Two Thousand Blalock-Taussig Shunts: A Six-Decade Experience
8
DOI: 10.1016/j.athoracsur.2007.06.067 2007;84:2070-2075 Ann Thorac Surg Baumgartner and Duke E. Cameron D. Patel, Akhil K. Seth, Diane E. Alejo, Vincent L. Gott, Luca A. Vricella, William A. Jason A. Williams, Anshuman K. Bansal, Bradford J. Kim, Lois U. Nwakanma, Nishant Two Thousand Blalock-Taussig Shunts: A Six-Decade Experience http://ats.ctsnetjournals.org/cgi/content/full/84/6/2070 located on the World Wide Web at: The online version of this article, along with updated information and services, is Print ISSN: 0003-4975; eISSN: 1552-6259. Southern Thoracic Surgical Association. Copyright © 2007 by The Society of Thoracic Surgeons. is the official journal of The Society of Thoracic Surgeons and the The Annals of Thoracic Surgery by on June 4, 2013 ats.ctsnetjournals.org Downloaded from
Transcript of Two Thousand Blalock-Taussig Shunts: A Six-Decade Experience

DOI: 10.1016/j.athoracsur.2007.06.067 2007;84:2070-2075 Ann Thorac Surg
Baumgartner and Duke E. Cameron D. Patel, Akhil K. Seth, Diane E. Alejo, Vincent L. Gott, Luca A. Vricella, William A.
Jason A. Williams, Anshuman K. Bansal, Bradford J. Kim, Lois U. Nwakanma, Nishant Two Thousand Blalock-Taussig Shunts: A Six-Decade Experience
http://ats.ctsnetjournals.org/cgi/content/full/84/6/2070located on the World Wide Web at:
The online version of this article, along with updated information and services, is
Print ISSN: 0003-4975; eISSN: 1552-6259. Southern Thoracic Surgical Association. Copyright © 2007 by The Society of Thoracic Surgeons.
is the official journal of The Society of Thoracic Surgeons and theThe Annals of Thoracic Surgery
by on June 4, 2013 ats.ctsnetjournals.orgDownloaded from
TAJLVDD
vreo
pbria
pc2(e1F
OpTtnmBmc
thadts
A
PS
APWc
©P
CA
RD
IOV
ASC
ULA
R
wo Thousand Blalock-Taussig Shunts:Six-Decade Experience
ason A. Williams, MD, Anshuman K. Bansal, BS, Bradford J. Kim, BA,ois U. Nwakanma, MD, Nishant D. Patel, BA, Akhil K. Seth, BS, Diane E. Alejo, BA,incent L. Gott, MD, Luca A. Vricella, MD, William A. Baumgartner, MD, anduke E. Cameron, MD
ivision of Cardiac Surgery, The Johns Hopkins Medical Institutions, Baltimore, Maryland
qthtrdpdsndiv
igi
Background. The Blalock-Taussig shunt (BTS) remainsaluable for palliation of congenital heart disease, but itsole has evolved. We reviewed our total institutionalxperience with BTS to examine changes in its use andutcomes.Methods. A retrospective review was performed of all
atients undergoing BTS at our institution from Novem-er 1944 to May 2006. Hospital records and autopsyecords were evaluated to determine patient demograph-cs, diagnoses, operative data, hospital complications,nd long-term outcomes.Results. During the last 62 years, 2,016 BTS were
erformed by 28 surgeons on 1,880 patients from 35ountries. Classic BTS were performed in 75% (1,503 of,016 BTS). Diagnosis was tetralogy of Fallot in 72%1,294 of 1,802), although diagnoses were imprecise in thearly part of the series. Overall operative mortality was4% (227 of 1,574). On follow-up, 32% of tetralogy of
allot patients (411 of 1,294 patients) underwent subse-hci
sEdcpcecd
P
PAwaH2tl
olfe St, Blalock 618, Baltimore, MD 21287; e-mail: [email protected].
2007 by The Society of Thoracic Surgeonsublished by Elsevier Inc
ats.ctsnetjournDownloaded from
uent total correction at our institution, and an addi-ional 116 patients for whom follow-up was availablead total correction of tetralogy of Fallot at other institu-
ions, a combined total correction of tetralogy of Fallotate of 41%. Of patients with complex congenital heartefects, 26% (106 of 404 patients) had subsequent cavo-ulmonary connection or atrial or arterial switch proce-ures. A comparison of the first and second halves of theeries revealed several trends: decreasing mean annualumber of BTS (66/year versus 9/year, respectively),ecreasing operative mortality (16% versus 9%), and
ncreasing proportion of single-ventricle diagnoses (5%ersus 34%).Conclusions. Evolution of the BTS has seen a decrease
n overall use, particularly in tetralogy of Fallot, butreater application to single-ventricle cardiac lesions andmproved operative survival.
(Ann Thorac Surg 2007;84:2070–5)
© 2007 by The Society of Thoracic Surgeonsn November 29, 1944, Dr Alfred Blalock performedthe first successful palliation of a “blue baby” with
ulmonic stenosis. Six months later, Drs Blalock andaussig submitted a report of the first surgical series for
he treatment of cyanotic heart disease involving pulmo-ary stenosis or atresia [1]. This landmark accomplish-ent was made possible by the collaboration of Alfred
lalock, Helen Taussig, and Vivian Thomas, and ulti-ately set the stage for rapid development of the field of
ardiac surgery [2].Since the 1940s, countless patients have benefited from
he shunt procedure. Although the majority of patientsad tetralogy of Fallot (TOF), this operation was quicklydapted to treat patients with a variety of cyanotic heartiseases, including tricuspid atresia, truncus arteriosus,
ransposition of the great vessels, and various forms ofingle ventricle [3–7]. Although operative techniques
ccepted for publication June 21, 2007.
resented at the Forty-third Annual Meeting of The Society of Thoracicurgeons, San Diego, CA, Jan 29–31, 2007.
ddress correspondence to Dr Cameron, Division of Cardiac Surgery,ediatric Cardiac Surgery, The Johns Hopkins Medical Institutions, 600 N
ave evolved during the past six decades, outcomesontinue to be excellent, and many patients are palliatedndefinitely or until definitive repair can be undertaken.
