
The high burden of cervical cancer in Fiji, 2004?07
8
The high burden of cervical cancer in Fiji, 2004–07 Irwin Law A,B,H , James J. Fong C , Eka M. Buadromo C , Josaia Samuela C , Mahomed S. Patel A , Suzanne M. Garland D,E , E. Kim Mulholland F,G and Fiona M. Russell B A National Centre for Epidemiology and Population Health, Australian National University, Acton, ACT 0200, Australia. B Centre for International Child Health, Department of Paediatrics, University of Melbourne, Australia Murdoch Childrens Research Institute, Royal Children’s Hospital, Parkville, Vic. 3052, Australia. C Ministry of Health, Suva, Fiji. D Department of Obstetrics and Gynaecology, University of Melbourne, The Royal Women’s Hospital and Murdoch Childrens Research Institute, Parkville, Vic. 3052, Australia. E Regional WHO HPV Reference Laboratory, Department of Microbiology and Infectious Disease, The Royal Women’s Hospital, Parkville, Vic. 3052, Australia. F London School of Hygiene and Tropical Medicine, University of London, Keppel Street, London, WC1E7HT, UK. G Menzies School of Health Research, Charles Darwin University, Darwin, NT 0811, Australia. H Corresponding author. Email: [email protected] Abstract. Background: There are few population-based data on the disease burden of cervical cancer from developing countries, especially South Pacific islands. This study aimed to determine the incidence and mortality associated with cervical cancer and the coverage of Papanicolaou (Pap) cervical cytology in 20- to 69-year-old women in Fiji from 2004 to 2007. Methods: National data on the incident cases of histologically confirmed cervical cancer and the associated deaths, and on Pap smear results were collected from all pathology laboratories, and cancer and death registries in Fiji from 2004 to 2007. Results: There were 413 incident cases of cervical cancer and 215 related deaths during the study timeframe. The annualised incidence and mortality rates in 20- to 69-year-old Melanesian Fijian women, at 49.7 per 100 000 (95% confidence interval (CI): 43.7–56.4) and 32.3 per 100 000 (95% CI: 26.9–38.4) respectively, were significantly higher than among 20- to 69-year-old Indo-Fijian women at 35.2 per 100 000 (P < 0.001, 95% CI: 29.5–41.7) and 19.8 per 100 000 (P = 0.002, 95% CI: 15.1–25.5) respectively. Of 330 cases diagnosed between 2004 and 2006, 186 (56%) had died by 31 December 2006. Pap smear coverage for this period was 8.0% (95% CI: 7.9–8.1) of the target population. Conclusions: The incidence and mortality related to cervical cancer in Fiji is high, whereas Pap smear coverage is very low. Greater investment in alternative screening strategies and preventive measures should be integrated into a comprehensive, strategic cervical cancer control program in Fiji. Additional keywords: epidemiology, human papillomavirus, Pap smear, South Pacific. Received 16 August 2012, accepted 2 December 2012, published online 5 April 2013 Introduction Cervical cancer is the third most common cancer in women worldwide, affecting 1.4 million, with a reported 529 000 incident cases and 275 000 deaths annually. 1 More than 85% of new cases and related deaths occur in developing countries, with more than 50% occurring in the Asia–Oceanic region. It is also the most common cancer in women from Eastern Africa, South and Central Asia, and Melanesia. However, incidence varies among countries and among subpopulations within countries. 2–4 Cervical cancer screening programs have been very effective in providing secondary prevention, and in reducing the incidence and mortality due to cervical cancer in developed countries. 5,6 Irrespective of the available screening tests, such programs have its greatest impact when they are highly organised (i.e. a national policy implemented with efficient mechanisms for recall and reminders, and quality assurance). However in developing countries, constraints in skilled human and laboratory resources, low coverage rates in high-risk groups, a lack of health care access and follow-up, inadequate quality screening and treatment facilities, and economic costs limit the effectiveness of cytological screening. 7 More than 80% of women from developed countries (e.g. the United Kingdom and Australia) within a given 5-year period have at least one CSIRO PUBLISHING Sexual Health http://dx.doi.org/10.1071/SH12135 Journal compilation Ó CSIRO 2013 www.publish.csiro.au/journals/sh
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of The high burden of cervical cancer in Fiji, 2004?07

The high burden of cervical cancer in Fiji, 2004–07
Irwin LawA,B,H, James J. FongC, Eka M. BuadromoC, Josaia SamuelaC, Mahomed S. PatelA,Suzanne M. GarlandD,E, E. Kim MulhollandF,G and Fiona M. RussellB
ANational Centre for Epidemiology and Population Health, Australian National University, Acton,ACT 0200, Australia.
BCentre for International Child Health, Department of Paediatrics, University of Melbourne,Australia Murdoch Childrens Research Institute, Royal Children’s Hospital,Parkville, Vic. 3052, Australia.
CMinistry of Health, Suva, Fiji.DDepartment of Obstetrics and Gynaecology, University of Melbourne, The Royal Women’s Hospital andMurdoch Childrens Research Institute, Parkville, Vic. 3052, Australia.
ERegional WHO HPV Reference Laboratory, Department of Microbiology and Infectious Disease,The Royal Women’s Hospital, Parkville, Vic. 3052, Australia.FLondon School of Hygiene and Tropical Medicine, University of London, Keppel Street, London,WC1E7HT, UK.GMenzies School of Health Research, Charles Darwin University, Darwin, NT 0811, Australia.HCorresponding author. Email: [email protected]
Abstract. Background: There are few population-based data on the disease burden of cervical cancer from developingcountries, especially South Pacific islands. This study aimed to determine the incidence and mortality associated withcervical cancer and the coverage of Papanicolaou (Pap) cervical cytology in 20- to 69-year-old women in Fiji from 2004 to2007. Methods: National data on the incident cases of histologically confirmed cervical cancer and the associated deaths,and on Pap smear results were collected from all pathology laboratories, and cancer and death registries in Fiji from 2004to 2007. Results: There were 413 incident cases of cervical cancer and 215 related deaths during the study timeframe.The annualised incidence and mortality rates in 20- to 69-year-old Melanesian Fijian women, at 49.7 per 100 000 (95%confidence interval (CI): 43.7–56.4) and 32.3 per 100 000 (95% CI: 26.9–38.4) respectively, were significantly higher thanamong 20- to 69-year-old Indo-Fijian women at 35.2 per 100 000 (P< 0.001, 95% CI: 29.5–41.7) and 19.8 per 100 000(P = 0.002, 95% CI: 15.1–25.5) respectively. Of 330 cases diagnosed between 2004 and 2006, 186 (56%) had died by 31December 2006. Pap smear coverage for this period was 8.0% (95% CI: 7.9–8.1) of the target population. Conclusions:The incidence and mortality related to cervical cancer in Fiji is high, whereas Pap smear coverage is very low. Greaterinvestment in alternative screening strategies and preventive measures should be integrated into a comprehensive, strategiccervical cancer control program in Fiji.
