The Role of Significant Others in Adolescent Diabetes: A Qualitative Study
10
Aaron E. Carroll, MD, MS David G. Marrero, PhD From the Children’s Health Services Research, Indiana University School of Medicine, and the Regenstrief Institute for Health Care, Indianapolis, Indiana (Dr Carroll), and the Diabetes Prevention and Control Center, Indiana University School of Medicine, and the Regenstrief Institute for Health Care, Indianapolis, Indiana (Dr Marrero). Correspondence to Aaron E. Carroll, MD, MS, Riley Research 330, 699 West Drive, Indianapolis, IN 46074 ([email protected]). Acknowledgment: We are grateful to the adolescents who were willing to share with us their experiences of living with diabetes so that we can better understand and provide care for them. We also want to thank Terri Matousek of Matousek and Associates for conducting all of the focus groups; Heather Herdman, RN, PhD, for her assistance with data analysis; and Melinda Swenson, RN, PhD, for her help in the design of the study. This research was funded by grants from the National Institutes of Health to A.E.C. (1 K23 DK067879-01) and from Clarian Health Partners to A.E.C. (VFR-190). DOI: 10.1177/0145721706286893 Role of Significant Others in Adolescent Diabetes 243 Carroll and Marrero The Role of Significant Others in Adolescent Diabetes A Qualitative Study Purpose The purpose of this study was to explore perceptions of how diabetes influences adolescents’ perceptions of quality of life in general and their relationships with par- ents, peers, school, and their physician. Methods The authors recruited adolescents between the ages of 13 and 18 years living with type 1 diabetes mellitus from a midwestern metropolitan area. Qualitative analysis of the focus group data followed a set procedure: (1) audio review of the tapes, (2) reading through the transcrip- tions, (3) discussions among investigators, (4) determi- nation of conceptual themes, and (5) assignment of relevant responses to appropriate thematic constructs. Results The 5 focus groups involved 31 adolescents. From the discussions that occurred within the 5 focus groups, the following themes were identified: personal perceptions of living with diabetes (which included living with dia- betes, testing and injections, and blood sugar fluctua- tions), impact on relationships (which included relationships with their parents, their friends/peers, and their physician), and impact on school. Conclusions Diabetes in adolescence is fraught with equal and oppo- site demands. One consequence of this internal push/pull is that adolescents become more afraid to do appropriate developmental activities. This can have a significant
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of The Role of Significant Others in Adolescent Diabetes: A Qualitative Study
Aaron E. Carroll, MD, MS
David G. Marrero, PhD
From the Children’s Health Services Research, IndianaUniversity School of Medicine, and the Regenstrief Institute forHealth Care, Indianapolis, Indiana (Dr Carroll), and the DiabetesPrevention and Control Center, Indiana University School ofMedicine, and the Regenstrief Institute for Health Care,Indianapolis, Indiana (Dr Marrero).
Correspondence to Aaron E. Carroll, MD, MS, Riley Research330, 699 West Drive, Indianapolis, IN 46074([email protected]).
Acknowledgment: We are grateful to the adolescents who werewilling to share with us their experiences of living with diabetesso that we can better understand and provide care for them.We also want to thank Terri Matousek of Matousek andAssociates for conducting all of the focus groups; HeatherHerdman, RN, PhD, for her assistance with data analysis; andMelinda Swenson, RN, PhD, for her help in the design of thestudy. This research was funded by grants from the NationalInstitutes of Health to A.E.C. (1 K23 DK067879-01) and fromClarian Health Partners to A.E.C. (VFR-190).
DOI: 10.1177/0145721706286893
Role of Significant Others in Adolescent Diabetes
243
Carroll and Marrero
The Role of Significant Others in Adolescent DiabetesA Qualitative Study
Purpose
The purpose of this study was to explore perceptions of
how diabetes influences adolescents’ perceptions of
quality of life in general and their relationships with par-
ents, peers, school, and their physician.
Methods
The authors recruited adolescents between the ages of 13
and 18 years living with type 1 diabetes mellitus from a
midwestern metropolitan area. Qualitative analysis of
the focus group data followed a set procedure: (1) audio
review of the tapes, (2) reading through the transcrip-
tions, (3) discussions among investigators, (4) determi-
nation of conceptual themes, and (5) assignment of
relevant responses to appropriate thematic constructs.
Results
The 5 focus groups involved 31 adolescents. From the
discussions that occurred within the 5 focus groups, the
following themes were identified: personal perceptions
of living with diabetes (which included living with dia-
betes, testing and injections, and blood sugar fluctua-
tions), impact on relationships (which included
relationships with their parents, their friends/peers, and
their physician), and impact on school.
