The effects of essential oil mouthrinses with or without alcohol ...
10
RESEARCH ARTICLE Open Access The effects of essential oil mouthrinses with or without alcohol on plaque and gingivitis: a randomized controlled clinical study Michael C. Lynch 1 , Sheila Cavalca Cortelli 2 , James A. McGuire 1 , Jane Zhang 1* , Danette Ricci-Nittel 1 , Carolyn J. Mordas 1 , Davi Romeiro Aquino 2 and Jose Roberto Cortelli 2 Abstract Background: The efficacy of several variants of essential oil mouthrinses has been studied extensively. This is the first study to compare the anti-plaque and anti-gingivitis efficacy of two marketed essential oil mouthrinses: one is an alcohol containing mouthrinse and the other one is an alcohol-free mouthrinse. Methods: This examiner-blind, parallel-group study randomized subjects to three groups: 1) Mechanical Oral Hygiene (MOH) only; 2) MOH plus Alcohol-Containing essential oil Mouthrinse (ACM); 3) MOH plus Alcohol-Free essential oil Mouthrinse (AFM). Primary endpoint was whole-mouth mean Modified Gingival Index (MGI) at six months. Secondary endpoints included whole-mouth mean MGI at one and three months, and whole-mouth mean Plaque Index (PI) and whole-mouth mean Bleeding Index (BI) at one, three and six months. Safety assessments were conducted at all time points. Results: A total of 370 subjects were enrolled; 348 subjects completed the study. After six months, subjects using essential oil mouthrinses with or without alcohol showed significant reduction (p < 0.001) in gingivitis (28.2% and 26. 7%, respectively) and significant reduction (p < 0.001) in plaque (37.8% and 37.0%, respectively), compared to those performing MOH only. Significant reductions in MGI, PI, and BI (p < 0.001) were observed at one and three months and also at six months for mean BI. No statistically significant differences were observed for all measured indices between ACM and AFM groups at any time point. Both mouthrinses were well tolerated. Conclusions: No significant differences were observed in the efficacy of ACM and AFM to reduce plaque and gingivitis, when used in addition to MOH, over six months. Trial registration: The trial was registered on clinicaltrials.gov on November 30, 2016. The registration number is NCT02980497. Keywords: Essential oils, Mouthrinse, Alcohol-free, Plaque, Gingival bleeding, Gingivitis * Correspondence: [email protected] 1 Johnson & Johnson Consumer Inc.,, 199 Grandview Road, Skillman, New Jersey 08558, USA Full list of author information is available at the end of the article © The Author(s). 2018 Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated. Lynch et al. BMC Oral Health (2018) 18:6 DOI 10.1186/s12903-017-0454-6
-
Upload
khangminh22 -
Category
Documents
-
view
2 -
download
0
Transcript of The effects of essential oil mouthrinses with or without alcohol ...

RESEARCH ARTICLE Open Access
The effects of essential oil mouthrinseswith or without alcohol on plaque andgingivitis: a randomized controlled clinicalstudyMichael C. Lynch1, Sheila Cavalca Cortelli2, James A. McGuire1, Jane Zhang1* , Danette Ricci-Nittel1,Carolyn J. Mordas1, Davi Romeiro Aquino2 and Jose Roberto Cortelli2
Abstract
Background: The efficacy of several variants of essential oil mouthrinses has been studied extensively. This is thefirst study to compare the anti-plaque and anti-gingivitis efficacy of two marketed essential oil mouthrinses: one isan alcohol containing mouthrinse and the other one is an alcohol-free mouthrinse.
Methods: This examiner-blind, parallel-group study randomized subjects to three groups: 1) Mechanical Oral Hygiene(MOH) only; 2) MOH plus Alcohol-Containing essential oil Mouthrinse (ACM); 3) MOH plus Alcohol-Free essential oilMouthrinse (AFM). Primary endpoint was whole-mouth mean Modified Gingival Index (MGI) at six months. Secondaryendpoints included whole-mouth mean MGI at one and three months, and whole-mouth mean Plaque Index (PI) andwhole-mouth mean Bleeding Index (BI) at one, three and six months. Safety assessments were conducted at all timepoints.
Results: A total of 370 subjects were enrolled; 348 subjects completed the study. After six months, subjects usingessential oil mouthrinses with or without alcohol showed significant reduction (p < 0.001) in gingivitis (28.2% and 26.7%, respectively) and significant reduction (p < 0.001) in plaque (37.8% and 37.0%, respectively), compared to thoseperforming MOH only. Significant reductions in MGI, PI, and BI (p < 0.001) were observed at one and three months andalso at six months for mean BI. No statistically significant differences were observed for all measured indices betweenACM and AFM groups at any time point. Both mouthrinses were well tolerated.
Conclusions: No significant differences were observed in the efficacy of ACM and AFM to reduce plaque andgingivitis, when used in addition to MOH, over six months.
Trial registration: The trial was registered on clinicaltrials.gov on November 30, 2016. The registration number isNCT02980497.