Our institutional experience with Blalock-Taussighunt (BTS) began with the first operation performed onileen Saxon in 1944. However, the indications andiagnoses for patients undergoing this procedure havehanged markedly since then. More than 30 years haveassed since we last reported our results with this pro-edure [6]. We sought to review our total institutionalxperience with BTS to identify changes that have oc-urred in its use and outcomes during the past sixecades.
atients and Methods
atient Selectionfter obtaining institutional review board approval andaiver of consent, retrospective review was performed of
ll patients undergoing the BTS procedure at The Johnsopkins Hospital from November 1944 through May
006. All patients who underwent some form of systemico pulmonary shunting procedure were included, regard-
ess of whether this was a part of a larger procedure or set0003-4975/07/$32.00doi:10.1016/j.athoracsur.2007.06.067
by on June 4, 2013 als.org
ococoDMattetwt
DIo
oac
SSw1ttricwwtsscga
R
PDsas(ehppivpi
DTfaw
TB
V
R
S
D
C
TC
O
123
B
T
1111112
B
2071Ann Thorac Surg WILLIAMS ET AL2007;84:2070–5 TWO THOUSAND BLALOCK-TAUSSIG SHUNTS
CA
RD
IOV
ASC
ULA
R
f procedures. The exceptions were patients undergoingentral shunts, such as Potts or Waterston shunts. The listf patients was generated from a compilation of theardiac surgery database, operative logs from the generalperating room, and personal records and archives ofrs Blalock and Taussig, which are kept in the Division ofedical Archives at our institution. Patients in whom an
nastomosis was found to be technically impossible athe time of thoracotomy or sternotomy before attemptinghe anastomosis were excluded from this study. How-ver, patients were included who expired intraopera-ively during an attempted anastomosis or who under-ent an attempted anastomosis that was found to be
echnically impossible or inadequate.
ata Collection and Patient Variablesnformation on patient demographics, diagnosis, type(s)f procedure(s), hospital complications, and long-term
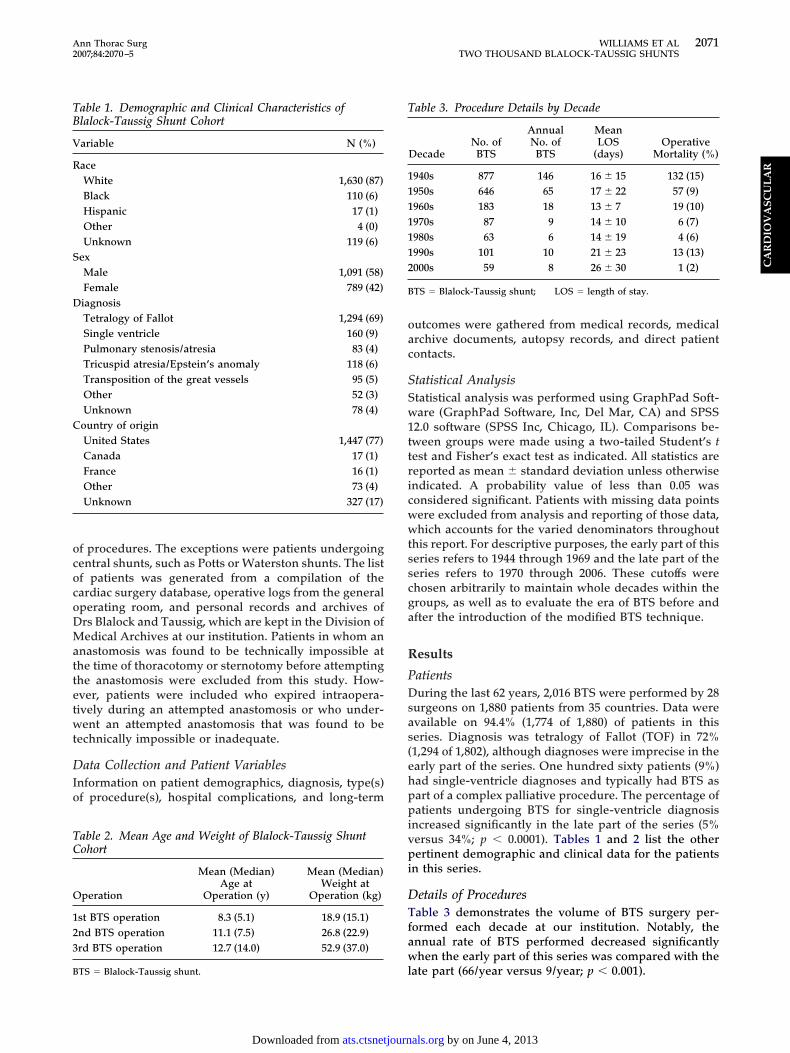
able 1. Demographic and Clinical Characteristics oflalock-Taussig Shunt Cohort
ariable N (%)
aceWhite 1,630 (87)Black 110 (6)Hispanic 17 (1)Other 4 (0)Unknown 119 (6)
exMale 1,091 (58)Female 789 (42)iagnosisTetralogy of Fallot 1,294 (69)Single ventricle 160 (9)Pulmonary stenosis/atresia 83 (4)Tricuspid atresia/Epstein’s anomaly 118 (6)Transposition of the great vessels 95 (5)Other 52 (3)Unknown 78 (4)
ountry of originUnited States 1,447 (77)Canada 17 (1)France 16 (1)Other 73 (4)Unknown 327 (17)
able 2. Mean Age and Weight of Blalock-Taussig Shuntohort
peration
Mean (Median)Age at
Operation (y)
Mean (Median)Weight at
Operation (kg)
st BTS operation 8.3 (5.1) 18.9 (15.1)nd BTS operation 11.1 (7.5) 26.8 (22.9)rd BTS operation 12.7 (14.0) 52.9 (37.0)
lTS � Blalock-Taussig shunt.
