The Koori Growing Old Well Study: investigating aging and dementia in urban Aboriginal Australians
11
International Psychogeriatrics: page 1 of 11 C International Psychogeriatric Association 2014 doi:10.1017/S1041610213002561 PROTOCOL-ONLY PAPER The Koori Growing Old Well Study: investigating aging and dementia in urban Aboriginal Australians ........................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................... Kylie Radford, 1,2,3 Holly A. Mack, 1 Hamish Robertson, 2 Brian Draper, 1,2,4 Simon Chalkley, 1,2,5 Gail Daylight, 6 Robert Cumming, 1,7 Hayley Bennett, 1 Lisa Jackson Pulver 1,8 and Gerald A. Broe 1,2,5 1 Neuroscience Research Australia, Sydney, Australia 2 Prince of Wales Hospital, Randwick, Sydney, Australia 3 School of Medical Sciences, University of New South Wales, Sydney, Australia 4 School of Psychiatry, University of New South Wales, Sydney, Australia 5 Geriatric Medicine, University of New South Wales, Sydney, Australia 6 South Eastern Sydney Local Health District, Sydney, Australia 7 School of Public Health, University of Sydney, Sydney, Australia 8 Muru Marri Indigenous Health Unit, University of New South Wales, Sydney, Australia ABSTRACT Background: Dementia is an emerging health priority in Australian Aboriginal communities, but substantial gaps remain in our understanding of this issue, particularly for the large urban section of the population. In remote Aboriginal communities, high prevalence rates of dementia at relatively young ages have been reported. The current study is investigating aging, cognitive decline, and dementia in older urban/regional Aboriginal Australians. Methods: We partnered with five Aboriginal communities across the eastern Australian state of New South Wales, to undertake a census of all Aboriginal men and women aged 60 years and over residing in these communities. This was followed by a survey of the health, well-being, and life history of all consenting participants. Participants were also screened using three cognitive instruments. Those scoring below designated cut-offs, and a 20% random sample of those scoring above (i.e. “normal” range), completed a contact person interview (with a nominated family member) and medical assessment (blind to initial screening results), which formed the basis of “gold standard” clinical consensus determinations of cognitive impairment and dementia. Conclusion: This paper details our protocol for a population-based study in collaboration with local Aboriginal community organizations. The study will provide the first available prevalence rates for dementia and cognitive impairment in a representative sample of urban Aboriginal people, across city and rural communities, where the majority of Aboriginal Australians live. It will also contribute to improved assessment of dementia and cognitive impairment and to the understanding of social determinants of successful aging, of international significance. Key words: Aboriginal health, Indigenous health, dementia, cognitive impairment, aging Introduction Around the world, the number of dementia cases is rising rapidly with population aging. However, some variability in the prevalence of dementia has been found across national, geographic, and cultural groups. The research of the 10/66 Group has found dementia prevalence rates vary from 4.8% (rural Correspondence should be addressed to: Dr Kylie Radford, Neuroscience Research Australia, PO Box 1165, Randwick, NSW 2031, Australia. Phone: +02-9399- 1269; Fax: +02-9399-1082. Email: [email protected]. Received 3 Apr 2013; revision requested 26 May 2013; revised version received 2 Jul 2013; accepted 10 Dec 2013. China) to 12.6% (Cuba), using a well-validated and consistent methodology across populations (Llibre Rodriguez et al., 2008). Dementia prevalence in the Indigenous Cree population in Canada was found to be 4.2%, with rates of Alzheimer’s dementia particularly low (0.5%; Hendrie et al., 1993). The nature and extent of dementia and other cognitive disorders are largely unknown in urban Australian Aboriginal communities, as are the experience and meaning of dementia for Aboriginal people, the risk factors for cognitive decline, and the need for and provision of appropriate dementia services (Arkles et al., 2010).
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of The Koori Growing Old Well Study: investigating aging and dementia in urban Aboriginal Australians

International Psychogeriatrics: page 1 of 11 C© International Psychogeriatric Association 2014doi:10.1017/S1041610213002561
P R O T O C O L- O N LY PA P E R
The Koori Growing Old Well Study: investigating aging anddementia in urban Aboriginal Australians
...........................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................................
Kylie Radford,1,2,3 Holly A. Mack,1 Hamish Robertson,2 Brian Draper,1,2,4
Simon Chalkley,1,2,5 Gail Daylight,6 Robert Cumming,1,7 Hayley Bennett,1
Lisa Jackson Pulver1,8 and Gerald A. Broe1,2,5
1Neuroscience Research Australia, Sydney, Australia2Prince of Wales Hospital, Randwick, Sydney, Australia3School of Medical Sciences, University of New South Wales, Sydney, Australia4School of Psychiatry, University of New South Wales, Sydney, Australia5Geriatric Medicine, University of New South Wales, Sydney, Australia6South Eastern Sydney Local Health District, Sydney, Australia7School of Public Health, University of Sydney, Sydney, Australia8Muru Marri Indigenous Health Unit, University of New South Wales, Sydney, Australia
ABSTRACT
Background: Dementia is an emerging health priority in Australian Aboriginal communities, but substantialgaps remain in our understanding of this issue, particularly for the large urban section of the population. Inremote Aboriginal communities, high prevalence rates of dementia at relatively young ages have been reported.The current study is investigating aging, cognitive decline, and dementia in older urban/regional AboriginalAustralians.
Methods: We partnered with five Aboriginal communities across the eastern Australian state of NewSouth Wales, to undertake a census of all Aboriginal men and women aged 60 years and over residingin these communities. This was followed by a survey of the health, well-being, and life history of allconsenting participants. Participants were also screened using three cognitive instruments. Those scoringbelow designated cut-offs, and a 20% random sample of those scoring above (i.e. “normal” range), completeda contact person interview (with a nominated family member) and medical assessment (blind to initialscreening results), which formed the basis of “gold standard” clinical consensus determinations of cognitiveimpairment and dementia.