Conclusions
Diabetes in adolescence is fraught with equal and oppo-
site demands. One consequence of this internal push/pull
is that adolescents become more afraid to do appropriate
developmental activities. This can have a significant

The Diabetes EDUCATOR
244
Volume 32, Number 2, March/April 2006
impact on their normal progression to independence and
adulthood, ironically at odds with the increased respon-
sibility they have had to assume throughout their lives to
care for their disease. Much of the clinical time and
research still focuses on the devices of diabetes care:
testing and treatment. While these are important tools in
improving the outcomes of people with diabetes, they
will have little impact on the adolescent until the devel-
opmental consequences of diabetes on their lives are
simultaneously addressed.
Dealing with diabetes is perhaps most difficult
and challenging for children and adoles-
cents.1 By its very nature, diabetes requires a
higher degree of behavioral regulation than
is normal for similar aged children.2 Adolescence is a
particularly difficult period.3-6 Research has shown that
adolescent patients with diabetes are susceptible to a
number of issues that make management troublesome.
Children with diabetes miss more school than their
healthy siblings and are more likely to have behavioral
problems.7 Parental involvement can lead to better con-
trol of disease, but older children are less likely to have
close parental involvement.8,9 Moreover, the presence of
the disease can exert more conflicted family dynamics
and stressful adolescent-parent interaction.4,5 More fre-
quent assessment of blood glucose levels is a predictor
of glycemic control; unfortunately, adolescents moni-
tor their blood sugars less frequently than do younger
children.8
Normal social development during adolescence
requires that a young person begins to reject parental
control as they strive to build an integrated self-identity.
This involves some rejection of parental and societal
controls, with greater attention to peers as a source of
rules for “normative” behavior and identity.2 The pres-
ence of diabetes, however, can significantly jeopardize
this process, particularly as parents, concerned over the
many negative consequences of poor diabetes manage-
ment, are reluctant to relinquish control of adolescent
behavior.6,10-12 In addition, many nondiabetic peers can pro-
vide influences that, although normal and age-appropriate,
may conflict with good diabetes care practices.13,14 Risk-
seeking behavior in adolescence can only complicate
this situation.13
Unfortunately, little is known about the dynamics of
adolescents and their family and environment, particu-
larly from the perspective of the adolescent with dia-
betes.15 Because the researchers wanted to observe
attitudes and reported behavior to construct theory, a
qualitative research method was decided on. A series of
focus groups with adolescents with diabetes was con-
ducted to explore their perceptions of how having dia-
betes influences their perceptions of quality of life in
general and their relationships with the 4 main social
influences that contribute to both their social develop-
ment and their therapeutic lives: parents, peers, school,
and their physician.
Methods
Research Design
A qualitative design was employed in which focus
groups were used to elicit data from adolescents living
with type 1 diabetes, with emphasis on how the disease
affects relationships with parents, peers, physicians, and
school. A focus group methodology was chosen because
it is an excellent means to gather opinions and beliefs in
a cost-effective manner with acceptable validity.16 The
focus groups were conducted by a professional facilita-
tor experienced in working with health care populations
(see the acknowledgments). A prepared set of open-
ended qualitative questions were used to solicit respons-
es during a 2-hour session (eg, “What is it like to be a
teenager with diabetes and how does it affect your life?
What is it like dealing with parents and diabetes?”).
Permission to tape record the sessions was asked and
received to allow for later transcription. All subjects vol-
untarily responded within the groups or when called on
to answer questions.
Sample
Adolescent patients with type 1 diabetes (aged 13 to
18 years) were recruited from physicians’ offices in a
midwestern metropolitan area. A total of 5 focus groups
were conducted with 18 males and 13 females. Both sub-
jects and parents gave informed consent and were paid
$40 to participate. This study was approved by the
Institutional Review Board of Indiana University.
Qualitative Analysis
Qualitative analysis of the focus group data followed
a set procedure: (1) audio review of the tapes, (2) read-
ing through the transcriptions, (3) discussions among
investigators regarding key elements of subjects’ percep-
tions of living with diabetes and how it affects relation-
ships, (4) determination of conceptual themes, and (5)
assignment of relevant responses to thematic constructs.
The study team was composed of a pediatric physician,
a social ecologist, and a nurse practitioner with medical
sociology training. All 3 members have experience with
qualitative methods. In particular, the social ecologist
(D.G.M.) is experienced with focus group methods and
has published studies using similar quantitative methods
to those reported here. All 3 are experienced with the
target population through both care and previous
research efforts. All 3 members, along with another
group consisting of 8 clinicians and 2 experienced qual-
itative researchers, contributed to the development of the
group questions used by the facilitator (see the acknowl-
edgments). The pediatrician was also present during the
sessions, contributed additional questions when appro-
priate, and took detailed notes. Transcription was done
by trained personnel within a week or two of each focus
group, and audiotapes were reviewed within 1 week of
session completion.