ats.ctsnetjournDownloaded from
utcomes were gathered from medical records, medicalrchive documents, autopsy records, and direct patientontacts.
tatistical Analysistatistical analysis was performed using GraphPad Soft-are (GraphPad Software, Inc, Del Mar, CA) and SPSS
2.0 software (SPSS Inc, Chicago, IL). Comparisons be-ween groups were made using a two-tailed Student’s test and Fisher’s exact test as indicated. All statistics areeported as mean � standard deviation unless otherwisendicated. A probability value of less than 0.05 wasonsidered significant. Patients with missing data pointsere excluded from analysis and reporting of those data,hich accounts for the varied denominators throughout
his report. For descriptive purposes, the early part of thiseries refers to 1944 through 1969 and the late part of theeries refers to 1970 through 2006. These cutoffs werehosen arbitrarily to maintain whole decades within theroups, as well as to evaluate the era of BTS before andfter the introduction of the modified BTS technique.
esults
atientsuring the last 62 years, 2,016 BTS were performed by 28
urgeons on 1,880 patients from 35 countries. Data werevailable on 94.4% (1,774 of 1,880) of patients in thiseries. Diagnosis was tetralogy of Fallot (TOF) in 72%1,294 of 1,802), although diagnoses were imprecise in thearly part of the series. One hundred sixty patients (9%)ad single-ventricle diagnoses and typically had BTS asart of a complex palliative procedure. The percentage ofatients undergoing BTS for single-ventricle diagnosis
ncreased significantly in the late part of the series (5%ersus 34%; p � 0.0001). Tables 1 and 2 list the otherertinent demographic and clinical data for the patients
n this series.
etails of Proceduresable 3 demonstrates the volume of BTS surgery per-
ormed each decade at our institution. Notably, thennual rate of BTS performed decreased significantlyhen the early part of this series was compared with the
able 3. Procedure Details by Decade
DecadeNo. of
BTS
AnnualNo. of
BTS
MeanLOS
(days)Operative
Mortality (%)
940s 877 146 16 � 15 132 (15)950s 646 65 17 � 22 57 (9)960s 183 18 13 � 7 19 (10)970s 87 9 14 � 10 6 (7)980s 63 6 14 � 19 4 (6)990s 101 10 21 � 23 13 (13)000s 59 8 26 � 30 1 (2)
TS � Blalock-Taussig shunt; LOS � length of stay.
ate part (66/year versus 9/year; p � 0.001).
by on June 4, 2013 als.org
pdaBetvroa
uIirraupmhuws
EO(Bw(tpr
smPeuo
p
pts2o
LOwtait
(ocmu
3fvh(cslchiudov
C
Ip1tppatt
F(
2072 WILLIAMS ET AL Ann Thorac SurgTWO THOUSAND BLALOCK-TAUSSIG SHUNTS 2007;84:2070–5
CA
RD
IOV
ASC
ULA
R
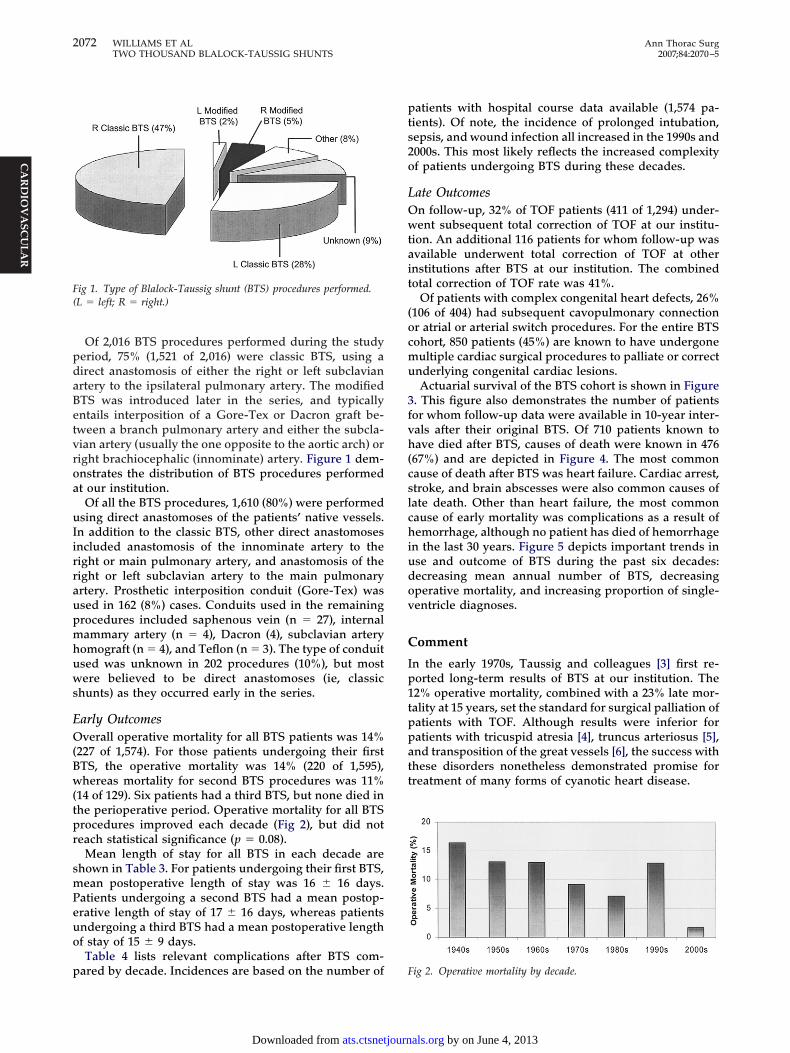
Of 2,016 BTS procedures performed during the studyeriod, 75% (1,521 of 2,016) were classic BTS, using airect anastomosis of either the right or left subclavianrtery to the ipsilateral pulmonary artery. The modifiedTS was introduced later in the series, and typicallyntails interposition of a Gore-Tex or Dacron graft be-ween a branch pulmonary artery and either the subcla-ian artery (usually the one opposite to the aortic arch) oright brachiocephalic (innominate) artery. Figure 1 dem-nstrates the distribution of BTS procedures performedt our institution.Of all the BTS procedures, 1,610 (80%) were performed
sing direct anastomoses of the patients’ native vessels.n addition to the classic BTS, other direct anastomosesncluded anastomosis of the innominate artery to theight or main pulmonary artery, and anastomosis of theight or left subclavian artery to the main pulmonaryrtery. Prosthetic interposition conduit (Gore-Tex) wassed in 162 (8%) cases. Conduits used in the remainingrocedures included saphenous vein (n � 27), internalammary artery (n � 4), Dacron (4), subclavian artery
omograft (n � 4), and Teflon (n � 3). The type of conduitsed was unknown in 202 procedures (10%), but mostere believed to be direct anastomoses (ie, classic
hunts) as they occurred early in the series.
