
The safety of tracheostomy speaking valve use during sleep in children: A pilot study
21
The Safety of Tracheostomy Speaking Valve Use During Sleep In Children: A Pilot Study Giselle Barraza MD, Claudia Fernandez MD, Claudia Halaby MD, C.C.C.- S.L.P,.T.S.H.H. Sara Ambrosio MS, Edwin F. Simpser MD, Melodi Pirzada MD PII: S0196-0709(14)00105-7 DOI: doi: 10.1016/j.amjoto.2014.04.011 Reference: YAJOT 1386 To appear in: American Journal of Otolaryngology–Head and Neck Medicine and Surgery Received date: 19 March 2014 Accepted date: 27 April 2014 Please cite this article as: Barraza Giselle, Fernandez Claudia, Halaby Claudia, Sara Ambrosio MS CCC-SLP,TSHH, Simpser Edwin F., Pirzada Melodi, The Safety of Tracheostomy Speaking Valve Use During Sleep In Children: A Pilot Study, American Journal of Otolaryngology–Head and Neck Medicine and Surgery (2014), doi: 10.1016/j.amjoto.2014.04.011 This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of The safety of tracheostomy speaking valve use during sleep in children: A pilot study

�������� ����� ��
The Safety of Tracheostomy Speaking Valve Use During Sleep In Children:A Pilot Study
Giselle Barraza MD, Claudia Fernandez MD, Claudia Halaby MD, C.C.C.-S.L.P,.T.S.H.H. Sara Ambrosio MS, Edwin F. Simpser MD, Melodi PirzadaMD
PII: S0196-0709(14)00105-7DOI: doi: 10.1016/j.amjoto.2014.04.011Reference: YAJOT 1386
To appear in: American Journal of Otolaryngology–Head and Neck Medicine and Surgery
Received date: 19 March 2014Accepted date: 27 April 2014
Please cite this article as: Barraza Giselle, Fernandez Claudia, Halaby Claudia,Sara Ambrosio MS CCC-SLP,TSHH, Simpser Edwin F., Pirzada Melodi, The Safetyof Tracheostomy Speaking Valve Use During Sleep In Children: A Pilot Study,American Journal of Otolaryngology–Head and Neck Medicine and Surgery (2014), doi:10.1016/j.amjoto.2014.04.011
This is a PDF file of an unedited manuscript that has been accepted for publication.As a service to our customers we are providing this early version of the manuscript.The manuscript will undergo copyediting, typesetting, and review of the resulting proofbefore it is published in its final form. Please note that during the production processerrors may be discovered which could affect the content, and all legal disclaimers thatapply to the journal pertain.
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
1
Barraza, Fernandez, Halaby, Ambrosio, Simpser, Pirzada
The Safety of Tracheostomy Speaking Valve Use During Sleep In
Children: A Pilot Study
AUTHORS
Giselle Barraza, MD Winthrop University Hospital
259 1st Street
Mineola, NY 11501
(914)-843-5678
Claudia Fernandez, MD Kidz Pulmonary Center
Miami Children’s Hospital
6280 SW 72nd
Street, Suite 607
South Miami, FL 33143
(305)342-0525
Claudia Halaby, MD Winthrop University Hospital
259 1st Street

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
2
Barraza, Fernandez, Halaby, Ambrosio, Simpser, Pirzada
Mineola NY 11501
(516)-663-4600
Sara Ambrosio, MS, CCC-SLP, TSHH St. Mary’s Hospital for Children
29-01 216th Street
Bayside, NY11360
(718) 281-8800
Edwin F. Simpser, MD St. Mary’s Hospital for Children
29-01 216th St
Bayside, NY 11360
(718) 281-8701
Melodi Pirzada, MD Winthrop University Hospital
259 1st Street
Mineola NY 11501
(516)-663-4600

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
3
Barraza, Fernandez, Halaby, Ambrosio, Simpser, Pirzada
Presentations:
Chest Conference 2013 - Poster Presentation (Chicago, Illinois)

