
The Psychosocial Challenges of Establishing the Field of Psychosocial Studies
Upload
independentCategory
view
7download
0
The influence of diabetes psychosocial attributes and self-management practices on change in diabetes status
Donna M. Zulman, MD, MS1,2,3, Ann-Marie Rosland, MD, MS2,3, HwaJung Choi, PhD1,2,Kenneth M. Langa, MD, PhD2,3, and Michele Heisler, MD, MPA1,2,3,4
1The Robert Wood Johnson Foundation Clinical Scholars Program, University of Michigan, AnnArbor, MI, USA2Department of Internal Medicine, University of Michigan, Ann Arbor, MI, USA3Department of Veterans Affairs, Health Services Research and Development Center ofExcellence, Ann Arbor, MI, USA4Department of Health Behavior and Health Education, School of Public Health, University ofMichigan, Ann Arbor, MI, USA
AbstractObjective—To examine the influence of diabetes psychosocial attributes and self-managementon glycemic control and diabetes status change.
Methods—Using data from the Health and Retirement Study, a nationally-representativelongitudinal study of U.S. adults > 51 years, we examined cross-sectional relationships amongdiabetes psychosocial attributes (self-efficacy, risk awareness, care understanding, prioritization ofdiabetes, and emotional distress), self-management ratings, and glycemic control. We thenexplored whether self-management ratings and psychosocial attributes in 2003 predicted change indiabetes status in 2004.
Results—In multivariate analyses (N = 1834), all diabetes psychosocial attributes wereassociated with self-management ratings, with self-efficacy and diabetes distress having thestrongest relationships (adj coeff = 8.1, p < 0.01 and −4.1, p < 0.01, respectively). Lower self-management ratings in 2003 were associated cross-sectionally with higher hemoglobin A1C (adjcoeff = 0.16, p < 0.01), and with perceived worsening diabetes status in 2004 (adj OR = 1.36, p <0.05), with much of this latter relationship explained by diabetes distress.
Conclusion—Psychosocial attributes, most notably diabetes-related emotional distress,contribute to difficulty with diabetes self-management, poor glycemic control, and worseningdiabetes status over time.
Practice Implications—Self-management and adherence interventions should targetpsychosocial attributes such as disease-related emotional distress.
Corresponding Author: Donna M. Zulman, MD, MS RWJ Clinical Scholars Program 6312 Medical Science Building I 1150 W.Medical Center Drive Ann Arbor, MI 48109-5604 USA Phone: 734-647-4844 Fax: 734-647-3301 [email protected]'s Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to ourcustomers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review ofthe resulting proof before it is published in its final citable form. Please note that during the production process errors may bediscovered which could affect the content, and all legal disclaimers that apply to the journal pertain.Conflict of Interest: None disclosed
NIH Public AccessAuthor ManuscriptPatient Educ Couns. Author manuscript; available in PMC 2013 April 1.
Published in final edited form as:Patient Educ Couns. 2012 April ; 87(1): 74–80. doi:10.1016/j.pec.2011.07.013.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Keywordsdiabetes; self-management; self-efficacy; diabetes distress
INTRODUCTIONEffective patient self-management is necessary to prevent adverse clinical outcomes indiabetes [1, 2]. A number of psychosocial attributes have been associated with diabetes self-management. For example, individuals with higher levels of diabetes self-efficacy [3–8],more knowledge about diabetes [9–11], and better understanding of their diabetes status andrisk for complications [12, 13] have better diabetes self-management and glycemic control.
Other attributes, such as diabetes-related emotional distress, are associated with poordiabetes self-management and glycemic control [14–16]. Distress about diabetes canencompass a range of emotions, including feeling discouraged about a treatment plan,worrying about low blood sugar or long-term disease complications, and having difficultypaying for medications or defining concrete goals for diabetes care. Not surprisingly, there isoften substantial overlap between levels of distress and depressive symptoms [17], whichhave also been shown to influence glycemic control [18].
Many of these diabetes-related psychosocial attributes are modifiable through interventions[3, 19–23], suggesting a potential opportunity to improve patient outcomes by targetingthese attributes. Little is known, however, about the relative contributions of thesepsychosocial attributes to a person's performance of self-management tasks [24]. In addition,it is unclear whether patients' self-assessment of these attributes and of their self-management can reliably predict changes in their diabetes status over time.
To address these deficiencies, we developed a conceptual model illustrating hypothesizedassociations among psychosocial attributes, self-reported performance of self-managementtasks, and patient-perceived diabetes status change (Figure 1). Using this model, we soughtto answer two related research questions: 1) What is the relative contribution of key diabetespsychosocial attributes, such as disease-specific self-efficacy and distress, to performance ofself-management tasks, and 2) To what degree does a person's assessment of their self-management and psychosocial attributes predict patient-perceived diabetes status over time.We examined these relationships using the Health and Retirement Study (HRS), a nationallyrepresentative longitudinal study of middle-aged and older adults.
METHODSStudy Population
The HRS is a nationally representative longitudinal study of adults over the age of 50 [25].In-depth health and economic information is gathered from more than 22,000 individualsthrough biennial surveys. In 2003, the HRS conducted a substudy of individuals withdiabetes. HRS participants who reported a diagnosis of diabetes in 2002 and were notparticipating in other concurrent HRS substudies were eligible. Of the 2,514 eligibleparticipants, 129 were determined to have died prior to the October 2003 start of theDiabetes Study. Questionnaires were returned by 1,901 of the remaining eligible individuals(response rate 79.7%). The survey covered a wide range of topics including diabetes historyand status, performance of self-management tasks, and knowledge and feelings aboutdiabetes. A subset of 1,233 participants (64.9% of those who returned questionnaires)returned a valid blood specimen using a self-administered hemoglobin A1C fingerstickkit. Individuals with certain characteristics (males, non-blacks, and those with higher levels
Zulman et al. Page 2
Patient Educ Couns. Author manuscript; available in PMC 2013 April 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
of education, higher income, fewer limitations in activities of daily living, shorter durationof diabetes, better health status, and lower levels of depression) were significantly morelikely to return the hemoglobin A1C assay. Individuals with type 1 diabetes (n = 50) andthose under the age of 51 at the time of the 2003 survey (n = 17) were excluded, resulting ina total sample of 1,834, including 1,187 individuals with hemoglobin A1C values.
Study VariablesDiabetes Status Change—The main outcome of interest was perceived diabetes statuschange. This was assessed in the 2004 core HRS survey by asking, “Since we interviewedyou last, is your diabetes better, worse, or about the same?” Responses were dichotomizedas “worse” vs. “better” or “about the same.”
Baseline Measures of Self-Management and Psychosocial Attributes—Self-management was assessed in the 2003 diabetes survey using a well-validated measure inwhich participants were asked to rate their difficulty with and ability to complete tasks overthe past six months in five domains (medication adherence, diet, exercise, blood sugarmonitoring, and checking feet for ulcers) (Appendix Table A) [26, 27]. Responses on a 5-point scale ranged from “So difficult: I couldn't do it at all,” to “Not difficult: I got it exactlyright.” The sum of responses to the five self-management questions, which could rangefrom 0 to 25, was converted to a 100-point scale and used as a dependent variable in cross-sectional analyses. For purposes of presentation clarity, this measure was categorized whenused as an independent variable in longitudinal analyses. For the categorical variable, anindividual's overall self-management rating was considered low, moderate, or high based onwhether the individual ranked 0 to 1, 2 to 3, or 4 to 5 self-care tasks as “Not difficulty: I gotit exactly right.”
