Thirty-second Board meeting - Public Health Wales
371
32 00 1 Thirty-second Board meeting Date of meeting: 26 June 2014 Time of meeting: 10.00 – 16.00 Venue for meeting: Room 1DM2, Pembrokeshire County Council, County Hall, Haverfordwest SA61 1TP Version: 1 Time Reference Preliminary matters 1. 10.00 Welcome and apologies Professor Sir Mansel Aylward Oral 2. 10.05 Declarations of interest Professor Sir Mansel Aylward Oral 3. 10.10 Minutes from thirty-first Board meeting on 29 April 2014 Professor Sir Mansel Aylward 32 01 a) Approval of minutes b) Action points c) Matters arising 4. 10.20 Chair report Professor Sir Mansel Aylward 32 02 (to follow) 5. 10.40 Chief Executive / Interim Chief Executive report Dr Tracey Cooper / Mr Huw George 32 03 For decision 6. 11.00 Integrated medium term plan: one year operational plan Mr Mark Dickinson 32 04 (to follow) 7. 11.45 Policies for approval a) Statutory and mandatory training Ms Ruth Davies, Director of Workforce and Organisational Development 32 05 8. 11.55 Governance and accountability module 32 06
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Thirty-second Board meeting - Public Health Wales

32 00
1
Thirty-second Board meeting Date of meeting: 26 June 2014
Time of meeting: 10.00 – 16.00
Venue for meeting: Room 1DM2, Pembrokeshire County Council,
County Hall, Haverfordwest SA61 1TP
Version: 1
Time Reference
Preliminary matters
1. 10.00 Welcome and apologies Professor Sir Mansel Aylward
Oral
2. 10.05 Declarations of interest
Professor Sir Mansel Aylward
Oral
3. 10.10 Minutes from thirty-first Board meeting on
29 April 2014 Professor Sir Mansel Aylward
32 01
a) Approval of minutes
b) Action points
c) Matters arising
4. 10.20 Chair report
Professor Sir Mansel Aylward
32 02
(to follow)
5. 10.40 Chief Executive / Interim Chief Executive
report
Dr Tracey Cooper / Mr Huw George
32 03
For decision
6. 11.00 Integrated medium term plan: one year operational plan
Mr Mark Dickinson
32 04 (to follow)
7. 11.45 Policies for approval
a) Statutory and mandatory training
Ms Ruth Davies, Director of Workforce and Organisational Development
32 05
8. 11.55 Governance and accountability module 32 06

32 00
2
Mr Keith Cox
For ratification
9. 12.00 Annual accounts and Annual Governance Statement
Mr Huw George
32 07
10. 12.10 Public Health Wales response to Public
Health Bill white paper Sir Mansel Aylward
32 08
(to follow)
12.20 LUNCH
For scrutiny and discussion
11. 12.50 Performance reports
a) Finance performance report
Mr Huw George
32 09
b) Update from Public Health Wales and Welsh
Government Joint Executive Team meeting Mr Mark Dickinson
32 10
13.
13.20 Governance report
Mr Keith Cox
32 11
a) Plan of Board business 32 12
b) Corporate Risk Register 32 13 (to follow)
14. 13.40 Trusted to Care: assurance to Board
Dr Tracey Cooper
32 14
15. 13.50 Hywel Dda local public health team
Dr Teresa Owens, Executive Director of Public Health, Hywel Dda University Health Board
Oral
16. 14.35 Committee meeting reports
a) Audit Committee
Mr Terence Rose
Oral
b) Information Governance Committee Mr John Spence
Oral
17. 14.45 Audit Committee annual report Mr Terence Rose
32 15
For information
18. 14.55 Non Executive Director reports Oral
19.
15.05 Annual reports
a) Safeguarding annual report 32 16
b) Emergency planning annual report 32 17
20.
Correspondence
a) Dr Tracey Cooper, Accountable Officer
letter
32 18
b) Dr Tracey Cooper, Joint Executive Team
letter
32 19
21. Committee meeting
a) Audit Committee minutes from meeting 32 20

32 00
3
held on 12 March 2014
b) Audit Committee minutes from meeting held on 8 May 2014
32 21
c) Information Governance Committee
minutes from meeting held on 12 March 2014
32 22
22. 15.15 Any other business and meeting close Professor Sir Mansel Aylward
23. Papers for information
a) Executive Team reports presented at the 41st meeting of the Public Health Wales
Executive Team held on 21 May 2014 Planning and Performance report
Board Secretary report Workforce and Organisational Development
report
Public Health Services report Public Health Development report
Nursing report Communications report
b) Public Health Wales and Welsh Government Joint Executive Team meeting presentation
32 23
PRIVATE SESSION
1. 15.20 Remuneration of senior managers Sir Mansel Aylward
32 24
2. 15.25 Proposal for appointing a deputy Chief
Executive Dr Tracey Cooper
Oral
3. 15.35 NATO Dr Quentin Sandifer
Oral
Items containing commercially sensitive information
4. 15.40 Ratification of decision: microbiology total bacteriology automation equipment for
north Wales Dr Quentin Sandifer
32 25
5. 15.45 WEDINOS
Sir Mansel Aylward
Oral
6. 15.50 Managed service contract for serology and
Chlamydia laboratory testing Dr Quentin Sandifer
32 26
7. 15.55 Death Certification and medical examiners
Dr Quentin Sandifer
32 27
16.00 Meeting close

32 01
Date: 16 June 2014 Version: 0a Page: 1 of 16
Minutes from the thirty-first
meeting of the Public Health
Wales Board Date of meeting: 29 April 2014
Venue for meeting: Council Chamber, Temple of Peace and Health, Cardiff
Version: 0a
Present:
Professor Sir Mansel Aylward Chair
Professor Peter Bradley Executive Director of Public Health Development
Dr Carl Clowes Non Executive Director
Mr Mark Dickinson Executive Director of Planning and Performance
Mr Huw George Interim Chief Executive
Ms Tamira Rolls Interim Executive Director of Finance
Mr Terence Rose Non Executive Director
Dr Quentin Sandifer Executive Director of Public Health
Services
Mr John Spence Non Executive Director
Professor Simon Smail Non Executive Director
In attendance:
Ms Rhiannon Beaumont-Wood
Director of Nursing
Professor Mark Bellis Director of Policy, Research and
Development
Mr Hugh Bennett Consultant in Dental Public Health, Team
Leader Dental Public Health and Dental Governance Team
Dr Tracey Cooper Incoming Chief Executive, Public Health
Wales

32 01
Date: 16 June 2014 Version: 0a Page: 2 of 16
Mr Keith Cox Board Secretary
Ms Margaret Foster Chair, NHS Wales Shared Services Partnership
Dr Rosemary Fox Director of Screening Services
Mr Neil Frowe Director, NHS Wales Shared Services Partnership
Ms Eleanor Higgins Corporate Governance Manager
Mr Chris Lines Director of Communications
Mr Chris Orr Business Support Manager
Ms Stephanie Wilkins Unite representative, Public Health Wales
Apologies:
Dr Carl Clowes Non Executive Director
Mrs Ruth Davies Director of Workforce and Organisational
Development
Renata Leonardi-Jones Unison representative, Public Health
Wales
Professor Gareth Williams Non Executive Director
PART A
1. Welcome and apologies for absence
Professor Sir Mansel Aylward all in attendance to the thirty first meeting of the Public Health Wales Board.
Apologies were received from Dr Carl Clowes, Professor Gareth
Williams and Ms Renata Leonardi-Jones.
2. Declarations of interest
No declarations of interest were received.
3. Minutes from Public Health Wales Board meeting held on 27
March 2014
a) Approval of minutes
The minutes (paper 31 01) from the last meeting of the Public
Health Wales Board were approved subject to one amendment.
Ms Stephanie Wilkins alerted the Board to an omission in the minutes under section 5 ‘interim Chief Executive’s report’ on page
4. It was agreed to add the following text to this section:

32 01
Date: 16 June 2014 Version: 0a Page: 3 of 16
Ms Stephanie Wilkins mentioned that, while the Statutory and Mandatory training compliance rates had improved, staff
had felt pressure from a number of areas towards the end of the financial year, for example, annual appraisals, the need
to take annual leave, and the request to undertake statutory and mandatory training. It was requested that better
planning take place throughout the year to avoid undue pressure at year-end.
Decision: Minutes from the last meeting of the Public Health Wales
Board were approved.
b) Actions:
Mr Keith Cox provided the Board with an update on actions which
were marked as ‘in progress’. Further information on each action is provided in the action table at the end of the minutes.
c) Matters arising
Dr Quentin Sandifer updated the Board on Diabetic Retinopathy
Screening Services Wales. At the last Board meeting, the Board had approved the recommendation for the Diabetic Retinopathy
Screening Service to transfer to Public Health Wales from Cardiff and Vale University Health Board subject to assurances against
revenue funding, capital funding and a start date of 1 April 2015.
As a result of Public Health Wales’ request for these assurances, the Welsh Government has requested more detailed analysis on
the revenue and capital funding.
4. Introduce new Chief Executive – Dr Tracey Cooper
Professor Sir Mansel Aylward introduced Dr Tracey Cooper to the Board. Dr Cooper would be taking up the appointment of Chief
Executive on 1 June 2014.
Dr Cooper thanked Sir Mansel for the kind words of welcome. Dr
Cooper also thanked everyone she had met from Public Health Wales. She noted the huge opportunity Public Health Wales has in
making a difference to the public health agenda in the Welsh health system.
Dr Cooper offered particular thanks to Sir Mansel, Mr John Spence
and Mr Huw George for facilitating her visit to Public Health Wales.

32 01
Date: 16 June 2014 Version: 0a Page: 4 of 16
5. Chair’s report
Professor Sir Mansel Aylward presented the Chair’s report (paper
31 02).
Sir Mansel informed the Board that he had recently had a meeting with representatives from the BMA (Dr Richard Lewis, Dr Andrew
Cross and Dr Mark Temple), Mr John Spence, Mr Huw George and Mr Keith Cox. The meeting was arranged to discuss whether the
BMA would nominate a member to attend Public Health Wales Board meetings. Both parties agreed that it would be beneficial to
for a representative of the BMA to attend Public Health Wales
Board meetings. It was agreed that Mr Cox and Dr Temple would draft a framework to support the nominated representative.
6. Interim Chief Executive’s report
Mr Huw George presented his Interim Chief Executive’s report
(paper 31.03).
Mr George commented on the considerable improvement in
compliance with statutory and mandatory training. He offered particular thanks to the Microbiology Division which had started
with a very low compliance rate.
The Board recorded its appreciation for all those involved in improving compliance rates. They were pleased to see a
substantial improvement against what had previously been significantly poor rates.
Professor Simon Smail reminded the Board that the Quality and
Safety Committee had shown concern about the low level of compliance. He mentioned that compliance with mandatory
training was still problematic as there was a lack of clarity over what denominators should be used to establish which staff groups
require which training. Mr George suggested that Claire Barley,
Head of Professional and Organisational Development, should report to Quality and Safety Committee and start identifying which
training is not needed by certain members of staff.
Action: invite Claire Barley to attend Quality and Safety Committee and begin identifying which training is not
needed by certain members of staff.
7. Proposal to transfer dental practice advisors from Public Health Wales to Health Boards

32 01
Date: 16 June 2014 Version: 0a Page: 5 of 16
Mr Hugh Bennett presented the Board with a proposal to transfer
dental practice advisors from Public Health Wales to Health Boards (paper 31 04).
The Board accepted the recommendations outlined in the paper.
8. Social media strategy review
Mr Chris Lines introduced the social media strategy review (paper 31 05).
Mr Lines explained that social media has provided a platform to
capture the work of staff selling powerful stories.
Ms Stephanie Wilkins raised some concerns that Unite has about people misusing social media. Mr Lines reassured Ms Wilkins that
he did not want to create unnecessary bureaucracy by restricting use of social media for staff and explained that full training would
be given to staff before accessing social media.
The Board approved the recommendations in the review.
9. Standing orders and standing financial instructions
Mr Keith Cox presented the Board with revised Standing Orders
and Standing Financial Instructions (paper 31 06). The revisions had been made to reflect the requirement for Public Health Wales
to produce an Integrated Medium Term Plan.
The Board approved the amended Standing Orders and Standing Financial Instructions.
10. Nursing and midwifery strategy
Ms Rhiannon Beaumont Wood presented the Board with the nursing and midwifery strategy (paper 31 07).
Ms Beaumont-Wood explained that the strategy had been
developed by a task and finish group comprising nursing and midwifery staff. If approved, the strategy would be launched on 12
May 2014, which was International Nursing Day.
The Board approved the strategy.
11. Policies for approval
a) Home working policy
32 01
Date: 16 June 2014 Version: 0a Page: 6 of 16
Mr Huw George presented the Board with the Home Working policy
in the absence of Ms Ruth Davies (paper 31 08).
Ms Tamira Rolls highlighted an error on page 16. It had previously been agreed to remove the last sentence on that page.
Mr Chris Lines suggested that the definition of ‘occasional home
working’ on page 7 should include a reference to appendix 3.
Ms Stephanie Wilkins requested a review date be added to the policy.
The Board agreed that the implementation of the policy would be crucial and a review should take place to establish whether it was
being implemented in a pragmatic way.
The Board approved the policy subject to the amendments mentioned above.
b) Domestic abuse policy
Mr Huw George presented the Domestic Abuse policy to the Board
(paper 31 09).
Ms Rhiannon Beaumont-Wood confirmed that she was the Executive Lead for the policy. Ms Beaumont-Wood also highlighted
that, under the terms of the policy, the HR team would be the main
source of advice for staff who wanted to use the policy. The team would, therefore, require significant training to undertake this role.
It was suggested that an implementation plan should accompany the policy.
Ms Stephanie Wilkins supported Ms Beaumont-Wood and informed
the Board that Unite members had also raised the issue about whether training would be provided for staff.
The Board approved the policy subject to an implementation plan
being developed to accompany the policy.
Action: ensure an implementation plan is developed to accompany the policy.
12. Quality and Delivery framework performance report
Mr Mark Dickinson presented the Board with the Quality and Delivery framework performance report (paper 31 10). Mr
Dickinson informed the Board that the format of the report had

32 01
Date: 16 June 2014 Version: 0a Page: 7 of 16
been revised to reflect the integrated medium term plan. The aim
was to increase objectivity rather than subjectivity.
He explained that section two would report against specific indicators in a colour coded way and provide data on the previous
four quarters and the latest quarter. Section three would report against the priorities for action from the integrated medium term
plan.
Professor Peter Bradley drew the Board’s attention to the 5 per cent target for the percentage of smokers treated by all smoking
cessation services. He explained that Public Health Wales was
responsible for a proportion of this target, with the Directors of Public Health in Health Boards taking responsibility for the rest of
the target through other methods such as pharmacy services and GP services. He informed the Board that Public Health Wales
would not meet the target in the first quarter of the year, but would deliver more in the second half of the year.
Dr Quentin Sandifer drew the Board’s attention to the uptake rate
for Breast Screening being only 0.5 percent above target. He informed the Board that there was a long term trend of the uptake
rate decreasing over the previous 20 years. He explained that whilst the uptake may be decreasing, the impact of Breast
Screening is increasing with the introduction of higher resolution imaging meaning more cancers are being recognised. The
coverage of Breast Screening was below target and Dr Sandifer
explained that work was underway to address inequalities and access hard to reach groups.
In relation to flu vaccination rates Professor Sir Mansel Aylward
queried what role Public Health Wales has in contributing to the vaccination of NHS staff. Dr Sandifer responded that Public Health
Wales has the following responsibilities through the Vaccine Preventable Disease Programme:
Attendance at national vaccination steering committee
Providing direct advice to the Welsh Government Immunisation lead
A team of staff dedicated to supporting health board local policy and practices and procedures
Running a network of immunisation coordinators
Leading the flu campaign in Wales.
The Board welcomed the revised version of the report.

32 01
Date: 16 June 2014 Version: 0a Page: 8 of 16
13. Finance performance
Ms Tamira Rolls provided an oral update on the year end financial
position. She confirmed that it was likely the final accounts would show a £25,000 - £30,000 underspend.
She also informed the Board that Public Health Wales had not
managed to achieve the target for Public Sector Payment Performance. This had been reported to the Board in July 2013
and the performance against this target had improved following the first quarter of the financial year and consistently achieved the
target.
14. Governance report
Mr Keith Cox presented the governance report (paper 31 11) to the
Board.
Mr Cox reminded the Board that the Chairman is required to sign the annual accounts before they are submitted to the Wales Audit
Office on 6 June 2014. The Chairman will, unfortunately, be out of
the country on this date and will be unable to sign the accounts. Mr Cox confirmed that the Standing Orders state that the Vice
Chair can be given full delegated authority by the Chairman. It has, therefore, been agreed that Mr John Spence will sign the
annual accounts on behalf of Sir Mansel Aylward.
Mr Cox also informed the Board that Dr Tracey Cooper would be taking up post as Chief Executive and therefore will become
Accountable Officer on 1 June 2014 and is required to sign the accounts and Annual Governance Statement on 6 June 2014. Mr
Cox informed the Board that a sentence would be added to the Annual Governance Statement explaining that Dr Cooper was
relying on assurances provided to her by the interim Chief Executive.
a) Plan of Board Business
Mr Keith Cox presented the latest plan of Board business (paper 31 12). Executive Directors have inputted into the plan of Board
business and meetings have been set up with Non-Executive Directors to discuss the plan before it is finalised.
b) Corporate Risk Register
Mr Keith Cox updated the Board on the latest corporate risk
register (paper 31 13).

32 01
Date: 16 June 2014 Version: 0a Page: 9 of 16
14. Medical revalidation
Dr Quentin Sandifer provided the Board with an update on medical revalidation (paper 31 14).
The Committee received the report.
15. Wales Audit Office report into management arrangements in microbiology – update to Board
Dr Quentin Sandifer provided the Board with an update on
progress being made against the recommendations which had been made in the Wales Audit Office report into management
arrangements in microbiology (Paper 31 15).
Mr Huw George asked the Board to nominate a lead Non Executive Director for the microbiology service redesign. It was agreed that
Professor Simon Smail should take up this role as the Quality and Safety Committee had already agreed to take on a monitoring role
for this area. Professor Smail would provide a link between the Board and the project group.
Action: Professor Simon Smail to take up role as lead Non Executive Directors for the microbiology service redesign.
16. Committee Meeting Reports
a) Audit Committee
Mr Terence Rose provided an update on the Audit Committee
meeting which took place on 12 March 2014.
The Committee approved revised terms of reference for the
Committee. A paragraph had been added to clarify the relationship between the Audit Committee and Quality and Safety Committee.
The Committee also approved its work plan for the next 12 – 18 months.
Mr Rose informed the Board that the Committee had discussed a
draft outline of the Annual Governance Statement and noted the timetable for completion of the annual accounts.
b) Information Governance Committee
Mr John Spence provided an update on the Information

32 01
Date: 16 June 2014 Version: 0a Page: 10 of 16
Governance Committee meeting which took place on 12 March
2014.
The Committee received a report about MeetingSphere, which informed the Committee that this was no longer considered a risk
to the organisation. The Committee also received updates on EU data protection legislation, Section 251, and Mail Marshall.
c) Quality and Safety Committee
Professor Simon Smail provided an update on the Quality and
Safety Committee meeting which took place on 22 April 2014.
Professor Smail explained that the agenda for the meeting on 22 April was essentially a double meeting. This was because the
meeting scheduled for 6 February had been cancelled.
The Committee received a number of reports on serious incidents, one of which related to a Bowel Screening Wales colonoscopist who
was currently under surveillance and supervision. The Committee requested further consideration of this case before the
colonoscopist be allowed to return to practice.
The Committee also received an update on a seminar which had been arranged to provide learning from incidents in colposcopy.
The afternoon session of the meeting focused on Microbiology
performance.
17. Non Executive Director Reports
Mr Terence Rose informed the Board that he had attended a
Cervical Screening conference.
Mr John Spence attended the Joint Chairs and Chief Executives of NHS Wales meeting in April. At the meeting the following items
were discussed:
Complaints handling CRB checks of Non Executive Board members
Working together Role of the NHS Wales Chief Executive.
Mr Spence had also attended a meeting of Vice Chairs with the
Minister to discuss mental health.
18. Public Health Bill white paper
Professor Mark Bellis attended the meeting to provide an update on

32 01
Date: 16 June 2014 Version: 0a Page: 11 of 16
what action Public Health Wales was taking in response to the
Public Health Bill white paper.
Professor Bellis advised the Board that a number of engagement events were being organised where people could feed in their
responses to the white paper. He confirmed that Public Health Wales would be consulting with staff and also with key
stakeholders including local authorities and Directors of Public Health.
The Board expressed disappointment that the white paper
appeared to omit some important areas. They referred to Public
Health Wales’ response to the Public Health Bill green paper which had been submitted to the Welsh Government in January 2013. In
particular there was no mention of health impact assessments, or health in all policies.
Professor Bellis informed the Board that the suggestion to place a
minimum price on alcohol was a considerable step forward for public health.
It was agreed that the Public Health Wales response to the Public
Health Bill white paper should be closely aligned to the Public Health Wales response to the Future Generations Bill.
Action: ensure the Public Health Wales response to the
Public Health Bill white paper is closely aligned to the Public
Health Wales response to the Future Generations Bill.
The Board were reminded that there would be a further discussion on Public Health Wales’ response to the white paper at a special
meeting arranged for 5 June 2014.
19. NHS Wales Shared Services Partnership
Mrs Margaret Foster and Mr Neil Frowe from the NHS Wales Shared
Services Partnership attended the Board meeting to provide an update on the Shared Services Partnership.
The presentation provided an opportunity for feedback on what
areas the Shared Services Partnership needed to improve on, and also to discuss any new functions which could be taken on by the
Shared Services Partnership which could benefit all in the NHS in Wales.
It was mentioned that Public Health Wales needs to receive more
up to date performance data from the NHS Wales Shared Services

32 01
Date: 16 June 2014 Version: 0a Page: 12 of 16
Partnership so that any issues can be flagged up as early as
possible. The Board had already discussed that the Public Sector Payment Policy target would not be met for 2013/14. The issues
were experienced at the beginning of the financial year and were rectified as soon as Public Health Wales became aware of the
target not being met. If Public Health Wales had received more timely performance data from Shares Services Partnership then
action could have been taken more promptly and the target may have been met for the financial year.
Mrs Stephanie Wilkins asked for advice on how staff can provide
feedback to the NHS Wales Shared Services Partnership. Mr Keith
Cox informed the Board that he was the Public Health Wales representative on the Shared Services Partnership Committee and
that he could pass on any feedback he received from staff. Mr Neil Frowe requested that feedback include actual examples so that
they can make changes where necessary.
Ms Rhiannon Beaumont-Wood queried whether the Shared Services Partnership would consider taking on the role of providing
Occupational Health Services to NHS Wales. Mrs Margaret Foster agreed that this was an area they could take on.
20. Any other business
No other business was noted.
21. Papers for information
Sir Mansel drew the Board’s attention to the following papers for information:
Audit Committee minutes from meeting held on 18 December 2013
Information Governance Committee minutes from meeting held on 18 December 2013
Board Secretary report; Director of Workforce and Organisational Development
report; Executive Director of Public Health Services report;
Executive Director of Public Health Development report; Executive Director of Planning report;
Director of Nursing report; and Director of Communications report.
PART B – Private Session
32 01
Date: 16 June 2014 Version: 0a Page: 13 of 16
1. C.Difficile investigation in north Wales
Dr Quentin Sandifer updated the Board on the C.Difficile investigation in Betsi Cadwaladr University Health Board.
2. Health Advisory structure review
Dr Quentin Sandifer informed the Board that the Welsh
Government had undertaken a consultation in relation to the structure of committees and groups providing health advice to the
Welsh Government. He explained that the existing structure was large and complex and the intention of the consultation was to
simplify the structure. Dr Sandifer had responded to the consultation in his role as Medical Director.
3. Welsh emerging drugs and identification of novel substances project (WEDINOS)
Professor Sir Mansel Aylward brought the Board’s attention to some recent media interest about WEDINOS which is hosted by
Public Health Wales.
The Board requested further assurance that the evidence base for the public health benefit of WEDINOS was balanced and robust. It
was, therefore, agreed that a rapid review of WEDINOS should take place to provide assurance to the Board.
Action: undertake rapid review of WEDINOS to provide
assurance to the Board that the evidence base is balanced and robust.
4. Bevan Commission
Professor Sir Mansel Aylward provided the Board with a copy of a remit letter he had received from the Minister for Health and Social
Services inviting him to refresh the Bevan Commission with a focus on Prudent Healthcare.

32 01
Date: 16 June 2014 Version: 0a Page: 14 of 16
No Action Who Start
Date
Due Date Status Action taken to
date
Revised
due date
27.09 Share dates of Chair/Chief Executive meetings with teams
and Executive Director of Public Health
Development/Director of Nursing meetings with teams.
EH 19/09/13 30/01/14 In progress Executive team are
reviewing the
visibility and
engagement of
Exec team
members are
having further
discussions about
the best way to
incorporate
visibility and
engagement from
non Executive
Directors
29/07/14
28.02 Sir Mansel Aylward to provide Mr Terence Rose with
further information regarding occupational health provision
in Wales.
MA 21/11/13 30/01/14 In progress Meeting scheduled
for 22 July and
feedback will be
provided after that
meeting
25/09/14
28.06 Include discussion on the revised accountability
arrangements for Public Health Wales at a future Board
meeting.
KC/
EH
21/11/13 30/01/14 In progress Discussions will be
held once draft has
been agreed.
Public Health Wales
is awaiting
comments from
Welsh Government
29/07/14
32 01
Date: 16 June 2014 Version: 0a Page: 15 of 16
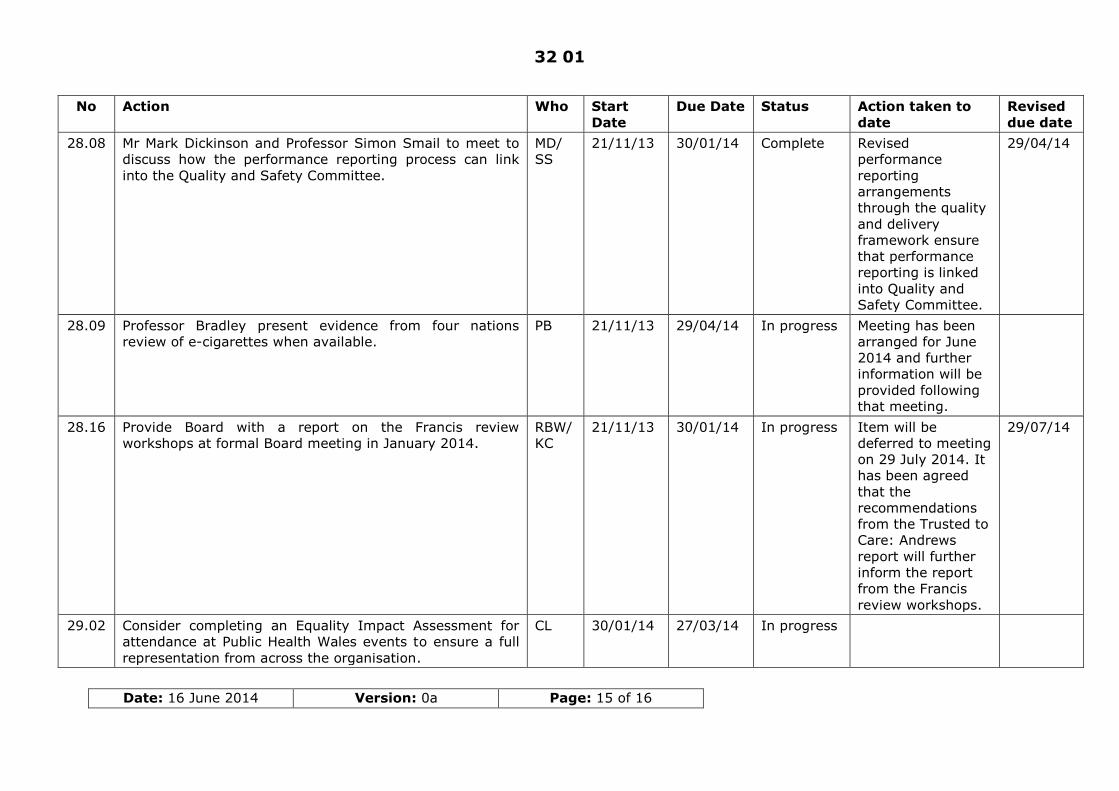
No Action Who Start
Date
Due Date Status Action taken to
date
Revised
due date
28.08 Mr Mark Dickinson and Professor Simon Smail to meet to
discuss how the performance reporting process can link
into the Quality and Safety Committee.
MD/
SS
21/11/13 30/01/14 Complete Revised
performance
reporting
arrangements
through the quality
and delivery
framework ensure
that performance
reporting is linked
into Quality and
Safety Committee.
29/04/14
28.09 Professor Bradley present evidence from four nations
review of e-cigarettes when available.
PB 21/11/13 29/04/14 In progress Meeting has been
arranged for June
2014 and further
information will be
provided following
that meeting.
28.16 Provide Board with a report on the Francis review
workshops at formal Board meeting in January 2014.
RBW/
KC
21/11/13 30/01/14 In progress Item will be
deferred to meeting
on 29 July 2014. It
has been agreed
that the
recommendations
from the Trusted to
Care: Andrews
report will further
inform the report
from the Francis
review workshops.
29/07/14
29.02 Consider completing an Equality Impact Assessment for
attendance at Public Health Wales events to ensure a full
representation from across the organisation.
CL 30/01/14 27/03/14 In progress

32 01
Date: 16 June 2014 Version: 0a Page: 16 of 16
No Action Who Start
Date
Due Date Status Action taken to
date
Revised
due date
31.01 Invite Claire Barley to attend Quality and Safety
Committee and begin identifying which training is not
needed by certain members of staff.
KC 29/04/14 29/07/14 In progress Next Quality and
Safety Committee
meeting is
scheduled for 22
July 2014
31.02 Ensure an implementation plan is developed to accompany
the policy.
RBW 29/04/14 26/06/14 In progress
31.03 Professor Simon Smail to take up role as lead Non
Executive Directors for the microbiology service redesign.
SS 29/04/14 26/06/14 Complete Professor Simon
Smail has taken on
the role
31.04 Ensure the Public Health Wales response to the Public
Health Bill white paper is closely aligned to the Public
Health Wales response to the Future Generations Bill.
MB 29/04/14 26/06/14 Complete Discussions have
been held with
Welsh Government
officials and the
Minister for Health
and Social Services
Public Health Wales
will submit a
supplementary
response to the
public health bill
once the Future
Generations Bill has
been published.
31.05 Undertake rapid review of WEDINOS to provide assurance
to the Board that the evidence base is balanced and
robust.
QS 29/04/14 26/06/14 Complete Rapid review has
been completed
and there is an
item on the agenda
on 26 June 2014 to
update the Board.
Date: 17 June 2014 Version: 1 Page: 1 of 7
Chief Executive Report June 2014
Purpose of Document:
The purpose of this paper is to provide the Public Health Wales Board with a report on key issues from the Chief Executive
Board/Committee to- (Please indicate)
To decide- Paper will outline recommendations or issues to
be approved by the Board or Committee.
To discuss- Board or Committee will be asked to discuss
and scrutinise the paper and provide feedback and comments.
X
To inform- Board or Committee will be asked to note the
paper for information only
Other relevant information
The Chief Executive’s Report will be presented to the Board at each formal
meeting.
Link to Public Health Wales commitment and priorities for action: (please tick which commitment(s) is/are relevant)
X
X
X
X
Priorities for action All priorities are relevant to this paper.
Author: Tracey Cooper, Chief Executive
Date: 17 June 2014 Version: 1
Who will present: (If appropriate) Tracey Cooper, Chief Executive
Documents attached: (If appropriate)
Report of the Chief Executive Officer
Date of meeting: 26 June 2014
Committee/Groups that have
received or considered this
paper:
N/A
Paper 32 03

Date: 17 June 2014 Version: 1 Page: 2 of 7
Link to standards
for health services
N/A
Link to risk
register
N/A
Equality impact assessment
N/A
Financial implications
N/A
Service user
engagement
N/A

Date: 17 June 2014 Version: 1 Page: 3 of 7
Chief Executive
Report –
June 2014 Author: Tracey Cooper, Chief Executive (from 2 June 2014)
Date: 16 June 2014 Version: 1
Distribution:
Public Health Wales Executive Team
Public Health Wales Board
Public Health Wales Internet
Purpose and summary of document:
The purpose of this paper is to provide the Public Health Wales Board, Executive Team and Senior Management Forum with a report on key
issues from the Chief Executive.
The Chief Executive’s report will be presented to the Board at each formal
meeting.
Date of Board Meeting: 26 June 2014

Public Health Wales Chief Executive Report – April 2014
Date: 17 June 2014 Version: 1 Page: 4 of 7
1 Welcoming
I would like to thank the Board, the Executive Team, Julie Lake and all of
our staff who I have had the opportunity to meet and work with since I started on 1 June 2014.
I have been made to feel extremely welcome and have been overwhelmed
by the obvious talent and expertise that we have across our various teams.
I very much look forward to working with the Board and our various teams
across the organisation as we continue to drive improvements in the health of our population.
2 Joint Executive Team (JET) meeting with
Welsh Government
The most recent JET meeting took place with Welsh Government on the 4
June 2014. It was a constructive meeting which focused predominantly around a presentation that our Executive Team gave containing a review
of our successes and areas for improvement in our 2013/2014 performance and also priorities for 2014/2015. This presentation is
enclosed in the information papers for the Board for information. It enabled a helpful discussion and challenge around a number of priority
areas that included the following:
Smoking cessation
Screening services Microbiology Health Improvement
Workforce
During the meeting we also discussed areas of challenge for us including
smoking cessation targets and the need for support from Welsh Government in areas that may require escalation where the achievement
of targets is not solely within our control. The establishment of effective ‘service level agreements’ with other stakeholders was also discussed and
identified as a priority for us in the immediate to medium term.
3 Integrated Medium Term Plan and
Operational Plan 2014/2015
As the Board is aware, the Integrated Medium Term Plan has not been approved by the Minister and discussions are ongoing to develop a
2014/2015 Operational Plan which is before the Board. This needs to be submitted by the 4 July 2014.

Public Health Wales Chief Executive Report – April 2014
Date: 17 June 2014 Version: 1 Page: 5 of 7
A substantial amount of work has been done across the organisation in
order to focus on SMART objectives with clear targets where applicable and focused actions to deliver on the targets. We have also expanded the
risks within each section.
Following submission of the Operational Plan, and subject to approval, we
will need to develop a process and timeline to develop a new Integrated Medium Term Plan for submission in January 2015 which will span the
period from 2015 to 2018.
4 Clinical Governance, Trusted to Care Report
and the Francis Report
The Board is familiar with the Trusted to Care Report and may also be
aware that each Health Board and NHS Trust was required to self-assess itself against the recommendations in the report and for the respective
Boards to assure themselves that any gaps in this assessment were being actively managed and met. It was unclear as to whether Public Health
Wales was being asked to do so and therefore a letter was sent to the
Minister outlining our actions taken to date. This letter can be seen in the correspondence section of the Board papers.
The Director of Nursing, Executive Director of Public Health Services/Medical Director and Board Secretary/Director of Corporate
Services have been undertaking an assessment of both the Francis Report and the Trusted to Care report across the organisation and an action plan
is being developed to consolidate the applicable recommendations of both into one plan. This will be presented to the Board in July.
During this process it has been identified that we would benefit from reviewing our clinical governance arrangements – which are taking place
albeit in a somewhat fragmented manner, with the purpose of developing a coherent clinical governance framework for the organisation. The
Director of Nursing and Executive Director of Public Health Services/Medical Director are in the process of developing proposals for
this which will be available to the Board in July.
5 Relationships with Stakeholders
With the increasing requirements for performance and delivery by Welsh Government and expanding roles for Public Health Wales, it has become
increasingly apparent that we need to develop more formalised arrangements with our partners. This is particularly important where there
are shared targets to be achieved by us and other partners which may be compromised by the inability to deliver on the part of either party. An
example of this is the smoking cessation targets and the need for a complementary and collaborative approach by Public Health Wales and

Public Health Wales Chief Executive Report – April 2014
Date: 17 June 2014 Version: 1 Page: 6 of 7
Health Boards through their Directors of Public Health. This collaborative
approach is variable across the country.
As a result of this, and is previously referred to in item 2 above, we will be
progressing the development of agreed service level agreements with key partners over the coming weeks and months that clearly outline the
respective accountabilities, responsibilities and authorities for each party with escalation measures in the case of persistent difficulties in achieving
a combined target. These will be established on the basis of collaboration and combined goals that should be mutually beneficial.
6 Bevan Commission
Progress has been made in relation to securing funding and clarity on the hosting arrangements for the Bevan Commission.
7 Designation as an Accountable Officer
I received the transfer of accountability letter from Andrew Goodall on 12 June 2014 and will respond accordingly. The letter is enclosed in the
correspondence section of the Board papers.
8 Nursing and Midwifery Strategy
The first Public Health Wales Nursing and Midwifery Strategy was launched on the 12 May in the Millennium Centre in Cardiff. The event, which was
planned to coincide with International Nursing Day, was attended by Professor Jean White Chief Nursing Officer for Wales, who confirmed how
pleased she was that Public Health Wales now has a Director of Nursing in post to provide internal and external leadership to represent nursing and
midwifery perspectives at Board level. Raising The Profile: Public Health Wales Nursing and Midwifery Strategy 2014-2017 .
The ten themes of the strategy aim to reflect key approaches to ensure that the nursing and midwifery professionals can respond and adapt to the
changing needs of the NHS in Wales and the aims Public Health Wales.
Huw George, in his role as interim Chief Executive spoke of his new
awareness of the variety of contributions made by nurses and midwives
every day in contributing to the aims of Public Health Wales, which may not always be apparent. He went on to state the profile is now raised,
with this as well as the expectations.
The strategy provides the vision to take forward a number of governance,
developmental and professional requirements such as changes to revalidation which will be expected to come into force during 2015.

Public Health Wales Chief Executive Report – April 2014
Date: 17 June 2014 Version: 1 Page: 7 of 7
Recent reports such as Trusted to Care and the Mid Staffordshire enquiry
highlight the need to ensure that nurses and midwives are well supported in adhering to their professional codes, in all working environments.
Nurses involved in co creating the strategy shared their positive experiences in developing the strategy with colleagues attending the
launch. An implementation plan is now being developed led by the Director of Nursing, which the Board will be able to receive updates on.
9 DEMOS
DEMOS, a cross-party think-tank, has published a report, Behind the Screen: Revealing the true cost of cervical cancer…, that contends that
increased screening rates would save the NHS £10m a year, and halve the number of deaths. The report was launched at a Ministerial event on 18
June. Public Health Wales was not approached before the report was written, nor was it asked for data. A few days before the launch we
discovered that the report incorrectly reported that the 2010-11 5-year
coverage rate for women aged 25-64 in Wales was 76.3%, which would suggest that Wales had the lowest coverage in the UK. In fact, the correct
figure for Wales is 79.6% and the best in the UK. DEMOS agreed to take down the online version of the report until it had corrected this error and
made another amendment we requested. They also agreed not to print any copies without correction and to insert an errata sheet in the printed
copies prepared for the launch event. The chief executive will be writing to the chief executive of DEMOS to follow-up on our concerns.

Statutory and Mandatorytraining policy
Purpose of Document:
A new Statutory and Mandatory training policy has been developed and has beenpublished for staff to comment on.
The policy identifies the type and frequency of statutory and mandatory training thatPublic Health Wales will provide in order to help promote safer working practices. Itsets out the roles and responsibilities of staff in relation to attendance of trainingcourses, the arrangements in relation to record keeping and the approach to inrelation to the design and delivery of statutory/mandatory training programmes.
The training is in line with the UK Core Skills Training Framework which has beendeveloped by Skills for Health for use by all health organisations to help guide andstandardise the focus and the key delivery of key statutory and mandatory trainingskills.
All staff are required by law, to undertake the training which is classified asstatutory. Staff must also undertake any mandatory training detailed in the policy asrelevant to their role, as this has been identified as necessary by the NHS and PublicHealth Wales.
Board/Committee to- (Please indicate)
To decide- Paper will outline recommendations or issues to beapproved by the Board or Committee.
x
To discuss- Board or Committee will be asked to discuss andscrutinise the paper and provide feedback and comments.
To inform- Board or Committee will be asked to note the paper forinformation only
Other relevant information
Next StepsOnce approved this policy will be circulated to all staff within Public HealthWales.
Link to Public Health Wales commitment and priorities for action:(please tick which commitment(s) is/are relevant)
x
Priorities for action include relevant priority for action(s)
Paper 32 05

Public Health Wales Paper Submission Cover Sheet
Date: 13 January 2013 Version:0g Page: 2 of 2
Link to standards forhealth services
Standard 22 - Managing Risk and Health andSafety
Link to risk register
Equality impactassessment
Has an equality impact assessment beencompleted? If so, please indicate here and includeas an appendix to the paper. If not, pleaseindicate here and explain why an equality impactassessment is not required.
Financial implications It may be necessary to engage the services of anexternal company to provide training to staff.
Service userengagement
Have you completed a service user engagementplan? If yes, please attach a copy.
Author:
Date: 16 June 2014 Version: 0a
Sponsoring Executive Director: Ruth Davies, Director of Workforceand Organisational Development
Who will present: (If appropriate) Ruth Davies, Director of Workforceand Organisational Development
Documents attached:(If appropriate)
Statutory and Mandatory trainingpolicy and summary of commentsfrom staff consultation
Date of meeting: 26 June 2014
Committee/Groups that havereceived or considered this paper:
This policy has been circulated inline with the Public Health Walespolicy consultation process

Date: 9 May 2013 Version: v0b Page 1 of 17
Statutory & MandatoryTraining Policy
Policy type: Public Health Wales wide
Policy reference number: PHW04
Policy classification: Human Resources
Author: Professional and Organisational Development Team
Policy lead: Claire Barley, Head of Professional and OrganisationalDevelopment
Executive lead: Ruth Davies, Director of Workforce and OD
Date: 14 May 2014 Version: 0g
Publication/ Distribution:
Public (Internet)
Review Date: TBC
Approval date:
Approving body: Quality and Safety Committee
Purpose and Summary of Document:
This policy covers the training the organisation must provide, and staff mustattend, in order for Public Health Wales to meet and comply with itsstatutory and mandatory requirements.
Intended audience: All staff
Interdependencies with other policies (this is should not be taken as anexhaustive list of relevant and related policies):
Health and Safety Policy Induction Policy (under development)Appraisal and Continuous Development Policy (under development)Welsh Language strategy
Public Health Wales Statutory and Mandatory Training Policy
Date: 14 May 2014 Version: v0d Page 2 of 17
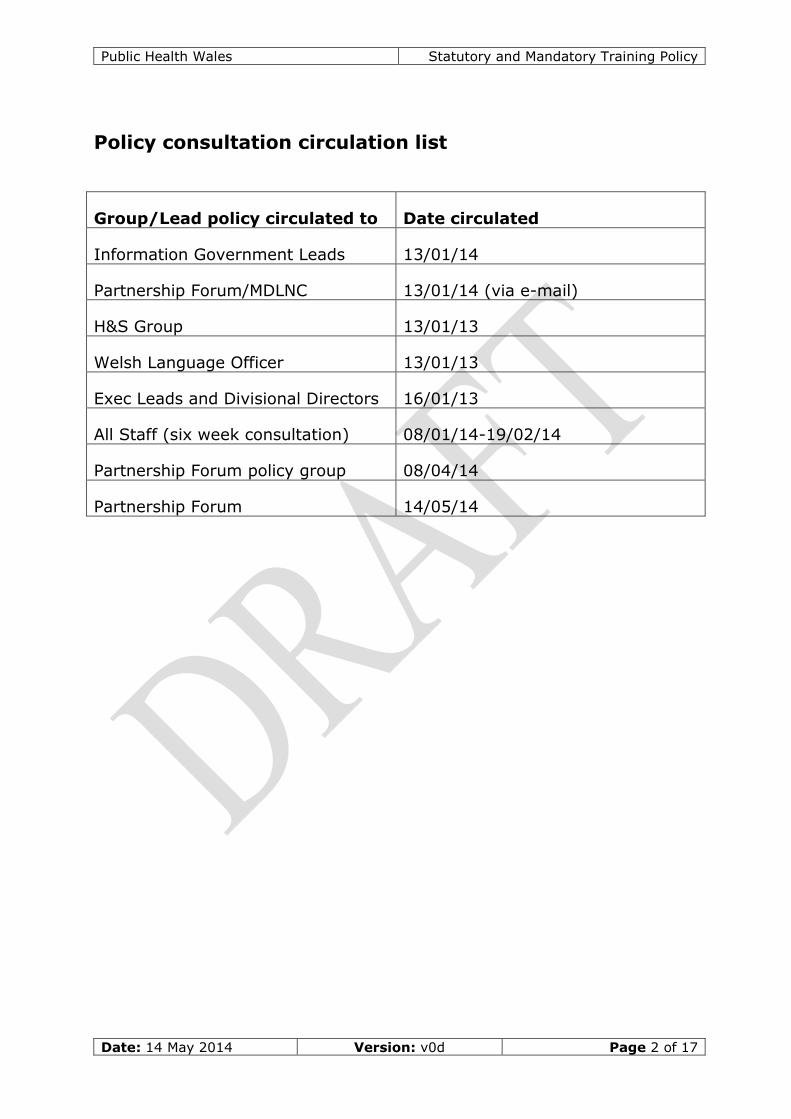
Policy consultation circulation list
Group/Lead policy circulated to Date circulated
Information Government Leads 13/01/14
Partnership Forum/MDLNC 13/01/14 (via e-mail)
H&S Group 13/01/13
Welsh Language Officer 13/01/13
Exec Leads and Divisional Directors 16/01/13
All Staff (six week consultation) 08/01/14-19/02/14
Partnership Forum policy group 08/04/14
Partnership Forum 14/05/14

Public Health Wales Statutory & Mandatory Training Policy
Date: 9 May 2013 Version: v0b Page 3 of 17
Contents
1 SUMMARY................................................................................4
2 INTRODUCTION ......................................................................4
3 POLICY AIM ............................................................................4
4 SCOPE .....................................................................................5
5 LEGISLATIVE AND NATIONAL INITIATIVES ............................6
6 DEFINITIONS..........................................................................66.1 Statutory Training............................................................66.2 Mandatory Training ..........................................................66.3 Additional Mandatory Training for specific roles....................6
7 ROLES AND RESPONSIBILITIES ..............................................6
8 A SYSTEMATIC APPROACH TO STATUTORY AND MANDATORYTRAINING ...............................................................................88.1 Training Needs Analysis (TNA)...........................................88.2 Training Action Plan(s)......................................................88.3 Training Programme.........................................................98.4 Recording Attendance at Training.......................................98.5 Non-attendance at Training ............................................. 10
9 MONITORING AND AUDITING ...............................................109.1 Quality Assurance .......................................................... 10
10 APPENDICES .........................................................................1210.1 Appendix A References to Legislation............................... 12

Public Health Wales Statutory and Mandatory Training Policy
Date: 14 May 2014 Version: v0d Page 4 of 17
1 Summary
Organisations have a moral, economic and legal responsibility to provide a safeand healthy environment for their staff, contractors and visiting members of thepublic and patients. They are required to provide a range of learning anddevelopment that ensures their workforce has the correct level of knowledge andskills to operate safely and that a safe and healthy working environment ismaintained. Although there is legislation that requires statutory training to beidentified, organisations need to establish their own minimum standards for safepractice tailored to the demands and requirements of their business.
2 Introduction
Public Health Wales has staff based across Wales, including sessional and loneworkers in a wide range of locations and environments. The organisation istherefore committed to equipping staff with the knowledge and skills required toundertake their roles competently and confidently. Staff are expected to takeresponsibility for developing and using these skills and participating in thelifelong learning process as they have a contractual responsibility to ensure they,and in turn, the organisation remains compliant with legislation and requiredstandards:
Section 35 of the Public Health Wales NHS Trust Contract of Employmentspecifically notes the employee’s duty to take reasonable care of the health andsafety of yourself and of others who may be affected by your acts or omissionsat work. Sections 6.6 and 6.7 of the Public Health Wales Health and SafetyPolicy specifically set out Managers’ and Employees’ responsibilities with regardto training attendance; subsequent failure to comply with these responsibilitiesmay lead to disciplinary action being taken.
Implied into every employment contract is the common law term of carrying outreasonable instructions given by the employer. Mandatory training is trainingthat the organisation (or wider NHS/Welsh Government) has deemed essentialfor either all staff or specific groups. Attendance at and/or completion ofmandatory training is considered a reasonable instruction; any subsequentfailure to do so may again lead to disciplinary action being taken.
The Disciplinary policy sets out examples of misconduct which include (atvarying levels), failure and/or refusal to carry out reasonable instructions,negligence. Employees would be advised to refer to the policy for full details.
3 Policy aim
The purpose of this policy is to:
Provide information about statutory and mandatory training; Set out the roles and responsibilities in respect of design and delivery of
statutory/mandatory training programmes in these areas;

Public Health Wales Statutory and Mandatory Training Policy
Date: 14 May 2014 Version: v0d Page 5 of 17
Identify training requirements in terms of programme and frequency; Set out the arrangements for ensuring all staff are able to attend relevant
training; Set out arrangements for record keeping of attendance and monitoring; Set out arrangements for following up those who fail to attend;
This policy specifies those areas of training that are driven by statute and thosethat have been made mandatory by the NHS and Public Health Wales in line withthe adoption of the UK Core Skills Training Framework, developed by Skills forHealth. The UK Core Skills Training Framework sets out a framework for use byhealth organisations to help guide and standardise the focus and the keydelivery of key statutory and mandatory training skills.
4 Scope
Statutory training is compulsory, by law, for all staff All staff must complete mandatory training appropriate for their post e.g.
a higher level of infection control for some laboratory staff, training in linewith professional standards as appropraite
The requirement to complete statutory and mandatory training is apriority over other forms of learning and development
Temporary staff employed via agencies and contractors must have hadtheir statutory and mandatory training requirements met by theiremployer with the exception of fire safety which should be provided aspart of their induction programme Contractors will be provided withrelevant information to ensure that they meet the requirements of firesafety.
Relating to this policy, the UK Core Skills Training Framework informs staffof the minimum training requirements for all identified statutory andmandatory topics (plus Welsh Language Awareness which is not includedin the framework)
These requirements have been collated on the basis of legislativerequirements (statutory training) and external assurance frameworks thatfeed into Public Health Wales policy documents (mandatory training). Therequirements will be subject to change on the basis of internal andexternal developments and will be reviewed in the event of any significantchange and reissued as necessary
Changes to Public Health Wales’ statutory and mandatory trainingrequirements and subsequently to this policy must be made via thesubject specialist lead, using the Public Health Wales template andsubmitting it to the Learning, Education and Development Group (LEaD)who will quality assure before working with the approving Quality andSafety Committee. No subject can be defined as mandatory unless it hasbeen approved via this process.

Public Health Wales Statutory and Mandatory Training Policy
Date: 14 May 2014 Version: v0d Page 6 of 17
5 Legislative and national initiatives
A comprehensive list of legislation, policy and guidance can be found inAppendix A.
6 Definitions
6.1 Statutory Training
Statutory training is training that is required by law and is governed by astatutory instrument. It is part of a package of measures to ensure thehealth, safety and welfare of employees when carrying out their professionalduties. The law applies equally to directly managed staff and employees ofindependent contractors.
6.2 Mandatory Training
Mandatory training is training that the NHS in Wales and Public Health Waleshas identified as essential for all staff to undertake to enable them to work torequired standards and for the organisation to achieve its objectives asdetermined by national, local and professional guidelines. All mandatorytraining requirements will have been agreed at Public Health Wales Board intheir adoption of new organisational policies.It is the responsibility of independent contractors who provide services toPublic Health Wales to identify and provide mandatory training to theiremployees related to the nature of the services they offer.
6.3 Additional Mandatory Training for specific roles
This is mandatory training, as defined above, that Public Health Wales hasidentified as essential for specific groups of staff, relating to their job role.
7 Roles and Responsibilities
Employers
Employers have a duty under the Health & Safety at Work Act 1974 to takereasonable measures to ensure the health, safety and welfare of their employeesat work. They also have a duty towards people who are not their employees butuse their premises.
The implications of failure to comply with the regulations are extremely seriousand can result in premises closure or significant fines being levied against theorganisation. In a serious breach of statutory regulations, responsible individualsmay be personally culpable and this can result in fines or even jail terms beinggiven if the organisation is found guilty.

Public Health Wales Statutory and Mandatory Training Policy
Date: 14 May 2014 Version: v0d Page 7 of 17
To ensure that Public Health Wales is, and remains, compliant with all statutoryregulations staff at all levels in the organisation have differing responsibilities asdetailed below.
Chief Executive and Executive Team
The Chief Executive is responsible for ensuring that all Public Health Wales staffhave the opportunity to participate in statutory and mandatory training.
The Director of Workforce and Organisational Development has an overallresponsibility for advising the Executive Team and through this group the Boardon statutory and mandatory training for all staff and for ensuring that systemsare in place to:
Monitor the implementation of the policy; Investigate and report back to Executive Team any issues of non-
compliance with suggested solutions Provide statutory and mandatory training to all staff Ensure that processes are in place to commission, plan and coordinate
statutory and mandatory courses Communicate Public Health Wales statutory and mandatory courses
appropriately Process applications for statutory and mandatory training and ensure staff
maintain their records on the Electronic Staff Record (ESR) system; Notify manager/reviewers should any staff member fail to attend a booked
training event Quality assure training through the monitoring of course evaluations and
as required (i.e. changes in legislation, ensure Public Health Walesmaintains compliance).
Line Managers
It is the responsibility of line managers to ensure that:
All staff undertake statutory and mandatory training and to take anyaction necessary to ensure compliance
All newly appointed staff undertake corporate induction or equivalentalternative within specified timescales
As part of the annual objective setting process line manager/reviewersmust ensure that attendance at relevant statutory and mandatory trainingrequired for their role has taken place and that accurate records aremaintained
Staff are given the opportunity to attend statutory and mandatory training Reviews are undertaken with members of staff where appropriate to
ensure the work environment complies with health and safety regulationsand also with any recommendations made during statutory andmandatory training
When a member of staff is unable to attend a booked statutory andmandatory training session another training date is arranged as soon aspossible

Public Health Wales Statutory and Mandatory Training Policy
Date: 14 May 2014 Version: v0d Page 8 of 17
Should a member of staff fail to attend a booked statutory and mandatorytraining course on more than one occasion, other than for reasons of illhealth, a review is undertaken to identify the difficulty
Statutory and mandatory training is up to date or clear plans are in placeto address training needs before considering any further study leaveapplications
Staff
It is the responsibility of staff to:
Review their required statutory and mandatory training and ensure that alltraining is up-to-date and notify their line manager where they have gaps
Plan statutory and mandatory training attendance as part of their annualobjective setting
Maintain an acceptable statutory and mandatory training record e.g. usingthe ESR, Faculty of Public Health tool and portfolios as appropriate
Set a high priority to statutory and mandatory training over other forms oflearning and development and make every effort to attend any trainingevents provided and arranged for this purpose
Advise their manager/reviewer and the course organiser as soon asreasonably possible if they are unable to attend a booked statutory andmandatory training session
Highlight any additional support or needs they may have with regards tounderstanding and benefiting from statutory and mandatory training
Ensure that all statutory training attendance is up to date before applyingfor further protected learning time (including study leave)
8 A Systematic Approach to Statutory andMandatory Training
Where new posts are established the line manager needs to identify statutoryand mandatory requirements for the post when the job description is beingwritten. This should then be reviewed with the post holder during the firstmonth of employment
8.1 Training Needs Analysis (TNA)
Training identified by managers/reviewers should be entered on to the ESR.Reports identifying training needs are gathered from the system and used todevelop a schedule of statutory and mandatory training.
8.2 Training Action Plan(s)
A statutory and mandatory training plan which will inform the structure anddetail of the rolling programme will be developed by the Professional andOrganisational Development team.

Public Health Wales Statutory and Mandatory Training Policy
Date: 14 May 2014 Version: v0d Page 9 of 17
8.3 Training Programme
A blended programme of training will be made available to include e-learning,classroom and work-based activities where appropriate. In order to ensurethat all training provided achieves the required outcomes, is of a consistentstandard for all subjects and provides value for money the following critera willbe applied.
Training events will have identified aims and learning outcomes Training will be designed taking into account the range of learning styles
likely to be useful to participants Where possible training should be delivered by someone with knowledge
of adult learning methods Training events will be evaluated by one or more of the following methods
as appropriate:o End of course participant evaluation form (with opportunity for
anonymity)o End of course test of knowledgeo End of course evaluation form completed by the trainer
Follow-up participant evaluation form or interview Other valid evaluation method Evaluations of each training event will be collated into a report Training evaluation reports will be reviewed on a regular basis and will
form part of the quarterly management report.
There will be a blended approach to the delivery of training providing flexibleopportunities for staff to undertake the necessary statutory and mandatorytraining.
Public Health Wales’ Welsh Language Scheme states the following:‘Public Health Wales is committed to assessing the need for vocational trainingthrough the medium of Welsh. Where the need for vocational training throughthe medium of Welsh is identified and suitable training is accessible it will besupported in order to facilitate implementation of the Scheme’.
8.4 Recording Attendance at Training
A guide to statutory and mandatory training relevant to various job roles can befound at Appendix B and C to assist manager/reviewers and staff members inidentifying their individual statutory and mandatory training requirements. Allbookings for training will need to be completed through the ESR system. E-learning programmes are self enrolling and can be undertaken at a time agreedwith the manager/reviewer.
An attendance register will be completed at all classroom based training and willbe signed by the individual delegates. The registers will be retained by thetrainer and a copy forwarded to the training organiser.

Public Health Wales Statutory and Mandatory Training Policy
Date: 14 May 2014 Version: v0d Page 10 of 17
Completion of e-learning packages will also be monitored by the Learning,Education and Development (LEaD) Group.
Attendance figures and e-learning package completion data will form part of thequarterly performance monitoring report provided to Executive Team throughthe Professional and Organisational Development Team, including a break downby division of compliance rates.
Individual training records should be maintained through the Electronic StaffRecord (ESR) by the individual and their line manager. Whilst ESR is beingrolled out across the organisation the Professional and OrganisationalDevelopment Team maintain a spreadsheet of current training dates(compliance) which is updated monthly and held in a confidential folder.
8.5 Non-attendance at Training
A copy of the attendance registers are returned to the training organisers at theend of each training programme by the tutor. Should a delegate not be presentat the course the training organiser will inform the delegate’s line manager
Persistent non attendance should be managed through the line manager and willbe recorded in the quarterly report.
Non attendance by division will be reported as part of the quarterly performancemonitoring process to the Executive Team.
Previous Training - Newly appointed staff from across the NHS may transfer anypreviously attended statutory and mandatory training (linked to the UK CoreSkills Frameowrk) attendance provided they are compliant with Public HealthWales requirements as determined by the policy. Details of training undertakenand evidence of attendance must be provided by the new employee and be inline with the requirements of the UK Core Skills Training Framework.
9 Monitoring and Auditing
Adherence to the statutory and mandatory training policy and the effectivenessof the training provided will be reviewed on an annual basis and in line with therequirements of the organisation’s self assessment against the Standards forHealth Services.
9.1 Quality Assurance
The statutory and mandatory training provisions will be evaluated using the annualand mid-year declaration of assurance against Standards for Health Services andany other mechanism felt appropriate by the Director of Workforce andOrganisational Development.
The length and frequency of provision of the various training coursescomprising the statutory and mandatory training programme will be reviewed

Public Health Wales Statutory and Mandatory Training Policy
Date: 14 May 2014 Version: v0d Page 11 of 17
against the effectiveness of outcomes and amended as required in line withthe requirements of the UK Core Skills Training Framework.

