The effects of community policies to reduce youth access to tobacco
6
The Effects of Community Policies to Reduce Youth Access to Tobacco Jean L. Forster, PhD, David M. Murray, PhD, Mark Wolfson, PhD, Therese M. Blaine, MA, Alexander C. Wagenaar, PhD, and Deborah J. Hennrikus, PhD Introduction A number of studies have shown that enforcing tobacco age-of-sale laws results in merchants' altering their practices and in reductions in illegal tobacco sales to minors.' It is believed that, consequently, young peo- ple who are experimenting with tobacco or considering initiation of tobacco use will be less likely to find a reliable and convenient source and thus will be discouraged from establishing the habit of regular use. New policies and enforcement practices also are believed to establish a normative climate in which provision of tobacco to minors and use of tobacco by youth are not acceptable.2 These assumptions led the US Department of Health and Human Services, in January 1996, to issue rules to implement the Synar amendment, which requires that each state receiving a federal Substance Abuse Preven- tion and Treatment Block Grant adopt and enforce a tobacco age-of-sale law and show progressive reductions in tobacco sales to minors.3 Following the same reasoning, the Food and Drug Administration issued regu- lations in August 1996 designed to restrict youth access to tobacco, including a require- ment that retailers request identification of purchasers, a ban on tobacco vending machines and self-service displays in most locations, and a prohibition against free tobacco samples.4 These actions came after a period of almost a decade during which sim- ilar provisions were adopted and/or enforced by hundreds of local jurisdictions and many state legislatures.'lo Despite this intensive activity, little is known about the effects of these policies on tobacco use by youth. Reductions in smok- ing prevalence among youth in single com- munities before and after policy adoption and/or enforcement have been reported.'"-'3 Recently, Rigotti et al. reported that after intensive enforcement of local youth access laws, retailer compliance with the laws was significantly higher in intervention commu- nities than in comparison communities, but youth smoking rates were unchanged.'4 Tobacco Policy Options for Prevention (TPOP) is a randomized community trial designed to test the effects of changes in local policies to limit youth access to tobacco. The study hypothesizes that local policy change brought about by community mobilization will have a positive effect on adolescent tobacco use through reductions in commer- cial availability. This paper reports the effects of the intervention on ordinances in TPOP communities, on cigarette purchase success by youth, and on adolescents' per- ceptions of availability and self-reported smoking behavior. Methods Design Fourteen communities in Minnesota were randomly assigned to experimental or control conditions. Criteria for inclusion of communities in the study were 90 or more students in each of grades 8, 9, and 10; loca- tion outside the primary Minnesota American Stop Smoking Intervention Study (ASSIST) geographic area; and no recent ordinance changes regarding tobacco. With the exception The authors, with the exception of Mark Wolfson, are with the Division of Epidemiology, School of Public Health, University of Minnesota, Minneapolis. Mark Wolfson is with the Department of Public Health Sciences, School of Medicine, Wake Forest University, Winston-Salem, NC. Requests for reprints should be sent to Jean L. Forster, PhD, Division of Epidemiology, School of Public Health, University of Minnesota, 1300 S Sec- ond St, Suite 300, Minneapolis, MN 55454-1015. This paper was accepted January 30, 1998. *: ~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~. . .. . .. ......... .... ....~~~~~~~~~~~~~~~~~~~~~. *: : :: :: :: :: :::e. ::. . ~~~~~~~~~~~~~~. . ... :::. :.. .:: ..... : .=-- -. '. ;:., :f ::":.;, .I; r. "Iff, .-. :.. ii V7 :, .::,: t:.'. Al, '.4s--f ff 'f="f -51.. ..f'r..": .......... 'if y::v ............... ji; American Joumal of Public Health 1193
Transcript of The effects of community policies to reduce youth access to tobacco

The Effects of Community Policies toReduce Youth Access to Tobacco
Jean L. Forster, PhD, David M. Murray, PhD, Mark Wolfson, PhD, Therese M. Blaine, MA,Alexander C. Wagenaar, PhD, and Deborah J. Hennrikus, PhD
Introduction
