The Arab Republic of Egypt Detailed Study for Egypt Japan ...
Upload
independentCategory
view
3download
0
Pergmon o277-~05)oooo1-1
Soc. Sci. Med. Vol. 40, No. 10, pp. S1-$30, 1995 Copyright © 1995 Elsevier Science Ltd
Printed in Great Britain. All rights rvaervod 0277-9536/95 $9.50 + 0.00
THE EFFECT OF A NATIONAL CONTROL OF DIARRHEAL DISEASES PROGRAM ON MORTALITY:
THE CASE OF EGYPT
PETER MILLER ~ and NORBERT HIRSCHHORN 2 tPopulation Council, No. 55 Street One, Sector F6/3, Islamabad, Pakistan and 2john Snow, Inc.,
210 Lincoln Street, Boston, MA 02111, U.S.A.
Abstract--The National Control of Diarrheal Diseases Project (NCDDP) of Egypt began in 1981, became fully operational nation-wide by 1984, and concluded in 1991. The project was designed as a campaign to lower mortality from diarrheal disease in children under five by at least 25% within five years. The principal strategy employed was to improve case-management of diarrhea through rehydration and better feeding: through assured production and distribution of oral rehydration salts, education of families through mass media and health workers through training programs, and creation of rehydration comers throughout the established primary health care and hospital network. A detailed plan for evaluation and research was designed at the start of the project. By its own terms, the NCDDP appears to have succeeded in improving case management; by several local and national mortality surveys, overall infant and childhood mortality fell by at least one-third with the majority proportion in diarrheal deaths. The declines coincided with the peak of NCDDP activities and results in improved case-management. The detailed analyses of this monograph seek to demonstrate that: (a) the mortality decline and the diarrheal mortality decline in particular were actual events; (b) that case-management improved with plausible sufficiency to account for most of the diarrheal mortality reduction; and (c) that changes in other proximate determinants to lowered mortality, such as host resistance or diarrheal incidence, do not plausibly account for the magnitude of the reductions seen. Data are also presented on general socio-economic changes in the decade of the Project. We conclude that improvements in primary care delivery and the use of mass media would have been facilitating factors to NCDDP efforts, while the overall deterioration of economic status would have tended to reduce the benefits.The monograph details the strengths and weaknesses of the available data, and also makes recommendations for sustained efforts in the control of diarrheal diseases.
I. INTRODUCTION
It is not often possible to measure the impact of a single health intervention on mortality. Most health projects are too small or deal with changes in mortality undetectable at levels of statistical significance within usual year-to-year fluctuations. Nearly all health projects in the past three decades have been carried out against a steady secular reduction in mortality among infants and children [1]. Nonetheless, when a large project ambitiously aims to reduce mortality from one or more causes, it is crucial that attempts be made to demonstrate impact before long-lasting policies are fixed.
The National Control of Diarrheal Diseases Project (NCDDP) was such a project. The NCDDP began in September 1981 with a five-year grant-agreement, later extended to ten, between the United States Agency for International Development and the Government of Egypt; one year later the project became operational when the Government of Egypt awarded a contract for technical assistance to John Snow, Inc. of Boston U.S.A.
The grant-agreement followed on a controlled trial of oral rehydration therapy (ORT) [2] in rural Egypt which demonstrated reduced mortality from di- a r rhea - the leading cause of death in infants and
children--by 40% [3]. NCDDP was thus designed as a campaign to implement the research findings on a national scale. The total grant assistance expended amounted to U.S.$32 million.
The initial project grant agreement specified three principal outcomes expected by 1986:
(1) 90% of mothers would become aware of ORT, and 75% understand its use;
(2) more than half of serious cases seen by the health system would get ORT; and
(3) diarrhea mortality in children under five years of age would decline by at least 25%.
Strategies planned and implemented to meet these targets included: in-country production and distri- bution of oral rehydration salts (ORS); the innovative use of mass media to promote and teach the use of ORT; training of health workers on a large scale; establishment of rehydration rooms in Ministry of Health and University hospitals and clinics. In the extended phase of the Project, a plan was implemented for eventual integration of the semi-autonomous NCDDP into the regular Ministry of Health structure by the end of the ten-year grant period.
Summary reports of the Project's strategies and impact have been presented elsewhere [4, 5]. These
S1

$2 Peter Miller and Norbert Hirschhorn
reports, however, could not do justice to the volume and complexity of the information available. This monograph intends to provide critical analyses of the change in infant and child mortality during the Project years and its relationship to changes in treatment of diarrheal disease. The monograph will bring together all of the available body of data considered of reasonable quality, from surveys, vital statistics, hospital records and local area studies collected since the late 1970s; to which NCDDP added substantially through its program of research and evaluation. The monograph therefore cites raw data and information from unpublished reports as well as formally published peer-reviewed studies. It therefore presents data of uneven quality but to do otherwise would mean telling less than the whole story. While rigorous proof of NCDDP impact on mortality is difficult to attain, the circumstantial evidence is plentiful.
The main body of the monograph is arranged in six sections:
I. The strategy of impact evaluation: how NCDDP organized evaluation and how this monograph models the analyses by a 'proximate-determinants' model.
II. The accomplishments of the NCDDP--a review: the principal inputs of the NCDDP.
III. Changes in mortality and its patterns: the evidence that infant and child mortality fell more than expected during the period of the NCDDP, particularly diarrheal mortality.
IV. Other factors potentially influencing mor- tality: based on the proximate-determinants model, other potential causes for the mortality decline.
V. Discussion: what was the impact of the NCDDP?: A summary of the information and analyses.
VI. Recommendations for the future.
H. THE STRATEGY OF IMPACT EVALUATION
1. The evaluation plan
To show a link between the activities of the NCDDP and changes in infant and childhood mortality, it is necessary to demonstrate the following:
(a) that program accomplishments were suffi- cient to have plausibly caused a decline in mortality;
(b) that such a mortality decline occurred; and (c) that no other major event occurred at the
same time, independent of the NCDDP, that could have plausibly caused the decline.
Rigorous proof of such hypotheses ideally is found through a randomized, controlled trial with strict control of inputs; causal interpretations of results can then be made with quantifiable levels of probability. (In fact, the following sections discuss two such experiments conducted at local levels in Egypt in
1979-80--one successful, the other not). Such a design was clearly impossible at the national level, yet criteria of proof are still necessary, to demonstrate: that the intended strategies and operations of the NCDDP were carried out to some effect; that new program strategies, such as use of mass media, could change how diarrhea was treated; and that improved treatment with ORT could lower mortality on a national scale even without much change in the incidence of diarrhea [6].
To these ends a detailed evaluation plan was created at the outset of the Project to measure inputs (such as production of ORS, training of health workers, understanding and acceptance of media messages), behavior change (such as improved feeding, knowl- edge and proper use of ORS, self-referral for serious illness) and outcomes (such as severity of illness seen in sentinel hospitals and changes in mortality).
The principal instruments for measurement in- cluded periodic knowledge-and-practice surveys, successive national household surveys before and after the summer diarrhea season [7], review of the national civil register and local area controlled trials done in the identical locations of those of 1979-1980. NCDDP also took advantage of data reported by independent studies such as the national Demographic and Health Surveys.
2. A proximate-determinants model as guide to the analysis
The precise measurement of mortality decline is difficult. A general decline in infant and childhood mortality can be well documented by surveys but this is insufficient--measurement of diarrhea-specific mortality is also needed. The civil register in principle provides this; however in Egypt infant deaths are incompletely reported, and cause of death is often inaccurate. Therefore establishing the degree and nature of a mortality decline must be attempted with considerable caution.
While the difficulties in measuring a program's effect on mortality are considerable, some positive aspects exist. For one, numerous data sources are available so the findings of a given study can usually be verified or contradicted by others. Also, great precision is not necessary: if the presence of a project as large and extensive as NCDDP has not been associated with substantial and measurable impact on the leading cause of death in children under five, then it has been a failure. Even if an impact is established, however, it is impossible to be absolutely certain, in the absence of experimental design, that no other factor plausibly explains all or any of the decline.
Some of the complexities can be simplified through logical modelling. To help clarify the logic of this evaluation, a simple 'proximate-determinants' model is proposed for diarrheal mortality (Fig. 1). This model is not intended to mathematically apportion relative factors influencing mortality change--neither the data or our theoretical understanding are adequate.

Diarrhea control: impact on mortality in Egypt
Background Determinants Intermediate Proximate Dqmwmlmlnts Determinants
$3
Economic Factors
Cultural Factors
Environmental/ Geographic Factors
Educational Levels
CDD Efforts
Non-Program Factors
Diarrhea Incidence
~ _ ~ Case ~ Infant/Child CDD Efforts Management Mortality
Non-Program Factors
Non-Program Factors
Host Resistance
Fig. 1. A 'proximate-determinants' model to evaluate the potential impact on mortality of a control of diarrheal diseases (CDD) program. Diarrhea incidence (including etiology), treatment and the children's resistance are considered the principal proximate determinants affected by program and non-program
factors which, in turn, are influenced by pervasive background determinants.
Rather, the model is to assist in sorting out how the myriad factors which influence diarrheal mortality might operate and interact. The model is useful in apportioning change only if some elements are zero or nearly so.
In this model, three classes of proximate-determi- nants directly influence diarrheal mortality: changes in incidence of diarrheal disease, changes in host resistance in case of diarrheal infection and changes in treatment. Each of these is affected by a variety of intermediate determinants, such as improved water supply, better hygienic practices, measles vaccination, availability of ORS, among others. These have not been listed individually but have been broadly divided into CDD (Control of Diarrheal Diseases) program and non-program factors. Each intermediate determi- nant is in turn affected by various background factors that form the basic structure within which either program or non-program factors operate. If a proximate determinant is unchanged during the period in question, then reduction in mortality did not occur as a result of factors influencing that proximate determinant through that path. If a proximate determinant does change, then the intermediate determinants associated with it must be examined in detail to discover why.
The model has its limitations. It does not distinguish explicitly between direct and indirect mortality from diarrhea, and does not address the non-mortality consequences of morbidity. Also, the proximate determinants can interact. It is known, for instance,
that improved treatment protects a child's nutrition [8], which should lead to improved host resistance-- perhaps not only to diarrhea but other infections as well. The model's main utility, therefore, is as a guide to logic for the questions posed in this analysis and not as an estimable model. At best, the model allows for the evaluation of a large body of circumstantial evidence.
3. The role of improved treatment in mortality reduction
We should first summarize how improved treatment (also known as 'case management') of diarrhea potentially reduces mortality. Various attempts have been made to define diarrhea precisely, but the layman's concept of passing frequent loose or watery stools is adequate for our purposes. Diarrheal episodes are typically classified as acute, lasting less than two weeks, or persistent, lasting two weeks or more. A brief episode characterized by loose, rather than watery, stools is rarely dangerous, regardless of how treated.
Approximately 90% of diarrheal episodes in Egypt are acute and about half are watery. Acute episodes with watery stools result in some degree of dehydration, even if not clinically detectable. Detectable dehydration can be fatal or when not can lead to undernutrition, reducing a child's chance for later survival. Children with dehydration but still able to drink, should be rehydrated with ORS, fed and watched for deterioration requiring intravenous (i.v.) fluids. ORS, by restoring electrolyte balance, stops vomiting and helps return appetite. ORT--rehydra-

$4 Peter Miller and Norbert Hirsehhorn
tion plus feeding---during watery diarrhea limits the severity of dehydration, and hastens recovery by reducing nutritional loss and healing the intestine. Antimicrobial drugs are useful in only about 10% of episodes, mainly for dysentery, constipative drugs ('antidiarrheais') and antiemetics hardly ever.
Persistent diarrhea usually has an acute onset--but for any of a variety of reasons, including inadequate treatment, persists for longer periods than usual and requires more intense management. Death results more from inanition and secondary infection than from dehydration.
Dysentery is diarrhea with visible blood in the stools often caused by the bacterial species Shigella. Death may occur from dehydration, systemic toxicity, inanition or some combination. Antimicrobial drugs are indicated; ORT is a useful adjunct treatment.
Children with measles are predisposed to all forms of diarrheal disease during and for months after the acute illness, and often in severe form. Improved coverage with measles vaccination (given at age nine months) will reduce diarrheal mortality, particularly in the one- to two-year olds [9].
In the developing world diarrheal diseases have had an extremely high incidence but low case-fatality, resulting in a high toll of direct mortality, and an unknown level of later, indirect mortality. By the same token, improved case management affects direct mortality and also an unknown level of the indirect. Thus evaluation of program impact on mortality necessarily includes both kinds of impact which are not dissectable into component parts, although direct mortality is by far the greater. Direct diarrheal mortality and most of the indirect is highly concentrated among children under two years of age.
4. Hypothetical interventions, anticipated consequences
A diarrheal disease control program could affect mortality in a variety of ways. Preventive measures could lower diarrheal incidence, averting some of the acute fatalities, and--by diminishing the weakening effects of illness--reduce delayed mortality from any cause. The correct use of ORT during diarrheal episodes in the population-at-large would similarly prevent or correct potentially fatal dehydration in acute cases; possibly prevent some acute cases from becoming persistent; help prevent death in some persistent cases; and improve the nutritional status of many children who would not otherwise have died from a particular episode. Correct emergency care for severe dehydration, with i.v. fluids, will also save lives, at least for the short-term.
All of these effects can be predicted qualitatively, but in no case can the number of lives saved by a particular intervention be credibly quantified. It is known, however, that nearly all diarrheal deaths represent some failure of case management; there would be few diarrheal deaths if all cases were properly treated, even in the absence of effective prevention.
5. An analytic strategy
With these considerations in mind, a strategy for an impact evaluation of NCDDP can be established as follows:
(a) Establish baselines for mortality, diarrheal epidemiology, childhood nutrition and medical and popular patterns of diarrhea case management.
(b) Quantify the accomplishments of NCDDP, focusing on the effect of the Project on those variables that can be predicted to affect mortality.
(c) Examine mortality patterns during the period of the Project. If the Project has been successful, a significant drop in diarrheal mortality should be evident coincident with the timing of Project accomplishments.
(d) If mortality decline is found, examine other possible causes. In particular, look for changes in diarrheal incidence, and in host resistance (such as improvement in nutrition, or measles vaccination). Finally, review the broader changes in the socio-economic standing in the 1980s which might have influenced diarrhea mortality in either direction independently, or as factors affecting the efforts of the NCDDP.
6. A note on data sources
This study is based on a comprehensive review of information bearing on the topic, from both Project and non-Project sources, from the late-1970s up to 1991. A number of studies and service statistics are not reported here, either because of problems of quality or because the data were too fragmentary to be of value. Most of their information supports the case presented in the monograph; considerable effort was made to identify and include data which might suggest otherwise. One potential body of studies not completely reviewed comes from doctoral and master's theses from the 13 Egyptian medical schools, although the authors did examine all relevant theses from the best-known schools (Cairo University, AI Azhar University, Alexandria University, Ain Shams University, Suez Canal University). During the life of the Project many of these theses were, in fact, prompted and supported by NCDDP. Most were either clinical studies, service statistics, hospital-based studies of etiology or local studies of mothers' treatment knowledge and practices. Data on mor- tality, however, came from NCDDP-sponsored evaluation and research, from the civil register back to 1970 and from independent national demographic surveys. The Project also examined--not reported here in detail--existing ethnographic studies pub- lished or known to anthropologists in Egypt, and commissioned additional focused ethnographic stud- ies to inform the program strategy.

