Higher Homologues of Mesomorphic Benzylidene Anilines. Manifestation of Smectic Polymorphism
The Skeletal Manifestation
of Malaria
A Clinical Case-Control Study
Nicole E. Smith, Dept. of Anthropology, University of Arkansas

Identifying Malaria in the Past
aDNA and antigen detection
Cribra orbitalia and/or porotic hyperostosis
association
Other lesions? Postcranial?

Identifying Malaria in the Past
• Etiology and scope of malaria’s skeletal
manifestation is poorly understood
• Clinical comparison needed → present study
Epidemiological Approach
• Case-control study:
• Endemic and non-endemic sample populations
• Lesion association testing
• Diagnostic power testing
• Sensitivity and Specificity
• Diagnostic outcome algorithm
Illustration: Alexander Bertram Powell

Endemic Sample
• 98 skeletons: known age, sex, tribe, cause of death
• Holoendemic area for malaria
Democratic Republic of
Congo (DRC)
Tanzania
Uganda
Rwanda
BurundiMaleFemale
RwandaUgandaBurundiTanzaniaDRC
Age0-15
16-25
26-35
36-45
46-55
56+
Endemic Sample
Phases of data collection:
• Phase I: Malarial/anemic sample
• Phase II: Matched sample to Phase I
• Phase III: All remaining with skulls present
I
II
III

Non-Endemic Sample
• 352 skeletons from LSU’s FACES lab collection
• Used 106 individuals of African-American
descent – similar rates of sickle cell
• Includes cases from 1980-2013
MaleFemale
Age0-15
16-25
26-35
36-45
46-55
56+

Anemic vs. Non-Anemic Samples
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Cribra
orbitalia
Porotic
hyperostosis
Humeral
cribra
Femoral
cribra
Spinal
porosity
Periostitis Alveolar
resorption
LEHs
Non-anemic
Anemic

