The Family Health Book - UPecon Foundation
375
The Family Health Book Aleli D. Kraft, Jhiedon L. Florentino, Rhodora A. Tiongson, and Orville Solon, editors
-
Upload
khangminh22 -
Category
Documents
-
view
3 -
download
0
Transcript of The Family Health Book - UPecon Foundation
The Family Health Book
Aleli D. Kraft, Jhiedon L. Florentino, Rhodora A. Tiongson, and Orville Solon, editors
Aleli D. Kraft, Jhiedon L. Florentino, Rhodora A. Tiongson and Orville Solon, editors
The Family Health Book
Published by the UPecon-Health Policy Development Program (HPDP), School of Economics, University of the Philippines Diliman, Quezon City, Philippines. Telephone: +632 927-9686 loc 322. E-mail: [email protected]. April 2012.
The mention (if any) of specific companies or of certain manufacturer’s products does not imply that they are endorsed or recommended by the publisher in preference over others of a similar nature. Articles may be reproduced in full or in part for non-profit purposes without prior permission, provided credit is given to HPDP and/or the individual authors for original pieces. A copy of the reprinted or adapted version will be appreciated.
Suggested Citation:
Kraft, A.D., J.L. Florentino, R.A. Tiongson, and O. Solon eds. The Family Health Book. Quezon City, UPecon-Health Policy Development Program, 2012.
This volume was made possible by the support of the American people through the U.S. Agency for International Development (USAID) to the UPecon-Health Policy Development Program under the terms of Cooperative Agreement No. 492-A-00-06-00031. The contents of this volume are the sole responsibility of the authors and do not necessarily reflect the views of the USAID, UPecon Foundation Inc., and the Department of Health (DOH).
Style editing: Wystan de la Peña
Cover design and lay-out: Giselle de la Peña and Judith Camille Rosette
Cover photos courtesy of Maria Gracia Alcantara and the Provincial Health Office of Compostela Valley
Acknowledgements
The UPecon-Health Policy Development Program (HPDP) would like to express its deepest appreciation to the province of Compostela Valley, headed by Governor Arturo Uy, for support in the implementation of the FHB Operations Research.
We would also like to acknowledge the officers and staff of the Compostela Valley Provincial Health Office, DOH-CHD 12, and PhilHealth Regional Office 12 for their invaluable support. The assistance and efforts of Dr. Alexis Cayoca, Dr. January Yabut, and Ms. Cheryl Osorio in running the operations research are also acknowledged.
Table of Contents
LIST OF TABLES 7
LIST OF FIGURES 17
LIST OF ABBREVIATIONS AND ACRONYMS 18
EDITORIAL OVERVIEW 21
1 THE FAMILY HEALTH BOOK OPERATIONS RESEARCH DESIGN 24
Abstract 24
What problems are the FHB trying to solve? 25
What causes can and cannot be affected by FHB interventions? 26
What critical set of services will be promoted by the FHB? 32
What family level barriers to the utilization of critical services can and cannot be influenced by the FHB? 37
What gaps and bottlenecks in the delivery system can and cannot be influenced by the FHB? 39
What are FHB interventions? 48
How will we measure changes due to FHB interventions? 64
How can we validate if observed changes can be attributed to the FHB? 81
What instruments and activities will be conducted to measure observed changes and validate that these changes are due to the FHB?
85
How will the FHB pilot be implemented? 96
How will the FHB pilot be managed? 104
Inter-CA collaboration on FHB 106
References 112
Appendix 1. Log frame of FHB interventions by intermediate outcome 115
Appendix 2. Summary Listing of Forms, Process Flow, and Timing of Collection 141
2 “GIYA SA MAAYONG PANGLAWAS”: THE FAMILY HEALTH BOOK IMPLEMENTATION IN COMPOSTELA VALLEY 144
Abstract 144
Introduction 145
FHB field testing 146
Listing of families 151
Navigator recruitment, training and development 154
Outreach 169
Other complementary and supporting activities 174
References 189
Appendix 1. Counts of Families 191
Appendix 2. Number of Navigators trained per barangay 197
Appendix 3. Family-Navigator Matching, by barangay 200
3 AN ANALYSIS OF THE IMPACTS OF THE FAMILY HEALTH BOOK INTERVENTIONS 204
Abstract 204
Introduction 205
Operations Research Setting 207
Methods 212
Results 222
DIscussion 235
Limitations 242
Conclusions 244
References 246
Appendix 1. Timing of Interventions in FHB municipalities 248
Appendix 2. FHB data collection efforts 250
Appendix 3. Logit runs: MFP 251
Appendix 4. Logit runs: At least one ANC visit 252
Appendix 5. Multinomial logit: SBA at facility 253
Appendix 6. Logit runs: FIC 254
4 BASELINE FAMILY HEALTH BOOK (FHB) SURVEY DOCUMENTATION REPORT 255
Abstract 255
Background 256
Description of the FHB Baseline Survey 258
Highlights of the FHB Household Survey 270
Highlights of Health Provider Survey 298
Highlights of Health Facilities Survey 314
Highlights of Patient Exit Survey 343
ABOUT THE AUTHORS AND EDITORS 372
List of Tables
1The Family Health Book Operations Research Design
Table 1.1 Indicators of Service Use by Wealth Quintile 31
Table 1.2 Number of facilities offering specific services, Compostela Valley
41
Table 1.3 Average score for vignettes, Compostela Valley 43
Table 1.4 Average patient satisfaction, Compostela Valley 44
Table 1.5 Average case load, Compostela Valley 45
Table 1.6 Indicator levels and corresponding health risks 50
Table 1.7 Measures of maternal, infant, and child deaths 64
Table 1.8 Interventions and Barriers Addressed, by Intermediate Outcomes
66
Table 1.9 Measures of intervention inputs received by unintended beneficiaries
71
Table 1.10 Measures and baseline data sources of environmental HH factors outside the control of FHB interventions
74
Table 1.11 Baseline education and income profile of households in Compostela, Mabini, Maco, and Montevista
76
Table 1.12 Measures and data sources of provider factors not covered by the FHB interventions
78
Table 1.13 Measures of other environmental factors not related to the household and providers that are outside the control of the FHB interventions
80
Table 1.14 Schedule of implementation of FHB interventions 83
Table 1.15 Benchmarks and timelines for October 2008-June 2010
100
8
2“Giya sa Maayong Panglawas” The Family Health Book Implementation in Compostela Valley
Table 2.1 Reasons for Family FHB Format 149
Table 2.2 Number of Families Targeted and Given Books 154
Table 2.3 Number of navigators trained 156
Table 2.4 Family-Navigator Matching 157
Table 2.5 Tally of Families by FHB Process 160
Table 2.6 Number of Families and Health Use Plans, as of August to September 2009 tally
161
Table 2.7 Number of Families and Health Use Plans, as of April to June 2010 tally
162
Table 2.8 Number of Families and MFP use 164
Table 2.9 Use of Modern FP of non-pregnant mothers, With RH Plan vs No RH Plan
164
Table 2.10 Number of pregnant mothers who delivered during FHB
165
Table 2.11 Use of Skilled Birth Attendance With Birth Plan vs No Birth Plan
165
Table 2.12 ANC use among mothers who were pregnant during the FHB
166
Table 2.13 With at least one ANC With Birth Plan vs No Birth Plan
166
Table 2.14 FIC among number of infants needing immunization
167
Table 2.15 FIC rates, With and Without Well Baby Plan 167
Table 2.16 Number of families accessing planned services from outreach
173
9
Table 2.17 FHB Developmental Costs 181
Table 2.18 FHB Pilot Implementation Costs 183
Table 2.19 Costs of FHB Operations Research 186
Table 2.20 Total Costs of FHB Implementation 188
Table 2.21 Estimated Unit Costs of Roll-Out 188
3An Analysis of the Impacts of the Family Health Book Interventions
Table 3.1 Descriptive statistics of variables use of any modern family planning method
223
Table 3.2 Marginal effects of regression runs on utilization of any modern FP method (MFP)
224
Table 3.3 Descriptive statistics of variables ANC 227
Table 3.4 Marginal effects of regression runs on utilization of at least one ANC
227
Table 3.5 Descriptive statistics of variables SBA 230
Table 3.6 Marginal effects of FHB interventions on SBA 231
Table 3.7 Descriptive statistics of variables FIC 233
Table 3.8 Marginal effects of regression runs on FIC 233
4Baseline Family Health Book (FHB) Survey Documentation Report
Table 4.1 Sample barangays and number of sample households per municipality
260
Table 4.2 Vignettes and number of respondents for the health provider survey
264
Table 4.3 Sample of facilities and number of patients 267
Table 4.4 General information of households 270
10
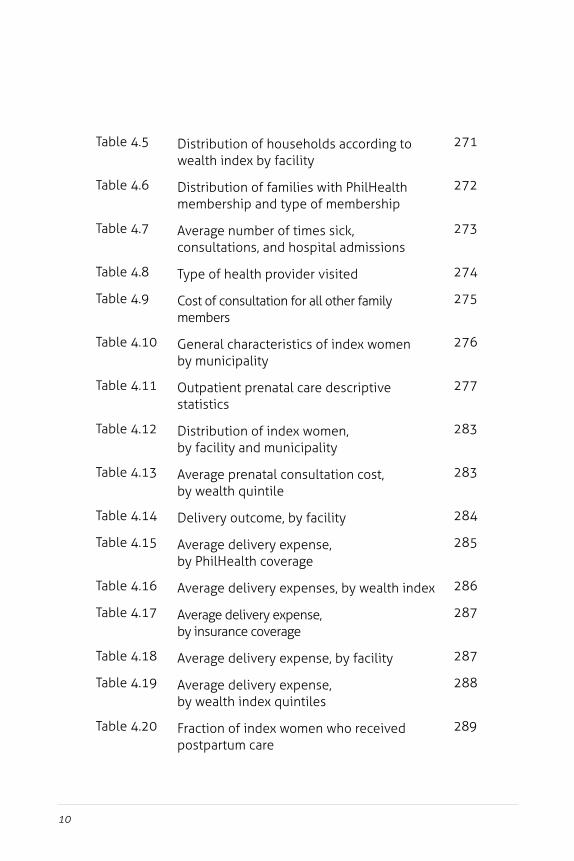
Table 4.5 Distribution of households according to wealth index by facility
271
Table 4.6 Distribution of families with PhilHealth membership and type of membership
272
Table 4.7 Average number of times sick, consultations, and hospital admissions
273
Table 4.8 Type of health provider visited 274
Table 4.9 Cost of consultation for all other family members
275
Table 4.10 General characteristics of index women by municipality
276
Table 4.11 Outpatient prenatal care descriptive statistics
277
Table 4.12 Distribution of index women, by facility and municipality
283
Table 4.13 Average prenatal consultation cost, by wealth quintile
283
Table 4.14 Delivery outcome, by facility 284
Table 4.15 Average delivery expense, by PhilHealth coverage
285
Table 4.16 Average delivery expenses, by wealth index 286
Table 4.17 Average delivery expense, by insurance coverage
287
Table 4.18 Average delivery expense, by facility 287
Table 4.19 Average delivery expense, by wealth index quintiles
288
Table 4.20 Fraction of index women who received postpartum care
289
11
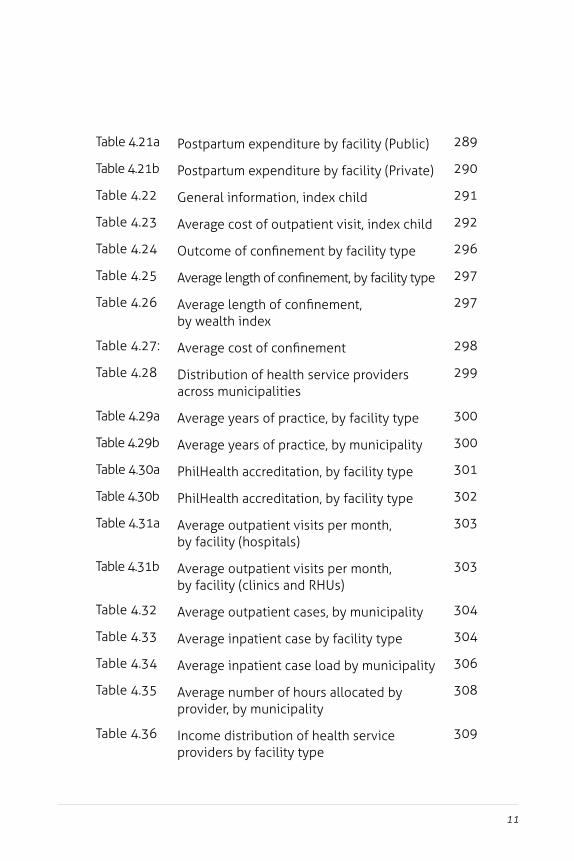
Table 4.21a Postpartum expenditure by facility (Public) 289
Table 4.21b Postpartum expenditure by facility (Private) 290
Table 4.22 General information, index child 291
Table 4.23 Average cost of outpatient visit, index child 292
Table 4.24 Outcome of confinement by facility type 296
Table 4.25 Average length of confinement, by facility type 297
Table 4.26 Average length of confinement, by wealth index
297
Table 4.27: Average cost of confinement 298
Table 4.28 Distribution of health service providers across municipalities
299
Table 4.29a Average years of practice, by facility type 300
Table 4.29b Average years of practice, by municipality 300
Table 4.30a PhilHealth accreditation, by facility type 301
Table 4.30b PhilHealth accreditation, by facility type 302
Table 4.31a Average outpatient visits per month, by facility (hospitals)
303
Table 4.31b Average outpatient visits per month, by facility (clinics and RHUs)
303
Table 4.32 Average outpatient cases, by municipality 304
Table 4.33 Average inpatient case by facility type 304
Table 4.34 Average inpatient case load by municipality 306
Table 4.35 Average number of hours allocated by provider, by municipality
308
Table 4.36 Income distribution of health service providers by facility type
309
12
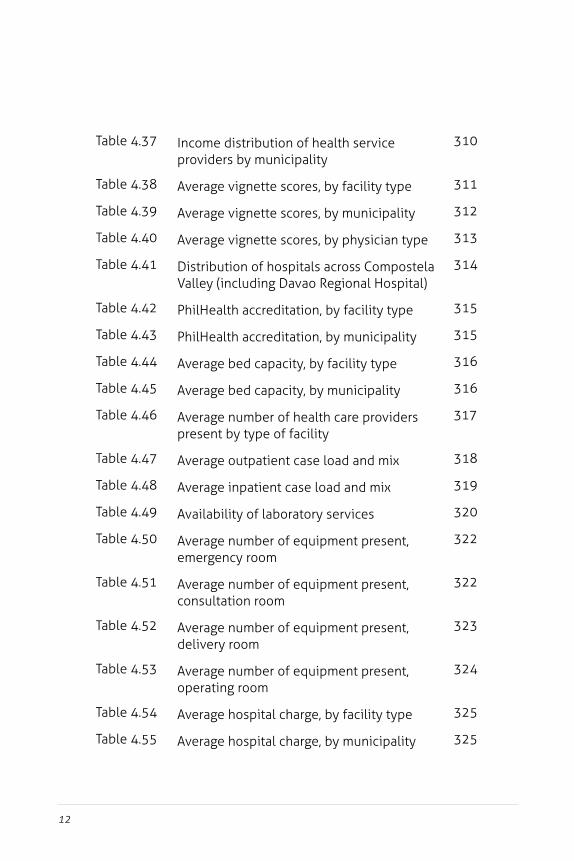
Table 4.37 Income distribution of health service providers by municipality
310
Table 4.38 Average vignette scores, by facility type 311
Table 4.39 Average vignette scores, by municipality 312
Table 4.40 Average vignette scores, by physician type 313
Table 4.41 Distribution of hospitals across Compostela Valley (including Davao Regional Hospital)
314
Table 4.42 PhilHealth accreditation, by facility type 315
Table 4.43 PhilHealth accreditation, by municipality 315
Table 4.44 Average bed capacity, by facility type 316
Table 4.45 Average bed capacity, by municipality 316
Table 4.46 Average number of health care providers present by type of facility
317
Table 4.47 Average outpatient case load and mix 318
Table 4.48 Average inpatient case load and mix 319
Table 4.49 Availability of laboratory services 320
Table 4.50 Average number of equipment present, emergency room
322
Table 4.51 Average number of equipment present, consultation room
322
Table 4.52 Average number of equipment present, delivery room
323
Table 4.53 Average number of equipment present, operating room
324
Table 4.54 Average hospital charge, by facility type 325
Table 4.55 Average hospital charge, by municipality 325
13
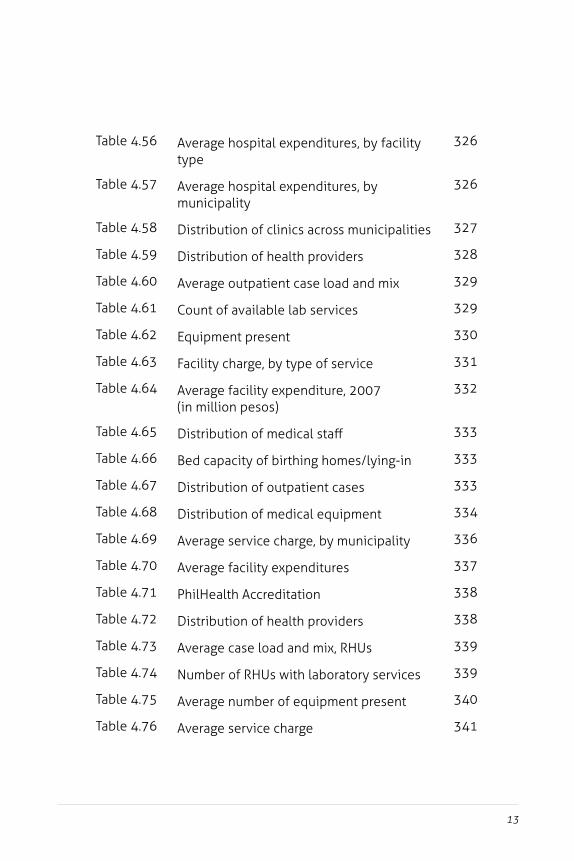
Table 4.56 Average hospital expenditures, by facility type
326
Table 4.57 Average hospital expenditures, by municipality
326
Table 4.58 Distribution of clinics across municipalities 327
Table 4.59 Distribution of health providers 328
Table 4.60 Average outpatient case load and mix 329
Table 4.61 Count of available lab services 329
Table 4.62 Equipment present 330
Table 4.63 Facility charge, by type of service 331
Table 4.64 Average facility expenditure, 2007 (in million pesos)
332
Table 4.65 Distribution of medical staff 333
Table 4.66 Bed capacity of birthing homes/lying-in 333
Table 4.67 Distribution of outpatient cases 333
Table 4.68 Distribution of medical equipment 334
Table 4.69 Average service charge, by municipality 336
Table 4.70 Average facility expenditures 337
Table 4.71 PhilHealth Accreditation 338
Table 4.72 Distribution of health providers 338
Table 4.73 Average case load and mix, RHUs 339
Table 4.74 Number of RHUs with laboratory services 339
Table 4.75 Average number of equipment present 340
Table 4.76 Average service charge 341
14
Table 4.77 Average facility expenditure (in million Pesos)
342
Table 4.78 Average facility expenditure, by municipality (in million Pesos)
342
Table 4.79 General characteristics 344
Table 4.80 General characteristics Facility visited for consultation
345
Table 4.81 Distribution of outpatients, by wealth quintiles
345
Table 4.82 Average household expenditures, by municipality
346
Table 4.83 Average household expenditure, by wealth quintile
347
Table 4.84 Patient’s reason for visit 348
Table 4.85 Physician visited by wealth quintile 348
Table 4.86 Average consultation cost by type of facility 350
Table 4.87 Average consultation cost, by municipality 350
Table 4.88 Average consultation costs, by patient type 351
Table 4.89 Average consultation costs, by wealth index 351
Table 4.90 Capacity to pay (average household) 352
Table 4.91 Average capacity to pay, by wealth quintiles 353
Table 4.92 Average patient satisfaction scores, by facility type
354
Table 4.93 Average patient satisfaction scores, by municipality
354
Table 4.94 Average patient satisfaction component scores, by facility type
355
15
Table 4.95 Average patient satisfaction component scores, by municipality
356
Table 4.96 Average patient satisfaction component scores, by patient type.
356
Table 4.97 General characteristics, inpatients 357
Table 4.98 Average length of confinement, by case 359
Table 4.99 Average length of confinement, by facility type
359
Table 4.100 Average length of stay, by municipality 359
Table 4.101 Average length of stay, by wealth quintile 360
Table 4.102 Average household expenditure, by municipality
360
Table 4.103 Average household expenditure, by wealth index
361
Table 4.104 Reason of confinement with attending specialist 361
Table 4.105 Attending specialists, by wealth index quintile 362
Table 4.106 Average miscellaneous costs of confinement, by municipality
363
Table 4.107 Average miscellaneous costs, by type of patient
363
Table 4.108 Average hospital charges, by type of patient 363
Table 4.109 Average hospital charges, by wealth index 364
Table 4.110 Average capacity to pay, by facility setting 365
Table 4.111 Average capacity to pay, by facility type 365
Table 4.112 Average capacity to pay, by wealth index quintiles
366
16
Table 4.113 Outcome of confinement, by facility setting 367
Table 4.114 Outcome of confinement, by facility type 367
Table 4.115 Outcome of confinement, by municipality 367
Table 4.116 Patient satisfaction score, by facility type 369
Table 4.117 Patient satisfaction, by facility 369
Table 4.118 Patient satisfaction, by type of patient 370
Table 4.119 Patient satisfaction component scores, by facility type
370
Table 4.120 Patient satisfaction component scores,by municipality
371
Table 4.121 Patient satisfaction component scores, by type of patient
371
List of Figures
1The Family Health Book Operations Research Design
Figure 1.1 Scatterplot for MMR-IMR, Philippines 2007 27
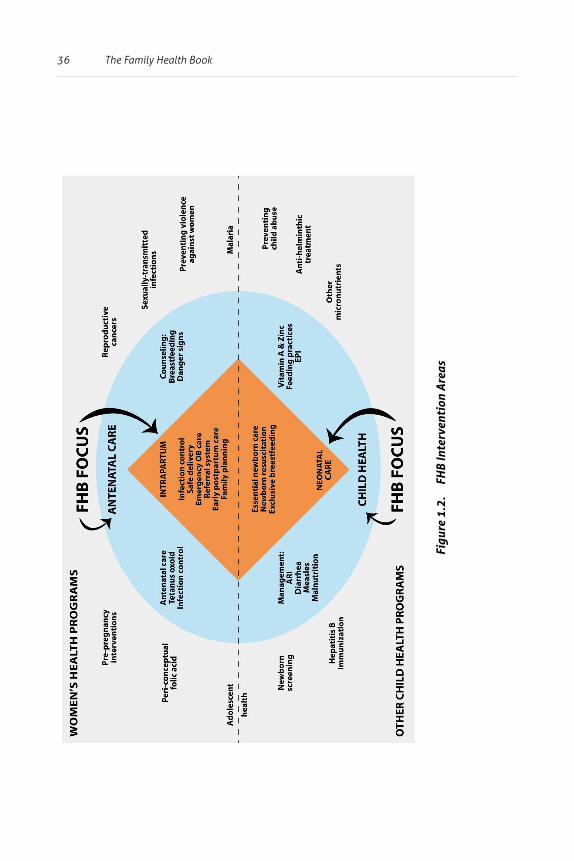
Figure 1.2 FHB Intervention Areas 36
2“Giya sa Maayong Panglawas”: The Family Health Book Implementation in Compostela Valley
Figure 2.1 Stages of Interaction of Families and Navigators 159
3An Analysis of the Impacts of the Family Health Book Interventions
Figure 3.1 Predicted probabilities, MFP use 225
Figure 3.2 Predicted probabilities, at least one ANC visit 228
Figure 3.3 Predicted probabilities: SBA 232
Figure 3.4 Predicted probabilities: FIC 234
18
ANC Antenatal care AOP Annual Operational PlanARI Acute Respiratory InfectionBCC Behavior Change Communication BCG Bacillus Calmette-Guerin BHWs Barangay Health Workers BTL Bilateral Tubal LigationBOY Beginning-of-Year CA Cooperating AgencyCA Cooperating Agency CEmONC Comprehensive Emergency Obstetric and Newborn Care CHD Center for Health Development CO Capital OutlayCoNECT Compostela Network of Communications and Transport CPR Contraceptive Prevalence RateCS Cesarean Section CVPH Compostela Valley Provincial Hospital DMPA Depot Medroxyprogesterone AcetateDOH Department of Health DOTS Directly Observed Treatment, Short-Course DPT Diphtheria Pertussis Tetanus EM Emergency Transport and CommunicationEmONC Emergency Obstetric and Neonatal Care EOY End-of-Year FCS Family Call SheetsFGD Focus Group DiscussionFHB Family Health Book FHSIS Field Health Service Information System FIC Fully Immunized Child FP Family Planning FPS Family Planning SurveyGP General PractitionerHH Household HPDP Health Policy Development Program HUP Health Use PlanIEC Information and Education Campaign
List of Abbreviations and Acronyms
19
IMCI Integrated Management of Childhood IllnessesIP Inpatient IRA Internal Revenue Allotments KII Key Informant InterviewsKSFI Kinasang’an Foundation IncorporatedLCEs Local Chief Executives LGU Local Government Unit MCP Maternal Care Package MFP Modern Family PlanningMHO Municipal Health Office/rMNCHN Maternal, Neonatal and Child Health and NutritionMOOE Maintenance and Other Operating ExpensesNSO National Statistics OfficeNDHS National Demographic and Health SurveyOH Office of HealthOB-Gyn Obstetrician-GynecologistOP OutpatientOPB Outpatient Benefit PackageOPV Oral Polio Vaccine OR Operations Research ORS Oral Rehydration Salts PHO Provincial Health Office/rPhP Philippine PesoPHS Philippine Health StatisticsPNC Prenatal CarePPC Postpartum CarePRO PhilHealth Regional OfficePS Personal Services RH Reproductive HealthRHM Rural Health MidwivesSBA Skilled Birth Attendants SDExH Service Delivery for Excellence in HealthTB TuberculosisTBA Traditional Birth AttendantsTEV Travel Expense Voucher
20
TT Tetanus ToxoidTWG Technical Working GroupUNICEF United Nations Children’s FundUSAID United States Agency for International DevelopmentUTI Urinary Tract InfectionWHO World Health Organization
21
EDITORIAL OVERVIEW:
The Family Health Book
The Family Health Book (FHB) is a behavior change package of interventions which aims to improve utilization of critical services to reduce the risk of maternal and child morbidity and mortality. The FHB was conceived in response to the observation that while the direct causes of maternal and child mortality are clinical in nature, the likelihood of dying from these causes are amplified by the risks of having mistimed and unplanned pregnancies and inadequate antenatal care, of lacking skilled birth attendance during and after delivery, and of low immunization rates among children.
These risks are mitigated through the utilization of critical Maternal, Neonatal and Child Health and Nutrition (MNCHN) services at the pre-pregnancy, pregnancy, delivery, and early childhood phases. FHB interventions thus aim to lessen these risks by addressing at least some family-level barriers to using health services, including the lack of information on what services to access, where and how these services can be accessed, and the means through which these services can be financed, as well as the lack of logistical support to accessing care.
The FHB Operations Research was designed to
(1) establish evidence on whether FHB interventions result in more utilization of MNCHN services and
(2) guide the refinement of specific interventions proven to have positively contributed to increased utilization, before such approaches are recommended for adoption by the Department of Health (DOH) and Centers for Health Development (CHDs).
This volume thus describes the design, implementation, and results of the FHB Operations Research.
22 The Family Health Book
The first article in this volume describes the FHB Operations Research design. It starts with the identification of the barriers that prevent the utilization of critical MNCHN services and details of FHB interventions that seek to address those barriers, to wit:
(1) Provision of information through a “Book” and deployment of “Navigators” to assist families and reinforce information from the book;
(2) Creation of emergency transportation and communication networks; and
(3) Organization of outreach activities which are described in detail.
The article also outlines the methodology for measuring and evaluating the impact of the initiative on key process and intermediate outcome indicators.
The second article in this volume reports on the implementation of the Family Health Book Operations Research (OR) in the province of Compostela Valley. The Family Health Book is known locally as Giya sa Maayong Panglawas. The results of field testing of the book prototype and the family-navigator interaction are described, and revisions on the form of the book, the Navigator’s Kit, and training modules are discussed. Discussion of the highlights of the implementation of each of the interventions, including adjustments made as field operations commenced, follows. Results of monitoring activities, specifically on indicators of input and FHB processes, are then reported, supplemented by results of qualitative assessments.
The third article in this volume presents the methodology for assessing the operations research’s impacts and results. The article begins, by recalling the OR setting and interventions, before detailing data sources and the multivariate models estimated to show the impacts.
The article also reports on the positive impact of FHB interventions on modern family planning (FP) use, antenatal care visits, skilled birth attendance, and immunization of children. For modern family
23
planning (MFP) and skilled birth attendance (SBA), the provision of key information through the Book and the Navigator resulted in increased utilization further amplified by the development of appropriate health use plans (HUPs).
In the case of antenatal care (ANC), the impacts manifested only when appropriate HUPs were developed in response to the information provision. These results suggest that providing key information through a physical medium, supported by personalized guidance and assistance from Navigators that eventually result in families developing plans to address their health risks, are effective in addressing informational barriers to utilization of key MNCHN services.
The Family Health Book Baseline Surveys provided critical information that aided in designing FHB interventions and the operations research, and analyzing its findings. Conducted in Compostela Valley in 2007-2008, the surveys consisted of household, patient exit, and facility surveys that provided baseline information on Compostela Valley residents’ health-seeking behavior and the barriers to care they faced.
The fourth article in this volume describes the surveys’ methodology, the instruments, and summary statistics.
The FHB operations research revealed that provision of information through the Book and Navigators allowed families to understand their health risks and act on them. Subsequently, this informed the development of the DOH Maternal, Neonatal, and Child Health and Nutrition (MNCHN) Strategy Manual of Operations (MOP), and in particular, the definition of the roles and functions of Community Health Teams (CHTs).
CHT navigational functions have been patterned largely after those of the FHB Navigator. In turn, Administrative Order (AO) 2010-0036, “The Aquino Health Agenda: Achieving Universal Health Care for All Filipinos,” provides for the deployment of such CHTs that shall actively assist families in assessing and acting on their health needs. Specific targets for the training and deployment of CHTs are specified in Department Order (DO) 2011-0188, “Kalusugang Pangkalahatan: Execution Plan and Implementation Arrangements.”
24
1 The Family Health Book Operations Research Design
Health Policy Development Program (HPDP)UPecon Foundation Inc. 1
Abstract1
The decline in the maternal and child mortality rates in the Philippines has slowed down over the past few years. While maternal and child mortality can be tied up with direct or clinical causes of death, the likelihood of dying from these causes are amplified by four risks:
1) mistimed and unplanned pregnancies; 2) inadequate antenatal care; 3) lack of skilled birth attendance during and after delivery; and 4) low immunization rates among children.
The Family Health Book (FHB) provides families with information and support mechanisms to access MNCHN services. Information is given through a “Book” and a health “Navigator.”
The Navigator assists families
• on how to use critical information contained in the book, such as health risks and action messages, health emergency contacts, and PhilHealth benefits and availment procedures; and
1 The following contributed to the development of the FHB Operations Research design: Orville Solon, Mary Anne Lansang, Carlo Panelo, Rhodora Tiongson, Jocelyn Ilagan, Aleli D. Kraft, Jhiedon Florentino, Maria Gracia Alcantara, Donabelle de Guzman, Ruth Francisco and Loyd Brendan Norella.
25The Family Health Book Operations Research Design
• how to address their health risks through the development of health use plans.
To facilitate physical access of families to these providers, setting up an emergency transport and communication (EM) network is included among the FHB interventions. The conduct of regular and targeted outreach services is one innovative approach to service delivery in far-flung areas with limited or no access to health providers. .
The Family Health Book (FHB) Operations Research intends to establish evidence on the effects of FHB interventions on the use of services deemed critical to reducing maternal and infant deaths–modern family planning (FP) use, antenatal care visits, safe deliveries, and full immunization of children. The province of Compostela Valley was chosen as the operations research site because of its high maternal and infant mortality despite the presence of basic service delivery structures.
This paper discusses the framework, design, and interventions of the FHB operations research and describes the methodology for measuring and evaluating the impact of the initiative on modern family planning use, antenatal care visit, facility-based delivery, and full immunization of children. It also describes the governance and monitoring arrangements for the field-level implementation of the operations research.
What problems are the FHB trying to solve?
In light of the high incidence of maternal and child mortality in the Philippines, FHB interventions are intended to promote and ensure access to life-saving services. In 2006, 162 mothers died per 100,000 live births and 32 children died per 1,000 live births (NSO, 2007). Around three out of four of these under-five deaths are due to infant mortality (24 per 1,000 live births, of which 13 are neonatal deaths). In the 2007 maternal and child death review for Compostela Valley, a total of 24 mothers and 75 under-five deaths were reported. Of these deaths, 27 were infants (36%) and eight (11%) were newborns.
26 The Family Health Book
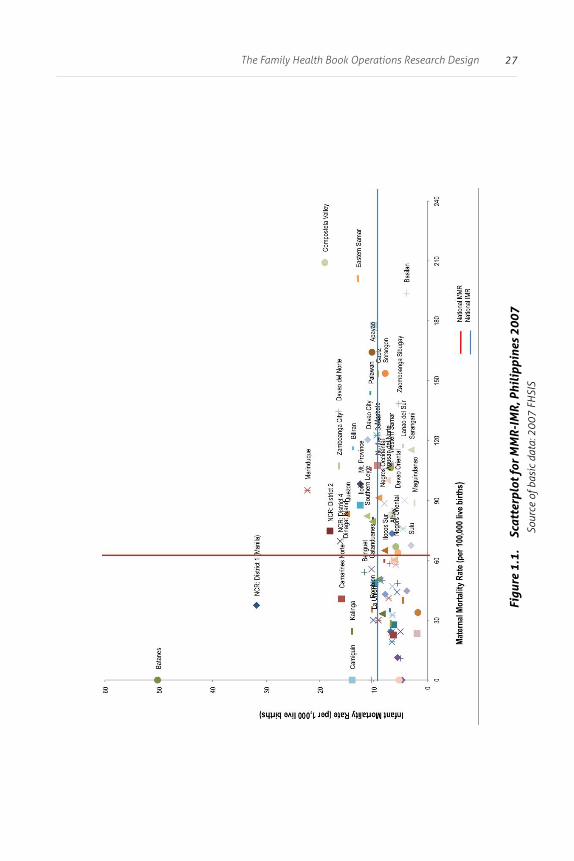
The rate of decline in maternal and infant mortality indicators has also slowed down in the past 10 years, resulting in wide variations in outcomes across income groups and localities in the country (Figure 1.1).
The need to rapidly reduce maternal and child mortality cannot be overstated, as these indicators serve as sensitive indices of performance and equity in any health system. Furthermore, mothers’ and children’s welfare are critical to overall development due to inter-generational impact on human capital development, which in turn is required for families to escape the poverty trap.
What causes can and cannot be affected by FHB interventions?
Direct causes of maternal and child mortality
The direct causes of maternal mortality arise from complications associated with hypertension (28%), postpartum hemorrhage (17%), and complications from abortion (8%) (PHS, 2004). The rest of the direct causes of maternal deaths are due to infection (sepsis) and obstructed labor (DOH, 2005).
Most maternal deaths occur during or within 24 hours after childbirth. In Compostela Valley, most maternal deaths were due to hypertension (33%), followed by hemorrhage (25%) and sepsis (25%). The average age at death of mothers in Compostela Valley was 29 years (range of 15 to 43) (Compostela Valley Provincial Health Office, 2007).
27The Family Health Book Operations Research Design
Figu
re 1
.1.
Scat
terp
lot f
or M
MR-
IMR,
Phi
lipp
ines
200
7So
urce
of b
asic
dat
a: 2
007
FHSI
S
28 The Family Health Book
Leading causes of under-five mortality include pneumonia, accidents, acute gastroenteritis, measles, and congenital anomalies (DOH, 2004). Of the 75 reported child deaths in Compostela Valley, diarrhea accounted for 25%; pneumonia, 21%; and accidents, 13%. The average age at death for under-five children was 1.9 years (Compostela Valley Provincial Health Office, 2007).
On the other hand, common causes of infant death include sepsis, respiratory distress of the newborn, pneumonia, disorders related to prematurity and low birth weight, congenital pneumonia, and congenital malformations (DOH, 2004). Most neonatal deaths occur within the first two days of life (WHO, 2000).
In Compostela Valley province, 48% and 30% of the 27 infant deaths reported were due to diarrhea and pneumonia, respectively. Half of the eight reported neonatal deaths were due to birth asphyxia while another 40% were due to congenital conditions (Compostela Valley Provincial Health Office, 2007).
Risk factors leading to maternal and child mortality
While the direct causes of maternal and child mortality are clinical in nature, the likelihood of dying from these conditions is amplified by four risks:
1. The risk of having a mistimed and unplanned pregnancy. Half of the estimated three million pregnancies that occur each year can be considered mistimed and unplanned. Mothers who have mistimed and unplanned pregnancies are less likely to avail of antenatal services and skilled attendance during delivery (NSO and ORC Macro, 2004). Unwanted and mistimed pregnancies are also more likely to be terminated by induced abortion.
29The Family Health Book Operations Research Design
In Compostela Valley, only one out of four women practiced modern family planning and almost one out of three births was said to be mistimed and unplanned -- despite the expressed desired spacing interval of 4.5 years. This highlights the substantial unmet need for family planning and the risk of mortality (HPDP, 2007b).
2. Inadequate and poor quality care. Once pregnant, the woman and her fetus face the risk of inadequate and poor quality care during the course of the pregnancy.
Nearly half of pregnant women suffer from iron deficiency anemia, a fourth are considered undernourished, and a fifth lack vitamin A. On the average, only 70% of mothers would have at least four prenatal visits during the course of the pregnancy (NSO and ORC Macro, 2004).
In Compostela Valley, only 45% of mothers had at least three antenatal care (ANC) visits. There is a large variation in quality of care among providers serving the province (HPDP, 2007a).
3. Delivery without skilled birth attendants (SBA). Home deliveries, attended mostly by traditional birth attendants (TBAs), currently account for 63% of deliveries in the country (NSO and ORC Macro, 2004).
In Compostela Valley, home-based TBA births account for nearly 70% of all deliveries. According to the Compostela Valley Maternal Death Report, all births that led to maternal deaths were initially managed at home by TBAs.
30 The Family Health Book
Home-based TBA births are risky because the non-sterile home environment increases the likelihood of infections. In addition, the TBA may not be able to promptly handle and refer complications like excessive bleeding and fetal distress to trained medical practitioners. Delivering mothers in home-based TBA birth settings usually do not have ready access to Comprehensive Emergency Obstetric and Neonatal Care (CEmONC) services in the event of complications.
4. Absence of child survival services. Child survival include promotion of and support for exclusive breastfeeding for at least six months, and immunizations and other services included in the Integrated Management of Childhood Illnesses (IMCI) strategy. In Compostela Valley, the fully-immunized child (FIC) rate was only 83% (DOH, 2007), way below the national target of 95% (HPDP, 2007b).
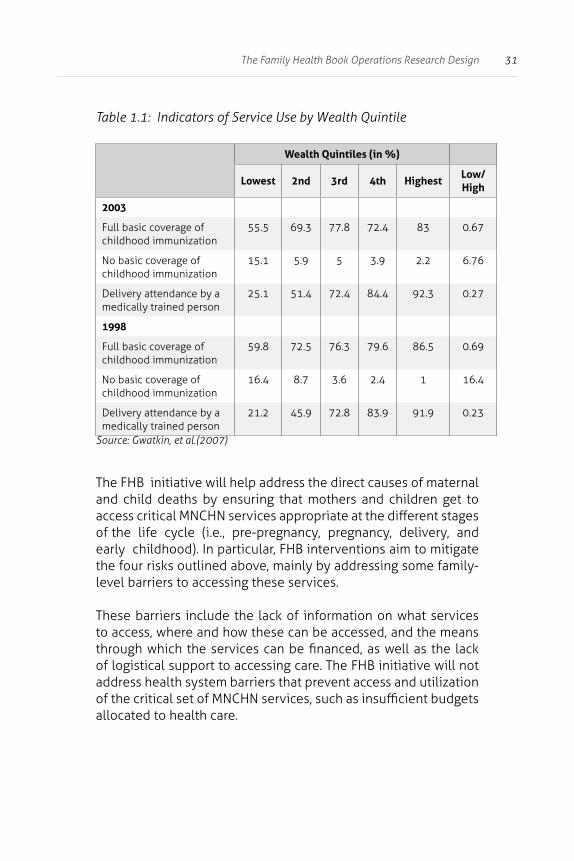
The magnitude of these risks increases across socio-economic groups and varies with other structural factors. Poor mothers were around three times less likely to avail of SBA services during delivery compared to those in the highest income quintile (Table 1.1). Moreover, children from poor families were less likely to complete their immunization schedule compared to those in the richest quintiles (NSO and ORC Macro, 2004).
31The Family Health Book Operations Research Design
Table 1.1: Indicators of Service Use by Wealth Quintile
Wealth Quintiles (in %)
Lowest 2nd 3rd 4th HighestLow/High
2003
Full basic coverage of childhood immunization
55.5 69.3 77.8 72.4 83 0.67
No basic coverage of childhood immunization
15.1 5.9 5 3.9 2.2 6.76
Delivery attendance by a medically trained person
25.1 51.4 72.4 84.4 92.3 0.27
1998
Full basic coverage of childhood immunization
59.8 72.5 76.3 79.6 86.5 0.69
No basic coverage of childhood immunization
16.4 8.7 3.6 2.4 1 16.4
Delivery attendance by a medically trained person
21.2 45.9 72.8 83.9 91.9 0.23
Source: Gwatkin, et al.(2007)
The FHB initiative will help address the direct causes of maternal and child deaths by ensuring that mothers and children get to access critical MNCHN services appropriate at the different stages of the life cycle (i.e., pre-pregnancy, pregnancy, delivery, and early childhood). In particular, FHB interventions aim to mitigate the four risks outlined above, mainly by addressing some family-level barriers to accessing these services.
These barriers include the lack of information on what services to access, where and how these can be accessed, and the means through which the services can be financed, as well as the lack of logistical support to accessing care. The FHB initiative will not address health system barriers that prevent access and utilization of the critical set of MNCHN services, such as insufficient budgets allocated to health care.
32 The Family Health Book
What critical set of services will be promoted by the FHB?
FHB interventions seek to improve utilization of a critical set of MNCHN services accessed as a package, reflecting the continuum of care from pre-pregnancy, pregnancy, delivery and postpartum, to neonatal and early childhood. Efforts to increase utilization will focus on a core set of critical services identified to have the greatest impact on maternal and child mortality based on best available evidence and accepted standards of practice (Habana, Mantaring, et al., 2008).
Modern Family Planning
Use of modern family planning methods can prevent mistimed and unplanned pregnancies which contribute to maternal mortality by unnecessarily increasing fertility rates. Fertility reduction has been identified as the most cost-effective intervention in preventing maternal and infant mortality in Bangladesh (NIPORT et al., 2003).
Furthermore, mistimed and unplanned pregnancies also decrease the likelihood of availing of antenatal care services and skilled attendance during deliveries, thus increasing the risk of complications and death. The following modern family planning methods shall be promoted by the FHB:
1. lactational amenorrhea method; 2. temperature or thermometer method; 3. cervical mucus method; 4. sympto-thermal method; 5. standard days method; 6. oral contraceptive pills;7. condom; 8. injectable hormones or DMPA; 9. intrauterine device; 10. bilateral tubal ligation (a permanent
method); and 11. non-scalpel vasectomy (a permanent
method).
33The Family Health Book Operations Research Design
Antenatal Care (ANC)
ANC services help avoid missed opportunities in providing a set of services aimed at preventing maternal morbidity and infant mortality. In the course of undertaking at least four ANC visits, the mother needs to at least receive the following interventions:
1) counseling on danger signs;
2) tetanus immunization to prevent maternal and neonatal infections;
3) micronutrient supplementation, such as iron (to prevent anemia) and folate (to prevent congenital malformations in the fetus);
4) screening for complications that will require early referral to specialized care facilities; and
5) planning for SBA during delivery.
While prevailing evidence downplays antenatal care’s role in maternal mortality reduction, it remains distinctly clear that components of prenatal care remain effective in reducing perinatal deaths (Bale et al., 2003).
Safe Delivery and Postpartum Care
Access to SBA during deliveries, including Comprehensive Emergency Obstetric and Newborn Care (CEmONC) services, addresses most direct causes of maternal and infant mortality (Campbell and Graham, 2006).
Delivery by non-skilled attendants hampers early detection of complications, referral to higher facilities, and early treatment of complications, thus increasing the risk of death.
34 The Family Health Book
Furthermore, improper postpartum and postnatal care also contribute significantly to increased maternal and neonatal morbidity and mortality. The following interventions crucial to reduce maternal deaths should be part of health providers’ protocols:
1) active management of the third stage of labor using oxytocin and proper cord traction;
2) use of antibiotics in prolonged labor or prolonged rupture of membranes;
3) use of the anticonvulsant magnesium sulfate;
4) use of partographs for monitoring progress of labor;
5) post-abortion care, including removal of retained products of conception, treatment of infection, correction of anemia, and anti-tetanus injections; and
6) administration of steroids for pre-term labor.
Newborn and Early Childhood Care
Reducing neonatal mortality requires the following procedures:
1) neonatal resuscitation;
2) STABLE (sugar, temperature, artificial breathing, blood pressure, laboratory work, and emotional support);
3) delayed cord clamping;
4) early latching on;
35The Family Health Book Operations Research Design
5) Routine newborn care (cord care, thermoregulation, weighing of the infant, application of erythromycin eye ointment, administration of vitamin K, hepatitis B vaccination, BCG vaccination); and
6) advanced pediatric life support.
Vaccine-preventable diseases like measles, polio, diphtheria, pertussis, tetanus, tuberculosis, and Hepatitis B can be fatal, but are preventable through vaccination. In countries where fully–immunized child (FIC) rates are low and herd immunity is not achieved, these diseases account for a significant cause of morbidity and mortality, aside from neonatal causes.
Other causes of child mortality, such as acute respiratory infections, benefit from early detection, referral, and antibiotic treatment. Acute gastroenteritis is highly preventable through breastfeeding, proper hygiene, and use of oral rehydration salts (ORS).
Other necessary services will still be implemented subject to the local health systems’ capacity to provide. A critical list of services was disseminated to providers and served as basis for developing the vignettes to assess for quality of care during the facility survey at baseline. Figure 1.2 shows how core FHB interventions relate with the rest of MNCHN and related interventions addressing maternal and child mortality.
36 The Family Health Book
Figu
re 1
.2.
FHB
Inte
rven
tion
Are
as
37The Family Health Book Operations Research Design
What family level barriers to the utilization of critical services can and cannot be influenced by the FHB?
Barriers to families’ utilization of health services significantly contribute to poor health outcomes. Even where health facilities, services, and supplies are available, many families do not use appropriate services because
• they do not recognize health risks; • they do not know the services they need, • they do not know where these services are available, • they do not know how to finance their access to these services.
Data from Compostela Valley illustrate examples of these barriers.
Lack of knowledge on risks and conse-quences
Information from focus group discussions (FGDs) from Compostela Valley illustrates the importance of cultural factors and the possession of information on the risks and consequences related to providers and services (HPDP and SDRC, 2008; Acuin, 2008).
FGD results show that only about one in every three reproductive-age women practiced modern family planning. More than half of those who did not were afraid of side effects. One out of ten was not aware of family planning. Close to half of pregnant participants did not undergo at least three ANC visits, with 16% of mothers thinking the visits were not necessary (HPDP, 2007b).
Close to eight of ten births were delivered at home under the care of TBAs. Many women preferred delivery with TBAs because it had been the practice in the family. Mothers who depended on TBAs for a long time would pass on this custom to their daughters.

38 The Family Health Book
The FGD also revealed that mothers find TBAs convenient since they are easier to summon and are willing to visit them even in the middle of the night. TBAs are also more considerate of expectant mothers’ needs and comfort. Respondents point out that they can scream during delivery without being scolded, and their husbands are allowed to stay by their side during delivery. Home deliveries also provide them with a sense of privacy and comfort, as the woman is not forced to lie on a delivery table with her genitals exposed.
The family does not need to worry about care support for the other children during home-based deliveries, unlike during facility-based deliveries when the father and/or other family members have to leave children at home to take care of the mother and her newborn.
FGD findings also reveal that decisions to seek care from health facilities were often made only when the delivery had become difficult or when complications arose (HPDP and SDRC, 2008). One out of four mothers also believed that delivering with TBAs was safe (HPDP, 2007b).
The FHB will address this barrier through the provision of vital information on health needs and health risks contained in a convenient media. Assigned Navigators can further explain these messages, dispel misconceptions and allay concerns of families.
39The Family Health Book Operations Research Design
Inacces-sibility of facilities
While only one out of twenty reported that distance and accessibility of facilities hampered family planning use, four out of ten mothers who did not avail of antenatal care services said going to the facilities was an inconvenience.
Another 15% said the facilities were inaccessible (HPDP, 2007b). Certain areas in Compostela Valley are difficult to reach due to terrain. In areas where public transportation is available, the trips are often long, infrequent, and costly. These barriers affect access patterns for routine and emergency care.
FHB intervention will address this barrier through the establishment of transportation and communication support networks for emergencies, and organization of outreach programs that provide regular public health services. However, the FHB will not intervene in improving transport and road conditions or providing subsidies for transportation costs.
What gaps and bottlenecks in the delivery system can and cannot be influenced by the FHB?
There are also delivery system gaps and bottlenecks that prevent families from accessing services. These include:
1) lack of available services and providers; 2) poor quality of services provided; 3) inadequate supply of health goods and commodities; 4) high user fees; 5) lack of access to emergency transport and communications; 6) insufficient health budgets; 7) unstable peace and order conditions;
40 The Family Health Book
8) geographic isolation; and 9) environmental hazards.
Lack of availability of services and providers
Access to services was largely contingent on the availability of services and qualified providers in the area. A survey of Compostela Valley services and facilities shows wide variations in accessibility of specific types of services across municipalities (see Table 1.2).
Of the 79 physicians practicing in the province, there were nine obstetrician-gynecologists, seven surgeons, five pediatricians, three internists, and one anesthesiologist. The remaining 54 physicians were generalists.
At the time of the survey, Cesarean section deliveries and blood banking services were usually done at the Davao Regional Hospital in Tagum City (HPDP and SDRC, 2008). Furthermore, the ability of PhilHealth members to avail of their privileges depended in part on the availability of accredited facilities.
Of the 38 health facilities in Compostela Valley, only 17 had PhilHealth accreditation. None of the 14 private clinics were PhilHealth-accredited or had Sentrong Sigla certification. Although all 11 RHUs had Sentrong Sigla certifications, 4 RHUs were not PhilHealth Outpatient Benefit (OPB)-accredited.
Only 33% of physicians and 14% of midwives had PhilHealth accreditation (HPDP, 2007a). During the provider orientations, one hospital was found to be operating without a license and was dropped from the FHB list of providers.
41The Family Health Book Operations Research Design
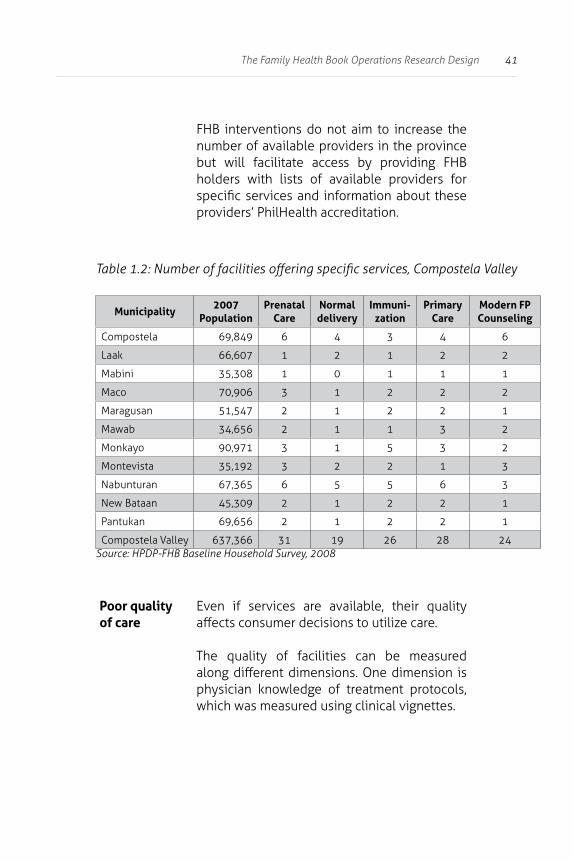
FHB interventions do not aim to increase the number of available providers in the province but will facilitate access by providing FHB holders with lists of available providers for specific services and information about these providers’ PhilHealth accreditation.
Table 1.2: Number of facilities offering specific services, Compostela Valley
Municipality2007
PopulationPrenatal
CareNormal delivery
Immuni-zation
Primary Care
Modern FP Counseling
Compostela 69,849 6 4 3 4 6
Laak 66,607 1 2 1 2 2
Mabini 35,308 1 0 1 1 1
Maco 70,906 3 1 2 2 2
Maragusan 51,547 2 1 2 2 1
Mawab 34,656 2 1 1 3 2
Monkayo 90,971 3 1 5 3 2
Montevista 35,192 3 2 2 1 3
Nabunturan 67,365 6 5 5 6 3
New Bataan 45,309 2 1 2 2 1
Pantukan 69,656 2 1 2 2 1
Compostela Valley 637,366 31 19 26 28 24Source: HPDP-FHB Baseline Household Survey, 2008
Poor quality of care
Even if services are available, their quality affects consumer decisions to utilize care.
The quality of facilities can be measured along different dimensions. One dimension is physician knowledge of treatment protocols, which was measured using clinical vignettes.
42 The Family Health Book
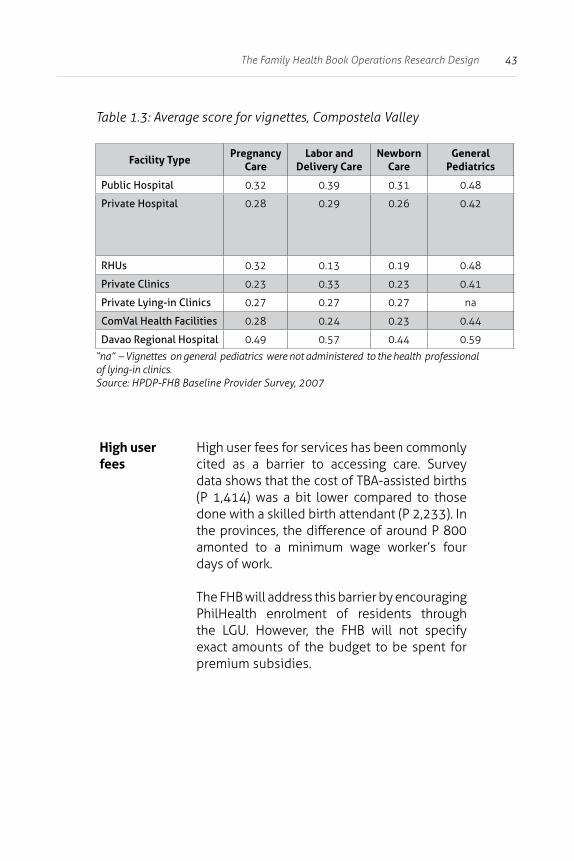
Data from the Compostela Valley baseline indicated that the providers on the average scored less than 30% for pregnancy-related vignettes and less than 50% for general pediatrics. Both fell short of the 55% cut-off score set at baseline (Table 1.3).
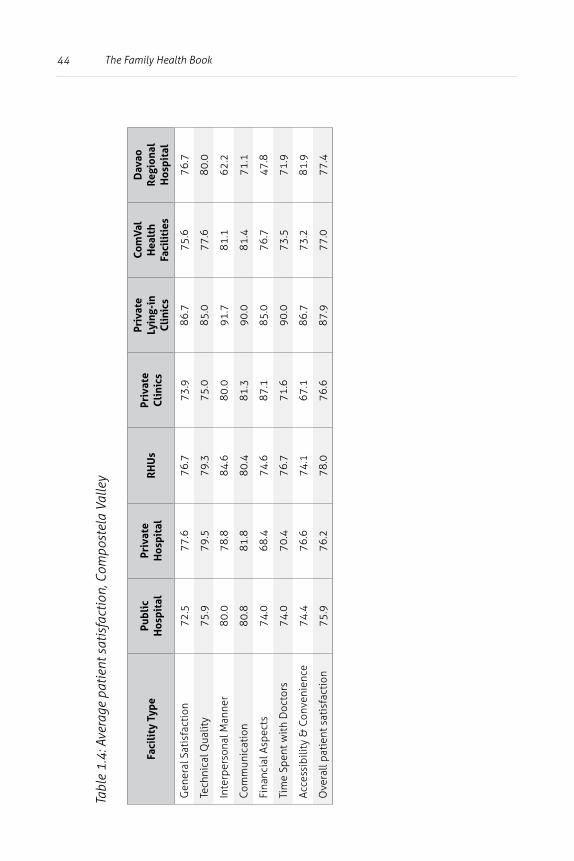
Another dimension of quality is the level of patient satisfaction for services rendered. Table 1.4 indicates that in general, close to three out of every four patients were satisfied with services they received. While patient satisfaction did not differ much across public and private facilities, private lying-in clinics registered higher satisfaction levels.
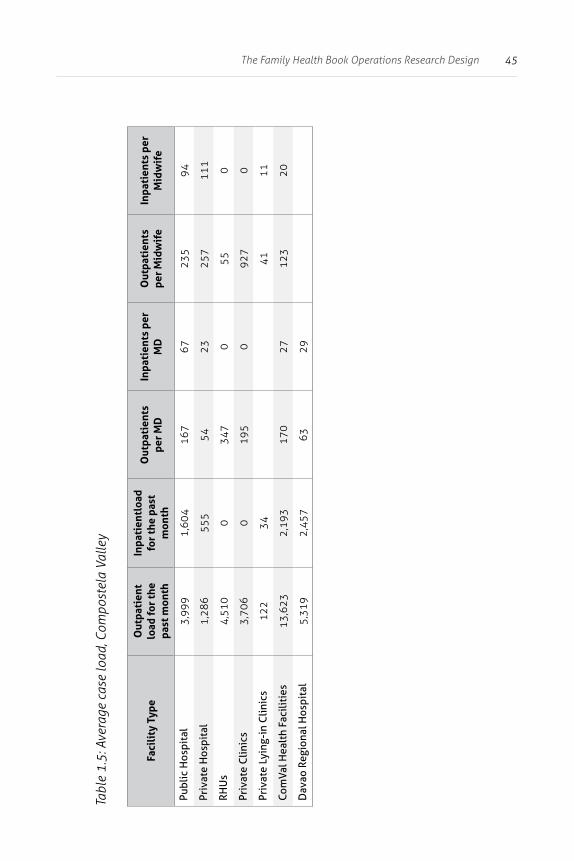
The facility’s patient load was also used as an indicator of quality of services. Table 1.5, which indicates the average case load of Compostela Valley providers, shows that public facilities had relatively higher patient load than private facilities.
The FHB can partly mitigate this barrier by facilitating access to resources needed to upgrade selected facilities. In particular, the focus of support will be the Compostela Valley Provincial Hospital (CVPH) to enable it to better provide CEmONC services. However, FHB will not do this for all facilities in the province.
Inadequate supplies and commodities
In the FGDs, many families reported not going to facilities because either services or supplies were not available. While service and supply inventory indicators such as drug stock out rates are not routinely collected, a proxy index of the lack of supplies could be that 88% of Compostela Valley residents resort to self-medication when ill (HPDP, 2007b). FHB interventions will not purchase nor supplement the commodities in the facilities.
43The Family Health Book Operations Research Design
Table 1.3: Average score for vignettes, Compostela Valley
Facility TypePregnancy
CareLabor and
Delivery CareNewborn
CareGeneral
Pediatrics
Public Hospital 0.32 0.39 0.31 0.48
Private Hospital 0.28 0.29 0.26 0.42
RHUs 0.32 0.13 0.19 0.48
Private Clinics 0.23 0.33 0.23 0.41
Private Lying-in Clinics 0.27 0.27 0.27 na
ComVal Health Facilities 0.28 0.24 0.23 0.44
Davao Regional Hospital 0.49 0.57 0.44 0.59
“na” – Vignettes on general pediatrics were not administered to the health professional of lying-in clinics.Source: HPDP-FHB Baseline Provider Survey, 2007
High user fees
High user fees for services has been commonly cited as a barrier to accessing care. Survey data shows that the cost of TBA-assisted births (P 1,414) was a bit lower compared to those done with a skilled birth attendant (P 2,233). In the provinces, the difference of around P 800 amonted to a minimum wage worker’s four days of work.
The FHB will address this barrier by encouraging PhilHealth enrolment of residents through the LGU. However, the FHB will not specify exact amounts of the budget to be spent for premium subsidies.
44 The Family Health Book
Tabl
e 1.
4: A
vera
ge p
atie
nt s
atis
fact
ion,
Com
post
ela
Valle
y
Faci
lity
Typ
ePu
blic
H
ospi
tal
Priv
ate
Hos
pita
lR
HU
sPr
ivat
e C
lini
cs
Priv
ate
Lyin
g-in
Cl
inic
s
Com
Val
Hea
lth
Faci
liti
es
Dav
ao
Regi
onal
H
ospi
tal
Gen
eral
Sat
isfa
ctio
n72
.577
.676
.773
.986
.775
.676
.7
Tech
nica
l Qua
lity
75.9
79.5
79.3
75.0
85.0
77.6
80.0
Inte
rper
sona
l Man
ner
80.0
78.8
84.6
80.0
91.7
81.1
62.2
Com
mun
icat
ion
80.8
81.8
80.4
81.3
90.0
81.4
71.1
Fina
ncia
l Asp
ects
74.0
68.4
74.6
87.1
85.0
76.7
47.8
Tim
e Sp
ent w
ith
Doc
tors
74.0
70.4
76.7
71.6
90.0
73.5
71.9
Acce
ssib
ility
& C
onve
nien
ce74
.476
.674
.167
.186
.773
.281
.9
Ove
rall
pati
ent s
atis
fact
ion
75.9
76.2
78.0
76.6
87.9
77.0
77.4
45The Family Health Book Operations Research Design
Tabl
e 1.
5: A
vera
ge c
ase
load
, Com
post
ela
Valle
y
Faci
lity
Typ
eO
utpa
tien
t lo
ad fo
r th
e pa
st m
onth
Inpa
tien
tloa
d fo
r th
e pa
st
mon
th
Out
pati
ents
pe
r M
DIn
pati
ents
per
M
DO
utpa
tien
ts
per
Mid
wif
eIn
pati
ents
per
M
idw
ife
Publ
ic H
ospi
tal
3,99
91,
604
167
6723
594
Priv
ate
Hos
pita
l1,
286
555
5423
257
111
RHU
s4,
510
034
70
550
Priv
ate
Clin
ics
3,70
60
195
092
70
Priv
ate
Lyin
g-in
Clin
ics
122
3441
11
Com
Val H
ealt
h Fa
cilit
ies
13,6
232,
193
170
2712
320
Dav
ao R
egio
nal H
ospi
tal
5,31
92,
457
6329

46 The Family Health Book
Lack of access to emergency transporta-tion and communi-cation
Compostela Valley residents usually resort to private means of transportation and communication -- if ever these are available -- during emergencies. While there were at least six government ambulances and an undetermined number of private vehicles with informal arrangements with communities, these were not organized as a formal network to serve the needs of the province.
Neither did households know how to access emergency transport. Emergency communications was mainly done through a radio network connecting the four public hospitals. While cellular phone access has increased over the past few years, only about one in three households had access to cellular phones in some areas. The peculiarity of single-side band radio system and cellular phones’ private nature limit household access to communication facilities to connect with the rest of the health system, especially during emergencies.
FHB interventions will address these barriers, not through the provision of vehicles and communication equipment, but through the establishment of a transport and communications network using local resources and initiatives.
Local health budget levels and allocations
The 2007 province-wide health budgets amounted to P 135.7 million, or 11% of total internal revenue allotments (IRA). Most of these monies (61%), was spent on personal services (PS) followed by maintenance and other operating expenses (MOOE) (30%) and capital outlay (CO) (2%). Around 7% was spent on programs.
47The Family Health Book Operations Research Design
Close to 60% of the IRA allocation is spent on the four hospitals, leaving very little for public health functions. Of these amounts, 54% goes to PS, 43% to MOOE, and only 3% to CO. The FHB will be able to generate estimates of service demands, which can guide LGUs on how to allocate these budgets, given fiscal constraints. The FHB, however, will not intervene in terms of increasing LGU budgets for health.
Peace and order
Implementation of FHB interventions depends largely on the peace and order situation in the area. Family access to Navigators, health emergency networks, health facilities, and outreach activities hinges on the feasibility and safety of operations in the area and the continuing support of the local government as well as other stakeholders. No FHB intervention was identified to address the special needs of internally displaced persons or people in conflict with the law.
Geographic and envi-ronmental hazards
Transport and communication providers, as well as Navigators and health facilities, may not venture in far-flung or hard-to-reach areas for logistical and practical reasons. This puts families in these locations in a disadvantaged position since they cannot use services they are entitled to receive nor fully tap the assistance Navigators should routinely provide. Despite FHB interventions, accessibility factors resulting from beneficiaries’ geographical locations and the environmental hazards these bring effectively limit their utilization of health care services.
48 The Family Health Book
What are the FHB interventions?
The FHB initiative is a package of interventions directed at addressing health care use barriers. This package provides essential health information backed by a supportive environment that enables target families to initiate and sustain the targeted behavior, i.e., the utilization of critical maternal and child health care services. Thus, FHB interventions include the linking of families to emergency transportation and communication services and mitigating the effects of geographic isolation and cost of transportation for routine health care.
FHB interventions are designed to inform and guide families in understanding health risks, in knowing and deciding on what services to access, in planning for and using these services, in knowing where to access transport and communication networks for emergency care services, and in identifying facilities where they can avail of essential family planning and MNCHN services.
In addition, the FHB initiative has complementary activities designed to address the lack of quality providers for safe deliveries, postpartum and neonatal care, and the lack of social health insurance that would effectively reduce out-of-pocket expenses. The FHB will accomplish this through three complementary interventions:
1) providing information through a book and deploying Navigators to assist families and reinforce information from the book;
2) establishing emergency transportation and communication networks; and
3) organizing outreach activities.

49The Family Health Book Operations Research Design
Providing vital information through the Family Health Book and Navigators
The FHB provides information to families in a way that allows them to understand and recognize health risks resulting from mistimed and unplanned pregnancies; inadequate or lack of prenatal and postpartum care; deliveries not attended by SBAs; unimmunized children and poor infant and childcare. Such information will guide families in determining the essential health services they need and identifying the health providers available in their area (i.e.,licensed and accredited providers, fee schedule, location, and their contact numbers) to address such risks and plan for the eventual utilization and financing of such services. Providing this information to families allows them to take effective responsibility for their own health.
This intervention proposes to use Navigators to reinforce the information contained in the book. The Surveys and FGD findings have validated the idea of engaging families to assist them and reinforce information they receive.
Both the HealthGov survey and baseline survey results point to barangay health workers (BHWs) and health volunteers as likely candidates for this navigation role, being the traditional and preferred conduits of information. Mothers in one Family Planning FGD expressed preference for face-to-face interaction when relaying family planning information (Acuin, 2008). The combined use of information and a health worker to complement the intervention has been proven effective in a pilot implemented in Davao del Norte and Compostela Valley (Costello et al., 2001).
Book
The Book is organized into sections which allow the families, with the help of their Navigator and providers, to go through the following FHB cycle:
1) orientation; 2) needs assessment; 3) health use planning; and 4) adherence to developed health use plans.
50 The Family Health Book
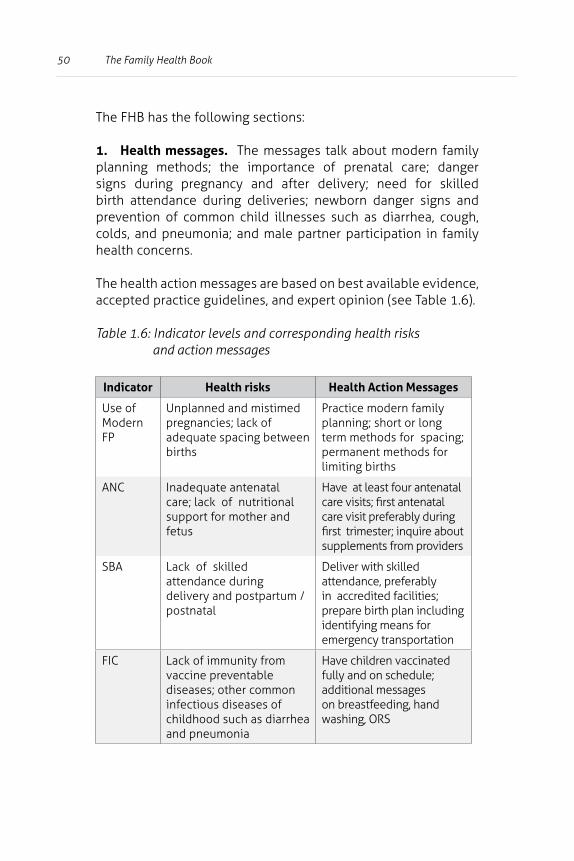
The FHB has the following sections:
1. Health messages. The messages talk about modern family planning methods; the importance of prenatal care; danger signs during pregnancy and after delivery; need for skilled birth attendance during deliveries; newborn danger signs and prevention of common child illnesses such as diarrhea, cough, colds, and pneumonia; and male partner participation in family health concerns.
The health action messages are based on best available evidence, accepted practice guidelines, and expert opinion (see Table 1.6).
Table 1.6: Indicator levels and corresponding health risks and action messages
Indicator Health risks Health Action Messages
Use of Modern FP
Unplanned and mistimed pregnancies; lack of adequate spacing between births
Practice modern family planning; short or long term methods for spacing; permanent methods for limiting births
ANC Inadequate antenatal care; lack of nutritional support for mother and fetus
Have at least four antenatal care visits; first antenatal care visit preferably during first trimester; inquire about supplements from providers
SBA Lack of skilled attendance during delivery and postpartum / postnatal
Deliver with skilled attendance, preferably in accredited facilities; prepare birth plan including identifying means for emergency transportation
FIC Lack of immunity from vaccine preventable diseases; other common infectious diseases of childhood such as diarrhea and pneumonia
Have children vaccinated fully and on schedule; additional messages on breastfeeding, hand washing, ORS
51The Family Health Book Operations Research Design
To allow customization of the various health messages to individual families and help determine what services are needed, the families, guided by their respective Navigators, need to assess their health status and anticipated health risks.
This can be done with the Health Risk and Needs Assessment tool in the Navigator’s kit. This tool allows the family, with the assistance from their Navigator, to better understand what health risks threaten their family, to identify critical health needs, and more importantly, to prompt them for action based on the applicable health messages. A summary report on the assessment will be given to the family. It will also be shown to a health provider for the development of a health use plan. The use of a health needs assessment form builds on the experience on the use of self-assessment tools such as growth charts that prompt users to act on specific findings.
The development of the health assessment tool builds on the experience with similar diagnostic checklists that ask questions from users based on characteristics or symptom patterns, including the triage or systematic screening checklists used by clinic staff (FHI, 2003) and a combination of patient education booklets and symptom checklist forms for TB patients (Datta and Nichter, 2003).
2. Health Use Plan. This will help families, assisted by the Navigator and in consultation with their provider, determine the steps necessary to act on identified health risks and needs.
The health use plan serves as a guide and reminder for families and providers in achieving desired goals. These health use plans will help the Navigator remind families and monitor their adherence to these plans.
Health use plans are an expanded application of birth plans -- drawn up by mothers in preparation for delivery -- being promoted by the DOH. The FHB contains separate health use plans for reproductive health and family planning needs, birth and delivery, sick child consultations, well-baby visits, and health emergency situations. A guide on how to avail of PhilHealth benefits will be integrated into the health use plan so that families, their Navigator, and their health providers can plan ahead and prepare specific requirements to access PhilHealth benefits.
52 The Family Health Book
3. Providers’ list. This includes information on locally-available providers, their location, contact numbers, fees, DOH licensing and PhilHealth/Sentrong Sigla accreditation status and available services.
This section addresses survey data and FGD findings that point to the lack of awareness on where services are being provided, who the licensed and accredited providers are and what services are being offered as important obstacles to health care utilization.
4. PhilHealth information. Significant gains could be generated from providing adequate PhilHealth information considering that a third of members are not aware of PhilHealth benefits and that half of mothers were not able to file claims. Inserts of PhilHealth information materials are included in the FHB. Reminders to PhilHealth members for them to seek care in accredited facilities and prepare documents required to file for claims are also mentioned in applicable health use plans the families will develop.
5. Contact information of the emergency transport and communication network. This information will provide families with the name of the person to contact during emergencies. These persons either operate the vehicle itself, or have authority to deploy transport. In some cases, these same persons listed may be the designated communication “hub” in isolated localities where cell phone access is limited.
To come up with the book, the following tasks and activities need to be undertaken:
• identify families who would most benefit from the information to be provided;
• develop the appropriate content and the form to ensure usefulness and acceptability to families;
• reproduce the book;
• distribute copies of the book to targeted beneficiaries; and
• regularly update the book’s contents to ensure continuing relevance.
53The Family Health Book Operations Research Design
In the identification of families, analysis of FHB Baseline Survey data undertaken with support from HPDP indicated that families which would benefit from use of the book are those with mothers who did not finish high school and those which satisfy the following criteria:
1) pregnant;
2) below 25 years old and with at least one child below five years old; and
3) 25 years old and above with at least two children below five years old.
Mothers belonging to low-income families or those with less than high school education are to be given priority since they are vulnerable to adverse health conditions, being unable to afford minimum basic needs for food, health, and other social amenities. National Statistics Office (NSO) data show that the poor spent more on food, fuel, and utilities in 2006, which took away 66% of the family budget. Given the worsening food and energy crisis in the last two years, we expect the poor to dig deeper into their pockets to cover food essentials, leaving very little for education and health.
The FHB Navigators
Navigators are expected to orient families and assist them in determining their health risks and assessing their health needs. They are also expected to guide families, together with the health providers, in developing health use plans, and do follow-up visits to monitor adherence to those plans. The Navigator links the families to providers and the emergency transport and communication network. In addition, Navigators also report families’ needs to the midwife and municipal health officer and help coordinate and organize FHB outreach activities.
Interaction between the families and the Navigators will allow families to become comfortable about discussing further any health risks and needs, and about choosing providers and
54 The Family Health Book
actually going to the identified provider. Constant reminders by Navigators will also increase families’ adherence to health use plans, hence, increasing the utilization of appropriate services.
Critical activities for the deployment of Navigators include the following:
1) selection and recruitment of Navigators;
2) matching of families with Navigators;
3) Navigator training including the development of instruction materials;
4) provision of continuous capacity building activities for Navigators;
5) provision of logistical support and incentives including support to their PhilHealth enrolment; and
6) monitoring and supervision of Navigators.
Selection and recruitment of Navigators
As a source of information for the family, recruited Navigators should be credible and be able to provide sufficient attention to the families they are managing.
Each Navigator will be assigned around 20 families in the community, which is consistent with the DOH standard. Simple application of this ratio identifies the minimum number of Navigators to be trained to cover the identified families. However, this number can be increased to ensure coverage of all FHB families in all puroks. The distribution of Navigators is to be based on the number of FHB families identified per barangay.
55The Family Health Book Operations Research Design
The initial 40 Navigators recruited for the FHB were chosen using the following criteria:
1) with at least two years of health-related activities in the community;
2) able to work with local officials;
3) with at least two years of high school education;
4) able and willing to regularly visit the households covered;
5) with good interpersonal communication skills and highly motivated; and
6) respected in the community.
The criteria were later relaxed due to a very limited number of Navigators who met the educational criteria. Those who finished elementary education were considered qualified provided that they had more than two years of health-related experience. HPDP assisted in identifying, recruiting, and training 40 Navigators. Out of these, 12 (three per municipality) were trained and tapped to participate in the FHB field testing. Results of the field assessment suggested limiting the number of families to be managed by Navigators (hence the need to recruit more Navigators) or delegating some of the Navigator tasks to other families.
56 The Family Health Book
Matching of families with Navigators
Careful matching of Navigators and families is crucial to the smooth implementation of the FHB initiative.
The process should take due consideration on the cultural context of a particular group or community (e.g., indigenous population, religious groups, etc.).
Navigator training
This entails the development of the following:
1) a training module (facilitator’s guide) for the core trainers who will be training the rest of the Navigators;
2) training modules for Navigators; and
3) the Navigator’s kit or instruction manual for the Navigators.
The core set of trainers came from the DOH, selected municipal health officers (MHOs), nurses, midwives, and other trainers, including from among Navigators themselves. The trainers are expected to provide mentoring support to the Navigators.
The module for Navigators shall consist of:
1) an overview of the health situation in the province;
2) the FHB Initiative and its components,
3) an orientation on FHB concepts including family planning and maternal and child health;
57The Family Health Book Operations Research Design
4) steps in engaging the families to participate in the FHB Initiative;
5) training for enhancing communication
and health teaching skills;
6) an orientation on PhilHealth benefits availment; and
7) training on the development and monitoring of related forms.
Navigators should have relational skills development in their training. Improvement in Navigators’ presentation, facilitation, and relational and negotiation skills using both non-verbal and verbal approaches will enable them to better explain health messages and health use plans in the FHB.
The Navigator’s Kit serves as an instructional manual for effectively engaging families, monitoring their compliance to health use plans and coordinating with midwife supervisors for technical and operational guidance (HPDP, 2008). The first part of the kit gives an FHB backgrounder while the second part shows how to engage families.
The key processes described in the second part include orienting families, assessing and determining health risks and needs, assisting families in developing their health use plans, encouraging families to access appropriate services, and following up on families.
58 The Family Health Book
Navigators should follow an appropriate communications strategy in talking to the families to help them better understand and act on key health messages. This strategy is discussed in the Navigator’s Kit, which gives concrete guidelines on how to maximize attention, like suggested scripts and scenarios. Navigators can employ these guidelines to contextualize messages to the families’ particular situation, and reinforce messages.
Provision of continuous and sustained capacity-building
The Navigator’s work requires continuous and sustained capability building on maternal and child health.
LGUs and concerned cooperating agencies (CA) should conduct re-orientation and refresher training on these essential public health programs on a staggered or modular basis to constantly update and build the knowledge among Navigators on MNCHN concepts and standards.
These capability-building activities are expected to help Navigators guide FHB families in health needs assessment, health planning, and accessing of health services.
Logistical support and incentives
As local issuances are critical to sustain Navigator community activities, LGU should make budgetary appropriations for these activities.
Local advocacies, policies, and resolutions to strengthen LGU-private partnerships (e.g., private sponsors supporting FHB Navigators) are essential to generate additional support for Navigators. In addition, incentives such as enroling Navigators in PhilHealth and giving them performance awards have been instituted to sustain Navigator support to the Initiative.
59The Family Health Book Operations Research Design
Navigator monitoring and supervision
To ensure that FHB Navigators are properly supervised and assisted, monitoring tools are needed.
The monitoring plan should come with adequate logistical support (e.g., travel expense vouchers or TEV) to ensure the regular conduct of monitoring activities.
Establishing emergency transport and communication networks
Unavailability and unaffordability of transport services explain families’ inability to reach facilities and utilize their services on time during emergencies. An emergency transport and communication (EM) network promotes rapid response to health emergencies and facilitates referrals and transfers to appropriate facilities. As barangays make arrangements for their constituents for these contingencies, the FHB initiative attempts to build on these community initiatives and facilitate broader coordination between communities and health facilities.
This intervention seeks to promote and expedite access of families to MNCHN services by providing them with the names and contact numbers of barangay officials, health workers, and other transport providers, as well as companies in their areas which allow use of their vehicles during emergency referrals. The FHB initiative seeks to make such a network functional in selected municipalities.
To establish a functional health emergency transport and communication network, the province must:
1) assess any current emergency system and network;
2) secure commitments of emergency contacts and different stakeholders to be involved in the FHB initiative;
60 The Family Health Book
3) work out arrangements on use, cost, repairs, maintenance and schedule of emergency vehicles with local officials, health and transport providers;
4) regularly update list of health emergency contacts;
5) continue to provide funds, mobilize support for emergency vehicles’ maintenance and repairs, and coordinate actively with health providers, transport groups, and the private sector to ensure availability of emergency vehicles 24 hours a day, seven days a week.
The overall responsiveness of the different pilot municipalities to health emergencies helps determine the right approach for the establishment of a functional health emergency transport and communication network in the area. To jumpstart this, HPDP conducted a survey to help the Provincial Health Office (PHO) to
• assess the accessibility of the nearest CEmONC facility from the different barangays;
• determine transport and communications costs in the different municipalities;
• identify the common response of different barangays to health emergencies; and
• map out all existing transport and communications providers in the area.
In an initial survey conducted in December 2008 on emergency arrangements in Compostela Valley, barangay captains reported that they were most often called for emergencies. Hence, they are more likely to be in charge of the emergency transport and communication network in each barangay. Part of the FHB/Giya sa Maayong Panglawas (GMP, or “Guide to Good Health”) kit is a booklet with a list of emergency contact persons (most are barangay captains) and their respective contact numbers.
61The Family Health Book Operations Research Design
Earlier, HPDP assisted the province in listing available health emergency contacts in selected barangays of the four pilot sites. This work was expanded to cover all barangays and to validate and update existing FHB health emergency directories. Intensive advocacy and collaboration with local health staff, community leaders, transport groups and private sector partners should be done to secure commitments for transport and communication arrangements in the municipality where the EM intervention is to be done.
Organizing outreach services
Geographic isolation, constraints of transportation systems and road networks, and transportation costs as barriers to accessing care will be addressed through periodic outreach services that provide critical services to FHB holders and their communities. The Municipal Health Office (MHO) shall coordinate and organize outreach activities based on needs identified by Navigators during the risk identification and health needs assessment and in the families’ health use plans developed for their reproductive health requirements, sick child care, and well-baby care.
The specific needs identified shall determine the kind of services and commodities to be delivered, the timing of the activity, and targeted beneficiaries (men and women of reproductive age, pregnant mothers, postpartum mothers, newborn infants and under-5 children). Outreach services, to be done on a quarterly basis, should be so scheduled to not interfere with major activities during the planting, harvesting and fiesta seasons, and important weekday or weekend activities. Regular outreach services to be conducted as part of the FHB initiative will target hard-to-reach and highly-mobile communities. Since these groups are most likely not frequently reached by Navigators, outreach activities are expected to bring the needed services closer to these FHB holders, increasing their adherence to health use plans, such as the reproductive health plan, well child plan, and sick child plan.
This intervention intends to increase the number of families utilizing antenatal care (ANC), family planning, and immunization services. Once the most vulnerable, high-risk and hard-to-reach
62 The Family Health Book
communities with very low access to and utilization of MNCHN services are mapped and identified, the outreach services are to be conducted in selected barangays or puroks. These barangays or puroks should
1) be located no more than two hours of time hours from the RHU or hospital using the most common mode of transportation;
2) have as patients at least 30% of the total number of FHB/GMP holders in the barangay;
3) be accessible by a motorcycle;
4) pose no security concerns for the medical teams;
5) have barangay officials committed to the outreach activities.
Moreover, the medical team involved should be willing and capable of rendering needed services and there should be available funds for the outreach activities.
Outreach services may include health navigational support, health education and promotion services, family planning counseling and distribution of prenatal care commodities, Vitamin A and iron folate supplements, immunizations and child health and nutrition counseling, and ancillary services like PhilHealth orientation and birth registration.
Outreach activities shall be organized only whenever there are enough attending families and there is an ample mix of cases that will require the services of a multi-function health team. The Navigators, together with the midwives, will review the summary call sheets to determine the number of FHB families and the corresponding services they need.
63The Family Health Book Operations Research Design
Key activities include the following:
1) Identifying hard-to- reach and highly-mobile communities;
2) Summarizing and analyzing families’ health use plans;
3) Planning the scope of services to be provided and the ideal mix of health providers during outreach activities, preparing health commodities needed by patients, and identifying units (PHO/RHU/others) and sponsors for a particular outreach activity;
4) Identifying coordination arrangements among the PHO, CHD, providers, local officials and other stakeholders in the conduct of the activity; and
5) Providing or soliciting resources for the conduct of such outreach activities.
HPDP provided technical assistance to the province to guide the conduct of outreach programs during the FHB pilot in Compostela Valley. The assistance includes a review of the design and conduct of existing health-related outreach services in the different municipalities to determine best practices from different models; the development of community outreach protocol to be organized for the FHB pilot; and creation of criteria for selecting families and communities to be targeted by the outreach activities. This protocol will also guide Compostela Valley in organizing, managing, and monitoring its outreach services.
There is ongoing technical assistance seeking potential local and private sector sponsorships for the different outreach services. Assistance can also be provided for advocacy for resources from both provincial and municipal governments as well as from private sponsors.

64 The Family Health Book
How will we measure changes due to FHB interventions?
FHB interventions aim to improve health outcomes, in particular the reduction of maternal, neonatal, infant, and child mortality rates. Effects on health outcomes can only be validated after implementing interventions after quite some time.
In the meantime, initial impact will still be measured by monitoring the actual counts of maternal, neonatal, infant, and child deaths in Compostela Valley, particularly in the municipalities where FHB interventions are implemented (see Table 1.7).
Table 1.7: Measures of maternal, infant, and child deaths
Outcome Baseline Data Sources
Number of MaternalDeaths
Compostela 9 PHO FHSIS Records; EOY Assessment ReportsMabini 0
Maco 2
Montevista 2
4 Pilot Sites 13
Number of Infant Deaths
Compostela 47 PHO FHSIS Records; EOY Assessment ReportsMabini 14
Maco 39
Montevista 12
4 Pilot Sites 112
Number of Child Deaths
Compostela 4 PHO FHSIS Records; EOY Assessment ReportsMabini 2
Source: Compostela Valley PHO, 2007 FHSIS
65The Family Health Book Operations Research Design
Intermediate outcomes
Parallel to the goal of improving health outcomes is the utilization of critical MNCHN services measured in terms of intermediate outcomes. The FHB initiative focuses on these four intermediate outcomes:
• Modern Family Planning (MFP) Method use;• Fully-Immunized Children (FIC);• Antenatal care (ANC); and • Skilled-Birth Attendance (SBA).
These will be monitored by the following intermediate outcome indicators:
• MFP: Number of users who continued to use family planning (FP), number of new acceptors of modern FP methods, and shifters from traditional to modern FP methods;
• FIC: Number of children fully immunized, and with immunization being on-schedule;
• ANC: Number of pregnant women with at least four antenatal visits, number of pregnant women with first antenatal visit during the first trimester, and number of women who received iron and folate supplementation; and
• SBA: Number of mothers who were assisted by skilled birth attendants.
However, there are barriers to utilization of MNCHN services, which eventually contribute to poor health outcomes. The three FHB interventions aim to address these barriers by providing information and supplementing it with a supportive environment that enables families to exhibit targeted behavior.
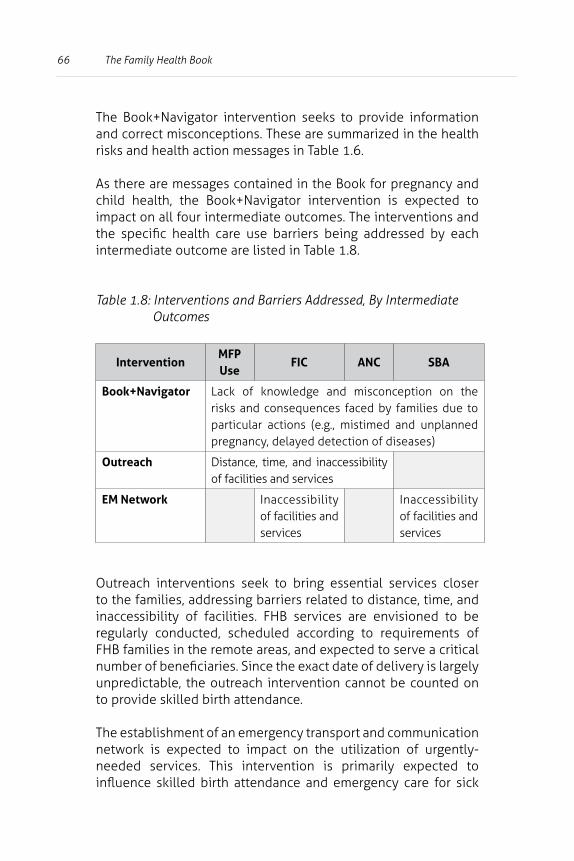
66 The Family Health Book
The Book+Navigator intervention seeks to provide information and correct misconceptions. These are summarized in the health risks and health action messages in Table 1.6.
As there are messages contained in the Book for pregnancy and child health, the Book+Navigator intervention is expected to impact on all four intermediate outcomes. The interventions and the specific health care use barriers being addressed by each intermediate outcome are listed in Table 1.8.
Table 1.8: Interventions and Barriers Addressed, By Intermediate Outcomes
InterventionMFP Use
FIC ANC SBA
Book+Navigator Lack of knowledge and misconception on the risks and consequences faced by families due to particular actions (e.g., mistimed and unplanned pregnancy, delayed detection of diseases)
Outreach Distance, time, and inaccessibility of facilities and services
EM Network Inaccessibility of facilities and services
Inaccessibility of facilities and services
Outreach interventions seek to bring essential services closer to the families, addressing barriers related to distance, time, and inaccessibility of facilities. FHB services are envisioned to be regularly conducted, scheduled according to requirements of FHB families in the remote areas, and expected to serve a critical number of beneficiaries. Since the exact date of delivery is largely unpredictable, the outreach intervention cannot be counted on to provide skilled birth attendance.
The establishment of an emergency transport and communication network is expected to impact on the utilization of urgently-needed services. This intervention is primarily expected to influence skilled birth attendance and emergency care for sick
67The Family Health Book Operations Research Design
children. Support to access to CEmONC facility is expected to influence utilization of services related to births, in particular skilled birth attendance.
FHB intermediate results /outputs
The processes and activities for each intervention are expected to attain FHB outputs (see Appendix 1 for the detailed logframe and indicators). The major outputs of FHB interventions are
• the number of completed health use plans; and
• the number of adhered-to health use plans.
Families that have been oriented by Navigators and informed of their health risks and consequences, and thus have identified their family health needs, are expected to develop health use plans corresponding to their identified health needs.
Health use plans serve as concrete manifestations of families’ intentions to use the identified critical MNCHN services. Depending on health needs, beneficiaries should have one or more health use plans (i.e., reproductive health, birth plan and emergency plan, and well baby and sick child plan).
Families who intend to limit or space pregnancy, for instance, should have a reproductive health (RH) health use plan, which will indicate the desired method of choice. Meanwhile, families with a pregnant mother should have a birth plan which will indicate when and where the pregnant mother should complete at least four ANC visits and other necessary maternal care services, the intended place of delivery and type of delivery assistance needed, and other details that are important, especially in case of emergency.
68 The Family Health Book
Families with infants should have a well-baby plan that includes three doses of the Diphtheria Pertussis Tetanus (DPT) vaccine, three doses of Oral Polio Vaccine (OPV), measles vaccines, and a Bacillus Calmette-Guerin (BCG) vaccine shot before the infants turn 12 months old. The health use plan will also serve as an important guide for Navigators when to remind and conduct a follow-up visit to the family to promote adherence to the health use plan.
Since FHB interventions are also intended to address barriers to utilization of services aside from the lack of information, families are expected to adhere to developed health use plans, utilizing identified services from the provider identified in the plan and during the specified time.
For instance, FHB families in remote barangays can still comply with antenatal care visits and immunization schedules, and utilize family planning services provided through outreach services. Those who identified a specific birth attendant to be consulted should be able to do so, as the contact numbers of emergency transport and communication networks are provided and a functional network is established in a selected municipality.
FHB intervention inputs and processes
The success of the FHB interventions can further be measured in terms of its objectives regarding
• the level of expended input; and
• the quantity and quality of FHB intervention processes and activities.
69The Family Health Book Operations Research Design
For example, the Book+Navigator intervention includes various inputs like health messages, a PhilHealth brochure, a list of health providers, and trained Navigators. Quantity and quality indicators at these levels can be used to gauge the interventions’ operational aspect and the potential effect on both intermediate and final outcomes.
FHB intervention inputs are indicators of the level of effort exerted in implementation. Different measures of inputs are assigned for each of the FHB interventions.
For the Book+Navigator intervention, books will be produced and distributed to households identified and validated based on criteria. The 300-plus Navigators will each receive a Navigator’s Kit and will have to orient all of these households. All barangays shall have a list of emergency transportation and communication networks, and these lists will be made available to all FHB holders.
Functional networks shall be established in selected areas. Outreach missions shall be systematically organized and targeted, and resources and sponsors for outreach services and commodities tapped.
The quantity and the quality of these processes/activities are to be assessed using process indicators. For example, the level of effort exerted on recruiting and developing the Navigators can be measured by the number of Navigators recruited, the number of Navigators who are trained and who passed post-training evaluation, and the number of Navigators who quit. Once Navigators are on-board, the next activity is the actual matching between families and Navigators and eventual family-Navigator contacts.
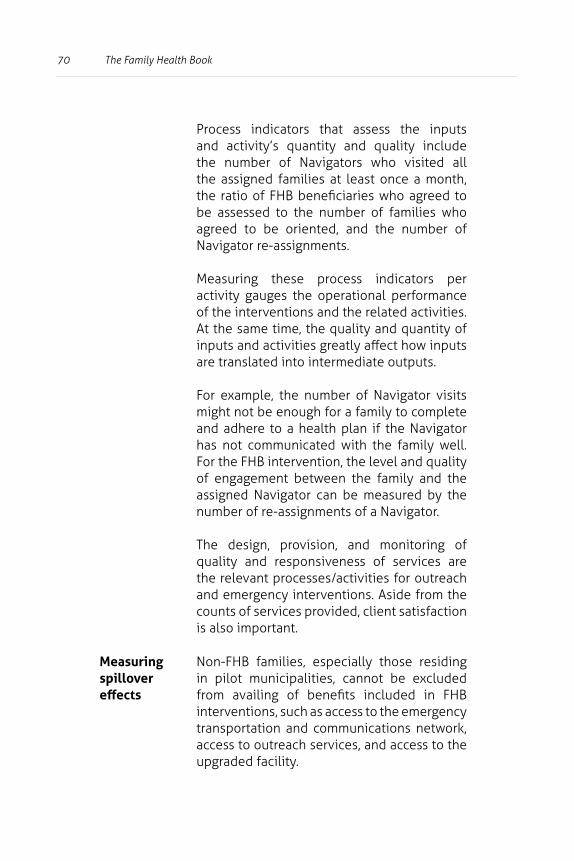
70 The Family Health Book
Process indicators that assess the inputs and activity’s quantity and quality include the number of Navigators who visited all the assigned families at least once a month, the ratio of FHB beneficiaries who agreed to be assessed to the number of families who agreed to be oriented, and the number of Navigator re-assignments.
Measuring these process indicators per activity gauges the operational performance of the interventions and the related activities. At the same time, the quality and quantity of inputs and activities greatly affect how inputs are translated into intermediate outputs.
For example, the number of Navigator visits might not be enough for a family to complete and adhere to a health plan if the Navigator has not communicated with the family well. For the FHB intervention, the level and quality of engagement between the family and the assigned Navigator can be measured by the number of re-assignments of a Navigator.
The design, provision, and monitoring of quality and responsiveness of services are the relevant processes/activities for outreach and emergency interventions. Aside from the counts of services provided, client satisfaction is also important.
Measuring spillover effects
Non-FHB families, especially those residing in pilot municipalities, cannot be excluded from availing of benefits included in FHB interventions, such as access to the emergency transportation and communications network, access to outreach services, and access to the upgraded facility.
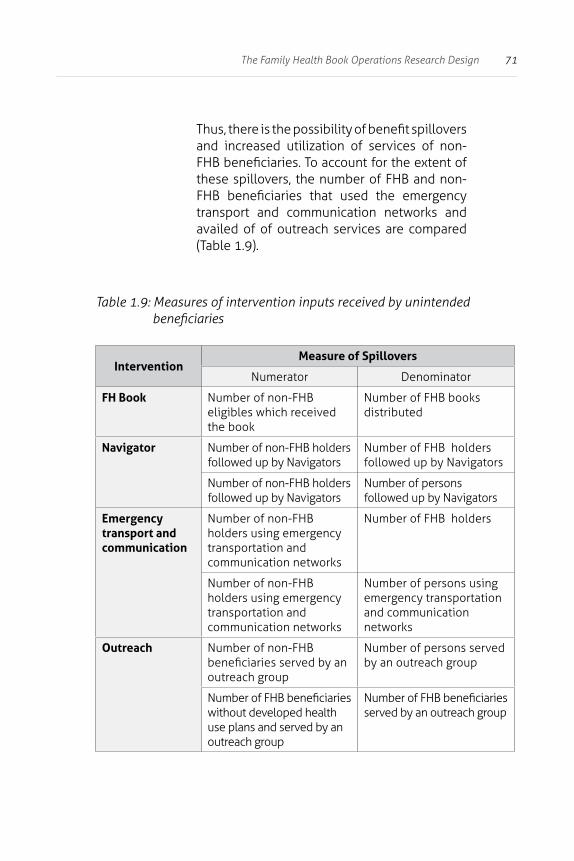
71The Family Health Book Operations Research Design
Thus, there is the possibility of benefit spillovers and increased utilization of services of non-FHB beneficiaries. To account for the extent of these spillovers, the number of FHB and non-FHB beneficiaries that used the emergency transport and communication networks and availed of of outreach services are compared (Table 1.9).