Additional keywords: epidemiology, human papillomavirus, Pap smear, South Pacific.
Received 16 August 2012, accepted 2 December 2012, published online 5 April 2013
IntroductionCervical cancer is the third most common cancer in womenworldwide, affecting 1.4million, with a reported 529 000incident cases and 275 000 deaths annually.1 More than 85%of new cases and related deaths occur in developing countries,with more than 50% occurring in the Asia–Oceanic region. It isalso the most common cancer in women from Eastern Africa,South and Central Asia, and Melanesia. However, incidencevaries among countries and among subpopulations withincountries.2–4
Cervical cancer screening programs have been very effectivein providing secondary prevention, and in reducing the
incidence and mortality due to cervical cancer in developedcountries.5,6 Irrespective of the available screening tests, suchprograms have its greatest impact when they are highlyorganised (i.e. a national policy implemented with efficientmechanisms for recall and reminders, and quality assurance).However in developing countries, constraints in skilled humanand laboratory resources, low coverage rates in high-risk groups,a lack of health care access and follow-up, inadequate qualityscreening and treatment facilities, and economic costs limit theeffectiveness of cytological screening.7 More than 80% ofwomen from developed countries (e.g. the United Kingdomand Australia) within a given 5-year period have at least one
CSIRO PUBLISHING
Sexual Healthhttp://dx.doi.org/10.1071/SH12135
Journal compilation ! CSIRO 2013 www.publish.csiro.au/journals/sh

Papanicolaou (Pap) smear, whereas participation is less than5% in low-income countries.5,8 Similarly, inequities insocioeconomic status impact on screening coverage, not onlyamong but also within countries.9 Given the challenges ofimplementing a quality-assured cytology-based screeningmethod in low-resourced countries, screening modalitiesbased on visual inspection and treatment methods, andhuman papillomavirus (HPV) DNA testing hold significantpromise.10–14
Since 1995, Fiji has been one of the few lower-middleincome countries in the world to implement cytology-basedcervical cancer screening. Over the past decade, cervical cancerwas the most common cancer, accounting for 19% of all cancersin Fiji, and the leading cause of cancer-related deaths (FijianMinistry of Health (MoH), unpubl. data). However, thepopulation-based cancer register was known to have majorunder-reporting of all types of cancer cases, with manyincomplete registrations.15
Primary prevention of cervical cancer includes the vaccinesdirected at the causal agent, the oncogenic types ofHPV. Although both the currently licensed HPV vaccines arehighly effective in preventing the high-grade cervical lesionsassociated with HPV-16 and HPV-18, the affordability, cost-effectiveness and sustainability of their implementationinfluences policy making.16,17 Country-based epidemiologicaldata are therefore needed to determine the burden of cervicalcancer to inform such vaccination policies. The current data oncervical cancer are primarily from developed countries, withvery few published studies documenting the extent of the diseasein South Pacific island countries and territories, especially inrecent decades.15,18–23 Thus in order to address these issues, wedetermined the incidence and mortality associated with cervicalcancer, as well as Pap smear coverage, in Fiji.
MethodsEthical approvalThe study was approved by the Fiji National Research EthicsReview Committee (no. 010–2007) and the University ofMelbourne Human Research Ethics Committee (no. 0715797.1).
Study siteThe South Pacific island nation of Fiji has a populationof 837 271 across more than 300 islands.24 It is primarilycomprised of indigenous Fijians (57%), who arepredominantly Melanesian with mixed Polynesian ethnicity;and Indo-Fijians (37%), who are of Indian ethnicity. Chinese,Europeans, Rotumans and other Pacific Islanders make up theremainder. Approximately two-thirds of the population areover 15 years of age and half the population lives in ruralareas.24 At present, Fiji is a lower-middle income country with4% of its GDP spent on health, with an under-5 mortality rateof 18 per 1000 live births, a maternal mortality ratio of 26 per100 000 live births and has a physician-to-population ratio of4.5 per 10 000.25 The government provides all health services forfree, with the private sector making up a very small proportion ofservices.
National cervical cancer screening guidelines weredeveloped as part of Fiji’s overall cancer control program
policy in 1995. The MoH recommends that Pap smears beundertaken once every 3 years in women of childbearing age,starting 2 years after sexual debut. However, due to limitations inhuman resources, the MoH has limited the number of Papsmears undertaken to ~20 000 per annum. There is no formalpatient reminder and recall system currently in place for Papsmears, with limited advocacy and mobilisation activities. Papsmears are usually performed at one of the 16 subdivisionalhospitals, 76 health centres or 101 nursing stations. Histologicaldiagnosis and management of high-grade smears are onlyundertaken by specialist gynaecologists at one of the threedivisional hospitals in the country. General practitioners canperform Pap smears but most are done in the public sector.Visual inspection and treatment methods, and HPVDNA testingare not routinely available. Cancer management comprises ofcone biopsies, large loop excision of the transformation zoneand hysterectomies. Some chemotherapy is available, but noradiotherapy services are available in Fiji. A very small numberof patients are diagnosed with cervical cancer and receivetreatment overseas. Very few women have hysterectomies inFiji due to the limited availability of nonemergency surgical andanaesthetic services.