A number of studies have shown thatenforcing tobacco age-of-sale laws results inmerchants' altering their practices and inreductions in illegal tobacco sales to minors.'It is believed that, consequently, young peo-ple who are experimenting with tobacco orconsidering initiation of tobacco use will beless likely to find a reliable and convenientsource and thus will be discouraged fromestablishing the habit of regular use. Newpolicies and enforcement practices also arebelieved to establish a normative climate inwhich provision of tobacco to minors anduse of tobacco by youth are not acceptable.2These assumptions led the US Departmentof Health and Human Services, in January1996, to issue rules to implement the Synaramendment, which requires that each statereceiving a federal Substance Abuse Preven-tion and Treatment Block Grant adopt andenforce a tobacco age-of-sale law and showprogressive reductions in tobacco sales tominors.3 Following the same reasoning, theFood and Drug Administration issued regu-lations in August 1996 designed to restrictyouth access to tobacco, including a require-ment that retailers request identification ofpurchasers, a ban on tobacco vendingmachines and self-service displays in mostlocations, and a prohibition against freetobacco samples.4 These actions came after aperiod of almost a decade during which sim-ilar provisions were adopted and/or enforcedby hundreds of local jurisdictions and manystate legislatures.'lo
Despite this intensive activity, little isknown about the effects of these policies ontobacco use by youth. Reductions in smok-ing prevalence among youth in single com-munities before and after policy adoptionand/or enforcement have been reported.'"-'3Recently, Rigotti et al. reported that afterintensive enforcement of local youth access
laws, retailer compliance with the laws wassignificantly higher in intervention commu-nities than in comparison communities, butyouth smoking rates were unchanged.'4
Tobacco Policy Options for Prevention(TPOP) is a randomized community trialdesigned to test the effects of changes in localpolicies to limit youth access to tobacco. Thestudy hypothesizes that local policy changebrought about by community mobilizationwill have a positive effect on adolescenttobacco use through reductions in commer-cial availability. This paper reports theeffects of the intervention on ordinances inTPOP communities, on cigarette purchasesuccess by youth, and on adolescents' per-ceptions of availability and self-reportedsmoking behavior.
Methods
Design
Fourteen communities in Minnesotawere randomly assigned to experimental orcontrol conditions. Criteria for inclusion ofcommunities in the study were 90 or morestudents in each of grades 8, 9, and 10; loca-tion outside the primary Minnesota AmericanStop Smoking Intervention Study (ASSIST)geographic area; and no recent ordinancechanges regarding tobacco. With the exception
The authors, with the exception of Mark Wolfson, arewith the Division of Epidemiology, School of PublicHealth, University of Minnesota, Minneapolis. MarkWolfson is with the Department of Public HealthSciences, School of Medicine, Wake Forest University,Winston-Salem, NC.
Requests for reprints should be sent to Jean L.Forster, PhD, Division of Epidemiology, School ofPublic Health, University of Minnesota, 1300 S Sec-ond St, Suite 300, Minneapolis, MN 55454-1015.
This paper was accepted January 30, 1998.
*: ~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~. . .. . .. ......... ........~~~~~~~~~~~~~~~~~~~~~.*: : :: :: :: :: :::e. ::. . ~~~~~~~~~~~~~~. . ... :::. :.. .:: ..... :.=-- -. '. ;:., :f ::":.;, .I; r."Iff,.-. :.. ii V7 :, .::,: t:.'.Al,
'.4s--f
ff
'f="f
-51 .. ..f' r. .": ..........'if y::v ...............
ji;
American Joumal of Public Health 1193

Forster et al.
of school officials, from whom permissionwas needed to survey students, no one wascontacted in potential communities before theintervention was begun. Twenty-two schooldistricts (representing 22 communities) werecontacted to achieve the desired sample sizeof 14 communities. The 8 districts thatrefused our invitation cited the burden ofother surveys in the schools. Study communi-ties ranged in size from 3200 to 13 100 resi-dents, and each was the largest community inits rural county. Communities were stratifiedprior to randomization by population andbaseline student smoking rate. All communi-ties in the TPOP study required that tobaccoretailers be licensed at the beginning of thestudy, as did approximately 94% of Min-nesota communities.6
Intervention
The goals of the 32-month interventionwere to make tobacco access by youth asalient community issue, to change localordinances to more effectively restrict youthaccess to tobacco, to change retailers' andother adults' practices regarding provision oftobacco to youth, and to promote enforce-ment of tobacco age-of-sale laws. The inter-vention followed a direct action communityorganizing model that called for mobilizinglarge numbers of people, encouraging indi-viduals to take active roles as citizens and tohold leaders accountable for public deci-sions, highlighting conflicts between citi-zens' values and the status quo, and usingthat conflict to move individuals to action.15The process in each community was thesame, but the implementation varied as thecommunities developed ownership of theproject.
