The Effect of Multidimensional Exercises on Balance, Mobility ...
12
The Effect of Multidimensional Exercises on Balance, Mobility, and Fall Risk in Community-Dwelling Older Adults Background and Purpose. This prospective clinical investigation exam- ined the effects of a multidimensional exercise program on balance, mobility, and risk for falls in community-dwelling older adults with a history of falling. Factors used to predict adherence and a success- ful response to exercise were identified. Subjects. A total of 105 community-dwelling older adults (165 years of age) with a history of two or more falls in the previous 6 months (no neurologic diagnosis) participated. They were classified into (1) a control group of fallers (n=21), (2) a fully adherent exercise group (n=52), and (3) a partially adherent exercise group (n=32). Methods. Following evaluation, each patient received an individualized exercise program addressing the impairments and functional disabilities identified during the assess- ment. The control group received no intervention. Changes in perfor- mance on five clinical tests of balance and mobility and fall risk were compared among groups. Results. Both exercise groups scored better than the control group on all measures of balance and mobility. Although both exercise groups showed a reduction in fall risk com- pared with the control group, the greatest reduction was found in the fully adherent exercise group. Factors associated with successful response to exercise included degree of adherence to exercise pro- gram and pretest score on the Tinetti Mobility Assessment. Conclusion and Discussion. Exercise can improve balance and mobility function and reduce the likelihood for falls among community-dwelling older adults with a history of falling. The amount of exercise needed to achieve these results, however, could not be determined from this study. [Shumway-Cook A, Gruber W, Baldwin M, Liao S. The effect of multidimensional exercises on balance, mobility, and fall risk in community-dwelling older adults. Phys Ther. 1997;77:46-57.1 Key Words: Balance, Exercise, Fall prevention. Anne Shumway-Cook William Gmber Margaret Baldwin Shiquan Liao Physical Therapy . Volume 77 . Number 1 . January 1997 Downloaded from https://academic.oup.com/ptj/article/77/1/46/2633046 by guest on 31 May 2022
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of The Effect of Multidimensional Exercises on Balance, Mobility ...
The Effect of Multidimensional Exercises on Balance, Mobility, and Fall Risk in Community-Dwelling Older Adults
Background and Purpose. This prospective clinical investigation exam- ined the effects of a multidimensional exercise program on balance, mobility, and risk for falls in community-dwelling older adults with a history of falling. Factors used to predict adherence and a success- ful response to exercise were identified. Subjects. A total of 105 community-dwelling older adults (165 years of age) with a history of two or more falls in the previous 6 months (no neurologic diagnosis) participated. They were classified into (1) a control group of fallers (n=21), (2) a fully adherent exercise group (n=52), and (3) a partially adherent exercise group (n=32). Methods. Following evaluation, each patient received an individualized exercise program addressing the impairments and functional disabilities identified during the assess- ment. The control group received no intervention. Changes in perfor- mance on five clinical tests of balance and mobility and fall risk were compared among groups. Results. Both exercise groups scored better than the control group on all measures of balance and mobility. Although both exercise groups showed a reduction in fall risk com- pared with the control group, the greatest reduction was found in the fully adherent exercise group. Factors associated with successful response to exercise included degree of adherence to exercise pro- gram and pretest score on the Tinetti Mobility Assessment. Conclusion and Discussion. Exercise can improve balance and mobility function and reduce the likelihood for falls among community-dwelling older adults with a history of falling. The amount of exercise needed to achieve these results, however, could not be determined from this study. [Shumway-Cook A, Gruber W, Baldwin M, Liao S. The effect of multidimensional exercises on balance, mobility, and fall risk in community-dwelling older adults. Phys Ther. 1997;77:46-57.1
Key Words: Balance, Exercise, Fall prevention.
Anne Shumway-Cook
William Gmber
Margaret Baldwin
Shiquan Liao
Physical Therapy . Volume 77 . Number 1 . January 1997
Dow
nloaded from https://academ
ic.oup.com/ptj/article/77/1/46/2633046 by guest on 31 M
ay 2022

lie risk for falls increases dramatically with age.'-3 Approximately 25% to 35% of people over the age of 65 years experiences one or more falls each The consequences of
falls among older adults are devastating. In people over the age of 65 years, falls are the leading cause of death from injury." Falls also lead to substantial morbidity among older adults. Nearly 70% of all emergency department visits by people over the age of 75 years are related to falls." Forty percent of hospital admissions in this age group are the result of fall-related injuries, resulting in an average length of stay of 11.6 days.6 Approxi~nately one half of older adults hospitalized for fall-related injuries are discharged to nursing homes.7
Because of the devastating effects of falls among older adults, risk factors for predicting falls and fall-related injuries have been studied extensively."-" Factors con- tributing to increased risk for falls have been categorized into intrinsic factors (those internal to the individual) and extri~nsic factors (those associated with environmen- tal features) . I 2 Intrinsic factors associated with increased likelihood for falls include changes in muscular strength,'"14 decreased joint flexibility,'~~~rnpaired visual sensation,I7 a decline in vestibular f u n c t i ~ n , ' ~ . ~ ~ and decreased vibratory sense.ZO
R e ~ e a r c h e r s ~ ~ ) . ~ , ~ ' ~ have shown that among intrinsic factors, impaired stance balance and mobility greatly increase the probability for falls, fractures, and func- tional dependency among older adults. It has been estimated that between 10% and 25% of all falls are associated with poor balance and gait abn0rmalities.2~ Deficits within the postural control system controlling stance balance that have been reported include changes in the temporal and spatial sequencing of muscles responding to loss of balan~e,Z+.2~ increased dependence on visual cues for postural ~ o n t r o l , ~ " 2 h n d a decreased ability to organize and select sensory information for postural control. 2"27
Despite the apparent relationship between impaired balance and increased likelihood for falls among elderly individuals, studies examining the effects of exercise on improving balance and reducing risk for falls in this population have had mixed result^.^^-^^ One possible reason for this inconsistency is the variation in exercise programs utilized in these studies. In addition, many researchers have incorporated exercise into a multifac- eted intervention approach, making it difficult to deter- mine the relative contribution of exercise to improving balance and decreasing fall risk.'
The purpose of this study was to prospectively examine the effects of a multidimensional exercise program on balance, mobility, and risk for falls among community- dwelling older adults with a history of falls. The research questions were: (1) Does a multidimensional exercise program improve stance balance and mobility and reduce the likelihood for falls in older community- dwelling adults? (2) What factors can be used to predict a successful response to exercise, defined as a reduction in probability for falls? and (3) What factors can be used to predict adherence to an exercise program for elderly persons?
Method
Subjects The quasi-experimental study involved two groups of community-dwelling older adults, over the age of 65 years, with no known neurologic diagnoses and a self- reported history of two or more falls in the previous 6 months. Subjects involved in the exercise program were selected from among the first 101 patients referred by their physicians to the Safety and Gait Enhancement Program (a fall-intervention program for older adults) of Northwest Hospital (Seattle, Wash) who met the study criteria and agreed to participate. Seventeen participants (14%) in the exercise program dropped out within the first 3 weeks; therefore, the number of exercisers
A Shumway-Cook, PhD, PT, is Research Coordinator, Department of Physical Therapy, Northwest Hospital, 10330 Meridian Ave N, Suite 110, Seattle, WA 98133 (USA) ([email protected]). Address all correspondence to Dr Shumway-Cook.
W Ckuber. MD, is Medical Director, Safety and Gait Enhancement Program, Northwest Hospital.