Keywords: Essential oils, Mouthrinse, Alcohol-free, Plaque, Gingival bleeding, Gingivitis
* Correspondence: [email protected] & Johnson Consumer Inc.,, 199 Grandview Road, Skillman, NewJersey 08558, USAFull list of author information is available at the end of the article
© The Author(s). 2018 Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, andreproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link tothe Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver(http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
Lynch et al. BMC Oral Health (2018) 18:6 DOI 10.1186/s12903-017-0454-6

BackgroundWhen used in conjunction with mechanical oral hygiene(MOH), the use of mouthrinses to help reduce plaque andgingivitis has been well documented and their efficacy is at-tributed to chemical agents, such as CetylpyridiniumChloride (CPC), Chlorhexidine (CHX), and Essential Oils(EO) contained in these products [1–9]. Commonly usedinactive ingredients include alcohol, water, bufferingagents, flavouring agents and surfactants. In EO mou-thrinses, alcohol serves as a preservative but also solubi-lizes the essential oils, thus maintaining their bioavailability[10, 11]. A 2015 meta-analysis of 29 clinical trials with du-rations of six months or longer further demonstrated theefficacy of essential oil mouthrinses [7].The inclusion of alcohol in mouthrinse has historically
limited its use in certain patient populations, such aschildren, alcoholics, people with strong taste prefer-ences, those of certain religious beliefs, and patients withoral mucositis [12].To address these limitations, an Alcohol-Free EO-
mouthrinse (AFM) was developed. Its antimicrobialproperties were demonstrated in vitro [13] and invivo [14] initially. This was followed by demonstrationof its efficacy in reducing plaque and gingivitis inclinical trials [15, 16]. However, no long-term studies(i.e., at least six months in duration) have directlycompared alcohol containing EO mouthrinses (ACM)to its Alcohol-Free counterpart, AFM. The objectiveof the current study is to compare the long-term effi-cacy of twice-daily rinsing with either an AFM or anACM, in conjunction with usual MOH, for the reduc-tion of plaque and gingivitis.
MethodsStudy designThis randomized, controlled, single-centre, examiner-blind, parallel-group study was conducted between 11September 2013 and 16 March 2014 (recruitmentperiod July 2013–September 2013) at the University ofTaubate, São Paulo, Brazil. The study was conducted inaccordance with the International Conference on Har-monisation (ICH) Harmonised Tripartite Guideline forGood Clinical Practice (ICH E6, 1996), in agreementwith the Declaration of Helsinki (2000), applicable localregulations, and the American Dental Association(ADA) Seal of Acceptance Program Guidelines for Che-motherapeutic Products for Control of Gingivitis [17].The study protocol was approved by the InstitutionalEthics Committee on research involving humans(CAAE: 20,402,713.1.00005501). The trial was regis-tered on clinicaltrials.gov. The registration number isNCT02980497. Written informed consent was obtainedfrom all subjects.
SubjectsSubjects from Taubate and neighbouring areas were se-lected from a database or recruited through advertisingand were consecutively enrolled in the study. Males andfemales aged ≥18 years, in good general and oral health,with the exception of mild to moderate gingivitis, andwith a minimum of 20 natural teeth having scorable fa-cial and lingual surfaces, were included. Each subjectwas required to have a whole-mouth mean gingivitisscore of ≥1.95, according to the Modified Gingival Index(MGI) [18], and a whole-mouth mean plaque score of≥1.95, according to the Turesky modification of theQuigley-Hein Plaque index (PI) [19] on six surfaces pertooth [20]. Other study inclusion criteria included theabsence of moderate/advanced periodontitis (ADA typesIII and IV), absence of significant oral soft tissue path-ology other than plaque-induced gingivitis; and no fixedor removable orthodontic appliance or removable den-tures. Periodontitis patients were excluded based onTanner’s early periodontitis definition [21], which re-quired one or more periodontal sites with >2 mm peri-odontal attachment loss in a given subject with meanclinical attachment level ≤ 1.5 mm. Key exclusion criteriaincluded regular use of products such as triclosan denti-frices and mouthrinses containing EO, CPC, or CHXwithin two weeks prior to baseline; use of antibiotic,anti-inflammatory, or anticoagulant therapy during thestudy or within two weeks prior to baseline; history ofsignificant adverse effects, including allergies followinguse of oral hygiene products; known sensitivity to the in-vestigational product ingredients; current, or history ofalcohol or drug abuse; and participation in a clinical trialwithin 30 days of the start of the study.
InterventionsAt baseline, after abstaining from oral hygiene for atleast eight hours, but no more than 18 h, pre-screenedsubjects underwent an oral examination, and gingivitisand plaque assessments. A disclosing dye (0.5% basicfuchsin neutral red solution [Byoformula, Taubate, SãoPaulo, Brazil]) was used to assess plaque. Eligible sub-jects received a dental prophylaxis to remove plaque,calculus and stain, and were randomly assigned to oneof the three treatment groups:1) a negative control group, or a Mechanical Oral Hy-
giene (MOH) only group, received a fluoridated tooth-paste (Colgate Cavity Protection, Colgate-PalmoliveCompany, New York, USA) and REACH® Soft-bristledtoothbrush (Johnson & Johnson, New Jersey USA);2) a test group received the same toothpaste and tooth-
brush, plus LISTERINE® ZERO™, an Alcohol Free Mou-thrinse (AFM) (Johnson & Johnson, New Jersey, USA);3) a positive control group received the same tooth-
paste and toothbrush, plus LISTERINE® COOL MINT®,
Lynch et al. BMC Oral Health (2018) 18:6 Page 2 of 10

an Alcohol Containing Mouthrinse (ACM) (Johnson &Johnson, New Jersey, USA).Both AFM and ACM contain a fixed combination of
four essential oils [eucalyptol (0.092%), menthol (0.042%),methyl salicylate (0.060%), and thymol (0.064%)], as wellas sorbitol, poloxamer, buffer, flavour and dye. AFM alsocontains Sodium Lauryl Sulphate and propylene glycol.At the start of the study, all subjects received REACH®
Soft-bristled toothbrush, Colgate® anticavity fluoridetoothpaste and were instructed to brush with one ribbonof toothpaste in their usual manner twice daily. Colgateanticavity fluoride toothpaste contained Sodium Mono-fluorophosphate (0.76% or 0.15% w/v Fluoride Ion),Dicalcium Phosphate Dihydrate, Water, Glycerin, So-dium Lauryl Sulfate, Cellulose Gum, Flavor, TetrasodiumPyrophosphate, Sodium Saccharin. Subjects in the ACMor AFM groups also received the assigned mouthrinseand plastic dosage cups marked at 20 mL level and wereinstructed to rinse with 20 mL of full strength mou-thrinse for 30 s after brushing twice daily. All subjectsreceived diaries to document compliance with the home-care regimen. Diaries were checked monthly and bottleswere weighed monthly to match the number of rinsesreported in the diaries to the actual used volume. Ab-sence of >3 consecutive rinses or >5 rinses within each30-day interval between study visits constituted a proto-col violation and the subject could be removed from thestudy at the discretion of the clinical investigator or theSponsor.Randomization was based on a block randomization
scheme devised by the Biometrics and Clinical Data Sys-tems Department at Johnson & Johnson, with a blocksize of six. Each subject was assigned a uniquerandomization number that determined the treatmentassigned to that subject according to a randomizationschedule. The randomization number was assigned se-quentially in ascending order and could not be reas-signed to another subject. Investigational supplies werekept separate from the site personnel involved in exam-ining the subjects. The dental examiner was, therefore,blinded to treatment throughout the study period. Sub-jects received investigational products in blinded pack-aging, and personnel dispensing the investigationalsupplies or supervising their use did not participate inthe examination of subjects to minimize potential bias.The first rinsing and the rinsing on the examinationvisits were under supervision at the study site. All otherrinsing was unsupervised.
