
The ICF as a framework to collect and interpret data on the ...
89
NeuroRehabilitation 36 (2015) 17–22 DOI:10.3233/NRE-141186 IOS Press 17 The ICF as a framework to collect and interpret data on the extent and variety of disability in neurological conditions A. Raggi * , M. Leonardi, V. Covelli, D. Sattin, C. Scaratti, S. Schiavolin, M. Willems and P. Meucci Neurology, Public Health and Disability Unit, Neurological Institute C. Besta IRCCS Foundation, Milan, Italy Abstract. INTRODUCTION: Neurological conditions are associated with high levels of disability. OBJECTIVES: The aim of this study was to describe, using the International Classification of Functioning, Disability and Health (ICF), the most relevant aspects of disability in patients with neurological conditions. We collated data from previous studies on myasthenia gravis, migraine, Parkinson’s disease, multiple sclerosis, traumatic brain injury, stroke, epilepsy, vegetative state and minimally conscious state, and identified as relevant those ICF categories reported by at least 50% of patients in each condition. CONCLUSIONS: Records from 1310 patients were available. A total of 97 ICF categories were reported, and 21 were commonly addressed in more than five conditions. Approximately half of the categories in body functions were related to mental and movement-related functions and more than 25% of the activities-related categories involved activities that require the support from a caregiver. Environmental factors were mostly reported as facilitators. Our data indicate a residual mind-body dichotomy, the relevance of disability not only for the patients but also for their caregivers, and the difficulties in addressing barriers in the environment. Keywords: Disability, ICF classification, mental functions, mobility, barriers 1. Introduction Neurological conditions are among the leading causes of disability. A recent report on a population survey of a sample of persons applying for disability certification showed that neurological conditions repre- sent approximately 40% of the conditions in the group of persons with the most severe disability (Leonardi et al., 2012). In terms of years lived with dis- ability (YLD), they account for approximately 687 YLD/100.000 (including stroke and brain cancers) with a 14.7% increase for the period 1990–2010 (Vos et al., 2012). YLDs are adequate for population- * Address for correspondence: Alberto Raggi, Psy.D., Neurology, Public Health and Disability Unit, Neurological Institute C. Besta IRCCS Foundation, Via Celoria 11, 20133 Milan, Italy. Tel.: +39 02 2394 3105 2521; Fax: +39 02 2394 2442; E-mail: [email protected]. based analyses and can be used to address how long people with sequelae of a condition experience a disability status, but are not suitable at the single individual level. Several assessment tools exist that enable us to measure and classify the severity of disability associated with a health condition. However, these instruments address only part of the possible impairments and activity limitations due to a health condition. A different approach to data collection and interpre- tation is needed to get a wider and more complete profile of the lived experience of having a disability, i.e., an approach that accounts for the presence of impairments, their impact upon daily activities and the extent to which factors in the person’s environment have a facilitating or hindering effect. Such an approach is provided by the International Classification of Functioning, Disability and Health (ICF) (World Health Organization, 2001). 1053-8135/15/$35.00 © 2015 – IOS Press and the authors. All rights reserved
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of The ICF as a framework to collect and interpret data on the ...
NeuroRehabilitation 36 (2015) 17–22DOI:10.3233/NRE-141186IOS Press
17
The ICF as a framework to collect andinterpret data on the extent and varietyof disability in neurological conditions
A. Raggi!, M. Leonardi, V. Covelli, D. Sattin, C. Scaratti, S. Schiavolin, M. Willems and P. MeucciNeurology, Public Health and Disability Unit, Neurological Institute C. Besta IRCCS Foundation, Milan, Italy
Abstract.INTRODUCTION: Neurological conditions are associated with high levels of disability.OBJECTIVES: The aim of this study was to describe, using the International Classification of Functioning, Disability and Health(ICF), the most relevant aspects of disability in patients with neurological conditions. We collated data from previous studies onmyasthenia gravis, migraine, Parkinson’s disease, multiple sclerosis, traumatic brain injury, stroke, epilepsy, vegetative state andminimally conscious state, and identified as relevant those ICF categories reported by at least 50% of patients in each condition.CONCLUSIONS: Records from 1310 patients were available. A total of 97 ICF categories were reported, and 21 were commonlyaddressed in more than five conditions. Approximately half of the categories in body functions were related to mental andmovement-related functions and more than 25% of the activities-related categories involved activities that require the supportfrom a caregiver. Environmental factors were mostly reported as facilitators. Our data indicate a residual mind-body dichotomy,the relevance of disability not only for the patients but also for their caregivers, and the difficulties in addressing barriers in theenvironment.
Keywords: Disability, ICF classification, mental functions, mobility, barriers
1. Introduction
Neurological conditions are among the leadingcauses of disability. A recent report on a populationsurvey of a sample of persons applying for disabilitycertification showed that neurological conditions repre-sent approximately 40% of the conditions in the groupof persons with the most severe disability (Leonardiet al., 2012). In terms of years lived with dis-ability (YLD), they account for approximately 687YLD/100.000 (including stroke and brain cancers) witha 14.7% increase for the period 1990–2010(Vos et al., 2012). YLDs are adequate for population-
!Address for correspondence: Alberto Raggi, Psy.D., Neurology,Public Health and Disability Unit, Neurological InstituteC. Besta IRCCS Foundation, Via Celoria 11, 20133 Milan, Italy.Tel.: +39 02 2394 3105 2521; Fax: +39 02 2394 2442; E-mail:[email protected].
based analyses and can be used to address how longpeople with sequelae of a condition experience adisability status, but are not suitable at the singleindividual level. Several assessment tools exist thatenable us to measure and classify the severity ofdisability associated with a health condition. However,these instruments address only part of the possibleimpairments and activity limitations due to a healthcondition.
A different approach to data collection and interpre-tation is needed to get a wider and more complete profileof the lived experience of having a disability, i.e., anapproach that accounts for the presence of impairments,their impact upon daily activities and the extent to whichfactors in the person’s environment have a facilitatingor hindering effect. Such an approach is provided by theInternational Classification of Functioning, Disabilityand Health (ICF) (World Health Organization, 2001).
1053-8135/15/$35.00 © 2015 – IOS Press and the authors. All rights reserved

18 A. Raggi et al. / The ICF as a framework to collect and interpret data
Since ICF was released, researchers have begun using itas a taxonomy to describe disability in patients with dif-ferent conditions; more than 40% of the ICF literaturedescribed the development of ICF-based instruments orICF use in clinical contexts, with the field of neurologybeing one of the most productive (Cerniauskaite et al.,2011). One of the reasons for this is likely due to thesubstantive impact of neurological conditions over avariety of body functions, in particular the mental andthe movement-related ones, and activities, with mobil-ity and communication-related activities as the mostprominent examples. Secondly, the prevalence, costsand disability associated with neurological conditionsare steadily increasing as a consequence of an ageingpopulation. In the last update of the study of the costsof disorders of the brain in Europe referred to the year2010, conditions with a typical old-age onset, suchas dementia or stroke, increased by 28.6% and 18.2%respectively, compared to the 2004 estimates, and thecorresponding increase in overall costs was 90.6%for dementia and 21.7% for stroke (Gustavsson et al.,2011). Despite these alarming figures, the similaritiesand dissimilarities, in terms of ICF categories, acrossneurological conditions have never been addressed.With this paper we provide a description of the extentand variety of disability features in the followingneurological conditions: myasthenia gravis (MG),migraine, Parkinson’s disease (PD), multiple sclerosis(MS), traumatic brain injury (TBI), stroke, epilepsy,vegetative state (VS) and minimally conscious state(MCS).
2. Paper selection and data analysis
We collated information on the use of ICF cate-gories that were reported in previous publications onthe selected conditions (Leonardi et al., 2009; Leonardiet al., 2010a; Raggi et al., 2010; Goljar et al., 2010;Svestkova et al., 2010a; Svestkova et al., 2010b; Cerni-auskaite et al., 2012; Sattin et al., 2014), which includeda total sample of 1310 patients, of whom approximately70% had Italian citizenship. The subsample sizes variedbetween 49 patients (epilepsy) and 396 patients (VS).We employed a descriptive approach to address thevariety of disability features, and selected those ICFcategories that were reported to be affected in at least50% of patients in each subsample. Within the activitiesand participation (A&P) domain, the selection thresh-old was calculated over the capacity qualifier. The mostcommonly reported categories for disability description
were defined as those reported by more than 50% ofsubjects in at least five of the nine health conditions.
3. Main findings
Out of 1310 patients, 45.7% were females, rang-ing between 23.8% (stroke) and 85.3% (migraine); themean age varied between 36.1 years (TBI) and 64.1years (PD), with an aggregate mean age of 52.5 years.
Table 1 reports the ICF categories from the compo-nents of body functions and structures (BF and BS)that were reported to be affected by more than 50%of patients in each condition. In total, 32 BF andseven BS were reported: the most frequent were mentalfunctions (9 categories) and movement-related func-tions (8 categories). The most frequently reported BFwere b130-Energy and drive, b140-Attention, b152-Emotional functions, b210-Seeing, b280-Sensation ofpain, and b730-Muscle power. S110-Brain was the onlyfrequently reported BS.
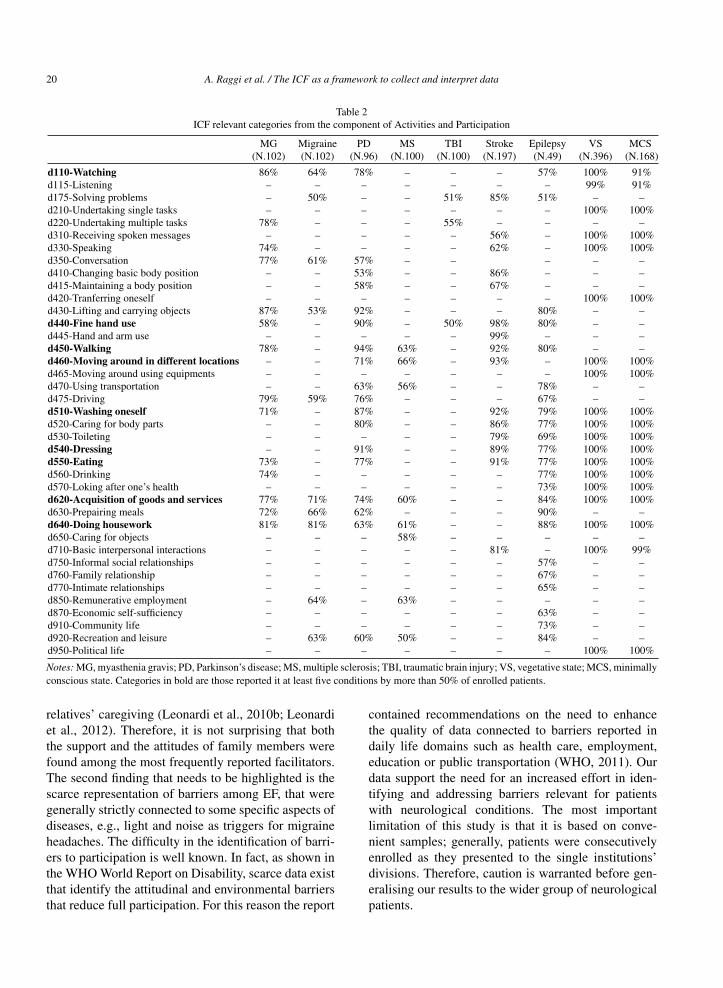
Table 2 reports the ICF categories from the com-ponent of A&P that were reported to be affectedby more than 50% of patients in each condition. Intotal, 39 categories were reported: the most frequentwere from the mobility (11 categories) and self-caredomains (7 categories). The most frequently reportedA&P were d110-Watching, d440-Fine hand use, d450-Walking, d460-Moving around in different locations,d510-Washing oneself, d540-Dressing, d550-Eating,d620-Acquisition of goods and services, and d640-Doing housework.
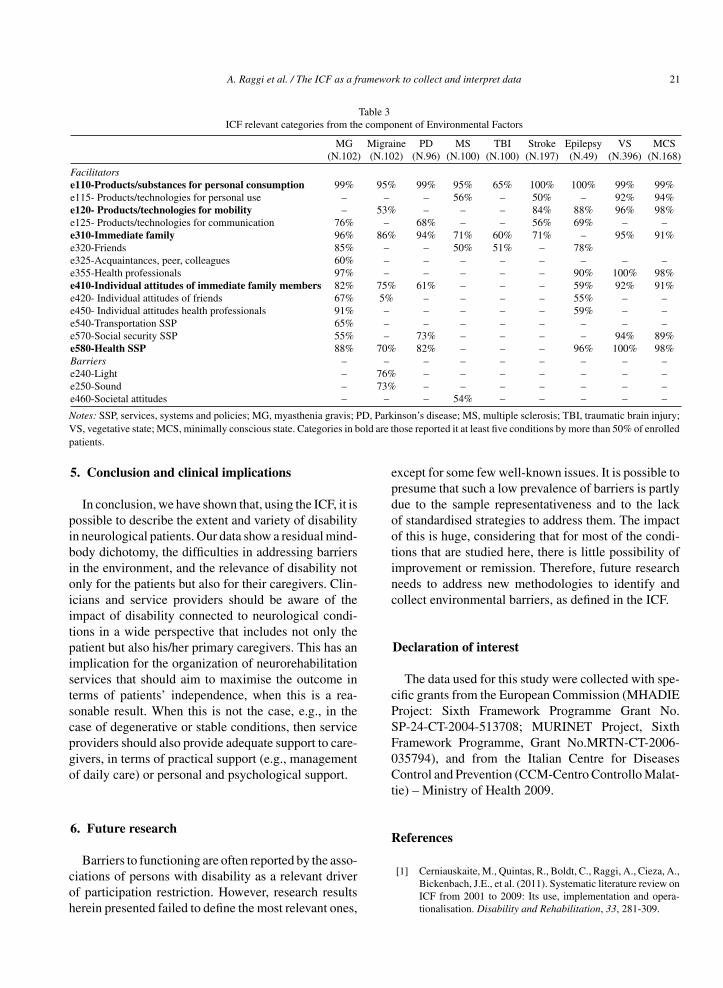
Table 3 reports the ICF categories from the compo-nent of environmental factors (EF) that were reportedto be affected by more than 50% of patients in eachcondition. In total, 17 categories – of which threespecifically as barriers – were reported: the mostfrequent were from products and technologies, andfrom support and relationships (four categories each).The most commonly reported facilitators were e110-Products/substances for personal consumption, e120-Products/technologies for mobility, e310-Immediatefamily, e410-Individual attitudes of immediate familymembers, and e580-Health SSP.
4. Discussion
The aim of this study was to provide a descrip-tion of the extent and variety of disability in selectedneurological conditions, using the ICF. Our data showthat 97 ICF categories were involved in the process of

A. Raggi et al. / The ICF as a framework to collect and interpret data 19
Table 1ICF relevant categories from the components of Body Functions and Body Structures
MG Migraine PD MS TBI Stroke Epilepsy VS MCS(N.102) (N.102) (N.96) (N.100) (N.100) (N.197) (N.49) (N.396) (N.168)
Body Functionsb110-Consciousness – – – – – – – 100% 100%b114-Orientation – – – – – – – 100% 100%b117-Intellectual – – – – – – – 100% 100%b130-Energy and drive 63% 63% 57% 52% 70% – – 100% 100%b134-Sleep 59% 64% – 60% – – – – –b140-Attention – 56% – – 59% – 55% 100% 100%b144-Memory – 59% – – 53% 95% – – –b152-Emotional 73% 77% 77% – 67% 54% 71% – –b167-Language – – – – – – – 100% 100%b210-Seeing 83% 70% 73% 65% 51% 67% 73% 87% 59%b230-Hearing – – – – – – – 82% 53%b235-Vestibular – – – 65% – – – – –b260-Proprioceptive functions – – – – – 68% – – –b265-Touch functions – – – – – 85% – – –b280-Sensation of pain 61% 96% 60% – – 85% 73% 83% 74%b310-Voice – – – – – – – 98% 95%b420-Blood pressure – – – – – 80% – – –b435-Immunological system 100% – – – – – – – –b440-Respiration – – – – – – – 57% –b455-Exercise tolerance functions – – – – – 60% – – –b510-Ingestion 62% – – – – – – 98% 95%b525-Defecation – – – – – – – 88% 81%b620-Urination – – – 70% – – – 91% 89%b640-Sexual – – – 58% – – – – –b710-Mobility of joint – – – – – 88% – 93% 97%b730-Muscle power 55% – 56% – – 99% – 97% 98%b735-Muscle tone – – 78% – – 78% – 99% 98%b740-Muscle endurance 77% – – – – – – – –b750-Motor reflex functions – – – – – 55% – – –b760-Control of voluntary movement – – – – – 99% – 97% 99%b765-Involuntary movement – – 79% – – 95% – 55% 63%b770-Gait pattern – – – 54% – 88% – – –Body Structuress110-Brain – – – 97% 89% 96% – 99% 97%s120-Spinal cord – – – 97% – – – – –s2-Eye, ear and related structures 68% 59% 59% – – – 59% – –s420-Structure of immune system 64% – – – – – – – –s430-Respiratory system – – – – – – – 77% 60%s530-Stomach – – – – – – – 95% 87%s810-Skin areas – – – – – – – 81% 76%
Notes: MG, myasthenia gravis; PD, Parkinson’s disease; MS, multiple sclerosis; TBI, traumatic brain injury; VS, vegetative state; MCS, minimallyconscious state. Categories in bold are those reported in at least five conditions by more than 50% of patients.
disability description; however, only 21 were frequentlyreported. Taken together, results seem to move in thedirection of a mind-body dichotomy. In fact, within BF,approximately half of the reported categories are eithermental or movement-related functions. Within A&P thesame is observable, as mobility categories (e.g. d440-Fine hand use, d450-Walking) or categories relatedto activities in which a relevant cognitive-relationalcomponent is needed (e.g. d175-Solving prob-lems, d350-Conversation, d710-Basic interpersonalinteractions) represent more than half of the totalamount of reported ICF categories.
Two other aspects deserve discussion. First, our datademonstrate that the burden of neurological condi-tions does not only affect the individual patient, butalso those persons around him/her. In fact, 11 outof 39 categories from A&P were related to self-careand domestic life activities, such as washing oneself,dressing, eating, acquiring goods and services or doinghousework. If people have major difficulties in thesekinds of activities, it is obvious that someone else willhave to perform them. Previous research findings showthat family members are usually the persons that, atleast in European contexts, carry the heavy burden of
20 A. Raggi et al. / The ICF as a framework to collect and interpret data
Table 2ICF relevant categories from the component of Activities and Participation
MG Migraine PD MS TBI Stroke Epilepsy VS MCS(N.102) (N.102) (N.96) (N.100) (N.100) (N.197) (N.49) (N.396) (N.168)
d110-Watching 86% 64% 78% – – – 57% 100% 91%d115-Listening – – – – – – – 99% 91%d175-Solving problems – 50% – – 51% 85% 51% – –d210-Undertaking single tasks – – – – – – – 100% 100%d220-Undertaking multiple tasks 78% – – – 55% – – – –d310-Receiving spoken messages – – – – – 56% – 100% 100%d330-Speaking 74% – – – – 62% – 100% 100%d350-Conversation 77% 61% 57% – – – – –d410-Changing basic body position – – 53% – – 86% – – –d415-Maintaining a body position – – 58% – – 67% – – –d420-Tranferring oneself – – – – – – – 100% 100%d430-Lifting and carrying objects 87% 53% 92% – – – 80% – –d440-Fine hand use 58% – 90% – 50% 98% 80% – –d445-Hand and arm use – – – – – 99% – – –d450-Walking 78% – 94% 63% – 92% 80% – –d460-Moving around in different locations – – 71% 66% – 93% – 100% 100%d465-Moving around using equipments – – – – – – – 100% 100%d470-Using transportation – – 63% 56% – – 78% – –d475-Driving 79% 59% 76% – – – 67% – –d510-Washing oneself 71% – 87% – – 92% 79% 100% 100%d520-Caring for body parts – – 80% – – 86% 77% 100% 100%d530-Toileting – – – – – 79% 69% 100% 100%d540-Dressing – – 91% – – 89% 77% 100% 100%d550-Eating 73% – 77% – – 91% 77% 100% 100%d560-Drinking 74% – – – – – 77% 100% 100%d570-Loking after one’s health – – – – – – 73% 100% 100%d620-Acquisition of goods and services 77% 71% 74% 60% – – 84% 100% 100%d630-Prepairing meals 72% 66% 62% – – – 90% – –d640-Doing housework 81% 81% 63% 61% – – 88% 100% 100%d650-Caring for objects – – – 58% – – – – –d710-Basic interpersonal interactions – – – – – 81% – 100% 99%d750-Informal social relationships – – – – – – 57% – –d760-Family relationship – – – – – – 67% – –d770-Intimate relationships – – – – – – 65% – –d850-Remunerative employment – 64% – 63% – – – – –d870-Economic self-sufficiency – – – – – – 63% – –d910-Community life – – – – – – 73% – –d920-Recreation and leisure – 63% 60% 50% – – 84% – –d950-Political life – – – – – – – 100% 100%
Notes: MG, myasthenia gravis; PD, Parkinson’s disease; MS, multiple sclerosis; TBI, traumatic brain injury; VS, vegetative state; MCS, minimallyconscious state. Categories in bold are those reported it at least five conditions by more than 50% of enrolled patients.
relatives’ caregiving (Leonardi et al., 2010b; Leonardiet al., 2012). Therefore, it is not surprising that boththe support and the attitudes of family members werefound among the most frequently reported facilitators.The second finding that needs to be highlighted is thescarce representation of barriers among EF, that weregenerally strictly connected to some specific aspects ofdiseases, e.g., light and noise as triggers for migraineheadaches. The difficulty in the identification of barri-ers to participation is well known. In fact, as shown inthe WHO World Report on Disability, scarce data existthat identify the attitudinal and environmental barriersthat reduce full participation. For this reason the report
contained recommendations on the need to enhancethe quality of data connected to barriers reported indaily life domains such as health care, employment,education or public transportation (WHO, 2011). Ourdata support the need for an increased effort in iden-tifying and addressing barriers relevant for patientswith neurological conditions. The most importantlimitation of this study is that it is based on conve-nient samples; generally, patients were consecutivelyenrolled as they presented to the single institutions’divisions. Therefore, caution is warranted before gen-eralising our results to the wider group of neurologicalpatients.
A. Raggi et al. / The ICF as a framework to collect and interpret data 21
Table 3ICF relevant categories from the component of Environmental Factors
MG Migraine PD MS TBI Stroke Epilepsy VS MCS(N.102) (N.102) (N.96) (N.100) (N.100) (N.197) (N.49) (N.396) (N.168)
Facilitatorse110-Products/substances for personal consumption 99% 95% 99% 95% 65% 100% 100% 99% 99%e115- Products/technologies for personal use – – – 56% – 50% – 92% 94%e120- Products/technologies for mobility – 53% – – – 84% 88% 96% 98%e125- Products/technologies for communication 76% – 68% – – 56% 69% – –e310-Immediate family 96% 86% 94% 71% 60% 71% – 95% 91%e320-Friends 85% – – 50% 51% – 78%e325-Acquaintances, peer, colleagues 60% – – – – – – – –e355-Health professionals 97% – – – – – 90% 100% 98%e410-Individual attitudes of immediate family members 82% 75% 61% – – – 59% 92% 91%e420- Individual attitudes of friends 67% 5% – – – – 55% – –e450- Individual attitudes health professionals 91% – – – – – 59% – –e540-Transportation SSP 65% – – – – – – – –e570-Social security SSP 55% – 73% – – – – 94% 89%e580-Health SSP 88% 70% 82% – – – 96% 100% 98%Barriers – – – – – – – – –e240-Light – 76% – – – – – – –e250-Sound – 73% – – – – – – –e460-Societal attitudes – – – 54% – – – – –
Notes: SSP, services, systems and policies; MG, myasthenia gravis; PD, Parkinson’s disease; MS, multiple sclerosis; TBI, traumatic brain injury;VS, vegetative state; MCS, minimally conscious state. Categories in bold are those reported it at least five conditions by more than 50% of enrolledpatients.
5. Conclusion and clinical implications
In conclusion, we have shown that, using the ICF, it ispossible to describe the extent and variety of disabilityin neurological patients. Our data show a residual mind-body dichotomy, the difficulties in addressing barriersin the environment, and the relevance of disability notonly for the patients but also for their caregivers. Clin-icians and service providers should be aware of theimpact of disability connected to neurological condi-tions in a wide perspective that includes not only thepatient but also his/her primary caregivers. This has animplication for the organization of neurorehabilitationservices that should aim to maximise the outcome interms of patients’ independence, when this is a rea-sonable result. When this is not the case, e.g., in thecase of degenerative or stable conditions, then serviceproviders should also provide adequate support to care-givers, in terms of practical support (e.g., managementof daily care) or personal and psychological support.
6. Future research
Barriers to functioning are often reported by the asso-ciations of persons with disability as a relevant driverof participation restriction. However, research resultsherein presented failed to define the most relevant ones,
except for some few well-known issues. It is possible topresume that such a low prevalence of barriers is partlydue to the sample representativeness and to the lackof standardised strategies to address them. The impactof this is huge, considering that for most of the condi-tions that are studied here, there is little possibility ofimprovement or remission. Therefore, future researchneeds to address new methodologies to identify andcollect environmental barriers, as defined in the ICF.
Declaration of interest
The data used for this study were collected with spe-cific grants from the European Commission (MHADIEProject: Sixth Framework Programme Grant No.SP-24-CT-2004-513708; MURINET Project, SixthFramework Programme, Grant No.MRTN-CT-2006-035794), and from the Italian Centre for DiseasesControl and Prevention (CCM-Centro Controllo Malat-tie) – Ministry of Health 2009.
References
[1] Cerniauskaite, M., Quintas, R., Boldt, C., Raggi, A., Cieza, A.,Bickenbach, J.E., et al. (2011). Systematic literature review onICF from 2001 to 2009: Its use, implementation and opera-tionalisation. Disability and Rehabilitation, 33, 281-309.
22 A. Raggi et al. / The ICF as a framework to collect and interpret data
[2] Cerniauskaite, M., Ajovalasit, D., Quintas, R., Alvarez, A.,Franceschetti, S., Casazza, M., et al. (2012). Functioning anddisability in persons with epilepsy. American Journal of Phys-ical Medicine and Rehabilitation, 91, S22-S30.
[3] Goljar, N., Burger, H., Vidmar, G., Marincek, C., Krizaj, J.,Chatterji, S., et al. (2010). Functioning and disability in stroke.Disability and Rehabilitation, 32, S50-S58.
[4] Gustavsson, A., Svensson, M., Jacobi, F., Allgulander, C.,Alonso, J., Beghi, E., et al. (2011). Cost of disorders of thebrain in Europe 2010. European Neuropsychopharmacology,21, 718-779.
[5] Leonardi,M.,Raggi,A.,Antozzi,C.,Confalonieri,P.,Maggi,L.,Cornelio,F., etal. (2009). Identificationof internationalclassifi-cationoffunctioning,disabilityandhealthrelevantcategories todescribe functioning and disability of patients with MyastheniaGravis. Disability and Rehabilitation, 31, 2041-2046.
[6] Leonardi, M., Raggi, A., Ajovalasit, D., Bussone, G., &D’Amico, D. (2010a). Functioning and disability in migraine.Disability and Rehabilitation, 32, S23-S32.
[7] Leonardi, M., Chatterji, S., Newton, A., Bjorck-Akesson, E.,Hollenweger, J., Francescutti, C., et al. (2010b). Integratingresearch into policy planning: MHADIE policy recommenda-tions, Disability and Rehabilitation, 32, S139-S147.
[8] Leonardi, M., Martinuzzi, A., Meucci, P., Sala, M., Russo, E.,Buffoni, M., et al. (2012). A population survey in Italy basedon the ICF Classification: Recognizing persons with severedisability. The Scientific World Journal, 2012, 189097
[9] Raggi, A., Leonardi, M., Ajovalasit, D., Carella, F.,Soliveri, P., Albanese, A., et al. (2010). Functioning and dis-ability in Parkinson’s disease, Disability and Rehabilitation,32, S33-S41.
[10] Sattin, D., Covelli, V., Pagani, M., Giovannetti, A.M.,Raggi, A., Meucci, P., Cerniauskaite, M., et al. (2014). Dodiagnostic differences between Vegetative state and Minimallyconscious state patients’ correspond to differences in func-tioning and disability profiles? Results from a national study,European Journal Physical and Rehabilitation Medicine, 50,309-21
[11] Svestkova, O., Angerova, Y., Sladkova, P., Bickenbach, J., &Raggi, A. (2010a). Functioning and disability in traumaticbrain injury, Disability and Rehabilitation, 32, S68-S77
[12] Svestkova, O., Angerova, Y., Sladkova, P., Keclikova, B., Bick-enbach, J., & Raggi, A. (2010b). Functioning and disability inmultiple sclerosis, Disability and Rehabilitation, 32, S59-S67.
[13] Vos, T., Flaxman, A.D., Naghavi, M., Lozano, R., Michaud,D., Ezzati, M., et al. (2012). Years lived with disability (YLDs)for 1160 sequelae of 289 diseases and injuries 1990–2010: Asystematic analysis for the Global Burden of Disease Study2010, Lancet, 380, 2163-2196
[14] World Health Organization (2001). The International Classi-fication of Functioning, Disability and Health (ICF). Geneva:World Health Organization.
[15] World Health Organization (2011). World report on disability2011. Geneva: World Health Organization.
Copyright of NeuroRehabilitation is the property of IOS Press and its content may not becopied or emailed to multiple sites or posted to a listserv without the copyright holder'sexpress written permission. However, users may print, download, or email articles forindividual use.
POINTS
TOTAL
M E M O R Y
N A M I N G
VISUOSPATIAL / EXECUTIVE
ATTENTION
LANGUAGE
ABSTRACTIONDELAYED RECALL
ORIENTATION
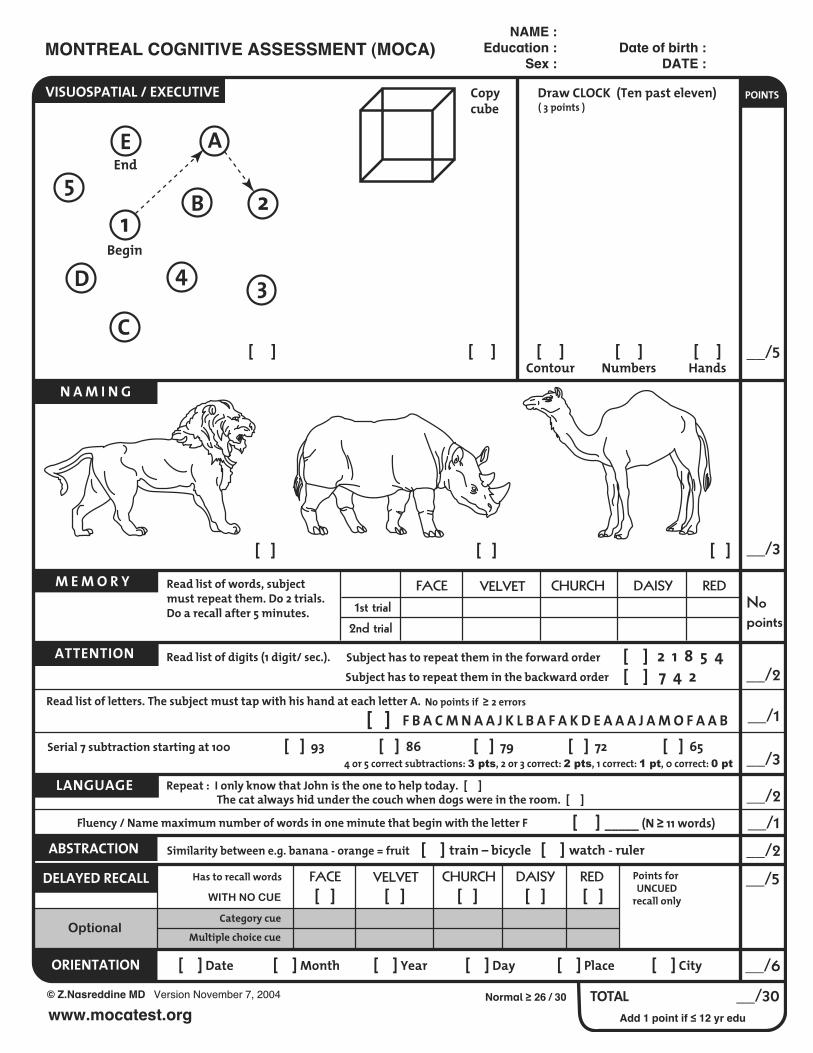
Read list of words, subject must repeat them. Do 2 trials. Do a recall after 5 minutes.
Subject has to repeat them in the forward order [ ] 2 1 8 5 4 Subject has to repeat them in the backward order [ ] 7 4 2
Read list of letters. The subject must tap with his hand at each letter A. No points if ! 2 errors[ ] F B A C M N A A J K L B A F A K D E A A A J A M O F A A B
Serial 7 subtraction starting at 100 [ ] 93 [ ] 86 [ ] 79 [ ] 72 [ ] 65
Repeat : I only know that John is the one to help today. [ ]The cat always hid under the couch when dogs were in the room. [ ]
Similarity between e.g. banana - orange = fruit [ ] train – bicycle [ ] watch - ruler
Draw CLOCK (Ten past eleven)Copy cube
__/5
__/3
No points
1st trial 2nd trial
FACE VELVET CHURCH DAISY RED
__/5
__/2
__/1
__/3
__/2Fluency / Name maximum number of words in one minute that begin with the letter F _____ [ ] (N ! 11 words) __/1
__/2
__/6
__/30
BBegin
End5
E
1
A
2
4 3C
D
Read list of digits (1 digit/ sec.).
NAME :Education :
Sex :Date of birth :
DATE :
© Z.Nasreddine MD Version November 7, 2004
www.mocatest.orgNormal ! 26 / 30
Add 1 point if " 12 yr edu
MONTREAL COGNITIVE ASSESSMENT (MOCA)
[ ] Date [ ] Month [ ] Year [ ] Day [ ] Place [ ] City
[ ]Contour
[ ][ ] [ ]Numbers
[ ]Hands
[ ] [ ] [ ]
4 or 5 correct subtractions: 3 pts, 2 or 3 correct: 2 pts, 1 correct: 1 pt, 0 correct: 0 pt
( 3 points )
Category cue
Points for UNCUED
recall onlyWITH NO CUE
Optional
Has to recall words
Multiple choice cue
FACE VELVET CHURCH DAISY RED [ ] [ ] [ ] [ ] [ ]

