
Visualization of music impression in facial expression to represent emotion

Neuropsycholoy~o, Vol 24. No 2, pp. 169.-1X0. 1986. Prmted m Great Britam
002&393?R6 53 OO/O.oO c 1986 Pergamon Press Ltd
THE EXPRESSION AND PERCEPTION OF FACIAL EMOTION IN BRAIN-DAMAGED PATIENTS
JOAN C. BOROD,*? E~.ISSA KOFF,~ MARJORIE PERLMAN LORCH? and MARJORIE NlCHOLASt
*Department of Psychiatry, New York University School of Medicine; tAphasia Research Center and Department of Neurology, Boston University School of Medicine; + +Department of Psychology, Wellesley
College
(Accrpted 24 July 1985)
Abstract&This study examined the expression and perception of facial emotion in patients with unilateral cerebrovascular pathology. Subjects were 12 right brain-damaged (RBD). I5 left brain- damaged (LBD) aphasic, and 16 normal control (NC) right-handed males. Expressions were elicited during posed and spontaneous conditions. Both positive and negative emotions were studied. RBDs were significantly impaired. relative to LBDs and NCs, in expressing and perceiving facial emotion. There were no group difierences as a function of condition, but there were differences as a function of emotional valence. Qualitative performance differences also were observed. There was no evidence that the ability to produce a particular emotion was related to the ability to identify the Same emotion. Overall, these findings support the notion that the right cerebral hemisphere is dominant for expressing and perceiving facial emotion.
INTRODUCTION
A SPECIAI~ role for the right hemisphere has recently been suggested for both the perception and expression of facial emotion (for review, see [9]). In normals, perception studies have demonstrated a left visual-field (i.e. right hemisphere) advantage for perceiving emotional facial expression [35,45,47, 58, 593. Expression studies with normals have documented that the left hemiface (presumably controlled by the right hemisphere) moves more extensively [4. 6, 1 I, 491 and appears more intense [ 16,26.37,54,56] during emotional expression than the right hemiface.
Clinical studies have suggested that deficits in the perception of emotional facial expression are associated primarily with right-hemisphere brain damage 12, 19. 24, 30). Studies of the production of emotional facial expression in brain-damaged patients are less common. and tend to focus on spontaneous, in contrast to posed. expression. BWX and DUWY [ 151 and BOROI), KOFF, PERI.MAN LORCH and NICHWAS [IO] found that spontaneous emotional facial expressions were less likely to occur in right brain-damaged patients than in left brain-damaged patients and normal controls. In a case study of two right brain-damaged patients. Ross and MESULAM [53] observed that spontaneous facial expression seldom occurred. On the other hand, KOLR and MII.NER [43] reported that spontaneous facial expressions and movements (it is not clear what percent of these were emotional) occurred with equal frequency in a group of right and left brain-damaged patients. but less frequently
‘Dr Bored IS now in the Departments of Psychology. Queens College, and Neurolog>, Mount Sinai School of Medicine. City University ofNew Yorh. Addresscorrespondence to: DrJoan C. Borod, Department of Psychology. Queens College. Flushing. NY 11367, U.S.A.
lh9

in those patients with frontal, relative to posterior, damage. In the only report (anecdotal) of posed facial expression among brain-damaged subjects, HEILMAN and VALENSTEIN [36] observed no performance differences between a small number of right and left brain- damaged patients. Since posed and spontaneous expressions are considered to reflect separate and possibly independent neuroanatomical pathways and origins [21, 32, 41, 48, 601, both types of expression should be studied in the same patients.
While perception and expression have been of great interest, none of the above studies examined both functions in the same individuals. In the case of brain-damaged patients, one would like to know whether a deficit in one function co-occurs with a deficit in the other. In the case of normals, one would like to know if the two functions are correlated. It could be argued that individuals with deficits in classifying or perceiving a particular emotional expression would have difficulty in producing or modeling that same expression.
While the bulk of the evidence suggests an overall right-hemisphere dominance for emotion [9, 46, 611, recent studies have speculated about right-hemisphere dominance for negative emotions and either left-hemisphere or bilateral involvement for positive ones [ 1, 5, 8, 13, 23. 25, 42, 51, 551. One possible explanation for this apparent inconsistency with respect to emotional valence is that the type of behavior (i.e. perception or expression) being observed might affect the results. HIRSCHMAN and SAFER [38], in fact, have speculated that valence is a more salient variable in studies ofexpression than in studies ofperception. Recent literature (e.g. [22. 621) has suggested that the site of lesion within a single hemisphere could moderate emotional processing as well.
The current study was designed to examine expression and perception of facial emotion within the same individuals. Subjects were patients with right- and left-hemisphere lesions in whom location of lesion could be determined. A demographically similar normal control group was also included. Both positive and negative emotions were studied. and posed and spontaneous expressions were elicited.
METHODS
‘Twelve males with unilateral right (RBD) and 15 males with unilateral left (LBD) hcmiaphcre pathology sxved a> subjects; 16 normal males (NC) served as controla. Patient\ were recruited from the ncurolog) kards of the Boston VA ?dedical Center. All subJects were right-handed by beif-report or familial-report. The three groups did not dilkr on formal a\scssment of lateral dominance [X)1: the m+;urity of sublects were right-footed (X6?;,) and rlpht-eyed (X6”‘u). The three subject groups did not differ signiticantly on demographic variables. v,ith an overall mean age of 57 g(S.D. =X.1), 13 yr ofcducation(S.D. =2.X), ~tndanoccupational level 1391 of3.‘)(S.D. = 1.5). The typical <ocio- economic occupational level was that of middle-class white collar worker.
