
Procalcitonin to Predict Severity of Acute Cholangitis ... - MDPI
Upload
independentCategory
view
0download
0
Gut 1993; 34: 242-246
Ulcerative colitis disease activity following treatmentof associated primary sclerosing cholangitis withcyclosporin
W J Sandborn, R H Wiesner, W J Tremaine, N F Larusso
AbstractThirty five adult patients with precirrhoticprimary sclerosing cholangitis were randomlyallocated to treatment for at least one year withlow dose (4.1 mg/kg/day) cyclosporin orplacebo in a double blind trial. Thirty patientshad coexisting ulcerative colitis, includingthree who had previously undergone colectomyand one who discontinued treatment afterthree months. Of the remaining 26 patients, 16received cyclosporin and 10 received placebo.Endoscopy was performed at entry to confirmthe diagnosis of inflammatory bowel disease.The ulcerative colitis disease activity wasprospectively classified annually as remission/mild, moderate, or severe using the Trueloveand Witt's criteria. Before treatment therewere no differences between the cyclosporinand placebo groups in the number of patientswith remission/mild colitis, 14/16 (88%) v 9/10(90%), and moderate colitis, 2/16 (12%) v 1/10(10%). During treatment, a remission/milddisease course was present in 15/16 (94%) v6/10 (60%), p=005 and a moderate diseasecourse in 1/16 (6%) v 4/10 (40%), p=005. It isconcluded that patients treated with cyclo-sporin for primary sclerosing cholangitis whohave coexisting ulcerative colitis have a morebenign course of colitis resulting both fromimprovement of moderately active colitis andfrom fewer flares of remission/mildly activecolitis. These findings suggest that cyclosporinmay be of benefit to the colon in patients withulcerative colitis who are being treated withcyclosporin for primary sclerosing cholangitis.(Gut 1993; 34: 242-246)
Ulcerative colitis and primary sclerosingcholangitis (PSC) are chronic disorders ofunknown cause which are presumed to bechronic immune inflammatory in nature.Primary sclerosing cholangitis occurs in 1-6% ofpatients with ulcerative colitisl-3 and, conversely,
Division ofGastroenterology andInternal Medicine, MayoClinic and MayoFoundation, Rochester,Minnesota, USAW J SandbornR H WiesnerW J TremaineN F LarussoCorrespondence to:Dr R H Wiesner, Mayo Clinic,200 First St SW, Rochester,MN 55905, USA.Accepted for publication3 August 1992
TABLE I Comparison ofpatient characteristics at studyentry*
Cyclosporin PlaceboVariable (n= 16) (n= 10)
Age (years) 36 (9) 45 (10)Men (%) 63 60Duration of PSC (years) 2-1 (4 5) 1-5 (2 2)Duration of colitis (years) 8-4 (8 2) 13-9 (11-4)Pancolitis (%) 94 90Systemic steroids (%) 0 0Steroid enemas (%) 0 10Sulphasalazine (%) 75 90
*Indicates no statistically significant differences betweencyclosporin and placebo.
ulcerative colitis occurs in 56-82% of patientswith primary sclerosing cholangitis.7 It is likelythat immunosuppressive treatment of primarysclerosing cholangitis may have some impact oncoexisting ulcerative colitis, but this has neverbeen studied.
Cyclosporin is a potent immunosuppressiveagent used to prevent allograft rejection in solidorgan transplantation. Cyclosporin is alsoeffective treatment in a number of autoimmunediseases, including uveitis, psoriasis, rheuma-toid arthritis, myasthenia gravis, chronic activehepatitis, and primary biliary cirrhosis.8-'3 Themechanism of action is inhibition of T lympho-cyte synthesis of interleukin 2.'4
Preliminary reports suggest that cyclosporin iseffective treatment for Crohn's disease' -20 andthis has been confirmed in a controlled trial.2'Other studies suggest that cyclosporin is oftherapeutic value in ulcerative colitis,2022-28 butthere have been no controlled trials. The mecha-nism of action of cyclosporin in Crohn's diseaseand ulcerative colitis is not known but maybe related to its effects on intestinal cellularimmunity.29 Cyclosporin has been shown tointerfere with the interleukin 2 pathway ofimmune activation in Crohn's disease.30 Thisstudy evaluates the disease activity of ulcerativecolitis during treatment of coexisting primarysclerosing cholangitis with low dose oral cyclo-sporin or placebo.