Conclusion: This paper details our protocol for a population-based study in collaboration with local Aboriginalcommunity organizations. The study will provide the first available prevalence rates for dementia and cognitiveimpairment in a representative sample of urban Aboriginal people, across city and rural communities, wherethe majority of Aboriginal Australians live. It will also contribute to improved assessment of dementia andcognitive impairment and to the understanding of social determinants of successful aging, of internationalsignificance.
Key words: Aboriginal health, Indigenous health, dementia, cognitive impairment, aging
Introduction
Around the world, the number of dementia casesis rising rapidly with population aging. However,some variability in the prevalence of dementia hasbeen found across national, geographic, and culturalgroups. The research of the 10/66 Group has founddementia prevalence rates vary from 4.8% (rural
Correspondence should be addressed to: Dr Kylie Radford, Neuroscience ResearchAustralia, PO Box 1165, Randwick, NSW 2031, Australia. Phone: +02-9399-1269; Fax: +02-9399-1082. Email: [email protected]. Received 3 Apr2013; revision requested 26 May 2013; revised version received 2 Jul 2013;accepted 10 Dec 2013.
China) to 12.6% (Cuba), using a well-validated andconsistent methodology across populations (LlibreRodriguez et al., 2008). Dementia prevalence in theIndigenous Cree population in Canada was foundto be 4.2%, with rates of Alzheimer’s dementiaparticularly low (0.5%; Hendrie et al., 1993). Thenature and extent of dementia and other cognitivedisorders are largely unknown in urban AustralianAboriginal communities, as are the experience andmeaning of dementia for Aboriginal people, the riskfactors for cognitive decline, and the need for andprovision of appropriate dementia services (Arkleset al., 2010).

2 K. Radford et al.
Aboriginal Australians have the poorest healthand greatest disadvantage in mortality rates ofall other Indigenous populations in comparablewealthy nations (Hill et al., 2007). Yet, despite this,the number of older Aboriginal and Torres StraitIslander people is increasing rapidly; Aboriginal“survivors” do reach old age in both urbanand remote communities; and at 75 years andover (when dementia risk is rising) Aboriginaland Torres Strait Islander people have a lifeexpectancy close to that of non-IndigenousAustralians (Australian Bureau of Statistics, 2010).Moreover, there is evidence to suggest that thepattern of excess morbidity and mortality in early–mid life is finally improving (Thomas et al.,2006; Australian Bureau of Statistics, 2010),which will result in a longer adult lifespan andpopulation aging in coming decades. This is ahealth transition that took place in the non-Indigenous community some 50 years previously(Broe, 2003). In the Aboriginal population thereis a pressing need to: (i) determine dementiaprevalence, (ii) improve dementia services, and(iii) work towards population-based objectives fordementia prevention and healthy aging, in the sameway as current research addresses these issues inother populations.
In remote Aboriginal communities, two studieshave shown high prevalence rates of dementia(Zann, 1994; Smith et al., 2008). One studyin the remote Kimberley region of WesternAustralia (Smith et al., 2008), used a validatedinstrument for remote Aboriginal communities –the Kimberley Indigenous Cognitive Assessment(KICA; LoGiudice et al., 2006). The KICA wasspecifically developed to work with Aboriginalpeople whose first language is not English, whoseliteracy rates are low, and whose lifestyles arenot comparable to urbanized populations. Thisstudy found a dementia prevalence of 12.4% inthe Aboriginal population aged 45 years and older(23.8% at 60 years and above; Smith et al.,2008), five times higher than the comparable overallAustralian dementia rate. Potential dementia riskfactors (associations) identified in the Kimberleystudy included lack of formal education, headinjury, stroke, epilepsy, and current smoking;dementia was also more common in men(Smith et al., 2010). Another study, in farnorth Queensland, using a non-validated modifiedinstrument, found a dementia prevalence rate ofapproximately 20% in Aboriginal and Torres StraitIslander peoples over the age of 65 years (Zann,1994).
The large majority of Aboriginal people,however, live in non-remote areas (i.e. major cities,regional cities/towns, and near rural locales, herein
referred to as “urban”), and the largest proportionin New South Wales (NSW), where 43% reside inmajor cities, 52% in regional areas, and only 5%in remote settings (Australian Bureau of Statistics,2010). This urban majority are primarily Englishspeaking and literate, but have also been exposed tomultiple social and biomedical risk factors across thelife course (Arkles et al., 2010), many of which mightcontribute to early cognitive decline and dementia.
Both urban and remote Aboriginal populationshave a disproportionate burden of mid-latelife disease, notably diabetes and cardiovasculardisease, compared to non-Indigenous Australians,attributable to higher rates of smoking, obesity,and physical inactivity (Vos et al., 2009). Thisparallels with recent research highlighting thatup to half the cases of Alzheimer’s dementiaworldwide could be attributed to modifiable factors(e.g. smoking, physical inactivity; Barnes andYaffe, 2011) and may go part way to explainingthe higher rates of dementia seen in remoteAboriginal Australians. However, it is increasinglyacknowledged that childhood environmental factorsare also associated with dementia onset (e.g.education, socioeconomic status, abuse, and otheradverse experiences; Moceri et al., 2001; Ansteyand Sargent-Cox, 2009). Older urban Aboriginalpopulations may have experienced a greaterstandard of living in terms of housing andaccess to education and health services whencompared to remote populations, though stillwell below that of mainstream Australia. Thisurban population has also commonly experienceddiscrimination (e.g. inequitable education andhealthcare, segregation of public space) anddispossession of traditional culture (i.e. throughforced settlement on reserves/missions, suppressionof traditional language and cultural practices,removal of children from families, and othergovernment assimilation policies), particularly intheir early years (Arkles et al., 2010). While remotepopulations have been affected by these thingstoo, the relative isolation from non-Indigenouscommunities and historically more recent exposureto white culture have contributed to greaterendurance of ancient languages and culturalpractices in remote communities. This connectionto traditional ways of life has been shown to bebeneficial to health (Burgess et al., 2009), andmay also protect against dementia. Thus, urbanAboriginal populations will likely have similarly highrates of dementia as seen in remote populations,but the pattern of associated risk factors, includingthe relative contribution of early social and mid-latelife biomedical factors, may differ. Moreover, giventhe hitherto limited awareness of dementia in theseAboriginal communities (Garvey et al., 2011), as

Dementia in urban Aboriginal Australians 3
well as in clinicians/service providers (Pollitt, 1997),we predict that access to dementia care services andsupports will be reduced, placing a greater strain onfamily caregivers.
