immuneresponse towards potential microbial pathogens.Greater the suppression of viral replication,lesser is the chance of emergence of drugresistant virus. Effective ART reduces infectivityof the patient for other persons, thus serves tolimit transmission.
Initiating antiretroviral therapy Althoughit is attractive to treat all symptomatic andasymptomatic HIV positive patients, little long-term clinical benefit has been demonstrated inasymptomatic cases with reasonable immunecompetence (CD4 cell count > 350/µl).Arguments against early treatment in asympto-matic stable patients include:• Deleterious effect of anti-HIV drugs on
quality of life, their side effects and toxicity,especially lipid abnormalities and druginteractions.
• Risk of drug resistance limiting futuretreatment options.
• Limited durability of available regimens.• Risk of dissemination of resistant virus.• High cost.The best time to initiate anti-HIV therapy remainsuncertain. Various professional bodies and healthauthorities have framed treatment guidelinesfrom time-to-time. Highlights of the same are:
CD4 cell count is the major determinant ofinitiating therapy in asymptomatic cases. ARTshould be started before the immune system is
precariously damaged and the patient becomesill or develops opportunistic infection. Increasedmortality occurs when treatment is begun afterCD4 count has fallen below 200/µl, and responseto anti-HIV drugs is suboptimal.
The US Department of Health and HumanServices guidelines (2010) recommendinstituting ART to:(a) All symptomatic HIV disease patients.(b) Asymptomatic patients when the CD4 cellcount falls to 350/μl or less.(c) All HIV patients coinfected with HBV/HCVrequiring treatment.(d) All pregnant HIV positive women.(e) All patients with HIV-nephropathy.In addition to above, the current NACOguidelines give priority in treatment to:• All HIV-positive persons in WHO-clinical
stage 3 and 4.• All persons who tested HIV positive 6–8 years
ago.• Patients with history of pulmonary TB and/
or Herpes zoster.• HIV infected partners of AIDS patients.• All HIV positive children < 15 years of age.In developed countries some authorities now recommendinitiating ART in asymptomatic subjects at CD4 count < 500/μL,and not wait till it falls below 350/μL.Greater potency andbetter tolerability of newer anti-HIV drugs has prompted suchrecommendation in the hope of offering life expectancyapproaching that of noninfected persons.
Therapeutic regimens Whenever treatmentis instituted, it should be aggressive (HAART)with at least 3 anti-HIV drugs. The optimumresponse to any regimen is reduction of plasmaHIV-RNA to undetectable levels (<50 copies/μl)within 6 months. In treatment-naive patients,therapy with 3 drugs is considered optimal.Addition of a fourth drug affords no additionalbenefit; may be tried in failed patients only. Dueto availability of multiple drugs, a variety ofcombination regimens are possible and have beenemployed. However, no specific combination canbe considered optimal initial regimen for allpatients. Choice has to be made on the basisof efficacy, durability, tolerability, convenience,

813C
HA
PTER58
ANTIVIRAL DRUGS
drug interactions, impact on future options andcost.
Taking into consideration the above factorsand the experience gained so far, the first lineregimens universally include 2 NRTIs + 1 NNRTI.In developed countries, placing emphasis ontolerability and efficacy over cost and otherconstraints, preferred NRTIs are lamivudine,abacavir, tenofovir and sometimes emtricitabine.Efavirenz is preferred over nevirapine as theNNRTI. However, NACO selects first lineregimens for untreated patients on the followingprinciples:• All regimens should have 2 NRTI+1NNRTI.• Include lamivudine in all regimens.• The other NRTI can be zidovudine or
stavudine.• Choose one NNRTI from nevirapine or
efavirenz.• Choose efavirenz in patients with hepatic
dysfunction and in those concurrentlyreceiving rifampin. Do not use efavirenz inpregnant women or in those likely to getpregnant.
The first-line NACO recommended regimens arelisted in the box.The other important general points are:• The 3 drugs in the regimen should belong
to at least 2 different classes. Single class
regimens are inferior. There is convincingevidence that 3 NRTI regimens are clinicallyless effective than those which include 2 NRTI+ 1 NNRTI.
• The 3 NRTI regimen is employed only whena NNRTI cannot be used.
• For treatment-naive patients, only PI sparingregimens (2 NRTI + NNRTI) are chosen. Theyare more convenient with lower pill burden,simpler dosing schedules, more acceptable,better tolerated and produce less metaboliccomplications.
• The PI containing regimens (2 NRTI + PI orNRTI + NNRTI + PI) are reserved for advan-ced cases who have failed earlier regimens.
• Low dose ritonavir boosted PIs are preferredover higher dose single PI due to lower pillburden and better tolerability.
• If drug toxicity develops, either the entireregimen should be interrupted or theoffending drug should be changed. No dosereduction should be tried.
• ‘Drug holidays’ or ‘structured treatmentinterruptions’ may briefly improve well being(by absence of side effects), but allow viralreplication and increase risk of drugresistance; are not recommended.
• Treatment is life-long.• Institution of HAART in patients with latent
or partially treated opportunistic infectionmay produce ‘immune reconstitution syn-drome’ characterized by marked inflammatoryreaction against residual organisms andconstitutional symptoms due to ‘reestablish-ment of immune function.
• Pregnancy in women does not contraindicateART. Drugs considered relatively safe duringpregnancy are: zidovudine, lamivudine,nevirapine, nelfinavir, saquinavir.
• The ARV drug combinations that should notbe employed are given in the box on p. 814.Durability of the regimens depends
mainly on adherence of the patient to it.Compliance is a major determinant of outcome.Use of combined drug formulations greatlyimproves convenience and adherence, and are
First-line antiretroviral regimens*
Preferred regimen
1. Lamivudine + Zidovudine + Nevirapine
Alternative regimens1. Lamivudine + Zidovudine + Efavirenz2. Lamivudine + Stavudine1 + Efavirenz3. Lamivudine + Stavudine + Nevirapine
Other options1. Lamivudine + Tenofovir2 + Nevirapine2. Lamivudine + Tenofovir2 + Efavirenz3. Lamivudine3 + Zidovudine + Tenofovir
* Recommended by NACO1. Stavudine is substituted for zidovudine if patient isanaemic2. Tenofovir is included when there is toxicity or othercontraindication to both zidovudine and stavudine3. 3NRTI regimen is only for patients unable to tolerateboth nevirapine and efavirenz.

814S
EC
TIO
N12
ANTIMICROBIAL DRUGS
recommended, unless doses have to beindividualized for specific reasons. Therapyshould not be discontinued during an acute oppor-tunistic infection, except in case of intolerance,interactions or toxicity. Since multiple antiretro-viral, anti-P. jiroveci, antitoxoplasma, anti-CMV/herpes virus, antitubercular, antifungal or otherdrugs may have to be used in a patient, carefulattention to drug interactions and toxicities hasto be paid.
Changing a failing regimen An ART regimenis considered to have failed when:• Plasma HIV-RNA count is not rendered
undetectable (<50 copies/μl) within 6 monthstherapy.
• Repeated detection of virus in plasma afterinitial suppression to undetectable levelsdespite continuation of the drug regimen.
• Clinical deterioration, fall in CD4 cell count,serious opportunistic infection whilecontinuing drug therapy.
Failure is due to development of resistance toone or more components of the regimen. Treatmentfailures are to be anticipated and occur invariablyafter one to few years. The failed regimen shouldbe changed entirely (all 3 drugs changed) to drugsthat have not been administered earlier. A singledrug should not be changed or added to a failedregimen.
In designing second line regimens, drugs withknown overlapping viral resistance should beavoided, e.g. indinavir should not be substitutedfor nelfinavir or saquinavir; efavirenz should notbe replaced by nevirapine. Viral resistance testingis recommended for selecting the salvage regimen.A boosted PI is nearly always included in 2nd lineregimens. Because an NNRTI is nearly alwaysused in 1st line regimens, and resistance to one
NNRTI means resistance to all NNRTIs, this classis practically out for 2nd line regimens. Withrepeated failures it may become more difficultto construct an active combination. The integraseinhibitor, CCR5 inhibitor or fusion inhibitor maybe considered at this stage. The 2nd line regimenssuggested by NACO are listed in the box.
Antiretroviral drug combinations to be avoided
1. Zidovudine + stavudine: Pharmacodynamicantagonism
2. Stavudine + didanosine: Increased toxicity(neuropathy, lacticacidosis)
3. Lamivudine + didanosine: Clinically not additive
List of second line regimens*(in order of preference)
NRTI components PI component
Standard regimens1. Tenofovir + Abacavir 1. Lopinavir/r£
2. Didanosine + Abacavir 2. Atazanavir/r3. Tenofovir + Zidovudine 3. Saquinavir/r4. Tenofovir + Lamivudine 4. Indinavir/rSpecial circumstances 5. Nelfinavir1. Didanosine + Zidovudine2. Didanosine + Lamivudine
* Suggested by NACO£ r-low dose ritonavir boosted
Prophylaxis of HIV infectionPost-exposure prophylaxis (PEP) Healthcare workers and others who get accidentallyexposed to the risk of HIV infection by needle-stick or other sharp injury or contact with blood/biological fluid of HIV patients or blood trans-fusion should be considered for PEP. The aimof PEP is to suppress local viral replication priorto dissemination, so that the infection is aborted.However, PEP is not necessary when the contactis only with intact skin, or with mucous membraneby only a few drops for short duration. It is alsonot indicated when the source is known to beHIV negative. The NACO recommends 2 typesof regimens (see box) for PEP depending on themagnitude of risk of HIV transmission.
In developed countries, where a large numberof source HIV patients have received one ormore anti-HIV regimens and may be harbouringdrug-resistant virus, alternative prophylacticregimens using stavudine, didanosine, abacavir,efavirenz have also been used. If the drugsreceived by the source person is known, prophy-lactic regimen may be individualized to includeat least 2 drugs that the source has not received.

815C
HA
PTER58
ANTIVIRAL DRUGS
there is no data to evaluate the value ofprophylaxis after sexual exposure, the sameregimen as for needle stick may be used.
Perinatal HIV prophylaxis HIV may betransmitted from the mother to the child eitherthrough the placenta, or during delivery, or bybreastfeeding. The highest risk (>2/3rd) oftransmission is during the birth process. As percurrent recommendation, all HIV positivewomen, who are not on ART, should be put onthe standard 3 drug ART. This should be continuedthrough delivery and into the postnatal period,and has been shown to prevent verticaltransmission of HIV to the neonate, as well asbenefit mother’s own health. The first line NACOregimen for pregnant women is:
Zidovudine + Lamivudine + Nevirapine
However, women with CD4 count > 250 cells/μLface a higher risk of hepatotoxicity due to NVPand should be closely watched. EFV is terato-genic, and not used, particularly in the firsttrimester. In HIV-positive women who are nottaking ART, Zidovudine (300 mg BD) startedduring 2nd trimester and continued throughdelivery to postnatal period, with treatment ofthe neonate for 6 weeks has been found toreduce mother-to-child transmission by 2/3rd.Combination therapy is even more effective. Evenif not started earlier, AZT administered duringlabour and then to the infant is also substantiallyprotective. Breastfeeding by HIV-positive motheris contraindicated, because it carrys substantialrisk of transmission to the infant.
Post-exposure prophylaxis of HIV
Basic (2 drug) regimen (for low risk)*
Zidovudine 300 mg + Twice dailyLamivudine 150 mg for 4 weeks
Expanded (3 drug) regimen (for high risk)$
Zidovudine 300 mg + Twice dailyLamivudine 150 mg
+Indinavir 800 mg Thrice daily(or another PI) All for 4 weeks
*Low risk• When the source is HIV positive, but asymptomatic
with low HIV-RNA titre and high CD4 cell count.• Exposure is through mucous membrane, or super-
ficial scratch, or through thin and solid needle.$High risk• When the source is symptomatic AIDS patient
with high HIV-RNA titre or low CD4 count.• Exposure is through major splash or large area
contact of longer duration with mucous membraneor abraded skin or through large bore hollow needle,deep puncture, visible patient’s blood on the needle.
⎫⎬⎭
⎫⎬⎭
Nevirapine is not recommended for PEP due toits hepatotoxic potential.
When indicated, PEP should be started assoon as possible, preferably within 1–2 hoursof exposure. The likelihood of preventing infec-tion declines with the delay; some guidelinesdo not recommend starting it beyond 72 hoursof exposure. According to others, in case ofdefault, PEP may be started even 1–2 weekslater. Though HIV infection may not be preven-ted, onset of AIDS may be delayed by the late-start PEP.
Prophylaxis after sexual exposure Though
PROBLEM DIRECTED STUDY
58.1 A dental surgeon consults you with the following problem:During a dental procedure he got exposed to a 26-year-old female patient’s blood and salivathrough a piercing injury on the finger. A needle had penetrated across his gloves and skinto a depth of 2–3 mm, but was withdrawn immediately and the area washed under runningwater. On enquiry, the patient revealed that one year back she had tested HIV positive, butwas asymptomatic and not taking any anti-HIV medication.(a) Should the dental surgeon be advised to take post-exposure prophylactic medication forHIV, or no medication is indicated under the circumstances?(b) If medication is advised, which drug/drugs, doses and duration of use would be appropriate?(see Appendix-1 for solution)

Antimalarial DrugsChapterChapterChapterChapterChapter 5959595959
These are drugs used for prophylaxis, treatmentand prevention of relapses of malaria.
Malaria, caused by 4 species of the protozoalparasite Plasmodium, is endemic in most partsof India and other tropical countries. It is oneof the major health problems. As per latest WHOestimates (2011)* between 149–274 (median216) million clinical cases and ~ 0.655 milliondeaths occur globally due to malaria each year,90% of which are in Africa. This amounts toone malaria death every minute. In India theNational Malaria Eradication Programme(NMEP), started in 1958, achieved near completedisappearance of the disease in 1960s (from 75million cases in 1950s to 0.1 million cases in1960s). However, due to the development ofinsecticide resistance among mosquitoes andother factors, it staged a comeback in the mid1970s (6.47 million cases in 1976), andcontinues to prevail in endemic/subendemicproportions, so that 80% indian population livesin malaria risk areas. Conceding that eradicationof malaria is not possible, NMEP was renamedNational Antimalaria Programme (NAMP), whichnow is ‘National vector borne diseases controlprogramme’ (NVBDCP) with a wider diseasecoverage. For the year 2010, the NVBDCP hasreported 1.49 million slide proven malaria casesin India, out of which 0.78 million (52%) werefalciparum malaria with 767 recorded deaths.The WHO estimates that actual number ofmalaria cases in India is much higher, and anexpert committee has estimated that about40,000 malaria deaths occur annually.The bark of Cinchona tree, growing in Peru, was introducedin Europe in the early 17th century as a cure for fevers. Laterit was realized to be a specific remedy for malaria. Quinine,isolated from Cinchona bark in 1820, replaced the crude
preparation and continued to be the major antimalarial drugtill 1942. The world’s supply of Cinchona bark for producingquinine was met by Java and neighbouring countries. Thiswas cut off from the Germans during World War I and fromthe Allies during World War II. Due to enormous militaryimportance of malaria and its treatment, intense activity wasinitiated for the development of antimalarial drugs. Mepacrinewas produced in Germany in 1926 and extensively field testedby the Allies during World War II. Chloroquine was producedin USA soon after as a less toxic alternative to mepacrine.It had already been synthesized and used by Germans in 1934as ‘Resochin’. Proguanil was introduced in 1945 by the Britishas a well tolerated clinical curative.
None of the above drugs were found to be capable ofpreventing relapses in vivax malaria. Pamaquine was the first8-aminoquinoline to be tested in Germany in the 1920s.However, no attention was paid to it because of its poorschizontocide action. This class of drugs was retested duringWorld War II as radical curative and Primaquine emergedas the most desirable drug. Pyrimethamine was produced in1951 under a planned post-war research programme forantimalarial drugs. Subsequently, chloroquine resistanceemerged in P. falciparum and several drugs were developedto combat it; the important ones are Mefloquine, Lumefantrine,Atovaquone, Pyronaridine, etc. However, the most significantadvance is the Chinese herb derived fast acting Artemisinincompounds, the latest one of which is a synthetic derivativeArterolane developed in India.
CLASSIFICATION
1. 4-Aminoquinolines Chloroquine (CQ)Amodiaquine (AQ)Piperaquine
2. Quinoline-methanol Mefloquine3. Cinchona alkaloid Quinine, Quinidine4. Biguanide Proguanil
(Chloroguanide)5. Diaminopyrimidine Pyrimethamine6. 8-Aminoquinoline Primaquine
Tafenoquine7. Sulfonamides Sulfadoxine
and sulfone SulfamethopyrazineDapsone* WHO: World Malaria Report, Dec. 2011

817C
HA
PTER59
ANTIMALARIAL DRUGS
8. Antibiotics TetracyclineDoxycyclineClindamycin
9. Sesquiterpine Artesunatelactones Artemether
ArteetherArterolane
10. Amino alcohols HalofantrineLumefantrine
11. Naphthyridine Pyronaridine12. Naphthoquinone Atovaquone
OBJECTIVES AND USE OFANTIMALARIAL DRUGS
The aims of using drugs in relation to malarialinfection are:
(i) To prevent clinical attack of malaria(prophylactic).
(ii) To treat clinical attack of malaria (clinicalcurative).
(iii) To completely eradicate the parasite fromthe patient’s body (radical curative).
(iv) To cutdown human-to-mosquito transmis-sion (gametocidal).
Fig. 59.1: The life cycle of malarial parasite in man. Stages and forms ofthe parasite at which different types of antimalarial drugs act are indicated.

818S
EC
TIO
N12
ANTIMICROBIAL DRUGS
TABLE 59.1 Comparative properties of antimalarial drugs
PRE-ERYTHRO. ERYTHROCYTIC PHASE HYPNO- GAMETES RESIS- TOXICITYDRUG Fal. Viv. Activity Onset Duration ZOITE TANCE GRADING
1. Chloroquine – – + Fast Long – – Slow +
2. Mefloquine – – + Int Long – – Minor ++
3. Quinine – – + Int Short – – Minor +++
4. Proguanil + – + Int Short – * Rapid ±
5. Pyrimethamine – – + Slow Long – – Rapid +
6. Primaquine + + – – – + + Minor ++
7. Sulfonamides – – ± Slow Long – – Minor +±
8. Tetracyclines – – + Slow Short – – Nil +
9. Clindamycin – – + Slow Short – – Nil +
10. Artemisinin – – + Fastest Short – + Nil +
11. Lumefantrine – – + Int Long – – Nil +
*Do not kill gametes but may inhibit their development in mosquito.Pre-erythro. — Preerythrocytic stage;Fal. — P. falciparum; Viv — P. vivax; Int — Intermediate
These are achieved by attacking the parasite atits various stages of life cycle in the human host(see Fig. 59.1). Antimalarials that act onerythrocytic schizogony are called erythrocyticschizontocides, those that act on preerythrocyticas well as exoerythrocytic (P. vivax) stages inliver are called tissue schizontocides, whilethose which kill gametocytes in blood are calledgametocides. Antimalarial drugs exhibit consi-derable stage selectivity of action (see Table59-1). Antimalarial therapy is given in thefollowing forms.
1. Causal prophylaxis The preerythrocyticphase (in liver), which is the cause of malarialinfection and clinical attacks, is the target forthis purpose.• Primaquine is a causal prophylactic for all
species of malaria, but has not been used inmass programmes, because of its toxicpotential.Trials in Kenya and Irian Jaya have successfully usedprimaquine 0.5 mg/kg daily against both P. f. and P. v.in subjects with normal G-6-PD levels. The CDC (USA)recommends it for short duration travel to P.vivaxpredominant endemic areas, and for subjects who cannottake any other prophylactic drug.
• Proguanil is a causal prophylactic, primarilyfor P.f., but is not used in India, because ofweak activity against liver stages of P.v., andrapid development of resistance when usedalone.
A combined formulation of atovaquone (250 mg) + proguanil(100 mg) is commonly used as a prophylactic by Americansand other western travellers visiting malaria endemic areas.Atovaquone also is active against preerythrocytic stage ofP.f., but is not approved in India.
2. Suppressive prophylaxis The schizonto-cides which suppress the erythrocytic phase andthus attacks of malarial fever can be used asprophylactics. Though the exoerythrocytic phasein case of vivax and other relapsing malariascontinues, clinical disease does not appear.• Chloroquine (CQ) 300 mg (base*) or 5 mg/
kg weekly. In travellers, start one week beforewith a loading dose of 10 mg/kg and continuetill one month after return from endemic area.However, it can be used as a prophylactic onlyin areas with CQ-sensitive P.f. (Mexico,Argentina, etc.). Since CQ-resistant P.f. is now
* All doses expressed in terms of base, e.g. chloroquinephosphate 250 mg = 150 mg base.

819C
HA
PTER59
ANTIMALARIAL DRUGS
widespread in India, and there are no exclu-sively P.v. areas, CQ is no longer employedas prophylactic in India.
• Mefloquine 250 mg started 1–2 weeks beforeand taken weekly till 4 weeks after returnfrom endemic area, has been used for areaswhere CQ-resistant P.f. is prevalent. In India,use of mefloquine for prophylaxis is notallowed among residents, but may be usedby travellers.If tolerated, mefloquine is a prophylactic with provenefficacy, even for long-term travellers and is useful exceptfor mefloquine-resistant P.f. areas (Myanmar, Thailand,Cambodia).
• Doxycycline 100 mg daily starting day beforetravel and taken till 4 weeks after return fromendemic area for CQ-resistant P.f., is analternative regimen for short-term (maximum6 weeks) visitors and those unable to takemefloquine. It is contraindicated in pregnantwomen and children < 8 yr.
• Proguanil 200 mg daily with chloroquine 300 mg weeklyaffords substantial protection against moderately CQ-resistant P. falciparum, but less than that afforded bymefloquine. This has been successfully used in Africa,but found ineffective, and not employed in India.Chemoprophylaxis of malaria should be
limited to short-term use in special risk groups,such as — nonimmune travellers, nonimmunepersons living in endemic areas for fixed periods(army units, labour forces), infants, children andpregnant women (falciparum malaria has seriousconsequences in the pregnant).
Intermittent preventive therapy (IPTp) in theform of one dose pyrimethamine (75 mg) +sulfadoxine (1500 mg) each is 2nd and 3rd
trimester (gap not < 1 month) is recommendedby WHO only in areas with high P.f. endemicity(P.f. >30%) for pregnant women.
3. Clinical cure The erythrocytic schizonto-cides are used to terminate an episode of malarialfever. The available drugs can be divided into:(a) High-efficacy drugs: Artemisinin, CQ,amodiaquine, quinine, mefloquine, halofantrine,lumefantrine and atovaquone. These drugs canbe used singly to treat attacks of malarial fever,but are now generally combined.
(b) Low-efficacy drugs: Proguanil, pyrimethamine,sulfonamides, tetracyclines and clindamycin.These drugs are used only in combination forclinical cure.
The faster acting drugs are preferred,particularly in falciparum malaria where delayin treatment may result in death even if theparasites are cleared from blood by the drug.The exoerythrocytic phase (hypnozoites) ofvivax and ovale persists which can causerelapses subsequently without reinfection. Thus,the erythrocytic schizontocides are radicalcuratives for falciparum, but not for vivax orovale malaria. However, recrudescences occurin falciparum infection if the blood is not totallycleared of the parasites by the drug.
The drugs and regimens used for uncompli-cated falciparum and vivax malaria are given inthe box (p. 820). Only oral drugs are used foruncomplicated malaria.
Relapses of vivax/ovale malaria are treatedin the same way as the primary attack becausethe parasite remains sensitive to the drug.Recrudescence in falciparum malaria indicatesresistant infection: should be treated with analternative drug as per local needs. However,recrudescences and failures with artemisinin-based combination therapy (ACT), used properly,are infrequent.
Falciparum malaria during pregnancy Anattack of falciparum malaria occurring duringpregnancy has serious implications both for themother as well as the foetus. It must be treatedpromptly and aggressively. Drugs recommendedare:1. Quinine 600 mg TDS × 7 days + clindamycin
300 mg TDS/QID (20 mg/kg) for 7 days; canbe used during all trimesters, especiallythe 1st.
2. Artemisinin-based therapy (ACT; see box) isa better tolerated 3 day regimen, which maybe used during the 2nd and 3rd trimester asan alternative to 7 day quinine + clindamycintherapy.

820S
EC
TIO
N12
ANTIMICROBIAL DRUGS
Treatment of uncomplicated malaria
A. Vivax (also ovale, malariae) malaria
1. Chloroquine 600 mg (10 mg/kg) followed by 300 mg (5 mg/kg) after 8 hours and then for next 2 days(total 25 mg/kg over 3 days) + Primaquine 15 mg (0.25 mg/kg) daily × 14 days
In occasional case of chloroquine resistance2. Quinine 600 mg (10 mg/kg) 8 hourly × 7 days + Doxycycline 100 mg daily × 7 days or
+ Clindamycin 600 mg 12 hourly × 7 days+ Primaquine (as above)
orArtemisinin-based combination therapy (see below)+ Primaquine (as above)
B. Chloroquine-sensitive falciparum malaria£
1. Chloroquine (as above) + Primaquine 45 mg (0.75 mg/kg) single dose (as gametocidal)
C. Chloroquine-resistant falciparum malaria
1.* Artesunate 100 mg BD (4 mg/kg/day) × 3 days +Sulfadoxine# 1500 mg (25 mg/kg) + Pyrimethamine 75 mg (1.25 mg/kg) single dose
or2. Artesunate 100 mg BD (4 mg/kg/day) × 3 days +
Mefloquine# 750 mg (15 mg/kg) on 2nd day and 500 mg (10 mg/kg) on 3rd day.or
3. Artemether 80 mg + Lumefantrine 480 mg twice daily × 3 days (child 25–35 kg BW ¾ dose;15–25 kg BW ½ dose; 5–15 kg BW ¼ dose)
or4. Arterolane (as maleate) 150 mg + Piperaquine 750 mg once daily × 3 days
or5. Quinine 600 mg (10 mg/kg) 8 hourly × 7 days
+ Doxycycline 100 mg daily × 7 days or + Clindamycin 600 12 hourly × 7 days
*First line ACT under NVBDCP#Sulfadoxine-pyrimethamine (S/P) alone and mefloquine alone are also used, but should preferably be combinedwith artesunate.£In India (including under NVBDCP) all P.f. cases, irrespective of CQ-resistance status, are treated with artemisinin-based combination therapy (ACT).
Severe and complicated falciparum malariaThis includes P. falciparum infection attendedby any one or more of—hyperparasitaemia,hyperpyrexia, fluid and electrolyte imbalance,acidosis, hypoglycaemia, prostration, cardio-vascular collapse, jaundice, severe anaemia,spontaneous bleeding, pulmonary edema,haemoglobinuria, black water fever, renal failureand cerebral malaria. Parenteral (i.m./i.v.) drugshave to be used; oral drugs may be substitutedwhen the condition improves. Drugs and regimensemployed are detailed in the box (p. 821).
4. Radical cure In case of vivax and ovalemalaria, drugs which attack the exoerythrocyticstage (hypnozoites) given together with a clinical
curative achieve total eradication of the parasitefrom the patient’s body. A radical curative isneeded in relapsing malaria, while in falciparummalaria — adequate treatment of clinical attackleaves no parasite in the body (there is nosecondary exoerythrocytic tissue phase).
Drug of choice for radical cure of vivax andovale malaria is:• Primaquine 15 mg daily for 14 days. A shorter
course of 5 days used earlier by NAMP inIndia has been found inadequate, and is nolonger recommended. This treatment shouldbe given concurrently with or immediatelyafter chloroquine/other schizontocide only toindividuals who test negative for G-6-PDdeficiency.

821C
HA
PTER59
ANTIMALARIAL DRUGS
(b) Patients treated during an epidemic and inareas undergoing eradication programme witheffective vector control measures to cut downtransmission.
5. Gametocidal This refers to eliminationof the male and female gametes of Plasmodiaformed in the patient’s blood. Gametocidal actionis of no benefit to the patient being treated, butwill reduce the transmission to mosquito.
Primaquine is gametocidal to all species ofPlasmodia, while artemisinins have weak lethalaction on early-stage but not mature gametes.Gametes exposesd to proguanil or pyrimetha-mine may fail to carry on the life cyle normallyin the mosquito. Adequate control of clinicalattacks will reduce formation of gametes.• A single 45 mg (0.75 mg/kg) dose of prima-
quine is employed immediately after clinicalcure of falciparum malaria to kill the gametesand cut down transmission to mosquito. Thisshould be given even when an artemisinin isused for clinical cure because artemisininsdo not kill all the gametes. Primaquine usedfor radical cure of vivax malaria eliminatesP.vivax gametes as well.
Chloroquine
It is a rapidly acting erythrocytic schizontocideagainst all species of plasmodia; controls mostclinical attacks in 1–2 days with disappearanceof parasites from peripheral blood in 1–3 days.Therapeutic plasma concentrations are in therange of 15–30 ng/ml. However, it has no effecton primary and secondary hepatic stages of theparasite—does not prevent relapses in vivax andovale malaria. CQ has no clinically usefulgametocidal activity.
The mechanism of action of CQ is notcompletely known. Plasmodia derive nutritionby digesting haemoglobin in their acidicvacuoles. CQ is actively concentrated bysensitive intraerythrocytic plasmodia; higher con-centration is found in infected RBCs than innoninfected ones. By accumulating in the acidic
Treatment of severe and complicatedfalciparum malaria*
1. Artesunate: 2.4 mg/kg i.v. or i.m., followed by 2.4mg/kg after 12 and 24 hours, and then once dailyfor 7 days. Switchover to 3 day oral ACT inbetweenwhenever the patient can take and tolerate oralmedication.
or2. Artemether: 3.2 mg/kg i.m. on the 1st day, followed
by 1.6 mg/kg daily for 7 days. Switchover to 3day oral ACT inbetween whenever the patient isable to take oral medication.
or3. $Arteether: 3.2 mg/kg i.m. on the 1st day, followed
by 1.6 mg/kg daily for the next 4 days. Switchoverto 3 day oral ACT inbetween whenever the patientis able to take oral medication.
or4. Quinine diHCl: 20 mg/kg (loading dose) diluted in
10 ml/kg 5% dextrose/dextrose-saline and infusedi.v. over 4 hours, followed by 10 mg/kg(maintenance dose) i.v. infusion over 4 hours (inadults) or 2 hours (in children) every 8 hours, untillpatient can swallow. Switchover to oral quinine 10mg/kg 8 hourly to complete the 7 day course.
————————$Arteether (i.m.) is slower acting than artesunate (i.v.),and appears to be less efficacious. It is used onlyin India.1. Volume of fluid for i.v. infusion of quinine shouldbe reduced in patients with volume overload/pulmonary edema.2. If possible, oral quinine should be substituted by3 day oral ACT, or doxycycline 100 mg daily shouldbe combined with it.3. Chloroquine HCl i.v. to be used only if none ofthe above is available and only in adults.
* Adopted from Regional guidelines for the managementof severe falciparum malaria in large hospitals (2006);WHO, Regional office for South-East Asia, New Delhi.
• Tafenoquine, a new long-acting 8-aminoquinolineexoerythrocytic schizontocide, is being developed as asingle dose antirelapse drug for vivax malaria.
There is no point in antirelapse treatment inhighly endemic areas, because chances ofreinfection would be high; a subsequent attackmay be erroneously labelled as failure of radicalcure. Antirelapse treatment of vivax malariashould be restricted to:(a) Areas with low level of transmission (whereonly sporadic cases occur).

822S
EC
TIO
N12
ANTIMICROBIAL DRUGS
vecuoles of the parasite and because of its weaklybasic nature, it raises the vacuolar pH and therebyinterferes with degradation of haemoglobin byparasitic lysosomes. Polymerization of toxichaeme generated from digestion of haemoglobinto nontoxic parasite pigment haemozoin is inhi-bited by the formation of CQ-haeme complex.Haeme itself or its complex with CQ thendamages the plasmodial membranes. Clumpingof pigment and changes in parasite membranesfollow. Other related antimalarials like quinine,mefloquine, lumefantrine, pyronaridine appear toact in an analogous manner.
Chloroquine-resistance among P.vivax hasbeen slow in developing, but P. falciparum hasacquired significant resistance, and resistantstrains have become prevalent in India(especially the east and north east), South EastAsia, China, Africa and South America. Someof these have also acquired resistance to sulfa-pyrimethamine (S/P), proguanil and may bemefloquine, quinine, etc. (multidrug resistantstrains). Because P. falciparum produces themore severe forms of malaria with considerablemortality, emergence of such strains is thebiggest threat to the antimalaria programmes, andis the focus of attention for current researchefforts.
Chloroquine-resistance among P. falciparumis now widespread in India, and no entirelysensitive areas can be indentified. The largestnumber of CQ failures are reported from theNortheastern part of India where 24–83% P.falciparum cases are resistant to CQ, and someof these (particularly in areas borderingMyanmar) are multidrug resistant. Due to spreadof CQ-resistant P.f. to most parts of India, withNortheast, Orissa, Karnataka, etc. reporting highrates of resistance, the NVBDCP has switchedover to ACT as the first line treatment of P.f.cases counrtywide. Resistance in P. falciparumis associated with a decreased ability of theparasite to accumulate CQ.
An efflux transporter encoded by the pfcrt (P.f.chloroquine-resistance transporter) gene, has been identifiedin the membranes of the acidic vacuoles of CQ-resistant P.f.It serves to pumpout CQ from the vacuoles and thus protects
the haeme detoxifying mechanism of the resistant parasite.This appears to be the most important mechanism of CQ-reistance. The pfmdr gene encoded P-glycoprotein is anenergy-dependent ABC transporter which confers resistanceto many antimalarials like quinine, mefloquine, and halofantrine.This transporter is also involved in certain cases of P.f.resistance to CQ.
Chloroquine-resistance among P. vivax wasfirst reported from Papua New Guinea in 1989.It has now been confirmed from Indonesia,Myanmar, Peru, Columbia, Ethiopia and detectedin India, but is focal and sporadic, reported fromChennai, Mathura, tribal areas of MadhyaPradesh, Mumbai and Bihar. It manifests asrecrudescence within 1–3 weeks of treating vivaxmalaria with standard dose of chloroquine. Suchcases can be treated by quinine given along withdoxycycline/clindamycin or by ACT, followedby primaquine to effect radical cure (see boxon p. 820). However, CQ given in standard dosesremains the first line treatment of vivax malariaas per NVBDCP guidelines.
Other actions Chloroquine is active againstEntamoeba histolytica and Giardia lamblia aswell.It has antiinflammatory, local irritant and localanaesthetic (on injection), weak smooth musclerelaxant, antihistaminic and antiarrhythmicproperties.
Pharmacokinetics Oral absorption of CQ isexcellent. About 50% gets bound in the plasma.It has high affinity for melanin and nuclearchromatin: gets tightly bound to these tissueconstituents and is concentrated in liver, spleen,kidney, lungs (several hundred-fold), skin,leucocytes and some other tissues. Its selectiveaccumulation in retina is responsible for theocular toxicity seen with prolonged use.
Chloroquine is partly metabolized by liverand slowly excreted in urine. The early plasmat½ varies from 3–10 days. Because of tighttissue binding, small amounts persist in the bodywith a terminal t½ of 1–2 months.
Adverse effects Toxicity of CQ is low, butside effects like nausea, vomiting, anorexia, un-controllable itching, epigastric pain, uneasiness,

823C
HA
PTER59
ANTIMALARIAL DRUGS
difficulty in accommodation and headache arefrequent and quite unpleasant. Weekly sup-pressive doses have been safely given for 3 years.• Prolonged use of high doses (as needed for rheumatoid
arthritis, DLE, etc.) may cause loss of vision due to retinaldamage. Corneal deposits may also occur and affect vision,but are reversible on discontinuation.
• Loss of hearing, rashes, photoallergy, mental disturbances,myopathy and graying of hair can occur on long-termuse.
• Intravenous injection of CQ (rarely given now) can causehypotension, cardiac depression, arrhythmias and CNStoxicity including seizures (more likely in children).
CQ can be used for treatment of malaria duringpregnancy: no abortifacient or teratogeniceffects have been reported.
Caution is to be exercised in the presenceof liver damage, severe g.i., neurological, retinaland haematological diseases. Attacks of seizures,porphyria and psoriasis may be precipitated.
CQ should not be coadministered with meflo-quine, amiodarone and other antiarrhythmics.
Preparations and administration
Chloroquine phosphate: (250 mg = 150 mg base) bitter, tabletshould not be chewed. RESOCHIN, CLOQUIN, LARIAGO,NIVAQUIN-P 250 mg tab, 500 mg forte tab, 100 mg (base)per 10 ml oral susp., 40 mg (base)/ml inj in 2 and 5 ml amp,30 ml vial.There is hardly any indication now for parenteral (i.v.)chloroquine. It should not be injected i.m. due to its localtissue toxicity.
Uses
1. CQ causes rapid fever clearance anddisappearance of parasitaemia in patients ofmalaria caused by all P.ovale and P.malariae,most P.vivax and some P.falciparum that arestill sensitive. It is the drug of choice forclinical cure of vivax, ovale and malariaemalaria. However, its use for P.falciparumis restricted to few areas that still havesusceptible P.f., but not in India. It is no longerused as a suppressive prophylactic in India,and such use is made only in vivaxpredominant countries or in those which haveCQ-sensitive P.f.
2. Extraintestinal amoebiasis (Ch. 60).3. Rheumatoid arthritis (Ch. 15).
4. Discoid lupus erythematosus—very effective;less valuable in systemic LE.
5. Lepra reaction (see p. 786).6. Photogenic reactions.7. Infectious mononucleosis: affords sympto-
matic relief.
Amodiaquine (AQ) It is almost identical toCQ in properties and is less bitter. Studies overthe past 30 years in Africa have found it to besomewhat faster acting than CQ.In the mid 1980s some fatal cases of toxic hepatitis andagranulocytosis were reported among travellers using AQ forprophylaxis, and WHO in 1990 recommended that it shouldnot be used for prophylaxis of malaria as well as for treatmentof CQ failures. The 19th WHO expert committee on malaria(1992) did not accept this recommendation totally, andpermitted use of AQ for treatment of clinical attacks. Countrieswhich had continued to use short courses of AQ (25–35mg/kg over 3 days) for clinical cure did not report any severereaction, and a subsequent metaanalysis (2003) concludedthat such use is as safe as CQ. Thus, it is possible that thesuspected hepatotoxicity and agranulocytosis are specificadverse effects of long-term AQ use made for prophylacticpurpose.Experience in Africa over the past 3 decadessupports use of AQ in uncomplicated falciparummalaria, but it is not recommended for prophy-laxis. There is evidence now that AQ is effectiveeven in areas with CQ-resistant P. falciparum.Coformulated with artesunate (AS/AQ) thecombined amodiaquine-artesunate tablet hasbecome 1st line treatment of falciparum malariain many African countries. On the basis ofsuccessful clinical trials in India, the combinedformulation of this ACT has been recentlyapproved for use in falciparum malaria,irrespective of CQ-resistance status.
Side effects of AQ are similar to that ot CQ;itching may be less common, though still themost common complaint. Neutropenia has beenassociated with AQ when it is used in childrenand in HIV patient receiving antiretroviral therapy.Dose: for treatment of acute attack of malaria: 25–35 mg/kg over3 days; CAMOQUIN 200 mg (as HCl = 150 mg base) tab;BASOQUIN 150 mg (base) per 5 ml susp.
Piperaquine (see under ACT, p. 834)

824S
EC
TIO
N12
ANTIMICROBIAL DRUGS
Mefloquine
This quinoline drug was originally tested duringWorld War II, but introduced for use only in1963 when it was reinvestigated and foundeffective against CQ-resistant P.f. Mefloquine(MQ) is intrinsically fast acting erythrocyticschizontocide, but slower than CQ or quininedue to prolonged absorption after oral ingestion.It is effective against CQ-sensitive as well asresistant plasmodia. A single dose (15 mg/kg)controls fever and eliminates circulating parasitesin infections caused by P. falciparum or P. vivaxin partially immune as well as nonimmuneindividuals. However, it neither has gametocidalactivity, nor kills vivax hypnozoites. Like CQrelapses occur subsequently in vivax malaria. Itis also an efficacious suppressive prophylacticfor multiresistant P. falciparum and other typesof malaria. Due to extensive use as monotherapy,MQ-resistance among P. falciparum has becomecommon in Thailand, Cambodia and Myanmar,but is sporadic in Africa, South America andMiddleeast. Since it has not been widely usedin India, MQ-resistance is not a problem,but due to its long t½ chances of selection ofresistant strains are high; MQ-resistantP. falciparum isolates have been reported fromNortheast, Gujarat and Andhra Pradesh.Resistance to MQ confers cross resistance toquinine and halofantrine.
The mechanism of action of MQ is notknown, but the morphological changes producedin the intraerythrocytic parasite resemble qui-nine and CQ induced changes. Like CQ itaccumulates in infected RBCs (including thosewith CQ-resistant P.f.), binds to haeme and thiscomplex may be damaging the parasite mem-branes. However, recent evidence suggests thatthe site of action of MQ is in the parasiticcytosol rather than in the acidic vacuole. Themajor mechanism by which P.f. develops MQ-resistance is by enhanced translation of pfmdr1gene, though Pfcrt mutation may also be involved.
Pharmacokinetics Oral absorption of MQ isgood but peak concentrations are reached slowly.
It is highly plasma protein bound and concen-trated in many organs including liver, lung andintestines. Extensive metabolism occurs in liverand it is primarily secreted in bile. Considerableenterohepatic circulation of MQ and its tissuebinding accounts for the long t½ which is2–3 weeks.
Adverse effects MQ is bitter in taste; commonreaction is dizziness, nausea, vomiting, diarrhoea,abdominal pain, sinus bradycardia and Q-Tprolongation. These are usually mild and largelydose related, but may be severe in some. Majorconcern has been a variety of neuropsychiatricreactions (disturbed sense of balance, ataxia,errors in operating machinery, strange dreams,anxiety, hallucinations, rarely convulsions) occur-ring in some recipients. These are dose relatedand subside over 1–3 weeks on discontinuation.Rare events are haematological, hepatic andcutaneous toxicity. MQ appears to be safe duringpregnancy, but should be avoided in 1st trimesterunless absolutely essential. MQ is contraindicatedin patients with anxiety, depression, psychosis,and in those with cardiac conduction defects.
Interactions Halofantrine or quinidine/quinineor CQ given to patients who have received MQcause QTc lengthening—cardiac arrests arereported. These drugs should not be administeredif MQ has been given < 12 hours earlier.
Use Mefloquine is an effective drug for multi-resistant P. falciparum. Because of its potentialtoxicity, cost and long t½, its use is restricted.To check the spread of MQ-resistance, currentrecommendation is to use it only in combinationwith artesunate as ACT for uncomplicatedfalciparum malaria, including CQ-resistant andCQ + sulfa-pyrimethamine (S/P) resistant cases.In Southeast Asia artesunate-MQ ACT has beenthe first line treatment of falciparum malaria.For vivax malaria, it should be used only in therare case of the parasite being both CQ andquinine + doxycycline resistant. MQ cannot begiven parenterally and is not used in complicated/severe malaria.

825C
HA
PTER59
ANTIMALARIAL DRUGS
For prophylaxis of malaria among travellersto areas with multidrug resistance; 5 mg/kg(adults 250 mg) per week is started preferably1–2 weeks before travel to assess side effectsin the individual. It is not recommended forprophylaxis in residents of the endemic area.MEFQUE, CONFAL, FACITAL 250 mg tab; to be taken withplenty of water after meals.
Mepacrine (Quinacrine, Atabrine) It is an acridinederivative erythrocytic schizontocide, more toxic and lesseffective than chloroquine. It is obsolete as an antimalarial,but is also active against giardia and tapeworms.
QuinineQuinine is the levo rotatory alkaloid obtainedfrom cinchona bark. Its d-isomer quinidine isused as an antiarrhythmic (and for malaria aswell in some countries).
Quinine is an erythrocytic schizontocide forall species of plasmodia, but less effective andmore toxic than CQ. Resurgence of interest inquinine is due to the fact that most CQ andmultidrug-resistant strains of P. falciparum stillrespond to it. However, even quinine-resistancehas been described in certain parts of SoutheastAsia and in Brazil where quinine + tetracyclinehas been the standard treatment of complicatedmalaria. Quinine-resistance has been encounte-red sporadically in India, particularly alongMyanmar border where in a sample study 6%falciparum malaria cases did not respondsequentially to CQ, S/P and quinine. There ispartial cross resistance between quinine and MQ,but many MQ-resistant cases respond to quinine.Though effective in terminating an acute attackof falciparum malaria, quinine may not preventrecrudescence—indicating incomplete clearanceof the parasites. Doxycycline or clindamycin ismostly added to it for complete parasiteclearance.
Quinine has no effect on preerythrocyticstage and on hypnozoites of relapsing malaria,but kills vivax gametes. Like CQ it is a weakbase, and acts in an analogous manner to inhibitpolymerization of haeme to hemozoin; freehaeme or haeme-quinine complex damages
parasite membranes and kills it. However, theexact mechanism of action is not known.Resistance to quinine in P.f. appears to involve both enhancedtranslation as well as mutation of Pfmdr gene among differentstrains.
Quinine has many other actions:
1. Local irritant and anaesthetic Quinine is intenselybitter and irritant. Orally it causes nausea, vomiting, epigastricdiscomfort. Injections can cause pain and local necrosis inthe muscle and thrombosis in the vein. Local inflammationmay be followed by fibrosis.
2. Systemic actions Gastric secretion is increased.Quinine is a weak analgesic and antipyretic; affects hearingand vision at higher doses. Cardiodepressant, antiarrhythmicand hypotensive actions are similar to quinidine (see Ch. 38).Rapid i.v. injection can produce marked fall in BP andcardiovascular collapse.
Quinine directly decreases contractile power of skeletalmuscle fibre (see Ch. 25). It stimulates the myometrium andcan cause abortion in early pregnancy. However, it is nota dependable abortifacient. Blood sugar is slightly lowereddue to release of insulin from the pancreas. Rapid i.v. injectionof quinine has caused hypoglycaemia.
Pharmacokinetics Quinine is rapidly andcompletely absorbed orally. It is 70% bound toplasma proteins, especially α1 acid glycoprotein,which increases during acute malarial infection.CSF concentrations are low. A large fraction ofthe dose is metabolized in the liver by CYP3A4and excreted in urine with a t½ of 10–12 hours.Quinine is noncumulative.
Adverse effects Toxicity of quinine is highand dose related; 8–10 g taken in a single dosemay be fatal.
Cinchonism A large single dose or highertherapeutic doses taken for a few days producea syndrome called ‘cinchonism’. It consists ofringing in ears, nausea, vomiting (due to bothgastric irritation and CTZ stimulation), headache,mental confusion, vertigo, difficulty in hearingand visual defects (due to direct neurotoxicityas well as constriction of retinal and auditoryvessels). Diarrhoea, flushing and marked perspi-ration may also appear. The syndrome subsidescompletely if the drug is stopped.
Poisoning with still higher doses results in the abovesymptoms in an exaggerated form. In addition, delirium, fever,

826S
EC
TIO
N12
ANTIMICROBIAL DRUGS
tachypnoea followed by respiratory depression, pulmonaryedema, hypoglycaemia, marked weakness and prostration canoccur. Hypotension, cardiac arrhythmias develop only on rapidi.v. injection — the patient may die. Watch Q-T prolongationduring i.v. infusion of quinine; stop if it exceeds 25%.
Few individuals are idiosyncratic/hypersensitive toquinine; cinchonism may appear after a single therapeuticdose. Purpura, rashes, itching, angioedema of face andbronchoconstriction may develop.
Quinine occasionally causes haemolysis, especially inpregnant women and in patients of falciparum malaria, resultingin haemoglobinuria (black water fever) and kidney damage.
During pregnancy it should be used only for life-threatening infection, with special care to preventhypoglycaemia.
Uses
1. Malaria Quinine is used orally for uncomp-licated CQ-resistant malaria, and i.v. forcomplicated/cerebral malaria.
(a) Uncomplicated resistant falciparum mala-ria: Quinine may be used orally as an alternativeto S/P-ACT in uncomplicated CQ-resistantfalciparum malaria. It acts more rapidly thanS/P alone. The 7 day quinine + doxycycline/clindamycin regimen (see box on p. 820) is the2nd line treatment of CQ-resistant malaria (bothfalciparum and vivax) under NVBDCP. CertainCQ-resistant strains are also resistant to S/P, butrespond to quinine.
(b) Complicated and severe malaria includingcerebral malaria: Quinine (i.v.) has been thedrug of choice for cerebral malaria (falciparummalaria with impaired consciousness) and otherforms of complicated malaria. However, recentstudies indicate that parenteral artemisinins arefaster acting, more effective, better tolerated andmore conveniently administered. Therefore,artesunate (i.v./i.m.) or artemether (i.m.) orarteether (i.m.) are now preferred over quininefor severe malaria. The dosage and schedule fori.v. infusion of quinine for severe malaria is givenin the box on p. 821. Hypoglycaemia due tohyperinsulinemia is the most important sideeffect which can be prevented by infusing quininein 5% dextrose.
Supportive treatment needed in cerebralmalaria is cooling for fever, i.v. diazepam for
convulsions, correction of fluid and electrolytebalance and acidosis. Corticosteroids are use-less, may be harmful—avoid them.2. Nocturnal muscle cramps: a single tablet of quinine (300mg) at bed time may benefit some, but not all cases, andrisks may not justify use. Quinine is also effective in myotoniacongenita.
REZOQUIN, QUININE, QUINARSOL 300, 600 mg tab, 600 mg/2 ml inj.
Proguanil (Chloroguanide)
It is a relatively slow-acting erythrocytic schizontocide forboth P.f. and P.v. In addition, it inhibits the preerythrocyticstage of P.f. Gametocytes exposed to proguanil are not killedbut may fail to develop properly in the mosquito. Proguanilis cyclized in the body to a triazine derivative (cycloguanil)which inhibits plasmodial DHFRase-thymidylate synthase inpreference to the mammalian DHFRase. Resistance to proguanildevelops rapidly due to mutational changes in the plasmodialDHFRase-thymidylate synthase enzyme. There is partial cross-resistance between proguanil and pyrimethamine, which isa directly acting plasmodial DHFRase inhibitor.
Absorption of oral proguanil is slow, but almost complete.It is partly metabolized and excreted in urine; t½ is 16–20hr; noncumulative. It is very well tolerated; side effects areless compared to CQ. Mild abdominal symptoms, vomiting,occasional stomatitis, haematuria, rashes and transient lossof hair are reported.
In the late 1940s and early 1950s it was extensively usedas a clinical curative for vivax malaria, especially in endemicareas with partially immune population. However, proguanilalone cannot be depended upon in nonimmune patients,particularly those with falciparum malaria, due to slowresponse and chances of rapid resistance. Currently in India,proguanil has little role either in prophylaxis or in clinical cureof malaria. However, its combination with atovaquone (seep. 831) is commonly used in Thailand, USA and some othercountries as a fast-acting erythrocytic schizontocide fortreatment of multidrug resistant falciparum malaria. Proguanil(without conversion to cycloguanil) by a DHFRase unrelatedaction potentiates the schizontocidal action of atovaquone.Moreover, P.f. does not easily develop resistance to thiscombination.
Atovaquone-proguanil is also used by western travellersas a causal prophylactic while visiting CQ-resistant/multidrug-resistant P.f. endemic areas. In Africa proguanil combined withCQ has been used as a suppressive prophylactic in moderatelyCQ-resistant P.f. areas.PROGUMAL 100 mg tab.
PyrimethamineIt is a directly acting inhibitor of plasmoidalDHFRase (does not require conversion to a cyclic

827C
HA
PTER59
ANTIMALARIAL DRUGS
triazine, as is the case with proguanil). Selectiveantimalarial action depends on high affinity forplasmodial enzyme (~2000 times greater thanfor the mammalian enzyme). In contrast totrimethoprim, it has very poor action on bacterialDHFRase. Under the influence of pyrimethamine,schizogony of malarial parasite in blood graduallystops. At high doses, it inhibits Toxoplasma gondii.
Pyrimethamine is more potent than proguanil,and a slowly acting erythrocytic schizontocide,but does not eliminate the preerythrocytic phaseof P. falciparum or the exoerythrocytic phaseof P.vivax. If used alone, resistance developsrather rapidly by mutation in the DHFRaseenzyme of the parasite wiith reduced affinity.These organisms exhibit cross resistance toproguanil.
Pharmacokinetics Absorption of pyrimetha-mine from g.i.t. is good but slow. Certain organslike liver, spleen, kidney and lungs concentratepyrimethamine. It is metabolized and excretedin urine with a t½ of 4 days. Prophylacticconcentrations remain in blood for 2 weeks.
Adverse effects Pyrimethamine is relativelysafe. The only side effects are occasional nauseaand rashes. Folate deficiency is rare; megalo-blastic anaemia and granulocytopenia may occurwith higher doses, especially in those withmarginal folate stores. This can be treated byfolinic acid.
Use Pyrimethamine is used only in combi-nation with a sulfonamide (S/P) or dapsone (seebelow) for treatment of falciparum malaria.
Sulfonamide-pyrimethamine (S/P)Sulfonamides/dapsone are not particularlyeffective antimalarial drugs in their own right;have some inhibitory influence on the erythro-cytic phase, especially of P. falciparum.However, they form supra-additive synergisticcombination with pyrimethamine due tosequential block (as in case of cotrimoxazole:p. 706). Though, both components are slowacting, the combination acts faster, so that it can
be employed as a clinical curative, particularlyfor P. falciparum. Efficacy against P. vivax israther low. By the addition of sulfonamide,development of resistance to pyrimethamine isretarded. There is no cross-resistance with othergroups of antimalarial drugs.The popular combinations are:Sulfadoxine 500 mg + pyrimethamine 25 mg tab: RIMODAR,FANCIDAR, LARIDOX, MALOCIDE; REZIZ 500 mg + 25 mgtab and per 10 ml susp; REZIZ FORTE 750 mg + 37.5 mgtab.Sulfamethopyrazine 500 mg + pyrimethamine 25 mg tab:METAFIN, MALADEX.Dapsone 100 mg + pyrimethamine 25 mg tab; MALOPRIM.
As clinical curative: Sulfadoxine 1500 mg +pyrimethamine 75 mg (3 tab) single dose(children 9–14 yr 2 tab, 5–8 yr 1½ tab, 1–4yr 1 tab).
Sulfadoxine and sulfamethopyrazine are ultra-long acting sulfonamides — attain low bloodconcentrations, but are able to synergise withpyrimethamine which also has long t½. Thecombination has the potential to cause seriousadverse effects (exfoliative dermatitis, Stevens-Johnson syndrome, etc.) due to the sulfonamide.Therefore, use is restricted to single dosetreatment of uncomplicated CQ-resistant falci-parum malaria. Prophylactic use, needingmultiple unsupervised doses is not approved. Itis contraindicated in infants and in individualsallergic to sulfonamide. There is no evidencethat single dose of the combination used fortreating malaria harms the foetus duringpregnancy, but should be avoided if possible.
The major importance of this combinationis due to its efficacy against CQ-resistant P.falciparum. Compliance is good due to singledose therapy and few acute side effects.Resistance to S/P among P. falciparum was firstnoted in 1980, and has spread globally now. Itis high in South East Asia, South America andSouthern Africa, so much that it is no longeremployed in these countries. In India, S/Presistance appears to be sporadic, except in theNorth east. A sample study from Assam found9% CQ-resistant P. falciparum cases to be

828S
EC
TIO
N12
ANTIMICROBIAL DRUGS
nonresponsive to S/P as well, while in the areabordering Myanmar 35–44% S/P failures wererecorded. To contain further spread of S/Presistance in India, the National drug policy onmalaria mandates compulsory use of artesunatealong with S/P for treatment of all falciparummalaria cases.
It is not an effective drug for vivax malaria.S/P is the first choice treatment for toxoplasmosis, whichmainly occurs in immunocompromised patients.
Primaquine
Unlike other antimalarial drugs, primaquine isa poor erythrocytic schizontocide: has weakaction on P. vivax, but blood forms ofP. falciparum are totally insensitive. On the otherhand, it is more active against the preerythrocyticstage of P. falciparum than that of P. vivax.Primaquine differs from all other availableantimalarials in having a marked effect onprimary as well as secondary hepatic phases ofthe malarial parasite. It is highly active againstgametocytes and hypnozoites.
The mechanism of action of primaquine isnot known. However, it is different from thatof CQ. Though, resistance among P. vivax againstprimaquine can be induced, it is not a clinicalproblem.
Pharmacokinetics Primaquine is readilyabsorbed after oral ingestion. It is oxidized inliver with a plasma t½ of 6–8 hrs and excretedin urine within 24 hours. It is not a cumulativedrug.Adverse effects The usual doses ofprimaquine produce only abdominal pain, g.i.upset, weakness or uneasiness in chest as sideeffect. These can be minimized by taking thedrug with meals. CNS and cardiovascularsymptoms are infrequent. Leucopenia occursrarely with larger doses.
The most important toxic potential is doserelated haemolysis, methaemoglobinaemia,tachypnoea and cyanosis. These are due to theoxidant property of primaquine. Its metabolitesare more potent in this regard. However, in normal
individuals doses < 60 mg (base) produce littlehaemolysis. Those with G-6-PD deficiency arehighly sensitive and haemolytic anaemia canoccur with 15–30 mg/day. There are severalvariants of G-6-PD deficiency, and the defectis graded. Massive haemolysis is associated onlywith the Mediterranean and few other variants.The incidence of G-6-PD deficiency is lowamong Indians, except in some tribal people ofJharkhand, Andhra Pradesh, Madhya Pradesh andAssam. It is high among black races andMediterranean people. Spot tests are availablefor detecting G-6-PD deficiency. Passage of darkurine is an indication of haemolysis; primaquineshould be promptly stopped if it occurs. Therisk of haemolysis and leucopenia is increasedin patients of rheumatoid arthritis, SLE and inthose acutely ill.
Primaquine should not be given duringpregnancy, because foetus is G-6-PD deficient.
Use
Vivax malaria: The primary indication ofprimaquine is for radical cure of relapsing (vivax)malaria.The dose used in most countries is 30mg/day, but in India 15 mg/day (children 0.25mg/kg/day) for 2 weeks is given along with fullcurative dose of CQ or another blood schizon-tocide to eliminate the erythrocytic phase.Relapse rate with 5 day primaquine treatment,employed earlier by NAMP (India), has beenfound similar to no treatment; therefore notrecommended now. The G-6-PD status of thepatient should be tested before giving 14 dayprimaquine course. It is to be taken with foodto reduce g.i. side effects.
Falciparum malaria: A single 45 mg dose ofprimaquine is given with the curative dose ofCQ or ACT to kill the gametes and cut downtransmission to mosquito. This use is restrictedto low transmission areas or where effectivevector control is implimented.MALIRID, EVAQUIN (as phosphate 26 mg = 15 mg base) 2.5,7.5, 15, 45 mg tab.
Primaquine 15 mg/day given with clindamycin 600 mg TDSis an alternative drug for Pneumocystis jiroveci pneumonia inAIDS patients.

829C
HA
PTER59
ANTIMALARIAL DRUGS
Tafenoquine
This new 8-aminoquinoline is being developed as a single doseantirelapse drug for vivax malaria. The need for 14 daily dosesof primaquine for effective relapse prevention is the biggesthurdle in implementing antirelapse therapy. Tafenoquine has along plasma t½ of 16–19 days (t½ of primaquine is 6–8 hours).Thus, it continues to act for weeks. In phase 3 clinical trials1–3 day treatment (along with CQ) has achieved upto 100%relapse prevention.
Tafenoquine is highly active against vivax hypnozoites. Ithas also shown some activity against asexual erythrocyticstages of P.v. and P.f. (including CQ-resistant strains), butclearance of fever and parasitaemia were slow. Therefore, itmust be accompanied by CQ or another rapidly actingerythrocytic schizontocide for vivax malaria. Tafenoquine shareswith primaquine the potential to cause haemolysis in G-6-PDdeficient individuals. Incidents of anaemia, haemolysis andmethaemoglobinemia are reported, but overall tolerabilityappears to be good.
Tafenoquine is undergoing phase-3 dose titration trial inIndia (along with standard 3 day CQ) for relapse prevention invivax malaria, and is likely to emerge as a single dose radicalcurative.
Tetracycline and Doxycycline
These antibiotics have slowly acting and weakerythrocytic schizontocidal action against allplasmodial species including CQ, MQ and S/Presistant P. falciparum. However, no clinicallyuseful action is exerted on the preerythrocyticstage. Gametocytes and vivax hypnozoites arealso not killed. Tetracyclines are never used aloneto treat malaria, but only in combination withquinine for the treatment of CQ-resistantfalciparum as well as vivax malaria. Tetracycline250 mg QID or doxycycline 100 mg OD areequally efficacious. Doxycycline 200 mg/day hasalso been combined with artesunate to treatmefloquine/chloroquine/S/P-resistant falciparummalaria in Thailand.
Doxycycline 100 mg/day is used as a 2ndline prophylactic for short-term travellers to CQ-resistant P. falciparum areas. Tetracyclines arenot to be given to children and pregnant women.
Clindamycin (see p. 756)
This is another bacteriostatic antibiotic that has slow actingerythrocytic schizontocidal property against all speciesof plasmodia including multidrug resistant strains ofP. falciparum. Liver stages and gametocytes are not affected.
It markedly potentiates the antimalarial activity of quinine andartemisinin, and is always used in combination with one ofthese. Clindamycin is a second choice drug to doxycyclinefor adding to quinine or to artesunate for the treatment ofmultidrug resistant falciparum malaria, or CQ-resistant vivaxmalaria. In contrast to doxycycline, it can be used in childrenand pregnant women. However, clindamycin is not used forprophylaxis of malaria, because of thrice daily dosing andrisk of adverse effects.
ARTEMISININ DERIVATIVES
Artemisinin is the active principle of the plantArtemisia annua used in Chinese traditionalmedicine as ‘Quinghaosu’. It is a sesquiterpinelactone endoperoxide active against P.falciparum resistant to all other antimalarialdrugs as well as sensitive strains and othermalarial species. Potent and rapid bloodschizontocide action is exerted eliciting quickerdefervescence and parasitaemia clearance (<48hr) than CQ or any other drug. In the erythrocyticschizogony cycle, artemisinins exert action ona wide range of stages—from ring forms to earlyschizonts; thus have the broadest time windowof antimalarial action.
Artemisinin is poorly soluble in water as wellas in oil. Several derivatives have been producedfor clinical use. Artemether is soluble in oil,while Artesunate (sod.) is water soluble. Bothcan be given orally as well as i.m., but artesunatesod. can also be given i.v. Their active meta-bolite generated in the body Dihydroartemisinin(DHA) is also used orally. An injectablecompound Arteether (i.m. in oil) was producedin India in the 1990s, and recently a totallysynthetic oral compound Arterolane has been

830S
EC
TIO
N12
ANTIMICROBIAL DRUGS
developed here. All these drugs are collectivelyreferred to as ‘Artemisinins’.
In addition to their potent schizontocidalaction, these drugs are lethal to early stagemalarial gametes but not mature ones. Bydecreasing the population of gametes, theyreduce but do not totally interrupt diseasetransmission. Artemisinins do not kill primaryliver forms or vivax hypnozoites.
The duration of action is short and recru-descence rate is high when they are used alonein short courses. Recrudescence depends uponthe dose and duration of therapy as well as onseverity of disease. Resistance among P.f. toartemisinins is not a clinical problem yet, butin some areas (Cambodia, Thailand, Myanmar)delayed parasitaemia clearance has been noted,that is indicative of decreased responsiveness.This reemphasizes the need to use artemisininsonly in combination (as ACT) with a drug whichacts by a different mechanism. No cross resis-tance with any other class of antimalarial drugsoccurs.
Because artemisinins are short acting drugs,monotherapy needs to be extended beyond thedisappearance of the parasites to prevent recru-descence. After 5 days treatment recrudescencerate is ~10%, while with a 3 day course it is~50%. Recrudescence can be totally preventedby combining 3 day artemisinin with a long-acting drug (see ACT later).
Mechanism of action of artemisinin is notdefinitely known. The endoperoxide bridge inits molecule appears to interact with haeme inthe parasite. Ferrous iron-mediated cleavage ofthe bridge releases a highly reactive free radicalspecies that binds to membrane proteins, causeslipid peroxidation, damages endoplasmicreticulum, and ultimately results in lysis of theparasite. Another line of evidence has shown thatthe artemisinin free radicals specifically inhibita plasmodial sarcoplasmic-endoplasmic calciumATPase labelled ‘Pf ATP6’.
Pharmacokinetics Data on pharmacokineticsof artemisinin derivatives is limited and
incomplete. Both artesunate and artemether areprodrugs.
Artesunate Its sodium salt is water-solubleand is administered by oral, i.m. or i.v. routes.In addition, rectal route has been tried. Afteroral ingestion, absorption is incomplete but fast,reaching peak in <60 min. It is rapidly convertedto the active metabolite DHA with a t½ of30–60 min. The t½ of DHA is 1–2 hours. Afterrepeated dosing, artesunate causes autoinductionof its own metabolism by CYP2B6 and CYP3A4.FALCIGO, FALCYNATE, ARTINATE 50 mg tab, 60 mg/vial inj;LARINATE, ARNATE 50 mg tab.
Artemether It is lipid-soluble and is adminis-tered orally or i.m., but not i.v. Absorption afteroral as well as i.m. dosing is slower taking2–6 hours. It undergoes substantial first passmetabolism and is converted to DHA. Extensivemetabolism by CYP3A4 yields a variable t½ of3–10 hours.PALUTHER, LARITHER, MALITHER 80 mg inj (in 1 ml arachisoil).
ααααα/βββββ Arteether This compound developed inIndia is available for i.m. administration only toadults for complicated malaria. Because of itslonger elimination t½ (23 hours), it is recom-mended in a 3 day schedule, but is consideredless dependable in severe/complicated malaria.The WHO recommends a 5 day course (see boxp. 821).Dose: 150 mg i.m. daily for 3 days in adults.E-MAL, FALCY, RAPITHER-AB 150 mg/2 ml amp (box of 3amp).
Dihydroartemisinin and Arterolane These areavailable for oral use only in combination, andare considered with ACT (see p. 833, 834).Adverse effects Data from >10000 monitoredpatients shows that artesunate/artemether producefew adverse effects; most are mild: nausea,vomiting, abdominal pain, itching and drug fever.Headache, tinnitus, dizziness, bleeding, dark urine,S-T segment changes, Q-T prolongation, firstdegree A-V block, transient reticulopenia andleucopenia are rare and subside when the patientimproves or drug is stopped. Millions of patients

831C
HA
PTER59
ANTIMALARIAL DRUGS
have been treated so far without any seriousneurological or other toxicity, but closemonitoring of the patient is advocated. Intravenousartesunate is much safer than i.v. quinine.
Interactions Concurrent administration ofartemisinins with drugs prolonging Q-T, likeastemizole, antiarrhythmics, tricyclic antidepres-sants and phenothiazines may increase the riskof cardiac conduction defects. However, nointerference with the ACT partner drugs has beennoted.
UseUncomplicated falciparum malaria Oralartemisinins are indicated for the treatment ofall cases of uncomplicated falciparum malaria(CQ-resistant as well as sensitive) as ACT. Evenwhen used alone, they are almost 100%effective, but because of short duration of actionrecrudescence rates are high. In order to preservetheir powerful antimalarial activity and to reducerecrudescence rates, they must be used incombination with a long-acting schizontocidewhich acts by a different mechanism. The DrugsController General of India has prohibited useof oral artemisinins as single drugs. Fixed-dosedrug combination formulations of ACT are beingencouraged.
For vivax malaria, artemisinins (as ACT) areindicated only in case of CQ-resistant infectionand when quinine + doxycycline/clindamycin alsocannot be used. Use of artemisinins for pro-phylaxis of malaria is not allowed. They haveshort duration of action and higher potentialtoxicity. Moreover, wide spread prophylactic usewill foster resistance. Their cidal action on earlystage gametes reduces transmission of resistantP.f. infection, but does not totally interrupt it.Single dose primaquine is recommended afterACT to kill all circulating gametes.
Severe and complicated falciparum malariaParenteral artemisinins are higly effective andare the drugs of choice irrespective of CQ-reistance status. Quinine infused i.v. had beenthe drug of choice for severe and complicated
malaria, including cerebral malaria, but now i.v./i.m. artemisinins are preferred, while quinine isused only as an alternative when artemisininscannot be used. Quinine (i.v.) continues to bethe drug used for severe falciparum malariaduring 1st trimester of pregnancy, because safetyof artemisinins is not yet proven. Artesunate (i.v.)offers several advantages:• It causes faster parasite clearance than i.v.
quinine.• It is safer and better tolerated than i.v. quinine.• Its dosing schedule is simpler.• Recent evidence indicates higher efficacy and
lower mortality.*Because i.v. injection achieves more rapid peakconcentration, and only artesunate sod. can begiven i.v., the NVBDCP has decided to use onlyi.v. artesunate for severe malaria.
Halofantrine It is a phenanthrene methanol bloodschizontocide having activity comparable to mefloquine withwhich it exhibits cross resistance. It is effective againstP. falciparum resistant to CQ and S/P, as well as against P.vivax. It is not active against gametocytes or hepatic stagesof the malarial parasite.
Oral absorption of halofantrine is low and erratic, andside effects are relatively common. Prolongation of QTc intervalis seen even at therapeutic doses and few cases of seriousventricular arrhythmia (some fatal) are on record.
It is not approved in India, but in other countries it hasbeen used for multiresistant falciparum malaria when no othereffective alternative is available.
Lumefantrine (see below under ACT)Pyronaridine (see below under ACT)
Atovaquone This synthetic naphthaquinone is a rapidlyacting erythrocytic schizontocide as well as active againstpreerythrocytic stage of P. falciparum and other plasmodia.Pneumocystis jiroveci and Toxoplasma gondii are alsosusceptible to atovaquone. It collapses plasmodial mito-chondrial membranes and interferes with ATP production.Proguanil potentiates its antimalarial action and preventsemergence of resistance. A fixed dose oral combination ofthe two drugs is used for 3 day treatment of uncomplicatedCQ-resistant P. falciparum as well as P. vivax malaria in theUSA and some other countries, but not in India.Taken oncedaily with food, this combination is also used as a prophylacticby nonimmune travellers visiting endemic areas.
* Artesunate versus quinine for treatment of severe falciparummalaria: a randomized trial. Lancet, 2005; 366: 717-25. (Trialconducted in India, Bangladesh, Myanmar and Indonesia).

832S
EC
TIO
N12
ANTIMICROBIAL DRUGS
Atovaquone is also employed as a second line drug foropportunistic infections with P. jiroveci and T. gondii in AIDSpatients. It produces few side effects—diarrhoea, vomiting,headache, rashes, fever, and is contraindicated duringpregnancy.
ARTEMISININ-BASED COMBINATIONTHERAPY (ACT)
Noting that use of antimalarial drugs singly hasfailed to curtail the prevalence of malariaglobally, particularly due to emergence of CQ-resistant, followed by multidrug-resistant P.falciparum, the WHO has recommended that allcases of acute uncomplicated falciparum malariashould be treated only by combining one of theartemisinin compounds with another effectiveerythrocytic schizontocide. In choosing thecompanion drug, the most important consi-deration is its elimination t½ (governing stayin the body), because effective concentrationsin blood must be maintained for at least 3–4asexual cycles of the parasite, i.e. 6–8 days, toexhaust the parasite burden. Therefore, short t½drugs have to be given for 7 days, while longeracting drugs can be given for 1–3 days. However,long t½ drugs allow subinhibitory concentrationsto persist in the blood facilitating selection ofresistant mutants. Combining a short t½ drugwith a long t½ drug in the conventional 3 dayregimen runs the risk of de facto monotherapyafter the short t½ drug is eliminated. This riskis minimized by choosing a short t½ drug thatreduces the parasite load rapidly and drastically.Artemisinin compounds fillin this requirement,as they rapidly kill > 95% plasmodia. They leaveonly a small biomass of the parasites to beeliminated by the long t½ drug, reducing thechances of selecting resistant mutants.Advantages of ACT over other antimalarials are:• Rapid clinical and parasitological cure.• High cure rates (>95%) and low recrudes-
cence rate.• Absence of parasite resistance (the compo-
nents prevent development of resistance toeach other).
• Good tolerability profile.
The ACT regimens for oral treatment ofuncomplicated falciparum malaria that arealready in use in India, or are WHO approved,or have completed clinical trial are given in thebox on p. 833. Oral ACTs are not to be usedin severe or complicated malaria, for whichparenteral drugs are needed.
1. Artesunate-sulfadoxine + pyrimetha-mine (AS-S/P) This ACT has been adopted asthe first line drug for uncomplicated falciparummalaria under the ‘National antimalaria drugpolicy’ of India, and has replaced CQ throughoutthe country. This does not imply that it is themost effective/best ACT, because it is not effec-tive against multidrug-resistant strains which arenonresponsive to S/P. However, treatmentfailures with AS-S/P ACT are mostly restrictedto Northeast areas bordering Myanmar; while inrest of India so far this ACT appears to beworking satisfactorily with >96% success rate.As such, NVBDCP continues to use AS-S/P ACTas the firstline therapy, including that during 2ndand 3rd trimester of pregnancy. This ACT appearsto produce fewer side effects than artesunate/mefloquine. Private clinics, however, are usingother ACTs. Most other malaria endemiccountries have found AS-S/P ACT to be inferior.2. Artesunate-mefloquine (AS/MQ) Thisis the standard and most extensively used ACTin Thailand, Myanmar and other Southeast Asiancountries as well as South-America and Africa.It was found highly effective and well toleratedin uncomplicated falciparum malaria. However,many areas in far East already have MQ-resistantP. f., but by combining with AS, further spreadof MQ resistance was checked. Nevertheless,some of them have switched over to alternativeACTs. In India AS/MQ has been used to a limitedextent, but small studies have shown ~ 100%efficacy. A kit with separate As and MQ tabletsis available and a FDC formulation has beenapproved. Side effects of MQ need to be watchedfor.3. Artemether-lumefantrine Lumefantrineis an orally active, high efficacy, long-acting

833C
HA
PTER59
ANTIMALARIAL DRUGS
ACT regimens for uncomplicated falciparum malaria*
1. Artesunate-mefloquine (AS/MQ)£
Artesunate 100 mg BD (4 mg/kg/day) × 3 days + mefloquine 750 mg (15 mg/kg) on 2nd day and 500mg (10 mg/kg) on 3rd day (total 25 mg/kg).FALCIGO PLUS kit (Artesunate 50 mg tab + Mefloquine 250 mg tab kit), (a FDC tablet has been approvedin India).
2. Artemether-lumefantrine (1:6)£
Artemether (80 mg BD) + lumefantrine (480 mg BD) × 3 daysCOARTEM, COMBITHER, LUMETHER (artemether 20 mg + lumefantrine 120 mg tab.) to be taken withfatty meal.Adult and child >35 kg 4 tab BD; child 25–35 kg 3 tab BD; 15–25 kg 2 tab BD; 5–15 kg 1 tab BD,all for 3 days.FALCIMAX PLUS, ARTE PLUS (artemether 80 mg + lumefantrine 480 mg tab) 1 tab BD × 3 days for adults.
3. Artesunate-sulfadoxine + pyrimethamine (AS/S/P)£
Artesunate 100 mg BD (4 mg/kg/day) × 3 days + sulfadoxine 1500 mg (25 mg/kg) and pyrimethamine75 mg (1.25 mg/kg) single dose.ZESUNATE kit, MASUNATE kit, FALCIART kit (Artesunate 100 mg × 6 tab + sulfadoxine 500 mg/pyrimethamine25 mg × 3 tab kit)
4. Arterolane-piperaquineArterolane (as maleate) 150 mg + piperaquine 750 mg daily × 3 daysSYNRIAM (arterolane 150 mg + piperaquine 750 mg) cap, 1 cap OD × 3 days
5. Dihydroartemisinin-piperaquine (DHA/PPQ 1:8)£ (ARTEKIN)DHA 120 mg (2 mg/kg) + piperaquine 960 mg (16 mg/kg) daily × 3 days
6. Artesunate-amodiaquine (AS/AQ)£
Artesunate 200 mg (4 mg/kg) + amodiaquine 600 mg (10 mg/kg) per day × 3 daysArtesunate 25 mg/50 mg/100 mg +Amodiaquine 67.5 mg/135 mg/270 mg fixed dose combination tabletshave been approved in India.
7. Artesunate-pyronaridine (1:3)Artesunate 100–200 mg (2–4 mg/kg) + pyronaridine 300–600 mg (6–12 mg/kg) per day × 3 days
* All drugs are administered orally£ WHO approved ACTs
erythrocytic schizontocide, related chemicallyand in mechanism of action to halofantrine andMQ. Additionally, nucleic acid and proteinsynthesis of the parasite is affected. Like theothers, vivax hypnozoites are not affected.Lumefantrine is highly lipophilic; absorptionstarts after 2 hours of ingestion and peaks at6–8 hours. Antimalarial action is slower thanCQ. Plasma protein binding is 99%, and it ismetabolized predominantly by CYP3A4.Terminal t½ is 2–3 days, which is prolongedto 4–6 days in malaria patients.
Lumefantrine is used only in combinationwith artemether, as FDC tablets. The twocomponents protect each other from plasmodialresistance. As such, no clinically relevant
resistance has developed so far. Clinical efficacyis high achieving 95–99% cure rate, which iscomparable to AS/MQ. Artemether-lumefantrineis active even in multidrug resistant P.f. areasincluding MQ-resistant. It has been extensivelyemployed in Southeast Asia and Africa. In Indiait is frequently used by private doctors. Whileartemether quickly reduces parasite biomass andresolves symptoms, lumefantrine preventsrecrudescence. Gametocyte population isreduced, checking transmission.
Artemether-lumefantrine must be adminis-tered with fatty food or milk, which markedlyenhances lumefantrine (and to some extentartemether) absorption, and ensures adequateblood levels. Failure to take it with fat rich food

834S
EC
TIO
N12
ANTIMICROBIAL DRUGS
limits absorption and may result in recrudes-cence. This ACT is generally well tolerated; sideeffects are—headache, dizziness, sleep distur-bances, abdominal pain, arthralgia, myalgia,pruritus and rash. Some studies indicate that itis better tolerated than AS/MQ. Artemether-lumefantrine should not be given with drugsmetabolized by CYP2D6 (metoprolol, neuro-leptics, tricyclic antidepressants, etc), becauselumefantrine inhibits the isoenzyme CYP2D6.Lumefantrine shares with halofantrine thepotential to prolong QTc, but the risk is muchless. Since artemether can also prolong Q-Tcto some extent, artemether-lumefantrine ACTshould not be given to patients receiving Q-Tcprolonging drugs. It is contraindicated infirst trimester of pregnancy and during breast-feeding.
4. Dihydroartemisinin (DHA)-piperaquinePiperaquine is a bisquinoline congener of CQdeveloped in China as a high efficacy long-acting(t½ 3–4 weeks) erythrocytic schizontocide witha slower onset of action because of largervolume of distribution. The mechanism of actionis similar to CQ, and it is equally active againstCQ-sensitive, but more active against CQ-resistant P. falciparum. In 1978, piperaquinereplaced CQ in China, where it has beenextensively used for mass prophylaxis as wellas treatment of malaria.
Piperaquine has been coformulated with DHAin a dose ratio of 8:1 (ARTEKIN) and extensivelyevaluated in multidrug resistant P.f. areas ofCambodia, Thailand, Vietnam, etc. with highsuccess rate. In clinical trials, efficacy of DHA-piperaquine fixed dose combination has beenfound comparable to artemether-lumefantrine orAS/MQ. Safety profile of DHA-piperaquine isgood and it is well tolerated even by children.However, dizziness, vomiting and other g.i.symptoms are common; rashes are rare. DHA-piperaquine FDC has completed clinical trialsin India producing > 98% response rate inuncomplicated falciparum malaria, and is likelyto be approved soon.
5. Artesunate-amodiaquine (AS/AQ)Amodiaquine (AQ; see p. 823) has long been usedparallel to CQ. While AQ itself has a short t½due to rapid metabolism, its metabolite, an equallypotent antimalarial has long t½ of 10–18 days.Because of close structural resemblance of AQto CQ, it was apprehended that AQ may not bean effective antimalarial in areas with CQ-resistant P.f. However, trials in Africa showed thatAQ produced satisfactory response in such areas.Addition of artesunate further improved the curerate. Trials were conducted in Africa with AS/AQcoformulated as FDC tablets, which produced highcure rates, and now this ACT has become the first-line therapy of uncomplicated falciparum malariain many African countries. Recent trial in Indiaalso yielded ~ 97% cure of falciparum malaria.This ACT has been approved in India as FDCtablets in 3 strengths for different age groups(see box on p. 833), to be taken twice daily for3 day treatment of uncomplicated falciparummalaria.
6. Arterolane-piperaquine Arterolane is anovel orally active synthetic trioxolane congenerof artemisinin that has been developed in Indiaand recently marketed in combination withpiperaquine. Arterolane acts rapidly at all stagesof asexual schizogony of malarial parasiteincluding multidrug resistant P.f., but has noeffect on the hepatic stages. It accumulates inthe food vacuole of the parasite, and thus differsfrom artemisinins which do not accumulate atthis site. It also has moderate gametocidal activitysimilar to that of artemether-lumefantrine.
Both arterolane and piperaquine are wellabsorbed orally, and absorption is unaffected byfood. Peak plasma arterolane concentration isreached in 3–5 hours and it has a large volumeof distribution. The major metabolic pathway isoxidation, mainly by CYP3A4, which is also theprimary isoenzyme responsible for piperaquinemetabolism. Arterolane is short acting and itsplasma t½ varies between 1–3 hours.
Arterolane-piperaquine FDC has undergonemulticentric clinical trials in India, Bangladesh

835C
HA
PTER59
ANTIMALARIAL DRUGS
and Thailand. In uncomplicated falciparummalaria this ACT has produced ≥ 95% cure ratewith a fever and parasitaemia clearance time of24–48 hours. In a comparative trial its efficacyand tolerability has been found equivalent toartemether-lumefantrine. Side effects aregenerally mild headache, postural dizziness,vomiting, abdominal pain and diarrhoea. Thus,arterolane-piperaquine appears to be an effectiveand well tolerated alternative ACT.7. Artesunate-pyronaridine Pyronaridine is a water-soluble naphthyridine Mannich base erythrocyticschizontocide with high efficacy and mechanism of action
PROBLEM DIRECTED STUDY
59.1 A 20-year-old girl reported to the district hospital OPD with irregular episodes of highfever for the past 3 days. The fever is preceded by chills and shivering and attended by headache,body ache, pain in abdomen, nausea and weakness. The fever lasts 4–6 hours and subsidesafter sweating. On enquiry she informed that she belongs to a village in the tribal area ofMadhya Pradesh. About a month back she had returned from her home after a 3 weeksvacation and she works as a house maid in the city. Blood smear examination showed presenceof intraerythrocytic P. vivax parasites. She was treated with the standard 1.5 g chloroquine(base) course over 3 days, and was given primaquine 15 mg tab to be taken once daily for14 days, after she tested negative for G-6PD deficiency. She was afebrile on the 4th day, butreturned back 7 days later with similar episode of chills and fever. Finger prick blood smearwas positive for P. vivax. She confirmed continuing to take daily primaquine medication.(a) What is the most likely cause of recurrence of fever and parasitaemia?(b) How should the 2nd episode of fever be treated?(c) Should primaquine medication be continued or stopped?(see Appendix-1 for solution)
similar to CQ, that has been used in China for ~ 40 years.It is active against both CQ-sensitive and CQ-resistant P.falciparum and other malarial species. The onset of actionis slower and duration long. It is concentrated in RBCs andmetabolized with a terminal t½ of 7 days. Weak analgesic-antipyretic action is produced at higher doses.
Clinical efficacy of artesunate-pyronaridine FDC (doseratio 1:3) has been tested in falciparum malaria in China,Thailand and Africa with >95% success and no recrudescencein 28 days. Multidrug-resistant P. falciparum and P. vivaxalso respond. Clinical trials have been completed in India with> 95% cure rate. Artesunate-pyronaridine is well tolerated.Side effects noted are abdominal pain, vomiting, headache,dizziness, loss of appetite, palpitation and transient ECGchanges, but no serious reactions have occurred. However,this ACT has not yet been approved for use in India.