The intervention was staffed by a half-time community organizer in each commu-nity. After interviewing about 100 people intheir community, organizers recruited a teamof 8 to 15 members to lead the policy changeeffort. Team members came from varyingbackgrounds but participated as individuals,not organizational representatives.
The local team planned and executedactivities to raise community awarenessabout youth tobacco access and use and todevelop and demonstrate broad support forpolicy change. Teams conducted group pre-sentations, letter and petition drives, mediacampaigns, and tobacco purchase attemptswith underaged youth. Technical assistanceand materials were provided by Universityof Minnesota staff, but the local teamsdecided how to use these resources.
Teams drafted their own ordinancebased on models from other communities,introduced the ordinance to their city council,
and then marshaled the support of commu-nity leaders and the public for their proposal.Team members and community supporterslobbied city councilors, met with tobaccoretailers, and attempted to obtain the supportof law enforcement officials for the proposedordinance.
Following ordinance passage, teamsworked to ensure enforcement of the ordi-nances, including mobilizing citizens again ifthe police delayed enforcement. The inter-vention implementation and process evalua-tion measures have been described in moredetail elsewhere.'6
Evaluation
Data were collected regarding adoles-cent tobacco use, tobacco acquisition behav-iors, and perceptions about tobacco availabil-ity via surveys administered in spring 1993and at the end of the intervention in spring1996. University staff administered the sur-vey during school time to all students ingrades 8 through 10. Details of the surveyhave been reported elsewhere.2 The finalsample consisted of 6014 students in 1993and 6269 students in 1996. Surveys werecompleted by 91.8% of eligible students in1993 and 92.9% in 1996. More than 94% ofthe students in both the baseline and follow-up samples were White. There were no dif-ferences between students from treatmentand control communities at baseline on anyof the outcome variables.
Tobacco purchase attempts were com-pleted at all retail tobacco outlets in eachcommunity in June 1993 and June 1996, fol-lowing a standard protocol.2 A list of all busi-nesses (over the counter and vendingmachine) licensed to sell tobacco wasobtained from each city clerk. Two purchaseattempts were carried out at each business(one each on successive days) by 2 different15-year-old female buyers from outside thestudy communities. Buyers were accompa-nied by an adult employee of the study.Immediately following the purchase attempt,buyers and supervisors recorded data aboutthe purchase attempt and the store environ-ment, including location and types of tobaccodisplays.
Measures
Prevalence of smoking among studentswas based on a smoking index constructedby combining answers to questions aboutlifetime smoking, smoking in the previous 7days, and smoking in the previous 24hours.'7 This index was used to classify stu-dents as never, monthly, weekly, or dailysmokers. Students were asked to indicate
how hard or easy it would be to obtain ciga-rettes from a variety of sources. The propor-tion who responded 1 (not at all difficult) to3 (little difficulty) on a 7-point scale was cal-culated for each community. Students whohad smoked were also asked how they hadobtained their most recent cigarette. Thosewho selected either salesperson or vendingmachine were classified as having used acommercial source, while friend, sibling,parent, and another teenager or adult wereconsidered social sources. Students werealso asked how many times they had tried tobuy cigarettes in the past 30 days, and thepercentages of respondents who indicatedone or more attempt were calculated for eachcommunity.