Assessments and outcomesEfficacy assessments were performed at baseline and atthe one-, three- and six-month visits. This involved vis-ual assessment of gingival inflammation, supragingivalplaque, and gingival bleeding, as measured by MGI, PI,
and gingival bleeding index (BI) [22, 23], respectively.Subjects were asked to abstain from oral hygiene for atleast eight hours, but no more than 18 h prior to theirclinical examinations.A trained and calibrated dental examiner performed
all examinations in the following order: oral tissues as-sessment, MGI, BI and PI. One examiner was usedthroughout the study.Gingivitis was assessed using the MGI on the buccal
and lingual marginal gingiva and interdental papillae ofall scorable teeth as follows: 0 - normal (absence of in-flammation); 1 - mild inflammation of any portion of thegingival unit; 2 - mild inflammation of the entire gingivalunit; 3 - moderate inflammation of the gingival unit; 4-severe inflammation of the gingival unit.To assess gingival bleeding, a periodontal probe was
inserted into the gingival crevice, and swept from distalto mesial around the tooth at an angle of approximately60°, while in contact with the sulcular epithelium. Eachof four gingival areas (distobuccal, mid-buccal, mid-lingual, and mesiolingual) around each tooth wasassessed. After approximately 30 s, bleeding at each gin-gival unit was recorded according to the following scale:0 - absence of bleeding after 30 s; 1 – bleeding after30 s; 2 – immediate bleeding.The plaque area was scored on six surfaces per tooth
[20] (distobuccal, midbuccal and mesiobuccal, distolin-gual, midlingual and mesiolingual) of all scorable teeth asfollows: 0 - no plaque; 1 - separate flecks or discontinuousband of plaque at the gingival margin; 2 - up to 1 mmcontinuous band of plaque at the gingival margin; 3 - bandof plaque wider than 1 mm but less than 1/3 of surface; 4- plaque covering 1/3 or more, but less than 2/3 of surface;5 - plaque covering 2/3 or more of surface.Safety assessments included oral examinations con-
ducted at baseline, and at monthly visits, to monitor theeffect of the mouthrinse formulations on soft and hardtissues. Changes from the baseline and previous visitswere recorded at each subsequent clinic visit. Clinicallysignificant findings were recorded as adverse events(AEs) and an assessment was made regarding relation-ship to investigational product at the discretion of amedically qualified clinical examiner.During the study, subjects were instructed to follow
their usual dietary habits and normal oral care regimen,incorporating only the toothpaste, toothbrush, and mou-thrinse provided to them. Subjects were also allowed tocontinue use of an interdental cleaning device to removeimpacted food between the teeth if it was part of theirusual oral care regimen. No other oral hygiene proce-dures were permitted, including teeth cleaning or dentalwork, except in an emergency.The primary efficacy endpoint was the mean MGI at
six months, while the secondary endpoints included
Lynch et al. BMC Oral Health (2018) 18:6 Page 3 of 10

mean MGI at one and three months; and mean PI andBI at one, three, and six months. Safety was assessed bysummarizing all AEs considered related to treatment.
Statistical analysesThe planned sample size of 330 subjects (110 per treat-ment group) provided 90% power to detect a between-treatment difference of 0.08, assuming a standard devi-ation [SD] of 0.180, based on previous studies [16, 24]for whole-mouth mean MGI at a 0.05 significance level(two-sided). Demographic and baseline characteristics
were compared across treatment groups using analysisof variance (ANOVA), Chi-square test, or Fisher’s exacttest. Efficacy analysis was based on the full analysis set(FAS), following the Intent-to-Treat principle, defined asall randomized subjects who used the study product andhad baseline and at least one post-baseline data point formean MGI. Missing data was assumed Missing At Ran-dom. No imputation of missing data was performed.Statistical comparisons for primary and secondary vari-ables were based on one-way analysis of covariance(ANCOVA), with treatment as a factor and the
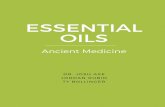
Fig. 1 Subject disposition/CONSORT flow diagram. MOH: mechanical oral hygiene; AFM: alcohol-free essential oil mouthrinse; ACM: alcohol-containingessential oil mouthrinse
Table 1 Subject demographic and baseline characteristics
Parameters MOH AFM ACM Total Overall
(n = 123) (n = 124) (n = 123) (n = 370) p-value
Age (years) 38.8 ± 11.75 35.1 ± 14.43 35.2 ± 13.83 36.4 ± 13.46 0.053a
Sex n (%) 0.757b
Male 50 (40.7) 46 (37.1) 51 (41.5) 147 (39.7)
Female 73 (59.3) 78 (62.9) 72 (58.5) 223 (60.3)
Race n (%) >0.999c
White 112 (91.1) 113 (91.1) 112 (91.1) 337 (91.1)
Black or African- American 1 (<1.0) 1 (<1.0) 1 (<1.0) 3 (<1.0)
Asian 1 (<1.0) 0 0 1 (<1.0)
Other 9 (7.3) 10 (8.1) 10 (8.1) 29 (7.8)
Smoker n (%) 0.876b
Yes 13 (10.6) 11 (8.9) 11 (8.9) 35 (9.5)
No 110 (89.4) 113 (91.1) 112 (91.1) 335 (90.5)
Whole-mouth scores
Baseline Mean MGI 2.439 ± 0.147 2.454 ± 0.149 2.462 ± 0.146 2.452 ± 0.147 0.450a
Baseline Mean PI 2.976 ± 0.224 2.991 ± 0.228 3.014 ± 0.269 2.994 ± 0.241 0.456a
Baseline Mean BI 0.604 ± 0.132 0.628 ± 0.183 0.623 ± 0.163 0.618 ± 0.161 0.474a
Data are mean ± SD unless otherwise specifiedACM Alcohol-containing essential oil mouthrinse, AFM Alcohol-free essential oil mouthrinse, BI Bleeding index, MGI Modified gingival index, MOH Mechanical oralhygiene, PI Plaque index, SD Standard deviationap-values are based on ANOVA model with term for treatmentbp-values are based on Chi-square testcbased on Fisher’s exact test
Lynch et al. BMC Oral Health (2018) 18:6 Page 4 of 10

corresponding baseline value as a covariate. Compari-sons were made in the following sequential manner tocontrol the family-wise error rate of 0.05: ACM versusMOH with respect to mean MGI; AFM versus MOHwith respect to mean MGI and; ACM versus AFM withrespect to mean MGI. All comparisons were madeusing a 0.05 level test (two-sided) and secondary end-points were analysed in the same manner. Safety ana-lysis was based on all randomized subjects who usedthe study product.