Antiamoebic and OtherAntiprotozoal Drugs
ChapterChapterChapterChapterChapter 6060606060
ANTIAMOEBIC DRUGS
These are drugs useful in infection caused bythe anaerobic protozoa Entamoeba histolytica.Other Entamoeba species are generally non-pathogenic.
Amoebiasis has a worldwide distribution(over 50 million people are infected), but it isendemic in most parts of India and otherdeveloping countries. Poor environmentalsanitation and low socio-economic status areimportant factors in the spread of the disease,which occurs by faecal contamination of foodand water. Amoebic cysts reaching the intestinetransform into trophozoites which either live onthe surface of colonic mucosa as commensals—form cysts that pass into the stools (luminalcycle) and serve to propagate the disease, orinvade the mucosa—form amoebic ulcers (Fig.60.1) and cause acute dysentery (with blood andmucus in stools) or chronic intestinal amoebiasis(with vague abdominal symptoms, amoeboma).
Occasionally the trophozoites pass into thebloodstream, reach the liver via portal vein andcause amoebic liver abscess. Other organs likelung, spleen, kidney and brain are rarely involvedin extraintestinal amoebiasis. In the tissues, onlytrophozoites are present; cyst formation doesnot occur. Tissue phase is always secondary tointestinal amoebiasis, which may be asympto-matic. In fact, most chronic cyst passers areasymptomatic. In the colonic lumen, theEntamoebae live in symbiotic relationship withbacteria, and a reduction in colonic bacteriareduces the amoebic population.
The ‘Brazil root’ or Cephaelis ipecacuanha was usedfor the treatment of dysentery in the 17th century. The purealkaloid emetine obtained from it was found to be a potentantiamoebic in 1912. Emetine remained the most efficaciousand commonly used drug for amoebiasis till 1960. Many 8-hydroxyquinolines (quiniodochlor, etc.) became very populardrugs for diarrhoea and amoebic dysentery, but have comeunder a cloud since they were held responsible for causingepidemics of ‘Subacute myelo-optic neuropathy’ (SMON) inJapan in 1970s.
Fig. 60.1: The luminal cycle and invasive forms of amoebiasis.T—trophozoite; C—cyst

837C
HA
PTER60
ANTIAMOEBIC AND OTHER ANTIPROTOZOAL DRUGS
Soon after its triumph as an antimalarial in 1948,chloroquine was found to be an effective and safe drug forhepatic amoebiasis. Diloxanide furoate was a useful additionin 1960, covering mainly chronic intestinal forms of the disease.However, the most remarkable development was thedemonstration of antiamoebic property of metronidazole inthe early 1960s. This drug had been introduced a few yearsback as a well tolerated, orally effective agent for trichomonasvaginitis. Of the many congeners of metronidazole that weretested, tinidazole has emerged in the 1970s as a goodalternative, and others have been added subsequently.
CLASSIFICATION1. Tissue amoebicides
(a) For both intestinal and extraintestinalamoebiasis:Nitroimidazoles: Metronidazole,Tinidazole, Secnidazole, Ornidazole,SatranidazoleAlkaloids: Emetine, Dehydroemetine
(b) For extraintestinal amoebiasis only:Chloroquine
2. Luminal amoebicides(a) Amide : Diloxanide furoate, Nitazoxanide(b) 8-Hydroxyquinolines: Quiniodochlor
(Iodochlorohydroxyquin, Clioquinol),Diiodohydroxyquin (Iodoquinol)
(c) Antibiotics: Tetracyclines, Paromomycin
NITROIMIDAZOLES
Metronidazole
It is the prototype nitroimidazole introduced in1959 for trichomoniasis and later found to bea highly active amoebicide. It has broad-spectrumcidal activity against anaerobic protozoa,including Giardia lamblia in addition to theabove two. Many anaerobic and microaerophilicbacteria, such as Bact. fragilis, Fusobacterium,Clostridium perfringens, Cl. difficile, Helico-bacter pylori, Campylobacter, peptococci,spirochetes and anaerobic Streptococci aresensitive. Though, it does not directly inhibit thehelminth Dracunculus medinensis, extraction ofthe worm from under the skin is facilitated.Metronidazole does not affect aerobic bacteria.Clinically significant resistance has notdeveloped among E. histolytica, but decreased
responsiveness of T. vaginalis has been observedin some areas. Anaerobic bacteria and G. lambliaalso can develop metronidazole resistance, butthis is a clinical problem only in the case ofH. pylori.
Metronidazole is selectively toxic toanaerobic and microaerophilic microorganisms.After entering the cell by diffusion, its nitro groupis reduced by certain redox proteins operativeonly in anaerobic microbes to a highly reactivenitro radical which exerts cytotoxicity. The nitroradical of metronidazole acts as an electron sinkwhich competes with the biological electronacceptors of the anaerobic organism for theelectrons generated by the pyruvate : ferredoxinoxidoreductase (PFOR) enzyme pathway ofpyruvate oxidation. The energy metabolism ofanaerobes that have no mitochondria is thus,disrupted. Aerobic environment attenuates cyto-toxicity of metronidazole by inhibiting itsreductive activation. Moreover, O2 competes withthe nitro radical of metronidazole for the freeelectrons generated during energy metabolism ofanaerobes. Anaerobes which develop metro-nidazole resistance become deficient in themechanism that generates the reactive nitroradical from it or have lower levels of PFOR.
Metronidazole, in addition, has been foundto inhibit cell mediated immunity, to inducemutagenesis and to cause radiosensitization.
Pharmacokinetics Metronidazole is almostcompletely absorbed from the small intestines;little unabsorbed drug reaches the colon. It iswidely distributed in the body, attaining thera-peutic concentration in vaginal secretion, semen,saliva and CSF. Metabolism occurs in liverprimarily by oxidation and glucuronide conju-gation followed by renal excretion. Plasma t½is 8 hrs.
Adverse effects Side effects of metroni-dazole are relatively frequent and unpleasant, butmostly nonserious.• Anorexia, nausea, metallic taste and abdo-
minal cramps are the most common. Loose-ness of stool is occasional.

838S
EC
TIO
N12
ANTIMICROBIAL DRUGS
• Less frequent side effects are—headache,glossitis, dryness of mouth and dizziness.
• Urticaria, flushing, heat, itching, rashes andfixed drug eruption occur in allergic subjects,warrant discontinuation of the drug andpreclude future use of nitroimidazoles.
• Prolonged administration may cause peri-pheral neuropathy and CNS effects. Seizureshave followed very high doses. Leucopeniais likely with repeated courses.
• Thrombophlebitis of the injected vein occursif the solution is not well diluted.
Contraindications Metronidazole is contraindi-cated in neurological disease, blood dyscrasias,first trimester of pregnancy (though no terato-genic effect has yet been demonstrated, itsmutagenic potential warrants caution). Cautioususe in chronic alcoholics.
Interactions A disulfiram-like intolerance toalcohol occurs in some patients taking metro-nidazole.Alcohol-metronidazole interaction occurs only in someindividuals, while majority of those taking it can consumealcohol without any reaction. There is no convincing evidenceof disulfiram-like action of metronidazole, but manufacturesadvise caution in drinking during metronidazole therapy.Enzyme inducers (phenobarbitone, rifampin)may reduce its therapeutic effect.Cimetidine can reduce metronidazole meta-bolism: its dose may need to be decreased.Metronidazole enhances warfarin action byinhibiting its metabolism. It can decrease renalelimination of lithium and precipitate toxicity.
PreparationsFLAGYL, METROGYL, METRON, ARISTOGYL ALDEZOLE200, 400 mg tab, 200 mg/5 ml susp. (as benzoyl metronidazole:tasteless); 500 mg/100 ml i.v. infusion; UNIMEZOL 200, 400 mgtabs, 200 mg/5 ml susp. METROGYL GEL, LUPIGYL GEL: 1%gel for vaginal/topical use.
Uses
1. Amoebiasis: Metronidazole is a first linedrug for all forms of amoebic infection. Manydosage regimens have been tried; the currentrecommendations are:
For invasive dysentery and liver abscess—800mg TDS (children 30–50 mg/kg/day) for 7–10days.In severe cases of amoebic dysentery or liverabscess 500 mg may be infused i.v. slowly every6–8 hours for 7–10 days or till oral therapycan be instituted.For mild intestinal disease—400 mg TDS for5–7 days. Metronidazole is less effective thanmany luminal amoebicides in eradicatingamoebic cysts from the colon, because it isnearly completely absorbed from the upperbowel.2. Giardiasis It is highly effective in a doseof 400 mg TDS for 7 days. A shorter courseof 3 days with 2 g/day is equally effective.3. Trichomonas vaginitis It is the drug ofchoice; 2.0 g single dose is preferred. Alterna-tively 400 mg BD–TDS may be used for 7 days.Additional intravaginal treatment is needed onlyin refractory cases. Repeated courses may benecessary in some patients, but should be givenwith gaps of 4–6 weeks. The male partner shouldbe treated concurrently in cases of recurrentinfections.Nonspecific bacterial vaginosis also responds.
4. Anaerobic bacterial infections Theyoccur mostly after colorectal or pelvic surgery,appendicectomy, etc. Brain abscesses andendocarditis may be caused by anaerobicorganisms.
Metronidazole is an effective drug for theseand is generally used in combination withgentamicin or cephalosporins (many are mixedinfections). For serious cases i.v. administrationis recommended: 15 mg/kg infused over 1 hrfollowed by 7.5 mg/kg every 6 hrs till oraltherapy can be instituted with 400–800 mg TDS.Prophylactic use in high risk situations(colorectal/biliary surgery) is recommended.Other drugs effective in anaerobic infections areclindamycin and chloramphenicol.
5. Pseudomembranous enterocolitis due toCl. difficile is generally associated with use of

839C
HA
PTER60
ANTIAMOEBIC AND OTHER ANTIPROTOZOAL DRUGS
antibiotics. Oral metronidazole 400–800 mgBD–TDS for 10–14 days is more effective, moreconvenient, less toxic, and therefore preferredover vancomycin which may be used in non-responsive cases, or when the infection recurs.
6. Acute necrotizing ulcerative gingivitis(ANUG) Metronidazole/tinidazole are the drugsof choice for ANUG (also called ‘trench mouth’)which is caused by anaerobes like fusobacteria,spirochetes and bacteroides. Metronidazole200–400 mg TDS (15–30 mg/kg/day) is oftencombined with amoxicillin, tetracycline orerythromycin. The response is rapid withdisappearance of the spirochete-fusobacteriumcomplex from the lesions and resolution of pain,bleeding, ulceration and bad breath within 2–3days; but treatment must be continued for at least5 days.
7. Helicobacter pylori gastritis/peptic ulcer(see p. 657) Metronidazole or tinidazole aloneare ineffective in eradicating H. pylori;resistance develops. Metronidazole 400 mg TDSor tinidazole 500 mg BD are combined withamoxicillin/clarithromycin and a proton pumpinhibitor in triple drug 2 week regimens.8. Guinea worm infestation Niridazole is considered tobe the drug of choice, but because it is not available in India,metronidazole is used. A 7 day course with 200– 400 mg TDSproduces symptomatic relief. The local reaction to the wormmay be suppressed by its antiinflammatory action, andextraction is facilitated. (This infestation is now rare in India).
Tinidazole It is an equally efficaciouscongener of metronidazole, similar to it in everyway except:• Metabolism is slower; t½ is ~12 hr; duration
of action is longer; dosage schedules aresimpler. Thus, it is more suited for singledose or once daily therapy.
• Some comparative trials in amoebiasis havereported higher cure rates.
• It appears to be better tolerated; the incidenceof side effects is lower: metallic taste (2%),nausea (1%), rash (0.2%).
TINIBA 300, 500, 1000 mg tabs; 800 mg/400 ml i.v. infusion;TRIDAZOLE 300, 500 mg tab; FASIGYN 0.5 g and 1 g tab., TINI0.3 g, 0.5 g, 1.0 g tabs, 75 mg/5 ml and 150 mg/5 ml oral susp.
Recommended schedules are—Intestinal amoebiasis: 2 g OD for 3 days(children 30–50 mg/kg/day) or 0.6 g BD for5–10 days.Amoebic liver abscess: The 2 g daily dose maybe continued for 3–6 days.Trichomoniasis and giardiasis: 2 g single doseor 0.6 g OD for 7 days.Anaerobic infections:
prophylactic—2 g single dose before colo-rectal/biliary surgery;therapeutic—2 g followed by 0.5 g BD for5 days.
H. pylori: 500 mg BD for 2 weeks in triplecombination.
Secnidazole A congener of metronidazolewith the same spectrum of activity and potency.Absorption after oral administration is rapid andcomplete, but metabolism is slower resulting ina plasma t½ of 17–29 hours. After 48 hr ofa single 2 g dose, plasma secnidazole concen-tration may still remain within the range of MICvalues against sensitive organisms. In intestinalamoebiasis a single 2 g dose has been foundto yield high cure rates. Side effect profile issimilar to metronidazole and reported incidenceis 2–10%.Dose: 2 g single dose (children 30 mg/kg) for mild intestinalamoebiasis, giardiasis, trichomonas vaginitis and nonspecificbacterial vaginosis. For acute amoebic dysentery 0.5 g TDS for5 days is recommended.SECNIL, SECZOL 0.5, 1.0 g tabs; NOAMEBA-DS 1.0 g tab.
Ornidazole It has activity similar to metro-nidazole, but it is slowly metabolized—has longert½ (12–14 hr). Dose and duration of regimensfor amoebiasis, giardiasis, trichomoniasis,anaerobic infections and bacterial vaginosisresemble those for tinidazole. In chronic intestinalamoebiasis and asymptomatic cyst passers 0.5twice daily for 5 to 7 days has also been used.Side effect profile is also similar to tinidazole.DAZOLIC 500 mg tab, 500 mg/100 ml vial for i.v. infusion.ORNIDA 500 mg tab, 125 mg/5 ml susp.
Satranidazole Another nitroimidazole havinglonger t½ (14 hr). Advantages claimed are: better

840S
EC
TIO
N12
ANTIMICROBIAL DRUGS
tolerability—no nausea, vomiting or metallictaste, absence of neurological and disulfiram-like reactions and that it does not produce theacetamide metabolite which is a weakcarcinogen.Dose: Amoebiasis 300 mg BD for 3–5 days, giardiasis andtrichomoniasis 600 mg single dose.SATROGYL 300 mg tab.
ALKALOID
EmetineIt is an alkaloid from Cephaelis ipecacuanha. Emetine is apotent and directly acting amoebicide—kills trophozoites buthas no effect on cysts. It acts by inhibiting protein synthesisin amoebae by arresting intraribosomal translocation of tRNA-amino acid complex.
In acute dysentery the stool is rapidly cleared of thetrophozoites and symptomatic relief occurs in 1–3 days (evenfaster than metronidazole), but it is not curative in the sensethat the patient continues to pass cysts in the stool. It ishighly efficacious in amoebic liver abscess also.
Emetine cannot be given orally because it will be vomitedout. It is administered by s.c. or i.m. injection: 60 mg OD.It is a local irrirant and has high systemic toxicity, viz, nausea,vomiting (due to CTZ stimulation and gastric irritation),abdominal cramps, diarrhoea, weakness, stiffness of muscles,myositis, hypotension, ECG changes and myocarditis.
Use Emetine is now rarely used for acute amoebic dysenteryor for amoebic liver abscess, only in patients not toleratingmetronidazole. A luminal amoebicide must always followemetine to eradicate the cyst forming trophozoites.It is also effective in liver fluke infestation.EMETINE HCl: 60 mg /2 ml inj; for not more than 10 days toavoid cumulative toxicity.
Dehydroemetine It is equally effective but less cumulativeand less toxic to the heart. Thus, it is usually preferred overemetine.Dose: 60–100 mg s.c./i.m.OD for not more than 10 days.DEHYDROEMETINE HCl: 30 mg/ml inj, 1 and 2 ml amps.
ChloroquineThe pharmacology of chloroquine is described in Ch. 59. Itkills trophozoites of E. histolytica and is highly concentratedin liver. Therefore, it is used in hepatic amoebiasis only.Because it is completely absorbed from the upper intestineand not so highly concentrated in the intestinal wall—it isneither effective in invasive dysentery nor in controlling theluminal cycle (cyst passers).
Efficacy of chloroquine in amoebic liver abscessapproaches that of emetine, but duration of treatment is longerand relapses are relatively more frequent, but amoebae donot develop resistance to chloroquine. A luminal amoebicidemust always be given with or after chloroquine to abolishthe luminal cycle.
Dose for amoebic liver abscess: 600 mg (base) for twodays followed by 300 mg daily for 2–3 weeks. Thoughchloroquine is relatively safe, side effects are frequent. The2–3 week course is poorly tolerated. It is employed only whenmetronidazole fails to clear the infection or is not tolerated.
AMIDES
Diloxanide furoate
It is a highly effective luminal amoebicide whichdirectly kills trophozoites responsible for pro-duction of cysts. The furoate ester is hydrolysedin intestine and the released diloxanide is largelyabsorbed. Diloxanide is a weaker amoebicide thanits furoate ester. No systemic antiamoebicactivity is evident despite its absorption. It isprimarily metabolized by glucuronidation and isexcreted in urine.
Diloxanide furoate exerts no antibacterialaction. It is less effective in invasive amoebicdysentery, because of poor tissue amoebicidalaction. However, a single course produces high(80–90%) cure rate in mild intestinal amoebiasisand in asymptomatic cyst passers.Dose: 500 mg TDS for 5–10 days; children 20 mg/kg/day.FURAMIDE, AMICLINE 0.5 g tab; in TINIBA-DF 250 mg + 150mg tinidazole and TINIBA-DF FORTE 500 mg + 300 mg tabs; inENTAMIZOLE 250 mg + 200 mg metronidazole andENTAMIZOLE FORTE 500 mg + 400 mg tabs.
Diloxanide furoate is very well tolerated; theonly side effects are flatulence, occasionalnausea, itching and rarely urticaria. It is apreferred drug for mild intestinal/asymptomaticamoebiasis, and is given after or along with anytissue amoebicide to eradicate cysts. Combineduse with metronidazole/tinidazole is quitepopular. Some chronic cases require repeatcourses for eradication.
Nitazoxanide This salicylamide congener ofthe anthelmintic niclosamide, introduced for thetreatment of giardiasis and cryptosporidiosis isalso active against many other protozoa andhelminths including E. histolytica, T. vaginalis,Ascaris, H. nana, etc. It is a prodrug which onabsorption is converted to the active formtizoxanide, an inhibitor of PFOR enzyme thatis an essential pathway of electron transport

841C
HA
PTER60
ANTIAMOEBIC AND OTHER ANTIPROTOZOAL DRUGS
energy metabolism in anaerobic organisms.Activity against metronidazole-resistant Giardiahas also been demonstrated. Tizoxanide generatedfrom nitazoxanide is glucuronide conjugated andexcreted in urine and bile.
Nitazoxanide is the most effective drug forCryptosporidium parvum infection (upto 88%cure), which causes diarrhoea, especially inchildren and AIDS patients. It is also indicatedin giardiasis, and in amoebic dysentery as luminalamoebicide. Abdominal pain, vomiting andheadache are mild and infrequent side effects.Dose: 500 mg (children 7.5 mg/kg) BD × 3 daysNITACURE, NITCOL, NITARID 200 mg, 500 mg tabs, 100 mg/5ml dry syrup.
8-HYDROXYQUINOLINES
Several 8-hydroxyquinolines including Quinio-dochlor and Iodoquinol were widely employedin the past: have similar properties; are activeagainst Entamoeba, Giardia, Trichomonas,some fungi (dermatophytes, Candida) and somebacteria. They kill the cyst forming amoebictrophozoites in the intestine, but do not havetissue amoebicidal action. Like diloxanidefuroate, they are not very effective in acuteamoebic dysentery but afford relief in chronicintestinal amoebiasis. Their efficacy to eradicatecysts from asymptomatic carriers is rated lowerthan that of diloxanide furoate. They are totallyvalueless in extraintestinal amoebiasis.
Absorption of 8-hydroxyquinolines from theintestine is variable. The absorbed fraction isconjugated in liver with glucuronic acid andsulfate and excreted in urine; t½ ~12 hours.Therapeutic concentrations are not attained inthe intestinal wall or in liver. The unabsorbedpart reaches lower bowel and acts on luminalcycle of amoebae.
Being inexpensive, these drugs have beenwidely and injudiciously used for the prophylaxisand treatment of nonspecific diarrhoeas,traveller’s diarrhoea, dietary indiscretion, etc.,but are infrequently prescribed now, except insome poor localities.
8-Hydroxyquinolines produce few sideeffects—nausea, transient loose and greenstools, pruritus, etc. but carry toxic potential ifimproperly used.
Iodism (furunculosis, inflammation ofmucous membranes) may occur due to chroniciodine overload. Goiter may develop. Individualssensitive to iodine may experience acute reactionwith chills, fever, angioedema and cutaneoushaemorrhages.
Prolonged/repeated use of relatively high doses ofquiniodochlor caused a neuropathic syndrome called‘subacute myelo-optic neuropathy’ (SMON) in Japan in anepidemic form, affecting several thousand people in 1970. Other8-hydroxyquinolines have also produced neuropathy andvisual impairment. However, despite widespread use in thepast, only sporadic and unconfirmed cases have been reportedfrom India. These drugs have been banned in Japan and fewother countries, but in India they are prohibited only forpediatric patients, because their use for chronic diarrhoeasin children has caused blindness. Their fixed dosecombinations, except for external application, are banned inIndia, and a cautionary note is inserted that use of high dosesfor more than 14 days can cause neuritis and optic damage.
8-Hydroxyquinolines are cheap and have goodpatient acceptability. They may be employed inintestinal amoebiasis as alternative to diloxanidefuroate.
Other uses are—giardiasis; local treatmentof monilial and trichomonas vaginitis, fungal andbacterial skin infections.Quniodochlor (Iodochlorohydroxyquin, Clioquinol): 250–500mg TDS; (not to exceed 1.5 g/day for 14 days).ENTEROQUINOL, QUINOFORM, DEQUINOL 250 mg tab.Diiodohydroxyquin (Iodoquinol): 650 mg TDS;, (not to exceed2.0 g/day for 14 days).DIODOQUIN 650 mg tab, 210 mg/5 ml susp.
ANTIBIOTICS
TetracyclinesTetracyclines have modest direct inhibitoryaction on Entamoeba. In addition the older tetra-cyclines are incompletely absorbed in the smallintestine, reach the colon in large amountsand inhibit the bacterial flora with whichEntamoebae live symbiotically. Thus, theyindirectly reduce proliferation of entamoebae inthe colon and are especially valuable in chronic,difficult to treat cases who have only the luminal

842S
EC
TIO
N12
ANTIMICROBIAL DRUGS
cycle with little mucosal invasion. Tetracyclineshave an adjuvant role in the management of suchcases, in conjunction with a more efficaciousluminal amoebicide. They have also been addedas the third drug along with a nitroimidazole +a luminal amoebicide in the treatment ofamoebic dysentery, but have no role in hepaticamoebiasis.
Paromomycin
It is an aminoglycoside antibiotic which closely resemblesneomycin. Distinctively, paromomycin is active against manyprotozoa like Emtamoeba, Giardia, Cryptosporidium,Trichomonas, Leishmania and some tape worms, in additionto having antibacterial spectrum like neomycin. In the 1960san oral formulation of paromomycin was introduced as aluminal amoebicide and was briefly marketed in India as well.However, it was soon overshadowed by metronidazole,became commercially unviable and was discontinued. It hasgained popularity again and is being frequently used in USAand some other countries. In India and Africa, parenteral (i.m.)paromomycin is being used in resistant Kalaazar (see p. 847).
The mechanism of antiprotozoal action of paromomycinappears to be the same as its antibacterial action; viz. bindingto 30S ribosome and interference with protein synthesis. Orallyadministered paromomycin acts only in the gut lumen. It isneither absorbed nor degraded in the intestines, and iseliminated unchanged in the faeces. Thus, it is free fromsystemic toxicity. Its effect on gut flora resembles that ofneomycin. Paromomycin can substitute for neomycin inhepatic coma and for preoperative preparation of bowel.
Paromomycin is an efficacious luminal amoebicide,achieving similar or even better clearing of cysts from stoolscompared to diloxanide furoate in asymptomatic cyst passers.Good symptomatic relief and cyst clearance is obtained inchronic amoebic colitis. It can be given along withmetronidazole in acute amoebic dysentery as well as in hepaticamoebiasis to eradicate the luminal cycle.
Paromomycin is an alternative drug for giardiasis,especially during 1st trimester of pregnancy whenmetronidazole and other drugs are contraindicated. It has beenused in cryptosporidiosis, but efficacy is uncertain. Topically,it may used in trichomonas vaginitis and dermal leishmaniasis.Dose: Oral: 500 mg (children 10 mg/kg) TDS, for 7 days foramoebiasis/giardiasis/cryptosporidiosis.Side effects are limited to the g.i.t.; nausea, vomiting, abdominalcramps, diarrhoea; rarely rashes.
NOTES ON THE TREATMENT OFAMOEBIASIS
1. Acute amoebic dysentery Most cases ofamoebic dysentery respond to a single adequate
course of treatment. Metronidazole/tinidazole arethe drugs of choice. Secnidazole, ornidazole,are the alternatives. Adjuvant measures fordiarrhoea and abdominal pain may be needed.Dehydroemetine is rarely used in the most severecases or when metronidazole produces severeallergic reaction or neurotoxicity. It should bediscontinued as soon as acute symptoms arecontrolled (2–3 days) and metronidazole started.
The above treatment should be followed bya course of luminal amoebicide to eradicateE. histolytica from the colon and to preventcarrier (cyst passing) state. A tetracycline, addedas the third drug, may have adjuvant value.
2. Mild intestinal amoebiasis/asympto-matic cyst passersNitroimidazoles afford rapid symptomatic reliefin mildly symptomatic intestinal amoebiasis aswell, and are the first line drugs. However, theymostly fail to clear cysts, and the standardpractice is to give diloxanide furoate or anotherluminal amoebicide, either concurrently orimmediately after. Luminal amoebicides aloneare generally slower in action, but avoid sideeffects of metronidazole. Asymptomatic cystpassers are mostly treated wtih only luminalamoebicide. Chronic cases may require 2–3repeated courses in which drugs may be alter-nated. A tetracycline may be given concurrentlywith the luminal amoebicide in cases which failto clear completely.
3. Amoebic liver abscess It is a seriousdisease; complete eradication of trophozoitesfrom the liver is essential to avoid relapses.Metronidazole/tinidazole are the first choicedrugs effective in > 95% cases. Critically illpatients may be treated with i.v. metronidazolefor the entire course, or at least initially,followed by oral dosing. Dehydroemetine is tobe used only if metronidazole cannot be givenfor one reason or the other, and in patients notcured by metronidazole. Large abscesses usuallytake months to resolve, even if all trophozoitesare killed. If a big abscess has formed, it maybe aspirated.

843C
HA
PTER60
ANTIAMOEBIC AND OTHER ANTIPROTOZOAL DRUGS
Treatment of different forms of amoebic infection
Drugs of Choice Alternative Drugs
Acute Amoebic Dysentery
• Metronidazole 800 mg oral TDS × 7–10 days • Ornidazole 2.0 g oral daily × 3 days(in severe cases 500 mg slow i.v. 6 hourly till ororal therapy can be instituted) • Secnidazole 0.5 g oral TDS × 5 days or Alternative luminal amoebicides
• Tinidazole 2.0 g oral daily × 3 days • Quiniodochlor 250–500 mg oral TDS × 7–14 days + or Luminal amoebicide • Iodoquinol 650 mg oral TDS × 7–14 days
• Diloxanide furoate 500 mg TDS × 5–10 days or• Paromomycin 500 mg oral TDS × 7–10 days +• Tetracycline 250 mg TDS × 7–10 days (adjuvant)
Mild intestinal amoebiasis/Asymptomatic cyst passers*
• Metronidazole 400 mg oral TDS × 5–7 days • Ornidazole 0.5 g oral BD × 5–7 days or or• Tinidazole 2.0 g oral OD × 2–3 days • Secnidazole 2.0 g oral single dose
+ Alternative luminal amoebicides Luminal amoebicide (as above) (as above) ±
Tetracycline 250 mg TDS × 7–10 days (adjuvant)
Amoebic liver abscess
• Metronidazole 800 mg oral TDS × 10 days • Emetine/Dehydroemetine 60 mg i.m./s.c. × 8–10 days(in serious cases 500 mg slow i.v. Followed by/alternatively6 hourly × 10 days) • Chloroquine 600 mg (base) oral daily × 2 days, followed or by 300 mg daily for 2–3 weeks.
• Tinidazole 2.0 g oral daily × 3–6 days +
Luminal amoebicide Alternative luminal amoebicides (as above) (as above, but no role of tetracycline)
* In asymptomatic cases, a luminal amoebicide alone may be used (the nitroimidazole may be omitted).Repeat courses after a gap of 2–3 weeks may be needed with the same or alternative drugs to eradicatethe chronic luminal cycle.
A luminal amoebicide must be given laterto finish the intestinal reservoir of infection.A course of chloroquine may be administeredafter that of metronidazole/dehydroemetine inthose with incomplete response or to ensure thatno motile forms survive in the liver.
DRUGS FOR GIARDIASIS
Giardia lamblia is a flagellate protozoon whichinfects children and adults by oro-faecalcontamination and mostly lives as a commensalin the intestine. It sometimes invades the mucosaand causes acute watery short duration diarrhoeawith foul smellling stools, gas and abdominal
cramps. If untreated, it may pass on to chronicdiarrhoea with greasy or frothy stools but noblood or mucus. Many drugs useful in amoebiasisare also effective in giardiasis.1. Metronidazole 400 mg TDS (children 15mg/kg/day) for 5–7 days or 2 g daily for 3 days
Ortinidazole 0.6 g daily for 7 days or 2 g singledose
Orsecnidazole 2 g single dose
These may be considered as the drugs of choice,but ~ 10% patients may not be cured, and asecond course or alternative drug may be needed.

844S
EC
TIO
N12
ANTIMICROBIAL DRUGS
2. Nitazoxanide (see p. 840) This prodrugof the PFOR enzyme inhibitor tizoxanide hasbecome available for the treatment of diarrhoeaand dysentery caused by Cryptosporidiumparvum, Giardia lamblia, E. histolytica. Thedosage schedule is convenient—500 mg(children 7.5 mg/kg) twice daily for 3 days,efficacy (~80%) approaches that of metroni-dazole and tolerability is good.3. Quiniodochlor 250 mg TDS for 7 days isa somewhat less effective alternative.4. Paromomycin In a dose of 500 mg TDS for 5–7 days,it is somewhat less effective than metronidazole, but is freeof systemic side effects and can be used during pregnancy.However, oral formulation is not available in India.
5. Furazolidone It is a nitrofuran compoundactive against many gram-negative bacilliincluding Salmonella and Shigella, also Giardiaand Trichomonas. For giardiasis 100 mg TDSfor 5–7 days has been used, but is inferior tometronidazole or tinidazole. It has also been usedin bacterial enteritis, food poisoning diarrhoeasand bacillary dysentery, but is not a first linetreatment for any of these.
Furazolidone is partly absorbed from intes-tines and excreted in urine which turns orange—patients should be told about it. Side effects aremild and infrequent—nausea, headache, dizziness.FUROXONE 100 mg tab, 25 mg/5 ml susp.
DRUGS FOR TRICHOMONIASIS
Trichomonas vaginalis is another micro-aerophilic flagellate protozoon which causesvulvovaginitis. It is a common sexually trans-mitted disease affecting ~ 10% sexually activewomen. Several drugs are partly effective byvaginal application, but may not entirely clearthe infection; recurrences are frequent; repeatcourses are required.
1. Drugs used orallyMetronidazole 400 mg TDS for 7 days or2 g single dose, or Tinidazole 600 mg dailyfor 7 days or 2 g single dose or Secnidazole2 g single dose, are the drugs of choice. They
produce upto 90% cure. However, vaginitis dueto nitroimidazole resistant T. vaginalis is beingreported. Some resistant cases respond to higherdoses, particularly of tinidazole. Additional intra-vaginal treatment is required only in refractorycases. A hard core of recurrent cases may remain.A repeat course can be given after 6 weeks.Additional treatment for nonspecific vaginosisoften helps. In some cases recurrences are dueto reinfection from the male partner whoharbours the parasite in the seminal vesicles butremains asymptomatic. In such cases, bothpartners should be treated concurrently to preventcross infection of each other.
2. Drugs used intravaginally1. Diiodohydroxyquin 200 mg inserted intra-
vaginally at bed time for 1–2 weeks;FLORAQUIN 100 mg vaginal pessaries.
2. Quiniodochlor 200 mg inserted in the vaginaevery night for 1–3 weeks;GYNOSAN 200 mg vaginal tab.
3. Povidone-iodine 400 mg inserted in thevagina daily at night for 2 weeks;BETADINE VAGINAL 200 mg pessaries.
DRUGS FOR LEISHMANIASISVisceral leishmaniasis (VL; kala-azar) caused by Leishmaniadonovani (and other Leishmania species) occurs in severaltropical and subtropical regions of the world. According toWHO the global burden of VL is ~0.5 million new cases and~50,000 deaths annually. About 90% of the cases occur inIndia, Bangladesh, Nepal, Sudan and Brazil, but the diseaseis also present in other countries of East Africa, South America,Mediterranean basin and central Asia. In india, leishmaniasisis prevalent in Bihar, West Bengal, Jharkhand and easternUP; the worst affected being Bihar which contributes 50%cases that occur world over. The geographical location isimportant, because the species of Leishmania causing VLand its responsiveness to different drugs differs betweendifferent regions. The disease is highly concentrated in NorthBihar and the parasite is resistant to sodium stibogluconate(SSG), the first line drug in many other countries.
Leishmaniasis is transmitted by the bite ofthe female sandfly phlebotomus. In the fly theparasite exists in the flagellate extracellular(promastigote) form, while in man it is foundonly intracellularly within macrophages in the

845C
HA
PTER60
ANTIAMOEBIC AND OTHER ANTIPROTOZOAL DRUGS
nonflagellate (amastigote) form. Mucocutaneousand dermal leishmaniasis are caused respectivelyby L. braziliensis and L. tropica (also otherspecies). Visceral leishmaniasis (VL) is fatalunless treated.The currently used drugs for treatment of VLare:1. Sodium stibogluconate (SSG)
(or Meglumine antimonate—in Frenchspeaking countries)
2. Amphotericin B (AMB)3. Miltefosine4. ParomomycinPentamidine was used in resistant kala-azar till 10 years backbut not now. Ketoconazole and Allopurinol have weak anti-leishmania action, but are not used now.Kala-azar is primarily a disease of the econo-mically poor class, and the areas affected areunderdeveloped. India launched a kala-azarcontrol programme in 1990, which was upgradedin the year 2000 to aim at elimination of thedisease. The programme is implemented under
the NVBDCP, which has laid down its owntreatment guidelines, and provides free treatment.Under the programme 33,043 cases of VL weretreated in 2011 with 80 deaths. However, theactual number of cases is much greater. Onlyconfirmed cases (by ‘rapid diagnostic test’ orsplenic aspirate examination) are to be treatedwith antileishmania drugs.
The choice of drugs, doses and regimens ascurrently recommended by WHO and NVBDCPare summarized in the box.
Cure is indicated by clinical improvementand absence of relapse within 6 months. Thiscan be confirmed by absence of leishmania insplenic aspirate smear examination.1. Sodium stibogluconate (SSG) It has been thestandard first line drug for VL in most parts of the worldachieving > 90% cure rate, and is still used in East Africa,Central Asia, Mediterranean basin and South America, butis no longer effective in India and Nepal because of extensiveresistance. Over 60% cases in Bihar are unresponsive. SSGis a water soluble pentavalent antimonial, the supplied solution
* Recommended treatment regimens for visceral leishmaniasis (Kala-azar) caused byL. donovani in the Indian subcontinent
£1. Amphotericin B deoxycholate (AMB-DOC): 0.75–1.0 mg/kg i.v. infusion over 4 hours daily or on alternatedays till 15 mg/kg total dose.
¥2. Liposomal amphotericin B (L-AMB): 3–5 mg/kg i.v. infusion daily for 3–5 days (total dose 15 mg/kg)or
L-AMB 10 mg/kg single dose i.v. infusion$3. Miltefosine (all doses given orally with meals for 28 days)
Adults (>12 years) weighing > 25 kg: 100 mg/day (50 mg cap twice daily)€
Adults (>12 years) weighing < 25 kg: 50 mg/day (50 mg cap once daily)Children (2–11 years): 2.5 mg/kg/day (as 10 mg caps)
4. Paromomycin sulfate: 15 mg (11 mg base) per kg/day i.m. for 21 days5. Sodium stibogluconate (SSG): 20 mg (Sb5+)/kg i.m. or slow i.v. daily for 30 days (only in areas where
the Leishmania is still sensitive to SSG).
COMBINATIONS (co-administered drugs)1. L-AMB (5 mg/kg i.v. infusion single dose) + Miltefosine (as above) for 7 days.2. L-AMB (5 mg/kg i.v. infusion single dose) + Paromomycin (as above) for 10 days.3. Miltefosine (as above) daily for 10 days + Paromomycin (as above) daily for 10 days.
RESCUE TREATMENT (of failure/non-responsive cases)1. AMB-DOC or L-AMB at higher doses.
* Adopted from Report of meeting of the WHO Expert Committee on control of leishmaniasis, March22–26, 2010; WHO Technical Report Series No. 949 (2010)
$ Used as 1st line treatment under NVBDCP£ Used as 2nd line treatment by NVBDCP.¥ 1st preference regimen recommended by WHO.€ The WHO in additon recommends miltefosine dose to be 150 mg/day for adults weighing > 50 kg, while
NVBDCP treats all adults above 25 kg with 100 mg/day

846S
EC
TIO
N12
ANTIMICROBIAL DRUGS
contains 10% (100 mg/ml) antimony, and doses areexpressed in terms of elemental Sb. The mechanism ofaction and the basis of selective toxicity to the leishmaniaamastigotes is unclear. It was believed that -SH dependentenzymes are inhibited by antimony and bioenergetics ofthe parasite is interfered with. This occurs due to blockingof glycolytic and fatty acid oxidation pathways. However,recent evidence indicates that a specific reductase enzyme,present in leishmania amastigots, reduces pentavalent-Sb of SSG to the toxic trivalent form, which thenpromotes efflux of glutathione and other reduced thiolsfrom the parasite residing within macrophages, exposingthem to oxidative damage. Resistance to SSG may involvereduced capacity of the parasite to convert it to thetrivalent form, and/or alteration in thiol metabolism ofthe parasite.
Sod. stibogluconate is rapidly absorbed from the site ofi.m. injection and excreted unchanged in urine within 6–12 hrs.A small fraction enters tissues and remains stored for longperiods. Repeated doses are cumulative. Accumulation of SSGwithin macrophages accounts for its prolonged inhibitory effecton leishmania residing there. SSG is administered by deep i.m.injection (into buttocks) or by slow i.v. injection daily or onalternate days.
Adverse effects Though, antimonials are toxic drugs, butthe pentavalent compounds (particularly SSG) are bettertolerated. Nausea, vomiting, metallic taste, cough, painabdomen, pain and stiffness of injected muscle, sterileabscesses, and mental symptoms often occur. Pancreatitis,liver and kidney damage, myelosuppression are possible, butare seldom severe. Q-T prolongation may herald arrhythmias.Few cases of shock and death are on record.
Sod. stibogluconate, nevertheless, is less toxic thanamphotericin B. Used alone or in combination withparomomycin, SSG is still a 1st line drug in East Africa, CentralAsia and South America. However, response is relatively poorin older and malnourished patients as well as in those coinfectedwith TB, HIV and other immunodeficient states.
2. Amphotericin B (AMB) (see Ch. 57) Thisantifungal antibiotic is available in two types ofpreparations. The older and less expensive oneis formulated with deoxycholate (AMB-DOC),while in the newer one it is incorporated inliposomes (L-AMB), and is very expensive. Likefungi, leishmania has high percentage ofergosterol and is susceptible to this antibioticwhich has high affinity for ergosterol and actsby binding to it. Presently, AMB is the drug withhighest cure rate in kala-azar: up to 99% clinicaland parasitological cure has been reported fromIndia in SSG resistant cases, and it is treatedas the ‘reference drug’ while comparing theefficacy of other drugs. However, high toxicity
and need for prolonged hospitalization, moni-toring and repeated slow i.v. infusions limit itsapplication. Therefore, it is the 2nd line treat-ment of VL under NVBDCP, though the WHOrecommendations accord it higher preferenceover miltefosine. Because miltefosine isteratogenic, AMB is the drug of choice inpregnant women and breast feeding mothers.
Liposomal AMB is particularly suited for kala-azar because it delivers the drug inside thereticuloendothelial cells in spleen and liver wherethe amastigotes live, but high cost is prohibitive.As such, use of L-AMB in India is largely limitedto clinical trial setting. Using L-AMB, the totaldose of 15 mg/kg can be administered over3–5 days with ~ 98% cure, and WHO has accordedit the highest preference. Even a single dosetreatment has been tried, reporting 90% cure at5 mg/kg, and 98% cure at 10 mg/kg.
AMB is also useful in mucocutaneousleishmaniasis.
3. Miltefosine It is a derivative of alkyl phos-phocholine with potent antileishmania activitythat has been tested in India since the 1980s, butwas approved only in 2002 as the first orally activedrug for kala-azar. Due to spread of SSGresistance in Bihar and neighbouring areas,NVBDCP is now using miltefosine as the 1st linetreatment of VL in India. A 4 week course ofmiltefosine has achieved >95% cure rate in Indiaand 90% in Ethiopia. Curaneous leishmaniasiscan also be cured by 4 week therpy. Miltefosineis available in India only through NVBDCP. It isalso available in few other countries of the Indianregion and in South America.
The mechanism of antileishmania action ofmiltefosine is not known. However, studies suggestthat it may be interfering with lipid metabolism ofthe parasite or prevent synthesis of some criticalcell surface anchor molecules, or alter signaltransduction. Leishmania can develop resistanceto miltefosine and this may be due to mutationlimiting transport of the drug into the parasite cell.To prevent development of resistance to this usefuldrug, combination therapy with paromomycin orAMB is being promoted.

847C
HA
PTER60
ANTIAMOEBIC AND OTHER ANTIPROTOZOAL DRUGS
Miltefosine is rapidly absorbed after oralmedication, and widely distributed in the body.It is a long acting drug with biphasic elimination.In the early phase, t½ is ~7 days while theterminal t½ is ~ 4 weeks. Anorexia, vomitingand diarrhoea are the commonest side effectsoccurring in over 50% patients. However, theseare generally brief and resolve with continueduse. Skin allergy and rise in hepatic transami-nases occurs in some recipients indicatinghepatic derangement, but this is usually mild andreverses on stopping the drug. Reversible kidneydysfunction with rise in serum creatinine hasalso been noted. Miltefosine is teratogenic. Itis contraindicated in pregnant women. Whenmiltefosine is given, it should be ensured thatfemale patients do not get pregnant during andtill 3 months after miltefosine course.
4. Paromomycin This aminoglycoside anti-biotic is described with antiamoebic drugs onp.842. In intestinal protozoal infections, it is usedby the oral route and remains confined to thegut. It has been later (in 2006) approved in Indiafor use in VL by the i.m. route. Over the pastdecade paromomycin has been widely tried inIndia and Africa for kala-azar and found to beeffective in SSG-resistant cases. The WHOrecommends 21 day paromomycin treatment asan alternative to miltefosine.
In a recent phase III trial on 667 kala-azar patients in Bihar,*paromomycin 11 mg/kg/day × 21 days has yielded 95% cure rate,which was not inferior to 99% cure rate obtained with AMB1 mg/kg × 15 injections over 30 days. Mortality was <1% withboth the drugs. Several other trials have confirmed the efficacyof paromomycin in VL. In Sudan, a 17 day course of SSG +paromomycin has become the 1st choice treatment of kala-azar,because it yielded higher initial cure rate and better survival thanmonotherapy with 30 day course of SSG. However, in India,combination of SSG + paromomycin has not been encouraging.
Though paromomycin produces ototoxicity(in 2% recipients), reversible elevation of serumtransaminase and injection site pain, but renaltoxicity is rare. It has proven to be an effective,less expensive and easier to use alternative toAMB in kala-azar.
Topical paromomycin is effective in dermalleishmaniasis.
Combination therapyLike in the case of TB, leprosy, HIV and malaria,combination therapy with 2 effective drugs hasseveral advantages in the treatment of VL. Theseare:• Limiting risk of development of drug
resistance, thereby prolonging the effectivelife-time of available medicines.
• Attaining higher efficacy and cure rate.• Shortening of duration of therapeutic regimen;
better compliance and convenience.• Reduction of overall dose; lower toxicity and
cost.Clinical studies in India have testified to the highefficacy of drug combinations, and have shownthat duration of treatment can be reduced by halfor more. The 3 combinations tested were:a. L-AMB (5 mg/kg i.v. single dose) +
Miltefosine (oral) daily × 7 daysb. L-AMB (5 mg/kg i.v. single dose) +
Paromomycin (i.m.) daily × 10 daysc. Miltefosine (oral) daily × 10 days +
Paromomycin (i.m.) daily × 10 days.Each of these combinations yielded 98–99%cure rate. As such, these combinations arerecommended with high preference by WHO.However, cost of L-AMB (even single dose) ishigh.
HIV and Leishmania coinfectionHIV and leishmania infections worsen each other.In endemic areas, HIV positive subjects are morelikely to develop VL, harbour higher anddisseminated leishmania load, and have poorerprognosis. Similarly, occurrence of VL in a HIVpositive subject is regarded to be a sign of AIDSand warrants initiation of antiretroviral treatmentirrespective of CD4+ count. Coinfected patientshave a poorer response to antileishmania as wellas anti-HIV drugs. Therapy of such patients isdifficult and mortality is high.
* Sundar S et al: Injectable paromomycin for visceralleishmaniasis in India. N Engl J Med. 2007;356: 2571-2581.

848S
EC
TIO
N12
ANTIMICROBIAL DRUGS
Drugs used locally for dermalleishmaniasis (oriental sore)Dermal leishmaniasis is not a life-threateningcondition; many cases are treated by localapplication of drugs.1. Sodium stibogluconate: Infiltrate 2 ml of the
solution (100 mg antimony/ml) round the sore.
2. Paromomycin (15%) ointment: appliedtopically on the sore, twice daily for 20 days.
Small and mild lesion may heal by itself in a fewmonths. Multiple sores and severe cases shouldbe treated by systemic drugs as for kala-azar.
Antibiotics may be needed for secondaryinfection of the sore.
PROBLEM DIRECTED STUDY
60.1 A 50-year-old gardner weighing 58 kg was admitted to the hospital with fever for 4days, severe pain in right upper part of abdomen, loss of appetite, vomiting and markedweakness. He was not well for the past 2–3 weeks and had lost weight. There was no historyof chronic diarrhoea. Palpation of abdomen revealed soft tender enlargement of liver 2 cmbelow costal margin. Marked tenderness was noted in the lower right intercostal region.Ultrasound showed a solitary 2.5 cm diameter abscess with sharp margins in the right lobeof liver. Stool examination was negative for any kind of ova and cysts. A clinical diagnosisof amoebic liver abscess was made and he was treated with:Injection Metronidazole 500 mg i.v. over 1 hour every 8 hours for 5 days along with infusionof glucose-saline and vitamins. The fever and vomiting subsided and he started eating food.The injections were substituted by oral metronidazole 800 mg 3 times a day for another5 days, and the patient became well, except weakness and mild tenderness in the right lowerchest. Repeat ultrasound showed abscess cavity size to decrease to 1.5 cm. The patient wasdischarged with advise for vitamins and food.(a) Was the choice of medication and route correct, or a better drug/route of administrationis available?(b) Should metronidazole therapy be extended or a repeat course given?(c) Should the patient be given any other antiamoebic medication in addition to or followingmetronidazole?(see Appendix-1 for solution)

Anthelmintic DrugsChapterChapterChapterChapterChapter 6161616161
Anthelmintics are drugs that either kill (vermi-cide) or expel (vermifuge) infesting helminths.
Helminthiasis is prevalent globally (1/3rd ofworld’s population harbours them), but is morecommon in developing countries with poorerpersonal and environmental hygiene. Multipleinfestations in the same individual are notinfrequent. In the human body, g.i.t. is the abodeof many helminths, but some also live in tissues,or their larvae migrate into tissues. They harmthe host by depriving him of food, causingblood loss, injury to organs, intestinal orlymphatic obstruction and by secreting toxins.Helminthiasis is rarely fatal, but is a major causeof ill health.
The choice of drug for each worm infestationis based not only on efficacy, but also on lackof side effects/toxicity, ease of administration(preferably single dose) and low cost. Develop-ment of resistance has not been a problem inthe clinical use of anthelmintics. The currentchoice of drugs for worm infestations commonin the Indian subcontinent is given in Table 61.1.
MebendazoleIt is a benzimidazole introduced in 1972. Thiscongener of thiabendazole became very popularbecause it retained the broad-spectrum anthel-mintic activity but not the toxicity of itspredecessor. It has produced nearly 100% curerate/reduction in egg count in roundworm, hookworm (both species), Enterobius and Trichurisinfestations, but is much less active on Strongy-loides. Upto 75% cure has been reported in tape-worms, but H. nana is relatively insensitive. Itexpels Trichinella spiralis from intestines, butefficacy in killing larvae that have migrated tomuscles is uncertain. Prolonged treatment has
been shown to cause regression of hydatid cystsin the liver. Treatment after resection of the cystmay prevent its regrowth.
The immobilizing and lethal action of meben-dazole on worms is rather slow: takes 2–3 daysto develop. The site of action of mebendazoleappears to be the microtubular protein ‘β-tubulin’of the parasite. It binds to β-tubulin of suscep-tible worms with high affinity and inhibits itspolymerization. Intracellular microtubules in thecells of the worm are gradually lost. In addition,it probably blocks glucose uptake in the parasiteand depletes its glycogen stores. Hatching ofnematode eggs and their larvae are also inhibited.Ascaris ova are killed.
Pharmacokinetics Absorption of mebendazolefrom intestines is minimal; 75–90% of an oraldose is passed in the faeces. The fractionabsorbed is excreted mainly as inactivemetabolites in urine/faeces.
Adverse effects Mebendazole is well toleratedeven by patients in poor health. Diarrhoea, nauseaand abdominal pain have attended its use in heavyinfestation. Incidents of expulsion of Ascarisfrom mouth or nose have occurred, probably dueto starvation of the parasite and their slow death.Allergic reactions, loss of hair and granulocy-topenia have been reported with high doses.
Safety of mebendazole during pregnancy isnot known, but it is contraindicated on the basisof animal data.
Uses and administration Mebendazole isavailable as: MEBEX, WORMIN 100 mg chewable tab and100 mg/5 ml suspension. MEBAZOLE 100 mg tab. The doseand duration of treatment is the same for childrenabove 2 years as for adults; ½ dose for 1–2yr age.

850S
EC
TIO
N12
ANTIMICROBIAL DRUGS
TABLE 61.1 Choice of drugs for helminthiasis
Worm First choice drugs Alternative drugs
1. ROUNDWORM Mebendazole, Albendazole, Piperazine, LevamisoleAscaris lumbricoides Pyrantel Ivermectin
2. HOOKWORMAncylostoma Pyrantel, Mebendazole, Levamisole
duodenale AlbendazoleNecator americanus Mebendazole, Albendazole Pyrantel
3. PIN WORM Pyrantel, Mebendazole, PiperazineEnterobius (Oxyuris) Albendazole
vermicularis
4. THREAD WORMStrongyloides stercoralis Ivermectin Albendazole
5. WHIPWORMTrichuris trichiura Mebendazole Albendazole
6. Trichinella spiralis Albendazole Mebendazole
7. FILARIA Diethyl carbamazine, AlbendazoleWuchereria bancrofti, IvermectinBrugia malayi
8. GUINEAWORM Metronidazole MebendazoleDracunculus medinensis
9. TAPEWORMSTaenia saginata Praziquantel, Niclosamide AlbendazoleTaenia solium Praziquantel Niclosamide, AlbendazoleHymenolepis nana Praziquantel Niclosamide, NitazoxanideNeurocysticercosis Albendazole Praziquantel
10. HYDATID DISEASEEchinococcus granulosus, Albendazole MebendazoleE. multilocularis Albendazole
RoundwormHookwormWhipworm
Upto 7 day treatment may be needed in heavytrichuriasisPin worm (Enterobius) 100 mg single dose,repeated after 2–3 weeks (to kill the ova thathave developed later). Strict hygienic measuresand simultaneous treatment of all children in thefamily or class is advocated to cut downautoinfection and person to person infection.This holds true of enterobiasis, irrespective ofdrug used.Trichinosis: 200 mg BD for 4 days; less effectivethan albendazole.Hydatid disease: 200–400 mg BD or TDS for3–4 weeks; less effective than albendazole.
Guinea worm: Mebendazole is an alternativedrug to metronidazole for facilitating extractionof the worm, when the latter cannot be given.
Mebendazole is one of the preferred drugsfor treatment of multiple infestations and is moreeffective than albendazole in trichuriasis. It hasalso been used for mass treatment, but need formultiple doses is a drawback.
AlbendazoleIt is a subsequently introduced congener ofmebendazole: retains the broad-spectrum activityand excellent tolerability of its predecessor, andhas the advantage of single dose administrationin many infestations. One dose treatment hasproduced cure rates in ascariasis, hookworm (bothspecies) and enterobiasis which are comparable
100 mg twice a day for 3 consecutivedays. No fasting, purging or any otherpreparation of the patients is needed.
⎫⎬⎭

851C
HA
PTER61
ANTHELMINTIC DRUGS
to 3 day treatment with mebendazole. Resultsin trichuriasis have been inferior to mebendazole.In strongyloidosis, it is more effective thanmebendazole: a 3 day course has achieved nearly50% cure, and a second course repeated after3 weeks cured practically all patients. Three daytreatment has been found necessary for tapewormsincluding H. nana. Results in hydatid diseaseand hookworm have been superior to mebendazole.Albendazole has weak microfilaricidal action, killscysticerci, hydatid larvae, ova of ascaris/hookworm and is also effective in cutaneous larvamigrans. The mechanism of action of albendazoleis similar to that of mebendazole.
Pharmacokinetics Absorption of albendazoleafter oral administration is significant, butinconsistent. It is enhanced when the drug is takenwith fatty meal (this may help in treatingneurocysticercosis and hydatid disease). Thefraction absorbed is converted by first passmetabolism to its sulfoxide metabolite whichhas potent anthelmintic action. In contrast, themetabolites of mebendazole and thiabendazoleare inactive. Albendazole sulfoxide is widelydistributed in the body, enters brain and isexcreted in urine with a t½ of 8.5 hours. Thus,albendazole is able to exert antihelmintic activityin tissues as well.
Side effects Albendazole is well tolerated;only gastrointestinal side effects have beennoted. Few patients have felt dizziness.Prolonged use, as in hydatid or in cysticercosis,has caused headache, fever, alopecia, jaundiceand neutropenia.ZENTEL, ALMINTH, ALBEZOLE, COMBANTRIN-A 400 mgtab, 200 mg/5 ml suspension.
Uses No preparation or postdrug fasting/purging is required. For intestinal worms itshould be given on empty stomach, while forcysticercosis, hydatid and cutaneous larvamigrans it should be given with a fatty meal.• Ascaris, hookworm, Enterobius and
Trichuris: a single dose of 400 mg (for adultsand children above 2 yrs, 200 mg for 1–2yr age). Three day treatment may be neededin heavy trichuriasis.
• Tapeworms and strongyloidosis: 400 mg dailyfor 3 consecutive days. Efficacy in strongy-loidosis is low, and it is the 2nd choice drugto ivermectin.
• Trichinosis: Three day treatment expels theadult worm from intestine, but has limitedeffect on larvae that have migrated to muscles.They are not killed but symptomatic reliefoccurs. Corticosteroids are added if systemicmanifestations are severe.
• Neurocysticercosis: Albendazole is theanthelmintic of choice for the treatment ofneurocysticercosis (see later). Usually 8–15days course of 400 mg BD (15 mg/kg/day)is employed. Cysticercosis of other tissues(muscles, subcutaneous area) also responds,but no drug should be given for ocularcysticercosis—blindness can occur due to thereaction.
• Cutaneous larva migrans: Albendazole 400 mgdaily for 3 days is the drug of choice; killslarvae and relieves symptoms.
• Hydatid disease: 400 mg BD for 4 weeks,repeat after 2 weeks (if required), up to 3 cour-ses. It is the preferred treatment given beforeand after surgery as well as to inoperable cases.
• Filariasis: Added to diethylcarbamazine(DEC) or ivermectin, albendazole has adjuvantvalue in treating lymphatic filariasis. A singledose of its combination with either DEC orivermectin given yearly has been used in massprogrammes to suppress microfilaraemia anddisease transmission.
Because it has exhibited embryotoxicity in ani-mals, use in pregnant women is contraindicated.It should be given with caution to patients withhepatic or renal disease.
Thiabendazole
It was the first benzimidazole polyanthelmintic introduced in1961, which covered practically all species of nematodesinfesting the g.i.t.—roundworm, hookworm, pin worm,Trichuris, Strongyloides and Trichinella spiralis. It alsoinhibits development of the eggs of worms and kills larvae.Thiabendazole affords symptomatic relief in cutaneous larvamigrans and skeletal muscle symptoms produced by migrationof Trichinella spiralis larvae to muscles, because it hasantiinflammatory action as well. Symptomatic relief also occursin guinea worm disease.

852S
EC
TIO
N12
ANTIMICROBIAL DRUGS
Since thiabendazole is well absorbed from g.i.t., systemicadverse effects like nausea, vomiting, abdominal pain,diarrhoea, giddiness, impairment of alertness, itching, etc. arecommon. Thiabendazole has gone out of use, due to theavailability of better tolerated mebendazole and albendazole.
Pyrantel pamoateIt was introduced in 1969 for pin worminfestation in children; use soon extended toroundworm and hookworm as well. Efficacyagainst Ascaris, Enterobius and Ancylostoma ishigh and comparable to that of mebendazole.Lower cure rates (about 60%) have been obtainedin case of Necator infestation. It is less activeagainst Strongyloides and inactive againstTrichuris and other worms.
Pyrantel causes activation of nicotiniccholinergic receptors in the worms resulting inpersistent depolarization → slowly developingcontracture and spastic paralysis. Worms are thenexpelled. An anticholinesterase action has alsobeen demonstrated. Because piperazine causeshyperpolarization and flaccid paralysis, itantagonizes the action of pyrantel. Cholinergicreceptors in mammalian skeletal muscle havevery low affinity for pyrantel.
Only 10–15% of an oral dose of pyrantelpamoate is absorbed: this is partly metabolizedand excreted in urine.
Adverse effects Pyrantel pamoate is remark-ably free of side effects: occasional g.i.symptoms, headache and dizziness is reported.It is tasteless, nonirritant; abnormal migrationof worms is not provoked. Its safety in pregnantwomen and in children below 2 years has notbeen established.
Use and administration For Ascaris,Ancylostoma and Enterobius: a single dose of10 mg/kg is recommended. A 3 day course forNecator and for Strongyloides has beensuggested.No fasting, purging or other preparation of thepatient is needed.NEMOCID, ANTIMINTH, EXPENT 250 mg tab, 50 mg/mlsuspension (10 ml bottle).
Piperazine
Introduced in 1950, it is a highly active drug against Ascarisand Enterobius; achieves 90–100% cure rates. However,because of the availability at more convenient and bettertolerated albendazole/mebendazole it is now considered asecond choice drug. Piperazine causes hyperpolarization ofAscaris muscle by a GABA agonistic action. Opening of Cl¯channels causes relaxation and depresses responsiveness tocontractile action of ACh. Flaccid paralysis occurs and wormsare expelled alive. They recover if placed in piperazine freemedium. Therefore, often a purgative (senna) is given with it,but is not necessary. No fasting or patient preparation isrequired. Piperazine does not excite Ascaris to abnormalmigration. It does not affect neuromuscular transmission in man.
A considerable fraction of the oral dose of piperazine isabsorbed. It is partly metabolized in liver and excreted in urine.Piperazine is safe, but nausea, vomiting, abdominal discomfortand urticaria may be felt. Dizziness and excitement occur athigh doses; toxic doses produce convulsions; death is due torespiratory failure. It is contraindicated in renal insufficiencyand in epileptics, but is safe in the pregnant.
Dose: For roundworm infestation 4 g once a day for 2consecutive days; children 0.75 g/year of age (max. 4 g) isconsidered curative. Because of its capacity to relax ascarids,it is of particular value in intestinal obstruction due toroundworms. It can be used during pregnancy while otherdrugs cannot be used.Pin worm: 50 mg/kg (max. 2 g) once a day for 7 days or75 mg/kg (max. 4 g) single dose, repeated after 3 weeks.PIPERAZINE CITRATE 0.75 g/5 ml elixir in 30 ml,115 ml bottle; 0.5 g (as phosphate) tablets;Combination of any other anthelmintic (except piperazine) witha purgative in the same formulation is banned in India.
Levamisole, Tetramisole
Tetramisole was developed in the late 1960s. It is racemic; itslevo isomer (levamisole) was found to be more active and ispreferred now. Both are active against many nematodes, butuse is restricted to ascariasis and ancylostomiasis as a secondline drug. The ganglia in worms are stimulated causing tonicparalysis and expulsion of live worms. Interference withcarbohydrate metabolism (inhibition of fumarate reductase) mayalso be contributing.Dose: Ascariasis—Single dose 150 for adults, 100 mg for children20–39 kg body weight, 50 mg for 10–19 kg.Ancylostomiasis—Two doses at 12 hour intervals. It is lesseffective against Neccator: not indicated.Tetramisole: DECARIS 50, 150 mg tab.Levamisole: DEWORMIS, VERMISOL 50,
150 mg tab, 50 mg/5 ml syr.Levamisole is an immunomodulator as well: restores depressedT cell function. It was used as a disease modifying drug inrheumatoid arthritis and as an adjunct in malignancies, aphthousulcers and recurrent herpes, but repeated doses produce severereactions; not used now.

853C
HA
PTER61
ANTHELMINTIC DRUGS
Adverse effects One or two doses used in helminthiasisare well tolerated. Incidence of side effects—nausea,abdominal pain, giddiness, fatigue, drowsiness or insomniais low.
Diethylcarbamazine citrate (DEC)Developed in 1948, it is the first drug forfilariasis caused by the nematodes Wuchereriabancrofti (90% cases) and Brugia malayi. DECis absorbed after oral ingestion, distributed allover the body (V = 3–5 L/kg), metabolized inliver and excreted in urine. Excretion is fasterin acidic urine. Plasma t½ of usual clinical dosesis 4–12 hours, depending on urinary pH.
Diethylcarbamazine is microfilaricidal. It hasa highly selective effect on microfilariae (Mf).A dose of 2 mg/kg TDS clears Mf of W. bancroftiand B. malayi from peripheral blood in 7 days.However, Mf present in nodules and transudates(hydrocoele) are not killed. The most importantaction of DEC appears to be alteration oforganelle membranes of the Mf promoting celldeath. It is also suggested that muscular activityof Mf and adult worms is affected so that theyare dislodged. Prolonged treatment may kill adultB. malayi and probably W. bancrofti worms also.Thus, DEC is slow acting macrofilaricidal.
DEC is active against Mf of Loa loa andOnchocerca volvulus as well. The adult wormof L. loa but not O. volvulus is killed. DECreduces worm burden in ascariasis, but efficacyis low.
Uses
1. Filariasis: DEC 2 mg/kg TDS is a first linedrug: produces rapid symptomatic relief; Mfdisappear from blood and patient becomesnoninfective to mosquitoes in 7 days. However,the adult worm survives in the lymphatics andgives rise to intermittent microfilaraemia andsymptoms. Prolonged treatment with differentschedules has been found to achieve radical curein most patients. A total dose of 72–126 mg/kgspread over 12 days to 3 weeks has been foundsatisfactory; more than one course may be needed
with a gap of 3–4 weeks. Elephantiasis due tochronic lymphatic obstruction is not affected byDEC, because fibrosis of lymphatics isirreversible. Yearly treatment with a combinationof DEC (6 mg/kg) and albendazole (400 mg)single dose on mass scale has brought down trans-mission of filariasis by reducing microfilaraemia.2. Tropical pulmonary eosinophilia: DEC(2–4 mg/kg TDS) for 2–3 weeks produces dramaticimprovement in the signs and symptoms ofeosinophilic lung or tropical eosinophilia. Thebenefit probably reflects anti-microfilarial action:the symptoms of the disease being presumablydue to reaction to the Mf.The associated cough may respond to inhaledcorticosteroids.HETRAZAN, BANOCIDE 50, 100 mg tab, 120 mg/5 ml syr;50 mg/ 5 ml pediatric syr; to be taken after meals.
Loa loa and O. volvulus infections can also betreated with DEC, but the risk of life-threateningreaction to dying Mf is high. It is imperativeto give small (25–50 mg) test dose initiallywhich avoids severe reaction. Ivermectin doesnot produce such severe reactions and ispreferred for initial treatment.
Adverse effects Side effects are common butgenerally not serious. Nausea, loss of appetite,headache, weakness and dizziness are the usualcomplaints.
A febrile reaction with rash, pruritus, enlarge-ment of lymph nodes, bronchospasm and fall inBP may occur due to mass destruction of Mfand adult worms. This is usually mild, but maybe severe. The reaction can be minimized bystarting with a low dose (0.5 mg/kg). When itoccurs, DEC should be temporarily withheld andantihistaminics and/or corticosteroids given.Subsequent administration of DEC does notcause such reaction. Leukocytosis and mildalbuminuria are also noted.
Ivermectin It is an extremely potent semisyn-thetic derivative of the antinematodal principleobtained from Streptomyces avermitilis.Ivermectin is the drug of choice for single dosetreatment of onchocerciasis and strongyloidosis,

854S
EC
TIO
N12
ANTIMICROBIAL DRUGS
and is comparable to DEC for bancroftian andbrugian filaria. It is microfilaricidal but notmacrofilaricidal. Ivermectin is also highlyeffective in cutaneous larva migrans andascariasis, while efficacy against Enterobius andTrichuris is moderate; has been used as addondrug to albendazole/mebendazole in heavytrichuriasis. Certain insects, notably scabies andhead lice are killed by ivermectin.
Nematodes develop tonic paralysis whenexposed to ivermectin. It acts through a specialtype of glutamate gated Cl¯ channel found onlyin invertebrates. Such channels are not involvedin the motor control of flukes and tapewormswhich are unaffected by ivermectin. Potentiationof GABAergic transmission in the worm has alsobeen observed. The lack of GABA-related actionsin man could be due to its low affinity formammalian GABA receptors and its exclusionfrom the brain, by P-glycoprotein mediated effluxat the blood-brain barrier.
A single 10–15 mg (0.2 mg/kg) oral dose ofivermectin, preferably with 400 mg albendazole,given annually for 5–6 years has been used forfilariasis. Single 0.15–0.2 mg/kg dose has yieldedhighest cure rate in strongyloidosis and reducesburden of other intestinal nematodes as well.
Ivermectin has replaced DEC for onchocerciasis and hasbeen used in the ‘river blindness’ control programme of WHOin Africa and Latin America. One dose of ivermectin is givenat 6–12 month intervals—produces long lasting reduction ofMf counts in eye and skin, without affecting the adult worm.Though it does not cure O. volvulus infection, ocularinflammation/damage as well as lymphadenopathy aresuppressed with only mild ocular or systemic reactions.
Ivermectin is the only drug effective orallyin scabies and pediculosis. Single 0.2 mg/kg dosecures most patients.IVERMECTOL, IVERMEC, VERMIN 3, 6 mg tabs; to be takenon empty stomach.
Ivermectin is well absorbed orally, widelydistributed in the body, but does not enter CNS,sequestrated in liver and fat, and has a longterminal t½ of 48–60 hours. It is metabolizedby CYP3A4, but no drug interactions related tothis isoenzyme are known. Side effects have beenmild—pruritus, giddiness, nausea, abdominalpain, constipation, lethargy and transient ECG
changes, but more important are the reactionsdue to degeneration products of the Mf, whichare similar to those occurring after DEC. Safetyof ivermectin in pregnant women and youngchildren is not established.
NiclosamideNiclosamide is a highly effective drug againstcestodes infesting man—Taenia saginata,T. solium, Diphyllobothrium latum andHymenolepis nana, as well as pin worm. The drugappears to act by inhibiting oxidative phosphory-lation in mitochondria and interfering withanaerobic generation of ATP by the tapeworm.Injured by niclosamide, the tapeworms are partlydigested in the intestine. In cases of T. solium,digestion of the dead segments can be hazardous,because the ova released from them may developinto larvae in the intestine, penetrate its wall andcause visceral cysticercosis. Though, the magni-tude of such risk is uncertain, many experts donot use niclosamide now for T. solium infestation.Regimen for tapeworm Niclosamide is available as 0.5 gtab (NICLOSAN). After a light breakfast, 2 tablets are to bechewed and swallowed with water, followed by another 2tablets after 1 hr (total 2 g); total dose for children 2–6 yearsis 1 g. A saline purge is given 2 hours after the later doseto wash off the worm. The scolex should be searched in thestools to be sure that the worm will not grow again. Curerate of 85–95% has been obtained by one day treatment. Athorough purge is essential in the cases of T. solium so thatall segments are passed out and cysticercosis does not occur.Because praziquantel does not lead to digestion of the wormand kills encysted larvae as well, it is the drug of choicefor T. solium.
For H. nana, the 2 g dose is repeated daily for 5 days.This is needed because cysticerci of H. nana (which are notaffected by niclosamide) develop in the jejunal villi of thesame host and worms appear in the intestinal lumen after4 days. However, no purgative is required. In some casestreatment may have to be repeated after 10 days. Praziquantelis now preferred due to single dose treatment.
Adverse effects Niclosamide is tasteless andnonirritating. It is minimally absorbed fromg.i.t.—no systemic toxicity occurs. It is welltolerated; minor abdominal symptoms areproduced occasionally. Malaise, pruritus and lightheadedness are rare. Niclosamide is safe duringpregnancy and in patients with poor health.