Methods
PATIENTSFrom 27 June 1985 to 13 July 1988, 35 patientswith precirrhotic primary sclerosing cholangitiswere randomly allocated to receive low dosecyclosporin (initial dose 5 mg/kg/day) or placeboin a double blind trial. All patients had histo-logical and cholangiographic findings consistentwith primary sclerosing cholangitis, otherinclusion and exclusion criteria have beendescribed previously.'3 Patients were classifiedaccording to the severity of their liver disease.'3The study was approved by the institutionalreview board of the Mayo Clinic and all patientsgave written consent.
Thirty of the 35 patients (80%) had concomi-tant primary sclerosing cholangitis andulcerative colitis; 19 received cyclosporin and11 received placebo. Three of these 30 patients(two in the cyclosporin group and one in theplacebo group) were excluded because they hadpreviously undergone colectomy for refractorycolitis. In addition, one patient receiving cyclo-sporin was excluded because treatment was
242
group.bmj.com on July 12, 2011 - Published by gut.bmj.comDownloaded from
Ulcerative colitis disease activityfollowing treatment ofassociated primary sclerosing cholangitis with cyclosporin
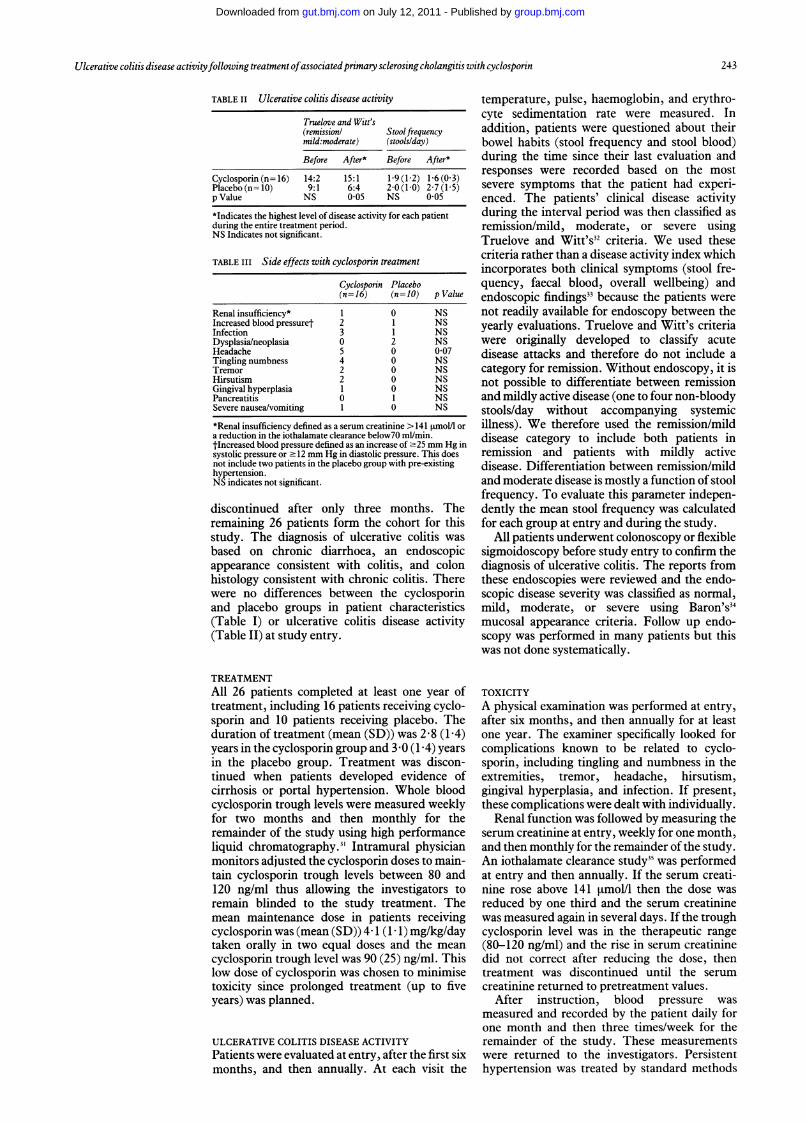
TABLE II Ulcerative colitis disease activity
Truelove and Wilt's(remission! Stool frequencymild:moderate) (stoolslday)
Before After* Before After*
Cyclosporin(n=16) 14:2 15:1 19(12) 1-6(0-3)Placebo (n= 10) 9:1 6:4 2-0 (1-0) 2-7 (1-5)p Value NS 0-05 NS 0-05
*Indicates the highest level of disease activity for each patientduring the entire treatment period.NS Indicates not significant.