Post-hoc analysisAn exploratory post-hoc analysis was conducted toevaluate the non-inferiority (defined as “at least as goodas”) of AFM compared with ACM. Using Fieller’s the-orem [25, 26], 90% confidence intervals (CIs) for the ra-tio of observed mean MGI scores of AFM and ACM atmonths 1, 3, and 6 were constructed. According to ADAguidelines (American Dental Association Council on Sci-entific Affairs 2011), the criterion for non-inferiority wassatisfied when the entire 90% Fieller CI consisted ofvalues no greater than 110%.
ResultsOf the 370 subjects enrolled in the study and random-ized, 348 completed the study, while 22 withdrew orwere lost to follow up (Fig. 1). There were no protocolviolations leading to removal from the study. In total,123, 124, and 123 subjects were included in the MOH,AFM, and ACM groups, respectively; 122, 121, and 122subjects who had both baseline and post-baseline datawere included in the FAS. The mean (SD) age of subjectswas 36.4 (13.46) years and the majority were females(60.3%), Caucasian (91.1%), and non-smokers (90.5%).Overall, mean (SD) MGI, PI, and BI were 2.452 (0.147),2.994 (0.241), and 0.618 (0.161), respectively. Baselineand demographic characteristics were comparable be-tween the three study groups (Table 1).
EfficacyPrimary endpointAt six months, ACM use resulted in a 28.2% reduction(between treatment difference [95% CI]; p value) (−0.62[−0.670, −0.570]; p < 0.001) in gingivitis, as measured byMGI, compared to MOH. AFM showed a 26.7% reduc-tion (−0.59 [−0.637, −0.538]; p < 0.001) in mean MGI
Table 2 Whole-mouth mean modified gingival index (MGI) at months 1, 3, and 6 (full analysis set)
Mean MGI MOH(n = 122)
AFM(n = 121)
ACM(n = 122)
Baseline
Mean ± SE 2.438 ± 0.013 2.452 ± 0.013 2.463 ± 0.013
Month 1
Adj. mean ± SE 2.191 ± 0.014 1.832 ± 0.014 1.838 ± 0.014
Difference between treatments (95% CI) Percent difference (%) p- valuea
AFM vs MOH −0.359 (−0.399, −0.319) −16.4 <0.001
ACM vs MOH −0.353 (−0.393, −0.313) −16.1 <0.001
ACM vs AFM 0.006 (−0.034, 0.046) 0.3 0.756
Month 3b
Adj. mean ± SE 2.257 ± 0.018 1.772 ± 0.018 1.768 ± 0.018
Difference between treatments (95% CI) Percent difference (%) p- value
AFM vs MOH −0.486 (−0.535, −0.437) −21.5 <0.001
ACM vs MOH −0.489 (−0.539, −0.440) −21.7 <0.001
ACM vs AFM −0.004 (−0.053, 0.045) −0.2 0.878
Month 6c
Adj. mean ± SE 2.201 ± 0.018 1.614 ± 0.018 1.581 ± 0.018
Difference between treatments (95% CI) Percent difference (%) p- value
AFM vs MOH −0.587 (−0.637, −0.538) −26.7 <0.001
ACM vs MOH −0.620 (−0.670, −0.570) −28.2 <0.001
ACM vs AFM −0.033 (−0.083, 0.017) −2.0 0.198
ACM Alcohol-containing essential oil mouthrinse, AFM Alcohol-free essential oil mouthrinse, CI Confidence interval, MGI Modified gingival index, MO Mechanicaloral hygiene, SE Standard errorap-values are based on ANCOVA model with term for treatment and baseline value as covariatebAt month 3, data for MOH, AFM, and ACM groups were obtained from 119 subjects in each groupcAt month 6, data for MOH, AFM, and ACM groups were obtained from 118, 116, and 114 subjects, respectively
Lynch et al. BMC Oral Health (2018) 18:6 Page 5 of 10

versus MOH. However, no significant difference in gin-givitis reduction was found between ACM and AFMtreatments after six months of use (−0.033 [−0.083,0.017]; p = 0.198) (Table 2).