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
4
Barraza, Fernandez, Halaby, Ambrosio, Simpser, Pirzada
ABSTRACT
Purpose
One of the disadvantages of having a tracheostomy tube is not being able to vocalize. Speaking valves
connected to a tracheostomy tube allow patients to vocalize. Some studies have shown that tracheostomy-
speaking valve can improve swallowing, respiratory secretion management, and expedite decannulation.
There is scant research about its use during sleep. The aim of this study is to evaluate the safety of
tracheostomy-speaking valve overnight, during sleep.
Materials and Methods
Children, ages 1 to 18 years, with tracheostomy tubes who were using a tracheostomy-speaking valve
during daytime/awake periods, were included in this study. The subjects had baseline monitoring of their
heart rate, respiratory rate, oxygen saturation, and end tidal carbon dioxide measurement the night prior to
the intervention, throughout the night at scheduled intervals. The tracheostomy-speaking valve was placed
the following night and the same parameters were monitored and recorded throughout the study night.
Results
A total of 9 patients were recruited. In all subjects, the mean values of the overnight parameters showed
no significant clinical variations between the baseline night and the study night. Repeated measure
ANOVA analysis revealed no significant changes in the parameters over the 8 hours of recorded time. No
major adverse events were recorded during the study night.
Conclusion
This pilot study reveals that extended use of a tracheostomy-speaking valve, while the children were
asleep, was not associated with adverse cardiopulmonary events. This is the first study to show that a
tracheostomy-speaking valve might be safely used during sleep, in children.

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
5
Barraza, Fernandez, Halaby, Ambrosio, Simpser, Pirzada
Introduction
Tracheostomy has become an increasingly common procedure performed in pediatric patients.
Indications for tracheostomy have changed in recent years and include upper airway obstruction
secondary to congenital birth anomalies or acquired anatomic abnormalities such as subglottic stenosis,
and anticipated need for prolonged ventilation [1-4]. Currently, the most common indication is prolonged
need for ventilation due to neuromuscular diseases or respiratory conditions such as chronic lung disease
[1, 2, 4, 5]. The most common pediatric age group in which this procedure is performed is under 1 year of
age [1, 2], probably due to increased survival of preterm infants [3, 5].
A tracheostomy-speaking valve (TSV) is a one way valve that attaches to the outside opening of the
tracheostomy tube. When the patient inhales, the valve opens to let air flow through the tracheostomy
tube and into the lungs. During exhalation, the valve closes without a leak and the air is directed around
the tracheostomy tube and through the vocal cords, larynx, oral and nasal cavities, enabling speech. The
closed position of the valve allows for a normal uninterrupted respiratory system which in turn allows for
generation of positive subglottic pressure. Exhaling around the tracheostomy tube is harder than through
it, and some children may need time to adapt and build the strength and ability to do this.
The literature is scant regarding the use of speaking valves in children and infants. Passy et al. evaluated
the efficacy of a one-way speaking valve in 15 adult ventilator-dependent patients. They concluded that
the TSV is a safe and effective adjunct to ventilator-dependent patients in improving communication
skills, speech flow and volume [6].
The goal of using a speaking valve in children with tracheostomy is to provide early vocalization practice
and to enable speech production. A retrospective review of 64 charts examined documented evidence of
tolerance of the TSV in infants and children younger than 2 years of life. 83% of these children tolerated
the TSV and 75% produced vocalization on their first trial [7]. A later retrospective study in 55
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
6
Barraza, Fernandez, Halaby, Ambrosio, Simpser, Pirzada
tracheostimized children, infants to 18 years, concluded that many of them (95%) tolerated the TSV. The
subjects may have needed 2 or more trials with the TSV until the patient and family were comfortable
with it. The most common reasons for failure in the TSV trials were inadequate leak around the
tracheostomy tube, childhood behavioral problems related to the placement of the valve, limited parental
behavioral management skills or parental problems with the TSV care and use, and inadequate pulmonary
toilet once the valve was placed [8].
Having a tracheostomy predisposes the patient to aspiration due to reduced laryngeal elevation, reduced
cough effectiveness, relative esophageal obstruction, disruption of phasic glottis function and blunting of
glottis closure reflex (resulting in loss of proprioception) [9,10]. In addition to its use for vocalization,
studies have shown that the use of TSV may decrease the risk of aspiration [11, 12, 13]. The TSV seams
to ameliorate some of these adverse effects of the tracheostomy tube.
Another possible benefit of using the TSV is that it decreases the respiratory secretions in
tracheostomized patients. Lichtman et al. studied 8 adult patients and found a significant decrease in
respiratory secretions when wearing the TSV. This study demonstrated a reduction in the collected
secretions by manual suctioning. The mechanism is unknown, but the authors hypothesize that the
secretion reduction is a result of the redirection of airflow to the oral and nasal passages, causing
evaporation of secretions in these pathways. They also found an improvement in olfaction with the use of
the TSV [14].
Lastly, the use of TSV was shown to decrease the time to decannulation. Le et al. examined 10 adult
patients and compared the rate of successful decannulation using conventional cap versus one-way valve.
They revealed that the time to decannulation was slightly shorter with the use of one-way valve (median
18 days) compared to conventional capping (median 23 days). However, this difference did not achieve
statistical significance due to the small number of patients enrolled in the study [15].

