
Two or six hyperthermia treatments as an adjunct to radiation therapy yield similar tumor responses:...
15
In, J Radmrron Oncology Bwl Phm Vol. 19. pp. 1481-1495 0360-3016/90 $3.00 + .oO Printed in the U.S.A. All nghts resened. CopyrIght ICI lY90 Pergamon Press plc ?? Phase I/II Clinical Trial TWO OR SIX HYPERTHERMIA TREATMENTS AS AN ADJUNCT TO RADIATION THERAPY YIELD SIMILAR TUMOR RESPONSES: RESULTS OF A RANDOMIZED TRIAL DANIEL S. KAPP, PH.D., M.D., IVY A. PETERSEN, M.D., RICHARD S. Cox, PH.D., GEORGE M. HAHN, PH.D., PETER FESSENDEN, PH.D., STAVROS D. PRIONAS, PH.D., ERIC R. LEE, B.S., JOHN L. MEYER, M.D., THADDEUS V. SAMULSKI, PH.D. AND MALCOLM A. BAGSHAW, M.D. Department of Radiation Oncology. Stanford University School of Medicine. Stanford. CA 94305 From March 1984 to February 1988.70 patients with 179 separate treatment fields containing superficially located (~3 cm from surface) recurrent or metastatic malignancies were stratified based on tumor size, histology, and prior radiation therapy and enrolled in prospective randomized trials comparing two versus six hyperthermia treatments as an adjunct to standardized courses of radiation therapy. A total of 165 fields completed the combined hyperthermia- radiation therapy protocols and were evaluable for response. No statistically significant differences were observed between the two treatment arms with respect to tumor location; histology: initial tumor volume; patient age and pretreatment performance status; extent of prior radiation therapy, chemotherapy, hormonal therapy. or immu- notherapy; or concurrent radiation therapy. The means for all fields of the averaged minimum, maximum, and average measured intratumoral temperatures were 40.2”C, 44.8”C, 42.5”C. respectively, and did not differ signif- icantly between the fields randomized to two or six hyperthermia treatments. The treatment was well tolerated with an acceptable level of complications. At 3 weeks after completion of therapy, complete disappearance of all measurable tumor was noted in 52% of the fields, ~50% tumor reduction was noted in 7% of the fields, ~50% tumor reduction was noted in 21% of the fields, and continuing regression (monotonic regression to ~50% of initial volume) was noted in 20% of the fields. No significant differences were noted in tumor responses at 3 weeks for fields randomized to two versus six hyperthermia treatments (p = 0.89). Cox regression analyses were performed to identify pretreatment or treatment parameters that correlated with duration of local control. Tumor histology, concurrent radiation dose, and tumor volume all correlated with duration of local control. The mean of the minimum intratumoral temperatures (~41°C vs. 241°C) was of borderline prognostic significance in the univariate analysis, and added to the power of the best three covariate model. Neither the actual number of hyperthermia treatments administered nor the hyperthermia protocol group (two versus six treatments) correlated with duration of local control. The development of thermotolerance is postulated to be, at least in part, responsible for limiting the effectiveness of multiple closely spaced hyperthermia treatments. Hyperthermia, Superficial lesions, Local control, Number of treatments, Thermotolerance, Prognostic parameters, Complications. INTRODUCTION Local-regional hyperthermia (HT) is being frequently used as an adjuvant to radiation therapy (XRT) in the treat- ment of locally advanced, recurrent, or metastatic super- ficially-located malignancies. Non-randomized and matched-paired studies have suggested improved complete response rates when HT was used in conjunction with XRT compared with the results obtained by similar treat- ment regimens using XRT alone (3. 35). Furthermore, superficially-located metastatic lesions ~3 cm in diameter that were treated with combined HT plus XRT revealed improved probability of local control at 12 months when compared to similar lesions randomized to XRT alone (23). Numerous pretreatment and treatment parameters have been shown to influence the outcome in combined XRT-HT treatment regimens ( 14. 33) and optimum use Presented in part at the 3 I st Annual Meeting of the American Society for Therapeutic Radiology and Oncology, San Francisco. CA, 2-6 October 1989. Reprint requests to: Daniel S. Kapp. Ph.D., M.D. Acknowledgments-The authors wish to acknowledge Allen Lohrbach for providing technical support, Walter Cox for aiding 1481 in the data analyses, and Sharon Clarke for preparing this manuscript. Particular thanks is extended to all the referring physicians and to the patients, for without their support and cooperation, this trial could not have been performed. Supported by NC1 grant CA-44665. Accepted for publication 2 1 June 1990.
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Two or six hyperthermia treatments as an adjunct to radiation therapy yield similar tumor responses:...

In, J Radmrron Oncology Bwl Phm Vol. 19. pp. 1481-1495 0360-3016/90 $3.00 + .oO
Printed in the U.S.A. All nghts resened. CopyrIght ICI lY90 Pergamon Press plc
??Phase I/II Clinical Trial
TWO OR SIX HYPERTHERMIA TREATMENTS AS AN ADJUNCT TO RADIATION THERAPY YIELD SIMILAR TUMOR RESPONSES:
RESULTS OF A RANDOMIZED TRIAL
DANIEL S. KAPP, PH.D., M.D., IVY A. PETERSEN, M.D., RICHARD S. Cox, PH.D.,
GEORGE M. HAHN, PH.D., PETER FESSENDEN, PH.D., STAVROS D. PRIONAS, PH.D.,
ERIC R. LEE, B.S., JOHN L. MEYER, M.D., THADDEUS V. SAMULSKI, PH.D.
AND MALCOLM A. BAGSHAW, M.D.
Department of Radiation Oncology. Stanford University School of Medicine. Stanford. CA 94305
From March 1984 to February 1988.70 patients with 179 separate treatment fields containing superficially located (~3 cm from surface) recurrent or metastatic malignancies were stratified based on tumor size, histology, and prior radiation therapy and enrolled in prospective randomized trials comparing two versus six hyperthermia treatments as an adjunct to standardized courses of radiation therapy. A total of 165 fields completed the combined hyperthermia- radiation therapy protocols and were evaluable for response. No statistically significant differences were observed between the two treatment arms with respect to tumor location; histology: initial tumor volume; patient age and pretreatment performance status; extent of prior radiation therapy, chemotherapy, hormonal therapy. or immu- notherapy; or concurrent radiation therapy. The means for all fields of the averaged minimum, maximum, and average measured intratumoral temperatures were 40.2”C, 44.8”C, 42.5”C. respectively, and did not differ signif- icantly between the fields randomized to two or six hyperthermia treatments. The treatment was well tolerated with an acceptable level of complications. At 3 weeks after completion of therapy, complete disappearance of all measurable tumor was noted in 52% of the fields, ~50% tumor reduction was noted in 7% of the fields, ~50% tumor reduction was noted in 21% of the fields, and continuing regression (monotonic regression to ~50% of initial volume) was noted in 20% of the fields. No significant differences were noted in tumor responses at 3 weeks for fields randomized to two versus six hyperthermia treatments (p = 0.89). Cox regression analyses were performed to identify pretreatment or treatment parameters that correlated with duration of local control. Tumor histology, concurrent radiation dose, and tumor volume all correlated with duration of local control. The mean of the minimum intratumoral temperatures (~41°C vs. 241°C) was of borderline prognostic significance in the univariate analysis, and added to the power of the best three covariate model. Neither the actual number of hyperthermia treatments administered nor the hyperthermia protocol group (two versus six treatments) correlated with duration of local control. The development of thermotolerance is postulated to be, at least in part, responsible for limiting the effectiveness of multiple closely spaced hyperthermia treatments.
Hyperthermia, Superficial lesions, Local control, Number of treatments, Thermotolerance, Prognostic parameters, Complications.
INTRODUCTION
Local-regional hyperthermia (HT) is being frequently used as an adjuvant to radiation therapy (XRT) in the treat- ment of locally advanced, recurrent, or metastatic super- ficially-located malignancies. Non-randomized and matched-paired studies have suggested improved complete response rates when HT was used in conjunction with XRT compared with the results obtained by similar treat-
ment regimens using XRT alone (3. 35). Furthermore, superficially-located metastatic lesions ~3 cm in diameter that were treated with combined HT plus XRT revealed improved probability of local control at 12 months when compared to similar lesions randomized to XRT alone (23). Numerous pretreatment and treatment parameters have been shown to influence the outcome in combined XRT-HT treatment regimens ( 14. 33) and optimum use
Presented in part at the 3 I st Annual Meeting of the American Society for Therapeutic Radiology and Oncology, San Francisco. CA, 2-6 October 1989.
Reprint requests to: Daniel S. Kapp. Ph.D., M.D. Acknowledgments-The authors wish to acknowledge Allen Lohrbach for providing technical support, Walter Cox for aiding
1481
in the data analyses, and Sharon Clarke for preparing this manuscript. Particular thanks is extended to all the referring physicians and to the patients, for without their support and cooperation, this trial could not have been performed.