Diarrhea control: impact on mortality in Egypt $5
10 -
.o
o~
o=
3 ?
[ ] 27.5g Local
• 27.5g Imported
[ ] 5.5g Local
i
78 79 80 81 82 83 84 85 86 87 88 89
Year
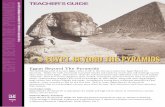
Fig. 2. Oral rehydration salts come in packets in Egypt. Initial importation (via UNICEF) and production for the public sector were of a packet for 11 of solution. For the private sector a 200 ml packet was
manufactured in-country and became the NCDDP standard in 1983.
In Section IV (Changes in mortality levels and patterns) and in Appendix A (On the relationship between classification error in cause of death and seasonality in evaluating diarrheal mortality) we will indicate our confidence in the data.
HI. T H E A C C O M P L I S H M E N T S O F N C D D P - - A R E V I E W
In terms of the proximate determinants model, the NCDDP placed primary emphasis on improved case management, secondary emphasis on activities designed to reduce diarrheal incidence and no direct emphasis on activities designed directly to improve host resistance (although proper treatment of diarrhea may itself have that effect).
To improve case management, NCDDP worked in three ways. First, the Project ensured that ORS was produced and distributed sufficiently to make packets universally accessible for all cases of diarrhea--both through the public and private sectors. The Project also sponsored the production and distribution to hospitals of a physiologically correct electrolyte solution for emergency i.v. treatment. Second, the Project tried to train properly all categories of personnel in the public health sector in the management of acute diarrhea. Third, the Project educated the population about the linkage of diarrhea to dehydration, and therefore its danger, and what to do when a child had diarrhea (proper feeding, use of ORS for watery diarrhea, seeking a physician's help
when a child was visibly dehydrated or the illness persisted).
NCDDP did not advocate home-mixing of sugar-salt solutions for fear of serious errors in mixing. It said little in its television campaigns against the various useless pharmaceuticals to avoid antago- nizing the medical profession (the correct approach was stressed, however, in all health worker training and Project documents). The Project dealt little with persistent diarrhea until the last three years when the problem became more apparent.
1. Production and distribution of ORS
The increase in use of ORS is reflected in data on production and importation (Fig. 2). From 1978, production and importation rose quickly to a level of about 4.5 million liter-equivalents in 1980 and 1981, declined in 1982 and 1983, but with the full implementation of NCDDP in 1984, increased to 8.6 million in 1985 before dropping off again. The temporary peak in 1980-81 is misleading as a considerable number of 1-1 packets were either not distributed from the warehouses or else not prescribed in the clinics (NCDDP internal reports). The mixing of liter packets also produced much more solution than was commonly used, yielding a higher proportion of wastage. A second peak in 1985 probably reflects to some extent a build-up of inventory. Since 1986, when distribution became demand-driven, production has more accurately reflected actual use.
SSM 40/lO~I

$6 Peter Miller and Norbert Hirschhorn
2. Training providers
Curative practices outside the range of modern medicine had gradually become less common by the time of the Project, and few Egyptians could be described as full-time traditional healers. The longer a diarrheal episode lasted, the more likely it was to be attributed to magical or other non-physical causes but as cases became more serious or chronic, physicians were increasingly likely to be consulted.
Before the Project, physicians uniformly tried to stop diarrhea with antibiotics and antidiarrheal agents [10, 11]. Physicians also told mothers to stop giving food or breast milk for at least 24-48 hr or until the diarrhea stopped [12, 13]. Dehydration was generally treated, if at all, with i.v. solutions [11]. ORS was accepted by the Ministry of Health in 1977, and packets distributed to MOH units in 1978, yet ORS was not widely used: between 1980 and 1983 local surveys estimated ORS use from 7 to 36% of episodes, even in governorates where the MOH was making extra efforts (details to follow).
The training unit of NCDDP had to try change medical practice throughout the country for the long-term. Training was necessary for persons in medical, nursing and pharmacy schools as well as for those already in practice. A wide variety of audio-visual and print training materials were produced and distributed by NCDDP, and seminars staged, geared to each profession. Each of the medical schools was contacted by senior academic pedia- tricians to introduce new concepts, provide teaching materials and negotiate curriculum changes. Nearly all 13 medical schools now include a question on diarrheal disease control on their final examinations in both pediatrics and public health. Diarrheal disease training, including ORT, is included in all house officer training programs. All 182 nurse training programs and the two High Institutes of Nursing follow revised MOH curricula and include diarrhea management questions on final examinations. Faculty from all the medical schools, the High Institutes of Nursing and the principal pharmacy schools were intimately involved in NCDDP-sponsored research and training.
For in-service training, NCDDP established rehydration training centers at all University and governorate Central Hospitals, as well as a number of Fever Hospitals, urban polyclinics and Ministry of Health Teaching Hospitals. By 1990, a total of 47 rehydration training centers had been created by refurbishing existing space near patient intake areas. Faculty included local physicians and nurses trained as trainers, as well as Ministry and Project staff. In addition, each of the 26 governorates has an official public health Training Center to which NCDDP contributed audio-visual and print materials. During the life of the Project, nearly 10,000 physicians and 14,000 nurses were trained for diarrheal disease management work.
Despite this massive effort, training was considered the most problematic component of the Project, particularly among physicians. For one, the concept of hands-on, 'competency-based training' was not entirely familiar to physician-trainers, and attempts to introduce this system widely were still on-going at the Project's close. Second, 3000-4000 new physicians graduated annually, all of whom received six weeks of in-service training by the Ministry of Health before posting to health centers; training in diarrhea treatment was but a small component and, because of the intake schedule, usually done in the season of lowest diarrhea incidence. Third, the NCDDP was not a line-organization and had only limited influence on the quality of the actual teaching. Finally, physicians in private practice were seldom reached by on-going training--and the majority of cases are attended by physicians in private practices.
As a result, a Health Facility Review conducted in 1990 by the Ministry of Health and WHO found that while health worker knowledge was reasonably good, actual practices in diagnosis, treatment and health education were much less than desired either by WHO or NCDDP. On the positive side, 82% of physicians checked for two or more signs of dehydration and 84% of mild to moderately dehydrated children were kept in the rehydration unit and given at least some ORS. Depending on the type of facility, antibiotics were used inappropriately in 5-31% of cases. Among mothers in the same health facilities, 95% knew how to mix ORS correctly and 73% knew how to administer it. Compared to the time before NCDDP these findings are entirely encouraging [4, 14].
The crucial question in relation to diarrheal mortality is whether health worker practices, insufficient as they were, were still enough to have plausibly contributed to the reductions in mortality we report.
3. Mass media and public education
The primary means of educating the public, especially mothers, about management of diarrhea were the mass media, and the primary medium was television. NCDDP launched its second annual campaign of TV spots during the middle of the diarrhea season of 1984 featuring the well-known motherly character actress Karima Mokhtar. The campaign was an enormous success. Everybody saw the TV spots and talked about them; Karima Mokhtar's acting and the well-crafted scripts had mothers all over Egypt demanding ORS.
The results of surveys recount the success of the TV spots in conveying the following key concepts: diarrhea is dangerous; diarrhea can lead to dehydration; what the signs of dehydration look like; how to give ORS and to continue specific foods and fluids; when to go for help; how to prevent diarrhea by personal hygiene and by breastfeeding. After 1985, nearly 100% of mothers knew about ORS and dehydration [15-21]. Remarkably, by 1988 nearly 90% of randomly

Diarrhea control: impact on mortality in Egypt $7
sampled mothers could mix ORS correctly on the spot [16-21]. The data on feeding are presented in the next section.
The television campaign was reinforced by other approaches. Radio continued to be used, articles on diarrheal disease control were regularly placed in popular magazines, billboards were erected, posters were put up in rehydration comers. The NCDDP logo, used in all visual media and printed on ORS boxes, helped to reinforce the content of the messages.
The mass media campaign had its limits. TV spots of one minute or less could not entirely be expected to convey modern medical ideas to a population with its own ideas about the nature and cause of disease. Many mothers never really understood the idea of dehydration as a loss of salts and water and ORS as a form of rehydration--rather than as a 'cure' for diarrhea [22]. Taxonomies of diarrhea associated with traditional cures continued to compete with modern ones [22, 23]. Messages about prevention of diarrhea stressing hygiene did not appear to have had much effect despite their prominent place in media messages throughout the Project.
Nonetheless, the mass media campaign must be regarded as a considerable success: mothers knew about ORT and knew how and when to use it. Coupled with the ready availability of ORS and with health workers increasingly supportive of and knowledgeable about proper care for diarrhea, a real improvement in case management could be expected.
4. Case management of acute diarrhea
In all the training and mass media messages, ORT was defined as rehydration with ORS plus continued feeding. In this section we separate these components only for the purpose of understanding the changes in case management. We are unable to say what proportion of life-saving (or child-strengthening in the instance of the child who would have survived anyway) either component contributed. A comprehensive review of this subject has been published [14].
Feeding patterns. Traditionally, diarrhea has been seen as a disease requiring some combination of home remedies, traditional medicine and modem medicine. Regardless of the source of treatment, the aim was to stop the diarrhea [12J--attempted with drugs and fasting. Three modem concepts were largely unknown to caregivers and health workers at the start of the Project: first that diarrhea is in most cases self-limiting and only about 10% of cases benefit from antibiotics, none from constipative drugs. Second, that the real problem of diarrhea is the loss of fluids and nutrients that must be restored. Third, that ORT itself helps slow diarrhea and heal the gut.
Mothers, often on advice from physicians, commonly stopped or reduced the amount of breast milk to infants or solid foods to older children and in their stead offered small amounts of herbal teas for as long as the episode lasted. Since with even mild dehydration and nausea a child loses appetite, the mothers' response appeared rational. As rehydration with ORS restores appetite and eliminates nausea, the Project advice to continue feeding could be more readily accepted: it was not simple exhortation. Table 1 shows data from studies before and after the Project on the proportions of mothers who discontinued (or reduced) food and fluids during the most recent diarrheal episode. In several surveys in Menoufia during 1980-82, between 51% and 65% of lactating mothers reported discontinuing breastfeed- ing during the last diarrhea episode, and between 34% and 65% of mothers reported discontinuing solid food to children between ages one and four [24]. In Dakahlia in 1980, 58% of mothers in a group of control villages discontinued breastfeeding during the last episode of diarrhea [25]. By 1985, those proportions had dropped to under 20%.
Fewer data are available for non-ORS fluids. Egyptian mothers have always given a variety of tisanes during diarrheal episodes but as constipatives and not for rehydration. Recent data indicate that re- duction or stopping of other fluids is now uncommon
Table 1. Feeding behavior during episodes of childhood diarrhea, Egypt, various survey data, 1979-91 Percent stopping feeding mode
Survey and reference Year Breast feeding Bottle feeding Other fluids Other foods Menoufia [24] 1979-82 51-65 Dakahlia [25] 1980 58 Five-Community Study [26] 1983 41' Menshiet Nasser [76] 1984 II b 63 b National K.A.P. Surveys 1984 32
[15-18] 1985 18 1986 14 1988 17 52 1989 5 36
Alexandria-Assiut [37] 1985 12 National ¢ DRSs [32, 33] 1985 12
1986 4 Menoufia [20] 1988 9 Menoufia [30] 1990--91
Stopped: 3 15 Reduced: 12 10
34-65
37 b
37 13 13
3 b 28
3 6 11 23
• On first day; 31% on subsequent days if diarrhea persisted. b Stopped or reduced. c DRS--Donble Round Survey.

$8 Peter Miller and Norbert Hirschhorn
Table 2. Percent use of ORS in last episode by recall period: Egypt, various survey data, 1980s Recall period
Survey (Re0 Year Past !-2 weeks Longer Ever-use Children under 5-6 Menoufia [34] 1979 Dakahlia [25] 1980 NNS [36] 1980 ~
Beni Suef [88] 1983 Alexandria [37] 1983 Assiut [37] 1983 Fayoum [89] 1984 NDH Survey [19] 1988 c Menoufia [30] 1990-91 a Arab League [90] 199 ! ~
Children under 2 WHO/EPI [91] 1984 44 Media Survey [92] 1984 35 57
1985 50 National DRSs [31-33] 1984 70
1985 78 1986 82
Sohag/Dakahlia [35] 1986 71 National KAP Surveys 1984 50
[15-18, 21] 1985 58 64 1986 50 68 1988 c 16 51 66 1989 46
NDH Survey [19] 1988 c 34 Menoufia [20] 1988 45 52 80 Menoufia [30] 1990-91 d 46 79
21 6 Lower Egypt b 18 Upper Egypt b
7 36 37 29 40 26
17'
19" 37"
• ORS plus home mixtures. b Menoufia, Dakahlia, Beni Suef, Alexandria in Lower Egypt; Assint, Fayoum, Sohag in Upper
Egypt. c Late Fall/Winter surveys. d Year-round average. Note: This table excludes surveys undertaken during or immediately following specific CDD
activities other than the national program.
and substantial proportions of mothers report increasing fluid intake, except in two studies where the majority of mothers feeding cows' milk said they discontinued the milk during the last episode (Table 1).
We recognize that answers to survey questions may reflect what the respondent thinks the questioner wants to hear, that is, the current received wisdom. Daily visits during the Five-Community Study, for instance, found that after five and ten days of diarrhea, 30% and 32%, respectively, still withheld breastmilk [26]; but some ethnographic studies indicated that breast milk was typically withheld only for a day [12, 13]. Complete fasting of children appears to have been rare [26]. The Project's advice appears to have been generally accepted as correct: a recent ethnographic study in six communities confirms that mothers now believe that children should continue to be given nutrients, particularly fluids, and should be fed well unless they are truly unwilling to eat [22].
Feeding practices reported by the mothers are generally similar to those which physicians in a Cairo-based study say they advise [27]. Of a sample of general practitioners and pediatricians, 12 % said that they generally advise decreasing breastfeeding, 66% advise decreasing bottle feeding, 2.4% advise decreasing fluids and 33.3% advise decreasing other foods. (The remainder in each category advise maintaining, increasing, or changing type).
In sum, during the course of the 1980s there is evidence of a marked improvement in maintaining proper feeding of children during diarrheal episodes, supported by a change in physicians' attitudes. The exception may be in discontinuation of cows' milk based-formulas; here, N C D D P was silent in its television campaign, not wishing to imply support for artificial milk. In physician-training, the N C D D P advised diluting formula milk or offering smaller portions.
Use o f ORS. A variety of large-sample household surveys, both sponsored by N C D D P and indepen- dently conducted, have studied the prevalence of use of ORS; several studies have looked at treatment in rehydration centers. Table 2 shows trends in the use of ORS from a variety of household surveys from 1979 up to the close of the Project. These include percentages of those who have ever used ORS as well as those who have used ORS during the most recent episodes at various intervals. Table 2 includes all studies we could find with reasonable samples from the period except two: the Five-Community Study obtained proportions of ORS use in current episodes during 15 monthly canvasses in six scattered communities just before and during full implemen- tation of the national program in 1983-84; the use rate rose from four percent in August 1983 to 48% in October 1984 [26]. A 1985 study found fairly high use

Diarrhea control: impact on mortality in Egypt $9
rates in Alexandria and Qcna, but its reference period is unclear [28].
Interpretation of the results is complicated by several factors which strongly influence reported use rates: the recall period, the age of the child and the season. ORS is less likely to be reported in the treatment if the episode occurred in the recent past rather than longer ago [18-20], a fact which has also been noted in international studies [29]. The main reason is probably recall bias: mothers are more likely to recall mild cases which have occurred recently, in which ORS is less likely to be used, and more likely to remember severe cases from the distant past when ORS was more often used. Hence estimates of use of ORS based on episodes in the last week or two weeks are preferable to those based on the more distant past, and may also be reasonably accurate.
ORS is also more likely to be used for children between six months and two years of age, so questions asked about all children under five will tend to show lower use rates than for children under two. Two studies of children under five give age breakdowns [19, 30], as shown in Table 2, indicating the extent of the influence of age.
A surprising differential in seasonal use of ORS was shown in a recent year-long study of ORS use and mortality in Menoufia [30] with differences of 10-20 percentage points between summer and late fall or winter. A prospective observational study by trained ethnographers in six scattered communities in January 1991 [22] found ORS used in 18 of 55 cases studied (33%) which may be reasonably compared to the Menoufia 49% use-rate in November/December 1990, and 23% use-rate in February 1991. This seasonal difference in use explains some seemingly anomalous low rates of ORS use seen on Table 2.
Taking these factors into consideration, one finds indications of change over time, particularly with respect to 'ever-use': moderately low rates through 1983, rapid increases in 1984 and 1985 and stable rates to the close of the Project. It seems likely that ORS has been used in one-third to one-half of all diarrhea episodes during the late 1980s. (We regard the anomalously high use-rates reported in the Double Round Surveys [31-33] as inaccurate. The surveyors were nurses from local Ministry of Health clinics who, while likely to gain easier entry into people's homes, were likely as well to be given the 'correct' answer).
Two local-area studies have more cleanly docu- mented the increase in ORS use where early, well-measured interventions were followed by long periods without special efforts. In 12 villages in Menoufia in 1979, 17% of mothers of children under two had used some form of ORT at some point ('ever-use'). By 1988, ever-use had risen to 80% in those same villages, and in 1990, was at 79% [20, 30, 34]. Similarly, a survey in Dakahlia in 1980 found ORS used in 21% of episodes in the control area for an experimental program; in the same villages in 1986, the proportion was 77% [25, 4].
ORS-use is also strongly determined by how the mother perceives the seriousness of the episode. Two recent studies [18, 20] have asked mothers whether they considered the episode 'simple' (basit) or 'strong' (shadid), whether dehydration (gafafl) was present, whether the child's stool was watery, and whether signs of dehydration such as vomiting, fever, diminished skin elasticity were present. Mothers' observations tended to correlate well with presen- t a t i o n - t h a t is, cases described as 'strong' tended to have more reported signs and symptoms of dehydration. ORS was far more likely to be used when cases were considered 'strong' or the mother perceived signs and symptoms of dehydration. Table 3 shows the associations with dehydration and with 'strong' diarrhea: some of the association is likely because a greater variety of treatments are attempted in serious cases, and also because ORS is seen by both mothers and physicians to be particularly necessary in more serious cases [22, 23].
Most diarrheal episodes are seen by a physician. For example, in three studies between 1986 and 1988 [18, 20, 35], between 64% and 76% of mothers said their child's most recent episode was attended by a physician. In one of these studies, ORS was given in 63% of cases seen by a physician compared with 29% not seen by a physician [18]; in another, the comparable figures were 66% and 26% [20]. Since serious cases are more likely to be seen by a physician than mild ones, part of the propensity of physicians to prescribe ORS is due to their seeing more serious cases.
Children taken to public health centers are more likely to receive ORS than children taken to private doctors [18, 20, 21, 30, 35]. The differential in Menoufia's year-long study was 80% use in public facilities, 67% in private practice [30] and a child was three times as likely to be seen by a private physician. Use of ORS is standard policy in the public health system, while in the private sector its use is more open to the physician's judgment. In a study in Cairo in 1990, however, physicians interviewed in their public practice reportedly were no more likely to have prescribed ORS in their last case of diarrhea than when interviewed in their private practice [27]. Physicians with both public and private practice may prescribe differently for patients coming to a public clinic than for their private patients, but no data are available on this topic.
ORS is somewhat more likely to be given in rural than in urban areas and least likely to be given in metropolitan areas such as Cairo and Alexandria
Table 3. Percent use of ORS in last episode by mothers' perceived characteristics of episode, Survey Data, Egypt, 1988-90
National KAP [18] Menoutia [20] Menoufia [19] 1988 1988 1990
'Strong' diarrhea 70 72 66 'Simple' diarrhea 25 39 37 Dehydrated 83 89 Not dehydrated 33 33