VAMCSLUMS EXAMINATIONQuestions about this assessment tool? E-mail [email protected]
Name___________________________________________________________ Age______________________Is the patient alert?____________________ Level of education________________________________________
1. What day of the week is it?
2. What is the year?
3. What state are we in?
4. Please remember these five objects. I will ask you what they are later. Apple Pen Tie House Car
5. You have $100 and you go to the store and buy a dozen apples for $3 and a tricycle for $20.How much did you spend?How much do you have left?
6. Please name as many animals as you can in one minute. 0-4 animals 5-9 animals 10-14 animals 15+ animals
7. What were the five objects I asked you to remember? 1 point for each one correct.
8. I am going to give you a series of numbers and I would like you to give them to me backwards. For example, if I say 42, you would say 24. 87 648 8537
9. This is a clock face. Please put in the hour markers and the time at ten minutes to eleven o’clock. Hour markers okay Time correct
10. Please place an X in the triangle.
Which of the above figures is largest?
11. I am going to tell you a story. Please listen carefully because afterwards, I’m going to ask you some questions about it.
Jill was a very successful stockbroker. She made a lot of money on the stock market. She then met Jack, a devastatingly handsome man. She married him and had three children. They lived in Chicago. She then stopped work and stayed at home to bring up her children. When they were teenagers, she went back to work. She and Jack lived happily ever after.
What was the female’s name? What work did she do? When did she go back to work? What state did she live in?
TOTAL SCORE
__/1
__/1
__/1
__/3
__/3
__/5
__/2
__/4
__/2
__/8
1
1
1
12
0 1 2 3
22
0 1 1
1
1
22
22
SCORING
SH Tariq, N Tumosa, JT Chibnall, HM Perry III, and JE Morley. The Saint Louis University Mental Status (SLUMS) Examination for detecting mild cognitive impairment and dementia is more sensitive than the Mini-Mental Status Examination (MMSE) - A pilot study. Am J Geriatr Psych 14:900-10, 2006.
CLINICIAN’S SIGNATURE DATE TIME
HIGH SCHOOL EDUCATION LESS THAN HIGH SCHOOL EDUCATION
27-30 NORMAL 25-30 21-26 MILD NEUROCOGNITIVE DISORDER 20-24 1-20 DEMENTIA 1-19

Patient Name: ____________________________________________ Date: _______________________
The Activities-specific Balance Confidence (ABC) Scale*
Instructions to Participants: For each of the following activities, please indicate your level of confidence in doing the activity without losing your balance or becoming unsteady from choosing one of the percentage points on the scale from 0% to 100% If you do not currently do the activity in question, try and imagine how confident you would be if you had to do the activity. If you normally use a walking aid to do the activity or hold onto someone, rate your confidence as if you were using these supports.
0% 10 20 30 40 50 60 70 80 90 100% No Confidence Completely Confident
How confident are you that you will not lose your balance or become unsteady when you…
1. …walk around the house? _____% 2. …walk up or down stairs? _____% 3. …bend over and pick up a slipper from the front of a closet floor? _____% 4. …reach for a small can off a shelf at eye level? _____% 5. …stand on your tip toes and reach for something above your head? _____% 6. …stand on a chair and reach for something? _____% 7. …sweep the floor? _____% 8. …walk outside the house to a car parked in the driveway? _____% 9. …get into or out of a car? _____% 10. …walk across a parking lot to the mall? _____% 11. …walk up or down a ramp? _____% 12. …walk in a crowded mall where people rapidly walk past you? _____% 13. …are bumped into by people as you walk through the mall? _____% 14. …step onto or off of an escalator while you are holding onto a railing? _____% 15. …step onto or off an escalator while holding onto parcels such that you cannot hold onto the
railing? _____% 16. …walk outside on icy sidewalks? _____%
*Powell LE & Myers AM. The Activities-specific Balance Confidence (ABC) Scale. Journal of Gerontology Med Sci 1995; 50(1):M28-34.
Total ABC Score: __________
Scoring: _____________ / 16 = Total ABC Score Patient Signature: ___________________________________________ Date: _____________________ Therapist Signature: __________________________________________ Date: _____________________
__________% of self confidence
MEDICARE PATIENTS ONLY 100% - _____% Function = _____% Impairment
Downloaded from www.rehabmeasures.org Test instructions provided courtesy of Mary E. Tinetti, MD Page 1
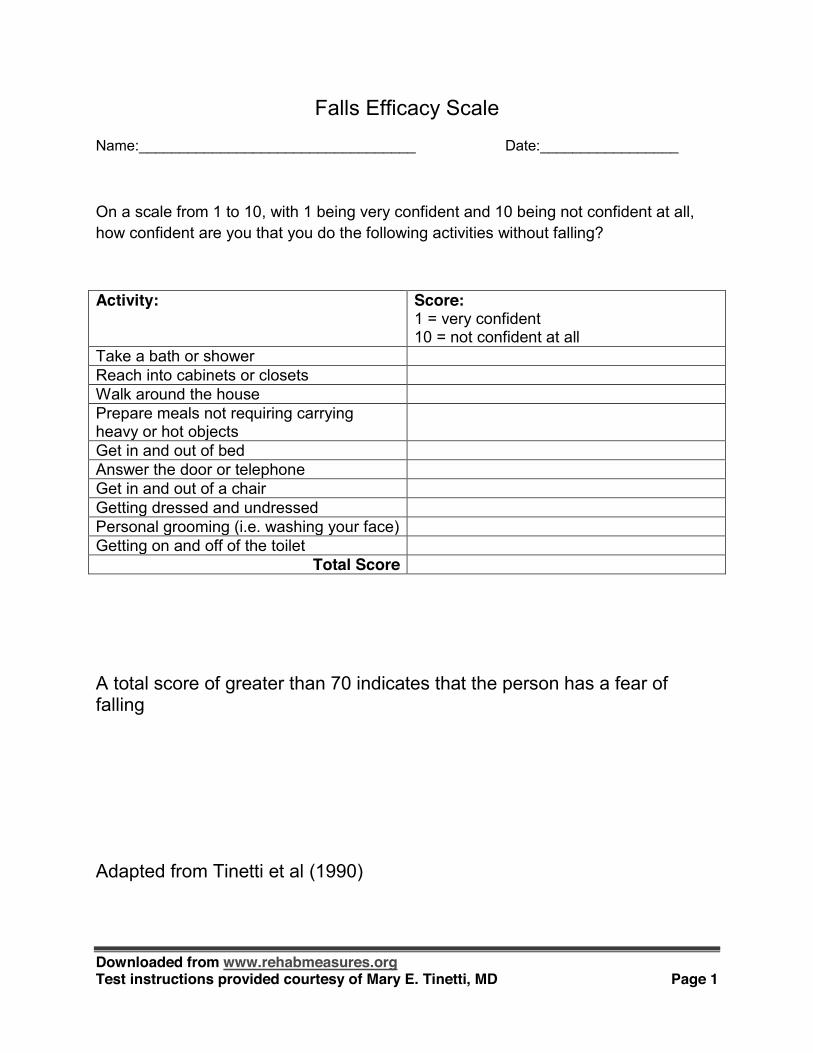
Falls Efficacy Scale
Name:__________________________________ Date:_________________
On a scale from 1 to 10, with 1 being very confident and 10 being not confident at all, how confident are you that you do the following activities without falling?
Activity: Score: 1 = very confident 10 = not confident at all
Take a bath or shower Reach into cabinets or closets Walk around the house Prepare meals not requiring carrying heavy or hot objects
Get in and out of bed Answer the door or telephone Get in and out of a chair Getting dressed and undressed Personal grooming (i.e. washing your face) Getting on and off of the toilet
Total Score
A total score of greater than 70 indicates that the person has a fear of falling
Adapted from Tinetti et al (1990)

Downloaded from www.rehabmeasures.org Test instructions provided courtesy of Mary E. Tinetti, MD Page 2
References: Tinetti, M., D. Richman, et al. (1990). "Falls efficacy as a measure of fear of falling." Journal of
gerontology 45(6): P239.
From The Hartford Institute for Geriatric Nursing, New York University, College of Nursing
Best Practices in Nursing Care to Older Adults
general assessment series
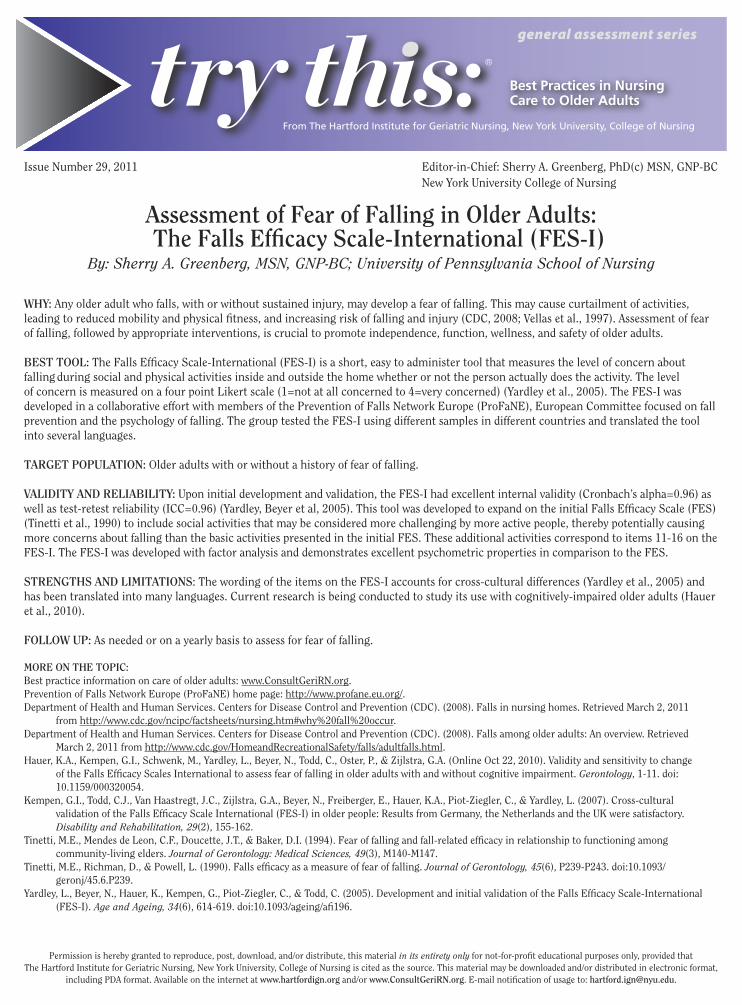
Issue Number 29, 2011 Editor-in-Chief: Sherry A. Greenberg, PhD(c) MSN, GNP-BC New York University College of Nursing
Assessment of Fear of Falling in Older Adults: 4HE&ALLS%FlCACY3CALE )NTERNATIONAL&%3 )
By: Sherry A. Greenberg, MSN, GNP-BC; University of Pennsylvania School of Nursing
WHY: Any older adult who falls, with or without sustained injury, may develop a fear of falling. This may cause curtailment of activities, leading to reduced mobility and physical fitness, and increasing risk of falling and injury (CDC, 2008; Vellas et al., 1997). Assessment of fear of falling, followed by appropriate interventions, is crucial to promote independence, function, wellness, and safety of older adults.
"%344//,The Falls Efficacy Scale-International (FES-I) is a short, easy to administer tool that measures the level of concern about falling during social and physical activities inside and outside the home whether or not the person actually does the activity. The level of concern is measured on a four point Likert scale (1=not at all concerned to 4=very concerned) (Yardley et al., 2005). The FES-I was developed in a collaborative effort with members of the Prevention of Falls Network Europe (ProFaNE), European Committee focused on fall prevention and the psychology of falling. The group tested the FES-I using different samples in different countries and translated the tool into several languages.
4!2'%40/05,!4)/.Older adults with or without a history of fear of falling.
6!,)$)49!.$2%,)!"),)49Upon initial development and validation, the FES-I had excellent internal validity (Cronbach’s alpha=0.96) as well as test-retest reliability (ICC=0.96) (Yardley, Beyer et al, 2005). This tool was developed to expand on the initial Falls Efficacy Scale (FES) (Tinetti et al., 1990) to include social activities that may be considered more challenging by more active people, thereby potentially causing more concerns about falling than the basic activities presented in the initial FES. These additional activities correspond to items 11-16 on the FES-I. The FES-I was developed with factor analysis and demonstrates excellent psychometric properties in comparison to the FES.
342%.'4(3!.$,)-)4!4)/.3: The wording of the items on the FES-I accounts for cross-cultural differences (Yardley et al., 2005) and has been translated into many languages. Current research is being conducted to study its use with cognitively-impaired older adults (Hauer et al., 2010).
&/,,/750As needed or on a yearly basis to assess for fear of falling.
-/2%/.4(%4/0)#Best practice information on care of older adults: www.ConsultGeriRN.org.Prevention of Falls Network Europe (ProFaNE) home page: http://www.profane.eu.org/.Department of Health and Human Services. Centers for Disease Control and Prevention (CDC). (2008). Falls in nursing homes. Retrieved March 2, 2011
from http://www.cdc.gov/ncipc/factsheets/nursing.htm#why%20fall%20occur.Department of Health and Human Services. Centers for Disease Control and Prevention (CDC). (2008). Falls among older adults: An overview. Retrieved
March 2, 2011 from http://www.cdc.gov/HomeandRecreationalSafety/falls/adultfalls.html.Hauer, K.A., Kempen, G.I., Schwenk, M., Yardley, L., Beyer, N., Todd, C., Oster, P., & Zijlstra, G.A. (Online Oct 22, 2010). Validity and sensitivity to change
of the Falls Efficacy Scales International to assess fear of falling in older adults with and without cognitive impairment. Gerontology, 1-11. doi: 10.1159/000320054.
Kempen, G.I., Todd, C.J., Van Haastregt, J.C., Zijlstra, G.A., Beyer, N., Freiberger, E., Hauer, K.A., Piot-Ziegler, C., & Yardley, L. (2007). Cross-cultural validation of the Falls Efficacy Scale International (FES-I) in older people: Results from Germany, the Netherlands and the UK were satisfactory. Disability and Rehabilitation, 29(2), 155-162.
Tinetti, M.E., Mendes de Leon, C.F., Doucette, J.T., & Baker, D.I. (1994). Fear of falling and fall-related efficacy in relationship to functioning among community-living elders. Journal of Gerontology: Medical Sciences, 49(3), M140-M147.
Tinetti, M.E., Richman, D., & Powell, L. (1990). Falls efficacy as a measure of fear of falling. Journal of Gerontology, 45(6), P239-P243. doi:10.1093/geronj/45.6.P239.
Yardley, L., Beyer, N., Hauer, K., Kempen, G., Piot-Ziegler, C., & Todd, C. (2005). Development and initial validation of the Falls Efficacy Scale-International (FES-I). Age and Ageing, 34(6), 614-619. doi:10.1093/ageing/afi196.
Permission is hereby granted to reproduce, post, download, and/or distribute, this material in its entirety only for not-for-profit educational purposes only, provided that The Hartford Institute for Geriatric Nursing, New York University, College of Nursing is cited as the source. This material may be downloaded and/or distributed in electronic format,
including PDA format. Available on the internet at www.hartfordign.org and/or WWW#ONSULT'ERI2.ORG. E-mail notification of usage to: HARTFORDIGN NYUEDU.

Best Practices in Nursing Care to Older Adults
A series provided by The Hartford Institute for Geriatric Nursing, New York University, College of Nursing
EMAIL [email protected] HARTFORD INSTITUTE WEBSITE www.hartfordign.org CLINICAL NURSING WEBSITE www.ConsultGeriRN.org
general assessment series
&ALLS%FlCACY3CALE )NTERNATIONAL%NGLISHI would like to ask some questions about how concerned you are about the possibility of falling. For each of the following activities, please circle the opinion closest to your own to show how concerned you are that you might fall if you did this activity. Please reply thinking about how you usually do the activity. If you currently don’t do the activity (example: if someone does your shopping for you), please answer to show whether you think you would be concerned about falling IF you did the activity.
Not at all concerned
1
Somewhat concerned
2
Fairly concerned
3
Very concerned
4
1 Cleaning the house (e.g. sweep, vacuum, dust)
2 Getting dressed or undressed
3 Preparing simple meals
4 Taking a bath or shower
5 Going to the shop
6 Getting in or out of a chair
7 Going up or down stairs
8 Walking around in the neighborhood
9 Reaching for something above your head or on the ground
10 Going to answer the telephone before it stops ringing
11 Walking on a slippery surface (e.g. wet or icy)
12 Visiting a friend or relative
13 Walking in a place with crowds
14 Walking on an uneven surface (e.g. rocky ground, poorly maintained pavement)
15 Walking up or down a slope
16 Going out to a social event (e.g. religious service, family gathering, or club meeting)
3UB4OTAL
4/4!, /64
Reprinted with permission from publisher.Reference: Yardley, L., Beyer, N., Hauer, K., Kempen, G., Piot-Ziegler, C., & Todd, C. (2005). Development and initial validation of the Falls Efficacy Scale-
International (FES-I). Age and Ageing, 34(6), 614-619. doi:10.1093/ageing/afi196.
Sherry Greenberg wishes to acknowledge that the development of this document was funded in part by a Ruth L. Kirschstein National Research Service Award (NRSA) Institutional Research Training Grant (T32) Individualized Care for At-Risk Older Adults, NewCourtland Center for Transitions and Health and the Center for Integrative Science in Aging, NIH/NINR (T32-NR009356) University of Pennsylvania School of Nursing.

Patient Identification. ___ ___-___ ___ ___-___ ___ ___
Pt. Date of Birth ___ ___/___ ___/___ ___
Hospital ________________________(___ ___-___ ___)
Date of Exam ___ ___/___ ___/___ ___
Interval: [ ] Baseline [ ] 2 hours post treatment [ ] 24 hours post onset of symptoms ±20 minutes [ ] 7-10 days [ ] 3 months [ ] Other ________________________________(___ ___)
Time: ___ ___:___ ___ [ ]am [ ]pm Person Administering Scale _____________________________________ Administer stroke scale items in the order listed. Record performance in each category after each subscale exam. Do not go back and change scores. Follow directions provided for each exam technique. Scores should reflect what the patient does, not what the clinician thinks the patient can do. The clinician should record answers while administering the exam and work quickly. Except where indicated, the patient should not be coached (i.e., repeated requests to patient to make a special effort).
Instructions Scale Definition Score
1a. Level of Consciousness: The investigator must choose a response if a full evaluation is prevented by such obstacles as an endotracheal tube, language barrier, orotracheal trauma/bandages. A 3 is scored only if the patient makes no movement (other than reflexive posturing) in response to noxious stimulation.
0 = Alert; keenly responsive. 1 = Not alert; but arousable by minor stimulation to obey,
answer, or respond. 2 = Not alert; requires repeated stimulation to attend, or is
obtunded and requires strong or painful stimulation to make movements (not stereotyped).
3 = Responds only with reflex motor or autonomic effects or totally unresponsive, flaccid, and areflexic.
______
1b. LOC Questions: The patient is asked the month and his/her age. The answer must be correct - there is no partial credit for being close. Aphasic and stuporous patients who do not comprehend the questions will score 2. Patients unable to speak because of endotracheal intubation, orotracheal trauma, severe dysarthria from any cause, language barrier, or any other problem not secondary to aphasia are given a 1. It is important that only the initial answer be graded and that the examiner not "help" the patient with verbal or non-verbal cues.
0 = Answers both questions correctly. 1 = Answers one question correctly. 2 = Answers neither question correctly.
______
1c. LOC Commands: The patient is asked to open and close the eyes and then to grip and release the non-paretic hand. Substitute another one step command if the hands cannot be used. Credit is given if an unequivocal attempt is made but not completed due to weakness. If the patient does not respond to command, the task should be demonstrated to him or her (pantomime), and the result scored (i.e., follows none, one or two commands). Patients with trauma, amputation, or other physical impediments should be given suitable one-step commands. Only the first attempt is scored.
0 = Performs both tasks correctly. 1 = Performs one task correctly. 2 = Performs neither task correctly.
______
2. Best Gaze: Only horizontal eye movements will be tested. Voluntary or reflexive (oculocephalic) eye movements will be scored, but caloric testing is not done. If the patient has a conjugate deviation of the eyes that can be overcome by voluntary or reflexive activity, the score will be 1. If a patient has an isolated peripheral nerve paresis (CN III, IV or VI), score a 1. Gaze is testable in all aphasic patients. Patients with ocular trauma, bandages, pre-existing blindness, or other disorder of visual acuity or fields should be tested with reflexive movements, and a choice made by the investigator. Establishing eye contact and then moving about the patient from side to side will occasionally clarify the presence of a partial gaze palsy.
0 = Normal. 1 = Partial gaze palsy; gaze is abnormal in one or both eyes,
but forced deviation or total gaze paresis is not present. 2 = Forced deviation, or total gaze paresis not overcome by the
oculocephalic maneuver.
______
Rev 10/1/2003

Patient Identification. ___ ___-___ ___ ___-___ ___ ___
Pt. Date of Birth ___ ___/___ ___/___ ___
Hospital ________________________(___ ___-___ ___)
Date of Exam ___ ___/___ ___/___ ___
Interval: [ ] Baseline [ ] 2 hours post treatment [ ] 24 hours post onset of symptoms ±20 minutes [ ] 7-10 days [ ] 3 months [ ] Other ________________________________(___ ___)
3. Visual: Visual fields (upper and lower quadrants) are tested by confrontation, using finger counting or visual threat, as appropriate. Patients may be encouraged, but if they look at the side of the moving fingers appropriately, this can be scored as normal. If there is unilateral blindness or enucleation, visual fields in the remaining eye are scored. Score 1 only if a clear-cut asymmetry, including quadrantanopia, is found. If patient is blind from any cause, score 3. Double simultaneous stimulation is performed at this point. If there is extinction, patient receives a 1, and the results are used to respond to item 11.
0 = No visual loss. 1 = Partial hemianopia. 2 = Complete hemianopia. 3 = Bilateral hemianopia (blind including cortical blindness).
______
4. Facial Palsy: Ask – or use pantomime to encourage – the patient to show teeth or raise eyebrows and close eyes. Score symmetry of grimace in response to noxious stimuli in the poorly responsive or non-comprehending patient. If facial trauma/bandages, orotracheal tube, tape or other physical barriers obscure the face, these should be removed to the extent possible.
0 = Normal symmetrical movements. 1 = Minor paralysis (flattened nasolabial fold, asymmetry on
smiling). 2 = Partial paralysis (total or near-total paralysis of lower
face). 3 = Complete paralysis of one or both sides (absence of
facial movement in the upper and lower face).
______
5. Motor Arm: The limb is placed in the appropriate position: extend the arms (palms down) 90 degrees (if sitting) or 45 degrees (if supine). Drift is scored if the arm falls before 10 seconds. The aphasic patient is encouraged using urgency in the voice and pantomime, but not noxious stimulation. Each limb is tested in turn, beginning with the non-paretic arm. Only in the case of amputation or joint fusion at the shoulder, the examiner should record the score as untestable (UN), and clearly write the explanation for this choice.
0 = No drift; limb holds 90 (or 45) degrees for full 10 seconds. 1 = Drift; limb holds 90 (or 45) degrees, but drifts down before
full 10 seconds; does not hit bed or other support. 2 = Some effort against gravity; limb cannot get to or
maintain (if cued) 90 (or 45) degrees, drifts down to bed, but has some effort against gravity.
3 = No effort against gravity; limb falls. 4 = No movement. UN = Amputation or joint fusion, explain: _____________________ 5a. Left Arm 5b. Right Arm
______ ______
6. Motor Leg: The limb is placed in the appropriate position: hold the leg at 30 degrees (always tested supine). Drift is scored if the leg falls before 5 seconds. The aphasic patient is encouraged using urgency in the voice and pantomime, but not noxious stimulation. Each limb is tested in turn, beginning with the non-paretic leg. Only in the case of amputation or joint fusion at the hip, the examiner should record the score as untestable (UN), and clearly write the explanation for this choice.
0 = No drift; leg holds 30-degree position for full 5 seconds. 1 = Drift; leg falls by the end of the 5-second period but does
not hit bed. 2 = Some effort against gravity; leg falls to bed by 5
seconds, but has some effort against gravity. 3 = No effort against gravity; leg falls to bed immediately. 4 = No movement. UN = Amputation or joint fusion, explain: ________________ 6a. Left Leg
6b. Right Leg
______
Rev 10/1/2003

Patient Identification. ___ ___-___ ___ ___-___ ___ ___
Pt. Date of Birth ___ ___/___ ___/___ ___
Hospital ________________________(___ ___-___ ___)
Date of Exam ___ ___/___ ___/___ ___
Interval: [ ] Baseline [ ] 2 hours post treatment [ ] 24 hours post onset of symptoms ±20 minutes [ ] 7-10 days [ ] 3 months [ ] Other ________________________________(___ ___)
______
7. Limb Ataxia: This item is aimed at finding evidence of a unilateral cerebellar lesion. Test with eyes open. In case of visual defect, ensure testing is done in intact visual field. The finger-nose-finger and heel-shin tests are performed on both sides, and ataxia is scored only if present out of proportion to weakness. Ataxia is absent in the patient who cannot understand or is paralyzed. Only in the case of amputation or joint fusion, the examiner should record the score as untestable (UN), and clearly write the explanation for this choice. In case of blindness, test by having the patient touch nose from extended arm position.
0 = Absent. 1 = Present in one limb. 2 = Present in two limbs. UN = Amputation or joint fusion, explain: ________________
______
8. Sensory: Sensation or grimace to pinprick when tested, or withdrawal from noxious stimulus in the obtunded or aphasic patient. Only sensory loss attributed to stroke is scored as abnormal and the examiner should test as many body areas (arms [not hands], legs, trunk, face) as needed to accurately check for hemisensory loss. A score of 2, “severe or total sensory loss,” should only be given when a severe or total loss of sensation can be clearly demonstrated. Stuporous and aphasic patients will, therefore, probably score 1 or 0. The patient with brainstem stroke who has bilateral loss of sensation is scored 2. If the patient does not respond and is quadriplegic, score 2. Patients in a coma (item 1a=3) are automatically given a 2 on this item.
0 = Normal; no sensory loss. 1 = Mild-to-moderate sensory loss; patient feels pinprick is
less sharp or is dull on the affected side; or there is a loss of superficial pain with pinprick, but patient is aware of being touched.
2 = Severe to total sensory loss; patient is not aware of
being touched in the face, arm, and leg.
______
9. Best Language: A great deal of information about comprehension will be obtained during the preceding sections of the examination. For this scale item, the patient is asked to describe what is happening in the attached picture, to name the items on the attached naming sheet and to read from the attached list of sentences. Comprehension is judged from responses here, as well as to all of the commands in the preceding general neurological exam. If visual loss interferes with the tests, ask the patient to identify objects placed in the hand, repeat, and produce speech. The intubated patient should be asked to write. The patient in a coma (item 1a=3) will automatically score 3 on this item. The examiner must choose a score for the patient with stupor or limited cooperation, but a score of 3 should be used only if the patient is mute and follows no one-step commands.
0 = No aphasia; normal. 1 = Mild-to-moderate aphasia; some obvious loss of fluency
or facility of comprehension, without significant limitation on ideas expressed or form of expression. Reduction of speech and/or comprehension, however, makes conversation about provided materials difficult or impossible. For example, in conversation about provided materials, examiner can identify picture or naming card content from patient’s response.
2 = Severe aphasia; all communication is through fragmentary
expression; great need for inference, questioning, and guessing by the listener. Range of information that can be exchanged is limited; listener carries burden of communication. Examiner cannot identify materials provided from patient response.
3 = Mute, global aphasia; no usable speech or auditory
comprehension.
______
10. Dysarthria: If patient is thought to be normal, an adequate sample of speech must be obtained by asking patient to read or repeat words from the attached list. If the patient has severe aphasia, the clarity of articulation of spontaneous speech can be rated. Only if the patient is intubated or has other physical barriers to producing speech, the examiner should record the score as untestable (UN), and clearly write an explanation for this choice. Do not tell the patient why he or she is being tested.
0 = Normal. 1 = Mild-to-moderate dysarthria; patient slurs at least some
words and, at worst, can be understood with some difficulty.
2 = Severe dysarthria; patient's speech is so slurred as to be unintelligible in the absence of or out of proportion to any dysphasia, or is mute/anarthric.
UN = Intubated or other physical barrier, explain:_____________________________
______
Rev 10/1/2003

Patient Identification. ___ ___-___ ___ ___-___ ___ ___
Pt. Date of Birth ___ ___/___ ___/___ ___
Hospital ________________________(___ ___-___ ___)
Date of Exam ___ ___/___ ___/___ ___
Interval: [ ] Baseline [ ] 2 hours post treatment [ ] 24 hours post onset of symptoms ±20 minutes [ ] 7-10 days [ ] 3 months [ ] Other ________________________________(___ ___)
11. Extinction and Inattention (formerly Neglect): Sufficient information to identify neglect may be obtained during the prior testing. If the patient has a severe visual loss preventing visual double simultaneous stimulation, and the cutaneous stimuli are normal, the score is normal. If the patient has aphasia but does appear to attend to both sides, the score is normal. The presence of visual spatial neglect or anosagnosia may also be taken as evidence of abnormality. Since the abnormality is scored only if present, the item is never untestable.
0 = No abnormality. 1 = Visual, tactile, auditory, spatial, or personal inattention
or extinction to bilateral simultaneous stimulation in one of the sensory modalities.
2 = Profound hemi-inattention or extinction to more than
one modality; does not recognize own hand or orients to only one side of space.
______
______ ______
Rev 10/1/2003


You know how. Down to earth. I got home from work. Near the table in the dining
room. They heard him speak on the
radio last night.