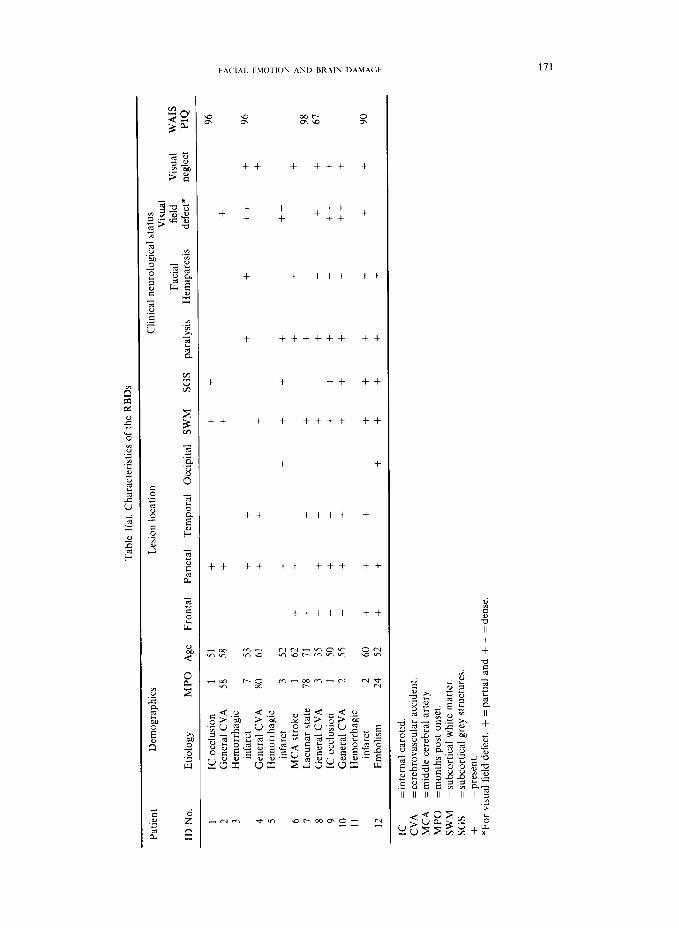
Table i describes the characteristics and symptomatology of the brain-damapod patients v,lth respect to apt. education. occupational level. etiology. number of months post onset. Icsion localization. facial paralysis. hcmiplcpia. visual field defect, and WAIS-R Pcrformuncc IQ (PIQ) score [_63] (when available). For RBDs. visual neglect IS reported. and for LBDs. aphasia type and the Boston Diagnostic Aphasia Examination (BDAf) auditory comprehrnsion z-score 1-141 arc reported.
P,itients were tested at Icast I month post onset of~llncss (median -9 months). and the tuo patlcnt groups did not differ significantly in number of months post onset. Patients uerc included for stud! if their lesions were the result of cercbrovaxular pathology, e.g. occlusion. emh~~lism, thrombosis. hemorrhagic Infarct. Patients with history of psychlatrlc disorder. psychotropicdrug treatment. or secondary neurological disordcr(c.g. epilepsy. dcmcntia)were excluded from the study. Evidence ofthe unilateral nature ofthe lesion was confirmed hy CT scan in a11 hut two cases (\ubjects No. 2 and 6). whcrc clinical data from neurological examination were used. Slutj-three pcrccnt of the patients had lesions restricted to the cortex ar&or subcortical white matter. while the remainder had cortical lcs~ons that ertendcd to hubcortical grcy matter structures (e.g. basal ganglia. thalamua). The tuo patient groups had comparable proportions of subject5 with lesions in particular regions. The folIowIng percentages indicate the distribution of lesion slteh for RBDa and LBDs. rcspectlvely: frontal 5X”&. 60”%: tcrnporal 5X”‘“. 67”1,. parietal 92’,;,. 67%: occipital 17”/,. 7”4,: subcortlcal white matter 83”,0. hO’/,,: and subcortical grcy structurch SO”;,. 27%. At the time of testing. the m;(Jorlty ofeach patient group had clinIcally-detcrmincd deficit\
Tab
le
l(a)
. C
hara
cter
istic
s of
the
R
BD
s
Patie
nt
Dem
ogra
phic
s L
esto
n lo
catio
n C
linic
al
neur
olog
ical
st
atus
V
isua
l Fa
cial
fi
eld
Vis
ual
WA
IS
ID
No.
E
tiolo
gy
MPO
A
ge
Fron
tal
Pane
tal
Tem
pora
l O
ccip
ital
SWM
SG
S pa
raly
sis
Hem
ipar
esis
de
fect
* ne
glec
t PI
Q
1 IC
occ
lusi
on
1 51
+
+ +
96
2 G
ener
al
CV
A
58
58
+ +
+ ;
3 H
emor
rhag
ic
? s in
farc
t 7
53
+ +
+ +
++
+ 96
-
4 G
ener
al
CV
A
80
61
+ +
+ +
2 5
Hem
orrh
agic
c
infa
rct
3 52
+
+ +
+ +
++
z z 6
MC
A
stro
ke
1 62
+
+ +
+ +
1 L
acun
ar
stat
e 78
71
+
+ +
+ 98
5
67
c 8
Gen
eral
C
VA
3
35
+ +
+ +
+ +
+ +
IC o
cclu
sion
1
50
+ +
++
+ =:
9
+ +
+ +
+ 2
IO
Gen
eral
C
VA
2
55
+ +
+ +
+ +
+ ++
+
L
11
Hem
orrh
agic
2
infa
rct
2 60
+
+ +
+ +
+ +
+ +
90
I
I2
Em
bolis
m
24
52
+ +
+ +
+ +
+ 5
IC
=int
erna
l ca
rotid
. C
VA
=c
ereb
rova
scul
ar
acci
dent
. M
CA
=
mid
dle
cere
bral
ar
tery
. M
PO
=mon
ths
post
on
set.
SWM
=s
ubco
rtic
al
whi
te
mat
ter.