TABLE III Side effects with cyclosponin treatment
Cyclosporin Placebo(n-16) (n=10) p Value
Renal insufficiency* 1 0 NSIncreased blood pressuret 2 1 NSInfection 3 1 NSDysplasia/neoplasia 0 2 NSHeadache 5 0 0-07Tingling numbness 4 0 NSTremor 2 0 NSHirsutism 2 0 NSGingival hyperplasia 1 0 NSPancreatitis 0 1 NSSevere nausea/vomiting 1 0 NS
*Renal insufficiency defined as a serum creatinine > 141 smolUl ora reduction in the iothalamate clearance below7O ml/min.tIncreased blood pressure defined as an increase of >25 mm Hg insystolic pressure or -12 mm Hg in diastolic pressure. This doesnot include two patients in the placebo group with pre-existinghypertension.NS indicates not significant.
discontinued after only three months. Theremaining 26 patients form the cohort for thisstudy. The diagnosis of ulcerative colitis wasbased on chronic diarrhoea, an endoscopicappearance consistent with colitis, and colonhistology consistent with chronic colitis. Therewere no differences between the cyclosporinand placebo groups in patient characteristics(Table I) or ulcerative colitis disease activity(Table II) at study entry.
TREATMENTAll 26 patients completed at least one year oftreatment, including 16 patients receiving cyclo-sporin and 10 patients receiving placebo. Theduration of treatment (mean (SD)) was 2-8 (1-4)years in the cyclosporin group and 3 0 (1 4) yearsin the placebo group. Treatment was discon-tinued when patients developed evidence ofcirrhosis or portal hypertension. Whole bloodcyclosporin trough levels were measured weeklyfor two months and then monthly for theremainder of the study using high performanceliquid chromatography.3' Intramural physicianmonitors adjusted the cyclosporin doses to main-tain cyclosporin trough levels between 80 and120 ng/ml thus allowing the investigators toremain blinded to the study treatment. Themean maintenance dose in patients receivingcyclosporin was (mean (SD)) 4- 1 (1 1) mg/kg/daytaken orally in two equal doses and the meancyclosporin trough level was 90 (25) ng/ml. Thislow dose of cyclosporin was chosen to minimisetoxicity since prolonged treatment (up to fiveyears) was planned.
ULCERATIVE COLITIS DISEASE ACTIVITYPatients were evaluated at entry, after the first sixmonths, and then annually. At each visit the
temperature, pulse, haemoglobin, and erythro-cyte sedimentation rate were measured. Inaddition, patients were questioned about theirbowel habits (stool frequency and stool blood)during the time since their last evaluation andresponses were recorded based on the mostsevere symptoms that the patient had experi-enced. The patients' clinical disease activityduring the interval period was then classified asremission/mild, moderate, or severe usingTruelove and Witt's32 criteria. We used thesecriteria rather than a disease activity index whichincorporates both clinical symptoms (stool fre-quency, faecal blood, overall wellbeing) andendoscopic findings33 because the patients werenot readily available for endoscopy between theyearly evaluations. Truelove and Witt's criteriawere originally developed to classify acutedisease attacks and therefore do not include acategory for remission. Without endoscopy, it isnot possible to differentiate between remissionand mildly active disease (one to four non-bloodystools/day without accompanying systemicillness). We therefore used the remission/milddisease category to include both patients inremission and patients with mildly activedisease. Differentiation between remission/mildand moderate disease is mostly a function of stoolfrequency. To evaluate this parameter indepen-dently the mean stool frequency was calculatedfor each group at entry and during the study.
All patients underwent colonoscopy or flexiblesigmoidoscopy before study entry to confirm thediagnosis of ulcerative colitis. The reports fromthese endoscopies were reviewed and the endo-scopic disease severity was classified as normal,mild, moderate, or severe using Baron's34mucosal appearance criteria. Follow up endo-scopy was performed in many patients but thiswas not done systematically.
TOXICITYA physical examination was performed at entry,after six months, and then annually for at leastone year. The examiner specifically looked forcomplications known to be related to cyclo-sporin, including tingling and numbness in theextremities, tremor, headache, hirsutism,gingival hyperplasia, and infection. If present,these complications were dealt with individually.