M Baldwin, PT, is Staff Physical Therapist, Department of Physical Therapy, Stevens Memorial Hospital, 21601 76th Ave W, Edmonds, WA 98026.
S Liao. PhD, is Biostatistician, CARE Management Department, Northwest Hospital.
This study was approved by the Institutional Review Board at Northwest Hospital.
Results frcm this study were presented at the Comhined Sections Meeting of the American Physical Therapy Association; February 8-12, 1995; Reno, NV. In addition, they have appeared in abstract form in the June 1995 issue of Neurolog, w o r t .
This investigation was supported by a grant from Northwest Hospital Foundation, Seattle, WA.
7717, artzclc war submzttrd A t ~ p s t 29, 1995, and was acreptrrl March 27, 1996.
Physical Therapy . Volume 77 . Number 1 . January 1997 Shumway-Cook et 01.47
Dow
nloaded from https://academ
ic.oup.com/ptj/article/77/1/46/2633046 by guest on 31 M
ay 2022
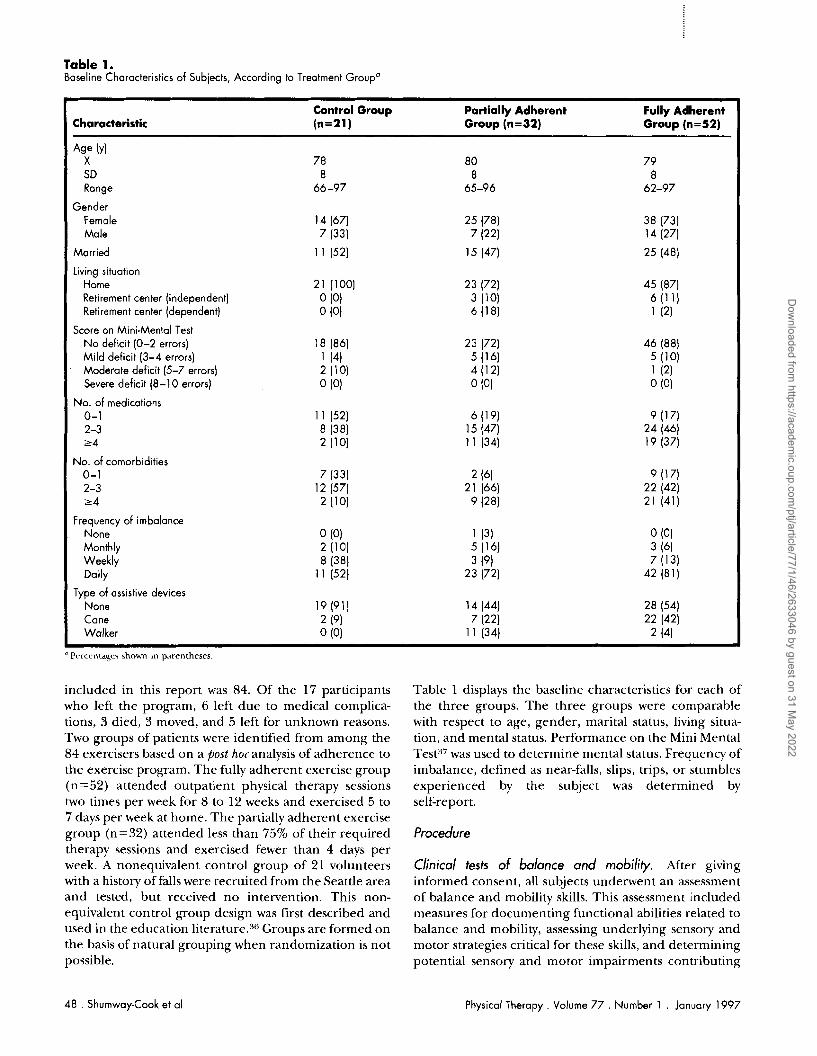
Table 1. Baseline Characteristics of Subiects, According to Treatment Groupo
Control Group Paltially Adherent Fully Adherent Characteristic (n=2l) Group (n=32) Group (n=52)
Ag_e (Y) X 78 80 79 SD 8 8 8 Range 66-97 65-96 62-97
Gender Female 14 (67) 25 (78) 38 (73) Male 7 (33) 7 (22) 1 4 (27)
Married 11 (52) 15 (47) 25 (48)
living situation Home 21 (100) 23 (72) 45 (87) Retirement center (independent) 0 (0) 3 (10) 6 (1 1 ) Retirement center (dependent) 0 (0) 6 (18) 1 (2)
Score on Mini-Mental Test N o deficit (0-2 errors) 18 (86) 23 (72) 46 (88) Mild deficit (3-4 errors) 1 (4) 5 (16) 5 (10) Moderate deficit (5-7 errors) 2 (10) 4 ( 1 2) 1 (2) Severe deficit (8-10 errors) 0 (0) 0 (0) 0 (0)
No. of medications 0-1 1 1 (52) 6 (19) 9 (171 2-3 8 (38) 15 (47) 24 (46) , 2 4 2 (10) 1 1 (34) 19 (37)
No. of comorbidities 0-1 7 (33) 2 (61 9 (1 7) 2-3 12 (57) 21 (66) 22 (42) r 4 2 (10) 9 (28) 21 (41)
Frequency of imbalance None 0 (0) 1 (3) 0 (0) Monthly 2 (10) 5 (16) 3 (6) Weekly 8 (38) 3 (9) 7 (131 Daily 11 (52) 23 (72) 42 (81)
Type of assistive devices None 19 (91) 14 (44) 28 (54) Cane 2 (9) 7 (22) 22 (42) Walker 0 (0) 1 1 (34) 2 (41
"Pr~crntacp shown in p~rentheses
included in this report was 84. Of the 17 participants who left the program, 6 left due to medical complica- tions, 3 died, 3 moved, and 5 left for unknown reasons. Two groups of patients were identified from among the 84 exercisers based on a post hoc analysis of adherence to the exercise program. The fully adherent exercise group (n=52) attended outpatient physical therapy sessions two times per week for 8 to 12 weeks and exercised 5 to 7 days per week at home. The partially adherent exercise group (n=32) attended less than 75% of their required therapy sessions and exercised fewer than 4 days per week. A nonequivalent control group of 21 volunteers with a history of falls were recruited from the Seattle area and tested, but received no intervention. This non- equivalent control group design was first described and used in the education literat~re.:~Wroups are formed on the basis of natural grouping when randomization is not possible.
Table 1 displays the baseline characteristics for each of the three groups. The three groups were comparable with respect to age, gender, marital status, living situa- tion, and mental status. Performance on the Mini Mental TesP7was used to determine mental status. Frequency of imbalance, defined as near-falls, slips, trips, or stumbles experienced by the subject was determined by self-report.
Procedure
Clinical tests of balance and mobility. After giving informed consent, all subjects underwent an assessment of balance and mobility skills. This assessment included measures for documenting functional abilities related to balance and mobility, assessing underlying sensory and motor strategies critical for these skills, and determining potential sensory and motor impairments contributing
48 . Shumway-Cook et al Physical Therapy . Volume 77 . Number 1 . January 1997
Dow
nloaded from https://academ
ic.oup.com/ptj/article/77/1/46/2633046 by guest on 31 M
ay 2022

to instability and gait impairment~.~s Subjects provided a medical history and a self-report of fall and balance history. Subjects then completed the Mini Mental Test and the Balance Self-Perceptions Test, a short question- naire in which subjects rate their perceived confidence when performing common activities of daily living. Sub- jects were asked to rate (on a scale of 1-5, where 1 =no confidence and 5=extreme confidence) their degree of confidence in performing 20 basic activities of daily living ancl instrumental activities of daily living without fear of loss of balance. The questionnaire was a modifi- cation of one developed by Tinetti et alS9 in their study examining the relationship between fear of falling and measures of basic and instrumental activities of daily living.
