
THE IMPACT OF SELF-DETERMINED MOTIVATION AND PERFECTIONISM ON EXERCISE DEPENDENCE IN EXPERIENCED...
79
THE IMPACT OF SELF-DETERMINED MOTIVATION AND PERFECTIONISM ON EXERCISE DEPENDENCE IN EXPERIENCED MALE ADULT WEIGHTLIFTERS LUKE I. WILKIN BA (Hons) A REPORT PRESENTED IN THE FACULTY OF HEALTH AND LIFE SCIENCES, COVENTRY UNIVERSITY, TOWARDS THE DEGREE OF MASTERS OF SCIENCE IN PSYCHOLOGY August 2012 0
Transcript of THE IMPACT OF SELF-DETERMINED MOTIVATION AND PERFECTIONISM ON EXERCISE DEPENDENCE IN EXPERIENCED...

THE IMPACT OF SELF-DETERMINED MOTIVATION AND PERFECTIONISM ON EXERCISE DEPENDENCE IN EXPERIENCED MALE ADULT WEIGHTLIFTERS
LUKE I. WILKIN BA (Hons)
A REPORT PRESENTED IN THE FACULTY OF HEALTH AND LIFE SCIENCES, COVENTRY UNIVERSITY, TOWARDS THE DEGREE OF MASTERS OF SCIENCE IN PSYCHOLOGY
August 2012
0

THE IMPACT OF SELF-DETERMINEDMOTIVATION AND PERFECTIONISM ON
EXERCISE DEPENDENCE IN EXPERIENCEDMALE ADULT WEIGHTLIFTERS
LUKE I. WILKIN BA (Hons)
COVENTRY UNIVERSITY
1

Acknowledgements
First of all I would like to thank the staff Coventry University for
their help and support which has surpassed my expectations.
Secondly, my supervisor Magdalena Marczak has been fantastic and has
provided me with guidance that has greatly improved my work. I feel
strongly that the input of all the staff I have worked with this
year has improved both my overall academic understanding and my
research report. Finally, I would like to thank my family and
friends for their motivational and emotional support that has
spurred me on towards completion of this course when the going got
tough.
2
Dedicated to my niece Rylee and nephew Jonah.
Abstract
Physical exercise is often used as a means to sustain and improve
physical and psychological wellbeing. However, excessive exercise
can become detrimental to one’s health. Utilising the Exercise
Dependence Scale [EDS], Frost Multidimensional Perfectionism Scale*
[FMPS*] and the Sport Motivation Scale-6 [SMS-6] as measurement
tools. The current study assessed the ability of perfectionism and
self-determined motivation to predict exercise dependence group
classification using a multinomial logistic regression. Model-1
(including perfectionism and self-determined motivation) did not
significantly predict exercise dependence group classification (p =
0.262). The prevalence rate for the at-risk group for exercise
dependence was 10.1%, which falls within the range found in previous
research. The results suggest that symptomatic and at-risk for
exercise dependence individuals can vary on levels of perfectionism
and self-determined motivation. Further research should assess
different sporting activities using the same measures as the current
study and examine the impact of directed activities in order to
reduce exercise dependence symptoms in weightlifters.
3

OR
Exercise dependence is a maladaptive behaviour with negative
connotations for physical and psychological well being. It is
important to understand the correlates of such a disorder to aid its
treatment and prevention. This study assessed the ability of
perfectionism (Frost Multidimensional Perfectionism Scale* [FMPS*])
and self-determined motivation (Sport Motivation Scale-6 [SMS-6]) to
exercise dependence (Exercise Dependence Scale [EDS]) group
classification. The prevalence rate for the at-risk group for
exercise dependence was 10.1%, which falls within the range found in
previous research. A multinomial logistic regression found Model-1
(including perfectionism and self-determined motivation) did not
significantly predict exercise dependence group classification (p =
0.262).. The results suggest that symptomatic and at-risk for
exercise dependence individuals can vary on levels of perfectionism
and self-determined motivation. Further research should assess
different sporting activities using the same measures as the current
study and examine the impact of directed activities in order to
reduce exercise dependence symptoms in weightlifters.
Table of Contents
Page numberTitle Pages
4

Acknowledgements 1
Abstract 2
Contents 3
1. Introduction 4
2. Review of Literature 6
2.1 Exercise Dependence
6
2.2 Perfectionism
8
2.3 Self-Determined Motivation
10
3. Hypothesis 13
4. Methodology 13
4.1 Design 13
4.2 Participants
13
4.3 Measures 14
4.4 Procedure 15
4.5 Data Analysis
15
5. Results 17
6. Discussion 29
7. References 36
8. Appendix 41
8.1 Gatekeeper Approval Letter
415
8.2 Ethical Approval Form 42
8.3 Informed Consent Form 43
8.4 Exercise Dependence Scale-21 (EDS)
44
8.5 Frost Multidimensional Perfectionism Scale* (FMPS*)
45
8.6 Sport Motivation Scale-6 (SMS-6)
46
8.7 Draft Dissertation Feedback
47
Introduction
Physical exercise is used by many people as an integral part of a
healthy lifestyle to sustain and improve well being. There are many
health related benefits of regular exercise participation (Biddle
and Mutrie, 2001); aiding the prevention of type 2 diabetes, obesity
(Warburton et al., 2006), reducing anxiety and depression (Smits et
al., 2008) and improve cardio-vascular health (Brene et al., 2007).
However, there can become a point where exercise develops into a
compulsive disorder, at which point the benefits gained from regular
exercise may be lost and the development of negative health effects
may occur.
An over-reliance on exercise is known as exercise dependence (ED),
defined as “craving for leisure-time physical activity that results
in uncontrollable excessive exercise behaviour and that manifests in
6

physiological and psychological symptoms” (Hausenblas and Symons
Downs, 2002a: 90). Common symptoms of excessive exercise include
athlete burnout (Cresswell and Ekland, 2003), injuries (Cumella,
2005), exhaustion (Raedeke, 1997) and withdrawal symptoms - when
unable to exercise (e.g. depression, irritability and anxiety)
(Allegre, Souville, Therme, and Griffiths, 2006).
There is great emphasis placed on increasing exercise participation
in an attempt to address the issues of obesity and depression,
amongst other ailments of sedentary individuals due to the effects
physical activity may have on an individual with regards to
combating such problems. Conversely, due to the maladaptive nature
of excessive exercise, it posits that research into the antecedents
of exercise dependence is of equal importance based on the
detrimental health effects that can ensue from overzealous exercise
engagement.
Researchers have put forward a variety of explanations in an attempt
to account for the development of exercise dependence; Physiological
factors (e.g. Tolerance [Hausenblas and Symons-Downs, 2002a],
withdrawal [Glasser, 1976; Thaxton, 1982] and the “thermogenic
regulation hypothesis” [de Vries, 1981]). Psychological factors
(e.g. Personality traits [Carron, Hausenblas and Estabrooks, 2003],
7

the “cognitive appraisal hypothesis” [Szabo, 1995] and the “affect
regulation hypothesis” [Hamer and Karageorhis, 2007]). The
personality trait explanation has received vast academic interest
based upon the premise that exercise dependant individuals exhibit
certain personality characteristics that either predispose an
individual to or occur as a result of exercise dependence. Many
personality characteristics have been linked to exercise dependence.
In light of the current study, one personality trait that has been
linked to exercise dependence is perfectionism (Hausenblas and
Giacobbi, 2004). Perfectionism entails the setting of excessively
high standards for performance which collude with over-critical self
evaluations of that performance (Frost, Marten, Lahart and
Rosenblate, 1990).
Motivation is another area in psychology that has been used to
ascertain why certain individuals become exercise dependence.
Motivation itself plays a substantial role in determining an
individual’s exercise behaviour i.e. the amount of exercise they
participate in (Wilson et al., 2004), making it an obvious factor to
examine when looking for antecedents of both a lack of and excessive
exercise participation. Self-Determination Theory (Ryan and Deci,
2002) is one measure of motivation that has been adapted to the
sport context in previous research. Self-determined motivation (SDM)
8
is measured on a continuum varying in degree of self-determinedness.
Amotivation is the lowest self-determined aspect, representing an
individual who can no longer identify valid reasons for
participation in an activity. Conversely, intrinsic motivation is
the most self-determined category of motivation and describes when
an individual gains pleasure from active involvement in an activity
(Lonsdale, Hodge and Rose, 2008).
Both perfectionism and motivation are considered to be key
determinants of exercise dependence (Hausenblas and Giacobbi, 2004;
Ogles, Masters, and Richardson, 1995) and have been linked
previously in the sporting context (e.g. McArdle and Duda, 2004).
Moreover, researchers have discovered found links between
perfectionism and ED (e.g. Hagan and Hausenblas, 2003) and SDM and
ED (Edmunds, Ntoumanis and Duda, 2006). However, there has been
little research into how the groups of exercise dependence (i.e.
non-dependent asymptomatic, non-dependent symptomatic and at-risk
for exercise dependence) differ in terms of their motivation
(Edmunds, Ntoumanis and Duda, 2006) and levels of perfectionism.
Moreover, the fact that perfectionism and motivation are said to be
antecedents of exercise dependence suggests certain levels of these
factors could predispose or signify an individual to be at a greater
risk of becoming dependent on exercise. Previous research has
9
assessed the variables dually in the sporting domain, but no study
to date has assessed all three constructs at the same time or upon
the same population. A better understanding of what motivates people
to participate in exercise and their levels of perfectionism could
aid in the detection and treatment of individuals identified as
being at-risk for exercise dependence.
10

Review of Literature
It is generally accepted that there is an “optimal level” of regular
exercise where individuals can receive both physical and
psychological benefits from participation. The U.S. Department of
Health and Human Services (2008) recommend 300 minutes a week of
moderate intensity or 150 vigorous intensity exercise in order to
best utilise to benefits from exercise, with a view maintaining
and/or improving well being (Warburton, Nicol and Bredin, 2006).
Individuals exercising at a greater frequency and/or intensity than
the ‘optimal level’ may incur negative consequences of such
excessive participation. In some cases, Exercise is used as a coping
strategy or to regain some control over one’s life (*) however
excessive exercise to combat a short term problem leads to a more
long term issue. Persons engaging in a behaviour that provides
pleasure or relief from distress within the self (i.e. stress,
anxiety etc.) coupled with a consistent inability to refrain from
such activity despite negative consequences signifies an addictive
behaviour (Goodman, 1990). This syndrome, otherwise known as
11
exercise dependence has been evident within the academic literature
since the 1970’s and interest in the area has increased dramatically
during the last decade.
Exercise Dependence
The landmark paper within the exercise dependence literature was
written by De Coverley Veale (1987). De Coverley Veale was the first
author to make the division between primary and secondary exercise
dependence. The distinguishing factor between the two is the
underlying reason for exercise participation. An individual
exercising for the enjoyment they receive from such participation,
where dieting or weight loss is used for performance enhancement
would be defined as primary ED. Here, a physical activity is an end
in itself (i.e. individuals are intrinsically motivated). On the
other hand, secondary ED individuals use exercise as a control
measure for an eating disorder, i.e. using exercise to control
weight i.e. calorie management and/or weight loss (American
Psychological Association [APA], 1994).
The main concern of early ED research was the use of poor research
techniques and unsound, invalidated self-report scales (Hausenblas
and Symons Downs, 2002b). The advancement of universal measures of
ED that were flexible, reliable and valid was paramount to develop a
better understanding of ED. The Exercise Dependence Scale [EDS],
12
developed Hausenblas and Symons Downs (2002b) is highly regarded as
a one of the best measures of ED and has been used in many studies
(Monok et al., 2012). The creation of a measurement tool that could
be utilised by various researchers allowed for comparisons across
both, different studies and populations. The EDS is based on the
DSM-IV criteria for substance dependence, consisting of 7 subscales;
tolerance, withdrawal, intention effects, loss of control, time,
conflict and continuance. The EDS comprehends that an individual can
be attributed to one of three categories based on the existence of
ED symptoms. Persons exhibiting no ED symptoms are classified as
‘nondependent-asymptomatic’. In comparison, the ‘nondependent-
symptomatic’ category encompasses individuals that exhibit some
symptoms of ED. Finally, individuals exhibiting high levels of ED
symptoms (high in 3 or more of the subscales) are categorised in the
‘at-risk for exercise dependence’ group (Downs, Hausenblas and Nigg,
2004).
A number of researchers have used to EDS as a measurement tool for
examining the prevalence rates of people at-risk for exercise
dependence. Hausenblas and Symons Downs (2002b) found the occurrence
of individuals at-risk for exercise dependence to be between 3.1%
and 13.4%, across 4 studies on university students. The authors
suggested the dispersion of scores was based on the changes made to
the EDS during its development within the 4 studies and the variety
13