MAMA
TIP – TOP
FIFTY – FIFTY
THANKS
HUCKLEBERRY
BASEBALL PLAYER

Rehabilitation Medicine, University of Gothenburg
Approved by Fugl-Meyer AR 2010 1
FUGL-MEYER ASSESSMENT ID: UPPER EXTREMITY (FMA-UE) Date: Assessment of sensorimotor function Examiner: Fugl-Meyer AR, Jaasko L, Leyman I, Olsson S, Steglind S: The post-stroke hemiplegic patient. A method for evaluation of physical performance. Scand J Rehabil Med 1975, 7:13-31.
A. UPPER EXTREMITY, sitting position
I. Reflex activity none can be elicited Flexors: biceps and finger flexors Extensors: triceps
0 0
2 2
Subtotal I (max 4)
II. Volitional movement within synergies, without gravitational help none partial full Flexor synergy: Hand from contralateral knee to ipsilateral ear. From extensor synergy (shoulder adduction/ internal rotation, elbow extension, forearm pronation) to flexor synergy (shoulder abduction/ external rotation, elbow flexion, forearm supination). Extensor synergy: Hand from ipsilateral ear to the contralateral knee
Shoulder Elbow Forearm
retraction elevation abduction (90°) external rotation flexion supination
0 0 0 0 0 0
1 1 1 1 1 1
2 2 2 2 2 2
Shoulder Elbow Forearm
adduction/internal rotation extension pronation
0 0 0
1 1 1
2 2 2
Subtotal II (max 18)
III. Volitional movement mixing synergies, without compensation none partial full Hand to lumbar spine cannot be performed, hand in front of SIAS
hand behind of SIAS (without compensation) hand to lumbar spine (without compensation)
0 1
2
Shoulder flexion 0°-90° elbow at 0° pronation-supination 0°
immediate abduction or elbow flexion abduction or elbow flexion during movement complete flexion 90°, maintains 0° in elbow
0 1
2
Pronation-supination elbow at 90° shoulder at 0°
no pronation/supination, starting position impossible limited pronation/supination, maintains position complete pronation/supination, maintains position
0 1
2
Subtotal III (max 6)
IV. Volitional movement with little or no synergy none partial full Shoulder abduction 0 - 90° elbow at 0° forearm pronated
immediate supination or elbow flexion supination or elbow flexion during movement abduction 90°, maintains extension and pronation
0 1
2 Shoulder flexion 90°- 180° elbow at 0° pronation-supination 0°
immediate abduction or elbow flexion abduction or elbow flexion during movement complete flexion, maintains 0° in elbow
0 1
2
Pronation/supination elbow at 0° shoulder at 30°-90° flexion
no pronation/supination, starting position impossible limited pronation/supination, maintains extension full pronation/supination, maintains elbow extension
0 1
2
Subtotal IV (max 6)
V. Normal reflex activity evaluated only if full score of 6 points achieved on part IV biceps, triceps, finger flexors
0 points on part IV or 2 of 3 reflexes markedly hyperactive 1 reflex markedly hyperactive or at least 2 reflexes lively maximum of 1 reflex lively, none hyperactive
0 1
2
Subtotal V (max 2)
Total A (max 36)
Rehabilitation Medicine, University of Gothenburg
Approved by Fugl-Meyer AR 2010 2
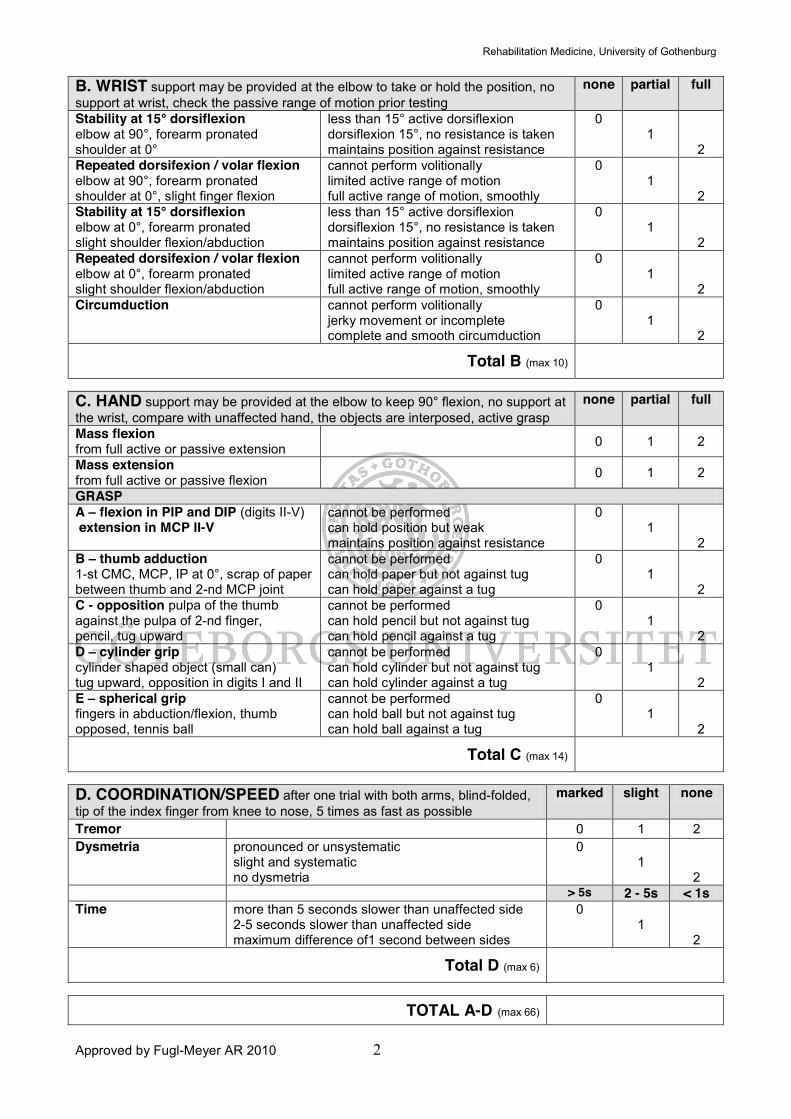
B. WRIST support may be provided at the elbow to take or hold the position, no support at wrist, check the passive range of motion prior testing
none partial full
Stability at 15° dorsiflexion elbow at 90°, forearm pronated shoulder at 0°
less than 15° active dorsiflexion dorsiflexion 15°, no resistance is taken maintains position against resistance
0 1
2
Repeated dorsifexion / volar flexion elbow at 90°, forearm pronated shoulder at 0°, slight finger flexion
cannot perform volitionally limited active range of motion full active range of motion, smoothly
0 1
2
Stability at 15° dorsiflexion elbow at 0°, forearm pronated slight shoulder flexion/abduction
less than 15° active dorsiflexion dorsiflexion 15°, no resistance is taken maintains position against resistance
0 1
2
Repeated dorsifexion / volar flexion elbow at 0°, forearm pronated slight shoulder flexion/abduction
cannot perform volitionally limited active range of motion full active range of motion, smoothly
0 1
2
Circumduction cannot perform volitionally jerky movement or incomplete complete and smooth circumduction
0 1
2
Total B (max 10)
C. HAND support may be provided at the elbow to keep 90° flexion, no support at the wrist, compare with unaffected hand, the objects are interposed, active grasp
none partial full
Mass flexion from full active or passive extension 0 1 2
Mass extension from full active or passive flexion 0 1 2
GRASP A – flexion in PIP and DIP (digits II-V) extension in MCP II-V
cannot be performed can hold position but weak maintains position against resistance
0 1
2
B – thumb adduction 1-st CMC, MCP, IP at 0°, scrap of paper between thumb and 2-nd MCP joint
cannot be performed can hold paper but not against tug can hold paper against a tug
0 1
2
C - opposition pulpa of the thumb against the pulpa of 2-nd finger, pencil, tug upward
cannot be performed can hold pencil but not against tug can hold pencil against a tug
0 1
2 D – cylinder grip cylinder shaped object (small can) tug upward, opposition in digits I and II
cannot be performed can hold cylinder but not against tug can hold cylinder against a tug
0 1
2
E – spherical grip fingers in abduction/flexion, thumb opposed, tennis ball
cannot be performed can hold ball but not against tug can hold ball against a tug
0 1
2
Total C (max 14)
D. COORDINATION/SPEED after one trial with both arms, blind-folded, tip of the index finger from knee to nose, 5 times as fast as possible
marked slight none
Tremor 0 1 2 Dysmetria pronounced or unsystematic
slight and systematic no dysmetria
0 1
2
> 5s 2 - 5s < 1s Time more than 5 seconds slower than unaffected side
2-5 seconds slower than unaffected side maximum difference of1 second between sides
0 1
2
Total D (max 6)
TOTAL A-D (max 66)

Rehabilitation Medicine, University of Gothenburg
Approved by Fugl-Meyer AR 2010 3
H. SENSATION, upper extremity blind-folded, compared with unaffected side
anesthesia hypoesthesia dysesthesia
normal
Light touch
upper arm, forearm palmar surface of the hand
0 0
1 1
2 2
absence less than 3/4
correct
3/4 correct considerable
difference
correct 100% little or no difference
Position small alterations in the position
shoulder elbow wrist thumb (IP-joint)
0 0 0 0
1 1 1 1
2 2 2 2
Total H (max12)
J. PASSIVE JOINT MOTION, upper extremity J. JOINT PAIN during passive
motion, upper extremity Sitting position, compare with unaffected side
only few degrees (less
than 10° in shoulder)
decreased normal pronounced constant pain during or at the
end of movement
some pain
no pain
Shoulder Flexion (0° - 180°) Abduction (0°-90°) External rotation Internal rotation
0 0 0 0
1 1 1 1
2 2 2 2
0 0 0 0
1 1 1 1
2 2 2 2
Elbow Flexion Extension
0 0
1 1
2 2
0 0
1 1
2 2
Forearm Pronation Supination
0 0
1 1
2 2
0 0
1 1
2 2
Wrist Flexion Extension
0 0
1 1
2 2
0 0
1 1
2 2
Fingers Flexion Extension
0 0
1 1
2 2
0 0
1 1
2 2
Total (max 24) Total (max 24)
A. UPPER EXTREMITY /36
B. WRIST /10
C. HAND /14
D. COORDINATION / SPEED / 6
TOTAL A-D (motor function) /66
H. SENSATION /12
J. PASSIVE JOINT MOTION /24
J. JOINT PAIN /24

Rehabilitation Medicine, University of Gothenburg
Approved by Fugl-Meyer AR 2010 1
FUGL-MEYER ASSESSMENT ID: LOWER EXTREMITY (FMA-LE) Date: Assessment of sensorimotor function Examiner: Fugl-Meyer AR, Jaasko L, Leyman I, Olsson S, Steglind S: The post-stroke hemiplegic patient. 1. a method for evaluation of physical performance. Scand J Rehabil Med 1975, 7:13-31.
E. LOWER EXTREMITY
I. Reflex activity, supine position none can be elicited Flexors: knee flexors Extensors: patellar, Achilles
0 0
2 2
Subtotal I (max 4)
II. Volitional movement within synergies, supine position none partial full Flexor synergy: Maximal hip flexion (abduction/external rotation), maximal flexion in knee and ankle joint (palpate distal tendons to ensure active knee flexion). Extensor synergy: From flexor synergy to the hip extension/adduction, knee extension and ankle plantar flexion. Resistance is applied to ensure active movement, evaluate both movement and strength.
Hip Knee Ankle
flexion flexion dorsiflexion
0 0 0
1 1 1
2 2 2
Hip Knee Ankle
extension adduction extension plantar flexion
0 0 0 0
1 1 1 1
2 2 2 2
Subtotal II (max 14)
III. Volitional movement mixing synergies, sitting position, knee 10cm from the edge of the chair/bed none partial full
Knee flexion from actively or passively extended knee
no active motion no flexion beyond 90°, palpate tendons of hamstrings knee flexion beyond 90°, palpate tendons of hamstrings
0 1
2
Ankle dorsiflexion compare with unaffected side
no active motion limited dorsiflexion complete dorsiflexion
0 1
2
Subtotal III (max 4)
IV. Volitional movement with little or no synergy, standing position, hip at 0° none partial full
Knee flexion to 90° hip at 0°, balance support is allowed
no active motion / immediate and simultaneous hip flexion less than 90° knee flexion or hip flexion during movement at least 90° knee flexion without simultaneous hip flexion
0 1
2 Ankle dorsiflexion compare with unaffected side
no active motion limited dorsiflexion complete dorsiflexion
0 1
2
Subtotal IV (max 4)
V. Normal reflex activity supine position, evaluated only if full score of 4 points achieved on earlier part IV, compare with unaffected side Reflex activity knee flexors, Achilles, patellar
0 points on part IV or 2 of 3 reflexes markedly hyperactive 1 reflex markedly hyperactive or at least 2 reflexes lively maximum of 1 reflex lively, none hyperactive
0 1
2
Subtotal V (max 2)
Total E (max 28)

Rehabilitation Medicine, University of Gothenburg
Approved by Fugl-Meyer AR 2010 2
F. COORDINATION/SPEED, supine, after one trial with both legs, blind-folded, heel to knee cap of the opposite leg, 5 times as fast as possible
marked slight none
Tremor 0 1 2 Dysmetria pronounced or unsystematic
slight and systematic no dysmetria
0 1
2
> 5s 2 - 5s < 1s Time more than 5 seconds slower than unaffected side
2-5 seconds slower than unaffected side maximum difference of 1 second between sides
0 1
2
Total F (max 6)
H. SENSATION, lower extremity blind-folded, compared with unaffected side
anesthesia hypoesthesia dysesthesia
normal
Light touch leg foot
0 0
1 1
2 2
absence, less than 3/4
correct
3/4 correct considerable
difference
correct 100% little or no difference
Position small alterations in the position
hip knee ankle great toe (IP-joint)
0 0 0 0
1 1 1 1
2 2 2 2
Total H (max12)
J. PASSIVE JOINT MOTION, lower extremity J. JOINT PAIN during passive
motion, lower extremity compare with unaffected side
only few degrees
decreased normal pronounced constant pain during or at the end of
movement
some pain
no pain
Hip
Flexion Abduction External rotation Internal rotation
0 0 0 0
1 1 1 1
2 2 2 2
0 0 0 0
1 1 1 1
2 2 2 2
Knee
Flexion Extension
0 0
1 1
2 2
0 0
1 1
2 2
Ankle
Dorsiflexion Plantar flexion
0 0
1 1
2 2
0 0
1 1
2 2
Foot
Pronation Supination
0 0
1 1
2 2
0 0
1 1
2 2
Total (max 20) Total (max 20)
E. LOWER EXTERMTY /28
F. COORDINATION / SPEED /6
TOTAL E-F (motor function) /34
H. SENSATION /12
J. PASSIVE JOINT MOTION /20
J. JOINT PAIN /20

The Trunk Impairment Scale: a new tool to measure
motor impairment of the trunk after stroke
G Verheyden, A Nieuwboer Department of Rehabilitation Sciences, Faculty of Physical Education and Physiotherapy,Katholieke Universiteit Leuven, Belgium, J Mertin Neurologic Rehabilitation Unit of the Kiliani-Klinik, Bad Windsheim,R Preger Neurologic Rehabilitation Unit of the Klinik Kipfenberg, Germany, C Kiekens Physical Medicine and RehabilitationUnit of the University Hospital Pellenberg, Katholieke Universiteit Leuven and W De Weerdt Department of RehabilitationSciences, Faculty of Physical Education and Physiotherapy, Katholieke Universiteit Leuven, Belgium
Received 17th December 2002; returned for revisions 2nd April 2003; revised manuscript accepted 15th June 2003.
Objective: To examine the clinimetric characteristics of the Trunk Impairment Scale(TIS). This newly developed scale evaluates motor impairment of the trunk afterstroke. The TIS scores, on a range from 0 to 23, static and dynamic sitting balance aswell as trunk co-ordination. It also aims to score the quality of trunk movement and tobe a guide for treatment.Design: Two physiotherapists observed each patient simultaneously, but scoredindependently. Each patient was re-examined by one of the therapists.Subjects: Twenty-eight patients in a rehabilitation setting.Results: Kappa and weighted kappa values for item per item reliability ranged for allbut two, from 0.62 to 1. All percentages of agreement exceeded 81%. Intraclasscorrelations (ICC) for the summed scores of the different subscales were between0.85 and 0.99. Test]/retest and interobserver reliability for the TIS total score (ICC)was 0.96 and 0.99, respectively. The 95% limits of agreement for the test]/retest andinterexaminer measurement error were 2/2.90, 3.68 and 2/1.84, 1.84, respectively.Cronbach alpha coefficients for internal consistency ranged from 0.65 to 0.89.Content validity was defined. Spearman rank correlations with the Barthel Index(r5 /0.86) and the Trunk Control Test (r5 /0.83) was used to examine construct andconcurrent validity, respectively.Conclusions: Analysis of different clinimetric parameters support the use of the TISin both clinical use and future stroke research. Guidelines for treatment and level ofquality of trunk activity can be derived from the assessment.
Introduction
Most literature concerning motor rehabilitationafter stroke focuses on the upper and lowerextremity.1] 3 Trunk rehabilitation receives only
little attention. Davies4 associates the loss ofselective control in the trunk with problems ofbreathing, speech, balance, gait, arm and handfunction. Sitting balance is also reported as apredictor of motor and functional recovery afterstroke.5] 8 The importance of recovery of trunkfunction, although often stated by clinical experts,needs to be confirmed by scientific research.
In the literature, the use of a clinical tool tomeasure trunk function is poorly documented.Sometimes a 3-, 4- or 5-point ordinal scale is
Address for correspondence: Geert Verheyden, KatholiekeUniversiteit Leuven, Faculty of Physical Educat ion andPhysiotherapy, Department of Rehabilitation Sciences, Tervuur-sevest 101, B-3000 Leuven, Belgium. e-mail: [email protected]
Clinical Rehabilitation 2004; 18: 326]/334
# Arnold 2004 10.1191/0269215504cr733oa

used without mentioning origin or basic statistica lcharacteristics.5,7,9 The Sitting Balance Scale devel-oped by Nieuwboer et al .10 showed poor reliability,especially for the items evaluating the quality oftrunk activity. The Trunk Control Test by Collinand Wade is a quick and reliable measure withpredictive validity.11,12 Limitations of the test arethat it does not take the quality of movement intoaccount11 as well as the moderate correlation withtrunk strength,13 measured using a hand dyna-mometer. The latter was explained by Bohannonbecause it needs more than trunk muscle strengthto complete the tasks of the Trunk Control Test.13
In several existing scales, (isolated) trunk activity isscored as one component. Examples are the legand trunk’ scale of the Rivermead Motor Assess-ment,14 the `balanced sitting’ item of the MotorAssessment Scale,15 the `postural control’ part ofthe Chedoke-McMaster Stroke Assessment,16 thelying and sitting’ tests of the Postural AssessmentScale for Stroke Patients17 and the `verticality’ and`abdominal manual muscle testing’ items of theStroke Impairment Assessment Set.18
The aim of this study was to develop acomprehensive tool to measure motor impairmentof the trunk after stroke, the Trunk ImpairmentScale (TIS), and to examine reliability, internalconsistency and validity of the TIS. The scaleshould include the observation of quality of trunkmovement and be a guide for the treatment of thetrunk in stroke patients.
Methods
The TIS consists of three subscales: static sittingbalance, dynamic sitting balance and co-ordina-tion. Each subscale contains between three andten items. The TIS score ranges from a minimumof 0 to a maximum of 23.
In a preliminary study, scoring the symmetryand manual lengthening of the hemiplegic andnonhemiplegic side of the trunk were considered aswell. Due to poor reliability, these items wereremoved from the scoring system. Other parts ofthe scale were redefined. The current scale is givenin the Appendix.
Stroke patients were recruited in rehabilitationcentres and were included if they were allowed to
sit upright. Exclusion criteria were a hip prosthesisat the nonhemiplegic side or a score of 0 on thecomprehension or speech item of the EuropeanStroke Scale.19 Further data collection to definethe population consisted of patient’s age, sex,hemiplegic side, type of stroke, days since stroke,Barthel Index,20 BrunnstroÈm-Fugl-Meyer test21 forupper and lower extremity and Trunk ControlTest.11
Twenty-eight patients (14 female and 14 male)were included in the study. Eleven had a righthemiplegia, 15 a left hemiplegia and two werebilaterally affected. Eight patients suffered froma haemorrhagic stroke, 20 had an ischaemicaccident. Median age was 63 years, median dayssince stroke 61 (Table 1). The majority of patientshad moderate ADL function and limited motorrecovery (Table 1).
Ethical approval was obtained from the EthicalCommission, Medical Faculty, K.U.Leuven, Bel-gium. Informed consent was obtained from allpatients.
For the reliability study, each patient wasexamined twice. On one occasion, two phy-siotherapists scored the TIS concurrently butindependently. On another occasion, one of thetherapists assessed the patient alone. The therapistwho examined the patient alone also instructed thepatient when both observers were scoring simulta-neously. The two observations were always on thesame day, separated by 1 or 2 hours of recoverytime. During that time no treatment was offered.The observations were planned every half hour, soat least two different patients were evaluated beforeseeing the same patient again. To further minimizerecall bias, the observers filled in the score sheetbut did not add up the scores. Allocation of the
Table 1 Patient characteristics
Median (Q1,Q3)a Range
Age (years) 63 (47,71) 32]/87Days since stroke 61 (46,94) 21]/2341Barthel Index 60 (33,80) 5 ]/100BrunnstroÈ m-Fugl-Meyer
Test (arm)9 (4,54) 0 ]/66
BrunnstroÈ m-Fugl-MeyerTest (leg)
19 (6,25) 0 ]/31
Trunk Control Test 75 (43,94) 0 ]/100
aQ1 means quartile one; Q3 means quartile three.
The Trunk Impairment Scale 327

patients to the observers as well as the order of thetwo observations were randomized. Each observerexamined a group of 14 patients twice, amountingto 28 patients in total.
In this study, every item of the scale wasperformed three times to avoid a possible scoringbias if a patient reached the maximum score afterone or two attempts.
Test ]/retest reliability was measured by compar-ing the results of the therapists who examined thepatient twice. To determine inter-rater reliability,the results of both therapists who observed thepatient simultaneously were compared.
Test ]/retest and interobserver reliability weredetermined for all scale items. Kappa and weightedkappa values were calculated for dichotomous andordinal scales, respectively. Percentage of agree-ment was also determined for all items. Test ]/retestand interobserver reliability for the subtotals andtotal score was examined by means of intraclasscorrelation (ICC). The 95% test ]/retest and inter-examiner measurement error interval according toHaas22 was determined. Cronbach’s alpha wascalculated to check for internal consistency of thesubscales and total scale. Content validity wasevaluated. The TIS total score was compared withthe Barthel Index by means of Spearman rankcorrelations for determining construct validity andwith the Trunk Control Test for concurrentvalidity.
Item per item reliability was established whenthe kappa or weighted kappa statistic exceeded0.6023 or when more then 80% agreement wasobserved. Test ]/retest and interobserver reliabilityof the subtotals and TIS total was reached whenthe ICC was 0.80 or higher. Cronbach’s alphashould exceed 0.70, which is suggested as a value ofscale reliability and indicates underlying con-struct.24
Results
As seen in Table 2, most kappa or weighted kappavalues ranged from 0.62 to 1. Test ]/retest agree-ment of item 2 of static sitting balance (0.51) anditem 2 of co-ordination (0.46) were insufficient.For these items, a high percentage of agreement,89% and 93% respectively, was observed. Nokappa or weighted kappa values could be calcu-
lated for item 3 (test ]/retest reliability) and item 4(test ]/retest and inter-rater reliability) of co-ordi-nation because of a skewed distribution of thedata. Percentage of agreement for these itemsranged from 86% to 100%.
ICCs for static and dynamic sitting balance,co-ordination and the total TIS are presented inTable 3 and were between 0.85 and 0.99. The 95%test ]/retest and interexaminer measurement errorinterval on the total TIS score was 2/2.90, 3.68and 2/1.84, 1.84, respectively.
Internal consistency by means of Cronbach’salpha was calculated for the subscales static sittingbalance (0.79), dynamic sitting balance (0.86) andco-ordination (0.65). Cronbach’s alpha for thetotal Trunk Impairment Scale was 0.89.
Content validity of the TIS was achievedthrough literature review, observing stroke pa-tients, clinical experience of the authors anddiscussing the content of the scale with specialistswithin the field of stroke rehabilita tion. Spearmanrank correlation between the TIS and the BarthelIndex (construct validity) was 0.86, between theTIS and the Trunk Control Test (concurrentvalidity) 0.83.
The time needed to complete the TIS rangedfrom 2 to 18 minutes. All obtained scores rangedbetween 0 and 21. The median score (quartile 1,quartile 3) was 14 (10, 16).
Discussion
The aim of this study was to develop a measure-ment tool to evaluate the impairment of the trunk
Clinical messages
. The Trunk Impairment Scale (TIS) is a newtool to measure motor impairment of thetrunk after stroke.
. The TIS evaluates static and dynamic sittingbalance as well as co-ordination of trunkmovement.
. The TIS has sufficient reliability, internalconsistency and validity for use in clinicalpractice and stroke research.
328 G Verheyden et al.
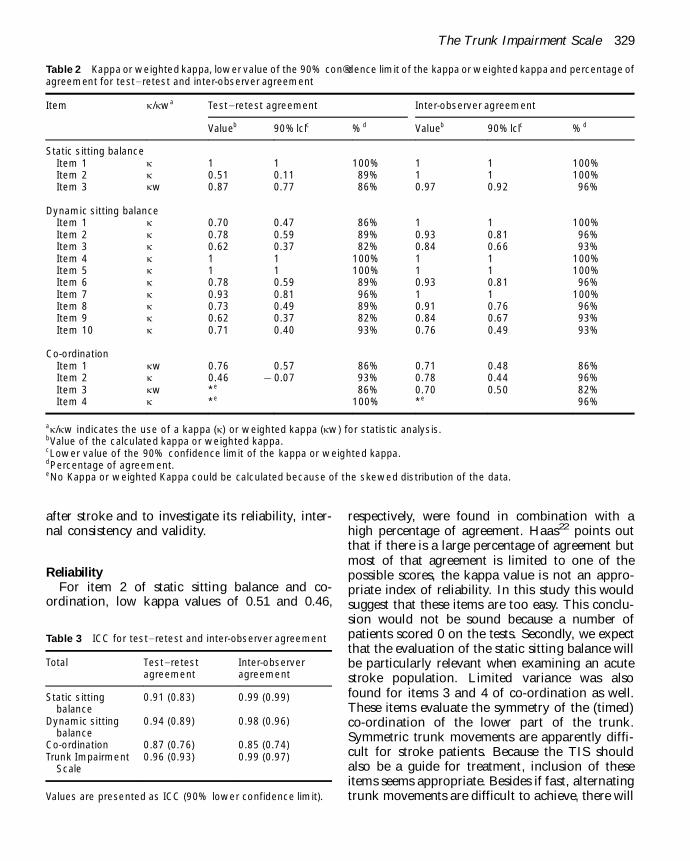
after stroke and to investigate its reliability, inter-nal consistency and validity.
Reliability
For item 2 of static sitting balance and co-ordination, low kappa values of 0.51 and 0.46,
respectively, were found in combination with ahigh percentage of agreement. Haas22 points outthat if there is a large percentage of agreement butmost of that agreement is limited to one of thepossible scores, the kappa value is not an appro-priate index of reliability. In this study this wouldsuggest that these items are too easy. This conclu-sion would not be sound because a number ofpatients scored 0 on the tests. Secondly, we expectthat the evaluation of the static sitting balance willbe particularly relevant when examining an acutestroke population. Limited variance was alsofound for items 3 and 4 of co-ordination as well.These items evaluate the symmetry of the (timed)co-ordination of the lower part of the trunk.Symmetric trunk movements are apparently diffi-cult for stroke patients. Because the TIS shouldalso be a guide for treatment, inclusion of theseitems seems appropriate. Besides if fast, alternatingtrunk movements are difficult to achieve, there will
Table 2 Kappa or weighted kappa, lower value of the 90% con®dence limit of the kappa or weighted kappa and percentage ofagreement for test]/retest and inter-observer agreement
Item j/jwa Test]/retest agreement Inter-observer agreement
Valueb 90%lclc %d Valueb 90%lclc %d
Static sitting balanceItem 1 j 1 1 100% 1 1 100%Item 2 j 0.51 0.11 89% 1 1 100%Item 3 jw 0.87 0.77 86% 0.97 0.92 96%
Dynamic sitting balanceItem 1 j 0.70 0.47 86% 1 1 100%Item 2 j 0.78 0.59 89% 0.93 0.81 96%Item 3 j 0.62 0.37 82% 0.84 0.66 93%Item 4 j 1 1 100% 1 1 100%Item 5 j 1 1 100% 1 1 100%Item 6 j 0.78 0.59 89% 0.93 0.81 96%Item 7 j 0.93 0.81 96% 1 1 100%Item 8 j 0.73 0.49 89% 0.91 0.76 96%Item 9 j 0.62 0.37 82% 0.84 0.67 93%Item 10 j 0.71 0.40 93% 0.76 0.49 93%
Co-ordinationItem 1 jw 0.76 0.57 86% 0.71 0.48 86%Item 2 j 0.46 2/0.07 93% 0.78 0.44 96%Item 3 jw *e 86% 0.70 0.50 82%Item 4 j *e 100% *e 96%
aj/jw indicates the use of a kappa (j) or weighted kappa (jw) for statistic analysis.bValue of the calculated kappa or weighted kappa.cLower value of the 90% confidence limit of the kappa or weighted kappa.dPercentage of agreement.eNo Kappa or weighted Kappa could be calculated because of the skewed distribution of the data.
Table 3 ICC for test]/retest and inter-observer agreement
Total Test]/retestagreement
Inter-observeragreement
Static sittingbalance
0.91 (0.83) 0.99 (0.99)
Dynamic sittingbalance
0.94 (0.89) 0.98 (0.96)
Co-ordination 0.87 (0.76) 0.85 (0.74)Trunk Impairment
Scale0.96 (0.93) 0.99 (0.97)
Values are presented as ICC (90% lower confidence limit).
The Trunk Impairment Scale 329

