Treatment Outcomes in the STAR Study: A Subanalysis of Solifenacin 5 mg and Tolterodine ER 4 mg
9
Neuro-urology Treatment Outcomes in the STAR Study: A Subanalysis of Solifenacin 5 mg and Tolterodine ER 4 mg Christopher R. Chapple a, *, Aino Fianu-Jonsson b , Mark Indig c , Vik Khullar d , Jose ´ Rosa e , Roberto M. Scarpa f , Arun Mistry g , D. Mark Wright g , John Bolodeoku g , for the STAR study group 1 a Urology Research Office, Royal Hallamshire Hospital, Sheffield, UK b Enheten fo ¨ r Obstetrik & Gynekologi, Karolinska Universitetssjukhuset Hudd, Stockholm, Sweden c Dr Indig, Private Practitioner, Kutzbach str.7, Trier, Germany d Department of Obstetrics and Gynaecology St Mary’s Hospital, London, UK e Department of Urology, Hospital Comarcal Santiago Apo ´ stol, Miranda de Ebro-Burgos, Spain f Clinica Urologica Universita ` di Torino, ASO S. Luigi Gonzaga, Orbassano (Torino) Italy g Medical Affairs Europe, Astellas Pharma Europe Ltd, Staines, UK european urology 52 (2007) 1195–1203 available at www.sciencedirect.com journal homepage: www.europeanurology.com Article info Article history: Accepted May 29, 2007 Published online ahead of print on June 6, 2007 Keywords: Antimuscarinic Solifenacin Tolterodine Overactive bladder Abstract Objective: To compare OAB symptom outcomes following initial randomised treat- ment with solifenacin 5 mg or tolterodine ER 4 mg at the 4-week clinic-visit and again at 12 weeks for patients choosing to remain on this treatment dose from 4 weeks. Methods: A prospective, double blind, double-dummy, two-arm, parallel-group, 12-week study (The STAR study) was conducted to compare the efficacy and safety of solifenacin 5/10 mg and tolterodine extended release (ER) 4 mg in OAB patients. Results: At 4 weeks mean improvements in OAB symptoms, including urgency, fre- quency (primary variable), incontinence and nocturia, were larger in patients rando- mised to solifenacin 5 mg; with the difference for incontinence being statistically significant (mean reduction in incontinence episodes/24 hrs in the solifenacin group of 1.30 vs. 0.90 ( p = 0.0181); the mean result for solifenacin 5 mg amounted to a 44% additional improvement.) There was an associated significant reduction in pad use (reduced by 1.21 vs. 0.80; p = 0.0089); the mean result for solifenacin 5 mg amounted to a 51% additional improvement over that of tolterodine ER 4 mg. For patients choosing to remain on these treatments improvements in favour of solifenacin were maintained at study end (12-weeks). Treatments were well tolerated. Conclusions: Within 4 weeks solifenacin 5 mg was statistically significantly better than tolterodine ER 4 mg in improving incontinence and reducing incontinence pad use. Differences in efficacy in favour of solifenacin 5 mg were maintained from 4 weeks for the duration of the study for patients choosing to remain on their starting dose. # 2007 European Association of Urology. Published by Elsevier B.V. All rights reserved. * Corresponding author. Tel. +44 114 2712559. E-mail address: c.r.chapple@sheffield.ac.uk (C.R. Chapple). 1 See Appendix A for complete list of contributors. 0302-2838/$ – see back matter # 2007 European Association of Urology. Published by Elsevier B.V. All rights reserved. doi:10.1016/j.eururo.2007.05.027 244477
Transcript of Treatment Outcomes in the STAR Study: A Subanalysis of Solifenacin 5 mg and Tolterodine ER 4 mg
Neuro-urology
Treatment Outcomes in the STAR Study: A Subanalysis ofSolifenacin 5 mg and Tolterodine ER 4 mg
Christopher R. Chapple a,*, Aino Fianu-Jonsson b, Mark Indig c, Vik Khullar d,Jose Rosa e, Roberto M. Scarpa f, Arun Mistry g, D. Mark Wright g, John Bolodeoku g,
for the STAR study group1
aUrology Research Office, Royal Hallamshire Hospital, Sheffield, UKbEnheten for Obstetrik & Gynekologi, Karolinska Universitetssjukhuset Hudd, Stockholm, SwedencDr Indig, Private Practitioner, Kutzbach str.7, Trier, GermanydDepartment of Obstetrics and Gynaecology St Mary’s Hospital, London, UKeDepartment of Urology, Hospital Comarcal Santiago Apostol, Miranda de Ebro-Burgos, SpainfClinica Urologica Universita di Torino, ASO S. Luigi Gonzaga, Orbassano (Torino) ItalygMedical Affairs Europe, Astellas Pharma Europe Ltd, Staines, UK
e u r o p e a n u r o l o g y 5 2 ( 2 0 0 7 ) 1 1 9 5 – 1 2 0 3
avai lab le at www.sciencedi rect .com
journa l homepage: www.europeanurology.com
Article info
Article history:Accepted May 29, 2007Published online ahead ofprint on June 6, 2007
Keywords:AntimuscarinicSolifenacinTolterodineOveractive bladder
Abstract
Objective: To compare OAB symptom outcomes following initial randomised treat-
ment with solifenacin 5 mg or tolterodine ER 4 mg at the 4-week clinic-visit and again
at 12 weeks for patients choosing to remain on this treatment dose from 4 weeks.
Methods: A prospective, double blind, double-dummy, two-arm, parallel-group,
12-week study (The STAR study) was conducted to compare the efficacy and safety
of solifenacin 5/10 mg and tolterodine extended release (ER) 4 mg in OAB patients.
Results: At 4 weeks mean improvements in OAB symptoms, including urgency, fre-
quency (primary variable), incontinence and nocturia, were larger in patients rando-
mised to solifenacin 5 mg; with the difference for incontinence being statistically
significant (mean reduction in incontinence episodes/24 hrs in the solifenacin group of
�1.30 vs. �0.90 (p = 0.0181); the mean result for solifenacin 5 mg amounted to a 44%
additional improvement.) There was an associated significant reduction in pad use
(reduced by�1.21 vs.�0.80; p = 0.0089); the mean result for solifenacin 5 mg amounted
to a 51% additional improvement over that of tolterodine ER 4 mg. For patients
choosing to remain on these treatments improvements in favour of solifenacin were
maintained at study end (12-weeks). Treatments were well tolerated.