SG
S =s
ubco
rtic
al
grey
st
ruct
ures
. +
= pr
esen
t. *F
or
visu
al
fiel
d de
fect
. +
= pa
rtia
l an
d +
+ =
dens
e

Tab
le
lfbt
. C
hara
cter
istic
s of
the
L
BD
s
Patie
nt
Dem
ogra
phic
s L
esio
n io
catio
n C
linic
al
neur
olog
ical
st
atus
W
AIS
L
angu
age
Vis
ual
Faci
al
ID
No.
fi
eld
Etio
log\
M
PG
Age
B
DA
E
Aph
asia
Fr
onta
l Pa
rict
al
Tem
pora
l O
ccip
ital
SWM
SG
S pa
raly
sis
Hem
ipar
esis
de
fect
* PI
Q
z-sc
ore
type
.-
-__
-_l_
_-
13
MC
A
stro
ke
22
56
+ +
i-
14
100
IC o
cclu
sion
75
5X
+
~-2.
0 G
loba
l f
i
15
MC
A
stro
ke
‘9
63
: B
roca
’s
i-
I6
+ +
105
Thr
ombo
sis
X44
t
+ 0.
5 B
roca
’s
t A
i
+ 72
-
1.5
Glo
bal
”
17
++
MC
A
stro
ke
2 5X
-t
-r
i
18
106
MC
A
stro
ke
- I .
5 W
erni
cke’
s 3j
2X
hi
-I
-c
10
1 -
1 .O
W
erni
cke’
s E
19
H
emor
rhag
ic
infa
rct
9
t
71
+ +
+ 94
-0
.5
Wer
nick
e’s
2
20
MC
A
stro
ke
22
57
i-
+ f
+ 21
6;
+
+ 95
~
1.3
Wer
nick
e’s
:
Gen
eral
C
VA
6
,- +
+ +
22
122
IC o
cclu
sion
3
42
-0.5
C
ondu
ctio
n f
+ +
23
+ ++
10
4 M
CA
st
roke
3
54
- -
1.3
Con
duct
ion
+ +
24
+ 72
G
ener
al
CV
A
XX
54
-0
.3
Mix
ed
+ +
54
_i
+ 25
+
+ IC
occ
lusi
on
20
+0.3
B
roca
’s
26
+ +
+ +
++
66
IC o
cclu
sion
49
55
i
~ 1.
3 M
ixed
i-
+
+ t
+ +
27
100
IC o
cclu
sion
M
ixed
no
nflu
ent
38
49
+ &
t
+ +
i +
X9
- I .
O
Mix
ed
nonf
luen
t
Key
as
Tab
le
l(a)
.
FA(‘I4L EMOTION AND RR 4lN 1?.4bMGF 173
on the side contralateral to their lesion: these were hemiplegia (58% of RBDs, 60% of LBDs); facial paralysis (75% of RBDs, 80% of LBDs); and visual field loss (58% of RBDs, 47% of LBDs).
Although all of the LBDs were aphasic [34] (three Broca’s, two Mixed Non-fluents, two Globals, two Conductions, four Wernicke’s, two Mixed or Uncategorized), all had sufficient auditory comprehension (mean BDAE 1343 z-score= -0.88, SD. =0.7) and cognitive functioning (mean WAIS-R Performance IQ =94, S.D. = 16) to perform the experimental tasks. All subjects had adequate visuo-perceptual skill, as assessed by the ability to correctly describe two practice slides-the TAT card 3GF [SO] and a scene from a kindergarten classroom [14].
Research design
All subjects were tested for expression (both posed and spontaneous) and perception of positive and negative facial emotions. All subjects were tested by the same examiner in the following task order: spontaneous expression, posed- verbal expression, perception, and posed-visual expression. Demographic and lateral dominance data were collected at the end of the session.
Expression procedures
Spontaneous condition. Slides designed to elicit spontaneous expressions of positive (pleasant) and negative (unpleasant) emotion [14] were presented to each subject; there were 10 positive and six negative slides. Positiue slides included exemplars from each of the following categories: pleasant scenes, e.g. a little baby picking flowers; scenic views, e.g. a beautiful sunset; sexual material, e.g. a nude couple embracing; and familiar people, e.g. a photograph of the examiner. Negatioe slides were selected from the following categories: disgusting materials, e.g. a surgical procedure; sad scenes, e.g. a young victim of starvation; and unusual photographs, e.g. a photographic double exposure. There were two slides from each category, except for familiar people, where there were four. Valence categories were based on findings from earlier studies of normal adults [7, 1 I] in which facial expressions in response to these stimulus slides were rated by trained judges for the degree of pleasant vs unpleasant affect on a seven-point Likert scale. A significant majority of the responses to ‘positive’ slides were rated as pleasant (73% for pleasant scenes, 64% for scenic views, 77% for sexual material), and a significant majority of the responses to ‘negative’ slides were rated as unpleasant (83% for disgusting materials, 85% for sad scenes, 66% for unusual photographs).
Slides were presented on a Singer Caramate projector positioned directly in front of the subject and slightly below eye level, using procedures developed by BUCK 1141 and by BOROD et al. [l 11. The order and orientation (original and mirror-reversed) of the slides were counterbalanced across subjects. Subjects were seated facing a one-way mirror covered with a dressing screen, behind which was a videocamera for recording facial expressions. The examiner sat beside to the subject, and side ofsubject was counterbalanced. A headrest was used to keep the subject’s head upright and relatively immobile, to ensure that the camera could record the full face for later ratings. The subject wore a microphone around his neck for voice recording. Each slide was presented for 6 set, after which the subject was requested to describe his feelings about and reactions to the slide. The slide was then left on the screen for l&15 set during which time the subject talked about these feelings. After describing his feelings, the subject was asked to respond to the question-“Does this picture make you feel good, bad, or indifferent?“* Following this response was a 3-set intertrial interval to allow the subject’s face to return to a neutral expression, to allow the examiner to check the headrest position, and to advance to the next slide.
Posed condition. There were two posed subconditions, verbal and visual. Both auditory verbal and visual nonverbal instructions were used to avoid a bias toward one hemisphere or input modality. The same expressions were used in both subconditions. Positive expressions included happiness, pleasant surprise and sexual arousal; negative expressions included sadness, anger, fear. disgust and confusion. Again. expressions were classified as positive or negative in light of ratings of posed expressions (under both verbal and visual conditions) made during earlier studies [7, Ill. A significant majority of the posed positive expressions were rated as pleasant (98% for happiness, 92% for sexual arousal), and a significant majority of the posed negative expressions were rated as unpleasant (91% for sadness. 90% for disgust, 82% for confusion).