Study period and populationData were collected for the period from 1 January 2004 to 18October 2007 on all women in Fiji who had biopsy-confirmedcervical cancer or a Pap smear. Registered deaths due tocarcinoma of the cervix uteri were collected from 1 January2004 to 31 December 2006. This difference in case and deathascertainment timeframes was related to about a year’s timelag between actual deaths and the recording of these deaths inthe relevant registries. No data from the private hospital orlaboratories were included, as these were estimated to compriseless than 5% of all Pap smears and cervical cancer cases(Dr N. Sharma. Minister for Health, Fiji; pers. comm.). Datawere limited to these timeframes on account of human resourcesand logistics.
Data sources and case definitionsData were collected from registries based at the three divisionalhospitals in Fiji. Specifically, enumerations of cervical cancercases were obtained from histology registries, and all recordedPap smear tests and their respective results were obtainedfrom cytology registries. A case of cervical cancer had to behistologically proven by biopsy. Histological classificationsof cervical cancer included squamous cell carcinoma,adenocarcinoma, adenosquamous carcinoma and small cellcarcinoma. Squamous cell carcinoma in situ was classified asa precursor lesion. Total Pap smears taken and smears diagnosedas cervical cancer were enumerated. Registered deaths wereidentified from two official sources: the Registrar-General’soffice and the MoH’s death registry. Death certificates areissued by the treating doctors, usually based on theirknowledge of the person’s medical history or the historyoffered by relatives (i.e. verbal autopsy), and InternationalClassification of Diseases (ICD) edition 10 codes are usedto code all deaths. To ensure cases were not duplicated,
B Sexual Health I. Law et al.

data linkages were created between all databases using Excel2007 (Microsoft, Bellevue, WA, USA) based upon name, dateof birth, hospital of diagnosis, national hospital number, anddate of diagnosis or date of Pap smear. The earliesthistological diagnosis of cancer or the first diagnostic Papsmear without histological confirmation was retained fromeach duplicate set.
Statistical methodsPopulation data were obtained from the last completed decennialcensus in 2007.24 Incidence and mortality rates related to womenof all ages with a focus on the 20- to 69-year-old age group.A correction factor of 0.8 was used for 2007 rate calculations,given that data were only collected for the first 290 days of 2007.Women of ‘other races’ were excluded from the rate estimationby ethnicity, as they represented less than 6% of all people in Fijiand are of wide ethnic diversity. Data were standardised to theWorld Health Organisation’s world standard population to allowfor regional comparisons.26 A case fatality ratio, whichrepresents the ratio of age-standardised mortality to incidencefor all ages, was determined as an estimate of the 5-year survivalrate. Pap smear coverage was defined as the proportion ofwomen in Fiji between 20 and 69 years who had at least onePap smear during 2004 to 2006. At the time of the survey, therewere insufficient data to exclude women from the targetpopulation who had a hysterectomy and did not requirefurther Pap smears. The Mann–Whitney U-test was used forbetween-group comparisons of median age. Incident andmortality rate ratios and confidence interval (CI) estimationutilised the Poisson distribution for cancer data but binomialdistributions for Pap smear coverage estimations. Kaplan–Meiercurves were compared for time to death from initial diagnosis,adjusted for age, using the log-rank test. A two-tailed level ofsignificance of P< 0.05 was used for all tests. Data wereanalysed using Stata ver. 10.0 (StataCorp, College Station,TX, USA).
ResultsIncidence
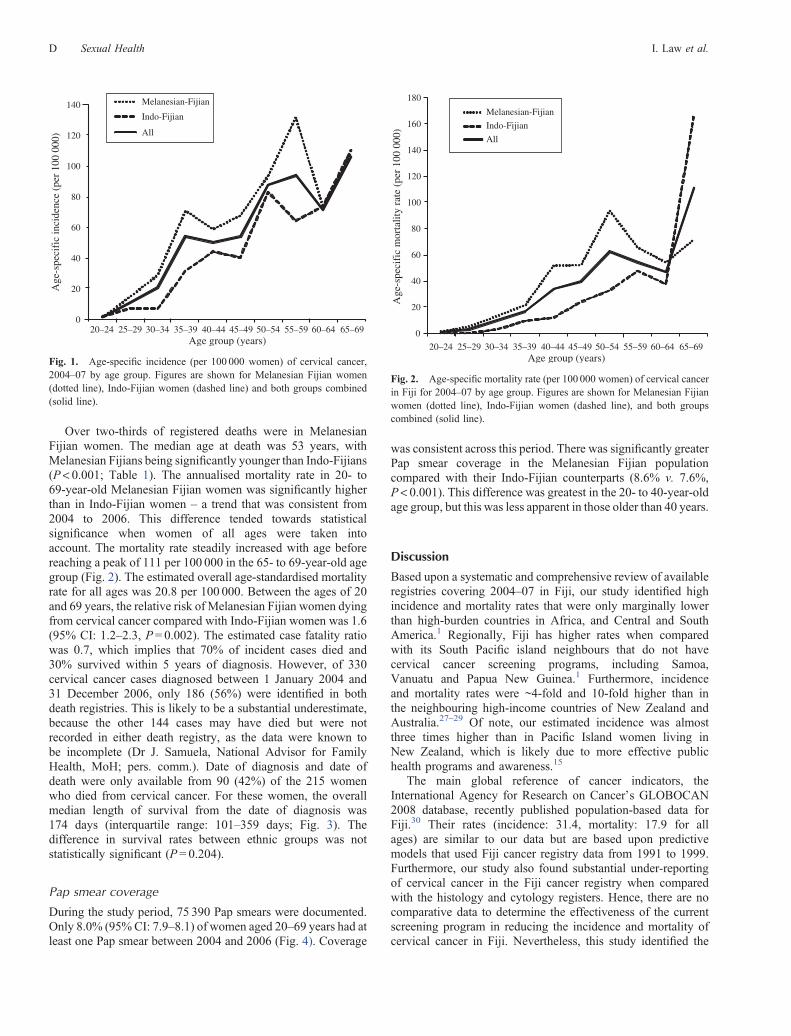
In total, 413 cases of cervical cancer were diagnosed between1 January 2004 and 18 October 2007. The median age atdiagnosis was 50 years, with Melanesian Fijians beingsignificantly younger at diagnosis than Indo-Fijians(P< 0.001; Table 1). The majority of women had squamouscell carcinoma (n= 370, 89.6%), followed by adenocarcinoma(n= 35, 8.5%), adenosquamous (n= 7, 1.7%) and small cellcarcinoma (n= 1, 0.2%). The incidence in Melanesian Fijianwomen aged 20–69 years was significantly higher than that inIndo-Fijian women (P< 0.05) for each year of the study (data notshown) and in all age groups, except those aged 60–69 years(Fig. 1). The highest incidence was in the older age groups, witha progressive rise in incidence with age. When women of allages were considered, there was no statistically significantdifference in incidence between the two ethnic groups. Theestimated age-standardised incidence for all ages was 29.7 per100 000. Between the ages of 20 and 69 years, the relative riskof Melanesian Fijian women developing cervical cancercompared with Indo-Fijian women was 1.4 (95% CI: 1.1–1.8,P = 0.001).