Five diabetes-specific psychosocial attributes were assessed in the 2003 diabetes survey(Appendix Table A). Diabetes self-efficacy, risk awareness, and care understanding wereevaluated using validated measures adapted from the Diabetes Care Profile [28]. Diabetesself-efficacy was measured based on participants' reported confidence in their ability toperform six key diabetes care activities. Diabetes risk awareness, a measure of a person'sperception of potential adverse consequences of diabetes and their ability to modify theseoutcomes, was assessed by asking participants whether they agreed that following theirprescribed diabetes treatment plan closely would help prevent six potential adverseconsequences of diabetes. Diabetes care understanding was assessed by asking participantsto rate how well they understood ten different aspects of their diabetes care [26].Prioritization of diabetes was assessed by asking participants whether they agreed with thestatement, “Taking care of my diabetes is my top priority right now” [29]. Diabetes-specificemotional distress was assessed through questions adapted from the Problem Areas inDiabetes scale, in which participants were asked to rate whether ten potential diabetes-related psychosocial stressors were a problem for them [15]. For purposes of presentationclarity, psychosocial attributes were analyzed as categorical variables that were constructeda priori by dichotomizing item responses, summing the items into a single score, and thendividing the scores into three categories that ensured a reasonable sample size in each group(Appendix Table A).
Covariates—Measures of baseline diabetes status included duration of diabetes, treatmentregimen, and diabetes severity. Duration of diabetes was ascertained by subtracting age atdiabetes diagnosis from age at the time of the 2003 diabetes survey. Missing values werereplaced using the diabetes diagnosis year from the HRS 2006 or 2008 core surveys, or byidentifying the last HRS core survey in which the participant reported not having diabetes.Antihyperglycemic treatment regimen was obtained from the 2003 diabetes survey and was
Zulman et al. Page 3
Patient Educ Couns. Author manuscript; available in PMC 2013 April 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
categorized as no medications, oral medications with no insulin treatment, and insulintreatment with or without oral medications. Diabetes severity was evaluated using diabetes-related components of the Total Illness Burden Index (TIBI) score; a composite measure thatwas developed to assess comorbid illness in older adults using self-reported symptoms andmedical event history [30].
Baseline self-rated health status was assessed using a single-item validated measure takenfrom the 2002 HRS core survey [31]. Baseline functional status was assessed through acount of activities of daily living limitations as reported in the 2002 HRS core survey. Non-diabetes comorbidities were assessed through reports of hypertension, cancer, non-asthmachronic lung disease, coronary heart disease or heart failure, stroke or TIA, or arthritis in the2002 HRS core survey. Tobacco use over the past ten years was determined using data fromHRS core surveys between 1992 and 2002. Depression was assessed in the 2003 HRS coresurvey through a modified version of the Center for Epidemiologic Studies Depression Scale(CES-D) that incorporates 8 of the original 20 items [32, 33].
Sociodemographics obtained from the 2002 HRS core survey were race (white, black,other), sex, years of formal education (<12, 12, >12), and income (analyzed in quartiles ofratio of family income to the poverty threshold). Age was assessed at the time of the 2003diabetes survey and was analyzed as a continuous variable.
Hemoglobin A1CA hemoglobin A1C value was obtained via a 2003 mail-in assay (At-Home; FlexSiteDiagnostics Inc, Palm City, Florida) that uses the Roche Unimate immunoassay and theCobas Integra analyzer (F. Hoffmann-La Roche Ltd, Basel, Switzerland) calibrated to asynthetic hemoglobin A1C standard.
Statistical AnalysisCross-sectional relationships between each psychosocial attribute and individuals' overallself-management ratings were examined with multivariate regression analyses adjusting forbaseline sociodemographics, health, and diabetes covariates. For the subset of participantswith a 2003 measure of glycemic control, bivariate and multivariate cross-sectionalrelationships were examined between individuals' psychosocial attributes and self-management ratings, and their hemoglobin A1C values. In addition, ANOVA analyses wereused to explore the relationship between participants' age and their levels of self-management, psychosocial attributes, and glycemic control.
Multivariate logistic regression models were utilized to assess predictors of worseningperceived diabetes status in 2004. First, a model was constructed to examine the relationshipbetween poor self-reported self-management and worsening diabetes status, adjusting forsociodemographics (age, race, sex, education, income) and baseline health, function, anddiabetes characteristics. Next, the five diabetes-specific psychosocial attributes (self-efficacy, care understanding, prioritization of diabetes, risk awareness, and emotionaldistress) were added to the model to determine how these attributes influenced therelationship between self-management and diabetes status change. Secondary analyses weresubsequently conducted to examine the predicted probability of diabetes status change in thepresence or absence of key explanatory variables, with all covariates set at the populationmeans. Additional post-hoc analyses were conducted to determine whether significantfindings in patients with high levels of diabetes distress were sensitive to the presence ofdepression symptoms.
Missing items from multiple-item scales were imputed using person mean imputation, wherean individual's mean score over observed scale items replaces a missing scale item. Rates of
Zulman et al. Page 4
Patient Educ Couns. Author manuscript; available in PMC 2013 April 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
item-level missing data were less than 10% for all covariates used in analyses except fordepression, which was included only in secondary analyses and had a missing rate of 10.5%.Regression diagnostic procedures yielded no evidence of multicollinearity in any of theregression models. Diabetes survey weights were utilized in analyses with diabetes statuschange to adjust for the oversampling design of HRS. Cross-sectional analyses did notutilize survey weights, thus these results are not nationally representative. All analyses wereperformed using Stata 11.0 (StataCorp 2009, College Station, Texas). All data weredeidentified and publicly available (http://hrsonline.isr.umich.edu/), and the surveys wereapproved by an institutional review board at the University of Michigan.