Table 1.9: Measures of intervention inputs received by unintended beneficiaries
InterventionMeasure of Spillovers
Numerator Denominator
FH Book Number of non-FHB eligibles which received the book
Number of FHB books distributed
Navigator Number of non-FHB holders followed up by Navigators
Number of FHB holdersfollowed up by Navigators
Number of non-FHB holders followed up by Navigators
Number of persons followed up by Navigators
Emergency transport and communication
Number of non-FHB holders using emergency transportation and communication networks
Number of FHB holders
Number of non-FHB holders using emergencytransportation and communication networks
Number of persons using emergency transportationand communication networks
Outreach Number of non-FHB beneficiaries served by anoutreach group
Number of persons served by an outreach group
Number of FHB beneficiaries without developed healthuse plans and served by an outreach group
Number of FHB beneficiariesserved by an outreach group

72 The Family Health Book
In addition, FHB interventions may have effects on FHB families’ utilization of other health care services, such as dental care, TB, and minor surgery. This is possible because FHB families are more closely linked to providers through the Navigators. For instance, families are not limited to PhilHealth MNCHN service benefits. They can avail of other services during the intervention and their utilization is tracked.
Change in confounding / environ-mental factors
Confounding or environmental factors will also be measured even if the FHB has no direct interventions to address these concerns. Confounding factors are grouped into the following:
• household factors such as income and education;
• provider factors such as quality, resources, accreditation etc.;
• local delivery and financing systems;
• PhilHealth accreditation policy changes and enrolment campaigns;
• DOH and LGU regulations;
• peace and order conditions; and
• exposure to natural phenomena, like landslides.
A summary of the measures and baseline data sources is given in Table 1.10. Baseline profiles of education and income measures for the four pilot sites are shown in Table 1.11. A year into the implementation, these profiles will be compared with profiles of FHB beneficiaries at the end of the intervention to detect any significant changes in their income and education profiles, which, other than the influence of FHB interventions, may affect family planning and MNCHN service use.

73The Family Health Book Operations Research Design
Since FHB beneficiaries were chosen on the basis of the mother’s educational attainment unlike the baseline sample, comparisons of income and employment status changes would have to be made for the same levels of educational attainment.
Assessment of provider factors will entail collecting measures of quality, resource availability and capacity, attitudes, prices and fees, and accreditation status of health facilities in Compostela Valley and the Davao Regional Hospital in Tagum City. Changes in these provider factors will be detected by comparing health provider profiles from the HPDP-FHB facility patient exit surveys, FHB baseline vignettes, and the profiles of Compostela Valley health facilities and providers, and the Davao Regional Hospital with post-intervention facility surveys, vignettes, and information from key informant interviews (KII) and focus group discussions (FGDs).
Measures on other environmental factors can be obtained from LGU records, PhilHealth records, project reports, key informant interviews, and news reports. They will be compared with gathered information on these environmental factors between beginning-of-year 2009 and post-intervention 2009 (see Tables 1.12 and 1.13).
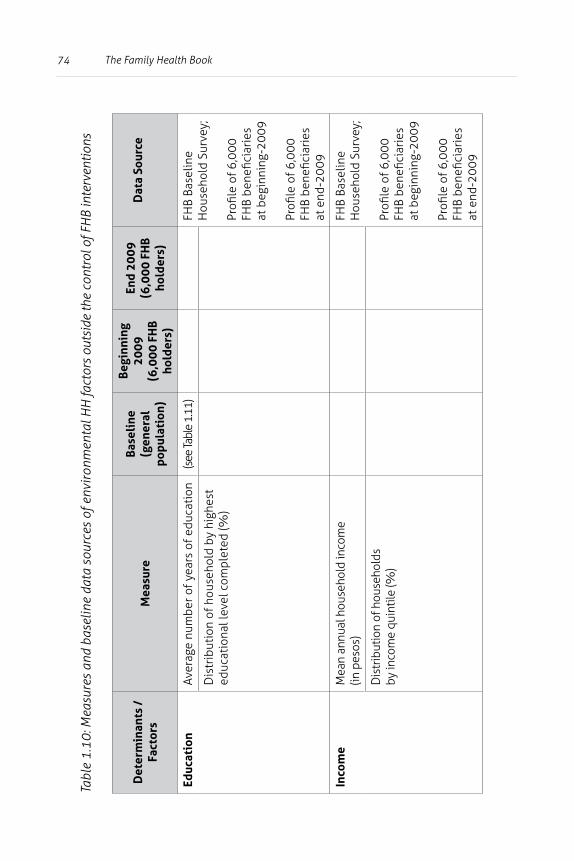
74 The Family Health Book
Tabl
e 1.
10: M
easu
res
and
base
line
data
sou
rces
of e
nvir
onm
enta
l HH
fact
ors
outs
ide
the
cont
rol o
f FH
B in
terv
entio
ns
Det
erm
inan
ts /
Fa
ctor
sM
easu
reBa
seli
ne
(gen
eral
po
pula
tion
)
Begi
nnin
g 20
09
(6,0
00 F
HB
hold
ers)
End
2009
(6
,000
FH
B ho
lder
s)
Dat
a So
urce
Educ
atio
nAv
erag
e nu
mbe
r of y
ears
of e
duca
tion
(see
Tabl
e 1.
11)
FHB
Base
line
Hou
seho
ld S
urve
y;
Profi
le o
f 6,0
00
FHB
bene
ficia
ries
at
beg
inni
ng-2
009
Profi
le o
f 6,0
00FH
B be
nefic
iari
es
at e
nd-2
009
Dis
trib
utio
n of
hou
seho
ld b
y hi
ghes
t ed
ucat
iona
l lev
el c
ompl
eted
(%)
Inco
me
Mea
n an
nual
hou
seho
ld in
com
e (in
pes
os)
FHB
Base
line
Hou
seho
ld S
urve
y;
Profi
le o
f 6,0
00
FHB
bene
ficia
ries
at
beg
inni
ng-2
009
Profi
le o
f 6,0
00FH
B be
nefic
iari
es
at e
nd-2
009
Dis
trib
utio
n of
hou
seho
lds
by
inco
me
quin
tile
(%)
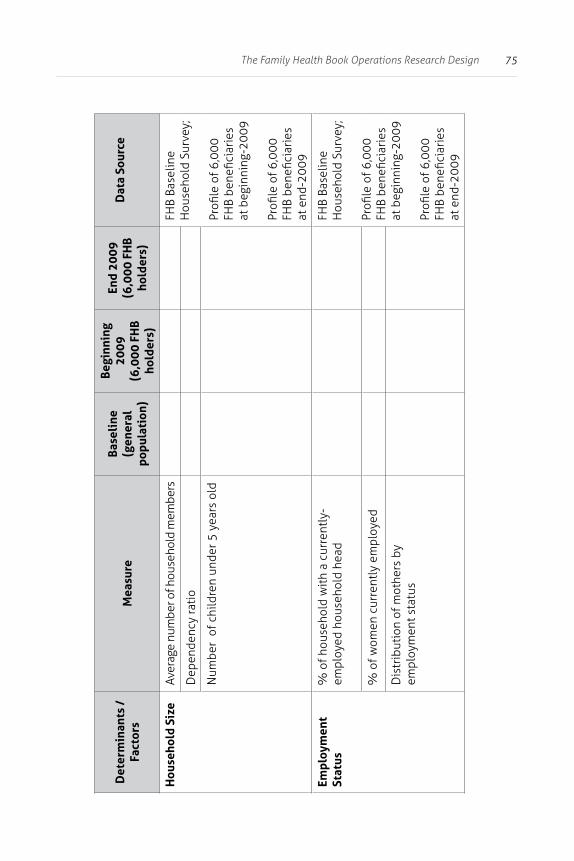
75The Family Health Book Operations Research Design
Det
erm
inan
ts /
Fa
ctor
sM
easu
reBa
seli
ne
(gen
eral
po
pula
tion
)
Begi
nnin
g 20
09
(6,0
00 F
HB
hold
ers)
End
2009
(6
,000
FH
B ho
lder
s)
Dat
a So
urce
Hou
seho
ld S
ize
Aver
age
num
ber o
f hou
seho
ld m
embe
rsFH
B Ba
selin
e H
ouse
hold
Sur
vey;
Profi
le o
f 6,0
00
FHB
bene
ficia
ries
at
beg
inni
ng-2
009
Profi
le o
f 6,0
00FH
B be
nefic
iari
es
at e
nd-2
009
Dep
ende
ncy
rati
o
Num
ber
of c
hild
ren
unde
r 5 y
ears
old
Empl
oym
ent
Stat
us%
of h
ouse
hold
wit
h a
curr
entl
y-em
ploy
ed h
ouse
hold
hea
dFH
B Ba
selin
e H
ouse
hold
Sur
vey;
Profi
le o
f 6,0
00
FHB
bene
ficia
ries
at
beg
inni
ng-2
009
Profi
le o
f 6,0
00FH
B be
nefic
iari
es
at e
nd-2
009
% o
f wom
en c
urre
ntly
em
ploy
ed
Dis
trib
utio
n of
mot
hers
by
empl
oym
ent s
tatu
s
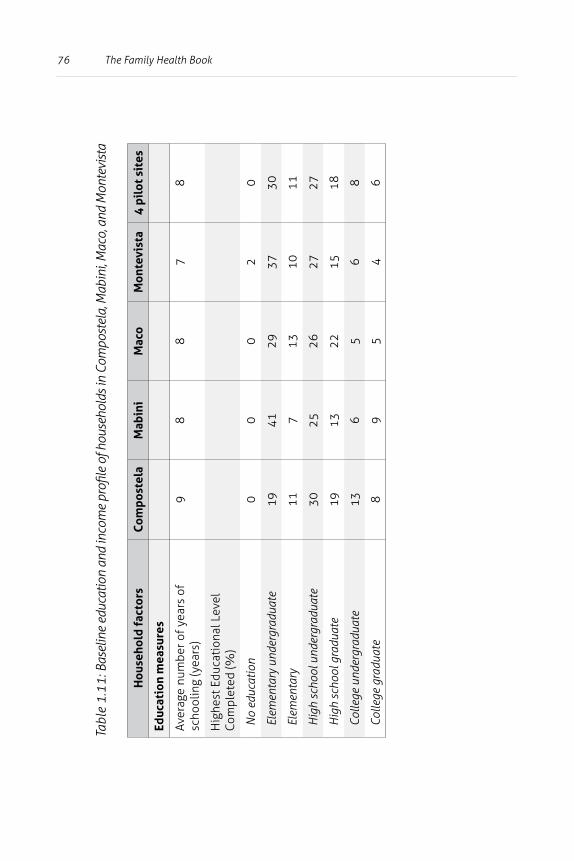
76 The Family Health Book
Tabl
e 1.
11: B
asel
ine
educ
atio
n an
d in
com
e pr
ofile
of h
ouse
hold
s in
Com
post
ela,
Mab
ini,
Mac
o, a
nd M
onte
vist
a
Hou
seho
ld fa
ctor
sCo
mpo
stel
aM
abin
iM
aco
Mon
tevi
sta
4 pi
lot s
ites
Educ
atio
n m
easu
res
Aver
age
num
ber o
f yea
rs o
f sc
hool
ing
(yea
rs)
98
87
8
Hig
hest
Edu
cati
onal
Lev
el
Com
plet
ed (%
)
No
educ
atio
n0
00
20
Elem
enta
ry u
nder
grad
uate
1941
2937
30
Elem
enta
ry11
713
1011
Hig
h sc
hool
und
ergr
adua
te30
2526
2727
Hig
h sc
hool
gra
duat
e19
1322
1518
Colle
ge u
nder
grad
uate
136
56
8
Colle
ge g
radu
ate
89
54
6
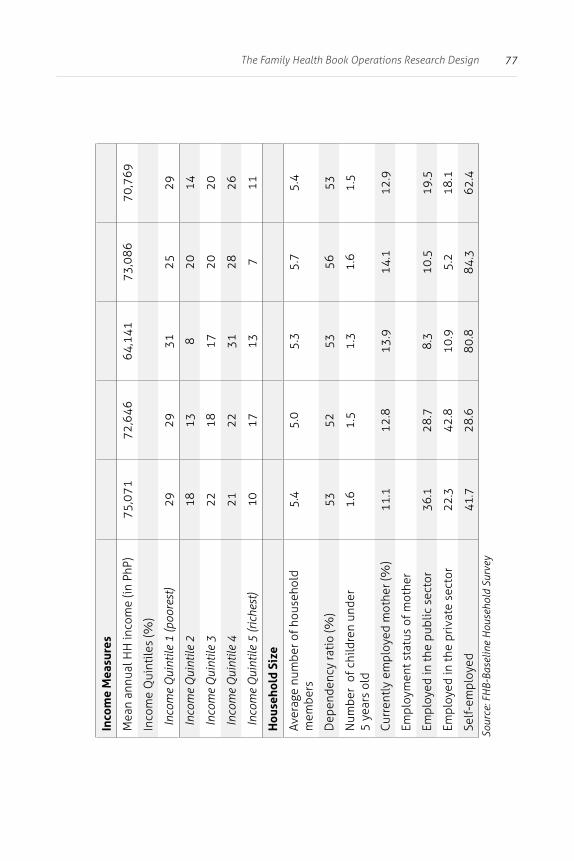
77The Family Health Book Operations Research Design
Inco
me
Mea
sure
s
Mea
n an
nual
HH
inco
me
(in P
hP)
75,0
7172
,646
64,1
4173
,086
70,7
69
Inco
me
Qui
ntile
s (%
)
Inco
me
Qui
ntile
1 (p
oore
st)
2929
3125
29
Inco
me
Qui
ntile
218
138
2014
Inco
me
Qui
ntile
322
1817
2020
Inco
me
Qui
ntile
421
2231
2826
Inco
me
Qui
ntile
5 (r
iche
st)
1017
137
11
Hou
seho
ld S
ize
Aver
age
num
ber o
f hou
seho
ld
mem
bers
5.4
5.0
5.3
5.7
5.4
Dep
ende
ncy
rati
o (%
)53
5253
5653
Num
ber
of c
hild
ren
unde
r 5
year
s ol
d1.
61.
51.
31.
61.
5
Curr
entl
y em
ploy
ed m
othe
r (%
)11
.112
.813
.914
.112
.9
Empl
oym
ent s
tatu
s of
mot
her
Empl
oyed
in th
e pu
blic
sec
tor
36.1
28.7
8.3
10.5
19.5
Empl
oyed
in th
e pr
ivat
e se
ctor
22.3
42.8
10.9
5.2
18.1
Self
-em
ploy
ed41
.728
.680
.884
.362
.4So
urce
: FH
B-Ba
selin
e H
ouse
hold
Sur
vey
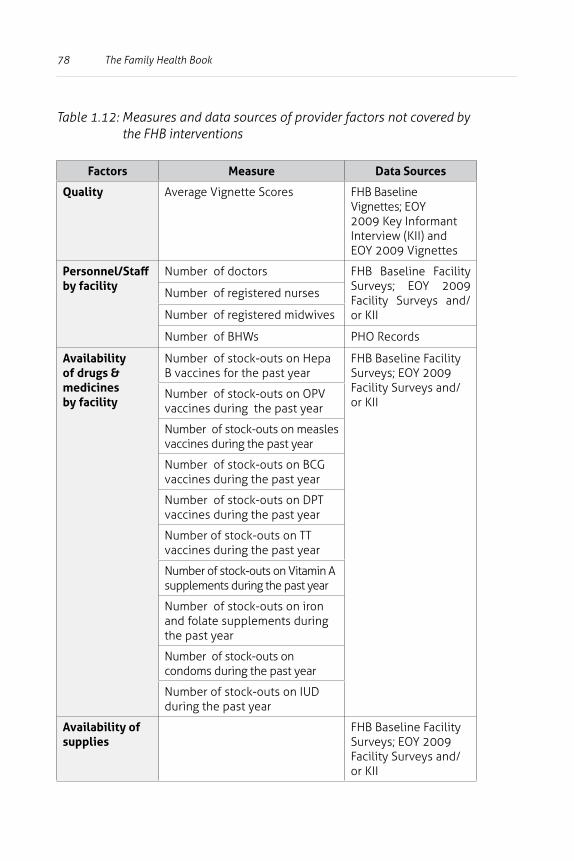
78 The Family Health Book
Table 1.12: Measures and data sources of provider factors not covered by the FHB interventions
Factors Measure Data Sources
Quality Average Vignette Scores FHB Baseline Vignettes; EOY 2009 Key Informant Interview (KII) and EOY 2009 Vignettes
Personnel/Staff by facility
Number of doctors FHB Baseline Facility Surveys; EOY 2009 Facility Surveys and/or KII
Number of registered nurses
Number of registered midwives
Number of BHWs PHO Records
Availability of drugs & medicines by facility
Number of stock-outs on Hepa B vaccines for the past year
FHB Baseline Facility Surveys; EOY 2009 Facility Surveys and/or KII
Number of stock-outs on OPV vaccines during the past year
Number of stock-outs on measles vaccines during the past year
Number of stock-outs on BCG vaccines during the past year
Number of stock-outs on DPT vaccines during the past year
Number of stock-outs on TT vaccines during the past year
Number of stock-outs on Vitamin A supplements during the past year
Number of stock-outs on iron and folate supplements during the past year
Number of stock-outs on condoms during the past year
Number of stock-outs on IUD during the past year
Availability of supplies
FHB Baseline Facility Surveys; EOY 2009 Facility Surveys and/or KII
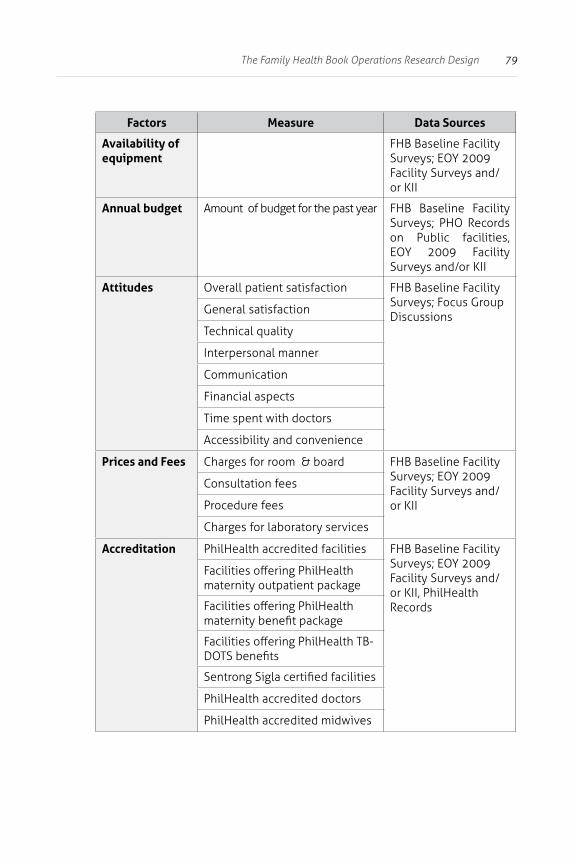
79The Family Health Book Operations Research Design
Factors Measure Data Sources
Availability of equipment
FHB Baseline Facility Surveys; EOY 2009 Facility Surveys and/or KII
Annual budget Amount of budget for the past year FHB Baseline Facility Surveys; PHO Records on Public facilities, EOY 2009 Facility Surveys and/or KII
Attitudes Overall patient satisfaction FHB Baseline Facility Surveys; Focus Group Discussions
General satisfaction
Technical quality
Interpersonal manner
Communication
Financial aspects
Time spent with doctors
Accessibility and convenience
Prices and Fees Charges for room & board FHB Baseline Facility Surveys; EOY 2009 Facility Surveys and/or KII
Consultation fees
Procedure fees
Charges for laboratory services
Accreditation PhilHealth accredited facilities FHB Baseline Facility Surveys; EOY 2009 Facility Surveys and/or KII, PhilHealth Records
Facilities offering PhilHealth maternity outpatient package
Facilities offering PhilHealth maternity benefit package
Facilities offering PhilHealth TB- DOTS benefits
Sentrong Sigla certified facilities
PhilHealth accredited doctors
PhilHealth accredited midwives
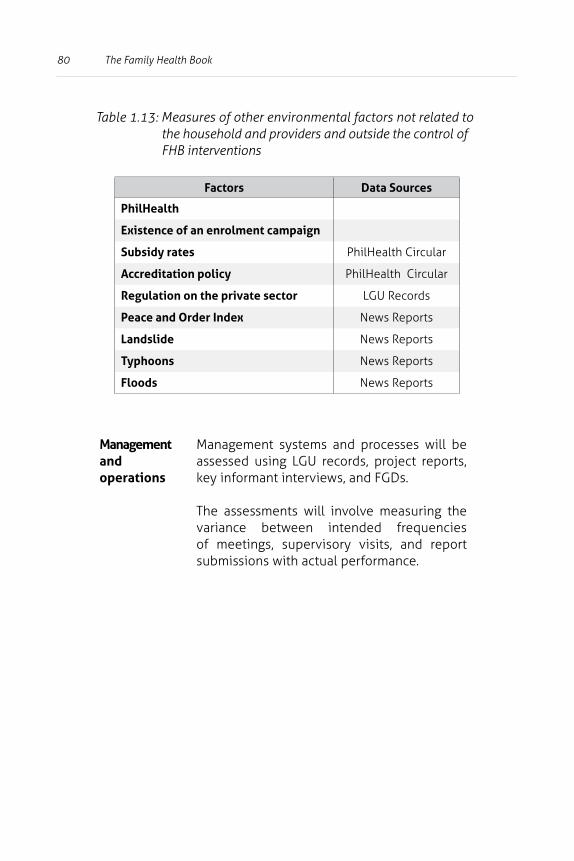
80 The Family Health Book
Table 1.13: Measures of other environmental factors not related to the household and providers and outside the control of FHB interventions
Factors Data Sources
PhilHealth
Existence of an enrolment campaign
Subsidy rates PhilHealth Circular
Accreditation policy PhilHealth Circular
Regulation on the private sector LGU Records
Peace and Order Index News Reports
Landslide News Reports
Typhoons News Reports
Floods News Reports
Management and operations
Management systems and processes will be assessed using LGU records, project reports, key informant interviews, and FGDs.
The assessments will involve measuring the variance between intended frequencies of meetings, supervisory visits, and report submissions with actual performance.
81The Family Health Book Operations Research Design
How can we validate if observed changes can be attributed to the FHB initiative?
Five comparisons are to be used to determine the incremental impact of FHB interventions:
1. Comparison of the utilization of families from the baseline survey with that of FHB families.
• Utilization rates of households with the same characteristics as FHB holders will be generated using the FHB household baseline survey. These will be compared with the actual use rates of FHB households.
2. Analysis of the utilization of FHB households, controlling for household characteristics and health risks.
• This requires an analysis of individual characteristics of FHB families’ patterns against actual adherence to health use plans. A critical factor here is the drawing up of a health profile of recipient families during orientation.
3. Post-intervention examination of changes in the status of FHB holders and the status of the comparable population in the same municipalities.
• This involves comparing non-FHB holders with FHB families in the same municipalities using a post-intervention household survey. This comparison will assume that non-FHB holders’ pre-intervention status is to be obtained in the baseline survey, while FHB holders’ baseline status is to be established at the beginning of the intervention (later than the baseline).
• Secondly, the comparison will have to account for contaminations or leaks of the interventions into the non-FHB population in the same municipalities. The second issue is particularly important for the use of emergency transport and communication, enrolment, and outreach. The FHB initiative will not deny non-FHB families access to these services.
82 The Family Health Book
4. Examination of changes in the status of families from both FHB and non-FHB municipalities.
• The non-FHB municipality serves as a control municipality that would allow the isolation of temporal and spillover effects. This will mean the conduct of a post-intervention survey of a sample of families from a non-FHB municipality. The results will be compared with those of the baseline survey for that municipality (as the pre-intervention status).
• A non-FHB municipality with relatively accessible health facilities should be chosen to ensure no overstating of the observed FHB effect. As resources permit, the post-intervention survey may be extended to cover more than one non-FHB municipality.
5. Comparison of changes in factors outside the control of the FHB such as health budgets, provider quality levels, and other confounding factors need to be compared.
• How such changes affect the observed incremental FHB effect need to be determined. This comparison will contribute to the proper attribution of impacts.
In undertaking any of the five comparisons, the analysis should take on a difference-in-difference approach even when doing qualitative assessment of possible FHB effects. The difference in difference approach compares the changes in outcomes over time between the FHB families (the ones receiving the interventions) and the non-FHB families (the comparison group). This would allow us to take into account any differences in the FHB families and non-FHB families that are constant over time.
A key concern with any operations research that tries to implement a package of interventions is the determination of each intervention’s incremental contribution. The FHB faces the same challenge. Ideally, different combinations of the interventions should be randomly assigned among the study sites. However, LGU commitments and support as well as operational bottlenecks prevent the FHB from being implemented like a randomized experiment.
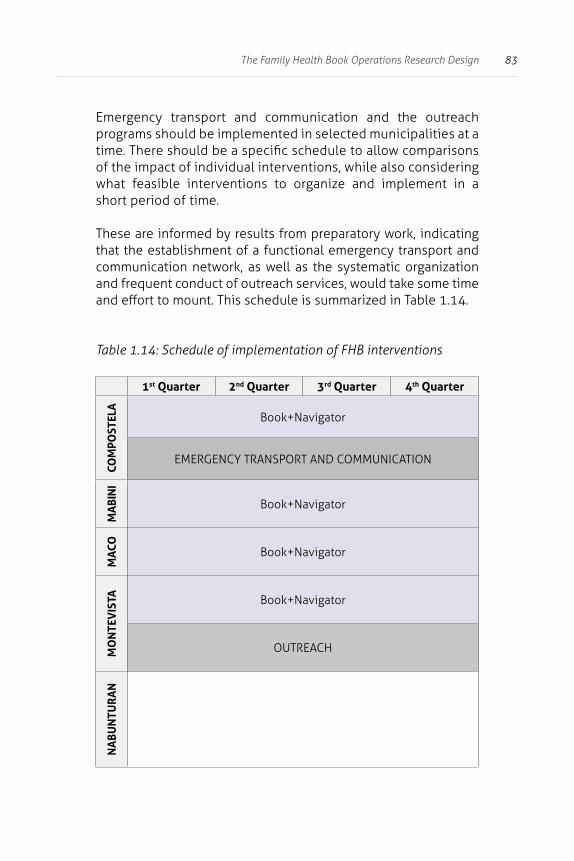
83The Family Health Book Operations Research Design
Emergency transport and communication and the outreach programs should be implemented in selected municipalities at a time. There should be a specific schedule to allow comparisons of the impact of individual interventions, while also considering what feasible interventions to organize and implement in a short period of time.
These are informed by results from preparatory work, indicating that the establishment of a functional emergency transport and communication network, as well as the systematic organization and frequent conduct of outreach services, would take some time and effort to mount. This schedule is summarized in Table 1.14.
Table 1.14: Schedule of implementation of FHB interventions
1st Quarter 2nd Quarter 3rd Quarter 4th Quarter
COM
POST
ELA
Book+Navigator
EMERGENCY TRANSPORT AND COMMUNICATION
MA
BIN
I
Book+Navigator
MA
CO Book+Navigator
MO
NTE
VIS
TA Book+Navigator
OUTREACH
NA
BUN
TUR
AN
84 The Family Health Book
The selective implementation of the interventions described in Table 1.14 allows for the following specific comparisons to be made:
1) The effect of the Book+Navigator – comparison of outcomes in Mabini and Maco with those in Nabunturan (as the non-FHB municipality).
2) The joint effect of the Book+Navigator and the functional emergency transport and communication network – comparison of the outcomes in Compostela with those in Nabunturan.
3) The joint effect of the Book+Navigator and outreach services – comparison of outcomes in Montevista with those in Nabunturan.
4) The effect of a functional emergency transport and communication network – comparison of outcomes in Compostela with those in Mabini and Maco.
5) The effect of outreach services – comparison of outcomes in Montevista with those in Mabini and Maco.
There is a possibility that in the current design, the effects of the outreach and emergency interventions may be completely confounded with the effects of unobserved factors specific to the municipalities where these interventions are implemented. A suggested adjustment to partly mitigate this is the utilization of the barangay as an alternative unit for implementing interventions.
For instance, emergency interventions are suggested for selected barangays in Maco, Mabini, and Montevista, and outreach interventions for selected barangays in Maco, Mabini and Compostela. The impact of these interventions can also be assessed by looking at the outcomes in these barangays.
85The Family Health Book Operations Research Design
These suggestions are under review, as they entail additional resource requirements. The political ramifications are also being considered, since it may be hard to convince local chief executives to limit implementation to the selected barangays.
To partly address the confounding factor, comparison of utilization patterns of non-FHB families with those of FHB families in these municipalities is suggested. The difference in the outcomes is expected to isolate the impact of the interventions from the impact of unobserved factors.
What instruments and activities will be conducted to measure observed changes and validate that these changes are due to the FHB?
In order to monitor the implementation of FHB interventions and evaluate their effects, several instruments and activities are proposed. These include:
1) Baseline and post-intervention surveys;
2) Forms accomplished by families and Navigators as part of the Book+Navigator intervention;
3) Profile forms for families and Navigators;
4) Intervention- and activity-specific forms to gather information on process indicators and the conduct of the interventions;
5) Focus group discussions; and
6) Meetings that form part of the management and governance of the FHB, like meetings of the FHB Technical Working Group (TWG) and the Steering Committee.
86 The Family Health Book
Surveys
Baseline surveys
Baseline surveys were conducted to generate information that will guide project planning and design, and provide basis for setting targets.
The following FHB baseline surveys were conducted with households, physicians, midwives, health facilities, and pharmacies across the 11 Compostela Valley municipalities:
1) Household survey and preliminary mapping of health facilities in Compostela Valley. This entailed a province-wide survey of sample households and a preliminary mapping of location of health facilities and other providers of health services where the sample households usually go to access maternal, neonatal, and child health services, as well as family planning counseling and commodities.
Sample barangays were randomly chosen and the survey focused only among index families with either a pregnant woman or a child below 12 months of age (called the index child). Eligible index families are further limited to families whose primary decision-maker is either the husband of the pregnant woman/father of the index child or his spouse.
This survey generates information like socio-economic characteristics, demographic characteristics and the household’s general health utilization pattern, health status of both the woman-respondent and the index child, and utilization of maternal, neonatal and childcare, nutrition, and family planning services.
The household survey was conducted from January 2007 to February 2008, with the preceding month as the reference period for utilization. A total of 2021 households were covered, distributed as follows: Compostela (203), Mabini (109), Maco (219), Montevista (110), and Nabunturan (216).
87The Family Health Book Operations Research Design
Data generated by the baseline household survey will also be useful in isolating the incremental contribution of each intervention and will be the main source of information for
• the health status and utilization patterns of families with the same characteristics as FHB beneficiaries, i.e., the expected use rates that would be utilized for the comparison with the actual use rates of FHB beneficiaries;
• the pre-intervention status and utilization patterns of households with the same characteristics as non-FHB and FHB families in the four pilot municipalities; and
• the pre-intervention status and utilization patterns of households with the same characteristics as non-FHB and FHB families in the control municipality of Nabunturan.
2) Physician and midwife survey and quality-of-care (QOC) assessment using vignettes. The survey aims to map health care professionals in Compostela Valley and measure quality of their maternal and child health care services. This survey provided information on the characteristics, income sources, and clinical and non-clinical practices of health professionals in their delivery of family planning, maternal, and child health services in Compostela Valley.
A total of 85 health professionals -- physicians (general practitioners and specialists), midwives, and nurses -- were randomly selected to answer vignettes and a provider survey. Thirty health professionals from the four FHB municipalities and 11 health professionals from Nabunturan participated. A total of 400 vignettes were administered.
VIGNETTES
Vignettes were administered among physicians, midwives and nurses to measure quality-of-care across family health providers. While these had five common cases, those vignettes for doctors had two additional ones. The cases which the vignettes touched on were
• Antenatal care;• UTI in pregnancy;• Uncomplicated birth delivery; • Postpartum hemorrhage; and• Newborn resuscitation.
Physician vignettes also covered neonatal sepsis and diarrhea (with mild/severe dehydration), two cases not found in the version for midwives and nurses.
88 The Family Health Book
3) Survey of patients, health facilities, and other health care providers in Compostela Valley. Patient exit interviews were conducted in public and private hospitals, RHUs, and lying-in and private clinics. This survey collects information on patients’ socio-economic and demographic characteristics, and contains a description of the confinement/consultation, services received, and expenditures. It also has results of a records review, information on patients’ health status, and satisfaction of maternal and pediatric patients.
Surveys were also conducted in public and private hospitals, RHUs, lying-in and private clinics, free-standing diagnostic facilities, and pharmacies. These surveys intend to map out health facilities, in terms of availability, affordability and quality of health services, and proximity and accessibility particularly to poor households. This mapping aims at forming an integrated network of facilities and professionals who will provide FHB services.
Patients from 13 inpatient facilities, which included public and private hospitals and lying-in/birthing homes, were included in the exit survey. Of the 61 inpatient respondents 16 were from FHB municipalities while nine came from Nabunturan.
From the 40 outpatient facilities, 155 outpatients were included in the patient exit survey. Of these outpatients, 29 were from FHB municipalities while 18 were from Nabunturan.
This baseline provider-side information would be utilized to measure pre-intervention levels of quality of care, most especially for the Compostela Valley Provincial Hospital and the other providers in the four FHB municipalities.
89The Family Health Book Operations Research Design
Post-intervention surveys
Ideally, the post-intervention survey should be conducted after a reasonable amount of time has elapsed following the start of implementation of the interventions. A year would be sufficient to assess the impact of, say, the full cycle of pregnancy and birth.
For the FHB initiative, post-intervention impact assessment surveys were conducted at around the ninth month (February 2010) after the start of the interventions. This was due more to practical and political realities. As general elections were scheduled in May, survey firms were expected to be fully occupied by March and April.
A household survey of families from the four FHB municipalities and Nabunturan was the major post-intervention survey conducted. A second set of surveys would be conducted on facilities and providers.
1) Post-intervention household survey. Unlike the province-wide baseline household survey, the proposed coverage of the post-intervention household survey was limited to the four FHB municipalities, one non-intervention site, the current control municipality (Nabunturan), and an additional municipality.
Resource limitations, including the need to finish the survey in a short time, constrained the coverage. Restricting the number of municipalities to be covered allowed for increasing the sample number of families in each site.
The post-intervention survey is to follow the sampling scheme used in the baseline household survey -- families with currently pregnant women (or were pregnant within the last year as of the reference period) or families with children under a year (or were one year old as of the reference period) -- to allow for direct comparison with baseline households.
90 The Family Health Book
This sampling scheme allowed previously-listed comparisons, since it could capture households that were
1) FHB beneficiaries;
2) Non-FHB beneficiaries;
3) Households with similar characteristics as the FHB and non-FHB beneficiaries in the control municipality; and
4) Households that may have received Navigator-less books or participated in FHB activities and interventions.
However, some FHB-eligible families may not qualify (i.e., those with children under 5 years but over a year old and the wife is not currently pregnant) and would not be sampled under this scheme.
The analysis for the outcomes of these families would just be a comparison of their status before and after the FHB initiative, as reflected in the forms filled out as part of the interventions.
The sampling scheme and sample size should also allow sufficient numbers of observations assessing the impact of the FHB interventions. The final sample size is still to be determined based on appropriate power calculations. As resources permit, oversampling of FHB families may be considered.
The post-intervention household survey would be:
a) a source of information for the health status and actual use rates of FHB beneficiaries for the first comparison;
b) the main source of information on the post-intervention status and utilization patterns of non-FHB households in the four FHB municipalities for the third comparison; and
c) the main source of information on the post-intervention status and utilization patterns of households in the control municipality of Nabunturan for the fourth comparison.
91The Family Health Book Operations Research Design
These information would also be utilized in analyzing the incremental impact of specific interventions. The post-intervention survey is also the backup information source should the collection of the Book+Navigator forms be hampered by non-functioning of the Navigators or the breakdown of the family-Navigator relationship.
The survey instrument to be used in the post-intervention household survey would be longer than the one used in the baseline survey. Two major additional sections would be included to measure spill-over effects of the interventions on non-FHB households in the FHB municipalities and in the control municipality, and to measure adherence to health use plans and some process indicators on the interventions (e.g., Navigator visits) for sampled FHB families.
2. Post-intervention facility survey and patient exits, provider vignettes. These surveys would be the main source of information for tracking changes in provider quality levels and other provider factors (changes in prices and presence of facilities and staff that could affect utilization of facilities by FHB and non-FHB families). Like the post-intervention household survey, the post-intervention facility survey would be limited to those providers identified in the baseline as being utilized by the households in the four FHB municipalities and in Nabunturan. A limited set of questionnaires and instruments sufficient to give indications on provider quality levels and factors would be administered.
Book+Navigator Forms
Forms that are required to be accomplished in the course of implementing the Book+Navigator intervention are also sources of information on utilization and other process indicators. These forms include:
1) the family health risk assessment form;2) the family journal;3) the family call sheet (FCS); 4) the health use plans; and5) GMP Navigator reporting form (see Appendix 2 for a summary
listing, the process flow and the timing of their collection).
92 The Family Health Book
These accomplished forms are the main sources of information for comparison of the status of FHB families before and after the intervention. These forms (or their photocopies) are to be collected at specified periods and encoded.
The family health risk assessment form
The Navigator uses this to assess the family’s health needs and risks and thus enables the Navigator to identify necessary services that the family should utilize.
The information it captures is useful for monitoring and evaluation purposes.
This form is to be collected at the beginning of the intervention period since it is a baseline indicator of FHB beneficiaries’ health needs. For additional health needs like pregnancy, the Navigators will have to make special reports.
The family journal
This is a monthly record of the Navigator’s visits with the family, recording activities undertaken during those visits, and other services accessed by the family during a current month.
This would show if Navigators visited at least once a month, and show what other services, aside from MNCHN-related ones, were accessed by the FHB families.
The health use plan form
This is accomplshed by the family, the Navigator, and the provider. It details the services that need to be accessed, the services actually accessed, when these were accessed, and identifies the provider of services. It records the family’s actual utilization of services.
Unlike the health risk assessment form, the health use plan would indicate whether FHB families actually obtained needed services as indicated by the risk assessment.
93The Family Health Book Operations Research Design
Since these serve as guides for the families and are accomplished in the course of accessing services, they cannot be collected from the families at the beginning or mid-term. These plans are only collected towards the end of the intervention period, near or at the time of the post-intervention survey.
To monitor intermediate-term service utilization of families based on their health use plans, family call sheets accomplished by the Navigators would be collected and used.
The information in the family call sheets are obtained from the health use plans and provide a family-level summary of services needed in a month, when and where these were obtained, what problems were encountered in accessing these services, and what were the adjustments carried out by the families and Navigators.
Navigators are to provide extra copies of these forms and these copies would be collected towards the middle of the intervention year. This is an alternative source of information available before the collection of health use plans.
GMP Navigator reporting form
This is another monitoring tool for process indicators.
It is a monthly reporting form that Navigators submit to their supervisor midwives, who in turn detail the summary tallies of the number of families who were given orientations, developed health use plans, utilized services, and claimed from PhilHealth.
Information from these reporting forms will be collected quarterly, although Navigators accomplish the forms monthly.
94 The Family Health Book
Profile forms for families and Navigators
In order to assess the impact of FHB interventions on utilization, socio-economic factors that could possibly influence utilization need to be controlled. Information on the socio-economic characteristics of FHB families can be seen in the socio-economic survey (SES), which elicits basic information on respondents’ educational and employment status, housing characteristics, assets, and household roster.
The form was patterned after the socio-economic part of the baseline household survey form. These are accomplished during the first meeting of Navigators and families. The information from these forms would be used to compare the status of FHB families at the beginning and at the end of the interventions. They would also be partly utilized in comparing utilization patterns of FHB holders with that of non-FHB holders from the baseline household survey.
Observed differences in utilization patterns of FHB families can be largely influenced by the performance of the Navigators, which in turn may be related to their skill levels, experience, and the possible incentives they expect to receive.
To control for these factors in the assessment, a similar socio-economic profile of Navigators is obtained through the Navigator profile form, which includes basic information on educational attainment, years of experience, as well as information on incentives and compensation they receive from the LGUs. The results of post-training assessment of the Navigators, which were composed of a post-training skills score and an assessment of family-Navigator interaction and skills in accomplishing forms conducted on a sample of Navigators, would also be integrated into the Navigator database.
Interventions and activity specific forms
Some of the services needed by families in far-flung areas are expected to be provided through outreach services interventions. To monitor how outreach activities effectively deliver the required services, an outreach monitoring form would be developed and administered during outreach activities.
95The Family Health Book Operations Research Design
The form would resemble a “patient chart” detailing services actually delivered and patients’ satisfaction with the services. It would have additional questions, specifically for FHB families, to obtain information needed to link with other family-level based data. This form would be an important source of spillovers of FHB services to non-FHB families.
A similar monitoring form will be developed for emergency services. The form would have to be accomplished by all those utilizing the emergency services, including non-FHB families.
Focus group discussions
Conducting focus group discussions (FGDs) to obtain qualitative information on the conduct of the interventions including feedback from families, is being planned. Select FHB families and Navigators would constitute the FGD participants. FGD topics would include operational concerns, families’ feedback on Navigators, outreach services conducted in Montevista, and emergency services in Compostela. The FGDs are proposed to be conducted a quarter after the interventions are implemented.
Maternal death reviews, specifically for FHB mothers who died during the intervention period, are also being considered.
Meetings that form part of the FHB governance structure
The FHB pilot has two working groups, the FHB Steering Committee and the FHB Technical Working Group (TWG). The FHB TWG is to meet monthly, while the FHB Steering Committee is to meet quarterly to discuss FHB concerns. Minutes and discussion notes from these meetings are envisioned to document important decisions and field level circumstances that may have an impact on the conduct of the interventions. Information in the forms submitted as part of the Book and Navigator interventions, particularly the GMP Navigator reporting form, are important inputs to these meetings.

96 The Family Health Book
How will the FHB pilot be implemented?
The FHB needs to be piloted to provide evidence on the FHB’s impact on health care use and on MNCHN outcomes. Specific evidence has to be generated to determine which features of the initiative contribute significantly to achievement of FHB outcomes. Moreover, necessary management and operational arrangements for FHB implementation cannot be effectively designed without field experience acquired from the pilot. Those arrangements are to guide the development of operational guidelines for future FHB implementation and roll-out.
Site selection
The provinces of Bulacan, Davao del Norte, Bukidnon, and Compostela Valley were originally considered for FHB piloting because of their commitment to health programs and the presence of DOH and USAID support. Compostela Valley was chosen because of its high maternal and infant mortality and low rates for contraceptive prevalence (CPR), antenatal care (ANC), skilled birth attendance (SBA), and fully immunized children (FIC) despite the presence of basic service delivery infrastructures.
The municipalities of Montevista, Maco, Compostela, and Mabini in Compostela Valley were selected for the distribution of the FHBs on the basis of their high maternal and infant mortality and low utilization rates of the health services, despite access to a full network of services including tertiary services.
97The Family Health Book Operations Research Design
Phases of the FHB pilot
The FHB pilot in Compostela Valley will be implemented in four phases:
1) preparation and baseline setting;
2) FHB design and validation;
3) implementation and measurement of effectiveness of the FHB on health care utilization; and
4) roll-out throughout the rest of the province.
Phase 1: Preparation and baseline setting
During the first phase, buy-in from DOH, Center for Health Development (CHD) XI, Compostela Valley, and partners will be secured. Baseline surveys and FGDs will be conducted to provide preliminary analyses relevant to FHB design and interventions. Providers will be oriented on their roles and expectations from them, especially concerning quality of care.
A steering committee headed by Governor Uy will be established. The Steering Committee, to be composed of the CHD, PhilHealth, mayors, and other local officials, is responsible for managing FHB pilot’s implementation.
A TWG composed of provincial and municipal health staff will assist the Steering Committee. The consultations and findings from surveys and FGDs done in the first phase will inform the FHB’s specific design in Compostela Valley.
98 The Family Health Book
Phase 2: FHB design and validation
Phase 2, which will run through February 2009, includes an assessment of the book’s prototype on the following areas:
1) effectiveness of the FHB form (carrier versus book); 2) effectiveness of content and form, including ease of use; 3) language; and 4) effectiveness of initial Navigator recruitment and training.
Initially, 24 families will be given books/carriers; and 12 Navigators will be trained to assist them. Assessment will be conducted in late November through December through FGDs and KIIs. Results of the assessment will be used in the FH Book’s revision, which is to be submitted to the Office of Health (OH).
Phase 3: Implementation and measurement of effectiveness of FHB on health care utilization
In Phase 3, many Navigators will be recruited, trained, and assigned to the initial 6,000 FHB recipients to maintain a 1:20 Navigator-family ratio. Navigators will be recruited from the pool of barangay health workers and other community-based volunteers, including mothers. They will be trained on how to orient families in using the FHB, how to assess family health needs, and how to support the development and accomplishment of family health use plans. The Rural Health Midwives (RHM) will supervise and monitor Navigators.
Phase 4 – Roll-out to the rest of the province
Roll-out throughout Compostela Valley depends on accomplishing FHB targets. Monitoring and evaluation schemes should thus be integrated in FHB operations. While the province, the municipalities, the CHD Davao Region, and USAID-cooperating agencies led by HPDP are to share the cost of implementing the initial FHBs in pilot municipalities, the cost of rolling out the FHB throughout the province is expected to be largely financed by commitments from local authorities, the CHD, and local sponsors.
99The Family Health Book Operations Research Design
Benchmarks and timelines for the FHB pilot’s implementation are shown on Table 1.15.
Expected lessons from the FHB pilot
The pilot is expected to draw out lessons from the various phases of the initiative and to recommend appropriate sequence and strategies for implementing various FHB interventions.
Specifically, it aims to:
1) determine strategic ways of securing local buy-in from national and local officials and stakeholders;
2) draw out lessons on how to establish and sustain local FHB management structure and operations;
3) determine each intervention’s contribution to the initiative’s desired outcomes;
4) improve each intervention’s design or develop a more appropriate one to local needs and conditions;
5) identify areas for improvement in the FHB implementation; and
6) guide the finalization of the FHB design for future roll-out to the rest of the province.
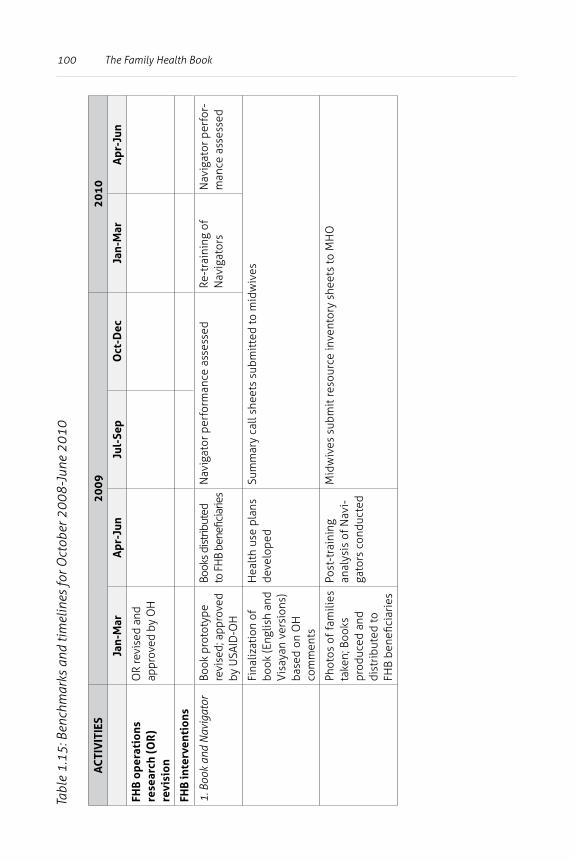
100 The Family Health BookTa
ble
1.15
: Ben
chm
arks
and
tim
elin
es fo
r Oct
ober
200
8-Ju
ne 2
010
AC
TIV
ITIE
S20
0920
10
Jan-
Mar
Apr
-Jun
Jul-
Sep
Oct
-Dec
Jan-
Mar
Apr
-Jun
FHB
ope
rati
ons
rese
arch
(OR
) re
visi
on
OR
revi
sed
and
appr
oved
by
OH
FHB
inte
rven
tion
s
1. B
ook
and
Nav
igat
orBo
ok p
roto
type
re
vise
d; a
ppro
ved
by U
SAID
-OH
Book
s dis
tribu
ted
to F
HB
bene
ficia
ries
Nav
igat
or p
erfo
rman
ce a
sses
sed
Re-t
rain
ing
of
Nav
igat
ors
Nav
igat
or p
erfo
r-m
ance
ass
esse
d
Fina
lizat
ion
of
book
(Eng
lish
and
Vis
ayan
ver
sion
s)
base
d on
OH
co
mm
ents
Hea
lth
use
plan
s de
velo
ped
Sum
mar
y ca
ll sh
eets
sub
mit
ted
to m
idw
ives
Phot
os o
f fam
ilies
ta
ken;
Boo
ks
prod
uced
and
di
stri
bute
d to
FH
B be
nefic
iari
es
Post
-tra
inin
g an
alys
is o
f Nav
i-ga
tors
con
duct
ed
Mid
wiv
es s
ubm
it re
sour
ce in
vent
ory
shee
ts to
MH
O
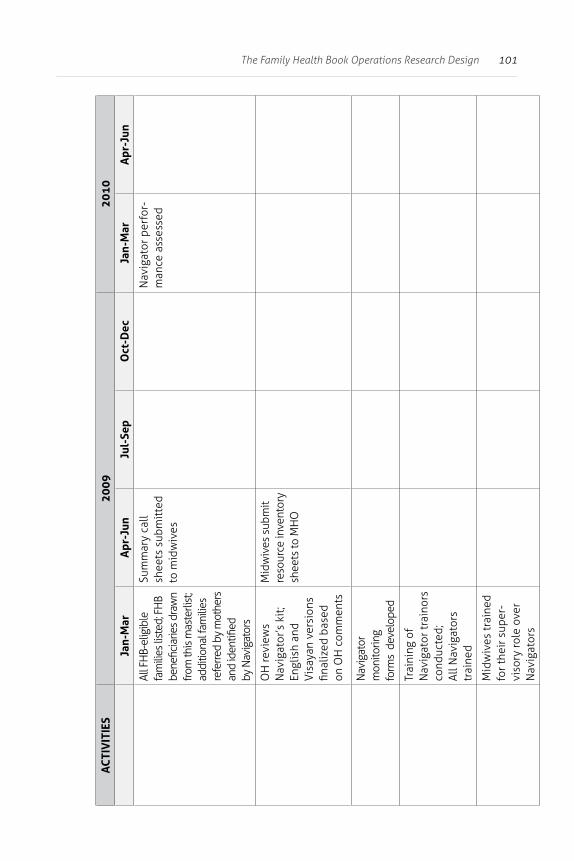
101The Family Health Book Operations Research Design
AC
TIV
ITIE
S20
0920
10
Jan-
Mar
Apr
-Jun
Jul-
Sep
Oct
-Dec
Jan-
Mar
Apr
-Jun
All F
HB-
elig
ible
fa
mili
es li
sted
; FH
B be
nefic
iarie
s dra
wn
from
this
mas
terli
st;
addi
tiona
l fam
ilies
re
ferre
d by
mot
hers
an
d id
entifi
edby
Nav
igat
ors
Sum
mar
y ca
ll sh
eets
sub
mit
ted
to m
idw
ives
Nav
igat
or p
erfo
r-m
ance
ass
esse
d
OH
revi
ews
Nav
igat
or’s
kit
; En
glis
h an
d V
isay
an v
ersi
ons
final
ized
bas
ed
on O
H c
omm
ents
Mid
wiv
es s
ubm
it re
sour
ce in
vent
ory
shee
ts to
MH
O
Nav
igat
or
mon
itorin
g fo
rms
dev
elop
ed
Trai
ning
of
Nav
igat
or tr
aino
rs
cond
ucte
d;
All N
avig
ator
s tr
aine
d
Mid
wiv
es tr
aine
d fo
r the
ir s
uper
-vi
sory
role
ove
r N
avig
ator
s
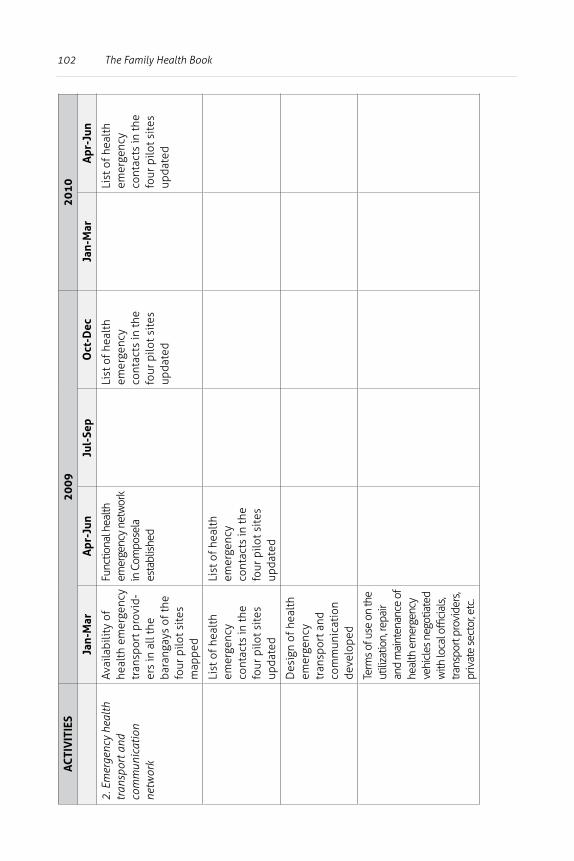
102 The Family Health BookA
CTI
VIT
IES
2009
2010
Jan-
Mar
Apr
-Jun
Jul-
Sep
Oct
-Dec
Jan-
Mar
Apr
-Jun
2. E
mer
genc
y he
alth
tr
ansp
ort a
nd
com
mun
icat
ion
netw
ork
Avai
labi
lity
of
heal
th e
mer
genc
y tr
ansp
ort p
rovi
d-er
s in
all
the
bara
ngay
s of
the
four
pilo
t sit
es
map
ped
Func
tiona
l hea
lth
emer
genc
y ne
twor
k in
Com
pose
la
esta
blis
hed
List
of h
ealt
h em
erge
ncy
cont
acts
in th
e fo
ur p
ilot s
ites
up
date
d
List
of h
ealt
h em
erge
ncy
cont
acts
in th
e fo
ur p
ilot s
ites
up
date
d
List
of h
ealt
h em
erge
ncy
cont
acts
in th
e fo
ur p
ilot s
ites
up
date
d
List
of h
ealt
h em
erge
ncy
cont
acts
in th
e fo
ur p
ilot s
ites
up
date
d
Des
ign
of h
ealt
h em
erge
ncy
tran
spor
t and
co
mm
unic
atio
n de
velo
ped
Term
s of u
se o
n th
e ut
iliza
tion,
repa
ir an
d m
aint
enan
ce o
f he
alth
em
erge
ncy
vehi
cles
neg
otia
ted
with
loca
l offi
cial
s,
trans
port
prov
ider
s,
priv
ate
sect
or, e
tc.
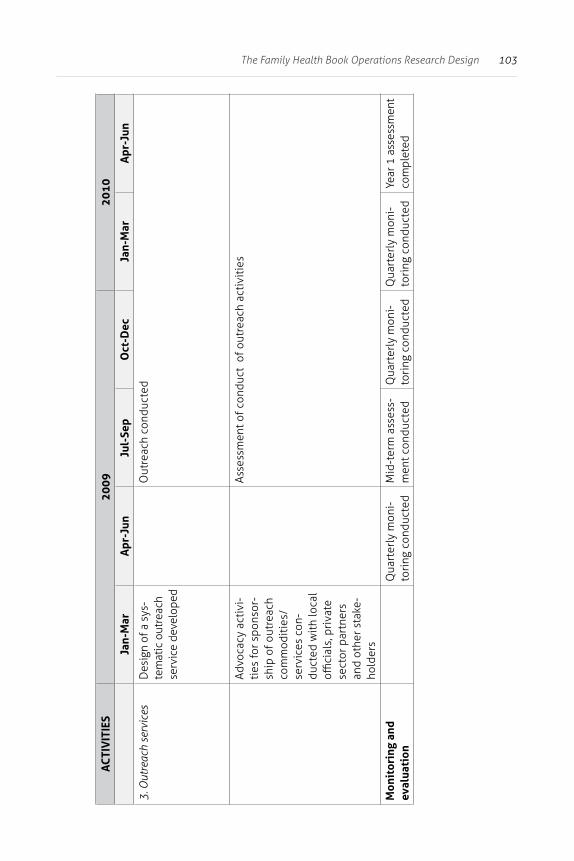
103The Family Health Book Operations Research Design
AC
TIV
ITIE
S20
0920
10
Jan-
Mar
Apr
-Jun
Jul-
Sep
Oct
-Dec
Jan-
Mar
Apr
-Jun
3. O
utre
ach
serv
ices
Des
ign
of a
sys
-te
mat
ic o
utre
ach
serv
ice
deve
lope
d
Out
reac
h co
nduc
ted
Advo
cacy
act
ivi-
ties
for s
pons
or-
ship
of o
utre
ach
com
mod
itie
s/se
rvic
es c
on-
duct
ed w
ith
loca
l offi
cial
s, p
riva
te
sect
or p
artn
ers
and
othe
r sta
ke-
hold
ers
Asse
ssm
ent o
f con
duct
of o
utre
ach
acti
viti
es
Mon
itor
ing
and
eval
uati
onQ
uart
erly
mon
i-to
ring
con
duct
edM
id-t
erm
ass
ess-
men
t con
duct
edQ
uart
erly
mon
i-to
ring
con
duct
edQ
uart
erly
mon
i-to
ring
con
duct
edYe
ar 1
ass
essm
ent
com
plet
ed
104 The Family Health Book
How will the FHB pilot be managed?
Compostela Valley
• Sustaining governance structures for FHB. The FHB Steering Committee, headed by the governor, will exercise oversight function in FHB implementation. Every quarter, the Technical Working Group (TWG) tasked with managing the pilot, will provide reports to the Steering Committee regarding the following:
1) status of FHB distribution;
2) status of Navigator deployment;
3) feedback on Navigator performance;
4) status of process and output indicators (i.e., families oriented, family health needs assessed, health use plans made and completed); and
5) issues/difficulties encountered by families and Navigators in developing and adhering to health use plans.
To generate this report, the TWG, headed by the PHO, shall meet at least once a month and consolidate findings into a quarterly report after convening the quarterly meeting of Navigators.
• Managing and sustaining FHB interventions. The province will be responsible for implementing the various FHB interventions, including updating and printing of the Book, recruitment and training of Navigators, maintaining and sustaining the health emergency transport and communication network, conducting periodic outreach services, building the CEmONC capacities of the Compostela Valley Provincial Hospital (CVPH), enroling FHB families in PhilHealth, and assisting critical facilities to comply with PhilHealth accreditation standards.
105The Family Health Book Operations Research Design
• Matching demand with the corresponding supply of needed FHB services and commodities. Navigators shall consolidate monthly the family call sheets which record the family’s health needs. They will submit a summary call sheet to the supervising rural health midwife, who will summarize all the health commodity and service requirements of families through the resource inventory sheet which is to be submitted to the MHO. This instrument guides the MHO in estimating the service and commodity requirements for a particular period. Should the expected requirements exceed local capacity to provide, the MHO may request assistance from the PHO or from CHD Davao Region for augmentation of its budget on specific MNCHN concerns.
CHD-Davao Region
CHD-Davao Region will assist in capacitating Navigators and in monitoring compliance of facilities with DOH licensing standards. It will also provide technical leadership on matters related to maternal, newborn and child health, and guiding FHB implementation towards the achievement of desired MNCHN outcomes.
PhilHealth
PhilHealth Region XI will support FHB intervention on PhilHealth enrolment with campaigns for universal health insurance coverage and the conduct of orientation sessions on PhilHealth benefits. The agency will become a strategic partner in facilitating accreditation of facilities for PhilHealth OPB, TB-DOTS and maternal and child packages (MCP).
106 The Family Health Book
Inter-CA collaboration on FHB
HPDP As the lead agency for the initiative, HPDP shall provide overall support to the management and operations, as well as the monitoring of the FHB in Compostela Valley.
It has assisted the province in getting baseline information needed for identifying the type and design of interventions needed in the province. This guided the selection of appropriate sites and beneficiaries, as well as the setup of structures and systems needed for the implementation of various FHB interventions (such as the Book and Navigator, the health emergency transport and communication network, regular outreach services, access to CEmONC facility, and support to PhilHealth accreditation and enrolment).
In line with its policy development thrust, HPDP jointly developed the core maternal and neonatal standards with the DOH. These now serve as the gold standard for the delivery of MNCHN services in Compostela Valley. Orientations were made with CHD XI and the PHO to update public and private health providers on these standards.
For the pre-implementation phase, HPDP is assisting the province in recruiting and training Navigators, selecting families, designing and printing the books, establishing a functional health emergency transport and communication network, designing the outreach activity, linking CVPH to funding sources, facilitating PhilHealth accreditation and renewal, and seeking sponsorships for various FHB activities.
107The Family Health Book Operations Research Design
To track the progress of the various interventions and immediately address impending operational problems, HPDP will conduct quarterly monitoring as well as mid-year and end-of year program evaluations. This entails conduct of surveys as well as FGDs with families, Navigators, midwives and other stakeholders in the initiative. Results of the surveys shall guide HPDP in making the necessary program adjustments and design improvement.
HPDP shall continue to monitor and evaluate the impact of FHB interventions in the four pilot municipalities until 2011.
HPDP will be the principal source of support during the first year of FHB implementation. Assistance from other CAs will come mostly in the roll-out phase.
HealthGov Assistance to FHB pilot sites. To sustain HPDP support for PhilHealth accreditation of critical facilities in the four pilot sites, HealthGov will provide the province with technical assistance on fund management.
Consultations will be made with the governor, mayors, and service providers in developing arrangements for managing PhilHealth capitation funds and reimbursements in a way that will sustain desired health outcomes. For instance, a local resolution may be issued enjoining health providers to share part of their reimbursements and capitation funds with the health emergency transport providers who brought the patient to the facility, and the TBAs who made the referrals. HealthGov can help organize sessions on this and can guide the province in drafting such issuance.
108 The Family Health Book
As part of its resource mobilization support, HealthGov will assist the province in generating funds for sustaining FHB interventions. It shall provide technical assistance to the province in developing grant applications and establishing resource generation schemes such as introduction of user’s fees in a public health facility.
Support can also be given in terms of identifying sources of FHB funds within the local budget and allocating portions of the 20% development fund, local taxes, and other similar coffers for the initiative.
Additionally, HealthGov will assist the Compostela MHO in securing a supplemental budget for setting up and maintaining its health emergency transport and communication network, and the Montevista MHO for the conduct of periodic outreach services.
Consultations with the mayors and barangay captains of the four pilot municipalities will likewise be made to leverage their share in the PhP 1.5 million family planning grant given to Compostela Valley for increased budgetary support for Navigator/BHW transport and training allowances and incentives as well as for procurement of MNCHN-related commodities.
HealthGov shall ensure that activities and investment requirements for Navigators, health emergency transport and communication network, outreach services, CVPH upgrades, and PhilHealth enrolment and accreditation are integrated in their 2010 Annual Investment Plan (AIP) and Province-wide Investment Plan for Health (PIPH) Annual Operational Plan (AOP).
109The Family Health Book Operations Research Design
To enhance the CVPH’s CEmONC capacity, HealthGov, at the province’s request, will roll out the Service Delivery for Excellence in Health (SDExH) to encourage a positive attitude towards patients among health personnel and to improve the quality of service delivery in the pilot sites.
This activity aims not only to help providers analyze the gap in their performance, but also to update them on clinical and service delivery standards and offer coaching and mentoring sessions in between workshops. The SDExH initially targeted the CVPH OB-Gynecology and Surgery personnel.
However, with the implementation of HealthGov’s Quality Assurance Partnership Committee (QAPC) initiative starting in April 2009, this initiative would be integrated with the FHB initiative in Compostela Valley. The QAPC is a governance mechanism that brings together local government officials, health service providers, members of civil society, and community representatives to address issues on accessibility, availability, and quality of MNCHN-related services in local health facilities.
Unlike other quality assurance programs where only service providers assess the quality of services, the QAPC intervention not only provides a venue for civil society to give feedback on health service delivery and quality, but also holds local officials and providers accountable to their communities for services delivered.
110 The Family Health Book
The QAPC is envisioned to provide oversight and problem-solving actions to improve MNCHN services in the facility. In Compostela Valley, a QAPC is proposed to be organized in the CVPH. In line with this, the QAPC orientation workshops will include an orientation on the SDExHH program. There are proposals to integrate into the QAPC the core maternal standards developed under the FHB.
Assistance to roll-out areas. For roll-out areas, HealthGov will coordinate with PhilHealth Regional Office (PRO) XI and the PHO in organizing sessions to orient heath service providers and LCEs on how they can benefit from PhilHealth by maximizing reimbursements. This is to encourage them to apply for or renew PhilHealth accreditation of their facilities and fast track PhilHealth enrolment of families to ensure optimal PhilHealth reimbursements.
HealthGov will also support municipalities in lobbying for supplemental budget for investments needed for MCP accreditation. Through SDExHH, support will also be provided for workshops and coaching/mentoring sessions aimed at improving the quality of services provided by RHUs.
HealthPRO To promote an environment conducive to the behavior change expected to result from the FHB interventions, HealthPRO will assist in a number of behavior change communication (BCC) on sensitive areas and issues.
Local champions and influential persons are keys to the promotion of healthy behaviors of target beneficiaries. Hence, the FHB initiative intends to engage them to endorse and promote the use of FHB and to help forge good relationships between families and the Navigators.
111The Family Health Book Operations Research Design
Arming these local champions and opinion leaders with appropriate health messages and information materials, and improved presentation and relational skills, will help families better understand the value of FHB interventions.
HealthPRO, through their Gabay, Damay, at Hawak Kamay programs which focus on developing and enhancing the network or areas of contact points, will help identify and develop local champions and opinion leaders. Through these programs, HealthPRO will also assist in the promotion and popularization through strategic brand development of the planned “FHB hour”–envisioned to be a “tag” or “brand” for all activities related to FHB implementation.
HealthPRO’s Gabay, Damay, at Hawak Kamay programs will also boost the planned promotion of CVPH and its services as a Center for Health and Wellness.
While the FHB remains a very good source of health messages and information on good health behavior and various health use plans, it remains a reading material without the Navigator. HPDP thus made the FHB+Navigator one package of behavior change intervention.
These necessary skills and interventions will be made possible through HealthPRO’s special assistance to the FHB initiative. Specifically, it will help in developing modules aimed at improving health service providers’ basic relational skills and in motivating them to value their work and role in the community.
112 The Family Health Book
References
Acuin, C. 2008. Conduct of Focus Group Discussions (FGDs) on Family Planning Behaviors among Men and Women in Selected Municipalities of Compostela Valley Province. Report submitted to the Health Policy Development Program, Quezon City, Philippines.
Bale, J., Stoll, B., and Lucas, O. (eds.) 2003. Improving Birth Outcomes: Meeting the Challenges in the Developing World. Washington, DC: National Academy of Sciences and Institute of Medicine.
Campbell, O.M. and Graham, W.J. 2006. “Strategies for reducing maternal mortality: getting on with what works.” The Lancet, 368 (9543): 1284-1299.
Compostela Valley Provincial Health Office. 2007. Maternal and Child Death Report. Manila, Philippines: Field Health Service Information System.
Costello, M., Lacuesta, M., RamaRao, S. and Jain, A. 2001. ”A Client-Centered Approach to Family Planning: The Davao Project.” Studies in Family Planning, 32: 302–314. Retrieved from http://www.jstor.org/pss/2696318.
Datta, M. and Nichter, M. 2003. Introducing Culturally Sensitive Tuberculosis Education and Context Specific Patient Screening. 1-30. Retrieved from http://www.tnmmu.ac.in/edu.pdf.
Department of Health (DOH). 2000. Philippine Health Statistics. Manila, Philippines: DOH.
____________________. 2004. Philippine Health Statistics. Manila, Philippines: DOH.
____________________. 2005. The National Objectives for Health 2005-2010. Manila, Phillipines: DOH.
____________________. 2007. Field Health Service Information System 2007. Manila, Philippines: DOH.
113The Family Health Book Operations Research Design
Family Health International Institute for HIV/AIDS (FHI). 2003). Baseline Assessment Tools for Preventing Mother to Child Transmission of HIV. Arlington, VA: Family Health International. Retrieved from http://www.fhi.org/en/hivaids/pub/guide/baseline+assessment+tools+for+pmtct.htm.
Gwatkin, D., Rutstein, S., Johnson, K., Suliman, E., Wagstaff, A., and Amouzou, A. 2007. Socio- economic Differences in Health, Nutrition and Population in the Philippines. Washington, DC: World Bank.
Habana, M., Mantaring, J. et al. 2008. The Family Health Book: Maternal, Neonatal and Child Health Care Packages and Standards for Practice and Facilities. Manila, Philippines: Foundation for the Advancement of Clinical Epidemiology, Inc. and Health Policy Development Program.
Health Policy Development Program (HPDP). 2007a. Family Health Book Baseline Facility Survey. Quezon City, Philippines: UPecon Foundation, Inc.-Health Policy Development Program..
____________________. 2007b. Family Health Book Baseline Household Survey. Quezon City, Philippines: UPecon Foundation, Inc.-Health Policy Development Program.
____________________. 2008. The Family Health Book Navigator’s Kit. Quezon City, Philippines: UPecon Foundation, Inc.-Health Policy Development Program.
Health Policy Development Program (HPDP) and Social Development Research Center (SDRC). 2008. Focus Group Discussion Report. Quezon City, Philippines: UPecon Foundation, Inc.-Health Policy Development Program.
National Institute of Population Research and Training (NIPORT), ORC Macro, Johns Hopkins University and ICDDR, B. (2003). Bangladesh Maternal Health Services and Maternal Mortality Survey 2001. Dhaka, Bangladesh and Calverton, Maryland: NIPORT, ORC Macro, Johns Hopkins University, and ICDDR, B. Retrieved from http://www.measuredhs.com/pubs/pub_details.cfm?ID=456.
114 The Family Health Book
National Statistics Office (NSO). 2006. Family Income and Expenditure Survey. Manila, Philippines. Retrieved from http://www.census.gov.ph/data/pressrelease/2008/ie06frtx.html.
____________________. 2007. Family Planning Survey 2006. Metro Manila: NSO.
National Statistics Office (NSO) and ORC Macro. 2004. National Demographic and Health Survey 2003. Calverton, Maryland: NSO and ORC Macro. World Health Organization (WHO). 2000. Core Health Indicators for Philippines. Washington, DC: World Health Organization. Retrieved from http://www.who.int/whosis/indicators.