Secondary endpointsStatistically significant reductions in gingivitis com-pared to MOH were also seen at one and three monthsin both the ACM and AFM mouthrinse groups (Table2). Similar to the results at six months, no significantdifferences were observed in gingivitis reduction be-tween the two mouthrinse groups at one month (0.006[−0.034, 0.046]; p = 0.756) or three months (−0.004[−0.053, 0.045] p = 0.878) of use.Both mouthrinses significantly reduced plaque and
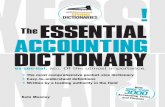
gingival bleeding compared to MOH at months one,three, and six (p < 0.001) (Tables 3 and 4). No significantdifference was seen in the reduction in plaque or gin-gival bleeding between ACM and AFM groups at one,three, and six months. Figure 2 illustrates the reductionin whole-mouth mean MGI, PI, and BI over the studyduration across all treatment groups.
Post hoc analysisA post-hoc statistical analysis was conducted to demon-strate that AFM is “at least as good as” ACM. The ratioof least square means of whole-mouth MGI betweenAFM and ACM at six months was 1.021 or 102% (90%Fieller CI [99%, 105%]) (Table 5).
SafetyAll treatments were well tolerated by the subjects. Thereported AEs were mild or moderate in severity and noserious AEs were reported, nor did any subject withdrawfrom the study due to AEs. Three subjects (0.8%) experi-enced AEs that were judged as related to the study prod-uct. This included one subject each in the ACM andAFM groups who experienced sensitivity of teeth, andone subject in the ACM group who reported dyspepsia.All investigation product–related AEs resolved withoutany treatment.
DiscussionHistorically, a key concern with formulating EO mou-thrinses without alcohol was the subsequent reductionin the solubility of these essential oils, leading to their
Table 3 Whole-mouth mean plaque index (PI) at months 1, 3, and 6 (full analysis set)
Mean PI MOH (n = 122) AFM (n = 121) ACM (n = 122)
Baseline
Mean ± SE 2.976 ± 0.020 2.991 ± 0.021 3.017 ± 0.024
Month 1
Adj. mean ± SE 2.781 ± 0.024 2.186 ± 0.024 2.206 ± 0.024
Difference between treatments (95% CI) Percent difference (%) p- valuea
AFM vs MOH −0.595 (−0.662, −0.527) −21.4 <0.001
ACM vs MOH −0.574 (−0.641, −0.507) −20.6 <0.001
ACM vs AFM 0.021 (−0.047, 0.088) 1.0 0.544
Month 3b
Adj. mean ± SE 2.806 ± 0.022 2.084 ± 0.022 2.032 ± 0.022
Difference between treatments (95% CI) Percent difference (%) p- valuea
AFM vs MOH −0.723 (−0.785, −0.661) −25.8 <0.001
ACM vs MOH −0.775 (−0.837, −0.712) −27.6 <0.001
ACM vs AFM −0.052 (−0.114, 0.010) −2.5 0.102
Month 6c
Adj. mean ± SE 2.881 ± 0.019 1.815 ± 0.019 1.791 ± 0.019
Difference between treatments (95% CI) Percent difference (%) p- valuea
AFM vs MOH −1.065 (−1.118, −1.012) −37.0 <0.001
ACM vs MOH −1.090 (−1.143,-1.036) −37.8 <0.001
ACM vs AFM −0.024 (−0.078, 0.029) −1.3 0.371
ACM Alcohol-containing essential oil mouthrinse, AFM Alcohol-free essential oil mouthrinse, CI Confidence interval, MGI Modified gingival index, MOH Mechanicaloral hygiene, SE Standard errorap-values are based on ANCOVA model with term for treatment and baseline value as covariatebAt month 3, data for MOH, AFM, and ACM groups were obtained from 119 subjects in each groupcAt month 6, data for MOH, AFM, and ACM groups were obtained from 118, 116, and 114 subjects, respectively
Lynch et al. BMC Oral Health (2018) 18:6 Page 6 of 10

diminished bioactivity and ultimately antimicrobial effi-cacy. The formulation of an alcohol-free EO mouthrinsetherefore required the replacement of alcohol withequally effective solubilisers, while maintaining a balancebetween all active and inactive ingredients for optimalantimicrobial efficacy.Contrary to common perception, rinsing with a vehicle
that contains alcohol at levels found in mouthrinses,does not provide any clinical benefit. For example, Lam-ster, et al. [27] demonstrated that a vehicle rinse contain-ing the same amount of alcohol (26.9%) as a marketedACM performed similarly to rinsing with a water controlafter six months of use. In that supervised clinical trial,the ACM group had significantly greater reductions inplaque and gingivitis levels when compared to the alco-hol vehicle and water control groups. These findingshave since been further validated in a systematic reviewand meta-analysis [28].To develop the AFM, systematic evaluation of multiple
non-alcoholic delivery systems in saliva-derived mixed-
species in vitro biofilm models [29] helped identify theprecise combination of a sodium lauryl sulphate, poloxa-mer, propylene glycol, and sorbitol delivery system thatwas effective in maintaining bioavailability and bioactiv-ity of EOs. At a range of 0.20%–0.35% w/w sodiumlauryl sulphate, and a total oil phase content of approxi-mately 0.36% w/w, the propylene glycol concentrationwas found to be optimum between 5% and 13% w/w,while sorbitol was optimum between 10% and 25% w/w(when added as a 70% sorbitol solution) [30, 31] BothAFM and ACM contain a fixed combination of four es-sential oils [eucalyptol (0.092%), menthol (0.042%), me-thyl salicylate (0.060%), and thymol (0.064%)], as well asother formulation ingredients.