Supported by NC1 grant CA-44665. Accepted for publication 2 1 June 1990.

I482 1. J. Radiation Oncology 0 Biology 0 Physics December 1990. Volume 19, Number 6
of HT will require carefully designed Phase II studies to define these treatment factors better. Since HT treatments are costly, time-consuming, and may result in untoward complications, and since most retrospective studies failed to demonstrate the added benefit of more than two HT treatments when administered with XRT in the treatment of superficially-located tumors (14, 33) a prospective randomized trial was undertaken to compare standardized XRT-HT treatment regimens of two HT versus six HT treatments.
Protocol design
The purpose of this study was to determine the possible influence of the number of HT treatments on tumor re- sponse rate, duration of local control, and complications. In addition, a detailed analysis of the results was under- taken in an attempt to identify any pretreatment or treat- ment parameters that correlated with the duration of local control.
METHODS AND MATERIALS
Between March 1984 and February 1988, a prospec- tively randomized Phase II trial was conducted at Stanford University Medical Center comparing standardized hy- perthermia-radiation treatment regimens consisting of two HT treatments with identical XRT treatment regimens using six HT treatments. Patients were eligible for the study if they had: biopsy-confirmed persistent, recurrent, or metastatic malignancies located within 3 cm of the surface in a region that had received a dose of less than 8000 cGy; lesions of any surface area that were measurable in at least two perpendicular diameters; age 18 years or greater; and a life expectancy of 3 months or more. The patients were advised of the investigational nature of the study and informed consent forms approved by the Stan- ford University Medical Committee for the Protection of Human Subjects were signed by all patients.
A treatment field was defined as a discrete region con- taining malignancy that could be treated with a single applicator: a field could contain one or more discrete tu- mors or could be diffusely infiltrated with tumor (16). Patients were stratified based on prior XRT to the treat- ment field, tumor histology (squamous cell carcinoma, adenocarcinoma, malignant melanoma, sarcoma and other), and maximum tumor diameter (13 cm vs. >3 cm). They were allocated to a standardized XRT regimen and randomized to receive either two or six HT treatments (Table 1). In patients with two or more eligible treatment fields, the fields were “paired” on the basis of tumor size and location, and one field in each pair was randomized to receive either two (or six) HT treatments whereas the other of the paired fields received six (or two) HT treat- ments. This permitted patients with multiple fields to serve as their own internal controls. The XRT-HT treatment regimens used for both paired and unpaired fields were determined by tumor histology and extent of prior irra- diation.
Putirnt rhaructrristics A total of 179 fields in 70 patients met the eligibility
criteria and were randomized on the protocol studies. A total of 14 fields in eight patients were excluded from final analysis. Progressive disease and death prior to the first follow-up was the cause for exclusion in five patients (ten fields), one patient (three fields) refused to continue XRT- HT after he developed progressive distant metastases, and temperature data were not obtained in one (of five fields) in a single patient. The remaining 165 fields in 64 patients form the cohort for analysis in this study. Patients that failed to complete the prescribed course of HT but com- pleted their XRT and were available for follow-up were analyzed in the study in the HT treatment category for
Table 1. Radiation therapy-hyperthermia treatment regimens
Protocol*
MA2 MA6
MB2 MB6
MC2
MC6
Prior radiation therapy
None None
Yes Yes
None
None
Histology
Melanoma Melanoma
All All
All except melanoma+
All except melanoma+
HT treatment XRT treatment
Fract./ Dose per Fract./ Total dose No. fields No. wk fract. (cGy) wk CCGY) analyzed
2 1 350 2 4200 II 6 I 350 2 4200 JO
2 1 180 4-5 2 160-3600 13 6 2 180 4-5 2160-3600 14
2 I 200 5 6000-6600 25
6 1 200 5 6000-6600 23
MD2
MD6
Yes
Yes
All-multiple fields
All-multiple fields
2 1 180 4-5 2 160-3600 34
6 2 180 4-5 2160-3600 35
HT = Hyperthermia; XRT = Radiation therapy; wk = Week. * Lesions stratified based on tumor histology and tumor size (~3 cm vs >3 cm). + Single or multiple fields per patient.

Radiation therapy and 2 vs. 6 hyperthermia treatments 0 D. S. KAPP ef a/. 1483
which they had been randomized. The causes for failure to complete the prescribed number of HT treatments were documented.
The extent and type of prior treatment (surgery, radia- tion, chemotherapy, hormonal therapy, immunotherapy, HT) was recorded for each treatment field as were the anatomical sites, tumor histology, and tumor dimensions. The anatomical sites were classified as head and neck, thorax, abdomen, pelvis. and extremities as previously defined (27). Tumor measurements were made in at least two orthogonal dimensions (three wherever possible) by vernier calipers at the time of initiation of therapy and confirmed by CT scans where applicable. Patients with irregularly-shaped, superficially-located tumors of varying thicknesses that diffusely filled the treatment field were scored as having “diffuse” disease. For patients with dis- crete measurable lesion(s) in their fields, tumor volume (V) was calculated by the formula:
V = i.a.b.c
where a, b, and c are orthogonal tumor diameters. When multiple tumor nodules were included within a treatment field, the total tumor volume was taken as the sum of the individual tumor volumes. Discrete tumor(s) could be measured and tumor volumes calculated in 136 fields. An additional 29 fields had diffuse disease.
Radiation therap?, treatment XRT was delivered with orthovoltage, electron beam
(6 MeV- 16 MeV) or megavoltage (4 MV- 15 MV) tech- niques. Choice of equipment was dependent on tumor location, prior radiation to the tumor site, and adjacent normal tissues. Since many of the fields had received prior megavoltage treatments that had delivered near tolerance doses to adjacent normal tissues, multiple field electron beam techniques were frequently used to minimize ad- ditional dose to these treatment-limiting normal tissues (e.g., spinal cord in the case of head and neck tumors and lung in the case of chest wall sites).
For the treatment of metastatic melanomas in previ- ously untreated fields, a dose fractionation of 350 cGy per fraction was delivered twice per week until a total dose of 4200 cGy was given. Tumors of all other histol- ogies were treated at doses of 180-200 cGy per fraction, four to five times per week to total doses of 2 160-3600 cGy if the field had received prior XRT, and 6000-6600 cGy if the field had not been previously irradiated (Table 1). Radiation field size was chosen to include the recurrent tumor with generous margins (2-3 cm minimum). For patients with recurrences of breast cancer on the chest wall, the entire ipsilateral chest wall and adjacent supra- clavicular areas were included whenever possible.
HJperthermia HT was delivered using horn and spiral microstrip mi-
crowave as well as planar ultrasound applicators with techniques as previously described (16, 26). Based on tu- mor size, site, and the nature of the surrounding normal tissues, applicators were chosen that were felt to be best able to heat the tumors within an individual field. The HT treatment was instituted as soon after the radiation treatment as possible (usually 30-45 minutes). Depending on the individual treatment protocol (Table I), the HT treatments were given at intervals of at least 3 and at most 7 days. The heating objectives were to elevate intratumoral temperatures rapidly to at least 43°C (typically within 3 to 6 minutes) while maintaining adjacent normal tissue temperatures to less than 43”C-43.5”C. Temperatures were maintained at these levels for 45 minutes after steady- state conditions had been obtained ( 16). The power was reduced when necessary to prevent any monitored intra- tumoral temperatures from exceeding 50°C. HT appli- cators were coupled through temperature controlled deionized water, which served as an intervening bolus between the applicator and the tissue. Skin cooling was used in situations in which the skin was not directly in- volved with tumor. However, in areas where the tumor extended through the skin, it was attempted to heat the tumor surface to the same temperatures as the remainder of the tumor. and the temperature of the bolus was ad- justed accordingly.
Thcrmometr~~ All treatments were monitored using at least one tem-
perature sensor placed in an interstitially located catheter. Multiple surface temperatures were also monitored. Thermistors* and fiberoptic probest were used during the microwave treatments, and thermocouples were used in cases of ultrasound treatments. Intratumoral and adjacent subcutaneous normal tissue temperatures were measured by manually or mechanically moving the thermistors or fiberoptic probes at 0.5 cm or 1 .O cm intervals along the catheters at least two times during treatment. If only two thermal maps were taken, the first was obtained shortly after steady-state conditions were obtained, and the second was taken towards the end of the treatment session (usually after at least 30 minutes at steady-state temperatures). Up to 16 additional temperature probes were placed on the skin surface or subcutaneously in and around the treat- ment field. These were monitored continuously during treatment. Both the intratumoral and surface tempera- tures were used to adjust the power in an attempt to obtain more uniform temperatures and to achieve the desired intratumoral and normal tissue temperature goals (26). In six of the fields treated. the individual tumor nodules were too small to be directly monitored, so the adjacent normal tissue and scar temperatures were monitored
* Bowman. BSD Medical Corporation, Salt Lake City, IJT 84108.