In addition to the self-report measure, the Balance Self-Perceptions Test, performance-based tests were cho- sen to evaluate functional balance and walking skills. The Berg Balance Scale rates balance during the perfor- mance of 14 tasks, including sitting, standing, reaching, leaning over, turning, and stepping.40 The Three-Minute Walk Test requires subjects to walk at their preferred pace for 3 minutes over a 91.4m (300-ft) indoor course.3s The course is carpeted, and involves four different turns. Balance and gait deviations were scored using the Performance-Oriented Mobility Test.41 The Dynamic Gait Index was used to evaluate the ability to adapt gait to changes in task demands, including chang- ing speeds, head turns in the vertical or horizontal direction, stepping over or around obstacles, and stair ascent and de~cent .~s All clinical tools have previously been shown to have good interrater and test-retest reliabilit~.~~-4l
Tests to document sensory and motor impairments included a manual muscle test of strength,4* range of
static postural alignment in sitting and stand- ing positions," presence or absence of coordinated multijoint movements for recovery of perturbed stance balan~e,"~ cerebellar coordination, sensation-vibration, stereognosis, vision, and presence or absence of dizziness.44
All subjects involved in the exercise program were reassessed using the same testing format approximately 8 to 12 weeks following the initial evaluation, just prior to discharge. Control group subjects were reassessed approximately 8 weeks following the initial evaluation.
Reliability testing of assessment protocol. Five physical therapists participated in this study. To ensure reliability and consistency among therapists, all were trained in both the evaluation and treatment procedures. A conve- nience sample of five community-dwelling older adults (3 female, 2 male, mean age=75 years) with varying
balance abilities were used to test reliability of the assessment procedures in a pilot study. Each of the therapists assessed the subjects and was blinded to the results of the other therapists' assessments. Two of the subjects underwent two tests, 1 week apart, in order to determine test-retest reliability.
Interrater reliability was assessed using the ratio of subject variability to the total variability (ie, variability among subjects divided by total variability). A large ratio close to 1.0 would indicate high interrater reliability. There were two components of variability, one contrib uted by the differences among the subjects and the rest contributed by the multiple raters. Ideally, the propor- tion of variability contributed by the raters is small relative to the total variability (or equivalently, the subject variability is large proportionally to the total variability). For our study involving five subjects and five raters, the interrater reliability ranged from 0.96 to 1.00 for the assessment procedure of five clinical measures of balance and mobility, indicating excellent interrater reliability.
Intervention. Following evaluation, each patient received an individualized multidimensional exercise program addressing the specific impairments and func- tional disabilities identified during the assessment. Because each patient presented a different constellation of problems, treatment was not limited to a single form of exercise. However, because all patients participating in the program were referred with balance and mobility problems, they all received a progression of exercises designed to improve balance and mobility skills. Balance exercises focused on improving postural alignment in sitting and standing positions, developing coordinated movement strategies for recovery of balance in sitting and standing, improving the use of senses for postural orientation, improving the ability to make effective anticipatory postural adjustments prior to volunt;~~?. movements, and integrating appropriate sensory and motor strategies for controlling posture and balance into functionally related balance and mobility tasks. Mobility retraining focused on improving stability during a variety of gait tasks, including unperturbed gait, perturbed gait, transfers, and stair climbing. In addition, exercises were prescribed in other areas of need, as determined by the evaluating therapist. For example, patients who scored less than 5 on manual muscle testing were given progres- sive resistive strength training exercises, whereas thosr who showed a significant impairment in range of motion in the trunk or lower extremities were given flexibility exercises.
In addition to exercises performed twice a week in physical therapy, a home exercise program was estah lished for each patient. All patients maintained a daily
Physical Therapy . Volume 77 . Number 1 . January 1997 Shumway-Cook et al .49
Dow
nloaded from https://academ
ic.oup.com/ptj/article/77/1/46/2633046 by guest on 31 M
ay 2022

log of exercise compliance and kept a record of falls or near-falls for the duration of the program and for 6 months following discharge.
Data Analysis Scores on the five measures of balance and mobility were obtained before and after participation in the exercise program. Fall rirk, a surrogated measure defined as the predicted probability for falling, was calculated for each patient based on a logistic regression model that was developed and tested on a different cohort of 44 subjects (22 older adults with a history of falls and 22 older adults without a history of falls) (unpublished research). In the development of the fall-risk model, univariate analyses were first applied to select variables that could poten- tially be used to identify older adults with a high risk for falling. Potential predictors included demographic vari- ables; variables related to the subjects' medical and balance history; current balance and mobility status as determined by five different clinical tests; and impair- ments in specific sensory and motor systems such as visual, vibratory or touch/pressure sense, range of motion, strength, and static alignment. Six variables that emerged to be individually and importantly associated with faller and nonfaller status were then used in a stepwise logistic regression analysis. Two variables, self- reported history of imbalance (IMBALANCE) and per- formance on the Berg Balance Scale (BERG), were identified by the stepwise logistic regression analysis as highly predictive of falling. The resulting logistic model was
= 10.459 + 2.324 IMBALANCE -0.249 BERG
where P = probability of falling and IMBALANCE = 1 if there is a history of instability or 0 if there is no history of instability. Of the 22 fallers, 18 subjects were correctly classified with a predicted probability of 10.5 (sensitivi- ty = 82%). Of the 22 nonfallers, 20 subjects were correctly classified using a predicted probability of C0.5 (specificity = 91 %).
An analysis of pretest balance and gait scores was done to determine whether differences existed between the con- trol group and the exercise groups. To control for the disparity in initial performance, percentage-of-change scores were used. To assess the effect of exercise on balance, mobility, and fall risk, differences in test scores following intervention were expressed by the percentage of change in test scores: (posttest-pretest)/pretest. Descriptive analyses indicated that outliers existed on the original percentage-of-change scores for all six mea- sures. To reduce the potential influence of outliers on the statistical analysis, a logit transformation was applied:
exp(x)/[l +exp(x)]. All six measures were transformed into a comparable scale between 0 and 1. Univariate analyses showed that each of the six transformed change scores had an approximately normal distribution, with no outliers. Statistical analyses were then carried out on the transformed scores. For convenience of interpreta- tion, the changes and confidence intervals (CIS) for all measures were then displayed as original percentage of change using inverse transformation (ie, transformed back to the original scales).
Statistical analyses included a multivariate analysis of variance (MANOVA, Wilk's criterion) performed on the five balance and gait measures c ~ m b i n e d . ~ ~ ? ~ ~ The results of the MANOVA would indicate whether a differ- ence existed among the three groups when the percent- ages of change in all five clinical measures were consid- ered together. An analysis of variance (ANOVA) was used to assess the difference among the three groups on each of the individual tests. Fall risk was analyzed sepa- rately using a univariate analysis of variance. A Tukey's post hoc pair-wise comparison was used to examine dif- ferences between each pair of the three groups if the overall difference was significant among the three groups. A probability value of less than .05 was consid- ered statistically significant, unless otherwise stated in this report.