Public Health Wales Statutory and Mandatory Training Policy
Date: 14 May 2014 Version: v0d Page 12 of 17
10 Appendices
10.1 Appendix A References to Legislation
Subject Legislation or Policy
Child Protection The Children Act 2004.Working Together 2006.Laming Report 2003.Children's NSF 2003.'Every Child Matters' 2003.RCP & CH Guidelines HCC CP Performance Indicators 2006-07.
Violence andAggression
Conflict Resolution Training - Implementing the National Syllabus 2004(NHSLA st3)A Professional Approach to Managing Security in the NHS 2003Welsh Violence and Aggression Passport Scheme
CorporateInduction
Standards for Health Services in Wales.Risk Management in the NHS
COSHH Health and Safety at Work Act (1974)Management of Health and Safety at Work Regulations (1999)COSHH Regulations 2004
Display ScreenEquipment
Health and Safety at Work Act (1974)Management of Health and Safety at Work Regulations (1999)DSE Regulations 1992
Equality &Diversity
Race Relations Amendment Act (2000) (NHSLA st3)Code of Practice for Racial Equality P32:3.20
Fire Safety Fire Precautions Act (1971) amended (1999)Management of Health and Safety at Work Regulations (1999)Health and Safety at Work Act 1974Regulatory Reform (Fire Safety) Order 2005Firecode HTM 83 - Fire Safety in Healthcare Premises 1994.
Infection Control Clinical Negligence Scheme for TrustsStandards for Health Services in Wales.MRSA Reduction (Key local and national target) (NHSLA st2 & 4)National Infection Control Training.
InformationGovernance
Caldicott Principles into PracticeData Protection Act 1998Health and Social Care Act 2008Confidentiality: Code of Practice for Health and Social Care in WalesAccess to Health Records Act 1990Freedom of Information Act 2000Human Rights Act 1998Wales Accord for the Sharing of Personal Information (WASPI)Section 251 of the National Health Service Act 2006
Manual Handling Health and Safety at Work Act (1974) (NHSLA st2)Management of Health and Safety at Work Regulations (1999)Manual Handling Operations Regulations (1992).Welsh Manual Handling Passport Scheme
Mental Capacity Mental Capacity Act 2005
RiskManagement
Risk Management in the NHSManagement of Health and Safety at Work Regulations (1999)Health and Safety at Work Act (1974
VulnerableAdults
Patient Safety (NHSLA st3)
Welsh Language Welsh Language Act 2004Welsh Language (Wales)measure 2011

Public Health Wales Statutory & Mandatory Training Policy
Date: 9 May 2013 Version: v0b Page 13 of 17
Appendix B Statutory and Mandatory Compliance List (shaded are based on UK Core Skills Frameworkguidance)
Course Staff Frequency Additional Notes
RelatedPublicHealthWalesPolicy
Fire Safety ALL STAFF
Induction/ classroominitiallyminimum every 2 yearsrenewal possible throughe learning
For those staff with responsibility forevacuating others e.g. patients, theywill need to receive training on anannual basis and identification of thiswill be based upon local riskassessment.
Fire Marshall/WardenTraining Nominated fire wardens Annually
Only required for staff nominated asfire wardens or first aidersFirst Aid at Work
Certificate Nominated first aiders Every 3 years
Health, Safety &Welfare
ALL STAFF
Initially classroomsession with renewalpossible through elearning - every 3 years
Laboratory staff - induction only anddemonstrated through on goingcompletion of appropriateaccreditation
Moving and Handling(level 1)
ALL STAFF
Induction via classroomor e learning Level 1 is deemed once only unless a
risk assessment deems the individualshould attend more regularly
Level 2 requirements should reviewedthrough a local risk assessmentprocess regularly
Moving and Handling(level 2)
All staff, including unpaid andvoluntary staff, whose role involvespatient handling activities
Organisation todetermine any requiredrefresher periods basedupon local assessment
Resuscitation
Level 1: All staff, including unpaidand voluntary staff involved in directpatient care
Level 1: Once atinduction
Sta
tuto
ry

Public Health Wales Statutory and Mandatory Training Policy
Date: 14 May 2014 Version: v0d Page 14 of 17
Level 2: Staff with direct clinical careresponsibilities including all qualifiedhealthcare professionals who deliverpatient services
Level 3: Registered healthcareprofessionals with a responsibility toparticipate as part of the resuscitationteam
Level 2: Every year
Level 3: Every year
Using display screenequipment:
AwarenessDSE Assessment
Staff identified as DSE users
At induction and/orfollowing a change of ITor general officeequipment or move toanother location. Also,identified need followinga risk assessment, returnfrom long term sicknessor pregnancy
When an individual has a DSEassessment undertaken, this countsas training
Radiation ProtectionLevel 1
Radiation ProtectionLevel 2
Screening Services only see separateguidance from screening
Screening Services onlysee separate guidancefrom screening
Screening Services only see separateguidance from screening
Violence andAggression Module A –Induction andAwareness Raising
ALL STAFF
Leaflet issued for all newstaff with offer letters orat inductionLeaflet also available toread on line
Job role risk assessed by linemanager to identify where modules Band C are required
Violence andAggression Modules B –Theory of PersonalSafety and De-escalation
Required staff based upon local riskassessment and training needsanalysis
Induction as identifiedthrough a riskassessment which shouldalso identify requiredrefresher periods for jobroles
Violence andAggression Module CBreakaway
Required staff based upon local riskassessment and training needsanalysis
Mandato
ry

Public Health Wales Statutory and Mandatory Training Policy
Date: 14 May 2014 Version: v0d Page 15 of 17
Infection Preventionand Control Level 1
ALL STAFF including contractors,unpaid and voluntary staff
All staff (Level 1) Every 3years
All healthcare staffproviding direct care:every year
Job role risk assessed by linemanager to identify where level 1 and2 are requiredInfection Prevention
and Control Level 2
All healthcare staff groups involved indirect patient care or services
Safeguarding level 1All non-clinical staff working in healthcare settings
At induction and every 3years in classroom or elearning
Job role risk assessed by linemanager to identify where levels 2and 3 are required
Also refer totheSafeguardingTraining Policy
Safeguarding Level 2
Clinical staff who have some degreeof contact with children and youngpeople and/or parents/carers.
Staff that MAY come into contact withchildren, vulnerable adults andfamilies. Staff that supervise otherswho may come into contact withchildren, vulnerable adults and theirfamilies, have recruitmentresponsibilities or deal withcomplaints. Staff who deal withsensitive information relating tochildren and / or vulnerable adults.
Those who have a strategic andmanagerial responsibility forcommission and delivering services,including CEO, directors and boardmembers
Classroom based (2.5hours), every 3 years
Safeguarding Level 3
Health professionals in regularcontact with children, young peopleand/or vulnerable adults or whoprovide direct care. Staff taking alead for children, young people orvulnerable adults
This training should beaccessed on an annualbasis where available.
InformationGovernance (and ITsecurity)
ALL STAFF Every 3 years
InformationGovernancePolicy

Public Health Wales Statutory and Mandatory Training Policy
Date: 14 May 2014 Version: v0d Page 16 of 17
Safeguarding adultsAll staff, including unpaid andvoluntary staff
Induction and no longerthan every 3 years
Welsh LanguageAwareness ALL STAFF
At induction / once onlyby DVD or e learning
Equality, Diversity andHuman Rights ALL STAFF Every 3 years
Dignity at WorkALL STAFF Every 3 years
Stress Awareness forManagers All line managers
Once only/every threeyears
Stress Awareness forStaff ALL STAFF
At induction/every threeyears
Course Staff Frequency Additional NotesPHWRelatedpolicy
Man
dato
ry
Improving QualityTogether All staff via e learning Once only
Welsh Government target
Bronze
SilverIdentified individuals via classroomlearning
Once only
GoldIdentified individuals via classroomlearning Once only
Putting Things RightAll staff modules 1, 2 and 5
Managers all 7 modules
Risk Managementtraining Managers and other staff as needed.
Good Clinical Practice(GCP) training forresearch
Individuals undertaking research
AnaphylaxisClinical staff - Screening
LidnocaineClinical staff - Screening

Public Health Wales Statutory and Mandatory Training Policy
Date: 14 May 2014 Version: v0d Page 17 of 17
Asbestos awarenessAll staff
Once only
Customer CareScreening
Mental CapacityScreening
Please note that this is not an exhaustive list of mandatory training for all staff groups across the organisation. Therewill be additional requirements in line with different professional bodies and roles and its an individuals and their linemanagers responsibility to ensure that they are aware of their statutory and mandatory training requirements.

1
PUBLIC HEALTH WALES
Statutory and Mandatory Training Policy – Summary of staff consultation comments
Contents Comments received Response
1. Introduction Include patients as they are recipients of PublicHealth Wales services
included
2. Aims andObjectives
3. Scope Recommendation: That the following should be
included in the list of criteria: ‘Training will be
designed to take account of the language needs and
preferences (Welsh or English) of employees’.
PHW has no control over the design ofmuch of the training on line which isdeveloped on a national basis.
An additional line in the policy hasbeen included which has been takenfrom the Welsh Language Scheme.
4. Legislative andNational Initiatives
Need to reference the Welsh Language measure 2011as well as Welsh Language Act
the framework could state that such training is to beprovided only by NHS organisations in Wales.
It is stated that there may (in the future) be arequirement for training in Welsh where required andthis would be a statutory requirement
Welsh language skills for staff
Included in the list
The content of the UK core SkillsFramework is out of the scope ofcontrol of the POD team or PublicHealth Wales.
The policy will have a review periodand flexibility to be updated shouldlegislation change.
The policy should be read inconjunction with relevant others, i.e,.Welsh Language Skills Strategy whendeveloped.
5. Definitions

2
6. Roles andResponsibilities
Include something on the quality of the trainingprovision
Query the tone on the policy and responsibilitiesbeing top down and that “calls to training” are ofteninaccurate.
the policy states that should a member of staff notattend a training course (on more than one occasion)for reasons other than ill health, then the managershould undertake a review. Clarity needs to beprovided on what this review would look like, whowould be involved and how would it be managed.There needs to be a system in place to inform themanager that staff have missed training on morethan one occasion.
This is more to do with theimplementation of the policy andquality of provision will be considered
This is a data management issue
which will be addressed with the
adoption of the Electronic Staff Record
and Self Serve.
Should a manager require support to
carry out their role, this should be
discussed with their line manager,
human resources or the learning and
development.
7. Main body ofpolicy (pleaseinsert appropriatetitle)
Please can you also include Putting Things Right e-learning training on the list and the compliance rateswithin the training report that you submit to the Q&SCommittee as this is mandatory for all staff and weare audited on compliance by the Welsh Risk Pool onan annual basis.
Section 8.5 reference Welsh NHS training – could thisnot be NHS UK?
Putting things right is included in the
list of mandatory training
requirements.
Yes – wording changed
8. Training &communicationwith staff
Add asbestos awareness to mandatory list Resuscitation – is this really needed for all staff?
Added
Added “those involved in direct patient
care”
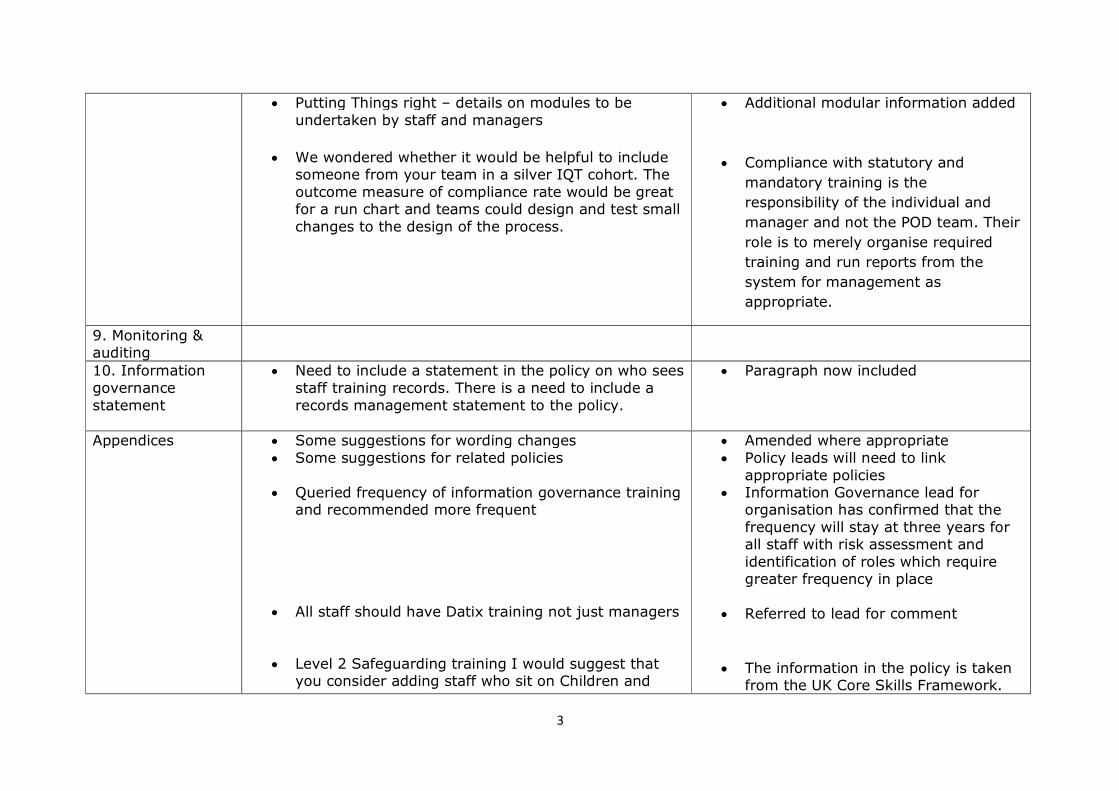
3
Putting Things right – details on modules to beundertaken by staff and managers
We wondered whether it would be helpful to includesomeone from your team in a silver IQT cohort. Theoutcome measure of compliance rate would be greatfor a run chart and teams could design and test smallchanges to the design of the process.
Additional modular information added
Compliance with statutory and
mandatory training is the
responsibility of the individual and
manager and not the POD team. Their
role is to merely organise required
training and run reports from the
system for management as
appropriate.
9. Monitoring &auditing
10. Informationgovernancestatement
Need to include a statement in the policy on who seesstaff training records. There is a need to include arecords management statement to the policy.
Paragraph now included
Appendices Some suggestions for wording changes Some suggestions for related policies
Queried frequency of information governance trainingand recommended more frequent
All staff should have Datix training not just managers
Level 2 Safeguarding training I would suggest thatyou consider adding staff who sit on Children and
Amended where appropriate Policy leads will need to link
appropriate policies Information Governance lead for
organisation has confirmed that thefrequency will stay at three years forall staff with risk assessment andidentification of roles which requiregreater frequency in place
Referred to lead for comment
The information in the policy is takenfrom the UK Core Skills Framework.

4
Young People’s Partnership groups and HealthySchools Coordinators
Query the amount of statutory and mandatorytraining required and comments that some isduplicated
Additional information is available inthe Public Health Wales Safeguardingpolicy and perhaps these examplescould be picked up in that document?
It has been acknowledged that the listof mandatory training is quiteextensive. Work will be undertaken inthe new financial year to work withthe policy leads to review policyrequirements and consider removingthe requirement for “mandatory”
A process needs to be developed toconsider training requirements in newand amended policies prior tosubmission to the Board / forapproval.

Date: 16 June 2014 Version: 1 Page: 1 of 45
Governance and Accountability module
Purpose of Document: The Governance and Accountability Module is a framework that Boards are required to
self assess against to establish how well the organisation is governed. It is also a requirement of the Welsh Government and forms part of the supporting information
for the Annual Governance Statement. The self assessment covers the period April 2013 – March 2014.
Board/Committee to- (Please indicate)
To decide- Paper will outline recommendations or issues to be approved by the Board or Committee.
X
To discuss- Board or Committee will be asked to discuss and scrutinise the
paper and provide feedback and comments.
To inform- Board or Committee will be asked to note the paper for
information only
Other relevant information
The Board has approved the Governance and Accountability module ‘out of Committee’ and are being asked to ratify that decision.
Next Steps
The Board are asked to ratify the approval of the Governance and Accountability
module.
Link to Public Health Wales commitment and priorities for action:
(please tick which commitment(s) is/are relevant)
X
Priorities for action Put in place a comprehensive governance framework
Author: Eleanor Higgins, Corporate Governance Manager
Date: 16 June 2014 Version: 1
Sponsoring Executive Director: Keith Cox, Board Secretary
Who will present: (If appropriate) Keith Cox, Board Secretary
Documents attached:
(If appropriate)
Governance and Accountability module
Date of meeting: 26 June 2014
Committee/Groups that have
received or considered this paper:
Executive Team
Board
Paper reference – 32 06

Public Health Wales Governance and accountability module
2
Link to standards
for health services
Standard 1: Governance and accountability
Link to risk
register
N/A
Equality impact assessment
N/A
Financial implications
N/A
Service user
engagement
N/A

Public Health Wales Governance and accountability module
3
Governance and
Accountability Module
Self Assessment Author: Eleanor Higgins, Corporate Governance Manager
Date: 16 June 2014 Version: 1
Purpose and Summary of Document:
The Governance and Accountability Module is a framework that Boards are required to self assess against to establish how well the organisation is
governed. It is also a requirement of the Welsh Government and forms part of the supporting information for the Annual Governance Statement. The self
assessment covers the period April 2013 – March 2014.

V1 16/06/14
4
Note: In establishing your level of agreement in relation to each of the statements made, you must be able to
demonstrate through your supporting narrative not only what your organisation or business is doing, but how well it is
working and the resulting impact on organisational performance.
Theme 1 - Setting the Direction
Desired Outcomes:
We place the people who use our services at the heart of our work We make sure our purpose is clear and know to develop and deliver our services to improve overall health and well being We are a value based organisation/business and carry out our work openly, honestly, ethically and with integrity
Public Health Wales Governance and accountability module
5
a) We make an effective contribution to the achievement of the strategic vision for health services in Wales
Str
on
gly
dis
ag
ree
Dis
ag
ree
Neith
er
ag
ree n
or
dis
ag
ree
Ag
ree
Str
on
gly
ag
ree
Supporting narrative
Public Health Wales plays a pivotal role in improving health in Wales and is committed to setting the
direction in Wales for reducing inequality resulting from the socio-economic determinants of health.
In September 2013, the Minister for Health and Social Services approved the recommendations set out in
the review of health improvement programmes in Wales. The recommendations refocused investment
and future action to improve health and wellbeing and reduce health inequalities. This work is now being
taken forward as ‘transforming health improvement in Wales’.
Public Health Wales continues to play a key role in contributing to the development of a public health bill
for Wales. The organisation is also a member of the reference and advisory groups for the Future
Generations Bill.
Last year we sought to establish clear system leadership on critical public health issues. We have
achieved this in some areas, for example work undertaken by the Public Health Wales Observatory; the
‘Add to Your Life’ over 50s health check; WCISU; vaccination via the measles outbreak; a position
statement on e-cigarettes; public health research and development; and the health improvement review.
An integrated medium term plan has been developed which documents where Public Health Wales plans to
contribute to the overall strategic vision for health services in Wales and how the progress and
achievements will be measured.
Public Health Wales has lead the work on Prudent Healthcare, following a request from the Minister for
Health and Social Services. Through 1000 Lives improvement we will collaborate closely with health
boards.
Discussions are ongoing to develop revised accountability arrangements between Public Health Wales, the
Welsh Government and wider public health system. This work will continue in 2014/15.
√

Public Health Wales Governance and accountability module
6
Supporting evidence
Integrated Medium Term Plan
Together for Health
Establishment Order
Our Healthy Future
Fairer Health Outcomes for All
Public Health Wales strategy and priorities for action
Long Term Agreement between Public Health Wales and Welsh Government
Heads of Agreement between Public Health Wales, health boards and local government
Public Health Wales Public Health Strategic Frameworks
Health Board Local Public Health Strategic Frameworks
Public Health Wales Strategic Delivery Plans
Planning and performance framework – quality and delivery framework
Health Improvement Review / Transforming Health Improvement in Wales programme
1000 Lives improvement service
Improving Quality Together
Briefings to Ministers
Chair, Chief Executive, Executive Team and Chair of Committees’ membership of All Wales peer
group meetings
Nursing and midwifery strategy

Public Health Wales Governance and accountability module
7
b) We have a clear purpose, vision and overall strategic direction that effectively aligns our local needs with the national strategy for health services in Wales
Str
on
gly
dis
ag
ree
Dis
ag
ree
Neith
er
ag
ree n
or
dis
ag
ree
Ag
ree
Str
on
gly
ag
ree
Supporting narrative
A healthier, happier and fairer Wales: Public Health Wales strategy was refreshed during 2013. It was
launched at the staff conference in October 2013. The strategy sets out the organisation’s aim, purpose,
approach, and commitments and is underpinned by priorities for action. In 2012/13 we identified the need
to refresh the Public Health Wales strategy to reflect the changes which had taken place in the
organisation.
Public Health Wales has a dual role, both locally and nationally in contributing to the national strategy for
health services in Wales.
We have contributed to the reconfiguration of services in Betsi Cadwaladr, Hywel Dda and the South Wales
programme.
The Public Health Wales Board has approved an integrated medium term plan which guides our strategy
and the achievement of a healthier, happier and fairer Wales. It demonstrates financial balance and
covers a three year period from 2014/15 – 2016/17. The plan fits within the NHS Wales planning
framework and supports the aims and policies if the Welsh Government.
There is a particular issue about lack of alignment with health boards, local public health teams and the
wider health improvement sector and we need to improve this area.
Supporting evidence
Public Health Wales documents which contribute to health services in Wales
Integrated medium term plan
Establishment order
Public Health Wales strategy and priorities for action
Public Health Wales Strategic Delivery Plans
√

Public Health Wales Governance and accountability module
8
Heads of Agreement between Public Health Wales, health boards and local government
Public Health Wales Public Health Strategic Frameworks
Planning and performance framework
Health Improvement Review
1000 Lives Plus
Improving Quality Together
Briefings to Ministers
Welsh Government documents within which Public Health Wales operates
Long Term Agreement between Public Health Wales and WG
Programme Level Agreements between Public Health Wales and WG
Together for Health
Our Healthy Future
Fairer Health Outcomes for All
c) Our citizens, staff and other stakeholders inform and influence our organisation/ business’s purpose, strategic vision and direction
Str
on
gly
dis
ag
ree
Dis
ag
ree
Neith
er
ag
ree n
or
dis
ag
ree
Ag
ree
Str
on
gly
Ag
ree
Supporting narrative
Citizens
Public Health Wales has long established links with various groups for engagement. The Screening
Engagement Team works in partnership with a variety of agencies at a local level including local
authorities, health boards, minority groups, community and development teams and third sector agencies.
A Public and Stakeholder Engagement strategy is in place, which seeks to ensure that the ongoing
development of Public Health Wales’ strategic direction is informed and influenced systematically by
citizens and other stakeholders. This was identified as an area for improvement last year and more work
is needed to evaluate whether staff are complying with the strategy.
A Service User Experience and Learning Panel, is in the process of being fully established and embedded.
√

Public Health Wales Governance and accountability module
9
The Director of Nursing will provide Executive level leadership on this agenda and will chair the panel.
Welsh Government requests on the organisations progress in implementing the framework for Assuring
Service User Experience (Action 5 of Achieving Excellence, the Quality Delivery Plan), have been provided
as requested at various intervals during this reporting period. A Non Executive Director champion has
been identified together with a Community Health Council representative.
There are plans in place to bring the monitoring of complaints, concerns and incidents together with the
Service user experience and learning panel, in addition to monitoring at local levels within teams and
divisions. It is anticipated that this will provide more clarity over how complaints and analysis from
service users is used to inform our business purpose, strategic vision and direction. We will be looking at
improving this during 2014/15.
We have recognised that there are a number of areas for improvement in relation to citizens informing
and influencing our purpose, strategic direction and vision. We will also develop a performance framework
which will be integrated into the Quality and Delivery performance report. Therefore, we have provided a
lower score than previous years. Once we have embedded learning from service user engagement into
the organisation, we will be able to increase the score.
Staff
The NHS Wales Staff survey results were received in May 2013. Engagement workshops were held to
discuss results of survey with staff and an action plan has been developed and approved by the Board.
The action plan provides details on how staff have informed and influenced the organisation. A number of
staff engagement events have been held across the organisation to consider the Mid Staffordshire inquiry
recommendations, in the context to Public Health Wales. Staff have provided their views on a range of
themes, this will be considered in light of what is already in place to support any required changes and will
highlight gaps which will need further work and focus during 2014-15.
We engage with staff representatives through the partnership forum. We have invited members of trade
unions and BMA to attend Board meetings as full non-voting members to contribute fully to discussions
and decisions at Board level. In 2012/13 we reported that there was no trade union representation at
Board level. We are pleased to report that the partnership forum has nominated two representatives to
attend Board meetings. They will alternate their attendance at each meeting. We are in discussions with
the BMA about securing a representative at Board meetings.
The Board and Executive team are supported by a leadership and delivery group comprising of Divisional
Directors, a national forum of professional and managerial staff and an annual staff conference.

Public Health Wales Governance and accountability module
10
Staff have been fully engaged in a review of accommodation. A series of workshops were held where staff
were invited to pass on their views and opinions to inform the future direction of the project.
Stakeholders
We regularly engage with partners and stakeholders. The Health Improvement Review engaged with
stakeholders who contributed to the final report and recommendations for service reconfiguration. The
implementation of the recommendations ‘transforming health improvement in Wales’ will be shaped and
informed by stakeholder groups.
Regular meetings of all Wales peer groups eg Chairs, Chief Executives, Vice Chairs, Directors of Planning,
Directors of Finance, Medical Directors, Directors of Public Health etc.
We also hold the annual Welsh Public Health Conference which has become well regarded amongst
professionals in Wales and the UK.
In 2012/13 we identified the need to improve links with Community Health Councils, third sector and local
government. We have established a link with Community Health Councils and are working with the third
sector and local government. The local government vacancy on our Board is still a risk to the organisation
and we are working with Welsh Government to fulfil the vacancy.
We have poor strategic links with local government and have not paid sufficient attention to stakeholder
and service user experience and feedback in developing our plans and services. This is highlighted as a
weakness in our integrated medium term plan.
Supporting evidence
Public and stakeholder engagement strategy
Content on internet and intranet sites including large number of page views and engagement on
interactive forums
Terms of reference and meetings of the NHS Wales Chief Executives group
Terms of reference and meetings of the Partnership Forum
Social media strategy
Staff engagement sessions
Regular meetings of Director of Public Health Development, Director of Public Health Services with
Chief Medical Officer, Health Board Directors of Public Health
Monthly meetings of the Chairs of the health boards and trusts
Frequent meetings between Executive Team; Board members and Chief Medical Officer
Service user experience reports submitted to Welsh Government

Public Health Wales Governance and accountability module
11
Screening services implementation of service user action plan
Stop Smoking Wales focus on improving efficiency of service in response to service user feedback
d) We carry out our work instilled with a strong sense of values, supported by clear standards of ethical behaviour
Str
on
gly
dis
ag
ree
Dis
ag
ree
Neith
er
ag
ree n
or
dis
ag
ree
Ag
ree
Str
on
gly
Ag
ree
Supporting narrative
In all our actions, whether with colleagues, stakeholders or partners, Public Health Wales seeks to be
professional, persuasive, open, reflective and responsive.
We have a strongly professionalised workforce who work with a strong sense of values which are
supported by clear standards of ethical behaviour, with a strong commitment to health inequalities. The
Medical Director oversees medical revalidation for the medical workforce and the Director of Nursing
provides a professional lead for nursing and midwifery staff.
Public Health Wales adopted a full set of policies and procedures when it was established on 1 October
2009. These policies and procedures are systematically reviewed in order of priority. Regular policy and
partnership forum meetings have been established to progress and agree policies between management
and trade union representatives. It has recently been noted by the Executive Team that some of these
policies are out of date and action is required to update them.
Board members adhere to the standards of good governance set for the NHS in Wales, which are based on
the Welsh Government’s Citizen Centred Governance Principles.
In the NHS staff survey 510 completed questionnaires were received from Public Health Wales staff, a
response rate of 39%, which was the second highest in Wales. The overall response rate for all LHBs and
Trusts was 27%. In the survey a large proportion of Public Health Wales staff confirmed that they were
prepared to ‘go the extra mile’ and were prepared to report incidences of harm. An action plan has been
approved by the Board to take forward issues identified in the staff survey.
Supporting evidence
Board and Committee Arrangements
√

Public Health Wales Governance and accountability module
12
Corporate Policies
Declaration of Interest
Standing Orders
Standing Financial Instructions
Scheme of Delegations
WAO reviews
WAO Structured Assessment
Internal Audit reviews
Appraisals / Performance Reviews
Other external reviews
Public Health Wales vision and values
Nursing and midwifery strategy
e) We promote equality and recognise diversity across all our services and activities S
tro
ng
ly
dis
ag
ree
Dis
ag
ree
Neith
er
ag
ree n
or
dis
ag
ree
Ag
ree
Str
on
gly
Ag
ree
Supporting narrative
We have put in place a revised Strategic Equalities Plan (SEP) and a working group to action the plan
which has representation from across Public Health Wales. The SEP considers equality issues affecting all
aspects of our work as well as our workforce. The group aims to facilitate learning across directorates and
divisions to actively engage staff in strategic decisions. The group will investigate embedding the
promotion of equality and diversity across all services and activity. There are equality internet pages
available for staff as a reference tool. An Equality Officer has been recruited on a part time basis to work
on embedding equality and diversity across the organisation.
The NHS Wales Equality Unit transferred into Public Health Wales on 1 April 2013.
All Public Health Wales accommodation has been audited to be compliant with the Disability Discrimination
Act.
Dignity at work and equality and diversity training is mandatory for all Public Health Wales staff.
Compliance of uptake of training needs to improve. We continue to focus efforts on improving compliance
√
Public Health Wales Governance and accountability module
13
rates. There is a dignity at work policy in place which is one of the main drivers for managing incidents of
harassment as well as being a management tool.
The recruitment of staff is supported by the two tick system whereby anyone applying for a post who self
declares themselves as disabled can receive automatic shortlisting when applying for jobs within the NHS,
providing they meet the essential criteria for the post, as set out in the person specification. This is
further supported by HR policies and procedures.
A range of equality and diversity data is collected from service users eg Screening. However, this is not
available for analysis of the workforce. The roll out of Electronic Staff Record will allow staff to update
their equality and diversity information directly. This will, in turn, provide more accurate information for
analysis.
We have an approved Welsh language scheme and action plan which demonstrates the organisations
commitment to offering bilingual services to the public of Wales.
We are working to develop a consistent approach for carrying out equality impact assessments (EqIA).
The central message is that EqIA activity should be started at the beginning of planning a new policy or
when substantially revising an existing policy. We are also looking to improve access to our services and
to be more inclusive in the way in which we engage with the wider public.
Supporting evidence
Equality Impact Assessments (EQIA) completed for all Public Health Wales policies
DDA audits
Single Equality Scheme
Welsh Language Scheme
Welsh Language Scheme Annual Monitoring Report
Dignity at Work Policy
Strategic Equality Plan

Public Health Wales Governance and accountability module
14
f) We apply and embed professional standards and quality requirements in a way that meets the needs and expectations of patients, service users, citizens and other stakeholders
Str
on
gly
dis
ag
ree
Dis
ag
ree
Neith
er
ag
ree n
or
dis
ag
ree
Ag
ree
Str
on
gly
Ag
ree
Supporting narrative
We receive regular scrutiny from internal and external auditors and other regulatory bodies to ensure that,
as a minimum, our services and activities comply with the national standards. We have also adopted and
embedded the Standards for Health Services which set national benchmarks for all our services and
activities. The Executive Team receives quarterly updates on how we are progressing our improvement
programme. This is then reported into the Quality and Safety Committee who have an oversight role.
Throughout the year the Quality and Safety Committee has received updates and presentations from each
division on their approaches to quality and any quality assurance systems in place.
CPA accreditation applies to microbiology and screening for compliance with national standards and
ongoing audit arrangements. The standards for health services have also been mapped to the CPA
standards.
Over a quarter of staff in Public Health Wales have taken up the Improving Quality Together challenge to
develop their quality improvement skills.
2012/13 was the first year that Public Health Wales produced an Annual Quality Statement. The
Statement provides an open and honest assessment of what Public Health Wales is doing to ensure all its
services are meeting the needs of the population of Wales and reaching high standards. It also provides a
summary highlighting how the organisation is striving to continuously improve the quality of the services it
provides and commissions in order to drive both improvements in population health and the quality and
safety of healthcare services. Public Health Wales participated in a peer review of all Annual Quality
Statement’s across NHS Wales. The Director of Nursing led a review team consisting of the Board
Secretary, Corporate Support Manager and Head of Nursing Screening. The team from Public Health
Wales reviewed the Powys Annual Quality Statement. Our statement was reviewed by the Welsh
Ambulance Service Trust. The review included a round table event chaired by the Chair of the Quality and
Safety Committee and contributions from staff who had detailed knowledge of specific areas across the
√

Public Health Wales Governance and accountability module
15
organisation. Learning from the peer review process will be used when preparing the statement for
2013/14.
The development of a Nursing and Midwifery strategy for Public Health Wales is underway and will
identify, underpin and support regulatory and fitness to practice requirements. This will be ratified at the
Public Health Wales Board in May 2014.
Further work will be progressed for other regulated health professional groups, Health Care Support
Workers and those in non medical Public Health roles.
2013/14 was the first full year of revalidation for the medical workforce. At the end of March 2014 25
percent of the workforce with a prescribed connection underwent revalidation. All received a positive
recommendation with no deferrals. Revalidation for medical staff will continue in 2014/15.
There is currently no systematic way for talking to the public about health, although it does work well in
some areas. Inroads have been made through the social media strategy where feedback has been sought
via social media channels. The ‘Add to Your Life’ over 50s health check has been developed following
close discussions with the public and service users and provides an example of how this can be taken
forward in others areas of the organisation.
Supporting evidence
Annual Quality Statement
Doctor / Nurse registration
CPA and UKAS accreditation
Screening Quality Standards
HSE Regulations / Regulatory Bodies
Medical revalidation
Annual performance reviews
1000 Lives improvement
Public Health Workforce Development programmes

Public Health Wales Governance and accountability module
16
Theme 1- Setting the direction: Your overall assessment
In relation to this particular theme, what is your overall assessment of where and how you:
are governing well
need to strengthen your arrangements
have noteworthy practice which you may wish to share
Governing well
Public Health Wales has an established Board and governance arrangements in place. We have refreshed our strategy to continue to
provide a clear purpose. We continue to develop and deliver our services to improve overall health and wellbeing. This can be evidenced
through the Health Improvement Review, introduction of new screening programmes, modernisation of screening programmes and
microbiology services.
Strengthen arrangements
We need to strengthen our learning from service users and stakeholders to inform service improvement and focus on embedding equality
and diversity within the organisation.
Noteworthy practice for sharing
The Health Improvement Review was a key piece of work where collaboration and engagement led to recommendations for service
improvement.
What maturity level have you demonstrated you have reached for this theme overall: 3
‘We are developing plans and processes and can demonstrate progress with some of our key areas for improvement.’
In relation to this particular theme, what are your priorities for improvement, what action are you going to take (and
when) and how will you measure your success?
Priorities for improvement Action to be taken Timescale Measure of success
Foster learning from service user
experience and complaints
Service user group
Service user engagement
strategy
Patient stories at Board
meetings
To be completed by March
2015
Service user feedback
performance reports will be
embedded into the reporting
system
Board will have opportunities to

Public Health Wales Governance and accountability module
17
hear from service users directly.
Strengthen equality and diversity
within organisation
Identify and deliver appropriate
training and development in
relation to equality and
diversity
Implement strategic equality
plan
To be completed by March
2015
Equality and diversity will be
embedded within the
organisation
Strengthen the lines of
professional accountability.
Develop nursing and midwifery
strategy
Clarify lines of accountability
To be completed by March
2015
Approved nursing and midwifery
strategy
Strengthen engagement with
service users and stakeholders
Review stakeholder
communications and
engagement strategy and
actions
Year 2 of Integrated Medium
Term Plan – 2015/16
Stakeholders, service users and
the public will be engaged in our
planning and all that we do.

Public Health Wales Governance and accountability module
18
Theme 2 – Enabling delivery Desired outcomes: We make sure that everyone involved in delivering health services understands each others contribution, and how together we can deliver a better service
We work constructively in partnership with others to improve the quality and safety of services for our patients, service users and the wider community We foster innovation and make the best use of all the resources available to us, including our
people, facilities and finances

Public Health Wales Governance and accountability module
19
a) We have the right people, with the right skills, doing the right things, in the right place, and at the right time to meet our responsibilities for the provision of safe, high quality care
Str
on
gly
dis
ag
ree
Dis
ag
ree
Neith
er
ag
ree n
or
dis
ag
ree
Ag
ree
Str
on
gly
Ag
ree
Supporting narrative
We have developed an integrated medium term plan, which includes workforce development and has been
approved by the Board.
As a result of engagement sessions with staff and the feedback from the NHS Wales staff survey, we have
developed a leadership and management development programme. This will strengthen the skills set for
many members of staff.
The Wales Audit Office reviewed the management arrangements for the Screening Division, and found
that while management was effective it was not efficient and would not be sustainable with the increased
portfolio of programmes. Management arrangements were amended and an overarching senior
management team was developed for the division. A similar Wales Audit Office review was also completed
for the management arrangements in the Microbiology Division which identified a number of areas for
improvement. An action plan has been put in place to address the issues raised.
A number of divisions are undergoing service redesign / modernisation. There is a risk that the results of
the changes in these service areas may leave people in the wrong place with the wrong skills. The Public
Health Development Directorate was significantly understaffed a consultant level at the beginning of the
year. Plans have been developed to increase the number of consultants in the Directorate and
recruitment processes have started.
All staff are required to undertake statutory and mandatory training. This has previously been identified
as an area which needs to improve. Further resource is needed to enable delivery of training where
necessary and work is being done to encourage line managers to take responsibility for making sure their
staff are up to date with their training requirements. The existing training database does not contain
accurate and up to date training records and further work is needed to establish whether all staff require
all levels of statutory and mandatory training. The Board has agreed to continue to monitor progress in
√

Public Health Wales Governance and accountability module
20
this area. Work is in hand to identify which areas of the organisation are falling below the expected level
of activity so attention can be focussed on the highest risk area. The Board feels that the level of marking
in this section reflects the level of improvement needed in this area. A higher marking will only be
achieved once this area has improved.
Supporting evidence
Integrated medium term plan to include finance, workforce and delivery plans
Professional registration
Defined and Practitioner registration
Performance Policies
Concerns and incident reporting policy and process
Medical revalidation
Annual performance reviews
Nursing and midwifery strategy
b) The different services and parts of our organisation/business work well together, and everyone understands who does what and why
Str
on
gly
dis
ag
ree
Dis
ag
ree
Neith
er
ag
ree n
or
dis
ag
ree
Ag
ree
Str
on
gly
Ag
ree
Supporting narrative
An organisational development plan has been shaped by the Executive Team which is closely aligned with
a three year delivery plan and financial plan.
Feedback from staff has been received via the staff survey and other engagement events which have
identified that staff feel more work is needed to ensure all parts of the organisation are working well
together. A Director of Health and Healthcare Improvement and Director of Policy, Research and
Development have been recruited which goes some way towards helping to resolve this issue.
Difficulties are experienced from working across multiple sites and this was highlighted in 2012/13 as an
issue. The ‘our space’ programme was launched in 2013 and aims to align flexible working practices, new
technology and the organisation’s accommodation strategy to enable Public Health Wales to move toward
√

Public Health Wales Governance and accountability module
21
developing a workplace for the future. An early part of the programme invited staff to attend a series of
workshops where they could feed in their views about how the organisation works together.
A new leadership and delivery group has been established to support the Executive Team and this will be
further supported by an operational group comprising corporate services. This will foster collaborative
working between areas of the organisation.
Supporting evidence
Public Health Wales Board structure
Public Health Wales Executive Team structure, terms of reference and papers
Divisional Director and Assistant Director structures
Executive Director monthly reports to Executive Team
Internal consultation documents
Service Delivery Model project documents
Terms of reference for the leadership and delivery group
Naming and branding strategy
Corporate communications strategy
Public Health Wales Staff e-bulletins
Public Health Wales intranet site
Information exchange process
Terms of reference and documents for the National Forum
Staff Conference feedback reports

Public Health Wales Governance and accountability module
22
c) We properly safeguard all those who work in or access our health services (including those who may accompany patients or service users), paying particular attention to the needs of children and vulnerable adults
Str
on
gly
dis
ag
ree
Dis
ag
ree
Neith
er
ag
ree n
or
dis
ag
ree
Ag
ree
Str
on
gly
Ag
ree
Supporting narrative
Those who work in our services
All Public Health Wales staff are provided with a job description, which contains specific responsibilities
and common responsibilities, relating to risk management, competence, supervision and health & safety
and in addition all staff must attend mandatory training in safeguarding adults and children every 3 years
All relevant staff receive a Disclosure and Barring check prior to taking up employment.
Safeguarding Children and Safeguarding Adults with Vulnerabilities policies have been developed to assist
staff in recognising and acting on abuse and neglect as well as Guidance on working with sexually active
young people and adults with vulnerabilities. Staff can raise concerns in a number of ways, including via
the Whistleblowing Policy, (section 5 page 6 of the policy which details the three steps that staff can follow
to escalate their concern) and if staff have concerns regarding professional abuse there is a policy for
Managing Allegations of Abuse by Staff. Staff are encouraged to raise issues via any mechanism they feel
comfortable with. This can include raising issues with staff representatives, line managers and in local
team meetings. If the issue cannot be dealt with at a local level, they should be escalated up to a
Director, or, to one of the relevant Governance Committees or Corporate Leads.
A Domestic Abuse and Sexual Violence Policy is in place to assist mangers and staff in dealing with
domestic violence in the workplace and an implementation plan is being developed which will include
training.
A Health and Safety Lead was appointed in August 2012. This appointment further strengthens the
safeguarding and protection of all assets, including the staff within the organisation. The individual left
the organisation in November 2013 and an interim arrangement was put in place to ensure there was no
√

Public Health Wales Governance and accountability module
23
risk to the organisation. More permanent arrangements will be put in place as soon as possible.
A Named Nurse for Safeguarding provides leadership, expert advice and ensures procedures are in place
to support staff in relation to responsibilities in safeguarding. A safeguarding strategy ‘Safeguarding in
Public Health Wales’ has been developed which includes safeguarding children and vulnerable adults. This
strategy also specifies that training is mandatory for all staff and Board members. This is an area which
required improvement, as compliance rates are below target.
Those who access our services
The Named Nurse Safeguarding ensures that there are safeguards in place to provide assurance that the
services provided by Public Health Wales are safe for children and adults with vulnerabilities. In addition
the Safeguarding Children Service is an independent service of designated professional experts, providing
assistance in keeping children safe to the wider NHS in Wales.
HealthWRAP training to support the Prevent anti-terrorist strategy is delivered to relevant staff.
Complaints and concerns raised by children, young people and vulnerable adults are dealt with under the
Putting Things Right – handling concerns, complaints and claims policy. There has been no significant
increase in the number of complaints received to date compared to last year.
Supporting evidence
Quality and Safety Committee terms of reference
Risk Management Group terms of reference
Safeguarding in Public Health Wales strategy
Safeguarding Children Policy and supporting procedures
Safeguarding Adults with Vulnerabilities Policy
Managing Allegations of Abuse by Staff
Domestic Abuse and Sexual Violence Policy
Guidance for working with sexually active young people and adults with vulnerabilities
Safeguarding Group terms of reference
Named Nurse for Safeguarding
Safeguarding Annual Report submitted to Quality and Safety Committee
Cross ref to Standards 11 – Safeguarding Children and Vulnerable Adults
Reports routinely received by Executive Team and Committees: incident reporting; complaints and
concerns; legal claims; DATIX.
Safeguarding Children Service

Public Health Wales Governance and accountability module
24
d) We have the right facilities (equipment and environment) to enable us to consistently deliver safe, high quality services across all the communities we serve
Str
on
gly
dis
ag
ree
Dis
ag
ree
Neith
er
ag
ree n
or
dis
ag
ree
Ag
ree
Str
on
gly
Ag
ree
Supporting narrative
A facilities Manager was appointed in early 2013 to ensure that existing facilities are maintained to the
highest standards. An estates database has been created to provide a central reference point for all
information available on the buildings occupied by Public Health Wales. This also includes a list of fire
wardens for each location and, in completing this work, the facilities manager has secured sufficient fire
wardens for each location. An asbestos management plan has also been developed for the organisation
which has assisted in minimising the risk of asbestos to the workforce and users of our facilities. An
internal audit report into asbestos was completed in 2014. It confirmed that work was underway to
address asbestos management arrangements in the organisation, but also identified a number of areas for
improvement. An action plan has been developed and will be implemented during 2014/15.
The organisation does experience some difficulties from working across multiple sites, which was identified
last year. Results from the staff survey and other engagement fora have highlighted that difficulties are
experienced by staff willing to work together. A review of accommodation is underway as part of a wider
project entitled ‘our space’. Workshops have concluded where staff were invited to pass on their views
and opinions to inform the future direction of the project. The project aims to create a modern fit for
purpose working environment that will make better use of space; incorporate new technology and flexible
working practices to support the delivery of organisational priorities and the revised healthier, happier and
fairer Wales strategy. It is hoped the review of accommodation can assist in improving cohesion and
understanding across the organisation of different team’s contributions and priorities.
Microbiology and Screening laboratories are subject to formal standards for health and safety and work to
standing operating procedures and this is assessed via CPA accreditation.
Supporting evidence
Business planning
Capital programme
√

Public Health Wales Governance and accountability module
25
Estates SLA
Estates consultation
Estates strategy
Standard 22 – Risk, Health and Safety Management
H&S and Infection Control Policy
Accommodation Strategy
e) We support the development and delivery of high quality, safe and accessible services through strong, effective financial planning and management
Str
on
gly
dis
ag
ree
Dis
ag
ree
Neith
er
ag
ree n
or
dis
ag
ree
Ag
ree
Str
on
gly
Ag
ree
Supporting narrative
Regular finance reports are forwarded to the Board and monthly financial performance reports are
submitted to the Welsh Government along with monthly Director of Finance commentary. Monthly
financial position / performance reports are also presented to the Public Health Wales Executive Team and
to individual divisional directors.
The Wales Audit Office audits the accounts on an annual basis and provide assurance in the form of an a
structured assessment and annual audit report. For 2013/14 the WAO made some minor
recommendations for improvement but overall concluded that governance arrangements for the
organisation were sound. In addition, the NHS Wales Shared Services Partnership – Audit & Assurance
Services undertake regular audits of financial and associated systems, along with providing assurance on
internal control.
Regular training sessions on budgetary control are provided and all new budget holders are required to
complete this training. The Trust has a budgetary control procedure and a finance guide is available on
the intranet, which includes information on both budgetary and financial control.
An integrated medium term plan has been developed which includes a financial plan.
Supporting evidence
√

Public Health Wales Governance and accountability module
26
Board reports;
WAO Structured Assessment
Budget strategy for 2012/13
Annual Governance Statement
Annual accounts letter
Vacancy control process
WAO and Internal Audit Reports
f) Our workforce at all levels in the organisation/business are equipped with the information they need to help them carry out their work effectively, and this information is shared appropriately and securely held
Str
on
gly
dis
ag
ree
Dis
ag
ree
Neith
er
ag
ree n
or
dis
ag
ree
Ag
ree
Str
on
gly
Ag
ree
Supporting narrative
Staff can access information from a wide variety of sources, including:
Specific information systems used by specific services (eg laboratory information management
systems (LIMS), screening programme call/recall systems)
Internal websites and document databases
Library and knowledge management service and Observatory
External sources facilitated by internet and intranet access
There is a strong informatics function specialising in areas specific to the organisations activity (including
screening, surveillance, microbiology). All staff have access to IT equipment for them to carry out their
work. The Wales Audit Office undertook a review of the organisation’s approach to data quality in
2012/13 and the outcome of this is being used to inform future developments, in particular, the reporting
mechanisms for data quality. During 2013/14 the Wales Audit Office carried out an audit of data backup
arrangements and identified some areas for improvement, but also noted that action was already
underway to address these areas which required improvement.
The Information Governance Committee; Information Governance Working Group; and local Information
Governance contacts all contribute to the effecting sharing of information and secure storage of
√

Public Health Wales Governance and accountability module
27
information. The Committee is reassured by the low number of complaints and errors which are reported
in relation to Information Governance.
The ‘Our Space’ programme is also considering ways of working across the organisation and part of this
work will look at accessing and sharing of information for staff. Staff feedback has identified that some
staff experience issues with the IT infrastructure in the organisation. This has prompted the informatics
team to set up a process for staff to use their own devices for work purposes, whilst retaining full security
of data and information, which goes some way to addressing the concerns raised.
Supporting evidence
Intranet
Internet
E-bulletin
Information Governance Committee minutes and Terms of Reference
Information Governance Working Group minutes and Terms of Reference
Policies and Procedures
g) We are an innovative organisation/ business that takes proper account of the risks
(both opportunities and threats) to the achievement of our aims and objectives S
tro
ng
ly
dis
ag
ree
Dis
ag
ree
Neith
er
ag
ree n
or
dis
ag
ree
Ag
ree
Str
on
gly
Ag
ree
Supporting narrative
Public Health Wales has a risk management strategy in place which includes a risk management
framework. The strategy involves 5 key areas: developing risk management in Public Health Wales;
embedding key risk management systems and processes; ensuring statutory compliance; ensuring Public
Health Wales is risk aware and staff are appropriately trained and skilled in risk management; ensuring
compliance with regulation and monitoring.
The Audit Committee receives the corporate risk register at each meeting. As part of a self assessment of
the Committee’s effectiveness, it has identified that it must start reviewing the assurances which are in
place for each risk. Internal audit has identified issues surrounding the reporting of risk within
organisational flows and made recommendations for improvement in relation to screening programmes
√

Public Health Wales Governance and accountability module
28
and asbestos management in particular. The Information Governance Committee reviews and scrutinises
all information governance risks and the Quality and Safety Committee review all risks relating to quality
and safety.
All incidents are reported to the Quality and Safety Committee. Any risks that are identified as a result of
reported incidents, are discussed in detail and appropriate risk assessments and action plans developed.
The Executive Team has questioned the way risks are managed in the organisation and have sought
independent advice and support on how to improve and embed risk management within the organisation.
Supporting evidence
Corporate Risk Register
Board and Committee structure and terms of reference
Executive Team Terms of Reference
Research & Development Committee terms of reference
Risk Management Group terms of reference
Health & Safety Group terms of reference
Champions for Health
Improving Quality Together
Digital Mammography
Health Protection
Early Years work
Sustainable Communities work
h) We have strong, effective relationships with our workforce, partners, citizens and other stakeholders
Str
on
gly
dis
ag
ree
Dis
ag
ree
Neith
er
ag
ree n
or
dis
ag
ree
Ag
ree
Str
on
gly
Ag
ree
Supporting narrative
Workforce
√

Public Health Wales Governance and accountability module
29
We work closely in partnership with staff and staff representatives through the Partnership Forum and
local negotiating arrangements. Representatives from the partnership forum have been invited to attend
Board meetings as a full, non-voting, Board member.
Staff engagement events have taken place to discuss the organisation’s response to the Francis Review
and to take part in a conversation about what is expected of leaders and managers and through the staff
survey. Action plans and proposals have been developed to address the issues raised by staff.
Partners / stakeholders
Staff within the organisation work closely with health boards and local authorities. The main contact with
local authorities is through the local public health teams. We have a long-standing vacancy on the Board
for a local authority Board member. This poses a considerable risk to our relationship with local
authorities in Wales. Efforts are continuing to recruit to this position and an interim appointment is
currently being sought.
There are well established health protection partnership arrangements with Consultants in Communicable
Disease Control appointed as ‘responsible officers’
Staff representatives are members of all Wales peer groups eg NHS Wales Chairs, Vice Chairs, Chief
Executives, Directors of Finance, Medical Directors, etc. Chairs of Committees also attend meetings with
their respective all Wales Committee Chairs.
A Public and Stakeholder Engagement Strategy is in place but more work is needed to establish whether
staff are following the actions.
Citizens
A Public and Stakeholder Engagement Strategy was developed after working with communications officers
from local health boards, local authorities, the Welsh Government and other public sector organisations to
map public engagement channels and methods with a view to sharing them for collective use.
We regularly use social media to communicate with citizens and stakeholders. We established successful
routes of communication during measles outbreak and this included an effective use of social media. WE
are reviewing our use of social media to ensure we are maximising every opportunity for engagement
through this medium.
It has been identified that the organisation would benefit from a forum/mechanisms for planning,
developing or getting a public mandate for health improvement.
Public Health Wales Governance and accountability module
30
Supporting evidence
Partnership Forum terms of reference
Naming and branding strategy
Staff engagement workshops and other fora
Heads of Agreement between Public Health Wales, the Welsh Government, Health Boards and Local
Authorities
Microbiology Service Level Agreements
Terms of reference for the NHS Wales Chief Executives Group
Screening Engagement Annual Report
Public and Stakeholder Engagement Strategy
Service user experience reports submitted to Welsh Government

Public Health Wales Governance and accountability module
31
i) Decisions taken throughout our organisation are made by those best placed to do so, are well informed, timely and are effectively communicated
Str
on
gly
dis
ag
ree
Dis
ag
ree
Neith
er
ag
ree n
or
dis
ag
ree
Ag
ree
Str
on
gly
Ag
ree
Supporting narrative
All decisions taken by the Board and Committees are made openly and transparently.
The Wales Audit Office produce a structured assessment each year for Public Health Wales. Last year
(2012) they concluded that the governance arrangements and functioning of the Board were sound, but
that there some recommendations which could further strengthen the organisation’s decision making
processes. All recommendations made have now been completed.
The structured assessment for 2013 concluded that in general, the Trust has good arrangements for
governance and board assurance but work remains to strengthen some components of the governance
framework. Improvements were identified for:
Internal controls in relation to statutory and mandatory training need to improve.
The Trust’s draft backup and recovery polices have yet to be formally agreed and some plans and
procedures for individual systems are out of date.
there are gaps in information on service user experience to help improve and shape services.
the Trust’s approach to identifying and recording divisional risks needs to be reviewed and
improved. It is not clear that risk registers are reviewed regularly
Board, Committee and Executive Team paper are published routinely on the Public Health Wales website.
A new leadership and delivery group has been established and will be supported by an operation group.
The National Forum will continue to meet quarterly.
Supporting evidence
Board intranet page
Executive Team terms of reference
Board Committees terms of reference
Executive Team communications process and paper
√

Public Health Wales Governance and accountability module
32
National Forum papers
Standing Orders & Standing Financial Instructions
Scheme of Delegation
Screening services implementation of service user action plan
Stop Smoking Wales focus on improving efficiency of service in response to service user feedback
Theme 2 – Enabling delivery:
Your overall assessment
In relation to this particular theme, what is your overall assessment of where and how you:
are governing well
need to strengthen your arrangements
have noteworthy practice which you may wish to share
Governing well
We continue to achieve high quality, safe and accessible services through sound financial planning and management. The organisation is
forecast to a balanced position for 2013/14 and has even identified areas of savings to broker some funds back to Welsh Government to
assist the wider NHS Wales financial position.
Our governance arrangements are generally sound.
Strengthen arrangements
A number of issues have been identified with staff working across different locations and a project is underway to address these issues
and propose options to improve accommodation and ways of working.
Compliance rates for statutory and mandatory training continue to be a concern and risk to the organisation. Work is continuing to
improve compliance rates and this remains a priority for 2014/15.
The Executive Team has identified the need to review risk management across the organisation and has sought independent advice.
Noteworthy practice for sharing
The 1000 Lives improvement service continues to support health boards in national and local improvement work.
The microbiology and screening divisions engage with others in the same business.

Public Health Wales Governance and accountability module
33
What maturity level have you demonstrated you have reached for this theme overall: 3
We are developing plans and processes and can demonstrate progress with some of our key areas for improvement.
In relation to this particular theme, what are your priorities for improvement, what action are you going to take (and
when) and how will you measure your success?
Priorities for improvement Action to be taken Timescale Measure of success
Consider ways to improve issues
arising from staff working across
different locations
Our Space programme Phase 1 and 2 to be
completed by March 2015
Reduce number of buildings
occupied by Public Health Wales
and co-locate staff
Improve compliance rates for
statutory and mandatory training
Implementation of statutory
and mandatory training policy
Work with managers to ensure
increase in compliance
March 2015 Compliance rates should either
meet, or exceed, target.
Recruit to local authority Non
Executive Director
Appoint interim position for 12
months, whilst awaiting
amendment to regulations to
allow full appointment
June 2014 Successful interim appointment
to be made.
Review risk management
arrangements
Good Governance Institute to
undertake a review of risk
management arrangements
Refresh approach to risk
management to ensure it is
embedded across the
organisation
Good Governance Institute
report due in June 2014
Refreshed, embedded
approach to be complete by
March 2015
Risk management arrangements
to be embedded across
organisation with divisional risk
registers feeding into corporate
risk register and linked to
integrated medium term plan.

Public Health Wales Governance and accountability module
34
Theme 3 – Delivering results, achieving excellence
Desired outcomes: We provide high quality and accessible health services in a manner that ensures equity of access and minimises waste, harm and variation We build on our strengths and take early, decisive action to improve services where we need to. We learn from our own and others experiences to continuously improve the provision of health services We contribute to the overall improvement of health services in Wales by sharing our learning with others

Public Health Wales Governance and accountability module
35
a) We have a clear understanding of how well we are performing overall, what services are doing well, and what services need improving (including those services that are carried out by others on our behalf)
We respond quickly and effectively to address areas of concern, including those relating to individuals’ performance S
tro
ng
ly
dis
ag
ree
Dis
ag
ree
Neith
er
ag
ree n
or
dis
ag
ree
Ag
ree
Str
on
gly
Ag
ree
Supporting narrative
We have developed a revised planning and performance framework during the year, which has helped to
inform development of an integrated medium term plan. A Quality and Delivery Framework has been
developed which sets out a mixture of quantitative and qualitative measures to assess performance
internally and externally against strategic objectives. Performance reporting to the Board has improved
greatly throughout the year.
The Quality and Safety Committee places emphasis on identifying, reviewing and assessing quality
performance measures.
The Board has scrutinised performance data and commended areas which are doing well. They have
requested further assurance for areas which need improving and regularly monitor progress against
improvements. For example the Board noted a reduction in performance for breast screening and length
of time to recall women to screening. They requested a full and comprehensive briefing on performance
and what measures were in place to improve matters. The Board have continued to monitor this area
closely.
We collect service user feedback, however we need to improve on how we will use the feedback to
improve services. Patient stories or a mechanism for reviewing outward facing services to give an
overview of how the organisation is performing.
All medical staff are required to comply with medical revalidation. Non medical staff are required to
√
Public Health Wales Governance and accountability module
36
undergo regular performance review and personal development.
Engagement sessions with staff have identified a desire for more structured management and leadership
development. A programme has been approved by the Board and implementation will begin in 2014/15.
Supporting evidence
Standards for Health Services and CPA mapping
Quality management systems
Workforce and Organisational Development reports
Quality and Safety Committee reports
Audit Committee reports
Public Health Wales Strategy
Screening services implementation of service user action plan
Stop Smoking Wales focus on improving efficiency of service in response to service user feedback
b) We operate in accordance with all legal and other requirements placed on us S
tro
ng
ly
dis
ag
ree
Dis
ag
ree
Neith
er
ag
ree n
or
dis
ag
ree
Ag
ree
Str
on
gly
Ag
ree
Supporting narrative
The standing orders, standing financial instructions and scheme of delegation are reviewed periodically by
the Board and are available on the Public Health Wales internet.
The Annual Governance Statement is prepared in line with Welsh Government requirements and takes
account of best practice issued by HM Treasury. The Statement provides an assurance of the governance
arrangements in the organisation. The Audit Committee play a key role in the completion of the
statement and by providing assurance to the Board that the organisation is operating in accordance with
all requirements placed on us.
A Local Counter Fraud specialist is in place and reports regularly to the Audit Committee. They provide
specialist criminal investigation, surveillance capability and financial investigation services.
√

Public Health Wales Governance and accountability module
37
A Board Assurance Framework was approved by the Board in September 2013.
A review of the Terms of Reference for the Audit, Information Governance and Quality & Safety Committee
was completed in 2013/14 and has confirmed that there is no overlap in responsibilities between the
Committees. This has also clarified which information needs to be received by which committee.
Workplans for each Committee will be developed together to ensure clarity of roles.
The Wales Audit Office audits our accounts on an annual basis and provides assurance in the form of an
annual audit report and structured assessment. Internal audit arrangements are provided by NHS Wales
Shared Services Partnership – Audit and Assurance Services.
Statutory and mandatory training is required of all staff. However, improvements are needed in this area
because compliance rates are lower than expected.
Public Health Wales policies and procedures highlight any legislation relevant to the policy and efforts are
focused on improving compliance.
Recruitment and selection is undertaken in regard of legal, professional and best practice requirements to
ensure staff are aware and act in accordance with the legislation.
In the last year we have put in place a revised Strategic Equalities Plan (SEP) and a working group to
action the plan which has representation from across Public Health Wales. The SEP considers equality
issues affecting all aspects of our work as well as our workforce.
We also ensure all our facilities comply with the Disability Discrimination Act.
The Welsh Language Board approved our Welsh Language Scheme which demonstrates the commitment
to communicating with the public in the Welsh and English languages on the basis of equality and
championing the Welsh Language.
Supporting evidence
Board and Committee structure
Standing Orders
Standing Financial Instructions
Risk Management structure
Statutory requirements
Policies and procedures
Scheme of Delegations

Public Health Wales Governance and accountability module
38
Welsh Audit Office Structured Assessment report
Agreement with NHS Wales Shared Services Partnership
Counter-Fraud SLA
Health & Safety Professional Lead
Radiation advice provided by Velindre NHS Trust
Register of interests
CPA
UKAS (annual review meeting)
Standards for Health Services
Professional registration
Code of Conduct
Support Criminal Record Bureau checks
Welsh Language Scheme monitoring reports
Medical revalidation
c) We know what our citizens and others (including our workforce) think of us, and this influences what we do and how we do it
Str
on
gly
dis
ag
ree
Dis
ag
ree
Neith
er
ag
ree n
or
dis
ag
ree
Ag
ree
Str
on
gly
Ag
ree
Supporting narrative
A Public and Stakeholder Engagement strategy has been approved by the Board. Work is underway to
assess stakeholder and service user satisfaction more systematically and in line with the strategy. A
service user engagement group is being established which will assist with learning from service user
feedback and influence what we do and how we do it.
Currently feed back is received via the following routes:
The screening programmes conduct satisfaction surveys for some of the populations they invite for
screening.
The screening programmes also have a public information group which include user representatives and
which develop public information materials
As part of its quality management system, Public Health Wales microbiology services conduct
√

Public Health Wales Governance and accountability module
39
stakeholder satisfaction surveys.
The Public Health Wales Networks evaluate each of their conferences and have themselves been
externally evaluated
Other conferences are also evaluated
Stop Smoking Wales get user feedback from survey sheets
All Public Health Wales websites have a feedback facility
The Equality Group has received ‘patient stories’
In each of the above cases, views are fed into the relevant management groups for consideration and
action. These only represent part of the organisation and work is underway to make this routine across
the entire organisation.
Representatives from the partnership forum have been invited to attend Board meetings as full, non-
voting Board members. We are still establishing representation from professional groups.
As an all Wales organisation we have experienced difficulties in engaging with Community Health Council.
We identified this as an area for improvement last year and engagement has started. We aim to link with
Community Health Councils wherever possible.
The Trust is exploring opportunities to develop staff stories that can be shared with the Board, which
would ensure that geographically dispersed staff can raise concerns with the Board. Although the nature of
the Trust’s business makes it difficult for executives and non-executives to carry out regular planned and
unplanned walkarounds to see first-hand staff experience, the Board has taken positive action to travel
and meet staff deployed in different parts of the Trust and at different locations.
A number of improvements have been identified for how the organisation can learn from citizens and
others. Therefore, the scoring has been reduced from last year.
Supporting evidence
Screening Engagement annual report
Reports on the Screening Services satisfaction surveys
Public Health Wales websites feedback facilities
Web forum
Open blog
Putting things right
Staff survey
Equality Group
Service user experience reports submitted to Welsh Government

Public Health Wales Governance and accountability module
40
Screening services implementation of service user action plan
Stop Smoking Wales focus on improving efficiency of service in response to service user feedback
d) We measure our performance against ‘best practice’ and other standards set for the services we provide and we use the results to drive improvement in the provision of high quality, safe and accessible services
Str
on
gly
dis
ag
ree
Dis
ag
ree
Neith
er
ag
ree n
or
dis
ag
ree
Ag
ree
Str
on
gly
Ag
ree
Supporting narrative
Performance is regularly measured against ‘best practice’ from the UK and internationally. Screening
services, for example, regularly compare screening programmes with those taking place in England,
Scotland and Northern Ireland. Each programme is developed and improved using international evidence
and research. The all Wales pathology modernisation work programme has drawn upon international best
practice.
All screening programmes operate a total quality management framework and standards for delivery are
outlined in each programme specific quality manual. There is also an ongoing programme of evaluation
and all reports and statistics are published annually on the Screening website. Programme performance
and individual performance are monitored on an ongoing basis as this enables the service to target re-
training or interventions as required. Screening programmes are being developed further so that they
continue to meet performance standards.
Public Health Wales has strong links with international colleagues and members of staff regularly attend
international meetings and conferences where best practice and innovation is shared. An example is
Public Health Wales membership of Eurohealthnet and staff attendance at the European Public Health
Association (EUPHA) conference. The International Health Coordination Centre strengthens international
links and opportunities.
The 1000 Lives improvement service regularly draws on international work and comparisons when
introducing new service improvement initiatives. The target for smoking cessation is based on an
international benchmark.
Members of the Board, Executive Team and staff within the organisation attend all Wales and international
√

Public Health Wales Governance and accountability module
41
meetings where best practice and experience is openly shared.
The Health and Healthcare Improvement Division has undertaken a series of tobacco control workshops
where best practice and other standards can be developed and shared amongst those working on smoking
cessation.
Supporting evidence
Standards for Health Services
Internal and External audit reviews
Reviews and inspections by regulatory bodies
UK and worldwide published data
WG guidance and instructions
Quality Delivery Plan
Internal performance data
NHS Wales Shared Services Partnership Committee
Staff involvement with professional groups
Staff Membership of professional bodies
International conferences and activities
Sharing of best practice within and between professional groups via regular monthly / quarterly
meetings
1000 Lives improvement service quarterly Learning Sessions and Webex meetings

Public Health Wales Governance and accountability module
42
e) We learn from our own and others experiences, and in turn share our learning with others
Str
on
gly
dis
ag
ree
Dis
ag
ree
Neith
er
ag
ree n
or
dis
ag
ree
Ag
ree
Str
on
gly
Ag
ree
Supporting narrative
We foster a sense of learning through engagement with others.
Board meetings are planned to foster learning from others and sharing experiences. Alternate Board
meetings take place in localities across Wales and individuals are invited to present to the Board to share
learning experiences. We hold an annual general meeting which provides an opportunity for staff and
stakeholders to reflect on the work undertaken during the year. A leadership and delivery group has
been established to facilitate learning across divisions and directorates.
We play a full part in the all Wales networks and are engaged in all areas where experiences are shared
and discussed.
We have strong links with the Chief Medical Officer and Chief Nursing Officerin Welsh Government, Public
Health England and public health colleagues in England, Scotland and Northern Ireland. The Director for
Public Health Development attends meetings of the ‘5 nations’ (Wales, England, Scotland, Northern
Ireland, Republic of Ireland) and the Director for Public Health Services attends meetings of the Public
Health England Advisory Board and Director of Nursing is developing stronger links with counterparts
within the four nations.
The Welsh Public Health conference is coorganised by Public Health Wales and provides a forum for
sharing of experiences and learning and is highly regarded amongst professionals in Wales and the UK.
The health protection team take part in formal reviews in relation to health protection and regular debriefs
during and after outbreaks. The measles outbreak has provided an opportunity to share learning with
others and a delegation attended and presented at the American Public Health Conference in Boston.
Supporting evidence
√

Public Health Wales Governance and accountability module
43
Welsh Government reviews
Annual General Meeting (AGM)
Stakeholder meetings
Director of Public Health meetings
All Wales Medical Director meetings
All Wales Nurse Director meetings
Board meetings
Committee meetings
Bevan Commission
Advisory committees
Regular meetings of Chief Executives; Executive Directors; Chairs; Board members etc.