Results
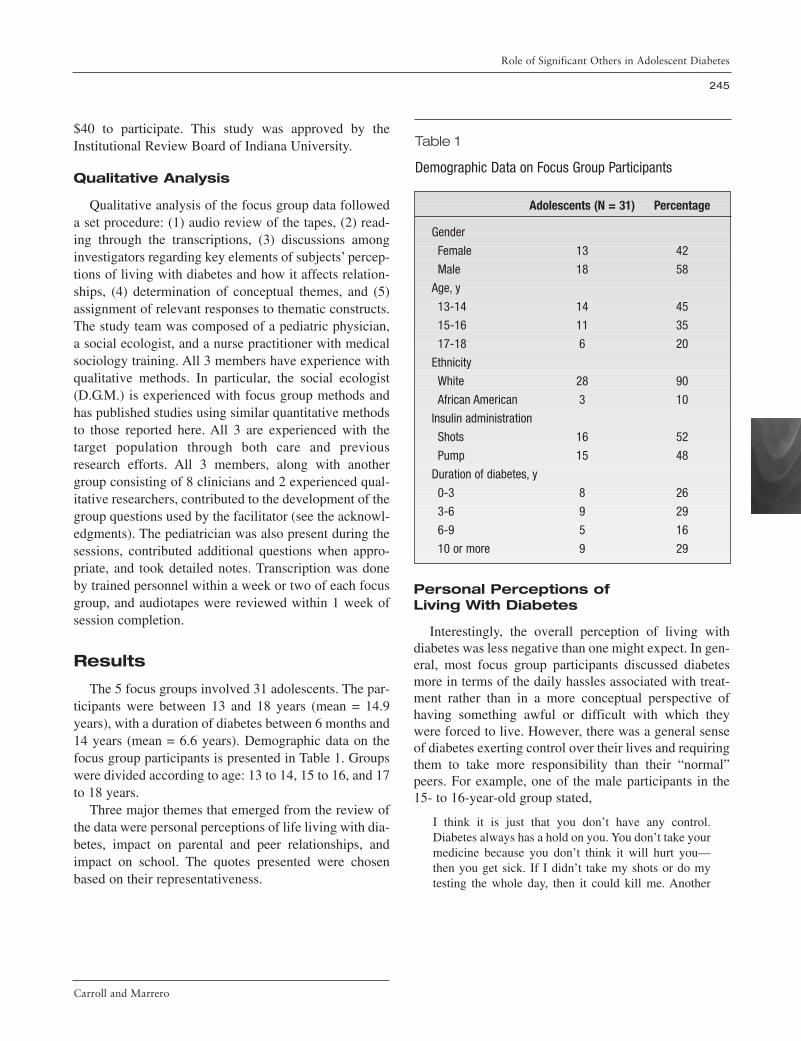
The 5 focus groups involved 31 adolescents. The par-
ticipants were between 13 and 18 years (mean = 14.9
years), with a duration of diabetes between 6 months and
14 years (mean = 6.6 years). Demographic data on the
focus group participants is presented in Table 1. Groups
were divided according to age: 13 to 14, 15 to 16, and 17
to 18 years.
Three major themes that emerged from the review of
the data were personal perceptions of life living with dia-
betes, impact on parental and peer relationships, and
impact on school. The quotes presented were chosen
based on their representativeness.
Personal Perceptions ofLiving With Diabetes
Interestingly, the overall perception of living with
diabetes was less negative than one might expect. In gen-
eral, most focus group participants discussed diabetes
more in terms of the daily hassles associated with treat-
ment rather than in a more conceptual perspective of
having something awful or difficult with which they
were forced to live. However, there was a general sense
of diabetes exerting control over their lives and requiring
them to take more responsibility than their “normal”
peers. For example, one of the male participants in the
15- to 16-year-old group stated,
I think it is just that you don’t have any control.
Diabetes always has a hold on you. You don’t take your
medicine because you don’t think it will hurt you—
then you get sick. If I didn’t take my shots or do my
testing the whole day, then it could kill me. Another
Role of Significant Others in Adolescent Diabetes
245
Carroll and Marrero
Table 1
Demographic Data on Focus Group Participants
Adolescents (N = 31) Percentage
Gender
Female 13 42
Male 18 58
Age, y
13-14 14 45
15-16 11 35
17-18 6 20
Ethnicity
White 28 90
African American 3 10
Insulin administration
Shots 16 52
Pump 15 48
Duration of diabetes, y
0-3 8 26
3-6 9 29
6-9 5 16
10 or more 9 29

The Diabetes EDUCATOR
246
Volume 32, Number 2, March/April 2006
example would be not taking my Humulin® one time or
not counting this one time.
Members of the older adolescent groups noted that
they are required to “watch what I eat . . . do my bolus-
es . . . do my equation . . . exercise . . . make sure I carry
sugar with me just in case I go low.” Many subjects
believed that living with diabetes had forced them to
“grow up faster” and that they see themselves as more
mature than some in their peer group. The following
statements from 2 of the female participants reflect this
theme:
It is like any other disease, no matter what, it is going
to have an impact on your life. At least when I got it
[diabetes] I came to a realization about things. I look at
things a lot differently and I know that I have matured.
It really has created who I am.
I pay attention to it. But, after a while it is like when
you are driving. You don’t really concentrate on the
driving because it becomes natural after a while. We
don’t have to concentrate on it [diabetes] anymore.