arly Outcomesverall operative mortality for all BTS patients was 14%
227 of 1,574). For those patients undergoing their firstTS, the operative mortality was 14% (220 of 1,595),hereas mortality for second BTS procedures was 11%
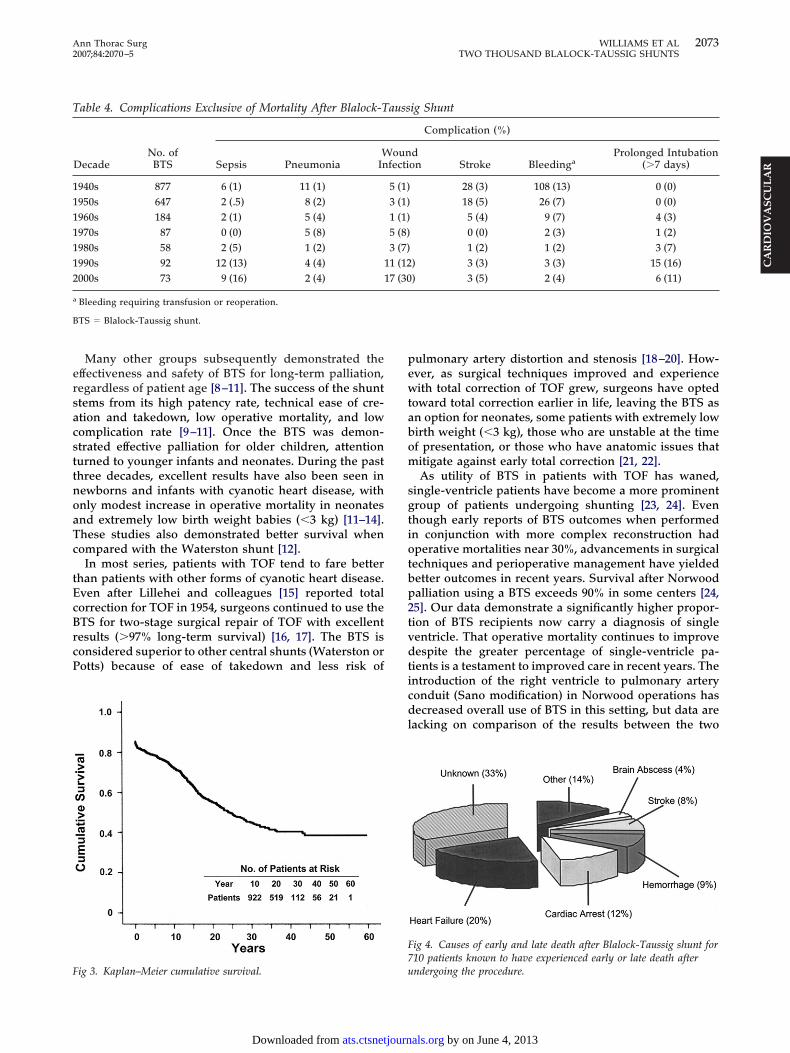
14 of 129). Six patients had a third BTS, but none died inhe perioperative period. Operative mortality for all BTSrocedures improved each decade (Fig 2), but did noteach statistical significance (p � 0.08).
Mean length of stay for all BTS in each decade arehown in Table 3. For patients undergoing their first BTS,ean postoperative length of stay was 16 � 16 days.
atients undergoing a second BTS had a mean postop-rative length of stay of 17 � 16 days, whereas patientsndergoing a third BTS had a mean postoperative lengthf stay of 15 � 9 days.Table 4 lists relevant complications after BTS com-
ig 1. Type of Blalock-Taussig shunt (BTS) procedures performed.L � left; R � right.)
ared by decade. Incidences are based on the number of F
ats.ctsnetjournDownloaded from
atients with hospital course data available (1,574 pa-ients). Of note, the incidence of prolonged intubation,epsis, and wound infection all increased in the 1990s and000s. This most likely reflects the increased complexityf patients undergoing BTS during these decades.
ate Outcomesn follow-up, 32% of TOF patients (411 of 1,294) under-ent subsequent total correction of TOF at our institu-
ion. An additional 116 patients for whom follow-up wasvailable underwent total correction of TOF at othernstitutions after BTS at our institution. The combinedotal correction of TOF rate was 41%.