Table 4 Whole-mouth mean gingival bleeding index (BI) atmonths 1, 3, and 6 (full analysis set)
Mean BI MOH (n = 122) AFM (n = 121) ACM (n = 122)
Baseline
Mean ± SE 0.605 ± 0.012 0.630 ± 0.017 0.623 ± 0.015
Month 1
Adj. mean ± SE 0.447 ± 0.008 0.309 ± 0.008 0.304 ± 0.008
Difference between treatments (95% CI) p- valuea
AFM vs MOH −0.137 (−0.160, −0.114) <0.001
ACM vs MOH −0.142 (−0.165, −0.119) <0.001
ACM vs AFM −0.005 (−0.028, 0.018) 0.657
Month 3b
Adj. mean ± SE 0.545 ± 0.009 0.299 ± 0.009 0.304 ± 0.009
Difference between treatments (95% CI) p- valuea
AFM vs MOH −0.246 (−0.271, −0.221) <0.001
ACM vs MOH −0.241 (−0.266, −0.216) <0.001
ACM vs AFM 0.006 (−0.019, 0.030) 0.661
Month 6c
Adj. mean ± SE 0.477 ± 0.007 0.180 ± 0.007 0.185 ± 0.007
Difference between treatments (95% CI) p- valuea
AFM vs MOH −0.297 (−0.316, −0.278)
ACM vs MOH −0.292 (−0.311, −0.272)
ACM vs AFM 0.005 (−0.014, 0.025)
ACM Alcohol-containing essential oil mouthrinse, AFM Alcohol-free essential oilmouthrinse, CI Confidence interval, MGI Modified gingival index, MOH Mechan-ical oral hygiene, SE Standard errorap-values are based on ANCOVA model with term for treatment and baselinevalue as covariatebAt month 3, data for MOH, AFM, and ACM groups were obtained from 119subjects in each groupcAt month 6, data for MOH, AFM, and ACM groups were obtained from 118,116, and 114 subjects, respectively
Fig. 2 a Mean modified gingival index (MGI), b plaque index (PI),and c gingival bleeding index (BI) at baseline, 1, 3, and 6 monthsacross all treatment groups. Baseline values were based on raw scores,and post-baseline means were based on adjusted means. MOH:mechanical oral hygiene; AFM: alcohol-free essential oil mouthrinse;ACM: alcohol-containing essential oil mouthrinse; SE: standarderror; *** p < 0.001
Lynch et al. BMC Oral Health (2018) 18:6 Page 7 of 10

The first proof-of-principle, human study on AFMsused a two-week, no-oral-hygiene, experimental gingi-vitis model in which the AFM group showed a reductionin plaque by 23.9% and gingivitis by 10.4%, compared tothe negative control rinse group [15]. However, whilethe results provided an indication of product perform-ance, the restrictions on mechanical oral hygiene limitthe applicability of the results.It is typical to demonstrate the efficacy of a mou-
thrinse in long-term clinical trials of at least six monthsin duration, a time period consistent with common rec-ommendations to patients for regular dental visits. A re-cent meta-analysis identified 35 clinical trials of six-month or longer on EO mouthrinses [7] and included29 trials that met the inclusion criteria. Two of these 29studies included an AFM but it was not compared withACM. One of these two studies was published [16]. Inthis published six-month study, the efficacy of AFM wasassessed in comparison to a negative control mouthrinseand an alcohol-free 0.05% CPC mouthrinse. Subjectsperformed their daily mechanical oral hygiene (MOH).The EO mouthrinse significantly reduced plaque (31.6%)and gingivitis (24.0%) at six months, compared to thecontrol rinse, and was found to be superior to the CPCmouthrinse. The results of the current study show thatboth the AFM and ACM provide a statistically and clin-ically significant additional benefit in subjects who per-formed their daily MOH. After one month, use of eitherthe AFM or ACM showed significant reduction inplaque (21.4% and 20.6%, respectively) and gingivitis(16.4% and 16.1%, respectively) compared to MOHalone. By month six, further reduction in plaque wasnoted; up to 37.0% and 37.8% in the AFM and ACMgroups, respectively, and gingivitis reduction up to 26.7%and 28.2%, respectively.No significant difference was found between the ACM
and AFM in plaque and gingivitis reduction (p = 0.371and p = 0.198, respectively) or in gingival bleeding (p =0.590), reinforcing the evidence that this alcohol-free de-livery system was successful in retaining the EO activityto prevent and reduce gingivitis and plaque.While the post-hoc analysis should be judged with the
caveat that it was exploratory in nature, the results (90%Fieller CI [99%, 105%]) suggest that since the upper 90%
Fieller CI is below 110% as specified by the ADA Guide-lines for Determination of Efficacy in Product Evaluation(American Dental Association Council on Scientific Af-fairs 2011), AFM is at least as good as ACM, adding tothe evidence supporting the use of AFM. Thus, the in-clusion of either ACM or AFM to an individual’s oralhygiene regimen can play a valuable role in reducingplaque, gingivitis, and gingival bleeding beyond usingMOH alone. Overall, improving patients’ oral hygienemay also help to improve gingival inflammation.A limitation of this study is the absence of a placebo
rinse in the MOH control group. This was due to the in-ability to provide a placebo rinse within the timeframe theclinical site had available to conduct the study. The biasintroduced by the placebo effect in clinical trials has beenwell documented [32, 33], so it is possible that the act ofrinsing/not rinsing itself may have had some modest effecton outcomes. However, the results of the MOH group inthe current study are similar to results from controlgroups using mechanical oral hygiene plus placebo mou-thrinses in previously published studies [16, 34–37] andother studies have shown that placebo rinses with alcoholwere not statistically different from water control rinses.
ConclusionsAlcohol-free and alcohol-containing EO mouthrinses wereable to reduce plaque, gingivitis, and gingival bleeding incomparison to the use of mechanical oral hygiene alone ina six-month, randomized study. No significant differencesin efficacy in reducing plaque, gingivitis and gingivalbleeding were found between alcohol containing and alco-hol free essential oil mouthrinse formulations.