855C
HA
PTER61
ANTHELMINTIC DRUGS
PraziquantelThis anthelmintic has wide ranging activityagainst Schistosomes, other trematodes,cestodes and their larval forms but notnematodes. It is rapidly taken up by susceptibleworms and appears to act by causing leakageof intracellular calcium from the membranes →contracture and paralysis. Selectivity of actionof praziquantel on tapeworms and flukes maybe dependent on the presence of a specificvariant of Ca2+ channel sensitive to praziquantelin these worms. The tapeworms lose grip of theintestinal mucosa and are expelled. Flukes andschistosomes are also dislodged in tissues andveins. Praziquantel is active against adult as wellas juvenile and larval stages of tapeworms.
At relatively higher concentrations, it causesvacuolization of the tegument and release of thecontents of tapeworms and flukes followed bytheir destruction by immune mechanisms of thehost. This action appears to be more importantin cases of schistosomes and flukes.
Pharmacokinetics Praziquantel is rapidlyabsorbed from intestines; absorption is enhancedif it is ingested with food. High first pass meta-bolism in liver limits its systemic bioavailability.Phenytoin, carbamazepine and dexamethasoneinduce praziquantel metabolism and furtherdecrease its bioavailability. Patients of neuro-cysticercosis are mostly receiving these drugswhich may contribute to therapeutic failure ofpraziquantel. It crosses blood-brain barrier andattains therapeutic concentrations in the brainand CSF. The plasma t½ is short (1.5 hours).Metabolites are excreted chiefly in urine.
Adverse effects Despite systemic absorption,praziquantel has exhibited no systemic toxicity.It tastes bitter: can produce nausea and abdo-minal pain. Other side effects are headache,dizziness and sedation. When used for schisto-somes and visceral flukes, symptoms like itching,urticaria, rashes, fever and bodyache occur asa reaction to the destroyed parasites. Destructionof cysticerci in the brain may produceneurological complications (see below).
No interaction with food, alcohol or tobaccohas been noted.
Uses
1. Tapeworms: Praziquantel administered asa single dose has achieved 90–100% cure ratein all human tapeworms. This level of efficacyis similar to that of niclosamide and even betterin case of H. nana.
T. saginata, T. solium: 10 mg/kg single dosein the morning. It is especially valuable in caseof T. solium, because it kills the tapeworm larvaewithin the cysts and there are no chances ofsystemic cysticercosis developing.
H. nana, D. latum: 15–25 mg/kg single dosein the morning. This is much simpler comparedto 5 day treatment needed with niclosamide foreradication of H. nana. In case of heavy infes-tation, retreatment after one week is desirable.2. Neurocysticercosis: The role of anthelminticsin this condition is controversial; only selectedcases should be treated with them. Praziquantelwas the first drug found to be effective in neuro-cysticercosis: 50 mg/kg daily in 3 divided dosesfor 15–30 days kills the larvae lodged in brainand other tissues. However, it is now the 2ndchoice drug to albendazole (see below).Praziquantel or albendazole are contraindicatedin ocular cysticercosis.3. Schistosomes: All 3 species can be treatedwith 40–75 mg/kg given once or in instalmentsover one day.4. Other flukes: Praziquantel is the drug ofchoice for all schistosome and fluke infestationsexcept Fasciola hepatica. The flukes respondto 75 mg/kg single day treatment in most cases,and on two occasions in the remaining.CYSTICIDE 500 mg tab, DISTOCIDE 600 mg tab.
Anthelmintic treatment ofneurocysticercosis
Cysticercosis of various organs, including brain,occurs in T. solium infestation due to migrationof the larvae from the gut to various tissuesvia blood stream. Anthelmintic treatment of

856S
EC
TIO
N12
ANTIMICROBIAL DRUGS
neurocysticercosis may or may not beappropriate, because the cysts do not cause anyproblem unless the larva dies and its productsinduce an intense focal reaction. The anthel-mintic kills the larvae and precipitates thereaction, resulting in meningeal irritation, risein intracranial pressure, seizures and otherneurological phenomena. However, it preventsfuture episodes due to spontaneous death of thecysticerci. The decision whether or not to givethe anthelmintic may be taken depending on thenumber, location and viability of the cysts. Activecysts, multiple parenchymal cysts, orintraventricular cysts likely to enlarge and causehydrocephalus are better treated. Inactive andcalcified cysts may be left alone.
Out of the two anthelmintics effective inkilling cysticerci, albendazole is now preferredover praziquantel for the following reasons:• The course of treatment is shorter (8–15 day)
compared to praziquantel (15–30 days).• Cure rates in terms of resolution of symptoms
and disappearance of cysts are higher (75–85%with albendazole) than praziquantel (50–60%).
• Corticosteroids (which have to be givenconcurrently) enhance the absorption ofalbendazole, but lower the blood levels of
praziquantel. Phenytoin and carbamazepinealso lower praziquantel levels.
• Albendazole is cheaper.Whichever anthelmintic is used, corticosteroids(prednisolone 40–60 mg/day or dexamethasone8–12 mg/day) must be started 2 days before andcontinued till 2 weeks after completing theanthelmintic course. This is necessary to suppressthe inflammatory reaction to the products of killedlarvae. Absorption of both albendazole andpraziquantel is enhanced by ingesting them withfood, particularly fatty food. For patients withseizures (as most of them are), adequateanticonvulsant treatment should be givenbeforehand and the fits controlled. Phenytoin andcarbamazepine are the most commonly useddrugs. They induce the metabolism of praziquan-tel, which may necessitate use of higher doses.The anticonvulsant must be continued through thecourse of anthelmintic medication and for anindefinite period (mostly 1–6 months) after it.While parenchymal cysts respond to albendazolein 8–15 days, intraventricular and subarachnoidcysts may require treatment for a month or longer.It is very important to kill and expel the adultworm from the gut to eliminate the source offuture cysticerci.
PROBLEM DIRECTED STUDY
61.1 A 40-year-old male weighing 60 kg presented with history of 2 episodes of suddenonset fits over the past 3 days. There is no past history of fits or any nervous disorder. Thepatient has been having headache for the last one month or so which responds to paracetamol.His wife who witnessed the fits gave a description which fitted tonic-clonic seizures. The wifealso informed of noticing some behavioural changes for the last 2 months. The fits were followedby confused behaviour and drowsiness for 2–3 hours. There is no family history of fits ormental illness. MRI scan of the brain revealed 4 active cortical parenchymal cysticerci. A diagnosisof neurocysticercosis was made.(a) Should this patient be treated with specific anthelmintic drug, or only symptomatic treatmentof seizures is indicated?(b) If anthelmintic therapy is to be given, should antiseizure drug also be given? If both areto be given, should they be given concurrently or one after the other or in overlapping mannerstarting with one first? What should be the sequence?(c) If anthelmintic is to be given, which drug, dose and duration of treatment would be appropriateand why?(d) Whether any other medication needs to be given? If so which, when, how long and why?(see Appendix-1 for solution)

Anticancer DrugsChapterChapterChapterChapterChapter 6262626262
SECTION 13
CHEMOTHERAPY OF NEOPLASTIC DISEASES
The anticancer drugs either kill cancer cells ormodify their growth. However, selectivity ofmajority of drugs is limited and they are oneof the most toxic drugs used in therapy.
Treatment of malignant diseases with drugsis a rather recent development—started after 1940when nitrogen mustard was used, but progresshas been rapid, both in revealing pathobiologyof the diseases and in discovery of new drugs.The latest innovations target growth factors,specific signaling pathways, angiogenesis, tumourantigens, etc. to introduce a different spectrumof drugs. In addition, attempts have been madeto define optimal combinations, treatment strate-gies and patient support measures. Cancerchemotherapy is now of established value anda highly specialized field to be handled byoncology specialists supported by a multi-disciplinary team. Only the general principles andan outline will be presented here.
In addition to their prominent role inleukaemias and lymphomas, drugs are used inconjunction with surgery, radiotherapy andimmunotherapy in the combined modalityapproach for many solid tumours, especiallymetastatic. In malignant diseases, drugs are usedwith the aim of:
1. Cure or prolonged remission Chemo-therapy is the primary treatment modality thatcan achieve cure or prolonged remission in:
Acute leukemias ChoriocarcinomaWilm’s tumour Hodgkin’s diseaseEwing’s sarcoma LymphosarcomaRetinoblastoma Burkitt’s lymphomaRhabdomyosarcoma Testicular teratomas
SeminomaMycosis fungoides
2. Palliation Gratifying results are obtained(shrinkage of evident tumour, alleviation of symp-toms) and life is prolonged by chemotherapy in:
Breast cancer Chronic lymphatic leukemiaOvarian carcinoma Chronic myeloid leukemiaEndometrial carcinoma Non-Hodgkin lymphomasMyeloma Head and neck cancersProstatic carcinoma Lung (small cell) cancer
Many other malignant tumours are less sensitiveto drugs—life may or may not be prolonged bychemotherapy. Tumours that are largely refrac-tory to presently available drugs are:
Colorectal carcinoma Malignant melanomasCarcinoma pancreas Bronchogenic carcinomaCarcinoma stomach (non small cell)Carcinoma esophagus HepatomaRenal carcinoma Sarcoma
3. Adjuvant chemotherapy Drugs are usedto mop up any residual malignant cells (micro-metastases) after surgery or radiotherapy. Thisis routinely employed now and may achieve
in c
hild
ren⎫⎬⎭

858S
EC
TIO
N13
CHEMOTHERAPY OF NEOPLASTIC DISEASES
apparent cure, especially in early breast, lung andcolonic cancers.
CLASSIFICATIONA. Cytotoxic drugs1. Alkylating agents Mechlorethamine
Nitrogen mustards (Mustine HCl)Cyclophosphamide,Ifosfamide,Chlorambucil,Melphalan
Ethylenimine Thio-TEPAAlkyl sulfonate BusulfanNitrosoureas Carmustine (BCNU),
Lomustine (CCNU)Triazine Dacarbazine (DTIC),
TemozolomideMethylhydrazine Procarbazine
2. Platinum Cisplatin,coordination Carboplatin,complexes Oxaliplatin
3. AntimetabolitesFolate Methotrexate (Mtx)
antagonist PemetrexedPurine 6-Mercaptopurine (6-MP),
antagonist 6-Thioguanine (6-TG),Azathioprine, Fludarabine
Pyrimidine 5-Fluorouracil (5-FU),antagonist Capecitabine, Cytarabine
(cytosine arabinoside)4. Microtubule Vincristine (Oncovin),
damaging Vinblastine, Vinorelbineagents Paclitaxel, Docetaxel
Estramustine5. Topoisomerase-2 Etoposide
inhibitors6. Topoisomerase-1 Topotecan,
inhibitors Irinotecan7. Antibiotics Actinomycin D
(Dactinomycin),Doxorubicin,Daunorubicin(Rubidomycin),Epirubicin,Mitoxantrone,Bleomycins,Mitomycin C
8. Miscellaneous Hydroxyurea,L-Asparaginase,Tretinoin,Arsenic trioxide
B. Targeted drugs1. Tyrosine protein- Imatinib,
kinase inhibitors Nilotinib2. EGF receptor Gefitinib, Erlotinib
inhibitors Cetuximab3. Angiogenesis Bevacizumab
inhibitors Sunitinib4. Proteasome Bortezomib
inhibitor5. Unarmed Rituximab,
monoclonal Trastuzumabantibody
C. Hormonal drugs1. Glucocorticoids Prednisolone and
others2. Estrogens Fosfestrol,
Ethinylestradiol3. Selective estrogen Tamoxifen,
receptor modulators Toremifene4. Selective estrogen Fulvestrant
receptor downregulators
5. Aromatase Letrozole,inhibitors Anastrozole,
Exemestane6. Antiandrogen Flutamide,
Bicalutamide7. 5-α reductase Finasteride,
inhibitor Dutasteride8. GnRH analogues Nafarelin, Leuprorelin
Triptorelin9. Progestins Hydroxyprogesterone
acetate, etc.
GENERAL TOXICITY OFCYTOTOXIC DRUGS
Majority of the cytotoxic drugs have moreprofound effect on rapidly multiplying cells,because the most important target of action arethe nucleic acids and their precursors, and rapid

859C
HA
PTE
R62
ANTICANCER DRUGS
nucleic acid synthesis occurs during cell division.Many cancers (especially large solid tumours)have a lower growth fraction (lower percentageof cells are in division) than normal bone marrow,epithelial linings, reticuloendothelial (RE) systemand gonads. These tissues are particularly affectedin a dose-dependent manner by majority of drugs;though, there are differences in susceptibility toindividual members.
1. Bone marrow Depression of bone marrowresults in granulocytopenia, agranulocytosis,thrombocytopenia, aplastic anaemia. This is themost serious toxicity; often limits the dose thatcan be employed. Infections and bleeding are theusual complications.
2. Lymphoreticular tissue Lymphocytopeniaand inhibition of lymphocyte function results insuppression of cell mediated as well as humoralimmunity.
Because of action (1) and (2) + damage toepithelial surfaces, the host defence mechanisms(specific as well as nonspecific) are broken down→ susceptibility to all infections is increased. Ofparticular importance are the opportunistic infec-tions due to low pathogenicity organisms.Infections by fungi (Candida and others causingdeep mycosis), viruses (Herpes zoster, cytomegalovirus), Pneumocystis jiroveci (a fungus) andToxoplasma are seen primarily in patients treatedwith anticancer drugs.
3. Oral cavity: The oral mucosa is particularlysusceptible to cytotoxic drugs because of highepithelial cell turnover. Many chemotherapeuticdrugs, particularly fluorouracil, methotrexate,daunorubicin, doxorubicin produce stomatitis asan early manifestation of toxicity. The gums andoral mucosa are regularly subjected to minortrauma, and breaches are common during chewing.Oral microflora is large and can be the sourceof infection. Neutropenia and depression ofimmunity caused by the drug indirectly increasethe chances of oral infections. Thrombocytopeniamay cause bleeding gums. Xerostomia due to thedrug may cause rapid progression of dental caries.
4. GIT Diarrhoea, shedding of mucosa,haemorrhages occur due to decrease in the rateof renewal of the gastrointestinal mucous lining.Drugs that prominently cause mucositis are—bleomycin, actinomycin D, daunorubicin,doxorubicin, fluorouracil and methotrexate.
Nausea and vomiting are prominent with manycytotoxic drugs. This is due to direct stimulationof CTZ by the drug, as well as generation ofemetic impulses/mediators from the upper g.i.t.and other areas (see Ch. 47).
Emetogenic potential of cytotoxic drugs
High Moderate Mild
Cisplatin Carboplatin BleomycinMustine Cytarabine ChlorambucilCyclophosphamide Procarbazine BusulfanActinomycin D Vinblastine FluorouracilDacarbazine Doxorubicin 6-ThioguanineLomustine Daunorubicin Hydroxyurea
Ifosfamide Vincristine6-Mercapto- Methotrexatepurine EtoposidePaclitaxel l-Asparaginase
5. Skin Alopecia occurs due to damage to thecells in hair follicles. Dermatitis is anothercomplication.
6. Gonads Inhibition of gonadal cells causesoligozoospermia and impotence in males;inhibition of ovulation and amenorrhoea arecommon in females.
Damage to the germinal cells may result inmutagenesis.
7. Foetus Practically all cytotoxic drugs givento pregnant women profoundly damage thedeveloping foetus → abortion, foetal death,teratogenesis.
8. Carcinogenicity Secondary cancers,especially leukaemias, lymphomas and histocytictumours appear with greater frequency many yearsafter the use of cytotoxic drugs. This may bedue to depression of cell mediated and humoralblocking factors against neoplasia.
9. Hyperuricaemia This is secondary tomassive cell destruction (uric acid is a product

860S
EC
TIO
N13
CHEMOTHERAPY OF NEOPLASTIC DISEASES
of purine metabolism) and is especially likely tooccur in leukaemias and bulky lymphomas. Acuterenal failure, gout and urate stones in the urinarytract may develop. Allopurinol is protective bydecreasing uric acid synthesis.
In addition to these general toxicities,individual drugs may produce specific adverseeffects, e.g. neuropathy by vincristine, cardio-myopathy by doxorubicin, cystitis and alopeciaby cyclophosphamide.
NOTES ON INDIVIDUAL DRUGS
ALKYLATING AGENTS
These compounds produce highly reactivecarbonium ion intermediates which transfer alkylgroups to cellular macromolecules by formingcovalent bonds. The position 7 of guanine residuesin DNA is especially susceptible, but othermolecular sites are also involved. They may reactwith carboxyl, hydroxyl, amino, sulfhydryl andphosphate groups of biomacromolecules.Alkylation results in cross linking/abnormal basepairing/scission of DNA strand. Cross linking ofnucleic acids with proteins can also take place.
Alkylating agents have cytotoxic and radio-mimetic (like ionizing radiation) actions. Mostare cell cycle non-specific, i.e. act on dividingas well as resting cells. Some have CNS stimulantand cholinergic properties.
Mechlorethamine (Mustine HCl) It is thefirst nitrogen mustard; highly reactive and localvesicant—can be given only by i.v. route. Itproduces many acute effects like nausea, vomitingand haemodynamic changes. Extravasation duringi.v. injection may cause sloughing. Hodgkin andnon-Hodgkin lymphomas are the main indications.It has been a component of erstwhile MOPPregimen.Dose: 0.1 mg/kg i.v. daily × 4 days; courses may be repeatedat suitable intervals.MUSTINE 10 mg dry powder in vial.
Cyclophosphamide It is inactive as such:produces few acute effects and is not locallydamaging. Transformation into active metabolites
(aldophosphamide, phosphoramide mustard)occurs in the liver, and a wide range of antitumouractions is exerted. It has prominent immuno-suppressant property. Thus, it is one of the mostpopular alkylating agents useful in many solidtumours. It is less damaging to platelets, butalopecia and cystitis (due to another metaboliteacrolein) are prominent. Chloramphenicol retardsthe metabolism of cyclophosphamide.Dose: 2–3 mg/kg/day oral; 10–15 mg/kg i.v. every 7–10 days,i.m. use also possible.ENDOXAN, CYCLOXAN 50 mg tab; 200, 500, 1000 mg inj.
Ifosfamide This congener of cyclophospha-mide has a longer and dose-dependent t½. It hasfound utility in bronchogenic, breast, testicular,bladder, head and neck carcinomas, osteogenicsarcoma and some lymphomas. The dose limitingtoxicity of ifosphamide is haemorrhagic cystitis.To prevent the same, mesna is routinely givenwith it. Mesna is a –SH compound that is excretedin urine—binds and inactivates the vasicotoxicmetabolites of ifosfamide and cyclophosphamide.Ifosfamide causes less alopecia and is lessemetogenic than cyclophosphamide.HOLOXAN-UROMITEXAN 1 g vial + 3 amps of mesna 200mg inj.; HOLOXAN, IPAMIDE 1 g inj.
Chlorambucil It is a very slow actingalkylating agent, especially active on lymphoidtissue: Myeloid tissue is largely spared. It is thedrug of choice for long-term maintenance therapyfor chronic lymphatic leukaemia; non-Hodgkinlymphoma and few solid tumours also resolve.It has some immunosuppressant property.Dose: 4–10 mg (0.1–0.2 mg/kg) daily for 3–6 weeks, then 2mg daily for maintenance; LEUKERAN 2, 5 mg tab.
Melphalan It is very effective in multiplemyeloma and has been used in advanced ovariancancer. Bone marrow depression is the mostimportant toxicity. Infections, diarrhoea andpancreatitis are the complications.Dose: 10 mg daily for 7 days or 6 mg/day for 2–3 weeks—4weeks gap—2 to 4 mg daily for maintenance orally. Also usedfor regional perfusion in malignant melanoma. ALKERAN 2,5 mg tab, 50 mg per vial for inj.
Thio-TEPA It is an ethylenimine: does notrequire to form an active intermediate. It has high

861C
HA
PTE
R62
ANTICANCER DRUGS
toxicity: seldom used now in ovarian and bladdercancer.Dose: 0.3–0.4 mg/kg i.v. at 1–4 week intervals.THIOTEPA 15 mg per vial inj.
Busulfan It is highly specific for myeloidelements; granulocyte precursors being the mostsensitive, followed by those of platelets and RBC.It produces little effect on lymphoid tissue andg.i.t. Hyperuricaemia is common; pulmonaryfibrosis and skin pigmentation are the specificadverse effects. Sterility also occurs. It is the drugof choice for chronic myeloid leukaemia.Dose: 2–6 mg/day (0.06 mg/kg/day) orally.MYLERAN, BUSUPHAN 2 mg tab.
Nitrosoureas These are highly lipid solublealkylating agents with a wide range of antitumouractivity. They cross blood-brain barrier—areeffective in meningeal leukaemias and braincancer. Nausea, vomiting are common and CNSeffects also occur. Bone marrow depression ispeculiarly delayed, taking nearly 6 weeks todevelop. Visceral fibrosis and renal damage canoccur:Lomustine (CCNU): 100–130 mg/m2 BSA single oraldose every 6 weeks; LOMUSTINE 40, 100 mg cap.
Dacarbazine (DTIC) After activation in liver,it acts by methylating DNA and interfering withits function. The most important indication ismalignant melanoma; also used in Hodgkin’sdisease. Nausea, vomiting, flu-like symptoms,neuropathy and myelosuppression are theprominent adverse effects.Dose: 3.5 mg/kg/day i.v. for 10 days, repeat after 4 weeks.DACARIN 100, 200, 500 mg inj; DACARZINE 200 mg/vialinj.
Temozolamide This orally active triazinemethylating agent is the drug of choice for gliomaand other malignant brain tumours; also utilizedin melanoma. Adverse effects are similar todacarbazine.Dose: 100–250 mg/day; GLIOZ 20, 100, 250 mg caps.
Procarbazine It is not a classical alkylatingagent, but has similar properties. After metabolicactivation (it is inactive as such), procarbazinemethylates and depolymerizes DNA causing
chromosomal damage. Inhibition of nucleic acidsynthesis also occurs. Beause of damage to DNA,mutagenic and carcinogenic potential has beendetected. It is a component of MOPP regimenfor Hodgkin’s and related lymphomas, and is analternative drug for brain tumours.
Procarbazine is a weak MAO inhibitor;produces sedation and other CNS effects, andcan interact with foods and drugs. Alcohol causeshot flushing and a disulfiram-like reaction inpatients taking procarbazine. Males may suffersterility. Vomiting, leucopenia, thrombocytopeniaare the prominent toxicities.Dose: 100 mg/m2/day for 14 days in 28 days cycles.INDICARB 20 mg cap, NEOZINE, P-CARZINE 50 mg cap.
PLATINUM COORDINATION COMPLEXES
Cisplatin It is hydrolysed intracellularly toproduce a highly reactive moiety which causescross linking of DNA. The favoured site is N7
of guanine residue. It can also react with –SHgroups of cytoplasmic and nuclear proteins. Effectsresemble those of alkylating agents and radiation.It is bound to plasma proteins, penetrates tissuesand is slowly excreted unchanged in urine with at½ of about 72 hrs. Negligible amounts enter brain.
A copper transporter CTR1 is involved in the entry ofplatinum complexes into the tumour cells. The same areextruded from the cells by the transporter MRP1 as well as bycopper efflux proteins. Resistance to cisplatin can be impartedby variation in the levels of these proteins.
Cisplatin is very effective in metastatic testi-cular and ovarian carcinoma. It is widely usedin many other solid tumours like lung, bladder,esophageal, gastric, hepatic, head and neckcarcinomas.Cisplatin is administered by slow i.v. infusion 50–100mg/m2 BSA every 3–4 weeks; CISPLATIN, CISPLAT,PLATINEX 10 mg/10 ml, 50 mg/50 ml vial.
Cisplatin is a highly emetic drug. Antiemeticsare routinely administered before infusing it. Themost important toxicity is renal impairment whichis dependent on total dose administered. Renaltoxicity can be reduced by maintaining goodhydration. Tinnitus, deafness, sensory neuropathyand hyperuricaemia are other problems. A shock-like state sometimes occurs during i.v. infusion.

862S
EC
TIO
N13
CHEMOTHERAPY OF NEOPLASTIC DISEASES
Carboplatin It is a less reactive second genera-tion platinum compound that is better toleratedand has a toxicity profile different from cisplatin,but mechanism of action and clinical utility aresimilar. Nephrotoxicity, ototoxicity and neuro-toxicity are low. Nausea and vomiting is milderand is delayed: only infrequently limits the dose.The dose-limiting toxicity is thrombocytopeniaand less often leucopenia. Liver dysfunction mayoccur. Because of less plasma protein binding,it is rapidly eliminated by the kidney with a plasmat½ of 2–4 hours. A small fraction that is boundis excreted over days. It is primarily indicatedin ovarian carcinoma of epithelial origin, and hasshown promise in squamous carcinoma of headand neck, small cell lung cancer, breast cancerand seminoma.ONCOCARBIN 150 mg inj, KEMOCARB 150, 450 mg/vialinj. 400 mg/m2 as an i.v. infusion over 15–60 min, to berepeated only after 4 weeks.
Oxaliplatin This third generation platinumcomplex differs significantly from cisplatin. Itappears to target different biomolecules. Pathwayswhich confer resistance to cisplatin are notoperative in its case. Resistance does not easilydevelop to oxaliplatin, and it retains activityagainst tumours that have become resistant tocisplatin. Oxaliplatin is highly effective in colo-rectal cancer; 5-fluorouracil markedly synergiseswith it. Gastroesophageal and pancreatic cancersalso respond.
The dose limiting toxicity is peripheral neuro-pathy. Sensory paresthesias involving arms, legs,mouth and throat are common. An acute formof neuropathy is usually triggered by exposureto cold. Myelosuppression is modest, but diarrhoeaand acute allergic reactions are reported.Dose: 85 mg/m2 i.v. every 2 weeks.KINAPLAT, OPLATIN 50 mg in 25 ml and 100 mg in 50 mlvial.
ANTIMETABOLITES
These are analogues related to the normal compo-nents of DNA or of coenzymes involved innucleic acid synthesis. They competitivelyinhibit utilization of the normal substrate or get
themselves incorporated forming dysfunctionalmacromolecules.
1. Folate antagonistMethotrexate (Mtx)This folic acid analogue is one of the oldestand highly efficacious antineoplastic drugs whichacts by inhibiting dihydrofolate reductase(DHFRase)—blocking the conversion of dihydro-folic acid (DHFA) to tetrahydrofolic acid (THFA).Utilizing the folate carrier it enters into cellsand is transformed to more active polyglutamateform by the enzyme folypolyglutamate synthase(FPGS). Tetrahydrofolic acid is an essentialcoenzyme required for one carbon transferreactions in de novo purine synthesis and aminoacid interconversions. The inhibition is pseudo-irreversible because Mtx has 50,000 times higheraffinity for the enzyme than the normal substrate.
Methotrexate has cell cycle specific action—kills cells in S phase; In addition to DHFRaseit inhibits thymidylate synthase as well so thatDNA synthesis is primarily affected. However,synthesis of RNA and protein also suffers. It exertsmajor toxicity on bone marrow—low doses givenrepeatedly cause megaloblastic anaemia, but highdoses produce pancytopenia. Mucositis anddiarrhoea are common side effects. Desquamationand bleeding may occur in g.i.t.
Methotrexate is absorbed orally, 50% plasmaprotein bound, little metabolized and largelyexcreted unchanged in urine. Salicylates,sulfonamides, dicumerol displace it from proteinbinding sites. Aspirin and sulfonamides enhancetoxicity of Mtx by decreasing its renal tubularsecretion.
The toxicity of Mtx cannot be overcome byfolic acid, because it will not be converted tothe active coenzyme form. However, Folinic acid(N5 formyl THFA, cirtrovorum factor) rapidlyreverses the effects. Thymidine also counteractsMtx toxicity.
Methotrexate is apparently curative inchoriocarcinoma: 15–30 mg/day for 5 days orallyor 20–40 mg/m2 BSA i.m. or i.v. twice weekly.

863C
HA
PTE
R62
ANTICANCER DRUGS
In a dose of 2.5–15 mg/day it is highly effectivein maintaining remission in children with acuteleukaemias, but it is not good for inducingremission: Mtx is widely used in non-Hodgkinlymphoma, breast, bladder, head and neck cancers,osteogenic sarcoma, etc. It has prominent immuno-suppressant property useful in rheumatoid arthritis,psoriasis and many other antoimmune disorders(see Ch. 63).NEOTREXATE 2.5 mg tab, 50 mg/2 ml inj; BIOTREXATE2.5 mg tab, 5, 15, 50 mg/vial inj.
The use of folinic acid rescue has permitted muchhigher doses of Mtx and has enlarged its scopeto many difficult-to-treat neoplasms. A nearly100 times higher dose (250–1000 mg/m2 BSA)of Mtx is infused i.v. over 6 hours, followed by3–15 mg i.v. calcium leucovorin within 3 hours,repeated as required. This procedure can berepeated weekly.
Pemetrexed This newer congener of Mtxprimarily targets the enzyme thymidylate synthase.Though, it is also a DHFRase inhibitor, the poolof THFA is not markedly reduced. Like Mtx itutilizes the folate carrier to enter cells and requirestransformation into polyglutamate form by FPGSfor activity enhancement. Adverse effects(mucositis, diarrhoea, myelosuppression) aresimilar to Mtx, but a painful, itching erythematousrash, mostly involving the hands and feet, ‘hand-foot syndrome’ is quite common. Dexamethasonecan relieve it, and pretreatment can reduce itsincidence. Low dose folic acid and vit B12 pre-treatment is recommended to limit pemetrexedinduced myelosuppression. NSAIDs should beavoided as they decrease pemetrexed clearanceand may increase toxicity.
In combination with cisplatin, pemetrexed isapproved for treatment of mesoepithelioma andnon-small cell lung carcinoma.Dose: 500 mg/m2 i.v. every 3 weeks.PEMEX 500 mg vial for i.v. inj.
2. Purine antagonistsMercaptopurine (6-MP) and thioguanine(6-TG) These are highly effective antineoplastic
drugs. After synthesis in the body to the corres-ponding monoribonucleotides, they inhibit theconversion of inosine monophosphate to adenineand guanine nucleotides that are the buildingblocks for RNA and DNA. There is also feedbackinhibition of de novo purine synthesis. They alsoget incorporated into RNA and DNA which aredysfunctional.
6-MP and 6-TG are especially useful inchildhood acute leukaemia, choriocarcinoma andhave been employed in some solid tumours aswell. In acute leukaemia, both have been usedin combination regimens to induce remission and6-MP for maintaining remission as well.
All antipurines are absorbed orally (thoughincompletely). Azathioprine and 6-MP areoxidised by xanthine oxidase; their metabolismis inhibited by allopurinol; dose has to be reducedto ¼–½ if allopurinol is given concurrently.Thioguanine is not a substrate for xanthineoxidase; follows a different (S-methylation)metabolic path and its dose need not be reducedif allopurinol is given.
Methylation by thiopurine methyl transferase(TPMT) is an additional pathway of 6-MPmetabolism. Genetic deficiency of TPMT makesthe individual more susceptible to 6-MP inducedmyelosuppression, mucositis and gut damage,while over expression of TPMT is an importantmechanism of 6-MP resistance in acute leukaemiacells. Toxicity of azathioprine is also enhancedin TPMT deficiency.
The main toxic effect of antipurines is bonemarrow depression, which develops slowly.Mercaptopurine causes more nausea and vomitingthan 6-TG. It also produces a high incidence ofreversible jaundice. Hyperuricaemia occurs withboth, and can be reduced by allopurinol.Dose: 6-Mercaptopurine: 2.5 mg/kg/day, half dose formaintenance; PURINETHOL, EMPURINE, 6-MP, 50 mg tab.6-Thioguanine: 100–200 mg/m2/day for 5–20 days; 6-TG40 mg tab.
Azathioprine This antipurine acts by gettingconverted to 6-MP, but has more prominentimmunosuppressant action (see p. 882), probablybecause of selective uptake into immune cells

864S
EC
TIO
N13
CHEMOTHERAPY OF NEOPLASTIC DISEASES
and intracellular conversion to 6-MP. This isfurther synthesized into the nucleic acid inhibitoryneucleotides. Azathioprine primarily suppressescell mediated immunity (CMI) and is used mainlyin autoimmune diseases (rheumatoid arthritis,ulcerative colitis) as well as in organ trans-plantation.Dose: Azathioprine 3–5 mg/kg/day, maintenance 1–2 mg/kg/day; IMURAN, TRANSIMUNE, AZOPRINE 50 mg tab.
Fludarabine This newer purine antimetaboliteis phosphorylated intracellularly to the activetriphosphate form which then inhibits DNApolymerase and ribonucleotide reductase,interferes with DNA repair as well as getsincorporated to form dysfunctional DNA.Tumour cell apoptosis is promoted by multiplemechanisms confering activity even in slowgrowing neoplasms. It is indicated in chroniclymphatic leukaemia and non-Hodgkin’slymphoma that have recurred after treatment.Prominent adverse effects are chills, fever,myalgia, arthralgia and vomiting after injection,myelosuppression and opportunistic infections (itis a potent suppressant of CMI).Dose: 25 mg/m2 BSA daily for 5 days every 28 days by i.v.infusionFLUDARA 50 mg/vial inj.
3. Pyrimidine antagonistsPyrimidine analogues have varied applications asantineoplastic, antifungal and antipsoriatic agents.
Fluorouracil (5-FU) is converted in thebody to the corresponding nucleotide 5-fluoro-2-deoxyuridine monophosphate, which forms acovalent ternary complex with methyl-THFA andtymidylate synthase (TS) resulting in irreversibleinhibition of TS. Consequently conversion ofdeoxyuridilic acid to deoxythymidylic acid isblocked. Selective failure of DNA synthesisoccurs due to non-availability of thymidylate.Accordingly, thymidine can partially reverse5-FU toxicity. 5-FU itself gets incorporated intoRNA, interferes with RNA synthesis and functioncontributing to its cytotoxicity. Even resting cellsare affected, though rapidly multiplying ones aremore susceptible. Since inhibition of TS by
5-FU is dependednt on the prsence of THFA,concurrent infusion of leucovorin enhances theefficacy of 5-FU. Cisplatin and oxaliplatin alsosynergise with 5-FU. Most protocols now employ5-FU along with leucovorin and cisplatin/oxaliplatin.
Currently, 5-FU is a commonly used anticancerdrug for many solid malignancies, especially ofcolon, rectum, stomach, pancreas, liver, urinarybladder, head and neck. Oral absorption of5-FU is unreliable. It is primarily used by i.v.infusion. 5-FU is rapidly metabolized by dihydro-pyrimidine dehydrogenase (DPD) resulting in aplasma t½ of 15–20 min after i.v. infusion. Geneticdeficiency of DPD predisposes to severe 5-FUtoxicity. Major toxicity of 5-FU is exerted onthe bone marrow and g.i.t. causing myelosuppres-sion, mucositis, diarrhoea, nausea and vomiting.Peripheral neuropathy (hand-foot syndrome) alsooccurs.Dose: 500 mg/m2 i.v. infusion over 1–3 hours weekly for 6–8weeks, or 12 mg/kg/day i.v. for 4 days followed by 6 mg/kgi.v. on alternate days, 3–4 doses.FLURACIL, FIVE FLURO, FIVOCIL 250 mg/5 ml and 500mg/10 ml vial.
A 1% topical solution applied twice dailyfor 3–6 weeks has yielded gratifying results insuperficial basal cell carcinoma, and in actinickeratosis.
Capecitabine It is an orally active prodrug of 5-FU. Afterabsorption it is converted to deoxy-5-fluorouridine in theliver and released in blood. Taken up by cells, it is hydrolysedto 5-FU by thymidine phosphorylase. Because many breastand colorectal cancer cells express large quantity of thisenzyme, they generate more 5-FU and suffer higher toxicitythan normal cells. A combined regimen of capecitabine +oxaliplatin is frequently used in metastatic colorectal cancer.It has also been utilized in 2nd line treatment of metastaticbreast cancer along with taxanes. Hand-foot syndrome anddiarrhoea are prominent adverse effects, but bone marrowdepression and mucositis are less marked.
Cytarabine (Cytosine arabinoside) Thiscytidine analogue is phosphorylated in the bodyto the corresponding nucleotide which inhibitsDNA synthesis. The triphosphate of cytarabineis an inhibitor of DNA polymerase, as well asblocks production of cytidilic acid. However, itsincorporation into DNA is now considered to be

865C
HA
PTE
R62
ANTICANCER DRUGS
more important for the expression of its cyto-toxicity. DNA repair is also affected. Cytarabineis cell cycle specific and acts primarily during‘S’ phase. Cytarabine is useful only in leukaemiasand lymphomas, and is not effective in solidtumours. Primary use is induction of remissionin acute myelogenous as well as lymphoblasticleukaemia in children and in adults. It is alsoused for blast crisis in chronic myelogenousleukaemia and non-Hodgkin’s lymphoma. Becausecytarabine is rapidly deaminated and cleared fromplasma, it is administered either by rapid i.v.injection (100 mg/m2) once or twice daily for5–10 days, or by continuous i.v. infusion over5–7 days. A high dose regimen of 1–3 g/day hasalso been used.CYTABIN, CYTOSAR, BIOBIN, REMCYTA 100, 500, 1000mg inj.Major toxic effects are due to bone marrowsuppression—leukopenia, thrombocytopenia,anaemia and mucositis, diarrhoea.
MICROTUBULE DAMAGING AGENTS
Vinca alkaloids
These are mitotic inhibitors, bind to microtubularprotein—‘tubulin’, prevent its polymerization andassembly of microtubules, cause disruption ofmitotic spindle and interfere with cytoskeletalfunction. The chromosomes fail to move apartduring mitosis: metaphase arrest occurs. They arecell cycle specific and act in the mitotic phase.Vincristine and vinblastine, though closely relatedchemically, have different spectrum of antitumouractivity and toxicity.
Vincristine (oncovin) It is a rapidly actingdrug, very useful for inducing remission in child-hood acute lymphoblastic leukaemia, but is notgood for maintenance therapy. Other indicationsare acute myeloid leukaemia, Hodgkin’s disease,Wilms’ tumour, Ewing’s sarcoma, neuroblastomaand carcinoma lung. Prominent adverse effectsare peripheral neuropathy and alopecia. It alsocauses ataxia, nerve palsies, autonomic dysfunction(postural hypotension, paralytic ileus, urinaryretention) and seizures. Bone marrow depression
is minimal, but syndrome of inappropriate secretionof ADH (SIADH) can occur.Dose: 1.5–2 mg/m2 BSA i.v. weekly.ONCOCRISTIN, CYTOCRISTIN 1 mg/vial inj.
Vinblastine It is primarily employed along withother drugs in Hodgkin’s disease, Kaposi sarcoma,neuroblastoma, non-Hodgkin’s lymphoma, breastand testicular carcinoma. Bone marrow depressionis more prominent, while neurotoxicity andalopecia are less marked than with vincristine.SIADH has been noted. It can cause local tissuenecrosis if extravasation occurs during i.v. infusion.Dose: 0.1–0.15 mg/kg i.v. weekly × 3 doses.UNIBLASTIN, CYTOBLASTIN 10 mg/vial inj.
Vinorelbine This is a newer semisyntheticvinblastine analogue with similar mechanism ofaction inhibiting microtubule assembly andcausing metaphase arrest. As a single agent orcombined with others, its primary indication isnon-small cell lung cancer. As a second line drug,it is useful in advanced breast and ovariancarcinoma. Neutropenia is the dose limitingtoxicity. Thrombocytopenia and neurotoxicity areless marked.Dose: 25–30 mg/m2 weekly by slow i.v. injection over 10 min.VINOTEC, RELBOVIN 10 mg, 50 mg vial.
Taxanes
Paclitaxel It is a complex diterpin taxaneobtained from bark of the Western yew tree,which exerts cytotoxic action by a novelmechanism. It binds to β-tubulin and enhancesits polymerization: a mechanism opposite to thatof vinca alkaloids. The microtubules are stabilizedand their depolymerization is prevented. Thisstability results in inhibition of normal dynamicreorganization of the microtubule network thatis essential for interphase and mitotic functions.Abnormal arrays or ‘bundles’ of microtubules areproduced throughout the cell cycle. Cytotoxicaction of paclitaxel emphasizes the importanceof tubulin-microtubule dynamic equilibrium.
The approved indications of paclitaxel aremetastatic ovarian and breast carcinoma afterfailure of first line chemotherapy and relapsecases. It has also shown efficacy in advanced

866S
EC
TIO
N13
CHEMOTHERAPY OF NEOPLASTIC DISEASES
cases of head and neck cancer, small cell lungcancer, esophageal adenocarcinoma, urinary andhormone refractory prostate cancer. AIDS relatedKaposi’s sarcoma also responds.Dose: 135–175 mg/m2 by i.v. infusion over 3 hr, repeated every3 weeks.ALTAXEL, MITOTAX, ONCOTAXEL 30 mg, 100 mg, 260mg as 6 mg/ml in cremophor (polyoxyethylated castor oil +alcohol + water) emulsion.Acute anaphylactoid reactions occur because of the cremophorsolvent. Pretreatment with dexamethasone, H1 and H2antihistaminics is routinely used to suppress the reaction.The major toxicity is reversible myelosuppres-sion (mainly granulocytopenia) and ‘stocking andglove’ neuropathy. Nausea, chest pain, arthralgia,myalgia, mucositis and edema can be troublesome.
Docetaxel More potent congener of paclitaxelwith the same mechanism of action. It has beenfound effective in breast and ovarian cancerrefractory to first line drugs. Small cell cancerlung, pancreatic, gastric and head/neck carcinomasare the other indications. Major toxicity isneutropenia (more than paclitaxel), but neuropathyis less frequent. Arrhythmias, fall in BP and fluidretention occur with repeated courses.Dose: 75–100 mg/m2 i.v. over 1 hr; repeat at 3 weeks.DOCECAD, DOCETERE, DOXEL 20 mg, 80 mg, 120 mg/vial inj.Docetaxel is formulated in polysorbate mediumwhich produces less acute hypersensitivityreactions.
Estramustine It is a complex of estradiol witha nitrogen mustard normustine, which has weakestrogenic but no alkylating property. However,it binds to β-tubulin and interferes with itsorganization into microtubules exerting antimitoticaction. Estramustine gets concentrated in prostateand the only indication is advanced or metastaticprostate cancer that is nonresponsive to hormonetherapy. It is orally active, undergoes first passmetabolism in liver into active as well as inactivemetabolites, which are mainly eliminated in faeces.A small amount is hydrolysed into estradiol andnormustine producing myelosuppression andestrogenic adverse effects, viz. gynaecomastia,impotence, fluid retention, increased risk of
thromboembolism and impaired glucose tolerance.Angioedema and other hypersensitivity reactionsalso occur.Dose: 4–5 mg/kg orally 3 times daily.ESMUST, ESTRAM 140 mg cap.
TOPOISOMERASE-2 INHIBITOR
Etoposide It is a semisynthetic derivative ofpodophyllotoxin, a plant glycoside. It is not amitotic inhibitor, but arrests cells in the G2 phaseand causes DNA breaks by affecting DNAtopoisomerase-2 function. While the cleaving ofdouble stranded DNA is not interfered, thesubsequent resealing of the strand is prevented.Etoposide is used in testicular tumours, lungcancer, Hodgkin’s and other lymphomas, carci-noma bladder and stomach. Alopecia, leucopeniaand g.i.t. disturbances are the main toxicity. Oralbioavailability is 50%; oral dose is double thani.v. dose.Dose: 50–100 mg/m2/day i.v. for 5 days, 100–200 mg/day oral.PELTASOL 100 mg in 5 ml inj., LASTET 25, 50, 100 mg cap,100 mg/5 ml inj, ACTITOP 50, 100 mg cap, 100 mg/5 ml inj.
TOPOISOMERASE-1 INHIBITORS
Camptothecin analoguesTopotecan, Irinotecan are two semisyntheticanalogues of camptothecin, an antitumourprinciple obtained from a Chinese tree. They actin a manner similar to etoposide, but interact witha different enzyme (DNA topoisomerase-1). Theirbinding to this nuclear enzyme allows single strandbreaks in DNA, but not its resealing after thestrand has untwisted. They damage DNA duringreplication; act in the S phase and arrest cell cycleat G2 phase.
Topotecan is used in metastatic carcinoma ofovary and small cell lung cancer after primarychemotherapy has failed. Combined with cisplatin,it has been used in cervical cancer. The majortoxicity is bone marrow depression, especiallyneutropenia. Other adverse effects are painabdomen, vomiting anorexia and diarrhoea.Dose: 1.5 mg/m2 i.v. over 30 min daily for 5 days every 3weeks, 4 or more cycles. TOPOTEC, CANTOP 2.5 mg inj.

867C
HA
PTE
R62
ANTICANCER DRUGS
Irinotecan It is a prodrug which is decarboxy-lated in liver to the active metabolite SN-38.Cholinergic effects are produced in some patientsbecause it inhibits AChE. These effects can besuppressed by prior atropinization. Irinotecan isprimarily indicated in metastatic/advancedcolorectal carcinoma; also in cancer lung/cervix/ovary and stomach. It has been combined with5-FU and leucovorin. Dose limiting toxicity isdiarrhoea. Neutropenia, thrombocytopenia,haemorrhage, bodyache and weakness are theother adverse effects.The active metabolite SN-38 is inactivated by glucuronidationin the liver. Individuals expressing the UGT1A1*28 allele ofglucuronyl transferase enzyme are more susceptible toirinotecan induced diarrhoea and neutropenia, because theyfail to inactivate SN-38.Dose: 125 mg/m2 i.v. over 90 min, weekly for 4 weeks.IRINOTEL, IRNOCAM 40 mg (2 ml), 100 mg (5 ml) inj.
ANTIBIOTICS
These are products obtained from microorganismsand have prominent antitumour activity. Practicallyall of them intercalate between DNA strands andinterfere with its template function.
Actinomycin D (Dactinomycin) It is a verypotent antineoplastic drug, highly efficacious inWilms’ tumour and childhood rhabdomyosarcoma.Good results have also been obtained in Mtxresistant choriocarcinoma, Ewing’s sarcoma andmetastatic testicular carcinoma. In addition toblocking RNA transcription (due to interferencewith template function of DNA) dactinomycincauses single strand breaks in DNA. Prominentadverse effects are vomiting, stomatitis, diarrhoea,erythema and desquamation of skin, alopecia andbone marrow depression.Dose: 15 µg/kg i.v. daily for 5 days.DACMOZEN 0.5 mg/vial inj.
Daunorubicin (Rubidomycin), DoxorubicinThese are anthracycline antibiotics having anti-tumour activity. However, utility of daunorubicinis limited to acute myeloid as well as lympho-blastic leukaemia (in which it is highly active),while doxorubicin, in addition, is effective in many
solid tumours, such as breast, thyroid, ovary,bladder and lung cancers, sarcomas andneuroblastoma. They intercalate between DNAstrands and block DNA as well as RNA synthesis.They are also capable of causing breaks in DNAstrands by activating topoisomerase-2 andgenerating quinone type free radicals. As such,they have mutagenic and carcinogenic potential.Maximum action is exerted at S phase, but toxicityis usually exhibited in G2 phase.
Both these antibiotics produce cardiotoxicityas a unique adverse effect. This can manifesteither acutely within 2–3 days, causing ECGchanges, arrhythmias and hypotension, all of whichare reversible; or be delayed—congestive heartfailure (related to the total dose administered).CHF is due to cardiomyopathy and may be fatal.Marrow depression, alopecia, stomatitis, vomitingand local tissue damage (on extravasation) areother adverse effects. Urine may be coloured red.Daunorubicin: 30–50 mg/m2 BSA i.v. daily for 3 days, repeatevery 3–4 weeks.DAUNOCIN, DAUNOMYCIN 20 mg/vial inj.Doxorubicin: 60–75 mg/m2 BSA slow i.v. injection every 3weeks; ADRIAMYCIN, DOXORUBICIN, ONCODRIA 10mg, 50 mg per vial inj.
Epirubicin This is a recently introducedanthracycline with mechanism of action andproperties similar to doxorubicin. Epirubicin hasbeen primarily used as a component of regimenfor adjuvant therapy of breast carcinoma. Otherindications are gastroesophageal, pancreatic,hepatic and bladder carcinoma. Alopecia,hyperpigmentation of skin and oral mucosa,painful oral ulcers, fever and g.i. symptoms arethe common adverse effects. Urine may turn red.Cardiotoxicity is dose related.Dose: 60–90 mg/m2 i.v. over 5 min, repeated at 3 weeks, totaldose < 900 mg/m2 to avoid cardiotoxicity.ALRUBICIN, EPIRUBITEC 10, 50 mg vials, for reconstitutionas 2 mg/ml soln. with diluent.
Mitoxantrone It is an anthracycline derivativerelated to doxorubicin with lower cardiotoxicity,probably because it does not produce quinone typefree radicals. However, it does bind to DNAcausing strand breaks and inhibiting DNA as well

868S
EC
TIO
N13
CHEMOTHERAPY OF NEOPLASTIC DISEASES
as RNA synthesis. Clinical utility is relativelynarrow, restricted mostly to acute myeloidleukaemia, advanced hormone refractory prostatecancer and occasionally in breast and hepaticcarcinoma, non-Hodgkin lymphoma. It has beenfound useful in late stage multiple sclerosis as well.Though cardiomyopathy can occur, major toxicityis marrow depression and mucosal inflammation.Discolouration of nails and eye may occur.ONCOTRON 20 mg/10 ml inj; 14 mg/m2 single i.v. dose,repeat at 3 weeks. For induction in acute leukaemia 12 mg/m2/day for 5 days.
Bleomycin This is a mixture of closely relatedglycopeptide antibiotics having potent antitumouractivity. It chelates copper or iron, producessuperoxide ions and intercalates between DNAstrands—causes chain scission and inhibits repair.It is highly effective in testicular tumour andsquamous cell carcinoma of skin, oral cavity, headand neck, genitourinary tract and esophagus; alsouseful in Hodgkin’s lymphoma. Rate of fluidcollection in malignant pleural or peritonealeffusion can be reduced by intrapleural/intra-peritoneal injection of bleomycin.
Mucocutaneous toxicity and pulmonaryfibrosis, but minimal myelosuppression are thespecial features. Allergic and hypotensive reactioncan occur after bleomycin injection. It can beinjected i.m. as well.Dose: 30 mg twice weekly i.v. or i.m. (total dose 300–400mg); BLEOCIN, ONCOBLEO 15 mg inj.
Mitomycin C This highly toxic drug is usedonly in resistant cancers of stomach, cervix, colon,rectum, breast, etc. It is usually combined with5-FU and radiation. Superficial bladder tumoursare treated by intravesical instillation of mitomycinC. It is transformed intracellularly to a form whichacts as an alkylating agent and crosslinks DNA.It also generates free radicals which damage DNA.Bone marrow and g.i.t. are the primary targetsof toxicity. Myelosuppression is typically delayed.Injections are repeated only after 6 weeks or more.A haemolytic-uremic syndrome is reported.Dose: 10 mg/m2 BSA, infused i.v. in one day or divided in 5and infused over 5 days. MITOCIN, ALMITO, LYOMIT 2, 10mg inj.
MISCELLANEOUS CYTOTOXIC DRUGS
These drugs (except L-asparaginase) have beendeveloped by random synthesis and testing forantitumour activity.
Hydroxyurea It blocks the conversion ofribonucleotides to deoxyribonucleotides by inhi-biting the enzyme ribonucleoside diphosphatereductase—thus interferes with DNA synthesis;exerts S-phase specific action. Its primarytherapeutic value is in chronic myeloid leukaemia,psoriasis, polycythaemia vera and occasionally insome solid tumours. It is also employed as aradiosensitizer before radiotherapy, and is afirst-line drug for sickle cell disease in adults.Hydroxyurea is well absorbed orally and iseliminated in urine with a plasma t½ of ~ 4 hours.Myelosuppression is the major toxicity.Gastrointestinal disturbances and cutaneousreactions including pigmentation also occur.Dose: 20–30 mg/kg daily or 80 mg/kg twice weekly;CYTODROX, HONDREA, UNIDREA 500 mg cap.
L-Asparaginase (L-ASPase) This enzyme wasintroduced on the basis of a difference observedbetween normal cells and those from childhoodlymphoblastic leukaemia, viz. the leukaemia cellswere found to be deficient in L-asparaginesynthase enzyme and depended on the supply ofL-asparagine from the medium. The enzymeL-ASPase (from E. coli.) degrades L-asparagineto L-aspartic acid, depriving the leukaemic cellsof an essential metabolite, and causes cell death.L-asparaginase is a component of regimen forinducing remission in acute lymphoblastic leukae-mia along with Mtx., prednisolone, vincristine,etc. However, resistance develops to L-ASPasemostly by induction of L-asparagine synthase inthe leukaemic cells. Moreover, L-ASPase isantigenic, produces neutralizing antibodies whichinactivate and clear the enzyme rapidly, so thatclinical response is lost. A polyethylene glycolconjugated L-ASPase (Peg-asparaginase) has beenproduced which has very slow clearance fromthe body, is injected every 2 weeks and is moreeffective. It is also less antigenic.

869C
HA
PTE
R62
ANTICANCER DRUGS
Many of the typical adverse effects of anti-cancer drugs are not seen with L-ASPase (noleukopenia, alopecia, or mucosal damage), butit produces effects due to defective proteinsynthesis—hyperglycaemia, raised triglyceridelevels, pancreatitis, liver damage, clotting defectsand CNS symptoms. A significant number ofrecipients develop allergic reactions (urticaria,chills, fever, rash), including anaphylaxis; deathsare reported.Dose: 50–200 KU/kg i.v., also i.m. daily or twice weekly for3–4 weeks.LEUNASE, HOILASP 10,000 KU per vial inj.
Tretinoin It is all trans-retinoic acid, a form of vit A acid(see Ch. 64) which acts as a differentiating agent and hasrecently emerged as a highly effective treatment (usually incombination with a daunorubicin or doxorubicin) for acutepromyelocytic leukaemia (APL). This subtype of acutemyelocytic leukaemia (AML) is associated with productionof a fusion gene PML-RARα due to a specific chromosomaltranslocation. The normal retinoic acid receptor RARα-RXRdimerization needed for cell differentiation is prevented andAPL is produced. Tretinoin given in relatively higher dosesbinds tightly to RARα-RXR diamer and prevents formationof PML-RARα dimerization. It also promotes degradation ofalready formed PML-RARα fusion gene. As a result, blockadeof myeloid precursor cell differentiation into cells of differentlineages is overcome and prolonged remission is induced inAPL. Though, tretinoin alone can induce temporary remissionin APL, induction therapy with tretinoin + an anthracyclineproduces complete remission in upto 95% patients of APL.Tretinoin has also been shown to promote stem cell renewalin bone marrow. A course of 45 mg/m2/day tretinoin is adminis-tered till one month after remission occurs (or max. 90 days).
Adverse effects of tretinoin are dryness of skin, eye, nose,mouth, pruritus, epistaxis, rise in serum lipids, hepatic trans-aminases and intracranial pressure. The most serious adverseeffect is ‘retinoic acid syndrome’ comprising of breathlessness,fever, pleural/pericardial effusion and pulmonary infiltrates.Pretreatment with dexamethasone largely prevents occurrenceof this syndrome.
Arsenic trioxide Arsenic has been a traditional poisonfor ages. Ehrlich produced organic arsenicals for cure ofsyphilis, and some organic arsenicals were used in amoebiasistill 1960s. Recently, therapeutic value of small doses of arsenictrioxide in APL has been recognized. It probably acts byenhancing reactive oxygen free radical generation in APLcells. It is primarily used in resistant/relapsed cases of APLafter tretinoin treatment. Lately, arsenic trioxide is also beingincluded in the 1st line therapy of APL along with tretinoin+ an anthracycline, particularly in high risk cases and inthose who have initial WBC count of > 10,000/μL. Withsuch triple therapy ~ 90% APL patients have remained inlong-term remission.
Though, arsenic trioxide is absorbed orally, it isadministered as 0.15 mg/kg daily i.v. infusion till remissionis induced or maximum 2 months. Further treatment maybe given after a gap. Adverse effects of arsenic are nausea,dizziness, malaise, fatigue, sensory disturbances, effusions,breathlessness, hyperglycaemia, Q-T prolongation, A-V block.Corticosteroid treatment provides considerable relief of theseadverse effects.
TARGETED DRUGS
In the recent years fundamental studies of cancerbiology and molecular mechanisms of carcinoge-nesis have identified several targets which canbe attacked to selectively kill/inhibit cancer cells.Designing and development of drugs to attackthese targets is an active area of current research.Several new drugs have been introduced whilea large number are in the pipe line. These drugsare primarily of two types:• Specific monoclonal antibodies that need to
be given parenterally, and attack cell surfacetargets or tumour antigens.
• Synthetic compounds, given orally, whichpenetrate cells and affect cancer-specificenzymes or processes.Only a sample of these drugs, especially those
available in India, are presented here.
1. Tyrosine-protein kinase inhibitorsImatinib It is the first selectively targeted drugto be introduced for treatment of a malignancy.It inhibits a specific tyrosine protein kinase labelled‘Bcr-Abl’ tyrosine kinase expressed by chronicmyeloid leukaemia (CML) cells and relatedreceptor tyrosine kinases including platelet derivedgrowth factor (PDGF) receptor that is constitutivelyactive in dermatofibrosarcoma protuberans, stemcell receptor and c-kit receptor active in gastro-intestinal stromal tumour (GIST) which is a raretumour. Imatinib is found to be strickinglysuccessful in chronic phase of CML (remissionin >90% cases) and in metastatic c-kit-positiveGIST, in which it is the drug of choice. A relativelyhigher dose may elicit response in accelerated phaseof CML as well. It is also indicated in dermato-fibrosarcoma protuberans. Resistance to imatinibdevelops by point mutations in Bcr-Abl tyrosinekinase affecting its affinity for imatinib.

870S
EC
TIO
N13
CHEMOTHERAPY OF NEOPLASTIC DISEASES
Imatinib is well absorbed orally, metabolizedin liver, one active metabolite is also produced.The major degrading enzyme is CYP3A4, andpotential interactions can occur with inducers andinhibitors of this isoenzyme. All metabolites areexcreted in faeces through bile. The t½ of imatinibis 18 hours while that of its active metaboliteis double. Adverse effects are abdominal pain,vomiting, fluid retention, periorbital edema,pleural effusion, myalgia, liver damage and CHF.Dose: 400 mg/day with meals; accelerated phase of CML600–800 mg/day.SHANTINIB, GLEE-VEC, IMATIB α 100 mg cap; UNITINIB100, 400 mg cap.
Nilotinib It is a second generation Bcr-Abl, PDGF-receptor βand c-kit receptor tyrosine kinase inhibitor with 20–50 foldhigher affinity for these kinases than imatinib. Thus, it canovercome resistance to imatinib due to Bcr-Abl mutationand is effective in chronic CML nonresponsive to imatinib.It is only 30% bioavailable orally, but absorption is improvedby food. It is also useful in accelerated phase of CML. Thus,it is an alternative drug in imatinib nontolerant or resistantcases of CML, and has now been used as a first line drugas well. Adverse effects are similar to imatinib; Q-Tprolongation has also been noted.
2. EGF receptor inhibitorsGefitinib Epidermal growth factor (EGF)receptor is a transmembrane receptor-tyrosine-kinase which regulates growth and differentiationof epitheilal cells. Binding of ligand (EGF) tothe extracellular domain of the receptor inducesdimerization leading to activation of tyrosinekinase activity of the intracellular domain (seeFig. 4.8) → autophosphorylation of the kinaseand phosphorylation of several cytoplasmic regu-latory proteins which modify gene transcriptionto regulate growth. Certain epithelial cancers overexpress EGF receptor or have an active EGFRmutation, and their growth is critically dependentupon activation of this receptor.
Gefitinib is a synthetic compound that pene-trates cells, binds to the tyrosine kinase domainof the EGF receptor (also Erbβ1, or HER1) andprevents phosphorylation of regulatory proteins.Gefitinib has been found effective in selectedpatients of non-small cell lung cancer which hasEGFR activating mutation. Lung cancers in non-
smokers and in women are generally of this mutanttype. In such cases, it has been found to be moreeffective than cytotoxic drugs. However, responsein non-mutant type of lung cancer is disappointing.Gefitinib monotherapy has been used for locallyadvanced or metastatic lung cancers after cisplatinand docetaxal have failed.
Oral bioavailability of gefitinib is 60%. It isprimarily metabolized by CYP3A4 with t½ of~ 40 hours. Drug interactions with inducers/inhibitors of CYP3A4 are likely.Dose: 250 mg/day orally;GEFONIB, GEFTINAT 250 mg tab/cap.The most common adverse effect is skin rashand diarrhoea. Others are nausea, anorexia, itchingand rise in serum transaminase. Interstitial lungdisease is an infrequent, but serious complication.
Erlotinib It is similar to gefitinib in action,pharmacokinetics, adverse effects and efficacy ina subtype of non-small cell lung cancer. It hasbeen combined with gemcitabine for advanced/metastatic pancreatic cancer as well. Few casesof serious hepatic dysfunction have occured inpatients with preexisting liver disease.Dose: 100–150 mg OD to be taken 1 hour before or 2 hoursafter meal.ERLOTEC 100, 150 mg tabs.
Cetuximab This inhibitor of EGF receptor is a chimericmonoclonal antibody directed to the extracellular domain ofthe EGF receptor. Binding to the receptor, it preventstransmembrane signalling resulting in blockade of cell growth,proliferation and metastasis. Survival of tumour cells isjeopardised. Infused i.v. in a loading dose followed by weeklyor fortnightly maintenance doses, cetuximab is approved foradvanced/metastatic squamous carcinoma of head and neckin combination with radiation and/or cisplatin basedchemothrapy. EGF receptor positive metastatic colorectalcancer is another indication, either in combination withirinotecan + cisplatin or as monotherapy in resistant cases.Adverse effects are acneform skin rash, itching, headache anddiarrhoea. Anaphylactoid reactions may occur during infusion.Hypomagnesemia and interstitial lung disease are infrequent.
3. Angiogenesis inhibitorsAngiogenesis (proliferation of new blood vessels)is essential for growth and metastasis ofcancers. The vascular endothelial growth factor(VEGF) is the most important stimulus for

871C
HA
PTE
R62
ANTICANCER DRUGS
neovascularization and increase in microvesseldensity within solid tumours. VEGF interacts withcell surface VEGF receptor, that is another recep-tor tyrosine kinase, which promotes angiogenesisby phosphorylating intracellular regulatoryproteins. Several cancers over express VEGFreceptor and inhibitors of this receptor have beendeveloped as antitumour drugs.
Bevacizumab It is a humanized monoclonal antibody thatbinds VEGF-A and hinders its access to the VEGF receptor,interrupting angiogenic signalling. Combined with 5-FU,bevacizumab is used in metastatic colorectal cancer. Addedto conventional chemotherapy, it improves survival inmetastatic non-small cell lung cancer, breast cancer, clearcell renal carcinoma and glioblastoma. Deafness due toneurofibromatosis can be reversed by growth inhibitory effectof bevacizumab.
Being an antibody, bevacizumab is administered by i.v.infusion every 2–3 weeks. Adverse effects are—rise in BP,arterial thromboembolism leading to heart attack and stroke,vessel injury and haemorrhages, heart failure, proteinurea,gastrointestinal perforations, and healing defects.
Sunitinib This is a small molecular synthetic VEGFreceptor-2 inhibitor, which enters cells and competitivelyblocks ATP binding to the tyrosine kinase domain, therebypreventing phosphorylation of angiogenic regulatory proteins.Sunitinib inhibits multiple receptor tyrosine kinases likeplatelet derived growth factor (PDGF) receptor α and β,c-KIT, RET, etc.). It is used in metastatic renal cell carcinomaand resistant g.i. stromal tumour (GIST). Sunitinib isadministered orally daily in 4 week cycles. Adverse effectsare hypertension, rashes, diarrhoea, weakness, bleeding,proteinurea, hypothyroidism, neutropenia, rarely CHF.
4. Proteasome inhibitorProteasomes are packaged complexes of proteo-lytic enzymes which degrade several intracellularsignalling proteins that control cell cycle,apoptosis and survival response.
Bortezomib It is a unique boron containingcompound that covalently binds to proteasomeand inhibits its proteolytic activity disrupting manyintracellular signalling pathways. The mostimportant of these is nuclear factor-κB (NF-κB)mediated signalling. NF-κB is a transcriptionfactor that normally resides in the cytoplasm boundto an inhibitory protein IκB. Hypoxia, cytotoxicdrugs, DNA breaks and other stressful stimuliactivate proteasome which cleaves and degrades
IκB to release NF-κB which then translocatesto the nucleus and transcripts certain genes toproduce molecules that oppose apoptosis andpromote cell proliferation. Some neoplasmsoverexpress NFκΒ which plays an important rolein their survival. By inhibiting proteasome,bortezomib prevents the breakup and degradationof IκB, so that NFκB is not released to transcriptsurvival molecules. It also causes build up of‘Bax’, an apoptosis promoting protein, and affectsother regulators of cell cycle.
The prime indication of bortezomib is multiplemyeloma, both for first line combined therapy(along with cytotoxic drugs), as well as forrelapsed disease. It is also used for refractorymantle cell lymphoma. The most prominentadverse effect is peripheral neuropathy. Othersare diarrhoea, fatigue, bone marrow depression,especially thrombocytopenia.Dose: 1.3 mg/m2 i.v. bolus injection, 4 doses at 3 day intervalsin cycles of 3 weeks.EGYBORT 3.5 mg vial for inj.
5. Unarmed monoclonal antibodiesMonoclonal antibodies (MAbs) are sourced fromhybridomas created by fusing a continuouslyproliferating cell line from mouse myeloma withantibody producing B lymphocytes sensitized toproduce antibody against a particular antigen. Thishybridoma is then cloned so that the single speciesantibody is obtained in large quantity. Separatehybridomas are created for each antibody.Chimerized MAbs are produced by substitutingmajor portion with human IgG molecule for themouse antibody. These MAbs are part human-part mouse. Totally human MAbs are calledhumanized MAbs. Chimerization and humani-zation of MAbs prolongs their sojourn in the bodyand reduces/eliminates their antigenicity.
Malignant cells express certain uniqueantigens on their surface to which MAbs couldbe directed. These unmodified (also calledunarmed or naked) MAbs kill the target cells byseveral mechanisms including direct signalling ofapoptosis, or antibody-dependent cellularcytotoxicity (ADCC), or complement-dependent

872S
EC
TIO
N13
CHEMOTHERAPY OF NEOPLASTIC DISEASES
cytotoxicity (CDC). They could also be used asmissiles to carry biological bombs (toxins) andare called immunotoxins, or a radioactive isotopeas radiopharmaceuticals. These are called ‘armed’MAbs.
Rituximab It is a chimerized MAb that binds to the CD20B-cell antigen expressed on the surface of B-lymphocytesand B-cell lymphomas. Rituximab binding to the antigenpromotes apoptosis through transmembrane signalling as wellas by ADCC and CDC mechanisms. It is indicated inB-cell lymphoma, non-Hodgkin lymphoma and chroniclymphocytic leukaemia, both as single agent as well as incombination with cytotoxic chemotherapy. Survival benefitshave been obtained both when it is used as initial therapyas well as in relapsed cases. Rituximab is also being usedin some autoimmune diseases. It is administered as slowi.v. infusion weekly or at 3–4 week intervals. Maintenancedoses have been given 6 monthly. Adverse effects are infusionreactions consisting of chills, fever, urticarial rashes, pruritus,dyspnoea and hypotension. Severity of the reaction varies,and is also related to rate of infusion. Pretreatment withantihistaminics dampens the reaction. Late onset neutropeniaand depletion of B-lympocytes are the other problems.
Other unarmed antitumour MAbs are:Trastuzumab, Bevacizumab, Alemtuzumab, Cetuximab
Toxin-linked MAbs are:Ozogamicin, Gemtuzumab
Radioisotope carrying MAbs are:Ibritumomab (90Y), Tositumomab (131I)
HORMONAL DRUGS
They are not cytotoxic, but modify the growthof hormone-dependent tumours. All hormones areonly palliative.
Glucocorticoids They have marked lympho-lytic action—are primarily used in acute child-hood leukaemia and lymphomas. They induceremission rapidly but relapses inevitably occurafter variable intervals and gradually the respon-siveness is lost. Considerable palliative effectsare obtained in Hodgkin’s disease. Glucocorticoidshave a secondary role in some hormone responsivebreast cancers.
Corticosteroids are also valuable for thecontrol of malignany/chemotherapy associatedcomplications like hypercalcaemia, haemolysis,bleeding due to thrombocytopenia, retinoic acidsyndrome, increased intracranial tension and
mediastinal edema due to radiotherapy. Moreover,they afford symptomatic relief by antipyretic andmood elevating action and potentiate the anti-emetic action of ondansetron/metoclopramide.Prednisolone/dexamethasone are most commonlyused; doses are high—hypercorticism may occur(see Ch. 20).
Estrogens They produce symptomatic reliefin carcinoma prostate (see p. 312), which is anandrogen-dependent tumour. However, relapsesoccur, but life is prolonged. Estrogens have beensuperseded in carcinoma prostate by GnRHagonists used with an antiandrogen.
Fosfestrol It is the phosphate derivative of stilbestrol;has been specifically used in carcinoma prostate.Dose: 600–1200 mg i.v. initially, maintenance 120–240 mgorally.HONVAN 120 mg tab, 300 mg/5 ml inj.
Selective estrogen receptor modulators(tamoxifen)Selective estrogen receptor down regulators(fulvestrant)Aromatase inhibitors (letrozole, etc).
The above three classes of drugs are the sheetanchor of adjuvant and palliative therapy ofcarcinoma breast, as well as for primary and secon-dary prevention of breast cancer (see Ch. 22).
Antiandrogen Flutamide and bicalutamide(see p. 302) antagonise androgen action on prostatecarcinoma and have palliative effect in advanced/metastatic cases. Because they increase androgenlevels by antiandrogenic action in pituitary,combination with orchiectomy or GnRH analoguesis required to produce full therapeutic effect.
5-ααααα reductase inhibitor Finasteride anddutasteride (see p. 303) inhibit conversion oftestosterone to dihydrotestosterone in prostate (andother tissues), have palliative effect in advancedcarcinoma prostate; occasionally used.
GnRH agonists (see p. 242) They indirectlyinhibit estrogen/androgen secretion by suppres-sing FSH and LH release from pituitary and havepalliative effect in advanced estrogen/androgen

873C
HA
PTE
R62
ANTICANCER DRUGS
dependent carcinoma breast/prostate. They aregenerally used in combination with antiandrogensor SERMs.
Progestins (see p. 319) They bring abouttemporary remission in some cases of advanced,recurrent (after surgery/radiotherapy) andmetastatic endometrial carcinoma. High doses areneeded. They have also been used in palliativetreatment of metastatic carcinoma breast that hasbecome unresponsive to tamoxifen.
GENERAL PRINCIPLES INCHEMOTHERAPY OF CANCER
1. In cancer chemotherapy, analogy is drawn withbacterial chemotherapy; the malignant cell beingviewed as an invader. However, there are twomain differences—
(a) Bacterial metabolism differs markedly fromthat of the host, while malignant cells are infact host cells with deranged regulation ofgrowth and differentiation and relativelyminor other differences. Therefore, selecti-vity of drugs is limited. A number ofmeasures which enhance selectivity of drugsfor the tumour need to be utilized. However,lately some unique tumour antigens andoncogenes (like the CML-tyrosine proteinkinase gene) have been identified, whichprovide specific targets for drug therapy.
(b) Infecting microorganisms are amenable toimmunological and other host defencemechanisms. This is absent or minimalagainst cancer cells.
Human interferon α-2 (see p. 804) and other cytokines(interleukin-2, tumour necrosis factor, etc.) that can modifythe biological responses to tumour cells are being used asadjuvants in treating neoplasms. They appear to have somedirect inhibitory effect on malignant cells, in addition toreinforcing immunological defence against these.
2. A single clonogenic malignant cell is capableof producing progeny that can kill the host. Toeffect cure, all malignant cells must be killed orremoved. Survival time is related to the numberof cells that escape chemotherapeutic attack.3. In any cancer, subpopulations of cells differin their rate of proliferation and susceptibility to
cytotoxic drugs. These drugs kill cancer cells byfirst order kinetics, i.e. a certain fraction of cellspresent are killed by one treatment.4. Drug regimens or number of cycles ofcombined chemotherapy which can effectivelypalliate large tumour burdens may be curativewhen applied to minute residual tumour cell popu-lation after surgery and/or irradiation. This is thebasis of the combined modality approach (seeFig. 62.1).5. Whenever possible, complete remissionshould be the goal of cancer chemotherapy: drugsare often used in maximum tolerated doses.Intensive regimens used at an early stage in thedisease yield better results.6. Formerly cancers were treated with one drugat a time. Now a combination of 2–5 drugs isgiven in intermittent pulses to achieve total tumourcell kill, giving time in between for normal cellsto recover (Fig. 62.1). However, few tumours arestill treated with a single drug.
Synergistic combinations and rationalsequences are devised by utilizing:
(a) Drugs which are effective when used alone.(b) Drugs with different mechanisms of action.(c) Drugs with differing toxicities.(d) Empirically by trial and error; optimal
schedules are mostly developed by thisprocedure.
(e) Drugs with different mechanisms of resis-tance.
(f) Drugs with known synergistic biochemicalinteractions.
(g) Kinetic scheduling: On the basis of cell cyclespecificity/nonspecificity of the drugs and thephase of cell cycle (see box, p. 875) at whichthe drug exerts its toxicity.
Cytotoxic drugs are either cell cycle nonspecific(CCNS) or cell cycle specific (CCS).
(a) Cell cycle nonspecific Kill resting as wellas dividing cells, e.g. mustine, cyclophosphamide,chlorambucil, carmustine, dacarbazine, busulfan,L-asparaginase, cisplatin, procarbazine, actino-mycin D.

874S
EC
TIO
N13
CHEMOTHERAPY OF NEOPLASTIC DISEASES
Fig. 62.1: Illustration of cancer cell dynamics with three chemotherapeutic approaches. The shaded area depictssymptoms, before which the cancer remains subclinical. The broken purple line indicates no treatment.A. A rationally designed combination of 2–5 chemotherapeutic drugs (red bar) is given cyclically. Each cycle kills99% tumour cells, reducing the tumour cell mass by 2 log units each time. Some regrowth occurs during the restinterval, but the rate of cell kill is more than regrowth and resistance does not develop. If the cycles are continued wellbeyond all symptoms disappear, cure may be achieved. Radiation may be used to supplement chemotherapy.B. The cancer (in case of solid tumours) is resected surgically and the small number of residual cancer cells (at theprimary site or in metastasis) are killed by relatively few cycles of adjuvant combination chemotherapy (blue bar). Thismay be supplemented by radiation (in case of radiosensitive tumours).C. The chemotherapy is begun relatively late with a single but effective drug given continuously (green bar). Itcauses slower tumour cell kill, but symptom relief may occur. Resistance soon develops, and the tumour startsregrowing even with continued chemotherapy. Symptoms reappear and increase in severity. Ultimately failure oftherapy and death occur.
(b) Cell cycle specific Kill only actively dividingcells. Their toxicity is generally expressed in Sphase. However, these drugs may show consi-derable phase selectivity, e.g.—
G1: Vinblastine.S : Mtx, cytarabine, fludarabine, 6-TG,
6-MP, 5-FU, hydroxyurea, mitomycin C,doxorubicin, daunorubicin.
G2: Daunorubicin, bleomycin, etoposide,topotecan.
M: Vincristine, vinblastine, vinorelbine,paclitaxel, docetaxel.
It is logical to use cell cycle specific drugs inshort courses (pulses) of treatment. This allowsnoncycling cells (which are generally lesssusceptible to drugs) to re-enter the cycle betweendrug courses. The CCS drugs are generallyscheduled after a course of CCNS drug(s) toimprove the cell kill. The CCS drugs are moreeffective in haematological malignancies and

875C
HA
PTE
R62
ANTICANCER DRUGS
in solid tumours with a large growth fraction,while the CCNS drugs are effective in these aswell as in solid cancers with a small growthfraction.
Many regimens have been devised by takinginto consideration the above factors and byobserving patient response.
Cyclic treatment is given, and for optimumremission 6–11 cycles may be needed. It has beenfound that maintenance therapy thereafter doesnot produce additional benefit.
One combination that has produced almost100% response in Ewing’s sarcoma is illustratedin Fig. 62.2.
Similarly many other regimens have beendevised for different tumours.VAMP : Vincristine + Amethopterine (Mtx) + 6-MP
+ Prednisolone (used in acute leukaemia).COAP : Cyclophosphamide + Oncovin (Vincristine) +
Ara-C (Cytarabine) + Prednisolone.FOLFIRI : 5-FU + Leucovorin + Irinotecan
(for colon cancer)FOLFOX : 5-FU + Leucovorin + Oxaliplatin
(for colon cancer).ABVD : Adriamycin (Doxorubicin) + Bleomycin +
Vinblastine + Dacarbazine(for Hodgkin’s disease).
CHOP-R : Cyclophosphamide + Hydroxydaunorubicin(Doxorubicin) + Oncovin (Vincristine) +Prednisolone + Rituximab(for non-Hodgkin’s lymphoma)
BEP : Bleomycin + Etoposide + Platinum (Cisplatin)(for testicular cancer).
7. Tumours often become resistant to any drugthat is used repeatedly due to selection of lessresponsive cells. Such selection is favoured iflow dose of a single drug is used.
Several mechanisms of tumour resistance havebeen recognized. Mutations altering the targetbiomolecule confer specific (to single drug)resistance. An important mechanism of multidrugresistance is overexpression of MDR 1 gene whichincreases the concentration of P-glycoprotein (anefflux transporter) on the surface of cancer cells,resulting in pumping out of the chemotherapeuticagents, especially natural products like vincaalkaloids, anthracycline antibiotics, taxanes, etc.
Phases of cell cycle
Pre (nucleic acid) synthesisinterval.
Synthesis of DNA occurs.
Post synthetic interval.
Mitosis occurs—two G1 cells areproduced, which either directlyre-enter next cycle or pass intothe nonproliferative (G0) phase.
Nonproliferating cells; a fractionof these are clonogenic—mayremain quiescent for variableperiods, but can be recruited incell cycle if stimulated later.
Fig. 62.2: Combined modality treatment for Ewing’s sarcoma

876S
EC
TIO
N13
CHEMOTHERAPY OF NEOPLASTIC DISEASES
Toxicity ameliorationHigh doses and intensive regimens are beingemployed aiming at cure of the malignancy. Theassociated toxicity may be ameliorated to someextent by—1. Toxicity blocking drugs: Folinic acid rescuehas permitted administration of > 100 fold doseof Mtx (see p. 863). It is professed that normalcells are rescued more than the cancer cells—therapeutic index is increased.• Cystitis caused by cyclophosphamide and
ifosphamide can be blocked by systemicallyadministered mesna and by irrigating thebladder with acetylcysteine. Both these are –SH containing compounds that combine withand detoxify the toxic metabolites in thebladder. Generous fluid intake and frequentbladder voiding also helps.
• For controlling cytotoxic drug inducedvomiting, ondansetron, a 5-HT3 antagonist, hassurpassed the efficacy of metoclopramide,which nevertheless is still used (see Ch. 47).Addition of dexamethasone and/or lorazepamor aprepitant further enhances the protectionagainst vomiting.
• The anthracycline antibiotics (doxorubicin,etc.) produce cumulative total dose relatedcardiotoxicity (usually at doses >300 mg/m2).Dexrazoxane is an iron chelating agent whichinfused i.v. before doxorubicin has been foundto reduce risk of such toxicity. However, itmay also compromise the anticancer efficacyof doxorubicin Dexrazoxane can also be usedto ameliorate anthracycline infusion sitereaction due to extravasation.
2. Amifostine It is an organic thiophosphatewhich on activation by alkaline phosphatase actsas a cytoprotective against cancer chemotherapyand radiotherapy. It is particularly used forprophylaxis of cisplatin induced neuro/nephro-toxicity, and radiotherapy related xerostomia.Dose: 910 mg/m2 i.v. before cisplatin infusion
200 mg/i.v. before radiotherapyCYTOFOS, NAPROFOS 500 mg/vial inj.Short term side effects of amifostine itself arenausea, vomiting, hypotension and infusion relatedreaction. Delayed adverse effect is hypocalcaemia.
Vigorous hydration of the patient before,during and after cisplatin infusion also reducesnephrotoxicity.3. Hyperuricaemia occurring as a consequenceof rapid destruction of bulky tumour masses anddegradation of large amount of purines can bereduced by allopurinol, alkalinization of urineand plenty of fluids. Corticosteroids also reducehyperuricemia.4. Hypercalcaemia occurring as a complicationof certain malignancies like myeloma, cancerbreast/prostate, etc. may be aggravated bychemotherapy. It is treated by vigorous hydrationand i.v. bisphosphonates (see Ch. 24).5. Drugs given in pulses with 2–3 week intervalsfor normal cells to recover improve the efficacyof therapy: malignant cells recovering more slowly.6. Selective exposure of tumour to the drugby intraarterial infusion into a limb or head andneck; intrapleural/intraperitoneal injection—especially for rapidly accumulating pleuraleffusion or ascitis; topical application on thelesion—on skin, buccal mucosa, vagina, etc. mayreduce systemic toxicity.7. Platelet and/or granulocyte transfusion aftertreatment—to prevent bleeding or infection.8. Use of biological agents like recombinantGM-CSF/G-CSF hastens recovery from cytotoxicdrug induced myelosuppression.
Filgrastim (GRAFEEL, NEUPROGEN 300 μg/vial orprefilled syringe.It is a human recombinant granulocyte-colonystimulating factor. Started one day after myelo-suppressive chemotherapy and injected s.c. or i.v.(5 μg/kg) daily, till neutrophil count normalizes,may be used to shorten recovery time fromneutropenia.
Molgramostim (LEUCOMAX 150, 300, 400 µg/vialfor s.c./i.v. inj) is a colony stimulating factor. Injecteddaily beginning one day after last dose ofmyelosuppressant chemotherapy, it hastensrecovery of neutrophil count.
Interleukin-2 (Il-2) is a cytokine biologicalagent that itself has antitumour property byamplifying killer T-cell response.

877C
HA
PTE
R62
ANTICANCER DRUGS
9. Bone marrow transplantation after treatmentwith high doses of myelosuppressant drugs.10. Thalidomide (banned in 1960 for itsteratogenic effect, but reintroduced as immuno-modulator, and angiogenesis inhibitor antitumourdrug) has anxiolytic, antiemetic, adjuvant
analgesic/antipyretic properties and has beenfound to counteract cancer associated cachexiaand retard tumour growth by inhibiting angiogene-sis. It probably acts by suppressing TNFα and bymodulating IL-2. Thalidomide is also useful inerythema nodosum leprosum (ENL), (see p. 786).

Immunosuppressant DrugsChapterChapterChapterChapterChapter 6363636363
SECTION 14
MISCELLANEOUS DRUGS
Immunosuppressants are drugs which inhibitcellular/humoral or both types of immuneresponses, and have their major use in organtransplantation and autoimmune diseases. Theimportant drugs are:
1. Calcineurin inhibitors(Specific T-cell inhibitors)
Cyclosporine (Ciclosporin), Tacrolimus
2. m-TOR inhibitorsSirolimus, Everolimus
3. Antiproliferative drugs (Cytotoxic drugs)Azathioprine, Methotrexate,Cyclophosphamide, Chlorambucil,Mycophenolate mofetil (MMF)
4. GlucocorticoidsPrednisolone and others
5. Biological agents(a) TNFα inhibitors: Etanercept,
Infliximab, Adalimumab(b) IL-1 receptor antagonist: Anakinra(c) IL-2 receptor antagonists: Daclizumab,
(anti CD-25 antibodies) Basiliximab(d) Anti CD-3 antibody: Muromonab CD3(e) Polyclonal antibodies: Antithymocyte
antibody (ATG), Rho (D) immune globulin.
Several other immunosuppressants and immunomodulatorshave also been produced.The development of immune response and thesites of action of different immunosuppressantsis summarized in Figure 63.1.
CALCINEURIN INHIBITORS(Specific T-cell inhibitors)
Cyclosporine It is a cyclic polypeptide with11 amino acids, obtained from a fungus and intro-duced in 1977 as a highly selective immunosup-pressant which has markedly increased the successof organ transplantations. It profoundly andselectively inhibits T lymphocyte proliferation,IL-2 and other cytokine production as well asresponse of inducer T cells to IL-1, without anyeffect on suppressor T-cells. Lymphocytes arearrested in G0 or G1 phase.
The CD4 molecule associated with T cellreceptor on helper T cells anchors the majorhistocompatibility complex class II (MHC II)carrying the antigen peptide so that it is able toactivate the T cell receptor (Fig. 63.2). Stimulationof T cell receptor phosphorylates PLc, whichhydrolyses PIP2 to generate DAG and IP3. WhileDAG activates PKc to produce MAPkinasedependent and other actions, IP3 releasesintracellular Ca2+. After binding to calmodulin this

879C
HA
PTE
R63
IMMUNOSUPPRESSANT DRUGS
Fig. 63.1: Generation of humoral and cell-mediated immune response and sites of action of immunosuppressantdrugs
The antigen (Ag) is processed by macrophages or other antigen presenting cells (APC), coupled with class IImajor histocompatibility complex (MHC) and presented to the CD4 helper T-cell which are activated by interleukin-I(IL-1), proliferate and secrete cytokines—these in turn promote proliferation and differentiation of antigen activated Bcells into antibody (Ab) secreting plasma cells. Antibodies finally bind and inactivate the antigen.
In cell-mediated immunity—foreign antigen is processed and presented to CD4 helper T cell which elaborateIL-2 and other cytokines that in turn stimulate proliferation and maturation of precursor cytotoxic lymphocytes (CTL)that have been activated by antigen presented with class I MHC. The mature CTL (Killer cells) recognize cellscarrying the antigen and lyse them.1. Glucocorticoids inhibit MHC expression and IL-1, IL-2, IL-6 production so that helper T-cells are not
activated.2. Cytotoxic drugs block proliferation and differentiation of T and B cells.3. Cyclosporine, tacrolimus and sirolimus inhibit antigen stimulated activation and proliferation of helper T cells as
well as expression of IL-2 and other cytokines by them.4. Antibodies like muromonab CD3, antithymocyte globulin specifically bind to helper T cells, prevent their
response and deplete them.