The current study addresses the pressing needto investigate aging, cognition, and dementia inurban Australian Aboriginal communities. Here,we describe the study protocol, with relevantbackground information and an overview of thedevelopment of the methodology of the study.
ObjectivesThe Koori Growing Old Well Study (KGOWS)primarily aims to: (i) determine, in urban Aboriginalpopulations aged 60 years and over, the prevalenceof dementia and cognitive impairment; (ii) assessthe relative performance of a number of standardas well as adapted cognitive screening instrumentsfor the assessment of dementia and cognitiveimpairment in this population; and (iii) examineassociated factors for dementia and cognitiveimpairment in this population. In addition, thisresearch will examine the use of formal dementiaservices and community services by Aboriginalpeople with dementia; describe the burden ofdementia in their caregivers; and build capacity indementia assessment and care, risk factor detectionand prevention.
We will test the following hypotheses: (i) Theoverall prevalence of dementia in urban Aboriginalpeople aged 60 years and over is higher thanthat found in prevalence studies in non-Indigenouspeople in this age group and is similar to thatfound in studies in remote Aboriginal communities(Zann, 1994; Smith et al., 2008;). (ii) Thecommon types of dementia in the urban Aboriginalpopulation are those found in non-Indigenouspopulations; however, the proportion of dementiasub-types will differ in Aboriginal and TorresStrait Islander people, reflecting the younger ageof onset of dementia and their additional riskfactor exposures (i.e. less Alzheimer’s dementia, arelative preponderance of vascular dementia, andmore secondary dementias). (iii) The prevalenceof cognitive impairment will be higher than inthe general Australian population, in parallel todementia prevalence. (iv) Cognitive screening fordementia in the urban Aboriginal populationwill be made by standard as well as culturallyappropriate instruments. (v) Dementia diagnosiswill be associated with early-life adverse events andestablished midlife dementia risk factors. (vi) Wealso predict that the use of formal dementia servicesand community services by Aboriginal people withdementia and their caregivers will be low, and thecaregiver burden will be high.
Table 1. Aboriginal and Torres Strait Islanderpopulation by KGOWS site based on AustralianBureau of Statistics (ABS) census data of 2006 and2011
ABORIGINALAND T ORRES
S T R A I TISLANDER
POPULATIONA G E D 60+
TOTALABORIGINALAND T ORRES
S T R A I TISLANDER
POPULATION
KGOWS SITES 2006 2011 2006 2011........................................................................................................................................................
Kempsey 143 206 2,540 3,115Coffs Harbour 111 148 2,310 2,817Nambucca 57 112 1,025 1,358La Perouse
(Randwick andBotany Bay)
184 240 2,107 2,456
Campbelltown 114 218 3,833 4,729Total 609 924 11,815 14,475
A further objective is to establish partnershipswith local Aboriginal Community ControlledHealth Organizations (ACCHOs) and to recruitAboriginal Research Assistants (ARAs) and othercommunity members into the study team toraise awareness and build capacity in dementiaassessment, risk factor prevention, and need fordementia services.
Methods
We partnered with five Aboriginal communitiesacross NSW as collaborating study sites. Study siteswere geographically defined by Local GovernmentAreas (LGAs) in conjunction with self-defined localAboriginal communities. The selected LGAs hadsignificant numbers of urban Aboriginal peopleaged 60 years and over (Australian Bureau ofStatistics (ABS) data; see Table 1). There weretwo sites in metropolitan Sydney (La Perouse[Randwick/Botany Bay LGAs], Campbelltown)and three in regional/rural coastal areas of NSW(Kempsey, Nambucca, Coffs Harbour). Eachof these had an ACCHO and a mainstreamAboriginal Health Manager, as well as Eldersgroups, Aboriginal Land Council, and othercommunity organizations with which our researchteam established a working relationship in healthservice delivery and/or research.
EthicsThe study received ethical approval from theAboriginal Health and Medical Research Council(AHMRC; 615/07), The University of New

4 K. Radford et al.
South Wales Human Research Ethics Committee(HREC 08003), and NSW Population & HealthServices Research Ethics Committee (AU RED Ref:HREC/09/CIPHS/65; Cancer Institute NSW Ref:2009/10/187).
Community engagement and study oversightThis study originated from our involvement withservice delivery to the La Perouse Aboriginalcommunity. Community consultations suggesteda need for aged care and dementia services fora growing older population and a major need forchild services and health promotion. Aboriginalresearchers with backgrounds and experience inAboriginal health, including the study leadership,associate investigators, and ARAs were involvedfrom the outset. ARAs were local Aboriginalpeople employed to support census and recruitmentactivities, and as part of our aims to build capacityin research and dementia knowledge/services. ARAswere an invaluable asset to the study, and we hadmost success with recruiting ARAs who were same-age “peers” as the study participants. Communityconsultation, consent, and partnerships (with localACCHOs) were established within each study siteprior to the recruitment of participants to thisstudy. A local community guidance group wasalso formed at each site, consisting of three to sixlocal Elders. These local guidance groups supportedand advised the study team on fieldwork matterssuch as approach to recruitment, nominationof ARA candidates, cultural appropriateness,and understanding local community networks. Adesignated leader of each local guidance group wasalso a member of the study’s Aboriginal ReferenceGroup (ARG). The ARG included communityElders and prominent Aboriginal people frommedicine, academia, and public policy, who wereotherwise independent of KGOWS. The ARGprovided advice and guidance to the research team,supported and monitored its capacity building indementia assessment and care for the Aboriginalworkers and communities.