SI0 Peter Miller and Norbert Hirsehhorn
[17-19]. This is partly because private physicians are more likely to be consulted in more urbanized areas, but the difference remains after controlling for type of physicians. There is some indication that prior to NCDDP ORS was more widely used in Upper Egypt than in Lower Egypt [36, 37]; more recent studies have shown the reverse [17-19], and the reasons for these changes are not well understood. The socio-economic status of mothers shows little consistent variation in use of ORS except that mothers with secondary school education or more are less likely to use ORS [19, 20, 30, 37] reflecting, perhaps, less serious illness and greater attendance by private practitioners.
Although studies have repeatedly shown that most mothers know how to mix ORS properly [15-21], it is necessary to examine whether ORS is used in sufficient amounts or for a long-enough time. 'Sufficiency' was studied in children rehydrated at two large rehydration centers: after initial rehydration, 300 children took an average of 327 ml ORS daily for five days, 520 ml if diarrhea was watery (one Egyptian packet yields 200 ml); one child died who should not have been treated at home (0.3% case-fatality rate, confidence interval 0-0.9%), and two others needed hospitaliz- ation [38]. In the 1988 national KAP survey, ORS was given on the first or second day of the episode in 70% of cases, but two-thirds gave only one or two packets, and one half continued for no more than two days [18]. The year-long Menoufia study showed ORS given in the first two days in 82% of cases, used for three days in 74%, in an average amount of 2.7 packets per day (540 ml, if all was consumed). This pattern of use was sufficient to yield an infant mortality rate from diarrhea of 14.4/1000 live births, and a 1-4 mortality from diarrhea of 2.4/1000 mid-year population. These figures may be compared to the 1979-80 study where little ORS was used, and the respective death rates were 71.2 and 9.5 [30].
While the average reported intakes appear sufficient for dramatic mortality reduction, many children are still insufficiently rehydrated. Underhydration was present in at least 66% of the diarrhea deaths in which rehydration was attempted according to a verbal autopsy in Menoufia in 1988 (Hirschhorn, unpub- lished), indicating considerable margin for improve- ment in case management. Moreover, a recent ethnographic study in Upper Egypt suggests that a 'packet consumed' may mean only one or two spoonfuls from that packet, even in some dehydrated cases [22]. From the mothers point of view, ORS use has several constraints. The use of ORS has to be integrated into a matrix of pre-existing concepts of child care, both in general and for diarrhea specifically [12]. For example, the ethnographic study found that the use of ORS depends on the categorization of the diarrhea according to the local terminology. ORS would be used for some types of diarrhea that caused dehydration (and are greatly feared) but other types of diarrhea were perceived to have different symptoms and causes, so ORS would not be considered.
Moreover, surveys show that while both diarrhea and dehydration are understood, the relation between the two remains hazy. Mothers who like ORS say so because it stops diarrhea; those who do not like it complain that it does not stop diarrhea [18, 20]. The notion that diarrhea itself is generally self-limiting and that the primary emphasis should be on maintaining fluids and nutritional balance is still not widely understood.
ORS also takes more time to give than ordinary 'medicine'. Two to four cups of solution at one teaspoon a minute requires up to nearly 3 hr to give, a considerable investment of a mother's time. She is less likely, therefore, to use ORS if the diarrhea seems not so serious. A study at Abou E1-Riche Hospital in Cairo, supported by casual observation, indicates that some mothers do not give ORS slowly, one spoonful a minute, but simply give it as a drink [39]. In practice, this may make ORS more likely to be used but may also induce more vomiting.
Why physicians often fail to prescribe ORS is not entirely clear. In surveys, physicians rarely report not using ORS [40,41], although community-based studies consistently indicate otherwise. Certainly the mother's point of view is a factor in physician prescription, and some mothers refuse to accept ORS [39]. Also, at least at the beginning of the Project, they did not consider ORS useful if clinical dehydration was not already present. This is probably still true to some extent, as suggested in the survey data that show that physicians are less likely to prescribe ORS in mild cases.
Consequences of failure to prescribe ORS have been described in a study at Bab E1-Sha'reya Hospital in Cairo [42]. Of cases presenting to Bab E1-Sha'reya Hospital with moderate or severe dehydration, 38% had seen one or more physicians prior to coming to Bab E1-Sha'reya Hospital who had made no attempt at rehydration. Among controls with no or mild dehydration, 14% had such a history. After appropriate controls in analysis, the authors conclude that in a substantial number of cases, the effect of taking a diarrhea-sick child to a physician was to delay appropriate treatment to the point of serious danger to the child.
Use of antimicrobials and other drugs. The use of antimicrobials, constipatives and antiemetic drugs, with or without ORS, ranges from 42% of cases in the public facilities to 59% by private physicians [30]. The 1988 national KAP survey gave the figure as 62% of episodes occurring in the past two weeks [18], and the Demographic Health Survey yielded a figure of 57% [19]. Since only about 10% of episodes need any kind of medication these figures indicate widespread incorrect treatment. It is probable, however, that the situation has improved somewhat from before NCDDP: one study presented in 1984 showed 96% of episodes receiving medicines in the public clinics of the Upper Egyptian governorate of Fayoum [14]. The Five-Community Study showed 83% of episodes

Diarrhea control: impact
Table 4. Numbers of children with severe dehy- dration, EI-Shatby and Bab El-Sha'reya Hospitals,
1981-90
Year EI-Shatby ° Bab ei-Sha'reya [43]
1981 5072 1982 5986 1983 5623 40 b 1984 5246 50 1985 4595 29 1986 2906 37 1987 2627 27 1988 2870 13 1989 1553 16 1990 1247 14 1991 13
,Communication to NCDDP. bMay-December only.
treated with some drug [26]. The ORS intervention study in Dakahlia in 1980 showed inappropriate prescription of antimicrobials in 65% of episodes in the control area, and in 48% of episodes in the intervention area; while in the repeated experiment in 1986 the figures were 45 and 14%, respectively [4].
In sum, it appears that since NCDDP began, children with acute diarrhea have been fed better, have been more likely to receive ORS, have been more likely attended by a physician whose case management has improved since NCDDP began. Each of these statements must be qualified--lack of a firm baseline prevents us from saying precisely how much feeding has improved; ORS is often not used well and sometimes not at all; and doctors still do not treat as well as they should. Nonetheless, it is clear that acute diarrhea cases, especially serious ones, are being treated better than they used to be.
Hospital severity data. From the data available on case management, the degree of clinical improvement resulting from appropriate management is difficult to predict with any precision. Nonetheless, proper management should manifest itself in reduced levels of serious dehydration. For ethical reasons, sound community-based studies on this cannot be done but a lower incidence of dehydration would likely be apparent in hospitals. Since the population has become more aware of and afraid of dehydration, and since mothers are seeking care more readily, one would expect, if anything, a higher proportion of dehydration cases to be brought to hospital for treatment. Hence a substantial reduction in the number of cases seen in hospitals with serious dehydration is likely to indicate a lower incidence of dehydration in the population.
The limited time series data available, backed by general clinical opinion, indicates that hospitals are indeed seeing fewer cases of severe dehydration (Table 4). With consistent and comparable criteria, the number of severely dehydrated children declined by 71% between 1984 and 1990 at Bab E1-Sha'reya Hospital (AI-Azhar University) in Cairo [43], while at EI-Shatby Hospital (University of Alexandria), the number has declined by 78% between 1983 and 1990 (NCDDP, unpublished statistics). Neither the number
on mortality in Egypt S11
of diarrhea outpatients nor the total number of outpatients declined substantially during this period.
A less positive series has been observed at Abou EI-Reeche Hospital in Cairo, the largest and most famous pediatric hospital in Egypt (NCDDP, unpublished statistics). Here statistics date back only to 1985, and are not kept on severity of dehydration. The number of patients treated with i.v. solution decreased between 1985 and 1987 but then increased in 1989 and again increased sharply in 1990. There are insufficient data to know whether the staff's inclina- tion to use i.v. rehydrated changed during this period.
5. A summary
The pillars of the NCDDP as a special project included guaranteed ORS production and distri- bution, a targeted mass media campaign, mass training of health workers, establishment of rehydra- tion centers, research and evaluation--all integrated into a mostly coherent whole. The Egyptian and American planners of this project believed that the effort could not have been achieved within the normal national health services, at least not within the time-frame given. We believe this judgment was correct but must now turn to the evidence that the hoped-for impact was indeed achieved.
IV. CHANGES IN MORTALITY AND ITS PATTERNS
1. Overall infant and childhood mortality pre-NCDD P
Infant mortality in Egypt has been declining since the mid-1940s. More recently, from 1970 to 1983, the civil register records a decline from 1169/oo to 659/00 [44-46], Table 5. The decline was more rapid between 1970 and 1977, after which the pace of the decline up to 1983 slowed. An extensive body of demographic analysis summarized by Central Agency for Public Mobilization and Statistics (CAPMAS) [48] sup- plements data from the civil register and the census to
Table 5. Infant deaths per 1000 live births and age-specific death rates for children aged I-4, 1970-90
Year Infant mortality Mortality age 1-4
1970 116 32 1971 103 27 1972 116 31 1973 98 24 1974 101 22 1975 89 22 1976 87 18 1977 75 19 1978 73 13 1979 76 17 1980 76 II 1981 70 II 1982 70 14 1983 65 10 1984 62 lO 1985 49 lO 1986 47 8 1987 45 8 1988 43 7 1989 41 6 1990 34 5

S12 Peter Miller and Norbert Hirschhorn
Table 6. Infant deaths per 1000 live births and ase-specitic death rates for children aged i-4, by cause, 1970-90 Infant mortality Childhood mortality
Year Diarrhea Non-diarrhea % As diarrhea Diarrhea Non*diarrhea % As diarrhea
1970 65.9 50.0 57 17.0 15.2 53 1971 48.6 54.4 47 11.6 15.4 43 1972 60.8 55.6 52 14.4 16.4 47 1973 55.8 42.2 57 11.6 12.0 49 1974 59.6 41.4 59 11.8 10.0 54 1975 49.3 39.7 55 10.3 11.2 48 1976 52.8 34.2 61 9.6 8.5 53 1977 49.0 36.3 57 9.7 9.1 52 1978 43.7 29.8 59 6.7 6.3 52 1979 42.3 34.1 55 9.5 7.6 56 1980 39.2 36.8 52 5.7 5.5 51 1981 35.8 34.2 51 4.9 6.3 44 1982 33.0 37.0 47 5.9 7.7 43 1983 29.1 35.6 45 4.0 6.0 40 1984 25.7 36.3 41 4.0 6.4 38 1985 15.3 33.9 31 2.7 6.9 28 1986 15.2 32.0 32 2.6 5.2 32 1987 12.3 32.8 27 2.3 5.5 29 1988 12.1 31.2 28 1.9 4.7 29 1989 11.8 28.7 29 1.6 4.5 26 1990 9.3 24.5 28 1.1 3.4 24
document this change, which is unchallenged in outline. Exact levels, however, remain in doubt, particularly for infant mortality.
Registration of infant mortality is known to be incomplete. The most comprehensive estimates of completeness are indirect estimates by Rashad [49] and the U.S. National Academy of Sciences [50] on the basis of the 1976 national census. Both sources estimated about 75% completeness for the period around 1975, which Bucht and EI-Badry [51] consider somewhat low. A recent attempt to repeat this procedure using data from the 1986 census in selected governorates [52] suggests that completeness of registration may have improved.
A second source of mortality estimation, typically showing higher levels, is from national demographic surveys, notably the Egyptian Fertility Survey (EFS) of 1980 [53] and the Demographic and Health Survey (DHS) of 1988 [19]. These estimates are of two types: indirect estimates, using children-ever-born to chil- dren-surviving ratios; and direct estimates derived from birth history data. The latter tend to be lower and are probably more accurate. The two studies show similar rates for the period they have approximately in common: the EFS estimates an IMR of 132 in 1975-79, compared with 124 for the DHS in 1974-78. Combined, the two surveys indicate a decline from 146 in 1970-74 to 119 in 1979-83, or 18%. The decline in the civil register, taking the average decline during the two periods, was 33%.
According to both civil registration and survey data, mortality for children aged one to four also declined between 1970 and 1983, and both sources agree on the approximate levels. The civil register shows an uneven but generally rapid decline between 1970 and 1978, with little overall change until 1983. The DHS shows a decline in childhood mortality (ages 1-4) of about 40% between the periods 1974-78 and 1979-83, compared with 32% in the civil register.
The civil register is the only pre-1980 source for cause-of-death data. Table 6 shows that somewhat over one half of all infant and child deaths between 1970 and 1979 were caused by diarrhea. In addition to underreporting, inaccuracy in cause of death classification is acknowledged, although the level has not been assessed. A limited body of other data, however, supports the general magnitude of these proportions. For example, a verbal autopsy conducted over a one year period (1979-80) in Menoufia [54] showed that 49% of 343 deaths to children aged five and under were caused by diarrhea. In Dakahlia, 1980, verbal autopsies on 179 summer (May-October) deaths of children aged one to 59 months, found 84% caused by diarrhea [3]. In 1983, diarrhea was said to be present the week before death for 36% of 53 deaths to children under five in Alexandria and 49% of 177 deaths in Assiut.
The two verbal autopsy studies from Dakahlia and Menoufia governorates in Lower Egypt shed light on the circumstances surrounding diarrheal mortality. The pattern suggested primarily acute rather than chronic diarrhea. In Dakahlia, diarrhea during the fatal episode lasted less than one week in 47 of 60 diarrhea deaths, and 14 days or longer in only three cases (Hirschhorn, unpublished). For 171 cases in Menoufia, the average clinical course of the terminal diarrheal episode was about four days [54]. In nearly all cases in both studies the child had been taken to a doctor, often to a hospital. In Menoufia, oral rehydration had not been attempted in 73% of fatal cases, and no rehydration at all in 42% [54]; in Dakahlia, no fluids were prescribed in the treatment of the final illness for 58% [3].
Infant and childhood mortality had a definite seasonality. In the four-month period between May and August, between 46% (in 1970) and 51% (in 1977) of all registered infant deaths occurred each year between 1970 and 1983. This seasonality was primarily