of population’s assessed. Other studies have also found differing
prevalence rates of at-risk for exercise dependence individuals;
Edmunds, Ntoumanis and Duda (2006) 3.4%, Monok et al., (2012) 1.9%
and Gonzalez-Cutre and Sicilia (2012) 7%. Only one study to date has
used the EDS to access ED on a weightlifting population. In Hale et
al. (2010) study, 15.1% of the participants were classified as at-
risk for exercise dependence. Hale et al’s study criticised previous
research on ED, citing the use of college age participants as a
possible reason for the lower prevalence rates, Hale et al. examined
older/ more experienced as well as younger, less experienced
bodybuilder, power lifters and fitness lifters in their sample.
There is some debate whether weightlifters and bodybuilders exercise
dependence symptoms increase or are reduced with time. Moreover, do
weightlifters gain greater satisfaction over their body the longer
they have trained for (Szabo, 2000) or in fact do they feel they
need to continuously train in order to address body image concerns
(Hurst, Hale, Smith and Collins, 2000). Both Edmunds et al. (2006)
and Gonzalez-Cutre and Sicilia (2012) suggest that as a person
begins to gain the desired body shape and size they are more liable
to become exercise dependent
14
These findings suggest that exercise dependence symptoms would show
greater prevalence as a person got older. However, research has
posited that younger individuals show a greater propensity to be
classified as exercise dependent (Edmunds et al., 2006; Allegre,
Therme and Griffiths, 2007). There is vast societal pressure on
young people especially, to have the ‘perfect figure’. For women, a
slim, toned and slender looking body while men desire to be
athletic, lean and muscular (Gonzalez- Cutre and Sicilia, 2012). It
may seem of little surprise that exercise dependence symptoms may
being to foster from an earlier age based of the social demands
placed on young people today.
Other researchers have utilised a specific bodybuilding ED scale,
named the bodybuilding dependence Scale [BDS] (Smith, Hale and
Collins, 1998) to examine ED within a bodybuilding/ weightlifting
population. The BDS consists of 9 items assessing three subscales;
social dependence, training dependence and mastery dependence. Hurst
et al. (2000) found experienced bodybuilders (EXPBB) to be
significantly higher on all 3 subscales of the BDS than
inexperienced bodybuilders and weightlifters. Suggesting EXPBB
become dependent on the process of lifting weights as well as the
social/ personal aspects of lifting weights. Hale et al. (2010)
found Bodybuilders to be significantly higher on ED than power
15

lifters and fitness lifters. Furthermore, bodybuilders were found to
be significantly higher in the drive for muscularity (DM) than
fitness lifters. The results show that ED is linked to the DM and
that DM is more evident in young males which may lead to greater
exposure to the exercise dependence symptoms. The reduction of DM
with age is perhaps based around the muscular increases over time
from weight training, which aids the reduction of social physique
anxiety and body image concerns. This Adds to the suggestions that
older BB may in fact become addicted to the process of lifting
weight. It seems plausible to suggest that younger BB may become
preoccupied with the drive for muscularity and this may be an
influencing factor in early exercise dependence symptoms. A
suggestion somewhat supported by Hausenblas and Symons Downs’s
(2002b) study that found individuals classified as at-risk for
exercise dependence reported a significantly heavier ideal weight
than that of the two non-dependent groups who reported they ideally
wanted to lose weight. This finding regarding at-risk for ED
individuals striving to gain weight could be applied to the before
mentioned drive for muscularity in young weightlifters.
Due to the maladaptive nature of exercise dependence it is important
to understand the factors that contribute to the creation,
development and maintenance of its symptoms. A greater understanding
16

of possible causes of ED will allow for a more successful treatment
and prevention of such a disorder (Gonzalez-Cutre and Sicilia,
2012).
Perfectionism
Academics have posited a number of possible causes and correlates
for ED that either manifest themselves as predisposing traits or
develop as part of regular exercise and lead to ED. A number of
different personality traits have been positively linked to exercise
dependence; trait anxiety (Coen and Ogles, 1993), extroversion
(Yates, Leehey and Shisslak, 1983) and obsessive compulsiveness
(Spano, 2001). Negative correlations have also been found between
ED; Neuroticism (Hausenblas and Giacobbi, 2004) and self-esteem
(Rudy and Estok, 1987; Carron et al., 2003). Another personality
trait strongly linked to exercise dependence is perfectionism.
“Perfectionism has been described as a personality disposition
characterized by striving for flawlessness and setting excessively
high standards for performance accompanied by tendencies for overly
critical evaluations of one’s behaviour” (Stöber, Feast and Hayward,
2009: 1-4).
There are two well validated measurement tools for perfectionism.
Firstly, Hewitt and Flett (1991a) suggested perfectionism was
17

comprised of 3 parts within the Multidimensional Perfectionism Scale
(MPS); self-orientated, socially-prescribed and other-orientated.
Self-orientated perfectionism details the propensity of an
individual to set abnormally high performance standards and focusing
or poor elements of his or her performance. Socially-prescribed
perfectionism states others set high performance standards for an
individual, and will consequently be disappointed if they are not
fulfilled. Other-orientated perfectionism entails the setting of
excessively high performance criteria for others and a critical
evaluation of their performance.
The second measure of perfectionism is the Frost Multidimensional
Perfectionism Scale [FMPS] (Frost, Marten, Lahart and Rosenblate
(1990) which was revised by Stöber et al. (1998) to contain 4
instead of the original 6 subscales; Concerns over Mistakes and
Doubts (CMD), Parental Expectations and Criticism (PEC), Personal
Standards (PS), and Organization (O). CMD measures the tendency of
becoming overly concerned with and react badly too mistakes as well
as experiencing uncertainty over a performance. PEC encompasses the
individuals perceptions of parental expectations and the over
critical nature of their parents when assessing a performance. PS
measures an individual’s creation of high performance standards and
goals. O measures a person’s neatness (Hachon, 2010).
18

With reference to the nature of perfectionism it can be adaptive or
maladaptive personality trait depending on the existence of
unwarranted self-critical evaluation and disproportionate high
standards (Frost et al., 1990). Adaptive perfectionists are
characterised by the setting of high PS and a preference for O
(Hachon, 2010). However, adaptive perfectionists are driven to
achieve these performance standards but can accept they may have
personal limitations (Blatt, 1995). Conversely, maladaptive
perfectionists also have high PS but are overly concerned about
making mistakes and have no other desire than to avoid failure
(Blatt, 1995). Maladaptive perfectionism includes an over-awareness
in the differences between actual and expected high PS with little
leeway for mistakes (Coen and Ogles, 1993). Adaptive perfectionism
refers to more positive influence of the personality trait “compared
to CMD but not always as adaptive as an absence of perfectionism”
(Mouratidis and Michou, 2011: 356). PS are considered to be more
adaptive in nature as opposed to CMD, and have shown to improve
performance (Stoll, Lau and Stöber, 2008) and reduce burnout
(Lemyre, Hall and Roberts, 2008). The striving to satisfy high PS
can lead to motivational benefits, as been demonstrated in both an
educational (Stöber and Rambow, 2007) and sports setting (Ommundsen
et al., 2005).
19

In relation to ED, a positive relationship has been fond with
perfectionism in three studies. Coen and Ogles (1993) found
obligatory runners to be significantly higher on perfectionism than
their non-obligatory counterparts. Hausenblas and Symons Downs
(2002b) stated the at-risk for exercise dependence group scored
significantly higher on perfectionism than both of the non-dependent
ED groups. Hagan and Hausenblas, 2003) found the high ED group
reported significantly higher levels of perfectionism than the low
ED group.
Although these studies provide evidence for a relationship between
high exercise dependence symptoms and high levels of perfectionism,
none of the papers used a multidimensional measure of perfectionism
or the finalised Exercise dependence scale.
Self-Determined Motivation
Another variable, linked to exercise dependence is motivation. A
person’s level of motivation determines the initiation, maintenance
and completion of exercises (Gonzalez-Cutre and Sicilia, 2012)
Furthermore, motivation has been described as one of the key
antecedents of exercise dependence (Ogles, Masters and Richardson,
1995). It so forth posits that a better understanding of the types
and nature of person’s motivation to participate in exercise can
lead to a greater understanding of ED and aid the development of
20

preventative strategies. Self-determination theory (SDT) devised by
Deci and Ryan (2000) is one theory of motivation that has been
applied within the sporting domain and has been correlated with
exercise behaviour (Lonsdale et al., 2008), athlete burnout
(Lonsdale, Hodge and Rose, 2009) and coping strategies (Mouratidis
and Michou, 2011).
Self-determination theory states that humans have three basic
psychological needs (adapted to exercise), Competence i.e. ability
to be effective in a given sport, Autonomy i.e. volition and choice
and Relatedness i.e. connections to others (Deci and Ryan, 2000).
“The extent to which these needs are satisfied determines the degree
to which an athlete’s behaviour is regulated by processes that are
congruent with the individual’s sense of self, known as self-
determined motivation” (Deci and Ryan, 1985, in Lonsdale et al.,
2009: 786). Satisfying these psychological demands leads to optimal
well-being (e.g. subjective vitality [Ryan and Frederick, 1997]),
where as failure leads to representations of ill-being (e.g. Burnout
[Perreault *et al., 2007]).
In accordance with SDT theory, human motivation can be depicted upon
a continuum with varying degrees of self-determination (Deci and
Ryan, 1985). The level of self-determination diminishes throughout
21

the continuum from intrinsic motivation to extrinsic motivation to
Amotivation (figure 1).
Figure 1. Self-Determination Continuum (Lonsdale, Hodge and Rose, 2008: 324) Amotivati
on Extrinsic MotivationIntrinsicMotivation
Controlled Motivation Autonomous Motivation
ExternalRegulation
Introjected
Regulation
IdentifiedRegulation
Integrated
Regulation
Low self-determination High self-determination
The most self-determined of the SDT continuum is intrinsic
motivation. Here motivation is derived from the pleasure and
satisfaction of participating in a given activity to pursue new
challenges in e.g. lifting weights for the feeling of being ‘pumped’
(Ryan and Deci, 2000). Extrinsic motivation exists when an
individual participates to achieve external goals and comprises of 2
super-ordinate parts; autonomous motivation (AM) and controlled
motivation (CM) and 4 sub-ordinate parts; Integrated Regulation,
Identified Regulation, Introjected Regulation and External
Regulation. Autonomous behaviours are freely determined and
originate within one’s self (Reeve, 2002) where as controlled
behaviours are derived from an external source and are non-
volitional in nature (Edmunds et al., 2006). When the needs of
competence, autonomy and relatedness are met, individuals become
22