In the posed-verbal subcondition, subjects were requested to pose each of the eight expressions upon oral command from the examiner, e.g. “Look happy”. In the posed-visual subcondition, subjects were shown slides from the EKMAN and FKIESEN series 1291 of an adult male posing prototypical facial emotional expressions. For ‘sexual arousal’, a happiness photograph 1291 was used, and for ‘confusion’, a photograph of a puzzled expression [4,6] was used. Subjects were required to pose each expression in turn. As the subjects were viewing the slides, they were
*To assess the correspondence between our valence labels, and the feelings reported by the subjects, we assigned ratings of 1 to bad, 2 to neutral (i.e. indifferent or descriptive rather than affective) and 3 to good, and submitted these ratings to a two-way analysis of variance for Group(3) x Valence(Z). There was no effect for Group, and a main effect for Valence (F= 16.61; df= 1, 40; P<O.OOl) such that the positive slides (X=2.76) were rated, appropriately, as more pleasant than the negative ones (x= 1.39). In the earlier study of normal adults [I 11, when emotional feelings about these slides were rated on a seven-point Likert scale, from 1 (unpleasant) to 7 (pleasant) with 4 as neutral, again, the positive slides (R= 5.65) were rated as more pleasant than the negative ones (X=2.57).

174 .I. C‘. BOKOI) (‘, r/l.
simultaneously instructed to look like the man in the picture: the following type oforal command, “Look happy, like the man in the picture looks” was used. They were told that a direct imitation of the poser’s facial pattern was not essential.
To facilitate deliberate control over the expressions produced in the posed conditron and to ensure that the patients understood the task and were sufficiently motivated and attentive for each pose, subjects were required to practice each expression before it was actually filmed. For the verbal subcondition, if the subject were unable to pose to command, coaching was used to facilitate a response. e.g. “Show me how you would look if you found a large sum of money and were very happy”. There was a standard vignette for each of the eight expressions. During actual filming of the posed subconditions, subjects were requested to make each expression immediately following a command of “Ready. go”, to make one complete expression, and to then return to a neutral baseline (i.e. a resting face). The pose following “Ready, go” was used for data analysis.
Prrcrption procedures
For the perception task, subjects viewed slides of the same photographs of the adult male posers used during the posed-visual subcondition. The same positive (happiness, sexual arousal, surprise) and negative (sadness, anger. fear, disgust, confusion) expressions were used. along with a neutral one [29]. The subjects were required to label/identify each expression being portrayed in the nine slides. Responses were recorded verbatim. If an LBD aphasic had unscorable speech output, a multiple-choice format with three options was used.
For the posed-visual expression task and the perception task, the slides were presented to the subject on the Caramate TV screen. The order and orientation (original and mirror-reversed) of the slides were randomized and counterbalanced across subjects.
Expression. Two judges viewed the videotapes of the experimental sessions and rated each facial expression for accuracy. For the spontaneous condition, the videotape was run from the onset ofeach slide until the occurrence of the first complete facial expression, determined by rater consensus. For the posed condition, the expression following “Ready, go” was rated. Each videotape segment was played through and reviewed several times to identify the point at which maximum or peak expression occurred; ratings were made at that point. To rule out the possibility that the ratings might be affected by a bias on the part of the perceiver to attend preferentially to the left hemispace (e.g. [ 17, 33, 44]), half of the videotapes were rated under mirror-image conditions on a TV monitor especially modified to reverse the video image.
For both the spontaneous and posed conditions, each expression was scored as accurate,‘successful (score= I) or unsuccessful (score=O). To be rated as successful, an expression had to be appropriate to the stimulus. Prior to rating, the judges were trained as follows. For the .spontunrous task. the judges were familiarized with the emotionally-laden slides 1141 used in the actual experiment and shown a training tape of two adult subjects responding appropriately to these slides. For the posed task, the judges examined the stimulus photographs used in the posed-visual subcondition and the perception task. In addition, they were familiarized with exemplars of prototypical expressions of happiness, surprise, sadness, anger, fear. disgust [28.40]. sexual arousal and confusion [4, I I]. Interrater agreement, determined from a sample of 244 observations, yielded complete agreement in 95% of the judgments. If the judges could not agree, the expression was scored as unsuccessful.
Prrcuptim Each subject’s labeling of the photographed expressions was scored as accurate (score= I) or inaccurate (score = 0). Synonyms and literal paraphasras were acceptable for all expressions: ‘happiness’ was acceptable for sexual arousal. For the aphastc LBDs. a modified scoring system was used whereby a score of I was assigned to a correct free response or a correct forced choice response when no free response had heen produced.
RESULTS
E.upre.ssion. Accuracy scores for individual expressions were examined within valence categories (positive, negative) using x2 tests. Since almost all comparisons were nonsignih- cant, expressions were pooled according to valence. For the sponturwous condition, each subject received separate mean scores for positive and for negative emotions. For the pc~ed condition, each subject received separate mean scores for positive emotions under verbal and visual subconditions. Since there were no significant differences between subconditions for positive (I;=O.Ol; d[= 1, 40; P>O.500) or for negative (F=O.27: iI’= I. 40; P>OSOO) emotions, scores were averaged across subconditions. Table 2 displays the mean accuracy scores for the expression variables (spontaneous positive, spontaneous negative, posed positive, posed negative) by subject group.
Prrcrption. Accuracy scores for individual perception trials were examined within valence

Table 2. Mean accuracy scores for expression and perception tasks, by subject group
Task Variable
RBDs (N= 12)
B SD.
LBDs (N= 15)
x S.D.