Conclusions: Within 4 weeks solifenacin 5 mg was statistically significantly better than
tolterodine ER 4 mg in improving incontinence and reducing incontinence pad use.
Differences in efficacy in favour of solifenacin 5 mg were maintained from 4 weeks for
the duration of the study for patients choosing to remain on their starting dose.
# 2007 European Association of Urology. Published by Elsevier B.V. All rights reserved.
* Corresponding author. Tel. +44 114 2712559.E-mail address: [email protected] (C.R. Chapple).1 See Appendix A for complete list of contributors.
244477
0302-2838/$ – see back matter # 2007 European Association of Urology. Published by Elsevier B.V. All rights reserved. doi:10.1016/j.eururo.2007.05.027

e u r o p e a n u r o l o g y 5 2 ( 2 0 0 7 ) 1 1 9 5 – 1 2 0 31196
1. Introduction
Overactive bladder (OAB) syndrome is a commonsymptom complex that affects millions of peopleworldwide, occurring with an increasing prevalencewith advancing age [1]. OAB may be defined asurgency, with or without urgency incontinence,usually accompanied by frequency and nocturia.(Urgency incontinence is an evolution of the termurge incontinence and provides a more precisecharacterization of incontinence in OAB.) Thesesymptoms have been shown to be bothersome topatients, to affect their well-being [1] and have animpact on quality of life [2]. Accordingly, in recentyears a number of therapeutic agents, all with anantimuscarinic mode of action, have been developedand have received regulatory approval; includingoxybutynin, tolterodine, propiverine, trospium andrecently launched drugs such as darifenacin andsolifenacin. However OAB is both under-reported bypatients and under-treated by clinicians [1,3] despiteclear evidence that antimuscarinics reduce OABsymptoms [4]. Furthermore antimuscarinics suchas solifenacin [5] achieve a good balance of efficacyand tolerability and as a consequence is associatedwith good long term compliance and patient satisfac-tion [6] The therapeutic profile however may differbecause antimuscarinics have differing profiles ofreceptor interaction on the five subtypes of muscari-nic receptor that represent targets for OAB treat-ments [7]. It is likely that selectivity for, or tissuepenetration of the drug onto, antimuscarinic recep-tors in the bladder as contrasted to those present inother peripheral tissues may be useful in achieving abalance between efficacy and side-effects such as drymouth and may result in differences in the efficacyand adverse event profiles of the different antimus-carinics.
The STAR study [8] was a comparative, double-blind, international pan-European study designed tocompare the therapeutic profiles of two antimus-carinics, solifenacin and tolterodine. A challenge forthe design of this study and similar studies is posedby the availability of different doses of the com-parators. Solifenacin is available at a dose of 5 mgwith the option to increase the dose to 10 mg ifneeded whereas the recommended dose of tolter-odine ER is 4 mg once daily with no option toincrease the dose if needed (higher doses wereassociated with increases in residual urinaryvolume and adverse events [8]). Accordingly, thedesign addressed this difference in dosing recom-mendations by offering all patients under double-blind conditions the option to request a doseincrease after 4 weeks of the 12 week active
treatment period but only increasing the dose forthose in the solifenacin group. Accordingly theprimary analysis [8] compared treatments accordingto the approved dosing regimens (solifenacin 5 mgrising to 10 mg if needed; tolterodine ER 4 mg) andthus reflected outcomes that the physician mightencounter in clinical practice after the establish-ment of treatment with either antimuscarinic.
Treatment outcomes prior to the option torequest a dose increase in the STAR study, i.e. whenall patients were treated with either solifenacin 5 mgor tolterodine ER 4 mg, reflect those that might beencountered by physicians in normal clinical prac-tice at the first clinic visit after initiating treatment.This would be a decision point when reviewingprogress and determining whether the treatmentwas optimal or could be improved by a dose increaseor treatment switch. The purpose of the presentarticle concerns this decision point and providesaspects of the secondary analysis concerned withimprovements at the first clinic visit in the STARstudy 4-weeks after initiation of treatment. Addi-tionally exploratory analysis is also presented tofollow the comparative outcomes for the subgroupsof patients who subsequently decided not to requesta dose increase and thus to remain on these dosesfor the duration of the STAR study.
2. Methods
The STAR study was conducted across Europe between May
2003 (first patient first visit) and October 2004 (last patient last
visit) and involved 17 countries, 117 study sites and screened
1355 patients. The study was performed in accordance with
the International Conference on Harmonisation Good Clinical
Practice guidelines, and the principles of the Declaration of
Helsinki. Both central and local ethics committee approved
the study protocol.
Patients enrolled were men and women aged at least
18 years who had OAB symptoms (including urinary frequency,
urgency or urgency incontinence) for 3 months or more and
being treated as outpatients.
2.1. Study design
The study followed a prospective, double-blind, 2-arm, parallel
group design with a 12-week active treatment period. The
screening visit was designated as Visit 1 and the inclusion
criteria included: (1) an average of�8 micturitions per 24 hours;
(2) an average of �1 incontinence episode per 24 hours, or an
average of �1 urgency episode per 24 hours. Eligibility was
confirmed for the above at the end of the 2-week, single-blind,
placebo run-in (Visit 2) using the results recorded in the 3-day
voiding diary period prior to the visit. Patients were then
randomised to receive as double-blind treatment either
solifenacin 5 mg or tolterodine ER 4 mg. The treatment regimen
throughout the study was double-blind and consisted of two

e u r o p e a n u r o l o g y 5 2 ( 2 0 0 7 ) 1 1 9 5 – 1 2 0 3 1197
tablets and one capsule regardless of treatment or dose.