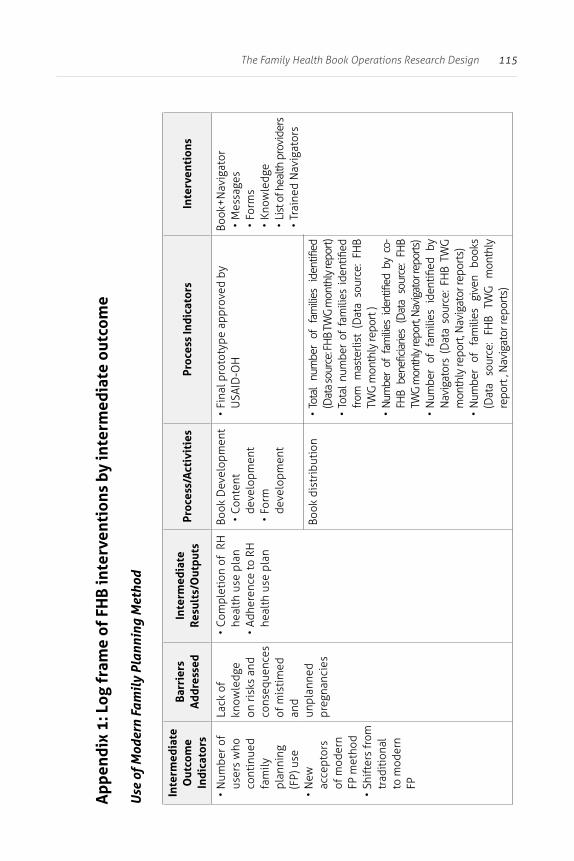
115The Family Health Book Operations Research Design
App
endi
x 1:
Log
fra
me
of F
HB
inte
rven
tion
s by
inte
rmed
iate
out
com
e
Use
of M
oder
n Fa
mil
y Pl
anni
ng M
etho
d
Inte
rmed
iate
Out
com
e In
dica
tors
Barr
iers
A
ddre
ssed
Inte
rmed
iate
Resu
lts/
Out
puts
Proc
ess/
Act
ivit
ies
Proc
ess
Indi
cato
rsIn
terv
enti
ons
• N
umbe
r of
user
s w
ho
cont
inue
d fa
mily
pl
anni
ng
(FP)
use
• N
ew
acce
ptor
s of
mod
ern
FP m
etho
d•
Shift
ers
from
tr
aditi
onal
to
mod
ern
FP
Lack
of
know
ledg
e on
risk
s an
d co
nseq
uenc
es
of m
isti
med
an
d un
plan
ned
preg
nanc
ies
• Co
mpl
etio
n of
RH
he
alth
use
pla
n •
Adhe
renc
e to
RH
he
alth
use
pla
n
Book
Dev
elop
men
t•
Cont
ent
deve
lopm
ent
• Fo
rm
deve
lopm
ent
• Fi
nal p
roto
type
app
rove
d by
U
SAID
-OH
Book
+Nav
igat
or•
Mes
sage
s•
Form
s•
Know
ledg
e•
List
of h
ealth
pro
vide
rs•
Trai
ned
Nav
igat
ors
Book
dis
trib
utio
n•
Tota
l nu
mbe
r of
fam
ilies
ide
ntifi
ed
(Dat
a so
urce
: FH
B TW
G m
onth
ly re
port)
• To
tal
num
ber
of f
amili
es i
dent
ified
fr
om m
aste
rlist
(D
ata
sour
ce:
FHB
TWG
mon
thly
repo
rt )
• N
umbe
r of
fam
ilies
ide
ntifi
ed b
y co
-FH
B be
nefic
iarie
s (D
ata
sour
ce:
FHB
TWG
mon
thly
repo
rt, N
avig
ator
repo
rts)
• N
umbe
r of
fam
ilies
ide
ntifi
ed b
y N
avig
ator
s (D
ata
sour
ce: F
HB
TWG
m
onth
ly re
port
, Nav
igat
or re
port
s)•
Num
ber
of
fam
ilies
gi
ven
book
s (D
ata
sour
ce:
FHB
TWG
m
onth
ly
repo
rt ,
Nav
igat
or re
port
s)
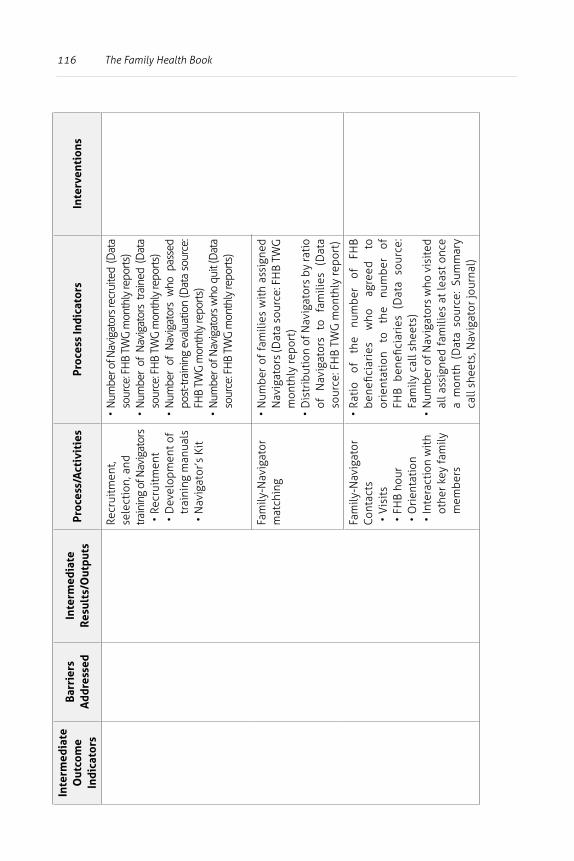
116 The Family Health BookIn
term
edia
teO
utco
me
Indi
cato
rs
Barr
iers
A
ddre
ssed
Inte
rmed
iate
Resu
lts/
Out
puts
Proc
ess/
Act
ivit
ies
Proc
ess
Indi
cato
rsIn
terv
enti
ons
Recr
uitm
ent,
sele
ctio
n, a
nd
train
ing
of N
avig
ator
s•
Recr
uitm
ent
• D
evel
opm
ent o
f tr
aini
ng m
anua
ls•
Nav
igat
or’s
Kit
• N
umbe
r of N
avig
ator
s rec
ruite
d (D
ata
sour
ce: F
HB
TWG
mon
thly
repo
rts)
• N
umbe
r of
Nav
igat
ors
train
ed (
Dat
a so
urce
: FH
B TW
G m
onth
ly re
ports
)•
Num
ber
of N
avig
ator
s w
ho p
asse
d po
st-tr
aini
ng e
valu
atio
n (D
ata
sour
ce:
FHB
TWG
mon
thly
repo
rts)
• N
umbe
r of N
avig
ator
s w
ho q
uit (
Dat
a so
urce
: FH
B TW
G m
onth
ly re
ports
)
Fam
ily-N
avig
ator
m
atch
ing
• N
umbe
r of
fam
ilies
wit
h as
sign
ed
Nav
igat
ors
(Dat
a so
urce
: FH
B TW
G
mon
thly
repo
rt)
• D
istr
ibut
ion
of N
avig
ator
s by
rati
o of
N
avig
ator
s to
fa
mili
es
(Dat
a so
urce
: FH
B TW
G m
onth
ly re
port
)
Fam
ily-N
avig
ator
Co
ntac
ts•
Vis
its
• FH
B ho
ur•
Ori
enta
tion
• In
tera
ctio
n w
ith
othe
r key
fam
ily
mem
bers
• Ra
tio
of
the
num
ber
of
FHB
bene
ficia
ries
w
ho
agre
ed
to
orie
ntat
ion
to
the
num
ber
of
FHB
bene
ficia
ries
(D
ata
sour
ce:
Fam
ily c
all s
heet
s)•
Num
ber o
f Nav
igat
ors
who
vis
ited
al
l ass
igne
d fa
mili
es a
t le
ast
once
a
mon
th (
Dat
a so
urce
: Su
mm
ary
call
shee
ts, N
avig
ator
jour
nal)
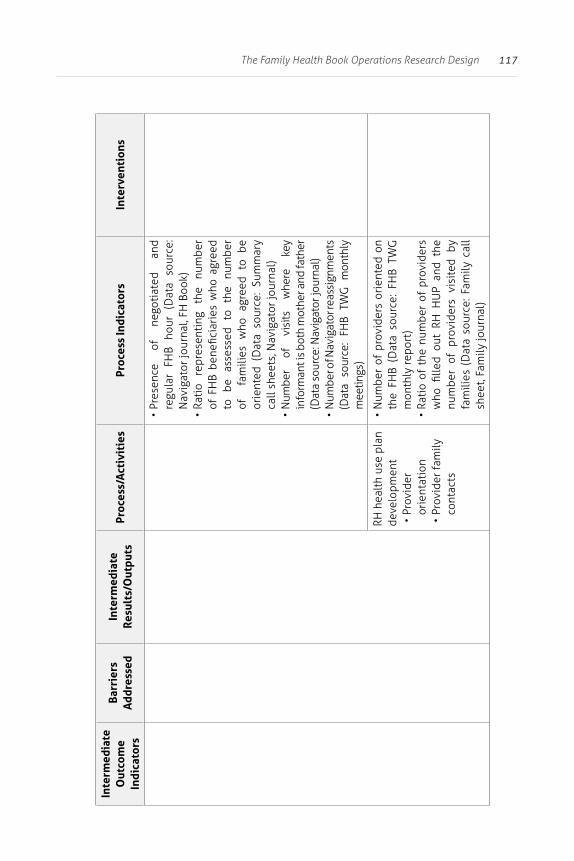
117The Family Health Book Operations Research Design
Inte
rmed
iate
Out
com
e In
dica
tors
Barr
iers
A
ddre
ssed
Inte
rmed
iate
Resu
lts/
Out
puts
Proc
ess/
Act
ivit
ies
Proc
ess
Indi
cato
rsIn
terv
enti
ons
• Pr
esen
ce
of
nego
tiat
ed
and
regu
lar
FHB
hour
(D
ata
sour
ce:
Nav
igat
or jo
urna
l, FH
Boo
k)•
Rati
o re
pres
enti
ng
the
num
ber
of F
HB
bene
ficia
ries
who
agr
eed
to
be
asse
ssed
to
th
e nu
mbe
r of
fa
mili
es w
ho a
gree
d to
be
orie
nted
(D
ata
sour
ce:
Sum
mar
y ca
ll sh
eets
, Nav
igat
or jo
urna
l)•
Num
ber
of
visi
ts
whe
re
key
info
rman
t is
both
mot
her a
nd fa
ther
(D
ata
sour
ce: N
avig
ator
jour
nal)
• N
umbe
r of N
avig
ator
reas
sign
men
ts
(Dat
a so
urce
: FH
B TW
G m
onth
ly
mee
tings
)
RH h
ealt
h us
e pl
an
deve
lopm
ent
• Pr
ovid
er
orie
ntat
ion
• Pr
ovid
er fa
mily
co
ntac
ts
• N
umbe
r of
pro
vide
rs o
rien
ted
on
the
FHB
(Dat
a so
urce
: FH
B TW
G
mon
thly
repo
rt)
• Ra
tio
of t
he n
umbe
r of
pro
vide
rs
who
fille
d ou
t RH
HU
P an
d th
e nu
mbe
r of
pro
vide
rs v
isit
ed b
y fa
mili
es (
Dat
a so
urce
: Fam
ily c
all
shee
t, Fa
mily
jour
nal)
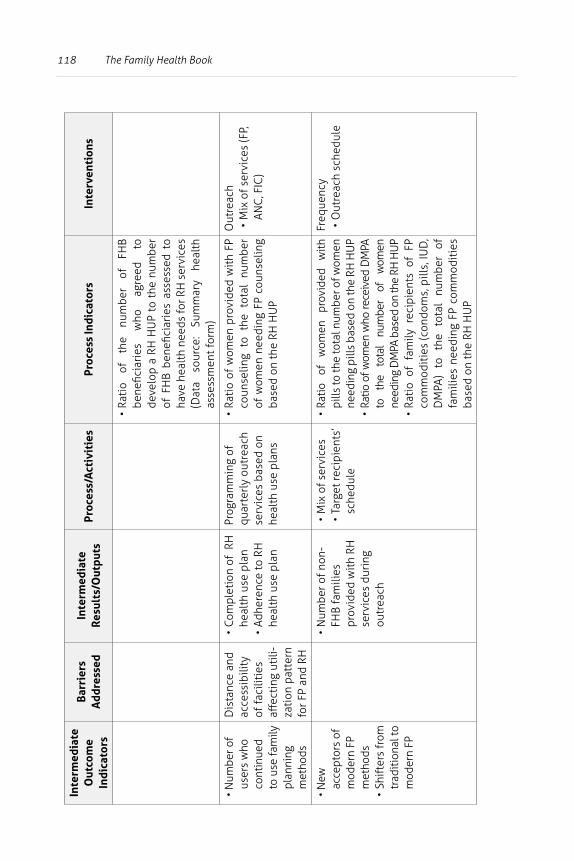
118 The Family Health BookIn
term
edia
teO
utco
me
Indi
cato
rs
Barr
iers
A
ddre
ssed
Inte
rmed
iate
Resu
lts/
Out
puts
Proc
ess/
Act
ivit
ies
Proc
ess
Indi
cato
rsIn
terv
enti
ons
• Ra
tio
of
the
num
ber
of
FHB
bene
ficia
ries
w
ho
agre
ed
to
deve
lop
a RH
HU
P to
the
num
ber
of F
HB
bene
ficia
ries
ass
esse
d to
ha
ve h
ealt
h ne
eds
for R
H s
ervi
ces
(Dat
a so
urce
: Su
mm
ary
heal
th
asse
ssm
ent f
orm
)
• N
umbe
r of
user
s w
ho
cont
inue
d
to u
se fa
mily
pl
anni
ng
met
hods
Dis
tanc
e an
d ac
cess
ibili
ty
of fa
cilit
ies
affec
ting
uti
li-za
tion
pat
tern
fo
r FP
and
RH
• Co
mpl
etio
n of
RH
he
alth
use
pla
n •
Adhe
renc
e to
RH
he
alth
use
pla
n
Prog
ram
min
g of
qu
arte
rly
outr
each
se
rvic
es b
ased
on
heal
th u
se p
lans
• Ra
tio
of w
omen
pro
vide
d w
ith
FP
coun
selin
g to
the
tot
al n
umbe
r of
wom
en n
eedi
ng F
P co
unse
ling
base
d on
the
RH H
UP
Out
reac
h•
Mix
of s
ervi
ces
(FP,
AN
C, F
IC)
• N
ew
acce
ptor
s of
m
oder
n FP
m
etho
ds•
Shift
ers
from
tr
aditi
onal
to
mod
ern
FP
• N
umbe
r of n
on-
FHB
fam
ilies
pr
ovid
ed w
ith
RH
serv
ices
dur
ing
outr
each
• M
ix o
f ser
vice
s•
Targ
et re
cipi
ents
’ sc
hedu
le
• Ra
tio
of
wom
en
prov
ided
w
ith
pills
to th
e to
tal n
umbe
r of w
omen
ne
edin
g pi
lls b
ased
on
the
RH H
UP
• Ra
tio o
f wom
en w
ho re
ceiv
ed D
MPA
to
th
e to
tal
num
ber
of
wom
en
need
ing
DM
PA b
ased
on
the
RH H
UP
• Ra
tio
of f
amily
rec
ipie
nts
of F
P co
mm
odit
ies
(con
dom
s, p
ills,
IUD
, D
MPA
) to
th
e to
tal
num
ber
of
fam
ilies
nee
ding
FP
com
mod
itie
s ba
sed
on th
e RH
HU
P
Freq
uenc
y•
Out
reac
h sc
hedu
le
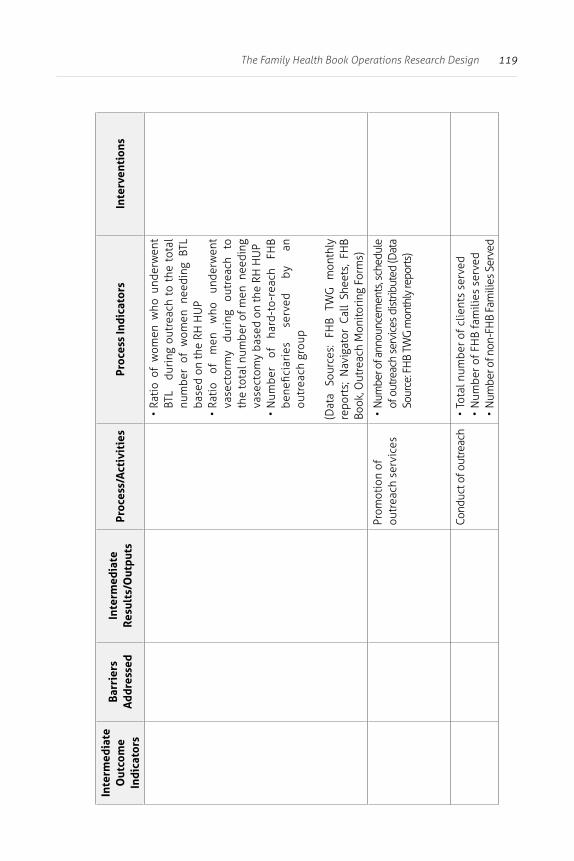
119The Family Health Book Operations Research Design
Inte
rmed
iate
Out
com
e In
dica
tors
Barr
iers
A
ddre
ssed
Inte
rmed
iate
Resu
lts/
Out
puts
Proc
ess/
Act
ivit
ies
Proc
ess
Indi
cato
rsIn
terv
enti
ons
• Ra
tio
of w
omen
who
und
erw
ent
BTL
du
ring
out
reac
h to
the
tot
al
num
ber
of w
omen
nee
ding
BTL
ba
sed
on th
e RH
HU
P•
Rati
o of
m
en
who
un
derw
ent
vase
ctor
my
duri
ng
outr
each
to
th
e to
tal n
umbe
r of m
en n
eedi
ng
vase
ctom
y ba
sed
on th
e RH
HU
P•
Num
ber
of
hard
-to-
reac
h FH
B be
nefic
iari
es
serv
ed
by
an
outr
each
gro
up
(Dat
a So
urce
s:
FHB
TWG
m
onth
ly
repo
rts;
Nav
igat
or C
all
Shee
ts,
FHB
Book
, Out
reac
h M
onito
ring
For
ms)
Prom
otio
n of
ou
trea
ch s
ervi
ces
• N
umbe
r of a
nnou
ncem
ents
, sch
edul
e of
out
reac
h se
rvic
es d
istri
bute
d (D
ata
Sour
ce: F
HB
TWG
mon
thly
repo
rts)
Cond
uct o
f out
reac
h•
Tota
l num
ber o
f clie
nts
serv
ed•
Num
ber o
f FH
B fa
mili
es s
erve
d•
Num
ber o
f non
-FH
B Fa
mili
es S
erve
d
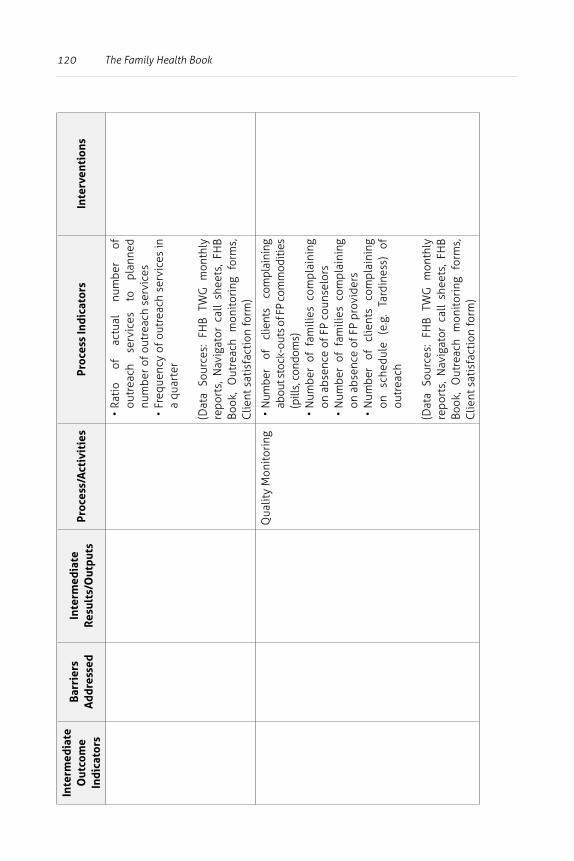
120 The Family Health BookIn
term
edia
teO
utco
me
Indi
cato
rs
Barr
iers
A
ddre
ssed
Inte
rmed
iate
Resu
lts/
Out
puts
Proc
ess/
Act
ivit
ies
Proc
ess
Indi
cato
rsIn
terv
enti
ons
• Ra
tio
of
actu
al
num
ber
of
outr
each
se
rvic
es
to
plan
ned
num
ber o
f out
reac
h se
rvic
es•
Freq
uenc
y of
out
reac
h se
rvic
es in
a
quar
ter
(Dat
a So
urce
s: F
HB
TWG
mon
thly
re
port
s, N
avig
ator
cal
l sh
eets
, FH
B Bo
ok,
Out
reac
h m
onit
orin
g fo
rms,
C
lient
sat
isfa
ctio
n fo
rm)
Qua
lity
Mon
itor
ing
• N
umbe
r of
cl
ient
s co
mpl
aini
ng
abou
t sto
ck-o
uts o
f FP
com
mod
ities
(p
ills,
con
dom
s)•
Num
ber
of f
amili
es c
ompl
aini
ng
on a
bsen
ce o
f FP
coun
selo
rs•
Num
ber
of f
amili
es c
ompl
aini
ng
on a
bsen
ce o
f FP
prov
ider
s•
Num
ber
of
clie
nts
com
plai
ning
on
sc
hedu
le
(e.g
. Ta
rdin
ess)
of
ou
trea
ch
(Dat
a So
urce
s: F
HB
TWG
mon
thly
re
port
s, N
avig
ator
cal
l sh
eets
, FH
B Bo
ok,
Out
reac
h m
onit
orin
g fo
rms,
C
lient
sat
isfa
ctio
n fo
rm)
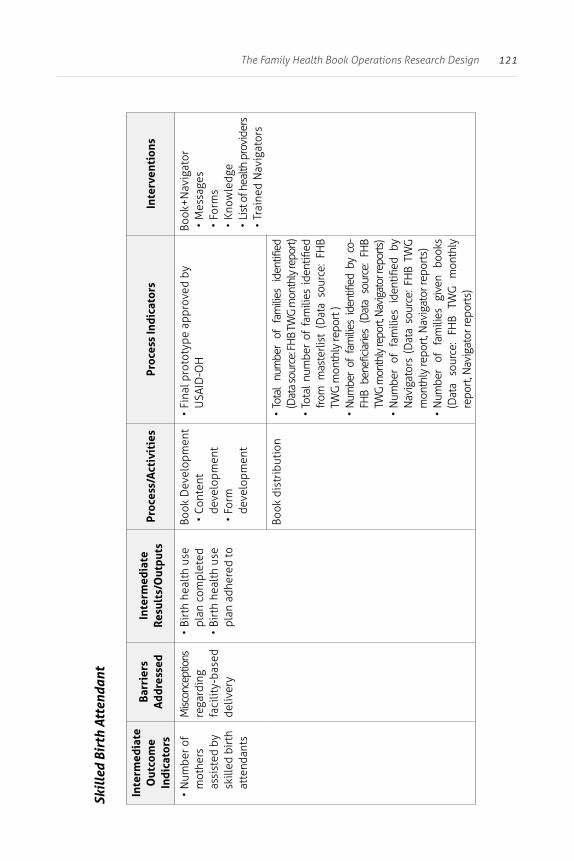
121The Family Health Book Operations Research Design
Skil
led
Birt
h At
tend
ant
Inte
rmed
iate
Out
com
e In
dica
tors
Barr
iers
A
ddre
ssed
Inte
rmed
iate
Resu
lts/
Out
puts
Proc
ess/
Act
ivit
ies
Proc
ess
Indi
cato
rsIn
terv
enti
ons
• N
umbe
r of
mot
hers
as
sist
ed b
y sk
illed
birt
h at
tend
ants
Misc
once
ptio
ns
rega
rdin
g fa
cilit
y-ba
sed
deliv
ery
• Bi
rth
heal
th u
se
plan
com
plet
ed•
Birt
h he
alth
use
pl
an a
dher
ed to
Book
Dev
elop
men
t•
Cont
ent
deve
lopm
ent
• Fo
rm
deve
lopm
ent
• Fi
nal p
roto
type
app
rove
d by
U
SAID
-OH
Book
+Nav
igat
or•
Mes
sage
s•
Form
s•
Know
ledg
e•
List
of h
ealth
pro
vide
rs•
Trai
ned
Nav
igat
ors
Book
dis
trib
utio
n•
Tota
l nu
mbe
r of
fam
ilies
ide
ntifi
ed
(Dat
a so
urce
: FH
B TW
G m
onth
ly re
port)
• To
tal
num
ber
of f
amili
es i
dent
ified
fr
om m
aste
rlist
(D
ata
sour
ce:
FHB
TWG
mon
thly
repo
rt )
• N
umbe
r of
fam
ilies
ide
ntifi
ed b
y co
-FH
B be
nefic
iarie
s (D
ata
sour
ce:
FHB
TWG
mon
thly
repo
rt, N
avig
ator
repo
rts)
• N
umbe
r of
fam
ilies
ide
ntifi
ed b
y N
avig
ator
s (D
ata
sour
ce: F
HB
TWG
m
onth
ly re
port
, Nav
igat
or re
port
s)•
Num
ber
of
fam
ilies
gi
ven
book
s (D
ata
sour
ce:
FHB
TWG
m
onth
ly
repo
rt, N
avig
ator
repo
rts)
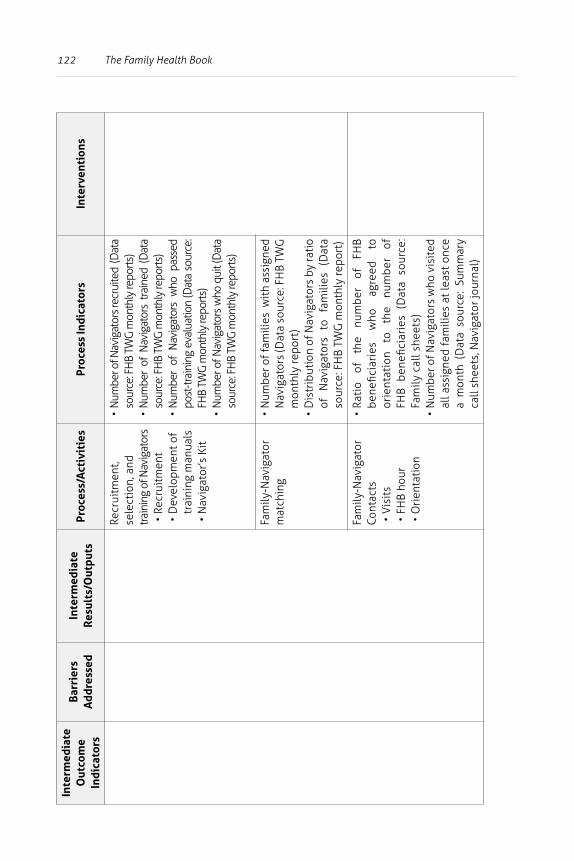
122 The Family Health BookIn
term
edia
teO
utco
me
Indi
cato
rs
Barr
iers
A
ddre
ssed
Inte
rmed
iate
Resu
lts/
Out
puts
Proc
ess/
Act
ivit
ies
Proc
ess
Indi
cato
rsIn
terv
enti
ons
Recr
uitm
ent,
sele
ctio
n, a
nd
train
ing
of N
avig
ator
s•
Recr
uitm
ent
• D
evel
opm
ent o
f tr
aini
ng m
anua
ls•
Nav
igat
or’s
Kit
• N
umbe
r of N
avig
ator
s rec
ruite
d (D
ata
sour
ce: F
HB
TWG
mon
thly
repo
rts)
• N
umbe
r of
Nav
igat
ors
train
ed (
Dat
a so
urce
: FH
B TW
G m
onth
ly re
ports
)•
Num
ber
of N
avig
ator
s w
ho p
asse
d po
st-tr
aini
ng e
valu
atio
n (D
ata
sour
ce:
FHB
TWG
mon
thly
repo
rts)
• N
umbe
r of N
avig
ator
s w
ho q
uit (
Dat
a so
urce
: FH
B TW
G m
onth
ly re
ports
)
Fam
ily-N
avig
ator
m
atch
ing
• N
umbe
r of f
amili
es w
ith
assi
gned
N
avig
ator
s (D
ata
sour
ce: F
HB
TWG
m
onth
ly re
port
)•
Dis
trib
utio
n of
Nav
igat
ors
by ra
tio
of
Nav
igat
ors
to
fam
ilies
(D
ata
sour
ce: F
HB
TWG
mon
thly
repo
rt)
Fam
ily-N
avig
ator
Co
ntac
ts•
Vis
its
• FH
B ho
ur•
Ori
enta
tion
• Ra
tio
of
the
num
ber
of
FHB
bene
ficia
ries
w
ho
agre
ed
to
orie
ntat
ion
to
the
num
ber
of
FHB
bene
ficia
ries
(D
ata
sour
ce:
Fam
ily c
all s
heet
s)•
Num
ber o
f Nav
igat
ors
who
vis
ited
al
l ass
igne
d fa
mili
es a
t le
ast
once
a
mon
th (
Dat
a so
urce
: Su
mm
ary
call
shee
ts, N
avig
ator
jour
nal)
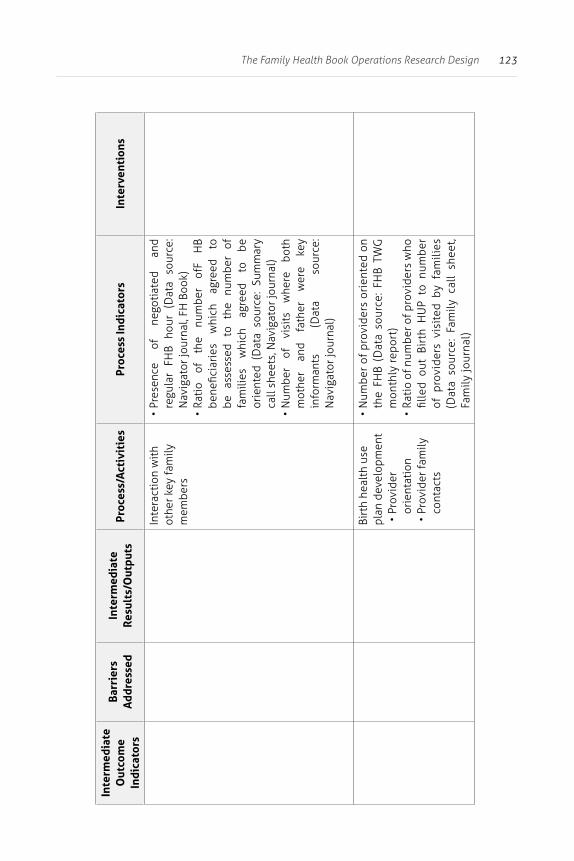
123The Family Health Book Operations Research Design
Inte
rmed
iate
Out
com
e In
dica
tors
Barr
iers
A
ddre
ssed
Inte
rmed
iate
Resu
lts/
Out
puts
Proc
ess/
Act
ivit
ies
Proc
ess
Indi
cato
rsIn
terv
enti
ons
Inte
ract
ion
wit
h ot
her k
ey fa
mily
m
embe
rs
• Pr
esen
ce
of
nego
tiat
ed
and
regu
lar
FHB
hour
(D
ata
sour
ce:
Nav
igat
or jo
urna
l, FH
Boo
k)•
Rati
o of
th
e nu
mbe
r of
F H
B be
nefic
iari
es
whi
ch
agre
ed
to
be
asse
ssed
to
th
e nu
mbe
r of
fa
mili
es
whi
ch
agre
ed
to
be
orie
nted
(D
ata
sour
ce:
Sum
mar
y ca
ll sh
eets
, Nav
igat
or jo
urna
l)•
Num
ber
of
visi
ts
whe
re
both
m
othe
r an
d fa
ther
w
ere
key
info
rman
ts
(Dat
a so
urce
: N
avig
ator
jour
nal)
Birt
h he
alth
use
pl
an d
evel
opm
ent
• Pr
ovid
er
orie
ntat
ion
• Pr
ovid
er fa
mily
co
ntac
ts
• N
umbe
r of
pro
vide
rs o
rien
ted
on
the
FHB
(Dat
a so
urce
: FH
B TW
G
mon
thly
rep
ort)
• Ra
tio
of n
umbe
r of p
rovi
ders
who
fil
led
out
Birt
h H
UP
to n
umbe
r of
pro
vide
rs v
isit
ed b
y fa
mili
es
(Dat
a so
urce
: Fa
mily
cal
l sh
eet,
Fam
ily jo
urna
l)
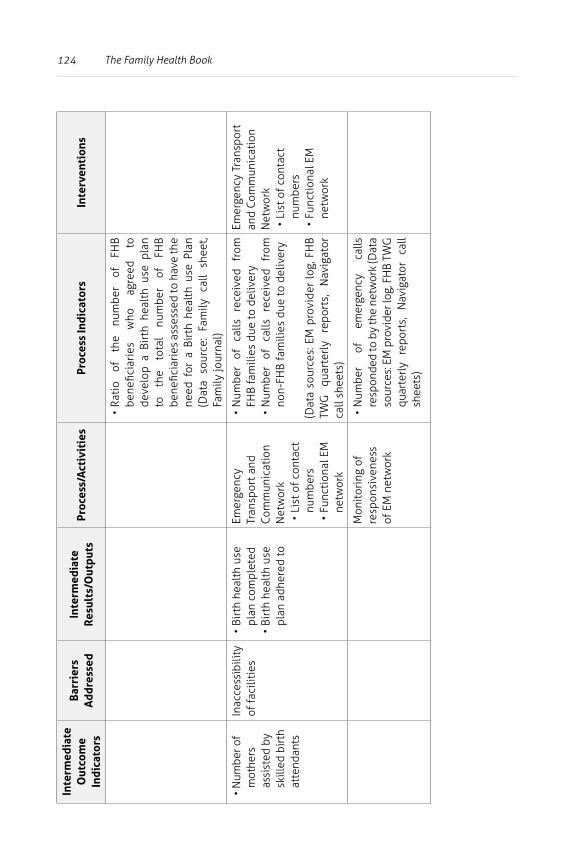
124 The Family Health BookIn
term
edia
teO
utco
me
Indi
cato
rs
Barr
iers
A
ddre
ssed
Inte
rmed
iate
Resu
lts/
Out
puts
Proc
ess/
Act
ivit
ies
Proc
ess
Indi
cato
rsIn
terv
enti
ons
• Ra
tio
of
the
num
ber
of
FHB
bene
ficia
ries
w
ho
agre
ed
to
deve
lop
a Bi
rth
heal
th u
se p
lan
to
the
tota
l nu
mbe
r of
FH
B be
nefic
iari
es a
sses
sed
to h
ave
the
need
for
a B
irth
hea
lth
use
Plan
(D
ata
sour
ce:
Fam
ily c
all
shee
t, Fa
mily
jour
nal)
• N
umbe
r of
mot
hers
as
sist
ed b
y sk
illed
birt
h at
tend
ants
Inac
cess
ibili
ty
of fa
cilit
ies
• Bi
rth
heal
th u
se
plan
com
plet
ed•
Birt
h he
alth
use
pl
an a
dher
ed to
Emer
genc
y Tr
ansp
ort a
nd
Com
mun
icat
ion
Net
wor
k•
List
of c
onta
ct
num
bers
• Fu
ncti
onal
EM
ne
twor
k
• N
umbe
r of
ca
lls
rece
ived
fr
om
FHB
fam
ilies
due
to d
eliv
ery
• N
umbe
r of
ca
lls
rece
ived
fr
om
non-
FHB
fam
ilies
due
to d
eliv
ery
(Dat
a so
urce
s: E
M p
rovi
der
log,
FH
B TW
G
quar
terl
y re
port
s,
Nav
igat
or
call
shee
ts)
Emer
genc
y Tr
ansp
ort
and
Com
mun
icat
ion
Net
wor
k•
List
of c
onta
ct
num
bers
• Fu
ncti
onal
EM
ne
twor
k
Mon
itor
ing
of
resp
onsi
vene
ss
of E
M n
etw
ork
• N
umbe
r of
em
erge
ncy
calls
re
spon
ded
to b
y th
e ne
twor
k (D
ata
sour
ces:
EM
pro
vide
r log
, FH
B TW
G
quar
terl
y re
port
s,
Nav
igat
or
call
shee
ts)
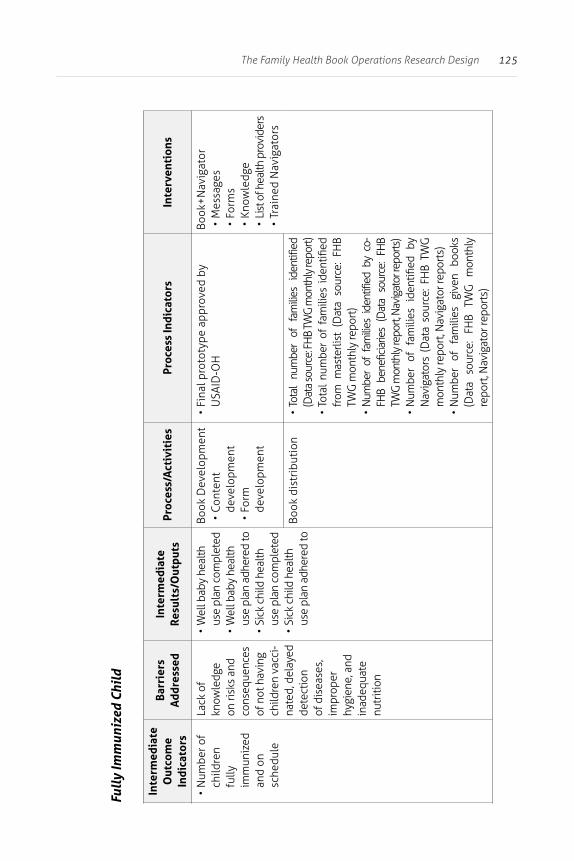
125The Family Health Book Operations Research Design
Full
y Im
mun
ized
Chi
ld
Inte
rmed
iate
Out
com
e In
dica
tors
Barr
iers
A
ddre
ssed
Inte
rmed
iate
Resu
lts/
Out
puts
Proc
ess/
Act
ivit
ies
Proc
ess
Indi
cato
rsIn
terv
enti
ons
• N
umbe
r of
child
ren
fully
im
mun
ized
an
d on
sc
hedu
le
Lack
of
know
ledg
e on
risk
s an
d co
nseq
uenc
es
of n
ot h
avin
g ch
ildre
n va
cci-
nate
d, d
elay
ed
dete
ctio
n of
dis
ease
s,
impr
oper
hy
gien
e, a
nd
inad
equa
te
nutr
ition
• W
ell b
aby
heal
th
use
plan
com
plet
ed•
Wel
l bab
y he
alth
us
e pl
an a
dher
ed to
• Si
ck c
hild
hea
lth
use
plan
com
plet
ed•
Sick
chi
ld h
ealth
us
e pl
an a
dher
ed to
Book
Dev
elop
men
t•
Cont
ent
deve
lopm
ent
• Fo
rm
deve
lopm
ent
• Fi
nal p
roto
type
app
rove
d by
U
SAID
-OH
Book
+Nav
igat
or•
Mes
sage
s•
Form
s•
Know
ledg
e•
List
of h
ealth
pro
vide
rs•
Trai
ned
Nav
igat
ors
Book
dis
trib
utio
n•
Tota
l nu
mbe
r of
fam
ilies
ide
ntifi
ed
(Dat
a so
urce
: FH
B TW
G m
onth
ly re
port)
• To
tal
num
ber
of f
amili
es i
dent
ified
fr
om m
aste
rlist
(D
ata
sour
ce:
FHB
TWG
mon
thly
repo
rt)
• N
umbe
r of
fam
ilies
ide
ntifi
ed b
y co
-FH
B be
nefic
iarie
s (D
ata
sour
ce:
FHB
TWG
mon
thly
repo
rt, N
avig
ator
repo
rts)
• N
umbe
r of
fam
ilies
ide
ntifi
ed b
y N
avig
ator
s (D
ata
sour
ce: F
HB
TWG
m
onth
ly re
port
, Nav
igat
or re
port
s)•
Num
ber
of
fam
ilies
gi
ven
book
s (D
ata
sour
ce:
FHB
TWG
m
onth
ly
repo
rt, N
avig
ator
repo
rts)
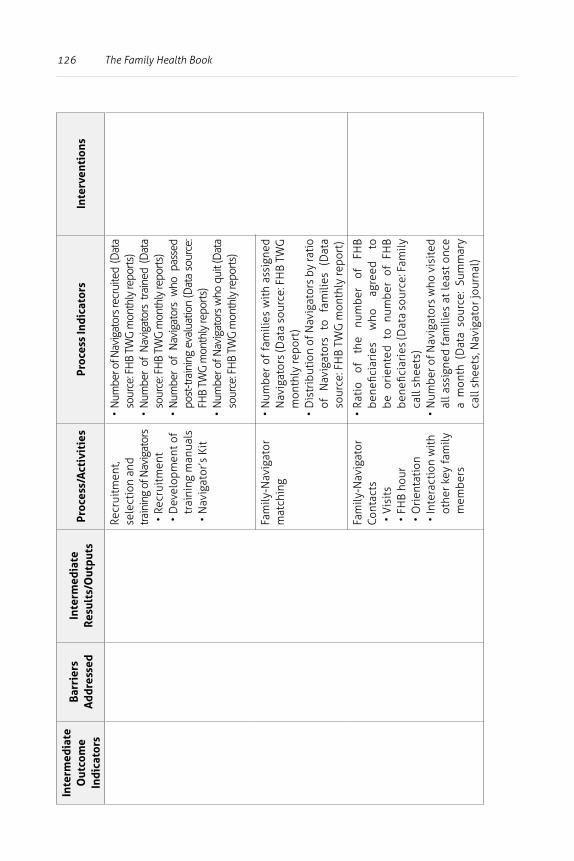
126 The Family Health BookIn
term
edia
teO
utco
me
Indi
cato
rs
Barr
iers
A
ddre
ssed
Inte
rmed
iate
Resu
lts/
Out
puts
Proc
ess/
Act
ivit
ies
Proc
ess
Indi
cato
rsIn
terv
enti
ons
Recr
uitm
ent,
sele
ctio
n an
d tra
inin
g of
Nav
igat
ors
• Re
crui
tmen
t•
Dev
elop
men
t of
trai
ning
man
uals
• N
avig
ator
’s K
it
• N
umbe
r of N
avig
ator
s rec
ruite
d (D
ata
sour
ce: F
HB
TWG
mon
thly
repo
rts)
• N
umbe
r of
Nav
igat
ors
train
ed (
Dat
a so
urce
: FH
B TW
G m
onth
ly re
ports
)•
Num
ber
of N
avig
ator
s w
ho p
asse
d po
st-tr
aini
ng e
valu
atio
n (D
ata
sour
ce:
FHB
TWG
mon
thly
repo
rts)
• N
umbe
r of N
avig
ator
s w
ho q
uit (
Dat
a so
urce
: FH
B TW
G m
onth
ly re
ports
)
Fam
ily-N
avig
ator
m
atch
ing
• N
umbe
r of
fam
ilies
wit
h as
sign
ed
Nav
igat
ors
(Dat
a so
urce
: FH
B TW
G
mon
thly
repo
rt)
• D
istr
ibut
ion
of N
avig
ator
s by
rati
o of
N
avig
ator
s to
fa
mili
es
(Dat
a so
urce
: FH
B TW
G m
onth
ly re
port
)
Fam
ily-N
avig
ator
Co
ntac
ts•
Vis
its
• FH
B ho
ur•
Ori
enta
tion
• In
tera
ctio
n w
ith
othe
r key
fam
ily
mem
bers
• Ra
tio
of
the
num
ber
of
FHB
bene
ficia
ries
w
ho
agre
ed
to
be o
rien
ted
to n
umbe
r of
FH
B be
nefic
iari
es (D
ata
sour
ce: F
amily
ca
ll sh
eets
)•
Num
ber o
f Nav
igat
ors
who
vis
ited
al
l ass
igne
d fa
mili
es a
t le
ast
once
a
mon
th (
Dat
a so
urce
: Su
mm
ary
call
shee
ts, N
avig
ator
jour
nal)
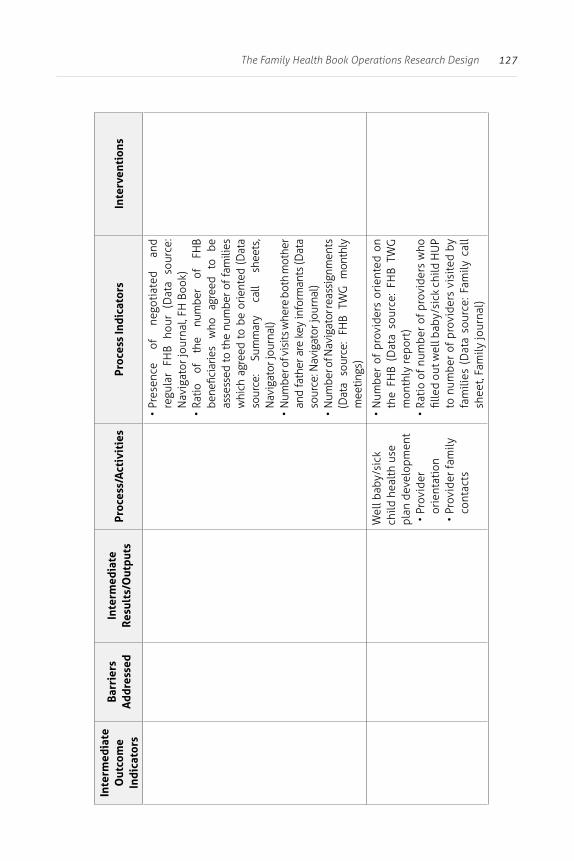
127The Family Health Book Operations Research Design
Inte
rmed
iate
Out
com
e In
dica
tors
Barr
iers
A
ddre
ssed
Inte
rmed
iate
Resu
lts/
Out
puts
Proc
ess/
Act
ivit
ies
Proc
ess
Indi
cato
rsIn
terv
enti
ons
• Pr
esen
ce
of
nego
tiat
ed
and
regu
lar
FHB
hour
(D
ata
sour
ce:
Nav
igat
or jo
urna
l, FH
Boo
k)•
Ratio
of
th
e nu
mbe
r of
FH
B be
nefic
iarie
s w
ho
agre
ed
to
be
asse
ssed
to th
e nu
mbe
r of f
amili
es
whi
ch a
gree
d to
be
orie
nted
(Dat
a so
urce
: Su
mm
ary
call
shee
ts,
Nav
igat
or jo
urna
l)•
Num
ber o
f vis
its w
here
bot
h m
othe
r an
d fa
ther
are
key
info
rman
ts (D
ata
sour
ce: N
avig
ator
jour
nal)
• N
umbe
r of N
avig
ator
reas
sign
men
ts
(Dat
a so
urce
: FH
B TW
G m
onth
ly
mee
tings
)
Wel
l bab
y/si
ck
child
hea
lth
use
plan
dev
elop
men
t•
Prov
ider
or
ient
atio
n•
Prov
ider
fam
ily
cont
acts
• N
umbe
r of
pro
vide
rs o
rien
ted
on
the
FHB
(Dat
a so
urce
: FH
B TW
G
mon
thly
repo
rt)
• Ra
tio
of n
umbe
r of
pro
vide
rs w
ho
fille
d ou
t wel
l bab
y/si
ck c
hild
HU
P to
num
ber
of p
rovi
ders
vis
ited
by
fam
ilies
(D
ata
sour
ce: F
amily
cal
l sh
eet,
Fam
ily jo
urna
l)
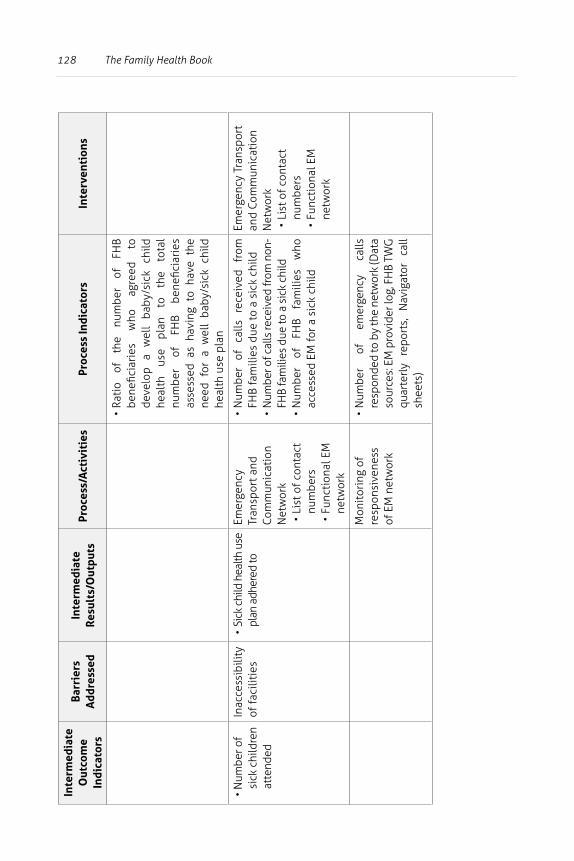
128 The Family Health BookIn
term
edia
teO
utco
me
Indi
cato
rs
Barr
iers
A
ddre
ssed
Inte
rmed
iate
Resu
lts/
Out
puts
Proc
ess/
Act
ivit
ies
Proc
ess
Indi
cato
rsIn
terv
enti
ons
• Ra
tio
of
the
num
ber
of
FHB
bene
ficia
ries
w
ho
agre
ed
to
deve
lop
a w
ell
baby
/sic
k ch
ild
heal
th
use
plan
to
th
e to
tal
num
ber
of
FHB
bene
ficia
ries
as
sess
ed a
s ha
ving
to
have
the
ne
ed f
or a
wel
l ba
by/s
ick
child
he
alth
use
pla
n
• N
umbe
r of
sick
chi
ldre
n at
tend
ed
Inac
cess
ibili
ty
of fa
cilit
ies
• Si
ck c
hild
hea
lth u
se
plan
adh
ered
toEm
erge
ncy
Tran
spor
t and
Co
mm
unic
atio
n N
etw
ork
• Li
st o
f con
tact
nu
mbe
rs•
Func
tion
al E
M
netw
ork
• N
umbe
r of
ca
lls
rece
ived
fr
om
FHB
fam
ilies
due
to a
sic
k ch
ild•
Num
ber o
f cal
ls re
ceiv
ed fr
om n
on-
FHB
fam
ilies
due
to a
sic
k ch
ild
• N
umbe
r of
FH
B fa
mili
es
who
ac
cess
ed E
M fo
r a s
ick
child
Emer
genc
y Tr
ansp
ort
and
Com
mun
icat
ion
Net
wor
k•
List
of c
onta
ct
num
bers
• Fu
ncti
onal
EM
ne
twor
k
Mon
itor
ing
of
resp
onsi
vene
ss
of E
M n
etw
ork
• N
umbe
r of
em
erge
ncy
calls
re
spon
ded
to b
y th
e ne
twor
k (D
ata
sour
ces:
EM
pro
vide
r log
, FH
B TW
G
quar
terl
y re
port
s,
Nav
igat
or
call
shee
ts)
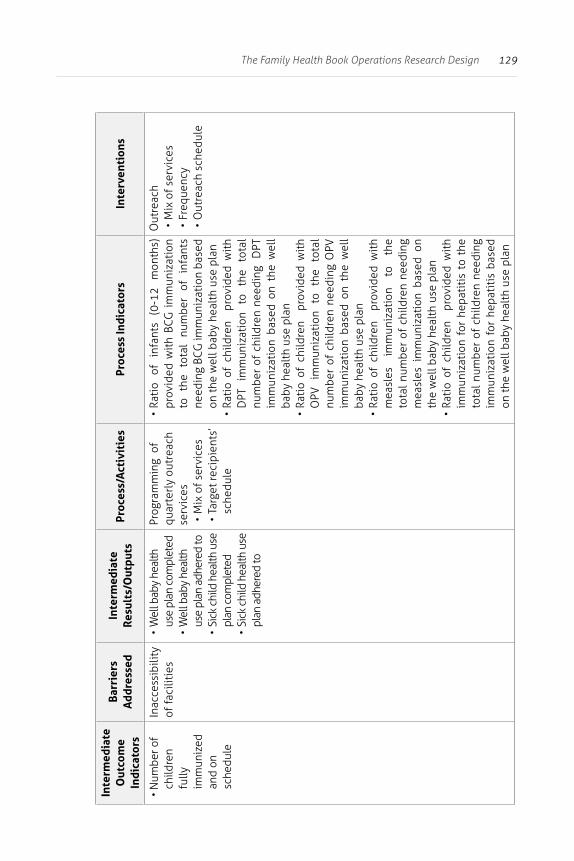
129The Family Health Book Operations Research Design
Inte
rmed
iate
Out
com
e In
dica
tors
Barr
iers
A
ddre
ssed
Inte
rmed
iate
Resu
lts/
Out
puts
Proc
ess/
Act
ivit
ies
Proc
ess
Indi
cato
rsIn
terv
enti
ons
• N
umbe
r of
child
ren
fully
im
mun
ized
an
d on
sc
hedu
le
Inac
cess
ibili
ty
of fa
cilit
ies
• W
ell b
aby
heal
th
use
plan
com
plet
ed•
Wel
l bab
y he
alth
us
e pl
an a
dher
ed to
• Si
ck c
hild
hea
lth u
se
plan
com
plet
ed•
Sick
chi
ld h
ealth
use
pl
an a
dher
ed to
Prog
ram
min
g o
f qu
arte
rly
outr
each
se
rvic
es•
Mix
of s
ervi
ces
• Ta
rget
reci
pien
ts’
sche
dule
• Ra
tio
of
infa
nts
(0-1
2 m
onth
s)
prov
ided
wit
h BC
G i
mm
uniz
atio
n to
th
e to
tal
num
ber
of
infa
nts
need
ing
BCG
imm
uniz
atio
n ba
sed
on th
e w
ell b
aby
heal
th u
se p
lan
• Ra
tio
of c
hild
ren
pro
vide
d w
ith
DPT
im
mun
izat
ion
to
the
tota
l nu
mbe
r of
chi
ldre
n ne
edin
g D
PT
imm
uniz
atio
n ba
sed
on t
he w
ell
baby
hea
lth
use
plan
• Ra
tio
of c
hild
ren
pro
vide
d w
ith
OPV
im
mun
izat
ion
to
the
tota
l nu
mbe
r of
chi
ldre
n ne
edin
g O
PV
imm
uniz
atio
n ba
sed
on t
he w
ell
baby
hea
lth
use
plan
• Ra
tio
of c
hild
ren
pro
vide
d w
ith
mea
sles
im
mun
izat
ion
to
the
tota
l num
ber
of c
hild
ren
need
ing
mea
sles
im
mun
izat
ion
base
d on
th
e w
ell b
aby
heal
th u
se p
lan
• Ra
tio
of c
hild
ren
pro
vide
d w
ith
imm
uniz
atio
n fo
r he
pati
tis
to t
he
tota
l num
ber
of c
hild
ren
need
ing
imm
uniz
atio
n fo
r he
pati
tis
base
d on
the
wel
l bab
y he
alth
use
pla
n
Out
reac
h•
Mix
of s
ervi
ces
• Fr
eque
ncy
• O
utre
ach
sche
dule
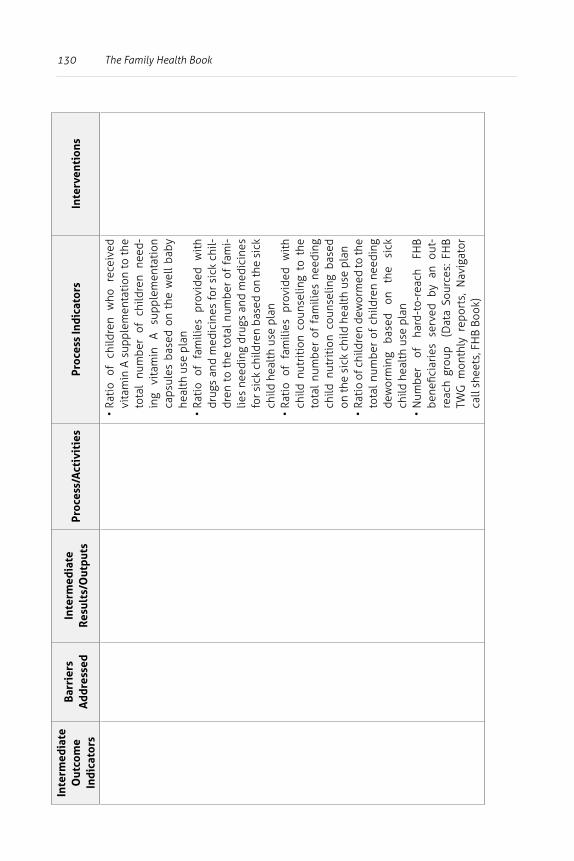
130 The Family Health BookIn
term
edia
teO
utco
me
Indi
cato
rs
Barr
iers
A
ddre
ssed
Inte
rmed
iate
Resu
lts/
Out
puts
Proc
ess/
Act
ivit
ies
Proc
ess
Indi
cato
rsIn
terv
enti
ons
• Ra
tio
of
child
ren
who
re
ceiv
ed
vita
min
A s
uppl
emen
tati
on t
o th
e to
tal
num
ber
of c
hild
ren
need
-in
g vi
tam
in
A su
pple
men
tati
on
caps
ules
bas
ed o
n th
e w
ell
baby
he
alth
use
pla
n•
Rati
o of
fam
ilies
pro
vide
d w
ith
drug
s an
d m
edic
ines
for
sick
chi
l-dr
en t
o th
e to
tal n
umbe
r of
fam
i-lie
s ne
edin
g dr
ugs
and
med
icin
es
for s
ick
child
ren
base
d on
the
sick
ch
ild h
ealt
h us
e pl
an•
Rati
o of
fam
ilies
pro
vide
d w
ith
child
nut
riti
on c
ouns
elin
g to
the
to
tal
num
ber
of f
amili
es n
eedi
ng
child
nut
riti
on c
ouns
elin
g ba
sed
on th
e si
ck c
hild
hea
lth
use
plan
• Ra
tio
of c
hild
ren
dew
orm
ed to
the
tota
l num
ber
of c
hild
ren
need
ing
dew
orm
ing
base
d on
th
e si
ck
child
hea
lth
use
plan
• N
umbe
r of
ha
rd-t
o-re
ach
FHB
bene
ficia
ries
ser
ved
by a
n ou
t-re
ach
grou
p (
Dat
a So
urce
s: F
HB
TWG
mon
thly
rep
orts
, N
avig
ator
ca
ll sh
eets
, FH
B Bo
ok)
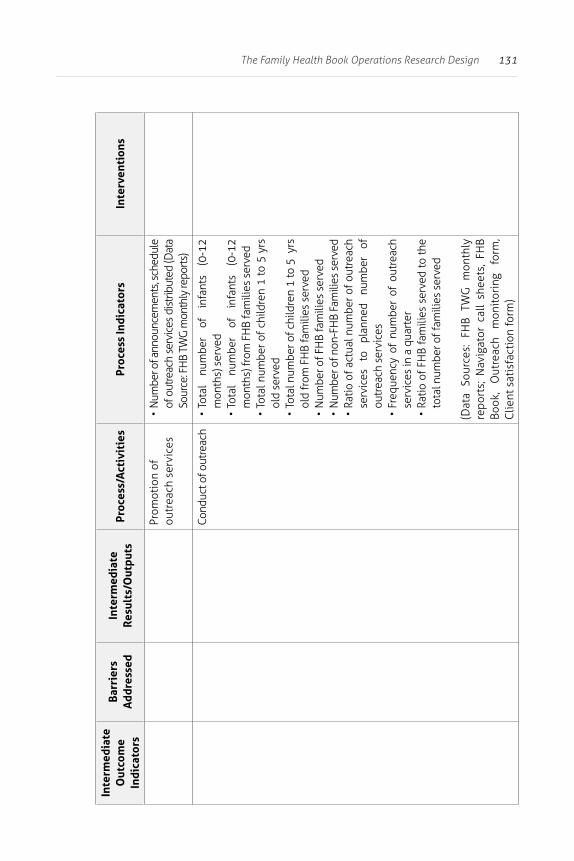
131The Family Health Book Operations Research Design
Inte
rmed
iate
Out
com
e In
dica
tors
Barr
iers
A
ddre
ssed
Inte
rmed
iate
Resu
lts/
Out
puts
Proc
ess/
Act
ivit
ies
Proc
ess
Indi
cato
rsIn
terv
enti
ons
Prom
otio
n of
ou
trea
ch s
ervi
ces
• N
umbe
r of a
nnou
ncem
ents
, sch
edul
e of
out
reac
h se
rvic
es d
istri
bute
d (D
ata
Sour
ce: F
HB
TWG
mon
thly
repo
rts)
Cond
uct o
f out
reac
h•
Tota
l nu
mbe
r of
in
fant
s (0
-12
mon
ths)
ser
ved
• To
tal
num
ber
of
infa
nts
(0-1
2 m
onth
s) fr
om F
HB
fam
ilies
ser
ved
• To
tal n
umbe
r of
chi
ldre
n 1
to 5
yrs
ol
d se
rved
• To
tal n
umbe
r of c
hild
ren
1 to
5 y
rs
old
from
FH
B fa
mili
es s
erve
d•
Num
ber o
f FH
B fa
mili
es s
erve
d•
Num
ber o
f non
-FH
B Fa
mili
es s
erve
d•
Ratio
of a
ctua
l num
ber o
f out
reac
h se
rvic
es
to
plan
ned
num
ber
of
outr
each
ser
vice
s•
Freq
uenc
y of
num
ber
of o
utre
ach
serv
ices
in a
qua
rter
• Ra
tio o
f FH
B fa
mili
es s
erve
d to
the
tota
l num
ber o
f fam
ilies
ser
ved
(Dat
a So
urce
s: F
HB
TWG
mon
thly
re
port
s; N
avig
ator
cal
l sh
eets
, FH
B Bo
ok,
Out
reac
h m
onit
orin
g fo
rm,
Clie
nt s
atis
fact
ion
form
)
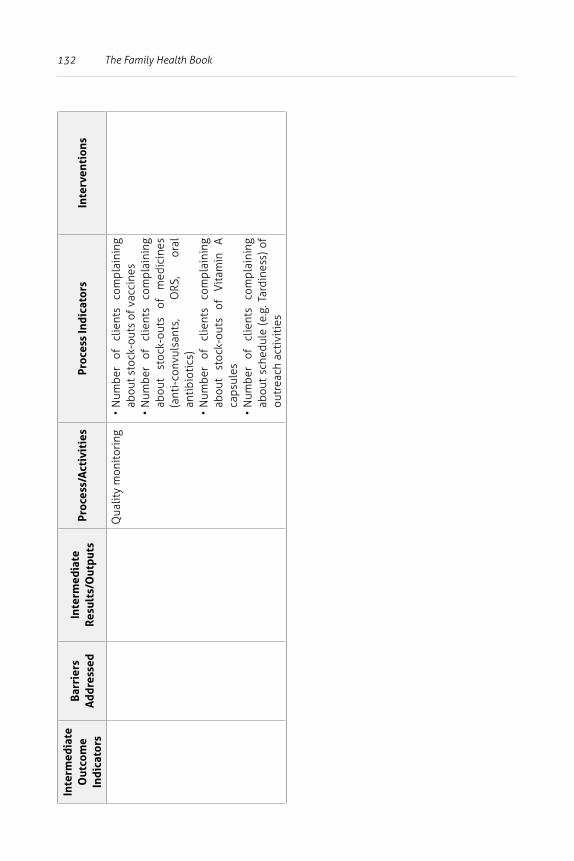
132 The Family Health BookIn
term
edia
teO
utco
me
Indi
cato
rs
Barr
iers
A
ddre
ssed
Inte
rmed
iate
Resu
lts/
Out
puts
Proc
ess/
Act
ivit
ies
Proc
ess
Indi
cato
rsIn
terv
enti
ons
Qua
lity
mon
itor
ing
• N
umbe
r of
cl
ient
s co
mpl
aini
ng
abou
t sto
ck-o
uts
of v
acci
nes
• N
umbe
r of
cl
ient
s co
mpl
aini
ng
abou
t st
ock-
outs
of
m
edic
ines
(a
nti-
conv
ulsa
nts,
O
RS,
oral
an
tibi
otic
s)•
Num
ber
of
clie
nts
com
plai
ning
ab
out
stoc
k-ou
ts
of
Vit
amin
A
caps
ules
• N
umbe
r of
cl
ient
s co
mpl
aini
ng
abou
t sc
hedu
le (
e.g.
Tar
dine
ss)
of
outr
each
act
ivit
ies
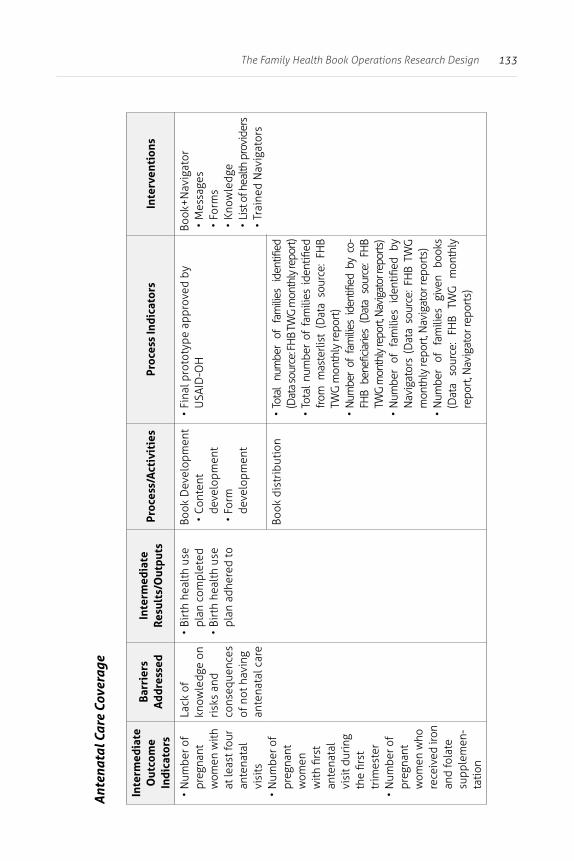
133The Family Health Book Operations Research Design
Ant
enat
al C
are
Cove
rage
Inte
rmed
iate
Out
com
e In
dica
tors
Barr
iers
A
ddre
ssed
Inte
rmed
iate
Resu
lts/
Out
puts
Proc
ess/
Act
ivit
ies
Proc
ess
Indi
cato
rsIn
terv
enti
ons
• N
umbe
r of
preg
nant
w
omen
with
at
leas
t fou
r an
tena
tal
visi
ts•
Num
ber o
f pr
egna
nt
wom
en
with
firs
t an
tena
tal
visi
t dur
ing
the
first
tr
imes
ter
• N
umbe
r of
preg
nant
w
omen
who
re
ceiv
ed ir
on
and
fola
te
supp
lem
en-
tatio
n
Lack
of
know
ledg
e on
ri
sks
and
cons
eque
nces
of
not
hav
ing
ante
nata
l car
e
• Bi
rth
heal
th u
se
plan
com
plet
ed•
Birt
h he
alth
use
pl
an a
dher
ed to
Book
Dev
elop
men
t•
Cont
ent
deve
lopm
ent
• Fo
rm
deve
lopm
ent
• Fi
nal p
roto
type
app
rove
d by
U
SAID
-OH
Book
+Nav
igat
or•
Mes
sage
s•
Form
s•
Know
ledg
e•
List
of h
ealth
pro
vide
rs•
Trai
ned
Nav
igat
ors
Book
dis
trib
utio
n•
Tota
l nu
mbe
r of
fam
ilies
ide
ntifi
ed
(Dat
a so
urce
: FH
B TW
G m
onth
ly re
port)
• To
tal
num
ber
of f
amili
es i
dent
ified
fr
om m
aste
rlist
(D
ata
sour
ce:
FHB
TWG
mon
thly
repo
rt)
• N
umbe
r of
fam
ilies
ide
ntifi
ed b
y co
-FH
B be
nefic
iarie
s (D
ata
sour
ce:
FHB
TWG
mon
thly
repo
rt, N
avig
ator
repo
rts)
• N
umbe
r of
fam
ilies
ide
ntifi
ed b
y N
avig
ator
s (D
ata
sour
ce: F
HB
TWG
m
onth
ly re
port
, Nav
igat
or re
port
s)•
Num
ber
of
fam
ilies
gi
ven
book
s (D
ata
sour
ce:
FHB
TWG
m
onth
ly
repo
rt, N
avig
ator
repo
rts)

134 The Family Health BookIn
term
edia
teO
utco
me
Indi
cato
rs
Barr
iers
A
ddre
ssed
Inte
rmed
iate
Resu
lts/
Out
puts
Proc
ess/
Act
ivit
ies
Proc
ess
Indi
cato
rsIn
terv
enti
ons
Recr
uitm
ent,
sele
ctio
n an
d tra
inin
g of
Nav
igat
ors
• Re
crui
tmen
t•
Dev
elop
men
t of
trai
ning
man
uals
• N
avig
ator
’s K
it
• N
umbe
r of N
avig
ator
s rec
ruite
d (D
ata
sour
ce: F
HB
TWG
mon
thly
repo
rts)
• N
umbe
r of
Nav
igat
ors
train
ed (
Dat
a so
urce
: FH
B TW
G m
onth
ly re
ports
)•
Num
ber
of N
avig
ator
s w
ho p
asse
d po
st-tr
aini
ng e
valu
atio
n (D
ata
sour
ce:
FHB
TWG
mon
thly
repo
rts)
• N
umbe
r of N
avig
ator
s w
ho q
uit (
Dat
a so
urce
: FH
B TW
G m
onth
ly re
ports
)
Fam
ily-N
avig
ator
m
atch
ing
• N
umbe
r of f
amili
es w
ith
assi
gned
N
avig
ator
s (D
ata
sour
ce: F
HB
TWG
m
onth
ly re
port
)•
Dis
trib
utio
n of
Nav
igat
ors
by ra
tio
of
Nav
igat
ors
to
fam
ilies
(D
ata
sour
ce: F
HB
TWG
mon
thly
repo
rt)
Fam
ily-N
avig
ator
Co
ntac
ts•
Vis
its
• FH
B ho
ur•
Ori
enta
tion
• In
tera
ctio
n w
ith
othe
r key
fam
ily
mem
bers
• Ra
tio
of
the
num
ber
of
FHB
bene
ficia
ries
w
ho
agre
ed
to
orie
ntat
ion
to
the
num
ber
of
FHB
bene
ficia
ries
(D
ata
sour
ce:
Fam
ily c
all s
heet
s)•
Num
ber o
f Nav
igat
ors
who
vis
ited
al
l ass
igne
d fa
mili
es a
t le
ast
once
a
mon
th (
Dat
a so
urce
: Su
mm
ary
call
shee
ts, N
avig
ator
jour
nal)
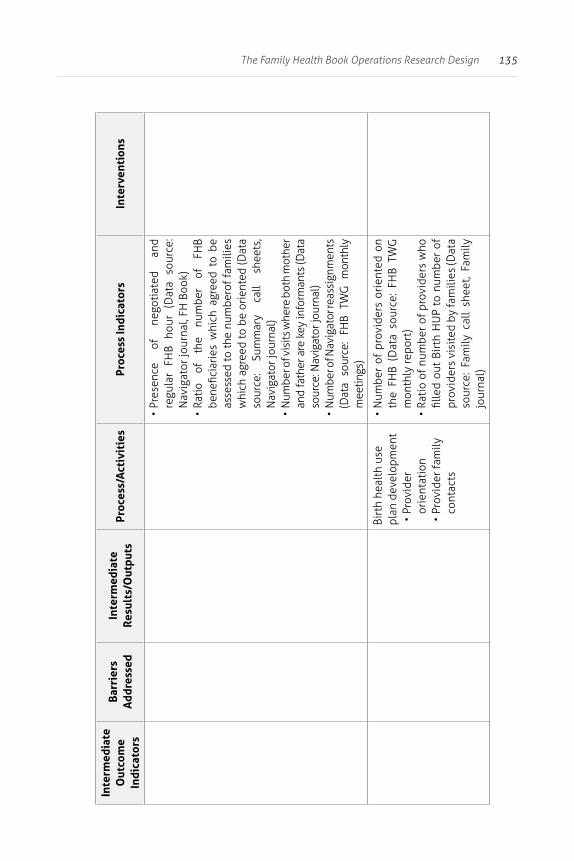
135The Family Health Book Operations Research Design
Inte
rmed
iate
Out
com
e In
dica
tors
Barr
iers
A
ddre
ssed
Inte
rmed
iate
Resu
lts/
Out
puts
Proc
ess/
Act
ivit
ies
Proc
ess
Indi
cato
rsIn
terv
enti
ons
• Pr
esen
ce
of
nego
tiat
ed
and
regu
lar
FHB
hour
(D
ata
sour
ce:
Nav
igat
or jo
urna
l, FH
Boo
k)•
Ratio
of
th
e nu
mbe
r of
FH
B be
nefic
iari
es w
hich
agr
eed
to b
e as
sess
ed to
the
num
bero
f fa
mili
es
whi
ch a
gree
d to
be
orie
nted
(Dat
a so
urce
: Su
mm
ary
call
shee
ts,
Nav
igat
or jo
urna
l)•
Num
ber o
f vis
its w
here
bot
h m
othe
r an
d fa
ther
are
key
info
rman
ts (D
ata
sour
ce: N
avig
ator
jour
nal)
• N
umbe
r of N
avig
ator
reas
sign
men
ts
(Dat
a so
urce
: FH
B TW
G m
onth
ly
mee
tings
)
Birt
h he
alth
use
pl
an d
evel
opm
ent
• Pr
ovid
er
orie
ntat
ion
• Pr
ovid
er fa
mily
co
ntac
ts
• N
umbe
r of
pro
vide
rs o
rien
ted
on
the
FHB
(Dat
a so
urce
: FH
B TW
G
mon
thly
repo
rt)
• Ra
tio
of n
umbe
r of
pro
vide
rs w
ho
fille
d ou
t Bi
rth
HU
P to
num
ber
of
prov
ider
s vi
site
d by
fam
ilies
(Dat
a so
urce
: Fa
mily
cal
l sh
eet,
Fam
ily
jour
nal)
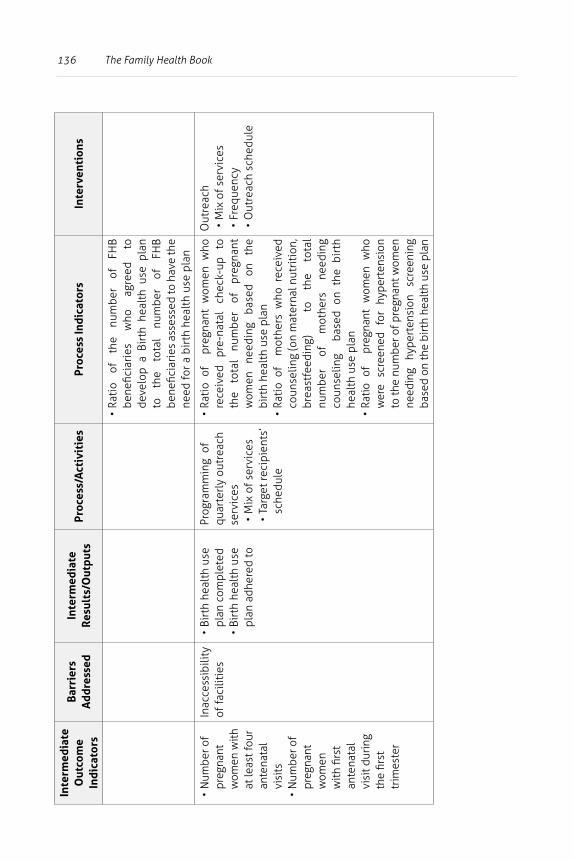
136 The Family Health BookIn
term
edia
teO
utco
me
Indi
cato
rs
Barr
iers
A
ddre
ssed
Inte
rmed
iate
Resu
lts/
Out
puts
Proc
ess/
Act
ivit
ies
Proc
ess
Indi
cato
rsIn
terv
enti
ons
• Ra
tio
of
the
num
ber
of
FHB
bene
ficia
ries
w
ho
agre
ed
to
deve
lop
a Bi
rth
heal
th u
se p
lan
to
the
tota
l nu
mbe
r of
FH
B be
nefic
iari
es a
sses
sed
to h
ave
the
need
for a
bir
th h
ealt
h us
e pl
an
• N
umbe
r of
preg
nant
w
omen
with
at
leas
t fou
r an
tena
tal
visi
ts•
Num
ber o
f pr
egna
nt
wom
en
with
firs
t an
tena
tal
visi
t dur
ing
the
first
tr
imes
ter
Inac
cess
ibili
ty
of fa
cilit
ies
• Bi
rth
heal
th u
se
plan
com
plet
ed•
Birt
h he
alth
use
pl
an a
dher
ed to
Prog
ram
min
g o
f qu
arte
rly
outr
each
se
rvic
es•
Mix
of s
ervi
ces
• Ta
rget
reci
pien
ts’
sche
dule
• Ra
tio
of
preg
nant
wom
en w
ho
rece
ived
pr
e-na
tal
chec
k-up
to
th
e to
tal
num
ber
of
preg
nant
w
omen
ne
edin
g ba
sed
on
the
birt
h he
alth
use
pla
n•
Rati
o of
m
othe
rs w
ho r
ecei
ved
coun
selin
g (o
n m
ater
nal n
utri
tion
, br
east
feed
ing)
to
the
tota
l nu
mbe
r of
m
othe
rs
need
ing
coun
selin
g b
ased
on
the
birt
h he
alth
use
pla
n•
Ratio
of
pre
gnan
t w
omen
who
w
ere
scre
ened
fo
r hy
pert
ensi
on
to th
e nu
mbe
r of p
regn
ant w
omen
ne
edin
g hy
pert
ensi
on
scre
enin
g ba
sed
on th
e bi
rth
heal
th u
se p
lan
Out
reac
h•
Mix
of s
ervi
ces
• Fr
eque
ncy
• O
utre
ach
sche
dule
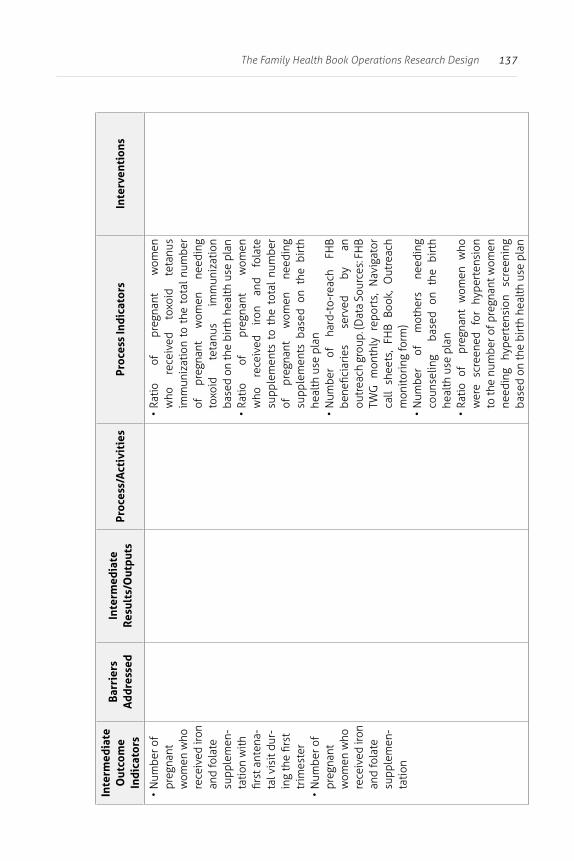
137The Family Health Book Operations Research Design
Inte
rmed
iate
Out
com
e In
dica
tors
Barr
iers
A
ddre
ssed
Inte
rmed
iate
Resu
lts/
Out
puts
Proc
ess/
Act
ivit
ies
Proc
ess
Indi
cato
rsIn
terv
enti
ons
• N
umbe
r of
preg
nant
w
omen
who
re
ceiv
ed ir
on
and
fola
te
supp
lem
en-
tatio
n w
ith
first
ant
ena-
tal v
isit
dur-
ing
the
first
tr
imes
ter
• N
umbe
r of
preg
nant
w
omen
who
re
ceiv
ed ir
on
and
fola
te
supp
lem
en-
tatio
n
• Ra
tio
of
preg
nant
w
omen
w
ho
rece
ived
to
xoid
te
tanu
s im
mun
izat
ion
to t
he t
otal
num
ber
of
preg
nant
w
omen
ne
edin
g to
xoid
te
tanu
s im
mun
izat
ion
base
d on
the
birt
h he
alth
use
pla
n•
Ratio
of
pr
egna
nt
wom
en
who
re
ceiv
ed
iron
and
fola
te
supp
lem
ents
to
the
tota
l nu
mbe
r of
pr
egna
nt
wom
en
need
ing
supp
lem
ents
bas
ed o
n th
e bi
rth
heal
th u
se p
lan
• N
umbe
r of
ha
rd-t
o-re
ach
FHB
bene
ficia
ries
se
rved
by
an
ou
trea
ch g
roup
. (D
ata
Sour
ces:
FH
B TW
G m
onth
ly r
epor
ts,
Nav
igat
or
call
shee
ts,
FHB
Book
, O
utre
ach
mon
itori
ng fo
rm)
• N
umbe
r of
m
othe
rs
need
ing
coun
selin
g b
ased
on
the
birt
h he
alth
use
pla
n•
Ratio
of
pre
gnan
t w
omen
who
w
ere
scre
ened
fo
r hy
pert
ensi
on
to th
e nu
mbe
r of p
regn
ant w
omen
ne
edin
g hy
pert
ensi
on
scre
enin
g ba
sed
on th
e bi
rth
heal
th u
se p
lan
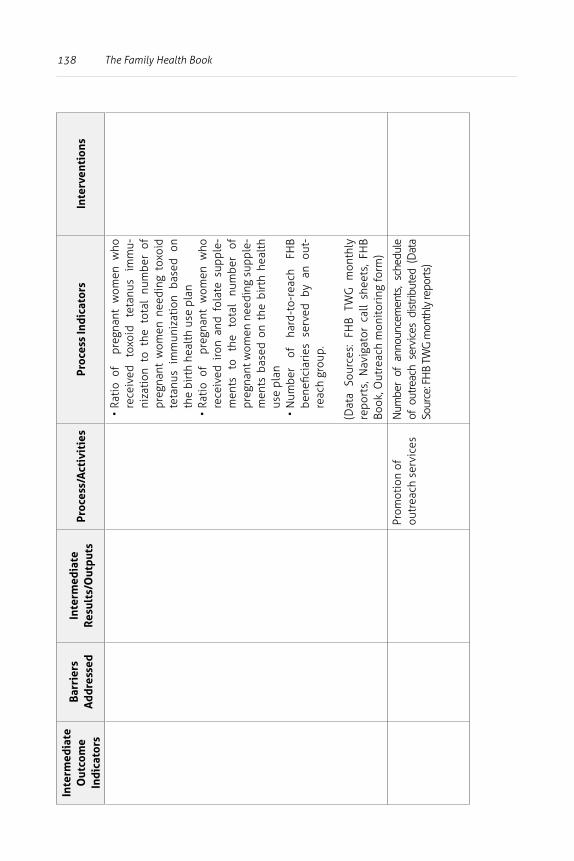
138 The Family Health BookIn
term
edia
teO
utco
me
Indi
cato
rs
Barr
iers
A
ddre
ssed
Inte
rmed
iate
Resu
lts/
Out
puts
Proc
ess/
Act
ivit
ies
Proc
ess
Indi
cato
rsIn
terv
enti
ons
• Ra
tio
of
preg
nant
wom
en w
ho
rece
ived
to
xoid
te
tanu
s im
mu-
niza
tion
to
the
tota
l nu
mbe
r of
pr
egna
nt w
omen
nee
ding
tox
oid
teta
nus
imm
uniz
atio
n ba
sed
on
the
birt
h he
alth
use
pla
n•
Rati
o of
pr
egna
nt w
omen
who
re
ceiv
ed i
ron
and
fola
te s
uppl
e-m
ents
to
th
e to
tal
num
ber
of
preg
nant
wom
en n
eedi
ng s
uppl
e-m
ents
bas
ed o
n th
e bi
rth
heal
th
use
plan
• N
umbe
r of
ha
rd-t
o-re
ach
FHB
bene
ficia
ries
ser
ved
by a
n ou
t-re
ach
grou
p.
(Dat
a So
urce
s: F
HB
TWG
mon
thly
re
port
s, N
avig
ator
cal
l sh
eets
, FH
B Bo
ok, O
utre
ach
mon
itor
ing
form
)
Prom
otio
n of
ou
trea
ch s
ervi
ces
Num
ber
of a
nnou
ncem
ents
, sc
hedu
le
of o
utre
ach
serv
ices
dis
tribu
ted
(Dat
a So
urce
: FH
B TW
G m
onth
ly re
ports
)
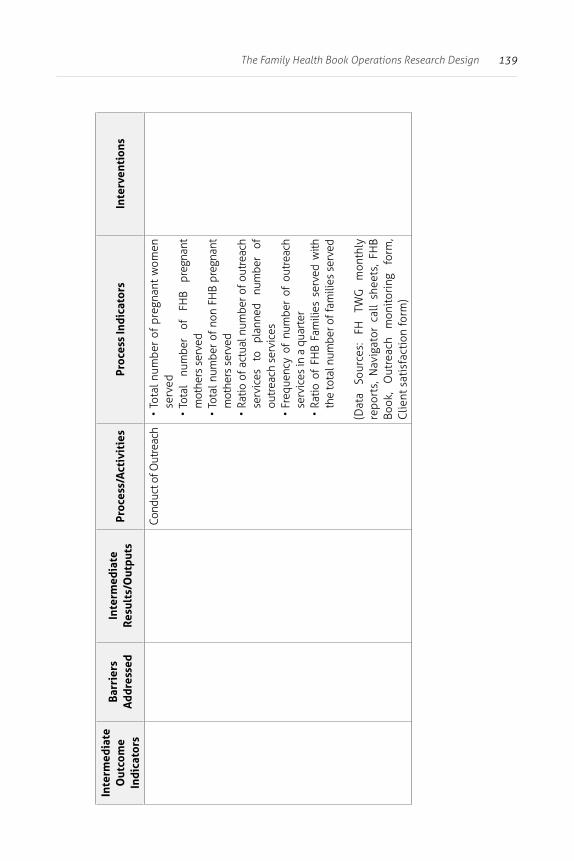
139The Family Health Book Operations Research Design
Inte
rmed
iate
Out
com
e In
dica
tors
Barr
iers
A
ddre
ssed
Inte
rmed
iate
Resu
lts/
Out
puts
Proc
ess/
Act
ivit
ies
Proc
ess
Indi
cato
rsIn
terv
enti
ons
Cond
uct o
f Out
reac
h•
Tota
l num
ber
of p
regn
ant
wom
en
serv
ed•
Tota
l nu
mbe
r of
FH
B pr
egna
nt
mot
hers
ser
ved
• To
tal n
umbe
r of
non
FH
B pr
egna
nt
mot
hers
ser
ved
• Ra
tio o
f act
ual n
umbe
r of o
utre
ach
serv
ices
to
pl
anne
d nu
mbe
r of
ou
trea
ch s
ervi
ces
• Fr
eque
ncy
of n
umbe
r of
out
reac
h se
rvic
es in
a q
uart
er•
Ratio
of
FHB
Fam
ilies
ser
ved
with
th
e to
tal n
umbe
r of f
amili
es s
erve
d
(Dat
a So
urce
s:
FH
TWG
m
onth
ly
repo
rts,
Nav
igat
or c
all
shee
ts,
FHB
Book
, O
utre
ach
mon
itor
ing
form
, C
lient
sat
isfa
ctio
n fo
rm)
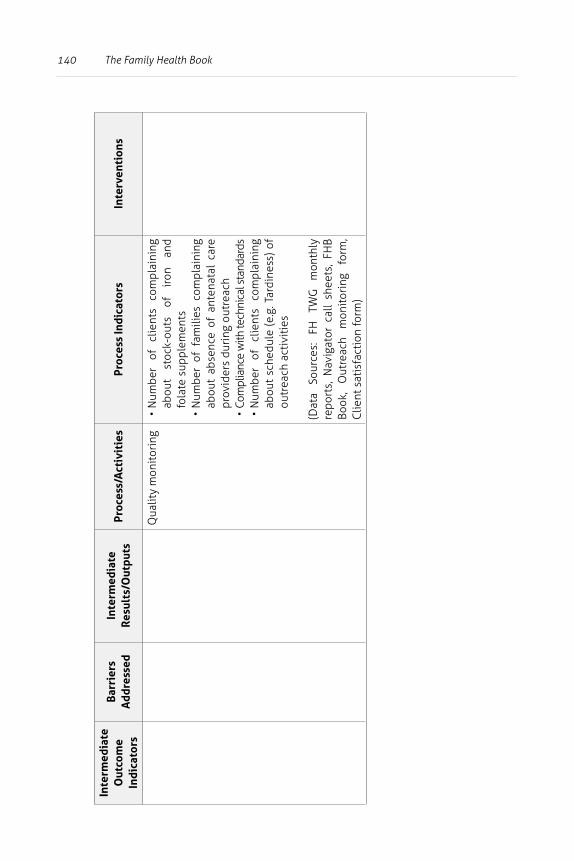
140 The Family Health Book
Inte
rmed
iate
Out
com
e In
dica
tors
Barr
iers
A
ddre
ssed
Inte
rmed
iate
Resu
lts/
Out
puts
Proc
ess/
Act
ivit
ies
Proc
ess
Indi
cato
rsIn
terv
enti
ons
Qua
lity
mon
itor
ing
• N
umbe
r of
cl
ient
s co
mpl
aini
ng
abou
t st
ock-
outs
of
ir
on
and
fola
te s
uppl
emen
ts•
Num
ber
of f
amili
es c
ompl
aini
ng
abou
t ab
senc
e of
ant
enat
al c
are
prov
ider
s du
ring
out
reac
h•
Com
plia
nce
with
tech
nica
l sta
ndar
ds•
Num
ber
of
clie
nts
com
plai
ning
ab
out
sche
dule
(e.
g. T
ardi
ness
) of
ou
trea
ch a
ctiv
itie
s
(Dat
a So
urce
s:
FH
TWG
m
onth
ly
repo
rts,
Nav
igat
or c
all
shee
ts,
FHB
Book
, O
utre
ach
mon
itor
ing
form
, C
lient
sat
isfa
ctio
n fo
rm)
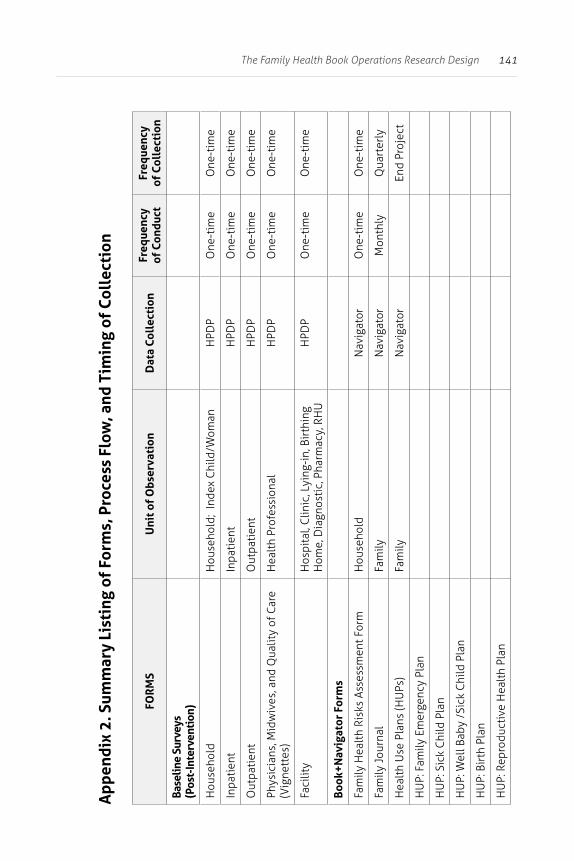
141The Family Health Book Operations Research Design
App
endi
x 2.
Sum
mar
y Li
stin
g of
For
ms,
Pro
cess
Flo
w, a
nd T
imin
g of
Col
lect
ion
FOR
MS
Uni
t of
Obs
erva
tion
Dat
a Co
llec
tion
Freq
uenc
y of
Con
duct
Freq
uenc
y of
Col
lect
ion
Base
line
Surv
eys
(Pos
t-In
terv
enti
on)
Hou
seho
ldH
ouse
hold
; In
dex
Chi
ld/W
oman
HPD
PO
ne-t
ime
One
-tim
e
Inpa
tien
tIn
pati
ent
HPD
PO
ne-t
ime
One
-tim
e
Out
pati
ent
Out
pati
ent
HPD
PO
ne-t
ime
One
-tim
e
Phys
icia
ns, M
idw
ives
, and
Qua
lity
of C
are
(Vig
nett
es)
Hea
lth
Prof
essi
onal
HPD
PO
ne-t
ime
One
-tim
e
Faci
lity
Hos
pita
l, C
linic
, Lyi
ng-i
n, B
irth
ing
Hom
e, D
iagn
osti
c, P
harm
acy,
RH
UH
PDP
One
-tim
eO
ne-t
ime
Book
+Nav
igat
or F
orm
s
Fam
ily H
ealt
h Ri
sks
Asse
ssm
ent F
orm
Hou
seho
ldN
avig
ator
One
-tim
eO
ne-t
ime
Fam
ily J
ourn
alFa
mily
Nav
igat
orM
onth
lyQ
uart
erly
Hea
lth
Use
Pla
ns (H
UPs
)Fa
mily
Nav
igat
orEn
d Pr
ojec
t
HU
P: F
amily
Em
erge
ncy
Plan
HU
P: S
ick
Chi
ld P
lan
HU
P: W
ell B
aby
/Sic
k C
hild
Pla
n
HU
P: B
irth
Pla
n
HU
P: R
epro
duct
ive
Hea
lth
Plan
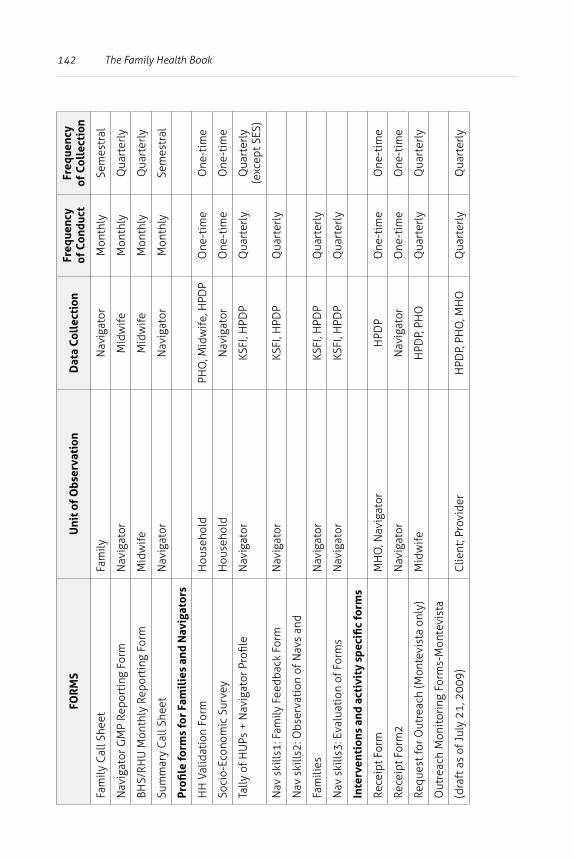
142 The Family Health BookFO
RM
SU
nit o
f O
bser
vati
onD
ata
Coll
ecti
onFr
eque
ncy
of C
ondu
ctFr
eque
ncy
of C
olle
ctio
n
Fam
ily C
all S
heet
Fam
ilyN
avig
ator
Mon
thly
Sem
estr
al
Nav
igat
or G
MP
Repo
rtin
g Fo
rmN
avig
ator
Mid
wife
Mon
thly
Qua
rter
ly
BHS/
RHU
Mon
thly
Rep
orti
ng F
orm
Mid
wife
Mid
wife
Mon
thly
Qua
rter
ly
Sum
mar
y C
all S
heet
Nav
igat
orN
avig
ator
Mon
thly
Sem
estr
al
Profi
le fo
rms
for
Fam
ilie
s an
d N
avig
ator
s
HH
Val
idat
ion
Form
Hou
seho
ldPH
O, M
idw
ife, H
PDP
One
-tim
eO
ne-t
ime
Soci
o-Ec
onom
ic S
urve
yH
ouse
hold
Nav
igat
orO
ne-t
ime
One
-tim
e
Tally
of H
UPs
+ N
avig
ator
Pro
file
Nav
igat
orKS
FI, H
PDP
Qua
rter
lyQ
uart
erly
(e
xcep
t SES
)
Nav
ski
lls1:
Fam
ily F
eedb
ack
Form
Nav
igat
orKS
FI, H
PDP
Qua
rter
ly
Nav
ski
lls2:
Obs
erva
tion
of N
avs
and
Fam
ilies
Nav
igat
orKS
FI, H
PDP
Qua
rter
ly
Nav
ski
lls3:
Eva
luat
ion
of F
orm
sN
avig
ator
KSFI
, HPD
PQ
uart
erly
Inte
rven
tion
s an
d ac
tivi
ty s
peci
fic
form
s
Rece
ipt F
orm
MH
O, N
avig
ator
HPD
PO
ne-t
ime
One
-tim
e
Rece
ipt F
orm
2N
avig
ator
Nav
igat
orO
ne-t
ime
One
-tim
e
Requ
est f
or O
utre
ach
(Mon
tevi
sta
only
)M
idw
ife
HPD
P, P
HO
Qua
rter
lyQ
uart
erly
Out
reac
h M
onit
orin
g Fo
rms-
Mon
tevi
sta
(dra
ft a
s of
Jul
y 21
, 200
9)C
lient
; Pro
vide
rH
PDP,
PH
O, M
HO
Qua
rter
lyQ
uart
erly
143The Family Health Book Operations Research Design
FOR
MS
Uni
t of
Obs
erva
tion
Dat
a Co
llec
tion
Freq
uenc
y of
Con
duct
Freq
uenc
y of
Col
lect
ion
Out
reac
h1_R
egis
trat
ion
Form
s
Out
reac
h2_S
urve
y of
Pro
vide
rs
Out
reac
h3_I
nven
tory
of S
uppl
ies
Out
reac
h4 F
eedb
ack
form
s
Out
reac
h5 R
epor
ting
For
m
Emer
genc
y fo
rms
144
2 “Giya sa Maayong Panglawas”:The Family Health Book Implementation in Compostela Valley
Rhodora A. Tiongson, Jhiedon Florentino, and Aleli D. Kraft
Abstract
The Family Health Book was implemented in Compostela Valley as Giya sa Maayong Panglawas (Guide to Good Health). Launched in September 3, 2008, implementation began with field testing of the Book prototypes and Navigator-family interactions.
The GMP carrier emerged as the preferred form for information documentation, and the Navigator’s Kit and training were revised based on feedback from the pilot implementation. Listing of GMP-eligible families was conducted. In areas where high mobility of families was noted, the lists were validated. Navigators were recruited and trained, and book distribution among the assigned families marked the start of full-scale implementation in May 2009.
Adjustments were made as field implementation proceeded, which included issuing advisories in handling mobile families as a response to family move-outs; partially substituting years of experience for educational requirements to come up with the required number of Navigators; and varying the number of assigned families per Navigator depending on the distance and density of families.
A demonstration training on the draft outreach protocol produced an outreach plan that included the selection of three target barangays with its GMP families for outreach services, outreach
145“Giya sa Maayong Panglawas”:
The Family Health Book Implementation in Compostela Valley
schedules, logistical arrangements, and resource-sharing among barangays, the municipality, and the province.
Assistance was provided in drafting the draft protocol for the health emergency transport and communication system in Compostela, and in advocating for the passage of barangay ordinances in support of the Compostela Network of Communications and Transport (CoNECT). Counterpart funds from the province were also released for operations. The total cost of FHB implementation was expected to amount to about PhP 53 million, which is the sum of developmental, pilot operations, and operations research costs. Of this amount, the pilot operations costs is the one relevant for the LGU roll-out of the initiative.
Implementation was monitored through data collection from family-Navigator interactions and qualitative mid-term assessments, and through random visits to families and outreach activities. These activities revealed that majority of target families had been profiled, their health risks assessed, and their health use plans developed. Outreach activities reached target recipients and enabled families to access services listed in their health use plans. Differences in utilization of GMP families with and without health use plans were also noted.
Introduction
Giya sa Maayong Panglawas (Guide to Good Health), the FHB, was launched in September 3, 2008 with the ceremonial gathering of selected family beneficiaries in the provincial capitol in Nabunturan. Full-scale implementation began in May 2009 with the distribution of books by the Navigators. This also signaled the start of family-Navigator interaction for health risk assessment, health use planning, and health care use.
Meanwhile, field testing was conducted to assess the Book prototypes, the contents and format of the Navigator training, and the process of family-Navigator engagement. Listing beneficiary families was done to determine their number and identify, recruit, and train the required number of Navigators to match the families.
146 The Family Health Book
Implementation of GMP was monitored through data collection on input and process indicators as well as through a qualitative mid-term assessment. Feedback from the families, Navigators, and local officials on difficulties encountered on the ground resulted in adjustments in the implementation of the operations research.
Section 2 of this report describes the conduct and results of the FHB field testing exercise, which determined the final form of the FHB and led to revisions of the training modules for Navigators and midwives.
Section 3 describes the steps undertaken in listing the families and the difficulties accompanying their high mobility. Section 4 describes the process of Navigator recruitment and training.
Section 5 reports on the process and results of family-Navigator interaction as implemented in Compostela Valley.
Sections 6 and 7 describe the actual implementation of the emergency and outreach interventions.
Section 8 describes complementary and supporting activities.
Section 9 reports on observations from the mid-project assessment and random visits.
Section 10 concludes with a report on the costs of the operations research and an illustration of the possible costs of rolling out the initiative in other areas.
FHB Field Testing
Prior to the FHB OR’s full-scale implementation in Compostela Valley, field testing of the FHB prototypes, the Navigator’s training course and kit, and the family-Navigator interaction was conducted for two weeks in November 2008. Six families were selected from each of the municipalities of Compostela, Mabini, Maco, and Montevista to assess the usefulness of the Book’s contents and to determine which format was more useful and
147“Giya sa Maayong Panglawas”:
The Family Health Book Implementation in Compostela Valley
acceptable to the families and Navigators. The families used the book format for a week and then switched to the carrier2 format for another week.
Three field testing Navigators were also selected from each of the four municipalities to assess the usefulness of the training process, the Navigator’s Kit, and the ease of use of the various health forms. The Navigators were trained using the developed materials. They also interacted with the families chosen for the field testing (HPDP, 2008a).
The field testing also determined the possible role of midwives in the FHB initiative. FGDs were conducted at the midpoint and end of the field testing period to get feedback from families, Navigators, midwives, and MHOs. The highlights of the field testing are presented below, drawing heavily from a 2008 HPDP report (Acuin, 2008).
2 The carrier is a foldable bag which can be hung on the door or wall. It contains materials similar to those found in the book: family picture, letter to the family, health emergency contacts, key health messages, health use plans, health provider information and useful references such as the Mother and Child Book and Family Guide on PhilHealth Benefits.
148 The Family Health Book
Book At the end of field testing, most families favored the carrier over the book format. Families opting for the carrier format said the carrier could be easily seen and checked. Moreover, as the carrier with the family picture could be hung on a wall, it attracts visitors’ attention and at the same time is kept out of children’s reach.
Families felt that they could easily choose things they wanted to read in the carrier format, unlike in the book version. However, compared with the book format, the families said the carrier was bulky and not portable. Its pages could get disorganized, and some sections could be lost (see Table 2.1).
Overall, the pilot families found the FHB materials attractive, useful, and very helpful. The families suggested that the carrier be of a darker color and that the pages of the materials should be bound in order to keep them intact. They also suggested the use of tabs to separate and identify topics.
Pilot families and Navigators appreciated the use of the Visayan language in the writing of the Books. They also found the language easy to understand, clear, and inoffensive. Interestingly, families generally felt that the FHB contained new and more comprehensive information compared with the Mother and Child Book of UNICEF and WHO. Specifically, the families cited the following topics as memorable and interesting:
1) birth spacing, 2) child feeding, 3) delivery in a facility, and 4) immunization.
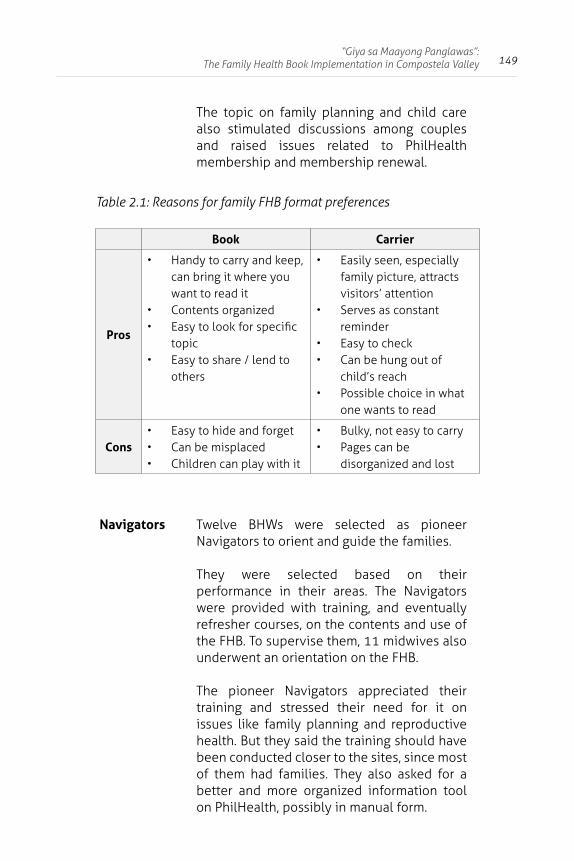
149“Giya sa Maayong Panglawas”:
The Family Health Book Implementation in Compostela Valley
The topic on family planning and child care also stimulated discussions among couples and raised issues related to PhilHealth membership and membership renewal.
Table 2.1: Reasons for family FHB format preferences
Book Carrier
Pros
• Handy to carry and keep, can bring it where you want to read it
• Contents organized• Easy to look for specific
topic• Easy to share / lend to
others
• Easily seen, especially family picture, attracts visitors’ attention
• Serves as constant reminder
• Easy to check• Can be hung out of
child’s reach• Possible choice in what
one wants to read
Cons• Easy to hide and forget• Can be misplaced• Children can play with it
• Bulky, not easy to carry• Pages can be
disorganized and lost
Navigators Twelve BHWs were selected as pioneer Navigators to orient and guide the families.
They were selected based on their performance in their areas. The Navigators were provided with training, and eventually refresher courses, on the contents and use of the FHB. To supervise them, 11 midwives also underwent an orientation on the FHB.
The pioneer Navigators appreciated their training and stressed their need for it on issues like family planning and reproductive health. But they said the training should have been conducted closer to the sites, since most of them had families. They also asked for a better and more organized information tool on PhilHealth, possibly in manual form.
150 The Family Health Book
Selection of Navigators and their training
Midwives said the FHB initiative would give more responsibilities to BHWs as Navigators and this would pose a difficulty in recruiting Navigators.
During the field testing, midwives said only 25-30% of BHWs would be able to do FHB work well enough. They suggested that Navigators should at least be high school graduates.
Neither were they keen on hiring new staff to serve as Navigators since this would involve barangay captains, a process perceived as a political matter. The midwives also suggested that the training of Navigators include the development of interpersonal skills, especially for the younger and newer BHWs.
Family-Navigator contact
Couples felt that ideally, both husband and wife should be present during Navigator visits. But the husbands’ irregular work schedules made it difficult for couples to find a common time for the FHB intiative’s activities. To ensure the husbands’ availability, at least during the orientation, group orientations should be conducted instead of individual family visits.
Many families said the Navigators helped them understand how to use the FHB. Though most families felt that the forms were relatively easy to fill out, those with members of limited education relied heavily on the Navigators in working with the forms.
The families also said the Navigators were most helpful during follow-up activities and in giving referrals to health centers and facilities (the Navigators accompanied the families to these places). Most families said they strongly preferred Navigators they already knew and who lived nearby.
151“Giya sa Maayong Panglawas”:
The Family Health Book Implementation in Compostela Valley
Management of Navigators
During the field testing, while a number of midwives accompanied Navigators during family orientations on the FHB, participating families said Navigators could conduct the orientation even without the midwives.
The Navigators also felt the same way. They were also concerned that the midwives would find it difficult to attend individual family orientations especially if the FHB initiative would be scaled up.
Outreach During field testing, the midwives felt that monthly outreach activities, like immunization, may be difficult to conduct, given the requirements needed.
Very frequent outreach activities may be taxing for midwives, who have other functions and duties. The midwives said the holding of quarterly activities was more feasible, as LGUs do have far-flung areas.
Listing of families
Books
Analysis of FHB Baseline Survey data showed that families with mothers who did not finish high school and which satisfy the following criteria would benefit most from the information provided by the FHB:
1) pregnant; or
2) non-pregnant, below 25 years old and with at least one child below five years of age; or
3) non-pregnant, 25 years old and above, and with at least two children below five years of age.

152 The Family Health Book
These conditions ultimately became the FHB eligibility criteria. Thus, identification and listing of families that satisfied the FHB eligibility criteria was one of the important preliminary activities.
Prior to the actual listing of families, national census data were used to project the number of women of reproductive age who qualified under the FHB eligibility criteria in the barangays of the intervention municipalities. The projected number was used as a guide in the actual listing of eligible families. To ensure that all areas in the municipalities would be covered, a listing of puroks within the covered barangays was conducted.
The FHB initiative engaged a team to coordinate with the municipalities’ midwives and barangay health workers (BHWs) on the identification of families which met the eligibility criteria for FHB interventions. The listing of families was conducted from December 2008 to February 2009. Using the list of families provided by the BHWs as an initial guide, the team visited the covered barangays and gathered the following data:
1) list of families residing in the barangays; 2) ages and number of children in the families; 3) mothers’ current pregnancy status; 4) families’ PhilHealth status; and 5) educational attainment of the mother and the father.
The team used a snowball approach, where information on other potential beneficiaries was solicited from residents to ensure full listing of families meeting FHB eligibility criteria. To ensure that households that were difficult to reach or which lived some distance from barangay and municipality centers would be listed, the team had quotas of families to enlist at the purok level.
The original eligibility criteria specified that qualified families should have mothers with less than high school education. However, initial feedback indicated that this requirement severely limited the number of potential beneficiaries. There were also reports that special programs (i.e., Sunday school and special certification programs) allowed residents to obtain a high school diploma. The educational criteria were thus changed to include families with mothers who had at most a high school diploma.
153“Giya sa Maayong Panglawas”:
The Family Health Book Implementation in Compostela Valley
The initial listing of families resulted in a registry with 5,347 families (see Table 2.2). Field validation, at the BHW and midwife levels, was conducted and supervised by the FHB Coordinator based in Compostela Valley from February to March 2009. The midwives and BHWs validated information specific to the eligibility criteria (see Appendix 1).
The midwives and the BHWs also conducted minor corrections on the names and the purok addresses of the validated families. The barangay workers and the FHB Coordinator also did validation of households on randomly chosen puroks.
From the validation and visits on the randomly chosen puroks, the list of families satisfying the eligibility criteria was further trimmed down, due to the following reasons: 1) moving out of families or mothers; 2) double entry of families and mothers on the original list; 3) refusals; and 4) non-eligibility based on the criteria.
However, only 4,815 families of 5,347 target beneficiaries were actually given books, largely due to the high mobility of families in the municipalities. Between the listing of families to the validation of the list, new families migrated in and out of the FHB municipalities. Some families initially identified during the listing activities were found to have permanently migrated to other FHB sites or other areas.
Cases of double-listing of families or of a family member in two different barangays were also discovered. New families identified by the BHWs and midwives were added. The validated list of BHWs was used during the actual distribution of Books.
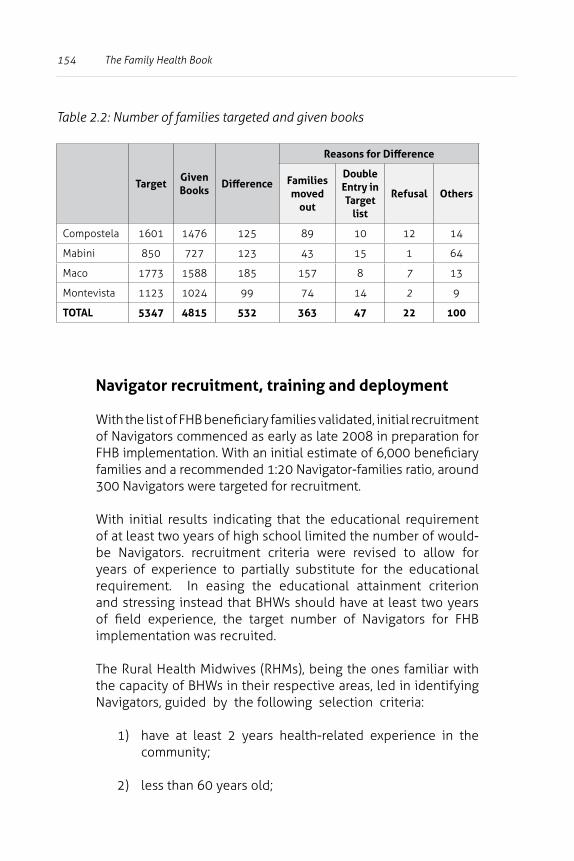
154 The Family Health Book
Table 2.2: Number of families targeted and given books
TargetGiven Books
Difference
Reasons for Difference
Families moved
out
Double Entry in Target
list
Refusal Others
Compostela 1601 1476 125 89 10 12 14
Mabini 850 727 123 43 15 1 64
Maco 1773 1588 185 157 8 7 13
Montevista 1123 1024 99 74 14 2 9
TOTAL 5347 4815 532 363 47 22 100
Navigator recruitment, training and deployment
With the list of FHB beneficiary families validated, initial recruitment of Navigators commenced as early as late 2008 in preparation for FHB implementation. With an initial estimate of 6,000 beneficiary families and a recommended 1:20 Navigator-families ratio, around 300 Navigators were targeted for recruitment.
With initial results indicating that the educational requirement of at least two years of high school limited the number of would-be Navigators. recruitment criteria were revised to allow for years of experience to partially substitute for the educational requirement. In easing the educational attainment criterion and stressing instead that BHWs should have at least two years of field experience, the target number of Navigators for FHB implementation was recruited.
The Rural Health Midwives (RHMs), being the ones familiar with the capacity of BHWs in their respective areas, led in identifying Navigators, guided by the following selection criteria:
1) have at least 2 years health-related experience in the community;
2) less than 60 years old;
155“Giya sa Maayong Panglawas”:
The Family Health Book Implementation in Compostela Valley
3) able and willing to regularly visit the households assigned to them; and
4) with good interpersonal communication skills and highly motivated and respected in the community.
The selection process included the listing of FHB beneficiaries, to ensure easy access and familiarity of Navigators and families with each other.
Together with CHD XI, HPDP assisted the Compostela Valley Provincial Health Office (PHO) in preparing midwives for their roles in the GMP. A Midwife’s Kit was drafted and pre-tested before it was used in the midwives’ training (HPDP, 2008b). On March 20-21 and 26-27, all 43 midwives in the four FHB pilot municipalities were oriented on how to supervise Navigators, plan and manage the needed MNCHN commodities/services, including those for FHB families, coordinate outreach services, and serve as primary service providers.
HPDP – in cooperation with CHD XI, Compostela Valley PHO, the PhilHealth Davao Region, and other partners – conducted a training for Navigator trainors on March 23-26, 2009 to help prepare around 400 Navigators in the four FHB pilot municipalities in orienting families on the use of the GMP and assist them in developing and accomplishing their health use plans.
The training design developed for Navigator trainors also included orientation on MNCHN standards, principles of informed choice and voluntarism, relational skills training for effectively engaging families, and preparations on conducting health risk assessment, developing health use plans and correctly filling out FHB monitoring forms.
The series of trainings for around 400 Navigators from the four pilot sites were completed by the end of April. However, a spot check conducted in the first week of June 2009, revealed that there were GMP beneficiaries in certain puroks who still had to be assigned Navigators, or whose assigned Navigators had failed to participate in the Navigators’ training.
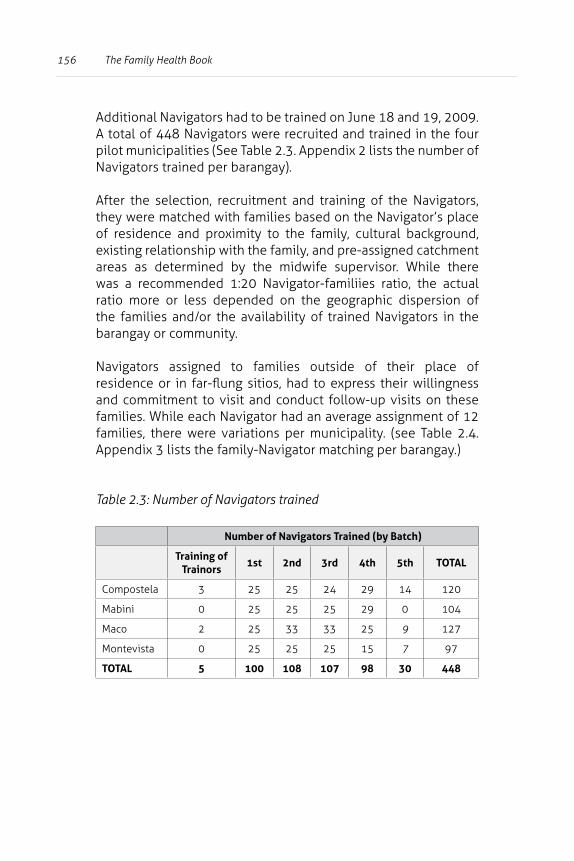
156 The Family Health Book
Additional Navigators had to be trained on June 18 and 19, 2009. A total of 448 Navigators were recruited and trained in the four pilot municipalities (See Table 2.3. Appendix 2 lists the number of Navigators trained per barangay).
After the selection, recruitment and training of the Navigators, they were matched with families based on the Navigator’s place of residence and proximity to the family, cultural background, existing relationship with the family, and pre-assigned catchment areas as determined by the midwife supervisor. While there was a recommended 1:20 Navigator-familiies ratio, the actual ratio more or less depended on the geographic dispersion of the families and/or the availability of trained Navigators in the barangay or community.
Navigators assigned to families outside of their place of residence or in far-flung sitios, had to express their willingness and commitment to visit and conduct follow-up visits on these families. While each Navigator had an average assignment of 12 families, there were variations per municipality. (see Table 2.4. Appendix 3 lists the family-Navigator matching per barangay.)
Table 2.3: Number of Navigators trained
Number of Navigators Trained (by Batch)
Training of Trainors
1st 2nd 3rd 4th 5th TOTAL
Compostela 3 25 25 24 29 14 120
Mabini 0 25 25 25 29 0 104
Maco 2 25 33 33 25 9 127
Montevista 0 25 25 25 15 7 97
TOTAL 5 100 108 107 98 30 448
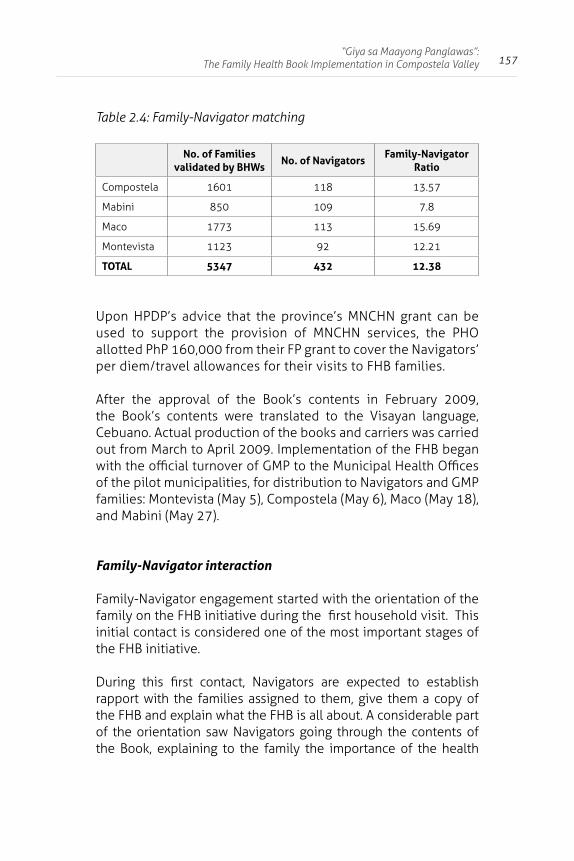
157“Giya sa Maayong Panglawas”:
The Family Health Book Implementation in Compostela Valley
Table 2.4: Family-Navigator matching
No. of Families validated by BHWs
No. of NavigatorsFamily-Navigator
Ratio
Compostela 1601 118 13.57
Mabini 850 109 7.8
Maco 1773 113 15.69
Montevista 1123 92 12.21
TOTAL 5347 432 12.38
Upon HPDP’s advice that the province’s MNCHN grant can be used to support the provision of MNCHN services, the PHO allotted PhP 160,000 from their FP grant to cover the Navigators’ per diem/travel allowances for their visits to FHB families.
After the approval of the Book’s contents in February 2009, the Book’s contents were translated to the Visayan language, Cebuano. Actual production of the books and carriers was carried out from March to April 2009. Implementation of the FHB began with the official turnover of GMP to the Municipal Health Offices of the pilot municipalities, for distribution to Navigators and GMP families: Montevista (May 5), Compostela (May 6), Maco (May 18), and Mabini (May 27).
Family-Navigator interaction
Family-Navigator engagement started with the orientation of the family on the FHB initiative during the first household visit. This initial contact is considered one of the most important stages of the FHB initiative.
During this first contact, Navigators are expected to establish rapport with the families assigned to them, give them a copy of the FHB and explain what the FHB is all about. A considerable part of the orientation saw Navigators going through the contents of the Book, explaining to the family the importance of the health
158 The Family Health Book
messages, what health use plans (HUPs) were, and how to use the list of providers as information on their options on which facility to go to for the appropriate health service indicated in the HUP. During this orientation, Navigators were expected to ask the families to fill in the family profile or socio-economic form (HPDP, 2008d).
After the first contact with the families, the Navigators’ next visit sought to identify health risks and needs. Using the health risks assessment (HRA) forms, Navigators were to elicit information which would eventually be used in the development of HUPs.
The HRA has three main parts, namely: Maternal and Newborn Health, Reproductive Health, and Child Health. Through the HRA, Navigators administer screening and follow-up questions, which gauge the families’ awareness of and their current health practices. The HRA also includes questions on immunization, current family planning methods, and utilization of ANC services.
After the health risks assessment, subsequent visits were made for the development of HUPs appropriate for the families. During this stage, the Navigator assisted the family in identifying services and commodities they need based on the risk assessment. Families are also assisted by Navigators in identifying health providers where they can avail of services for delivery, ANC, immunization, and FP counseling. All of these choices and information are reflected in the families’ HUPs, specifically the dates when the services and commodities should be accessed and the appropriate health provider.
Family-Navigator contacts: Results of monitoring activities
Most Navigators assigned to far-flung families administered the socio-economic status (SES) profile and health risks assessment (HRA) during the initial contact, the same time the Book was issued to the families. Some Navigators administered the SES and HRA during a different visit.