880S
EC
TIO
N14
MISCELLANEOUS DRUGS
Fig. 63.2: Interaction between macrophage antigen presenting cell (APC) and helper T-cell in the immune responseand mechanism of action of cyclosporine, tacrolimus and sirolimus.
Cyclosporine binds to an intracellular protein ‘Cyclophilin’ and this complex inhibits Ca2+-Calmodulin (Ca2+-CAM)activated phosphatase ‘Calcineurin’. Tacrolimus also inhibits calcineurin, but after binding to a different protein FKBP(FK binding protein). Normally, after activation through T-cell receptor, calcineurin dephosphorylates a ‘nuclear factorof activated T-cells’ (NFAT) which translocates to the nucleus and triggers transcription of cytokine genes resulting inproduction of IL-2 and other cytokines. IL-2 diffuses out and acts on IL-2 receptor to stimulate T-cell proliferation andother processes, carrying forward the immune response.
Sirolimus also binds to FKBP, but this complex acts at a later stage. It binds to and inhibits a kinase termedm-TOR (mammalian target of rapamycin) which is a key factor for progression of cell proliferation.PLC—phospholipase C; PIP2—phosphatidyl inositol bisphosphate; DAG—diacyl glycerol; PKC—protein kinase C.
Ca2+ activates a membrane associated serine/threonine phosphatase called calcineurin whichdephosphorylates regulatory protein ‘nuclearfactor of activated T-cell’ (NFAT), permitting itsintranuclear migration and transcription ofcytokine genes leading to production of IL-2 alongwith other interleukins, GM-CSF, TNFα, inter-feron, etc. IL-2 is the major cytokine for T-cellmultiplication and differentiation. Cyclosporineenters target cells and binds to cyclophilin, animmunophilin class of protein. The complex thenbinds to and inactivates calcineurin → responseof the helper T cell to antigenic stimulation fails.Cyclosporine also enhances expression of
transforming growth factor β (TGFβ), an inhibitorof IL-2 which attenuates IL-2 stimulated T-cellproliferation and production of killer lymphocytes.Cyclosporine is most active when administeredbefore antigen exposure, but can, in addition,suppress the responses of primed helper T cells;hence useful in autoimmune diseases as well.
Cyclosporine selectively suppresses cell-mediated immunity (CMI), prevents graft rejectionand yet leaves the recipient with enough immuneactivity to combat bacterial infection. Unlikecytotoxic immunosuppressants, it is free of toxiceffects on bone marrow and RE system. Humoralimmunity remains intact. However, it is nephro-

881C
HA
PTE
R63
IMMUNOSUPPRESSANT DRUGS
toxic—the major limitation, and impairs liverfunction. Other adverse effects are sustainedrise in BP, precipitation of diabetes, anorexia,lethargy, hyperkalaemia, hyperuricaemia, oppor-tunistic infections, hirsutism, gum hyperplasia,tremor and seizures.
Cyclosporine is the most effective drug forprevention and treatment of graft rejection reaction.It is routinely used in renal, hepatic, cardiac, bonemarrow and other transplantations. For inductionit is started orally 12 hours before the transplantand continued for as long as needed. When graftrejection has started, it can be given i.v., becauseoral bioavailability is low, dependent on presenceof bile and is highly variable. Blood levelmonitoring is required for effective therapy. It isconcentrated in WBCs and RBCs, metabolizedin liver by CYP3A4 and excreted in bile. Theplasma t½ is biphasic 4–6 hr and 12–18 hr.Dose: 10–15 mg/kg/day with milk or fruit juice till 1–2 weeksafter transplantation, gradually reduced to maintenance doseof 2–6 mg/kg/day. Therapy may be started with 3–5 mg/kgi.v. infusion.IMUSPORIN 25, 50, 100 mg soft gelatin cap. Absorption fromthis preparation is slower and more variable. A newer micro-emulsion formulation SANDIMMUN NEORAL, PANIMUNBIORAL 25, 50, 100 mg caps, has more consistent bio-availability. For i.v. use cyclosporine is dispersed in cremaphoremulsion: SANDIMMUN, PANIMUN 100 mg/ml inj in 1 ml,5 ml, 50 ml vial, which is diluted and infused over 4–6 hours.An acute reaction consisting of chills, fever, bodyache anddyspnoea often occurs because of the solvent; i.v. cyclosporineis used only in emergency, and is substituted by oral medicationas soon as possible.
Cyclosporine is a second line drug in autoimmunediseases, like severe rheumatoid arthritis, uveitis,bronchial asthma, inflammatory bowel disease,dermatomyositis, etc. and in psoriasis, especiallyto suppress acute exacerbations. It is generallyused along with corticosteroids or Mtx. Goodresults have been obtained in some cases ofaplastic anaemia. For these conditions, lower doses(2–5 mg/kg/day) are needed and adverse effectsare milder. However, it is not curative and relapsesoccur when the drug is withdrawn.
Drug interactions Cyclosporine can interactwith a large number of drugs. All nephrotoxicdrugs like aminoglycosides, vancomycin,amphotericin B and NSAIDs enhance its toxicity.
By depressing renal function, it can reduceexcretion of many drugs. Phenytoin, pheno-barbitone, rifampin and other enzyme inducerslower its blood levels so that transplant rejectionmay result. On the other hand, CYP3A4 inhibitorserythromycin, ketoconazole and related drugsinhibit its metabolism to increase bioavailabilityand cause toxicity. Potassium supplements andK+ sparing diuretics can produce markedhyperkalaemia in patients on cyclosporine.
Tacrolimus (FK506) This immunosuppressantis chemically different from cyclosporine, but hasthe same mechanism of action, and is ~100 timesmore potent. It binds to a different cytoplasmicimmunophilin protein labelled ‘FK 506 bindingprotein (FKBP)’, but the subsequent steps arethe same, i.e. inhibition of helper T cells viacalcineurin.
Tacrolimus is administered orally as well asby i.v. infusion. Oral absorption is variable anddecreased by food. It is metabolized by CYP3A4and excreted in bile with a t½ of 12 hour.Therapeutic application, clinical efficacy as wellas toxicity profile are similar to cyclosporine.Tacrolimus also requires blood level monitoringfor dose adjustment. However, due to higherpotency and easier monitoring of blood levels,it is generally preferred now for organ transplan-tations. Tacrolimus may be useful in patients whoserejection reaction is not suppressed by cyclo-sporine. It is particularly valuable in liver trans-plantation because its absorption is not dependenton bile. Being more potent, it is also suitable forsuppressing acute rejection that has set in.
Tacrolimus has been used in fistulatingCrohn’s disease. A 10 week course may induceremission. Topically, it is useful in atopic der-matitis. Hypertension, hirsutism, gum hyperplasiaand hyperuricaemia are less marked than withcyclosporine, but tacrolimus is more likely toprecipitate diabetes, cause neurotoxicity, alopeciaand diarrhoea. Dose limiting toxicity is renal.Dose: 0.05–0.1 mg/kg BD oral (for renal transplant), 0.1–0.2mg/kg BD (for liver transplant). It can also be given i.v. (noi.v. preparation is available in India); 0.03–0.1% topically.TACROMUS, PANGRAF 0.5, 1.0, 5.0 mg caps;TACRODERM, TACREL 0.03, 0.1% oint.

882S
EC
TIO
N14
MISCELLANEOUS DRUGS
mTOR INHIBITORS
Sirolimus This new and potent immunosup-pressant is a macrolide antibiotic (like tacrolimus),which was earlier named Rapamycin. It binds tothe same immunophillin FKBP as tacrolimus, butthe sirolimus-FKBP complex inhibits anotherkinase called ‘mammalian target of rapamycin’(mTOR), and does not interact with calcineurin(Fig. 63.2). The mTOR is an important link inthe cascade of signalling pathways which leadto proliferation and differentiation of T-cellsactivated by IL-2 and other cytokines. Sirolimusarrests the immune response at a later stage thancyclosporine.
Sirolimus is absorbed orally, but fatty mealreduces absorption. It is extensively metabolized,mainly by CYP3A4, so that systemic bioavailabi-lity is only 15–20%. Elimination occurs primarilyby the biliary route; the t½ is ~60 hours. Inhibitorsand inducers of CYP3A4 significantly alter itsblood level, which needs to be monitored.Cyclosporine shares the same isoenzyme andraises the blood level of sirolimus. For prophylaxisand therapy of graft rejection reaction, sirolimuscan be used alone, but is generally combined withlower dose of cyclosporine/tacrolimus and/orcorticosteroids and mycophenolate mofetil. Thelatter combination avoids use of a calcineurininhibitor, and is particularly suitable for patientsdeveloping renal toxicity with cyclosporine.Sirolimus is effective in some steroid refractorycases, and has been used in stem cell transplantas well. However, it is not recommended for livertransplant. Sirolimus coated stents are being usedto reduce the incidence of coronary arteryrestenosis, by inhibiting endothelial proliferationat the site.
Significantly, sirolimus is not nephrotoxic, butit can suppress bone marrow, mainly causingthrombocytopenia. Rise in serum lipids iscommon. Other adverse effects are diarrhoea, liverdamage and pneumonitis.Dose: Initially loading dose 1 mg/m2 daily, followed by titratedlower doses for maintenance.RAPACAN 1 mg tab.
Everolimus It is similar to sirolimus in mechanism, clinicalefficacy, doses, toxicity and drug interactions, but is betterabsorbed orally and has more consistent bioavailability. Thet½ is shorter (~40 hours) so that steady state levels canbe reached earlier.
ANTIPROLIFERATIVE DRUGS(Cytotoxic immunosuppressants)Certain cytotoxic drugs used in cancer chemo-therapy exhibit prominent immunosuppressantproperty, mainly by preventing clonal expansionof T and B lymphocytes (see Fig. 63.1).
Azathioprine (see p. 863) It is a purine antime-tabolite which has more marked immuno-suppressant than antitumour action. The basis forthis difference is not clear, but may be due toits selective uptake into immune cells andintracellular conversion to the active metabolite6-mercaptopurine, which then undergoes furthertransformations to inhibit de novo purine syn-thesis and damage to DNA. It selectively affectsdifferentiation and function of T cells and inhibitscytolytic lymphocytes; CMI is primarilydepressed.
The most important application of azathio-prine is prevention of renal and other graftrejection, but it is less effective than cyclosporine;generally combined with it or used in patientsdeveloping cyclosporine toxicity. Relatively lowerdoses (1–2 mg/kg/day) are used in progressiverheumatoid arthritis (see p. 211), and it isfrequently employed for maintening remission ininflammatory bowel disease (see p. 685). It maybe an alternative to long-term steroids in someother autoimmune diseases as well.
Methotrexate (Mtx. see p. 862) This folateantagonist is a potent immunosuppressant whichmarkedly depresses cytokine production andcellular immunity, and has antiinflammatoryproperty. It has been used as a first line drugin many autoimmune diseases like rapidly progres-sing rheumatoid arthritis (see p. 210), severepsoriasis, pemphigus, myasthenia gravis, uveitis,chronic active hepatitis. Low dose Mtx mainte-nance therapy is relatively well tolerated.

883C
HA
PTE
R63
IMMUNOSUPPRESSANT DRUGS
Cyclophosphamide (see p. 860) Thiscytotoxic drug has more marked effect on B cellsand humoral immunity compared to that on T cellsand CMI. It has been particularly utilized in bonemarrow transplantation in which a short coursewith high dose is generally given. In other organtransplants it is employed only as a reserve drug.In rheumatoid arthritis, it is rarely used, only whensystemic manifestations are marked. Low dosesare occasionally employed for maintenance therapyin pemphigus, systemic lupus erythematosus andidiopathic thrombocytopenic purpura.Chlorambucil It has relatively weak immuno-suppressant action which is sometimes utilizedin autoimmune diseases and transplant main-tenance regimens.
Mycophenolate mofetil (MMF) It is a newerimmunosuppressant; prodrug of mycophenolicacid which selectively inhibits inosine monophos-phate dehydrogenase, an enzyme essential for denovo synthesis of guanosine nucleotides in theT and B cells (these cells, unlike others, do nothave the purine salvage pathway). Lymphocyteproliferation, antibody production and CMI areinhibited. As ‘add on’ drug to cyclosporine +glucocorticoid in renal transplantation, it has beenfound as good or even superior to azathioprine,but should not be combined with azathioprine.It can help to reduce the dose of cyclosporineand thus its toxicity. MMF + glucocorticoid +sirolimus is a non-nephrotoxic combination thatis utilized in patients developing renal toxicitywith cyclosporine/tacrolimus. MMF is rapidlyabsorbed orally and quickly converted to the activemetabolite mycophenolic acid. This is then slowlyinactivated by glucuronidation with a t½ of~ 16 hours. The glucuronide is excreted in urine.Vomiting, diarrhoea, leucopenia and predispositionto CMV infection, g.i. bleeds are the prominentadverse effects.Dose: 1.0 g BD oral; CELLMUNE, MYCEPT, MYCOPHEN250, 500 mg tab/cap.
Glucocorticoids (see Ch. 20)
Glucocorticoids have potent immunosuppressantand antiinflammatory action, inhibit several
components of the immune response (see p. 286).They particularly inhibit MHC expression (Fig.63.1) and activation/proliferation of T lympho-cytes. Expression of several IL and other cytokinegenes is regulated by corticosteroids and produc-tion of adhesion molecules is depressed. The short-lived rapid lymphopenic effect of steroids is dueto sequestration of lymphocytes in tissues.Accordingly, they have marked effect on CMIbut little effect on humoral immunity.
The corticosteroids are widely employed ascompanion drug to cyclosporine or other immuno-suppressants in various organ transplants. In casegraft rejection sets in—large doses of corticoidsi.v. are employed for short periods. They are usedin practically all cases of severe autoimmunediseases, especially during exacerbation. Long-term complications are the greatest limitations ofsteroid use; and it is maintenance of remissionfor which other immunosuppressants often provesafer.
BIOLOGICAL AGENTSThese are biotechnologically produced recom-binant proteins or polyclonal/monoclonal anti-bodies directed to cytokines or lymphocyte surfaceantigens which play a key role in immuneresponse. They are important recent additions,mostly as supplementary/reserve drugs for severeand refractory cases of autoimmune diseases andgraft versus host reaction.
TNFααααα inhibitorsTNFα is secreted by activated macrophages andother immune cells to act on TNF receptors(TNFR1, TNFR2) which are located on the surfaceof neutrophils, fibroblasts, endothelial cells as wellas found in free soluble form in serum and serousfluids. TNFα amplifies immune inflammation byreleasing other cytokines and enzymes likecollagenases and metalloproteinases. The TNFαinhibitors are mainly used in autoimmune diseases,and are briefly described with disease modifyingdrugs for rheumatoid arthritis in Ch.15.
Etanercept This fusion protein of human TNF receptorand Fc portion of human IgG1 neutralizes both TNFα andTNFβ. It prevents activation of macrophages and T-cells

884S
EC
TIO
N14
MISCELLANEOUS DRUGS
during immune reaction. It is used mostly in combinationwith Mtx in rheumatoid arthritis patients who fail to respondadequately to the latter (see p. 212). It is also approvedfor severe/refractory ankylosing spondylitis, polyarticularidiopathic juvenile arthritis and plaque psoriasis.Infliximab It is chimeral monoclonal antibody against TNFαwhich binds and inactivates TNFα. Used by s.c. injectionevery 4–8 weeks along with Mtx and other conventionaltherapy, it has proven useful in refractory rheumatoid arthritis,fistulating Crohn’s disease, ulcerative colitis, psoriasis andankylosing spondylitis.Adalimumab It is fully human recombinant anti-TNFαantibody indicated in the same range of autoimmune diseasesas infliximab, and like the latter, does not bind TNFβ, butis less antigenic. It can be added to Mtx or other conventionaldrugs for additional benefit.
IL-1 receptor antagonistStimulated macrophages and other mononuclear cells elaborateIL-1 which activates helper T-cells and induces productionof other ILs, metalloproteinases, etc. An endogenous IL-1receptor antagonist has been isolated and several of itsrecombinant variants have been produced for clinical use.Anakinra This recombinant human IL-1 receptor antagonistprevents IL-1 binding to its receptor and has been approvedfor use in refractory rheumatoid arthritis (see p. 212) notcontrolled by conventional DMARDs. Anakinra along withcontinued Mtx has been used alone as well as added to TNFαantagonists, because its clinical efficacy as monotherapyappears to be lower.
IL-2 receptor antagonistThe CD-25 molecule is expressed on the surface ofimmunologically activated, but not resting T-cells. It actsas a high affinity receptor for IL-2 through which cellproliferation and differentiation are promoted. Some antiCD-25 antibodies have been developed as IL-2 receptorantagonist to specifically arrest the activated T-cells.Daclizumab It is a highly humanized chimeric monoclonalanti CD-25 antibody which binds to and acts as IL-2 receptorantagonist. Combined with glucocorticoids, calcineurinantagonists and/or azathioprine/MMF, it is used to preventrenal and other transplant rejection reaction. The plasma t½of daclizumab is long (3 weeks), and it has also been usedin combination regimens for maintenance of graft.Basiliximab This is another anti CD-25 antibody withhigher affinity for the IL-2 receptor, but shorter plasma t½(1 week). Clinical use of basiliximab is similar to that ofdaclizumab.
Both daclizumab and basiliximab can cause anaphylacticreactions and promote opportunistic infection.
Anti-CD3 antibodyMuromonab CD3 It is a murine monoclonalartibody against the CD3 glycoprotein expressednear to the T cell receptor on helper T cells (seeFig. 63.2). Binding of muromonab CD3 to the
CD3 antigen obstructs approach of the MHCII-antigen complex to the T-cell receptor.Consequently, antigen recognition is interfered,and participation of T-cells in the immune responseis prevented. Following antibody binding, theT-cell receptor is internalized and the T-cells getrapidly depleted from blood, partly by cytolysisand partly by their migration to non-lymphoidorgans. An immune blocked state results.
Muromonab CD3 is the oldest (developed inthe 1980s) monoclonal antibody that is stilloccasionally used clinically, though newerhumanized anti CD3 monoclonal antibodies havebeen produced which are less antigenic.Muromonab CD3 is now primarily used for acutetransplant rejection reaction, particularly insteroid-resistant cases. Daily i.v. injection ofmuromonab CD3 is given for 2 weeks along withcorticosteroids and other immunosuppressants.Subsequent courses are not recommended,because the first course produces antibodiesagainst mouse protein which neutralise it. Useof muromonab CD3 for induction therapy of organtransplantation is infrequent now, since betteralternatives are available. It has also been usedto deplete T cells from the donor bone marrowbefore transplantation.
Initial doses of muromonab CD3 areassociated with ‘cytokine release syndrome’ withflu-like symptoms, viz. chills, rigor, high fever,wheezing, malaise, etc. which is due to releaseof TNFα, ILs and interferon. The symptomsdecrease in severity with subsequent doses.Occasionally aseptic meningitis, intragraftthrombosis, life-threatening pulmonary edema,seizures and a shock-like state are produced. High-dose corticosteroid pretreatment attenuates thereaction, and is a part of the usual protocol whileadministering muromonab CD3.
Polyclonal antibodies
Antithymocyte globulin (ATG) It is a polyclonalantibody purified from horse or rabbit immunizedwith human thymic lymphocytes which containsantibodies against many CD antigens as well asHLA antigens. It binds to T lymphocytes anddepletes them. It is a potent immunosuppressant

885C
HA
PTE
R63
IMMUNOSUPPRESSANT DRUGS
and has been used primarily to suppress acuteallograft rejection episodes, especially in steroid-resistant cases, by combining with other immuno-suppressants, including steroids. It can also be usedin induction regimens, but this has the potentialto produce serum sickness or anaphylaxis.LYMPHOGLOBULIN (equine) 100 mg/vial inj.; 10 mg/kg/day i.v.;THYMOGLOBULIN (rabbit) 25 mg/vial inj.; 1.5 mg/kg/day.ATG 100 mg inj; 200 mg i.v./day.
Anti-D immune globulin It is human IgGhaving a high titer of antibodies against Rh (D)antigen. It binds the Rho antigens and does notallow them to induce antibody formation in Rhnegative individuals. It is used for prevention ofpostpartum/post-abortion formation of antibodiesin Rho-D negative, DU negative women who havedelivered or aborted an Rho-D positive, DUpositive baby/foetus. Administered within 72 hoursof delivery/ abortion, such treatment prevents Rhhaemolytic disease in future offspring. It has alsobeen given at 28th week of pregnancy.Dose: 250–350 µg i.m. of freez dried preparation.RHESUMAN, RHOGAM, IMOGAM 300 µg per vial/prefilledsyringe.
Higher doses (1000–2000 µg) are needed for Rhnegative recipients of inadvertantly administeredRh positive blood. It should never be given tothe infant or to Rho-D positive, DU positiveindividuals.
IMMUNOSUPPRESSION IN ORGANTRANSPLANTATIONUse of immunosuppressants is essential for suc-cessful organ transplantation. In general 3 typesof regimens are used depending upon the stageof transplantation.
1. Induction regimen This is given in theperioperative period: starting just before thetransplant to about 2–12 weeks after it.Accelerated rejection develops in the first week,while acute rejections are most likely from2–12 weeks. The most common regimens includetriple therapy with cyclosporine/tacrolimus/sirolimus + prednisolone + MMF/azathioprine.The sirolimus + prednisolone + MMF combinationavoids risk of renal toxicity. Two drug and single
drug regimens are also used. Many experts donot give cyclosporine preoperatively, and try todelay its induction as far as possible to avoidnephrotoxicity, particularly in renal transplan-tation. If no rejection develops, the doses aregradually reduced after 2 weeks and this phasemerges imperceptably with maintenance phase.
2. Maintenance regimen This is given forprolonged periods, may be life-long. Triple drugregimen consisting of maintenance doses of anythree of the following choices—cyclosporine/tacrolimus, sirolimus, prednisolone, azathioprine/MMF are generally favoured, because eachcomponent is needed in lower doses—reducestoxicity and cost. Nephrotoxicity is often thelimiting factor with cyclosporine/tacrolimus, whilelong-term steroid therapy has its own problems.The component which produces toxicity in a givenpatient is curtailed or dropped. Two drug andone drug regimens are also used, but are associatedwith more episodes of acute rejection. After1 year, cyclosporine is generally dropped, butits continuation is associated with fewer acuterejections. In case of intolerance to the first linedrugs viz. cyclosporine, tacrolimus, sirolimus,MMF, azathioprine and prednisolone, the secondline drugs like cyclophosphamide, chlorambucilor daclizumab are substituted.3. Antirejection regimen This is given tosuppress an episode of acute rejection. Steroidpulse therapy (methylprednisolone 0.5–1 g i.v.daily for 3–5 days) is effective in majority ofcases. In case of no response, muromonab CD3/ATG is given as rescue therapy or the antibodiesare combined with steroids. Tacrolimus, sirolimus,MMF have also been used in rescue therapy ofsteroid resistant rejection. If the maintenanceregimen had not included cyclosporine, its additioncan treat acute rejection, but can be damagingto the transplanted kidney.
Adverse effects The two general untowardeffects of immunosuppressant therapy are:(a) Increased risk of bacterial, fungal, viral (espe-cially CMV) as well as opportunistic infections.(b) Development of lymphomas and relatedmalignancies after a long latency.

Drugs Acting on Skin andMucous Membranes
ChapterChapterChapterChapterChapter 6464646464
A variety of drugs applied topically to the skinor mucous membranes produce therapeutic effectslocalized to the site of application. They act pri-marily by virtue of their physical/mechanical/chemical/biological attributes and may be dividedinto several categories designated by the mostprominent action.
DEMULCENTS
Demulcents are inert substances which soothinflamed/denuded mucosa or skin by preventingcontact with air/irritants in the surroundings. Theyare, in general, high molecular weight substancesand are applied as thick colloidal/viscid solutionsin water. Some, like gum acacia, gum tragacanthproduce foam with water, reduce surface tensionand act as suspending/emulsifying agents.
Glycyrrhiza is a sweet tasting root (liquorice);used in cough lozenges to sooth the throat andas sweetening/flavouring agent in mixtures. Itcontains a glycoside glycyrrhizin which has steroidlike salt retaining action when taken orally.
Methylcellulose It is a synthetic cellulose deri-vative used as bulk purgative, in nose drops andcontact lens solutions.
CADILOSE 0.5% drops in 10 ml bottle.Propylene glycol is a clear, viscous liquid,
miscible with water as well as some oils thatis used in cosmetics and as occlusive dressingfor ichthyosis, etc.
Glycerine is a clear, sweet, viscous liquid.Undiluted glycerine has dehydrating property—produces a warm sensation and irritates mucousmembranes. Applied to anal canal as suppositoryit induces evacuation. Applied to dry skin andcracked lips (50% in water) it acts as emollientand is a popular vehicle for gum/throat paints.It is also used orally/per rectum (50–75%) or
intravenously (10%) to reduce intraocular/intracranial tension.
EMOLLIENTS
Emollients are bland oily substances which soothand soften skin. They form an occlusive film overthe skin, preventing evaporation, thus restoringelasticity of cracked and dry skin. Olive oil, arachisoil, sesame oil, cocoa butter, hard and soft paraffin,liquid paraffin, wool fat, bees wax and spermacetiare the commonly employed emollients. They arealso used as vehicles for topically applied medica-ments and as ointment bases.
Wool fat may cause allergy in some patients.
ADSORBANTS AND PROTECTIVES
Adsorbants are finely powdered, inert andinsoluble solids capable of binding to their sur-face (adsorbing) noxious and irritant substances.They are also called protectives because theyafford physical protection to the skin or mucosa.Other protectives form a continuous, adherent andflexible occlusive coating on the skin. Demulcentsand emollients also serve as protectives.
Magnesium/zinc stearate They have verysmooth surface—prevent friction, and are notwater wettable—can be used on exuding surfacesbecause they allow evaporation of water and donot form a crust.
Talc It is native hydrous magnesium silicate,which spreads easily—used in talcum/facepowders. Entering raw surfaces, it can formgranulomas—should not be sprinkled on woundor used for surgical gloves.
Calamine It is native zinc carbonate tinted pinkwith ferric oxide. Calcined calamine is zinc oxide.

887C
HA
PTE
R64
DRUGS ACTING ON SKIN AND MUCOUS MEMBRANES
It has mild astringent and antiseptic action andis a good soothing and protective agent. Usedin calamine lotion along with zinc oxide andbentonite (native hydrated aluminium silicate)which have similar properties, as cosmetic, onsunburn, insect bite, urticaria and contactdermatitis.CALACREME 5% cream, CALAMINOL 5% and CALAMYL10% emulsion, CALAK 15% with zinc oxide 5%, bentonite3% sodium citrate 0.5%, glycerol 5% (calamine lotion).
Starch It is used in dusting powders and forsurgical gloves, but should not be used on exudingsurfaces because it absorbs moisture, crusts ondrying and encourages fermentation.
Boric acid It is a smooth and fine powder: hasmild antiseptic (see Ch. 65), antipruritic anddeodorant actions. It is a common ingredient ofprickly heat powders.
Aloe vera gel It is a mucilaginous preparationfrom the fleshy leaves of Aloe vera plant withsoothing and moisturising property, widelyincluded in cosmetic and skin care products.Therapeutic claims in acne, psoriasis and manyother conditions have been made.ALOVIT: Aloe extract 10% + vit E 0.5% cream.
Polyvinyl polymer On drying its solution formsan occlusive pellicle-like coating on abraded skin.Used as a spray on abrasions and minor cuts,it protects from dust and exposure.HEALEX SPRAY: 2.5% + benzocaine 0.36% as aerosol wounddressing.
Feracrylum It is a water-soluble biodegradablepolymer which forms gel-like complexes oncoming in contact with blood. Applied to freshabrasions, it stops oozing of blood and protectsthe wound by acting as a physical barrier. A mildantiseptic action is also exerted.SEPGARD GEL: 1% gel, to be applied as a thin film on theabrasion/wound.
Dimethicone (Dimethyl polysiloxane, Simethi-cone) It is a silicone polymer—a viscous,amphiphilic liquid. It is pharmacologically inert,has water repellent and surface tension reducingproperties (collapses froth). Applied to the skin,it adheres and protects it; special use—to prevent
maceration and excoriation of skin due to soilingwith urine (suprapubic cystostomy). Also used onbedsores, ulcers and burns.BARRIER-SF: Dimethiocone 15%, vit E 0.18% cream.
Sucralfate (topical) This aluminium salt ofsulfated sucrose used primarily as peptic ulcerprotective (see p. 656), has been formulated asa topical gel. Applied on burns, bedsores, diabetic/radiation/aphthous ulcers, excoriated skin, sores,etc. it adheres and serves to protect damagedtissue—facilitates healing.PEPSIGARD LIGHT GEL 10% gel; to be applied on the ulcer3-4 times a day.
ASTRINGENTS
Astringents are substances that precipitate proteins,but do not penetrate cells, thus affecting thesuperficial layer only. They toughen the surfacemaking it mechanically stronger and decreaseexudation. Drugs are:
Tannic acid and tannins Tannic acid is presentin many plants but is generally obtained fromnutgalls of oak. Tannins are found in tea, catechu,nutmeg, areca nut (betel nut), etc. They denatureproteins forming protein tannate. Uses are:Bleeding gums—as glycerine of tannic acid.Bleeding piles—as tannic acid suppository.Alkaloidal poisoning—precipitates ingestedalkaloids as tannates.(Its use on burns has been abandoned because it forms a crustunder which bacteria could grow. Sufficient systemicabsorption often occurred to cause centrilobular necrosis ofthe liver.)
Alcohol Ethanol and methanol are goodastringents at 50–90% concentration. Denaturedspirit rubbed on the skin prevents bedsores, butshould not be applied on the sores once thesehave formed, as it is highly irritating to rawsurfaces. Ethanol is also used as after-shave andon minor cuts.
Mineral astringents Heavy metal ions areastringent and antiseptic. Alum has been used asafter-shave and as local haemostatic on minorcuts. Other aluminium, zinc and zirconium salts

888S
EC
TIO
N14
MISCELLANEOUS DRUGS
are used as antiperspirants. They diffuse throughthe sweat ducts, reduce secretion from glands andpartially block the ducts as well. Their antibacterialaction prevents decomposition of sweat bybacteria, reducing body odour.
IRRITANTS AND COUNTER-IRRITANTS
Irritants stimulate sensory nerve endings andinduce inflammation at the site of application.Depending on their nature, concentration andsensitiveness of the site, they produce coolingsensation or warmth, pricking and tingling,hyperaesthesia or numbness and local vasodila-tation. Irritants which cause local hyperemiawith little sensory component are calledRubefacients. Stronger irritants which in additionincrease capillary permeability and causecollection of fluid under the epidermis (formingraised vesicles) are termed Vesicants. Certainirritants also produce a remote effect which tendsto relieve pain and inflammation in deeperorgans—called Counter-irritants.
Mechanism of counterirritation Cutaneoussensations are precisely localized. Deepersensations from muscles, joints and viscera areperceived more diffusely. A spinal segment,receiving afferent impulses from the surface aswell as from deeper organs, modulates them—preferentially conducting the former to the highercenters. When a counter-irritant is applied to thearea of skin supplied by nerves from the samesegment as the deeper organ from which painimpulses are coming, the cutaneous impulsesobscure the deeper sensation.
Irritation of afferent nerve endings producesarteriolar dilatation in the adjoining areas of skinby axon reflex (which mediates flare in tripleresponse). Through segmental association ofafferents, vasodilatation also occurs in thecorresponding deeper organ. Increased bloodsupply helps to fight the cause of pain andinflammation in the deeper organ.
Counterirritants are generally massaged torelieve headache, muscular pain (torticollis,backache, sprain), joint pain, pleural/peritonealpain, colics, etc. Drugs are:
Volatile oils (essential oils) are terpenehydrocarbons of plant origin having a charac-teristic odour. They have variable properties, butall are irritants. Stearoptenes are solid volatileoils.
Turpentine oil Obtained by distilling Pinusoleoresin; used as counterirritant in the form ofliniment or ‘stupes’.
Clove oil Applied by cotton swab for toothache.
Eucalyptus oil Used in pain balms.
Camphor It is obtained from the bark ofCinnamomum camphora or produced synthe-tically. Produces cooling sensation on skin andis mildly anaesthetic—relieves itching. It is addedin liniments and pain balms. Taken internally—small doses produce a warm and comforting sensa-tion in epigastrium; large doses are emetic.Systemically it produces excitement and con-vulsions (especially in children).
Thymol Obtained from Thymus vulgaris, hasa pungent taste. It is included in pain balms.
Menthol From mint or prepared synthetically,has cooling and soothing action. It is added topain balms, throat paints, throat lozenges andinhalers for relief of nasal congestion. It is alsoa carminative.
Mustard seeds It contains a glycoside sinigrinand an enzyme myrosin. When ground seeds aresoaked in water, myrosin hydrolyses sinigrin torelease allyl isothiocyanate which is a strongirritant. Mustard plaster has been used asrubefacient and counterirritant. As a suspensionin water 4–8 g of ground seeds are emetic.
Capsicum (Chillies) It is a powerful irritant,hot in taste. The active principle is capsaicin.It is a popular condiment in Indian cooking, andis included in some counterirritant preparations.After initial stimulation, capsaicin depletes afferentnerve endings of the transmitter substance P;may relieve post-herpetic neuralgia on localapplication.

889C
HA
PTE
R64
DRUGS ACTING ON SKIN AND MUCOUS MEMBRANES
Canthridin A crystalline solid obtained fromSpanish fly. It is a strong irritant, higherconcentrations damage the epithelium and causevesication—has been used to remove warts, etc.It is added to hair tonics—claimed to increasevascularity of scalp and promote hair growth.
Methyl salicylate (oil of wintergreen) Incontrast to other salicylates, it is not used internally(induces vomiting, gastritis and systemic toxicity).It is combined with other irritants in linimentsand ointments for muscle and joint pain.
Alcohol Produces rubefaction when rubbed onskin and is a vehicle for liniments.
Some counterirritant combinationsALGIPAN: Capsicum oleoresin 0.1%, histamine 0.1%, methylnicotinate 1%, glycol salicylate 5% cream.ARJET SPRAY: Methyl salicylate 875 mg, menthol 1.6 g,camphor 1.5 g, benzyl nicotinate 20 mg, squalance 250 mg,glycol salicylate 875 mg per 50 ml spray.RELISPRAY: Winter green oil 20%, clove oil 1%, menthol4%, nilgiri oil 6%, camphor 10%, cinnamon oil 0.5%,turpentine oil 10% spray.EUTHERIA: Eucalyptol 7.2%, menthol 4.7%, methylsalicylate11.25% balm.MEDICREME: Methylsalicylate 8%, menthol 2%, adrenaline0.03%, mephenesin 2.5%, chlorpheniramine 0.2%, cream.RELAXYL: Capsicum oleoresin 0.05%, mephenesin 10%methyl nicotinate 1% ointment.VICKS VAPORUB: Menthol 2.8%, camphor 5.25%, thymol0.1% turpentine oil 5.5% ointment.IODEX: Methylsalicylate 5%, iodine 4% nonstaining ointment.AMRUTANJAN: Eucalyptus oil 17%, camphor 10%, thymol1%, menthol 4.5%, methylsalicylate 7% ointment.CAPSIGYL-D: Capsaicin 0.075%, methyl salicylate 20%,menthol 10%, camphor 5%, eucalyptus oil 5%, diclofenac 1%gel.
CAUSTICS AND ESCHAROTICS
Caustic means corrosive and Escharotic meanscauterizer. These chemicals cause local tissuedestruction and sloughing. An escharotic, inaddition, precipitates proteins that exude to forma scab—gets fibrosed to form a tough scar. Theyare used to remove moles, warts (including genitalwarts) condylomata, papillomas and on keratoticlesions. Care is needed in their application toavoid ulceration. It is believed that all micro-
organisms are killed during cauterization, but thisis not always so.
Podophyllum resin As 10–25% alcoholic solu-tion or suspension in mineral oil.PODOWART 20% paint; CONDYLINE 0.5% podophyllotoxinsoln.
Silver nitrate As toughened silver nitrate sticksor pencils.
Phenol As 80% w/w solution.
Trichloroacetic acid As crystals or 10–20%solution to cauterise adenoids; dilute solution isused to promote peeling of frackled skin.
Glacial acetic acid Undiluted.
KERATOLYTICSKeratolytics dissolve the intercellular substancein the horny layer of skin. The epidermal cellsswell, soften and then desquamate. These drugsare used on hyperkeratotic lesions like corns,warts, psoriasis, chronic dermatitis, ringworm,athletes foot, etc.
Salicylic acid As 10–20% solution in alcoholor propylene glycol for dissolving corns. Moreeffective when applied under occlusive dressing.Propylene glycol is hygroscopic. Applied underpolyethylene occlusive dressing, it causesmaceration of skin and acts as a keratolytic,supplementing the action of salicylic acid.CORNAC 16.5% liquid, CORN CAP 40% oint in adhesivetape.
Lower concentrations (3–5%) are used in otherconditions, e.g. in Whitfield’s ointment.RINGCUTTER 3% ointment with 5% benzoic acid.It is also mildly antiseptic and antifungal.
Resorcinol Has antiseptic, antifungal, localirritant and keratolytic properties; 3–10% is usedin eczema, seborrheic dermatitis, ringworm, etc.
Urea Applied at a concentration of 5–20% incream/ointment base, urea acts as a humectantby its hygroscopic and water retaining property.It causes softening and solubilization of keratin,facilitating its removal from hyperkeratinizedlesions like ichthyosis, lichen planus. Inclusion

890S
EC
TIO
N14
MISCELLANEOUS DRUGS
of urea enhances the penetration of theconcurrently applied topical steroid.
ANTI-SEBORRHEICS
These are drugs effective in seborrheic dermati-tis which affects areas rich in sebaceous glands(scalp, face, trunk) and is characterized byerythematous, scaling lesions. Dandruff is thecommonest complaint. A causal role of the yeastPityrosporum ovale has been shown, but varioustrigger factors like change in quantity andcomposition of sebum, increase in alkalinity ofskin (due to increased sweating), external localfactors, emotional stress, genetic predispositionappear to be needed to transform the yeast froma commensal to a noninvasive pathogenicorganism. Drugs used are:Selenium sulfide Applied to the scalp as a2.5% lotion or shampoo, it slows epidermalproliferation and scaling. It is also antikeratolyticand fungicidal to P. ovale. Dryness, folliculitisand dandruff are benefited, but > 50% patientsrelapse on discontinuation. Systemic absorptionand toxicity can occur if it is applied to inflamedor damaged skin. Some individuals developsensitivity reactions.SELSUN 2.5% susp., SELDRUFF PLUS 2.5% susp. withclotrimazole 1%.
Zinc pyrithione It reduces epidermal turnoverand inhibits P. ovale. Weekly shampoo (1%)reduces dandruff, but symptoms do not resolvecompletely.
It is often combined with ketoconazole.SCALPE: Zinc pyrithione 1%, Ketoconazole 2% shampoo.
Corticosteroids Massaged in the scalp as alotion, topical steroids are highly effective inrelieving symptoms of seborrheic dermatitisincluding dandruff. Pityrosporal yeasts are reducedin the affected skin. However, relapse rates arehigh on discontinuation and prolonged use canproduce adverse effects like atrophy, poor healing,purpura, etc.
Imidazole antifungals Among several of thesecompounds, ketoconazole (KTZ) was found to
be the most effective against P. ovale. Orally (200mg/day for 4 weeks) it has been found to improveseborrhoea. But because this is often a chronicrelapsing condition and prolonged oral KTZtherapy is considered unwarranted, KTZ has beenformulated into 2% cream/shampoo/scalp gel.Good to excellent results have been obtained withthese preparations without skin irritation, contactsensitivity, phototoxicity or systemic adverseeffects.KETOVATE, NIZRAL, OCONA 2% cream, 2% shampoo.
Clotrimazole 1% solution may be used in itsplace.Sulfur, Resorcinol, Coaltar, Ammoniatedmercury These drugs are mildly effective. Theyhave minimal antiyeast action: may benefit sebor-rhoea by keratolytic and antiseptic properties.
Salicylic acid It is keratolytic, has mild effectin seborrhoea, probably by removing the scalesand by improving penetration of other drugs.
MELANIZING AGENTS
Melanizing agents are drugs that increasesensitivity to solar radiation and promoterepigmentation of vitiliginous areas of skin.Psoralens are furocoumarins which on photo-activation stimulate melanocytes and induce theirproliferation.
Psoralen It is obtained from fruit of Ammimajus.MANADERM 10 mg tablet, 1% ointment, PSORLINE5 mg tablet, 0.25% solution and ointment.
Methoxsalen (MACSORALEN 10 mg tab, 1%solution, MALANOCYL 10 mg tab, 0.75% soln.) andTrioxsalen (NEOSORALEN 5 mg, 25 mg tablets and0.2% lotion) are synthetic psoralens.
They sensitize the skin to sunlight which theninduces erythema, inflammation and pigmenta-tion. They are applied topically as well as givenorally. Methoxsalen is absorbed better, undergoesless first pass metabolism and is more effectivethan trioxsalen. Their plasma t½ is short (~ 1 hr);sensitization of skin is maximal at 1–2 hours,but lasts for 8 hours or more.

891C
HA
PTE
R64
DRUGS ACTING ON SKIN AND MUCOUS MEMBRANES
Topical therapy The solution/ointment iscarefully painted on the small well definedvitiliginous lesion—which is then exposed tosunlight for 1 minute and then occluded bybandage or sun screen ointment. Weekly treat-ment with longer exposures is given. Pigmenta-tion usually begins to appear after a few weeks;months are needed for satisfactory results. Thenperiodic maintenance treatment may be needed.This therapy should be undertaken only underdirect supervision of physician because longerexposure causes burning and blistering.
Oral therapy On alternate days after 2 hoursof a 0.3–0.6 mg/kg (usually 20 mg) oral doseof a psoralen, skin is exposed to sunlight (orartificial UV light), initially for 15 minutes—gradually increasing to 30 minutes over days.Eyes, lips and other normally pigmented areasshould be protected during exposure to sunlight.
DRUGS FOR PSORIASIS
Psoriasis is an immunological disorder manifestingas localized or widespread erythematous scalinglesions or plaques. There is excessive epidermalproliferation attended by dermal inflammation.Periodic flareups are common. Drugs can diminishthe lesions, but cannot cure the disease. Therapyhas to be prolonged and adjusted to the severityof disease. Topically applied emollients, kerato-lytics, antifungals afford variable symptomaticrelief, but topical corticosteroids are the primarydrugs used. They are very effective in mild-to-moderate disease, and initially even in severecases. Most patients respond within 3 weeks, andthe response may be hastened by applying thesteroid under occlusion. Therapy is started witha potent steroid which is substituted afterimprovement by either weekly application or bya milder preparation. However, they carry theirown local and systemic adverse effects, and lesionsmay progressively become refractory. Systemictherapy with corticosteroids and/or immunosup-pressants is reserved for severe and refractorycases. Other topically used drugs are:
Calcipotriol It is a synthetic nonhypercalcaemicvit D analogue effective topically in plaque typepsoriasis. It binds to the intracellular vit D receptorin epidermal keratinocytes and suppresses theirproliferation while enhancing differentiation. Onabsorption through the skin, it is inactivatedrapidly by metabolism so that little systemic effecton calcium metabolism is exerted. Benefit inpsoriasis is slow; but most cases respond in4–8 weeks. Response is maintained till treatmentis continued. Efficacy of calcipotriol in psoriasisis rated comparable to a moderate potency topicalsteroid. Combination with a steroid is moreeffective than either drug alone. Side effects areskin irritation, erythema and scaling. Hyper-calcaemia is rare. It is a safe and effectivealternative to steroids, but expensive.DAIVONEX 0.005% oint; apply over psoriatic lesions twicedaily.
Tazarotene This synthetic retinoid applied asa topical gel (0.05–0.1%) is moderately effectivein psoriasis. It is a prodrug which is hydrolysedin the skin to tezarotenic acid that exertsantiproliferative and antiinflammatory action bybinding to the intracellular retinoic acid receptorand modification of gene function. Combinationwith a topical steroid/calcipotriol may benefitrefractory cases. Skin irritation, burning sensation,peeling are common. These can be minimizedby careful application to the plaques only. It isteratogenic.LATEZ 0.05%, 0.1% gel; TAZRET 0.05% gel, 0.1% cream;0.05–0.1% application once daily in the evening.
Coaltar This crude preparation containingmany phenolic compounds exerts a phototoxicaction on the skin when exposed to light, especiallyUVA, and retards epidermal turnover. Applied asointment or alcoholic solution on psoriatic plaques(generally with salicylic acid) and exposed tosunlight daily, it induces resolution of psoriaticlesions in majority of cases, but relapses arecommon. Its use has declined now because ofstrong smell, cosmetic unacceptability, skin irri-tation, allergy, and potential for photosensitivityand carcinogenicity.

892S
EC
TIO
N14
MISCELLANEOUS DRUGS
EXETAR: coaltar 6%, salicylic acid 3%, sulfur ppt. 3%, oint.TARSYL: coaltar 1%, salicylic acid 3% lotion. IONAX-T:coaltar 4.25%, salicylic acid 2% scalp lotion.
Photochemotherapy (PUVA: Psoralenultraviolet A) Photoactivated psoralenundergoes O2 independent as well as O2 dependentreactions and binds to pyrimidine bases—interferes with DNA synthesis and epithelial cellturnover. PUVA therapy has produced gratifyingresults in severely debilitating psoriasis, butrelapses occur when treatment is stopped. Oralmethoxasalen is followed 1–2 hours later by UVAexposure on alternate days. There are seriousconcerns regarding potential of PUVA to causeskin cancer, cataracts and immunological damage.Being inconvenient and carrying risks, it isreserved for severe cases of psoriasis only.
Psoralens have also been used to acceleratetanning—a maximum of 2 weeks treatment hasbeen advised for this purpose. Other applicationsof PUVA are in lichen planus, urticaria pigmen-tosa, atopic dermatitis and cutaneous T celllymphoma.
Adverse effects: Mottling, erythema, burns,blistering, premature ageing of skin, gastricdiscomfort, nervousness and insomnia.
Acitretin It is a synthetic retinoid for oral usein psoriasis, lichen planus, severe ichthyosis, etc.It acts by binding to ‘retinoic acid receptor’ inepidermal cells and regulating their proliferationand maturation. Inflammation is suppressed.Because of frequent and potentially seriousadverse effects, use of acitretin is restricted torecalcitrant, pustular and other forms of severepsoriasis. Combination with topical antipsoriaticdrugs is advised.Dose: 0.5–0.75 mg/kg/day oral;ACITRIN, ACETEC, ACERET 10, 25 mg tab.
Dryness of skin and eyes, gingivitis, erythemaand scaling of skin, alopecia, arthralgia, myalgia,lipid abnormalities and liver damage are theimportant adverse effects. Elimination of acitretinis very slow (taking months) because of accu-mulation in body fat. It is highly teratogenic.Women taking acitretin must not conceive during
and till 3 years after stopping it. Drinking alcoholshould be prohibited during and till 3 monthsafter acitretin use.
Etanercept It is a TNFα inhibitor immuno-suppressive drug, also used in psoriasis. It isdescribed in Ch. 15 and Ch. 63.
DEMELANIZING AGENTS
They lighten hyperpigmented patches on skin.
Hydroquinone It is a weak hypopigmentingagent. It inhibits tyrosinase and other melaninforming enzymes, decreases formation of andincreases degradation of melanosomes. Regularapplication (as 2–6% lotion or cream) for monthsis required in melasma, chloasma of pregnancy,etc. The response is often incomplete and pig-mentation may recur when it is discontinued,especially if exposed to sunlight; sunscreens arefrequently combined. Skin irritation, rashes andallergy are possible. Care is to be taken to avoidits entry in eyes.EUKROMA 4% cream, MELALITE: Hydroquinone 2% withglycerylester of PABA 2.8% cream. BRITE: hydroquinone 4%,glyceryl PABA 2.8% cream.
Monobenzone A derivative of hydroquinone;potent demelanizing agent—destroys melanocytesand may cause permanent depigmentation. Fulleffect takes 4–6 months; treated areas should beprotected from sunlight by a sunscreen. Itsbleaching action is somewhat irregular: uglydepigmented patches can appear. Erythema andeczema may also result. Therefore, its use shouldbe restricted to patients with widespread vitiligo—to reduce the colour contrast between pigmen-ted and nonpigmented areas and for post-inflammatory melasma; 5% lotion or 20%ointment is applied 2–3 times daily.BENOQUIN 20% ointment.
Azelaic acid It is a drug for acne (see p. 894)that is also effective in hyperpigmentary disordersincluding melasma. It appears to act by inhibitingthe melanin forming enzyme tyrosinase. However,it is a weak demelanizing agent with reversiblehypopigmentary action.

893C
HA
PTE
R64
DRUGS ACTING ON SKIN AND MUCOUS MEMBRANES
Azelaic acid is used as a 10%, 20% cream.The only side effect is mild and transient localirritation.AZIDERM 10%, 20% cream.
SUNSCREENSSunscreens are substances that protect the skinfrom harmful effects of exposure to sunlight.
(a) Chemical sunscreens They absorb andscatter UV rays that are responsible for sunburnand phototoxicity, but allow longer wave lengthsto penetrate, so that tanning occurs.
Efficacy of a sunscreen formulation isquantified by its ‘Sun protection factor’ (SPF)which is the ratio of the dose of UVB radiationthat will produce minimal erythema on protectedskin to the dose required for the same onunprotected skin. Most commercial preparationshave a SPF of 15. Period for which they remaineffective depends on the vehicle.
Para-aminobenzoic acid (PABA) and itsesters: glyceryl mono amino benzoate. Theyabsorb UVB (290–320 nm). PABA is used as5% solution in alcohol/propylene glycol(PABALAK) or as 10% cream (PARAMINOL).
Benzophenones (such as oxybenzone 2–6%)block UVA (320–400 nm); are highly protective;thus higher concentrations prevent tanning also.
Cinnamates (such as octyl methoxy cinnamate)are included in sunscreens.SUNSHIELD: Octyl methoxy cinnamate 5%, vit E 0.25%lotion. EUKROMA-SG: Oxybenzone 3%, Octylmethoxycinnamate 5%, hydroquinone 2% cream.
Uses Chemical sunscreens are used as adjunctsin vitiligo therapy, drug induced phototoxicity andto facilitate tanning while preventing sunburn.There is some evidence that they can preventskin cancer and premature ageing of skin.
(b) Physical sunscreens Heavy petroleumjelly, titanium dioxide, zinc oxide and calamineare opaque substances that stop and scatter notonly UV but also visible light. They are also called‘sun shades’ and have to be applied as a thicklotion/cream which may be cosmetically
disagreeable. They withhold longer wave lengthsalso, which are mostly involved in photoallergy.Not only sunburn, but tanning as well is prevented.
Chloroquine taken orally is effective in actiniceruptions, but should be reserved for severe casesonly.
DRUGS FOR ACNE VULGARISAcne vulgaris is the most common skin diseasein adolescent boys and girls. Under androgenicstimulation the sebaceous follicles of face andneck produce excess of sebum and get colonizedby bacteria and yeast (Propionibacterium acnes,Staph. epidermidis, Pityrosporum ovale). Bacteriallipases produce fatty acids which irritate thefollicular ducts causing retention of secretions andhyperkeratosis— ‘comedones’ are formed whichmay rupture into the dermis causing inflammationand pustulation.
1. Topical Therapy
1. Benzoyl peroxide It is one of the mosteffective and widely used drugs in acne: graduallyliberates oxygen (in the presence of water) whichkills bacteria, especially anaerobic/microaerophilicones: used almost exclusively for acne becauseof its high efficacy against P. acnes and additionalkeratolytic and comedolytic properties. P. acnesor other bacteria do not develop resistance tobenzoyl peroxide. It induces mild desquamation,the comedone caps are shed and production ofirritant fatty acids in the sebum is reduced. Benzoylperoxide is a mild irritant of the skin—burningand stinging sensation is often felt initially,localized erythema may occur. Most patientsgradually develop tolerance to these actions; ifnot, use should be discontinued. Avoid contactwith eyes, lips, mucous membranes and denudedskin. It can bleach hair and coloured fabric.
Adverse effects are excessive dryness of skin,marked scaling, erythema, edema and contactsensitization (in 1–2% patients). It is used as5–10% cream, gel or lotion; duration andfrequency of application is guided by the degreeof irritation produced and tolerated; start with15 min once daily.

894S
EC
TIO
N14
MISCELLANEOUS DRUGS
PERSOL, PERNOX, BENZAC-AC 2.5% and 5% gel; inPERSOL FORTE 10% cream with sulfur ppt. 5%.
2. Retinoic acid (all trans vitamin A acid,Tretinoin) It is a potent comedolytic: promoteslysis of keratinocytes, prevents horny cells frombinding to each other, hence comedones, whichare horny impactions in follicles, cannot form.Epidermal cell turnover is stimulated resultingin peeling. No antibacterial action is exerted. Itis highly efficacious in acne, but response isdelayed (may take 6–10 weeks). Tretinoin hasthe potential to irritate the skin; start with thelower concentration applied once daily.
Side effects are feeling of warmth, stinging,excessive redness, edema and crusting. Used asa 0.025–0.05% gel or cream, it can be alternatedwith benzoyl peroxide (one in the morning theother at night), but both should not be appliedtogether because benzoyl peroxide acceleratesdegradation of tretinoin. Teratogenic risk withtopical retinoic acid is minor because of low bloodlevels produced; but it should be used duringpregnancy only if essential.
Tretinoin has been shown to preventphotoageing of skin. Dry scaly surface, mottling,wrinkles, rough and leathery texture, sagging ofloose skin that develop due to excessive exposureto sun are arrested and pigmented spots tend tofade. However, the risk-benefit ratio of long-termprophylactic therapy is not clear.EUDYNA 0.05% cream. RETINO-A 0.025% and 0.05%cream.
3. Adapalene It is a newer synthetic tretinoin-like drug which binds directly to the nuclearretinoic acid receptor and modulates keratinizationand differentiation of follicular epithelial cells.It also exerts antiinflammatory action; comedoneformation is suppressed. In acne vulgaris it isas effective but less irritating than tretinoin. Itremains stable in the presence of benzoyl peroxide;can be combined with it.ADAFERIN, ADAPEN, ADAPLE, ACLENE 0.1% gel; applyonce daily at bed time.
Tazarotene (see p. 891) is another topicalretinoid with therapeutic effect in acne vulgarisin addition to that in psoriasis.
4. Topical antibiotics Clindamycin, erythro-mycin and tetracyclines are less effective againstP. acnes than benzoyl peroxide. They are appro-priate for cases with inflamed papules, rather thanin non-inflamed comedones. They do not irritateskin but can cause sensitization.Erythromycin: ACNEDERM 2% lotion and oint; ERYTOP 3%lotion and cream; ACNESOL 4% gel, 2% lotion, ACNELAK-Z 4% lotion and gel with zinc acetate 2%.Clindamycin: CLINDAC-A, CLINCIN 1% gel.
Nadifloxacin is a newer topical quinolone broad-spectrum antibiotic which has exerted therapeuticbenefit in inflamed acne and folliculitis.NADIBACT, NADOXIN 1% cream for topical application.
5. Azelaic acid It is a natural product fromPityrosporum ovale that has been developed fortopical treatment of acne. Many aerobic andanaerobic microorganisms, especially P. acnespresent on acne bearing skin are inhibited. Azelaicacid reduces cutaneous bacterial density, free fattyacid content of skin surface lipids and proliferationof keratinocytes. Used as 10%, 20% cream, itsefficacy in acne approaches that of benzoylperoxide, but response is delayed. It has alsobenefited melasma (p. 892).AZIDERM 10%, 20% cream
II. Systemic TherapySystemic use of drugs in acne is indicated onlyin severe cases with cysts and pustules whichare likely to form scars.
1. Antibiotics Tetracycline, minocycline orerythromycin have been used. After initial control,smaller maintenance doses may be continued formonths. However, long-term systemic antibiotictherapy has its own complications. Recently riskof intracranial hypertension after use of tetra-cyclines for > 2 months has been emphasized.
2. Isotretinoin (13-cis retinoic acid) is anorally administered retinoid that reducesproduction of sebum (skin bacteria decreasesecondarily), corrects abnormal keratinization offollicles and causes dramatic improvement. A 20week course of 0.5–1 mg/kg daily brings aboutremission in most cases of cystic acne. Relapses

895C
HA
PTE
R64
DRUGS ACTING ON SKIN AND MUCOUS MEMBRANES
occur after variable intervals; can be treatedsimilarly. Side effects are frequent—cheilitis,dryness of skin, eyes, nose and mouth, epistaxis,pruritus, conjunctivitis, paronychia, rise in serumlipids and intracranial tension, and musculoskeletalsymptoms. Therefore, it should be reserved forunresponsive cases of severe acne.
Isotretinoin is highly teratogenic; upto 25%exposed foetuses had birth defects—craniofacial,heart and CNS abnormalities (ACCUTANEembryopathy). It is contraindicated in womenlikely to become pregnant during therapy and onemonth after. The t½ of isotretinoin is ~18 hours,and it is not accumulated like other retinoids.ISOTROTIN, SOTRET 10, 20 mg cap, IRET 20 mg cap.
Isotretinoin is also effective in the prevention andtreatment of skin cancers. Oral leucoplakia, actinic keratosesand other premalignant lesions can be treated, but benefit-risk ratio is not clear.
TOPICAL STEROIDS
Glucocorticoids are used topically for a largevariety of dermatological conditions. They bene-fit by virtue of their antiinflammatory, immuno-suppressive, vasoconstrictor and antiproliferative(for scaling lesions) actions. The intensity of actiondepends on the extent of absorption to the deeperlayers, thus lipophilicity of the compounddetermines potency to a great extent. Fluorinatedcompounds and lipid soluble esters, e.g. hydro-cortisone butyrate are potent. The availablepreparations may be roughly graded as:
Potent
Beclomethasone 0.025% BECLATE cream.dipropionate
Betamethasone 0.025% TOPICASONE cream,benzoate oint.
Betamethasone 0.12% BETNOVATE cream,valerate oint.
BETASONE cream.Halcinonide 0.1% CORTILATE,
HALOG, creamClobetasol 0.05% LOBATE, TENOVATE,
propionate DERMOTYL creamDexamethasone 0.1% DECADRON cream
sod. phosphate (with Neomycin 0.35%).Dexamethasone 0.1% MILLICORTENOL
trimethyl-acetate cream.
Fluocinolone 0.025% FLUCORT oint.,acetonide LUCI oint.
Fluocortolone 0.5% ULTRALAN oint.Triamcinolone 0.1% LEDERCORT oint.
acetonide
Moderately potent
Fluocinolone 0.01% FLUCORT-H oint.acetonide and skin lotion.
Clobetasol butyrate 0.05% EUMOSONE creamFluocortolone 0.25% COLSIPAN oint.Mometasone 0.1% MOMATE, CUTIZONE
oint, creamFluticasone 0.05% FLUTIVATE,
propionate MOLIDERM creamPrednicarbate 0.1-0.25% DERMATOP,
STEROTOP creamTriamcinolone 0.05% DESOWEN,
acetonide DESONIDE cream/lotion
Hydrocortisone 1% COTARYL-H cream.+ urea 12%
Hydrocortisone 2.5% WYCORT oint.acetate
MildHydrocortisone 0.1– LYCORTIN 1% oint.,acetate 1.0% in CORTOQUINOL
1% with quiniodochlor4% cream,GENTACYN-HCTOPICAL 1% withgentamicin 0.1%.CORTISON-KEMICETINE 0.5%with chloramphenicol0.5%.
Hydrocortisone 0.001% LOCOID creambutyrate
General guidelines for theuse of topical steroids(i) Penetration of the steroid at different sitesdiffers markedly—high at axilla, groin, face, scalpand scrotum; medium at limbs and trunk: lowat palm, sole, elbow and knee. Areas of high pene-tration easily develop adverse effects—potentpreparations should be avoided. Areas of lowpenetration do not generally respond to milderagents.(ii) Absorption into the skin also depends on thenature of lesion—high in atopic and exfoliativedermatitis, low in hyperkeratinized and plaque

896S
EC
TIO
N14
MISCELLANEOUS DRUGS
forming lesions. Milder drugs should be used onacute lesions, stronger ones reserved for chroniclesions.(iii) Choice of vehicle is important. Lotions andcreams (to some extent) are better for exudativelesions—they allow evaporation, have a cooling,drying and antipruritic effect. Sprays and gelsare appropriate for hairy regions. Ointments forman occlusive film and are good for chronic, scalyconditions.(iv) Occlusive dressing markedly enhancesabsorption of the steroid (as much as 10 fold),retains moisture and results in maceration of thehorny layer. Chronic, hypertrophied lesions maybe occluded intermittently (12 hours at a time).Continuous occlusion promotes bacterial and fungalgrowth.(v) Absorption is greater in infants and youngchildren—milder agents should be used.
(vi) Routine use of potent steroids is not justified.Very potent preparations should be restrictedto severe inflammatory conditions, unresponsiveeczema, psoriasis, etc., and that too only for shortperiods till the lesion resolves. The mildest prepa-ration that will control the lesion should be used.
(vii) Use of potent preparations should be shortterm or intermittent to prevent adverse effectsand tachyphylaxis. Sudden discontinuation shouldbe avoided. Upon improvement a less potent
preparation may be substituted or the steroid maybe alternated with an emollient till the lesionresolves.
(viii) More than 2 applications a day do notafford additional benefit. Generally twice dailyapplication is satisfactory.
A combination of steroid with an antimicrobialmay be used for—impetigo, furunculosis, secon-dary infected dermatoses, napkin rash, otitisexterna, intertriginous eruptions.
Local adverse effects of topical steroids
Thinning of epidermisDermal changes—atrophyTelangiectasia, StriaeEasy bruisingHypopigmentationDelayed wound healingFungal and bacterialinfections
Systemic adverse effects of topical steroidsAdrenal pituitary suppression can occur if largeamounts are applied repeatedly. Infants andchildren are particularly susceptible. Rarely,Cushing’s syndrome has been reported. Withproper use, the systemic risks are minimal.Popular combinations are:Containing Neomycin (0.3–0.5%): BECLATE-N,BETASONE-N, COLSIPAN-N, DECADRON, KENACOMB,KENALOG-S SKIN, TOPICASONE.
Containing Chinoform or Quiniodochlor (3–4%):BECLATE-C, BETASONE-C, BETNOVATE-C,CORTOQUINOL, FLUCORT-C
Containing Gentamicin (0.1%): GENTICYN-HCTOPICAL, DERMOTYL-G, LOBATE-G
Containing Chloramphenicol (1%): CORTISON-KEMICETINE
Containing Providone iodine (1%): ECZO-BETADINE
Containing Miconazole (2%): FLUCORT-MZ,TENOVATE-M
Containing Clotrimazole (1%): CLOBEN
Indications for topical steroids
Lesions that usually Lesions requiring potentrespond well steroids, respond slowly
Atopic eczema Cystic acneAllergic contact Alopecia areata
dermatitis Discoid LELichen simplex Hypertrophied scars,Primary irritant keloids
dermatitis Lichen planusSeborrheic dermatitis Nail disordersPsoriasis of face, Psoriasis of palm, sole,
flexures elbow, kneeVaricose eczema
Related to thepotency of prepara-tion and duration oftreatment; skin offace is moresusceptible. Potenthalogenated steroidsnot to be used on face.

Antiseptics, Disinfectants andEctoparasiticides
ChapterChapterChapterChapterChapter 6565656565
ANTISEPTICS AND DISINFECTANTS
The terms antiseptic and disinfectant connote anagent which inhibits or kills microbes on contact.Conventionally, agents used on living surfaces(skin, mouth) are called antiseptics while thoseused for inanimate objects (instruments, privies,water supply) are called disinfectants. There isconsiderable overlap and many agents are usedin either way. A practical distinction between thetwo on the basis of a growth inhibiting versusdirect lethal action is futile because these areoften concentration dependent actions. The termGermicide covers both category of drugs.
There, however, is difference between ‘dis-infection’ and ‘sterilization’. While sterilizationmeans complete killing of all forms of micro-organisms, disinfection refers to reduction in thenumber of viable pathogenic microbes to a levelthat they do not pose a risk to individuals withnormal host defence. The terms ‘sanitization’ and‘decontamination’ also have similar connotation.Thus, in ordinary usage, disinfectants do noteliminate all microbes.
The era of antiseptics and disinfectants was heraldedby Semmelweiss (washing of hands in chlorinated lime) andLister (antiseptic surgery by the use of phenol) in the 19thcentury. These germicides differ from systemically usedantimicrobials by their low parasite selectivity—are too toxicfor systemic use. However, many systemic antimicrobialsare applied topically as well, and some antibiotics (bacitracin,neomycin) are restricted to topical use, but are generallynot enumerated with the antiseptics. A strict distinction isthus impossible.
A good antiseptic/disinfectant should be:(i) Chemically stable.
(ii) Cheap.(iii) Nonstaining with agreeable colour and
odour.(iv) Cidal and not merely static, destroying spores
as well.
(v) Active against all pathogens—bacteria,fungi, viruses, protozoa.
(vi) Require brief time of exposure.(vii) Able to spread through organic films and
enter folds and crevices.(viii) Active even in the presence of blood, pus,
exudates and excreta.
A disinfectant in addition should not corrode orrust instruments and be easily washable. Anantiseptic in addition should be:
• Rapid in action and exert sustainedprotection.
• Nonirritating to tissues, should not delayhealing.
• Nonabsorbable, produce minimum toxicityif absorbed.
• Nonsensitizing (no allergy).• Compatible with soaps and other detergents.
Spectrum of activity of majority of antiseptic-disinfectants is wide, reflecting nonselectivity ofaction. However, some are rather selective, e.g.hexachlorophene, chlorhexidine, quaternaryammonium antiseptics, gentian violet andacriflavin are more active on gram-positive thangram-negative bacteria; silver nitrate is highlyactive against gonococci and benzoyl peroxideagainst P. acnes.
Mechanisms of action of germicides are varied,but can be grouped into:
(a) Oxidation of bacterial protoplasm.(b) Denaturation of bacterial proteins including
enzymes.(c) Detergent like action increasing permeability
of bacterial membrane.
Factors which modify the activity of germicidesare:
• Temperature and pH.

898S
EC
TIO
N14
MISCELLANEOUS DRUGS
• Period of contact with the microorganism.• Nature of microbe involved.• Size of innoculum.• Presence of blood, pus or other organic
matter.
Potency of a germicide is generally expressedby its phenol coefficient or Rideal Walkercoefficient, which is the ratio of the minimumconcentration of test drug required to kill a 24hour culture of B. typhosa in 7.5 minute at 37.5°Cto that of phenol under similar conditions. Thistest has only limited validity, particularly inrelation to antiseptics which have to be testedon living surfaces.
Therapeutic index of an antiseptic is definedby comparing the concentration at which it actson microorganisms with that which produces localirritation, tissue damage or interference withhealing.
CLASSIFICATION1. Phenol derivatives: Phenol, Cresol,
Hexylresorcinol, Chloroxylenol,Hexachlorophene.
2. Oxidizing agents: Pot. permangnate,Hydrogen peroxide, Benzoyl peroxide.
3. Halogens: Iodine, Iodophores, Chlorine,Chlorophores.
4. Biguanide: Chlorhexidine.5. Quaternary ammonium (Cationic): Cetri-
mide, Benzalkonium chloride, Dequaliniumchloride.
6. Soaps: of Sod. and Pot.7. Alcohols: Ethanol, Isopropanol.8. Aldehydes: Formaldehyde, Glutaraldehyde.9. Acids: Boric acid, Acetic acid.
10. Metallic salts: Silver nitrate, Silversulfadiazine, Mild silver protein, Zincsulfate, Calamine, Zinc oxide.
11. Dyes: Gentian violet, Acriflavine, Proflavine.12. Furan derivative: Nitrofurazone.
1. PHENOLS
Phenol (Carbolic acid) It is one of the earliestused antiseptics and still the standard for com-paring other germicides. It is a relatively weakagent (static at 0.2%, cidal at >1%, poor actionon bacterial spores). It is a general protoplasmicpoison, injuring microbes and tissue cells alike—at higher concentrations causes skin burns andis a caustic. It acts by disrupting bacterialmembranes and denaturing bacterial proteins.Organic matter diminishes its action slightly whilealkalies and soaps do so profoundly (carbolicsoaps are not more germicidal than soap itself).It is now seldom employed as an antiseptic, butbeing cheap, it is used to disinfect urine, faeces,pus, sputum of patients and is sometimes includedin antipruritic preparations because of its mildlocal anaesthetic action.
Cresol It is methyl-phenol; more active (3–10times) and less damaging to tissues. Used fordisinfection of utensils, excreta and for washinghands.LYSOL is a 50% soapy emulsion of cresol.
Hexylresorcinol It is a more potent derivative of thephenolic compound resorcinol that is odourless andnonstaining; used as mouthwash, lozenge and as anti-fungal.
Chloroxylenol It has a phenol coefficient of70; does not coagulate proteins, is noncorrosive,nonirritating to intact skin, but efficacy is reducedby organic matter. It is poorly water soluble; thecommercial 4.8% solution (DETTOL) is preparedin 9% terpinol and 13% alcohol; used for surgicalantisepsis. A 0.8% skin cream and soap, 1.4%lubricating obstetric cream (for vaginal examina-tion, use on forceps, etc.), and a mouthwash(DETTOLIN 1% with menthol 0.45%) are also available.These preparations lose activity if diluted withwater and kept for a time.
Hexachlorophene This chlorinated phenolacts by inhibiting bacterial enzymes and (in highconcentration) causing bacterial lysis. It isodourless, nonirritating and does not stain. Itsactivity is reduced by organic matter but not by

899C
HA
PTE
R65
ANTISEPTICS, DISINFECTANTS AND ECTOPARASITICIDES
soap. It is commonly incorporated in soap andother cleansing antiseptics for surgical scrub,patient’s skin, etc., but is narrow spectrum; killsgram-positive but not gram-negative bacteria orspores. The degerming action is slow but persistentdue to deposition on the skin as a fine film thatis not removed by rinsing with water. Incorporatedin toilet products, it is a good deodorant.
Use of a 3% solution for baby bath markedlyreduced the incidence of staphylococcal infec-tions, but produced brain damage (especially inpremature neonates). Around 1970 several fata-lities occurred in USA. Since then use ofpreparations containing > 2% hexachlorophenehave been banned.
2. OXIDIZING AGENTS
Potassium permanganate It occurs aspurple crystals, highly water soluble, liberatesoxygen which oxidizes bacterial protoplasm. Theavailable oxygen and germicidal capacity is usedup if much organic matter is present—the solutiongets decolourised. A 1:4000 to 1:10,000 solution(Condy’s lotion) is used for gargling, douching,irrigating cavities, urethra and wounds. The actionis rather slow and higher concentrations causeburns and blistering—popularity therefore hasdeclined.
It has also been used to disinfect water (wells,ponds) and for stomach wash in alkaloidalpoisoning (except atropine and cocaine which arenot efficiently oxidized). It promotes rusting andis not good for surgical instruments.
Hydrogen peroxide It liberates nacent oxygen whichoxidizes necrotic matter and bacteria. A 3.0% solutionproduces 10 volumes of oxygen, much of which escapesin the molecular form. Catalase present in tissues speedsdecomposition resulting in foaming—helps in loosening andremoving slough, ear wax, etc. Hydrogen peroxide has poorpenetrability and a weak, transient action. It loses potencyon keeping. Use therefore is much restricted.
Benzoyl peroxide It is specifically activeagainst P. acnes and used on acne vulgaris (seep. 893).
3. HALOGENS
Iodine It is a rapidly acting, broad-spectrum(bacteria, fungi, viruses) microbicidal agent; hasbeen in use for more than a century. Acts byiodinating and oxidizing microbial protoplasm.A 1 : 20,000 solution kills most vegetative formswithin 1 min. Even bacterial spores are killedwith higher concentrations/longer contact. Organicmatter retards but does not abolish its germicidalaction.
Solid iodine is corrosive, stronger solutions(> 5%) cause burning and blistering of skin.Tincture iodine (2% in alcohol) stings on abrasions.It is used on cuts, for degerming skin beforesurgery, and to treat ring worm, etc. Mandel’s paint(1.25% iodine dissolved with the help of Pot.iodide forming soluble I3̄ -ions) is applied on sorethroat. A nonstaining iodine ointment (IODEX 4%)is popular as antiseptic and counterirritant. Someindividuals are sensitive to iodine—rashes andsystemic manifestations occur in them.
Iodophores These are soluble complexes ofiodine with large molecular organic compoundsthat serve as carriers—release free iodine slowly.The most popular—Povidone (Polyvinyl-pyrrolidone) iodine: is nonirritating, nontoxic,nonstaining and exerts prolonged germicidalaction. Treated areas can be bandaged or occludedwithout risk of blistering. It is used on boils,furunculosis, burns, otitis externa, ulcers, tinea,monilial/trichomonal/ nonspecific vaginitis and forsurgical scrubbing, disinfection of endoscopes andinstruments.BETADINE 5% solution, 5% ointment, 7.5% scrub solution,200 mg vaginal pessary; PIODIN 10% solution, 10% cream,1% mouthwash; RANVIDONE AEROSOL 5% spray withfreon propellant.
Chlorine A highly reactive element and arapidly acting potent germicide, 0.1–0.25 ppmkills most pathogens (but not M. tuberculosis)in 30 sec. However, the degerming action is soonexhausted, and it lacks substantivity. It is usedto disinfect urban water supplies. Organicmatter binds chlorine, so that excess has to beadded to obtain free chlorine concentration of

900S
EC
TIO
N14
MISCELLANEOUS DRUGS
0.2–0.4 ppm. This is known as the ‘chlorinedemand’ of water. Chlorine is more active in acidicor neutral medium.
Chlorophores These are compounds thatslowly release hypochlorous acid (HOCl). Becauseof ease of handling, they are used in preferenceto gaseous chlorine.
(i) Chlorinated lime (bleaching powder) Itis obtained by the action of chlorine on lime;resulting in a mixture of calcium chloride andcalcium hypochlorite. On exposure, it decomposesreleasing 30–35% W/W chlorine. It is used asdisinfectant for drinking water, swimming poolsand sanitizer for privies, etc.
(ii) Sodium hypochlorite solution Contains4–6% sodium hypochlorite. It is a powerfuldisinfectant used in dairies for milk cans, otherequipment and for infant feeding bottles. It isunstable and too irritant to be used as antiseptic,except for root canal therapy in dentistry.
4. BIGUANIDE
Chlorhexidine A powerful, nonirritating,cationic antiseptic that disrupts bacterial cellmembrane. A secondary action is denaturation ofmicrobial proteins. It is relatively more activeagainst gram-positive bacteria. Like hexachloro-phene it persists on the skin. Present in SAVLON(see below), it is extensively used for surgicalscrub, neonatal bath, mouthwash, obstetrics andas general skin antiseptic.
Chlorhexidine is the most widely employedantiseptic in dentistry. As 0.12–0.2% oral rinseor 0.5–1% toothpaste, it is highly active in preven-ting/treating gingivitis. Twice daily chlorhexidineoral rinse markedly reduces oral infections inimmunocompromised patients, including AIDS.However, it may leave an unpleasant after taste,and repeated application causes brownishdiscolouration of teeth.
5. QUATERNARY AMMONIUM (CATIONIC) ANTISEPTICS
These are detergents; cidal to bacteria, fungi andviruses. However, many gram-negative bacteria
(especially Pseudomonas), M. tuberculosis andbacterial spores are relatively resistant. They actby altering permeability of cell membranes anddenaturing of bacterial proteins. Soaps, beinganionic, neutralize their action, while alcoholpotentiates. They spread through oil and grease,have cleansing and emulgent properties. They arenonirritating and mildly keratolytic. However, thegermicidal action is rather slow and bacteria maythrive under a film formed by them on the skin.Pus, debris and porous material like cotton,polyethylene reduce their activity. Occasionallysensitization occurs. These disadvantages notwithstanding, they are widely used as sanitizers,antiseptic and disinfectant for surgical instruments,gloves, etc, but should not be consideredsterilizing.
Cetrimide A soapy powder with a faint fishyodour. Used as 1–3% solution, it has good clean-sing action, efficiently removing dirt, grease, tarand congealed blood from road side accidentwounds. Alone or in combination with chlorhexi-dine, it is one of the most popular hospitalantiseptic and disinfectant for surgical instruments,utensils, baths, etc.CETAVLON CONCENTRATE: Cetrimide 20%SAVLON LIQUID ANTISEPTIC: Chlorhexidine gluconate1.5% + Cetrimide 3%.SAVLON/CETAVLEX CREAM: Chlorhexidine HCl 0.1% +Cetrimide 0.5%.SAVLON HOSPITAL CONCENTRATE: Chlorhexidine gluco-nate 7.5% + Cetrimide 15%.
Benzalkonium chloride (Zephiran) It is highly solublein water and alcohol. A 1:1000 solution is used for sterilestorage of instruments and 1 in 5000 to 1 in 10,000 fordouches, irrigation, etc.
Dequalinium chloride Has been used in gum paints andlozenges.DEQUADIN 0.25 mg lozenges.
6. SOAPS
Soaps are anionic detergents; weak antiseptics,affect only gram-positive bacteria. Their useful-ness primarily resides in their cleansing action.Washing with soap and warm water is one ofthe most effective methods of preventingtransmission of infection by removing/diluting

901C
HA
PTE
R65
ANTISEPTICS, DISINFECTANTS AND ECTOPARASITICIDES
pathogenic bacteria. Soaps can be medicated byother antiseptics.
7. ALCOHOLS
Ethanol It is an effective antiseptic andcleansing agent at 40–90% concentration. Therapidity of action increases with concentrationupto 70% and decreases above 90%. It acts byprecipitating bacterial proteins. A cotton swabsoaked in 70% ethanol rubbed on the skin kills90% bacteria in 2 min.; has been used beforehypodermic injection and on minor cuts. Lowconcentrations enhance the antiseptic activity ofiodine and chlorhexidine when used as solventfor these. It is an irritant and should not be appliedto mucous membranes or to delicate skin(scrotum), ulcers, etc. On open wounds it producesa burning sensation, injures the surface and formsa coagulum under which bacteria could grow. Itis a poor disinfectant for instruments—does notkill spores and promotes rusting.
Isopropanol It is less volatile; can be usedin place of ethanol.
8. ALDEHYDES
Formaldehyde It is a pungent gas—sometimesused for fumigation. A 37% aqueous solutioncalled Formalin is diluted to 4% and used forhardening and preserving dead tissues. It denaturesproteins and is a general protoplasmic poison,but acts slowly. A broad-spectrum germicide, butuse as antiseptic is restricted by its irritating natureand pungent odour. It is occasionally employedto disinfect instruments and excreta. Those whohandle formalin can develop eczematoid reactions.The urinary antiseptic methenamine acts byreleasing formaldehyde in acidic urine (seep. 760). Formaline is also used to precipitatetoxoids from toxins.
Glutaraldehyde It is less volatile, less pungent,less irritating and better sterilizing agent thanformalin, but needs to be activated by alkaliniza-tion of the solution. It exerts broad-spectrumactivity against bacteria, fungi and viruses. Organic
matter does not inactivate it. A 2% solution isused to disinfect surgical instruments andendoscopes, but prolonged contact is needed.Repeated application on skin can cause sensitiza-tion. The alkalinized solution has a short shelflife (2 weeks) unless stablilizing agents are added.
9. ACIDS
Boric acid It is only bacteriostatic and a veryweak antiseptic. But being nonirritating even todelicate structures, saturated aqueous solutions(4%) have been used for irrigating eyes,mouthwash, douche, etc. Boroglycerine paint(30%) is used for stomatitis and glossitis. A 10%ointment (BOROCIDE) is available for cuts andabrasion. It is included in prickly heat powdersand ear drops. However, boric acid is notinnocuous; systemic absorption causes vomiting,abdominal pain, diarrhoea, visual disturbances andkidney damage. Hence its use for irrigatingbladder, large wounds, as ointment on extensiveburnt areas, liberal use of powder for infants isnot recommended.
Acetic acid It is a relatively weak antiseptic, bactericidalonly above 5%. Pseudomonas is especially susceptible. Itis occasionally used for burn dressing and for douche in1–3% strength.
10. METALLIC SALTS
Silver compounds These are astringent andcaustic. They react with SH, COOH, PO4 andNH2 groups of proteins.
(i) Silver nitrate rapidly kills microbes, actionpersisting for long periods because of slow releaseof Ag+ ions from silver proteinate formed byinteraction with tissue proteins. Tissues get stainedblack due to deposition of reduced silver. Silvernitrate touch is used for hypertrophied tonsillitisand aphthous ulcers. It is highly active againstgonococci—1% solution is used for ophthalmianeonatorum.(ii) Silver sulfadiazine (see p. 706) is highlyactive against Pseudomonas and has been usedon burns.