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
7
Barraza, Fernandez, Halaby, Ambrosio, Simpser, Pirzada
Currently, the TSV are FDA approved to be used only during the daytime while the patient is awake.
There is scant data on its safety use at night, during sleep. To our knowledge there are no studies
published that address the safety of the TSV use during sleep in children. As the valve has multiple
advantages, in this study we aim to assess the safety of TSV use in children during sleep.
Materials and methods
A prospective, case-control, descriptive study was conducted to assess the safety of TSV during sleep in
tracheostomized children, from May 2011 through July 2013, in St. Mary’s Hospital for Children in
Bayside, NY. Children ages 1 to 18 years who had a tracheostomy tube and were using a speaking valve
or cap during daytime, were eligible to enter the study.
Our inclusion criteria followed St. Mary’s Hospital for Children written policy evaluating children
candidates for speech valve trial, in effect since December 2006 (lastly revised in April 2011). A
multidisciplinary team of a pediatrician, an ENT or pulmonary specialist, a nurse, a Speech Language
Pathologist (SLP), and a Respiratory Therapist (RT), evaluated the patient’s eligibility for the device. In
order to be eligible to use a speech valve during the day, the patient’s tracheostomy should have been
placed at least 48 hours earlier, and upper airway patency should have been evaluated by direct
observation. The candidate had to be alert and responsive, and should not have any acute respiratory tract
infections.
Once a subject was approved to use the valve during the day, while awake, the family was offered the
opportunity to participate in this study. After obtaining parental consent, patients were included in the
study if they were wearing the tracheostomy speaking valve or capping during their awake time,
throughout the day. If the subject had an acute intercurrent illness, like an upper respiratory infection
(URI), he/she was not allowed to participate in the study for a period of 2 weeks and needed to be cleared
by his/her primary physician in order to participate in the study.

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
8
Barraza, Fernandez, Halaby, Ambrosio, Simpser, Pirzada
The night prior to the study, the subject’s respiratory rate (RR), heart rate (HR), oxygen saturation
(SpO2), end tidal carbon dioxide (EtCO2) and baseline sleeping status were monitored and documented
every hour from 10 pm to 2 am and thereafter, every 2 hours from 2am to 6am. Hourly intervals were
chosen for the first 4 hours to make sure that the patient tolerated the speaking valve, thereafter every two
hours for the following 4 hours. The following night, subjects had the TSV attached to the tracheostomy
tube (with a deflated cuff, if applicable) from 10pm to 6am (8 hours) and the same parameters were
monitored at the same time intervals. The monitoring was done and recorded by one of the physicians
involved in the study. Any change in vital signs, improvement in oxygen saturation, and adverse events
were also recorded. In addition, the general appearance of the patient, and work of breathing were
assessed by a physician.
In our study, the patients used the Passy-Muir tracheostomy-speaking valve (Irvine, CA). Humidification
was delivered via a tracheostomy collar mask during both nights. The subject’s baseline continuous heart
rate and oxygen saturation were monitored using the Masimo Radical-7 (Irvine, CA). End tidal carbon
dioxide was measured using a Novametrix "Tidal Wave" model 610 (Respironics Inc. Louisville, KY).
This is a handheld device that attaches to the tracheostomy and provides a reading within 15 seconds
without interfering with the oxygen supply.
The protocol for this study was reviewed and approved by the Institutional Review Board of the St.
Mary’s Healthcare System for Children in Bayside, NY. The study was allowed to proceed by the FDA
on January 6th, 2011 for studying the safety of TSV during sleep in children, using a Passy-Muir valve.
Statistical analysis
Continuous variables were presented as mean (standard deviation). Variables were tested for normal
distribution by using Kolmogorov-Smirnov test. Pre and Post average values were calculated for each
variable over time (10pm to 6AM) then the dataset was analyzed using paired t-test. Non-parametric test
for paired data signed-rank test was also used to analyze data. P-values were reported from both the tests.