Analysis
Mixed-model regression procedures,implemented via SAS PROC MIXED (ver-sion 6.11),18 were used in analyzing theschool survey data. For each dependent vari-able, the primary analysis was conducted in 2stages. The full model included fixed effectsfor condition, time, the time x conditioninteraction, and covariates identified asrelated to the dependent variable in questionbased on preliminary analyses (e.g., gender,age, grade, family structure, socioeconomicstatus, presence of an adult in the home afterschool, and discretionary income). Randomeffects were included for community (condi-tion), for the time X community (condition)interaction, and for residual error. Thereduced model eliminated covariates found tobe nonsignificant in the full model(P> .05). The intervention effect, estimatedas the net change over time between the 2conditions, was represented by the time xcondition interaction. The standard error forthat effect reflected the multiple sources ofrandom variation in the data and was basedon the time x community (condition) inter-action. Degrees offreedom were based on thenumber of communities. All random effectswere presumed to be independently and iden-tically distributed Gaussian effects, based onthe recent report that this assumption isappropriate for data from group-randomizedtrials even when the observation-level dataare dichotomous.'9
Following the primary analysis for theschool survey data, the reduced model wasrepeated after separate post hoc stratificationby gender and grade. In those models, fixed-effect terms were added for the condition Xstratum, time x stratum, and time x condi-tion X stratum interactions, and random-effect terms were added for the stratum xcommunity (condition) and time X stratumx community (condition) interactions. The
August 1998, Vol. 88, No. 81194 American Journal of Public Health

Youth Access to Tobacco
TABLE 1-Ordinances Passed in Tobacco Policy Options for Prevention (TPOP) Intervention Communities and PenaltiesApplied Following Enforcement: Minnesota, 1993-1996
Vending Self- Compliance PenaltyDate License Vendor Clerk Machine Service Purchaser Checks Following
Community Adopted Fee Penalty Penalty Ban Ban Penalty Required Enforcement
A 2/16/95 and3/11/96
B 8/11/95C 2/22/95D 7/10/95E 4/3/95F 12/12/94G 10/17/95
$50
$100$15$25$36$250$50
Yes
YesYesYesYesYesYes
Yes
NoYesNoYesYesNo
Yes No Yes
Yes YesYes YesYes YesYes YesYes NoYes Yes
NoYesNoYesYesNo
Yes
YesYesYesYesNoYes
Warning
FineFine
WarningFine
Fine/suspensionWarning
intervention effect in the stratified analyseswas represented by the time X condition Xstratum interaction and was assessed againstthe time x stratum x community (condition)interaction. Degrees of freedom were basedon the number ofcommunities and strata.
The tobacco purchase attempt datawere analyzed via similar procedures, modi-fied to reflect the slightly different designused in this survey. Fixed effects wereincluded for condition, time, and the time Xcondition interaction. Covariates were typeof outlet and age and gender of seller. Fordependent variables in which the valuecould vary between the 2 visits to each out-let, visit was included as a random effect.For all dependent variables, community(condition), time x community (condition),and residual error were included as randomeffects; in addition, the confederate's identi-fication number was included as a random-effect covariate. The intervention effect,estimated as the net change over timebetween the intervention and comparisonconditions, was represented by the time Xcondition interaction. The standard error forthat effect reflected the multiple sources ofrandom variation in the data and was basedon the time x community (condition) inter-action. Degrees of freedom were based onthe number ofcommunities.
Results
By the end of the intervention period,all 7 TPOP intervention communities hadadopted a comprehensive ordinance aimed atensuring merchant compliance with tobaccoage-of-sale laws and reducing youth accessto tobacco. The provisions of the ordinancesare shown in Table 1. All communitiesincreased the license fee to cover administra-tive costs, added a graduated system of civilpenalties for the license holder, and bannedtobacco vending machines, and 6 requiredthat at least 2 unannounced compliancechecks be carried out annually. In addition, 5
communities prohibited self-service displaysof tobacco products, and 4 included fines forboth salespersons who made illegal sales andminors who attempted to purchase tobacco.By the end of the intervention period, com-pliance checks had been carried out bypolice in all 7 intervention communities,according to police records. In 4 communi-ties, violators were given fines or licensesuspensions; in the other 3 communities,only warnings were issued.
During the intervention period, 3 con-trol communities adopted modifications oftheir tobacco ordinance: one communityadopted a self-service ban to take effect inAugust 1997, another adopted civil penaltiesfor tobacco sales to minors, and a thirdadopted a model ordinance proposed by thetobacco retail industry. The latter prohibitedtobacco self-service displays and vendingmachines except when they were in view ofan employee and permitted the communityto conduct compliance checks. Ordinances
30
25
20
15 -
10
5.0
passed in the control communities wereweaker and much less comprehensive thanthose passed in intervention communities.