Of patients with complex congenital heart defects, 26%106 of 404) had subsequent cavopulmonary connectionr atrial or arterial switch procedures. For the entire BTSohort, 850 patients (45%) are known to have undergoneultiple cardiac surgical procedures to palliate or correct
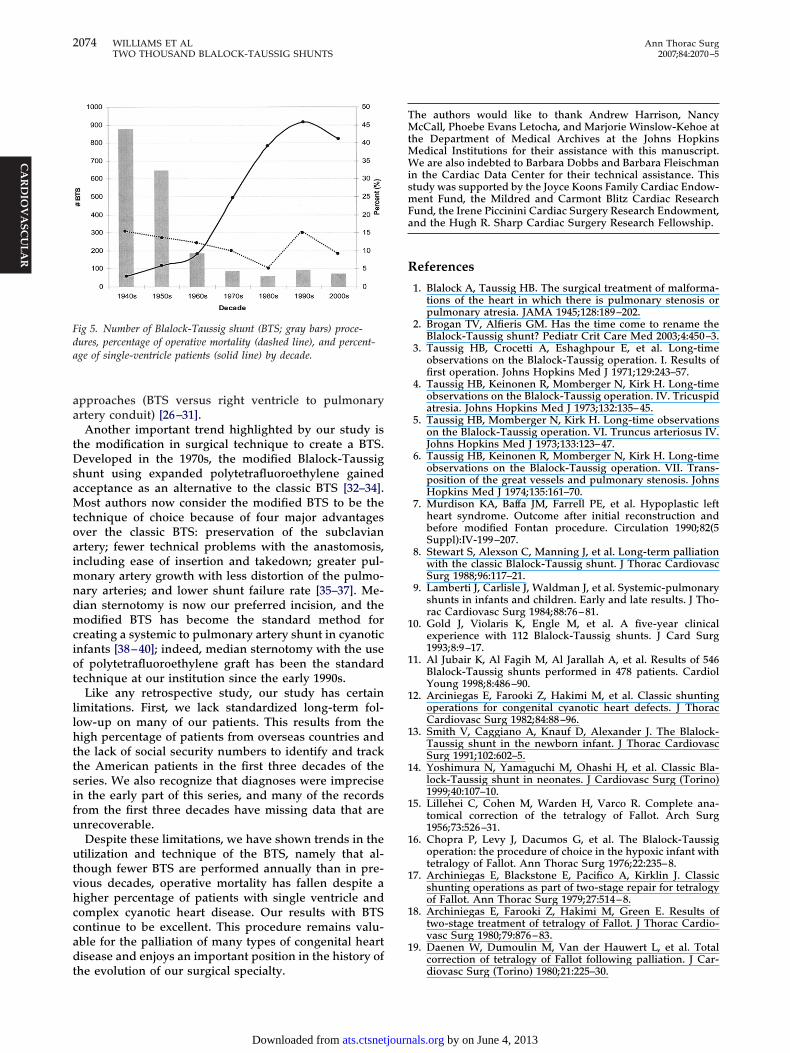
nderlying congenital cardiac lesions.Actuarial survival of the BTS cohort is shown in Figure
. This figure also demonstrates the number of patientsor whom follow-up data were available in 10-year inter-als after their original BTS. Of 710 patients known toave died after BTS, causes of death were known in 476
67%) and are depicted in Figure 4. The most commonause of death after BTS was heart failure. Cardiac arrest,troke, and brain abscesses were also common causes ofate death. Other than heart failure, the most commonause of early mortality was complications as a result ofemorrhage, although no patient has died of hemorrhage
n the last 30 years. Figure 5 depicts important trends inse and outcome of BTS during the past six decades:ecreasing mean annual number of BTS, decreasingperative mortality, and increasing proportion of single-entricle diagnoses.
omment
n the early 1970s, Taussig and colleagues [3] first re-orted long-term results of BTS at our institution. The2% operative mortality, combined with a 23% late mor-ality at 15 years, set the standard for surgical palliation ofatients with TOF. Although results were inferior foratients with tricuspid atresia [4], truncus arteriosus [5],nd transposition of the great vessels [6], the success withhese disorders nonetheless demonstrated promise forreatment of many forms of cyanotic heart disease.
ig 2. Operative mortality by decade.
by on June 4, 2013 als.org
ersacsttnoaTc
tEcBrcP
pewtabom
sgtiotbp2tvdticdl
F7
T
1111112
a
B
F
2073Ann Thorac Surg WILLIAMS ET AL2007;84:2070–5 TWO THOUSAND BLALOCK-TAUSSIG SHUNTS
CA
RD
IOV
ASC
ULA
R
Many other groups subsequently demonstrated theffectiveness and safety of BTS for long-term palliation,egardless of patient age [8–11]. The success of the shunttems from its high patency rate, technical ease of cre-tion and takedown, low operative mortality, and lowomplication rate [9–11]. Once the BTS was demon-trated effective palliation for older children, attentionurned to younger infants and neonates. During the pasthree decades, excellent results have also been seen inewborns and infants with cyanotic heart disease, withnly modest increase in operative mortality in neonatesnd extremely low birth weight babies (�3 kg) [11–14].hese studies also demonstrated better survival whenompared with the Waterston shunt [12].
In most series, patients with TOF tend to fare betterhan patients with other forms of cyanotic heart disease.ven after Lillehei and colleagues [15] reported totalorrection for TOF in 1954, surgeons continued to use theTS for two-stage surgical repair of TOF with excellentesults (�97% long-term survival) [16, 17]. The BTS isonsidered superior to other central shunts (Waterston orotts) because of ease of takedown and less risk of
able 4. Complications Exclusive of Mortality After Blalock-T
DecadeNo. of
BTS Sepsis PneumoniaW
In
940s 877 6 (1) 11 (1)950s 647 2 (.5) 8 (2)960s 184 2 (1) 5 (4)970s 87 0 (0) 5 (8)980s 58 2 (5) 1 (2)990s 92 12 (13) 4 (4) 1000s 73 9 (16) 2 (4) 1
Bleeding requiring transfusion or reoperation.