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
9
Barraza, Fernandez, Halaby, Ambrosio, Simpser, Pirzada
Repeated measure ANOVA was used to analyze data in longitudinal fashion. All calculations were
performed using SAS 9.3 (SAS Institute, Carry, NC). Since this is a pilot study with a small sample size
(n=9), any significance value should be interpreted with caution as the study does not have enough power
to detect any statistically significant difference.
Results
A total of nine patients were recruited in the study. Six patients were males and three were females. The
mean age of the subjects was 5.6 years. The subjects had different medical indications for the
tracheostomy tube placement (Table 1).
In all subjects, the mean values of the overnight parameters showed no significant clinical changes
between the baseline night and study night (Table 2). Repeated measure ANOVA analysis did not reveal
any significant differences in the HR, RR, SpO2 and EtCO2 over an 8 hour period (10pm to 6am) (Table
3).
During the study night, none of the patients had any clinical respiratory adverse events while using the
TSV. Two subjects were requiring oxygen at baseline and it was continued on the study night. One
subject (subject #4) was noticed to have an increased heart rate prior to the start of the study night. At 12
am due to the constant increased heart rate, his temperature was checked and was 100.6 °F. However, this
subject did not have any clinical symptoms of an upper respiratory tract infection. One subject (subject
#3) needed to be suctioned on the study night due to increased secretions and did not sleep the rest of the
night from 12 pm to 6 am after being suctioned. This subject was known to have increased secretion at
baseline. The other 8 subjects, except subject #3, did not have any disturbance in their sleep while using
the TSV.
None of the subjects had decreases in oxygen saturation on the study night, while wearing the TSV. One
subject (subject #5) had an episode of desaturation into the 50’s the night prior to the study because of

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
10
Barraza, Fernandez, Halaby, Ambrosio, Simpser, Pirzada
increased secretions, but did not have any desaturations on the study night. One subject’s (subject #8) had
a recorded oxygen saturation the night prior to the study ranging from 90 to 93% and on the study night
ranging from 95 to 98%, suggesting an improvement in oxygen saturation with the TSV use. Finally,
none of the 9 subjects had witnessed apneas during the time that they used the TSV.
Discussion:
Our study suggests that it is safe to use the TSV valve during sleep in children, once a subject tolerates it
while awake. The results revealed no significant changes in the subjects mean values between the baseline
and study night parameters (HR, RR, SpO2, EtCO2). There was also no significant difference between
the baseline and study night parameters when they were measured longitudinally over the eight hour
study period.
One limitation of our study is the small number of patients that we were able to enroll. However, the
overall number of children that are tracheotomized is small in the general pediatric population. We also
had a short period of observation of only one night. Observing subjects on subsequent nights can give us a
better understanding of its safety use during the night. We also had a selected population that had no acute
intercurrent illness making it difficult to assess the safety and tolerance of the TSV during acute illness.
Lastly, we did not have an objective measure to evaluate any sleep disturbance with the use of the TSV
valve. Patients’ sleep quality and variations may have been assessed better if overnight polysomnography
had been performed at baseline and on the study night.
To our knowledge, this is the first study that assessed the safety of TSV during sleep in children. Previous
studies have demonstrated the tolerance of the TSV in children but did not assess its safety during sleep.
In the adult population, much research has been accomplished on the use of the TSV. A small prospective
study done on 10 tracheostomized adult patients with a mean age of 70 years showed that the use of the