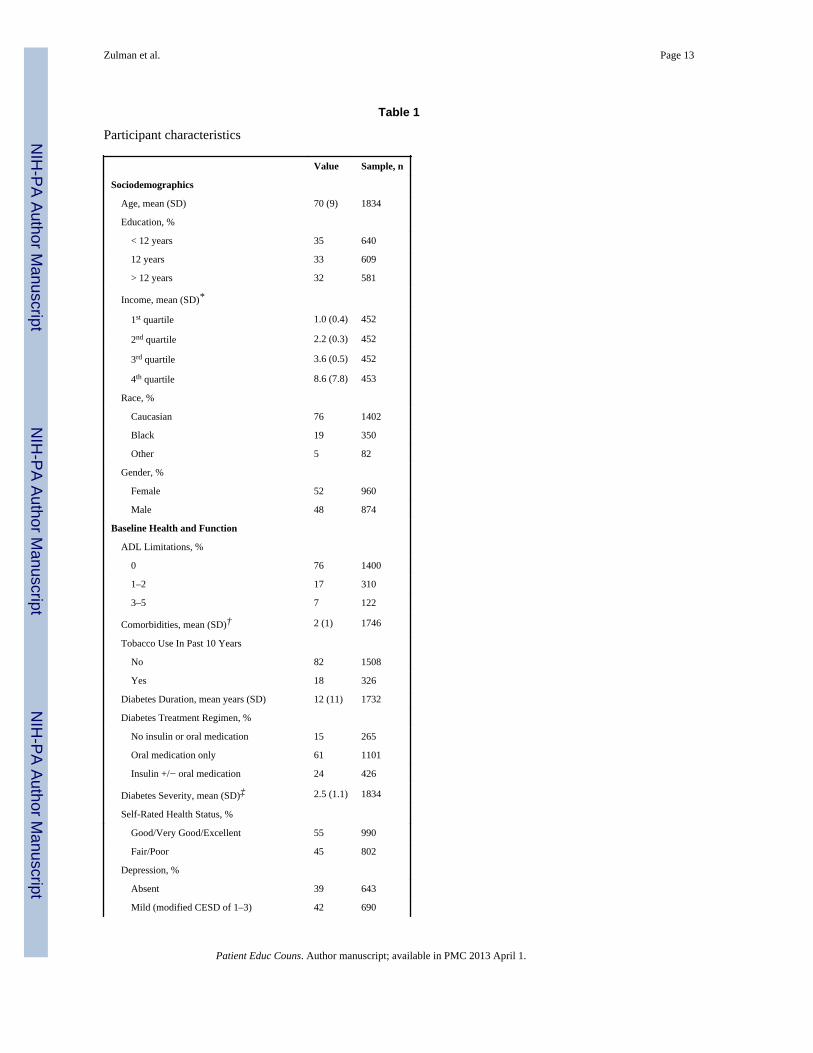
RESULTSTable 1 summarizes the baseline characteristics of the 1,834 participants who completed the2003 diabetes survey. Self-reported self-management ratings and psychosocial attributes ofthese respondents are provided in Appendix Table A.
Self-Reported Self-ManagementThere were 448 (26%) individuals who reported performing four or five of the five self-management tasks exactly right over the past six months and were categorized as havinghigh levels of self-management, and 545 (31%) who reported performing none or only oneof these tasks exactly right over this time period and were categorized as having low levelsof self-management (Appendix Table A). Exercise and diet were the two most challengingself-management activities, with 54% and 35% of individuals reporting difficulty executingthese tasks as recommended, respectively (Appendix Table B). Self-reported self-management increased steadily, and significantly, with age (F-statistic 8.56, p < 0.001)(Appendix Table C).
Diabetes-Specific Psychosocial AttributesPrioritization of diabetes was high, with 1,173 (67%) respondents reporting that taking careof their diabetes was one of their top priorities (Appendix Table A). A similar proportion ofrespondents had high levels of diabetes care understanding in at least 9 of 10 domains (1163,66%), and high levels of risk awareness regarding the long-term complications associatedwith uncontrolled diabetes (1,262, 72%). Levels of diabetes self-efficacy were also high,with 1,092 respondents (61%) indicating that they were confident in their ability to performat least seven of eight diabetes tasks. Diabetes-specific emotional distress, however, waspresent to some degree in 62% of individuals, with 657 (38%) participants stating that 1 to 3diabetes issues were currently a moderate problem for them, and 423 (24%) participantsstating that 4 to 10 diabetes issues were currently a serious problem for them. The mostcommon issues causing distress were finding money to pay for medications and supplies(25%), feelings of food deprivation (32%), and worrying about the future and thepossibility of serious complications (38%) (Appendix Table D).
Several attributes had significant relationships with age. Emotional distress decreasedsignificantly as age increased (F statistic 7.37, p < 0.001). Risk awareness and careunderstanding also decreased significantly with age, while self-efficacy and prioritization ofdiabetes did not change substantially (Appendix Table C).
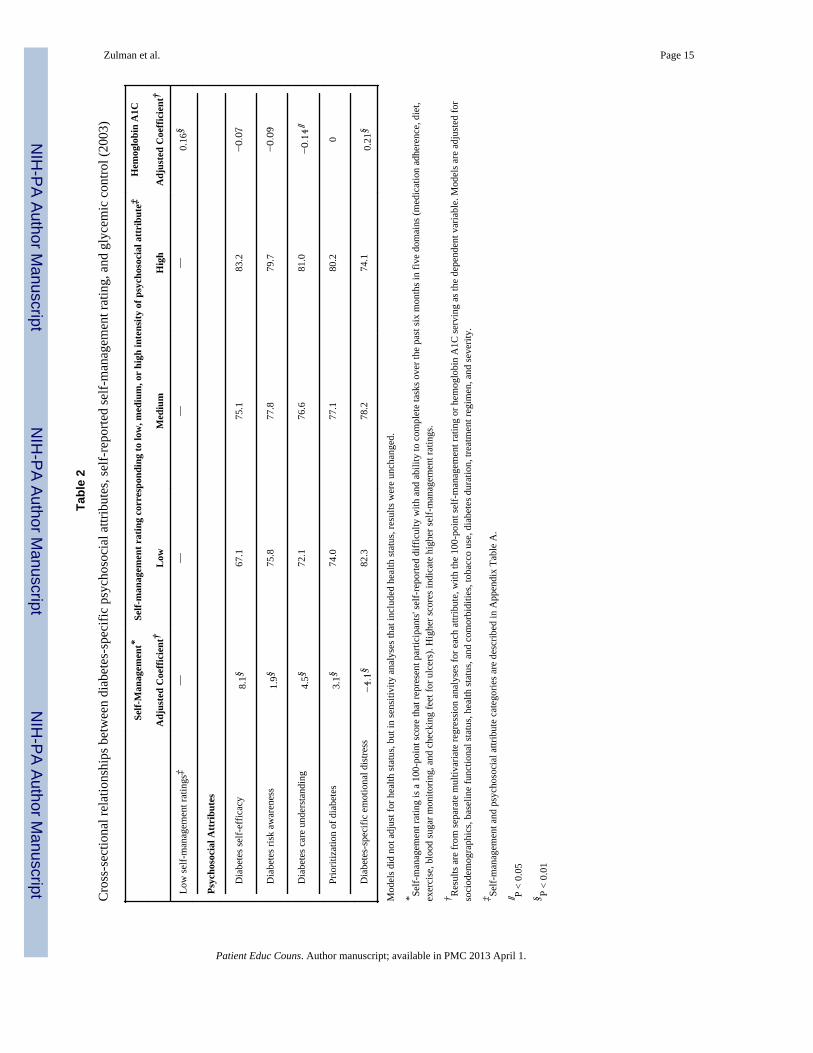
Associations among Psychosocial Attributes, Self-Management, and Glycemic ControlIn multivariate cross-sectional analyses that adjusted for baseline sociodemographics andhealth covariates, all diabetes-specific attributes were independently associated with self-reported self-management, with diabetes self-efficacy having the strongest positiverelationship (adjusted coefficient = 8.1, p < 0.01) and diabetes distress having the strongest
Zulman et al. Page 5
Patient Educ Couns. Author manuscript; available in PMC 2013 April 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
negative relationship (adjusted coefficient = −4.1, p < 0.01) (Table 2). Among the subset ofindividuals with cross-sectional hemoglobin A1C levels, lower self-management ratings andhigher levels of diabetes distress were associated with worse glycemic control (adj coeff forhemoglobin A1C = 0.16, p < 0.01 and 0.21, p < 0.01, respectively). Higher levels of diabetescare understanding were associated with better glycemic control (adjusted coefficient −0.14,p < 0.05), and there was a non-significant trend suggesting a correlation between self-efficacy and risk awareness with lower hemoglobin A1C as well (adjusted coefficients−0.07, p = 0.22 and −0.09, p = 0.14, respectively).