autonomously motivated. Conversely, if the basic psychological needs
are not achieved then a person will exhibit controlled motivation
(Ryan and Deci, 2002). The most self-determined dimension of
extrinsic motivation is integrated regulation, which represents an
individual’s belief that certain behaviours are part of their
individual identity and conform to their personal values (Ryan and
Deci, 2000). The second part of autonomous motivation is identified
regulation, which accounts for an individual’s participation in
exercise to achieve goals that he or she finds morally important
(Lonsdale et al., 2009). Introjected regulation describes the need
for intrapersonal rewards such as pride and the avoidance self-
inflicted punishments such as guilt (Duncan et al., 2010). External
regulation is the least self-determined aspect of extrinsic
motivation and states that an individual wishes to obtain rewards/
avoid punishment to satisfy significant others such as parents or
coaches (Duncan et al., 2010). The final aspect of the SD continuum
is Amotivation, characterised by an individual that mat no longer
have the ability identify the reasons for participation in an given
activity (Lonsdale et al., 2009).
Despite the pivotal role of motivation in determining exercise
behaviour, to date only four studies to the authors knowledge have
directly assessed the relationship between SD motivation and the
23
three exercise dependence groups. Hamer, Karageorghis and
Vlachopoulos (2002) were the first authors to assess the
relationship between SD motivation and ED. Their results showed
introjected and identified regulation to be the only positive
predictors of high exercise dependence individuals, a finding that
was mirrored by Fortier and Farrell (2009). Edmunds et al. (2006)
also found introjected regulation approached significance as a
positive predictor of strenuous exercise behaviour for symptomatic
individuals. Identified regulation was found to be a positive
predictor of strenuous exercise for asymptomatic individuals. In
addition, Gonzalez-Cutre and Sicilia (2012) established introjected
regulation to be a positive predictor of ED. Moreover, and somewhat
surprisingly external regulation and integrated regulation were also
found to be positive and significant predictors of ED in an ego-
involving climate (i.e. where a person’s ability is compared to that
of others). Although this study did not assess a weightlifting
population it seems reasonable to suggest that in sports (such as
weightlifting), where judgment is often made on a person’s body
size, shape and strength they may become addicted towards such an
activity in an effort to outdo others around them or to avoid
negative feelings about one’s self, which may create self doubt and
lower self-esteem.
24
There are clear links a between motivation and perfectionism
demonstrated in the study above. Other researchers have also
discovered a relationship between the two constructs. High personal
standards have been found to be positively correlated with both
autonomous and controlled motivation. The degree of SD depends on
the perception of the PS; whether they are seen as a challenge or as
a performance level norm to maintain self-worth (DiBartolo, Frost,
Chang, LaSota, and Grills, 2004). When PS are seen as a challenge,
they are more likely to manifest as an intrinsic motivator due to
the challenge-seeking nature of IM (Chatzisarantis and Hagger,
2007). Conversely, Personal standards that are seen as a
prerequisite to gain self-worth may manifest as a restraint of one’s
self-regulated behaviour and will therefore lead to presentation of
controlled motivation (Mouratidis and Michou, 2011). Other
researchers such as Stöber, Feast and Hayward (2009) found self-
orientated perfectionism (internal form) to be positively linked
with the more self-determined aspects of motivation and socially-
orientated perfectionism (external form) to be positively related
with the lesser self-determined aspects. Concerns over mistake are
likely to lead controlled motivation Gaudreau and Antl (2008). Due
to the internal stresses which evoke controlled forms of motivation.
Based on the impact of a critical approach towards making mistakes
and failing, athletes will often become and/ or remain controlled
25
motivated (DiBartolo et al., 2004). Other studies have used the
relationship between the two constructs to assess other variables
such as coping strategies (Mouratidis and Michou, 2011).
The papers outlined above provide supporting evidence for the use of
SDT in the assessment of exercise dependence. The current literature
review has shed light upon the three constructs however no research
to date has directly assessed them on the same population. There is
still a lack of research comparing the three groups of exercise
dependence (i.e. non-dependent asymptomatic, non-dependent
symptomatic and at-risk for exercise dependence) and how they differ
in terms of their motivation and perfectionism Edmonds et al.
(2006). As stated above motivation and personality traits play a
pivotal role in the development of ED symptoms. A study that
assesses the relationship and predictability of such antecedents of
ED would be beneficial in aiding the prevention and treatment of
such a psychological disorder.
The majority of research on ED has been undertaken on long distance
runners (e.g. Allegre et al., 2007), with only two studies to date
(Hurst, Hale, Smith and Collings, 2000; Hale, Roth, DeLong and
Briggs, 2010) having directly assessed exercise dependence on
weightlifters. For that reason, the primary aim of the current study
26

was to assess whether an individual’s level of perfectionism and
self-determined motivation could predict the group classification of
exercise dependence (i.e. non-dependent asymptomatic [low ED], non-
dependent symptomatic [moderate ED] and at-risk for exercise
dependence [high ED]). Secondly, further analysis will be undertaken
between participant’s scores of the three constructs with a view to
identifying any possible patterns between the variables and to
conflict or confer with previous research findings. Tests will also
be included to examine any mediating relationship that age and the
amount of hours a person spends weightlifting may have and affect on
their exercise dependence classification.
Hypothesis
Can exercise dependence group classification be determined/
predicted by an individual’s level of perfectionism and self-
determined motivation?
27
Methodology
Design
The current study adopted a non-experimental, quantitative approach.
A logistical regression design enabled the author to identify any
relationships between the two categorical, independent variables
(i.e. self-determined motivation and perfectionism) and the
categorical, dependent (i.e. exercise dependence). Specifically,
multinomial logistic regression was used to provide the estimated
predictability of an individual belonging to a specific population
(i.e. exercise dependence group) based on their scores on the two
independent/ predictor variables. The two independent (IV)/predictor
variables were perfectionism (three levels [used during data
analysis]: low, moderate and high) and self-determined motivation
(six levels: Amotivation, Extrinsic regulation, Introjected
regulation, Integrated regulation, Identified regulation and
Intrinsic motivation). The dependent (DV)/ outcome variable was
exercise dependence. (The three levels of exercise dependence are;
28

non-dependent asymptomatic, non-dependent symptomatic and at-risk
for exercise dependence).
Participants
A total of 69 experienced* male weightlifters (M = 23.86, SD =5.62)
participated in the current study. Ethical Approval (see appendix 1)
and gatekeeper approval (see appendix 2) were received prior to any
data collection being undertaken. An opportunity sampling method was
employed to recruit participants. Individuals were approached by the
researcher upon entry to the leisure centre and asked if they would
like to participant in the study once they had finished their
workout. All participants provided voluntary participation and
informed consent to partake in the current study. Informed consent
was obtained from each participant via the informed consent form
(see appendix 3). Participants were assigned to one of three groups
on the exercise dependence continuum (non-dependent asymptomatic,
non-dependent symptomatic, and at-risk for exercise dependence)
based on their score on the Exercise Dependence Scale (EDS).
* Experienced weightlifters are characterised as having a minimum of
12 months weightlifting participation.
Measures
29

The Exercise Dependence Scale [EDS] Hausenblas and Symons Downs, 2002) – was
used to measure participants exercise dependence symptoms. The 21-
item scale contains seven sub-categories based on the seven
criterions for which substance dependence is based (American
Psychiatric Association [APA], 1994). Withdrawal effects (e.g., I
exercise to avoid feeling irritable), continuance (e.g. I exercise
when injured), tolerance (e.g. I continually increase my exercise
duration to achieve the desired effects. Benefits), lack of control
(e.g. I am unable to reduce how long I exercise), reduction is other
activities (e.g. I would rather exercise than spend time with my
family/ friends), time (e.g. I spend most of my free time
exercising), and intention effects (e.g. I exercise longer than I
plan). Participants provided responses to questions using a 6-point
Likert scale with 1 (never) and 6 (always) at the extremes. A higher
score indicates higher levels of exercise dependence symptoms.
Responses can be studied as an overall ED score and as individuals
subscale. A distinction between physiological and non-physiological
dependence can also be demonstrated based on scores from the
tolerance and withdrawal effects subscales (see appendix 4).
(to
The Frost Multidimensional Perfectionism Scale [FMPS] Stöber (1998) – was used to
measure participant’s levels of perfectionism. The original FMPS
30

(Frost et al., 1990) consists of 35 items with 6 dimensions:
Concerns over Mistakes (9-items) (, Doubts about Actions (4-
items) (, Parental Expectations (5-items) (
Parental Criticism (4-items) (, Personal Standards (7-
items) (, and Organisation (6-items) ( However,
Stöber’s (1998) revised model uses four dimensions: Concerns over
Mistakes and Doubts (CMD), Parental Expectations and Criticism
(PEC), Personal Standards (PS) and Organisation (O). Due to the
remit of the current study, the inclusion of PEC and organisation O
may have affect the face validity of the study as they are not
directly related to the weightlifting context under investigation.
Henceforth, the current study only assessed responses to CMD [13-
items] (e.g. I hate being less than the best at things), and PS [7-
items] (e.g. I have extremely high goals). A similar method has
previously been utilised in the sporting domain (Dunn et al., 2002;
Mouratidis and Michou, 2011). The correlation between CMD and PS was
found to be adequately reliable (. The modified questionnaire
will now be referred to as FMPS* (rather than FMPS, which is used to
identify the original scale). Responses were provided using a 7-
point Likert scale for which scores can be calculated for each
dimension as well as an aggregate score for perfectionism. Higher
scores signify higher levels of perfectionism (see appendix 5).
31

The Sport Motivation Scale-6 [SMS-6] (Mallett et al., 2007) – was used to
identify participant’s underlying reasons for exercise participation
(i.e. motivation). The SMS-6 consists of 24-items, which measures
self-determined motivation along a continuum. The original SMS
(Pelletier et al., 1995) outlined 7 self-determined categories
however the SMS-6 only has 6. Each of the 24 items was is response
to the question “Why do you practise your sport”, with 4 items for
each category; amotivation (e.g. I don’t know anymore; I have the
impression of being incapable of succeeding in this sport) (,
external regulation (e.g. Because it allows me to be well regarded
by people that I know) (, introjected regulation (e.g.
Because I must do sports to feel good about myself) (,
identified regulation (e.g. Because training hard will improve my
performance) (, integrated regulation (e.g. Because it is an
extension of me) (, and intrinsic motivation (e.g. For the
excitement I feel when I am really involved in the activity)
(. Responses are given on a 7-point Likert scale with 1 (Does
not correspond at all) and 7 (corresponds exactly) at the extremes
(see appendix 6). (
Procedure
Before commencing the study, ethical approval was received by
Coventry University Ethics Committee (see appendix 1). Prior to any
32
data being collected, the manager of Trilogy Health and Fitness
Leisure Centres was contacted in order to gain approval to use its
members as participants in the study described above, gatekeeper
approval can be found in appendix 2. Gym members were approached
upon entry to the leisure centre, given a brief overview of the
study and were asked if they would like to participate in the study
once they had completed their workout. Each participant was screened
to ensure they met the entry criteria for the study (i.e.
Participants were required to be male, over 18 years of age and have
one year’s weightlifting experience as a minimum). Participants
meeting the criteria and wishing to take part were given a
questionnaire pack consisting of a participant information sheet
(PIS), informed consent form (IC), demographic sheet (DS) [age, sex,
hours spent weightlifting per week], EDS, FMPS*, SMS-6 and debrief
sheet. Participants were advised that the questionnaire pack would
take around 15 minutes to complete and were asked to read all of the
information presented to them carefully. Participants were taken to
a quiet room in the leisure centre and completed the entire
questionnaire pack. The researcher remained with the participant in
order to address any questions or difficulties they may encounter
regarding the completion of the questionnaire pack. The researcher
collected the IC, DS and questionnaires once completed. The
researcher then explained the purpose of the study in greater
33

detail, handed a debrief sheet to each participant and asked if they
had any further questions about the research project. Participants
were advised to keep their PIS and debrief sheet safe in case they
would like to withdraw their consent for participation in the study
or contact the researcher.
Data Analysis
All data returned to the author was collated and input into SPSS
statistics software for data analysis. Basic descriptive and
frequency analysis was undertaken. T-tests were used to compare
means of age and average hours spent weightlifting. Following this,
a Multinomial Logistic Regression (MLR) analysis was carried out in
order to assess the impact of the two independent/ predictor
variables upon the prediction model. A base line prediction was
made, to which the MLR test adds each predictor variable to assess
whether or not it improves the models ability to successfully
predict categorisation of an individual on the dependent/ outcome
variable of exercise dependence (i.e. non-dependent asymptomatic,
non-dependent symptomatic, and at-risk for exercise dependence).
Multinomial logistic regression does not make any assumptions of
normality, linearity, and homogeneity of variance for the
independent variables. The significance level was set at .05 for the
current study.
34