For the 84 exercisers, a stepwise regression analysis was used to determine which factors predicted a successful response to exercise, as measured by the reduction in probability for falls. A stepwise logistic regression analy- sis was used to determine which factors predicted adher- ence to the prescribed exercise program (ie, fully adher- ent versus partially adherent, as defined earlier). All statistical analyses were performed using SPSS for Win- dows, Release 6 . 0 . ~ ' ~
Results Table 2 displays the pretest and posttest values, percent- age of change, and 95% CI for each of the three groups on six dependent measures. Results of the MANOVA showed that a significant difference (P<.001) existed among the three groups when the five balance and mobility measures were combined.
Effect of Exercise on Functional Balance Skills Figure 1 graphs the percentage of change (group mean and 95% CI) of the two balance measures: the Berg Balance Scale and the Balance Self-Perceptions Test. Both exercise groups showed a significant improvement (P<.001) compared with the control group on both measures of balance. There was no difference between
' SPSS Inc, 444 N Michigan Ave, Chicagi~. 11. 60611
50 . Shumway-Cook et al Physical Therapy . Volume 77 . Number 1 . January 1997
Dow
nloaded from https://academ
ic.oup.com/ptj/article/77/1/46/2633046 by guest on 31 M
ay 2022
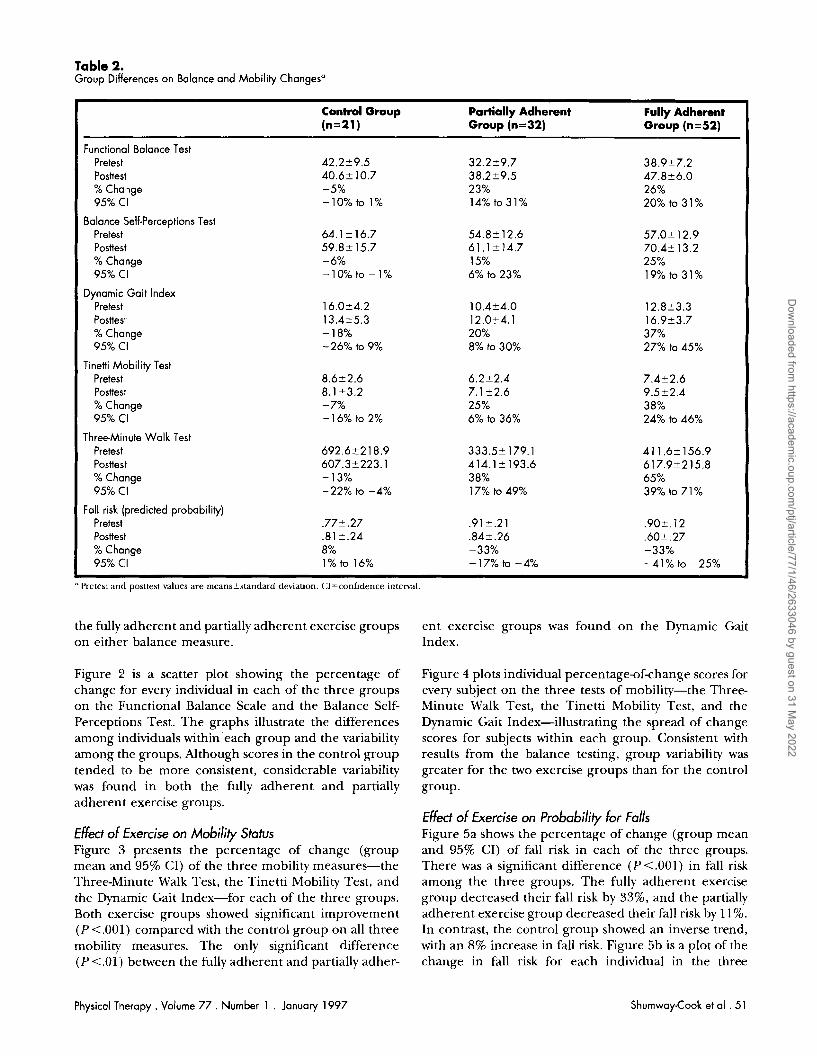
Table 2. Group Differences on Balance and Mobility Changesa
Control Group Partially Adherent Fully Adherent (n=2l) Group (n=32) Group (n=52)
Functional Balance Test Pretest Posttest % Change 95% CI
Balance Self-Perceptions Test Pretest Posttesl % Change 95% CI
Dynamic Gait Index Pretest Posttest % Change 95% CI
Tinetti Mobility Test Pretest Posttest % Change 95% C'I
ThreeMinute Walk Test Pretest Posttest % Change 95% CI
Foll risk (predicted probability) Pretest Posttest % Change 95% CI
"Pretest anti posttest values are meanakstandard deviation. CI=confidence intenral.
the fully adherent and partially adherent exercise groups ent exercise groups was found on the Dynamic Gait on either balance measure. Index.
Figure :! is a scatter plot showing the percentage of change for every individual in each of the three groups on the Functional Balance Scale and the Balance Self- Perceptions Test. The graphs illustrate the differences among individuals within each group and the variability among the groups. Although scores in the control group tended to be more consistent, considerable variability was found in both the fully adherent and partially adherent exercise groups.
Effect OF Exercise on Mobility Status Figure 3 presents the percentage of change (group mean and 95% CI) of the three mobility measures-the Three-Minute Walk Test, the Tinetti Mobility Test, and the Dynamic Gait Index-for each of the three groups. Both exercise groups showed significant improvement (P <.001) compared with the control group on all three mobility measures. The only significant difference (P <.01:) between the fully adherent and partially adher-
Figure 4 plots individual percentage-of-change scores for every subject on the three tests of mobility-the Three- Minute Walk Test, the Tinetti Mobility Test, and the Dynamic Gait Index-illustrating the spread of change scores for subjects within each group. Consistent with results from the balance testing, group variability was greater for the two exercise groups than for the control group.