Census and recruitmentAn important issue in this study was how tocarry out scientifically acceptable research wherestandard recruitment methods (e.g. random digitdialing, census district door knock techniques,electoral rolls, etc.) were not appropriate. InNSW, Aboriginal and Torres Strait Islander peoplecomprise 2.5% of the overall population, and thisproportion is particularly low in major cities. TheAboriginal and Torres Strait Islander populationis interspersed within the wider community andthus not as accessible as in remote regions,
where the Aboriginal and Torres Strait Islanderpopulation is proportionally much higher (i.e. 30–90%; Australian Bureau of Statistics, 2010).
For each study site we generated a samplingframe based on three strategies. (i) Where available,currently existing lists identifying Aboriginal andTorres Strait Islander people aged 60 and over weresought in the development of the sampling frame;the most comprehensive of these was identifiedin collaboration with our ACCHO partners, ARGand local health service. (ii) The second strategyentailed augmenting any currently available lists bya snowball sampling technique to capture thoseindividuals who were not represented on existinglists. This technique is appropriate in populationswith incomplete and/or unavailable identification,and where people are likely to know each other(Kalton and Anderson, 1986). Snowball samplingwas conducted in parallel with study recruitmentand with the assistance of local ARAs, communityhealth workers, and other community members.(iii) Third, we compared these augmented datawith known data from the ABS Census, 2006,for evidence of comprehensiveness. In keepingwith national Australian ethical guidelines, thefinal study list belonged to the local Aboriginalcommunity and was allowed to be used by us forthe purposes of this study only.
The study census process was initiated at thefirst site in September 2008, progressively rolled-out across all sites, and continued alongsidestudy recruitment. Formal study recruitment beganin early 2010, following community engagementand pilot work throughout 2008–09 (outlinedbelow).
Our approach to recruitment was gentle,culturally appropriate, and multifaceted. A directapproach from non-Aboriginal researchers wasgenerally avoided. Our researchers investedconsiderable time in maintaining a “presence”in communities, participating in key communityactivities (as appropriate), and generally givingtime to build trust and rapport, and allow forthe many obstacles to participation that couldarise even for those very willing to take part.We connected with community members throughARAs, local community guidance groups, localservices, media outlets, and periodic mail-outs usingour study census list. In some cases, the recruitmentprocess, from time of first contact with the potentialparticipant until they were interviewed, took twoyears. Some of the key issues that constrainedor guided our recruitment activities includedtemporary/seasonal relocation and extended periodsaway with family in connected (but geographicallydistant) communities; difficulty contacting somepotential participants via conventional means (e.g.

Dementia in urban Aboriginal Australians 5
phone connections unavailable); and inaccuraterecords of identification for Aboriginal and TorresStrait Islander individuals (e.g. Aboriginality notasked about or not documented correctly, as wellas fears of being identified). Establishing andmaintaining contact via community home visitsby ARAs was important for participation in thestudy.
Sample and inclusion/exclusion criteriaWe aimed to recruit a total of 366 Aboriginal andTorres Strait Islander people 60 years of age andolder – that is, 60% of a target total populationof 609 (ABS Census of 2006, see Table 1).Additionally, if the true dementia prevalence ratein the community were as high as rates found inremote communities in the same age range (i.e.�24%; Smith et al., 2008), this sample size wouldbe adequate to ensure a 95% probability that asample estimate between 19.6% and 28.4% wouldbe obtained.
The study included all participants who wereidentified on the study lists, self-identified asAboriginal and/or Torres Strait Islander (and wererecognized by the community as such; as peraccepted Australian definition), aged 60 years orolder, dwelling in the urban environment for mostof their lives (and at least six months in therelevant LGA at time of study enrolment), willingto participate, and capable of providing writteninformed consent. Verbal assent was obtained fromparticipants assessed as unable to consent butcapable of participating in the study; proxy consentwas also obtained from their closest relative orfriend (“person responsible” as defined by the1987 Guardianship Act in NSW). Individuals wereexcluded from the study if they had a stroke in thepast three months; they presently were incarcerated;their “person responsible” did not want them toparticipate (as applicable); or, in the case of thosewho agreed to participate but were unable toconsent, if they had no “person responsible” toconsent for them. All participants received a giftpack with health information, local service listings,grocery voucher, and bag (valued at AU$15).
For each participant who progressed to StudyPhase 2 (see Procedure, below), we also recruitedone designated family- or community-based“Contact Person” (CP), as nominated by the studyparticipant. CPs could include family members,people residing with the participant, key membersof the community, etc. CPs were people who hadknown our participants and their family-networkswell and, as far as possible, known them overmuch of their lifespan. CPs did not need to beAboriginal.