Diarrhea control: impact on mortality in Egypt S13
due to diarrheal mortality, but registered mortality from other causes also tended to increase slightly during the summer. For example, in 1983, 56% of infant diarrheal deaths occurred during the third of the year from May to August, compared with 44% of respiratory deaths, 36% of deaths from perinatal causes, and 40% of deaths from other causes. The excess of registered respiratory mortality in summer is counter to common clinical impression but not incompatible with the poorer nutrition (wasting) found in summer [36].
2. Overall infant and childhood mortality after NCDDP
The data on Table 5 show the registered infant and childhood deaths for the period of 1983-90. During the first five years of national implementation of NCDDP, infant and childhood mortality each declined by about one-third. For infant mortality, most of the decline took place between 1984 and 1985, whereas for childhood mortality the largest drop was from 1985 to 1986. The average annual decline in infant mortality was somewhat faster between 1983 and 1989 than between 1970 and 1983. For childhood mortality the pace of the decline was about the same. Rashad has modeled the linear trend in infant mortality from 1965 and shows a significant discontinuity after 1984 due to a change in the intercept but not in the slope of decline [55].
Retrospective data from the DHS support the finding of recent rapid mortality declines [19]. Between 1979-83 and 1984-88, there was a decline of 39% for infant mortality and 43% for childhood mortality, somewhat greater than the decline shown in the civil register for the same period. This also suggests that the completeness of the civil register may have improved somewhat during the period in question, a conclusion consistent with analysis using 1986 national census data [52].
A third source of documentation for a national mortality decline for part of the period in question is a series of Double Round Surveys (DRS), commis- sioned by NCDDP in 1984-86 [31-33]. Three annual cycles were undertaken, designed to enumerate about 10,700 children from birth to two years of age at the beginning of peak diarrhea season. The children were then followed up after six months to determine survivorship, and in case of death to ascertain whether diarrhea was present in the week before death. The study was done in a quasi-probability cluster sample of eight governorates, intended to be broadly representative of Egypt. The six-month mortality rate declined from 17.5/1000 in 1984 to 11.5/1000 in 1985 to 10.9/1000 in 1986. The decline of 34% during 1984-85 is greater than the 21% indicated in the civil register, while the decline during 1985-86 is about the same (5 and 4%, respectively). The nature of the study does not allow direct calculation of an infant mortality rate but estimates can be made from model life tables and are quite consistent with the levels of the DHS. Rashad analyzed the DRS data for 1984 and 1985 by
logistic regression analysis and found that age of child (younger), year of survey (1984), and sanitation of household (poorer)--in that order of magnitude-- significantly contributed to the risk of mortality [56]. There were serious weaknesses in the DRS--less than ideal supervision and hurried execution due to the Ramadan, for instance--and we would not base our final conclusions on these surveys alone.
In sum, three independent data sources--the civil register, DHS and DRS--indicate that infant and childhood mortality declined rapidly during 1983-88, including a particularly sharp decline in 1985. For infant mortality, the decline has been more rapid than for the period 1970-83. In itself, this does not indicate NCDDP effect, but it does suggest that some factor or factors continued to operate to reduce the force of mortality during the period of the Project. The next step is to determine whether the decline was concentrated in diarrheal mortality.
3. Cause of death and seasonality
In principle, the most compelling mortality evidence for NCDDP impact should be found in the data on cause of death for infants and children. I fNCDDP has had an impact, there should be decreases both in the rates and in the proportions of infant and child deaths from diarrhea. A particularly troublesome possibility, for which some anecdotal support exists, is that in the context of a national program, some local physicians may underreport diarrheal mortality in order to make local efforts appear successful. If widespread, such a practice would introduce a spurious decline in registered diarrheal mortality at a time when NCDDP activities were being vigorously implemented. We will deal with the problem of misclassification in this section and in greater detail in Appendix A.
Figure 3 and Table 6 show the ratios of infant diarrheal and non-diarrheal deaths to births from 1970 to 1990 [57]. Diarrheal and non-diarrheal mortality declined at approximately the same pace between 1970 and 1978. Thereafter, non-diarrheal mortality in- creased slightly, while diarrheal mortality declined steadily until 1984, at which point the decline accelerated [58]. In exponential terms, from 1970 to 1977 infant mortality from diarrhea declined by a mean of 4.2% per year. From the Ministry's first use of ORS in 1978 until implementation of NCDDP in 1983, the average decline was 7.8% per year. From 1983 to 1990 the average annual decline was 15.9%. A similar pattern is observable in childhood mortality (Fig. 4, Table 6) with corresponding period declines in diarrheal mortality averaging 8.0, 9.9 and 21.0% per year. Diarrhea is no longer the leading cause of registered infant and child death in Egypt, replaced in 1985 by respiratory infection--which had accounted for fewer than one half as many deaths prior to 1978.
Change in cause of death was also measured in the DRSs (Table 7). Deaths were considered diarrhea- associated if diarrhea was reported as present during

S14 Peter Miller and Norbert Hirschhom
70 ~ • Diarrheal
e01\ . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4"_ Non_-D_ia_r~_eal _
. . . . . . . . . . . . . . . . . . . . . . . . . . . .
40 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
i
70 71 72 73 74 75 76 77 78 79 80 81 82 83 84 85 86 87 88 89 90
Year Fig. 3. Infant deaths per 1000 live births, diarrhea and non-diarrhea, from 1970 to 1990, according to the
civil register.
the week prior to the child's death. The proportion of diarrhea-associated deaths during the diarrhea season fell from 62% in 1984 to 51% in 1986, a decline statistically significant at the 0.05 level. Eighty-two percent of the decline in mortality between 1984 and
1986 was in diarrhea-associated mortality. By comparison, 71% of the decline in infant mortality in the civil register between 1984 and 1986 was due to diarrheal mortality. Rashad's regression discontinuity analysis shows this also to be a significant departure
20 j • Diarrhea
1 5 ~ ~ l ~ . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . _-F_ Non:Dia_r _rh;a_ _ _ _
I- o iii i_iiiiiiiiiiiiii--iiiiii ....
-•,,.,,
0 70 71 72 73 74 75 76 77 78 79 80 81 82 83 84 85 86 87 88 89
Year
Fig. 4. Age-specific child mortality, diarrhea and non-diarrhea, from 1970 to 1990, according to the civil register.
9 0

Diarrhea control: impact on mortality in Egypt
Table 7. Changes in proportions dead after six months from initial cohorts of children aged 0-23 months, DRS, 1984-86
S15
Diarrhea Year Children Total deaths Rate/1000 related deaths Rate/1000 Other deaths Rate/1000
1984 10,739 188 17.5 117 10.9 71 6.6 1985 10,738 124 11.5 73 6.8 51 4.7 1986 8704 95 10.9 48 5.5 47 5.4
Refs: [31-33, 56].
from the previous trend-line in the civil register data [55].
Another data source for comparison to the civil register, bearing on the cause of death nationally, is the 1988 DHS. This survey found that 29% of deaths occurring to children under five during the five years preceding the survey were associated with diarrhea during the week prior to death [19]. For the same period, the civil register indicated that 33% of deaths occurring in children under five were caused by diarrhea.
As an internal check on the validity of cause of death information in the civil register, one can examine seasonality of mortality. As noted before, diarrheal disease is the most highly seasonal of major causes of infant and childhood mortality in Egypt, with well over one half of the deaths from diarrhea occurring during the four-month period from May through August. Moreover, the month of death is more accurately reported than the cause, and it is implausible that the month of death would be misreported as a result of NCDDP activities. Hence a decline in the degree of summer seasonality of mortality would provide strong support for the
validity of the decline in registered diarrheal mortality. Seasonality data for infant mortality are shown in
Fig. 5 from 1970 through 1989. The degree of excess summer mortality tended to rise during the 1970s until 1978, after which it declined through 1987, with a particularly strong and sustained decrease after 1984. Between 1979 and 1987, nearly two-thirds of the seasonality of infant mortality in Egypt disappeared. There is a slight increase in seasonality of mortality in 1988-89, as non-diarrheal mortality decreased more than diarrheal mortality for infants.
Further information can be obtained by joint analysis of cause of death and seasonality in the civil register, considering possible effects of classification error in cause of death. Table 8 shows cause (diarrheal vs other) and season of death for infants between 1983 and 1988. The rapid drop in total infant deaths between 1983 and 1985 is primarily due to a sharp decline in summer diarrhea mortality, without a corresponding increase in summer mortality from other causes. Diarrheal mortality in each season fell rapidly during 1985, and continued to decline slowly. Non-diarrheal mortality has shown no clear trend, but
• May - August I No seasonality
1
45
40-
3 5 . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
I I I I I ', ', ', ~ = ', ', ~ = = = I
30 70 71 72 73 74 75 76 77 78 79 80 81 82 83 84 85 86 87 88 89
Y e a r
Fig. 5. Proportionate infant mortality, according to the civil register, in the months of May through August (which includes the peak diarrhea season), 1970-1989. In any four-month period 33% of annual deaths
would occur were there no seasonality of deaths.

S16
Table 8. Infant deaths (000) by cause and season, Egypt, 1983-88
Peter Miller and Norbert Hirschhom
Birth ratio Year Cause Jan -Apr May-Aug Sep-Dec Total ('83 ffi 100)
1983 DD 7.4 27.2 13.9 48.5 100.0 N D D 16.5 24.5 18.3 59.3
1984 DD 8.6 23.7 14.1 46.3 107.8 N D D 19.9 24.6 20.8 65.3
1985 DD 5.7 14.6 8.9 29.2 114.2 N D D 17.2 24.5 22.9 64.5
1986 D D 5.6 14.2 9.2 29.0 ! 14.5 N D D 17.3 22.1 21.5 61.0
1987 D D 4.6 12.1 8.9 25.6 125.2 N D D 20.1 24.5 23.9 68.4
1988 D D 4.6 12.0 6.6 23.2 114.7 N D D 17.5 23.2 19.0 59.7
DD = Diarrheal deaths ( x 1000). N D D = Non-diarrheal deaths ( x 1000).
is generally consonant with the overall increase in births. To account for these patterns by changes in patterns of misclassification of cause of death would require impressive coincidence.
The data were also examined by individual governorate and showed similar patterns except in two: In Sohag Governorate a sharp decline in summer infant mortality between 1984 and 1985 was counterbalanced by a rise in non-diarrheal summer mortality, suggesting deliberate misclassification on a substantial scale. In Menoufia Governorate the proportion of deaths from diarrhea in 1983 was already much lower than in any other governorate, and remained approximately constant. Other data, as well as field observation, indicate gross underreporting of diarrheal mortality in the Menoufia civil register starting in the early 1980s, prior to NCDDP. Strong declines in seasonality of both diarrheal and non-diarrheal mortality suggest that, in fact, the proportion of diarrheal mortality in Menoufia declined as it did in the rest of the country.
Closer observation of the seasonality data shows that the decline in seasonality is greater than can be accounted for by the observed decline in diarrheal mortality, and that seasonality has declined for both diarrheal and non-diarrheal mortality. Human and biological factors could explain this decline--but continuing and random two-way misclassification
could as well. Appendix A examines this possibility in detail, one implication of such misclassification is that the real decline in the proportion of deaths due to diarrhea during the period was actually understated in the civil register.
Analysis of seasonality of mortality thus strongly supports the cause of death data in the civil register. Misreporting could potentially account for the change in reported cause of death but implausibly accounts for change in seasonality, which occurs in patterns consistent with a large, real drop in diarrheal mortality. This is not to say that underreporting of diarrheal deaths did not occur even outside Menoufia and Sohag--doubtless it did--but that this does not appear to account for the observed decline in diarrheal mortality during the period in question.
4. Mortality data from local area studies
Two controlled community trials of rehydration with ORS were carried out in 1979-80 (Table 9). The NCDDP sponsored a replication of both trials seven to nine years later, after a period of no special activity other than the implementation of the national program. In Dakahlia Governorate in 1980, 29 villages were randomly allocated to experimental or control treatments. In experimental areas, ORS use in the last diarrhea episode was 53 %, compared with 21% in the control areas, and diarrhea mortality to children ages one to 59 months, as measured by verbal autopsy, was substantially lower [3]. In the 1986 trial, there was no longer any significant difference between the two areas in either ORS use or mortality--but in both areas ORS use was higher and diarrhea mortality lower than even in the 1980 intervention area [4]. Ninety-one percent of the decline in the six-month (diarrhea) season mortality between 1980 and 1986 was in diarrheal mortality. Examination of the civil register for the 29 villages showed that the decline in mortality was concentrated during 1983-85. Civil registration data for the whole governorate showed that the proportion of deaths occurring during the four summer months declined from 49% in 1980 to 37% in 1986, with nearly one half of the decline occurring in 1984.
A partially comparable situation existed in Menoufia Governorate, where an experimental ORS home distribution experiment was conducted in six villages, matched with six control villages, in 1979-80.
Table 9. Changes in diarrheal and non-diarrheal mortality in two local studies, pre- and post -NCDDP
(A) Dakahfia [3, 4]: six month summer mortality in children aged 1-5 months, control and experimental areas in 1980 vs experimental and control areas combined in 1986
Area Children Total deaths Rate/1000 DD deaths Rate/1000 Other deaths Rate/1000
Control 1980 10,418 189 18.1 159 15.3 30 2.9 Exper., 1980 16,359 171 10.5 125 7.6 46 2.9 Comb., 1986 31,243 193 6.2 115 3.7 78 2.5
(B) Menonfia [20, 54]: Estimated deaths per 1000 children under five years of age, combined study areas, 1979-80 and 1987-88
Period Children Total deaths Rate/1000 DD deaths Rate/1000 Other deaths Rate/1000 i 979-80 7650 343 44.7 172 22.4 171 22.3 1987-88 8925 144 16.1 56 5.9 88 10.2
DD ffi Diarrheal disease.

Diarrhea control: impact on mortality in Egypt S17
A carefully conducted mortality study using verbal autopsies found that the experiment had no effect on mortality. Tekce [54] concluded that either the design was inappropriate--the local medical community was not involved nor was there effective training or public education--or that the potential of ORS is limited as long the incidence of diarrhea remains the same. The nationwide implementation of NCDDP is a test of the former hypothesis, so the study area was revisited in 1988 to investigate both mortality and case management of diarrhea after full implementation of NCDDP. By 1987, mortality of children 0--4 had declined by about 64% [20] with most of the decline occurring in 1985-86. According to verbal autopsy findings, 38% of the past year's infant and child deaths was due to diarrhea, compared to the 1979-80 verbal autopsy study in which the proportion was 50%. Overall, diarrheal mortality had declined by 72%, non-diarrheal mortality by 56%, with lower diarrheal mortality accounting for 56% of the mortality decline.
Both diarrheal and non-diarrheal death rates have declined in Menoufia at a faster rate than the rest of Egypt. Even if diarrheal mortality had gone to zero, non-diarrheal mortality would have had to decline by 25% to account for the overall drop. We have no certain explanation for this event except to suggest that as home governorate to both Presidents Sadat and Mubarak, Menoufia may have benefitted from a greater level of public investment.
A major prospective study has recently been completed in the same 12 villages, with more careful mortality estimation procedures for both retrospective and prospective periods [30]. Whereas the 1979-80 survey estimated infant mortality at 115%o and child mortality at 67%0, these values in 1990-91 were 42 and 18, respectively. The proportion of all infant and child deaths due to diarrhea in 1990-91 was 41%.
5. Changes in the circumstances of diarrheal mortality
In comparison to the wealth of data on mortality change in general, there is relatively little information on the details of the diarrheal deaths themselves. Most of the information comes from four verbal autopsy studies, two each from Dakahlia and Menoufia. These verbal autopsies have not been written up in sufficient detail either to know the extent to which the same procedures are used, or to learn as much as we would like about the circumstances of death. Nonetheless, fragmentary evidence suggests that persistent diarrhea has become increasingly common in fatal cases. In Dakahlia in 1980, in only 5% of deaths caused by diarrhea did the episode last more than 14 days [3], and in Menoufia in 1979-80 the average clinical course of the fatal diarrheal episode was four days [54]. In Menoufia in 1987-88, on the other hand, diarrhea lasting for 14 days or more occurred in 25% of all deaths for which diarrhea was the direct cause or a contributing cause [20]. If case management has indeed improved, its major impact should be on acute diarrhea; persistent diarrhea should then form a higher
proportion of diarrhea deaths than previously. This phenomenon, if true, might have contributed to the slowing in the decline of mortality after 1985: the easier was accomplished first.
It is unlikely that the prevalence of persistent diarrhea has markedly increased, coming perhaps from an enlarging pool of weakened survivors of acute illness. At Bab EI-Sha'reya Hospital in Cairo, for instance, no important change was observed over time in the proportion of patients with persistent diarrhea reporting to the rehydration center, approx. 2% each year [43]. Evidence in the literature would suggest that ORT actually protects a child's nutrition for several months after an episode [8].
The most important change in the treatment of fatal cases seems to be in the use of ORS. Most fatal cases, both before and during NCDDP, were taken to a physician at least once during the fatal illness; but most died at home: in Menoufia 35% of fatal cases were hospitalized during the final illness in 1979-80 compared with 42% in 1987-88 [20, 54]. ORS, however, was given in only 33% of diarrhea deaths in 1979-80, compared with 91% in 1987-88. This indicates that emergency treatment of cases has improved.
6. Summary
Beyond question, a major decline in infant and childhood mortality has taken place since the initiation of NCDDP, primarily due to a rapid drop in deaths, specifically from diarrheal disease. According to the civil register, between 1983 and 1988 infant and childhood mortality each declined by one-third. In the same period, registered diarrheal mortality fell by 58% for infants, 53% for children ages 1-4. Seventy-nine percent of the drop in infant mortality and 62% of the drop in childhood mortality was due to diarrheal disease. Data from other sources including national surveys and local area investigations suggest that both the overall decline in mortality and the proportion due to diarrheal disease may be understated in the civil register. These other sources are independent from each other and have complementary strengths and weaknesses. While the exact level of the changes can be debated, it is wholly implausible that they could all be wrong.
In contrast to the abundance of demographic data, details on the circumstances of diarrheal deaths are scanty, allowing only limited inferences as to why the change occurred. The next section will address this question in detail.
V. OTHER FACTORS POTENTIALLY INFLUENCING MORTALITY
At the beginning of this investigation, the proximate determinants of diarrheal mortality were divided into three classes: case management; incidence/prevalence (including etiology); and host resistance. Thus far only case management has been examined in detail which