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
11
Barraza, Fernandez, Halaby, Ambrosio, Simpser, Pirzada
speaking valve for one night in seriously ill patients was not associated with apneas or significant
desaturations [16]. A cohort study of 32 tracheostomized patients showed that 14 patients were able to
tolerate a speaking valve for 24 hours; even during sleep [17].
Using the TSV at night, during sleep may have many potential benefits for tracheostomized children. It
allows noise/speech production in case of an emergency during night. It improves olfaction and decreases
airway secretions. Wearing the valve for 24 hours would be beneficial for the children who are at risk for
aspiration, since aspiration may occur at any time during the day or night.
In summary, our findings suggest that the TSV can be safely used during sleep in children. However,
future research is needed to observe the effect over longer periods of time and during intercurrent
illnesses.
Conclusion:
Based on our findings, the extended use of TSV while the child is asleep was not associated with adverse
cardiopulmonary events. This is the first study to show that a speaking valve can be safely used during
sleep in children with tracheostomy tubes.

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
12
Barraza, Fernandez, Halaby, Ambrosio, Simpser, Pirzada
References:
1. Corbett HJ, Mann KS, Mitra I, et al. Tracheostomy – a 10 year experience from a UK
pediatric surgical center. J Pediat Surg. 2007;42:1251-4.
2. Butnaru CS, Colreavy MP, Ayari S, et al. Tracheotomy in children: Evolution in indications.
Int J Pediatr Otorhinolaryngol. 2006;70:115-9. Epub 2005 Sep 16.
3. Alladi A, Rao S, Das K, et al. Pediatric tracheostomy: A 13-year experience. Pediatr Surg Int.
2004;20: 695-8. Epub 2004 Sep 21.
4. Hadfield PJ, Lloyd-Faulconbridge RV, Almeyda J, et al. The changing indications for
paediatric tracheostomy. Int J Pediatr Otorhinolaryngol. 2003;67:7-10.
5. Carron JD, Derkay CS, Strope GL, et al. Pediatric tracheotomies: Changing indications and
outcomes. Laryngoscope. 2000;110:1099-104.
6. Passy V, Baydur A, Prentice W, et al. Passy-Muir tracheostomy speaking valve on ventilator-
dependent patients. Larygoscope 1993; 103.
7. Engleman SG, Turnage-Carrier C. Tolerance of the Passy-Muir speaking valve in infants and
children less than 2 years of age. Pediatr Nurs. 1197 Nov-Dec; 23(6):571-3
8. Cho Lieu JE, Muntz HR, Prater D, et al. Passy-Muir valve in children with tracheostomy. Int.
J. Pediatr. Otorhinolarygnol. 50 (1999) 197-203.
9. Eibling DE and Gross RD. Subglottic air pressure: A key component of swallowing
efficiency.Annals of Otology, Rhinology and Laryngology, 1996; (in press).
10. Gross RD, Mahlmann JE and Grayhack JP. Physiologic effects of open and closed
tracheostomy on the pharyngeal swallow. Ann Otol Rhinol Laryngol 112:2003
11. Dettelbach MA, Gross, RD, Mahlmann J, et al. Effect of the passy-muir valve on aspiration
in patients with tracheostomy. Head & Neck, Vol 17(4): 297-302,1995
12. Stachler RJ, Hamlet SL, Choi J, et al. Scintigraphic quantification of aspiration reduction
with the passy-muir valve. Laryngoscope. 1996;106:231-234.
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
13
Barraza, Fernandez, Halaby, Ambrosio, Simpser, Pirzada
13. Elpern EH, Borkgren M, Bacon M, et al. Effect of the passy-muir valve on pulmonary
aspiration in adults. Heart Lung, 2000; Jul-Aug 29(4):287-93.
14. Lichtman SW, Birnbaum IL, Sanfilippo MR, et al. Effect of a tracheostomy speaking valve
on secretions, arterial oxygenation, and olfaction: a quantitative evaluation. J Speech Hear
Res. 1995 Jun; 38 (3):549-55
15. Minh Le H, Aten JL, Chiang JT, et al. Comparison between conventional cap and one –way
valve in the decannulation of patients with long-term tracheostomies. Respir Care 1993;
38(11):1161-1167.
16. Gross RD, Atwood C. Safety of tracheostomy speaking valve use during sleep. Otolaryngol
Head Neck Surg. 2007;137:209.
17. Oliveira Silveira, AR, Soki MN, Chone CT, et al. Brazilian tracheotomy speech valve:
Diaphragm pressure standardization. Braz J Otorhinolaryngol 2009; 75 (1): 107-10.