AbbreviationsACM: Alcohol-containing mouthrinse; ADA: American Dental Association;AE: Adverse Event; AFM: Alcohol-free mouthrinse; ANCOVA: Analysis ofcovariance; ANOVA: Analysis of Variance; BI: Bleeding index;CHX: Chlorhexidine; CI: Confidence Interval; CPC: Cetylpyridinium Chloride;EO: Essential Oils; FAS: Full Analysis Set; MGI: Modified Gingival Index;MOH: Mechanical oral hygiene; PI: Plaque index; SD: Standard Deviation
AcknowledgmentsEditorial support, in the form of medical writing, assembling tables based onauthors’ detailed directions, collating author comments, copyediting, factchecking, and referencing, was provided by Michelle Rebello, PhD, andNamita Bose, PhD, of Cactus Communications, and was funded by Johnsonand Johnson Consumer Inc. The authors would like to acknowledge LisaFitzgerald for managing the study, Jose Pelino for supporting the study,
Table 5 Post-hoc analysis: Fieller confidence interval (CI) for whole-mouth mean gingival indexa
Treatment Mean MGI
Month 1 Month 3 Month 6
AFM 1.832 ± 0.0144 1.772 ± 0.0176 1.614 ± 0.0179
ACM 1.838 ± 0.0144 1.768 ± 0.0177 1.581 ± 0.0181
AFM/ACM (90% CI) 0.997 (0.978, 1.015) 1.002 (0.979, 1.026) 1.021 (0.994, 1.048)
Data are adj. Mean ± standard error. ACM Alcohol-containing essential oil mouthrinse, AFM Alcohol-free essential oil mouthrinse, CI Confidence interval;aResults are based on ANCOVA model with term for treatment and baseline value as covariate
Lynch et al. BMC Oral Health (2018) 18:6 Page 8 of 10

Ratna Revankar for supporting study design and statistical analysis, and MaryLynn Bosma for critically reviewing the manuscript.
FundingFunding for this study was provided by Johnson & Johnson Consumer Inc.
Availability of data and materialsThe datasets used and/or analysed during the current study available fromthe corresponding author on reasonable request.
Authors’ contributionsDr. Lynch (MCL), Dr. Sheila Cortelli (SCC), Ms. Ricci-Nittel (DRN), Dr. Aquino (DRA)and Dr. Jose Cortelli (JRC) contributed to the design and execution of the study.Mr. McGuire (JAM) contributed to the study design and statistical analysis. Dr.Mordas contributed (CJM) to the formulation and related discussion. Dr. Zhang(JZ) led the development of the manuscript and served as the correspondingauthor. All authors contributed to the development of the manuscript andapproved the manuscript.
Ethics approval and consent to participateThe study protocol was approved by the Institutional Ethics Committee onresearch involving humans (CAAE: 20,402,713.1.00005501), University ofTaubate, Taubaté, São Paolo, Brazil. Written informed consent was obtainedfrom all subjects in agreement with the Declaration of Helsinki.
Consent for publicationNot applicable.
Competing interestsMichael Lynch, Danette Ricci-Nittel, James McGuire, Carolyn J. Mordas, andJane Zhang are employees of Johnson & Johnson Consumer Inc. Sheila CavalcaCortelli, Davi Romeiro Aquino and Jose Roberto Cortelli are employees ofUniversity of Taubate, Taubaté, São Paolo, Brazil and have received grants fromJohnson & Johnson Consumer Inc. to conduct this study. The authors declarethat they have no competing interests.
Publisher’s NoteSpringer Nature remains neutral with regard to jurisdictional claims inpublished maps and institutional affiliations.
Author details1Johnson & Johnson Consumer Inc.,, 199 Grandview Road, Skillman, NewJersey 08558, USA. 2Nucleus of Periodontal Research, Dental School,University of Taubate, Taubaté, São Paolo, Brazil.
Received: 17 May 2017 Accepted: 10 December 2017
References1. Escribano M, Figuero E, Martín C, Tobías A, Serrano J, Roldán S, Herrera D.
Efficacy of adjunctive anti-plaque chemical agents: a systematic review andnetwork meta-analyses of the Turesky modification of the Quigley and Heinplaque index. Journal of Clinical Periodontology. 2016;43:1059–73.
2. Gunsolley JC. A meta-analysis of six-month studies of antiplaque andantigingivitis agents. The journal of the American dental association. 2006;137:1649–57.
3. Gunsolley JC. Clinical efficacy of antimicrobial mouthrinses. Journal ofdentistry 2010;Vol. 38, pp. Suppl 1, S6–10.
4. Haps S, Slot D, Berchier C, van der Weijden G. The effect of cetylpyridiniumchloride-containing mouth rinses as adjuncts to toothbrushing on plaqueand parameters of gingival inflammation: a systematic review. InternationalJournal of Dental Hygiene. 2008;6:290–303.
5. Serrano J, Escribano M, Roldán S, Martín C, Herrera D. Efficacy of adjunctiveanti-plaque chemical agents in managing gingivitis: a systematic reviewand meta-analysis. Journal of clinical periodontology. 2015;42:S106–38.
6. Van Leeuwen M, Slot D, van der Weijden G. Essential oils comparedto chlorhexidine with respect to plaque and parameters of gingivalinflammation: a systematic review. Journal of periodontology. 2011;82:174–94.
7. Araujo MW, Charles CA, Weinstein RB, McGuire JA, Parikh-Das AM, Du Q,Zhang J, Berlin JA, Gunsolley JC. Meta-analysis of the effect of an essential
oil-containing mouthrinse on gingivitis and plaque. The journal of theAmerican dental association. 2015;146:610–22.
8. Chapple ILC, Van der Weijden F, Doerfer C, Herrera D, Shapira L, Polak D.Primary prevention of periodontitis: managing gingivitis. J Clin Periodontol2015;42(Suppl 16):S71–S76.
9. Van der Weijden FA, Van der Sluijs E, Ciancio SG, Slot DE. Can ChemicalMouthwash Agents Achieve Plaque/Gingivitis Control? Dent Clin North Am.2015;59:799–829.
10. Boyle P, Koechlin A, Autier P. Mouthwash Use and the Prevention of Plaque,Gingivitis and Caries. Oral Diseases. 2014;20:1–68.
11. Claffey N. Essential oil mouthwashes: a key component in oral healthmanagement. Journal of clinical periodontology. 2003;30:22–4.