TS � Blalock-Taussig shunt.
uig 3. Kaplan–Meier cumulative survival.
ats.ctsnetjournDownloaded from
ulmonary artery distortion and stenosis [18–20]. How-ver, as surgical techniques improved and experienceith total correction of TOF grew, surgeons have opted
oward total correction earlier in life, leaving the BTS asn option for neonates, some patients with extremely lowirth weight (�3 kg), those who are unstable at the timef presentation, or those who have anatomic issues thatitigate against early total correction [21, 22].As utility of BTS in patients with TOF has waned,
ingle-ventricle patients have become a more prominentroup of patients undergoing shunting [23, 24]. Evenhough early reports of BTS outcomes when performedn conjunction with more complex reconstruction hadperative mortalities near 30%, advancements in surgicalechniques and perioperative management have yieldedetter outcomes in recent years. Survival after Norwoodalliation using a BTS exceeds 90% in some centers [24,5]. Our data demonstrate a significantly higher propor-ion of BTS recipients now carry a diagnosis of singleentricle. That operative mortality continues to improveespite the greater percentage of single-ventricle pa-
ients is a testament to improved care in recent years. Thentroduction of the right ventricle to pulmonary arteryonduit (Sano modification) in Norwood operations hasecreased overall use of BTS in this setting, but data are
acking on comparison of the results between the two
ig 4. Causes of early and late death after Blalock-Taussig shunt for10 patients known to have experienced early or late death after
ig Shunt
Complication (%)
don Stroke Bleedinga
Prolonged Intubation(�7 days)
28 (3) 108 (13) 0 (0)18 (5) 26 (7) 0 (0)5 (4) 9 (7) 4 (3)0 (0) 2 (3) 1 (2)1 (2) 1 (2) 3 (7)
) 3 (3) 3 (3) 15 (16)) 3 (5) 2 (4) 6 (11)
auss
ounfecti
5 (1)3 (1)1 (1)5 (8)3 (7)1 (127 (30
ndergoing the procedure.
by on June 4, 2013 als.org
aa
tDsaMtoaimndmciot
llhttsifu
utvhccadt
TMtMWismFa
R
1
1
1
1
1
1
1
1
1
1
Fda
2074 WILLIAMS ET AL Ann Thorac SurgTWO THOUSAND BLALOCK-TAUSSIG SHUNTS 2007;84:2070–5
CA
RD
IOV
ASC
ULA
R
pproaches (BTS versus right ventricle to pulmonaryrtery conduit) [26–31].Another important trend highlighted by our study is
he modification in surgical technique to create a BTS.eveloped in the 1970s, the modified Blalock-Taussig
hunt using expanded polytetrafluoroethylene gainedcceptance as an alternative to the classic BTS [32–34].ost authors now consider the modified BTS to be the
echnique of choice because of four major advantagesver the classic BTS: preservation of the subclavianrtery; fewer technical problems with the anastomosis,ncluding ease of insertion and takedown; greater pul-
onary artery growth with less distortion of the pulmo-ary arteries; and lower shunt failure rate [35–37]. Me-ian sternotomy is now our preferred incision, and theodified BTS has become the standard method for
reating a systemic to pulmonary artery shunt in cyanoticnfants [38–40]; indeed, median sternotomy with the usef polytetrafluoroethylene graft has been the standardechnique at our institution since the early 1990s.
Like any retrospective study, our study has certainimitations. First, we lack standardized long-term fol-ow-up on many of our patients. This results from theigh percentage of patients from overseas countries and
he lack of social security numbers to identify and trackhe American patients in the first three decades of theeries. We also recognize that diagnoses were imprecisen the early part of this series, and many of the recordsrom the first three decades have missing data that arenrecoverable.Despite these limitations, we have shown trends in the
tilization and technique of the BTS, namely that al-hough fewer BTS are performed annually than in pre-ious decades, operative mortality has fallen despite aigher percentage of patients with single ventricle andomplex cyanotic heart disease. Our results with BTSontinue to be excellent. This procedure remains valu-ble for the palliation of many types of congenital heartisease and enjoys an important position in the history of
ig 5. Number of Blalock-Taussig shunt (BTS; gray bars) proce-ures, percentage of operative mortality (dashed line), and percent-ge of single-ventricle patients (solid line) by decade.
he evolution of our surgical specialty.
ats.ctsnetjournDownloaded from
he authors would like to thank Andrew Harrison, NancycCall, Phoebe Evans Letocha, and Marjorie Winslow-Kehoe at
he Department of Medical Archives at the Johns Hopkinsedical Institutions for their assistance with this manuscript.e are also indebted to Barbara Dobbs and Barbara Fleischman
n the Cardiac Data Center for their technical assistance. Thistudy was supported by the Joyce Koons Family Cardiac Endow-ent Fund, the Mildred and Carmont Blitz Cardiac Research
und, the Irene Piccinini Cardiac Surgery Research Endowment,nd the Hugh R. Sharp Cardiac Surgery Research Fellowship.
eferences
1. Blalock A, Taussig HB. The surgical treatment of malforma-tions of the heart in which there is pulmonary stenosis orpulmonary atresia. JAMA 1945;128:189–202.
2. Brogan TV, Alfieris GM. Has the time come to rename theBlalock-Taussig shunt? Pediatr Crit Care Med 2003;4:450–3.
3. Taussig HB, Crocetti A, Eshaghpour E, et al. Long-timeobservations on the Blalock-Taussig operation. I. Results offirst operation. Johns Hopkins Med J 1971;129:243–57.