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
14
Barraza, Fernandez, Halaby, Ambrosio, Simpser, Pirzada
Fig. 1. Airflow pathway during breathing when valve is attached to external opening of tracheostomy. (included
with permission of Passy-Muir Inc.)
Placement: Page 4

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
15
Barraza, Fernandez, Halaby, Ambrosio, Simpser, Pirzada
Fig. 2. The “no leak” position of the tracheostomy-speaking valve versus other valve with a leak (included with
permission of Passy-Muir Inc)
Placement: Page 4

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
16
Barraza, Fernandez, Halaby, Ambrosio, Simpser, Pirzada
Table 1- Patient Characteristics
Subjects Age (in
years)
Sex Primary Indication for a
Tracheostomy Tube *
Medical Diagnosis
1 11.5 M Prolonged need for ventilation due to
apneas
Mental retardation, Cerebral palsy
with muscular weakness
2 7.5 M Prolonged need for ventilation due to
obstructive sleep apnea
Inability to handle and clear
secretions
Lissencephaly, seizure disorder,
developmental delay
3 3.5 F Prolonged need for ventilation due to
obstructive sleep apnea
Inability to handle and clear
secretions
Lissencephaly
4 2.5 M Inability to handle and clear
secretions (chronic
aspiration/pneumonia)
Cerebral atrophy, seizure disorder,
developmental delay
5 8.5 M Prolonged need for ventilation due to
central apneas
Freeman Sheldon syndrome, Ebstein
abnormality, chronic lung disease,
persuasive disorder, asthma, GERD
6 5.5 M Prolonged need for ventilation due to
chronic respiratory failure
Congenital heart disease w/ Shone’s
complex and pulmonary
hypertension, GERD

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
17
Barraza, Fernandez, Halaby, Ambrosio, Simpser, Pirzada
Subjects Age (in
years)
Sex Primary Indication for a
Tracheostomy Tube *
Medical Diagnosis
7 2.5 F Prolonged need for ventilation due to
respiratory failure
Chronic lung disease of prematurity,
developmental delay
8 3 F Prolonged need for ventilation
due to respiratory failure
Hypoxic-ischemic encephalopathy,
asthma, developmental delay, seizure
disorder
9 6 M Prolonged need for ventilation due to
respiratory failure
Chronic lung disease of prematurity,
asthma, developmental delay
*None of the subjects were chronically ventilated at the enrollement of the study
F = female, M = male
Placement: Page 8

ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
18
Barraza, Fernandez, Halaby, Ambrosio, Simpser, Pirzada
Table 2. Evaluating effect of intervention by comparing baseline night and study night values of clinical parameters
recorded
Variable
Baseline night:
mean(SD)
Study night:
mean(SD)
Difference,
mean(SD)
p-value
(paired t-test)
p-value
(signed-rank)
HR 93(20) 91(26) -2(22) 0.795 0.441
RR 26(6) 26(6) 0(5) 0.853 0.672
O2SAT 96(3) 97(2) 1(3) 0.228 0.336
ETCO2 35(4) 35(3) 0(1) 0.500 0.656
Note: Mean value of all time points (10PM, 11PM, 12AM, 1AM, 2AM, 4AM and 6AM) was calculated for each
patient. This mean of overnight values per patients were used for pre and post comparisons. SD= standard deviation,
HR= heart rate, RR= respiratory rate, O2SAT= oxygen saturation, ETCO2= end tidal carbon dioxide.
Placement: Page 8
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
19
Barraza, Fernandez, Halaby, Ambrosio, Simpser, Pirzada
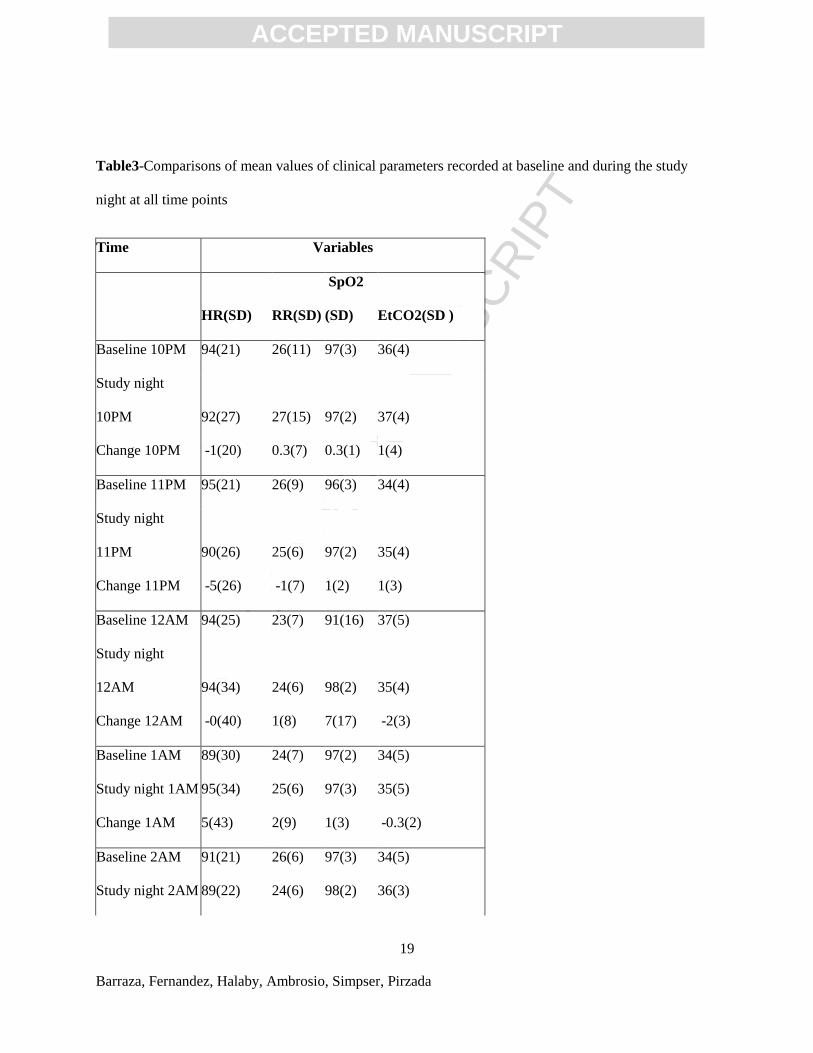
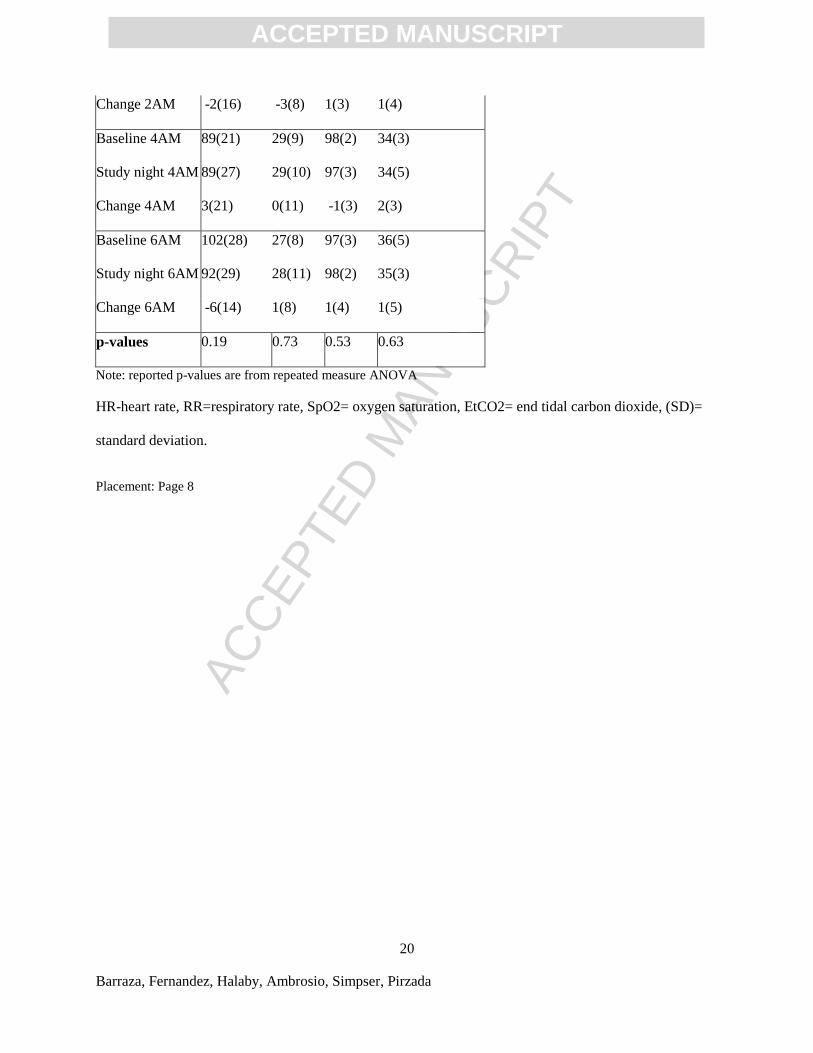
Table3-Comparisons of mean values of clinical parameters recorded at baseline and during the study
night at all time points
Time Variables
HR(SD) RR(SD)