Mortality
The MoH’s death registry listed 212 women from 1 January2004 to 31 December 2006 whose primary cause of death wascervical cancer. By contrast, the Registrar-General’s office listedonly 14 deaths from cervical cancer between1 January 2004 and31 December 2005, with no deaths recorded thereafter. Only 3 ofthese 14 deaths were not listed in the MoH’s death registry. Thusthe total number of deaths due to cervical cancer between 1January 2004 and 31 December 2006 was 215. Of these, 29deaths were not recorded in the histology cancer registries; it wastherefore assumed that they were diagnosed before January2004. No secondary causes of death due to cervical cancerwere known.
Table 1. Annualised incidence of and mortality rates from cervical cancer in Fiji by ethnicityIQR, interquartile range; CI, confidence interval. P-value compares Melanesian Fijian women with Indo-Fijian women
Melanesian Fijian Indo-Fijian Other Total P-value
Cases20–69 years 244 133 13 390All ages 254 145 14 413Median age at diagnosis in years (IQR) 47 (38–56) 52 (43–61.3) 46 (36–52) 50 (40–57.5) <0.001
Annualised incidence per 100 000 (95% CI)A
20–69 years 49.7 (43.7–56.4) 35.2 (29.5–41.7) – 42.4 (38.3–46.9) 0.001All ages 28.7 (25.2–32.4) 24.8 (20.9–29.2) 26.5 (24.0–29.2) 0.163
Deaths20–69 years 125 59 8 192All ages 138 68 9 215Median age at death in years (IQR) 50.5 (42–59) 58 (50–66) 47 (44–62) 53 (44–63) <0.001
Annualised mortality rate per 100 000 (95% CI)B
20–69 years 32.3 (26.9–38.4) 19.8 (15.1–25.5) – 26.5 (22.9–30.5) 0.002All ages 19.7 (16.6–23.3) 14.5 (11.4–18.7) – 17.5 (15.2–20.0) 0.05
AAge-standardised incidence (world): 46.1 per 100 000 (for women aged 20–69 years); 29.7 per 100 000 (all ages).BAge-standardised mortality rate (world) 29.4 per 100 000 (for women aged 20–69 years); 20.8 per 100 000 (all ages).
Cervical cancer in Fiji Sexual Health C
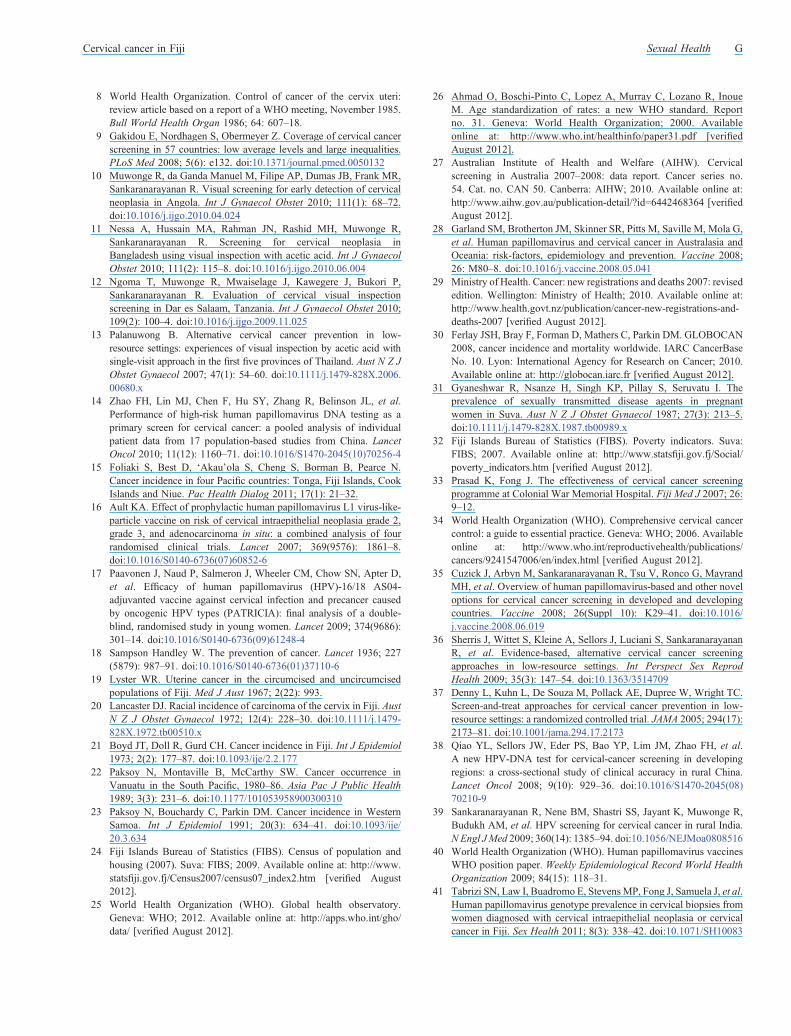
Over two-thirds of registered deaths were in MelanesianFijian women. The median age at death was 53 years, withMelanesian Fijians being significantly younger than Indo-Fijians(P < 0.001; Table 1). The annualised mortality rate in 20- to69-year-old Melanesian Fijian women was significantly higherthan in Indo-Fijian women – a trend that was consistent from2004 to 2006. This difference tended towards statisticalsignificance when women of all ages were taken intoaccount. The mortality rate steadily increased with age beforereaching a peak of 111 per 100 000 in the 65- to 69-year-old agegroup (Fig. 2). The estimated overall age-standardised mortalityrate for all ages was 20.8 per 100 000. Between the ages of 20and 69 years, the relative risk of Melanesian Fijian women dyingfrom cervical cancer compared with Indo-Fijian women was 1.6(95% CI: 1.2–2.3, P= 0.002). The estimated case fatality ratiowas 0.7, which implies that 70% of incident cases died and30% survived within 5 years of diagnosis. However, of 330cervical cancer cases diagnosed between 1 January 2004 and31 December 2006, only 186 (56%) were identified in bothdeath registries. This is likely to be a substantial underestimate,because the other 144 cases may have died but were notrecorded in either death registry, as the data were known tobe incomplete (Dr J. Samuela, National Advisor for FamilyHealth, MoH; pers. comm.). Date of diagnosis and date ofdeath were only available from 90 (42%) of the 215 womenwho died from cervical cancer. For these women, the overallmedian length of survival from the date of diagnosis was174 days (interquartile range: 101–359 days; Fig. 3). Thedifference in survival rates between ethnic groups was notstatistically significant (P = 0.204).