Tolterodine ER 4 mg (or equivalent placebo) was blinded by
over-encapsulation (without back-filler). Patients returned after
4-weeks active treatment (Visit 3), when they had the option of
requesting a dose increase, based on their satisfaction with
treatment efficacy and tolerability, and discussion with the
investigator. Only patients randomised to solifenacin received
an actual dose increase. The primary analysis was comparison
at end point between patients treated with solifenacin or
tolterodine ER as per the SPC dosing recommendations and has
been reported previously [8]. Pre-specified secondary analyses
included time course comparisons for the Randomised Treat-
ment (RT) groups and for treatment subgroups arising from the
patient selection at the dose increase request option of the
4 week visit (Visit 3) and are presented here.
2.1.1. Patient populations, treatment groups and subgroupscomparedIn order to compare the efficacy and safety of solifenacin 5 mg
and tolterodine ER 4 mg only results are presented here for:
1. R
andomised Treatment Groups at Visit 3, i.e. after the initial4 week treatment period and before the dose increase
option.
2. N
o Dose Increase (NDI) subgroups at endpoint, i.e. after thefinal 8 week treatment period (12 weeks total) and after the
dose increase option.
The NDI subgroups were formed from the Randomised
Treatment groups by the subtraction of all patients who
requested, rather than were randomised to, a dose increase.
Thus the NDI comparison should be viewed as exploratory and
hypothesis-generating.
The study population for each was the Full Analysis Set
(FAS) an Intent-To-Treat (ITT) population modified by the
requirement for efficacy data at both baseline (V2, end of
placebo run-in) and during double-blind treatment as the
variables are ‘change from baseline’.
2.1.2. Statistical methodsData is presented as between-treatment differences in changes
from baseline to 4 Weeks in the primary and secondary efficacy
variables. Analytical methods for Randomised Treatment
groups and NDI subgroups differed. Inferential analysis was
applied to the Randomised Treatment groups as these groups
were created by randomisation and subjected to sample size
calculations. Comparisons for the Randomised Treatment
groups at 4 weeks were formally tested using an Analysis of
Covariance (ANCOVA). The testing described here was for
superiority. Descriptive analysis was applied to the NDI
subgroup as these subgroups were created by patient choice
and were not subjected to sample size calculations. Compar-
isons for the NDI subgroup at study endpoint described here are
numerical based upon calculated means.
2.2. Efficacy assessments
Efficacy assessments, which were derived from the 3-day
voiding diary, included baseline and change from baseline in
episodes/24 h of micturition (primary endpoint), urgency,
urgency incontinence, incontinence (with and without the
sensation of urgency) and nocturia. Other endpoints included:
patient pad usage per 24 hours, the volume voided per
micturition, Perception of Bladder Condition (PBC) for patient
assessment of the severity of the problems caused by their
OAB.
2.3. Safety assessments
Adverse events (AEs) were evaluated for individuals receiving
at least one dose of active study medication. At each clinic visit
any AE reported in response to general and non-specific
questioning by the investigator, or volunteered by the patient,
was recorded in the appropriate page of the Case Report Form.
An AE was counted when the event occurred after the first
dose of study medication, or was an exacerbation of an AE that
was present before the first dose of the study medication. The