SpO2
(SD) EtCO2(SD )
Baseline 10PM 94(21) 26(11) 97(3) 36(4)
Study night
10PM 92(27) 27(15) 97(2) 37(4)
Change 10PM -1(20) 0.3(7) 0.3(1) 1(4)
Baseline 11PM 95(21) 26(9) 96(3) 34(4)
Study night
11PM 90(26) 25(6) 97(2) 35(4)
Change 11PM -5(26) -1(7) 1(2) 1(3)
Baseline 12AM 94(25) 23(7) 91(16) 37(5)
Study night
12AM 94(34) 24(6) 98(2) 35(4)
Change 12AM -0(40) 1(8) 7(17) -2(3)
Baseline 1AM 89(30) 24(7) 97(2) 34(5)
Study night 1AM 95(34) 25(6) 97(3) 35(5)
Change 1AM 5(43) 2(9) 1(3) -0.3(2)
Baseline 2AM 91(21) 26(6) 97(3) 34(5)
Study night 2AM 89(22) 24(6) 98(2) 36(3)
ACC
EPTE
D M
ANU
SCR
IPT
ACCEPTED MANUSCRIPT
20
Barraza, Fernandez, Halaby, Ambrosio, Simpser, Pirzada
Change 2AM -2(16) -3(8) 1(3) 1(4)
Baseline 4AM 89(21) 29(9) 98(2) 34(3)
Study night 4AM 89(27) 29(10) 97(3) 34(5)
Change 4AM 3(21) 0(11) -1(3) 2(3)
Baseline 6AM 102(28) 27(8) 97(3) 36(5)
Study night 6AM 92(29) 28(11) 98(2) 35(3)
Change 6AM -6(14) 1(8) 1(4) 1(5)
p-values 0.19 0.73 0.53 0.63
Note: reported p-values are from repeated measure ANOVA
HR-heart rate, RR=respiratory rate, SpO2= oxygen saturation, EtCO2= end tidal carbon dioxide, (SD)=
standard deviation.
Placement: Page 8




