Results
All participants were male, ageing between 18 and 45 (M =23.85, SD =
5.62). The frequencies for each variable were calculated to show how
many individuals were found to be in each group (Table 1).
Table 1. Group populations for ED, SD motivation and PerfectionismNumber of
Participants
Scale Group(N
= ) %Exercise Dependence Scale Non-Dependent Asymptomatic 1 1.4( EDS) Non-Dependent Symptomatic 61 88.4
At-Risk for Exercise Dependence 7 10.1
Frost Multidimensional Low 23 33.33Perfectionism Scale* Moderate 23 33.33(FMPS*) High 23 33.33Sport Motivation Scale-6 Amotivation 0 0 (SMS-6) External Regulation 3 4.3 Introjected Regulation 14 20.3 Identified Regulation 8 11.6 Integrated Regulation 18 26.1 Intrinsic Motivation 26 37.7Note: perfectionism groups created during data analysis (see below)
The majority of participants were classified as non-dependent
symptomatic (N = 61, 88.4%; M = 68.54, SD = 12.10) for exercise
dependence, followed by at-risk for exercise dependence (N = 7,
10.4%) M = 97.71, SD = 9.78 and non-dependent Asymptomatic (N = 1,
1.4%).
35
For ease of data interpretation, perfectionism total scores were
transformed from a continuous to a categorical scale. The newly
formed perfectionism groups (low, moderate and high) were calculated
using the best cut-points created using SPSS transform visual
binning. Three groups were found to be more reliable as they
provided less empty cases in the final output (3 groups, n = 21; 5
groups, n = 42) and an equal distribution of individuals to each
category compared to 5 groups. The results were as follows; Low
perfectionism (N = 23, 33.3%; M = 58.22, SD = 7.54), Moderate
perfectionism (N = 23, 33.3%; M = 76.10, SD = 4.35) and High
perfectionism (N = 23, 33.3%; M = 93.80, SD = 9.13).
In terms of self-determined motivation, Intrinsic motivation was
found to be the most common group amongst the current population (N
= 26, 37.7%), followed by integrated regulation (N =18, 26.1 %),
identified regulation (N =8, 11.6 %), introjected regulation (N =14,
20.3%), external regulation (N = 3, 4.3%). Finally, none of the 69
participants were found to belong to the amotivation category of
self-determined motivation.
Secondly, cross tabulations were conducted to assess whether any
relationship or pattern could be found between the three variables
based on the group populations (Tables 2, 3 and 4).
36

Table 2. Cross tabulations for ED and SD motivation groups for low perfectionism
Exercise Dependence group (N = )
Self-DeterminedMotivation group
Non-Dependent
AsymptomaticNon-DependentSymptomatic
At-risk forExercise
DependenceTota
lExternal Regulation 0 0 0 0Introjected Regulation 0 3 0 3Identified Regulation 0 2 0 2Integrated Regulation 0 6 1 7Intrinsic Motivation 0 11 0 11Total 0 22 1 23
Table 3. Cross tabulations for ED and SD motivation groups for moderate perfectionism
Exercise Dependence group (N = )
Self-DeterminedMotivation group
Non-Dependent
Asymptomatic
Non-Dependent
Symptomatic
At-risk forExercise
DependenceTota
lExternal Regulation 0 1 0 1Introjected Regulation 1 4 0 5Identified Regulation 0 1 1 2Integrated Regulation 0 5 2 7Intrinsic Motivation 0 8 0 8Total 1 19 3 23
Table 4. Cross tabulations for ED and SD motivation groups for high perfectionism
Exercise Dependence group (N = )
Self-DeterminedMotivation group
Non-Dependent
AsymptomaticNon-DependentSymptomatic
At-risk forExerciseDependence
Total
External 0 1 1 2
37

RegulationIntrojected Regulation 0 6 0 6Identified Regulation 0 4 0 4Integrated Regulation 0 3 1 4Intrinsic Motivation 0 6 1 7Total 0 20 3 23
The at-risk for exercise dependence group is of particular interest
as 4 of the 7 individuals identified as at-risk for exercise
dependence were classified into the integrated regulation category
for SD motivation. These 4 individuals are spread across all three
groups for perfectionism. Moreover, only 1 of the 7 high exercise
dependence individuals was found to exhibit low perfectionism, with
the other 6 spread equally between the moderate and high
perfectionism groups.
Based on the findings of previous research, a prediction was made
for each Ed group with regards to the expected levels of
perfectionism and self-determined motivation individuals classified
within that group were likely to exhibit.
(1) Individuals classified as at-risk for exercise dependence will
score highly on perfectionism and the autonomous/ more self-
determined motivation categories (i.e. intrinsic motivation,
38

integrated regulation and identified regulation) as well as external
regulation. (2) Individuals classified as non-dependent symptomatic
will score high to moderate on perfectionism and be classified
within the high SD end of controlled motivation and both parts of
autonomous motivation (i.e. introjected regulation, identified
regulation and integrated motivation). (3) Individuals classified as
non-dependent asymptomatic for exercise dependence will score low to
moderate on perfectionism and classified mainly as identified
regulation for self-determined motivation.
Prediction 1 was partially correct for the at-risk for exercise
dependence group. Perfectionism was found to be scattered across the
three groups, with the majority of individuals classified as high or
moderate. All of the 7 individuals categorised in the high ED group
fell within the four of the five categories (intrinsic motivation,
integrated regulation, identified regulation and external
regulation. Prediction 2 was also somewhat incorrect. Non-dependent
symptomatic individuals were dispersed almost equally across the
three perfectionism groups. In terms of motivation, intrinsic
motivation was the most heavily populated category, also introjected
and integrated groups housed large amounts of individuals compared
to external and identified regulation. Prediction 3 was again
partially correct in terms of perfectionism, as the individual
39
identified with the low asymptomatic group yielded a moderate
perfectionisms total. Moreover, the individual was not correctly
predicted in terms of motivation (i.e. introjected rather than
identified regulation). The results for the non-dependent
asymptomatic category however should be disregarded as only one
individual populated this category, making generalisability of the
findings invalid.
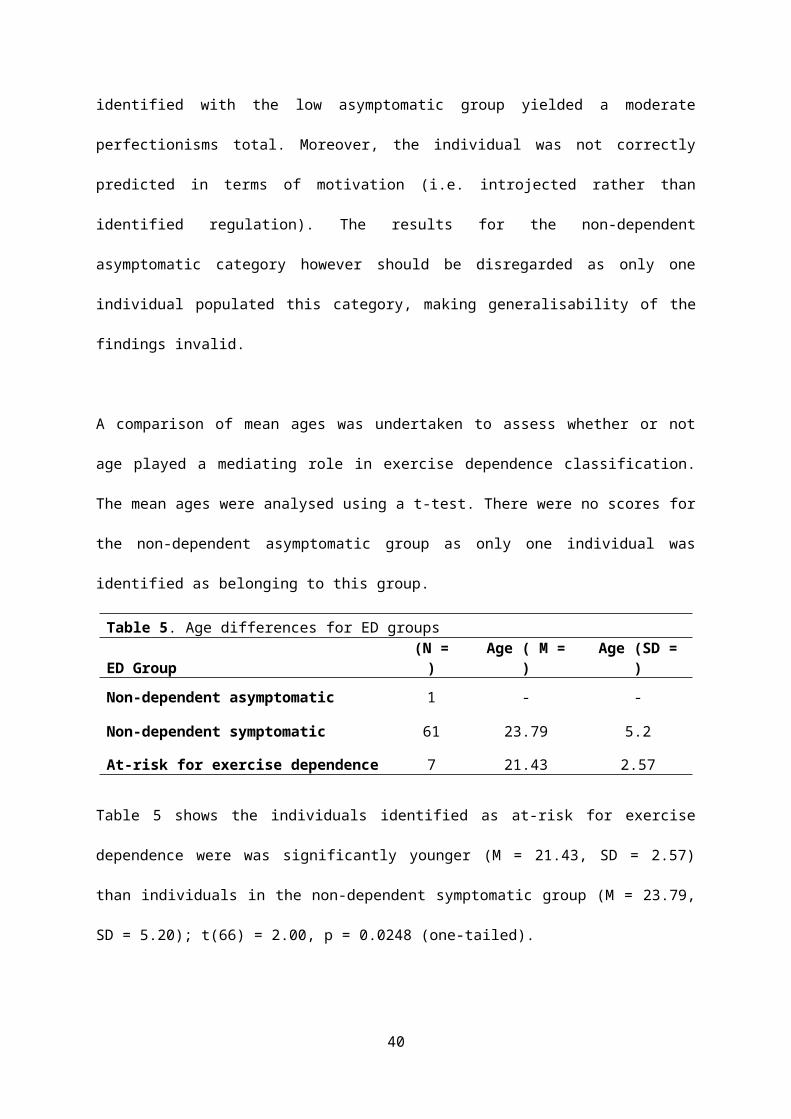
A comparison of mean ages was undertaken to assess whether or not
age played a mediating role in exercise dependence classification.
The mean ages were analysed using a t-test. There were no scores for
the non-dependent asymptomatic group as only one individual was
identified as belonging to this group.
Table 5. Age differences for ED groups
ED Group(N =)
Age ( M =)
Age (SD =)
Non-dependent asymptomatic 1 - -
Non-dependent symptomatic 61 23.79 5.2
At-risk for exercise dependence 7 21.43 2.57
Table 5 shows the individuals identified as at-risk for exercise
dependence were was significantly younger (M = 21.43, SD = 2.57)
than individuals in the non-dependent symptomatic group (M = 23.79,
SD = 5.20); t(66) = 2.00, p = 0.0248 (one-tailed).
40

The ability of perfectionism and self-determined motivation scores
to predict exercise dependence group classification was assessed
using a multinomial logistic regression (MLR). The relationship test
between the independent variables of self-determined motivation and
perfectionism and the dependent variable, exercise dependence was
based on the reduction in likelihood values for the model with
(model-1) and without the independent variables(model-0). The
difference in likelihood is described as a chi-square distribution.
The model containing the independent variables as predictors is
known as the model chi-square. The results of prediction model are
presented below.
Table 6. Model fitting information
Model-2 Log
Likelihood Chi-square df sigIntercept Only 32.901Model 18.273 16.268 12 0.262
The distribution (table 6) shows that the probability of the model
chi-square (16.268) was 0.262, greater than the significance level
set at .05. Therefore, model-1 was underperforming in comparison to
model-0. Consequently, the hypothesis was rejected as this finding
provides no supporting evidence for the existence of a relationship
between the dependent variable (ED) and the combination of
41
independent variables (SD motivation and perfectionism) in terms of
a prediction model.
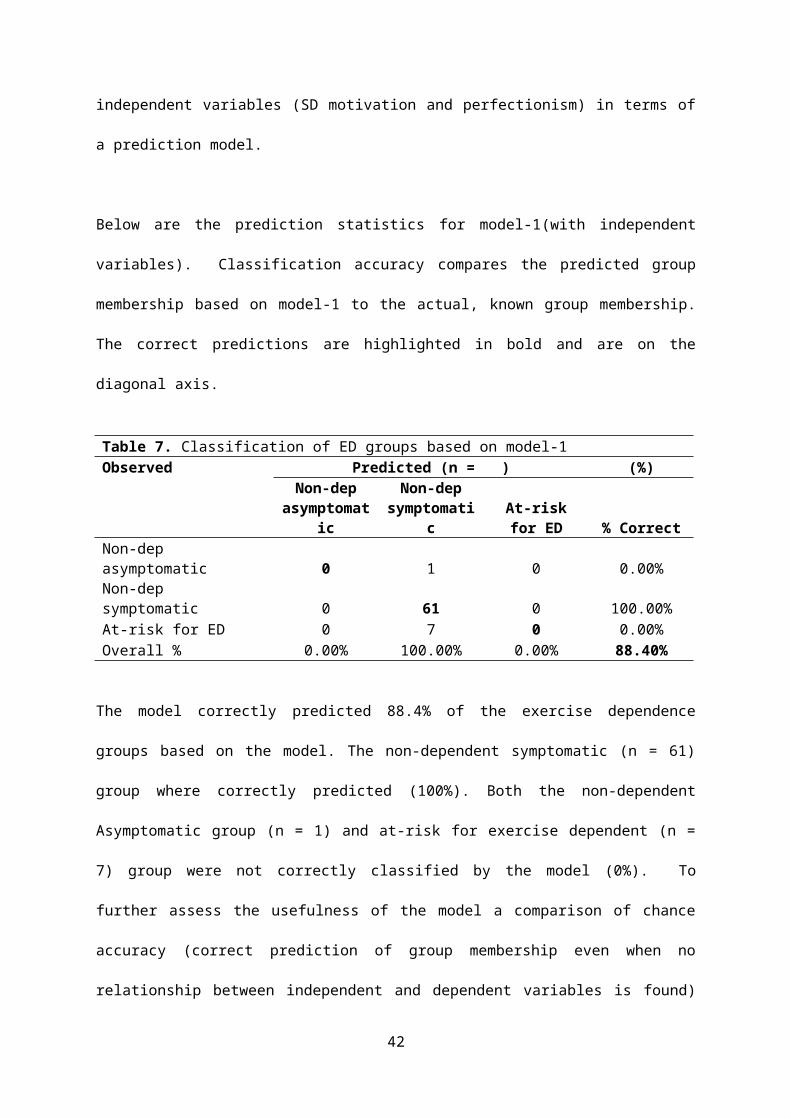
Below are the prediction statistics for model-1(with independent
variables). Classification accuracy compares the predicted group
membership based on model-1 to the actual, known group membership.
The correct predictions are highlighted in bold and are on the
diagonal axis.
Table 7. Classification of ED groups based on model-1Observed Predicted (n = ) (%)
Non-depasymptomat
ic
Non-depsymptomati
cAt-riskfor ED % Correct
Non-dep asymptomatic 0 1 0 0.00%Non-dep symptomatic 0 61 0 100.00%At-risk for ED 0 7 0 0.00%Overall % 0.00% 100.00% 0.00% 88.40%
The model correctly predicted 88.4% of the exercise dependence
groups based on the model. The non-dependent symptomatic (n = 61)
group where correctly predicted (100%). Both the non-dependent
Asymptomatic group (n = 1) and at-risk for exercise dependent (n =
7) group were not correctly classified by the model (0%). To
further assess the usefulness of the model a comparison of chance
accuracy (correct prediction of group membership even when no
relationship between independent and dependent variables is found)
42