Pap smear coverage
During the study period, 75 390 Pap smears were documented.Only 8.0% (95%CI: 7.9–8.1) of women aged 20–69 years had atleast one Pap smear between 2004 and 2006 (Fig. 4). Coverage
was consistent across this period. There was significantly greaterPap smear coverage in the Melanesian Fijian populationcompared with their Indo-Fijian counterparts (8.6% v. 7.6%,P < 0.001). This difference was greatest in the 20- to 40-year-oldage group, but this was less apparent in those older than 40 years.
DiscussionBased upon a systematic and comprehensive review of availableregistries covering 2004–07 in Fiji, our study identified highincidence and mortality rates that were only marginally lowerthan high-burden countries in Africa, and Central and SouthAmerica.1 Regionally, Fiji has higher rates when comparedwith its South Pacific island neighbours that do not havecervical cancer screening programs, including Samoa,Vanuatu and Papua New Guinea.1 Furthermore, incidenceand mortality rates were ~4-fold and 10-fold higher than inthe neighbouring high-income countries of New Zealand andAustralia.27–29 Of note, our estimated incidence was almostthree times higher than in Pacific Island women living inNew Zealand, which is likely due to more effective publichealth programs and awareness.15
The main global reference of cancer indicators, theInternational Agency for Research on Cancer’s GLOBOCAN2008 database, recently published population-based data forFiji.30 Their rates (incidence: 31.4, mortality: 17.9 for allages) are similar to our data but are based upon predictivemodels that used Fiji cancer registry data from 1991 to 1999.Furthermore, our study also found substantial under-reportingof cervical cancer in the Fiji cancer registry when comparedwith the histology and cytology registers. Hence, there are nocomparative data to determine the effectiveness of the currentscreening program in reducing the incidence and mortality ofcervical cancer in Fiji. Nevertheless, this study identified the
0
20
40
60
80
100
120
140
Age
-spe
cifi
c in
cide
nce
(per
100
000
)
Melanesian-Fijian
Indo-Fijian
All
20–24 25–29Age group (years)
30–34 35–39 40–44 45–49 50–54 55–59 60–64 65–69
Fig. 1. Age-specific incidence (per 100 000 women) of cervical cancer,2004–07 by age group. Figures are shown for Melanesian Fijian women(dotted line), Indo-Fijian women (dashed line) and both groups combined(solid line).
0
20
40
60
80
100
120
140
160
180
Age
-spe
cifi
c m
orta
lity
rate
(per
100
000
)
Melanesian-FijianIndo-FijianAll
20–24 25–29Age group (years)
30–34 35–39 40–44 45–49 50–54 55–59 60–64 65–69
Fig. 2. Age-specific mortality rate (per 100 000 women) of cervical cancerin Fiji for 2004–07 by age group. Figures are shown for Melanesian Fijianwomen (dotted line), Indo-Fijian women (dashed line), and both groupscombined (solid line).
D Sexual Health I. Law et al.

high burden of cervical cancer despite an existing screeningstrategy.
It is unknown why Melanesian Fijian women have a greaterrisk of developing and dying from cervical cancer comparedwith Indo-Fijian women, the reason is likely to be multifactorial.This difference is commonly observed in the notification datafor all types of cancer in both men and women over the pastdecade (MoHCancer Registry, unpubl. data). However, possibleexplanations may include differences of public knowledge andawareness, access to health services, prevalence of risk factorssuch as smoking and sexual behaviour, prevalence of sexuallytransmitted diseases, health-seeking behaviours, and stigmaassociated with seeking care for sexually transmissibleinfections and cervical cancer.31 Socioeconomic factors areless likely to account for disease rate differences given thesimilarity of poverty rates and rural versus urban residencebetween the two groups.32 It is of interest that the latest
GLOBOCAN estimates for age-standardised rates in India(incidence: 27.0, mortality: 15.2) were comparable to those ofIndo-Fijian women in our study.30 Indeed, further explorationinto such differences is required. Nonetheless, the high burden ofdisease in both ethnic groups calls for greater public healthinitiatives that are equitable and effective.