Public Health Wales Governance and accountability module
44
Theme 3 – Delivering results, achieving excellence: Your overall assessment
In relation to this particular theme, what is your overall assessment of where and how you:
are governing well
need to strengthen your arrangements
have noteworthy practice which you may wish to share
Governing well
We have developed revised performance and planning arrangements.
We operate within all legal and other requirements placed upon us.
Strengthen arrangements
We need to improve learning from service user engagement.
Noteworthy practice for sharing
We have applied learning from the measles outbreak and presented findings at conference in Boston
What maturity level have you demonstrated you have reached for this theme overall: 3
We are developing plans and processes and can demonstrate progress with some of our key areas for improvement.
In relation to this particular theme, what are your priorities for improvement, what action are you going to take (and
when) and how will you measure your success?
Priorities for improvement Action to be taken Timescale Measure of success
Learning from service user
experience
Service user group
Service user engagement
strategy
Patient stories at Board
meetings
To be completed by March
2015
Service user feedback
performance reports will be
embedded into the reporting
system
Board will have opportunities to
hear from service users directly.
Improve compliance with
statutory and mandatory training
Implementation of statutory
and mandatory training policy
Work with managers to ensure
increase in compliance
March 2015 Compliance rates should either
meet, or exceed, target.

Public Health Wales Governance and accountability module
45
Standards for Health Services Governance and Accountability Maturity Matrix
1 2 3 4 5
We do not yet have a clear, agreed
understanding of where we are (or how we are
doing) and what / where we need to improve
We are aware of the improvements that
need to be made and have prioritised them,
but are not yet able to demonstrate
meaningful action.
We are developing plans and processes
and can demonstrate progress with some of
our key areas for improvement
We have well developed plans and
processes and can demonstrate
sustainable improvement
throughout the organisation /
business
We can demonstrate sustained good
practice and innovation that is
shared throughout the organisations /
business, and which others can learn from

Public Health Wales Annual accounts and Annual GovernanceStatement 2013/14
Date: 16 June 2014 Version:1 Page: 1 of 2
Annual accounts andAnnual Governance Statement 2013/14
Purpose of Document:The annual accounts and Annual Governance Statement for 2013/14 were approvedby the Public Health Wales Audit Committee on 5 June 2014 and submitted to theWelsh Government on 6 June 2014. The Board are asked to ratify the approval of theaccounts and governance statement.
Board/Committee to- (Please indicate)
To decide- Paper will outline recommendations or issues to be approved bythe Board or Committee.
X
To discuss- Board or Committee will be asked to discuss and scrutinise thepaper and provide feedback and comments.
To inform- Board or Committee will be asked to note the paper forinformation only
Other relevant information
Please include any recommendations/details of decisions Board/Committees are askedto make.Next Steps
The Board are asked to ratify the approval of the annual accounts and AnnualGovernance Statement for 2013/14.
Link to Public Health Wales commitment and priorities for action:(please tick which commitment(s) is/are relevant)
x
Priorities for action Put in place an effective governanceframeworkEnsure financial sustainability
Author: Ms Tamira Rolls, Assistant Director of Finance and Ms Eleanor Higgins,Corporate Governance ManagerDate: 16 June 2014 Version: 1
Sponsoring Executive Director: Mr Huw George, Executive Director ofFinance and Mr Keith Cox, BoardSecretary
Paper reference – 32 07

Public Health Wales Annual accounts and Annual GovernanceStatement 2013/14
Date: 16 June 2014 Version:1 Page: 2 of 2
Who will present: (If appropriate) Mr Huw George / Mr Keith CoxDocuments attached:(If appropriate)
Annual accounts 2013/14Annual Governance Statement 2013/14
Date of meeting: 26 June 2014Committee/Groups that havereceived or considered this paper:
Audit Committee
Link to standardsfor health services
Standard 1: Governance and Accountability
Link to risk register Risk ID 87: Failure to meet statutory brake even duty. Failureto full savings targets outstanding WG funding Cost of wageawardsRisk ID 102: Ensuring the Public Health WalesGovernance/assurance and performance managementframework evolves to reflect the changing organisation andchanging external governance environment whilst continuingto meet statutory obligations.
Equality impactassessment
N/A
Financialimplications
N/A
Service userengagement
N/A

Public Health Wales NHS Trust Annual Accounts 2013-14
Foreword
Public Health Wales NHS Trust
These accounts for the period ended 31 March 2014 have been prepared to comply with International Financial Reporting Standards (IFRS) adopted by the European Union, in accordance with HM Treasury's I-FReM by the Public Health Wales NHS Trust under schedule 9 section 178 Para 3 (1) of the National Health
Service (Wales) Act 2006 (c.42) in the form in which the Welsh Ministers, with the approval of the Treasury, directed.
The establishment of Public Health Wales in 2009, created for the first time, an
independent NHS body with a clear and specific public health focus, and a remit to act across all the domains of public health practice. The Minister for Health and Social Services confirmed Public Health Wales would provide the national resource for the effective delivery of public health services at national, local and community level. Public Health Wales originally incorporated the functions and services previously provided by the National Public Health Service (NPHS), Wales Centre for Health
(WCfH), Welsh Cancer Intelligence Surveillance Unit (WCISU), Congenital Anomaly Register and Information Service (CARIS) and Screening Services Wales.
Since 2009, we have continued to grow, taking on a range of additional functions
and services from both the Welsh Government and NHS Wales, including the Programme Management Unit, several Health Improvement Programmes, Newborn Bloodspot Screening, Abdominal Aeortic Aneurism Screening and the Wrexham Microbiology Laboratory. One of the outcomes of the review into the former National Leadership and Innovation Agency for Healthcare (NLIAH), was that the improvement functions within NLIAH transferred into Public Health Wale on April 1st 2013, along with the
functions of equality and human rights.
The overall income level for Public Health Wales has increased by over 25 per cent over the last four years, from just over £80m in 2010/11 to £105m in 2013/14.
Furthermore, the National Cancer Service Advisory Group (NCSAG) will be transferring into Public Health Wales from Velindre NHS Trust on April 1st 2014,
with a budget of £240k. The financial target of payment of 95% of all invoices (by number) was not met in 2013/14, with the actual performance at 93.9%; missing the target by just 1.2%. This is a direct result of a several changes to both the reporting requirements and
the operating arrangements for the payment of invoices. Although performance increased during the second half of the financial year, following several
improvements to operational arrangements, the cummulative performance for the year remains below the 95%. The payment of 95% of all invoices by value has
been met. However both statutory targets of acheiving financial balance and remaining within
our EFL have been met again in 2013/14. The accounts that follow present a balanced position, with a small retained surplus of £15k.

Public Health Wales NHS Trust Annual Accounts 2013-14
STATEMENT OF COMPREHENSIVE INCOME FOR THE YEAR ENDED 31 March 2014
2013-14 2012-13
Note £000 £000
Revenue from patient care activities 2 83,044 79,098
Other operating revenue 3 22,038 19,299
Operating expenses 6 (105,033) (98,314)
Operating surplus/(deficit) 49 83
Investment revenue 7 16 55
Other gains and losses 8 0 (86)
Finance costs 9 (50) (42)
Retained surplus/(deficit) 33.1 15 10
Other Comprehensive Income
Items that will not be reclassified to net operating costs:
Net gain/(loss) on revaluation of property, plant and equipment 56 0
Net gain/(loss) on revaluation of intangible assets 0 0
Net gain/(loss) on revaluation of financial assets 0 0
Net gain/(loss) on revaluation of PPE and Intangible assets held for sale 0 0
Impairments and reversals 0 (187)
Movements in other reserves 0 0
Transfers between reserves 0 0
Net gain/loss on Other Reserve 0 0
Reclassification adjustment on disposal of available for sale financial assets 0 0
Sub total 56 (187)
Items that may be reclassified subsequently to net operating costs
Net gain/(loss) on revaluation of financial assets held for sale 0 0
Sub total 0 0
Total other comprehensive income for the year 56 (187)
Total comprehensive income for the year 71 (177)
1
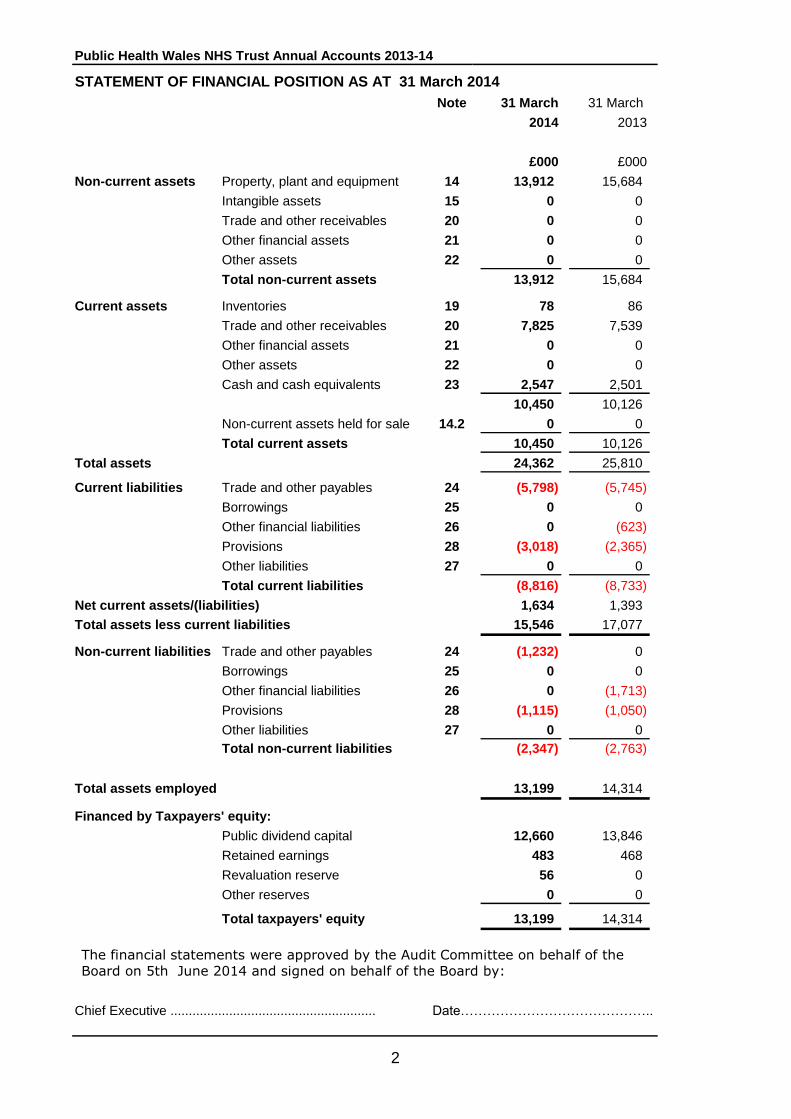
Public Health Wales NHS Trust Annual Accounts 2013-14
Note 31 March 31 March
2014 2013
£000 £000
Non-current assets Property, plant and equipment 14 13,912 15,684
Intangible assets 15 0 0
Trade and other receivables 20 0 0
Other financial assets 21 0 0
Other assets 22 0 0
Total non-current assets 13,912 15,684
Current assets Inventories 19 78 86
Trade and other receivables 20 7,825 7,539
Other financial assets 21 0 0
Other assets 22 0 0
Cash and cash equivalents 23 2,547 2,501
10,450 10,126
Non-current assets held for sale 14.2 0 0
Total current assets 10,450 10,126
Total assets 24,362 25,810
Current liabilities Trade and other payables 24 (5,798) (5,745)
Borrowings 25 0 0
Other financial liabilities 26 0 (623)
Provisions 28 (3,018) (2,365)
Other liabilities 27 0 0
Total current liabilities (8,816) (8,733)
Net current assets/(liabilities) 1,634 1,393
Total assets less current liabilities 15,546 17,077
Non-current liabilities Trade and other payables 24 (1,232) 0
Borrowings 25 0 0
Other financial liabilities 26 0 (1,713)
Provisions 28 (1,115) (1,050)
Other liabilities 27 0 0
Total non-current liabilities (2,347) (2,763)
Total assets employed 13,199 14,314
Financed by Taxpayers' equity:
Public dividend capital 12,660 13,846
Retained earnings 483 468
Revaluation reserve 56 0
Other reserves 0 0
Total taxpayers' equity 13,199 14,314
Chief Executive ........................................................ Date……………………………………..
STATEMENT OF FINANCIAL POSITION AS AT 31 March 2014
The financial statements were approved by the Audit Committee on behalf of the
Board on 5th June 2014 and signed on behalf of the Board by:
2

Public Health Wales NHS Trust Annual Accounts 2013-14
STATEMENT OF CHANGES IN TAXPAYERS' EQUITY
2013-14
Public
Dividend
Capital
Retained
earnings
Revaluation
reserve
Other
reserves Total
£000 £000 £000 £000 £000
Balance at 1 April 2013 13,846 468 0 0 14,314
Changes in taxpayers' equity for 2013-
14
Retained surplus/(deficit) for the year 15 15Net gain/(loss) on revaluation of property,
plant and equipment 0 56 0 56
Net gain/(loss) on revaluation of intangible
assets 0 0 0 0
Net gain/(loss) on revaluation of financial
assets 0 0 0 0
Net gain/(loss) on revaluation of PPE and
Intangible assets held for sale 0 0 0 0
Net gain/(loss) on revaluation of financial
assets held for sale 0 0 0 0
Impairments and reversals 0 0 0 0
Movements in other reserves 0 0 0 0
Transfers between reserves 0 0 0 0
Net gain/loss on Other Reserve (specify) 0 0 0 0
Reclassification adjustment on disposal of
available for sale financial assets 0 0 0 0
Reserves eliminated on dissolution 0 0
New Public Dividend Capital received 62 62
Public Dividend Capital repaid in year (1,186) (1,186)
Public Dividend Capital
extinguished/written off 0 0
Other movements in PDC in year (62) (62)
Balance at 31 March 2014 12,660 483 56 0 13,199
The notes on pages 6 to 89 form part of these accounts.
3
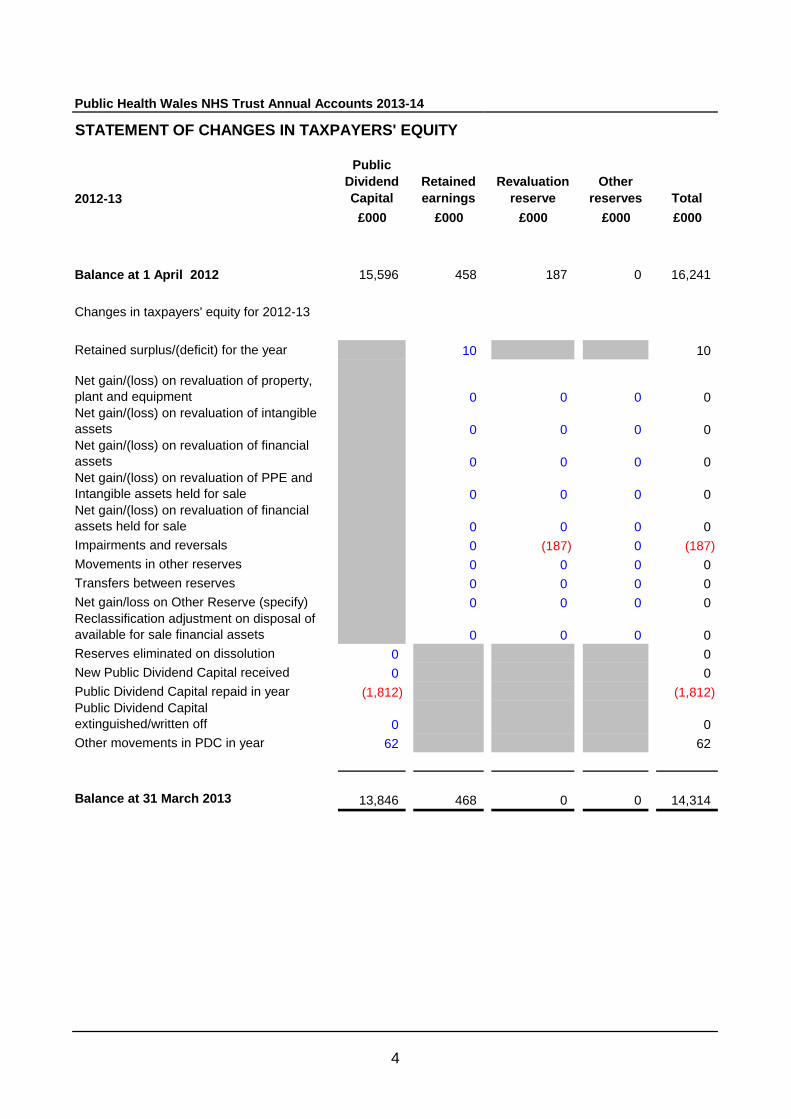
Public Health Wales NHS Trust Annual Accounts 2013-14
STATEMENT OF CHANGES IN TAXPAYERS' EQUITY
2012-13
Public
Dividend
Capital
Retained
earnings
Revaluation
reserve
Other
reserves Total
£000 £000 £000 £000 £000
Balance at 1 April 2012 15,596 458 187 0 16,241
Changes in taxpayers' equity for 2012-13
Retained surplus/(deficit) for the year 10 10
Net gain/(loss) on revaluation of property,
plant and equipment 0 0 0 0
Net gain/(loss) on revaluation of intangible
assets 0 0 0 0
Net gain/(loss) on revaluation of financial
assets 0 0 0 0
Net gain/(loss) on revaluation of PPE and
Intangible assets held for sale 0 0 0 0
Net gain/(loss) on revaluation of financial
assets held for sale 0 0 0 0
Impairments and reversals 0 (187) 0 (187)
Movements in other reserves 0 0 0 0
Transfers between reserves 0 0 0 0
Net gain/loss on Other Reserve (specify) 0 0 0 0
Reclassification adjustment on disposal of
available for sale financial assets 0 0 0 0
Reserves eliminated on dissolution 0 0
New Public Dividend Capital received 0 0
Public Dividend Capital repaid in year (1,812) (1,812)
Public Dividend Capital
extinguished/written off 0 0
Other movements in PDC in year 62 62
Balance at 31 March 2013 13,846 468 0 0 14,314
4

Public Health Wales NHS Trust Annual Accounts 2013-14
2013-14 2012-13
Note £000 £000
Cash flows from operating activities
Operating surplus/(deficit) SOCI 49 83
Depreciation and amortisation 6 2,798 2,438
Impairments and reversals 6 0 1,783
Release of PFI deferred credits 0 0
Donated Assets received credited to revenue but non-cash 3 0 0
Government Granted Assets received credited to revenue but non-cash 3 0 0
Interest paid (50) (42)
(Increase)/decrease in inventories 8 25
(Increase)/decrease in trade and other receivables (348) (1,984)
(Increase)/decrease in other current assets 0 0
Increase/(decrease) in trade and other payables 1,216 418
Increase/(decrease) in other current liabilities (2,336) 223
Increase/(decrease) in provisions 718 20
Net cash inflow/(outflow) from operating activities 2,055 2,964
Cash flows from investing activities
Interest received 17 55
(Payments) for property, plant and equipment (742) (1,924)
Proceeds from disposal of property, plant and equipment 0 0
(Payments) for intangible assets 0 0
Proceeds from disposal of intangible assets 0 0
(Payments) for investments with Welsh Government 0 0
Proceeds from disposal of investments with Welsh Government 0 0
(Payments) for financial assets. (304) (780)
Proceeds from disposal of financial assets. 0 0
Rental proceeds 0 0
Net cash inflow/(outflow) from investing activities (1,029) (2,649)
Net cash inflow/(outflow) before financing 1,026 315
Cash flows from financing activities
Public Dividend Capital received 62 0
Public Dividend Capital repaid (1,186) (1,812)
Loans received from Welsh Government 0 0
Other loans received 0 0
Loans repaid to Welsh Government 0 0
Other loans repaid 0 0
Other capital receipts 0 0
Capital elements of finance leases and on-SOFP PFI 144 30
Cash transferred (to)/from other NHS Wales bodies 0 0
Net cash inflow/(outflow) from financing activities (980) (1,782)
Net increase/(decrease) in cash and cash equivalents 46 (1,467)
Cash [and] cash equivalents [and bank overdrafts] 23 2,501 3,968
at the beginning of the financial year
Cash [and] cash equivalents [and bank overdrafts]
at the end of the financial year 23 2,547 2,501
The notes on pages 6 to 89 form part of these accounts.
STATEMENT OF CASH FLOWS FOR THE YEAR ENDED 31 MARCH 2014
5

Public Health Wales NHS Trust Annual Accounts 2013-14 13/06/2014
Notes to the Accounts
Accounting policies
1. The Welsh Minister for Health and Social Services has directed that the financial statements of NHS Trusts in Wales shall meet the accounting requirements of the NHS Trust Manual for Accounts. Consequently, the following financial statements have been prepared in accordance with the 2013-14 NHS Trusts Manual for Accounts. The accounting policies contained in that manual follow the European Union version of the International Financial Reporting Standards to the extent that they are meaningful and appropriate to the NHS, as determined by HM Treasury, which is advised by the Financial Reporting Advisory Board. Where the NHS Trusts Manual for Accounts permits a choice of accounting policy, the accounting policy which is judged to be most appropriate to the particular circumstances of the trust for the purpose of giving a true and fair view has been selected. The particular policies adopted by the trust are described below. They have been applied consistently in dealing with items considered material in relation to the accounts. 1.1 Accounting convention These accounts have been prepared under the historical cost convention modified to account for the revaluation of property, plant and equipment, intangible assets and inventories. 1.2 Acquisitions and discontinued operations Activities are considered to be ‘acquired’ only if they are taken on from outside the public sector. Activities are considered to be ‘discontinued’ only if they cease entirely. They are not considered to be ‘discontinued’ if they transfer from one public sector body to another. 1.3 Pooled budgets The trust has not entered into any pooled budget arrangements with Local Authorities.
1.4 Revenue
Revenue in respect of services provided is recognised when, and to the extent that,
performance occurs, and is measured at the fair value of the consideration receivable. The
main source of revenue for the trust is from the Welsh Government and the Health Boards.
This revenue is recognised in the period in which services are provided.
Where income is received from Non NHS bodies for a specific activity that is to be delivered
in the following year, that income is deferred.
The Trust receives no income under the NHS Injury Cost Recovery Scheme.
1.5 Employee Benefits
Salaries, wages and employment-related payments are recognised in the period in which the
service is received from employees. The cost of leave earned but not yet taken by
employees at the end of the period is recognised in the financial statements to the extent
that employees are permitted to carry forward leave into the following period.
Retirement benefit costs
Past and present employees are covered by the provisions of the NHS Pensions Scheme.
The scheme is an unfunded, defined benefit scheme that covers NHS employers, General
Practices and other bodies, allowed under the direction of the Secretary of State, in England
and Wales. The scheme is not designed to be run in a way that would enable NHS bodies to
identify their share of the underlying scheme assets and liabilities. Therefore, the scheme is
accounted for as if it were a defined contribution scheme: the cost to the NHS body of
participating in the scheme is taken as equal to the contributions payable to the scheme for
the accounting period.
6

Public Health Wales NHS Trust Annual Accounts 2013-14 13/06/2014
For early retirements other than those due to ill health the additional pension liabilities are
not funded by the scheme. The full amount of the liability for the additional costs is
charged to expenditure at the time the trust commits itself to the retirement, regardless
of the method of payment.
1.6 Other expenses
Other operating expenses for goods or services are recognised when, and to the extent
that, they have been received. They are measured at the fair value of the consideration
payable.
1.7 Property, plant and equipment
Recognition
Property, plant and equipment is capitalised if:
it is held for use in delivering services or for administrative purposes;
it is probable that future economic benefits will flow to, or service potential will be
supplied to, the trust;
it is expected to be used for more than one financial year;
the cost of the item can be measured reliably; and
the item has cost of at least £5,000; or
Collectively, a number of items have a cost of at least £5,000 and individually have a
cost of more than £250, where the assets are functionally interdependent, they had
broadly simultaneous purchase dates, are anticipated to have simultaneous disposal dates
and are under single managerial control; or
● Items form part of the initial equipping and setting-up cost of a new building, ward or
unit, irrespective of their individual or collective cost.
Where a large asset, for example a building, includes a number of components with
significantly different asset lives, the components are depreciated over their own useful
economic lives.
Valuation
All property, plant and equipment are measured initially at cost, representing the cost
directly attributable to acquiring or constructing the asset and bringing it to the location
and condition necessary for it to be capable of operating in the manner intended by
management.
Land and buildings used for the trust’s services or for administrative purposes are stated
in the balance sheet at their revalued amounts less any subsequent accumulated
depreciation and impairment losses. Revaluations are performed with sufficient regularity
to ensure that carrying amounts are not materially different from those that would be
determined at the balance sheet date. Fair values are determined as follows:
- Land and non specialised buildings – market value for existing use
- Specialised buildings – depreciated replacement cost
From 1 April 2009 the depreciated replacement cost valuation applies the Modern
Equivalent Asset (MEA) cost basis of estimation to arrive at the cost of replacing the
capacity and utility of a building rather than a like for like replacement cost.
7

Public Health Wales NHS Trust Annual Accounts 2013-14 13/06/2014
Properties in the course of construction for service or administration purposes are carried
at cost, less any impairment loss. Cost includes professional fees but not borrowing costs,
which are recognised as expenses immediately, as allowed by IAS 23 for assets held at fair
value. Assets are revalued and depreciation commences when they are brought into use.
For 2012-13 a formal revaluation exercise by the District Valuation Office was applied to
the Land and Properties of NHS Wales Trusts from 1 April 2012. In 2013-14 indexation
has been applied to property plant and equipment based on indices supplied by the District
Valuation Office. The carrying value of existing assets at that date will be written off over
their remaining useful lives and new fixtures and equipment are carried at depreciated
historic cost as this is not considered to be materially different from fair value.
An increase arising on revaluation is taken to the revaluation reserve except when it
reverses an impairment for the same asset previously recognised in expenditure, in which
case it is credited to expenditure to the extent of the decrease previously charged there. A
revaluation decrease that does not result from a loss of economic value or service potential
is recognised as an impairment charged to the revaluation reserve to the extent that there
is a balance on the reserve for the asset and, thereafter, to expenditure. Impairment
losses that arise from a clear consumption of economic benefit should be taken to
expenditure. This is a change in accounting policy from previous years where all
impairments were taken to the revaluation reserve to the extent that a balance was held
for that asset and thereafter to expenditure. However, to ensure that the outcome as
reflected in the reserves figure on the Statement of Financial Position is consistent with the
requirements of IAS 36 had this adaptation not been applied, the balance on any
revaluation reserve (up to the level of the impairment) to which the impairment would
have been charged under IAS 36 should be transferred to Retained earnings.
Subsequent expenditure
Where subsequent expenditure enhances an asset beyond its original specification, the
directly attributable cost is capitalised. Where subsequent expenditure restores the asset
to its original specification, the expenditure is capitalised and any existing carrying value of
the item replaced is written-out and charged to operating expenses.
1.8 Intangible assets
Recognition
Intangible assets are non-monetary assets without physical substance, which are capable
of sale separately from the rest of the trust’s business or which arise from contractual or
other legal rights. They are recognised only when it is probable that future economic
benefits will flow to, or service potential be provided to, the trust; where the cost of the
asset can be measured reliably, and where the cost is at least £5.000.
8

Public Health Wales NHS Trust Annual Accounts 2013-14 13/06/2014
Intangible assets acquired separately are initially recognised at fair value. Software
that is integral to the operating of hardware, for example an operating system, is
capitalised as part of the relevant item of property, plant and equipment. Software
that is not integral to the operation of hardware, for example application software, is
capitalised as an intangible asset. Expenditure on research is not capitalised: it is
recognised as an operating expense in the period in which it is incurred. Internally-
generated assets are recognised if, and only if, all of the following have been
demonstrated:
the technical feasibility of completing the intangible asset so that it will be
available for use
the intention to complete the intangible asset and use it
the ability to sell or use the intangible asset
how the intangible asset will generate probable future economic benefits or
service potential
the availability of adequate technical, financial and other resources to complete
the intangible asset and sell or use it
the ability to measure reliably the expenditure attributable to the intangible asset
during its development
Measurement
The amount initially recognised for internally-generated intangible assets is the sum
of the expenditure incurred from the date when the criteria above are initially met.
Where no internally-generated intangible asset can be recognised, the expenditure
is recognised in the period in which it is incurred.
Following initial recognition, intangible assets are carried at fair value by reference
to an active market, or, where no active market exists, at amortised replacement
cost (modern equivalent assets basis), indexed for relevant price increases, as a
proxy for fair value. Internally-developed software is held at historic cost to reflect
the opposing effects of increases in development costs and technological advances.
1.9 Research and development
Research and development expenditure is charged to operating costs in the year in
which it is incurred, except insofar as it relates to a clearly defined project, which
can be separated from patient care activity and benefits there from can reasonably
be regards as assured. Expenditure so deferred is limited to the value of future
benefits expected and is amortised through the SOCNI on a systematic basis over
the period expected to benefit from the project.
1.10 Depreciation, amortisation and impairments
Freehold land, properties under construction and assets held for sale are not
depreciated.
Otherwise, depreciation and amortisation are charged to write off the costs or
valuation of property, plant and equipment and intangible non-current assets, less
any residual value, over their estimated useful lives, in a manner that reflects the
consumption of economic benefits or service potential of the assets. The estimated
useful life of an asset is the period over which the Trust expects to obtain economic
benefits or service potential from the asset. This is specific to the Trust and may be
shorter than the physical life of the asset itself. Estimated useful lives and residual
values are reviewed each year end, with the effect of any changes recognised on a
prospective basis. Assets held under finance leases are depreciated over the shorter
9

Public Health Wales NHS Trust Annual Accounts 2013-14 13/06/2014
At each reporting period end, the trust checks whether there is any indication that any of
its tangible or intangible non-current assets have suffered an impairment loss. If there is
indication of an impairment loss, the recoverable amount of the asset is estimated to
determine whether there has been a loss and, if so, its amount. Intangible assets not yet
available for use are tested for impairment annually.
Impairment losses that do not result from a loss of economic value or service potential
are taken to the revaluation reserve to the extent that there is a balance on the reserve
for the asset and, thereafter, to the Statement of Comprehensive Net Income.
Impairment losses that arise from a clear consumption of economic benefit are taken to
the Statement of Comprehensive Net Income. The balance on any revaluation reserve (up
to the level of the impairment) to which the impairment would have been charged under
IAS 36 are transferred to retained earnings.
1.11 Borrowing costs
Borrowing costs are recognised as expenses as they are incurred.
1.12 Donated assets
Following the accounting policy change outlined in the Treasury FREM for 2011-12, a
donated asset reserve is no longer maintained. Donated non-current assets are
capitalised at their fair value on receipt, with a matching credit to Income. They are
valued, depreciated and impaired as described above for purchased assets. Gains and
losses on revaluations, impairments and sales are as described above for purchased
assets. Deferred income is recognised only where conditions attached to the donation
preclude immediate recognition of the gain.
1.13 Government grants
Following the accounting policy change outlined in the Treasury FREM for 2011-12, a
government grant reserve is no longer maintained. The value of assets received by
means of a government grant are credited directly to income. Deferred income is
recognised only where conditions attached to the grant preclude immediate recognition of
the gain.
1.14 Non-current assets held for sale
Non-current assets are classified as held for sale if their carrying amount will be recovered
principally through a sale transaction rather than through continuing use. This condition
is regarded as met when the sale is highly probable, the asset is available for immediate
sale in its present condition and management is committed to the sale, which is expected
to qualify for recognition as a completed sale within one year from the date of
classification. Non-current assets held for sale are measured at the lower of their
previous carrying amount and fair value less costs to sell. Fair value is open market value
including alternative uses.
10

Public Health Wales NHS Trust Annual Accounts 2013-14 13/06/2014
The profit or loss arising on disposal of an asset is the difference between the sale proceeds
and the carrying amount and is recognised in the Statement of Comprehensive Net Income.
On disposal, the balance for the asset on the revaluation reserve is transferred to retained
earnings.
Property, plant and equipment that is to be scrapped or demolished does not qualify for
recognition as held for sale. Instead, it is retained as an operational asset and its economic
life is adjusted. The asset is de-recognised when it is scrapped or demolished.
1.15 Leases
Leases are classified as finance leases when substantially all the risks and rewards of
ownership are transferred to the lessee. All other leases are classified as operating leases.
The trust as lessee
Property, plant and equipment held under finance leases are initially recognised, at the
inception of the lease, at fair value or, if lower, at the present value of the minimum lease
payments, with a matching liability for the lease obligation to the lessor. Lease payments
are apportioned between finance charges and reduction of the lease obligation so as to
achieve a constant rate on interest on the remaining balance of the liability. Finance
charges are recognised in calculating the trust’s surplus/deficit.
Operating lease payments are recognised as an expense on a straight-line basis over the
lease term. Lease incentives are recognised initially as a liability and subsequently as a
reduction of rentals on a straight-line basis over the lease term.
Contingent rentals are recognised as an expense in the period in which they are incurred.
Where a lease is for land and buildings, the land and building components are separated
and individually assessed as to whether they are operating or finance leases.
The trust as lessor
Amounts due from lessees under finance leases are recorded as receivables at the amount
of the trust’s net investment in the leases. Finance lease income is allocated to accounting
periods so as to reflect a constant periodic rate of return on the trust’s net investment
outstanding in respect of the leases.
Rental income from operating leases is recognised on a straight-line basis over the term of
the lease. Initial direct costs incurred in negotiating and arranging an operating lease are
added to the carrying amount of the leased asset and recognised on a straight-line basis
over the lease term.
1.16 Private Finance Initiative (PFI) transactions
The Trust has no PFI arrangements.
11

and the carrying amount and is recognised in the Statement of Comprehensive Net Income.
11

Public Health Wales NHS Trust Annual Accounts 2013-14 13/06/2014
1.17 Inventories
Inventories are valued at the lower of cost and net realisable value using the first in
first out cost formula. This is considered to be a reasonable approximation to fair value
due to the high turnover of stocks.
1.18 Cash and cash equivalents
Cash is cash in hand and deposits with any financial institution repayable without
penalty on notice of not more than 24 hours. Cash equivalents are investments that
mature in 3 months or less from the date of acquisition and that are readily convertible
to known amounts of cash with insignificant risk of change in value.
In the Statement of Cash Flows, cash and cash equivalents are shown net of bank
overdrafts that are repayable on demand and that form an integral part of the trust’s
cash management.
1.19 Provisions
Provisions are recognised when the trust has a present legal or constructive obligation
as a result of a past event, it is probable that the trust will be required to settle the
obligation, and a reliable estimate can be made of the amount of the obligation. The
amount recognised as a provision is the best estimate of the expenditure required to
settle the obligation at the end of the reporting period, taking into account the risks and
uncertainties. Where a provision is measured using the cash flows estimated to settle
the obligation, its carrying amount is the present value of those cash flows using
discount rates supplied by HM Treasury.
When some or all of the economic benefits required to settle a provision are expected to
be recovered from a third party, the amount receivable is recognised as an asset if it is
virtually certain that reimbursements will be received and the amount of the receivable
can be measured reliably.
Present obligations arising under onerous contracts are recognised and measured as a
provision. An onerous contract is considered to exist where the trust has a contract
under which the unavoidable costs of meeting the obligations under the contract exceed
the economic benefits expected to be received under it.
A restructuring provision is recognised when the trust has developed a detailed formal
plan for the restructuring and has raised a valid expectation in those affected that it will
carry out the restructuring by starting to implement the plan or announcing its main
features to those affected by it. The measurement of a restructuring provision includes
only the direct expenditures arsing from the restructuring, which are those amounts
that are both necessarily entailed by the restructuring and not associated with ongoing
activities of the entity.
1.20 Clinical Negligence Costs
The Welsh Risk Pool (WRP) operates a risk pooling scheme which is currently funded by
the Welsh Government. The WRP is hosted by Velindre NHS Trust.
1.21 Carbon Reduction Commitment Scheme
The trust is not a member of the Carbon Reduction Commitment Scheme.
12

Public Health Wales NHS Trust Annual Accounts 2013-14 13/06/2014
1.22 Contingencies
A contingent liability is a possible obligation that arises from past events and whose
existence will be confirmed only by the occurrence or non-occurrence of one or more
uncertain future events not wholly within the control of the trust, or a present obligation
that is not recognised because it is not probable that a payment will be required to settle
the obligation or the amount of the obligation cannot be measured sufficiently reliably. A
contingent liability is disclosed unless the possibility of a payment is remote.
A contingent asset is a possible asset that arises from past events and whose existence will
be confirmed by the occurrence or non-occurrence of one or more uncertain future events
not wholly within the control of the trust. A contingent asset is disclosed where an inflow
of economic benefits is probable.
Where the time value of money is material, contingencies are disclosed at their present
value.
1.23 Financial assets
Financial assets are recognised when the trust becomes party to the financial instrument
contract or, in the case of trade receivables, when the goods or services have been
delivered. Financial assets are derecognised when the contractual rights have expired or
the asset has been transferred.
Financial assets are initially recognised at fair value.
Financial assets are classified into the following categories: financial assets ‘at fair value
through SoCNI’; ‘held to maturity investments’; ‘available for sale’ financial assets, and
‘loans and receivables’. The classification depends on the nature and purpose of the
financial assets and is determined at the time of initial recognition.
Financial assets at fair value through SoCNI
Embedded derivatives that have different risks and characteristics to their host contracts,
and contracts with embedded derivatives whose separate value cannot be ascertained, are
treated as financial assets at fair value through SoCNI. They are held at fair value, with
any resultant gain or loss recognised in calculating the trust’s surplus or deficit for the
accounting period. The net gain or loss incorporates any interest earned on the financial
asset.
The Trust has no embedded derivatives. (Delete as appropriate).
Held to maturity investments
Held to maturity investments are non-derivative financial assets with fixed or determinable
payments and fixed maturity, and there is a positive intention and ability to hold to
maturity. After initial recognition, they are held at amortised cost using the effective
interest method, less any impairment. Interest is recognised using the effective interest
method.
Available for sale financial assets
The Trust does not have any available for sale financial assets.
13

Public Health Wales NHS Trust Annual Accounts 2013-14 13/06/2014
Loans and receivables
Loans and receivables are non-derivative financial assets with fixed or determinable
payments which are not quoted in an active market. After initial recognition, they are
measured at amortised cost using the effective interest method, less any impairment.
Interest is recognised using the effective interest method.
Fair value is determined by reference to quoted market prices where possible, otherwise
by valuation techniques
The effective interest rate is the rate that exactly discounts estimated future cash receipts
through the expected life of the financial asset, to the initial fair value of the financial
asset.
The Trust has no financial assets, other than those held at ‘fair value through profit and
loss’ that will need to be impaired.
1.24 Financial liabilities
Financial liabilities are recognised on the statement of financial position when the trust
becomes party to the contractual provisions of the financial instrument or, in the case of
trade payables, when the goods or services have been received. Financial liabilities are
de-recognised when the liability has been discharged, that is, the liability has been paid or
has expired.
Loans from the Welsh Government are recognised at historical cost. Otherwise, financial
liabilities are initially recognised at fair value.
Financial guarantee contract liabilities
Financial guarantee contract liabilities are subsequently measured at the higher of:
- the premium received (or imputed) for entering into the guarantee less cumulative
amortisation;
- the amount of the obligation under the contract, as determined in accordance with IAS
37 Provisions, Contingent Liabilities and Contingent Assets.
Financial liabilities at fair value through SoCNI
Embedded derivatives that have different risks and characteristics to their host contracts,
and contracts with embedded derivatives whose separate value cannot be ascertained, are
treated as financial liabilities at fair value through profit and loss. They are held at fair
value, with any resultant gain or loss recognised in the trust’s surplus/deficit. The net
gain or loss incorporates any interest payable on the financial liability.
The Trust does not have any financial guarantee contract liabilities nor any financial
derivatives requiring to be stated at fair value through profit and loss.
Other financial liabilities
After initial recognition, all other financial liabilities are measured at amortised cost using
the effective interest method, except for loans from the Welsh Government, which are
carried at historic cost. The effective interest rate is the rate that exactly discounts
estimated future cash payments through the life of the asset, to the net carrying amount
of the financial liability. Interest is recognised using the effective interest method.
14

Public Health Wales NHS Trust Annual Accounts 2013-14 13/06/2014
1.25 Value Added Tax
Most of the activities of the trust are outside the scope of VAT and, in general, output tax
does not apply and input tax on purchases is not recoverable. Irrecoverable VAT is
charged to the relevant expenditure category or included in the capitalised purchase cost
of fixed assets. Where output tax is charged or input VAT is recoverable, the amounts
are stated net of VAT.
1.26 Foreign currencies
The trust's functional currency and presentational currency is sterling. Transactions
denominated in a foreign currency are translated into sterling at the exchange rate ruling
on the dates of the transactions. At the end of the reporting period, monetary items
denominated in foreign currencies are retranslated at the spot exchange rate on 31
March. Resulting exchange gains and losses for either of these are recognised in the
trust’s surplus/deficit in the period in which they arise.
1.27 Third party assets
Assets belonging to third parties (such as money held on behalf of patients) are not
recognised in the accounts since the trust has no beneficial interest in them.
1.28 Public Dividend Capital (PDC) and PDC dividend
Public Dividend Capital represents taxpayers equity in the NHS Trust. At any time the
Welsh Minister for Health and Social Services with the approval of HM Treasury can issue
new PDC to, and require repayments of, PDC from the NHS Trust. PDC is recorded at the
value received. As PDC is issued under legislation rather than under contract, it is not
treated as an equity financial instrument.
From 1 April 2010 the requirement to pay a public dividend over to the Welsh
Government ceased.
1.29 Losses and Special Payments
Losses and special payments are items that the Welsh Government would not have
contemplated when it agreed funds for the health service or passed legislation. By their
nature they are items that ideally should not arise. They are therefore subject to special
control procedures compared with the generality of payments. They are divided into
different categories, which govern the way each individual case is handled.
Losses and special payments are charged to the relevant functional headings in the
income statement on an accruals basis, including losses which would have been made
good through insurance cover had NHS Trusts not been bearing their own risks (with
insurance premiums then being included as normal revenue expenditure). However, the
note on losses and special payments is compiled directly from the losses and
compensations register which is prepared on a cash basis.
The Trust accounts for all losses and special payments gross (including assistance from
the Welsh Risk Pool). The Trust accrues or provides for the best estimate of its future
payouts for certain or probable liabilities and discloses all other potential payments as
contingent liabilities, unless the probability of the liabilities becoming payable is remote.
All claims for losses and special payments are provided for, where the probability of
settlement of an individual claim is over 50%. Where reliable estimates can be made,
incidents of clinical negligence against which a claim has not, as yet, been received are
provided in the same way. Expected reimbursements from the Welsh Risk Pool are
included in debtors. For those claims where the probability of settlement is below 50%,
the liability is disclosed as a contingent liability.
15

Public Health Wales NHS Trust Annual Accounts 2013-14 13/06/2014
1.30 Critical Accounting Judgements and key sources of estimation uncertainty
In the application of the Trust's accounting policies, management is required to make
judgements, estimates and assumptions about the carrying amounts of assets and liabilities
that are not readily apparent from other sources. The estimates and associated
assumptions are based on historical experience and other factors that are considered to be
relevant. Actual results may differ from those estimates and the estimates and underlying
assumptions are continually reviewed. Revisions to accounting estimates are recognised in
the period in which the estimate is revised if the revision affects only that period, or the
period of the revision and future periods if the revision affects both current and future
periods.
1.31 Critical Judgements in applying accounting policies
There are no critical judgements that management has made in the process of applying the
Trust's accounting policies.
1.32 Key sources of estimation uncertainty
The following are the key assumptions concerning the future, and other key sources of
estimation uncertainty at the end of the reporting period, that have a significant risk of
causing a material adjustment to the carrying amounts of assets and liabilities within the
next financial year
Annual Leave Provision
1.33 Subsidiaries
Material entities over which the trust has the power to exercise control so as to obtain
economic or other benefits are classified as subsidiaries and are consolidated. Their income
and expenses; gains and losses; assets, liabilities and reserves; and cash flows are
consolidated in full into the appropriate financial statement lines. Appropriate adjustments
are made on consolidation where the subsidiary’s accounting policies are not aligned with
the trust’s or where the subsidiary’s accounting date is before 1 January or after 30 June.
Subsidiaries that are classified as ‘held for sale’ are measured at the lower of their carrying
amount or ‘fair value less costs to sell’
For 2013/14 the Trust has not consolidated the NHS charitable funds for which it is the
corporate trustee as the control lies with Velindre NHS Trust; the funds are therefore
subsumed within Velindre NHS Trust's charitable funds.
16

judgements, estimates and assumptions about the carrying amounts of assets and liabilities
16

Public Health Wales NHS Trust Annual Accounts 2013-14 13/06/2014
1.34 Absorption Accounting
Transfers of function are accounted for as either by merger or by absorption accounting, dependent upon the treatment prescribed in the FReM. Absorption accounting requires that entities account for their transactions in the period in which
they took place with no restatement of performance required. For transfers of functions involving NHS Wales Trusts in receipt of PDC the double entry for the fixed asset NBV value and the net movement in assets is PDC or General Reserve as
appropriate. 1.35 Accounting standards that have been issued but have not yet been
adopted The following accounting standards have been issued by the IASB and IFRIC but have not been adopted because they are not yet required to be adopted by the FReM
IFRS 9 Financial Instruments - subject to consultation. IFRS 10 Consolidated Financial Statements - subject to consultation.
IFRS 11 Joint Arrangements - subject to consultation. IFRS 12 Disclosure of Interests in Other Entities - subject to consultation. IFRS 13 Fair Value Measurement - subject to consultation.
IPSAS 32 Service Concession Arrangements - subject to consultation.
1.36 Accounting standards issued that have been adopted early No accounting standards issued have been adopted early
17

Public Health Wales NHS Trust Annual Accounts 2013-14
2. Revenue from patient care activities 2013-14 2012-13
£000 £000
Welsh Government 83,044 79,098
Welsh Health Specialised Services Committee (WHSSC) 0 0
Local health boards 0 0
Welsh NHS Trusts 0 0
Other NHS trusts 0 0
Strategic health authorities and primary care trusts 0 0
Foundation Trusts 0 0
Welsh Local Authorities 0 0
Local authorities 0 0
Non NHS:
Private patient income 0 0
Overseas patients (non-reciprocal) 0 0
Injury Costs Recovery (ICR) Scheme 0 0
Other revenue from activities 0 0
Total 83,044 79,098
ICR income is subject to a provision for impairment of 15.8% to reflect expected rates of collection.
3. Other operating revenue 2013-14 2012-13
£000 £000
Patient transport services 0 0
Education, training and research 1,750 1,490
Charitable and other contributions to expenditure 0 0
Receipt of donations for capital acquisitions 0 0
Receipt of government grants for capital acquisitions 0 0
Non-patient care services to other bodies 0 0
Income generation 38 43
Rental revenue from finance leases 0 0
Rental revenue from operating leases 0 0
Other revenue:
Provision of pathology services 13,327 12,495
Accommodation and catering charges 0 0
Mortuary fees 0 0
Staff payments for use of cars 0 0
Business unit 0 0
Other 6,923 5,271
Total 22,038 19,299
Other revenue of £6,923k (2012-13 £5,271k) comprises
1 Excellence Awards 284 335
2 Grants - other 529 373
3 Grants - LA 186 254
4 WG - non Core Income 3,622 1,990
5 Staff Recharges 2,149 2,065
6 Other 153 254
Total 6,923 5,271
18

Public Health Wales NHS Trust Annual Accounts 2013-14
4. Revenue
Revenue is almost totally from the supply of services. Revenue from the sale of goods is immaterial.
5. Income generation activities
2013-14 2012-13
£000 £000
Income 0 0
Full cost 0 0
Surplus/(deficit) 0 0
The Trust does not undertakes income generation activities with an aim of achieving profit, which is then used in patient care.
19

Public Health Wales NHS Trust Annual Accounts 2013-14
6. Operating expenses 2013-14 2012-13
6.1 Operating expenses £000 £000
Welsh Government 81 49
WHSSC 0 0
Local Health Boards 13,420 13,692
Welsh NHS Trusts 1,377 1,160
Other NHS Trusts 282 382
Goods and services from other NHS bodies 0 0
Purchase of healthcare from non-NHS bodies 0 0
Welsh Local Authorities 4,572 4,912
Other Local Authorities 0 0
Directors' costs 1,252 1,203
Staff costs 59,877 53,302
Supplies and services - clinical 8,061 7,524
Supplies and services - general 231 247
Consultancy Services 415 397
Establishment 6,178 5,388
Transport 530 471
Premises 3,574 3,534
Impairments and Reversals of Receivables 0 0
Depreciation 2,798 2,438
Amortisation 0 0
Impairments and reversals of property, plant and equipment 0 1,783
Impairments and reversals of intangible assets 0 0
Impairments and reversals of financial assets 0 0
Impairments and reversals of non current assets held for sale 0 0
Audit fees 151 155
Other auditors' remuneration 0 0
Losses, special payments and irrecoverable debts 181 149
Research and development 0 0
Other operating expenses 2,053 1,528
Total 105,033 98,314
Both Staff costs and Establishment cost have increased significantly (£6.6m and £800k respectively) as a result of several service transfering into Public Health Wales during 2013/14. 48 staff joined Public Health Wales from the formal NLIAH, and a further 20 staff transferred into Public Health Wales within theWrexham Microbiology Laboratory from Betsi Cadwalidr University LHB. This has resulted in the increased expenditure on both staff costs and establishment costs, and in addition - the increase in expenditure on clinical supplies and services. This increase in expenditure has been covered by an increased level of core income, along with additional microbiology contract income. There have been no impairments of fixed assets during 2013/14
20

Public Health Wales NHS Trust Annual Accounts 2013-14
6. Operating expenses (continued)
6.2 Losses, special payments and irrecoverable debts:
Charges to operating expenses 2013-14 2012-13
Increase/(decrease) in provision for future payments: £000 £000
Clinical negligence 893 448
Personal injury 36 373
All other losses and special payments 21 20
Defence legal fees and other administrative costs 125 67
Gross increase/(decrease) in provision for future payments 1,075 908
Contribution to Welsh Risk Pool 0 0
Premium for other insurance arrangements 0 0
Irrecoverable debts 8 3
Less: income received/ due from Welsh Risk Pool (902) (762)
Total charge 181 149
Personal injury includes £135k (2012-13 £80k) in respect of permanent injury benefits.
21

Public Health Wales NHS Trust Annual Accounts 2013-14
7. Investment revenue 2013-14 2012-13
£000 £000
Rental revenue :
PFI finance lease revenue:
Planned 0 0
Contingent 0 0
Other finance lease revenue 0 0
Interest revenue:
Bank accounts 16 55
Other loans and receivables 0 0
Impaired financial assets 0 0
Other financial assets 0 0
Total 16 55
8. Other gains and losses 2013-14 2012-13
£000 £000
Gain/(loss) on disposal of property, plant and equipment 0 (86)
Gain/(loss) on disposal of intangible assets 0 0
Gain/(loss) on disposal of assets held for sale 0 0
Gain/(loss) on disposal of financial assets 0 0
Gains/(loss) on foreign exchange 0 0
Change in fair value of financial assets at fair value through income statement 0 0
Change in fair value of financial liabilities at fair value through income statement 0 0
Recycling of gain/(loss) from equity on disposal of financial assets held for sale 0 0
Total 0 (86)
9. Finance costs 2013-14 2012-13
£000 £000
Interest on loans and overdrafts 0 0
Interest on obligations under finance leases 50 42
Interest on obligations under PFI contracts:
Main finance cost 0 0
Contingent finance cost 0 0
Interest on late payment of commercial debt 0 0
Other interest expense 0 0
Total interest expense 50 42
Provisions unwinding of discount 0 0
Other finance costs 0 0
Total 50 42
22

Public Health Wales NHS Trust Annual Accounts 2013-14
10. Operating leases
10.1 Trust as lessee
2013-14 2012-13
Payments recognised as an expense £000 £000
Minimum lease payments 883 832
Contingent rents 0 0
Sub-lease payments 0 0
Total 883 832
Total future minimum lease payments 2013-14 2012-13
Payable: £000 £000
Not later than one year 850 735
Between one and five years 1,136 1,293
After 5 years 66 191
Total 2,052 2,219
Total future sublease payments expected to be received 0 0
There are some significant leasing arrangements where the Trust is the lessee; the trust leases a number of buildings where the lease agreement exceeds 5 years.
23
Public Health Wales NHS Trust Annual Accounts 2013-14
10. Operating leases (continued)
10.2 Trust as lessor
2013-14 2012-13
Receipts recognised as income £000 £000
Rent 0 0
Contingent rent 0 0
Other 0 0
Total rental revenue 0 0
Total future minimum lease payments 2013-14 2012-13
Receivable: £000 £000
Not later than one year 0 0
Between one and five years 0 0
After 5 years 0 0
Total 0 0
There are no leasing arrangement where the Trust is the lessor.
24

Public Health Wales NHS Trust Annual Accounts 2013-14
11. Employee costs and numbers
2013-14 2012-132008-09
11.1 Employee costs Permanently Agency Staff on £000 £000
employed Staff Inward
staff Secondment
£000 £000 £000 £000 £000
Salaries and wages 46,793 423 4,015 51,231 45,712
Social security costs 3,741 0 0 3,741 3,340
Employer contributions to NHS Pensions Scheme 6,071 0 0 6,071 5,361
Other pension costs 0 0 0 0 0
Other post-employment benefits 0 0 0 0 0
Termination benefits 0 0 0 0 0
Total 56,605 423 4,015 61,043 54,413
Of the total above:
Charged to capital 0 0
Charged to revenue 61,043 54,413
Total 61,043 54,413
11.2 Average number of employees
Permanently Agency Staff on Total Total
Employed Staff Inward
Secondment
Number Number Number Number Number
Medical and dental 95 1 29 125 118
Ambulance staff 0 0 0 0 0
Administrative and estates 720 9 14 743 619
Healthcare assistants and other support staff 0 0 0 0 0
Nursing, midwifery and health visiting staff 49 0 3 52 48
Nursing, midwifery and health visiting learners 0 0 0 0 0
Scientific, therapeutic and technical staff 377 1 2 380 393
Social care staff 0 0 0 0 0
Other 0 0 0 0 3
Total 1,241 11 48 1,300 1,181
11.3 Employee benefits
The Trust operates a lease car policy and 3 salary sacrifice schemes (childcare vouchers, bikes and computer scheme) scheme for employees.
25

Public Health Wales NHS Trust Annual Accounts 2013-14
11.4 Reporting of other compensation schemes - exit packages
Total number Total number
of exit of exit
packages by packages by
cost band cost band
Number Number
2013-14 2012-13
Exit package cost band
<£10,000 0 1
£10,000 to £25,000 1 1
£25,000 to £50,000 0 2
£50,000 to £100,000 1 1
£100,000 to £150,000 0 0
£150,000 to £200,000 0 0
£200,000+ 0 0
Total number of exit packages by type 2 5
Total resource cost £ 73 102
The above exit packages all relate to the nationally agreed NHS Wales Voluntary Early Release Scheme (VERS) This disclosure reports the number and value of exit packages taken by staff leaving in the year
26

Public Health Wales NHS Trust Annual Accounts 2013-14
11.5 Remuneration Relationship
Reporting bodies are required to disclose the relationship between the
remuneration of the highest-paid director in their organisation and the median
remuneration of the organisation’s workforce.
The banded remuneration of the highest-paid director in Public Health Wales in the
financial year 2013-14 was £155k-£160k (2012-13, £155k-£160k). This was 5.25
times (2012-13, 5.25) the median remuneration of the workforce, which was
£30,054 (2012-13, £29,464k).
In 2013-14, 0 (2012-13, 1) employees received remuneration in excess of the
highest-paid director. Remuneration ranged from £14,292 to £157,884 (2012-13
£10,029-£155,477).
Total remuneration includes salary, non-consolidated performance-related pay and
benefits-in-kind. It does not include severance payments, employer pension
contributions and the cash equivalent transfer value of pensions.
The figures above are annualised figures
Overtime payments are included for the calculation of both elements of the
relationship.
27

Public Health Wales NHS Trust Annual Accounts 2013-14
12. Pensions
Pension costs
Past and present employees are covered by the provisions of the NHS Pensions Scheme. Details of the benefits payable under these provisions can be found on the NHS Pensions website at www.nhsbsa.nhs.uk/pensions. The scheme is an unfunded, defined benefit scheme that covers NHS employers, GP practices and other bodies, allowed under the direction of the Secretary of State, in England and Wales. The scheme is not designed to be run in a way that would enable NHS bodies to identify their share of the underlying scheme assets and liabilities. Therefore, the scheme is accounted for as if it were a defined contribution scheme: the cost to the NHS Body of participating in the scheme is taken as equal to the contributions payable to the scheme for the accounting period.
In order that the defined benefit obligations recognised in the financial statements do not differ materially from those that would be determined at the reporting date by a formal actuarial valuation, the FReM requires that “the period between formal valuations shall be four years, with approximate assessments in intervening years”. An outline of these follows:
a) Accounting valuation A valuation of the scheme liability is carried out annually by the scheme actuary as at the end of the reporting period. This utilises an actuarial assessment for the previous accounting period in conjunction with updated membership and financial data for the current reporting period, and are accepted as providing suitably robust figures for financial reporting purposes. The valuation of the scheme liability as at 31 March 2014, is based on valuation data as 31 March 2013, updated to 31 March 2014 with summary global member and accounting data. In undertaking this actuarial assessment, the methodology prescribed in IAS 19, relevant FReM interpretations, and the discount rate prescribed by HM Treasury have also been used.
The latest assessment of the liabilities of the scheme is contained in the scheme actuary report, which forms part of the annual NHS Pension Scheme (England and Wales) Pension Accounts, published annually. These accounts can be viewed on the NHS Pensions website. Copies can also be obtained from The Stationery Office.
b) Full actuarial (funding) valuation The purpose of this valuation is to assess the level of liability in respect of the benefits due under the scheme (taking into account its recent demographic experience), and to recommend the contribution rates.
The last published actuarial valuation undertaken for the NHS Pension Scheme was completed for the year ending 31 March 2004. Consequently, a formal actuarial valuation would have been due for the year ending 31 March 2008. However, formal actuarial valuations for unfunded public service schemes were suspended by HM Treasury on value for money grounds while future scheme terms are developed as part of the reforms to public service pension provision due to be implemented in 2015. The Scheme Regulations allow contribution rates to be set by the Secretary of State for Health, with the consent of HM Treasury, and after consideration of the advice of the Scheme Actuary. A formal valuation for funding purposes as at March 2012 is currently close to completion and will be used to inform the contribution rates applicable from 1 April 2015. c) Scheme provisions The NHS Pension Scheme provides defined benefits, which are summarised below. This list is an illustrative guide only, and is not intended to detail all the benefits provided by the Scheme or the specific conditions that must be met before these benefits can be obtained:
28