Expression Spontaneous positive 0.25 0.26 0.54 0.30 Spontaneous negative 0.42 0.36 0.57 0.32 Posed positive 0.63 0.35 0.81 0.18 Posed negative 0.67 0.19 0.59 0.21
Perception Positive 0.83 0.25 0.79 0.26 Negative 0.38 0.28 0.76 0.19 Neutral 0.42 0.52 0.93 0.27
NCs (N= 16)
R SD.
0.45 0.27 0.54 0.32 0.89 0.21 0.79 0.20 0.94 0.20 0.71 0.26 0.81 0.40
categories (positive, negative) using x2 tests. Since most comparisons were nonsignificant, scores were pooled according to valence. Table 2 displays the mean accuracy scores by subject group, for positive and negative emotions and for the neutral expression.
Analyses of variance
We conducted a series of analyses of variance (ANOVAs) on the expression and perception data. For expression, the effects of Group (RBD, LBD, NC), Condition (posed, spontaneous) and Valence (positive, negative) were examined. For perception, the effects of Group and Valence (positive, negative, neutral) were examined. Post hoc tests, with the conventional significance level (PI 0.05), were performed using the Newman-Keuls multiple comparison procedure [64].
Expression. A three-way repeated measures ANOVA was conducted to examine the effects of Group (3), Condition (2) and Valence (2) on the mean accuracy ratings. Overall, there was a main effect of Group (F=4.89; df=2, 40; P<O.Ol). Using post hoc tests, RBDs (x=0.49) were significantly less accurate in their expression of facial emotion than LBDs (T= 0.62) or NCs (X=0.67). There was also a significant Group by Valence interaction (F=3.33; df=2, 40; P~0.05). Using post hoc tests to examine group differences for each valence category, RBDs (x=0.44) were significantly more impaired than LBDs (x=0.72) or NCs (x=0.67) for positive emotions, and RBDs (x=0.54) were significantly more impaired than NCs (X=0.67) for negative emotions. Using post hoc tests to examine valence differences within each group, there were no significant differences for LBDs or NCs, but RBDs had significantly more difficulty with positive (X=0.44) than with negative (8=0.54) emotions. None of the other interactions with the Group variable were significant (P>O.300).
There was also a main effect of Condition (F= 23.98; df= 1, 40; PC O.OOl), such that posed expressions (x=0.73) were expressed more accurately than spontaneous expressions (x=0.46). Finally, there was a significant Condition by Valence interaction (F= 12.39; df’= 1, 40; P<O.O05), with mean accuracy scores ordered as follows-posed positive (0.77) posed negative (0.68) spontaneous negative (0.51) and spontaneous positive (0.42). When post hoc tests were computed for all possible comparisons of means, all were significant.
Since sexual arousal and confusion are not considered part of the canon of basic emotions 127, 281, the three-way ANOVA was repeated with these expressions removed, in case they were somehow affecting the results. Again, there were significant main effects for Group (F=4.20; df=2, 40; PcO.05) and Condition (F=35.97; df= 1, 40; P<O.OOl) and similar interactions for Group by Valence (F= 2.59; df = 2, 40; P < 0.10) and Condition by Valence (F= 9.99; df= 1, 40; P < 0.005). Post hoc tests yielded the same pattern of results as reported above.

176 J. C. &)ROl, <‘I t/l.
Perception. A two-way repeated measures ANOVA on the identification accuracy scores was performed for Group (3) and Valence (3). There was a main effect of Group (F= 8.17; df=2, 39; P~O.005). Using the post hoc Newman-Keuls procedure, overall, the RBDs (8= 0.55) were significantly less accurate in their perception of facial emotion than either the LBDs (x=0.82) or the NCs (x=0.82). There was also a significant Group by Valence interaction (F= 4.63; df= 4, 78; P < 0.005). Using the post hoc Newman-Keuls procedure to test group differences for each valence category, RBDs were significantly less accurate than LBDs and NCs in their perception of negative and neutral expressions; the groups did not differ, however, in their perception of positive expressions. Post hoc tests were used to examine valence differences within each group. There were no significant differences for LBDs, but negative emotions were identified less accurately than positive ones by NCs, and negative and neutral emotions were identified less accurately than positive ones by RBDs. Finally, there was a main effect of Valence (F= 9.13; cEf=2, 78; P<O.O05), with mean accuracy scores ordered as follows-negative (X= 0.62), neutral (8= 0.72) and positive (x=0.85) expressions. Using post hoc tests, all possible comparisons were significant.
When the ANOVA was recomputed, omitting sexual arousal and confusion, there were main effects for Group (F=5.96; df=2, 39; PcO.01) and Valence (F=6.92; d’=2. 78; P<O.O05) and, again, a Group by Valence interaction (F= 3.56; 4f= 4, 78; P~0.01). Post hoc
tests yielded the same pattern of results as reported above. The findings suggest that these two expressions were not unduly affecting the results.
The relationship between expression and perception
To examine the relationship between performance on the expression and perception tasks. expression accuracy scores were correlated with perception accuracy scores, separately for the three subject groups. Since there were four expression variables (posed positive, posed negative, spontaneous positive, spontaneous negative) and three perception variables (positive, negative, neutral), each of the three subject group correlation matrices had 12 entries. Of the 36 resulting correlations, only two were significant, and no systematic patterns emerged. When the data for all subjects were combined, only two of the 12 correlations were significant.
To look more closely at the relationship between perception and production of emotional expression, the distribution for each of the posed expressions was compared to the distribution for its perceptual analogue (e.g. posed verbal happiness vs perceived happiness, posed visual happiness vs perceived happiness); Fisher Tests of Exact Probability [57] were carried out on these comparisons. Of the 16 analyses conducted (eight emotions for posed- verbal plus eight emotions for posed-visual) for each of the three subject groups, all but two (of 48) were nonsignificant.