+ Luxtron Inc., Mountain View. CA 94043.

1484 1. J. Radiation Oncology 0 Biology 0 Physics December 1990. Volume 19. Number 6
through the subcutaneously placed catheters. For all the censored in those patients who subsequently received remaining 159 fields, intratumoral temperatures were chemotherapy. Complications of treatment were scored monitored as noted above. by type and outcome as previously described ( 15, 16).
Individual HT treatments were characterized by the average (Tave), maximum (Tmax), and minimum (Tmin) of the mapped intratumoral tissue temperatures. Tave, Tmax, and Tmin are the average, maximum, and mini- mum temperatures, respectively, of all the mapped intra- tumoral temperatures for a given treatment once steady- state conditions were obtained. In addition, the percentage ofthe temperatures measured that were >43.5”C (Pmax) or ~41 “C (Pmin) were also determined as previously de- scribed ( 16). Averages of these parameters were calculated over all treatments for a given treatment field (e.g., Tave indicating the mean of the average of all measured intratumoral temperatures for all treatments within a given field). Distributions of the percentage of fields with --v
Statistical considerations
Tmax, Tave, Tmm greater than or equal to a given index temperature for all fields randomized to receive two HT treatments were compared with those obtained for all fields randomized to six HT treatments.
The differences in the distributions of pretreatment pa- rameters, treatment parameters, and initial responses be- tween fields randomized to either two or six HT treatments were tested for statistical significance by contingency tables or the Student’s 1 test. The actuarial probability of local control was plotted from the time of initiation of treatment using the Kaplan-Meier method (13). Univariate analyses were used to identify pretreatment or treatment param- eters correlated with duration of local control, and the significance of differences between patient subgroups was evaluated by either the method of Gehan ( 10) or Cox (7). Subsets of patients with values of parameters yielding similar local control curves were then grouped and mul- tivariate analyses performed (7) to determine those pa- rameters most predictive of duration of local control.
Study endpoints The endpoints of this study were the initial tumor re-
sponses, duration of local tumor control, and complica- tions of treatment for the fields randomized to either two or six HT treatments. All patients were scheduled for ini- tial follow-up at 3 weeks after completion of XRT-HT. monthly for the next 3 months, and at 3 month intervals thereafter. Vernier caliper measurements of all tumors treated, as well as evidence for treatment related toxicities, were recorded at each follow-up, and color photographs were taken to document responses and toxicities.
Initial response was evaluated at the time of the first follow-up (3 weeks after treatment completion). A com- plete response (CR) was defined as the clinical complete disappearance of all disease within the treatment field, a partial response (PR) was defined as a ~50% tumor re- duction, and no response (NR) was defined as a ~50% reduction in tumor volume. An additional category of continuing regression, similar to the designation of “per- sistent regression” used by Overgaard and Overgaard (22), was employed to indicate those tumors which had ob- tained at least a 50% reduction in tumor volume and had monotonically continued to regress throughout treatment.
The duration of local control was measured from the date of initiation of treatment. All fields that were either CR or in continuing regression at 3 week follow-up were scored as locally controlled at time zero. All other re- sponses at 3 weeks (either PR or NR) were scored as local failures. Fields that after 3 weeks exhibited: (a) new disease developing within or extending into the treatment field, or (b) an increase of 25% in volume of tumor in fields with continuing regression, were scored as failures of local control. Patients who had local control in the treatment field at the time of their death were considered locally controlled and censored at that date. Responses were not
RESULTS
Pretreatment characteristics The distribution of the 165 fields as per protocol is
summarized in Table 1. The fields were evenly distributed between the two and six HT treatment regimens (p = 0.98). No significant differences between the two HT treatment regimens were noted in the distribution of the pretreatment parameters investigated, which included site of disease, histology, age, performance status, tumor vol- ume, and prior treatment (Table 2). The distribution of sites and histologies reflects our interest in the treatment of chest wall recurrences from metastatic adenocarcinoma of the breast. The averages of the parameters were cal- culated by averaging over the 165 fields rather than over the 64 patients.
Treatment parameters All but two of the HT treatments were delivered using
microwave applicators ( 16, 26). Fifty-eight percent of the total of 6 17 treatments used the scanning double spiral microstrip antenna applicator, 22% used the scanning single spiral microstrip antenna applicator, 19% used sta- tionary spiral microstrip antenna applicators, and 1% used the single or dual horn applicators. Two of the fields were treated with a 6 cm diameter aperture planar ultrasound applicator. A total of 26 fields had HT treatments with more than one type of applicator used throughout the treatment course, whereas the remainder of the fields had all treatments for a given field delivered with a single type of applicator.
The actual number of HT treatments delivered and the reasons for failure to complete the prescribed number of treatments are summarized in Table 3. All but four of the 83 fields randomized to the two treatment HT groups received the prescribed two HT treatments. Fifty-four of

Radiation therapy and 2 vs. 6 hyperthermia treatments 0 D. S. KAPP et ai. 1485
the 82 fields randomized to the six treatment HT groups received all six HT treatments. Nineteen fields received only five HT treatments usually because of patient un- willingness to undergo the final treatment or because of difficulties in scheduling the final HT treatment during the prescribed XRT regimen.
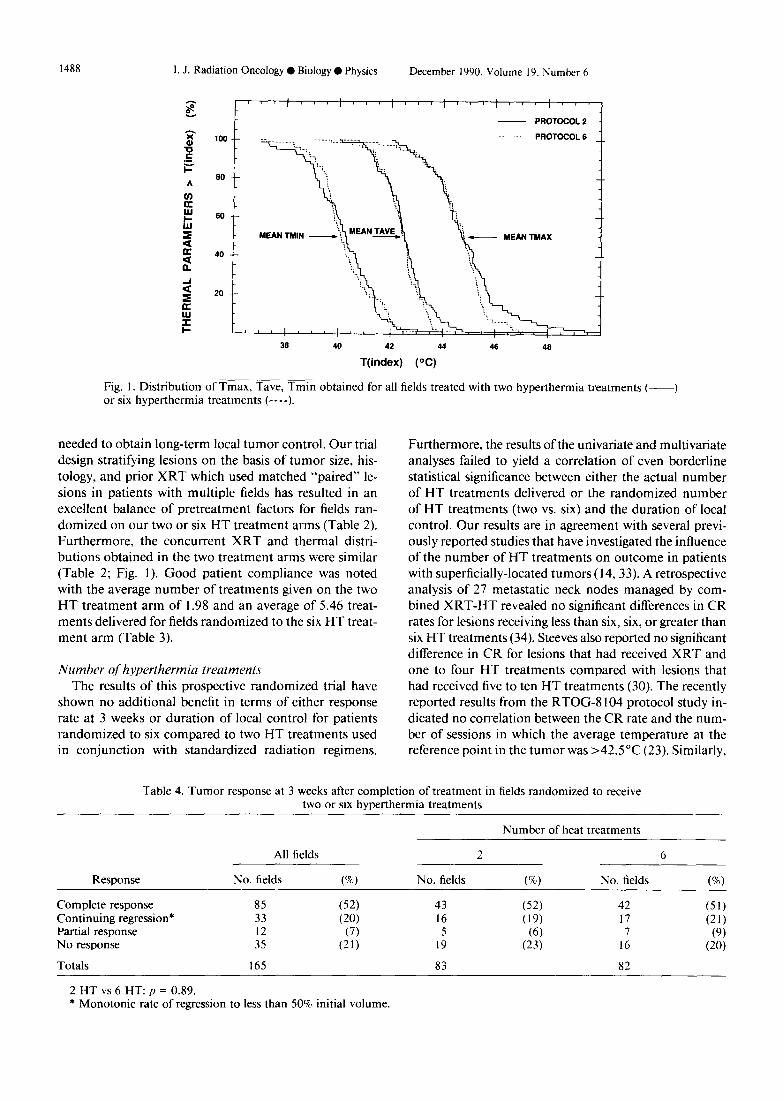
The radiation and HT treatment parameters for fields randomized to two versus six HT are summarized in Table 2 and revealed no statistically significant differences be- tween the two HT groups. Three patients with a total of four fields received concurrent chemotherapy during their XRT-HT treatments and 18 patients with 42 fields re- ceived concurrent hormonal therapy. An average of 2.8 temperature maps were taken for each treatment and the distributions of monitored intratumoral mean maximum, mean average, and mean minimum tumor temperatures for all fields randomized to six HT treatments were vir- tually superimposable to those obtained for all fields ran- domized to two HT treatments (Fig. 1).