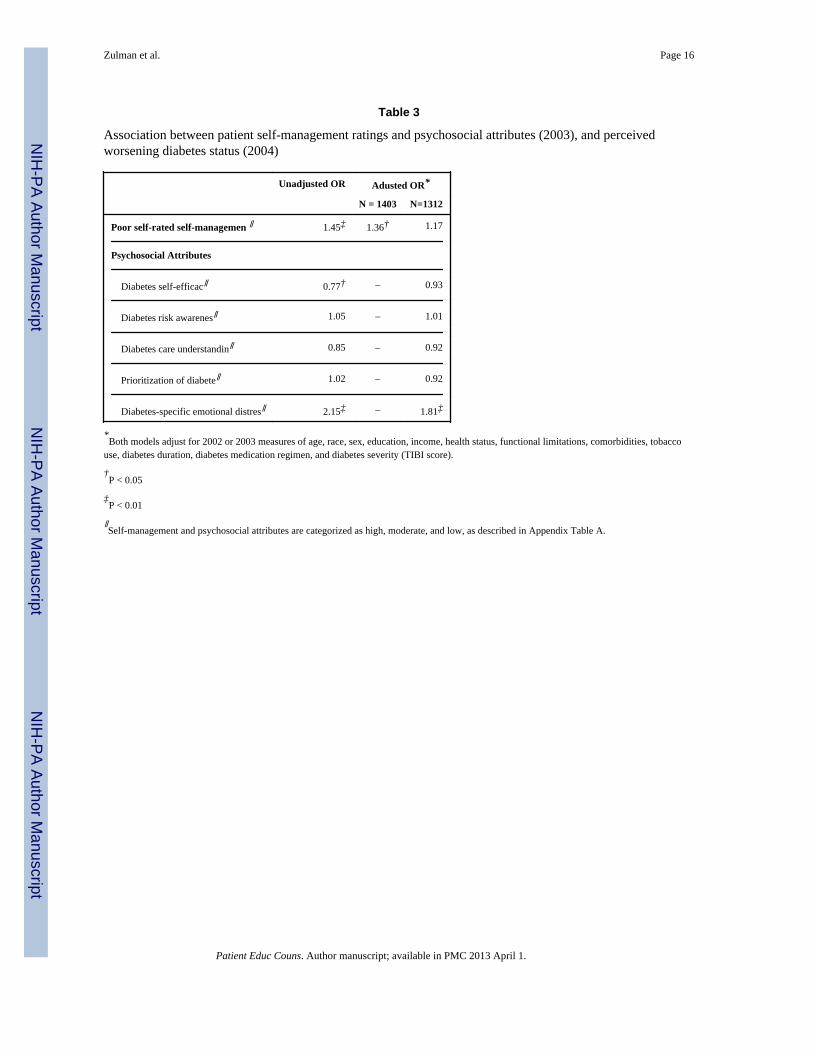
Predictors of Worsening Diabetes Status Over TimeLow self-reported ratings of self-management in 2003 were associated with a greaterlikelihood of perceived worsening diabetes status the following year (adjusted OR 1.36, p <0.05) (Table 3). When the model was adjusted for psychosocial attributes, however, thisassociation was no longer significant (adjusted OR 1.17, p = 0.34), suggesting that theattributes account for some of the observed relationship between self-management anddiabetes status change. Of the psychosocial attributes that were evaluated, only diabetesdistress independently influenced diabetes status change in the full multivariable model,with higher levels of distress resulting in greater likelihood of perceived worsening diabetesstatus in 2004 (adjusted OR 1.81, p < 0.01).
Several post-hoc analyses were conducted to further explore the relationship betweendiabetes distress and worsening diabetes status. Figure 2 illustrates how this relationshipremains fairly consistent across all self-reported ratings of self-management. For example,the predicted probability of worsening diabetes status ranges from 3.9% with no diabetesdistress to 11.7% with severe diabetes distress among individuals with high self-management ratings, and ranges from 5.2% to 15.4% among individuals with low self-management ratings. Given the known clinical association between depression and diabetesdistress [14], the relationship between these constructs was also evaluated. There was amoderate correlation between continuous measures of these variables (r = 0.32). Whendepression was included in the full model, however, a significant association betweendiabetes distress and worsening diabetes status persisted (OR 1.70, p < 0.01).
DISCUSSION AND CONCLUSIONDiscussion
In this study of middle-aged and older individuals with type 2 diabetes, we identified astrong cross-sectional relationship between multiple diabetes-specific psychosocial attributes(including self-efficacy, care understanding, and disease-related distress) and self-management. We also confirmed that poor self-management ratings correlate with worseglycemic control cross-sectionally and are strongly associated with worsening perceiveddiabetes status over one year. Much of this latter relationship may be attributed to highlevels of diabetes-related emotional distress and other psychosocial attributes.
Our findings build on over two decades of work examining how individuals' self-management behaviors are influenced by specific attributes, such as their understandingabout their diabetes care [11], their confidence in their ability to manage their disease [4, 5,7, 34–36], and their diabetes-related emotional distress [15]. One of the strengths of thisstudy is the simultaneous evaluation of multiple psychosocial attributes in a large nationalsample of middle-aged and older adults, which enabled a comparison of the relative impactof these characteristics on both self-management and glycemic control. Of the fivepsychosocial attributes that were assessed, high levels of diabetes self-efficacy, followed byhigh levels of diabetes care understanding and low levels of diabetes-related emotionaldistress, appeared to have the strongest association with performance of self-management
Zulman et al. Page 6
Patient Educ Couns. Author manuscript; available in PMC 2013 April 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
tasks. This study also verifies previous findings that effective self-management [27, 28, 37],better diabetes care understanding [9, 10], and low levels of diabetes distress [14–16], areassociated with better glycemic control. Our results support a previously cited relationshipbetween self-efficacy and glycemic control as well [8, 23], although the association was notstatistically significant in this study.
Our finding that poor self-management ratings were significantly associated with worseningperceived diabetes status over one year builds on previous research demonstrating arelationship between self-management and glycemic control over short time periods [38,39]. Interestingly, in our sample, much of this relationship appears to be explained by highlevels of diabetes distress. Furthermore, the effect of distress was virtually unchanged whenthe model accounted for concurrent depression, indicating that diabetes distress exerts anindependent effect on perceived diabetes status [14]. These results suggest that a central aimof diabetes self-management interventions should be to address and reduce some of thefeelings of anxiety, worry, guilt, and fear that frequently accompany this condition. Thismay be especially important among middle-aged patients, who we found to have higherlevels of emotional distress.