S18 Peter Miller and Norbert Hirsehhorn
leads to the conclusion that NCDDP had a considerable effect on case management, despite serious remaining weaknesses. The following section discusses changes in etiology, incidence and preva- lence, and host resistance to examine the influence each may have had on diarrheal mortality, and to understand why these changes, if any, may have occurred.
1. Etiology, incidence and prevalence of diarrhea
The etiology of diarrhea. Some information is available regarding the etiology of diarrhea in Egypt during the pre-Project period but comparisons are difficult. The data before 1980, for instance, cannot be easily compared to the period of the NCDDP as microbiologic techniques became more precise and several new etiologic agents have been discovered. It is likely, however, that shigellosis was more common in earlier times: in the 1950s Shigella species were isolated in 8% of asymptomatic children and in over one-third of diarrheal episodes in village children under five [59-61], with an overall annual attack rate of 2.8 episodes per child and a diarrhea death rate of 50/1000. An out-patient clinic study in 1962 in children under two gave a 22% isolation rate for Shigella [62]. By 1983-84 the isolation rate in cases of diarrhea was only 2-8% [63,64]. The former situation is reminiscent of Bangladesh today, a function, perhaps, of the overall state of nutrition [65].
National profiles of etiology are not available as most of the data are from single community or hospital-based studies [66, 67] which use different sampling bases and time periods; routine stool cultures are seldom done in cases of diarrhea. Nonetheless, some recent comparisons are of interest:
--Children admitted with diarrhea to EI-Shatby (Alexandria University) Pediatric Hospital (1981-82) had the following proportionate isolations: rotavirus 19%, Campylobacter 11%, Shigella 8%, enterotoxigenic E. coli 10%, enteropathogenic E. coli 6%, Salmonellae 4% [63].
- - I n fatal or near fatal cases of diarrhea in children in Cairo under 18 months old (1982), isolations were Giardia lamblia 35%, rotavirus 33%, enterotoxigenic E. coli 31%, en- teropathogenic E. coli 8%, Salmonellae 5% [66].
--Rotavirus isolation totaled 20% in children visiting the rehydration center at Alexandria University E1-Shatby Hospital (1982) [68].
- - I n eight rural villages of Lower Egypt (1983-84) the isolations of microorganisms from cases of diarrhea detected on home-visits (the majority in children) were Giardia lamblia 44%, enterotoxigenic E. coli 27%, en- teropathogenic E. coli 4%, rotavirus 3%, Shigella 2%, Campylobacter 2%, Salmonellae 1%. [69].
- - I n urban Alexandria, in children under two (1983-84), the isolations from outpatient eases of diarrhea were rotavirus 29%, Giardia lamblia 21%, Campylobacter 21%, enterotoxi- genic E. coli 9%, Entameba histolytica 4%, Salmonellae 3%, Shigella 2% [64].
- - A t Bab EI-Sha'reya Hospital (AI Azhar University) in 1986, children under two had rotavirus isolated in 40% of cases [70].
(One expects rotavirus and enterotoxigenic E. coli to be more common in children visiting a hospital as both produce a more acute illness and severer dehydration. The consistently high prevalence of Giardia, however, probably represents adventitious carriage as it is so common in asymptomatic cases; its role in acute illness has not been well determined in Egypt. When first infecting a child, however, Giardia tends to produce an acute, watery diarrhea).
The profiles are reasonably consistent with those in other developing countries in 0-3 year olds: rotavirus 16%, Shigella 11%, enterotoxigenic E. coli 16%, Campylobacter 11%, enteropathogenic E. coli 9%, Salmonellae 3%, V. cholerae 1%, Giardia lamblia 3%, and other viruses 7% [71].
We cannot conceive of what changes in microbio- logic profile would account for the substantially lower mortality rates over a one or two-year period--in particular rotavirus and enterotoxigenic E. coli--un- less the incidence of diarrhea had also dropped significantly and selectively for the more serious etiologies. We turn now to a consideration of diarrhea incidence.
Incidence and prevalence. Incidence and prevalence of diarrheal disease in Egypt at any time depend on a variety of factors, most notably time of year (diarrhea is most common in summer [26]), age of child (most frequent among children between six months and two years [26, 36, 72]), and geographic location (preva- lence generally increases as one moves south [15-19]). Estimates also vary depending on the survey methods. The length of the recall period is important, both because it determines the length of exposure, and because episodes from the more distant past, especially mild ones, are more likely to be forgotten [18-20, 29]. The definition and terminology used for diarrhea, and the manner and context in which questions are asked, may also affect estimates [29]. Finally, real incidence and prevalence may vary for reasons which are in effect random to an observer, perhaps as particular etiological agents wax and wane within, say, the ranges of the profiles given above. Under such circumstances, the precise determination of diarrheal disease incidence or prevalence is not possible. Characteriz- ation of general levels and patterns, however, is feasible and represents a valuable contribution.
Prevalence estimates for the period between 1978 and 1983 from six retrospective surveys and two prospective studies could be found. Two of the retrospective studies and one prospective study were

Diarrhea control: impact on mortality in Egypt
Table t0. Seasonally adjusted percentage of children with diarrhea within specified recall periods, by age, household survey, date, 1978-91
Prevalence interval Study Last 24 hr 1 Week 2 Weeks
Children under five NNSs °,b [36, 72] 1978
1980 Menoufia ¢ 1980--81 Dakahlia [25] 1980
1981 Alexandria [37] 1983 Assiut [37] 1983 NDH Survey [19] 1988 Menoufia [30] 1990
Children under two
NNS [36, 72]
Five-Community Study [26] National DRSs [31-33]
National K.A.P. Surveys [16-18, 21]
Dakahlia [35] Sohag [35] NDH Survey [19] Menoutia [20] Menoniia [30]
9 19 9
1978 1980
1983-84 12 1984 1985 1986 1985 1986 1988 10 1989 8 1986 1986 1988 17 1988 6
1990-91 d
16 12 7
13 7
22
27 20
30 29 26 39 38 31
20 39
25
45 21 38 32 36 38 28
IAge 6-71 months for under-fives, and 6-23 months for under-twos. bMenoufia, Dakahlia, Alexandria in lower Egypt; Assiut, Sohag in upper Egypt. °Menoufia 1980-81 data from N. Nosseir, unpublished. dFull-year longitudinal survey.
S19
conducted on a national level, or at least covered several geographic areas, while the others were conducted in only one or two locations.
The Five-Community Study. The richest body of data comes from a NCDDP-sponsored and designed study conducted in five varied communities between August 1983 and October 1984 [26]. In this study, 1079 diarrhea cases found in August 1983 were followed daily for up to 11 days, and a monthly canvass was made of all children under 3 years old between August 1983 and October 1984 to study seasonal variation in day-point prevalence. The study thus gives data on clinical characteristics of cases, management patterns and seasonality. It should be noted, however, that locating all cases active on a given day tends to oversample cases of longer duration. Essential features of this study were repeated in 1987-88.
From the monthly canvasses, annualized and averaged day-point prevalence was about 12%, or about 43 diarrhea-days per child per year. Age- specific attack rates (diarrhea present on the canvass day) fell off only in the third year of life. Watery diarrhea occurred on 57% of diarrhea days, vomiting on 19%, and bloody stools on 2% of diarrhea days. On day-one of the August 1983 follow-up, vomiting occurred in 15% of cases, the child was less active in 22%, and inelastic skin was noted in 5% of cases. Eight percent of cases persisted, continuously or intermittently, for at least ten days after the canvass day. Estimation of a true frequency distribution of
duration or proportions of persistent diarrhea is uncertain due to selection of cases during rather than at the beginning of episodes, and truncation of observation at ten days. Seasonality followed expected patterns: prevalence in summer was more than twice as high as in winter.
Using these seasonal data, combined with data from the 1987-88 study (which showed little change in either level or seasonality), approximate adjustment factors by month were prepared for the cross-sectional studies of prevalence or incidence. (The calculations are shown in Appendix B). Seasonally adjusted prevalence estimates from the retrospective surveys are shown by recall period in Table 10. The 12% day-point prevalence from the Five-Community Study looks reasonable in relation to other studies. Day-point prevalence is lower than weekly prevalence, which is lower than bi-weekly prevalence. Prevalence for under-fives is lower than that for under-twos.
The only prospective study yielding numbers of episodes per year was in a rural Lower Egyptian community in 1981 to 1983, which found averages of 5.3 episodes per year for children under 6 months, 5.9 per year at 6-11 months, and 2.1 per year at 1-4 years [73]. Accepting the calculation of 43 diarrhea-days per year from the Five-Community Study implies a mean duration of 7-8 days per episode, quite similar to data from studies in other countries [74]. Five episodes per child per year is therefore a reasonable average estimate for children under two.

$20 Peter Miller and Norbert Hirschhorn
Since the pre-Project data did not allow a firm estimate of diarrhea incidence or prevalence, it is difficult to make a precise statement about change. A small increase or decrease in prevalence would be impossible to confirm, but a substantial, sustained change ought to be apparent. The information available, adjusted for the time of year of the fieldwork and organized within comparable cat- egories of age and prevalence interval, show no consistent trend over time. In most cases there are insufficient data to examine trends over time within a single age group and prevalence interval. What might be considered an exception is in one-week prevalence for children under two. Here the data from 1984 and after are consistently higher than from the 1978 and 1980 nutrition surveys. (The exclusion of children under six months from the nutrition survey data would actually tend to bias that study's prevalence upwards compared with all children under two).
Three opportunities exist for us to look at time series data for which the same groups of researchers collected data over two or more years using (nearly) the same methodologies, in the same places, at the same approximate times of year. Both the Double Round Surveys from 1984-86 and the KAP studies from 1985-88 show modest declines over three rounds, 13 and 21%, respectively, in diarrhea prevalence over the past week. The 1987-88 Five-Community Study, however, shows a trivial increase in day-point prevalence over the estimates from 1983-84. If the decreases in the DRS and KAP studies were due to selective waning of rotavirus and enterotoxigenic E. coil--for which, however, we have no evidence-- this could account for some of the mortality decline [751.
It is noteworthy that similar patterns of variability in prevalence rates found in the pre-Project data are seen in the late 1980s. Rates are higher for children between six months and two years, for children of disadvantaged families, and (slightly) for boys, rural dwellers, and those living in Upper Egypt. The highest rates geographically are likely to be found in metropolitan slums: the 1978 National Nutrition Survey supports this [72], as do data from Menshiet Nasser, one of the poorest areas of Cairo, with a
seasonally adjusted two-week incidence of 64% in children under three [76].
In summary, we cannot demonstrate substantial reductions in the incidence of diarrhea in small children or in the etiology; smaller changes could easily escape the analyses.
2. Changes in host resistance
Changes in the predisposition of children to survive an attack of diarrhea, apart from case management, can be manifested essentially in two ways: change in nutrition, which affects the ability of the child to tolerate a given degree of illness or nutritional loss without threat to life; and change in the capacity of the intestine to absorb food and withstand infection.
Nutritional status. Substantial improvement in the overall nutritional status of infants and children might have a substantial impact on diarrheal mortality. In turn, nutritional status should be improved to some extent by better treatment of diarrhea since diarrhea is so common and has such important nutritional consequences. More specifically, a reduction in wasting (fewer children with low weight for height) would likely result in a lower case fatality for diarrhea, and improvements in routine patterns of care for diarrhea would, over time, cause a reduction in stunting (fewer children with low height for age) as the long-term nutritional consequences of repeated diarrheal attacks are eased.
The relevant data on changes over time in nutritional status are few, but fortunately exist in almost the exact form most needed. Anthropometric measurements have been conducted using similar methodologies on large national samples of infants and children in 1978 (the National Nutritional Survey, or NNS) [72] and 1988 (DHS) [36]. Data from both studies using standard deviations from the median of the NCHS/CDC/WHO international reference popu- lation are partially reproduced in Table 11.
The data show cumulative distributions of proportions of children whose nutritional level is less than a specified level in relation to the standard normal distribution in the reference population, in terms of weight-for-height, height-for-age and weight-for-age. The higher the percent, the greater the proportion under the specified level, that is, the poorer the
Table 11. Cumulative percentages of children with anthropometric measures less than specified number of standard deviations from reference median, NNS a 1978 and DHS b 1988
Weight/height Height/age Weight/age Median NNS DHS NNS DHS NNS DHS Reference
< - 4 0.0 3.8 0.6 0.0 b < - 3 0A 0.1 12.9 12.0 3.1 2.5 0.1 < - 2 1.0 IA 36.3 30.8 14.6 13.3 2.3 < - l 9.4 9.8 69.8 59.8 44.5 41.8 15.9 < 0 40.7 91.9 79.0 50.0 < + 1 82.7 82.9 98.5 95.9 96.2 93.9 84.1 < +2 97.6 96.8 99.6 98.6 99.5 98.8 97.7 < +3 99.7 99.9 100.0 99.9 < +4 99.9 100.0 100.0
"National Nutrition Survey [72]. bNational Demographic and Health Survey [19].

Diarrhea control: impact on mortality in Egypt S21
nutrition. The proportions in the reference population are shown for comparison.
Two relevant methodological differences separate the two studies. The 1978 NNS was conducted in January-April, the 1988 DHS in November-January. This should not make much difference: the major source of seasonal variation in nutrition is diarrheal disease and both studies were done in the off-season; but if anything the timing might lead to slightly less wasting in the NNS as diarrhea incidence is higher in November-January than January-April. The NNS was conducted on children ages 6-71 months, the DHS on children 3-36 months. Since, by age breakdowns not comparable to those shown in the DHS, malnutrition was more common in the NNS for children under age three, the effect of including older children would be to reduce the level of malnutrition in the NNS relative to the DHS. Thus, both potentially significant methodological differences between the two studies should tend to produce greater levels of malnutrition in the 1988 DHS; but the biases should be quite small.
The distributions are strikingly similar. Virtually no difference shows up in weight-for-height, wasting. In the DHS, a modest improvement in height-for-age, stunting, appears. Weight-for-age, representing a combination of the two, is intermediate. After neutralizing the biases indicated above, the suggestion is that there may have been a small improvement in wasting and a modest improvement in stunting.
The improvement in stunting may be partially due to improvements in case management of diarrhea, as the cumulative effect of better nutrition through several episodes is felt. It is the wasted child, however, for whom diarrhea is particularly dangerous. The absence of any noticeable improvement in weight-for- height suggests that nutritional improvement did not contribute substantially to the fall in diarrheal mortality.
An separate predictor of susceptibility to illness is low birth weight. Data from UNICEF show, if anything, a greater proportion with LBW in 1990 (10%) than in the period 1979-83 [77] ([1], p. 66).
We cannot, of course, rule out unmeasured improvements in children's blood and tissue levels of such micronutrients as zinc, folic acid and vitamin A that could positively affect intestinal integrity and immune status; but then we also do not know whether low enough levels existed in 1978 to account for the higher mortality seen then.
Measles. Measles vaccination coverage increased from 41% of children ages 12-23 months in 1984, to 76% in 1987, and to 86% in 1990 [78]. A major push to improve coverage was initiated in September 1986. Feachem and Koblinsky have suggested that a measles vaccination program that achieves a 60% coverage of children at 9-11 months of age, with a vaccine having 85% efficacy, might reduce the diarrhea mortality rate by 13% among children under five years of age [9]. Hence the Egyptian achievement probably con-
tributed to the reduction in child mortality from diarrhea. Measles vaccination begins at nine months, however, preventing measles episodes which would occur later, and thus preventing diarrheal deaths during and months after the episode; measles vaccination could not therefore have had a significant effect on infant mortality, which declined nearly as rapidly as childhood mortality. Moreover, the measles campaign began after most of the diarrheal mortality decline had already occurred in both age-groups.
3. Other changes during the Project period
While insufficient change seems to have occurred in the proximate determinants of diarrhea prevalence or in host resistance to explain the mortality decline, it is necessary to examine other general changes in Egypt and examine how these might have affected diarrheal mortality.
Socioeconomic changes. On the negative side, public spending by government (including food subsidies) declined beginning in 1984-85, private consumption spending slowed in 1985-86, while inflationary pressures were severe throughout all the 1980s [79]. Real agricultural wages peaked in 1985 but began a serious and continuing decline in 1986 [80]. The GNP per capita fell during the Project years, from U.S.$700 in 1983, to U.S.$680 in 1987, to U.S.$610 in 1990 ([77], p. 142; [81], [1], p. 74), and the proportion of persons below absolute poverty level rose from 21%/25% (urban/rural) in 1977-83 to 34% nationally ([77], p. 142; [1], p. 74). These economic changes would have had a greater negative impact on the health of that segment of the population from which most of diarrheal mortality must come. The population also became more urban: between 1980 and 1988 the proportion of households in urban areas went from 42% to 48% [19, 53]. To the degree that the new arrivals occupied the worst housing, incidence of illness could be expected to increase, though access to emergency care in hospitals would improve.
Other changes were more positive: between 1980 and 1986, the proportion of homes with electricity increased from 65% to 87%, the proportion with piped water (outside or in) from 70% to 73% [53, 82]. The NCDDP's Double Round Surveys showed 39, 43 and 35% with indoor piped water in 1984/85/86, respectively [56, 33]. According to UNICEF, access to safe water rose from 88%/64% (urban/rural) in 1980 to 95%/86% ([77], p. 186; [1], p.68). By 1988, 20% of women of reproductive age were working, compared with 17% in 1980; 26% had completed primary school, doubled from 13% [19, 53]. Illiteracy in women over age 15, however, fell only slightly during the time of the Project: 73% in 1980 [83], 70% in 1985 ([81], p. 82), and 66% in 1990 ([1], p. 70). Ownership of television, an essential precondition for the mass media campaign, seems to have increased dramatically. In the 12-village Menoufia study area, TV ownership increased from 12% in 1979 to 80% in 1988 [20]. Nationally, 38% of households had TVs in 1980 [53],
SSM 40/lO~J