be no ceiling effect of the scale. The level ofdifficulty for the various items could be determinedby means of a Rasch analysis. However a very largenumber of patients is needed for this analysis.
Although the percentage of observer agreementis high and exceeds the proposed limit, severalauthors point out that the agreement due tochance alone is not taken into account whenpercentage agreement is presented.22,25 To establishthe reliability of items 1 and 2 of static sittingbalance (easy items) and items 2, 3 and 4 of co-ordination (difficult items), a new study should beset up examining the TIS on an acute ward withseverely impaired stroke patients and on a nearlyfully recovered stroke population, respectively.
Measurement error
In this study, values for inter-rater reliabilityexceeded those for test ]/retest agreement. Thiscould be explained by the fact that in the case ofthe inter-rater reliability, both observers werescoring the patient at the same time, so all possibleareas of bias and variability were minimized.Variation within the patient’s performance canalso be a possible reason for lower test ]/retestreliability. This is confirmed by the higher test ]/
retest examiner measurement error, 3.68 (16% ofTIS total) in comparison with the 1.84 (8% of TIStotal) for the interexaminer measurement error.The latter is comparable with the reported limits ofagreement of the Action Research Arm test(between 10 and 10.88%) and the BrunnstroÈm-Fugl-Meyer assessment scale (between 7.58 and10%).26 For the Sickness Impact Profile, Becker-man et al .27 also found a minimum decrease of9.26% before an unbiased improvement can beconsidered. The test ]/retest examiner measurementerror of the TIS (3.68) was based on a methodsuggested by Haas,22 an alternative to the methodof Altman and Bland.28 An increase of 4 points onthe TIS can be seen as an improvement withoutreproducibility bias.
Internal consistency
Cronbach’s alpha for the subscale co-ordinationwas under the suggested value of 0.70. This reflectsonly moderate reliability according to Nunnally.24
Still the ICC values for the subscale co-ordinationare well above the critical value. Further, 0.70 isonly a rule of thumb. Hatcher and Stepanski29
describe literature where useful alpha coefficientsare reported under 0.70 or 0.60. In this studyCronbach’s alpha was mainly used to examine theunderlying construct of the subscales and totalTIS, which seems confirmed by the presented data.
Comparison with other scales
Kappa and weighted kappa values for the test ]/
retest and inter-rater agreement of the individualitems of the TIS ranged from 0.46 to 1 and from0.70 to 1, respectively. Kappa values reportedfor the lying and sitting items of the PosturalAssessment Scale for Stroke Patients17 are similar.They ranged between 0.45 and 1 for intra- andbetween 0.64 and 1 for inter-rater reliability.Nieuwboer et al .10 reported lower values from0.20 to 1. Items regarding quality of movementranged from 0.20 to 0.64. The previous two studiesdo not mention percentage of agreement if therewas a low kappa value. Total scale score of the TISis highly reliable. Reported Spearman rho correla-tion coefficients for the inter-rater agreement ofthe Trunk Control Test11 was 0.76, for the sittingbalance item of the Motor Assessment Scale30
0.99. Product moment and rank order correlationcoefficients only have a limited value as indices ofreliability. Systematic errors are not taken intoaccount.22,25,31,32 Adding up dichotomous andordinal items is a widely used method in scaledevelopment. The total score can thus be seen as acontinuous variable. Therefore ICC can be used asan appropriate statistic for examining reliability.
Franchignoni et al .12 reported for the TrunkControl Test Cronbach’s alpha coefficients of 0.83and 0.86. Benaim et al .17 found for the PosturalAssessment Scale for Stroke Patients 0.95 ascoefficient of internal consistency. These are inline with the results for the TIS in this study (0.89).
Content, construct (r5 /0.86 with Barthel Index)and concurrent validity (r5 /0.83 with Trunk Con-trol Test) of the TIS were established. Constructvalidity of the Trunk Control Test was examinedby comparison with the Functional IndependenceMeasure (F IM). Correlation coefficients rangedfrom 0.71 to 0.79 and from 0.82 to 0.86 for thetotal F IM and for the motor part of the F IM,respectively.12 Benaim et al .17 found a correlationof 0.73 between the Postural Assessment Scale forStroke Patients and the FIM. A correlation of 0.28was found between the sitting balance item of the
330 G Verheyden et al.
Motor Assessment Scale and the BrunnstroÈm-Fugl-Meyer assessment.30
An additional aim of the TIS was to score thequality of trunk movement and to be a guide fortreatment. The four tasks of the subscale dynamicsitting balance evaluate an appropriate shorteningor lengthening of both sides of the trunk as wellas the use of compensation strategies. In thepresent study, this method was found more reliablethan scoring a symmetrical or asymmetrical per-formance as index of quality of movement.10 Staticand dynamic sitting balance as well as the co-ordination of the trunk are considered. Althoughnot all aspects of trunk function are covered by theTIS, it can be used as a guideline for treatment.Proprioception of the trunk and muscle strengthfor instance are not evaluated in the TIS. Thereforefurther validation of the TIS is required to evaluateits value as a measure of total trunk function.
Conclusion
This study reports the development of the TrunkImpairment Scale, a clinical test to measure motorimpairment of the trunk after stroke. The TISmeasures static and dynamic sitting balance andco-ordination of the trunk. Item per item relia-bility, subtotal and scale total agreement wereestablished as well as the internal consistency ofthe subscales and the total scale. Content, con-struct and concurrent validity were evaluated.Statistica l analysis of the different clinimetricparameters of the TIS endorse its further use inclinical practice as well as in research. The assess-ment can be used as a guideline for treatment andtakes the quality of trunk movement into account.To the best of our knowledge, the TIS is a uniquemeasurement of its kind in stroke literature.
Acknowledgements
The authors would like to thank Inge Taillieuand Ilse Baert for helping to collect the data. Weare also grateful for the logistic support of L Lutter(Kiliani-K linik Bad Windsheim, Germany),F Roelandt (Klinik Kipfenberg, Germany) andP Popelier (U niversitair Ziekenhuis Pellenberg,Belgium).
References
1 Moreland J, Thomson MA. Ef®cacy ofelectromyographic biofeedback compared withconventional physical therapy for upper-extremityfunction in patients following stroke: a researchoverview and meta-analysis. Phys Ther 1994;
74
:534]/47.
2 Moreland JD, Thomson MA, Fuoco AR.Electromyographic biofeedback to improve lowerextremity function after stroke: a meta-analysis.Arch Phys M ed Rehabil 1998;
79
: 134]/40.3 van der Lee JH, Snels IAK, Beckerman H,
Lankhorst GJ, Wagenaar RC, Bouter LM. Exercisetherapy for arm function in stroke patients: asystematic review of randomized controlled trials.Clin Rehabil 2001;
15
: 20]/31.4 Davies PM. Problems associated with the loss of
selective trunk activity in hemiplegia. In: Right in
the middle. Berlin, Heidelberg: Springer-Verlag,1990: 31]/65.
5 Wade DT, Skilbeck CE, Langton Hewer R.Predicting Barthel ADL score at 6 months after anacute stroke. Arch Phys M ed Rehabil 1983;
64
: 24]/
28.6 Loewen SC, Anderson BA. Predictors of stroke
outcome using objective measurement scales.Stroke 1990;
21
: 78]/81.7 Sandin KJ, Smith BS. The measure of balance in
sitting in stroke rehabilitation prognosis. S troke
1990;21
: 82]/86.8 Kwakkel G, Wagenaar RC, Kollen BJ, Lankhorst
GJ. Predicting disability in stroke ]/ a critical reviewof the literature. Age Ageing 1996;
25
: 479]/89.9 Bohannon RW. Lateral trunk ¯exion strength:
impairment, measurement reliability andimplications following unilateral brain lesion. Int J
Rehabil Res 1992;15
: 249]/51.10 Nieuwboer A, Feys H, De Weerdt W, Nuyens G, De
Corte E. Developing a clinical tool to measuresitting balance after stroke: a reliability study.Physiotherapy 1995;
81
: 439]/45.11 Collin C, Wade D. Assessing motor impairment
after stroke: a pilot reliability study. J Neurol
Neurosurg Psychiatry 1990;53
: 576]/79.12 Franchignoni FP, Tesio L, Ricupero C, Martino
MT. Trunk control test as an early predictor ofstroke rehabilitation outcome. S troke 1997;
28
:1382]/85.
13 Bohannon RW. Recovery and correlates of trunkmuscle strength after stroke. Int J Rehabil Res 1995;18
: 162]/67.14 Lincoln N, Leadbitter D. Assessment of motor
function in stroke patients. Physiotherapy 1979;65
:48]/51.
The Trunk Impairment Scale 331

15 Carr JH, Shepherd RB, Nordholm L, Lynne D.Investigation of a new motor assessment scale forstroke patients. Phys Ther 1985;
2
: 175]/80.16 Gowland CA. Staging motor impairment after
stroke. S troke 1990;21
: II-19]/II-21.17 Benaim C, PeÂrennou DA, Villy J, Rousseaux M,
Pelissier JY. Validation of a standardizedassessment of postural control in stroke patients.The postural assessment scale for stroke patients(PASS). Stroke 1999;
30
: 1862]/68.18 Tsuji T, Liu M, Sonoda S, Domen K, Chino N. The
stroke impairment assessment set: its internalconsistency and predictive validity. Arch Phys M ed
Rehabil 2000;81
: 863]/68.19 Hantson L, De Weerdt W, De Keyser J et al . The
European stroke scale. Stroke 1994;25
: 2215]/19.20 Mahoney F, Barthel D. Functional evaluation: the
Barthel index. M d M ed J 1965;14
: 61]/65.21 Fugl-Meyer AR , JaÈaÈskoÈ L, Leyman I, Olsson S,
Steglind S. The post-stroke hemiplegic patient.Scand J Rehabil M ed 1975;
7
: 13]/31.22 Haas M. Statistical methodology for reliability
studies. J M anip Physiol Ther 1991;14
: 119]/32.23 Landis RJ, Koch GG. The measurement of observer
agreement for categorical data. Biometrics 1977;33
:159]/74.
24 Nunnally J. Psychometric theory. New York:McGraw-H ill, 1978.
25 Kramer MS, Feinstein AR. Clinical biostatistics.LIV. The biostatistics of concordance. Clin
Pharmacol Ther 1981;29
: 111]/23.26 van der Lee JH, Beckerman H, Lankhorst GJ,
Bouter LM. The responsiveness of the actionresearch arm test and the Fugl-Meyer assessment inchronic stroke patients. J Rehabil M ed 2001;
33
:110]/13.
27 Beckerman H, Roebroeck ME, Lankhorst GJ,Becher JG, Bezemer PD, Verbeek AL. Smallest realdifference, a link between reproducibility andresponsiveness. Qual L ife Res 2001;
10
: 571]/78.28 Altman DG, Bland JM. Measurement in medicine:
the analysis of method comparison studies.Statistician 1983;
32
: 307]/17.29 Hatcher L, Stepanski EJ. Assessing scale reliability
with coef®cient alpha. In: A step-by step approach to
using the SAS
Òsystem for univariate and
multivariate statistics. Cary, NC: SAS Institute Inc.,1994: 505]/16.
30 Poole JL, Whitney SL. Motor assessment scale forstroke patients: concurrent validity and interraterreliability. Arch Phys M ed Rehabil 1988;
69
: 195]/
97.31 Haas M. The reliability of reliability. J M anip
Physiol Ther 1991;14
: 199]/208.32 Bland JM, Altman DG. Statistical methods for
assessing agreement between two methods ofclinical measurement. Lancet 1986;
1
: 307]/10.
332 G Verheyden et al.
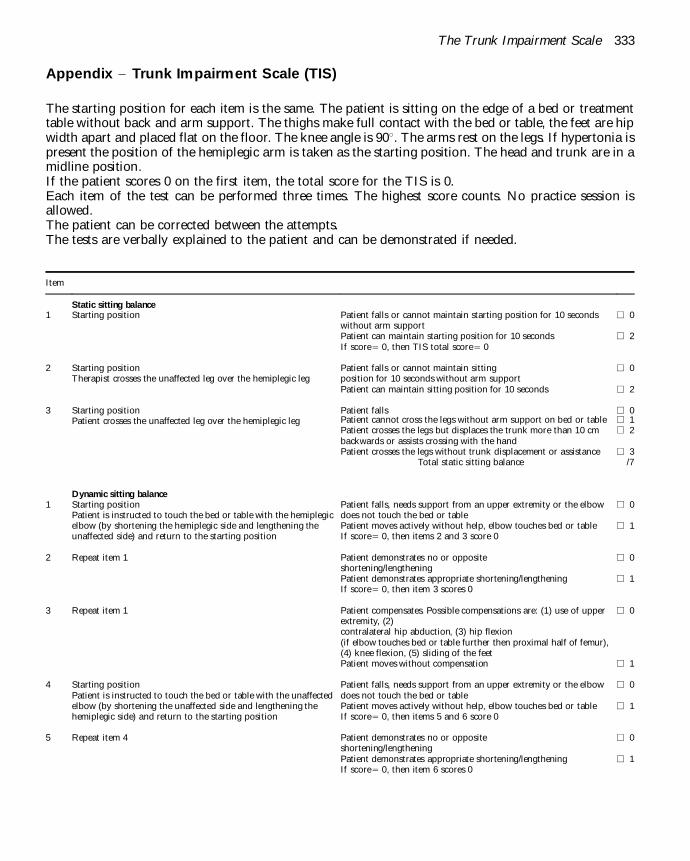
Appendix ]/ Trunk Impairment Scale (TIS)
The starting position for each item is the same. The patient is sitting on the edge of a bed or treatmenttable without back and arm support. The thighs make full contact with the bed or table, the feet are hipwidth apart and placed flat on the floor. The knee angle is 908. The arms rest on the legs. If hypertonia ispresent the position of the hemiplegic arm is taken as the starting position. The head and trunk are in amidline position.If the patient scores 0 on the first item, the total score for the TIS is 0.Each item of the test can be performed three times. The highest score counts. No practice session isallowed.The patient can be corrected between the attempts.The tests are verbally explained to the patient and can be demonstrated if needed.
Item
Static sitting balance
1 Starting position Patient falls or cannot maintain starting position for 10 secondswithout arm support
e 0
Patient can maintain starting position for 10 seconds e 2If score5 /0, then TIS total score5 /0
2 Starting positionTherapist crosses the unaffected leg over the hemiplegic leg
Patient falls or cannot maintain sittingposition for 10 seconds without arm support
e 0
Patient can maintain sitting position for 10 seconds e 2
3 Starting positionPatient crosses the unaffected leg over the hemiplegic leg
Patient falls e 0Patient cannot cross the legs without arm support on bed or table e 1Patient crosses the legs but displaces the trunk more than 10 cmbackwards or assists crossing with the hand
e 2
Patient crosses the legs without trunk displacement or assistance e 3Total static sitting balance /7
Dynamic sitting balance
1 Starting positionPatient is instructed to touch the bed or table with the hemiplegicelbow (by shortening the hemiplegic side and lengthening theunaffected side) and return to the starting position
Patient falls, needs support from an upper extremity or the elbowdoes not touch the bed or table
e 0
Patient moves actively without help, elbow touches bed or table e 1If score5 /0, then items 2 and 3 score 0
2 Repeat item 1 Patient demonstrates no or oppositeshortening/lengthening
e 0
Patient demonstrates appropriate shortening/lengthening e 1If score5 /0, then item 3 scores 0
3 Repeat item 1 Patient compensates. Possible compensations are: (1) use of upperextremity, (2)contralateral hip abduction, (3) hip flexion(if elbow touches bed or table further then proximal half of femur),(4) knee flexion, (5) sliding of the feet
e 0
Patient moves without compensation e 1
4 Starting positionPatient is instructed to touch the bed or table with the unaffectedelbow (by shortening the unaffected side and lengthening thehemiplegic side) and return to the starting position
Patient falls, needs support from an upper extremity or the elbowdoes not touch the bed or table
e 0
Patient moves actively without help, elbow touches bed or table e 1If score5 /0, then items 5 and 6 score 0
5 Repeat item 4 Patient demonstrates no or oppositeshortening/lengthening
e 0
Patient demonstrates appropriate shortening/lengthening e 1If score5 /0, then item 6 scores 0
The Trunk Impairment Scale 333

Item
6 Repeat item 4 Patient compensates. Possible compensations are: (1) use of upperextremity, (2)contralateral hip abduction, (3) hip flexion(if elbow touches bed or table further then proximal half of femur),(4) knee flexion, (5) sliding of the feet
e 0
Patient moves without compensation e 1
7 Starting positionPatient is instructed to lift pelvis from bed or table at thehemiplegic side (by shortening the hemiplegic side and lengtheningthe unaffected side) and return to the starting position
Patient demonstrates no or oppositeshortening/lengthening
e 0
Patient demonstrates appropriate shortening/lengthening e 1If score5 /0, then item 8 scores 0
8 Repeat item 7 Patient compensates. Possible compensations are: (1) use of upperextremity, (2) pushing off with the ipsilateral foot (heel loses contactwith the floor)
e 0
Patient moves without compensation e 1
9 Starting positionPatient is instructed to lift pelvis from bed or table at theunaffected side (by shortening the unaffected side and lengtheningthe hemiplegic side) and return to the starting position
Patient demonstrates no or opposite shortening/lengthening e 0Patient demonstrates appropriate shortening/lengthening e 1If score5 /0, then item 10 scores 0
10 Repeat item 9 Patient compensates. Possible compensations are: (1) use of upperextremities, (2) pushing off with the ipsilateral foot (heel losescontact with the floor)
e 0
Patient moves without compensation e 1Total dynamic sitting balance /10
Co-ordination
1 Starting positionPatient is instructed to rotate upper trunk 6 times (every shouldershould be moved forward 3 times), first side that moves must behemiplegic side, head should be fixated in starting position
Hemiplegic side is not moved three times e 0Rotation is asymmetrical e 1Rotation is symmetrical e 2If score5 /0, then item 2 scores 0
2 Repeat item 1 within 6 seconds Rotation is asymmetrical e 0Rotation is symmetrical e 1
3 Starting positionPatient is instructed to rotate lower trunk 6 times (every kneeshould be moved forward 3 times), first side that moves must behemiplegic side, upper trunk should be fixated in starting position
Hemiplegic side is not moved three times e 0Rotation is asymmetrical e 1Rotation is symmetrical e 2If score5 /0, then item 4 scores 0
4 Repeat item 3 within 6 seconds Rotation is asymmetrical e 0Rotation is symmetrical e 1
Total co-ordination /6
Total Trunk Impairment Scale /23
334 G Verheyden et al.

Reproducedwith permission of the copyright owner. Further reproduction prohibitedwithout permission.

BERG Patient Name: ____________________________ BALANCE Rater Name: ____________________________ SCALE Date: ____________________________
Balance Item Score (0-4)
1. Sitting unsupported _______
2. Change of position: sitting to standing _______
3. Change of position” standing to sitting _______
4. Transfers _______
5. Standing unsupported _______
6. Standing with eyes closed _______
7. Standing with feet together _______
8. Tandem standing _______
9. Standing on one leg _______
10. Turning trunk (feet fixed) _______
11. Retrieving objects from floor _______
12. Turning 360 degrees _______
13. Stool stepping _______
14. Reaching forward while standing _______ TOTAL (0–56): _______
Interpretation
0–20, wheelchair bound 21–40, walking with assistance 41–56, independent
References Berg K, Wood-Dauphinee S, Williams JI, Maki, B: Measuring balance in the elderly: Validation of an instrument. Can. J. Pub. Health, July/August supplement 2:S7-11, 1992. Berg K, Wood-Dauphinee S, Williams JI, Gayton D: Measuring balance in the elderly: Preliminary development of an instrument. Physiotherapy Canada, 41:304-311, 1989.
Provided by the Internet Stroke Center — www.strokecenter.org
Downloaded from www.rehabmeasures.org Test instructions provided courtesy of Virgil Mathiowetz, PhD, OTR/L Page 1
Box and Blocks Test Instructions
General Information (derived from Mathiowetz et al, 1985): The patient is allowed a 15-second trial period prior to testing Immediately before testing begins, the patient should place his/her hands on the
sides of the box When testing begins, the patient should grasp one block at a time with the dominant
hand, transport the block over the partition, and release it into the opposite compartment
The patient should continue doing this for one minute The procedure should then be repeated with the nondominant hand After testing, the examiner should count the blocks If a patient transports two or more blocks at the same time, this should be noted and
the number subtracted from the total No penalty should be made if the subjects transported any blocks across the
partition and the blocks bounced from the box to the floor or table
Set-up: A test box with 150 blocks and a partition in the middle is placed lengthwise along
the edge of a standard-height table The patient should be seated on a standard height chair facing the box 150 blocks should be in the compartment of the test box on the side of the patient’s
dominant hand The examiner should face the patient so she or he could view the blocks being
transported
Patient Instructions (derived from Mathiowetz et al, 1985): “I want to see how quickly you can pick up one block at a time with your right (or left) hand [point to the hand]. Carry it to the other side of the box and drop it. Make sure your fingertips cross the partition. Watch me while I show you how.” Transport three cubes over the partition in the same direction you want the patient to move them. After a demonstration say the following: “If you pick up two blocks at a time, they will count as one. If you drop one on the floor or table after you have carried it across, it will still be counted, so do not waste time picking it up. If you toss the blocks without your fingertips crossing the partition, they will not be counted. Before you start, you will have a chance to practice for 15 seconds. Do you have any questions?”

Downloaded from www.rehabmeasures.org Test instructions provided courtesy of Virgil Mathiowetz, PhD, OTR/L Page 2
“Place your hands on the sides of the box. When it is time to start, I will say ready and then go.” Trial period: Start the stop watch at the word go. When 15 seconds has passed, say "stop." If mistakes are made during the practice period, correct them before the actual testing begins. On completion of the practice period, transport the cubes to the original compartment. Continued with the following directions: “This will be the actual test. The instructions are the same. Work as quickly as you can. Ready.” [Wait 3 seconds] “Go.” “Stop.” [After 1 minute, count the blocks and record as described above] “Now you are to do the same thing with your left (or right) hand. First you can practice. Put your hands on the sides of the box as before. Pick up one block at a time with your hand, and drop it on the other side of the box.” “Ready.” [Wait 3 seconds] “Go.” “Stop.” [After 15 seconds] Return the transported blocks to the compartment as described above. “This will be the actual test. The instructions are the same. Work as quickly as you can.” “Ready.” [Wait 3 seconds] “Go.” “Stop.” [After 1 minute, count the blocks and record as described above] Scoring The score is the number of blocks carried from one compartment to the other in one minute. Score each hand separately.

Downloaded from www.rehabmeasures.org Test instructions provided courtesy of Virgil Mathiowetz, PhD, OTR/L Page 3
Box and Blocks Testing Form
Name: ___________________________________________________________
Dominant Hand (circle one): Right Left
Number of blocks transported in one minute:
Date: ________ Dominant Hand: __________ Non-Dominant Hand: _______
Date: ________ Dominant Hand: __________ Non-Dominant Hand: _______
Date: ________ Dominant Hand: __________ Non-Dominant Hand: _______
Date: ________ Dominant Hand: __________ Non-Dominant Hand: _______

Downloaded from www.rehabmeasures.org Test instructions provided courtesy of Virgil Mathiowetz, PhD, OTR/L Page 4
Reference: Mathiowetz, V., G. Volland, et al. (1985). "Adult norms for the Box and Block Test of manual dexterity." Am J Occup Ther 39(3160243): 386-391.

Downloaded from www.rehabmeasures.org Test instructions derived from Mathiowetz et al, 1985 The NHPT is provided courtesy of Virgil Mathiowetz, PhD, OTR/L, FAOTA Page 1
Nine Hole Peg Test Instructions
General Information: The Nine Hole Peg Test should be conducted with the dominant arm first. One practice trial (per arm) should be provided prior to timing the test. Timing should be performed with a stopwatch and recorded in seconds. The stop watch is started when the patient touches the first peg. The stop watch is stopped when the patient places the last peg in the container.
Set-up (Mathiowetz et al, 1985):
A square board with 9 holes, o holes are spaced 3.2 cm (1.25 inches) apart o each hole is 1.3 cm (.5 inches) deep
9 wooden pegs should be .64 cm (.25 inches) in diameter and 3.2 cm (1.25 inches) long
A container that is constructed from .7 cm (.25 inches) of plywood, sides are attached (13 cm x 13 cm) using nails and glue
The peg board should have a mechanism to decrease slippage. Self-adhesive bathtub appliqués were used in the study.
The pegboard should be placed in front of the patient, with the container holding the pegs on the side of the dominant hand.
Patient Instructions (Mathiowetz et al, 1985):
The instructions should be provided while the activity is demonstrated. The patient’s dominant arm is tested first. Instruct the patient to:
o “Pick up the pegs one at a time, using your right (or left) hand only and put them into the holes in any order until the holes are all filled. Then remove the pegs one at a time and return them to the container. Stabilize the peg board with your left (or right) hand. This is a practice test. See how fast you can put all the pegs in and take them out again. Are you ready? Go!”
After the patient performs the practice trial, instruct the patient: o “This will be the actual test. The instructions are the same. Work as
quickly as you can. Are you ready? Go!” (Start the stop watch when the patient touches the first peg.)
o While the patient is performing the test say “Faster” o When the patient places the last peg on the board, instruct the patient
“Out again…faster.” o Stop the stop watch when the last peg hits the container.
Place the container on the opposite side of the pegboard and repeat the instructions with the non-dominant hand.
Downloaded from www.rehabmeasures.org Test instructions derived from Mathiowetz et al, 1985 The NHPT is provided courtesy of Virgil Mathiowetz, PhD, OTR/L, FAOTA Page 2
Nine Hole Peg Test
Name:___________________________________________________________
Dominant Hand (circle one): Right Left
Time to complete the test in seconds:
Date: ________ Dominant Hand: __________ Non-Dominant Hand: _______
Date: ________ Dominant Hand: __________ Non-Dominant Hand: _______
Date: ________ Dominant Hand: __________ Non-Dominant Hand: _______
Date: ________ Dominant Hand: __________ Non-Dominant Hand: _______

Downloaded from www.rehabmeasures.org Test instructions derived from Mathiowetz et al, 1985 The NHPT is provided courtesy of Virgil Mathiowetz, PhD, OTR/L, FAOTA Page 3
References: Mathiowetz V, Weber K, Kashman N, Volland G. Adult Norms for the Nine Hole Peg Test of Finger Dexterity. The Occupational Therapy Journal of Research. 1985;5:24-33.

Stroke Impact ScaleVERSION 3.0
The purpose of this questionnaire is to evaluate how stroke has impacted your health and life. We want to know from YOUR POINT OF VIEW how stroke has affected you. We will ask you questions about impairments and disabilities caused by your stroke, as well as how stroke has affected your quality of life. Finally, we will ask you to rate how much you think you have recovered from your stroke.

