Today's Objectives - Community Physical Therapy
129
Plante Moran, PLLC 2013 614-222-9020 plantemoran.com Presented by: Jane Belt, RN, MS, RAC-MT Plante & Moran, PLLC [email protected] Members Sign-in Medicare Reviews and Successful Medicare Documentation } } plantemoran.com Today’s Objectives Today’s Objectives 2 Review history of the federally mandated Recovery Auditor program from the 2005 pilots to the present national roll-out Identify the three (3) major audit issues found in the pilot project that generated the greatest SNF Medicare overpayments Delineate strategies for development of internal or external audits
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of Today's Objectives - Community Physical Therapy

Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
Presented by:
Jane Belt, RN, MS, RAC-MT
Plante & Moran, [email protected]
Members Sign-in
Medicare Reviews and
Successful Medicare Documentation}
}
plantemoran.com
Today’s ObjectivesToday’s Objectives
2
� Review history of the federally mandated
Recovery Auditor program from the 2005
pilots to the present national roll-out
� Identify the three (3) major audit issues found
in the pilot project that generated the greatest
SNF Medicare overpayments
� Delineate strategies for development of
internal or external audits
Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
Today’s ObjectivesToday’s Objectives
3
� Discuss the strategies and tools for the nursing
facility to prepare for the Medicare audits
� Discuss key elements in successful Medicare
documentation
� Detail the risks associated with inadequate
documentation
� Review current audit trends
plantemoran.com
What is the Medicare What is the Medicare RA Program?RA Program?
4
� “RA” stands for Recovery Auditor
� Efforts by CMS to “identify improper payments and fight fraud, waste and abuse in the Medicare
Program”
� 3 year, 3 state demonstration/pilot program identified ~$1.0 billion in improper claims across all healthcare providers
� Demonstration focused on highest Medicare utilization states: NY, CA, and FL in 2005
Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
What is the MedicareWhat is the MedicareRA Program? RA Program?
5
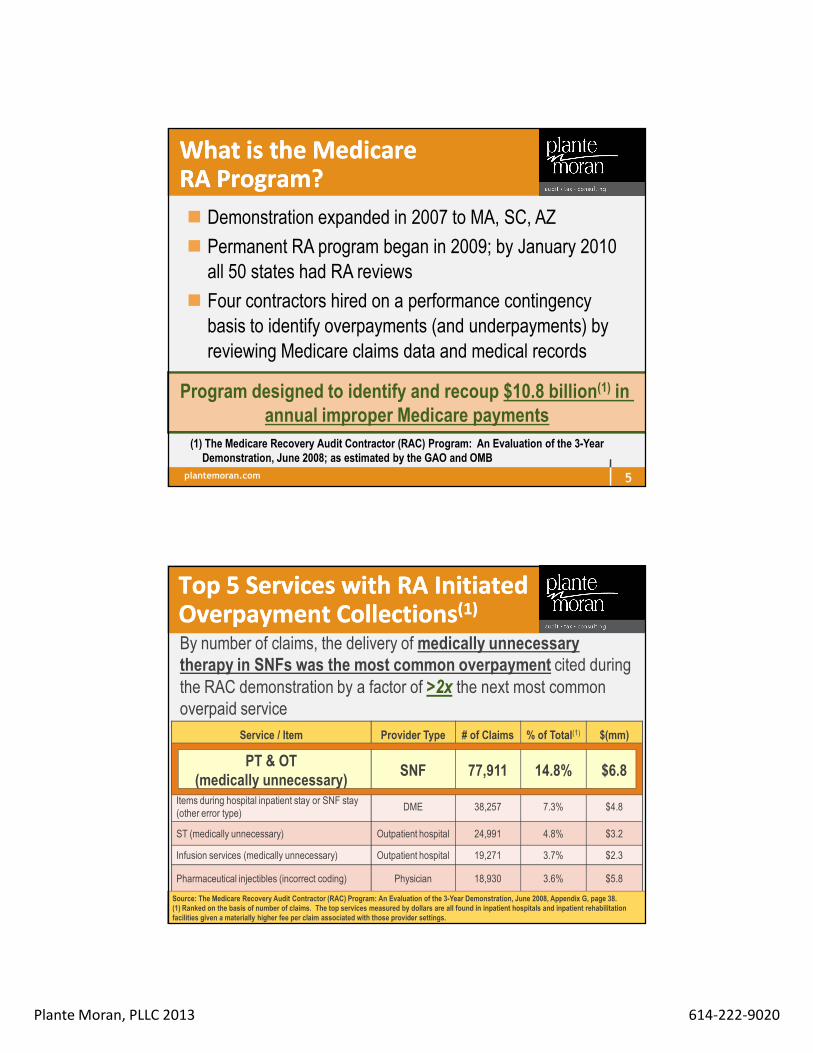
� Demonstration expanded in 2007 to MA, SC, AZ
� Permanent RA program began in 2009; by January 2010
all 50 states had RA reviews
� Four contractors hired on a performance contingency
basis to identify overpayments (and underpayments) by
reviewing Medicare claims data and medical records
Program designed to identify and recoup $10.8 billion(1) in annual improper Medicare payments
(1) The Medicare Recovery Audit Contractor (RAC) Program: An Evaluation of the 3-Year Demonstration, June 2008; as estimated by the GAO and OMB
plantemoran.com
Top 5 Services with RA Initiated Top 5 Services with RA Initiated Overpayment CollectionsOverpayment Collections(1)(1)
6
By number of claims, the delivery of medically unnecessary therapy in SNFs was the most common overpayment cited during the RAC demonstration by a factor of >2x the next most common overpaid service
Service / Item Provider Type # of Claims % of Total(1) $(mm)
PT & OT (medically unnecessary)
SNF 77,911 14.8% $6.8
Items during hospital inpatient stay or SNF stay(other error type)
DME 38,257 7.3% $4.8
ST (medically unnecessary) Outpatient hospital 24,991 4.8% $3.2
Infusion services (medically unnecessary) Outpatient hospital 19,271 3.7% $2.3
Pharmaceutical injectibles (incorrect coding) Physician 18,930 3.6% $5.8
Source: The Medicare Recovery Audit Contractor (RAC) Program: An Evaluation of the 3-Year Demonstration, June 2008, Appendix G, page 38.(1) Ranked on the basis of number of claims. The top services measured by dollars are all found in inpatient hospitals and inpatient rehabilitation facilities given a materially higher fee per claim associated with those provider settings.
Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
Most Common Improper Most Common Improper Payment Areas for SNFsPayment Areas for SNFs
7
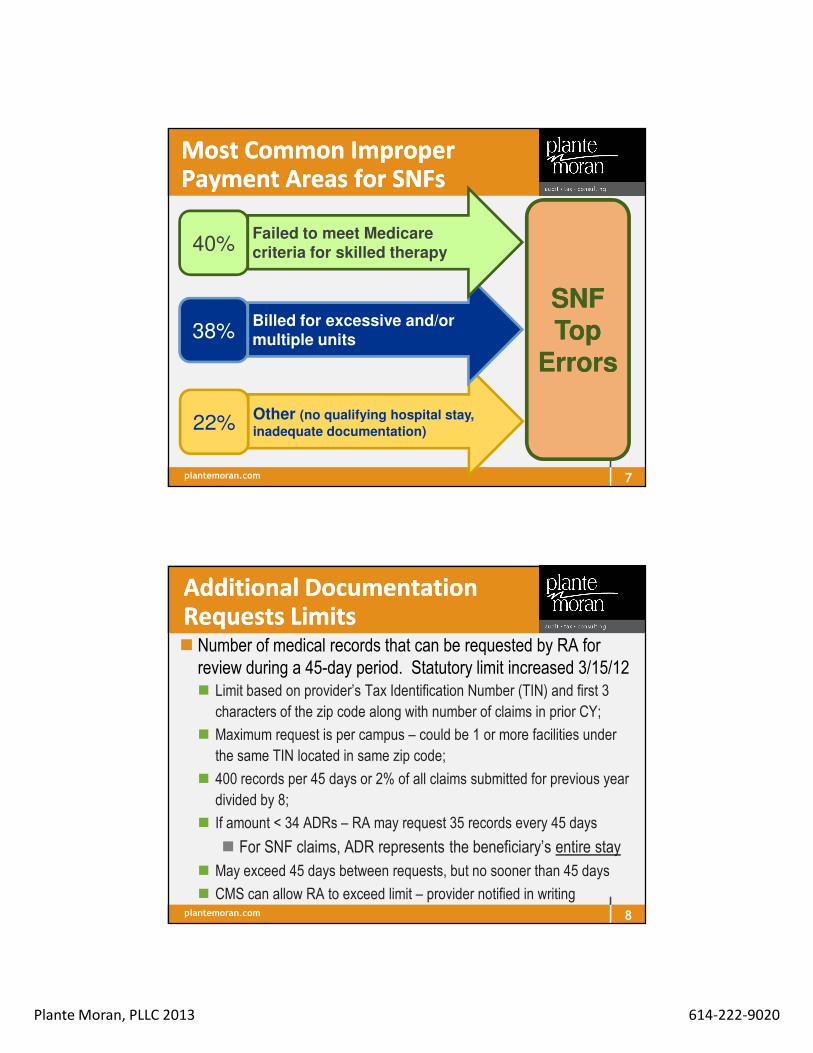
22%Other (no qualifying hospital stay,
inadequate documentation)
SNF SNF Top Top
ErrorsErrors
38%Billed for excessive and/or
multiple units
40%Failed to meet Medicare
criteria for skilled therapy
plantemoran.com
Additional Documentation Additional Documentation Requests LimitsRequests Limits
8
� Number of medical records that can be requested by RA for review during a 45-day period. Statutory limit increased 3/15/12� Limit based on provider’s Tax Identification Number (TIN) and first 3
characters of the zip code along with number of claims in prior CY;
� Maximum request is per campus – could be 1 or more facilities under
the same TIN located in same zip code;
� 400 records per 45 days or 2% of all claims submitted for previous year
divided by 8;
� If amount < 34 ADRs – RA may request 35 records every 45 days
� For SNF claims, ADR represents the beneficiary’s entire stay
� May exceed 45 days between requests, but no sooner than 45 days
� CMS can allow RA to exceed limit – provider notified in writing

Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
Good News Good News –– Some RA Some RA ImprovementsImprovements
9
� Reduction of fee-driven motivation� In the demo, RAs required to return contingency fee
only if overpayment determination overturned on the first-level appeal.
� National program requires fees to be returned if determination is overturned at ANY level
� RAs must disclose areas of focus when looking for overpayments www.cms.hhs.gov/RAC
plantemoran.com
A Powerful Financial Incentive for A Powerful Financial Incentive for RAs to Find OverpaymentsRAs to Find Overpayments
10
� The RA program is CMS’s first foray into contingent-based contractor payment structures
� Incentivizes contractors to find improper payments (bounty hunters)
Contingency Fee Schedule(1)
Region A 12.45%
Region B 12.50%
Region C 9.00%
Region D 9.49%
RAs earned over $187m in contingency fees during the demonstration
(1) Federal Business Opportunities web site: www.fbo.gov; www.cms.hhs.gov/RAC/
Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
How do RA Reviews Work?How do RA Reviews Work?
11
� There are 2 types of RA reviews —
1. Automated
2. Complex
“These two review processes—automated review and complex review—are similar to those employed by the Medicare claims processing
contractors to identify improper payments.”
Medicare Recovery Audit Contract (RAC) Program: An Evaluation of the 3-Year Demonstration, June 2008
plantemoran.com
Review TypesReview Types
12
�� Automated ReviewsAutomated Reviews = RAs identified improper
payments via automation where the provider clearly
billed in violation of Medicare policy
� Certainty that service is not covered or is
incorrectly coded ANDAND
� A written Medicare policy, Medicare article or
Medicare-sanctioned coding guideline (e.g., CPT
statement) exists
Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
More on Automated More on Automated ReviewsReviews
13
Automated Reviews Automated Reviews
� Completed when “improper payment” can be identified without “human analysis”
� Can be done without a facility being notified until an “error” is found and payment adjusted or denied
� Uses the facility submission UB-04 or electronic submissions and looks for coding errors or looks for missing validation of acceptance into federal repository
� Payment due within 40 days or recoupment becomes automatic (with interest accrued from date of demand letter)
plantemoran.com
Examples of Reasons for Examples of Reasons for Automated RA ReviewsAutomated RA Reviews
14
� Coding errors HIPPS and modifiers (RUG scores and
reason for assessment)
� ARD on MDS doesn’t match ARD on the UB-04
� Duplicate claims
� Bill submitted prior to MDS transmitted to QIES ASAP
� Pricing mistakes
� Missing codes
� Mistakes in coverage periods

Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
Reviews TypesReviews Types
15
Complex ReviewsComplex Reviews = RA identifies likely improper payment and
requests records from provider to conduct more in-depth review
� Improper payment suspected, but record review needed to make determination
� Performed by clinical personnel and medical directors� Medical directors must discuss claim denial with the provider if
requested
� Medical record limits based on type of provider
� Providers will have 45 days to provide requested medical records; RA will have 60 days from receipt of records to make a final determination
plantemoran.com
Examples of Reasons for Examples of Reasons for Complex RA ReviewsComplex RA Reviews
16
� Diagnosis code inconsistent
� Inconsistency with therapy minutes and ADL score
(RUA)
� Static therapy treatment (holding at the same RUG
level for lengthy treatment periods)
� Medical necessity
Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
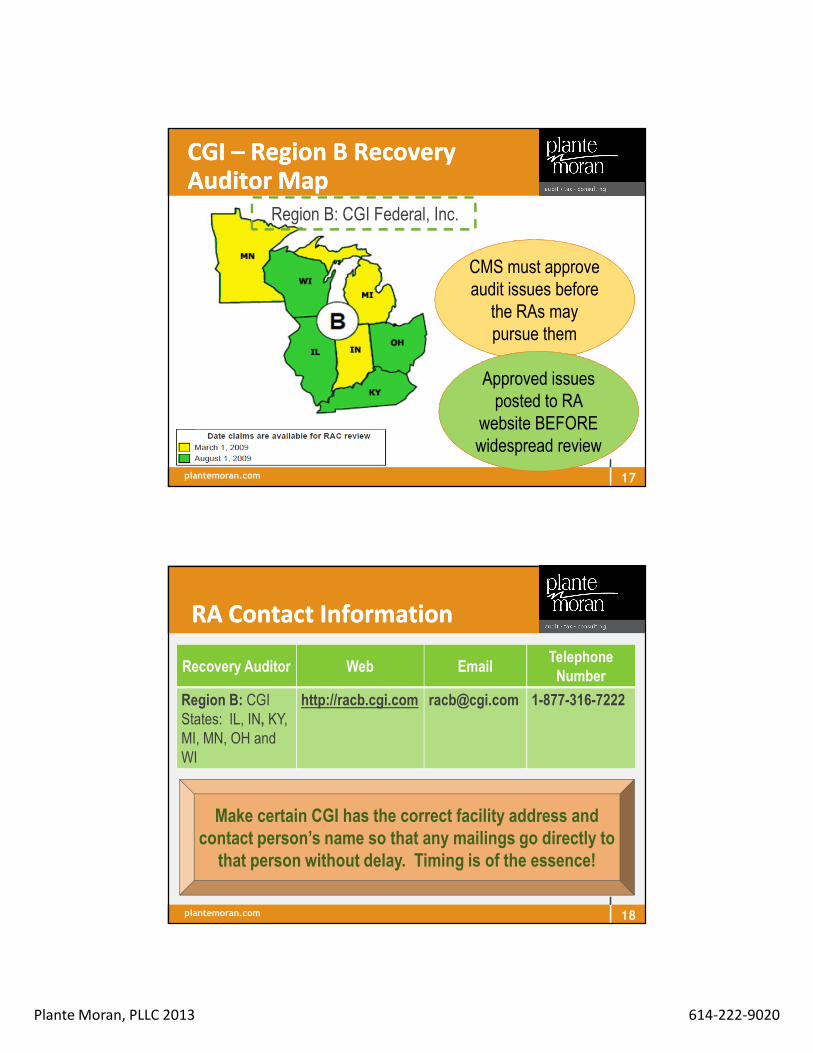
CGI CGI –– Region B Recovery Region B Recovery Auditor MapAuditor Map
17
Region B: CGI Federal, Inc.
CMS must approve CMS must approve audit issues before
the RAs may pursue them
widespread review
Approved issues posted to RA
website BEFORE widespread review
plantemoran.com
Recovery Auditor Web EmailTelephone Number
Region B: CGIStates: IL, IN, KY, MI, MN, OH and WI
http://racb.cgi.com [email protected] 1-877-316-7222
RA Contact InformationRA Contact Information
18
Make certain CGI has the correct facility address and contact person’s name so that any mailings go directly to that person without delay. Timing is of the essence!
Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
More About CGI More About CGI -- MissionMission
� Identify improper payments through detection and
collection of overpayments, the identification of
underpayments, and the implementation of actions
that will prevent future improper payments utilizing
their Customized Auditing Software (CAS) 5.0
software for “data mining” to identify unusual patterns
19
plantemoran.com
What is an Improper Payment?What is an Improper Payment?
20
Payments made for services that do not meet
Medicare’s medical necessity criteria
Payments made for services that are incorrectly coded
Providers failed to submit documentation when
requested or enough documentation to support the
claim
Provider was paid twice because duplicate claims were
submitted
Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
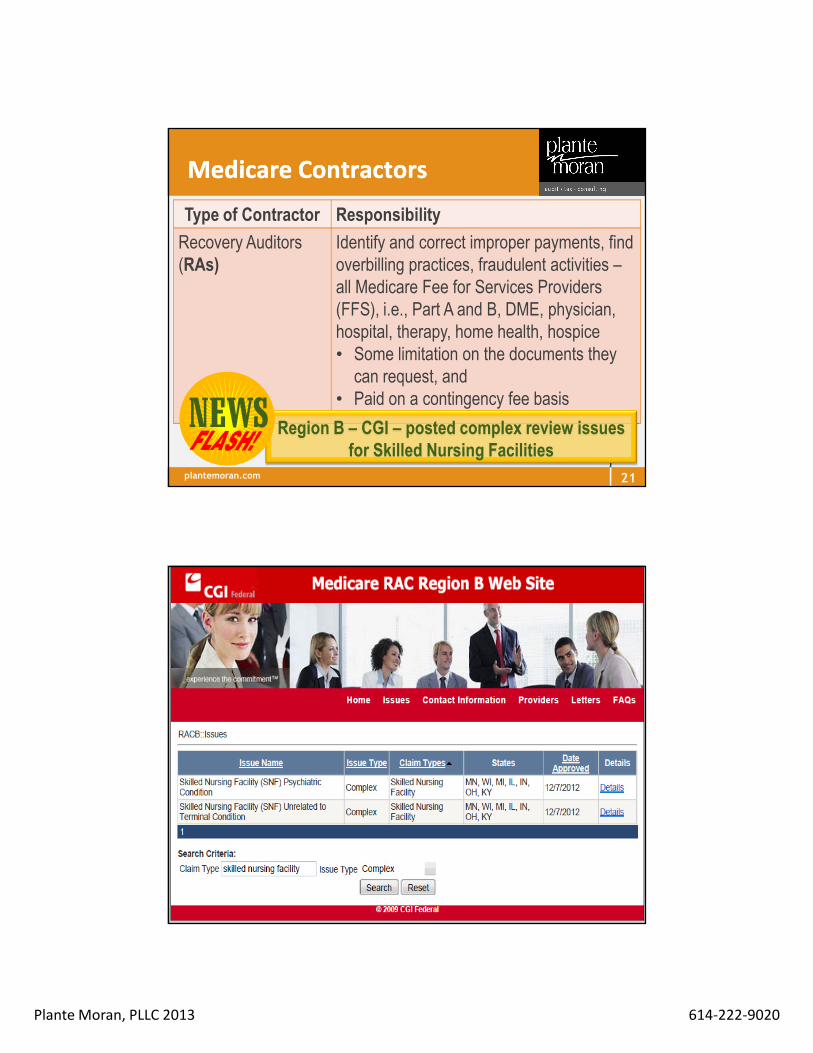
Type of Contractor Responsibility
Recovery Auditors (RAs)
Identify and correct improper payments, find overbilling practices, fraudulent activities –all Medicare Fee for Services Providers (FFS), i.e., Part A and B, DME, physician, hospital, therapy, home health, hospice• Some limitation on the documents they
can request, and• Paid on a contingency fee basis
Medicare ContractorsMedicare Contractors
21
Region B – CGI – posted complex review issues for Skilled Nursing Facilities
plantemoran.com 22

Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
Skilled Nursing Facility (SNF) Psychiatric Condition
ComplexSkilled Nursing Facility
MN, WI, MI, IL, IN, OH, KY
12/7/2012 Details
Skilled Nursing Facility (SNF) Unrelated to Terminal Condition
23
Patients with only a psychiatric condition who are transferred from a psychiatric hospital to a participating SNF are likely to receive only non-covered care. Also, patients whose primary condition/needs are psychiatric in nature often require considerably more specialized, sophisticated nursing techniques and physician attention than is available in most participating SNFs. (SNFs primarily engaged in treating psychiatric disorders are precluded by law from participating in Medicare.) Skilled Nursing Facility (SNF) Psychiatric Condition
plantemoran.com 24
Date Approved
12/7/12
A hospice beneficiary certified as having a terminal illness with a life expectancy of 6 months or less waives all rights to Medicare payment for services related to the terminal condition. Services unrelated to the terminal condition may still be payable and are designated by the presence of condition code 07. SNF Part A claims with a condition code 07 will be reviewed to validate that the services did not relate to the patient’s terminal condition and met SNF coverage criteria.
SNF Unrelated to Terminal Condition
Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
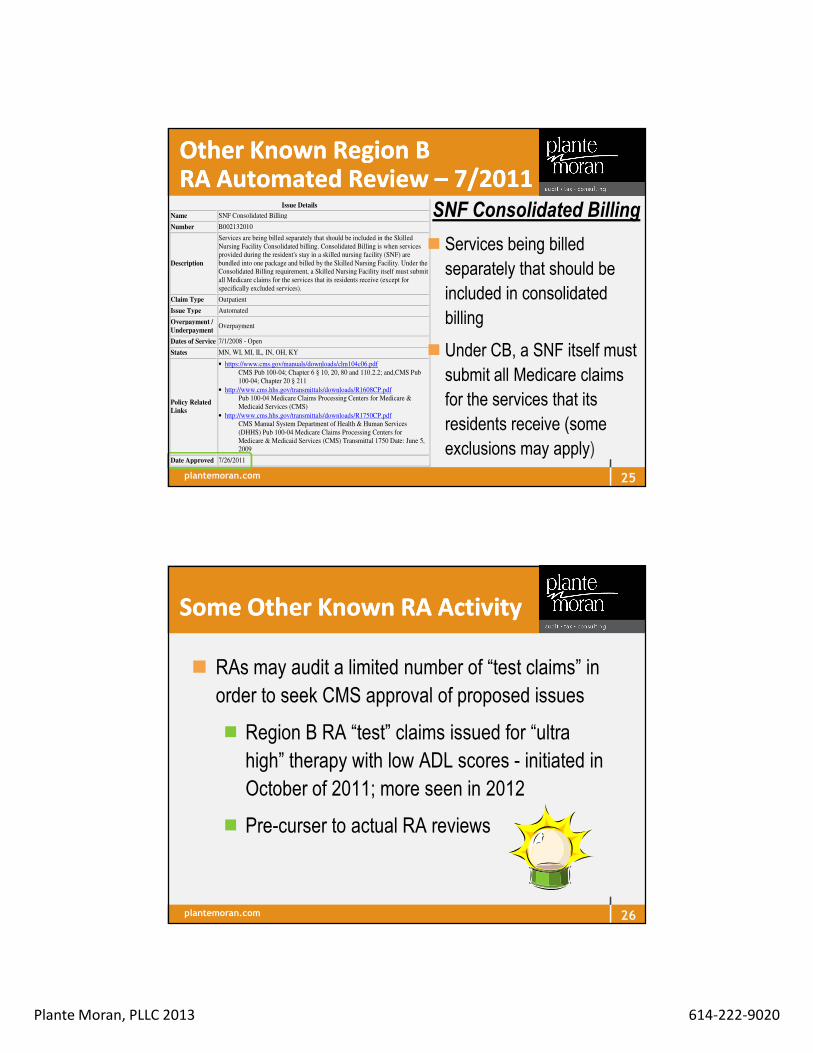
Issue Details
Name SNF Consolidated Billing
Number B002132010
Description
Services are being billed separately that should be included in the Skilled
Nursing Facility Consolidated billing. Consolidated Billing is when services
provided during the resident's stay in a skilled nursing facility (SNF) are
bundled into one package and billed by the Skilled Nursing Facility. Under the
Consolidated Billing requirement, a Skilled Nursing Facility itself must submit
all Medicare claims for the services that its residents receive (except for
specifically excluded services).
Claim Type Outpatient
Issue Type Automated
Overpayment /
Underpayment Overpayment
Dates of Service 7/1/2008 - Open
States MN, WI, MI, IL, IN, OH, KY
Policy Related
Links
• https://www.cms.gov/manuals/downloads/clm104c06.pdf
CMS Pub 100-04; Chapter 6 § 10, 20, 80 and 110.2.2; and,CMS Pub
100-04; Chapter 20 § 211
• http://www.cms.hhs.gov/transmittals/downloads/R1608CP.pdf
Pub 100-04 Medicare Claims Processing Centers for Medicare &
Medicaid Services (CMS)
• http://www.cms.hhs.gov/transmittals/downloads/R1750CP.pdf
CMS Manual System Department of Health & Human Services
(DHHS) Pub 100-04 Medicare Claims Processing Centers for
Medicare & Medicaid Services (CMS) Transmittal 1750 Date: June 5,
2009
Date Approved 7/26/2011
Other Known Region B Other Known Region B RA Automated Review RA Automated Review –– 7/20117/2011
SNF Consolidated Billing
� Services being billed
separately that should be
included in consolidated
billing
� Under CB, a SNF itself must
submit all Medicare claims
for the services that its
residents receive (some
exclusions may apply)
25
plantemoran.com
Some Other Known RA ActivitySome Other Known RA Activity
� RAs may audit a limited number of “test claims” in
order to seek CMS approval of proposed issues
� Region B RA “test” claims issued for “ultra
high” therapy with low ADL scores - initiated in
October of 2011; more seen in 2012
� Pre-curser to actual RA reviews
26

Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
What Does the RA Mean What Does the RA Mean
For ProviderFor Provider ??
27
� Increased scrutiny
� Negative cash flow implications
� Potential for declining profit margins
� Administrative burden to comply with documentation requests
� Expensive and lengthy appeals processes
� Current and historical exposure (not before 10/01/07)
Potential for significant financial exposure
plantemoran.com
Getting the DataGetting the Data
� All FFS paid claims subject to RA review – except
those that have already been reviewed by another
Medicare entity (i.e., MAC or ZPIC)
� No Medicare Advantage claims
� No Medicare Part D claims
� RAs search CMS data looking for:
� Coding errors
� Patterns and trends in the claims
28

Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
� Increased competition to recoup Medicare dollars
However, the RA Is Not Our However, the RA Is Not Our Only Concern!!Only Concern!!
29
“CMS will not limit either carriers/FIs/MACs or RACs but instead will rely on a ‘first come first serve’ philosophy for post payment reviews.”
--CMS Final RAC RFP Solicitation Questions & Answers(1)
� Since same claim cannot be reviewed by multiple Medicare reviewers (i.e., MACs and RAs), likely will create competition to mine a finite set of claims
� $1.9 billion in denied claims by claims reviewers in NY, CA, and FL plus ~$1.0 billion in RAC recouped funds during pilot
� Other claims contractors have added checks into their claims processing systems to deny claims with certain obvious errors based on RA demonstration findings
plantemoran.com
� Centers for Medicare & Medicaid Services (CMS) has
implemented numerous initiatives to prevent improper
payments before a claim is processed and to identify and
recoup improper payments after the claim is processed
� Overall goal of CMS’ claim review programs is to reduce
payment error by identifying billing errors (coverage and
billing) made by providers
� Government estimates that 8.6% of all Medicare Fee-For-
Service (FFS) claim payments are improper
Improper Payment InitiativeImproper Payment Initiative
30
Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
� On 11/20/09 President issued Executive Order -
Reducing Improper Payments aimed at intensifying
efforts to eliminate payment error, waste, fraud, and
abuse in the major federal programs, while continuing to
ensure that the right people receive the right payment for
the right reason at the right time
� Improper Payments Elimination and Recovery Act of
2010 requires agencies to assess every federal program
and dollar for improper payment risk, measure payment
accuracy annually, and initiate improvements to ensure
payment errors are reduced
Improper Payment InitiativeImproper Payment Initiative
31
plantemoran.com
Improper Payment InitiativeImproper Payment Initiative
� As required by the President’s Executive Order, a website was created with information about: � Current and historical rates and amounts of improper
payments� Why improper payments occur� What agencies are doing to reduce and recover improper
payments
http://paymentaccuracy.gov/about-site
32
Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
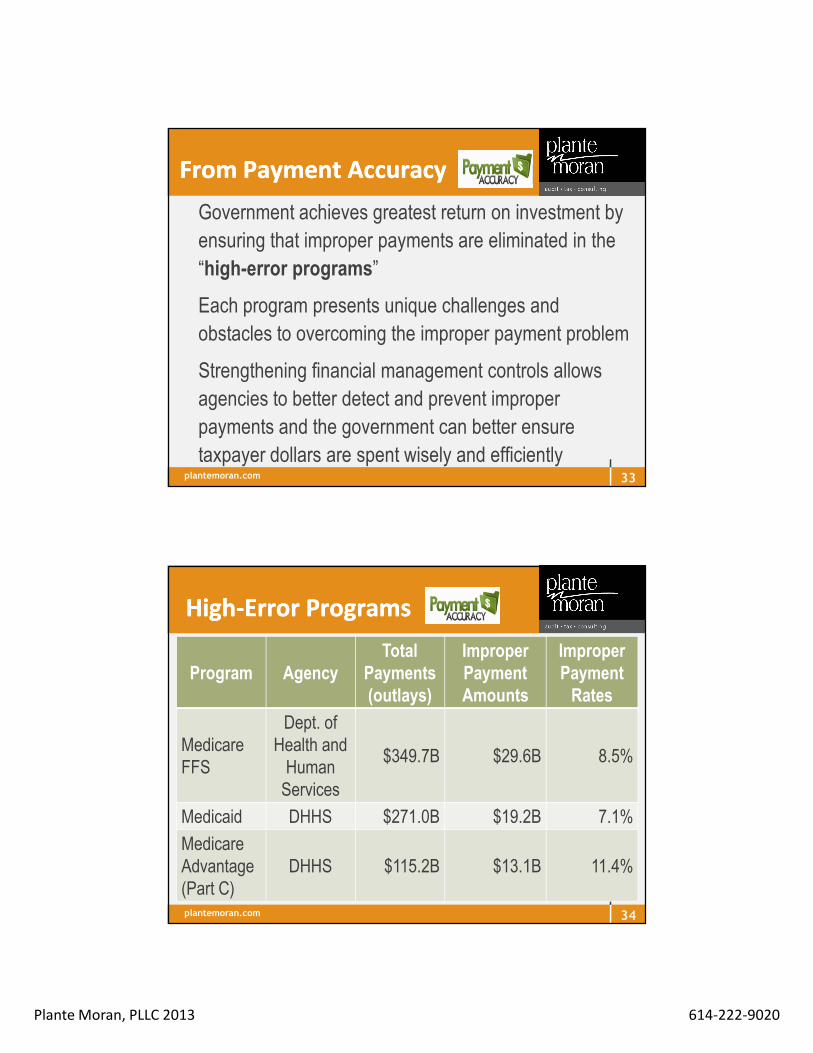
From Payment AccuracyFrom Payment Accuracy
� Government achieves greatest return on investment by
ensuring that improper payments are eliminated in the
“high-error programs”
� Each program presents unique challenges and
obstacles to overcoming the improper payment problem
� Strengthening financial management controls allows
agencies to better detect and prevent improper
payments and the government can better ensure
taxpayer dollars are spent wisely and efficiently33
plantemoran.com
HighHigh--Error Programs Error Programs
Program AgencyTotal
Payments (outlays)
Improper Payment Amounts
Improper Payment Rates
Medicare FFS
Dept. of Health and
Human Services
$349.7B $29.6B 8.5%
Medicaid DHHS $271.0B $19.2B 7.1%
Medicare Advantage (Part C)
DHHS $115.2B $13.1B 11.4%
34
Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
� The problem:
� Funds go to the wrong recipient;
� The right recipient receives the incorrect amount of
funds (including overpayments and
underpayments);
� Documentation is not available to support a
payment; or
� The recipient uses funds in an improper manner
Improper PaymentsImproper Payments
35
plantemoran.com
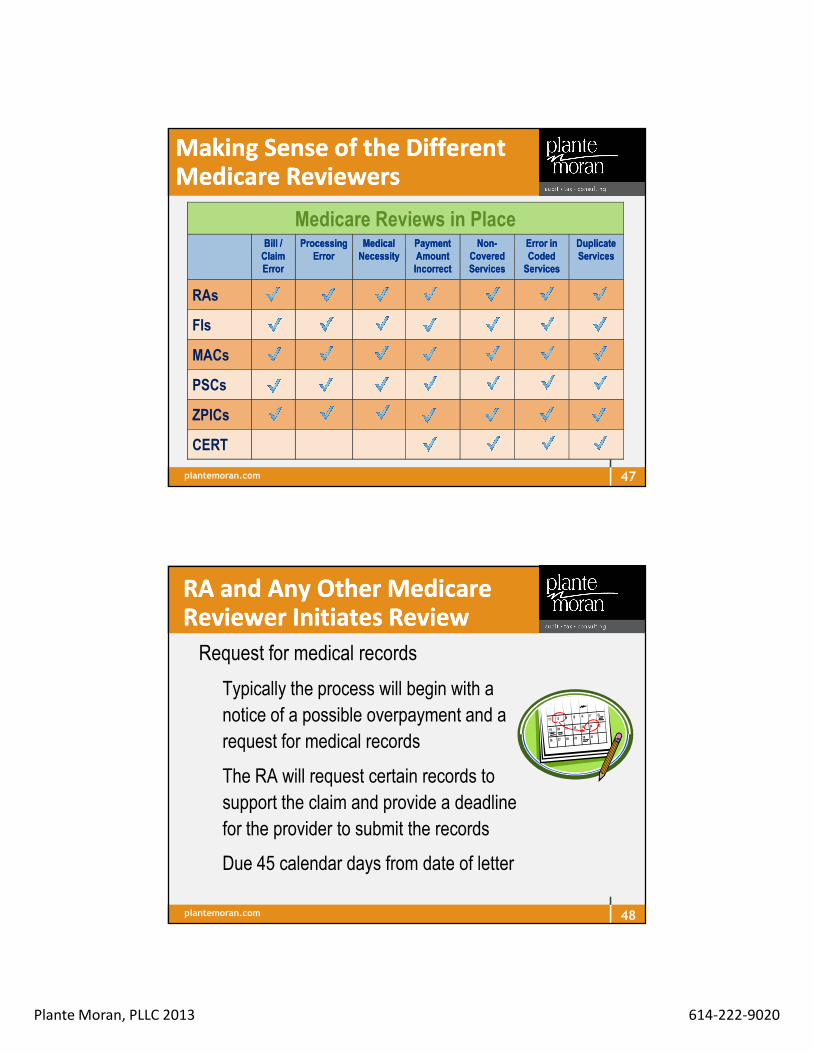
Percentage Distribution of Percentage Distribution of Improper Payments (FY 2012)Improper Payments (FY 2012)
Medicaid 17.9%
MA (Part C) 12.2%
Medicare FFS 27.5%
36

Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
Long Term Care Scrutinized Long Term Care Scrutinized From All SidesFrom All Sides
The Health Care Reform Act provides $350 million to fight fraud, waste and abuse
LTC
37
plantemoran.com
The Focus on Skilled Nursing The Focus on Skilled Nursing FacilitiesFacilities
The Federal Government zeroed in on Medicare
payments to SNFs as initially identified in 2010 Office of
the Inspector General (OIG) report. Subsequent reports
maintain the scrutiny
� SNFs increasingly billed Medicare for higher paying
RUGs from 2006-2008 even though the OIG states
beneficiary characteristics remained the same
� Reported that for-profit SNFs were more likely to bill for
higher paying RUGs than for nonprofit SNFs
38

Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
Skilled Nursing Facility FocusSkilled Nursing Facility Focus
OIG recommendations to CMS included:
�Monitor payments to SNFs;
�Strengthen monitoring of SNFs that are
billing for higher paying RUGs
(Comparative Billing Reports recently
issued to providers);
� Follow-up on the SNFs identified as having
questionable billing
39
plantemoran.com
� CMS employs a variety of contractors to process claims
and submits payment to providers in accordance with
the Medicare and Medicaid rules and regulations
Who Else Is Watching?Who Else Is Watching?
40
And the private sector managed care insurance reviews are very busy scrutinizing as well

Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
Type of Contractor Responsibility
Affiliated Contractors (ACs) – Medicare claims processing contractors such as carriers and Fiscal Intermediaries (FIs) and Medicare Administrative Contractors (MACs)
Process claims submitted by physicians, hospitals, and other HC providers/suppliers, and submit payment to those providers in accordance with Medicare regulations. This includes identifying and correcting underpayments and overpayments. The purpose of MACs is to educate providers, process and conduct billing, correct the behavior in need of change and prevent future inappropriate billing, and recover payments.
Medicare Contractors Medicare Contractors
41
plantemoran.com
6
Current State & Workload Cutover Date
NGSIllinois – Part AWisconsin – Part A
July 13, 2013
WPSWisconsin – Part BIllinois – Part B
September 7, 2013
Transitioning to National Government Services

Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
Contractor Responsibility
Zone Program Integrity Contractors (ZPICs) / Program Safeguard Contractors (PSCs)
Identify cases of suspected fraud and take appropriate corrective actions across entire MCR program. Take place of 2 auditors – Program Safeguard Contractors (PSC) and Medicare Drug Integrity Contractors (MEDIC). ZPIC responsible for program integrity – Part A & B, hospitals, home health, hospice, DME, Part C - Medicare Advantage & Part D.• Do not conduct random audits• No specification regarding look-back periods• Can make unlimited document requests• Not paid on a contingency fee basis, although
they do get performance bonuses
RAs Bark, but ZPICs Bite
plantemoran.com
1. Safeguard Services: American Samoa, California, Guam, Hawaii, Mariana Islands,
Nevada
2. NCI (previously AdvanceMed Corp.): Alaska, Arizona, Idaho, Iowa, Kansas, Missouri,
Montana, Nebraska, North Dakota, Oregon, South Dakota, Utah, Washington, Wyoming
3. Cahaba Safeguard Administrators: Illinois, Indiana, Kentucky, Michigan, Minnesota,
Ohio, Wisconsin
4. Health Integrity: Colorado, New Mexico, Oklahoma, Texas
5. NCI: Alabama, Arkansas, Georgia, Louisiana, Mississippi, North Carolina, South Carolina,
Tennessee, Virginia, West Virginia
6. Cahaba Safeguard Administrators: Connecticut, Delaware, District of Columbia, Maine,
Maryland, Massachusetts, New Hampshire, New Jersey, New York, Pennsylvania, Rhode
Island, Vermont
7. SafeGuard Services: Florida, Puerto Rico, U.S. Virgin Islands
ZPIC ZPIC Zones (7 Compared to the Zones (7 Compared to the Previous 17 PSCs)Previous 17 PSCs)
44

Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
Type of Contractor Responsibility
Comprehensive Error Rate Testing (CERT)
Collect documentation; perform reviews on a statistically-valid random sample of Medicare FFS claims to produce annual improper payment rate FIs & MACs, but still review SNFs’ claims and the providers have to repay any overpayments found
Payment Error Rate Measurement (PERM)
Perform statistical calculations, data processing reviews of FFS, managed care and beneficiary eligibility in both the Medicaid program and CHIP (Children’s Health Insurance Program)
Medicare ContractorsMedicare Contractors
plantemoran.com
Contractor Responsibility
Medicaid Integrity Contractors (MICs)
Payment watchdogs auditing nursing homes and other providers. The MICs will use a data-driven approach to focus efforts on aberrant billing practices. Facilities may be more likely to get medical requests the MICs than the RACs. Three types of contractors:1. Review – mine the data to find issues indicative
of erroneous claims2. Audit – conducts audits onsite or as desk audits3. Education – Pick up concerns from the other 2 to
educate providers and others
And Last but Certainly And Last but Certainly Not LeastNot Least
46
Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
Making Sense of the DifferentMaking Sense of the DifferentMedicare ReviewersMedicare Reviewers
Medicare Reviews Already in Place
Bill/Claim
Error
Processing
Error
Medical
Necessity
Payment
Amount
Incorrect
Non-
Covered
Services
Error in
Coded
Services
Duplicate
Services
RACs
FIs
Carriers
MACs
PSCs
CERT
Medicare Reviews in PlaceBill / Bill / Claim Claim ErrorError
Processing Processing ErrorError
Medical Medical NecessityNecessity
Payment Payment Amount Amount IncorrectIncorrect
NonNon--Covered Covered ServicesServices
Error in Error in Coded Coded ServicesServices
Duplicate Duplicate ServicesServices
RAs
FIs
MACs
PSCs
ZPICs
CERT
47
plantemoran.com
RA and Any Other Medicare RA and Any Other Medicare Reviewer Initiates ReviewReviewer Initiates Review
� Request for medical records
� Typically the process will begin with a
notice of a possible overpayment and a
request for medical records
� The RA will request certain records to
support the claim and provide a deadline
for the provider to submit the records
� Due 45 calendar days from date of letter
48
Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
This Is This Is NotNot Junk MailJunk Mail
49
plantemoran.com
Sample ADR Sample ADR Letter from CGILetter from CGI
50
Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
More of the Sample LetterMore of the Sample Letter
51
Entire letter on web site
and is 5 pages in
length
plantemoran.com
Responding to Record RequestsResponding to Record Requests
� Was the request sent to the right place?
� CGI received a data file over a secured data
line from each MAC/FI/Carrier containing
facility/provider information. CGI uses this
contact information, unless provider supplies
an update via e-mail or call CGI and since
1/1/2012 CGI uses the information from the
web site. Keep contact information currentKeep contact information current
� Check to make sure the RA did not exceed
the record request limit
52
Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
Responding to Record RequestsResponding to Record Requests� Review all records before they are released
� Permits early identification of issues
� Establishes priority for appeals
� Intensive work
� Must have a team and must be organized with a system of
collection and organization
� Has the claim been reviewed by another contractor
� Did the RA follow the “New Issue Review” Process?
� Letter should clearly state basis for the request
� Look at CMS and RA websites; confirm issue was posted53
plantemoran.com
Responding to Record RequestsResponding to Record Requests
� Stamp date and time received
� Calculate 45 calendar days from date of letter
� Can request an extension with explanation of need
� Notify reviewer if significant discrepancy between
date of letter and date of receipt
� Identify any internal issues in expeditiously getting the
mail for processing
54

Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
Responding to Record RequestsResponding to Record Requests
� Document Management
� Bates stamp number on each page
� Scan/copy everything produced to Medicare reviewer
and keep separate from the original medical record
� RAs will accept imaged medical records on CD/DVD
(follow instructions at website) – check letters from
other reviewers for details
� Use cover letter itemizing contents of box or CD
� Send certified mail or, if regular mail, complete
affidavit of service by mail – time frame = 45 days
55
plantemoran.com
CheckCheck Your Review Status and Your Review Status and Additional Documentation LimitsAdditional Documentation Limits
� If disagree with the Additional Documentation
Limits calculation, contact CGI and they will
work with the provider to help explain what
constitutes the limits that were calculated
� RAs were required to have provider access on
the website to monitor status of review
� If ever not available, can call RA for status report
� CMS has urged providers to keep up with the
status of their record reviews
56
Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
Finding OutFinding OutReview Results LetterReview Results Letter
� Comes from the Medicare reviewer to facility: reason
for the review and details their findings
� Narrative description of improper payment issues
� Specific explanation of why services determined not to
be covered or were incorrectly coded
� No review letter for automated – demand letter from RA
– amount, policy, summary, time frames for
recoupment, and how to stop recoupment (appeal)
57
plantemoran.com
Review Results LetterReview Results Letter
� No appeal information in this letter
� **New** CGI has changed process for the discussion
period. Experience indicates that discussions requested
following audits handled more effectively if a written request
and additional documentation are sent to us rather than
receiving the request by phone
� We have also found that many of the requests, particularly
when additional documentation is submitted to support the
claim, can be resolved without the need for a teleconference
58
Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
� Updated PROVIDER REQUEST FOR DISCUSSION form
� Send documents to location shown on Request for Discussion
form
� When request received, the auditor and Medical Director will
determine if phone call is needed, or if response can be put in
writing based on the submitted documentation.
� If a phone call is needed, facility contacted to set a time. Letter
sent detailing the outcome of each written or oral discussion
� The auditors involve the Medical Director as needed in the initial
review and discussion process, whether the discussion is
completed as a written review or a teleconference.
New Process for New Process for Discussion PeriodDiscussion Period
59
plantemoran.com 60

Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
Notification on the Remittance Notification on the Remittance AdviceAdvice� When RA finds overpayment either during an automated or
complex review, Remark Code N432 will appear on the
Remittance Advice
If found, notify other members of RA team
Review other claims for the denial issue
Adjust claims as needed or contact FI/MAC
� The Remittance Advice with N432 will be followed by the
demand letter
� Date of demand letter starts the timing for recoupment and
appeals 61
plantemoran.com
Demand Letter Demand Letter -- Date Starts Date Starts 41 day Clock for Recoupment41 day Clock for Recoupment� Arrives directly from the Medicare reviewer
� Contains list of claims (over or underpaid) and reason the
claims denied and:
� Amount of denial and calculation method
� Reason original payment incorrect
� Cites regulatory basis
� Describes appeal rights
� Recoupment, payment and interest options and the
associated timelines62
Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
Key TimeframesKey Timeframes
� Rebuttal
� Opportunity to submit rebuttal statement and accompanying
evidence why the overpayment will cause a financial
hardship and
� Not intended to review supporting medical documentation
nor disagreement with the overpayment decision
� Claims Processing Contractor will make the decision
� Time frame is 15 days beginning with the date of the
demand letter
63
plantemoran.com
Key TimeframesKey Timeframes
� 30 days
� Full payment – no interest
� Interest begins to accrue on 31st day – assessed for each full 30-day
period
� If unable to pay the entire amount, contact to determine possibility of
approval of repayment plan
� After 40 days Medicare will begin withholding – applies to
current and future claims until full overpayment and
applicable interest has been recouped or acceptable
repayment request received64
Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
Stopping RecoupmentStopping Recoupment
� Even if overpayment not paid in full, recoupment can
be stopped – how?
� Medicare receives a valid and timely request for
redetermination within 30 days of the demand letter
� If the appeal is later than 30 days, recoupment stopped
at whatever point that an appeal is received – however
– Medicare may not refund any recoupment already
taken
65
plantemoran.com
Stopping RecoupmentStopping Recoupment
� If redetermination decision is not favorable, Medicare
can begin to recoup no earlier than 61st day from the
date of the redetermination notice, or
� If decision partially favorable, can begin to recoup no
earlier than the 61st day from the date of the Medicare
revised overpayment Notice/Revised Demand Letter
� Can resume recoupment following reconsideration by
the QIO
66

Plante Moran, PLLC 2013 614-222-9020
plantemoran.com 67
NO
YES
RA requests medical records
Provider has up to 45 days +/- 10 calendar days to
respond
RA has up to 60 days to review medical records
RA makes a claim
determination
Complex Review
AutomatedReview
RA makes a claim
determination
RAC issues Review Results Review Results
LetterLetterto provider (does NOT communicate
improper amount or appeal rights; and/or including “no findings”)
RA decides whether medical records are required to make determinations
If nofindingsSTOP
Complex Review Discussion Period Begins
plantemoran.com 68
On Day 41On Day 41,
Carrier/FI/MACrecoupsby offset
Day 1 Day 1
RAC issues Demand Demand LetterLetter which includes amount and appeal
rights
Complex Review Discussion Period Continues
Automated ReviewDiscussion Period
NOTE: Detailed review results letter
and claims information to
Carrier/FI/MAC are done simultaneously
RA sends claim info to
Carrier/FI/MAC
NOTE: This is an informational
entry only on the RA. No actual money taken at
this point
Carrier/FI/MAC adjusts & issues RemittanceRemittanceAdviceAdvice to provider.
Code “N432”Code “N432”
NOTE: The date of the demand letter starts the
41 day clock for recoupment
NOTE: Offset occurs if the provider has not submitted an appeal
request within 30 days of the date on the demand letter. No claim detail for the overpayment appears on the Remittance Advice
at the time the recoupment occurs

Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
Provider Options Regarding RA Provider Options Regarding RA Overpayment DeterminationsOverpayment Determinations
69
plantemoran.com
Identify Your RA RisksIdentify Your RA Risks
70
�Medicare daily rate exceeds peers
�How does the facility stand compared to others in your
CBSA (core-based statistical area)
�Are there patterns or trends that are easily identified –
same RUG category for several of the Medicare required
assessments for the same resident
�High percentage of resident treated exactly to RUG
minimum
�Medical necessity not substantiated in medical record

Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
� PSCs and now ZPICs use extrapolation with audit findings. The RAs can
use it, too, but one difference is that they have to obtain CMS approval
� In many extrapolations, claims reviewed frequently span a 12- to 24-month
period. The review date or date of the medical record request occurred
more than a year after most claims in the sample were paid by Medicare.
The Medicare contractor calculates an error rate and applies that error rate
to all similar claims within the sample period to produce an overpayment
estimate that greatly exceeds the combined value of the individually denied
claims, sometimes by more than 100 times the actual amount.
� Overpayment amounts assessed by reviewers are huge and, after a
certain level of appeal has been exhausted, CMS may recoup the
overpayment from future reimbursements while the appeal continues
Added Risk of Claim Reviews = Added Risk of Claim Reviews = ExtrapolationExtrapolation
71
plantemoran.com
Greatest RisksGreatest Risks
72
DOJDOJOIGOIG
ZPICZPIC
RARA
MMICIC
MACMAC
QIOQIOCERTCERT Routine
business
Compliance
Legal

Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
The Microscope of MedicareThe Microscope of Medicare
73
Criteria
plantemoran.com
� All four of the following factors must be met:
1. Requires skilled nursing or skilled rehabilitation services
2. Requires these skilled services on a daily basis
3. Daily skilled services can only be provided only on
inpatient basis in SNF
4. Services must be reasonable and necessary for
treatment of patient’s illness or injury
Requirements for SNF CoverageRequirements for SNF Coverage
74
Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
� Facility primarily engaged in providing skilled
nursing care and related services for residents who
require medical or nursing care, or rehabilitation
services for injured, disabled, or sick persons based
on Medicare requirements
What Is a Skilled Nursing What Is a Skilled Nursing Facility?Facility?
75
CMS IOM Publication 100-01,Medicare General Information, Eligibility and Entitlement Manual, Chapter 5, Section 30
plantemoran.com
Principles of DeterminingPrinciples of DeterminingSkilledSkilled
� Service must be so inherently complex inherently complex of a service
prescribed for a patient that it can be performed safely
and/or effectively only by or under the general supervision
of skilled nursing or skilled rehabilitation personnel; then
the documentation must reflect medical complications that documentation must reflect medical complications that
require the provision of the services by skilled personnelrequire the provision of the services by skilled personnel
� Medical condition is a valid factor, but diagnosis or
prognosis should never be the sole factor in deciding that
a service is not skilled
76

Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
“Reasonable and Necessary”“Reasonable and Necessary”
� From Medicare Policy Manual, Chapter 8: Services
must be:
� consistent with nature/severity of illness and
individual’s needs
� within accepted standards of medical practice
� appropriate as per level of caregiver
� appropriate intensity of service
77
plantemoran.com
Practical MatterPractical Matter
� Daily skilled services can be provided only in an SNF
� They are not available on an outpatient basis in the area in which the individual resides
� Transportation to the closest facility would be:
� An excessive physical hardship;
� Less economical; or
� Less efficient or effective than an inpatient institutional setting
78
Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
Related ConditionRelated Condition
� Services are needed for a condition which was
treated during the qualifying hospital stay
OR
� For a condition that arose while in the SNF and while
the beneficiary was still under treatment for a
condition for which the patient was previously treated
in the hospital
79
plantemoran.com
Benefit PeriodBenefit Period
� Up to 100 days per “Spell of Illness”
� Benefit period is not based on calendar year
� Days 1 to 20
� 100% paid by Medicare
� Days 21 – 100
� Coinsurance billing required
� 2013 rate = $148.00/day
80
Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
Medicare Benefit PeriodMedicare Benefit Period
� The beginning and ending of a benefit period is
based on the level of care that the patient requires
Beginning of a Benefit Period:
� Begins when a patient is admitted to a hospital for
inpatient care, and the beneficiary has not received
skilled services for at least 60 days
81
plantemoran.com
Medicare Benefit PeriodMedicare Benefit Period
Continuing a Benefit Period:
� Continues as the patient is admitted to a skilled nursing facility as an inpatient and requires a skilled level of care
� As long as the patient continues to require a Medicare skilled level of care, the benefit period does not end even if the patient exhausts their 100 days of Part even if the patient exhausts their 100 days of Part A coverageA coverage
82

Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
Medicare Benefit PeriodMedicare Benefit Period
Ending a Benefit Period:
� Ends when the care required by the patient no
longer meets the requirement for a Medicare skilled
level of care
� Patient must remain at a non-skilled level of care for
60 consecutive days before being eligible for a new
benefit period
83
plantemoran.com
� Begins
� Beneficiary enters qualified hospital or SNF as inpatient
by a qualified provider in a month for which the patient
is entitled to hospital insurance benefits
Starting and Ending a Benefit Starting and Ending a Benefit PeriodPeriod
84
� Ends
� 60 consecutive days from date of discharge and was
not in the hospital OR
� If the beneficiary stays in the facility, but does not
receive skilled care for at least 60 days

Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
Spell Of IllnessSpell Of Illness
• 3 day hospital stay• 30 day transfer rule
• Assigned to 1 of top 52 RUGs (5-day PPS) (presumption of coverage) and
• After that must meet the skilled level of care criteria
May receive up to 100 days per spell of illness
• At a non-skilled level of care for 60 consecutive days
85
plantemoran.com
Teaching &
Training
Direct Skilled CareNURSINGNURSINGOr Or
THERAPYTHERAPY
Skilled Care Building BlocksSkilled Care Building Blocks
86

Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
SNF SNF –– Medicare Part A Medicare Part A ––What’s Skilled?What’s Skilled?� Resident requires the skills of a licensed nurse or therapist
� Often a continuation of care for the reason of hospitalization
� Skilled care is delivered through:
� Direct nursing (7 days/week) OROR
therapy (5 days/week) services
� Teaching and Training
� Nursing Observation and Assessment
� Care Plan Management87
plantemoran.com
Direct Skilled CareDirect Skilled Care
�� NursingNursing - 7 days per week7 days per week
� IV, IM Injections and IV feedings
� Tube Feedings*
� Suprapubic Catheter Care
� Suctioning (tracheal, nasopharyngeal)
� Dressing Changes
� Ulcer/Surgical Wound Care
� Heat treatments
� Initial phases of medical gases (oxygen)
� Restorative nursing (2 programs each 15 minutes/day for 6 days)
/week)
�� TherapyTherapy
� PT
� OT
� SLP
� RT (provided by a nurse or
respiratory therapist)
5 days per 5 days per
weekweek
88*TF = 51% daily calories or at least 26% of total calories and 501cc of fluid
Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
� Several from CMS Transmittal 161 (CR 8044) for
MBPM, Chapter 8: Coverage of SNF Services
� Extended care services must have been treatment for which
the beneficiary was receiving inpatient hospital services
(including ER) or a condition which arose while in the SNF
for treatment for which was previously hospitalized. In other
words, the applicable hospital condition need not have been
the principal diagnosis that actually precipitated the
beneficiary’s admission to the hospital, but could be any one
of the conditions present during the qualifying hospital stay
Some Medicare A Manual Some Medicare A Manual Changes for April 2013Changes for April 2013
89
plantemoran.com
� Daily basis requirement for skilled services (7 days) and therapy services (5 days):� The daily requirement for therapy must be a single type of
skilled services on at least 5 days per week. It can be met by the single type of service daily or by furnishing various types of skilled services on different days of the week that collectively add up to “daily” skilled services. However, arbitrarily staggering the times of various therapy modalities during the week in order to have some type of therapy occur each day, would not satisfy the SNF coverage requirement for daily services. To meet this requirement –the resident must actually NEED services furnished daily.
Some Medicare A Manual Some Medicare A Manual Changes for April 2013Changes for April 2013
90Continued

Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
� Daily basis requirement for skilled services (7 days) and therapy services (5 days):
� Not sufficient to arrange the therapy so that it is furnished each day – unless there is a resident medical need. For example, if PT is furnished on 3 days each week and OT is furnished on 2 other days each week, the “daily basis” requirement would be satisfied only if there is a valid medical reason why both cannot be furnished on the same day.
Some Medicare A Manual Some Medicare A Manual Changes for April 2013Changes for April 2013
91
plantemoran.com
� HIQA not HIPAA compliant and replaced now with Medicare
Health Insurance Portability and Accountability (HIPAA)
compliant Eligibility Transaction System (HETS)
� In real–time mode handles requests for eligibility verification for
Part A and/or Part B; determines payment responsibility with
regard to deductible/co-payment; determines eligibility for
preventive services; determines if Medicare is primary or
secondary payer; MCR plan, MA plan or Part D; proper billing
� Check with your software vendor with any questions about
HETS http://www.cms.gov/Outreach-and-Education/Medicare-
Learning-Network-MLN/MLNMattersArticles/downloads/SE1249.pdf
Reminder about Verifying Reminder about Verifying Benefits Benefits –– After 4/1/2013 After 4/1/2013
92

Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
Documents Needed At Documents Needed At AdmissionAdmission
� Benefit eligibility confirmation – HETS
� Admission agreement with authorization to treat;
� Authorization to bill Medicare or insurance;
� Medicare Secondary Payor form;
� Copies of Medicare and Insurance cards
93
plantemoran.com
� Physician Documentation
� Therapy Evaluation and Documentation
� Nursing Documentation
� Ancillary Documentation
So What Documentation So What Documentation Do We Need?Do We Need?
94
Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
� Order to admit for skilled services
� Initial certification of skilled care as a continuation of a service or need arising during the hospitalization
� Orders for skilled care
� History and Physical detailing the skilled need
� Progress notes to support ongoing skilled services
Physician DocumentationPhysician Documentation
95
plantemoran.com
Physician CertificationPhysician CertificationRecertificationRecertification
Requirements
� Content of Certification – Post hospital SNF care is or was required because the individual needs or needed on a daily basis skilled nursing care (furnished directly by or requiring supervision of skilled nursing personnel) or other skilled rehabilitation services that, as a practical matter, can only be provided in a SNF on an inpatient basis; and and
96
Remember :
Physician
signature and
date should
be in the
same
handwriting
Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
Physician CertificationPhysician CertificationRecertificationRecertification
� The care is needed for a condition for which the patient received inpatient hospital services
� Timing of Certification – the certification must be obtained at the time of admission or as soon thereafter as is reasonable and practicable which is no later than the third day following the day of admission. This provides for consideration of weekend admissions
� Remember – faxed signatures are acceptable
97
plantemoran.com
Physician CertificationPhysician CertificationRecertificationRecertification
� Content of recertifications
� Reasons for continued need of SNF care
� Estimated time the individual will need to remain in the SNF
� Plans for home care, if any and
� If appropriate, the fact that continued services are needed for a condition that arose after admission to the SNF and while the individual was still under treatment for the condition for which he or she had received inpatient hospital services
98

Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
� The recertification statement must contain an adequate
written record of the reasonsreasons for the continued need
for services, the estimated period of time required for
the patient to remain in the facility, and any plans,
where appropriate, for home care. The recertification
statement made by the physician does not have to
include this entire statement if, for example, all of the
required information is in fact included in progress.
40.3 40.3 -- Recertifications Recertifications for Extended for Extended Care Services Care Services ((Rev. 1, 09Rev. 1, 09--1111--02)02)
99
plantemoran.com
� NOTE: In such a case, the physician's statement could
indicate that the individual's medical record contains
the required information and that continued post-
hospital extended care services are medically
necessary. A statement reciting only that continued
extended care services are medically necessary is not,
in and of itself, sufficient.
40.3 40.3 -- Recertifications Recertifications for Extended for Extended Care Services Care Services ((Rev. 1, 09Rev. 1, 09--1111--02)02)
100
Medicare General Information, Eligibility, and Entitlement Chapter 4 - Physician Certification and Recertification of Services
(Rev. 76, 01-13-12)

Plante Moran, PLLC 2013 614-222-9020
plantemoran.com 101
Must be signed and dated within 30 days of the previous date
plantemoran.com
Physician CertificationPhysician CertificationTiming and DocumentationTiming and Documentation� Upon admission
� By day 14
� Every 30 days thereafter (from the
physician signature date)
� Certification must include:
� Reason for certification (skilled care)
� Estimated of time services needed
� Discharge plans
can be signed at same timecan be signed at same time
102
Who Can Sign?
� Attending physician
� Physician on the staff who has knowledge of the case
� Physician extender who is not employed by the facility, but working in collaboration with a physician

Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
� No less than monthly for residents receiving skilled
care – especially Medicare Part A and replacement
plans;
� Must reflect an awareness of the treatment plan;
� Must reflect an awareness of the resident’s goals
and status;
� Include all skilled care provided at the time of the
visit
Physician DocumentationPhysician Documentation
103
plantemoran.com
Documentation Documentation
� Should “paint a picture” of the resident and their ability
� Must reflect the skilled service provided
� Assessment of acute medical conditions – spell it out
� Description of delivered services and resident’s response
� Teaching and training
� Provision of skilled care
� Show the interdisciplinary approach to skilled services
104
Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
Direct Skilled Therapy ServicesDirect Skilled Therapy Services
� Reasonable and necessary to the treatment of the illness or injury
� Documentation components:
� Evaluation
� Treatment plan = established by a physician after consultation by a qualified therapist
� Progress notes
� Updated treatment plan (recertification)
� Discharge Summary
105
plantemoran.com
� Must be of such a level of complexity and
sophistication or the condition of the resident must
be such that the services required can be safely
and effectively performed only by a qualified
therapist or under his/her supervision
Therapy ServicesTherapy Services
106

Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
� Reason for Referral – supporting hospital documentation or decline as noted in the nursing documentation
� Should include the medical diagnosis resulting in the need for therapy services
� Should include the treatment diagnosis that describes the symptoms or problems to be treated and needs to be supported by objective or descriptive documentation
TherapyTherapyEvaluationEvaluation
107
plantemoran.com
� Prior Level of Function (PLOF) – very important in
establishing why therapy treatment is warranted
� Should establish baseline data necessary for
assessing expected rehab potential
� Should incorporate standardized tests that can be
repeated throughout the POC process
TherapyTherapyEvaluationEvaluation
108

Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
� Should include impressions and clinical summary of the deficits identified during the evaluation:
“What is wrong with the resident?”
� Should establish why the resident has a “NEED” for therapy from a functional standpoint
TherapyTherapyEvaluationEvaluation
109
plantemoran.com
� Should include:
� Goals
� Resident focused with resident’s input
� Functional, objective and measureable
� Long term (LTG) – reflective of final level resident
is expected to achieve
� Short term (STG) – components of the LTGs with
a 2-3 week timeframe
Plan of CarePlan of Care(aka Treatment Plan)(aka Treatment Plan)
110

Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
� Should include:
� Specific treatment – description of the treatment or intervention (modalities):
� Gait training
� Therapeutic exercise
� ADL training
� Frequency – number of times in a week treatment will be provided
� Duration – number of weeks (Part A) or treatment sessions (Part B) for the Plan of Care (PoC)
Plan of Care Plan of Care (aka Treatment Plan) (aka Treatment Plan) (continued)(continued)
111
plantemoran.com
� Daily –
� Describes what was done in the treatment session
that day
� Supports why a code was billed and supports length
of time they were billed
� Requires a signature WITH credentials
� Does not need to support medical necessity
TherapyTherapyProgress NotesProgress Notes
112
Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
� Weekly –
� Provides justification for ongoing treatment
� Must show complexity of treatment and service provided
� Should detail significant progress
� If not – detail the barriers to the progress
� If no progress by the second weekly note – consider
change in treatment plan or determine need to transition
out of therapy. Progress needs to be monitored from the
initiation of treatment – not 3-4 weeks into treatment
TherapyTherapyProgress NotesProgress Notes
113
plantemoran.com
� Describe the skilled components of the intervention,
activity or technique that only the clinician has the
knowledge to provide
� “Skill” is not shown by only documenting the following:
� What patient or therapist did
� Exercise name, number of repetitions, amount of weight,
amount of assistance and distance ambulated
� Skilled treatment requires more documentation that just
“therapeutic activities”
Documenting Skilled Documenting Skilled TreatmentTreatment
114

Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
� When you read the therapy note – why does this
resident need the skills of the therapist to do this?
The medical record must justify all of the modalities
and services being provided to that individual resident
� Example – for gait training the regulation states that
the resident has to have a deficiency in orthopedic,
neurological, or musculoskeletal problem to qualify for
skilled gait training
Tips for Therapy Tips for Therapy DocumentationDocumentation
115
plantemoran.com
OneOne--onon--One TreatmentOne Treatment
� Need information to prove that services billed were
provided, medically necessary and required the skills of
a therapist or assistant under supervision of a therapist
� Type of exercises or activities performed
� Sets and repetitions of exercise
� Weight or resistance used
� Variations and progression of specific interventions
� Gait distance
� Assistive device used
� Patient/caregiver training
� Observations made before, during and after116

Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
CPT 97110 CPT 97110 Therapeutic ExercisesTherapeutic Exercises
� Supportive documentation recommendations include but are not limited to:
� Objective measurements of loss of strength and range of motion and effect on function
� If used for pain – include pain rating, location, effect of pain on function
� Specific exercises performed, number of sets and reps, amount of weight or resistance, purpose of exercise related to function, instruction provided and any assistance provided
� Any vital sign monitoring required related to clinical condition (pulse oximetry, heart rate, blood pressure)
117
plantemoran.com
CPT 97112 CPT 97112 Neuromuscular ReNeuromuscular Re--educationeducation
� Supportive documentation recommendations include
but are not limited to:
� Objective loss of ADLs, mobility, balance,
coordination deficits, hypo and/or hypertonicity
and posture and effect on function.
� Specific exercises/activities performed, purpose of
the exercise as it relates to function, instruction
provided, and assistance needed
118
Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
CPT 97116 CPT 97116 Gait TrainingGait Training
� Supportive documentation recommendations include but
are not limited to:
� Objective measurements of balance and gait distance,
assistive devices used, assistance required, gait deviations
and limitations being addressed, use of orthotics or
prosthesis, need for and description of verbal cueing
� Presence of complicating factors (pain, balance deficits, gait
deficits, stairs, architectural or safety concerns)
� Specific gait training techniques used, instructions provided,
and/or assistance needed, resident response to interventions
119
plantemoran.com
CPT 97535 SelfCPT 97535 Self--Care Home Care Home Management TrainingManagement Training
� Supportive documentation recommendations include but are not limited to:
� Objective measurements of the patient’s ADL and instrumental activity of daily living (IADL) impairment to be addresses
� The specific ADL and/or compensatory training provided, specific safety procedures addressed, specific adaptive equipment/assistive technology utilized, instruction provided, assistance provided and resident response to the interventions to support the services provided required the skills of the therapist
120
Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
CPT 97530 CPT 97530 Therapeutic ActivitiesTherapeutic Activities
� Supportive documentation recommendations include
but are not limited to:
� Objective measurements of loss of ADLs, balance,
strength, coordination, range of motion, mobility
and effect on function
� Specific activities performed and amount and type
of assistance to demonstrate the skills and
expertise of the therapist were required
121
plantemoran.com
CPT 97542 CPT 97542 Wheelchair ManagementWheelchair Management
� Supportive documentation recommendations include but are not limited to:
� Recent event prompting the need for a skilled w/c assessment
� Any previous w/c assessments completed
� Most recent prior level of function
� Any previous interventions attempted by the nursing staff, caregivers and/or resident that may have failed
� Functional deficits related to poor positioning or seating
� Objective assessments of applicable impairments such as range of motion, strength, sitting balance, skin integrity, sensation and tone
� Response of the resident or caregiver to the fitting and training
122
Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
� Should outline the progress demonstrated since treatment initiated;
� Should include impact on resident’s functional status
� Should include the reason for continued need of therapy – LTGs as it relates to the resident’s return to community or transition to long term care
� What still needs to be accomplished?
ReRe--certificationcertification
123
plantemoran.com
Includes the following:
� Criteria to discontinue treatment
� Current functional status
� Detail goals achieved
� Details reasons for unmet goals
� Describe plan related to resident’s continuing care (restorative, home care, out-patient)
� Referrals for additional services
� Equipment provided or ordered
Discharge SummaryDischarge Summary
124
Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
Skilled Nursing DocumentationSkilled Nursing Documentation
� Must be completed no less than daily
� Describe skilled care was provided � Medication administration record (MAR)
� Treatment administration record (TAR)
� IV sheet
� Behavior grids
� Wound grids
� Nurses notes/progress notes
� Assessments pertaining to skilled services – what, why, action taken, resident’s response
125
plantemoran.com
� Describe resident’s response
� Tolerance
� Discomfort
� Side effects experienced
� Describe need for change of treatment or physician
notification
� Must detail what skilled care the resident received
� Should include ADL status
Skilled Nursing DocumentationSkilled Nursing Documentation
126
Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
Documentation of ServicesDocumentation of Services
� Reflect resident self performance and staff
support for activities of daily living (ADLs) – note
what the resident can or cannot do
� Walking
� Dressing/am and pm care
� Toileting
� Eating
� Bed mobility and transfers
127
plantemoran.com
� Therapy will document what the resident does in therapy
� Nursing must document:
� Therapy attendance
� Pain related to therapy (if reported)
� Compliance
� If the resident refuses therapy – let someone know immediately
� Safety factors observed
� Resident self performance of care in and out of room
� Document the problems the resident is having caring for self (if
present
Nursing DocumentationNursing Documentation(As It Relates to Therapy)(As It Relates to Therapy)
128
Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
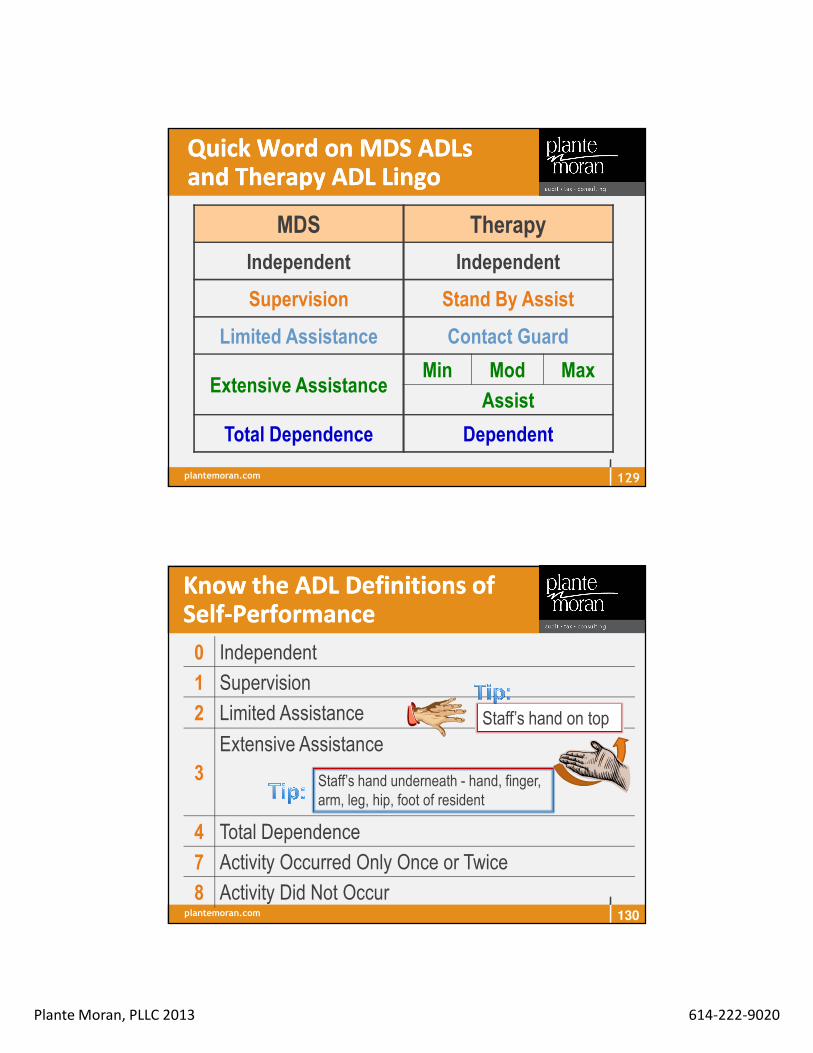
Quick Word on MDS Quick Word on MDS ADLs ADLs and Therapy ADL Lingoand Therapy ADL Lingo
MDS Therapy
Independent Independent
Supervision Stand By Assist
Limited Assistance Contact Guard
Extensive AssistanceMin Mod Max
Assist
Total Dependence Dependent
129
plantemoran.com
Know the ADL Definitions of Know the ADL Definitions of SelfSelf--PerformancePerformance
0 Independent
1 Supervision
2 Limited Assistance
3
Extensive Assistance
4 Total Dependence
7 Activity Occurred Only Once or Twice
8 Activity Did Not Occur
Staff’s hand on top
Staff’s hand underneath - hand, finger, arm, leg, hip, foot of resident
130

Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
ADL Values for Bed Mobility, ADL Values for Bed Mobility, Toilet Use, TransferToilet Use, Transfer
RUGs IV
Support
Performance None (0)/
Setup (1)
1-person (2)
2-person (3)
Independent(0)/Supervision (1) 0
LimitedAssistance (2) 1
Extensive Assistance (3) 2
4TotalDependence (4) 3
Includes self-performance codes (7) and (8)
131
What makes HUGE difference in ADL scoring?
Column 2: Support
One or two staff person assistance
plantemoran.com
RUGs IV
Support
Performance None (0)/
Setup (1)
None (8)
1-person
(2)
2-person
(3)
Independent(0)/Supervision (1)
0 2Limited
Assistance (2)1 or 2 times (7)None (8)
Extensive
Assistance (3)
23
TotalDependence (4) 4
ADL Values for EatingADL Values for Eating
132
Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
� Office of the Inspector General in November 2012 report called
“Inappropriate Payments to Skilled Nursing Facilities Cost
Medicare More than a Billion Dollars in 2009” focused on
importance of medical record supporting the need for skilled
care and the accuracy of MDS coding. The RUG system forces
them to be connected. Some statistics:
� SNFs reported inaccurate information not supported in
medical record for at least one MDS item for 47% of claims.
Therapy was the source of most errors, but also special
care and ADLs showed mistakes
Speaking of the MDSSpeaking of the MDS
133
plantemoran.com
� Another report from the OIG (February 2013) called “Skilled
Nursing Facilities Often Fail to Meet Care Planning and
Discharge Planning Requirements” reported that 37% of stays,
SNF did not develop care plans that met requirements or did
not provide services based on the plans of care. Reviewers
found that therapy played a significant role and either provided
more or less services than care planned.
� The area that had the most common problems of not
addressing needs identified in the assessments was the
care area of ADLs – impacting 86% of resident stays.
Speaking of More Hits from Speaking of More Hits from the OIGthe OIG
134
Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
Observation and Observation and AssessmentAssessment
� Nursing
� Resident condition is unstable for medical reasons
� Risk for occurrence of acute problem
� Skills of a licensed nurse are required on a daily basis to assure resident safety
� Examples: COPD, CHF, recent MI, medication changes
135
plantemoran.com
� If admitted for skilled observation but did not develop
a further acute episode or complication, skilled
observation services are covered so long as there
was reasonable probability for such a complication or
further acute episode
� "Reasonable probability" means that a potential
complication or further acute episode was a likely
possibility
Observation and AssessmentObservation and Assessment
136
Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
A patient with arteriosclerotic heart disease with congestive heart failure requires close observation by skilled nursing personnel for signs of decompensation, abnormal fluid balance, or adverse effects resulting from prescribed medication. Skilled observation is needed to determine whether the digitalis dosage should be reviewed or whether other therapeutic measures should be considered until the patient's treatment regimen is essentially stabilized
Observation and AssessmentObservation and AssessmentExample 1Example 1
137
plantemoran.com
A frail 85-year-old man was hospitalized for pneumonia. The infection was resolved, but the patient, who had previously maintained adequate nutrition, will not eat or eats poorly.The patient is transferred to a SNF for monitoring of fluid and nutrient intake, assessment of the need for tube feeding if required. Observation and monitoring by skilled nursing personnel of the patient's oral intake is required to prevent dehydration.
Observation and AssessmentObservation and AssessmentExample 2Example 2
138
Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
Care Plan ManagementCare Plan Management
� Nursing
� Multitude of non-skilled services (which are
able to be performed by non-licensed persons)
� Licensed nurse required to manage the care
� Potential for complications with relation to those
services
139
plantemoran.com
Care Plan ManagementCare Plan Management
� Development, management, and evaluation of a patient care plan, based on the physician's orders
� In terms of the patient's physical or mental condition
� Services require the involvement of skilled nursing personnel to:
� Meet medical needs
� Promote recovery
� Ensure medical safety
140

Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
Care Plan Management Care Plan Management Example 1Example 1
An aged patient with a history of Diabetes Mellitus and angina is recovering from hip surgery requires:
� Careful skin care
� Oral medications
� Diabetic diet
� Therapeutic exercise program to preserve muscle tone and body condition
� Observation to notice signs of deterioration in his condition or complications resulting from his restricted (but increasing) mobility
141
plantemoran.com
� Since the nature of the patient's condition, his age and his immobility create a high potential for serious complications, such an understanding is essential to assure the patient's recovery and safety.
� The management of this plan of care requires skilled nursing personnel until the treatment regimen is essentially stabilized.
� Even though the individual services involved are supportive in nature and do not require skilled nursing personnel
Care Plan Management Care Plan Management Example 1 (continued)Example 1 (continued)
142

Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
An aged patient is recovering from pneumonia, is
lethargic, disoriented, has residual chest congestion,
is confined to bed as a result of debilitation, and
requires restraints at times. To decrease the chest
congestion, the Dr. has prescribed:
� Frequent changes in position
� Coughing and deep breathing
Care Plan Management Care Plan Management Example 2Example 2
143
plantemoran.com
� The residual chest congestion alone would not
represent a high risk factor, but immobility and
confusion represent complicating factors which, when
coupled with the chest congestion, could create high
probability of a relapse
� Skilled overseeing of the non-skilled services would
be reasonable and necessary, pending the
elimination of the chest congestion, to assure the
patient's medical safety
Care Plan Management Care Plan Management Example 2 (continued)Example 2 (continued)
144
Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
Teaching and TrainingTeaching and Training
� Learn self-maintenance skills, such as:
� Restorative programs � G-tube feedings, flushes� Dressing changes� Medication administration� Skin treatment � Self-catheterization, ostomy or catheter� Diabetic diet, foot care, blood glucose monitoring � Oxygen administration, adjustments of equipment
145
� Incorporate into
treatment plan from
beginning
� Document patient’s
response
� Do not add extra days
on for education
� Improve resident’s functional status by
teaching new techniques
� Nursing
plantemoran.com
Who Reads Your ChartingWho Reads Your Charting
� Remember charting is not just for the next shift to read, it’s for:
� Doctors
� Administrative staff
� Consultants
� Medicare Administrative Contractors
� State Surveyors
� Medical Staff outside facility
� Medicare and/or Medicaid reviewers – RA, MIC, ZPIC,
exception reviewers, CERT, PERM
� Attorneys
146

Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
Charting TipsCharting Tips
� Take time to gather your thoughts before beginning to document
� Don’t take shortcuts – use only approved abbreviations by your facility, write it out for a clear understanding
� Be complete – describe the event in complete sentences with enough detail that the reader will get a clear picture
147
plantemoran.com
Charting TipsCharting Tips
� Documentation of preceding events is helpful
� If it’s important enough to be in shift report then it’s
important enough to document in the medical record
� Chart about the resident not yourself, with focus on
resident’s reaction to treatment and outcome
� Document phone calls to the physician as the
resident’s advocate and the persistence in expressing
the resident’s needs
148
Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
Charting TipsCharting Tips
� Remember to chart:
� What you see
� Action taken
� Effectiveness of the interventions implemented
� Discrepancies between therapy and nursing need
to be investigated and clarified
149
plantemoran.com
Medicare providers are faced with the challenges of providing quality healthcare while meeting ever increasing regulatory and compliance regulations. Many are investing in Electronic Health Records (EHR) to increase the quality of their documentation, decrease or minimize documentation time and improve their overall record keeping capabilities. Providers need to be aware that EHR can inadvertently cause some documentation pitfalls such as making the documentation appear cloned. Cloned documentation could cause payment to be denied in the event of a medical review audit of records.lllll
Documentation is considered cloned when it is worded exactly like or similar to previous entries. It can occur when the documentation is exactly the same from patient to patient. Individualized patient notes for each patient encounter are required. Documentation must reflect the patient condition necessitating treatment, the treatment rendered and if applicable the overall progress of the patient to demonstrate medical necessity.
150
Cloned Documentation Could Resultin Medicare Denials for Payment 08/12
Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
An EHR allows default options. Defaults cause a provider to overlook
significant new findings that may result in safety/quality issues. Default data
may document a more extensive history and physical exam than is medically
necessary and may not differentiate new findings or changes in condition. It is
important to document patient progress. Cloned documentation also applies
to disciplines where the documentation must demonstrate the patient is
making progress towards goals, or documenting the findings or changes
in a patient’s condition to meet Medicare medical necessity.l
No matter if the documentation resulted from EHR, a pre-printed template, or
handwritten documentation, cloned documentation will be considered
misrepresentation of medical necessity requirement due to the lack of specific
individual information for each unique patient. Identification of this type of
documentation will lead to denial of services for lack of medical necessity and
the recoupment of all overpayments made 151
Cloned Documentation Could Resultin Medicare Denials for Payment 08/12
plantemoran.com
� Patient slept well all night, alert and verbally
responsive. Noted episodes of incontinence,
kept clean and dry, assisted in using the bed
pan. Bed placed in the lowest position, bed
alarm in place. Call light in reach.
� Patient slept well all night, alert and oriented,
continent of b/b, assisted to the bathroom.
Scheduled meds given as ordered. Call light in
reach, needs attended to. Afebrile
Sample Skilled Nursing NotesSample Skilled Nursing Notes
152
SkilledServices
SkilledServices

Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
� Pt. alert and ambulatory w/walker. No c/o
pain during shift. All meds administered
w/o any adverse effect. Pt. ate in the dining
room w/ good appetite. Continue w/therapy
services w/o any issues. Pt. showered
w/staff assistance. Will follow up
Sample Skilled Nursing NotesSample Skilled Nursing Notes
153
SkilledServices
plantemoran.com
� Pt. assessed to be alert and oriented x 3. No distress noted. Right knee
incision, assessed to be clean, intact and dry. Has order for weight bearing
as tolerated on right LE. Limited weight bearing assistance is needed for
ADLs of bed mobility, transfer, dressing, toileting & positioning. On
anticoagulant therapy as post-op. precaution, monitored for signs and
symptoms of bleeding which were negative at this time. Meds given as
ordered. Fall precautions observed. Copy of Transition Summary &
Recapitulation form given to patient with instructions, verbalized
understanding. Patient assisted & supervised with ADLs. Pain assessed
and evaluated and managed with prn pain medication, polar care
application, and rest. Patient on modified independence, ambulates with
the use of cane with steady gait. Patient denies any chest pain/heaviness.
No SOB/dizziness at this time. Call light within reach. Needs attended. 154
Sample Skilled Nursing NotesSample Skilled Nursing NotesSkilled Services

Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
� Interventions provided: Therapeutic exercises 2# weighted bar for
chest press, bicep curls, shoulder flexion and shoulder horizontal
abduction/adduction. Omnicycle x 15 minutes. Therapeutic activities:
fine motor coordination training, buttoning, zipping and hooking
clothing fasteners to improve fine motor coordination,
throwing/catching activities to facilitate strength, coordination,
balance and dynamic function activities to increase strength, ROM,
flexibility in a progressive manner. OmniVR for sit to stand activities.
Neuromuscular Re-Ed and dynamic standing balance training and
facilitation of weight shift/dynamic stability. Self-care mgmt.: dressing
techniques and analysis of sequencing during ADLs. W/C Mgmt.:
training in locking/unlocking brakes to facilitate safety.155
Sample Skilled Therapy NotesSample Skilled Therapy Notes
continued
plantemoran.com
Pt. and caregiver training: Instructed patient in safe transfer
techniques to reduce the risk for falls.
Continued Skill: Reason for skilled Services: Patient requires skilled
OT services to assess safety and independence with self care and
functional tasks of choice, facilitate dynamic standing balance and
increase functional activity tolerance in order to enhance patient’s
quality of life by improving ability to facilitate ability to live in
environment w/least amount of supervision and assistance.
Patient demonstrates good rehab potential as evidenced by high
PLOF.
156
Sample Skilled Therapy NotesSample Skilled Therapy Notescontinued
Was NOT from Alden facility
Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
� Pt. progressing toward goals/continue per
POC.
� Balance, gait, transfer, strength & ROM.
Continue with current tx.
� Pt. has achieved STG #2 & STG #1.
Continue to work to achieve LT goals
� Progressing Therapeutic ex & progressing
gait training, continue with current tx
strategies.
157
Sample Skilled Therapy NotesSample Skilled Therapy Notes
Progress notes do not provide justification for the medical necessity of treatment
Individual Resident Therapy Notes
� The facility utilizes a check-off sheet, in addition to a note, for exercises and modalities provided; this lacks objective measurement; e.g., grey Thera-band checked off without any indication of why it is useful or the resident’s response.
Additional Comments
plantemoran.com
� Resident name must match that reflected on the Medicare
card
� Correct Medicare number
� Days of Therapy – no longer units
� HIPPS and Modifier coding matches the MDS
� Diagnosis selection and coding
� Consolidated billing requirements
� Cannot be submitted until the MDS is accepted for
residents in a Medicare Part A stay
UBUB--04 Completion and 04 Completion and SubmissionSubmission
158

Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
So Let’s Talk About So Let’s Talk About Diagnosis CodingDiagnosis Coding
159
Now – Don’t Get THAT Excited!!
What we will cover:� Types of diagnoses� Describe what is the
“primary/principal” diagnosis for LTC
� Secondary and supporting diagnoses
� Risks for miscoding� Strategies for success
plantemoran.com
� Accuracy of the MDS
� Reimbursement
� Audit risks
Why IsWhy IsDiagnosis Coding Important? Diagnosis Coding Important?
160
Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
� ICD 9 – International Statistical Classification of
Diseases and Related Health Problems approved
by:
� CMS
� American Hospital Association
� American Health Information Association
� National Center for Health Statistics
ICDICD--9 9 –– What is it?What is it?
161
plantemoran.com
� Updates every October 1 – although 2011 seems
to be the last publication for the Official Guidelines
� Scheduled to adopt ICD-10 in October 1, 2014 to
be in line with the World Health Organization
� Expands codes from 17,000 to 155,000
ICDICD--9 9 –– What is it?What is it?
162
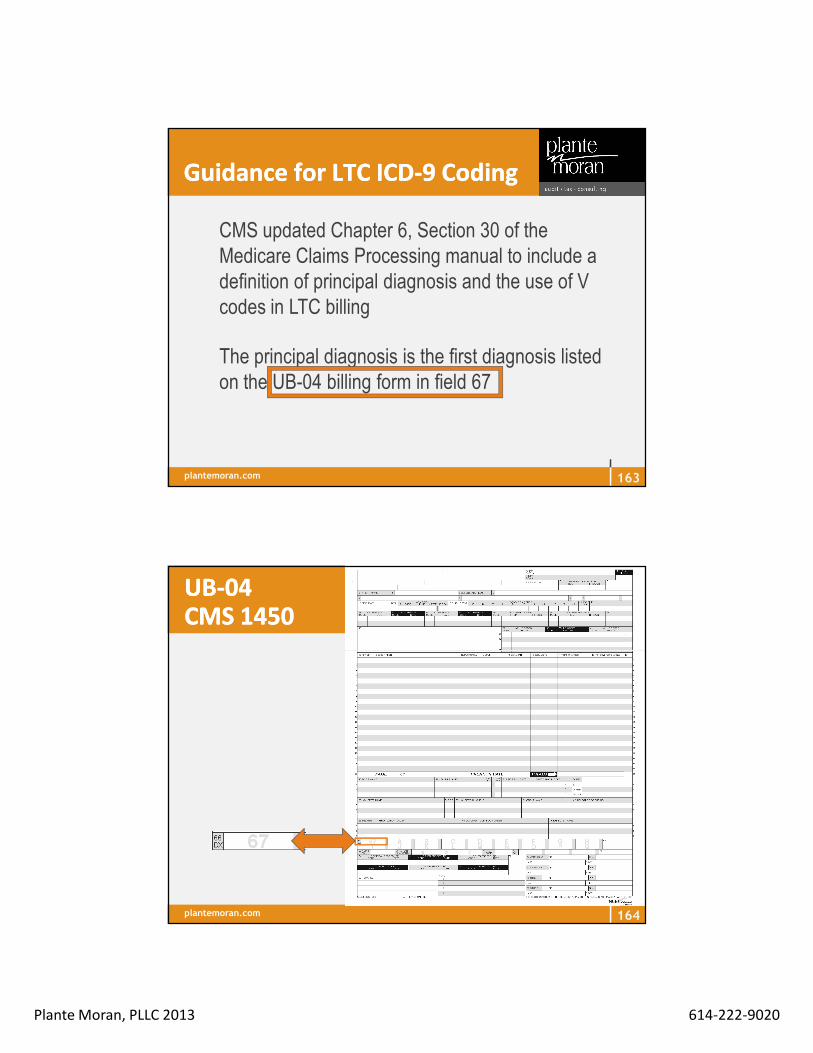
Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
Guidance for LTC ICDGuidance for LTC ICD--9 Coding9 Coding
� CMS updated Chapter 6, Section 30 of the Medicare Claims Processing manual to include a definition of principal diagnosis and the use of V codes in LTC billing
� The principal diagnosis is the first diagnosis listed on the UB-04 billing form in field 67
163
plantemoran.com
UBUB--0404CMS 1450CMS 1450
164

Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
� Secondary diagnoses can be listed in the additional fields, with no sequencing requirements
� Supportive treatment diagnoses can be listed in no sequencing order
Guidance for LTC ICDGuidance for LTC ICD--9 9 CodingCoding
165
plantemoran.com
Medlearn Matter MM3664Medlearn Matter MM3664
� Principal Diagnosis Code – Code must be reported according to Official ICD-9-CM Guidelines, including appropriate use of V-codes
� Other Diagnosis Codes Required – CMS does not have additional requirements regarding reporting or sequencing of codes
www.cdc.gov/nchs/data/icd9/icdguide09.pdf
166
Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
� Section I: General Coding Guidelines for Late Effects
� Residual condition (late effect) = condition that remains after
acute phase of an illness
� Sequenced first unless otherwise instructed
� Cause of late effect listed second
� Do not use code for the acute phase of illness
Ex: Quadriplegia (344.00) following Cervical Fracture (907.2)
Guidance for Guidance for LTCLTCICDICD--9 Coding9 Coding
167
plantemoran.com
� Section II: Selection of principal diagnosis applies to
all inpatient care settings including LTC
� Principal diagnosis for LTC: Condition chiefly
responsible for resident’s admission to the facility
(therapy, aftercare or diagnosis), or reason for
resident remaining in the facility
� In LTC where claims are submitted for extended stays,
the principal diagnosis listed may change to the reason
for which the resident remains in the facility
Guidance for LTC ICDGuidance for LTC ICD--9 Coding9 Coding
168
Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
� Section III: Reporting Additional Diagnoses applies to
all inpatient care settings including LTC. The definition
for “other diagnoses” is interpreted as additional
conditions that affect patient care in terms of requiring:
clinical evaluation; or therapeutic treatment; or
diagnostic procedures; or extended length of hospital
stay; or increased nursing care
Guidance for LTC Guidance for LTC ICDICD--9 Coding9 Coding
169
plantemoran.com
� Create a listing of diagnoses and codes
� Select principal diagnosis and list first
� List additional diagnoses that reflect services
provided or clinical conditions
� Do not list diagnoses that are not pertinent to
nursing facility stay
� Do not list diagnoses that have been resolved or
are historical unless clinically significant to staff
Tips for LTC ICDTips for LTC ICD--9 Coding9 Coding
170
Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
� Use of Diagnoses on the MDS
� V-codes can be reported in I8000
� Do not report V57.xx codes for therapies (captured
elsewhere on the MDS [Section O])
� DO NOT include code if already captured in other
sections of MDS (therapies, g-tube)
More Tips for LTC ICDMore Tips for LTC ICD--9 Coding9 Coding
171
plantemoran.com
Coding Process in LTCCoding Process in LTC
� High acuity residents (i.e., Medicare or managed care)� Review codes monthly
Codes on MDS, billing claim forms (i.e., UB-04) and in medical record need to support:� Medical necessity� Skilled services provided (may include therapy
treatment diagnosis)� Resource Utilization Group (RUG) selection as
applicable
172

Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
Chart diagnosis list
UB-04MDS
Develop Consistency of DataDevelop Consistency of Data
173
plantemoran.com
� Accurate reporting of ICD-9-CM codes affects:
� Medicare billing
� Quality Measures
� Data collected for long term care residents
� Overall accuracy of the MDS/RUG categories
Develop Consistency of DataDevelop Consistency of Data
174

Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
� Not all diagnoses reported on MDS are appropriate
for billing claim forms (i.e., UB-04);
� Not all diagnoses on the MDS relate to the reason(s)
for Medicare coverage;
� Keep in mind time frame of MDS vs. billing claim form
Accurately Reporting ICDAccurately Reporting ICD--99Codes: MDS vs. Billing Claim FormsCodes: MDS vs. Billing Claim Forms
175
plantemoran.com
� Use I8000 to report additional diagnoses not listed in
Section I – Diagnoses Items I0100 to I6500 that affect
current status
� Consider listing therapy treatment diagnoses in I8000
I8000 I8000 –– Other Current or More Other Current or More Detailed Diagnoses and ICDDetailed Diagnoses and ICD--9 Codes9 Codes
176

Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
I8000 I8000 –– Other Current or More Other Current or More Detailed Diagnoses and ICDDetailed Diagnoses and ICD--9 Codes9 Codes
� Annual ICD-9 code updates take effect on October 1 of each year
�� V codes may be used if they affect resident’s V codes may be used if they affect resident’s current statuscurrent status
� American Health Information Management Association coding and practice guidelines resource: www.ahima.org/infocenter/guidelines/ltcs/
177
plantemoran.com
I8000 I8000 –– Using VUsing V--CodesCodes
� V Codes – Aftercare� Used when
� Initial treatment of disease or injury has been performed ANDAND
� Continued care required during the healing or recovery phase OROR
� Continued care required for the long-term consequences of the disease
178

Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
I8000 Using VI8000 Using V--CodesCodes
� Supplementary Classification of factors influencing health status and contact with health services
� ICD-9-CM Official Guidelines for Coding and Reporting: Section I, General Coding Guidelines –Categories of V codes, Aftercare
179
plantemoran.com
I8000 I8000 –– Using VUsing V--CodesCodes
� V Codes – Aftercare� DO NOT use if treatment is directed at a current,
acute disease or injury� Use diagnosis code for current disease or
injury (the code must be the full ICD-9-CM diagnosis code, including all five digits where applicable)
180
Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
VV--Codes (V01Codes (V01--V82)V82)
� Assign V-code as first listed, or principal diagnosis when main reason for resident’s admission or continued stay is for:� Rehab services (V57) – Can only be used as first listed code
� Orthopedic aftercare (V54) – can be listed first or additional
� Surgical aftercare (V58.4x and V58.7x) – can be listed first or additional diagnosis
181
plantemoran.com
VV--Codes (V01Codes (V01--V82)V82)
� Other V-codes that can be assigned as first listed or principal diagnosis but are typically used as secondary diagnosis in LTC include:� Attention and management of artificial openings
(V55)� Amputation status (V49.6x or V49.7x)� Acquired absence of organ (V45.7x)� Monitoring therapeutic drug uses – i.e., Coumadin
(V58.83)
182
Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
VV--Codes (V01Codes (V01--V82)V82)
� While it is technically possible to assign the following V codes as “first-listed” or principal diagnosis, it is extremely rare and should be discussed with manager prior to coding:� “History” of impacts or affects current care of the
resident� Personal history codes (range V10 – V13)� Family history (V16 – V19)
183
plantemoran.com
V Codes (V01V Codes (V01--V82)V82)
� V codes that can ONLYONLY be listed as secondary diagnosis include:� Drug resistance present (V09)� Personal history codes (range V14 – V15) except except
V15.88 history of fall which can be first listed or additional
� Organ replacement status (V42 or V43)� Long term (current) drug use (V58.6x)� Hospice (V66.7)
184
Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
More on Using Code V57.xxMore on Using Code V57.xxin LTCin LTC
� Assign code from V57.xx (care involving use of rehabilitative procedures) if resident is admitted specifically for rehabilitative therapy:� Use V57.89 (multiple therapies) when two or
more therapies services are provided� Use additional code(s) to identify underlying
condition(s)
185
plantemoran.com
More on Using Code V57.xx More on Using Code V57.xx in LTCin LTC
� V57.xx is:� First listed or principal diagnosis for admission if
resident admitted primarily for therapy intervention. Can only be used as first listed
� Coupled with codes for medical conditions (related to the need for therapy) and a treatment diagnosis
� Not used as a therapy medical diagnosis
186
Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
Coding ExamplesCoding Examples
A resident is admitted for physical therapy following a hip replacement for an intertrochanteric right hip fracture due to a fall
187
plantemoran.com
Coding ExamplesCoding Examples
Physical therapy:� V57.1 = Physical Therapy: Hip replacement:� V54.81 Aftercare following joint replacement due
to fracture (fractured not coded since repaired with prosthesis)
� V43.64 Joint replacement, hip� Due to a fall: V15.88 History of a fall
188
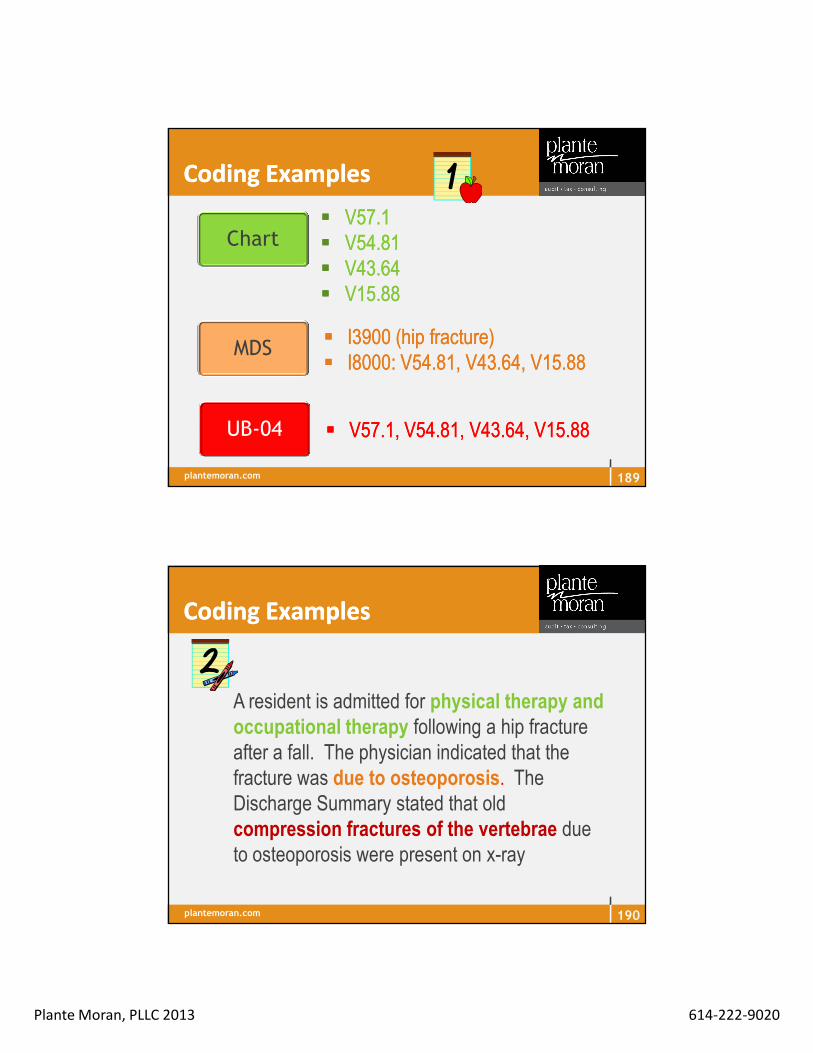
Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
Coding ExamplesCoding Examples
�� V57.1V57.1�� V54.81V54.81�� V43.64V43.64�� V15.88V15.88
Chart
MDS
UB-04
�� I3900 (hip fracture)I3900 (hip fracture)�� I8000: V54.81, V43.64, V15.88I8000: V54.81, V43.64, V15.88
�� V57.1, V54.81, V43.64, V15.88V57.1, V54.81, V43.64, V15.88
189
plantemoran.com
Coding ExamplesCoding Examples
A resident is admitted for physical therapy and occupational therapy following a hip fracture after a fall. The physician indicated that the fracture was due to osteoporosis. The Discharge Summary stated that old compression fractures of the vertebrae due to osteoporosis were present on x-ray
190

Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
Coding ExamplesCoding Examples
Physical and occupational therapy:� V57.89 Multiple therapies
Hip fracture (due to osteoporosis):� V54.23 Aftercare for continuing treatment of healing
pathological fracture of hip
Osteoporosis:� 733.00 Osteoporosis
Compression fractures of vertebrae:� V54.27 Pathological fractures of vertebrae
191
plantemoran.com
Coding ExamplesCoding Examples
�� V57.89V57.89�� V54.23V54.23�� 733.00733.00�� V54.27V54.27
Chart
MDS
UB-04
�� I3900(hip fracture); I4000 I3900(hip fracture); I4000 (pathological (pathological fracture); fracture); I3800 I3800 (osteoporosis)(osteoporosis)
�� I8000: V54.23, V54.27, I8000: V54.23, V54.27,
�� V57.89, V54.23, 733.00, V54.27V57.89, V54.23, 733.00, V54.27
192

Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
Coding ExamplesCoding Examples
A resident is admitted for physical therapy and occupational therapy following a below knee amputation of the left leg due to peripheral vascular disease secondary to Type II Diabetes Mellitus
193
plantemoran.com
Coding ExamplesCoding Examples
Physical and occupational therapy:� V57.89 = Multiple therapies
Below knee amputation:� V54.89 Aftercare for amputation stump� V49.75 Lower limb amputation status, below knee
Peripheral vascular disease 2° to Type II diabetes� 250.70 Diabetes w/ peripheral circulatory disorders� 443.81 PVD 2° Type II Diabetes Mellitus
194
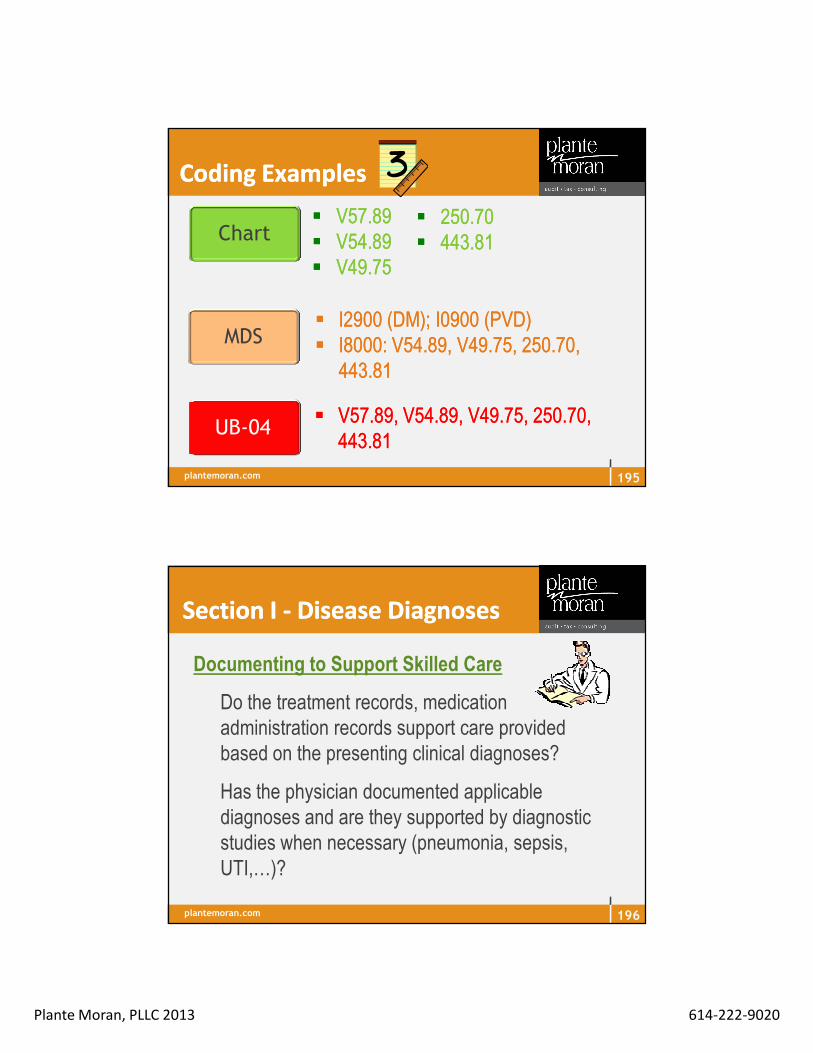
Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
Coding ExamplesCoding Examples
�� V57.89V57.89�� V54.89V54.89�� V49.75V49.75
Chart
MDS
UB-04
�� I2900 (DM); I0900 (PVD)I2900 (DM); I0900 (PVD)�� I8000: V54.89, V49.75, 250.70, I8000: V54.89, V49.75, 250.70,
443.81 443.81
�� V57.89, V54.89, V49.75, 250.70, V57.89, V54.89, V49.75, 250.70, 443.81443.81
�� 250.70250.70�� 443.81443.81
195
plantemoran.com
Documenting to Support Skilled Care
� Do the treatment records, medication administration records support care provided based on the presenting clinical diagnoses?
� Has the physician documented applicable diagnoses and are they supported by diagnostic studies when necessary (pneumonia, sepsis, UTI,…)?
Section I Section I -- Disease DiagnosesDisease Diagnoses
196

Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
Section I Section I –– Active DiagnosesActive Diagnoses
� Code diseases that have a relationship to the
resident’s:
� Current functional status
� Cognitive status
� Mood or behavior status
� Medical treatments
� Nursing monitoring
� Risk of death
197
plantemoran.com
Section I Section I –– Active DiagnosesActive Diagnoses
� Diagnoses required to have documentation from a
physician or other authorized licensed staff as
permitted by the state (PA, NP, CNS)
� 12 major divisions
� Use a 60-day look-back period to identify diagnoses
� Determine diagnosis status
� Active or inactive
� Use a 7-day look-back period
198

Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
Section I Section I –– Active DiagnosesActive Diagnoses
� Step 1 = include ONLY diagnoses identified in the
last 60 days
� Step 2 = active or inactive (7-day look-back)• Transfer documents • Nursing care plans
• Physician progress notes • Medication sheets
• Recent History & Physical • Doctor’s orders
• Recent discharge summaries • Consults
• Nursing assessments • Official diagnostic reports
• Physician order sheets
199
plantemoran.com
� Specific documentation of active diagnosis in medical record
� Recent onset or acute exacerbation indicated by a positive study,
test, or procedure, hospitalization for acute symptoms and/or
recent change in therapy
� Symptoms and abnormal signs indicating ongoing or
decompensated disease
� Symptoms must be specifically attributable to a disease
� Ongoing therapy with medications or other interventions to
manage a condition that requires monitoring for therapeutic
efficacy or to monitor potential adverse effects
Indicators of Active DiagnosisIndicators of Active Diagnosis
200
Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
� Determine whether diagnoses are active – do not include
conditions that have been resolved or have no longer
affected the resident’s function or care plan
� Adds definition to what is an active disease process as
“physician documented diagnoses in the last 60 days
that have a direct relationship to the residents functional
status, cognitive status, mood or behavior, medical
treatments, nursing monitoring or risk of death in the 7-
day look back period
More on Section I More on Section I
201
plantemoran.com
� Admissions
� Director of Nursing (or designee)
� MDS Nurse
� Therapy
� Billing
So Who Is Responsible?So Who Is Responsible?
202
Diagnosis Coding

Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
� Provide preliminary referral information
� Check on any observation days in the hospital
� Obtain hospital information for team review
� Complete face sheet with appropriate primary
diagnosis listed
AdmissionsAdmissions
203
plantemoran.com
� Review diagnosis for referrals in clinical stand up (if available)
� Review diagnosis for new admissions first day after admission to validate team awareness of primary diagnosis
AdmissionsAdmissions
204
Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
� Review referrals pre-admission
� Assign primary diagnosis (reason admitted to SNF)
� Discuss new admissions in clinical stand up (confirm
diagnosis)
� Communicate with clinical team reason for admission
and primary diagnosis at time of admission
Director of NursingDirector of Nursing
205
plantemoran.com
� Include primary diagnosis on MDS
� Conduct Medicare/PPS meeting - review primary
diagnosis each meeting (it may/should change
during the stay)
MDSMDS
206

Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
� Obtain therapy treatment diagnosis for
inclusion on the MDS (use I8000)
� Validate primary diagnosis use within
nursing documentation
� Attend end of the month pre claim release
audit
MDSMDS
207
plantemoran.com
� Review referral information
� Review hospital therapy documentation
(if available)
� Confirm and include primary diagnosis
on therapy evaluation
TherapyTherapy
208

Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
� Provide resident specific treatment codes to MDS
� Include primary and treatment codes on all
therapy documentation
� Attend Medicare/PPS meetings
� Attend end of the month pre claim release audit
TherapyTherapy
209
plantemoran.com
� Complete UB-04
� Include primary diagnosis as selected
by clinical team on UB-04
� Validate primary diagnosis is
consistent with services provided
BillingBilling
210

Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
� Include secondary and supportive diagnoses on the
UB-04 best reflective of reasonreason for SNF stay
� Attend Medicare/PPS meeting
� Review with team all the diagnoses used on the UB-
04 at end of the month pre-claim release audit
BillingBilling
211
plantemoran.com
� Education – ongoing – ALL disciplines, including the
physicians and physician extenders - Medicare basics,
ADL coding and documentation
� Communication – physician, therapy, nurse, MDS, and
billing, condition and status
� Collaboration – PPS meetings, nursing and therapy,
scheduling
� Audits – all skilled documentation and Medicare billing
components – internal and external; therapy
Basic Strategies For Success toBasic Strategies For Success toReducing Review RiskReducing Review Risk
212

Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
� Communication must start prior to resident admission
� Discuss primary diagnosis for admission
� Obtain and review hospital treatment information
(therapy) if available
� Share referral information with team
� Communication between therapy and MDS is critical
� Part of communication is continued discussion of
diagnoses to be used on MDS, chart, and the UB-04s
Strategies for Reducing Risks Strategies for Reducing Risks of an Auditof an Audit
213
plantemoran.com
Communication Is EssentialCommunication Is Essential
Admissions
Billing
Ancillary Providers
Clinical
214
Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
Communication IsCommunication IsEssentialEssential
�� Admissions must supplyAdmissions must supply::
� Correct Medicare numbers and coverage eligibility
� Correct qualifying hospital stay dates
� Correct and verified information regarding coinsurance billing sources
� Correct information regarding MSP status
� Correct info re: prior use of Part-A days in benefit period or status of resident during the last 60 days to determine eligibility of a new benefit period
215
plantemoran.com
Communication IsCommunication IsEssentialEssential
�� Clinical must supplyClinical must supply::
� Immediate notification of any resident who is technically eligible for Medicare A, but does not meet medical criteria
� Immediate notification of any resident who has Medicare A days remaining in his/her benefit period, but no longer meets medical criteria
� Weekly summary that includes accurate list of Medicare A residents with correct RUGs IV codes, HIPPS codes, and assessment reference dates
� Notification of changed RUG IV categories based on MDS Correction Policy
216

Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
Communication Is EssentialCommunication Is Essential
�� Ancillary Provider must supplyAncillary Provider must supply::
� Timely and accurate charges for Medicare A residents
� Pharmacy
� Radiology
� Lab
� Therapy
� Ambulance, if applicable
� Outpatient Hospital Services, if applicable
217
plantemoran.com
Communication IsCommunication IsEssentialEssential
�� Billing must supplyBilling must supply::
� Timely information to ancillary providers of admission date and termination/exhaust date of all Medicare A residents
� Immediate notice to clinical and admissions of rejection or termination of MSP pay sources so that the MDS process will begin without default
� Immediate notice to admissions if coinsurance source is invalid or terminated
� Immediate notice to clinical and admissions if prior use of Medicare A days is different than anticipated so that the MDS schedule can be adjusted
218

Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
� SNF managers can ensure that care is
interdisciplinary and that therapy is aligned with the
rest of the IDT is to set aside time for more in-depth
discussion, especially at the Medicare meetings
� Assessment Reference Date
� RUG level
� ADL abilities – performance in nursing versus therapy
Communication is EssentialCommunication is Essential
219
plantemoran.com
� End of the month review to include� MDS
� Validation report and RUG scores� Diagnosis coding
� Therapy� Treatment/MDS/UB-04
� Business � HIPPs and modifiers� Therapy units� Diagnosis� HCPCs
� Administrator (monitor processes for completion)
Another Strategy For Reducing Another Strategy For Reducing Medicare AuditsMedicare Audits
220

Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
� What do we check?
� ARD and type of assessment
� Signature verification and completed forms – orders, certs
and re-certs, treatment evaluations, MDS
� Therapy ARD, days and minutes – match logs and MDS
� Primary diagnosis – UB-04, MDS, therapy evaluations
� Treatment diagnoses – UB-04, MDS, therapy evaluations
� RUG group and assessment modifier
� Date MDS accepted into QIES ASAP
Internal Checking SystemInternal Checking System
221
plantemoran.com
Find or develop a list that works for
your team – as team
progresses should be able to reduce time involved and
items to check
222
Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
� Audit using RA targets and/or identified risks
� Facility based audits
� Internal by corporate (should not be facility
staff)
� External provider
� Identify corrective actions for compliance
� Watch the trends within the clinical areas
� Compare facility to peer groups
� Analyze effectiveness of Medicare meetings
Strategies for Reducing the RiskStrategies for Reducing the Riskof Auditsof Audits
223
plantemoran.com
Therapy ReviewsTherapy Reviews
224
� Signed and dated plans of care
� Documentation supports the minutes and the RUG level billed
� Progress notes completed within required period
� Demonstrate skilled therapy within the context of documentation
� Documentation supports medical necessity of interventions
� Required components in place and timely
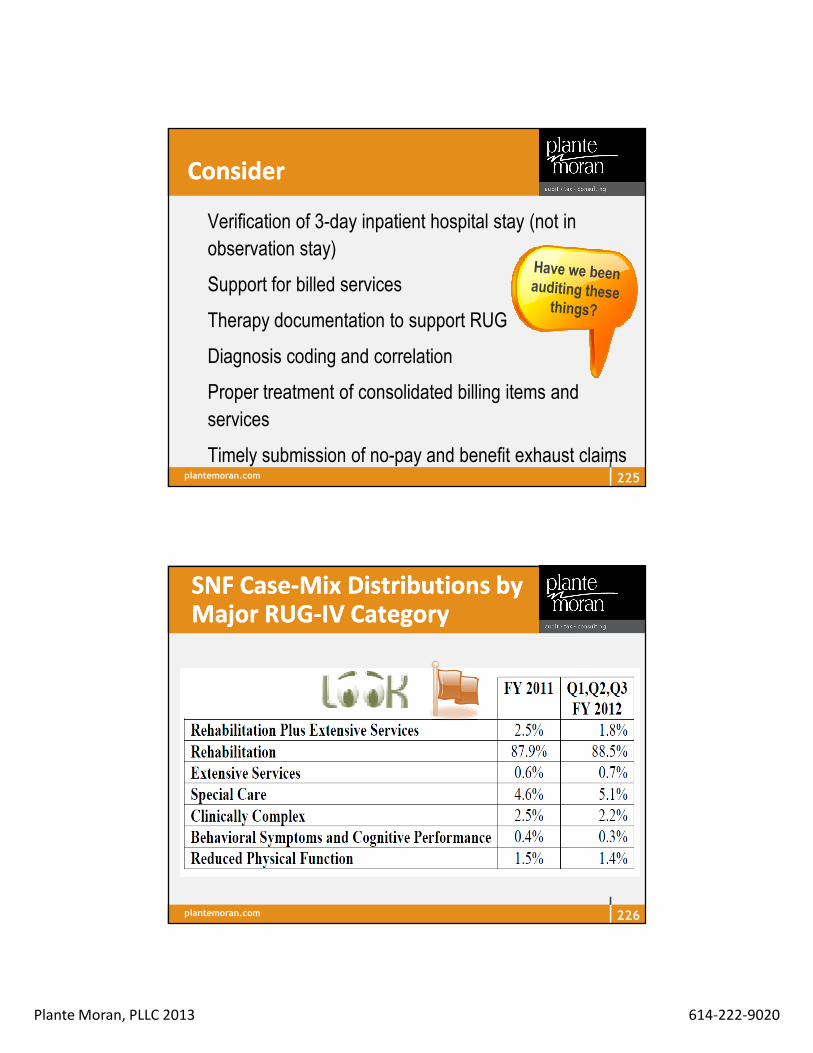
Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
ConsiderConsider
� Verification of 3-day inpatient hospital stay (not in
observation stay)
� Support for billed services
� Therapy documentation to support RUG
� Diagnosis coding and correlation
� Proper treatment of consolidated billing items and
services
� Timely submission of no-pay and benefit exhaust claims225
plantemoran.com
SNF CaseSNF Case--Mix Distributions by Mix Distributions by Major RUGMajor RUG--IV CategoryIV Category
226

Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
SNF CaseSNF Case--Mix Distributions by Mix Distributions by Minor RUG Therapy CategoriesMinor RUG Therapy Categories
How Does Your Facility Compare?
227
plantemoran.com
Flags for a Medicare Flags for a Medicare Claim ReviewClaim Review
� Claim history for treatment of same diagnosis
� Medicare daily rate exceeds peers
� Patterns or trends that are easily identified –
same RUG category for several of the
Medicare required assessments
� High percentage of resident treated exactly to
RUG minimum
� Exceeding RUG trends
228

Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
Flags for a Medicare Flags for a Medicare Claim ReviewClaim Review
� Inconsistent documentation from therapy to
MDS to UB-04 (Medicare claim - bill)
� Improper diagnosis codes
� High rehab index
� Exceptionally high average ADL score
� Low ADL scores and a high Medicare rate
(RUA, RVA)
229
plantemoran.com
LearnLearn from Others’ Mistakesfrom Others’ Mistakes
230
� Know where to find other improper payments found by
the RAs
� Demonstration findings: www.cms.hhs.gov/rac
� Permanent RA findings: will be listed on the RAs’ websites
� Look to see what improper payments have been found
in OIG and CERT reports
� OIG reports: www.oig.hhs.gov/reports.asp
� CERT reports: www.cms.hhs.gov/cert

Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
� No support for service provided – services not of
complexity requiring skilled professional
� Conflicting information
� Documentation supports lower level of service delivery
– no need for the therapist
� Illegible documentation
� Missing daily documentation
� No indication of decline in condition prior to Part B
therapy pick-up
Identified Denial Reasons Identified Denial Reasons
231
plantemoran.com
Identified Denial ReasonsIdentified Denial Reasons
� Excessive therapy services – resident’s condition does
not support the frequency of treatment and or the
amount of treatment provided in a given day
� Certification not signed prior to the claim being billed –
certification is a condition for payment
� Resident reached maximum benefit of PT/OT and care
can be performed by supportive personnel
� Documentation did not support medical necessity
232
Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
� No supporting therapy diagnosis on the UB-04
� Therapy goals not measurable or not clearly defined
� Services considered unskilled, such as activities usually conducted through repetitive activity or exercises:
� Increasing general activity tolerance
� Improving overall endurance
� Improving general fitness
� Increasing distance ambulation or of w/c propulsion
� Increasing upright tolerance
Identified Denial ReasonsIdentified Denial Reasons
233
plantemoran.com
Identified Denial ReasonsIdentified Denial Reasons
� Documentation did not support a significant decline in
function for PT/OT and did not appear reasonable or
necessary for the condition or diagnosis of the resident
� Documentation did not support the statutory
requirement for the physician’s certification of the plan
of care was met
� Discrepancy in record regarding resident’s function
between nursing and PT/OT
234
Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
Identified Denial ReasonsIdentified Denial Reasons
� Resident did not make significant measurable progress or
improvement with PT/OT
� Notes did not indicate a valid expectation of improvement
when PT/OT were initiated
� Resident reached maximum benefit of PT/OT and care can
be performed by supportive personnel
� Signature/credentials were illegible or missing and
therefore unable to determine if the appropriate personnel
provided the treatment PT/OT
235
plantemoran.com
Psychology of Maintaining a Psychology of Maintaining a Successful Medicare ProgramSuccessful Medicare Program
� No one individual or discipline is responsible for entire
process
� Involve team members
� Encourage participation/communication and
discussion about timing, ADLs, diagnoses, RUGs
� Maintain physical log of ongoing activities
� Regular review of activities
� Keep up-to-date with all regulatory changes236

Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
Are These Pieces Are These Pieces in Place?in Place?
237
� Educate facility staff about MDS accuracy both in
the clinical sense and reimbursement
� Make sure most recent RAI Manual on hand (v1.09)
� Clear policies for required documentation
� Routinely check MDS Validation Reports – compare
acceptance date with billing date
� MDS Validation Reports warning messages may
indicate a trend in the MDS process
plantemoran.com
Is Your Review Is Your Review Team Ready?Team Ready?
238
� Establish internal Medicare Review team
– who is lead
� Who’s the team? Interdisciplinary Team:
Legal, Finance, Clinical, Compliance, IT
� Prepare a system in advance of RA audits or ANY Medicare review
� Designate a lead person to organize and track audit requests
� Develop central tracking mechanisms/database for all reviews

Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
Look at Your Medicare Review Look at Your Medicare Review Team ProgramTeam Program� Coordinate the tracking mechanism with communications
structure – record reviews and appeal of recoupment deadlines
� Create a response “file format” – easy to read and easy to use - - incoming and outgoing (who)
� Identify the RA process for Region B – CGI – who is responsible and how often is web site monitored?
� Who is monitoring the MAC web site? Any other helpful site
� Knowledge is power – training on billing, coding and documentation – critical! Training is an ongoing process
239
plantemoran.com
Look at Your Medicare Review Look at Your Medicare Review Team ProgramTeam Program� Conduct self audits to identify potential problems
� Participate in RA trainings and outreach
� Monitor news sources, CMS, associations, and your own reports to stay abreast of trends
� If desired, development of unique forms for Redeterminations and other appeal levels once issues identified
� Make sure Corporate Compliance Committee activeactive
� Develop a QAPI process to learn from findings240
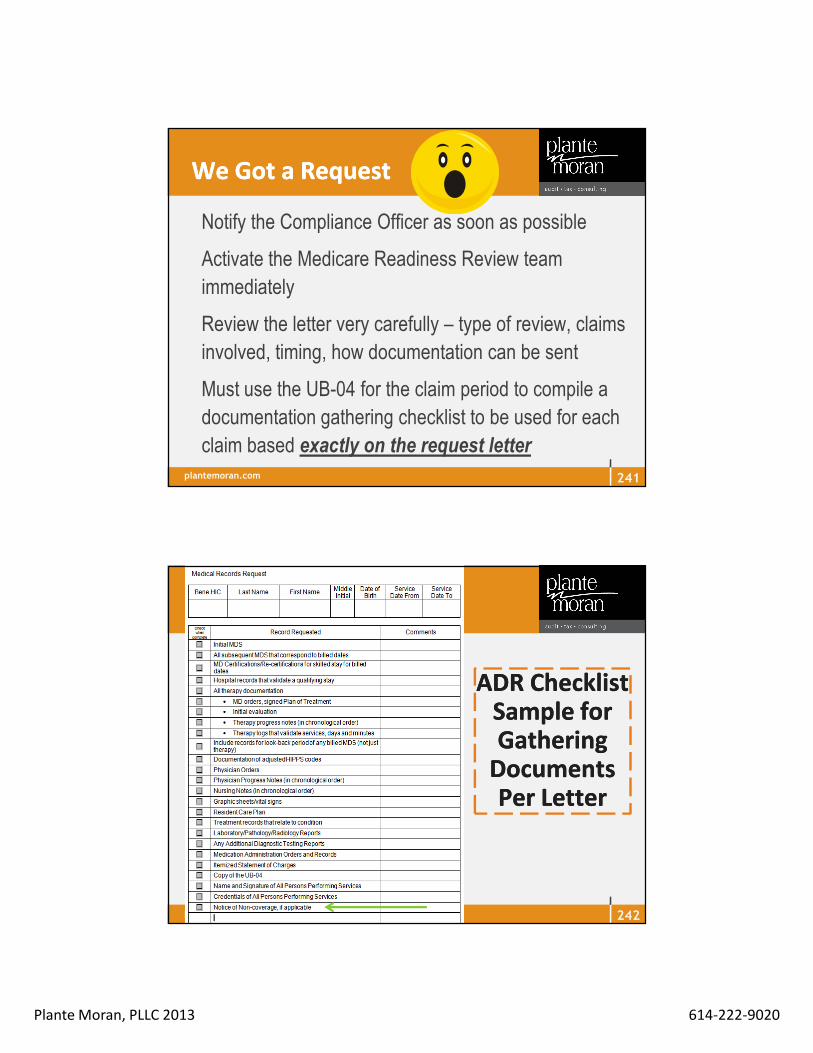
Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
� Notify the Compliance Officer as soon as possible
� Activate the Medicare Readiness Review team
immediately
� Review the letter very carefully – type of review, claims
involved, timing, how documentation can be sent
� Must use the UB-04 for the claim period to compile a
documentation gathering checklist to be used for each
claim based exactly on the request letter
We Got a RequestWe Got a Request
241
plantemoran.com
ADR Checklist ADR Checklist Sample for Sample for Gathering Gathering
Documents Documents Per LetterPer Letter
242

Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
ABN Guideline ABN Guideline SheetSheet
243
plantemoran.com
� Team approach – billing, nursing, and therapy gather
appropriate and requested documentation
� Consider not only the claim time frame for
documentation, but the look-back period of any billed
MDS. Documentation needs to be provided for the
look-back period even if not in the claim period
� Arrange the packet in the order that the documents
were requested in the letter received
We Got a RequestWe Got a Request
244

Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
� Set a target date for mailing
� Provide every piece of documentation requested
� Have an outside set of eyes review packet for
completeness, risk areas
� Maintain a copy of each packet sent to the review
contractor – put original documents back in medical
record, but keep a copy of the packet separate. You
need to know exactly what was sent to the reviewer
We Got a RequestWe Got a Request
245
plantemoran.com
� Once an initial claims determination is made by a
contractor, providers have the right to appeal the
determination
� All appeal requests must be writing
� All time frames critical for process to have success at
all
Medicare Appeals ProcessMedicare Appeals Process
246
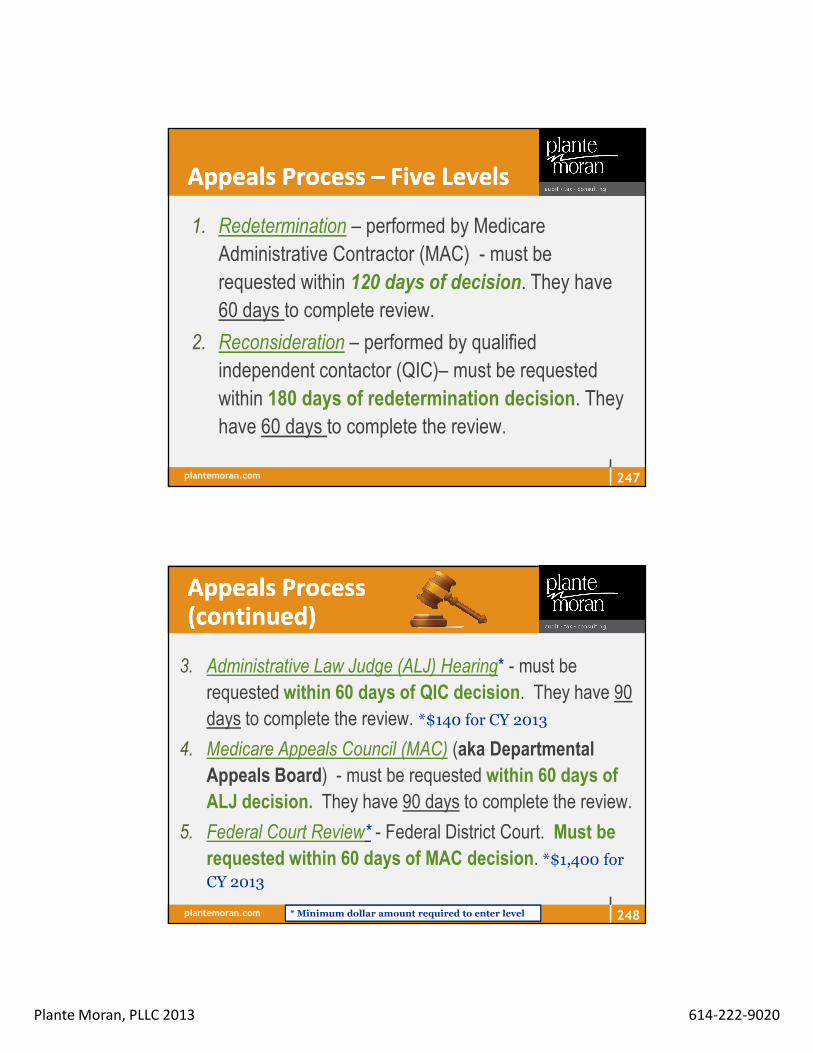
Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
Appeals Process Appeals Process –– Five LevelsFive Levels
1. Redetermination – performed by Medicare
Administrative Contractor (MAC) - must be
requested within 120 days of decision. They have
60 days to complete review.
2. Reconsideration – performed by qualified
independent contactor (QIC)– must be requested
within 180 days of redetermination decision. They
have 60 days to complete the review.
247
plantemoran.com
Appeals ProcessAppeals Process(continued)(continued)
3. Administrative Law Judge (ALJ) Hearing* - must be
requested within 60 days of QIC decision. They have 90
days to complete the review. *$140 for CY 2013
4. Medicare Appeals Council (MAC) (aka Departmental
Appeals Board) - must be requested within 60 days of
ALJ decision. They have 90 days to complete the review.
5. Federal Court Review* - Federal District Court. Must be
requested within 60 days of MAC decision. *$1,400 for CY 2013
* Minimum dollar amount required to enter level 248
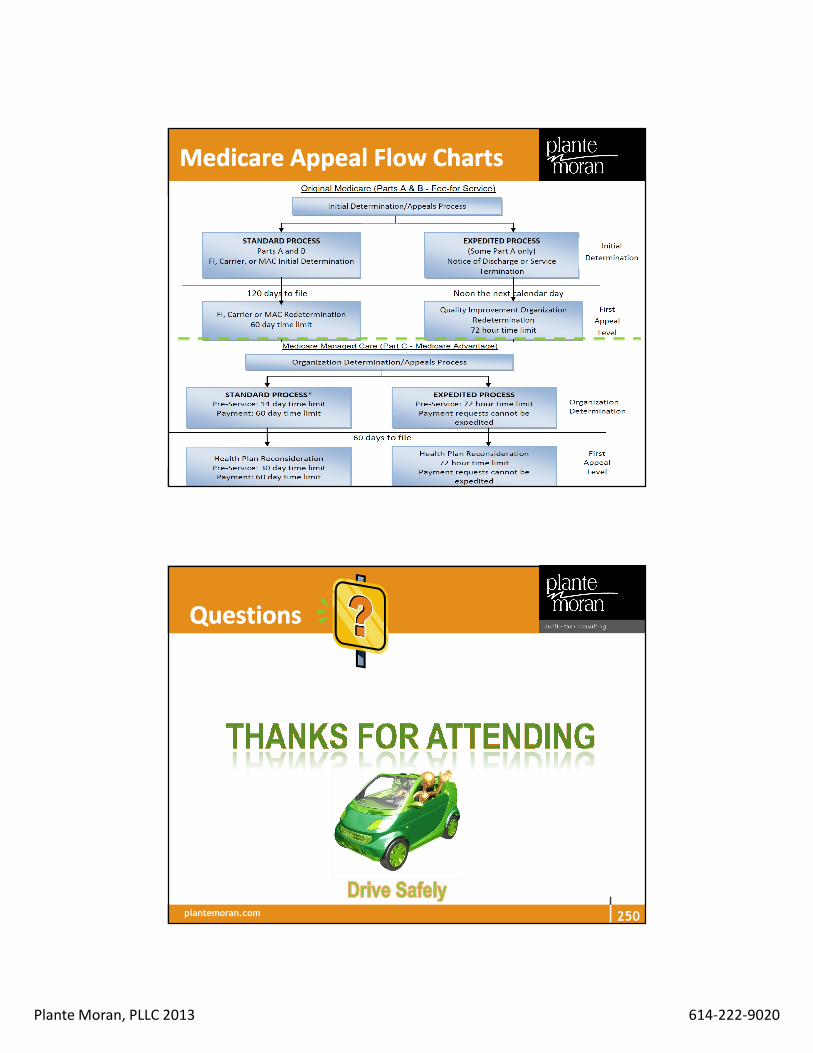
Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
Medicare Appeal Flow ChartsMedicare Appeal Flow Charts
plantemoran.com
QuestionsQuestions
250

Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
Jane Belt
614-222-9020
Regina Loncaric
614-222-9070
Mary Poplstein
216-274-6544
Brenda Sowash
419-842-6204
Judy Vogel
513-744-4768
Plante Plante MoranMoran Clinical GroupClinical Group
251
plantemoran.com
� HETS information:
http://www.cms.gov/Outreach-and-Education/Medicare-Learning-
Network-MLN/MLNMattersArticles/downloads/SE1249.pdf
� RAI MDS Manual http://www.cms.gov/Medicare/Quality-
Initiatives-Patient-Assessment-
Instruments/NursingHomeQualityInits/MDS30RAIManual.html
� Guidelines for Therapy Certification: Medicare Benefit Policy
Manual Chapter 15 – Covered Medical and Other Health
Services (Rev. 161, 10-26-12); Section 220.3
ResourcesResources
252
Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
� CMS IOM Publication 100-01, Medicare General
Information, Eligibility and Entitlement Manual, Chapter
5, Section 30http://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/Downloads/ge101c05.pdf
� CMS IOM Publication 100-02, Medicare Benefit Policy Manual, Chapter 8 - Coverage of Extended Care (SNF) Services Under Hospital Insurancehttp://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/Downloads/bp102c08.pdf
ResourcesResources
253
plantemoran.com
� CMS IOM Publication 100-02, Medicare Benefit Policy
Manual Chapter 15, Covered Medical and Other Health
Services, Sections 220-230
http://www.cms.gov/Regulations-and-
Guidance/Guidance/Manuals/Downloads/bp102c15.pdf
� CGI https://racb.cgi.com/Issues.aspx
� Signature Guidelines for Medical Reviews
http://www.cms.gov/Outreach-and-Education/Medicare-
Learning-Network-
MLN/MLNMattersArticles/downloads/MM6698.pdf
ResourcesResources
254

Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
� UB-04 Fact Sheet: http://www.cms.gov/Outreach-and-
Education/Medicare-Learning-Network-
MLN/MLNProducts/downloads/ub04_fact_sheet.pdf
� CGI: Additional Documentation Letter
http://racb.cgi.com/Docs/Letters/ADRDUAL-
Additional%20Documentation%20Letter%20Dual%20Sample%2002
122013.pdf
� Medicare General Information, Eligibility, and Entitlement,
Chapter 4 - Physician Certification and Recertification of
Services http://www.cms.gov/Regulations-and-
Guidance/Guidance/Manuals/downloads/ge101c04.pdf
ResourcesResources
255
plantemoran.com
� Cloned Documentation http://www.ngsmedicare.com/wps/portal/ngsmedicareEducation and Training, Part B, Posted 09/05/2012
� ICD-9 Official Guidelines for Coding and Reporting
http://www.cdc.gov/nchs/data/icd9/icd9cm_guidelines_2011.pdf
� Medicare Claims Processing Manual, Chapter 6 - SNF Inpatient Part A Billing and SNF Consolidated Billing, (Rev. 2573, 10-26-12); Section 30: http://www.cms.gov/Regulations-
and-Guidance/Guidance/Manuals/Downloads/clm104c06.pdf
ResourcesResources
256

Plante Moran, PLLC 2013 614-222-9020
plantemoran.com
� Davis, Caralyn; AANAC LTC Leader, January 9, 2013;
“Upcoming Medicare A Manual Changes for April 2013”, pages
1, 2, and 8
� Shephard, Rena: AANAC LTC Leader, January 23, 2013; “Part
A Skilled Care: Keys to Success”; pages 1, 2, 9
� CMS BPM, Chapter 8; Section 30.4.I.2; Application of
Guidelines
� Belt, Jane: AANAC LTC Leader, March 21, 2013, OIG:
“Therapy a Culprit in Medicare Care Planning, Quality Issues”
page 2
ResourcesResources
257