902S
EC
TIO
N14
MISCELLANEOUS DRUGS
Zinc salts They are astringent and mild anti-septics.(i) Zinc sulfate: is highly water soluble,0.1–1% is used for eyewash and in eye/ear drops(Zinc-boric acid drops—in ZINCO-SULFA 0.1% eyedrop). Applied to skin, it decreases perspiration.White lotion containing 4% each of zinc sulfateand sulfurated potash has been used for acne andimpetigo; (THIOSOL 2.5%, THIOSOL FORTE 4% lotion).(ii) Calamine and zinc oxide: are insoluble. Inaddition to being mildly antiseptic, they arepopular dermal protectives and adsorbants.
11. DYES
Gentian violet (crystal violet) A rosanilinedye active against staphylococci, other gram-positive bacteria and fungi, but gram-negativeorganisms and mycobacteria are insensitive.Aqueous or alcoholic solution (0.5–1%) is usedon furunculosis, bedsores, chronic ulcers, infectedeczema, thrush, Vincent’s angina, ringworm, etc.It has become unpopular due to deep staining.
Acriflavine and Proflavine These are orange-yellow acridine dyes active against gram-positivebacteria and gonococci. Their efficacy is notreduced by organic matter and is enhanced inalkaline medium. Solutions lose efficacy onexposure to light—store in amber bottles. Theyare nonirritant and do not retard healing—parti-cularly suitable for chronic ulcers and wounds.Bandage impregnated with acriflavine-vaseline isused for burn dressing;ACRINOL 0.1% acriflavine cream.
The triple dye lotion contains gentian violet0.25% + brilliant green 0.25% + acriflavine 0.1%(TRIPLE DY), has been used for burns and fordressing umbilical stump in neonates.
12. FURAN DERIVATIVES
Nitrofurazone (Nitrofural) It is cidal to bothgram-positive and negative, aerobic and anaerobicbacteria, even in high dilutions, but activity isreduced in the presence of serum. Acts byinhibiting enzymes necessary for carbohydratemetabolism in bacteria. It is highly efficacious
in burns and for skin grafting. Its local toxicityis negligible—but sensitization occurs frequently.FURACIN 0.2% cream, soluble ointment, powder.Nitrofurantoin and Furazolidone are other furan derivativesused for urinary and intestinal infections respectively.
ECTOPARASITICIDES
These are drugs used to kill parasites that liveon body surface. Lice (Pediculus sp.—winglessinsects) and mites (Sarcoptes/Acarus scabiei—arachnids) are minute arthropods infesting humanskin and hair.
Scabies It is highly contagious; the mite bur-rows through the epidermis, laying eggs whichform papules that itch intensely. Lesions may getsecondarily infected requiring systemic antimicro-bial therapy. The finger webs are the preferredsites of entry, but may soon spread to forearms,trunk, genitals and lower legs. Other membersof the patient’s family should be treatedconcurrently; garments and bed linen should bewashed in hot water and put in sun to preventcross infection and re-infection.
Pediculosis The lice thrive on head (P. capitis),body (P. corporis) or pubic region (P. pubis).They cause itching, suck blood and transmit typhusand relapsing fever. The eggs called nits getattached to the hair and clothing by a chitin likecement.
Drugs used are:Permethrin SulfurLindane (BHC) Dicophane (DDT)Benzyl benzoate IvermectinCrotamiton
1. Permethrin This broad-spectrum andpotent pyrethoid insecticide is currently the mostefficacious and most convenient drug for bothscabies and lice. It causes neurological paralysisin insects, probably by delaying depolarization.Toxicity of permethrin in humans is very low;apparently 40–400 times lower than that oflindane. After application, permethrin persists onthe skin for days; systemic absorption is minimal.Nearly 100% cure rates have been obtained in

903C
HA
PTE
R65
ANTISEPTICS, DISINFECTANTS AND ECTOPARASITICIDES
scabies and pediculosis; comparative studies havefound it to be more effective than lindane, benzylbenzoate and crotamiton. Single application isneeded in most cases. Resistance to permethrinis very rare and it is effective in lindane nonres-ponsive cases. Few patients may experience mildand transient burning, itching, tingling, erythemaor rash.For scabies: PERMITE, OMITE, NOMITE 5% cream; applyall over the body except face and head; wash after 8–12 hours.SCABERID 5% cream, 1% soap; SCABPER 5% lotion.For head lice: PERLICE, KERALICE 1% cream rinse, ELICE5% lotion, SCALTIX 1% lotion; massage about 30 g into thescalp, washoff after 10 min.Thus, permethrin is now the 1st choice drug forscabies and pediculosis
2. Lindane (Gamma benzene hexachloride,BHC) Another broad-spectrum insecticide whichkills lice and mites by penetrating through theirchitinous cover and affecting the nervous system.Lindane is highly effective in treating headlice(67–92% cure) and scabies (84–92% cure) bysingle treatment. However, efficacy is lower thanpermethrin. Both lice and mites can developresistance to lindane. Combining it with benzylbenzoate precludes resistance and improves curerate to nearly 100%.GAB 1% lotion, ointment; GAMADERM, SCABOMA 1%lotion; GAMASCAB 1% lotion, cream; ASCABIOL 1%emulsion with cetrimide 0.1%; BENZO 1% lotion, 1% soap.For pediculosis: apply to scalp and hair (taking care not toenter eyes), leave for 12–24 hr. (a shower cap may be used forlong hair) and then wash off. If lice are still present, repeattreatment after 1 week.For scabies: the lotion/cream is rubbed over the body (belowneck) and a scrub bath taken 12–24 hr later. Singletreatment suffices in most patients; can be repeated only aftera week, if the mite is still present.
The disadvantages of lindane are:Being highly lipid soluble it can be absorbedthrough the skin (especially from oily vehiclesand in small children)— can produce systemictoxicity —CNS stimulation, vertigo, convulsions(especially in children) and cardiac arrhythmias.
Absorbed lindane is widely distributed in thebody, especially in fat; is metabolised and elimina-ted with a t½ ~24 hr. It can induce CYP isoenzymesin liver and affect metabolism of many drugs.
Though well tolerated by most patients ifinstructions are followed, it is less favoured fortreatment of scabies—because application overlarge body surface is required—possibility ofsystemic absorption is more. It should be avoidedin infants, young children and during pregnancy.Skin irritation is not prominent.3. Benzyl benzoate It is an oily liquid withfaint aromatic smell; has been popular fortreatment of scabies. The emulsion is applied allover except face and neck after a cleansing bath.A second coat is applied next day which is washedafter 24 hours. The treatment is convenient anddoes not interfere with routine activities. It hasachieved 76–100% cure in scabies. Benzylbenzoate is minimally absorbed through the skin;systemic toxicity is low, but neurologicalsymptoms have occurred in children—contraindi-cated in them. Skin irritation is common, especiallyin children. Contact dermatitis is possible.BENZYLBENZOATE APPLICATION 25% lotion; DERMIN25% lotion; SCABINDON 25% oint with DDT 1% andbenzocaine 2%
For pediculosis, it can be applied to the scalp,taking care not to enter eyes, and is washed offafter 24 hours. Benzyl benzoate is now a 2ndchoice drug for scabies and seldom used forpediculosis. Its combination with lindane is highlyeffective.
4. Crotamiton It is an effective scabicide,pediculocide and antipruritic, but has producedlower cure rates (60–88%) in scabies. Betterresults have been obtained by extended 5 dayapplication in children. It is less prone to causeskin irritation and has low systemic toxicity despiteabsorption through the skin—may be preferredfor children. It is applied twice at 24 hr intervaland washed off day after that.CROTORAX, CROTON 10% cream, lotion
Because of lower efficacy and need for repeatapplication, it is a second choice drug for scabiesand pediculosis.5. Sulfur It is the oldest scabicide and weak pediculo-cide, antiseptic, fungicide and keratolytic. Applied to skinit is slowly reduced to H2S and oxidized to SO2 andpentathionic acid. These, especially the latter, dissolve the

904S
EC
TIO
N14
MISCELLANEOUS DRUGS
cuticle of itch mite and kill it. The reactions are carriedout by epidermal cells and the arthropods themselves.
Sublimed sulfur or precipitated sulfur is used as a 10%ointment. After a warm scrubbing bath (to open the burrows)the ointment is massaged over the entire body (below theneck) for 3 consecutive days, followed by soap water bathon the fourth day. It is cheap but has disadvantages:(a) Treatment is messy.(b) Produces bad odour—socially unacceptable —may
interfere with patient’s vocation.(c) Repeated applications are required.
Sulfur has been superseded by better drugs.
6. Dicophane (DDT) It has been a popular insecticidefor mosquitoes, flies and other pests. For this purpose, itis used in the dust or watery suspension form, which ispoorly absorbed through skin. For pediculosis and scabiesa 1–2% lotion or ointment is applied and washed off after12–24 hours. It penetrates through the exoskeleton and actsas a neurotoxin for the arthropods. When oily vehicles areused, significant amounts may be absorbed through the skinand cause rashes, muscle weakness, tremor. Very high dosesproduce BHC like convulsions. It gets stored in body fat
and induces microsomal enzymes. Combination with benzylbenzoate (SCABINDON oint) is more effective. It is rarelyused.
7. Ivermectin This anthelmintic drug (seep. 854) has been found highly effective in scabiesand pediculosis as well. It is the only orallyadministered drug used for ectoparasitosis. Asingle 0.2 mg/kg (12 mg in adults) dose has curedupto 91–100% patients of scabies. AIDS patientswith scabies also respond. Most cases of head/body lice have been successfully treated.
Ivermectin is very well tolerated by scabies/pediculosis patients, with few if any side effects.However, it is not to be given to children < 5 yr,pregnant and lactating women. Only limited useof ivermectin has been made in scabies and pedi-culosis because of the availability of efficacioustopical agents.

Chelating AgentsChapterChapterChapterChapterChapter 6666666666
These are drugs which complex metallic ions,forming ring structures within their molecule(Greek Chele = Crab; the compound holds themetal like a crab’s claw). They are primarily usedin heavy metal poisonings.
Those compounds which form stable, non-toxic and easily excreted complexes with toxicmetals are valuable in poisonings. The usefulagents contain two or more reactive groups(ligands) which can hold the metal from at leasttwo sides so that a ring is formed. When thering is 5–7 membered, it is most stable.Ligand is a functional group capable of formingcoordinate bond, i.e. a covalent bond in whichboth the shared electrons are donated by theligand—generally O, N, or S atoms in hydroxyl,carboxyl, keto, sulfhydryl, disulfide, amino orphosphate groups.
Heavy metals exert their toxic effects bycombining with and inactivating functional groups(ligands) of enzymes or other critical biomole-cules. Chelating agents compete with bodyligands for the heavy metal. They differ in theiraffinity for different metals. Clinically usefulagents should have a higher affinity for thetoxic metal than for calcium, because Ca2+
is readily available in plasma and extracellularfluid. They should also have higher affinitythan the body ligands for the toxic metal.Moreover, to be effective in metal poisoning, theirdistribution in the body should correspond to thatof the metal to be chelated, and they should bewater soluble.
Efficacy of all chelating agents in promotingexcretion of the toxic metal and in reversing toxicmanifestations declines rapidly as the intervalbetween entry of the metal in the body and theadministration of the chelator increases.
Chelating agents useful as drugs are:Dimercaprol (BAL) Calcium disodium DTPADimercaptosuccinic Penicillamine
acid (Succimer) DesferrioxamineDisodium edetate DeferiproneCalcium disodium
edetate
Dimercaprol (British antilewisite; BAL)It is an oily, pungent smelling, viscous liquid,developed during World War II by Britishers asan antidote to the arsenical war gas lewisite. Thetwo SH groups of dimercaprol bind those metalswhich produce their toxicity by interacting withsulfhydryl containing enzymes in the body, i.e.As, Hg, Au, Bi, Ni, Sb, Cu. The complex of2 molecules of dimercaprol with one metal ionis more stable than 1:1 complex. It is, therefore,desirable to maintain excess of dimercaprol inplasma to allow formation of 2 : 1 complex. Thedimercaprol-metal complex spontaneously disso-ciates releasing the metal at a slow rate; alsodimercaprol is partly oxidized in the body: furtheremphasizing the necessity to have excessdimercaprol available. But due to dose dependenttoxicity of dimercaprol, large amounts should notbe given at a time.
H H H| | |
H — C — C — C — H| | |
SH SH OH
DIMERCAPROL
Uses
1. Poisoning by As, Hg, Au, Bi, Ni, Sb: it isadministered i.m., 5 mg/kg stat, followed by2–3 mg/kg every 4–8 hours for 2 days, then once

906S
EC
TIO
N14
MISCELLANEOUS DRUGS
or twice a day for 10 days. It is partly oxidizedand glucuronide conjugated, but mainly excretedas such in 4–6 hours. Earlier the treatment isinstituted, the better it is. Because the dimercaprol-metal complex dissociates faster in acidic urineand the released metal can damage the kidney,urine is alkalinized during dimercaprol therapy.2. As an adjuvant to Cal. disod. edetate in leadpoisoning.3. As an adjuvant to penicillamine in Cupoisoning and in Wilson’s disease—300 mg/dayi.m. for 10 days every second month.BAL INJ 100 mg/2 ml (in arachis oil) inj.
It is contraindicated in iron and cadmiumpoisoning, because the dimercaprol-Fe anddimercaprol-Cd complex is itself toxic.
Adverse effects These are frequent, dose relatedand distressing, but generally not damaging.Rise in BP, tachycardia, vomiting, tingling andburning sensations, inflammation of mucousmembranes, sweating, cramps, headache andanxiety.Antihistaminics given 30 min before dimercaprolinjection, reduce the intensity of adverse effects.
Dimercaptosuccinic acid (Succimer) It is similar todimercaprol in chelating properties, water soluble, less toxicand orally effective. Its efficacy has been demonstrated inAs, Hg and Pb poisoning. It has been marketed in USAand some other countries, but not in India for the treatmentof lead intoxication. Side effects are nausea, anorexia andloose motions.
Disodium edetate (Na2EDTA) It is the disodium saltof ethylene diamine tetraacetic acid (EDTA). It is a potentchelator of calcium—causes tetany on i.v. injection. Whena slow infusion is given, tetany does not occur, becausecalcium is withdrawn from bones. It can be used for emergencycontrol of hypercalcaemia: 50 mg/kg i.v. infusion over2–4 hours, but bisphosphonates are preferred.
NaOOCH2C CH2 COONa N CH2—CH2 N
HOOCH2C CH2 COOH
DISODIUM EDETATE
Calcium disodium edetate (Ca Na2 EDTA)It is the calcium chelate of Na2 EDTA. Becausethis chelating agent has higher affinity for metals
like Pb, Zn, Cd, Mn, Cu and some radioactivemetals, it can remove them from the body byexchanging with Ca held by it. It is highly ionized,therefore distributed only extracellularly andrapidly excreted in urine by glomerular filtration(t½ < 1 hour) carrying the toxic metal along. Itis not metabolized. Because of its ionic nature,Ca Na2 EDTA is not absorbed from the g.i.t.—must be given parenterally. Since i.m. injectionis painful, preferred route is i.v. It does not enterbrain or CSF. Thus, it can remove toxic metalsonly from accessible sites.
Uses
1. Lead poisoning This is the most importantindication for CaNa2EDTA; 1 gm is diluted to200–300 ml in saline or glucose solution andinfused i.v. over 1 hour twice daily for 3–5 days.The urinary excretion of Pb is promptly increased,but declines quickly as the metal is removed fromaccessible sites (primarily bone). A second courseof CaNa2EDTA may be repeated after 5–7 days,allowing time for Pb to redistribute to extracellularsites.2. It is also useful in Fe, Zn, Cu, Mn andradioactive metal, but not Hg poisoning, becauseHg is more firmly bound to body constituentsand is localized in areas not accessible to CaNa2
EDTA.
Adverse effects CaNa2 EDTA does not producetetany and is relatively safe.Kidney damage with proximal tubular necrosisis the most important problem. This is roughlydose-related and may be due to the toxic metalpartly dissociating in the tubule. It can beminimized by maintaining high urine flow.An acute febrile reaction with chills, bodyache,malaise, tiredness occurs in some individuals.Anaphylactoid reaction with fall in BP andcongestion of eyes and nose is also reported.Calcium disodium DTPA Diethylene triamine pentaacetic acid (DTPA, Pentetic acid) is a congener of EDTA.It has higher affinity for many heavy metals than EDTA.Its calcium chelate has been used in metal poisonings(especially radioactive metals like uranium, plutonium) which

907C
HA
PTE
R66
CHELATING AGENTS
do not respond to CaNa2EDTA. However, because of itslimited distribution in the body, results are not impressive.
PenicillamineIt is dimethyl cysteine, obtained as a degradationproduct of penicillin. It was found to have strongcopper chelating property and was used in 1956for Wilson’s disease. It selectively chelates Cu,Hg, Pb and Zn. The d-isomer is used therapeu-tically, because the l-isomer and the recemateproduce optic neuritis and are more toxic. It isadequately absorbed after oral administration, littlemetabolized in the body and excreted in urineand faeces. When given to patients with heavymetal toxicity, excretion of the metal is enhanced.
tion in the urinary tract, because penicillamine-cysteine complex is more soluble than dicysteine(cystine).5. Scleroderma: Penicillamine benefits byincreasing soluble collagen.It was used as a disease modifying drug inrheumatoid arthritis, but has been replaced nowby safer drugs (see p. 212).
Adverse effects Short-term administration (asmetal chelator) of penicillamine does not causemuch problem. Various cutaneous reactions,itching and febrile episodes may occur. However,long-term use produces pronounced toxicity. Der-matological, renal, haematological and collagentissue toxicities are prominent.
DesferrioxamineFerrioxamine is a long chain iron containing comp-lex obtained from an actinomycete. Chemicalremoval of iron from it yields desferrioxaminewhich has very high affinity for iron: 1g is capableof chelating 85 mg of elemental iron. The straightchain desferrioxamine molecule winds round ferriciron and forms a stable nontoxic complex whichis excreted in urine. It removes loosely boundiron as well as that from haemosiderin and ferritin,but not from haemoglobin or cytochrome. Anotherdesirable property is its low affinity for calcium.
Little of orally administered desferrioxamineis absorbed. Parenterally administered desferrioxa-mine is partly metabolized and rapidly excretedin urine.
Uses
1. Acute iron poisoning: mostly in children. Thisis the most important indication—may be lifesaving (see p. 606).
2. Transfusion siderosis: occurs in thalassemiapatients who receive repeated blood trans-fusion. Desferrioxamine 0.5–1 g/day i.m. helpsto excrete the chronic iron overload; may alsobe infused i.v. concurrently with bloodtransfusion—2 g per unit of blood.
Adverse effects Desferrioxamine can causehistamine release → fall in BP, flushing, itching,
CH3
|H3C — C — CH — C O
| | |SH NH2 OH
PENICILLAMINE
Uses
1. Wilson’s disease (Hepatolenticular degene-ration): This is due to genetic deficiency ofceruloplasmin, a protein which normally bindsand disposes off Cu from the body. In its absence,plasma concentration of free Cu is high whichgets deposited in liver, substantia nigra, basalganglia of brain, and causes local degeneration.Life long therapy is needed to prevent progres-sion of the disease.Dose: 0.5–1 g daily in divided doses 1 hour before or 2 hourafter meals to avoid chelation of dietary metals.ARTAMIN, CILAMIN 250 mg cap, ARTIN 150, 250 mg cap.Pot. sulfide 20–40 mg may be given with eachmeal to decrease the absorption of dietary copper.2. Copper/mercury poisoning: 1–1.5 g/day isgiven for a few days. It is the drug of choicefor Cu poisoning and alternative drug to dimerca-prol/succimer for Hg poisoning.3. Chronic lead poisoning: It may be used asan adjuvant to CaNa2EDTA, but succimer ispreferred.4. Cystinuria and cystine stones: It promotes theexcretion of cysteine and prevents its precipita-

908S
EC
TIO
N14
MISCELLANEOUS DRUGS
urticaria, rashes. A variety of allergic reactionsare reported. Changes in lens and retina can occuron repeated use.Other side effects are abdominal pain, loosemotions, muscle cramps, fever and dysuria.DESFERAL 0.5 g/vial inj.
DeferiproneIt is an orally active iron chelator which hassimplified the treatment of transfusion siderosisin thalassemia patients. Excessive haemolysisoccurs in these patients, and they have to be givenrepeated blood transfusions. An iron chelator has
to be used to clear the resulting iron overload.Oral deferiprone is a somewhat less effectivealternative to injected desferrioxamine. Sideeffects and cost of treatment are reduced.Deferiprone has also been indicated for acute ironpoisoning (less effective than desferrioxamine)and for iron load in liver cirrhosis.Dose: 50–100 mg/kg daily in 2–4 divided doses.KELFER 250, 500 mg caps.
Side effects are anorexia, vomiting, alteredtaste, joint pain, reversible neutropenia, rarelyagranulocytosis. However, long-term safety is notyet known.

VitaminsChapterChapterChapterChapterChapter 6767676767
Vitamins are nonenergy yielding organic com-pounds, essential for normal human metabolism,that must be supplied in small quantities in thediet. This definition excludes the inorganicessential trace minerals and essential amino acidsand fatty acids which are required in much largerquantities. Other substances needed for propergrowth of microorganisms or cells in culture arecalled ‘growth factors’. The different chemicalforms and precursors of a vitamin can be calledits Vitamers (analogy—isomers).
The importance of vitamins as drugs is pri-marily in the prevention and treatment ofdeficiency diseases. Some vitamins do have otherempirical uses in pharmacological doses. Vitamindeficiencies occur due to inadequate intake,malabsorption, increased tissue needs, increasedexcretion, certain genetic abnormalities and drug-vitamin interactions.
Vitamins, as a class, are over-promoted, over-prescribed and over-used. Myths like ‘vitaminsenergise the body’, ‘any physical illness is accom-panied by vitamin deficiency’, ‘vitamin intake innormal diet is precariously marginal’, ‘vitaminsare harmless’, are rampant.
Vitamins are traditionally divided into twogroups:
(a) Fat-soluble (A, D, E, K): These (except vitK) are stored in the body for prolonged periodsand are liable to cause cumulative toxicity afterregular ingestion of large amounts. Some interactwith specific cellular receptors analogous tohormones.
(b) Water-soluble (B complex, C): These aremeagerly stored: excess is excreted with littlechance of toxicity. They act as cofactors forspecific enzymes of intermediary metabolism.
Chemical forms and preparations of vitamins arelisted in Table 67.1.
FAT-SOLUBLE VITAMINS
VITAMIN A
Chemistry and source Vitamin A occurs innature in several forms. Retinol (Vit. A1) is anunsaturated alcohol containing an ‘ionone’ ring.Marine fish (cod, shark, halibut) liver oils arerich sources. Appreciable amounts are present inegg yolk, milk and butter.
Dehydroretinol (Vit A2) is present in fresh waterfishes. Carotenoids are pigments found in greenplants (carrot, turnip, spinach), β Carotene is themost important carotenoid. It is inactive as such,one molecule splits to provide two molecules ofretinol. Man on normal diet gets half of hisvit A as retinol esters and half from carotenoids.
1 µg of retinol = 3.3 IU of vit. A activityIt is now called 1 Retinol Equivalent = 6 µgof dietary carotene (because of incomplete utiliza-tion of the provitamin).
Absorption and fate Retinyl palmitate, the chief retinylester in diet, is hydrolysed in intestines to retinol which isabsorbed by carrier transport and reesterified. Aided by bile,it passes into lacteals. Absorption is normally complete, butnot in steatorrhoea, bile deficiency and from protein poordiet. Retinol ester circulates in chylomicrons and is storedin liver cells. Free retinol released by hepatocytes combineswith retinol binding protein (RBP a plasma globulin) andis transported to the target cells. On entering them, it getsbound to the cellular retinol binding protein (CRBP). Smallamount is conjugated with glucuronic acid, excreted in bile,undergoes enterohepatic circulation. Minute quantities of watersoluble metabolites are excreted in urine and faeces.
In contrast to retinol, only 30% of dietary β caroteneis absorbed. It is split into two molecules of retinal in theintestinal wall; only half of this is reduced to retinol andutilized.

910S
EC
TIO
N14
MISCELLANEOUS DRUGS
Physiological role and actions(a) Visual cycle Retinal generated by reversibleoxidation of retinol is a component of thelight sensitive pigment Rhodopsin which issynthesized by rods during dark adaptation. Thispigment gets bleached and split into its compo-nents by dim light and in the process generatesa nerve impulse through a G-protein calledTransducin. Retinal so released is reutilized. Asimilar pigment (Iodopsin) is synthesized in thecones—responsible for vision in bright light,colour vision and primary dark adaptation. In vit.A deficiency rods are affected more than cones;irreversible structural changes with permanentnight blindness occur if the deprivation is long-term.
(b) Epithelial tissue Vit. A promotes differen-tiation and maintains structural integrity ofepithelia all over the body. It also promotesmucus secretion, inhibits keratinization andimproves resistance to infection. It appears to havethe ability to retard development of malignanciesof epithelial structures. Vit A is also required forbone growth.
(c) Reproduction Retinol is needed for mainte-nance of spermatogenesis and foetal development.
(d) Immunity Increased susceptibility to infec-tion occurs in vit A deficiency. Physiologicalamount of vit A appears to be required for properantibody response, normal lymphocyte prolife-ration and killer cell function.
Deficiency symptoms Since vit. A is storedin liver, deficiency symptoms appear only afterlong-term deprivation, but vit A deficiency is quiteprevalent, especially among infants and childrenin developing countries. Manifestations are:• Xerosis (dryness) of eye, ‘Bitot’s spots’, kerato-
malacia (softening of cornea), corneal opacities,night blindness (nyctalopia) progressing to totalblindness.
• Dry and rough skin with papules (phryno-derma), hyperkeratinization, atrophy of sweatglands.
• Keratinization of bronchopulmonary epithe-lium, increased susceptibility to infection.
• Unhealthy gastrointestinal mucosa, diarrhoea.• Increased tendency to urinary stone formation
due to shedding of ureteric epithelial liningwhich acts as a nidus.
• Sterility due to faulty spermatogenesis,abortions, foetal malformations.
• Growth retardation, impairment of specialsenses.
Therapeutic uses1. Prophylaxis of vit A deficiency during infancy,
pregnancy, lactation, hepatobiliary diseases,steatorrhoea: 3000–5000 IU/day.
2. Treatment of established vit A deficiency:50,000–100,000 IU i.m or orally for 1–3 daysfollowed by intermittent supplemental doses.
3. Skin diseases like acne, psoriasis, ichthyosis.Retinoic acid (see below) and 2nd or 3rdgeneration retinoids are used.
Interactions
(i) Vit E promotes storage and utilization ofretinol and decreases its toxicity.
(ii) Regular use of liquid paraffin by carryingthrough with it vit A can result in deficiency.
(iii) Long-term oral neomycin induces steator-rhoea and interferes with vit A absorption.
Hypervitaminosis A Regular ingestion of grossexcess of retinol (100,000 IU daily for months)has produced toxicity—nausea, vomiting, itching,
Fig. 67.1: The role of vit. A in visual cycle

911C
HA
PTE
R67
VITAMINS
erythema, dermatitis, exfoliation, hair loss, boneand joint pains, loss of appetite, irritability,bleeding, increased intracranial tension andchronic liver disease. Excess retinol is also tera-togenic in animals and man. Daily intake shouldnot exceed 20,000 IU.
Acute poisoning has been described after consumptionof polar bear liver which contains 30,000 IU/g vit A. Singlemassive ingestion (> 1 million IU) produces intense headache,drowsiness, irritability, rise in intracranial tension, vomiting,liver enlargement and shedding of skin. Due to saturationof RBP, excess retinol esters circulate in the free state orloosely associated with lipoprotein. These have surfactantproperty which damages tissues.
Treatment consists of stopping further ingestion, supportivemeasures, and vit E which promotes storage of retinol intissues and speeds recovery. Most signs regress in a week,some persist for months. Excess intake of carotenoids doesnot produce hypervitaminosis A, because conversion to retinolhas a ceiling.
Retinoic acid (vit A acid) Retinoic acid hasvit A activity in epithelial tissues and promotesgrowth, but is inactive in eye and reproductiveorgans. All-trans retinoic acid (Tretinoin) is usedtopically, while 13-cis retinoic acid (Isotretinoin)is given orally for acne (see Ch. 64). Unlikeretinol, it is not stored but rapidly metabolizedand excreted in bile and urine.
The cellular retinoic acid binding protein(CRABP) is different from CRBP, is present inskin and other tissues but not in retina—this maybe the reason for the inability of retinoic acidto participate in visual cycle.
Retinoid receptors Retinol and retinoic acidact through nuclear retinoid receptors whichfunction in a manner analogous to the steroidreceptors: activation results in modulation ofprotein synthesis. In the target cells (epithelial,gonadal, fibroblast) synthesis of certain proteinsis enhanced while that of other proteins isdepressed—accounting for the structural andfunctional changes. Two distinct families ofretinoid receptors, viz. Retinoic acid receptors(RARs) and Retinoid X receptors (RXRs) havebeen identified with differing affinities for differentretinoids.
VITAMIN E
Chemistry and source A number of toco-pherols, of which α tocopherol is the mostabundant and potent, have vit E activity. Thed-isomer is more potent than l-isomer. Wheat germoil is the richest source, others are cereals, nuts,spinach and egg yolk.
1 mg of d α-tocopherol is called α-tocopherolequivalent = 1.49 IU of vit E.
The daily requirement of vit. E is estimatedat 10 mg. It is increased by high intake of poly-unsaturated fats.Absorption and fate Vit. E is absorbed from intestinethrough lymph with the help of bile; it circulates in plasmain association with β-lipoprotein, is stored in tissues andexcreted slowly in bile and urine as metabolites.
Physiological role and actions Vit E actsas antioxidant, protecting unsaturated lipids incell membranes, coenzyme Q, etc. from freeradical oxidation damage and curbing generationof toxic peroxidation products. Feeding animalswith polyunsaturated fats increases vit Erequirement, while antioxidants like cystein,methionine, selenium, chromenols prevent somevit E deficiency symptoms in animals. However,vit E might be having some more specific actionor a structural role in biological membranes,because other deficiency symptoms are notrelieved by these unrelated antioxidants.
Deficiency symptoms Experimental vit E defi-ciency in animals produces recurrent abortion,degenerative changes in spinal cord, skeletalmuscles and heart, and haemolytic anaemia. Noclear-cut vit E deficiency syndrome has beendescribed in humans, but vit E deficiency hasbeen implicated in certain neuromuscular diseasesin children, neurological defects in hepatobiliarydisease and some cases of haemolytic anaemia.
Therapeutic uses1. Primary vit E deficiency does not occur clini-
cally. Supplemental doses (10–30 mg/ day) maybe given to patients at risk (see above).
2. G-6-PD deficiency—prolonged treatment with 100mg/day increases survival time of erythrocytes.

912S
EC
TIO
N14
MISCELLANEOUS DRUGS
3. Acanthocytosis—100 mg /week i.m: normalizes oxidativefragility of erythrocytes.
4. The risk of retrolental fibroplasia in premature infantsexposed to high oxygen concentrations can be reducedby 100 mg/kg/day oral vitamin E.
5. Alongwith vit A to enhance its absorption and storage,and in hypervitaminosis A to reduce its toxicity.
6. Large doses (400–600 mg/day) have been reported toafford symptomatic improvement in intermittentclaudication, fibrocystic breast disease and nocturnalmuscle cramps.For its antioxidant property, vit E has been
promoted for recurrent abortion, sterility,menopausal syndrome, toxaemia of pregnancy,atherosclerosis, ischaemic heart disease, cancerprevention, several skin diseases, prevention ofneurodegenerative disorders, postherpetic neura-lgia, scleroderma and many other conditions, butwithout convincing evidence of benefit.
Toxicity Even large doses of vit E for longperiods have not produced any significant toxicity,but creatinuria and impaired wound healing havebeen reported; abdominal cramps, loose motionsand lethargy have been described as side effectsof vit. E.Vit E can interfere with iron therapy.
Antioxidant vitamins (vit E, βββββ carotene,vit C) in prevention of cardiovasculardisease and cancerAntioxidants are believed to quench free radicals.Free radicals are atoms or molecules with ‘singlet’,i.e. unpaired electron which makes them highlyreactive. Oxidative free radicals are generated bymetabolic reactions—create a chain reactionleading to membrane lipid peroxidation, DNAdamage, etc. Free radical oxidation has beenimplicated in atherosclerosis (oxidized LDL ismore atherogenic), cancers, neurodegenerativediseases and inflammatory bowel diseases. Manyendogenous and dietary compounds like super-oxide dismutase, ferritin, transferrin, ceruloplas-min, α tocopherol, β carotene and ascorbic acidhave antioxidant and free radical scavengingproperties. On this theoretical basis supported bysome epidemiological observations, cohort studiesand prospective trials β carotene, vit C and
especially vit E have been claimed to protectagainst atherosclerosis leading to coronary arterydisease as well as many types of cancers (lung,breast, mouth, skin, esophagus, stomach, etc.).As a result, vit E and others are being aggressivelypromoted and many physicians are prescribingthem for prophylaxis of these conditions. Learningfrom mass media, people on their own also areconsuming them on a large scale. However, theevidence of a beneficial effect is highlycontradictory.
Several large observational studies (involvingtens of thousands of subjects) and their meta-analysis have failed to demonstrate any benefitof antioxidant vitamins in terms of cardiovascularevent/cancer prevention in well nourishedpopulation. On the other hand, there is someindication of increased risk of CHF with>400 mg/day α tocopherol and increased risk ofhip fracture among postmenopausal women withhigh dose of vit A. Therefore, it would be welladvised to adopt a healthy lifestyle, viz. eatingsufficient fruits and vegetables, doing regularexercise, avoiding overweight and smoking, ratherthan consuming antioxidant medications.
A large number of antioxidant proprietarypreparations (ANTOXID, CAROFIT, GLACE, VITOXID,REVOX, CARNITOR, CARNIVIT-E, etc.) containingwidely variable amounts of β-carotene, vit Aacetate, vit E, vit C, selenium, zinc, copper,manganese, carnitine (a substance synthesized inliver and kidney, and involved in intracellulartransport of long-chain fatty acids) are brisklypromoted and consumed, but with no credibleevidence of benefit, and may be some potentialharm.
WATER-SOLUBLE VITAMINS
THE VITAMIN B COMPLEX GROUP
Thiamine (Aneurine, vit B1)Chemistry and source A colourless, crystallinecompound containing a pyrimidine and a thiazolering. It is present in the outer layers of cereals(rice polishing), pulses, nuts, green vegetables,yeasts, egg and meat.

913C
HA
PTE
R67
VITAMINS
TABLE 67.1 Chemical forms, stability, daily allowance and non-combination preparations of vitamins
Vitamin Chemical forms Thermostability Daily allowance Preparations(adult males)
Fat-Soluble Vitamins
Retinol (A1) Stable in 1000 µg AQUASOL-A 50,000 IU cap, 100,000 IU in 2 ml inj.A Dehydroretinol (A2) absence of air (4000 IU) AROVIT 50,000 IU tab, 150,000 IU/ml drops, 100,000 IU/ 2 ml inj.
β-Carotene (provit) CAROFRAL 50,000 IU tab, 100,000 IU/2 ml inj.
Calciferol (D2) Stable 5 µg ACRACHITOL, OSTELIN FORTE 300,000 IU/ml & 600,000 IU/mlD Cholecalciferol (D3) (200 IU) inj (1 ml amp.), CALCIROL 60,000 IU in 1 g granules.
Calcitriol 1 µg CALTROL, ROCALTROL 0.25 µg cap, CALCIBEST 1 μg/ml inj.
E α-Tocopherol Stable; air and 10 mg EVION 100, 200, 400, 600 mg pearls, 50 mg/ml paed. drops.UV light VITEOLIN, ECAP 200, 400 mg pearls, cap.,decompose EROVIT, ETOPLEX, EPHYNA 200, 400 mg caps.
Phytonadione (K1) Stable, 50–100 µg VITAMIN-K, KENADIONE 10 mg/ml inj.(Phylloquinone) decomposed
K Menaquinones (K2) by lightMenadione (K3)Acetomenaphthone KAPILIN 10 mg tab., ACETOMENADIONE 5, 10 mg tab.
Water-Soluble Vitamins
B1 Thiamine Relatively labile 1.5 mg BERIN 50, 100 mg tab, 100 mg/ml inj. (10 ml vial)BENEURON 5 mg cap., BETABION 100 mg tab.
B2 Riboflavin Relatively stable 1.7 mg LIPABOL 20 mg tab.RIBOFLAVIN 10 mg/ml inj.
Nicotinic acidNiacin
NICOTINIC ACID 25, 50 mg tab., NIALIP 250, 375, 500 mg tabB3 Nicotinamide Stable 20 mg NICOTINAMIDE 25, 50 mg tab.
Tryptophan (provit.)
Pyridoxine Stable in 2 mg PYRIDOXINE HCl 50 mg/2 ml inj., 10 mg tab.B6 Pyridoxal absence of air BENADON 40 mg tab, PYRICONTIN 100 mg tab
Pyridoxamine
Pantothenic acid Labile 4–7 mg CALCIUM PANTOTHENATE 50 mg tab., 50 mg/2 ml inj.
Biotin Stable 0.1–0.2 mg
Folic acid Labile 0.2 mg FOLVITE, FACITAB 5 mg tab.Folinic acid CALCIUM LEUCOVORIN 3 mg/ml inj.
B12 Cyanocobalamin Stable 2 µg MACRABIN 35 µg/ml liq: 100, 500, 1000 µg inj.,Hydroxocobalamin REDISOL-H, MACRABIN-H 500, 1000 µg inj.
VITAMIN B12 500, 1000 µg in 10 ml vial.Methylcobalamin METHYLCOBAL, BIOCOBAL, DIACOBAL, 500 µg cap
C Ascorbic acid Labile in 60 mg CECON 500 mg tab, 100 mg/ml drops.solution CELIN 50, 100, 500 mg tab., CHEWCEE 500 mg tab
REDOXON 200, 500 mg tab, 500 mg/5 ml inj.
⎫⎬⎭
Absorption and fate Physiological amounts are absorbedby active transport. When large doses are given orally, somepassive diffusion also occurs. Limited amounts are storedin tissues. About 1 mg/day is degraded in the body, excessis rapidly excreted in urine.
Physiological role After conversion in the bodyto Thiamine pyrophosphate, it acts as a coenzymein carbohydrate metabolism: decarboxylation of
ketoacids and hexose monophosphate shunt.Requirement is dependent upon carbohydrateintake—about 0.3 mg/ 1000 K cal. It also appearsto play some role in neuromuscular transmission.
Pyrithiamine and oxythiamine are syntheticthiamine antagonists. Tea also contains a thiamineantagonist.

914S
EC
TIO
N14
MISCELLANEOUS DRUGS
Deficiency symptoms The syndrome ofthiamine deficiency beriberi is seen in dry andwet forms:
Dry beriberi: Neurological symptoms are promi-nent—polyneuritis with numbness, tingling,hyperesthesia, muscular weakness and atrophyresulting in ‘wrist drop’, ‘foot drop’, paralysisof whole limb, mental changes, sluggishness, poormemory, loss of appetite and constipation.
Wet beriberi: Cardiovascular system is primarilyaffected—palpitation, breathlessness, high outputcardiac failure and ECG changes. Proteindeficiency is commonly associated and adds tothe generalised anasarka due to CHF.
Therapeutic uses
1. Prophylactically (2–10 mg daily) in infants,pregnant women, chronic diarrhoeas, patients onparenteral alimentation. Glucose infusion unmasksmarginal thiamine deficiency.2. Beriberi—100 mg/day i.m. or i.v. till symp-toms regress—then maintenance doses orally.3. Acute alcoholic intoxication: thiamine 100 mgis added to each vac of glucose solution infused.Most neurological symptoms in chronic alcoholicsare due to thiamine deficiency—peripheralneuritis, Wernick’s encephalopathy, Korsakoff’spsychosis: give 100 mg/day parenterally.4. In neurological and cardiovascular disorders,hyperemesis gravidarum, chronic anorexia andobstinate constipation—thiamine has been usedeven without definite proof of its deficiency—symptoms improve dramatically if thiaminedeficiency has been causative.
Adverse effects Thiamine is nontoxic. Sensi-tivity reactions sometimes occur on parenteralinjection.
Riboflavin (vit B2)Chemistry and source A yellow flavone com-pound found in milk, egg, liver, green leafyvegetables, grains.
Absorption and fate Well absorbed by active transportand phosphorylated in the intestine. Riboflavin phosphate(Flavin mononucleotide: FMN) is formed in other tissuesas well. Body does not significantly store riboflavin; largerdoses are excreted unchanged in urine. Thiamine andriboflavin are both synthesized by colonic bacteria but thisdoes not become available to the host.
Actions and physiological role Flavin adeninedinucleotide (FAD) and flavin mononucleotide(FMN) are coenzymes for flavoproteins involvedin many oxidation-reduction reactions. Thiamineand riboflavin are devoid of pharmacologicalactions.Deficiency symptoms Riboflavin deficiencygenerally occurs in association with otherdeficiencies. Characteristic lesions are angularstomatitis; sore and raw tongue, lips, throat, ulcersin mouth; vascularization of cornea. Dry scalyskin, loss of hair; anaemia and neuropathy developlater.Therapeutic uses To prevent and treat aribo-flavinosis (2–20 mg/day oral or parenteral),generally along with other B complex members.There is no proof of benefit in any other condition.
Niacin (vit B3)Chemistry and source Niacin refers toNicotinic acid as well as Nicotinamide—pyridinecompounds, initially termed pellagra preventingfactor. Sources are liver, fish, meat, cereal husk,nuts and pulses.
The amino acid tryptophan (mainly fromanimal protein) can be regarded as a provitamin,as it is partially converted in the body to nicotinicacid (60 mg tryptophan = 1 mg nicotinic acid).Maize eaters have suffered from pellagra becausecorn flour is poor in tryptophan and it is believedto contain a niacin antagonist. Thus, dailyrequirement of niacin is affected by the amountof tryptophan in diet.
Absorption and fate Niacin is completely absorbed fromgastrointestinal tract. Physiological amounts are metabolizedin the body, while large doses are excreted unchanged inurine. Modest amounts are stored in liver.
Physiological role and actions Nicotinic acidis readily converted to its amide which is a

915C
HA
PTE
R67
VITAMINS
component of the coenzyme Nicotinamide-adenine-dinucleotide (NAD) and its phosphate(NADP) involved in oxidation-reduction reactions.These pyridine nucleotides act as hydrogenacceptors in the electron transport chain in tissuerespiration, glycolysis and fat synthesis.Flavoproteins regenerate them by oxidizingNADH and NADPH.
Nicotinic acid (but not nicotinamide) in largedoses is a vasodilator, particularly of cutaneousvessels. It also lowers plasma lipids (see Ch. 45).
Deficiency symptoms Niacin deficiencyproduces ‘Pellagra’, cardinal manifestations ofwhich are:
Dermatitis—sunburn like dermal rash on hands,legs and face which later turn black, crack andpeal.
Diarrhoea—with enteritis, stomatitis, glossitis,salivation, nausea and vomiting.
Dementia—with hallucinations preceded byheadache, insomnia, poor memory, motor andsensory disturbances.
Anaemia and hypoproteinaemia are commonin pellagra. Chronic alcoholics are particularlyat risk of developing pellagra, because in additionto dietary deficiency, niacin absorption is impairedin them. Other B vitamin deficiencies are oftenassociated.
Therapeutic uses
1. Prophylactically (20–50 mg/day oral) inpeople at risk of developing pellagra.2. Treatment of pellagra—200 to 500 mg/dayin divided doses orally or parenterally. Strikingimprovement occurs in 1–2 days, but skinlesions take weeks to months. Nicotinamide ispreferred, especially for injection, because it doesnot cause flushing and other side effects seenwith nicotinic acid.3. Hartnup’s disease: in which tryptophantransport is impaired, and in carcinoid tumourswhich use up tryptophan for manufacturing5-HT, need niacin supplementation.
4. Nicotinic acid (not nicotinamide) has beenused in peripheral vascular disease and ashypolipidaemic (Ch. 45).
Adverse effects Nicotinic acid, in pharmacolo-gical doses, has many side effects and toxicities(p. 640). Nicotinamide is innocuous.
Pyridoxine (vit B6)Chemistry and source Pyridoxine, Pyriodoxaland Pyridoxamine are related naturally occurringpyridine compounds that have vit B6 activity.Dietary sources are—liver, meat, egg, soybean,vegetables and whole grain.Absorption and fate All three forms of the vitamin arewell absorbed from the intestine. They are oxidized in thebody and excreted as pyridoxic acid. Little is stored.
Physiological role and actions Pyridoxine andpyridoxamine are readily oxidized to pyridoxal,which is then phosphorylated to pyridoxalphosphate—the coenzyme form. Pyridoxal depen-dent enzymes include transaminases and decar-boxylases involved in synthesis of nonessentialamino acids, tryptophan and sulfur containingamino acid metabolism, formation of 5-HT,dopamine, histamine, GABA and aminolevulinicacid (first step in the synthesis of haeme). Highprotein diet increases pyridoxine requirement.
Pyridoxine has been shown to interact withsteroid hormone receptors, but its clinicalimplication is not clear. Prolonged intake of largedoses of pyridoxine can give rise to dependence,and mega doses (0.2–2.0 g/day) have been linkedwith sensory neuropathy. Otherwise, pyridoxineis free from pharmacological actions and sideeffects. However, suppression of lactation has beennoted in nonsuckling postpartal women given highdoses of pyridoxine: may be due to increaseddopamine action on pituitary lactotropes.
Drug interactions
1. Isoniazid reacts with pyridoxal to form ahydrazone, and thus inhibits generation ofpyridoxal phosphate. Isoniazid also combines withpyridoxal phosphate to interfere with its coenzyme

916S
EC
TIO
N14
MISCELLANEOUS DRUGS
function. Due to formation of hydrazones, therenal excretion of pyridoxine compounds isincreased. Thus, isoniazid therapy produces apyridoxine deficiency state.2. Hydralazine, cycloserine and penicillaminealso interfere with pyridoxine utilization andaction.3. Oral contraceptives reduce pyridoxalphosphate levels in some women.4. Pyridoxine, by promoting formation ofdopamine from levodopa in peripheral tissues,reduces its availability in the brain, abolishingthe therapeutic effect in parkinsonism, but notwhen a peripheral decarboxylase inhibitor iscombined with it.5. 4-deoxypyridoxine is a vit B6 antagonist.
Deficiency symptoms Deficiency of vit B6
usually occurs in association with that of otherB vitamins. Symptoms ascribed to pyridoxinedeficiency are—seborrheic dermatitis, glossitis,growth retardation, mental confusion, loweredseizure threshold or convulsions (due to fall inbrain GABA levels), peripheral neuritis andanaemia.
Therapeutic uses
1. Prophylactically (2–5 mg daily) in alcoholics,infants and patients with deficiency of other Bvitamins.2. To prevent and treat (10–50 mg/day) isoniazid,hydralazine and cycloserine induced neurologicaldisturbances. Acute isoniazid poisoning has beensuccessfully treated with massive doses (in grams)of pyridoxine.3. To treat mental symptoms in women on oralcontraceptives (50 mg daily).4. Pyridoxine responsive anaemia (due todefective haeme synthesis) and homocystinuriaare rare genetic disorders that are benefited bylarge doses of pyridoxine (50–200 mg/day).5. Convulsions in infants and children.
Pantothenic acid
Pantothenic acid is an organic acid, widely distributed infood sources, especially liver, mutton, egg yolk and vegetables.
It is quickly absorbed and excreted unchanged in urine withlittle storage.
It is a component of coenzyme-A which functions incarbohydrate, fat, steroid and porphyrin metabolism bycatalysing acetate transfer reactions. Clinical deficiency ofpantothenic acid is not known. Experimental deficiency inman causes insomnia, intermittent diarrhoea, flatulence,vomiting, leg cramps and paresthesias. Calcium/sodiumpantothenate is included in B complex and multivitaminpreparations. Intravenous calcium pantothenate has been triedin paralytic ileus.
Biotin
Biotin is a sulfur containing organic acid found in egg yolk,liver, nuts and many other articles of food. Some of thebiotin synthesized by intestinal bacteria is also absorbed.It is well absorbed from intestine and excreted mainlyunchanged in urine. Not much is stored in the body. Avidin,a heat labile protein in egg white, binds and prevents theabsorption of biotin. Some other biotin antagonists are alsoknown.
Biotin is a coenzyme for several carboxylases involvedin carbohydrate and fat metabolism. Deficiency symptomsinclude seborrheic dermatitis, alopecia, anorexia, glossitisand muscular pain. Spontaneous deficiency of biotin hasbeen noted only in subjects consuming only raw egg whiteand in patients on total parenteral nutrition. Except for theseunusual instances and rare genetic abnormalities of biotindependent enzymes, there are no clearly defined therapeuticuses of biotin. It is present in some multivitamin prepara-tions.
VITAMIN C (ASCORBIC ACID)
Chemistry and source Ascorbic acid is a6 carbon organic acid with structural similarityto glucose. It is a potent reducing agent andl-form is biologically active. Citrus fruits (lemons,oranges) and black currants are the richest sources;others are tomato, potato, green chillies, cabbageand other vegetables. Human milk is richer invit C (25–50 mg/L) than cow’s milk.Absorption and fate It is nearly completely absorbedfrom g.i.t. and widely distributed extra- and intracellularly.Plasma concentration and total body store of vit C is relatedto daily intake. The usual 60 mg/day intake results in about0.8 mg/dl in plasma and 1.5 g in the body as a whole.Increasing proportions are excreted in urine with higherintakes. Body is not able to store more than 2.5 g. It ispartly oxidized to active (dehydroascorbic acid) and inactive(oxalic acid) metabolites.
Physiological role and actions Vit C playsa role in many oxidative and other metabolic

917C
HA
PTE
R67
VITAMINS
TAB
LE 6
7.2
Com
bina
tion
prep
arat
ions
of v
itam
ins
Pro
prie
tary
nam
eD
ose
unit
Vit.
AV
it. D
Vit.
ETh
iam
ine
Rib
ofla
vin
Nia
cin
Pyr
idox
ine
Pan
toth
enic
Bio
tinFo
lic a
cid
B12
Vit.
C(I
U)
(IU
)(m
g)(m
g)(m
g)(m
g)(m
g)(m
g)(m
g)(m
g)(µ
g)(m
g)
AB
DE
C D
RO
PS
per
0.6
ml
5,00
040
0 –
11
100.
63
––
–50
AD
EX
OLI
Nca
ppe
r ca
p.5,
000
400
– –
––
––
––
– –
AQ
UA
SO
L-A
-Ddr
ops
per
ml
24,0
001,
000
––
––
––
––
––
AQ
UA
SO
L-A
-Eca
ppe
r ca
p.30
,000
–50
––
––
––
––
–
BE
CO
SU
LES
cap
per
cap.
––
– 1
010
503
12.5
–1
515
0
“sy
rup
per
5 m
l–
––
2 2
.520
26
––
–75
BE
CO
ZYM
E C
FO
RTE
tab.
per
tab.
––
–15
1550
316
.30.
15–
10
150
BE
JEC
TAL
inj.
per
ml
––
–10
2 7
55
5–
––
–
ED
INO
Lca
ppe
r ca
p.10
,000
1,00
015
1010
503
10–
15
150
MU
LTIV
ITA
PLE
Xel
ixir
per
5 m
l2,
500
200
–2
2.5
201
5–
––
50
“ FO
RTE
cap.
per
cap.
10,0
0040
015
55
50
1.5
5–
15
75
CO
BA
DE
X F
OR
TEca
p.pe
r ca
p–
––
1010
100
350
–1.
515
–
CO
BA
DE
X S
YR
UP
syr
per
5 m
l–
––
52.
550
1.5
5–
––
–
KIN
ETO
NE
liq.
per
15 m
l20
0020
07.
52
3–
1.5
––
–1
–
OP
TIN
EU
RO
Nin
j.pe
r 3
ml
––
–10
05
100
100
50–
–10
00–
STR
ES
S C
AP
Sca
p.pe
r ca
p–
––
1010
100
220
––
515
0
NE
UR
OX
IN-1
2in
j.pe
r 10
ml
––
–30
––
14–
––
500
–
“ F
OR
TEin
j.pe
r 3
ml
––
–10
0 5
100
100
50–
–10
00–
NE
UR
OB
ION
tab
per
tab
––
–10
1045
350
––
15–
PO
LYB
ION
cap.
per
cap.
––
– 1
010
100
350
–1.
515
150
“in
j.pe
r 2
ml
––
–10
4 4
04
6–
–8
–
RO
VIG
ON
tab.
per
tab.
10,0
00–
70–
––
––
––
––
SC
LER
OB
ION
tab.
per
tab.
10,0
00–
25 –
––
3–
––
– –
VIM
AG
NA
drop
spe
r m
l2,
000
200
–0.
80.
8 1
30.
81.
7–
––
20
Com
bine
d fo
rmul
atio
ns o
f vita
min
s w
ith a
nalg
esic
s, a
ntiin
flam
mat
ory
drug
s, tr
anqu
ilize
rs a
nd a
ntitu
berc
ular
dru
gs (
exce
pt is
onia
zid
+ py
ridox
ine)
are
ban
ned
in In
dia.

918S
EC
TIO
N14
MISCELLANEOUS DRUGS
reactions, e.g. hydroxylation of proline and lysineresidues of protocollagen—essential for forma-tion and stabilization of collagen triple helix;hydroxylation of carnitine, conversion of folic acidto folinic acid, biosynthesis of adrenal steroids,catecholamines, oxytocin and vasopressin andmetabolism of cyclic nucleotides and prostag-landins. It directly stimulates collagen synthesisand is very important for maintenance ofintercellular connective tissue. A number of ill-defined actions have been ascribed to ascorbicacid in mega doses, but none is proven.
Deficiency symptoms Severe vit Cdeficiency Scurvy, once prevalent among sailorsis now seen only in malnourished infants, children,elderly, alcoholics and drug addicts. Symptomsstem primarily from connective tissue defect:increased capillary fragility—swollen and bleedinggums, petechial and subperiosteal haemorrhages,deformed teeth, brittle bones, impaired woundhealing, anaemia and growth retardation.
Therapeutic uses1. Prevention of ascorbic acid deficiency in
individuals at risk (see above) and in infants:50–100 mg/ day. Vit C or orange juice canbe routinely included in infant diet.
2. Treatment of scurvy—0.5–1.5 g/day.3. Postoperatively (500 mg daily): though vit C
does not enhance normal healing, suboptimalhealing can be guarded against. It has alsobeen found to accelerate healing of bedsores
and chronic leg ulcers. Requirement of ascorbicacid is increased in postinjury periods.
4. Anaemia: Ascorbic acid enhances iron absorp-tion and is frequently combined with ferroussalts (maintains them in reduced state).Anaemia of scurvy is corrected by ascorbicacid, but it has no adjuvant value in otheranaemias.
5. To acidify urine (1 g TDS–QID) in urinarytract infections (see Ch. 54).
6. Large doses (2–6 g/day) of ascorbic acid havebeen tried for a variety of purposes (commoncold to cancer) with inconsistent results. Nodefinite beneficial effect has been noted inasthma, cataract, cancer, atherosclerosis, psy-chological symptoms, infertility, etc. However,severity of common cold symptoms may besomewhat reduced, but not the duration of illnessor its incidence. Improved working capacity atsubmaximal workloads has been found inathletes but endurance is not increased.
Adverse effects Ascorbic acid is welltolerated in usual doses. Mega doses given forlong periods can cause ‘rebound scurvy’ on stop-page—probably due to enhancement of its ownmetabolism or tissue acclimatization. The risk ofurinary oxalate stones may be increased. Highdoses may also be cytotoxic when added to ironpreparations.
Vitamin D (Ch. 24), vit K (Ch. 44), folic acidand vit B12 (Ch. 43) have been considered inearlier chapters.

Vaccines and SeraChapterChapterChapterChapterChapter 6868686868
Vaccines and sera are biological products whichact by reinforcing the immunological defence ofthe body against foreign agencies (mostly infectingorganisms or their toxins).Vaccines impart active immunity—act as antigenswhich induce production of specific antibodiesby the recipient himself.Antisera and Immune globulins impart passiveimmunity—readymade antibodies (produced byanother person or animal who has been activelyimmunized) are transferred.
Active immunization is more efficacious andlonger lasting than passive immunization, but theformer needs a latent period of one to many weeks,whereas the latter affords immediate protection.Antisera are, therefore, curative also, whereasvaccines are only prophylactic. Acutely ill,debilitated or immunocompromised individualsmay not be able to generate an adequate antibodyresponse and require passive protection.
Vaccines and sera are potentially dangerousproducts and mostly used in public health pro-grammes—their manufacture, quality control,distribution and sale is strictly supervised by Statehealth authorities. These biologicals are standar-dized by bioassay and need storage in cold tomaintain potency.
VACCINES
Vaccines are antigenic materials consisting of thewhole microorganism or one of its products.Vaccines are of 3 types:(i) Killed (Inactivated) vaccines: consist ofmicroorganisms killed by heat or chemicals. Theygenerally require to be given by a series ofinjections for primary immunization. Theimmunity is relatively shorter-lasting; booster
doses are mostly needed at intervals of monthsor years.(ii) Live attenuated vaccines: consist of live bac-teria or viruses which have been renderedavirulent. They nevertheless grow and multiplyin the body of the host to a limited extent. Livevaccines usually produced long-lasting immunity.In individuals with impaired host defence, e.g.
(a) Leukaemia or other malignancies, especiallythose receiving cytotoxic chemotherapy.
(b) Systemic lupus erythematosus.(c) Corticosteroid recipients.(d) AIDS and other immune deficiency states.
The limited virulence of organisms in the livevaccine may be sufficient to cause a disease; livevaccines are contraindicated in them.
Two live vaccines, if not given together, shouldpreferably be administered with a gap of 1 month.(iii) Toxoids: are modified bacterial exotoxins sothat toxicity is lost but antigenicity is retained.The term ‘vaccine’ is sometimes restricted topreparations of whole microorganisms and toxoidsare enumerated separately.
Active immunization with vaccines may failto ‘take’ during corticosteroid or immunosuppres-sant medication and should be avoided.Vaccination should be deferred in the presenceof any acute (especially respiratory) infection andduring pregnancy. Antibiotics added duringproduction of vaccines and present in traceamounts in viral vaccines may cause reaction inindividuals sensitive to these. Egg proteins (invaccines prepared on chick embryo) and othermaterials used for vaccine culture may beresponsible for allergic reactions. Adrenalineinjection (1 in 1000) should be available tocontrol allergic reaction to the vaccine, if itoccurs.

920S
EC
TIO
N14
MISCELLANEOUS DRUGS
Killed (inactivated) vaccines Live attenuated vaccines
BACTERIALTyphoid-paratyphoid (TAB) Bacillus Calmette-Guérin (BCG)Vi Typhoid polysaccharide Typhoid-Ty 21aCholeraWhooping cough (Pertussis)MeningococcalHaemophilus influenzae type bPlague
VIRALPoliomyelitis inactivated (IPV, Salk) Poliomyelitis oral live (OPV, Sabin)Rabies (Neural tissue) Mumps (live attenuated)Rabies (Chick embryo cell, PCEV) Measles (live attenuated)Rabies (Human diploid cell, HDCV) Rubella (live attenuated)Rabies (Vero cell, PVRV) Varicella (live attenuated)InfluenzaHepatitis BHepatitis A
TOXOIDSTetanus (fluid/adsorbed)Diphtheria (adsorbed)
COMBINED VACCINESDouble antigen (DT-DA)Triple antigen (DPT)Measles, mumps, rubella (MMR)
Pentavalent vaccine (DPT + Hepatitis B + H. influenzae type b)
The antibodies developed in response to liveor killed vaccines inactivate the bacteria/viruswhen it subsequently enters the body, while thoseinduced by toxoids neutralize the elaboratedexotoxin. The latent period between vaccinationand development of immunity and the period forwhich it lasts depends primarily on the organism,but varies somewhat in different individuals. Viralvaccines and toxoids generally afford moreprolonged protection than bacterial vaccines. Theimportant vaccines are described briefly.
BACTERIAL VACCINES
1. Typhoid-Paratyphoid A, B (TABvaccine) It is a sterile suspension, 1 mlcontaining 1 × 109 S. typhi and 7.5 × 108 eachof S. paratyphi A and B organisms in 5, 10 mlvials. Dose—0.5 ml s.c., 2–3 injections at2–4 weeks intervals. Local tenderness, fever andmalaise lasting 1–2 days are common after thefirst dose. It is estimated to be 70% effective
in preventing enteric fever for 1 year. Boosterdoses may be given every 2–3 years.
2. Vi Typhoid polysaccharide vaccine Itcontains purified Vi capsular antigen of S. typhi.A single 0.5 ml s.c./i.m. dose affords 72%protection at 18 months and 60% protection at3 years. It produces much less local and systemicside effects than TAB and induces longer lastingimmunity, but does not protect against paraty-phoid A and B. Thus, it is an improvement overthe whole cell TAB vaccine. However, it is notapproved for use in children below 2 years andin pregnant women.VACTYPH, TYPHIM Vi, TYPHIVAX 0.025 mg in 0.5 ml inj;repeat after 3 years.
3. ‘Typhoid-Ty21a’ oral vaccine This is anewer live oral typhoid vaccine prepared fromTy 21a attenuated strain of S. typhi which lacksthe Vi polysaccharide and is nonpathogenic. Theattenuation is due to absence of the enzyme

921C
HA
PTE
R68
VACCINES AND SERA
Uridine diphosphate galactose-4 epimerase whichis essential for the production of lipopolysaccha-ride ‘O’ antigens. It is avirulent. By lodging inthe intestinal mucosa it protects against S. typhiinvasion of the gut in addition to imparting sys-temic immunity. High cell mediated and modestantibody mediated immunity is produced.Administered as 3 doses on alternate days in theform of enteric coated capsules it affords pro-tection for 3 years. Efficacy is better than TAB.Trials in India and other countries have reported67–90% protection at 3 years. Side effects arenegligible: only 2% cases have reported diarrhoea,abdominal pain or rashes. It is much more con-venient, safer and longer acting. It is not approvedfor use in children below 5 years and in pregnantwomen.TYPHORAL S. typhi strain Ty21A 109 organism per cap; 3caps taken in 3 doses on alternate days in between meals.
4. Cholera vaccine It is a suspension ofphenol/formalin killed Inaba and Ogawa strainsof V. cholerae, each ml containing 8 × 109
organisms in 5, 10, 30 ml vials. Dose: 0.5 mls.c. or i.m. followed by 1 ml 1–4 weeks later,or a single dose of 1 ml for mass innoculation.Immunity, sufficient to prevent clinical disease,is produced only in 50% of those innoculated,and lasts 6 months or so—sufficient to tide overan epidemic. Cholera innoculation duringcongregations (melas) has not reduced theincidence of the disease (because it takes 2–3weeks for immunity to develop): this practice hasbeen discontinued. It also does not prevent carrierstate. Transient local soreness, low grade fever,aches and pains lasting 1–2 days are common.Neurological complications are rare.Two new oral cholera vaccines have been produced: killedwhole cell/recombinant B subunit (WC/r BS) and live CVD-103 HgR vaccine. Both these vaccines are highly immuno-genic, safer than the present cholera vaccine and provideimmunity upto 3 years. Cumulative protective efficacy of 86%at 3 weeks and 50% at 3 years have been estimated. They havebeen made available in Europe, but not yet in India.
5. Whooping cough (pertussis) vaccineIt is killed 2 × 1010 organisms/ml suspension ofB. pertussis organisms. Dose 0.25–0.5 ml s.c. or
i.m. thrice at 4 week intervals in infants andchildren below 5 years (whooping cough is veryrare after 5 years age).
It also induces a state of diminished βadrenergic reactivity and aids sensitization to otherantigens.
In addition to local pain and induration, severesystemic (even fatal) reactions have been reported,but extremely rarely—high fever with hypotonichyporesponsive child, convulsions, alterations ofconsciousness and focal neurological signs. Onceany such reaction has occurred, further doses arecontraindicated. It is also contraindicated inchildren with history of convulsions or otherneurological disease.
It is a component of triple antigen: seldomused separately.
6. Meningococcal A&C vaccine It containspurified capsular polysaccharide of N. meningitidisgroup A and C, 50 µg of each per unit in singledose and 10 dose vials. One dose (0.5 ml s.c.or i.m.) is indicated for prophylaxis of meningitisduring an epidemic caused by group A or Cmeningococci.MENINGOCOCCAL A & C, MENCEVAX A & C 0.5 ml amp,5 ml vial.
7. Haemophilus influenzae type b (Hib)vaccine It contains medium oligosaccharide ofH. influenzae type b (10 µg) conjugated withnontoxic protein (25 µg) of CRM197 mutant C.diphtheriae toxin along with alum. hydrox.adjuvant. It is indicated for protection of infantsand children against H. influenzae meningitis,pneumonia, etc. Infants 2–6 months are given3 doses (0.5 ml i.m.) at 8 week gaps, 7–11 months2 doses, while those older than 1 yr require only1 dose. Good antibody response and protectionhas been obtained in > 90% recipients.VAXEM-HIB, HIB-TITER 0.5 ml and 5 ml vials8. Antiplague vaccine formalized It contains 2 × 109
Y. pestis organisms per ml, killed by formaline, in 10 mlvial. Dose—1 ml i.m. twice 1–2 weeks apart or 2 ml singledose. Local and systemic reactions are relatively frequentand increase with the number of booster doses. Immunitylasts 6–8 months—sufficient to cover an epidemic. Plagueis now rare, so is the need for this vaccine.

922S
EC
TIO
N14
MISCELLANEOUS DRUGS
9. Bacillus Calmette-Guérin (BCG) vac-cine It is a live vaccine bearing an attenuatedbovine strain of M. tuberculosis, developed in 1921by Calmette and Guérin in France. It is suppliedas 0.5–1 mg dry powder (1–2.5 × 107 colonyforming units) in ampules to be suspended in1 ml of sterile water; 0.05 ml (in neonate)0.1 ml (older individuals) is injected intracuta-neously in the left deltoid region at birth. In childrenand adults tuberculine testing is done beforehandand BCG is given only to negative responders.
A red painless papule appears after 7–10 days;reaches about 8 mm diameter in 5 weeks withswelling of axillary lymph node; may ulcerate,but scales and dries in 3 months; totally healsin 6 months. The protection afforded by BCGis partial and neither permanent nor entirelypredictable. It has been widely used to enhanceresistance to tubercular infection, but doubt hasbeen cast about its utility in adults, though childrenappear to be benefited.
BCG has also been used to enhance immunitynonspecifically by stimulating the reticuloendo-thelial system: employed as adjuvant in immu-notherapy of cancer and some other conditions.It is contraindicated in tuberculine positiveindividuals, in those with compromised hostdefence including HIV positive children, andduring pregnancy.
VIRAL VACCINES
1. Poliomyelitis The virus (type 1, 2, 3) isgrown in monkey kidney cell culture and twovaccines are prepared from it.
(a) Oral poliovirus vaccine (OPV; Sabinvaccine) It is the live virus available in 10 mland 50 ml vials; each dose is 2 drops, droppeddirectly in the mouth. The virus multiplies in theintestines and produces active immunity,simulating natural infection, without producingsymptoms of the disease. For primary immuni-zation OPV is now generally given at birth andthen at 6, 10 and 14 weeks. Booster doses aregiven between 15–18 months and at schoolentry. OPV is the vaccine of choice for active
immunization of children because it is simple toadminister, is well accepted, induces systemic aswell as intestinal immunity (the portal of entryof disease virus) and is highly efficacious. Theintestinal immunity also eliminates carrier stateand thus limits spread of the disease. It is advisedto postpone the vaccine in presence of vomitingand diarrhoea. Vaccine associated paralysis occursextremely rarely.
Simultaneous vaccination of all infants andchildren upto 5 years age (pulse polio programme)has eradicated the wild virus in many countriesby colonizing all susceptible intestines by thevaccine virus. This programme is underway inIndia.
(b) Inactivated poliomyelitis vaccine (IPV, Salkvaccine) It is inactivated suspension of the virus whichis preferred over OPV only for:
(i) primary immunization in adults (risk of vaccineassociated paralysis following OPV is higher in adults).
(ii) in persons with compromized immune system.Three doses of 1 ml each are injected s.c. in the deltoidregion at 4–6 week intervals and a fourth is given 6–12months later. Booster doses are given every 5 years. Feverand local pain are common. Allergic reactions sometimesoccur, probably to the animal protein present in the vaccine.
2. Rabies Four rabies vaccines have been pro-duced.a. Antirabic vaccine carbolized (Semple vaccine) Alsocalled ‘Neural tissue vaccine’ (NTV), it is a 5% suspensionof sheep brain substance containing carbolic acid fixed rabiesvirus. Though long considered obsolete because of poorerefficacy, need for 14 daily painful large volume (2–5 ml)injections into the anterior abdominal wall, and risk of serious(even fatal) vaccine associated allergic encephalomyelitis,it continued to be used in Government hospitals in Indiatill mid 2005, after which it has been discontinued.
b. Purified chick embryo cell vaccine(PCEV) It consists of Flury-LEP strain of rabiesvirus grown on chick fibroblasts and inactivatedby β-propiolactone; available as 2.5 IU in 1 mlamp (RABIPUR). The efficacy of this vaccine isnearly equal to HDCV, and it produces localreactions in ~5% cases. However, rare neuro-paralytic complications have been reported. Localpain, erythema, swelling and lymph nodeenlargement can occur.

923C
HA
PTE
R68
VACCINES AND SERA
c. Human diploid cell vaccine (HDCV) Itis lyophilized inactivated rabies virus grown inhuman diploid cell culture. The vial containing2.5 IU is freshly suspended in 1 ml of diluent.
A local reaction—redness and slight indurationlasting 1–2 days occurs in 10% cases. Fever andarthralgia is reported in 1%. HDCV is ~100%effective and well tolerated. Vaccine associatedencephalitis does not occur.
d. Purified vero cell rabies vaccine (PVRV)This contains inactivated wistar rabies PM/WI38-1-503-3M strain grown on vero continuous cellline (VERORAB 1 ml; VEROVAX-R 0.5 ml).
Post-exposure prophylaxis: This is given to allnonimmunised animal-bite cases suspected to havebeen exposed to the rabies virus. The intradermal(i.d.) regimen for all tissue culture rabies vaccinescalled the ‘Thai regimen’ that has beenrecommended by the WHO since 1992, has beenapproved and notified by the Government of Indiain 2006. This regimen requires only 1/5 dose ofthe earlier used i.m. regimen, is less expensive,more convenient and equally efficacious. In thisregimen 0.1 ml of PCEV or PVRV or 0.2 mlof HDCV is injected i.d. at 2 sites (over deltoidof both arms) on days 0, 3 and 7 followed by1 site injection on day 28 (or 30) and day 90,(2 + 2 + 2 + 1 + 1 = 8 injections). Thus, noinjection is given on day 14 as in earlier i.m.regimen which employed 1 ml PCEV/HDCV or0.5 ml PVRV per injection on days 0, 3, 7, 14,30, 90.
Because rabies vaccines take 10–14 days todevelop protective antibodies, concurrentadministration of rabies immunoglobulin (RIG)is recommended in category III bites, where riskof contacting rabies is high.
An alternative 8 site i.d. regimen (Oxford regimen) isadvocated for an earlier antibody response, particularly whenRIG is not available for postexposure treatment. In this regimen0.1 ml of PCEV or HDCV (but not PVRV) is injected at8 sites (over both deltoids, suprascapular region, thighs andabdomen) on day 0. On 7th day 4 sites are injected followedby one site injection on day 28 and 90 (total 14 injections).
Pre-exposure prophylaxis (Primary vaccination):This is usually recommended for veterinary
workers and animal handlers, who are at highrisk of animal bites. Three i.d. injections of 0.1ml each of PCEV/HDCV/PVRV are given on days0, 7 and 28. Booster doses are recommendedevery 2 years so long as the person remains atrisk.
Post-exposure prophylaxis in already vaccinatedsubjects: This is given when an immunized personis bitten by a suspected animal. Three 0.1 mli.d. injections are given on days 0, 3 and 7.
Local treatment of bite wound: Early localtreatment of bite wound is essential in additionto the vaccine ± RIG. The wound should bethoroughly washed with soap under running waterfor at least 5 min, followed by application ofan antiseptic (alcohol/povidone iodine/cetrimide).Cauterization with carbolic acid is contraindicated.In category III bites, RIG should be infiltratedlocally in the depth and around the wound toinactivate the locally present virus. Suturing ofthe wound should be avoided, at least for 2 days.3. Influenza virus vaccine Contains inactivatedinfluenza virus A and B. Immunization may be done annuallyor during an epidemic: 2 injections of 0.5–1 ml i.m. 1–2 months apart. Influenza virus undergoes frequent antigenicchanges; hence the efficacy of the vaccine is inconsistent.It is indicated only in high risk cases.
Adverse reactions are commoner in children—localtenderness and induration occurs in 30%. Fever, malaise andmyalgia lasting 1–2 days is less frequent. Allergic reactionsto the egg protein present in the vaccine occur rarely.
4. Hepatitis B vaccine The new hepatitisB vaccine (ENGERIX-B) is prepared in yeast cellsby recombinant DNA technique and containsaluminium hydroxide adsorbed hepatitis B virussurface antigen 20 µg in 1 ml suspension. Three1 ml injections in the deltoid muscle given at0, 1 and 6 months produce protective antibodytiters in 99% subjects. Children <10 yr are given0.5 ml doses in the thigh. Now included inuniversal immunization for all, but is especiallyindicated in persons who come in contact withblood, blood products and other body fluids(surgeons, dentists, blood bank personnel,laboratory technicians and other health careworkers, haemophilics, haemodialysis patients,

924S
EC
TIO
N14
MISCELLANEOUS DRUGS
drug addicts, etc). Induration and soreness atinjection site and occasional fever and malaiseare the adverse effects.
5. Hepatitis A vaccine It is prepared byinactivating with formaldehyde hepatitis A virusgrown in human diploid cell culture. A single0.5 ml i.m. injection in deltoid muscle affordsprotection, but a booster dose ater 6 month isrecommended.AVAXIM 0.5 ml prefilled syringe, HAVRIX 0.5 ml inj.
6. Mumps virus vaccine live attenuatedIt is prepared from mumps virus grown in cellculture of chick embryo. A single dose of 5000TCID50 (tissue culture infectious dose 50%)affords protection for 10 years; revaccination isnot required. Clinical disease may occur if thevaccine is given after exposure to natural mumps.It is generally combined with measles and rubellavaccine (MMR), and is not recommended below1 year of age. A mild febrile reaction occursoccasionally.
7. Measles vaccine live attenuated Thisis also a vaccine grown on chick embryo; availablein single dose vials containing 1000 TCID50 ofEdmonston Schwarz strain (ROUVAX, RIMEVAX) orEdmonston zagreb strain (M-VAC) for s.c. injectionover right deltoid region. It produces a modifiedinfection—fever, rash and coryza may appear after5–10 days; immunity lasts 8 years and no boosterdoses are required. It is recommended in children9 months or older. Ordinarily, adults need not beimmunized. Malnourished, chronically ill andtuberculous children must be protected to minimizethe risk of serious complications of natural measles.Some protection is afforded even if given afterexposure. It should be given with caution tochildren with history of febrile convulsions orparental history of epilepsy.8. Rubella vaccine (R-VAC) It contains liveattenuated rubella virus Wistar RA27/3 strain 1000TCID50 per 0.5 ml inj. for deep s.c. or i.m.injection in upper arm. It is used especially ingirls from 1 yr age to puberty—for immunizationagainst German measles; mostly as combined
MMR vaccine. It is contraindicated during preg-nancy, febrile illness and in untreated tuberculosispatients. Reactions are fever, malaise, sore throat,joint pain and lymphadenopathy.9. Measles-Mumps-Rubella (MMR) vac-cine Two preparations of this combined livevaccine are available: have similar efficacy.TRIMOVAX lyophilized measles 1000 TCID50 of Schwarzstrain, mumps 5000 TCID50 and rubella 1000 TCID50 per unitdose (0.5 ml) vial.TRESIVAC lyophilized measles 5000 TCID50 of EdmonstonZagreb strain, mumps 5000 TCID50 and rubella 4000 TCID50
per unit dose (0.5 ml) vial.
A single dose injected s.c. over right deltoid isindicated in children older than 12 months forprotection against these 3 diseases. Mild fever,rash, enlargement of cervical/occipital lymphnodes and parotid glands and local indurationmay occur after ~5 days. It is absolutely contra-indicated during pregnancy; adult femalevaccinees should not conceive for at least2 months.
10. Varicella vaccine It is lyophilised liveattenuated OKa strain of varicella-zoster virusgrown in human diploid cell culture, containing103.3 PFU (plaque forming units) of the virus.A single dose induces antibody response in> 98% children and affords protection for 10 years.Dose: 0.5 ml s.c. single dose for children 1–12 years, and2 doses 6–10 weeks apart in those >12 years.VARILRIX, OKAVAX 0.5 ml inj.Contraindicated during pregnancy, in those withlymphocytopenia and within 1 month of measlesvaccination. Mild local reaction, papular eruptionand short-lasting fever occurs in 4–5% children.
TOXOIDS
1. Tetanus toxoid It is formaline treatedexotoxin of tetanus bacilli; indicated for routineimmunization in all children and adults. Two typesof preparations—fluid and adsorbed are available.The adsorbed toxoid is superior—induces higherantibody titers and more prolonged immunity.Dose: 0.5 ml, preferable route is i.m., can alsobe given s.c.

925C
HA
PTE
R68
VACCINES AND SERA
For primary immunization—Tetanus toxoidadsorbed (0.5 ml amp. 10 ml vial), 2 doses aregiven 4–6 weeks apart, or Tetanus toxoid fluid(1 ml amp, 10 ml vial) 3 doses at interval of3–4 weeks. Booster dose should be given after1 year and then every 10 years. In non-immunizedor inadequately immunized individuals the toxoidshould be given after any injury likely to intro-duce tetanus bacilli. Concomitant administrationof chloramphenicol is avoided, as it may interferewith antibody response.
Reactions—Local erythema, pain and indurationis not uncommon. Axillary lymph nodes mayenlarge. Fever, chills, malaise, aches and painsoccur occasionally, especially in adults. Paresisand other neurological complications are rare.
2. Diphtheria toxoid adsorbed It is modi-fied diphtheria exotoxin adsorbed onto aluminiumhydroxide. It is indicated in infants and childrenbelow 6 years of age. Older individuals seldomrequire protection against diphtheria. For primaryimmunization 2–3 injections of 0.5 ml i.m. aregiven 4–6 weeks apart, booster dose after 1 yearand then at school entry. Reactions are similarto those caused by tetanus toxoid.
MIXED ANTIGENS
1. Double antigen (DT-DA) It consists ofalum precipitated toxoids of tetanus anddiphtheria, available in 0.5 ml ampule and 5 mlvial (DUAL ANTIGEN). It is used in children above5 years and in younger children in place of tripleantigen when pertussis vaccine is contraindicated.Dose: 0.5 ml i.m.
2. Triple antigen (DPT) It is a mixture oftoxoids of tetanus and diphtheria with pertussisvaccine (TRIPVAC: Diphtheria toxoid 25 Lf, tetanus toxoid5 Lf, B. pertussis 20,000 million in 0.5 ml amp; also 10ml multidose vial).
It is the preparation of choice for primaryactive immunization against the 3 diseases inchildren below 5 years age. Dose–0.5 ml i.m.in the anterolateral aspect of mid thigh or rightdeltoid, 2–3 injections 4–8 weeks apart, between3–9 months age and one at 18 months. Reactions,
precautions and contraindications mentioned underthe individual vaccines apply to triple antigenas well.
3. Pentavalent vaccine It contains toxoidsof tetanus and diphtheria along with pertussisvaccine, hepatitis B vaccine and Haemophilusinfluenzae type b (Hib) vaccine. Used in placeto triple antigen for primary immunization ofinfants, it affords protection against two additionalcommon infections, and reduces the total numberof injections that the infant receives for protectionagainst these 5 infections. Pentavalent vaccinehas been used in many countries, and nowGovernment of India is introducing it in a phasedmanner in its universal immunization programmefor infants and children. However, recently fewinfant deaths have been reported, though therelationship between these and the vaccine is notclear. Nevertheless, some experts have raisedconcern about its safety.
A routine immunization schedule for infantsand children is given in the box.
Routine immunization schedule for infants andchildren
At birth BCG + OPV (first dose) +Hepatitis B (after 12–24 hours)
At 6 weeks DPT + OPV + Hepatitis BAt 10, 14 weeks DPT + OPVAt 6 months Hepatitis BAt 9 months MeaslesAt 15–18 months DPT + MMR + OPV
(booster dose)At 4–5 years DT-DA + OPV (booster dose)(School entry) Typhoid (TAB 2 doses/
Vi 1 dose/Ty 21a 3 doses)optional
At 10 years TT + TAB/Vi/Ty 21a (optional)At 16 years TT
For pregnant women16–24 weeks TT (1st dose)24–34 weeks TT (2nd dose)
ANTISERA AND IMMUNE GLOBULINS
Antisera are purified and concentrated prepara-tions of serum of horses actively immunizedagainst a specific antigen.