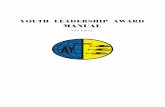
As Figure 1 indicates, the interventionresulted in a lower net prevalence of smok-ing in the intervention communities than inthe control communities. The prevalence ofdaily, weekly, and monthly smoking climbedsharply in the control communities over thecourse of the study. However, the increase inthe intervention communities was less pro-nounced, with net differences between inter-vention and control communities of -4.9%for daily smoking (95% confidence interval[CIl= -9.0, -0.7), -5.6% for weekly smok-ing (95% CI = -11.7, 0.5), and -6.7% formonthly smoking (95% CI = -14.9, 1.5). Inaddition to the main effects models, stratifiedmodels were examined to determine whetherthe effects were homogeneous across genderand grade. The intervention was equallyeffective in slowing the rate of increase inmale and female students. For monthly and
* 1993* 1996
I CDaily Smokingnet difference = -4.995% CI = -9.0, -0.7
I CWeekly Smokingnet difference = -5.695% CI = -1 1.7,+0.5
I CMonthly Smoldngnet difference - -6.795% CI = -14.9, +1.5
I = InterventionC = Control
FIGURE 1-Prevalence of smoking, by time and treatment condition: TobaccoPolicy Options for Prevention (TPOP) intervention, Minnesota,1993-1996.
American Journal of Public Health 1195August 1998, Vol. 88, No. 8

Forster et al.
TABLE 2-Perceived Availability and Sources of Cigarettes, by Time and Treatment Condition (Student Survey): Minnesota,1993-1996
Intervention, % Control, % Net 95% ConfidenceStratum 1993 1996 1993 1996 Difference, % Interval
High perceived availability fromsocial sources
High perceived availability fromcommercial sources
Commercial source for mostrecent cigarette (smokers)
Any purchase attempt in past month
weekly smokers, the intervention was alsoequally effective across grades 8 through 10.For daily smokers, there was a nonsignifi-cant trend toward greater effectivenessamong younger students.
Differences in perceived availability andcigarette acquisition pattems reported on thestudent survey were also noted (Table 2). Theintervention had no effect on the perceivedavailability of cigarettes from social sources,with most students in both conditions report-ing that it was easy to obtain cigarettes fromfamily members, friends, or acquaintances.Perceived availability of cigarettes from com-mercial sources showed a net decrease amongstudents in the intervention condition. Therewas a net decline among boys in reporting acommercial source for their most recent ciga-rette; the trend among girls was also favor-able. The proportion of adolescents whoreported at least one purchase attempt in theprevious month declined in the interventioncommunities, while it increased in the controlcommunities. This was true among studentswho had smoked at least once in the previousmonth as well as among all students.
There was a sharp decline in the suc-cess of underaged confederate buyers inpurchasing cigarettes from 1993 to 1996(P = .00 14) (Table 3). The trend in purchasesuccess differences between interventionand control communities was consistentwith expectations but statistically nonsignif-icant. Similarly, there was a sharp increasein the proportion of purchase attempts inwhich the seller requested age identification(P = .0099); that trend also was the same inboth the intervention and control communi-ties. The proportion of outlets that stored cig-arettes behind the counter or in locked cabi-nets increased sharply in the interventioncommunities. Finally, there was a modestincrease in the proportion of outlets thatposted signs announcing state, local, and storeage-of-sale policies in the intervention com-munities relative to the control communities.
In summary, the results indicate thatcomprehensive ordinances passed in all
All 79.9 85.1 81.2 84.1
All 79.8 77.2 80.1 83.9
Male studentsFemale studentsAllSmokers
2.3
-6.4
28.5 19.5 24.0 27.2 -12.217.3 14.3 18.0 20.5 -5.59.0 6.5 8.0 9.9 -4.4
34.9 23.8 31.8 33.3 -12.5
intervention communities resulted in a lowersmoking prevalence among young adoles-cents in these communities than in controlcommunities. This net reduction in smokingprevalence was associated with a lower per-ceived availability of tobacco from commer-cial sources, a reduction in commercialsources of cigarettes, and fewer cigarettepurchase attempts reported by adolescents inintervention than in control communities.Cigarettes were more likely to be displayedbehind a counter in intervention communi-ties, and stores were more likely to postsigns about age-of-sale policies.