Stroke Impact Scale
These questions are about the physical problems which may have occurred as a result of your stroke.
1. In the past week, how would you rate the strength of your....
A lot of strength
Quite a bit of strength
Some strength
A little strength
No strength at
alla. Arm that was most affected by your stroke?
5 4 3 2 1
b. Grip of your hand that was most affected by your stroke?
5 4 3 2 1
c. Leg that was most affected by your stroke?
5 4 3 2 1
d. Foot/ankle that was most affected by your stroke?
5 4 3 2 1
These questions are about your memory and thinking.
2. In the past week, how difficult was it for you to...
Not difficult at
all
A little difficult
Somewhat difficult
Very difficult
Extremely difficult
a. Remember things that people just told you?
5 4 3 2 1
b. Remember things that happened the day before?
5 4 3 2 1
c. Remember to do things (e.g. keep scheduled appointments or take medication)?
5 4 3 2 1
d. Remember the day of the week? 5 4 3 2 1
e. Concentrate? 5 4 3 2 1
f. Think quickly? 5 4 3 2 1
g. Solve everyday problems? 5 4 3 2 1
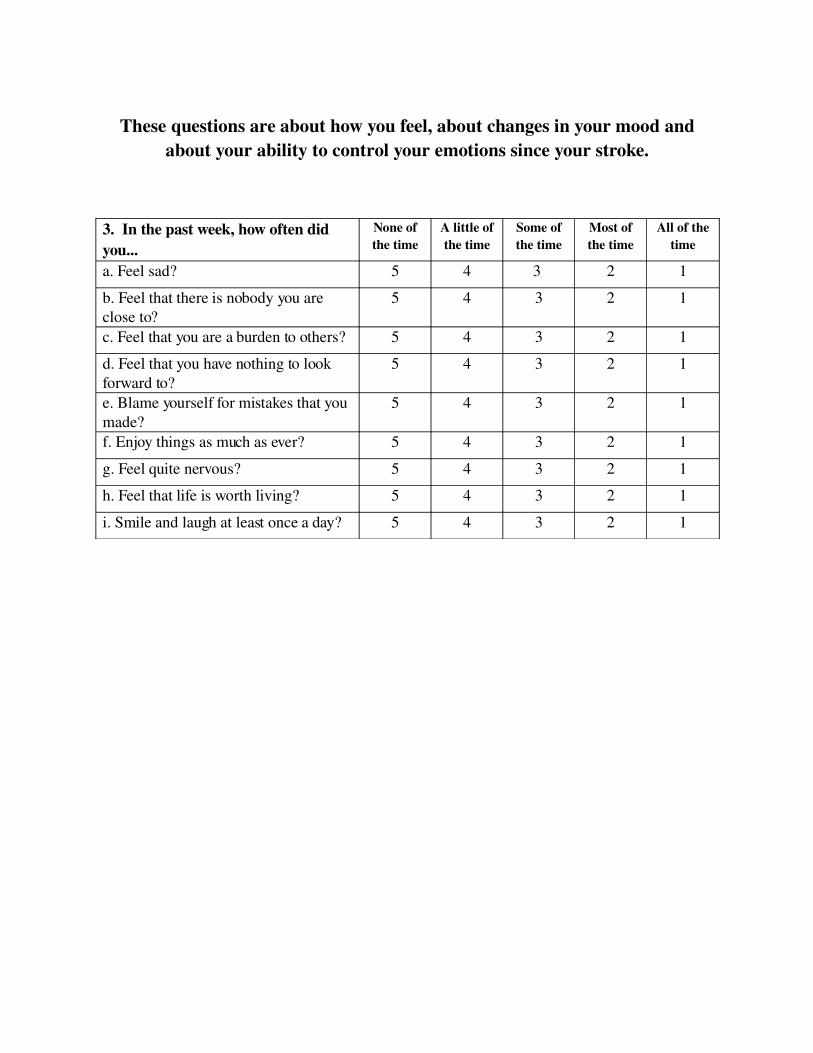
These questions are about how you feel, about changes in your mood and about your ability to control your emotions since your stroke.
3. In the past week, how often did you...
None of the time
A little of the time
Some of the time
Most of the time
All of the time
a. Feel sad? 5 4 3 2 1
b. Feel that there is nobody you are close to?
5 4 3 2 1
c. Feel that you are a burden to others? 5 4 3 2 1
d. Feel that you have nothing to look forward to?
5 4 3 2 1
e. Blame yourself for mistakes that you made?
5 4 3 2 1
f. Enjoy things as much as ever? 5 4 3 2 1
g. Feel quite nervous? 5 4 3 2 1
h. Feel that life is worth living? 5 4 3 2 1
i. Smile and laugh at least once a day? 5 4 3 2 1
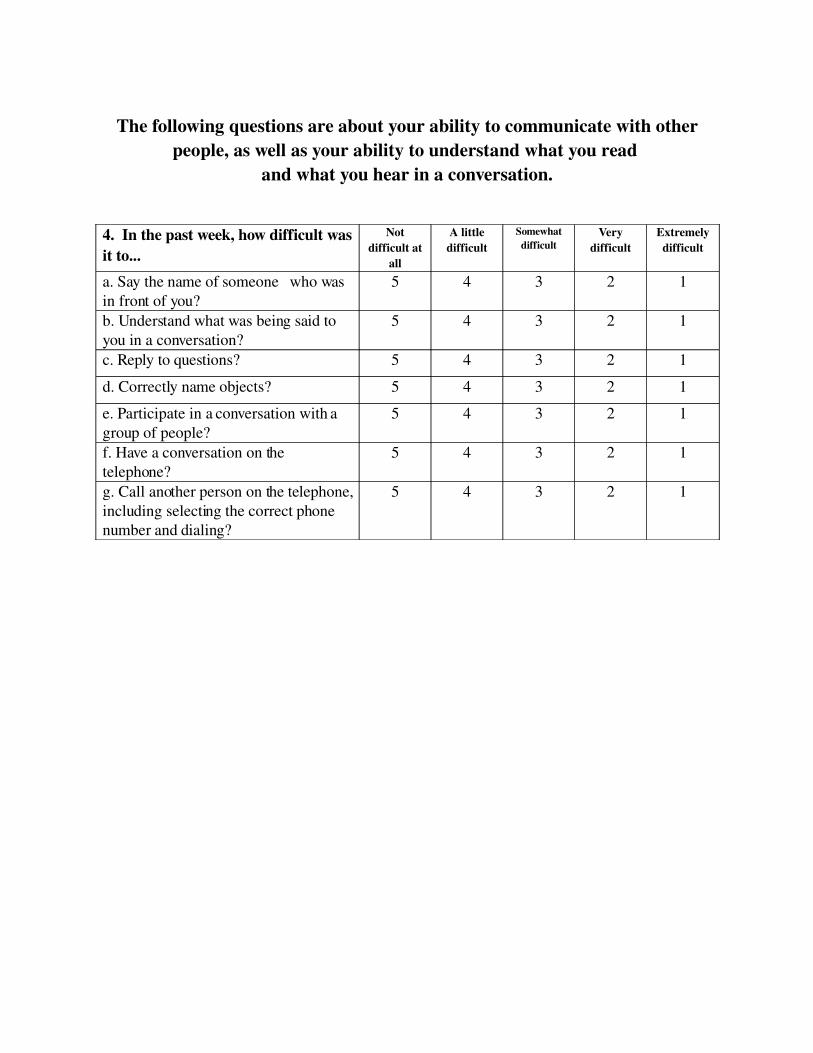
The following questions are about your ability to communicate with other people, as well as your ability to understand what you read
and what you hear in a conversation.
4. In the past week, how difficult was it to...
Not difficult at
all
A little difficult
Somewhat difficult
Very difficult
Extremely difficult
a. Say the name of someone who was in front of you?
5 4 3 2 1
b. Understand what was being said to you in a conversation?
5 4 3 2 1
c. Reply to questions? 5 4 3 2 1
d. Correctly name objects? 5 4 3 2 1
e. Participate in a conversation with a group of people?
5 4 3 2 1
f. Have a conversation on the telephone?
5 4 3 2 1
g. Call another person on the telephone, including selecting the correct phone number and dialing?
5 4 3 2 1

The following questions ask about activities you might doduring a typical day.
5. In the past 2 weeks, how difficult was it to...
Not difficult at all
A little difficult
Somewhat difficult
Very difficult
Could not do at all
a. Cut your food with a knife and fork? 5 4 3 2 1
b. Dress the top part of your body? 5 4 3 2 1
c. Bathe yourself? 5 4 3 2 1
d. Clip your toenails? 5 4 3 2 1
e. Get to the toilet on time? 5 4 3 2 1
f. Control your bladder (not have an accident)?
5 4 3 2 1
g. Control your bowels (not have an accident)?
5 4 3 2 1
h. Do light household tasks/chores (e.g. dust, make a bed, take out garbage, do the dishes)?
5 4 3 2 1
i. Go shopping? 5 4 3 2 1
j. Do heavy household chores (e.g. vacuum, laundry or yard work)?
5 4 3 2 1
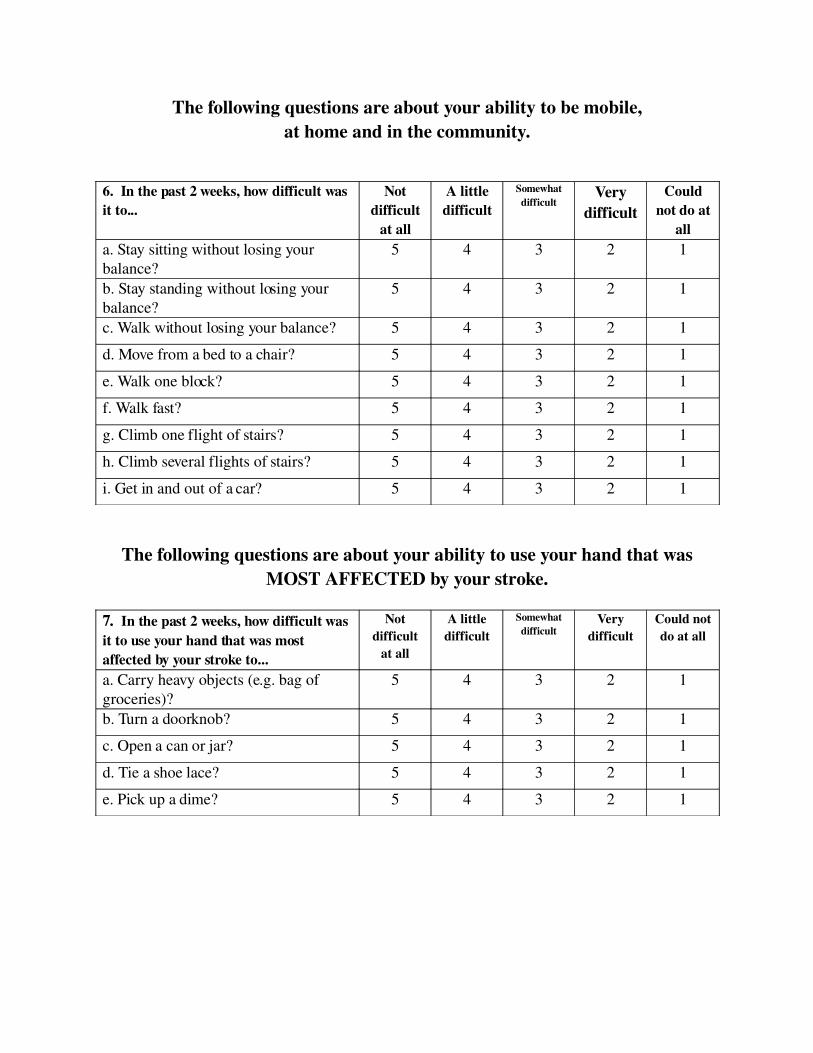
The following questions are about your ability to be mobile,at home and in the community.
6. In the past 2 weeks, how difficult was it to...
Not difficult
at all
A little difficult
Somewhat difficult
Very difficult
Could not do at
alla. Stay sitting without losing your balance?
5 4 3 2 1
b. Stay standing without losing your balance?
5 4 3 2 1
c. Walk without losing your balance? 5 4 3 2 1
d. Move from a bed to a chair? 5 4 3 2 1
e. Walk one block? 5 4 3 2 1
f. Walk fast? 5 4 3 2 1
g. Climb one flight of stairs? 5 4 3 2 1
h. Climb several flights of stairs? 5 4 3 2 1
i. Get in and out of a car? 5 4 3 2 1
The following questions are about your ability to use your hand that was MOST AFFECTED by your stroke.
7. In the past 2 weeks, how difficult was it to use your hand that was most affected by your stroke to...
Not difficult
at all
A little difficult
Somewhat difficult
Very difficult
Could not do at all
a. Carry heavy objects (e.g. bag of groceries)?
5 4 3 2 1
b. Turn a doorknob? 5 4 3 2 1
c. Open a can or jar? 5 4 3 2 1
d. Tie a shoe lace? 5 4 3 2 1
e. Pick up a dime? 5 4 3 2 1

The following questions are about how stroke has affected your ability to participate in the activities that you usually do, things that are meaningful to
you and help you to find purpose in life.
8. During the past 4 weeks, how much of the time have you been limited in...
None of the time
A little of the time
Some of the time
Most of the time
All of the time
a. Your work (paid, voluntary or other) 5 4 3 2 1
b. Your social activities? 5 4 3 2 1
c. Quiet recreation (crafts, reading)? 5 4 3 2 1
d. Active recreation (sports, outings, travel)?
5 4 3 2 1
e. Your role as a family member and/or friend?
5 4 3 2 1
f. Your participation in spiritual or religious activities?
5 4 3 2 1
g. Your ability to control your life as you wish?
5 4 3 2 1
h. Your ability to help others? 5 4 3 2 1

9. Stroke Recovery
On a scale of 0 to 100, with 100 representing full recovery and 0 representing no recovery, how much have you
recovered from your stroke?
100 Full Recovery __
90 __ 80 __ 70 __ 60 __ 50 __ 40 __ 30 __ 20 __ 10
________ 0 No Recovery

Item Clarifications
1. If patient says “I don’t have an affected side”, then instruct them to score using their perceived weaker side. If they still insist there is no affected, or weaker, side instruct them to score using their dominant side.
4. If patient says s/he does not do any or all of the items listed, code item(s) as Extremely Difficult.
(Item f) If patient does not call but is handed the phone this is OK.(Item g) If patient cannot hold a phone book, if they can read it this is OK. This item addresses whether the patient is able to initiate a phone call, look up the number, and dial this number correctly.
5. If patient says s/he does not do any or all of the items listed, code item(s) as Cannot do at all.(Item a) If person is on pureed food, even if they feel they could cut the food, code as Cannot do at All (1/5/98)(Item c) Bathing oneself does not include getting into the tub.(Item e) This question is associated with movement. Does the person have the physical ability to get to the bathroom quickly enough?(Item f) Losing a little urine/dribbling is considered an accident.
If person has intermittent catheter and is having no leaking problems code them as per report. (1/5/98) If person has an in-dwelling Foley catheter, code as Cannot do at all. (1/5/98)
(Item g) Constipation is not counted here, person has to have an accident.(Item i) “Shopping” means any type of shopping and does not include driving.
6. If patient hasn’t done any of the items in the past two weeks code as Cannot do at all. (Item h) If patient hasn’t “climbed several flights of stairs” in two weeks, they may be prompted by saying “have you gone up and down one flight of stairs a couple of times in a row.” If they still say they have not done it then they must be coded as Cannot do at all.(Item i) If the patient wants to know what kind of car say “your car” or “the car you ride in most.”
7. If patient says “I don’t have an affected side”, then instruct them to score using their perceived weaker side. If they still insist there is no affected, or weaker, side instruct them to score using their dominant side.
(Item a) If the patient says s/he has not been to the grocery store say “have you carried anything heavy with that hand.”(Item d) This item is to tie a shoelace/bow using both hands.
8. If patient does not do any of the specific items (and has never done), code interference as None of the time.
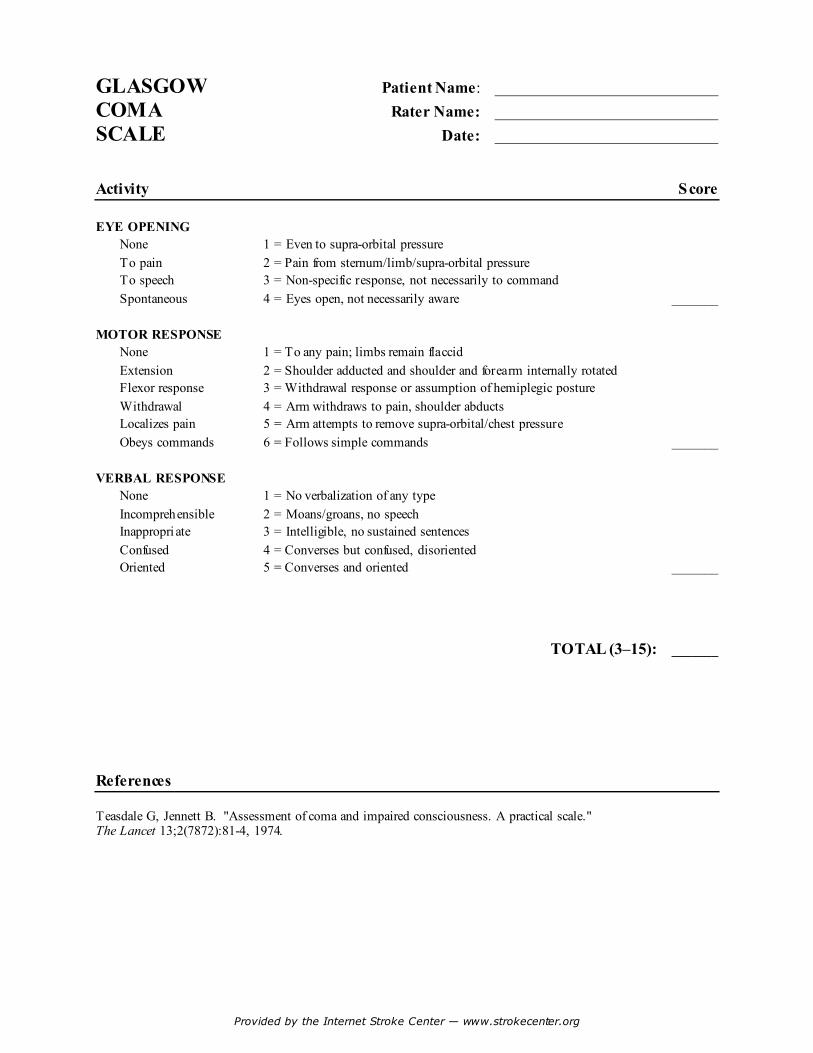
Provided by the Internet Stroke Center — www.strokecenter.org
GLASGOW Patient Name: ____________________________ COMA Rater Name: ____________________________ SCALE Date: ____________________________
Activity Score EYE OPENING
None 1 = Even to supra-orbital pressure To pain 2 = Pain from sternum/limb/supra-orbital pressure To speech 3 = Non-specific response, not necessarily to command Spontaneous 4 = Eyes open, not necessarily aware _______
MOTOR RESPONSE
None 1 = To any pain; limbs remain flaccid Extension 2 = Shoulder adducted and shoulder and forearm internally rotated Flexor response 3 = Withdrawal response or assumption of hemiplegic posture Withdrawal 4 = Arm withdraws to pain, shoulder abducts Localizes pain 5 = Arm attempts to remove supra-orbital/chest pressure Obeys commands 6 = Follows simple commands _______
VERBAL RESPONSE
None 1 = No verbalization of any type Incomprehensible 2 = Moans/groans, no speech Inappropri ate 3 = Intelligible, no sustained sentences Confused 4 = Converses but confused, disoriented Oriented 5 = Converses and oriented _______
TOTAL (3–15): _______ References Teasdale G, Jennett B. "Assessment of coma and impaired consciousness. A practical scale." The Lancet 13;2(7872):81-4, 1974.

RANCHO LOS AMIGOS SCALEAKA Level of Cognitive Functioning Scale (LCFS)
____ (1) Level I - No Response .
Patient does not respond to external stimu li and appears asleep.
____ (2) Level II - Genera lized Response .
Patient reacts to external stimu li in nonspecific, inconsistent, and nonpurposefu l manner w ith
stereotyp ic and lim ited responses.
____ (3) Level III - Loca lized Response .
Patient responds specifically and inconsistently w ith delays to stimu li, but may fo llow simp le
com mands for motor action.
____ (4) Level IV - Confused , Ag itated Response.
Patient exh ib its b izarre, nonpurposefu l, incoherent or inappropriate behav iors, has no short-
term recall, attention is short and nonselective.
____ (5) Level V - Confused , Inappropriate, Nonag itated Response.
Patient gives random , fragmented, and nonpurposefu l responses to complex or unstructured
stimu li - S imp le com mands are fo llowed consistently , memory and selective attention are
impaired, and new information is not retained.
____ (6) Level VI - Confused , Appropriate Response.
Patient g ives context appropriate, goal-d irected responses, dependent upon external input for
d irection. There is carry-over for relearned, but not for new tasks, and recent memory
prob lems persist.
____ (7) Level VII - Automatic, Appropriate Response .
Patient behaves appropriately in fam iliar settings, performs daily routines automatically, and
shows carry-over for new learn ing at lower than normal rates. Patient in itiates social
interactions, but judgment remains impaired.
____ (8) Level VIII - Purposefu l, Appropriate Response.
Patient oriented and responds to the env ironment but abstract reason ing ab ilities are
decreased re lative to premorb id leve ls.

30
25
20
15
10
5
0
Date
Time
City
Month
Date
Year
Clock Time
Kind of Place
Name of Hospital
Day of Week
Etiology/Event
Pathology Deficits
Patient Name:
The Orientation Log (O-Log) Key: 3=spontaneous/free recall2=logical cuing1=multiple choice, phonemic cuing0=unable, incorrect, inappropriate

UAB Spain Rehabilitation Center: The Orientation Log (O-Log)(Jackson & Novack, 1994)
DEMOGRAPHIC INFORMATION:
Name: Medical Record #:
Age: DOB: Sex: Marital Status: Race:
Education (years): Occupation:
Rehabilitation diagnosis and brief medical history:
Current medications:
ADMINISTRATION AND SCORING:The Orientation Log (O-Log) is designed to be a quick quantitative measure of orienta-tional status for use at bedside with rehabilitation inpatients. Place, time, and situation-al (Etiology/Event + Pathology/Deficits) domains are assessed. Patient responses arescored according to the following criteria:
3 = correct spontaneously or upon first free recall attempt; 2 = correct upon logical cueing (e.g., "That was yesterday, so today must be …"); 1 = correct upon multiple choice or phonemic cuing; and 0 = incorrect despite cueing, inappropriate response, or unable to respond.
Incorrect responses should be followed by cuing at the next highest level. In the placedomain, "Hospital" in any context is sufficient for Kind of Place. In the domain of time,Month, Date, Year, and Day of Week must be exact; however, Clock Time can be correctto within 30 minutes (plus or minus). Patients are allowed to look at a clock withoutpenalty when responding to the Clock Time item. For situation, the patient must be ori-ented to both Etiology/Event (e.g., "What brought you into the hospital?") andPathology/Deficits (e.g., "What kind of injuries did you have?" or "How did the strokeaffect you?"). Situational responses must demonstrate awareness of head/brain injuryand how the injury was sustained (e.g., MVA, fall, assault, GSW). Add scores down eachcolumn and plot total.

© reserved 1989, The Ohio State University
AGITATED BEHAVIOR SCALE Patient Period of Observation: a.m. Observ. Environ. From: p.m. / / a.m. Rater/Disc. To: p.m. / / At the end of the observation period indicate whether the behavior described in each item was present and, if so, to what degree: slight, moderate or extreme. Use the following numerical values and criteria for your ratings.
1 = absent: the behavior is not present. 2 = present to a slight degree: the behavior is present but does not prevent
the conduct of other, contextually appropriate behavior. (The individual may redirect spontaneously, or the continuation of the agitated behavior does not disrupt appropriate behavior. )
3 = present to a moderate degree: the individual needs to be redirected from an agitated to an appropriate behavior, but benefits from such cueing.
4 = present to an extreme degree: the individual is not able to engage in appropriate behavior due to the interference of the agitated behavior, even when external cueing or redirection is provided.
DO NOT LEAVE BLANKS. 1. Short attention span, easy distractibility, inability to concentrate. 2. Impulsive, impatient, low tolerance for pain or frustration. 3. Uncooperative, resistant to care, demanding. 4. Violent and or threatening violence toward people or property. 5. Explosive and/or unpredictable anger. 6. Rocking, rubbing, moaning or other self-stimulating behavior. 7. Pulling at tubes, restraints, etc. 8. Wandering from treatment areas. 9. Restlessness, pacing, excessive movement. 10. Repetitive behaviors, motor and/or verbal. 11. Rapid, loud or excessive talking. 12. Sudden changes of mood. 13. Easily initiated or excessive crying and/or laughter. 14. Self-abusiveness, physical and/or verbal.
Total Score
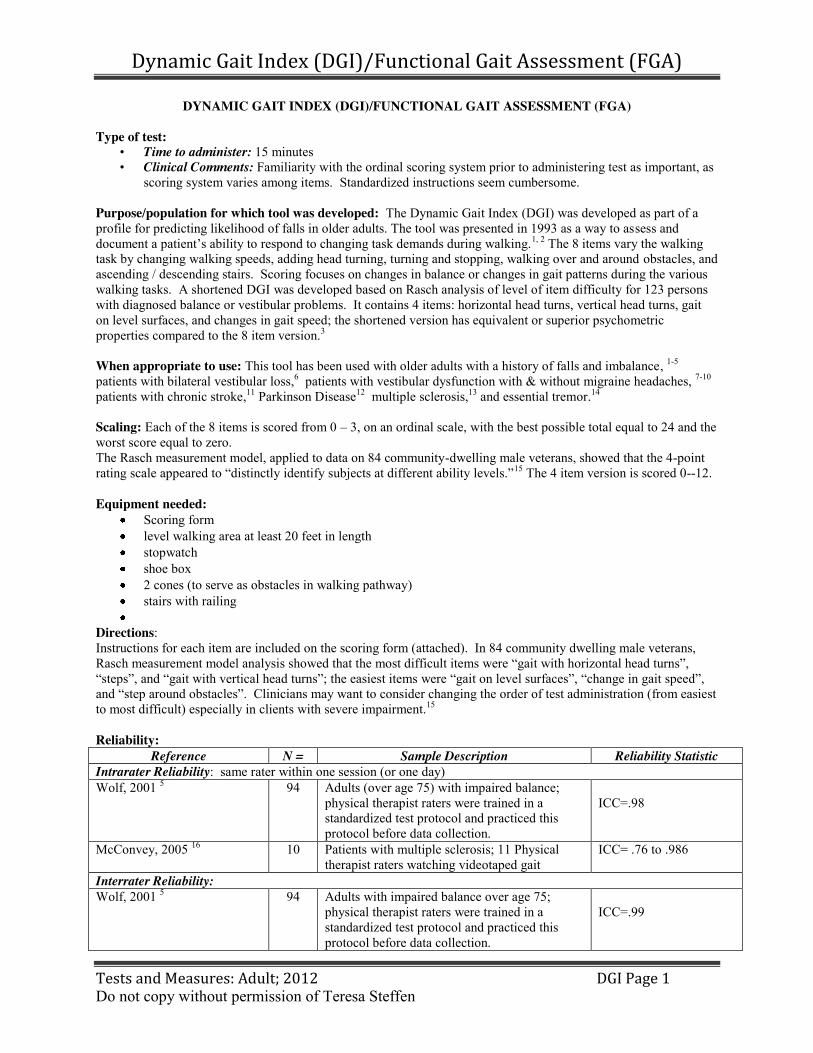
Dynamic Gait Index (DGI)/Functional Gait Assessment (FGA)
Tests and Measures: Adult; 2012 DGI Page 1 Do not copy without permission of Teresa Steffen
DYNAMIC GAIT INDEX (DGI)/FUNCTIONAL GAIT ASSESSMENT (FGA) Type of test:
• Time to administer: 15 minutes • Clinical Comments: Familiarity with the ordinal scoring system prior to administering test as important, as
scoring system varies among items. Standardized instructions seem cumbersome. Purpose/population for which tool was developed: The Dynamic Gait Index (DGI) was developed as part of a profile for predicting likelihood of falls in older adults. The tool was presented in 1993 as a way to assess and document a patient’s ability to respond to changing task demands during walking.1, 2 The 8 items vary the walking task by changing walking speeds, adding head turning, turning and stopping, walking over and around obstacles, and ascending / descending stairs. Scoring focuses on changes in balance or changes in gait patterns during the various walking tasks. A shortened DGI was developed based on Rasch analysis of level of item difficulty for 123 persons with diagnosed balance or vestibular problems. It contains 4 items: horizontal head turns, vertical head turns, gait on level surfaces, and changes in gait speed; the shortened version has equivalent or superior psychometric properties compared to the 8 item version.3 When appropriate to use: This tool has been used with older adults with a history of falls and imbalance, 1-5 patients with bilateral vestibular loss,6 patients with vestibular dysfunction with & without migraine headaches, 7-10 patients with chronic stroke,11 Parkinson Disease12 multiple sclerosis,13 and essential tremor.14 Scaling: Each of the 8 items is scored from 0 – 3, on an ordinal scale, with the best possible total equal to 24 and the worst score equal to zero. The Rasch measurement model, applied to data on 84 community-dwelling male veterans, showed that the 4-point rating scale appeared to “distinctly identify subjects at different ability levels.”15 The 4 item version is scored 0--12. Equipment needed:
Scoring form level walking area at least 20 feet in length stopwatch shoe box 2 cones (to serve as obstacles in walking pathway) stairs with railing
Directions: Instructions for each item are included on the scoring form (attached). In 84 community dwelling male veterans, Rasch measurement model analysis showed that the most difficult items were “gait with horizontal head turns”, “steps”, and “gait with vertical head turns”;; the easiest items were “gait on level surfaces”, “change in gait speed”, and “step around obstacles”. Clinicians may want to consider changing the order of test administration (from easiest to most difficult) especially in clients with severe impairment.15 Reliability:
Reference N = Sample Description Reliability Statistic Intrarater Reliability: same rater within one session (or one day) Wolf, 2001 5 94 Adults (over age 75) with impaired balance;
physical therapist raters were trained in a standardized test protocol and practiced this protocol before data collection.
ICC=.98
McConvey, 2005 16 10 Patients with multiple sclerosis; 11 Physical therapist raters watching videotaped gait
ICC= .76 to .986
Interrater Reliability: Wolf, 2001 5 94 Adults with impaired balance over age 75;
physical therapist raters were trained in a standardized test protocol and practiced this protocol before data collection.
ICC=.99