severity of AEs was determined by the investigator, according
the following guidelines: a mild AE caused discomfort but no
disruption of normal daily activity; a moderate AE caused
discomfort sufficient to reduce or affect normal daily activity;
and a severe AE was one that resulted in inability to work or
perform daily activity. Discontinuations due to AEs were also
recorded.
3. Results
3.1. Comparisons of the Randomised Treatment groups at
4 weeks (improvements before the dose increase request option)
The Randomised Treatment groups, i.e. patientsrandomised to solifenacin (FAS n = 578) or tolter-odine (FAS n = 599), were comparable in demo-graphic and baseline data [8].
At 4 weeks mean improvements in OAB symp-toms, including urgency, frequency (primary vari-able), incontinence and nocturia, were larger inpatients randomised to solifenacin 5 mg (seeTable 1), although only the difference for incon-tinence was statistically significant (mean reductionin incontinence episodes/24 hrs in the solifenacingroup of�1.30 vs.�0.90 ( p = 0.0181); the mean resultfor solifenacin 5 mg amounted to a 44% additionalimprovement.) There was an associated significantreduction in pad use (reduced by �1.21 vs. �0.80;p = 0.0089); the mean result for solifenacin 5 mgamounted to a 51% additional improvement overthat of tolterodine ER 4 mg. See Fig. 1.
3.2. Comparisons of the NDI subgroups at endpoint
(improvements in OAB variables after the dose increase
option)
After 4 weeks (Visit 3) 52% of solifenacin patientsand 49% of tolterodine ER patients in the FASpopulation chose to continue as previously and
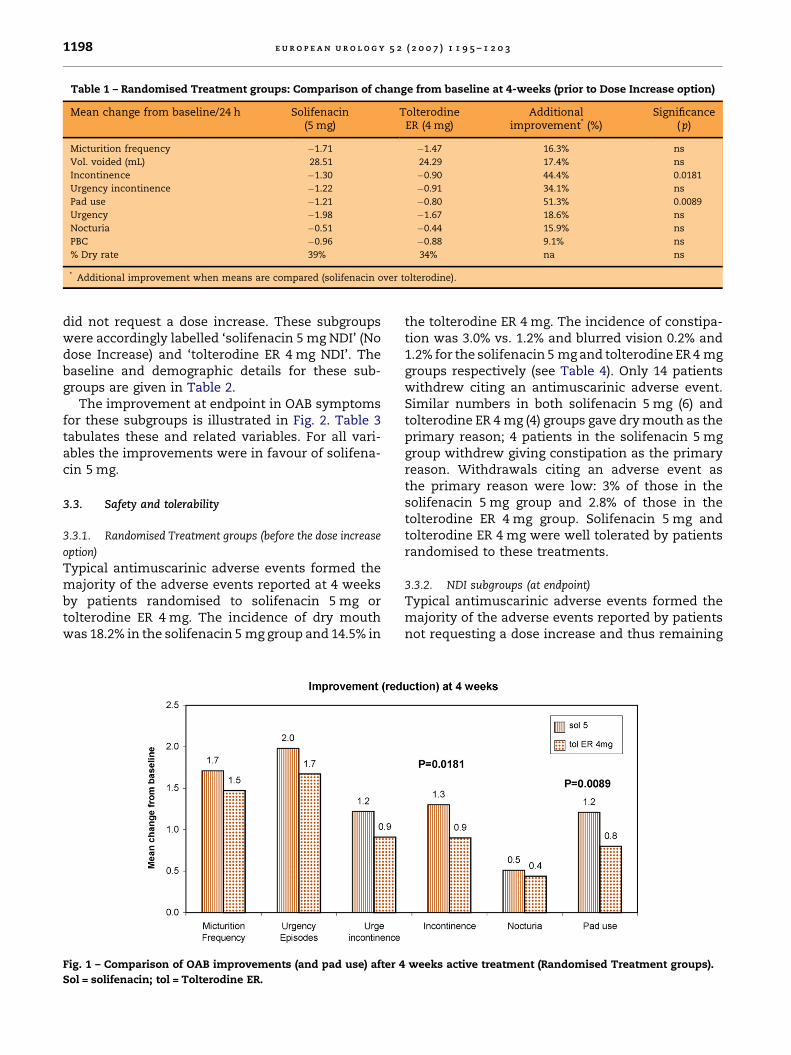
Table 1 – Randomised Treatment groups: Comparison of change from baseline at 4-weeks (prior to Dose Increase option)
Mean change from baseline/24 h Solifenacin(5 mg)
TolterodineER (4 mg)
Additionalimprovement* (%)
Significance(p)
Micturition frequency �1.71 �1.47 16.3% ns
Vol. voided (mL) 28.51 24.29 17.4% ns
Incontinence �1.30 �0.90 44.4% 0.0181
Urgency incontinence �1.22 �0.91 34.1% ns
Pad use �1.21 �0.80 51.3% 0.0089
Urgency �1.98 �1.67 18.6% ns
Nocturia �0.51 �0.44 15.9% ns
PBC �0.96 �0.88 9.1% ns
% Dry rate 39% 34% na ns
* Additional improvement when means are compared (solifenacin over tolterodine).
e u r o p e a n u r o l o g y 5 2 ( 2 0 0 7 ) 1 1 9 5 – 1 2 0 31198
did not request a dose increase. These subgroupswere accordingly labelled ‘solifenacin 5 mg NDI’ (Nodose Increase) and ‘tolterodine ER 4 mg NDI’. Thebaseline and demographic details for these sub-groups are given in Table 2.
The improvement at endpoint in OAB symptomsfor these subgroups is illustrated in Fig. 2. Table 3tabulates these and related variables. For all vari-ables the improvements were in favour of solifena-cin 5 mg.
3.3. Safety and tolerability
3.3.1. Randomised Treatment groups (before the dose increase
option)
Typical antimuscarinic adverse events formed themajority of the adverse events reported at 4 weeksby patients randomised to solifenacin 5 mg ortolterodine ER 4 mg. The incidence of dry mouthwas 18.2% in the solifenacin 5 mg group and 14.5% in
Fig. 1 – Comparison of OAB improvements (and pad use) after 4
Sol = solifenacin; tol = Tolterodine ER.
the tolterodine ER 4 mg. The incidence of constipa-tion was 3.0% vs. 1.2% and blurred vision 0.2% and1.2% for the solifenacin 5 mg and tolterodine ER 4 mggroups respectively (see Table 4). Only 14 patientswithdrew citing an antimuscarinic adverse event.Similar numbers in both solifenacin 5 mg (6) andtolterodine ER 4 mg (4) groups gave dry mouth as theprimary reason; 4 patients in the solifenacin 5 mggroup withdrew giving constipation as the primaryreason. Withdrawals citing an adverse event asthe primary reason were low: 3% of those in thesolifenacin 5 mg group and 2.8% of those in thetolterodine ER 4 mg group. Solifenacin 5 mg andtolterodine ER 4 mg were well tolerated by patientsrandomised to these treatments.