and classification accuracy from SPSS MLR output was undertaken.
Chance accuracy was found to be 98.98% compared to the SPSS MLR of
88.4% (see table 3.). This finding signifies that model-1 is not
helpful in predicting group categorisation.
To survey the usefulness of the two independent variables
separately, the likelihood ratio tests were extracted and examined
from the MLR output. These figures (table 8) are important to check
in order to evaluate whether one of the variables was in fact a
significant predictor of exercise dependent group classification but
was adversely affected by the other variable in the model-1
prediction total.
Table 8. Likelihood Ratio tests
Effect-2 Log likelihood of
Reduced Model Chi-Square df Sig.Intercept 18.273 a
SDM 29.154 10.881 8 0.209PERF 21.962 3.689 4 0.450
a – The Intercept reduced model is equivalent to the final model as omitting the effect doesnot increase the degrees of freedom
Likelihood ratio tests demonstrated that neither perfectionism nor
self-determined motivation contributed to improving the original
prediction model (Intercept). A result which shows there is no
significant relationship between SD motivation and ED (p = 0.209) or
perfectionism (PERF) and ED (p = 0.450).
The findings presented in table 9 describe the relationship between
the IV categories and the DV. The parameter estimates show whether
or not each category on the two independent variables can
43
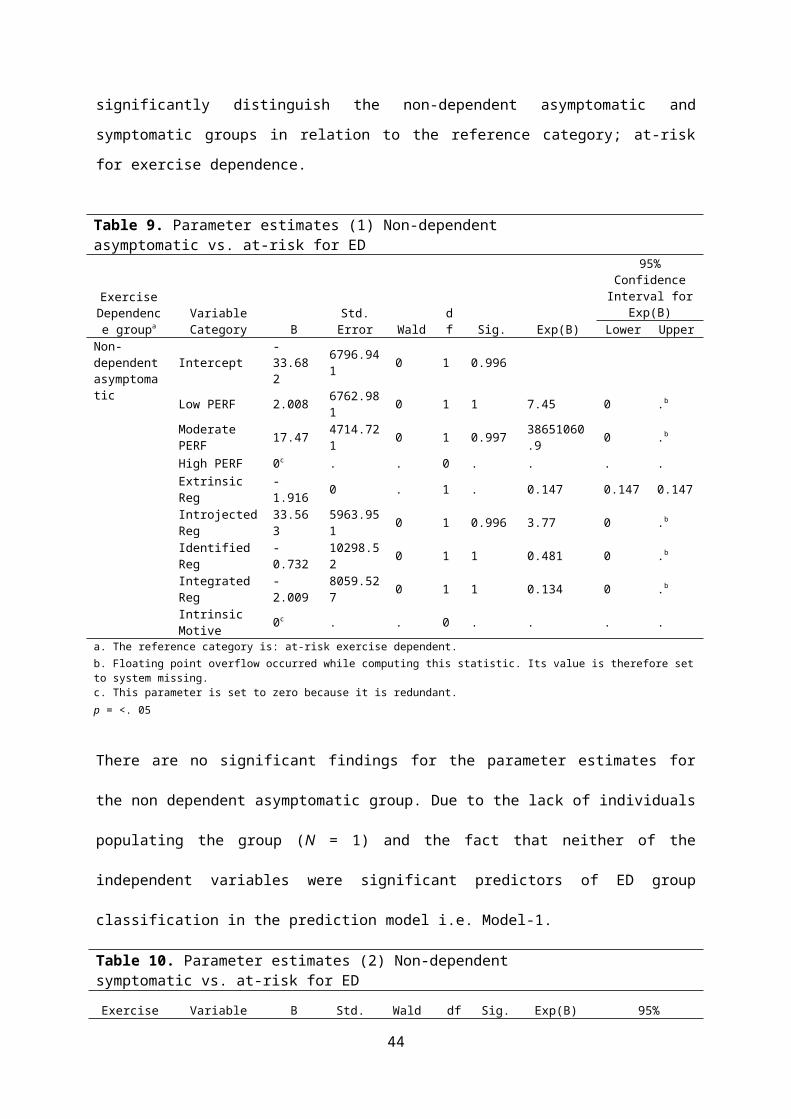
significantly distinguish the non-dependent asymptomatic and
symptomatic groups in relation to the reference category; at-risk
for exercise dependence.
Table 9. Parameter estimates (1) Non-dependent asymptomatic vs. at-risk for ED
ExerciseDependence groupa
VariableCategory B
Std.Error Wald
df Sig. Exp(B)
95%Confidence
Interval forExp(B)
Lower UpperNon-dependentasymptomatic
Intercept-33.682
6796.941 0 1 0.996
Low PERF 2.008 6762.981 0 1 1 7.45 0 .b
Moderate PERF 17.47 4714.72
1 0 1 0.997 38651060.9 0 .b
High PERF 0c . . 0 . . . .Extrinsic Reg
-1.916 0 . 1 . 0.147 0.147 0.147
IntrojectedReg
33.563
5963.951 0 1 0.996 3.77 0 .b
Identified Reg
-0.732
10298.52 0 1 1 0.481 0 .b
Integrated Reg
-2.009
8059.527 0 1 1 0.134 0 .b
Intrinsic Motive 0c . . 0 . . . .
a. The reference category is: at-risk exercise dependent.b. Floating point overflow occurred while computing this statistic. Its value is therefore setto system missing.c. This parameter is set to zero because it is redundant.p = <. 05
There are no significant findings for the parameter estimates for
the non dependent asymptomatic group. Due to the lack of individuals
populating the group (N = 1) and the fact that neither of the
independent variables were significant predictors of ED group
classification in the prediction model i.e. Model-1.
Table 10. Parameter estimates (2) Non-dependent symptomatic vs. at-risk for ED Exercise Variable B Std. Wald df Sig. Exp(B) 95%
44

Dependence groupa Category Error
ConfidenceInterval for
Exp(B)Lower Upper
Non-dependentsymptomatic
Intercept 2.765 1.159 5.687 1 0.017
Low PERF 1.371 1.294 1.122 1 0.289 3.94 0.312 49.79
7Moderate PERF 0.148 0.975 0.023 1 0.88 1.159 0.171 7.836
High PERF 0c . . 0 . . . .Extrinsic Reg -2.12 1.622 1.709 1 0.19
1 0.12 0.005 2.883
IntrojectedReg
15.825
3405.72 0 1 0.99
67459422.28 0 .b
Identified Reg -1.09 1.502 0.527 1 0.46
8 0.336 0.018 6.379
Integrated Reg
-1.995 1.184 2.84 1 0.09
2 0.136 0.013 1.385
Intrinsic Motive 0c . . 0 . . . .
a. The reference category is: at-risk exercise dependent.b. Floating point overflow occurred while computing this statistic. Its value is therefore setto system missing.c. This parameter is set to zero because it is redundant.p = <. 05
The only significant finding within the parameter estimates output
was that of the intercept (model without IV’s), which could
significantly distinguish between individuals in the non-dependent
symptomatic and at-risk for exercise dependence groups (p=0.017),
providing further evidence that Model-1 is not a good prediction
model for classifying individuals into exercise dependence groups.
45

Discussion
The aim of the present study was to assess the impact of
perfectionism and self-determined motivation on exercise dependence.
Specifically, was it possible to predict which category of exercise
dependence an individual would classified into based on their levels
of perfectionism and self-determined motivation.
The current study found that Model-1 (model with independent
variables) was underperforming in comparison to Model-0 (model with
no independent variables). In other words, self-determination and
perfectionism were found not too significantly predict an
individual’s exercise dependence group classification (p = 0.262).
In light of the results discussed above, the research hypothesis was
rejected.
Note: Due to only 1 participate populating the non-dependent
asymptomatic group; the subsequent discussion will disregard all
findings surrounding this category as no generalisations can be
drawn from such results.
46

Exercise dependence
In the current study, 7 participants (10.1%) were categorised in the
at-risk for exercise dependence group and were all found to have a
physiological dependence toward exercise (i.e. evidence of tolerance
and withdrawal). The prevalence rate found in the current study fits
in line with those found across the ED literature; Monok et al.,
(2012) 1.9%; Edmunds et al., (2006) 3.4%; Symons Downs et al. (2004)
3.6%-5%; Gonzalez-Cutre and Sicilia (2012) 7%; Hausenblas and Symons
Downs (2002b) 3.1%-13.4%; and Hale et al. (2010) 15.1%.
Perhaps surprising is the lack of individuals categorised as non-
dependent asymptomatic in the current population (1.4%). Previous
research has found the percentage for this group to be much higher;
7.5% in Hale et al. (2010); 11.7-69.5% in Hausenblas and Symons
Downs (2002).
The contrast in prevalence rates from the current study and the
majority of previous research is attributed to the type of activity
that has been examined in the present study. The Hausenblas and
Symons Downs, (2002b) studies focused on college athletes who
participated in a variety of activities and as noted, found a range
of at-risk prevalence rates. This adds weight to the belief that the
47
activity has a bearing on the development of ED. Gonzalez-Cutre and
Sicilia 2012) suggest the type of activity plays an important role
in the development of ED symptoms. Gonzalez-Cutre and Sicilia (in
press) found individuals participating in semi-directed activities
(instructor plans and supervises weight training program) and free
activities (person trains alone e.g. free weight or fitness
training) exhibited higher levels of exercise dependence compared to
people participating in directed tasks (instructor present to
monitor activity e.g. aerobics and indoor cycling) .
All participants used in the current study were participating in
either semi-directed activities (training program given to them
during their induction) or free activities (using their own weight
training program) which may explain the increase seen for
symptomatic and at-risk prevalence rates and the extremely low
population of the asymptomatic group. The main premise of
weightlifting participation is to improve ones physique and in order
to judge ones progress, comparisons are constantly made. This ego-
involving climate and an obsession with how others physiques compare
to your own are the perfect environment for exercise dependence
symptoms to thrive.
48

It was originally believed that ED symptoms would increase with age,
Hale et al. (2010) suggested the higher prevalence rate found within
their study was due to the fact that they had assessed ‘older adult
weightlifters’ as opposed to ‘college-ages lifters’ in Hausenblas
and Symons Downs (2002b). However, findings within this study
contradict such a belief as the symptomatic group was found to be
significantly older the at-risk for exercise dependence group. There
are a number of factors that are closely related to exercise
dependence; especially in weightlifters are in young lifters more
so. These include a greater drive for muscularity, higher social
physique anxiety and peer pressure. Media sources also put pressure
on young men to have an athletic, lean and muscular appearance and
for women to be slim, toned and slender (Gonzalez- Cutre and
Sicilia, 2012).
In pursuit of this ideal physique, persons exhibiting high ED
symptoms will participate in more frequent bouts of exercise and at
a greater intensity than non-dependent individuals (Hagan and
Hausenblas, 2003). It is of little surprise that individuals
identified as at-risk for exercise dependence individuals spent on
average more hours weightlifting every week than non-dependent
individuals.
Perfectionism
49