$22 Peter Miller and Norbert Hirsehhom
but by the mid-1980s television sets appeared to be in a majority of homes. The evidence for social change is therefore mixed but positive structural changes were of the sort that would have facilitated the work of the NCDDP.
The public health system. While there appears to have been a modest improvement in safe water supply, overall changes in environmental sanitation are difficult to assess but do not appear to have changed greatly. The public health system was for the most part structurally in place by 1980 but a considerable increase in the numbers of personnel in health centers and improvements in logistics and supply took place over the decade. The number of physicians in private practice has also increased, particularly in rural areas--a trend most noticed toward the end of the decade. The number of pharmacy outlets exceeds 6000, many also now in the rural areas.
In addition to the NCDDP, several major health projects have strengthened particular aspects of the health system. Noteworthy among these have been the four-governorate Strengthening of Rural Health Delivery project which ran from 1978 to 1988, the Urban Health Project (Cairo) in the same period, major ongoing EPI and family planning efforts, and since 1987, a large, national Child Survival Project. Coverage for all immunizable diseases increased greatly between 1984 and 1990; by the latter year about three-fourths of all children ages 12-23 months had been fully immunized. Prevalence of contraception increased from 30% in 1980 to 38% in 1988 [19, 53], and seems recently to be increasing at a faster pace.
In sum, the decade of the 1980s saw steady progress in development in ways that might have been expected to reduce general mortality. On the other hand, economic deterioration beginning in the mid-1980s could have acted in the opposite direction. Important improvements in health services have also occurred, particularly during the latter part of the decade. Some of the more noteworthy improvements were important to the success of NCDDP, such as increases in television ownership, and availability of health providers. Such factors were certainly not part of the NCDDP program but surely facilitated improved case management; recent evidence from Africa could not find much mortality impact from ORT but neither was it taken up as well as immunization [84]. The experience in Nicaragua suggests that a primary health care infrastructure was essential to the initiation and continuation of the decline in infant mortality [85].
VI. DISCUSSION--WHAT WAS THE IMPACT OF THE NCDDP?
1. Sorting out the evidence
In the beginning of this monograph it was proposed that to demonstrate impact it would be necessary to show:
(a) sufficient program accomplishments to have plausibly caused a mortality decline;
(b) (c)
the actual occurrence of such a decline; and proof that the program was the principal cause of the decline. (We accepted the evidence that ORT, when properly adminis- tered in a controlled experiment, did reduce mortality).
Assuming that mortality did decline, it was argued we could simplify the attribution of the decline to the program or something outside the program by examining the proximate determinants of diarrheal mortality. These were put in three categories: case management; etiology/incidence/prevalence; and host resistance. If any of these changed, it would be important to determine why.
The clearest part of the picture is the mortality decline itself. Several sources conclusively document a rapid and nation-wide drop in diarrheal mortality in the middle 1980s, sustained since, and concomitant with the timing of implementation of NCDDP. Diarrheal mortality fell by more than one half during the first five years of NCDDP. Non-diarrheal mortality also declined but--nation-wide--much more slowly.
The Project was able to document substantial improvements in case management. ORS is more likely to be used, and children are better fed during diarrheal episodes, though the situation--especially regarding use of ORS--is not ideal. Children coming to two University hospitals (in Cairo and Alexandria) were, over the years of the project, progressively less likely to show up visibly dehydrated--indicating, perhaps, better case management at home. We believe that there has also been an improvement in emergency care for cases of moderate and severe dehydration.
Definitively determining diarrheal disease preva- lence proved impossible but so many different studies addressed the issue that it was possible to conclude with reasonable confidence that no substantial decline occurred during the 1980s; fragmentary evidence suggests no major change in diarrheal pathogens--but neither would such a change in a one-year period be credible. Likewise, there appar- ently was little if any improvement in childhood nutrition, particularly in wasting; and while measles vaccination coverage improved, this appears to have been a lesser factor in reducing diarrheal mortality, particularly in infants. Yet before we can conclude that a major decline in diarrheal mortality was caused primarily by improved case management, and as a result of the efforts of NCDDP, we must review the quality of the evidence.
All of the conclusions above are based on a substantial but nevertheless flawed body of evidence. Virtually all data on social issues are inaccurate to some extent; the question here is: are the errors in the data sufficient to cast serious doubt on the fundamental conclusions?
Measurement of mortality in general, and cause of death in particular, are notoriously problematic in

Diarrhea control: impact on mortality in Egypt $23
developing countries. In the present situation this is complicated by the possibility that both the cause of death data in the civil register and the results of the DRS of 1984-1986 might have been biased towards showing a decline in diarrheal mortality where none occurred. The logic here has been to present data from a variety of studies, each of which is either of uncertain accuracy or of limited geographic scope, to see whether they are convincing collectively. All sources which bear on the issue agree that there has been a substantial decline in infant and child mortality concentrated in the early Project period, and that most of this decline was due to decline in diarrheal mortality. The different designs and sources of these studies, coupled with internal consistencies, make it implausible that the agree- ments are the result of coincidental biases. For example, within the civil register the cause-specific decline, which might have been caused by deliberate failure to report diarrheal deaths, is broadly consistent both at national and governorate levels with declines in the seasonality of mortality, for which such a bias is implausible. The mortality decline in the DRS, commissioned by the NCDDP, could have been a contractor's desire to please, but the DHS, conducted independently, was not. Mortality declines were established by continuous registration, by prospective surveillance, and by retrospective survey. Cause of death data from the civil register are backed by local-area verbal autopsy information. Differences in degree are not sufficient to call into question the conclusions of this analysis.
Was the use of ORT of such quality as to justify the rubric, ' improved case management?' The evidence for continued feeding is clear enough, and the majority of mothers learned to mix ORS correctly. We have no way, however, to estimate the increase in ORS use or improvement in feeding necessary during diarrheal episodes for a given change in mortality. There is evidence that indicates ORS is not much used in mild cases of diarrhea but is more extensively and intensively used in serious cases, precisely from where most mortality would come.
Identification and measurement of other factors which might plausibly have caused the mortality decline is the most problematic part of the analysis. The most substantial evidence is on broad measures of diarrheal etiology, incidence and prevalence, and on these topics it can be said with some confidence that major changes did not take place. Unmeasured change in some key factor cannot be completely ruled out. For example, there could have been a major and sudden change in etiology or in the virulence of one or more diarrheagenic organisms; or by an improvement in micronutrient nutrition not detected by anthropomet- ric measures; or an improvement in some other unsuspected, and hence unmeasured, factor contribut- ing to host resistance. That such events might have occurred, undetected, at precisely the time that NCDDP was having its large and measurable impact
on case management seems implausible but cannot be disproved with the evidence at hand.
As for background determinants, important social changes occurred in the 1980s but most were oftbe sort to facilitate the work of the NCDDP: the spread of television, improved availability and access to medical care and pharmaceuticals, slight improvements in safe water supply and in female literacy. Economic conditions, however, began to deteriorate substan- tially in the mid-1980s.
We conclude that problems of measurement do not call into question the conclusions that NCDDP caused a substantial improvement in the treatment of diarrheal disease, or that a major decline in diarrheal mortality occurred coincident with that improvement. The scope and quality of the data do not permit us to say that no other factors could have been responsible; for this we must weigh the circumstantial evidence, bearing in mind both the limitations of the data and the plausibility of alternative explanations.
2. On the replacement hypothesis
There is a well-known hypothesis, associated in particular with Mosley [87], that argues that some specifically targeted health interventions, such as ORT, will have less net effect on mortality than the direct effect would imply. This is because many of the children saved arc basically weak and sick, and in the absence of treatment for more fundamental problems, they are likely to dic later in childhood after being saved from a particular bout of diarrhea by ORS. The standard reply goes: yes, but on the other hand, many children who would not have died from a particular bout of diarrhea would have been more severely weakened if not for ORT, and might have gone on to die later. When expressed in this manner, the argument is one of a balance of probabilities. When seen as such a balance, Egypt presents little evidence for the replacement hypothesis. Changes in diarrheal and non-diarrheal mortality rates over time tend to be correlated in a weakly positive manner, rather than negatively as the replacement hypothesis would suggest. Sharp drops in diarrheal mortality in local-area experiments were not associated with an increase in non-diarrheal mortality. Neither is there any evidence that overall nutrition worsened between 1978 and 1988; if anything, it showed modest improvement in stunting (Table 11).
The replacement hypothesis, however, is not just about probabilities; it is also about appropriate health strategies and about proper treatment for children at risk. The strategy pursued by NCDDP worked in part because it was not simply an ORS campaign, but a broad-based program of diarrheal management that has had important public health benefits well beyond keeping particular children alive. There seems to be no conflict between this kind of activity and the aims of improving fundamental primary health care systems.
The Egyptian health care system is at its best in preventing and treating well-defined, acute diseases

$24 Peter Miller and Norbert Hirsehhorn
Table 12. E~ect of reduction in diarrheal mortality rates on deaths to children 0-4, 1982-89 Infant deaths Deaths to children !--4
Year Observed Expected Diff . Obse rved Expected Diff. 1982 53,135 53,135 0 28,262 28,262 0 1983 48,485 55,313 6828 20,369 28,998 8269 1984 46,316 59,637 13,321 20,868 29,753 8885 1985 29,152 63,148 33,996 14,555 30,527 15,972 1986 28,953 63,313 34,360 14,571 31,322 16,751 1987 25,599 63,134 37,535 12,892 32,137 19,245 1988 23,170 63,472 40,302 11,462 32,973 21,511 1989 19,787 55,558 35,771 9,966 33,832 23,866 Total by age 202,113 114,499 Total 316,612 Note : For infant mortality, calculations based on registered births and infant diarrheal deaths.For
children 1-4, calculations based on official CAPMAS estimates of children aged 1-4 and o n registered diarrhea deaths for those ages.
but is less adequately prepared to respond to the needs of frail, chronically-ill children. The child with a long-term infection-malnutrition complex is unlikely to get the sustained care needed. In a recent ethnographic observational study of 55 children with diarrhea [22], four were classified as not expected by the mother to live. Each had been sick for a long time, and the mother, having tried all the doctors and remedies she could find, had given up. She was convinced that God was going to take her child. The problem is not one of resources or technology, but of adjusting the system to handle a different kind of problem. After initial successes, continued reduction in infant mortality requires more complex interven- tions [86]. It is one of the more formidable problems still facing the Egyptian health care system.
3. Deaths averted
The calculation of deaths averted by any health project is a problematic undertaking. It involves the inclusion not only of data on mortality reduction, but also estimation of the project's share in that reduction. In brief, it is simply not possible to say what would have happened in the absence of the Project. Nonetheless the number of infants and children saved after a given year through reduction of infant and child mortality from diarrheal disease can be estimated without specifying what would have happened in the absence of NCDDP or approximating the share that NCDDP might have had in that reduction. This is done by comparing the infant and child diarrhea deaths that actually occurred with the deaths that would have occurred had diarrheal mortality rates remained constant. To do this, we make the following assumptions:
(1) Coverage of mortality to children under five is complete. Violation of this assumption will result in underestimation of the mortality reduction by the proportion of underregis- tration, given constant underregistration during the period in question.
(2) Cause of death data in the civil register are accurate regarding diarrheal disease. This
assumption is discussed at some length above and in Appendix A.
(3) The numbers of births and of children 1-4 are correct.
Violations of these assumptions to the degree plausible would have relatively minor effect on the estimates.
Using these data and assumptions, Table 12 shows the reduction in numbers of diarrheal deaths implied by changes in registered death rates after any given year, using as a base the 1982 diarrheal mortality rates of 33.2%0 for infants and 5.6%0 for children aged 1-4. Cumulatively, over 300,000 fewer children had died by 1989 than would have died if the 1982 rates had stayed constant.
It must be re-emphasized that this is not an estimate of lives saved by NCDDP, but a simple translation of reduced diarrheal mortality rates into fewer diarrheal deaths (some reduction in non-diarrheal deaths is expected as well by improved case management of diarrhea). Estimating lives saved would require an estimate of what would have happened had there been no NCDDP.
4. Had there been no NCDDP
It may never be fully understood why mortality fell but we offer the following speculations: first, mothers were never comfortable withholding breastmilk and other nutrients, and probably continued feeding more than they admitted. When NCDDP came with its highly attractive TV campaign, mothers were delighted to hear that they should continue to feed their children and promptly complied (easier as well to do as ORS stops vomiting and improves appetite). At the same time, they became frightened of the new problem---dehydration--and quickly learned to rec- ognize it and its link to diarrhea, and thus began to take action sooner. Meanwhile, doctors' practice was changing. Before NCDDP, there was only gradually increasing awareness that the danger from diarrhea was dehydration, and the proper response was rehydration. NCDDP, with widespread training, propaganda, and insistence on Ministry policy, reinforced these ideas, and the ready availability of

Diarrhea control: impact on mortality in Egypt $25
ORS made rehydration much easier than before. Moreover, when doctors saw a child in real danger, they were more likely to know what to do. As a result, fewer children became dehydrated, and of those, fewer died. In short, ORT and emergency care, the key elements of proper case management, were more frequently practiced than before.
Undoubtedly some of these changes would have occurred, to some degree, in the absence of the NCDDP, either through some different project, differently designed, or simply by gradual diffusion in Egypt of international knowledge and practice. The path of mortality, in turn, would have depended to a great extent on the nature of these efforts. Diarrheal mortality fell in the 1980s because of factors operating during the 1980s, and our analysis suggests that those factors largely involved case management.
It is legitimate to ask if the 32 million dollars spent over ten years could have been put to better use? In other words, were there foregone economic opportuni- ties? In terms of people reached per unit time and behavior changed, the NCDDP must be considered highly cost-efficient. Nevertheless, as this was the first program to improve case management on a national scale it had to create its own lessons and while much should have gone better, there is no comparable example to inform us that it couldhave gone better. As for the approach: when NCDDP was designed in 1981 there was no experimental evidence at hand for any other approach that could go to national scale quickly and, to our knowledge, none yet exists.
Within its own set of initial objectives--90% of mothers become aware of ORT and 75% understand its use; more than half of serious cases seen by the health system get ORT; and diarrhea mortality in children under five years of age reduced by at least 25%-- the NCDDP can be considered a success.
5. More work necessary
This monograph seeks to avoid self-congratulation: many problems remain. Mothers may still diagnose diarrhea and dehydration improperly. Serious cases are often brought to the doctor at late stages and inappropriate care sometimes causes further delays. Continuity of care is difficult to maintain. Most doctors are unwilling to abandon futile attempts to treat diarrhea with antimicrobials and antidiarrheals in response to mothers' frequent requests for 'real' medicine rather than ORS. The careful nutritional management necessary to treat persistent diarrheas is rarely understood or implemented. All of the usual problems of interaction between patients and the medical system continue to stand in the way of proper care. Finally, diarrheal incidence, with its huge effect on the welfare and development of children, remains largely unaffected, probably until major socioeco- nomic development changes the hygienic conditions in which young children are raised. However, enough important and positive concepts of management of acute diarrhea have taken root in both the public and
the medical profession to have caused a dramatic, and probably permanent, reduction in the damage caused by diarrhea.
VII. RECOMMENDATIONS
1. Institutionalization
The NCDDP has made an orderly transition to a General Directorate for Disease Control within the Ministry of Health-- the first time a donor-funded project has been so incorporated in Egypt. It has the tasks of ensuring the regular supply of ORS, enhancing education through mass media, upgrading the training of new health personnel. At the time of this writing (April 1994), there had been considerable slippage in program activity and ORS use rate although the situation is now correctly recognized by a new Minister of Health. The problem of diarrheal disease is by no means resolved. Given the new cohorts of parents and health workers arising each year, the Ministry of Health will need to sustain the activities of the NCDDP at a substantial level.
2. Improving use o f ORS
ORS is not always used when needed, particularly in milder cases, and less in private medical practice. Since nearly three-fourths of diarrhea cases are now being seen in the private sector [30], the General Directorate will need to evolve a plan to reach those practitioners.
A number of clinical studies sponsored by NCDDP have shown the equivalence or superiority of rice-based ORS in reducing the duration and volume of diarrhea. Since stopping diarrhea is what both parents and physicians ardently desire, such a product should be brought into the market, and probably through the private sector. It can be profitable even at a cost still affordable by the majority of the population, and could help drive out the unnecessary or dangerous antidiarrheal drugs.
3. Misuse o f antimicrobials and other drugs
NCDDP was unable to stop the widespread prescription and use of unneeded medicines, the bulk of which are produced by State-owned firms. To what degree physicians, pharmacists and the public can be convinced to use fewer drugs through standard education approaches is unknown. Any approach that lessens the severity of diarrhea--such as rice-based ORS or marked improvement in sanitation and hygiene---is likely to work better.
4. Persistent diarrhea
As death from acute dehydration becomes less frequent, persistent diarrhea will emerge as a larger component of mortality. The illness is largely a nutritional one. It is treatable: by feeding, with ORS to clear up existing dehydration, antimicrobials on occasion for attendant infections, and careful