Dynamic Gait Index (DGI)/Functional Gait Assessment (FGA)
Tests and Measures: Adult; 2012 DGI Page 2 Do not copy without permission of Teresa Steffen
Shumway Cook, 1997 4 5 Community-dwelling older adults with varying balance abilities; 5 physical therapist raters.
.96 to 1.00 (ratio of subject variability to total variability)
McConvey, 2005 16 10 Patients with multiple sclerosis; 11 Physical therapist raters watching videotaped gait
ICC = .983
Marchetti, 2006 3 39 Adults in tertiary-care setting, test and control; 6 paired physical therapist raters on 8 item version.
.54 to .80 Kappa
Internal Consistency: how items in a scale relate to each other and to the group of items as a whole
Marchetti, 2006 3 226
123 of the subjects had known balance disorders; 103 subjects were controls without balance or vestibular dysfunction. All were community dwellers.
Chronbach’s alpha 8 item version: 0.92 4 item version: 0.89
Chiu, 2006 15 84 Community-dwelling male veterans (mean age = 75)
Person separation reliability .80
Test-Retest Reliabilty Hall,200610 16 Adults with peripheral vestibular
disorders,(same day, same raters). ICC (3,1) = .86
Validity: Construct / Concurrent Validity: It is difficult to always differentiate between these 2 types of validity. Evaluating this property requires a “gold standard” measure with which to compare the tests results. Such a “gold standard” is often not available.
Population N = Support for Validity Community-dwelling older adults with and without hx of falls
105 DGI is correlated with: the Berg Balance Scale (BBS) (0.67), with a balance self-perceptions test (0.76), with use of an assistive device ( -0.44), and with a history of imbalance (-0.46).1
Patients with unilateral vestibular dysfunction (retrospective review)
137
DGI scores correlated with: ABC scale for persons with mild – moderate vestibular weakness (0.72); ABC scale for persons with severe vestibular weakness (0.48).17
Multiple sclerosis 10 DGI scores correlated inversely with: time to walk six meters (-0.80)16 Persons with and without balance or vestibular disorders (retrospective review)
81 (with balance disorders)
DGI scores correlated inversely with 5-timed-sit-to-stand test scores (-0.68). 18
93 (without balance disorders)
Persons with vestibular disorders (Age range 14 – 88, mean=65)
32 DGI correlates with Gait speed (0 .82) measured as time to walk 11 meters, inversely with Four Square Step Test (-0.51), inversely with Timed Up and Go (TUG) (-0.56).19
Persons with vestibular dysfunction (Mean age = 64) (retrospective review)
70
DGI correlates with BBS (0.71).20
Multiple Sclerosis (Mean age = 45)
51 DGI correlates with BBS (0.78), ABC (0.54) and inversely with TUG (0.72) Dizziness Handicap Index (DHI) (-0.39), and Deambulation Index (0.8). 13
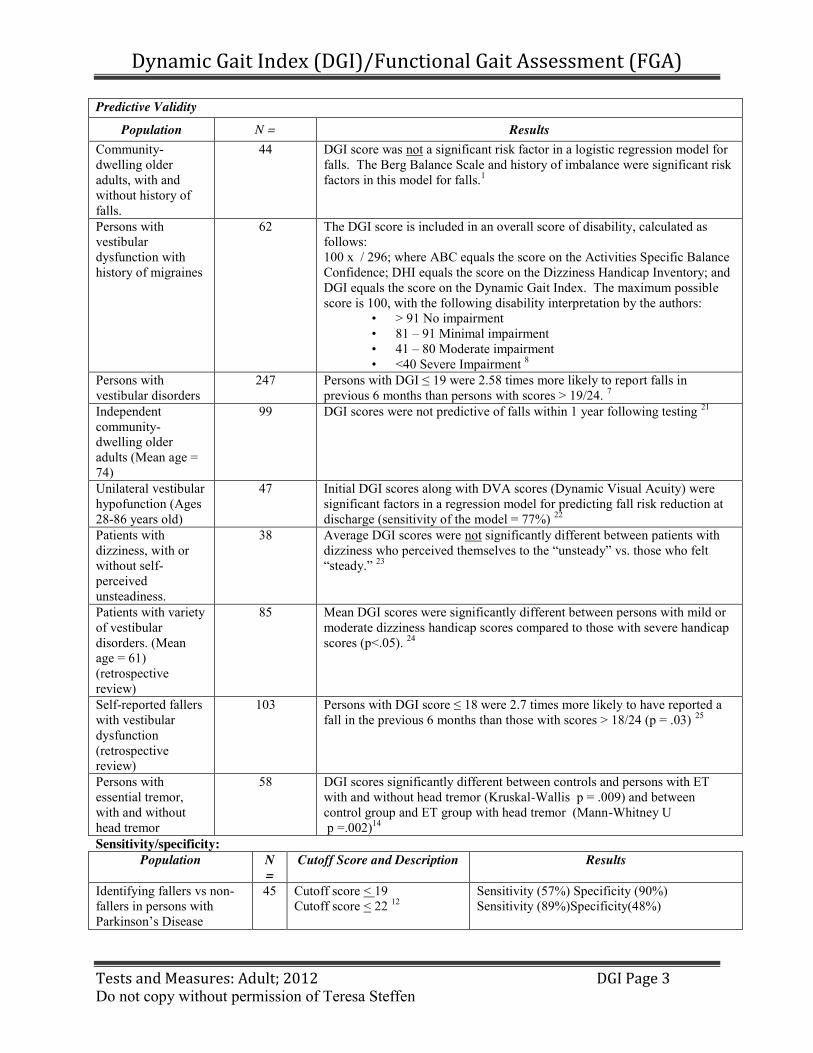
Dynamic Gait Index (DGI)/Functional Gait Assessment (FGA)
Tests and Measures: Adult; 2012 DGI Page 3 Do not copy without permission of Teresa Steffen
Predictive Validity
Population N = Results Community-dwelling older adults, with and without history of falls.
44 DGI score was not a significant risk factor in a logistic regression model for falls. The Berg Balance Scale and history of imbalance were significant risk factors in this model for falls.1
Persons with vestibular dysfunction with history of migraines
62 The DGI score is included in an overall score of disability, calculated as follows: 100 x / 296; where ABC equals the score on the Activities Specific Balance Confidence; DHI equals the score on the Dizziness Handicap Inventory; and DGI equals the score on the Dynamic Gait Index. The maximum possible score is 100, with the following disability interpretation by the authors:
• > 91 No impairment • 81 – 91 Minimal impairment • 41 – 80 Moderate impairment • <40 Severe Impairment 8
Persons with vestibular disorders
247 Persons with DGI ≤ 19 were 2.58 times more likely to report falls in previous 6 months than persons with scores > 19/24. 7
Independent community-dwelling older adults (Mean age = 74)
99 DGI scores were not predictive of falls within 1 year following testing 21
Unilateral vestibular hypofunction (Ages 28-86 years old)
47 Initial DGI scores along with DVA scores (Dynamic Visual Acuity) were significant factors in a regression model for predicting fall risk reduction at discharge (sensitivity of the model = 77%) 22
Patients with dizziness, with or without self-perceived unsteadiness.
38 Average DGI scores were not significantly different between patients with dizziness who perceived themselves to the “unsteady” vs. those who felt “steady.” 23
Patients with variety of vestibular disorders. (Mean age = 61) (retrospective review)
85
Mean DGI scores were significantly different between persons with mild or moderate dizziness handicap scores compared to those with severe handicap scores (p<.05). 24
Self-reported fallers with vestibular dysfunction (retrospective review)
103
Persons with DGI score ≤ 18 were 2.7 times more likely to have reported a fall in the previous 6 months than those with scores > 18/24 (p = .03) 25
Persons with essential tremor, with and without head tremor
58 DGI scores significantly different between controls and persons with ET with and without head tremor (Kruskal-Wallis p = .009) and between control group and ET group with head tremor (Mann-Whitney U p =.002)14
Sensitivity/specificity: Population N
= Cutoff Score and Description Results
Identifying fallers vs non-fallers in persons with Parkinson’s Disease
45 Cutoff score < 19 Cutoff score < 22 12
Sensitivity (57%) Specificity (90%) Sensitivity (89%)Specificity(48%)
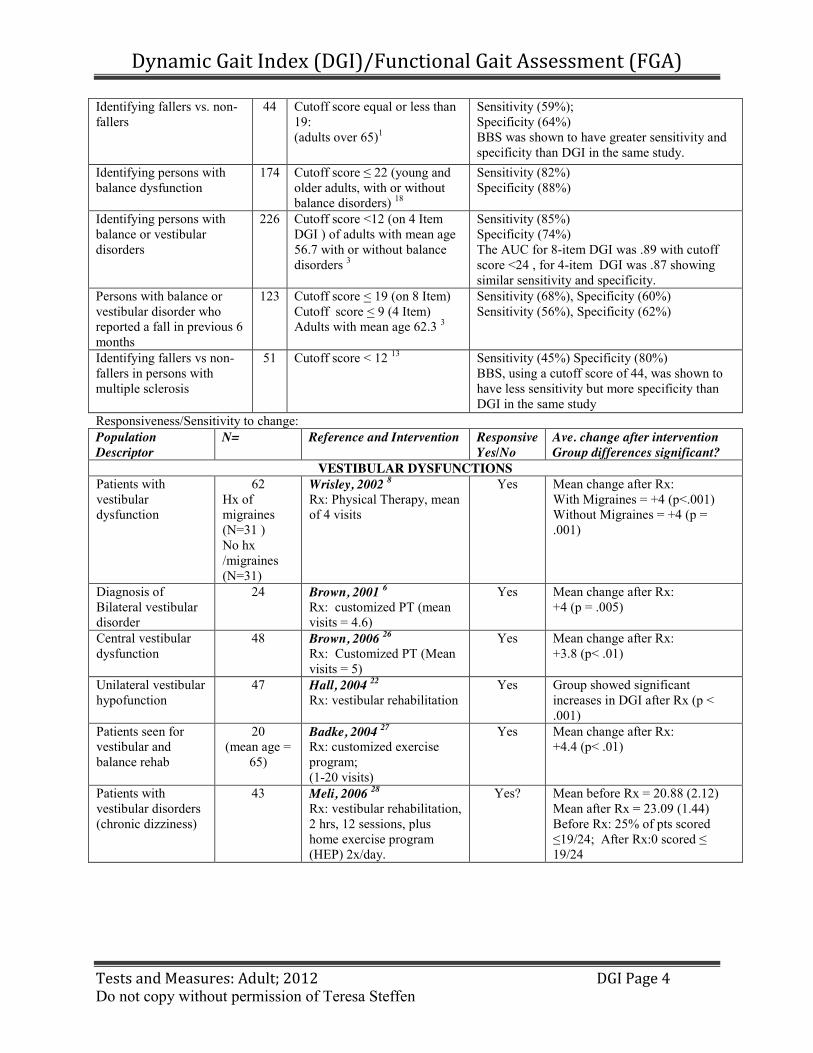
Dynamic Gait Index (DGI)/Functional Gait Assessment (FGA)
Tests and Measures: Adult; 2012 DGI Page 4 Do not copy without permission of Teresa Steffen
Identifying fallers vs. non-fallers
44 Cutoff score equal or less than 19: (adults over 65)1
Sensitivity (59%); Specificity (64%) BBS was shown to have greater sensitivity and specificity than DGI in the same study.
Identifying persons with balance dysfunction
174 Cutoff score ≤ 22 (young and older adults, with or without balance disorders) 18
Sensitivity (82%) Specificity (88%)
Identifying persons with balance or vestibular disorders
226 Cutoff score <12 (on 4 Item DGI ) of adults with mean age 56.7 with or without balance disorders 3
Sensitivity (85%) Specificity (74%) The AUC for 8-item DGI was .89 with cutoff score <24 , for 4-item DGI was .87 showing similar sensitivity and specificity.
Persons with balance or vestibular disorder who reported a fall in previous 6 months
123 Cutoff score < 19 (on 8 Item) Cutoff score < 9 (4 Item) Adults with mean age 62.3 3
Sensitivity (68%), Specificity (60%) Sensitivity (56%), Specificity (62%)
Identifying fallers vs non-fallers in persons with multiple sclerosis
51 Cutoff score < 12 13 Sensitivity (45%) Specificity (80%) BBS, using a cutoff score of 44, was shown to have less sensitivity but more specificity than DGI in the same study
Responsiveness/Sensitivity to change: Population Descriptor
N= Reference and Intervention Responsive Yes/No
Ave. change after intervention Group differences significant?
VESTIBULAR DYSFUNCTIONS Patients with vestibular dysfunction
62 Hx of migraines (N=31 ) No hx /migraines (N=31)
Wrisley, 2002 8 Rx: Physical Therapy, mean of 4 visits
Yes Mean change after Rx: With Migraines = +4 (p<.001) Without Migraines = +4 (p = .001)
Diagnosis of Bilateral vestibular disorder
24 Brown, 2001 6 Rx: customized PT (mean visits = 4.6)
Yes Mean change after Rx: +4 (p = .005)
Central vestibular dysfunction
48 Brown, 2006 26 Rx: Customized PT (Mean visits = 5)
Yes Mean change after Rx: +3.8 (p< .01)
Unilateral vestibular hypofunction
47 Hall, 2004 22 Rx: vestibular rehabilitation
Yes Group showed significant increases in DGI after Rx (p < .001)
Patients seen for vestibular and balance rehab
20 (mean age =
65)
Badke, 2004 27 Rx: customized exercise program; (1-20 visits)
Yes Mean change after Rx: +4.4 (p< .01)
Patients with vestibular disorders (chronic dizziness)
43 Meli, 2006 28 Rx: vestibular rehabilitation, 2 hrs, 12 sessions, plus home exercise program (HEP) 2x/day.
Yes? Mean before Rx = 20.88 (2.12) Mean after Rx = 23.09 (1.44) Before Rx: 25% of pts scored ≤19/24;; After Rx:0 scored ≤ 19/24
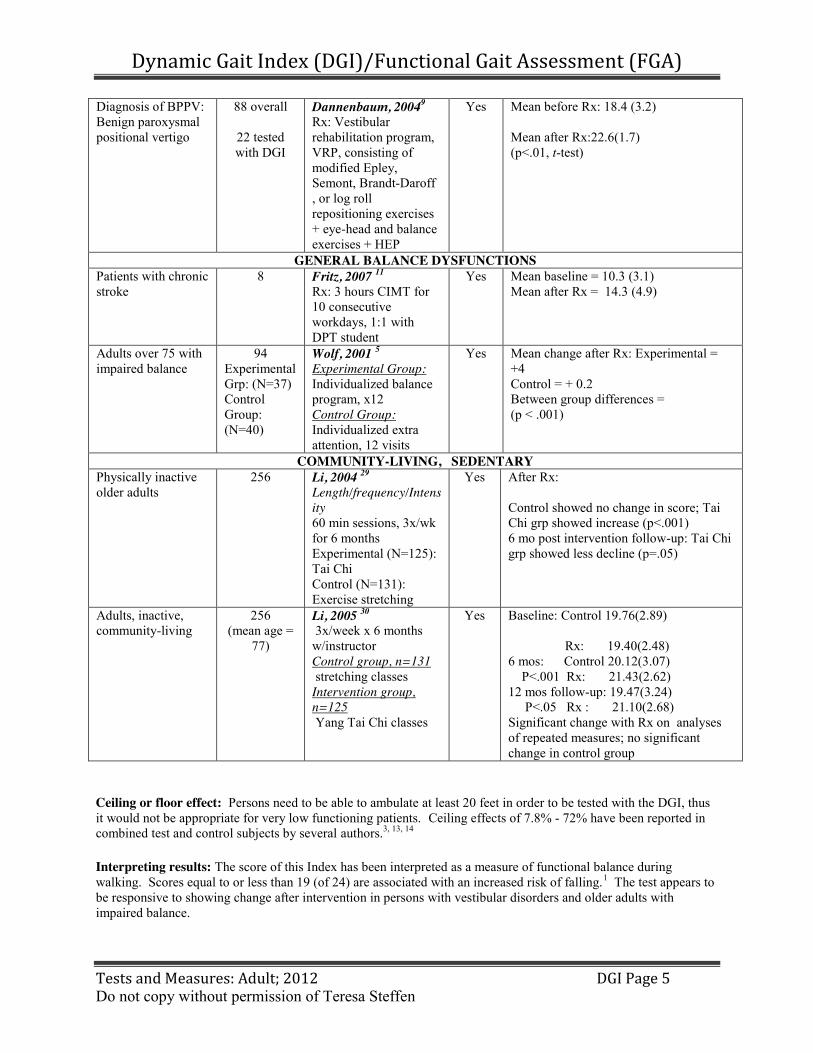
Dynamic Gait Index (DGI)/Functional Gait Assessment (FGA)
Tests and Measures: Adult; 2012 DGI Page 5 Do not copy without permission of Teresa Steffen
Diagnosis of BPPV: Benign paroxysmal positional vertigo
88 overall
22 tested with DGI
Dannenbaum, 20049 Rx: Vestibular rehabilitation program, VRP, consisting of modified Epley, Semont, Brandt-Daroff , or log roll repositioning exercises + eye-head and balance exercises + HEP
Yes Mean before Rx: 18.4 (3.2)
Mean after Rx:22.6(1.7) (p<.01, t-test)
GENERAL BALANCE DYSFUNCTIONS Patients with chronic stroke
8 Fritz, 2007 11 Rx: 3 hours CIMT for 10 consecutive workdays, 1:1 with DPT student
Yes Mean baseline = 10.3 (3.1) Mean after Rx = 14.3 (4.9)
Adults over 75 with impaired balance
94 Experimental Grp: (N=37) Control Group: (N=40)
Wolf, 2001 5 Experimental Group: Individualized balance program, x12 Control Group: Individualized extra attention, 12 visits
Yes Mean change after Rx: Experimental = +4 Control = + 0.2 Between group differences = (p < .001)
COMMUNITY-LIVING, SEDENTARY Physically inactive older adults
256 Li, 2004 29 Length/frequency/Intensity 60 min sessions, 3x/wk for 6 months Experimental (N=125): Tai Chi Control (N=131): Exercise stretching
Yes After Rx:
Control showed no change in score; Tai Chi grp showed increase (p<.001) 6 mo post intervention follow-up: Tai Chi grp showed less decline (p=.05)
Adults, inactive, community-living
256 (mean age =
77)
Li, 2005 30 3x/week x 6 months w/instructor Control group, n=131 stretching classes Intervention group, n=125 Yang Tai Chi classes
Yes Baseline: Control 19.76(2.89)
Rx: 19.40(2.48) 6 mos: Control 20.12(3.07) P<.001 Rx: 21.43(2.62) 12 mos follow-up: 19.47(3.24) P<.05 Rx : 21.10(2.68) Significant change with Rx on analyses of repeated measures; no significant change in control group
Ceiling or floor effect: Persons need to be able to ambulate at least 20 feet in order to be tested with the DGI, thus it would not be appropriate for very low functioning patients. Ceiling effects of 7.8% - 72% have been reported in combined test and control subjects by several authors.3, 13, 14 Interpreting results: The score of this Index has been interpreted as a measure of functional balance during walking. Scores equal to or less than 19 (of 24) are associated with an increased risk of falling.1 The test appears to be responsive to showing change after intervention in persons with vestibular disorders and older adults with impaired balance.
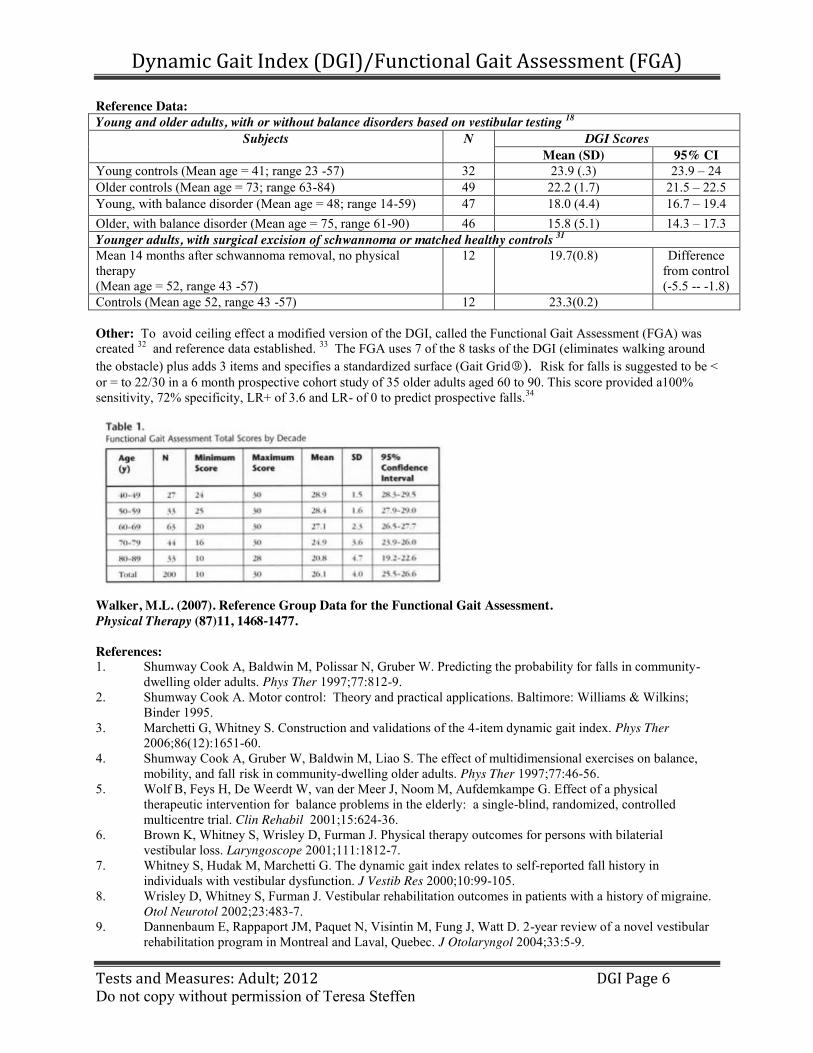
Dynamic Gait Index (DGI)/Functional Gait Assessment (FGA)
Tests and Measures: Adult; 2012 DGI Page 6 Do not copy without permission of Teresa Steffen
Reference Data: Young and older adults, with or without balance disorders based on vestibular testing 18
Subjects N DGI Scores Mean (SD) 95% CI
Young controls (Mean age = 41; range 23 -57) 32 23.9 (.3) 23.9 – 24 Older controls (Mean age = 73; range 63-84) 49 22.2 (1.7) 21.5 – 22.5 Young, with balance disorder (Mean age = 48; range 14-59) 47 18.0 (4.4) 16.7 – 19.4 Older, with balance disorder (Mean age = 75, range 61-90) 46 15.8 (5.1) 14.3 – 17.3 Younger adults, with surgical excision of schwannoma or matched healthy controls 31 Mean 14 months after schwannoma removal, no physical therapy (Mean age = 52, range 43 -57)
12 19.7(0.8) Difference from control (-5.5 -- -1.8)
Controls (Mean age 52, range 43 -57) 12 23.3(0.2) Other: To avoid ceiling effect a modified version of the DGI, called the Functional Gait Assessment (FGA) was created 32 and reference data established. 33 The FGA uses 7 of the 8 tasks of the DGI (eliminates walking around the obstacle) plus adds 3 items and specifies a standardized surface (Gait Grid). Risk for falls is suggested to be < or = to 22/30 in a 6 month prospective cohort study of 35 older adults aged 60 to 90. This score provided a100% sensitivity, 72% specificity, LR+ of 3.6 and LR- of 0 to predict prospective falls.34
Walker, M.L. (2007). Reference Group Data for the Functional Gait Assessment. Physical Therapy (87)11, 1468-‐1477. References: 1. Shumway Cook A, Baldwin M, Polissar N, Gruber W. Predicting the probability for falls in community- dwelling older adults. Phys Ther 1997;77:812-9. 2. Shumway Cook A. Motor control: Theory and practical applications. Baltimore: Williams & Wilkins; Binder 1995. 3. Marchetti G, Whitney S. Construction and validations of the 4-item dynamic gait index. Phys Ther 2006;86(12):1651-60. 4. Shumway Cook A, Gruber W, Baldwin M, Liao S. The effect of multidimensional exercises on balance, mobility, and fall risk in community-dwelling older adults. Phys Ther 1997;77:46-56. 5. Wolf B, Feys H, De Weerdt W, van der Meer J, Noom M, Aufdemkampe G. Effect of a physical therapeutic intervention for balance problems in the elderly: a single-blind, randomized, controlled multicentre trial. Clin Rehabil 2001;15:624-36. 6. Brown K, Whitney S, Wrisley D, Furman J. Physical therapy outcomes for persons with bilaterial vestibular loss. Laryngoscope 2001;111:1812-7. 7. Whitney S, Hudak M, Marchetti G. The dynamic gait index relates to self-reported fall history in individuals with vestibular dysfunction. J Vestib Res 2000;10:99-105. 8. Wrisley D, Whitney S, Furman J. Vestibular rehabilitation outcomes in patients with a history of migraine. Otol Neurotol 2002;23:483-7. 9. Dannenbaum E, Rappaport JM, Paquet N, Visintin M, Fung J, Watt D. 2-year review of a novel vestibular rehabilitation program in Montreal and Laval, Quebec. J Otolaryngol 2004;33:5-9.

Dynamic Gait Index (DGI)/Functional Gait Assessment (FGA)
Tests and Measures: Adult; 2012 DGI Page 7 Do not copy without permission of Teresa Steffen
10. Hall C, SJ H. Reliability of clinical measures used to assess patients with peripheral vestibular disorders. J Neurol Phys Ther 2006;30(2):74-81. 11. Fritz SL, Pittman AL, Robinson AC, Orton SC, Rivers ED. An intense intervention for improving gait, balance, and mobility for individuals with chronic stroke: a pilot study J Neurol Phys Ther 2007;31:71-6. 12. Dibble L, Lange M. Predicting falls in individuals with Parkinson disease: a reconsideration of clinical balance measures J Neurol Phys Ther 2006;30(2):60-7. 13. Cattaneo D, Regola A, Meotti M. Validity of six balance disorders scales in persons with multiple sclerosis. Disabil Rehabil 2006;28(12):789-95. 14. Parisi S, Heroux M, Gulham E, Norman K. Functional mobility and postural control in essential tremor. Arch Phys Med Rehabil 2006;87:1357-64. 15. Chiu Y, Fritz S, Light K, Velozo C. Use of item response analysis to investigate measurement properties and clinical validity of data for the dynamic gait index. Phys Ther 2006;86(6):778-87. 16. McConvey J, Bennett S. Reliability of the dynamic gait index in individuals with multiple sclerosis. Arch Phys Med Rehabil 2005;86:130-3. 17. Legters K, Whitney S, Porter R, Buczek F. The relationship between the activities-specific balance confidence scale and the dynamic gait index in peripheral vestibular dysfunction. Physio Research Inter 2005;10(1):10-22. 18. Whitney S, Wrisley D, Marchetti G, Gee M, Redfern M, Furman J. Clinical measurement of sit-to-stand performance in people with balance disorders: validity of data for the five-times-sit-to-stand test. Phys Ther 2005;85(10):1034-45. 19. Whitney S, G. Marchetti, L. O. Morris, Sparto PJ. The reliability and validity of the four square step test for people with balance deficits secondary to a vestibular disorder. Arch Phys Med Rehabil 2007;88:99-104. 20. Whitney S, Wrisley D, Furman J. Concurrent validity of the berg balance scale and the dynamic gait index in people with vestibular dysfunction. Physiother Res Int 2003;8(4):178-86. 21. Boulgarides L, McGinty S, Willett J, Barnes C. Use of clinicaland impairment- Based tests to predict falls by community-dwelling older adults. Phys Ther 2003;83(4):328-9. 22. Hall C, Shubert M, Herdman S. Prediction of fall risk reduction as measured by dynamic gait index in individuals with unilateral vestibular hypofunction. Otol Neurotol 2004;25:746-51. 23. Lin S, Tsai T, Lee I, Wu Y. Perception of unsteadiness in patients with dizziness: Association with handicap and imbalance. J Biomed Sci 2002;9:428-35. 24. Whitney S, Wrisley D, Brown K, Furman J. Is perception of handicap related to functional performance in persons with vestibular dysfunction? Otol Neurotol 2004;25:139-43. 25. Whitney S, Marchetti G, Schade A, Wrisley D. The sensitivity and specificity of the timed "up and go" and the dynamic gait index for self-reported falls in persons with vestibular disorders. J Vestib Res 2004;14:397-409. 26. Brown K, Whitney S, Marchetti G, Wrisley D, Furman J. Physical therapy for central vestibular dysfunction. Arch Phys Med Rehabil 2006;87:76-81. 27. Badke M, Shea T, Miedaner J, Grove C. Outcomes after rehabilitation for adults with balance dysfunction. Arch Phys Med Rehabil 2004;85(February):227-33. 28. Meli A, Zimatore G, Badaracco C, De Angelis E, Tufarelli D. Vestibular rehabilitation and 6-month follow-up using objective and subjective measures. Acta OtoLaryngologica 2006;126:259-66. 29. Li F, Harmer P, Fisher K, Mcauley E. Tai Chi: improving functional balance and predicting subsequent falls in older persons. Med Sci Sports Exerc 2004;36(12):2046-52. 30. Li F, Harmer P, Fisher KJ, McAuley E, Chaumeton N, Eckstrom E et al. Tai chi and fall reductions in older adults: a randomized controlled trial. J Gerontol A Biol Sci Med Sci 2005;60A(2):187-94. 31. Low Choy N, Johnson N, Treleavan J, Jull G, Panizza B, Brown-Rothwell D. Balance, mobility and gaze stability deficits remain following surgical removal of vestibular schwannoma (acustic neuroma): An observational study. Aust J Physiother 2006:211-6. 32. Wrisley DM, Marchetti GF, Kuharsky DK, Whitney SL. Reliability, internal consistency, and validity of data obtained with the functional gait assessment. Phys Ther 2004;84(10):906-18. 33. Walker ML, Austin AG, Banke GM, Foxx SR, Gaetano L, Gardner LA et al. Reference group data for the functional gait assessment. Phys Ther 2007;87(11):1468-77. 34. Wrisley, DM, Kumar,NA. Functional gait assessment: Concurrent, discriminative, and predictive validity in community-dwelling older adults. Phys Ther 2010: 90(5):761-773.
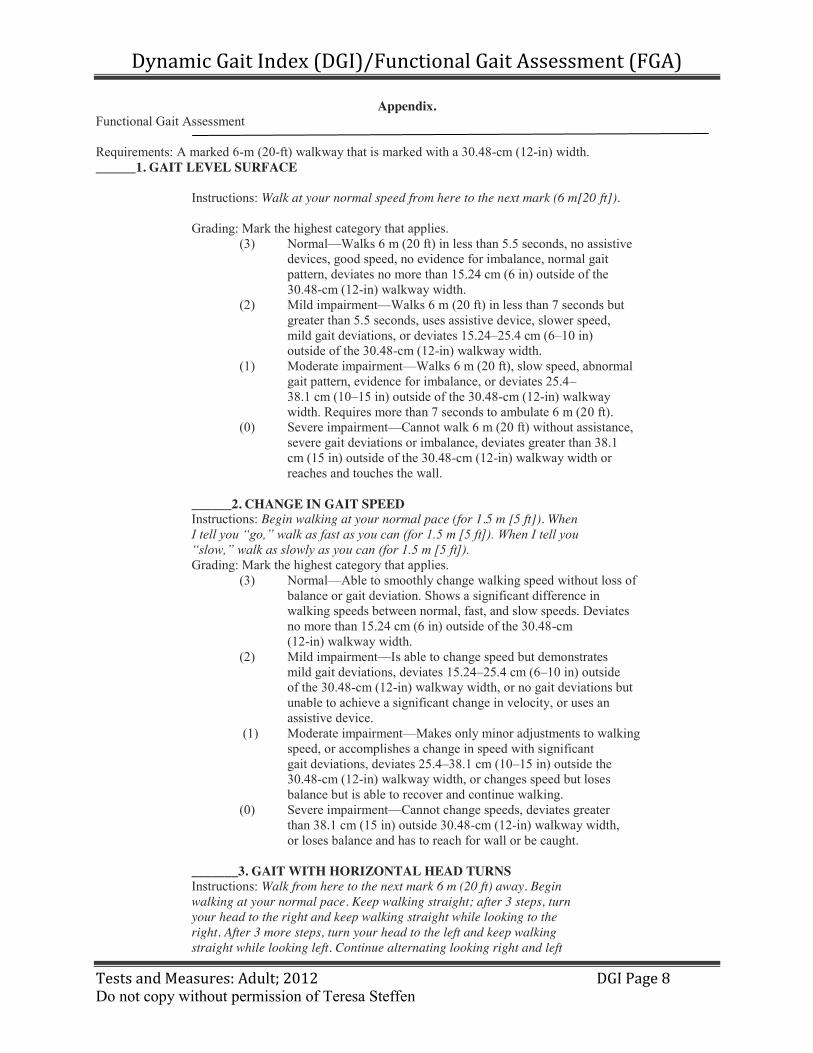
Dynamic Gait Index (DGI)/Functional Gait Assessment (FGA)
Tests and Measures: Adult; 2012 DGI Page 8 Do not copy without permission of Teresa Steffen
Appendix. Functional Gait Assessment
Requirements: A marked 6-m (20-ft) walkway that is marked with a 30.48-cm (12-in) width. ______1. GAIT LEVEL SURFACE
Instructions: Walk at your normal speed from here to the next mark (6 m[20 ft]).
Grading: Mark the highest category that applies. (3) Normal—Walks 6 m (20 ft) in less than 5.5 seconds, no assistive devices, good speed, no evidence for imbalance, normal gait pattern, deviates no more than 15.24 cm (6 in) outside of the 30.48-cm (12-in) walkway width. (2) Mild impairment—Walks 6 m (20 ft) in less than 7 seconds but greater than 5.5 seconds, uses assistive device, slower speed, mild gait deviations, or deviates 15.24–25.4 cm (6–10 in) outside of the 30.48-cm (12-in) walkway width. (1) Moderate impairment—Walks 6 m (20 ft), slow speed, abnormal gait pattern, evidence for imbalance, or deviates 25.4– 38.1 cm (10–15 in) outside of the 30.48-cm (12-in) walkway width. Requires more than 7 seconds to ambulate 6 m (20 ft). (0) Severe impairment—Cannot walk 6 m (20 ft) without assistance, severe gait deviations or imbalance, deviates greater than 38.1 cm (15 in) outside of the 30.48-cm (12-in) walkway width or reaches and touches the wall. ______2. CHANGE IN GAIT SPEED Instructions: Begin walking at your normal pace (for 1.5 m [5 ft]). When I tell you “go,” walk as fast as you can (for 1.5 m [5 ft]). When I tell you “slow,” walk as slowly as you can (for 1.5 m [5 ft]). Grading: Mark the highest category that applies. (3) Normal—Able to smoothly change walking speed without loss of balance or gait deviation. Shows a significant difference in walking speeds between normal, fast, and slow speeds. Deviates no more than 15.24 cm (6 in) outside of the 30.48-cm (12-in) walkway width. (2) Mild impairment—Is able to change speed but demonstrates mild gait deviations, deviates 15.24–25.4 cm (6–10 in) outside of the 30.48-cm (12-in) walkway width, or no gait deviations but unable to achieve a significant change in velocity, or uses an assistive device. (1) Moderate impairment—Makes only minor adjustments to walking speed, or accomplishes a change in speed with significant gait deviations, deviates 25.4–38.1 cm (10–15 in) outside the 30.48-cm (12-in) walkway width, or changes speed but loses balance but is able to recover and continue walking.
(0) Severe impairment—Cannot change speeds, deviates greater than 38.1 cm (15 in) outside 30.48-cm (12-in) walkway width, or loses balance and has to reach for wall or be caught. _______3. GAIT WITH HORIZONTAL HEAD TURNS Instructions: Walk from here to the next mark 6 m (20 ft) away. Begin walking at your normal pace. Keep walking straight; after 3 steps, turn your head to the right and keep walking straight while looking to the right. After 3 more steps, turn your head to the left and keep walking straight while looking left. Continue alternating looking right and left

Dynamic Gait Index (DGI)/Functional Gait Assessment (FGA)
Tests and Measures: Adult; 2012 DGI Page 9 Do not copy without permission of Teresa Steffen
every 3 steps until you have completed 2 repetitions in each direction. Grading: Mark the highest category that applies. (3) Normal—Performs head turns smoothly with no change in gait. Deviates no more than 15.24 cm (6 in) outside 30.48-cm (12-in) walkway width. (2) Mild impairment—Performs head turns smoothly with slight change in gait velocity (eg, minor disruption to smooth gait path), deviates 15.24–25.4 cm (6–10 in) outside 30.48-cm (12-in) walkway width, or uses an assistive device. (1) Moderate impairment—Performs head turns with moderate change in gait velocity, slows down, deviates 25.4–38.1 cm (10–15 in) outside 30.48-cm (12-in) walkway width but recovers, can continue to walk. (0) Severe impairment—Performs task with severe disruption of gait (eg, staggers 38.1 cm [15 in] outside 30.48-cm (12-in) walkway width, loses balance, stops, or reaches for wall). _______4. GAIT WITH VERTICAL HEAD TURNS Instructions: Walk from here to the next mark (6 m [20 ft]). Begin walking at your normal pace. Keep walking straight; after 3 steps, tip your head up and keep walking straight while looking up. After 3 more steps, tip your head down, keep walking straight while looking down. Continue alternating looking up and down every 3 steps until you have completed 2 repetitions in each direction. Grading: Mark the highest category that applies. (3) Normal—Performs head turns with no change in gait. Deviates no more than 15.24 cm (6 in) outside 30.48-cm (12-in) walkway width. (2) Mild impairment—Performs task with slight change in gait velocity (eg, minor disruption to smooth gait path), deviates 15.24–25.4 cm (6–10 in) outside 30.48-cm (12-in) walkway width or uses assistive device. (1) Moderate impairment—Performs task with moderate change in gait velocity, slows down, deviates 25.4–38.1 cm (10–15 in) outside 30.48-cm (12-in) walkway width but recovers, can continue to walk.
(0) Severe impairment—Performs task with severe disruption of gait (eg, staggers 38.1 cm [15 in] outside 30.48-cm (12-in) walkway width, loses balance, stops, reaches for wall). _______5. GAIT AND PIVOT TURN Instructions: Begin with walking at your normal pace. When I tell you, “turn and stop,” turn as quickly as you can to face the opposite direction and stop. Grading: Mark the highest category that applies. (3) Normal—Pivot turns safely within 3 seconds and stops quickly with no loss of balance. (2) Mild impairment—Pivot turns safely in _3 seconds and stops with no loss of balance, or pivot turns safely within 3 seconds and stops with mild imbalance, requires small steps to catch balance. (1) Moderate impairment—Turns slowly, requires verbal cueing, or requires several small steps to catch balance following turn and stop.