159“Giya sa Maayong Panglawas”:
The Family Health Book Implementation in Compostela Valley
Figure 2.1. Stages of interaction of families and navigators
SES and HRA administration lasted from late May to August 2009. Several families were reported to have changed residence by the end of this period, resulting in a decreased number of families with SES and HRA data (see Table 2.5).
In response, the Provincial Health Office advised midwives on what to do upon finding out about a family which changed residence or is about to do so. The FHB Coordinator listed the names of relocated families or those about to move out, including their destinations, and endorsed them to the receiving midwives within the FHB sites.
The mobility of some of the families was believed to be seasonal, due to the sources of livelihood in the province (e.g., some families would move out to mining sites during the rainy season, moving back to their farms during harvesting months). Given this temporary nature of movements, Navigators and midwives were advised not to permanently remove families from their assigned lists.
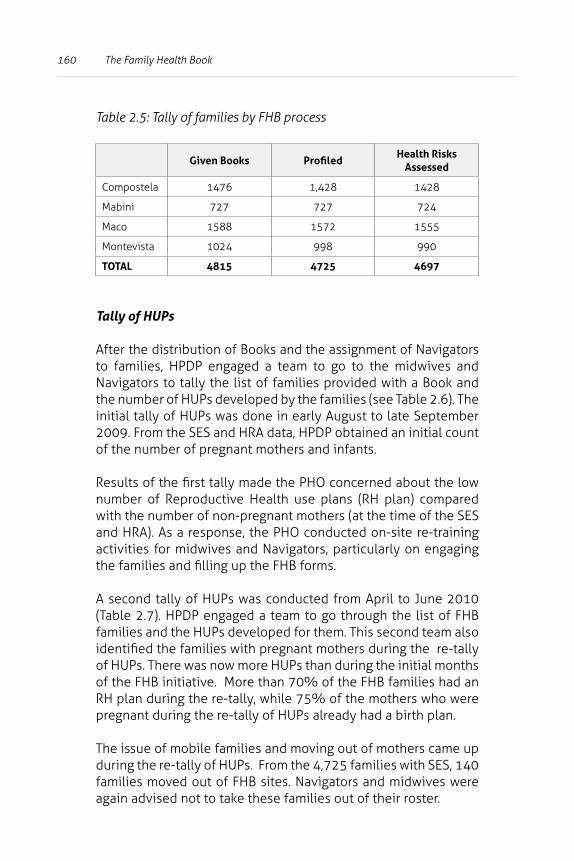
160 The Family Health Book
Table 2.5: Tally of families by FHB process
Given Books Profiled Health Risks
Assessed
Compostela 1476 1,428 1428
Mabini 727 727 724
Maco 1588 1572 1555
Montevista 1024 998 990
TOTAL 4815 4725 4697
Tally of HUPs
After the distribution of Books and the assignment of Navigators to families, HPDP engaged a team to go to the midwives and Navigators to tally the list of families provided with a Book and the number of HUPs developed by the families (see Table 2.6). The initial tally of HUPs was done in early August to late September 2009. From the SES and HRA data, HPDP obtained an initial count of the number of pregnant mothers and infants.
Results of the first tally made the PHO concerned about the low number of Reproductive Health use plans (RH plan) compared with the number of non-pregnant mothers (at the time of the SES and HRA). As a response, the PHO conducted on-site re-training activities for midwives and Navigators, particularly on engaging the families and filling up the FHB forms.
A second tally of HUPs was conducted from April to June 2010 (Table 2.7). HPDP engaged a team to go through the list of FHB families and the HUPs developed for them. This second team also identified the families with pregnant mothers during the re-tally of HUPs. There was now more HUPs than during the initial months of the FHB initiative. More than 70% of the FHB families had an RH plan during the re-tally, while 75% of the mothers who were pregnant during the re-tally of HUPs already had a birth plan.
The issue of mobile families and moving out of mothers came up during the re-tally of HUPs. From the 4,725 families with SES, 140 families moved out of FHB sites. Navigators and midwives were again advised not to take these families out of their roster.
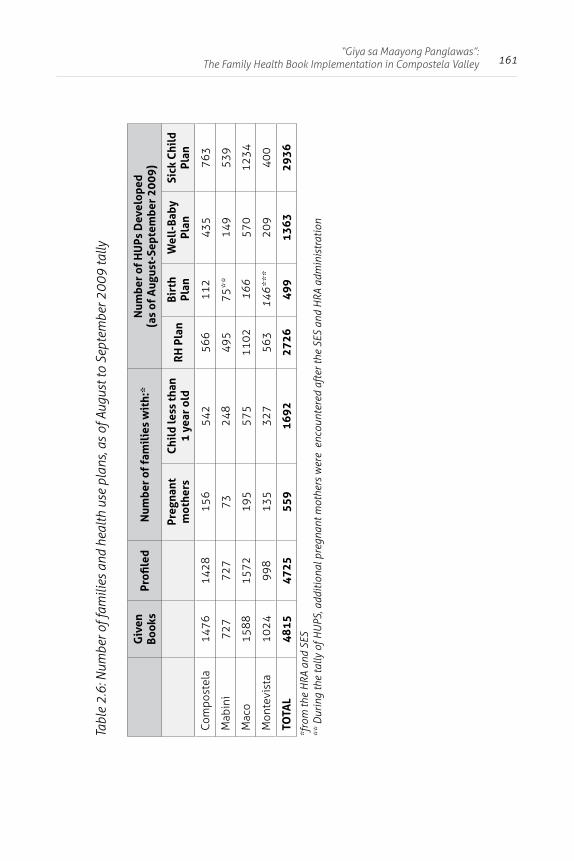
161“Giya sa Maayong Panglawas”:
The Family Health Book Implementation in Compostela Valley
Tabl
e 2.
6: N
umbe
r of f
amili
es a
nd h
ealth
use
pla
ns, a
s of
Aug
ust t
o Se
ptem
ber 2
009
tally
Giv
en
Book
sPr
ofile
d N
umbe
r of
fam
ilie
s w
ith:
*N
umbe
r of
HU
Ps D
evel
oped
(a
s of
Aug
ust-
Sept
embe
r 20
09)
Preg
nant
m
othe
rsC
hild
less
than
1
year
old
RH
Pla
nBi
rth
Plan
Wel
l-Ba
by
Plan
Sick
Chi
ld
Plan
Com
post
ela
1476
1428
156
542
566
112
435
763
Mab
ini
727
727
7324
849
575
**14
953
9
Mac
o15
8815
7219
557
511
0216
657
012
34
Mon
tevi
sta
1024
998
135
327
563
146*
**20
940
0
TOTA
L48
1547
2555
916
9227
2649
913
6329
36
*fro
m th
e H
RA a
nd S
ES**
Dur
ing
the
tally
of H
UPS
, add
ition
al p
regn
ant m
othe
rs w
ere
enc
ount
ered
aft
er th
e SE
S an
d H
RA a
dmin
istr
atio
n
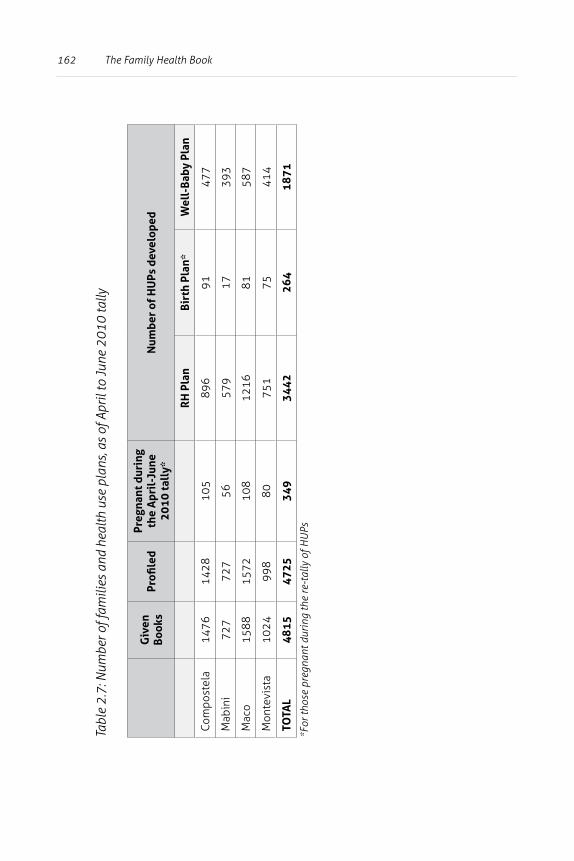
162 The Family Health Book
Tabl
e 2.
7: N
umbe
r of f
amili
es a
nd h
ealth
use
pla
ns, a
s of
Apr
il to
June
201
0 ta
lly
Giv
en
Book
sPr
ofile
d Pr
egna
nt d
urin
g th
e A
pril
-Jun
e 20
10 ta
lly*
Num
ber
of H
UPs
dev
elop
ed
RH
Pla
nBi
rth
Plan
*W
ell-
Baby
Pla
n
Com
post
ela
1476
1428
105
896
9147
7
Mab
ini
727
727
5657
917
393
Mac
o15
8815
7210
812
1681
587
Mon
tevi
sta
1024
998
8075
175
414
TOTA
L48
1547
2534
934
4226
418
71
*For
thos
e pr
egna
nt d
urin
g th
e re
-tal
ly o
f HU
Ps
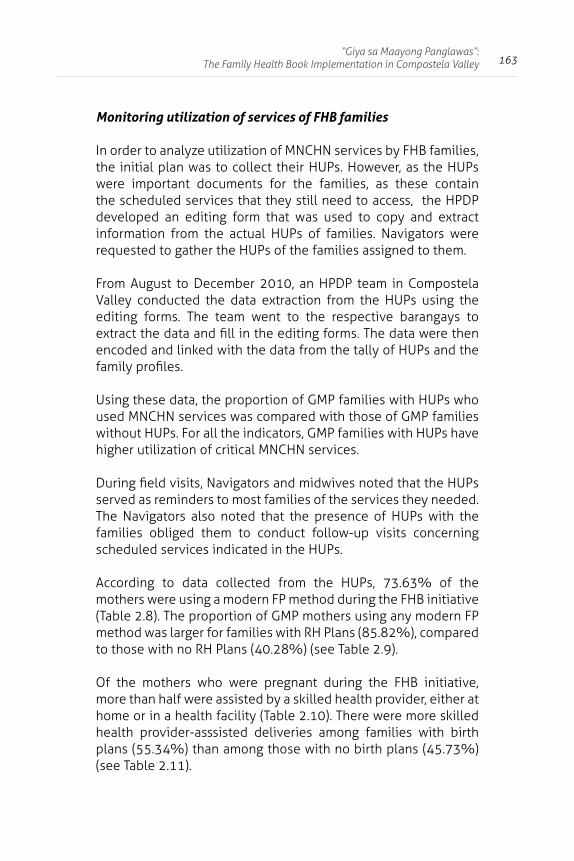
163“Giya sa Maayong Panglawas”:
The Family Health Book Implementation in Compostela Valley
Monitoring utilization of services of FHB families
In order to analyze utilization of MNCHN services by FHB families, the initial plan was to collect their HUPs. However, as the HUPs were important documents for the families, as these contain the scheduled services that they still need to access, the HPDP developed an editing form that was used to copy and extract information from the actual HUPs of families. Navigators were requested to gather the HUPs of the families assigned to them.
From August to December 2010, an HPDP team in Compostela Valley conducted the data extraction from the HUPs using the editing forms. The team went to the respective barangays to extract the data and fill in the editing forms. The data were then encoded and linked with the data from the tally of HUPs and the family profiles.
Using these data, the proportion of GMP families with HUPs who used MNCHN services was compared with those of GMP families without HUPs. For all the indicators, GMP families with HUPs have higher utilization of critical MNCHN services.
During field visits, Navigators and midwives noted that the HUPs served as reminders to most families of the services they needed. The Navigators also noted that the presence of HUPs with the families obliged them to conduct follow-up visits concerning scheduled services indicated in the HUPs.
According to data collected from the HUPs, 73.63% of the mothers were using a modern FP method during the FHB initiative (Table 2.8). The proportion of GMP mothers using any modern FP method was larger for families with RH Plans (85.82%), compared to those with no RH Plans (40.28%) (see Table 2.9).
Of the mothers who were pregnant during the FHB initiative, more than half were assisted by a skilled health provider, either at home or in a health facility (Table 2.10). There were more skilled health provider-asssisted deliveries among families with birth plans (55.34%) than among those with no birth plans (45.73%) (see Table 2.11).
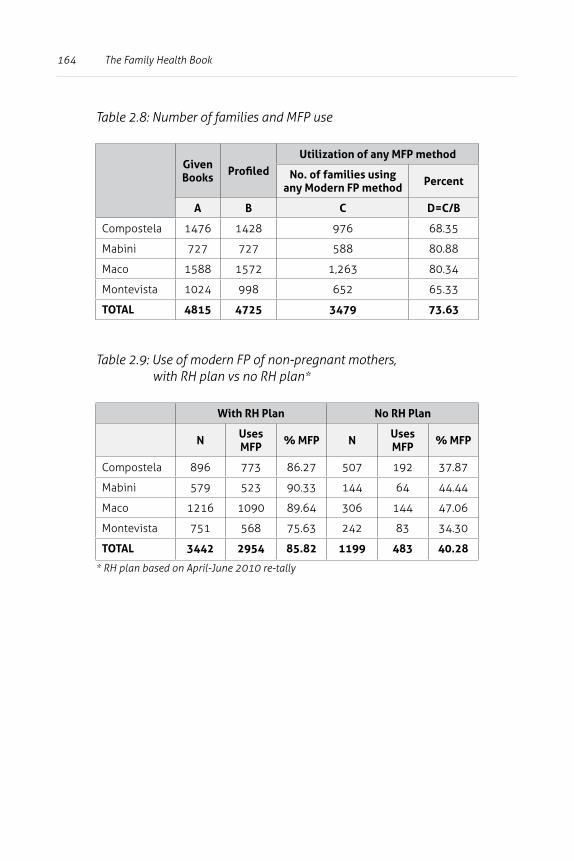
164 The Family Health Book
Table 2.8: Number of families and MFP use
Given Books Profiled
Utilization of any MFP method
No. of families using any Modern FP method Percent
A B C D=C/B
Compostela 1476 1428 976 68.35
Mabini 727 727 588 80.88
Maco 1588 1572 1,263 80.34
Montevista 1024 998 652 65.33
TOTAL 4815 4725 3479 73.63
Table 2.9: Use of modern FP of non-pregnant mothers, with RH plan vs no RH plan*
With RH Plan No RH Plan
N Uses MFP % MFP N Uses
MFP % MFP
Compostela 896 773 86.27 507 192 37.87
Mabini 579 523 90.33 144 64 44.44
Maco 1216 1090 89.64 306 144 47.06
Montevista 751 568 75.63 242 83 34.30
TOTAL 3442 2954 85.82 1199 483 40.28
* RH plan based on April-June 2010 re-tally
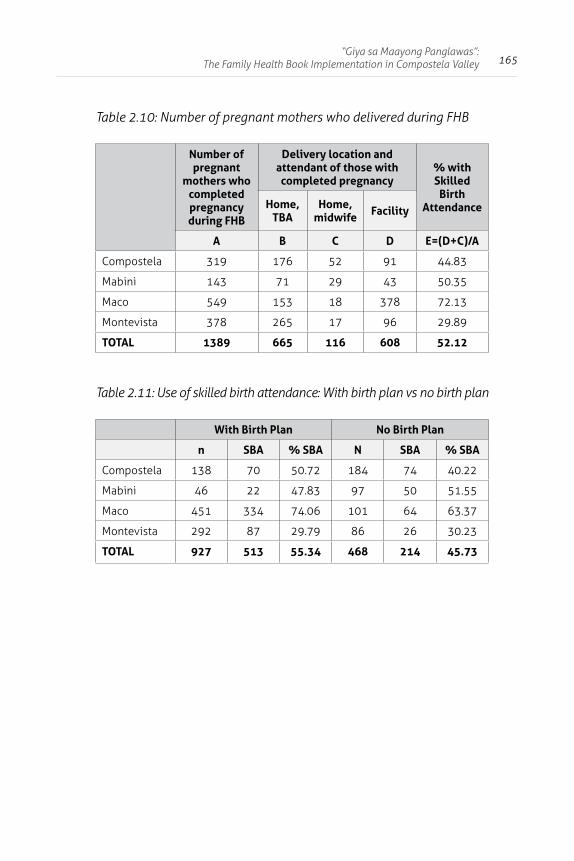
165“Giya sa Maayong Panglawas”:
The Family Health Book Implementation in Compostela Valley
Table 2.10: Number of pregnant mothers who delivered during FHB
Number of pregnant
mothers who completed pregnancy during FHB
Delivery location and attendant of those with completed pregnancy
% with Skilled
Birth AttendanceHome,
TBAHome,
midwife Facility
A B C D E=(D+C)/A
Compostela 319 176 52 91 44.83
Mabini 143 71 29 43 50.35
Maco 549 153 18 378 72.13
Montevista 378 265 17 96 29.89
TOTAL 1389 665 116 608 52.12
Table 2.11: Use of skilled birth attendance: With birth plan vs no birth plan
With Birth Plan No Birth Plan
n SBA % SBA N SBA % SBA
Compostela 138 70 50.72 184 74 40.22
Mabini 46 22 47.83 97 50 51.55
Maco 451 334 74.06 101 64 63.37
Montevista 292 87 29.79 86 26 30.23
TOTAL 927 513 55.34 468 214 45.73
166 The Family Health Book
Nine in every ten pregnant mothers during the FHB initiative utilized at least one ANC (Table 2.12). Moreover, the proportion of pregnant mothers with at least one ANC was also larger among families with birth plans compared to families with no birth plans (Table 2.13).
Table 2.12: ANC use among mothers who were pregnant during the FHB initiative
Number of pregnant women
during FHB
With at least one ANC
% with at least one ANC
A B C=A/B
Compostela 363 320 88.15
Mabini 150 112 74.67
Maco 584 544 93.15
Montevista 396 373 94.19
TOTAL 1493 1349 90.35
Table 2.13: With at least one ANC: With birth plan vs no birth plan*
With Birth Plan No Birth Plan
N W/ANC % SBA n W/ANC % SBA
Compostela 165 159 96.36 196 165 84.18
Mabini 51 49 96.08 99 66 66.67
Maco 477 477 100.00 98 71 72.45
Montevista 305 299 98.03 92 77 83.70
TOTAL 998 984 98.60 485 379 78.14
*cumulative (from 2009 to 2010)
While the FIC rate was high during the FHB initiative, with 78% of infants needing immunization able to complete all the services (Table 2.14), there were no significant differences in FIC rates between those with and without well baby plans (Table 2.15).
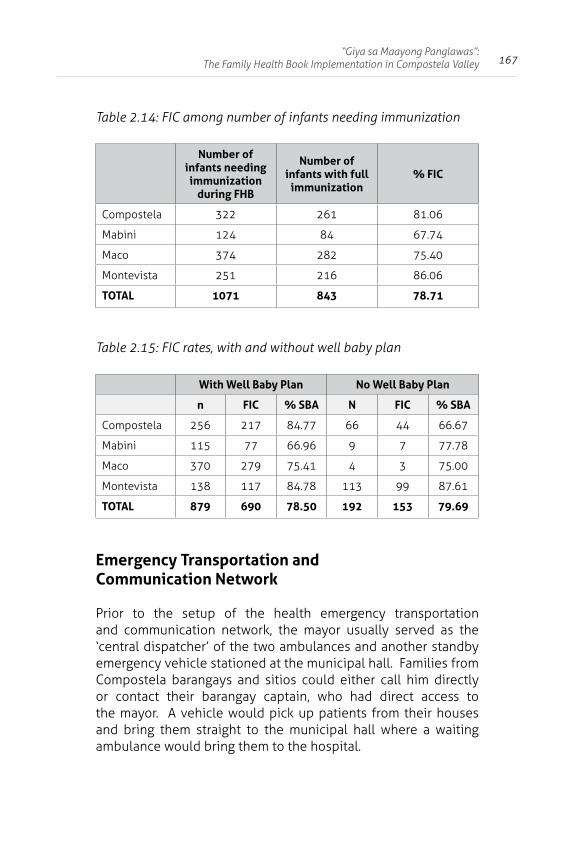
167“Giya sa Maayong Panglawas”:
The Family Health Book Implementation in Compostela Valley
Table 2.14: FIC among number of infants needing immunization
Number of infants needing immunization
during FHB
Number of infants with full
immunization% FIC
Compostela 322 261 81.06
Mabini 124 84 67.74
Maco 374 282 75.40
Montevista 251 216 86.06
TOTAL 1071 843 78.71
Table 2.15: FIC rates, with and without well baby plan
With Well Baby Plan No Well Baby Plan
n FIC % SBA N FIC % SBA
Compostela 256 217 84.77 66 44 66.67
Mabini 115 77 66.96 9 7 77.78
Maco 370 279 75.41 4 3 75.00
Montevista 138 117 84.78 113 99 87.61
TOTAL 879 690 78.50 192 153 79.69
Emergency Transportation and Communication Network
Prior to the setup of the health emergency transportation and communication network, the mayor usually served as the ‘central dispatcher’ of the two ambulances and another standby emergency vehicle stationed at the municipal hall. Families from Compostela barangays and sitios could either call him directly or contact their barangay captain, who had direct access to the mayor. A vehicle would pick up patients from their houses and bring them straight to the municipal hall where a waiting ambulance would bring them to the hospital.
168 The Family Health Book
In the case of far-flung barangays, the municipality designated a Center that served as a health emergency base, and with a direct link to the mayor. It is equipped with a functional vehicle. Depending on their capacity to pay, families are asked to pay for full or partial cost of gasoline expenses3. The municipal government gives full subsidy to extremely poor families.
Since travel from the remotest barangay to the Poblacion takes an entire day, expectant mothers in those areas usually make arrangements to stay with relatives in the Poblacion two days before their expected delivery date to ensure availability of transportation that can immediately take them to hospital facilities.
HPDP provided the four pilot municipalities with health emergency contacts in the GMP book and provided assistance in organizing the Compostela Network of Communications and Transport (CoNECT), a network of transport and communication providers that the families of Compostela could tap during emergencies. HPDP helped in the development of a protocol for CoNECT.
A pamphlet containing the assigned providers per barangay within the municipality was also produced and translated into the local language. The protocol integrated suggestions from various groups, such as local transport providers and the private sector.
Majority of the 16 barangays of Compostela passed ordinances supporting CoNECT. The Memorandum of Agreement among the provincial LGU, Compostela, and other stakeholders, was finalized prior to endorsement to the Sangguniang Bayan/Panlalawigan (Municipal and Provincial Councils) for approval in November 2009. The governor committed to provide PhP 150,000 counterpart funds to sustain CoNECT operations.
3 About PhP 102 from Poblacion, Compostela to Compostela Valley Provincial Hospital [CVPH]; PhP 450 to Davao Regional Hospital [DRH]; and PhP 1,020 to Davao Medical Center.
169“Giya sa Maayong Panglawas”:
The Family Health Book Implementation in Compostela Valley
Outreach
FHB outreach services were conducted regularly and targeted hard-to-reach communities to ensure their access to health services and adherence of families to health use plans.
In consultation with Municipal Health Offices, CHD XI, PHO, and other stakeholders, HPDP assisted in drafting the manual of operations for the regular conduct of outreach services in Montevista. It specified which core MNCHN services are to be offered during outreach activities and the criteria for selecting recipient barangays, and offered a guide for estimating logistical requirements and directions on how to conduct the outreach activity.
A demonstration training on the use of the manual was conducted on the third week of July 2009. This led to the crafting of an outreach plan for Montevista, which was carried out in August 2009. Lessons from this initial outreach were used to improve and finalize the manual of operations (Alcantara, 2009a).
Other salient parts of the manual of operations:
1. Creation of teams to plan, prepare, conduct, and monitor outreach activities:
• the planning team composed of the municipal LGU budget officer, procurement officer, PHO representative, and concerned barangay captains – to be headed by the MHO;
• the medical team composed of the PHO, MHO, and health workers of participating NGOs;
• the support team composed of the Navigators, barangay officials/volunteers, and NGOs; and
• the monitoring team from PHO and HPDP.
170 The Family Health Book
2. Barangays which meet the following selection criteria are chosen for outreach services:
• those with areas/sitios no more than 2 hours away, using the common modes of transportation, from the nearest RHU or government hospital;
• those with considerable number of FHB families (at least 30% of FHB families in the barangay residing in far-flung sitios);
• those with areas accessible by motorcycle or “habal-habal”; and
• those which pose no safety risks to the medical team.
Other factors to be considered in determining the number of barangays for outreach activities:
• the municipality’s budget; and• the capacity and willingness of the medical team and
barangay officials.
During the demonstration training, three barangays in Montevista (Mayaon, Banglasan, and San Vicente) were found to satisfy the criteria. GMP holders living in far-flung sitios in these barangays -- the target families for the outreach services -- numbered 57, 32, and 29 families, respectively.
Core MNCHN and other ancillary services were offered during the outreach activities:
1) prenatal/postnatal care (tetanus immunization, iron and folate supplementation, hypertension screening,etc.);
2) child care services (immunization, nutrition counseling);
3) reproductive health services (counseling and provision of FP commodities); and
4) birth registration and PhilHealth orientation.
171“Giya sa Maayong Panglawas”:
The Family Health Book Implementation in Compostela Valley
The actual range of health services provided depended on the health needs identified by the health use plans. These were expected to be collected by end-July in the three barangays. The midwife in-charge of the barangay, assisted by the partner Navigators, consolidated these health use plans.
Outreach activities were so scheduled to not conflict with residents’ major activities during the planting, harvesting and fiesta seasons, and important weekday or weekend activities. The outreach activities in these barangays were branded as “GMP Day” to differentiate from other activities of the community. GMP families were prioritized in the availment of services, which were also available for non-GMP families which need them.
The Municipal Health Officer (who heads the planning and medical team) prepared the schedule, identified the venue and the participants, and prepared the logistic requirements for the outreach activities. Depending on the available budget, the MHO had the option to procure and/or request the assistance of other agencies (Provincial Health Office/Department of Health/other government offices and NGOs) to ensure availability of services and commodities.
The support team, headed by the barangay captain, prepared the venue and conducted promotional activities to ensure that GMP families attended and availed of the health services offered during the outreach activities.
The first GMP outreach activities -- jointly sponsored by the MHO and PHO -- were conducted in Barangay Banglasan on August 14, 2009 and in Barangay Mayaon on September 4, 2009. At least three rounds of outreach services were conducted at quarterly intervals up to April 2010. An average of about 75 percent of targeted families attended the outreach services. Although GMP families were the priority, non-GMP families also received services. A patient flow protocol ensured adequate and orderly provision of services.
172 The Family Health Book
Navigational support to families (how to update health use plans, health education, and referrals to appropriate providers) was also provided and patient and provider feedbacks gathered for improvement of subsequent outreach activities.
Unlike typical outreach activities conducted by LGUs in the province, FHB outreach activities mainly provided MNCHN services. The outreach services also provided the opportunity for families in the selected outreach puroks to utilize services indicated in their developed health use plans (see Table 2.16).
Random visits were also conducted to gather inputs and feedback from midwives handling the FHB outreach activities. Though ideally, these should be conducted in the puroks where the target families resided, logistical concerns made it difficult to do so. The puroks of the target families were only accessible by motorcycle or were reached after at least 30 minutes of walking.
One remedy adopted was to fetch the target families from their residences just before or on the day of the outreach activities and bring them to a more central location. To guarantee attendance, midwives ensured that the Navigators informed the target families days ahead of the FHB outreach dates.
The Navigators and midwives also reported that compared with regular outreach activities, there was less overestimation of supply requirements in FHB outreach activitites, as only services and commodities indicated in the HUPs were prepared.
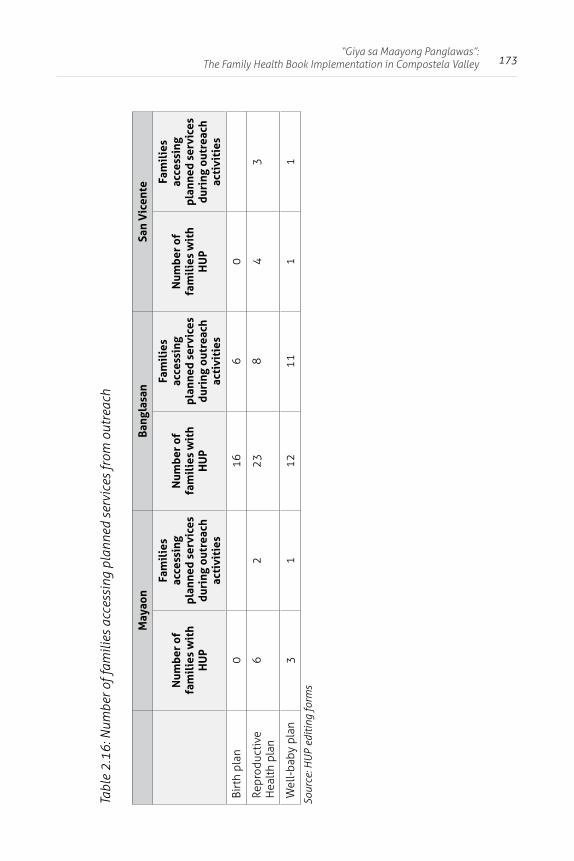
173“Giya sa Maayong Panglawas”:
The Family Health Book Implementation in Compostela Valley
Tabl
e 2.
16: N
umbe
r of f
amili
es a
cces
sing
pla
nned
ser
vice
s fr
om o
utre
ach
May
aon
Bang
lasa
nSa
n V
icen
te
Num
ber
of
fam
ilie
s w
ith
HU
P
Fam
ilie
s ac
cess
ing
plan
ned
serv
ices
du
ring
out
reac
h ac
tivi
ties
Num
ber
of
fam
ilie
s w
ith
HU
P
Fam
ilie
s ac
cess
ing
plan
ned
serv
ices
du
ring
out
reac
h ac
tivi
ties
Num
ber
of
fam
ilie
s w
ith
HU
P
Fam
ilie
s ac
cess
ing
plan
ned
serv
ices
du
ring
out
reac
h ac
tivi
ties
Birt
h pl
an0
166
0
Repr
oduc
tive
H
ealt
h pl
an6
223
84
3
Wel
l-ba
by p
lan
31
1211
11
Sour
ce: H
UP
editi
ng fo
rms
174 The Family Health Book
Other complementary and supporting activities
Providers’ orientation
The Provincial Health Office of Compostela Valley conducted providers’ orientation of the MNCHN services last May 22, 2009. The participants were providers from the local government units (LGUs) such as the PHO of Compostela Valley, the MHOs of the municipalities of Mabini, Nabunturan, Montevista, and Compostela, as well as the private providers. The FHB initiative and the role of providers in the initiative were discussed. Kits were distributed to the providers, containing the FHB primer, a CD of the maternal and child health standards, and the GMP carrier. Unfortunately, the core referral hospitals such as the CVPH and DRH were not able to send their representatives.
Hence, the FHB orientation for the staff of the CVPH was held by the PHO last June 4, 2009. During the said orientation, it was discovered that the staff of CVPH were unaware of the FHB initiative. While the Chief of CVPH has been informed of the FHB, the information was not echoed to his staff. As a result of the orientation, CVPH physicians agreed to provide the information needed in the FHB. Commitment to provide the FHB Navigators and CoNECT operatives free basic laboratory procedures and consultations were secured.
Support to Compostela Valley Provincial Hospital
In a Memorandum of Agreement between the Department of Health and the province on the implementation of PIPH, Compostela Valley invested PhP10 million as local counterpart for the upgrading of CVPH. It was a priority intervention in the PIPH because CVPH served as the end-referral facility for the province on MNCHN services. Upon the request of the province, HPDP also facilitated the conduct of a meeting among the Compostela Valley PHO and DOH officials to follow up on the DOH counterpart to the upgrading of CVPH last July 1, 2009.
175“Giya sa Maayong Panglawas”:
The Family Health Book Implementation in Compostela Valley
In addition, HPDP assisted HealthGov in introducing the “Quality Assurance Partnership Committees” (QAPC) to the province and CVPH on June 16, 2009, contextualizing it within the FHB initiative in the province. The creation of QAPC is part of the Health Systems 20/20 Initiative which aims to address issues on access and quality of MNCHN services in local facilities. Institutionalizing QAPC in CVPH, the end-referral facility for maternity care services in the province, forms part of HealthGov’s support to FHB. HealthGov will develop the QAPC workplan for Compostela Valley with technical inputs from HPDP. It will also provide SDExH training for CVPH as part of QAPC.
As part of its support to CVPH and upon the request from CHD XI Regional Director Baluma as well as Compostela Valley provincial LGU/PHO, HPDP linked the province to La Union Medical Center to expose the former to the experience of the latter in converting hospitals into economic enterprises. In line with this, HPDP supported the participation of selected Compostela Valley officials in the Study Tour Program in La Union from June 30 to July 1, 2009. The Compostela Valley team was composed of the Governor’s Executive Assistant on Fiscal Matters, Sangguniang Panlalawigan Board Member and Committee on Health Chair, CVPH Chief, and the Provincial Planning and Development Officer.
PhilHealth benefit delivery
HPDP assisted the PHO in terms of securing accreditation of critical facilities in the province through the assessment of PhilHealth accreditation deficiencies and operational hindrances of critical facilities. Following the assessment, technical support was provided to fast-track accreditation of RHUs in the four pilot municipalities for OPB, TB-DOTS, and MCP by facilitating preliminary evaluation of their facilities by PhilHealth, estimating resource requirements for RHUs’ accreditation, and linking the RHUs with key officials from the MHOs, local Sanggunians, and the PhilHealth Regional Office in the course of troubleshooting technical and operational bottlenecks in accreditation. HPDP further assisted in advocating with the Sangguniang Bayan and Panlalawigan budgetary allocations for the enhancement and
176 The Family Health Book
construction of maternity care centers needed to facilitate MCP accreditation. Assistance for the renewal of accreditation of the district and provincial hospitals as primary and secondary level facilities was given as well. Moreover, support was provided to local Sanggunians in drafting Appropriation Ordinances for the estimated resource requirements.
Part of the assistance of HPDP was advocacy with LGUs for the need and advantages of enroling their indigent population to PhilHealth. HPDP assisted in advocating with the Mayors and local Sanggunians for budget allocations for the PhilHealth enrolment of FHB families and Navigators. While these were considered in the municipal LGUs’ 2009 Supplemental Budget, allocations were not sufficient to cover all proposed enrolees given current local budget limitations. On the whole, the province needed to cover the PhilHealth premium counterpart payment for around 5,153 of the 5,347 GMP families and 396 Navigators. However, total funds from the provincial LGU, the municipal LGUs, and the Priority Development Assistance Fund (PDAF) were not enough to enrol around 976 families and Navigators.
Application of families in PhilHealth was slowed down by the tedious process of identifying which FHB families will be sponsored by the municipal LGUs, assisting families in accomplishing the family data survey forms, and checking the accuracy and completeness of these forms by the Municipal Social Welfare and Development Officers (MSWDOs). Since the FHB families were not included in the enrolment of sponsored program families at the start of the year, the MSWDOs perceived this as an additional burden on their part. The determination of the criteria for selection of families for enrolment has largely been left to the local government units.
Mid-project assessment and random visits
A mid-project assessment was conducted for the FHB after the distribution of Book in May to July 2009 (Acuin, 2009). A series of FGDs were conducted among the early recipients of the Book. For Maco, the families for the FGD were from the most remote barangays; for Montevista, families from the poblacion were
177“Giya sa Maayong Panglawas”:
The Family Health Book Implementation in Compostela Valley
included; while for Compostela and Mabini, it was a mix of poblacion and remote barangay residents. All the families in the FGD had a mother who was pregnant during the FGD or recently delivered during the FHB period.
FGDs were also conducted among the Navigators. Navigators in Maco handling more than 20 families were included for the FGD, while Navigators assigned to far-flung areas and were handling less than 20 families were drawn from the other three municipalities.
Random visits to the field were also conducted to determine and address concerns related with the FHB interventions. In particular, visits on outreach sites were conducted to check whether FHB outreach activities were regularly conducted. Visits to far-flung areas and barangays were also done to determine whether Navigator visits were regularly performed
Book and Navigator
During the FGDs, the families expressed their appreciation of the efforts exerted by the Navigators, especially during the orientation and follow-up visits. Families, especially those residing in far-flung barangays and who have never been to the RHU, felt that after a long time someone is paying attention to their health needs. Most families felt that Navigators are better than the BHWs since the former conduct actual home visits.
However, an issue that arose was the variation in terms of the number of Navigators‘ visits experienced by families. Families with Navigators who were also neighbors and relatives experienced weekly visits. However, families located in far-flung areas and were assigned to Navigators residing in different puroks expressed that visits were done at most once a month. Families from remote barangays in Maco, in fact, were not immediately visited by their Navigator.
One of the concerns raised by the families was that the FHB carrier was difficult to carry around. Some couples with limited educational attainment, expressed that a discussion by the Navigator should be done instead of them actually reading the contents. Another concern was that the fathers’ participation, at
178 The Family Health Book
least during the orientation, was difficult to ensure. The mothers felt that their partners’ presence during the orientation and Navigator visits was relevant since the discussion during the FHB visits brought up the role of the fathers in health care.
The health workers and volunteers felt that being Navigators made them more involved with the health issues and problems of families under their care. They also noticed that people were treating them with higher regard as Navigators. Most of the Navigators gave credit to the training they received, particularly those on family planning, PhilHealth, and newborn screening.
Though health workers realized that they were better appreciated as Navigators, they were concerned of their heavier responsibility relative to their BHW tasks. In particular, they worried about the implications on their workload. Also, at the start of the FHB, it was found out that some Navigators were initially assigned with more than 20 families. Moreover, some Navigators suggested that they should handle at the most ten families, and preferably those near their residences.
Some Navigators admitted that some families assigned to them were visited late and infrequently followed-up. These Navigators cited that some families were not accessible by basic transportation and required travel by foot (one to two hours required walking). In selected barangays and puroks, transportation cost was a big factor. Especially in the far-flung areas of Maco, like the Masaralines, a one-way trip can reach up to PhP400 to PhP600 per person. Due to this, Navigators handling families in these types of areas requested additional compensation or transportation allowance.
179“Giya sa Maayong Panglawas”:
The Family Health Book Implementation in Compostela Valley
Cost of the FHB OR
Costs associated with the FHB initiative can be classified into three components;
• developmental costs;• costs of pilot implementation • operations research costs.
The developmental costs include one-time expenses associated with technical assistance obtained to define and design the FHB interventions including prototype development of the Books and Navigators’ Kits, training design for Navigators, development of PhilHealth guides for families and providers, protocol design for emergency and outreach services, and field coordination and management to secure buy-in of local officials. Detailed costs for these developmental activities are given in Table 2.17. Around PhP 13 million was incurred for the development of the FHB intervention packages, which were shared by HPDP and other CAs.
The costs of implementing the pilot include expenses incurred for the following: 1) the listing and validation of eligible families; 2) the translation, production, and distribution of the Books and forms; 3) the selection, training, and deployment of Navigators (e.g., transportation expense vouchers); 4) the investments required for accreditation of facilities; 5) premium payments for PhilHealth enrolment; 6) the investments for the hospital upgrade; 7) marketing and social advocacy; and 8) management costs including Steering Committee and TWG meetings. Because of the pilot nature of the implementation, some of the costs that are expected to be shouldered by LGUs in a normal implementation were initially shouldered by HPDP. Some of these costs, for instance, PhilHealth premium payments, would have been incurred by LGUs even without the FHB interventions. It would be primarily from this cost component where the roll-out costs would be extracted.
180 The Family Health Book
Around PhP 30.8 million is the estimated cost of running the FHB pilot (see Table 2.18), a significant amount of which represents the estimated cost of supporting the upgrade of the hospital. Around half of these costs were shouldered by the provincial and municipal LGUs, with around one-third being shouldered by HPDP and by the DOH.
The operations research costs pertain to those related to assessing the impacts of the FHB interventions, i.e., the monitoring and evaluation activities. These are costs that are not expected to be incurred by the LGUs in the roll-out. Around PhP 9.5 million was expected to be spent for these activities (see Table 2.19).
Thus, the FHB implementation in Compostela Valley was to cost around a total of PhP 53 million (see Table 2.20).
However, not all of these expenses are expected to be incurred by provinces wishing to implement the interventions, particularly the developmental costs and the operations research costs. The expected roll-out costs for LGUs would mainly be extracted from the costs of implementing the pilot. Preliminary estimates of these unit costs are given in Table 2.21. These were derived by simply dividing the estimates of the operational costs of the pilot by the applicable number of units in Compostela Valley.
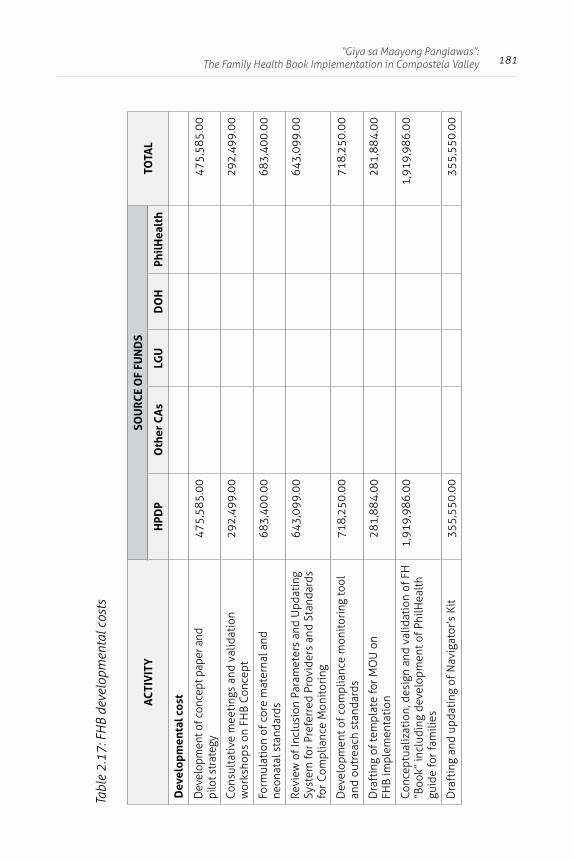
181“Giya sa Maayong Panglawas”:
The Family Health Book Implementation in Compostela Valley
Tabl
e 2.
17: F
HB
deve
lopm
enta
l cos
ts
AC
TIV
ITY
SOU
RCE
OF
FUN
DS
TOTA
LH
PDP
Oth
er C
As
LGU
DO
HPh
ilH
ealt
h
Dev
elop
men
tal c
ost
Dev
elop
men
t of c
once
pt p
aper
and
pi
lot s
trat
egy
475,
585.
0047
5,58
5.00
Cons
ulta
tive
mee
ting
s an
d va
lidat
ion
wor
ksho
ps o
n FH
B Co
ncep
t29
2,49
9.00
292,
499.
00
Form
ulat
ion
of c
ore
mat
erna
l and
ne
onat
al s
tand
ards
683,
400.
0068
3,40
0.00
Revi
ew o
f Inc
lusi
on P
aram
eter
s an
d U
pdat
ing
Syst
em fo
r Pre
ferr
ed P
rovi
ders
and
Sta
ndar
ds
for C
ompl
ianc
e M
onit
orin
g
643,
099.
0064
3,09
9.00
Dev
elop
men
t of c
ompl
ianc
e m
onit
orin
g to
ol
and
outr
each
sta
ndar
ds71
8,25
0.00
718,
250.
00
Dra
ftin
g of
tem
plat
e fo
r MO
U o
n FH
B im
plem
enta
tion
281,
884.
0028
1,88
4.00
Conc
eptu
aliz
atio
n, d
esig
n an
d va
lidat
ion
of F
H
“Boo
k” in
clud
ing
deve
lopm
ent o
f Phi
lHea
lth
guid
e fo
r fam
ilies
1,91
9,98
6.00
1,91
9,98
6.00
Dra
ftin
g an
d up
dati
ng o
f Nav
igat
or’s
Kit
355,
550.
0035
5,55
0.00
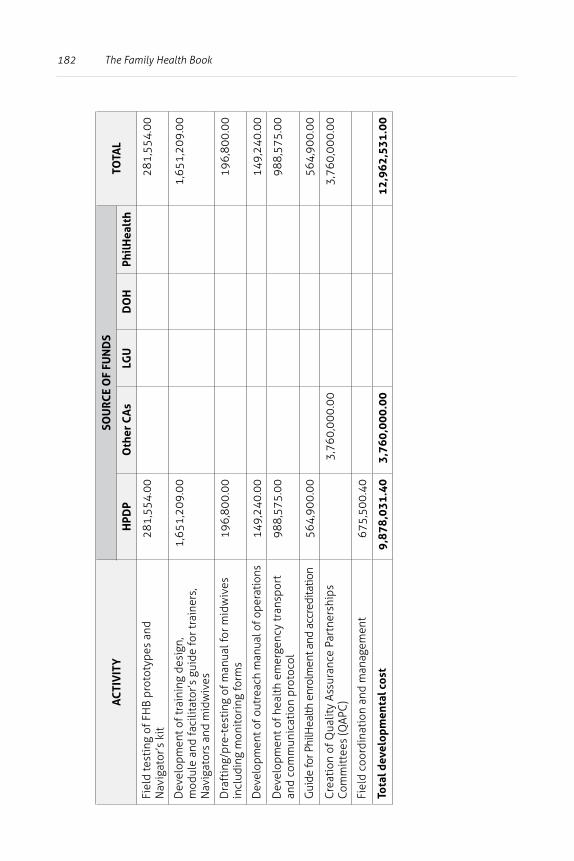
182 The Family Health Book
AC
TIV
ITY
SOU
RCE
OF
FUN
DS
TOTA
LH
PDP
Oth
er C
As
LGU
DO
HPh
ilH
ealt
h
Fiel
d te
stin
g of
FH
B pr
otot
ypes
and
N
avig
ator
’s k
it28
1,55
4.00
281,
554.
00
Dev
elop
men
t of t
rain
ing
desi
gn,
mod
ule
and
faci
litat
or’s
gui
de fo
r tra
iner
s,
Nav
igat
ors
and
mid
wiv
es
1,65
1,20
9.00
1,65
1,20
9.00
Dra
ftin
g/pr
e-te
stin
g of
man
ual f
or m
idw
ives
in
clud
ing
mon
itor
ing
form
s19
6,80
0.00
196,
800.
00
Dev
elop
men
t of o
utre
ach
man
ual o
f ope
ratio
ns14
9,24
0.00
149,
240.
00
Dev
elop
men
t of h
ealt
h em
erge
ncy
tran
spor
t an
d co
mm
unic
atio
n pr
otoc
ol98
8,57
5.00
988,
575.
00
Gui
de fo
r Phi
lHea
lth e
nrol
men
t and
acc
redi
tatio
n56
4,90
0.00
564,
900.
00
Cre
atio
n of
Qua
lity
Assu
ranc
e Pa
rtne
rshi
ps
Com
mit
tees
(QAP
C)
3,76
0,00
0.00
3,76
0,00
0.00
Fiel
d co
ordi
nati
on a
nd m
anag
emen
t67
5,50
0.40
Tota
l dev
elop
men
tal c
ost
9,87
8,03
1.40
3,76
0,00
0.00
12,9
62,5
31.0
0
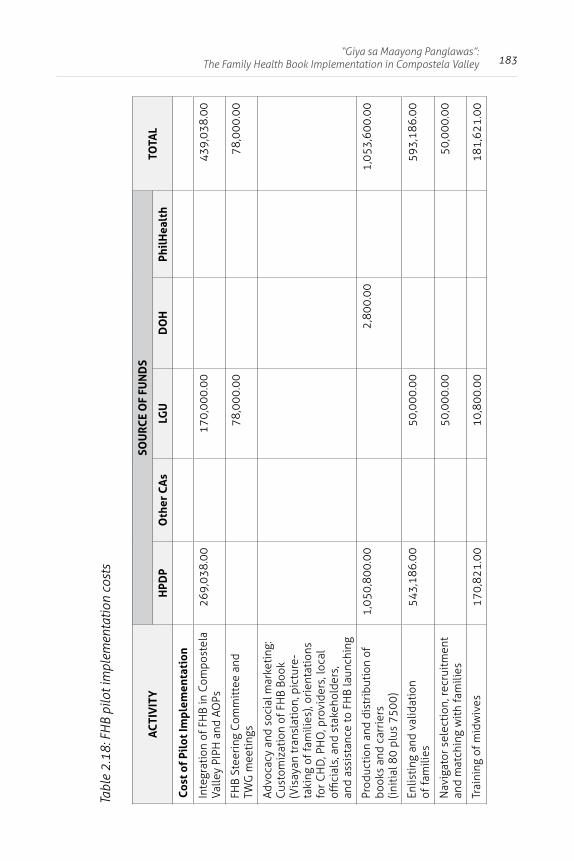
183“Giya sa Maayong Panglawas”:
The Family Health Book Implementation in Compostela Valley
Tabl
e 2.
18: F
HB
pilo
t im
plem
enta
tion
cost
s
AC
TIV
ITY
SOU
RCE
OF
FUN
DS
TOTA
LH
PDP
Oth
er C
As
LGU
DO
HPh
ilH
ealt
h
Cost
of
Pilo
t Im
plem
enta
tion
Inte
grat
ion
of F
HB
in C
ompo
stel
a Va
lley
PIPH
and
AO
Ps26
9,03
8.00
170,
000.
0043
9,03
8.00
FHB
Stee
ring
Com
mit
tee
and
TWG
mee
ting
s78
,000
.00
78,0
00.0
0
Advo
cacy
and
soc
ial m
arke
ting
: Cu
stom
izat
ion
of F
HB
Book
(V
isay
an tr
ansl
atio
n, p
ictu
re-
taki
ng o
f fam
ilies
), or
ient
atio
ns
for C
HD
, PH
O, p
rovi
ders
, loc
al
offici
als,
and
sta
keho
lder
s,
and
assi
stan
ce to
FH
B la
unch
ing
Prod
ucti
on a
nd d
istr
ibut
ion
of
book
s an
d ca
rrie
rs
(init
ial 8
0 pl
us 7
500)
1,05
0,80
0.00
2,80
0.00
1,05
3,60
0.00
Enlis
ting
and
val
idat
ion
of fa
mili
es54
3,18
6.00
50,0
00.0
059
3,18
6.00
Nav
igat
or s
elec
tion
, rec
ruit
men
t an
d m
atch
ing
wit
h fa
mili
es50
,000
.00
50,0
00.0
0
Trai
ning
of m
idw
ives
170,
821.
0010
,800
.00
181,
621.
00
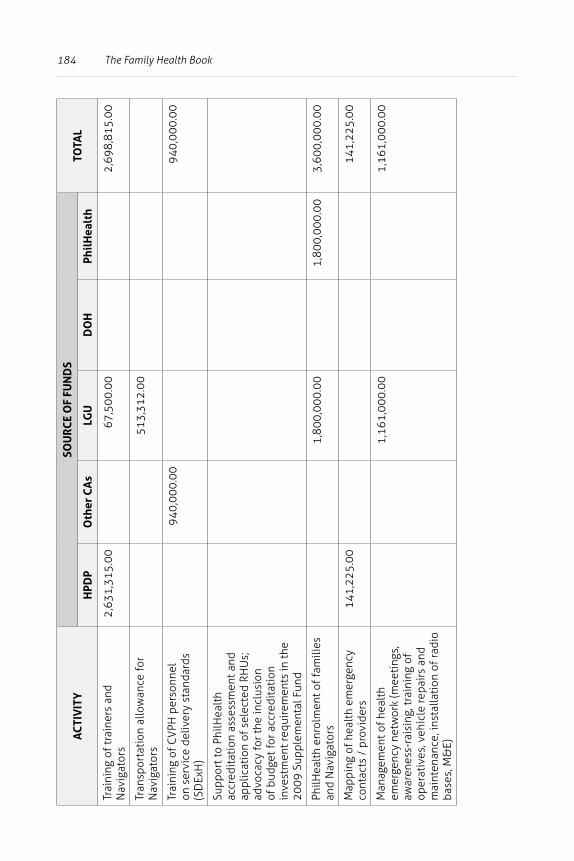
184 The Family Health Book
AC
TIV
ITY
SOU
RCE
OF
FUN
DS
TOTA
LH
PDP
Oth
er C
As
LGU
DO
HPh
ilH
ealt
h
Trai
ning
of t
rain
ers
and
Nav
igat
ors
2,63
1,31
5.00
67,5
00.0
02,
698,
815.
00
Tran
spor
tati
on a
llow
ance
for
Nav
igat
ors
513,
312.
00
Trai
ning
of C
VPH
per
sonn
el
on s
ervi
ce d
eliv
ery
stan
dard
s (S
DEx
H)
940,
000.
0094
0,00
0.00
Supp
ort t
o Ph
ilHea
lth
accr
edit
atio
n as
sess
men
t and
ap
plic
atio
n of
sel
ecte
d RH
Us;
ad
voca
cy fo
r the
incl
usio
n of
bud
get f
or a
ccre
dita
tion
in
vest
men
t req
uire
men
ts in
the
2009
Sup
plem
enta
l Fun
d
PhilH
ealt
h en
rolm
ent o
f fam
ilies
an
d N
avig
ator
s1,
800,
000.
001,
800,
000.
003,
600,
000.
00
Map
ping
of h
ealt
h em
erge
ncy
cont
acts
/ p
rovi
ders
141,
225.
0014
1,22
5.00
Man
agem
ent o
f hea
lth
emer
genc
y ne
twor
k (m
eeti
ngs,
aw
aren
ess-
rais
ing,
trai
ning
of
oper
ativ
es, v
ehic
le re
pair
s an
d m
aint
enan
ce, i
nsta
llati
on o
f rad
io
base
s, M
&E)
1,16
1,00
0.00
1,16
1,00
0.00
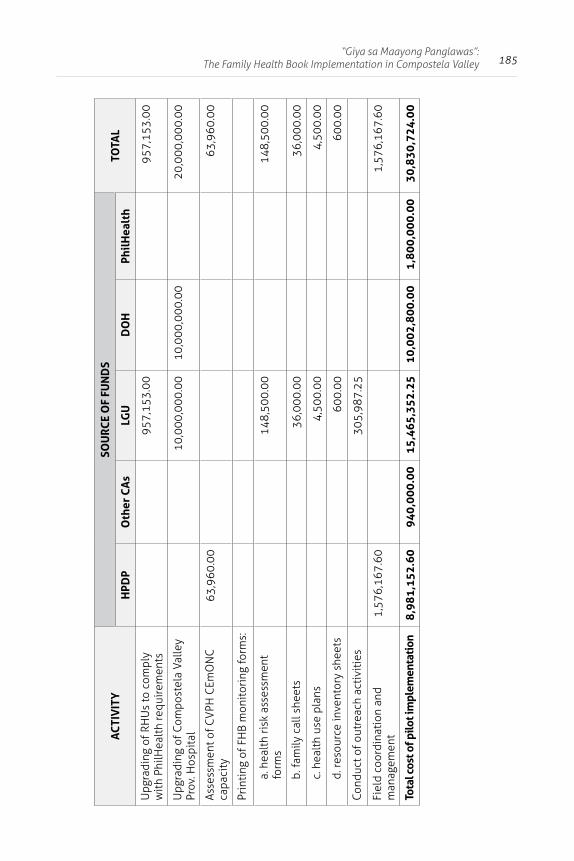
185“Giya sa Maayong Panglawas”:
The Family Health Book Implementation in Compostela Valley
AC
TIV
ITY
SOU
RCE
OF
FUN
DS
TOTA
LH
PDP
Oth
er C
As
LGU
DO
HPh
ilH
ealt
h
Upg
radi
ng o
f RH
Us
to c
ompl
y w
ith
PhilH
ealt
h re
quir
emen
ts95
7,15
3.00
957,
153.
00
Upg
radi
ng o
f Com
post
ela
Valle
y Pr
ov. H
ospi
tal
10,0
00,0
00.0
010
,000
,000
.00
20,0
00,0
00.0
0
Asse
ssm
ent o
f CV
PH C
EmO
NC
ca
paci
ty63
,960
.00
63,9
60.0
0
Prin
ting
of F
HB
mon
itor
ing
form
s:
a. h
ealt
h ri
sk a
sses
smen
t fo
rms
148,
500.
0014
8,50
0.00
b. fa
mily
cal
l she
ets
36,0
00.0
036
,000
.00
c. h
ealt
h us
e pl
ans
4,50
0.00
4,50
0.00
d. re
sour
ce in
vent
ory
shee
ts60
0.00
600.
00
Cond
uct o
f out
reac
h ac
tivi
ties
305,
987.
25
Fiel
d co
ordi
nati
on a
nd
man
agem
ent
1,57
6,16
7.60
1,57
6,16
7.60
Tota
l cos
t of p
ilot i
mpl
emen
tati
on8,
981,
152.
6094
0,00
0.00
15,4
65,3
52.2
510
,002
,800
.00
1,80
0,00
0.00
30,8
30,7
24.0
0
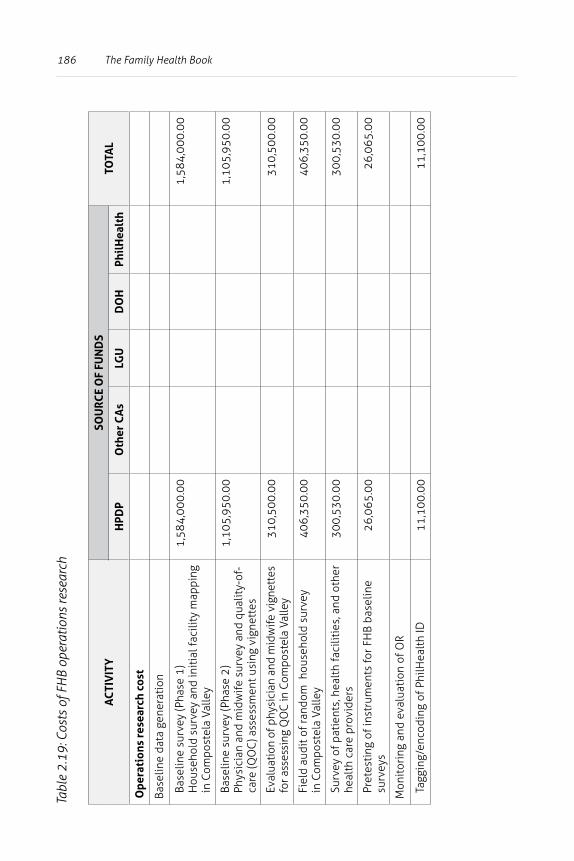
186 The Family Health BookTa
ble
2.19
: Cos
ts o
f FH
B op
erat
ions
rese
arch
AC
TIV
ITY
SOU
RCE
OF
FUN
DS
TOTA
LH
PDP
Oth
er C
As
LGU
DO
HPh
ilH
ealt
h
Ope
rati
ons
rese
arch
cos
t
Base
line
data
gen
erat
ion
Base
line
surv
ey (P
hase
1)
Hou
seho
ld s
urve
y an
d in
itia
l fac
ility
map
ping
in
Com
post
ela
Valle
y
1,58
4,00
0.00
1,58
4,00
0.00
Base
line
surv
ey (P
hase
2)
Phys
icia
n an
d m
idw
ife s
urve
y an
d qu
alit
y-of
-ca
re (Q
OC
) ass
essm
ent u
sing
vig
nett
es
1,10
5,95
0.00
1,10
5,95
0.00
Eval
uatio
n of
phy
sici
an a
nd m
idw
ife v
igne
ttes
fo
r ass
essi
ng Q
OC
in C
ompo
stel
a Va
lley
310,
500.
0031
0,50
0.00
Fiel
d au
dit o
f ran
dom
hou
seho
ld s
urve
y in
Com
post
ela
Valle
y40
6,35
0.00
406,
350.
00
Surv
ey o
f pat
ient
s, h
ealt
h fa
cilit
ies,
and
oth
er
heal
th c
are
prov
ider
s30
0,53
0.00
300,
530.
00
Pret
esti
ng o
f ins
trum
ents
for F
HB
base
line
surv
eys
26,0
65.0
026
,065
.00
Mon
itor
ing
and
eval
uati
on o
f OR
Tagg
ing/
enco
ding
of P
hilH
ealt
h ID
11,1
00.0
011
,100
.00
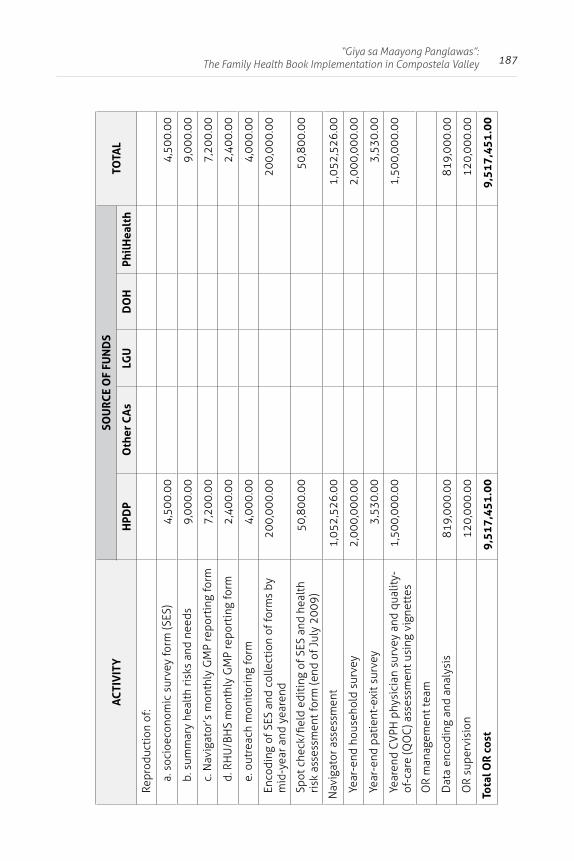
187“Giya sa Maayong Panglawas”:
The Family Health Book Implementation in Compostela Valley
AC
TIV
ITY
SOU
RCE
OF
FUN
DS
TOTA
LH
PDP
Oth
er C
As
LGU
DO
HPh
ilH
ealt
h
Repr
oduc
tion
of:
a. s
ocio
econ
omic
sur
vey
form
(SES
)4,
500.
004,
500.
00
b. s
umm
ary
heal
th ri
sks
and
need
s9,
000.
009,
000.
00
c. N
avig
ator
’s m
onth
ly G
MP
repo
rtin
g fo
rm7,
200.
007,
200.
00
d. R
HU
/BH
S m
onth
ly G
MP
repo
rtin
g fo
rm2,
400.
002,
400.
00
e. o
utre
ach
mon
itor
ing
form
4,00
0.00
4,00
0.00
Enco
ding
of S
ES a
nd c
olle
ctio
n of
form
s by
m
id-y
ear a
nd y
eare
nd20
0,00
0.00
200,
000.
00
Spot
che
ck/fi
eld
edit
ing
of S
ES a
nd h
ealt
h ri
sk a
sses
smen
t for
m (e
nd o
f Jul
y 20
09)
50,8
00.0
050
,800
.00
Nav
igat
or a
sses
smen
t1,
052,
526.
001,
052,
526.
00
Year
-end
hou
seho
ld s
urve
y2,
000,
000.
002,
000,
000.
00
Year
-end
pat
ient
-exi
t sur
vey
3,53
0.00
3,53
0.00
Year
end
CV
PH p
hysi
cian
sur
vey
and
qual
ity-
of-c
are
(QO
C) a
sses
smen
t usi
ng v
igne
ttes
1,50
0,00
0.00
1,50
0,00
0.00
OR
man
agem
ent t
eam
Dat
a en
codi
ng a
nd a
naly
sis
819,
000.
0081
9,00
0.00
OR
supe
rvis
ion
120,
000.
0012
0,00
0.00
Tota
l OR
cos
t9,
517,
451.
009,
517,
451.
00
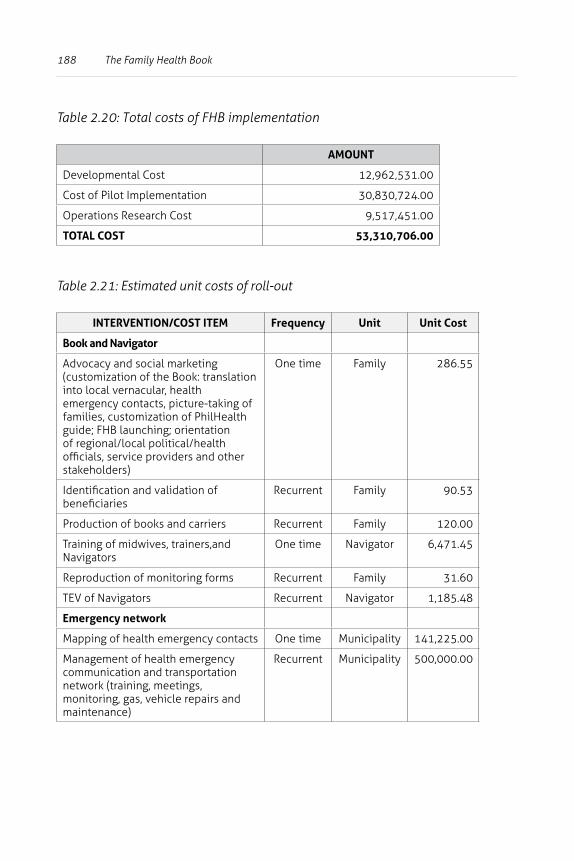
188 The Family Health Book
Table 2.20: Total costs of FHB implementation
AMOUNT
Developmental Cost 12,962,531.00
Cost of Pilot Implementation 30,830,724.00
Operations Research Cost 9,517,451.00
TOTAL COST 53,310,706.00
Table 2.21: Estimated unit costs of roll-out
INTERVENTION/COST ITEM Frequency Unit Unit Cost
Book and Navigator
Advocacy and social marketing (customization of the Book: translation into local vernacular, health emergency contacts, picture-taking of families, customization of PhilHealth guide; FHB launching; orientation of regional/local political/health officials, service providers and other stakeholders)
One time Family 286.55
Identification and validation of beneficiaries
Recurrent Family 90.53
Production of books and carriers Recurrent Family 120.00
Training of midwives, trainers,and Navigators
One time Navigator 6,471.45
Reproduction of monitoring forms Recurrent Family 31.60
TEV of Navigators Recurrent Navigator 1,185.48
Emergency network
Mapping of health emergency contacts One time Municipality 141,225.00
Management of health emergency communication and transportation network (training, meetings, monitoring, gas, vehicle repairs and maintenance)
Recurrent Municipality 500,000.00
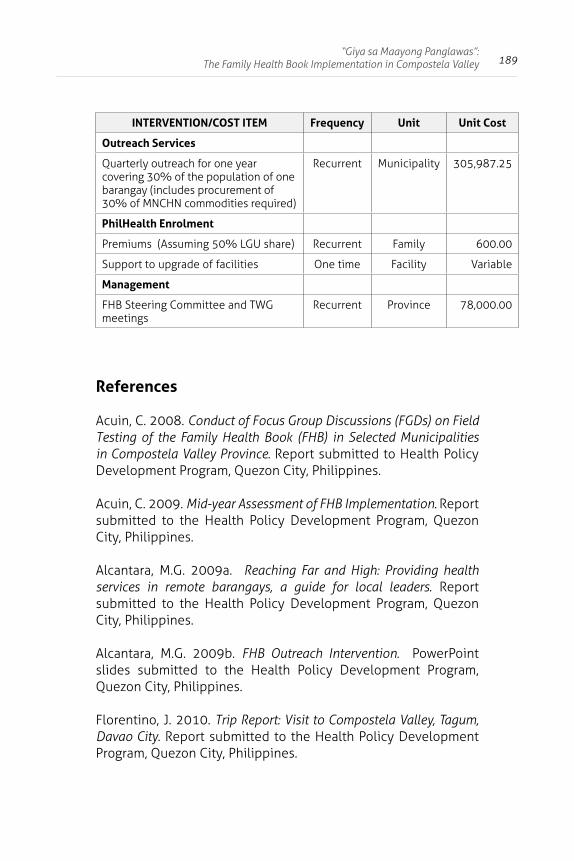
189“Giya sa Maayong Panglawas”:
The Family Health Book Implementation in Compostela Valley
INTERVENTION/COST ITEM Frequency Unit Unit Cost
Outreach Services
Quarterly outreach for one year covering 30% of the population of one barangay (includes procurement of 30% of MNCHN commodities required)
Recurrent Municipality 305,987.25
PhilHealth Enrolment
Premiums (Assuming 50% LGU share) Recurrent Family 600.00
Support to upgrade of facilities One time Facility Variable
Management
FHB Steering Committee and TWG meetings
Recurrent Province 78,000.00
References
Acuin, C. 2008. Conduct of Focus Group Discussions (FGDs) on Field Testing of the Family Health Book (FHB) in Selected Municipalities in Compostela Valley Province. Report submitted to Health Policy Development Program, Quezon City, Philippines.
Acuin, C. 2009. Mid-year Assessment of FHB Implementation. Report submitted to the Health Policy Development Program, Quezon City, Philippines.
Alcantara, M.G. 2009a. Reaching Far and High: Providing health services in remote barangays, a guide for local leaders. Report submitted to the Health Policy Development Program, Quezon City, Philippines.
Alcantara, M.G. 2009b. FHB Outreach Intervention. PowerPoint slides submitted to the Health Policy Development Program, Quezon City, Philippines.
Florentino, J. 2010. Trip Report: Visit to Compostela Valley, Tagum, Davao City. Report submitted to the Health Policy Development Program, Quezon City, Philippines.
190 The Family Health Book
Health Policy Development Program. 2008a. The Family Health Book Navigator’s Kit. Quezon City, Philippines, UPecon Foundation, Inc.-Health Policy Development Program.
__________. 2008b. The Family Health Book Midwives’ Kit. Quezon City, Philippines, UPecon Foundation, Inc.-Health Policy Development Program.
__________. 2008c. Navigator’s Training Modules. Quezon City, Philippines, UPecon Foundation, Inc.-Health Policy Development Program.
__________. 2008d. FHB Collection of Forms. Excel file submitted to the Health Policy Development Program, Quezon City, Philippines.
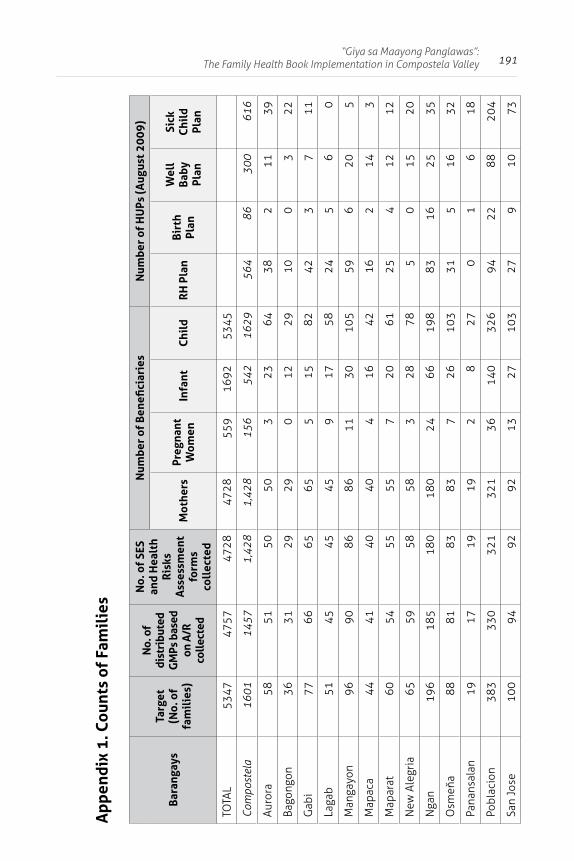
191“Giya sa Maayong Panglawas”:
The Family Health Book Implementation in Compostela Valley
App
endi
x 1.
Cou
nts
of F
amil
ies
Bara
ngay
sTa
rget
(N
o. o
f fa
mil
ies)
No.
of
dist
ribu
ted
GM
Ps b
ased
on
A/R
co
llect
ed
No.
of
SES
and
Hea
lth
Ris
ks
Ass
essm
ent
form
s co
llec
ted
Num
ber
of B
enefi
ciar
ies
Num
ber
of H
UPs
(Aug
ust 2
009)
Mot
hers
Preg
nant
W
omen
Infa
ntC
hild
RH
Pla
nBi
rth
Plan
Wel
l Ba
by
Plan
Sick
C
hild
Pl
an
TOTA
L53
4747
5747
2847
28 5
5916
92
5345
Com
post
ela
1601
1457
1,42
81,
428
156
542
1629
564
8630
061
6
Auro
ra58
5150
503
2364
382
1139
Bago
ngon
3631
2929
012
2910
03
22
Gab
i77
6665
655
1582
423
711
Laga
b51
4545
459
1758
245
60
Man
gayo
n96
9086
8611
3010
559
620
5
Map
aca
4441
4040
416
4216
214
3
Map
arat
6054
5555
720
6125
412
12
New
Ale
gria
6559
5858
328
785
015
20
Nga
n19
618
518
018
024
6619
883
1625
35
Osm
eňa
8881
8383
726
103
315
1632
Pana
nsal
an19
1719
192
827
01
618
Pobl
acio
n38
333
032
132
136
140
326
9422
8820
4
San
Jose
100
9492
9213
2710
327
910
73
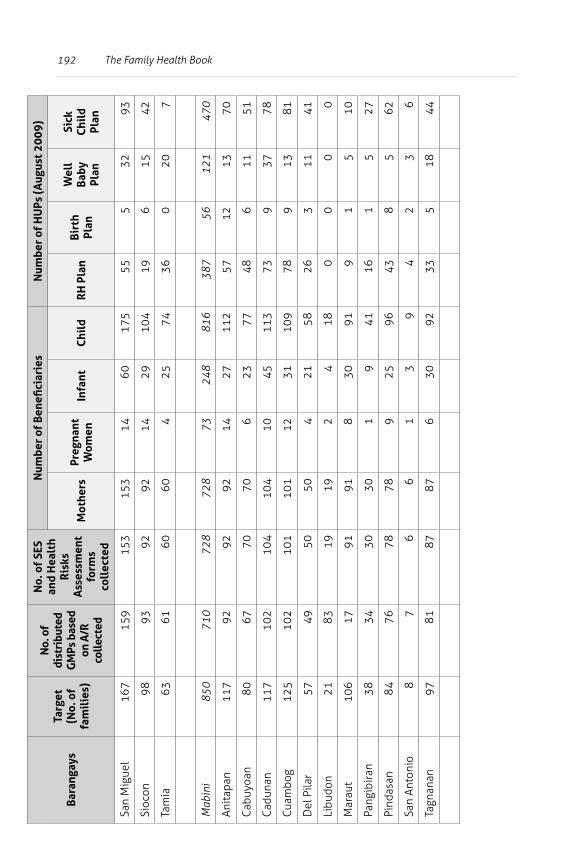
192 The Family Health BookBa
rang
ays
Targ
et
(No.
of
fam
ilie
s)
No.
of
dist
ribu
ted
GM
Ps b
ased
on
A/R
co
llect
ed
No.
of
SES
and
Hea
lth
Ris
ks
Ass
essm
ent
form
s co
llec
ted
Num
ber
of B
enefi
ciar
ies
Num
ber
of H
UPs
(Aug
ust 2
009)
Mot
hers
Preg
nant
W
omen
Infa
ntC
hild
RH
Pla
nBi
rth
Plan
Wel
l Ba
by
Plan
Sick
C
hild
Pl
an
San
Mig
uel
167
159
153
153
1460
175
555
3293
Sioc
on98
9392
9214
2910
419
615
42
Tam
ia63
6160
604
2574
360
207
Mab
ini
850
710
728
728
7324
881
638
756
121
470
Anit
apan
117
9292
9214
2711
257
1213
70
Cab
uyoa
n80
6770
706
2377
486
1151
Cad
unan
117
102
104
104
1045
113
739
3778
Cuam
bog
125
102
101
101
1231
109
789
1381
Del
Pila
r57
4950
504
2158
263
1141
Libu
don
2183
1919
24
180
00
0
Mar
aut
106
1791
918
3091
91
510
Pang
ibir
an38
3430
301
941
161
527
Pind
asan
8476
7878
925
9643
85
62
San
Anto
nio
87
66
13
94
23
6
Tagn
anan
9781
8787
630
9233
518
44
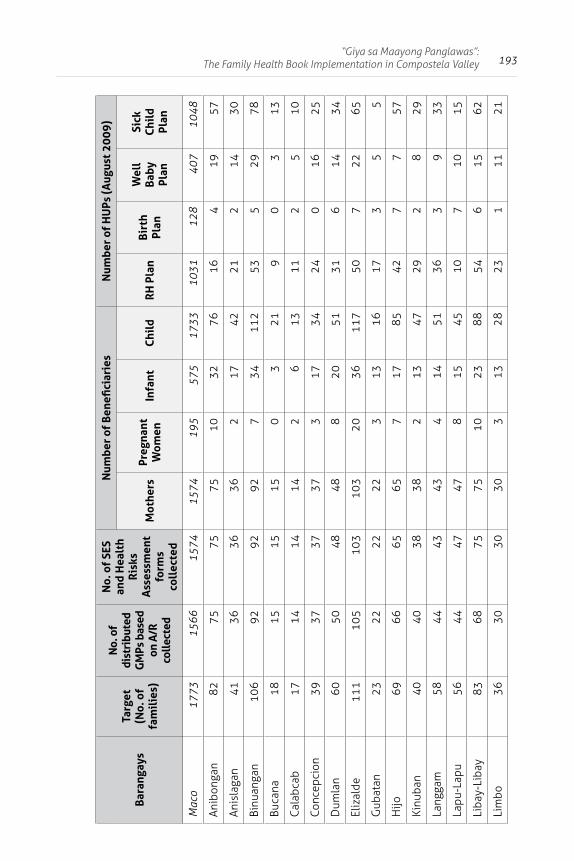
193“Giya sa Maayong Panglawas”:
The Family Health Book Implementation in Compostela Valley
Bara
ngay
sTa
rget
(N
o. o
f fa
mil
ies)
No.
of
dist
ribu
ted
GM
Ps b
ased
on
A/R
co
llect
ed
No.
of
SES
and
Hea
lth
Ris
ks
Ass
essm
ent
form
s co
llec
ted
Num
ber
of B
enefi
ciar
ies
Num
ber
of H
UPs
(Aug
ust 2
009)
Mot
hers
Preg
nant
W
omen
Infa
ntC
hild
RH
Pla
nBi
rth
Plan
Wel
l Ba
by
Plan
Sick
C
hild
Pl
an
Mac
o17
7315
6615
7415
7419
557
517
3310
3112
840
710
48
Anib
onga
n82
7575
7510
3276
164
1957
Anis
laga
n41
3636
362
1742
212
1430
Binu
anga
n10
692
9292
734
112
535
2978
Buca
na18
1515
150
321
90
313
Cal
abca
b17
1414
142
613
112
510
Conc
epci
on39
3737
373
1734
240
1625
Dum
lan
6050
4848
820
5131
614
34
Eliz
alde
111
105
103
103
2036
117
507
2265
Gub
atan
2322
2222
313
1617
35
5
Hijo
6966
6565
717
8542
77
57
Kinu
ban
4040
3838
213
4729
28
29
Lang
gam
5844
4343
414
5136
39
33
Lapu
-Lap
u56
4447
478
1545
107
1015
Liba
y-Li
bay
8368
7575
1023
8854
615
62
Lim
bo36
3030
303
1328
231
1121
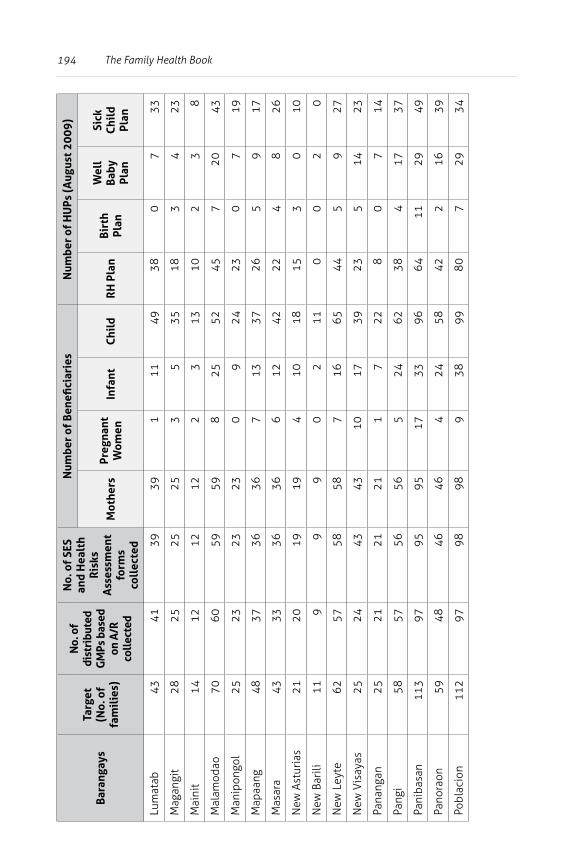
194 The Family Health Book
Bara
ngay
sTa
rget
(N
o. o
f fa
mil
ies)
No.
of
dist
ribu
ted
GM
Ps b
ased
on
A/R
co
llect
ed
No.
of
SES
and
Hea
lth
Ris
ks
Ass
essm
ent
form
s co
llec
ted
Num
ber
of B
enefi
ciar
ies
Num
ber
of H
UPs
(Aug
ust 2
009)
Mot
hers
Preg
nant
W
omen
Infa
ntC
hild
RH
Pla
nBi
rth
Plan
Wel
l Ba
by
Plan
Sick
C
hild
Pl
an
Lum
atab
4341
3939
111
4938
07
33
Mag
angi
t28
2525
253
535
183
423
Mai
nit
1412
1212
23
1310
23
8
Mal
amod
ao70
6059
598
2552
457
2043
Man
ipon
gol
2523
2323
09
2423
07
19
Map
aang
4837
3636
713
3726
59
17
Mas
ara
4333
3636
612
4222
48
26
New
Ast
uria
s21
2019
194
1018
153
010
New
Bar
ili11
99
90
211
00
20
New
Ley
te62
5758
587
1665
445
927
New
Vis
ayas
2524
4343
1017
3923
514
23
Pana
ngan
2521
2121
17
228
07
14
Pang
i58
5756
565
2462
384
1737
Pani
basa
n11
397
9595
1733
9664
1129
49
Pano
raon
5948
4646
424
5842
216
39
Pobl
acio
n11
297
9898
938
9980
729
34
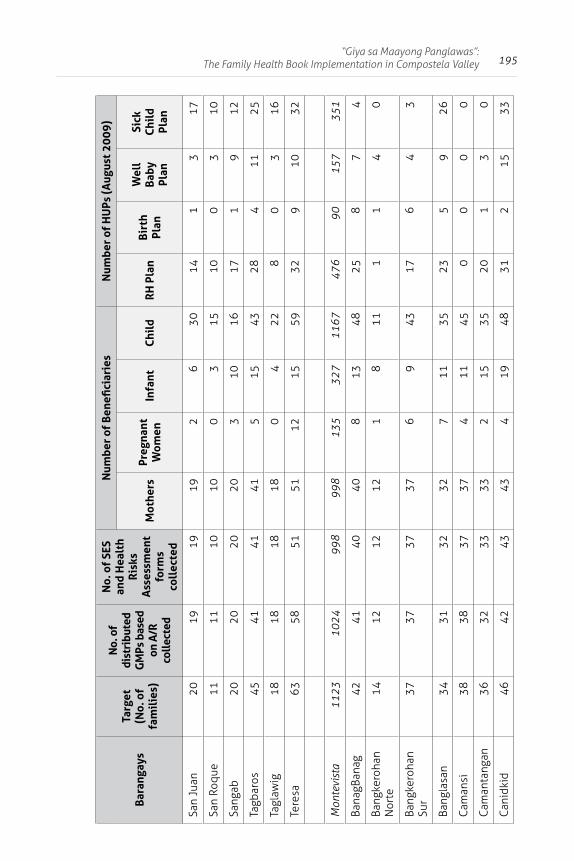
195“Giya sa Maayong Panglawas”:
The Family Health Book Implementation in Compostela Valley
Bara
ngay
sTa
rget
(N
o. o
f fa
mil
ies)
No.
of
dist
ribu
ted
GM
Ps b
ased
on
A/R
co
llect
ed
No.
of
SES
and
Hea
lth
Ris
ks
Ass
essm
ent
form
s co
llec
ted
Num
ber
of B
enefi
ciar
ies
Num
ber
of H
UPs
(Aug
ust 2
009)
Mot
hers
Preg
nant
W
omen
Infa
ntC
hild
RH
Pla
nBi
rth
Plan
Wel
l Ba
by
Plan
Sick
C
hild
Pl
an
San
Juan
2019
1919
26
3014
13
17
San
Roqu
e11
1110
100
315
100
310
Sang
ab20
2020
203
1016
171
912
Tagb
aros
4541
4141
515
4328
411
25
Tagl
awig
1818
1818
04
228
03
16
Tere
sa63
5851
5112
1559
329
1032
Mon
tevi
sta
1123
1024
998
998
135
327
1167
476
9015
735
1
Bana
gBan
ag42
4140
408
1348
258
74
Bang
kero
han
N
orte
1412
1212
18
111
14
0
Bang
kero
han
Sur
3737
3737
69
4317
64
3
Bang
lasa
n34
3132
327
1135
235
926
Cam
ansi
3838
3737
411
450
00
0
Cam
anta
ngan
3632
3333
215
3520
13
0
Can
idki
d46
4243
434
1948
312
1533
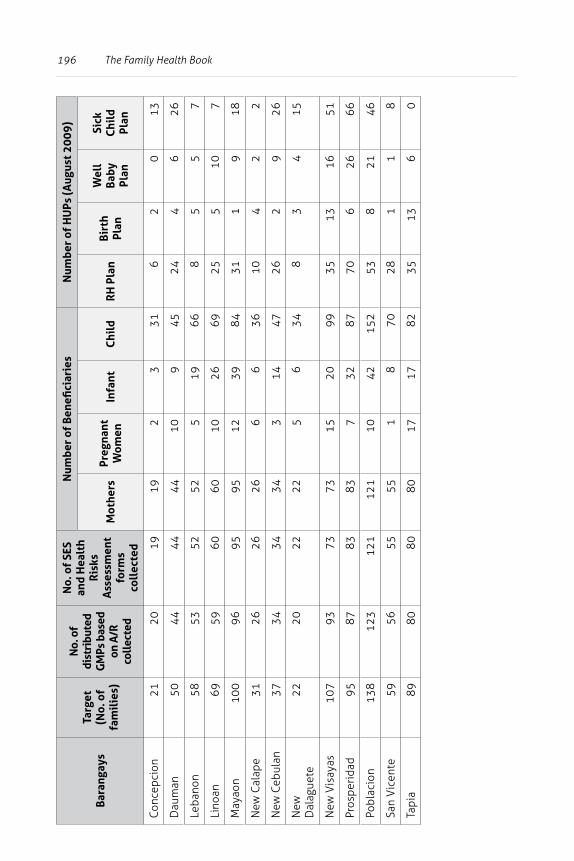
196 The Family Health Book
Bara
ngay
sTa
rget
(N
o. o
f fa
mil
ies)
No.
of
dist
ribu
ted
GM
Ps b
ased
on
A/R
co
llect
ed
No.
of
SES
and
Hea
lth
Ris
ks
Ass
essm
ent
form
s co
llec
ted
Num
ber
of B
enefi
ciar
ies
Num
ber
of H
UPs
(Aug
ust 2
009)
Mot
hers
Preg
nant
W
omen
Infa
ntC
hild
RH
Pla
nBi
rth
Plan
Wel
l Ba
by
Plan
Sick
C
hild
Pl
an
Conc
epci
on21
2019
192
331
62
013
Dau
man
5044
4444
109
4524
46
26
Leba
non
5853
5252
519
668
55
7
Lino
an69
5960
6010
2669
255
107
May
aon
100
9695
9512
3984
311
918
New
Cal
ape
3126
2626
66
3610
42
2
New
Ceb
ulan
3734
3434
314
4726
29
26
New
D
alag
uete
2220
2222
56
348
34
15
New
Vis
ayas
107
9373
7315
2099
3513
1651
Pros
peri
dad
9587
8383
732
8770
626
66
Pobl
acio
n13
812
312
112
110
4215
253
821
46
San
Vic
ente
5956
5555
18
7028
11
8
Tapi
a89
8080
8017
1782
3513
60
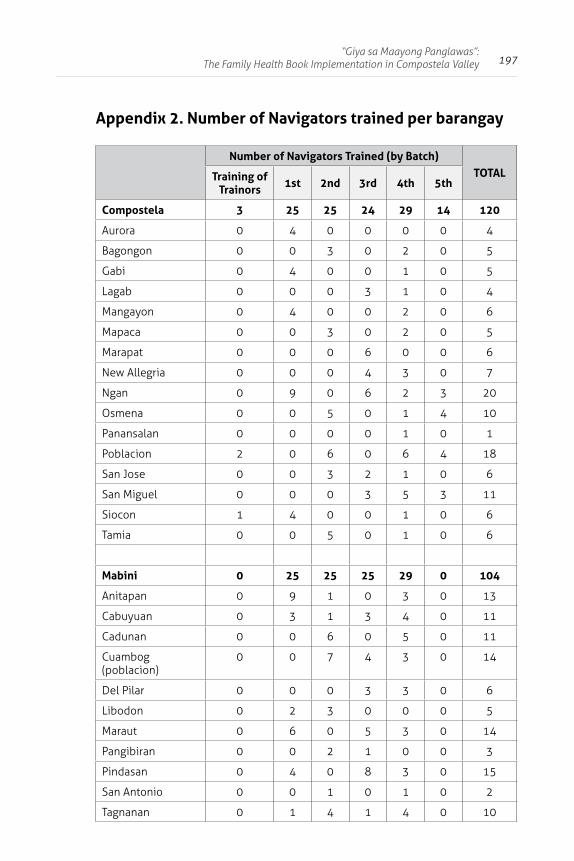
197“Giya sa Maayong Panglawas”:
The Family Health Book Implementation in Compostela Valley
Appendix 2. Number of Navigators trained per barangay
Number of Navigators Trained (by Batch)TOTALTraining of
Trainors 1st 2nd 3rd 4th 5th
Compostela 3 25 25 24 29 14 120
Aurora 0 4 0 0 0 0 4
Bagongon 0 0 3 0 2 0 5
Gabi 0 4 0 0 1 0 5
Lagab 0 0 0 3 1 0 4
Mangayon 0 4 0 0 2 0 6
Mapaca 0 0 3 0 2 0 5
Marapat 0 0 0 6 0 0 6
New Allegria 0 0 0 4 3 0 7
Ngan 0 9 0 6 2 3 20
Osmena 0 0 5 0 1 4 10
Panansalan 0 0 0 0 1 0 1
Poblacion 2 0 6 0 6 4 18
San Jose 0 0 3 2 1 0 6
San Miguel 0 0 0 3 5 3 11
Siocon 1 4 0 0 1 0 6
Tamia 0 0 5 0 1 0 6
Mabini 0 25 25 25 29 0 104
Anitapan 0 9 1 0 3 0 13
Cabuyuan 0 3 1 3 4 0 11
Cadunan 0 0 6 0 5 0 11
Cuambog (poblacion)
0 0 7 4 3 0 14
Del Pilar 0 0 0 3 3 0 6
Libodon 0 2 3 0 0 0 5
Maraut 0 6 0 5 3 0 14
Pangibiran 0 0 2 1 0 0 3
Pindasan 0 4 0 8 3 0 15
San Antonio 0 0 1 0 1 0 2
Tagnanan 0 1 4 1 4 0 10
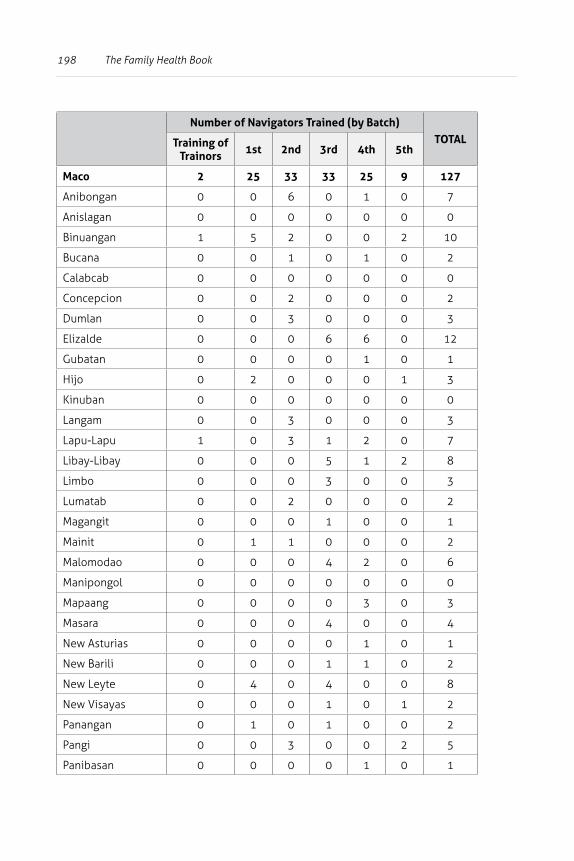
198 The Family Health Book
Number of Navigators Trained (by Batch)TOTALTraining of
Trainors 1st 2nd 3rd 4th 5th
Maco 2 25 33 33 25 9 127
Anibongan 0 0 6 0 1 0 7
Anislagan 0 0 0 0 0 0 0
Binuangan 1 5 2 0 0 2 10
Bucana 0 0 1 0 1 0 2
Calabcab 0 0 0 0 0 0 0
Concepcion 0 0 2 0 0 0 2
Dumlan 0 0 3 0 0 0 3
Elizalde 0 0 0 6 6 0 12
Gubatan 0 0 0 0 1 0 1
Hijo 0 2 0 0 0 1 3
Kinuban 0 0 0 0 0 0 0
Langam 0 0 3 0 0 0 3
Lapu-Lapu 1 0 3 1 2 0 7
Libay-Libay 0 0 0 5 1 2 8
Limbo 0 0 0 3 0 0 3
Lumatab 0 0 2 0 0 0 2
Magangit 0 0 0 1 0 0 1
Mainit 0 1 1 0 0 0 2
Malomodao 0 0 0 4 2 0 6
Manipongol 0 0 0 0 0 0 0
Mapaang 0 0 0 0 3 0 3
Masara 0 0 0 4 0 0 4
New Asturias 0 0 0 0 1 0 1
New Barili 0 0 0 1 1 0 2
New Leyte 0 4 0 4 0 0 8
New Visayas 0 0 0 1 0 1 2
Panangan 0 1 0 1 0 0 2
Pangi 0 0 3 0 0 2 5
Panibasan 0 0 0 0 1 0 1
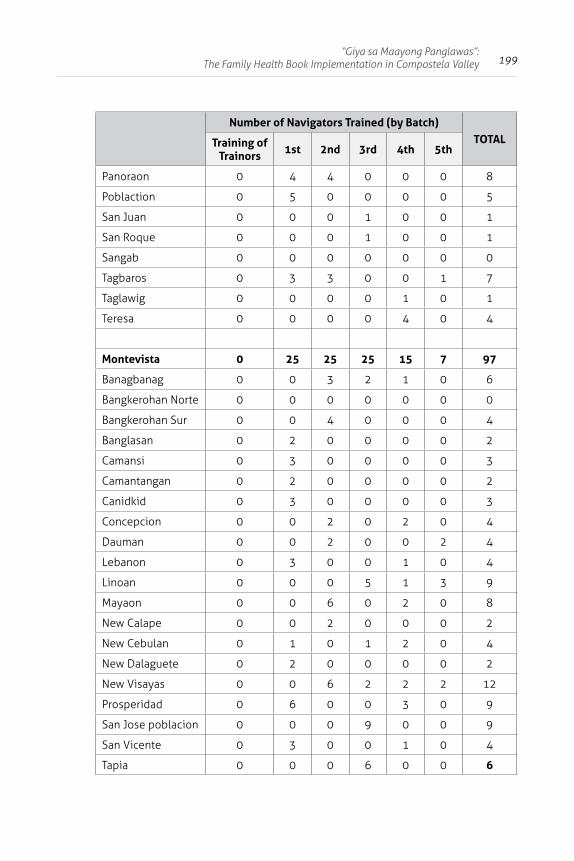
199“Giya sa Maayong Panglawas”:
The Family Health Book Implementation in Compostela Valley
Number of Navigators Trained (by Batch)TOTALTraining of
Trainors 1st 2nd 3rd 4th 5th
Panoraon 0 4 4 0 0 0 8
Poblaction 0 5 0 0 0 0 5
San Juan 0 0 0 1 0 0 1
San Roque 0 0 0 1 0 0 1
Sangab 0 0 0 0 0 0 0
Tagbaros 0 3 3 0 0 1 7
Taglawig 0 0 0 0 1 0 1
Teresa 0 0 0 0 4 0 4
Montevista 0 25 25 25 15 7 97
Banagbanag 0 0 3 2 1 0 6
Bangkerohan Norte 0 0 0 0 0 0 0
Bangkerohan Sur 0 0 4 0 0 0 4
Banglasan 0 2 0 0 0 0 2
Camansi 0 3 0 0 0 0 3
Camantangan 0 2 0 0 0 0 2
Canidkid 0 3 0 0 0 0 3
Concepcion 0 0 2 0 2 0 4
Dauman 0 0 2 0 0 2 4
Lebanon 0 3 0 0 1 0 4
Linoan 0 0 0 5 1 3 9
Mayaon 0 0 6 0 2 0 8
New Calape 0 0 2 0 0 0 2
New Cebulan 0 1 0 1 2 0 4
New Dalaguete 0 2 0 0 0 0 2
New Visayas 0 0 6 2 2 2 12
Prosperidad 0 6 0 0 3 0 9
San Jose poblacion 0 0 0 9 0 0 9
San Vicente 0 3 0 0 1 0 4
Tapia 0 0 0 6 0 0 6
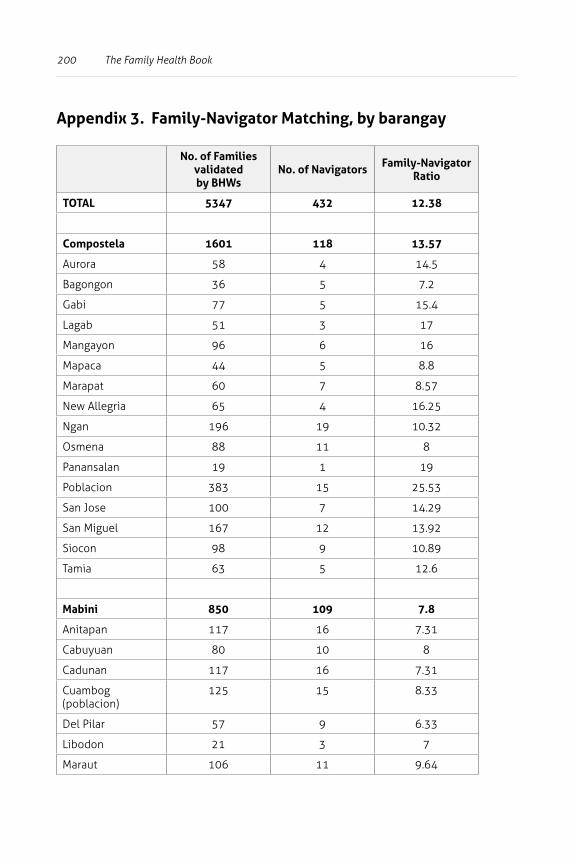
200 The Family Health Book
Appendix 3. Family-Navigator Matching, by barangay
No. of Families validated by BHWs
No. of Navigators Family-Navigator Ratio
TOTAL 5347 432 12.38
Compostela 1601 118 13.57
Aurora 58 4 14.5
Bagongon 36 5 7.2
Gabi 77 5 15.4
Lagab 51 3 17
Mangayon 96 6 16
Mapaca 44 5 8.8
Marapat 60 7 8.57
New Allegria 65 4 16.25
Ngan 196 19 10.32
Osmena 88 11 8
Panansalan 19 1 19
Poblacion 383 15 25.53
San Jose 100 7 14.29
San Miguel 167 12 13.92
Siocon 98 9 10.89
Tamia 63 5 12.6
Mabini 850 109 7.8
Anitapan 117 16 7.31
Cabuyuan 80 10 8
Cadunan 117 16 7.31
Cuambog (poblacion)
125 15 8.33
Del Pilar 57 9 6.33
Libodon 21 3 7
Maraut 106 11 9.64
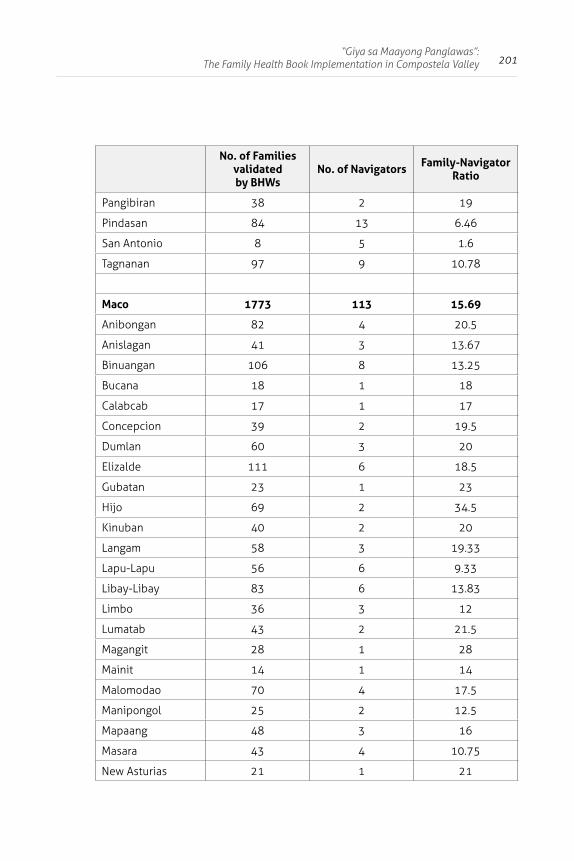
201“Giya sa Maayong Panglawas”:
The Family Health Book Implementation in Compostela Valley
No. of Families validated by BHWs
No. of Navigators Family-Navigator Ratio
Pangibiran 38 2 19
Pindasan 84 13 6.46
San Antonio 8 5 1.6
Tagnanan 97 9 10.78
Maco 1773 113 15.69
Anibongan 82 4 20.5
Anislagan 41 3 13.67
Binuangan 106 8 13.25
Bucana 18 1 18
Calabcab 17 1 17
Concepcion 39 2 19.5
Dumlan 60 3 20
Elizalde 111 6 18.5
Gubatan 23 1 23
Hijo 69 2 34.5
Kinuban 40 2 20
Langam 58 3 19.33
Lapu-Lapu 56 6 9.33
Libay-Libay 83 6 13.83
Limbo 36 3 12
Lumatab 43 2 21.5
Magangit 28 1 28
Mainit 14 1 14
Malomodao 70 4 17.5
Manipongol 25 2 12.5
Mapaang 48 3 16
Masara 43 4 10.75
New Asturias 21 1 21
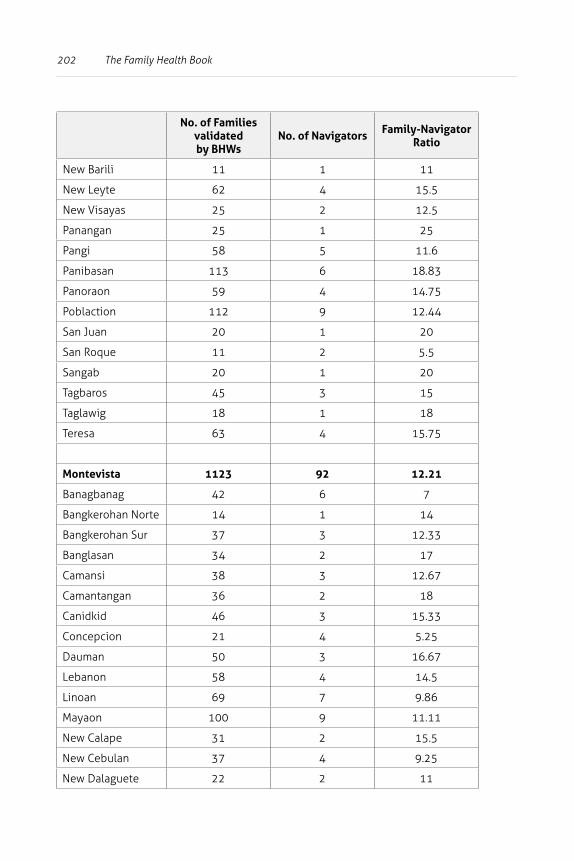
202 The Family Health Book
No. of Families validated by BHWs
No. of Navigators Family-Navigator Ratio
New Barili 11 1 11
New Leyte 62 4 15.5
New Visayas 25 2 12.5
Panangan 25 1 25
Pangi 58 5 11.6
Panibasan 113 6 18.83
Panoraon 59 4 14.75
Poblaction 112 9 12.44
San Juan 20 1 20
San Roque 11 2 5.5
Sangab 20 1 20
Tagbaros 45 3 15
Taglawig 18 1 18
Teresa 63 4 15.75
Montevista 1123 92 12.21
Banagbanag 42 6 7
Bangkerohan Norte 14 1 14
Bangkerohan Sur 37 3 12.33
Banglasan 34 2 17
Camansi 38 3 12.67
Camantangan 36 2 18
Canidkid 46 3 15.33
Concepcion 21 4 5.25
Dauman 50 3 16.67
Lebanon 58 4 14.5
Linoan 69 7 9.86
Mayaon 100 9 11.11
New Calape 31 2 15.5
New Cebulan 37 4 9.25
New Dalaguete 22 2 11
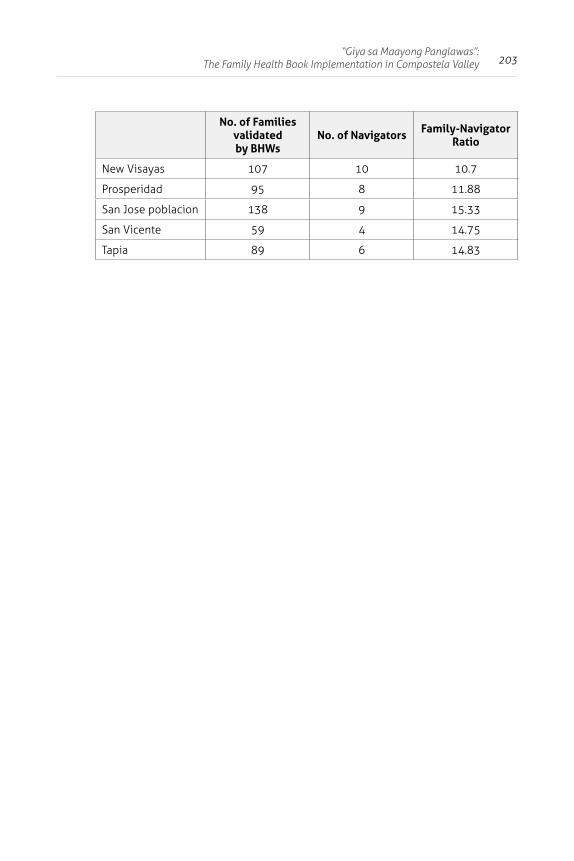
203“Giya sa Maayong Panglawas”:
The Family Health Book Implementation in Compostela Valley
No. of Families validated by BHWs
No. of Navigators Family-Navigator Ratio
New Visayas 107 10 10.7
Prosperidad 95 8 11.88
San Jose poblacion 138 9 15.33
San Vicente 59 4 14.75
Tapia 89 6 14.83
204
3 An Analysis of the Impacts of the Family Health Book Interventions
Jhiedon L. Florentino, Aleli D. Kraft, Julio M. Galvez, and Orville Solon
Abstract
This paper presents evidence from the Family Health Book (FHB) operations research on the impact of the FHB interventions on:
1) modern family planning (MFP), 2) antenatal care (ANC) by pregnant women; 3) skilled birth attendance (SBA) at home or in a facility; and 4) immunization (as determined by the number of fully-
immunized children, or FIC).