The e&t qf lesion location on task performance
Since our two patient groups were not matched for lesion distribution within each hemisphere, the data were examined for effects of intrahemispheric location of lesion. Patients were classified as ‘posterior’ (five RBDs, six LBDs) if their lesions were confined to parietal, temporal, and/or occipital lobe structures; as ‘anterior’ (four LBDs) if their lesions involved pre-Rolandic structures; and as ‘anterior,‘posterior’(seven RBDs. five LBDs) if their lesions involved frontal and parietal, temporal, or occipital structures. The medians were determined for the total accuracy scores for the expression variable (mean of posed positive, posed negative, spontaneous positive and spontaneous negattve scores) and for the perception variable (mean of positive, negative, and neutral scores) and are listed by lesion

FACIAL EMOTION AYD RRAlh DAMAGE 177
subgroup in Table 3. As can be seen in Table 3, the presence of an anterior/posterior lesion had opposite effects within the two brain-damaged groups. Among RBDs, impairment appeared to be related to the presence of lesions in both anterior and posterior regions, while among LBDs, impairment appeared more related to the presence of lesions in the posterior region only.
Table 3. Median total accuracy scores for expression and perception tasks, by lesion side and site
Side Lesion
Site Expression Perception
N median median
Right Anterior/posterior 7 0.43 0.40 Posterior 5 0.49 0.69
Left Posterior 6 0.50 0.82 Anterior 4 0.72 0.88 Anterior/posterior 5 0.73 0.89
DISCUSSION
These data suggest that patients with right-hemisphere pathology have deficits in processing facial emotion when compared to patients with left-hemisphere pathology or normal controls. This appears to be the case for both perception, and for spontaneous and posed expression, of emotion. The data are in agreement with previous studies that have examined either perception (e.g. [24]) or expression (e.g. [15]) of facial emotion. To our knowledge, this is the first study to assess both of these functions in the same subjects.
In examining the correlations between expression and perception accuracy scores, no systematic relationships emerged for the total group or for any of the individual subject groups. Thus, the ability to pose a particular emotion did not appear related to the ability to identify the emotion. The fact that there were negligible correlations between expression and perception variables suggests that these two types of performance may be tapping relatively separate aspects of emotional processing.
Several studies indicate that the two hemispheres might process emotional valence somewhat differently. In the current study, there was a relationship between affected hemisphere and valence for both expression and perception, but not in the same direction. For perception, the finding that RBDs, relative to LBDs, were impaired for negative but not for positive emotions is consistent with findings in normals that the right hemisphere is specialized for negative emotion (e.g. Cl]). For expression, the findings were more complex: RBDs, relative to LBDs, were impaired for positive but not negative emotions-but only for the posed condition. Despite the lack of a significant interaction between Group, Condition, and Valence, we thought that post hoc analyses might elucidate this complex relationship. Post hoc tests revealed that RBDs were significantly more impaired than LBDs for posed positive, spontaneous positive, and spontaneous negative emotions. For posed negative emotions, the two groups did not differ.
Lesion location within a hemisphere also appeared to have an effect on both expression and perception. Among patients with right-hemisphere pathology, those with lesions involving both anterior and posterior structures were more impaired in performance on tasks of facial emotion than patients with posterior lesions. However, among patients with left-hemisphere pathology, those with posterior lesions were more impaired than patients

178 J. C‘. ,k)ROI) (‘I (I/.
with anterior, or anterior plus posterior, lesions. It is important to note that the intrahemispheric effects were examined with regard to location only and not extent or size of lesion. Size of lesion is a relevant variable, which we were not able to control in this study because our neuroanatomical data were not amenable to this type of analysis.
The data for the LBD aphasics appear consistent with reports of emotional behavior in aphasics [3, 12, 31, 521 in which some anterior aphasics are observed to display illness- appropriate (though often extreme) emotional reactions, while some posterior aphasics are described as unconcerned with, or unaware of, their illness. It occurred to us that aphasia subtype and/or auditory comprehension difficulties might underlie the deficits among the posterior aphasics. Since the four Wernicke’s and the two Conduction aphasics included in this study were the only LBDs with exclusively posterior lesions, it is difficult to separate the effects of lesion location from diagnostic type among these LBDs. When the BDAE comprehension z-scores were correlated with the total mean accuracy scores for the perception and expression variables, there was no relationship between auditory comprehen- sion and facial perception (p = +0.07, P>O.50) but a substantial negative correlation between auditory comprehension and facial expression (p= -0.59. Pt0.05). The more impaired a patient’s comprehension, the more emotionally expressive he was. There are reports in the clinical literature (e.g. [IS]) that aphasics can communicate nonverbally, even in the face of severe language disturbances.
One might also raise the question of whether bucco-facial apraxia was present among these LBD aphasics. These LBDs demonstrated significant (PtO.O1) impairments, relative to the NCs and RBDs, on praxis tasks (using standard procedures developed by GOOD~;LASS
and KAPLAN [34]). When performance scores for the praxis tasks were correlated with posed and spontaneous expression accuracy scores, no significant relationships emerged for any of the groups.
In addition to quantitative differences in the performance of RBDs relative to LBDs on tasks of facial emotion, the quality of responses also differed. On the expression task, a variety of inappropriate responses were observed. Among these were what we have termed ‘paramotias’ (i.e. a part of the total facial expression was inaccurate), unrecognizable facial expressions, facial groping (i.e. a disorganized performance of multiple facial movements without production of any one specific or recognizable configuration), and vocalization (e.g. saying “happy” when requested to look happy). RBDs demonstrated significantly (P < 0.05. one-tailed r-test) more paramotias, unrecognizable facial expressions, and facial groping than NCs, and RBDs tended (P-CO. 10) to show more paramotias and unrecognizable expressions than LBDs. LBDs produced significantly more vocalization responses than RBDs or NCs. On the perception task, when the NCs and LBDs erred, they tended to give responses
that approximated the target, e.g. “fear” for surprise, “concerned” for confusion, “anger” for disgust. The incorrect responses of the RBDs, however, were harder to reconcile with the target, e.g. “happy” for confusion, “sexually aroused” for sadness and “jerky” for disgust.