Effect OF Exercise on Probability For Falls Figure 5a shows the percentage of change (group mean and 95% CI) of fall risk in each of the three groups. There was a significant difference (P<.001) in fall risk among the three groups. The fully adherent exercise group decreased their fall risk by 33%, and the partially adherent exercise group decreased their fall risk by 11%. In contrast, the control group showed an inverse trend, with an 8% increase in fall risk. Figure 5b is a plot of the change in fall risk for each individual in the three
Physical Therapy . Volume 77 . Number 1 . January 1997 Shumway-Cook et a1 . 51
Dow
nloaded from https://academ
ic.oup.com/ptj/article/77/1/46/2633046 by guest on 31 M
ay 2022
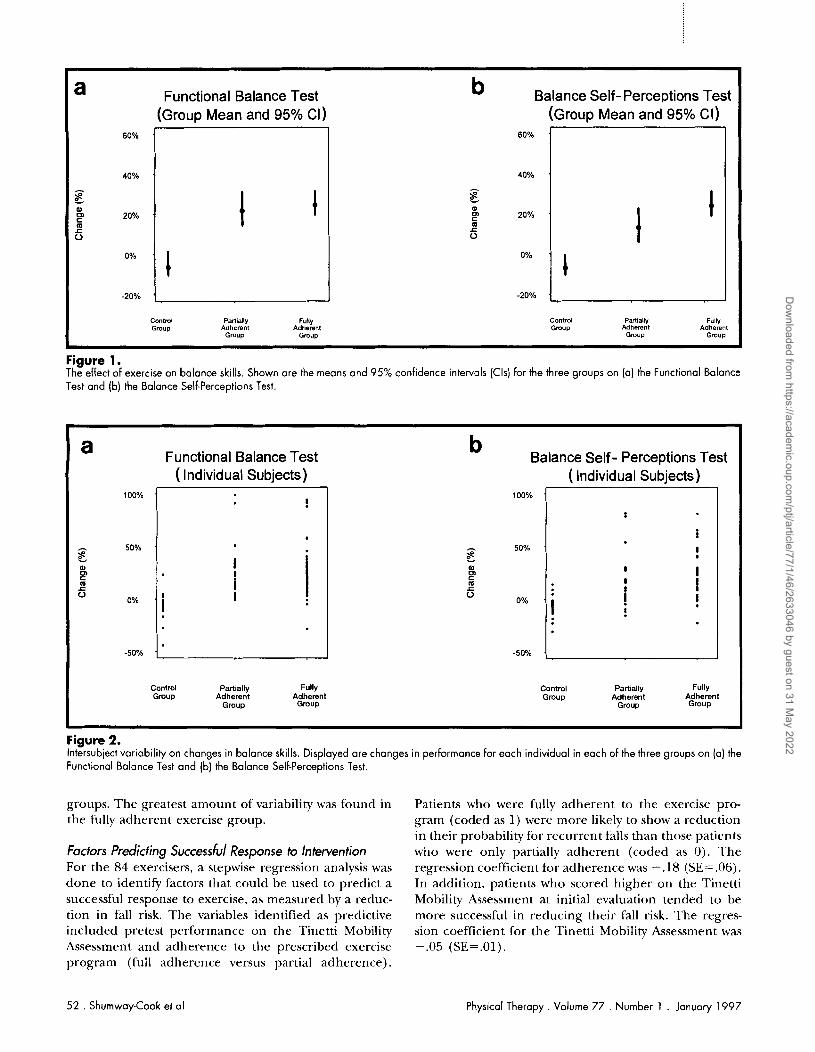
Figure 1. The effect of exercise on balance skills. Shown are the means and 95% confidence intervals (Cls) for the three groups on (a) the Functional Balance
a Functional Balance Test b Balance Self- Perceptions Test (Group Mean and 95% CI) (Group Mean and 95% CI)
Test and (b) the Balance Self-Perceptions Test.
I
I ,
Figure 2. Intersubject variability on changes in balance skills. Displayed are changes in performance for each individual in each of the three groups on (a) the Functional Balance Test and (b) the Balance Self-Perceptions Test.
Contml Partially FuHy Contml Partially Fully Gmup Adherent Adherent Gmup Adherent Adherent
Group Gmup Group Gmup
60% '
40% . - E ?4 20% . m 5
% '
-20%
60% .
40% ' - al c m C 20% . m 5
O, '
-20% .
-
a Functional Balance Test b
Balance Self- Perceptions Test ( Individual Subjects) ( Individual Subjects)
groups. The greatest amount of variability was found in the fully adherent exercise group.
I
I
Factors Predicting Successb/ Response to Intervention For the 84 exercisers, a stepwise regression analysis was done to identify factors that could be used to predict a successful response to exercise, as measured by a reduc- tion in fall risk. The variables identified as predictive included pretest performance on the Tinetti Mobility Assessment and adherence to the prescribed exercise program (full adherence versus partial adherence).
100% .
A 50% . E. al
F 6
0% .
-50% .
Patients who were fully adherent to the exercise pro- gram (coded as 1) were more likely to show a reduction in their probability for recurrent falls than those patients who were only partially adherent (coded as 0). The regression coefficient for adherence was - .18 (SE = .06). In addition, patients who scored higher on the Tinetti Mobility Assessment at initial evaluation tended to be more successful in reducing their fall risk. The regres- sion coefficient for the Tinetti Mobility Assessment was -.05 (SEz.01).
Control Partially Fully Control Partially Fully Group Adherent Adherent Group Adherent Adherent
Group Group Group Group
?
. I I i I i
100% '
50% . E. al m
m 6
O,
-50% .
52 . Shumway-Cook et al Physical Therapy. Volume 77 . Number 1 . January 1997
i
! I I
I i .I
i !
Dow
nloaded from https://academ
ic.oup.com/ptj/article/77/1/46/2633046 by guest on 31 M
ay 2022
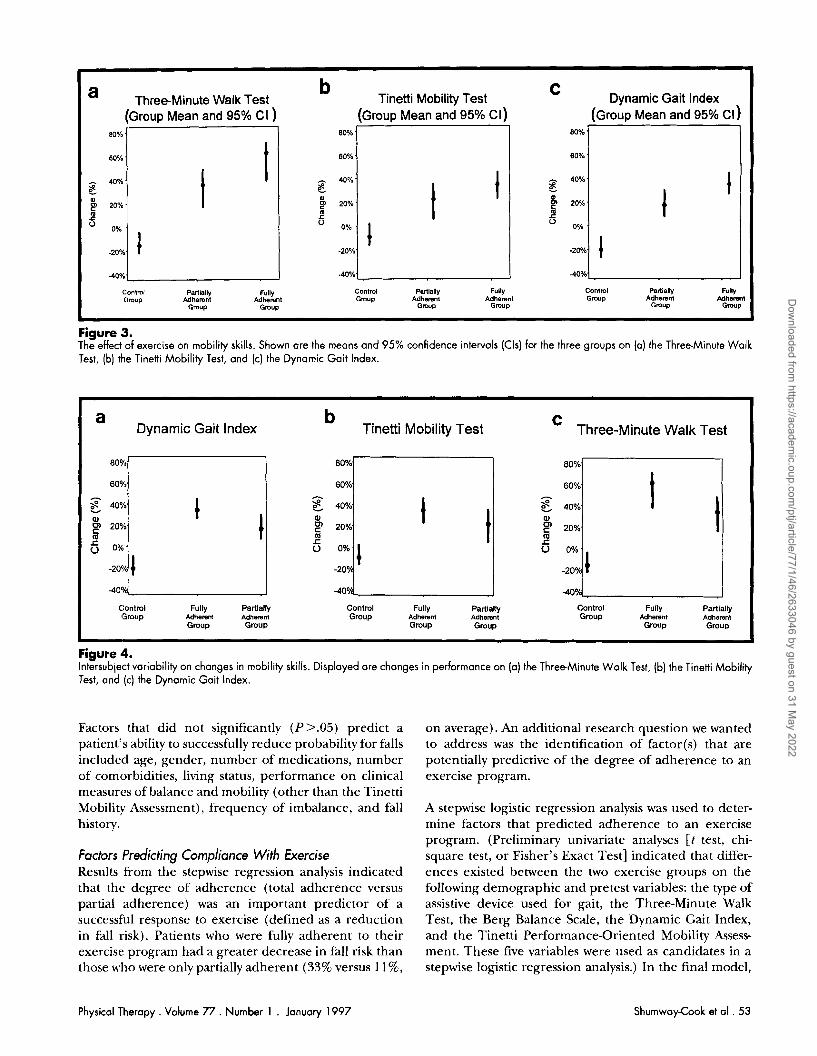
Figure 3. The effect of exercise on mobility skills. Shown are the means and 95% confidence intervals (Cls) for the three groups on (a) the Three-Minute Walk
a Three-Minute Walk Test b
Tinetti Mobility Test C Dynamic Gait lndex
(Group Mean and 95% Cl ) (Group Mean and 95% CI) (Group Mean and 95% CI )
Test, (b) the Tinetti Mobility ~es;, and (c) the Dynamic Gait Index.
I I
I
Figure 4. lntersubiect variability on changes in mobility skills. Displayed are changes in performance on (a) the ThreeMinute Walk Test, (b) the Tinetti Mobility Test, and (c) the Dynomic Gait Index.