MeasuresWe used a combination of standard, as wellas adapted, instruments to determine diagnosisof dementia, dementia types, and cognitiveimpairment. We made extensive use of themethodology of the Sydney Older Persons Study(SOPS; Waite et al., 2001), the KICA study (Smithet al., 2008), and the results of our pilot study.We used these previous protocols primarily toinform our study procedure and assessment ofmedical history, daily functioning, and decline, interms of scope and culturally appropriate waysof posing these questions. We also drew onABS surveys for demographic items (includingsocioeconomic status). In contrast to these previousstudies, we included a more comprehensive earlylife history section and several standardized self-report scales. The pilot study involved 30 Aboriginalpeople (aged 41–79 years; 22 women and 8 men)from two of the current KGOWS sites (city andregional). Participants had ten years of formaleducation on average (range: 6–14 years) andall participants spoke English as their preferredlanguage. We sought feedback from participantsand fieldworkers as to the cultural appropriatenessand feasibility of the proposed instruments. Themain pilot feedback themes were that the initialsurvey was too long, sometimes not structured inan appropriate way (i.e. not user friendly or pursuedtoo many personally irrelevant questions), and someof the standardized scales did not “speak to” oradequately capture participants’ experiences (e.g.originally selected racism and resilience scales).The pilot study outcomes were work-shoppedwith Aboriginal and non-Indigenous researchers,and instruments retained, modified or replaced,accordingly. The overall length of the survey wasreduced by 30% (in line with the majority feedback),while current service use was assessed in greaterdetail. Participants were generally willing to provideinformation and respond to questions, includingthose of a sensitive nature (e.g. childhood abuse,separation from family, and discrimination).
COGNITIVE FUNCTION
A key methodological challenge was how toeffectively and appropriately assess cognitiveimpairment in this population (Pollitt, 1997).We reviewed the literature on the design andmodification of cognitive assessment tools for usewith specific cultural and language populations,including those with reduced literacy and/orpoor formal education; as well as standardinstruments used in our own, and other, clinicaland population studies, taking into accountthe high level of basic literacy in our urban

6 K. Radford et al.
Table 2. Summary of Kimberley IndigenousCognitive Assessment (KICA) modifications
I T E M(S)N E W I T E M
(mKICA)O R I G I N A L I T E M
(KICA-COG)........................................................................................................................................................
1 What month is it? Is this week pension week?2 What season is it? What time of year is it
now?4–6 Cup Pannikin8 First point to the
ceiling and thenpoint to the floor
. . . sky . . . ground
9 All animalsaccepted.Prompts not givenduring verbalfluency task
“Animals you can hunt”required. Can promptwith: Any more? Whatabout in the air? In thewater?
Aboriginal population. We included two standard(RUDAS and MMSE) and one adapted (mKICA)cognitive screening tests to evaluate their relativeperformance to detect cognitive impairment against“gold standard” medical diagnosis. The RowlandUniversal Dementia Assessment Scale (RUDAS)is a six-item cognitive screening tool developed inAustralia to detect dementia in culturally diversepopulations, which appears to be culturally fairand not influenced by language, education, orgender (Storey et al., 2004). The RUDAS isscored out of 30 points. The Mini-Mental StateExamination (MMSE; Folstein et al., 1975), a 20-item screening tool that is also scored out of 30, wasincluded for comparison as a common and effectivecognitive screening tool used in clinical practiceand dementia research across many culturesand language groups. The modified KimberleyIndigenous Cognitive Assessment (mKICA) wasadapted from the original KICA cognitive section(LoGiudice et al., 2006; developed for remote non-literate Aboriginal people with English as a secondlanguage). Changes were made in consultation withthe KICA developers, to improve face validity fornon-remote populations. Modifications includedadjustment to the wording and administrationinstructions for some items, but no substantivechanges to task content (see Table 2). The mKICAhas 16 items and is scored from a total of 39 points.
The cultural appropriateness and preliminaryvalidity of these cognitive screening tools wereinvestigated in our pilot study (Radford and Mack,2012). All tests were well tolerated and acceptableto participants, and discriminated between normalfunctioning and cognitive impairment (includingdementia) at the group level. Significantly lowertest scores were found for those classified as havingcognitive impairment (n = 9; RUDAS: M = 24.9,
SD = 4.8; MMSE: M = 24.5, SD = 7.0; mKICA:M = 34.8, SD = 4.9) compared to those without(n = 10; RUDAS: M = 28.2, SD = 1.4; MMSE:M = 28.4, SD = 1.5; mKICA: M = 38.2, SD =1.0). Scores were not significantly correlated witheducation. The proposed study screening cut-offs(RUDAS � 25, MMSE � 26, and/or mKICA �35) selected 33% of participants. Overall, including20% of those scoring above these cut-offs, wecalculated an approximate 50% (n = 183) projectedselection rate for Phase 2 of the main study(see Procedure, below). In the pilot sample, thesescreening criteria successfully detected all dementiacases and 2/4 MCI cases. The two MCI cases notdetected had very high scores (e.g. 29 and 30 onMMSE), thus it would not have been feasible toraise the cut-offs to such a level given the resourcesavailable.
R I S K F A C T O R S
To examine the role of early-life adverse events,education, and established midlife biomedical riskfactors for cognitive impairment and dementia,we developed a comprehensive survey instrumentbased on those from SOPS and KICA, as well as theABS. These were piloted and adapted accordingly.This survey covered socioeconomic risk factorsincluding education, childhood social environment,and employment history; and medical risk factorsincluding hearing loss, alcohol and drug use, headinjury, vascular risk factors, and midlife chronicsystemic diseases (e.g. cardiovascular disease,stroke, diabetes). Our survey instrument alsoincluded standardized measures to assess childhoodtrauma and abuse, racial discrimination, resilienceand coping, mental health, and alcohol use. Furtherdetails on the scales used and their reliability andvalidity, particularly as this relates to AboriginalAustralians, are provided in Table S1, publishedas supplementary material online attached to theelectronic version of this paper at http://journals.cambridge.org/ipg.
O T H E R M E A S U R E S
Functional status (activities of daily living) wasassessed using the Kilsyth Disability Rating Scale(Akhtar et al., 1973). A comprehensive survey ofhealth and social service use was devised, examininga range of health, aged care, and dementiaservices, including mainstream and Aboriginalcommunity controlled services; frequency of use,quality of service, and barriers to services wereassessed. In addition, caregiver burden (in CPs) wasmeasured using the modified Caregiver Strain Index(Thornton and Travis, 2003).