12. Lemos-Júnior CA, Villoria GEM. Reviewed evidence about the safety of thedaily use of alcohol-based mouthrinses. Brazilian oral research. 2008;22:24–31.
13. Fourre T, Quieiroz D, Mordas CJ, McGuire JA Ilg D. In vitro efficacy of analcohol-free essential oil containing mouthrinse. Journal of Dental Research2011;Vol. 90, p. Abstr 793.
14. Ilg D, Junker L, Queiroz D, Mordas CJ, McGuire J, Ricci-Nittel D. In vivoefficacy of an alcohol-free essential oil containing mouthrinse. Journal ofDental Research 2012;Vol. 91, p. Abstr 791.
15. Charles CA, Amini P, Gallob J, Shang H, McGuire JA, Costa R. Antiplaque andantigingivitis efficacy of an alcohol-free essential-oil containing mouthrinse:a 2-week clinical trial. American Journal of Dentistry. 2012;25:195–8.
16. Cortelli SC, Cortelli JR, Shang H, McGuire JA, Charles CA. Long-termmanagement of plaque and gingivitis using an alcohol-free essential oilcontaining mouthrinse: a 6-month randomized clinical trial. AmericalJournal of Dentistry. 2013;26:149–55.
17. American Dental Association. Seal of Acceptance Program Guidelines forChemotherapeutic Products for Control of Gingivitis. s.l. : American DentalAssociation (ADA), 2011.
18. Lobene RR, Weatherford T, Ross NM, Lamm RA, Menaker L. A modifiedgingival index for use in clinical trials. Clinical preventive dentistry. 1986;8:3–6.
19. Turesky S, Gilmore ND, Glickman I. Reduced plaque formation by thechloromethyl analogue of victamine C. Journal of Periodontology. 1970;41:41–3.
20. Lobene RR, Soparkar P, Newman M. Use of dental floss. Effect on plaqueand gingivitis. Clinical preventive dentistry. 1982;4:5–8.
21. Tanner AC, Kent R Jr, Van Dyke T, Sonis ST, Murray LA. Clinical and other riskindicators for early periodontitis in adults. Journal of periodontology. 2005;76:573–81.
22. Ainamo J, Bay I. Problems and proposals for recording gingivitis and plaque.International dental journal. 1975;25:229–35.
23. Saxton CA, van der Ouderaa FJ. The effect of a dentifrice containing zinccitrate and Triclosan on developing gingivitis. J Periodontol Research. 1989;24:75–80.
24. Cortelli SC, Cortelli JR, Shang H, Costa R, Charles CA. Gingival health benefitsof essential-oil and cetylpyridinium chloride mouthrinses: a 6-monthrandomized clinical study. Americal journal of dentistry. 2014;27:119–26.
25. Fieller EC. The distribution of the index in a normal bivariate population.Biometrika. 1932;24:428–40.
26. Koch GG, Tangen CM. Nonparametric analysis of covariance and its role innoninferiority clinical trials. Drug information journal. 1999;33:1145–59.
27. Lamster IB, Alfano MC, Seiger MC, Gordon JM. The Effect of ListerineAntiseptic on Reduction of Existing Plaque and Gingivitis. Clinical preventivedentistry. 1983;5(6):12–6.
28. Van Leeuwen M, Slot D, van der Weijden G. The effect of an essential-oilsmouthrinse as compared to a vehicle solution on plaque and gingivalinflammation: a systematic review and meta-analysis. International Journalof Dental Hygiene. 2014;12:160–7.
29. Pan PC, Harper S, Ricci-Nittel D, Lux R, Shi W. In-vitro evidence for efficacyof antimicrobial mouthrinses. Journal of dentistry. 2010;38:S16–20.
30. Mordas CJ, Gambogi RJ. Non-alcohol bioactive essential oil mouth rinses.2015. US Patent 9084902:B2. https://www.google.com/patents/US9084902.
31. Mordas CJ, Queiroz DR, Tsai PB. Methods of preparing non-alcohol bioactiveessential oil mouth rinses. US Patent. 2014;20140322146:A1.
32. Brown WA. Expectation, the placebo effect and the response to treatment.Rhode Island medical journal. 2015;98:19–21.
33. Kienle GS, Kiene H. The powerful placebo effect: fact or fiction? Journal ofclinical epidemiology. 1997;50:1311–8.
34. Bauroth K, Charles CH, Mankodi SM, Simmons K, Zhao Q, Kumar LD. Theefficacy of an essential oil antiseptic mouthrinse vs. dental floss in
Lynch et al. BMC Oral Health (2018) 18:6 Page 9 of 10

controlling interproximal gingivitis: a comparative study. The Journal of theAmerican Dental Association. 2003;134:359–65.
35. Charles CA, Mostler K, Bartels L, Mankodi S. Comparative antiplaque andantigingivitis effectiveness of a chlorhexidine and an essential oilmouthrinse: 6-month clinical trial. Journal of clinical periodontology. 2004;31:878–84.
36. Charles CA, McGuire JA, Qaqish J, Amini P. Increasing antiplaque/antigingivitis efficacy of an essential oil mouthrinse over time: an in vivostudy. General Dentistry. 2013;61:23–8.
37. Sharma N, Charles CH, Lynch MC, Qaqish J, McGuire JA, Galustians JG,Kumar LD. Adjunctive benefit of an essential oil-containing mouthrinse inreducing plaque and gingivitis in patients who brush and floss regularly: asix-month study. The Journal of the American Dental Association. 2004;135:496–504.
• We accept pre-submission inquiries
• Our selector tool helps you to find the most relevant journal
• We provide round the clock customer support
• Convenient online submission
• Thorough peer review
• Inclusion in PubMed and all major indexing services
• Maximum visibility for your research
Submit your manuscript atwww.biomedcentral.com/submit
Submit your next manuscript to BioMed Central and we will help you at every step:
Lynch et al. BMC Oral Health (2018) 18:6 Page 10 of 10