Renal function was followed by measuring theserum creatinine at entry, weekly for one month,and then monthly for the remainder of the study.An iothalamate clearance study33 was performedat entry and then annually. If the serum creati-nine rose above 141 [imol/I then the dose wasreduced by one third and the serum creatininewas measured again in several days. If the troughcyclosporin level was in the therapeutic range(80-120 ng/ml) and the rise in serum creatininedid not correct after reducing the dose, thentreatment was discontinued until the serumcreatinine returned to pretreatment values.
After instruction, blood pressure wasmeasured and recorded by the patient daily forone month and then three times/week for theremainder of the study. These measurementswere returned to the investigators. Persistenthypertension was treated by standard methods
243
group.bmj.com on July 12, 2011 - Published by gut.bmj.comDownloaded from

Sandborn, Wiesner, Tremaine, Larusso
and if it did not resolve then the dose of the studydrug was reduced.
STATISTICAL ANALYSISParametric (Student's t test) and non-parametric(Fisher's exact test) methods were used whereappropriate to compare the cyclosporin andplacebo groups before and after treatment. Atwo tailed p value below 0 05 was consideredsignificant.
Results
Changes in serum creatininelevels and iothalamateclearance. Solid lines indicatethe cyclosporin group anddashed lines indicate theplacebo group. The verticalbars represent one standarddeviation. The p values shownarefor differences between thegroups. NS indicates notsignificant.
CLINICAL DISEASE ACTIVITYAt entry, remission/mild colitis was present in 14of 16 patients in the cyclosporin group and nineof 10 in the placebo group. Of these patients, 13in the cyclosporin group and six in the placebogroup continued to have remission/mild diseasethroughout the study. Colitis flares of moderateseverity occurred during the study in one patientreceiving cyclosporin (two flares) and in threepatients receiving placebo (one flare/patient).Two of 16 patients in the cyclosporin group
and one of 10 patients in the placebo group hadmoderately active colitis at entry into the study.Both patients receiving cyclosporin had areduction in disease severity from moderate toremission/mild. The patient receiving placebocontinued to have moderately active disease.This patient had a previous left hemi-colectomywith a transverse colon rectal anastomosis for acolonic stricture. We elected to include thispatient in the study since the entire remainingright colon had active ulcerative colitis.
Overall, out of 16 patients in the cyclosporingroup, 15 had a remission/mild disease course
Month
and one had a moderate disease course duringtreatment (Table II). In comparison, out of10 patients in the placebo group, six had aremission/mild disease course and four had amoderate disease course during the study. Thedifferences in disease severity during the studywere paralleled by a higher mean stool frequencyfor the placebo group as compared with thecyclosporin group, 2-7 v 1 6 stools/day (TableII). None of the patients in either group hadsevere colitis at entry or developed a severe flareduring the study. Classification of the diseasecourse (remission/mild, moderate or severe) andcalculation of the mean stool frequency wereboth based on the highest level of disease activityexperienced during the entire study. Patientsreceiving sulphasalazine at study entry (cyclo-sporin group 75%, placebo group 90%) con-tinued to take the drug throughout the study anddid not reduce the dose. All the patients whoexperienced disease flares were taking sulpha-salazine. The sulphasalazine dose was increasedin some of these patients but this increase alwaysoccurred after the flare started when the colitishad already been classified as moderately active.No patients required corticosteroid treatmentfor colitis flares.
ENDOSCOPIC DISEASE ACTIVITYAt entry, quiescent or mildly active colitis wasseen at endoscopy in 15 of 16 patients in thecyclosporin group and nine of 10 in the placebogroup. Follow up endoscopy was performed inmany patients but this was not done systematic-ally. Cyclosporin treated patients had 22 followup endoscopies: 10 at one year; six at two years;four at three years; and two at four years. Placebotreated patients had 12 follow up endoscopies:eight at one year; and four at two years. Theoverall concordance between the clinical andendoscopic level of severity was 93% (cyclo-sporin group 97%, placebo group 86%). Becauseendoscopic follow up was inconsistent, we didnot attempt to make an assessment of endoscopicdisease activity during the treatment period.
TOXICITYSide effects occurred in both the cyclosporin andplacebo groups but were more common inpatients receiving cyclosporin (Table III).Nephrotoxicity (defined in the study protocol asa serum creatinine >141 imol/I or a reduction inthe iothalamate clearance below 70 ml/min)occurred only in the cyclosporin treated group.One patient (6%) had a rise in serum creatinine to203 iimol/l and none of the patients had aniothalamate clearance less than 70 ml/min. Therewas a rise in the mean serum creatinine whichreached statistical significance after two years anda trend towards a decline in the mean iothalamateclearance in cyclosporin treated patients (Fig 1).In most cases, however, the magnitude of thesechanges was not sufficient to qualify as nephro-toxicity.