Dementia in urban Aboriginal Australians 7
Census How many Aboriginal
people aged 60 years andover live in the community?
Eligible participants give informed consent
Phase 1: Life span survey and cognitive
screening
Screened positive MMSE ≤ 26 &/or mKICA ≤ 35 &/or
RUDAS ≤ 25
Screened negative MMSE > 26 & mKICA > 35 & RUDAS > 25
Phase 2: Medical assessment and contact
person interview
20% randomly selected Phase 2: Medical
assessment and contact person interview
80% end-study participation
End-study participation and case reviewed by consensus panel for
diagnosis
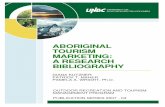
Figure 1. Study flow diagram.
ProcedureFollowing the sharing of key existing communitylists by partner Aboriginal organizations underAHMRC guidelines, the generation of study censuslists proceeded in parallel with study recruitmentand data collection, until all available sources ofinformation were exhausted. Data collection wasconducted in two phases (see Figure 1).
PHASE 1All consenting participants were interviewed bya trained researcher (accompanied by the localARA, as appropriate) using our structured surveyinstrument. Participants were also screened usingthe three cognitive instruments (RUDAS, MMSE,and mKICA).
PHASE 2The second phase was limited to participants whoscored below a predetermined cut-off score onany one of the three cognitive instruments and a20% random sample of those who scored abovethese cut-offs. A positive screening result was
RUDAS � 25, MMSE � 26, and/or mKICA� 35. In Phase 2, a separate CP Interview wascompleted for each participant, to complementthe information on potential risk factors acrossthe lifespan collected during the initial (Phase 1)participant interview. A medical assessment bya geriatrician or physician experienced in agedcare was also conducted, including social andmedical history, neurological examination, briefcognitive assessment, and assessment of functionalstatus. A CP was also consulted as part of themedical assessment. For further details of themedical assessment, see Table S2 published assupplementary material online attached to theelectronic version of this paper at http://journals.cambridge.org/ipg.
OutcomesFinal dementia diagnosis was determined, basedon results of Phase 2 medical assessment, byclinical consensus with a panel of three or moreclinicians, including at least one geriatrician andone clinical neuropsychologist. Clinicians involved

8 K. Radford et al.
in Phase 2 medical assessments and consensusdeterminations were blind to all data collectedin study Phase 1, including the outcome ofcognitive screening. This was the “gold standard”for determining prevalence rates. Dementia wasdiagnosed using National Institute on Agingand Alzheimer’s Association Workgroup “all-causedementia” criteria (McKhann et al., 2011). Specifictypes of dementia were also diagnosed: Alzheimer’sdementia (American Psychiatric Association, 2000;McKhann et al., 2011), vascular dementia (Amer-ican Psychiatric Association, 2000), frontotemporaldementia (Neary et al., 1998), dementia with Lewybodies (McKeith et al., 2005), dementia due toother medical conditions (American PsychiatricAssociation, 2000), dementia due to the persistingeffect of substance abuse (American PsychiatricAssociation, 2000), along with dementia nototherwise specified or “mixed dementia,” asapplicable. Diagnosis of mild cognitive impairment(MCI; Winblad et al., 2004) was made forthose with reported cognitive decline not meetingdementia criteria.
Statistical analysisUsing Phase 2 “gold standards,” the performanceof the three cognitive screening tests will beevaluated using ROC-analyses, logistic regression,and/or discriminant analyses. By inverse-weightingdiagnoses for the 20% who were randomlyselected for Phase 2 (i.e. screened negative), suchresults can be generalized to the wider studysample to determine dementia prevalence rates.Age standardized prevalence rates will also becalculated. Analysis of associated factors will becarried out using logistic and linear regressionmethods.
Results
Participation rate and sample characteristicsThe study census process yielded a list of546 eligible participants, of which 336 (62%)participated in the study. Of the 210 peopleidentified who did not participate, 123 refused, 31could not be contacted, 11 moved away beforethey were interviewed, nine died before interviewed,and 36 could not be scheduled for other reasonsprior to the end of data collection. There were nosignificant differences in age, sex, or urban/regionaldistribution between those who participated in thestudy and those who did not. The distribution ofthe study sample across urban Sydney (n = 140;42%) and other regional/rural sites (n = 196; 58%)was also comparable to ABS Census figures shown
in Table 1. The median age of participants was 66years (range: 60–92 years) and 60% were female.All participants spoke English, which was reportedto be their first language in 98% of cases. Only asmall proportion (1%; n = 3) reported receivingno formal education; (39%; n = 131) reported atleast ten years of education. Approximately halfthe participants screened “positive” (i.e. belowstudy cut-off on at least one cognitive test; n =171; 51%). Including the 20% random sampleof those who screened negative, 204 (61%) wereselected for Phase 2. Of these, 153 (75%) completedPhase 2 medical assessment. Reasons for notcompleting Phase 2 included: 39 refused, sixdied, two were lost to follow-up, and four wereunable to be scheduled before the end of datacollection. Compared to non-completers, those whocompleted a medical assessment were more likelyto be from a regional/rural site (64% vs. 45%,χ2 = 5.69, p = 0.017, ϕ = 0.17), but there were nosignificant differences in age, sex or MMSE scoresbetween these groups. Further sample descriptionand results pertaining to our specific hypotheses willbe presented in subsequent reports.