$26 Peter Miller and Norbert Hirschhorn
followup. The WHO definition of persistent diarrhea is any bout lasting two weeks or more: we recommend that children with diarrhea exceeding one week be considered at high risk and put on special treatment.
5. Prevention
NCDDP was unable to make a substantial impact on diarrheal incidence. A recently completed study by the Ministry of Health and UNICEF (co-funded by NCDDP) in rural Egypt indicates reductions are achievable with a concerted and integrated program of water supply, latrines, and intense home-based health education (UNICEF/Cairo, personal communi- cation). Whether the approach can be brought to scale and maintained would be the subject of another national program.
6. Monitoring, research and evaluation
The NCDDP from the start saw the need for well-designed and organized methods of data collection, focussed research, monitoring and evalu- ation. Much of this was put into effect; much was also ad hoc and opportunistic, late in implementation, less than ideal in execution. We wish it could have been neater. In general, we do not recommend that major resources be routinely spent on estimating causal effects of national CDD efforts on mortality. From our experience in Egypt, the small and community-based longitudinal study can provide cleaner data to guide policy, and should certainly be a necessary component of any national program intending to implement changes. Small-scale operations-research studies should help guide specific management decisions. Ideally, national trends should be monitored not by special CDD efforts, but by national-level periodic health surveys documenting childhood morbidity, mortality, and health practices generally. Only under special circumstances should evaluations go beyond this to attempt causal analysis of program impact.
7. Integration of health programs
Midway through the tenure of the NCDDP, Egypt launched a successful immunization campaign. Rational treatment of pneumonia is also being promoted by a special child survival program. Years of education and promotion in family planning have begun to bear fruit. Since all public health programs must train health workers, educate the public, deal with logistics of supply, manage evaluation and supervision, there are likely economies of scale in integrating at least some of these inputs.
Given peace, continued development and more equitably shared resources among all citizens, we are confident that Egypt will continue to make important strides in bringing health to its people.
Acknowledgements--A work of synthesis like this one cannot be written by just two persons. In the most fundamental sense it rests on the labors of all who worked for the NCDDP, and all the health and medical workers, media persons and
international agency staff who helped carry out the vision. Academically, it is a work of secondary analysis, relying on the authors of all the studies in the references, and some uncited. Our thinking was enriched in discussions with many scholars: Hoda Rashad, Belgin Teckce, Ahmed Nagaty and Ray Langsten were particularly noteworthy. Earlier drafts were considerably improved in analysis and clarity by Drs Mervat EI-Rafie, Said Madkour (NCDDP), Mark Robbins (John Snow, Inc.), and two anonymous reviewers; all errors of omission and commission, however, are ours. Basic funding was supplied by the United States Agency for International Development through Grant No. 263-0137. Additional support came from John Snow, Inc. (Joel Lamstein, President), and the Population Council in Cairo (Dr Barbara Ibrahim) and Dhaka (Dr Kim Streatfield).Our profoundest appreciation is reserved for the families of Egypt who struggle daily to do what is best for their children. We hope we have served them well.
REFERENCES
1. UNICEF. The State of the World's Children 1994, pp. 80-81. Oxford University Press, Oxford, 1994.
2. An important distinction must be made between oral rehydration salts (ORS) and oral rehydration therapy (ORT): the latter refers to the total management of an episode of acute diarrhea with rehydration using ORS, and continued feeding. Reduced use of unnecessary antidiarrheal drugs is an ideal component of OPT but not as often carried out.
3. Kielmann A. A., Mobarek A. B., Hammamy M. T., Gomaa A. I., Abou-El-Saad, S., Lotfi R. K., Mazen I. and Nagaty A. Control of deaths from diarrheal disease in rural communities. I. Design of an intervention study and effects on child mortality. Trop. Med. Parasit. 36, 191, 1985.
4. National Control of Diarrheal Diseases Project. Impact of the National Control of Diarrheal Diseases Project on infant and child mortality in Dakahlia, Egypt. Lancet II, 145, 1988.
5. EI-Raiie M., Hassouna W. A., Hirschhorn N., Loza S., Miller P., Nagaty A., Nasser S. and Riyad S. Effect of diarrhoeal disease control on infant and child mortality in Egypt. Lancet 335, 334, 1990.
6. Messages to prevent diarrhea by improved personal hygiene were regularly broadcast. The Project could not, however, undertake a national program to supply the hardware for clean water and sanitation.
7. The baseline measurement was made in 1984, not 1983. In NCDDP's first full year the resources for national sampling were only sufficient to determine the commonest available household container and families' preferences so that a crucial decision could be made as to the size of the ORS packet. In 1983 a vigorous debate existed between those promoting a one-liter packet (UNICEF, WHO) and those advocating a cup-sized packet. Research demonstrated the superiority of the latter.
8. International Study Group. A positive effect on the nutrition of Philippine children of an oral glucose-elec- trolyte solution given at home for the treatment of diarrhoea. Bull. Wld Hlth Org. 55, 87, 1977.
9. Feachem R. G. and Koblinsky M. A. Interventions for the control of diarrhoeal diseases among young children: measles immunization. Bull. WldHIth Org. 61,641, 1983.
10. Kamel N. The Morbidity and Mass Media Survey: Final Report. NCDDP, Cairo, 1984.
11. Radar Public Relations and Research Co. Oral Rehydration Therapy Focus Group: General Prac- titioners. NCDDP, Cairo, 1983.
12. Hirschhorn N. A Summary of Ethnographic Research in Egypt with Respect to Diarrheal Diseases in Children. NCDDP, Cairo, 1984.

Diarrhea control: impact on
13. Hodfar H. Child care and child survival in low-income neighborhoods of Cairo. West Asia and North Africa Regional Papers. The Population Council, Cairo, 1986.
14. Miller P. Trends in the manag~aent of childhood diarrhoea in Egypt: 1979-1990. J. Diarrhoeal Dis. Res. 10, 193, 1992.
15. Social Planning, Analysis, and Administration Consul- tants. Final Report: Evaluation of NCDDP National Campaign, KAP of Mothers. NCDDP, Cairo, 1985.
16. Social Planning, Analysis, and Administration Consult- ants. Final Report: Evaluation of NCDDP National Campaign, KAP of Mothers. NCDDP, Cairo, 1986.
17. Social Planning, Analysis, and Administration Consult- ants. Final Report: Evaluation of NCDDP National Campaign, KAP of Mothers. NCDDP, Cairo, 1987.
18. Social Planing, Analysis, and Administration Consult- ants. Final Report: Evaluation of NCDDP National Campaign, KAP of Mothers. NCDDP, Cairo, 1988.
19. Sayed H. A-A., Osman M. I., EI-Zanaty F. and Way A. A. Egypt Demographic and Health Survey 1988. Egypt National Population Council and Institute for Resource Development/Macro Systems, Inc., 1989.
20. Miller P., Loza S., Terreri N., Nagaty A., Bayoumi M., Hirschhorn N. and Gibson R. Diarrhea and mortality in Menoufia, Egypt. J. Diarrhoeal Dis. Res. 12, 173, 1994.
21. Sinai Consultation Group. Knowledge, Attitude, and Practice Survey: Final Report. NCDDP, Cairo, 1990.
22. Social Planning, Analysis, and Administration Consult- ants. Case Management for Diarrheal Disease in Children under Age Three: Ethnographic Summary Report. NCDDP, Cairo, 1991.
23. UNICEF. Sociocultural Factors Influencing the Preva- lence of Diarrheal Disease in Rural Upper Egypt. An Ethnographic Study in Six Villages. UNICEF, Cairo, November 1990.
24. Gadalla S., Nossair N. and McCarthy J. Comprehensive Report of the Integrated Social Service Delivery System Project in Menoufia Governorate, Egypt. Social Research Center, American University in Cairo, and Hopkins Population Center, The Johns Hopkins University, Baltimore, 1983.
25. Kielmann A. A., Nagaty A. and AjeUo C. A. Control of deaths from diarrheal diseases in rural communities. II. Motivating and monitoring the community. Trop. Med. Parasit. 36, 191, 1985.
26. National Control of Diarrheal Diseases Project. The clinical epidemiology of acute diarrhoeal disease in Egyptian children. J. Trop. Ped. 34, 150, 1988.
27. Unpublished data from a study of the knowledge, attitudes and practices of Cairo physicians. NCDDP, Cairo, 1990.
28. Riyad S. Behavioral Determinants of the Incidence of Diarrhoea and Mothers' Beliefs and Traditional Self Help Practices for Diarrhoeal Disease Treatment. NCDDP, Cairo, 1987.
29. Larson A. and Mitra S. N. Usage of oral rehydration solutions (ORS): a critical assessment of utilization rates. Hlth Pol. Planning 7, 251, 1992.
30. Langsten R. and Hill K. Child Survival in Rural Egypt: Final Report. Social Research Center, American University in Cairo, Johns Hopkins University, Baltimore, 1992.
31. Sinai Consultation Group. Incidence of Diarrheal-associ- ated Illness in Children Aged Two Years and Under in Eight Egyptian Governorates: Final Report 1984. NCDDP, Cairo, 1985.
32. Sinai Consultation Group. Incidence of Diarrheal-associ- ated Illness in Children Aged Two Years and Under in Eight Egyptian Governorates: Final Report 1985. NCDDP, Cairo, 1986.
33. Sinai Consultation Group. Incidence of Diarrheal- associated Illness in Children Aged Two Years and
mortality in Egypt $27
Under in Eight Egyptian Governor ares: Final Report 1986. NCDDP, Cairo, 1987.
34. Gadalla S., Nosseir N. and McCarthy J. Integrated Social Service Delivery System Project In Menoufia Governorate, Egypt: Results of the First and Second Rounds of a Socio-demographic Survey. Social Research Center, The American University in Cairo, and Hopkins Population Center, The Johns Hopkins University, Baltimore, 1982.
35. Sinai Consultation Group. Diarrheal Diseases: Mothers' Treatment Seeking Behavior and Treatment Choice. NCDDP, Cairo, 1988.
36. Nutrition Institute, Arab Republic of Egypt. Nutrition Status Survey H. Cairo, 1980.
37. EI-Sayyad L., Hassouna W. A. and Taylor M. T. Incidence of diarrhea-associated illness and mortality in under.five year olds in two Egyptian goveruorates. Hlth Researcher 5, (1), 1984. Hammamy D. M. T. Oral rehydration salts: patterns of usage in Cairo, Egypt. Doctoral Thesis, Harvard University, 1986.
38. Riyad S., EI-Mougl M., Wahsh A. A. E. R. and Hirschhorn N. After rehydration: what happens to the child? J. Trop. Ped. 37, 220, 1991.
39. Kalenshian N. Maternal perceptions and attitudes towards diarrheal diseases. Master's Thesis, American University in Cairo, May 1990.
40. Sinai Consultation Group. ORS Survey of Service Providers: Physicians, Nurses, and Pharmacists in Eight Egyptian Governorates: Final Report. NCDDP, Cairo, 1986.
41. E1-Rafie M., Abdelmonem H. and Saleeb S. A. Knowledge, attitudes, and practices (KAP) of doctors in Cairo Governorate---1990. NCDDP Diarrhea Control Newslett. Snmmer, No. 11, 1990.
42. Langsten R. and E1-Mougi M. The physician as risk factor in moderate and severe dehydration. Paper presented at the Annual Meeting of the Population Association of America, Toronto, 3 May, 1990.
43. E1-Mougi M., Hendawi A., Gomaa M. H., E1-Abhar A., Amer A., Shobair I., Hanafy R. M. K. and EI-Shafie M. Patterns of diarrhoeal diseases at a University Hospital in Cairo: a seven-year experience. J. Trop. Ped. 37, 85, 1991.
44. All numbers of registered births and deaths are from official data published by the Central Agency for Public Mobilization and Statistics (CAPMAS). Data through 1987 are published in annual vital statistics reports; more detailed tables for 1982-88 were provided specially to NCDDP by CAPMAS. Most essential data are published in Refs [45] and [46]. In the absence of officially published estimates of numbers of children by single year of age, most estimates of age-specific death rates to children 1-4 use base populations derived from Nounou [47]
45. Central Agency for Public Mobilization and Statistics. The State of the Egyptian Child. CAPMAS, Cairo, 1988.
46. Central Agency for Public Mobilization and Statistics. Infant and Child Mortality Rates in Egypt, 1980-87. CAPMAS, Cairo, 1989.
47. Nounou N. M. Evaluation of Age and Sex Composition in 1976 Population Census of Egypt. CAPMAS Population Studies and Research Centre Working Paper No. 6. CAPMAS, Cairo, 1984.
48. Central Agency for Public Mobilization and Statistics. CAPMAS Population Studies and Research Center: Infant and Child Mortality in Egypt. CAPMAS, Cairo, 1986.
49. Rashad H. Evaluation of the Completeness of Mortality Registration in Egypt. The Population Council, West Asia and North Africa Regional Papers. Population Council, Cairo, 1981.
50. National Academy of Sciences, Committee on Popu- lation and Demography. The Estimation of Recent