Those in the youngest group of participants (13-14
years) tended to describe having diabetes more in terms
of it being “a pain,” “stressful,” and “annoying” than did
the older groups. Most of the older teens (15-18 years)
seemed to accept their condition without a great deal of
anger or frustration. Statements such as, “It’s so easy. It
is a part of your life,” and “I am just used to it . . . it is
all pretty much normal to me,” are indicative of this
acceptance. Indeed, many of the participants stated that
diabetes is something to which they have grown accus-
tomed: “It is who you are. You make it your life. You
work around it.” Other participants indicated that with
the exception of testing and injections, diabetes does not
affect them in a distinct or drastic way. Some of the par-
ticipants noted that diabetes is time-consuming because
of the need to calculate insulin, test blood glucose, track
what foods are being eaten, and so forth. Frequent physi-
cian’s office visits and research participation also take up
more time for them than for their nondiabetic peers.
Others spoke of the need to be organized and responsible
prior to going anywhere, which makes it more difficult
to be spontaneous. One of the male participants
described it in this manner:
Well, you have to be more responsible. You have to
remember your insulin, tester, sugar foods and to count
everything you eat. You can’t just eat whatever and
whenever you want, which is something I did before I
was diagnosed.
Several of the participants indicated that greater expe-
rience with self-management makes living with diabetes
less stressful. They became more aware of their bodies
and how they respond to high and low blood glucose and
are better able to anticipate things. For example, one of
the females in the 15- to 16-year-old group stated,
“When I was newly diagnosed I was scared to death to
go low. Then I went low, and I can identify it now.”
Many of the participants identified that they could
“guess” their blood glucose levels and were able to stop
themselves from going too low or too high because they
were aware of their own warning signs. This seemed to
make the experience of living with diabetes less scary
and more controllable. However, the teens acknowl-
edged that one of the hardest things to accept is that there
simply is no cure for the disease.
Many of the participants noted that diabetes exerted
some negative influences, particularly regarding partici-
pation in sports, driving, and potentially diminished
career choices. Some, but not all, of the teens felt that
their ability to participate competitively in sports had
been hampered by their diabetes. Complaints included
being more tired, having to pay attention to and/or test-
ing blood glucose levels during games, needing to
request to come out of a game, and going low during
sporting events. One male in the 15- to 16-year-old
group stated that his blood glucose dropped too low dur-
ing a football practice and that he had a seizure. Others
note that parents bring them food during their sport
events or that they eat or drink to get their blood glucose
levels higher before an event to prevent potential low-
blood-glucose episodes. Driving was viewed to be a bit
of a hassle by the older group of teens (17-18 years)
“because you get in the car you have to check your blood
sugar and its too high then you are not legal to drive and
then you have to have someone else drive you.” One
male participant in the 15- to 16-year-old group noted
that he had hoped to be a fighter pilot but has learned that
he cannot enter the US Armed Services.
Impact on Relationships
Participants in all groups were asked to discuss how
their diabetes has affected relationships with their par-
ents, their friends/peers, and their physician. Each of

those relationships had subthemes as well, which are dis-
cussed in detail below.
Parental Relationships
Participants were queried regarding how having dia-
betes influenced their relationships with their parents.
Three subthemes emerged from the data: parental con-
cern and overbearing behaviors, parental support, and
letting go of control.
Parental concern and overbearing behaviors. Most
participants across all focus groups discussed situations
in which their parents demonstrated concern regarding
their ability to manage their diabetes. The adolescents
stated that their parents’ behaviors as a result of this con-
cern could be overbearing or “annoying,” “stressful,”
“controlling,” “nagging,” and “overprotective.” Others
stated that their parents would “freak out” or “go nuts” if
their blood glucose readings were abnormal. One partic-
ipant stated that these types of parental behaviors made
her feel “like I’m drowning.” Another suggested, “they
get concerned too much.”
One issue raised was the inability to do “normal
teenage things” because of overbearing parental behav-
iors. For example, teens spoke about being prohibited
from spending the night with friends and going on camp-
ing trips and school trips because of fear that their blood
glucose levels might go too high or low. Others stated
that if they did get to participate in these events, they had
to check in with their parents repeatedly. One of the 13-
to 14-year-old females gave this example: “When I get
invited to a friend’s house, my mom tells me to call her
every time that I eat and every time that I give myself a
shot.” However, when questioned further, the same teen
acknowledged that she would probably rather have to
call than not call, because “if you fainted at your friend’s
house and she didn’t know what to do then you would
probably die.”
Some of the participants noted that one parent was
more knowledgeable about diabetes and how it affected
them specifically than the other parent was and that this
could be a source of conflict. One of the female partici-
pants in the 17- to 18-year-old group described it in this
manner:
My dad is constantly telling me that I am not doing
what I am supposed to be doing and that I am doing
things wrong. He just doesn’t understand my case.
When you first go to the hospital they teach you how
to handle it for you. My dad wasn’t there so he just
doesn’t know what I am supposed to do for my case.