Humeral Cribra
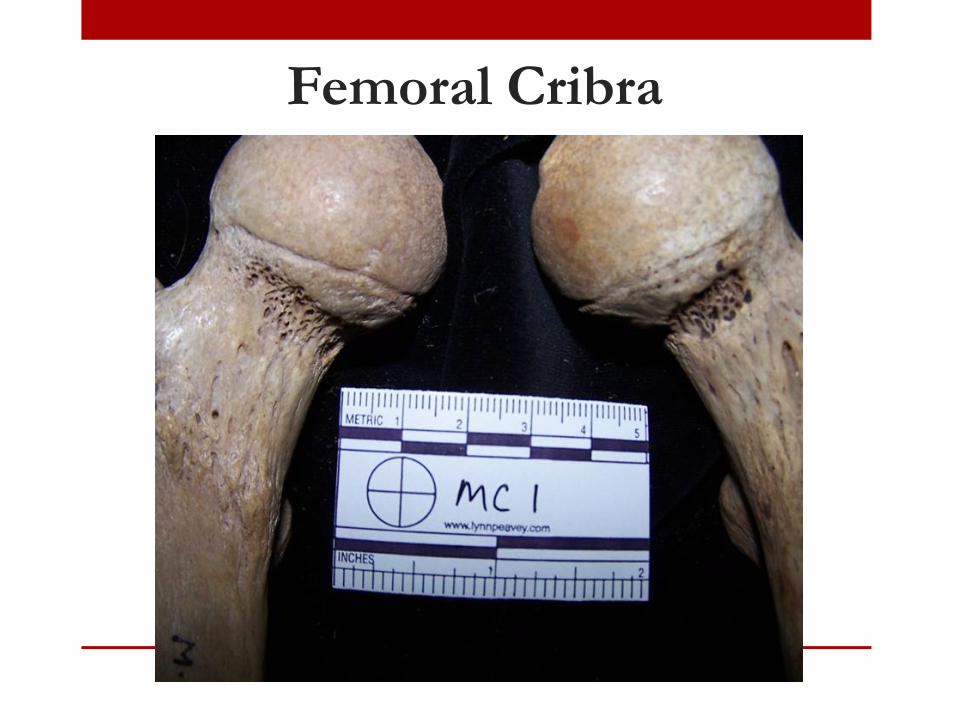
Femoral Cribra

Spinal Porosity
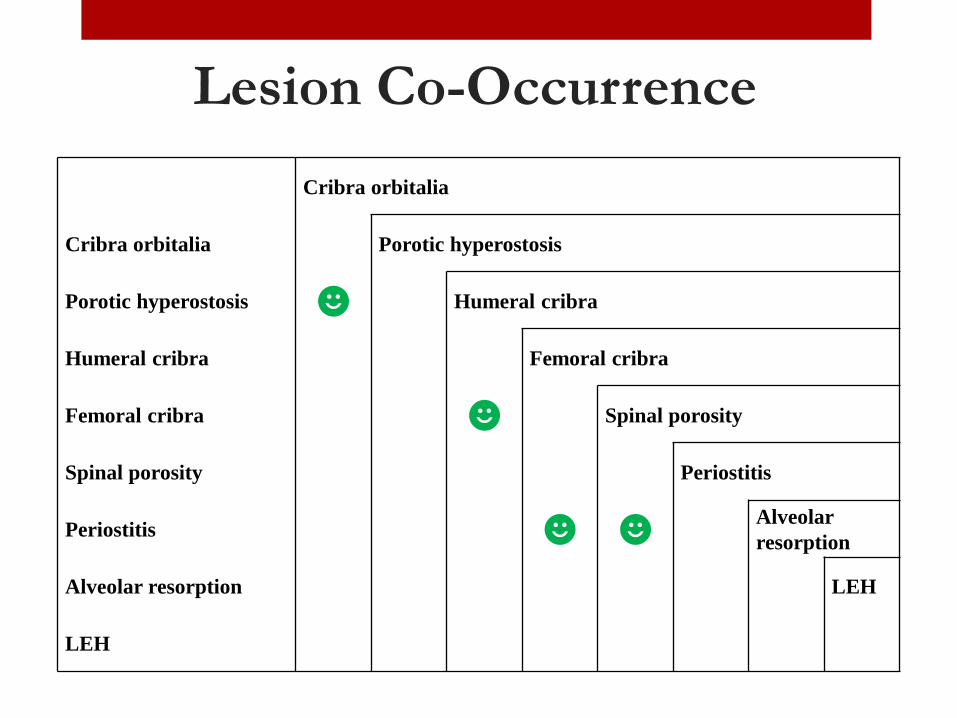
Lesion Co-Occurrence
Cribra orbitalia
Cribra orbitalia Porotic hyperostosis
Porotic hyperostosis ☻ Humeral cribra
Humeral cribra Femoral cribra
Femoral cribra ☻ Spinal porosity
Spinal porosity Periostitis
Periostitis ☻ ☻Alveolar
resorption
Alveolar resorption LEH
LEH