In terms of perfectionism, at-risk and symptomatic individuals were
predicted to exhibit moderate to high and asymptomatic individuals
to exhibit low to moderate perfectionism levels. These predictions
however, were only partially correct as individuals categorised as
at-risk for ED were found to score predominantly moderate to high on
perfectionism with a group mean off 86 which was higher than that of
the total participants mean of 76. A rather surprising result was
that 1 at-risk individual was was found to be low on perfectionism.
Although in terms of applying the results to the wider population
based on the fact that 1 individual scored low of perfectionism is
unjust, it offers an alternative view to that found in other
research that states that at-risk for ED individuals are
characterised by solely high levels of perfectionism. For non-
dependent symptomatic individuals, perfectionism categorisation was
split almost equally between the low, moderate and high groups;
however the symptomatic group mean was 74.93, slightly below that of
the population mean. This suggests that individuals showing symptoms
of ED may not necessarily be driven by high perfectionist tendencies
but may in fact be directed by other factors that may determine
their level of ED.
It is possible to suggest that the high number of individuals in the
symptomatic category and moderate levels of perfectionism are
50
because individuals participating in weightlifting are doing so for
a variety of different reasons (as found in the scattering across
the 5 populated groups of SD motivation). Although, everyone may
have aspirations for the ‘perfect’ physique, many people are aware
of their personal limitations so instead seek to improve their
physical and psychological well being without being overly concerned
of meeting these distorted images of the faultless body, often
portrayed.
Self-determined motivation
As Deci and Ryan (1985) outline, self-determined motivation is
measured along a continuum with 6 categories varying in self-
determinedness. Amotivation, being the least self-determined aspect
of the continuum is linked to behavioural disengagement and negative
psychological outcomes (Ryan and Deci, 2000). It was therefore
unsurprising that no participants were categorised as amotivated
from the current population. A weightlifter exhibiting amotivation
would be likely to cease participation in favour of a different
activity or give up completely. Intrinsic motivation has been linked
to persistent task engagement and improvements of one’s
psychological well-being (Deci and Ryan, 1985). Consequently it was
found that the most self-determined aspects, intrinsic motivation
(37.7%) and integrated regulation (26.1%). were the two most
51

populated categories was found to be the most populated category and
Integrated regulation. The two upper echelons of self-determined
motivation contain almost two thirds of the current population,
findings that correspond with Li’s (1999) research stating ‘more
frequent exercisers’ exhibit higher levels of intrinsic motivation
and autonomous, extrinsic motivation than ‘less frequent
exercisers’. Extrinsic regulation was found to be the lowest of the
populated SD groups (4.3%). Suggesting that participants in the
current study are generally motivated by more self-determined/
internal reasons rather than external reasons such as the
appeasement of significant others or other goals outside the
activity itself (Deci, 1971).
With relation to exercise dependence, 4 of the 7 (57.14%)
individuals categorised as at-risk for exercise dependence were
categorised in the integrated regulation SD group. Integrated
regulation details how exercise becomes an integral part of an
individual’s identity and has only been found as a positive
predictor of high ED in one study to date (Gonzalez-Cutre and
Sicilia, 2012). With this said, it seems viable to suggest the
integrated regulation could be seen as a strong positive predictor
for high ED symptoms in activities that support an ego-involving
climate, such as weightlifting. The other three individuals
52
identified as at-risk for ED were categorised into intrinsic
motivation, identified regulation and external regulation with one
in each group. The four groups mentioned above have all been found
to positively predict at-risk for ED individuals in previous
research (Hamer et al, 2002; Edmunds et al, 2006; Fortier* and
Farrell, 2009; Gonzalez-Cutre and Sicilia, 2012). However,
contradictory to previous research none of the individual’s
identified as at-risk for exercise dependence were categorised as
introjected regulated. Hamer et al. (2002), Edmunds et al. (2006),
Fortier and Farrell (2009) and Gonzalez-Cutre and Sicilia, (2012)
all found introjected regulation to significantly predict high ED
symptoms. Persons guided by introjected regulation would participate
in weightlifting because of feelings of guilt or about from not
doing so (Edmunds et al., 2006).
In a motivational sense, a belief that weightlifting is a part of
who you are as a person and the importance participating in
weightlifting has with regards to improving ones physique may play a
larger role in determining exercise behaviour. It would be unwise to
suggest that feelings of guilt from missing training sessions do not
reside within at-risk for ED and or some symptomatic individuals.
Feelings of guilt from missing a weight training session (i.e.
withdrawal) it would be easy for an individual to stop weightlifting
53

if they lost enthusiasm for the activity. With this said, it may not
seem so unexpected that 6 of the 7 at-risk individuals were
classified in the top 3 SD aspects of the continuum as intrinsic
motivation (most SD form) has been positively linked to increased
exercise behaviour (Edmunds et al., 2006)
Limitations and Future Research
There are a number of limitations and issues with the current study
that the author wishes to address. Firstly, although the sample size
for this study (N = 69) was adequate for its purpose as a research
project, the utilisation of a much larger sample would of been
greatly beneficial. It would of allowed for greater generalisability
of the findings in terms of the prevalence rates of each ED group.
It would of helped to support or refute the findings discovered in
this study that do not mirror those found in previous research such
as the low prevalence rate of the asymptomatic group. Furthermore,
if more people would have been identified within the asymptomatic
group if would of allowed this group to be included in data analysis
and the discussion sections, due to only one person being in their
group it provided the author with no viable findings.
54

Secondly, the sample used in the current study was of adequate size
for the purpose of the research project although a larger sample
would have beneficial sought after if time would have permitted.
Increasing the number of participants would have perhaps allowed for
better inter group comparisons and may have reduced the
categorisation disparity as it may have added more cases to the
asymptomatic group which would of allowed the author to use the
group during the data analysis. Previous research suggest many more
people should of been found to populate the non-dependent
asymptomatic group however, as noted earlier activities where an
ego-involving climate is apparent may differ in terms of the ratio
between the three ED groups. A larger sample size in future research
would aid the generalisability of such findings. Furthermore,
mediating factors such as hours spent weightlifting per week and age
could provide more significant findings if in fact, they have a
bearing on ED symptoms
With regards to the scoring of the FMPS*, it was unclear whether to
use a continuous or categorical scale to categorise people in terms
of perfectionism. For ease of data interpretation scale was graded
using a categorical scale with three groups (low, moderate and high
perfectionism). The groups were created using SPSS visual binning,
after the data had been interpreted. This created the groups with an
55

equal amount of people in each group for perfectionism. However, in
hindsight it may have yielded more interesting findings had these
boundaries been created prior to the data input stage. This was
however not a simple task as creating the cut points could severely
affect the results if put in the wrong place. The author of the
original scale Dr. Stöber was contacted regarding the best way to
calculate the scale however the information provided did not shed
light on this issue. Further research assessing perfectionism should
seek to address this issue as it would be beneficial for assessing
the construct in the sporting domain.
Due to nature of the current study (i.e. regression), it is not
possible to infer causality from the results. Future research should
seek to utilise a longitudinal design in order to assess whether
variables such as perfectionism and motivation are a cause or an
affect derived from ED. Longitudinal studies provide many problems
for researchers such as high dropout rates as well as time and
monetary constraints, which is why such studies are yet to
undertaken. Furthermore, studies adopting a mixed design (i.e.
qualitative and quantitative) would be beneficial to gain a better
understanding of other factors that may directly relate to ED and
with the use of qualitative research, could offer up new avenues for
researchers to test experimentally. Although the current ED research
56

has examined a variety of different populations it would be
advantageous to compare results across different sporting activities
using the same measurement scales in order to confirm or refute the
suggestions that the type of activity a person participates in can
influence the existence of ED.
In conclusion, no significant findings were discovered during this
research project. Perfectionism and self-determination were not
significant predictors of exercise dependence group classification.
This is not to say that they are not influencing factors of such a
maladaptive behaviour but suggest exercise dependence is a much more
complex phenomena as cannot be individuals cannot be categorised in
a certain group for based on their scores of perfectionism and self-
determined motivation and even for the at-risk group, individual
varied between all 3 groups of perfectionism and 4 groups of self-
determined motivation
This study has found higher prevalence rates for the at-risk group
than in all but one study and the highest population rate for the
symptomatic group of any study that has utilised the EDS as a
measurement tool. These findings may be influenced by both the type
of activity (i.e. weightlifting) and the fact that all participants
in the current study were participating in semi-directed or free
57

activities that have little or no supervision, which have been
synonymous of higher levels of ED (Gonzalez-Cutre and Sicilia, in
Press). The use of personal trainers could benefit both the
symptomatic and at-risk for ED groups as it would allow them to
restructure their exercise programs and regain control over the
amount of time, the intensity and frequency they lift weights lift,
as these are key areas that are characteristic of an individual
exhibiting exercise dependence symptoms. Furthermore, personal
trainer input would allow for people to participate in directed
activities (as opposed to their current semi-directed and/of free
activities) which have been linked to lower levels of ED symptoms
(Gonzalez-Cutre and Sicilia, in Press).
References
Allegre, B., Therme, P., and Griffiths, M. D. (2007) ‘Individualfactors and the context of physical activity in exercise dependence:A prospective study of “ultra-marathoners”’ International Journal of MentalHealth and Addiction 5, 233–243
American Psychiatric Association (1994) Diagnostic and statistical manual ofmental disorders (4th ed). Washington, DC: American PsychiatricAssociation
Bamber, D. J., Cockerill, I., and Carroll, D. (2000) ‘Thepsychological status of exercise dependence’. British Journal of SportsMedicine 34, 125–132
Biddle, J. H., and Mutrie, N. (2001) Psychology of physical activity:Determinants, well-being and interventions. London & New York: Routledge
Blatt, S. J. (1995). ‘The destructiveness of perfectionism:Implications for the treatment of depression’. American Psychologist 50,1003–1020
58
Brene, S., Bjornebekk, A., Aberg, E., Mathe, A. A., Olson, L., andWerme, M. (2007) ‘Running is rewarding and antidepressive’ Physiologyand Behavior 92, 136–140
Carron, A.V., Hausenblas, A.H., and Estabrooks, P.A. (2003) ThePsychology of Physical Activity. McGraw-Hill, New York
Chatzisarantis, N. L. D., and Hagger, M. S. (2007) ‘Mindfulness andthe Intention-Behavior Relationship Within the Theory of PlannedBehavior’ Personality and Social Psychology Bulletin 33, 663 -676
Coen, S. P., and Ogles, B. M. (1993) ‘Psychological characteristicsof the obligatory runner: a critical examination of the anorexiaanalogue hypothesis’. Journal of Sport & Exercise Psychology 15, 338–354
Cresswell, S. L., and Eklund, R. C. (2003) ‘The athlete burnoutsyndrome: A practitioner’s guide’ New Zealand Journal of Sports Medicine 31,4–9.
Cumella, E. J. (2005) ‘The heavy weight of exercise addiction’Behavioral Health Management 25/ 26 (31) *
Deci, E. L. (1971) ‘Effects of externally mediated rewards onintrinsic motivation’. Journal of Personality and Social Psychology18, 105-115
Deci, E.L., and Ryan, R.M. (1985) Intrinsic motivation and self-determination inhuman behavior New York, NY: Plenum Press
Deci, E. L., and Ryan, R. M. (2000) ‘The ‘‘what’’ and ‘‘why’’ ofgoal pursuits: Human needs and the self-determination of behavior’Psychological Inquiry 11, 227–268
de Coverley Veale, D. M. W. (1995) ‘Does primary exercise dependencereally exist?’ in Exercise addiction: motivation for participation in sport andexercise. ed. by Annett, J., Cripps, B., and Steinberg, H. Leicester,UK: British Psychological Society, 1-5
De Vries, H. A. (1981) ‘Tranquilizer effect of exercise: A criticalreview’ The Physician and Sports Medicine 9(11), 47–53
DiBartolo, P.M., Frost, R.O., Chang, P., LaSota, M., and Grills,A.E. (2004) ‘Shedding light on the relationship between personalstandards and psychopathology: The Case of contingent self-worth’.Journal of Rational-Emotive and Cognitive-Behavioural Therapy 22, 241-254
59
Downs, D. S., Hausenblas, H. A., and Nigg, C. R. (2004) ‘Factorialvalidity and psychometric examination of the exercise dependencescale-revised’ Measurement in Physical Education and Exercise Science 8(4), 183–201
Duncan, L. R., Hall. C. R., Wilson, P. M., Jenny, O. (2010)‘Exercise motivation: a cross-sectional analysis examining itsrelationships with frequency, intensity, and duration of exercise’International Journal of Behavioral Nutrition and Physical Activity 7 (7), 1-9
Dunn, J.G.H., Causgrove Dunn, J., and Syrotuik, D. G. (2002)‘Relationship between Multidimensional Perfectionism and GoalOrientations in Sport’. Journal of Sport & Exercise Psychology 24, 376-395
Edmunds, J. K., Ntoumanis, N., and Duda, J. L. (2006) ‘A test ofself-determination theory in the exercise domain’. Journal of AppliedSocial Psychology 36, 2240–2265
Fortier, M. S., and Farrell, R. J. (2009) ‘Comparing self-determination and body image between excessive and healthyexercisers’ Hellenic Journal of Psychology 6, 223-243
Frost, R. O., Marten, P. A., Lahart, C., and Rosenblate, R. (1990)‘The dimensions of perfectionism’. Cognitive Therapy and Research 14, 449–478
Garner, D. M. (1991) Eating Disorder Inventory--2 manual. Odessa, FL:Psychological Assessment Resources
Gaudreau, P., and Antl, S. (2008) ‘Athletes’ broad dimensions ofdispositional perfectionism: examining changes in life satisfactionand the mediating role of sport-related motivation and coping’.Journal of Sport & Exercise Psychology 30, 356-382
Glasser, W. (1976) Positive Addiction. New York, Harper & Row
Godin, G., Jobin, J., and Bouillon, J. (1986) ‘Assessment of leisuretime exercise behavior by self-report: A concurrent validity study’Canadian Journal of Public Health 77, 359-361
Goodman, A. (1990) ‘Addiction: Definition and implications’ BritishJournal of Addiction 85 (11), 1403–1408
Hachon, T. A., (2010) ‘The relations between perfectionism andachievement goals’ Personality and Individual differences 49, 885-890
60