Dynamic Gait Index (DGI)/Functional Gait Assessment (FGA)
Tests and Measures: Adult; 2012 DGI Page 10 Do not copy without permission of Teresa Steffen
(0) Severe impairment—Cannot turn safely, requires assistance to turn and stop. _______6. STEP OVER OBSTACLE Instructions: Begin walking at your normal speed. When you come to the shoe box, step over it, not around it, and keep walking. Grading: Mark the highest category that applies. (3) Normal—Is able to step over 2 stacked shoe boxes taped together (22.86 cm [9 in] total height) without changing gait speed; no evidence of imbalance. (2) Mild impairment—Is able to step over one shoe box (11.43 cm [4.5 in] total height) without changing gait speed; no evidence of imbalance.
(0) Moderate impairment—Is able to step over one shoe box (11.43 cm [4.5 in] total height) but must slow down and adjust steps to clear box safely. May require verbal cueing. (0) Severe impairment—Cannot perform without assistance. _______7. GAIT WITH NARROW BASE OF SUPPORT Instructions: Walk on the floor with arms folded across the chest, feet aligned heel to toe in tandem for a distance of 3.6 m [12 ft]. The number of steps taken in a straight line are counted for a maximum of 10 steps. Grading: Mark the highest category that applies. (3) Normal—Is able to ambulate for 10 steps heel to toe with no staggering. (2) Mild impairment—Ambulates 7–9 steps. (1) Moderate impairment—Ambulates 4–7 steps. (0) Severe impairment—Ambulates less than 4 steps heel to toe or cannot perform without assistance. _______8. GAIT WITH EYES CLOSED Instructions: Walk at your normal speed from here to the next mark (6 m [20 ft]) with your eyes closed. Grading: Mark the highest category that applies. (3) Normal—Walks 6 m (20 ft), no assistive devices, good speed, no evidence of imbalance, normal gait pattern, deviates no more than 15.24 cm (6 in) outside 30.48-cm (12-in) walkway width. Ambulates 6 m (20 ft) in less than 7 seconds. (2) Mild impairment—Walks 6 m (20 ft), uses assistive device, slower speed, mild gait deviations, deviates 15.24–25.4 cm (6–10 in) outside 30.48-cm (12-in) walkway width. Ambulates 6 m (20 ft) in less than 9 seconds but greater than 7 seconds. (1) Moderate impairment—Walks 6 m (20 ft), slow speed, abnormal gait pattern, evidence for imbalance, deviates 25.4–38.1 cm (10–15 in) outside 30.48-cm (12-in) walkway width. Requires more than 9 seconds to ambulate 6 m (20 ft). (0) Severe impairment—Cannot walk 6 m (20 ft) without assistance, severe gait deviations or imbalance, deviates greater than 38.1 cm (15 in) outside 30.48-cm (12-in) walkway width or will not attempt task. ______9. AMBULATING BACKWARDS Instructions: Walk backwards until I tell you to stop. Grading: Mark the highest category that applies. (3) Normal—Walks 6 m (20 ft), no assistive devices, good speed, no evidence for imbalance, normal gait pattern, deviates no

Dynamic Gait Index (DGI)/Functional Gait Assessment (FGA)
Tests and Measures: Adult; 2012 DGI Page 11 Do not copy without permission of Teresa Steffen
more than 15.24 cm (6 in) outside 30.48-cm (12-in) walkway width. (2) Mild impairment—Walks 6 m (20 ft), uses assistive device, slower speed, mild gait deviations, deviates 15.24–25.4 cm (6–10 in) outside 30.48-cm (12-in) walkway width. (1) Moderate impairment—Walks 6 m (20 ft), slow speed, abnormal gait pattern, evidence for imbalance, deviates 25.4–38.1 cm (10–15 in) outside 30.48-cm (12-in) walkway width. (0) Severe impairment—Cannot walk 6 m (20 ft) without assistance, severe gait deviations or imbalance, deviates greater than 38.1 cm (15 in) outside 30.48-cm (12-in) walkway width or will not attempt task. ________10. STEPS Instructions: Walk up these stairs as you would at home (ie, using the rail if necessary). At the top turn around and walk down. Grading: Mark the highest category that applies. (3) Normal—Alternating feet, no rail. (2) Mild impairment—Alternating feet, must use rail. (1) Moderate impairment—Two feet to a stair; must use rail. (0) Severe impairment—Cannot do safely. TOTAL SCORE: ______ MAXIMUM SCORE 30 a Adapted from Dynamic Gait Index.1 Modified and reprinted with permission of authors and Lippincott Williams & Wilkins (http://lww.com). Walker, M.L. (2007). Reference Group Data for the Functional Gait Assessment. Physical Therapy (87)11, 1468-‐1477.

HiMAT: HIGH LEVEL MOBILITY ASSESSMENT TOOL
PATIENT
ID LABEL
DATE…………………………………
DATE OF ACCIDENT………………
DIAGNOSIS……………………..…..
AFFECTED SIDE LEFT / RIGHT
SCORE
ITEM PERFORMANCE 0 1 2 3 4 5 WALK sec X > 6.6 5.4-6.6 4.3-5.3 < 4.3 X WALK BACKWARD sec >13.3 8.1-13.3 5.8-8.0 < 5.8 X WALK ON TOES sec > 8.9 7.0 - 8.9 5.4-6.9 < 5.4 X WALK OVER OBSTACLE sec > 7.1 5.4-7.1 4.5-5.3 < 4.5 X RUN sec > 2.7 2.0-2.7 1.7-1.9 < 1.7 X SKIP sec > 4.0 3.5-4.0 3.0-3.4 < 3.0 X HOP FORWARD (AFFECTED) sec > 7.0 5.3-7.0 4.1-5.2 < 4.1 X BOUND (AFFECTED) 1) cm
2) 3)
< 80 80-103 104-132 > 132 X
BOUND (LESS-AFFECTED) 1) cm 2) 3)
< 82 82-105 106-129 > 129 X
UP STAIRS DEPENDENT (Rail OR not reciprocal: if not, score 5 and rate below)
sec >22.8 14.6-22.8 12.3-14.5 <12.3
UP STAIRS INDEPENDENT (No rail AND reciprocal: if not score 0 and rate above)
sec > 9.1 7.6-9.1 6.8-7.5 < 6.8 X
DOWN STAIRS DEPENDENT (Rail OR not reciprocal: if not score 5 and rate below)
sec >24.3 17.6-24.3 12.8-17.5 <12.8
DOWN STAIRS INDEPENDENT (No rail AND reciprocal: if not score 0 and rate above)
sec > 8.4 6.6-8.4 5.8-6.5 < 5.8 X
SUBTOTAL
TOTAL HiMAT SCORE /54
Please notify Gavin Williams at [email protected] or [email protected] so that the use of the HiMAT can be tracked.

HiMAT: High-level Mobility Assessment Tool
Instructions
Subject suitability: The HiMAT is appropriate for assessing people with high-level balance and mobility problems. The minimal mobility requirement for testing is independent walking over 20m without gait aids. Orthoses are permitted.
Item testing: Testing takes 5-10 minutes. Patients are allowed 1 practice trial for each item. Instructions: Patients are instructed to perform at their maximum safe speed except for the
bounding and stair items. Walking: The middle 10m of a 20m trial is timed. Walk backward: As for walking. Walk on toes: As for walking. Any heel contact during the middle 10m is recorded as a fail. Walk over obstacle: As for walking. A house brick is placed across the walkway at the mid-point. Patients must
step over the brick without contacting it. A fail is recorded if patients step around the brick or make contact with the brick.
Run: The middle 10m of a 20m trial is timed. A fail is recorded if patients fail to have a consistent
flight phase during the trial. Skipping: The middle 10m of a 20m trial is timed. A fail is recorded if patients fail to have a consistent
flight phase during the trial. Hop forward: Patients stand on their more affected leg and hop forward. The time to hop10m meters is
recorded. Bound (affected). A bound is a jump from one leg to the other with a flight phase. Patients stand behind a line
on their less affected leg, hands on hips, and jump forward landing on their more affected leg. Each bound is measured from the line to the heel of the landing leg. The average of three trials is recorded.
Bound (less-affected). Patients stand behind a line on their more affected leg, hands on hips, and jump forward
landing on their less affected leg. The average of three trials is recorded. Up stairs: Patients are asked to walk up a flight of 14 stairs as they normally would and at their normal
speed. The trial is recorded from when the patient starts until both feet are at the top. Patients who use a rail or a non-reciprocal pattern are scored on Up Stairs Dependent. Patients who ascend the stairs reciprocally without a rail are scored on Up Stairs Independent and get an additional 5 points in the last column of Up Stairs Dependent.
Down stairs: As for Up stairs. Scoring: All times and distances are recorded in the ‘performance’ column. The
corresponding score for each item is then circled and each column is then subtotaled. Subtotals are then added to calculate the HiMAT score.

UPDRS, Hoehn & Yahr, Scwab & England_SVUH_MedEl_tools 1/4
Scales in Parkinson’s disease Introduction The UPDRS (Unified Parkinson’s disease rating score), Hoehn & Yahr and Schwab & England scales are the scales in common practice for Parkinson’s disease. Their utility is that they objectively rate an individual patient’s disability at a particular moment in time. Each scale score is a reflection of disease burden on the individual patient and is useful in describing disease progression and treatment response with time. The UPDRS is scored from a total of 195 points; higher scores reflect worsening disability.
Modified Hoehn and Yahr staging Stage 0 No signs of disease Stage 1 Unilateral disease Stage 1.5 Unilateral plus axial involvement Stage 2 Bilateral disease, without impairment of balance Stage 2.5 Mild bilateral disease, with recovery on pull test Stage 3 Mild to moderate bilateral disease; some postural instability; physically
independent Stage 4 Severe disability; still able to walk or stand unassisted Stage 5 Wheelchair bound or bedridden unless aided
Schwab & England Activities of Daily Living scale 100% Completely independent. Able to do all chores w/o slowness, difficulty, or
impairment. Essentially normal. Unaware of any difficulty.
90% Completely independent. Able to do all chores with some degree of slowness, difficulty and impairment. May take twice as long. Beginning to be aware of difficulty.
80% Completely independent in most chores. Takes twice as long. Conscious of difficulty and slowing.
70% Not completely independent. More difficulty with some chores. X 3-4 as long in some. May spend a large part of the day with chores.
60% Some dependency. Can do most chores, but exceedingly slowly and with much effort. Errors, some impossible.
50% More dependent. Help with 1/2 of chores. Difficulty with everything.
40% Very dependant. Can assist with all chores but few alone.
30% With effort, now and then does a few chores alone or begins alone. Much help needed.
20% Nothing alone. Can do some slight help with some chores. Severe invalid.
10% Totally dependant, helpless. Complete invalid.
0% Vegetative functions such as swallowing, bladder and bowel function are not functioning. Bedridden.

UPDRS, Hoehn & Yahr, Scwab & England_SVUH_MedEl_tools 2/4
Unified Parkinson’s disease Rating Scale (UPDRS) I 1 2 3 4 II 5 6 7 8 9
Mentation, Behaviour & Mood Intellectual impairment 0 = none 1 = mild, consistent forgetfulness 2 = moderate, difficulty with complex problems 3 = severe, disorientation for time & place 4 = severe, help with personal care. Cannot be left alone Thought disorder 0 = none 1 = vivid dreaming 2 = “benign" hallucination with insight retained 3 = hallucination or delusions without insight 4 = persistent hallucination, delusions, or florid psychosis Depression 0 = not present 1 = periods of sadness or guilt > normal, never sustained for days/weeks 2 = sustained depression for >1 week 3 = vegetative symptoms (insomnia, anorexia, weight loss) 4 = vegetative symptoms and suicidal thoughts Motivation/Initiative 0 = normal 1 = less assertive than usual, more passive 2 = loss of initiative/disinterest in elective activities 3 = loss of initiative/disinterest in routine activities 4 = withdrawn, complete loss of motivation Activities of Daily Living Speech 0 = Normal 1 = Mildly affected 2 = Moderately affected. Sometimes asked to repeat statements 3 = Severely affected. Frequently asked to repeat statements 4 = Unintelligible most of the time Salivation 0 = Normal 1 = Slight saliva excess. Some night-time drooling 2 = Moderately excessive saliva; minimal drooling 3 = Marked excess saliva with some drooling 4 = Marked drooling, requires constant tissue/handkerchief Swallowing 0 = Normal 1 = Rare choking 2 = Occasional choking 3 = Requires soft food 4 =Requires nasogastric tube or gastrostomy feeding Handwriting 0 = Normal 1 = Slightly slow or small 2 = Moderately slow/small; all words are legible 3 = Severely affected; not all words are legible 4 = The majority of words are not legible Cutting food and handling utensils 0 = Normal 1 = Somewhat slow and clumsy, but no help needed 2 = Can cut most foods slowly; some help needed 3 = Food must be cut by someone, but can still feed slowly 4 = Needs to be fed
10 11 12 13 14 15 16 17 III 18 19
Dressing 0 = Normal 1 = Somewhat slow, but no help needed 2 = Occasional assistance with buttons, arms in sleeves 3 = Considerable help, can do some things alone 4 = Helpless Hygiene 0 = Normal 1 = Somewhat slow, no help needed 2 = Help to shower/bathe 3 = Assistance for washing hair, brushing teeth & hair 4 =Foley catheter or pads Turning in bed & adjusting bed clothes 0 = Normal 1 = Somewhat slow & clumsy, no help needed 2 = Turns alone or adjusts sheets, but with difficulty 3 = Can initiate, but not turn or adjust sheets alone 4 = Helpless Falling 0 = None 1 = Rare falling 2 = Occasionally falls, < 1 per day 3 = Falls on average once per day 4 = Falls > once per day Freezing when walking 0 = None 1 = Rare freezing; may have start-hesitation 2 = Occasional freezing when walking 3 = Frequent freezing. Occasional falls resulting 4 = Frequent falls from freezing Walking 0 = Normal 1 = Mild difficulty. May not swing arm or may drag leg 2 = Moderate difficulty, but requires no assistance 3 = Severe disturbance, requires assistance 4 = Cannot walk, even with assistance Tremor (Symptomatic complaint in any body part) 0 = Absent 1 = Slight & infrequently present 2 = Moderate; bothersome to patient 3 = Severe; interferes with many activities 4 = Marked; interferes with most activities Sensory complaints relating to parkinsonism 0 = None 1 = Occasional numbness, tingling or aching 2 = Frequent numbness, tingling or aching 3 = Frequent painful sensations 4 = Excruciating pain Motor examination Speech 0 = Normal 1 = Slight loss of expression, diction or volume 2 = Monotone, slurred but understandable 3 = Marked impairment, difficult to understand 4 = Unintelligible Facial expression 0 = Normal 1 = Minimal hypomimia, could be ‘poker face’ 2 = Definite diminution of expression 3 = Moderate hypomimia; lips parted some of the time 4 = Masked or fixed facies; lips parted ¼ inch or more

UPDRS, Hoehn & Yahr, Scwab & England_SVUH_MedEl_tools 3/4
20 21 22
Tremor at rest - Right upper limb 0 = Absent 1 = Slight, infrequently present 2 = Mild amplitude & persistent or moderate & intermittent 3 = Moderate amplitude, present most of the time 4 = Marked amplitude, present most of the time Tremor at rest - Left upper limb 0 = Absent 1 = Slight, infrequently present 2 = Mild amplitude & persistent or moderate & intermittent 3 = Moderate amplitude, present most of the time 4 = Marked amplitude, present most of the time Tremor at rest - Right lower limb 0 = Absent 1 = Slight, infrequently present 2 = Mild amplitude & persistent or moderate & intermittent 3 = Moderate amplitude, present most of the time 4 = Marked amplitude, present most of the time Tremor at rest – Left lower limb 0 = Absent 1 = Slight, infrequently present 2 = Mild amplitude & persistent or moderate & intermittent 3 = Moderate amplitude, present most of the time 4 = Marked amplitude, present most of the time Action or posture tremor of hands – Right hand 0 = Absent 1 = Slight, present with action 2 = Moderate in amplitude, present with action 3 = Moderate in amplitude, with posture holding & action 4 = Marked in amplitude; interferes with feeding Action or posture tremor of hands – Left hand 0 = Absent 1 = Slight, present with action 2 = Moderate in amplitude, present with action 3 = Moderate in amplitude, with posture holding & action 4 = Marked in amplitude; interferes with feeding Rigidity (judged on passive movement of major joints with patient relaxed in the sitting position) Rigidity - neck 0 = Absent 1 = Slight, detectable only with mirror movements 2 = Mild to moderate 3 = Marked, but full range of movement easily achieved 4 = Severe, range of movement achieved with difficulty Rigidity – Right upper limb 0 = Absent 1 = Slight, detectable only with mirror movements 2 = Mild to moderate 3 = Marked, but full range of movement easily achieved 4 = Severe, range of movement achieved with difficulty Rigidity – left upper limb 0 = Absent 1 = Slight, detectable only with mirror movements 2 = Mild to moderate 3 = Marked, but full range of movement easily achieved 4 = Severe, range of movement achieved with difficulty
23 24 25
Rigidity – right lower limb 0 = Absent 1 = Slight, detectable only with mirror movements 2 = Mild to moderate 3 = Marked, but full range of movement easily achieved 4 = Severe, range of movement achieved with difficulty Rigidity – left lower limb 0 = Absent 1 = Slight, detectable only with mirror movements 2 = Mild to moderate 3 = Marked, but full range of movement easily achieved 4 = Severe, range of movement achieved with difficulty Finger taps (patient taps thumb with index finger in rapid succession with widest amplitude possible) Finger taps - Right hand 0 = Normal 1 = Mild slowing and/or reduction in amplitude 2 = Definite & early fatiguing; occasional arrests 3 = Frequent hesitation in initiation or arrests in movement 4 = Can barely perform the task Finger taps - Left hand 0 = Normal 1 = Mild slowing and/or reduction in amplitude 2 = Definite & early fatiguing; occasional arrests 3 = Frequent hesitation in initiation or arrests in movement 4 = Can barely perform the task Hand movements (Patient opens & closes hands in rapid succession with widest amplitude possible) Hand movements – Right hand 0 = Normal 1 = Mild slowing and/or reduction in amplitude 2 = Definite & early fatiguing; occasional arrests 3 = Frequent hesitation in initiation or arrests in movement 4 = Can barely perform the task Hand movements – Left hand 0 = Normal 1 = Mild slowing and/or reduction in amplitude 2 = Definite & early fatiguing; occasional arrests 3 = Frequent hesitation in initiation or arrests in movement 4 = Can barely perform the task Rapidly alternating hand movements (pronation-supination movements with as large an amplitude as possible) Rapidly alternating hand movements – Right hand 0 = Normal 1 = Mild slowing and/or reduction in amplitude 2 = Definite & early fatiguing; occasional arrests 3 = Frequent hesitation in initiation or arrests in movement 4 = Can barely perform the task Rapidly alternating hand movements – Left hand 0 = Normal 1 = Mild slowing and/or reduction in amplitude 2 = Definite & early fatiguing; occasional arrests 3 = Frequent hesitation in initiation or arrests in movement 4 = Can barely perform the task

UPDRS, Hoehn & Yahr, Scwab & England_SVUH_MedEl_tools 4/4
26 27 28 29 30 31
Leg agility (rapid heel tapping. Amplitude ≥ 3 inches) Leg agility – Right heel 0 = Normal 1 = Mild slowing and/or reduction in amplitude 2 = Definite & early fatiguing; occasional arrests 3 = Frequent hesitation in initiation or arrests in movement 4 = Can barely perform the task Leg agility – Left heel 0 = Normal 1 = Mild slowing and/or reduction in amplitude 2 = Definite & early fatiguing; occasional arrests 3 = Frequent hesitation in initiation or arrests in movement 4 = Can barely perform the task Arising from a chair (patient’s arms across chest) 0 = Normal 1 = Slow; or may need more than 1 attempt 2 = Pushes self up from arms of seat 3 = May fall back or try more than once to get up 4 =Unable to arise without help Posture 0 = Normal erect 1 = Slightly stooped; could be normal for older person 2 = Moderately stooped; can be slightly leaning to 1 side 3 = Severely stooped with kyphosis; can be moderately leaning to one side 4 = Marked flexion with extreme abnormality of posture Gait 0 = Normal 1 = Walks slowly, short steps but no festination 2 = Walks with difficulty but without assistance; festination, short steps or propulsion 3 = Severely disturbed gait; requires assistance 4 =Cannot walk even with assistance Postural stability (pull test, may have practice runs) 0 = Normal 1 = Retropulsion, but recovers unaided 2 = Absence of posture response, would fall if not caught 3 = Very unstable, spontaneous loss of balance 4 = Unable to stand without assistance Body bradykinesia & hypokinesia (slowness, hesitancy, decreased arm swing, small amplitude & poverty of movement) 0 = None 1 = Minimal slowness, deliberate character, possibly reduced amplitude 2 = Mild slowness, poverty or small amplitude of movement 3 = Moderate slowness, poverty or small amplitude of movement 4 = Marked slowness, poverty or small amplitude of movement
IV A 32 33 34 35 B 36 37 38 39 C 40 41 42
Complications of therapy (in the past week) DYSKINESIAS Duration: What proportions of the waking day are dyskinesias present? 0 = None 1 = 1 – 25% of the day 2 = 26 – 50% of the day 3 = 51 – 75% of the day 4 =76 – 100% of the day Disability: How disabling are the dyskinesias? 0 = Not disabling 1 = Mildly disabling 2 = Moderately disabling 3 = Severely disabling 4 =Completely disabled Painful dyskinesias: How painful are the dyskinesias? 0 = None 1 = Slight 2 = Moderate 3 = Severe 4 =Marked Presence of early morning dystonias 0 = No 1 = Yes CLINICAL FLUCTUATIONS Are any ‘off’ periods predictable as to timing after medication dosing? 0 = No 1 = Yes Are any ‘off’ periods unpredictable as to timing after medication dosing? 0 = No 1 = Yes Do any of the ‘off’ periods come on suddenly (seconds)? 0 = No 1 = Yes What percentage of the waking day is the patient ’off’ on average? 0 = None 1 = 1 – 25% of the day 2 = 26 – 50% of the day 3 = 51 – 75% of the day 4 =76 – 100% of the day OTHER COMPLICATIONS Does the patient have anorexia nauseas or vomiting? 0 = No 1 = Yes Does the patient have any sleep disturbance? 0 = No 1 = Yes Does the patient have symptomatic orthostasis? 0 = No 1 = Yes

053 McKinly Lab University of Delaware Newark, Delaware 19716-2590 Ph: (302) 831-8893 Fax: (302) 831-4468 www.udel.edu/PT/
5X Sit-to-Stand Test (5XSST)
Description: Assesses functional lower extremity strength, transitional movements, balance, and fall risk. Equipment: Stopwatch; standard height chair with straight back (16 inches high); Therapist Instructions: Have the patient sit with their back against the back of the chair. Count each stand aloud so that the patient remains oriented. Stop the test when the patient achieves the standing position on the 5th repetition. Patient Instructions: “Please stand up straight as quickly as you can 5 times, without stopping in between. Keep your arms folded across your chest. I’ll be timing you with a stopwatch. Ready, begin.” Interpretation:
Lower times = better scores MDC: 3.6-4.2 sec1, 2
MCID: 2.3 sec3 Age-Matched Norms4:
Age Bracket Time (sec) 60-‐69 yo 11.4 70-‐79 yo 12.6 80-‐89 yo 14.8
Fall Risk:
Geriatrics -need for further assessment of fall risk: ≥ 12 sec5 -recurrent falls: > 15 sec6
Vestibular Disorders -fall risk: > 15 sec7
Parkinson’s Disease -fall risk: > 16 sec8
1 Schaubert, K. L. and Bohannon, R. W. (2005). "Reliability and validity of three strength measures obtained from community-dwelling elderly persons." J Strength Cond Res 19(3): 717-720. 2 Mong, Y., Teo, T. W., et al. (2010). "5-repetition sit-to-stand test in subjects with chronic stroke: reliability and validity." Archives of Physical Medicine and Rehabilitation 91(3): 407-413. 3 Meretta, B. M., Whitney, S. L., et al. (2006). "The five times sit to stand test: responsiveness to change and concurrent validity in adults undergoing vestibular rehabilitation." Journal of Vestibular Research 16(4-5): 233-243. 4 Bohannon RW. Reference values for the five-‐repetition sit-‐to-‐stand test: a descriptive metaanalysis of data from elders. Percept Mot Skills 2006; 103(1):215-‐222. 5 Tiedemann, A., Shimada, H., et al. (2008). "The comparative ability of eight functional mobility tests for predicting falls in community-dwelling older people." Age and Ageing 37(4): 430-435. 6 Buatois, S., Perret-Guillaume, C., et al. (2010). "A simple clinical scale to stratify risk of recurrent falls in community-dwelling adults aged 65 years and older." Physical Therapy 90(4): 550-560. 7 Buatois, S., Miljkovic, D., et al. (2008). "Five times sit to stand test is a predictor of recurrent falls in healthy community-living subjects aged 65 and older." Journal of the American Geriatrics Society 56(8): 1575-1577. 8 Duncan, R. P., Leddy, A. L., et al. (2011). "Five times sit-to-stand test performance in Parkinson's disease." Arch Phys Med Rehabil 92(9): 1431-1436.
PHYSICAL THERAPY CLINIC

Kurtzke Expanded Disability Status Scale (EDSS)
! 0.0 - Normal neurological exam (all grade 0 in all Functional System (FS) scores*). ! 1.0 - No disability, minimal signs in one FS* (i.e., grade 1). ! 1.5 - No disability, minimal signs in more than one FS* (more than 1 FS grade 1). ! 2.0 - Minimal disability in one FS (one FS grade 2, others 0 or 1). ! 2.5 - Minimal disability in two FS (two FS grade 2, others 0 or 1). ! 3.0 - Moderate disability in one FS (one FS grade 3, others 0 or 1) or mild disability in three or
four FS (three or four FS grade 2, others 0 or 1) though fully ambulatory. ! 3.5 - Fully ambulatory but with moderate disability in one FS (one grade 3) and one or two FS
grade 2; or two FS grade 3 (others 0 or 1) or five grade 2 (others 0 or 1). ! 4.0 - Fully ambulatory without aid, self-sufficient, up and about some 12 hours a day despite
relatively severe disability consisting of one FS grade 4 (others 0 or 1), or combination of lesser grades exceeding limits of previous steps; able to walk without aid or rest some 500 meters.
! 4.5 - Fully ambulatory without aid, up and about much of the day, able to work a full day, may
otherwise have some limitation of full activity or require minimal assistance; characterized by relatively severe disability usually consisting of one FS grade 4 (others or 1) or combinations of lesser grades exceeding limits of previous steps; able to walk without aid or rest some 300 meters.
! 5.0 - Ambulatory without aid or rest for about 200 meters; disability severe enough to impair
full daily activities (e.g., to work a full day without special provisions); (Usual FS equivalents are one grade 5 alone, others 0 or 1; or combinations of lesser grades usually exceeding specifications for step 4.0).
! 5.5 - Ambulatory without aid for about 100 meters; disability severe enough to preclude full
daily activities; (Usual FS equivalents are one grade 5 alone, others 0 or 1; or combination of lesser grades usually exceeding those for step 4.0).
! 6.0 - Intermittent or unilateral constant assistance (cane, crutch, brace) required to walk about
100 meters with or without resting; (Usual FS equivalents are combinations with more than two FS grade 3+).

! 6.5 - Constant bilateral assistance (canes, crutches, braces) required to walk about 20 meters without resting; (Usual FS equivalents are combinations with more than two FS grade 3+).
! 7.0 - Unable to walk beyond approximately 5 meters even with aid, essentially restricted to
wheelchair; wheels self in standard wheelchair and transfers alone; up and about in wheelchair some 12 hours a day; (Usual FS equivalents are combinations with more than one FS grade 4+; very rarely pyramidal grade 5 alone).
! 7.5 - Unable to take more than a few steps; restricted to wheelchair; may need aid in transfer;
wheels self but cannot carry on in standard wheelchair a full day; May require motorized wheelchair; (Usual FS equivalents are combinations with more than one FS grade 4+).
! 8.0 - Essentially restricted to bed or chair or perambulated in wheelchair, but may be out of
bed itself much of the day; retains many self-care functions; generally has effective use of arms; (Usual FS equivalents are combinations, generally grade 4+ in several systems).
! 8.5 - Essentially restricted to bed much of day; has some effective use of arm(s); retains some
self-care functions; (Usual FS equivalents are combinations, generally 4+ in several systems).
! 9.0 - Helpless bed patient; can communicate and eat; (Usual FS equivalents are
combinations, mostly grade 4+). ! 9.5 - Totally helpless bed patient; unable to communicate effectively or eat/swallow; (Usual FS
equivalents are combinations, almost all grade 4+). ! 10.0 - Death due to MS.
*Excludes cerebral function grade 1. Note 1: EDSS steps 1.0 to 4.5 refer to patients who are fully ambulatory and the precise step
number is defined by the Functional System score(s). EDSS steps 5.0 to 9.5 are defined by the impairment to ambulation and usual equivalents in Functional Systems scores are provided.
Note 2: EDSS should not change by 1.0 step unless there is a change in the same direction of at
least one step in at least one FS. Sources: Kurtzke JF. Rating neurologic impairment in multiple sclerosis: an expanded disability status scale (EDSS).
Neurology. 1983 Nov;33(11):1444-52. Haber A, LaRocca NG. eds. Minimal Record of Disability for multiple sclerosis. New York: National Multiple
Sclerosis Society; 1985.