3.3.2. NDI subgroups (at endpoint)
Typical antimuscarinic adverse events formed themajority of the adverse events reported by patientsnot requesting a dose increase and thus remaining
weeks active treatment (Randomised Treatment groups).
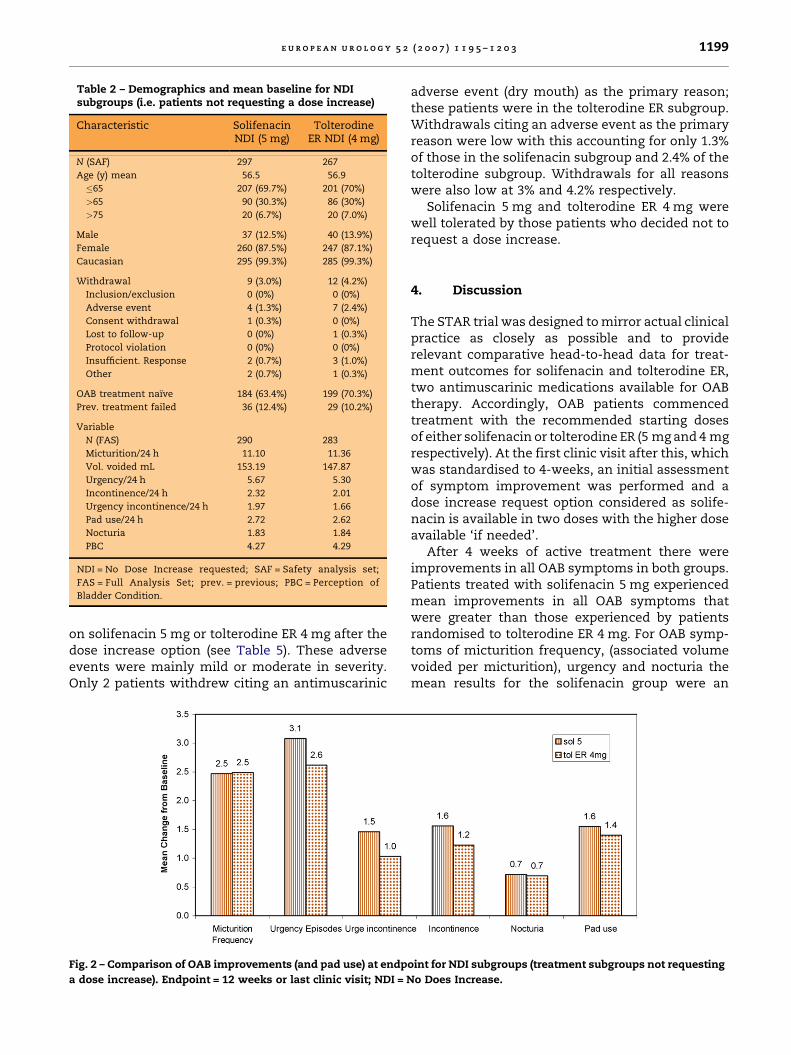
Table 2 – Demographics and mean baseline for NDIsubgroups (i.e. patients not requesting a dose increase)
Characteristic SolifenacinNDI (5 mg)
TolterodineER NDI (4 mg)
N (SAF) 297 267
Age (y) mean 56.5 56.9
�65 207 (69.7%) 201 (70%)
>65 90 (30.3%) 86 (30%)
>75 20 (6.7%) 20 (7.0%)
Male 37 (12.5%) 40 (13.9%)
Female 260 (87.5%) 247 (87.1%)
Caucasian 295 (99.3%) 285 (99.3%)
Withdrawal 9 (3.0%) 12 (4.2%)
Inclusion/exclusion 0 (0%) 0 (0%)
Adverse event 4 (1.3%) 7 (2.4%)
Consent withdrawal 1 (0.3%) 0 (0%)
Lost to follow-up 0 (0%) 1 (0.3%)
Protocol violation 0 (0%) 0 (0%)
Insufficient. Response 2 (0.7%) 3 (1.0%)
Other 2 (0.7%) 1 (0.3%)
OAB treatment naıve 184 (63.4%) 199 (70.3%)
Prev. treatment failed 36 (12.4%) 29 (10.2%)
Variable
N (FAS) 290 283
Micturition/24 h 11.10 11.36
Vol. voided mL 153.19 147.87
Urgency/24 h 5.67 5.30
Incontinence/24 h 2.32 2.01
Urgency incontinence/24 h 1.97 1.66
Pad use/24 h 2.72 2.62
Nocturia 1.83 1.84
PBC 4.27 4.29
NDI = No Dose Increase requested; SAF = Safety analysis set;
FAS = Full Analysis Set; prev. = previous; PBC = Perception of
Bladder Condition.
e u r o p e a n u r o l o g y 5 2 ( 2 0 0 7 ) 1 1 9 5 – 1 2 0 3 1199
on solifenacin 5 mg or tolterodine ER 4 mg after thedose increase option (see Table 5). These adverseevents were mainly mild or moderate in severity.Only 2 patients withdrew citing an antimuscarinic
Fig. 2 – Comparison of OAB improvements (and pad use) at endp
a dose increase). Endpoint = 12 weeks or last clinic visit; NDI = N
adverse event (dry mouth) as the primary reason;these patients were in the tolterodine ER subgroup.Withdrawals citing an adverse event as the primaryreason were low with this accounting for only 1.3%of those in the solifenacin subgroup and 2.4% of thetolterodine subgroup. Withdrawals for all reasonswere also low at 3% and 4.2% respectively.
Solifenacin 5 mg and tolterodine ER 4 mg werewell tolerated by those patients who decided not torequest a dose increase.
4. Discussion
The STAR trial was designed to mirror actual clinicalpractice as closely as possible and to providerelevant comparative head-to-head data for treat-ment outcomes for solifenacin and tolterodine ER,two antimuscarinic medications available for OABtherapy. Accordingly, OAB patients commencedtreatment with the recommended starting dosesof either solifenacin or tolterodine ER (5 mg and 4 mgrespectively). At the first clinic visit after this, whichwas standardised to 4-weeks, an initial assessmentof symptom improvement was performed and adose increase request option considered as solife-nacin is available in two doses with the higher doseavailable ‘if needed’.
After 4 weeks of active treatment there wereimprovements in all OAB symptoms in both groups.Patients treated with solifenacin 5 mg experiencedmean improvements in all OAB symptoms thatwere greater than those experienced by patientsrandomised to tolterodine ER 4 mg. For OAB symp-toms of micturition frequency, (associated volumevoided per micturition), urgency and nocturia themean results for the solifenacin group were an
oint for NDI subgroups (treatment subgroups not requesting
o Does Increase.