There are several potential limitations of this study that should be noted. HRS focuses onindividuals aged 51 years and older, so results should not be generalized to youngerindividuals. All independent variables were based on HRS survey data, and are thereforesubject to errors associated with self-reported information. In particular, social desirabilitybias may have influenced individuals' responses about their self-management behaviors.Another limitation is that given the breadth of HRS, some of the validated scales forpsychosocial attributes (e.g., self-efficacy and diabetes distress) and other characteristics(e.g., depression) were shortened such that measurement error may have been introduced.
An additional limitation of this study is that certain relevant outcomes could not beevaluated. For example, although the HRS has recently started tracking hemoglobin A1C forall respondents, the sample of individuals with repeat measures of hemoglobin A1C iscurrently too small to examine change in glycemic control over time. We also did not haveinformation after 2003 about the presence of diabetes complications such as retinopathy andneuropathy, which have been associated with poor glycemic control [40]. Thus, the onlyoutcome that specifically measured a change in diabetes severity was the measure ofperceived change in diabetes status; a valuable patient-centered outcome, but one that hasnot been validated against objective measures of disease control.
ConclusionOur findings suggest that multiple diabetes-specific psychosocial attributes, including self-efficacy, care understanding, and diabetes-related distress, are strongly associated with aperson's self-management of their disease and their glycemic control. Diabetes distress, inparticular, also appears to account for a substantial component of the relationship betweenself-management and perceived diabetes status change over a one year period. Futureresearch should examine repeated patient assessments of these constructs to clarify thestability of these measures and the consistency of their relationship with glycemic controland other measures of disease status.
Practice ImplicationsInterventions aiming to improve diabetes self-management activities and adherence shouldtarget psychosocial attributes that might account for difficulties with these tasks, such asdisease-related emotional distress. Emphasizing these attributes may lead to improved
Zulman et al. Page 7
Patient Educ Couns. Author manuscript; available in PMC 2013 April 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
glycemic control, and reduce the likelihood of complications and declining health secondaryto diabetes.
Supplementary MaterialRefer to Web version on PubMed Central for supplementary material.
AcknowledgmentsThe authors thank Michelle Housey for her assistance with manuscript preparation, and Rod Hayward and JeremySussman for their thoughtful comments regarding analyses and study findings. All of the above individuals areaffiliated with the University of Michigan.
Funding: The National Institute on Aging (NIA) provided funding for the Health and Retirement Study (HRS)(U01 AG09740), data from which were used for this analysis. The HRS is performed at the Institute for SocialResearch, University of Michigan. Dr. Zulman is supported by the Robert Wood Johnson Foundation ClinicalScholars Program and an associated VA Advanced Fellowship.
REFERENCES1. The Diabetes Control and Complications Trial Research Group. The effect of intensive treatment of
diabetes on the development and progression of long-term complications in insulin-dependentdiabetes mellitus. N Engl J Med. Sep 30; 1993 329(14):977–986. [PubMed: 8366922]
2. UK Prospective Diabetes Study (UKPDS) Group. Intensive blood-glucose control withsulphonylureas or insulin compared with conventional treatment and risk of complications inpatients with type 2 diabetes (UKPDS 33). Lancet. Sep 12; 1998 352(9131):837–853. [PubMed:9742976]
3. Anderson RM, Funnell MM, Butler PM, Arnold MS, Fitzgerald JT, Feste CC. Patientempowerment. Results of a randomized controlled trial. Diabetes Care. Jul; 1995 18(7):943–949.[PubMed: 7555554]
4. King DK, Glasgow RE, Toobert DJ, Strycker LA, Estabrooks PA, Osuna D, Faber AJ. Self-efficacy,problem solving, and social-environmental support are associated with diabetes self-managementbehaviors. Diabetes Care. Apr; 2010 33(4):751–753. [PubMed: 20150299]