Public Health Wales NHS Trust Annual Accounts 2013-14
12.1 Retirement costs due to ill-health
The Scheme is a “defined benefit” scheme. Annual pensions are normally based on 1/80th for the 1995 section and of the best of the last three years pensionable pay for each year of service, and 1/60th for the 2008 section of reckonable pay per year of membership. Members who are practitioners as defined by the Scheme Regulations have their annual pensions based upon total pensionable earnings over the relevant pensionable service. With effect from 1 April 2008 members can choose to give up some of their annual pension for an additional tax free lump sum, up to a maximum amount permitted under HMRC rules. This new provision is known as “pension commutation”.
Annual increases are applied to pension payments at rates defined by the Pensions (Increase) Act 1971, and are based on changes in inflation in the twelve months ending 30 September in the previous calendar year. From 2011-12 the Consumer Price Index (CPI) has been used as the measure of inflation and replaced the Retail Prices Index (RPI).
Early payment of a pension, with enhancement, is available to members of the scheme who are permanently incapable of fulfilling their duties effectively through illness or infirmity. A death gratuity of twice final year’s pensionable pay for death in service, and five times their annual pension for death after retirement is payable.
For early retirements other than those due to ill health the additional pension liabilities are not funded by the scheme. The full amount of the liability for the additional costs is charged to the employer.
Members can purchase additional pension in the NHS Scheme and contribute to money purchase AVC’s run by the Scheme’s approved providers or by other Free Standing Additional Voluntary Contributions (FSAVC) providers.
Other Pensions Disclosure National Employment Savings Trust (NEST) NEST is a not-for-profit workplace pension scheme established by law to support the introduction of automatic enrolment providing defined contribution pension schemes. NEST was established by legislation and is treated as a trust-based scheme. The Trustee responsible for running the scheme is NEST Corporation. It’s a non-departmental public body (NDPB) that operates at arm’s length from government and is accountable to Parliament through the Department for Work and Pensions (DWP).
NEST Corporation has agreed a loan with the Department for Work and Pensions (DWP). This has paid for the scheme to be set up and will cover expected shortfalls in scheme costs during the earlier years while membership is growing. Currently, the legal minimum contribution level is 2 per cent of a jobholder’s qualifying earnings for employers whose legal duties have started. Of this the employer needs to pay at least 1 per cent, though they can pay more if they elect to do so. By 2018 the minimum contribution will rise to 8 per cent of qualifying earnings, of which the employer must pay at least 3 per cent. The National Employment Savings Trust has an annual contribution limit. It is reviewed annually and adjusted in line with average earnings. The annual contribution limit is currently up to £4,500 for the 2013/14 tax year.
The annual contribution limit includes member contributions, money from their employer and any tax relief. It also includes any money paid in by someone else on behalf of the member,
such as a member’s partner or spouse .
During 2013-14 there were 2 (2012-13 0)early retirements from the trust agreed on the grounds of ill-health. The estimated additional pension costs of these ill-health retirements will be £81,413 (2012-13 £0). The cost of these ill-health retirements will be borne by the NHS Business Services Authority - Pensions Division.
29

Public Health Wales NHS Trust Annual Accounts 2013-14
13. Public Sector Payment Policy
13.1 Prompt payment code - measure of compliance
2013-14 2013-14 2012-13 2012-13
Number £000 Number £000
NHS
Total bills paid in year 2,147 20,135 1,614 20,079
Total bills paid within target 2,001 19,444 1,501 18,756
Percentage of bills paid within target 93.2% 96.6% 93.0% 93.4%
Non-NHS
Total bills paid in year 21,755 27,600 21,117 25,574
Total bills paid within target 20,416 26,222 20,316 25,226
Percentage of bills paid within target 93.8% 95.0% 96.2% 98.6%
Total
Total bills paid in year 23,902 47,735 22,731 45,653
Total bills paid within target 22,417 45,666 21,817 43,982
Percentage of bills paid within target 93.8% 95.7% 96.0% 96.3%
13.2 The Late Payment of Commercial Debts (Interest) Act 1998 2013-14 2012-13
£ £
Amounts included within finance costs from claims made under legislation 0 0
Compensation paid to cover debt recovery costs under legislation 0 0
Total 0 0
The Welsh Government requires that trusts pay all their trade creditors in accordance
with the CBI prompt payment code and Government Accounting rules. The Welsh
Government has set as part of the trust financial targets a requirement to pay 95% of
the number of non-NHS creditors within 30 days of delivery or receipt of a valid invoice,
The financial target of payment of 95% of all invoices (by number) has not been
met in 2013/14. This is a direct result of a several changes to both the reporting requirements and the operating arrangements for the payment of invoices. It should be noted that Public Health Wales does not make any contractor
payments which would have the effect of increasing performance substantially.
ALthough performance increased during the second half of the financial year, following several improvements to operational arrangement, the cummulative
performance for the year remains below the 95%. The payment of 95% of all invoices by value has been met.
30

Public Health Wales NHS Trust Annual Accounts 2013-14
14. Property, plant and equipment :
2013-14
Cost or valuation £000 £000 £000 £000 £000 £000 £000 £000 £000
At 1 April 2013 935 3,745 0 476 10,600 45 6,144 533 22,478
Indexation 0 74 0 0 0 0 0 0 74
Revaluation 0 0 0 0 0 0 0 0 0
Additions - purchased 0 22 0 0 317 12 619 0 970
Additions - donated 0 0 0 0 0 0 0 0 0
Additions - government granted 0 0 0 0 0 0 0 0 0
Transfers from/(into) other NHS bodies 0 0 0 0 0 0 0 0 0
Reclassifications 0 0 0 (476) 476 0 0 0 0
Reclassified as held for sale 0 0 0 0 0 0 0 0 0
Disposals other than by sale 0 0 0 0 (310) 0 (149) (10) (469)
Impairments 0 0 0 0 0 0 0 0 0
Reversal of impairments 0 0 0 0 0 0 0 0 0
At 31 March 2014 935 3,841 0 0 11,083 57 6,614 523 23,053
Depreciation
At 1 April 2013 0 908 0 0 3,213 29 2,276 368 6,794
Indexation 0 18 0 0 0 0 0 0 18
Revaluation 0 0 0 0 0 0 0 0 0
Transfers from/(into) other NHS bodies 0 0 0 0 0 0 0 0 0
Reclassifications 0 0 0 0 0 0 0 0 0
Reclassified as held for sale 0 0 0 0 0 0 0 0 0
Disposals other than by sale 0 0 0 0 (310) 0 (149) (10) (469)
Impairments 0 0 0 0 0 0 0 0 0
Reversal of impairments 0 0 0 0 0 0 0 0 0
Charged during the year 0 266 0 0 1,322 3 1,125 82 2,798
At 31 March 2014 0 1,192 0 0 4,225 32 3,252 440 9,141
Net book value
At 1 April 2013 935 2,837 0 476 7,387 16 3,868 165 15,684
Net book value
At 31 March 2014 935 2,649 0 0 6,858 25 3,362 83 13,912
Net book value at 31 March 2014 comprises :
Purchased 935 2,535 0 0 6,858 25 3,362 83 13,798
Donated 0 114 0 0 0 0 0 0 114
Government Granted 0 0 0 0 0 0 0 0 0
At 31 March 2014 935 2,649 0 0 6,858 25 3,362 83 13,912
Asset Financing:
Owned 935 2,649 0 0 6,858 25 1,407 83 11,957
Held on finance lease 0 0 0 0 0 0 1,955 0 1,955
On-SoFP PFI contract 0 0 0 0 0 0 0 0 0
PFI residual interest 0 0 0 0 0 0 0 0 0
At 31 March 2014 935 2,649 0 0 6,858 25 3,362 83 13,912
The net book value of land, buildings and dwellings at 31 March 2014 comprises :
£000
Freehold 2,415
Long Leasehold 292
Short Leasehold 877
Total 3,584
Land
Buildings,
excluding
dwellings
Dwellings
Assets under
construc-tion
and
payments on
account
TotalPlant &
machinery
Transport
Equipment
Information
Technology
Furniture
and fittings
Of the totals at 31 March 2010, £nil related to land valued at open market value and £nil related to buildings, installations and fittings valued at open market
Of the totals at 31 March 2010, £nil related to land valued at open market value and £nil related to buildings, installations and fittings valued at open market
Building have been revalued using indices published by the the District Valuation (DV) Office. The price index for building
for 2013/14 is 102 (ie and increase of 2%) which reflects the increase in market value of buildings during 2013/14.
31

Public Health Wales NHS Trust Annual Accounts 2013-14
14. Property, plant and equipment :
2012-13
Cost or valuation £000 £000 £000 £000 £000 £000 £000 £000 £000
At 1 April 2012 1,060 5,574 0 1,848 9,763 45 4,907 535 23,732
Indexation 0 0 0 0 0 0 0 0 0
Revaluation 0 (74) 0 0 0 0 0 0 (74)
Additions - purchased 0 374 0 476 369 0 1,314 54 2,587
Additions - donated 0 0 0 0 0 0 0 0 0
Additions - government granted 0 0 0 0 0 0 0 0 0
Transfers from/(into) other NHS bodies 0 0 0 0 0 0 0 0 0
Reclassifications 0 15 0 (1,848) 1,824 0 9 0 0
Reclassified as held for sale 0 0 0 0 0 0 0 0 0
Disposals 0 0 0 0 (1,356) 0 (86) (56) (1,498)
Impairments (125) (2,144) 0 0 0 0 0 0 (2,269)
Reversal of impairments 0 0 0 0 0 0 0 0 0
At 31 March 2013 935 3,745 0 476 10,600 45 6,144 533 22,478
Depreciation
At 1 April 2012 0 1,109 0 0 3,259 25 1,399 350 6,142
Indexation 0 0 0 0 0 0 0 0 0
Revaluation 0 (233) 0 0 0 0 0 0 (233)
Transfers from/(into) other NHS bodies 0 0 0 0 0 0 0 0 0
Reclassifications 0 0 0 0 0 0 0 0 0
Reclassified as held for sale 0 0 0 0 0 0 0 0 0
Disposals 0 0 0 0 (1,270) 0 (86) (56) (1,412)
Impairments 0 (209) 0 0 68 0 0 0 (141)
Reversal of impairments 0 0 0 0 0 0 0 0 0
Charged during the year 0 241 0 0 1,156 4 963 74 2,438
At 31 March 2013 0 908 0 0 3,213 29 2,276 368 6,794
Net book value
at 1 April 2012 1,060 4,465 0 1,848 6,504 20 3,508 185 17,590
Net book value
at 31 March 2013 935 2,837 0 476 7,387 16 3,868 165 15,684
Net book value at 31 March 2013 comprises :
Purchased 935 2,697 0 476 8,587 16 2,668 165 15,544
Donated 0 140 0 0 0 0 0 0 140
Government Granted 0 0 0 0 0 0 0 0 0
Total 31 March 2013 935 2,837 0 476 8,587 16 2,668 165 15,684
Asset Financing:
Owned 935 2,837 0 476 8,587 16 2,668 165 15,684
Held on finance lease 0 0 0 0 0 0 0 0 0
On-SoFP PFI contract 0 0 0 0 0 0 0 0 0
PFI residual interest 0 0 0 0 0 0 0 0 0
Total 31 March 2013 935 2,837 0 476 8,587 16 2,668 165 15,684
The net book value of land, buildings and dwellings at 31 March 2013 comprises :
£000
Freehold 1,250
Long Leasehold 849
Short Leasehold 1,673
3,772
Land
Buildings,
excluding
dwellings
Dwellings
Assets under
construc-tion
and payments
on account
TotalPlant &
machinery
Transport
Equipment
Information
Technology
Furniture
and fittings
Of the totals at 31 March 2010, £nil related to land valued at open market value and £nil related to buildings, installations and fittings valued at open market
Of the totals at 31 March 2010, £nil related to land valued at open market value and £nil related to buildings, installations and fittings valued at open market
32

Public Health Wales NHS Trust Annual Accounts 2013-14
Disclosures:
i) Donated Assets
Public Health Wales NHS Trust did not receive any donated assets during the year.
ii) Valuations
The Trusts Land and Buildings were revalued by the District Valuation Service with an
effective date of 1st April 2012. The valuation has been prepared in accordance with the
terms of the Royal Institution of Chartered Surveyors' Valuation Standards, 6th edition.
The Trust is required to apply the revaluation model set out in IAS 16 and value its
capital assets to fair value. Fair value is defined by IAS16 as the amount for which an
asset could be exchanged between knowledgeable, willing parties in an arms length
transaction.
This has been undertaken on the assumption that the property is sold as part of the
continuing enterprise in occupation.
iii) Asset Lives
Land is not depreciated
Buildings as determined by the District Valuation service
Equipment 5-20 years
iv) Compensation
There has been no compensation received from third parties for assets impaired, lost or
given up, that is included in the income statement
v) Write Downs
There have been no write downs
vi) The Trust does not hold any property where the value is materially different from its
open market value.
vii) Assets Held for Sale or sold in the period
There are no assets held for sale or sold in the period
33

Public Health Wales NHS Trust Annual Accounts 2013-14
14.2 Non-current assets held for sale
£000 £000 £000 £000 £000 £000
Balance b/f 1 April 2013 0 0 0 0 0 0
Plus assets classified as held for
sale in year 0 0 0 0 0 0
Revaluation 0 0 0 0 0 0
Less assets sold in year 0 0 0 0 0 0
Less impairment for assets held for
sale 0 0 0 0 0 0
Plus reversal of impairments 0 0 0 0 0 0
Less assets no longer classified as
held for sale for reasons other than
disposal by sale 0 0 0 0 0 0
Balance c/f 31 March 2014 0 0 0 0 0 0
Balance b/f 1 April 2012 0 0 0 0 0 0
Plus assets classified as held for
sale in year 0 0 0 0 0 0
Revaluation 0 0 0 0 0 0
Less assets sold in year 0 0 0 0 0 0
Less impairment for assets held for
sale 0 0 0 0 0 0
Plus reversal of impairments 0 0 0 0 0 0
Less assets no longer classified as
held for sale for reasons other than
disposal by sale 0 0 0 0 0 0
Balance c/f 31 March 2013 0 0 0 0 0 0
Other assets TotalLand
Buildings,
including
dwellings
Other
property
plant and
equipment
Intangible
assets
34

Public Health Wales NHS Trust Annual Accounts 2013-14
15. Intangible assets
2013-14
Cost or valuation £000 £000 £000 £000 £000 £000 £000
At 1 April 2013 0 0 0 0 0 0 0
Revaluation 0 0 0 0
Additions
- purchased 0 0 0 0 0 0 0
- internally generated 0 0 0 0 0 0 0
- donated 0 0 0 0 0 0 0
- government granted 0 0 0 0 0 0 0
Transfers from/(into) other NHS bodies 0 0 0 0 0 0 0
Reclassifications 0 0 0 0 0 0 0
Reclassified as held for sale 0 0 0 0 0 0 0
Disposals other than by sale 0 0 0 0 0 0 0
Impairments 0 0 0 0 0 0 0
Reversal of impairments 0 0 0 0 0 0 0
Gross cost at 31 March 2014 0 0 0 0 0 0 0
Amortisation
Accumulated amortisation at
1 April 2013 0 0 0 0 0 0 0
Revaluation 0 0 0 0
Transfers from/(into) other NHS bodies 0 0 0 0 0 0 0
Reclassifications 0 0 0 0 0 0 0
Reclassified as held for sale 0 0 0 0 0 0 0
Disposals other than by sale 0 0 0 0 0 0 0
Impairments 0 0 0 0 0 0 0
Reversal of impairments 0 0 0 0 0 0 0
Charged during the year 0 0 0 0 0 0 0
Accumulated amortisation at
31 March 2014 0 0 0 0 0 0 0
Net book value at 1 April 2013 0 0 0 0 0 0 0
Net book value at 31 March 2014 0 0 0 0 0 0 0
Net book value
Purchased 0 0 0 0 0 0 0
Internally Generated 0 0 0 0 0 0 0
Donated 0 0 0 0 0 0 0
Government granted 0 0 0 0 0 0 0
Total at 31 March 2014 0 0 0 0 0 0 0
Develop-ment
expenditure
internally
generated
Total
Computer
software
purchased
Computer
software
internally
developed
Licenses
and trade-
marks
Patents
CRC
Emission
Trading
Scheme
35

Public Health Wales NHS Trust Annual Accounts 2013-14
15. Intangible assets
2012-13
Cost or valuation £000 £000 £000 £000 £000 £000 £000
At 1 April 2012 0 0 0 0 0 0 0
Revaluation 0 0 0 0
Additions
- purchased 0 0 0 0 0 0 0
- internally generated 0 0 0 0 0 0 0
- donated 0 0 0 0 0 0 0
- government granted 0 0 0 0 0 0 0
Transfers from/(into) other NHS bodies 0 0 0 0 0 0 0
Reclassifications 0 0 0 0 0 0 0
Reclassified as held for sale 0 0 0 0 0 0 0
Disposals other than by sale 0 0 0 0 0 0 0
Impairments 0 0 0 0 0 0 0
Reversal of impairments 0 0 0 0 0 0 0
Gross cost at 31 March 2013 0 0 0 0 0 0 0
Amortisation
Accumulated amortisation at
1 April 2012 0 0 0 0 0 0 0
Revaluation 0 0 0 0
Transfers from/(into) other NHS bodies 0 0 0 0 0 0 0
Reclassifications 0 0 0 0 0 0 0
Reclassified as held for sale 0 0 0 0 0 0 0
Disposals other than by sale 0 0 0 0 0 0 0
Impairments 0 0 0 0 0 0 0
Reversal of impairments 0 0 0 0 0 0 0
Charged during the year 0 0 0 0 0 0 0
Accumulated amortisation at
31 March 2013 0 0 0 0 0 0 0
Net book value at 1 April 2012 0 0 0 0 0 0 0
Net book value at 31 March 2013 0 0 0 0 0 0 0
Net book value
Purchased 0 0 0 0 0 0 0
Internally Generated 0 0 0 0 0 0 0
Donated 0 0 0 0 0 0 0
Government granted 0 0 0 0 0 0 0
Total at 31 March 2013 0 0 0 0 0 0 0
Develop-
ment
expenditure
internally
generated
Total
Computer
software
purchased
Computer
software
internally
developed
Licenses
and trade-
marks
Patents
CRC
Emission
Trading
Scheme
36

Public Health Wales NHS Trust Annual Accounts 2013-14
15. Intangible assets
16. Revaluation reserve balance for intangible assets
2013-14 2012-13
£000 £000
At 1 April 0 0
0 0
At 31 March 0 0
Public Health Wales has no intangible assets
37
Public Health Wales NHS Trust Annual Accounts 2013-14
17. Impairments
Impairments in the period arose from: Property, plant Intangible Property, plant Intangible
& equipment assets & equipment assets
£000 £000 £000 £000
Loss or damage from normal operations 0 0 0 0
Abandonment of assets in the course of construction 0 0 0 0
Over specification of assets (Gold Plating) 0 0 0 0
Loss as a result of a catastrophe 0 0 0 0
Unforeseen obsolescence 0 0 0 0
Changes in market price 0 0 1,676 0
Other (specify) 0 0 107 0
Impairments charged to operating expenses 0 0 1,783 0
Impairments charged in the year to
0 0 1,783 0
0 0 187 0
Total 0 0 1,970 0
18. Capital commitments
Commitments under capital expenditure contracts at the statement of financial position sheet date were:
31 March 31 March
2014 2013
£000 £000
Property, plant and equipment 0 0
Intangible assets 0 0
Total 0 0
Operating expenses in Statement of Comprehensive
Income
Revaluation reserve
2013-14 2012-13
38
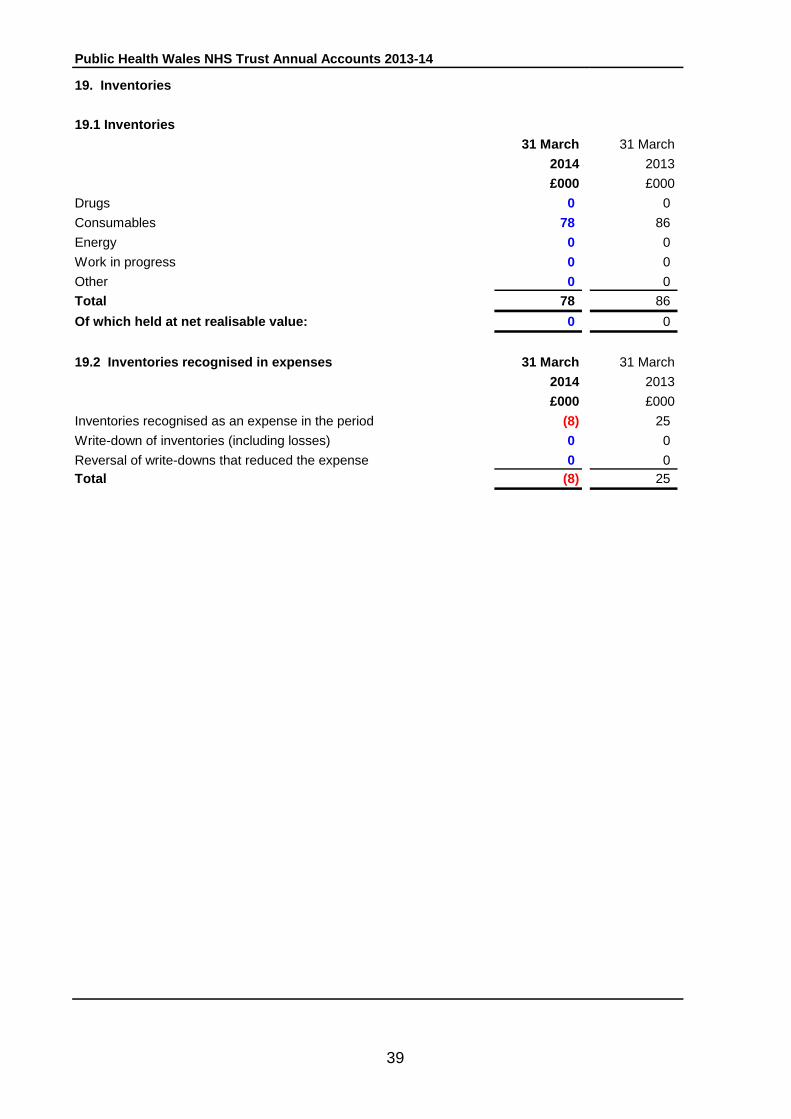
Public Health Wales NHS Trust Annual Accounts 2013-14
19. Inventories
19.1 Inventories
31 March 31 March
2014 2013
£000 £000
Drugs 0 0
Consumables 78 86
Energy 0 0
Work in progress 0 0
Other 0 0
Total 78 86
Of which held at net realisable value: 0 0
19.2 Inventories recognised in expenses 31 March 31 March
2014 2013
£000 £000
Inventories recognised as an expense in the period (8) 25
Write-down of inventories (including losses) 0 0
Reversal of write-downs that reduced the expense 0 0
Total (8) 25
39

Public Health Wales NHS Trust Annual Accounts 2013-14
20. Trade and other receivables
20.1 Trade and other receivables
31 March 31 March
2014 2013
Current £000 £000
Welsh Government 641 848
Welsh Health Specialised Services Committee 12 60
Welsh Health Boards 2,165 2,554
Welsh NHS Trusts 15 10
Non - Welsh Trusts 22 43
Other NHS 0 0
Welsh Risk Pool 3,105 2,314
Welsh Local Authorities 159 131
Other Local Authorities 0 0
Capital debtors 0 0
Other debtors 832 1,112
Provision for impairment of trade receivables (49) (41)
Pension Prepayments
NHS Pensions Agency 0 0
NEST 0 0
Other prepayments and accrued income 923 508
Sub-total 7,825 7,539
Non-current
Welsh Government 0 0
Welsh Health Specialised Services Committee 0 0
Welsh Health Boards 0 0
Welsh NHS Trusts 0 0
Non - Welsh Trusts 0 0
Other NHS 0 0
Welsh Risk Pool 0 0
Welsh Local Authorities 0 0
Other Local Authorities 0 0
Capital debtors 0 0
Other debtors 0 0
Provision for impairment of trade receivables 0 0
Pension Prepayments
NHS Pensions Agency 0 0
NEST 0 0
Other prepayments and accrued income 0 0
Sub-total 0 0
Total trade and other receivables 7,825 7,539
No interest is charged on trade receivables. The value of trade receivables that are past their due payment date but not impaired is £239k. (£550k in 2012-13)
40

Public Health Wales NHS Trust Annual Accounts 2013-14
20.2 Receivables VAT 31 March 31 March
2014 2013
£000 £000
Trade receivables 172 130
Other 0 0
Total 172 130
20.3 Receivables past their due date but not impaired
31 March 31 March
2014 2013
£000 £000
By up to 3 months 71 279
By 3 to 6 months 17 89
By more than 6 months 102 182
Balance at end of financial year 190 550
20.4 Allowance for bad and doubtful debts
31 March 31 March
2014 2013
£000 £000
Balance at beginning of the year (41) (38)
Transfer to other NHS Wales body 0 0
Provision utilised (Amount written off during the year) 0 0
Provision written back during the year no longer required 0 0
Increase/(decrease) in provision during year (8) (3)
Bad debts recovered during year 0 0
Balance at end of financial year (49) (41)
In determining whether a debt is impaired consideration is given to the age of the debt
and the results of actions taken to recover the debt, including reference to credit
agencies.
41

Public Health Wales NHS Trust Annual Accounts 2013-14
21. Other financial assets
31 March 31 March
2014 2013
Non-current £000 £000
Finance lease receivables 0 0
Financial assets carried at fair value through income statement 0 0
Held to maturity investments carried at amortised cost 0 0
Available for sale financial assets carried at fair value 0 0
Loans carried at amortised cost 0 0
Total 0 0
Current
Finance lease receivables 0 0
Financial assets carried at fair value through income statement 0 0
Held to maturity investments carried at amortised cost 0 0
Available for sale financial assets carried at fair value 0 0
Loans carried at amortised cost 0 0
Total 0 0
22. Other assets
31 March 31 March
2014 2013
Non-current £000 £000
Other assets 0 0
Total 0 0
Current
CRC Emissions trading scheme allowances 0 0
Other assets 0 0
Total 0 0
42

Public Health Wales NHS Trust Annual Accounts 2013-14
23. Cash and cash equivalents
31 March 31 March
2014 2013
£000 £000
Opening Balance 2,501 3,968
Net change in year 46 (1,467)
Closing Balance 2,547 2,501
Made up of:
Cash with Government Banking Service (GBS) 2,529 2,501
Cash with Commercial banks 0 0
Cash in hand 18 0
Total cash 2,547 2,501
Current investments 0 0
2,547 2,501
Bank overdraft - GBS 0 0
Bank overdraft - Commercial banks 0 0
Cash & cash equivalents as in Statement of Cash Flows 2,547 2,501
Cash and cash equivalents as in SoFP
43

Public Health Wales NHS Trust Annual Accounts 2013-14
24. Trade and other payables at the SoFP Date 31 March 31 March
2014 2013
Current £000 £000
Welsh Government 79 124
Welsh Health Specialised Services Committee 0 0
Welsh Health Boards 1,381 762
Welsh NHS Trusts 264 876
Other NHS 77 198
Welsh Local Authorities 293 214
Other Local Authorities 0 0
Taxation and social security payable / refunds:
Refunds of taxation by HMRC 0 0
VAT payable to HMRC 0 0
Other taxes payable to HMRC 0 0
National Insurance contributions payable to HMRC 0 0
Non-NHS trade payables - revenue 2,679 3,362
Non-NHS trade payables - capital 95 26
Rentals due under operating leases 53 74
Obligations due under finance leases and HP contracts 640 0
Imputed finance lease element of on SoFP PFI contracts 0 0
Pensions: staff 0 0
Accruals 170 24
Deferred Income:
Deferred income brought forward 67 85
Deferred income additions 0 0
Transfer to/from current/non current deferred income 0 0
Released to the Income Statement 0 0
Other liabilities - all other payables 0 0
Sub-total 5,798 5,745
44

Public Health Wales NHS Trust Annual Accounts 2013-14
24. Trade and other payables at the SoFP Date (cont)
31 March 31 March
2014 2013
Non-current £000 £000
Welsh Government 0 0
Welsh Health Specialised Services Committee 0 0
Welsh Health Boards 0 0
Welsh NHS Trusts 0 0
Other NHS 0 0
Welsh Local Authorities 0 0
Other Local Authorities 0 0
Taxation and social security payable / refunds:
Refunds of taxation by HMRC 0 0
VAT payable to HMRC 0 0
Other taxes payable to HMRC 0 0
National Insurance contributions payable to HMRC 0 0
Non-NHS trade payables - revenue 0 0
Non-NHS trade payables - capital 0 0
Rentals due under operating leases 0 0
Obligations due under finance leases and HP contracts 1,232 0
Imputed finance lease element of on SoFP PFI contracts 0 0
Pensions: staff 0 0
Accruals 0 0
Deferred Income:
Deferred income brought forward 0 0
Deferred income additions 0 0
Transfer to/from current/non current deferred income 0 0
Released to the Income Statement 0 0
Other liabilities - all other payables 0 0
Sub-total 1,232 0
Total 7,030 5,745
It is intended to pay all invoices within the 30 day period directed by the Welsh
Government.
45

Public Health Wales NHS Trust Annual Accounts 2013-14
25. Borrowings 31 March 31 March
Current 2014 2013
£000 £000
Bank overdraft - GBS 0 0
Bank overdraft - Commercial bank 0 0
Loans from:
Welsh Government 0 0
Other entities 0 0
PFI liabilities:
Main liability 0 0
Lifecycle replacement received in advance 0 0
Finance lease liabilities 0 0
Other 0 0
Total 0 0
Non-current
Bank overdraft - OPG 0 0
Bank overdraft - Commercial bank 0 0
Loans from:
Welsh Government 0 0
Other entities 0 0
PFI liabilities:
Main liability 0 0
Lifecycle replacement received in advance 0 0
Finance lease liabilities 0 0
Other 0 0
Total 0 0
25.2 Loan advance/strategic assistance funding
The NHS trust has received no loan advance or strategic funding from the Welsh
Government.
46

Public Health Wales NHS Trust Annual Accounts 2013-14
26. Other financial liabilities
Current 31 March 31 March
2014 2013
£000 £000
Financial liabilities carried at fair value through income statement. 0 623
Non-current
Financial liabilities carried at fair value through income statement. 0 1,713
27. Other liabilities
Current
31 March 31 March
2014 2013
£000 £000
Lease incentives 0 0
PFI asset - deferred credit 0 0
Other (Please specify) 0 0
Total 0 0
Non-current
Lease incentives 0 0
PFI asset - deferred credit 0 0
Other (Please specify) 0 0
Total 0 0
The Trust has no early retirement buy outs.
47

Public Health Wales NHS Trust Annual Accounts 2013-14
28. Provisions
2013-14
28.1 Public Health Wales NHS Trust including
Welsh Risk Pool
Current
£000 £000 £000 £000 £000 £000 £000 £000 £000 £000
Clinical negligence 1,922 0 0 0 0 980 (172) (87) 0 2,643
Personal injury 360 0 0 (65) 0 135 (147) (99) 0 184
All other losses and special payments 0 0 0 0 0 21 (21) 0 0 0
Defence legal fees and other administration 83 0 0 0 0 153 (17) (28) 191
Pensions relating to: former directors 0 0 0 0 0 0 0 0 0
Pensions relating to: other staff 0 0 0 0 0 0 0 0 0
Restructurings 0 0 0 0 0 0 0 0
Other 0 0 0 0 0 0 0 0
Total 2,365 0 0 (65) 0 1,289 (357) (214) 0 3,018
Non Current
Clinical negligence 0 0 0 0 0 0 0 0 0 0
Personal injury 1,050 0 0 65 0 0 0 0 0 1,115
All other losses and special payments 0 0 0 0 0 0 0 0 0 0
Defence legal fees and other administration 0 0 0 0 0 0 0 0 0
Pensions relating to: former directors 0 0 0 0 0 0 0 0 0
Pensions relating to: other staff 0 0 0 0 0 0 0 0 0
Restructurings 0 0 0 0 0 0 0 0
Other 0 0 0 0 0 0 0 0
Total 1,050 0 0 65 0 0 0 0 0 1,115
TOTAL
Clinical negligence 1,922 0 0 0 0 980 (172) (87) 0 2,643
Personal injury 1,410 0 0 0 0 135 (147) (99) 0 1,299
All other losses and special payments 0 0 0 0 0 21 (21) 0 0 0
Defence legal fees and other administration 83 0 0 0 0 153 (17) (28) 191
Pensions relating to: former directors 0 0 0 0 0 0 0 0 0
Pensions relating to: other staff 0 0 0 0 0 0 0 0 0
Restructurings 0 0 0 0 0 0 0 0
Other 0 0 0 0 0 0 0 0
Total 3,415 0 0 0 0 1,289 (357) (214) 0 4,133
Expected timing of cash flows:
Timing period yet to be confirmed In the remainder of spending Between Between Thereafter
review to 31 March 2015 1 April 2015 1 April 2020 Totals
31 March 2020 31 March 2025
£000 £000 £000 £000 £000
Clinical negligence 2,643 0 0 0 2,643
Personal injury 183 314 287 515 1,299
All other losses and special payments 0 0 0 0 0
Defence legal fees and other administration 191 0 0 0 191
Pensions - former directors 0 0 0 0 0
Pensions - other staff 0 0 0 0 0
Restructuring 0 0 0 0 0
Other 0 0 0 0 0
Total 3,017 314 287 515 4,133
At 31 March
2014
Transfers
to creditors
Utilised
during the
year
Transfers
(to)/from
other NHS
body
Unwinding
of discount
At 1 April
2013
Structured
settlement
cases
transferr-ed
to Risk Pool
Arising
during the
year
Reversed
unused
Transfers
between
current and
non current
The expected timing of cashflows are based on best available information; but they could change on the basis of individual ca se changes.
The "Personal Injury" category includes provisions for 3 Permanent Injury Benefit cases.
48

Public Health Wales NHS Trust Annual Accounts 2013-14
28. Provisions (continued)
2012-13
Current
£000 £000 £000 £000 £000 £000 £000 £000 £000 £000
Clinical negligence 2,186 0 0 0 0 591 (712) (143) 0 1,922
Personal injury 44 0 0 92 0 374 (149) (1) 0 360
All other losses and special payments 0 0 0 0 0 20 (20) 0 0 0
Defence legal fees and other administration 38 0 0 0 0 76 (22) (9) 83
Pensions relating to: former directors 0 0 0 0 0 0 0 0 0
Pensions relating to: other staff 0 0 0 0 0 0 0 0 0
Restructurings 0 0 0 0 0 0 0 0
Other 0 0 0 0 0 0 0 0
Total 2,268 0 0 92 0 1,061 (903) (153) 0 2,365
Non Current
Clinical negligence 0 0 0 0 0 0 0 0 0 0
Personal injury 1,127 0 0 (92) 0 0 15 0 0 1,050
All other losses and special payments 0 0 0 0 0 0 0 0 0 0
Defence legal fees and other administration 0 0 0 0 0 0 0 0 0
Pensions relating to: former directors 0 0 0 0 0 0 0 0 0
Pensions relating to: other staff 0 0 0 0 0 0 0 0 0
Restructurings 0 0 0 0 0 0 0 0
Other 0 0 0 0 0 0 0 0
Total 1,127 0 0 (92) 0 0 15 0 0 1,050
TOTAL
Clinical negligence 2,186 0 0 0 0 591 (712) (143) 0 1,922
Personal injury 1,171 0 0 0 0 374 (134) (1) 0 1,410
All other losses and special payments 0 0 0 0 0 20 (20) 0 0 0
Defence legal fees and other administration 38 0 0 0 0 76 (22) (9) 83
Pensions relating to: former directors 0 0 0 0 0 0 0 0 0
Pensions relating to: other staff 0 0 0 0 0 0 0 0 0
Restructurings 0 0 0 0 0 0 0 0
Other 0 0 0 0 0 0 0 0
Total 3,395 0 0 0 0 1,061 (888) (153) 0 3,415
At 31
March 2012
Structured
settlement
cases
transferr-ed
to Risk Pool
Arising
during the
year
Reversed
unused
Unwinding
of discount
At 31 March
2013
Transfer to
creditors
Utilised
during the
year
Transfers
(to)/from
other NHS
body
Transfer
between
current
and non
current
49

Public Health Wales NHS Trust Annual Accounts 2013-14
29. Finance leases
29.1 Finance leases obligations (as lessee)
Amounts payable under finance leases:
LAND 31 March 31 March
2014 2013
£000 £000
Minimum lease payments
Within one year 0 0
Between one and five years 0 0
After five years 0 0
Less finance charges allocated to future periods 0 0
Minimum lease payments 0 0
Included in:
Current borrowings 0 0
Non-current borrowings 0 0
Total 0 0
Present value of minimum lease payments
Within one year 0 0
Between one and five years 0 0
After five years 0 0
Total present value of minimum lease payments 0 0
Included in:
Current borrowings 0 0
Non-current borrowings 0 0Total 0 0
The Trust has a finance lease for the Picture Archive Computer System (PACS).
The inherent interest rate has been calculated at 2.77%. This has been used to discount the total future minimum lease payments of £2,016k to their
present value of £1,872k
Maintenance costs are charged directly to SOCI and are not included as part of the lease value.
50

Public Health Wales NHS Trust Annual Accounts 2013-14
29.1 Finance leases obligations (as lessee) continued
31 March 31 March
Amounts payable under finance leases: 2014 2013
BUILDINGS £000 £000
Minimum lease payments
Within one year 0 0
Between one and five years 0 0
After five years 0 0
Less finance charges allocated to future periods 0 0
Minimum lease payments 0 0
Included in: Current borrowings 0 0
Non-current borrowings 0 0
Total 0 0
Present value of minimum lease payments
Within one year 0 0
Between one and five years 0 0
After five years 0 0
Total present value of minimum lease payments 0 0
Included in: Current borrowings 0 0
Non-current borrowings 0 0
Total 0 0
OTHER 31 March 31 March
2014 2013
Minimum lease payments £000 £000
Within one year 690 671
Between one and five years 1,326 1,851
After five years 0 0
Less finance charges allocated to future periods 0 0
Minimum lease payments 2,016 2,522
Included in: Current borrowings 0 0
Non-current borrowings 0 0
Total 0 0
Present value of minimum lease payments
Within one year 640 623
Between one and five years 1,232 1,713
After five years 0 0
Total present value of minimum lease payments 1,872 2,336
Included in: Current borrowings 640 623
Non-current borrowings 1,232 1,713
Total 1,872 2,336
51
Public Health Wales NHS Trust Annual Accounts 2013-14
29.2 Finance lease receivables (as lessor)
Amounts receivable under finance leases:
31 March 31 March
2014 2013
£000 £000
Gross investment in leases
Within one year 0 0
Between one and five years 0 0
After five years 0 0
Less finance charges allocated to future periods 0 0
Present value of minimum lease payments 0 0
Included in:
Current borrowings 0 0
Non-current borrowings 0 0
Total 0 0
Present value of minimum lease payments
Within one year 0 0
Between one and five years 0 0
After five years 0 0
Total present value of minimum lease payments 0 0
Included in:
Current borrowings 0 0
Non-current borrowings 0 0Total 0 0
There are no finance lease receivables.
52

Public Health Wales NHS Trust Annual Accounts 2013-14
29.3 Rental Revenue 31 March 31 March
2014 2013
£000 £000
Contingent rent 0 0
Other 0 0
Total rental revenue 0 0
29.4 Finance Lease Commitment
30. Private finance transactions
Private Finance Initiatives (PFI) / Public Private Partnerships (PPP)
The Trust has no PFI or PPP schemes deemed to be "on or off SoFP."
Public Health Wales NHS Trust has no finance lease commitments for an asset which has not become fully operational during or prior to 2013-14.
53

Public Health Wales NHS Trust Annual Accounts 2013-14
31. Financial riskCertificate of Chief Financial Officer/Director of Finance
IFRS 7, Derivatives and Other Financial Instruments, requires disclosure of the role that
financial instruments have had during the period in creating or changing the risks an entity
faces in undertaking its activities.
NHS trusts are not exposed to the degree of financial risk faced by business entities.
Financial instruments play a much more limited role in creating or changing risk than would
be typical of the listed companies to which IFRS 7 mainly applies. NHS trusts have limited
powers to borrow or invest surplus funds and financial assets and liabilities are generated
by day to day operational activities rather than being held to change the risks facing NHS
trusts in undertaking its activities.
The NHS trust's treasury management operations are carried out by the finance department
within parameters defined formally within the NHS trust's standing financial instructions and
policies agreed by the board of directors. NHS trust treasury activity is subject to review by
the NHS trust's internal auditors.
Liquidity risk
NHS trust's net operating costs are incurred under annual service agreements with various
Health bodies, which are financed from resources voted annually by parliament. NHS trusts
also largely finance their capital expenditure from funds made available from the Welsh
Government under agreed borrowing limits. NHS trusts are not, therefore, exposed to
significant liquidity risks.
Interest-rate risks
The great majority of NHS trust's financial assets and financial liabilities carry nil or fixed
rates of interest. NHS trusts are not, therefore, exposed to significant interest-rate risk.
Foreign currency risk
NHS trusts have no or negligible foreign currency income or expenditure and therefore are
not exposed to significant foreign currency risk.
Credit Risk
Because the majority of the trust's income comes from contracts with other public sector
bodies, the trust has low exposure to credit risk. The maximum exposures are in
receivables from customers as disclosed in the Trade and other receivables note.
General
The powers of the NHS trust to invest and borrow are limited. The Board has determined
that in order to maximise income from cash balances held, any balance of cash which is not
required will be invested. The trust does not borrow from the private sector. All other
financial instruments are held for the sole purpose of managing the cash flow of the trust on
a day to day basis or arise from the operating activities of the trust. The management of
risks around these financial instruments therefore relates primarily to the trust's overall
arrangements for managing risks to their financial position, rather than the trust's treasury
management procedures.
54

Public Health Wales NHS Trust Annual Accounts 2013-14
32. Financial Instuments
Financial assets At "fair value" Loans and Available Total
through I&E receivables for sale
£000 £000 £000 £000
Embedded derivatives 0 0 0 0
NHS receivables 5,960 0 0 5,960
Cash at bank and in hand 2,547 0 0 2,547
Other financial assets 1,858 0 0 1,858
Total at 31 March 2014 10,365 0 0 10,365
Financial liabilities At "fair value" Other Total
through I&E
£000 £000 £000
Embedded derivatives 0 0 0
PFI and finance lease obligations 1,872 0 1,872
Other financial liabilities 5,158 0 5,158
Total at 31 March 2014 7,030 0 7,030
Financial assets At "fair value" Loans and Available Total
through I&E receivables for sale
£000 £000 £000 £000
Embedded derivatives 0 0 0 0
NHS receivables 5,829 0 0 5,829
Cash at bank and in hand 2,501 0 0 2,501
Other financial assets 0 0 0 0
Total at 31 March 2013 8,330 0 0 8,330
Financial liabilities At "fair value" Other Total
through I&E
£000 £000 £000
Embedded derivatives 0 0 0
PFI and finance lease obligations 2,336 0 2,336
Other financial liabilities 5,745 0 5,745
Total at 31 March 2013 8,081 0 8,081
Financial instruments play a much more limited role in creating or changing risk than
would be typical of listed companies. The NHS trust has limited powers to borrow or
invest surplus funds and financial assets and liabilities are generated by day-to-day
operational activities rather than being held to change the risks facing the NHS trust in
undertaking its activities.
The directors consider that the carrying amounts of financial assets and financial
liabilities recorded at amortised cost in the financial statements approximate their fair
value.
Only NHS receivables have been included in the financial assets as these have been
formally agreed through the NHS agreement process. The other financial liabilities
figure is the total liabilities from Note 23
55

Public Health Wales NHS Trust Annual Accounts 2013-14 13/06/2014
33. Financial performance targets
The Trust has met 2 out of 3 of its financial targets. Details are given below:
33.1 Breakeven 2013-14
£000
Target retained surplus 0
Actual retained surplus 15
Variance (15)
The Trust has broken even in 2013-14.
33.2 External financing 31 March 31 March
The Trust is given an external financing limit which it is permitted to undershoot 2014 2013
£000 £000 £000
External financing limit set by the Welsh Government (1,809) (1,720)
Cash flow financing (1,026) (1,750)
Finance leases taken out in the year (783) 30
Other capital receipts 0 0
External financing requirement (1,809) (1,720)
Undershoot (overshoot) 0 0
The Trust has achieved its external financing limit.
33.3 Creditor payment
The Trust is required to pay 95% of the number of non-NHS bills within 30 days of receipt of goods or
a valid invoice (whichever is the later). The Trust has achieved the following results: 2013-14
Total number of non-NHS bills paid 2013-14 21,755
Total number of non-NHS bills paid within target 20,416
Percentage of non-NHS bills paid within target 93.8%
The Trust has not met the target.
The in year breakeven target and actual surpluses are £0k and £15k respectively Public Health Wales NHS Trust has also achieved on-going breakeven requirement.
56
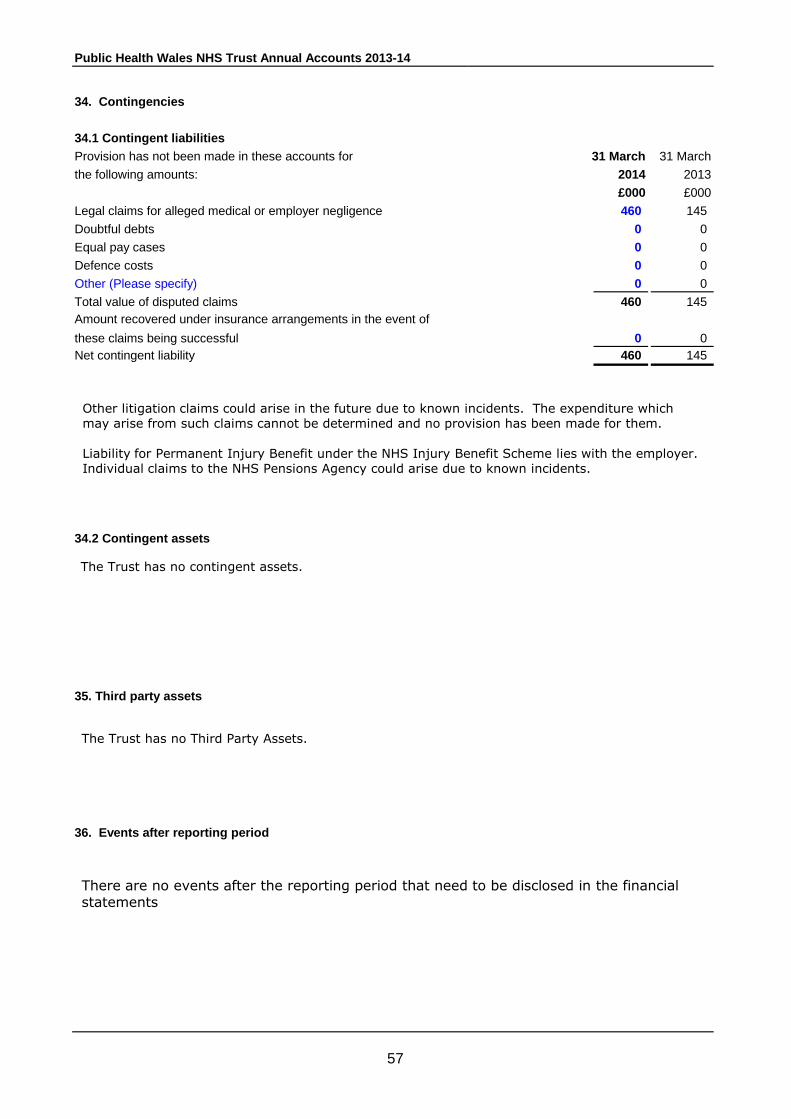
Public Health Wales NHS Trust Annual Accounts 2013-14
34. Contingencies
34.1 Contingent liabilities
Provision has not been made in these accounts for 31 March 31 March
the following amounts: 2014 2013
£000 £000
Legal claims for alleged medical or employer negligence 460 145
Doubtful debts 0 0
Equal pay cases 0 0
Defence costs 0 0
Other (Please specify) 0 0
Total value of disputed claims 460 145
Amount recovered under insurance arrangements in the event of
these claims being successful 0 0
Net contingent liability 460 145
34.2 Contingent assets
35. Third party assets
36. Events after reporting period
Other litigation claims could arise in the future due to known incidents. The expenditure which
may arise from such claims cannot be determined and no provision has been made for them.
Liability for Permanent Injury Benefit under the NHS Injury Benefit Scheme lies with the employer.
Individual claims to the NHS Pensions Agency could arise due to known incidents.
The Trust has no Third Party Assets.
The Trust has no contingent assets.
There are no events after the reporting period that need to be disclosed in the financial
statements
57

Public Health Wales NHS Trust Annual Accounts 2013-14
37. Related Party transactions
Payments to Receipts from Amounts owed Amounts due
related party related party to related party from related party
£000 £000 £000 £000
Payments to Receipts from Amounts owed Amounts due
related party related party to related party from related party
£000 £000 £000 £000
Welsh Government 274 87,864 79 641
FHoT 0 0 0 0
WHSSC 0 337 0 12
ABMU LHB 4,414 3,517 355 313
Aneurin Bevan LHB 3,012 745 314 220
Betsi Cadwaladwr LHB 3,636 3,104 324 256
Cardiff and Vale LHB 3,178 5,208 161 943
Cwm Taf LHB 1,597 217 50 127
Hywel Dda LHB 1,666 1,645 145 300
Powys LHB 217 128 31 6
Velindre NHS Trust 1,615 223 211 15
WAST 49 0 0 0
WRP 0 0 0 0
Cardiff University 809 905 106 212
Merthyr Tydfil CBC 155 1 48 0
Swansea University 464 23 3
Public Health England 271 74 16
21,357 103,991 1,824 3,064
'The Trust is a body corporate established by order of the Welsh Minster for Health and Social Services. 'During the year none of the board members or members of the key management staff or parties 'related to them has undertaken any material transactions with the Trust
The trust is a body corporate established by order of the Welsh Minister for Health and Social
Services. During the year none of the board members or members of the key management
staff or parties related to them has undertaken any material transactions with the trust
The Welsh Government is regarded as a related party. During the year the Trust has had a significant
number of material transactions with the Welsh Government and with other entities for which the Welsh Government is regarded as the parent body.In addition, those organisations which have been identified as related parties to board or executive team members are also listed below.
58

Public Health Wales NHS Trust Annual Accounts 2013-14
38. Intra Government balances and transactions
38.1 Intra Government Balances Receivables: Receivables: Payables: Payables:
Current Non-current Current Non-current
£000 £000 £000 £000
2013-14:
Welsh Government 641 0 79 0
Welsh Local Health Boards 2,165 0 1,381 0
Welsh NHS Trusts 15 0 264 0
WHSSC 12 0 0 0
All English Health Bodies 22 0 77 0
All N. Ireland Health Bodies 0 0 0 0
All Scottish Health Bodies 0 0 0 0
Miscellaneous 4639 0 3,704 1,232
Credit note provision 0 0 0 0
Sub total 7,494 0 5,505 1,232
Other Central Government Bodies
Other Government Departments 0 0 0 0
Revenue & Customs 172 0 0 0
Local Authorities 159 0 293 0
Balances with Public Corporations and trading funds 0 0 0 0
Balances with bodies external to Government 0 0 0 0
TOTAL 7,825 0 5,798 1,232
Receivables: Receivables: Payables: Payables:
Current Non-current Current Non-current
£000 £000 £000 £000
2012-13:
Welsh Government 848 0 124 0
Welsh Local Health Boards 2,554 0 762 0
Welsh NHS Trusts 10 0 876 0
WHSSC 60 0 0 0
All English Health Bodies 43 0 56 0
All N. Ireland Health Bodies 0 0 0 0
All Scottish Health Bodies 0 0 0 0
Miscellaneous 2,373 0 142 0
Credit note provision 0 0 0 0
Sub total 5,888 0 1,960 0
Other Central Government Bodies
Other Government Departments 52 0 0 0
Revenue & Customs 130 0 0 0
Local Authorities 131 0 214 0
Balances with Public Corporations and trading funds 0 0 0 0
Balances with bodies external to Government 1,338 0 3,571 0
TOTAL 7,539 0 5,745 0
59
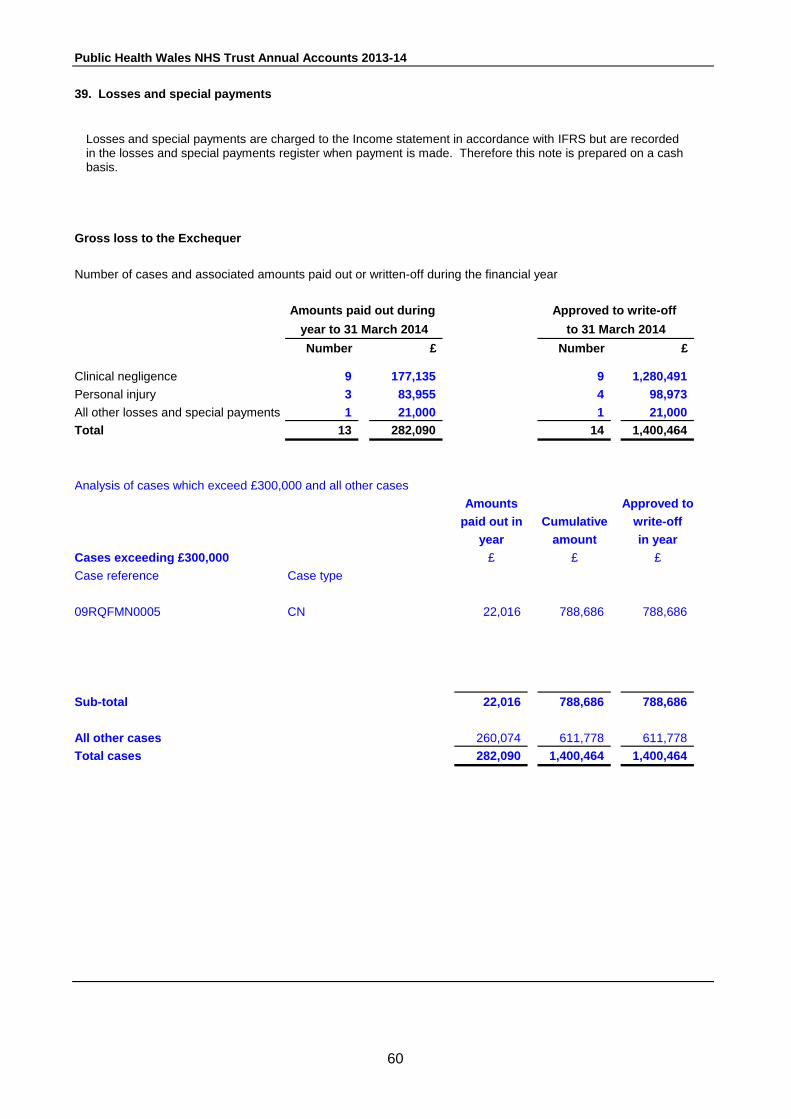
Public Health Wales NHS Trust Annual Accounts 2013-14
39. Losses and special payments
Gross loss to the Exchequer
Number of cases and associated amounts paid out or written-off during the financial year
Number £ Number £
Clinical negligence 9 177,135 9 1,280,491
Personal injury 3 83,955 4 98,973
All other losses and special payments 1 21,000 1 21,000
Total 13 282,090 14 1,400,464
Analysis of cases which exceed £300,000 and all other cases
Amounts Approved to
paid out in Cumulative write-off
year amount in year
Cases exceeding £300,000 £ £ £
Case reference Case type
09RQFMN0005 CN 22,016 788,686 788,686
Sub-total 22,016 788,686 788,686
All other cases 260,074 611,778 611,778
Total cases 282,090 1,400,464 1,400,464
Approved to write-off
to 31 March 2014
Amounts paid out during
year to 31 March 2014
Losses and special payments are charged to the Income statement in accordance with IFRS but are recorded in the losses and special payments register when payment is made. Therefore this note is prepared on a cash basis.
60
Public Health Wales NHS Trust Annual Accounts 2013-14
40. Pooled budgets
Public Health Wales NHS trust has no pooled budgets.
61

Public Health Wales NHS Trust Annual Accounts 2013-14
41. Operating segments
[Disclose: [Provide reconciliations of: [Desirable disclosures: Cash flow from:
The Trust’s primary remit is the provision of public health services throughout Wales and this is viewed as the only segment that is recognisable under this legislation. The Chief Operating Decision Maker (CODM) is considered to be the Trust Board. The CODM receives a variety of information dealing with various aspects of the Trust’s performance, however considers the provision of public health services to be ultimately generic, in terms of geography and service. The Trust therefore is deemed to operate as one segment.
62

Public Health Wales NHS Trust Annual Accounts 2013-14
42. Other
At 1 April the Improvement Functions of the former NLIAH, along with the functions of
equality and human rights, and their associated asset and liabilities were transferred
from ABMU LHB to Public Health Wales NHS Trust.
This resulted in an increase to the annual core funding for Public Health Wales of £4.4m.
48 staff were transferred into Public Health Wales and an opening creditor balance of
£10k, which was paid in year.
The transfer of functions were treated using absorption accounting adapted for the issue
of PDC.
All transactions and balances related to those functions pre 1st April 2013 are included in
the transferor accounts and post 1st April 2013 are included in Public Health Wales NHS
Trust’s financial statements:
63

Public Health Wales NHS Trust Annual Accounts 2013-14
1 4 2
(£10,4 5 1
(£15,
3
(£1
6 (£210,000)
Xxx LHB/NHS Trust
*Nu
mb
er
Number of
other
departures
Num
ber
of
Audit report of the Auditor General to the National Assembly for
Wales
I certify that I have audited the financial statements of Public Health Wales NHS Trust for
the year ended 31 March 2014 under Section 61 of the Public Audit (Wales) Act 2004.
These comprise the Statement of Comprehensive Income, the Statement of Financial
Position, the Cash Flow Statement and the Statement of Changes in Tax Payers Equity and
related notes. The financial reporting framework that has been applied in their preparation
is applicable law and HM Treasury’s Financial Reporting Manual based on International
Financial Reporting Standards (IFRSs). I have also audited the information in the
Remuneration Report that is described as having been audited.
Respective responsibilities of Directors, the Chief Executive and the Auditor
As explained more fully in the Statements of Directors’ and Chief Executive’s
Responsibilities set out on page 66, the Directors and the Chief Executive are responsible
for the preparation of financial statements which give a true and fair view.
My responsibility is to audit the financial statements in accordance with applicable law and
International Standards on Auditing (UK and Ireland). Those standards require me to
comply with the Auditing Practices Board’s Ethical Standards for Auditors.
Scope of the audit of financial statements
An audit involves obtaining evidence about the amounts and disclosures in the financial
statements sufficient to give reasonable assurance that the financial statements are free
from material misstatement, whether caused by fraud or error. This includes an
assessment of: whether the accounting policies are appropriate to Public Health Wales NHS
Trust’s circumstances and have been consistently applied and adequately disclosed; the
reasonableness of significant accounting estimates made by the Directors and Chief
Executive; and the overall presentation of the financial statements.
I am also required to obtain sufficient evidence to give reasonable assurance that the
expenditure and income have been applied to the purposes intended by the National
Assembly for Wales and the financial transactions conform to the authorities which govern
them.
In addition, I read all the financial and non-financial information in the annual report to
identify material inconsistencies with the audited financial statements. If I become aware of
any apparent material misstatements or inconsistencies I consider the implications for my
report.
Opinion on financial statements
In my opinion the financial statements:
- give a true and fair view of the state of affairs of Public Health Wales NHS Trust as at 31
March 2014 and of its surplus, its recognised gains and losses and cash flows for the year
then ended; and
- have been properly prepared in accordance with the National Health Service (Wales) Act
2006 and directions made there under by Welsh Ministers.
64

Public Health Wales NHS Trust Annual Accounts 2013-14
Opinion on Regularity
In my opinion in all material respects, the expenditure and income have been applied to
the purposes intended by the National Assembly for Wales and the financial transactions
conform to the authorities which govern them.
Opinion on other matters
In my opinion:
- the part of the remuneration report to be audited has been properly prepared in
accordance with the National Health Service (Wales) Act 2006 and directions made there
under by Welsh Ministers; and
- I have been unable to read the other information contained in the Annual Report and
consider whether it is consistent with the audited financial statements as it was not
available at the time of my audit.
Matters on which I report by exception
I have nothing to report in respect of the following matters, which I report to you, if, in my
opinion:
- the Annual Governance Statement does not reflect compliance with HM Treasury’s and
Welsh Ministers’ guidance;
- proper accounting records have not been kept;
- information specified by HM Treasury or Welsh Ministers regarding remuneration and
other transactions is not disclosed; or
- I have not received all the information and explanations I require for my audit.
Report
I have no observations to make on these financial statements.
Huw Vaughan Thomas
Auditor General for
Wales
24 June 2014
Wales Audit Office
24 Cathedral Road
Cardiff
CF11 9LJ
65

Public Health Wales NHS Trust Annual Accounts 2013-14
STATEMENT OF THE CHIEF EXECUTIVE'S RESPONSIBILITIES
AS ACCOUNTABLE OFFICER OF THE TRUST
The Welsh Ministers have directed that the Chief Executive should be the Accountable Officer to
the Trust. The relevant responsibilities of Accountable Officers, including their responsibility for the
propriety and regularity of the public finances for which they are answerable, and for the keeping of proper
records, are set out in the Accountable Officer's Memorandum issued by the Welsh Government.
To the best of my knowledge and belief, I have properly discharged the responsibilities set out in
my letter of appointment as an Accountable Officer.
Date: ........................ 2014 ............................................................Chief Executive
The total value of transactions with Board members and key senior
66