926S
EC
TIO
N14
MISCELLANEOUS DRUGS
use are—viral hepatitis A and B (prophylaxis),measles, mumps, poliomyelitis and chickenpox(prophylaxis and modification of course of illness),and has some beneficial action in burns. It isespecially valuable in agammaglobulinemia,premature infants and in patients of leukemia orthose undergoing immunosuppression. It canaugment the response to antibiotics in debilitatedpatients with bacterial infections.Dose: 0.02–1 ml/kg i.m. for different indications.GAMMALIN, GLOBUNAL, Sii GAMMA GLOBULIN,GAMAFINE 10%, 16.5% injection in 1, 2 ml amps.
An intravenous preparation (Sii I.V.GG 0.1–0.4 g/kg/day) has been made available for conditionsrequiring high doses which cannot be injected i.m.
2. Anti-D immune globulin (see p. 885).
3. Tetanus
(a) Tetanus immune globulin (human) It isindicated for prophylaxis in non-immunized personsreceiving a contaminated wound who are at highrisk of developing tetanus. The t½ of this antitoxinis 4 weeks and significant blood levels aremaintained for upto 14 weeks. It is more efficaciousand longer acting than the equine antitoxin (ATS).If tetanus toxoid is given at the same time (butat a different site), development of primary immuneresponse to the toxoid is not interfered with. Ithas also been used for the treatment of clinicaltetanus, but the efficacy is variable. Intrathecaladministration has also been tried.Dose: prophylactic 250–500 IU, therapeutic 3000–6000 IUi.m. and/or 250-500 IU intrathecal.Sii TIG 250 IU (liquid), 500 IU (lyophilized), TETNAL 250IU/2 ml inj., TETAGAM 250 IU/ml inj.
(b) Tetanus antitoxin (antitetanic serum,ATS) It is obtained from horse; is inferior tohuman antitoxin and should be used for the aboveindications only when tetanus immuneglobulin isnot available.Dose: prophylactic 1500–3000 IU, i.m. or s.c.;therapeutic 50,000–100,000 IU part i.v. and rest i.m.TETANUS ANTITOXIN 750 IU, 1500 IU, 5000 IU, 10,000IU, 20,000 IU, and 50,000 IU in 1–10 ml ampoules.TETANUS IMMUNE SERUM (enzyme refined, equine)10,000 and 20,000 IU vials.
Immediate type of allergic reactions (urticaria,angioedema, respiratory distress, anaphylaxis) canoccur with any antiserum; adrenaline (1:1000amp.) should be at hand while injecting them.Prior to each administration, history of reactionto any ‘serum’ preparation should be elicited andan intracutaneous/scratch test should be perfor-med. A positive test contraindicates administrationbut a negative test does not completely rule outsystemic sensitivity.Serum sickness with fever, rash, joint pain,lymphadenopathy appearing 7–12 days later ismore frequent after large doses and repeatedadministration. An overall incidence of 5–10%is reported.Local pain, erythema and arthus type reactionwithout constitutional symptoms may also occur7–10 days after i.m. injection.
Immune globulins (IGs) are separated humangamma globulins which carry the antibodies.These may be nonspecific (normal) or specific(hyperimmune) against a particular antigen. Theseare more efficacious than the correspondingantisera. Hypersensitivity reactions are very rarewith IGs. Skin tests may be misleading and arenot needed. However, large doses and repeatedinjections do increase risk; adrenaline should beavailable. Transient local tenderness and stiffnessof injected muscle is occasional. Serum sicknessdoes not occur with human IGs.
Antisera (from horse)
Tetanus antitoxin (ATS)Gas gangrene antitoxin (AGS)Diphtheria antitoxin (ADS)Antirabies serum (ARS)Antisnake venom polyvalent
Immune globulins (human)Normal human gamma globulinAnti-D immune globulinTetanus immune globulinRabies immune globulinHepatitis-B immune globulin
1. Normal human gamma globulin It isconcentrated IG obtained by fractionation in coldfrom pooled human plasma. Indications for its

927C
HA
PTE
R68
VACCINES AND SERA
4. Rabies
(a) Antirabies serum (ARS) Also called‘equine rabies immune globulin’ (ERIG) isrefined, concentrated and lyophilized serum fromhorses hyperimmunized by repeated injections offixed rabies virus. It is indicated promptly aftersuspected exposure and is given simultaneouslywith rabies vaccine to nonimmunized individuals.Dose—40 IU/kg infiltrated round the wound and excess isinjected i.m.; single dose at the initiation of antirabic therapyalong with rabies vaccine. It is inferior to HRIG and should beused only when HRIG is not available.IMORAB 1000 IU/5 ml inj.
(b) Rabies immune globulin human (HRIG)It is used in the same manner as ARS and issuperior to it with longer t½. Dose—20 IU/kg,on day 0 only, infiltrated round the bite; excessmay be injected i.m. elsewhere. Passive protectionwith HRIG or ARS is needed because activeimmunity takes 2 or more weeks to develop.BERIRAB-P 300 IU/2 ml and 750 IU/5 ml inj; RABGLOB300 IU/2 ml inj.
5. Hepatitis B immune globulin It is10–18% solution of human IG containing a hightiter of antibody to hepatitis B surface antigen.It is a better prophylactic than normal human gammaglobulin: indicated in individuals acutely exposedto HBsAg positive blood or blood products.Hepatitis B vaccine should be given concurrently.Dose: 1000–2000 IU (adults), 32–48 IU/kg (children) to beadministered within 7 days of exposure.HEPAGLOB 100 IU (0.5 ml) 200 IU (1 ml) per vial for i.m.inj.
6. Diphtheria antitoxin (Antidiphtheriticserum ADS) It is obtained from horse andis used therapeutically in clinical diphtheriawithout waiting for bacteriological report, becauseeach hour’s delay increases the dose requirementand decreases beneficial effects: damage alreadycaused by the toxin is not reversed. The antitoxinneutralizes the exotoxin released at the site of
infection and that circulating in blood but notthat fixed to tissues.Dose: 20,000–40,000 IU i.m. or i.v. for pharyngeal/laryngealdisease of upto 48 hour duration. Higher dose (upto 100,000IU may be needed).DIPHTHERIA ANTITOXIN 10,000 IU in 10 ml amp.
Appropriate antimicrobials should also be given.Unprotected child contacts should be given ADS(1000 IU) along with diphtheria toxoid forprophylaxis.7. Gas gangrene antitoxin (Anti gas gan-grene serum, AGS) It is enzyme refinedequine antitoxin against Cl. edematiens, Cl.perfringens and Cl. septicum.Dose: prophylactic 10,000 IU; therapeutic 30,000–75,000 IUs.c./i.m./i.v.AGGS 10,000 IU amp.
8. Antisnake venom (ASV) serum poly-valent It is available as purified, enzyme refinedand concentrated equine globulins in lyophilizedvials with 10 ml ampule of distilled water. Afterreconstitution, each ml neutralizes:
0.6 mg of standard Cobra (Naja naja) venom.0.6 mg of standard Russel’s viper (Viperarusselli) venom.0.45 mg of standard Sawscaled viper (Echiscarinatus) venom.0.45 mg of standard Krait (Bungaruscaeruleus) venom.
ANTISNAKE VENOM SERUM POLYVALENT, ASVSDose: 20 ml i.v. (1 ml/min injection) repeated at 1–6 hourlyintervals till symptoms of envenomation disappear: upto 300ml may be required in viper bites, while still larger amounts(upto 900 ml) have been used in cobra bites, but it is importantto continue ASV treatment till evidence of envenomationpersists. In case of viper bite some serum should also beinfiltrated around the site to prevent venom induced gangrene.
Allergic reactions, including anaphylacticshock, to the serum are possible. When time per-mits, sensitivity test should be done; otherwiseadrenaline may be injected s.c. concurrently. Anantihistaminic and a glucocorticoid may also begiven prophylactically.

Drug InteractionsChapterChapterChapterChapterChapter 6969696969
Drug interaction refers to modification of responseto one drug by another when they are adminis-tered simultaneously or in quick succession. Themodification is mostly quantitative, i.e. theresponse is either increased or decreased inintensity, but sometimes, it is qualitative, i.e. anabnormal or a different type of response isproduced. The possibility of drug interaction ariseswhenever a patient concurrently receives morethan one drug, and the chances increase with thenumber of drugs taken.
Many medical conditions are treated with acombination of drugs. The components of thecombination are so selected that they complementeach other’s action, e.g. an antibiotic is used alongwith an analgesic to treat a painful infectivecondition; adrenaline is combined with lidocainefor local anaesthesia; antitubercular drugs arecombined to prevent drug resistance; mixedaerobic-anaerobic bacterial infections are treatedwith a combination of antimicrobials. More com-monly, multiple drugs are used to treat a patientwho is suffering from two or more diseases atthe same time. The chances of unintended/adversedrug interactions are greater in this later situation,because an assortment of different drugs may beadministered to a patient depending on his/herdiseases/symptoms.
Several drug interactions are desirable anddeliberately employed in therapeutics, e.g. thesynergistic action of ACE inhibitors + diureticsto treat hypertension or sulfamethoxazole +trimethoprim to treat bacterial infection orfurosemide + amiloride to prevent hypokalaemia.These are well-recognized interactions and do notpose any undue risk to the patient. The focusof attention in this chapter are drug interactionswhich may interfere with the therapeutic outcomeor be responsible for adverse effects, or may even
be fatal (bleeding due to excessive anticoagulantaction).
The severity of drug interactions in most casesis highly unpredictable. However the doctor mustknow which drugs are not to be prescribedconcurrently. More importantly, a large sectionof patients may be receiving one or several drugsfor their chronic medical conditions likehypertension, diabetes, arthritis, etc. (see box forregular medication drug classes employedcommonly). The physician may prescribe certaindrugs which may interact with those already beingtaken by the patient and result in adverseconsequences. It is, therefore, imperative for thedoctor to elicit a detailed drug history of the patientand record all the medication that he/she iscurrently on. The list of potential adverse druginteractions is already quite long and constantlygrowing. It is practically impossible for anyoneto know/remember all possible drug interactions.Fortunately, the clinically important and commondrug interactions that may be encountered inroutine practice are relatively few. Some of theseare listed in Table 69.1. More exhaustive
Regular medication drugs(Likely to be involved in drug interactions)
1. Antidiabetics2. Antihypertensives3. Antianginal drugs4. Antiarthritic drugs5. Antiepileptic drugs6. Antiparkinsonian drugs7. Oral contraceptives8. Anticoagulants9. Antiasthmatic drugs
10. Psychopharmacological agents11. Antipeptic ulcer/reflux drugs12. Corticosteroids13. Antitubercular drugs14. Anti-HIV drugs

929C
HA
PTE
R69
DRUG INTERACTIONS
compilations and documentation are available inspecialized books, monographs, review articlesand computer database on the subject, but thesealso need constant updating.
Certain types of drugs (see box) can beidentified that are most likely to be involved inclinically important drug interactions. Thephysician may take special care and pay attentionto the possibility of drug interactions when thepatient is receiving one or more of suchmedications, or when the doctor intends toprescribe any of such drugs.
Types of drugs most likely to be involved inclinically important drug interactions
• Drugs with narrow safety margin, e.g. amino-glycoside antibiotics, digoxin, lithium
• Drugs affecting closely regulated body functions,e.g. antihypertensives, antidiabetics, anticoagulants
• Highly plasma protein bound drugs like NSAIDs,oral anticoagulants, sulfonylureas
• Drugs metabolized by saturation kinetics, e.g.phenytoin, theophylline
MECHANISM OF DRUG INTERACTIONSDrug interactions can be broadly divided intopharmacokinetic and pharmacodynamic intera-ctions. In certain cases, however, the mechanismsare complex and may not be well understood.Few interactions take place even outside the bodywhen drug solutions are mixed before adminis-tration.
Pharmacokinetic interactions
These interactions alter the concentration of theobject drug at its site of action (and consequentlythe intensity of response) by affecting itsabsorption, distribution, metabolism or excretion.
Absorption Absorption of an orally adminis-tered drug can be affected by other concurrentlyingested drugs. This is mostly due to formationof insoluble and poorly absorbed complexes inthe gut lumen, as occurs between tetracyclinesand calcium/iron salts, antacids or sucralfate.Phenytoin absorption is decreased by sucralfatedue to binding in the g.i. lumen. Such interactions
Pharmacokinetic interactions
• Alteration of absorption or first-pass metabolism• Displacement of plasma protein bound drug• Alteration of drug binding to tissues affecting
volume of distribution and clearance• Inhibition/induction of metabolism• Alteration of excretion
can be minimized by administering the twodrugs with a gap of 2–3 hours so that they donot come in contact with each other in the g.i.t.Ketoconazole absorption is reduced by H2
blockers and proton pump inhibitors becausethey decrease gastric acidity which promotesdissolution and absorption of ketoconazole.Antibiotics like ampicillin, tetracyclines,cotrimoxazole markedly reduce gut flora thatnormally deconjugates oral contraceptive steroidssecreted in the bile as glucuronides and permitstheir enterohepatic circulation. Several instancesof contraceptive failure have been reportedwith concurrent use of these antibiotics due tolowering of the contraceptive blood levels.Alteration of gut motility by atropinic drugs,tricyclic antidepressants, opioids and prokineticdrugs like metoclopramide or cisapride can alsoaffect drug absorption.
Distribution Interactions involving drug distri-bution are primarily due to displacement of onedrug from its binding sites on plasma proteinsby another drug. Drugs highly bound to plasmaproteins that have a relatively small volume ofdistribution like oral anticoagulants, sulfonylureas,certain NSAIDs and antiepileptics are particularlyliable to displacement interactions. Anotherrequirement is that the displacing drug shouldbind to the same sites on the plasma proteinswith higher affinity. Displacement of bound drugwill initially raise the concentration of the freeand active form of the drug in plasma that mayresult in toxicity. However, such effects are usuallybrief, because the free form rapidly getsdistributed, metabolized and excreted, so thatsteady-state levels are only marginally elevated.The clinical outcome of displacement interactions

930S
EC
TIO
N14
MISCELLANEOUS DRUGS
is generally significant only when displacementextends to tissue binding sites as well, or isaccompanied by inhibition of metabolism and/or excretion. Quinidine has been shown to reducethe binding of digoxin to tissue proteins as wellas its renal and biliary clearance by inhibing theefflux transporter P-glycoprotein, resulting innearly doubling of digoxin blood levels andtoxicity.
Metabolism Certain drugs reduce or enhancethe rate of metabolism of other drugs. They maythus affect the bioavailability (if the drugundergoes extensive first pass metabolism in liver)and the plasma half-life of the drug (if the drugis primarily eliminated by metabolism). Inhibitionof drug metabolism may be due to competitionfor the same CYP450 isoenzyme or cofactor, andattains clinical significance mostly for drugs thatare metabolized by saturation kinetics. Macrolideantibiotics, azole antifungals, chloramphenicol,omeprazole, SSRIs, HIV-protease inhibitors,cimetidine, ciprofloxacin and metronidazole aresome important inhibitors of metabolism ofmultiple drugs. Risk of statin induced myopathyis increased by fibrates, niacin, erythromycin,azole antifungals and HIV-protease inhibitors,probably due to inhibition of statin metabolism.Because lidocaine metabolism is dependent onhepatic blood flow, propranolol has been foundto prolong its t½ by reducing blood flow to theliver.
A number of drugs induce microsomal drugmetabolizing enzymes and enhance biotrans-formation of several drugs (including their ownin many cases). Induction involves gene mediatedincreased synthesis of certain CYP450isoenzymes; takes 1–2 weeks of medication withthe inducer to produce maximal effect (contrastinhibition of metabolism which develops quickly)and regresses gradually over 1–3 weeks afterdiscontinuation of the inducer. Barbiturates,phenytoin, carbamazepine, rifampin, cigarettesmoking, chronic alcoholism and certain pollutantsare important microsomal enzyme inducers.Instances of failure of antimicrobial therapy with
metronidazole, doxycycline or chloramphenicolhave occurred in patients who are on long-termmedication with an inducing drug. Contraceptivefailure and loss of therapeutic effect of many otherdrugs have occurred due to enzyme induction.On the other hand, the toxic dose of paracetamolis lower in chronic alcoholics and in those onenzyme inducing medication, because one of themetabolites of paracetamol is responsible for itsoverdose hepatotoxicity.
Excretion Interaction involving excretion areimportant mostly in case of drugs actively secretedby tubular transport mechanisms, e.g. probenecidinhibits tubular secretion of penicillins andcephalosporins and prolongs their plasma t½. Thisis particularly utilized in the single dose treatmentof gonorrhoea. Aspirin blocks the uricosuric actionof probenecid and decreases tubular secretion ofmethotrexate. Change in the pH of urine can alsoaffect excretion of weakly acidic or weakly basicdrugs. This has been utilized in the treatment ofpoisonings. Diuretics and to some extenttetracyclines, ACE inhibitors and certain NSAIDshave been found to raise steady-state blood levelsof lithium by promoting its tubular reabsorption.
Pharmacodynamic interactionsThese interactions derive from modification of theaction of one drug at the target site by anotherdrug, independent of a change in its concentration.This may result in an enhanced response(synergism), an attenuated response (antagonism)or an abnormal response. The phenomena ofsynergism and antagonism are described in Chapter4, and are deliberately utilized in therapeutics forvarious purposes. Of clinical significance are theinadvertent concurrent administration of synergisticor antagonistic pair of drugs with adverseconsequences. Some examples are:
1. Excessive sedation, respiratory depression,motor incoordination due to concurrent ad-ministration of a benzodiazepine (diazepam),a sedating antihistaminic (promethazine), aneuroleptic (chlorpromazine), an opioid

931C
HA
PTE
R69
DRUG INTERACTIONS
TABLE 69.1 Selected clinically important drug interactions
Precipitant drug* Object drug£ Likely interaction and comments
1. Ampicillin Oral contraceptives Interruption of enterohepatic circulation of the estrogen →Amoxicillin failure of contraception; Advise alternative contraception.
Oral anticoagulants Inhibition of gut flora → decreased vit K production ingut → risk of bleeding; Monitor INR and reduce anticoagu-lant dose if needed.
2. Probenecid Penicillin Inhibition of tubular secretion → prolongation of antibioticAmpicillin action; Desirable interaction utilized for single dose therapy.Cephalosporins
3. Allopurinol Ampicillin Increased incidence of rashes; Avoid concurrent use.6-Mercaptopurine Inhibition of metabolism; Reduce dose of 6-MP/azathioprineAzathioprine to 1/3.Warfarin Inhibition of metabolism; Monitor and reduce dose of objectTheophylline drug.
4. Carbenicillin Aspirin and other Perturbation of surface receptors on platelets → additiveTicarcillin antiplatelet drugs platelet inhibition → risk of bleeding; Avoid concurrent use.
5. Ceftriaxone Oral anticoagulants Additive hypoprothrombinaemia → bleeding; Monitor INRCefoperazone and reduce dose of anticoagulant.
6. Sulfonamides Phenytoin Displacement$ + inhibition of metabolism → phenytoinCotrimoxazole toxicity; Avoid concurrent use.
Warfarin Displacement + inhibition of metabolism + decreasedproduction of vit K in gut → risk of bleeding; Monitor INRand reduce dose of warfarin.
Sulfonylureas Displacement + inhibition of metabolism → hypoglycaemia;Avoid concurrent use.
Thiazide diuretics Increased incidence of thrombocytopenia; Avoid concurrentuse.
Oral contraceptives Interruption of enterohepatic circulation of the estrogen →failure of contraception; Advise alternative contraception.
7. Metronidazole Alcohol Possibly accumulation of acetaldehyde → disulfiram-like orTinidazole bizarre reactions; Warn the patient not to drink alcohol.Cefoperazone
8. Metronidazole Lithium salts Decreased excretion → Li+ toxicity; Monitor Li+ level andTinidazole reduce lithium dose.
Warfarin Inhibition of metabolism → risk of bleeding; Avoidconcurrent use.
9. Ciprofloxacin Theophylline Inhibition of metabolism → toxicity of object drug; MonitorNorfloxacin Warfarin and reduce dose of object drug.Pefloxacin
10. Erythromycin Terfenadine Inhibition of metabolism by CYP3A4 → rise in blood levelClarithromycin Astemizole of object drug → dangerous ventricular arrhythmia;Ketoconazole Cisapride Concurrent use contraindicated.Itraconazole PhenytoinFluconazole CarbamazepineProtease inhibitors Warfarin
Sulfonylureas Inhibition of metabolism by CYP3A4 → toxicity of objectDiazepam drug; Avoid concurrent use or readjust dose of object drug.TheophyllineCyclosporineHIV protease inhibitorsStatins Inhibition of metabolism, higher risk of myopathy;
Avoid concurrent use.* Precipitant drug is the drug, which alters the action/pharmacokinetics of the other drug. Contd...£ Object drug is the drug whose action/pharmacokinetics is altered.$ Displacement of plasma protein bound drug.

932S
EC
TIO
N14
MISCELLANEOUS DRUGS
TABLE 69.1 Contd...
11. Gemfibrozil Statins Increased risk of myopathy; Caution in concurrent use.Nicotinic acid
12. Tetracyclines Oral contraceptives Interruption of enterohepatic circulation of the estrogen →failure of contraception; Advise alternative contraception.
Lithium salts Rise in plasma Li+ level due to decreased excretion; Avoiduse of tetracycline or monitor and reduce dose of lithium.
13. Iron salts Tetracyclines Decreased absorption due to formation of complexes inCalcium salts Fluoroquinolones g.i.t. → failure of antibiotic therapy; Stager drugAntacids administration by 2–3 hours.Sucralfate
14. Furosemide Minocycline Enhanced vestibular toxicity; Avoid concurrent use.Aminoglycoside Additive ototoxicity and nephrotoxicity; Avoid concurrentantibiotics use.
15. Diuretics Tetracycline Antianabolic effect of tetracycline increases urea productionwhich is retained by the diuretic; Avoid concurrent use.
Lithium Decreased excretion—rise in Li+ level—toxicity; Reducedose of lithium and monitor level.
Digoxin Hypokalaemia caused by diuretic increases digoxin toxicity;Give K+ sparing diuretic/K+ supplements.
16. Tetracyclines Penicillins Bactericidal action of penicillins and cephalosporins mayChloramphenicol Cephalosporins be antagonized by the bacteriostatic antibiotics; AvoidMacrolide antibiotics concurrent use.Clindamycin
17. Clindamycin Erythromycin Mutual antagonism of antibacterial action due to proximalClarithromycin binding sites on bacterial ribosomes; Avoid concurrent use.AzithromycinChloramphenicol
18. Phenobarbitone MetronidazolePhenytoin DoxycyclineCarbamazepine Chloramphenicol Induction of metabolism → loss of efficacy of object drug;Rifampin Protease inhibitors Avoid concurrent use or increase dose of object drug with
Warfarin monitoring.CorticosteroidsOral contraceptivesSulfonylureasAntidepressants
19. Chloramphenicol Warfarin Inhibition of metabolism → toxicity of the object drug.Phenytoin Avoid concurrent use or monitor and reduce dose of objectSulfonylureas drug.
20. NSAIDs Ciprofloxacin and Enhanced CNS toxicity, seizures; Avoid concurrent use.other fluoroquinolones
21. Aspirin and Sulfonylureas Displacement and/or reduced elimination → toxicity ofother NSAIDs Phenytoin object drug; Avoid concurrent use/substitute NSAID with
Valproate paracetamol.MethotrexateWarfarin Enhanced risk of bleeding due to antiplatelet action andHeparin gastric mucosal damage; Avoid concurrent use.ACE inhibitors Reduced antihypertensive effect due to inhibition of renalβ blockers PG synthesis; Avoid concurrent use.Thiazide diureticsFurosemide Reduced diuretic action due to PG synthesis inhibition in
kidney; Avoid concurrent use.
Precipitant drug* Object drug£ Likely interaction and comments
Contd...

933C
HA
PTE
R69
DRUG INTERACTIONS
TABLE 69.1 Contd...
Aspirin and Alcohol Increased risk of gastric mucosal damage and gastricother NSAIDs Corticosteroids bleeding; Concurrent use contraindicated.
22. Aspirin Spironolactone Reduced K+ conserving action due to decreased tubularsecretion of canrenone (active metabolite of spironolactone);Avoid concurrent use.
23. Chronic Paracetamol Hepatotoxic dose of paracetamol is reduced; dosesalcoholism < 3 g/day are safe.
24. Chlorpromazine MorphineImipramine and Pethidine Enhanced CNS and respiratory depression; Avoidother TCAs Codeine concurrent use.
25. Chlorpromazine Levodopa-carbidopa Antagonism of antiparkinsonian effect; Concurrent useHaloperidol contraindicated.Metoclopramide
26. Levodopa-carbidopa ACE inhibitors Excessive postural hypotension; Reduce dose ofVasodilators antihypertensives.Prazosin
27. TCAs Adrenaline (added to Potentiation due to neuronal uptake inhibition → rise inlocal anaesthetic) BP; Use plain local anaesthetic solution.
28. PromethazineAlcohol Diazepam and other Additive CNS and respiratory depression, motorOpioids benzodiazepines impairment; Avoid concurrent use.Antipsychotics
29. Cimetidine Diazepam and Inhibition of metabolism → exaggerated CNS depression;Isoniazid other benzodiazepines Avoid concurrent use or reduce benzodiazepine dose.
30. Sildenafil Nitrates Marked potentiation → precipitous fall in BP;Tadalafil Concurrent use contraindicated.
31. Propranolol Adrenaline (injected with Rise in BP due to blockade of vasodilator action of adrenalinelocal anaesthetic) that enters systemic circulation; Avoid adrenaline containing
local anaesthetic.Lidocaine Reduced hepatic clearance of lidocaine; Ceiling amount
used in local anaesthesia is reduced.32. Lidocaine β-blockers Enhanced bradycardia and hypotension; Avoid concurrent
use.Quinidine and other Exaggerated cardiac depression, precipitation ofantiarrhythmic drugs arrhythmias; Avoid concurrent use.
NSAIDs: Nonsteroidal antiinflammatory drugsTCAs: Tricyclic antidepressants
Precipitant drug* Object drug£ Likely interaction and comments
(morphine) or drinking alcoholic beveragewhile taking any of the above drugs.
2. Excessive fall in BP and fainting due toconcurrent administration of α1 adrenergicblockers, vasodilators, ACE inhibitors, highceiling diuretics and cardiac depressants.
3. Pronounced and asymptomatic hypogly-caemia can occur when propranolol isadministered to diabetics receiving insulin/sulfonylureas, due to blockade of β adreno-
ceptors which contribute to recovery fromhypoglycaemia as well as some hypogly-caemic symptoms.
4. Additive prolongation of prothrombin timeand bleeding by administration of ceftriaxoneor cefoperazone to a patient on oral anti-coagulants.
5. Excessive platelet inhibition resulting inbleeding due to simultaneous use of aspirin/ticlopidine/clopidogrel and carbenicillin.

934S
EC
TIO
N14
MISCELLANEOUS DRUGS
6. Increased risk of bleeding due to concurrentuse of antiplatelet drugs (aspirin, clopido-grel) with anticoagulants (warfarin).
7. Marked bradycardia due to administrationof propranolol in digitalized patients.
8. Precipitous fall in BP and myocardialischaemia due to use of sildenafil by patientsreceiving organic nitrates, because nitratesincrease generation of cGMP, whilesildenafil prevents its degradation byinhibiting PDE 5.
9. Severe hyperkalaemia by concurrent use ofACE inhibitors and K+ sparing diuretics.
10. Additive ototoxicity due to use of an amino-glycoside antibiotic in a patient receivingfurosemide.
11. Antagonism of bactericidal action ofβ-lactam antibiotic by combining it with abacteriostatic drug like tetracycline, erythro-mycin or clindamycin.
12. Mutual antagonism of antibacterial action ofmacrolides, clindamycin and chloram-phenicol due to interference with each other’sbinding to the bacterial 50S ribosome.
13. Reduction in antihypertensive action ofclonidine by chlorpromazine and imipra-mine, possibly due to blockade of centralaction of clonidine.
14. Attenuation of antihypertensive effect ofACE inhibitors/β blockers/diuretics byNSAIDs due to inhibition of renal PGsynthesis.
15. Blunting of K+ conserving action ofspironolactone by aspirin, because it inhibitsthe tubular secretion of canrenone (an activemetabolite of spironolactone).
16. Blockade of antiparkinsonian action oflevodopa by neuroleptics and metoclopra-mide having antidopaminergic action.
Abnormal responses sometimes result frompharmacodynamic interaction between certaindrugs, e.g. bizarre somewhat disulfiram-likedistressing symptoms are experienced by certainsubjects when they drink alcoholic beverages
while taking metronidazole or cefoperazone. Itis not known whether this is due to inhibitionof aldehyde dehydrogenase. The basis of certaininteractions is not explained, e.g. ampicillin hasproduced high incidence of skin rashes in patientstreated with allopurinol.
Drug interactions before administration
Certain drugs react with each other and getinactivated if their solutions are mixed beforeadministration. In combined oral or parenteralformulations, the manufacturers take care that suchincompatibilities do not take place. In practicesituations, these in vitro interactions occur wheninjectable drugs are mixed in the same syringeor infusion bottle. Some examples are:• Penicillin G or ampicillin mixed with genta-
micin or another aminoglycoside antibiotic• Thiopentone sodium when mixed with
succinylcholine or morphine• Heparin when mixed with penicillin/
gentamicin/hydrocortisone• Noradrenaline when added to sodium
bicarbonate solution.In general, it is advisable to avoid mixing of
any two or more parenteral drugs before injecting.
Comment Not all patients taking interactingdrugs experience adverse consequences, but it isadvisable to take due precautions to avoid mishapsin all cases where interactions are possible. Thattwo drugs have the potential to interact does notnecessarily contraindicate their concurrent use.In many cases, knowledge of the nature andmechanism of the possible interaction may permittheir concurrent use provided appropriate doseadjustments are made or other corrective measuresare taken. A list of significant and common druginteractions that may be encountered in clinicalpractice is given in Table 69.1, along with thesuggested corrective measure. However, it isprudent to consider the possibility of druginteraction whenever two or more drugs areprescribed to a patient, or any drug is added towhat the patient is already taking.

Solution to Problem DirectedStudy
AppendixAppendixAppendixAppendixAppendix 11111
APPENDICES
SOLUTION 1.1
a. Since the child is seriously ill, a fast and more predictable action of the antibiotic is needed;a parenteral route of administration is appropriate. Moreover, oral dosing may be difficultin this case as the child is dull and irritable. Entering a vein for i.v. injection is relativelydifficult in children, particularly in the presence of dehydration. Therefore, the antibioticmay be injected i.m. However, if an i.v. line is set up for rehydration, the antibiotic maybe administered through the i.v. line.
b. In this case the provisionally selected antibiotic should be started as early as possible, becausethe child is seriously ill. Waiting for the lab. reports to confirm the diagnosis/select thedefinitive antibiotic may compromise the prognosis.
SOLUTION 2.1
a. Gastric acid is required for the absorption of oral iron salts. Concurrent ingestion of antacidtablets could have interfered with iron absorption. Hence, the anaemia failed to improve.
SOLUTION 2.2
a. Aspirin displaces sulfonylureas from plasma protein binding sites. Therefore, plasmaconcentration of unbound (and active) glibenclamide would have risen after aspirin ingestioncausing hypoglycaemia which produced the symptoms. As such, glucose ingestion relievedthe symptoms.
b. Paracetamol and ibuprofen are analgesics equally effective in toothache as aspirin, and donot displace or otherwise interact with sulfonylureas. As such, these analgesics are moresuitable for the given patient.

936 APPENDICESA
PP
EN
DIC
ES
SOLUTION 3.1
a. Rifampin is known to induce the metabolism of contraceptive steroids. Thus, after regularintake of rifampin for more than 2 weeks (needed for enzyme induction) the steady-stateblood level of levonorgestrel and ethinylestradiol could have fallen below the threshold forinhibition of ovulation/contraception. As such, fertility was restored and the woman conceived.
b. In view of the essentiality of rifampin (and other antitubercular drugs) in this patient andthe likelihood of failure of the oral contraceptive, the couple should have been advised totake additional/alternative contraceptive measure such as condom or intrauterine contraceptivedevice.
SOLUTION 3.2
The total volume of distribution and total body clearance for this patients has to be calculatedfirst.
Total V = 1.4 L/kg × 60 kg = 84 LTotal body clearance (CL) = 80 ml/hr/kg × 60 kg
= 4.8 L/hr 70
Fractional bioavailability (F) = = 0.7 100
Applying the formula: target Cp × V
Loading dose =F
Or 6 mg/L X 84 L = 720 mg
0.7Maintenance dose rate = Cpss × CL
FOr 6 mg/L × 4.8 L/hr
= 41 mg/hr0.7
Or 41 mg/hr × 24 hr = 984 mg/day
For this patient: Loading dose 720 mg initially; or practically 3½ tablets of 200 mg each.
Maintenance dose: 984 mg/day.
To be practical, the maintenance dose could be one 400 mg tab. in the morning and 1½ tab.(600 mg) in the evening.
SOLUTION 4.1
a. Since Mtx binds to the same site of DHFRase as the endogenous metabolite DHFA, it willact as a competitive inhibitor. However, because the binding affinity of Mtx for the enzymeis 50,000 times greater, even excess DHFA will not be able to displace it from the enzymeand nonequilibrium type of inhibition will be produced.
b. Folic acid administered as a drug will not be able to counteract Mtx toxicity becauseit will not be converted to the active coenzyme form THFA. On the other hand, folinicacid will supply readymade active coenzyme THFA and will be able to overcome Mtx toxicity.

937SOLUTION TO PROBLEM DIRECTED STUDYA
PP
EN
DIX
1
SOLUTION 5.1
a. The most likely pathogenesis of the symptoms on the 3rd day of brisk diuretic therapy inthis patient is occurrence of hypokalaemic alkalosis, which precipitated hepatic encephalopathy.In cirrhotics with moderate to severe hepatic dysfunction, ammonia (NH3) produced by gutbacteria is not completely detoxified (by conversion to urea) in the liver. Blood NH3 tendsto rise. This ionizes partly to NH4
+ and is excreted in urine as NH4Cl. The NH4+ ions do not
cross the blood-brain barrier. During alkalosis, NH3 ionizes to a lesser extent, raising bloodNH3 level which enters brain to cause encephalopathy. Weakness and postural hypotensionare the other manifestations of hypokalaemic alkalosis.
b. The diuretic should be withheld till the fluid electrolyte and acid-base balance is restored.Intravenous infusion of KCl along with normal saline can hasten recovery from hypokalaemiaand alkalosis. Oral lactulose (a nonabsorbable disaccharide) helps in reducing blood NH3
level by producing acidic degradation products in the gut which convert NH3 into poorlyabsorbed NH4
+ ions. Moreover, lowering of stool pH by lactulose has a suppressant effecton NH3 producing gut bacteria.
SOLUTION 6.1
a. The patient has a serious disease for which many effective drugs are available. As such,antitubercular treatment should be continued, albeit with nonhepatotoxic drugs.
b. The criteria for causality assessment, viz. temporal relationship, previous knowledge, dechallengeand rechallenge should be applied to identify the causative drug. In this case, the reactionoccurred in the 4th week of drug therapy which is consistent with the time-sequencing ofdrug-induced hepatitis. The reaction can be confirmed and the actual causative drug identifiedby dechallenge and rechallenge.• Stop all suspected drugs (H, R and Z); treat the patient with E and two other nonhepatotoxic
drugs, preferably streptomycin (i.m.) and a fluoroquinolone (e.g. levofloxacin). If the jaundiceclears in the subsequent weeks, dechallenge is positive (one or more of the 3 stoppeddrugs had caused hepatitis).
• Rechallenge by reintroducing the stopped drugs, one at a time, and repeatedly monitorliver function tests.
• Generally, R is started first followed by H after 7–10 days. If both are tolerated, Z couldhave been the causative drug. In any case, after completing the intensive phase withH+R+E, the continuation phase with H+R should be extended to 9 months.
• If R is implicated, it should be stopped as soon as the liver function tests become abnormal.Start H and continue H+E+S for 2 months followed by H+E for 10 months.
• If H is implicated, it should be stopped immediately, and R+E+Z may be given for 9 months.
In this way, the implicated drug can be identified and antitubercular therapy completed withminimal use of parenteral/2nd line drugs.

938 APPENDICESA
PP
EN
DIC
ES
SOLUTION 7.1
a. The diagnosis of myasthenia gravis can be confirmed by the ‘edrophonium test’. Edrophoniumis injected i.v. (2 mg initially which if tolerated; followed by 8 mg after 30–60 sec). Reversalof ptosis, diplopia and increase in the strength of affected muscles lasting 5–10 min constitutesa positive result.In case edrophonium is not available, the test can be performed with neostigmine 1.5 mgi.v. Atropine 0.6 mg may be given i.m./i.v. to block the muscarinic side effects of edrophonium/neostigmine.
b. Myasthenia gravis is an autoimmune disorder due to production of antibodies against the nicotinicreceptor at the muscle end-plate. No drug is curative. Both anticholinesterases (neostigmine,etc.) and corticosteroids (other immunosuppressants as well) afford only symptomatic relieftill administered. The former preserve ACh and improve neuromuscular transmission, whilethe latter inhibit the immunological reaction, without removing the cause of the illness.
c. In many cases (especially older men), thymus is the source of the nicotinic receptor antigen.As such, thymectomy has been found to lower disease activity and even induce long-lastingremission.
SOLUTION 8.1
a. Dimenhydrinate is a H1 antihistaminic-antivertigo drug with potent antimuscarinic action.Since muscarinic cholinoceptors mediate neurogenic contraction of the detrusor muscle,antimuscarinic drugs interfere with vesical contractions needed for urination. Elderly menwith benign hypertrophy of prostate have bladder neck obstruction and are prone to developurinary retention as a side effect of antimuscarinic drugs. This patient has history indicativeof prostatic hypertrophy. As such, all drugs having antimuscarinic activity must be givencautiously to elderly males.
SOLUTION 9.1
a. The symptoms and intraocular pressure (i.o.p.) of this patient indicate that she is havinggluaucoma in both eyes. Phenylephrine (10%) eyedrop would be the suitable mydriatic forher. Phenylephrine is an α1 adrenergic agonist that dilates the pupil by increasing the toneof radial muscles of iris, which are adrenergically innervated. It does not produce cycloplegiabecause the ciliary muscles lack adrenergic motor innervation. Cycloplegia causes blurringof near vision and is not required in this patient. Phenylephrine is not likely to raise i.o.p.in glaucoma patients. On the other hand, antimuscarinic mydriatics like tropicamide,cyclopentolate, etc. produce both mydriasis and cycloplegia, and tend to raise i.o.p. in glaucomapatients. Therefore, antimuscarinics are to be avoided in glaucoma patients.
SOLUTION 10.1
a. The smooth muscles of the bladder neck and prostatic urethra are constricted by sympatheticinnervation via α1 adrenergic receptors. Terazosin being α1 receptor blocker reduces thedynamic component of urinary obstruction in benign prostatic hypertrophy, improves urinaryflow and affords symptomatic relief. Contd...

939SOLUTION TO PROBLEM DIRECTED STUDYA
PP
EN
DIX
1
b. The α1 adrenergic receptors also mediate reflex vasoconstriction in the lower extremity andtrunk which occurs on standing up from a reclining position to maintain cerebral bloodflow. Terazosin blocked these α1 receptors as well; reflex vasoconstriction failed to occurwhen this patient got up from bed to pass urine; blood supply to brain suffered and thepatient fainted. That is why he soon regained consciousness on being laid flat on the bed.Such an event is especially likely to occur after the first dose when compensatory haemodynamicadjustments have not taken effect.
c. The patient should have been advised not to spring up from the bed. He should first siton the bed for few minutes and then slowly assume the erect posture. This would allowtime for the reflex adjustments.
The 5 mg terazosin dose is a high starting dose. Therapy should have been initiated at 1 mgdaily dose, with upward titration every 1–2 weeks according to the symptomatic relief obtainedand the haemodynamic tolerance by the patient.
SOLUTION 10.2
a. Timolol is a potent lipophilic, nonselective (β1 + β2) adrenergic blocker. In this patient ofmild episodic asthma, the drug in the eyedrops appears to have been absorbed systemicallyduring drainage through the nasolacrimal ducts and precipitated severe bronchospasm byblocking bronchodilator adrenergic β2 receptors. Since timolol is a competitive antagonist,its action could be overcome by higher concentration of salbutamol in the nebulized aerosolsupplemented with the anticholinergic ipratropium bromide to block the reflex vagalbronchoconstriction.
b. This complication could have been prevented by eliciting the history of episodic asthmaand avoiding β-blocker ocular hypotensive drug. Latanoprost (a prostaglandin analogue) wouldbe a more suitable antiglaucoma drug for this patient. In case, it was imperative to usean ocular β-blocker, the β1 selective antagonist betaxolol would be a safer alternative. Itis also prudent to start with 0.25% timolol drops and change to 0.5% drops only whenneeded. In any case, the patient should be advised to apply mild pressure by fingertip forfew minutes at the inner canthus of the eye after each eyedrop instillation to prevent passageof the drug into the nasolacrimal duct.
SOLUTION 11.1
a. Since histamine is an important mediator of allergic rhinitis, the H1 antihistaminics affordrapid symptomatic relief. A non-sedating second generation antihistaminic like loratadine,des-loratadine or fexofenadine would be suitable for this patient, who is a taxi driver. Thesedrugs are least likely to impair alertness and driving. The first generation sedating antihistamineslike promethazine, hydroxyzine, chlorpheniramine, clemastine, etc. are contraindicated if therecipient has to drive. Even the second generation antihistaminic cetirizine impairs psychomotorperformance and should be avoided in this patient.However, antihistaminics have no prophylactic effect. Because the patient has recurrent episodesduring spring, he should in addition be prescribed a topical corticosteroid like budesonideor fluticasone nasal spray, starting just before and continuing all through the season to preventfurther attacks of rhinitis.

940 APPENDICESA
PP
EN
DIC
ES
SOLUTION 13.1
a. Prostaglandin E2 (Dinoprostone) has the property to soften the cervix and make it more compliantat term. Applied to the cervix or inserted into vagina, low doses of dinoprostone act withina few hours and help to ripen the cervix so that it is ‘taken up’ and dilates to allow passageof the presenting part. Side effects are minimal with these routes of administration. The preferredformulation for this purpose is the cervical gel containing 0.5 mg of dinoprostone in 2.5 mlgel. It should be inserted into the cervical canal. Alternatively, the vaginal gel containing 1.0mg in 2.5 ml should be deposited at the posterior fornix of vagina. These doses of PGE2
only affect the cervix and do not significantly augment uterine contractions.b. Since the patient has no anaemia or toxaemia of pregnancy or cephalopelvic disproportion,
presentation is correct and head is engaged, there are no contraindications to the use ofPGE2.
SOLUTION 14.1
a. Paracetamol taken in adequate doses (upto 2.6 g per day) is the most suitable analgesicfor relieving knee pain in the given patient. Unlike many NSAIDs, it does not increase therisk of myocardial infarction/stroke. Paracetamol does not inhibit endothelial PGI2 synthesis,does not affect platelet function and does not nullify the cardioprotective effect of low doseaspirin. Moreover, it is a first-line drug for osteoarthritic pain, and is well tolerated withminimal gastric side effects.
b. The selective COX-2 inhibitors (celecoxib, etoricoxib) are not suitable for this patient, becausethey increase the risk of heart attack and stroke by inhibiting endothelial PGI2 synthesis.Diclofenac is also not free of such risk. Though propionic acid NSAIDs (ibuprofen, etc.) arenonselective COX inhibitors which do not increase thrombotic risk, they block thecardioprotective effect of low dose aspirin that this patient is taking.
c. Topical NSAIDs, e.g. diclofenac/ketoprofen gel can afford adjuvant symptomatic relief in thispatient. Since blood levels of NSAIDs after local application are low, they are well toleratedand do not increase cardiovascular risk.
SOLUTION 16.1
a. The recently developed symptoms of the patient are indicative of early stage theophyllinetoxicity. Erythromycin is an inhibitor of several hepatic microsomal enzymes, including thosethat metabolize theophylline. As such, when the patient took erythromycin, metabolism oftheophylline appears to have been retarded, causing rise in its plasma concentration overthe next 2 days and producing overdose symptoms.
b. This complication could have been prevented in two ways, viz—i. When erythromycin was prescribed, the daily dose of theophylline should have been reduced
from 800 mg to 500 mg, and maintained at this level till the patient was taking erythromycin.Or
ii. An alternative antibiotic (e.g. a β-lactam like amoxicillin or cephalexin) which does notinhibit theophylline metabolism but is effective in sore throat, could have been selectedfor this patient.

941SOLUTION TO PROBLEM DIRECTED STUDYA
PP
EN
DIX
1
SOLUTION 18.1
a. Since carbimazole inhibits further synthesis of thyroid hormones (T3, T4) without affectingtheir release or action, the hormone stored in the gland continues to be released and produceeffects. Moreover, thyroxine has a long plasma t½ of 6–7 days. Thus, the effect of carbimazolestarts manifesting only after 2–3 weeks and peaks after 2–3 months.Many of the symptoms of thyrotoxicosis are due to sympathetic overactivity. Blockade ofβ adrenergic receptors (β1 and β2) by propranolol or similar drug affords rapid symptomaticrelief, without affecting thyroid status. A nonselective β-blocker given to her along withcarbimazole could have controlled palpitation, tremor, etc. within a few days. This drug couldbe withdrawn when carbimazole had taken effect.
b. The reappearance of neck swelling without any symptom of thyrotoxicosis indicates that itis due to deficient feedback inhibition of TSH by a suboptimal thyroid hormone level as aresult of higher maintenance dose of carbimazole. This is supported by the mild hypothyroidsymptoms experienced by the patient and the raised TSH level alongwith low normal FT4
level. The raised TSH is stimulating the thyroid so that despite its low functional status, deficiencyis not marked. Since the disease activity in Graves’ disease may decline after some time, themaintenance dose of carbimazole needs to be adjusted from time-to-time according to theassessed clinical and laboratory thyroid status of the patient. This patient requires temporarydiscontinuation of carbimazole followed by a lower maintenance dose as assessed later.
SOLUTION 19.1
a. According to the current recommendation of professional guidelines, the patient should beprescribed metformin therapy concurrently with dietary and lifestyle measures. This is basedon the finding that metformin can delay progression of diabetes and prevent microvascularas well as macrovascular (heart attack, stroke) complications. It does not increase circulatinginsulin, reduces insulin resistance, is unlikely to induce hypoglycaemia and may have a positiveinfluence on pancreatic B cell health. Lack of serious toxicity over several decades of useof metformin is well established. No other antidiabetic drug has all these favourable features,and therefore, it is considered the first-choice drug. Metformin is particularly suitable forthis patient who is overweight, because it can aid weight reduction. A combination of antidiabeticdrugs is not indicated at this stage. Another drug needs to be added only when the targetblood glucose and HbA1c levels are not attained by metformin alone.
SOLUTION 20.1
a. The patient has received supraphysiological doses of a corticosteroid for more than 3 weeks,and is likely to have developed hypothalamo-pituitary-adrenal (HPA) suppression. The injuryand surgery are a stress which need excess corticoid activity. The depressed HRA axis maynot be able to cope up with increased demand, and there is risk of developing acute adrenalinsufficiency. As such, hydrocortisone hemisuccinate 100 mg should be infused i.v. duringsurgery and repeated 8 hourly till the patient is stable.
b. Prednisolone therapy must not be stopped in the postoperative period apprehending spreadof infection and delayed healing. Effective antibiotic medication to prevent wound infectionshould be given and prednisolone dose should be increased temporarily (for a week or so)to 20 mg/day, till the stress of the trauma and surgery subsides.

942 APPENDICESA
PP
EN
DIC
ES
SOLUTION 21.1
a. This is a case of advanced metastatic prostate carcinoma, for which only palliativetherapy with androgen deprivation (tumour cells remain androgen dependent) ispossible. When orchidectomy has been refused, the most effective method of androgendeprivation is to give a long acting GnRH agonist. Thus, the choice of triptorelin is correct.The GnRH agonists initially increase LH (also FSH) release for 1–2 weeks, followed by receptordesensitization and nearly total blockade of LH secretion by 3–4 weeks. The raised LH levelsin the beginning stimulate testis to secrete more testosterone which activates tumour cellsresulting in increased bone pain and bladder obstruction noticed after 1 week of therapyin this patient.
b. The initial flaring of symptoms can be avoided by pretreating with an antiandrogen bicalutamide50 mg orally daily for 3 days before starting triptorelin injection and then continuing bothdrugs together. The stimulatory effect of excess testosterone on tumour cells would be blockedby bicalutamide so that no flaring of symptoms would occur. The combined androgen blockadewith GnRH agonist + androgen antagonist is the favoured approach.
c. The patient can be given an antiresorptive drug in addition to relieve bone pain. A potentparenteral bisphosphonate like zoledronate infused i.v. over 15 min every 1–4 weeks is themost effective drug for this purpose. It may also retard growth of the bony metastasis forsome time.
SOLUTION 22.1
a. The most likely cause of endometrial thickening in this patient is tamoxifen therapy. Tamoxifenis a selective estrogen receptor modulator (SERM) which has estrogen antagonistic actionin the breast (basis of its use in breast carcinoma), but agonistic action on the endometriumwhich stimulates proliferation. Such unopposed (by progestin) hyperproliferation can producethickening and predisposes to endometrial carcinoma.
b. For the reason stated above, tamoxifen should not be continued in this patient. Total stoppageof adjuvant therapy is not advisable, because estrogen suppression therapy has been shownto exert protective effect for atleast 5 years. Aromatase inhibitors, which block synthesisof estrogens in the body, have been clearly demonstrated to prevent recurrence of breastcancer, without stimulating endometrial proliferation or predisposing to endometrial carcinoma.Therefore, in this case, tamoxifen should be replaced by letrozole 2.5 mg /day or anastrozole1.0 mg/day for the next 5 years. Due precautions to prevent osteoporosis and measuresto address arthritic symptoms, if they develop, should be taken concurrently.
SOLUTION 22.2
a. All diseases and conditions which contraindicate use of oral contraceptives or need cautionin their use have to be ruled out before prescribing one to this subject. Full medical history,including menstrual history and past pregnancy details should be elicited. Any thromboembolicepisode, jaundice or toxaemia of pregnancy should be ascertained. History of smoking, diabetes,hypertension, migraine, tuberculosis and gallbladder disease should be specifically asked.Any medication that she is taking and the reason for it should be taken into account to
Contd...

943SOLUTION TO PROBLEM DIRECTED STUDYA
PP
EN
DIX
1
foresee possible interactions with the contraceptive. Whether she is obese or very lean alsomatters in selecting the contraceptive preparation. General physical examination, includingpalpation of breast, for any lump and a per vaginum examination for fibroid/other tumour,should be done. Blood pressure should be recorded to rule out hypertension. Fasting andpostprandial blood glucose, lipid profile should be ordered to detect diabetes and dyslipidaemia.Ultrasound examination of pelvic organs should be performed for uterus size, fibroid, ovariancyst or malignancy.Only after all the above findings are favourable that an oral contraceptive be selected andprescribed.
SOLUTION 23.1
a. Though the progress of labour in this case is tardy and uterine contractions are relativelyweak, there are signs of foetal distress (passage of meconium stained liquor, rapid foetalheart becoming irregular during uterine contraction). Moreover, the mother is dehydratedand exhausted. As such, the best course of action is to deliver the baby by caesarean section.
b. The mother should not be administered an oxytocic drug, because stronger uterine contractionsare likely to worsen foetal distress and pose risk to the baby. The mother is also not ina fit condition to endure the stress of a difficult labour.
SOLUTION 25.1
a. Rocuronium is the preferred muscle relaxant for tracheal intubation and short lasting musclerelaxation in this patient. Succinylcholine (SCh), the fastest and shortest acting muscle relaxantwhich is most commonly used for aiding tracheal intubation, is not suitable for this patient,because it is a depolarizing blocker and releases K+ from skeletal muscles. Since this patienthas extensive burns and tissue injury, which itself causes hyperkalemia due to leakage ofK+ from injured cells, the K+ released by SCh will accentuate the hyperkalemia and exposethe patient to risk of cardiac arrhythmias and other complications.Rocuronium, on the other hand, is a nondepolarizing blocker which does not trigger lossof intracellular K+. It is the fastest acting nondepolarizing blocker with speed of actionapproaching that of SCh. Intubating conditions can be obtained in 60–90 sec. It also providessurgical grade relaxation for 25–40 min, along with good cardiovascular stability.
SOLUTION 26.1
a. Labour pain as well as that due to stretching of the birth canal can be largely relieved byspinal as well as epidural anaesthesia. It is desirable, at the same time, not to producemotor block so that the mother can actively participate in the process of labour. Since motorfibres are less sensitive to local anaesthetics (LAs) than sensory fibres, motor block of alower level is usually produced during spinal anaesthesia. Such separation is more pronouncedwith epidural anaesthesia. Lidocaine and bupivacaine are the two LAs commonly used forepidural anaesthesia. Out of these, bupivacaine is more suitable for this purpose for thefollowing reasons: Contd...

944 APPENDICESA
PP
EN
DIC
ES
• It provides greater separation of sensory from motor block. Separation is still larger whenlower concentration (0.25% bupivacaine) is used.
• Because of higher lipid solubility, its tissue distribution is large and maternal blood levelsare lower. Less drug is likely to cross to the foetus, reducing chances of neonatal depression.
• It is longer acting.Thus, epidural anaesthesia with 0.25% bupivacaine is most suitable for this patient.
SOLUTION 28.1
a. Alcohol exerts anticonvulsant action while its concentration in the brain is rising or ismaintained. This is followed by lowering of seizure threshold when the concentration fallsand becomes zero. Thus, recurrence of seizures in this patient could most likely be dueto the temporarily increased susceptibility to seizures caused by withdrawal of alcohol fromthe brain.
b. Since this lowering of seizure threshold is a short-term problem, no abrupt change in antiepilepticmedication or alteration of dose is warranted at this stage. The patient should be kept underobservation for few days/weeks and decision about further antiepileptic therapy taken onlyon the basis of the subsequent course of events. The patient also must be advised to strictlyavoid alcoholic drinks in future.
SOLUTION 29.1
a. Since this patient does not require a hypnotic on regular basis, there is no identifiable causeof occasional sleep onset difficulty and he has tried non-drug measures, he can be prescribeda hypnotic to be kept handy for use when required. Because there is only sleep onset difficulty,and he will take the drug only later at night (after going to bed as usual), he needs a shortacting hypnotic which would be free of residual effect next morning. Zaleplon would besuitable for this patient, as it has a short t½ (1 hour), does not cause next morning drowsiness,day time anxiety or rebound insomnia. Tolerance is unlikely to develop, because use is goingto be occasional.
SOLUTION 30.1
a. The husband of the patient should be instructed that at the first sign of a seizure attackthe patient should be laid on bed or ground in the prone or lateral position with neckextended to ensure free airway. A wooden/plastic gag should be placed between the teethto prevent biting of tongue. No emergency medicine is required during or just after thefit. Only reassurance and moral support are needed. These instructions should be sharedwill other family members, so that anyone who is closeby may do the needful.
b. Because the patient has a history of head trauma and two seizure attacks have occurredwithin one week, the probability of developing epilepsy is high. As such, antiepileptic medicationshould be started rightaway without waiting for test reports or further fits to occur.
Contd...

945SOLUTION TO PROBLEM DIRECTED STUDYA
PP
EN
DIX
1
c. Therapy should be initiated with a single antiepileptic drug. Antiepileptics with proven efficacyin post-head injury tonic-clonic seizures are phenobarbitone, phenytoin, carbamazepine andvalproate. Since the patient is a young active lady, phenobarbitone with sedative/cognitiveside effects, phenytoin with gum hyperplasia, hirsutism and other cosmetic side effects, andvalproate with tremor and weight gain would be less suitable. Carbamazepine appears tobe the most appropriate initial drug in this case.
SOLUTION 31.1
a. The parkinson’s disease of this patient appears to have advanced over the last 5 years andhe is now experiencing ‘wearing off effect’ of levodopa-carbidopa. He is also developingdyskinesia, a late adverse effect of the drug. At this stage, antiparkinsonian medication cannotbe withdrawn, because he will develop marked rigidity, immobility and tremor hamperinglife activities. He is already experiencing an adverse effect of his medication; therefore, thedose should not be increased further.Since levodopa-carbidopa is the most efficacious and cheapest medication for parkinsonism,it may be prudent to continue it at a reduced dose and supplement it with another longeracting drug to smoothen the therapeutic effect. The options available as supplementarymedication are:• A direct dopamine agonist like ropinirole/pramipexole can be gradually added to levodopa-
carbidopa whose dose should be reduced in steps. Both drugs can be taken concurrently3 times a day. Ropinirole/pramipexole being longer acting will smoothen symptom control.They also produce less dyskinesia.
• A MAO-B inhibitor like selegiline 5 mg twice a day or rasagiline 1 mg once a day inthe morning will prevent degradation of dopamine in the brain, prolonging and smootheningeffect of levodopa-carbidopa.
• Entacapone 200 mg with each dose of levodopa-carbidopa can also potentiate and prolonglevodopa action by inhibiting another metabolizing enzyme COMT. It can also be an additionalthird drug to levodopa-carbidopa + selegiline for greater symptomatic relief.
SOLUTION 32.1
a. The most likely cause of the motor restlessness exhibited by the patient after 4 weeksof haloperidol therapy is appearance of a common extrapyramidal side effect of theantipsychotic drug called ‘akathisia’. The symptom does not appear to be due to inadequatedose of haloperidol, because the psychotic symptoms have been relieved and theinitial psychomotor restlessness had been controlled. There is no return of anxiety, hallucinations,etc. As such, there is no need to increase the dose of haloperidol. Dose reduction maybe tried but return of psychotic symptoms is a risk. One of the atypical antipsychoticdrugs may be substituted for haloperidol. Quetiapine with its sleep promoting effect willbe more suitable in this case. The atypical antipsychotics have a low propensity to causeextrapyramidal motor side effects, including akathisia.
Contd...

946 APPENDICESA
PP
EN
DIC
ES
b. For early resolution of motor restlessness, a benzodiazepine, e.g. clonazepam 1 mg or diazepam(5 mg) 2–3 times a day may be given. This may be supplemented by trihexyphenidyl2 mg 3 times/day. In case the akathisia persists, propranolol 40 mg 2–3 times a day maybe added.
SOLUTION 33.1
a. Sertraline is a selective serotonin reuptake inhibitor (SSRI) and a first-line drug for majordepression. The choice of drug is correct and the 50 mg twice daily an average dose forinitiation of therapy. However, since antidepressant action of any drug (including sertraline)takes 2–4 weeks to manifest, it is too early at 1 week to expect any improvement in depressivesymptoms. The dose is not subtherapeutic as indicated by appearance of mild side effects,which nevertheless are quick to appear, but to whom gradual tolerance usually develops.Restlessness, nausea, dyspepsia, epigastric distress, anorexia are expected side effects of SSRIs.The patient and his family members should be counselled to continue the medication foranother 3–4 weeks by which time symptoms should start improving. The choice of drugis appropriate, and at this stage, there is no reason to change the medicine or its dose.No additional drug needs to be added at this stage.
SOLUTION 34.1
a. Symptoms and signs indicate that the patient is going into neurogenic shock due to theexcruciating pain of the crush injury. As such, the first priority is to relieve the acute pain.Morphine 5 mg should be injected i.v. immediately. It will not only lessen the pain andsuffering of the patient, but also allay apprehension and counteract neurogenic shock. Itwill facilitate proper examination and first aid measures as well. Supplemental doses maybe given every 2–3 hours. An i.v. infusion of saline should be started at the earliest to restoreblood pressure and maintain tissue perfusion.
SOLUTION 35.1
a. The primary reason for no improvement in the state of the patient is that all medicines,including donepezil, take weeks and months before any perceptible improvement in Alzheimer’ssymptoms become apparent. Moreover, donepezil (or any other drug) is not effective ina significant number of patients. However, one week is too short a time to know whetherthis patient is going to benefit or not. Since this patient has developed intolerable cholinergicside effects, they are due to donepezil which should be discontinued.No other anticholinesterase drug is likely to be tolerated by this patient. Therefore, a drugwhich acts by a different mechanism could be used in this patient. Memantine is the onlyother drug, with documented efficacy in moderate to severe Alzheimer’s disease, which isnot a cholinergic drug, and which probably acts by blocking glutamate excitotoxicity. It isbetter tolerated and does not produce cholinergic side effects. However, improvement inmemory and cognitive function is less likely, and it may only serve to slow the functionaldecline.

947SOLUTION TO PROBLEM DIRECTED STUDYA
PP
EN
DIX
1
SOLUTION 36.1
a. The weakness, nausea, sweating and fainting suffered by the patient is due to the markedrapid fall in BP caused by captopril (and augmented by furosemide). Congestive heart failurepatients have an overactive renin-angiotensin system (RAS) which helps in maintaininghaemodynamics in the face of low cardiac output. Captopril is a rapidly acting ACE inhibitor,which, given in doses used for hypertension, removes the RAS support (angiotensin II is notformed) and causes marked fall in BP. This is aggravated by Na+ loss caused by the diuretic.
b. Though, a slower acting ACE inhibitor, e.g. enalapril, would be less likely to cause rapid fallin BP, captopril cannot be considered a wrong choice of drug, provided it is initiated at1/4th dose. In CHF, captopril therapy should be initiated at 6.25 mg dose, which can be graduallyincreased as haemodynamic adjustments take place.
c. The reaction could have been avoided by initiating captopril at 6.25 mg twice daily dose. A sloweracting ACE inhibitor (at low starting dose) could be still less likely to produce acute hypotension.
d. The first measure to be taken in this case is to put the patient in 15° head low position.This could be supplemented by short-term fluid and electrolyte infusion. A pressor agentis rarely needed.
SOLUTION 37.1
a. This patient of moderate CHF is in a decompensated state with dilated heart. Though, thediuretic (furosemide) and ACE inhibitor (enalapril) will relieve symptoms slowly, they maynot be sufficient to restore a compensated cardiac status. Digoxin should be prescribedconcurrently as it is the most effective drug for restoring compensation by increasing cardiaccontractility. The features of this patient do not indicate any urgency. Therefore, the patientmay be started with an average maintenance dose 0.25 mg/day of digoxin. It is expectedto produce peak effect after 5–7 days. Dosage adjustment may be done after that dependingon the response.
b. Enalapril dose of 5 mg twice a day should be increased by 5 mg/day at 1–2 week intervalstill hypotension or other side effects appear or 40 mg/day dose is reached. For maximumprognostic benefit, ACE inhibitors have to be used at or near the highest permissible dosage.Enalapril should not be stopped unless compelled by an adverse effect, because it continuesto retard worsening of CHF and avoid complications.
c. Since the patient is in a decompensated state, a β blocker cannot be added at this stage,because chances of deterioration of cardiac status are high. However, after compensationhas been restored by digoxin, diuretic and enalapril and the patient is in a stable condition,a suitable β blocker may be started at a very low dose, to be upward titrated later, becauseβ blockers afford further morbidity and mortality benefits.
SOLUTION 38.1
a. The patient has been having atrial fibrillation (AF) for at least the past one month. He islikely to have developed thrombii in the fibrillating atria, and is at risk of embolic strokewhen sinus rhythm (SR) is restored. Therefore, he has been put on anticoagulant medicationwith warfarin to prevent thromboembolism. Contd...

948 APPENDICESA
PP
EN
DIC
ES
b. His heart (ventricular) rate can be controlled by a drug which depresses A-V conduction.For this purpose verapamil or diltiazem or propranolol should be given orally and dose adjustedto maintain a heart rate between 60–70/min. Digoxin (0.25 mg/day) may be prescribed inaddition if the target heart rate is not achieved by monotherapy.
c. If electrical cardioversion does not succeed, amiodarone 200 mg injected i.v. over 60 minmay be tried for reversal to SR.
d. After restoration of SR, the same may be maintained by continued treatment with one ofthe following drugs, viz. sotalol/propafenone/amiodarone/dronedarone or disopyramide.
SOLUTION 39.1
a. This patient is having one or more episodes of angina practically every day; therefore, heshould be prescribed regular medication to prevent the episodes. The first line drugs forthis purpose which can be given to this patient are:1. A long-acting nitrate viz. oral sustained release isosorbide mononitrate or similar drug
morning and afternoon or transdermal glyceryl trinitrate patch applied in the morningand taken off at night.
2. A long-acting calcium channel blocker, like amlodipine once a day.Alternative second line or add-on drugs are:
Nicorandil (K+ channel opener), or ranolazine (INa current inhibitor), or trimetazidine(LC3-KAT inhibitor) or ivabradine (If current inhibitor).
Since he is also suffering from COPD, he cannot be given a β blocker which is likely to precipitatesevere breathlessness.b. This patient is having coronary artery disease (CAD). None of the above drugs can alter
the course of CAD or prevent complications like MI or death. He should in addition be puton long-term treatment with the following to arrest/delay the progression of CAD and toafford cardioprotection:1. An antiplatelet drug, such as low-dose aspirin or clopidogrel.2. A hypolipidaemic statin, such as atorvastatin.3. An angiotensin converting enzyme (ACE) inhibitor, such as enalapril.
SOLUTION 40.1
a. Since the systolic BP is above 140 mm Hg and diastolic BP is below 90 mm Hg, this patienthas ‘isolated systolic hypertension’. Repeated measurements have confirmed the raised BP,therefore, antihypertensive medication is indicated. Therapy should be initiated with a singledrug because he is stage I hypertensive (systolic BP <160, and diastolic BP <100 mm Hg).Considering the age of the patient (>55 years), diagnosis of isolated systolic hypertension,history of stroke in the past, absence of diabetes/heart failure/ischaemic heart disease/chronickidney disease, the most suitable antihypertensive drug for this patient is a thiazide diuretic(hydrochlorothiazide/chlorthalidone) or a long-acting dihydropyridine calcium channel blocker(like amlodipine).Therapy may be initiated with either of these classes of drugs and later modified dependingon the response and tolerability.

949SOLUTION TO PROBLEM DIRECTED STUDYA
PP
EN
DIX
1
SOLUTION 41.1
a. Induction of brisk diuresis with furosemide alone is not the appropriate treatment of cirrhoticedema and ascites. Hepatic cirrhosis is associated with raised aldosterone and low plasmaK+ levels. Therefore, the aldosterone antagonist spironolactone is the drug of choice. It canbe supplemented by furosemide, because spironolactone alone is a weak diuretic. In thispatient, use of furosemide alone resulted in further hypokalaemia and alkalosis. This indirectlyraised blood NH3 levels which crosses to the brain resulting in deterioration of mental statusand neurological symptoms. Because of secondary hyperaldosteronism, the response tofurosemide decreased within few days.
b. At this stage, the patient should be managed by temporarily stopping furosemide and institutingspironolactone (50 mg 6 hourly) therapy along with appropriate i.v. fluid and electrolyteinfusion to correct the imbalance, guided by repeated plasma level monitoring. After restorationof the fluid/electrolyte balance and his mental status, the patient should be put on maintenancetherapy with spironolactone (100–400 mg/day) and furosemide (40–160 mg/day) with doseadjustment according to response. If hormonal side effects of spironolactone occur, it maybe substituted by the other aldosterone antagonist eplerenone. The potassium sparing non-aldosterone antagonist diuretic amiloride is an alternative.
SOLUTION 43.1
a. There are several reasons which could account for failure of this patient of iron deficiencyanaemia to respond to the oral iron medication she has been taking:• Taking 160 mg of ferric ammonium citrate (iron content 20%) would provide just 32 mg
of elemental iron/day. This is grossly inadequate to treat iron deficiency, for which 200mg of elemental iron/day is required to yield optimum response.
• Iron in ferric ammonium citrate needs to be reduced to ferrous form before absorption.Therefore, its bioavailability is lower compared to ferrous salts.
• Gastric acid is required to reduce ferric iron to ferrous iron and to facilitate iron absorption.This patient is taking acid suppressant medication (rabeprazole, a proton pump inhibitor).
As such absorption of iron from the medicine that she took could be very low.b. Since there are obvious factors in this case which can be tackled, it would be inappropriate
to abandon oral iron therapy at this stage and jump on to injectable iron. Proper selectionof oral iron preparation and its dose, and careful management of therapy may yield a responsein this patient. A ferrous salt with high iron content like ferrous sulphate or ferrous fumarate(both having ~33% iron) should be prescribed in a dose of 200 mg 3 times a day (total600 mg or 200 mg elemental iron/day). However, therapy should be initiated with a lowdose to be gradually increased as the gastrointestinal tract adjusts to the medication andtolerance to side effects develops. The doses should preferably be taken in empty stomach,but if gastric discomfort occurs, it may be given with food. Selection of ferrous salt wouldreduce dependence on gastric acid for absorption of iron. However, if tolerated, an effortshould be made to discontinue rabeprazole.

950 APPENDICESA
PP
EN
DIC
ES
SOLUTION 44.1
a. Passage of dark urine indicates bleeding in the kidney. This along with blood loss per vaginumhas resulted in acute fall in Hb level. The rise in INR value is indicative of excessive deficiencyof clotting factors, especially of prothrombin, factor X and factor VII due to relative warfarinoverdose. The obvious cause in this patient is the additive hypoprothrombinaemic actionof inj ceftriaxone given for treatment of pelvic infection.
This complication could have been prevented either by selecting an antibiotic that doesnot cause hypoprothrombinaemia/interact with warfarin or by reducing the dose of warfarinwhen ceftriaxone was started. The new warfarin dose should have been arrived at by repeateddetermination of INR value till ceftriaxone was being given.
b. Further warfarin dose must be stopped immediately and vit K 10 mg injected i.m. at theearliest. The patient must be put on bed rest to reduce bleeding. Because Hb level is9 g/dl, blood transfusion is not required at this stage, but must be kept handy in case shebleeds further. Repeat doses of vit K (5.0 mg i.m.) should be guided by frequent INR measurementand the severity of bleeding, avoiding too much vit K that would interfere with the protectiveeffect of warfarin subsequently. Changing the antibiotic to one which does not causehypoprothrombinaemia or bleeding may be considered on the basis of bacteriological sensitivityof the organism causing pelvic infection.
SOLUTION 45.1
a. This subject, though asymptomatic, has four risk factors for coronary artery disease (CAD),viz.(i) He is a male above 45-year age, (ii) his body mass index (BMI) is >25, (iii) total and
LDL-cholesterol (CH) are raised to values that are above the threshold for initiation ofhypolipidaemic drug therapy, (iv) the HDL-CH is low (<40 mg/dl). Thus, apart from life-style changes to regulate diet, reduce body weight and increase physical exercise, he requireslipid lowering medication.
b. In view of his lipid profile, he should be treated with a ‘statin’ drug to lower LDL-CH tobelow 130 mg/dl. Thus, a 40% reduction in LDL-CH should be aimed. This is likely to beachieved by atorvastatin 20 mg/day or simvastatin 40 mg/day. After treating with eitherof the above medication for 4–6 weeks, attainment of the goal LDL-CH (<130 mg/dl) shouldbe checked. In case, it is not met, the dose may be doubled. The aim should be to maintainhis LDL-CH below 130 mg/dl. With this therapy, the TG level, which is borderline, is alsoexpected to decrease and HDL-CH level to rise above 40 mg/dl.
SOLUTION 46.1
a. This patient is suffering from recurrent peptic ulcer disease. The earlier episode of similarsymptoms had responded to proton pump inhibitor (PPI) therapy. Therefore, it was also dueto peptic ulcer. Symptom relief and ulcer healing can be achieved this time as well with theuse of a PPI given for 4–8 weeks depending on endoscopic confirmation of ulcer healing.However, it alone cannot prevent recurrences, which most commonly are caused by persistent
Contd...

951SOLUTION TO PROBLEM DIRECTED STUDYA
PP
EN
DIX
1
colonization of upper gastrointestinal tract by H. pylori. Since the same cannot be confirmedin the absence of testing facility, he should be given the benefit of H. pylori eradication therapywhich largely prevents ulcer recurrences. A 3 drug, 2 week regimen would be the most effectiveoption. Since he has a history of metronidazole use in the recent past, chances of nitroimidazoleresistance are high, and he should be treated with a PPI (omeprazole 20 mg/lansoprazole30 mg/pantoprazole 40 mg/rabeprazole 20 mg) + amoxicillin 750 mg + clarithromycin 500mg, all given twice daily. The PPI should then be continued till endoscopic confirmation ofhealing is obtained, because the ulcer was larger than 10 mm in diameter.
SOLUTION 47.1
a. This child has developed acute muscular dystonia, an extrapyramidal motor reaction thatcan be caused by drugs with dopaminergic D2 receptor blocking action. Antiemetics withD2 blocking action are chlorpromazine and related neuroleptics like triflupromazine,prochlorperazine, etc. and prokinetic drug metoclopramide. It is likely that the girl was giveninjection of one of these drugs by the local doctor, following which the vomiting had subsidedand the dystonia had developed within 2–3 hours.
b. Though the dystonic reaction usually passes off within a few hours, it can be rapidly reversedby a parenterally administered centrally acting anticholinergic drug. Since the parents arealarmed and to afford quick relief, she may be given a deep intramuscular injection of10–15 mg of promethazine or hydroxyzine, which have anticholinergic, antihistaminergic,sedative and antiemetic properties. This can reverse the dystonia within 15–30 min.
SOLUTION 48.1
a. This patient of diarrhoea seems to have lost only small amount of fluid and there are nosigns of dehydration. Moreover, he is a young adult. Thus, there is no need of rehydrationtherapy, but normal fluid intake and nutrition should be continued.
b. The features of this patient including fever are indicative of moderately severe enteroinvasiveinfection. As such, antibiotic therapy is indicated. A well absorbed fluoroquinolone likeciprofloxacin or ofloxacin would be suitable first line antibiotic for empiric therapy.
c. Antimotility-antidiarrhoeal drug is contraindicated in this patient, because in all likelyhoodthere is enteroinvasive infection, so that restriction of bowel clearance can favour furtherbowel wall invasion and systemic spread of the pathogen.
d. Symptomatic relief of fever can be afforded by paracetamol 500 mg 6 hourly. Abdominalpain can be dampened by an antispasmodic drug like dicyclomine 20 mg 6–8 hourly.
SOLUTION 49.1
a. Since this is an elective surgery with no indication of any infection in the operative area,but where the biliary tract is going to be cut, with no/minimal spillage or contact withinfected material expected, it may be categorized as ‘clean-contaminated’ surgery. As such,she requires to be given antimicrobial prophylaxis.
Contd...

952 APPENDICESA
PP
EN
DIC
ES
b. The surgery involves cutting the biliary tract. Therefore, prophylaxis covering aerobic as wellas anaerobic organisms and both gram-negative as well as gram-positive bacteria would beappropriate. Drugs recommended are:
Cefuroxime 1.5 g i.v. + metronidazole 0.5 g i.v.or gentamicin 160 mg i.v.Single dose injected i.v. within 30 min before surgery. Normally, there is no need to repeatthe injection, but if the surgery lasts more than 2 hours, a repeat injection after surgerymay be given.
SOLUTION 50.1
a. Moxifloxacin is a 2nd generation fluoroquinolone (FQ) antibiotic with high activity againstgram positive cocci which are primarily involved in acute sinusitis. Moreover, it has a convenientonce a day oral dosing schedule and is generally well tolerated. It has been used in sinusitiswith high success rates. These could be the considerations on the basis of which the doctorhas decided to use moxifloxacin. However, moxifloxacin is not appropirate for this patientbecause she is receiving amitryptyline, a tricyclic antidepressant which has proarrhythmicpotential. Moxifloxacin can prolong Q-T interval and increase the risk of serious cardiacarrhythmias such as Torsades de pointes when given along with amitryptyline.
Other antibiotics which are active against gram-positive cocci and suitable for treatingsinusitis are amoxicillin alone or with clavulanic acid, a first generation cephalosporin orazithromycin. These antibiotics donot carry the risk of precipitating arrhythmias.
SOLUTION 51.1
a. In this patient antibiotic therapy should be started on the basis of clinical diagnosis, becausethe patient is quite sick. Rapid relief of symptoms and cure should be the aim. Moreover,blood culture is not necessarily positive in all cases of typhoid fever. Treatment cannot bewithheld for want of confirmation by culture.
b. The most appropriate antibiotic is ceftriaxone (or a similar 3rd generation cephalosporinlike cefoperazone, cefotaxime), becuase it produces the fastest and surest response. Moreover,being bactericidal it prevents relapse and the risk of carrier state. Being long acting, ceftriaxonecan be given as a once daily injection. The daily dose for this boy would be (75 mg/kgx 25 kg) = 1875 mg or rounded off to 2.0 g per day, given as slow i.v. injection once daily.The dose may be halved after 2 days or when fever subsides. It should be given till 2 daysafter the fever subsides totally.
c. In case of typhoid fever, a single antibiotic is sufficient, since addition of another antibiotichas not been found to hasten or improve the response.
⎫⎬⎭

953SOLUTION TO PROBLEM DIRECTED STUDYA
PP
EN
DIX
1
SOLUTION 52.1
a. The most appropriate drugs and regimens for treating chlamydial endocervicitis are:Azithromycin 1.0 g (2 tabs of 500 mg) single dose, or Doxycycline 100 mg twice daily for7 days. Both these regimens are adequate to treat uncomplicated gonococcal infection aswell as concurrent chlamydial and gonococcal infection. Both these antibiotics are oral andwell tolerated. While azithromycin has the advantage of single dose treatment, doxycyclineneeds twice daily dosing for one week, but is cheaper.Other first choice antibiotics like amoxicillin and ceftriaxone for gonorrhoea are not effectiveagainst chlamydia.
b. Both these infections are sexually transmitted diseases. Her husband is also likely to be infected.She must be counselled to get her husband examined and treated concurrently.
SOLUTION 53.1
a. The recommended dose range of gentamicin for a person with normal renal function is3–5 mg/kg/day (or 4 mg/kg/day on average). For a patient with creatinine clearance valueof 50 ml/min, the dose has to be reduced to 50%, or 2 mg/kg/day. In this patient weighing60 kg, it would be 120 mg/day. With renal impairment, this patient is not suitable for oncedaily dosing regimen, and he should be treated with the conventional 8 hourly regimen.As such, he may be injected with gentamicin 40 mg every 8 hours making it 120 mg/24hours. Since the patient is unconscious and in ICU, an i.v. line must have been maintained.Gentamicin may be injected through the i.v. line taking 30 min to complete the injection.Alternatively, it may be injected i.m.The usual dose-range of cefotaxime for an adult is 1–2 g every 6–12 hours (2–8 g/day). Thispatient has renal impairment, half life of cefotaxime is likely to be prolonged. Therefore, a dosenear the lower end the range would be appropriate for him. As such, a dose of 1 g every 8 hours(3 g/day) may be selected. This may be slowly injected in the i.v. line or given by i.m. route.
SOLUTION 54.1
a. Since the patient has distressing urinary symptoms and is febrile, empirical antimicrobialtreatment should be started after urine has been collected for bacteriological testing. Moreover,in a sexually active woman, lower urinary tract infections (UTI) are moslty treated empirically.The first line antimicrobials for this purpose are fluoroquinolones, cotrimoxazole, amoxicillin-clavulanate, an oral 1st or 2nd generation cephalosporin, or nitrofurantoin. Any of these maybe selected and prescribed for 3–5 days depending on symptom resolution. She should beavised to abstain from sexual intercouse in this period. Nitrofurantoin is usually not preferredbecause it needs at least 7 days treatment, and often causes nausea and gastric pain.
b. Phenazopyridine is a urinary analgesic with no antimicrobial activity. It relieves symptomsof bladder and uretheral irritation and can be given with the selected antimicrobial drug.
c. Because this patient has suffered >3 episodes of cystitis within one year, she should beadvised long term prophylactic therapy. The suitable prophylactic drug for her is cephalexin250 mg once daily at bed time, because it is not contraindicated in pregnant women. Thoughthis patient is not presently pregnant, she may conceive during use of the prophylacticdrug. The other recommended prophylactic drugs, viz cotrimoxazole, nitrofurantoin andnorfloxacin are all contraindicated during pregnancy.

954 APPENDICESA
PP
EN
DIC
ES
SOLUTION 55.1
a. Since the patient is a previously treated case of TB, it is important to find out the drugresistance status of the bacilli infecting him. Sputum culture for AFB and sensitivity testingshould be ordered. However, chemotherapy should be started immediately, because the cultureand sensitivity tests take 6 weeks or more and defering treatment for such a long timemay jeopardise outcome.
b. Selecting the anti-TB regimen for retreatment patients is guided by assessment of risk ofmultidrug resistance (MDR) TB. This is a defaulted patient who has taken isoniazid and rifampinonly for 3 months. As such, risk of MDR-TB may be categorized as low and he should betreated with the 8 month regimen of 1st line drugs. For the initial 2 months, he shouldbe given all 5 first line drugs, viz isoniazid 300 mg + rifampin 600 mg + pyrazinamide 1.5g + ethambutol 1.0 g all orally and streptomycin 1.0 g i.m. daily. Streptomycin should bestopped after that and the 4 oral drugs given for another 1 month. Pyrazinamide shouldbe discontinued and 3 drugs rifampin, isoniazid and ethambutol should be continued for5 more months. This is a retreatment case, who should be given drugs daily under supervision.The thrice weekly regimen carries higher risk of drug resistance in his case. The regimenmay be modified when the culture and sensitivity report becomes available.
SOLUTION 56.1
a. Since the patient had taken the standard multidrug therapy for the prescribed one year,and had responded clinically, the most likely cause of relapse is reactivation of dormant(persister) bacilli. Development of resistance to the multidrug regimen is very rare. Thereactivated persisters remain sensitive to the same drugs. As such, he should be treatedwith the same drugs, viz rifampin 600 mg + clofazimine 300 mg once a month alongwithdapsone 100 mg + clofazimine 50 mg daily for one year.
SOLUTION 57.1
a. The treatment of choice for Candida esophagitis is oral fluconazole 100 mg/day for 3 weeks,because it is highly effective and well tolerated. However, some cases do not respond dueto fluconazole resistance. These may be treated with itraconazole 200/day or voriconazole200 mg twice daily.
b. Uncontrolled diabetes is an important predisposing factor in the causation of esophagealcandidiasis, and appears to have played a role in this patient. Therefore, measures to achievequick glycaemia control are needed. Since the patient already had a complication of diabetes(Candida infection) it is desirable to shift her to insulin therapy (at least till the esophagitisis fully cured). The dose and frequency of insulin injections should be guided by repeatedblood glucose monitoring. Fluconazole (other azoles as well) inhibit CYP450 isoenzymes andraise the blood levels of salfonylureas. The intensity of action of glibenclamide (if continuedin this case) is likely to be affected unpredictably. Thus, even if this drug is continued, closemonitoring of blood glucose level and dose adjustment of the sulfonylurea is required.

955SOLUTION TO PROBLEM DIRECTED STUDYA
PP
EN
DIX
1
SOLUTION 58.1
a. Considering the facts of injury and exposure in this case, the risk of contacting HIV infectionby the dental surgeon is very low. However, HIV disease can only be prevented, but notcured, and has serious implications. Moreover, even a few virions entering the body canset up an infection. Therefore, it would be prudent to give prophylactic medication to furthercut down chances of acquiring the infection.
b. Because the given case is of the low risk category, and the source person is neither symptomaticnor taking any anti-HIV medication, the standard 2 drug prophylaxis would be appropriate.The dental surgeon should be advised to immediately start taking—Zidovudine 300 mg + Lamivudine 150 mg twice daily for 4 weeks.
SOLUTION 59.1
a. Recurrence of fever after being afebrile for 7 days indicates ‘recrudescence’ due to incompleteparasitaemia clearance by the treatment given for the 1st episode of fever. This occurs dueto low grade chloroquine-resistance. While majority of asexual schizonts are killed by chloroquineand the fever subsides, some survive and multiply to cause fever again. The second episodeof fever is not due to ‘relapse’ which is caused by vivax hypnozoites reinvading RBCs. Relapsegenerally occurs after 3 weeks to few months. Moreover, the patient is taking primaquinewhich kills hypnozoites.
b. As broughtout above, recrudescence indicates chloroquine-resistance, which is particularlylikely in this case, because the infection appears to be contacted from an area where chloroquine-resistance among P. vivax has been detected. As such, she should be treated with an alternativedrug effective against chloroquine-resistant P. vivax. These are:1. Quinine 600 mg three times a day for 7 days along with doxycycline 100 mg once daily
for 7 days.2. Artesunate 100 mg twice daily for 3 days, along with a single dose of sulfadoxine 1500
mg + pyrimethamine 75 mg.c. The primaquine therapy should be continued to complete the 14-day course, so as to totally
eradicate the P. vivax hypnozoites from the liver.
SOLUTION 60.1
a. Metronidazole is the drug of choice for amoebic liver abscess. Tinidazole is an equivalent,but not necessarily better alternative. Since the patient was seriously ill and was vomiting,the initial choice of i.v. route of administration was appropriate. It was correctly changedto oral route once the patient improved, because oral bioavailability of metronidazole isnearly complete.
b. Experience has shown that a single 10-day course of metronidazole is generally enough tokill all viable amoebae in the liver abscess, though the abscess cavity may persist for fewweeks and heal spontaneously. Since the patient has improved clinically, visualization ofpersisting abscess cavity on ultrasound is not in itself an indication to extend/repeatmetronidazole therapy.
Contd...