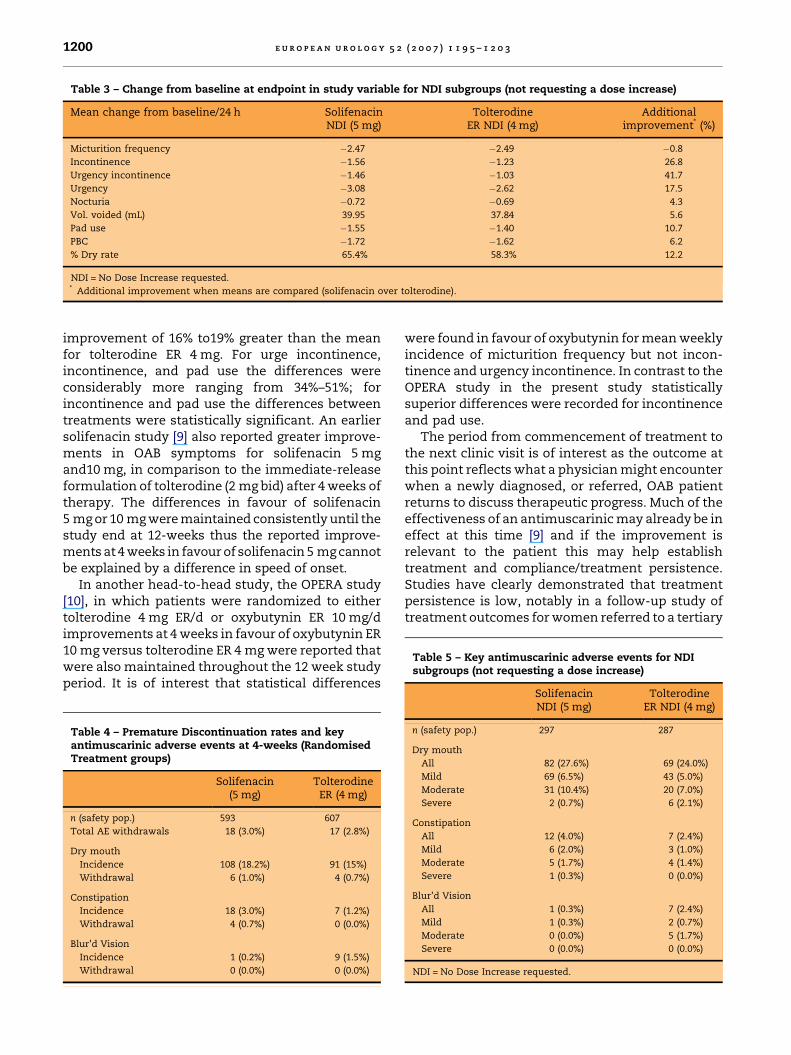
Table 3 – Change from baseline at endpoint in study variable for NDI subgroups (not requesting a dose increase)
Mean change from baseline/24 h SolifenacinNDI (5 mg)
TolterodineER NDI (4 mg)
Additionalimprovement* (%)
Micturition frequency �2.47 �2.49 �0.8
Incontinence �1.56 �1.23 26.8
Urgency incontinence �1.46 �1.03 41.7
Urgency �3.08 �2.62 17.5
Nocturia �0.72 �0.69 4.3
Vol. voided (mL) 39.95 37.84 5.6
Pad use �1.55 �1.40 10.7
PBC �1.72 �1.62 6.2
% Dry rate 65.4% 58.3% 12.2
NDI = No Dose Increase requested.* Additional improvement when means are compared (solifenacin over tolterodine).
Table 5 – Key antimuscarinic adverse events for NDIsubgroups (not requesting a dose increase)
e u r o p e a n u r o l o g y 5 2 ( 2 0 0 7 ) 1 1 9 5 – 1 2 0 31200
improvement of 16% to19% greater than the meanfor tolterodine ER 4 mg. For urge incontinence,incontinence, and pad use the differences wereconsiderably more ranging from 34%–51%; forincontinence and pad use the differences betweentreatments were statistically significant. An earliersolifenacin study [9] also reported greater improve-ments in OAB symptoms for solifenacin 5 mgand10 mg, in comparison to the immediate-releaseformulation of tolterodine (2 mg bid) after 4 weeks oftherapy. The differences in favour of solifenacin5 mg or 10 mg were maintained consistently until thestudy end at 12-weeks thus the reported improve-ments at 4 weeks in favour of solifenacin 5 mg cannotbe explained by a difference in speed of onset.
In another head-to-head study, the OPERA study[10], in which patients were randomized to eithertolterodine 4 mg ER/d or oxybutynin ER 10 mg/dimprovements at 4 weeks in favour of oxybutynin ER10 mg versus tolterodine ER 4 mg were reported thatwere also maintained throughout the 12 week studyperiod. It is of interest that statistical differences
Table 4 – Premature Discontinuation rates and keyantimuscarinic adverse events at 4-weeks (RandomisedTreatment groups)
Solifenacin(5 mg)
TolterodineER (4 mg)
n (safety pop.) 593 607
Total AE withdrawals 18 (3.0%) 17 (2.8%)
Dry mouth
Incidence 108 (18.2%) 91 (15%)
Withdrawal 6 (1.0%) 4 (0.7%)
Constipation
Incidence 18 (3.0%) 7 (1.2%)
Withdrawal 4 (0.7%) 0 (0.0%)
Blur’d Vision
Incidence 1 (0.2%) 9 (1.5%)
Withdrawal 0 (0.0%) 0 (0.0%)
were found in favour of oxybutynin for mean weeklyincidence of micturition frequency but not incon-tinence and urgency incontinence. In contrast to theOPERA study in the present study statisticallysuperior differences were recorded for incontinenceand pad use.
The period from commencement of treatment tothe next clinic visit is of interest as the outcome atthis point reflects what a physician might encounterwhen a newly diagnosed, or referred, OAB patientreturns to discuss therapeutic progress. Much of theeffectiveness of an antimuscarinic may already be ineffect at this time [9] and if the improvement isrelevant to the patient this may help establishtreatment and compliance/treatment persistence.Studies have clearly demonstrated that treatmentpersistence is low, notably in a follow-up study oftreatment outcomes for women referred to a tertiary
SolifenacinNDI (5 mg)
TolterodineER NDI (4 mg)
n (safety pop.) 297 287
Dry mouth
All 82 (27.6%) 69 (24.0%)
Mild 69 (6.5%) 43 (5.0%)
Moderate 31 (10.4%) 20 (7.0%)
Severe 2 (0.7%) 6 (2.1%)
Constipation
All 12 (4.0%) 7 (2.4%)
Mild 6 (2.0%) 3 (1.0%)
Moderate 5 (1.7%) 4 (1.4%)
Severe 1 (0.3%) 0 (0.0%)
Blur’d Vision
All 1 (0.3%) 7 (2.4%)
Mild 1 (0.3%) 2 (0.7%)
Moderate 0 (0.0%) 5 (1.7%)
Severe 0 (0.0%) 0 (0.0%)
NDI = No Dose Increase requested.

e u r o p e a n u r o l o g y 5 2 ( 2 0 0 7 ) 1 1 9 5 – 1 2 0 3 1201
urogynaecology clinic where only around 20% offemale patients with detrusor overactivity continuedwith anticholinergic treatment after 6 months [11].Similar findings were reported following an analysisof pharmacy prescriptions [12] which suggests thatpatients prescribed antimuscarinics exhibit poorpersistence and generally discontinue treatmentwithin a few months. Such findings, whilst contrast-ing with the higher persistency on trial therapy, (nodoubt at least in part due to patient selection and thecircumstances of a controlled study) are disappoint-ing, especially given the fact that OAB patients areoften reluctant to seek treatment in the first place.Accordingly, it appears that if not convinced of earlytherapeutic benefit and perhaps if subject to inade-quate follow-up, these patients may readily abandonhope of obtaining successful treatment. Even if theypersist in trying to obtain treatment benefit a recentUK epidemiological study [3] found that patientstrying a number of different anticholinergic medica-tions used more National Health Service resourcesand were often referred to secondary care; thusunsuccessful first-line treatment equated toincreased healthcare costs.