5. Nelson KM, McFarland L, Reiber G. Factors influencing disease self-management among veteranswith diabetes and poor glycemic control. J Gen Intern Med. Apr; 2007 22(4):442–447. [PubMed:17372790]
6. Norris SL, Engelgau MM, Narayan KM. Effectiveness of self-management training in type 2diabetes: a systematic review of randomized controlled trials. Diabetes Care. Mar; 2001 24(3):561–587. [PubMed: 11289485]
7. Sarkar U, Fisher L, Schillinger D. Is self-efficacy associated with diabetes self-management acrossrace/ethnicity and health literacy? Diabetes Care. Apr; 2006 29(4):823–829. [PubMed: 16567822]
8. Sousa VD, Zauszniewski JA, Musil CM, Price Lea PJ, Davis SA. Relationships among self-careagency, self-efficacy, self-care, and glycemic control. Res Theory Nurs Pract. Fall; 2005 19(3):217–230. [PubMed: 16144240]
9. McPherson ML, Smith SW, Powers A, Zuckerman IH. Association between diabetes patients'knowledge about medications and their blood glucose control. Res Social Adm Pharm. Mar; 20084(1):37–45. [PubMed: 18342821]
10. Panja S, Starr B, Colleran KM. Patient knowledge improves glycemic control: is it time to go backto the classroom? J Investig Med. Jul; 2005 53(5):264–266.
11. Persell SD, Keating NL, Landrum MB, Landon BE, Ayanian JZ, Borbas C, Guadagnoli E.Relationship of diabetes-specific knowledge to self-management activities, ambulatory preventivecare, and metabolic outcomes. Prev Med. Oct; 2004 39(4):746–752. [PubMed: 15351541]
12. Klungel OH, Storimans MJ, Floor-Schreudering A, Talsma H, Rutten GE, de Blaey CJ. Perceiveddiabetes status is independently associated with glucose monitoring behaviour among type 2diabetes mellitus patients. Prim Care Diabetes. Feb; 2008 2(1):25–30. [PubMed: 18684417]
Zulman et al. Page 8
Patient Educ Couns. Author manuscript; available in PMC 2013 April 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
13. Scollan-Koliopoulos M, Walker EA, Bleich D. Perceived risk of amputation, emotions, and footself-care among adults with type 2 diabetes. Diabetes Educ. May–Jun; 2010 36(3):473–482.[PubMed: 20181805]
14. Fisher L, Mullan JT, Arean P, Glasgow RE, Hessler D, Masharani U. Diabetes distress but notclinical depression or depressive symptoms is associated with glycemic control in both cross-sectional and longitudinal analyses. Diabetes Care. Jan; 2010 33(1):23–28. [PubMed: 19837786]
15. Polonsky WH, Anderson BJ, Lohrer PA, Welch G, Jacobson AM, Aponte JE, Schwartz CE.Assessment of diabetes-related distress. Diabetes Care. Jun; 1995 18(6):754–760. [PubMed:7555499]
16. Welch GW, Jacobson AM, Polonsky WH. The Problem Areas in Diabetes Scale. An evaluation ofits clinical utility. Diabetes Care. May; 1997 20(5):760–766. [PubMed: 9135939]
17. Fisher L, Skaff MM, Mullan JT, Arean P, Mohr D, Masharani U, Glasgow R, Laurencin G.Clinical depression versus distress among patients with type 2 diabetes: not just a question ofsemantics. Diabetes Care. Mar; 2007 30(3):542–548. [PubMed: 17327318]
18. Egede LE. Effect of depression on self-management behaviors and health outcomes in adults withtype 2 diabetes. Curr Diabetes Rev. 2005; 1(3):235–243. [PubMed: 18220600]
19. Anderson RM, Funnell MM, Aikens JE, Krein SL, Fitzgerald JT, Nwankwo R, Tannas CL, TangTS. Evaluating the Efficacy of an Empowerment-Based Self-Management ConsultantIntervention: Results of a Two-Year Randomized Controlled Trial. Ther Patient Educ. Jun 1; 20091(1):3–11. [PubMed: 20076768]
20. Maddigan SL, Majumdar SR, Guirguis LM, Lewanczuk RZ, Lee TK, Toth EL, Johnson JA.Improvements in patient-reported outcomes associated with an intervention to enhance quality ofcare for rural patients with type 2 diabetes: results of a controlled trial. Diabetes Care. Jun; 200427(6):1306–1312. [PubMed: 15161780]
21. Welch G, Weinger K, Anderson B, Polonsky WH. Responsiveness of the Problem Areas InDiabetes (PAID) questionnaire. Diabet Med. Jan; 2003 20(1):69–72. [PubMed: 12519323]
22. Fonda SJ, McMahon GT, Gomes HE, Hickson S, Conlin PR. Changes in diabetes distress relatedto participation in an internet-based diabetes care management program and glycemic control. JDiabetes Sci Technol. Jan; 2009 3(1):117–124. [PubMed: 20046656]
23. Trief PM, Teresi JA, Eimicke JP, Shea S, Weinstock RS. Improvement in diabetes self-efficacyand glycaemic control using telemedicine in a sample of older, ethnically diverse individuals whohave diabetes: the IDEATel project. Age Ageing. Mar; 2009 38(2):219–225. [PubMed: 19171951]
24. Heisler M, Faul JD, Hayward RA, Langa KM, Blaum C, Weir D. Mechanisms for racial and ethnicdisparities in glycemic control in middle-aged and older Americans in the health and retirementstudy. Archives of Internal Medicine. 2007; 167(17):1853–1860. [PubMed: 17893306]