Endemic vs. Non-endemic Samples
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Cribra
orbitalia
Porotic
hyperostosis
Humeral
cribra
Femoral
cribra
Spinal
porosity
Periostitis Alveolar
resorption
LEHs
Non-endemic
Endemic
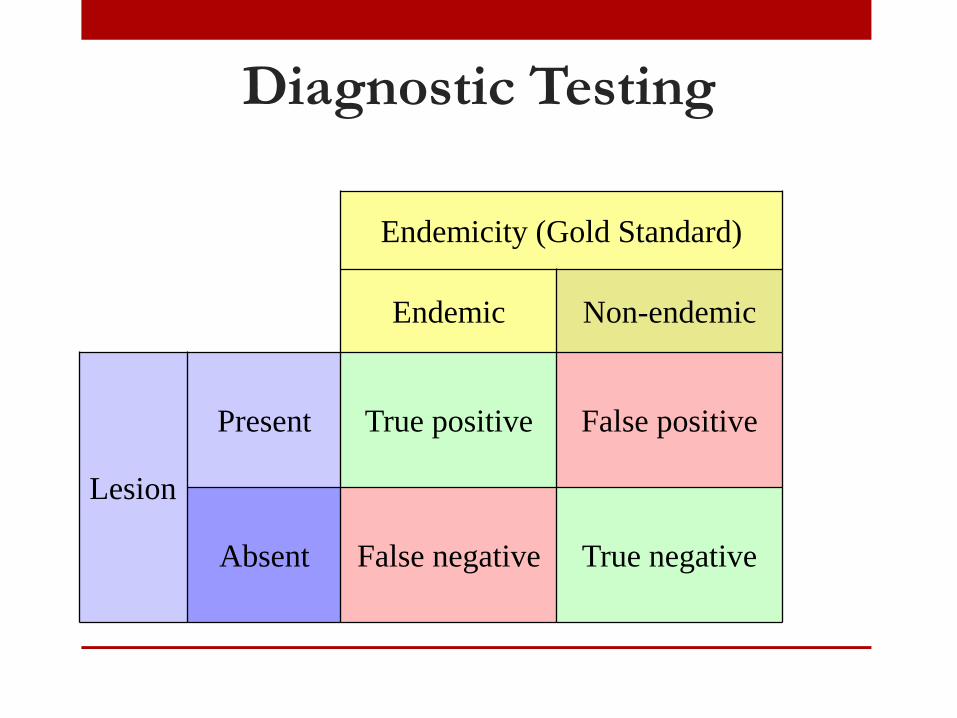
Diagnostic Testing
Endemicity (Gold Standard)
Endemic Non-endemic
Lesion
Present True positive False positive
Absent False negative True negative
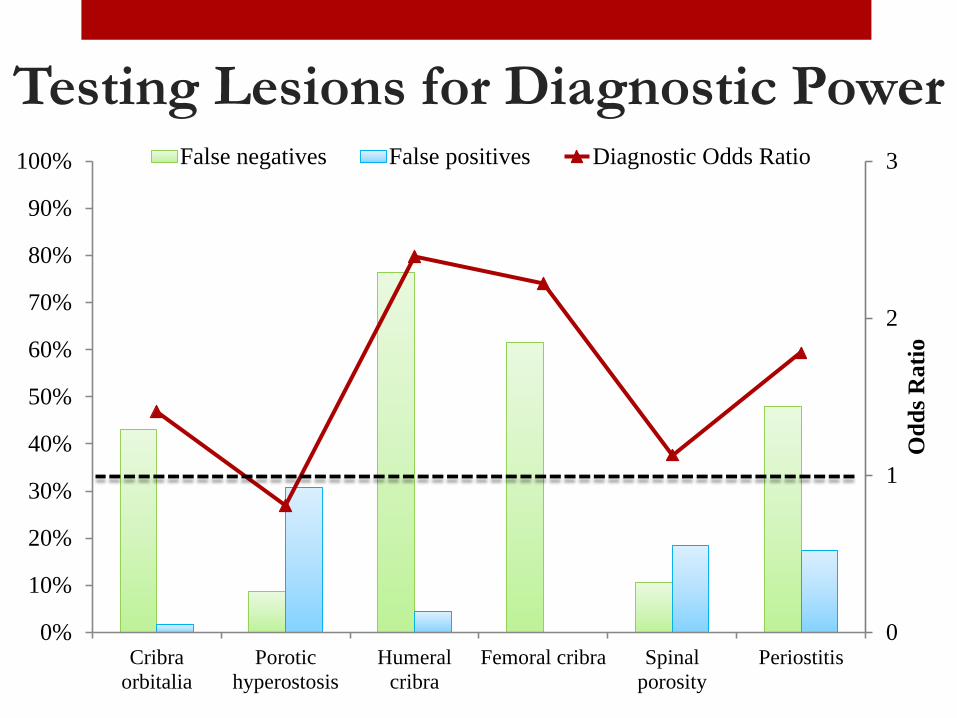
Testing Lesions for Diagnostic Power
0
1
2
3
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Cribra
orbitalia
Porotic
hyperostosis
Humeral
cribra
Femoral cribra Spinal
porosity
Periostitis
Od
ds
Rati
o
False negatives False positives Diagnostic Odds Ratio

Diagnostic Outcome Algorithm
• False negatives = 30%
• False positives = 3%
OROR OR +
Diagnostic Outcome Algorithm
Using only the individuals who died of malaria/anemia:
• False negatives = 15%
• False positives = 3%

Implications
• Malarial lesions: cribra orbitalia, humeral cribra,
femoral cribra, spinal porosity, and periostitis
• Possible etiological factors:
1. Severe malarial anemia
2. Imbalance in bone remodeling
3. General inflammation
Limitations
• Greater range of health problems likely affected
the Ugandan sample
• Malaria tends to co-infect with other diseases,
including dysentery and tuberculosis
• Need to test findings with more clinical samples
Acknowledgements
• Arkansas Graduate Fellowship in Anthropology,
Department of Anthropology, University of Arkansas
• Anatomy Department, Makerere University, Kampala
• Ginesse Listi and Nicole Klein, FACES Lab, LSU
Photo: National Library of Medicine
Copyright © 2022 FDOKUMEN