Aside from the key indicators of incidence and mortality indetermining the effectiveness of a cytology-based screeningprogram, the screening coverage of the target population isparamount. Despite the higher Pap smear coverage inMelanesian Fijian women compared with Indo-Fijian women,which may be explained by the former having greater parity andhence more opportunistic Pap smears at antenatal visits than thelatter, coverage was extremely low in both ethnic groups. Papsmear coverage is also a function of access to health services.Previous estimates identified that only 47% of women in Fijiwith high-grade abnormal Pap smears ever returned for follow-up management.33 Furthermore, at the time of the study, thescreening program in Fiji was functioning at full capacity withonly nine cytology technicians, three histopathologists andthree gynaecologists to process, review and manage all Papsmears nationwide. Assuming there were enough supplies andinfrastructure to perform more Pap smears, we estimated that a3- to 8-fold increase in staff numbers would be required tomanage a screening program that has 80% coverage of the targetpopulation, as recommended by WHO.34 This is likely to beunaffordable for a country with many competing health needsand priorities. Such collective evidence was not unexpected,given that programmatic constraints in Fiji are similar to thosein other low-income countries.7
Implementation of well designed and well organisedscreening programs can reduce the burden of cervicalcancer.35 However, as shown in our study, a cytology-basedscreening program is challenging to implement and manageefficiently in less well equipped environments. Focussing onPap smear screening in women post partum is opportunistic, buta more strategic approach should target older women. Othercost-effective alternative strategies that use a one-visit visualinspection with acetic acid method have been shown to be safe,acceptable and feasible, and, in some instances, to significantlyincrease screening coverage and reduce overall screening costsin resource-poor countries.10–13 This growing body of evidencehas led the Alliance for Cervical Cancer Prevention torecommend visual inspection with acetic acid as the mostefficient and effective screening method for use in low-resourced countries.36 The use of HPV DNA testing mayoffer another screening tool in the future.14,37–39 Nonetheless,no single screening strategy may be sufficient for Fiji, but basedupon the cost-utility of each, adopting a multistrategy programmay improve efficiency and cervical cancer outcomes, and iscurrently under discussion.
As recommended by WHO, such strategies may incorporatethe HPV vaccine as part of a country’s national immunisationschedules, especially where cervical cancer is a public healthpriority, and where vaccine implementation is feasible andfinancially sustainable.40 The prevalence of the two mostcommon HPV genotypes associated with cervical cancers inFiji, HPV-16 and -18, are similar to that described worldwide.41
Thus the current vaccines could potentially reduce the burden
1.00
0.75
0.50
0.25
0.00
0 200 400
Time since diagnosis (days)
Prop
ortio
n al
ive
600 800
Fig. 3. Kaplan-Meier curves comparing survival of Melanesian Fijianwomen (dotted line) and Indo-Fijian women (solid line) with cervicalcancer, 2004–2007.
0
2
4
6
8
10
12
14
Pap
smea
r cov
erag
e (%
)
Melanesian Fijian
Indo-Fijian
All
Age group (years)30–34 35–39 40–44 45–49 50–54 55–59 60–64 65–6920–24 25–29
Fig. 4. Pap smear coverage for Melanesian Fijian women (dotted line),Indo-Fijian women (dashed line), and both groups combined (solid line) for2004–2006 by age group.
Cervical cancer in Fiji Sexual Health E

of cervical cancer by more than 80% within Fiji. Allowingfor underascertainment and based on the incidence in 20- to69-year-old women and 100% lifelong efficacy of the vaccine,we estimated that with 90% vaccine coverage of HPV-naive10- to 14-year-old girls in Fiji (n= 40 015), between 14 and 17new cases of cervical cancer could be prevented each year. InSeptember 2008, Fiji commenced a one-off national campaignwith the quadrivalent HPV vaccine to vaccinate 9- to 12-year-old girls via a school-based immunisation program, and anextended campaign for women up to 20 years of age (Thethird HPV dose coverage was 55% (MoH, unpubl. data)). Anevaluation of the acceptability of the HPV vaccine has led to thedevelopment of a sustainable financial solution with donorsand in 2013, Fiji’s MoH commenced a national school-basedHPV vaccine program within the routine immunisationschedule. Despite early indications of the vaccine’s benefit inreductions of genital warts and high-grade abnormalities in Papsmears, the full beneficial impact of the vaccine with respectto cervical cancer may not be seen for possibly more than10 years.42–44 These modelling predictions are based uponlong-standing and effective screening programs with highvaccine coverage in developed countries. Therefore forcountries such as Fiji, the introduction of the HPV vaccineshould be in association with strengthening the cervical cancerscreening and disease surveillance system and creating greaterlinkages between cancer screening and histology registriesin order to evaluate effectiveness of the HPV vaccine.Nevertheless, the 2009 WHO HPV vaccine position paperstates that the introduction of the HPV vaccine should not bedelayed if these interventions cannot be implemented.40
The study has several limitations related tounderascertainment of cases and of deaths. All data werecollected from hospitals and public health registries, ofwhich only the latter were in an electronic format. Cervicalcancer cases may have been missed due to incompletetranscription of handwritten registries and manual datacollection. Nonetheless, it was assumed that a woman withcervical cancer remaining undiagnosed in the communitywould be uncommon. Deaths due to cervical cancer weresubject to potential coding errors, given the ongoingtransition from hard to soft copies and adaptation of ICDcodes. Furthermore, the incomplete processing of deathcertificates, delays caused by the legal formalities requiredto register deaths and possible misclassification of the causeof death contributed to underascertainment. The low medianlength of survival supported the claim from clinicians in Fijithat more than 95% of women diagnosed with cervical cancerwill die from their disease within 5 years due to latepresentation, limited treatment options for advanced diseaseand poor diagnostic follow-up (Dr J. Fong, consultantgynaecologist, MoH, pers. comm.). The estimated casefatality ratio, a proxy for 5-year survival rates, is muchlower than this claim, further supporting the inadequacy ofrecording registered cervical cancer deaths. Assessing thevalidity of the death registries by checking all deathcertificates in Fiji was beyond the scope of the study, butby inference, our estimates of mortality rates are likely to be asubstantial underestimate.
In summary, Fiji has a high burden of cervical cancer andvery low levels of Pap smear coverage. Its cytology-basedmultiple-visit screening program is currently not effective toreduce the cervical cancer burden. Further discussions arerequired to optimise the cervical cancer screening strategies,given the current resource restrictions, and to develop acomprehensive approach to cervical cancer control in Fiji.Despite the HPV vaccine’s enormous potential with nationalintroduction, there is still a need for more widespread screeningcoverage, which could possibly be addressed through alternativeand age-targeted screening strategies. Nonetheless, advances insystematic monitoring and evaluation are also required in orderto detect such future benefits.
Conflicts of interestsSMG has received advisory board fees and grant support fromCommonwealth Serum Laboratories and GlaxoSmithKline(GSK), and lecture fees from Merck, GSK and SanofiPasteur; in addition, she also has received funding throughher institution to conduct HPV vaccine studies for Merck andGSK. She is a member of the Merck Global Advisory Board aswell as the Merck Scientific Advisory Committee for HPV.