Kurtzke Functional Systems Scores (FSS)
! Pyramidal Functions 0 - Normal 1 - Abnormal signs without disability 2 - Minimal disability 3 - Mild to moderate paraparesis or hemiparesis (detectable weakness but most
function sustained for short periods, fatigue a problem); severe monoparesis (almost no function)
4 - Marked paraparesis or hemiparesis (function is difficult), moderate quadriparesis (function is decreased but can be sustained for short periods); or monoplegia
5 - Paraplegia, hemiplegia, or marked quadriparesis 6 - Quadriplegia 9 - (Unknown)
! Cerebellar Functions 0 - Normal 1 - Abnormal signs without disability 2 - Mild ataxia (tremor or clumsy movements easily seen, minor interference with
function) 3 - Moderate truncal or limb ataxia (tremor or clumsy movements interfere with function
in all shpheres) 4 - Severe ataxia in all limbs (most function is very difficult) 5 - Unable to perform coordinated movements due to ataxia 9 - (Unknown)
! Record #1 in small box when weakness (grade 3 or worse on pyramidal) interferes with testing.
! Brainstem Functions 0 - Normal 1 - Signs only 2 - Moderate nystagmus or other mild disability 3 - Severe nystagmus, marked extraocular weakness, or moderate disability of other
cranial nerves 4 - Marked dysarthria or other marked disability 5 - Inability to swallow or speak 9 - (Unknown)
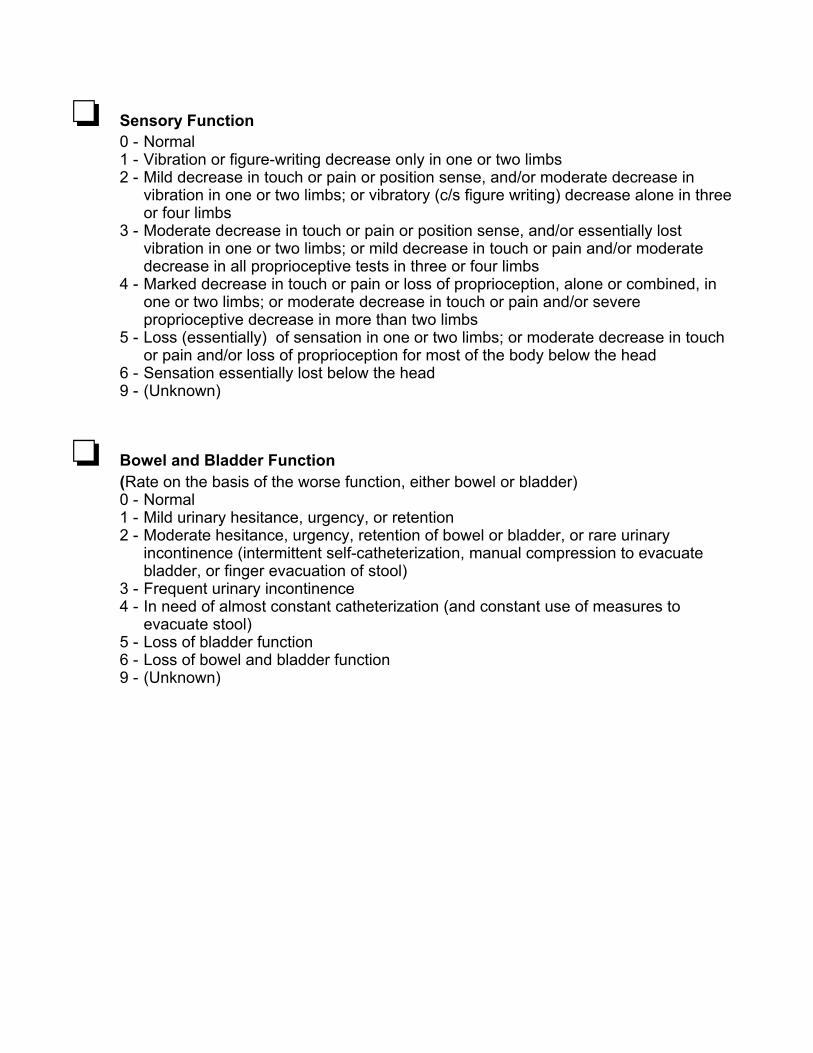
! Sensory Function 0 - Normal 1 - Vibration or figure-writing decrease only in one or two limbs 2 - Mild decrease in touch or pain or position sense, and/or moderate decrease in
vibration in one or two limbs; or vibratory (c/s figure writing) decrease alone in three or four limbs
3 - Moderate decrease in touch or pain or position sense, and/or essentially lost vibration in one or two limbs; or mild decrease in touch or pain and/or moderate decrease in all proprioceptive tests in three or four limbs
4 - Marked decrease in touch or pain or loss of proprioception, alone or combined, in one or two limbs; or moderate decrease in touch or pain and/or severe proprioceptive decrease in more than two limbs
5 - Loss (essentially) of sensation in one or two limbs; or moderate decrease in touch or pain and/or loss of proprioception for most of the body below the head
6 - Sensation essentially lost below the head 9 - (Unknown)
! Bowel and Bladder Function (Rate on the basis of the worse function, either bowel or bladder)
0 - Normal 1 - Mild urinary hesitance, urgency, or retention 2 - Moderate hesitance, urgency, retention of bowel or bladder, or rare urinary
incontinence (intermittent self-catheterization, manual compression to evacuate bladder, or finger evacuation of stool)
3 - Frequent urinary incontinence 4 - In need of almost constant catheterization (and constant use of measures to
evacuate stool) 5 - Loss of bladder function 6 - Loss of bowel and bladder function 9 - (Unknown)

! Visual Function 0 - Normal 1 - Scotoma with visual acuity (corrected) better than 20/30 2 - Worse eye with scotoma with maximal visual acuity (corrected) of 20/30ñ20/59 3 - Worse eye with large scotoma, or moderate decrease in fields, but with maximal
visual acuity (corrected) of 20/60ñ20/99 4 - Worse eye with marked decrease of fields and maximal visual acuity (corrected) of
20/100ñ20/200; grade 3 plus maximal acuity of better eye of 20/60 or less 5 - Worse eye with maximal visual acuity (corrected) less than 20/200; grade 4 plus
maximal acuity of better eye of 20/60 or less 6 - Grade 5 plus maximal visual acuity of better eye of 20/60 or less 9 - (Unknown)
! Record #1 in small box for presence of temporal pallor
! Cerebral (or Mental) Functions 0 - Normal 1 - Mood alteration only (does not affect EDSS score) 2 - Mild decrease in mentation 3 - Moderate decrease in mentation 4 - Marked decrease in mentation (chronic brain syndrome ñ moderate) 5 - Dementia or chronic brain syndrome ñ severe or incompetent 9 - (Unknown)
Sources: Kurtzke JF. Rating neurologic impairment in multiple sclerosis: an expanded disability status scale (EDSS). Neurology. 1983 Nov;33(11):1444-52.
Haber A, LaRocca NG. eds. Minimal Record of Disability for multiple sclerosis. New York: National
Multiple Sclerosis Society; 1985.
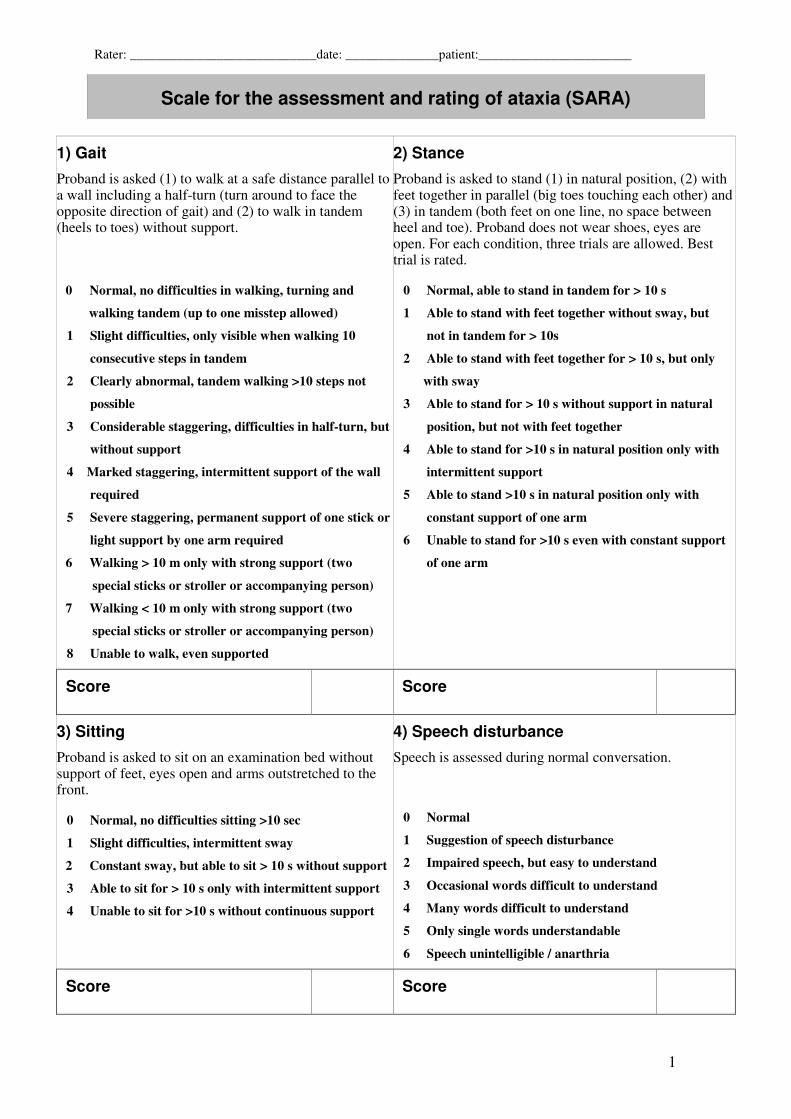
Rater: ____________________________date: ______________patient:_______________________
1
Scale for the assessment and rating of ataxia (SARA)
1) Gait
Proband is asked (1) to walk at a safe distance parallel to a wall including a half-turn (turn around to face the opposite direction of gait) and (2) to walk in tandem (heels to toes) without support.
0 Normal, no difficulties in walking, turning and
walking tandem (up to one misstep allowed)
1 Slight difficulties, only visible when walking 10
consecutive steps in tandem
2 Clearly abnormal, tandem walking >10 steps not
possible
3 Considerable staggering, difficulties in half-turn, but
without support
4 Marked staggering, intermittent support of the wall
required
5 Severe staggering, permanent support of one stick or
light support by one arm required
6 Walking > 10 m only with strong support (two
special sticks or stroller or accompanying person)
7 Walking < 10 m only with strong support (two
special sticks or stroller or accompanying person)
8 Unable to walk, even supported
2) Stance
Proband is asked to stand (1) in natural position, (2) with feet together in parallel (big toes touching each other) and (3) in tandem (both feet on one line, no space between heel and toe). Proband does not wear shoes, eyes are open. For each condition, three trials are allowed. Best trial is rated. 0 Normal, able to stand in tandem for > 10 s
1 Able to stand with feet together without sway, but
not in tandem for > 10s
2 Able to stand with feet together for > 10 s, but only
with sway
3 Able to stand for > 10 s without support in natural
position, but not with feet together
4 Able to stand for >10 s in natural position only with
intermittent support
5 Able to stand >10 s in natural position only with
constant support of one arm
6 Unable to stand for >10 s even with constant support
of one arm
Score Score
3) Sitting
Proband is asked to sit on an examination bed without support of feet, eyes open and arms outstretched to the front. 0 Normal, no difficulties sitting >10 sec
1 Slight difficulties, intermittent sway
2 Constant sway, but able to sit > 10 s without support
3 Able to sit for > 10 s only with intermittent support
4 Unable to sit for >10 s without continuous support
4) Speech disturbance
Speech is assessed during normal conversation. 0 Normal
1 Suggestion of speech disturbance
2 Impaired speech, but easy to understand
3 Occasional words difficult to understand
4 Many words difficult to understand
5 Only single words understandable
6 Speech unintelligible / anarthria
Score Score

Rater: ____________________________date: ______________patient:_______________________
2
5) Finger chase
Rated separately for each side Proband sits comfortably. If necessary, support of feet and trunk is allowed. Examiner sits in front of proband and performs 5 consecutive sudden and fast pointing movements in unpredictable directions in a frontal plane, at about 50 % of proband´s reach. Movements have an amplitude of 30 cm and a frequency of 1 movement every 2 s. Proband is asked to follow the movements with his index finger, as fast and precisely as possible. Average performance of last 3 movements is rated. 0 No dysmetria
1 Dysmetria, under/ overshooting target <5 cm
2 Dysmetria, under/ overshooting target < 15 cm
3 Dysmetria, under/ overshooting target > 15 cm
4 Unable to perform 5 pointing movements
6) Nose-finger test
Rated separately for each side Proband sits comfortably. If necessary, support of feet and trunk is allowed. Proband is asked to point repeatedly with his index finger from his nose to examiner’s finger which is in front of the proband at about 90 % of proband’s reach. Movements are performed at moderate speed. Average performance of movements is rated according to the amplitude of the kinetic tremor. 0 No tremor
1 Tremor with an amplitude < 2 cm
2 Tremor with an amplitude < 5 cm
3 Tremor with an amplitude > 5 cm
4 Unable to perform 5 pointing movements
Score Right Left Score Right Left
mean of both sides (R+L)/2 mean of both sides (R+L)/2
7) Fast alternating hand movements
Rated separately for each side Proband sits comfortably. If necessary, support of feet and trunk is allowed. Proband is asked to perform 10 cycles of repetitive alternation of pro- and supinations of the hand on his/her thigh as fast and as precise as possible. Movement is demonstrated by examiner at a speed of approx. 10 cycles within 7 s. Exact times for movement execution have to be taken. 0 Normal, no irregularities (performs <10s)
1 Slightly irregular (performs <10s)
2 Clearly irregular, single movements difficult
to distinguish or relevant interruptions, but
performs <10s
3 Very irregular, single movements difficult
to distinguish or relevant interruptions,
performs >10s
4 Unable to complete 10 cycles
8) Heel-shin slide
Rated separately for each side Proband lies on examination bed, without sight of his legs. Proband is asked to lift one leg, point with the heel to the opposite knee, slide down along the shin to the ankle, and lay the leg back on the examination bed. The task is performed 3 times. Slide-down movements should be performed within 1 s. If proband slides down without contact to shin in all three trials, rate 4. 0 Normal
1 Slightly abnormal, contact to shin maintained
2 Clearly abnormal, goes off shin up to 3 times
during 3 cycles
3 Severely abnormal, goes off shin 4 or more times
during 3 cycles
4 Unable to perform the task
Score Right Left Score Right Left
mean of both sides (R+L)/2 mean of both sides (R+L) / 2

FALL PROOF PROGRAM: CENTER FOR SUCCESSFUL AGING, CAL STATE FULLERTON
Modified Clinical Test of Sensory Interaction in Balance (CTSIB-M)
*Administer only one trial per condition if participant able to complete first trial without loss of balance.
Condition One: Eyes Open, Firm Surface Trial One Total Time: _______ / 30 sec
Trial Two Total Time: _______ / 30 sec Trial Three Total Time: _______ / 30 sec Condition Two: Eyes Closed, Firm Surface
Trial One Total Time: _______ / 30 sec Trial Two Total Time: _______ / 30 sec Trial Three Total Time: _______ / 30 sec Condition Three: Eyes Open, Foam Surface
Trial One Total Time: _______ / 30 sec Trial Two Total Time: _______ / 30 sec Trial Three Total Time: _______ / 30 sec Condition Four: Eyes Closed, Foam Surface
Trial One Total Time: _______ / 30 sec Trial Two Total Time: _______ / 30 sec Trial Three Total Time: _______ / 30 sec
TOTAL: _______ / 120 sec Purpose of Test: This test is designed to assess how well an older adult is using sensory inputs when one or more sensory systems are compromised. In condition one, all sensory systems (i.e., vision, somatosensory, and vestibular) are available for maintaining balance. In condition two, vision has been removed and the older adult must rely on the somatosensory and vestibular systems to balance. In condition three, the somatosensory system has been compromised and the older adults must use vision and the vestibular system to balance. In condition four, vision has been removed and the somatosensory system has been compromised. The older adults must not rely primarily on the vestibular inputs to balance. Begin timing each trial using a stopwatch. The trial is over when (a) the participant opens his/her eyes in an eyes closed condition, (b) raises arms from sides, (c) loses balance and requires manual assistance to prevent a fall. This test provides some insight into whether each of the sensory system available for balance are being used effectively. Failure to maintain balance in condition two indicates that the older adults is visually dependent. They are not using somatosensory inputs to maintain balance when eyes are closed. Failure to maintain balance in conditions 3 and 4 indicate that the visual and/or vestibular system is not being used to maintain balance. Poor performance on this test would suggest the need for multisensory training if the medial history does not indicate that

FALL PROOF PROGRAM: CENTER FOR SUCCESSFUL AGING, CAL STATE FULLERTON an actual problem(s) exists (e.g., peripheral neuropathy will affect our ability to use somatosensory inputs, etc.). Check medical history to determine whether the participants has a history of inner ear infections or an inner ear disorder (e.g., meniere’s disease, acoustic neuroma, etc.)
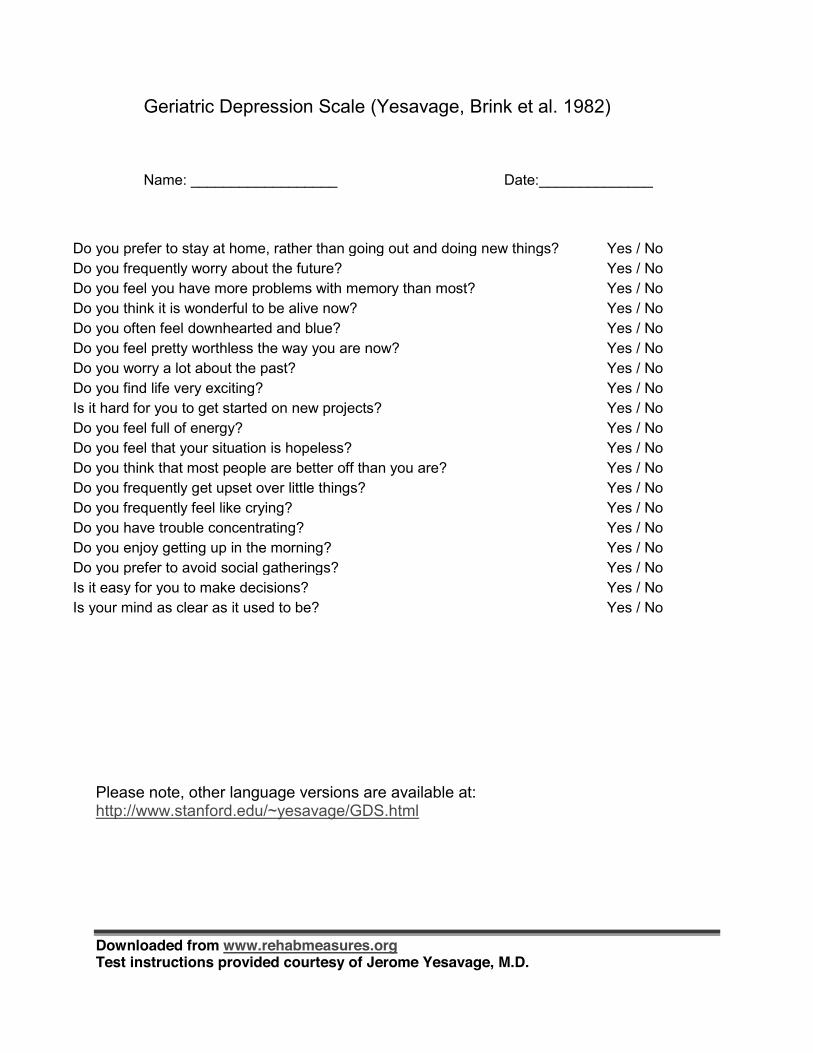
Downloaded from www.rehabmeasures.org Test instructions provided courtesy of Jerome Yesavage, M.D.
Geriatric Depression Scale (Yesavage, Brink et al. 1982)
Name: __________________ Date:______________
Do you prefer to stay at home, rather than going out and doing new things? Yes / No Do you frequently worry about the future? Yes / No Do you feel you have more problems with memory than most? Yes / No Do you think it is wonderful to be alive now? Yes / No Do you often feel downhearted and blue? Yes / No Do you feel pretty worthless the way you are now? Yes / No Do you worry a lot about the past? Yes / No Do you find life very exciting? Yes / No Is it hard for you to get started on new projects? Yes / No Do you feel full of energy? Yes / No Do you feel that your situation is hopeless? Yes / No Do you think that most people are better off than you are? Yes / No Do you frequently get upset over little things? Yes / No Do you frequently feel like crying? Yes / No Do you have trouble concentrating? Yes / No Do you enjoy getting up in the morning? Yes / No Do you prefer to avoid social gatherings? Yes / No Is it easy for you to make decisions? Yes / No Is your mind as clear as it used to be? Yes / No
Please note, other language versions are available at: http://www.stanford.edu/~yesavage/GDS.html
Downloaded from www.rehabmeasures.org Test instructions provided courtesy of Jerome Yesavage, M.D.
References: Yesavage, J. A., T. L. Brink, et al. (1982). "Development and validation of a geriatric depression screening
scale: a preliminary report." J Psychiatr Res 17(1): 37-49.
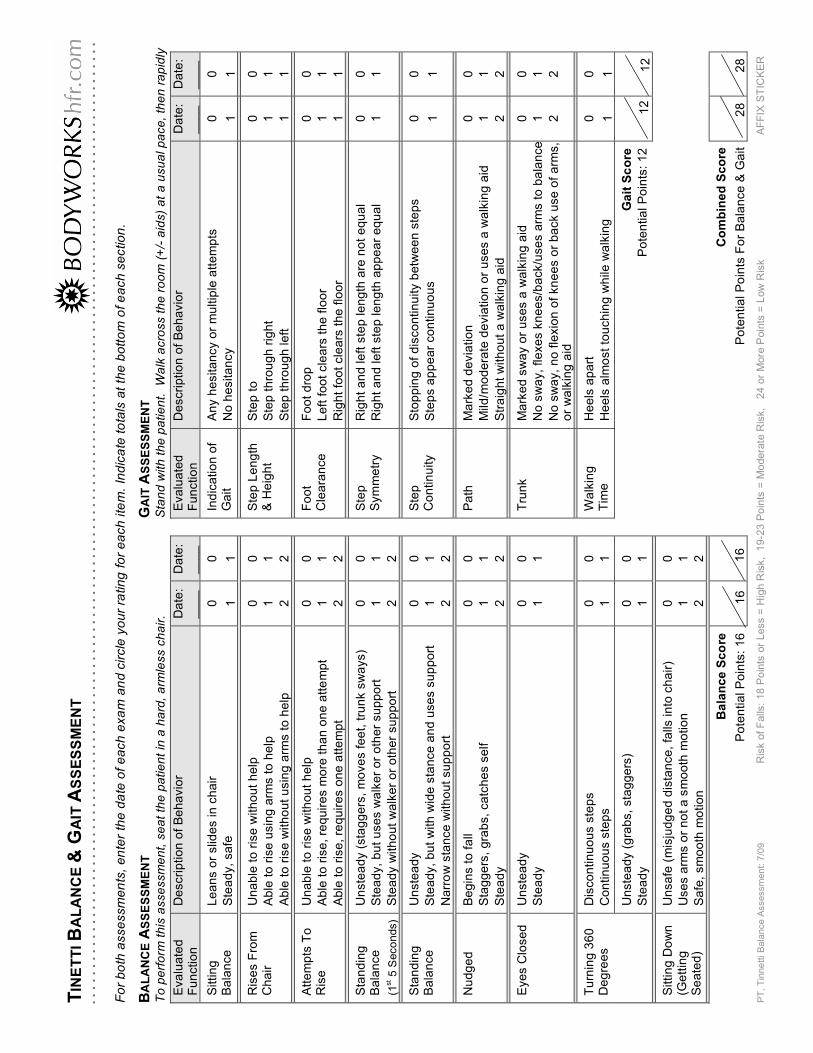
PT
, T
inne
tti B
ala
nce A
ssessm
ent: 7
/09
R
isk o
f F
alls
: 18 P
oin
ts o
r Less =
Hig
h R
isk, 1
9-2
3 P
oin
ts =
Mo
dera
te R
isk,
24 o
r M
ore
Poin
ts =
Low
Ris
k
AF
FIX
ST
ICK
ER
TIN
ET
TI B
AL
AN
CE
& G
AIT
AS
SE
SS
ME
NT
Fo
r b
oth
asse
ssm
en
ts,
en
ter
the
da
te o
f e
ach
exa
m a
nd
cir
cle
yo
ur
ratin
g f
or
ea
ch
ite
m.
Ind
ica
te t
ota
ls a
t th
e b
ott
om
of e
ach
se
ctio
n.
BA
LA
NC
E A
SS
ES
SM
EN
T
GA
IT A
SS
ES
SM
EN
T
To
pe
rfo
rm t
his
asse
ssm
en
t, s
ea
t th
e p
atie
nt
in a
ha
rd,
arm
less c
ha
ir.
Sta
nd
with
th
e p
atie
nt.
W
alk
acro
ss t
he
ro
om
(+
/- a
ids)
at
a u
su
al p
ace
, th
en
ra
pid
ly
Eva
lua
ted
F
un
ctio
n
De
scri
ptio
n o
f B
eh
avio
r D
ate
: _
__
_
Da
te:
__
__
Eva
lua
ted
F
un
ctio
n
De
scri
ptio
n o
f B
eh
avio
r D
ate
: _
__
_
Da
te:
__
__
Sittin
g
Ba
lan
ce
L
ea
ns o
r slid
es in
ch
air
Ste
ad
y,
sa
fe
0
1
0
1
In
dic
atio
n o
f G
ait
An
y h
esita
ncy o
r m
ultip
le a
tte
mp
ts
No
he
sita
ncy
0
1
0
1
Ris
es F
rom
C
ha
ir
Un
ab
le t
o r
ise
with
ou
t h
elp
Ab
le t
o r
ise
usin
g a
rms t
o h
elp
Ab
le t
o r
ise
with
ou
t u
sin
g a
rms t
o h
elp
0
1
2
0
1
2
S
tep
Le
ng
th
& H
eig
ht
Ste
p t
o
Ste
p t
hro
ug
h r
igh
t
Ste
p t
hro
ug
h le
ft
0
1
1
0
1
1
Att
em
pts
To
R
ise
U
na
ble
to
ris
e w
ith
ou
t h
elp
Ab
le t
o r
ise
, re
qu
ire
s m
ore
th
an
on
e a
tte
mp
t
Ab
le t
o r
ise
, re
qu
ire
s o
ne
att
em
pt
0
1
2
0
1
2
F
oo
t C
lea
ran
ce
F
oo
t d
rop
Le
ft f
oo
t cle
ars
th
e f
loo
r
Rig
ht
foo
t cle
ars
th
e f
loo
r
0
1
1
0
1
1
Sta
nd
ing
B
ala
nce
(1st 5
Seco
nds)
Un
ste
ad
y (
sta
gg
ers
, m
ove
s f
ee
t, t
run
k s
wa
ys)
Ste
ad
y,
bu
t u
se
s w
alk
er
or
oth
er
su
pp
ort
Ste
ad
y w
ith
ou
t w
alk
er
or
oth
er
su
pp
ort
0
1
2
0
1
2
S
tep
S
ym
me
try
Rig
ht
an
d le
ft s
tep
le
ng
th a
re n
ot
eq
ua
l
Rig
ht
an
d le
ft s
tep
le
ng
th a
pp
ea
r e
qu
al
0
1
0
1
Sta
nd
ing
B
ala
nce
U
nste
ad
y
Ste
ad
y,
bu
t w
ith
wid
e s
tan
ce
an
d u
se
s s
up
po
rt
Na
rro
w s
tan
ce
with
ou
t su
pp
ort
0
1
2
0
1
2
S
tep
C
on
tin
uity
Sto
pp
ing
of
dis
co
ntin
uity b
etw
ee
n s
tep
s
Ste
ps a
pp
ea
r co
ntin
uo
us
0
1
0
1
Nu
dg
ed
B
eg
ins t
o f
all
Sta
gg
ers
, g
rab
s,
ca
tch
es s
elf
Ste
ad
y
0
1
2
0
1
2
P
ath
M
ark
ed
de
via
tio
n
Mild
/mo
de
rate
de
via
tio
n o
r u
se
s a
wa
lkin
g a
id
Str
aig
ht
with
ou
t a
wa
lkin
g a
id
0
1
2
0
1
2
Eye
s C
lose
d
Un
ste
ad
y
Ste
ad
y
0
1
0
1
T
run
k
Ma
rke
d s
wa
y o
r u
se
s a
wa
lkin
g a
id
No
sw
ay,
fle
xe
s k
ne
es/b
ack/u
se
s a
rms t
o b
ala
nce
No
sw
ay,
no
fle
xio
n o
f kn
ee
s o
r b
ack u
se
of
arm
s,
or
wa
lkin
g a
id
0
1
2
0
1
2
Dis
co
ntin
uo
us s
tep
s
Co
ntin
uo
us s
tep
s
0
1
0
1
W
alk
ing
T
ime
H
ee
ls a
pa
rt
He
els
alm
ost
tou
ch
ing
wh
ile w
alk
ing
0
1
0
1
Tu
rnin
g 3
60
D
eg
ree
s
Un
ste
ad
y (
gra
bs,
sta
gg
ers
)
Ste
ad
y
0
1
0
1
Ga
it S
co
re
Po
ten
tia
l P
oin
ts:
12
12
1
2
Sittin
g D
ow
n
(Ge
ttin
g
Se
ate
d)
Un
sa
fe (
mis
jud
ge
d d
ista
nce
, fa
lls in
to c
ha
ir)
Use
s a
rms o
r n
ot
a s
mo
oth
mo
tio
n
Sa
fe,
sm
oo
th m
otio
n
0
1
2
0
1
2
B
ala
nc
e S
co
re
Po
ten
tia
l P
oin
ts:
16
16
16
Co
mb
ine
d S
co
re
Po
ten
tia
l P
oin
ts F
or
Ba
lan
ce
& G
ait
2
8
2
8
. .
. .
. .
. .
. .
. . .
. .
. .
. .
. .
. . .
. .
. .
. .
. .
. .
. .
. .
. .
. .
. .
. .
. .
. . .
. .
. .
. .
. .
. .
. .
. .
. .
. .
. .
. . .
. .
. .
. .
. .
. .
. .
. .
. . .
. .
. .
. .
. .
. . .
. .
. .
. .
. .
. . .
. .
. .
. .
. .
. .
. .
. .
. .
. .
.




