956 APPENDICESA
PP
EN
DIC
ES
c. Since amoebic liver abscess is always secondary to colonization of colon by amoebae(which may be asymptomatic) and because metronidazole does not effectively eradicatecyst forming trophozoites from the colon (it is completely absorbed in the upper intestine,and very little reaches the colonic lumen), a luminal amoebicide should be given alongwith or after metronidazole. Absence of cysts in stools does not ruleout colonization ofcolon by amoebae. The first choice luminal emoebicide that should have been given inaddition is:Diloxanide furoate 500 mg 3 times a day for 5–10 days alongwith or after metronidazole.
SOLUTION 61.1
a. This patient of neurocysticercosis is suitable for treatment with anthelmintic drug, becausethere are multiple active parenchymal cysticerci in the cerebral cortex which in additionto seizures can cause other focal reactions in the brain. Planned killing of the cysticerciunder corticosteroid cover may prevent future episodes of the reaction and may abolishthe cause of seizures, so that long term antiseizure therapy can be avoided.
b. The seizures must be controlled first before starting anthelmintic treatment. The preferreddrug is carbamazepine; start with 200 mg 3 times a day, increase by 200 mg/day if theseizures recur till they are fully suppressed or a maximum of 1200 mg/day dose is reached.A second antiseizure drug may be added in nonresponsive cases. However, most cases respondto carbamazepine alone. It should be continued during the course of anthelmintic medicationand for about 6 months thereafter, followed by gradual withdrawal over another 2–3 months.
c. Albendazole is the anthelmintic of choice in neurocysticercosis. To this patient, it shouldbe given in a dose of 400 mg twice daily with milk or fat-rich food (to enhance absorption)for 15 days. It is better than the alternative drug praziquantel, because cure rate with albendazoleis higher and praziquantel needs to be given for longer period (15–30 days). Carbamazepineinduces praziquantel metabolism and lowers its blood level, but not that of albendazole.Dexamethasone (which has to be given) also lowers praziquantel blood levels, but increasesalbendazole absorption.
d. Dexamethasone in a dose of 8–12 mg once daily in the morning should be started 2 daysbefore initiating albendazole, continued throughout the course and till 15 days thereafter,followed by gradual tapering of dose and final withdrawal. This is essential to suppress theinflammatory reaction to the dying cysticerci killed by albendazole therapy.

List of Essential Medicines(W): Included in WHO Model List of Essential Medicines (17th edition,March 2011)(I): Included in National List of Essential Medicines (2011), India
Appendix 2Appendix 2Appendix 2Appendix 2Appendix 2
AAbacavir (ABC) (W)Acenocoumarol (I)Acetazolamide (W,I)Acetic acid (W)Acetylcysteine (W)Acetyl salicylic acid (Aspirin) (W,I)Acriflavin + Glycerine (I)Actinomycin D (Dactinomycin) (W,I)Activated charcoal (W,I)Acyclovir (W,I)Adenosine (I)Albendazole (W,I)Albumin (I)Allopurinol (W,I)Alpha interferon (I)Alprazolam (I)Aluminium hydroxide + Magnesium hydroxide (I)Amidotrizoate (W)Amikacin (W,I)Amiloride (W)5-Aminosalicyclic acid (mesalamine) (I)p-Aminosalicylic acid (W)Amiodarone (W,I)Amitriptyline (W,I)Amlodipine (W,I)Amodiaquine (W)Amoxicillin (W,I)Amoxicillin + Clavulanic acid (W,I)Amphotericin B (W,I)Ampicillin (W,I)Anti-snake venom serum (polyvalent/specific) (W,I)Anti-D immunoglobulin (Human) (W,I)Anti-Tetanus immunoglobulin (Human) (W,I)Artemether (W)Artemether + Lumefantrine (W)Artesunate (W,I)Artesunate + amodiaquine (W,I)Ascorbic acid (W,I)Asparaginase (W)Atazanavir (W)Atenolol (W,I)Atorvastatin (I)Atracurium (W,I)Atropine (W,I)Azathioprine (W,I)Azithromycin (W,I)
BB.C.G. vaccine (W,I)Barium sulfate (W,I)Beclomethasone dipropionate (W,I)Benzathine benzylpenicillin (W,I)Benznidazole (W)Benzoin compound (I)Benzoyl peroxide (W)Benzyl benzoate (W,I)Benzyl Penicillin (W)Betamethasone (W,I)Betamethasone dipropionate (I)Betaxolol (I)Biperiden (W)Bisacodyl (I)Bisoprolol (W)Bleaching powder (I)Bleomycin (W,I)Bromocriptine (I)Budesonide (W)Bupivacaine (W,I)Busulfan (I)
CCaffeine (W)Calamine (lotion) (W,I)Calcium folinate (W)Calcium salts (gluconate, carbonate) (W,I)Calcium ipodate (I)Capreomycin (W)Carbamazepine (W,I)Carbimazole (I)Carboplatin (W,I)Cefazolin (W)Cefixime (W,I)Cefotaxime (W,I)Ceftazidime (W,I)Ceftriaxone (W,I)Cephalexin (W,I)Cetrimide (I)Cetrizine (I)Chlorambucil (W,I)Chloramphenicol (W,I)Chlorhexidine (W,I)Chloroquine (W,I)Chloroxylenol (W)Chlorpheniramine (W,I)

958 APPENDICESA
PP
EN
DIC
ES
Chlorpromazine (W,I)Cholera vaccine (W)Ciprofloxacin (W,I)Cisplatin (W,I)Clarithromycin (W)Clindamycin (W,I)Clofazimine (W,I)Clomiphene (W,I)Clopidogrel (I)Clomipramine (W)Clotrimazole (W,I)Cloxacillin (W,I)Coal tar (W,I)Codeine (W,I)Colchicine (I)Concentrated vit. A solution (Retinol) (W,I)Co-trimoxazole (W,I)
(Trimethoprim + Sulphamethoxazole)Cyclizine (W)Cyclophosphamide (W,I)Cycloserine (W)Cyclosporine (W,I)Cytosine arabinoside (cytarabine) (W,I)
DD.P.T. vaccine (I)Dacarbazine (W,I)Danazol (I)Dapsone (W,I)Daunorubicin (W,I)Deferoxamine (W,I)Dexamethasone (W,I)Dexchlorpheniramine (I)Dextran-40 (I)Dextran 70 (W,I)Dextromethorphan (I)Diazepam (W,I)Diclofenac (I)Dicyclomine HCl (I)Didanosine (ddl) (W,I)Diethylcarbamazine (W,I)Digoxin (W,I)Dihydro ergotamine (I)Diloxanide furoate (W,I)Diltiazem (I)Dimercaprol (W,I)Diphtheria antitoxin (W,I)Diphtheria vaccine (W)Dithranol (W,I)Dobutamine (I)Docetaxel (W)Docusate sodium (W)Domperidone (I)Dopamine (W,I)Doxorubicin (W,I)Doxycycline (W,I)
EEfavirenz (EFV or EFZ) (W,I)EMLA cream (I)Efavirenz + emtricitabine + tenofovir (W)Eflornithine (W)Emtricitabine (W)Emtricitabine + tenofovir (W)Enalapril (W,I)Enoxaparin (I)Ephedrine (W)Epinephrine (adrenaline) (W,I)Ergometrine (W)Erythromycin (W,I)Estradiol cypionate + medroxyprogesterone acetate (W)Esmolol (I)Ethambutol (W,I)Ether, anaesthetic (I)Ethinylestradiol (W,I)Ethinylestradiol + Levonorgestrel (W,I)Ethinylestradiol + Norethisterone (W,I)Ethionamide (W)Ethosuximide (W)Ethyl alcohol 70%, (Ethanol) (W,I)Etoposide (W,I)
FFactor IX complex (W,I)
(coagulation factors II,VII,IX,X)Factor VIII concentrate (W,I)Famotidine (I)Fentanyl (I)Ferrous salt (W,I)Ferrous salt + folic acid (W)Fluconazole (W,I)Flucytosine (W)Flumazenil (I)Fludrocortisone (W)Fluorescein (W,I)5-Fluorouracil (W)Fluoxetine (W,I)Fluphenazine (W)Flutamide (I)Folic acid (W,I)Folinic acid (I)Formaldehyde IP (I)Framycetin sulfate (I)Fresh frozen plasma (I)Furosemide (W,I)
GGemcitabine (I)Gentamicin (W,I)Gentian violet (I)Glibenclamide (W,I)Glucagon (W,I)Glucose (W,I)

959LIST OF ESSENTIAL MEDICINESA
PP
EN
DIX
2
Glucose with sodium chloride (W,I)Glutaraldehyde (Glutaral) (W,I)Glycerine IP (I)Glyceryl trinitrate (W,I)Griseofulvin (W,I)
HHaemophilus influenzae (b) vaccine (W)Haloperidol (W,I)Halothane (W,I)Heparin sodium (W,I)Hepatitis A vaccine (W)Hepatitis B vaccine (W,I)Homatropine (I)Hormone releasing IUD (I)Hydralazine (W)Hydrochlorothiazide (W,I)Hydrocortisone (W)Hydrocortisone sodium succinate (I)Hydrogen peroxide (I)Hydroxocobalamin (W)Hydroxycarbamide (W)Hydroxychloroquine PO4 (W,I)Hydroxyethyl starch (Hetastarch) (I)Hyoscine HCl (W)Hyoscine N butylbromide (I)
IIbuprofen (W,I)Imipenem + Cilastatin (W)Ifosphamide (W,I)Imatinib (I)Imipramine (I)Immunoglobulin (human, normal) (W)Indinavir (W,I)Influenza vaccine (W)Insulin injection (soluble) (W,I)Intermediate acting insulin (W,I)(Lente/NPH insulin/premix 30:70)Intraperitoneal dialysis solution (W,I)Iodine (W,I)Iohexol (W)Iopanoic acid (I)Ipratropium bromide (W,I)Iron dextran (W,I)Isoflurane (W,I)Isoniazid (W,I)Isoniazid + Ethambutol (W)Isoniazid + Ethambutol + Rifampicin (W)Isoniazid + Rifampicin (W)Isoniazid + Rifampicin + Pyrazinamide (W)Isoniazid + Rifampicin + Pyrazinamide + (W)
EthambutolIsosorbide dinitrate (W,I)Isosorbide-5-mononitrate (I)Isphagula (I)IUD containing Copper (W,I)
Ivermectin (W)
KKanamycin (W)Ketamine (W,I)
LLactulose (W)Lamivudine (3TC) (W,I)Lamivudine + zidovudine (W,I)Lamivudine + Stavudine (I)Lamivudine + Nevirapine + Zidovudine (W)Lamivudine + Nevirapine + Stavudine (W,I)L-Asparaginase (W,I)Leflunomide (I)Levamisol (W)Levodopa + Carbidopa (W,I)Levonorgestrel (W)Levothyroxine (W,I)Lidocaine (Lignocaine) (W,I)Lidocaine + Epinephrine (W,I)Lithium carbonate (W,I)Lopinavir (W)Lopinavir + Ritonavir (LPV/r) (W)Lorazepam (W,I)Losartan pot. (I)Lugols solution (W)
MMagnesium sulfate (W,I)Mannitol (W,I)Measles vaccine (W,I)Mebendazole (W)Medroxy progesterone acetate (depot) (W,I)Mefloquine (W,I)Meglumine iothalamate/iotroxate (W,I)Melarsoprol (W)Melphalan (I)Meningococcal vaccine (W)Mercaptopurine (W,I)Mesna (W,I)Metformin (W,I)Methadone (W)Methotrexate (W,I)Methyl cellulose (I)Methyldopa (W,I)Methyl ergometrine (I)Methylprednisolone (I)Methylrosalinium chloride (Gentian voilet) (I)Methylthioninium chloride
(methylene blue) (W,I)Metoclopramide (W,I)Metoprolol (I)Metronidazole (W,I)Miconazole (W,I)Midazolam (I)Mifepristone (W,I)

960 APPENDICESA
PP
EN
DIC
ES
Miltefosine (W)Misoprostol (W,I)Mitomycin-C (I)Morphine (W,I)Multivitamins (I)Mumps vaccine (W)Mupirocin (W)
NN-acetylcysteine (I)Naloxone (W,I)Nelfinavir (NFV) (I)Neomycin + Bacitracin (I)Neostigmine (I)Nevirapine (NVP) (W,I)Niclosamide (W)Nicotinamide (W,I)Nicotine replacement therapy (NRT) (W)Nifedipine (W,I)Nifurtimox (W)Nitrofurantoin (W,I)Nitrous oxide (W,I)Norethisterone (W,I)Nystatin (W,I)
OOfloxacin (W,I)Olanzapine (I)Omeprazole (W,I)Ondansetron (W,I)Oral Poliomyelitis vaccine (W,I)
(live attenuated)Oral rehydration salts (W,I)Oseltamivir (W)Oxamniquine (W)Oxaliplatin (I)Oxygen (W,I)Oxytocin (W,I)
PPaclitaxel (W,I)Pancreatic enzymes (W)Pantoprazole (I)Paracetamol (W,I)Paromomycin (W)Penicillamine (W,I)Pentamidine isothionate (W,I)Permethrin (W,I)Pertussis vaccine (W)Pheniramine (I)Phenobarbital (W,I)Phenylephrine (I)Phenoxymethyl penicillin (W)Phenytoin sodium (W,I)Phytomenadione (W,I)Pilocarpine (W,I)Piperazine (I)
Pneumococcal vaccine (W)Podophyllum resin (W)Polygeline (I)Potassium chloride (W,I)Potassium iodide (W)Potassium permanganate (W,I)Povidone iodine (W,I)Pralidoxime (2-PAM) (I)Praziquantel (W,I)Prednisolone (W,I)Prednisolone acetate/sodium phosphate (I)Primaquine (W,I)Procainamide (I)Procaine benzylpenicillin (W)Procarbazine (W,I)Proguanil (W)Promethazine (I)Propofol (W,I)Propranolol (W,I)Propylthiouracil (W)Prostaglandin E (W)Protamine sulfate (W,I)Prussian blue (W)Pyrantel pamoate (W)Pyrazinamide (W,I)Pyridostigmine (W,I)Pyridoxine (W,I)Pyrimethamine + Sulfadoxine (W,I)
QQuinine (W,I)
RRabies immunoglobulin (W,I)Rabies vaccine (W,I)Raloxifene (I)Ranitidine HCl (W,I)Retinol (Vit A) (W,I)Ribavirin (W)Riboflavin (W,I)Rifabutin (W)Rifampicin (W,I)Ringer lactate solution (I)Ritonavir (r) (W,I)Rotavirus vaccine (W)Rubella vaccine (W)
SSalbutamol (W,I)Salicylic acid (I)Saquinavir (SQV) (W,I)Selenium sulfide (W)Senna (W)Sevoflurane (I)Silver sulphadiazine (I)Simvastatin (W)Sodium calcium edetate (W)

961LIST OF ESSENTIAL MEDICINESA
PP
EN
DIX
2
Sodium chloride (W)Sodium fluoride (W)Sodium bicarbonate (W,I)Sodium iothalamate (I)Sodium lactate (W)Sodium nitrite (W,I)Sodium nitroprusside (W,I)Sodium stibogluconate (W,I)Sodium thiosulfate (W,I)Sodium valproate (valproic acid) (W,I)Spectinomycin (W)Spironolactone (W,I)Stavudine (d4T) (W,I)Streptokinase (W,I)Streptomycin (W,I)Succinyl choline (Suxamethonium) (W,I)Sulfacetamide sod. (I)Sulfadiazine (W,I)Sulfadoxine + pyrimethamine (W,I)Sulfasalazine (W,I)Suramin sod. (W)Surfactant (W)
TTamoxifen (W,I)Tenofovir disoproxil fumarate (W)Terbinafine (W)Terbutaline (I)Testosterone propionate (W,I)Tetanus toxoid (vaccine) (W,I)Tetracaine (W,I)Tetracycline (W,I)Thiamine (W,I)Thioguanine (W)Thiopental sodium (I)
Timolol (W,I)Tramadol (I)Tranexamic acid (W)Triclabendazole (W)Trihexyphenidyl (I)Trimethoprim (W)Tropicamide (W,I)Tuberculine purified protein derivative (W,I)Typhoid vaccine (W)
UUrea (W)Urokinase (I)
VVancomycin (W,I)Varicella vaccine (W)Vecuronium (W,I)Verapamil (W,I)Vinblastine (W,I)Vincristine (W,I)Vit B12 (Cyanocobalamin) (W,I)Vit D3 (Cholecalciferol) (W,I)
WWarfarin sodium (W,I)
XXylometazoline (W)
ZZidovudine (W,I)Zidovudine + lamivudine + nevirapine (W,I)Zinc oxide (I)Zinc sulfate (W,I)

Prescribing in Pregnancy
There are major concern of permanent harm (tcratogenesis in the I" trimester [sec p. 89] and clfoct on grow1h and development of foetus in 1he 2nd and 3ro 1rimes1er) to the baby whenever any drug is administered to prcgnam women. Maternal medication can also increa:.c the incidence of abonion. foetal death, premature/ delayed labour or create perinatal problems. Moreover. there arc pronounced and progressive physiological changes during pregnancy which can affect drug disposition (see p. 65). As such. prescribing for t11c pregnant woman requires a lot of skill and restraint. Possible harm to the foetus by the administered drug ha~ to be weighed against hann to both mother and the baby due 10 untremed disease. There 1s pauciiy ofdaw about safety of majority of drugs during pregnancy: largely because prospective drug trials in pregnant women arc fraught with ethical. legal. emotional
and practical di0icul1ies. lnfom1ation is mostly derived from anecdotal reports and retrospective sn1dics. The US-FDA categorization of drugs into 5 categories (see p. 90) according to increasing order of risk documentation during pregnancy is a useful (through in some cases outdated and incorrect) guide to therapeutic decision making during pregnancy.
While insufficient data arc available to make definitive n.-commcndations regarding choice of dnigs for trea1ing common problems likely to be encountered during pregnancy. the table on the succeeding pages attempts to delineate the relatively/probably afcr alternatives. The list is not exhaustive and manufacturers literature/ package inserts or other authoritative texts should be consulted. Drugs marked (X) arc contraindicated during pregnancy.
Pnnc1plos of proscribing during prcgmmcy
Where possible use nondrug therapy Prescribe drugs only when definitely needed.
Choose the drug having the best safety record over time. Avoid newer drugs, unless safety is clearty established Over-the-counter drugs cannot be assvmed to be safe. As far as possible, avoid medication in the initial 10 weeks of gestation. Use the lowest effective dose
Use drugs for the shortest penod necessary
If possable. 91110 drugs 1111enn1ttenUy

963PRESCRIBING IN PREGNANCYA
PP
EN
DIX
3
Choice of drugs for common problems during pregnancy
Drug class (condition)
1. Antiemetics(morning sickness,other types of vomiting)
2. Drugs for peptic ulcer andGERD
3. Laxatives(constipation)
4. Antidiarrhoeals
5. Analgesics(headache, bodyache, jointpain, visceral pain)
6. Cold-cough remedies
7. Antiallergics
8. Antibacterials(systemic bacterialinfections)
9. Antitubercular
10. Antiamoebic
11. Antimalarial
12. Anthelmintic
13. Antifungal(superficial and deepmycosis)
Safety uncertain/unsafe
Domperidone (X)Ondansetron
Cimetidine, LansoprazoleCisapride (X), Mosapride
Senna, Bisacodyl, DocusatesSaline purgatives
Diphenoxylate-atropine,Loperamide
Aspirin, Metamizol, NSAIDsCOX-2 inhibitors, CodeineDextropropoxyphene, Morphine(X) Pethidine, Tramadol
Codeine, DextromethorphanBromhexine, Expectorants
Cetirizine, LoratadineFexofenadine, Astemizole (X)
Cotrimoxazole, Fluoroquinolones(X), Tetracycline (X), Doxycycline(X), Chloramphenicol (X),Gentamicin, Streptomycin (X),Kanamycin (X), Tobramycin (X),Clarithromycin, Azithromycin,Clindamycin, Vancomycin,Nitrofurantoin
Pyrazinamide, Streptomycin (X)
Metronidazole, TinidazoleQuiniodochlor
Artemether, ArtesunatePrimaquine (X)
Albendazole (X), Mebendazole(X) Ivermectin, Pyrantel pamoate,Diethylcarbamazine (X)
Amphotericin B (X), FluconazoleItraconazole (X), Ketoconazole(X) Griseofulvin (X), Terbinafine
Safer alternative
Promethazine, DoxylamineDicyclomine, ProchlorperazineMetoclopramide
Ranitidine, FamotidineOmeprazole Pantoprazole,
Dietary fibre, IspaghulaLactulose
Oral rehydration salts
ParacetamolIbuprofen (low dose)
XylometazolineOxymetazoline Nasal dropsBudesonide
ChlorpheniraminePromethazine
Penicillin G, AmpicillinAmoxicillin-clavulanateCloxacillin, PiperacillinCephalosporinsErythromycin
Isoniazid, Rifampicin, Ethambutol
Diloxanide furoate, Paromomycin
Chloroquine, Mefloquine, ProguanilQuinine (only in 1st trimester),Pyrimethamine + Sulfadoxine(only single dose)
PiperazineNiclosamidePraziquantel
ClotrimazoleNystatin TopicalTolnaftate
Contd...
⎫⎬⎭

964 APPENDICESA
PP
EN
DIC
ES
Drug class (condition) Safety uncertain/unsafe Safer alternative
14. Antiretroviral(HIV-AIDS)
15. Antiviral(other than HIV)
16. Antihypertensives
17. Antianaemic
18. Antidiabetics
19. Corticosteroids
20. Thyroid hormone(hypothyroidism)
21. Antithyroid drugs(thyrotoxicosis)
22. Antipsychotic(schizophrenia)
23. Antimanic(bipolar illness)
24. Antidepressants
25. Anticoagulants(thromboembolism)
26. Antiasthmatic
Didanosine, Abacavir, IndinavirRitonavir, Efavirenz
Acyclovir, Ganciclovir (X)Foscarnet (X), Amantadine (X)Vidarabine (X), α-interferon (X)
ACE inhibitors (X), Angiotensinantagonists (X), Thiazide diureticsFurosemide, PropranololNitroprusside
—
Sulfonylureas (X), Metformin (X)Pioglitazone, Repaglinide,Nateglinide, Acarbose (X)
Betamethasone, Dexamethasone(high dose and prolonged use)
—
Carbimazole, Radioactiveiodine (X), Iodide
Chlorpromazine, Fluphenazine (X)Clozapine, Olanzapine, Risperidone
Lithium carbonate, ValproateCarbamazepine
Trimipramine (X), Dothiepin (X)Sertraline, Paroxetine, CitalopramTrazodone, VenlafaxineMoclobemide
Warfarin (X), AcenocoumarolPhenindione (X)
Theophylline, Ketotifen (X)Montelukast, ZafirlukastSystemic corticosteroids
Zidovudine, Lamivudine,Nevirapine, Nelfinavir, Saquinavir
—
Methyldopa, Hydralazine, AtenololMetoprolol, Pindolol, NifedipinePrazosin, Clonidine
Iron salts (oral), Iron dextran(i.m.) Folic acid, Vit B12
Insulin (preferably human insulin)
Inhaled corticosteroidsTopical corticosteroidsPrednisolone oral (low dose)
Thyroxine
Propylthiouracil
HaloperidolTrifluoperazine
—
Amitriptyline, Imipramine,Fluoxetine
Heparin (unfractionated)Heparin (LMW)
Salbutamol/SalmeterolIpratropium bromideBeclomethasone/ InhaledBudesonideSod. cromoglycate
Contd...
⎫⎬⎭

Drugs in BreastfeedingAppendix 4Appendix 4Appendix 4Appendix 4Appendix 4
AcetazolamideAlbendazoleAntacidsAntifungal drugs (topical)Aspirin (low dose)BaclofenBeclomethasone (Inhaled)Benzyl benzoate (topical)BupivacaineBuprenorphineCephalosporinsCloxacillinCodeineCromoglycate sod.DextropropoxypheneDiclofenacDigoxinDomperidoneErgometrineErythromycinEthambutolFolic acidGentamicinHeparinHydralazineIbuprofen
InsulinsIpratropium Br. (inhalation)Iron dextran (i.m.)Iron salts (oral)KetoprofenLidocaineLoperamideMebendazoleMethyldopaNaproxenNefopamNiclosamideParacetamolPermethrin (topical)PiperacillinPiperazinePiroxicamPraziquantelPyrantelPyrazinamideSalbutamol (inhalation)SucralfateTerbutaline (inhalation)Valproate sod.Vitamins (maintenance dose)Warfarin
A. Drugs whose amount in milk is too small to be harmful to the infant, orthose found to be safe in ordinary doses
Administration of drugs to women who arebreastfeeding may have ill effects on the sucklinginfant, and/or affect lactation. Estrogens (in oralcontraceptives) and bromocriptine (D2 agonist)decrease milk production. Toxic effects on theinfant are largely dependent on entry of the drugin milk in pharmacologically significant amounts.In the case of large number of drugs (except thoseacting on CNS and few others), the concentration
in milk is low, and the breastfed infant receivesinsufficient quantity to produce adverse effects.Maternal medication or breastfeeding should notbe interfered in case of such drugs. However,currently available data are insufficient to makespecific recommendations in the case of manydrugs and the list given below is not exhaustive.Manufacturer’s recommendations/package insertsshould be consulted.
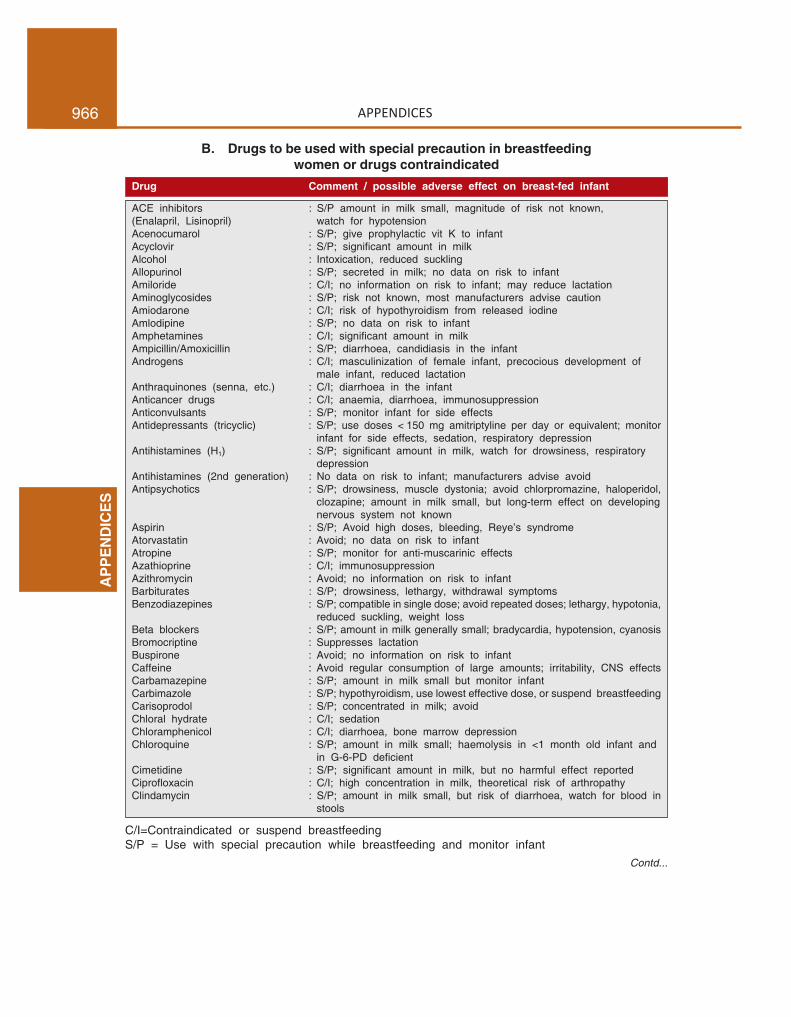
966 APPENDICESA
PP
EN
DIC
ES
B. Drugs to be used with special precaution in breastfeedingwomen or drugs contraindicated
Drug Comment / possible adverse effect on breast-fed infant
ACE inhibitors : S/P amount in milk small, magnitude of risk not known,(Enalapril, Lisinopril) watch for hypotensionAcenocumarol : S/P; give prophylactic vit K to infantAcyclovir : S/P; significant amount in milkAlcohol : Intoxication, reduced sucklingAllopurinol : S/P; secreted in milk; no data on risk to infantAmiloride : C/I; no information on risk to infant; may reduce lactationAminoglycosides : S/P; risk not known, most manufacturers advise cautionAmiodarone : C/I; risk of hypothyroidism from released iodineAmlodipine : S/P; no data on risk to infantAmphetamines : C/I; significant amount in milkAmpicillin/Amoxicillin : S/P; diarrhoea, candidiasis in the infantAndrogens : C/I; masculinization of female infant, precocious development of
male infant, reduced lactationAnthraquinones (senna, etc.) : C/I; diarrhoea in the infantAnticancer drugs : C/I; anaemia, diarrhoea, immunosuppressionAnticonvulsants : S/P; monitor infant for side effectsAntidepressants (tricyclic) : S/P; use doses < 150 mg amitriptyline per day or equivalent; monitor
infant for side effects, sedation, respiratory depressionAntihistamines (H1) : S/P; significant amount in milk, watch for drowsiness, respiratory
depressionAntihistamines (2nd generation) : No data on risk to infant; manufacturers advise avoidAntipsychotics : S/P; drowsiness, muscle dystonia; avoid chlorpromazine, haloperidol,
clozapine; amount in milk small, but long-term effect on developingnervous system not known
Aspirin : S/P; Avoid high doses, bleeding, Reye’s syndromeAtorvastatin : Avoid; no data on risk to infantAtropine : S/P; monitor for anti-muscarinic effectsAzathioprine : C/I; immunosuppressionAzithromycin : Avoid; no information on risk to infantBarbiturates : S/P; drowsiness, lethargy, withdrawal symptomsBenzodiazepines : S/P; compatible in single dose; avoid repeated doses; lethargy, hypotonia,
reduced suckling, weight lossBeta blockers : S/P; amount in milk generally small; bradycardia, hypotension, cyanosisBromocriptine : Suppresses lactationBuspirone : Avoid; no information on risk to infantCaffeine : Avoid regular consumption of large amounts; irritability, CNS effectsCarbamazepine : S/P; amount in milk small but monitor infantCarbimazole : S/P; hypothyroidism, use lowest effective dose, or suspend breastfeedingCarisoprodol : S/P; concentrated in milk; avoidChloral hydrate : C/I; sedationChloramphenicol : C/I; diarrhoea, bone marrow depressionChloroquine : S/P; amount in milk small; haemolysis in <1 month old infant and
in G-6-PD deficientCimetidine : S/P; significant amount in milk, but no harmful effect reportedCiprofloxacin : C/I; high concentration in milk, theoretical risk of arthropathyClindamycin : S/P; amount in milk small, but risk of diarrhoea, watch for blood in
stools
Contd...
C/I=Contraindicated or suspend breastfeedingS/P = Use with special precaution while breastfeeding and monitor infant

967DRUGS IN BREASTFEEDINGA
PP
EN
DIX
4
Clofazimine : S/P; skin discolourationClonidine : S/P; sedation, hypotensionCorticosteroids : S/P; compatible in single doses; pituitary-adrenal suppression possible
with >10 mg prednisolone daily to mother, impaired growthCotrimoxazole : S/P; folate deficiency, risk of kernicterus, haemolysis in G-6-PD deficient;
safe for healthy older infantsCyclosporine : C/I; significant amount in milkDapsone : S/P; haemolytic anaemia, jaundiceDepot medroxyprogesteron : Compatible with breastfeeding from 6 weeks postpartum
acetate (i.m.)Diltiazem : S/P; significant amount in milkDisopyramide : S/P; small amount in milk, antimuscarinic effectsDoxepin : S/P; sedation, respiratory depressionEphedrine : S/P; irritability, sleep disturbanceErgotamine : C/I; ergotism in the infant; may suppress lactationEstrogens : C/I; gynaecomastia in male infant, may suppress lactationEthosuccimide : C/I; hyperexcitability, poor sucklingFamotidine : S/P; present in milk, but harm to infant not knownFluconazole : C/I; secreted in milk, but harm to infant not knownFluoxetine : S/P; small amount in milk, but can accumulate in infant; avoid if possibleFurosemide : S/P; small amount in milk, electrolyte disturbances in the infantGemfibrozil : Avoid; no information on risk to infantIndomethacin : C/I; CNS effects, convulsionsIodine/Iodides : C/I; concentrated in milk, hypothyroidism and goiter in the infantIodine radioactive : C/I; suspend breastfeeding for 24 hr after diagnostic dose and for long-
term after therapeutic doseIsoniazid : S/P; neuropathy, convulsions, jaundice, give prophylactic pyridoxineItraconazole : Avoid unless essential; amount in milk smallKetoconazole : C/I; secreted in milk but harm to infant not known.Ketorolac : Avoid as no data on safetyLansoprazole : Avoid unless essential; no data on safetyLevodopa/Carbidopa : S/P; no data on safetyLithium carbonate : C/I; intoxication in the infant, cardiac arrhythmiasLosartan : S/P; magnitude of risk not known; avoid if possibleMefloquine : S/P; secreted in milk, but harm to infant unlikelyMetformin : C/I; secreted in milk; hypoglycaemia, lactic acidosisMesalazine : S/P; amount in milk small; watch for diarrhoeaMethotrexate : C/I; toxicity in infantMetoclopramide : S/P; watch for diarrhoea, dystonia in infantMetronidazole : Significant amount in milk: avoid high doses; suspend breastfeeding
for 12 hr after single dose therapyMontelukast : Avoid; no data on risk to infantMorphine : S/P; usual doses unlikely to affect infant; lethargy, poor growth,
(and other opioids) withdrawal symptoms in infants of dependent mothersNalidixic acid : S/P; small risk of haemolytic anaemia; avoid if possibleNeostigmine : S/P; small amount in milk but monitor infantNifedipine : S/P; small amount in milk but monitor infantNitrofurantoin : S/P; small amount in milk, haemolysis in G-6-PD deficient infantNorfloxacin : Avoid; no information on risk to infantOmeprazole : Not known to be harmful, manufacturer advises ‘avoid’Oral contraceptives : Avoid until 6 month after birth, see estrogensPenicillins : Toxicity unlikely but risk of allergyPhenolphthalein : C/I; diarrhoea, rashes
Drug Comment / possible adverse effect on breast-fed infant
Contd...

968 APPENDICESA
PP
EN
DIC
ES
Phenytoin : S/P; small amount in milk, but monitor infantProgestins : Low doses safe, may suppress lactation at high dosesPropylthiouracil : S/P; hypothyroidism with high doses onlyPyrimethamine-sulfadoxine : S/P; significant amount in milk; appears safe if infant is olderQuinidine : S/P; significant amount in milk but harm to infant not knownRanitidine : S/P; significant amount in milk but harm to infant not knownRifampin : S/P; amount in milk small, but monitor infant for jaundiceSertraline : S/P; present in milk but no harm reported in short-termSpironolactone : S/P; drowsiness, hirsutism, gynaecomastiaStreptomycin : Compatible with breastfeeding; monitor infant for diarrhoea and thrushSulfonamides : S/P; rashes, small risk of kernicterus in neonate, haemolysis in
G-6-PD deficient; safer for older infantsSulfonylureas : S/P; no adverse effect reported, but watch for hypoglycaemiaTetracyclines : C/I; growth retardation, candidiasis, tooth discolourationTheophylline : S/P; irritability, CNS effectsThiazide diuretics : S/P; amount in milk small; may reduce lactationThyroxine : S/P; monitor for hyperthyroidismTinidazole : S/P; present in milk; suspend breastfeeding till 3 days after stoppingVancomycin : S/P; present in milk, but absorption from infant’s gut unlikelyVerapamil : S/P; small amount in milk, but monitor infantVigabatrin : C/I; present in milk, no data on risk to infantVitamin A and D : Avoid high doses, risk of hypervitaminosisZolpidem : Avoid unless essential; amount in milk small, but watch for sedation
in infant
Drug Comment / possible adverse effect on breast-fed infant

Drugs and Fixed DoseCombinations Banned in India$
(updated till Dec. 2012)
Appendix 5Appendix 5Appendix 5Appendix 5Appendix 5
A. Single drug preparations(or combinations of)
1. Amidopyrine.2. Phenacetin.3. Nialamide.4. Methaqualone.5. Methapyriline (and its salts).6. Practolol.7. Penicillin skin/eye ointment.8. Tetracycline/Oxytetracycline/Demeclocycline
liquid oral preparations.9. Chloral hydrate.
10. Dover’s powder and Dover’s powder tablets I.P.11. Chloroform exceeding 0.5% w/w or v/v in
pharmaceutical preparations.12. Mepacrine HCl (Quinacrine and its salts) in any
dosage form for use for female sterilization orcontraception.
13. Fenfluramine14. Dexfenfluramine15. Terfenadine16. Astemizole17. Phenformin18. Rofecoxib19. Valdecoxib20. Rimonabant21. Rosiglitazone22. Nimesulide formulations for children below 12
years age23. Cisapride24. Phenylpropanolamine*25. Sibutramine and R-Sibutramine26. Gatifloxacin27. Tegaserod28. Human placental extract formulations, except
for:i. topical application for wound healingii. injection for pelvic inflammatory disease
29. Halogenated hydroxyquinolines in liquid oralantidiarrhoeals or any other dosage form forpediatric use.
30. Letrozole for induction of ovulation in ano-vulatory infertility.
B. Fixed dose combination with anyother drug
1. Corticosteroids with any other drug for internaluse, except for metered dose inhalers and drypowder inhalers.
2. Chloramphenicol with any other drug for internaluse.
3. Sodium bromide/chloral hydrate with other drugs.4. Crude ergot with any drug except preparations
containing ergotamine, caffeine, analgesics,antihistamines for treatment of migraine,headache.
5. Anabolic steroids with other drugs.6. Metoclopramide with other drugs (except with
aspirin/paracetamol).7. Pectin and/or kaolin with any drug which is
systemically absorbed from g.i. tract, except forcombination of pectin and/or kaolin with drugsnot systemically absorbed.
8. Hydroxyquinolines with any other drug exceptin preparations for external use.
9. Oxyphenbutazone or phenylbutazone with anyother drug.
10. Dextropropoxyphene with any other drug exceptantispasmodics and/or NSAIDs.
11. Analgin (metamizol) with any other drug.12. Fixed dose combination of haemoglobin in any
form.
C. Fixed dose drug combinations of
1. Penicillins with sulfonamides.2. Tetracyclines with vitamin C.
* Presently stayed by Highcourt.$ Drugs Control Organisation, Govt. of India; http//www.drugscontrol.org/ban_drugs.htm

970 APPENDICESA
PP
EN
DIC
ES
3. Antitubercular drugs with Vitamins (exceptIsoniazid with Pyridoxine HCl).
4. Vitamins with Analgesics/Antiinflammatorydrugs.
5. Vitamins with Tranquillisers.6. Atropine and Analgesic-antipyretics.7. Yohimbine and Strychnine with Testosterone and
Vitamins.8. Strychnine and Caffeine in tonics.9. Iron with Strychnine, Arsenic and Yohimbine.
10. Antihistaminics with Antidiarrhoeals.11. More than one Antihistamine in the same
preparation.12. Sedatives/Hypnotics/Anxiolytics with
Analgesic-antipyretics.13. H2 receptor antagonists with Antacids (except
those combinations approved by Drugs Con-troller, India).
14. Anthelmintics (except Piperazine) with aCathartic/Purgative.
15. Salbutamol (or any other bronchodilator) withcentrally acting Antitussive and/or an Antihista-mine.
16. Centrally acting Antitussives with Antihistamineshaving atropine like activity in expectorants.
17. Centrally acting Antitussive and/or Antihistaminein preparations for cough associated with asthma.
18. Laxatives and/or antispasmodic drugs in enzymepreparations.
19. Glycerophosphates and/or other phosphates, and/or CNS stimulant in liquid oral tonics.
20. Estrogen and Progestin (other than oralcontraceptives) containing per tablet estrogenmore than 50 µg ethinylestradiol (or equivalent)and progestin more than 3 mg of norethisteroneacetate (or equivalent), and all fixed dosecombination injectable preparations containingsynthetic estrogen and progesterone.
21. Ethambutol with Isoniazid, except in thefollowing daily doses:Isoniazid 200 mg + Ethambutol 600 mg orIsoniazid 300 mg + Ethambutol 800 mg.
22. Pyrazinamide with other antitubercular drugs,except that which provide the following dailydoses:Rifampicin 450 to 600 mgIsoniazid 300 to 400 mgPyrazinamide 1000 to 1500 mg
23. Essential oils with Alcohol having percentagehigher than 20% proof (except preparations givenin the I.P.).
24. Liquid oral tonic preparations containing alcoholmore than 20% proof.
25. Streptomycin with penicillin in parenteral pre-paration.
26. Antidiarrhoeals containing adsorbants likekalolin, pectin, attapulgite, activated charcoal etc.
27. Antidiarrhoeals containing phthalylsulfathiazole,succinyl sulfathiazole, sulfaguanidine, neomycin,streptomycin, dihydrostreptomycin.
28. Antidiarrhoeal formulations for pediatric usecontaining diphenoxylate, loperamide, atropine,hyoscyamine.
29. Antidiarrhoeals with electrolytes.30. Pancreatine or pancrelipase containing amylase,
protease and lipase with any other enzyme.31. Oral rehydration salts other than those
conforming to the following parameters:(a) Oral rehydration salts on reconstitution to one
litre shall contain: sodium–50 to 90 mM; totalosmolarity–240 to 290 mOsm; dextrose:sodium molar ratio–not less than 1:1 and notmore than 3:1.
(b) Cereal based ORS on reconstitution to onelitre shall contain: total osmolarity not morethan 2900 mOsm. Precooked rice equivalentto not less than 50 g and not more than 80 gas total replacement of dextrose.
(c) ORS may contain amino acids in addition toORS conforming to the parameters specifiedabove and labelled with the indication for“Adult Choleratic Diarrhoea” only.
(d) ORS shall not contain mono or poly-saccharides or saccharin sweetening agent.
32. A drug, standards of which are prescribed in the2nd schedule to Drugs and Cosmetics Act with anAyurvedic, Siddha or Unani drug.
33. Vitamin B1, vit B6, and vit B12 for human use.34. Diazepam with diphenhydramine HCl.35. Nitrofurantoin with trimethoprim.36. Phenobarbitone with any antiasthmatic drug, or
with hyoscine and/or hyoscyamine, or ergotamineand/or belladonna.
37. Haloperidol with any anticholinergic agentincluding propantheline Br.
38. Nalidixic acid with any antiamoebic includingmetronidazole.
39. Loperamide with furazolidone.40. Cyproheptadine with lysine or peptone.

Selected References forFurther Reading
1. Brunton LL, Chabner BA, Knollman BC (Eds):Goodman and Gilman’s The Pharmacological Basis ofTherapeutics: 12th edn: McGraw-Hill, New York, 2011.
2. McPhee SJ, Papadakis MA, Rabow MW (Eds): CurrentMedical Diagnosis and Treatment 2012: LangeMedical Books/McGraw-Hill, New York, 2012.
3. Sweetman SC (Ed): Martindale, The Complete DrugReference: 37th edn: The Pharmaceutical Press, TheRoyal Pharmaceutical Society of Great Britain, London,2011.
4. British National Formulary, No 62; BMJ PublishingGroup and RPS Publishing, London, 2011.
5. Katzung BG, Masters SB, Trevor AJ (Eds): Basic andClinical Pharmacology: 12th edn: Lange medical book,Tata McGraw-Hill, New Delhi, 2012.
6. Rang HP, Dale MM, Ritter JM, Flower RJ, HendersonG: Pharmacology: 7th edn: Elsevier, ChurchillLivingstone, Edinburgh, 2012.
7. Bennett PN, Brown MJ: Clinical Pharmacology: 10th
edn: Churchill Livingstone, Edinburgh, 2008.8. Essential Medicines, WHO Model List: 17th edn, WHO,
Geneva (March 2011).9. National List of Essential Medicines (2011). Govt. of
India, Ministry of Health & Family Welfare, DirectorateGeneral of Health Services, New Delhi, 2011 [http://www.cdsco.nic.in].
10. Agarwal AK, Singhal RK, Jain DG, Upadhyay R,Rewari BB (Eds): Emergency Medicine; Associationof Physicians of India, Delhi State Chapter, JaypeeBrothers, New Delhi, 2005.
11. Morgan GE, Mikhail MS, Murray MJ: ClinicalAnaesthesiology: 4th edn: Lange Book, Tata McGrawHill, New Delhi, 2006.
12. Kar HK, Kumar B: IAL Textbook of Leprosy: JaypeeBrothers Medical Publishers, New Delhi, 2010.
13. DOTS-Plus guidelines: Central TB Division,Directorate General of Health Services, Ministry ofHealth and Family Welfare, Govt. of India, New Delhi,2010.
14. Treatment of Tuberculosis: Guidelines, 4th edn: WHO,Geneva, 2010.
15. Girdhar BK, Girdhar A: Short course treatment ofleprosy: present status. ICMR Bulletin 32(2): 13-19,2002.
16. Antiretroviral therapy guidelines for HIV infectedadults and adolescents, including post-exposure;NACO, Department of AIDS Control, Min. of Health
and Family Welfare, Govt. of India, 2007 [http/www.nacoonline.org].
17. Guidelines for the Treatment of Malaria, 2nd edn:WHO, Geneva. 2010 [http://www.who.int/malaria/publications/atoz/978924154925/en/index.html]
18. National Drug Policy on Malaria (2010), Directorateof National Vector Borne Disease Control Programme,DGHS, Govt. of India, 2010.
19. Kala azar Treatment Policy (2011), Directorate ofNational Vector Borne Disease Control Programme.DGHS, Govt. of India, 2011.
20. Expert committee on control of Leishmaniasis; WHOTechnical Report Series No. 949: Geneva, 2010.
21. List of drugs banned for marketing in India; DrugsControl Organisation, Govt of India; http//www.drugscontrol.org/ban_drugs.htm.
22. Sharma HL, Sharma KK: Principles of Pharmacology:2nd edn; Paras Medical Publisher, Hyderabad, 2011.
23. Rubin P (Ed): Prescribing in Pregnancy: 3rd edn: BMJBooks, London, Jaypee Brothers, New Delhi (Indianedition 2001), 2000.
24. Project Team of the Resuscitation Council (UK):Emergency medical treatment of anaphylacticreactions: consensus guidelines; Resuscitation 41: 93-99, 1999.
25. Jiménez-Ruiz C, Berlin I, Hering T: Varenicline: a novelpharmacotherapy for smoking cessation. Drugs 69 (10),1319-38, 2009.
26. Breslier RS, et al: Cardiovascular events associatedwith rofecoxib in a colorectal adenoma chemopre-vention trial, Adenomatous polyp prevention on vioxx(APPROVe). N Engl J Med 352: 1092-1102, 2005.
27. Kearney PM, et al: Do selective COX-2 inhibitors andtraditional NSAIDs increase the risk of athero-thrombosis? Meta-analysis of randomized trials. BMJ332: 1302-1308, 2006.
28. Schnitzer TJ: Update on guidelines for the treatmentof chronic musculoskeletal pain. Clin Rheumatol 25:(Suppl 7) 22–29, 2006.
29. Heyneman CA, Lawless-Liday C, Wall GC: Oral versustopical NSAIDs in rheumatic diseases: a comparison;Drugs 60: 555-574, 2000.
30. Roy AD, Richard BH: Topical therapies forosteoarthritis. Drugs 71(10), 1259-79, 2011.
31. Diabetes control and complications trial (DCCT)Group: Effect of intensive therapy on the microvascularcomplications of type 1 diabetes mellitus; JAMA 287:2563-2569, 2002.

972 ESSENTIALS OF MEDICAL PHARMACOLOGY
32. UK Prospective Diabetes Study Group: Intensive blood-glucose control with sulfonylureas or insulin comparedwith conventional regimen and risk of complicationsin patients with type 2 diabetes (UKPDS 33); Lancet352: 837-853, 1998.
33. Diabetes Prevention Programme (DPP) research group:Reduction in the incidence of type 2 diabetes withlifestyle intervention or metformin. N Engl J Med 346:393-403, 2002.
34. Dormandy JA, et al: Secondary prevention ofmacrovascular events in patients with type 2 diabetesin the PRoactive study: A randomized controlled trial.Lancet 366: 1280, 2005.
35. Ramirej MA, Borja NL: Epalrestat: an aldose reductaseinhibitor for the treatment of diabetic neuropathy.Pharmacotherapy 28(5), 646-55, 2008.
36. Gupta V, Kalra S: Choosing a gliptin. Indian JEndocrinol Metab. 15 (4), 298-308, 2011.
37. Vandekerckhove P, Lilford R, et al: Withdrawn:Androgens versus placebo or no treatment foridiopathic oligo/asthenospermia. Cochrane DatabaseSyst Rev 2007 Jul 18; (4): CD000/150; http://www.ncbi.nlm.nih.gov/pubmed/17636603.
38. McKeage K, Croxtall JD: Ulipristal acetate: a reviewof its use in emergency contraception. Drugs 71 (7),935-45, 2011.
39. Anderson GL, et al: The Women’s Health Initiative(WHI) randomized controlled trial: Effect of conjugatedequine estrogens in post-menopausal women withhysterectomy. JAMA 291: 1701-1712, 2004.
40. Espeland MA, et al: The WHI-memory study:Conjugated equine estrogens and global cognitivefunction in postmenopausal women. JAMA 291: 2959-2968, 2004.
41. Rossouw JE, et al: The WHI trial, risks and benefits ofestrogens + progestin in healthy postmenopausalwomen; principal results. JAMA 288: 321-333, 2002.
42. Beral V, et al: Million Women Study (MWS): Breastcancer and hormone replacement therapy. Lancet 362:419-427, 2003.
43. Grady D, Herrington D, et al: Cardiovascular diseaseoutcomes during 6.8 years of hormone therapy: Heartand estrogen/progestin replacement study follow-up(HERS II); JAMA 288: 49-57, 2002.
44. Yang LPH, Keam SJ: Sugammadex: a review of its usein anaesthetic pratice. Drugs 69 (7), 919-42, 2009.
45. Parkinson Study Group: Pramipexole vs levodopa asinitial treatment for Parkinson’s disease, A randomizedcontrolled trial. JAMA 284: 1931-1938, 2000.
46. Hadjipavlou G, Mok H, Yatham LN: Pharmacotherapyof bipolar II disorder: a critical review of currentevidence. Bipolar Disord 6: 14-25, 2004.
47. Dhillon S: Aripiprazole: a review of its use in themanagement of mania in adults with bipolar I disorder.Drugs 72 (1), 133-62, 2012.
48. Lee F, Cundiff D: Meperidine vs morphine inpancreatitis and cholecystitis; Arch Intern Med 158:2399, 1998.
49. Yusuf S, Sleight P, et al: Effects of an angiotensin-converting enzyme inhibitor ramipril, on cardiovascularevents in high risk patients. The Heart OutcomesPrevention Evaluation (HOPE) study investigators; NEngl J Med 342: 145-153, 2000.
50. Packer M, Poole-Wilson PA, et al: Comparative effectsof low and high doses of the angiotensin convertingenzyme inhibitor, lisinopril, on morbidity and mortalityin chronic heart failure. ATLAS study Group;Circulation 100: 2312-2318, 1999.
51. EUROPA investigators: Efficacy of perindopril inreduction of cardiovascular events among patients withstable coronary artery disease; European trial on thereduction of cardiac events with perindopril in stablecoronary artery disease. Lancet 362: 782-788, 2003.
52. Pfeffer MA, et al: Valsartan, captopril or both inmyocardial infarction complicated by heart failure, leftventricular dysfunction or both; Valsartan in acutemyocardial infarction trial (VALIANT). New Engl JMed 349: 1893-1896, 2003.
53. Mc Murray JJ, et al: Effect of candesartan in patientswith chronic heart failure and reduced left ventricularsystolic function taking ACE inhibitors. The CHARM-Added Trial. Lancet 262: 767-771, 2003.
54. Chaitman BR: Ranolazine for the treatment of chronicangina and potential use in other cardiovascularconditions. Circulation 113: 2462-2472, 2006.
55. Chobanian AV, et al: The 7th report of the JointNational Committee on prevention, detection,evaluation and treatment of high blood pressure: TheJNC7 report; JAMA 289: 2560-2572, 2003.
56. Whitworth JA: World Health Organization (WHO)/International Society of Hypertension (ISH) statementon management of hypertension. J Hypertens 21: 1983,2003.
57. ALLHAT officers, et al: Major outcomes in high-riskhypertensive patients randomized to ACE inhibitor orcalcium channel blocker vs diuretic. The anti-hypertensive and lipid-lowering treatment to preventheart attack trial. JAMA 288: 2981-2997, 2002.
58. Arnold JMO, et al: Prevention of heart failure inpatients, in the HOPE study. Circulation 107: 1284-1290, 2003.
59. Varon J: Treatment of acute severe hypertension:current and newer agents. Drugs 68(3), 283-297, 2008.
60. Plosker GL: Tolvaptan. Drugs 70 (4), 443-454, 2010.61. Lyseng-Williamson, Katherine A, Keating GM: Ferric
carboxymaltose: a review of its use in iron-deficiencyanaemia: Drugs 69 (6), 739-756, 2009.
62. Walraven CV, Hart RG, et al: Oral anticoagulant vsaspirin in nonvalvular atrial fibrillation: an individualpatient meta-analysis. JAMA 288: 2441-2448, 2002.

973SELECTED REFERENCES
63. Mehta SR, Yusuf S, et al: The clopidogrel in unstableangina to prevent recurrent events (CURE) trialincluding a metaanalysis. Eur Heart J 21: 2033-2041,2000.
64. Grundy SM, et al: Implications of recent clinical trialsfor the National Cholesterol Education Programme,ATPIII guidelines. Circulation 110: 227-239, 2004.
65. Heart Protection Study collaborative group: Effects ofcholesterol lowering with simvastatin on stroke andother major vascular events in 20,536 people withcerebrovascular disease or other high-risk conditions.Lancet 363: 757-767, 2004.
66. Niebyl JR: Clinical practice. Nausea and vomiting inpregnancy; N Engl J Med 363 (16): 1544-1550, 2010.
67. Curran MP, Robinson DM: Aprepitant: a review of itsuse in the prevention of nausea and vomiting: Drugs69(13): 1853-1878, 2009.
68. Fischer Walker CL, Fontaine O, Young MW, Black RE:Zinc and low osmolarity oral rehydration salts fordiarrhoea: A renewed call to action; WHO Bull 87; 780-786, 2009.
69. Layer P, Andresen V: Review article: rifaximin, aminimally absorbed oral antibacterial for the treatmentof traveller’s diarrhoea; Aliment Pharmacol Ther.31(11); 1155-1164, 2010.
70. Sazawal S et al: Efficacy of probiotics in preventionof acute diarrhoea: a meta-analysis of masked, rando-mised, placebo-controlled trials: Lancet Infect Dis, 6;374-382, 2006.
71. Albanna AS, Menzies D: Drug resistant tuberculosis:what are the treatment options? Drugs 71(7): 815-825,2011.
72. India achieves National elimination of leprosy. Ind JLeprosy 78: 101, 2006.
73. Jefferson T, Demicheli, V, et al: Antivirals for influenzain healthy adults: systematic review. Lancet 367: 303-313, 2006.
74. Mohapatra PK, et al: Evaluation of chloroquine andsulphadoxine/pyrimethamine therapy in uncomplicatedfalciparum malaria in Indo-Myanmar border areas. TropMed and Internat Health 10: 478-483, 2005.
75. White NJ for SEAQUAMAT group: Artesunate versusquinine for treatment of severe falciparum malaria: arandomized trial. Lancet 366: 717-725, 2005.
76. Rueangweerayut R, Phyo AP, et al: Pyronaridine-artesunate versus mefloquine plus artesunate formalaria. N Engl J Med 366: 1298-1309, 2012.
77. Gargano N, et al: Therapeutic efficacy and safety ofdihydroartemisinin-piperaquine versus artesunate-mefloquine in uncomplicated Plasmodium falciparummalaria in India, Malaria Journal 11-233, 1-12,2012.
78. Anvikar AR, et al: Artesunate-amodiaquine fixed dosecombination for the treatment of Plasmodium falci-parum malaria in India. Malaria Journal 11: 97, 1-8,2012.
79. Melaku Y, et al. Treatment of kala-azar in SouthernSudan using a 17-day regimen of sodium stiboglu-conate combined with paromomycin: a retrospectivecomparison with 30-day sodium stibogluconatemonotherapy. Am J Trop Med Hyg 77: 89-94,2007.
80. Sundar S, et al: Injectable paromomycin for visceralleishmaniasis in India. N Engl J Med 356: 2571-2581,2007.
81. Patra P, et al: Efficacy of oral miltefosine in visceralleishmaniasis in rural West Bengal, India: Ind JPharmacol 44: 500-503, 2012.
82. Breastfeeding and maternal medication; WHO/CDR95.11, 1995.
83. National Formulary of India: 4th edn. IndianPharmacopoeia Commission, Ministry of Health andFamily Welfare, Govt. of India, 2010.


Index
AAbacavir, 798, 808, 814ABC (ATP-binding cassettee) transporters, 13Abciximab, 629, 631Abortion: drugs for, 189-90, 319-20, 332Absorbants, 685Absorption of drugs, 6, 14-16Acamprosate, 393Acarbose, 277, 279Acebutolol, 147, 148, 149Aceclofenac, 192, 204Acenocoumarol, 617, 621, 622Acetaminophen. See ParacetamolAcetazolamide, 155-56, 579, 586-87, 591Acetic acid, 898, 901Acetomenaphthone, 615, 913Acetylation, 24, 567, 767Acetylcholine (ACh), 93-94, 99-104Acetylcholinesterase (AChE), 96, 99-100, 106, 109Acetylsalicylic acid. See AspirinAcid neutralizing capacity (ANC), 654Acitretin, 892Acne vulgaris: drugs for, 738, 893-95, 899Acriflavine, 902Acromegaly, 237, 239-40ACTH (Adrenocorticotropic hormone), 234-36, 243-44,
282, 283, 294Actinomycin D, 858, 859, 867Action potential (AP)
effect of digitalis on, 513fast channel; slow channel, 493in heart, 492-93, 526in nerve, 361
Activation of drugs, 22-23Active transport of drugs, 13-14, 30Acute coronary syndsromes (ACS), 544, 556, 631, 632Acute left ventricular failure, 478, 520, 522, 545,
556, 581Acute necrotizing ulcerative gingivitis (ANUG),
720, 722, 839Acyclovir, 763, 798-800Adalimumab, 212, 685, 884Adapalene, 894Addiction: to drugs, 88Addison’s disease, 285, 290Adefovir dipivoxil, 798, 803
Adenosine, 536, 537, 538Adenylyl cyclase: cAMP pathway, 46, 47, 48, 132-33Adrenaline (Adr), 47, 124-33, 138, 563Adrenergic
blockers, 129, 140-51, also see Alfa adrenergicblockers, Beta adrenergic blockers
drugs, 129-39, 363neurone blockers, 140, 141, 568receptors, 47, 125-28transmission, 124-29
Adrenochrome monosemicarbazone, 616Adriamycin. See DoxorubicinAdult treatment panel III (ATP III), 642, 643Adverse drug effects, 82-91
causality assessment, 83Adverse drug event (ADE), 82Adverse drug reaction (ADR), 82Aeromatic chest rub, 221Affinity, 41, 42Agonist, 40, 41AIDS: drugs for. See Antiretrovirus drugsAkathisia, 444Albendazole, 850-51, 854, 856Albumin (human), 644Alcohol
drinking: motivation for, 393drinking: safe guidelines, 392ethyl, 388-94, 395, 901methyl, 394-95
Alcoholic beverages, 388Alcoholism, 388, 392-93Aldehyde dehydrogenase inhibitors, 394Aldosterone, 234, 282, 283, 284, 290, 523, 577, 588
antagonist, 520, 523-24, 587-89, also seeSpironolactone
Aldosterone induced protein (AIP), 284, 587, 588Alendronate, 343, 344, 345Alfa adrenergic blockers, 140-44, 564-65Alfacalcidol, 342, 343Alfa glucosidase inhibitors, 258, 269, 2775-Alfa reductase inhibitors, 302-03, 872Aliskiren, 508, 562Alkylating agents, 858, 860-61Allergy (hypersensitivity) to drugs, 85-87, 167, 719Allopurinol, 216-17, 845Allylestrenol, 316, 318

976 ESSENTIALS OF MEDICAL PHARMACOLOGY
Aloe vera gel, 887Alogliptin, 275Alopecia: drugs for, 302, 567Alprazolam, 405, 466, 468Alprostadil, 190, 304Alteplase (rt-PA), 626, 627Alum, 887Aluminium hydroxide, 655Alvimopan, 677Alzheimer’s disease: drugs for, 108, 488-91Amantadine, 432-33, 434, 801, 802Ambroxol, 219, 221Amethocaine. See TetracaineAmifostine, 876Amikacin (Am), 749, 765, 770, also See
Aminoglycoside antibioticsAmiloride, 561, 589-90, 591, 598Amineptine, 454, 463Aminoglycoside antibiotics, 743-50
common properties, 743-47mechanism of action, 743-44shared toxicities, 744-45
Aminopenicillins, 722-23Aminophylline, 222, 227, also See Theophylline5-Aminosalicylic acid (5-ASA). See MesalazineAmiodarone, 528, 529, 533-34, 537, 538Amisulpiride, 436, 443Amitriptyline, 454, 458, also See Tricyclic
antidepressantsAmlodipine, 540, 549, 550Ammonium chloride, 218Amodiaquine (AQ), 816, 823, 833, 834Amoebiasis: treatment of, 838, 839, 840, 841, 842,
843 Amoxapine, 457, 458, 460Amoxicillin, 657, 658, 702, 712, 721, 722, 723, 762,
763Amphetamine, 134-35, 137, 139, 487Amphotericin B (AMB), 787-89, 794, 845, 846
liposomal, 788, 845, 846Ampicillin, 657, 722-23, 762, 763Amrinone. See InamrinoneAnabolic steroids, 300-01Anaemia: drugs for, 599, 602, 605, 606, 607-10Anaesthesia: general, 372
complications of, 385local vs general, 360mechanism of, 372-73pharmacokinetics of : inhalational, 375-76stages of, 373-74techniques of: inhalational, 376-77techniques of: local, 367-71
Anakinra, 212, 878, 884Analeptics, 486, 487
Analgesic: definition, 469combinations, 209nonopioid, 192-209opioid, 469-78
Analgesic nephropathy, 195Anandamide, 183, 452Anaphylactic reaction, 86-87, 138, 719Anaphylactic shock: treatment of, 87, 138, 167, 291Anastrozole, 314, 315, 858Androgens, 296-300
transdermal, 299Androsterone, 296Angina pectoris, 150, 539, 543, 544, 545, 550Angiogenesis inhibitors, 858, 870-71Angiotensin II (Ang II), 495-500
antagonists, See Angiotensin receptor blockersconverting enzyme (ACE) inhibitors, 500-05,
520, 521-23, 557, 561receptor blockers (ARBs), 505-08, 520, 521-23,
557, 561-62Anidulafungin, 790Anorectic drugs, 137, 139Antacid, 654-56, 659
combinations, 655in peptic ulcer, 656
Antagonism, 57-60among antimicrobials, 698-99
Antagonist: competitive, 38, 42, 58, 59non competitive, 38, 58, 59
Anterior pituitary hormones, 235, 236-44Anthelmintic drugs, 849-56Anthraquinone purgatives, 674-75Anti H. pylori drugs, 657-58Antiamoebic drugs, 836-43Antiandrogens, 301-02Antianginal drugs, 539-54Antianxiety drugs, 402, 465-68Anti-aquaretic, 593Antiarrhythmic drugs, 526-38
choice of, 538Antibiotic: definition, 688
sources of, 690Anticancer: drugs, 857-76
antibiotics, 858, 867-68general principles in use of, 873-77general toxicity, 858-60
Anticholinergic drugs, 113-21, 386, 433, 654Anticholinesterases, 105-11
in Alzheimer’s disease, 498-90poisoning, 110-11
Anticoagulants, 616-25Anticonvulsants. See Antiepileptic drugsAntidepressants, 454-64
atypical, 454, 458, 462-63

977INDEX
Antidiarrhoeal drugs, 679-87Anti-D immune globulin, 885, 926Antidiuretics, 593-98Antidiuretic hormone (ADH), 329, 577, 593-97Antiemetics, 387, 662-70Antiepileptic drugs, 411-24Antiestrogens, 312-13Antifibrinolytic drugs, 628-29Antifungal drugs, 787-97Antihaemophilic factor, 613, 616Antihistamines
H1 blockers, 163-68H2 blockers, 169, 387, 649-51, 659H3 antagonists, 160, 169second generation, 166-67
Antihypertensive drugs, 558-74combinations of, 572in pregnancy, 572
Antileprotic drugs, 780-86Antimalarial drugs, 816-35
causal prophylactics, 818clinical curatives, 817, 819-20for chloroquine resistant falciparum malaria, 820,
824, 826, 827, 829-35gametocidal, 817, 821radical curative, 817, 819-20, 828, 829suppressive prophylactics, 818-19
Antimanic drugs, 447-51Antimetabolites, 858, 862-65Antimicrobial agent (AMA): definition, 688
choice of, 694-98combinations, 698-99failure of, 702in liver disease, 695in pregnancy, 695in renal failure, 695, 762mechanisms of action, 689-90prophylactic use of, 700-02resistance to, 691-93
Antimotility drugs, 686-87Antineoplastic. See AnticancerAntioxidant vitamins, 912Antiparkinsonian drugs, 118, 425-34Antiplatelet drugs, 629-33Antiprogestin, 319-21, 323Antipsychotic drugs, 436-47Antipyretic-analgesics, 192-209Anti-retrovirus (ARV) drugs, 798, 805-15Antiseborrheics, 890Antiseptics, 897-902
definition, 897mechanism of action of, 897potency of, 898properties of ideal, 897therapeutic index of, 898
Antisera, 919, 925-27diphtheria antitoxin (ADS), 927gasgangrene antitoxin (AGS), 927rabies (ARS), 927snake venom polyvalent, 927tetanus antitoxin (ATS), 926
Antithrombotic. See Antiplatelet drugsAntithymocyte globulin (ATG), 884Antithyroid drugs, 252-54Antitubercular drugs, 765-78Antitussives, 219-20Antiviral drugs, 798-815Anxiety, 435, 446, 465, 467-68
drugs for 402, 464, 465-68Apomorphine, 661Apraclonidine, 154, 157Aprepitant, 663, 669Ardeparin, 619Arecoline, 105Argatroban, 617, 620Aripiprazole, 436, 440, 442, 443, 444, 446, 451, 528Armodafinil, 486, 488Aromatase inhibitors, 314-15, 872Arsenic trioxide, 858, 869Arteether, 821, 829, 830, 833Artemether, 821, 829, 830Artemether-lumefantrine, 820, 832, 833Artemisinin, 818, 819, 829Artemisinin-based combination therapy (ACT), 819,
820, 832-35Arterolane, 820, 830, 833, 834-35Arterolane-piperaquine, 820, 833, 834-35Artesunate, 821, 829, 830, also See Artemisinin-
based combination therapy (ACT)Artesunate-amodiaquine, 823, 833, 834Artesunate-mefloquine, 820, 832, 833Artesunate-pyronaridine, 833, 835Artesunate-sulfadoxine/pyrimethamine (AS/SP), 820,
832, 833Ascariasis: drugs for, 850, 851, 582Ascorbic acid, 913, 916, 918Aspirin, 192, 195-99, 209, 544, 557, 629, 632, 633Astemizole, 164, 165, 166Asthma
bronchial, 119, 138, 189, 221-33cardiac, 478, also See Acute left ventricular failure
Astringents, 887Atazanavir (ATV), 798, 810Atenolol, 144, 148, 149, 540, 563Atomoxetine, 463, 464, 487Atorvastatin, 636, 637, also See StatinsAtosiban, 333Atovaquone, 818, 831-32Atracurium, 78, 352, 353-54

978 ESSENTIALS OF MEDICAL PHARMACOLOGY
Atrial fibrillation (AF), 518, 519, 527, 532, 534,535, 538, 625
Atrial flutter (Afl), 519, 527, 538Atrial natriuretic peptide (ANP), 50, 578, 593Atropine, 100, 101, 104, 111, 113-16, 118-21, 386,
429, 529, 537, 538Atropine methonitrate, 113, 116Attention deficit hyperkinetic disorder (ADHD),
139, 464, 487Atypical antidepressants, 454, 458, 462-63Atypical antipsychotics, 436, 440, 441, 442, 443, 451Auranofin, 212Autacoids: definition, 158Autonomic influences on heart, 494Autoreceptors, 125, 171, 172, 467A-V block, 138, 528, 529, 537AVP (Arginine-vasopressin), 329, 593-97, also See
Antidiuretic hormoneAzathioprine, 211, 685, 858, 863, 882Azelastine, 164, 167Azithromycin, 712, 754, 755, 763, 779Azelaic acid, 892, 894AZT (Azidothymidine). See ZidovudineAztreonam, 730
BBacampicillin, 723Bacitracin, 759, 760Baclofen, 358, 359Bactericidal AMAs, 690, 697, 698Bacteriological sensitivity testing, 696-97Bacteriostatic AMAs, 690, 697, 698BAL. See DimercaprolBalsalazide, 684Bambuterol, 222, 223BAN (British approved name), 3Banned drugs, 969-70Barbiturates, 398-401, 403, 404, 412-13Barbiturate poisoning, 400Basiliximab, 884Beclomethasone dipropionate, 222, 230, 231, 895Belladonna poisoning, 110, 120Benazepril, 500, 503Bendroflumethiazide, 579Benidipine, 540, 550Benign hypertrophy of prostate (BHP): drugs for, 143,
302Benoxinate, 367, 368Benserazide, 425, 429, 430Bentonite, 887Benzalkonium chloride, 900Benzathine penicillin, 719, 720Benzhexol. See TrihexyphenidylBenzocaine, 367, 368
Benzodiazepines (BZDs), 357, 383, 386, 393, 398,401-06, 407, 414, 418-19, 465-68, 670
antagonist, 403, 404, 408-09Benzoic acid, 796-97Benzothiadiazines. See ThiazidesBenzoyl peroxide, 893, 894, 899Benzthiazide, 579, 590Benzyl benzoate, 903-04Beta adrenergic blockers, 144, 151, 153, 179, 256, 520,
523, 532-33, 545-46, 556, 563-64, 570, 571ocular, 153-54
Beta-lactam antibiotics, 716-31Beta-lactamase, 692, 718, 724
inhibitors, 721, 724-25Betahistine, 163, 168Betamethasone, 288, 289, 292, also See
Corticosteroidsbenzoate, 895valarate, 895
Betaxolol, 144, 153, 154, also See Beta blockers:ocular
Bethanechol, 101, 104Bevacizumab, 858, 871Bezafibrate, 635, 636, 639, also See Fibric acid
derivativesBhang, 452Bicalutamide, 302, 858Bicuculline, 403, 404, 486Biguanide, 258, 275-76Bile acid sequestrants (Resins), 635, 638Bioavailability, 16-17Biological membrane, 10-11Biotin, 913, 916, 917Biotransformation, 22-27Biperiden, 113, 426, 433Bipolar disorder, 435, 450
drugs for, 416, 418, 442, 447-51Bird flu (avian-influenza): drugs for, 802-03Bisacodyl, 674, 676, 677Bishydroxycoumarin, 620, 621, 622Bismuth
colloidal, 656, 657subsalicylate, 686
Bisoprolol, 144, 147, 148, 149, 520, 523Bisphosphonates, 343-46Bivalirudin, 617, 620Bleaching powder, 900Bleomycin, 858, 868, 875Blood-brain barrier, 14, 18-19Boric acid, 887, 898, 901Bortezomib, 858, 871Botulinum toxin, 99, 100, 121Bradykinin, 509-11
antagonists, 511

979INDEX
Brain natriuretic peptide (BNP), 525Bran, 673Breast feeding and drugs, 28-29, 965-68Brimonidine, 154Brinzolamide, 155, 587Broad spectrum antibiotics, 690, 733-42Bromhexine, 219, 221Bromocriptine, 176, 239, 278, 430Bronchial asthma: drugs for, 189, 221-33
drug therapy, 232-33Bronchodilators, 116-17, 133, 220-21, 222-28Budesonide, 230, 231Buerger’s disease. See Peripheral vascular diseaseBufotenin, 451Bumetanide, 520, 579, 581Bupivacaine, 362, 364, 365, 366, 367, 368, 369, 371Buprenorphine, 479, 482Bupropion, 122, 454, 458, 463Buspirone, 171, 172, 465, 466-67, 468Busulfan, 858, 859, 861, 873Butamben, 360, 367, 368Butenafine, 787, 797Butorphanol, 479, 480, 482Butyrocholinesterase (BuChE). See Pseudocholinesterase
CCabergoline, 238, 239Caffeine, 224, 225, 226, 488Calamine, 886-87Calciferol, 340-42, 913, also See vit DCalcineurin inhibitors (T-cell inhibitors), 878-81Calcipotriol, 343, 891Calcitonin, 245, 339-40Calcitriol, 335, 336, 339, 340-43, 913Calcium, 335-37
carbonate, 336channel blockers, (CCBs), 180, 333, 354, 522, 529,
535-36, 540, 541, 546-51, 552, 562-63, 570channels, 546citrate, 336daily allowance, 337edetate (calcium EDTA), 906gluconate, 336lactate, 336
Camphor, 888Cancer chemotherapy. See Anticancer drugsCandesartan, 505-06Candidiasis: drugs for, 789Cannabinoid receptors, 452Cannabinoids, 452, 670Cannabis, 452Canthridin, 889Capecitabine, 858, 864Capreomycin (Cm), 765, 770
Capsicum, 888Captopril, 500-02, 573Captopril test, 505Carbachol, 100, 104Carbamazepine, 415-16, 421, 422, 423, 451, 598Carbapenems, 731Carbaryl, 105Carbenicillin, 723, 762Carbetocin, 331Carbidopa, 425, 429, 430Carbimazole, 246, 252, 253, 254Carbocisteine, 218, 219Carbolic acid. See PhenolCarbonic anhydrase inhibitors, 152, 155, 420, 586-87
topical, 155Carbonyl iron, 602, 603Carboplatin, 858, 859, 862Carboprost (15-methyl PGF2α), 189Carcinogenicity, 79, 90-91, 859Carcinoid syndrome, 173Cardiac arrhythmias, 526-28
drugs for, 150, 519, 526-38Cardiac electrophysiology, 492-94, 526-27Cardiac glycosides, 512-19, also See Digitalis/DigoxinCarisoprodol, 357Carrier transport, 12-14Carvedilol, 144, 150, 151, 523Cascara sagrada, 675Case-control study, 76, 77Caspofungin, 787, 789, 790Castor oil, 675, 677, 866Catecholamines (CAs), 124-26, also See Individual drugsCathartics, 672, also See LaxativesCaudal anaesthesia, 366Caustics, 889CCNU. See LomustineCefaclor, 726, 727Cefadroxil, 702, 726Cefazolin, 702, 726, 730Cefdinir, 726, 728Cefepime, 726, 729Cefixime, 726, 728, 763Cefoperazone, 712, 726, 728, 729, 931Cefotaxime, 712, 726, 727Cefpirome, 726, 729Cefpodoxime proxetil, 726, 728, 761Cefprozil, 726, 727Ceftamet pivoxil, 726, 728Ceftazidime, 726, 728Ceftibuten, 726, 728Ceftizoxime, 702, 726, 727, 730Ceftriaxone, 681, 712, 726, 727, 729, 730, 763Cefuroxime, 702, 726, 727, 763Cefuroxime axetil, 726, 727

980 ESSENTIALS OF MEDICAL PHARMACOLOGY
Celecoxib, 205-06, also See COX-2 inhibitorsCeliprolol, 144, 149Cell cycle, 875
nonspecific drugs, 873specific drugs, 874
Centchroman, 327Cephalexin, 702, 726, 761Cephalosporins, 695, 712, 725-30, 762, 931Cerebral malaria, 820, 826, 831, also See Malaria,
severe and complicatedCerebroactive drugs. See Cognition enhancersCervical priming (ripening), 189, 320Cetirizine, 164, 166CETP-inhibitors, 641Cetrimide, 900Cetuximab, 858, 870Chancroid: drugs for, 708, 711, 728, 730, 754, 755,
763Charas, 452Charcoal activated, 37, 85, 401Cheese reaction, 143, 455, 564, 565, 573Chelating agents, 37, 905-08Chemotherapy, See Antimicrobial agents
definition, 2, 688failure of, 702-03history of, 688-89of cancer, 857, 873-77
Chenodeoxycholic acid (chenodiol), 671Chickenpox: drug for, 800Child dose calculation, 63-64Chlamydia trachomatis urethritis, 713, 737, 755, 763Chlophedianol, 220Chloral hydrate, 397, 398Chlorambucil, 858, 859, 860, 873, 883Chloramphenicol, 712, 734, 739-42
palmitate, 740succinate, 740
Chlordiazepoxide, 401, 435, 466Chlorhexidine, 900Chlorinated lime, 900Chlorine, 899Chlormezanone, 357Chloroguanide. See ProguanilChlorophores, 900Chloroprocaine, 360, 361, 362Chloroquine (CQ), 211, 781, 816, 818, 820, 821-
23, 840, 843Chloroxylenol, 898Chlorpheniramine, 160, 164, 165, 221Chlorpromazine (CPZ), 435, 436, 437-39, 440, 665Chlorpropamide, 273, 598Chlorthalidone, 558, 559, 572, 579, 583, 584Chlorzoxazone, 357Cholecalciferol, 337, 341, 342, 913, also see Vit D
Cholera: drugs for, 682, 700, 711, 737vaccine, 921
Cholestyramine, 636, 638Choline esters, 102-04Cholinergic
crisis/weakness, 110drugs, 102-05transmission, 99-102
Cholinesterase reactivators, 111Cholinesterases, 99, 100, 101Choline theophyllinate, 227Cholinoceptors, 100-02Cholinomimetic alkaloids, 104-05Choriogonadotropin (rHCG), 241Chorionic gonadotropin (human, HCG), 241Chronic obstructive pulmonary disease (COPD), 116,
119, 138, 222, 224, 227, 228, 230Ciclesonide, 230, 231Ciclopirox olamine, 796Cidofovir, 798, 801Cilomilast, 226Cilostazole, 555Cimetidine, 649, 650, also See H2 antagonistsCinacalcet, 338Cinchonism, 825-26Cinnamates, 893Cinnarizine, 164, 168, 663Ciprofloxacin, 681, 682, 708, 709, 710-12, 761, 763,
766, 770Circus movement reentry, 527Cisapride, 174, 667, 753, also See Prokinetic drugsCisatracurium, 347, 352, 354Cisplatin, 858, 859, 861, 862, 864Citalopram, 454, 458, 461Citicoline, 491Citrovorum factor (folinic acid) rescue, 611, 863, 876Clarithromycin, 657, 754-55, 783, 931, 932Clavulanic acid, 724, 725, 761, 762Clearance of drug (CL), 30, 31, 32Clemastine, 164Clidinium, 113, 118Clindamycin, 756-57, 818, 829, 894Clinical pharmacology, 2, 61-70Clinical trial, 67, 73-75, 79-81
phase ‘0’ studies, 80Clioquinol. See QuiniodochlorClobazam, 418, 421Clobetasol butyrate, 895Clobetasol propionate, 895Clofazimine (Clo), 780, 781-82, 784, 785, 786Clofibrate, 639Clomiphene citrate, 312Clomipramine, 454, 456, 458, 464, also see
Tricyclic antidepressantsClonazepam, 402, 418, 421, 422