AcknowledgementsThe authors thank the staff from the Ministry of Health, the FijiPneumococcal Project, Colonial War Memorial Hospital, and Lautokaand Labasa Hospitals for their assistance. This work was supported bytheWorld Health Organisation (South Pacific). The funder did not play a rolein the study design; in the collection, analysis and interpretation of data; norin the writing of the manuscript or the decision to submit the manuscript forpublication.
References1 Ferlay J, Shin HR, Bray F, Forman D, Mathers C, Parkin DM.
Estimates of worldwide burden of cancer in 2008: GLOBOCAN2008. Int J Cancer 2010; 127(12): 2893–917. doi:10.1002/ijc.25516
2 Foliaki S, JeffreysM,Wright C, Blakey K, Pearce N. Cancer in Pacificpeople in New Zealand: a descriptive study. Pac Health Dialog 2004;11(2): 94–100.
3 McCracken M, Olsen M, Chen MS, Jemal A, Thun M, Cokkinides V,et al. Cancer incidence, mortality, and associated risk factorsamong Asian Americans of Chinese, Filipino, Vietnamese, Korean,and Japanese ethnicities. CA Cancer J Clin 2007; 57(4): 190–205.doi:10.3322/canjclin.57.4.190
4 Sankaranarayanan R. Overview of cervical cancer in the developingworld. FIGO 26th annual report on the results of treatment ingynecological cancer. Int J Gynaecol Obstet 2006; 95: S205–10.doi:10.1016/S0020-7292(06)60035-0
5 Canfell K, Sitas F, Beral V. Cervical cancer in Australia and the UnitedKingdom: comparison of screening policy and uptake, and cancerincidence and mortality. Med J Aust 2006; 185(9): 482–6.
6 Nygard JF, Skare GB, Thoresen SO. The cervical cancer screeningprogramme in Norway, 1992–2000: changes in Pap smear coverageand incidence of cervical cancer. J Med Screen 2002; 9(2): 86–91.doi:10.1136/jms.9.2.86
7 Sankaranarayanan R, Budukh AM, Rajkumar R. Effective screeningprogrammes for cervical cancer in low- and middle-incomedeveloping countries. Bull World Health Organ 2001; 79(10):954–62.
F Sexual Health I. Law et al.
8 World Health Organization. Control of cancer of the cervix uteri:review article based on a report of a WHO meeting, November 1985.Bull World Health Organ 1986; 64: 607–18.
9 Gakidou E, Nordhagen S, Obermeyer Z. Coverage of cervical cancerscreening in 57 countries: low average levels and large inequalities.PLoS Med 2008; 5(6): e132. doi:10.1371/journal.pmed.0050132
10 Muwonge R, da Ganda Manuel M, Filipe AP, Dumas JB, Frank MR,Sankaranarayanan R. Visual screening for early detection of cervicalneoplasia in Angola. Int J Gynaecol Obstet 2010; 111(1): 68–72.doi:10.1016/j.ijgo.2010.04.024
11 Nessa A, Hussain MA, Rahman JN, Rashid MH, Muwonge R,Sankaranarayanan R. Screening for cervical neoplasia inBangladesh using visual inspection with acetic acid. Int J GynaecolObstet 2010; 111(2): 115–8. doi:10.1016/j.ijgo.2010.06.004
12 Ngoma T, Muwonge R, Mwaiselage J, Kawegere J, Bukori P,Sankaranarayanan R. Evaluation of cervical visual inspectionscreening in Dar es Salaam, Tanzania. Int J Gynaecol Obstet 2010;109(2): 100–4. doi:10.1016/j.ijgo.2009.11.025
13 Palanuwong B. Alternative cervical cancer prevention in low-resource settings: experiences of visual inspection by acetic acid withsingle-visit approach in the first five provinces of Thailand. Aust N Z JObstet Gynaecol 2007; 47(1): 54–60. doi:10.1111/j.1479-828X.2006.00680.x
14 Zhao FH, Lin MJ, Chen F, Hu SY, Zhang R, Belinson JL, et al.Performance of high-risk human papillomavirus DNA testing as aprimary screen for cervical cancer: a pooled analysis of individualpatient data from 17 population-based studies from China. LancetOncol 2010; 11(12): 1160–71. doi:10.1016/S1470-2045(10)70256-4
15 Foliaki S, Best D, ‘Akau’ola S, Cheng S, Borman B, Pearce N.Cancer incidence in four Pacific countries: Tonga, Fiji Islands, CookIslands and Niue. Pac Health Dialog 2011; 17(1): 21–32.
16 Ault KA. Effect of prophylactic human papillomavirus L1 virus-like-particle vaccine on risk of cervical intraepithelial neoplasia grade 2,grade 3, and adenocarcinoma in situ: a combined analysis of fourrandomised clinical trials. Lancet 2007; 369(9576): 1861–8.doi:10.1016/S0140-6736(07)60852-6
17 Paavonen J, Naud P, Salmeron J, Wheeler CM, Chow SN, Apter D,et al. Efficacy of human papillomavirus (HPV)-16/18 AS04-adjuvanted vaccine against cervical infection and precancer causedby oncogenic HPV types (PATRICIA): final analysis of a double-blind, randomised study in young women. Lancet 2009; 374(9686):301–14. doi:10.1016/S0140-6736(09)61248-4
18 Sampson Handley W. The prevention of cancer. Lancet 1936; 227(5879): 987–91. doi:10.1016/S0140-6736(01)37110-6
19 Lyster WR. Uterine cancer in the circumcised and uncircumcisedpopulations of Fiji. Med J Aust 1967; 2(22): 993.
20 Lancaster DJ. Racial incidence of carcinoma of the cervix in Fiji. AustN Z J Obstet Gynaecol 1972; 12(4): 228–30. doi:10.1111/j.1479-828X.1972.tb00510.x
21 Boyd JT, Doll R, Gurd CH. Cancer incidence in Fiji. Int J Epidemiol1973; 2(2): 177–87. doi:10.1093/ije/2.2.177
22 Paksoy N, Montaville B, McCarthy SW. Cancer occurrence inVanuatu in the South Pacific, 1980–86. Asia Pac J Public Health1989; 3(3): 231–6. doi:10.1177/101053958900300310
23 Paksoy N, Bouchardy C, Parkin DM. Cancer incidence in WesternSamoa. Int J Epidemiol 1991; 20(3): 634–41. doi:10.1093/ije/20.3.634
24 Fiji Islands Bureau of Statistics (FIBS). Census of population andhousing (2007). Suva: FIBS; 2009. Available online at: http://www.statsfiji.gov.fj/Census2007/census07_index2.htm [verified August2012].