Hypertension, which was easily controlledwith anti-hypertensive treatment, occurred intwo patients treated with cyclosporin and onepatient treated with placebo. There were no
30
0E
0c
0)C
0)
25
20
15
10
5
0
-5
a)m -EE .'cuE
0'~CoC
CDc0
u-
4
0--
-4
-8
-12
-16
-20
-24
-28
-32Entry
244
group.bmj.com on July 12, 2011 - Published by gut.bmj.comDownloaded from

Ulcerative colitis disease activityfollowing treatment ofassociated primary sclerosing cholangitis with cyclosporin
significant differences in the mean systolic ordiastolic blood pressures at one and two yearswhen compared with entry for either the cyclo-sporin or placebo groups. Infections appeared tooccur more commonly in the cyclosporin group,although the difference was not statisticallysignificant. Recurrent oral and vaginal yeastinfections occurred in two patients receivingcyclosporin and oral thrush occurred in onepatient receiving placebo. All three patientsresponded to temporary withdrawal of the studydrug and topical nystatin treatment. One patientreceiving cyclosporin developed bacterialcholangitis. Cyclosporin treatment was stoppedbut the patient continued to deteriorate and diedfrom sepsis and shock in spite of antibiotictreatment.None of the patients who received cyclosporin
developed dysplasia or tumours. In the placebogroup one patient underwent colectomy afterhigh grade dysplasia of the colon was found atcolonoscopy and another patient developed acholangiocarcinoma, which resulted in death.Other side effects which occurred only in thecyclosporin group included headaches, tinglingand numbness in the extremities, tremor,hirsutism, and gingival hyperplasia. When thesecyclosporin specific side effects occurred, theremay have been a tendency for the study drug tobe disclosed. The number of patients with sideeffects was small, however (Table III), andseveral different investigators evaluatedpatients.36 These factors probably minimisedunblinding. One patient receiving cyclosporinhad severe nausea and vomiting and had todiscontinue the study after one year. Pancreatitisoccurred in one patient receiving placebo.
DiscussionUp to the present all patients treated withcyclosporin for ulcerative colitis have had severe,refractory disease and there are no publishedcontrolled trials. Several case reports have sug-gested that oral cyclosporin is effective in induc-ing clinical and endoscopic remission.2022-24 Twolarger series have shown conflicting results.Lichtiger25 reported that 11 of 15 patients withsevere ulcerative colitis responded to a shortcourse of intravenous (IV) cyclosporin (4 mg/kg!day) followed by oral cyclosporin (6-8 mg/kg!day) for six months, and that nine of the 11responders remained in remission during thefollow up period. In contrast, Bianchi Porro26reported five patients treated with oral cyclo-sporin (8-5 mg/kg/day) and fi've patients treatedwith IV cyclosporin (4 mg/kg/day) followed byoral azathioprine in the responders. All fivepatients receiving oral cyclosporin had a remis-sion but relapse occurred within three months ofdiscontinuing the drug. Three of the five patientstreated with IV cyclosporin had a remission andone of these three had a relapse nine months laterwhile receiving azathioprine. There are two pilotstudies suggesting that cyclosporin enemas areeffective for proctosigmoiditis.2728
Ulcerative colitis associated with primarysclerosing cholangitis is usually quiescent or onlymildly active but a few patients do have moder-ately active disease. Our results show that
patients treated with low dose cyclosporin forprimary sclerosing cholangitis are more likely tohave a disease course characterised by remissionor mild activity than are patients receivingplacebo. These results are the first controlleddata to suggest that cyclosporin may be of clinicalbenefit in patients with ulcerative colitis. Thesefindings are surprising since it is more difficult toshow efficacy when the majority of patients haveremission/mild disease. A clinical trial specific-ally designed to assess the efficacy of cyclosporintreatment for patients with mildly or moderatelyactive ulcerative colitis would be of interest.Such a trial would be unethical, however, giventhe unfavourable risk/benefit ratio of cyclosporintreatment in this setting. In spite of the method-ological problems discussed below, this studydesign is probably the only ethical way to obtainplacebo controlled data on the efficacy of cyclo-sporin in patients with mildly and moderatelyactive ulcerative colitis.The validity of comparing the effects of cyclo-
sporin and placebo on ulcerative colitis inpatients who were not randomly admitted to thestudy or removed from the study on the basis ofulcerative colitis disease activity can be justified asfollows. Firstly, although patients were randomlyadmitted to the study on the basis of severity ofliver disease, patients with ulcerative colitis in theplacebo and cyclosporin treated groups hadsimilar characteristics, including mean age, sexratio, mean duration of colitis, extent of colitis,concomitant therapy, and ulcerative colitisdisease severity (Tables I-II). Secondly, the meanduration of treatment before study terminationwas similar in both groups. This is not surprisingsince the groups were balanced at study entry forseverity of liver disease and cyclosporin was noteffective in altering the natural progression ofprimary sclerosing cholangitis to cirrhosis.6 Ourresults compare the disease activity at entry withthe most severe disease activity experiencedduring the entire treatment period for eachpatient. To confirm that differences in treatmentduration for individual patients did not affect theanalysis, we also compared ulcerative colitisdisease activity in the placebo and cyclosporingroups at one year when all patients were still inthe study. The ultimate clinical course of thecolitis became evident during the first year of thestudy and therewas no difference between the oneyear analysis and the final analysis (Table II) per-formed after a mean follow up of 2 8 years in theplacebo group and 3-0 years in the cyclosporingroup.