Public Health Wales NHS Trust Annual Accounts 2013-14
STATEMENT OF DIRECTORS' RESPONSIBILITIES IN RESPECT OF
The directors are required under the National Health Service Act (Wales) 2006 to prepare accounts for
each financial year. The Welsh Ministers, with the approval of the Treasury, direct that these accounts
give a true and fair view of the state of affairs of the NHS trust and of the income and expenditure of the
NHS trust for that period. In preparing those accounts, the directors are required to:
- apply on a consistent basis accounting principles laid down by the Welsh Ministers with the approval
of the Treasury
- make judgements and estimates which are responsible and prudent
- state whether applicable accounting standards have been followed, subject to any material departures
disclosed and explained in the account.
The directors confirm they have complied with the above requirements in preparing the accounts.
The directors are responsible for keeping proper accounting records which disclose with reasonable
accuracy at any time the financial position of the Trust and to enable them to ensure that the accounts
comply with requirements outlined in the above mentioned direction by the Welsh Ministers.
By Order of the Board
Signed:
Date: ............................2014 Chairman: .....................................................
Date: ............................2014 Chief Executive: ............................................
Date: ............................2014 Director of Finance: ........................................
67

Public Health Wales NHS Trust Annual Accounts 2013-14
1 4 2
(£10,4 5 1
(£15,
3
(£1
6 (£210,000)
Total
num3
(£25,
Xxx LHB/NHS Trust
*Nu
mb
er
Number of
other
departures
Num
ber
of
THE NATIONAL HEALTH SERVICE IN WALES ACCOUNTS DIRECTION GIVEN BY WELSH MINISTERS IN ACCORDANCE WITH SCHEDULE 9 SECTION 178 PARA 3(1) OF THE NATIONAL HEALTH SERVICE (WALES) ACT 2006 (C.42) AND WITH THE APPROVAL OF TREASURY NHS TRUSTS 1. Welsh Ministers direct that an account shall be prepared for the financial year ended 31 March 2010 and subsequent financial years in respect of the NHS Wales Trusts in the form specified in paragraphs [2] to [7] below. BASIS OF PREPARATION 2. The account of the NHS Wales Trusts shall comply with: (a) the accounting guidance of the Government Financial Reporting Manual (FReM), which is in force for the financial year for which the accounts are being prepared, as detailed in the NHS Wales Trust Manual for Accounts; (b) any other specific guidance or disclosures required by the Welsh Government. FORM AND CONTENT 3. The account of the Trust for the year ended 31 March 2010 and subsequent years shall comprise a foreword, an income statement, a statement of financial position, a statement of cash flows and a statement of changes in taxpayers’ equity as long as these statements are required by the FReM and applied to the NHS Wales Manual for Accounts, including such notes as are necessary to ensure a proper understanding of the accounts. 4. For the financial year ended 31 March 2010 and subsequent years, the account of the Trust shall give a true and fair view of the state of affairs as at the end of the financial year and the operating costs, changes in taxpayers’ equity and cash flows during the year. 5. The account shall be signed and dated by the Chief Executive. MISCELLANEOUS 6. The direction shall be reproduced as an appendix to the published accounts. 7. The notes to the accounts shall, inter alia, include details of the accounting policies adopted. Signed by the authority of Welsh Ministers Signed : Chris Hurst Dated : 17.06.2010 1 Please see regulation 3 of the 2009 No 1558(W.153); NATIONAL HEALTH SERVICE, WALES; The National Health Service Trusts (Transfer of Staff, Property Rights and Liabilities) (Wales) Order 2009
68

Public Health Wales NHS Trust Annual Accounts 2013-14
1 4 2
(£10,4 5 1
(£15,
3
(£1
6 (£210,000)
Xxx LHB/NHS Trust
*Nu
mb
er
Number of
other
departures
Num
ber
of
Annual Governance Statement
1 Scope of Responsibility
The Board is accountable for governance, risk management and internal control. As Chief Executive and Accountable Officer of Public Health
Wales, I have responsibility for maintaining appropriate governance structures and procedures as well as a sound system of internal control
that supports the achievement of the organisation’s policies, aims and objectives, whilst safeguarding the public funds and the organisation’s
assets, for which I am personally responsible. These are carried out in
accordance with the responsibilities assigned by the Accounting Officer of NHS Wales.
As Chief Executive and Accountable Officer, I have personal overall
responsibility for the management and staffing of the organisation. I am required to assure myself, and therefore the Board, that the
organisation’s executive management arrangements are fit for purpose and enable effective leadership. I have received assurances from the
Interim Chief Executive as to the controls, which were in place during the year. The following statement demonstrates the mechanisms and
methods used to enable me to gain that assurance.
2 Governance Framework
Public Health Wales has continued to develop a system of governance and
assurance. The Board functions as a corporate decision-making body, with Executive Directors and Non-Executive Directors being full and equal
members and sharing corporate responsibility for all the decisions of the Board.
In particular, the Board has responsibility for the strategic direction,
governance framework, organisational culture and development, developing strong relationships with key stakeholders and partners and
delivery of Public Health Wales’ aims and objectives. In addition,
Executive Directors have Board level responsibility for discharging Public Health Wales’ corporate and public health functions.
The Board is supported by the Board Secretary, who acts as principal
advisor on all aspects of governance within Public Health Wales.
The Board has established a standing Committee structure, which it has determined best meets the needs of the organisation whilst taking
account of any regulatory or Welsh Government requirements.
69

Public Health Wales NHS Trust Annual Accounts 2013-14
1 4 2
(£10,4 5 1
(£15,
3
(£1
6 (£210,000)
Xxx LHB/NHS Trust
*Nu
mb
er
Number of
other
departures
Num
ber
of
Diagram 1.1 below provides an overview of the governance framework
established by Public Health Wales, which operated during 2013/14.
These arrangements have been further strengthened by the introduction of a service user experience and learning panel with clearer senior management
oversight, which will be operational from April 2014 and will report directly to the Quality and Safety Committee. Further information on the development of the
panel appears later in this document.
At an operational level, the Executive Team has a robust governance structure
ensuring monitoring and control of the efficient and effective use of the Trust’s resources. Financial monitoring, service performance, quality and workforce information is scrutinised at meetings of the Trust Board, and at various
operational team meetings.
NHS Trusts in Wales must agree Standing Orders for the regulation of proceedings and business. They are designed to translate the statutory
requirements set out in the Public Health Wales NHS Trust (Membership and Procedures) Regulations 2009 into day-to-day operating practice. Together with the adoption of a scheme of decisions reserved for the Board, a scheme of
delegations to officers and others, and Standing Financial Instructions, they provide the regulatory framework for the business conduct of the Trust. These
documents, together with the range of corporate policies set by the Board and the adoption of the Values and Standards of Behaviour framework, make up the
Governance Framework.
Board
Audit Committee
Quality & Safety
Committee
Information Governance Committee
Remuneration and Terms of
Service Committee
Charitable Funds Committee
(administered by Velindre NHS Trust)
Information Governance
Working Group
Research & Development
Group
Infection Control Group
Health & Safety Group
Safeguarding Group
Executive Team
Senior Management
Forum
Risk Management
Group
Lines of accountability & information flow
Lines of information flow
70

Public Health Wales NHS Trust Annual Accounts 2013-14
1 4 2
(£10,4 5 1
(£15,
3
(£1
6 (£210,000)
Xxx LHB/NHS Trust
*Nu
mb
er
Number of
other
departures
Num
ber
of
During the year, a number of developments have been put in place, which will
further strengthen the governance framework for the organisation and test the robustness of the framework. In response to the Mid-Staffordshire NHS Foundation Trust Public Inquiry (the Francis Report), a Francis review team was
established. The review team has undertaken a series of engagement workshops with staff across the organisation. The workshops considered the
implications for Public Health Wales of the findings from the Mid-Staffordshire Inquiry. The themes identified in the workshops will be considered alongside
work being undertaken by the Workforce and Organisational Development team in response to the staff survey and the Public Health Wales Strategy and delivery planning. The emerging themes focus on organisational culture and ways of
working. More detailed findings are currently being considered by the Executive Team and will be reported to the Board on 26 June 2014.
We have also recognised that information on service user experience can help to improve and shape services in the organisation. This was also identified as an
area for improvement in the Wales Audit Office Structured Assessment for this year. Work has begun to establish a Service User Experience and Learning
Panel, which will bring scrutiny and emphasis on placing service users at the centre of improving, developing and planning services. The panel will also
consider concerns, incidents and complaints in conjunction with Service User Experience. This will provide a more joined up and coherent approach to understanding emerging issues from a citizen centred perspective leading to
service improvements. The panel will have representation from key areas where services are provided across the organisation. A representative from Community
Health Councils has also been identified to sit on the group. The group will report regularly against the Welsh Government’s Service User Experience Framework and the agreed national service user standards. A Non Executive Director has
been appointed as service user experience champion. This will assist quality improvements and service user experience whilst ensuring the user’s voice and
experience are heard and represented at Board level and also further strengthen the assurance arrangements for the organisation.
2.1 Board membership
The Board has been constituted to comply with the Public Health Wales National Health Service Trust (Membership and Procedure) Regulations 2009. In addition
to responsibilities and accountabilities set out in terms and conditions of appointment, Board members also fulfil a number of Champion roles where they act as ambassadors for these matters.
71

Public Health Wales NHS Trust Annual Accounts 2013-14
1 4 2
(£10,4 5 1
(£15,
3
(£1
6 (£210,000)
Xxx LHB/NHS Trust
*Nu
mb
er
Number of
other
departures
Num
ber
of
In addition to the Board members appointed in accordance with the Public Health Wales NHS Trust (Membership and Procedures) Regulations 2009, Public Health Wales has appointed four additional posts, which have an integral role in the
governance of the organisation. These include a Board Secretary, Director of Nursing, Director of Workforce and Organisational Development and Director of
Communications. Individuals appointed to these positions are members of the Executive Team and have a standing invitation to Board meetings where they
can contribute to discussions but do not have voting rights. The Director of Nursing post was a new post created in 2013. The Director of Nursing took up her post in April 2013. This new post provides an improved position for the
organisation in ensuring that appropriate arrangements are in place to ensure the necessary protection for the public, professional leadership and
accountability for registered nurses and midwives employed within the organisation. Professional lines of accountability are made clear and will be reflected in job descriptions for all registered nurses and midwives where
registration with the NMC is a pre requisite for employment within Public Health Wales. Table 1 outlines the membership of the Board for 2013/14 and also
highlights the membership of the Committees and areas of responsibilities that are championed by the members of the Board.
2.1.1 Vacant Board position
The Local Authority Non Executive Director position has remained vacant throughout 2013/14. The Public Health Wales NHS Trust (membership and
procedure) Regulations 2009 prescribe that this position must be filled using a nominee from local authorities in Wales. The Board had recognised that this nomination approach disadvantages people from under-represented groups and
does not promote the organisation’s commitment to openness and transparency. Following discussions with the Minister for Health and Social Services, it has
been agreed to amend the Regulations so that the post can be advertised through fair and open competition, rather than a nomination process. The Welsh
Government has agreed that until the Regulations have been amended, the post can be filled on an interim basis. This vacancy has added pressure to the time already given by existing Non Executive Directors and does not present the
Board with a rounded local government view. We are well into the process of appointing an interim Board member for a 12 month period that can provide a
strong link to local authorities in Wales. Local Government is a key partner in tackling public health issues in Wales and it is therefore a distinct disadvantage for the organisation not to have this link in place.
72

Public Health Wales NHS Trust Annual Accounts 2013-14
1 4 2
(£10,4 5 1
(£15,
3
(£1
6 (£210,000)
Xxx LHB/NHS Trust
*Nu
mb
er
Number of
other
departures
Num
ber
of
2.1.2 Recruitment of new Chief Executive Mr Bob Hudson left his post as Chief Executive of Public Health Wales in
November 2013. An interim arrangement was put in place whereby Mr Huw George took up the position as interim Chief Executive. There was a seamless
transition between Mr Hudson leaving the organisation and Mr George taking up the role of interim Chief Executive. Mr George’s substantive role as Executive
Director of Finance ensured a continuity of knowledge and did not present any risk to the organisation. Mr Huw George remained in post until I took up the position on 1 June 2014. Mrs Tamira Rolls was appointed as interim Executive
Director of Finance during this period.
2.1.3 Staff representation at Board meetings We have invited members of trade unions and BMA to attend Board meetings as
full non-voting members to contribute fully to discussions and decisions at Board level. In 2012/13 we reported that there was no staff representation at Board
level. We are pleased to report that the partnership forum has nominated two representatives to attend Board meetings. They will alternate their attendance
at each meeting and attendance started in January 2014. We are in discussions with the BMA about securing a representative at Board meetings.
73

Public Health Wales NHS Trust Annual Accounts 2013-14
74

Public Health Wales NHS Trust Annual Accounts 2013-14
* Attend Board / Committee meetings, but are not members of the Board / Committee
and therefore do not have voting rights.
The following table outlines dates of Board and Committee meetings held during 2013/14, highlighting any meetings that were inquorate:
Table 1.2 Board and Committee meetings held during 2013/14
Quorate
Inquorate
There were no inquorate meetings held during 2013/14. Where meetings have been inquorate in previous years, escalation arrangements were in place to ensure that any matters of significant concern that could not be brought to the
attention of the Committee could be raised with the Trust Chair.
2.2 Board Committees The Board has established four standing Board Committees, chaired by Non
Executive Directors, that have key roles in relation to the system of governance and assurance, decision making, scrutiny, development discussions, an
assessment of current risks and performance monitoring. Committee papers and minutes for each meeting are published on the Public Health Wales website.
The chairs of the Committees provide verbal reports to the Board meeting following each Committee meeting. Minutes of Committee meetings are also presented to the Board once approved by the relevant Committee. Each
Committee also produces an annual report, which provide a summary of business undertaken during the year. Copies of these reports are available on
the Public Health Wales website. The Committee annual reports provide the Board with assurance that the Committees are working effectively and contribute to the overall assessment of Board effectiveness.
75

Public Health Wales NHS Trust Annual Accounts 2013-14
There is common membership between the Committees to ensure integration
with each other in relevant areas. The Terms of Reference for the Committees were reviewed in January 2014 to ensure that there were no overlaps or obvious gaps in roles and responsibilities for each of the Committees. This was
undertaken in response to the Audit Committee’s review of its effectiveness. The outcome of the review was that few changes were needed to the Terms of
Reference, although some additional information was included to reinforce the need for Committees to ensure a connection between the business of key
committees and also seek to integrate assurance reporting. In addition, Public Health Wales has established a Charitable Funds Committee.
This Committee has not met, as charitable funds are currently administered by Velindre NHS Trust on Public Health Wales’ behalf. The Board has agreed that in
the interest of cost effectiveness, Velindre NHS Trust will continue to administer charitable funds on behalf of Public Health Wales.
The following paragraphs provide highlights of reports received by Committees throughout the year. These highlights provide evidence of the governance
framework working in practice.
2.2.1 The Audit Committee The Audit Committee met five times during 2013/14 and was quorate on each
occasion. The Audit Committee provides advice and assurance to the Board on the systems of internal control, governance and efficient and effective use of
resources by overseeing and monitoring a programme of internal and external audit. During the year, the Audit Committee received and discussed a number of reports produced by internal audit, which included sustainability reporting;
Annual Quality Statement; implementation of alert notices; Screening services – service modification; Welsh Risk Pool claims management; financial systems
review; and asbestos management. The Committee was pleased to note that, with the exception of the Welsh Risk Pool claims management report and the
asbestos report, each of these reports were rated ‘reasonable assurance’. The Welsh Risk Pool claims management report was rated ‘substantial assurance’. The asbestos management report was rated ‘limited assurance’. In relation to
the asbestos management report the Committee were informed of a number of issues highlighted in the report and noted the recommendations. At the end of
March 2014, a number of the recommendations had been addressed and the Committee agreed that Internal Audit should complete a further review in September 2014.
1. Further information regarding the ratings of assurance from internal audit is
provided at appendix A
76

Public Health Wales NHS Trust Annual Accounts 2013-14
In July 2013 the Board noted that the organisation was likely to miss the target
for public sector payment compliance. The Audit Committee requested further assurances on what measures were being taken to improve the situation and received a report at their meeting in September 2013. The Committee received
assurance that the issue had occurred early in the financial year and was due to a change over in systems. The organisation had achieved the target for the
majority of the year, however the issues earlier in the year would mean that the target across the year would not be met. The Committee noted that this would
be confirmed in the annual accounts for 2013/14. The Committee also undertook a self assessment exercise where they assured
themselves that the Committee was complying with the requirements set out in the Audit Committee handbook and identified areas for improvement for the
Committee. This self assessment exercise included further development sessions and a renewed focus on roles and responsibilities for the Committee. The Committee also received a presentation on risk assurance in the
organisation and discussed actions, which are currently in place to mitigate the high level corporate risks.
The organisation commissioned an external audit report into the management
arrangements in the Microbiology Division. The final version of that report was received and discussed in December 2013. Consequent to which the Committee requested regular updates on progress being made to address the
recommendations in the report. A similar audit report with recommendations was received by the Committee in March 2013 in relation to management
arrangements in the Screening Division. This was followed by the receipt of regular reports, which provided updates on progress being made against the recommendations in the Screening Division report.
NHS Wales Shared Services Partnership carries out a number of functions on
behalf of Public Health Wales. The Audit Committee receives reports from the internal audit function at NHS Wales Shared Services Partnership which provide
it with assurance that these functions are efficient and cost effective. Public Health Wales also has representation on the NHS Wales Shared Services Partnership Committee where any issues, which have been identified are shared
and fed back to the Committee.
2.2.2 The Quality and Safety Committee The Quality and Safety Committee met three times during 2013/14 and was
quorate on each occasion. However the Committee meeting scheduled for 8 February 2014 did not take place because the meeting did not have a full
quorum.
77

Public Health Wales NHS Trust Annual Accounts 2013-14
The Committee expressed concern about the low level of compliance of statutory
and mandatory training requirements and requested regular updates on actions to be taken, or already in place, substantially to improve compliance. The Committee has continued to monitor the situation and maintained to exert
pressure on managers across the organisation to soundly address and achieve the necessary improvement in compliance among their colleagues. A focus on
statutory training has been maintained by the Committee. Data subsequently received by the Committee demonstrated a welcome significant improvement in
compliance by end of March 2014. The Committee will maintain its focus on compliance with statutory and mandatory training and expect continuing improvement in 2014/15.
During the year the Committee received a programme of reports from Divisions
within the organisation on their quality assurance arrangements and how they are implemented and monitored. This series of reports also gave the Committee an opportunity to scrutinise thoroughly the performance frameworks within those
divisions and to request further assurance where necessary. The Committee were pleased to note that the microbiology division has robust quality assurance
arrangements in place. They monitored closely the division’s Clinical Pathology Accreditation (CPA), during 2012/13. CPA assesses and declares the competence
of medical laboratories in the UK. Adherence to the CPA standards for medical laboratories ensures a thorough assessment and evaluation of all aspects of an organisation’s operations. A small number of non conformances with the
Standards was identified. These were rectified and full CPA accreditation was received in June 2013. The microbiology laboratory in Wrexham transferred to
Public Health Wales in October 2013 and maintained its CPA accreditation. Public Health Wales is now recognised as the only fully accredited pathology service in Wales. The next scheduled assessment in Public Health Wales
Microbiology is expected in June 2014. This will be subject to the internationally recognised standard ISO15189:2012 medical laboratories – particular
requirements for quality, competence, which was introduced by CPA in October 2013.
During the year, the Committee recognised that further work was needed in the microbiology division to develop performance reporting within the division. The
Committee arranged a half-day session where they requested proposals on how performance reporting will be developed in the division and the link to the
already well-established quality assurance arrangements. This was arranged for February 2014, but was postponed to the meeting on 22 April 2014. The Committee will continue to monitor this closely during 2014/15.
78

Public Health Wales NHS Trust Annual Accounts 2013-14
The Committee also reviews and considers claims under the NHS Wales redress
scheme. No settlements under this scheme were made during 2013/14. 2.2.3 The Information Governance Committee
The Information Governance Committee met four times during 2013/14 and was
quorate on each occasion. Throughout the year the corporate risk register contained four high level information governance risks (see below). The
Committee received regular updates on each of these risks and discussed the actions being taken to mitigate the risks. The Committee were pleased to note that one risk, relating to all Wales patient consent forms, was removed as a risk
during the year. A second risk relating the removal of section 251 support (which ensured compliance with the data protection act, removing the need to
obtain explicit consent) has significantly reduced following action by, and pressure brought by the Committee. A third risk relating to EU data protection is still listed as a high risk and is being monitored closely by the Committee. The
fourth risk is an overarching one relating to the risk of failure to ensure appropriate governance of information. This is an organisational wide risk which
the Committee has discussed could possibly be reduced due to the robust controls which are now in place. The Committee has agreed to discuss this in
more detail at their meeting in June 2014. The Information Governance Committee receives summaries and reports on all
Information Governance incidents and ‘near misses’ reported through the Trust’s incident management system. All serious incidents are reported fully to the
Committee and Welsh Government and full Root Cause Analysis investigations are undertaken.
2.2.4 The Remuneration and Terms of Service Committee
The Remuneration and Terms of Service Committee met four times during 2013/14 and was quorate on each occasion. As a result of the national pay
freeze which has been observed in Public Health Wales, the Committee mostly considered applications in respect of the voluntary early release scheme. The Committee approved a 1 per cent cost of living pay award for senior managers in
line with that awarded to staff under Agenda for Change and medical and dental staff in April 2013. However, it was subsequently discovered that this payment
was made erroneously. This has now been rectified and reversed.
3 System of Internal Control The system of internal control is designed to manage risk to a reasonable level rather than to eliminate all risks; it can therefore only provide reasonable and
not absolute assurance of its effectiveness.
79

Public Health Wales NHS Trust Annual Accounts 2013-14
The system of internal control is based on an ongoing process designed to identify and prioritise the risks to the achievement of organisational policies, aims and objectives, to evaluate the likelihood of those risks being realised and
the impact should they be realised, and to manage them efficiently, effectively and economically.
The system of internal control has been in place in the Trust for the year ended 31 March 2014, and up to the date of approval of the Annual Report and
Accounts.
A Board Assurance Framework was approved by the Board in September 2013. The Board Assurance Framework is used to monitor, proactively seek assurance
and ensure shortfalls are addressed through the scrutiny of the Board and its Committees.
Key controls are defined as those controls and systems in place to assist in securing the delivery of the Board’s strategic objectives. Examples of key
controls include:
- Schemes of delegation
- Policies and procedures - Performance data
- Financial management information - Quality and Safety processes
4 Risk Management Public Health Wales has continued to develop and embed its approach to risk management but has identified a need to review the risk management process
to ensure risk is embedded across the organisation and linked to our three year integrated plan.
Public Health Wales has a risk management strategy in place, which includes a risk management framework. The strategy involves 5 key areas:
- developing risk management in Public Health Wales;
- embedding key risk management systems and processes; - ensuring statutory compliance;
- ensuring Public Health Wales is risk aware and staff are appropriately trained and skilled in risk management; - ensuring compliance with regulation and monitoring.
Risks are identified using an online risk management tool, which was launched in
April 2013. All staff have received training and are encouraged to report risks using the online reporting facility. Risks are captured at every level within the organisation, from day to day risks faced by the staff on the ground, to the
strategic risks at Board level.
80

Public Health Wales NHS Trust Annual Accounts 2013-14
Individual divisions, service areas, teams, programmes and laboratories are responsible for maintaining their own risk registers. These risks can then be prioritised according to a wide range of criteria, enabling principal risks to be fed
upwards to the Board. Divisional Directors review their divisional risks regularly and ensure an action plan is in place and monitor progress against the action
plan. A risk management group has responsibility for reviewing and commenting on the risk register and seeking assurance from those who have identified the
risk that action plans are in place to manage and reduce the risk. These arrangements will be further strengthened in 2014/15. Risks are allocated to Executive leads and are reviewed at each Executive Team meeting.
The Audit Committee receives the corporate risk register regularly and has been
reviewing the assurance in place for each risk. The Information Governance Committee review and scrutinise all information governance risks and the Quality and Safety Committee review all risks relating to quality and safety.
The corporate risk register contains ten high level risks. This is an increase on
the eight high level risks which were in place in at the beginning of 2013/14. The table below provides a breakdown of categories of risk. The risk register is
published on the Public Health Wales website with the Board papers for each Board meeting. The published register provides more details regarding the nature of the risk and the mitigating actions being taken by the organisation
Table 4.1 Category and number of risks
The corporate risk register is supported by an operational risk profile. The risks
on the operational risk profile arise from activities and processes undertaken within Divisions to achieve the organisation’s objectives. The risks are identified
during the normal course of work and are considered as they arise. They are managed at the time that they arise and reported
81

Public Health Wales NHS Trust Annual Accounts 2013-14
by staff locally. However, if necessary the risk can be escalated as appropriate.
The Wales Audit Office Structured Assessment recommended that ‘the trust’s approach to identifying and recording divisional risks needs to be reviewed and
improved. It is not clear that risk registers are reviewed regularly’. The Board has accepted this recommendation and recognises that more work is needed in
this area. The development of the integrated medium term plan (more detail of which is found later in this document) has linked to a new operational plan with
newly identified corporate risks, which are linked to the organisational priorities. The Board has also commissioned Academi Wales in conjunction with the Good Governance Institute to undertake a rapid review of governance behaviours and
systems in April 2014. This is in response to the recommendation from Wales Audit Office.
All serious incidents are reported fully to the Quality and Safety Committee and Welsh Government and full Root Cause Analysis investigations are undertaken.
The Committee is also responsible for the monitoring progress against actions identified to ensure that they are completed within the timescales set. In
2013/14 a total of seven Serious Incidents were reported to the Welsh Government. All Serious Incidents are reported by the Screening Division and
relate either to misdiagnosis or recognised procedural risks. Each case is reviewed thoroughly and reported to the Quality and Safety Committee through the Putting Things Right highlights report which can be found on the Quality and
Safety Committee website. The Quality and Safety Committee is also responsible for ensuring that lessons are learnt from serious incidents and that
these lessons are embedded in future practices. The NHS Wales Shared Services Partnership, Audit and Assurance Services
provide an internal audit function for Public Health Wales. Their programme of reviews provides an independent and objective opinion on the adequacy of the
systems of risk management, control and governance by measuring and evaluating effectiveness.
5 Doing Well, Doing Better: Standards for Health Services in Wales Public Health Wales uses the Doing Well, Doing Better: Standards for Health Services in Wales as its framework for gaining assurance on its ability to fulfil its
aims and objectives for the delivery of safe, high quality health services. This involves self assessment of performance against the standards across all
activities and at all levels throughout the organisation. An evaluation of this self assessment is undertaken by the Audit and Assurance Service and a plan for improvement is developed, which is further considered by the Quality and Safety
Committee.
82

Public Health Wales NHS Trust Annual Accounts 2013-14
As part of this process, the organisation has completed the Governance &
Accountability assessment module and has: - openly assessed its performance using the maturity matrix
- responded, where received, to feedback from Healthcare Inspectorate Wales - put plans in place to achieve the improvement actions identified within clearly
defined timescales proportionate to the risk.
For 2013/14 a more streamlined and focused assessment of the Governance and Accountability module has been completed. Areas for improvement have been identified and are reflected in the actions identified from the Standards for
Health Services in Wales self assessment. Progress against these actions will be monitored and reported on a quarterly basis to the Executive Team and the
Quality and Safety Committee and reports are available on the Public Health Wales website. The following improvements were identified and completed during the year:
Standard 1: Governance and Accountability
A Board Assurance Framework was approved by the Board in September 2013. The template for Board papers will be amended to include a requirement
to link any Board discussion to the revised strategic objectives and priorities and the relevant standards for health services
Standard 12: Environment A facilities database has been developed which now acts as the central point for
all estate related documentation and also to track any actions generated from inspections and audits. This database will help the organisation to determine best practice within our premises and also identify any gaps that require
addressing.
Standard 22: Risk, Health and Safety The online risk management system has been implemented across Public Health
Wales and the web based risk assessment form and escalation process has been made available to all staff to enable them to report risks identified. These risks are subject to review and approval prior to being included on the Team, Division
or Corporate risk register.
The organisation considered the following levels of performance for 2013/14. Also included is a comparison with scores achieved in previous years.
83

Public Health Wales NHS Trust Annual Accounts 2013-14
Table 4.1 Governance and Accountability Module
* 2011/12 ° 2012/13 X 2013/14
This process has been subject to independent internal assurance by the
organisation’s Head of Internal Audit. The Quality and Safety Committee is responsible for the monitoring of progress against the Corporate Standards for Health Services Improvement Plan. Public Health Wales is represented at the
Healthcare Standards Self Assessment Tool User Group.
Public Health Wales embeds the Standards for Health Services within its activities and structures as they develop. Each of the Corporate Standards for Health Services had an Executive Lead and nominated Corporate Lead, along
with a responsible Board Committee. In addition, the revised Healthcare Standards are built into relevant Public Health Policies and Procedures as
appropriate.
Divisional Directors are also required to develop and lead arrangements to cascade and embed the standards that are relevant to their work. To assist with this a protocol has been developed to provide staff with details
84
Public Health Wales NHS Trust Annual Accounts 2013-14
of their roles and responsibilities in relation to the management of the Standards
for Health Services.
6 UK Corporate Governance Code Public Health Wales Board is required to comply with ‘corporate governance in central government departments: code of good practice 2011’. The information
provided in this Governance Statement provides an assessment of how Public Health Wales Board complies with the main principles of the Code as they relate
to an NHS public sector organisation in Wales. This assessment has been informed by the organisation’s assessment against the Governance and
Accountability Module undertaken by the Board and also evidenced by internal and external audits. Public Health Wales is following the spirit of the Code to good effect and is conducting its business openly and in line with the Code. The
Board recognises that not all reporting elements of the Code are outlined in this Governance Statement but are reported more fully in the Trust’s wider Annual
Report. There have been no reported departures from the Corporate Governance Code.
The main principles of the code, which apply to Public Health Wales Board, include: role of the Board, Board composition, Board effectiveness and risk
management. Public Health Wales complies with the first three of each of the principles in the following ways. More information on how Public Health Wales
Board complies with risk management can be found in section 4. 6.1 Role of Board and Board composition
Public Health Wales is headed by a Board comprising five Executive and seven
Non Executive Board members. There is a clear division of roles and responsibilities. The Board is responsible for shaping strategy and non Executive Directors regularly challenge and scrutinise the work of the executive. The Chair
is accountable to the Minister for Health and Social Services and responsible for ensuring that the Board leads the organisation effectively so that the
organisation delivers against national objectives set by the Welsh Government.
The Chair of the Board is accountable and reports to the Minister for Health and Social Services in regard to the overall performance of the Trust and its strategic direction. The Chief Executive is accountable and reports to the Chair and the
Chief Executive of NHS Wales/Director General, Department for Health, Social Services and Children, Welsh Government. The Board itself is fully accountable
to the Minister for Health and Social Services, the Welsh Government. As a public body, it also has a responsibility to its’ partners and stakeholders, and the
85

Public Health Wales NHS Trust Annual Accounts 2013-14
general public. The risk management process is described earlier in this
document. Internal control principles are detailed and described in the Board Assurance Framework, which was approved by the Board in September 2013, and the organisation’s annual report and accounts provide an overview of
assurance reporting to the Welsh Government and Welsh Ministers.
6.2 Board Effectiveness
The composition of the Board provides an appropriate balance of skills, experience, independence and knowledge. The board has expressed concern about the gender imbalance of Board members and the lack of people from
under-represented groups. Work is being taken forward to ensure all future recruitment encourages applications from these under-represented groups and is
in line with Welsh Government policy in this area. Agendas and papers are issued ten calendar days before each formal Board
meeting. This provides members and those invited to attend the Board in an observer capacity with sufficient time to consider all relevant information and
papers for decision, discussion, guidance, information and intelligence so that they are aided and informed to discharge their duties and responsibilities
effectively. Inevitably, meetings have very full agendas necessitating a considerable amount of business is completed at each meeting. Nevertheless, the chair of the Board is satisfied that the Board has only very rarely had
insufficient time to fully consider and debate matters. In that rare circumstance less pressing matters are referred to the next meeting, or an agreed balanced
sub-group of board members are assigned to progress the task before the next meeting, report their deliberations to the Chair who ensures that the sub-group’s deliberations and outcomes are reported, discussed and endorsed or otherwise
at the next plenary session of the Board. Board members have also confirmed that they are not pressurised into making decisions without the full and relevant
information being made available to them.
Ongoing training and development for Board members, both Executive and Non Executive, is delivered through informal Board meetings. Non Executive Directors are involved in a variety of other ways which include attending
management meetings through to chairing conferences. The Board has identified the need for a bespoke development programme and has commissioned a
programme of Board development to assist it in evaluating its own performance. The Audit Committee have also undertaken an evaluation exercise which has resulted in a number of actions which will be addressed in Board development
sessions. This is supplemented by regular meetings between the Chair, Board Secretary and Chief Executive to identify areas requiring further development.
Furthermore, the need for specific areas for development of individual Board members and the
86

Public Health Wales NHS Trust Annual Accounts 2013-14
relevance to general Board development are identified and discussed at regular
performance development reviews of Board members carried out by the Chair and Chief Executive. During 2013/14 these discussions informed a series of informal Board meetings and away days, which provided an opportunity to
address development needs and to reflect on the Board and organisation’s strategic direction and performance since it was established in 2009.
In early 2013 the Board participated in a workshop where they discussed the
recommendations from the Mid Staffordshire NHS Foundation Trust Public Inquiry (Francis report). These discussions were used to inform the staff engagement events which are mentioned earlier in this document in section 2.
The Board continued these discussions throughout 2013/14 and reflected on their performance and effectiveness as a group and individually. The Wales Audit
Office and Healthcare Inspectorate Wales report into governance arrangements at Betsi Cadwaladr Health Board was also considered by the Board. The Board reflected on the findings from the report and undertook a piece of work to assure
themselves of the governance arrangements in Public Health Wales. As part of this reflection, the Board concluded that they are confident that Public Health
Wales has indeed been proactive in adopting an enduring review and strengthening of its governance and scrutiny arrangements in response to the
report into Betsi Cadwaladr Health Board. The assessment was submitted to David Sissling, Director General Directorate for Health and Social Services, Welsh Government and Chief Executive NHS Wales. Improvements have been
made to the structure of Board agendas and supporting papers to ensure absolute clarity of why an item is being brought to the Board and whether it is
for decision, scrutiny or information. There was also a renewed focus on Board development, as mentioned earlier in this document. Having undertaken the exercise above, the Board has satisfied itself that the quality of information and
data received at Board meetings is acceptable. An independent consultant from the Good Governance Institute attended the Board meeting on 30 January 2014
to provide feedback on the quality and level of information and data received by the Board. This provided a basis for the rapid review which has been
commissioned.
7 Integrated medium term plan
Public Health Wales has developed an integrated medium term plan, which supports the aims and policies of the Welsh Government and fits within the NHS Wales Planning Framework. The plan guides the delivery of our strategy and the
achievement of a healthier, happier and fairer Wales through our three commitments improve health and wellbeing and reduce health inequalities;
improve the quality, equity and effectiveness of healthcare services; and protect people from infectious and environmental hazards. It demonstrates financial
87

Public Health Wales NHS Trust Annual Accounts 2013-14
balance and covers a three year period from 2014/15 to 2016/17. The plan was
approved by the Public Health Wales Board in March 2014 and submitted to the Welsh Government for consideration and comment. Following feedback from the Welsh Government a one year, more detailed, plan will be submitted by 30 June
2014.
The plan sets out where we have come from; where we are now; where we want to go; and how we will get there.
This plan is our first under the 2013 NHS Wales Planning Framework. It is also the first under our refreshed strategy.
In early 2013, we started the current planning cycle from first principles, by
reviewing and refreshing the strategy that we had adopted following our establishment in 2009. This was because:
- we had developed as an organisation and had important new perspectives and ideas about our aims, our priorities and the best ways of contributing to them
- the environment in which we operate had changed, with new, more
challenging, expectations of us - we had grown by approximately 25%, by taking on new services and functions
- it was clear that some of the established ways of doing things were not having
a big enough impact on the health of the people of Wales Arising out of the development of our refreshed strategy, we have agreed and
adopted new priorities for action. These were agreed at the end of 2013 and have informed the development of the plan.
We will review our plan annually to ensure that it continues to meet our needs
and those of our partners, stakeholders and the citizens in Wales. Over the next year, we will ensure even greater alignment between our plan and the plans of stakeholders. We will do this by aligning public health priorities and actions to
address and tackle them across NHS Wales and beyond.
A Quality and Delivery Framework has been developed in support of the integrated plan, which sets out a mixture of quantitative and qualitative measures to assess performance internally and externally against the
organisation’s strategic objectives. This has driven an improvement in performance reporting to the Board. This has also assisted a more integrated
approach to finance, workforce and service planning and provides a clearer approach to demonstrating achievement of the organisation’s objectives.
88

Public Health Wales NHS Trust Annual Accounts 2013-14
8 Additional Assurance Disclosures 8.1 Ministerial Directions
Whilst Ministerial Directions are received by Local Health Boards, these are not
always applicable to Public Health Wales. All Ministerial Directions issued throughout the year are listed on the Welsh Governance website. During 2013/14 nine Non-Statutory Instruments were issued by the Welsh Government.
Public Health Wales was only required to take action on one of these Non-Statutory Instruments ‘establishment of the Emergency Ambulance Services
Committee (Wales). Under this direction the Chief Executive of Public Health Wales is appointed as an associate member of the joint Committee and as such
may not vote in any meetings or proceedings of the joint committee. In addition to the above Non-Statutory Instruments Public Health Wales receives
letters from the Minister where we are required to take action. Any letters which are received are reported at each Board meeting in the Board Secretary’s
Governance report, with further information on what action has been taken in response to the letter.
8.2 1000 Lives Plus
The organisation engages with the 1000 Lives Plus programme, and the Board promotes use of methodologies for improvement, and is aware of improvements
made and barriers to extending it. On 1 April 2013 staff from the National Leadership and Innovation Agency for
Healthcare (NLIAH) service improvement unit transferred into Public Health Wales. These staff, along with the staff working in the 1000 Lives Plus team in
Public Health Wales were brought together to form to 1000 Lives Improvement Service. There were no significant risks identified during the transition process and the staff are now embedded within the organisation.
Improving Quality Together (IQT) was launched by the Chief Medical Officer for
Wales and the Chair of Public Health Wales in March 2013 and is the national quality improvement programme for NHS Wales. It provides a common and
consistent approach to improving the quality of services in NHS organisations across Wales. Public Health Wales made a commitment for 25% of the workforce to be trained in IQT by 31 March 2014. Public Health Wales is pleased
to note that staff have exceeded the target with a current rate of 29% of staff having completed the training. All members of the Board have also completed
the training and were, in fact, the first Board in Wales to gain the bronze level stage of IQT.
89

Public Health Wales NHS Trust Annual Accounts 2013-14
8.3 Hosted Bodies
During 2013/14, Public Health Wales continued to host the Health and Wellbeing, Best Practice and Innovation Board. Public Health Wales put in place a hosting
agreement which provided details of the responsibilities of Public Health Wales Board and the hosted Board. Consisting of the Chair and two staff members, the
Board of the hosted body has evaluated the potential impact of innovations and developments and facilitated their adoption across the NHS, local government
and the third sector in Wales. The Board of the hosting body concluded their work and published a final report on 31 March 2014.
8.4 Civil Contingencies/Business Continuity
Public Health Wales’ Emergency Response Plan details the organisation’s response to a wide range of incidents and threats. The plan provides an overarching framework for the organisation’s response to incidents and
outbreaks, including the mobilisation of additional resources.
The organisation has undertaken risk assessments and Carbon Reduction Delivery Plans are in place in accordance with emergency preparedness and civil
contingency requirements as based on UKCIP 2009 weather projections to ensure that the organisation’s obligation under the climate change Act and the Adaptation Reporting requirements are complied with. We monitor our Carbon
footprint using 2013/14 as a baseline figure and we have adopted the Welsh Government initiative of ensuring sustainability is embedded in everything we
do. Public Health Wales has also adopted an Accommodation Strategy that embeds sustainable development as key principles.
Key divisions within Public Health Wales, such as Screening, Health Protection and Microbiology, have established business continuity arrangements in place.
As part of these arrangements, relevant staff are aware of their duties as described within the plans. The Information management and technology
installed infrastructure has been tested to ensure the network is available across multiple sites in the event of local emergencies or one or more buildings suffering unforeseen problems.
8.5 Sustainability
Public Health Wales fully supports proposals detailed in various Welsh Government consultation documents to embed sustainable development as the
central organising principle of public sector bodies in Wales by ensuring a clear focus on outcomes and that strategic decisions are informed by consideration of
the wider determinants of health and wellbeing. Public Health Wales recognises that sustainable development and public health are intrinsically linked and that
complementary and coordinated actions are necessary to address the key challenges facing Wales in relation to both.
90

Public Health Wales NHS Trust Annual Accounts 2013-14
Public Health Wales is fully engaged in the Welsh Government’s development of
the Future Generations Bill (previously the Sustainable Development Bill). The Bill aims to tackle the generational challenges Wales faces in a more robust, joined up and integrated way. It is expected that the Bill will place a new duty
on public services in Wales to make sustainable development their central organising principle. The Bill will also set out a number of long term economic,
social, and environmental wellbeing goals, many of which will link closely with work undertaken by Public Health Wales. A national conversation has been
launched by the Welsh Government to involve people across Wales in exploring what are for them the most important issues in improving their lives and those of their families and communities. Public Health Wales is fully engaged in the
national conversation and will be playing a key role in the development of the Bill.
8.6 Equality
A Strategic Equality Plan was adopted by the Trust Board in April 2012, with regular progress reports provided to the Board. The plan details the actions we
are taking to address and improve equality related issues in all parts of the organisations. The Strategic Equality Plan also laid out an additional objective to
‘embed Equalities into organisational performance and Executive and Board Decision Making’. As part of the Strategic Equality Plan, all new and revised policies and strategies are subject to an equality impact assessment (EQIA).
An equality group has been established to oversee the strategic equality plan, to
ensure under-represented groups are properly considered and that measures are in place to ensure that all the organisation’s obligations under equality, diversity and human rights legislation are complied with.
8.7 Staff
Public Health Wales engages staff systematically in a number of ways which are
part of the checks and balances Public Health Wales undertakes to enable good governance. Formal consultative fora are well established through the Partnership Forum, Joint Medical and Dental Negotiating Group, and the Joint
Negotiating Committee for Agenda for Change staff. These fora provide mechanisms which allow for feedback to senior management on organisational
performance or any other issues that staff wish to raise, which aids transparency. In addition to these formal mechanisms, we have a consultation process open to all staff for all new and revised organisational policies, a staff
conference, a senior management forum and a national forum, all of which are fully exploited and used to engage in conversations with staff at individual and
group levels. These mechanisms are used in parallel with an open blog, a web forum and other virtual ways for staff to share their work and opinions.
91

Public Health Wales NHS Trust Annual Accounts 2013-14
In 2013/14 we have focussed strongly on improving compliance with Statutory
and Mandatory training as this is a key way of ensuring staff have the appropriate knowledge and skills to enact organisational policies as well ensuring compliance with Health and Safety, Information Governance and other important
legislation. At the beginning of the year compliance against statutory training was considerably low and was identified as an issue by the Quality and Safety
Committee. Compliance figures have improved considerably during the year, for example Health and Safety training compliance has risen from 8 per cent
compliance to 85 per cent, manual handling has risen from 33 per cent to 72 per cent and fire safety has risen from 35 per cent to 70 per cent.
Recruiting the right people is critically important especially where we are providing services directly to members of the public. 2013/14 has seen a
renewed focus on selection methods, with assessment centres being adopted as the preferred method of assessment for all posts at Band 8a and above. This is a more robust method of understanding how job applicants match the competency
requirements and goes beyond asking for information to testing the application of some of the competencies in practice. New procedures to check job
candidates against new Vetting and Barring requirements have been developed and will be implemented in 2014/15.
Public Health Wales, as an employer with staff entitled to membership of the NHS Pension Scheme, control measures are in place to ensure all employer
obligations contained within the Scheme’s regulations are complied with. This includes ensuring that deductions from salary, employer’s contributions and
payments in to the Scheme’s are in accordance with the Scheme rules, and that member Pension Scheme records are accurately updated in accordance with the timescales detailed in the Regulations. Note 12 to the accounts provides details
of the scheme, how it operates and the entitlement of employees.
9 Review of effectiveness
As Accounting Officer, I have responsibility for reviewing the effectiveness of the systems of internal control. My review of the system of internal control is
informed by the work of the internal auditors and the executive officers within the organisation who have responsibility for the development and maintenance
of the internal control framework and comments made by external auditors in their audit letter and other reports. The following text provides examples of the review of effectiveness which has been undertaken throughout the year. In
addition the assessment of compliance with the UK Corporate Governance Code at section 6 contributes to the review of effectiveness.
92

Public Health Wales NHS Trust Annual Accounts 2013-14
9.1 Internal Audit
Internal Audit provides me as Accounting Officer, and the Board through the Audit Committee, with a flow of assurance on the system of internal control. I
have commissioned a programme of audit work which has been delivered in accordance with public sector internal audit standards by the NHS Wales Shared
Services Partnership. The scope of this work is agreed with the Audit Committee, and is focused on significant risk areas and local improvement
priorities approved by the Board. The overall opinion by the Head of Internal Audit, NHS Wales Shared Services
Partnership on governance, risk management and control is a function of this risk based audit programme and contributes to the picture of assurance available
to the Board in reviewing effectiveness and supporting our drive for continuous improvement.
The Head of Internal Audit has concluded:
“In my opinion the Board can take reasonable assurance that arrangements to secure governance, risk management and internal control, within those areas
under review, are suitably designed and applied effectively. Some matters require management attention in control design or compliance with low to moderate impact on residual risk exposure until resolved.”
In reaching this opinion the Head of Internal Audit has identified that the
majority of reviews during the year concluded positively, with the only exceptions being asbestos management and the lack of progress with implementing the recommendations relating to mandatory training.
During the year internal audit issued one report with limited assurance on
asbestos management. Five recommendations were made which have been accepted and an action plan is in place to address the issues raised and improve
the situation across the organisation.
93

Public Health Wales NHS Trust Annual Accounts 2013-14
9.2 Counter Fraud Cardiff and Vale Counter Fraud Service provides a service to Public Health Wales.
Their work plan for 2013/14 was completed and covered all the requirements under Welsh Government Directions. The counter fraud service provides regular
reports and updates to members of the Executive Team and directly to the Audit Committee. The Audit Committee received the counter fraud and corruption
annual report for 2013/14 and the local counter fraud specialist provided the following declaration:
I declare that the Anti-Fraud, Bribery and Corruption work carried out during the financial year 2013/14, within the Public Health Wales NHS Trust, has been self
reviewed against the NHS Protect Standards for Providers - Fraud, Bribery and Corruption/NHS Standard Contract and the rating as detailed in Appendix 4 (green for all standards) has been achieved.
9.3 External Audit – Wales Audit Office
The Auditor General for Wales is the statutory external auditor for the NHS in
Wales. The Wales Audit Office undertakes the external auditor role for Public Health Wales on behalf of the Auditor General. The Wales Audit Office completed their Structured Assessment for 2013/14 and overall they concluded
that the organisation has good arrangements for governance and board assurance but work remains to strengthen some components of the governance
framework. The Wales Audit Office highlighted the need for internal controls for statutory and mandatory training to improve and to review and improve the approach to identifying and recording divisional risks.
9.4 Information security
During 2013/14, Public Health Wales reported one significant data security
lapse; this incident involved the misdirection of Public Health Wales data by an external data processor. The Information Commissioner found that Public Health Wales and the data processor had taken the appropriate subsequent action and
decided that no further action was needed.
10 Conclusion
As Accounting Officer, I can confirm that no significant governance issues have been identified. Therefore, reasonable assurance can be given that there is a
sound governance framework, designed to meet the organisation’s objectives and that the framework is generally being applied consistently.
Signed: ___________________
Dr Tracey Cooper
94

Public Health Wales NHS Trust Annual Accounts 2013-14
Appendix A 2012/2013 Audit Assurance Ratings
95

30 09
Date: 16 June 2014 Version:1a Page: 1 of 11
Month 2 2014/15 finance performance report
Purpose of Document: To report on the year to date and projected outturn position of
Public Health Wales as at 31 May 2014
To provide an update on major budget movements, the capitalprogramme and the key financial performance indicators
To provide an update on the financial services function
Board/Committee to- (Please indicate)To decide- Paper will outline recommendations or issues tobe approved by the Board or Committee.
To discuss- Board or Committee will be asked to discussand scrutinise the paper and provide feedback andcomments.
X
To inform- Board or Committee will be asked to note thepaper for information only
Other relevant informationN/A
Next StepsN/A
Link to Public Health Wales commitment and priorities for action:(please tick which commitment(s) is/are relevant)
X
Priorities for action Ensure financial sustainability
Author: Mr Huw George, Executive Director of Finance, Ms Tamira Rolls,Assistant Director of Finance, Ms Margaret Krawiecka, Assistant Director ofFinance
Date: 16 June 2014 Version:1aSponsoring Executive Director: Mr Huw George, Executive Director
of Finance
Who will present: (If appropriate) Mr Huw George, Executive Directorof Finance
Documents attached:(If appropriate)
Finance performance report
Date of meeting: 26 June 2014
Paper reference 30 09

Public Health Wales Paper Submission Cover Sheet
Date: 15 March 2014 Version:1 Page: 2 of 11
Committee/Groups that havereceived or considered thispaper:
Executive Team
Link to standardsfor health services
Standard 1: Governance and accountability
Link to riskregister
Risk 87: Failure to meet statutory brake even duty.
Equality impactassessment
N/A
Financialimplications
See information in attached paper
Service userengagement
N/A

Public Health Wales Board Arrangements Paper
Date: 15 June 2014 Version: 1a Page: 3 of 8
Month 2 2014/15Finance Performance
ReportAuthors: Huw George , Tamira Rolls and Margaret Krawiecka
Date: 15 June 2014 Version: 1a
Distribution:
Public Health Wales Trust Board
Purpose and summary of document: To report on the month 2 position for Public Health Wales
To provide an update on major budget movements, the capitalprogramme and the key financial performance indicators

Public Health Wales Month 2 Finance Performance Report – May 2014
Date: 15 June 2014 Version: 1a Page: 4 of 8
1 Introduction
The content of this report reflects the Director of Finance commentarywhich was formally submitted to Welsh Government on 12 June 2014 aspart of the full financial monitoring return for month 2 (31 May 2014).
The report will cover the following areas:
Year to Date (YTD) Position and variance report (section 2) Budget movements and reconciliation to 2014/15 budget Strategy
(section 3) Risks and Issues (section 4) Balance Sheet Summary (section 5) Key Financial performance Indicators (Section 6) Capital Programme (Section 7)
2 YTD Position
The table below summarises the month 2 (to 31 May) financial position bydirectorate. A Divisional level summary is provided in the Appendix 1.
The reasons for the individual directorate and divisional variances are givenbelow. Further details are provided in the individual divisional financialreports.
Dir Type
AnnualBudget£000s
YTDBudget£000s
YTDActual£000s
YTDVariance
£000s
PH Services Income -60,766 -9,863 -9,923 -61
Pay 33,741 5,623 5,491 -132
Non Pay 28,247 4,447 4,664 217
PHS Total 1,222 208 232 24
PH Development Income -3,779 -630 -616 14
Pay 22,201 3,700 3,632 -68
Non Pay 10,633 1,772 1,659 -114
PH Dvt Total 29,055 4,842 4,675 -167
Corporate Income -40,187 -6,698 -6,686 12
Pay 7,182 1,189 1,209 20
Non Pay 2,729 459 488 29
Corp Total -30,276 -5,050 -4,989 62
Grand Total 0 0 -82 -82

Public Health Wales Month 2 Finance Performance Report – May 2014
Date: 15 June 2014 Version: 1a Page: 5 of 8
Summary:
Total Income -104,733 -17,190 -17,225 -35
Total Pay 63,123 10,512 10,332 -180
Total Non Pay 41,609 6,678 6,811 133
TOTAL 0 0 -82 -82
2.1 Public Health Services (£24k YTD overspent)
2.1.1 Microbiology Division (£77K overspent):
Income has over achieved at month 2 by £26k mainly due to ad hocincome.
Pay is under spent £66k mainly due to vacancies at various levels acrossall laboratories of £126k, with an offset of £60k of vacancy factor to date.
Non pay is over spent £168k due to chemicals and kits mainly in Cardifflaboratory. Over activity for the first two months of £46k has beenfactored into the financial statements: both income and non pay budgetshave been increased.
2.1.2 Screening Division (£37k under spent)
Income has over achieved by £32k due to having more trainee assistantradiographers than planned and over achieving course income formammography training.
Pay is £31k under spent due mainly to vacancies of radiography andmedical positions.
Non pay is £25k over spent by small amounts over various expenditureheadings.
2.1.3 Health Protection Division (£6k under spent)
Income is £3k under spent due to an over achievement of tonsillectomysurveillance income.
Pay is £25k under spent due to mainly consultant vacancies and maternityleave.
Non pay is £23k over spent mainly due to a payment for software. Budgetwill now be phased in to cover this payment.
2.1.4 Safeguarding Children (£10k under spent)
Pay budgets are showing an under spend of £11k due to slippage atadministration budget.

Public Health Wales Month 2 Finance Performance Report – May 2014
Date: 15 June 2014 Version: 1a Page: 6 of 8
Non pay is over budget by £2k mainly due to travel and subsistenceexpenditure.
2.2 Public Health Development (£167k YTD overspent)
Public Health Development has agreed a budget plan with a vacancy factorof £400k which is based on the historical pattern for staff turnover andfilling of vacancies. This target is not currently devolved to divisions andso they would expect to see a local pay underspend which is offset by thecentral vacancy target.
2.2.1 Health and Healthcare Improvement (£86K underspent):
The underspend to date is primarily due to vacant posts within thePharmaceutical and Stop Smoking Wales teams.
2.2.2 Health Intelligence (£30k under spent)
The underspend to date is mainly due to vacant posts within theEvidence Service and the Observatory Analytical teams.
2.2.4 Policy Research and Development (£18k under spent)
This underspend is primarily due to planned lower expenditure atthe beginning of the year within the Research and Developmentand the Public Health Networks teams. Expenditure levels willincrease in line with plans during the remainder of the financialyear.
2.2.5 Local Public Health Teams (£80k under spent)
£52k of the underspend to date is a result of vacant posts withinseveral local PH teams. A further £28k is due to planned lowerexpenditure at the beginning of the year with expenditure levelsplanned to increase during the remainder of the financial year.
2.2.3 PHD Management and 1,000 Lives Improvement Unit (£47kover spent)
This is primarily a result of an overspend against the staffturnover target for Public Health Development as described above.
2.3 Corporate (£61k YTD overspent)
There is a small overspend within the area of corporate budgets as theTrust has set higher targets for the management of vacancies in order toincrease development funds.

Public Health Wales Month 2 Finance Performance Report – May 2014
Date: 15 June 2014 Version: 1a Page: 7 of 8
3 Budget Changes
The table at appendix 2 reconciles the original Budget strategy figureswith the month 2 figures. The budget currently stands at £105,254m. Thechanges are due to movement of budgets between income andexpenditure lines and because the majority of the investment budget hasnot yet been allocated to the divisions and remain in the corporatedirectorate. There has been some additional noncore income.
4 Risks and Issues
4.1 Savings Plan
The 2014/15 budget strategy includes £2,255 savings, split between pay(£611k) and non pay (£1,644k). As in previous years, the savings will bemonitored on a regular basis with detailed performance reports on each ofthe savings programmes reported to the board on a quarterly basis.
Whilst every effort will be made to ensure the savings plans are achievedin full during 2014/15, there is nevertheless a risk that they are notachieved.
4.2 NHS Agreements and Contracts
All SLAs and contracts with other NHS Wales organisations are currently inthe process of being finalised and signed. We anticipate that all contractswill be agreed and signed by the end of June 2013.
PHW Income:
Public Health Wales has approximately £12.5m in Microbiology contractincome for tests carried out in the Microbiology labs. These contracts arebased on an historic baseline and are updated each year for anyanticipated changes to the activity. The LHBs receive activity reports on aquarterly basis, and are invoiced on a monthly basis.
PHW Expenditure:
The majority of our NHS Wales expenditure relates to Screening ServicesLTAs with other NHS Wales Organisations (approx £11.5m) which aregenerally multi-year LTAs and will therefore have been agreed pre2014/15.
4.3 Re-implementation of Oracle Financial andprocurement system
A new version (R12) of the all Wales Finance and procurement system wasimplemented on 1st April 2014. There were several problems with
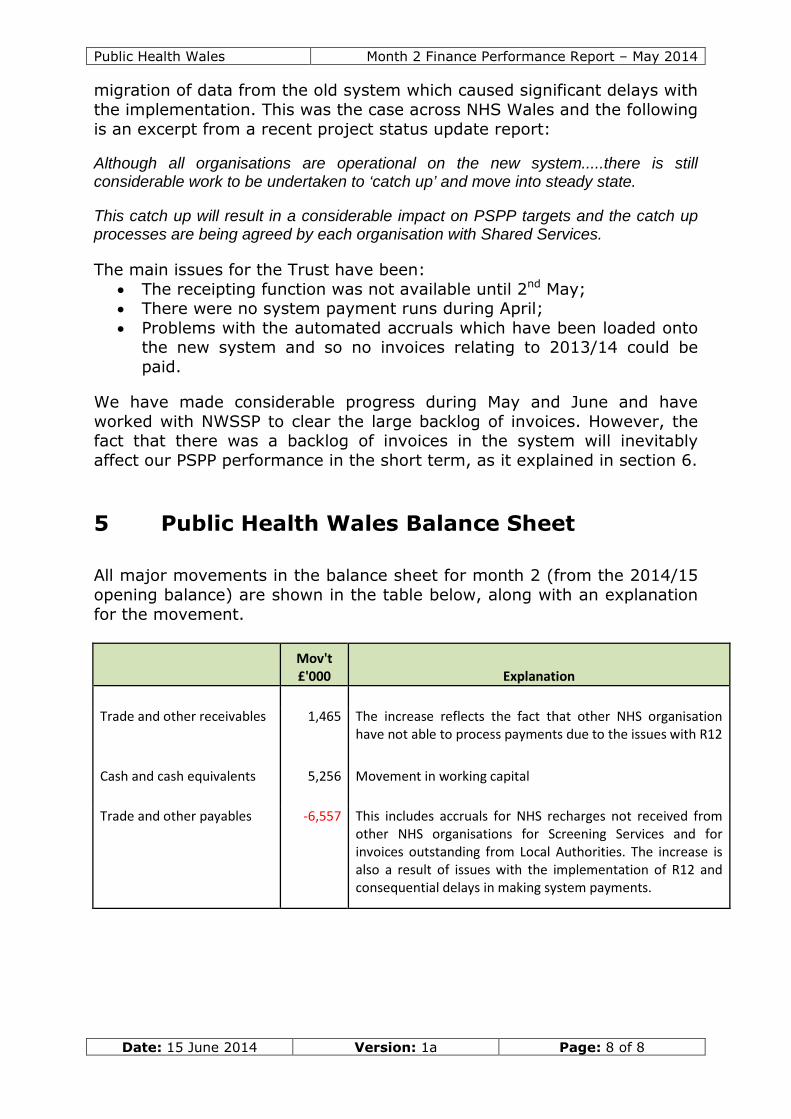
Public Health Wales Month 2 Finance Performance Report – May 2014
Date: 15 June 2014 Version: 1a Page: 8 of 8
migration of data from the old system which caused significant delays withthe implementation. This was the case across NHS Wales and the followingis an excerpt from a recent project status update report:
Although all organisations are operational on the new system.....there is stillconsiderable work to be undertaken to ‘catch up’ and move into steady state.
This catch up will result in a considerable impact on PSPP targets and the catch upprocesses are being agreed by each organisation with Shared Services.
The main issues for the Trust have been: The receipting function was not available until 2nd May; There were no system payment runs during April; Problems with the automated accruals which have been loaded onto
the new system and so no invoices relating to 2013/14 could bepaid.
We have made considerable progress during May and June and haveworked with NWSSP to clear the large backlog of invoices. However, thefact that there was a backlog of invoices in the system will inevitablyaffect our PSPP performance in the short term, as it explained in section 6.
5 Public Health Wales Balance Sheet
All major movements in the balance sheet for month 2 (from the 2014/15opening balance) are shown in the table below, along with an explanationfor the movement.
Mov't£'000 Explanation
Trade and other receivables 1,465 The increase reflects the fact that other NHS organisationhave not able to process payments due to the issues with R12
Cash and cash equivalents 5,256 Movement in working capital
Trade and other payables -6,557 This includes accruals for NHS recharges not received fromother NHS organisations for Screening Services and forinvoices outstanding from Local Authorities. The increase isalso a result of issues with the implementation of R12 andconsequential delays in making system payments.