Discussion
KGOWS is one of a number of studies occurringaround the world that aim to establish theprevalence of and risk factors for dementia andcognitive impairment in Indigenous people inhigh-, middle-, and low-income countries. Thisstudy will provide the first available prevalencerates for dementia and cognitive impairmentin a representative sample of older AboriginalAustralians residing in urban (non-remote) areas –specifically, across communities in metropolitanSydney and regional NSW. KGOWS will alsoexamine diagnostic instruments and criteria to makea culturally fair and validated dementia diagnosis inurban Aboriginal communities, taking into accountfactors such as education and socioeconomicdisadvantage. The study will provide informationon biomedical and socioeconomic factors associatedwith dementia; specifically it will provide objectivedata on the association between education andcognitive status in Aboriginal communities that willunderpin the move towards early and continuingaccess to education for Aboriginal and Torres StraitIslander people to improve cognitive and healthoutcomes. It will also provide information on thehealthcare needs of the participating communities,the use of formal dementia and community servicesby Aboriginal people with dementia and theircaregivers, and on the burden of dementia onAboriginal caregivers.

Dementia in urban Aboriginal Australians 9
In addition, KGOWS will report results to ourpartner Aboriginal communities and ACCHOs;build their capacity in dementia assessment, riskfactor detection, prevention, and dementia services;and extend this model to other urban Aboriginalcommunities through our networks, collaborators,and publications. As part of our study procedure,we provide results of study health checks forconsenting participants to their nominated primaryhealthcare provider. It has emerged that one ofthe most direct and rewarding ways we wereable to benefit individual study participants hasinvolved our local research teams (ARA, ProjectOfficer, non-Aboriginal interviewer, and medicalpersonnel) assisting participants with high needs toaccess crucial health, home care, and other supportservices.
KGOWS has led to an affiliated researchand capacity building program, including youngerparticipant groups and additional Aboriginalcommunities, using postgraduate researchers andsmall grants. This program is currently exploring:the experience and meaning of dementia fromAboriginal perspectives; the influence of educationand early learning experiences on cognition anddementia risk; and the relationship between earlylife stress, cognitive impairment, and brain aging.We are currently funded to develop strategiesfor dementia education and improved access toappropriate services for Aboriginal people withdementia and their caregivers, as part of ourcommitment to translate research into sustainablecommunity benefits. We also plan to extendKGOWS as a longitudinal study on the role ofdocumented early life social factors (such as adversechildhood events, parenting, and education) andmidlife biomedical risk factors (such as smoking,hypertension, diabetes) in cognitive decline withadvancing age. KGOWS and its associatedresearch program will contribute to the assessmentof dementia and cognitive impairment beingundertaken in Indigenous communities around theworld and improve the level of understanding ofthe social and biological determinants of successfulaging.
Conflict of interest
This study is supported by a National Healthand Medical Research Council Project Grant(510347). Initial piloting of instruments was fundedby Dementia Collaborative Research Centres(DCRC) and Alzheimer’s Australia Research. DrRadford is funded by the RW & JG Post-doctoralFellowship in Aboriginal Health and Ageing andthe project received donations through the Ageing
Research Centre at Prince of Wales Hospital,Sydney. The Koori Growing Old Well Study(KGOWS) is a collaboration between NeuroscienceResearch Australia (NeuRA), University of NSW,and Aboriginal and academic research partners.Our collaborators include: our Aboriginal partnercommunities, Aboriginal Health Managers in NSWArea Health Services (Gail Daylight, Vicki Wade,Tim Agius), Muru Marri Indigenous Health UnitUNSW, Dementia Collaborative Research Centres,Prince of Wales Hospital, KICA Research Groupat University of Western Australia, ARC-NHMRCAgeing Well Network, and the National Aboriginaland Torres Strait Islander Dementia AdvisoryGroup (NATSIDAG) at Alzheimer’s Australia.
Description of authors’ roles
K. Radford participated in the study designand implementation, fieldwork, and consensusdeterminations and drafted the paper. H. Mackmanaged the research team and data collection,participated in the study design, ethics approvals,implementation and community engagement, andhelped to draft the paper. H. Robertson participatedin the funding application and ethics approvals andhelped to draft the paper. B. Draper participatedin the study design and implementation, andhelped to draft the paper. S. Chalkley participatedin the study design, fieldwork, and consensusdeterminations. G. Daylight was integral in initialcommunity consultations and in guiding thecultural appropriateness of the study. R. Cummingparticipated in the study implementation andhelped to draft the paper. H. Bennett participatedin the study design and consensus determinations.L. Jackson Pulver participated in the design andimplementation of the study. G.A. Broe conceivedof and directed the study; he participated in itsdesign, community engagement, fieldwork, andconsensus determinations, and helped to draft thepaper. All authors read and approved the finalpaper.
Acknowledgments
This work relied on the assistance and supportof many individuals and organizations. We areparticularly grateful to our participants, ourlocal Elder guidance groups, KGOWS AboriginalReference Group, and our Aboriginal communitypartners who continue to offer their supportfor our research: Durri Aboriginal CorporationMedical Service in Kempsey, Darrimba MaarraAboriginal Health Clinic in Nambucca, Galambila

10 K. Radford et al.
Aboriginal Health Service in Coffs Harbour,La Perouse Local Aboriginal Land Council, LaPerouse Aboriginal Community Health Centre,and Tharawal Aboriginal Corporation in Camp-belltown. We wish to recognize the hard work ofour research team including Aboriginal researchassistants, project officers and interviewers, andmedical doctors. We thank Professor Leon Flicker,Associate Professor Dina Logiudice, and Dr KateSmith for their expert advice on adapting the KICAcognitive screening tool, along with Dr JeffreyRowland for guidance on use of the RUDAS withurban/regional Aboriginal communities. We alsothank Associate Professor Emeritus David Graysonfor his substantial contribution to the design andimplementation of the study, and ongoing supportwith data analyses.
References
Akhtar, A. J., Broe, G. A., Crombie, A., McLean,W. M., Andrews, G. R. and Caird, F. I. (1973).Disability and dependence in the elderly at home. Age andAgeing, 2, 102–111.
American Psychiatric Association (2000). Diagnostic andStatistical Manual of Mental Disorders: DSM-IV-TR.Washington, DC: American Psychiatric Association.