The FHB families’ use of these services is compared with that of similar families at baseline, using combined data from the FHB Baseline Survey and those collected from the FHB families as part of the operations research monitoring activities.
FHB interventions are represented by variables that indicate whether the families:
1) were given critical information through a “Book” and assigned to trained community health workers called “Navigators”;
2) developed appropriate health use plans (HUPs) for their health needs and risks; and
3) were recipients of outreach services.
205An Analysis of the Impacts of the Family Health Book Interventions
Multivariate techniques were used, and socio-economic, location, and supply side characteristics were controlled in estimating the impacts.
One year after the distribution of the Book and assignment of Navigators, improvements were noted in the utilization of MFP, SBA, and ANC services. Provision of key information through the Book and Navigator resulted in improvements in MFP and SBA service utilization. These improvements were amplified by the development of HUPs. In the case of ANC, the impacts emerged only after the development of appropriate HUPs in response to the information provision. No additional impacts were seen in the FIC when HUPs were developed.
The measured improvements in the utilization of key maternal, neonatal, and child health and nutrition (MNCHN) services are consistent with field observations of both clients and health workers from the municipalities where the FHB OR was implemented. These results also validate findings in the international literature on the effectiveness of “patient” Navigators in assisting families for both MNCHN and non-MNCHN concerns.
The results imply that providing key information through a physical medium, supported by personalized guidance and assistance from Navigators that eventually result in families developing plans to address their health risks, are effective in addressing information barriers to utilization of key MNCHN services.
Introduction
From 2008 to 2010, the HPDP conducted the FHB operations research in the province of Compostela Valley. This operations research sought to establish evidence on the impacts of the FHB integrated package of interventions that aimed at increasing the utilization of critical family planning, maternal, neonatal, and child health care services.
The framework, design and interventions of the FHB are described in the operations research document (see Chapter 1). This paper describes the data and methods used to estimate the impacts
206 The Family Health Book
and analyzes results of the FHB’s impact on critical intermediate outcomes of interest. It also discusses observations from the field that explain the results, as well as issues that may impact on future implementation.
Specifically, the FHB interventions’ impact on the utilization of the following services and commodities are evaluated:
• modern family planning (MFP);• antenatal care (ANC) by pregnant women;• skilled birth attendance at home or in a facility (SBA); and • immunization (as determined by the number of fully-
immunized children, or FIC).
The use of these services by FHB families is compared with that of similar families at baseline using the combined data from the FHB Baseline Survey and data collected from FHB families as part of the operations research monitoring activities. The latter includes data from forms accomplished in the course of the family and FHB Navigator interactions which form part of the FHB interventions, and special tallies used for mid-term assessment and monitoring.
FHB interventions are represented by variables that indicate whether the families:
1) were given critical information through a “Book” and assigned to trained community health workers called “Navigators”;
2) developed appropriate health use plans (HUPs) for their health needs and risks; and
3) were recipients of outreach services.
Multivariate techniques were used, and socio-economic, location, and supply side characteristics were controlled in estimating the impacts.
A year after the distribution of the Book and assignment of Navigators, improvements were noted in the utilization of MFP, SBA, and ANC services. Providing families with Books and assigning them to Navigators improved the likelihood of pregnant mothers delivering in a facility (with a skilled birth attendant) by more than 15 percentage points. If the families developed
207An Analysis of the Impacts of the Family Health Book Interventions
health use plans, there was a 35 percentage-point increase in the likelihood of delivering in a facility. Mothers in families which had Books and Navigators and also developed HUPs had increased likelihood by more than 25 percentage points of using a modern FP method. Receiving a Book, being assigned to Navigators, and developing a birth plan increased the likelihood of having at least one ANC visit by 10 percentage points. Families provided with information through the Books and Navigators increased FIC by 35 percentage points.
The paper also discusses issues related to the FHB operation, and insights from the Navigators, midwives, MHOs, and families to explain improvements seen in SBA and MFP use. Selected experiences from the field, such as dealing with mobile families and identification of beneficiaries, are also examined.
Section II reviews FHB interventions and study sites. Section III follows with a review of analysis methods, data and models. Section IV presents detailed results for MFP, ANC, SBA, and FIC. Section V discusses the study in the context of field operations and observations. Section VI presents the study’s conclusions.
Operations Research Setting
Study site and population
The FHB operations research was conducted in Compostela Valley from 2008 to 2010. Compostela Valley was chosen because of its high rates of maternal and infant mortality, and its low rates for contraceptive prevalence (CPR), antenatal care (ANC), skilled birth attendance (SBA), and fully-immunized children (FIC) despite the presence of basic service delivery infrastructures.
The municipalities of Compostela, Mabini, Maco, and Montevista were further chosen on the basis of high maternal and infant mortality rates and low utilization rates of health services. All the 81 barangays in these municipalities were included in the operations research.
208 The Family Health Book
Based on the FHB Baseline Survey results, families which would benefit most from the FHB interventions as they had the lowest rates of use of critical maternal and child health care services were those with mothers who did not finish high school education and were:
• pregnant; • below 25 with at least one child below
five years old; or• aged 26 and above, with at least two
children below five years old.
Some 6,940 potential FHB families met the initial screening. Community health workers validated the initial list and reduced the number to 5,361.
From this validated list, only some 4,730 were given Books and assigned to Navigators due to the very high mobility of target families. Some permanently transferred residence to non-FHB areas even before the distribution of the Books.
Interventions, sites, and timelines
All of the families in the four municipalities satisfying the eligibility criteria were provided with a “Book” and assigned to a “Navigator.”
The Book contains critical health information and health messages that prompt specific actions depending on the needs of the families. Health messages include modern family planning methods, discussion of the importance of prenatal care, danger signs during and after delivery, the need for skilled birth attendance during deliveries, and prevention of common child illnesses.
209An Analysis of the Impacts of the Family Health Book Interventions
Other information presented in the Book are:
1) the list of providers and services given;
2) information on PhilHealth, the country’s national health insurance program; and
3) contact information of persons who operate or deploy vehicles in cases of health emergencies.
To guide the families in understanding the Book, community health workers were recruited and trained as “Navigators.” Navigators were selected from the ranks of community health workers and volunteers who satisfied the following criteria:
1) with at least two years of health-related activities in the community;
2) able to work with local officials;
3) finished at least two years of high school education or had at least elementary education, but with at least two years of health-related experience;
4) able and willing to regularly visit assigned households;
5) with good inter-personal communication skills and highly motivated; and
6) respected in the community.
210 The Family Health Book
The community workers’ training for their navigational functions with FHB families involved the following components:
1) an overview of the over-all health situation in the province;
2) the FHB Initiative and its components;
3) family planning and maternal and child health concepts ;
4) PhilHealth benefit entitlements and claim procedures;
5) instructions on their key roles, such as health risk assessment, formulation of HUPs, and accomplishment of various FHB forms; and
6) modules on communication and relational skills.
The trained Navigators were matched with the FHB families, and on average, assigned to handle around 10 to 12 families. This was less than the originally-planned 20 families per Navigator.
The Navigators assisted the families in determining their health risks and needs. They also guided them, together with health providers, in developing their HUPs.
HUPs contain the list and schedule of identified commodities and services which families require for their health concerns. They also identify the provider of these services and where these may be accessed. The HUPs also serve as a basis for Navigators to remind families and monitor their utilization of critical MNCHN services.
211An Analysis of the Impacts of the Family Health Book Interventions
The FHB has five separate HUPs:
1) a Reproductive Health (RH) Plan for reproductive health and family planning needs;
2) a Birth Plan (BP) for antenatal care and delivery;
3) a Well-Baby plan (WBP) for immunization and other services for infants;
4) a Sick Child Plan (SCP) for consults and services for children 2 to 5 years old; and
5) an Emergency Plan (EP) that lists health emergency contacts.
The second FHB intervention sought to organize and conduct outreach services to address the health needs of families in far-flung areas. Unlike typical community outreach activities, FHB outreach services were regularly scheduled, targeted far-flung areas, and were based on identified health services and commodities in the HUPs of families in targeted barangays.
The targeted barangays were identified based on:
1) length of travel time to nearest rural health unit or health provider;
2) number of potential beneficiaries; and 3) accessibility to common transport.
The barangays of Banglasan, Mayaon, and San Vicente were selected based on the criteria while intervention was randomly assigned to Montevista. At least four rounds of outreach services were conducted during the FHB initiative (August 2009- March 2010).
212 The Family Health Book
The last FHB intervention sought to establish a functional health emergency communication and transport network that would actively coordinate with providers, transport groups and the private sector for availability of funding- and logistically-supported emergency transport 24 hours a day, 7 days a week.
The municipality of Compostela was randomly chosen to receive this intervention. After a baseline assessment of its capacity to respond to emergency cases, and consultation with the province’s and town’s health officers, a new round of meetings were held to design the protocol and to draft the Memorandum of Agreement between the province and Compostela for funding support to the network.
Eventually, the health emergency network operations were integrated into the municipality’s network for general emergencies (see Appendix 1 for the timing of the interventions).
Methods
Data To analyze the impacts of the FHB interventions, information from two main sources was merged -- the FHB Baseline Survey conducted as part of the design phase of the operations research, and the forms accomplished during family-Navigator interactions and during monitoring of FHB implementation activities.
213An Analysis of the Impacts of the Family Health Book Interventions
The latter source included:
• special tallies for monitoring the conduct of FHB activities and for the mid-year assessment of the FHB implementation;
• FHB forms used by the Navigators; and • collected and encoded HUPs.
The FHB Baseline Survey data represented pre-intervention scenarios while FHB forms and tallies from the field were used to gather information on post-intervention utilization of critical MNCHN services of recipient families.
The FHB baseline surveys consisted of household, facility, physician, midwife, and patient exit surveys that sought to provide baseline information on the health utilization and health-seeking behavior of Compostela Valley residents, as well as the status of Compostela Valley providers. The surveys, conducted from December 2007 to around March 2008, covered all the municipalities of the province.
Sample barangays were randomly selected and families with either a pregnant woman or a child below 12 months of age were sampled. Families eligible for the survey were further limited to those whose primary decision maker was either the husband of the pregnant woman or the father of the infant, or the spouse.
From the 2,021 sampled households in all the municipalities, only those from the four FHB municipalities were included; and from these families, only those that met the FHB eligibility criteria. This yielded a total of 402 households from the baseline survey, with 114 from Compostela, 76 from Mabini, 139 from Maco, and 73 from Montevista.
214 The Family Health Book
From May 2009 to September 2010, the FHB operations research conducted various data collection and monitoring activities. The effort was a collaboration between HPDP, the Navigators, midwives, and the provincial government (refer to Appendix 2 on data collection efforts).
Data on the socio-economic status (SES) of the families and Navigators were collected at about the same time the Books were distributed to the families in May 2009. Afterwards, Navigators simultaneously or in the next visit conducted health risk assessment for the families.
HPDP encoded data from the submitted accomplished HRA forms. These forms also provided information on the families’ previous use of MNCHN services and some indicators of the health risks they faced. However, resource constraints impeded collection of subsequent health risk assessment forms accomplished in the wake of changing family circumstances (delivery of children and new pregnancies, etc.).
The mobility of families and members became apparent during the collection of the HRA and SES. Families identified as mobile -- initial feedback from the field -- were still included in the list of families for subsequent data collection.
Data on utilization during the FHB OR were collected from three sources:
1) the monitoring forms used by the Navigators;
2) forms and tallies from HPDP monitoring activities; and
3) the HUPs kept by the families.
215An Analysis of the Impacts of the Family Health Book Interventions
Since the families retained the HUPs to remind them of scheduled utilization of services and commodities, Navigators’ monitoring forms were the initial data sources for the midterm monitoring of utilization patterns. The Navigators recorded and summarized in the Family Call Sheet (FCS) the scheduled and actual use of services indicated in the HUPs. HPDP began collecting and encoding data from FCS in December 2010. This provided information on the use of services from the start of Book distribution to the date of the collection.
In September 2009, HPDP inventoried the health use plans during the post-training assessment of Navigators. Relying heavily on Navigator reports validated by MHOs and nurses, HPDP complied a list of individuals who assisted (and where the assistance was done) in the delivery of those pregnant at the time of the FH Book distribution.
HPDP made another tally of health use plans -- supplemented by Navigator reports -- in the second quarter of 2010 to check whether FHB mothers who got pregnant after the Book distribution received visits and had health use plans, and whether infants born of mothers who were pregnant as of the book distribution had well-baby plans. HPDP also gathered information on utilization of modern family planning methods.
A year after the Book distribution and assignment of Navigators, a team of editors and encoders recorded all information found in the HUPs. The team obtained additional information on utilization (not required to be listed in the HUPs, such as the name of the actual birth attendant, place of delivery of FHB
216 The Family Health Book
mothers, dates of visits by the FHB families to facilities for services not reflected in the HUPs) from the families and the Navigators. Records, like target client lists for family planning services, in facilities visited by FHB familiies also provided utilization data. But data from these sources cannot be verified.
Data from the FHB Baseline Survey and the FHB monitoring forms did not allow for adequate assessment of the functional health emergency and communication network’s impacts. The FHB Baseline Survey made no inquiries on the use of emergency transport services during cases of illness, nor did FHB monitoring forms indicate the mode of transport used for emergency cases. With the use of emergency transport and communication services not limited to FHB families, a household survey would have been the better vehicle to assess whether FHB and non-FHB families benefited from this intervention.
Models and variables
To determine the impact of FHB interventions, FHB families’ utilization of services was compared with those of non-FHB families in similar situations at baseline. Regression models were estimated to determine the contribution of key FHB interventions on MFP use, antenatal care visits of pregnant women, delivery by skilled birth attendants at home and in facilities, and full immunization of children, controlling for family, Navigator, and area characteristics.
217An Analysis of the Impacts of the Family Health Book Interventions
The general form of the model used is:
Ui = α + φBi + κCi + λDi + θEi+ F’iυ + G’iπ + ϵi
where Ui is the utilization of services/commodity by individual family member i.
To represent the FHB interventions, the following variables were used:
Bi -- dummy variable denoting whether individual i belonged to a family which received the FHB Book and was assigned to a Navigator;
Ci -- dummy variable denoting whether the individual’s family was provided a Book, assigned to a Navigator, and developed an HUP applicable to the service/commodity as indicated by a specified health goal in the HUP3;
Di -- dummy variable denoting whether the individual’s family was provided a Book, assigned to a Navigator, and resided in an area targeted for FHB outreach services; and
Ei -- a dummy variable denoting whether the individual’s family was provided a Book, assigned to a Navigator, resided in an area targeted for outreach services, and developed the applicable HUP.
4
4 Having a health goal indicates that the family actually developed or filled out HUP forms.
218 The Family Health Book
The different coefficients capture the following information:
Coefficient B -- captures the impact of the information provided by the Book and the Navigator;
Coefficient C -- captures the impact of families developing appropriate HUPs in response to information provided by the Book and the Navigator;
Coefficient D -- captures the combined impact of having a Book and the Navigator and being in an area where FHB outreach services were conducted; and
Coefficient E -- captures the combined impact of families having Books and Navigators, developing their HUPs, and living in an area where outreach services were conducted.
The impacts of the HUP and the FHB outreach activities were always combined with the basic intervention of information provision through the Book and the Navigator.
In estimating these impacts, the effects of family characteristics (such as mother’s age, father or mother’s educational attainment, income, and PhilHealth membership status on utilization of services), F’, was controlled. These effects are captured by v.
219An Analysis of the Impacts of the Family Health Book Interventions
The vector G’ is composed of municipality dummies and the distance from the individual’s barangay residence to the municipality’s poblacion. These site characteristics are included to capture the effects of unobserved supply-side variables that may influence differences in utilization.
To capture modern FP use, a variable was constructed that took on a value of “1” in the tally of HUPs if the Navigator indicated that the mother was using modern FP or if there were records of modern FP utilization (e.g., restocking of pills, condoms) from the FCS and the encoded RH Plan. If not , the variable took on a “0” value.
For FHB baseline sample mothers, modern FP use took on a value of “1” based on the response to the questions on family planning methods used. Because there could be differences in the accuracy of FP utilization data from the various sources, another variable was added to control for the source of data, especially for the presence of the HUP.
In addition, previous use of FP by FHB mothers was also controlled by using a variable that took on a value of “1” if the mother had indicated modern FP use in the HRA. Unfortunately, previous FP use for the baseline sample could not be controlled, so the reference category for this dummy was FHB mothers without previous use and all sample mothers at baseline.

220 The Family Health Book
As family planning services were also provided during outreach services, variables that indicated whether the families resided in target outreach barangays were included. A logit regression model was used to estimate the impacts on the sample of FHB non-pregnant mothers and comparable non-pregnant mothers from the baseline.
For antenatal care visits, a variable was assigned a value of “1” if a mother had indicated at least one antenatal care visit for the current pregnancy (if currently pregnant) or for the last pregnancy (if non-pregnant) from the FHB Baseline Survey, or if there was at least one antenatal care visit recorded in the HRA or at least one antenatal care visit recorded in the birth plan.
An indicator of residence in outreach barangays was also included since antenatal care visits were also provided in such outreach activities. A logit regression model was used to estimate the impacts on the sample of mothers who were currently pregnant during the distribution of the Books or became pregnant in the course of the FHB intervention.
To capture place and attendant during delivery, a variable was constructed to indicate whether the pregnant mother had been assisted by a traditional birth attendant and delivered at home, assisted by a skilled birth attendant and delivered at home, or assisted by a skilled birth attendant and delivered in a health facility.
221An Analysis of the Impacts of the Family Health Book Interventions
For the baseline sample, the questions on birth attendance referred to the last birth. For the FHB sample, the names of the attendants and place of delivery were obtained from pregnant mothers who had already delivered by the time of the HUP encoding.
This consisted of mothers who were initially pregnant during the health risk assessment and mothers who became pregnant in the course of the FHB intervention. Midwives and Navigators validated the information on birth attendance and location. A multinomial logit regression model was estimated.
To determine whether infants and young children received all the basic immunizations, immunization records received before the health risk assessment for infants and those obtained from family call sheets, and the encoded HUPs were used.
Those infants who had already reached one year old and expected to have completed the immunizations were included in the sample. From baseline families, children who were at least nine months old and those whose immunization status were obtained from vaccination cards were included. An indicator of residence in target outreach areas was likewise included. A logit regression model was estimated.
222 The Family Health Book
Results
Modern FP Use
Only 23% of families comparable with those of the FHB were found to be users of any modern FP method (Table 3.1).
Mothers aged 18 years old or below accounted for 15% of baseline mothers, while FHB mothers in that age group only accounted for 2% of all the FHB mothers.
Mothers aged 35 years or above accounted for 12% of baseline mothers, while FHB mothers in that age group was 9% of all FHB mothers.
Baseline families had a slightly higher number of children under five years old; however, this might be due to the baseline survey’s sampling criteria. For both baseline and the FHB families, roughly 50% of fathers reached elementary level. FHB families were also poorer compared to the baseline. More than half of the number of FHB families had monthly incomes lower than PhP 3,000.
In comparing the groups, two regression models were used: one controlled for whether the FHB mother was already a modern FP user prior to the intervention; the other did not, although a non-FHB mother could not be tagged if she was a previous user of modern FP prior to the baseline interview. Since utilization of modern FP for the FHB mothers came from various data collection sources in the course of the operation of the FHB, data source was also controlled for when determining the impact of the intervention.
For both regression runs, more than 70% of mothers were found to be non-users of modern FP methods at baseline (see Table 3.2 for the marginal effects and refer to Appendix 3 for the estimated logit equation).
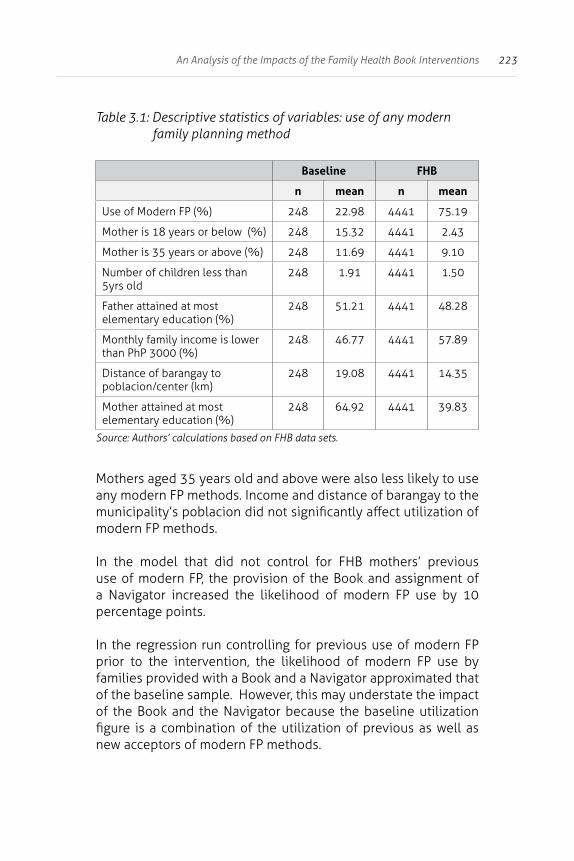
223An Analysis of the Impacts of the Family Health Book Interventions
Table 3.1: Descriptive statistics of variables: use of any modern family planning method
Baseline FHB
n mean n mean
Use of Modern FP (%) 248 22.98 4441 75.19
Mother is 18 years or below (%) 248 15.32 4441 2.43
Mother is 35 years or above (%) 248 11.69 4441 9.10
Number of children less than 5yrs old
248 1.91 4441 1.50
Father attained at most elementary education (%)
248 51.21 4441 48.28
Monthly family income is lower than PhP 3000 (%)
248 46.77 4441 57.89
Distance of barangay to poblacion/center (km)
248 19.08 4441 14.35
Mother attained at most elementary education (%)
248 64.92 4441 39.83
Source: Authors’ calculations based on FHB data sets.
Mothers aged 35 years old and above were also less likely to use any modern FP methods. Income and distance of barangay to the municipality’s poblacion did not significantly affect utilization of modern FP methods.
In the model that did not control for FHB mothers’ previous use of modern FP, the provision of the Book and assignment of a Navigator increased the likelihood of modern FP use by 10 percentage points.
In the regression run controlling for previous use of modern FP prior to the intervention, the likelihood of modern FP use by families provided with a Book and a Navigator approximated that of the baseline sample. However, this may understate the impact of the Book and the Navigator because the baseline utilization figure is a combination of the utilization of previous as well as new acceptors of modern FP methods.
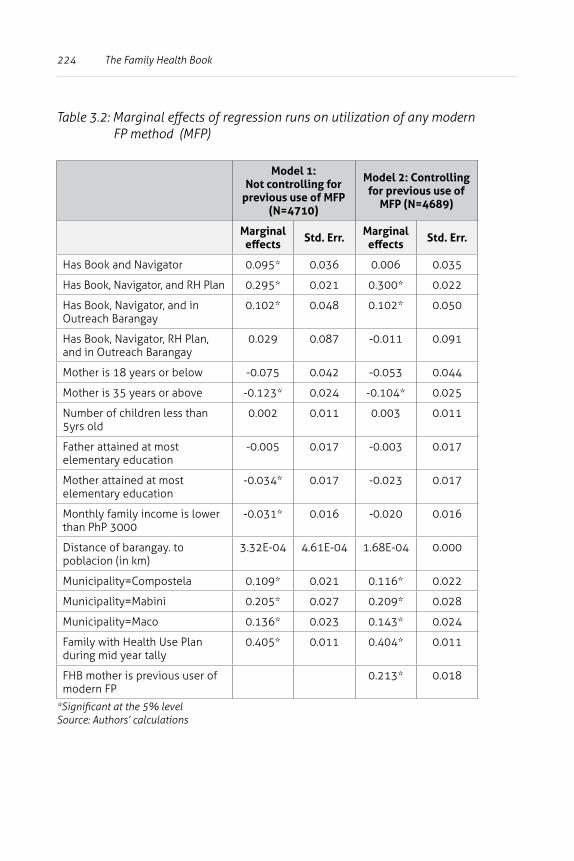
224 The Family Health Book
Table 3.2: Marginal effects of regression runs on utilization of any modern FP method (MFP)
Model 1: Not controlling for
previous use of MFP (N=4710)
Model 2: Controlling for previous use of
MFP (N=4689)
Marginal effects Std. Err. Marginal
effects Std. Err.
Has Book and Navigator 0.095* 0.036 0.006 0.035
Has Book, Navigator, and RH Plan 0.295* 0.021 0.300* 0.022
Has Book, Navigator, and in Outreach Barangay
0.102* 0.048 0.102* 0.050
Has Book, Navigator, RH Plan, and in Outreach Barangay
0.029 0.087 -0.011 0.091
Mother is 18 years or below -0.075 0.042 -0.053 0.044
Mother is 35 years or above -0.123* 0.024 -0.104* 0.025
Number of children less than 5yrs old
0.002 0.011 0.003 0.011
Father attained at most elementary education
-0.005 0.017 -0.003 0.017
Mother attained at most elementary education
-0.034* 0.017 -0.023 0.017
Monthly family income is lower than PhP 3000
-0.031* 0.016 -0.020 0.016
Distance of barangay. to poblacion (in km)
3.32E-04 4.61E-04 1.68E-04 0.000
Municipality=Compostela 0.109* 0.021 0.116* 0.022
Municipality=Mabini 0.205* 0.027 0.209* 0.028
Municipality=Maco 0.136* 0.023 0.143* 0.024
Family with Health Use Plan during mid year tally
0.405* 0.011 0.404* 0.011
FHB mother is previous user of modern FP
0.213* 0.018
*Significant at the 5% levelSource: Authors’ calculations
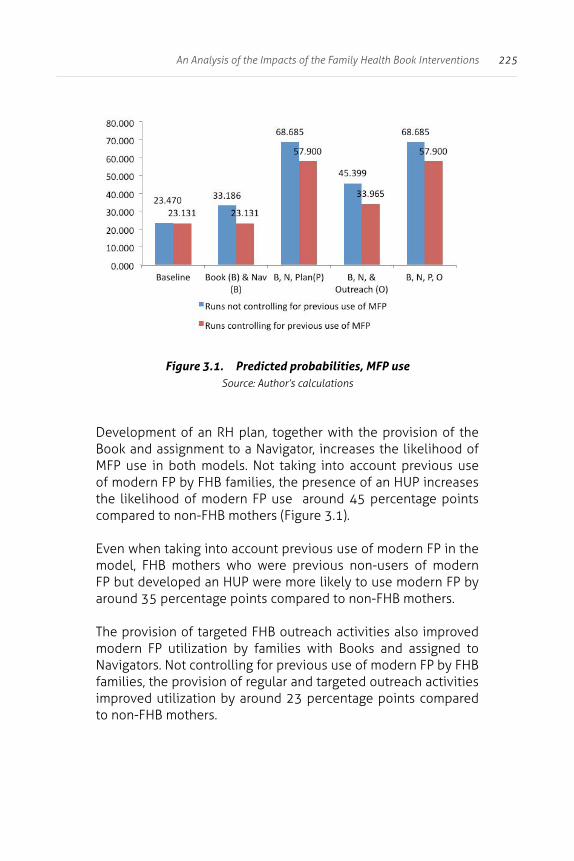
225An Analysis of the Impacts of the Family Health Book Interventions
Figure 3.1. Predicted probabilities, MFP useSource: Author’s calculations
Development of an RH plan, together with the provision of the Book and assignment to a Navigator, increases the likelihood of MFP use in both models. Not taking into account previous use of modern FP by FHB families, the presence of an HUP increases the likelihood of modern FP use around 45 percentage points compared to non-FHB mothers (Figure 3.1).
Even when taking into account previous use of modern FP in the model, FHB mothers who were previous non-users of modern FP but developed an HUP were more likely to use modern FP by around 35 percentage points compared to non-FHB mothers.
The provision of targeted FHB outreach activities also improved modern FP utilization by families with Books and assigned to Navigators. Not controlling for previous use of modern FP by FHB families, the provision of regular and targeted outreach activities improved utilization by around 23 percentage points compared to non-FHB mothers.
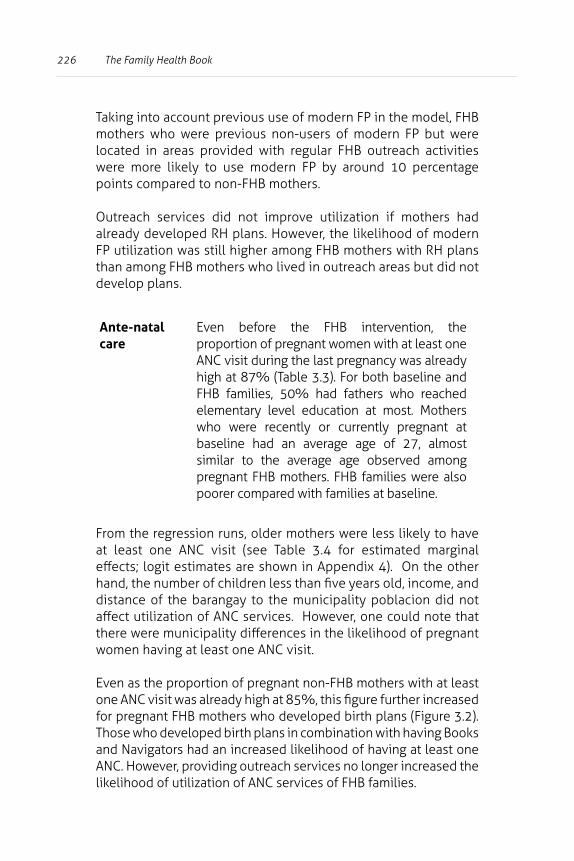
226 The Family Health Book
Taking into account previous use of modern FP in the model, FHB mothers who were previous non-users of modern FP but were located in areas provided with regular FHB outreach activities were more likely to use modern FP by around 10 percentage points compared to non-FHB mothers.
Outreach services did not improve utilization if mothers had already developed RH plans. However, the likelihood of modern FP utilization was still higher among FHB mothers with RH plans than among FHB mothers who lived in outreach areas but did not develop plans.
Ante-natal care
Even before the FHB intervention, the proportion of pregnant women with at least one ANC visit during the last pregnancy was already high at 87% (Table 3.3). For both baseline and FHB families, 50% had fathers who reached elementary level education at most. Mothers who were recently or currently pregnant at baseline had an average age of 27, almost similar to the average age observed among pregnant FHB mothers. FHB families were also poorer compared with families at baseline.
From the regression runs, older mothers were less likely to have at least one ANC visit (see Table 3.4 for estimated marginal effects; logit estimates are shown in Appendix 4). On the other hand, the number of children less than five years old, income, and distance of the barangay to the municipality poblacion did not affect utilization of ANC services. However, one could note that there were municipality differences in the likelihood of pregnant women having at least one ANC visit.
Even as the proportion of pregnant non-FHB mothers with at least one ANC visit was already high at 85%, this figure further increased for pregnant FHB mothers who developed birth plans (Figure 3.2). Those who developed birth plans in combination with having Books and Navigators had an increased likelihood of having at least one ANC. However, providing outreach services no longer increased the likelihood of utilization of ANC services of FHB families.
227An Analysis of the Impacts of the Family Health Book Interventions
Table 3.3: Descriptive statistics of variables: ANC
Baseline FHB
n mean n mean
Had at least one ANC visit (%) 392 86.99 1402 92.01
Age of mother 392 26.82 1402 25.85
Number of children less than 5 yrs old
392 1.52 1402 1.39
Monthly family income is lower than PhP 3000 (%)
392 45.15 1402 60.34
Distance of barangay to poblacion/center (km)
392 19.10 1402 16.99
Father attained at most elementary schooling (%)
392 51.79 1402 50.64
Mother attained at most elementary schooling (%)
392 64.80 1402 43.01
Source: Authors’ calculations based on FHB data sets.
Table 3.4: Marginal effects of regression runs on utilization of at least one ANC
Mother uses at least one ANC
Marginal effects Std. Err.
Has Book and Navigator 0.002 0.019
Has Book, Navigator, and Birth Plan
0.187* 0.045
Has Book, Navigator, and in Outreach Barangay
0.028 0.077
Age of Mother -0.005* 0.001
Number of children less than 5yrs old
-0.010 0.010
Monthly family income is lower than PhP 3000
0.007 0.017
Distance of barangay to poblacion (in km)
4.84E-05 0.000
Father attained at most elementary education
0.002 0.018
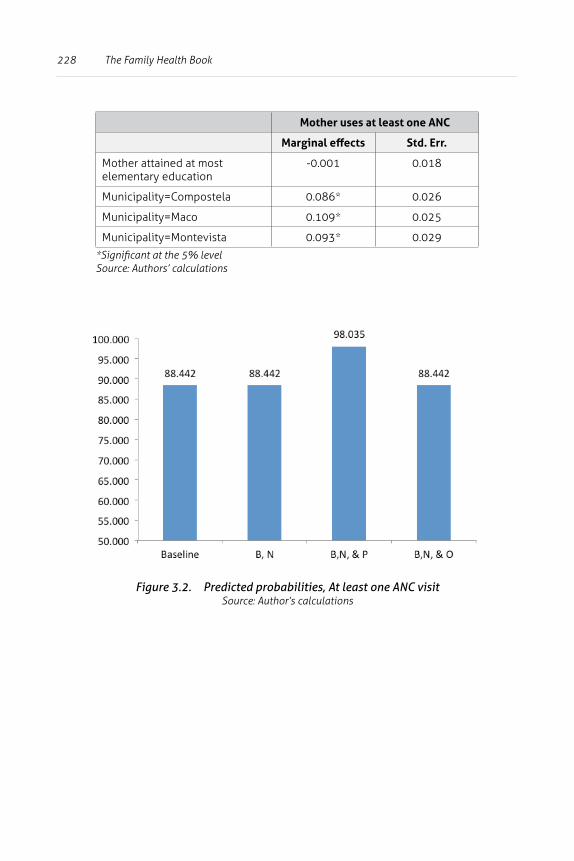
228 The Family Health Book
Mother uses at least one ANC
Marginal effects Std. Err.
Mother attained at most elementary education
-0.001 0.018
Municipality=Compostela 0.086* 0.026
Municipality=Maco 0.109* 0.025
Municipality=Montevista 0.093* 0.029
*Significant at the 5% levelSource: Authors’ calculations
Figure 3.2. Predicted probabilities, At least one ANC visitSource: Author’s calculations

229An Analysis of the Impacts of the Family Health Book Interventions
Skilled birth attendance in facilities
More than 70% of the mothers at baseline chose to deliver at home and sought the assistance of traditional birth attendants (TBAs) during delivery (Table 3.5).
Only 25% of baseline mothers sought assistance from trained health providers during delivery. During the FHB initiative, a large proportion of mothers gave birth with the assistance of a skilled birth attendant in a facility.
Baseline and FHB mothers who gave birth had an average age of 27. FHB families were poorer compared to baseline families.
More than 50% of FHB families with a mother who recently gave birth had a PhilHealth-covered member, a figure much higher compared to that of baseline families. This may be explained by enrolment efforts exerted by the provincial and municipal governments in enroling FHB families in PhilHealth.
Regression results revealed that mothers with more children aged less than five years were more likely to seek assistance of TBAs (see Table 3.6 for the marginal effects and Appendix 5 for the estimated equation).
Similarly, mothers from families with low incomes relied more on TBAs during delivery than on skilled birth attendants in facilities.
Location of the barangay where the family resides also figured significantly on the choice of provider during delivery. Mothers residing in barangays far from the poblacion center of the communities were more likely to be assisted by TBAs than by trained health providers.
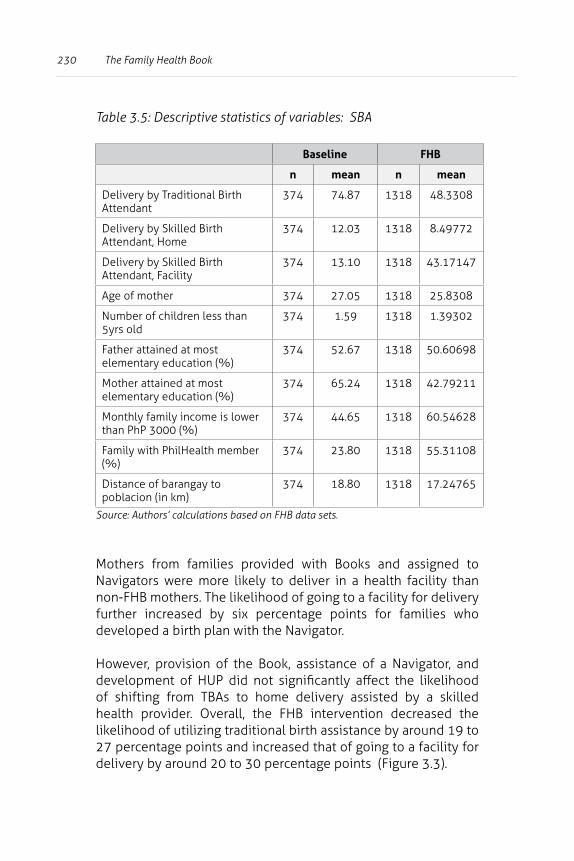
230 The Family Health Book
Table 3.5: Descriptive statistics of variables: SBA
Baseline FHB
n mean n mean
Delivery by Traditional Birth Attendant
374 74.87 1318 48.3308
Delivery by Skilled Birth Attendant, Home
374 12.03 1318 8.49772
Delivery by Skilled Birth Attendant, Facility
374 13.10 1318 43.17147
Age of mother 374 27.05 1318 25.8308
Number of children less than 5yrs old
374 1.59 1318 1.39302
Father attained at most elementary education (%)
374 52.67 1318 50.60698
Mother attained at most elementary education (%)
374 65.24 1318 42.79211
Monthly family income is lower than PhP 3000 (%)
374 44.65 1318 60.54628
Family with PhilHealth member (%)
374 23.80 1318 55.31108
Distance of barangay to poblacion (in km)
374 18.80 1318 17.24765
Source: Authors’ calculations based on FHB data sets.
Mothers from families provided with Books and assigned to Navigators were more likely to deliver in a health facility than non-FHB mothers. The likelihood of going to a facility for delivery further increased by six percentage points for families who developed a birth plan with the Navigator.
However, provision of the Book, assistance of a Navigator, and development of HUP did not significantly affect the likelihood of shifting from TBAs to home delivery assisted by a skilled health provider. Overall, the FHB intervention decreased the likelihood of utilizing traditional birth assistance by around 19 to 27 percentage points and increased that of going to a facility for delivery by around 20 to 30 percentage points (Figure 3.3).
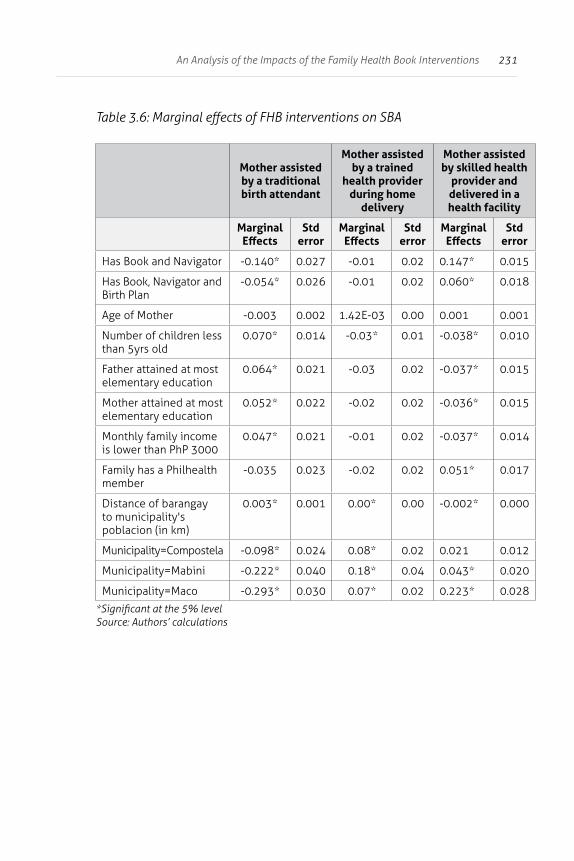
231An Analysis of the Impacts of the Family Health Book Interventions
Table 3.6: Marginal effects of FHB interventions on SBA
Mother assisted by a traditional birth attendant
Mother assisted by a trained
health provider during home
delivery
Mother assisted by skilled health
provider and delivered in a health facility
Marginal Effects
Std error
Marginal Effects
Std error
Marginal Effects
Std error
Has Book and Navigator -0.140* 0.027 -0.01 0.02 0.147* 0.015
Has Book, Navigator and Birth Plan
-0.054* 0.026 -0.01 0.02 0.060* 0.018
Age of Mother -0.003 0.002 1.42E-03 0.00 0.001 0.001
Number of children less than 5yrs old
0.070* 0.014 -0.03* 0.01 -0.038* 0.010
Father attained at most elementary education
0.064* 0.021 -0.03 0.02 -0.037* 0.015
Mother attained at most elementary education
0.052* 0.022 -0.02 0.02 -0.036* 0.015
Monthly family income is lower than PhP 3000
0.047* 0.021 -0.01 0.02 -0.037* 0.014
Family has a Philhealth member
-0.035 0.023 -0.02 0.02 0.051* 0.017
Distance of barangay to municipality's poblacion (in km)
0.003* 0.001 0.00* 0.00 -0.002* 0.000
Municipality=Compostela -0.098* 0.024 0.08* 0.02 0.021 0.012
Municipality=Mabini -0.222* 0.040 0.18* 0.04 0.043* 0.020
Municipality=Maco -0.293* 0.030 0.07* 0.02 0.223* 0.028
*Significant at the 5% levelSource: Authors’ calculations
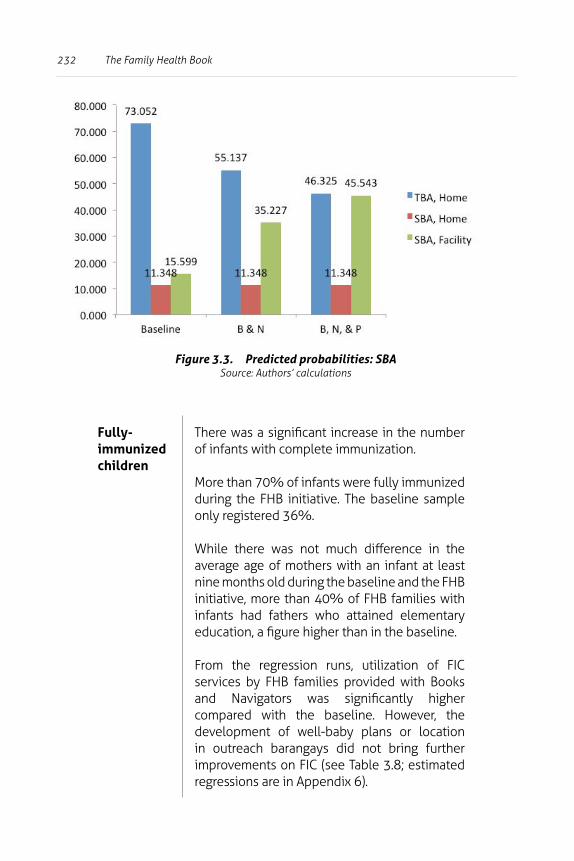
232 The Family Health Book
Figure 3.3. Predicted probabilities: SBASource: Authors’ calculations
Fully-immunized children
There was a significant increase in the number of infants with complete immunization.
More than 70% of infants were fully immunized during the FHB initiative. The baseline sample only registered 36%.
While there was not much difference in the average age of mothers with an infant at least nine months old during the baseline and the FHB initiative, more than 40% of FHB families with infants had fathers who attained elementary education, a figure higher than in the baseline.
From the regression runs, utilization of FIC services by FHB families provided with Books and Navigators was significantly higher compared with the baseline. However, the development of well-baby plans or location in outreach barangays did not bring further improvements on FIC (see Table 3.8; estimated regressions are in Appendix 6).
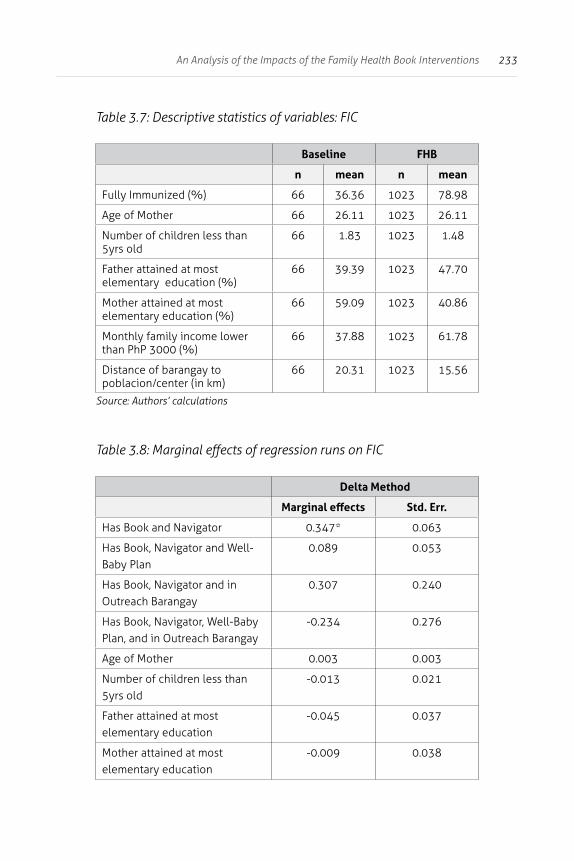
233An Analysis of the Impacts of the Family Health Book Interventions
Table 3.7: Descriptive statistics of variables: FIC
Baseline FHB
n mean n mean
Fully Immunized (%) 66 36.36 1023 78.98
Age of Mother 66 26.11 1023 26.11
Number of children less than 5yrs old
66 1.83 1023 1.48
Father attained at most elementary education (%)
66 39.39 1023 47.70
Mother attained at most elementary education (%)
66 59.09 1023 40.86
Monthly family income lower than PhP 3000 (%)
66 37.88 1023 61.78
Distance of barangay to poblacion/center (in km)
66 20.31 1023 15.56
Source: Authors’ calculations
Table 3.8: Marginal effects of regression runs on FIC
Delta Method
Marginal effects Std. Err.
Has Book and Navigator 0.347* 0.063
Has Book, Navigator and Well-Baby Plan
0.089 0.053
Has Book, Navigator and in Outreach Barangay
0.307 0.240
Has Book, Navigator, Well-Baby Plan, and in Outreach Barangay
-0.234 0.276
Age of Mother 0.003 0.003
Number of children less than 5yrs old
-0.013 0.021
Father attained at most elementary education
-0.045 0.037
Mother attained at most elementary education
-0.009 0.038
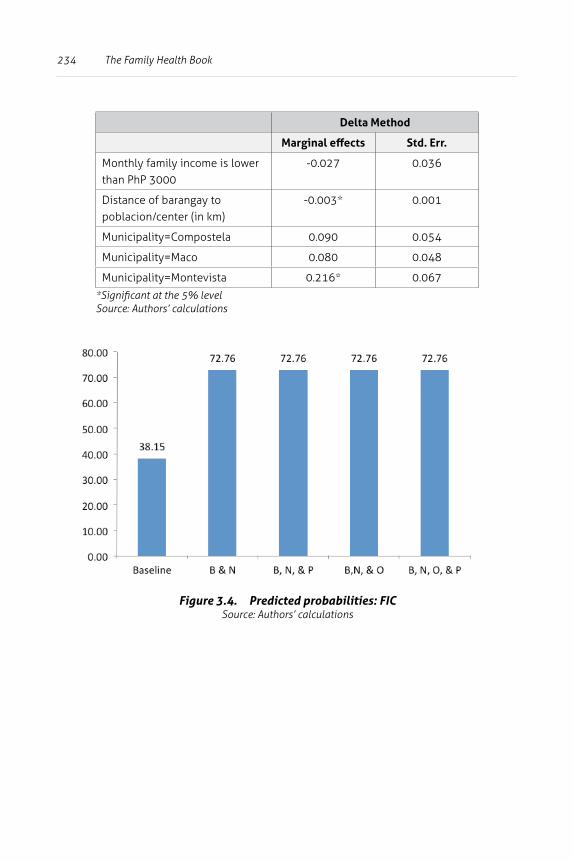
234 The Family Health Book
Delta Method
Marginal effects Std. Err.
Monthly family income is lower than PhP 3000
-0.027 0.036
Distance of barangay to poblacion/center (in km)
-0.003* 0.001
Municipality=Compostela 0.090 0.054
Municipality=Maco 0.080 0.048
Municipality=Montevista 0.216* 0.067
*Significant at the 5% levelSource: Authors’ calculations
Figure 3.4. Predicted probabilities: FICSource: Authors’ calculations
235An Analysis of the Impacts of the Family Health Book Interventions
Discussion
Whether the utilization of critical MNCHN services improved with the implementation of the FHB package of interventions was analyzed, using data from the FHB Baseline Survey and from the operations research monitoring activities.
Controlling for family characteristics and location characteristics, the provision of information through the Book and reinforcement by Navigators improved skilled attendance and facility delivery by 15 percentage points, and full immunization of children by about 34 percentage points.
Families acting on the information provided by appropriately-developed health use plans increased modern family planning use by about 27 percentage points, antenatal care use by 18 percentage points, and skilled birth attendance in a facility by an additional 6 percentage points.
Outreach services significantly increased utilization of modern FP services for families which received information even if these families did not develop plans. These findings showed that information provided in a way that would make families act on their health risks and needs (i.e., with visits, assistance, and monitoring of Navigators) could substantially increase utilization of MNCHN services.
Field observations and interviews validated these findings. The mid-project FGD conducted among recipient families after initial visits by the Navigators, elicited mainly positive reactions. Families expressed appreciation for Navigators’ efforts in conducting actual visits, information dissemination, and health risks assessment. The orientation process on the FHB, the Book, risks assessment, and the HUP development made families residing in far-flung areas feel that they were being looked after for the first time. Many of these families, especially those residing in upland barangays, have never been to the health stations or rural health units.
236 The Family Health Book
Field observations and random household visits conducted to determine the accuracy of the observed improvement in SBA among FHB mothers revealed that the ordinances in Maco and Compostela banning TBAs from assisting mothers during deliveries could not be fully credited for these improvements.
During random household visits in the municipality of Compostela5, the families said the Navigators were the sole source of information regarding implementation of the ordinance promoting SBAs. The mothers cited that Navigators referred them to midwives, facilities, and even emergency transport providers during delivery.
Mothers also said that the Navigators linked up pregnant mothers and health providers. This was crucial in dispelling notions regarding giving birth in RHUs and other facilities. Some mothers felt that doctors performed unnecessary and painful procedures during deliveries in facilities.
In one of the families randomly visited, a mother with five children who recently gave birth in the RHU said she was initially afraid of going to the facility to deliver because of stories she had heard from neighbors about the painful injections given during delivery. Her earlier pregnancies were all assisted by a TBA at home.
Encouraged by her Navigator, she delivered her fifth child in the RHU. This changed her ideas about doctors. She said she was immediately able to perform basic household chores a few days after delivery and did not suffer after delivery.
The Navigators were also instrumental in starting discussions among couples on health issues. In many families, the Navigator referred couples to the BHS and RHUs for FP counseling. Though Navigators in the FHB did not perform health service delivery functions, the families appreciated their efforts in referring them to health providers.
5 HPDP staff conducted random, unannounced household visits -- in July and November 2009; January and March 2010; and April 2011 -- to validate records and Navigators’ and midwives’ reports.
237An Analysis of the Impacts of the Family Health Book Interventions
A mother from one of the families randomly visited said her Navigator constantly reminded her of the importance of adhering to the schedule for taking birth control pills. In another family, the presence of a Navigator helped settle disagreements on limiting the number of children. The wife wanted to undergo ligation but the husband refused to sign the consent form for the procedure. Through the Navigator, the wife was referred to the midwife for counseling and was presented with options on various FP methods. The couple subsequently agreed on using an intra-uterine device (IUD).
Discussions with the MHOs were conducted to validate data extracted from monitoring forms and to draw observations from the provider viewpoint on the impacts of the FHB initiative on families. The MHO and other health personnel in the municipalities credited the improvements in the utilization of MFP commodities and services and SBAs to the efforts of the Navigators in referring mothers to health facilities and midwives for FP counseling.
Health providers in RHUs also noticed that early in the FHB initiative, many pregnant mothers from FHB families consulted for ANC during their first trimester. Midwives and doctors observed that some FHB families were familiar with the brand and prices of birth control pills.
According to the MHO, mothers visiting the RHUs credited the Navigators for giving them basic advice on taking pills. Mothers who recently gave birth cited the Navigator’s specific advice that lactating mothers could take birth control pills.
Navigators themselves recognized that their interaction with the families was the main difference between their tasks under the FHB initiative and their usual work as BHWs. Some Navigators cited that as BHWs, they did not individually visit families. Their previous interactions with families occurred mostly during community-level activities, such as vaccination drives and general outreach activities. They indicated that the training given to them boosted their morale and confidence in performing their FHB tasks.
238 The Family Health Book
However, provision of assistance to families entailed a significant level of effort on the part of the Navigators, depending on the number of families assigned. From the suggested ratio of 1 Navigator per 20 families, Navigator reassignments were made in consideration of actual difficulty and distance from the Navigator’s residence to the families being handled.
Navigators assigned to families living in the poblacion or lowland barangays were made to handle more families (some even up to 30), while those assigned to families living in small, upland areas with high degree of dispersion of families, and which required large transport costs were assigned less families (some even less than ten).
Despite these adjustments, Navigators still cited the difficulty of conducting regular visits due to the lack of transportation allowances, especially for those handling families in far-flung areas. This was consistent with the observations of some MHOs on the declining number of pregnant FHB mothers visiting the RHUs for their antenatal care, which they attributed to the failure of Navigators to conduct visits. Some Navigators overcame these difficulties by asking for transportation assistance from barangay officials.
Other challenges faced by Navigators:
• difficulty in using some of the FHB monitoring forms;• absence of the mother or father during monitoring visits; and• mobility of families.
To partly alleviate these, some midwives deployed other available community health workers to assist Navigators in follow-up activities.
239An Analysis of the Impacts of the Family Health Book Interventions
Outreach The additional impact of the FHB outreach services can be attributed to measures that ensured that families were informed ahead of time of outreach schedules and were able to attend outreach services.
For instance, as some of the far-flung areas proved to be inaccessible especially during the rainy months, the MHO and PHO conducted outreach activities in the poblacion areas of the targeted barangays but provided transportation to the outreach sites for families living in far-flung areas.
There were also difficulties encountered in conducting FHB outreach activities. During a random visit in one of the outreach barangays, midwives cited the need to be up-to-date on the scheduled services indicated in the HUPs of families.
Midwives also indicated the advantages of having cost-effective FHB outreach activities compared to regular outreach activities. According to one midwife, the usual practice of putting up a buffer, or over-projecting the need for commodities, would amount to more than 70% of the needs of the identified beneficiaries.
She said there was overprojection since there was no prior information on the needs, or even the actual counts of beneficiaries, on the ground. On the other hand, the HUPs provided them with prior information on the number of beneficiaries and the required commodities and services.

240 The Family Health Book
Evidence on other health Navigators
Findings in Compostela Valley were consistent with the international experience in the use of health Navigators and/or health navigational functions. There is a wide body of literature on the role of health Navigators in providing information for target groups, which ultimately affect behavior and health outcomes. In Bangladesh and Nepal, community health workers (Manandhar et al., 2004; Baqui et al., 2008; McPherson et al., 2006) were assigned to expectant mothers and assisted them in preparing for childbirth. Through focus group discussions, targeted women were given information about the importance of ANC and SBA.
In another intervention, health workers provided targeted women with keychains and flipcharts containing health messages on desired behaviors for birth-preparedness. (McPherson et al., 2006).
Results indicated that community health workers positively influence intermediate health outcomes. But, as some studies note, health services being promoted by health workers should be services actually available in the communities (McPherson et al., 2006).
Other studies assert that health Navigators should be sensitive to the cultures of the communities they serve (Garcia et al., 2009; Guadagnolo et al., 2011). Providing culturally competent Navigators who are able to provide appropriate solutions for their clients results in better client satisfaction, and consequently, improved intermediate health outcomes.

241An Analysis of the Impacts of the Family Health Book Interventions
In this regard, some patient Navigator programs in the USA (Hendren et al., 2010) require potential Navigators to be fluent in a language other than English; for instance, Spanish. Potential health Navigators are also required to attend training programs, where basic health diagnostics and patient Navigator roles are taught. Some studies indicate that while health Navigators might be effective, “overburdening” them with a large group of clients may result in dampened impact on behavior change, and ultimately on health outcomes.
A study on the National Family Planning program in Vietnam showed that patient Navigators, called “collaborators,” did not continue with follow-up meetings for women who adopted a long-term contraceptive method. The collaborators felt overburdened since they were also expected to be service providers aside from being patient Navigators (Tuan and Johnston, 2002).
Patient navigation is in fact a current trend in developed countries and even involves the private sector. Patient navigation programs have been successful in guiding breast cancer patients through the health care system, and survival rates of cancer patients have increased5 (Battaglia et al., 2006; Freeman, 2006).
6
6 The first patient Navigator program established in Harlem Hospital for breast cancer patients reported that five-year survival rates from 1995 to 2000 increased from 29% to 78%. The incidence of late-stage cancers dropped from 40% to 28%, then to 21%.
242 The Family Health Book
These services are being increasingly used in the United States as they provide cost savings for patients, particularly those afflicted with chronic diseases such as cancer, HIV/AIDS, and diabetes.
A study of diabetes patients in West Baltimore, Maryland, USA showed that patient Navigators resulted in cost savings of at least $2,245 per year (Fedder et al., 2003). Hourly wages may vary from as little as $15 to as much as $50 for community health worker (CHW) volunteers, shooting up to $200 per hour for private patient Navigators (Bank, 2009; Fayerman, 2011), which indicates that the provision of patient Navigator services constitutes a lucrative business.
Limitations
Our results show increased key intermediate outcomes for FHB families which received Books and were engaged by their Navigators. However, these results may be biased by the limited information obtained on eligible and highly-mobile families during the intervention period. These families, who would most likely benefit from the FHB interventions may be the less likely ones to utilize care.
The high mobility of the eligible population became apparent even before the distribution of Books: the initial list of families for the FHB needed to be validated twice to confirm the families’ addresses. There were less families who received the Book than those found in the validated lists, as some families were known to have moved out of the pilot sites.
243An Analysis of the Impacts of the Family Health Book Interventions
During follow-up visits by Navigators and midwives, the common types of mobility observed included the following:
1) permanent transfer of a family to a non-FHB site (either within or outside the province);
2) permanent transfer of a family within the FHB site; 3) temporary move-outs to non-FHB sites; and 4) temporary move-outs to FHB sites.
Given the mobility of families, the Provincial Health Office advised families to bring the Book and HUPs with them when transfering residence.
Endorsement among Navigators of families transferring residence within FHB sites was also recommended. Navigators were also instructed not to drop those families transferring residence from their rosters, just in case these return again to FHB sites. Despite these instructions, no more follow-ups were done on some families, especially those who have transferred to non-FHB sites.
Mobility of family members also included the following:
• temporary moving out of either the mother or father to non-FHB sites during specific months of the year;
• temporary move-outs of mothers from residence; and • permanent move-outs of mothers from residence.
Temporary transfer of residence within the province was a seasonal phenomenon. During rainy seasons, men went to the mining sites for gold panning. Some families only returned to their residences during the rainy season for harvesting.
Some mothers leave their families to work in nearby cities as household help. The general advice given by Navigators to families with mothers leaving behind children: endorse the Book and the HUP to the father or relatives living nearby.
Cases of temporary move-outs made it difficult for Navigators to conduct follow-up visits. Some families would not be in their usual addresses for months. In some cases, the mother would
244 The Family Health Book
bring along the Book and the family’s HUPs, where the children’s scheduled services were recorded. Navigators thus had to reconstruct HUPs by reviewing their records and logs.
Conclusions
The FHB operations research conducted in Compostela Valley sought to assess whether a package of demand-side interventions could increase utilization of critical MNCHN services. Families were given critical information through a Book, assigned to trained community health workers who assisted them in developing appropriate HUPs for their health needs and risks, and were recipients of outreach services.
Using multivariate techniques on a combined baseline household data set and data collected from FHB monitoring activities, the FHB package of interventions was shown as exerting a significant impact on the use of modern family planning, antenatal care visits, skilled birth attendance at a facility, and immunizations for children.
These results are robust even after controlling for the following:
• individual and family characteristics that affected demand;• distance and municipality characteristics that affected
supply conditions and geographic access; and • noise that arise from data sources.
In the case of MFP and SBA, the provision of key information through the Book and Navigators resulted in cases of better utilization which were further reinforced by the development of HUPs. The impacts were seen only in ANC cases when appropriate HUPs were developed. Meanwhile, no additional impacts were seen in the incidence of FIC even when HUPs were developed. But seen from a larger context, the results imply that addressing informational barriers to utilization of key MNCHN services by providing key information through a physical medium, then giving support to beneficiary families through personalized guidance and assistance from Navigators, are effective ways to persuade families to develop plans which address their health risks.

245An Analysis of the Impacts of the Family Health Book Interventions
Both clients and health workers validated the measured improvements in utilization of key MNCHN services. FHB families appreciated efforts of Navigators to assist them in understanding their risks and the available options to address these risks. Community health workers assigned to these families felt empowered by the training provided to them, and which boosted their morale and confidence to perform their navigational functions.
Field observations also highlighted that logistical support, specifically transportation allowances from both the provincial as well as municipal governments, was crucial in facilitating Navigators’ visits to their assigned families. Support from provincial, municipal, and barangay officials was also instrumental in ensuring the outreach activities’ success. Adjustments in the assignment of the number of families assigned to Navigators were also needed.
The high mobility of FHB families proved to be a challenge for Navigators and health workers. Advisories and operational adjustments prove insufficient to ensure that FHB families received the proper care in their new residence areas, especially in cases of permanent transfers and transfers to non-FHB municipalities.
The literature reveals that in both developed and non-developed country settings, the use of patient Navigators is effective in assisting families for both MNCHN as well as non-MNCHN concerns. Results from the FHB operations research in Compostela Valley reinforced the literature, with its findings that the provision of critical information through the Book, the Navigator, and through guided assistance in developing HUPs were effective interventions that could increase utilization of critical MNCHN services. Expanding these FHB interventions at the provincial, regional, and nationwide levels is something worth considering in order to improve MNCHN outcomes.
246 The Family Health Book
References
Acuin, C. 2008. Conduct of Focus Group Discussions (FGDs) on Family Planning Behaviors Among Men and Women in Selected Municipalities of Compostela Valley Province. Report submitted to the Health Policy Development Program, Quezon City, Philippines.
Bank, D. 2009. Encore ‘Navigators’ improve health, reduce costs. Retrieved from http://www.encore.org/news/encore-navigators-work-i.
Baqui, A., El-Arifeen, S., Darmstadt, G.L., Ahmed, S., Williams, E.K., Seraji, H., …, and Black, R. 2008. Effect of community-based newborn-care intervention package implemented through two service-delivery strategies in Sylhet district, Bangladesh: A cluster-randomised controlled trial. Lancet 371 (9628), 1936-1944.
Battaglia, T.A., Roloff, K., Posner, M. A., and Freund, K. M. 2006. Improving follow-up to abnormal breast cancer screening in an urban population. Cancer 109 (12), 359-367.
Fayerman, P. 2011. Canadians unwilling to pay for private care. Retrieved from http://www.vancouversun.com/news/patient-navigationseries/Canadians+unwilling+private+care/4374666/story.html.
Fedder, D.O., Chang, R., Curry, S., and Nichols, G. 2003. The effectiveness of a community health worker outreach program on healthcare utilization of West Baltimore City Medicaid patients with diabetes, with or without intervention. Ethnicity and Disease 13 (1), 22-27.
Freeman, H. 2006. Patient navigation: A community based strategy to reduce cancer disparities. Journal of Urban Health 83 (2), 139-141.
Garcia, E.L., Viveros, L., and Feldman, N. 2009. Patient navigation: Lay patient Navigators and delivery of breast cancer treatment to indigent Hispanic women. Abstract presented in the American Society of Clinical Oncology Breast Cancer Symposium, San Francisco, California.
247An Analysis of the Impacts of the Family Health Book Interventions
Guadagnolo, B.A., Boylan, A., Sargent, M., Koop, D., Brunette, D., Kanekar, S., and Petereit, D. G. 2011. Patient navigation for American Indians undergoing cancer treatment: Utilization and impact on care delivery in a regional healthcare center. Cancer 117 (12), 2754-2761.
Health Policy Development Program. 2009. The Family Health Book Operations Research Design. Quezon City, Philippines: UPecon Foundation, Inc.-Health Policy Development Program.
Hendren, S., Griggs J.J., Epstein, R.M., Humiston, S., Rousseau, S., Jean-Pierre, P., and Fiscella, K. 2010. Study protocol: a randomized controlled trial of patient navigation-activation to reduce cancer health disparities. BMC Cancer 10 (551).
Manandhar, D., Osrin, D., Shrestha, B.P., Mesko, N., Morrison, J., Tumbahangphe, K.M., and Costello, A.M. 2004. Effect of a participatory intervention with women’s groups on birth outcomes in Nepal: Cluster-randomised controlled trial. Lancet 364 (9438), 970-979.
McPherson, R., Khadka, N., Moore, J., and Sharma, M. 2006. Are birth-preparedness programs effective? Results from a field trial in Siraha district, Nepal. Journal of Health Population and Nutrition 24 (4), 479-488.
Palmer, L., Hill, I., and Magazimik, A. 2007. HealthConnect in our community: What do health Navigators, community health workers, and families say about the program? Washington, DC: The Urban Institute.
Simmons, J. 2011. Patient Navigator Improves Outcomes, Incomes. Retrieved from http://www.healthleadersmedia.com/page-2/MAG-246087/Patient-Navigator-Improves-Outcomes-Incomes.
Tuan, N. A., and Johnston, H. 2002. Can Vietnam’s Family Planning Collaborators Improve Grassroots Reproductive Health Services? Results of an assessment in two communes. Chapel Hill, North Carolina: Ipas.
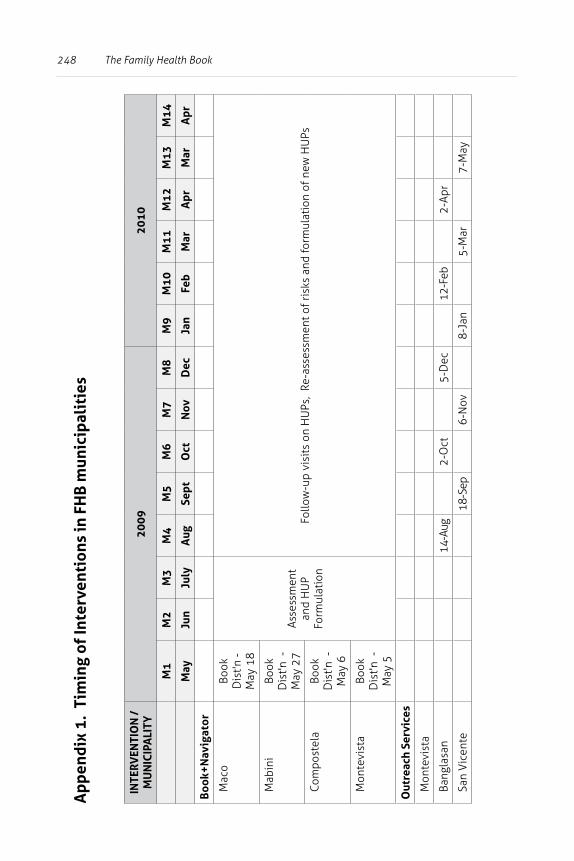
248 The Family Health Book
App
endi
x 1.
Tim
ing
of In
terv
enti
ons
in F
HB
mun
icip
alit
ies
INTE
RVEN
TIO
N /
M
UN
ICIP
ALI
TY20
0920
10
M1
M2
M3
M4
M5
M6
M7
M8
M9
M10
M11
M12
M13
M14
May
Jun
July
Aug
Sept
Oct
Nov
Dec
Jan
Feb
Mar
Apr
Mar
Apr
Boo
k+N
avig
ator
Mac
oBo
ok
Dis
t'n -
May
18
Asse
ssm
ent
and
HU
P Fo
rmul
atio
nFo
llow
-up
visi
ts o
n H
UPs
, Re
-ass
essm
ent o
f ris
ks a
nd fo
rmul
atio
n of
new
HU
Ps
Mab
ini
Book
D
ist'n
-
May
27
Com
post
ela
Book
D
ist'n
-
May
6
Mon
tevi
sta
Book
D
ist'n
-
May
5
Out
reac
h Se
rvic
es
Mon
tevi
sta
Bang
lasa
n
14-A
ug
2-O
ct
5-D
ec
12-F
eb
2-Ap
r
San
Vic
ente
18-S
ep
6-N
ov
8-Ja
n
5-M
ar
7-M
ay
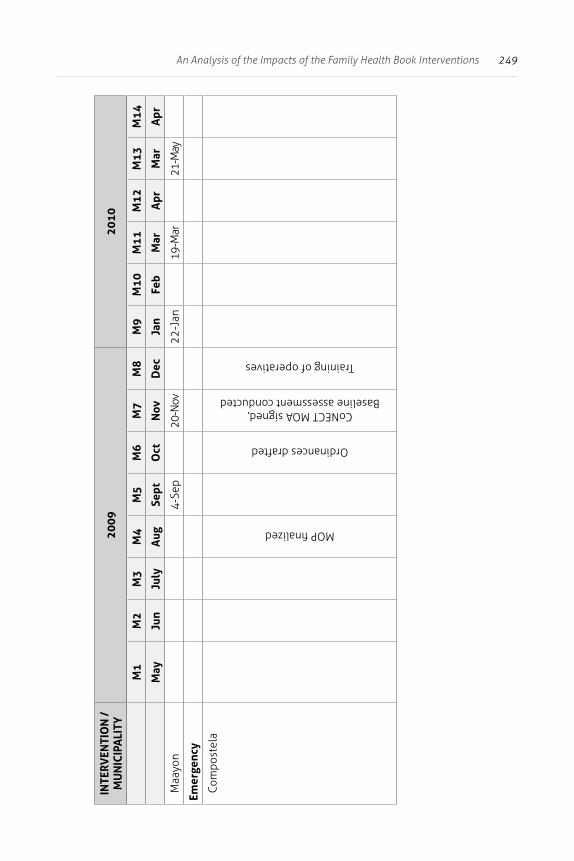
249An Analysis of the Impacts of the Family Health Book Interventions
INTE
RVEN
TIO
N /
M
UN
ICIP
ALI
TY20
0920
10
M1
M2
M3
M4
M5
M6
M7
M8
M9
M10
M11
M12
M13
M14
May
Jun
July
Aug
Sept
Oct
Nov
Dec
Jan
Feb
Mar
Apr
Mar
Apr
Maa
yon
4-Se
p
20-N
ov
22-J
an
19-M
ar
21-M
ay
Emer
genc
y
Com
post
ela
MOP finalized
Ordinances drafted
CoNECT MOA signed, Baseline assessment conducted
Training of operatives
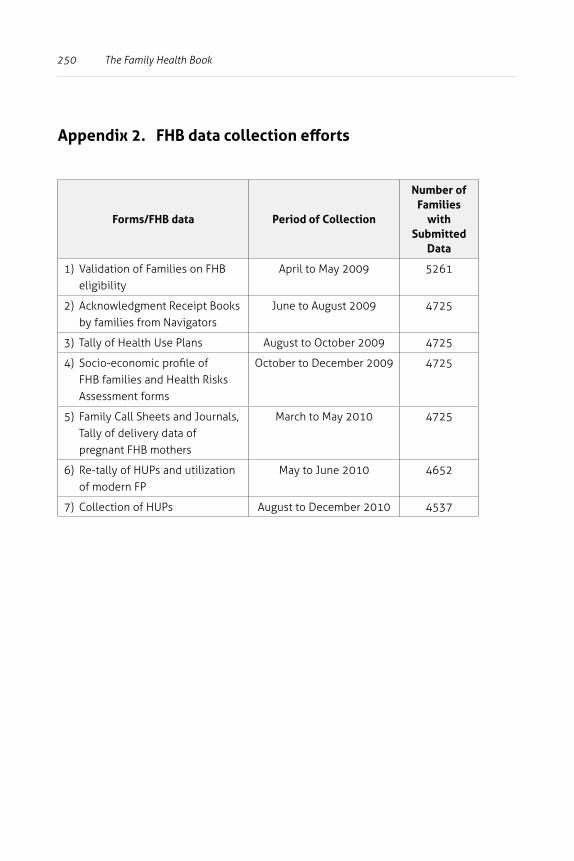
250 The Family Health Book
Appendix 2. FHB data collection efforts
Forms/FHB data Period of Collection
Number of Families
with Submitted
Data
1) Validation of Families on FHB eligibility
April to May 2009 5261
2) Acknowledgment Receipt Books by families from Navigators
June to August 2009 4725
3) Tally of Health Use Plans August to October 2009 4725
4) Socio-economic profile of FHB families and Health Risks Assessment forms
October to December 2009 4725
5) Family Call Sheets and Journals, Tally of delivery data of pregnant FHB mothers
March to May 2010 4725
6) Re-tally of HUPs and utilization of modern FP
May to June 2010 4652
7) Collection of HUPs August to December 2010 4537
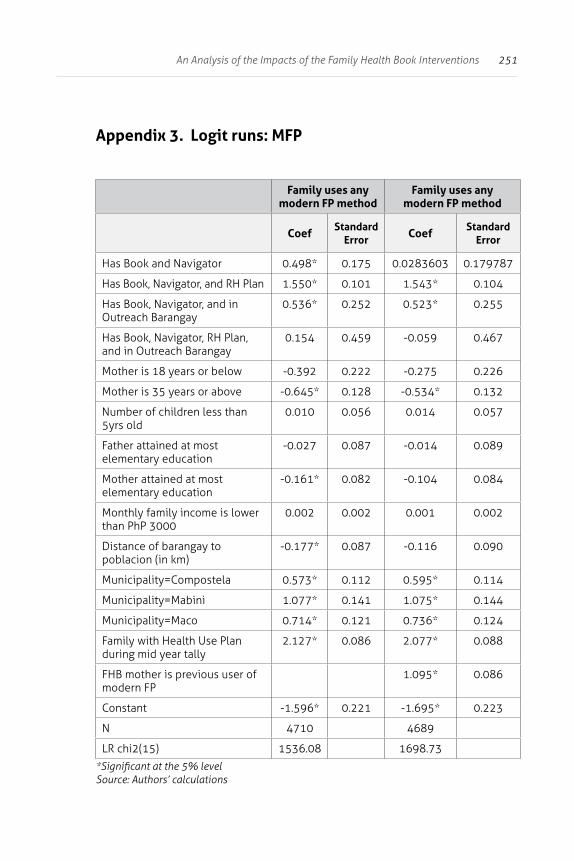
251An Analysis of the Impacts of the Family Health Book Interventions
Appendix 3. Logit runs: MFP
Family uses any modern FP method
Family uses any modern FP method
Coef Standard Error Coef Standard
Error
Has Book and Navigator 0.498* 0.175 0.0283603 0.179787
Has Book, Navigator, and RH Plan 1.550* 0.101 1.543* 0.104
Has Book, Navigator, and in Outreach Barangay
0.536* 0.252 0.523* 0.255
Has Book, Navigator, RH Plan, and in Outreach Barangay
0.154 0.459 -0.059 0.467
Mother is 18 years or below -0.392 0.222 -0.275 0.226
Mother is 35 years or above -0.645* 0.128 -0.534* 0.132
Number of children less than 5yrs old
0.010 0.056 0.014 0.057
Father attained at most elementary education
-0.027 0.087 -0.014 0.089
Mother attained at most elementary education
-0.161* 0.082 -0.104 0.084
Monthly family income is lower than PhP 3000
0.002 0.002 0.001 0.002
Distance of barangay to poblacion (in km)
-0.177* 0.087 -0.116 0.090
Municipality=Compostela 0.573* 0.112 0.595* 0.114
Municipality=Mabini 1.077* 0.141 1.075* 0.144
Municipality=Maco 0.714* 0.121 0.736* 0.124
Family with Health Use Plan during mid year tally
2.127* 0.086 2.077* 0.088
FHB mother is previous user of modern FP
1.095* 0.086
Constant -1.596* 0.221 -1.695* 0.223
N 4710 4689
LR chi2(15) 1536.08 1698.73
*Significant at the 5% levelSource: Authors’ calculations
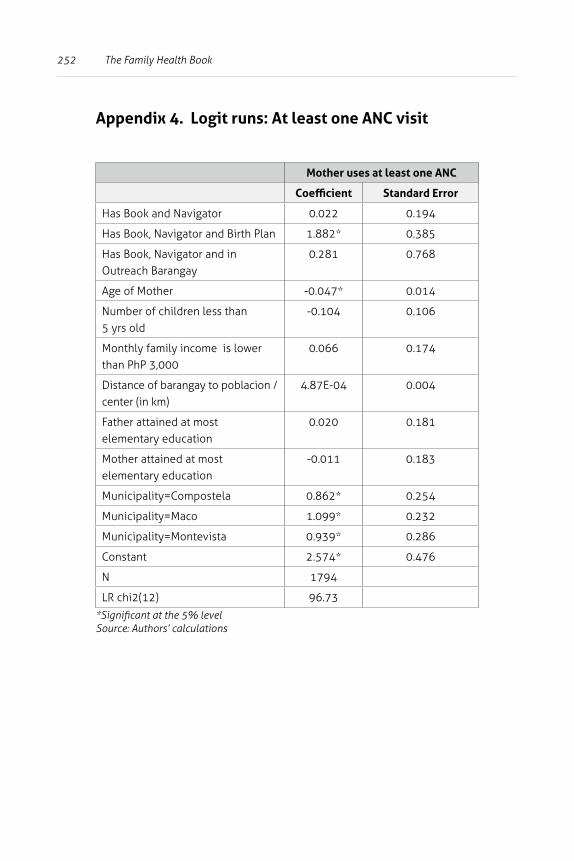
252 The Family Health Book
Appendix 4. Logit runs: At least one ANC visit
Mother uses at least one ANC
Coefficient Standard Error
Has Book and Navigator 0.022 0.194
Has Book, Navigator and Birth Plan 1.882* 0.385
Has Book, Navigator and in Outreach Barangay
0.281 0.768
Age of Mother -0.047* 0.014
Number of children less than 5 yrs old
-0.104 0.106
Monthly family income is lower than PhP 3,000
0.066 0.174
Distance of barangay to poblacion / center (in km)
4.87E-04 0.004
Father attained at most elementary education
0.020 0.181
Mother attained at most elementary education
-0.011 0.183
Municipality=Compostela 0.862* 0.254
Municipality=Maco 1.099* 0.232
Municipality=Montevista 0.939* 0.286
Constant 2.574* 0.476
N 1794
LR chi2(12) 96.73
*Significant at the 5% levelSource: Authors’ calculations
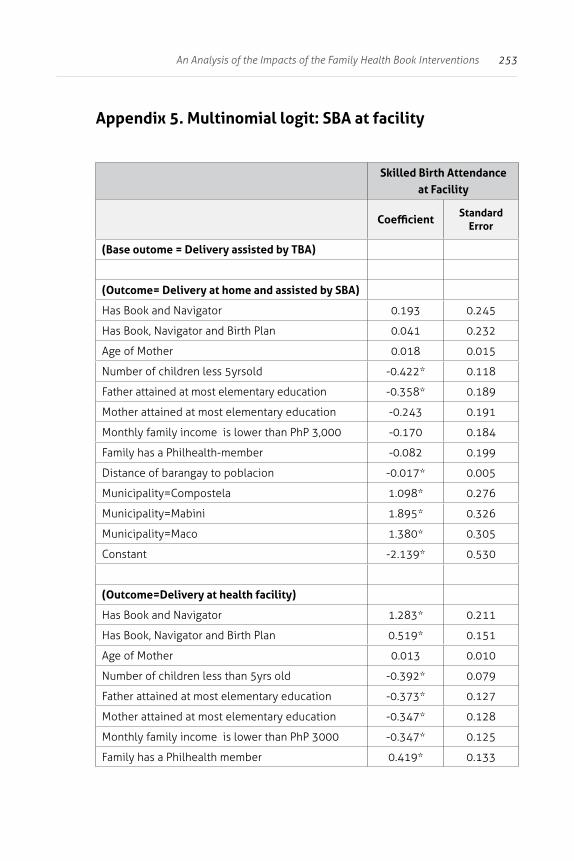
253An Analysis of the Impacts of the Family Health Book Interventions
Appendix 5. Multinomial logit: SBA at facility
Skilled Birth Attendance
at Facility
CoefficientStandard
Error
(Base outome = Delivery assisted by TBA)
(Outcome= Delivery at home and assisted by SBA)
Has Book and Navigator 0.193 0.245
Has Book, Navigator and Birth Plan 0.041 0.232
Age of Mother 0.018 0.015
Number of children less 5yrsold -0.422* 0.118
Father attained at most elementary education -0.358* 0.189
Mother attained at most elementary education -0.243 0.191
Monthly family income is lower than PhP 3,000 -0.170 0.184
Family has a Philhealth-member -0.082 0.199
Distance of barangay to poblacion -0.017* 0.005
Municipality=Compostela 1.098* 0.276
Municipality=Mabini 1.895* 0.326
Municipality=Maco 1.380* 0.305
Constant -2.139* 0.530
(Outcome=Delivery at health facility)
Has Book and Navigator 1.283* 0.211
Has Book, Navigator and Birth Plan 0.519* 0.151
Age of Mother 0.013 0.010
Number of children less than 5yrs old -0.392* 0.079
Father attained at most elementary education -0.373* 0.127
Mother attained at most elementary education -0.347* 0.128
Monthly family income is lower than PhP 3000 -0.347* 0.125
Family has a Philhealth member 0.419* 0.133
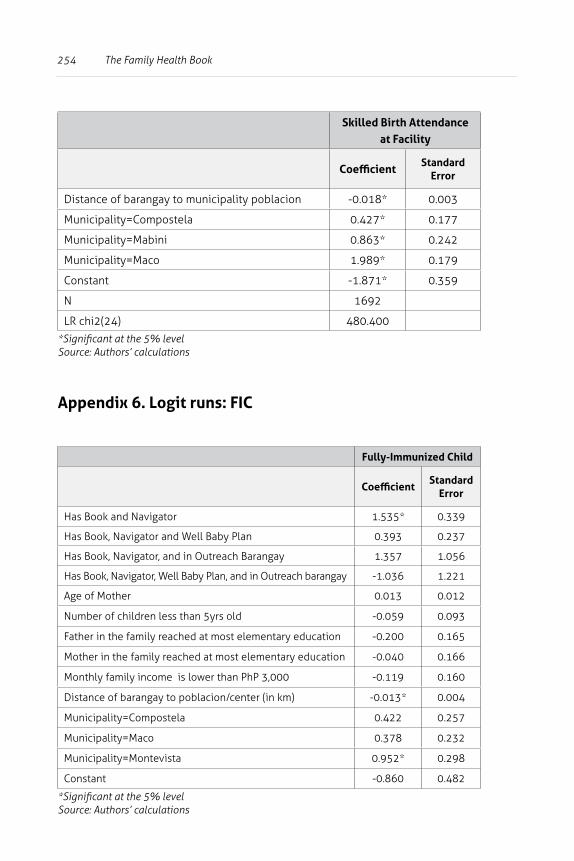
254 The Family Health Book
Skilled Birth Attendance
at Facility
CoefficientStandard
Error
Distance of barangay to municipality poblacion -0.018* 0.003
Municipality=Compostela 0.427* 0.177
Municipality=Mabini 0.863* 0.242
Municipality=Maco 1.989* 0.179
Constant -1.871* 0.359
N 1692
LR chi2(24) 480.400
*Significant at the 5% levelSource: Authors’ calculations
Appendix 6. Logit runs: FIC
Fully-Immunized Child
CoefficientStandard
Error
Has Book and Navigator 1.535* 0.339
Has Book, Navigator and Well Baby Plan 0.393 0.237
Has Book, Navigator, and in Outreach Barangay 1.357 1.056
Has Book, Navigator, Well Baby Plan, and in Outreach barangay -1.036 1.221
Age of Mother 0.013 0.012
Number of children less than 5yrs old -0.059 0.093
Father in the family reached at most elementary education -0.200 0.165
Mother in the family reached at most elementary education -0.040 0.166
Monthly family income is lower than PhP 3,000 -0.119 0.160
Distance of barangay to poblacion/center (in km) -0.013* 0.004
Municipality=Compostela 0.422 0.257
Municipality=Maco 0.378 0.232
Municipality=Montevista 0.952* 0.298
Constant -0.860 0.482
*Significant at the 5% levelSource: Authors’ calculations
255
4 Baseline Family Health Book (FHB) Survey Documentation Report
Health Policy Development Program (HPDP)UPecon Foundation Inc.
Abstract
This report details the contents of the FHB Baseline survey conducted to provide data for analysis of maternal and child health practices in Compostela Valley. The survey has three components: the household survey, physician and midwife survey, and hospital and clinic survey.
The household survey provided information on health care utilization and mapped health facilities and providers patronized by residents in Compostela Valley. The physician and midwife survey generated information on practice characteristics and health care providers’ case/patient load. The hospital and clinic survey yielded data on patient characteristics, their health use patterns, and satisfaction from provided health care services.
256 The Family Health Book
Background
The Health Policy Development Program (HPDP) is a five-year project funded by the United States Agency for International Development (USAID) and is mandated to assist the Department of Health (DOH) in shaping the policy environment towards achieving better health outcomes, a more responsive health system, and equitable health care financing. The HPDP is managed by the UPecon Foundation, Inc.—a private non-profit organization composed of faculty from the UP School of Economics.
The Family Health Book (FHB) initiative is one of HPDP’s flagship products. The FHB initiative aims to improve utilization of critical services to help reduce the risk of maternal and child morbidity and mortality. FHB interventions aim to mitigate these risks by addressing some family-level barriers to using critical services, which include
• lack of information on what services to access; • where these services can be accessed;• how these services can be accessed; • the means through which these services can be financed; and • the lack of logistical support to accessing care.
An innovation under the FHB initiative is the use of health Navigators to assist families recognize their health risks and plan for the utilization of health services to address those risks. To test the effectiveness and efficiency of the FHB intiative prior to a nationwide scale up, a pilot implementation was conducted In the province of Compostela Valley in partnership with the Center for Heath Development XI (CHD XI), and the Compostela Valley LGUs.
To support the conduct of the FHB pilot, a Baseline Survey was done to:
• identify pilot sites for the initial launching of the FHB initiative;• determine core services to be offered; and • define how providers should be linked together into
service delivery networks.
257Baseline Family Health Book (FHB) Survey Documentation Report
The Baseline Survey had three component surveys which generated data for situational analysis of maternal and child health practices in Compostela Valley. It also mapped health services providers and quality of care.
Component Surveys
Household survey
This component survey gathered information on health care utilization and mapped health facilities and providers patronized by residents in Compostela Valley. The information generated by the Household Survey also included access to maternal, newborn, and child health services, as well as family planning counseling and medical commodities.
Physician and midwife survey
This component survey, administered among physicians and midwives, generated information on practice characteristics and case/patient load.
It also included clinical vignettes that measured the quality of select maternal and child health care services provided by physicians and midwives in Compostela Valley.