Concern about nephrotoxicity has been themajor factor limiting more widespread investi-gational use of cyclosporin in ulcerative colitis.Most patients without renal disease receivingcyclosporin have a 20% or more decline in renalfunction during the first six months of treatmentwith little progression thereafter."7 3X Thesechanges are usually reversible within two weeksof stopping the drug. In the two largest studiesusing cyclosporin for inflammatory boweldisease the incidence of nephrotoxicity was7-10%. 125 In all instances the toxicity was easilyreversed by reducing the cyclosporin dose.Patients receiving cyclosporin in our study had a20% rise in mean serum creatinine and a 14%
245
group.bmj.com on July 12, 2011 - Published by gut.bmj.comDownloaded from

246 Sandborn, Wiesner, Tremaine, Larusso
reduction in mean iothalamate clearance at twoyears. Only one patient (6%) receiving cyclo-sporin met our criteria for nephrotoxicity andthat patient improved after reducing the dose.These findings suggest that low doses of cyclo-sporin can be given for prolonged periods topatients with ulcerative colitis with minimalnephrotoxicity.The incidence of minor infections including
thrush and candida vaginitis was slightly higherin patients receiving cyclosporin but the differ-ence was not statistically significant. Theseinfections cleared up after standard treatmentand temporary discontinuation of the cyclo-sporin. One patient died from cholangitis andsepsis. Since cholangitis is a frequent complica-tion of primary sclerosing cholangitis, it is notclear that cyclosporin contributed to this death.A further concern about treating ulcerative
colitis with cyclosporin is the carcinogenic risk inpatients who already have an increased incidenceof colonic dysplasia and carcinoma. In addition,there is a small risk of developing lymphomawith cyclosporin immunosuppression. Most ofthe reported cases had associated Epstein-Barrviral infection and occurred during treatmentwith high doses of cyclosporin in combinationwith corticosteroids and azathioprine.3839 Ourresults showed no increase in the incidence ofany malignancies in patients receiving cyclo-sporin, although the mean follow up is only 2-8years.
In conclusion, patients treated with cyclo-sporin for primary sclerosing cholangitis whohave coexisting ulcerative colitis have a morebenign course of colitis resulting both fromimprovement of moderately active colitis andfewer flares in patients with remission/mildcolitis. Significant cyclosporin toxicity duringprolonged treatment is minimal and does notappear to be a limiting factor at this dose ofcyclosporin. Further controlled trials are neededto define clearly the role of cyclosporin in thetreatment of ulcerative colitis.
Supported by grants from the Sandoz Corporation and the MayoFoundation.
Presented at the annual meeting of the American College ofGastroenterology, 12-16 October 1991, Boston.
1 Schrump E, Fausa 0, Kolmannskog F, Elgio G, Ritland S,Gjone E. Sclerosing cholangitis in ulcerative colitis. Afollow-up study. ScandJ Gastroenterol 1982; 17: 33-9.
2 Rasmussen HH, Fallingborg J, Mortensen PB, Freund L,Rasmussen SN. Primary sclerosing cholangitis in patientswith ulcerative colitis during a 12-year period. Scand JGastroenterol 1989; 24 (suppl 159): 57.