Discussion
This study provides evidence that acommunity mobilization intervention result-ing in policy adoption and enforcement toreduce youth access to tobacco can affectadolescent smoking rates. The effects wereconsistent across grades and genders. Amongdaily smokers, who would be expected to tryto purchase cigarettes most often, the effectwas greater for the younger students, whoseunderage status would be more apparent tomerchants. In addition, students in the inter-vention communities believed cigarettes weremore difficult to buy and were less likely totry to purchase cigarettes.
The magnitude of change in adolescentsmoking prevalence due to the TPOP inter-vention (a net reduction in daily smoking of28% of the baseline rate) is considerablylarger than the average effect sizes reportedfor school-based programs using social influ-ence or social or other skills-focused curric-ula and equal to the effects reported by themost effective programs.20 The interventionhad these effects even though it did notinclude any components targeted directly atadolescents.
Although more than 6000 children weresurveyed in both 1993 and 1996, all of theanalyses were conducted at the level of the
-2.5, 7.1
-12.6, -0.1
-21.4, -3.0-14.8, 3.9-8.2, -0.7
-25.6, 0.5
community (as was appropriate given thatcommunity was the unit of randomization).Thus, the degrees of freedom for all inter-vention effects reported here were based onthe number of communities in the study (14)rather than the number of students. Thisapproach to the analysis both protected thetype I error rate and provided the statisticalbasis for generalizing to communities similarto those included in the study.21 We believethat even though the confidence intervalsincluded zero at the upper bound, the differ-ences in weekly and monthly smokingprevalence in this study are noteworthygiven the limited degrees of freedom.
Our findings suggest that refusals bysellers at the time of purchase attempts byyoung people do not account for the loweradolescent smoking rates observed in theintervention communities. Both interventionand control communities showed reductionsin the proportion ofbusinesses that sold ciga-rettes to underaged study confederates. Sales-people in both treatment and control commu-nities were equally likely to ask thesestudents for age identification. However, thecommunity mobilization and awareness cam-paigns that were part of the intervention, aswell as the policies that were adopted, mayhave increased the perception among stu-dents that they would not be able to purchasetobacco and/or discouraged them from tryingto do so. Businesses in the intervention com-munities were more likely to display ciga-rettes behind a counter, thus requiring thatindividuals request the products from sales-people, and they were more likely to postsigns announcing local or store policiesregarding sale of tobacco to minors. Theseactions may account for the findings that stu-dents in the intervention communities wereless likely to try to purchase cigarettes thanstudents in control communities and that theybelieved cigarettes were more difficult to pur-chase. These findings are consistent with pre-vious studies reporting that stores with self-service displays of tobacco products are morelikely to sell tobacco to minors.222
1196 American Joumal of Public Health August 1998, Vol. 88, No. 8

Youth Access to Tobacco
TABLE 3-Purchase Success and Transaction Characteristics, by Time and Treatment Condition
Intervention, % Control, % Net 95% ConfidenceStratum 1993 1996 1993 1996 Difference, % Interval
Purchase success All 38.8 4.9 41.9 12.5 -4.5 -18.7, 9.7Over the counter 36.7 3.1 41.0 8.8 -1.5 -11.7, 8.6
Identification requested Over the counter 62.3 86.3 58.9 83.4 0.0 -11.2,10.3Cigarettes stored behind counter Over the counter 52.6 83.8 55.2 57.2 29.2 3.1, 55.3Signs posted on state, local, All 10.9 23.4 9.2 7.7 14.1 -3.0, 31.1and store age-of-sale policies
The reduction in tobacco purchase suc-cess across both the intervention and controlcommunities is not surprising given the levelof attention to the issue of youth access totobacco in Minnesota recently. During theintervention period (1993 through 1996), astrong effort to pass state legislation toreduce youth access to tobacco was accom-panied by statewide media attention. Stateretailers' associations and the tobacco indus-try launched statewide campaigns to educateretailers and their employees about the Min-nesota tobacco age-of-sale law and ways toavoid violating it. In addition, Minnesotaparticipates in both the ASSIST and Smoke-less States projects. Moreover, local healthagencies throughout the state became inter-ested in the issue and began implementingtobacco purchase attempts in their communi-ties. Other recent studies also suggest thatretailers respond to the changing policy andenforcement climate of a region rather thansimply to local efforts.23'24
Results from this study emphasize thevalue of local policy changes in the contextof intensive education for action, publicdebate, and involvement of hundreds ofcommunity members. In addition to the pol-icy and practice changes and law enforce-ment efforts, the mobilization processchanged perceptions of availability and (verylikely) community norms about tobaccosales to and use by youth. The effects onyouth tobacco use seen in this study must beattributed to effects of the local policies andtheir enforcement in the context of an inten-sive community organizing effort.