In conclusion, the finding that RBDs are impaired relative to both LBDs and NCs in expressing and perceiving facial emotion is consistent with the notion that the right hemisphere has a predominant role in the processing of emotional stimuli [9, 46, 613. This interhemispheric effect appeared to override the effects of elicitation condition but was moderated by the valence of the emotion and the location of the lesion within a hemisphere. This research demonstrates that facial behaviors are amenable to qualitative, as well as quantitative, analysis. While the data are suggestive, additional studies using a similar design and procedures are necessary to substantiate these conclusions.

Acknowledgements-Portions of this paper were presented at the International Neuropsychology Society Annual Meetings in Pittsburgh, 1982 and Mexico City, 1983. This research was supported by USPHS Grants NS06209 to the Aphasia Research Center of Boston University Medical School and MH37592 to New York University Medical School, and by Biomedical Research Support Grant No. 1-S07RR07186-02 to Wellesley College. We are grateful to Dr Ross Buck, Karen Olsen, Hope Heller, Nancy Lefkowitz, and Fern Cytryn for their assistance in this project, to Dr Joan Welkowitz for statistical assistance, to the reviewers for their comments, and to the Neurology and Medical Research Services of the Boston VA Medical Center.
I.
2.
1 4:
5.
6.
7. 8.
AHERN, G. L. and SCHWARTZ, G. E. Differential lateralization for positive versus negative emotion. Neuropsychologia 17, 693-698, 1979. BENOWITZ, L. I. Cerebral lateralization in the perception of nonverbal emotional cues. McLean Hosp. J. 5, 146-167, 1980. BENSON, D. F. Psychiatric aspects of aphasia. Br. J. Psychiat. 123, 555-566, 1973. BOROD, J. C. and CARON, H. S. Facedness and emotion related to lateral dominance, sex, and expression type. Neuropsychologia 18, 237-242, 1980. BOROD, J. C., CARON, H. S. and KOFF, E. Asymmetries in positive and negative facial expressions: Sex differences. Neuropsychologia 19, 819-824, 1981 BOROD, J. C., CARON, H. and KOFF, E. Asymmetry of facial expression related to handedness, footedness, and eyedness: a quantitative study. Cortex 17, 381-390, 1981. BOROD, J. C. and KOFF, E. Hemiface mobility and facial expression asymmetry. Cortex 19, 355-361, 1983. BOROD, J. C. and KOFF, E. Asymmetries in affective facial expression: anatomy and behavior. In The Psychobiology ofAflectiue Development N. Fox and R. DAVIDSON (Editors). Lawrence Erlbaum, Hillsdale, NJ, 1984.
9.
10.
11.
12. 13. 14.
15.
16. 17. 18. 19.
20.
21.
22.
BOROD, J. C., KOFF, E. and CARON, H. S. Right hemisphere specialization for the expression and appreciation of emotion: a focus on the face. In Cognitive Processes in the Right Hemisphere, E. PERECMAN (Editor). Academic Press, New York, 1983. BOROD, J. C., KOFF, E., PERLMAN LORCH, M. and NICHOLAS, M. Channels of emotional expression in patients with unilateral brain damage. Archs Neural. 42, 345-348, 1985. BOROD, J. C., KOFF, E. and WHITE, B. Facial asymmetry in posed and spontaneous expressions of emotion. Brain Cognit. 2, 165.-175, 1983. BROWN, J. Book review. J. nerv. ment. Dis. 172, 232-234, 1984. BRUYER, R. Asymmetry of facial expression in brain damaged subjects. Neuropsychologia 19, 615-624, 1981. BUCK, R. The slide-viewing technique for measuring nonverbal sending accuracy: a guide for replication. Catalog of Selected Documents in Psychology, Vol. 8, p. 63, 1978. BUCK, R. and DUFFY, R. J. Nonverbal communication of affect in brain-damaged patients. Cortex 16,351-362, 1980. CAMPBELL, R. Asymmetries in interpreting and expressing a posed facial expression. Cortex 14, 327-342, 1978. CAMPBELL, R. Asymmetries in moving faces. Br. J. Psychol. 73, 95-103, 1982. CHESTER, S. and EGOLF, D. Nonverbal communication and aphasia therapy. Rehabil. Lit. 35,231-233, 1974. CICONE, M., WAPNER, W. and GARDNER, H. Sensitivity to emotional expressions and situations in organic patients. Cortex 16, 145-158, 1980. COREN, S., PORAC, C. and DUNCAN, P. A behaviorally validated self-report inventory to assess four types of lateral preferences. .I. clin. NeuropsychoL 1, 55-64, 1979. DAMASIO, A. R. and MAURER, R. G. A neurological model for childhood autism. Archs Neural. 35, 777-786, 1978.
23.
24.
25.
26.
DAVIDSON, R. and Fox, N. Asymmetrical brain activity discrimination between positive and negative affective stimuli in human infants. Science 218, 1235-1237, 1982. DAVIDSON, R. J., SCHWARTZ, G. E.. SARON, C., BENNETT, J. and GOLEMAN, D. Frontal versus parietal EEG asymmetry during positive and negative affect. Paper presented at the Society for Psychophysiological Research, Madison, Wisconsin, 1978. DEKOSKY, S. T., HEILMAN, K. M., BOWERS, D. and VALENSTEIN, E. Recognition and discrimination ofemotional faces and pictures. Brain Lang. 9, 206214, 1980. DIMOND, S. J., FARRINGTON, L. and JOHNSON. P. Differing emotional response from right and left hemisphere. Nature 261, 689-691, 1976. DOPSON, W. G., BECKWITH, B. E., TUCKER, D. M. and BULLARD-BATES, P. C. Asymmetry of facial expression in spontaneous emotion. Cortex 20, 243-252, 1984,
27. EKMAN, P. Emotion in the Human Face. Cambridge University Press, Cambridge, 1983. 28. EKMAN, P. and FRIESEN, W. Unmasking the Face. Prentice-Hall, Englewood Cliffs, NJ, 1975. 29. EKMAN, P. and FRIESEN, W. Pictures of Facial A&r. Consulting Psychologists Press, Palo Alto, CA, 1976.