4. Taussig HB, Keinonen R, Momberger N, Kirk H. Long-timeobservations on the Blalock-Taussig operation. IV. Tricuspidatresia. Johns Hopkins Med J 1973;132:135–45.
5. Taussig HB, Momberger N, Kirk H. Long-time observationson the Blalock-Taussig operation. VI. Truncus arteriosus IV.Johns Hopkins Med J 1973;133:123–47.
6. Taussig HB, Keinonen R, Momberger N, Kirk H. Long-timeobservations on the Blalock-Taussig operation. VII. Trans-position of the great vessels and pulmonary stenosis. JohnsHopkins Med J 1974;135:161–70.
7. Murdison KA, Baffa JM, Farrell PE, et al. Hypoplastic leftheart syndrome. Outcome after initial reconstruction andbefore modified Fontan procedure. Circulation 1990;82(5Suppl):IV-199–207.
8. Stewart S, Alexson C, Manning J, et al. Long-term palliationwith the classic Blalock-Taussig shunt. J Thorac CardiovascSurg 1988;96:117–21.
9. Lamberti J, Carlisle J, Waldman J, et al. Systemic-pulmonaryshunts in infants and children. Early and late results. J Tho-rac Cardiovasc Surg 1984;88:76–81.
0. Gold J, Violaris K, Engle M, et al. A five-year clinicalexperience with 112 Blalock-Taussig shunts. J Card Surg1993;8:9–17.
1. Al Jubair K, Al Fagih M, Al Jarallah A, et al. Results of 546Blalock-Taussig shunts performed in 478 patients. CardiolYoung 1998;8:486–90.
2. Arciniegas E, Farooki Z, Hakimi M, et al. Classic shuntingoperations for congenital cyanotic heart defects. J ThoracCardiovasc Surg 1982;84:88–96.
3. Smith V, Caggiano A, Knauf D, Alexander J. The Blalock-Taussig shunt in the newborn infant. J Thorac CardiovascSurg 1991;102:602–5.
4. Yoshimura N, Yamaguchi M, Ohashi H, et al. Classic Bla-lock-Taussig shunt in neonates. J Cardiovasc Surg (Torino)1999;40:107–10.
5. Lillehei C, Cohen M, Warden H, Varco R. Complete ana-tomical correction of the tetralogy of Fallot. Arch Surg1956;73:526–31.
6. Chopra P, Levy J, Dacumos G, et al. The Blalock-Taussigoperation: the procedure of choice in the hypoxic infant withtetralogy of Fallot. Ann Thorac Surg 1976;22:235–8.
7. Archiniegas E, Blackstone E, Pacifico A, Kirklin J. Classicshunting operations as part of two-stage repair for tetralogyof Fallot. Ann Thorac Surg 1979;27:514–8.
8. Archiniegas E, Farooki Z, Hakimi M, Green E. Results oftwo-stage treatment of tetralogy of Fallot. J Thorac Cardio-vasc Surg 1980;79:876–83.
9. Daenen W, Dumoulin M, Van der Hauwert L, et al. Total
correction of tetralogy of Fallot following palliation. J Car-diovasc Surg (Torino) 1980;21:225–30.by on June 4, 2013 als.org

2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
3
3
4
D
DWlhtacbcrp2wlaoro
i
2075Ann Thorac Surg WILLIAMS ET AL2007;84:2070–5 TWO THOUSAND BLALOCK-TAUSSIG SHUNTS
CA
RD
IOV
ASC
ULA
R
0. Stanley P, Chartrand C, Davignon A, et al. Palliative surgeryin tetralogy of Fallot. Can J Surg 1981;24:475–9.
1. Sousa U, Chardigny C, Galetti L, et al. Surgery for tetralogyof Fallot at less than six months of age. Is palliation “old-fashioned?” Eur J Cardiothorac Surg 1995;9:453–60.
2. Fraser C, McKenzie E, Cooley D. Tetralogy of Fallot: surgicalmanagement individualized to the patient. Ann Thorac Surg2001;71:1556–63.
3. Pigott J, Murphy J, Barber G, Norwood W. Palliative recon-structive surgery for hypoplastic left heart syndrome. AnnThorac Surg 1988;45:122–8.
4. Duncan B, Rosenthal G, Jones T, Lupinetti F. First-stagepalliation of complex univentricular cardiac anomalies inolder infants. Ann Thorac Surg 2001;72:2077–88.
5. Maher K, Gidding S, Baffa J, et al. New developments in thetreatment of hypoplastic left heart syndrome. Minerva Pe-diatr 2004;56:41–9.
6. Malec E, Januszewska K, Kolez J, Mroczek T. Right ventricle-to-pulmonary artery shunt versus modified Blalock-Taussigshunt in the Norwood procedure for hypoplastic left heartsyndrome—influence on early and late haemodynamic sta-tus. Eur J Cardiothorac Surg 2003;23:728–33.
7. Bradley S, Simsic J, McQuinn T, et al. Hemodynamic statusafter the Norwood procedure: a comparison of right ventri-cle-to-pulmonary artery connection versus modified Bla-lock-Taussig shunt. Ann Thorac Surg 2004;78:933–41.
8. Pizarro C, Mroczek T, Malec E, Norwood W. Right ventricleto pulmonary artery conduit reduces interim mortality afterstage 1 Norwood for hypoplastic left heart syndrome. AnnThorac Surg 2004;78:1959–64.
9. Tabbut S, Dominguez T, Ravishankar C, et al. Outcomesafter the stage I reconstruction comparing the right ventricleto pulmonary artery conduit with the modified Blalock-Taussig shunt. Ann Thorac Surg 2005;80:1582–91.