Our results are relevant to the debateamong tobacco control advocates aboutwhether an emphasis on reducing youthaccess to tobacco is warranted given avail-able evidence concerning its effectiveness inreducing youth tobacco use.2927 This debateintensified in light of the finding of Rigottiand colleagues'4 that enforcement of thetobacco age-of-sale law was not associatedwith a reduction in adolescent smokingprevalence. In the Rigotti et al. study,
enforcement efforts resulted in a reduction intobacco sales to minors to about 20% in the 3intervention towns (vs 54% in control towns)after 1 year. In the TPOP study, purchase suc-cess in the intervention communities wasreduced to about 5%, as compared with12.5% in the control communities. Becauseof the intensive activity leading to policychanges in the study communities, our resultsdo not directly predict the effectiveness ofefforts focused specifically on enforcement.It is possible that the level of reduction inpurchase success achieved in our study iswhat is necessary to effectively reduce youthaccess, or it may be that an intensive commu-nity mobilization intervention is needed tochange the perceptions and behaviors ofyoung people.
Conclusions from this study are limitedby the fact that our results reflect short-termeffects only, based on data collected immedi-ately following the intervention. Further-more, all of the communities in the study arelocated in one state, and all are small townsin rural counties with relatively homoge-neous, almost entirely White populations.Clearly, longer-term studies in a variety ofcommunities are needed. Because of limita-tions in the standard purchase attemptmethodology, we cannot be sure whether ornot commercial access to tobacco was actu-ally reduced. Changes in purchase successrates in intervention communities cannot bereliably distinguished from temporal trends.Nevertheless, these results provide encourag-ing evidence that efforts to limit commercialaccess to tobacco by youth represent aneffective component of a multidimensionalapproach to reducing tobacco use. El
AcknowledgmentsThis study was supported by grant CA54893 fromthe National Institutes of Health.
Portions of these data were presented at the125th Annual Meeting of the American Public HealthAssociation, November 1997, Indianapolis, Ind.
We wish to acknowledge the community orga-nizers for their work on the project.
References1. Forster JL, Wolfson M. Youth access to
tobacco: policies and politics. Annu Rev PublicHealth. 1998;19:203-235.
2. Forster JL, Wolfson M, Murray DM, WagenaarAC, Claxton AJ. Perceived and measuredavailability of tobacco to youth in fourteenMinnesota communities: the TPOP study. Am JPrev Med. 1997;13:167-174.
3. US Dept of Health and Human Services.Tobacco regulation for substance abuse preven-tion and treatment block grants: final rule. Fed-eral Register 1996;61:1491-1509.
4. Kessler DA, Witt AM, Barnett PS, et al. TheFood and Drug Administration's regulation oftobacco products. N Engl J Med. 1996;335:988-994.
5. Shelton DM, Alciati MA, Chang MM, et al.State law on tobacco control-United States,1995. MMWR Morb Mortal Wkly Rep. 1995;44:1-30.
6. Forster JL, Komro K, Wolfson M. Survey ofcity ordinances and local enforcement regard-ing commercial availability of tobacco tominors. Tob Control. 1996;5:46-51.
7. State Tobacco Control Highlights 1996.Atlanta, Ga: Centers for Disease Control andPrevention; 1996.
8. Downey LA, Gardiner JA, Kreps BC. Reduc-ing Youth Access to Tobacco: A Partial Inven-tory ofState Initiatives. Chicago, Ill: Universityof Illinois at Chicago; 1996.
9. Tobacco Products Liability Project of theTobacco Control Research Center Inc. StopCigarette Sales to Kids: A Fifty State LegalManual. Boston, Mass: Northeastern Univer-sity School of Law; 1996.