Hagan, A. L., and Hausenblas, H. A., (2003) ‘’The relationshipbetween exercise dependence and perfectionism’ American Journal of HealthStudies 18, 133–137.
Hale, B. D., Roth, A. D., DeLong, R. E. and Briggs, M. S. (2010)‘Exercise dependence and the drive for muscularity in malebodybuilders, power lifters and fitness lifters’ Body Image 7, 234–239
Hall, H. K., Kerr, A. W., Kozub, S. A., and Finnie, S. B. (2007)‘Motivational antecedents of obligatory exercise: The influence ofachievement goals and perfectionism’. Psychology of Sport and Exercise 8(3), 297-316
Hamer, M., Karageorghis, C. I., and Vlachopoulos, S. P. (2002) ‘Motives of exercise participation as predictors of exercise dependence among endurance athletes’ Journal of Sports Medicine and Physical Fitness 42, 233–238
Hamer, M., and Karageorghis, C. I. (2007) ‘Psychobiologicalmechanisms of exercise dependence’ Sports Medicine 37 (6), 477–484
Hausenblas, H. A., and Symons Downs, D. (2002a) ‘Exercisedependence: A systematic review’. Psychology of Sport and Exercise 3, 89–123
Hausenblas, H. A., and Symons Downs, D. (2002b) ‘How much is toomuch? The development and validation of the Exercise DependenceScale’. Psychology and Health: An International Journal 17,387–404
Hausenblas, H., and Giacobbi, P. (2004) ‘Relationship betweenexercise dependent symptoms and personality’. Personality and IndividualDifferences 36, 1265–1273
Hurst, R., Hale, B., Smith, D., and Collins, D. (2000) ‘Exercisedependence, social physique anxiety, and social support inexperienced and inexperienced bodybuilders and weightlifters’ BritishJournal of Sports Medicine 34 (6), 431–435
Lemyre, P. N., Hall, H. K., and Roberts, G. C. (2008) ‘A socialcognitive approach to burnout in elite athletes’. Scandinavian Journal ofMedicine & Science in Sports 18, 221-234.
61
Li, F. (1999) ‘The exercise motivation scale: Its multifacetedstructure and construct validity’. Journal of Applied Sport Psychology 11,97-115
Lonsdale, C., Hodge, K., and Rose, E. A. (2008) ‘The develpoment ofthe behavioral regulation in sport questionnaire (BRSQ): instrumentdevelopment and initial validity evidence’. Journal of Sport & ExercisePsychology 30, 323-355
Lonsdale, C., Hodge, K., and Rose, E. (2009) ‘Athlete burnout inelite sport: A self-determinationPerspective’ Journal of Sports Sciences 27, 785–795
Mallett, C., Kawabata, M., Newcomebe, P., Otero-Forero, A., andJackson, S. (2007) ‘Sport motivation scale-6 (SMS-6): A revised six-factor sport motivation scale’. Psychology of Sport and Exercise 8, 600–614
McArdle, S., and Duda, J. L. (2004) ‘Exploring social-contextualcorrelates of perfectionism in adolescents: a multivariateperfectionism’. Cognitive Therapy and Research 28, 765-788
Mullan, E., Markland, D., and Ingledew, D. K. (1997) ‘A gradedconceptualization of self-determination in the regulation ofexercise behaviour: Development of a measure using confirmatoryfactor analytic procedures’ Personality and Individual Differences 23, 745 – 752
Monok, K., Berczik, K., Urban, R., Szabo, A., Griffiths, M. D.,Farkas, J., Magi, A. Eisinger, A., Kurimay, T., Kokonye, G., Kun,B., Paksi and Demetrovics, Z. (2012) ‘ Psychometric properties andconcurrent validity of two exercise addiction measures: A populationwide study’ Psychology of Sport and Exercise, 1-8
Ogles,B. M., Masters, K. S., and Richardson,S. A. (1995) ‘Obligatoryrunning and gender: An analysis of participation motives andtraining habits’. International Journal of Sports Psychology 26, 233–248
Ommundsen, Roberts, Lemyre, and Miller (2005) ‘Peer relationships inadolescent competitive soccer: Associations to perceivedmotivational climate, achievement goals and perfectionism’. Journal ofSports Sciences 23, 977–989.
Pargman, D., and Baker. M. C., (1980) ‘Running high: Enkephalin indicted’. Journal of Drug Issues 10, 341-349
62
Pelletier, L. G., Fortier, M. S., Vallerand, R. J., Tuson, K. M.,Brie` re, N. M., and Blais, M. R. (1995) ‘Toward a new measure ofintrinsic motivation, extrinsic motivation, and amotivation insports: The sport motivation scale (SMS)’. Journal of Sport and ExercisePsychology 17, 35–53
Perreault, S., Gaudreau, P., Lapointe, M.-C., and Lacroix, C. (2007)‘Does it take three to tango? Psychological need satisfaction andathlete burnout’ International Journal of Sport Psychology 38, 437–450
Raedeke, T. D. (1997) ‘Is athlete burnout more than just stress? Asport commitment perspective’ Journal of Sport and Exercise Psychology 19,396–417.
Reeve, J. (2002) ‘Self-determination theory applied to educational settings’. in Handbook of self-determination research. ed. by Deci, E. L., and Ryan., R. M. Rochester, NY: University of Rochester Press, 183–203
Rudy, E.B., and Estok, P.J. (1989) ‘Measurement and significance ofnegative addiction in runners’ Western Journal of Nursing Research 5, 325–336
Ryan, R. M., and Frederick, C. M. (1997) ‘On energy, personality,and health: Subjective vitality as a dynamic reflection ofwellbeing’ Journal of Personality 65, 529–565
Ryan, R. M., and Deci, E.L. (2000) ‘Self-determination theory andthe facilitation of intrinsic motivation, social development, andwell-being’ American Psychologist 55, 68-78
Ryan, R. M., and Deci, E. L. (2002) ‘An overview of self-determination theory: An organismic dialectical perspective’. inHandbook of self-determination research. ed. by Deci, E. L., and Ryan, R. M.Rochester, NY: University of Rochester, 3-33
Smith, D. K., Hale, B. D., and Collins, D. J. (1998) ‘Measurement ofexercise dependence in bodybuilders’ Journal of Sport Medicine and PhysicalFitness 38, 66–74
Smits, J. A. J., Berry, A. C., Rosenfield, D., Powers, M. B., Behar,and Otto, M. W. (2008) ‘Reducing anxiety sensitivity with exercise’Depression and Anxiety 25, 689–699
63

Spano, L. (2001) ‘The relationship between exercise and anxiety,obsessive-compulsiveness, and narcissism’ Personality and IndividualDifferences 30, 87-93
Stöber, J. (1998) ‘The Frost Multidimensional Perfectionism Scalerevisited: More perfect with four (instead of six) dimensions’.Personality and Individual Differences 24, 481-491
Stöber, J., and Otto, K. (2006) ‘Positive conceptions ofperfectionism: Approaches, evidence, challenges’. Personality and SocialPsychology Review 10, 295-319
Stöber, J., and Rambow, A. (2007) ‘Perfectionism in adolescentschool students: relations with motivation, achievement, and well-being’. Personality and Individual Differences 42, 1379-1389
Stöber, J., Feast, A. F., and Hayward, J. A. (2009) ‘Self-orientatedand socially prescribed perfectionism: Differential relationshipswith intrinsic and extrinsic motivation and test anxiety’ Personalityand Individual Differences 47, 425-428
Stoll, O., Lau, A., and Stöber, J. (2008) ‘Perfectionism andperformance in a new basketball training task: does striving forperfection enhance or undermine performance?’. Psychology of Sport andExercise 9, 620-629
Symons Downs, D., Hausenblas, H., and Nigg, C. (2004) ‘Factorialvalidity and psychometric examination of the exercise dependencescale—revised’. Measurement in Physical Education and Exercise Science 84 (4),183–201
Szabo, A. (1995) ‘The impact of exercise deprivation on wellbeing ofhabitual exercisers’. Australian Journal of Science and Medicine in Sport 27, 68–75
Szabo, A., Frenkl, R., and Caputo, A. (1997) ‘Relationships betweenaddiction to running, commitment to running and deprivation fromrunning: A study on the internet’. in European Yearbook of SportPsychology . ed. Seiler, R. Augustin: FEPSAC . 130-147
Szabo, A. (2010) Addiction to exercise: A symptom or a disorder? New York, NY:Nova Science Publishers
64
Thaxton, L. (1982) ‘Physiological and psychological effects ofshort-term exercise addiction on habitual runners’ Journal of SportPsychology 4, 73-80
U.S. Department of Health and Human Services. (2008). 2008 physicalactivity guidelines for Americans. Downloaded from.http://www.health.gov/paguidelines/pdf/paguide.pdf (09-06-2012).
Warburton D. E. R., Nicol, C.W., and Bredin, S. S. D. (2006) ‘Healthbenefits of physical activity: The evidence’ Canadian Medical AssociationJournal 174(6), 801–809
Wilson, P. M., Rodgers, W. M., Fraser, S. N., and Murray, T. C.(2004) ‘Relationships between exercise regulations and motivationalconsequences in university students’. Research Quarterly for Exercise andSport 75(1), 81-91
Yates, A., Leehey, K., and Shisslak, C. M. (1983) ‘Running – ananalogue of anorexia?’ New England Journal of Medicine 308 (5), 251–255
Appendix 1: Ethics Review Feedback Form REGISTRY RESEARCH UNIT
Name of applicant: Luke Wilkin.......
Faculty/School/Department: [Health and Life Sciences] HLS Psychology
Research project title: THE IMPACT OF SELF-DETERMINED MOTIVATION AND PERFECTIONISM ON EXERCISE DEPENDENCE IN EXPERIENCED MALE ADULT WEIGHTLIFTERS
65
Comments by the reviewer
1. Evaluation of the ethics of the proposal:
Good proposal
2. Evaluation of the participant information sheet and consent form:
Please check grammar on PIS and debrief e.g.
The aim of this study is to examine the relationship between exercise dependence, perfectionism and motivation. Specifically,to assess whether a person’s levels of perfectionism and self-determined motivation could predict exercise dependence group classification
Change grammatical error in PIS and debriefProvide relevant helpline and/or website for exercise dependenceon debrief formSubject to gatekeeper permission being gained.No need to resubmit - supervisor can sign off to say conditions have been met.
3. Recommendation:(Please indicate as appropriate and advise on any conditions. If there any conditions, the applicant will be required to resubmit his/her application and this will be sent to the same reviewer).
Approved - no conditions attached
X Approved with minor conditions (no need to re-submit)
Conditional upon the following – please use additional sheets if necessary (please re-submit application)
Rejected for the following reason(s) – please use other sideif necessary
Not required
66
Name of reviewer: Anonymous..................................
Date: 19/12/2011.............................................
Appendix 2: Gate Keeper Approval Letter
Luke, Sorry I have not responded to your request. I am nervous about letting you approach members, as I am not keen to disturb them whilst training and give them any reason to reconsider their membership, If I'm honest as well I cannotsee how this research would benefit Trilogy. However I am prepared to support you where I can. For Trilogy to allow you to proceed with this research you would need to confirm that it would take no longer than a week(& confirm dates), I would also stipulate that the research was completed only week days between 6.45am - 4.30pm and weekends, ensuring that you avoided the peak gym hours in the evening. Unfortunately Trilogy could not support you advertising the research, simply because we have limited advertising space & too much to advertise already - I would ask that you promoted the questionnaire verbally yourself when conducting the research. Also I would advise that if you did not stick to the above stipulations, or if there was any complaint or negative comments from members, I would have to ask you to stop the research. I apologise if I sound restrictive, but I need to put the interest of the members first. Please confirm a date you would like to work to. When you start you will need to speak with the Duty Manager and Gym Instructor on every visit and confirm you are in the building and what you are doing.
67