Hospital and clinics survey
This survey generated information on the operation of health facilities (including pharmacies).
It also included patient exit interviews that provided data on patient characteristics, their health use patterns, and satisfaction from provided health care services.
258 The Family Health Book
Description of the FHB Baseline Survey
Overview
The FHB Baseline Survey consisted of component surveys on households, health care providers, health facilities, and patient exits conducted between 2007 and 2008.
The household survey covered the following number of households:
Compostela 203 Monkayo 339
Laak 199 Montevista 110
Mabini 109 Nabunturan 216
Maco 219 New Bataan 144
Maragusan 147 Pantukan 223
Mawab 112
The health facilities survey covered practically all facilities in Compostela Valley except for hospital-based clinics, and the Davao Regional Hospital and its corporate clinics in Tagum City, which is in the adjoining province of Davao del Norte.
This survey enumerated 12 hospitals (five public and seven private) and 21 private clinics, 11 RHUs, and 21 pharmacies.
The health provider survey covered 94 health professionals (physicians, nurses, and midwives). Disaggregated by health facility where they practiced,
• 25 came from public hospitals; • 13 came from private hospitals;• 2 came from hospital-based clinics;• 17 came from free-standing clinics;• 34 from RHUs and satellite units; and • 3 from birthing home/lying-in clinics.
259Baseline Family Health Book (FHB) Survey Documentation Report
The patient exit survey enumerated respondents from all surveyed hospitals and clinics. They included the following:
• 6 inpatient and 5 outpatients from the regional hospital; • 4 inpatients and 5 outpatients from district and
municipal hospitals; • 4 inpatients and 3 outpatients from private hospitals; and • 3 outpatients from private clinics and RHUs.
In all, the patient exit survey covered a total of 61 inpatient (23 maternal and 38 pediatric cases) and 166 outpatient (48 maternal and 118 pediatric cases) respondents.
Sampling Design
Household Survey
To measure health care utilization (particularly of maternal, neonatal, and child health services) in Compostela Valley, a random survey of households was conducted in select barangays in each of its municipalities.
Respondent households were selected using multi-stage stratified sampling with clustering. Barangays from each municipality were selected using probability-proportional-to-size (PPS).
Random sampling of households was done in each cluster. In developing a barangay sampling frame, barangay officials, barangay health workers, social workers, and rural health center staff were consulted to identify households with pregnant women or children below 1 year old.
The survey allowed for a 20-percent maximum drop-out rate; thus, from the sampling frame, 52 households (104 for 2-cluster barangays) were randomly drawn. Attaining 43 respondent households (86 for 2-cluster barangays) sufficed for the quota for a barangay.
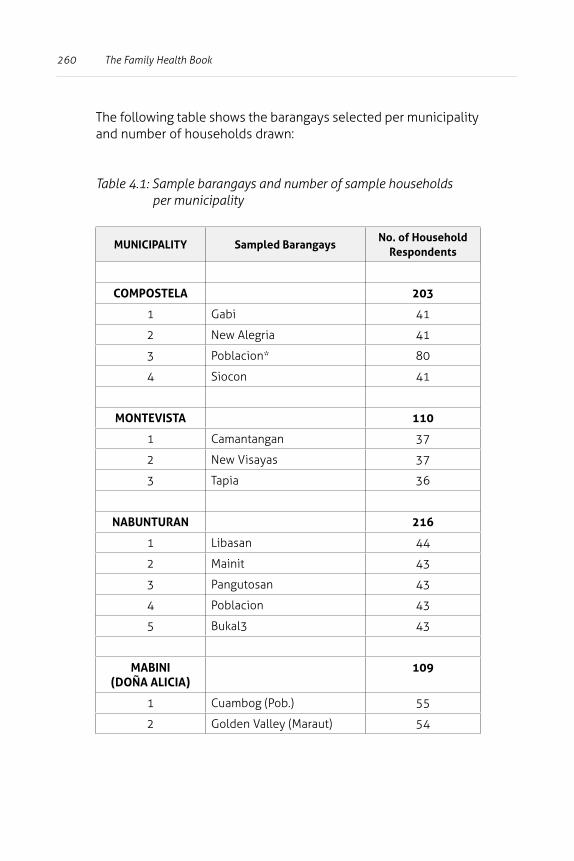
260 The Family Health Book
The following table shows the barangays selected per municipality and number of households drawn:
Table 4.1: Sample barangays and number of sample households per municipality
MUNICIPALITY Sampled BarangaysNo. of Household
Respondents
COMPOSTELA 203
1 Gabi 41
2 New Alegria 41
3 Poblacion* 80
4 Siocon 41
MONTEVISTA 110
1 Camantangan 37
2 New Visayas 37
3 Tapia 36
NABUNTURAN 216
1 Libasan 44
2 Mainit 43
3 Pangutosan 43
4 Poblacion 43
5 Bukal3 43
MABINI (DOÑA ALICIA)
109
1 Cuambog (Pob.) 55
2 Golden Valley (Maraut) 54
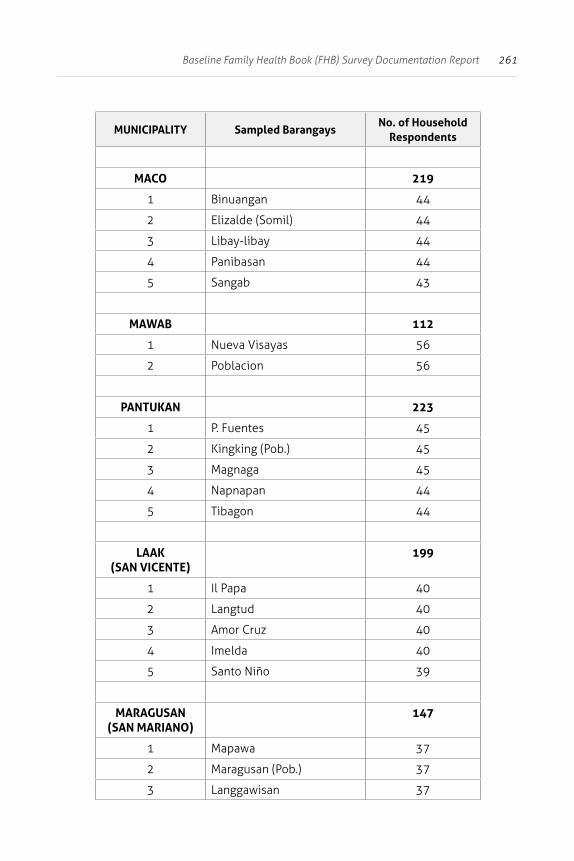
261Baseline Family Health Book (FHB) Survey Documentation Report
MUNICIPALITY Sampled BarangaysNo. of Household
Respondents
MACO 219
1 Binuangan 44
2 Elizalde (Somil) 44
3 Libay-libay 44
4 Panibasan 44
5 Sangab 43
MAWAB 112
1 Nueva Visayas 56
2 Poblacion 56
PANTUKAN 223
1 P. Fuentes 45
2 Kingking (Pob.) 45
3 Magnaga 45
4 Napnapan 44
5 Tibagon 44
LAAK (SAN VICENTE)
199
1 Il Papa 40
2 Langtud 40
3 Amor Cruz 40
4 Imelda 40
5 Santo Niño 39
MARAGUSAN(SAN MARIANO)
147
1 Mapawa 37
2 Maragusan (Pob.) 37
3 Langgawisan 37
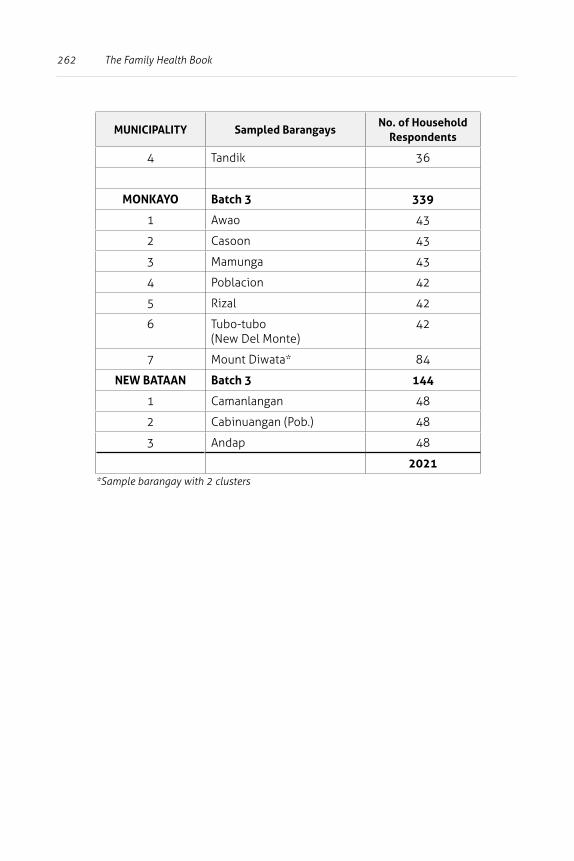
262 The Family Health Book
MUNICIPALITY Sampled BarangaysNo. of Household
Respondents
4 Tandik 36
MONKAYO Batch 3 339
1 Awao 43
2 Casoon 43
3 Mamunga 43
4 Poblacion 42
5 Rizal 42
6 Tubo-tubo (New Del Monte)
42
7 Mount Diwata* 84
NEW BATAAN Batch 3 144
1 Camanlangan 48
2 Cabinuangan (Pob.) 48
3 Andap 48
2021*Sample barangay with 2 clusters
263Baseline Family Health Book (FHB) Survey Documentation Report
Some households were dropped from the sample on the following bases:
1) respondent household could not be located; 2) respondent household refused to participate in the survey; 3) household number and name of household head did not
match with what is in the field; and4) the house was all closed up and the neighbor said no
one lived there, or the respondent household moved away permanently.
In these cases, the enumerator proceeded to the next household in the list. If household members were temporarily unavailable for interview, the enumerator scheduled a call back. A household was dropped from the sample only after six (6) failed call-backs.
In case the household transferred within the same barangay, the enumerator should find the household in the new location and administer the questionnaire.
Physician and Midwife Survey and Quality of Care Assessment Using Vignettes
This survey collected data on the characteristics and clinical and non-clinical practices of health care providers in Compostela Valley. Through clinical vignettes, it also measured the quality of maternal and child health care services provided.
All facility-based and free-standing/independent physicians attending to maternal, neonatal, and child-health/pediatric cases were considered eligible for the survey. The following table shows the vignettes and number of respondents selected in all public and private hospitals in Compostela Valley.
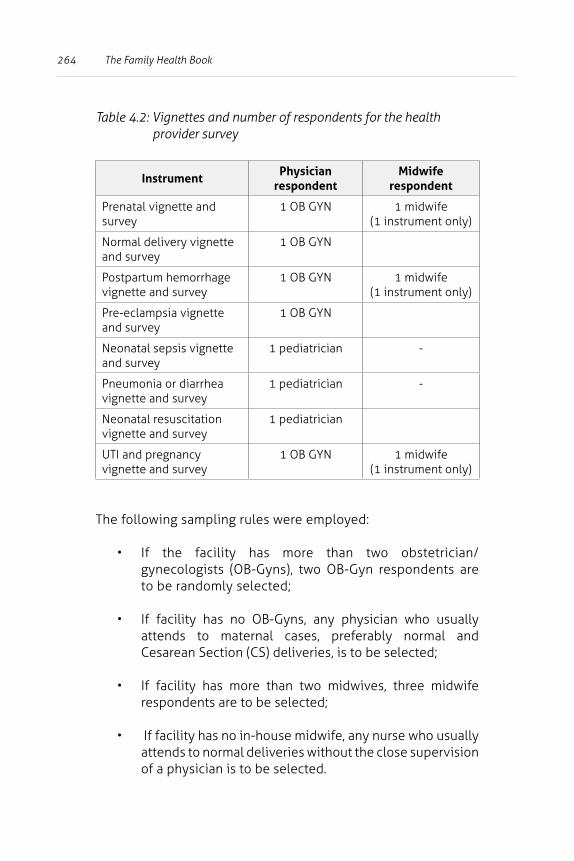
264 The Family Health Book
Table 4.2: Vignettes and number of respondents for the health provider survey
InstrumentPhysician
respondentMidwife
respondent
Prenatal vignette and survey
1 OB GYN 1 midwife (1 instrument only)
Normal delivery vignette and survey
1 OB GYN
Postpartum hemorrhage vignette and survey
1 OB GYN 1 midwife (1 instrument only)
Pre-eclampsia vignette and survey
1 OB GYN
Neonatal sepsis vignette and survey
1 pediatrician -
Pneumonia or diarrhea vignette and survey
1 pediatrician -
Neonatal resuscitation vignette and survey
1 pediatrician
UTI and pregnancy vignette and survey
1 OB GYN 1 midwife (1 instrument only)
The following sampling rules were employed:
• If the facility has more than two obstetrician/gynecologists (OB-Gyns), two OB-Gyn respondents are to be randomly selected;
• If facility has no OB-Gyns, any physician who usually attends to maternal cases, preferably normal and Cesarean Section (CS) deliveries, is to be selected;
• If facility has more than two midwives, three midwife respondents are to be selected;
• If facility has no in-house midwife, any nurse who usually attends to normal deliveries without the close supervision of a physician is to be selected.
265Baseline Family Health Book (FHB) Survey Documentation Report
• If facility has more than two pediatricians, two pediatrician respondents are to be randomly selected;
• If facility has no pediatrician, any physician who usually attends to pediatric cases is to be selected.
• For free-standing or independent physicians attending to maternal, neonatal, and pediatric cases, either prenatal or normal delivery vignette and survey AND either postpartum hemorrhage or preeclampsia vignette and survey should be administered to all independent OB-Gyns, Family Medicine practitioners, general practitioners (GPs), and midwives.
• Eligible respondents who cannot be located (after 6 call-backs), who refuse to participate in the survey and sign a waiver form, who are on leave for more than a week, or who have permanently relocated outside Compostela Valley are considered drop-outs.
In such a case, the enumerator should randomly choose another facility-based respondent. In addition, respondents who refuse to answer one or two vignettes should sign a waiver form.
266 The Family Health Book
Health Facility Survey
This survey covered all public and private hospitals in Compostela Valley, and included the Davao Regional Hospital in Tagum City. It also all pharmacies and RHUs. The survey aimed to collect data on facility staff, equipment inventory, and facility pricing and services. Table 4.3 shows the sampling design by facility type.In case of refusal by the selected facility, the enumerator should request the facility administrator to sign a waiver form. If the administrator refuses to sign, the enumerator should inform the HPDP field auditor as soon as possible for further instructions.
For refusals in the patient exit survey, the enumerator should list down the names of refusing respondents and their reasons for refusal. Another qualified respondent must be identified to replace the dropped respondent.
Description of Survey Instruments
Four questionnaires composed the FHB baseline survey:
1) household survey;2) health provider survey (for physicians, nurses, and
midwives);3) facility questionnaire (for public and private hospitals,
RHUs, facility-based and free-standing clinics, and birthing homes; and
4) patient exit survey (for inpatients and outpatients).
The household survey collect baseline data on characteristics of households and their health-seeking behavior, particularly that of pregnant mothers and children below a year old. The questionnaire is composed of the following blocks:
• sampling information; • household information (number of members, sex,
employment, lifestyle, among others); • socio-economic status;
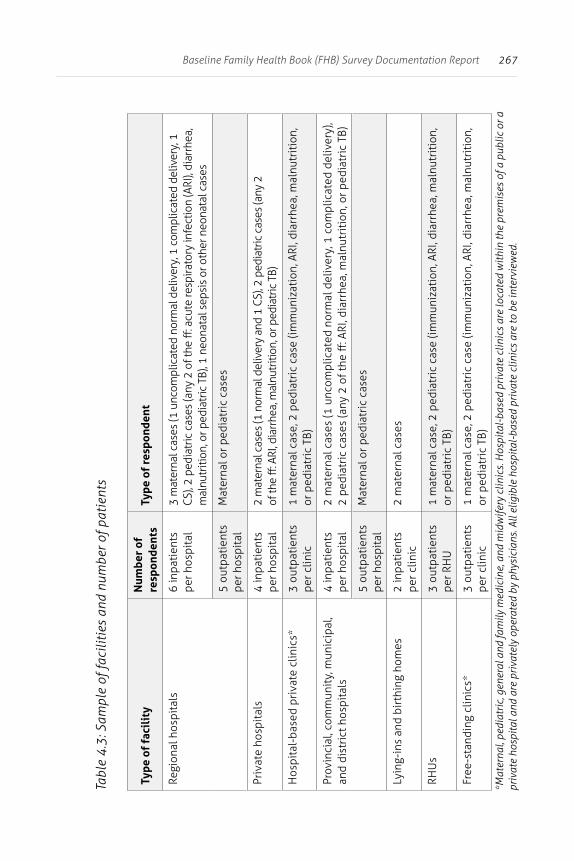
267Baseline Family Health Book (FHB) Survey Documentation Report
Tabl
e 4
.3: S
ampl
e of
faci
litie
s an
d nu
mbe
r of p
atie
nts
Type
of
faci
lity
Num
ber
of
resp
onde
nts
Type
of
resp
onde
nt
Regi
onal
hos
pita
ls6
inpa
tien
ts
per h
ospi
tal
3 m
ater
nal c
ases
(1 u
ncom
plic
ated
nor
mal
del
iver
y, 1
com
plic
ated
del
iver
y, 1
CS
), 2
pedi
atric
cas
es (a
ny 2
of t
he ff
: acu
te re
spira
tory
infe
ctio
n (A
RI),
diar
rhea
, m
alnu
triti
on, o
r ped
iatr
ic T
B), 1
neo
nata
l sep
sis
or o
ther
neo
nata
l cas
es
5 ou
tpat
ient
s pe
r hos
pita
lM
ater
nal o
r ped
iatr
ic c
ases
Priv
ate
hosp
ital
s4
inpa
tien
ts
per h
ospi
tal
2 m
ater
nal c
ases
(1 n
orm
al d
eliv
ery
and
1 CS
), 2
pedi
atric
cas
es (a
ny 2
of
the
ff: A
RI, d
iarr
hea,
mal
nutr
ition
, or p
edia
tric
TB)
Hos
pita
l-ba
sed
priv
ate
clin
ics*
3 ou
tpat
ient
s pe
r clin
ic1
mat
erna
l cas
e, 2
ped
iatr
ic c
ase
(imm
uniz
atio
n, A
RI, d
iarr
hea,
mal
nutr
itio
n,
or p
edia
tric
TB)
Prov
inci
al, c
omm
unit
y, m
unic
ipal
, an
d di
stri
ct h
ospi
tals
4
inpa
tien
ts
per h
ospi
tal
2 m
ater
nal c
ases
(1 u
ncom
plic
ated
nor
mal
del
iver
y, 1
com
plic
ated
del
iver
y),
2 pe
diat
ric
case
s (a
ny 2
of t
he ff
: ARI
, dia
rrhe
a, m
alnu
trit
ion,
or p
edia
tric
TB)
5 ou
tpat
ient
s pe
r hos
pita
lM
ater
nal o
r ped
iatr
ic c
ases
Lyin
g-in
s an
d bi
rthi
ng h
omes
2 in
pati
ents
pe
r clin
ic2
mat
erna
l cas
es
RHU
s3
outp
atie
nts
per R
HU
1 m
ater
nal c
ase,
2 p
edia
tric
cas
e (im
mun
izat
ion,
ARI
, dia
rrhe
a, m
alnu
trit
ion,
or
ped
iatr
ic T
B)
Free
-sta
ndin
g cl
inic
s*3
outp
atie
nts
per c
linic
1 m
ater
nal c
ase,
2 p
edia
tric
cas
e (im
mun
izat
ion,
ARI
, dia
rrhe
a, m
alnu
trit
ion,
or
ped
iatr
ic T
B)
*Mat
erna
l, pe
diat
ric,
gen
eral
and
fam
ily m
edic
ine,
and
mid
wife
ry c
linic
s. H
ospi
tal-
base
d pr
ivat
e cl
inic
s ar
e lo
cate
d w
ithin
the
prem
ises
of a
pub
lic o
r a
priv
ate
hosp
ital a
nd a
re p
riva
tely
ope
rate
d by
phy
sici
ans.
All
elig
ible
hos
pita
l-ba
sed
priv
ate
clin
ics
are
to b
e in
terv
iew
ed.
268 The Family Health Book
• health-status, health-seeking behavior, and health financing (health care expenditures of pregnant mothers and one-year-old children and below; preventive care and morbidity for infants; and
• family planning practices.
The physician and midwife survey questionnaire collected data on physician characteristics and the quality of their service. It contained the following information blocks:
• general provider information; • practice characteristics; • practice time allocation; • case load and mix; • referrals; • PhilHealth accreditation; and • income distribution by source.
The clinical vignettes measured provider quality and had the following domains:
• Routine/Normal pregnancy care;• Specialized/additional/complicated pregnancy care;• Outline/normal labor and delivery care;• Specialized/additional/complicated labor and delivery care;• Routine neonatal care (neonatal resuscitation);• Specialized/additional/complicated newborn care;• Routine general pediatric care (including immunization); and• Specialized/additional/complicated general pediatric care.
For the facility survey, different questionnaires were administered for hospitals, clinics, lying-in and birthing homes, and RHUs.
The RHU/clinic questionnaire had the following information blocks:
• general clinic characteristics; • facility management; • patient load and mix; • laboratory services; • equipment/supplies availability; • drugs and contraceptives availability;
269Baseline Family Health Book (FHB) Survey Documentation Report
• financing; • services packages; • networking; and • provider satisfaction.
The hospital survey questionnaire had the followinginformation blocks:
• general hospital characteristics; • hospital management;• patient load and mix; • laboratory services; • equipment availability; • drugs and medicine availability; • medical supplies availability; • networking; and • hospital administration satisfaction.
The patient exit survey is composed of inpatient and outpatient questionnaires designed to capture the following data:
• general information of patients; • health status; • pre-hospitalization events; • description of confinement; • services and medical expenditures; • records review; • provider satisfaction; • development and general well-being index; and • housing, assets, expenditure, and income.
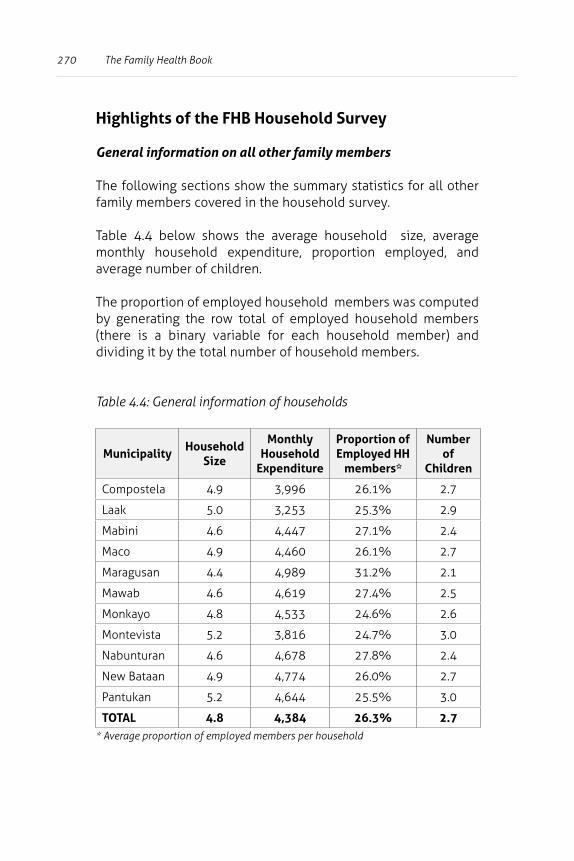
270 The Family Health Book
Highlights of the FHB Household Survey
General information on all other family members
The following sections show the summary statistics for all other family members covered in the household survey.
Table 4.4 below shows the average household size, average monthly household expenditure, proportion employed, and average number of children.
The proportion of employed household members was computed by generating the row total of employed household members (there is a binary variable for each household member) and dividing it by the total number of household members.
Table 4.4: General information of households
MunicipalityHousehold
Size
Monthly Household
Expenditure
Proportion of Employed HH
members*
Number of
Children
Compostela 4.9 3,996 26.1% 2.7
Laak 5.0 3,253 25.3% 2.9
Mabini 4.6 4,447 27.1% 2.4
Maco 4.9 4,460 26.1% 2.7
Maragusan 4.4 4,989 31.2% 2.1
Mawab 4.6 4,619 27.4% 2.5
Monkayo 4.8 4,533 24.6% 2.6
Montevista 5.2 3,816 24.7% 3.0
Nabunturan 4.6 4,678 27.8% 2.4
New Bataan 4.9 4,774 26.0% 2.7
Pantukan 5.2 4,644 25.5% 3.0
TOTAL 4.8 4,384 26.3% 2.7* Average proportion of employed members per household
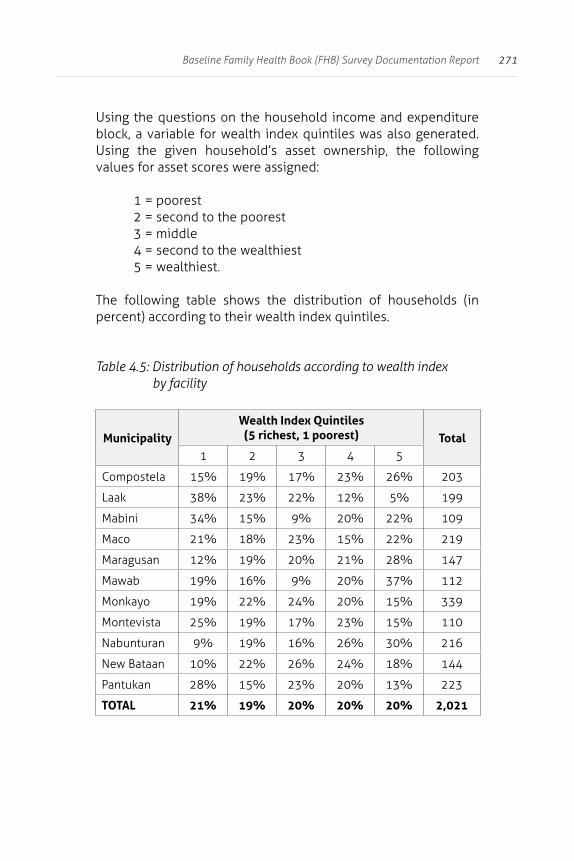
271Baseline Family Health Book (FHB) Survey Documentation Report
Using the questions on the household income and expenditure block, a variable for wealth index quintiles was also generated. Using the given household’s asset ownership, the following values for asset scores were assigned:
1 = poorest2 = second to the poorest3 = middle4 = second to the wealthiest 5 = wealthiest.
The following table shows the distribution of households (in percent) according to their wealth index quintiles.
Table 4.5: Distribution of households according to wealth index by facility
MunicipalityWealth Index Quintiles
(5 richest, 1 poorest) Total1 2 3 4 5
Compostela 15% 19% 17% 23% 26% 203
Laak 38% 23% 22% 12% 5% 199
Mabini 34% 15% 9% 20% 22% 109
Maco 21% 18% 23% 15% 22% 219
Maragusan 12% 19% 20% 21% 28% 147
Mawab 19% 16% 9% 20% 37% 112
Monkayo 19% 22% 24% 20% 15% 339
Montevista 25% 19% 17% 23% 15% 110
Nabunturan 9% 19% 16% 26% 30% 216
New Bataan 10% 22% 26% 24% 18% 144
Pantukan 28% 15% 23% 20% 13% 223
TOTAL 21% 19% 20% 20% 20% 2,021
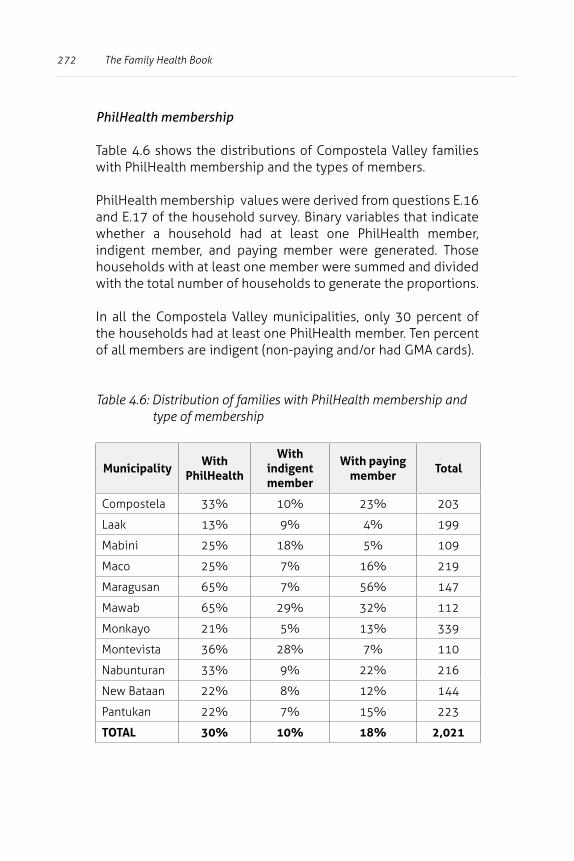
272 The Family Health Book
PhilHealth membership
Table 4.6 shows the distributions of Compostela Valley families with PhilHealth membership and the types of members.
PhilHealth membership values were derived from questions E.16 and E.17 of the household survey. Binary variables that indicate whether a household had at least one PhilHealth member, indigent member, and paying member were generated. Those households with at least one member were summed and divided with the total number of households to generate the proportions.
In all the Compostela Valley municipalities, only 30 percent of the households had at least one PhilHealth member. Ten percent of all members are indigent (non-paying and/or had GMA cards).
Table 4.6: Distribution of families with PhilHealth membership and type of membership
MunicipalityWith
PhilHealth
With indigent member
With paying member
Total
Compostela 33% 10% 23% 203
Laak 13% 9% 4% 199
Mabini 25% 18% 5% 109
Maco 25% 7% 16% 219
Maragusan 65% 7% 56% 147
Mawab 65% 29% 32% 112
Monkayo 21% 5% 13% 339
Montevista 36% 28% 7% 110
Nabunturan 33% 9% 22% 216
New Bataan 22% 8% 12% 144
Pantukan 22% 7% 15% 223
TOTAL 30% 10% 18% 2,021
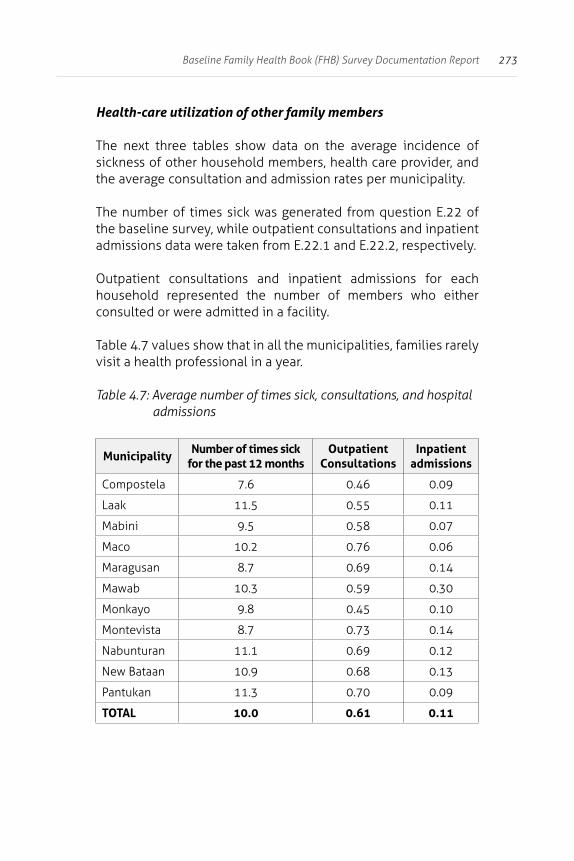
273Baseline Family Health Book (FHB) Survey Documentation Report
Health-care utilization of other family members
The next three tables show data on the average incidence of sickness of other household members, health care provider, and the average consultation and admission rates per municipality.
The number of times sick was generated from question E.22 of the baseline survey, while outpatient consultations and inpatient admissions data were taken from E.22.1 and E.22.2, respectively.
Outpatient consultations and inpatient admissions for each household represented the number of members who either consulted or were admitted in a facility.
Table 4.7 values show that in all the municipalities, families rarely visit a health professional in a year.
Table 4.7: Average number of times sick, consultations, and hospital admissions
MunicipalityNumber of times sick
for the past 12 monthsOutpatient
ConsultationsInpatient
admissions
Compostela 7.6 0.46 0.09
Laak 11.5 0.55 0.11
Mabini 9.5 0.58 0.07
Maco 10.2 0.76 0.06
Maragusan 8.7 0.69 0.14
Mawab 10.3 0.59 0.30
Monkayo 9.8 0.45 0.10
Montevista 8.7 0.73 0.14
Nabunturan 11.1 0.69 0.12
New Bataan 10.9 0.68 0.13
Pantukan 11.3 0.70 0.09
TOTAL 10.0 0.61 0.11
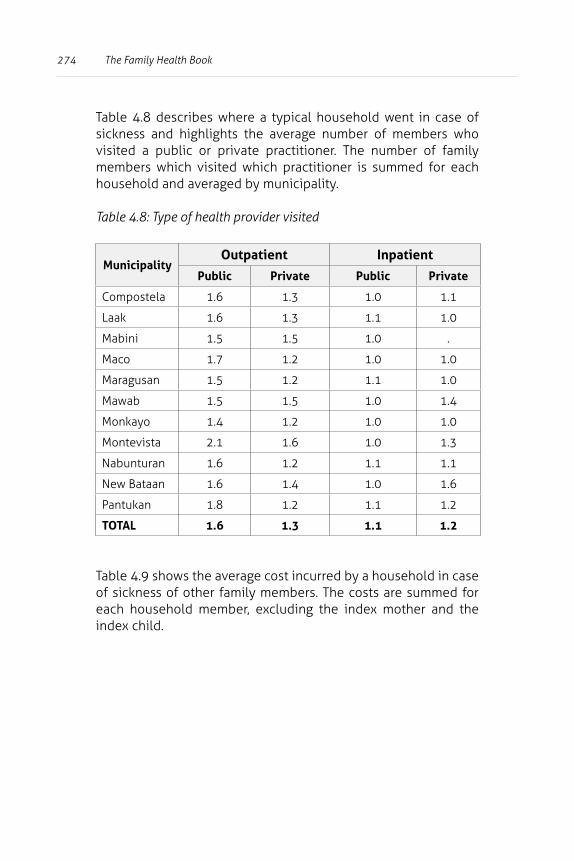
274 The Family Health Book
Table 4.8 describes where a typical household went in case of sickness and highlights the average number of members who visited a public or private practitioner. The number of family members which visited which practitioner is summed for each household and averaged by municipality.
Table 4.8: Type of health provider visited
MunicipalityOutpatient Inpatient
Public Private Public Private
Compostela 1.6 1.3 1.0 1.1
Laak 1.6 1.3 1.1 1.0
Mabini 1.5 1.5 1.0 .
Maco 1.7 1.2 1.0 1.0
Maragusan 1.5 1.2 1.1 1.0
Mawab 1.5 1.5 1.0 1.4
Monkayo 1.4 1.2 1.0 1.0
Montevista 2.1 1.6 1.0 1.3
Nabunturan 1.6 1.2 1.1 1.1
New Bataan 1.6 1.4 1.0 1.6
Pantukan 1.8 1.2 1.1 1.2
TOTAL 1.6 1.3 1.1 1.2
Table 4.9 shows the average cost incurred by a household in case of sickness of other family members. The costs are summed for each household member, excluding the index mother and the index child.
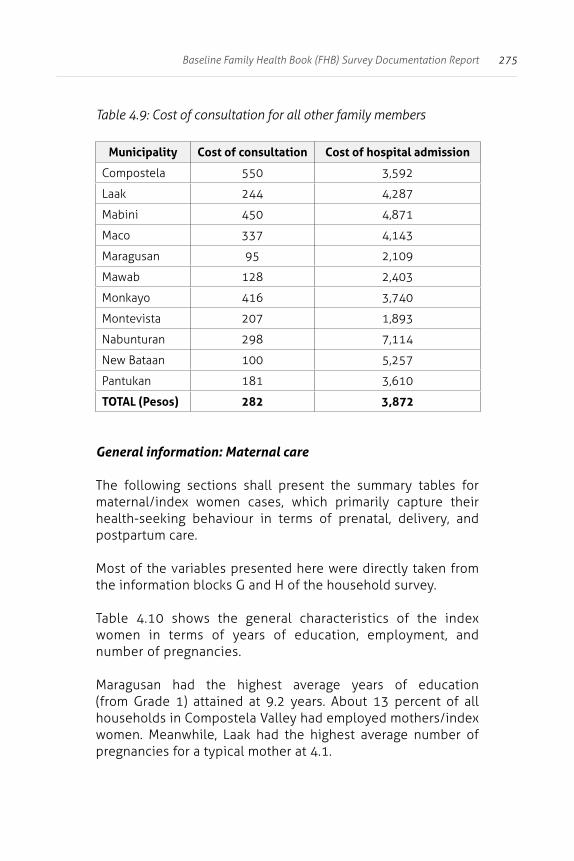
275Baseline Family Health Book (FHB) Survey Documentation Report
Table 4.9: Cost of consultation for all other family members
Municipality Cost of consultation Cost of hospital admission
Compostela 550 3,592
Laak 244 4,287
Mabini 450 4,871
Maco 337 4,143
Maragusan 95 2,109
Mawab 128 2,403
Monkayo 416 3,740
Montevista 207 1,893
Nabunturan 298 7,114
New Bataan 100 5,257
Pantukan 181 3,610
TOTAL (Pesos) 282 3,872
General information: Maternal care
The following sections shall present the summary tables for maternal/index women cases, which primarily capture their health-seeking behaviour in terms of prenatal, delivery, and postpartum care.
Most of the variables presented here were directly taken from the information blocks G and H of the household survey.
Table 4.10 shows the general characteristics of the index women in terms of years of education, employment, and number of pregnancies.
Maragusan had the highest average years of education (from Grade 1) attained at 9.2 years. About 13 percent of all households in Compostela Valley had employed mothers/index women. Meanwhile, Laak had the highest average number of pregnancies for a typical mother at 4.1.
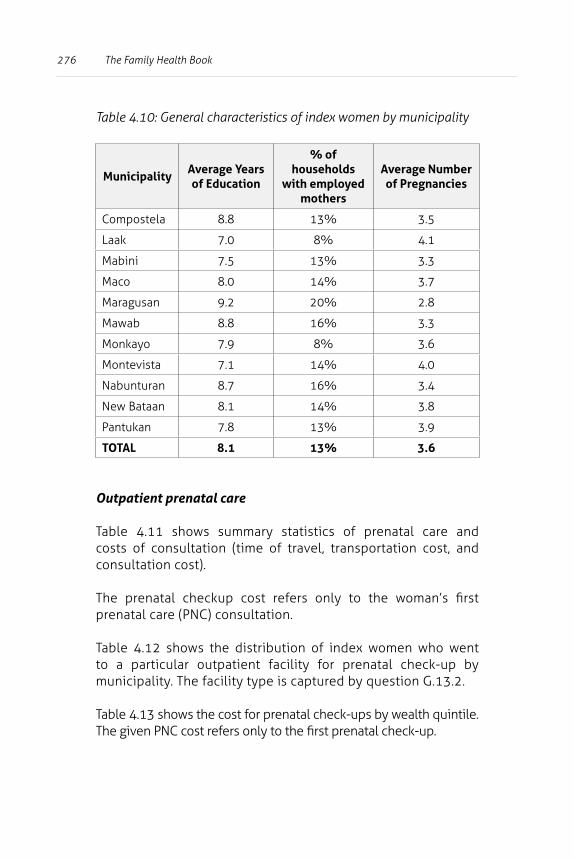
276 The Family Health Book
Table 4.10: General characteristics of index women by municipality
MunicipalityAverage Years of Education
% of households
with employed mothers
Average Number of Pregnancies
Compostela 8.8 13% 3.5
Laak 7.0 8% 4.1
Mabini 7.5 13% 3.3
Maco 8.0 14% 3.7
Maragusan 9.2 20% 2.8
Mawab 8.8 16% 3.3
Monkayo 7.9 8% 3.6
Montevista 7.1 14% 4.0
Nabunturan 8.7 16% 3.4
New Bataan 8.1 14% 3.8
Pantukan 7.8 13% 3.9
TOTAL 8.1 13% 3.6
Outpatient prenatal care
Table 4.11 shows summary statistics of prenatal care and costs of consultation (time of travel, transportation cost, and consultation cost).
The prenatal checkup cost refers only to the woman’s first prenatal care (PNC) consultation.
Table 4.12 shows the distribution of index women who went to a particular outpatient facility for prenatal check-up by municipality. The facility type is captured by question G.13.2.
Table 4.13 shows the cost for prenatal check-ups by wealth quintile. The given PNC cost refers only to the first prenatal check-up.
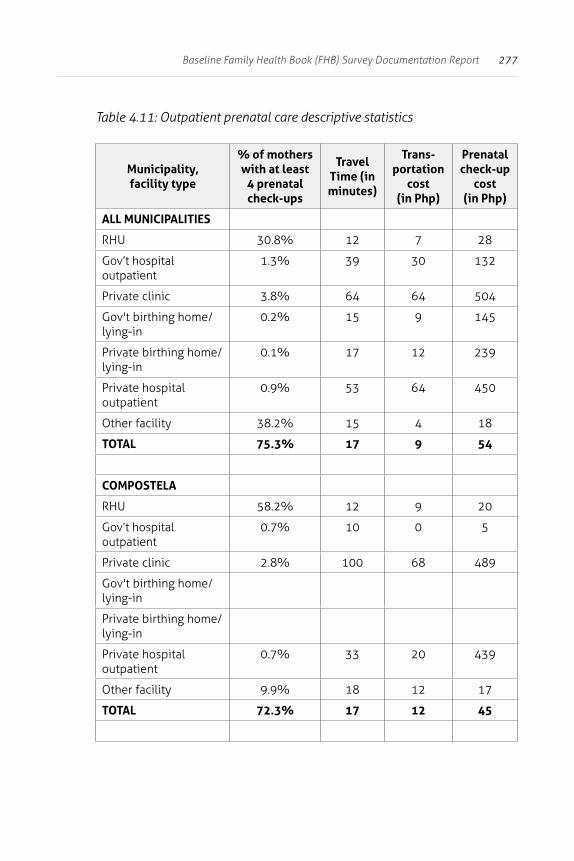
277Baseline Family Health Book (FHB) Survey Documentation Report
Table 4.11: Outpatient prenatal care descriptive statistics
Municipality, facility type
% of mothers with at least
4 prenatal check-ups
Travel Time (in minutes)
Trans-portation
cost (in Php)
Prenatal check-up
cost (in Php)
ALL MUNICIPALITIES
RHU 30.8% 12 7 28
Gov’t hospital outpatient
1.3% 39 30 132
Private clinic 3.8% 64 64 504
Gov't birthing home/lying-in
0.2% 15 9 145
Private birthing home/lying-in
0.1% 17 12 239
Private hospital outpatient
0.9% 53 64 450
Other facility 38.2% 15 4 18
TOTAL 75.3% 17 9 54
COMPOSTELA
RHU 58.2% 12 9 20
Gov’t hospital outpatient
0.7% 10 0 5
Private clinic 2.8% 100 68 489
Gov't birthing home/lying-in
Private birthing home/lying-in
Private hospital outpatient
0.7% 33 20 439
Other facility 9.9% 18 12 17
TOTAL 72.3% 17 12 45
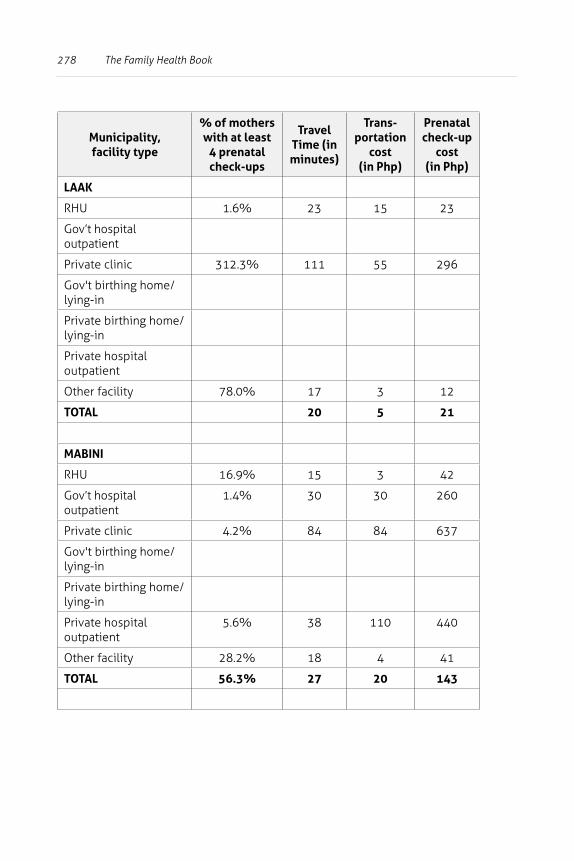
278 The Family Health Book
Municipality, facility type
% of mothers with at least
4 prenatal check-ups
Travel Time (in minutes)
Trans-portation
cost (in Php)
Prenatal check-up
cost (in Php)
LAAK
RHU 1.6% 23 15 23
Gov’t hospital outpatient
Private clinic 312.3% 111 55 296
Gov't birthing home/lying-in
Private birthing home/lying-in
Private hospital outpatient
Other facility 78.0% 17 3 12
TOTAL 20 5 21
MABINI
RHU 16.9% 15 3 42
Gov’t hospital outpatient
1.4% 30 30 260
Private clinic 4.2% 84 84 637
Gov't birthing home/lying-in
Private birthing home/lying-in
Private hospital outpatient
5.6% 38 110 440
Other facility 28.2% 18 4 41
TOTAL 56.3% 27 20 143
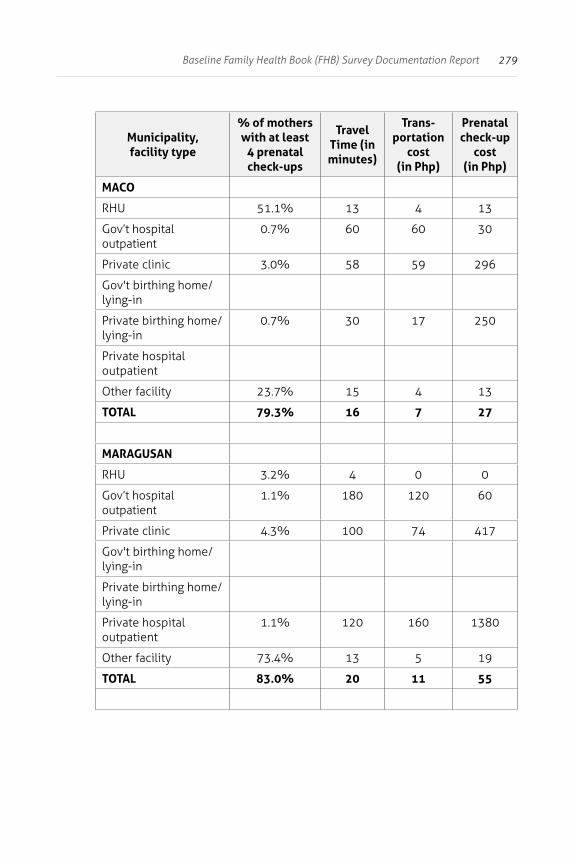
279Baseline Family Health Book (FHB) Survey Documentation Report
Municipality, facility type
% of mothers with at least
4 prenatal check-ups
Travel Time (in minutes)
Trans-portation
cost (in Php)
Prenatal check-up
cost (in Php)
MACO
RHU 51.1% 13 4 13
Gov’t hospital outpatient
0.7% 60 60 30
Private clinic 3.0% 58 59 296
Gov't birthing home/lying-in
Private birthing home/lying-in
0.7% 30 17 250
Private hospital outpatient
Other facility 23.7% 15 4 13
TOTAL 79.3% 16 7 27
MARAGUSAN
RHU 3.2% 4 0 0
Gov’t hospital outpatient
1.1% 180 120 60
Private clinic 4.3% 100 74 417
Gov't birthing home/lying-in
Private birthing home/lying-in
Private hospital outpatient
1.1% 120 160 1380
Other facility 73.4% 13 5 19
TOTAL 83.0% 20 11 55
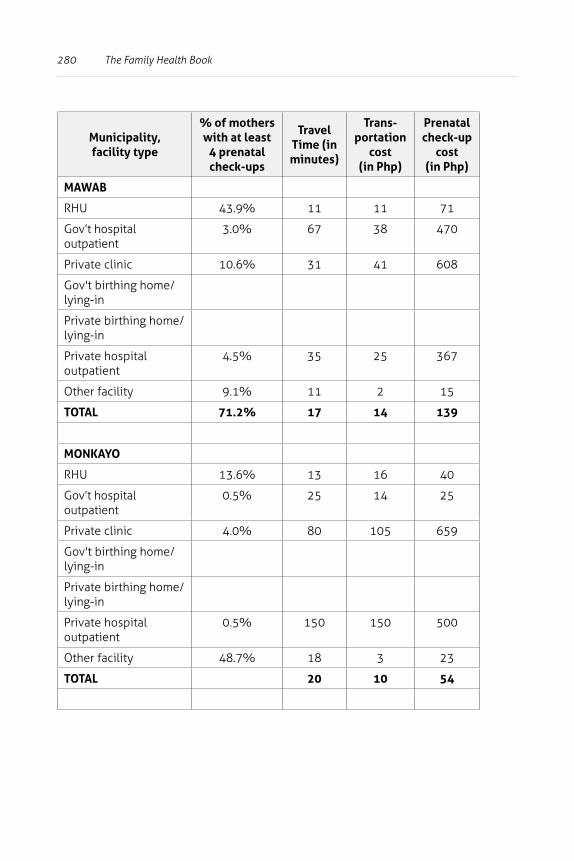
280 The Family Health Book
Municipality, facility type
% of mothers with at least
4 prenatal check-ups
Travel Time (in minutes)
Trans-portation
cost (in Php)
Prenatal check-up
cost (in Php)
MAWAB
RHU 43.9% 11 11 71
Gov’t hospital outpatient
3.0% 67 38 470
Private clinic 10.6% 31 41 608
Gov't birthing home/lying-in
Private birthing home/lying-in
Private hospital outpatient
4.5% 35 25 367
Other facility 9.1% 11 2 15
TOTAL 71.2% 17 14 139
MONKAYO
RHU 13.6% 13 16 40
Gov’t hospital outpatient
0.5% 25 14 25
Private clinic 4.0% 80 105 659
Gov't birthing home/lying-in
Private birthing home/lying-in
Private hospital outpatient
0.5% 150 150 500
Other facility 48.7% 18 3 23
TOTAL 20 10 54
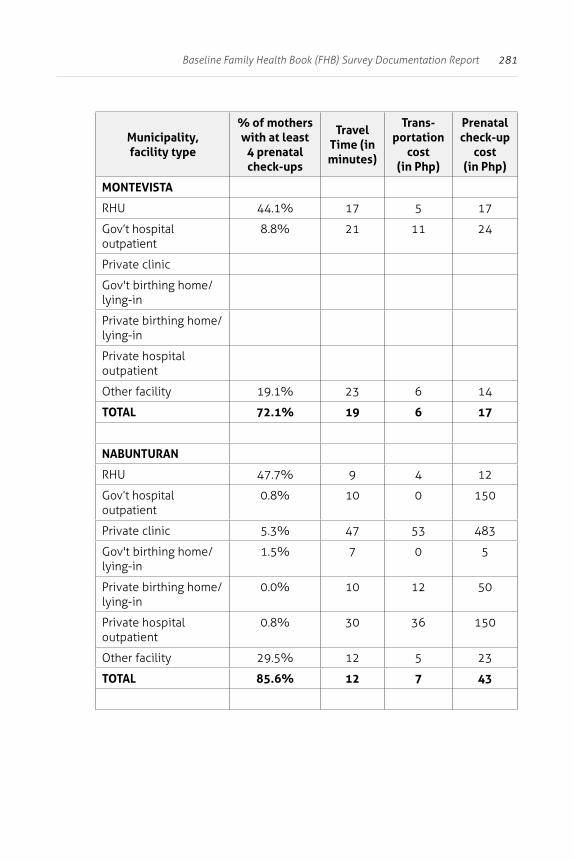
281Baseline Family Health Book (FHB) Survey Documentation Report
Municipality, facility type
% of mothers with at least
4 prenatal check-ups
Travel Time (in minutes)
Trans-portation
cost (in Php)
Prenatal check-up
cost (in Php)
MONTEVISTA
RHU 44.1% 17 5 17
Gov’t hospital outpatient
8.8% 21 11 24
Private clinic
Gov't birthing home/lying-in
Private birthing home/lying-in
Private hospital outpatient
Other facility 19.1% 23 6 14
TOTAL 72.1% 19 6 17
NABUNTURAN
RHU 47.7% 9 4 12
Gov’t hospital outpatient
0.8% 10 0 150
Private clinic 5.3% 47 53 483
Gov't birthing home/lying-in
1.5% 7 0 5
Private birthing home/lying-in
0.0% 10 12 50
Private hospital outpatient
0.8% 30 36 150
Other facility 29.5% 12 5 23
TOTAL 85.6% 12 7 43
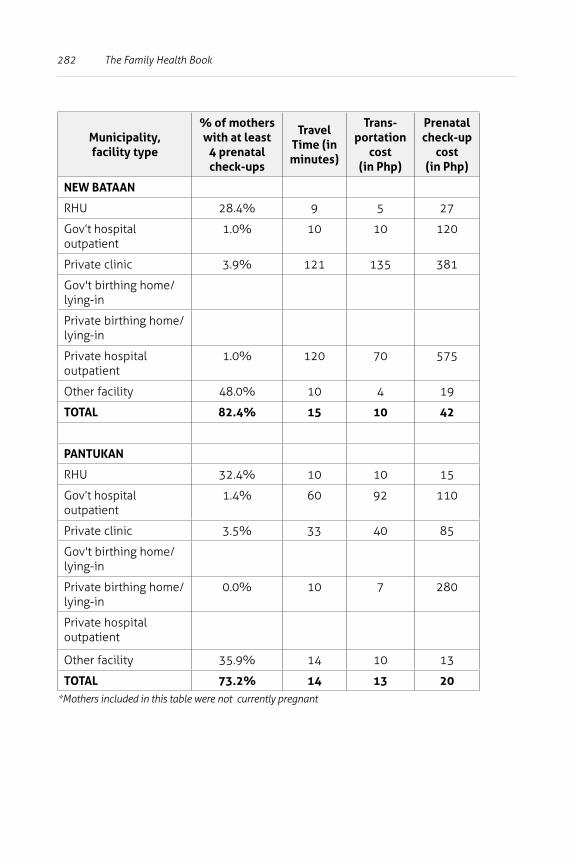
282 The Family Health Book
Municipality, facility type
% of mothers with at least
4 prenatal check-ups
Travel Time (in minutes)
Trans-portation
cost (in Php)
Prenatal check-up
cost (in Php)
NEW BATAAN
RHU 28.4% 9 5 27
Gov’t hospital outpatient
1.0% 10 10 120
Private clinic 3.9% 121 135 381
Gov't birthing home/lying-in
Private birthing home/lying-in
Private hospital outpatient
1.0% 120 70 575
Other facility 48.0% 10 4 19
TOTAL 82.4% 15 10 42
PANTUKAN
RHU 32.4% 10 10 15
Gov’t hospital outpatient
1.4% 60 92 110
Private clinic 3.5% 33 40 85
Gov't birthing home/lying-in
Private birthing home/lying-in
0.0% 10 7 280
Private hospital outpatient
Other facility 35.9% 14 10 13
TOTAL 73.2% 14 13 20*Mothers included in this table were not currently pregnant
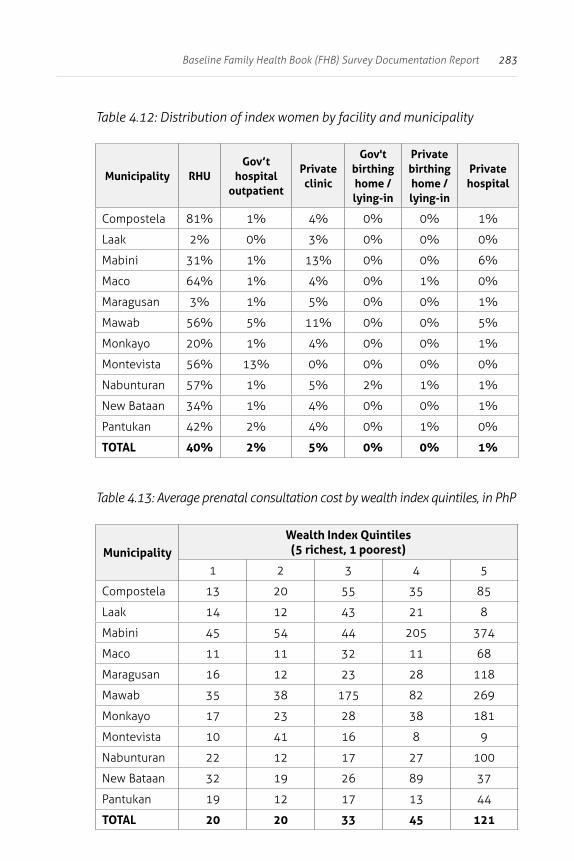
283Baseline Family Health Book (FHB) Survey Documentation Report
Table 4.12: Distribution of index women by facility and municipality
Municipality RHUGov’t
hospital outpatient
Private clinic
Gov't birthing home /lying-in
Private birthing home /lying-in
Private hospital
Compostela 81% 1% 4% 0% 0% 1%
Laak 2% 0% 3% 0% 0% 0%
Mabini 31% 1% 13% 0% 0% 6%
Maco 64% 1% 4% 0% 1% 0%
Maragusan 3% 1% 5% 0% 0% 1%
Mawab 56% 5% 11% 0% 0% 5%
Monkayo 20% 1% 4% 0% 0% 1%
Montevista 56% 13% 0% 0% 0% 0%
Nabunturan 57% 1% 5% 2% 1% 1%
New Bataan 34% 1% 4% 0% 0% 1%
Pantukan 42% 2% 4% 0% 1% 0%
TOTAL 40% 2% 5% 0% 0% 1%
Table 4.13: Average prenatal consultation cost by wealth index quintiles, in PhP
MunicipalityWealth Index Quintiles
(5 richest, 1 poorest)
1 2 3 4 5
Compostela 13 20 55 35 85
Laak 14 12 43 21 8
Mabini 45 54 44 205 374
Maco 11 11 32 11 68
Maragusan 16 12 23 28 118
Mawab 35 38 175 82 269
Monkayo 17 23 28 38 181
Montevista 10 41 16 8 9
Nabunturan 22 12 17 27 100
New Bataan 32 19 26 89 37
Pantukan 19 12 17 13 44
TOTAL 20 20 33 45 121
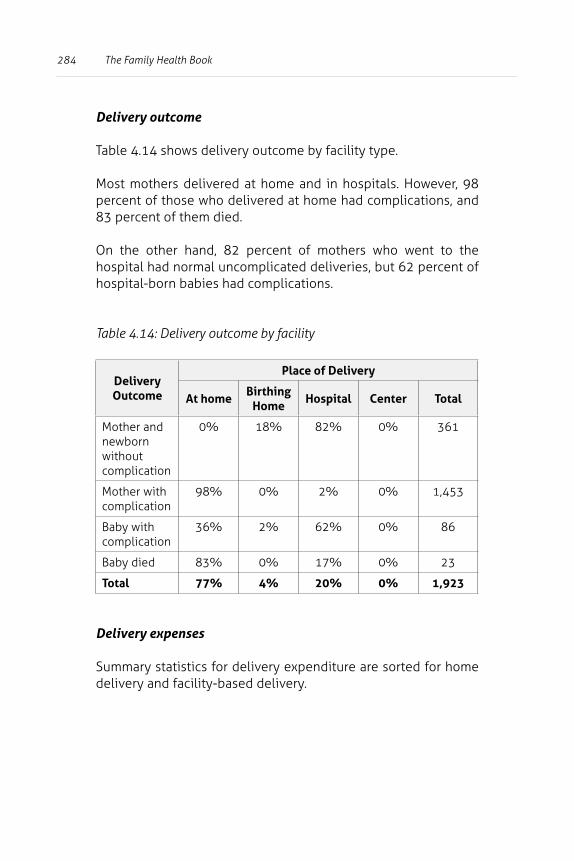
284 The Family Health Book
Delivery outcome
Table 4.14 shows delivery outcome by facility type.
Most mothers delivered at home and in hospitals. However, 98 percent of those who delivered at home had complications, and 83 percent of them died.
On the other hand, 82 percent of mothers who went to the hospital had normal uncomplicated deliveries, but 62 percent of hospital-born babies had complications.
Table 4.14: Delivery outcome by facility
Delivery Outcome
Place of Delivery
At homeBirthing
HomeHospital Center Total
Mother and newborn without complication
0% 18% 82% 0% 361
Mother with complication
98% 0% 2% 0% 1,453
Baby with complication
36% 2% 62% 0% 86
Baby died 83% 0% 17% 0% 23
Total 77% 4% 20% 0% 1,923
Delivery expenses
Summary statistics for delivery expenditure are sorted for home delivery and facility-based delivery.
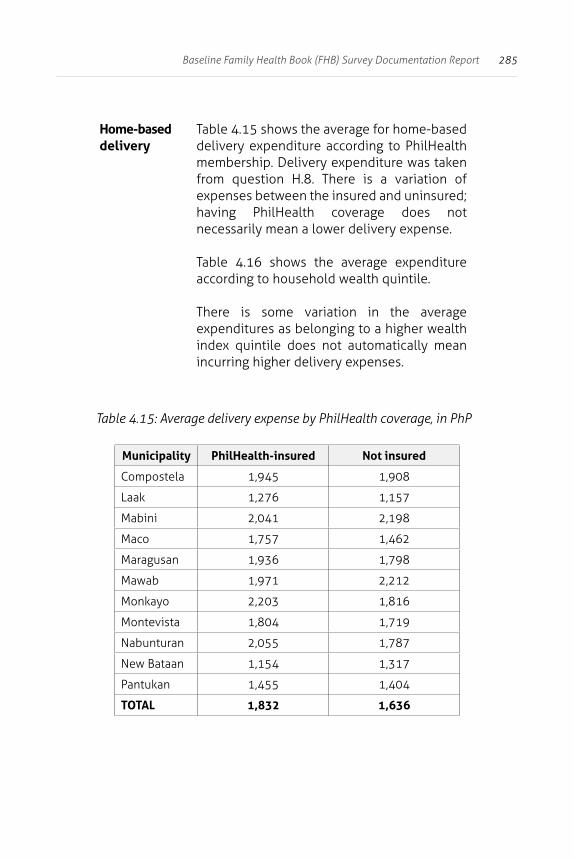
285Baseline Family Health Book (FHB) Survey Documentation Report
Home-based delivery
Table 4.15 shows the average for home-based delivery expenditure according to PhilHealth membership. Delivery expenditure was taken from question H.8. There is a variation of expenses between the insured and uninsured; having PhilHealth coverage does not necessarily mean a lower delivery expense.
Table 4.16 shows the average expenditure according to household wealth quintile.
There is some variation in the average expenditures as belonging to a higher wealth index quintile does not automatically mean incurring higher delivery expenses.
Table 4.15: Average delivery expense by PhilHealth coverage, in PhP
Municipality PhilHealth-insured Not insured
Compostela 1,945 1,908
Laak 1,276 1,157
Mabini 2,041 2,198
Maco 1,757 1,462
Maragusan 1,936 1,798
Mawab 1,971 2,212
Monkayo 2,203 1,816
Montevista 1,804 1,719
Nabunturan 2,055 1,787
New Bataan 1,154 1,317
Pantukan 1,455 1,404
TOTAL 1,832 1,636
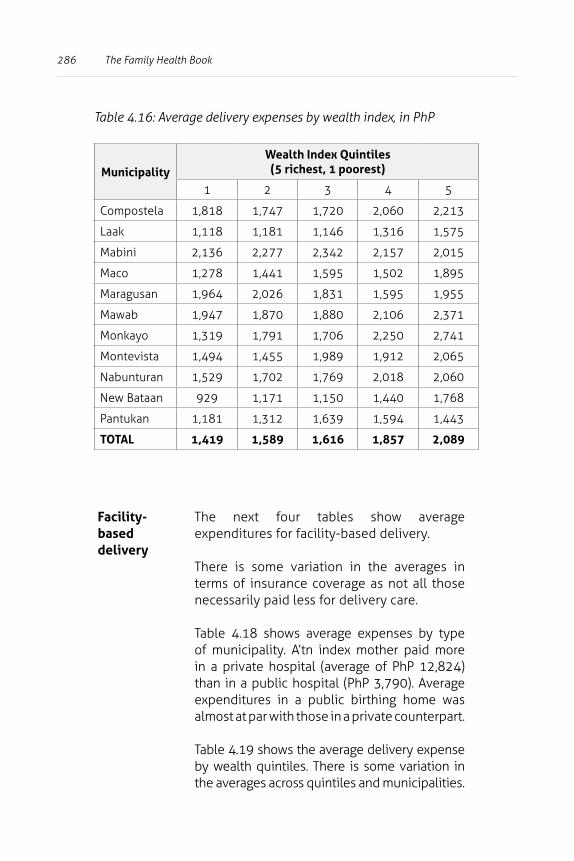
286 The Family Health Book
Table 4.16: Average delivery expenses by wealth index, in PhP
MunicipalityWealth Index Quintiles
(5 richest, 1 poorest)
1 2 3 4 5
Compostela 1,818 1,747 1,720 2,060 2,213
Laak 1,118 1,181 1,146 1,316 1,575
Mabini 2,136 2,277 2,342 2,157 2,015
Maco 1,278 1,441 1,595 1,502 1,895
Maragusan 1,964 2,026 1,831 1,595 1,955
Mawab 1,947 1,870 1,880 2,106 2,371
Monkayo 1,319 1,791 1,706 2,250 2,741
Montevista 1,494 1,455 1,989 1,912 2,065
Nabunturan 1,529 1,702 1,769 2,018 2,060
New Bataan 929 1,171 1,150 1,440 1,768
Pantukan 1,181 1,312 1,639 1,594 1,443
TOTAL 1,419 1,589 1,616 1,857 2,089
Facility-based delivery
The next four tables show average expenditures for facility-based delivery.
There is some variation in the averages in terms of insurance coverage as not all those necessarily paid less for delivery care.
Table 4.18 shows average expenses by type of municipality. A’tn index mother paid more in a private hospital (average of PhP 12,824) than in a public hospital (PhP 3,790). Average expenditures in a public birthing home was almost at par with those in a private counterpart.
Table 4.19 shows the average delivery expense by wealth quintiles. There is some variation in the averages across quintiles and municipalities.
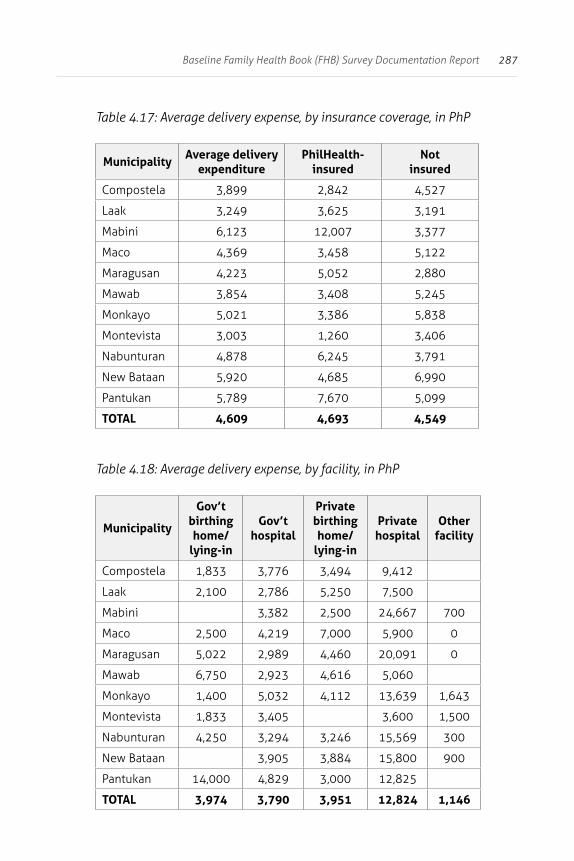
287Baseline Family Health Book (FHB) Survey Documentation Report
Table 4.17: Average delivery expense, by insurance coverage, in PhP
MunicipalityAverage delivery
expenditurePhilHealth-
insured Not
insured
Compostela 3,899 2,842 4,527
Laak 3,249 3,625 3,191
Mabini 6,123 12,007 3,377
Maco 4,369 3,458 5,122
Maragusan 4,223 5,052 2,880
Mawab 3,854 3,408 5,245
Monkayo 5,021 3,386 5,838
Montevista 3,003 1,260 3,406
Nabunturan 4,878 6,245 3,791
New Bataan 5,920 4,685 6,990
Pantukan 5,789 7,670 5,099
TOTAL 4,609 4,693 4,549
Table 4.18: Average delivery expense, by facility, in PhP
Municipality
Gov’t birthing home/
lying-in
Gov’t hospital
Private birthing home/
lying-in
Private hospital
Other facility
Compostela 1,833 3,776 3,494 9,412
Laak 2,100 2,786 5,250 7,500
Mabini 3,382 2,500 24,667 700
Maco 2,500 4,219 7,000 5,900 0
Maragusan 5,022 2,989 4,460 20,091 0
Mawab 6,750 2,923 4,616 5,060
Monkayo 1,400 5,032 4,112 13,639 1,643
Montevista 1,833 3,405 3,600 1,500
Nabunturan 4,250 3,294 3,246 15,569 300
New Bataan 3,905 3,884 15,800 900
Pantukan 14,000 4,829 3,000 12,825
TOTAL 3,974 3,790 3,951 12,824 1,146
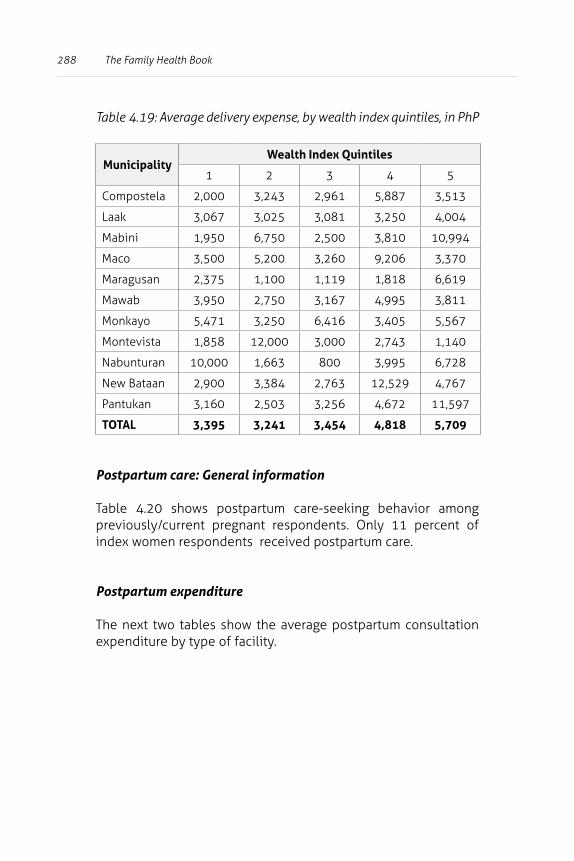
288 The Family Health Book
Table 4.19: Average delivery expense, by wealth index quintiles, in PhP
MunicipalityWealth Index Quintiles
1 2 3 4 5
Compostela 2,000 3,243 2,961 5,887 3,513
Laak 3,067 3,025 3,081 3,250 4,004
Mabini 1,950 6,750 2,500 3,810 10,994
Maco 3,500 5,200 3,260 9,206 3,370
Maragusan 2,375 1,100 1,119 1,818 6,619
Mawab 3,950 2,750 3,167 4,995 3,811
Monkayo 5,471 3,250 6,416 3,405 5,567
Montevista 1,858 12,000 3,000 2,743 1,140
Nabunturan 10,000 1,663 800 3,995 6,728
New Bataan 2,900 3,384 2,763 12,529 4,767
Pantukan 3,160 2,503 3,256 4,672 11,597
TOTAL 3,395 3,241 3,454 4,818 5,709
Postpartum care: General information
Table 4.20 shows postpartum care-seeking behavior among previously/current pregnant respondents. Only 11 percent of index women respondents received postpartum care.
Postpartum expenditure
The next two tables show the average postpartum consultation expenditure by type of facility.
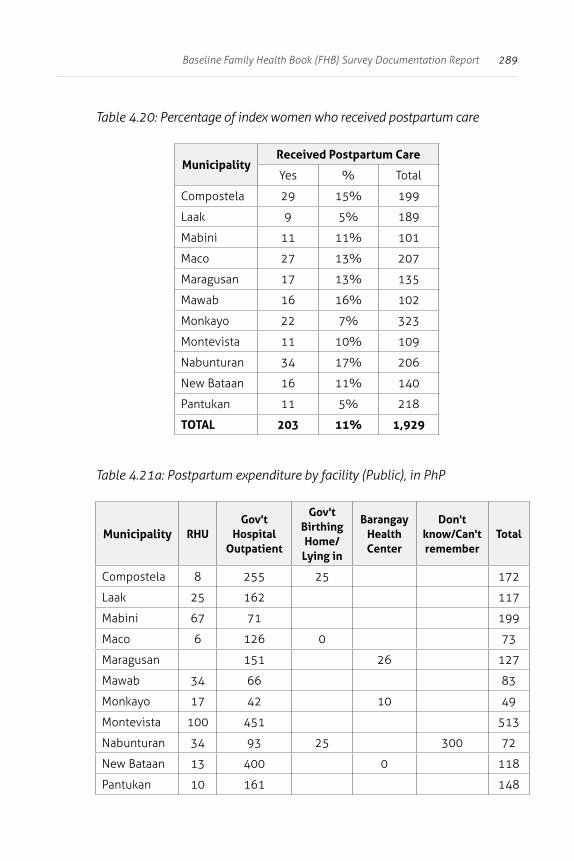
289Baseline Family Health Book (FHB) Survey Documentation Report
Table 4.20: Percentage of index women who received postpartum care
MunicipalityReceived Postpartum Care
Yes % Total
Compostela 29 15% 199
Laak 9 5% 189
Mabini 11 11% 101
Maco 27 13% 207
Maragusan 17 13% 135
Mawab 16 16% 102
Monkayo 22 7% 323
Montevista 11 10% 109
Nabunturan 34 17% 206
New Bataan 16 11% 140
Pantukan 11 5% 218
TOTAL 203 11% 1,929
Table 4.21a: Postpartum expenditure by facility (Public), in PhP
Municipality RHUGov't
Hospital Outpatient
Gov't Birthing Home/
Lying in
Barangay Health Center
Don't know/Can't remember
Total
Compostela 8 255 25 172
Laak 25 162 117
Mabini 67 71 199
Maco 6 126 0 73
Maragusan 151 26 127
Mawab 34 66 83
Monkayo 17 42 10 49
Montevista 100 451 513
Nabunturan 34 93 25 300 72
New Bataan 13 400 0 118
Pantukan 10 161 148
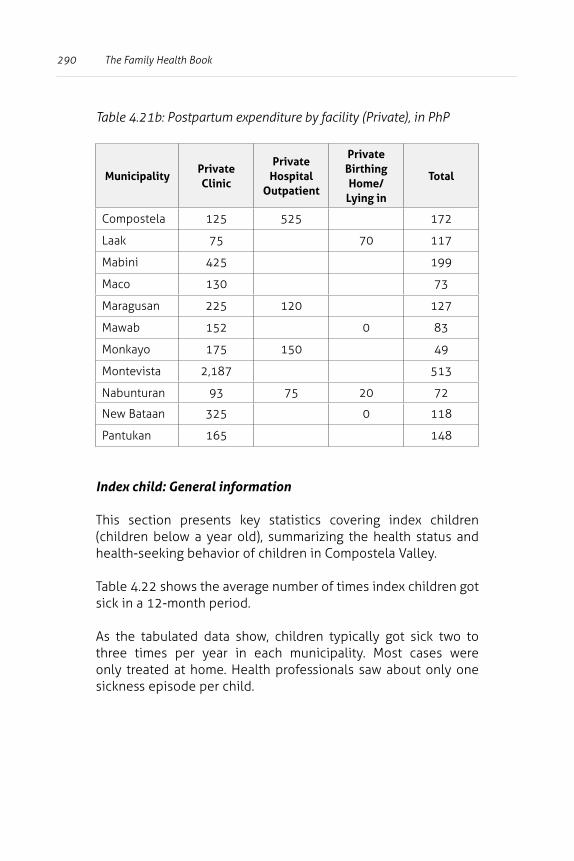
290 The Family Health Book
Table 4.21b: Postpartum expenditure by facility (Private), in PhP
MunicipalityPrivate Clinic
Private Hospital
Outpatient
Private Birthing Home/
Lying in
Total
Compostela 125 525 172
Laak 75 70 117
Mabini 425 199
Maco 130 73
Maragusan 225 120 127
Mawab 152 0 83
Monkayo 175 150 49
Montevista 2,187 513
Nabunturan 93 75 20 72
New Bataan 325 0 118
Pantukan 165 148
Index child: General information
This section presents key statistics covering index children (children below a year old), summarizing the health status and health-seeking behavior of children in Compostela Valley.
Table 4.22 shows the average number of times index children got sick in a 12-month period.
As the tabulated data show, children typically got sick two to three times per year in each municipality. Most cases were only treated at home. Health professionals saw about only one sickness episode per child.
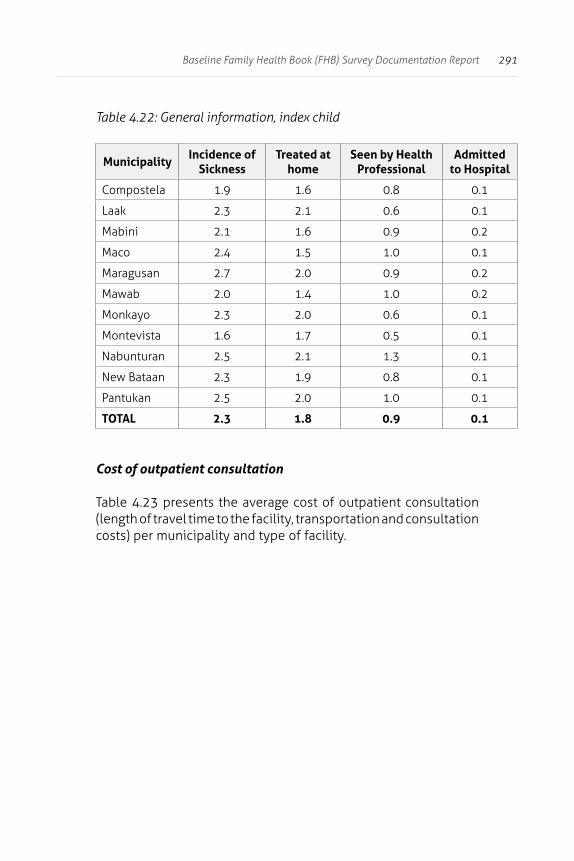
291Baseline Family Health Book (FHB) Survey Documentation Report
Table 4.22: General information, index child
MunicipalityIncidence of
SicknessTreated at
homeSeen by Health
ProfessionalAdmitted
to Hospital
Compostela 1.9 1.6 0.8 0.1
Laak 2.3 2.1 0.6 0.1
Mabini 2.1 1.6 0.9 0.2
Maco 2.4 1.5 1.0 0.1
Maragusan 2.7 2.0 0.9 0.2
Mawab 2.0 1.4 1.0 0.2
Monkayo 2.3 2.0 0.6 0.1
Montevista 1.6 1.7 0.5 0.1
Nabunturan 2.5 2.1 1.3 0.1
New Bataan 2.3 1.9 0.8 0.1
Pantukan 2.5 2.0 1.0 0.1
TOTAL 2.3 1.8 0.9 0.1
Cost of outpatient consultation
Table 4.23 presents the average cost of outpatient consultation (length of travel time to the facility, transportation and consultation costs) per municipality and type of facility.
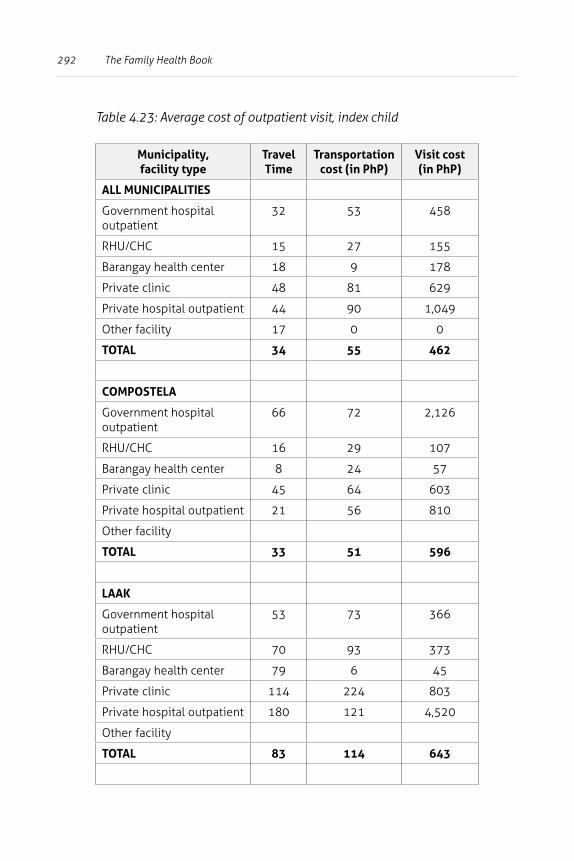
292 The Family Health Book
Table 4.23: Average cost of outpatient visit, index child
Municipality, facility type
Travel Time
Transportation cost (in PhP)
Visit cost (in PhP)
ALL MUNICIPALITIES
Government hospital outpatient
32 53 458
RHU/CHC 15 27 155
Barangay health center 18 9 178
Private clinic 48 81 629
Private hospital outpatient 44 90 1,049
Other facility 17 0 0
TOTAL 34 55 462
COMPOSTELA
Government hospital outpatient
66 72 2,126
RHU/CHC 16 29 107
Barangay health center 8 24 57
Private clinic 45 64 603
Private hospital outpatient 21 56 810
Other facility
TOTAL 33 51 596
LAAK
Government hospital outpatient
53 73 366
RHU/CHC 70 93 373
Barangay health center 79 6 45
Private clinic 114 224 803
Private hospital outpatient 180 121 4,520
Other facility
TOTAL 83 114 643
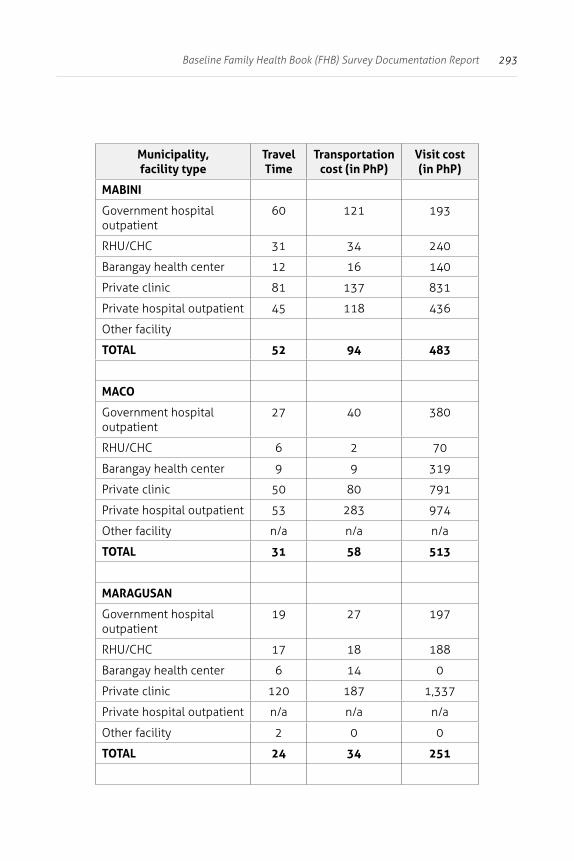
293Baseline Family Health Book (FHB) Survey Documentation Report
Municipality, facility type
Travel Time
Transportation cost (in PhP)
Visit cost (in PhP)
MABINI
Government hospital outpatient
60 121 193
RHU/CHC 31 34 240
Barangay health center 12 16 140
Private clinic 81 137 831
Private hospital outpatient 45 118 436
Other facility
TOTAL 52 94 483
MACO
Government hospital outpatient
27 40 380
RHU/CHC 6 2 70
Barangay health center 9 9 319
Private clinic 50 80 791
Private hospital outpatient 53 283 974
Other facility n/a n/a n/a
TOTAL 31 58 513
MARAGUSAN
Government hospital outpatient
19 27 197
RHU/CHC 17 18 188
Barangay health center 6 14 0
Private clinic 120 187 1,337
Private hospital outpatient n/a n/a n/a
Other facility 2 0 0
TOTAL 24 34 251
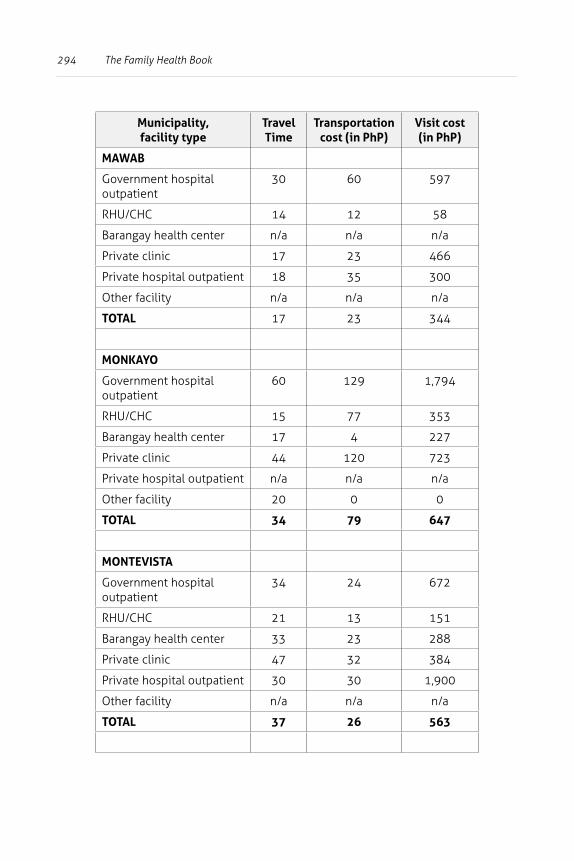
294 The Family Health Book
Municipality, facility type
Travel Time
Transportation cost (in PhP)
Visit cost (in PhP)
MAWAB
Government hospital outpatient
30 60 597
RHU/CHC 14 12 58
Barangay health center n/a n/a n/a
Private clinic 17 23 466
Private hospital outpatient 18 35 300
Other facility n/a n/a n/a
TOTAL 17 23 344
MONKAYO
Government hospital outpatient
60 129 1,794
RHU/CHC 15 77 353
Barangay health center 17 4 227
Private clinic 44 120 723
Private hospital outpatient n/a n/a n/a
Other facility 20 0 0
TOTAL 34 79 647
MONTEVISTA
Government hospital outpatient
34 24 672
RHU/CHC 21 13 151
Barangay health center 33 23 288
Private clinic 47 32 384
Private hospital outpatient 30 30 1,900
Other facility n/a n/a n/a
TOTAL 37 26 563
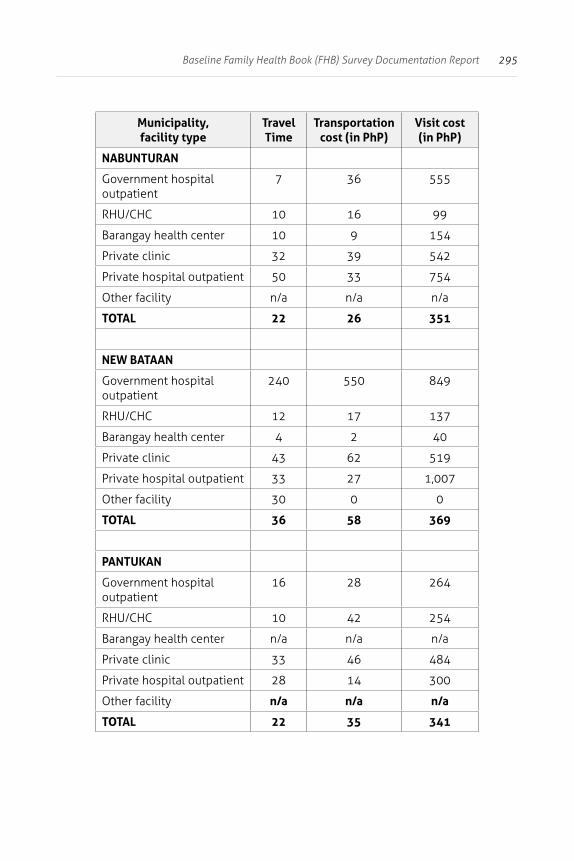
295Baseline Family Health Book (FHB) Survey Documentation Report
Municipality, facility type
Travel Time
Transportation cost (in PhP)
Visit cost (in PhP)
NABUNTURAN
Government hospital outpatient
7 36 555
RHU/CHC 10 16 99
Barangay health center 10 9 154
Private clinic 32 39 542
Private hospital outpatient 50 33 754
Other facility n/a n/a n/a
TOTAL 22 26 351
NEW BATAAN
Government hospital outpatient
240 550 849
RHU/CHC 12 17 137
Barangay health center 4 2 40
Private clinic 43 62 519
Private hospital outpatient 33 27 1,007
Other facility 30 0 0
TOTAL 36 58 369
PANTUKAN
Government hospital outpatient
16 28 264
RHU/CHC 10 42 254
Barangay health center n/a n/a n/a
Private clinic 33 46 484
Private hospital outpatient 28 14 300
Other facility n/a n/a n/a
TOTAL 22 35 341
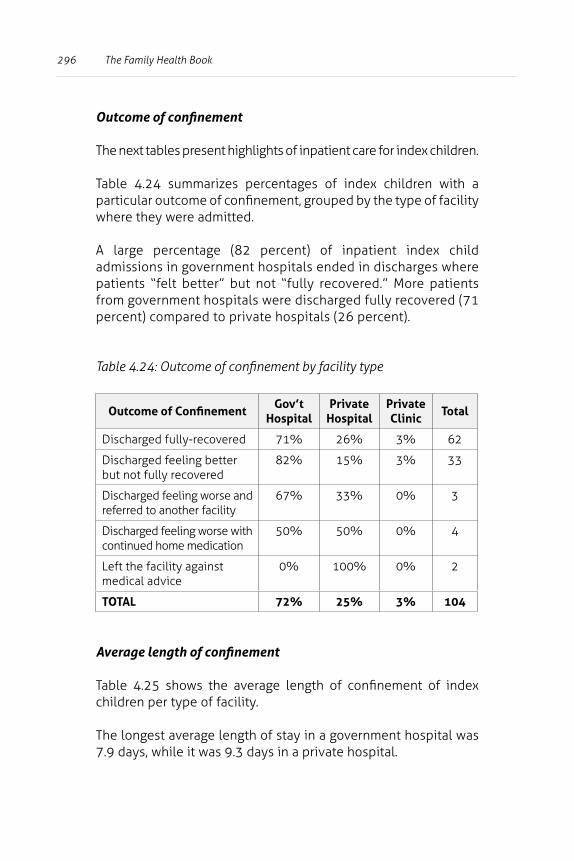
296 The Family Health Book
Outcome of confinement
The next tables present highlights of inpatient care for index children.
Table 4.24 summarizes percentages of index children with a particular outcome of confinement, grouped by the type of facility where they were admitted.
A large percentage (82 percent) of inpatient index child admissions in government hospitals ended in discharges where patients “felt better” but not “fully recovered.” More patients from government hospitals were discharged fully recovered (71 percent) compared to private hospitals (26 percent).
Table 4.24: Outcome of confinement by facility type
Outcome of ConfinementGov’t
HospitalPrivate
HospitalPrivate Clinic
Total
Discharged fully-recovered 71% 26% 3% 62
Discharged feeling better but not fully recovered
82% 15% 3% 33
Discharged feeling worse and referred to another facility
67% 33% 0% 3
Discharged feeling worse with continued home medication
50% 50% 0% 4
Left the facility against medical advice
0% 100% 0% 2
TOTAL 72% 25% 3% 104
Average length of confinement
Table 4.25 shows the average length of confinement of index children per type of facility.
The longest average length of stay in a government hospital was 7.9 days, while it was 9.3 days in a private hospital.
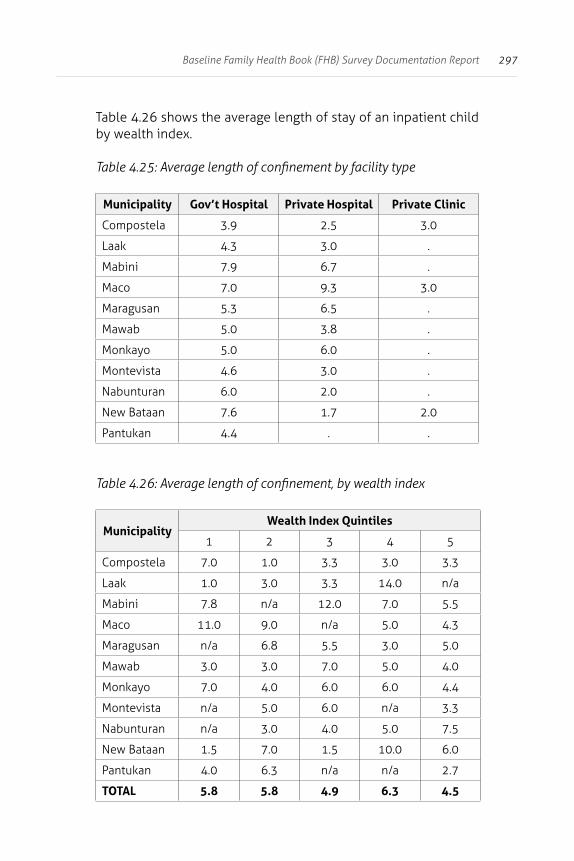
297Baseline Family Health Book (FHB) Survey Documentation Report
Table 4.26 shows the average length of stay of an inpatient child by wealth index.
Table 4.25: Average length of confinement by facility type
Municipality Gov’t Hospital Private Hospital Private Clinic
Compostela 3.9 2.5 3.0
Laak 4.3 3.0 .
Mabini 7.9 6.7 .
Maco 7.0 9.3 3.0
Maragusan 5.3 6.5 .
Mawab 5.0 3.8 .
Monkayo 5.0 6.0 .
Montevista 4.6 3.0 .
Nabunturan 6.0 2.0 .
New Bataan 7.6 1.7 2.0
Pantukan 4.4 . .
Table 4.26: Average length of confinement, by wealth index
MunicipalityWealth Index Quintiles
1 2 3 4 5
Compostela 7.0 1.0 3.3 3.0 3.3
Laak 1.0 3.0 3.3 14.0 n/a
Mabini 7.8 n/a 12.0 7.0 5.5
Maco 11.0 9.0 n/a 5.0 4.3
Maragusan n/a 6.8 5.5 3.0 5.0
Mawab 3.0 3.0 7.0 5.0 4.0
Monkayo 7.0 4.0 6.0 6.0 4.4
Montevista n/a 5.0 6.0 n/a 3.3
Nabunturan n/a 3.0 4.0 5.0 7.5
New Bataan 1.5 7.0 1.5 10.0 6.0
Pantukan 4.0 6.3 n/a n/a 2.7
TOTAL 5.8 5.8 4.9 6.3 4.5
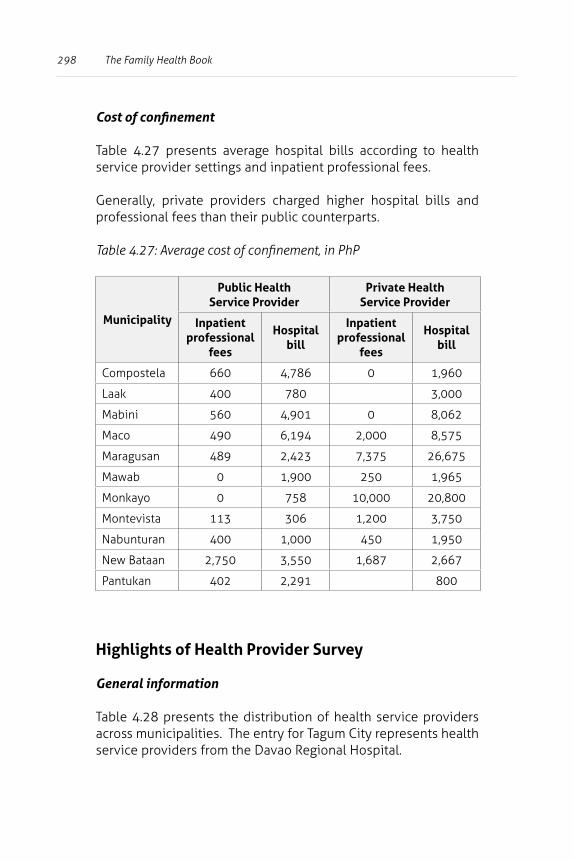
298 The Family Health Book
Cost of confinement
Table 4.27 presents average hospital bills according to health service provider settings and inpatient professional fees.
Generally, private providers charged higher hospital bills and professional fees than their public counterparts.