When I exercise I go low, and with most other people
that is the opposite. It takes 4 hours to actually catch up
with me. I am a very weird diabetic. My dad doesn’t
understand that so it gets frustrating.
Many of the participants, especially in the 17- to 18-
year-old group, wanted their parents to begin to give up
some of their control: “I would say, back off a little. They
always say that I am going to have to take care of myself
when I get older. I know that I can.” Those who felt their
parents tried to be in control stated that they “always tell
you what you can and cannot eat” or “how much insulin
to take and not to take.” One of the males in the 13- to
14-year-old group stated, “I want to be responsible and I
want to handle it on my own. My mom is always asking
me and checking my meter. It makes me feel like she
does not trust me.”
One issue of concern was the number of participants
who noted that to avoid parental conflicts, they some-
times chose not to test if they thought they were high or
low because of the expected negative parental reaction.
Parental support. Some of the participants acknowl-
edged that their parents have been incredibly supportive
of them as they have dealt with their diabetes. One of the
teens in the 13- to 14-year-old group acknowledged, “I
have found that they are usually right when they are con-
cerned.” There was some agreement that parents think
the diabetes is harder on their children than how the
teens perceive it themselves. One teen stated, “I think
that it bothers them more than it bothers me that I have
it. They are very supportive.” One of the male partici-
pants in the 17- to 18-year-old group described his rela-
tionship with his parents this way:
They are not bad at all. They have always been behind
me and very supportive. They don’t bug me about food
and that stuff but they will bug me about testing. All
they really do is ask, though, they don’t nag. They just
want to make sure that I am doing what I am supposed
to do.
Participants acknowledged that parents ensured that
they had all the supplies that they needed, scheduled
physician’s appointments, and placed calls to the physi-
cian’s office if there were any problems. One of the
females in the 13- to 14-year-old group offered, “My
Role of Significant Others in Adolescent Diabetes
247
Carroll and Marrero

The Diabetes EDUCATOR
248
Volume 32, Number 2, March/April 2006
parents try to answer questions that people ask the best
way they can so that I don’t have to.” One of the males
in the 15- to 16-year-old group described his relationship
with his mother in a positive manner: “My mom is will-
ing to do anything and everything that she can. She goes
with me every time to the doctor.”
Letting go of control. Participants talked about their
belief that their parents did not always acknowledge how
much they knew about their own disease. It seemed
important, especially as the teens aged, for parents to
relinquish some control and begin to trust their children
to control their own condition. One of the males in the
15- to 16-year-old group described a positive experience
of his mother letting go of control in this way:
My mom has gotten a lot better. I think that she is wor-
rying less because she has realized that I can take care
of myself. She started putting more responsibility on
me. Things like what I ate and when I tested.
Teens believed that it was important for them to feel
that their parents trusted their diabetic management.
They acknowledged that it was scary for parents to let go
of control and suggested keeping lines of communica-
tion open so that management could be discussed in a
way that was not punitive or “blaming.” One of the
females in the 15- to 16-year-old group described how
her parents have supported her by letting go of control:
They don’t know what insulin that I get or when I test
since I have gotten the pump. I do everything. I want to
have that control because I will be going to college. I
don’t want to have to be dependent on anybody else. It
wasn’t like they had to stay out of it, but it started out
with them doing everything. As soon as I had the free-
dom to do it myself I realized that I could do it. I need
their help sometimes but I want to be able to do it
myself.
Several of the participants acknowledged that they
felt their parents and other family members did not
understand as much about diabetes as they thought they
did. This can lead to misunderstandings and even fear
about honestly reporting blood glucose levels. One par-
ticipant in the 15- to 16-year-old group stated,
Everyone makes mistakes and sometimes parents pun-
ish them. If they don’t think that I was taking care of
my diabetes they will ground me. Parents need to real-
ize that we are going to make mistakes. I think that at
our age we want more responsibility. The fact that we
are 16 and driving shows that we are old enough to
have responsibility when it comes to our diabetes. We
need to know this stuff so that we can move out some
day.
Another of the males in that same group shared a similar
experience:
It seems that my mom is overbearing sometimes.
Sometimes I feel like she doesn’t want me to take con-
trol because I might screw something up. She doesn’t
let me make any decisions about my diabetes. If she
would let me deal with it now I wouldn’t have to be
thrown into it when I go to college.
Peer Relationships
The focus group facilitator queried participants
regarding their relationship with their peers, as it related
to their diabetes. Three subthemes emerged from the
data: peer support, peer intrusive behaviors, and peer
lack of understanding.
Peer support. In general, friends were positively per-
ceived in terms of support with diabetic management.
Participants spoke about how friends were aware of their
condition and were helpful if they were ever in trouble.
Many of the participants stated that their friends are sup-
portive of them testing. Some commented that their
friends “always want to try it [testing]” or “think it is cool
when I take shots in the middle of class.” One of the
females in the 17- to 18-year-old group gave this example:
I am really grateful for my friends because I was a
cheerleader and I played basketball and all of these
sports. They were always there when I was low. If I
couldn’t walk or something then they would help me
and give me juice or whatever I need.