Returning patients to continence or maximallyreducing incontinence is an important treatmentgoal [13]. It is well established that both solifenacin[6] and tolterodine ER [14] show clear superiority toplacebo in reducing incontinence. The apparentadditional benefit of solifenacin over tolterodine ERin this context is very encouraging since urinaryincontinence has a considerable social and emo-tional impact. Incontinent respondents in a USsurvey [15] were reported to be more functionallyimpaired, having poorer self-reported health, andwere lonelier and sadder than continent respond-ents. Likewise for physicians, incontinence is oftenthe key symptom associated with OAB symptomseverity and the decision to pharmacologically treatpatients [16]. Similarly for healthcare providersurinary incontinence represents a major financialburden as it has been estimated to be associatedwith considerable costs, for example $US26.3 billion($US3565 per individual) [17]. The cost of routinecare such as laundry and pads was estimated at$US11.4 billion. A recent study [18] of the cost of OABto five European countries (Germany, Italy, Spain,Sweden and the United Kingdom) produced anestimate of s4.2 billion in 2000 with the costsestimated to reach s5.2 billion by 2020. It wascalculated that the annual direct costs of OABmanagement ranged from s269–s706 with thelargest costs being the use of incontinence padsaccounting for an average of 63% of the annual perpatient OAB cost. Thus, consistent demonstrations
of a treatment advantage in addressing the problemof urinary incontinence is extremely importantattribute of a useful treatment. Furthermore theadvantage of solifenacin 5 mg over tolterodine ER4 mg at 4 weeks was also demonstrated for pad useand was supported by improvement outcomes infavour of solifenacin 5 mg for all other variables. Theuse of incontinence pads is often part of a patient’scoping strategy [19] and can be a ‘just in case’response to urgency whether or not the patientactually suffers from incontinence. Thus the effect onpad use, which demonstrates an economic advan-tage, implies that the reduction in incontinence wasnoticeable and meaningful to the patient. Discontin-uing pad use is a major step for a patient indicatingconfidence in the therapy and should ensure persis-tence in the therapy required for a chronic condition.
The efficacy benefits of any therapy must beconsidered in the context of both safety andtolerability. Clearly both solifenacin 5 mg andtolterodine ER 4 mg were well tolerated and pre-mature withdrawal due to adverse events after4 weeks treatment were very low (<3%) for bothsolifenacin 5 mg and tolterodine ER 4 mg. Dry mouthincidence, which was the most prevalent adverseevent, was associated with similar low levels ofwithdrawals (<1%).
In summary, at the end of the crucial first fourweeks after initiating treatment, greater improve-ments in OAB symptoms were experienced bypatients treated with solifenacin 5 mg versus thosetreated with tolterodine ER 4 mg. Solifenacin 5 mgwas statistically significantly more effective thantolterodine ER 4 mg both in reducing incontinence,an OAB symptom with a major social and emotionalimpact, and also incontinence pad use, indicating atangible and health-economic benefit.
Conflicts of interest
Professor Chapple is a consultant, investigator, andspeaker for Astellas Pharma Inc (Yamanouchi),Pfizer, Novartis, and Schwarz, and has acted as aconsultant to UCB.
This study was undertaken with a research grantfrom Yamanouchi Pharmaceutical Co, Ltd (nowAstellas Pharma Inc). Tokyo, Japan.
Acknowledgements
This study was undertaken with a research grantfrom Yamanouchi Pharmaceutical Co., Ltd. (nowAstellas Pharma Inc.) Tokyo, Japan.

e u r o p e a n u r o l o g y 5 2 ( 2 0 0 7 ) 1 1 9 5 – 1 2 0 31202
Appendix A. STAR Study Group
Belarus: Arkadiy Gres; Sergey Voskresenski.Belgium: Dr. Van Erps; Prof. Wyndaele; Dr. Ackaert;Prof. Everaert; Dr. Michielsen; Prof. Dr. Dhont; Prof.de Leval. Czech Republic: Richard Fiala; IvanHuvar; Josef Liehne; Viktor Vik; Michael Halaska;Jan Zmrhal; Jaroslav Zenısek. Denmark: GunnarLose; John B. Nielsen; Hans Madsen; Lasse Raaberg;Peter Thind; Jorgen Nordling; Torsten Sorensen;Hans Thyssen. France: Prof. Francois Richard; Prof.Michel Soulie; Dr. Pascal Glemain; Prof. FredericStaerman; Prof. Bernard Jacquetin; Prof. FrancoisDesgrandchamps; Prof. Jacques Tostain; Prof.Philippe Grise; Prof. Frank Bladou; Prof. PhilippeDescamps; Prof. Philippe Ballanger; Prof. JacquesBiserte. Germany: Dr. Stefan Carl; Dr. Heinz-PeterFischer; Dr. Matthias Heisler; Dr. Mark Indig; Dr.Wolfgang Jorger; Dr. Jorg Knipphals; Dr. UllrichKoppermann; Dr. Kai Scholermann; Dr. MichaelVoss; Dr. Wolfgang Warnack; Dr. Peter Weitz.Greece: Prof. Georgios Barbalias; Prof. Aris Giano-poulos; Dr. Charilaos Katsifotis; Prof. DemetriosHatzichristou; Prof. Michalis Melekos. Hungary: Dr.Gyula Fontos; Dr. Ferenc Katona; Dr. LaszloKisbenedek; Dr. Jozsef Kondas; Dr. Gabor Nagy.Italy: Prof. Walter Artibani; Prof. Francesco Cat-anzaro; Prof. Salvatore Dessole; Prof. RobertoMario Scarpa; Prof. Luigi Selvaggi; Prof. AlbertoMasala. The Netherlands: Dr. H. Vergunst; Dr. C.H.van der Vaart; Dr. P.H. van de Weijer; Dr. O.B. vanVierssen Trip; Dr. E.L. Koldewijn; Prof. H.J. Men-sink; Prof. R.J. Nijman; Dr. M.J. de Bruin; Dr. P.J. Kil.Norway: Sigurd Kulseng-Hanssen; Raymond Mor-tensen; Hjalmar Schiotz; Bjarne Eriksen. RussianFederation: Dmitry Pushkar; Leonid Gorilovsky;Nikolay Lopatkin; Vera Smetnik; Salman Al-Shukri;Vadim Surikov; Yuriy Zakhmatov. Slovakia: Prof. JanBreza; Prof. Jan Kliment; Dr. Jozef Marencak; Dr.Ivan Mincik; Dr. Ladislav Valansky. Spain: Dr. JoseM. Martınez-Sagarra; Dr. Luis Prieto; Dr. RobertoMartınez; Dr. Jose Rosa; Dr. Narcıs Serrallach-Mila;Dr. Carmen Zubiaur; Dr. Marceliano Garcıa; Dr.Lorenzo Perales; Dr. Antonio Marques. Sweden: IanMilsom; Aino Fianu-Jonasson; Martin Stjernquist.Ukraine: Victor Pirogov; Sergey Pasechnikov.United Kingdom: Mr. Christopher Chapple; Mr.Robert Freeman; Mr. Vikram Khullar; Mr. MalcolmLucas; Prof. James Malone-Lee; Mr. ChristopherMayne; Mr. Thomas McNicholas; Miss JoanPitkin; Mr. David Richmond; Mr. Julian Shah; Mr.Phillip Toozs-Hobson. Study Team: T. Drogendijk;M. Klaver; D. Macfarlane; H. Mollee; E. Vink;M. Wright.