Anstey, K. and Sargent-Cox, K. (2009). Growing healthybrains from birth and keeping them healthy duringadulthood: a life-course approach to cognitive epidemiologyand dementia. Australasian Epidemiologist, 16, 11–13.
Arkles, R., Jackson Pulver, L., Robertson, H., Draper,B., Chalkley, S. and Broe, G. (2010). Ageing, Cognitionand Dementia in Australian Aboriginal and Torres StraitIslander Peoples. Sydney: Neuroscience Research Australiaand Muru Marri Indigenous Health Unit, UNSW.
Australian Bureau of Statistics (2010). PopulationCharacteristics, Aboriginal and Torres Strait IslanderAustralians (Report No. 4713.0, reissue). Canberra:Australian Bureau of Statistics.
Barnes, D. E. and Yaffe, K. (2011). The projected effect ofrisk factor reduction on Alzheimer’s disease prevalence.Lancet Neurology, 10, 819–828.
Broe, G. A. (2003). Population ageing, human lifespan andneurodegenerative disorders: a fifth epidemiologictransition. In P. S. Sachdev (ed.), The Ageing Brain(pp. 11–31). Lisse, The Netherlands: Swets & Zeitlinger.
Burgess, C. P. et al. (2009). Healthy country, healthypeople: the relationship between Indigenous health statusand “caring for country”. Medical Journal of Australia, 190,567–572.
Folstein, M., Folstein, S. E. and McHugh, P. R. (1975).“Mini-mental state”: a practical method for grading thecognitive state of patients for the clinician. Journal ofPsychiatric Research, 12, 189–198.
Garvey, G. et al. (2011). Making sense of dementia:understanding amongst Indigenous Australians.International Journal of Geriatric Psychiatry, 26, 649–656.
Hendrie, H. C. et al. (1993). Alzheimer’s disease is rare inCree. International Psychogeriatrics, 5, 5–14.
Hill, K., Barker, B. and Vos, T. (2007). Excess Indigenousmortality: are Indigenous Australians more severelydisadvantaged than other Indigenous populations?International Journal of Epidemiology, 36, 580–589.
Kalton, G. and Anderson, D. W. (1986). Sampling rarepopulations. Journal of the Royal Statistical Society, Series A:Statistics in Society, 149, 65–82.
Llibre Rodriguez, J. J. et al. (2008). Prevalence of dementiain Latin America, India, and China: a population-basedcross-sectional survey. Lancet, 372, 464–474.
LoGiudice, D. et al. (2006). Kimberley IndigenousCognitive Assessment tool (KICA): development of acognitive assessment tool for older indigenous Australians.International Psychogeriatrics, 18, 269–280.
McKeith, I. G. et al. (2005). Diagnosis and management ofdementia with Lewy bodies: third report of the DLBConsortium. Neurology, 65, 1863–1872.
McKhann, G. M. et al. (2011). The diagnosis of dementiadue to Alzheimer’s disease: recommendations from theNational Institute on Aging-Alzheimer’s Associationworkgroups on diagnostic guidelines for Alzheimer’sdisease. Alzheimer’s and Dementia, 7, 263–269.
Moceri, V. M. et al. (2001). Using census data and birthcertificates to reconstruct the early-life socioeconomicenvironment and the relation to the development ofAlzheimer’s disease. Epidemiology, 12, 383–389.
Neary, D. et al. (1998). Frontotemporal lobar degeneration:a consensus on clinical diagnostic criteria. Neurology, 51,1546–1554.
Pollitt, P. A. (1997). The problem of dementia in AustralianAboriginal and Torres Strait Islander communities: anoverview. International Journal of Geriatric Psychiatry, 12,155–163.
Radford, K. and Mack, H. (2012). Dementia Screening forUrban Aboriginal Australians: The Modified KimberlyIndigenous Cognitive Assessment (mKICA). Sydney:Dementia Collaborative Research Centres.
Smith, K. et al. (2008). High prevalence of dementia andcognitive impairment in Indigenous Australians. Neurology,71, 1470–1473.
Smith, K. et al. (2010). Factors associated with dementia inAboriginal Australians. Australian and New Zealand Journalof Psychiatry, 44, 888–893.
Storey, J. E., Rowland, J. T., Basic, D., Conforti, D. A.and Dickson, H. G. (2004). The Rowland UniversalDementia Assessment Scale (RUDAS): a multiculturalcognitive assessment scale. International Psychogeriatrics, 16,13–31.
Thomas, D. P. et al. (2006). Long-term trends in Indigenousdeaths from chronic diseases in the Northern Territory: afoot on the brake, a foot on the accelerator. Medical Journalof Australia, 185, 145–149.
Thornton, M. and Travis, S. (2003). Analyisis of thereliability of the modfied caregiver strain index. Journals ofGerontology, Series B: Psychological Sciences and SocialSciences, 58B, 127–132.
Vos, T., Barker, B., Begg, S., Stanley, L. and Lopez,A. D. (2009). Burden of disease and injury in Aboriginaland Torres Strait Islander Peoples: the Indigenous healthgap. International Journal of Epidemiology, 38, 470–477.

Dementia in urban Aboriginal Australians 11
Waite, L. M., Broe, G. A., Grayson, D. A. and Creasey,H. (2001). The incidence of dementia in an Australiancommunity population: the Sydney Older Persons Study.International Journal of Geriatric Psychiatry, 16, 680–689.
Winblad, B. et al. (2004). Mild cognitive impairment –beyond controversies, towards a consensus: report of the
International Working Group on Mild CognitiveImpairment. Journal of Internal Medicine, 256, 240–246.
Zann, S. (1994). Identification of Support, Education andTraining Needs of Rural/Remote Health Care Service ProvidersInvolved in Dementia Care. RHSET Project ProgressReport. Queensland: Northern Regional Health Authority.