Rrsponse Evaluation of response at 3 weeks after completion of
treatment revealed no significant differences between the two versus the six hyperthermia treatment groups (p = 0.89: Table 4). CR were obtained in 52% of the fields and continuing regressions noted in 20%. Patients were followed for an average of 1.12 years. At the time of last follow-up, 18 of the 85 CR had failed in the treatment field (79% remained in continuous CR) and two fields that failed after CR were subsequently cleared of disease once again with additional therapy. Of the 33 fields with continuing regressions noted at 3 weeks, subsequent fol- low-up revealed that 14 fields became unequivocal CR and eight fields showed continued tumor regression (67% were, therefore, locally controlled fields); an additional five fields became CR and then failed (one was subse- quently salvaged), and six of the fields with initial con- tinuing regressions failed without ever obtaining a CR. None of the fields with either a NR or PR at 3 weeks exhibited subsequent CR or was salvaged with additional treatment.
The actuarial probability of local control did not differ significantly for those fields randomized to two versus six HT treatments (p = 0.76; Fig. 2). nor were any significant differences in the duration of local control noted between the fields randomized to two versus six HT treatments when analyzed separately by individual protocols.
Prognostic, fuctors fi,r duration of local control Analysis of local control by histology revealed similar
and relatively high local control durations for squamous cell carcinomas, melanomas, and tumors of other histol- ogies when compared with adenocarcinomas and sarco- mas (Fig. 3a). For subsequent regression analysis, there- fore, tumor histologies were combined into two groups; squamous cell carcinomas, melanomas, and other his- tologies versus adenocarcinomas and sarcomas. Fields
treated with radiation doses of > 3600 cGy showed a sug- gestion of improved local control compared with those treated with lower doses, although the difference was not statistically significant (Fig. 3b). No statistically significant differences were noted for fields treated with doses of >3600 cGy and randomized to two versus six HT treat- ments (p = 0.95) or for fields treated with ~3600 cGy and randomized to two versus six HT treatments (p = 0.52). Local control for the various anatomic sites re- vealed a suggestion of better local control for superficially located tumors of the extremities compared with those of the pelvis (p = 0.16). Intermediate but similar local-con- trol durations were noted for fields involving head and neck and thoracic sites (Fig. 3~). For subsequent analyses. therefore, fields were placed in three groups according to site: the extremities versus head and neck plus thorax ver- sus pelvic sites. Finally, an analysis of local control by tumor volume revealed statistically significant improved local control for tumors <l cc versus those 21 cc (p = 0.03). Fields containing diffuse disease behaved similarly to those with tumors of volume <l cc (Fig. 3d). Fields with tumors of volume <l cc randomized to two HT treatments compared to fields with tumors <l cc ran- domized to six HT treatments showed no significant dif- ference in local control durations (p = 0.77), and the number of HT treatments failed to influence the local control for fields with tumor volumes 2 1 cc as well (p = 0.36). For subsequent analysis, tumor volumes were grouped as diffuse plus < 1 cc versus volumes 2 1 cc. All thermal parameters were initially entered into the regres- sion analyses as continuous variables.
The results of univariate regression analyses, under- taken in an attempt to identify parameters correlating with the duration of local control, are summarized in order of their power in Table 5. The four covariates which showed a significant association with duration of local control were tumor histology, concurrent radiation dose, site of disease, and tumor volume.
None of the thermal parameters showed statistically significant correlations with the duration of local control; however, the strongest correlation found was with Tmin. Further regression analyses were performed inves- tigating the influence of dichotomizing Tmin at different points between 39.5”C and 4 1.5”C. This was done to help take into account any “threshold” for efficacy of heating as indicated by minimum intratumoral temperature. A division of Tmin at <4 1 “C versus 24 1 “C gave the lowest p-value (P = 0.08) in the univariate regression analyses.
None of the other covariates tested, including concur- rent hormonal therapy, showed statistically significant correlations with the duration of local control. In partic- ular, neither the actual number of HT treatments delivered nor the HT protocol group (two vs. six treatments) prog- nosticated for local control (p = 0.99 and a = 1 .OO, re- spectively).
Stepwise regression analyses with the parameters grouped as in the univariate analyses revealed that the

1486 1. J. Radiation Oncology 0 Biology 0 Physics December 1990, Volume 19. Number 6
Table 2. Patient characteristics and concurrent treatment parameters of fields randomized to 2 versus 6 hyperthermia treatments
Parameter Total no. fields or
range all fields 2HT 6HT p value*
Site (all superficial) Head and neck Thorax Pelvis Extremities
Histology Adenocarcinoma Squamous cell carcinoma Melanoma Sarcoma Other
Age (yrs) Minimum-maximum Average + SD
Karnofsky status (%) Minimum-maximum Average + SD
Prior radiation dose (cGy)+ Minimum-maximum Average t SD
Tumor volume (cc)* Minimum-maximum Average _t SD
Prior surgery Yes None
Prior chemotherapy Single agent Multiple agents None
Prior hormonal therapy Single agent Multiple agents None
Prior immunotherapy Yes None
Prior hyperthermia Yes None
Prior radiation therapy Yes None
Prior radiation sensitizers Yes None
Concurrent radiation (cGy) Minimum-maximum Average + SD
No. tumor temperature points measured per treatment
Minimum-maximum Average & SD
Maximum intratumoral temperature per field (“C)
Minimum-maximum Average + SD
Average intratumoral temperature per field (“C)
Minimum-maximum Average -+ SD
27 12 15 111 58 53
4 3
1; 2
23 12
107 54 53 II 6 5 25 14 II 17 8 9 5 I 4
27.8-84.2 27.8-84.2 29.2-84.2 57.4 + 13.0 57.5 -t 12.8 57.3 f 13.3
45-100 45-100 45-100 86.8 f 10.7 86.8 + 10.4 86.7 * 11.1
1000- 10,420 IOOO- 10,420 3000- 10.420 5386 f 1387 5280 -t 1364 5490 t 1415
0.01-I 11.4 0.01-61.4 0.01-I 11.4 6.15 f 15.4 5.31 -t 1 I.0 1.07 * 19.2
136 69 67 29 14 15
8 3 5 119 56 63 38 24 14
40 22
103
21 10 52
19 12 51
14 7 7 151 76 75
14 6 8 151 77 74
101 64
10 155
1260-6600 3603 + 1151
50 51 33 31
5 5 78 77
1260-6600 1260-6600 3670 t 1200 3535 + 1102
2-120 2-108 2-120 28.6 + 21.0 30.2 -t 22.8 28.1 + 20.2
40.7-53.6 42. I-53.6 40.7-47s 44.8 +- 1.4 45.0 f 1.7 44.6 f 1.3
39.7-47.1 40.1-47.1 39.7-44.7 42.5 +- 0.9 42.6 t 1.0 42.4 + 0.8
0.90
0.68
0.90
0.95
0.45
0.50
0.97
0.17
0.87
1.00
0.76
0.92
1.00
0.45
0.28
0.14
0.29

Parameter
Radiation therapy and 2 vs. 6 hyperthermia treatments 0 D. S. KAPP el al.
Table 2. (Contd)
Total no. fields or range all fields 2HT 6HT
I487
p value*
Minimum intratumoral temperature per field (“C)
Minimum-maximum Average ? SD
% intratumoral temperatures >43.5”C per field
Minimum-maximum Average f SD
%I intratumoral temperatures <4 1 “C per field
Minimum-maximum Average t SD
Number receiving hormones Number receiving chemotherapy
37.0-43.8 37.0-43.2 37.2-43.8 40.2 +- 1.2 40.2 & I.2 40.3 ?Y 1.1 0.75
0.0-88.9 0.0-83.3 0.0-88.9 26.7 -t 18.5 27.8 + 20.5 25.5 -t 16.7 0.43
0.0-77. I 0.0-65.9 0.0-77.1 18.1 Ifr 16.3 17.2 & 16.4 19.0 + 16.3 0.48
42 21 ?I I .oo 4 2 2 I .oo
* Student’s I test. ’ For the 101 fields that had prior radiation therapy. * For the I36 fields with discrete tumor(s): 12 fields on 2 HT arm and I7 fields on 6 HT arm had diffuse disease.
best three covariate model correlating with duration of local control included tumor histology, concurrent XRT dose, and tumor volume (p = 0.00044 for the model). The addition of a fourth covariate of either age or Tmin (~4 I “C vs. ~4 I “C) improved the model slightly: however, the covariate p-values for these additional parameters were not statistically significant (Table 6). The addition of either HT protocol group (two vs. six) or actual number of HT treatments delivered, when added as a fourth covariate, resulted in considerably poorer models.
No life-threatening sequelae resulted from the XRT- HT treatment regimens. A total of 30 complications were noted in 27 (of the 83) fields that were randomized to receive two HT treatments. This complication rate did not significantly differ from the finding of 28 complica- tions in 25 (of the 82) fields that were randomized to six HT treatments (p = 0.9 I ). The types of complications, their management, and their outcomes are summarized in Table 7 using the classification system previously de- scribed ( 16). The majority of complications were minor, causing minimal patient discomfort, and were similarly
distributed for the fields randomized to two versus six HT treatments. Subcutaneous induration/fibrosis developed in a total of 26 fields, often at sites of the catheter place- ment for temperature monitoring. Usually, this induration persisted for long periods of time without causing any significant patient discomfort. Ulcerations were noted in the sites of I5 tumors that had grossly invaded through the skin. Edema required medical treatment in only one instance, and this patient had undergone extensive prior treatment. One subcutaneous ulcer that developed in the site of a surgical scar required debridement and packing. The ulcer healed after approximately 9 months.