References
[1] Milsom I, Abrams P, Cardozo L, Roberts RG, Thuroff J,
Wein AJ. How widespread are the symptoms of an over-
active bladder and how are they managed? A population-
based prevalence study. BJU Int 2001;87:760–6.
[2] Jackson S. The patient with overactive bladder – symp-
toms and quality-of-life issues. Urology 1997;50(Suppl 6A):
18–22.
[3] Odeyemi I, Dakin HA, O’Donnell RA, Warner J, Jacobs A,
Dasgupta P. Epidemiology, prescribing patterns and
resource use associated with overactive bladder in UK
primary care. Int J Clin Pract 2006;60:949–58.
[4] Nabi G, Cody JD, Ellis G, Herbison P, Hay-Smith J. Anti-
cholinergic drugs versus placebo for overactive bladder
syndrome in adults. Cochrane Database Syst Rev. 2006:
CD003781.
[5] Haab F, Cardozo L, Chapple C, Ridder AM. Long-term
open-label solifenacin treatment associated with persist-
ence with therapy in patients with overactive bladder
syndrome. Eur Urol 2005;47:376–84.
[6] Abrams P, Swift S. Solifenacin is effective for the treat-
ment of OAB dry patients: a pooled analysis. Eur Urol
2005;48:483–7.
[7] Chapple CR. Muscarinic receptor antagonists in the treat-
ment of overactive bladder. Urology 2000;55(Suppl 5A):
33–46.
[8] ChappleCR,Martinez-GarciaR,SelvaggiL,Toozs-HobsonP,
Warnack W, Drogendijk T, et al. A comparison of the
efficacy and tolerability of solifenacin succinate and
extended release tolterodine at treating overactive
bladder syndrome: results of the STAR trial. Eur Urol
2005;48:464–70.
[9] Chapple CR, Rechberger T, Al-Shukri S, Meffan P, Everaert K,
Huang M, et al. Randomised, double-blind placebo- and
tolterodine-controlled trial of the once-daily antimuscari-
nic agent solifenacin in patients with symptomatic over-
active bladder. BJU Int 2004;93:303–10.
[10] Diokno AC, Appell RA, Sand PK, Dmochowski RR,
Gburek BM, Klimberg IW, et al. Prospective, randomised,
double-blind study of the efficacy and tolerability of the
extended-release formulations of oxybutynin and tolter-
odine for overactive bladder: results of the OPERA study.
Mayo Clin Proc 2003;78:687–95.
[11] Kelleher CJ, Cardozo LD, Khullar V, Salvatore S. A medium-
term analysis of the subjective efficacy of treatment
of women with detrusor instability and low bladder
compliance. Br J Obstet Gynaecol 1997;104:988–93.
[12] Cisternas M, Noe L, Patel B, Remigio-Baker, Williamson T,
Black L. Comparison of persistence among therapies for
overactive bladder: a retrospective pharmacy claims
analysis. Neurourol Urodyn 2005;24:580.
[13] Staskin DR, MacDiarmid SC. Pharmacologic management
of overactive bladder: practical options for the primary
care physician. Am J Med 2006;119(3 Suppl 1):245–85.
[14] Van Kerrebroeck P, Kreder K, Jonas U, Zinner N, Wein A.
Tolterodine once-daily: superior efficacy and tolerability
in the treatment of overactive bladder. Urology 2001;57:
414–21.

e u r o p e a n u r o l o g y 5 2 ( 2 0 0 7 ) 1 1 9 5 – 1 2 0 3 1203
[15] Fultz NH, Herzog R. Self reported and emotional impact
of urinary incontinence. J Am Geriatr Soc 2001;49:
892–9.
[16] Diokno A, Lee P, Zorn BH, Lenderking WR, Grossman MA,
Bull SA, et al. Factors associated with clinical assessment
of overactive bladder and selection of treatment. Clin
Ther 2001;23:1542–51.
[17] Wagner TH, Hu TW. Economic cost of urinary inconti-
nence in 1995. Urology 1998;51:355–61.
[18] Reeves P, Irwin D, Kelleher C, Milsom I, Kopp Z, Calvert N,
Lloyd A. The current and future burden and cost of over-
active bladder in five European countries. Eur Urol
2006;50:1050–7.
[19] Ricci JA, Baggish JS, Hunt TL, Stewart WF, Wein A,
Herzog AR, et al. Coping strategies and health care-
seeking behaviour in a US national sample of adults with
symptoms suggestive of overactive bladder. Clin Ther
2001;23:1245–59.