Contml Partially Fully Contml Parlially Fully Contml Partially Fully Cimup Adherent Adherent Gmup Adherent Adherent Gmvp Adherent Adherent
Gmup Gmup Group Gmup Gmup G ~ U P
a Dynamic Gait lndex
b Tinetti Mobility Test Three-Minute Walk Test
Factors that did not significantly (P>.05) predict a patient's ability to successfully reduce probability for falls included age, gender, number of medications, number of com'orbidities, living status, performance on clinical measures of balance and mobility (other than the Tinetti Mobility Assessment), frequency of imbalance, and fall history.
I 1 1
80% '
80% '
- 40%'
al
F 20% '
OUh 1 -20%
40%.
80% '
60% '
- 40%' C
m g 20%.
.20%'
-40%
80%
60% - 40%
w p 20% m 5 o.,.
-2OVti
4OCVe,
Factors Predicting Compliance With Exercise Results from the stepwise regression analysis indicated that the degree of adherence (total adherence versus partial adherence) was an important predictor of a successful response to exercise (defined as a reduction in fall risk). Patients who were fully adherent to their exercise program had a greater decrease in fall risk than those who were only partially adherent (33% versus 11%,
80% '
80% '
40%' r p 20%'
oO,O
-20%
40%'
I t l
on average). An additional research question we wanted to address was the identification of factor(s) that are potentially predictive of the degree of adherence to an exercise program.
C:ontml Fully Partially Control Fully Partially Control Fully Partially l h u p Adherent Adherant Group Adherent Adherent Gmup Adherent Adherent
Group Group Gmup Group Group Grow
I 1
A stepwise logistic regression analysis was used to deter- mine factors that predicted adherence to an exercise program. (Preliminary univariate analyses [ t test, chi- square test, or Fisher's Exact Test] indicated that differ- ences existed between the two exercise groups on the following demographic and pretest variables: the type of assistive device used for gait, the Three-Minute Walk Test, the Berg Balance Scale, the Dynamic Gait Index, and the Tinetti Performance-Oriented Mobility Assess- ment. These five variables were used as candidates in a stepwise logistic regression analysis.) In the final model,
Physical Therapy . Volume 77 . Number 1 . January 1997 ShumwayCook et a1 .53
80%
60% A
5 40% m
20%. m
-2OY
-40%
80%
60%. - 5 40% w 9 20% l a
-207 OOh.I
40Ye,
' I ,
Dow
nloaded from https://academ
ic.oup.com/ptj/article/77/1/46/2633046 by guest on 31 M
ay 2022
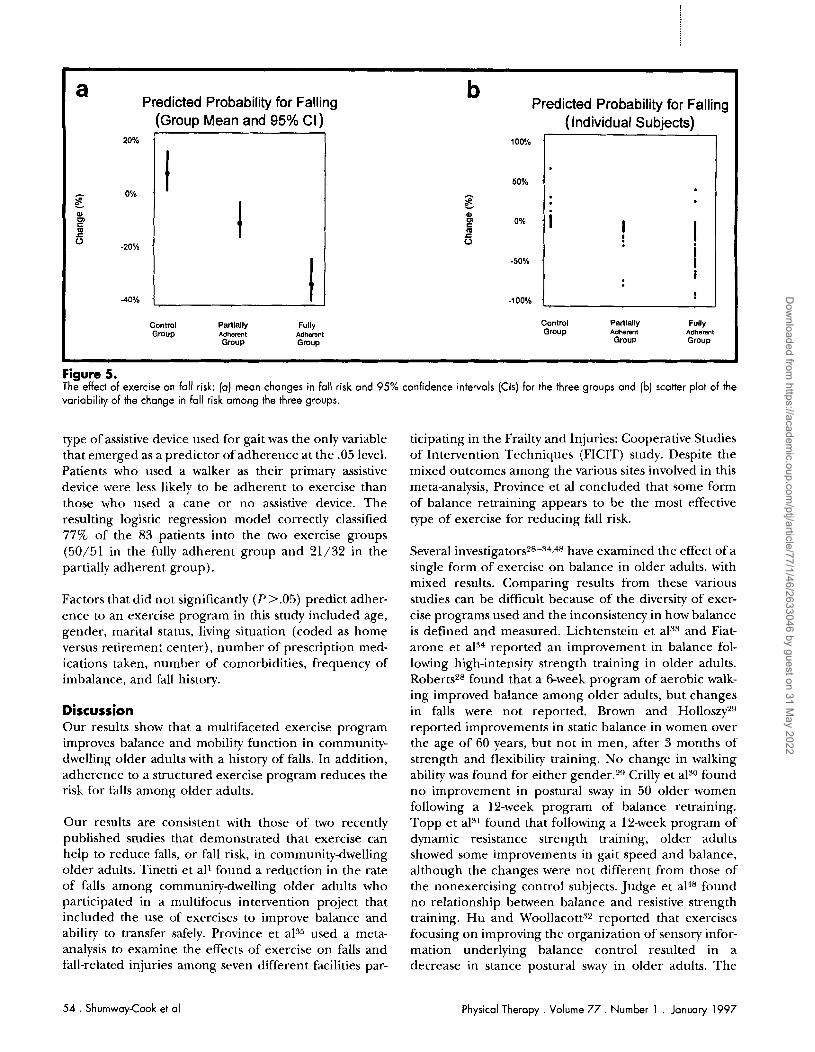
Figure 5. The effect of exercise on fall risk: (a) mean changes in fall risk and 95% confidence intervals (Cls) for the three groups and (b) scatter plot of the variability of the change in fall risk among the three groups.
a Predicted Probability for Falling b
Predicted Probability for Falling (Group Mean and 95% CI) (Individual Subjects)
type of assistive device used for gait was the only variable that emerged as a predictor of adherence at the .05 level. Patients who used a walker as their primary assistive device were less likely to be adherent to exercise than those who used a cane or no assistive device. The resulting logistic regression model correctly classified 77% of the 83 patients into the two exercise groups (50/51 in the fully adherent group and 21/32 in the partially adherent group).
Factors that did not significantly (P >.05) predict adher- ence to an exercise program in this study included age, gender, marital status, living situation (coded as home versus retirement center), number of prescription med- ications taken, number of comorbidities, frequency of imbalance, and fall history.
20%
A 0% '
E Q m m 5
-20% .
40% .
Discussion Our results show that a multifaceted exercise program improves balance and mobility function in community- dwelling older adults with a history of falls. In addition, adherence to a structured exercise program reduces the risk for falls among older adults.
Control Partially Fully Control Partially Fully Gmup Adherent Adherent Group Adherent Adherent
Gmup Gmup Gmup Gmup .
I
, I
100% .
50% . A
5 Q
P m 5
-50% .
-100% .
Our results are consistent with those of two recently published studies that demonstrated that exercise can help to reduce falls, or fall risk, in community-dwelling older adults. Tinetti et all found a reduction in the rate of falls among community-dwelling older adults who participated in a multifocus intervention project that included the use of exercises to improve balance and ability to transfer safely. Province et als5 used a meta- analysis to examine the effects of exercise on falls and fall-related injuries among seven different facilities par-
. i I ! I
i I i
!
ticipating in the Frailty and Injuries: Cooperative Studies of Intervention Techniques (FICIT) study. Despite the mixed outcomes among the various sites involved in this meta-analysis, Province et a1 concluded that some form of balance retraining appears to be the most effective type of exercise for reducing fall risk.