DISCUSSION
The increasing use of HT as an adjunct to XRT in the treatment of superficially-located malignancies, the con- siderable time and personnel commitment to the perfor- mance of high-quality treatments, the relatively high cost of equipment, patient discomfort during treatments, and late complications of treatment all lend justification for studies designed to optimize XRT-HT regimens and to determine the minimum number of HT treatments
Table 3. Number of hyperthermia sessions received by fields randomized to 2 or 6 hyperthermia treatments
Randomization (total no. fields)
2 HT (83) 6 HT (82)
1
3” 0
2
79 2’
Number HT delivered
3 4
0 ;,” 4c
5 6
0 0 19 54
Average f SD
1.98 ? 0.22 5.46 I 0.93 p < 0.0001
a Tumor necrosis after I HT. no residual to heat (1); refused 2”* treatment (2). h Technical malfunction during IS’ treatment. therefore 3 HT given. ’ Pts refused additional HT after developed infection in catheter site: completed prescribed course of radiation. d Additional HT not given due to infection (1) or progressive metastases outside of treatment fields (2). ’ Additional HT not given due to skin ulceration (2) or progressive metastases outside of treatment fields (2).
1488 1. J. Radiation Oncology 0 Biology 0 Physics December 1990. Volume 19. Number 6
~““,,,i,‘,i,,‘i’,‘i”‘i,,‘s - PROTOCOL2
PROTOCOL 6 __
60 --
60 --
38 40 42 44 46 40
T(index) (“C) ____
Fig. 1. Distribution of Tmax, Tave, ?%% obtained for all fields treated with two hyperthermia treatments (--) or six hyperthermia treatments (----).
needed to obtain long-term local tumor control. Our trial design stratifying lesions on the basis of tumor size, his- tology, and prior XRT which used matched “paired” le- sions in patients with multiple fields has resulted in an excellent balance of pretreatment factors for fields ran- domized on our two or six HT treatment arms (Table 2). Furthermore, the concurrent XRT and thermal distri- butions obtained in the two treatment arms were similar (Table 2; Fig. 1). Good patient compliance was noted with the average number of treatments given on the two HT treatment arm of 1.98 and an average of 5.46 treat- ments delivered for fields randomized to the six HT treat- ment arm (Table 3).
Number of hyperthermiu treatments The results of this prospective randomized trial have
shown no additional benefit in terms of either response rate at 3 weeks or duration of local control for patients randomized to six compared to two HT treatments used in conjunction with standardized radiation regimens.
Furthermore, the results of the univariate and multivariate analyses failed to yield a correlation of even borderline statistical significance between either the actual number of HT treatments delivered or the randomized number of HT treatments (two vs. six) and the duration of local control. Our results are in agreement with several previ- ously reported studies that have investigated the influence of the number of HT treatments on outcome in patients with superficially-located tumors (14,33). A retrospective analysis of 27 metastatic neck nodes managed by com- bined XRT-HT revealed no significant differences in CR rates for lesions receiving less than six, six, or greater than six HT treatments (34). Steeves also reported no significant difference in CR for lesions that had received XRT and one to four HT treatments compared with lesions that had received five to ten HT treatments (30). The recently reported results from the RTOG-8 104 protocol study in- dicated no correlation between the CR rate and the num- ber of sessions in which the average temperature at the reference point in the tumor was >42.5”C (23). Similarly,
Table 4. Tumor response at 3 weeks after completion of treatment in fields randomized to receive two or six hyperthermia treatments
Number of heat treatments
All fields 2 6
Response No. fields @) No. fields (W) No. fields (So)
Complete response 85 (52) 43 (52) 42 (51) Continuing regression* 33 (20) 16 (19) 17 (21) Partial response 12 (7) 5 (6) 7 (9) No response 35 (21) 19 (23) 16 (20)
Totals 165 83 82
2 HT vs 6 HT: p = 0.89. * Monotonic rate of regression to less than 50% initial volume.

Radiation therapy and 2 vs. 6 hyperthermia treatments 0 D. S. KAPP d al 1489
- 2 HEAT TREATMENTS (63)
- - - - - 100
i
6 HEAT TREATMENTS (82)
Gehan P-value: 0.7596
0.2 0.4 0.6 0.6 1.0 1.2 1.4 1.6 I.8 2.0 2.2 2.4 2.6 2.6 3.0
TIME (YEARS)
Fig. 2. Duration of local control for all analyzed fields (165) randomized to either two hyperthermia treatments (--) or six hyperthermia treatments (----).
the RTOG study reported by Scott ct (II., which investi- gated definitive XRT and HT in the treatment of super- ficially-located malignancy, failed to demonstrate a cor- relation between the number of heat sessions (~9, 29), or the number of “good” (243°C for at least 45 minutes) heat sessions (0, 1-8, ~9) and tumor response (29). Dun- lop ef al. also analyzed the influence of the number of “satisfactory” HT treatments (treatments obtaining a minimum thermal dose within the tumor equivalent to 20 minutes at 43°C) on CR in superficially-located tumors
that were treated with XRT-HT regimens (9). A statisti- cally significant improved CR rate was obtained in tumors that received two to four “satisfactory” HT treatments (86%; 19/22) compared to those which had received zero to one “satisfactory” treatments (35%: 8/23) (p I 0.001). No differences were noted in CR rates in tumors that received 2, 3, or 4 “satisfactory” HT treatments. In con- trast to these studies, Arcangeli et al., in a retrospective comparison of 23 lesions treated with XRT-HT. suggested an improvement in CR for ten HT treatments given twice
100 (a) HISTOLOGY
Onea CARCINOMA (5) MELAN,,,4A (25j 80 . . . ..I ..____.L_...**....._........~ -L-L__ .___ ___L__.____ _____ 0
SGUAMOUS CELL (11)
! SARCOMA (17)
ADENGCARCINWA (107)
L 1
(c) SITE OF DISEASE Gohan P~alues
100~ HNvr.TH 0.86 HN vs. PE 0.43 HN vs. EX 0.80 lHvs.PE 0.45
SO - Tn vs EX 0.77 PE v,. EX 0.15
20 I _,
t
THORAX (111) _L _____-__.c-.._-_-,
PELVIS (4, : I
0.5 1.0 1.5 2.0 2.5 3.0
I (d) INITIAL VOLUME ckhlll P-VAlun DF vs. -1 0.46 DF v,. 21 0.26 <, Ys .I 0.03
NODULAR -z 1 cc (72)
..,_,,_______._, _-__.._,
DIFFUSE (29) :..,
iNODULAR L= 1 cc (64) ;
0.5 10 1.5 2.0 2.5 3.0
TIME (YEARS)
Fig. 3. Duration of local control by (a) histology, (b) radiation dose, (c) site of disease, and (d) initial tumor volume.

1490 I. J. Radiation Oncology 0 Biology 0 Physics December 1990, Volume 19, Number 6
Table 5. Results of univariate regression analysis indicating the relative risk for local failure within a treatment held
Covariate Relative risk p value (Cox)
Tumor histology (SCC, melanoma, other vs adenoCA, sarcoma)
Concurrent radiation dose Site of disease
(extremity vs head and neck, thorax vs pelvis) Initial tumor volume
(diffuse. <I cc vs 21 cc) Prior radiation therapy (none vs yes) Average of minimum tumor temperature per field
(<4 1 “C vs 24 I “C) Average of minimum tumor temperature per field Average of % tumor temperatures < 4 I “C per field
(55% vs >S%) Average of % tumor temperatures > 43S”C per
field Average of % tumor temperatures < 41 “C per field Average of maximum tumor temperatures per field Age Concurrent hormone therapy (yes vs none) Karnofsky performance status Actual number hyperthermia treatments Lesion type
(diffuse vs discrete) Average of average tumor temperatures per field Average of standard deviations of all tumor
temperatures per field Hyperthermia protocol group
(2 vs 6)
12.58 0.77 (per 10 Gy)
1:1.88:3.53
I : I .60 0.048 l:l.61 0.053
1:0.62 0.080 0.90 per “C 0.31
]:I.33
1.05 per 10% 0.42 I .04 per 10% 0.64 1.03 per “C 0.75 I .02 per decade 0.81 I : 1.06 0.84 I .OO per 10% 0.88 I .O I per treatment 0.90
I :0.98 0.96 0.99 per “C 0.96
1.00 per “C
I : I .oo
0.002 I 0.016
0.029
0.32
0.99
1 .oo
weekly when compared with five HT treatments given once weekly (78% versus 64%, respectively) (5).