25. National Institute on Aging. [Accessed 5/17/11] Health and Retirement Study: A longitudinalstudy of health, retirement, and aging. 2011. http://hrsonline.isr.umich.edu/
26. Heisler M, Bouknight RR, Hayward RA, Smith DM, Kerr EA. The relative importance ofphysician communication, participatory decision making, and patient understanding in diabetesself-management. J Gen Intern Med. Apr; 2002 17(4):243–252. [PubMed: 11972720]
27. Heisler M, Smith DM, Hayward RA, Krein SL, Kerr EA. How well do patients' assessments oftheir diabetes self-management correlate with actual glycemic control and receipt of recommendeddiabetes services? Diabetes Care. Mar; 2003 26(3):738–743. [PubMed: 12610031]
28. Fitzgerald JT, Davis WK, Connell CM, Hess GE, Funnell MM, Hiss RG. Development andvalidation of the Diabetes Care Profile. Eval Health Prof. Jun; 1996 19(2):208–230. [PubMed:10186911]
29. Kerr EA, Heisler M, Krein SL, Kabeto M, Langa KM, Weir D, Piette JD. Beyond comorbiditycounts: How do comorbidity type and severity influence diabetes patients' treatment priorities andself-management? Journal of General Internal Medicine. 2007; 22:1635–1640. [PubMed:17647065]
30. Hayward RA, Manning WG, Kaplan SH, Wagner EH, Greenfield S. Starting insulin therapy inpatients with type 2 diabetes: effectiveness, complications, and resource utilization. JAMA. Nov26; 1997 278(20):1663–1669. [PubMed: 9388085]
Zulman et al. Page 9
Patient Educ Couns. Author manuscript; available in PMC 2013 April 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
31. DeSalvo KB, Fisher WP, Tran K, Bloser N, Merrill W, Peabody J. Assessing measurementproperties of two single-item general health measures. Qual Life Res. Mar; 2006 15(2):191–201.[PubMed: 16468076]
32. Steffic, D.; Group, HW. Documentation of Affective Functioning Measures in the Health andRetirement Study. Survey Research Center, University of Michigan; Ann Arbor: 2000.
33. Radloff LS. The CES-D Scale: A Self-Report Depression Scale for Research in the GeneralPopulation. Applied Psychological Measurement. June 1; 1977 1(3):385–401. 1977.
34. Kingery PM, Glasgow RE. Self-efficacy and outcome expectations in the self-regulation of non-insulin dependent diabetes mellitus. Health Educ. Dec; 1989 20(7):13–19. [PubMed: 2516067]
35. Lorig KR, Ritter PL, Laurent DD, Plant K. Internet-based chronic disease self-management: arandomized trial. Med Care. Nov; 2006 44(11):964–971. [PubMed: 17063127]
36. Hurley AC, Shea CA. Self-efficacy: strategy for enhancing diabetes self-care. Diabetes Educ. Mar–Apr; 1992 18(2):146–150. [PubMed: 1537242]
37. Weinger K, Butler HA, Welch GW, La Greca AM. Measuring diabetes self-care: a psychometricanalysis of the Self-Care Inventory-Revised with adults. Diabetes Care. Jun; 2005 28(6):1346–1352. [PubMed: 15920050]
38. Jones H, Edwards L, Vallis TM, Ruggiero L, Rossi SR, Rossi JS, Greene G, Prochaska JO, ZinmanB. Changes in diabetes self-care behaviors make a difference in glycemic control: the DiabetesStages of Change (DiSC) study. Diabetes Care. Mar; 2003 26(3):732–737. [PubMed: 12610030]
39. Karter AJ, Ackerson LM, Darbinian JA, D'Agostino RB Jr. Ferrara A, Liu J, Selby JV. Self-monitoring of blood glucose levels and glycemic control: the Northern California KaiserPermanente Diabetes registry. Am J Med. Jul; 2001 111(1):1–9. [PubMed: 11448654]
40. Stolar M. Glycemic control and complications in type 2 diabetes mellitus. Am J Med. Mar; 2010123(3 Suppl):S3–11. [PubMed: 20206730]
Zulman et al. Page 10
Patient Educ Couns. Author manuscript; available in PMC 2013 April 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
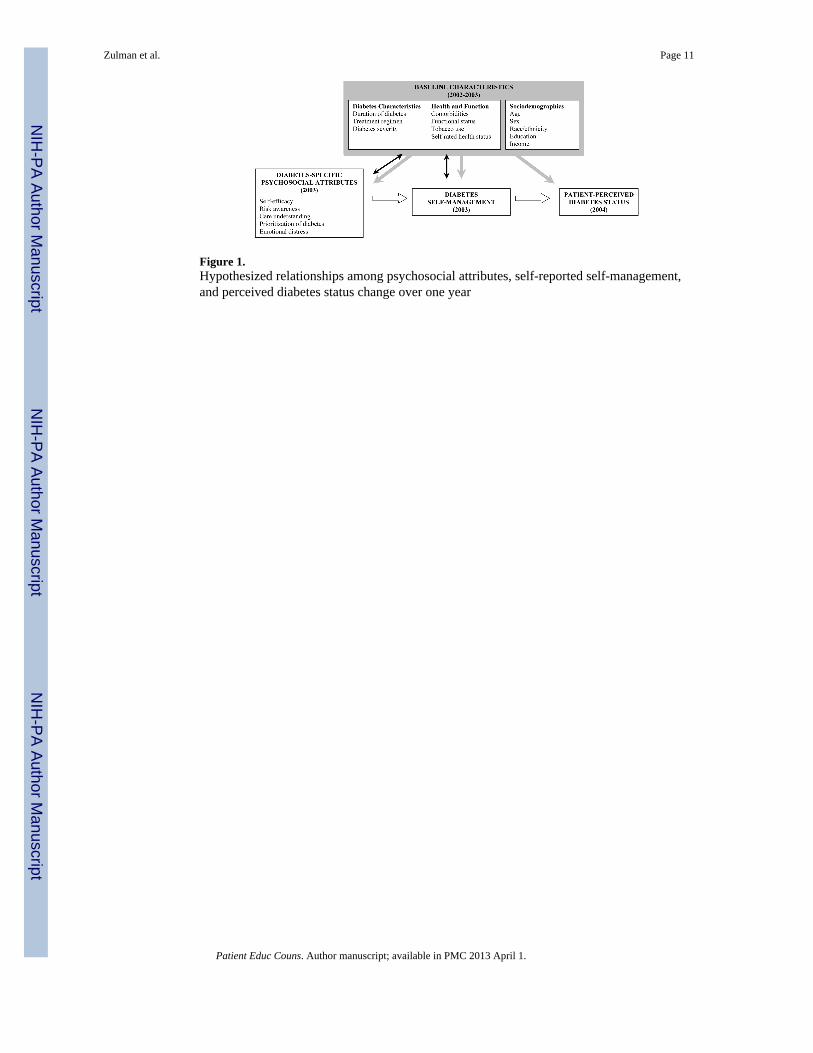
Figure 1.Hypothesized relationships among psychosocial attributes, self-reported self-management,and perceived diabetes status change over one year
Zulman et al. Page 11
Patient Educ Couns. Author manuscript; available in PMC 2013 April 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
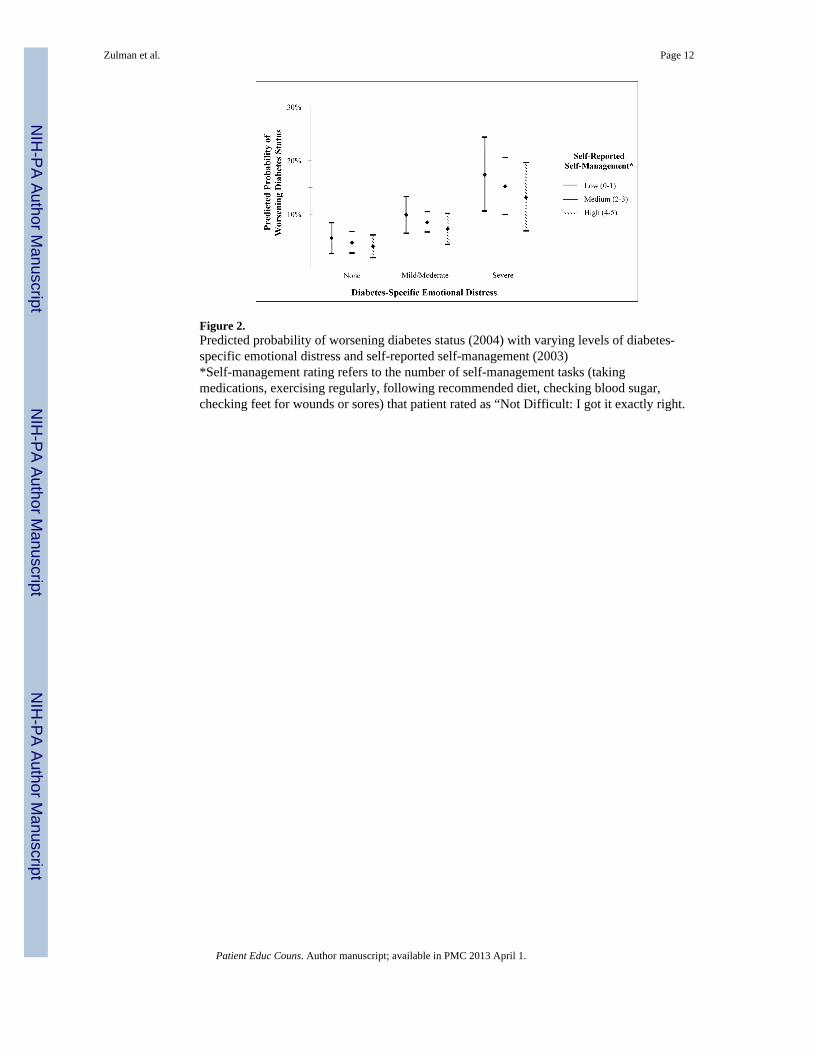
Figure 2.Predicted probability of worsening diabetes status (2004) with varying levels of diabetes-specific emotional distress and self-reported self-management (2003)*Self-management rating refers to the number of self-management tasks (takingmedications, exercising regularly, following recommended diet, checking blood sugar,checking feet for wounds or sores) that patient rated as “Not Difficult: I got it exactly right.