Several investigator^*^-^^,^^ have examined the effect of a single form of exercise on balance in older adults, with mixed results. Comparing results from these various studies can be difficult because of the diversity of exer- cise programs used and the inconsistency in how balance is defined and measured. Lichtenstein et a133 and Fiat- arone et a134 reported an improvement in balance fol- lowing high-intensity strength training in older adults. Roberts28 found that a Gweek program of aerobic walk- ing improved balance among older adults, hut changes in falls were not reported. Brown and Holloszp9 reported improvements in static balance in women over the age of 60 years, but not in men, after 3 months of strength and flexibility training. No change in walking ability was found for either gender.29 Crilly et also found no improvement in postural sway in 50 older women following a 12-week program of balance retraining. Topp et a131 found that following a 12-week program of dynamic resistance strength training, older adults showed some improvements in gait speed and balance, although the changes were not different from those of the nonexercising control subjects. Judge et a14Vound no relationship between balance and resistive strength training. Hu and Woollacotts2 reported that exercises focusing on improving the organization of sensory infor- mation underlying balance control resulted in a decrease in stance postural sway in older adults. The
54 . Shumway-Cook et al Physical Therapy . Volume 77 . Number 1 . January 1997
Dow
nloaded from https://academ
ic.oup.com/ptj/article/77/1/46/2633046 by guest on 31 M
ay 2022

exercise group had fewer falls during their experimental tests of balance compared with subjects who did not exercise; however, differences in number of falls in a natural environment were not reported.3*
A Multidimensional Approach to Retraining The results from our study suggest that a multi- dimensional exercise program can improve balance, mobility, and fall risk in older adults. Our multifaceted exercise approach was based on a systems model of postural control that suggests that stability emerges from a complex interaction of musculoskeletal and neural systems."' A systems approach to understanding balance function In elderly persons examines the extent to which deterioration in specific physiologic and musculoskeletal systems contributes to loss of stability and mobility in this populat ic~n.~~ Thus, a systems approach to assessment of balance and mobility uses a variety of tests and measure- ments to document functional abilities and to determine the underlying sensory, motor, and cognitive impair- ments contributing to functional disabilities." The goals of retraining are (1) to resolve or prevent underlying impairments, (2) to develop effective and efficient task- specific sensory and motor strategies, and (3) to adapt task-specific strategies so that functional tasks can be performed in changing environmental contexts." A multidimensional approach to retraining balance and mobility functions in older adults is intuitively appealing because it is consistent with current research indicating that most falls in older adults involve multiple risk factors artd that many of these factors may be remedi- ; ~ t e d . ~ ~ Until now, the effectiveness of this type of approach has not been tested scientifically. Results from our study suggest that a multidimensional approach is successful in improving balance and mobility skills and that these improvements are associated with a reduction in fall risk.
The Importance of Adherence Although both groups of exercisers showed a reduction in fall risk compared with the control group, who did not exercise, subjects who were completely adherent were more like'ly to reduce their fall risk than those who were partially adherent. Results showed that both exercise groups showed an improvement in balance and gait skills compared with the control group. Although the fully adherent exercisers performed better as a group on clinical measures of balance and mobility than the partially adherent exercisers, the differences were not statistically significant. Thus, the amount of exercise necessary to show an improvement in balance and mobility skills is not clear from this study.
Results from this study suggest that the type of assistive device used for ambulating was the only factor that predicted the degree of adherence. Patients who walked
with no assistive devices or with a cane tended to be more adherent than those who used a walker. This finding suggests that patients with more severe balance problems, as indicated by the use of a walker, do not appear to adhere as well as those patients with less severe balance problems. One reason could be that patients who are severely impaired do not believe that exercise can change their level of function and, therefore, are less likely to adhere.
An important and encouraging finding of this study was that age was not associated with the adherence to exercise and with the reduction of fall risk. Patients who were above the age of 80 years were its likely to be adherent and successful as those in thcir 60s. This finding suggests that balance and gait retraining pro- grams can be beneficial to very old individuals. Because this study was limited to adults over the age of 65 years who lived in their own homes or in retirement centers, the results may not apply to those under the age of 65 years or to older adults residing in nursing homes.
Limitations of the Study There were several limitations associated with this study. One limitation was the lack of randomization of subjects to the control group versus the experimental groups. Our study utilized patients who were specifically referred for balance and mobility retraining. It was therefore not possible to randomly assign patients to a noninterven- tion group. Thus, our study used a quasi-experimental, nonequivalent control group design. This design is reported to be an acceptable alternative to an experi- mental design when randomization is not p o s ~ i b l e . ~ ~ . . ~ ~ )
A second limitation of the study was that both pretesting and posttesting for each subject were carried out by the therapist responsible for treating that patient, introduc- ing the possibility of evaluator bias. Interrater reliability measurements suggest that all therapists were well trained in the evaluation procedures. In addition, ther- apists were not given access to pretest scores at the time of posttest evaluation, reducing the probability of evalu- ator bias.
Finally, our study examined the effects of exercise on fall risk, not on actual frequency of falls. The use of fall risk as a measure of intervention effectiveness has been reported by others as an alternative to reporting actual fall frequency (see Province et a135 for a review). In addition, our model for predicting fall risk has been shown to be highly related to actual fall frequency (unpublished research).
Conclusion The effects of falls are devastating, contributing to an increase in mortality and morbidity in adults over the
Physical Therapy. Volume 77 . Number 1 . January 1997 Shumway-Cook et al . 5 5
Dow
nloaded from https://academ
ic.oup.com/ptj/article/77/1/46/2633046 by guest on 31 M
ay 2022

age of 65 years. A multidimensional exercise program is an important factor in improving upright balance and gait function and in reducing the risk for falls in older community-dwelling adults. Both adherence to an exer- cise program and degree of balance and gait impairment appear to be important factors in determining a success- ful response to exercise. How much exercise is needed to achieve maximal effects, however, is unclear. Thus, further study is needed to determine the optimal rela- tionship between patient characteristics and exercise frequency and duration.
References 1 Tinetti ME, Baker DI, McAway G, et al. A multifactorial intervention to reduce the risk of' falling among elderly people living in the community. N Engl J Med. 1994;331:821-827.
2 Hornbrook MC, Stevens J, Wingfield DJ, et al. Preventing falls among communitydwelling older persons: results from a randomized trial. Gerontologist. 1994;34: 16-23.
3 Blake AJ, Morgan K, Bendall MJ, et al. Falls by elderly people at home: prevalence and associated factors. Age Ageing. 1988;17:365-372.
4 Nevitt MC, Cummings SR. Risk factors for recurrent non-syncopoal falls: a prospective study. J A M . 1989;261:2663-2668.
5 Tinetti ME, Ginter SF. Identifymg mobility dysfunctions in elderly patients: standard neuromuscular examination or direct assessment? J A M . 1988;259:1190-1193.
6 Sattin RW. Falls among older persons: a public health perspective. Annu Rnl Public Health. 1992;13:489-508.
7 Sattin RW, Lambert H, Devito CA, et al. The incidence of fall injury events among the elderly in a defined population. Am J ~p id th io l . 1990;131:1028-1037.
8 Campbell AJ, Borrie MJ, Spears GF. Risk factors for falls in a community-based prospective study of people 70 years and older. J h n l o l . 1989;44:M112-M117.
9 Kellogg International Work Group on the Prevention of Falls by the Elderly. The prevention of falls in later life. Dan Med Bull. 1987;34:1- 24.
10 Tinetti ME, Speechley M, Ginter SF. Risk factors for falls among elderly persons living in the community. N EnglJMed. 1988;319:1701- 1707.