10. State Legislated Actions on Tobacco Issues.Washington, DC: Coalition on Smoking orHealth; 1995.
11. DiFranza JR, Carlson RR, Caisser RE Jr.Reducing youth access to tobacco. Tob Control.1992;1:59.
12. Jason LA, Ji PY, Anes MD, Birkhead SH.Active enforcement of cigarette control laws inthe prevention of cigarette sales to minors.JAMA. 1991;266:3159-3161.
13. Hinds MW. Impact of local ordinance banningtobacco sales to minors. Public Health Rep.1992;107:355-358.
14. Rigotti NA, DiFranza JR, YuChiao C, TisdaleT, Kemp B, Singer DE. The effect of enforcingtobacco-sales laws on adolescents' access totobacco and smoking behavior. N Engl J Med.1997;337: 1044-1051.
August 1998, Vol. 88, No. 8 American Journal of Public Health 1197

Forster et al.
15. Hanna MG, Robinson B. Strategiesfor Com-munity Empowerment. Lewiston, NY: EdwinMellen Press; 1994.
16. Blaine TM, Forster JL, Hennrikus D, O'Neil S,Wolfson M, Phamn H. Creating tobacco controlpolicy at the local level: implementation of adirect action organizing approach. Health EducBehav. 1997;24:640-651.
17. Pechacek TF, Murray DM, Luepker RV, Mittel-mark MB, Johnson CA, Shultz JM. Measure-ment of adolescent smoking behavior: rationaleand methods. JBehav Med. 1984;7:123-140.
18. SAS/STAT Software: Changes and Enhance-ments, through Release 6.11. Cary, NC: SASInstitute Inc; 1990.
19. Hannan PJ, Murray DM. Gauss or Bernoulli? AMonte Carlo comparison of the performance of
the linear mixed model and the logistic mixedmodel analyses in simulated community trialswith a dichotomous outcome variable at theindividual level. Eval Rev. 1996;20:338-352.
20. Rooney BL, Murray DM. A meta-analysis ofsmoking prevention programs after adjustmentfor errors in the unit of analysis. Health Educ Q.1996;23:48-64.
21. Murray DM. Design and Analysis of Group-Randomized Trials. New York, NY: OxfordUniversity Press Inc; 1998.
22. Wildey MB, Woodruff SI, Pampalone SZ,Conway TL. Self-service sale of tobacco: howit contributes to youth access. Tob Control.1995;4:355-361.
23. Centers for Disease Control and Prevention.Estimates of retailers willing to sell tobacco to
minors-California, August-September 1995and June-July 1996. MMWR Morb MortalWkly Rep. 1996;45:1095-1099.
24. Cummings KM, Hyland A, Saunders-Martin T,Perna J, Coppola PR, Pechacek TF. Evaluation ofan enforcement program to reduce tobacco salesto minors. Am JPublic Health. 1998;88:932-936.
25. Glantz SA. Preventing tobacco use-the youthaccess trap. Am JPublic Health. 1996;86:156-157.
26. Lumpkin JR, Rice JR. State health agencies'role in a more balanced and sophisticatedtobacco control program. Am J Public Health.1996;86:1482.
27. Feder BJ. Battle on youth smoking brings hopeand caution. New York Times. November 19,1996:A13-A15.
War and Public HealthEdited by Barry S. Levy and Victor W. Sidel, 1996
For health professionals, educators or students of public health ormedicine, people Involved in intemational studies, diplomacy or the military
his is the first book that documents the impact of war on public health, and describes whathealth professionals can do to prevent war and to minimize its consequences. The effects of
war on health, human rights, and the environment are comprehensively described. Among the 26chapters are chapters on the Vietnam War, the Persian Gulf War, and the war in Central America, aswell as the roles of health professionals in the prevention of war and during war. Also discussed arethe health effects of nuclear, chemical and biological weapons systems and the public healthconsequences. The book deals with both the direct consequences of the use of conventional weaponsand the role of the international arms trade, including the diversion of resources that could otherwisebe used for health and human welfare. Separate chapters cover particularly vulnerable populations,such as women, children, and refugees.
Published by Oxford University Press in cooperation with APHA1996 * 398 pp. * hardcover * ISBN: 0-19-510814-0
American Public Health AssociationPublications SalesP.O. Box 753, Waldorf, MD 20604-0753Tel: 301/893-1894; Fax: 301/843-0159
1198 American Journal of Public Health August 1998, Vol. 88, No. 8