Participants stated that it is easier for them to tell their
friends about diabetes than to hide it. They can become
a safety mechanism for the teens, “They know when my
sugar is getting low and they get me something to eat
when I need it.”
Peer intrusive behaviors. Most of the comments
regarding intrusive behaviors were not specific to the
participant’s group of friends but to others in their school
or that they encountered in their daily lives. One female
participant in the 13- to 14-year-old group did state,
however, “My best friend acts like my mom. It gets on

my nerves.” The intrusiveness is generally related to
questioning. For example, one of the females in the 13-
to 14-year-old group shared this scenario: “It’s like at the
pool, when you have your side pump on and people ask
questions about it. Then you have to give a whole expla-
nation. It’s kind of annoying.” Other teens mentioned
that peers will repeatedly ask them if they are all right,
which can become annoying. Another teenage girl in the
13- to 14-year-old group discussed her irritation at her
diabetic management regimen being questioned by peers
who do not know much about the disease:
The only thing that really annoys me is when people
ask if I can have something to eat, because of my dia-
betes. They need to realize that I wouldn’t be eating it
if I couldn’t have it. It is annoying when people ask me
if it hurts to test. I don’t mind if they ask questions
about what I’m doing. I think curiosity is a good thing,
but when people ask you hundreds of times if some-
thing hurts, it gets tiresome.
Peer lack of understanding. Some of the participants
acknowledge that it is difficult for other teens to under-
stand their condition. “Sometimes when I have to leave
the same class before lunch kids say that I am only doing
it to skip class,” stated one of the 13- to 14-year-old
females. Others say that the diabetic teens are lucky if
they get to leave class early to test or because of a blood
glucose level fluctuation. One of the downfalls that the
teens acknowledged was that there are many individuals
who know very little about diabetes. The fact that others
may not know about the condition placed teens in a situ-
ation of feeling that they need to be more careful about
their own condition because others may not be able to
help them if something should go wrong. One of the
females in the 13- to 14-year-old age group stated,
“When I am away from home I get more nervous about
it and I test it more just to make sure it is fine.”
Physician Relationships
The focus group facilitator queried participants
regarding their relationship with their physicians, as it
related to their diabetes. Two subthemes emerged from
the data: physician demeanor and physician access/
communication.
Physician demeanor. It is clear that the “bedside
manner” or personal demeanor of the physician is a key
factor for these adolescents. A great deal of the conver-
sation regarding physicians centered on interpersonal
relationships the teens experienced with their provider. It
is very important to a participant that he or she be seen
as an individual first, then as someone who has a disease.
One of the teens in the 17- to 18-year-old group
explained it this way:
I like my doctor a lot. I am still with my pediatrician.
He is on a personal level with me. He asks about my
grades and other things in my life. It is nice to know he
actually cares about me. We have to see him so often
that it is important.
Other participants indicated that they were happier with
their physicians when they were able to talk to them
about nondiabetic situations and when they supported
them in living life in a way that worked for the teens
rather than merely “feeding you information.”
A concern that was voiced involved physicians and
staff members leaving the room to discuss a case and
then returning with the answer:
She and her staff always go out then come in and tell
me things and then go out and talk and then come in
and tell me more stuff. I just want them to talk about
stuff in front of me.
Others agreed that some physicians and medical students
treated them as a disease rather than as a person.
Comments included, “They look at you like you are the
disease,” “It’s not comforting,” and “They look at me in
a really crude way.”
Some of the suggestions made to physicians included,
“Look at each age group that you are dealing with. I am
18 so I should be treated like I’m 18 and not 13,” “Hear
us out and let us figure some things out,” and “Don’t talk
down to your patients—sometimes it feels like they
think I’m incompetent.” Others suggested, “Don’t
threaten your patients—just try to help them get it [their
diabetes] under control.”
Physician access/communication. Time spent with
the physician was important to some of the participants.
Not all of the teens felt that the physician took time to
answer all of their questions, although they might send in
another staff member to do so. One of the participants in
the 17- to 18-year-old group stated,
My doctor is a really good doctor but she only spends
20 minutes and sometimes there are a lot of things that
Role of Significant Others in Adolescent Diabetes
249
Carroll and Marrero

The Diabetes EDUCATOR
250
Volume 32, Number 2, March/April 2006
I would like to tell her. She is gone in 20 minutes and I
waited 2 hours to see her.
There was a clear age difference among the participants
in terms of how they wanted physicians to communicate:
with/to them primarily or with/to their parents. Not sur-
prisingly, those in the older age groups wanted more
communication channeled directly to them. One partici-
pant indicated, “Sometimes I wish that my doctor would
talk to me alone because all my mom does is give me a
lecture.”