0. Griselli M, McGuirk S, Stumper O, et al. Influence ofsurgical strategies on outcome after the Norwood procedure.
J Thorac Cardiovasc Surg 2006;131:418–26.s an ongoing use of the modified Blalock-Taussig shunt. I think
iihhtobvoswvcon
Hp
D
ats.ctsnetjournDownloaded from
1. Cua C, Thiagarajan R, Gauvreau K, et al. Early postoperativeoutcomes in a series of infants with hypoplastic left heartsyndrome undergoing stage I palliation operation with ei-ther modified Blalock-Taussig shunt or right ventricle topulmonary artery conduit. Pediatr Crit Care Med 2006;7:238–44.
2. Donahoo J, Gardner T, Zahka K, Kidd B. Systemic-pulmonary shunts in neonates and infants using micro-porous expanded polytetrafluoroethylene: immediate andlate results. Ann Thorac Surg 1980;30:146–50.
3. Di Benedetto G, Tiraboschi R, Vanini V, et al. Systemic-pulmonary artery shunt using PTFE prosthesis (Gore-Tex).Early results and long-term follow-up on 105 consecutivecases. Thorac Cardiovasc Surg 1981;29:143–7.
4. de Leval M, McKay R, Jones M, et al. Modified Blalock-Taussig shunt: use of subclavian artery orifice as flow regu-lator in prosthetic systemic-pulmonary artery shunts. J Tho-rac Cardiovasc Surg 1981;81:112–9.
5. Lawless C, Smith E, Hallidie-Smith K, Sapsford R. Themodified Blalock-Taussig shunt using microporous ex-panded polytetrafluoroethylene (PTFE). J Cardiovasc Surg(Torino) 1982;23:287–92.
6. Nanton M, Roy D, Murphy D, et al. Polytetrafluoroethyleneshunts in congenital heart disease. Can J Surg 1982;25:134–8.
7. Ullom R, Sade R, Crawford F, et al. The Blalock-Taussigshunt in infants: standard versus modified. Ann Thorac Surg1987;44:539–43.
8. Odim J, Portzky M, Zurakowski D, et al. Sternotomy ap-proach for the modified Blalock-Taussig shunt. Circulation1995;92(9 Suppl):II-256–61.
9. Bove E, Sondheimer H, Kavey R, et al. Subclavian-pulmonary artery shunts with polytetrafluoroethylene inter-position grafts. Ann Thorac Surg 1984;37:88–91.
0. Moulton A, Brenner J, Ringel R, et al. Classic versus modi-fied Blalock-Taussig shunts in neonates and infants. Circu-
lation 1985;72(3 Suppl):II-35–44.ISCUSSION
R DENTON A. COOLEY (Houston, TX): Well, thank you, Drilliams, for this interesting study, and it certainly brings to
ight some of the sequences and consequences of that earlyistoric operation in November 1944. I was privileged to be on
he original team and certainly cherish the memory. I havelways believed that that was the dawn of the modern era ofardiac surgery, and I was privileged to be present to witness theeginning. It has been interesting to see the evolution andhanges technically in the procedure. The concept, of course, hasemained pretty much the same, that is, a systemic-to-ulmonary shunt. I think the big revolution has come in the last0 years with the development of synthetic graft prostheses,hich make it possible for the surgeon to select not only the
ength but also the diameter of the shunt and to try to estimatend predict the volume of the shunt involved. I know in some ofur early trepidations we had much difficulty in all of thoseespects. For example current techniques do not require sacrificef brachiocephalic tributaries.I have noticed in our own Texas Children’s Hospital that there
t is probably a larger series than you report from Hopkins, butt is an integral part of our palliative treatment of congenitaleart disease. It is interesting to me to also note that it may evenave use as a destination therapy. Just last week I saw a patient
hat I had operated on in 1956 with a classic Blalock-Taussigperation for tricuspid atresia. This patient has gone throughirthing deliveries on two occasions uneventfully and now is aery active grandmother; however, she is facing the possibilityf a cardiac transplantation. Nevertheless, the classic Blalockhunt is still continuing to function. So some of these patientsith very complex congenital anomalies, particularly single-
entricle anomalies, where there is such a strong effort toonvert every one of them to a Fontan type of physiology, somef them probably could enjoy a reasonably comfortable life withothing more than the modified Blalock-Taussig operation.Thank you very much Dr Williams and your colleagues atopkins, and I compliment you on this very interestingresentation.
R WILLIAMS: Thank you for your kind comments.
by on June 4, 2013 als.org

DOI: 10.1016/j.athoracsur.2007.06.067 2007;84:2070-2075 Ann Thorac Surg
Baumgartner and Duke E. Cameron D. Patel, Akhil K. Seth, Diane E. Alejo, Vincent L. Gott, Luca A. Vricella, William A.
Jason A. Williams, Anshuman K. Bansal, Bradford J. Kim, Lois U. Nwakanma, Nishant Two Thousand Blalock-Taussig Shunts: A Six-Decade Experience
& ServicesUpdated Information
http://ats.ctsnetjournals.org/cgi/content/full/84/6/2070including high-resolution figures, can be found at:
References http://ats.ctsnetjournals.org/cgi/content/full/84/6/2070#BIBL
This article cites 40 articles, 20 of which you can access for free at:
Citations
shttp://ats.ctsnetjournals.org/cgi/content/full/84/6/2070#otherarticleThis article has been cited by 5 HighWire-hosted articles:
Subspecialty Collections
http://ats.ctsnetjournals.org/cgi/collection/congenital_cyanotic Congenital - cyanotic
following collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
[email protected]: orhttp://www.us.elsevierhealth.com/Licensing/permissions.jsp
in its entirety should be submitted to: Requests about reproducing this article in parts (figures, tables) or
Reprints [email protected]
For information about ordering reprints, please email:
by on June 4, 2013 ats.ctsnetjournals.orgDownloaded from