3 Olsson R, Danielsson A, Jarnerot G, Lindstrom E, Loof L,Rolny P, et al. Prevalence of primary sclerosing cholangitisin patients with ulcerative colitis. Gastroenterology 1991; 100:1319-23.
4 Wiesner RH, LaRusso NF. Clinicopathological features of thesyndrome of primary sclerosing cholangitis. Gastroenterology1980; 79: 200-6.
5 Chapman RWG, Marborgh BA, Rhodes JM, Summerfield JA,Dick R, Scheuer PJ, et al. Primary sclerosing cholangitis: areview of its clinical features, cholangiography, and hepatichistology. Gut 1980; 21: 870-7.
6 Helzberg JH, Peterson JM, Boyer JL. Improved survival withprimary sclerosing cholangitis. A review of clinicopathologicfeatures and a comparison of symptomatic and asympto-matic patients. Gastroenterology 1987; 92: 1869-75.
7 Aadland E, Schrumpf E, Fausa 0, Elgjo K, Heilo A, AakhusT, et al. Primary sclerosing cholangitis: a long-term follow-up study. ScandJr Gastroenterol 1987; 22: 655-64.
8 Nusenblatt RB, Palestine AG, Chan CC. Cyclosporin Atherapy in the treatment of intraocular inflammatory disease
resistant to systemic corticosteroids and cytotoxic agents.AmJ Ophthalmol 1983; 96: 275-82.
9 Ellis CN, Gorsulowsky DC, Hamilton TA, Billings JK, BrownMD, Headington JT, et al. Cyclosporine improves psoriasisin a double-blind study. JAMA 1986; 256: 3110-6.
10 Dougados M, Awada H, Amor B. Cyclosporin in rheumatoidarthritis: a double-blind, placebo-controlled study in 52patients. Ann Rheum Dis 1988; 47: 127-33.
11 Tindall RSA, Rollins JA, Phillips JT, Greenlee RG, Wells L,Belendiuk G. Preliminary results ofa double-blind, random-ized, placebo-controlled trial of cyclosporine in myastheniagravis. NEnglJrMed 1987; 316: 719-24.
12 Hyams JS, Ballow M, Leichtner AM. Cyclosporine treatmentof auto-immune chronic active hepatitis. Gastroenterology1987; 93: 890-3.
13 Wiesner RH, Ludwig J, Lindor KD, Jorgensen RA, BaldusWP, Homberger HA, et al. A controlled trial of cyclosporinein the treatment of primary biliary cirrhosis. N EnglJ3 Med1990; 322: 1419-24.
14 Hess AD, Tutschka PJ, Santos GW. Effect of cyclosporin A onhuman lymphocyte response in vitro. III. CsA inhibits theproduction of T lymphocyte growth factors in secondarymixed lymphocyte responses but does not inhibit theresponse of primed lymphocytes to TCGF. J Immunol 1982;128: 355-9.
15 Allison MC, Pounder RE. Cyclosporin for Crohn's disease.Aliment Pharmacol Therap 1987; 1: 39-43.
16 Peltekian KM, Williams CN, MacDonald AS, Roy PD,Czolpinska E. Open trial of cyclosporine in patients withsevere Crohn's disease refractory to conventional therapy.CanJfGastroenterol 1988; 2: 5-11.
17 Parrot NR, Taylor RMR, Venables CW, Record CO. Treat-ment of Crohn's disease in relapse with cyclosporin A.BrJSurg 1988; 75: 1185-8.
18 Fukushima T, Sugita A, Masuzawa S, Yamazaki Y, TsuchiyaS. Effects of cyclosporin A on active Crohn's disease.GastroenterolJpn 1989; 24: 12-5.
19 Brynskov J, Binder V, Riis P, Lauritsen K, Schaffalitzky DeMuckadell 0, Freund L, et al. Low-dose cyclosporin forCrohn's disease; implications for clinical trials. AlimentPharmnacol Therap 1989; 3: 135-42.
20 Stange EF, Fleig WE, Rehklau E, Ditschuneit H. CyclosporinA treatment in inflammatory bowel disease. Dig Dis Sci1989; 43:1387-92.
21 Brynskov J, Freund L, Rasmussen SN, Lauritsen K,Schaffalitzky De Muckadell 0, Williams N, et al. A placebo-controlled, double-blind, randomized trial of cyclosporinetherapy in active Crohn's disease. N EnglJ7 Med 1989; 321:845-50.