Public Health Wales Month 2 Finance Performance Report – May 2014
Date: 15 June 2014 Version: 1a Page: 9 of 8
6 Key Financial Indicators
6.1 Public Sector Payment Policy (PSPP) Compliance
As a result of issues with the R12 implementation, and the consequentialdelays in paying invoices, the PSPP figures are lower than expected.
The table below shows the month 2 (YTD) figures. These are also themonth 2 figures as no payments were made in month 1.
% of NHS Invoices Paid Within 30 Days - By Value 57.9%
% of NHS Invoices Paid Within 30 Days - By Number 53.5%
% of Non NHS Invoices Paid Within 30 Days - By Value 70.1%
% of Non NHS Invoices Paid Within 30 Days - By Number 86.0%
Although we have missed the Non NHS invoices by number at month 2,we had been making significant process during 2013/14 on increasing ourperformance, and we are hopeful that we will be able to achieve the targetof 95% percent by year end.
6.2 Agency Expenditure and WTE movement
The agency costs have reduced significantly during April and May 2014and are 0.4% of the total staff costs for both months 1 and 2.
The table below summarises the movement in all 3 categories betweenApril and May 2014.
Sum of WTE Contracted Sum of WTE Worked Sum of WTE Paid
Job Type April May Mvt April May Mvt April May Mvt
A&C & Board Members 738.10 739.68 1.58 710.96 709.44 -1.52 711.54 710.15 -1.39
Medical & Dental 96.23 95.63 -0.60 93.65 93.29 -0.36 93.65 93.29 -0.36
Registered 51.72 50.92 -0.80 50.16 49.33 -0.83 50.16 49.33 -0.83
Prof Scientific & Tech 12.56 12.81 0.25 12.56 12.81 0.25 12.56 12.81 0.25
Additional Clinical Servs 121.02 123.82 2.80 118.36 121.50 3.14 119.90 123.55 3.65
Allied Health Profs 53.04 52.94 -0.10 54.40 54.10 -0.30 54.57 54.38 -0.19
Healthcare Scientists 195.29 195.29 0.00 192.77 194.77 2.00 196.48 199.74 3.26
Estates & Ancilliary 1.91 1.91 0.00 1.91 1.91 0.00 1.91 1.91 0.00
1,269.87 1,273.00 3.13 1,234.77 1,237.15 2.38 1,240.77 1,245.16 4.39
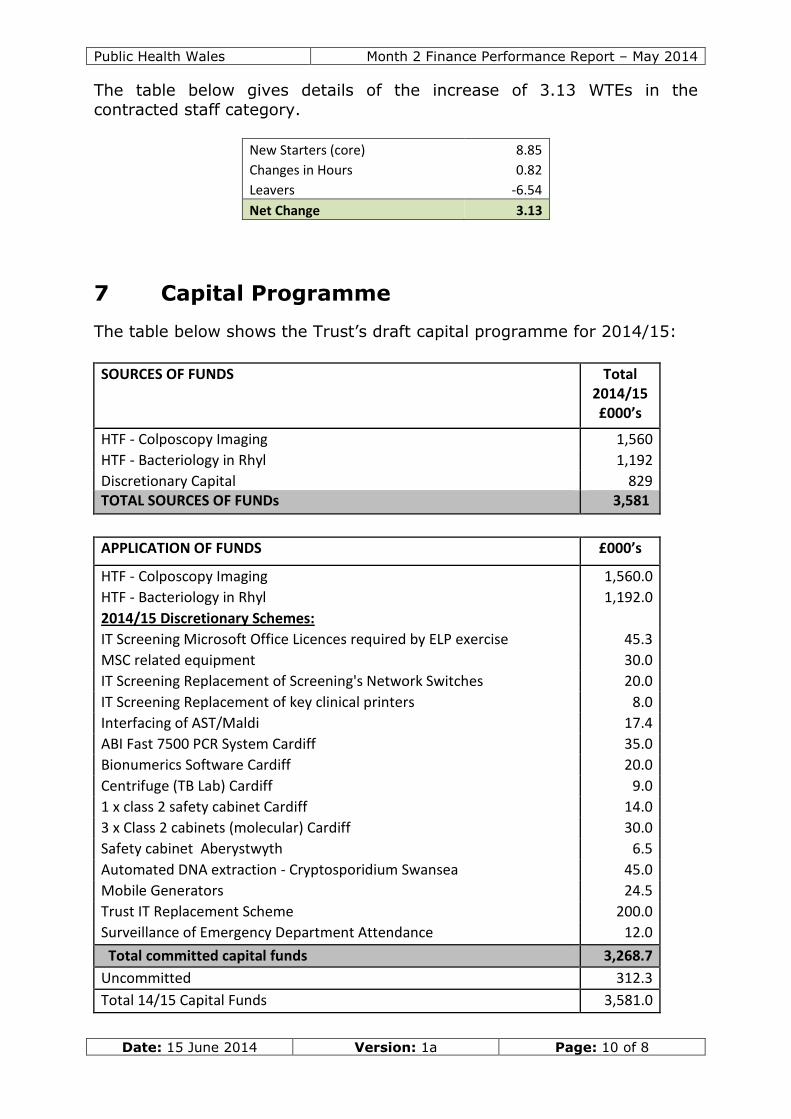
Public Health Wales Month 2 Finance Performance Report – May 2014
Date: 15 June 2014 Version: 1a Page: 10 of 8
The table below gives details of the increase of 3.13 WTEs in thecontracted staff category.
New Starters (core) 8.85
Changes in Hours 0.82
Leavers -6.54
Net Change 3.13
7 Capital Programme
The table below shows the Trust’s draft capital programme for 2014/15:
SOURCES OF FUNDS Total2014/15£000’s
HTF - Colposcopy Imaging 1,560
HTF - Bacteriology in Rhyl 1,192
Discretionary Capital 829TOTAL SOURCES OF FUNDs 3,581
APPLICATION OF FUNDS £000’s
HTF - Colposcopy Imaging 1,560.0
HTF - Bacteriology in Rhyl 1,192.0
2014/15 Discretionary Schemes:
IT Screening Microsoft Office Licences required by ELP exercise 45.3
MSC related equipment 30.0
IT Screening Replacement of Screening's Network Switches 20.0
IT Screening Replacement of key clinical printers 8.0
Interfacing of AST/Maldi 17.4
ABI Fast 7500 PCR System Cardiff 35.0
Bionumerics Software Cardiff 20.0
Centrifuge (TB Lab) Cardiff 9.0
1 x class 2 safety cabinet Cardiff 14.0
3 x Class 2 cabinets (molecular) Cardiff 30.0
Safety cabinet Aberystwyth 6.5
Automated DNA extraction - Cryptosporidium Swansea 45.0
Mobile Generators 24.5
Trust IT Replacement Scheme 200.0
Surveillance of Emergency Department Attendance 12.0
Total committed capital funds 3,268.7
Uncommitted 312.3
Total 14/15 Capital Funds 3,581.0

Public Health Wales Month 2 Finance Performance Report – May 2014
Date: 15 June 2014 Version: 1a Page: 11 of 8
Welsh Government has approved two technology bids: colposcopy andcolonoscopy imaging £1.56m and automation of bacteriology in our Rhyllaboratory £1.192m. The colposcopy imaging equipment was going to bepurchased in 13-14 however due to procurement uncertainties WelshGovernment have authorised the transfer of funding from 13-14 to 14-15to enable the investments to be made during 2014-15. Welsh Governmenthas confirmed the capital charges funding relating to these schemes for14-15.
8 Conclusion
The Trust is forecasting that it will fulfil its statutory break even duty for2014/15.
Work is ongoing to mitigate all risks and also to create opportunities fordevelopment of the organisation.

Appendix 1
2014/15 Financial Performance Report - Month 2 Variance Report by Division
PH DEVELOPMENT: Type Annual Budget YTD Budget YTD Actual YTD Variance
Hlth and HC Improvement Income -1,935,853 -322,644 -373,571 -50,927
Non Pay 7,324,351 1,220,730 1,264,363 43,633
Pay 5,717,103 952,866 873,792 -79,074
Hlth and HC Improvement Total 11,105,601 1,850,952 1,764,585 -86,367
Hlth Intelligence Income -283,740 -47,290 -47,315 -25
Non Pay 531,201 88,534 102,720 14,186
Pay 2,848,357 474,734 430,490 -44,244
Hlth Intelligence Total 3,095,818 515,978 485,895 -30,083
1,000 Lives Improvement Unit Income -591,751 -98,626 -40,500 58,126
Non Pay 1,263,005 210,502 104,133 -106,369
Pay 2,690,625 448,438 388,305 -60,133
Improvement Total 3,361,879 560,314 451,938 -108,376
Local PH Teams Income -717,264 -119,546 -119,746 -200
Non Pay 989,799 164,962 137,707 -27,255
Pay 7,997,013 1,332,840 1,280,574 -52,266
LPHTs Total 8,269,548 1,378,256 1,298,536 -79,720
Policy Research and Development Income -250,865 -41,810 -34,702 7,109
Non Pay 459,830 76,642 37,608 -39,034
Pay 1,179,746 196,628 210,250 13,622
Policy R&D Total 1,388,711 231,460 213,156 -18,304
PHD Management and Admin Non Pay 64,938 10,820 12,042 1,222
*includes staff turnover target* Pay 1,768,105 294,688 448,841 154,153 66,667
PHD Management and Admin Total 1,833,043 305,508 460,883 155,375
PH Dvt Total 29,054,600 4,842,468 4,674,993 -167,475
PH SERVICES: Type Annual Budget YTD Budget YTD Actual YTD Variance
Health Protection Income -4,754,978 -714,316 -717,177 -2,861
Non Pay 795,101 54,337 77,003 22,666
Pay 4,498,232 749,705 724,324 -25,382
Health Protection Total 538,355 89,726 84,149 -5,576
Microbiology Income -20,751,079 -3,532,383 -3,557,922 -25,539
Non Pay 6,427,507 1,149,267 1,317,278 168,011
Pay 14,894,633 2,482,439 2,416,661 -65,778
Microbiology Total 571,060 99,323 176,017 76,694

Safeguarding Children Services Income 0 0 -618 -618
Non Pay 16,316 2,719 4,641 1,921
Pay 987,488 164,581 153,667 -10,915
SCS Total 1,003,804 167,301 157,689 -9,612
Screening Services Income -35,260,429 -5,615,971 -5,647,646 -31,675
Non Pay 21,008,135 3,240,590 3,265,680 25,090
Pay 13,360,584 2,226,764 2,196,079 -30,685
Screening Services Total -891,710 -148,618 -185,888 -37,270
PHS Total 1,221,509 207,732 231,968 24,236
CORPORATE: Type Annual Budget YTD Budget YTD Actual YTD Variance
Board and Corporate (Inc Core Income) Income -38,990,364 -6,498,396 -6,496,122 2,274
Non Pay 1,054,186 171,517 219,125 47,608
*includes staff turnover target* Pay 2,838,795 473,132 544,747 71,615
Board and Corporate Total -35,097,383 -5,853,747 -5,732,250 121,497
Planning IM&T and PMU Income -379,971 -63,328 -63,328 0
Non Pay 325,710 54,287 66,845 12,559
Pay 1,569,576 261,597 253,094 -8,502
Planning IM&T and PMU Total 1,515,315 252,555 256,612 4,056
Estates Income -67,368 -11,228 -11,228 0
Non Pay 917,438 152,906 144,914 -7,992
Pay 34,289 5,714 5,775 61
Estates Total 884,359 147,392 139,461 -7,931
Finance Non Pay 75,000 12,500 9,162 -3,338
Pay 776,406 129,402 132,887 3,485
Finance Total 851,406 141,902 142,049 147
HR / Training and Development Non Pay 395,303 65,884 41,112 -24,772
Pay 761,351 126,892 130,340 3,448
HR / Training and Development Total 1,156,654 192,776 171,452 -21,324
SpRs Income -749,000 -124,834 -115,001 9,833
Non Pay 10,760 1,792 6,472 4,680
Pay 1,151,780 191,964 142,546 -49,418
SpRs Total 413,540 68,922 34,018 -34,904
Corp Total -30,276,109 -5,050,200 -4,988,660 61,540
Grand Total 0 0 -81,699 -81,699

Appendix 2
TOTAL
Investment
Budget Adj
Movement
between
Directorates
Capital
Charges
Adjustment
Other
Changes in
non core
Inc / Exp
Current
Month 2
Budget
Amended
Month 2
Budget
PHS Expenditure 62,328 -210 -130 61,988 61,988
PHS Income -60,896 0 130 -60,766 -60,766
Net PH Services 1,432 -210 0 0 0 1,222 1,222
PHD Expenditure 33,368 -396 -138 0 32,834 32,834
PHD Income -4,081 302 0 -3,779 -3,779
Net PH Development 29,287 -396 164 0 0 29,055 29,055
Corporate
Expenditure 9,305 606 138 -521 383 9,911 10,432
Corporate Income -40,024 -302 521 -383 -40,188 -40,709
Net Corporate -30,719 606 -164 0 0 -30,277 -30,277
Total Expenditure 105,001 0 0 -521 253 104,733 105,254
Total Income
-
105,001 0 0 521 -253 -104,733 -105,254

Date: 16 June 2014 Version: 1p Page: 1 of 2
Update from Public Health Wales and Welsh Government JointExecutive Team meeting
Purpose of Document:
The Public Health Wales and Welsh Government bi-annual Joint Executive Teammeeting took place on 4 June 2014. The attached quality and delivery frameworkperformance report was discussed at the meeting.
Board/Committee to- (Please indicate)
To decide - Paper will outline recommendations or issues to beapproved by the Board or Committee.
To discuss - Board or Committee will be asked to discuss andscrutinise the paper and provide feedback and comments.
X
To inform - Board or Committee will be asked to note the paper forinformation only
Other relevant information
Next Steps
Link to Public Health Wales commitment and priorities for action:(please tick which commitment(s) is/are relevant)
X
Priorities for action
Author: Mr Mark Dickinson, Executive Director of Planning and PerformanceDate: 16 June 2014 Version: 1p
Sponsoring Executive Director: Mr Mark Dickinson, Executive Director ofPlanning and Performance
Who will present: (If appropriate) Mr Mark Dickinson, Executive Director ofPlanning and Performance
Documents attached:(If appropriate)
Quality and delivery frameworkperformance report
Date of meeting: 26 June 2014Committee/Groups that havereceived or considered this paper:
Public Health Wales and WelshGovernment Joint Executive Team
Paper reference – 32 10

Public Health Wales Performance report 2013-14
Date: 16 June 2014 Version:1 Page: 2 of 2
Link to standardsfor health services
N/A
Link to risk register N/A
Equality impactassessment
N/A
Financialimplications
N/A
Service userengagement
N/A
Public Health Wales Quality and Delivery FrameworkPerformance Report – 2013/14
Date: 04/06/14 Version: 1p Page: 1 of 26
Quality and DeliveryFramework
Performance Report2013/14
Author: Public Health Wales
Date: 4 June 2014 Version: 1p(with additional material)
Distribution:
Welsh Government
Public Health Wales Intranet and Internet
Purpose and Summary of Document:
The purpose of this performance report is to provide the WelshGovernment with an update on performance, using the Public HealthWales’ Quality and Delivery Framework. This framework, agreed in 2013,consists of performance indicators and updates that Public Health Walesreports against internally and externally. The Performance Report ispresented in two sections:
1. Selected indicators from the latest Welsh Health Survey (outcomes),which illustrate the scale of the challenge faced by TransformingHealth Improvement in Wales
2. Performance indicators for a range of programmes and services andour internal enablers
The Public Health Wales Quality and Delivery Framework continues to bestrengthened and additional performance indicators, including foradditional programmes and services, will be added as they are developed.

Public Health Wales
Date: 04/06/14
1 Selected all-Welsh Health Survey
Smoking
Physically active on five or more days per
0
5
10
15
20
25
30
35
%
0
5
10
15
20
25
30
35
40
%
Quality and Delivery FrameworkPerformance Report
Version: 1p Page:
-Wales indicators from the latestWelsh Health Survey
Physically active on five or more days per week
Men 16+
Women 16+
All
Men 16+
Women 16 +
All
Quality and Delivery FrameworkPerformance Report – 2013/14
Page: 2 of 26
Wales indicators from the latest
week
Men 16+
Women 16+
Men 16+
Women 16 +
All

Public Health Wales
Date: 04/06/14
Overweight or obese
Alcohol consumption above guidelines
0
10
20
30
40
50
60
70
%
-
10
20
30
40
50
60
2008 2009
%
Quality and Delivery FrameworkPerformance Report
Version: 1p Page:
Overweight or obese
Alcohol consumption above guidelines
Men 16+
Women 16+
All
2009 2010 2011 2012 2013
Men 16+
Women 16+
All
Quality and Delivery FrameworkPerformance Report – 2013/14
Page: 3 of 26
Men 16+
Women 16+
Men 16+
Women 16+

Public Health Wales Quality and Delivery FrameworkPerformance Report – 2013/14
Date: 04/06/14 Version: 1p Page: 4 of 26
2 Performance indicators for existingprogrammes and services and our enablers
This section presents numerical performance indicators relating to existingPublic Health Wales programmes and services and to our internal enablers.Most indicators are reported on for the most recent year and the most recentquarter for which data is available, whilst some are only reported for the mostrecent year (where quarterly data is not relevant or available).
Because the indicators are reported on using the most recent data available,and reporting times vary from programme to programme, some indicators arereported for calendar year 2013 and some are reported for financial year2013/14. The periods being reported on are specified for each indicator.
Most indicators are reported against targets. In these cases, the performanceachieved is also colour coded using the following traffic light system:
Green Performance meets target
Amber Performance is within 10% of target value
Red Performance is more that 10% below target
Changes in performance from the previous year are also colour coded:
or Performance has improved
Performance is unchanged (and meets target)
Performance is unchanged (and below target)
or Performance has deteriorated (but meets target)
or Performance has deteriorated (and does not meet target)

Public Health Wales
Date: 04/06/14
2.1 Summary of performance indicators
Overall performance of all NHS Wales smokingcessation services (Tier 1 targets)
Smokers treated by all smoking cessation services
CO validated 4 week quit rate
Stop Smoking Wales performance
Number of smokers completing programme
Self reported 4 week quit rate
CO validated 4 week quit rate
52 week success rate
Client satisfaction rate
ASSIST performance
Number of secondary schools targeted
Number of pupils trained
Quality and Delivery FrameworkPerformance Report – 2013/14
04/06/14 Version: 1p Page: 5 of 26
of performance indicators
Wales smokingcessation services (Tier 1 targets)
Target
for 9m to end Q3 13/14
mokers treated by all smoking cessation services >=5%
>=40%
Target
2013Change
N/A 6,639
>=50% 52.8%
>=40% 37.3%
>=15% 33.7%
>=80% 93.2%
Target
2013/14
50 - 60 51
N/A 1,500
Quality and Delivery Framework2013/14
26
Actual
for 9m to end Q3 13/14
1.7%
36.5%
Actual
Change from2012
Q3 13/14
1,264
50.1%
34.2%
43.5%
94.9%
Actual
2013/14Change from
2012/13

Public Health Wales
Date: 04/06/14
National Exercise Referral Scheme performance
Number of referrals
Number of consultations
Take up
16 week retention (as a % of take up)
52 week retention (as a % of 16 week retention)
Healthy Working Wales performance
Organisations completing a Corporate Health Standard mock assessment
Private sector organisations completing a mock assessment
Organisations completing a full assessment
Private sector organisations completing a full assessment
Organisations achieving a Small Workplace Health Award
Number of Workboost interventions delivered
Alcohol Brief Intervention training
People trained to deliver alcohol brief interventions
Training sessions delivered
‘Train the trainer’ sessions delivered
Quality and Delivery FrameworkPerformance Report – 2013/14
04/06/14 Version: 1p Page: 6 of 26
National Exercise Referral Scheme performance Target
2013/14Change
2012/13
21,359 29,427
21,359 27,646
16,019 16,345
45% 53%
(as a % of 16 week retention) 50% 37%
Healthy Working Wales performance Target
2013/14
Organisations completing a Corporate Health Standard mock assessment 25 17
Private sector organisations completing a mock assessment 5 8
25 20
Private sector organisations completing a full assessment 5 9
Organisations achieving a Small Workplace Health Award 100 57
600 501
Alcohol Brief Intervention training performance Target
2013/14Change from
2012/13
People trained to deliver alcohol brief interventions 100 3,439
16 223
N/A 2
Quality and Delivery Framework2013/14
26
Actual
Change from2012/13
Q4 13/14
8,411
7,626
4,659
49%
35%
Actual
2013/14Change from
2012/13
Actual
Change from2012/13
Q4 13/14
1,271
51
1

Public Health Wales
Date: 04/06/14
Screening programme performance
Breast screening - uptake
Breast screening - coverage
Bowel screening - coverage
Bowel screening - CPA accreditation status
Cervical screening - coverage
Cervical screening - CPA accreditation status
Abdominal Aortic Aneurysm screening - uptake
Newborn hearing screening – percentage offered screening
Newborn hearing screening - uptake
Healthcare associated infections
Clostridium difficile rate (per 100,000 population)
MRSA rate (per 100,000 population)
Microbiology performance
Microbiology - CPA accreditation status
EQA performance – bacteriology
EQA performance – virology
Quality and Delivery FrameworkPerformance Report – 2013/14
04/06/14 Version: 1p Page: 7 of 26
performance Target
2013/14Change from
2012/13
>=70% 70.8%
>=70% 66.1%
>=60% 48.9%
Full Full
>=80% 79.0%
Full Full
>=80% 70.6% New programme
offered screening >=99% 100.0%
>=95% 99.4%
Target
by 09/1512m to March 2014
rate (per 100,000 population) <=31 50.71
<=2.6 5.20
Target
2013/14Change from
2012/13
Full Full
>=95% 98.1% Not
>=95% 98.0%
Quality and Delivery Framework2013/14
26
Actual
Change from2012/13
Q4 13/14
71.4%
66.1%
48.9%
Full
79.0%
Full
New programme 69.7%
100.0%
99.4%
Actual
12m to March 2014Change from
2012/13
Actual
Change from2012/13
Q4 13/14
Full
Not previouslyreported
98.1%
98.6%

Public Health Wales
Date: 04/06/14
Turnaround time compliance – bacteriology
Turnaround time compliance – virology
Turnaround time compliance – urgent samples
Non processed samples – bacteriology/virology
Number of samples processed – bacteriology
Number of samples processed – virology
Number of samples processed – reference units
Vaccination rates
Uptake of all scheduled vaccinations at age 4 (2013)
Influenza vaccine uptake among children aged 2
Influenza vaccine uptake among those aged 65 and over
Influenza vaccine uptake among high risk groups
Influenza vaccine uptake among pregnant women
Influenza vaccine uptake among healthcare workers
Quality and Delivery FrameworkPerformance Report – 2013/14
04/06/14 Version: 1p Page: 8 of 26
>=95% 95.0%
>=95% 93.8%
>=95% 95.0%
TBC 1.5%/0.6%
N/A 990,559
N/A 392,715
reference units N/A 37,735
Target
2013/14
2013) >=95% 87.5%
ptake among children aged 2-16 years >=75% Not yet available
65 and over >=75% 68.3%
Influenza vaccine uptake among high risk groups >=75% 51.1%
Influenza vaccine uptake among pregnant women >=75% 70.5%
Influenza vaccine uptake among healthcare workers >=50% 40.6%
Quality and Delivery Framework2013/14
26
95.5%
94.2%
Annual
1.9%/0.5%
260,496
102,930
7,549
Actual
2013/14Change from
2012/13
87.5%
ot yet available New programme
68.3%
51.1%
70.5%
40.6%

Public Health Wales
Date: 04/06/14
Enablers
Sickness absence rate
Number of written concerns/complaints received
Written concerns/complaints responded to within target
Number of serious untoward incidents (SUIs) reported
SUI investigations completed within target timescales
Quality and Delivery FrameworkPerformance Report – 2013/14
04/06/14 Version: 1p Page: 9 of 26
Target
2013/14
<=3.25% 3.52%
Number of written concerns/complaints received N/A 92
Written concerns/complaints responded to within target 100% 92.4%
incidents (SUIs) reported N/A 7
SUI investigations completed within target timescales 100% 100%
Quality and Delivery Framework2013/14
26
Actual
2013/14Change from
2012/13
3.52%
92.4%

Public Health Wales
Date: 04/06/14
2.2 Health improvement programmes
Overall performance of all NHS Wales smoking cessation services (Tier 1 targets)
Performance Indicator
Smokers treated by all smoking cessation services
CO validated 4 week quit rate
Stop Smoking Wales performance
Performance Indicator
Number of smokers completing programme
Self reported 4 week quit rate
CO validated 4 week quit rate
52 week success rate
Client satisfaction rate
Quality and Delivery FrameworkPerformance Report – 2013/14
04/06/14 Version: 1p Page: 10 of 26
Health improvement programmes
Overall performance of all NHS Wales smoking cessation services (Tier 1 targets)
Target
mokers treated by all smoking cessation services >=5%
>=40%
Stop Smoking Wales performance
Target
2013Change from
N/A 6,639
>=50% 52.8%
>=40% 37.3%
>=15% 33.7%
>=80% 93.2%
Quality and Delivery Framework2013/14
26
Overall performance of all NHS Wales smoking cessation services (Tier 1 targets)
Actual
for 9m to end Q3 13/14
1.7%
36.5%
Actual
Change from2012
Q3 13/14
1,264
50.1%
34.2%
43.5%
94.9%

Public Health Wales Quality and Delivery FrameworkPerformance Report – 2013/14
Date: 04/06/14 Version: 1p Page: 11 of 26
Performance trends (actual and planned)
Planned action to improve performance
Development of formal agreement withDsPH outlining set of agreed principlesaimed at improving uptake of smokingcessation services provided by SSW
Development and implementation of jointaction plans with local teams, includingtarget action at vulnerable groups andthose with increased prevalence
Monthly performance meetings with localteams to monitor real time local data
Review and undertake options appraisalon model for service delivery andimplement any recommended changes
Undertake rolling programme of briefinterventions training for health boards
Delivery of locally tailored socialmarketing project across Wales
Delivery of Stoptober campaign
Development of plans for online services,including apps etc
0
2000
4000
6000
8000
10000
12000
14000
16000
18000
13/14Q1
13/14Q2
13/14Q3
13/14Q4
14/15Q1
14/15Q2
14/15Q3
14/15Q4
Number of smokers treated byStop Smoking Wales
Target- Number of smokerstreated by Stop Smoking Walesannually
Cumulative number of smokerstreated by Stop Smoking Wales

Public Health Wales
Date: 04/06/14
ASSIST performance
Performance Indicator
Number of secondary schools targeted
Number of pupils trained
National Exercise Referral Scheme performance
Performance Indicator
Number of referrals
Number of consultations
Take up
16 week retention (as a % of take up)
52 week retention (as a % of 16 week retention)
Quality and Delivery FrameworkPerformance Report – 2013/14
04/06/14 Version: 1p Page: 12 of 26
Target
2013/14
50 - 60 51
N/A 1,500
Referral Scheme performance
Target
2013/14Change from
2012/13
21,359 29,427
21,359 27,646
16,019 16,345
45% 53%
(as a % of 16 week retention) 50% 37%
Quality and Delivery Framework2013/14
26
Actual
2013/14Change from
2012/13
Actual
Change from2012/13
Q4 13/14
8,411
7,626
4,659
49%
35%

Public Health Wales
Date: 04/06/14
Healthy Working Wales performance
Performance Indicator
Organisations completing a Corporate Health Standard mock
Private sector organisations completing a mock assessment
Organisations completing a full assessment
Private sector organisations completing a full assessment
Organisations achieving a Small Workplace Health Award
Number of Workboost interventions delivered
Alcohol Brief Intervention training
Performance Indicator
People trained to deliver alcohol brief interventions
Training sessions delivered
‘Train the trainer’ sessions delivered
Quality and Delivery FrameworkPerformance Report – 2013/14
04/06/14 Version: 1p Page: 13 of 26
performance
Target
2013/14
Organisations completing a Corporate Health Standard mock assessment 25 17
Private sector organisations completing a mock assessment 5 8
25 20
Private sector organisations completing a full assessment 5 9
Organisations achieving a Small Workplace Health Award 100 57
600 501
Alcohol Brief Intervention training performance
Target
2013/14Change from
2012/13
People trained to deliver alcohol brief interventions 100 3,439
16 223
N/A 2
Quality and Delivery Framework2013/14
26
Actual
2013/14Change from
2012/13
Actual
Change from2012/13
Q4 13/14
1,271
51
1

Public Health Wales
Date: 04/06/14
2.3 Screening programmes
Screening programme performance
Performance Indicator
Breast screening - uptake
Breast screening - coverage
Bowel screening - coverage
Bowel screening - CPA accreditation status
Cervical screening - coverage
Cervical screening - CPA accreditation status
Abdominal Aortic Aneurysm screening - uptake
Newborn hearing screening – percentage offered screening
Newborn hearing screening - uptake
Quality and Delivery FrameworkPerformance Report – 2013/14
04/06/14 Version: 1p Page: 14 of 26
performance
Target
2013/14Change from
2012/13
>=70% 70.8%
>=70% 66.1%
>=60% 48.9%
Full Full
>=80% 79.0%
Full Full
>=80% 70.6% New programme
percentage offered screening >=99% 100.0%
>=95% 99.4%
Quality and Delivery Framework2013/14
26
Actual
Change from2012/13
Q4 13/14
71.4%
66.1%
48.9%
Full
79.0%
Full
New programme 69.7%
100.0%
99.4%

Public Health Wales Quality and Delivery FrameworkPerformance Report – 2013/14
Date: 04/06/14 Version: 1p Page: 15 of 26
Performance trends (actual and planned)
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
12/13Q1
12/13Q2
12/13Q3
12/13Q4
13/14Q1
13/14Q2
13/14Q3
13/14Q4
14/15Q1
14/15Q2
14/15Q3
14/15Q4
Breast screening uptake
Target Breast screening uptake
Bowel screening coverage
Target bowel screening coverage
Cervical screening coverage
Target cervical screening coverage
Newborn hearing screening uptake
Target newborn hearing screeninguptake

Public Health Wales Quality and Delivery FrameworkPerformance Report – 2013/14
Date: 04/06/14 Version: 1p Page: 16 of 26
Planned action to improve performance
Action across all programmes to improve uptake and reduce inequalities
Launch ‘key messages’ for all programmes to be disseminated to the public by trusted advisers e.g. primary care, pharmacies, LocalPublic Health Teams, Communities First and secondary care
Ensure screening is incorporated into health board cancer action plans and Local Public Health Team work plans
Deliver Screening for Life month activities
Work with gypsy traveller groups to engage with communities and look at information needs
Develop ‘easy to read’ resources for participants with learning disabilities
Analyse latest annual uptake figures at health board, local authority, GP Practice and GP cluster level and discuss with partnersactions for improvement
Implement programme performance recovery action plans and undertake the following specific actions:
Breast screening
o Increase utilisation of static breast screening units to support improvements in screening round length
o Alter invitation schedule as mobile units come in to standard, to improve equity of round length
o Reduce numbers of cancelled clinics by work with health boards to improve surgical attendance at clinics
Bowel screening
o Work with health boards that have longest waits to improve provision of service to commissioned levels (bowel screeningcolonoscopy wait)
o Consider alternative provision where health boards are unable to provide service
o Support the implementation of the Welsh Government Endoscopy Action Plan, to improve waiting times for colonoscopy
o Trial introductory letters and evaluate impact on uptake and inequalities
o Distribute bowel screening key messages through pharmacies
Cervical screening
o Work with health boards (including primary care) and 1,000 Lives+ to map processes and identify areas where timeliness canbe improved
o Implement 28 day wait for results for cytology samples and undertake local intervention in health boards where performanceis outside standard for colposcopy, cytology or histology

Public Health Wales
Date: 04/06/14
2.4 Healthcare associated infections
Healthcare associated infection
Performance Indicator
Clostridium difficile rate (per 100,000 population)
MRSA rate (per 100,000 population)
Performance trends
89.24
0.0
10.0
20.0
30.0
40.0
50.0
60.0
70.0
80.0
90.0
100.0
Monthly rolling 12 month rates of Clostridium difficile (aged 2and over) diagnosed in Wales per 100,000 population, for the
period Apr 11 to Mar 14
Quality and Delivery FrameworkPerformance Report – 2013/14
04/06/14 Version: 1p Page: 17 of 26
Healthcare associated infections
Healthcare associated infections
Target
by 09/15 12m to March2014
rate (per 100,000 population) <=31 50.71
<=2.6 5.20
50.71
Monthly rolling 12 month rates of Clostridium difficile (aged 2and over) diagnosed in Wales per 100,000 population, for the
6.92
0.0
1.0
2.0
3.0
4.0
5.0
6.0
7.0
8.0
Monthly rolling 12 month rates of MRSA bacteraemiadiagnosed in Wales per 100,000 population, for the period
Apr 11 to Mar 14
Quality and Delivery Framework2013/14
26
Actual
12m to March2014
Change from2012/13
50.71
5.20
5.20
Monthly rolling 12 month rates of MRSA bacteraemiadiagnosed in Wales per 100,000 population, for the period

Public Health Wales Quality and Delivery FrameworkPerformance Report – 2013/14
Date: 04/06/14 Version: 1p Page: 18 of 26
Planned action to improve performance
Work with health boards to review HCAIaction plans and develop joint work plansto address challenges and barriers
Continued provision of advice andsupport through polices, guidelines andon an ad hoc basis
Provision of data reports and ad hocanalysis to support reductions in HCAI
Revise monthly reports/dashboards tomonitor progress against tier 1 target
Map infection rates alongsideantimicrobial usage for primary andsecondary care
Regularly review routine surveillance dataand notify organisations of any unusualactivity
Provision of educational and trainingtools, including: e-learning packages,forums, leaflets and specialist courses
Hold two HCAI learning events aimed atsharing experience and best practice
Provision of material, such as patientstories, to support local campaigns
Conduct stakeholder engagement eventand agree contributions in relation tocommunity based HCAI prevention andcontrol

Public Health Wales
Date: 04/06/14
2.5 Microbiology
Laboratory Performance Indicators
Performance Indicator
Microbiology - CPA accreditation status
EQA performance – bacteriology
EQA performance – virology
Turnaround time compliance – bacteriology
Turnaround time compliance – virology
Turnaround time compliance – urgent samples
Non processed samples – bacteriology/virology
Number of samples processed – bacteriology
Number of samples processed – virology
Number of samples processed – reference units
Quality and Delivery FrameworkPerformance Report – 2013/14
04/06/14 Version: 1p Page: 19 of 26
Laboratory Performance Indicators
Target
2013/14Change from
2012/13
Full Full
>=95% 98.1%
Not previously
>=95% 98.0%
>=95% 95.0%
>=95% 93.8%
>=95% 95.0%
TBC 1.5%/0.6%
N/A 990,559
N/A 392,715
reference units N/A 37,735
Quality and Delivery Framework2013/14
26
Actual
Change from2012/13
Q4 13/14
Full
Not previouslyreported
98.1%
98.6%
95.5%
94.2%
Reportedannually
1.9%/0.5%
260,496
102,930
7,549

Public Health Wales
Date: 04/06/14
2.6 Teenage pregnancy
Under 18 conceptions
Area
Wales
Abertawe Bro Morgannwg
Aneurin Bevan
Betsi Cadwaladr
Cardiff and Vale
Cwm Taf
Hywel Dda
Powys
Performance trend
Quality and Delivery FrameworkPerformance Report
Version: 1p Page:
Teenage pregnancy
Under 18 conceptions
2011
Number Rate per100,000
Number
1,885 34.2 1677
292 32.8 279
337 30.1 319
441 36.2 404
295 36.0 267
232 43.2 186
235 34.6 176
53 21.3 46
Quality and Delivery FrameworkPerformance Report – 2013/14
Page: 20 of 26
2012
Number Rate per100,000
30.8
31.5
28.7
33.5
33.0
34.7
26.9
19.1

Public Health Wales
Date: 04/06/14
2.7 Vaccination and immunisation
Childhood vaccination
Uptake of all scheduled childhood vaccinations at age 4
Area
Wales
Abertawe Bro Morgannwg
Aneurin Bevan
Betsi Cadwaladr
Cardiff and Vale
Cwm Taf
Hywel Dda
Powys
Trend of childhood vaccination uptake (1997
Quality and Delivery FrameworkPerformance Report
Version: 1p Page:
Vaccination and immunisation
vaccination uptake
Uptake of all scheduled childhood vaccinations at age 4
Target Actual
2013 Change from
>=95%
87.5%
86.7%
86.1%
90.5%
84.3%
89.9%
87.2%
90.2%
vaccination uptake (1997 – 2013)
Quality and Delivery FrameworkPerformance Report – 2013/14
Page: 21 of 26
Change from2012/13

Public Health Wales
Date: 04/06/14
Uptake of childhood vaccinations by type (as at end 2013)
(Summary of uptake rates for selected immunisations in resident children reaching1st, 2nd, 5th and 16th birthday between 01/10/13 and 31/12/13 and resident on31/12/13)
Planned action to address performance
Support improved uptake of vaccine inpre-school children
Support health boards in the iuniversal flu vaccine for children 2into the routine schedule –secondary schools
Quality and Delivery FrameworkPerformance Report
Version: 1p Page:
Uptake of childhood vaccinations by type (as at end 2013)
Summary of uptake rates for selected immunisations in resident children reaching1st, 2nd, 5th and 16th birthday between 01/10/13 and 31/12/13 and resident on
Planned action to address performance
Support improved uptake of vaccine in
Support health boards in the inclusion offor children 2-16y
phase 2
Rollout online training resource for allstaff groups responsible for theoperational delivery of immunisationprogrammes in Wales
Quality and Delivery FrameworkPerformance Report – 2013/14
Page: 22 of 26
Summary of uptake rates for selected immunisations in resident children reaching their1st, 2nd, 5th and 16th birthday between 01/10/13 and 31/12/13 and resident on
out online training resource for allstaff groups responsible for theoperational delivery of immunisation

Public Health Wales
Date: 04/06/14
Influenza vaccination uptake
Health Board/Trust
Target 65y+
Actual2013/14
Wales
>=75%
68.3%
Abertawe BroMorgannwg
65.5%
Aneurin Bevan 70.4%
Betsi Cadwaladr 70.7%
Cardiff and Vale 69.7%
Cwm Taf 66.4%
Hywel Dda 65.7%
Powys 67.1%
Public Health Wales
Velindre
Ambulance Service
Quality and Delivery FrameworkPerformance Report – 2013/14
04/06/14 Version: 1p Page: 23 of 26
uptake
65y+ High risk groups Pregnant women
Changefrom
12/13
Actual2013/14
Changefrom
12/13
Actual2013/14
Changefrom
12/13
Target
51.1% 70.5%
>=50%
45.3% 66.7%
55.3% 65.0%
53.5% 79.6%
52.4% 79.0%
51.7% 68.2%
47.5% 47.3%
49.7% 100.0%
N/A
Quality and Delivery Framework2013/14
26
NHS Staff
Target Actual2013/14
Changefrom
12/13
>=50%
40.6%
41.1%
39.4%
41.0%
41.0%
41.1%
41.2%
42.4%
33.9%
No data52.2%
30.2%

Public Health Wales Quality and Delivery FrameworkPerformance Report – 2013/14
Date: 04/06/14 Version: 1p Page: 24 of 26
Trend of flu vaccination uptake (2007/08 – 2013/14)
Percentage uptake of influenza vaccination in pregnant women by Health Board2013 and 2014
Planned action to improve performance
Provision of surveillance, epidemiologicalanalysis and interpretation of vaccinationuptake data by GP practice, cluster, localauthority, health board and all Wales.This will support NHS action, challengeby Welsh Government and public scrutiny
Support health boards and primary carein identifying low uptake and monitor theeffectiveness of interventions to improveuptake and reduce inequalities
Work with partner agencies (WelshGovernment, health boards, third sector)to support meeting targets
Promote uptake of influenza vaccinationto the public and NHS staff via targetedcampaigns
Continue working with WelshGovernment to inform on policy andguidance
0%
10%
20%
30%
40%
50%
60%
70%
80%
2007/08 2008/09 2009/10 2010/11 2011/12 2012/13 2013/14
65y+
High risk groups
Pregnant women
Target
NHS staff
Target (NHS staff)
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
ABMU AneurinBevan
BetsiCadwaladr
Cardiff &Vale
Cwm Taf Hywel Dda PowysTeaching
All Wales
2013
2014
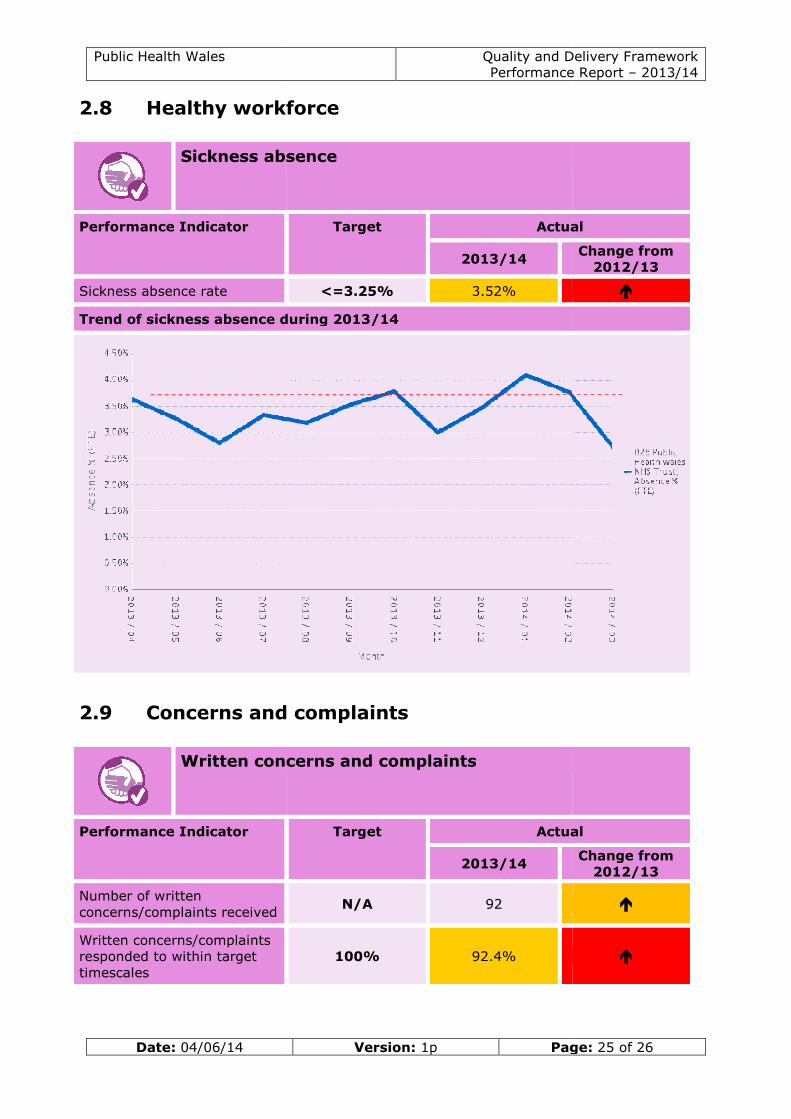
Public Health Wales
Date: 04/06/14
2.8 Healthy workforce
Sickness absence
Performance Indicator
Sickness absence rate
Trend of sickness absence during 2013/14
2.9 Concerns and complaints
Written concerns and complaints
Performance Indicator
Number of writtenconcerns/complaints received
Written concerns/complaintsresponded to within targettimescales
Quality and Delivery FrameworkPerformance Report
Version: 1p Page:
workforce
Sickness absence
Target Actual
2013/14
<=3.25% 3.52%
rend of sickness absence during 2013/14
Concerns and complaints
Written concerns and complaints
Target Actual
2013/14
N/A 92
100% 92.4%
Quality and Delivery FrameworkPerformance Report – 2013/14
Page: 25 of 26
Actual
Change from2012/13
Actual
Change from2012/13

Public Health Wales
Date: 04/06/14
2.10 Incidents
Serious untoward incidents (SUIs)
Performance Indicator
Number of serious untowardincidents (SUIs) reported
SUI investigations completedwithin target timescales
Quality and Delivery FrameworkPerformance Report
Version: 1p Page:
Serious untoward incidents (SUIs)
Target Actual
2013/14
N/A 7
100% 100%
Quality and Delivery FrameworkPerformance Report – 2013/14
Page: 26 of 26
Actual
Change from2012/13
Date: 17 June 2014 Version:1 Page: 1 of 7
Governance Report Purpose of Document: The purpose of this paper is to provide the Board with a report on Public Health
Wales’ key governance issues.
Board/Committee to-
To decide- Paper will outline recommendations or issues to be
approved by the Board or Committee.
To discuss- Board or Committee will be asked to discuss and
scrutinise the paper and provide feedback and comments.
√
To inform- Board or Committee will be asked to note the paper for information only
Other relevant information
No further relevant information
Link to Public Health Wales commitment and priorities for action: (please tick which commitment(s) is/are relevant)
√
Priorities for action Put in place a comprehensive governance
framework that addresses the issues raised in the Francis report
Develop and equip staff to work
effectively and in new ways by developing leadership and management skills,
including in support of our system leadership role and making more effective
use of accommodation
Review and update our business continuity arrangements
Author: Mr Keith Cox, Board Secretary
Date: 17 June 2014 Version: 1
Sponsoring Executive Director: Mr Keith Cox, Board Secretary
Who will present: (If appropriate) Mr Keith Cox, Board Secretary
Documents attached: Governance Report
Date of meeting: 26 June 2014
Committee/Groups that have
received or considered this paper:
N/A
PHW 32 11

Public Health Wales Governance Report
Date: 17 June 2014 Version: 1 Page: 2 of 7
Link to standards
for health services
Standard 1 – Governance and Accountability
framework
Link to risk
register
Risk ID 102
Equality impact assessment
An equality impact assessment is not required as the paper is to inform the Board of key governance
issues.
Financial
implications
No financial implications
Service user engagement
No

Public Health Wales Governance Report
Date: 17 June 2014 Version: 1 Page: 3 of 7
Governance
Report Author: Mr Keith Cox, Board Secretary
Date: 17 June 2014 Version: 1
Purpose and Summary of Document:
The purpose of this paper is to provide the Board with a report on Public
Health Wales’ key governance issues, which includes Board, Committees, and Audit Reports.

Public Health Wales Governance Report
Date: 17 June 2014 Version: 1 Page: 4 of 7
Public Health Wales Programme of Board
Business
The latest version of the Public Health Wales Programme of Board
Business is reproduced at Paper 32.12. The document sets out details of planned Board business which has been scheduled for both formal and
informal Board meetings over the next 12-15 months. The programme is reviewed and updated continuously.
List of External Consultations
A list of external consultations for July is attached at Appendix A.
Board Development
Interviews took place between Hilary Merrett from the Good Governance
Institute (GGI) and key Board and Executive Team members as part of the next phase of the Rapid Review being carried out by GGI as part of the
Board Development programme on 7, 8, 9 and 19 May 2014.
Ms Merrett has also carried out a review of key governance documents.
Feedback from the interviews and the document review will be discussed
at a meeting between John Bullivant and Andrew Corbett-Nolan from GGI and Tracey Cooper and Professor Sir Mansel Aylward on 19 June 2014.
Governance and Accountability Module
The Governance and Accountability Module has been completed following comments from Board members. The final version is presented under
Paper 32.07 for approval by the Board.
Risk Register
The Audit Committee expressed some concerns that the Corporate Risk
Register was not fully completed, particularly relating to actions. The Committee asked for the register to be reviewed.
The Executive Team has now reviewed their individual risks and updated the register accordingly. An updated version of the Risk Register is
reproduced at Paper 32.13.
Our Space - Accommodation Programme
Stage one of the Our Space programme has now been completed. A Next Steps paper, detailing the work done to date and what needs to be done
in Stage 2 has been submitted and approved by the Executive Team.

Public Health Wales Governance Report
Date: 17 June 2014 Version: 1 Page: 5 of 7
Information is being prepared for communication to managers, trade
unions and staff.
Francis Review
The assessment of the impact of the Francis review on Public Health Wales
is complementary to the work that is also now being undertaken on the Trusted to Care report. As a consequence, an action plan which
consolidates the outcomes from both pieces of work into one plan is now being prepared. This will be presented to the Board in July.
Next Board Meetings Dates for Board meetings throughout 2014 are attached at Appendix B.
The next Board meeting will be partly formal and partly informal and will
be held in the ground floor meeting room, 14 Cathedral Road on 29 July 2014.
Board Committees Meetings
The next Committee meetings are as follows:
Audit Committee: 11 September 2014
Information Governance Committee: 11 September 2014
Quality and Safety Committee: 24 July 2014

Public Health Wales Governance Report
Date: 17 June 2014 Version: 1 Page: 6 of 7
Appendix A – List of External Consultations
Title Category Organisation Comments to
Comments from
Public Health
Wales staff to be
received by:
Consultation closing date
The Active Travel
(Wales) Act 2013 – Design Guidance
Physical Activity
Welsh
Government
Malcolm
Ward
03 July
2014
04 August 2014
Guidance for the Delivery of the
Active Travel (Wales) Act 2013
Physical Activity
Welsh Government
Malcolm Ward
03 July 2014
04 August 2014
Active Travel
Action Plan
Physical
Activity
Welsh
Government
Malcolm
Ward
03 July
2014
04 August 2014

Date: 17 June 2014 Version: 1 Page: 7 of 7
Appendix B - Public Health Wales Board Meeting Dates 2014
Date Formal/Informal Venue
30 January 2014 Formal Cwm Taf Health Board Headquarters,
Ynysmeurig House, Unit 3, Navigation
Park, Abercynon
05 March 2014 Informal First floor meeting
room, Unit 1, Charnwood Court,
Nantgarw
27 March 2014 Formal Council Chamber, Temple of Peace
29 April 2014 Formal Council Chamber,
Temple of Peace
22 May 2014 Informal Boardroom, 14
Cathedral Road
26 June 2014 Formal Room 1DM2,
Pembrokeshire County Council
County Hall, Havorfordwest
29 July 2014 Informal Boardroom, 14
Cathedral Road
25 September 2014 + AGM (TBC)
Formal Council Chamber, Temple of Peace
28 October 2014 Informal Boardroom, 14 Cathedral Road
27 November 2014 Formal Aneurin Bevan Health Board
Headquarters, St Cadoc’s Hospital
18 December 2014 Informal Boardroom, 14 Cathedral Road

Date: 17 June 2014 Version:1 Page: 1 of 2
Plan of Board BusinessPurpose of Document:The Public Health Wales Plan of Board Business sets out details of planned Boardbusiness which has been scheduled for both formal and informal Board meetings overthe next 12-15 months. The programme is reviewed and updated continuously.
Board/Committee to-To decide- Paper will outline recommendations or issues to beapproved by the Board or Committee.
To discuss- Board or Committee will be asked to discuss andscrutinise the paper and provide feedback and comments.
√
To inform- Board or Committee will be asked to note the paper forinformation only
Other relevant information
No further relevant information
Link to Public Health Wales commitment and priorities for action:(please tick which commitment(s) is/are relevant)
√
Priorities for action Review and update our businesscontinuity arrangements
Author: Mr Keith Cox, Board SecretaryDate: 17 June 2014 Version: 1
Sponsoring Executive Director: Mr Keith Cox, Board Secretary
Who will present: (If appropriate) Mr Keith Cox, Board SecretaryDocuments attached: Plan of Board Business
Date of meeting: 26 June 2014
Committee/Groups that havereceived or considered this paper:
N/A
PHW 32 12
Public Health Wales Plan of Board Business Cover Sheet
Date: 17 June 2014 Version:1 Page: 2 of 2
Link to standardsfor health services
Standard 1 – Governance and Accountability framework
Link to risk register Risk ID 102
Equality impactassessment
An equality impact assessment is not required as the paper isan information tool for the Board.
Financialimplications
No financial implications
Service userengagement
No

De
cisi
on
Scru
tin
y an
d
Dis
cuss
ion
Info
rmat
ion
January Performance? X Mark Dickinson Mark Dickinson
(Formal) Budget Strategy X Huw George Huw George
Wales Audit Office structured
assessment
X Wales Audit Office Keith Cox / Tami Rolls
Local public health team - Cwm Taf X Nicola John Nicola John
Management learning and
development programme
X Barbara Busby Ruth Davies
Wales Audit Office report -
microbiology (private session)
X Quentin Sandifer Quentin Sandifer
Role of medical examiners and death
certification (private session)
X Quentin Sandifer Quentin Sandifer
Safeguarding Children Service X Aideen Naughton Quentin Sandifer
February Improving Quality Together - Board
development session
X
(Informal) Board themes and walkabouts X Keith Cox Keith Cox
Shared services X Margaret Foster Sir Mansel Aylward
Communities First X Peter Bradley
Public Health Development capacity to
deliver
X Mark Bellis / Pat Riordan Peter Bradley
Cervical Screening modernisation X Rose Fox Quentin Sandifer Improve cervical screening
through the use of HPV testingBowel Screening complex polypectomy X
Genomics X Quentin Sandifer
Medical Examiner Responsibility (part
formal)
X Quentin Sandifer Quentin Sandifer
March Integrated Medium Term Plan X Mark Dickinson Mark Dickinson
(Formal) Budget strategy X Huw George Huw George
Timetable for year end governance
documents
X Keith Cox Keith Cox
Welsh Langauge Commisioner's
response to annual monitoring report
X Chris Lines Chris Lines
Recruitment and retention protocol X Ruth Davies Ruth Davies
Employment break policy X Ruth Davies Ruth Davies
Presenter /Author Director Priority for action
Plan of Board Business 2014
Month Items
For
Additional Information
Corporate/Enablers
Protect the public from infectious and environmental hazards
Improve the quality, equity and effectiveness of healthcare services
Improve health and wellbeing and to reduce health in equalities
Healthcare Standard/Risk
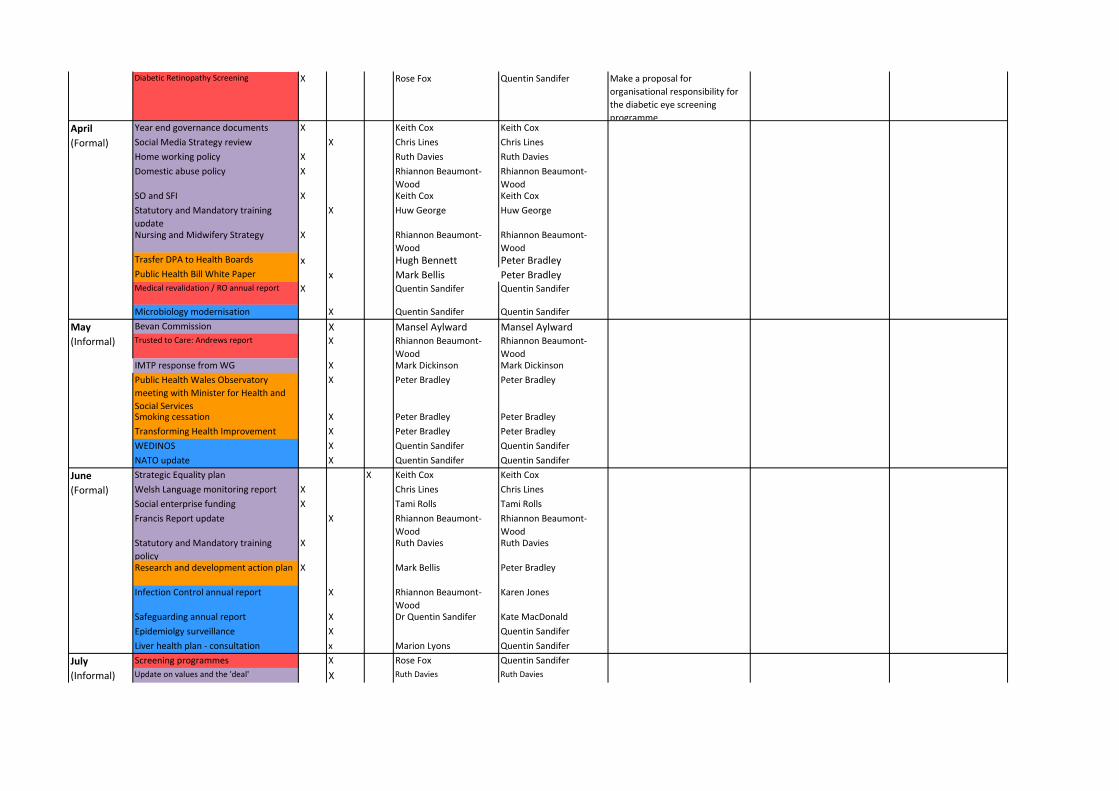
Diabetic Retinopathy Screening X Rose Fox Quentin Sandifer Make a proposal for
organisational responsibility for
the diabetic eye screening
programmeApril Year end governance documents X Keith Cox Keith Cox
(Formal) Social Media Strategy review X Chris Lines Chris Lines
Home working policy X Ruth Davies Ruth Davies
Domestic abuse policy X Rhiannon Beaumont-
Wood
Rhiannon Beaumont-
WoodSO and SFI X Keith Cox Keith Cox
Statutory and Mandatory training
update
X Huw George Huw George
Nursing and Midwifery Strategy X Rhiannon Beaumont-
Wood
Rhiannon Beaumont-
WoodTrasfer DPA to Health Boards x Hugh Bennett Peter BradleyPublic Health Bill White Paper x Mark Bellis Peter BradleyMedical revalidation / RO annual report X Quentin Sandifer Quentin Sandifer
Microbiology modernisation X Quentin Sandifer Quentin Sandifer
May Bevan Commission X Mansel Aylward Mansel Aylward
(Informal) Trusted to Care: Andrews report X Rhiannon Beaumont-
Wood
Rhiannon Beaumont-
WoodIMTP response from WG X Mark Dickinson Mark Dickinson
Public Health Wales Observatory
meeting with Minister for Health and
Social Services
X Peter Bradley Peter Bradley
Smoking cessation X Peter Bradley Peter Bradley
Transforming Health Improvement X Peter Bradley Peter Bradley
WEDINOS X Quentin Sandifer Quentin Sandifer
NATO update X Quentin Sandifer Quentin Sandifer
June Strategic Equality plan X Keith Cox Keith Cox
(Formal) Welsh Language monitoring report X Chris Lines Chris Lines
Social enterprise funding X Tami Rolls Tami Rolls
Francis Report update X Rhiannon Beaumont-
Wood
Rhiannon Beaumont-
WoodStatutory and Mandatory training
policy
X Ruth Davies Ruth Davies
Research and development action plan X Mark Bellis Peter Bradley
Infection Control annual report X Rhiannon Beaumont-
Wood
Karen Jones
Safeguarding annual report X Dr Quentin Sandifer Kate MacDonald
Epidemiolgy surveillance X Quentin Sandifer
Liver health plan - consultation x Marion Lyons Quentin Sandifer
July Screening programmes X Rose Fox Quentin Sandifer
(Informal) Update on values and the 'deal' X Ruth Davies Ruth Davies

International work X Peter Bradley To include links with Lesotho and
Betsi Cadwaladr University Health
BoardSudden infant deats X Judith Greenacre Peter Bradley
Child Measurement Programme x Peter Bradley
Working with academia X Mark Bellis Peter Bradley Improve intelligence and
evidence to support action by
strengthening collaboration with
academiaMental Health X Peter Bradley
1000 Lives improvement service and
prudent healthcare
X Alan Willson Peter Bradley
August
No Meeting
September Committee annual reports X Keith Cox Keith Cox
(AGM and
Formal)
Performance? X Mark Dickinson Mark Dickinson
PHW Annual report X Chris Lines Chris Lines
Approval of priorities for action
WCISU update X Judith Greenacre Peter Bradley
Capability- appriasals and performance
management
X Ruth Davies Ruth Davies
CARIS - general overview X Judith Greenacre Peter Bradley
Integrated public health network X Mark Bellis Peter Bradley
Responsible Officer revalidation update X Quentin Sandifer Quentin Sandifer
Public Health training X Brendan Mason Quentin Sandifer
Cervical Screening modernisation and HPV
testingX Rose Fox Rose Fox
Complex Polypectomy X Rose Fox Quentin Sandifer
Service user engagement action plan X TBC Rhiannon Beaumont-
WoodHealth Protection managed outbreaks-
Board brief
X Marion Lyons Quentin Sandifer
Flu Vaccine update report X Quentin Sandifer
Vaccine developments progress report X Richard Roberts Quentin Sandifer
Healthcare associated infections and
antimicrobial resistance
X Marion Lyons Quentin Sandifer
Vaccine developments progress report X Richard Roberts Quentin Sandifer
Liver implementation plan X Marion Lyons Quentin Sandifer
Environmental Health Protection report X Huw Brunt Quentin Sandifer

October Health, Wellbeing and Resilience X Ruth Davies Ruth Davies How the corporate standard
will be achieved, staff survey
work update, team and
individual resilience
(Informal) Medical Survey results X Ruth Davies Ruth Davies
November Declaration of interest X Keith Cox Keith Cox
(Formal) Gifts and hospitality X Keith Cox Keith Cox
Register of Seal X Keith Cox Keith Cox
Attraction and Selection Policy X Ruth Davies Ruth Davies
HCAIs X Marion Lyons Quentin Sandifer
Screening Annual Report X Rose Fox Quentin Sandifer
December Review of internal communications X Chris Lines Chris Lines
(Informal)

Trusted to care: letter to Ministerfor Health and Social Services
Purpose of Document:
On 13 May 2014 the Minister for Health and Social Services published‘Trusted to care’, a report by Professor June Andrews and Mark Butler. Thereport followed the review of the quality of care for older people at thePrincess of Wales and Neath Port Talbot hospitals. In the letter the Ministerrequested that the report be discussed by the Board and gave each Board afour week period to absorb the findings of the report and satisfy themselvesthat departures from basic professional standards highlighted in the reportare not present in their organisation.
The Board discussed the report at their informal Board meeting on 22 May2014. The Chief Executive has since written the attached letter to theMinister providing information on key pieces of work which are well underwaywhich directly correlate to improvements which the Trusted to Care reportalludes to.
An assurance template has been completed which will be shared with theBoard at regular intervals.
Board/Committee to- (Please indicate)
To decide- Paper will outline recommendations or issues to beapproved by the Board or Committee.
To discuss- Board or Committee will be asked to discuss and scrutinisethe paper and provide feedback and comments.
x
To inform- Board or Committee will be asked to note the paper forinformation only
Other relevant information
Next StepsThe Board are asked to scrutinise and discuss the letter.
Link to Public Health Wales commitment and priorities for action:(please tick which commitment(s) is/are relevant)
x
Priorities for action Identify and act on priorities for serviceimprovement, in collaboration with NHS WalesImprove healthcare quality by providingprofessional leadership
Paper reference – 32 14

Public Health Wales Trusted to Care: response to Minister forHealth and Social Services
Date: 10 June 2014 Version: 1 Page: 2 of 2
Author: Dr Tracey Cooper
Date: 10 June 2014 Version: 1Sponsoring Executive Director: Dr Tracey Cooper, Chief Executive
Who will present: (If appropriate) Dr Tracey Cooper, Chief Executive
Documents attached:(If appropriate)
Letter to Minister for Health and SocialServices
Date of meeting: 26 June 2014
Committee/Groups that havereceived or considered this paper:
N/A
Link to standards forhealth services
Standard 7: Safe and clinically effective careStandard 10: Dignity and respectStandard 11: Safeguarding children andsafeguarding vulnerable adultsStandard 15: Medicines managementStandard 14: nutritionStandard 23: Dealing with concerns and managingincidents
Link to risk register N/A
Equality impactassessment
N/A
Financial implications N/A
Service userengagement
N/A


Date: 16 June 2014 Version: 1 Page: 1 of 15
Audit Committee Annual report 2013/14
Purpose of Document: The Audit Committee has prepared annual report of its business to present to the
Public Health Wales Board. The report sets out how the Committee has met its terms of reference and what activity has taken place during the year.
Board / Committee to- (Please indicate)
To decide- Paper will outline recommendations or issues to be recommended to the Board for approval.
To discuss- Board / Committee will be asked to discuss and scrutinise the
paper and provide feedback and comments.
√
To inform- Board / Committee will be asked to note the paper for information
only
Other relevant information
Next Steps The Board are asked to receive the annual report from the Audit Committee.
Link to Public Health Wales commitment and priorities for action: (please tick which commitment(s) is/are relevant)
√
Priorities for action Put in place a comprehensive governance
framework
Author: Eleanor Higgins, Corporate Governance Manager
Date: 16 June 2014 Version: 1
Sponsoring Executive Director: Keith Cox, Board Secretary
Who will present: (If appropriate) Keith Cox, Board Secretary
Documents attached: (If appropriate)
Audit Committee annual report 2013/14
Date of meeting: 26 June 2014
Committee/Groups that have received or considered this paper:
N/A
Paper 32 15

Public Health Wales Audit Committee Annual Report
Date: 16 June 2014 Version: 1 Page: 2 of 15
Link to standards
for health services
Standard 1: Governance and accountability
Link to risk
register
N/A
Equality impact
assessment
N/A
Financial
implications
N/A
Service user engagement
N/A

Public Health Wales Audit Committee Annual Report
Date: 16 June 2014 Version: 1 Page: 3 of 15
Audit Committee
Annual report 2013/14
Author: Eleanor Higgins, Corporate Governance Manager
Date: 16 June 2014 Version: 1
Purpose and Summary of Document:
This Report summarises the key areas of business activity undertaken by
the Audit Committee over the past year and highlights some of the key issues which the Committee intend to give further consideration to over
the next 12 months.