Zulman et al. Page 12
Patient Educ Couns. Author manuscript; available in PMC 2013 April 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Zulman et al. Page 13
Table 1
Participant characteristics
Value Sample, n
Sociodemographics
Age, mean (SD) 70 (9) 1834
Education, %
< 12 years 35 640
12 years 33 609
> 12 years 32 581
Income, mean (SD)*
1st quartile 1.0 (0.4) 452
2nd quartile 2.2 (0.3) 452
3rd quartile 3.6 (0.5) 452
4th quartile 8.6 (7.8) 453
Race, %
Caucasian 76 1402
Black 19 350
Other 5 82
Gender, %
Female 52 960
Male 48 874
Baseline Health and Function
ADL Limitations, %
0 76 1400
1–2 17 310
3–5 7 122
Comorbidities, mean (SD)† 2 (1) 1746
Tobacco Use In Past 10 Years
No 82 1508
Yes 18 326
Diabetes Duration, mean years (SD) 12 (11) 1732
Diabetes Treatment Regimen, %
No insulin or oral medication 15 265
Oral medication only 61 1101
Insulin +/− oral medication 24 426
Diabetes Severity, mean (SD)‡ 2.5 (1.1) 1834
Self-Rated Health Status, %
Good/Very Good/Excellent 55 990
Fair/Poor 45 802
Depression, %
Absent 39 643
Mild (modified CESD of 1–3) 42 690
Patient Educ Couns. Author manuscript; available in PMC 2013 April 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Zulman et al. Page 14
Value Sample, n
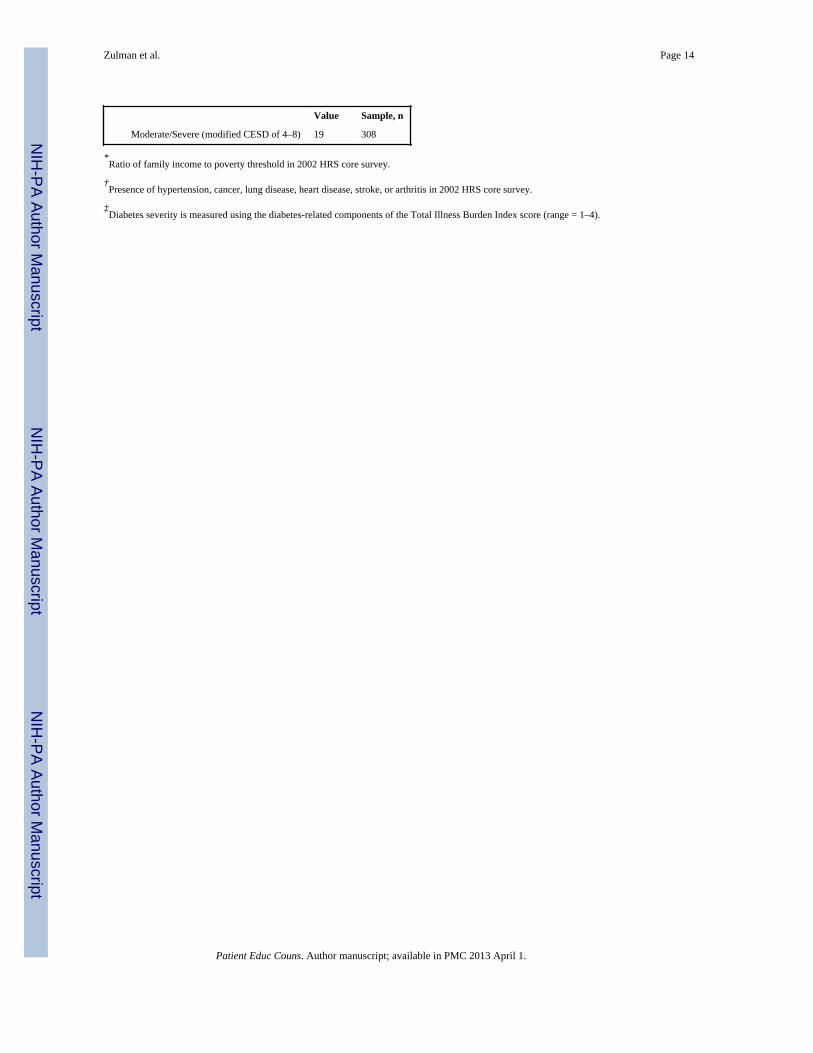
Moderate/Severe (modified CESD of 4–8) 19 308
*Ratio of family income to poverty threshold in 2002 HRS core survey.
†Presence of hypertension, cancer, lung disease, heart disease, stroke, or arthritis in 2002 HRS core survey.
‡Diabetes severity is measured using the diabetes-related components of the Total Illness Burden Index score (range = 1–4).
Patient Educ Couns. Author manuscript; available in PMC 2013 April 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Zulman et al. Page 15
Tabl
e 2
Cro
ss-s
ectio
nal r
elat
ions
hips
bet
wee
n di
abet
es-s
peci
fic p
sych
osoc
ial a
ttrib
utes
, sel
f-re
porte
d se
lf-m
anag
emen
t rat
ing,
and
gly
cem
ic c
ontro
l (20
03)
Self-
Man
agem
ent*
Self-
man
agem
ent r
atin
g co
rres
pond
ing
to lo
w, m
ediu
m, o
r hi
gh in
tens
ity o
f psy
chos
ocia
l attr
ibut
e‡H
emog
lobi
n A
1C
Adj
uste
d C
oeffi
cien
t†L
owM
ediu
mH
igh
Adj
uste
d C
oeffi
cien
t†
Low
self-
man
agem
ent r
atin
gs‡
——
——
0.16
§
Psyc
hoso
cial
Attr
ibut
es
D
iabe
tes s
elf-
effic
acy
8.1§
67.1
75.1
83.2
−0.07
D
iabe
tes r
isk
awar
enes
s1.
9§75
.877
.879
.7−0.09
D
iabe
tes c
are
unde
rsta
ndin
g4.
5§72
.176
.681
.0−0.14
∥
Pr
iorit
izat
ion
of d
iabe
tes
3.1§
74.0
77.1
80.2
0
D
iabe
tes-
spec
ific
emot
iona
l dis
tress
−4.1§
82.3
78.2
74.1
0.21
§
Mod
els d
id n
ot a
djus
t for
hea
lth st
atus
, but
in se
nsiti
vity
ana
lyse
s tha
t inc
lude
d he
alth
stat
us, r
esul
ts w
ere
unch
ange
d.
* Self-
man
agem
ent r
atin
g is
a 1
00-p
oint
scor
e th
at re
pres
ent p
artic
ipan
ts' s
elf-
repo
rted
diff
icul
ty w
ith a
nd a
bilit
y to
com
plet
e ta
sks o
ver t
he p
ast s
ix m
onth
s in
five
dom
ains
(med
icat
ion
adhe
renc
e, d
iet,
exer
cise
, blo
od su
gar m
onito
ring,
and
che
ckin
g fe
et fo
r ulc
ers)
. Hig
her s
core
s ind
icat
e hi
gher
self-
man
agem
ent r
atin
gs.
† Res
ults
are
from
sepa
rate
mul
tivar
iate
regr
essi
on a
naly
ses f
or e
ach
attri
bute
, with
the
100-
poin
t sel
f-m
anag
emen
t rat
ing
or h
emog
lobi
n A
1C se
rvin
g as
the
depe
nden
t var
iabl
e. M
odel
s are
adj
uste
d fo
rso
ciod
emog
raph
ics,
base
line
func
tiona
l sta
tus,
heal
th st
atus
, and
com
orbi
ditie
s, to
bacc
o us
e, d
iabe
tes d
urat
ion,
trea
tmen
t reg
imen
, and
seve
rity.
‡ Self-
man
agem
ent a
nd p
sych
osoc
ial a
ttrib
ute
cate
gorie
s are
des
crib
ed in
App
endi
x Ta
ble
A.
∥ P <
0.05
§ P <
0.01
Patient Educ Couns. Author manuscript; available in PMC 2013 April 1.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Zulman et al. Page 16
Table 3
Association between patient self-management ratings and psychosocial attributes (2003), and perceivedworsening diabetes status (2004)
Unadjusted OR Adusted OR*
N = 1403 N=1312
Poor self-rated self-managemen ∥ 1.45‡ 1.36† 1.17
Psychosocial Attributes
Diabetes self-efficac∥ 0.77† – 0.93
Diabetes risk awarenes∥ 1.05 – 1.01
Diabetes care understandin∥ 0.85 – 0.92
Prioritization of diabete∥ 1.02 – 0.92
Diabetes-specific emotional distres∥ 2.15‡ – 1.81‡
*Both models adjust for 2002 or 2003 measures of age, race, sex, education, income, health status, functional limitations, comorbidities, tobacco
use, diabetes duration, diabetes medication regimen, and diabetes severity (TIBI score).
†P < 0.05
‡P < 0.01
∥Self-management and psychosocial attributes are categorized as high, moderate, and low, as described in Appendix Table A.
Patient Educ Couns. Author manuscript; available in PMC 2013 April 1.
Copyright © 2022 FDOKUMEN




