981INDEX
Clonidine, 127, 129, 564, 565-66, 573Clopamide, 579, 584Clopidogrel, 630, 631, 632, 633, 933, 934Clorgyline, 454Clotrimazole, 763, 789, 792Clove oil, 888Cloxacillin, 721, 723, 762Clozapine, 171, 175, 436, 437, 440, 441, 442CNS stimulants, 486-88Coagulants, 613-16Coaltar, 890, 891Cobalt, 606Cobra bite, 110, 927Cocaine, 129, 364, 365, 366Codeine, 218, 220, 474, 686Codergocrine. See DihydroergotoxineCoffee, 224Cognition-enhancers, 488-91Cohort study, 76Colchicine, 213, 214Colestipol, 636, 638Colistin, 759Colloidal bismuth subcitrate (CBS), 656, 657Common cold, 138, 168, 918Complex regional pain syndrome (CRPS), 420COMT (Catechol-O-methyl transferase), 125, 126
inhibitors 425, 432Conditioned avoidance response (CAR), 437Congenital adrenal hyperplasia, 290Congestive heart failure (CHF), 517-18
drugs for, 134, 138, 150, 151, 504, 507, 508,518, 519-25
effect on drug kinetics, 69treatment of, 519-25
Conjugation reactions, 24Conscious sedation, 384-85Constipation: treatment of, 676-77Contraceptives, 321-27
emergency (postcoital), 320, 322-23, 324for females, 321-27for males, 327hormonal, 321-27implants, 323injectable, 323, 324once a month (oral), 320
Controlled ovarian hyperstimulation, 241, 242Controlled release tablet/capsule, 35Convulsants, 486Copper, 606Coronary artery disease (CAD)
antiplatelet drugs in, 632fibrinolytic drugs in, 628hypolipidaemic drugs in, 641, 642risk factors, 642
Coronary chemoreflex, 171, 172Coronary steal, 551, 553Corticosteroids, 109, 168, 213, 214, 229-33, 282-
95, 670, 684-85, 778, 856, 872, 883, 885,891, 895-96
Corticotropin. See ACTHCortisol. See HydrocortisoneCo-transmission, 97-98Cotrimazine, 708Cotrimoxazole, 682, 706-08, 712, 761, 762, 763Cough: drugs for, 168, 218-221
specific treatment approaches, 219Counter-irritants, 888-89COX-1/COX-2 (cyclooxygenase) isoenzymes, 78, 182,
192COX-2 (cyclooxygenase-2) inhibitors, 183, 187, 192-
94, 203-06Cresol, 898Cretinism, 251, 256Crohn’s disease:drugs for, 683-85, also See
Inflammatory bowel diseaseCromoglycate sod (Cromolyn sod), 229, 232Cross resistance, 693, 735, 743Cross tolerance, 70Crotamiton, 903Cryptorchidism, 241Cryptosporidiosis: nitazoxanide in, 840, 841Cumulation, 69Curare, 347, also See TubocurarineCutaneous larva migrans, 851, 854Cyanide poisoning, 545Cyanocobalamin, 606-09, 913, also See Vit. B12Cyclandelate, 555CyclicAMP(cAMP), 46, 47, 48, 127, 160, 225, 338,
481, 594, 595Cyclic GMP (cGMP), 160, 303, 541, 542, 678Cyclooxygenase (COX) inhibitor, 183, 192-95, also
See Nonsteroidal antiinflammatory drugsCyclopentolate, 113, 118, 119Cyclophosphamide, 858, 859, 860-61, 875, 883Cycloserine (Cs), 765, 771, 776Cyclosporine, 211, 685, 878-81Cyproheptadine, 164, 165, 168, 174Cyproterone acetate, 302Cytarabine, 858, 859, 864-65Cytochrome P 450(CYP) isoenzymes, 23, 25Cytotoxic drugs, 858-69, 878, 879, 882-83
DDabigatran etexilate, 617, 623Dacarbazine (DTIC), 858, 861Daclizumab, 878, 884Dactinomycin. See Actinomycin DDalfopristin/Quinupristin, 759

982 ESSENTIALS OF MEDICAL PHARMACOLOGY
Dalteparin, 619DAM (Diacetyl monoxime), 111Danaparoid, 617, 620Danazol, 301Dantrolene, 356, 359, 379, 444Dapagliflozin, 270, 278Dapoxetine, 454, 461-62, 464Dapsone (DDS), 780-81, 783, 784, 785, 786, 827Darbepoetin, 611Daunorubicin (Rubidomycin), 858, 867DDS. See DapsoneDDT. See DicophaneDecamethonium (C-10), 347, 348Deep vein thrombosis, 622, 624, 626, 627Deferiprone, 908Deflazacort, 289Dehydroemetine, 840, 843Demeclocycline, 735, 736, 737Demelanizing agents, 892Dementia, 488
drugs for, 489-91Demulcents, 886Denosumab, 346Depot preparations, 8, 9, 35Deprenyl. See SelegilineDepression (of function), 37
mental, 435, 450, 454Dequalinium chloride, 900Dermatophytosis: drugs for, 790, 791, 792, 793, 795,
796, 797Dermojet, 8Desamino oxytocin, 331Desensitization, 50, 52Desferrioxamine, 604, 907-08Desflurane, 375, 377, 380, 381Desloratadine, 164, 166Desmopressin, 596, 597, 616Desogestrel, 316, 318, 321, 322Dexamethasone, 288, 289, 670, 856, also See
Corticosteroidssod. phosphate, 287, 895trimethyl acetate, 895
Dexamphetamine, 134, 135Dexchlorpheniramine, 164Dexfenfluramine, 134, 137Dexmedetomidine, 384Dexrabeprazole, 653Dexrazoxane, 876Dextran, 645Dextromethorphan, 217, 220, 221Dextropropoxyphene, 476DFP. See DyflosDHE (Dihydroergotamine), 140, 175, 176, 178
Diabetesinsipidus, 584, 593, 597, 736, 737mellitus, 258-59, 266-67, 278-80
Diabetic hyperosmolar (nonketotic) coma, 269Diabetic ketoacidosis (Diabetic coma), 267-68Diabetic nephropathy, 505, 507Diacetylmorphine (Heroin), 474Diarrhoea: management of, 677-87
antimicrobials in, 681-82probiotics in, 682-83zinc in, 680
Diastase, 670Diazepam, 357, 358, 383, 385, 386, 398, 401,
404-05, 418-19, 421, 424, 466, also SeeBenzodiazepines
Diazinon (TIK-20), 105Diazoxide, 281, 552, 567Dibucaine, 360, 366, 367, 368Diclofenac sod., 204, 208Dicloxacillin. See CloxacillinDicophane (DDT), 902, 904Dicumarol. See BishydroxycoumarinDicyclomine, 117, 120, 663Didanosine, 798, 807, 814Dienestrol, 306, 308Dietary fibre, 672-73, 676Diethyl carbamazine (DEC), 850, 853Diethylstilbestrol (Stilbestrol), 306, 308, 309Diffusion: of drugs, 11-12Diffusion hypoxia, 376, 378Digestants, 670Digitalis, 512-19, 520, also See Digoxin
toxicity, 516, 531Digoxin, 512-19, 521, 529, 536, 538
antibody, 516Dihydralazine. See HydralazineDihydroartemisinin (DHA), 829, 830, also See
Dihydroatemisinin-piperaquineDihydroatemisinin-piperaquine, 833, 834Dihydroergotamine (DHE), 140, 175, 176, 178Dihydroergotoxine, 140, 141, 175, 176, 489, 491Dihydrofolate reductase (DHFRase) inhibitors, 706,
707, 826-27, 862-63Dihydropyridines (DHPs), 540, 546, 547, 549-50,
552, 562-63, 570, 571Dihydrotachysterol, 342, 343Dihydrotestosterone, 296, 297, 298, 299, 300Diiodohydroxyquin, 837, 841, 844Dilling’s formula, 63Diloxanide furoate, 682, 837, 840, 842, 843Diltiazem, 519, 522, 529, 535, 536, 537, 538, 546,
548-49, 551, 562, 570Dilutional hyponatremia, 585Dimenhydrinate, 164, 165, 168, 663
983INDEX
Dimercaprol (BAL), 905-06Dimercaptosuccinic acid (Succimer), 905, 906Dimethicone, 670, 887Dinoprost (PGF2α), 190Dinoprostone (PGE2), 189Dioctyl sulfo succinate (DOSS). See DocusatesDipeptidyl peptidase-4 (DPP-4) inhibitors, 270, 272,
274-75, 280Diphenhydramine, 164, 165, 168, 177, 663Diphenoxylate, 686Diphenylhydantoin. See PhenytoinDipivefrine, 154Dipyridamole, 553, 629-30, 633Dipyrone. See MetamizolDirect factor Xa inhibitor, 617, 623Direct renin inhibitor (DRI), 500, 508, 562Direct thrombin inhibitors, 617, 620, 623Disinfectants, 897-904Disopyramide, 528, 529, 531, 537, 538Dissociative anaesthesia, 378, 383Disulfiram, 394Diuretic therapy: complications of, 584-86Diuretics, 520-21, 559-61, 570, 571, 579-91Divalproex, 412, 418, 450DMCM, 403, 404DMPA (Depot Medroxy progesterone acetate), 323DMPP (Dimethyl phenyl piperazinium), 100, 102, 121Dobutamine, 127, 129, 134, 524DOCA (Desoxycorticosterone acetate), 287, 289,
290, also See MineralocorticoidDocetaxel, 858, 866Docusates, 672, 673, 677Dofetilide, 529, 534, 535Dog (animal) bite: treatment of, 923Domperidone, 663, 665, 666, also see Prokinetic drugsDonepezil, 105, 108, 489-90Donovanosis. See Granuloma inguinaleDopamine (DA), 124, 134, 137, 425, 524
receptor subtypes, 426theory of schizophrenia, 437-38transporter (DAT), 14, 40, 97
Doripenem, 731Dorzolamide, 155, 587Dose: of drug, 32-34, 61-62
for child, 63-64for elderly, 64loading, 33maintenance, 33
Dose-response relationship, 53-56DOTS (Directly observed treatment short course),
766, 773Dothiepin, 458, also See Tricyclic antidepressantsDoxacurium, 347, 352, 353Doxapram, 486
Doxazosin, 142, 144, 565Doxepin, 458, 465, also See Tricyclic antidepressantsDoxophylline, 222, 227Doxorubicin, 858, 859, 867, 869Doxycycline, 733, 735, 736, 737, 738, 763, 817, 820,
829Doxylamine, 662-63Dronabinol, 670Dronedarone, 529, 534, 538Drotaverine, 118Drug
absorption, 14-17, 929abuse, 88action, 37, 38, 44activation, 22, 23addiction, 88adverse effects, 82-91allergy, 85-87banned, 969-70combinations (fixed dose), 61-62combined effect of, 56-60compendia, 3-4definition, 2dependence, 87-88development, 77-81diffusion, 11-12distribution, 17-21, 931-31dosage, 33, 34, 61-64effect, 44, 47efficacy, 41, 54-55essential: medicines, 4, 957-61excretion, 27-30, 930factors modifying action of, 62-70formularies, 3habituation, 88induced diseases, 91interactions, 15, 20, 23, 30, 57-60, 69, 928-34nomenclature, 2-3non-prescription, 5orphan, 5over-the-counter (OTC), 5penetration into brain, 14, 18-19potency, 54-55prescription, 4-5resistance, 70, 691-93routes of administration, 5-9selectivity, 55-56specificity, 56storage in body, 20, 21targets of action, 37-38withdrawal reactions, 88, 89
DTPA cal. disod., 905, 906Duloxetine, 458, 462, 464Dutasteride, 303, 858

984 ESSENTIALS OF MEDICAL PHARMACOLOGY
Dydrogesterone, 316, 318Dyflos, 105, 108, also See OrganophosphatesDynorphins, 479, 484Dysfunctional uterine bleeding, 312, 319Dysmenorrhoea, 119, 184, 193-94, 201, 312
EEbastine, 164, 167, 528Echinocandins, 787, 790Echothiophate, 105, 108Econazole, 787, 792Ecstasy, 452Ectoparasiticides, 902-04Edema: drugs for, 518, 581, 584, 588Edrophonium, 108, 110EDTA (sod. edetate/Calcium disodium), 905, 906EDRF (Endothelium dependent relaxing factor), 103,
161, 171, also See Nitric oxideEfavirenz (EFV), 798, 808, 809, 813EGF receptor inhibitors, 870Eicosanoids, 181-90Elimination rate constant (K), 31Emergency (postcoital) contraception, 320, 322-23, 324Emesis, 661, 662
drugs for, 120, 168, 387, 446-47, 662-70Emetine HCl, 840, 843Emetics, 661-62Emollients, 886Enalapril, 501, 502-03, 558, 572, also See Angiotensin
converting enzyme (ACE) inhibitorsEndogenous (major) depression: treatment, 463-64Endometriosis, 242, 301, 319Endorphins, 479, 484Enfuvirtide, 798, 811Enkephalins, 479, 480, 484Enoxaparin, 619Entacapone, 425, 432, 434Enteric fever. See Typhoid feverEnteric nervous system (ENS), 93, 647, 648, 661, 665Enterobiasis (pinworm): drugs for, 850, 851, 852Enterohepatic cycling (of drugs), 28Enuresis (bed wetting): drugs for, 119, 139, 464, 597Enzyme
induction, 26-27, 38, 930inhibition, 25-26, 38-39, 930stimulation, 38
Epalrestat, 279Ephedrine, 129, 133, 134, 138, 224Epidural anaesthesia, 367, 370-71Epilepsies, 411
experimental models of, 411treatment, 421-24
Epinephrine. See AdrenalineEpirubicin, 858, 867
Eplerenone, 524, 561, 571, 579, 589Epoetin. See ErythropoietinEpoprostenol (PGI2), 190Epsilon amino caproic acid (EACA), 628Eptifibatide, 629, 631, 632Erectile dysfunction: drugs for, 303-04Ergometrine (Ergonovine), 141, 175, 176, 331-32Ergot alkaloids, 141, 174, 175-76, 178, 331-32Ergotamine, 141, 174, 175, 176, 178, 331Ergotoxine, 140, 141Erlotinib, 858, 870Erythema nodosum leprosum, 782, 786, 877Erythrityl tetranitrate, 540, 543, 544Erythromycin, 682, 752-54, 757, 763, 894
estolate, 753ethylsuccinate, 753stearate, 753
Erythropoietin (EPO), 611Escharotics, 889Escitalopram, 454, 458, 461Eserine. See PhysostigmineEsmolol, 144, 149, 529, 533, 537, 573Esomeprazole, 78, 649, 653, 657, also See Proton
pump inhibitorsEsophagitis. See Gastroesophageal refluxEssential medicines (drugs), 4Estradiol, 306, 308, also See EstrogensEstradiol-TTS (transdermal), 309Estramustine, 858, 866Estriol, 306, 308Estrogens, 306-12, 327, 335, 858, 872, also See
Oral contraceptivesconjugated, 308, 310
Estrone, 306Eszopiclone, 406Etanercept, 212, 883-84, 892Ethacridine, 332Ethambutol (E), 765, 766, 769, 774, 776, 779Ethamsylate, 616Ethanol. See Ethyl alcoholEther, 372, 373, 377, 378Ethical considerations in drug trials, 74, 79Ethinyl estradiol, 306, 308, 321, 322 also See Oral
contraceptivesEthinyl estranol. See LynestrenolEthionamide (Eto), 765, 766, 771, 776, 782Ethosuccimide, 414, 416-17, 421, 423Ethyl alcohol, 388-94, 395, 901 also See Alcohol ethylEthylbiscoumacetate, 621, 622Ethylene glycol poisoning, 396Ethylmorphine, 220, 474Etidronate, 343, 345Etodolac, 192, 204-05Etophylline, 227

985INDEX
Etoposide, 858, 866Etoricoxib, 192, 205, 206, 213, also See COX-2 inhibitorsEucalyptus oil, 888Eutectic lidocaine/prilocaine, 366, 368Everolimus, 882Evidence based medicine, 73-77Excretion: of drugs, 27-30, 930Exemestane, 314, 315Exenatide, 270, 273Exocytosis, 95, 124Expectorants, 218-19, 221Expiry date of pharmaceuticals, 73Extensively drug-resistant (XDR) TB, 776Ezetimibe, 635, 641
FFacilitated diffusion, 13Factors modifying drug action, 62-70False transmitter, 129, 566Famciclovir, 763, 800Famotidine, 169, 650, also See H2 antagonistsFaropenem, 731Febrile convulsions, 419, 421, 423Febuxostat, 213, 217Felodipine, 540, 549, 550Fenamate, 192, 201Fenofibrate, 636, 639, also See Fibric acid
derivativesFenfluramine, 134, 137Fentanyl, 382, 384, 385, 476, 478
transdermal, 476, 478Feracrylum, 887Ferric
ammonium citrate, 602, 603carboxymaltose, 604, 605glycerophosphate, 603hydroxide, 603
Ferritin curtain, 601Ferrous
aminoate, 602, 603fumarate, 602, 603gluconate, 602, 603succinate, 602, 603sucrose, 604, 605sulfate, 602, 603
Fexofenadine, 164, 166Fibric acid derivatives (Fibrates), 635, 636, 638-40, 644Fibrin, 616Fibrinogen, 613, 616Fibrinolytic drugs, 556, 625-28Filariasis: drugs for, 850, 851, 853, 854Filgrastim, 876Filtration: of drugs, 12, 29Finasteride, 302
First dose effect, 142, 564First pass (presystemic) metabolism, 27Fixed dose combinations (FDCs), 61-62Flavoxate, 113, 118Flecanide, 529, 532Fluconazole, 789, 793-94Flucytosine (5-FC), 787, 791Fludarabine, 858, 864Fludrocortisone, 288, 289, 290Flumazenil, 401, 403, 404, 408-09Flunarizine, 180Flunisolide, 231Fluocinolone acetonide, 895Fluocortolone, 895Fluoroquinolones (FQs), 682, 709-14, 761, 762,
765, 7705-Fluorouracil (5-FU), 611, 858, 864, 874, 875Fluoxetine, 458, 461Flupenthixol, 440, 441Fluphenazine, 439, 440
decanoate, 439Flurazepam, 404, 405Flurbiprofen, 200, 201, 208Flutamide, 302, 858Fluticasone propionate, 231Fluvoxamine, 454, 458, 461Folic acid, 609-11, 913, 917
antagonists. See Dihydrofolate reductase inhibitorFolinic acid (THFA, leucovorin), 395, 610, 862,
863, 864, 876, 913Follitropin α/β (rFSH), 241Fomepizole, 395Fomivirsen, 798, 801Fondaparinux, 617, 619-20, 625Formalin (Formaldehyde), 901Formoterol, 133, 224Formularies, 3Fosaprepitant, 670Foscarnet, 801Fosfestrol, 308, 872Fosinopril, 501, 503Fosphenytoin, 415, 421, 424Framycetin, 750Free radicals, 912Frovatriptan, 179Frusemide. See FurosemideFSH (Follicle stimulating hormone), 234, 240, 241Fulvestrant, 313Furazolidone, 844Furosemide, 520-21, 556, 559-60, 574, 579-82,
591, also See High ceiling diureticsFusidic acid (Fusidate sod.), 759Fusion inhibitor, 811

986 ESSENTIALS OF MEDICAL PHARMACOLOGY
GGABAA-benzodiazepine receptor, 358, 402-03, 404, 412
drugs affecting, 404GABAB receptor, 358GABA-transporter (GAT), 40, 414, 421Gabapentin, 419-20, 421Galantamine, 108, 110, 490Gallium nitrate, 345Gall stone dissolving drugs, 671Gamma benzene hexachloride (BHC, Lindane), 903Ganciclovir, 798, 801Ganglionic
blocking agents, 122-23stimulants, 121-22
Ganja, 452Gastric acid secretion: regulation of, 647-48Gastric hurrying agent, 664, 666Gastroesophageal reflux disease (GERD), 658
drugs for, 651, 652, 658-60, 666Gefitinib, 858, 870Gelatin
degraded polymer, 645foam, 616
Gemeprost, 190Gemfibrozil, 636, 639, also See Fibric acid derivativesGemifloxacin, 711, 714General anaesthetics (GA), 372-85
properties of ideal, 377Genetics: and drug action, 65-66Gentamicin, 698, 702, 744, 746, 747-48, 762, also
See Aminoglycoside antibioticsGentian violet, 902Gepirone, 465Germicide, 897Gestodene, 316Giardiasis: drugs for, 838, 839, 843-44Ginkgo biloba (Ginkgolide), 491Glaucoma: drugs for, 108, 151-57, 190, 587Glibenclamide, 270, 272, also See Oral
hypoglycaemic drugsGliclazide, 272Glimepiride, 272Glipizide, 272Glucagon, 260, 280-81Glucocorticoids, 283, 284-87, 288-94, 670, 684-85,
788, 856, 872, 883, 885, 890, 891, 895-96, also See Corticosteroids
antagonist, 295, 319, 320Glucuronide conjugation, 24Glutaraldehyde, 901Glyburide. See GlibenclamideGlycerol (Glycerine), 156, 591, 886Glyceryl trinitrate (GTN), 522, 540-43, 544, 573,
also See Nitrates
Glycopeptide antibiotics, 757-58Glycoprotein (GP) IIb/IIIa antagonists, 629, 631,
632Glycopyrrolate, 110, 117, 386Glycylcycline antibiotic, 733, 738-39Glycyrrhiza, 886GnRH agonists, 242-43, 302, 872GnRH antagonists, 243Goiter, 251, 252Goitrin, 252Goitrogens, 252Gold, 212Gonadotropins (Gns), 234, 240-41Gonadotropin releasing hormone (GnRH,
Gonadorelin), 235, 242Gonorrhoea: drugs for, 711, 720, 722, 728, 730, 738
755, 763Good clinical practice (GCP), 79Goserelin, 242Gossypol, 327Gout: drugs for, 213-17, 291
acute, 213-14chronic, 213, 215-17
G-6-PD deficiency: and drugs 66, 828G-proteins, 45, 46G-protein coupled receptor (GPCR), 44-48Granisetron, 175, 669Granuloma inguinale (Donovanosis), 737, 755, 763Grave’s disease, 254, 255, 256, 257Gray baby syndrome, 64, 741Griseofulvin, 787, 790-91Growth hormone (GH), 236-37Guaiaphenesin, 218, 221Guanethidine, 129, 568Guinea worm: drugs for, 839, 850Gum acacia, 886Gum tragacanth, 886
HHAART (Highly active antiretroviral therapy), 778,
811-14H1 antagonists, 160, 163-68H2 antagonists, 160, 169, 387, 649-51, 659H3 antagonists, 160, 169Habituation, 88Haematinics, 599-611Haemostatics: local, 616Haemophilia, 597, 616Halcinonide, 895Half life (t½), 31, 32Hallucinogens, 451-53Halofantrine, 817, 831Haloperidol, 436, 440, 441, 446, 664Halothane, 372, 377, 379

987INDEX
Hamycin, 790Harmine, 451Heart block. 537, See A-V blockHeavy metal antagonists (Chelating agents), 905-08Hemicholinium (HC3), 99, 100Heparin, 617-20, 624, 625
antagonist, 620low molecular weight, 619
Hepatic coma: drugs for, 676, 750Hepatitis B virus (HBV): drugs for, 798, 803-04, 808Hepatitis C virus: drugs for, 798, 804-05Hereditary angioneurotic edema, 300, 301Heroin, 474-75Herpes simplex: drugs for, 798-801
genital, 763, 799, 800Herpes zoster : drugs for, 800Hetastarch, 645Hexachlorophene, 897, 898-99Hexamethonium, 100, 102, 122Hexamine., 760, See MethenamineHexyl resorcinol, 898High-ceiling diuretics, 518, 520-21, 559-60, 579-82,
584-86Histamine, 158, 159-63
receptors, 159, 160releasers, 163
Hit and run drugs, 34, 455HIV infection: drugs for (Antiretrovirus drugs),
805-15prophylaxis of, 814-15treatment guidelines, 811-14
HMG-CoA reductase inhibitors (Statins), 635, 636-38,642, 643, 644
Hofmann elimination, 25, 353Homatropine, 118, 119Hook worm: drugs for, 849, 850, 851, 852Hormone: definition, 234
sites and mechanisms of action, 235Hormone replacement therapy (HRT), 309-11Human diploid cell vaccine (HDCV) 920, 923Human insulin, 259, 264Human teratogenic drugs, 89Hydatid disease: drugs for, 850, 851Hydralazine, 520, 522, 559, 566-67, 573Hydrochlorothiazide, 558, 559-60, 579, 583, 584,
also See Thiazide diureticsHydrocortisone, 87, 233, 256, 282, 283, 287, 288,
289, 290, also See Corticosteroidsacetate, 287, 288butyrate, 895
Hydroflumethiazide, 579, 588Hydrogen peroxide, 898, 899Hydrolysis: of drugs, 24Hydroquinone, 892
Hydroxocobalamin, 605, 606, 608, also See Vit B12Hydroxychloroquine, 210, 211Hydroxyethyl theophylline, 222, 227Hydroxyprogesterone caproate, 316, 3188-Hydroxyquinolines, 837, 8415-Hydroxytryptamine (5-HT), 170-73
receptor subtypes, 170-71, 1725-HT antagonists, 174-76, 180, 668-69Hydroxyurea, 858, 868, 874Hydroxyzine, 164, 165, 467Hyoscine, 113, 115, 116, 120, 386, 663
butyl bromide, 116Hypercalcaemia, 340, 344, 345, 582Hyperglycaemics, 280-81Hyperkinetic children. See Attention deficit
hyperkinetic disorderHyperparathyroidism, 338, 340Hypersensitivity (allergic) reactions, 86-87, 138, 162,
167, 291to penicillin, 719-20
Hypertension: drugs for, 143, 149, 503-04, 507,551, 558-68, 582, 584, 589
treatment of, 568-72Hypertensive emergencies/urgencies, 572-74Hyperthyroidism, 253-54, 255-56, also See
ThyrotoxicosisHypertrophic obstructive cardiomyopathy, 151, 551Hypervitaminosis A, 910Hypervitaminosis D, 335, 342Hypnotics, 397-409Hypoglycaemia, 199, 265, 271, 281Hypolipidaemic drugs, 634-44Hypoparathyroidism, 338, 339, 343Hypothalamic hormones/factors, 235, 237, 242, 244Hypothyroidism, 251
IIbandronate, 343Ibuprofen, 199, 200, 208, 209Ibutilide, 529, 535Icatibant, 511Idiosyncrasy, 85, 197, 472, 826Idoxuridine, 798Ifosphamide, 858, 860IL-1 antagonist, 210, 212Imatinib, 858, 869Imidapril, 503Imidazole antifungals, 787, 791-93, 890Imidazoline receptors, 565Imipenem, 731Imipramine, 454, 455, 458, also See Tricyclic
antidepressantsImmune globulins (IGs), 926-27
anti-D, 885, 926

988 ESSENTIALS OF MEDICAL PHARMACOLOGY
hepatitis B, 926, 927normal human, 926, 927rabies (HRIG), 926, 927tetanus, 926
Immunization schedule for infants and children, 925Immunosuppressant drugs, 878-85
in inflammatory bowel disease, 685, 881, 882, 884in organ transplantation, 885in rheumatoid arthritis, 210, 882, 883, 884
Impeded androgens, 301Implants: drug releasing, 36Inamrinone, 524-25Indapamide, 561, 579, 583, 584Indinavir (IDV), 798, 809, 810, 814, 815Indomethacin, 192, 202, 213, 598Infantile spasms, 411, 424Infertility: drugs for, 238, 241, 312, 313, 319Inflammatory bowel disease (IBD): drugs for, 683-
85, 881, 882, 884Infliximab, 212, 685, 884Influenza virus : drugs for, 798, 801-03INH. See Isoniazid, 766-67Inhaled asthma medication, 231Inhaled steroids, 230-31, 232Inhalation of drugs, 8, 375, 376Inhibin, 240, 296Inhibition of drug metabolism, 25-26Inodilator, 525Insomnia: drugs for, 407-08, 409Insulin, 259-70
analogues, 263, 264-65aspart, 263, 265assay, 259basal-bolus regimen, 267delivery devices, 269-70detemir, 263, 265glargine, 263, 265glulisine, 263, 265human, 259, 263, 264lispro, 263, 265preparations, 263-65reactions to, 265-66receptor, 261, 262resistance, 258, 269split-mixed regimen, 267
Insulin like growth factors (IGFs), 234, 237Integrase inhibitor, 798, 811Interaction: among drugs, 928-34, also See Drug
interactionsbefore administration, 934clinically important, 931-33pharmacodynamic, 930, 933, 934pharmacokinetic, 929-30
Interferon α, 798, 801-02
Intolerance, 85Intraarterial injection, 5Intradermal (i.d.) injection, 9, 923Intramuscular injection (i.m.), 9
absorption from, 15-16Intravenous anaesthetics, 381-85Intravenous injection (i.v.), 9Intravenous regional anaesthesia, 371Intrinsic activity, 41, 42Inverse agonists, 40, 42, 144, 403, 404Iodide. sod./pot., 218, 252, 254-55Iodine, 251, 252, 254-55, 898, 899
radioactive (131I), 252, 255-56Iodochlorohydroxyquin., 837, 841, See QuiniodochlorIodophores, 898, 899Iodoquinol., 841, See DiiodohydroxyquinIon channels : as target of drug action, 38, 39-40Ion trapping, 12IP3 (Inositol trisphosphate), 44, 46, 48, 49IP4 (Inositol tetrakisphosphate), 47Ipecacuanha (Ipecac), 661Ipratropium bromide, 113, 116, 119, 222, 227, 233Irbesartan, 506, 507Irinotecan, 66, 858, 866, 867Iron, 599-606
absorption, 600-07choline citrate, 603calcium complex, 602, 603dextran, 604dietary sources, 600hydroxy polymaltose, 602, 603poisoning, 606, 907-08sorbitol-citric acid, 604-05sucrose, 605
Irritable bowel syndrome (IBS), 673, 675, 681Irritants, 888Irritation, 37Ischaemic preconditioning, 552Isoflurane, 375, 377, 380Isoniazid (INH; H), 765, 766-67, 773, 774, 775, 777Isoprenaline, 127, 129, 131, 133, 138, 537Isopropamide, 113, 117Isopropanol, 898, 901Isosorbide, 591Isosorbide dinitrate, 540, 543-44Isosorbide mononitrate, 540, 543, 544Isotretinoin, 89, 894-95, 911Isoxsuprine, 134, 136, 139, 333Ispaghula, 37, 672, 673Ispapirone, 465Itopride, 663, 667Itraconazole (ITR), 787, 789, 794-95Ivabradine, 540, 554

989INDEX
Ivermectin, 850, 853-54, 902, 904
JJAK-STAT kinase binding receptors, 50, 236, 611, 804Jarisch-Herxheimer reaction, 720
KKala-azar. See Leishmaniasis, 844-47Kallidin, 158, 509-11Kallikreins, 509, 510Kanamycin (Km), 743, 744, 749, 765, 770, 776Keratolytics, 889-90Ketamine, 378, 382, 383-84Ketanserin, 174-75Ketoconazole (KTZ), 26, 787, 792-93, 845, 890Ketoprofen, 192, 200, 201Ketorolac, 192, 202Ketotifen, 222, 229Kidney disease and drugs, 68-69Kinetics of drug elimination, 30-34Kinins: plasma, 158, 509-11
receptors, 510Kinin antagonists, 511
LLabetalol, 144, 148, 151, 564, 573Labour: induction/augmentation, 189, 330-31Labour: suppression, 333Lacidipine, 540, 550Lacosamide, 421Lactulose, 672, 676, 677Lamivudine, 798, 803, 807-08, 811, 813, 815Lamotrigine, 412, 419, 421, 451Lanreotide, 238Lansoprazole, 649, 653, 657, also See Proton pump
inhibitorsLaropiprant, 640L-Asparaginase, 858, 868-69, 873Latanoprost, 154, 155, 190Laxatives, 672-77L-Dopa., 425, See Levodopa,Lead poisoning, 906Leflunomide, 210, 212Leishmaniasis: drugs for, 750, 789, 842, 844-48
dermal, 847, 848Lepirudin, 617, 620Lepra reaction, 786Leprosy: drugs for, 780-86
alternative regimens, 786multidrug therapy (MDT), 783, 784-85
Leptin, 139Leptospirosis: drugs for, 720, 738, 754Lercanidipine, 540, 550
Letrozole, 314-15, 872Leucovorin., 610, See Folinic acidLeukotrienes (LTs), 181, 182, 187-88, 189
antagonists, 189, 222, 228-29, 232Leuprolide, 243Levamisole, 850, 852Levarterenol. , 133, See NoradrenalineLevetiracetam, 412, 420, 421Levobunolol, 148, 154Levobupivacaine, 367Levocetirizine, 164, 167Levodopa, 425, 426-30, 433-34Levofloxacin, 709, 713, 765, 771, 776Levonorgestrel, 316, 318, 322LH (Luteinizing hormone), 234, 240, 241, also See
GonadotropinsLidocaine, 27, 360, 361, 364, 366, 368, 369, 370,
516, 530-31, also See Local anaestheticsLigand, 39, 41, 44, 49, 905Lignocaine. , 360, See LidocaineLinagliptin, 275Lincomycin, 757Lincosamide antibiotics, 756-57Lindane, 902, 903Linezolid, 758Liothyronine, 250, See TriiodothyronineLiposomal amphotericin B, 788, 845, 846Liposomes, 36, 788Liquid paraffin, 672, 673-74, 677Liquorice, 218, 886Liragutide, 270, 274Lisinopril, 500, 501, 503, 558, also See
Angiotensin converting enzyme inhibitorsLithium, 435, 447-50, 596
alternatives to, 450-51Liver disease and drugs, 67-68, 695Loading dose: of drug, 33Lobeline, 121Local anaesthetics (LAs), 360-71
with adrenaline, 363, 365, 369Lomefloxacin, 709, 714Lomustine (CCNU), 858, 859, 861Loperamide, 686-87Lopinavir (LPV), 798, 809, 811, 814Loratadine, 164, 165, 166Lorazepam, 383, 398, 419, 424, 466Losartan, 498, 506, 558, 561, also See
Angiotensin antagonistsLovastatin, 636, 637, also See StatinsLoxapine, 436, 440, 441Lubiprostone, 675Lugol’s solution, 255Lumefantrine, 818, 819, 832-33, also See
Artemether-lumefantrine

990 ESSENTIALS OF MEDICAL PHARMACOLOGY
Lutropin (rLH), 241Lymphogranuloma venereum, 737, 755, 763Lypressin, 593, 596Lynestrenol, 316, 318Lysergic acid amide, 451Lysergic acid diethylamide (LSD), 451
MMAC (Mycobacterium avium complex): drugs for, 779Macrolide antibiotics, 752-56Mafenide, 704, 705Magaldrate, 655Magnesium
hydroxide, 649, 655, 675stearate, 886sulfate, 37, 333, 675trisilicate, 649, 655
Maintenance dose of drug, 33-34Malaria
drugs for, 816-35prophylaxis of, 818-19radical cure of, 820-21treatment of severe and complicated, 820, 821,
826, 831treatment of uncomplicated, 819, 820, 833
Malathion, 105, also See OrganophosphatesMale contraceptive, 327Malignant hyperthermia, 355, 356, 379Malignant neuroleptic syndrome, 444Mania, 435, 446, 447-51Manic depressive illness (MDI). See Bipolar disorderMannitol, 156, 579, 590-91Maraviroc, 798, 811Marijuana, 452Masking of infection, 694Mast cell stabilizers, 222, 229Maturation factors, 606-11MDMA. , 452, See EcstasyMDR1 (Multidrug resistance1) gene, 14, 875Mebendazole, 849-50Mecamylamine, 123Mechanism of drug action, 37-53Mechlorethamine (Mustine HCl), 858, 860Meclozine (Meclizine), 164, 662, 663Medroxyprogesterone acetate (MPA), 316, 318, 319, 323Mefloquine, 816, 818, 819, 824-25, also See
Artesunate-mefloquineMegaloblastic anaemia, 606, 608, 609, 610Megestrol acetate, 316Meglitinide analogue, 270, 272, 273Melanizing agents, 890-91Melatonin, 409Meloxicam, 192, 204
Melphalan, 858, 860Memantine, 489, 490Menadione, 613, 615, 616
sodium bisulfite, 613, 615Méniére’s disease, 163, 168, 554Menopausal hormone therapy (MHT). See Hormone
replacement therapyMenotropins, 241Menthol, 888Mepacrine, 825Meperidine. See PethidineMephenamic acid, 192, 201Mephenesin, 357Mephentermine, 129, 133, 136Mercaptopurine (6-MP), 216, 858, 863, 874, 882Meropenem, 731Mesalazine (5-ASA, Mesalamine), 684
enema, 684Mescaline, 452Mesna, 860, 876Mesterolone, 296, 299Mestranol, 306, 308Metaanalysis, 75Metabolism., 22-27, See BiotransformationMetabolism: presystemic (first pass), 27Metamizol, 192, 203Metformin, 270, 275-76, 278, 279, 280, also See
BiguanidesMethacholine, 101, 102, 104Methadone, 474, 476Methamphetamine, 134, 135Methandienone, 300Methanol., 394-96, See Alcohol methylMethenamine, 760, 762Methicillin, 718, 721Methicillin resistant Staphylococcus aureus (MRSA),
718, 721drugs for, 757, 758, 759
Methimazole, 252, 253Methocarbamol, 357Methohexitone, 378, 382, 398Methotrexate (Mtx), 210-11, 230, 611, 685, 858,
862-63, 874, 882Methoxamine, 133, 136Methoxsalen, 890Methyl alcohol, 394-96Methyl cellulose, 672, 673, 886Methyl cobalamin, 607, 608, 913Methyldopa, 559, 566Methylergometrine, 331, 332Methyl naltrexone, 484Methylphenidate, 486, 487Methyl polysiloxane, 670, 887Methyl prednisolone, 288-89

991INDEX
Methyl salicylate, 889Methyl testosterone, 296Methyl xanthines, 222, 224-27Methysergide, 174Metoclopramide, 177, 387, 659, 663, 664-66Metolazone, 520, 579, 583, 584Metoprolol, 144, 148-49, 150, 523, 540, 558Metronidazole, 657, 658, 682, 702, 837-39, 842,
843, 844Metyrapone, 295Mezlocillin, 724Mianserin, 454, 458, 462Micafungin, 790Miconazole, 787, 792Microsomal enzymes, 25
induction, 26-27Microtubule damaging agents, 865-66Midazolam, 378, 383, 405Mifepristone, 295, 319-20, 323Miglitol, 270, 277Migraine:drugs for, 150, 173, 176-80, 418, 465, 488Milk-alkali syndrome, 655Milk ejection reflex, 330Milk: excretion of drugs in, 28-29, 965Milk of magnesia, 655, 675Milrinone, 519, 525Miltefosine, 845, 846-47Mineralocorticoid, 283-84, 293Minimal alveolar concentration (MAC), 372, 377Minimal brain dysfunction. See Attention deficit
disorderMinimum bactericidal concentration (MBC), 696 Minimum inhibitory concentration (MIC), 696Minocycline, 734, 735, 737, 780, 782-83, 786Minoxidil, 552, 567Miotic, 108, 152, 153, 155, 156Mirtazapine, 454, 458, 462Misoprostol, 190, 320, 332, 654Mitomycin C, 858, 868Mitoxantrone, 858, 867-68Mivacurium, 347, 352, 354Mizolastine, 164, 167Moclobemide, 129, 454, 455Modafinil, 486, 487, 488Molgramostim, 876Mometasone, 895Monoamine oxidase (MAO), 19, 124, 125, 126,
170, 428, 454non selective inhibitors (MAOI), 128, 456selective MAO-A inhibitor, 129, 174, 454, 455selective MAO-B inhibitor, 129, 425, 431-32, 454subtypes of, 431, 454
Monobactams, 730Monobenzone, 892
Monoclonal antibodies, 871-72, 884Montelukast, 189, 222, 228, 229Mood stabilizer, 436, 447-51Morning sickness, 117, 168, 447, 663, 664Morphine, 386, 469-74, 477-78, 479, 556
dependence, 473epidural/intrathecal, 477poisoning, 472-73
Mosapride, 663, 667, also See Prokinetic drugsMotion sickness, 120, 168, 663, 664Moxifloxacin, 709, 711, 714, 770, 780, 782, 786MPTP, 425MRP (Multidrug resistance associated protein), 14m-TOR inhibitors, 878, 882Mucokinetics. , 218, See ExpectorantsMucolytics, 218, 219Mupirocin, 759Muromonab CD3, 878, 884Muscarine, 100, 102, 104Muscarinic
actions, 103receptor, 100-02
Muscimol, 404Muscle relaxants, 347-59
centrally acting, 356-59Mushroom poisoning, 104Mustard seeds, 888Mutagenicity of drugs, 79, 90Mustine. , 858, 860, See MechlorethamineMyasthenia gravis, 109-10Mycobacterium avium complex (MAC) infection, 779Mycophenolate mofetil (MMF), 878, 883, 885Mydriatics, 113, 118, 119, 138Myocardial infarction (MI): drugs for, 150, 199,
477, 504-05, 507, 544, 556-57, 624-25,627, 631, 632
Myxoedema, 251, also see HypothyroidismMyxoedema coma, 251
NNabilone, 663, 670Nabumetone, 192, 203N-acetyl cysteine, 207Nadifloxacin, 894Nadroparin, 619Nafarelin, 242, 858Nalidixic acid, 66, 695, 708, 709, 760, 761Nalmefene, 480, 484Nalorphine, 479, 480Naloxone, 479, 480, 483Naltrexone, 393, 479, 480, 483-84Nandrolone, 300Naphazoline, 134, 136Naproxen, 192, 200, 201, 208, 213

992 ESSENTIALS OF MEDICAL PHARMACOLOGY
Naratriptan, 179Narcoanalysis, 382Narcolepsy, 139Narcotine. , 220, See NoscapineNasal decongestants, 134, 136-37, 138Nasal route of administration, 8, 242, 340, 597Nateglinide, 270, 272, 273Natural progesterone, 316, 318Nebivolol, 144, 147, 149, 150, 523Needlestick injury: prophylaxis after, 814-15Nefopam, 192, 207Nelfinavir (NFV), 798, 809, 810, 814Neomycin, 743, 750Neostigmine, 105, 107, 108, 109, 350, 354Nerve block anaesthesia, 368-69Nesiritide, 525Netilmicin, 743, 749-50Neuroadaptation, 88Neurocysticercosis: drugs for, 292, 850, 851, 855-56Neurohumoral transmission, 93-98Neurokinin NK1 receptor antagonists, 663, 669-70Neuroleptic drugs, 437, also See Antipsychotic drugsNeuromuscular blocking agents, 347-56Neuroses, 435New formula WHO-ORS, 679, 680Nevirapine (NVP), 798, 808, 809Niacin (Nicotinic acid, vit B3), 640, 913, 914Niclosamide, 850, 854Nicorandil, 522, 540, 552-53Nicotinamide. See Niacin, 913, 914Nicotine, 100, 121-22
chewing gum, 122transdermal, 122
Nicotinic acid (vit B3), 635, 636, 640, 913, 914Nicotinic actions, 103Nicotinic receptors, 102, 109, 348, 351Nicotinyl xanthinate, 555Nicoumalone. , 617, 621, 622, See AcenocoumarolNifedipine, 333, 522, 535, 546, 547, 548, 549,
558, 573Nilotinib, 858, 870Nimesulide, 192, 203-04, 208Nimodipine, 540, 550Nitazoxanide, 837, 840-41, 844, 850Nitrates, 522, 540-45Nitrate dependence/tolerance, 542Nitrazepam, 398, 405Nitrendipine, 547, 549, 558Nitric oxide (NO), 94, 97, 103, 161, 303, 541,
567-68, also See EDRFNitrofurantoin, 760, 761, 762, 764Nitrofurazone, 902Nitrogen mustards, 858, 860Nitroglycerine., 542, See Glyceryl trinitrate (GTN)
Nitroprusside sod., 522, 559, 567-68, 572, 573Nitrous oxide (N2O), 372, 373, 376, 377, 378, 385Nocebo, 67Nociceptin/Orphanin FQ (N/OFQ), 485Nomegestrol acetate, 316Nonadrenergic-noncholinergic (NANC) transmission,
97, 303, 665Non-benzodiazepine hypnotics, 398, 406-08Noncompetitive antagonism, 58, 59Nonmicrosomal enzymes, 25Nonnucleoside reverse transcriptase inhibitors
(NNRTIs), 798, 808-09, 813, 814Nonprescription drugs, 4-5Nonreceptor mediated action, 53Nonsedating antihistamines, 166, See
Antihistamines: second generationNonsteroidal antiinflammatory drugs (NSAIDs), 177,
192-209, 210, 213and PG synthesis inhibition, 192-95choice of, 208-09in gout, 213interactions with, 199shared toxicities, 193topical, 208
Nootropic drug, 490Noradrenaline (NA)
actions, 129-32as transmitter, 93, 94, 95, 96, 97, 124-129preparations and use, 133, 138
Noradrenergic and specific serotonergic antidepressant(NaSSA), 463
Norepinephrine. See Noradrenaline, 133Norepinephrine transporter (NET), 14, 40, 96, 97,
125, 128, 456Norethisterone, 316, See NorethindroneNorethindrone, 316, 318, 322
enanthate (NEE), 323Norfloxacin, 709, 711, 713, 761, 764Norgestimate, 316, 321Norgestrel, 316, 322Noscapine, 218, 220, 469Nortriptyline, 454, 458Nucleoside reverse transcriptase inhibitors (NRTIs),
798, 806-08, 813Nystatin, 787, 789-90
OOAT (organic anion transporter), 29, 40, 579, 583OATP (organic anion transporting polypeptide), 14,
28, 30, 215Obesity: drugs for, 139Obsessive compulsive disorder (OCD), 436, 460,
461, 462, 464, 465, 467

993INDEX
OCT (organic cation transporter), 14, 29, 30, 125Octreotide, 238, 686Ofloxacin, 709, 711, 712, 713, 763, 765, 770, 776,
780, 782, 786Oil of wintergreen. , 889, See Methyl salicylateOlanzapine, 436, 440, 442, 446Olestra, 139Olive oil, 886Olmesartan, 507Olsalazine, 684Omalizumab, 222, 231Omeprazole, 387, 649, 651-53, 657, 658, also See
Proton pump inhibitorsOndansetron, 171, 175, 387, 663, 668, 876On-off effect, 429, 431, 434Opioid
agonist-antagonists, 480-82analgesics, 469-78antagonists (pure), 483-84antidiarrhoeals, 687antitussives, 218, 220peptides, 484-85receptors, 478-80
Opium, 469Oral
absorption, of drugs, 7, 15anticoagulants, 615, 617, 620-23, 624, 625contraceptives (OCs), 321-23, 324-27direct thrombin inhibitor, 617, 623hypoglycaemic drugs, 270-79, 280iron preparations, 601-03rehydration salt/solution (ORS), 679-80route of administration, 6
Organ transplantation: immunosuppressants in, 885Organophosphates, 105, 106, 107, 108
poisoning, 111Orlistat, 139Ormeloxifene, 327Ornidazole, 837, 839Orphan drugs, 5Orphan receptors, 43Orphenadrine, 426, 433Oseltamivir, 798, 802Osmotic diuretics, 579, 590-91Osmotic (saline) purgatives, 672, 675-76Osteoarthritis:
analgesic-antiinflammatory drugs in, 199, 204,206, 207, 208, 209
corticosteroids in, 291Osteomalacia, 341, 342, 414Osteoporosis
anabolic steroids in, 301bisphosphonates in, 343-45calcitonin in, 340
calcium in, 337hormone replacement therapy in, 310raloxifene in, 314vit D in, 343
Over-the-counter drugs (OTC), 5Oxaliplatin, 858, 862Oxazepam, 398, 466Oxazolidinone antimicrobial, 758Oxcarbazepine, 412, 416Oxethazaine, 360, 367, 368Oxiconazole, 787, 792Oxidation (of drugs), 22-23Oximes, 111Oxotremorine, 100Oxpentifylline, 555, See PentoxiphyllineOxybenzone, 893Oxybutynin, 113, 117, 118Oxymetazoline, 134, 136Oxymetholone, 300Oxyphedrine, 554Oxyphenbutazone, 192, 203Oxyphenonium, 113, 117, 654Oxytetracycline, 733, 735, 736Oxytocics, 329-32Oxytocin, 329-31
antagonist, 333Oxytocin challenge test, 331
PPABA (Para amino benzoic acid), 893Paclitaxel, 858, 865-66, 874PAF antagonists, 191, 491Paget’s disease, 340, 344, 345Palonosetron, 663, 6692-PAM, 111, See PralidoximePamidronate, 343, 345Pancreatin, 670Pancuronium, 347, 352, 353Pantoprazole, 387, 649, 653, 657, also See
Proton pump inhibitorsPantothenic acid, 913, 916Papain, 670Papaverine, 144, 304, 469Para aminosalicylic acid (PAS), 765, 771Paracetamol, 192, 206-07
poisoning, 206-07Paraffin: soft/hard, 886
liquid, 673-74, 677Paraldehyde, 398Parasympathetic system, 93, 94Parasympathomimetic drugs, 102-05, See
Cholinergic drugsParathyroid hormone (PTH), 337-39

994 ESSENTIALS OF MEDICAL PHARMACOLOGY
Parecoxib, 192, 205, 206Parenteral routes, 8-9, 15Parkinsonism, 425, 433, 444
drugs for, 120, 168, 239, 425-34Parnaparin, 619Paromomycin, 743, 750, 842, 843, 845, 847Paroxetine, 454, 458, 461Paroxysmal supraventricular tachycardia (PSVT), 519,
527, 529, 535, 536, 538Partial agonist, 41, 42, 467, 479, 480, 565Patient controlled analgesia (PCA), 478Pediculosis: drugs for, 902-04Pefloxacin, 709, 711, 713Peginterferon, 804-05Pegvisomant, 238Pellet implantation, 8-9Pemetrexed, 858, 863Pemoline, 488Penfluridol, 436, 441Penicillamine, 212, 907Penicillinase, 718, 721Penicillins, 716-24
acid resistant, 721benzathine, 719, 720, 763benzyl (G), 716, 717-20extended spectrum, 721, 722-24penicillinase resistant, 721phenoxymethyl (V), 721procaine, 719semisynthetic, 720-24
Pentaerythritol tetranitrate, 543, 544Pentavalent vaccine, 920, 925Pentazocine, 479, 480-82Pentobarbitone, 398Pentolinium, 122Pentoxiphylline, 555Pentylene tetrazole (PTZ), 411, 486Pepsin, 670Peptic ulcer: drugs for, 117, 119, 647-58
treatment of, 651, 652, 654, 656, 657-58Perchlorate sod/pot., 252Perinatal HIV prophylaxis, 815Perindopril, 501, 503, 558Peripheral decarboxylase inhibitors, 425, 429-30,
433-34Peripheral vascular diseases (PVDs), 138, 144, 190,
555, 633Permethrin, 902-03Pernicious anaemia, 608, 610Pethidine, 386, 474, 475-76, 478P-glycoprotein, (P-gp), 13, 14, 15, 19, 28, 508,
517, 768, 875, 930Pharmaceutics, 2Pharmacodynamics, 1, 37-60
Pharmacogenetics, 65-66Pharmacogenomics, 65Pharmacokinetics, 1-2, 10-36Pharmacology: definition, 1Pharmacopoeias, 3Pharmacotherapeutics, 2Pharmacovigilance, 82-83Pharmacy: definition, 2Phase ‘0’ studies, 80Phenacetin, 206Phenazopyridine, 761Phencyclidine, 452Phenformin, 275Phenindione, 617, 621, 622Pheniramine, 164, 165Phenobarbitone, 398, 400, 412-13, also See BarbituratesPhenol, 889, 898Phenolphthalein, 672, 674Phenoxybenzamine, 140, 141, 144, 565Phentolamine, 140, 141-42, 143, 144, 304, 455,
565, 573Phenylbutazone, 192, 203Phenylephrine, 127, 129, 133, 134, 135-36, 138Phenyl propanolamine (PPA), 134, 137Phenytoin, 412, 413-15, 421, 422, 423, 424Pheochromocytoma, 143, 150, 151, 573Pholcodeine, 220, 474Phosphodiesterase-3 (PDE-3) inhibitors, 524-25, 555Phosphodiesterase-5 (PDE-5) inhibitors, 303-04Phospholipase C-IP3-DAG pathway, 46-48, 102,
160, 171, 593, 647Photochemotherapy (PUVA), 892Photosensitivity, 87Phylloquinone, 613, 913, See Vit. K1Physical dependence, 88Physostigmine, 105, 107, 108, 110Phytonadione (vit K1), 613Picrotoxin, 404, 486Pilocarpine, 102, 104, 108, 121, 154, 155, 156Pimozide, 436, 440, 441Pindolol, 144, 147, 148Pinocytosis, 14Pioglitazone, 270, 272, 276-77, 279, 280Pipecuronium, 347, 352, 353Pipenzolate, 113, 117Piperacillin, 721, 724Piperaquine, 823, 834, also See Arterolane-piperaquinePiperazine, 850, 852PIPE therapy, 144, 304Piracetam, 489, 490Pirenzepine, 101, 115, 117, 654Piribedil, 489, 491Piroxicam, 192, 201-02, 208, 213Pitavastatin, 636, 637

995INDEX
pKa, 11Placebo, 67Placental hormones, 235Placental transfer of drugs, 19, 89Plague: drugs for, 700, 738, 748Plasma concentration monitoring, 34Plasma expanders, 644-66Plasma half life (t½), 31-32Plasma kinins, 158, 509-11Plasma protein binding of drugs, 19-21Plateau principle, 33Platelet activating factor (PAF), 158, 190-91
antagonists, 191Pneumocystis jiroveci pneumonia: drugs for, 700, 707,
708, 756, 828Podophyllum resin, 889Poisoning, 84-85Polyene antibiotics, 787-90Polygeline, 645Polymyxin B, 759Polypeptide antibiotics, 759-60Polyvinyl polymer, 887Polyvinyl pyrrolidone (PVP), 163Posaconazole, 789, 795Post antibiotic effect (PAE), 697, 744Postexposure prophylaxis (PEP)
of HIV, 807, 814-15of rabies, 923
Postmarketing surveillance 77, 80-81, 83Post-partum haemorrhage (PPH), 189, 194, 331, 332Post-traumatic stress disorder (PTSD), 461, 464, 468Potassium
channel openers, 540, 552-53, 567chloride, 268, 395iodide, 218, 255permanganate, 899sparing diuretics, 561, 579, 587-90
Potentiation, 57Povidone iodine, 899Pralidoxime (2-PAM), 111Pramipexole, 425, 430-31Pramlintide, 270, 278Prasugrel, 629, 631, 632Pravastatin, 635, 637, also See StatinsPraziquantel, 850, 855, 856Prazosin, 127, 140, 142, 143, 559, 564-65Preanaesthetic medication, 117, 118-19, 168, 385-87Preclinical studies, 78-79Prednicarbate, 895Prednisolone, 230, 288, 289, 684, 872, also See
CorticosteroidsPregabalin, 419, 420Pregnancy: and drugs, 64-65, 89-90, 962-64
category of drugs, 90termination by drugs, 189-90, 320, 332
Premature ejaculation, 461-62, 464Premature labour, 319, 333Premenstrual dysphoric disorder (tension), 319, 462Prenoxdiazine, 218, 220Prescription drugs, 4-5Presystemic (first pass) metabolism, 27Prilocaine, 360, 361, 366Primaquine, 66, 816, 818, 820, 828Primidone, 412, 413, 421Prinzmetal’s angina, 539, See Variant anginaProbenecid, 30, 213, 215, 586, 718, 722, 763Probiotics in diarrhoea, 682-83Procainamide, 528, 529-30, 538Procaine, 360, 361, 364, 366Procarbazine, 858, 861, 873Prochlorperazine, 168, 662, 664Procyclidine, 113, 426, 433Prodrug, 22, 23Progesterone, 234, 316-19, 332-33
natural, 316Progestins, 316-19, 858, 873, also See Oral
contraceptivesProguanil (Chloroguanide), 816, 818, 819, 826Prokinetic drugs, 659-60, 663, 664-68Prolactin, 234, 238Prolonging drug action, 34-36Promethazine, 164, 168, 220, 386, 433, 662, 663
theoclate, 663Propafenone, 528, 529, 532, 538Propantheline, 113, 117, 654Propionic acid derivatives, 192, 199-201, 209Propiphenazone, 192, 203Propofol, 378, 382-83, 385Propoxur, 105Propranolol, 127
in akathisia, 444in angina pectoris, 150, 545in anxiety, 151, 467in cardiac arrhythmias, 150, 516, 532-33, 538in essential tremor, 151in hypertension, 149-50, 563, 572in hypertrophic obstructive cardiomyopathy, 151in migraine, 150, 179-80in myocardial infarction, 150, 556in pheochromocytoma, 150in thyrotoxicosis, 150, 256pharmacology of, 144-47, 148
Propylene glycol, 886, 889Propyl thiouracil, 252, 253, 254, 256Prorenin, 496-97(Pro) renin receptor (PRR), 496-97Prostacycline (PGI2), 181, 182, 183-87, 188, 190Prostaglandins (PGs), 158, 181-87, 188, 189-90,
304, 332

996 ESSENTIALS OF MEDICAL PHARMACOLOGY
analogues, 154-55, 190, 320, 654synthesis inhibitors, 183, 192-95, 203, 205-06,
629, also See Nonsteroidalantiinflammatory drugs
Prostanoid receptors, 188Protamine sulfate, 620, 624Protease inhibitors (PIs) 798, 809-11, 813, 814, 815Proteasome inhibitor, 858, 871Protectives, 886Prothionamide, 766, 771Proton pump inhibitors (PPIs), 387, 649, 651-53, 657-
58, 659Prucalopride, 675Prulifloxacin, 709, 711, 714Pseudocholinesterase (BuChE), 99, 101, 104
deficiency/atypical, 65, 350, 353Pseudoephedrine, 134, 136-37, 138Pseudomembranous enterocolitis, 682, 694, 737, 755,
756, 757, 838-39Psilocybin, 451Psoralen, 890-91, 892Psoriasis: drugs for, 891-92Psychological dependence, 88Psychopharmacological agents (Psychotropic drugs),
435-68Psychoses, 435, 445-46Psychostimulants, 486, 487-88Psychotogens, 451-53, See HallucinogensPsychotomimetics, 451-53, See HallucinogensPsyllium, 673Pulmonary arterial hypertension: drug for, 304Purgatives, 672-77
abuse, 677bulk forming, 672, 673mechanism of action, 672osmotic/saline, 675stimulant, 674-75
Purified chick embryo cell vaccine (PCEV), 922Purified vero cell rabies vaccine (PVRV), 923Purine antagonists, 858, 863-64, 882PUVA (Psoralen-Ultraviolet A), 892Pyrantel pamoate, 850, 852Pyrazinamide (Z), 765, 768-69, 774, 776, 777Pyrazolone derivatives, 192, 203Pyridostigmine, 105, 108, 109Pyridoxine (vit B6), 429, 606, 767, 771, 776, 913,
915-16, 917Pyrimethamine, 816, 818, 819, 826-27Pyrimethamine-sulfonamide combination, 820, 827-28,
832, 833Pyrimidine antagonists, 858, 864-65Pyritinol (Pyrithioxine), 490Pyronaridine, 817, 835
QQuaternary ammonium antiseptics, 898, 900Quetiapine, 436, 440, 442, 446, 451Quinapril, 503Quinidine, 528, 529Quinine, 356, 816, 818, 820, 821, 825-26, 831Quiniodochlor, 797, 841, 843, 844Quinolones, 708-14Quinupristin/Dalfopristin, 759
RRabeprazole, 649, 653, 657, also See Proton pump
inhibitorsRacecadotril, 685Raloxifene, 312, 314Reltegravir, 798, 811Ramelteon, 409Ramipril, 501, 503, also See Angiotensin converting
enzyme inhibitorsRamosetron, 663, 669Randomization, 74Ranitidine, 160, 649, 650, also See H2 antagonistsRanolazine, 540, 554Rapacuronium, 347Rasagiline, 425, 432Rasburicase, 217Rational use of medicines, 70-73Rauwolfia alkaloid, 568, See ReserpineRaynaud’s phenomenon, 144, 173, 190, 551, 555,
also See Peripheral vascular diseaseReboxetine, 454, 460Receptors, 38, 40-53
desensitization, 52, 53functions of, 53G-protein coupled (GPCRs), 44-49ion channel, 45, 49nature of, 43occupation theory, 41-42presynaptic (prejunctional), 125regulating gene expression, 50, 51regulation, 52-53silent, 44spare, 42subtypes, 43-44transducer mechanisms, 44-52transmembrane enzyme-linked, 49-50transmembrane JAK-STAT binding, 50tyrosine kinases (RTKs), 49, 261, 262two-state model, 42
Rectal administration, 6, 7Redistribution, 18, 381, 400, 404, 405Red man syndrome, 757Reduction, 23

997INDEX
Reflux esophagitis, 658, See Gastroesophageal refluxRefractory asthma, 233, See Status asthmaticusRehydration, 679-80Renal excretion of drugs, 29-30, 35Renin: Angiotensin system (RAS), 495-97, 521
drugs inhibiting, 500-08, 521-22Repaglinide, 270, 272, 273Renzapride, 171Reserpine, 128, 129, 435, 568Resistance: to AMAs, 691-93
prevention of, 693Resorcinol, 889Respiratory stimulants (Analeptics), 486Restless legs syndrome, 431Reteplase, 626, 627Retinoic acid, 894, 911Retinoid receptors, 911Retroviral protease inhibitors (PIs), 809-11. See
Protease inhibitorsReversal reaction: in leprosy, 786Reversible inhibitors of MAO-A (RIMAs), 454, 455Reviparin, 619Reye’s syndrome, 197Rheumatic fever, 198, 291, 700, 720, 721Rheumatoid arthritis, 210
corticosteroids in, 213, 291disease modifying antirheumatic drugs in, 210-13immunosuppressants in, 210-11, 881, 882, 883, 884nonsteroidal antiinflammatory durgs in, 198, 200,
201, 203, 204, 205, 209Ribavirin, 798, 804Riboflavin (vit B2), 606, 913, 914Rickets, 342, 343Rickettsial infections, 738, 741Rideal-Walker coefficient, 898Rifabutin, 765, 771-72, 779Ritonavir (RTV), 798, 809, 810, 814Rifaximin, 681-82Rifampin (Rifampicin, R), 765, 767-68, 772, 774,
775, 777, 778, 782, 784, 785Rimantadine, 798, 802Risedronate, 343, 345Risk-benefit ratio, 56Risperidone, 175, 436, 440, 441, 446Ritodrine, 134, 333Ritonavir, 798, 809, 810, 814Rituximab, 872Rivaroxaban, 617, 623Rivastigmine, 108, 110, 489Rizatriptan, 179Rocuronium, 347, 352, 354Rofecoxib, 205Roflumilast, 226Ropinirole, 425, 430, 431
Ropivacaine, 360, 367Rosuvastatin, 635, 636, 637, also See StatinsRound worm (Ascariasis): drugs for, 850, 851, 852Routes of administration, 5-9Roxatidine, 649, 650, also see H2 antagonistsRoxithromycin, 754Rubefacients, 888Rubidomycin, 858, 867, See DaunorubicinRupatadine, 164, 167Rutin, 613, 616Ryanodine receptor (RyR) calcium channel, 66, 356,
379, 514
SSABE (Subacute bacterial endocarditis), 720, 722, 748Salbutamol, 133, 136, 218, 222, 223, 233Salicylates, 195-99Salicylazosulfapyridine, 683. See SulfasalazineSalicylic acid, 797, 889, 890Saline purgatives, 675. See Osmotic purgativesSalmeterol, 133, 222, 223Saquinavir (SQV), 798, 809, 810, 814Satranidazole, 837, 839-40Saxagliptin, 270, 275Scabies: drugs for, 854, 902, 903Schizophrenia, 435
drugs for, 436, 440, also See Antipsychotic drugstreatment of, 445-46
Sclerosing agents, 616Scopolamine, 113, See HyoscineSecnidazole, 837, 839, 843Secondary effects, 84Second gas effect, 376, 378Sedative, 397Selective estrogen receptor down regulators (SERDs),
313, 872Selective estrogen receptor modulators (SERMs),
312, 313-15, 872Selective 5-HT1D/1B agonists, 178-79Selective serotonin reuptake inhibitors (SSRIs), 14,
40, 174, 454, 458, 460-62, 467, 668Selegiline, 425, 431-32, 433Selenium sulfide, 890Senna, 672, 675, 677Sequential trial, 75Serotonergic receptors, 170-71, 172Serotonin, 170, See 5-HydroxytryptamineSerotonin and noradrenaline reuptake inhibitor
(SNRI), 454, 458, 462, 467, 468Serotonin transporter (SERT), 14, 40, 170Sertraline, 454, 458, 461Sevoflurane, 377, 381Sexually transmitted diseases: treatment of, 763, 764Shelf-life (of drugs), 73

998 ESSENTIALS OF MEDICAL PHARMACOLOGY
Shift work disorder (SWD), 487Shock: drugs for, 87, 134, 137-38, 144, 645
septic: corticosteroids in, 292SIADH (syndrome of inappropriate secretion of ADH),
598Sialistic implants, 9Sibutramine, 137Side effects, 72, 84Sildenafil, 303-04Silver nitrate, 889, 901Silver sulfadiazine, 706, 898, 901Simethicone, 887, See DimethiconeSimvastatin, 635, 636, 637, also See StatinsSingle enantiomer drugs, 78Sirolimus, 878, 880, 882, 885Sisomicin, 743, 744, 749Sitagliptin, 270, 272, 274-75Skeletal muscle relaxants, 347-59SLC (solute carrier), transporter, 13, 14Sleep, 397, 398Slow acting antirheumatoid drugs (SAARDs), 210Smoking cessation: aid to, 122, 463SMON (subacute myelo-optic neuropathy), 836, 841SNP (single neucleotide polymorphism), 66Sodium
alginate, 659benzoate, 676bicarbonate, 268-69, 395, 556, 654citrate, 218, 617, 654, 680cromoglycate, 222, 229, 232edetate (EDTA), 617, 905, 906hypochlorite solution, 900nitrite, 545nitroprusside, 522, 559, 567-68, 572, 573oxalate, 617phenyl acetate, 676phosphate, 675picosulfate, 674pot. tartrate, 675stibogluconate (SSG), 845, 848sulfate, 675tetradecyl sulfate, 616thiosulfate, 797valproate (Valproic acid), 412, 417-18, 421,
422, 423, 424, 450Somatomedins, 237Somatostatin, 235, 237, 281Somatropin, 237Sotalol, 144, 148, 529, 533, 537, 538Sources of drugs, 77Sparfloxacin, 528, 709, 714Spectinomycin, 758-59Spermaceti, 886SPF (sun protection factor), 893
Spinal anaesthesia, 369-70Spirits, 388Spiramycin, 756Spironolactone, 520, 523-24, 558, 561, 579, 587-
89, 591SRS-A, 182, See LeucotrienesStanozolol, 300Starch, 887Statins (HMG-CoA reductase inhibitors), 635, 636-
38, 642, 643Status asthmaticus, 230, 233Status epilepticus, 413, 415, 421, 424Stavudine, 798, 807, 813, 814Stimulation, 37Stokes-Adams syndrome, 138Streptokinase (Stk), 626Streptomycin (S), 743, 744, 748, 765, 769-70, 774,
775, 777Streptozocin, 281Stroke (cerebrovascular disease), 625, 627-28, 633Strongyloidosis: drugs for, 850, 851, 853, 854Strontium ranelate, 346Strychnine, 486Styptics, 616Subcutaneous injection (s.c.), 8, 15-16
absorption from, 15Sublingual administration, 6Succimer, 905, 906Succinyl choline (SCh), 347, 348, 349, 350, 351,
352, 353, 355, 517Sucralfate, 649, 656, 887Sugamadex, 355Sulbactam, 724, 725, 728Sulfacetamide sod, 704, 705Sulfadiazine, 704, 705Sulfadoxine, 705, 816, 827, 832, 833Sulfamethoxazole, 704, 705, 706, also see
CotrimoxazoleSulfamethopyrazine, 704, 705, 816, 827Sulfanilamide, 704Sulfasalazine, 210, 211, 683-84, 706Sulfinpyrazone, 213, 215Sulfonamides, 704-06, 716, 818, also See
CotrimoxazoleSulfonamide-pyrimethamine (S/P), 820, 827-28, 832, 833Sulfone syndrome, 781Sulfonylureas (SUs), 258, 270-72, 273, 278, 279, 280Sulfur, 890, 903-04Sultamicillin tosylate, 725Sumatriptan, 171, 174, 178-79Sunitinib, 858, 871Sunscreens, 893Superactive Gn-RH agonists, 242-43, 301, 302, 319Superinfection (Suprainfection), 693-94

999INDEX
Supersensitivity, 52Surface anaesthesia, 367, 368Surface area and drug dose, 63Surgical site infection (SSI): prophylaxis of, 701-02Suxamethonium, 347, See SuccinylcholineSympathetic nervous system, 92, 93, 94Sympathomimetics, 129-39, 222-24, 537
directly acting, 129indirectly acting, 129
Synergism, 57among antimicrobials, 698, 699
Syphilis: drugs for, 720, 738, 754, 763
TTachyphylaxis, 70Tacrine, 105, 108, 489Tacrolimus, 878, 880, 881, 885Tadalafil, 303, 304Tafenoquine, 816, 821, 829Takadiastase, 670Talc, 886Tamoxifen citrate, 312, 313, 315, 872Tamsulosin, 140, 142, 144Tannic acid/Tannins, 887Tape worm: drugs for, 850, 854, 855Tardive dyskinesia, 444-45Targeted drug delivery, 36Targeted drugs, 858, 869-72Target level strategy, 33, 61Taxanes, 865-66Tazarotene, 891, 894Tazobactam, 725, 728Tea, 224Teicoplanin, 758Telmisartan, 507Temazepam, 398, 405Temozolamide, 858, 861Tenecteplase, 626, 627Tenofovir, 798, 803, 808, 813, 814Tenoxicam, 192, 202Teratogenecity, 89-90Terazosin, 140, 142, 144, 565Terbinafine, 787, 795Terbutaline, 133, 223Terfenadine, 166Teriparatide, 339Terizidone, 766, 771Terlipressin, 593, 596, 597Testosterone, 296-300, 303
undecanoate, 296, 299, 300Tetanus: drugs for, 359, 447, 720, 754
antitoxin, 926immune globulin, 926toxoid, 924-25
Tetany, 337Tetracaine, 360, 361, 364, 366, 368, 369Tetracyclines, 733-38, 762, 763, 817, 818, 829,
841-42, 843, 894Δ9 Tetrahydrocannabinol (Δ9 THC), 452, 670Tetramethyl ammonium (TMA), 121Tetramisole, 852Tetrodotoxin, 94Thalidomide, 89, 90, 786, 877Theobromine, 224Theophylline, 222, 224-27, 232, also See Methyl
xanthinesethanolate of piperazine, 227ethylene diamine. (Aminophylline), 227
Therapeutic drug monitoring (TDM), 34Therapeutic index, 55, 56Therapeutic window, 56, 457Thiabendazole, 851-52Thiacetazone (Tzn), 766, 771Thioamides, 252-54, See Antithyroid drugsThiamine (vit B1), 912, 913Thiazide diuretics, 520, 559-61, 570, 571, 579,
582-86, 591Thiazolidinediones, 258, 270, 272, 276-77, also See
PioglitazoneThiocolchicoside, 357, 358Thiocyanate sod./pot, 2526-Thioguanine (6-TG), 858, 863, 874Thiopentone sod., 18, 378, 381-82, 400Thioridazine, 436, 439, 440, 446Thio-TEPA, 858Threadworm, 850. See StrongyloidosisThreatened abortion, 139, 319, 332-33Thrombin, 616Thrombolytics, 625-28. See Fibrinolytic drugsThromboxane A2 (TXA2), 181-83, 185. See ProstaglandinsThymol, 888Thyroid disease: effect on drugs, 69Thyroid hormones, 245-52Thyroid inhibitors, 252-56Thyroid storm: treatment of, 150, 255, 256, 293Thyrotoxicosis, 252
drugs for, 150, 252-56Thyrotropin, 243. See TSHThyroxine (T4), 245-52Tiagabine, 412, 414, 421Tianeptine, 454, 463TIAs (Transient ischaemic attacks), 489, 555, 625,
631, 633Tibolone, 306, 311Ticlopidine, 630Tigecycline, 733, 738-39TIK-20, 105, also See DiazinonTiludronate, 343

1000 ESSENTIALS OF MEDICAL PHARMACOLOGY
Timolol, 144, 148, 153, 154, 157Tinea infection (dermatophytosis): drugs for, 790-91,
792, 794, 795, 796-97Tinidazole, 657, 658, 763, 837, 839, 842, 843, 844Tiotropium bromide, 113, 117, 227Tirofiban, 629, 631-32Tissue type plasminogen activator (rt-PA, Alteplase),
626, 627Titanium dioxide, 893Tizanidine, 357, 358TNFα inhibitors, 212, 685, 883-84Tobacco, 121, 122
amblyopia, 609Tobramycin, 743, 744, 749Tocolytics, 332, also See Uterine relaxantsTolbutamide, 270, 272Tolcapone, 129, 425, 432Tolerance, 70Tolnaftate, 787, 796Tolterodine, 113, 118Tolu balsum, 218, 221Tolvaptan, 525, 598Topical application of drugs, 5, 16Topical NSAIDs, 208Topical steroids, 895-96
adverse effect, 896Topiramate, 177, 180, 420, 421, 423Topoisomerase-1 inhibitors, 858, 866-67Topotecan, 866, 874Torcetrapib, 641Toremifene, 313Torasemide, 579, 581Torsades de pointes, 166, 528, 529, 530, 533, 667Toxic effects, 84Toxicity tests, 79Toxicology: definition, 2Toxoids, 919, 920, 924-25
diphtheria, 925tetanus (TT), 924-25, 926
TPMT-deficiency, 66, 863Trachoma: drugs for, 738, 755Tramadol, 474, 477Trandolapril, 503Tranexamic acid, 628Tranquillizer, 436Transdermal androgen, 299Transdermal fentanyl, 476, 478Transdermal therapeutic systems (TTS), 6, 8, 35Transduction: drug resistance by, 692Transporters, 12-14, 40Tranylcypromine, 129, 455Traveller’s diarrhoea, 681, 682, 687, 841Trazodone, 454, 458, 462
Trench mouth, 839. See Acute necrotizing ulcerativegingivitis
Tretinoin, 869, 894, 911Triamcinolone, 288, 289
acetonide, 287, 895Triamterene, 579, 589, 590Triazolam, 398, 405Triazole antifungals, 787, 791, 793-95Trichloroacetic acid, 889Trichomoniasis: drugs for, 763, 838, 839, 844Tricyclic antidepressants, 180, 454, 455-60, 463-65Trifluoperazine, 436, 439, 440Trifluperidol, 436, 440, 441Triflupromazine, 436, 439, 440Trifluridine, 798Trigeminal neuralgia, 413, 415, 470Trihexyphenidyl, 113, 426, 433Triiodothyronine (T3), 245, 246, 247, 248, 249-50, 251Trimetazidine, 540, 553-54Trimethaphan camforsulfonate, 123Trimethoprim+ sulfamethoxazole, 706-08.
See CotrimoxazoleTrimipramine, 454, 458, also See Tricyclic
antidepressantsTrioxsalen, 890Tripotassium dicitrato-bismuthate, 656. See Colloidal
bismuth subcitrateTriprolidine, 164, 165, also See H1 antagonistsTriptorelin, 242Tropical eosinophilia: drug for, 853Tropicamide, 113, 118, 119TSH (Thyroid stimulating hormone), 243, 245, 247, 248Tuberculosis, 765
biology of infection, 772chemoprophylaxis of, 777-78corticosteroids in, 292, 778extensively drug resistant (XDR), 776-77in AIDS patients, 778in breast feeding women, 777in pregnancy, 777, 963multidrug resistant (MDR), 765, 773, 775-76short course chemotherapy (SCC), 773-75treatment of, 772-78
Tubocurarine (d-TC), 100, 102, 347, 348, 349-53Tubular reabsorption/secretion of drugs, 29-30Turpentine oil, 888Typhoid fever: drugs for, 708, 711, 712, 722, 728,
741, 756Tyramine, 125, 129Tyrosine-protein kinase inhibitors, 869-70
UUlcerative colitis: drugs for, 683-85Ulcer protectives, 649, 656

1001INDEX
Ulipristal, 320-21, 322-23Undecylenic acid, 796Unstable angina (UA), 540, 546, 551, 556, 625,
631, 632Urea, 889Ureido penicillins, 721, 724Uricosuric drugs, 215-16Urinary antiseptics, 760Urinary pH and excretion of drugs, 29Urinary tract infection: drugs for, 708, 711, 714,
722, 723, 730, 742, 748, 760, 761-62prophylaxis, 764urinary pH and use of AMAs in, 762
Urofollitropin, 241Urokinase, 626Ursodeoxycholic acid (Ursodiol), 671USAN (United States adopted name), 2Uterine
inertia, 330-31relaxants, 332-33stimulants, 329-32
VVaccines, 919-25
bacterial, 920-22BCG, 920, 922, 925cholera:inactivated, 920, 921cholera: oral, 921double antigen (DT-DA), 920, 925haemophilus influenzae type b (Hib), 921, 925hepatitis A, 920, 924hepatitis B, 920, 923, 925influenza virus, 923killed (inactivated), 919, 920live attenuated, 919, 920measles: live attenuated, 920, 924meningococcal A & C, 921MMR (measles, mumps, rubella), 920, 924, 925mumps: live attenuated, 920, 924pentavalent, 920, 925plague, 920, 921polio: inactivated (IPV, Salk), 920, 922polio: oral (OPV, Sabin), 920, 922rabies: carbolized, (Semple/neural tissue vaccine), 922rabies: purified chick embryo cell vaccine
(PCEV), 920, 922rabies: human diploid cell (HDCV), 920, 923rabies: purified vero cell (PVRV), 920, 923rubella, 920, 924TAB, 920, 925triple antigen (DPT), 920, 925typhoid-Ty21a (oral), 920-21typhoid: Vi polysaccharide, 920varicella (live attenuated), 920, 924
viral, 920, 922-24whooping cough (pertussis), 920, 921
Valacyclovir, 763, 800Valethamate, 113, 117Valganciclovir, 798, 801Valproic acid (Sodium valproate), 412, 417-18, 421,
422, 423, 424, 450VAMP regimen, 875Valsartan, 507, 558, 561Vancomycin, 702, 717, 757Vardenafil, 303, 304Varenicline, 122Variant angina, 173, 332, 539-40, 544, 550, 551Vasaka, 218, 221Vasodilators, 522-23, 566-68Vasomotor reversal, 131, 140, 141Vasopressin. See AVP
receptors, 593-94, 595Vecuronium, 347, 352, 353Venereal diseases: treatment of, 763. See Sexually
transmitted diseasesVenlafaxine, 454, 458, 462Verapamil, 535, 536, 537, 538, 540, 546, 547, 548, 570Vertigo: drugs for, 163, 168Vesamicol, 99, 100Vesicular monoamine transporter (VMAT), 14, 40,
125, 128, 134, 135, 170, 568VIAGRA. See SildenafilVigabatrin, 412, 421, 424Vildagliptin, 270, 272, 275Vinblastine, 858, 865, 874Vinca alkaloids, 865Vincristine, 858, 865, 874Vinorelbine, 858, 865VRE (Vancomycin resistant enterococcus), 757, 758, 759VRSA (Vancomycin resistant Staphylococcus aureus),
757, 758, 759Visual cycle: vit A in, 910Vitamins, 909-18
definition, 909fat soluble, 909-12, 913vit A, 909-11, 913, 917vit B complex, 912-16vit B12, 606-09, 913, 917vit C, 916, 917, 918vit D, 340-43, 913, 917vit E, 911-12, 913vit K, 613-16, 913water soluble, 912, 913, 914-18
Voglibose, 270, 277Volatile oils, 888-89Volume of distribution (V), 17-18, 20, 21, 30, 32, 33, 64,
69, 929von Willebrand’s factor (vWF), 596, 597, 616Voriconazole, 787, 789, 794, 795

1002 ESSENTIALS OF MEDICAL PHARMACOLOGY
WWarfarin sod., 617, 620-23, 624, 625Whip worm (Trichuris): drugs for, 850, 851Whitefield’s ointment, 797, 889Whooping cough, 741, 754, 921Wilson’s disease: drug for, 906, 907Wines, 388, 392Withdrawal reactions, 88-89Wool fat, 886WPW (Wolff-Parkinson-White syndrome), 527, 530,
532, 533, 535, 538
XXantinol nicotinate, 555Xenobiotics, 11, 13Xipamide, 579, 583, 584Xylometazoline, 134, 136
YYaba, 452Yohimbine, 127, 140, 143
Young’s formula, 63Yuzpe method, 322
ZZafirlukast, 189, 222, 228-29Zaleplon, 398, 403, 407Zanamivir, 798, 802-03Zidovudine (AZT), 798, 806-07, 813, 814, 815Zileuton, 183, 229Zinc
in diarrhoea, 680oxide, 902pyrithione, 890stearate, 886sulfate, 902
Ziprasidone, 436, 440, 442-43, 446, 528Zoledronate, 343, 345Zollinger-EIlison syndrome, 651, 652-53Zolmitriptan, 179Zolpidem, 398, 403, 406-07Zonisamide, 412, 414, 420, 421, 423Zopiclone, 398, 406Zotepine, 436, 443





