Public Health Wales Audit Committee Annual Report
Date: 16 June 2014 Version: 1 Page: 4 of 15
Contents Foreword ..................................................................................... 5
1 Introduction ........................................................................... 6
2 Role and Responsibilities .......................................................... 6
3 Committee structure ................................................................ 7
3.1 Membership of Committee ................................................... 7
3.2 Others in attendance ........................................................... 7
3.3 Meeting frequency .............................................................. 8
4 Assurance .............................................................................. 8
4.1 Committee self assessment.................................................. 9
4.2 Risk .................................................................................. 9
4.3 Public sector payments policy ............................................... 9
5 Audit Committee Activity 2013/14 ............................................. 9
5.1 External audit .................................................................. 10
5.2 Internal audit ................................................................... 11
5.3 Financial reporting ............................................................ 13
5.4 Counter-fraud .................................................................. 13
5.5 Other Committee work ...................................................... 13
6 Relationship with other Committees ......................................... 14
7 Actions for next year 2014/15 ................................................. 14
8 Conclusions and Way forward ................................................. 14

Public Health Wales Audit Committee Annual Report
Date: 16 June 2014 Version: 1 Page: 5 of 15
Foreword
I am pleased to provide the foreword for the fourth Public Health Wales
Audit Committee annual report.
The report summarises the key areas of business activity undertaken by the Audit Committee over the past year.
Throughout the year the Committee has continued to provide
reassurance to the Board on the governance and systems of assurance of Public Health Wales, with a particular focus on the financial systems
and on management arrangements where change may impact on service provision (eg microbiology and screening).
The Committee has an important role in taking timely action when there are indications that all is not well. Examples during the year
include:
Taking early action and requesting reassurance in relation to the Public Sector Payment Policy and reporting the issue to the
Board. Commissioning the internal audit review of asbestos
management, prompted by the significant number of building locations and the need to ensure risks were being properly
addressed. Actions have been identified for improvement and will continue to be monitored by the Committee.
Audit Committees must never become complacent and satisfied with their own performance and for that reason during the year we have
undertaken a 'self assessment' and will be taking further actions in the
coming year relating to its outcome.
I would like to extend my thanks to all members of Committee and those who contribute to meetings on behalf of Public Health Wales,
internal audit, external audit and counter-fraud.
I am grateful to the support given to me by the Board Secretary, Corporate Governance Manager and Business Support Manager for
ensuring the Committee remains focused on matters relating to governance and assurance. I am particularly grateful to Ms Tamira
Rolls who took on the role of Acting Director of Finance for the second half of the year.
Mr Terence Rose
Audit Committee Chair

Public Health Wales Audit Committee Annual Report
Date: 16 June 2014 Version: 1 Page: 6 of 15
1 Introduction
This Report summarises the key areas of business activity undertaken by the Audit Committee over the past year and highlights some of the
key issues which the Committee intend to give further consideration to over the next 12 months.
The Audit Committee’s annual ‘business cycle’ ends on 30 June
following the closure and audit of the Trust’s annual accounts and reflects the Committee’s key role in the development and monitoring of
the Trust’s Governance and Assurance framework, the production of the Trust’s Annual Governance Statement and the relevant Financial
Statements.
2 Role and Responsibilities
The primary purpose of the Audit Committee is to provide advice and assurance to the Trust Board on whether effective arrangements are in
place - through the design and operation of the Trust’s assurance framework - to support the Board in its decision taking and in
discharging its accountability for achieving the Trust’s objectives, in accordance with standards of good governance determined for NHS
Wales.
Where appropriate, the Committee will advise the Board and the Accountable Officer on where, and how, its assurance framework may
be strengthened and developed further.
The core functions of the Audit Committee are as follows;
Consider the effectiveness of risk management arrangements,
the control environment, and the related anti-fraud and anti-corruption arrangements;
Seek assurances that action is being taken on risk related issues
identified by auditors, by regulatory bodies and by the Trust itself;
Be satisfied that the assurance statements properly reflect the
risk environment and any action required to improve it;
Approve the Internal Audit strategy, plan and monitor performance; review Internal Audit reports and the main issues
arising; seek assurance that action has been taken where
necessary; receive and consider the Annual Report from Internal Audit;

Public Health Wales Audit Committee Annual Report
Date: 16 June 2014 Version: 1 Page: 7 of 15
Review the reports of External Audit and other Regularity Bodies
and the main issues arising; seek assurance that action has been taken where necessary; receive and consider the Annual External
Audit Report;
Approve the Local Counter-fraud Services (LCS) strategy, plan and monitor performance; review LCS reports and the main
issues arising; seek assurance that action has been taken where necessary; receive and consider the Annual Report from LCS;
Review the financial statements and, acting under delegated
powers, approve the adoption of the accounts;
Consider the results of audit and assurance work specific to the
Trust and the implications of the findings of wider audit and assurance activity relevant to the Trust’s operations to secure the
ongoing development and improvement of the Organisation’s governance arrangements; and
Ensure an effective relationship with the Quality and Safety
Committee and any other Committees or sub-Committees of the Board so that it can understand the system of assurance for the
Board as a whole.
3 Committee structure
A key element of the Committee is that the membership comprises Non
Executive Directors only, this provides a basis for it to operate independently of any decision making process and to apply an objective
approach to the conduct of its business. Executive Directors and other
members of staff are invited to attend meetings to provide assurances and explanations to the Committee on specific issues.
3.1 Membership of Committee
The membership of the Committee during 2013/14 included:
Mr Terence Rose Chair and independent Non Executive Director
Mr John Spence independent Non Executive Director
Dr Carl Clowes third sector Non Executive Director
3.2 Others in attendance During 2013/14 the meetings were also regularly attended by the
following:

Public Health Wales Audit Committee Annual Report
Date: 16 June 2014 Version: 1 Page: 8 of 15
Mr Bob Hudson Chief Executive and Accountable Officer (until 30
November 2013)
Mr Huw George Director of Finance (until 30 November 2013)
Interim Chief Executive (from 1 December
2013)
Ms Tamira Rolls Assistant Director of Finance (until 30 November
2013) Interim Director of Finance (from 1 December
2013)
Mr Keith Cox Board Secretary
Mr James Johns Internal audit, NHS Wales Shared Services
Partnership
Ms Jayne Gibbon Internal audit, NHS Wales Shared Services
Partnership
Mr Matthew Coe Wales Audit Office
Mr Jeremy Saunders Wales Audit Office
Ms Gabby Smith Wales Audit Office
Mr Craig Greenstock Local Counter Fraud Service, Cardiff and Vale University Health Board
3.3 Meeting frequency
The terms of reference for the Committee require meetings to be held no less than quarterly and otherwise as the Chair of the Committee
deems necessary – consistent with the Trust’s annual plan of Board Business. During 2013/14 the Committee met five times and was
quorate on each occasion.
4 Assurance The work of the Audit Committee, through scrutiny of external audit,
internal audit, counter-fraud and other pieces of work, enable the Committee to provide reliable assurances to the Board and the
Accountable Officer. The Committee has reviewed the system of assurance and concluded that it is fit for purpose. There are no areas
of significant duplication or omissions in the systems of governance in the organisation that have come to the attention of the Committee or
which have not been adequately resolved.
The Committee has, on occasion, requested further information on particular items to allow further scrutiny of the issues and to enable
them to provide robust assurance to the Board and Accountable Officer.
Examples of this include:

Public Health Wales Audit Committee Annual Report
Date: 16 June 2014 Version: 1 Page: 9 of 15
4.1 Committee self assessment During the year the Committee completed a self assessment exercise in
order to assess the effectiveness of the Committee. The Committee used the Audit Committee Handbook as a starting point to establish
how far they complying with the requirements set out in the Handbook
and identified areas for improvement for the committee. The self assessment concluded that the Committee continued to operate
effectively but also identified a need for further development sessions and a renewed focus on roles and responsibilities for the Committee.
Actions arising from the self assessment included reviewing the terms of reference of the Committee and producing a plan of Committee
business.
4.2 Risk
During the year it was agreed that the Committee would received the corporate risk register at each Committee meeting. The Committee
requested further assurance on the system of risk management. In doing so the Committee concluded that the system was adequate in
identifying risks and allowing the Board to understand the appropriate management of those risks. However, there were some areas where
the Committee felt the system could be improved. They requested that further information be provided on what controls and actions are in
place to mitigate the risk. They also recommended that the Board should consider how corporate risks link to divisional risks. In order to
strengthen the system of risk management, the Board has commissioned a rapid review of the system by the Good Governance
Institute. The results will be provided in June 2014.
4.3 Public sector payments policy
The Committee noted that the organisation was likely to miss the target for public sector payment compliance and requested further
assurances on what measures were being taken to improve the situation. The Committee received assurance that the issue had
occurred early in the financial year and was due to a change over in
systems. The organisation had achieved the target for the majority of the year, however the issues earlier in the year would mean that the
target across the year would not be met. The Committee ensured that this was noted in the Annual Governance Statement and that it would
be confirmed in the annual accounts for 2013/14.
5 Audit Committee Activity 2013/14

Public Health Wales Audit Committee Annual Report
Date: 16 June 2014 Version: 1 Page: 10 of 15
The Audit Committee fulfilled its work plan for 2013/14 covering a wide
range of activity. This work can be summarised under the following headings:
External audit;
Internal audit; Financial reporting;
Counter-fraud; and Other Committee work.
5.1 External audit External audit services are provided to Public Health Wales by the
Wales Audit Office. The Committee received and agreed the Wales Audit Office annual plan for 2013/14 which set out specific areas to be
covered in relation to both the audit of financial systems and performance audit assignments. The plan of work was developed in
consultation with Executive Directors to ensure it was aligned to the organisational priorities and financial and operational risks facing the
organisation. The Committee received progress reports from WAO at each meeting in relation to this work. These reports also give details of
reviews undertaken at a national level.
The Wales Audit Office final accounts memorandum was received by
the Committee in June 2014 and summarised the findings from the work carried out during 2012/13 as follows:
I have issued an unqualified opinion on the 2013-14 financial statements of the Trust, although in doing so, I have brought several
issues to the attention of officers and the Audit Committee
The Wales Audit Office performance audit work forms the structured assessment for the organisation. The results of the structured
assessment for 2013 were: - The Trust’s financial planning and management work well and
have contributed to the Trust consistently meeting its savings and statutory break even targets
- The Trust continues to improve its arrangements to support good
governance. Work remains to strengthen some components of the governance framework, collect more feedback from service
users and further develop the information in the Annual Quality Statement
- In its approach to managing resources effectively, the Trust has made good progress with workforce planning and organisational
development

Public Health Wales Audit Committee Annual Report
Date: 16 June 2014 Version: 1 Page: 11 of 15
The Wales Audit Office concluded the following local audits which were
received by the Audit Committee:
- Data backup arrangements - Microbiology management arrangements
- External review of NHS Wales Shared Services Partnership
The actions agreed by Public Health Wales in response to the recommendations in WAO reports are recorded in an action log and the
Committee continues to monitor progress in addressing them.
5.2 Internal audit
Internal audit services are provided to Public Health Wales by NHS Wales Shared Services Partnership. The Audit Committee approved the
Internal Audit Plan for 2013/14 at the start of the year, ensuring that the plan was robust and specifically targeted to risks identified within
the organisation. The Committee also approved the revised internal audit strategy.
The work completed by internal audit provides assurance that risks are
managed and controls and governance arrangements are in place. The
internal audit plan was developed in consultation with the Executive Directors and reflected the key risks and strategic objectives identified
by the Board.
During the year the Committee received seven assurance reviews. The following levels of assurance were awarded:
Substantial assurance
1. Budgetary control The Board can take substantial
assurance that arrangements to
secure governance, risk
management and internal control,
within those areas under review,
are suitably designed and applied effectively. Few
matters require attention and are compliance or
advisory in nature with low impact on residual
risk exposure.
2. Welsh risk pool claims
3. Standards for Health Services
Reasonable assurance
4. Implementation of alerts
The Board can take reasonable
assurance that arrangements to
secure governance, risk
management and internal control,
5. Screening modernisation

Public Health Wales Audit Committee Annual Report
Date: 16 June 2014 Version: 1 Page: 12 of 15
6. Financial systems
review
within those areas under review, are suitably
designed and applied effectively. Some matters
require management attention in control design or
compliance with low to moderate impact on
residual risk exposure until resolved.
Limited assurance
7. Asbestos management The Board can take limited
assurance that arrangements to
secure governance, risk
management and internal control,
within those areas under review,
are suitably designed and applied effectively. More
significant matters require management attention
with moderate impact on residual risk exposure
until resolved.
The following reports were completed by Internal Audit but did not offer an assurance rating.
Sustainability
Annual Quality Statement
The Head of Internal Audit has concluded:
Reaso
nab
le
assu
ran
ce
- +
Yellow
The Board can take reasonable assurance that
arrangements to secure governance, risk management
and internal control, within those areas under review,
are suitably designed and applied effectively. Some
matters require management attention in control design
or compliance with low to moderate impact on
residual risk exposure until resolved.
In reaching this opinion the Head of Internal Audit has identified that the majority of reviews during the year concluded positively, with the
only exceptions being asbestos management and the lack of progress with implementing the recommendations relating to mandatory
training. The Audit Committee has responded to the exceptions noted by the Head of Internal Audit and has ensured that action has been
taken at Board level to improve the situation and work continues to
monitor the improvements. Significant progress has been made during the year to improve statutory and mandatory training compliance and
this will remain a priority for 2014/15.
The Committee is also scheduled to receive reports during the course of the year on the audits of financial systems operated by NHS Wales
Shared Services partnership, processing transactions on behalf of Public Health Wales. There were no reports of this nature presented to
the Committee during 2013/14.

Public Health Wales Audit Committee Annual Report
Date: 16 June 2014 Version: 1 Page: 13 of 15
Any areas identified for improvement by the reviews above are
recorded on the internal audit action log which is received by the Committee at each meeting. It is closely monitored and each action is
allocated to an Executive lead. During the year the committee requested that actions also be allocated an overseeing Committee.
5.3 Financial reporting The Audit Committee considered the annual accounts for 2013/14 in
May 2014, including the organisation’s Annual Governance Statement. The Committee subsequently approved the annual accounts and Annual
Governance Statement in June 2014, on behalf of the Board. In doing so, the Committee confirmed that the Annual Government Statement
was consistent with the Committee’s view on Public Health Wales’ system of internal control. The Committee did not identify any
reasonable limitations to draw to the attention of the Board.
5.4 Counter-fraud
The Committee approved the 2013/14 annual work plan of the Local Counter Fraud Specialist, provided to Public Health Wales by Cardiff
and Vale Counter Fraud Services. Regular reports were received by the Committee to monitor progress against the plan. The reports advised
the Committee about ongoing and concluded fraud investigations, policy and procedure reviews, action being taken to deter and prevent
fraud and to raise fraud awareness throughout the organisation.
5.5 Other Committee work
In addition to the work undertaken by Wales Audit Office, Internal Audit and Counter-fraud, the Committee completed the following pieces
of work:
Received and monitored a report into salary overpayments;
Responded consultation on the Auditor General’s revised Code of Audit Practice and a Statement of Practice for local government
improvement audit, assessment and special inspection work;
Received a report on clinical negligence and personal injury
claims;
Received and reviewed the reporting of single tender contracts and procurement activity at each Committee meeting;

Public Health Wales Audit Committee Annual Report
Date: 16 June 2014 Version: 1 Page: 14 of 15
The Audit Committee also received the formal report on the
ongoing work on the register of interest and the register of gifts and hospitality and the register of common seal; and
Reviewed the organisation’s first Annual Quality Statement.
6 Relationship with other Committees
The Audit Committee has worked closely with the Quality and Safety Committee during the year. Two members of the Audit Committee are
also members of the Quality and Safety Committee. This common membership ensures continuity across the two Committees and
provides the Chair of the Audit Committee with assurance that clinical quality and safety is being addressed appropriately by the Quality and
Safety Committee. Performance data has been improved during the
year and information flows relating to performance against Public Health Wales’ strategic objectives are improving.
The Audit Committee and Quality and Safety Committee have reviewed
their terms of reference to ensure that there were no overlaps or obvious gaps in roles and responsibilities for each of the Committees.
The outcome of the review was that few changes were needed, although some additional information was included to reinforce the
need for Committees to ensure a connection between the business of key committees and also seek to integrate assurance reporting.
7 Actions for next year 2014/15
The Committee has identified the following areas to focus on during the forthcoming year:
Continue to ensure that financial controls are operating
effectively;
Ensure continued development and improvement of effective risk
management and governance arrangements;
Continue to monitor progress against recommendations made in internal and external audit reports; and
Ensure continued development and effectiveness of Audit Committee.
8 Conclusions and Way forward

Public Health Wales Audit Committee Annual Report
Date: 16 June 2014 Version: 1 Page: 15 of 15
The Audit Committee is now well established and has undertaken all of
its core functions. The results of external reviews are pleasing and all recommendations are forming part of action plans which are actively
monitored. The Committee has concluded that the above programme of work provides a comprehensive and reliable assurance to support
the Board and Accountable Officer in discharging their accountability obligations.
The Audit Committee has established an active process which gives
oversight of all internal and external recommendations and their timely implementation.
Good working relationships continue between the Committee Members
and the colleagues from external and internal audit.

Date: 13 January 2013 Version:1 Page: 1 of 17
Safeguarding Annual Report 2013-2014 Purpose of Document: The purpose of this Annual Report is to provide an overview of safeguarding activity
across Public Health Wales NHS Trust over the last 12 months. In addition this report
will provide assurance to the Board that the Trust meets its statutory responsibilities in relation to safeguarding.
Board/Committee to- (Please indicate)
To decide- Paper will outline recommendations or issues to be
approved by the Board or Committee.
To discuss- Board or Committee will be asked to discuss and scrutinise the paper and provide feedback and comments.
To inform- Board or Committee will be asked to note the paper for information only
Other relevant information
Next Steps
Link to Public Health Wales commitment and priorities for action:
(please tick which commitment(s) is/are relevant)
Priorities for action include relevant priority for action(s)
Author: Kate McDonald, Named Nurse Safeguarding
Date: 25 March 2014 Version: 1
Sponsoring Executive Director: Dr Quentin Sandifer
Who will present: (If appropriate) Dr Quentin Sandifer
Documents attached: (If appropriate)
Safeguarding annual report
Date of meeting: 26 June 2014
Committee/Groups that have received or considered this paper:
Public Health Wales Safeguarding Group Quality and Safety Committee
Paper 32 16

Date: 13 January 2013 Version:1 Page: 2 of 17
Link to standards
for health services
Standard 11: Safeguarding children and
safeguarding vulnerable adults
Link to risk
register
N/A
Equality impact assessment
No, report is for internal purposes only
Financial implications
No
Service user
engagement
No

Public Health Wales Safeguarding Annual Report to Board 2013-2014
Date: 25 March 2014 Version: 1 Page: 3 of 17
ANNUAL REPORT
SAFEGUARDING
2013-2014
Author: Kate McDonald, Named Nurse Safeguarding
Date: 25 March 2014 Version: 1
Publication/ Distribution:
Public Health Wales Board
Sponsor: Dr Quentin Sandifer
Purpose and Summary of Document:
The purpose of this Annual Report is to provide an overview of safeguarding activity across Public Health Wales NHS Trust over the last
12 months. In addition this report will provide assurance to the Board that
the Trust meets its statutory responsibilities in relation to safeguarding.

Date: 13 January 2013 Version:1 Page: 4 of 17
1 INTRODUCTION
1.1 This is the annual safeguarding report to the Public Health Wales NHS Trust board for the period March 2013-2014. The purpose of
this report is to provide the board with an update of the assurance arrangements in place to discharge Public Health Wales’
safeguarding responsibilities. It is imperative for Public Health Wales to safeguard vulnerable persons in accordance with the
legislation framework of the Children Act 1989, Children Act 2004, and key principles and core values arising from ‘In Safe Hands’,
All Wales Interim Adult Protection Policies & Procedures (2013) and the Domestic Abuse Strategic Agenda.
1.2 Safeguarding children and vulnerable adults is a public duty, placed on key agencies across Wales by legislation and guidance.
The duty is a clear one, and to protect the most vulnerable
members of our society requires everyone within Public Health Wales to recognise their important role in helping prevent and
identify abuse and neglect. There were 2.950 children (including unborn children) on child protection registers in Wales at 31 March
2013, a rate of 47 children per 10,000 population aged under 18. The highest number of registrations was shown in categories
involving neglect (43 per cent) (Welsh Government, 2012).
1.3 Wales also has the highest share of over-60s than any other part
of the UK, with nearly one in four aged 60 or over. In 2009/10 there were 3,572 completed referrals alleging abuse of adults in
Wales (WG, 2011) and the number of referrals are increasing year on year. The most commonly reported victim of alleged
abuse was an older woman but it is understood that there is an under reporting of abuse in people who have mental health
problems or learning difficulties.
1.4 The continued high profile court cases relating to sexual abuse and the inquiries currently underway into the abuse perpetrated
by Jimmy Savile inside hospitals and other public institutions serve to underline the importance of ensuring that Public Health
Wales has robust systems in place to ensure that children and vulnerable people may be safeguarded effectively.
2 GOVERNANCE AND ACCOUNTABILITY
2.1 The combining of the safeguarding of children and vulnerable
adults into the remit of one professional has strengthened the governance arrangements and the Named Nurse now takes the

Public Health Wales Safeguarding Annual Report to Board 2013-2014
Date: 25 March 2014 Version: 1 Page: 5 of 17
lead for both groups within Public Health Wales in order to ensure
an equal focus. Safeguarding is however a dynamic process which is constantly evolving in line with changing legislation and
guidance as well as recommendations from current investigations and inquiries. Safeguarding is both highly emotive and politically
sensitive and the agenda is expected to increase significantly with the Social Services (Wales) Bill and the Ending Violence Against
Women, Domestic Abuse and Sexual Violence (Wales) Bill expected to reach the statute books in 2014.
2.2 In line with legislation and guidance as well as intercollegiate and professional competency frameworks and the Public Health Wales
Safeguarding in Public Health safeguarding strategy, the role of the Named Nurse Safeguarding for Public Health Wales comprises both
a strategic and operational function. The strategic role includes taking an overview to ensure that children and vulnerable adults
are safeguarded in the planning and development of services and
that there are appropriate policies and procedures in place to ensure their protection. In addition, there are operational duties
including providing advice and support to all levels of staff and training.
2.3 Central to safeguarding in Public Health Wales in 2013-2014 has been the Safeguarding Group which meets on a quarterly basis to
provide a forum and focus for the management of safeguarding in Public Health Wales. In line with the Terms of Reference the
Group is chaired by Dr Quentin Sandifer, lead Executive Director for Safeguarding, attended by Professor Simon Smail, lead Non-
Executive Director for Safeguarding and the Nurse Director and is constituted of representatives from all service areas. Evidence of
the functioning of the group is through the production of relevant minutes, plans, reports and other documentation. Reporting
responsibility is to the Quality and Safety Committee through the
Risk Management Group.
2.4 The Safeguarding Group ensures compliance with section 28,
27(2) (a) (b) and section 25 and section 31 of the Children Act 2004. Although there is no similar legislation for adults the
Human Rights Act 1998 places a positive duty upon ‘public bodies’ to act compatibly with the 1950 European Convention on
Human Rights which includes duties under Article 2: ‘The right to life’; Article 3: ‘Freedom from torture’ (including humiliating
and degrading treatment) and Article 8: ‘Right to family life’. In addition, the Safeguarding Group ensures compliance with safe
recruitment and monitoring arrangements as well as providing leadership, commitment and operational support to
safeguarding across Public Health Wales.

Public Health Wales Safeguarding Annual Report to Board 2013-2014
Date: 25 March 2014 Version: 1 Page: 6 of 17
2.5 The attendance at the group has been generally satisfactory in
2012–2013 and it has been a dynamic group with a committed membership which has contributed greatly to safeguarding in
Public Health Wales. The goal for the next year will be to ensure attendance from all service areas.
3 MONITORING AND AUDIT
3.1 The main monitoring and audit system within the NHS in Wales are the Standards for Health Services, and compliance with
Standard 11 is monitored to enable the annual self-assessment submission. Standard 11 is completed by all service areas, and in
considering this year’s submissions it is clear that more work remains to be undertaken with teams to ensure the submissions
are more meaningful going forward. The Safeguarding Group oversees the development, review and implementation of the
Standard 11 Improvement Plan. This will provide the basis for
planning safeguarding priorities in Public Health Wales; additional priorities may also be set by the Safeguarding Group.
3.2 To ensure a robust safeguarding culture it is important to learn from events happening internally or externally, this is achieved
through:
Risk management processes
Membership of the Risk Management Group
DATIX risk reporting system.
Raising concerns and incidents through the Safeguarding Group Recommendations from Serious Case Reviews across Wales are
shared with the Named Nurse Safeguarding Children by the Safeguarding Children Service and for adults via the adult
protection fora. Any risk areas or identified training needs within Public Health Wales would then be addressed.
3.3 The Local Safeguarding Children Boards (LSCBs) in Wales request
an annual audit against section 28 of the Children Act 2004 responsibilities. To avoid duplication across all LSCBs a Public
Health Wales s28 audit setting out Public Health Wales compliance with all statutory legislation and guidance was developed for
LSCBs and distributed in response to requests.
3.4 In his report ‘Safeguarding and Protecting Children in NHS Wales’
(Cardiff University, 2010) Professor Sir Mansel Aylward called for the establishment of an all Wales NHS clinical network for
safeguarding to be established under the leadership of the Safeguarding Children Service. The Named Nurse is a member of

Public Health Wales Safeguarding Annual Report to Board 2013-2014
Date: 25 March 2014 Version: 1 Page: 7 of 17
this group the ‘All Wales Safeguarding Children Clinical Network’
and reports back to the Safeguarding Group. He also identified the need for robust monitoring and evaluation in order to improve and
develop services. The acceptance of this recommendation by Welsh Government led to the development of the Quality
Outcomes Framework (QOF) by the Safeguarding Children Service, Public Health Wales. This was completed for the first time
in 2013. The timescales for completion were extremely tight and some of the information proved challenging for all Trusts and
Health Boards including Public Health Wales. A working group has been established to further develop the QOF for the 2013-2014
submission later this year.
4 PROGRESS AGAINST PRIORITIES
4.1 Disclosure and Barring checks
4.11 On the 12 September 2012, the definition of regulated activity for
a check changed and now covers a check against a barred list for children and/or adults.
The key changes that impact on Public Health Wales are:
The term ‘access’ to children or vulnerable adults only concerns
employees having direct, physical, day-to-day contact with patients; it does not include positions where there is no face to
face contact and therefore staff in positions of trust, advising on policies affecting children and vulnerable adults,
Safeguarding Nurses and the Board are not may not have
standard or enhanced checks.
Positions that purely involve having access to records or
sensitive information are not covered under the definition of regulated activity and checks may not be undertaken.
4.12 A Task and Finish Group was established and developed a manager checklist to be used by managers to assess if a position
requires a DBS check and to what level. The group considered the possibility that an audit be completed to ascertain whether a
current post-holder working in a position assessed to require a Disclosure and Barring (DBS) check currently has one. If they do
not have the appropriate DBS check, Public Health Wales would be in a strong position to justify why this has to be completed.
4.13 In order to further clarify the position in relation to performing a check on staff that don’t readily fall into one of the prescribed
categories, the Named Nurse is taking this issue forward with
Welsh Government via the Wales Safeguarding Clinical Network.

Public Health Wales Safeguarding Annual Report to Board 2013-2014
Date: 25 March 2014 Version: 1 Page: 8 of 17
4.2 Training
4.21 Safeguarding occurs in a culture that prioritises training and
therefore has a competent and safe workforce, and full engagement of managers and staff is required to increase
knowledge and ultimately reduce the risks to service users, employees and the organisation. A safeguarding training strategy
is currently being developed incorporating the competences
outlined in the RCPCH intercollegiate document ‘‘Safeguarding Children and Young people: roles and competences for health care
staff’ which has been adopted by WG as the safeguarding training standard for Wales. This contains a tool to assist managers to
assess the level of training each staff member requires.
4.22 Training in safeguarding children and vulnerable adults is
mandatory for all staff. A combined children and adult safeguarding training has been developed in line with standards
set in the All Wales Child Protection Procedures 2008, the RCPCH intercollegiate guidance on ‘Safeguarding Children and Young
people: roles and competences for health care staff’ and the ‘Wales Interim Policy and Procedures for the Protection of
Vulnerable Adults from Abuse’ (appendix 1). Safeguarding training is delivered at 3 levels in Public Health Wales. (Appendix 1), all
training is delivered by the Named Nurse Safeguarding.
4.23 Level 1 safeguarding children e learning is now available, but is not suitable for staff to use as there is no POVA element, however
there is an all Wales group currently developing this. Once available this would be useful for those staff new in post and
those whose post outline would only require them to have this level of training. In the interim the development of a POVA
workbook is underway to sit alongside the online training. Not all staff requiring level 1 would have ready access to a computer and
a level 1 training package has been developed which can be delivered by managers and trainers where available. It is hoped
that this will facilitate an increase in the number of staff accessing this training.
4.24 Level 2 training has been delivered to staff across Wales by the Named Nurse Safeguarding. This is face-to-face training delivered
in multidisciplinary sessions as well as to discrete teams. This has
been well-received (appendix 2).
4.25 The only training compliance figures currently reported on are for
level 1 safeguarding children training, which shows compliance across the organisation at 41% (505 staff members) to the end of
Public Health Wales Safeguarding Annual Report to Board 2013-2014
Date: 25 March 2014 Version: 1 Page: 9 of 17
January 2014. However, it must be noted that in the absence of
specific and defined training denominators, it is not possible to give accurate compliance figures, for example some staff may not
be required to attend level 1 as they require a higher level training.
The intention going forward is to accurately define and set out in the Safeguarding Training Strategy the staff requiring each level
of training and it would then be possible to report compliance against those denominators.
An additional challenge is that as ESR is not yet rolled out across the organisation a basic Excel database is the only method of
reporting training compliance. In the meantime until there is such accurate central reporting, POD will continue to maintain records
as accurately as possible, however with the implementation of the updated Safeguarding Training Strategy, it may be requested that
training records are maintained locally and fed into POD on a
quarterly basis.
4.26 HealthWRAP training which is part of the PREVENT counter-
terrorism strategy, continues in line with the Implementation Strategy. Another trainer has been trained and is also delivering
HealthWRAP. Four sessions have been delivered in 2013-14 but the attendance has been disappointing with some sessions having
been cancelled.
4.27 Level 3 training is available to staff on topics such as internet and
online abuse, domestic violence, neglect and substance misuse. This has been delivered successfully to discrete teams where
requested e.g. domestic violence, FGM and Sexual Exploitation training to Newborn Hearing Screeners. Three training sessions on
the Mental Capacity Act 2005 are scheduled across Wales in 2014. Training priorities in 2013 will be the roll-out of training on
Domestic Violence to accompany the launch of the Public Health
Wales ‘Domestic violence, violence against women and sexual violence policy, and training on female genital mutilation.
4.3 Policy and Procedures
4.31 The development of safeguarding policy and guidance for Public
Health Wales has been a priority. A ‘Safeguarding adults at risk’ policy’ has been developed and is in the final stages of
consultation prior to adoption by Public Health Wales.
4.32 The ‘Procedure for staff working with sexually active young people and vulnerable adults’ has been developed and is in the final
stages of consultation prior to adoption by Public Health Wales.

Public Health Wales Safeguarding Annual Report to Board 2013-2014
Date: 25 March 2014 Version: 1 Page: 10 of 17
This will assist staff in understanding the legislation and guidance
in this area of work. This is particularly timely having regard to the recent high profile cases.
4.33 The proposed legislation to end violence against women, domestic abuse and sexual violence (Wales) will place a duty on all public
sector employers to have a workplace policy for violence against women, domestic abuse and sexual violence. The Welsh
Government has therefore requested that the policy is developed and accompanied by staff training. This has been developed and is
nearing the end of the consultation process prior to adoption by Public Health Wales.
4.34 The all Wales Named Professionals Forum has developed a safeguarding Supervision Strategy which will be considered by the
Safeguarding Group and may be adopted by Public Health Wales.
4.35 National safeguarding policies and procedures, the All Wales Child
Protection Procedures 2008 and the All Wales Interim Adult
Protection Policy and Procedures 2010 are available to all staff on the intranet. In light of the proposed changes under the Social
Services and well-being (Wales) Bill 2012 it is inevitable that these policies may require further amendment to reflect any
changes arising from the final legislation.
4.4 Organisational Support
A key component in safeguarding is to provide advice and support to
Public Health Wales staff to promote good professional practice within Public Health Wales. To ensure that all staff are aware of their
responsibilities and know how to access advice on entry to the organisation safeguarding leaflets are given to staff at induction.
There are safeguarding children and vulnerable adults’ web pages which contain links to all relevant internal and external safeguarding documents
and policies, referral forms and contact details for advice and referrals.
4.41 Children
4.41.1 The Named Nurse is available to all staff to offer advice, however the nature of the work of Public Health Wales means less face-to-
face work with children than in other Health Boards and Trusts. In 2013 – 2014 there were 15 formal requests for advice which
resulted in 12 referrals on to other agencies.
4.41.2 Effective supervision is important in promoting good standards of
practice and supporting individual staff members. Supervision
allows time for reflective practice and is a vital component in the protection of children. A Safeguarding Children Supervision

Public Health Wales Safeguarding Annual Report to Board 2013-2014
Date: 25 March 2014 Version: 1 Page: 11 of 17
Procedure is in place which stipulates that direct supervision is
made available to staff dealing with a child protection case. This would also be the case with vulnerable adults and when this
procedure requires updating it will be amended as such.
4.41.3 Safeguarding supervision sessions have continued with all
Newborn Hearing Screeners and are greatly valued by staff and the Named Nurse. An evaluation of the supervision programme
has been completed and a report submitted to the service.
4.41.4 A Public Health Wales Safeguarding Children Handbook has been
developed to assist staff in recognition and the referral process. This is distributed to staff attending training and is available on
the intranet.
4.42 Vulnerable Adults
4.42.1 The Named Nurse Safeguarding is available via telephone or email to all staff to offer advice about any adult protection concern.
Each year there are thousands of adults who come into contact
with Public Health Wales services, however there have been few requests for advice. Due to the workload of the Named Nurse
there has been insufficient time to fully develop this part of the role. This is something which should be a priority for Public Health
Wales in 2014-15. It is envisaged that referrals will increase as awareness of POVA issues increases within Public Health Wales.
4.42.2 A Public Health Wales Safeguarding Vulnerable Adults Handbook has been developed to assist staff in recognition and the referral
process. This is distributed to staff attending training and is available on the intranet.
4.42.3 The Named Nurse Safeguarding is in a position to access the four multiagency adult protection fora in Wales but this is difficult due
to time constraints. This is unfortunate because this would afford the opportunity to keep updated with current legislation,
guidance, recommendations and trends in adult protection as well
as ‘networking’ opportunities. This will be a priority in 2014-15. In addition an all Wales Safeguarding Vulnerable Adults Health
Professionals Group has been established of which the Named Nurse is a member and attends meetings where possible.
5 Social Services and Well-being (Wales) Bill
5.1 The Deputy Minister for Children and Social Services has set out her approach to safeguarding and protecting people in Wales
which included a commitment to carry forward a Social Services and well-being (Wales) Bill in 2012. The bill was introduced on

Public Health Wales Safeguarding Annual Report to Board 2013-2014
Date: 25 March 2014 Version: 1 Page: 12 of 17
28/01/13 and is progressing through the Welsh Government for
implementation later this year. The Bill will include a statutory framework for protecting people (adults and children). It will
consolidate arrangements for children and encompass new duties to investigate, co-operate and share information in the field of
adult protection and will include a statutory definition of an adult at risk.
5.2 In addition, there is a rationale for fewer Local Safeguarding Children Boards, currently most of the existing LSCBs are merging
to form Regional Safeguarding Children Boards, some of which are operating in shadow form, and this is also the case for Adult
Protection Boards. The possibility has been mooted of the adult and children boards merging to form Safeguarding and Protection
Boards to reflect the holistic approach required to safeguard and protect people in Wales. If this were to happen it would only be
when ministers believe that these boards are operating effectively
and assessed to provide evidence to support integration.
6 Priorities for 2014 - 2015
6.1 The priorities for Public Health Wales have been identified
following completion of Section 11 of the Healthcare Standards for Wales and the subsequent action plan. These will be included in
the Named Nurse workplan and overseen by the Safeguarding Group.
6.2 The priorities fall under three headings:
1. Policy development:
Update, combine and complete the Training Strategy in
line with the RCPCH and Skills for Health competency
frameworks.
Update the Project and Partnership Risk Assessment Tools
2. Training:
Collaborate with POD to scope training needs and deliver
a training programme across Wales
Further develop training to utilise training-for-trainers and
e learning
3. Governance
Provide a paper for the Board outlining the challenges for
the Named Nurse in delivering adequate safeguards for
children, vulnerable adults and the organisation
Ensure that safeguarding advice is readily available to
staff

Public Health Wales Safeguarding Annual Report to Board 2013-2014
Date: 25 March 2014 Version: 1 Page: 13 of 17
Update and further develop the safeguarding web pages
Ensure compliance with Standards for Health 11
Attend meetings of the regional adult protection fora.
6.3 The overarching priority for the next year will be for Public Health Wales to continue to build on the work already in progress and to see substantial progress against issues highlighted in the
Healthcare Standards.
6.4 Personal priorities include increasing my knowledge-base on the
safeguarding of vulnerable adults and updating my job description to take account of my new role.
7 Conclusions
The clear aim of both the child and adult safeguarding functions within
Public Health Wales is to make a fundamental difference to the protection of children and young people, vulnerable adults and those subject to
domestic abuse and violence. There is a requirement to provide a coordinated response to ensure that all staff understand their
safeguarding responsibilities to both children and vulnerable adults and are aware of the nominated point of contact for support and advice when
they have a concern. It should be noted that as Public Health Wales is an all Wales organisation, safeguarding covers the whole of Wales and the
safeguarding of children and vulnerable adults is covered under one post, it is clear that this is a challenging remit for one individual to deliver.
8 References
1. CHILDREN ACT 2004. London: The Stationery Office.
2. HUMAN RIGHTS ACT 1998. London: The Stationery Office.
3. LOCAL SAFEGUARDING CHILDREN BOARDS (2008) All Wales Child
Protection Procedures
4. MENTAL CAPACITY ACT (2005). London: The Stationary Office.
5. ROYAL COLLEGE OF PAEDIATRICS AND CHILD HEALTH (2010)
Safeguarding Children and Young people: roles and competences for
health care staff. London: RCPCH
6. UNITED NATIONS CONVENTION ON THE RIGHTS OF A CHILD (1989)
General Assembly Resolution Document A/RES/44
7. WELSH ADULT PROTECTION FORA (2010). Wales Interim Policy and
Procedures for the Protection of Vulnerable Adults from Abuse. Cardiff:
Welsh Adult Protection Fora
8. WELSH ASSEMBLY GOVERNMENT (2006) Safeguarding Children:
Working Together under the Children Act 2004). Cardiff.

Public Health Wales Safeguarding Annual Report to Board 2013-2014
Date: 25 March 2014 Version: 1 Page: 14 of 17
9. WELSH ASSEMBLY GOVERNMENT (2006a) Healthcare Standards for
Wales. Cardiff.

Public Health Wales Safeguarding Annual Report to Board 2013-2014
Date: 25 March 2014 Version: 1 Page: 15 of 17
APPENDIX 1
Training Activities March 2013-2014 Public Health Wales
Staff Safeguarding Training
Training Sessions Delivered
Level 1 Training
Date Venue Trainer Region Number
Attended
28/1/2014 Microbiology Lab,
Bronglais Hospital, Aberystwyth
Kate
McDonald
Mid Wales 10
Total Number of Staff Trained to Level 1 10
Level 2 Training
Date Venue Trainer Region Number Attended
15/01/2013 AAA Screening Staff, Llantrisant
Kate McDonald
South Wales 20
19/02/2013 Morning
Newbridge PHT, Anvil Court,
Abertillery
Kate McDonald
South Wales 11
19/02/2013
Afternoon
Newbridge PHT,
Anvil Court, Abertillery
Kate
McDonald
South Wales 7
20/02/2013 Health Improvement Team, Nantgarw
Kate McDonald
South Wales 6
28/02/2013 Screening Staff, BTW Cardiff
Kate McDonald
South Wales 6
25/04/2013 Morning
14 Cathedral Road, Cardiff
Kate McDonald
South Wales 13
25/04/2013 Afternoon
14 Cathedral Road, Cardiff
Kate McDonald
South Wales 11
12/06/2013 Preswylfa, Mold
Kate McDonald
North Wales 11
17/06/2013 Stop Smoking Wales
Cardiff
Kate McDonald
South Wales 18
10/07/2013 Orchard Street,
Swansea
Kate
McDonald
South Wales Cancelled
11/07/2013 Public Health
Wales, Carmarthen (TBC)
Kate
McDonald
Mid Wales Cancelled
15/07/2013 Stop Smoking Wales Swansea
Kate McDonald
North Wales 6

Public Health Wales Safeguarding Annual Report to Board 2013-2014
Date: 25 March 2014 Version: 1 Page: 16 of 17
Level 2 Training
Date Venue Trainer Region Number
Attended
16/07/2013 Stop Smoking
Wales Swansea
Kate
McDonald
South Wales 13
17/09/2013 Public Health Wales, Merthyr Tydfil
Gloria Smith South Wales 20
02/10/2013 Preswylfa, Mold Kate McDonald
North Wales 11
08/10/2013 Morning
Programme Managing Unit,
Churchill Way, Cardiff
Kevin Hogan South Wales 14
08/10/2013 Afternoon
Programme Managing Unit,
Churchill Way, Cardiff
Kevin Hogan South Wales 5
23/10/2013 Morning
Innovation House, Llanharan
Kate McDonald
South Wales Cancelled
23/10/2013 Afternoon
Innovation House, Llanharan
Kate McDonald
South Wales Cancelled
13/02/2014 Preswylfa Kate McDonald
North Wales
4
19/02/2014 14 Cathedral Rd, Cardiff
Kate McDonald
South Wales
20
04/03/2014 BTW Boardroom Kate
McDonald
South Wales 0 (no
shows)
24/03/2014 BTW Llandudno Kate McDonald
North Wales 13
Total Number of Staff Trained to Level 2 209
Newborn Hearing Screeners POVA & Forced Marriage (Level 2/3)
Date Venue Trainer Region Number Attended
08/07/2013 Velindre HQ, Llantrisant
Kate McDonald
South Wales 24
13/11/2013 Royal Alexandra Hospital, Rhyl
Kate McDonald
North Wales 9
14/11/2013 Singleton Hospital, Swansea
Kate McDonald
South Wales 10
13/02/14 Preswylfa, Mold Kate McDonald
North Wales 6
Total Number of NBHS Staff Trained to Level 2/3 43
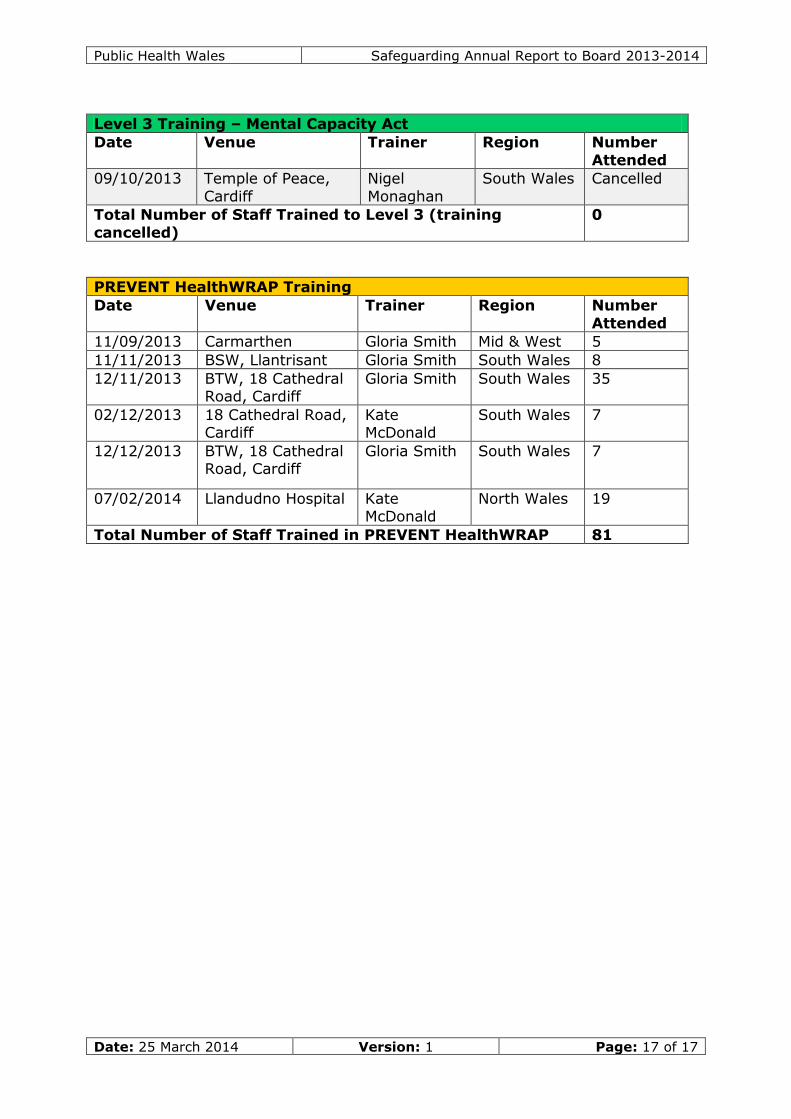
Public Health Wales Safeguarding Annual Report to Board 2013-2014
Date: 25 March 2014 Version: 1 Page: 17 of 17
Level 3 Training – Mental Capacity Act
Date Venue Trainer Region Number
Attended
09/10/2013 Temple of Peace,
Cardiff
Nigel
Monaghan
South Wales Cancelled
Total Number of Staff Trained to Level 3 (training
cancelled)
0
PREVENT HealthWRAP Training
Date Venue Trainer Region Number
Attended
11/09/2013 Carmarthen Gloria Smith Mid & West 5
11/11/2013 BSW, Llantrisant Gloria Smith South Wales 8
12/11/2013 BTW, 18 Cathedral Road, Cardiff
Gloria Smith South Wales 35
02/12/2013
18 Cathedral Road, Cardiff
Kate McDonald
South Wales 7
12/12/2013 BTW, 18 Cathedral Road, Cardiff
Gloria Smith South Wales 7
07/02/2014 Llandudno Hospital Kate McDonald
North Wales 19
Total Number of Staff Trained in PREVENT HealthWRAP 81

Date: 13 January 2013 Version:1 Page: 1 of 3
Health Emergency Planning Annual Report 2013Purpose of Document:
To present the Health Emergency Planning Annual Report 2013 and the report of theassessment by the Welsh Government.
Board/Committee to- (Please indicate)
To decide - Paper will outline recommendations or issues to beapproved by the Board or Committee.
To discuss - Board or Committee will be asked to discuss andscrutinise the paper and provide feedback and comments.
To inform - Board or Committee will be asked to note the paper forinformation only
X
Other relevant information
None
Next Steps
Link to Public Health Wales commitment and priorities for action:(please tick which commitment(s) is/are relevant)
X
Priorities for action Health emergency planning is a corefunction of a public health protectionservice.
Author: Dr Quentin Sandifer, Executive Director of Public Health Services
Date: 12 June 2014 Version: 1Sponsoring Executive Director: Dr Quentin Sandifer
Who will present: (If appropriate) Dr Quentin Sandifer
Documents attached:(If appropriate)
Public Health Wales Health EmergencyPlanning Annual Report for 2013
Health Emergency Planning Annual Reportfor 2013 – Summary Response
Date of meeting: 26 June 2014
Committee/Groups that havereceived or considered this paper:
Paper reference – 32 17

Public Health Wales Health Emergency Planning Annual Report 2013
Date: 12 June 2014 Version:1 Page: 2 of 3
Link to standardsfor health services
Standard 4 – Civil Contingency and Emergency Planningarrangements
Link to risk register
Equality impactassessment
N/A
Financialimplications
None
Service userengagement
N/A

Public Health Wales Health Emergency Planning Annual Report 2013
Date: 12 June 2014 Version:1 Page: 3 of 3
1 Introduction
Health emergency planning is the process by which Public Health Wales responds toincidents and outbreaks where escalation is required to mobilise additional capabilitiesbeyond the norm. It ensures that the organisation is able to fulfil its role as aCategory 1 Responder under the Civil Contingencies Act 2004. This Act places anumber of legal duties on Public Health Wales in respect of:
Risk assessment Maintenance of a risk register Planning arrangements for
o Prevention of emergencieso Response to emergencies
Planning arrangements for business continuity management Warning and informing Sharing information Co-operation with other agencies (planning, response and recovery)
The annual report follows a proforma provided by Welsh Government for self-completion by the Head of Emergency Planning and sign-off by the Chief Executive.The Head of Emergency Planning for Public Health Wales is Dr Gwen Lowe, aConsultant in Communicable Disease Control. The deadline for report submission was31 January 2014.
2 Updates since January 2014
Public Health Wales can report the following changes since submission of the annualreport in January 2014:
An updated Emergency Response Plan was published on 27 February 2014 The evaluation of the measles response centre referred to under Q12 is
complete and available on request Public Health Wales has established a secondary response centre at Magden
Park near Llantrisant An exercise, Exercise Stargate, was arranged to test the secondary centre on
10 June 2014 Public Health Wales, together with Aneurin Bevan and Cardiff and Vale Health
Boards, is working with Welsh Government on the health planningarrangements for the 2014 NATO Summit in September
As part of the planning arrangements for the NATO Summit Public Health Waleshas organised several exercises and training events for June and July 2014.
3 Recommendation
The Board is asked to receive and note the Health Emergency Planning Annual Reportfor 2013.

UUnneedd PPaarrooddrrwwyydddd aamm AArrggyyffyynnggaauu IIeecchhyydd
HHeeaalltthh EEmmeerrggeennccyy PPrreeppaarreeddnneessss UUnniitt
HHEEAALLTTHH EEMMEERRGGEENNCCYY PPLLAANNNNIINNGG AANNNNUUAALL RREEPPOORRTT FFOORR 22001133 Name of NHS
Organisation
Public Health Wales NHS
Trust Date 31/1/14
Signature of Chief
Executive Officer
Planning and Preparation
1. Please provide the name of your nominated Executive level lead for the organisation’s civil
contingency/emergency planning arrangements.
Dr Quentin Sandifer
2. Please provide the name of your nominated Executive level business continuity lead if
different to the above.
Mr Mark Dickinson
3. Please provide the name of your accountable emergency officer(s) with day to day
responsibilities for civil contingencies/emergency planning/business continuity
arrangements.
Health Protection- Dr Gwen Lowe Business Continuity- Mr Nathan Jones
4. Have you identified all posts and services critical to delivery of your Emergency Plans?
YES
As set out in the Emergency Response Plan which identifies the posts and services critical to delivery of a Public Health Wales Emergency Response. The Action Cards identify both the posts and other roles needing to be filled in an emergency and also capture these functions.
5. Does your business continuity planning address the resilience of all posts and services
critical to delivery of your key functions?
YES
The Emergency Response Plan also addresses resilience for key health protection team functions as most of the organisation’s other functions, apart from screening and microbiology, would be redirected to support the emergency response. Screening and microbiology services also have business continuity plans.
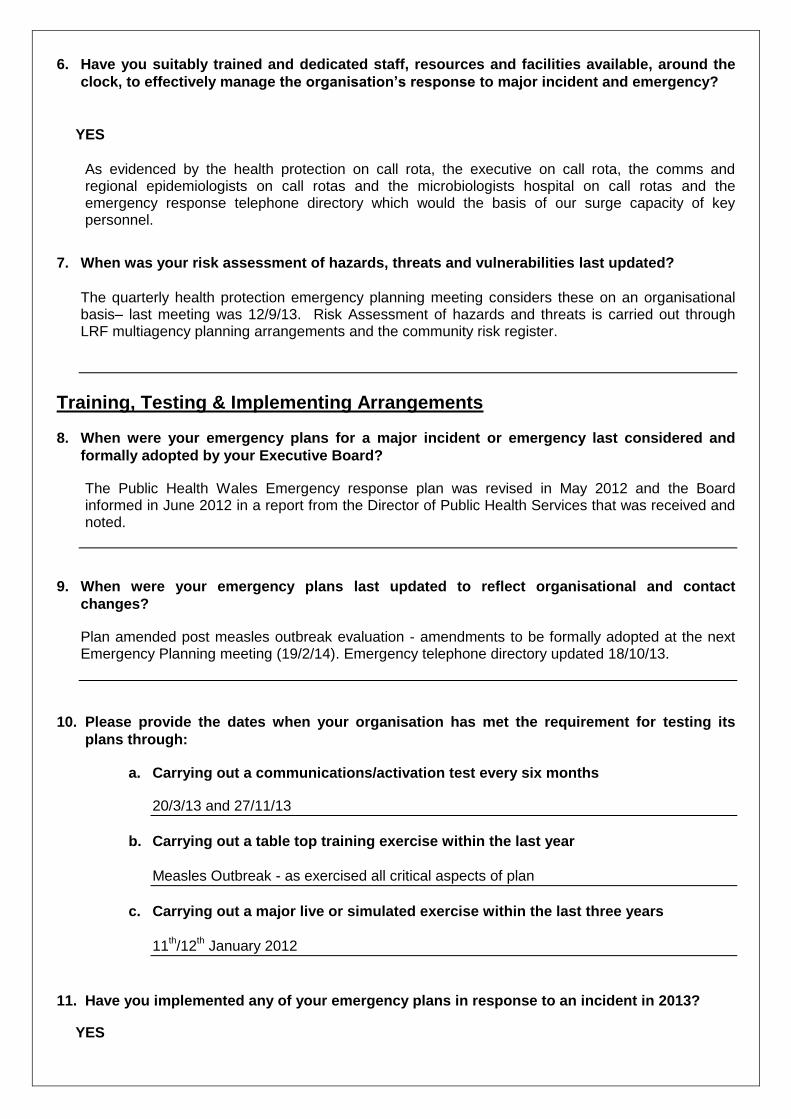
6. Have you suitably trained and dedicated staff, resources and facilities available, around the
clock, to effectively manage the organisation’s response to major incident and emergency?
YES
As evidenced by the health protection on call rota, the executive on call rota, the comms and regional epidemiologists on call rotas and the microbiologists hospital on call rotas and the emergency response telephone directory which would the basis of our surge capacity of key personnel.
7. When was your risk assessment of hazards, threats and vulnerabilities last updated?
The quarterly health protection emergency planning meeting considers these on an organisational basis– last meeting was 12/9/13. Risk Assessment of hazards and threats is carried out through LRF multiagency planning arrangements and the community risk register.
Training, Testing & Implementing Arrangements
8. When were your emergency plans for a major incident or emergency last considered and
formally adopted by your Executive Board?
The Public Health Wales Emergency response plan was revised in May 2012 and the Board informed in June 2012 in a report from the Director of Public Health Services that was received and noted.
9. When were your emergency plans last updated to reflect organisational and contact
changes?
Plan amended post measles outbreak evaluation - amendments to be formally adopted at the next Emergency Planning meeting (19/2/14). Emergency telephone directory updated 18/10/13.
10. Please provide the dates when your organisation has met the requirement for testing its
plans through:
a. Carrying out a communications/activation test every six months
20/3/13 and 27/11/13
b. Carrying out a table top training exercise within the last year
Measles Outbreak - as exercised all critical aspects of plan
c. Carrying out a major live or simulated exercise within the last three years
11
th/12
th January 2012
11. Have you implemented any of your emergency plans in response to an incident in 2013?
YES

If yes what was the nature of the incident?
Measles Outbreak
12. Have you undertaken an assessment of staff training needs in relation to your emergency
plans?
YES
Staff training needs are considered formally at quarterly emergency planning meetings as evidenced by meeting minutes. In addition we evaluate post major incident and are finalising collating the questionnaires sent out to staff in the measles response centre - one of the questions formally asks the staff drafted in if they had any further training needs following this.
13. Do you have a training programme relating to your emergency plans?
YES
The on-call training day 7
Feb 2013 and the on call training teleconference timetables and
proformas throughout the past year. In addition we are just finalising an e-learning induction training package on the plan and emergency response for all new starters and for all staff - the package is developed and been electronically tested and we are just negotiating with our OD team about rolling it out.
Communications
14. Have all relevant NHS organisations and partner agencies been consulted about their role in
your emergency plans?
YES
Relevant partners with specified roles in our emergency plan are Health Boards and CRCE. All are members of our emergency planning group that meets quarterly. The emergency plan and proposed amendments are circulated to these members for sign off at the meeting.
15. Is there a mechanism for discussing and co-ordinating health emergency planning
arrangements internally and with other NHS organisations serving the Local Resilience
Forum area?
YES
If yes please provide date of last meeting and health representation. Infectious Disease/pandemic flu Subgroups in all 4 LRF areas - attended by CCDCs and other local health organisations- SWLRF last meeting 12/12/13
16. Who represents your organisation at meetings of the Local Resilience Forum? The local CCDCs
Assessment
17. Are you satisfied with your organisation’s emergency preparedness and business continuity
arrangements?
YES
18. Are you satisfied that your organisation is fulfilling its requirements under the Civil
Contingencies Act 2004?
YES
Completed and signed forms to be returned by 31st January 2014
To: David Goulding, Health Emergency Planning Adviser, Floor 4, Cathays Park, Cardiff
CF10 3NQ or e-mail: [email protected]