Several of the participants indicated that they used e-
mail communication with their physicians; this was
viewed as a positive, even by those participants for
whom this was not available. E-mail communication was
used for things such as advice on changes to be made for
sporting events, questions that they have, and following
up on blood glucose readings.
Participants who felt they had a good relationship
with their physician noted that they were more careful
about their diabetes management before and after their
physician appointments. They stated that the physicians
have told them “everything we need to know,” and so it
is fresh in their minds and they are more careful. They
acknowledge that they “slowly drift” over the next few
months but that they are fairly set in their routines for the
first month after an appointment. These participants stat-
ed they “don’t want her to be disappointed” or “don’t
want my doctor to be mad at me.”
Impact on School
Many of the participants indicated that their diabetes
has had relatively little, if any, impact on their school
life. Others, however, shared some ways in which school
life has been affected. Participants that have trouble with
unstable blood glucose levels state that they miss a fair
amount of classes. One of the females in the 17- to 18-
year-old group shared the following:
I tend to have problems in the morning. So people
always ask me why I haven’t lost credit in that class. I
get exempted for things when I miss class and it is dia-
betes related. I hate that people think I am using it for
an excuse. I would rather be at school than be behind.
One of the females in the 13- to 14-year-old group
shared, “I have made friends with the school nurse. I hate
getting low, missing class, and having to catch up.”
Some of the students, however, resented the school nurs-
es, feeling that they “don’t trust me . . . they watch me do
everything and second-guess me all of the time.” Others
indicated that the nurses do not allow them to return to
classes until their blood glucose is stabilized, which
means that they miss a lot of classes and have more work
to make up.
A few of the participants found it difficult to deal with
their diabetes at school. It is uncomfortable to have their
blood glucose levels drop and have to leave class to get
to the school nurse’s office. Others indicated that there
are some problems with some of their teachers. They
may become angry or yell at students who need to leave
the classroom because of their blood glucose levels. For
example, one student shared,
The teachers accept what is going on, except for the
teacher I have right before lunch. I have to leave a lot
because that is when I get the lowest and he gets really
ticked at me.
Another participant in the 15- to 16-year-old group com-
mented on the lack of understanding:
I get annoyed when my teacher won’t let me go to the
bathroom when I want to because when my numbers
are high I have to go to the bathroom. Before I was
diagnosed I would drink a lot—which is a symptom—
and they wouldn’t let me go to the bathroom.
Some participants noted that they find it difficult to go to
gym class because they do not know how to eat prior to
class. One participant in the 13- to 14-year-old group
stated, “It affects my gym class because my teacher
hounds me. He asks me if I am okay and if I need to go
to the nurse after running a mile.”
Participants admitted to using their diabetes as an
excuse at times to get out of class. One of the 13- to 14-
year-olds admitted,
Sometimes I leave class 10 minutes before the end
because it is almost lunch and I can feel my blood
sugar getting too low, but I know I could wait. I have a
pass in my assignment book that says I can get a drink
or use the bathroom whenever I want. Sometimes when
there is nothing to do I get a pass to the bathroom and
walk really slowly.
Discussion
This qualitative focus group study provides insight
into adolescents living with type 1 diabetes, specifically

as it relates to relationships with parents, peers, physi-
cians, and school experiences. From the discussions that
occurred within the 5 focus groups, the following themes
were identified: personal perceptions of living with dia-
betes (which included living with diabetes, testing and
injections, and blood sugar fluctuations), impact on rela-
tionships (which included relationships with parents,
friends/peers, and physician), and impact on school.
The adolescents in this study were truly not much dif-
ferent from other children unaffected by chronic illness.
If one were to substitute the word homework for diabetes
in many of their statements, the feelings of frustration
and rebellion would not be altered radically. The critical
difference is that their struggle for independence has
more severe, and sometimes immediate, consequences.
They want to rebel but often know that they cannot. This
frustration is complicated by a hypervigilance on the part
of their parents to retain control—attention that the ado-
lescents often simultaneously appreciate and reject.
Diabetes in adolescence is fraught with equal and
opposite demands. One consequence of this internal
push/pull is that adolescents become more afraid to do
appropriate developmental activities. This can have a
significant impact on their normal progression to inde-
pendence and adulthood, ironically at odds with the
increased responsibility they have had to assume
throughout their lives to care for their disease. Their rela-
tionships with their peers are just as conflicted by their
diabetes as those with their parents. Many of their
friends and their families shy away from the potential
responsibilities of a relationship with a diabetic child;
others try and step into the role of caregiver, whether it
is welcome or not. Schools can fail to recognize that
some of these adolescents need to be given more of an
ability to care and make decisions for themselves while
simultaneously abdicating their responsibility to provide
a safe environment for these children. These conflicts,
and the adolescent’s inability to control many of the fac-
tors that influence his or her life, can lead to a feeling of
learned helplessness instead of one of emerging confi-
dence in their independence.