25 World Health Organization (WHO). Global health observatory.Geneva: WHO; 2012. Available online at: http://apps.who.int/gho/data/ [verified August 2012].
26 Ahmad O, Boschi-Pinto C, Lopez A, Murray C, Lozano R, InoueM. Age standardization of rates: a new WHO standard. Reportno. 31. Geneva: World Health Organization; 2000. Availableonline at: http://www.who.int/healthinfo/paper31.pdf [verifiedAugust 2012].
27 Australian Institute of Health and Welfare (AIHW). Cervicalscreening in Australia 2007–2008: data report. Cancer series no.54. Cat. no. CAN 50. Canberra: AIHW; 2010. Available online at:http://www.aihw.gov.au/publication-detail/?id=6442468364 [verifiedAugust 2012].
28 Garland SM, Brotherton JM, Skinner SR, Pitts M, Saville M, Mola G,et al. Human papillomavirus and cervical cancer in Australasia andOceania: risk-factors, epidemiology and prevention. Vaccine 2008;26: M80–8. doi:10.1016/j.vaccine.2008.05.041
29 Ministry of Health. Cancer: new registrations and deaths 2007: revisededition. Wellington: Ministry of Health; 2010. Available online at:http://www.health.govt.nz/publication/cancer-new-registrations-and-deaths-2007 [verified August 2012].
30 Ferlay JSH, Bray F, Forman D, Mathers C, Parkin DM. GLOBOCAN2008, cancer incidence and mortality worldwide. IARC CancerBaseNo. 10. Lyon: International Agency for Research on Cancer; 2010.Available online at: http://globocan.iarc.fr [verified August 2012].
31 Gyaneshwar R, Nsanze H, Singh KP, Pillay S, Seruvatu I. Theprevalence of sexually transmitted disease agents in pregnantwomen in Suva. Aust N Z J Obstet Gynaecol 1987; 27(3): 213–5.doi:10.1111/j.1479-828X.1987.tb00989.x
32 Fiji Islands Bureau of Statistics (FIBS). Poverty indicators. Suva:FIBS; 2007. Available online at: http://www.statsfiji.gov.fj/Social/poverty_indicators.htm [verified August 2012].
33 Prasad K, Fong J. The effectiveness of cervical cancer screeningprogramme at Colonial War Memorial Hospital. Fiji Med J 2007; 26:9–12.
34 World Health Organization (WHO). Comprehensive cervical cancercontrol: a guide to essential practice. Geneva: WHO; 2006. Availableonline at: http://www.who.int/reproductivehealth/publications/cancers/9241547006/en/index.html [verified August 2012].
35 Cuzick J, Arbyn M, Sankaranarayanan R, Tsu V, Ronco G, MayrandMH, et al. Overview of human papillomavirus-based and other noveloptions for cervical cancer screening in developed and developingcountries. Vaccine 2008; 26(Suppl 10): K29–41. doi:10.1016/j.vaccine.2008.06.019
36 Sherris J, Wittet S, Kleine A, Sellors J, Luciani S, SankaranarayananR, et al. Evidence-based, alternative cervical cancer screeningapproaches in low-resource settings. Int Perspect Sex ReprodHealth 2009; 35(3): 147–54. doi:10.1363/3514709
37 Denny L, Kuhn L, De Souza M, Pollack AE, Dupree W, Wright TC.Screen-and-treat approaches for cervical cancer prevention in low-resource settings: a randomized controlled trial. JAMA 2005; 294(17):2173–81. doi:10.1001/jama.294.17.2173
38 Qiao YL, Sellors JW, Eder PS, Bao YP, Lim JM, Zhao FH, et al.A new HPV-DNA test for cervical-cancer screening in developingregions: a cross-sectional study of clinical accuracy in rural China.Lancet Oncol 2008; 9(10): 929–36. doi:10.1016/S1470-2045(08)70210-9
39 Sankaranarayanan R, Nene BM, Shastri SS, Jayant K, Muwonge R,Budukh AM, et al. HPV screening for cervical cancer in rural India.NEngl JMed 2009; 360(14): 1385–94. doi:10.1056/NEJMoa0808516
40 World Health Organization (WHO). Human papillomavirus vaccinesWHO position paper. Weekly Epidemiological Record World HealthOrganization 2009; 84(15): 118–31.
41 Tabrizi SN, Law I, Buadromo E, Stevens MP, Fong J, Samuela J, et al.Human papillomavirus genotype prevalence in cervical biopsies fromwomen diagnosed with cervical intraepithelial neoplasia or cervicalcancer in Fiji. Sex Health 2011; 8(3): 338–42. doi:10.1071/SH10083
Cervical cancer in Fiji Sexual Health G

42 Brotherton JM, Fridman M, May CL, Chappell G, Saville AM, GertigDM. Early effect of the HPV vaccination programme on cervicalabnormalities in Victoria, Australia: an ecological study. Lancet 2011;377(9783): 2085–92. doi:10.1016/S0140-6736(11)60551-5
43 Cuzick J, Castanon A, Sasieni P. Predicted impact of vaccinationagainst human papillomavirus 16/18 on cancer incidence and cervicalabnormalities in women aged 20–29 in the UK. Br J Cancer 2010; 102(5): 933–9. doi:10.1038/sj.bjc.6605528
44 Donovan B, Franklin N, Guy R, Grulich AE, Regan DG, Ali H, et al.Quadrivalent human papillomavirus vaccination and trends in genitalwarts in Australia: analysis of national sentinel surveillance data.Lancet Infect Dis 2011; 11(1): 39–44. doi:10.1016/S1473-3099(10)70225-5
H Sexual Health I. Law et al.
www.publish.csiro.au/journals/sh




