REFERENCES
180 J. C. HOKOI) (‘I t/l
30 31 32
33 34
35
36
37
38
39 40. 41 42.
43
44
45
46.
47
48. 49
50. 51.
52.
53.
54.
55.
56.
57. 58. 59.
60.
61. 62.
63.
64.
ETCOFF, N. L. Selective attention to facial identity and facial emotion. Neuropsychologia 22, 281-295, 1984. GAINOTTI, G. Emotional behavior and hemispheric side of the lesion. Cortex 8, 41-55, 1972. GESCHWIND, N. The apraxias: neural mechanisms of disorders of learned movement. Am. Scient. 63, 188-195. 1975. GILBERT, C. and BAKAN, P. Visual asymmetry in perception of faces. Neuropsychologia 11, 355-362, 1973. GOODGLASS, H. and KAPLAN, E. The Assessment @Aphasia and Related Disorders. Lea & Febiger, Philadelphia, 1972. HANSCH, E. C. and PIROZZOLO, F. J. Task relevant effects on the assessment ofcerebral specialization for facial emotion. Brain Lang. 10, 51-59, 1980. HEILMAN, K. M. and VALENSTEIN. E. Cknical Neuropsychology, p. 427. Oxford Llniversity Press, New York, 1979. HELLER, W. and LEVY, J. Perception and expression of emotion in right-handers and left-handers. Neuropsychologia 19, 363-372, 1981. HIRSCHMANN, R. S. and SAFER, M. A. Hemisphere differences in perceiving positive and negative emotions. Cortex 18, 569-580. 1982. HOLLINGSHEAD, A. B. and REDLICH, F. C. Sociul Class and Mental Illness. Wiley, New York, 1958. IZARD, C. D. The Face ofEmotion. Appleton-Century-Crofts, New York, 1971. KAHN, E. A. Facial expression. Clin. Neurosurg. 12, 9-22, 1964. KARLIN, R., WEINAPPLE. M., ROCHFORD, J. and GOLDSTEIN, L. Quantitative EEG features of negative aflective states: Report of some hypnotic studies. Res. Commun. Psychol. 4, 397-413, 1979. KOLB, B. and MILNER, B. Observations on spontaneous facial expression after focal cerebral excisions and after intracarotid injection of sodium amytal. Neuropsycholoyia 19, 505-514, 1981. LEVY, J., HELLER, W., BANICH, M. T. and BURTON, L. A. Asymmetry of perception in free viewing of chimeric faces. Brain Cog&. 2, 404419, 1983. LEY, R. G. and BRYDEN, M. P. Hemispheric differences in processing emotions and faces. Brain Lung. 7, 127-138, 1979. LEY, R. G. and BRYDEN, M. P. Consciousness, emotion, and the right hemisphere. In Aspecrs ofConsriousn~.w. R. STEVENS and G. UNDERWIXD (Editors). Academic Press, New York, 1982. MCKEEVER, W. F. and DIXON, M. F. Right-hemisphere superiority for discriminating memorized from nonmemorized faces: affective imagery, sex, and perceived emotionality effects. Brain Lang. 12,24&260, 1981. MIEHLKE, A. Surgery of the Facial Nerenre. W. B. Saunders, Philadelphia, 1973. MOS~OVIT~H, M. and OLDS, J. Asymmetries in spontaneous facial expression and their possible relation to hemispheric specialization. Neuropsychologiu 20, 71-81. 1982. MURRAY, H. A. Explorations in Personality. Oxford University Press, New York. 1938. REUTER-LORENZ, P. and DAVIDSON, R. Differential contributions of the two cerebral hemispheres to the perception of happy and sad faces. Neuropsychologia 19, 609%61X 1981. ROBINSON, R. G. and BENSON, D. F. Depression in aphasic patients: frequency, severity, and clinical- pathological correlation. Brain Lang. 41, 282 291, 1981. Ross, E. D. and MESIJLAM, M. Dominant language functions of the right hemisphere’? Prosody and emotional gesturing. Archs Neural. 36, 144148, 1979. RUBIN, D. A. and RUBIN, R. T. Differences in asymmetry of facial expression between left- and right-handed children. Neuropsychologia 18, 373-377, 1980. SACKEIM, H.. GREENBERG. M.. WEIMAN, A., GUR, R., HUNGERBUHLER, J. and GES~HWIND, N. Functional brain asymmetry in the expression of positive and negative emotions: lateralization of insult in cases of uncontrollable emotional outbursts. Archs Neural. 19. 21@218. 1982. SACKEIM, H. and GUR, R. C. Lateral asymmetry in intensity of emotional expression. Nrurops~lchologlu 16, 473-381, 1978. SIEGEL, F. Nonparametric Statistics. McGraw-Hill, New York. 1956. STRAUSS. E. and MOS~OVIT~H, M. Perception of facial expressions. Brain Lung. 13, 308 332, 1981. SUBERI, M. and MCKEEVER, W. F. Differential right hemisphere memory storage of emotional and nonemotional faces. Neuropsychologia 15, 757 -768. 1977. TSCHIASSNY, K. Eight syndromes of facial paralysis and their significance in locating the lesion. Ann. Otol. Rhino/. Laryng. 62, 677 691, 1953. T~:CKER, D. M. Lateral brain function, emotion, and conceptualizatton. Psycho/. Bull 89, 19-46, 1981. TUCKER. D. M.. STENSLIE. C. E.. ROTH, R. S. and SHEARER, S. L. Right frontal lobe activation and right hemisphere performance: decrement during a depressed mood. Archs gin. Psychiur. 38, 169-l 74, 1981. WECHSLER, D. The Measurement and Appraisal o/Adult Intelliaencr. Williams & Wilkins, Baltimore, Maryland, 1958. WINER. B. J. Statistical Principles in Experimental Drsiyn. McGraw-Hill, New York, 1971
Copyright © 2022 FDOKUMEN




