If you have any questions please come back to me.
John FletcherBusiness Development Manager07766 725 823www.nleisure.co.uk
Appendix 3: Informed Consent Form
THE IMPACT OF SELF-DETERMINED MOTIVATION AND PERFECTIONISM ONEXERCISE DEPENDENCE IN EXPERIENCED MALE ADULT WEIGHTLIFTERS
Regular exercise can lead to a variety of physical andpsychological benefits. However, an over-reliance on exercisecan lead to a loss of these benefits and to the development ofnegative health effects. It is therefore important to look atvariables that can influence the likelihood of ahealthy/regular exercise, who reaps the health benefits fromexercise, becoming an individual who is exercise dependent andis exposed to the negative psycho-somatic problems associatedwith excessive exercising.
Please initial
1. I confirm that I have read and understood the participant information sheet (insert version number) for the above study and have had the opportunity to ask questions
68
Participant

2. I understand that my participation is voluntary andthat I am free to withdraw at anytime without giving areason
3. I understand that all the information I provide will be treated in confidence
4. I understand that I also have the right to change my mind about participating in the study for a short period after the study has concluded (insert deadline here)
5. I agree to take part in the research project
Participant: Name Signature
Date
Researcher: Name Signature
Date
Demographic Questions
Age:
Sex:
Average number of hours spent weightlifting per week(last 3 months):
Appendix 4: Exercise Dependence Scale-21 (Hausenblas and Symons Downs, 2002)
69

Using the scale provided below, please complete the following questions ashonestly as possible. The questions refer to current exercise beliefs andbehaviours that have occurred in the past 3 months. Please place your
answer in the blank space provided after each statement.
1 2 3 4 5 6 Never Sometimes Always
1. I exercise to avoid feeling irritable. 1 2 3 4 5 6 2. I exercise despite recurring physical problems. 1 2 3 4 5 6
3. I continually increase my exercise intensity to achievethe desired effects/benefits. 1 2 3 4 5 6
4. I am unable to reduce how long I exercise. 1 2 3 4 5 6
5. I would rather exercise than spend time with family/friends.1 2 3 4 5 6
6. I spend a lot of time exercising. 1 2 3 4 5 6
7. I exercise longer than I intend. 1 2 3 4 5 6
8. I exercise to avoid feeling anxious. 1 2 3 4 5 6
9. I exercise when injured. 1 2 3 4 5 6
10. I continually increase my exercise frequency to achieve the desired effects/benefits. 1 2 3 4 5 6
11. I am unable to reduce how often I exercise. 1 2 3 4 5 6
12. I think about exercise when I should be concentrating onschool/work. 1 2 3 4 5 6
70

StronglyagreeAgreeDisagr
ee
13. I spend most of my free time exercising. 1 2 3 4 5 6
14. I exercise longer than I expect. 1 2 3 4 5 6
15. I exercise to avoid feeling tense. 1 2 3 4 5 6
16. I exercise despite persistent physical problems.1 2 3 4 5 6
17. I continually increase my exercise duration to achieve thedesired effects/benefits. 1 2 3 4 5 6
18. I am unable to reduce how intense I exercise. 1 2 3 4 5 6
19. I choose to exercise so that I can get out of spending time with family/friends. 1 2 3 4 5 6
20. A great deal of my time is spent exercising. 1 2 3 4 5 6
21. I exercise longer than I plan. 1 23 4 5 6Appendix 5: The Frost Multidimensional Perfectionism Scale (FMPS)
Stöber (1998)
Please select which best reflects your opinion using the ratingscale below.
1 2 3 4 5 6 7
1. If I fail at work/school, I am a failure as a person. 1 2 3 4 5 6 7
2. I should be upset if I make a mistake. 1 2 3 4 5 6 7
71
AgreeSomewhat
Disagreesomewhat
Stronglydisagree
Undecide
3. I expect higher performance in my daily tasks than most people. 1 2 3 4 5 6 7
4. Even when I do something very carefully, I often feel that it is notquite right. 1 23 4 5 6 7
5. If someone does a task at work/school better than I, then I feel like
I failed the whole task. 1 2 3 4 5 6 7
6. It is important to me that I am thoroughly competent in everything
I do. 1 2 34 5 6 7
.7. If I fail partly, it is as bad as being a complete failure.
1 2 3 4 5 6 7
8. If I do not set the highest standards for myself, I am likely to endup a second-rate person. 1 2 3 4 5 6 7
9. It takes me a long time to do something "right." 1 2 3 4 5 6 7
10. I hate being less than the best at things. 1 2 3 4 5 6 7
11. I set higher goals than most people. 1 2 3 4 5 6 7
12. People will probably think less of me if I make a mistake. 1 2 3 4 5 6 7
13. I have extremely high goals. 1 2 3 4 5 6 7
14. If I do not as well as other people, it means I am an inferior humanbeing. 1 2 3 4 5 6 7
72

15. I tend to get behind in my work because I repeat things overand over. 1 2 3 4 5 6 7
16. I am very good at focusing my efforts on attaining a goal 1 2 3 4 5 6 7
17. If I do not do well all the time, people will not respectme. 1 2 3 4 5 6 7
18. Other people seem to accept lower standards than I do. 1 2 3 4 5 6 7
19. The fewer mistakes I make, the more people will like me. 1 2 3 4 5 6 7
20. I usually have doubts about the simple everyday things I do. 1 2 3 4 5 6 7
Appendix 6: Sport Motivation Scale-6Mallett, Kawabata, Newcombe, Otero-Foreroand Jackson, (2007)
Using the scale below, please indicate to what extent each ofthe following items corresponds to one of the reasons for
which you are presently practising your sport.
1 2 3 4 5 6 7
Why do you practice your sport?
1. For the excitement I feel when I am really involved in the activity 1 2 3 4 5 6 7
2. Because it’s part of the way in which I’ve chosen to live my life 1 2 3 4 5 6 7
3. Because it is a good way to learn lots of things which could be usefulto me in other areas of my life 1 2 3 4 5 6 7
4. Because it allows me to be well regarded by people that I know 1 2 3 4 5 6 7
73
Does notCorrespondat all
Corresponds
Corresponds
Corresponds
Corresponds

5. I don’t know anymore; I have the impression of being incapable ofsucceeding in this sport 1 2 3 4 5 6 7
6. Because I feel a lot of personal satisfaction while mastering certaindifficult training techniques 1 2 3 4 5 6 7
7. Because it is absolutely necessary to do sports if one wants to be inShape 1 2 3 4 5 6 7
8. Because it is one of the best ways I have chosen to develop otheraspects of my life 1 2 3 4 5 6 7
9. Because it is an extension of me 1 2 3 4 5 6 7
10. Because I must do sports to feel good about myself 1 2 3 4 5 6 7
11. For the prestige of being an athlete 1 2 3 4 5 6 7
12. I don’t know if I want to continue to invest my time and effort asmuch in my sport anymore 1 2 3 4 5 6 7
13. Because participation in my sport is consistent with my deepestPrinciples 1 2 3 4 5 6 7
14. For the satisfaction I experience while I am perfecting my abilities 1 2 3 4 5 6 7
15. Because it is one of the best ways to maintain good relationshipswith my friends 1 2 3 4 5 6 7
16. Because I would feel bad if I was not taking time to do it1 2 3 4 5 6 7
74

17. It is not clear to me anymore; I don’t really think my place is in sport 1 2 3 4 5 6 7
18. For the pleasure of discovering new performance strategies 1 2 3 4 5 6 7
19. For the material and/or social benefits of being an athlete 1 2 3 4 5 6 7
20. Because training hard will improve my performance 1 2 3 4 5 6 7
21. Because participation in my sport is an integral part of my life 1 2 3 4 5 6 7
22. I don’t seem to be enjoying my sport as much as I previously did 1 2 3 4 5 6 7
23. Because I must do sports regularly 1 2 3 4 5 6 7 24. To show others how good I am at my sport 1 2 3 4 5 6 7
75

Abstract There is nothing for me to comment in your abstract as there isn’t one (it should be relatively brief about why you explored this topicwhat you’ve done (results) and why this is important). The acknowledgements section is optional. You have contents page, I would make the introduction more concise and expand on the lit review in the table of contents so that it includes some of the information you’ve put in the introduction when you talk about exercise dependence, personality and so on.), similar to the way you’ve done it with Methodology.
Introduction
A nice opening paragraph. I would recommend using other subheadings in this section, which capture the content that follows and will addclarity – I make some suggestions in due course. Your introduction is a bit too long and it contains information that should go to the lit review part (example p. 5 line 19-24 when you talk about what groups individuals can be attributed to. This isn’t needed in the introduction but rather in the lit review section under a subheadingof exercise dependence) to give it more clarity. The whole section of what the lit review will do is not needed at all (p. 6 lines 25 –30).
When you start the sentence with ‘As noted earlier, p.6 line 31) yourefer to all the information you have included in the introduction. This information should be just here followed by what the rest of lit review on ED. You describe in details Hagan & Hausenblas (2003) study when all you need is their results and a link to what you wantto do. You also provide a lot of information of what kind of scales have been developed which is unnecessary as your research is not on developing yet another scale but on predictors of ED. Very similar when you describe Hurst et al research and Hale et al research– all
76

this details is not needed just the results and a link to why their results are important to what you want to measure.
Once you finish describing ED you can make a subheading for personality and talk about the traits (so take some of the information from your introduction and put it in here followed by what you have on p. 9 line 9 - perfectionism). Again similar thing with Hausenblas and Symons Downs (2002b) research as commented above. Once you finish with perfectionism you make another subheading on motivation (these are just a suggestions – the call isyour of course).
When you talk about the aims of the study, as well as throughout thedifferent part of the whole document you need to be consistent with the tense you are using (example p. 12 line 26 – 31). When you talkabout hypothesis you can’t state whether something will be successful or not. You can though elaborate on this in the sense that according to the literature this is what you expect.
Method You need to include: Design – whether it’s qualitative or quantitative to start with. Then you can talk about the analysis youdid and your variables – you say that ‘Due to the nature of the research project an alpha level was set at .05.’ – I think you mean the significance level? It’s usually set at this level so you don’thave to include an explanation for that.. Participants (you don’t need to specify which leisure centre the participants came from, theinclusion criteria should be in your procedure section), Materials used/measures – (this is fine but you need to add Cronbach alpha foreach of the scale), Procedure talk about it the way so it enable exact replication of the ‘testing procedure’ and not necessarily your ‘ethics procedure’. In fact, the only ethics document you ‘must’ include and refer to is the one from the committee (Appendix).
Results All the information you’ve put on p. 16 should be put in the tables and then described and interpreted below the tables. At this moment I’m not sure what I am looking at as some of the information you’ve put there is duplicated.
Discussion
Obviously you need to write this part.
General Comments
Just check that the format of your dissertation is entirely in accordance with the guidelines in the Module Guide on the M48PY Module Web. In this guide, there is also useful information on otherissues that you should take a look at prior to final submission e.g.what to include in a title page. There are some punctuation and paragraphing errors and sometimes a lack of clarity – read your dissertation carefully and make any necessary changes. I have not checked all references in depth, but even at a glance I have noticed
77

some errors – make sure you follow ‘Harvard style’ throughout.
Appendix 7: Dissertation Draft Feedback Sheet. Student Name: LW
78








![Positive and negative affect in adolescents: An investigation of the 2 x 2 model of perfectionism [2014]](https://static.fdokumen.com/doc/165x107/631650a6c32ab5e46f0db856/positive-and-negative-affect-in-adolescents-an-investigation-of-the-2-x-2-model.jpg)