Two additional non-randomized trials analyzed the in- fluence of the number of HT treatments on CR in com- bined XRT-HT treatment of spontaneous tumors in pet animals. Dewhirst and Sim noted no difference in out- come in tumors that had received one, two, three, or four HT treatments (8). However, Thompson et a/. reported an improved CR rate for tumors that had received two HT treatments (72%; 26/36) compared with tumors that had received only one HT treatment (33%: 5/15) (p = 0.0095) (3 1).
Preliminary results of two ongoing randomized studies also agree with our finding of no improved CR with greater numbers of HT treatments. Alexander et al., in combined XRT-HT regimens comparing four versus eight HT treatments, failed to show improvement with the higher number of HT treatments (1). Finally, Valdagni et al., in a randomized comparison involving the treatment of 17 neck node metastases with radical XRT and either two or six HT treatments, showed no statistically significant differences in CR rates between the two groups (86% vs. SO%, respectively) (32).
Less information is available concerning the influence
Table 6. Results of multivariate regression analyses indicating models best correlating with duration of local control
Relative risk Covariate p value
Model p value
Best 3 covariate model: Covariate Tumor histology
(XC, melanoma, other vs adeno, sarcoma) Concurrent radiation dose Initial tumor volume (diffuse, <I cc vs 21 cc)
4 Covariate models: adding Age Average of minimum tumor temperatures per
field (~4 I “C vs r4 1 “C) Hyperthermia protocol group (2 vs 6) Actual number hyperthermia treatments
112.43 0.0094 0.79 per 10 Gy 0.03 1 1:1.63 0.037
0.00044
1.02 per decade 0.096 0.00036
1:0.59 0.078 0.00026 1:0.93 0.77 0.0012 0.99 per treatment 0.81 0.0012

Radiation therapy and 2 vs. 6 hyperthermia treatments 0 D. S. KAPP 41 a/. 1491
Table 7. Complications of treatment noted at any time of follow-up for fields randomized to either 2 or 6 hyperthermia sessions
Outcome of complications
Hyperthermia Number Resolved Medical Surgical Type randomization complications Persistent spontaneously treatment treatment
Subcutaneous 2 HT I5 13 I I 0 induration/fibrosis 6HT II II 0 0 0
Tumor ulceration 2 HT 7 4 2 0 I 6 HT 8 5 3 0 0
Edema 2 HT 5 5 0 0 0 6 HT 7 5 I 1 0
Normal tissue 2 HT 2 0 2 0 0 ulceration 6 HT 2 1 0 0 I
Infection in 2 HT I 0 0 I 0 catheter site 6 HT 0 0 0 0 0
Totals 2 HT 30 22 5 2 I 6 HT 28 23 4 1 I
of the number of HT treatments in combined XRT-HT regimens for the treatment of deep-seated tumors. In a study reported by Hiraoka and colleagues that included some deeply-located tumors (32 were ~5 cm below the skin: eight were >5 cm below the skin) treated with XRT and radiofrequency capacitive heating, no significant dif- ference in CR rate was noted in tumors that received 2- 7 HT treatments (50%: 5/ 10) compared with those that received 8- 12 HT treatments (53%; 16/30) ( 12). Sapozink et ul., however, reported in a series of 43 patients with deep-seated pelvic malignancy that the number of “sat- isfactory” heat treatments (defined as having achieved in- tratumoral temperatures of >42”C at some time during the treatment) correlated with response (28). Leopold rt al. have recently reported the results of the treatment of resectable soft tissue sarcomas with preoperative XRT and one versus two HT treatments per week (averages of 4.4 and 7.3 HT treatments employed) (19). Using the end- point of severe histopathologic damage in the resection specimen, a statistically significant enhancement of dam- age was noted for tumors randomized to 2 HT treatments per week. Whether the 2 HT treatment per week group will experience improved local control or survival awaits additional patient accrual and follow-up. The far larger tumor volumes, their lack of prior treatment, and the use of a histopathological endpoint makes intercomparison between this sarcoma study and the studies on XRT-HT in superficially-located tumors difficult ( 19).
The development of thermotolerance (TT), that is, a transient resistance to heat killing following an initial heat exposure, provides a possible biological explanation for the general failure to demonstrate either improved CR rates or local-control rates for XRT-HT regimens using three or more HT treatments compared to those using two HT treatments (2 1). Recent studies on murine tumors and on human xenografts have demonstrated prolonged
persistence of TT following initial HT. Meyer et al. heated RIF tumors implanted in mice at 44.O”C for 20 minutes once per week for one to five treatments (20). Single HT treatments induced similar cure rates as did two to five HT treatments. Furthermore, in vitro HT treatment of cells dissociated from the RIF tumors left in situ and re- moved at 5. 10. or 15 days following three HT treatments (delivered once per week), all showed similar levels of TT (20). Prolonged persistence of TT was also exhibited by several of the human melanoma xenografts grown in BALB/c-nu/nu/BOM mice (25). Following an initial in rG heat challenge of 43.5”C for 30 minutes. the half- times of TT decay (as measured by the ratio of slopes of the dose-response curves for specific growth delay versus heating times) for the five human melanoma xenografts studied varied from 53 hours to 142 hours. In two of the five xenografts, the time to “complete” TT decay was greater than 14 days.
Recent in vitro studies on the induction and decay of TT in a human cell line derived from a fibrosarcoma have demonstrated that TT was continuously acquired during exposure to 43°C (O-l 50 minutes). When these cells were made fully TT and returned to 37°C. they did not show complete decay of TT until approximately 150 hours ( I 1). Furthermore, evidence for the development of TT in bi- opsy specimens in both a human mesothelioma and a human ovarian cancer were reported following HT ex- posure in vitro and subsequent incubation at 37°C using dansyl lysine staining as a measure of heat induced cy- totoxicity (36). Thus, TT may offer one explanation for our findings: two treatments may induce TT to the point that subsequent HT treatments are ineffective.
A second, but less likely, explanation for our failure to demonstrate improved CR or local-control rates with six versus two HT treatments is that the HT (as administered in this study) was not an effective adjunct to XRT. A

1492 I. J. Radiation Oncology 0 Biology 0 Physics December 1990. Volume 19. Number 6
thorough review of numerous uncontrolled, matched- paired, and prospectively randomized controlled studies has provided strong evidence that, at least for small (~3 cm) superficially-located lesions, HT when used in com- bination with XRT does result in improved CR rates and local control when compared to similar regimens of XRT alone (2). Although intercomparisons between and sum- mations of various studies are fraught with potential for error because of possible differences in patient selection criteria, XRT-HT treatment regimens, and other prog- nostic factors, a compilation of I1 separate studies in which direct comparison of XRT versus XRT-HT was undertaken in matched-paired lesions revealed an overall CR rate of 67% (242/362) quite similar to the initial local- control rate of 72% ( 118/165) obtained in our protocol study (35). These results compare favorably to the com- posite CR rate of 3 1% ( 108/35 1) reported for the matched lesions that were treated with XRT alone in the I 1 studies (35). Similarly, a separate analysis of 25 fields in our study treated with low-dose radiation ( 1900 cGy-2500 cGy) and HT revealed an initial local-control rate of 40%, superior to the CR rate of 7% for low-dose XRT alone (2000-2400 cGy) noted by van der Zee et al. for the retreatment of metastatic breast cancers (35). The 49 fields in our study treated with higher radiation doses (3000 cGy-3600 cGy) plus HT achieved an initial local-control rate of 82%, which also compares favorably with CR rates of 20% re- ported for XRT alone (3000-3600 cGy) for metastatic breast cancer (35). Furthermore, a local-control rate at 9 months of 75% was obtained for tumors of < 1 cc volume treated on our study with XRT-HT (radiation dose of ~3600 cGy), and a local-control rate of 80% was reported from the RTOG-8104 study for tumors < 3 cm in size treated with XRT (400 cGy X 8) and HT (23). Both of these local-control rates are superior to that of 15% re- ported at 9 months in the RTOG-8 104 study for lesions < 3 cm in diameter treated with XRT alone (23). For lesions of diameter > 3 cm, the RTOG trial noted local- control rates at 12 months of about 25% for both the radiation alone and the radiation plus HT treatments. For lesions 2 1 cc treated in our study, approximately 57% local control was noted at 1 year.
Prognostic,factors The results of our univariate regression analyses sug-
gesting a correlation of our ability to heat tumors (as mea- sured by Tmin) with the duration of local control are in agreement with other studies which have, in general, shown correlations between response rates and measures of either minimum or average intratumoral temperatures (14, 33). Furthermore, the results of our multivariate analyses demonstrated a significantly improved model when Tmin (dichotomized at <4 1 “C versus 24 1 “C) was added as a fourth covariate after histology, concurrent radiation dose, and tumor volume. However, inferences from this finding should not be too hastily drawn, since
considerable effort was directed towards finding a break- point in the average minimum temperature that would yield the most statistically significant results. While these findings are consistent with the existence ofa “threshold” average minimum temperature above which improve- ment in CR and duration of local control exists as reported by Arcangeli et ul. (4), there were too few fields for which Tmin was 241 “C (46 fields) in our study to make such an interpretation confidently.