Table 4.27: Average cost of confinement, in PhP
Municipality
Public Health Service Provider
Private Health Service Provider
Inpatient professional
fees
Hospital bill
Inpatient professional
fees
Hospital bill
Compostela 660 4,786 0 1,960
Laak 400 780 3,000
Mabini 560 4,901 0 8,062
Maco 490 6,194 2,000 8,575
Maragusan 489 2,423 7,375 26,675
Mawab 0 1,900 250 1,965
Monkayo 0 758 10,000 20,800
Montevista 113 306 1,200 3,750
Nabunturan 400 1,000 450 1,950
New Bataan 2,750 3,550 1,687 2,667
Pantukan 402 2,291 800
Highlights of Health Provider Survey
General information
Table 4.28 presents the distribution of health service providers across municipalities. The entry for Tagum City represents health service providers from the Davao Regional Hospital.
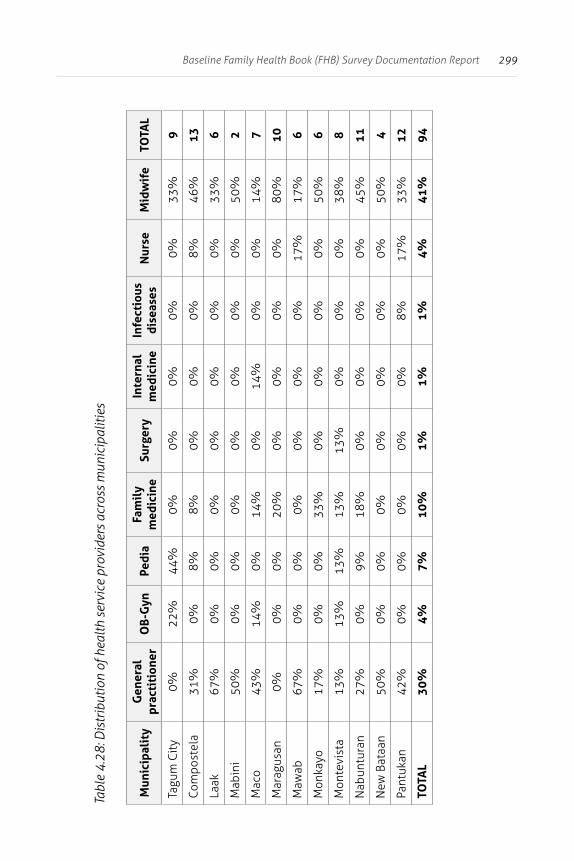
299Baseline Family Health Book (FHB) Survey Documentation Report
Tabl
e 4.
28: D
istr
ibut
ion
of h
ealth
ser
vice
pro
vide
rs a
cros
s m
unic
ipal
ities
Mun
icip
alit
yG
ener
al
prac
titi
oner
OB-
Gyn
Pedi
aFa
mil
y m
edic
ine
Surg
ery
Inte
rnal
m
edic
ine
Infe
ctio
us
dise
ases
Nur
seM
idw
ife
TOTA
L
Tagu
m C
ity
0%22
%44
%0%
0%0%
0%0%
33%
9
Com
post
ela
31%
0%8%
8%0%
0%0%
8%46
%13
Laak
67%
0%0%
0%0%
0%0%
0%33
%6
Mab
ini
50%
0%0%
0%0%
0%0%
0%50
%2
Mac
o43
%14
%0%
14%
0%14
%0%
0%14
%7
Mar
agus
an0%
0%0%
20%
0%0%
0%0%
80%
10
Maw
ab67
%0%
0%0%
0%0%
0%17
%17
%6
Mon
kayo
17%
0%0%
33%
0%0%
0%0%
50%
6
Mon
tevi
sta
13%
13%
13%
13%
13%
0%0%
0%38
%8
Nab
untu
ran
27%
0%9%
18%
0%0%
0%0%
45%
11
New
Bat
aan
50%
0%0%
0%0%
0%0%
0%50
%4
Pant
ukan
42%
0%0%
0%0%
0%8%
17%
33%
12
TOTA
L30
%4%
7%10
%1%
1%1%
4%41
%94
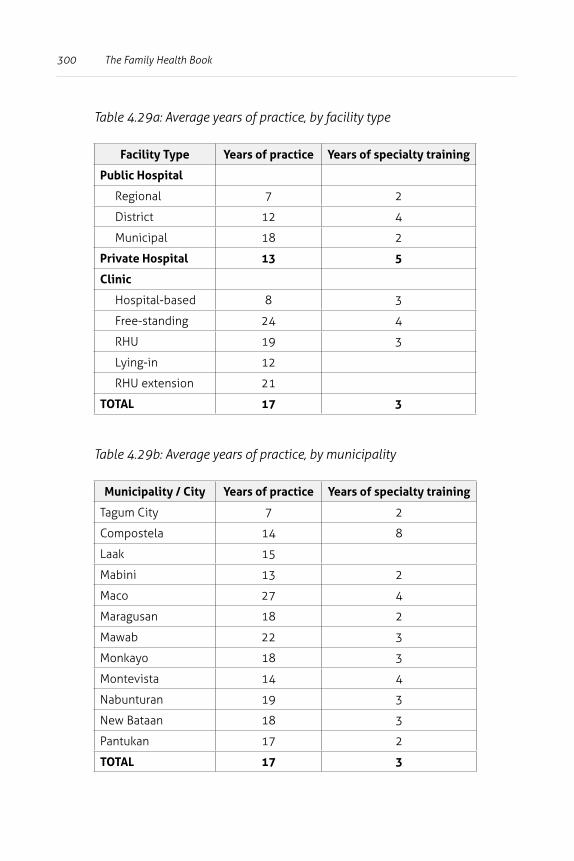
300 The Family Health Book
Table 4.29a: Average years of practice, by facility type
Facility Type Years of practice Years of specialty training
Public Hospital
Regional 7 2
District 12 4
Municipal 18 2
Private Hospital 13 5
Clinic
Hospital-based 8 3
Free-standing 24 4
RHU 19 3
Lying-in 12
RHU extension 21
TOTAL 17 3
Table 4.29b: Average years of practice, by municipality
Municipality / City Years of practice Years of specialty training
Tagum City 7 2
Compostela 14 8
Laak 15
Mabini 13 2
Maco 27 4
Maragusan 18 2
Mawab 22 3
Monkayo 18 3
Montevista 14 4
Nabunturan 19 3
New Bataan 18 3
Pantukan 17 2
TOTAL 17 3
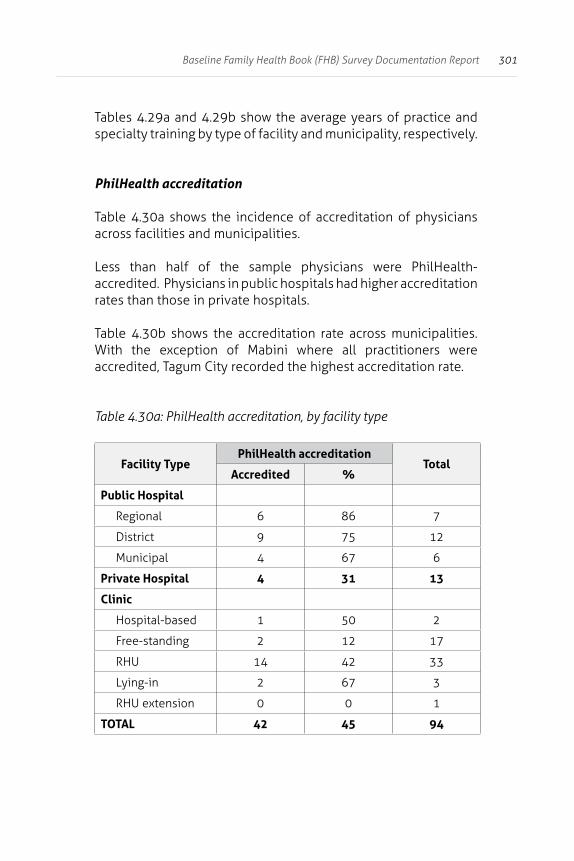
301Baseline Family Health Book (FHB) Survey Documentation Report
Tables 4.29a and 4.29b show the average years of practice and specialty training by type of facility and municipality, respectively.
PhilHealth accreditation
Table 4.30a shows the incidence of accreditation of physicians across facilities and municipalities.
Less than half of the sample physicians were PhilHealth-accredited. Physicians in public hospitals had higher accreditation rates than those in private hospitals.
Table 4.30b shows the accreditation rate across municipalities. With the exception of Mabini where all practitioners were accredited, Tagum City recorded the highest accreditation rate.
Table 4.30a: PhilHealth accreditation, by facility type
Facility TypePhilHealth accreditation
TotalAccredited %
Public Hospital
Regional 6 86 7
District 9 75 12
Municipal 4 67 6
Private Hospital 4 31 13
Clinic
Hospital-based 1 50 2
Free-standing 2 12 17
RHU 14 42 33
Lying-in 2 67 3
RHU extension 0 0 1
TOTAL 42 45 94
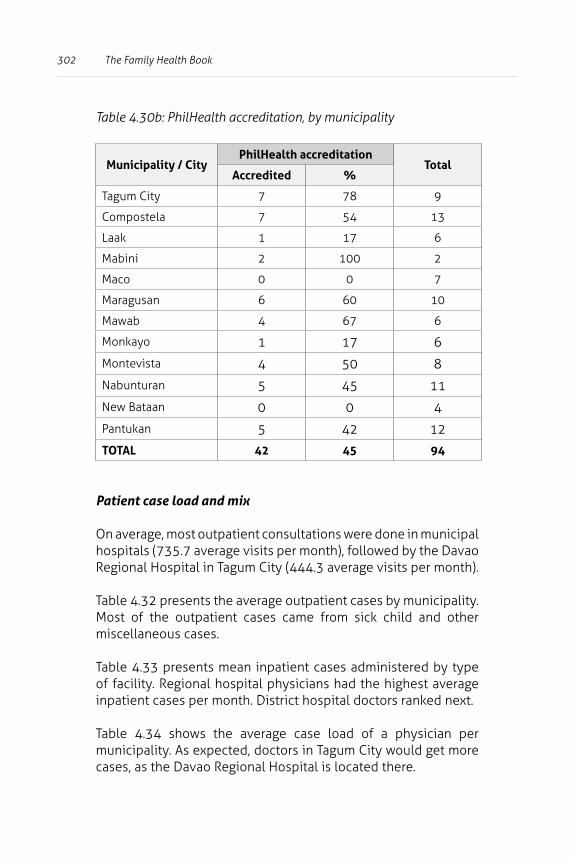
302 The Family Health Book
Table 4.30b: PhilHealth accreditation, by municipality
Municipality / CityPhilHealth accreditation
TotalAccredited %
Tagum City 7 78 9
Compostela 7 54 13
Laak 1 17 6
Mabini 2 100 2
Maco 0 0 7
Maragusan 6 60 10
Mawab 4 67 6
Monkayo 1 17 6
Montevista 4 50 8
Nabunturan 5 45 11
New Bataan 0 0 4
Pantukan 5 42 12
TOTAL 42 45 94
Patient case load and mix
On average, most outpatient consultations were done in municipal hospitals (735.7 average visits per month), followed by the Davao Regional Hospital in Tagum City (444.3 average visits per month).
Table 4.32 presents the average outpatient cases by municipality. Most of the outpatient cases came from sick child and other miscellaneous cases.
Table 4.33 presents mean inpatient cases administered by type of facility. Regional hospital physicians had the highest average inpatient cases per month. District hospital doctors ranked next.
Table 4.34 shows the average case load of a physician per municipality. As expected, doctors in Tagum City would get more cases, as the Davao Regional Hospital is located there.
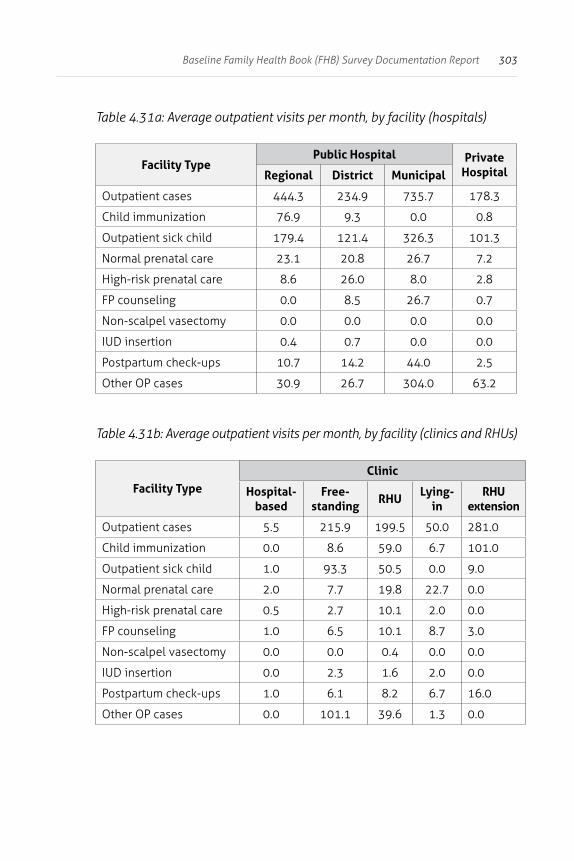
303Baseline Family Health Book (FHB) Survey Documentation Report
Table 4.31a: Average outpatient visits per month, by facility (hospitals)
Facility TypePublic Hospital Private
HospitalRegional District Municipal
Outpatient cases 444.3 234.9 735.7 178.3
Child immunization 76.9 9.3 0.0 0.8
Outpatient sick child 179.4 121.4 326.3 101.3
Normal prenatal care 23.1 20.8 26.7 7.2
High-risk prenatal care 8.6 26.0 8.0 2.8
FP counseling 0.0 8.5 26.7 0.7
Non-scalpel vasectomy 0.0 0.0 0.0 0.0
IUD insertion 0.4 0.7 0.0 0.0
Postpartum check-ups 10.7 14.2 44.0 2.5
Other OP cases 30.9 26.7 304.0 63.2
Table 4.31b: Average outpatient visits per month, by facility (clinics and RHUs)
Facility TypeClinic
Hospital-based
Free-standing
RHULying-
inRHU
extension
Outpatient cases 5.5 215.9 199.5 50.0 281.0
Child immunization 0.0 8.6 59.0 6.7 101.0
Outpatient sick child 1.0 93.3 50.5 0.0 9.0
Normal prenatal care 2.0 7.7 19.8 22.7 0.0
High-risk prenatal care 0.5 2.7 10.1 2.0 0.0
FP counseling 1.0 6.5 10.1 8.7 3.0
Non-scalpel vasectomy 0.0 0.0 0.4 0.0 0.0
IUD insertion 0.0 2.3 1.6 2.0 0.0
Postpartum check-ups 1.0 6.1 8.2 6.7 16.0
Other OP cases 0.0 101.1 39.6 1.3 0.0
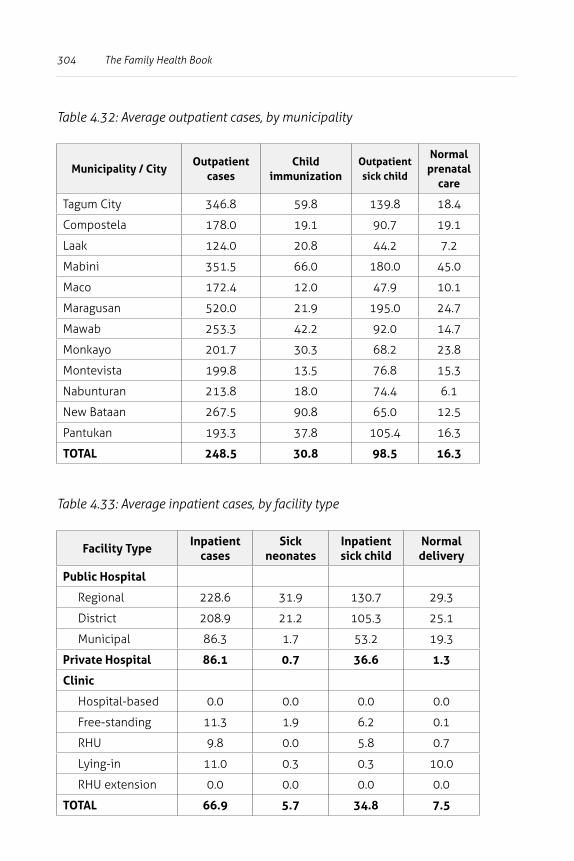
304 The Family Health Book
Table 4.32: Average outpatient cases, by municipality
Municipality / CityOutpatient
casesChild
immunizationOutpatient sick child
Normal prenatal
care
Tagum City 346.8 59.8 139.8 18.4
Compostela 178.0 19.1 90.7 19.1
Laak 124.0 20.8 44.2 7.2
Mabini 351.5 66.0 180.0 45.0
Maco 172.4 12.0 47.9 10.1
Maragusan 520.0 21.9 195.0 24.7
Mawab 253.3 42.2 92.0 14.7
Monkayo 201.7 30.3 68.2 23.8
Montevista 199.8 13.5 76.8 15.3
Nabunturan 213.8 18.0 74.4 6.1
New Bataan 267.5 90.8 65.0 12.5
Pantukan 193.3 37.8 105.4 16.3
TOTAL 248.5 30.8 98.5 16.3
Table 4.33: Average inpatient cases, by facility type
Facility TypeInpatient
casesSick
neonatesInpatient sick child
Normal delivery
Public Hospital
Regional 228.6 31.9 130.7 29.3
District 208.9 21.2 105.3 25.1
Municipal 86.3 1.7 53.2 19.3
Private Hospital 86.1 0.7 36.6 1.3
Clinic
Hospital-based 0.0 0.0 0.0 0.0
Free-standing 11.3 1.9 6.2 0.1
RHU 9.8 0.0 5.8 0.7
Lying-in 11.0 0.3 0.3 10.0
RHU extension 0.0 0.0 0.0 0.0
TOTAL 66.9 5.7 34.8 7.5
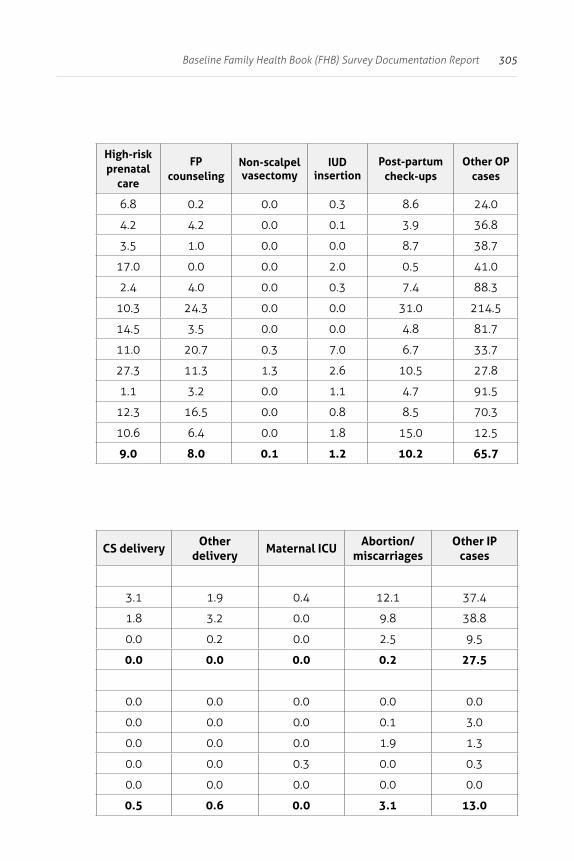
305Baseline Family Health Book (FHB) Survey Documentation Report
High-risk prenatal
care
FP counseling
Non-scalpel vasectomy
IUD insertion
Post-partum check-ups
Other OP cases
6.8 0.2 0.0 0.3 8.6 24.0
4.2 4.2 0.0 0.1 3.9 36.8
3.5 1.0 0.0 0.0 8.7 38.7
17.0 0.0 0.0 2.0 0.5 41.0
2.4 4.0 0.0 0.3 7.4 88.3
10.3 24.3 0.0 0.0 31.0 214.5
14.5 3.5 0.0 0.0 4.8 81.7
11.0 20.7 0.3 7.0 6.7 33.7
27.3 11.3 1.3 2.6 10.5 27.8
1.1 3.2 0.0 1.1 4.7 91.5
12.3 16.5 0.0 0.8 8.5 70.3
10.6 6.4 0.0 1.8 15.0 12.5
9.0 8.0 0.1 1.2 10.2 65.7
CS deliveryOther
deliveryMaternal ICU
Abortion/ miscarriages
Other IP cases
3.1 1.9 0.4 12.1 37.4
1.8 3.2 0.0 9.8 38.8
0.0 0.2 0.0 2.5 9.5
0.0 0.0 0.0 0.2 27.5
0.0 0.0 0.0 0.0 0.0
0.0 0.0 0.0 0.1 3.0
0.0 0.0 0.0 1.9 1.3
0.0 0.0 0.3 0.0 0.3
0.0 0.0 0.0 0.0 0.0
0.5 0.6 0.0 3.1 13.0
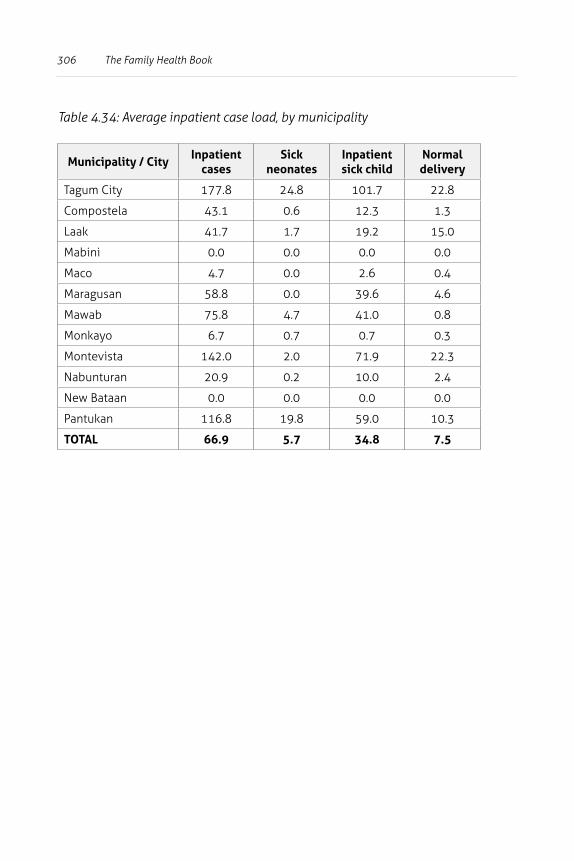
306 The Family Health Book
Table 4.34: Average inpatient case load, by municipality
Municipality / CityInpatient
casesSick
neonatesInpatient sick child
Normal delivery
Tagum City 177.8 24.8 101.7 22.8
Compostela 43.1 0.6 12.3 1.3
Laak 41.7 1.7 19.2 15.0
Mabini 0.0 0.0 0.0 0.0
Maco 4.7 0.0 2.6 0.4
Maragusan 58.8 0.0 39.6 4.6
Mawab 75.8 4.7 41.0 0.8
Monkayo 6.7 0.7 0.7 0.3
Montevista 142.0 2.0 71.9 22.3
Nabunturan 20.9 0.2 10.0 2.4
New Bataan 0.0 0.0 0.0 0.0
Pantukan 116.8 19.8 59.0 10.3
TOTAL 66.9 5.7 34.8 7.5
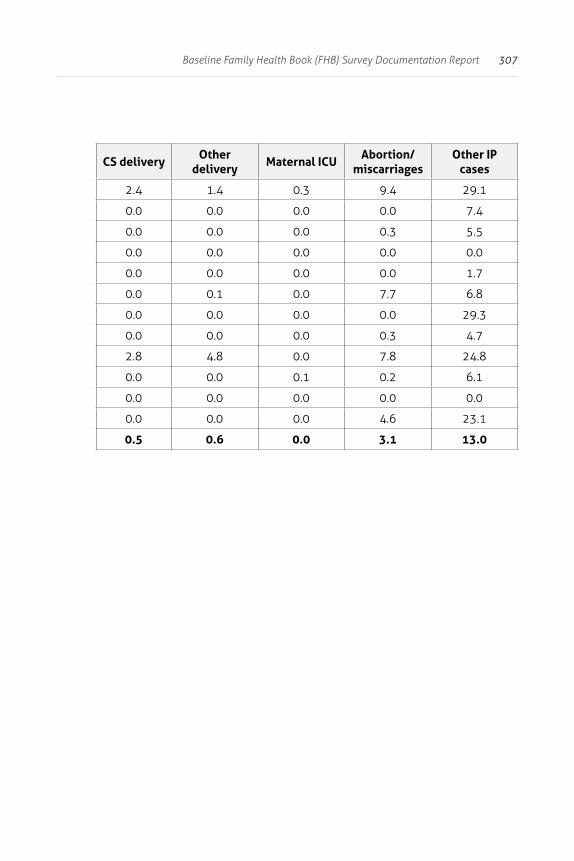
307Baseline Family Health Book (FHB) Survey Documentation Report
CS deliveryOther
deliveryMaternal ICU
Abortion/ miscarriages
Other IP cases
2.4 1.4 0.3 9.4 29.1
0.0 0.0 0.0 0.0 7.4
0.0 0.0 0.0 0.3 5.5
0.0 0.0 0.0 0.0 0.0
0.0 0.0 0.0 0.0 1.7
0.0 0.1 0.0 7.7 6.8
0.0 0.0 0.0 0.0 29.3
0.0 0.0 0.0 0.3 4.7
2.8 4.8 0.0 7.8 24.8
0.0 0.0 0.1 0.2 6.1
0.0 0.0 0.0 0.0 0.0
0.0 0.0 0.0 4.6 23.1
0.5 0.6 0.0 3.1 13.0
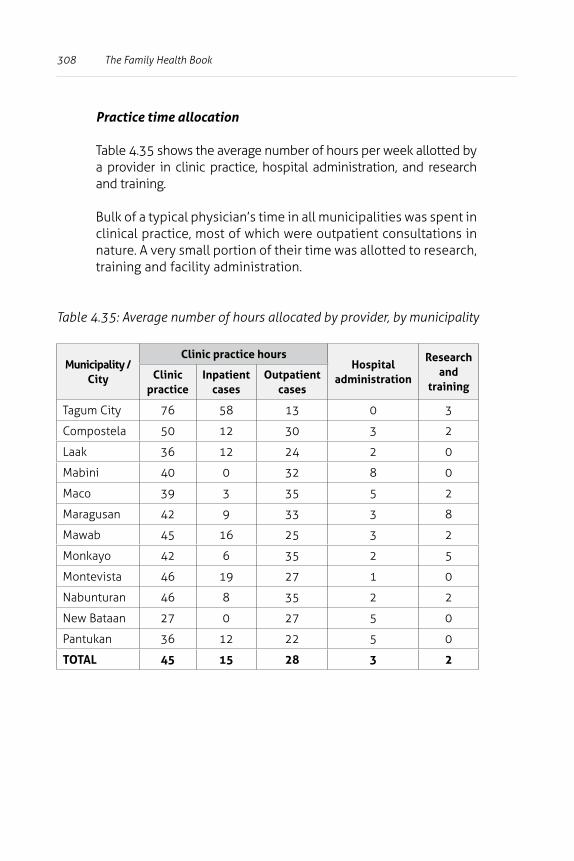
308 The Family Health Book
Table 4.35: Average number of hours allocated by provider, by municipality
Municipality / City
Clinic practice hoursHospital
administration
Research and
trainingClinic
practiceInpatient
casesOutpatient
cases
Tagum City 76 58 13 0 3
Compostela 50 12 30 3 2
Laak 36 12 24 2 0
Mabini 40 0 32 8 0
Maco 39 3 35 5 2
Maragusan 42 9 33 3 8
Mawab 45 16 25 3 2
Monkayo 42 6 35 2 5
Montevista 46 19 27 1 0
Nabunturan 46 8 35 2 2
New Bataan 27 0 27 5 0
Pantukan 36 12 22 5 0
TOTAL 45 15 28 3 2
Practice time allocation
Table 4.35 shows the average number of hours per week allotted by a provider in clinic practice, hospital administration, and research and training.
Bulk of a typical physician’s time in all municipalities was spent in clinical practice, most of which were outpatient consultations in nature. A very small portion of their time was allotted to research, training and facility administration.
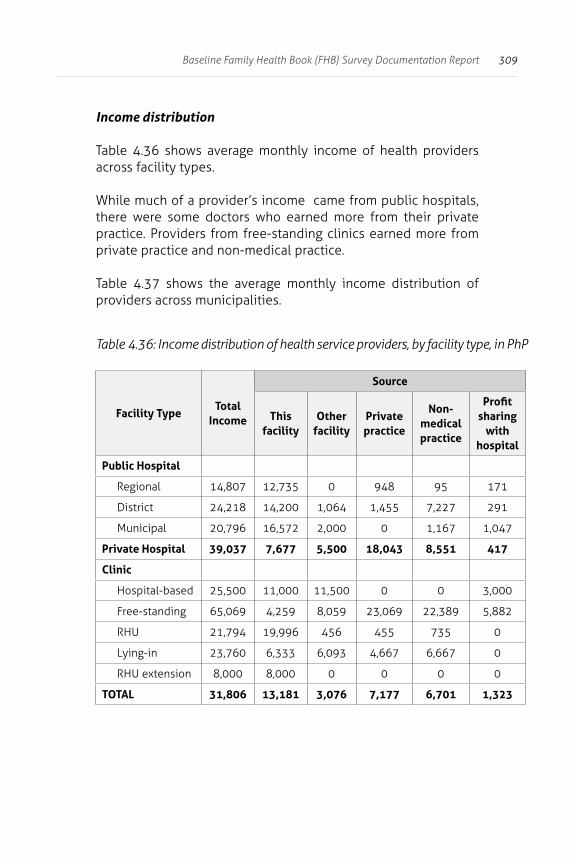
309Baseline Family Health Book (FHB) Survey Documentation Report
Income distribution
Table 4.36 shows average monthly income of health providers across facility types. While much of a provider’s income came from public hospitals, there were some doctors who earned more from their private practice. Providers from free-standing clinics earned more from private practice and non-medical practice.
Table 4.37 shows the average monthly income distribution of providers across municipalities.
Table 4.36: Income distribution of health service providers, by facility type, in PhP
Facility TypeTotal
Income
Source
This facility
Other facility
Private practice
Non-medical practice
Profit sharing
with hospital
Public Hospital
Regional 14,807 12,735 0 948 95 171
District 24,218 14,200 1,064 1,455 7,227 291
Municipal 20,796 16,572 2,000 0 1,167 1,047
Private Hospital 39,037 7,677 5,500 18,043 8,551 417
Clinic
Hospital-based 25,500 11,000 11,500 0 0 3,000
Free-standing 65,069 4,259 8,059 23,069 22,389 5,882
RHU 21,794 19,996 456 455 735 0
Lying-in 23,760 6,333 6,093 4,667 6,667 0
RHU extension 8,000 8,000 0 0 0 0
TOTAL 31,806 13,181 3,076 7,177 6,701 1,323
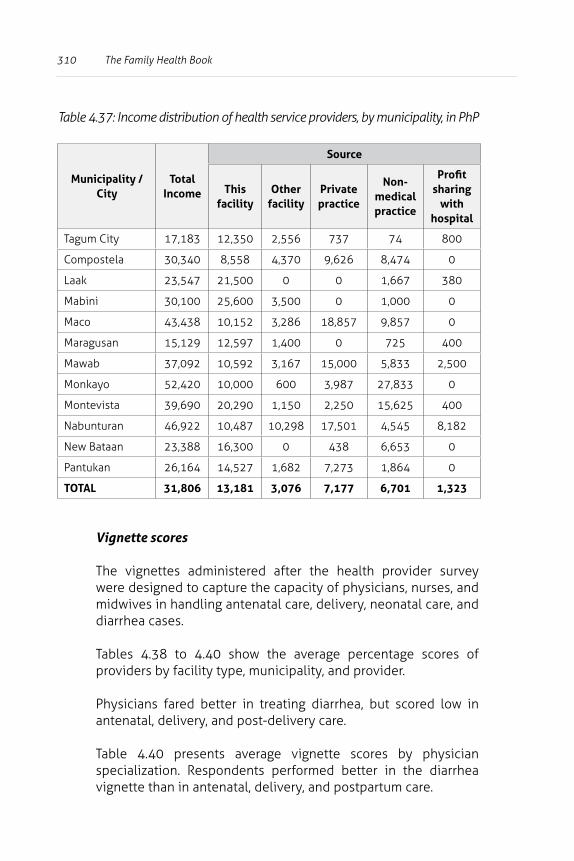
310 The Family Health Book
Table 4.37: Income distribution of health service providers, by municipality, in PhP
Municipality / City
Total Income
Source
This facility
Other facility
Private practice
Non-medical practice
Profit sharing
with hospital
Tagum City 17,183 12,350 2,556 737 74 800
Compostela 30,340 8,558 4,370 9,626 8,474 0
Laak 23,547 21,500 0 0 1,667 380
Mabini 30,100 25,600 3,500 0 1,000 0
Maco 43,438 10,152 3,286 18,857 9,857 0
Maragusan 15,129 12,597 1,400 0 725 400
Mawab 37,092 10,592 3,167 15,000 5,833 2,500
Monkayo 52,420 10,000 600 3,987 27,833 0
Montevista 39,690 20,290 1,150 2,250 15,625 400
Nabunturan 46,922 10,487 10,298 17,501 4,545 8,182
New Bataan 23,388 16,300 0 438 6,653 0
Pantukan 26,164 14,527 1,682 7,273 1,864 0
TOTAL 31,806 13,181 3,076 7,177 6,701 1,323
Vignette scores
The vignettes administered after the health provider survey were designed to capture the capacity of physicians, nurses, and midwives in handling antenatal care, delivery, neonatal care, and diarrhea cases.
Tables 4.38 to 4.40 show the average percentage scores of providers by facility type, municipality, and provider.
Physicians fared better in treating diarrhea, but scored low in antenatal, delivery, and post-delivery care.
Table 4.40 presents average vignette scores by physician specialization. Respondents performed better in the diarrhea vignette than in antenatal, delivery, and postpartum care.
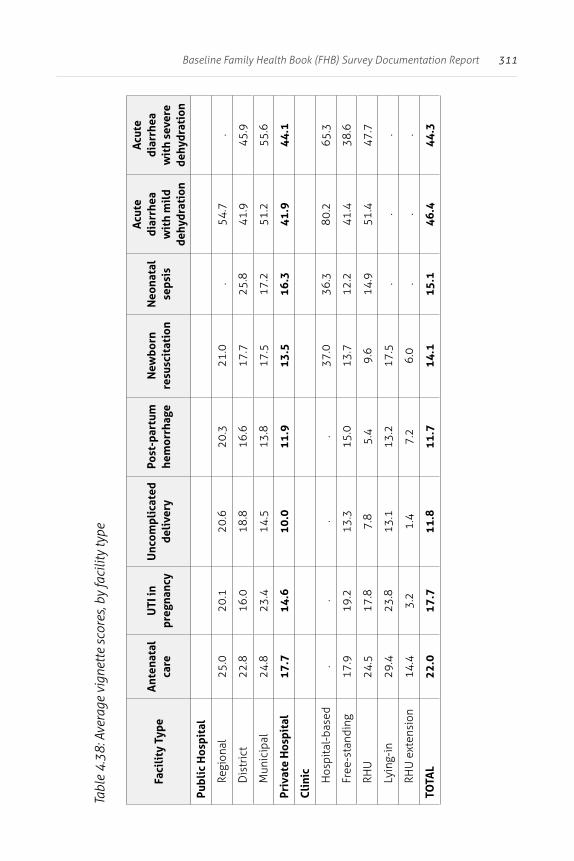
311Baseline Family Health Book (FHB) Survey Documentation Report
Tabl
e 4.
38: A
vera
ge v
igne
tte
scor
es, b
y fa
cilit
y ty
pe
Faci
lity
Typ
eA
nten
atal
ca
reU
TI in
pr
egna
ncy
Unc
ompl
icat
ed
deli
very
Post
-par
tum
he
mor
rhag
eN
ewbo
rn
resu
scit
atio
nN
eona
tal
seps
is
Acu
te
diar
rhea
w
ith
mil
d de
hydr
atio
n
Acu
te
diar
rhea
w
ith
seve
re
dehy
drat
ion
Publ
ic H
ospi
tal
Regi
onal
25.0
20.1
20.6
20.3
21.0
.54
.7.
Dis
tric
t22
.816
.018
.816
.617
.725
.841
.945
.9
Mun
icip
al24
.823
.414
.513
.817
.517
.251
.255
.6
Priv
ate
Hos
pita
l17
.714
.610
.011
.913
.516
.341
.944
.1
Cli
nic
Hos
pita
l-ba
sed
..
..
37.0
36.3
80.2
65.3
Free
-sta
ndin
g17
.919
.213
.315
.013
.712
.241
.438
.6
RHU
24.5
17.8
7.8
5.4
9.6
14.9
51.4
47.7
Lyin
g-in
29.4
23.8
13.1
13.2
17.5
..
.
RHU
ext
ensi
on14
.43.
21.
47.
26.
0.
..
TOTA
L22
.017
.711
.811
.714
.115
.146
.444
.3
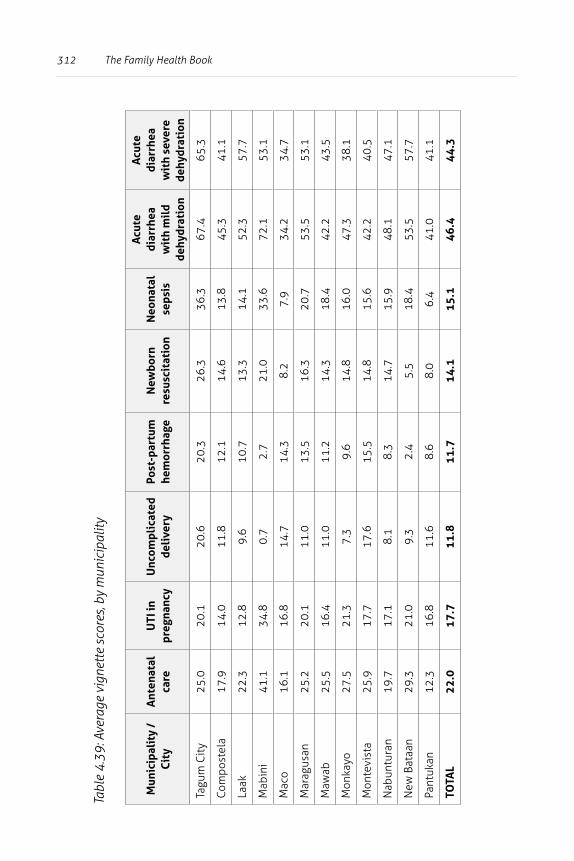
312 The Family Health Book
Tabl
e 4.
39: A
vera
ge v
igne
tte
scor
es, b
y m
unic
ipal
ity
Mun
icip
alit
y /
Cit
yA
nten
atal
ca
reU
TI in
pr
egna
ncy
Unc
ompl
icat
ed
deli
very
Post
-par
tum
he
mor
rhag
eN
ewbo
rn
resu
scit
atio
nN
eona
tal
seps
is
Acu
te
diar
rhea
w
ith
mil
d de
hydr
atio
n
Acu
te
diar
rhea
w
ith
seve
re
dehy
drat
ion
Tagu
m C
ity
25.0
20.1
20.6
20.3
26.3
36.3
67.4
65.3
Com
post
ela
17.9
14.0
11.8
12.1
14.6
13.8
45.3
41.1
Laak
22.3
12.8
9.6
10.7
13.3
14.1
52.3
57.7
Mab
ini
41.1
34.8
0.7
2.7
21.0
33.6
72.1
53.1
Mac
o16
.116
.814
.714
.38.
27.
934
.234
.7
Mar
agus
an25
.220
.111
.013
.516
.320
.753
.553
.1
Maw
ab25
.516
.411
.011
.214
.318
.442
.243
.5
Mon
kayo
27.5
21.3
7.3
9.6
14.8
16.0
47.3
38.1
Mon
tevi
sta
25.9
17.7
17.6
15.5
14.8
15.6
42.2
40.5
Nab
untu
ran
19.7
17.1
8.1
8.3
14.7
15.9
48.1
47.1
New
Bat
aan
29.3
21.0
9.3
2.4
5.5
18.4
53.5
57.7
Pant
ukan
12.3
16.8
11.6
8.6
8.0
6.4
41.0
41.1
TOTA
L22
.017
.711
.811
.714
.115
.146
.444
.3
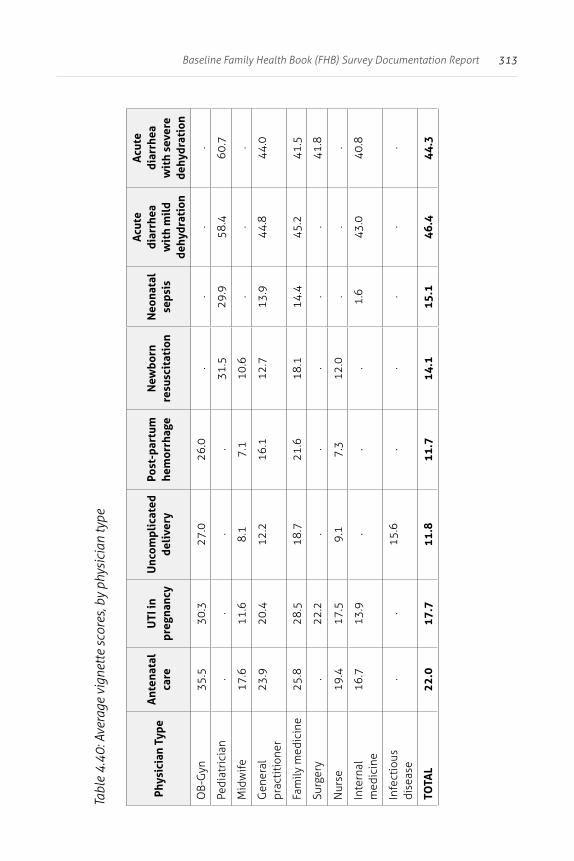
313Baseline Family Health Book (FHB) Survey Documentation Report
Tabl
e 4.
40: A
vera
ge v
igne
tte
scor
es, b
y ph
ysic
ian
type
Phys
icia
n Ty
peA
nten
atal
ca
reU
TI in
pr
egna
ncy
Unc
ompl
icat
ed
deli
very
Post
-par
tum
he
mor
rhag
eN
ewbo
rn
resu
scit
atio
nN
eona
tal
seps
is
Acu
te
diar
rhea
w
ith
mil
d de
hydr
atio
n
Acu
te
diar
rhea
w
ith
seve
re
dehy
drat
ion
OB-
Gyn
35.5
30.3
27.0
26.0
..
..
Pedi
atri
cian
..
..
31.5
29.9
58.4
60.7
Mid
wife
17.6
11.6
8.1
7.1
10.6
..
.
Gen
eral
pr
acti
tion
er23
.920
.412
.216
.112
.713
.944
.844
.0
Fam
ily m
edic
ine
25.8
28.5
18.7
21.6
18.1
14.4
45.2
41.5
Surg
ery
.22
.2.
..
..
41.8
Nur
se19
.417
.59.
17.
312
.0.
..
Inte
rnal
m
edic
ine
16.7
13.9
..
.1.
643
.040
.8
Infe
ctio
us
dise
ase
..
15.6
..
..
.
TOTA
L22
.017
.711
.811
.714
.115
.146
.444
.3
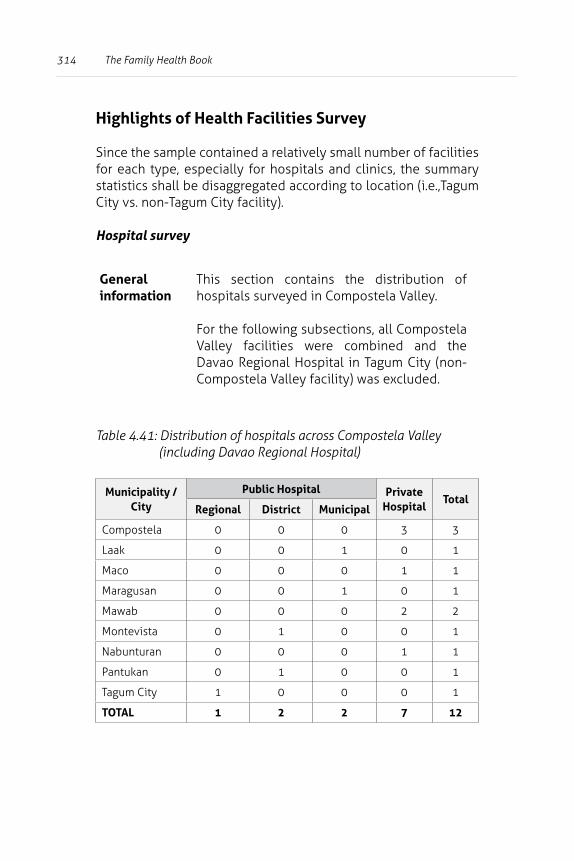
314 The Family Health Book
Highlights of Health Facilities Survey
Since the sample contained a relatively small number of facilities for each type, especially for hospitals and clinics, the summary statistics shall be disaggregated according to location (i.e.,Tagum City vs. non-Tagum City facility).
Hospital survey
General information
This section contains the distribution of hospitals surveyed in Compostela Valley.
For the following subsections, all Compostela Valley facilities were combined and the Davao Regional Hospital in Tagum City (non-Compostela Valley facility) was excluded.
Table 4.41: Distribution of hospitals across Compostela Valley (including Davao Regional Hospital)
Municipality / City
Public Hospital Private Hospital
TotalRegional District Municipal
Compostela 0 0 0 3 3
Laak 0 0 1 0 1
Maco 0 0 0 1 1
Maragusan 0 0 1 0 1
Mawab 0 0 0 2 2
Montevista 0 1 0 0 1
Nabunturan 0 0 0 1 1
Pantukan 0 1 0 0 1
Tagum City 1 0 0 0 1
TOTAL 1 2 2 7 12
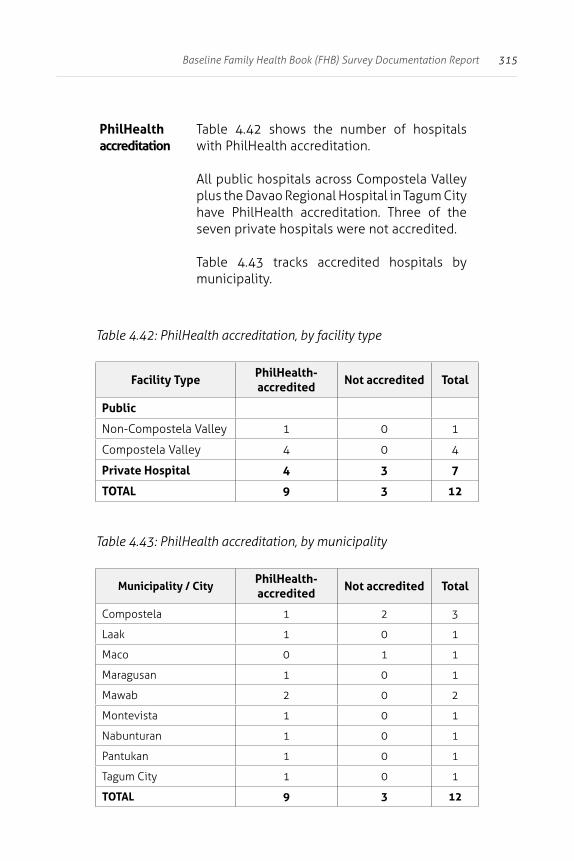
315Baseline Family Health Book (FHB) Survey Documentation Report
PhilHealth accreditation
Table 4.42 shows the number of hospitals with PhilHealth accreditation.
All public hospitals across Compostela Valley plus the Davao Regional Hospital in Tagum City have PhilHealth accreditation. Three of the seven private hospitals were not accredited.
Table 4.43 tracks accredited hospitals by municipality.
Table 4.42: PhilHealth accreditation, by facility type
Facility TypePhilHealth-accredited
Not accredited Total
Public
Non-Compostela Valley 1 0 1
Compostela Valley 4 0 4
Private Hospital 4 3 7
TOTAL 9 3 12
Table 4.43: PhilHealth accreditation, by municipality
Municipality / CityPhilHealth-accredited
Not accredited Total
Compostela 1 2 3
Laak 1 0 1
Maco 0 1 1
Maragusan 1 0 1
Mawab 2 0 2
Montevista 1 0 1
Nabunturan 1 0 1
Pantukan 1 0 1
Tagum City 1 0 1
TOTAL 9 3 12
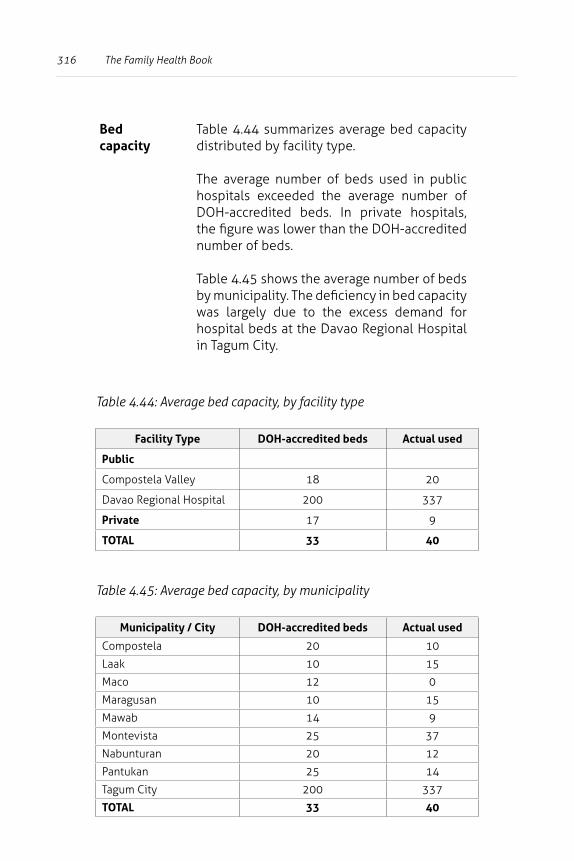
316 The Family Health Book
Bed capacity
Table 4.44 summarizes average bed capacity distributed by facility type.
The average number of beds used in public hospitals exceeded the average number of DOH-accredited beds. In private hospitals, the figure was lower than the DOH-accredited number of beds.
Table 4.45 shows the average number of beds by municipality. The deficiency in bed capacity was largely due to the excess demand for hospital beds at the Davao Regional Hospital in Tagum City.
Table 4.44: Average bed capacity, by facility type
Facility Type DOH-accredited beds Actual used
Public
Compostela Valley 18 20
Davao Regional Hospital 200 337
Private 17 9
TOTAL 33 40
Table 4.45: Average bed capacity, by municipality
Municipality / City DOH-accredited beds Actual used
Compostela 20 10
Laak 10 15
Maco 12 0
Maragusan 10 15
Mawab 14 9
Montevista 25 37
Nabunturan 20 12
Pantukan 25 14
Tagum City 200 337
TOTAL 33 40
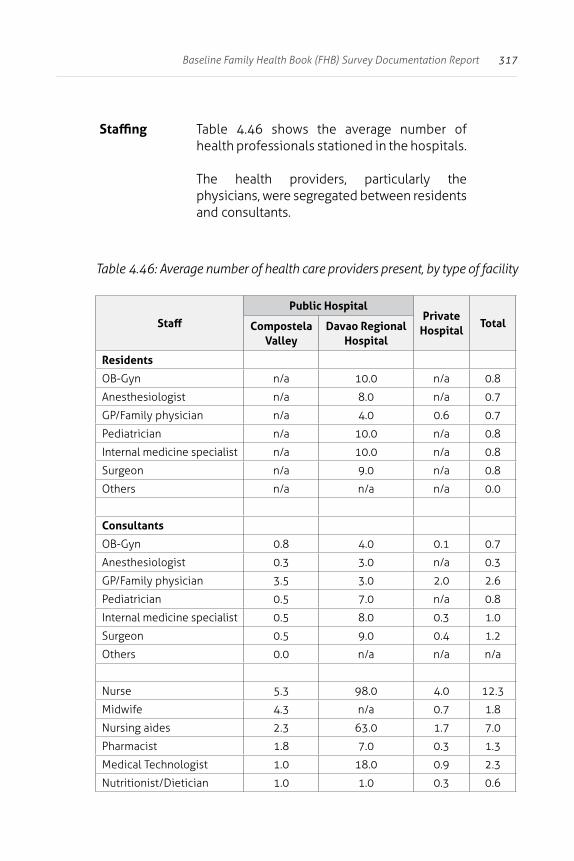
317Baseline Family Health Book (FHB) Survey Documentation Report
Staffing Table 4.46 shows the average number of health professionals stationed in the hospitals.
The health providers, particularly the physicians, were segregated between residents and consultants.
Table 4.46: Average number of health care providers present, by type of facility
Staff
Public HospitalPrivate
HospitalTotalCompostela
ValleyDavao Regional
Hospital
Residents
OB-Gyn n/a 10.0 n/a 0.8
Anesthesiologist n/a 8.0 n/a 0.7
GP/Family physician n/a 4.0 0.6 0.7
Pediatrician n/a 10.0 n/a 0.8
Internal medicine specialist n/a 10.0 n/a 0.8
Surgeon n/a 9.0 n/a 0.8
Others n/a n/a n/a 0.0
Consultants
OB-Gyn 0.8 4.0 0.1 0.7
Anesthesiologist 0.3 3.0 n/a 0.3
GP/Family physician 3.5 3.0 2.0 2.6
Pediatrician 0.5 7.0 n/a 0.8
Internal medicine specialist 0.5 8.0 0.3 1.0
Surgeon 0.5 9.0 0.4 1.2
Others 0.0 n/a n/a n/a
Nurse 5.3 98.0 4.0 12.3
Midwife 4.3 n/a 0.7 1.8
Nursing aides 2.3 63.0 1.7 7.0
Pharmacist 1.8 7.0 0.3 1.3
Medical Technologist 1.0 18.0 0.9 2.3
Nutritionist/Dietician 1.0 1.0 0.3 0.6
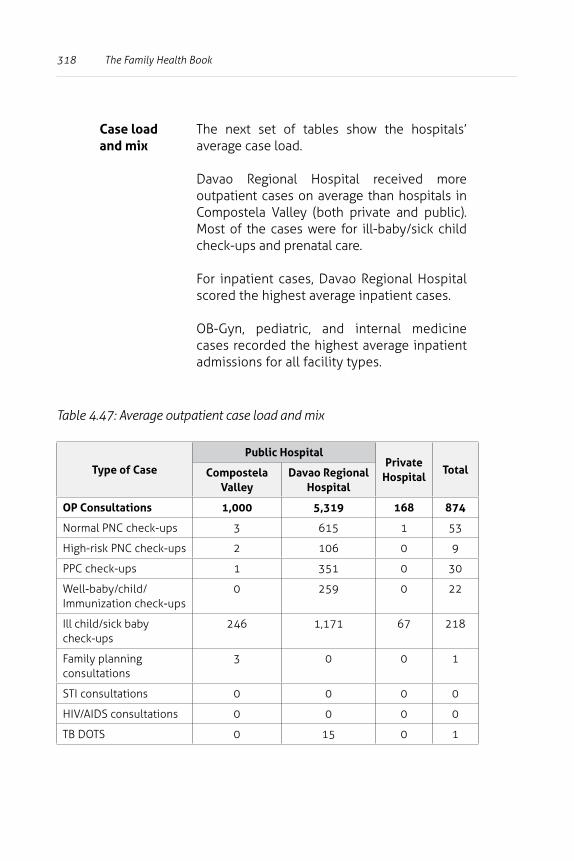
318 The Family Health Book
Case load and mix
The next set of tables show the hospitals’ average case load.
Davao Regional Hospital received more outpatient cases on average than hospitals in Compostela Valley (both private and public). Most of the cases were for ill-baby/sick child check-ups and prenatal care.
For inpatient cases, Davao Regional Hospital scored the highest average inpatient cases.
OB-Gyn, pediatric, and internal medicine cases recorded the highest average inpatient admissions for all facility types.
Table 4.47: Average outpatient case load and mix
Type of Case
Public HospitalPrivate
HospitalTotalCompostela
ValleyDavao Regional
Hospital
OP Consultations 1,000 5,319 168 874
Normal PNC check-ups 3 615 1 53
High-risk PNC check-ups 2 106 0 9
PPC check-ups 1 351 0 30
Well-baby/child/Immunization check-ups
0 259 0 22
Ill child/sick baby check-ups
246 1,171 67 218
Family planning consultations
3 0 0 1
STI consultations 0 0 0 0
HIV/AIDS consultations 0 0 0 0
TB DOTS 0 15 0 1
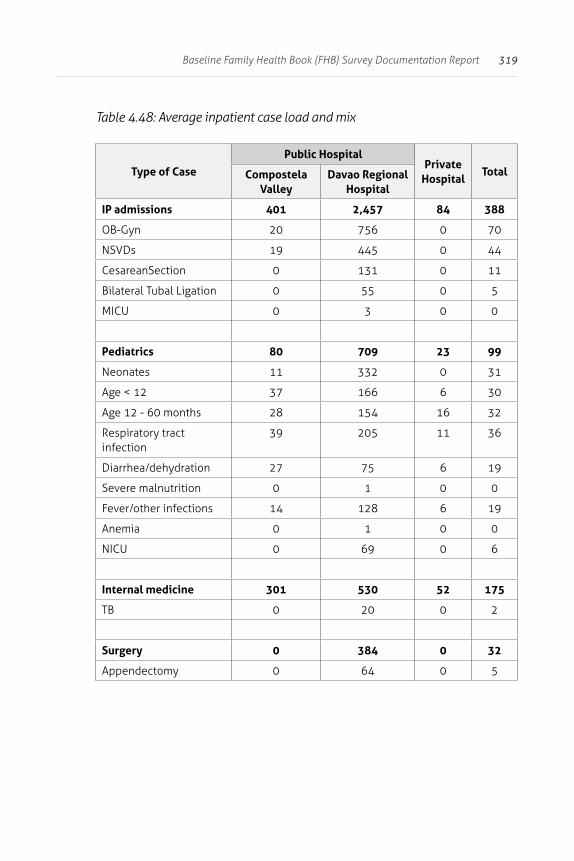
319Baseline Family Health Book (FHB) Survey Documentation Report
Table 4.48: Average inpatient case load and mix
Type of Case
Public HospitalPrivate
HospitalTotalCompostela
ValleyDavao Regional
Hospital
IP admissions 401 2,457 84 388
OB-Gyn 20 756 0 70
NSVDs 19 445 0 44
CesareanSection 0 131 0 11
Bilateral Tubal Ligation 0 55 0 5
MICU 0 3 0 0
Pediatrics 80 709 23 99
Neonates 11 332 0 31
Age < 12 37 166 6 30
Age 12 - 60 months 28 154 16 32
Respiratory tract infection
39 205 11 36
Diarrhea/dehydration 27 75 6 19
Severe malnutrition 0 1 0 0
Fever/other infections 14 128 6 19
Anemia 0 1 0 0
NICU 0 69 0 6
Internal medicine 301 530 52 175
TB 0 20 0 2
Surgery 0 384 0 32
Appendectomy 0 64 0 5
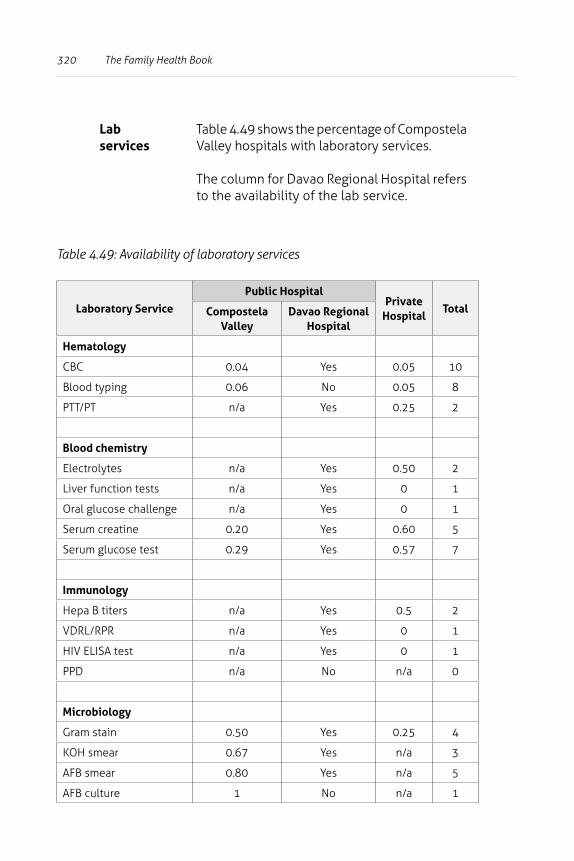
320 The Family Health Book
Lab services
Table 4.49 shows the percentage of Compostela Valley hospitals with laboratory services.
The column for Davao Regional Hospital refers to the availability of the lab service.
Table 4.49: Availability of laboratory services
Laboratory Service
Public HospitalPrivate
HospitalTotalCompostela
ValleyDavao Regional
Hospital
Hematology
CBC 0.04 Yes 0.05 10
Blood typing 0.06 No 0.05 8
PTT/PT n/a Yes 0.25 2
Blood chemistry
Electrolytes n/a Yes 0.50 2
Liver function tests n/a Yes 0 1
Oral glucose challenge n/a Yes 0 1
Serum creatine 0.20 Yes 0.60 5
Serum glucose test 0.29 Yes 0.57 7
Immunology
Hepa B titers n/a Yes 0.5 2
VDRL/RPR n/a Yes 0 1
HIV ELISA test n/a Yes 0 1
PPD n/a No n/a 0
Microbiology
Gram stain 0.50 Yes 0.25 4
KOH smear 0.67 Yes n/a 3
AFB smear 0.80 Yes n/a 5
AFB culture 1 No n/a 1
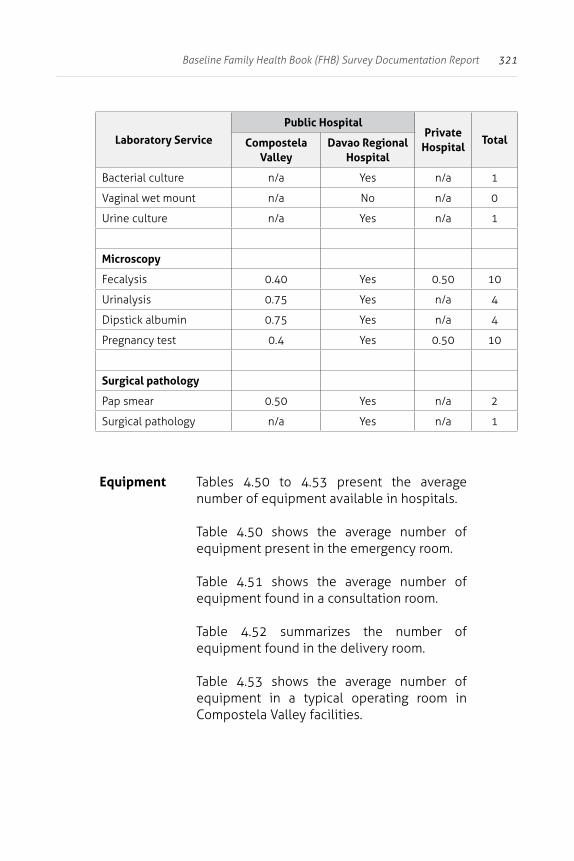
321Baseline Family Health Book (FHB) Survey Documentation Report
Laboratory Service
Public HospitalPrivate
HospitalTotalCompostela
ValleyDavao Regional
Hospital
Bacterial culture n/a Yes n/a 1
Vaginal wet mount n/a No n/a 0
Urine culture n/a Yes n/a 1
Microscopy
Fecalysis 0.40 Yes 0.50 10
Urinalysis 0.75 Yes n/a 4
Dipstick albumin 0.75 Yes n/a 4
Pregnancy test 0.4 Yes 0.50 10
Surgical pathology
Pap smear 0.50 Yes n/a 2
Surgical pathology n/a Yes n/a 1
Equipment Tables 4.50 to 4.53 present the average number of equipment available in hospitals.
Table 4.50 shows the average number of equipment present in the emergency room.
Table 4.51 shows the average number of equipment found in a consultation room.
Table 4.52 summarizes the number of equipment found in the delivery room.
Table 4.53 shows the average number of equipment in a typical operating room in Compostela Valley facilities.
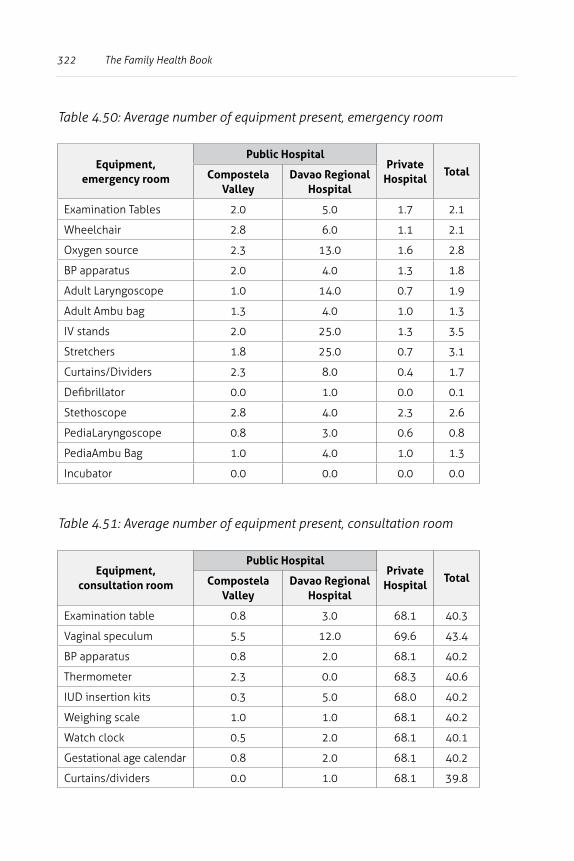
322 The Family Health Book
Table 4.50: Average number of equipment present, emergency room
Equipment, emergency room
Public HospitalPrivate
HospitalTotalCompostela
ValleyDavao Regional
Hospital
Examination Tables 2.0 5.0 1.7 2.1
Wheelchair 2.8 6.0 1.1 2.1
Oxygen source 2.3 13.0 1.6 2.8
BP apparatus 2.0 4.0 1.3 1.8
Adult Laryngoscope 1.0 14.0 0.7 1.9
Adult Ambu bag 1.3 4.0 1.0 1.3
IV stands 2.0 25.0 1.3 3.5
Stretchers 1.8 25.0 0.7 3.1
Curtains/Dividers 2.3 8.0 0.4 1.7
Defibrillator 0.0 1.0 0.0 0.1
Stethoscope 2.8 4.0 2.3 2.6
PediaLaryngoscope 0.8 3.0 0.6 0.8
PediaAmbu Bag 1.0 4.0 1.0 1.3
Incubator 0.0 0.0 0.0 0.0
Table 4.51: Average number of equipment present, consultation room
Equipment, consultation room
Public HospitalPrivate
HospitalTotalCompostela
ValleyDavao Regional
Hospital
Examination table 0.8 3.0 68.1 40.3
Vaginal speculum 5.5 12.0 69.6 43.4
BP apparatus 0.8 2.0 68.1 40.2
Thermometer 2.3 0.0 68.3 40.6
IUD insertion kits 0.3 5.0 68.0 40.2
Weighing scale 1.0 1.0 68.1 40.2
Watch clock 0.5 2.0 68.1 40.1
Gestational age calendar 0.8 2.0 68.1 40.2
Curtains/dividers 0.0 1.0 68.1 39.8
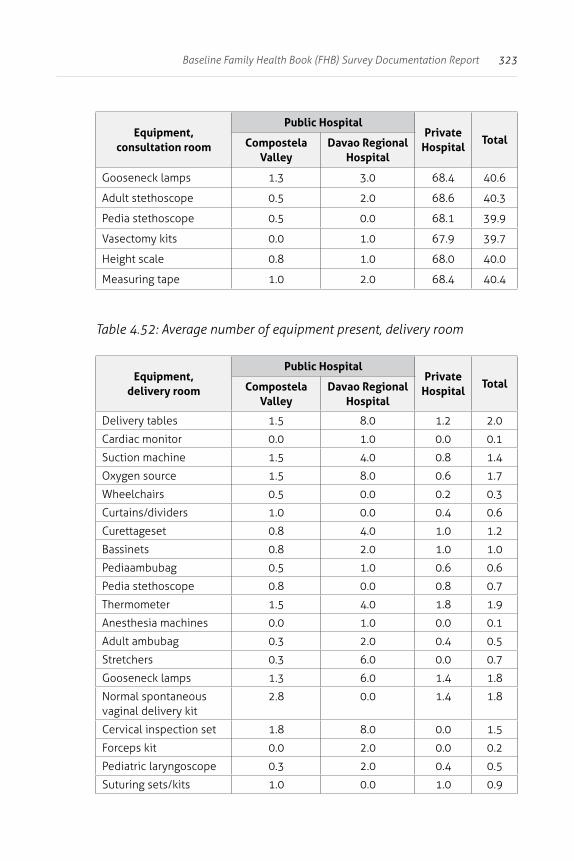
323Baseline Family Health Book (FHB) Survey Documentation Report
Equipment, consultation room
Public HospitalPrivate
HospitalTotalCompostela
ValleyDavao Regional
Hospital
Gooseneck lamps 1.3 3.0 68.4 40.6
Adult stethoscope 0.5 2.0 68.6 40.3
Pedia stethoscope 0.5 0.0 68.1 39.9
Vasectomy kits 0.0 1.0 67.9 39.7
Height scale 0.8 1.0 68.0 40.0
Measuring tape 1.0 2.0 68.4 40.4
Table 4.52: Average number of equipment present, delivery room
Equipment, delivery room
Public HospitalPrivate
HospitalTotalCompostela
ValleyDavao Regional
Hospital
Delivery tables 1.5 8.0 1.2 2.0
Cardiac monitor 0.0 1.0 0.0 0.1
Suction machine 1.5 4.0 0.8 1.4
Oxygen source 1.5 8.0 0.6 1.7
Wheelchairs 0.5 0.0 0.2 0.3
Curtains/dividers 1.0 0.0 0.4 0.6
Curettageset 0.8 4.0 1.0 1.2
Bassinets 0.8 2.0 1.0 1.0
Pediaambubag 0.5 1.0 0.6 0.6
Pedia stethoscope 0.8 0.0 0.8 0.7
Thermometer 1.5 4.0 1.8 1.9
Anesthesia machines 0.0 1.0 0.0 0.1
Adult ambubag 0.3 2.0 0.4 0.5
Stretchers 0.3 6.0 0.0 0.7
Gooseneck lamps 1.3 6.0 1.4 1.8
Normal spontaneous vaginal delivery kit
2.8 0.0 1.4 1.8
Cervical inspection set 1.8 8.0 0.0 1.5
Forceps kit 0.0 2.0 0.0 0.2
Pediatric laryngoscope 0.3 2.0 0.4 0.5
Suturing sets/kits 1.0 0.0 1.0 0.9
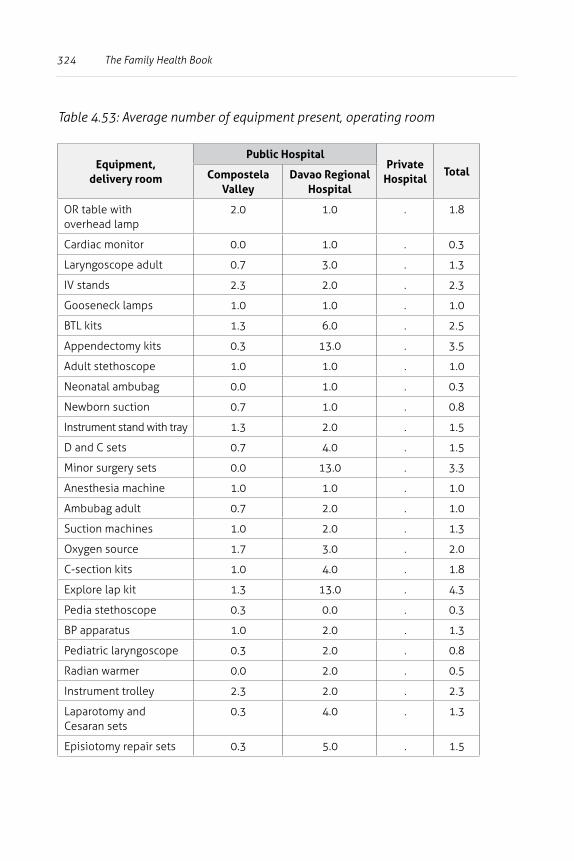
324 The Family Health Book
Table 4.53: Average number of equipment present, operating room
Equipment, delivery room
Public HospitalPrivate
HospitalTotalCompostela
ValleyDavao Regional
Hospital
OR table with overhead lamp
2.0 1.0 . 1.8
Cardiac monitor 0.0 1.0 . 0.3
Laryngoscope adult 0.7 3.0 . 1.3
IV stands 2.3 2.0 . 2.3
Gooseneck lamps 1.0 1.0 . 1.0
BTL kits 1.3 6.0 . 2.5
Appendectomy kits 0.3 13.0 . 3.5
Adult stethoscope 1.0 1.0 . 1.0
Neonatal ambubag 0.0 1.0 . 0.3
Newborn suction 0.7 1.0 . 0.8
Instrument stand with tray 1.3 2.0 . 1.5
D and C sets 0.7 4.0 . 1.5
Minor surgery sets 0.0 13.0 . 3.3
Anesthesia machine 1.0 1.0 . 1.0
Ambubag adult 0.7 2.0 . 1.0
Suction machines 1.0 2.0 . 1.3
Oxygen source 1.7 3.0 . 2.0
C-section kits 1.0 4.0 . 1.8
Explore lap kit 1.3 13.0 . 4.3
Pedia stethoscope 0.3 0.0 . 0.3
BP apparatus 1.0 2.0 . 1.3
Pediatric laryngoscope 0.3 2.0 . 0.8
Radian warmer 0.0 2.0 . 0.5
Instrument trolley 2.3 2.0 . 2.3
Laparotomy and Cesaran sets
0.3 4.0 . 1.3
Episiotomy repair sets 0.3 5.0 . 1.5
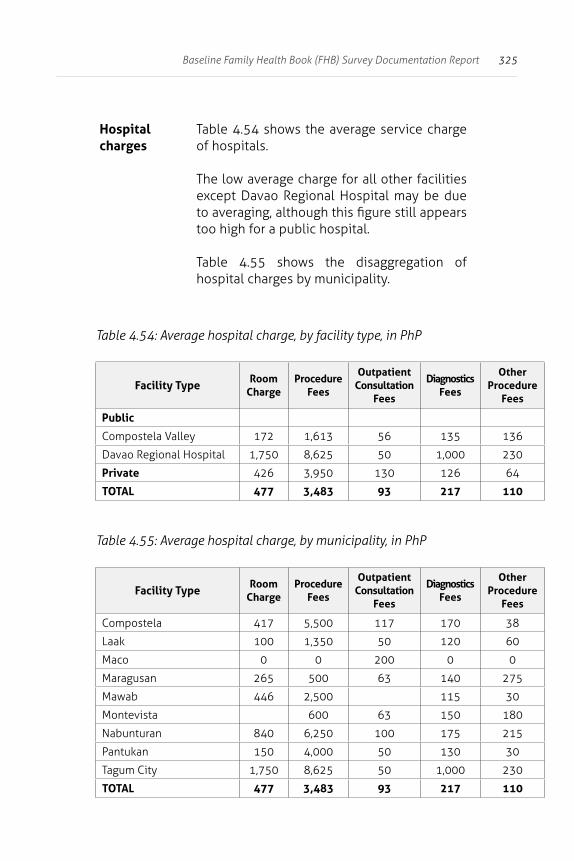
325Baseline Family Health Book (FHB) Survey Documentation Report
Hospital charges
Table 4.54 shows the average service charge of hospitals.
The low average charge for all other facilities except Davao Regional Hospital may be due to averaging, although this figure still appears too high for a public hospital.
Table 4.55 shows the disaggregation of hospital charges by municipality.
Table 4.54: Average hospital charge, by facility type, in PhP
Facility Type Room Charge
Procedure Fees
Outpatient Consultation
Fees
Diagnostics Fees
Other Procedure
Fees
Public
Compostela Valley 172 1,613 56 135 136
Davao Regional Hospital 1,750 8,625 50 1,000 230
Private 426 3,950 130 126 64
TOTAL 477 3,483 93 217 110
Table 4.55: Average hospital charge, by municipality, in PhP
Facility Type Room Charge
Procedure Fees
Outpatient Consultation
Fees
Diagnostics Fees
Other Procedure
Fees
Compostela 417 5,500 117 170 38
Laak 100 1,350 50 120 60
Maco 0 0 200 0 0
Maragusan 265 500 63 140 275
Mawab 446 2,500 115 30
Montevista 600 63 150 180
Nabunturan 840 6,250 100 175 215
Pantukan 150 4,000 50 130 30
Tagum City 1,750 8,625 50 1,000 230
TOTAL 477 3,483 93 217 110
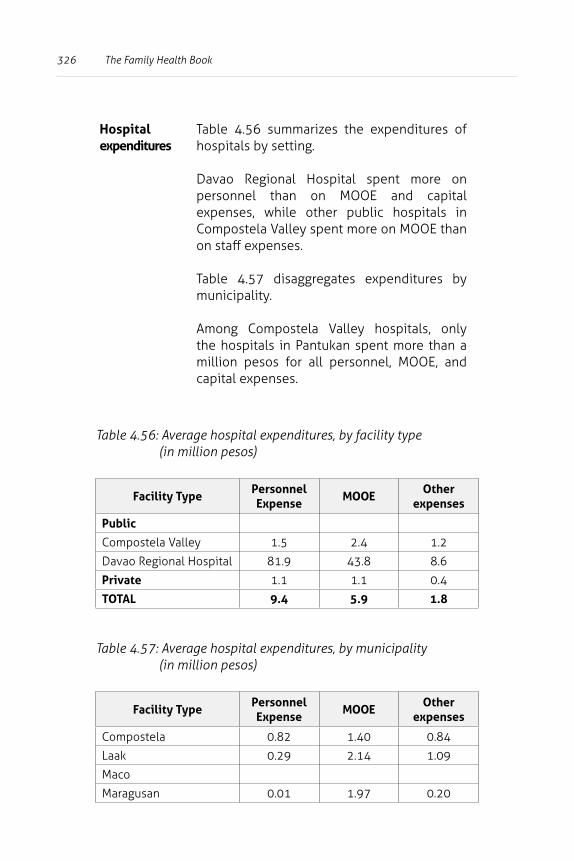
326 The Family Health Book
Hospital expenditures
Table 4.56 summarizes the expenditures of hospitals by setting.
Davao Regional Hospital spent more on personnel than on MOOE and capital expenses, while other public hospitals in Compostela Valley spent more on MOOE than on staff expenses.
Table 4.57 disaggregates expenditures by municipality.
Among Compostela Valley hospitals, only the hospitals in Pantukan spent more than a million pesos for all personnel, MOOE, and capital expenses.
Table 4.56: Average hospital expenditures, by facility type (in million pesos)
Facility TypePersonnel Expense
MOOEOther
expenses
Public
Compostela Valley 1.5 2.4 1.2
Davao Regional Hospital 81.9 43.8 8.6
Private 1.1 1.1 0.4
TOTAL 9.4 5.9 1.8
Table 4.57: Average hospital expenditures, by municipality (in million pesos)
Facility TypePersonnel Expense
MOOEOther
expenses
Compostela 0.82 1.40 0.84
Laak 0.29 2.14 1.09
Maco
Maragusan 0.01 1.97 0.20
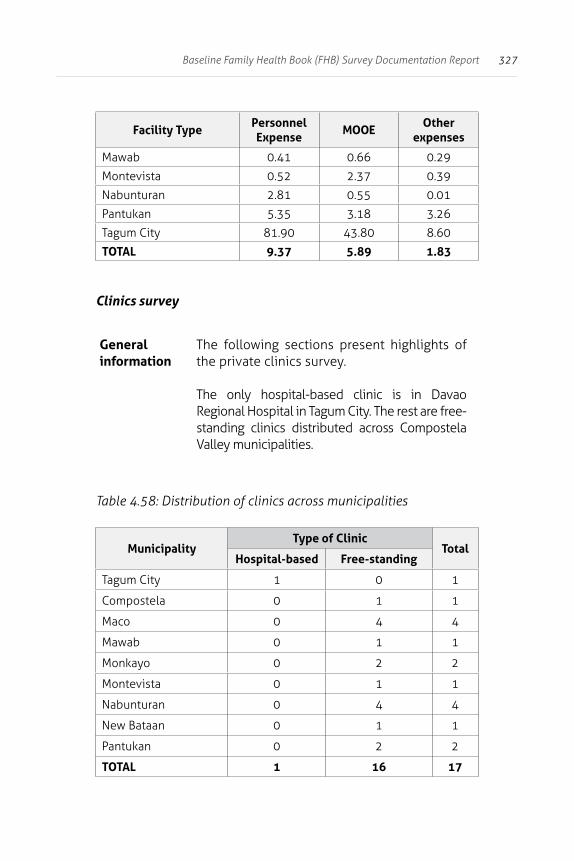
327Baseline Family Health Book (FHB) Survey Documentation Report
Facility TypePersonnel Expense
MOOEOther
expenses
Mawab 0.41 0.66 0.29
Montevista 0.52 2.37 0.39
Nabunturan 2.81 0.55 0.01
Pantukan 5.35 3.18 3.26
Tagum City 81.90 43.80 8.60
TOTAL 9.37 5.89 1.83
Clinics survey
General information
The following sections present highlights of the private clinics survey.
The only hospital-based clinic is in Davao Regional Hospital in Tagum City. The rest are free-standing clinics distributed across Compostela Valley municipalities.
Table 4.58: Distribution of clinics across municipalities
MunicipalityType of Clinic
TotalHospital-based Free-standing
Tagum City 1 0 1
Compostela 0 1 1
Maco 0 4 4
Mawab 0 1 1
Monkayo 0 2 2
Montevista 0 1 1
Nabunturan 0 4 4
New Bataan 0 1 1
Pantukan 0 2 2
TOTAL 1 16 17
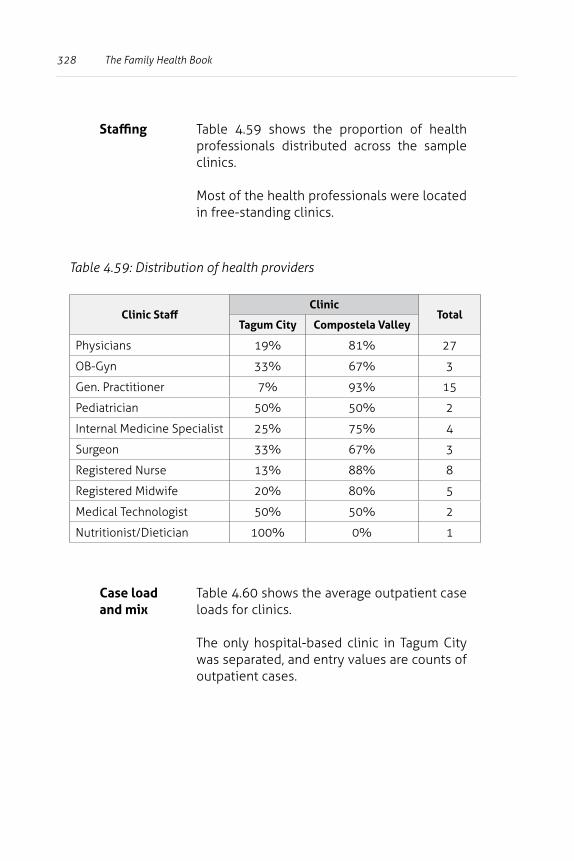
328 The Family Health Book
Staffing Table 4.59 shows the proportion of health professionals distributed across the sample clinics.
Most of the health professionals were located in free-standing clinics.
Table 4.59: Distribution of health providers
Clinic StaffClinic
TotalTagum City Compostela Valley
Physicians 19% 81% 27
OB-Gyn 33% 67% 3
Gen. Practitioner 7% 93% 15
Pediatrician 50% 50% 2
Internal Medicine Specialist 25% 75% 4
Surgeon 33% 67% 3
Registered Nurse 13% 88% 8
Registered Midwife 20% 80% 5
Medical Technologist 50% 50% 2
Nutritionist/Dietician 100% 0% 1
Case load and mix
Table 4.60 shows the average outpatient case loads for clinics.
The only hospital-based clinic in Tagum City was separated, and entry values are counts of outpatient cases.
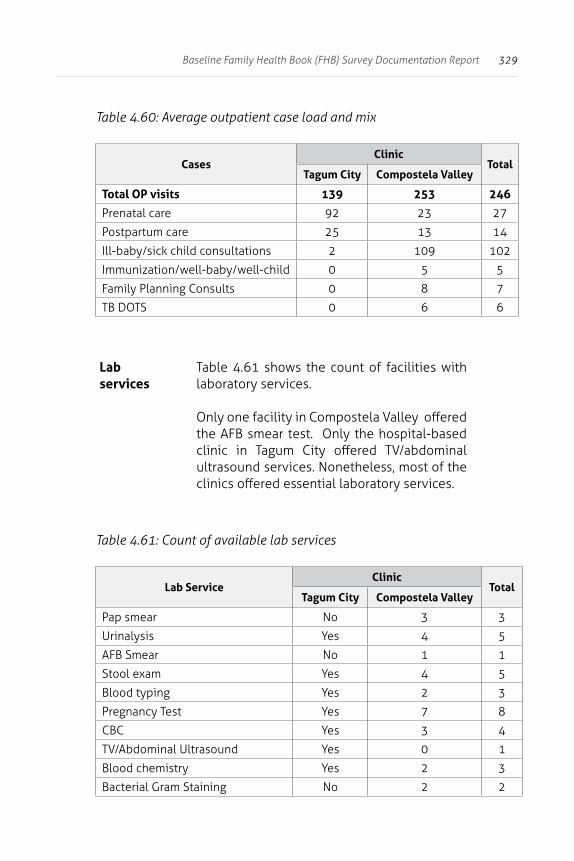
329Baseline Family Health Book (FHB) Survey Documentation Report
Table 4.60: Average outpatient case load and mix
CasesClinic
TotalTagum City Compostela Valley
Total OP visits 139 253 246
Prenatal care 92 23 27
Postpartum care 25 13 14
Ill-baby/sick child consultations 2 109 102
Immunization/well-baby/well-child 0 5 5
Family Planning Consults 0 8 7
TB DOTS 0 6 6
Lab services
Table 4.61 shows the count of facilities with laboratory services.
Only one facility in Compostela Valley offered the AFB smear test. Only the hospital-based clinic in Tagum City offered TV/abdominal ultrasound services. Nonetheless, most of the clinics offered essential laboratory services.
Table 4.61: Count of available lab services
Lab ServiceClinic
TotalTagum City Compostela Valley
Pap smear No 3 3
Urinalysis Yes 4 5
AFB Smear No 1 1
Stool exam Yes 4 5
Blood typing Yes 2 3
Pregnancy Test Yes 7 8
CBC Yes 3 4
TV/Abdominal Ultrasound Yes 0 1
Blood chemistry Yes 2 3
Bacterial Gram Staining No 2 2
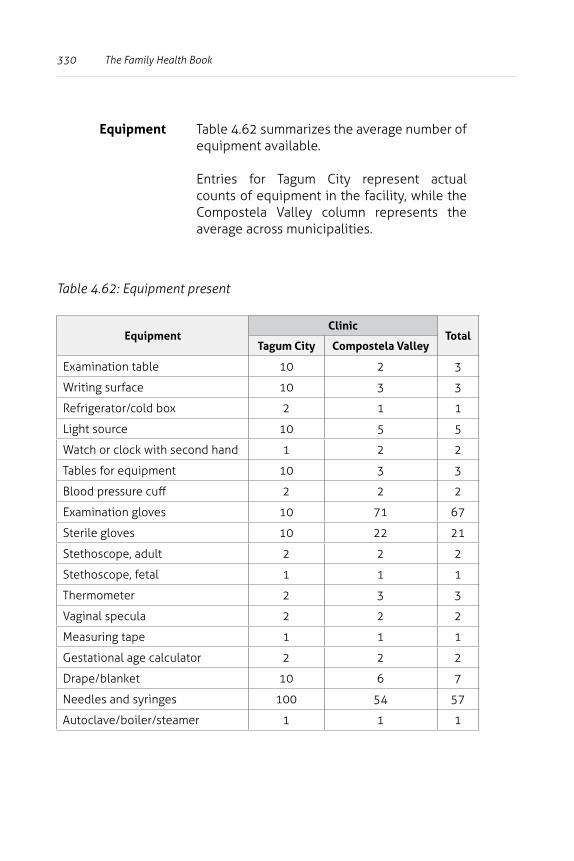
330 The Family Health Book
Equipment Table 4.62 summarizes the average number of equipment available.
Entries for Tagum City represent actual counts of equipment in the facility, while the Compostela Valley column represents the average across municipalities.
Table 4.62: Equipment present
EquipmentClinic
TotalTagum City Compostela Valley
Examination table 10 2 3
Writing surface 10 3 3
Refrigerator/cold box 2 1 1
Light source 10 5 5
Watch or clock with second hand 1 2 2
Tables for equipment 10 3 3
Blood pressure cuff 2 2 2
Examination gloves 10 71 67
Sterile gloves 10 22 21
Stethoscope, adult 2 2 2
Stethoscope, fetal 1 1 1
Thermometer 2 3 3
Vaginal specula 2 2 2
Measuring tape 1 1 1
Gestational age calculator 2 2 2
Drape/blanket 10 6 7
Needles and syringes 100 54 57
Autoclave/boiler/steamer 1 1 1
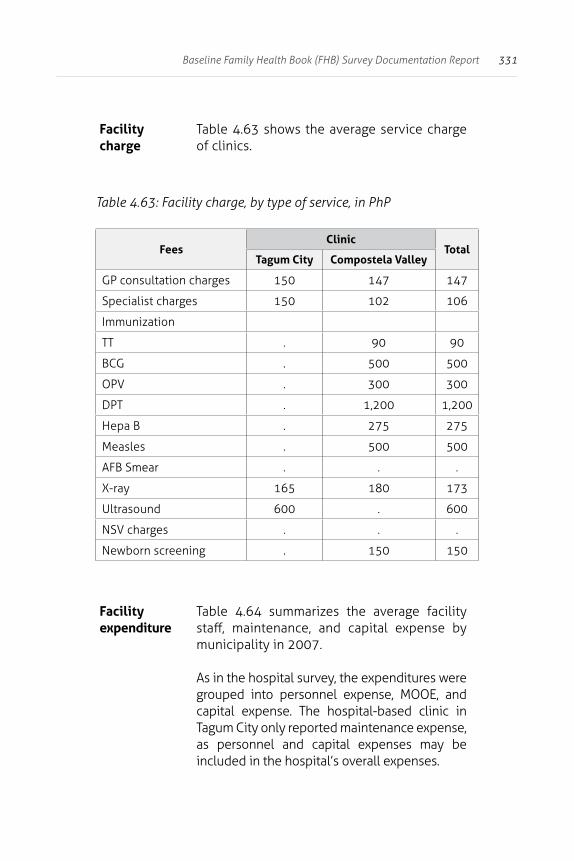
331Baseline Family Health Book (FHB) Survey Documentation Report
Facility charge
Table 4.63 shows the average service charge of clinics.
Table 4.63: Facility charge, by type of service, in PhP
FeesClinic
TotalTagum City Compostela Valley
GP consultation charges 150 147 147
Specialist charges 150 102 106
Immunization
TT . 90 90
BCG . 500 500
OPV . 300 300
DPT . 1,200 1,200
Hepa B . 275 275
Measles . 500 500
AFB Smear . . .
X-ray 165 180 173
Ultrasound 600 . 600
NSV charges . . .
Newborn screening . 150 150
Facility expenditure
Table 4.64 summarizes the average facility staff, maintenance, and capital expense by municipality in 2007.
As in the hospital survey, the expenditures were grouped into personnel expense, MOOE, and capital expense. The hospital-based clinic in Tagum City only reported maintenance expense, as personnel and capital expenses may be included in the hospital’s overall expenses.
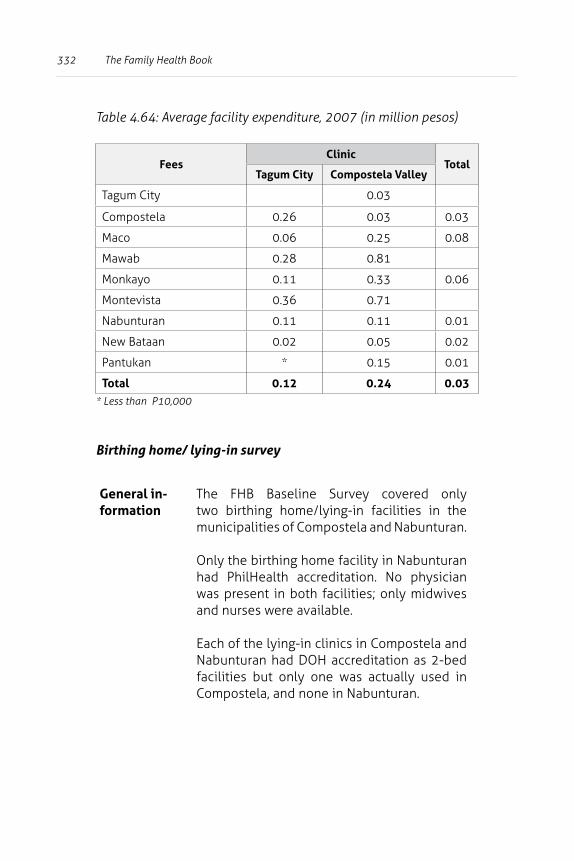
332 The Family Health Book
Table 4.64: Average facility expenditure, 2007 (in million pesos)
FeesClinic
TotalTagum City Compostela Valley
Tagum City 0.03
Compostela 0.26 0.03 0.03
Maco 0.06 0.25 0.08
Mawab 0.28 0.81
Monkayo 0.11 0.33 0.06
Montevista 0.36 0.71
Nabunturan 0.11 0.11 0.01
New Bataan 0.02 0.05 0.02
Pantukan * 0.15 0.01
Total 0.12 0.24 0.03* Less than P10,000
Birthing home/ lying-in survey
General in-formation
The FHB Baseline Survey covered only two birthing home/lying-in facilities in the municipalities of Compostela and Nabunturan.
Only the birthing home facility in Nabunturan had PhilHealth accreditation. No physician was present in both facilities; only midwives and nurses were available.
Each of the lying-in clinics in Compostela and Nabunturan had DOH accreditation as 2-bed facilities but only one was actually used in Compostela, and none in Nabunturan.
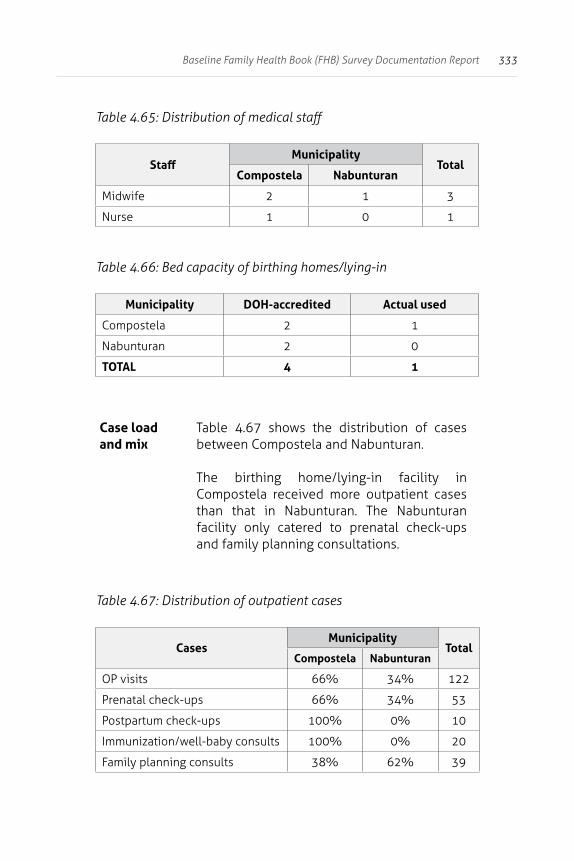
333Baseline Family Health Book (FHB) Survey Documentation Report
Table 4.65: Distribution of medical staff
StaffMunicipality
TotalCompostela Nabunturan
Midwife 2 1 3
Nurse 1 0 1
Table 4.66: Bed capacity of birthing homes/lying-in
Municipality DOH-accredited Actual used
Compostela 2 1
Nabunturan 2 0
TOTAL 4 1
Case load and mix
Table 4.67 shows the distribution of cases between Compostela and Nabunturan.
The birthing home/lying-in facility in Compostela received more outpatient cases than that in Nabunturan. The Nabunturan facility only catered to prenatal check-ups and family planning consultations.