11 Duncan PW, Studenski S, Chandler J, Prescott B. Functional reach: predictive validity in a sample of elderly male veterans. J Gerontol. 1992;47:M93-M98.
12 Nickens H. Intrinsic factors in falling among the elderly. Arch Intern Med. 1985;145: 1089-1093.
13 Whipple RH, Wolfson LI, Amerman PM. The relationship of knee and ankle weakness to falls in nursing home residents: an isokinetic study. J A m Geriatr Sor. 1987;35: 13-20.
14Aniansson A, Grimby F, Gedberg A. Muscle function in old age. Scand J Rehabil Med. 1978;6(suppl) :43- 49.
15 Guralnik JM, Ferrucci L, Simonsick E, et al. Lower-extremity func- tion in persons over the age of 70 years as a predictor of subsequent disability. N Engl J Med. 1995;332:556-561.
16 Lewis C, Bottomley J. Musculoskeletal changes with age. In: Lewis C, ed. Aging: Health Care's Chalknge. 2nd ed. Philadelphia, Pa: FA Davis Co: 1990: 145-146.
17 Kosnik W, Winslow L, Kline D, et al. Visual changes in daily life throughout adulthood. J Gerontol Psych Sci. 1988;43:63-70.
18 Sloane P, Baloh RW, I-Ionrubia V. The vestibular system in the elderly. Am J Otolalyngol. 1989;1:422-429.
19 Ochs AL, Newberry J, Lenhardt ML, Harkins SW. Neural and vestibular aging associated with falls. In: Birren JE, Schaie KW, eds. Handbook ofPsychology ofAging. New York, NY: Van Nostrand Reinhold; 1985:378-399.
20 Whanger A, Wang HS. Clinical correlates of the vibratory sense in elderly psychiatric patients. J Gerontol. 1974;29:39-45.
21 Woollacott MH, Shumway-Cook A. Changes in posture control across the life span: a systems approach. Phys Tho: 1990;70:799-807.
22 Maki B, Holliday PJ, Topper AK. Fear of falling and postural performance in the elderly. J Ckvntol. 1991;46:M123-M131.
23 Nelson RC, Amin MA. Falls in the elderly. Ernerg Med Clin North Am. 1990;8:309-324.
24 Woollacott MH, Shumway-Cook A, Nashner LM. Aging and posture control: changes in sensory organization and muscular coordination. Int JAgrng Hurn Dm. 1986;23:97-114.
25 Manchester D, Woollacott MH, Zederbauer-Hylton N, Marin 0 . Visual, vestibular, and somatosensory contributions to balance control in the older adult. J Gerontol. 1989:44:M118-hf127.
26 Horak F, Shupert C, Mirka A. Components of postural dyscontrol in the elderly: a review. Neurobiol Agrng. 1989;10:727-745.
27 Peterka RJ, Black FO. Age-related changes in human posture control: sensory organization tests. Journal of Vesfihlar Research. 1990; 1:73-85.
28 Roberts B. Effects of walking on balance among elders. Nurs Res. 1989;38:180-183.
29 Brown M, Holloszy JO. Effects of a low-intensity exercise program on selected physical performance characteristics of 60- to 70-year-olds. Aging (Milano). 1991;3: 129-1 39.
30 Crilly RG, Willems DA, Trenhold KJ, et al. Effect of exercise on postural sway in the elderly. Gerontology. 1989;35:137-143.
31 Topp R, Mikesky A, Wigglesworth J , et al. The effect of a 12-week dynamic resistance strength training program on gait velocity and balance of older adults. Geronlologrst. 1993;33:501-506.
32 Hu M, Woollacott MH. Multisensory training of standing balance in older adults, I: postural stability and one-leg stance balance. J Gerontol. 1994;49:M52-M61.
33 Lichtenstein MJ, Shields SL, Shiavi RG, Burger C. Exercise and balance in aged women: a pilot controlled clinical trial. Atzh Phys Med Rehabil. 1989;70:138-143.
34 Fiatarone MA, Marks EC, Ryan ND, et al. High-intensity strength training in nonagenarians: effects on skeletal muscle. JAhlrZ. 1990;263: 3029-3034.
35 Province MA, Hadley EC, Hornbrook MC, et al. The effects of exercise on falls in elderly patients. JAhZA. 1995;272:1341-1347.
36 Campbell D, Stanley J. Experimental and quasi-experimental designs for research on teaching. In: Gage NL, ed. Handbook ofliesearch on Teaching. Chicago, Ill: Rand McNally; 1963.
37 Pfeiffer E. Short portable mental status questionnaire. JArn Genntr Soc. 1975;23:433-441.
38 Shumway-Cook A, Woollacott MH. Motor Control: Theoly and Practical Applications. Baltimore, Md: Williams & Wilkins; 1995.
56 . Shumway-Cook et a1 Physical Therapy . Volume 77 . Number 1 . January 1997
Dow
nloaded from https://academ
ic.oup.com/ptj/article/77/1/46/2633046 by guest on 31 M
ay 2022
39 Tinetti ME, Mendes deleon CF, Doucette JT, Baker Dl. Fear of falling and fall-related efficacy in relationship to functioning among communityliving elders. J Gerontol. 1994;49:140-147.
40 Berg K. Mmsunng Balance in the Elderly: Validatio~i of an I~zstrumat. Montreal, Quebec, Canada: McGill University; 1993. Dissertation.
41 Tinetti ME. Performance-oriented assessment of mobility problems in elderlv patients. , ]Am Gen'ai~ Sor. 1986;34:l 19-126.
42 Kendall F, McCreaw EK. Musrles: Testfag and Fununctzon. Baltimore, Md: Willia~ns & Wilkins; 1983.
43 Saunders D. Evaluatton, Tre(itmnt, and Pralrnlzon of Musculoskeletal Dztolders. Minneapol~s, Minn: V~king Press; 1991.
44 Shumway-Cook A, Horak F. Rehabilltation strategies for patients with vest~bular deficits. Nruro/~gy Cl?ndrs of North A7nenca. 1990;8:441- 457.
46 Tabachnick BG, Fidell LS. Usi~zg hfziltivanate S~alistics. 2nd ed. New York, NY I-IarperCollins Publishers; 1989.
47 SPPFF'S for Windows: Advanced .S/cltistirs, Relrasr 6.0. Chicago, Ill: SPSS Inc; 1993.
48 Judge JO, U'hipple RH, M'olfso~l LI. Effects of resistive and balance exercises on isokinetic strength in older persons. J Am Geriatr Sor. 1994;42:937-946.
49 Lipsitz W, Jonssc~n PV, Kellev MM, Koestner JS. Causes and correlates of recurrent falls in ambulatory frail elderly. J Gerontol. 1991;46:M114-M122.
50 Kenny DA. A quasi-experimental approach to assessing treatment effects in the nonequiv.alent control group design. Psyrhol Bull. 1975; 82:345-362.
45 Fiqher L.D, Van Belle G. Biostotictics: A Mrthodology f ~ r the Health Scirnres. New York. NY John M'ilev & Sons Inc; 1993.
SATISFACTION INSTRUMENTS: A COMPENDIUM
from 8:30 am to 5:30 p m Eastern time,
Mastercard or VISA handy, O r e-mail your credit card order via the Internet to:
To fax or mail in your order, please refer to the order form found on page 119.
Physical Therapy . Volume 77 . Number 1 . January 1997 Shumway-Cook et al . 57
Dow
nloaded from https://academ
ic.oup.com/ptj/article/77/1/46/2633046 by guest on 31 M
ay 2022