Only brief discussion needs to be directed towards the other prognostic factors identified in this study since this subject has been extensively reviewed ( 14, 33). Most stud- ies in the literature have reported only univariate analyses and have failed to take into account the influence ofother associated pretreatment or treatment factors on outcome. Given the limitations of these retrospective analyses, it has been felt that no histologic groups were particularly sensitive to combined XRT-HT regimens. However, re- cent studies on superficially-located metastases of Hodg- kin’s disease add support to earlier trials suggesting ex- cellent CR for lymphomas (24). In our current study, a slightly higher initial response rate and improved duration of local control were found for melanomas, squamous cell carcinomas, and other histologies (including Merkel cell tumors) compared with adenocarcinomas and sar- comas. None of the differences between these groups were of statistical significance (Fig. 3a). The various histologies were then lumped into an apparently “favorable” group (consisting of melanomas, squamous cell carcinomas. and other histologies) and an “unfavorable” group (consisting of the adenocarcinomas and sarcomas) for further anal- yses. Univariate and multivariate analyses demonstrated that such a subgrouping resulted in a highly significant difference in duration of local control between the two groups. However, several factors influence this finding. First, the follow-up in the “favorable” group was consid- erably shorter than for the patients in the “unfavorable” group, which consisted primarily of patients with ade- nocarcinoma of the breast metastatic to the chest wall. This latter group of patients has relatively long survivals permitting reseeding into the treatment field or direct ex- tension back into the treatment fields from adjacent sub- cutaneous areas of involvement. Second, the better du- ration of local control in the “favorable” group was in- fluenced by the highly durable local control for melanomas in agreement with other investigations (22, 33) and the excellent response reported for Merkel cell tumors (18). Longer follow-up and larger patient numbers will be needed to substantiate the prognostic significance of the histological subgroups employed.
The strong influence of concurrent radiation dose on response duration confirms the findings of numerous other XRT-HT trials (14, 33) showing improved results with higher total radiation doses. Both our univariate and trivariate models indicated an approximate decrease in risk of local failure of 0.78 per 1000 cGy. Aside from

Radiation therapy and 2 vs. 6 hyperthermia treatments 0 D. S. KAPP et d. 1493
histology, concurrent XRT dose was the most important parameter predictive of local control. This finding should encourage the use of as high a dose of radiation as can be safely given in future combined XRT-HT trials. The au- thors strongly feel that it is premature to consider de- creasing the standard radiation dose that would have otherwise been used in the anticipation that the concurrent use of HT could more than adequately compensate for this dose reduction.
Finally, our finding of the negative influence of in- creasing tumor volume on outcome is also in agreement with the studies reported in the literature (14, 33). Previous analyses of our XRT-HT results have indicated poorer response rates for larger tumors whether the tumor size was characterized by maximum diameter, surface area, or tumor volume ( 17). In these previous studies, the mean minimal intratumoral temperatures obtained were sig- nificantly lower in the tumors that were at least 5 cc than in smaller tumors. The influence of tumor size on our ability to heat tumors requires additional study, and se- lection and availability of HT applicators capable of heat- ing larger surface tumors is of great importance in the design of future HT trials (23).
Other parameters, such as tumor site or prior XRT dose, that were significant or of borderline significance in the univariate analyses of our study failed to be of inde- pendent significance in the multivariate analyses. This is related to the correlation between these parameters and other significant covariates. Site of disease was strongly correlated with histology. The vast majority of the thorax fields contained adenocarcinomas (from metastatic breast cancers), and the head and neck sites contained mostly metastatic squamous cell cancers. Similarly, prior XRT was strongly correlated with concurrent XRT dose. Pa- tients who had previously received full-course XRT re- ceived lower doses of concurrent XRT with their HT treatments.
Complications Given the advanced nature of the patients’ disease and
their often extensive prior treatments, it was felt that our complication rate from XRT-HT was acceptable. There were no life-threatening complications, and only two complications required surgical repair-one for a normal tissue ulceration (in a scar) and one for persistent ulcer- ation after eradication of the tumor. A detailed analysis of factors associated with complications for our overall experience with the use of XRT-HT in patients with deep as well as superficially-located tumors has been recently reported ( 15). A correlation between both the Tmax and the number of HT treatments per field with the devel- opment of complications was noted ( 15). The studies re- ported here included only superficially-located tumors treated primarily with microwave applicators and two or six HT treatments, and no overall increase in complica- tions or alteration in the type or severity of complications
was noted with increased number of HT treatments. Our finding of an overall incidence of 16% (26/ 165) of fields showing area(s) of subcutaneous induration/fibrosis, often at sites of the insertion of catheters for subcutaneous tem- perature monitoring, is believed to be related to our gen- erous use of topical xylocaine for local anesthesia prior to the insertion of the catheters. This association is cur- rently being further investigated.
It is difficult to compare our complication rate directly with other studies because of the shorter follow-up in many studies, their lack of sufficient details on compli- cations, difference in subgroupings used to quantitate complications, and different definitions used to separate acute or subacute side effects from long-term complica- tions. Scott et a/., in a trial of full-dose XRT and HT, tabulated the “most severe complication reported” 6 months or more after the start of treatment in 58 patients with available information (29). Rates of minimum skin depigmentation/fibrosis of 24%. and moderate subcuta- neous fibrosis of 9%. were similar to the overall rate of 16% for subcutaneous fibrosis/induration noted at any follow-up (3 weeks post-treatment or longer) in our series. Scott ef al. also reported a 12% incidence of persistent ulceration and a 3% incidence of skin/subcutaneous ne- crosis, in close agreement with our rates of 9.1% ( 15/ 165) for tumor ulceration and 2.4% (4/165) for normal tissue (skin and subcutaneous tissue) ulcerations (29).
CONCLUSIONS
The results of this study involving 165 evaluable fields with superficially-located (~3 cm from the surface) ma- lignancies in 64 patients randomized to standardized XRT-HT regimens using two versus six HT treatments have demonstrated no significant influence of the number of HT treatments on either the response rate at 3 weeks or the duration of local control. The pretreatment and treatment parameters did not significantly differ between the fields randomized to two versus six HT treatments. ___ __ Tmax, Tave, Tmin of 44.8”C, 42.5”C. and 40.2”C. re- spectively, were obtained for the entire group. The treat- ments were well tolerated and the complication rate was felt to be acceptable. Univariate and multivariate regres- sion analyses identified tumor histology, concurrent ra- diation dose, initial tumor volume, and Tmin (when di- chotomized to <4 1 “C versus 24 1 “C) as correlating with duration of local control.
This study lends support for the value of HT when used in conjunction with XRT for the treatment of su- petficially-located malignancies and suggests the influence of thermotolerance in limiting the effectiveness of multiple relatively closely spaced HT treatments. It also points to the need to obtain higher m, use high XRT doses, and stratify patients based on tumor histology and size of le- sion. Additional XRT-HT trials are felt warranted to clar-

1494 I. J. Radiation Oncology 0 Biology 0 Physics December 1990. Volume 19. Number 6
ify further the value of HT and to optimize XRT-HT are new trials at Stanford designed to evaluate the influ- treatment regimens. Trials following strict guidelines for ence of TT (3). Participation in such randomized trials is quality assurance for HT treatments and comparing XRT to be encouraged: exciting and meaningful results from with and without HT in selected sites are ongoing (6), as these studies should be forthcoming.
REFERENCES
I. Alexander, G. A.; Moylan, D. J.; Waterman, F. M.; Nerlin- ger, R. E.; Leeper, D. B. Randomized trial of 1 vs. 2 adjuvant hyperthermia treatments in patients with superficial metas- tases. Presented at the 35th Annual Meeting of the Radiation Research Society, Atlanta, Georgia, February 2 I-26, 1987.
2. Anderson, R. L.; Kapp, D. S. Hyperthermia in cancer ther- apy: current status. Med. J. Australia 152:3 IO-3 15; 1990.
3. Anderson, R. L.; Kapp, D. S.; Woo, S. Y.; Rice, G. C.; Lee, K. J.; Hahn, G. M. Predictive assays for tumor response to single and multiple fractions of hyperthermia. Recent Re- sults in Cancer Res. 109:239-249; 1988.
4. Arcangeli, G.; Arcangeli, G.; Guerra. A.: Lovisolo. G.: Civ- idalli, A.; Marino, C.; Mauros, F. Tumor response to heat and radiation: prognostic variables in the treatment of neck node metastases from head and neck cancer. Int. J. Hy- perther. 1:207-217: 1985.