22 Gupta S, Keshavarzian A, Hodgson HJF. Cyclosporin inulcerative colitis. Lancet 1984; ii: 1277-8.
23 Shelly ED, Shelly WB. Cyclosporine therapy for pyodermagangrenosum associated with sclerosing cholangitis andulcerative colitis. J Am Acad Dermatol 1988; 18: 1084-8.
24 Hyams JS, Treem WR. Cyclosporine treatment of fulminantcolitis. J Pediatr Gastroenterol Nutr 1989; 9: 383-7.
25 Lichtiger S, Present DH. Preliminary report: cyclosporin intreatment of severe active ulcerative colitis. Lancet 1990;336: 16-9.
26 Bianchi Porro G, Petrillo M, Ardizzone S. Cyclosporinetreatment for severe active ulcerative colitis. Lancet 1990;336: 439.
27 Brynskov J, Freund L, Thomsen 00, Anderson CB,Rasmussen SN, Binder V. Treatment of refractory ulcera-tive colitis with cyclosporine enemas. Lancet 1989; i: 721-2.
28 Ranzi T, Campanini MC, Velio P, Quarto Di Palo F, BianchiPA. Treatment of chronic proctosigmoiditis with cyclo-sporin enemas. Lancet 1989; ii: 97.
29 MacDermott RP. Cell-mediated immunity in gastrointestinaldisease. Hum Pathol 1986; 17: 219-33.
30 Brynskov J, Tvede N. Plasma interleukin-2 and a soluble/shedinterleukin-2 receptor in serum of patients with Crohn'sdisease. Effect of cyclosporine. Gut 1990; 31: 795-9.
31 Sawchuk AJ, Cartier LL. Liquid chromatographic determina-tion of cyclosporine A in blood and plasma. Clin Chem 1981;27: 1368-71.
32 Truelove SC. Treatment of ulcerative colitis with localhemisuccinate sodium: a report on a controlled therapeutictrial. BMJ' 1958; ii: 1072-7.
33 Schroeder KW, Tremaine WJ, Ilstrup DM. Coated oral5-aminosalicylic acid therapy for mildly to moderately activeulcerative colitis: a randomized study. N EnglJ Med 1987;317: 1625-9.
34 Baron JH, Connell AM, Lennard-Jones JE. Variation betweenobservers in describing mucosal appearances in procto-colitis. BMJ 1964; i: 89-92.
35 Sigman EM, Elwood CM, Knox F. The measurement ofglomerular filtration rate in man with sodium iothalamateF'I (Conray). J7 Nucl Med 1966; 7: 60-8.
36 Wiesner RH, Steiner B, LaRusso NF, Lindor KD, BaldusWP. A controlled clinical trial evaluating cyclosporine in thetreatment of primary sclerosing cholangitis. Hepatology1991; 14: 63A.
37 Tegzess AM, Doorenbos BM, Minderhound JM, DonkerAJM. Prospective serial renal function studies in patientswith nonrenal disease treated with cyclosporine A.Transplant Proc 1988; 20 (suppl 2): 390-3 .
38 Palestine AG, Nussenblatt RB, Chan CC. Side effccts ofsystemic cyclosporine in patients not undergoing trans-plantation. AmJy Med 1984; 77: 652-6.
39 Cockburn I. Assessment of risks of malignancy andIymphomas developing in patients using Sandimmune.Transplant Proc 1987; 19: 1804-7.
group.bmj.com on July 12, 2011 - Published by gut.bmj.comDownloaded from

doi: 10.1136/gut.34.2.242 1993 34: 242-246Gut
W J Sandborn, R H Wiesner, W J Tremaine, et al. cholangitis with cyclosporin.treatment of associated primary sclerosing Ulcerative colitis disease activity following
http://gut.bmj.com/content/34/2/242Updated information and services can be found at:
These include:
serviceEmail alerting
box at the top right corner of the online article.Receive free email alerts when new articles cite this article. Sign up in the
CollectionsTopic
(6644 articles)Pancreas and biliary tract � (952 articles)Ulcerative colitis �
Articles on similar topics can be found in the following collections
Notes
http://group.bmj.com/group/rights-licensing/permissionsTo request permissions go to:
http://journals.bmj.com/cgi/reprintformTo order reprints go to:
http://group.bmj.com/subscribe/To subscribe to BMJ go to:
group.bmj.com on July 12, 2011 - Published by gut.bmj.comDownloaded from
Copyright © 2022 FDOKUMEN
