Health Emergency Planning Annual Report 2013 - Summary Response
Y% N%
1 Please provide the name of your nominated Executive level lead for the organisation’s civilcontingency/ emergency planning arrangements.
100 0
2 Please provide the name of your nominated Executive level business continuity lead if differentfrom the above.
100 0
3 Please provide the name of your accountable emergency officer(s) with day to dayresponsibilities for civil contingencies/emergency planning/business continuity arrangements
100 0
4 Have you identified all posts and services critical to delivery of your Emergency Plans? 100 0
5 Does your business continuity planning address the resilience of all posts and services criticalto delivery of your key functions?
90 10
6 Have you suitably trained and dedicated staff, resources and facilities available, around theclock to effectively manage the organisation’s response to major incident and emergency?
100 0
7 When was your risk assessment of hazards, threats and vulnerabilities last updated? 100 0
8 When were your emergency plans for a major incident or emergency last considered andformally adopted by your Executive Board?
100 0
9 When were your emergency plans last updated to reflect organisational and contact changes? 100 0
10 Please provide the dates when your organisation has met the requirement for testing its plansthrough:
a. Carrying out a communications/activation test every six months 70 30
b. Carrying out a table top exercise within the last year 80 20
c. Carrying out a major live or simulated exercise within the last three years 90 10
11 Have you implemented any of your emergency plans in response to an incident in 2013? 100 0
12 Have you undertaken an assessment of staff training needs in relation to your emergencyplans?
100 0
13 Do you have a training programme relating to your emergency plans? 100 0
14 Have all relevant NHS Organisations and partner agencies been consulted about their role inyour emergency plans?
100 0
15 Is there a mechanism for discussing and co-ordinating health emergency planningarrangements internally and with other NHS organisations serving the Local Resilience Forumarea?
100 0
16 Who represents your organisation at meetings of the Local Resilience Forum? 100 0
17 Are you satisfied with your organisation’s emergency preparedness and business continuityarrangements?
90 10
18 Are you satisfied that your organisation is fulfilling its requirements under the CivilContingencies Act 2004?
90 10
2013 Nominated Exec level EP lead-AB Mr Richard Bowen HD Mr Paul Hawkins/Stuart MoncurABMU Mr Paul Stauber PHW Dr Quentin SandiferBC Mr Neil Bradshaw Powys Ms Catherine WoodwardC&V Mrs Abigail Harris WAST Mr Mike CollinsCT Mr Robert Williams WBS / V Mr Carl James
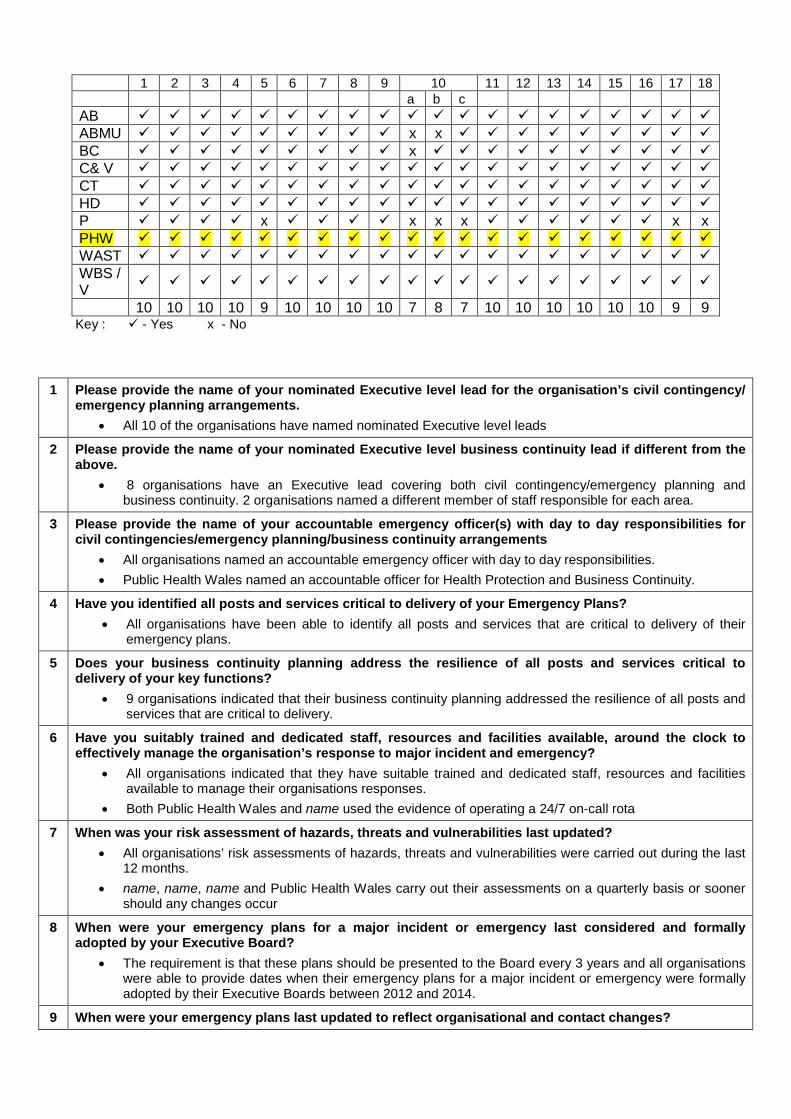
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18a b c
AB ABMU x x BC x C& V CT HD P x x x x x xPHW WAST WBS /V
10 10 10 10 9 10 10 10 10 7 8 7 10 10 10 10 10 10 9 9Key : - Yes x - No
1 Please provide the name of your nominated Executive level lead for the organisation’s civil contingency/emergency planning arrangements.
All 10 of the organisations have named nominated Executive level leads
2 Please provide the name of your nominated Executive level business continuity lead if different from theabove.
8 organisations have an Executive lead covering both civil contingency/emergency planning andbusiness continuity. 2 organisations named a different member of staff responsible for each area.
3 Please provide the name of your accountable emergency officer(s) with day to day responsibilities forcivil contingencies/emergency planning/business continuity arrangements
All organisations named an accountable emergency officer with day to day responsibilities.
Public Health Wales named an accountable officer for Health Protection and Business Continuity.
4 Have you identified all posts and services critical to delivery of your Emergency Plans?
All organisations have been able to identify all posts and services that are critical to delivery of theiremergency plans.
5 Does your business continuity planning address the resilience of all posts and services critical todelivery of your key functions?
9 organisations indicated that their business continuity planning addressed the resilience of all posts andservices that are critical to delivery.
6 Have you suitably trained and dedicated staff, resources and facilities available, around the clock toeffectively manage the organisation’s response to major incident and emergency?
All organisations indicated that they have suitable trained and dedicated staff, resources and facilitiesavailable to manage their organisations responses.
Both Public Health Wales and name used the evidence of operating a 24/7 on-call rota
7 When was your risk assessment of hazards, threats and vulnerabilities last updated?
All organisations’ risk assessments of hazards, threats and vulnerabilities were carried out during the last12 months.
name, name, name and Public Health Wales carry out their assessments on a quarterly basis or soonershould any changes occur
8 When were your emergency plans for a major incident or emergency last considered and formallyadopted by your Executive Board?
The requirement is that these plans should be presented to the Board every 3 years and all organisationswere able to provide dates when their emergency plans for a major incident or emergency were formallyadopted by their Executive Boards between 2012 and 2014.
9 When were your emergency plans last updated to reflect organisational and contact changes?
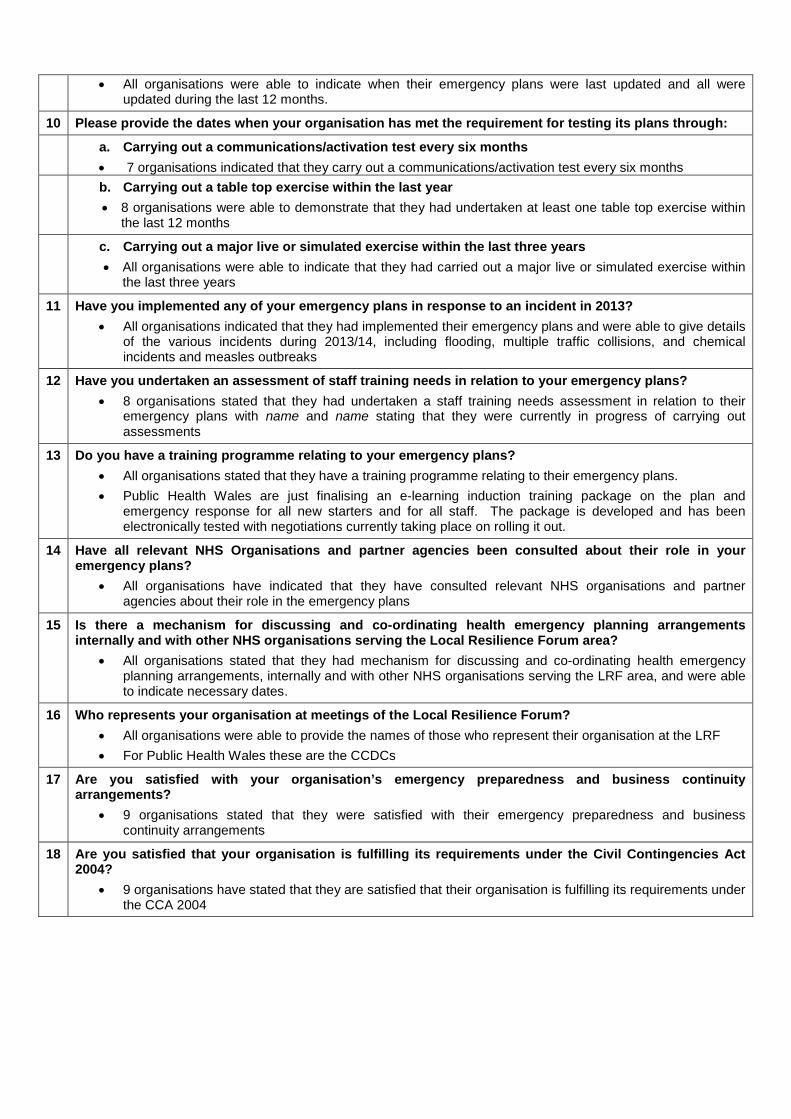
All organisations were able to indicate when their emergency plans were last updated and all wereupdated during the last 12 months.
10 Please provide the dates when your organisation has met the requirement for testing its plans through:
a. Carrying out a communications/activation test every six months
7 organisations indicated that they carry out a communications/activation test every six months
b. Carrying out a table top exercise within the last year
8 organisations were able to demonstrate that they had undertaken at least one table top exercise withinthe last 12 months
c. Carrying out a major live or simulated exercise within the last three years
All organisations were able to indicate that they had carried out a major live or simulated exercise withinthe last three years
11 Have you implemented any of your emergency plans in response to an incident in 2013?
All organisations indicated that they had implemented their emergency plans and were able to give detailsof the various incidents during 2013/14, including flooding, multiple traffic collisions, and chemicalincidents and measles outbreaks
12 Have you undertaken an assessment of staff training needs in relation to your emergency plans?
8 organisations stated that they had undertaken a staff training needs assessment in relation to theiremergency plans with name and name stating that they were currently in progress of carrying outassessments
13 Do you have a training programme relating to your emergency plans?
All organisations stated that they have a training programme relating to their emergency plans.
Public Health Wales are just finalising an e-learning induction training package on the plan andemergency response for all new starters and for all staff. The package is developed and has beenelectronically tested with negotiations currently taking place on rolling it out.
14 Have all relevant NHS Organisations and partner agencies been consulted about their role in youremergency plans?
All organisations have indicated that they have consulted relevant NHS organisations and partneragencies about their role in the emergency plans
15 Is there a mechanism for discussing and co-ordinating health emergency planning arrangementsinternally and with other NHS organisations serving the Local Resilience Forum area?
All organisations stated that they had mechanism for discussing and co-ordinating health emergencyplanning arrangements, internally and with other NHS organisations serving the LRF area, and were ableto indicate necessary dates.
16 Who represents your organisation at meetings of the Local Resilience Forum?
All organisations were able to provide the names of those who represent their organisation at the LRF
For Public Health Wales these are the CCDCs
17 Are you satisfied with your organisation’s emergency preparedness and business continuityarrangements?
9 organisations stated that they were satisfied with their emergency preparedness and businesscontinuity arrangements
18 Are you satisfied that your organisation is fulfilling its requirements under the Civil Contingencies Act2004?
9 organisations have stated that they are satisfied that their organisation is fulfilling its requirements underthe CCA 2004

Yr Adran Iechyd a Gwasanaethau Cymdeithasol Cyfarwyddwr Cyffredinol a Prif Weithredwr, GIG Cymru Department for Health and Social Services Director General and Chief Executive, NHS Wales
Parc Cathays ● Cathays Park Caerdydd ● Cardiff
CF10 3NQ
Ffôn ● Tel 02920 801182/1144
Gwefan ● website: www.wales.gov.uk
Dr Tracey Cooper Chief Executive Public Health Wales NHS Trust 14 Cathedral Road Cardiff CF11 9LJ
Our Ref: AG/ZE/RA
12 June 2014 Dear Tracey DESIGNATION AS AN ACCOUNTABLE OFFICER
It is a condition of your appointment to the role of Chief Executive, Public Health Wales NHS Trust that you must also be formally designated, by me, as an Accountable Officer. This letter formally designates you as the Accountable Officer for Public Health Wales NHS Trust with immediate effect. Full details of your responsibilities as an Accountable Officer are set out in the attached memorandum. Conditions You are directly accountable to me for the conduct of your role as Accountable Officer, and your continuing designation is dependent upon the following conditions, that you:
undertake appropriate training for Accountable Officers;
continue to keep yourself up to date with developments affecting your responsibilities as an Accountable Officer;
demonstrate to me that you meet the full range of your responsibilities set out in
the memorandum, and in a manner that displays a thorough understanding of propriety and accountability issues as they affect public services;

ensure that your Board members and Trust staff are aware of and understand your role and responsibilities as Accountable Officer; and
ensure that your responsibilities as Accountable Officer are reflected within the
Trust’s overall governance and accountability arrangements. Your designation as Accountable Officer may be withdrawn at any time if I consider that you have not met any of the conditions above or if I conclude that you are no longer a fit person to carry out the responsibilities of an Accountable Officer. In considering any such action, I would first consult with your Chair, to whom I am copying this letter. If your position as Chief Executive ceases, your appointment as Accountable Officer will automatically be withdrawn. Next steps You should familiarise yourself with the principles set out in Managing Welsh Public Money, as well as the standards of good governance set for the NHS in Wales - and embodied within the Assembly Government’s Citizen Centred Governance Principles - and the contents of the NHS Wales Governance e-manual www.NHSWalesGovernance.com I would be grateful if you could complete the form enclosed and return it to Zoe Elston within fourteen days to acknowledge receipt of this letter and acceptance of the responsibilities placed upon you as an Accountable Officer. Yours sincerely
Dr Andrew Goodall
cc Sir Mansel Aylward, Chair, Public Health Wales NHS Trust Enc

APPOINTMENT AS ACCOUNTABLE OFFICER
I acknowledge receipt of your letter appointing me as the Accountable Officer for: ………………………………………………………….. NHS Trust and confirm I have read the Accountable Officer Memorandum enclosed with your letter and accept the responsibilities placed upon me as an Accountable Officer. Signed: ……………………………………….. Date: ………………….. Please return completed form to: Zoe Elston Workforce and Organisational Development Department for Health and Social Services Welsh Government 2nd Floor Cathays Park CARDIFF CF10 3NQ

Yr Adran Iechyd a Gwasanaethau Cymdeithasol Dirprwy Brif Weithredwr Dros Dro, GIG Cymru Department for Health and Social Services Deputy Chief Executive, NHS Wales
Parc Cathays ● Cathays Park Caerdydd ● Cardiff
CF10 3NQ
Ffôn ● Tel 02920 801182/1144
Gwefan ● website: www.wales.gov.uk
Dr Tracey Cooper Chief Executive Public Health Wales 14 Cathedral Road Cardiff CF11 9LJ
Our Ref: SD/MR/DCL
17 June 2014 Dear Tracey Public Health Wales JET meeting Thank you for attending the JET meeting on 4 June 2014 with your Executive Team to discuss the end of year position against a number of key areas. I recognise this has been a challenging year for your organisation, with both the change in leadership during the year and dealing with the measles outbreak in ABMU. You recognised there were opportunities to strengthen the links between PHW and Welsh Government. You reported that your focus for the coming year was on smoking cessation, screening and building more effective relationships with Health Boards. We started our conversation discussing smoking cessation. You reported that a great deal of work had been done over the last year, including changing the service model which had resulted in waiting times reducing to six days, and that you are looking at ways to improve the data. You recognised there were issues around communication with Health Boards, and it was agreed that a meeting involving all parties would be set up to help resolve them. It was also agreed that further conversations would take place regarding the required increase in episodes of care planned for the coming year to meet the target. We discussed the MAMs smoking cessation project, and I would encourage you to ensure the evaluation of this project is carried out swiftly. You reported on the improvements made in immunisation rates, with the MMR1 figure the highest in the UK, and the MMR2 figure the 2nd highest. This improvement in performance is noted and welcomed. I recognise the improvements made in flu vaccination rates, particularly the improvement in the number of NHS staff receiving the vaccine. It is
important this improvement is continued into the coming year. You reported you have introduced three new vaccine programs this year, and you are committed to deliver further improvements, even though you only have a small team. I note you report you are doing additional work with local partners and communities, as well as working with Flying Start teams. You need to continue this collaborative approach going forward. On screening, you reported that there remain some long standing challenges, particularly with some of the cancer screening programmes, notably around provision of diagnostic assessments such as colonoscopies and cervical histology by Health Boards. You reported you are developing a suite of key messages to be used to support raising awareness, including some of the gender issues around bowel screening. You reported there are issues with working with Health Boards, and it is important that you resolve these issues as a priority. Your priority for the year was around improving efficiency, and are aiming for a 14 day turnaround for cervical screening. You reported that following a survey, 23% of patients were interested in breast screening at “unsocial” hours, and you are now looking at how this may be implemented. On health improvement, you reported that the mechanism to deliver has changed and that the working groups are due to report in July, with implementation then taking place up to the autumn. It is important that you have a representative from the Directors of Public Health on your group, and it was agreed that the CMO would follow this up. You reported a 19% drop in the number of c-difficile cases during the year, but recognise that the target is for zero. There has been a slight rise in the reported number of both MRSA and MSSA cases. You reported that you are in the process of formally establishing a group to develop a plan for antimicrobial resistance. Your main cause for concern going forward is the pace at which you will be able to implement as you only have a small team of people to do this. You reported that you are now carrying out e-coli surveillance after concerns had been raised. On microbiology, you reported that you now have a single service in place across North Wales, and have appointed a new Director of Operations. A new SLA with Health Boards needs to be developed. It is important that you look at prudent healthcare requirements in the number of tests that you are carrying out. I was pleased to hear that your microbiology network service has received CPA accreditation. We discussed user experience and you reported that you have implemented a new framework and have agreed action plans for each program. It is important for equality that you continue to aim to contact those hard to reach groups. It was noted that you are learning from the SUIs reported, and that action plans have been put in place, and that all SUIs are reported to the Quality & Safety Board. You reported that there are issues with autoclaves and estate management. It was agreed that this would be pursued further with relevant Chief Executives and Nursing Directors. You reported that a number of issues had been picked up over the last year in relation to health care quality, including prudent health, unscheduled care and the 1000 lives plus programme. You reported that a paper produced with McMillan had been supplied to the Minister on patient information, and it was agreed that a further discussion would take place outside of the meeting. I noted that you are working on developing your relationship with Health Boards, and are working with Sharon Hopkins, Director of Public Health in Cardiff to develop the SLA. You also reported that you are holding face to face meetings with organisations. It is clear that

this is an area that needs to be developed and improved in the coming year. On planning, you reported that you are working to the end of June to deliver your one year plan, and are learning lessons in preparing your IMTP for next year. You have established a new Policy, Research and Development division and appointed a Director. You recognise there is further work to do, including establishing further links with universities. You reported that you are aligning your workforce to the IMTP, and are developing the skills within the team so as to provide effective leadership. You are tackling staff appraisals and providing training where necessary. You reported that your medical appraisal rate is 100%. This is an important area and needs to be maintained. You reported that you had governance arrangements in place to cover both the vacancy created due to having no substantive Chief Executive, and to cover the absence of the Chair. You are working to get TUS representation on the Board, and there is a development programme on-going. You also reported that you are looking at accommodation issues, as the organisation is currently spread over 50 different locations across Wales. In summary, this has been a year with a number of successes. However, there are areas where further work is required, including the building of effective relationships with Health Boards. I would be grateful if I could have a response to the issues raised in my letter by 27 June 2014. Yours sincerely
Simon Dean

PHW AC 22:01
Date: 06/06/14 Version: 1 Page: 1 of 8
Minutes of the twenty
first meeting of the Public Health Wales Audit
Committee Date of meeting: 12 March 2014
Time of meeting: 13:00 – 15.00
Venue for meeting: Boardroom, 14 Cathedral Road, Cardiff
Version: 1
Present:
Mr Terry Rose (Chair)
Board Member, Public Health Wales
Dr Carl Clowes Board Member, Public Health Wales
Mr John Spence Board Member, Public Health Wales
Mr Huw George Interim Chief Executive Officer, Public Health Wales
Mr Mark Dickinson Director of Planning and Performance, Public Health Wales (in part)
Mrs Tamira Rolls Interim Director of Finance, Public Health Wales
Ms Gabby Smith Wales Audit Office
Mr Jeremy Saunders
Wales Audit Office
Mr Ian Virgil NHS Wales Shared Services Partnership – Audit & Assurance Services
Mr James Johns NHS Wales Shared Services Partnership – Audit & Assurance Services
Ms Eleanor Higgins Corporate Governance Manager, Public Health Wales
Mr Christopher Orr Business Support Manager, Public Health Wales
Ms Gay Reynolds Corporate Services Manager
Apologies:

Date: 06/06/14 Version: 1 Page: 2 of 8
Mr Matthew Coe Wales Audit Office
Mr Anthony Ford Wales Audit Office
Mr Keith Cox Board Secretary, Public Health Wales
Mr Craig Greenstock Cardiff and Vale University Health Board – Counter Fraud
Ms Jayne Gibbon NHS Wales Shared Services Partnership – Audit & Assurance Services
1. Welcome and apologies
The Chair welcomed all those in attendance to the twenty
first meeting of the Public Health Wales Audit Committee.
Apologies were received from Matthew Coe, Anthony Ford, Keith Cox, Craig Greenstock and Jayne Gibbon.
Ms Gay Reynolds was also in attendance.
2. Declarations of interest
There were no declarations of interest to register.
3. Minutes and matters arising
a) The minutes from the previous meeting were received
by the Committee and agreed as an accurate account subject to one minor amendment.
Action- Ms Gay Reynolds to provide the wording for
inclusion in the minutes to clarify the risk assurance process.
b) Ms Eleanor Higgins provided updates on the actions
currently in the action log
In the absence of Mr Cox no update on the review of library services arrangements could be provided however
it was agreed a short paper would be circulated to the
board members to provide them with an update. It was also agreed that the accountability arrangements with
Welsh Government are a Board and Chief Executive issue rather than solely for the Executive team.
Action-Mr Cox to include a paper regarding library
services arrangements at a future Board meeting.

Date: 06/06/14 Version: 1 Page: 3 of 8
4. Revised Terms of Reference
a) Audit Committee
Ms Higgins presented the revised terms of reference to the
Committee and highlighted the changes that have been made from the previous terms of reference. Ms Higgins
brought the paragraph regarding the relationship between the Audit Committee and Quality and Safety Committee to
the Committee’s attention. Inclusion of this paragraph was welcomed. It was also agreed that further work was
required to ensure this relationship between Committees
is maintained and how we give the Committees assurance this is happening. Work plans for each Committee should
be agreed annually and the Board Secretary should monitor these plans to ensure there are no omissions. A
column on which Committee is responsible for the action should be added to the internal and external audit action
logs . It was agreed that individuals would also not be named within the terms of reference. The wording relating
to the quorum of a Committee would also be amended.
Action- Names to be removed from the terms of reference and column added to the internal and
external audit action logs detailing which Committee is responsible for the action.
b) Quality and Safety Committee
Ms Higgins informed the Committee that similar changes had been made to the Quality and Safety terms of
reference. These will be reviewed at the next Quality and Safety meeting.
It was agreed that both sets of terms of reference would
be brought to the Board for approval in June 2014.
5. Audit Committee work plan
Ms Higgins introduced the Audit Committee work plan for
2014-2015. This document was welcomed by the Committee and set out the work of the Committee very
clearly. Wales Audit Office requested that local audit work is included within the work plan and the internal and
external audit log would be added as standing items.
Action- Ms Higgins to include additional items into

Date: 06/06/14 Version: 1 Page: 4 of 8
work plan.
6. Wales Audit Office
a) Audit outline plan
Mr Jeremy Saunders presented the draft audit outline plan
2014/2015. Mr George raised the issue regarding audit fees and the difficulty in setting budgets without knowing
these costs. Mr Saunders informed the Committee that confirmation of these fees was expected in the next couple
of weeks.
The planned audit work on early intervention and public behaviour change was raised as an item of interest for
Public Health Wales and the Committee were keen to ensure Public Health Wales are actively engaged in this
audit work.
The Committee approved the report subject to minor amendments.
7. Internal Audit
a) Internal Audit progress Report
The above report was received and noted by the Committee members for information. The report provided
an update of work against the internal audit plan. Mr Ian Virgil highlighted that the statutory and mandatory audit
had been followed up and there were slippages with regard to the recommendations and actions however these
were being addressed through the internal audit action
log. Mr Virgil also informed the Committee that the planned audit on performance reporting would now be
taking place in 2014/2015.
b) Final audit report for review of Screening
services
This paper was withdrawn from the meeting as response from management had yet to be agreed.
8. Counter Fraud progress report
The above report was received and noted by the Committee members for information. The report provided
Date: 06/06/14 Version: 1 Page: 5 of 8
an update of the key work carried out this year to date by
the Counter Fraud team.
Ms Tami Rolls on behalf of Mr Craig Greenstock informed the Committee that the one case that was open has now
been closed and no further action is to be taken.
9. Internal Audit action log
Ms Eleanor Higgins updated the Committee on the internal
audit action log.
The Committee were pleased to see the progress being made with statutory and mandatory training and were
informed a fuller update on business continuity arrangements will follow at the next meeting.
10. External Audit action log
Ms Tami Rolls updated the Committee on the external audit action log.
Ms Rolls informed the Committee that she had been
unable to get an update for action no.43 and this update will be provided at the next meeting.
11. Procurement report
Ms Tami Rolls presented the Procurement report to the Committee for information. The Committee received the
report.
12. Year end and annual accounts timetable
Ms Tami Rolls presented the year end accounts timetable to the Committee. This outlines the time table for the
production of the annual accounts and when they will be
received by various groups and Committees.
13. Draft Annual Governance Statement
Ms Eleanor Higgins presented a paper outlining the drafting process of the Annual Governance Statement for
2013/14. The annual governance statement will take into account all the recommendations received from the Wales
Audit Office last year and a draft will be circulated .
Date: 06/06/14 Version: 1 Page: 6 of 8
14. Audit fees letter
This paper was received for information.
15. Clinical Negligence and Personal Injury Claims
update
This paper was received for information.
16. Publication of papers
It was agreed by the Committee that all papers should be
published except the procurement report, year end and accounts timetable and draft annual governance
statement.
11 Any Other Business
There was no other business to be discussed.
12. Dates of next meetings
08 May 2014 05 June 2014
11 September 2014 11 December 2014

PHW AC 22:01
Date: 06/06/14 Version: 1 Page: 7 of 8
ACTIONS
No. Action Who Start End Status Revised Implementation
date
16.3 Develop an Action Plan to track
progress on implementation of recommendations from report
into management arrangements in Screening
Division.
RF 20.03.13 06.06.13 Complete- Action
plan presented at Board meeting on 29 April 2014.
19.8 Provide Board with more
information on the review of
library services arrangements
KC 18.09.13 18.12.13 Complete- This will
now be picked up as action 21.02
05.06.14
20.01 Audit Committee to take
forward identified actions as outlined in Appendix 1 of paper
20.02.
Audit
Committee
18.12.13 12.03.14 Complete
20.02 Arrange a development session for Audit Committee, internal
audit and external audit to discuss findings of the self
assessment.
CO/EH 18.12.13 12.03.14 This action will be addressed through the wider Board
development work which is currently
ongoing
20.03 Item to be added to agenda of
a future meeting to examine risk in more detail.
CO/EH 18.12.13 12.03.14 To be included
within the Audit Committee work plan
20.05 Board member survey and EH/CO 18.12.13 12.03.14 This action will be
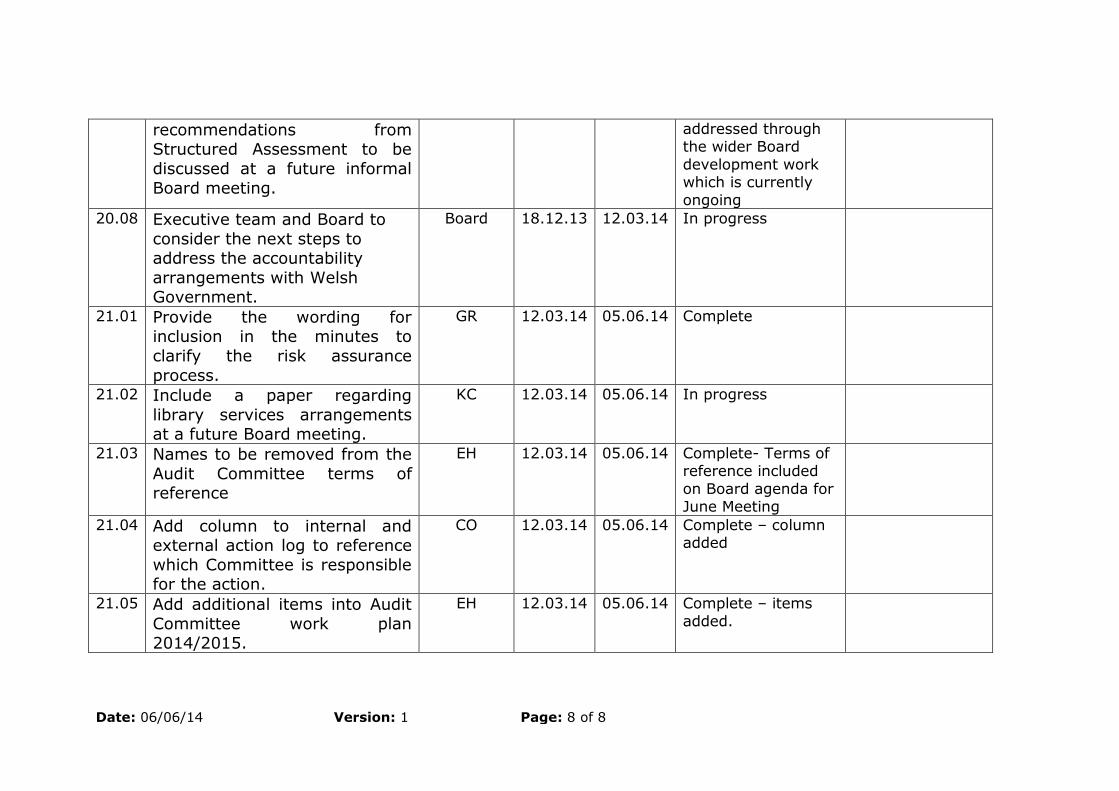
Date: 06/06/14 Version: 1 Page: 8 of 8
recommendations from Structured Assessment to be
discussed at a future informal
Board meeting.
addressed through the wider Board
development work which is currently
ongoing
20.08 Executive team and Board to
consider the next steps to address the accountability
arrangements with Welsh Government.
Board 18.12.13 12.03.14 In progress
21.01 Provide the wording for inclusion in the minutes to
clarify the risk assurance
process.
GR
12.03.14 05.06.14 Complete
21.02 Include a paper regarding
library services arrangements at a future Board meeting.
KC 12.03.14 05.06.14 In progress
21.03 Names to be removed from the
Audit Committee terms of reference
EH 12.03.14 05.06.14 Complete- Terms of reference included
on Board agenda for June Meeting
21.04 Add column to internal and external action log to reference
which Committee is responsible for the action.
CO 12.03.14 05.06.14 Complete – column added
21.05 Add additional items into Audit
Committee work plan 2014/2015.
EH 12.03.14 05.06.14 Complete – items
added.
PHW AC 23:01
Date: 06/06/14 Version: 1 Page: 1 of 8
Minutes of the twenty
second meeting of the Public Health Wales Audit
Committee Date of meeting: 08 May 2014
Time of meeting: 13:00 – 15.00
Venue for meeting: Boardroom, 14 Cathedral Road, Cardiff
Version: 1
Present:
Mr Terry Rose (Chair)
Board Member, Public Health Wales
Mr Huw George Interim Chief Executive Officer, Public Health Wales
Mr Keith Cox Board Secretary, Public Health Wales
Mrs Tamira Rolls Interim Director of Finance, Public Health Wales
Mr Matthew Coe Wales Audit Office
Mr Jeremy Saunders
Wales Audit Office
Ms Jayne Gibbon NHS Wales Shared Services Partnership – Audit & Assurance Services
Mr James Johns NHS Wales Shared Services Partnership – Audit & Assurance Services
Ms Eleanor Higgins Corporate Governance Manager, Public Health Wales
Mr Christopher Orr Business Support Manager, Public Health Wales
Apologies:
Dr Carl Clowes Board Member, Public Health Wales
Mr John Spence Board Member, Public Health Wales
Mr Anthony Ford Wales Audit Office
Ms Gabby Smith Wales Audit Office

Date: 06/06/14 Version:1 Page: 2 of 8
Mr Craig Greenstock Cardiff and Vale University Health Board – Counter
Fraud
1. Welcome and apologies
The Chair welcomed all those in attendance to the twenty second meeting of the Public Health Wales Audit
Committee.
Apologies were received from John Spence, Carl Clowes, Anthony Ford, Craig Greenstock and Gabby Smith.
The Chair informed the Committee that no decisions could
be made at the meeting as the Committee were not quorate.
2. Declarations of interest
There were no declarations of interest to register.
3. Minutes and matters arising
As the meeting was not quorate the minutes were not
discussed. These would be approved at the meeting on the 5 June 2014.
4. Draft annual accounts
Ms Rolls provided a short presentation to the Audit
Committee summarising the draft annual accounts that were submitted to the Wales Audit Office on 2 May 2014.
Ms Rolls also informed the Committee that Tracey Cooper, as the Accountable Officer and Huw George, as Director of
Finance, will sign off the accounts on the 6 June 2014.
Dr Clowes had provided comments to the Committee in
advance of the meeting and questioned why Public Health Wales was not a member of the Carbon Reduction
Commitment Scheme. It was agreed that Ms Rolls would look into this and feed back with additional information.
Action- Find out further information on the Carbon
Footprint reduction Scheme and why Public Health Wales is not a member.
Ms Rolls informed the Committee that the Remuneration

Date: 06/06/14 Version:1 Page: 3 of 8
paper had not been included in the papers but would be
circulated to Committee members.
Action- Circulate Remuneration Report to Audit Committee members.
Following the discussions, the Chair thanked Ms Rolls and
her team for the work that has been undertaken throughout the year to produce the draft accounts.
5. Annual Governance Statement
Ms Higgins presented the draft Annual Governance Statement to the Committee. The Committee noted a few
minor formatting amendments and were pleased with the content of the statement.
The Chair thanked Ms Higgins for her work on the Annual
Governance Statement to date.
6. Wales Audit Office
a) Audit Position Statement
Mr Saunders presented the Audit Position Statement. Work had commenced to audit the annual accounts and Mr
Coe informed the Committee that there were no further updates on the planned audit work on early intervention
and public behaviour change. He also informed the Committee that Ms Smith, following a conversation with Dr
Sandifer, has agreed that the Wales Audit Office review of Microbiology management arrangements will be published
later this month. Ms Higgins also informed the Committee
that the majority of the comments on the draft Annual Governance Statement had been included in the latest
version and work is underway to incorporate the remaining comments.
b) Outline of Audit work 2014
Mr Coe presented the outline of audit work 2014. The
Committee received the draft outline at the meeting in March 2014. Mr Coe brought the audit fee section to the
attention of the Committee. This outlines the increase in audit fees for 2014-2015 due to the new fee setting
requirements on Wales Audit Office that came into effect from 1 April 2014. The Chair questioned the justification
for the 5.7% increase in fee for next year. Mr Coe

Date: 06/06/14 Version:1 Page: 4 of 8
explained that this increase is proportionate and had to be
adjusted to fully comply with their statutory requirements.
Mr Huw George informed the Committee that discussions had taken place with the Wales Audit Office and it had
been agreed that the Wales Audit Office would provide Public Health Wales with a three year plan for the
performance audit work and would highlight added value.
The Committee accepted the increase in audit fees for 2014/2015.
The Committee received both reports.
7. Internal Audit
a) Internal Audit progress Report
The above report was received and noted by the Committee members for information. The report provided
an update of work against the internal audit plan. A draft
internal audit plan for 2014/2015 has been issued for comment.
b) Welsh Risk Pool claims management
The above report was received by the Committee. The
audit identified no weaknesses during the review and no areas identified that require management action. The
overall assurance rating for this review was substantial.
c) Financial systems review
The above report was received by the Committee. Internal audit provided reasonable assurance as to the
effectiveness of the system of internal control to manage
the risks associated with the objectives covered in this review. Mr George informed the Committee that the Board
were aware of the likely failure to meet the Public Sector Payment Policy(PSPP) target at an early stage and
appropriate processes were in place. The Committee also requested that this should be reflected in the Annual
Governance Statement. Ms Higgins confirmed that this was referred to in the Annual Governance Statement.
Action- Ensure Annual Governance Statement refers
to Audit Committee and Board’s early involvement in

Date: 06/06/14 Version:1 Page: 5 of 8
addressing the issues surrounding meeting the
(PSPP) target.
d) Screening Services – service modification
The above report was received by the Committee.
Reasonable assurance has been provided by Internal Audit as to the effectiveness of the system of internal control in
place to manage the risk associated with the modernisation of Breast Screening Services. The two key
findings were in relation to risk management and that the Implementation Project Board did not include a member of
the trust Board. Following discussions outside the meeting
it has been agreed that a lead Non-Executive Director will be nominated for each major programme however they
will not be required to attend every meeting and will receive updates from the relevant Executive Director. The
nominated Non-Executive Director will then report any issues or concerns at Board meetings.
e) Asbestos Management
The above report was received by the Committee. Internal
audit provided limited assurance to the effectiveness of the systems of internal control to manage the risk
associated with asbestos management. The Committee were informed of the significant improvements that have
been made in this area however at the time of review only
limited assurance could be provided as these systems have not been fully embedded. Internal audit will be
following up this review later in the year which will hopefully provide an improved position.
8. Procurement report
Ms Tami Rolls presented the procurement report to the
Committee for information. The Committee received the
report.
9. Any Other Business
There was no other business to be discussed.
10. Dates of next meetings
05 June 2014
11 September 2014

Date: 06/06/14 Version:1 Page: 6 of 8
11 December 2014
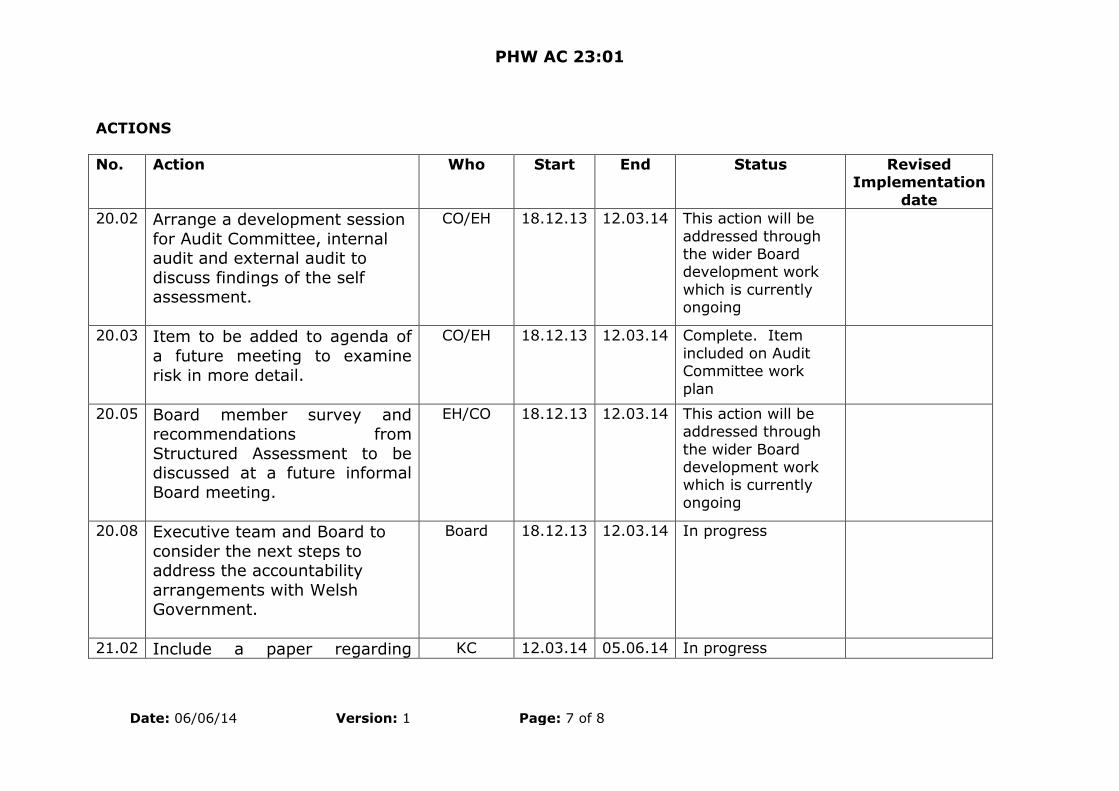
PHW AC 23:01
Date: 06/06/14 Version: 1 Page: 7 of 8
ACTIONS
No. Action Who Start End Status Revised Implementation
date
20.02 Arrange a development session
for Audit Committee, internal audit and external audit to
discuss findings of the self assessment.
CO/EH 18.12.13 12.03.14 This action will be
addressed through the wider Board development work
which is currently ongoing
20.03 Item to be added to agenda of
a future meeting to examine
risk in more detail.
CO/EH 18.12.13 12.03.14 Complete. Item
included on Audit Committee work
plan
20.05 Board member survey and recommendations from
Structured Assessment to be discussed at a future informal
Board meeting.
EH/CO 18.12.13 12.03.14 This action will be addressed through
the wider Board development work which is currently
ongoing
20.08 Executive team and Board to
consider the next steps to address the accountability
arrangements with Welsh Government.
Board 18.12.13 12.03.14 In progress
21.02 Include a paper regarding KC 12.03.14 05.06.14 In progress

Date: 06/06/14 Version:1 Page: 8 of 8
library services arrangements at a future Board meeting.
21.04 Add column to internal and
external action log to reference which Committee is responsible
for the action.
CO 12.03.14 05.06.14 Complete. Column
has been added to internal and external action log.
21.05 Add additional items into Audit
Committee work plan
2014/2015.
EH 12.03.14 05.06.14 Complete
22.01 Find out further information on
the Carbon Footprint reduction Scheme and why Public Health
Wales is not a member.
CO 08.05.14 05.06.14 Complete
22.02 Circulate Remuneration Report to Audit Committee members
TR 08.05.14 05.06.14 Complete
22.03 Ensure Annual Governance Statement refers to Audit
Committee and Board’s early involvement in addressing the
issues surrounding meeting the (PSPP) target
EH 08.05.14 05.06.14 Complete
PHW IGC 16:01
Minutes of the fifteenth Meeting of the Public Health Wales Information
Governance Committee Date of meeting: 12 March 2014
Time of meeting: 15.00 – 16.00
Venue for meeting: Boardroom, 14 Cathedral Road
Version: 1
Present:
Mr John Spence Board Member (Chair)
Mr Terry Rose Board Member Dr Carl Clowes Board Member
Mr Huw George Chief Executive
Mr Mark Dickinson Executive Director of Planning and Performance Mr John Morley Information Governance Manager
Mr Christopher Orr Business Support Manager Ms Jane Evans Information Governance Manager
Ms Eleanor Higgins Corporate Governance Manager Dr Quentin Sandifer
Director of Public Health Services
1. Welcome & apologies for absence
The Chair welcomed the Committee to their fifteenth
meeting.
No were no apologies for absence.
2. Declarations of Interest There were no declarations of interest to register.
3. Minutes from Information Governance Committee
meeting held on 18 December 2013
a) Approval of minutes
The minutes from the previous meeting were checked for

Public Health Wales Minutes – Information Governance
Committee
Date: 6 June 2014 Version: 1 Page: 2 of 6
accuracy and approved.
b) Actions arising
A verbal update on all actions arising was given by Mr Mark Dickinson.
4. Minutes from Information Governance Working Group meeting held on 4 February 2013
The minutes were noted by the Committee.
5. MeetingSphere
Mr Mark Dickinson informed the Committee that the relevant checks and enquiries had been made and that
MeetingSphere software was no longer considered an information governance risk regarding the use of cloud
services.
6. Information Governance Updates
a) EU Data Protection update
Mr Mark Dickinson informed the Committee that significant
progress had been made with regard to the EU Data
Protection Act. The Committee need to be clear what effect and impact this legislation will have on Public Health
Wales and a report will be provided to the next Committee meeting.
Action- provide a report to the Committee on the
potential impact and risks if the EU Data Protection Act is introduced.
b) Section 251 update
Mr Mark Dickinson informed the Committee that we are
currently awaiting a memorandum of understanding from the Confidentiality and Advisory group and the
Department of Health.
c) Mail Marshall update
The Committee were informed that a paper will be
submitted to the Exec team proposing the switch of Mail Marshall into ‘enforce mode’ with the aim to have this in
place by 1 May 2014.

Public Health Wales Minutes – Information Governance
Committee
Date: 6 June 2014 Version: 1 Page: 3 of 6
7. Information Governance Risk Register
The risk register was discussed by the Committee. It was
agreed that further discussions are required as to what risks are regarded as ‘tolerable’ and the language used
within the risk register needs to be reviewed.
Action: include an item on agenda for next meeting where risk appetite can be reviewed.
8. Freedom of Information Act Report
The above report was presented for information purposes.
The Committee received and discussed the paper.
9. Information Governance incident report
The above paper was presented for discussion.
The Committee were informed that Incident 1522 had now been closed and a letter from the Information
Commissioner’s Office has been received closing the
incident.
The Committee received the papers.
10. Information Governance incident trend report
Mr John Morley presented the incident trend report to the Committee. This will be a standing item on the agenda
every 6 months.
The Committee received the papers.
11. Information Governance training report
The Information Governance training report was presented to the Committee. The Committee were informed that
since the papers had been circulated the compliance rate had increased from 69% to 75%. The Committee were
assured that the target of 80% should be met by the end of March 2014.
There was also discussion with regard to how often the training needed to be completed. At present this is every 3
years however a discussion is needed to establish whether

Public Health Wales Minutes – Information Governance
Committee
Date: 6 June 2014 Version: 1 Page: 4 of 6
this is a suitable frequency or whether it should be
reduced to 1 or 2 years. It was agreed that the frequency of training would be discussed further after the end of this
financial year.
Action: arrange for discussion at next meeting on whether frequency of IG training should be reduced
from 3 years to 1 or 2 years.
12. ICO Closure Letter
This paper was received for information. The letter
confirms that no further action is to be taken with regard to this incident.
13. Care.data
This paper was received for information. The Committee were keen to find out how NWIS are using this
information. There is also the potential that if the EU Data Protection Act is passed, this legislation could override
care.data.
14. Publication of papers
It was agreed that all papers should be published except for the appendix to the information governance incidents
paper.
15. Dates of next meetings 05 June 2014
11 September 2014 11 December 2014
16. AOB
Mark Dickinson updated the Committee on two outstanding information governance incidents which had
been reported in the past week. Once concerned a complaint which had been made directly to the
Information Commissioner and the other concerned a complaint against inappropriate access to data. Further
information would be provided at the next meeting.

PHW IGC 16:01
ACTIONS
No. Action Who Start End Status
15.1 Provide an update on the CPIP-
improvement plan on a 6 monthly basis.
JM/JE 18.12.13 05.06.14 Complete
15.2 Review risk of using MeetingSphere
and report back to the Committee at the next meeting.
MD 18.12.13 12.03.14 Complete- Committee have been
assured that MeetingSphere is not considered as a risk.
15.3 Circulate letter from Mel Evans to
Committee members.
MD 18.12.13 12.03.14 Complete
15.4 Inform Welsh Government when information is released to the media
under FOI
JM 18.12.13 12.03.14 Complete- reported via two routes on a weekly basis. Internally this is done through the Communications team and
externally from the FOI group.
15.5 Prioritise statutory and mandatory
training and hold managers to account for staff attendance at
training
HG 18.12.13 12.03.14 Complete
16.1 Provide a report to the Committee on the potential impact and risks if
the EU Data Protection Act is introduced.
MD 12.03.14 11.09.14 In progress – will be discussed by refreshed Information Governance Working Group and further update
provided at Committee meeting in September.
16.02
Include an item on agenda for next meeting where risk appetite can be
CO 12.03.14 11.09.14 In progress – will be discussed by refreshed Information Governance

Public Health Wales Minutes – Information Governance
Committee
Date: 6 June 2014 Version: 1 Page: 6 of 6
reviewed Working Group and further update provided at Committee meeting in
September.
16.0
3 Arrange for discussion at next
meeting on whether frequency of IG training should be reduced from 3
years to 1 or 2 years.
CO 12.03.14 11.09.14 In progress – will be discussed by
refreshed Information Governance Working Group and further update
provided at Committee meeting in September.
Joint Executive TeamMeeting 2013/14
Insert name of presentation on MasterSlide
Meeting 2013/14
4 June 2014

Introduction• Overview of 2013/14
• Critical Issues in 2013/14 and challenges• Critical Issues in 2013/14 and challengesfor 2014/15
• Integrated Medium Term Plan
• Emerging and developing priorities
• Research Development and Innovation
• Workforce and Organisational Development• Workforce and Organisational Development
• Governance
• Conclusion
Presenter: Tracey Cooper

Overview 2013/14
• Refreshed strategy
• Health Improvement Review conclusion• Health Improvement Review conclusion
• New programmes implementation
• Excellent cancer detection rate
• Measles response
• Observatory reports• Observatory reports
• Health Technology Funding
• Another year balanced financially
Presenter: Huw George

Critical issues 2014/15
• Smoking rates
• Screening uptake• Screening uptake
• Immunisation
• Relationship with health boards and thewider system
• Focus on outcomes• Focus on outcomes
Presenter: Huw George

Insert name of presentation on MasterSlide
Smoking cessation
Presenter: Peter Bradley
Successes and concerns• Reduced waiting times to 6 days
• Increased appointment availability• Increased appointment availability
• Increased translation of contacts intotreated smokers
• Improved performance management
• New initiatives
• Smoking in pregnancy pilots potential• Smoking in pregnancy pilots potential
• Need to change service delivery model toreach 16% target
Presenter: Peter Bradley
Actions for 2014/15
• Formal agreement with DsPH and jointaction plans and performance meetingsaction plans and performance meetings
• Targeted action
• Service delivery model options appraisal
• Brief interventions training programme
• Social marketing campaign• Social marketing campaign
• ‘Stoptober’ campaign
• Online booking, apps etc
Presenter: Peter Bradley

Insert name of presentation on MasterSlide
Immunisation
Presenter: Quentin Sandifer

• Successful measles outbreak response
Successes and concerns
• Successful measles outbreak response
– 75,000 MMR vaccine doses delivered
• Highest ever MMR uptake for Wales
– 96.5% for MMR1 at 2 years
– 92.6% for MMR2 at 5 years
• Tier 1 target for childhood vaccination at• Tier 1 target for childhood vaccination atage 4: 87.5% (target: 95%)
Presenter: Quentin Sandifer

Successes and concerns
• Flu vaccination• Flu vaccination
– 2.5% increase in under 65 at risk
– No change in over 65 flu rates
– Only one NHS organisation on target
Presenter: Quentin Sandifer

Actions for 2014/15
• Surveillance of disease, epidemiologicalanalysis and interpretation of vaccination
• Surveillance of disease, epidemiologicalanalysis and interpretation of vaccinationuptake data
• Inform policy and guidance
• Support partner agencies to meettargetstargets
• Inform and educate NHS Wales and thepopulation
Presenter: Quentin Sandifer

Screening
Insert name of presentation on MasterSlide
Screening
Presenter: Quentin Sandifer

Successes and concerns
• Implemented AAA and newborn bloodspotand change in age range for cervical
• Implemented AAA and newborn bloodspotand change in age range for cervicalscreening
• Developed new sickle testing protocol
• First home nation to go fully digital inbreast screeningbreast screening
• Consistently highest cancer detection rateof any UK breast screening programme
Presenter: Quentin Sandifer

Successes and concerns
• Health board performance (timeliness)against provision of diagnostic
• Health board performance (timeliness)against provision of diagnosticassessment services e.g. colonoscopy(up to 11 weeks) and cervical histology(up to 6 weeks)
• Poor uptake in bowel programme and• Poor uptake in bowel programme andfalling uptake in breast programme
Presenter: Quentin Sandifer

Actions for 2014/15• Targeted support to health boards
• Formal project to address uptake• Formal project to address uptake
• Cervical modernisation programme andHPV ‘test of cure’ in September andplanning for triage in cytology
• 14-day turnaround time cervicalscreening methodologyscreening methodology
• Improving breast and cervical timeliness
• Transfer of diabetic retinopathy service
Presenter: Quentin Sandifer

Insert name of presentation on MasterSlide
Transforming healthimprovementPresenter: Peter Bradley
Successes and concerns
• Completed review: Transforming HealthImprovement in WalesImprovement in Wales
– Not reaching large proportion of thepopulation
– Some had no evidence base
• Established programme to overseeimplementation of recommendationsimplementation of recommendations
• Disinvestment process
• Ongoing delivery of ‘legacy’ programmes
Presenter: Peter Bradley

Actions for 2014/15
• Transforming Health Improvementprogramme on scheduleprogramme on schedule
– Infrastructure established
– Ongoing engagement with DsPH/local teams
– Expert groups to report by end July 2014
– Detailed work plans by November 2014
– Implementation of work plans from November– Implementation of work plans from November
• Health Improvement Alliance to promoteinnovation and advocacy
Presenter: Peter Bradley

Integrated Medium Term Plan &Budget Setting
Healthcare associatedinfections
Presenter: Quentin Sandifer
Successes and concerns
• Epidemiological intelligence, direct supportand published outputsand published outputs
• BCUHB Clostridium difficile outbreak
• Review of death certification associatedwith Clostridium difficile
• Health board targets and Code of Practice
• Downward trend in Clostridium difficile (-• Downward trend in Clostridium difficile (-19.2%); increase in MRSA (+2.5%);increase in MSSA (+3.2%)
Presenter: Quentin Sandifer

Actions for 2014/15
• Provide epidemiological analysis andinterpretation of bacterial infections
• Provide epidemiological analysis andinterpretation of bacterial infections
• Continue working with health boardsincluding support to large scale change
• Continue to advise and inform policy onHCAIsHCAIs
• Lead all-Wales action planning onantimicrobial resistance
Presenter: Quentin Sandifer

Insert name of presentation on MasterSlide
Clinical microbiology
Presenter: Quentin Sandifer

Successes and concerns
• Second ever network service to attainfull CPA accreditationfull CPA accreditation
• Single central laboratory established inRhyl, Wrexham service transfer andsingle North Wales microbiology service
• Modernisation programme to achieve asingle, national, managed microbiologysingle, national, managed microbiologyservice network
• Director of Operations
Presenter: Quentin Sandifer

Actions for 2014/15
• Automated technology into bacteriologyservice in North Walesservice in North Wales
• Develop formal commissioner-providermodel for microbiology services
• New performance management framework
• Secure full clinical microbiologistengagement in local HCAI actionengagement in local HCAI action
• ISO 15189 accreditation by June 2016
• Infectious diseases genomics service
Presenter: Quentin Sandifer
Insert name of presentation on MasterSlide
Service user experience
Presenter: Rhiannon Beaumont-Wood

Successes and concerns
• Improved organisational focus
• Service User and Learning Panel established• Service User and Learning Panel established
• User experience, complaints/concernslearning & monitoring now combined
• National core questions do not adequatelycapture requirements
• Planning/evaluating changes to services• Planning/evaluating changes to services
• Creation of agreed PIs
• Better use of existing IT products
Presenter: Rhiannon Beaumont-Wood
Successes and concerns
• Service example: Stop Smoking Walesclient feedback 1 Jan 2014 – 31 March
• Service example: Stop Smoking Walesclient feedback 1 Jan 2014 – 31 March2014
– 96% + of clients (263 individuals) weresatisfied or very satisfied with the supportthey received
Presenter: Rhiannon Beaumont-Wood

Actions for 2014/15
• Improve data capture• Improve data capture
• Agree approach to reporting
• Dedicated resource
• Improved methods for sharing learning
• Performance framework being developed
• Agree and start Board reporting• Agree and start Board reporting
• Identify methods to inform service users ofimprovements resulting from feedback
Presenter: Rhiannon Beaumont-Wood

Insert name of presentation on MasterSlide
Relationship with healthboardsPresenter: Huw George

Relationship with healthboards• Need clarity on roles and responsibilities
• Hold each other to account• Hold each other to account
• Pilot work with Cardiff and Vale
– Including key areas, specification based,agreed action, for implementation inSeptember
• Executive to Executive discussions• Executive to Executive discussions
– Betsi Cadwaladr
– Critical performance issues and ownership
Presenter: Huw George

Insert name of presentation on MasterSlide
Planning
Presenter: Mark Dickinson

Successes and concerns
• Refreshed strategy - Summer 2013
• Developed priorities for action - Autumn• Developed priorities for action - Autumn2013
• Developed initial draft IMTP - January 2014
• Refinement and strengthening of plan
• Plan and balanced budget approved byBoard - March 2014Board - March 2014
• Plan not approved and requirement toproduce one year plan by June 2014
Presenter: Mark Dickinson

Successes and concerns
• Development of, and reporting against,Quality and Delivery Framework
• Development of, and reporting against,Quality and Delivery Framework
• Contribution to Public Health OutcomesFramework
• Development of further performanceindicatorsindicators
Presenter: Mark Dickinson

Actions for 2014/15
• Operational Plan 2014/15• Operational Plan 2014/15
– Key areas to be further strengthened anddeveloped
– Updated sections on smoking and screeningperformance submitted
– Divisional Directors leading development ofrelevant sectionsrelevant sections
– To be approved by Board on 26 June
Presenter: Mark Dickinson

Actions for 2014/15
• Integrated Medium Term Plan
– Formal review of 2013/14 planning process– Formal review of 2013/14 planning process
– Key areas to be improved and specificactions
– Revised plan submitted by January 2015
• Further development of Quality andDelivery FrameworkDelivery Framework
• Complete Public Health OutcomesFramework
Presenter: Mark Dickinson

Insert name of presentation on MasterSlide
Emerging issues
Presenter: Peter Bradley

Emerging issues
• Unscheduled care• Unscheduled care
• Prudent healthcare
• Large-scale change in relation tophysical activity
• Primary care vision
• Health inequalities• Health inequalities
• Public Health Bill support and co-ordination
Presenter: Peter Bradley

Insert name of presentation on MasterSlide
Research and development
Presenter: Peter Bradley

Research and development
• New Policy, Research & DevelopmentDivision and Director
• New Policy, Research & DevelopmentDivision and Director
• Reorganisation including newgovernance structure and new strategy
• Research activity funds increase of£129k£129k
• Co-bidder for research grants
Presenter: Peter Bradley
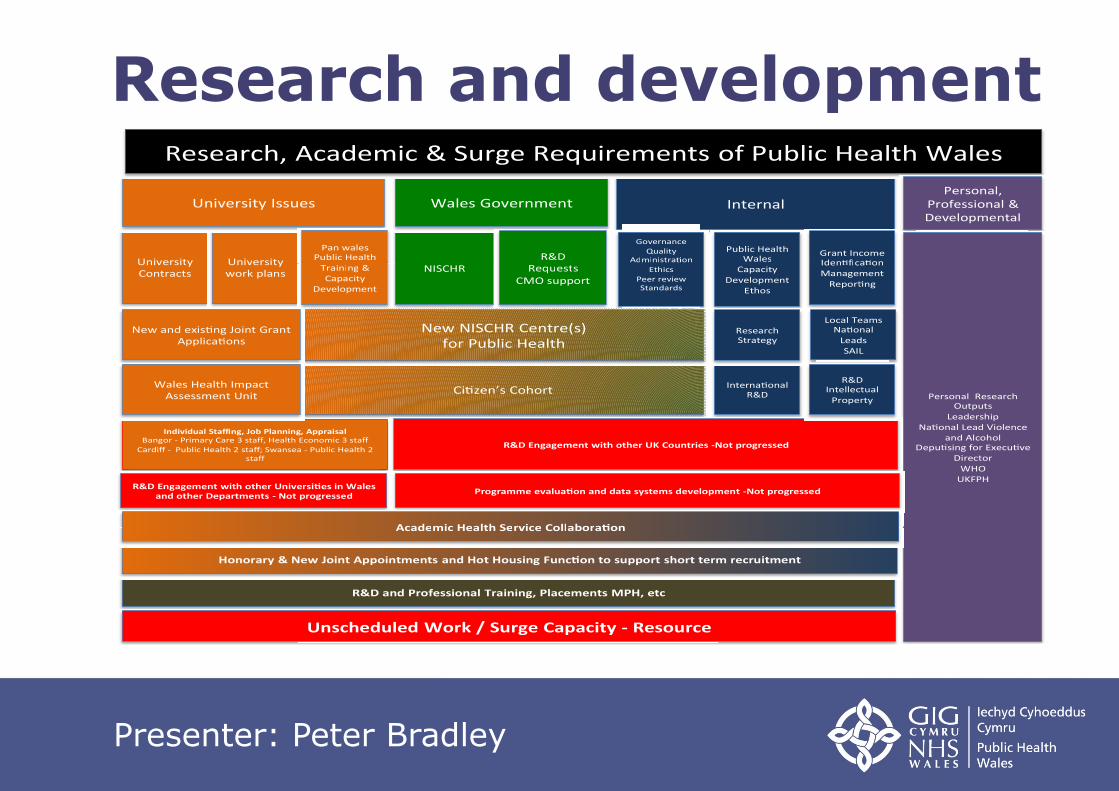
Research and development
NISCHRUniversity University
InternalUniversity Issues
Pan walesPublic Health
Training &
Wales Government
R&DRequests
Governance
QualityAdministra on
Public HealthWales
Grant IncomeIden fica on
Research, Academic & Surge Requirements of Public Health Wales
Personal,Professional &Developmental
NISCHRUniversityContracts
Universitywork plans
Training &Capacity
Development
Ci zen’s Cohort
RequestsCMO support
Administra on
Ethics
Peer reviewStandards
WalesCapacity
DevelopmentEthos
Iden fica onManagement
Repor ng
New NISCHR Centre(s)for Public Health
Interna onalR&D
ResearchStrategy
Local TeamsNa onal
LeadsSAIL
Individual Staffing, Job Planning, AppraisalBangor - Primary Care 3 staff, Health Economic 3 staff
Cardiff - Public Health 2 staff; Swansea - Public Health 2staff
New and exis ng Joint GrantApplica ons
Personal ResearchOutputs
LeadershipNa onal Lead Violence
and AlcoholDepu sing for Execu ve
DirectorWHO
UKFPHR&D Engagement with other Universi es in Wales
and other Departments - Not progressed
R&D Engagement with other UK Countries -Not progressed
Programme evalua on and data systems development -Not progressed
Wales Health ImpactAssessment Unit
Academic Health Service Collabora on
R&DIntellectual
Property
R&D and Professional Training, Placements MPH, etc
Unscheduled Work / Surge Capacity - Resource
Honorary & New Joint Appointments and Hot Housing Func on to support short term recruitment
Academic Health Service Collabora on
Presenter: Peter Bradley

Insert name of presentation on MasterSlide
Workforce and OrganisationalDevelopmentPresenter: Ruth Davies

Successes and concerns
• Work around culture and values• Work around culture and values
• Developing leadership and management
• Improved statutory and mandatorytraining
• Work on staff appraisals
Presenter: Ruth Davies

Actions for 2014/15
• Work on values and culture• Work on values and culture
• Leadership and managementdevelopment
• Learning and development plan
• Further work on mandatory training
• Upward feedback survey on staff• Upward feedback survey on staffappraisals
Presenter: Ruth Davies

Insert name of presentation on MasterSlide
Governance
Presenter: Keith Cox

Successes and concerns
• Interim arrangements to cover vacantChief Executive and absence of ChairChief Executive and absence of Chair
• Vacancy for local authority member
• Trade union/staff representation
• First Annual Quality Statement
• Staff engagement on Francis Review
• Programme to review accommodationneeds and ways in which we work
Presenter: Keith Cox

Actions for 2014/15
• Interim arrangements to cover the localauthority Board vacancy
• Interim arrangements to cover the localauthority Board vacancy
• Work to encourage BMA representation
• Good Governance Institute ‘rapid review’of Board, governance and riskmanagement arrangementsmanagement arrangements
• Work with Academi Wales
• Board Development programme
Presenter: Keith Cox

Actions for 2014/15
• Annual Quality Statement
• Francis Review report to Board in June• Francis Review report to Board in June
• Final decision on accommodation and waysof working options by September
Presenter: Keith Cox

A healthier, happier andfairer Wales
• Continued progress in 2013/14• Continued progress in 2013/14
• Build on our success
• Continue to develop the organisation andBoard
• Focus on delivery
• Focus on outcomes• Focus on outcomes
Presenter: Tracey Cooper