There are several limitations to this study. Some
include the focus group methodology itself: small con-
venience samples limit the generalizability of the find-
ings, group consensus may inhibit an individual from
stating his or her differing opinion, and introverted indi-
viduals may be more apt to keep silent about their opin-
ions. This particular study does not address perceptions
of the parents, peers, or physicians about the relation-
ships with the diabetic adolescents. However, a second
article does examine the perceptions of parents raising
adolescents with diabetes (in process). This is necessary
to provide corroboration with the adolescents’ percep-
tion of the parent-teen relationship.
The breadth and depth of the information gleaned
from these discussions has implications for those who
work with adolescents living with diabetes. These find-
ings reveal areas in which researchers could improve the
lives of teenagers with diabetes coping with their emerg-
ing independence into adulthood. Clinicians need to help
adolescents assume responsibility, perhaps as negotiators
between them and the other powers in their lives.
Clinicians may need to be more active participants in
refining the relationships teenagers have with their par-
ents and schools in the care of their diabetes. More time
needs to be spent on how to care for their diabetes than
on a focus of outcomes. Much of the clinical time and
research still focuses on the devices of diabetes care:
testing and treatment. While these are important tools in
improving the outcomes of people with diabetes, they
will have little impact on the adolescent until the devel-
opmental consequences of diabetes on their lives are
simultaneously addressed. These findings illustrate that
providers should consider the important role that parent-
child relationships play in how diabetes therapy is
accepted and acted on. They suggest that providers may
want to discuss relationship issues and determine
whether some compromises should be discussed to
improve therapeutic status. Important improvements and
an increased awareness of these factors have been
accomplished in the past 20 years; much more needs to
be done.
References
1. Curtis JA, Hagerty D. Managing diabetes in childhood and ado-
lescence. Can Fam Physician. 2002;48:499-502, 505-499.
2. Anderson BJ, Wolpert HA. A developmental perspective on the
challenges of diabetes education and care during the young adult
period. Patient Educ Couns. 2004;53:347-352.
3. Anderson BJ. Children with diabetes mellitus and family func-
tioning: translating research into practice. J Pediatr Endocrinol
Metab. 2001;14(suppl 1):645-652.
4. Gowers SG, Jones JC, Kiana S, North CD, Price DA. Family
functioning: a correlate of diabetic control? J Child Psychol
Psychiatry. 1995;36:993-1001.
Role of Significant Others in Adolescent Diabetes
251
Carroll and Marrero

The Diabetes EDUCATOR
252
Volume 32, Number 2, March/April 2006
5. Daneman D, Wolfson DH, Becker DJ, Drash AL. Factors affect-
ing glycosylated hemoglobin values in children with insulin-
dependent diabetes. J Pediatr. 1981;99:847-853.
6. Anderson BJ, Brackett J, Ho J, Laffel LM. An office-based inter-
vention to maintain parent-adolescent teamwork in diabetes man-
agement: impact on parent involvement, family conflict, and
subsequent glycemic control. Diabetes Care. 1999;22:713-721.
7. Kaufman FR, Halvorson M, Carpenter S. Association between
diabetes control and visits to a multidisciplinary pediatric dia-
betes clinic. Pediatrics. 1999;103(5 pt 1):948-951.
8. Anderson B, Ho J, Brackett J, Finkelstein D, Laffel L. Parental
involvement in diabetes management tasks: relationships to
blood glucose monitoring adherence and metabolic control in
young adolescents with insulin-dependent diabetes mellitus. J
Pediatr. 1997;130:257-265.
9. Koski ML. The coping processes in childhood diabetes. Acta
Paediatr Scand Suppl. 1969;198(suppl 198):1+.
10. Miller-Johnson S, Emery RE, Marvin RS, Clarke W, Lovinger R,
Martin M. Parent-child relationships and the management of
insulin-dependent diabetes mellitus. J Consult Clin Psychol.
1994;62:603-610.
11. Coyne JC, Anderson BJ. The “psychosomatic family” reconsid-
ered: diabetes in context. J Marital Fam Ther. 1988;14:113-123.
12. Minuchin S, Rosman BL, Baker L. Psychosomatic Families:
Anorexia Nervosa in Context. Cambridge, Mass: Harvard
University Press; 1978.
13. Frey MA, Guthrie B, Loveland-Cherry C, Park PS, Foster CM.
Risky behavior and risk in adolescents with IDDM. J Adolesc
Health. 1997;20:38-45.
14. Ludvigsson J. Socio-psychological factors and metabolic control
in juvenile diabetes. Acta Paediatr Scand. 1977;66:431-437.
15. Marrero DG, Golden MP, Kershnar A, Myers GC. Family dynam-
ics in adolescent diabetes mellitus: Parental behavior and meta-
bolic control. Psychological aspects of diabetes in children and
adolescents. In: Kaplan SA, ed. Clinical Pediatric and Adolescent
Endocrinology. Philadelphia, Pa: Saunders; 1982:ix, 392.
16. Morse JM, Field P-A, Field P-A. Qualitative Research Methods
for Health Professionals. 2nd ed. Thousand Oaks, Calif: Sage
Publications; 1995.