5. Arcangeli, G.; Nervi. C.; CividaIIi, A.; Lovisolo, G. A. Prob- lem of sequence and fractionation in the clinical application of combined heat and radiation. Cancer Res. 44(Suppl.): 4857s-4863s: 1984.
6. Arcangeli, G.; Overgaard. J.; Gonzalez-Gonzalez, D.; Shri- vastava, P. N. Hyperthermia trials. Int. J. Radiat. Oncol. BioI. Phys. 14:S93-S109; 1988.
7. Cox, D. R. Analysis of binary data. London: Chapman and Hall; 1970.
8. Dewhirst, M. W.: Sim, D. A. The utility of thermal dose as a predictor of tumor and normal tissue responses to com- bined radiation and hyperthermia. Cancer Res. 44(Suppl.): 4772s-4780s; 1984.
9. Dunlop, P. R. C.; Hand, J. W.; Dickinson, R. J.; Field, S. B. An assessment of local hyperthermia in clinical prac- tice. Int. J. Hyperther. 2:39-50; 1986.
10. Gehan. E. A. A generalized Wilcoxon test for comparing arbitrarily singly censored samples. Biometrika 52:203-233; 1965.
11. Hahn, G. M.; Ning. S. C.: Elizaga, M.: Kapp, D. S.; An- derson, R. L. A comparison of thermal responses of human and rodent cells. Int. J. Radiat. BioI. 56:817-825; 1989.
12. Hiraoka, M.: Jo, S.; Dodo. Y.; Ono. K.: Takahashi. M.: Nishida, H.; Abe, M. Clinical results of radiofrequency hy- perthermia combined with radiation in the treatment of radioresistant cancers. Cancer 54:2898-2904; 1984.
13. Kaplan, E. L.; Meier, P. Nonparametric estimation from incomplete observations. J. Am. Statist. Assoc. 53:457-48 I ; 1958.
14. Kapp, D. S. Areas of need for continued Phase 11 testing in human patients. In: Paliwal, B. R., Hetzel, F. W., Dewhirst, M. W., eds. Biological, physical and clinical aspects of hy- perthermia. Medical physics monograph No. 16. New York: American Institute of Physics, Inc.; 1988; 424-443.
15. Kapp, D. S.; Cox, R. S.; Fessenden, P.; Meyer, J. L.; Prionas, S. D.: Lee, E. R.: Bagshaw, M. A. Parameters predictive for complications of treatment with combined hyperthermia and radiation therapy. Int. J. Radiat. Oncol. Biol. Phys. lS(Suppl. 1):122-123: 1988.
16. Kapp, D. S.; Fessenden. P.: Samulski. T. V.; Bagshaw, M. A.; Cox, R. S.; Lee, E. R.; Lohrbach. A. W.; Meyer, J. L.; Prionas, S. D. Stanford University institutional report.
Phase I evaluation of equipment for hyperthermia treatment of cancer. Int. J. Hyperther. 4:75-l 15; 1988.
17. Kapp. D. S.; Samulski, T. V.; Fessenden, P.: Bagshaw, M. A.: Lee. E. R.: Lohrbach. A. W.: Cox. R. S. Prognostic significance of tumor volume on response following Iocal- regional hyperthermia and radiation therapy. Presented at the 35th Annual Meeting of the Radiation Research Society, Atlanta, Georgia, February 2 I-26. 1987.
18. Knox, S. J.; Kapp, D. S. Hyperthermia and radiation therapy in the treatment of recurrent Merkel cell tumors. Cancer 62:1479-1486; 1988.
19. Leopold, K. A.; Harrelson, J.; Prosnitz. L.: Samulski, T. V.: Dewhirst, M. W.; Oleson, J. R. Preoperative hyperthermia and radiation for soft tissue sarcomas: advantage of two vs one hyperthermia treatment per week. Int. J. Radiat. Oncol. Biol. Phys. 16:107-l 15: 1989.
20. Meyer, J. L.: van Kersen. I.; Hahn, G. M. Tumor responses following multiple hyperthermia and x-ray treatments: role of thermotolerance at the cellular level. Cancer Res. 46: 569 I-5695; 1986.
21. Overgaard. J.: Nielsen, 0. S. The importance of thermo- tolerance for the clinical treatment with hyperthermia. Ra- diother. Oncol. 1: 167- 178; 1983.
22. Overgaard, J.: Overgaard, M. Hyperthermia as an adjuvant to radiotherapy in the treatment of malignant melanoma. Int. J. Hyperther. 3:483-501: 1987.
23. Perez, C. A.; Gillespie, B.; Pajak, T.: Hornback, N. B.; Emami, B.: Rubin, P. Quality assurance problems in clinical hyperthermia and their impact on therapeutic outcome: a report by the Radiation Therapy Oncology Group. Int. J. Radiat. Oncol. Biol. Phys. 16:551-558: 1989.
24. Petersen. I. A.; Kapp, D. S. Local hyperthermia and radia- tion therapy in the retreatment of superficially located re- currences in Hodgkin’s disease. Int. J. Radiat. Oncol. Biol. Phys. 18:603-6 11; 1990.
25. Rofstad. E. K. Influence of cellular. microenvironmental, and growth parameters on thermotolerance kinetics in vivo in human melanoma xenografts. Cancer Res. 49:5027-5032: 1989.
26. Samulski, T. V.: Fessenden, P.: Lee. E. R.: Kapp, D. S.: Tanabe. E.; McEuen. A. Spiral microstrip hyperthermia ap- plicators: technical design and clinical performance. Int. J. Radiat. Oncol. BioI. Phys. 18233-242; 1990.
27. Sapozink. M. D.: Cetas. T.; Cony, P. M.: Egger. M. J.; Fes- senden, P.; and the NCI Hyperthermia Equipment Evalu- ation Contractors’ Group. Introduction to hyperthermia device evaluation. Int. J. Hyperther. 4: I-I 5: 1988.
28. Sapozink. M. D.; Gibbs, F. A.: Egger, M. J.; Stewart. J. R. Regional hyperthermia for chnically advanced deep-seated pelvic malignancy. Am. J. Clin. Oncol. (CTT) 9:162-169; 1986.
29. Scott, R.; Gillespie, B.; Perez, C. A.: Hornback, N. B.; John- son, R.: Emami, B.; Bauer. M.: Pakuris. E. Hyperthermia in combination with definitive radiation therapy: results of a phase I/II RTOG study. Int. J. Radiat. Oncol. Biol. Phys. 15:71 l-716; 1988.
30. Steeves. R. A. Local hyperthermia and electron therapy for recurrent breast cancer. In: Steeves. R. A., Paliwal. B. R..

Radiation therapy and 2 vs. 6 hyperthermia treatments 0 D. S. KAPP cf a/. 1495
eds. Syllabus: a categorical course in radiation therapy: hy- perthermia. Oak Brook, IL: Radiological Society of North America, Inc., 1987: 77-91.
3 I. Thompson. J. M.: Dhoodhat, Y. A.: Bleehen, N. M.; Gor- man. N. T. Microwave hyperthermia in the treatment of spontaneous canine tumors: an analysis of treatment pa- rameters and tumor response. Int. J. Hyperther. 4:383-399: 1988.
34. Valdagni. R.; Kapp, D. S.: Valdagni, C. NJ (TNM-UICC) metastatic neck nodes managed by combined radiation therapy and hyperthermia: clinical results and analysis of treatment parameters. Int. J. Hyperther. 2: 189-200: 1986.
32. Valdagni, R.; Amichetti, M.; Pani, G. Radical radiation alone versus radical radiation plus microwave hyperthermia for N3 (TNM-UICC) neck nodes: a prospective randomized clinical trial. Int. J. Radiat. Oncol. Biol. Phys. l5:13-24: 1988.
35. van der Zee, J.; Treurniet-Donker, A. D.; The. S. K.; Helle, P. A.; Seldenrath, J. J.: Meerwaldt, J. H.; Wijnmaalen, A. J.: van den Berg, A. P.; van Rhoon, G. G.; Broekmeyer- Reurink. M. P.. Reinhold, H. S. Low dose reirradiation in combination with hyperthermia: a palliative treatment for patients with breast cancer recurring in previously irradiated areas. Int. J. Radiat. Oncol. Biol. Phys. 15:1407-1413: 1988.
33. Valdagni. R.; Liu, F. F.: Kapp. D. S. Important prognostic 36. Woo, S. Y.; Rice, G. C.; Kapp, D. S.: Hahn, G. M. A pre- factors influencing outcome of combined radiation and hy- dictive assay for human tumor cellular response to hyper- perthermia. Int. J. Radiat. Oncol. Biol. Phys. 15:959-972: thermia using dansyl lysine staining and flow cytometry. 1988. Int. J. Radiat. Oncol. Biol. Phys. 14:361-365: 1988.




