Table 4.67: Distribution of outpatient cases
CasesMunicipality
TotalCompostela Nabunturan
OP visits 66% 34% 122
Prenatal check-ups 66% 34% 53
Postpartum check-ups 100% 0% 10
Immunization/well-baby consults 100% 0% 20
Family planning consults 38% 62% 39
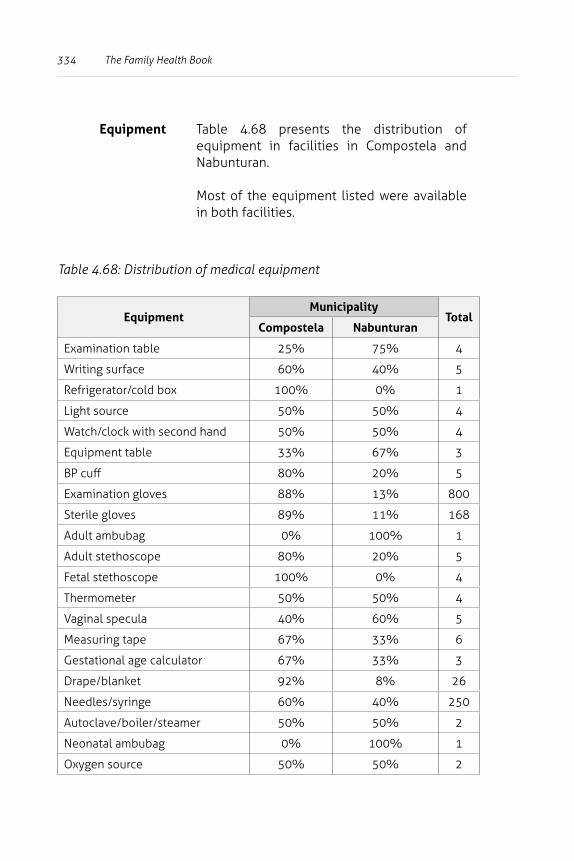
334 The Family Health Book
Equipment Table 4.68 presents the distribution of equipment in facilities in Compostela and Nabunturan.
Most of the equipment listed were available in both facilities.
Table 4.68: Distribution of medical equipment
EquipmentMunicipality
TotalCompostela Nabunturan
Examination table 25% 75% 4
Writing surface 60% 40% 5
Refrigerator/cold box 100% 0% 1
Light source 50% 50% 4
Watch/clock with second hand 50% 50% 4
Equipment table 33% 67% 3
BP cuff 80% 20% 5
Examination gloves 88% 13% 800
Sterile gloves 89% 11% 168
Adult ambubag 0% 100% 1
Adult stethoscope 80% 20% 5
Fetal stethoscope 100% 0% 4
Thermometer 50% 50% 4
Vaginal specula 40% 60% 5
Measuring tape 67% 33% 6
Gestational age calculator 67% 33% 3
Drape/blanket 92% 8% 26
Needles/syringe 60% 40% 250
Autoclave/boiler/steamer 50% 50% 2
Neonatal ambubag 0% 100% 1
Oxygen source 50% 50% 2
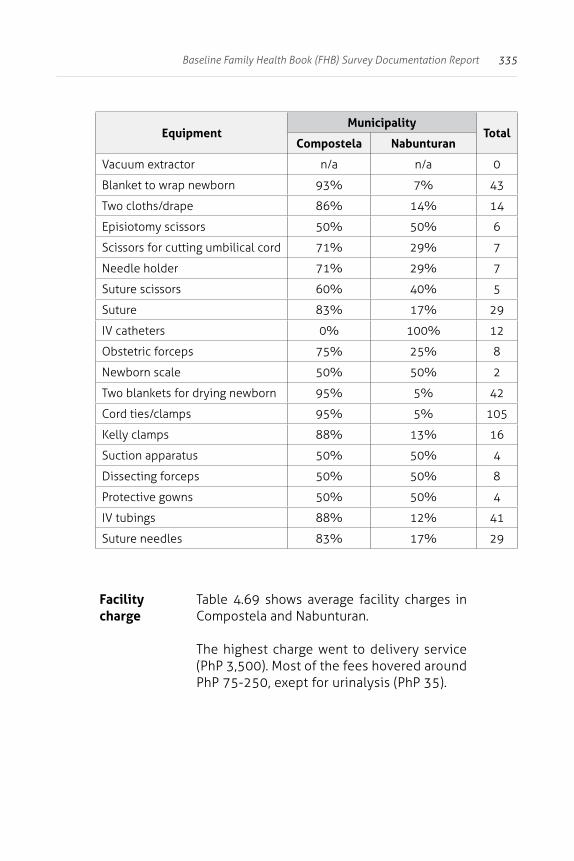
335Baseline Family Health Book (FHB) Survey Documentation Report
EquipmentMunicipality
TotalCompostela Nabunturan
Vacuum extractor n/a n/a 0
Blanket to wrap newborn 93% 7% 43
Two cloths/drape 86% 14% 14
Episiotomy scissors 50% 50% 6
Scissors for cutting umbilical cord 71% 29% 7
Needle holder 71% 29% 7
Suture scissors 60% 40% 5
Suture 83% 17% 29
IV catheters 0% 100% 12
Obstetric forceps 75% 25% 8
Newborn scale 50% 50% 2
Two blankets for drying newborn 95% 5% 42
Cord ties/clamps 95% 5% 105
Kelly clamps 88% 13% 16
Suction apparatus 50% 50% 4
Dissecting forceps 50% 50% 8
Protective gowns 50% 50% 4
IV tubings 88% 12% 41
Suture needles 83% 17% 29
Facility charge
Table 4.69 shows average facility charges in Compostela and Nabunturan.
The highest charge went to delivery service (PhP 3,500). Most of the fees hovered around PhP 75-250, exept for urinalysis (PhP 35).
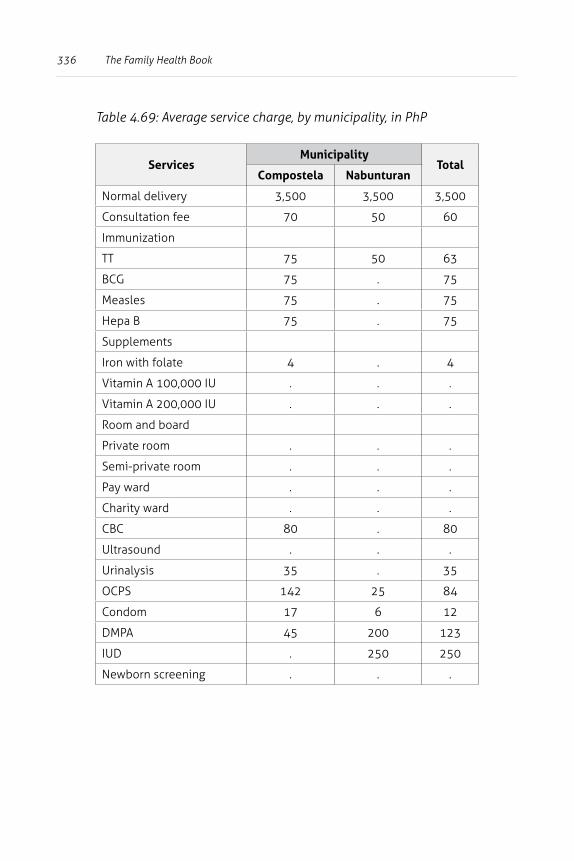
336 The Family Health Book
Table 4.69: Average service charge, by municipality, in PhP
ServicesMunicipality
TotalCompostela Nabunturan
Normal delivery 3,500 3,500 3,500
Consultation fee 70 50 60
Immunization
TT 75 50 63
BCG 75 . 75
Measles 75 . 75
Hepa B 75 . 75
Supplements
Iron with folate 4 . 4
Vitamin A 100,000 IU . . .
Vitamin A 200,000 IU . . .
Room and board
Private room . . .
Semi-private room . . .
Pay ward . . .
Charity ward . . .
CBC 80 . 80
Ultrasound . . .
Urinalysis 35 . 35
OCPS 142 25 84
Condom 17 6 12
DMPA 45 200 123
IUD . 250 250
Newborn screening . . .
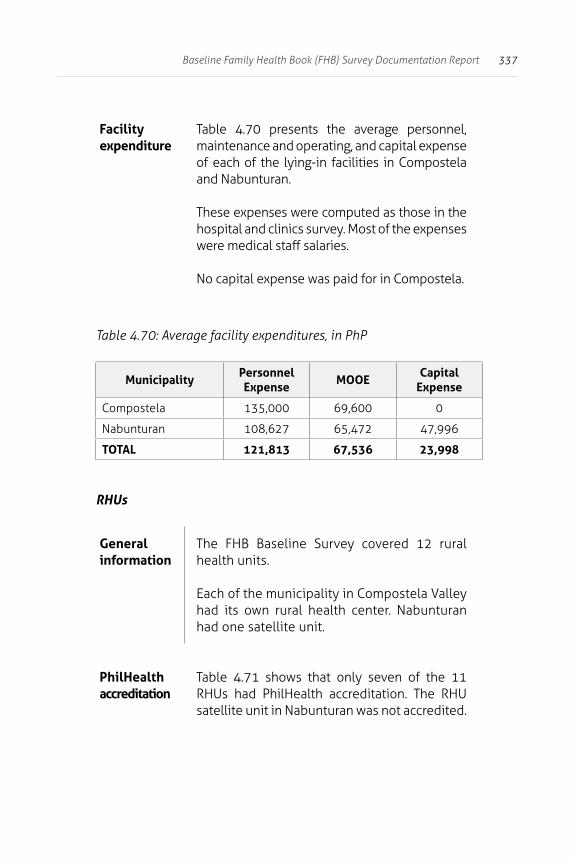
337Baseline Family Health Book (FHB) Survey Documentation Report
Facility expenditure
Table 4.70 presents the average personnel, maintenance and operating, and capital expense of each of the lying-in facilities in Compostela and Nabunturan.
These expenses were computed as those in the hospital and clinics survey. Most of the expenses were medical staff salaries.
No capital expense was paid for in Compostela.
Table 4.70: Average facility expenditures, in PhP
MunicipalityPersonnel Expense
MOOECapital
Expense
Compostela 135,000 69,600 0
Nabunturan 108,627 65,472 47,996
TOTAL 121,813 67,536 23,998
RHUs
General information
The FHB Baseline Survey covered 12 rural health units.
Each of the municipality in Compostela Valley had its own rural health center. Nabunturan had one satellite unit.
PhilHealth accreditation
Table 4.71 shows that only seven of the 11 RHUs had PhilHealth accreditation. The RHU satellite unit in Nabunturan was not accredited.
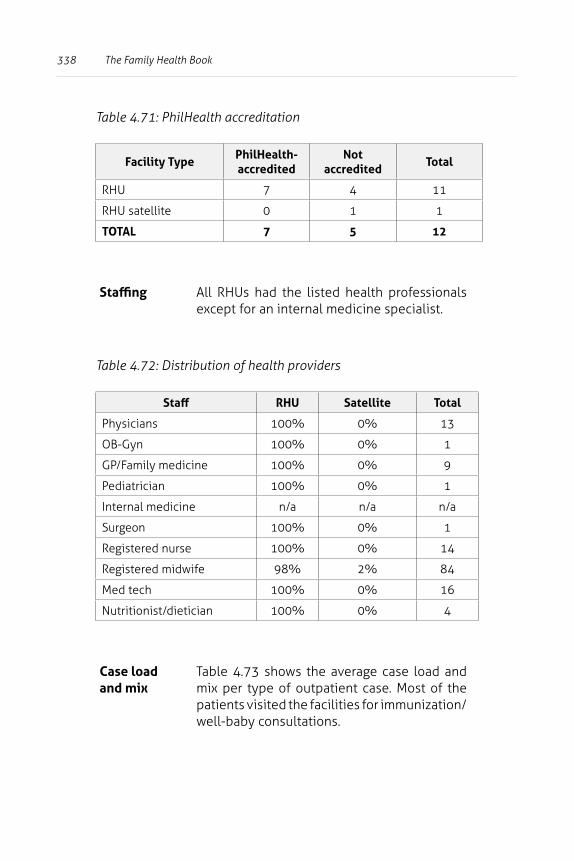
338 The Family Health Book
Table 4.71: PhilHealth accreditation
Facility TypePhilHealth-accredited
Not accredited
Total
RHU 7 4 11
RHU satellite 0 1 1
TOTAL 7 5 12
Staffing All RHUs had the listed health professionals except for an internal medicine specialist.
Table 4.72: Distribution of health providers
Staff RHU Satellite Total
Physicians 100% 0% 13
OB-Gyn 100% 0% 1
GP/Family medicine 100% 0% 9
Pediatrician 100% 0% 1
Internal medicine n/a n/a n/a
Surgeon 100% 0% 1
Registered nurse 100% 0% 14
Registered midwife 98% 2% 84
Med tech 100% 0% 16
Nutritionist/dietician 100% 0% 4
Case load and mix
Table 4.73 shows the average case load and mix per type of outpatient case. Most of the patients visited the facilities for immunization/well-baby consultations.
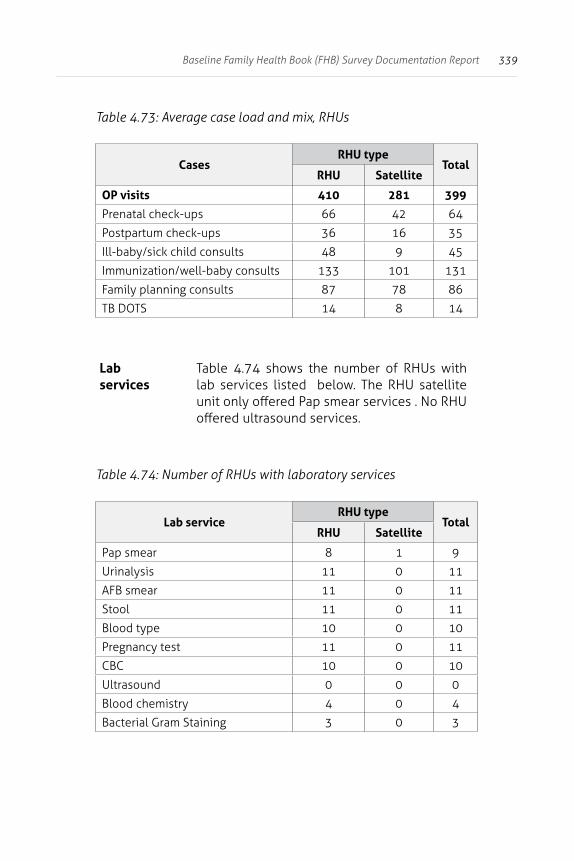
339Baseline Family Health Book (FHB) Survey Documentation Report
Table 4.73: Average case load and mix, RHUs
CasesRHU type
TotalRHU Satellite
OP visits 410 281 399
Prenatal check-ups 66 42 64
Postpartum check-ups 36 16 35
Ill-baby/sick child consults 48 9 45
Immunization/well-baby consults 133 101 131
Family planning consults 87 78 86
TB DOTS 14 8 14
Lab services
Table 4.74 shows the number of RHUs with lab services listed below. The RHU satellite unit only offered Pap smear services . No RHU offered ultrasound services.
Table 4.74: Number of RHUs with laboratory services
Lab serviceRHU type
TotalRHU Satellite
Pap smear 8 1 9
Urinalysis 11 0 11
AFB smear 11 0 11
Stool 11 0 11
Blood type 10 0 10
Pregnancy test 11 0 11
CBC 10 0 10
Ultrasound 0 0 0
Blood chemistry 4 0 4
Bacterial Gram Staining 3 0 3
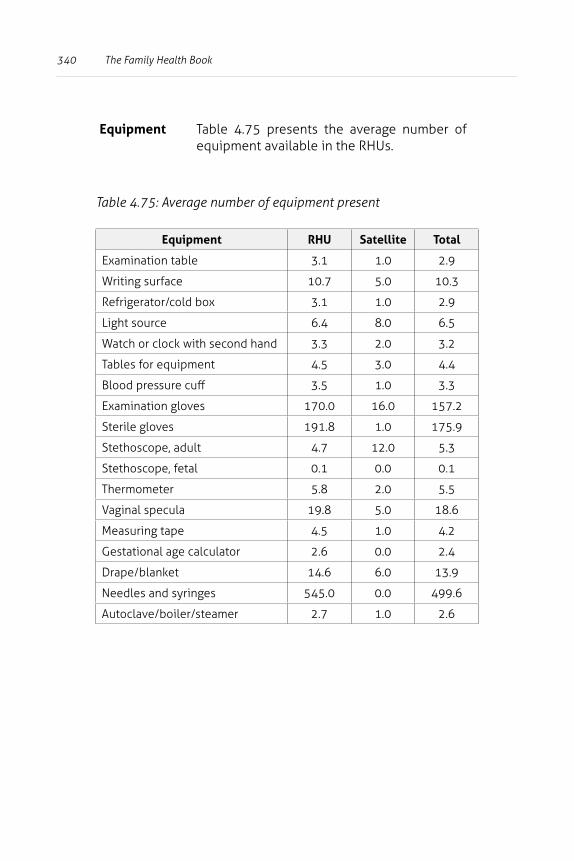
340 The Family Health Book
Equipment Table 4.75 presents the average number of equipment available in the RHUs.
Table 4.75: Average number of equipment present
Equipment RHU Satellite Total
Examination table 3.1 1.0 2.9
Writing surface 10.7 5.0 10.3
Refrigerator/cold box 3.1 1.0 2.9
Light source 6.4 8.0 6.5
Watch or clock with second hand 3.3 2.0 3.2
Tables for equipment 4.5 3.0 4.4
Blood pressure cuff 3.5 1.0 3.3
Examination gloves 170.0 16.0 157.2
Sterile gloves 191.8 1.0 175.9
Stethoscope, adult 4.7 12.0 5.3
Stethoscope, fetal 0.1 0.0 0.1
Thermometer 5.8 2.0 5.5
Vaginal specula 19.8 5.0 18.6
Measuring tape 4.5 1.0 4.2
Gestational age calculator 2.6 0.0 2.4
Drape/blanket 14.6 6.0 13.9
Needles and syringes 545.0 0.0 499.6
Autoclave/boiler/steamer 2.7 1.0 2.6
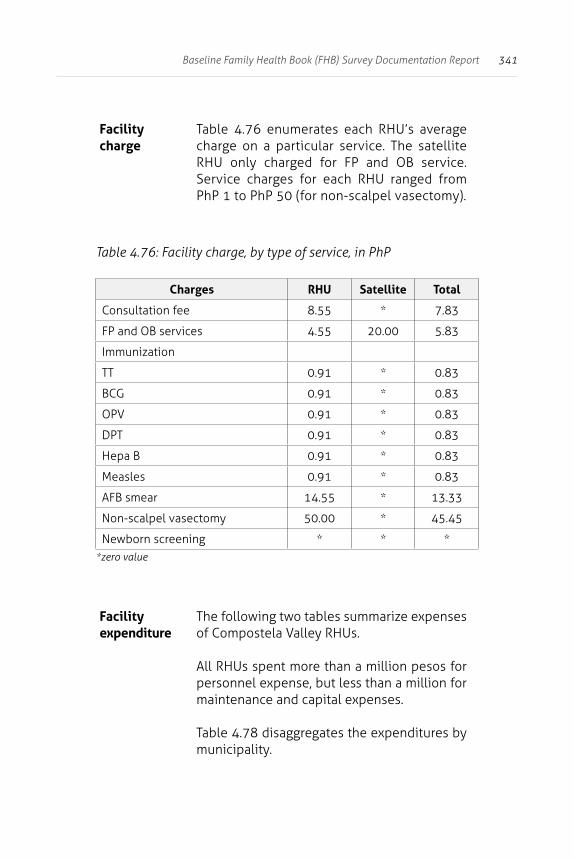
341Baseline Family Health Book (FHB) Survey Documentation Report
Facility charge
Table 4.76 enumerates each RHU’s average charge on a particular service. The satellite RHU only charged for FP and OB service. Service charges for each RHU ranged from PhP 1 to PhP 50 (for non-scalpel vasectomy).
Table 4.76: Facility charge, by type of service, in PhP
Charges RHU Satellite Total
Consultation fee 8.55 * 7.83
FP and OB services 4.55 20.00 5.83
Immunization
TT 0.91 * 0.83
BCG 0.91 * 0.83
OPV 0.91 * 0.83
DPT 0.91 * 0.83
Hepa B 0.91 * 0.83
Measles 0.91 * 0.83
AFB smear 14.55 * 13.33
Non-scalpel vasectomy 50.00 * 45.45
Newborn screening * * **zero value
Facility expenditure
The following two tables summarize expenses of Compostela Valley RHUs.
All RHUs spent more than a million pesos for personnel expense, but less than a million for maintenance and capital expenses.
Table 4.78 disaggregates the expenditures by municipality.
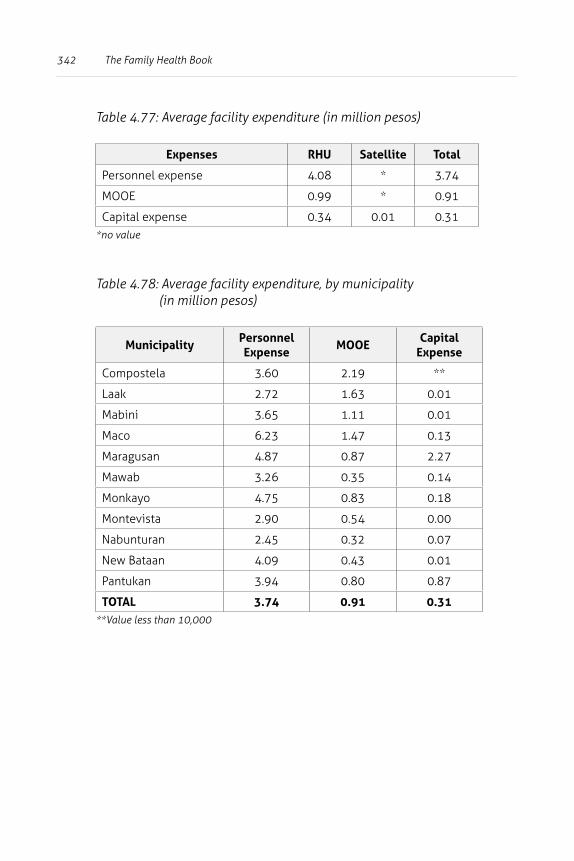
342 The Family Health Book
Table 4.77: Average facility expenditure (in million pesos)
Expenses RHU Satellite Total
Personnel expense 4.08 * 3.74
MOOE 0.99 * 0.91
Capital expense 0.34 0.01 0.31*no value
Table 4.78: Average facility expenditure, by municipality (in million pesos)
MunicipalityPersonnel Expense
MOOECapital
Expense
Compostela 3.60 2.19 **
Laak 2.72 1.63 0.01
Mabini 3.65 1.11 0.01
Maco 6.23 1.47 0.13
Maragusan 4.87 0.87 2.27
Mawab 3.26 0.35 0.14
Monkayo 4.75 0.83 0.18
Montevista 2.90 0.54 0.00
Nabunturan 2.45 0.32 0.07
New Bataan 4.09 0.43 0.01
Pantukan 3.94 0.80 0.87
TOTAL 3.74 0.91 0.31**Value less than 10,000
343Baseline Family Health Book (FHB) Survey Documentation Report
Highlights of the Patient Exit Survey
In this section, the socio-economic characteristics and satisfaction of inpatients and outpatients admitted in facilities included in the facilities survey are discussed.
Outpatient survey
General information
Table 4.79 presents the distribution of outpatients by type.
The cases covered were maternal and childcare. Majority of the cases were child care-related.
Table 4.80 summarizes the distribution of outpatients by type of facility. The regional hospital refers to the Davao Regional Hospital in Tagum City.
Table 4.81 shows the distribution by wealth quintiles of outpatients who visited either public or private facilities.
Wealth quintiles were computed using patients’ asset ownership.
Most of the poorer outpatients chose to visit a public facility (23 of the 166 outpatients). Richer patients chose to visit private facilities (22 of 166).
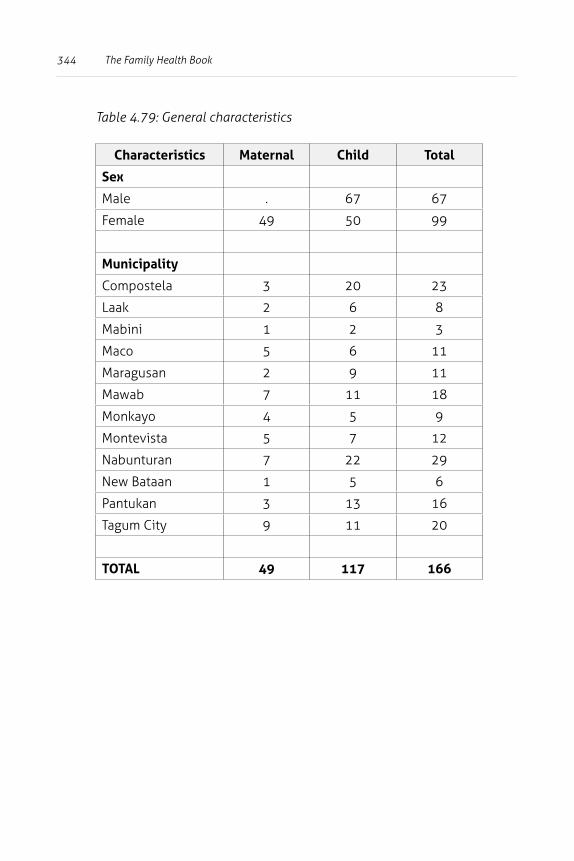
344 The Family Health Book
Table 4.79: General characteristics
Characteristics Maternal Child Total
Sex
Male . 67 67
Female 49 50 99
Municipality
Compostela 3 20 23
Laak 2 6 8
Mabini 1 2 3
Maco 5 6 11
Maragusan 2 9 11
Mawab 7 11 18
Monkayo 4 5 9
Montevista 5 7 12
Nabunturan 7 22 29
New Bataan 1 5 6
Pantukan 3 13 16
Tagum City 9 11 20
TOTAL 49 117 166
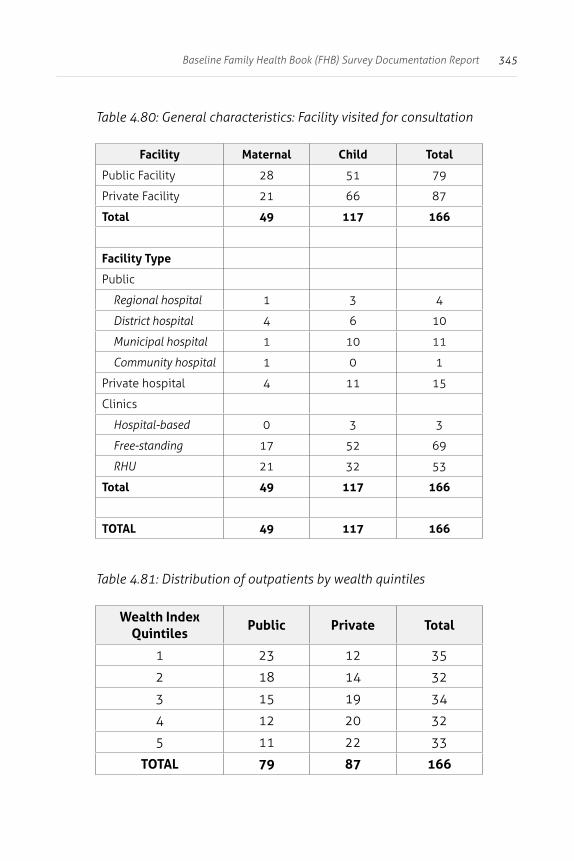
345Baseline Family Health Book (FHB) Survey Documentation Report
Table 4.80: General characteristics: Facility visited for consultation
Facility Maternal Child Total
Public Facility 28 51 79
Private Facility 21 66 87
Total 49 117 166
Facility Type
Public
Regional hospital 1 3 4
District hospital 4 6 10
Municipal hospital 1 10 11
Community hospital 1 0 1
Private hospital 4 11 15
Clinics
Hospital-based 0 3 3
Free-standing 17 52 69
RHU 21 32 53
Total 49 117 166
TOTAL 49 117 166
Table 4.81: Distribution of outpatients by wealth quintiles
Wealth Index Quintiles
Public Private Total
1 23 12 35
2 18 14 32
3 15 19 34
4 12 20 32
5 11 22 33
TOTAL 79 87 166
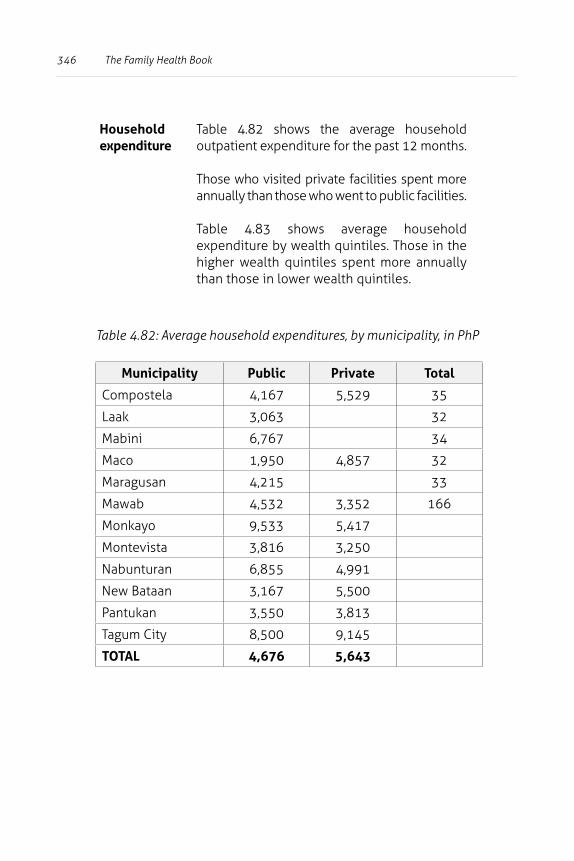
346 The Family Health Book
Household expenditure
Table 4.82 shows the average household outpatient expenditure for the past 12 months.
Those who visited private facilities spent more annually than those who went to public facilities.
Table 4.83 shows average household expenditure by wealth quintiles. Those in the higher wealth quintiles spent more annually than those in lower wealth quintiles.
Table 4.82: Average household expenditures, by municipality, in PhP
Municipality Public Private Total
Compostela 4,167 5,529 35
Laak 3,063 32
Mabini 6,767 34
Maco 1,950 4,857 32
Maragusan 4,215 33
Mawab 4,532 3,352 166
Monkayo 9,533 5,417
Montevista 3,816 3,250
Nabunturan 6,855 4,991
New Bataan 3,167 5,500
Pantukan 3,550 3,813
Tagum City 8,500 9,145
TOTAL 4,676 5,643
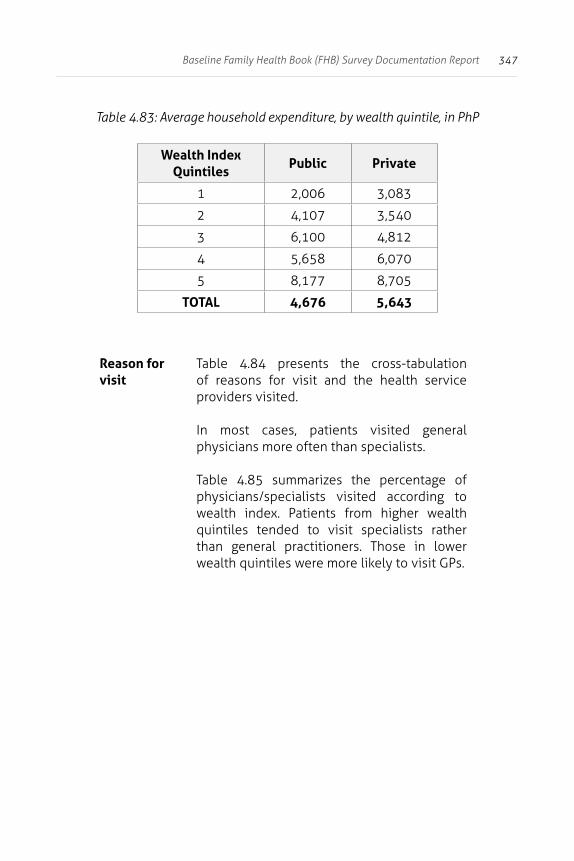
347Baseline Family Health Book (FHB) Survey Documentation Report
Table 4.83: Average household expenditure, by wealth quintile, in PhP
Wealth Index Quintiles
Public Private
1 2,006 3,083
2 4,107 3,540
3 6,100 4,812
4 5,658 6,070
5 8,177 8,705
TOTAL 4,676 5,643
Reason for visit
Table 4.84 presents the cross-tabulation of reasons for visit and the health service providers visited.
In most cases, patients visited general physicians more often than specialists.
Table 4.85 summarizes the percentage of physicians/specialists visited according to wealth index. Patients from higher wealth quintiles tended to visit specialists rather than general practitioners. Those in lower wealth quintiles were more likely to visit GPs.
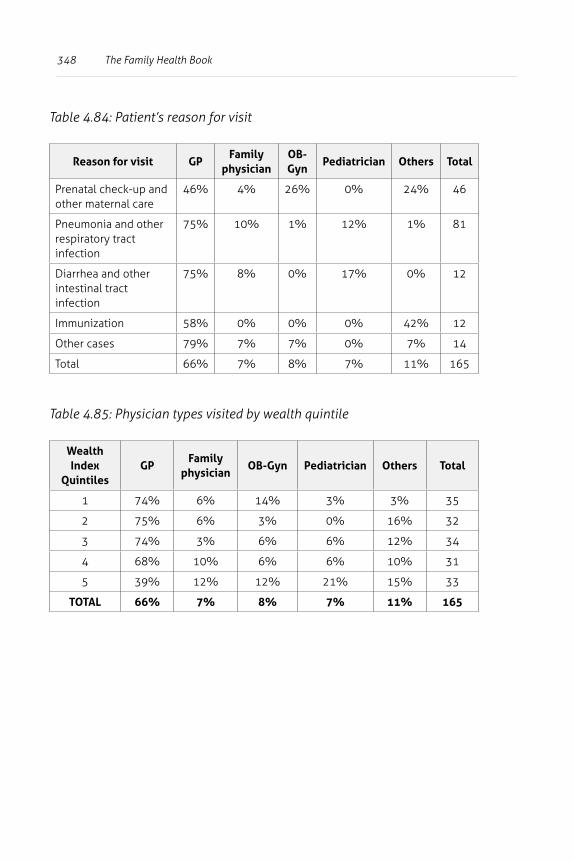
348 The Family Health Book
Table 4.84: Patient’s reason for visit
Reason for visit GPFamily
physicianOB-Gyn
Pediatrician Others Total
Prenatal check-up and other maternal care
46% 4% 26% 0% 24% 46
Pneumonia and other respiratory tract infection
75% 10% 1% 12% 1% 81
Diarrhea and other intestinal tract infection
75% 8% 0% 17% 0% 12
Immunization 58% 0% 0% 0% 42% 12
Other cases 79% 7% 7% 0% 7% 14
Total 66% 7% 8% 7% 11% 165
Table 4.85: Physician types visited by wealth quintile
Wealth Index
QuintilesGP
Family physician
OB-Gyn Pediatrician Others Total
1 74% 6% 14% 3% 3% 35
2 75% 6% 3% 0% 16% 32
3 74% 3% 6% 6% 12% 34
4 68% 10% 6% 6% 10% 31
5 39% 12% 12% 21% 15% 33
TOTAL 66% 7% 8% 7% 11% 165
349Baseline Family Health Book (FHB) Survey Documentation Report
Consultation cost
Table 4.86 shows average consultation costs, which also covered travel time to the facility and the transportation cost.
Patients typically had longer travel times and spent more to visit a public hospital than a private facility.
While private hospitals were more accessible to patients, they charged more on average than public facilities. This also applied to clinics and RHUs, as patients paid less for a consultation (PhP 19) in an RHU.
In Table 4.87, public and private facilities are aggregated and outpatient visits per municipality are summarized.
Consultations in private facilities cost more than in public facilities, although transportation costs going to public facilities were higher compared to those incurred in going to private facilities.
Table 4.88 shows the average consultation costs by patient type (child or maternal). Consultation costs in private facilities were higher than those in public facilities.
Table 4.89 shows average consultation costs by wealth quintiles. Relatively wealthier patients tended to spend more than the poor in both public and private facilities.
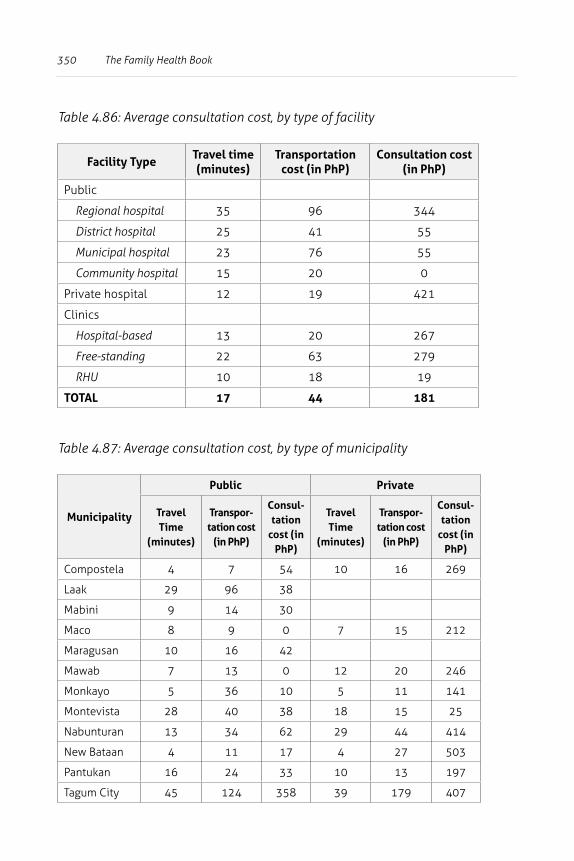
350 The Family Health Book
Table 4.86: Average consultation cost, by type of facility
Facility TypeTravel time (minutes)
Transportation cost (in PhP)
Consultation cost (in PhP)
Public
Regional hospital 35 96 344
District hospital 25 41 55
Municipal hospital 23 76 55
Community hospital 15 20 0
Private hospital 12 19 421
Clinics
Hospital-based 13 20 267
Free-standing 22 63 279
RHU 10 18 19
TOTAL 17 44 181
Table 4.87: Average consultation cost, by type of municipality
Municipality
Public Private
Travel Time
(minutes)
Transpor-tation cost
(in PhP)
Consul-tation
cost (in PhP)
Travel Time
(minutes)
Transpor-tation cost
(in PhP)
Consul-tation
cost (in PhP)
Compostela 4 7 54 10 16 269
Laak 29 96 38
Mabini 9 14 30
Maco 8 9 0 7 15 212
Maragusan 10 16 42
Mawab 7 13 0 12 20 246
Monkayo 5 36 10 5 11 141
Montevista 28 40 38 18 15 25
Nabunturan 13 34 62 29 44 414
New Bataan 4 11 17 4 27 503
Pantukan 16 24 33 10 13 197
Tagum City 45 124 358 39 179 407
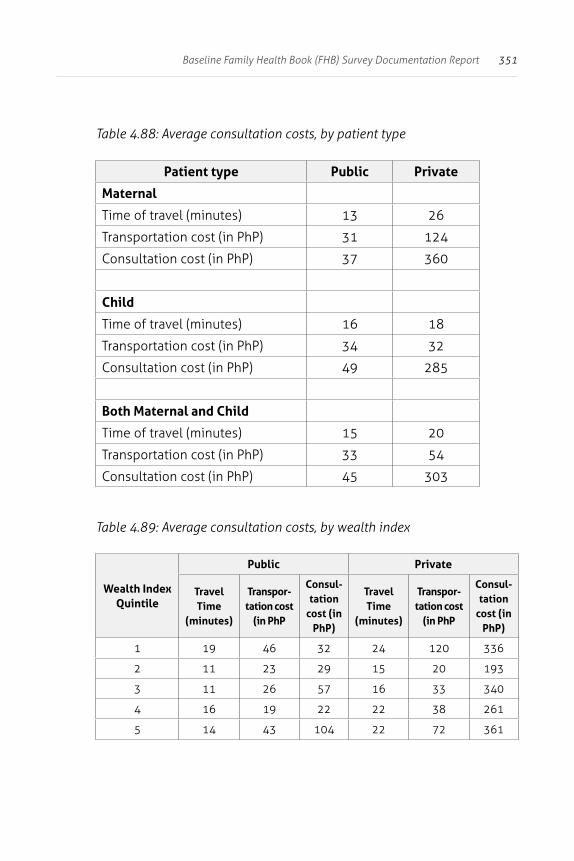
351Baseline Family Health Book (FHB) Survey Documentation Report
Table 4.88: Average consultation costs, by patient type
Patient type Public Private
Maternal
Time of travel (minutes) 13 26
Transportation cost (in PhP) 31 124
Consultation cost (in PhP) 37 360
Child
Time of travel (minutes) 16 18
Transportation cost (in PhP) 34 32
Consultation cost (in PhP) 49 285
Both Maternal and Child
Time of travel (minutes) 15 20
Transportation cost (in PhP) 33 54
Consultation cost (in PhP) 45 303
Table 4.89: Average consultation costs, by wealth index
Wealth Index Quintile
Public Private
Travel Time
(minutes)
Transpor-tation cost
(in PhP
Consul-tation
cost (in PhP)
Travel Time
(minutes)
Transpor-tation cost
(in PhP
Consul-tation
cost (in PhP)
1 19 46 32 24 120 336
2 11 23 29 15 20 193
3 11 26 57 16 33 340
4 16 19 22 22 38 261
5 14 43 104 22 72 361
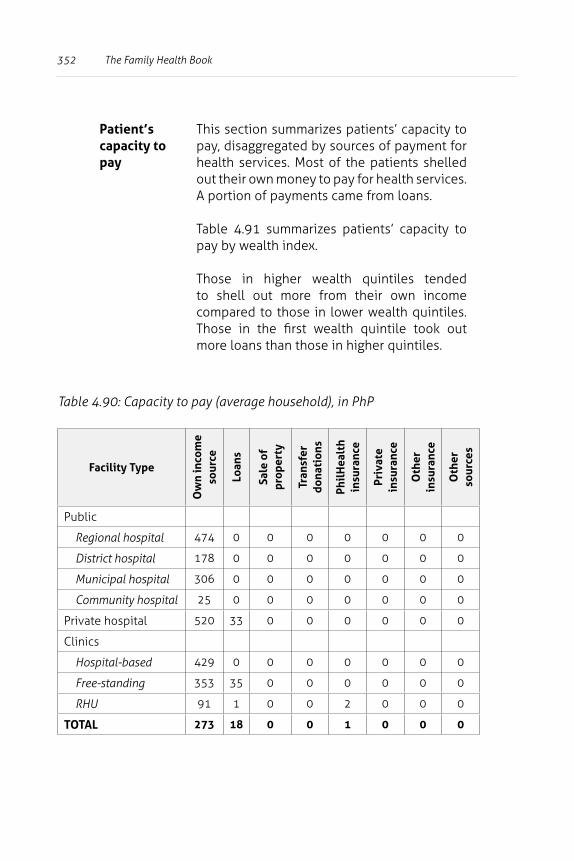
352 The Family Health Book
Patient’s capacity to pay
This section summarizes patients’ capacity to pay, disaggregated by sources of payment for health services. Most of the patients shelled out their own money to pay for health services. A portion of payments came from loans.
Table 4.91 summarizes patients’ capacity to pay by wealth index.
Those in higher wealth quintiles tended to shell out more from their own income compared to those in lower wealth quintiles. Those in the first wealth quintile took out more loans than those in higher quintiles.
Table 4.90: Capacity to pay (average household), in PhP
Facility Type
Ow
n in
com
e so
urce
Loan
s
Sale
of
prop
erty
Tran
sfer
do
nati
ons
Phil
Hea
lth
insu
ranc
e
Priv
ate
insu
ranc
e
Oth
er
insu
ranc
e
Oth
er
sour
ces
Public
Regional hospital 474 0 0 0 0 0 0 0
District hospital 178 0 0 0 0 0 0 0
Municipal hospital 306 0 0 0 0 0 0 0
Community hospital 25 0 0 0 0 0 0 0
Private hospital 520 33 0 0 0 0 0 0
Clinics
Hospital-based 429 0 0 0 0 0 0 0
Free-standing 353 35 0 0 0 0 0 0
RHU 91 1 0 0 2 0 0 0
TOTAL 273 18 0 0 1 0 0 0
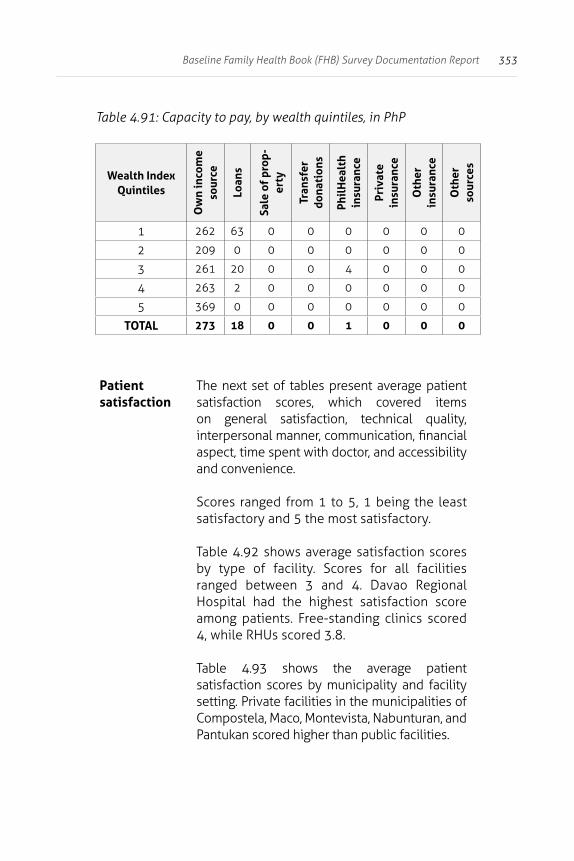
353Baseline Family Health Book (FHB) Survey Documentation Report
Table 4.91: Capacity to pay, by wealth quintiles, in PhP
Wealth Index Quintiles
Ow
n in
com
e so
urce
Loan
s
Sale
of
prop
-er
ty
Tran
sfer
do
nati
ons
Phil
Hea
lth
insu
ranc
e
Priv
ate
insu
ranc
e
Oth
er
insu
ranc
e
Oth
er
sour
ces
1 262 63 0 0 0 0 0 0
2 209 0 0 0 0 0 0 0
3 261 20 0 0 4 0 0 0
4 263 2 0 0 0 0 0 0
5 369 0 0 0 0 0 0 0
TOTAL 273 18 0 0 1 0 0 0
Patient satisfaction
The next set of tables present average patient satisfaction scores, which covered items on general satisfaction, technical quality, interpersonal manner, communication, financial aspect, time spent with doctor, and accessibility and convenience.
Scores ranged from 1 to 5, 1 being the least satisfactory and 5 the most satisfactory.
Table 4.92 shows average satisfaction scores by type of facility. Scores for all facilities ranged between 3 and 4. Davao Regional Hospital had the highest satisfaction score among patients. Free-standing clinics scored 4, while RHUs scored 3.8.
Table 4.93 shows the average patient satisfaction scores by municipality and facility setting. Private facilities in the municipalities of Compostela, Maco, Montevista, Nabunturan, and Pantukan scored higher than public facilities.
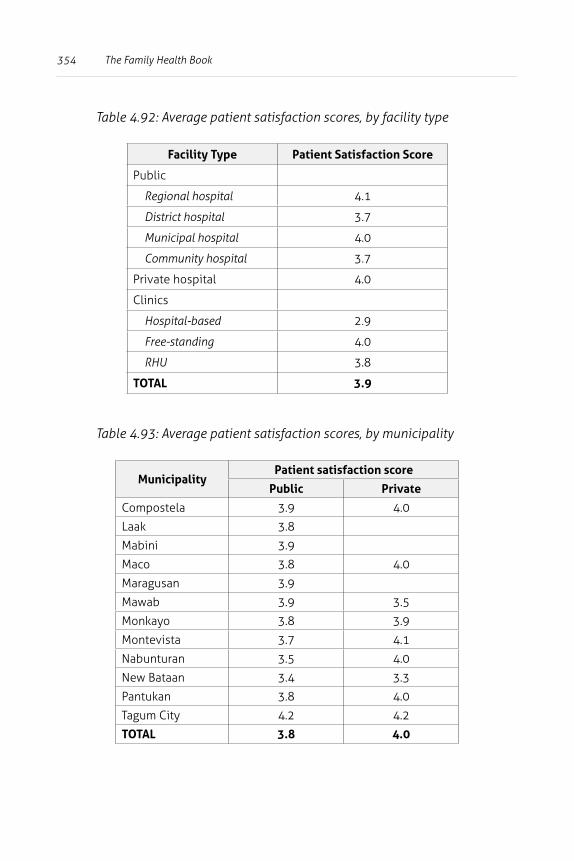
354 The Family Health Book
Table 4.92: Average patient satisfaction scores, by facility type
Facility Type Patient Satisfaction Score
Public
Regional hospital 4.1
District hospital 3.7
Municipal hospital 4.0
Community hospital 3.7
Private hospital 4.0
Clinics
Hospital-based 2.9
Free-standing 4.0
RHU 3.8
TOTAL 3.9
Table 4.93: Average patient satisfaction scores, by municipality
MunicipalityPatient satisfaction score
Public Private
Compostela 3.9 4.0
Laak 3.8
Mabini 3.9
Maco 3.8 4.0
Maragusan 3.9
Mawab 3.9 3.5
Monkayo 3.8 3.9
Montevista 3.7 4.1
Nabunturan 3.5 4.0
New Bataan 3.4 3.3
Pantukan 3.8 4.0
Tagum City 4.2 4.2
TOTAL 3.8 4.0
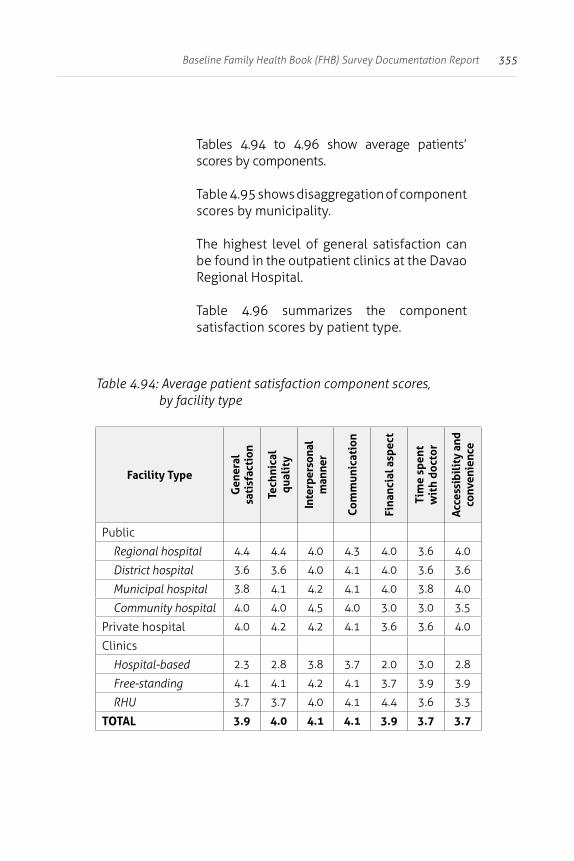
355Baseline Family Health Book (FHB) Survey Documentation Report
Tables 4.94 to 4.96 show average patients’ scores by components.
Table 4.95 shows disaggregation of component scores by municipality.
The highest level of general satisfaction can be found in the outpatient clinics at the Davao Regional Hospital.
Table 4.96 summarizes the component satisfaction scores by patient type.
Table 4.94: Average patient satisfaction component scores, by facility type
Facility Type
Gen
eral
sa
tisf
acti
on
Tech
nica
l qu
alit
y
Inte
rper
sona
l m
anne
r
Com
mun
icat
ion
Fina
ncia
l asp
ect
Tim
e sp
ent
wit
h do
ctor
Acc
essi
bili
ty a
nd
conv
enie
nce
Public
Regional hospital 4.4 4.4 4.0 4.3 4.0 3.6 4.0
District hospital 3.6 3.6 4.0 4.1 4.0 3.6 3.6
Municipal hospital 3.8 4.1 4.2 4.1 4.0 3.8 4.0
Community hospital 4.0 4.0 4.5 4.0 3.0 3.0 3.5
Private hospital 4.0 4.2 4.2 4.1 3.6 3.6 4.0
Clinics
Hospital-based 2.3 2.8 3.8 3.7 2.0 3.0 2.8
Free-standing 4.1 4.1 4.2 4.1 3.7 3.9 3.9
RHU 3.7 3.7 4.0 4.1 4.4 3.6 3.3
TOTAL 3.9 4.0 4.1 4.1 3.9 3.7 3.7
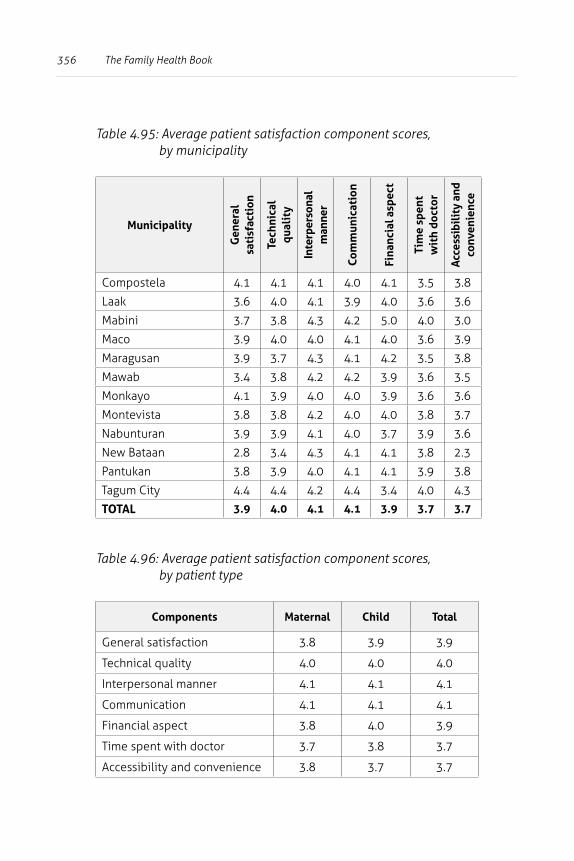
356 The Family Health Book
Table 4.95: Average patient satisfaction component scores, by municipality
MunicipalityG
ener
al
sati
sfac
tion
Tech
nica
l qu
alit
y
Inte
rper
sona
l m
anne
r
Com
mun
icat
ion
Fina
ncia
l asp
ect
Tim
e sp
ent
wit
h do
ctor
Acc
essi
bili
ty a
nd
conv
enie
nce
Compostela 4.1 4.1 4.1 4.0 4.1 3.5 3.8
Laak 3.6 4.0 4.1 3.9 4.0 3.6 3.6
Mabini 3.7 3.8 4.3 4.2 5.0 4.0 3.0
Maco 3.9 4.0 4.0 4.1 4.0 3.6 3.9
Maragusan 3.9 3.7 4.3 4.1 4.2 3.5 3.8
Mawab 3.4 3.8 4.2 4.2 3.9 3.6 3.5
Monkayo 4.1 3.9 4.0 4.0 3.9 3.6 3.6
Montevista 3.8 3.8 4.2 4.0 4.0 3.8 3.7
Nabunturan 3.9 3.9 4.1 4.0 3.7 3.9 3.6
New Bataan 2.8 3.4 4.3 4.1 4.1 3.8 2.3
Pantukan 3.8 3.9 4.0 4.1 4.1 3.9 3.8
Tagum City 4.4 4.4 4.2 4.4 3.4 4.0 4.3
TOTAL 3.9 4.0 4.1 4.1 3.9 3.7 3.7
Table 4.96: Average patient satisfaction component scores, by patient type
Components Maternal Child Total
General satisfaction 3.8 3.9 3.9
Technical quality 4.0 4.0 4.0
Interpersonal manner 4.1 4.1 4.1
Communication 4.1 4.1 4.1
Financial aspect 3.8 4.0 3.9
Time spent with doctor 3.7 3.8 3.7
Accessibility and convenience 3.8 3.7 3.7
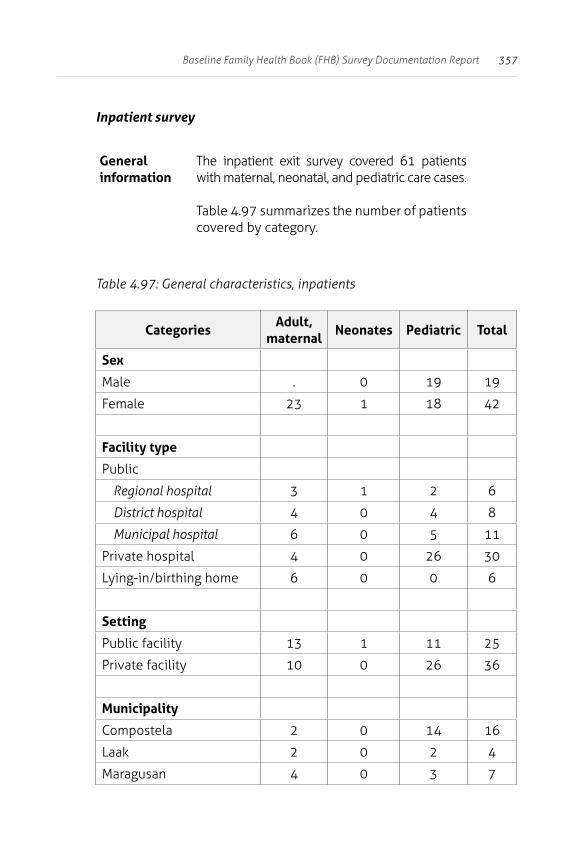
357Baseline Family Health Book (FHB) Survey Documentation Report
Inpatient survey
General information
The inpatient exit survey covered 61 patients with maternal, neonatal, and pediatric care cases.
Table 4.97 summarizes the number of patients covered by category.
Table 4.97: General characteristics, inpatients
CategoriesAdult,
maternalNeonates Pediatric Total
Sex
Male . 0 19 19
Female 23 1 18 42
Facility type
Public
Regional hospital 3 1 2 6
District hospital 4 0 4 8
Municipal hospital 6 0 5 11
Private hospital 4 0 26 30
Lying-in/birthing home 6 0 0 6
Setting
Public facility 13 1 11 25
Private facility 10 0 26 36
Municipality
Compostela 2 0 14 16
Laak 2 0 2 4
Maragusan 4 0 3 7
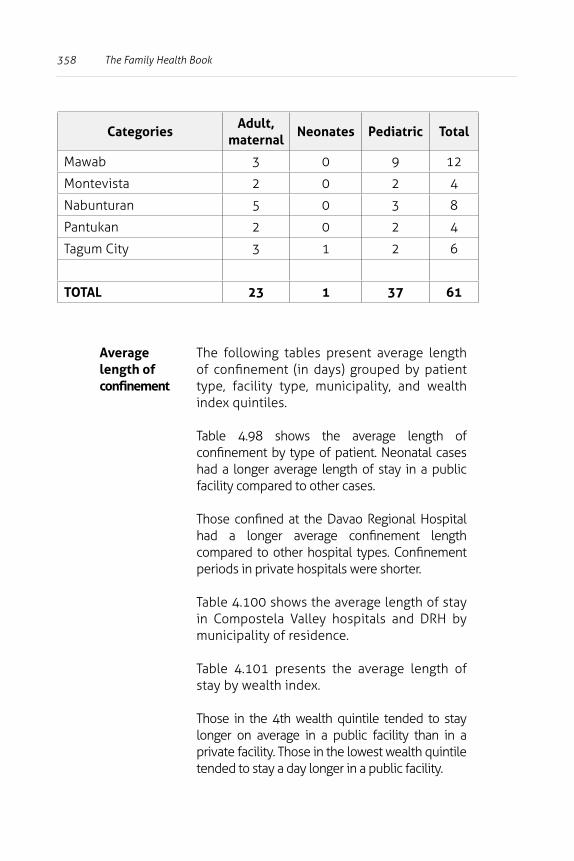
358 The Family Health Book
CategoriesAdult,
maternalNeonates Pediatric Total
Mawab 3 0 9 12
Montevista 2 0 2 4
Nabunturan 5 0 3 8
Pantukan 2 0 2 4
Tagum City 3 1 2 6
TOTAL 23 1 37 61
Average length of confinement
The following tables present average length of confinement (in days) grouped by patient type, facility type, municipality, and wealth index quintiles.
Table 4.98 shows the average length of confinement by type of patient. Neonatal cases had a longer average length of stay in a public facility compared to other cases.
Those confined at the Davao Regional Hospital had a longer average confinement length compared to other hospital types. Confinement periods in private hospitals were shorter.
Table 4.100 shows the average length of stay in Compostela Valley hospitals and DRH by municipality of residence.
Table 4.101 presents the average length of stay by wealth index.
Those in the 4th wealth quintile tended to stay longer on average in a public facility than in a private facility. Those in the lowest wealth quintile tended to stay a day longer in a public facility.
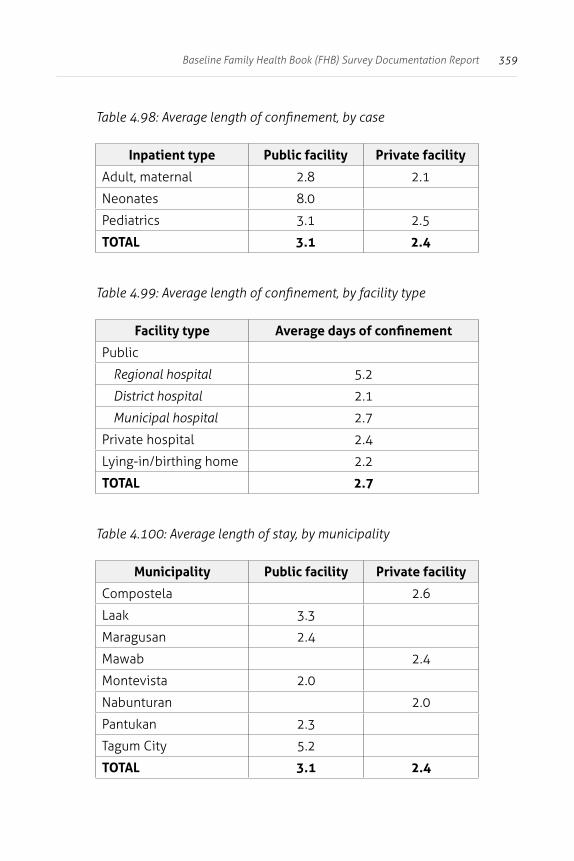
359Baseline Family Health Book (FHB) Survey Documentation Report
Table 4.98: Average length of confinement, by case
Inpatient type Public facility Private facility
Adult, maternal 2.8 2.1
Neonates 8.0
Pediatrics 3.1 2.5
TOTAL 3.1 2.4
Table 4.99: Average length of confinement, by facility type
Facility type Average days of confinement
Public
Regional hospital 5.2
District hospital 2.1
Municipal hospital 2.7
Private hospital 2.4
Lying-in/birthing home 2.2
TOTAL 2.7
Table 4.100: Average length of stay, by municipality
Municipality Public facility Private facility
Compostela 2.6
Laak 3.3
Maragusan 2.4
Mawab 2.4
Montevista 2.0
Nabunturan 2.0
Pantukan 2.3
Tagum City 5.2
TOTAL 3.1 2.4
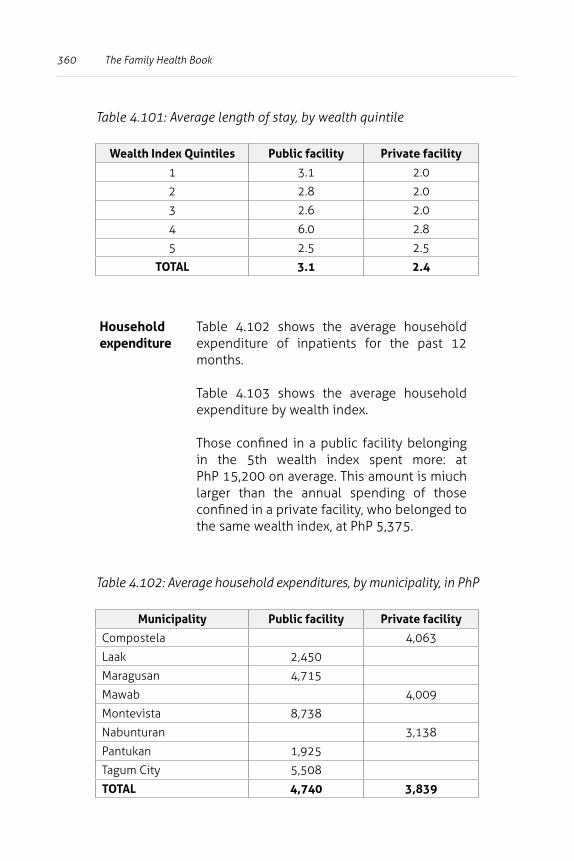
360 The Family Health Book
Table 4.101: Average length of stay, by wealth quintile
Wealth Index Quintiles Public facility Private facility
1 3.1 2.0
2 2.8 2.0
3 2.6 2.0
4 6.0 2.8
5 2.5 2.5
TOTAL 3.1 2.4
Household expenditure
Table 4.102 shows the average household expenditure of inpatients for the past 12 months.
Table 4.103 shows the average household expenditure by wealth index.
Those confined in a public facility belonging in the 5th wealth index spent more: at PhP 15,200 on average. This amount is miuch larger than the annual spending of those confined in a private facility, who belonged to the same wealth index, at PhP 5,375.
Table 4.102: Average household expenditures, by municipality, in PhP
Municipality Public facility Private facility
Compostela 4,063
Laak 2,450
Maragusan 4,715
Mawab 4,009
Montevista 8,738
Nabunturan 3,138
Pantukan 1,925
Tagum City 5,508
TOTAL 4,740 3,839
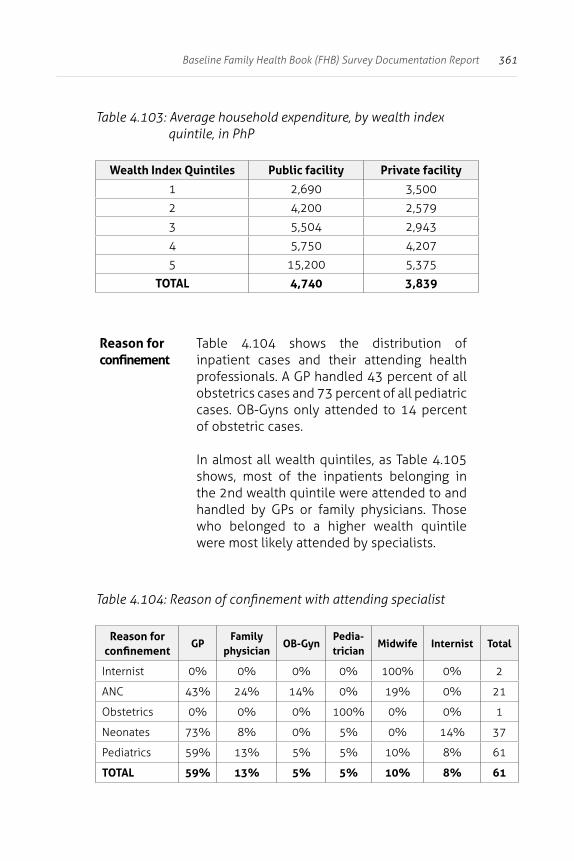
361Baseline Family Health Book (FHB) Survey Documentation Report
Table 4.103: Average household expenditure, by wealth index quintile, in PhP
Wealth Index Quintiles Public facility Private facility
1 2,690 3,500
2 4,200 2,579
3 5,504 2,943
4 5,750 4,207
5 15,200 5,375
TOTAL 4,740 3,839
Reason for confinement
Table 4.104 shows the distribution of inpatient cases and their attending health professionals. A GP handled 43 percent of all obstetrics cases and 73 percent of all pediatric cases. OB-Gyns only attended to 14 percent of obstetric cases.
In almost all wealth quintiles, as Table 4.105 shows, most of the inpatients belonging in the 2nd wealth quintile were attended to and handled by GPs or family physicians. Those who belonged to a higher wealth quintile were most likely attended by specialists.
Table 4.104: Reason of confinement with attending specialist
Reason for confinement
GPFamily
physicianOB-Gyn
Pedia-trician
Midwife Internist Total
Internist 0% 0% 0% 0% 100% 0% 2
ANC 43% 24% 14% 0% 19% 0% 21
Obstetrics 0% 0% 0% 100% 0% 0% 1
Neonates 73% 8% 0% 5% 0% 14% 37
Pediatrics 59% 13% 5% 5% 10% 8% 61
TOTAL 59% 13% 5% 5% 10% 8% 61
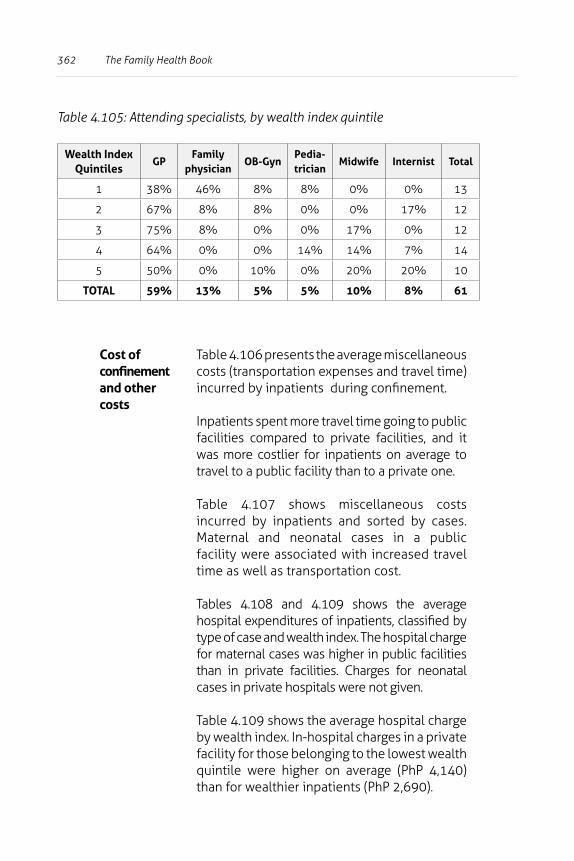
362 The Family Health Book
Table 4.105: Attending specialists, by wealth index quintile
Wealth Index Quintiles
GPFamily
physicianOB-Gyn
Pedia-trician
Midwife Internist Total
1 38% 46% 8% 8% 0% 0% 13
2 67% 8% 8% 0% 0% 17% 12
3 75% 8% 0% 0% 17% 0% 12
4 64% 0% 0% 14% 14% 7% 14
5 50% 0% 10% 0% 20% 20% 10
TOTAL 59% 13% 5% 5% 10% 8% 61
Cost of confinement and other costs
Table 4.106 presents the average miscellaneous costs (transportation expenses and travel time) incurred by inpatients during confinement.
Inpatients spent more travel time going to public facilities compared to private facilities, and it was more costlier for inpatients on average to travel to a public facility than to a private one.
Table 4.107 shows miscellaneous costs incurred by inpatients and sorted by cases. Maternal and neonatal cases in a public facility were associated with increased travel time as well as transportation cost.
Tables 4.108 and 4.109 shows the average hospital expenditures of inpatients, classified by type of case and wealth index. The hospital charge for maternal cases was higher in public facilities than in private facilities. Charges for neonatal cases in private hospitals were not given.
Table 4.109 shows the average hospital charge by wealth index. In-hospital charges in a private facility for those belonging to the lowest wealth quintile were higher on average (PhP 4,140) than for wealthier inpatients (PhP 2,690).
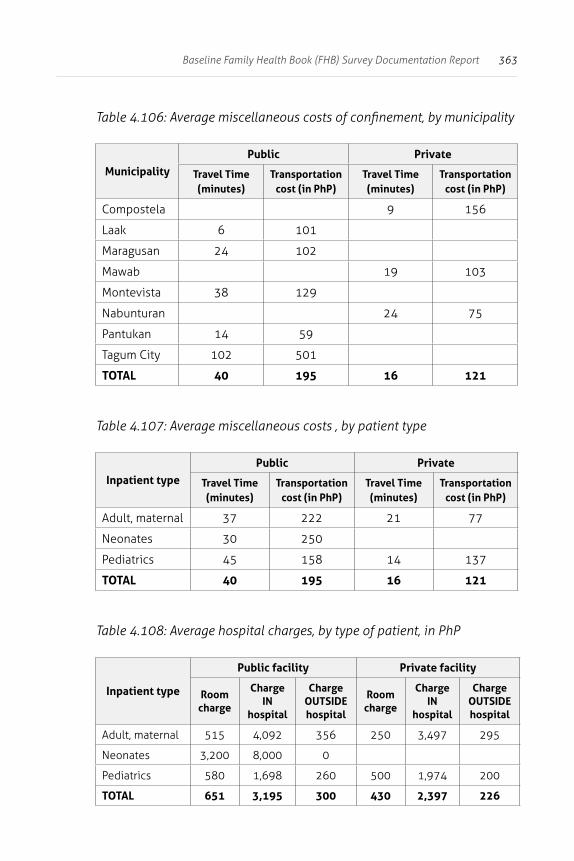
363Baseline Family Health Book (FHB) Survey Documentation Report
Table 4.106: Average miscellaneous costs of confinement, by municipality
MunicipalityPublic Private
Travel Time (minutes)
Transportation cost (in PhP)
Travel Time (minutes)
Transportation cost (in PhP)
Compostela 9 156
Laak 6 101
Maragusan 24 102
Mawab 19 103
Montevista 38 129
Nabunturan 24 75
Pantukan 14 59
Tagum City 102 501
TOTAL 40 195 16 121
Table 4.107: Average miscellaneous costs , by patient type
Inpatient typePublic Private
Travel Time (minutes)
Transportation cost (in PhP)
Travel Time (minutes)
Transportation cost (in PhP)
Adult, maternal 37 222 21 77
Neonates 30 250
Pediatrics 45 158 14 137
TOTAL 40 195 16 121
Table 4.108: Average hospital charges, by type of patient, in PhP
Inpatient type
Public facility Private facility
Room charge
Charge IN
hospital
Charge OUTSIDE hospital
Room charge
Charge IN
hospital
Charge OUTSIDE hospital
Adult, maternal 515 4,092 356 250 3,497 295
Neonates 3,200 8,000 0
Pediatrics 580 1,698 260 500 1,974 200
TOTAL 651 3,195 300 430 2,397 226
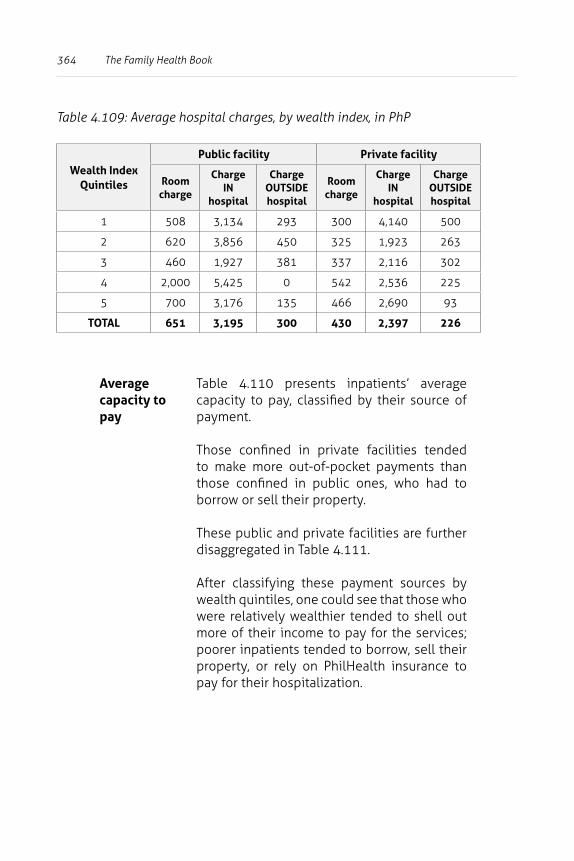
364 The Family Health Book
Table 4.109: Average hospital charges, by wealth index, in PhP
Wealth Index Quintiles
Public facility Private facility
Room charge
Charge IN
hospital
Charge OUTSIDE hospital
Room charge
Charge IN
hospital
Charge OUTSIDE hospital
1 508 3,134 293 300 4,140 500
2 620 3,856 450 325 1,923 263
3 460 1,927 381 337 2,116 302
4 2,000 5,425 0 542 2,536 225
5 700 3,176 135 466 2,690 93
TOTAL 651 3,195 300 430 2,397 226
Average capacity to pay
Table 4.110 presents inpatients’ average capacity to pay, classified by their source of payment.
Those confined in private facilities tended to make more out-of-pocket payments than those confined in public ones, who had to borrow or sell their property.
These public and private facilities are further disaggregated in Table 4.111.
After classifying these payment sources by wealth quintiles, one could see that those who were relatively wealthier tended to shell out more of their income to pay for the services; poorer inpatients tended to borrow, sell their property, or rely on PhilHealth insurance to pay for their hospitalization.
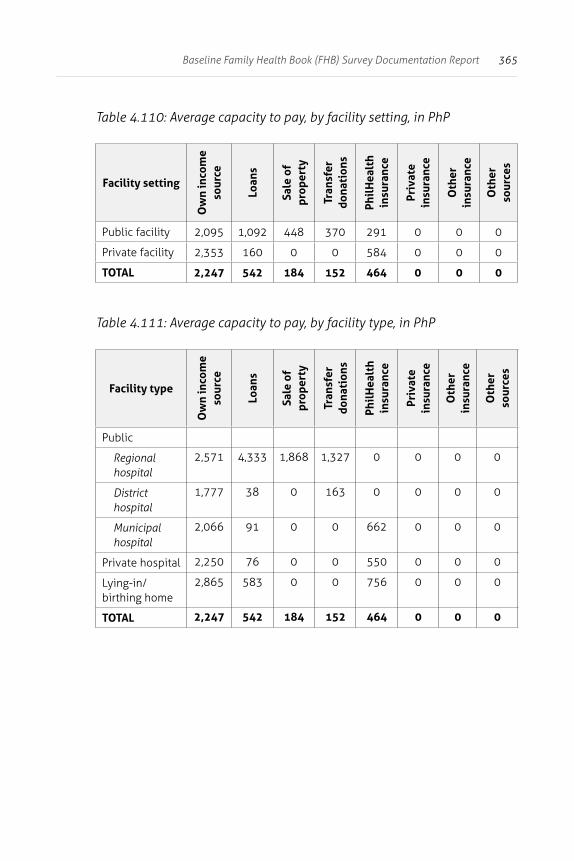
365Baseline Family Health Book (FHB) Survey Documentation Report
Table 4.110: Average capacity to pay, by facility setting, in PhP
Facility setting
Ow
n in
com
e so
urce
Loan
s
Sale
of
prop
erty
Tran
sfer
do
nati
ons
Phil
Hea
lth
insu
ranc
e
Priv
ate
insu
ranc
e
Oth
er
insu
ranc
e
Oth
er
sour
ces
Public facility 2,095 1,092 448 370 291 0 0 0
Private facility 2,353 160 0 0 584 0 0 0
TOTAL 2,247 542 184 152 464 0 0 0
Table 4.111: Average capacity to pay, by facility type, in PhP
Facility type
Ow
n in
com
e so
urce
Loan
s
Sale
of
prop
erty
Tran
sfer
do
nati
ons
Phil
Hea
lth
insu
ranc
e
Priv
ate
insu
ranc
e
Oth
er
insu
ranc
e
Oth
er
sour
ces
Public
Regional hospital
2,571 4,333 1,868 1,327 0 0 0 0
District hospital
1,777 38 0 163 0 0 0 0
Municipal hospital
2,066 91 0 0 662 0 0 0
Private hospital 2,250 76 0 0 550 0 0 0
Lying-in/birthing home
2,865 583 0 0 756 0 0 0
TOTAL 2,247 542 184 152 464 0 0 0
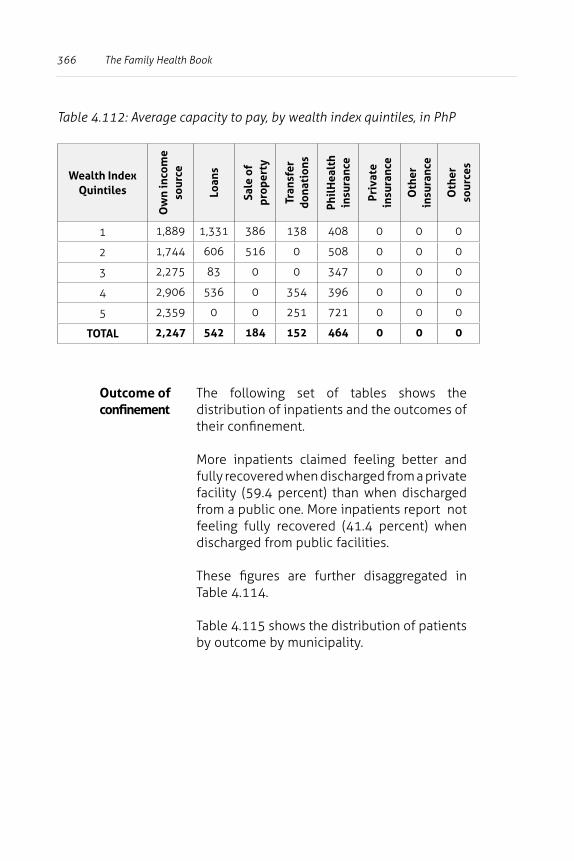
366 The Family Health Book
Table 4.112: Average capacity to pay, by wealth index quintiles, in PhP
Wealth Index Quintiles
Ow
n in
com
e so
urce
Loan
s
Sale
of
prop
erty
Tran
sfer
do
nati
ons
Phil
Hea
lth
insu
ranc
e
Priv
ate
insu
ranc
e
Oth
er
insu
ranc
e
Oth
er
sour
ces
1 1,889 1,331 386 138 408 0 0 0
2 1,744 606 516 0 508 0 0 0
3 2,275 83 0 0 347 0 0 0
4 2,906 536 0 354 396 0 0 0
5 2,359 0 0 251 721 0 0 0
TOTAL 2,247 542 184 152 464 0 0 0
Outcome of confinement
The following set of tables shows the distribution of inpatients and the outcomes of their confinement.
More inpatients claimed feeling better and fully recovered when discharged from a private facility (59.4 percent) than when discharged from a public one. More inpatients report not feeling fully recovered (41.4 percent) when discharged from public facilities.
These figures are further disaggregated in Table 4.114.
Table 4.115 shows the distribution of patients by outcome by municipality.
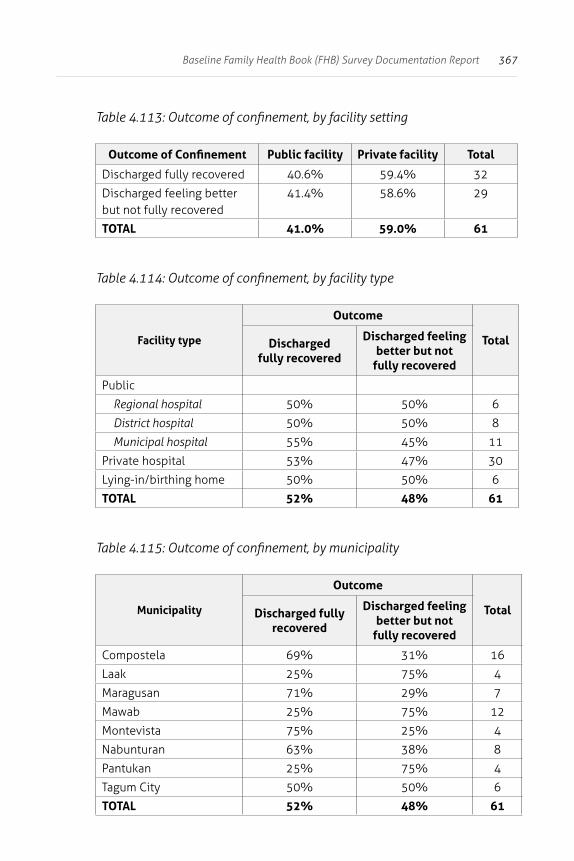
367Baseline Family Health Book (FHB) Survey Documentation Report
Table 4.113: Outcome of confinement, by facility setting
Outcome of Confinement Public facility Private facility Total
Discharged fully recovered 40.6% 59.4% 32
Discharged feeling better but not fully recovered
41.4% 58.6% 29
TOTAL 41.0% 59.0% 61
Table 4.114: Outcome of confinement, by facility type
Facility type
Outcome
TotalDischarged fully recovered
Discharged feeling better but not
fully recovered
Public
Regional hospital 50% 50% 6
District hospital 50% 50% 8
Municipal hospital 55% 45% 11
Private hospital 53% 47% 30
Lying-in/birthing home 50% 50% 6
TOTAL 52% 48% 61
Table 4.115: Outcome of confinement, by municipality
Municipality
Outcome
TotalDischarged fully recovered
Discharged feeling better but not
fully recovered
Compostela 69% 31% 16
Laak 25% 75% 4
Maragusan 71% 29% 7
Mawab 25% 75% 12
Montevista 75% 25% 4
Nabunturan 63% 38% 8
Pantukan 25% 75% 4
Tagum City 50% 50% 6
TOTAL 52% 48% 61
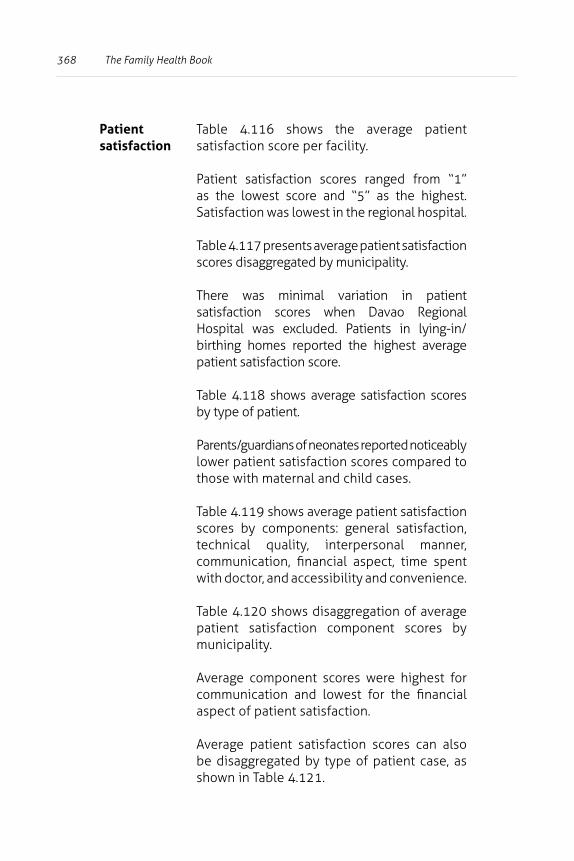
368 The Family Health Book
Patient satisfaction
Table 4.116 shows the average patient satisfaction score per facility.
Patient satisfaction scores ranged from “1” as the lowest score and “5” as the highest. Satisfaction was lowest in the regional hospital.
Table 4.117 presents average patient satisfaction scores disaggregated by municipality.
There was minimal variation in patient satisfaction scores when Davao Regional Hospital was excluded. Patients in lying-in/birthing homes reported the highest average patient satisfaction score.
Table 4.118 shows average satisfaction scores by type of patient.
Parents/guardians of neonates reported noticeably lower patient satisfaction scores compared to those with maternal and child cases.
Table 4.119 shows average patient satisfaction scores by components: general satisfaction, technical quality, interpersonal manner, communication, financial aspect, time spent with doctor, and accessibility and convenience.
Table 4.120 shows disaggregation of average patient satisfaction component scores by municipality.
Average component scores were highest for communication and lowest for the financial aspect of patient satisfaction.
Average patient satisfaction scores can also be disaggregated by type of patient case, as shown in Table 4.121.
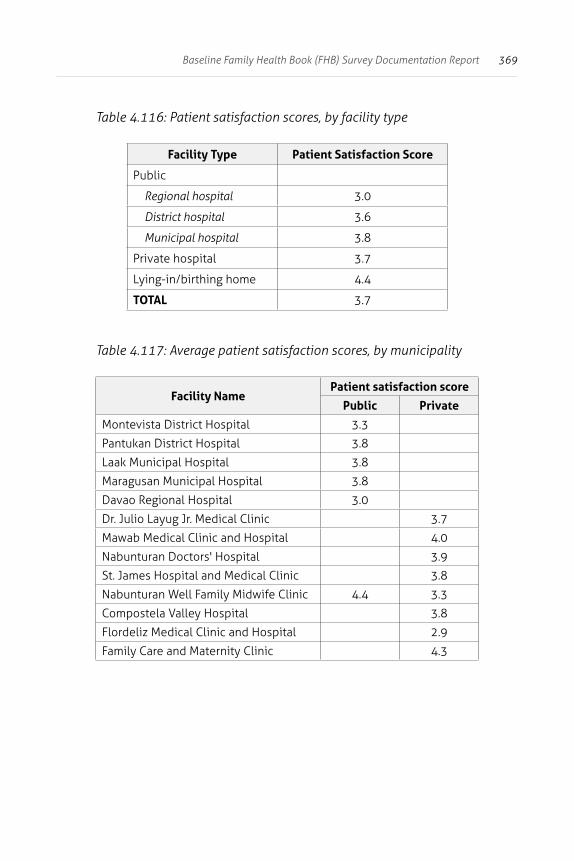
369Baseline Family Health Book (FHB) Survey Documentation Report
Table 4.116: Patient satisfaction scores, by facility type
Facility Type Patient Satisfaction Score
Public
Regional hospital 3.0
District hospital 3.6
Municipal hospital 3.8
Private hospital 3.7
Lying-in/birthing home 4.4
TOTAL 3.7
Table 4.117: Average patient satisfaction scores, by municipality
Facility NamePatient satisfaction score
Public Private
Montevista District Hospital 3.3
Pantukan District Hospital 3.8
Laak Municipal Hospital 3.8
Maragusan Municipal Hospital 3.8
Davao Regional Hospital 3.0
Dr. Julio Layug Jr. Medical Clinic 3.7
Mawab Medical Clinic and Hospital 4.0
Nabunturan Doctors' Hospital 3.9
St. James Hospital and Medical Clinic 3.8
Nabunturan Well Family Midwife Clinic 4.4 3.3
Compostela Valley Hospital 3.8
Flordeliz Medical Clinic and Hospital 2.9
Family Care and Maternity Clinic 4.3
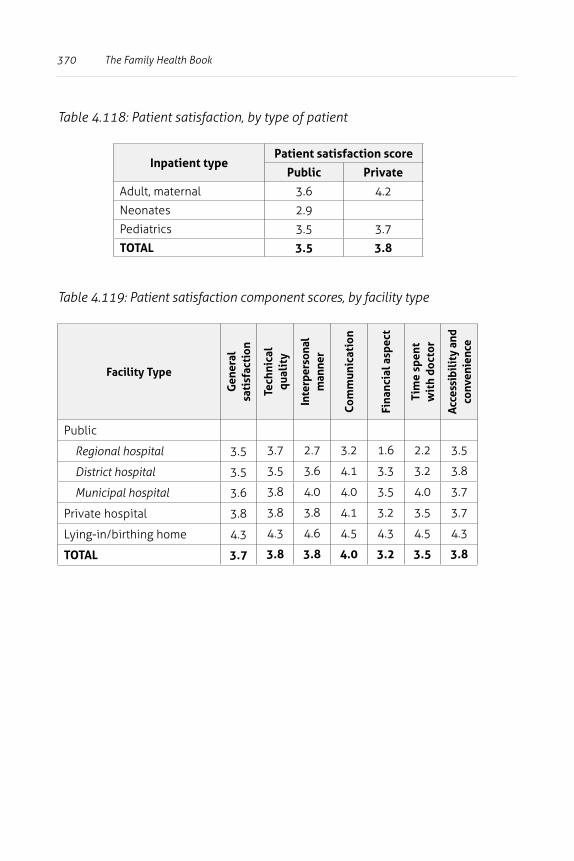
370 The Family Health Book
Table 4.118: Patient satisfaction, by type of patient
Inpatient typePatient satisfaction score
Public Private
Adult, maternal 3.6 4.2
Neonates 2.9
Pediatrics 3.5 3.7
TOTAL 3.5 3.8
Table 4.119: Patient satisfaction component scores, by facility type
Facility Type
Gen
eral
sa
tisf
acti
on
Tech
nica
l qu
alit
y
Inte
rper
sona
l m
anne
r
Com
mun
icat
ion
Fina
ncia
l asp
ect
Tim
e sp
ent
wit
h do
ctor
Acc
essi
bili
ty a
nd
conv
enie
nce
Public
Regional hospital 3.5 3.7 2.7 3.2 1.6 2.2 3.5
District hospital 3.5 3.5 3.6 4.1 3.3 3.2 3.8
Municipal hospital 3.6 3.8 4.0 4.0 3.5 4.0 3.7
Private hospital 3.8 3.8 3.8 4.1 3.2 3.5 3.7
Lying-in/birthing home 4.3 4.3 4.6 4.5 4.3 4.5 4.3
TOTAL 3.7 3.8 3.8 4.0 3.2 3.5 3.8
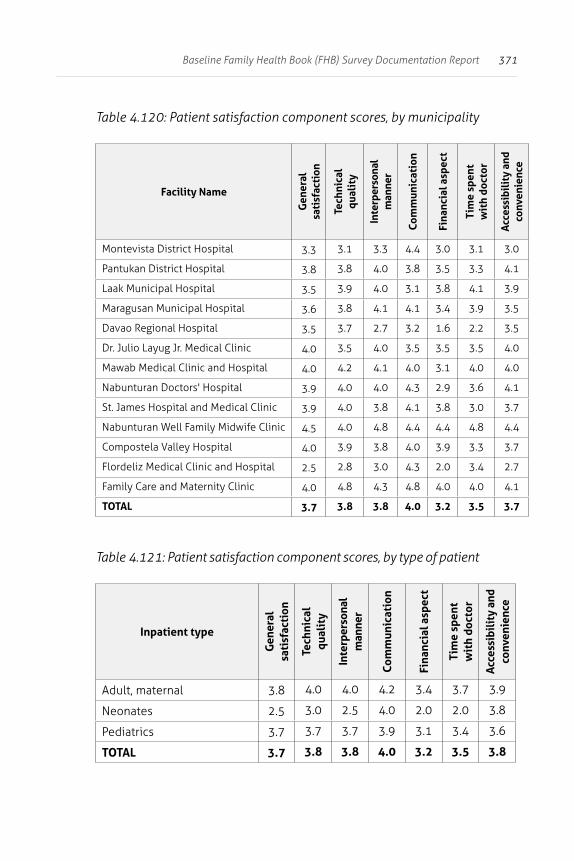
371Baseline Family Health Book (FHB) Survey Documentation Report
Table 4.120: Patient satisfaction component scores, by municipality
Facility Name
Gen
eral
sa
tisf
acti
on
Tech
nica
l qu
alit
y
Inte
rper
sona
l m
anne
r
Com
mun
icat
ion
Fina
ncia
l asp
ect
Tim
e sp
ent
wit
h do
ctor
Acc
essi
bili
ty a
nd
conv
enie
nce
Montevista District Hospital 3.3 3.1 3.3 4.4 3.0 3.1 3.0
Pantukan District Hospital 3.8 3.8 4.0 3.8 3.5 3.3 4.1
Laak Municipal Hospital 3.5 3.9 4.0 3.1 3.8 4.1 3.9
Maragusan Municipal Hospital 3.6 3.8 4.1 4.1 3.4 3.9 3.5
Davao Regional Hospital 3.5 3.7 2.7 3.2 1.6 2.2 3.5
Dr. Julio Layug Jr. Medical Clinic 4.0 3.5 4.0 3.5 3.5 3.5 4.0
Mawab Medical Clinic and Hospital 4.0 4.2 4.1 4.0 3.1 4.0 4.0
Nabunturan Doctors' Hospital 3.9 4.0 4.0 4.3 2.9 3.6 4.1
St. James Hospital and Medical Clinic 3.9 4.0 3.8 4.1 3.8 3.0 3.7
Nabunturan Well Family Midwife Clinic 4.5 4.0 4.8 4.4 4.4 4.8 4.4
Compostela Valley Hospital 4.0 3.9 3.8 4.0 3.9 3.3 3.7
Flordeliz Medical Clinic and Hospital 2.5 2.8 3.0 4.3 2.0 3.4 2.7
Family Care and Maternity Clinic 4.0 4.8 4.3 4.8 4.0 4.0 4.1
TOTAL 3.7 3.8 3.8 4.0 3.2 3.5 3.7
Table 4.121: Patient satisfaction component scores, by type of patient
Inpatient type
Gen
eral
sa
tisf
acti
on
Tech
nica
l qu
alit
y
Inte
rper
sona
l m
anne
r
Com
mun
icat
ion
Fina
ncia
l asp
ect
Tim
e sp
ent
wit
h do
ctor
Acc
essi
bili
ty a
nd
conv
enie
nce
Adult, maternal 3.8 4.0 4.0 4.2 3.4 3.7 3.9
Neonates 2.5 3.0 2.5 4.0 2.0 2.0 3.8
Pediatrics 3.7 3.7 3.7 3.9 3.1 3.4 3.6
TOTAL 3.7 3.8 3.8 4.0 3.2 3.5 3.8
372
About the Authors
Aleli KRAFT is a consultant at the UPecon-HPDP and an associate professor at the U.P. School of Economics.
Jhiedon FLORENTINO is a consultant at the UPecon-HPDP.
Julio M. GALVEZ is a research assistant at the UPecon-HPDP.
Orville SOLON is Chief of Party of UPecon-HPDP.
Carlos Antonio TAN Jr. is a consultant at the UPecon-HPDP.
Rhodora TIONGSON is a program associate at the UPecon-HPDP.