$28 Peter Miller and Norbert Hirschhorn
Trends in Fertility and Mortality in Egypt. Report No. 9. National Academy Press, Washington, 1982.
51. Bucht B. and EI-Badry M. A. Reflections on Recent Levels and Trends of Fertility and Mortality in Egypt. Pop. Stud. 40, 101, 1986.
52. Rashad H., El-Deeb B. and Mohamed A. Analysis of 1986 Census Data Related to Infant and Child Mortality. Unpublished, 1989.
53. Central Agency for Public Mobilization and Statistics. The Egyptian Fertility Survey, 1980. CAPMAS, Cairo, 1983.
54. Tekce B. Oral rehydration therapy: an assessment of mortality effects in rural Egypt. Stud. Family Planning 13, 315, 1982.
55. Rashad H. The mortality impact of oral rehydration therapy in Egypt: re-appraisal of evidence. In Child Health Priorities for the 1990s. Report of a Seminar held June 20-22, 1991 at the Johns Hopkins University School of Hygiene and Public Health (Edited by Hill K.), pp. 135-159. Johns Hopkins University, Baltimore, 1993.
56. Rashad H. Oral rehydration therapy and its effect on child mortality in Egypt. J. Biosoc. Sci. Suppl. 10, 105, 1989.
57. Analysis of mortality between 1982 and 1989 used detailed tabulations provided specially to the NCDDP by CAPMAS, the civil registration authority. A death was classified as 'diarrheal' if the ICD code (ninth revision) for the underlying cause of death was listed as any of the codes 001-009, i.e. infectious intestinal disorders. Most such deaths were classified in code 009, infectious intestinal disorders of unknown origin. Intestinal disorders of non-infectious origin, which in most years numbered less than 1,000 for children age (b-4, were not included.
58. One important caveat must be offered in respect to the timing of major decline in diarrheal mortality: It was recently discovered that between 1985 and 1987, for reasons not known, several thousand childhood deaths were classified in ICD code 558, non-infectious intestinal disorders of unknown origin. In 1988, the number again became negligible. It is likely that these deaths are miscoded and perhaps should have been coded as 009. If so, the large decline in diarrheal mortality in 1985 is somewhat reduced: 26 to 18%o instead of 26 to 15--and a larger drop then appears between 1987 and 1988 (16-12 instead of 12-12). (See Ref. [55]). The latter would suggest that more of the decline during the decade may have been due to accumulating understanding of treatment principles and somewhat less to the campaign of 1984-85. Since the other studies on mortality and seasonality data still support the larger drop in 1985--see text--we will not attempt to amend the data presented in the text.
59. Floyd T. M. Incidence of Shigella infections in Egyptian village children. Am. J. Trop. Med. Hyg. 3, 294, 1954.
60. Higgins A. R., Floyd T. M. and Kader M. A. Studies in shigeUosis. II. Observations on incidence and etiology of diarrheal disease in Egyptian village children. Am. J. Trop. Med. Hyg. 4, 271, 1955.
61. Floyd T. M., Higgins A. R. and Kader M. A. Studies in shigellosis. V. The relationship of age to the incidence of Shigella infections in Egyptian children, with special reference to shigellosis in the newborn and in infants in the first six months of life. Am. J. Trop. Med. Hyg. 5, 119, 1956.
62. Mohiedin M. S., Gabr M., E1-Hefny A., Sayed-Mah- moud S. and Abdallah A. Bacteriological and clinical studies in infantile diarrhoea. Part I. Known pathogens: Shigella, Salmonella and enteropathogenic E. coll. J. Trop. Ped. 11, 69, 1965.
63. Kassem A. S., El-Araby I., Massoud B., Madkour A., Abdou M., Micheal M. and Massoud M. Effect of
antibiotics on the duration and speed of rehydration. Gaz. Egypt Paed. Assoc. 31, 117, 1983.
64. Pazzaglia G., Bourgeois A. L., Araby I., Mikhail I., Podgore J. K., Mourad A., Riyad S., Gaffar T. and Ramadan A. M. Campylobacter-associated diarrhoea in Egyptian infants: epidemiology and clinical manifestations of disease and high frequency of concomitant infections. J. Diarrhoeal Dis. Res. 11, 6, 1993.
65. Victora C. G., Huttly S. R. A., Fuchs S. C., Barros F. C., Garenne M., Leroy O., Fontaine O., Beau J. P., Fauveau V., Chowdhury H. R., Yunus M., Chakraborty J., Sarder A. M., Kapoor S. K., Bhan M. K., Nath L. M. and Martines J. C. International differences in clinical patterns of diarrhoeal deaths: a comparison of children from Brazil, Senegal, Bangladesh, and India. J. Diarrhoeal Dis. Res. 11, 25, 1993.
66. Shukry S., Zaki A. M., DuPont H. L., Shoukry I., El Tagi M. and Hamed Z. Detection of enteropathogens in fatal and potentially fatal diarrhea in Cairo, Egypt. J. Clin. Microbiol. 24, 959, 1986.
67. Yahya A. E. Multicentre study ofaetiology of diarrhoea in Egypt in the first three years of life. Unpublished, no date.
68. Massoud B. Z., Kassem A. S., Omar N. Y. and Madkour A. Rotavirus and acute diarrhoeal disease in children in Alexandria. Gaz. Egypt Paed. Assoc. 31, 129, 1983.
69. Zaki, A. M., Dupont H. L., E1 Aiamy M. A., Arafat R. R., Amin K., Awad M. M., Bassiouni L., Imam I. Z., E1 Malih G. S., E1Marsafie A., Mohieldin M. S., Naguib T., Rakha M. A., Sidaros M., Wasef N., Wright C. E. and Wyatt R. G. The detection of enteropathogens in acute diarrhea in a family cohort population in rural Egypt. Am. J. Trop. Med. Hyg. 35, 1013, 1986.
70. EI-Mougi M., Amer A., El-Abhar A., Hughes J. and EI-Shafie A. Epidemiological and clinical features of rotavirus-associated acute infantile diarrhoea in Cairo, Egypt. J. Trop. Ped. 35, 230, 1989.
71. Huilan S., Zhen L. G., Mathan M. M., Mathew M. M., Olarte J., Espejo R., Maung U K., Ghafoor M. A., Khan M. A., Sami Z. and Sutton R. G. Etiology of acute diarrhoea among children in developing countries: a multicentre study in five countries. Bull. Wld Hlth Org. 69, 549, 1991.
72. Nutrition Institute, Arab Republic of Egypt. National Nutrition Survey, 1978. Cairo, no date.
73. El Alamy M. A., Thacker S. B., Arafat R. R., Wright C. E. and Zaki A. M. The incidence of diarrheal disease in a defined population of rural Egypt. Am. J. Trop. Med. Hyg. 35, 1006, 1986.
74. Hirschhorn N. Oral rehydration therapy: the programme and the promise. In Child Health and Survival. The UNICEF GOBI-FFF Program (Edited by Richard Cash, Gerald T. Keusch and Joel Lanstein), Table 2.5, pp. 32-33. Croon Helm, London, 1987.
75. If infant mortality rate for diarrhea was approx. 30/1000 in 1983 and each child had five episodes per year, this implies a case-fatality rate of approx. 0.6%. If the fall to a diarrhea-IMR of 15/1000 by 1985 was due to a 20% reduction in incidence we would have a case fatality rate of 0.375 % (15 deaths per 4000 episodes). If the incidence reduction consisted entirely of rotavirus and enterotoxi- genie E. coli episodes, it implies a case-fatality rate of 1.5 % for these organisms (I 5 deaths per 1000 episodes), a four-fold difference. This differential is reasonable and suggests that some of the continuing fall in mortality after 1985 could be related to etiologic prevalence changes. There is no evidence for change in etiology, however, between 1983 and 1985.
76. Tekce B. and Oldham L. Living conditions and child health in a self-help settlement of Cairo. Unpublished draft, data released with permission of the authors.

Diarrhea control: impact on mortality in Egypt $29
77. UNICEF. State of the World's Children 1986, p.134. Oxford University Press, Oxford, 1985.
78. Ministry of Health, and UNICEF. National Cluster Survey for Vaccination Coverage Egypt: 1990. UNICEF, Cairo, 1990.
79. World Bank World Tables, World Bank, Washington D.C., 1992.
80. Richards A. The Egyptian Farm Labor Market Revisited. J. Dev. Econ. 43, 239, 1994.
81. UNICEF. State of the World's Children 1990, p. 86. Oxford University Press, Oxford, 1990.
82. Central Agency for Public Mobilization and Statistics. 1986 General Census: Final Results. Volume 2, Comprehensive Listing: Population Characteristics. CAP- MAS, Cairo, 1990.
83. UNICEF. The State of the World's Children 1982-83, p. 132. Oxford University Press, Oxford, 1982.
84. Ewbank D. C. Impact of Health Programmes on child mortality in Africa: evidence from Zaire and Liberia. Int. J. Epidemiol. 22, $64, 1993.
85. Koch-Weser D. and Yankauer A. What makes infant mortality fall in developing countries? Am. J. Publ. Hlth 81, 12, 1991.
86. Hirschhorn N., Grabowsky M., Houston R. and Steinglass R. Are we ignoring different levels of mortality in the primary health care debate? Hlth Policy Planning 4, 343, 1989.
87. Mosely W. H. Will primary health care reduce infant and child mortality? In Health Policy, Social Policy, and Mortality Prospects (Edited by Vallin J. and Lopez A.). Ordina Editions, Liege, 1985.
88. Gadalla S., Nosseir N. and McCarthy J. Maternal and Child Health and Family Planning Services in Menoufia and Beni Suef Governorates, Egypt. Social Research Center, American University in Cairo, and Hopkins Population Center, The Johns Hopkins University, Baltimore, 1984.
89. Tawfik Y. Improving Oral Rehydration Salts: ORS Distribution in Rural Areas of Egypt. Ministry of Health, Strengthening of Rural Health Delivery Project, Cairo, 1985.
90. Pan Arab Project for Child Development. Egypt Maternal and Child Health Survey 1991 (Edited by Abdel-Azeem F., Farid S. M. and Khalifa A. M.). CAPMAS and League of Arab States, Cairo, 1993.
91. Ministry of Health of Egypt and World Health Organization. Expanded Programme on Immunization (EPI) and Primary Health Care (PHC) Programme Review. Ministry of Health of Egypt and World Health Organization, Egypt, 1984.
92. Middle East Advisory Group. Media Survey. NCDDP, Cairo, 1984, 1985.
APPENDIX A
On the Relationship Between Classification Error in Cause of Death and Seasonality in Evaluating Diarrheal Mortality
In the Egyptian situation, a strong seasonality of general infant and childhood mortality has traditionally been domi- nated by the seasonality of a single cause: diarrhea. Infant and childhood mortality is substantially higher in summer than in winter primarily because of the strong summer seasonality of diarrheal mortality. In such a situation, reduction in diarrheal mortality should have a predictable and quantifiable effect in reducing general seasonality of mortality, other things being equal. Among the factors that could affect that prediction is misclassification of cause of death. This note examines how misclassification error could affect estimates of diarrheal and non-diarrheal seasonality, and the implications for estimates of mortality by cause.
To set the problem in concrete terms, let us look at some civil registration data on the infant mortality decline between 1983 and 1985.
Year 1983 1984 1985
Proportion of deaths during May-August 0.480 0.433 0.417
Proportion of diarrhea deaths May-August 0.561 0.511 0.500
Proportion of non-diarrhea deaths May-August 0.413 0.377 0.379
Proportion of deaths due to diarrhea 0.450 0.415 0.311
The overall seasonality of infant mortality has declined, as one would expect if the proportion of mortality due to diarrhea has dropped. What is not expected, however, is that the seasonality of both diarrheal and non-diarrheal mortality has also declined. While various possibilities can be hypothesized, we know of no reason why this should have occurred in fact. Put another way, the decline in seasonality is greater than can be accounted for by the observed decline in the proportion of deaths due to diarrhea. Why?
Effects of misclassification error Misclassification of cause of death would affect observed
seasonality of mortality, to the extent that registered deaths in a cause category would include deaths actually due to another cause with different seasonality.
To the extent that deaths from diarrhea were misclassified as non-diarrheal deaths, seasonality of non-diarrheal mortality would tend to be upwardly biased, because some highly seasonal deaths would be added to less seasonal causes. (This may well explain much of the observed seasonality of non-diarrbeal mortality). To the extent that deaths from non-diarrheal causes were misclassified as diarrheal deaths, the seasonality of diarrheal mortality would be downwardly biased, as some less-seasonal deaths were added to highly seasonal ones. If both of these tendencies were operating continuously and if there were a real decline in diarrheal mortality, the result would be a decline in the observed seasonality of both diarrheal and non-diarrheal deaths. For diarrheal deaths, the proportion of registered diarrheal deaths actually due to diarrhea would be reduced, so the real seasonality would be 'watered down' with a higher proportion of non-diarrheal deaths. For non-diarrheal deaths, the proportion of registered deaths misclassified as diarrheal would also decline, so the upward bias in seasonality would be reduced.
This point is of particular interest, because in Egypt, considerable misclassification of death in the civil register is a well known phenomenon, leading to doubt as to the validity of observed changes in cause of death. To examine how misclassification might in practice affect observed seasonality, let us take a hypothetical example. Suppose that the reality of a situation were as follows:
(1) In year one, 50% of deaths were due to diarrhea. Of the diarrheal deaths, two-thirds occurred in May-August; of the non-diarrheal deaths, one- third occurred in May-August (i.e. no seasonal- ity).
(2) In year two, diarrheal mortality is reduced by half, but no change in non-diarrheal mortality and no change in seasonality of death, either diarrheal or non-diarrheal, occurs.
(3) Continuously throughout the period, one-quarter of all diarrheal deaths are misclassified as non-diarrheal, and one-quarter of all non-di- arrheal deaths are misclassified as diarrheal.
Then the appearance, as shown in the civil register, along with the hypothesized reality, would be as presented in the table below. Hence, in this hypothetical example (Table 13):
(l) misclassification error obscures part of the season- ality of diarrheal mortality and introduces a spurious seasonality into non-diarrbeal mortality;

$30 Peter Miller and Norbert Hirschhorn
Table 13. Reality vs observed registration data under hypothetical conditions described in text
Year I Year 2 Regist. Reality Regist. Reality
Percent DD May-August 58.3 66.7 53.3 66.7 Percent non-DD May-August 41.7 33.3 38.1 33.3 Percent all deaths May-August 50.0 50.0 44.4 44.4 Percent due to diarrhea 50.0 50.0 41.7 33.3
(2) the decline in real mortality from diarrhea reduces the observed seasonality of both diarrheal and non-diarrheal mortality, when no such change in fact occurred; and
(3) due to an unchanging pattern of misclassification error, the decline in diarrheal mortality is understated by half in the civil register.
This has occurred in a situation which, though hypothetical, is not implausible; indeed, the observed data in the hypothetical example above are not very far from the actual Egyptian registration data of 1983-85. Thus, the observed declines in seasonality within cause could be explained by plausible levels of misclassification error.
In sum, it is generally accepted that there is substantial error in classification of cause of death. To the extent that non-diarrheal deaths are misclassified as diarrheal deaths, seasonality of diarrheal mortality will be underestimated in the vital statistics; to the extent that diarrheal deaths are misclassified as non-diarrheal deaths, seasonality of non-diarrheal mortality will be overestimated in the vital statistics. If misclassification is occurring in both directions, a decline in the real proportion of deaths due to diarrhea will introduce a spurious decline in registered seasonality for both diarrheal and non-diarrheal deaths. The observed patterns of change in seasonality are consistent with this phenomenon, at plausible levels of misclassification error. A further implication is that in such a situation, the decline in the proportion of diarrheal mortality will be underestimated in the civil register.
APPENDIX B
Adjustment Factors for Seasonality in Diarrhea Prevalence Estimation
Because diarrhea prevalence varies in consistent patterns over the course of a year, the comparison of prevalence levels from different times of year requires adjustment for seasonality. If a survey conducted in July finds higher prevalence of diarrhea than one in December, this may be due only to the seasonality; we need some way to adjust any figures for the time of year at which they were collected, because otherwise it is difficult to interpret the results. In particular, we need to present evidence on whether there has indeed been a change over time when great fluctuations occur in measurements taken at different times of year.
To do this, we need data using a consistent methodology taken at all seasons of the year, over as large a part of the country as possible. The best data for this in Egypt are from the Five-Community Studies conducted by NCDDP in 1983-84 and again in 1987-88. These were done in several scattered communities in Egypt: in 1983-84, in Dakahlia, Menoufia, Fayyoum, Giza (rural) and Alexandria; and in 1987-88 in Dakahlia, Menoufia, Giza, Alexandria and Cairo. While not strictly representative, and in particular not covering Upper Egypt south of the Fayyoum, these communities provide substantial geographic variety. As part
Table 14. Computation of pooled prevalence levels and 'adjustment factors', from Five-Community Data from 1983-84 and 1987-88, by
month
Adjustment Month 1983-84 1987-88 median (n) Factor (k/n) Jan 7.6 7.5 7.6 1.65 Feb 7.1 7.4 7.3 1.72 Mar 7.6 6.6 7.1 1.75 Apr 11.2 12.3 11.8 1.06 May 14.3 16.6 15.5 0.81 Jun 13.8 21.3 17.6 0.71 Jul 15.2 19.3 17.3 0.72 Aug 19.4 15.2 17.3 0.72 Sep 15.8 15.8 15.8 0.79 Oct 14.5 12.8 13.7 0.91 Nov 10.3 9.9 10.1 1.23 Dec 8.0 9.0 8.5 1.46
Mean of means: 298.5/24 = 12.44 (=k).
of that study, each household was canvassed every month to determine whether any child aged under 36 months of age had diarrhea during the 24 hr prior to the canvass. The 1983-84 study lasted 15 months, so three months (August-October) were covered twice. The 1987-88 study lasted 12 months.
Raw data are not available for the 1983-84 study, and prevalence data are presented graphically rather than with numeric data. The 'mean', which is here assumed to mean the overall pooled prevalence, was published in a line graph generated by computer for each month. Assuming the computer placed the dots in the graph with reasonable precision, it is possible to get a good estimate of the numeric value by careful measurement of the height of the dots. This was done for all 15 months; for the three months with two readings, the midpoint of the two readings was used. For the 1987 study, each participating center prepared its own report; from each report, the number of children canvassed each month can be obtained, along with the number with diarrhea during the past 24 hr. Data were actually collected at four week intervals in some centers, so that in one month for each of these centers, two readings were taken during the month; both were included in the pooled data at full value. Data are missing for four months from the Cairo center, and some questions have been raised about the quality of the field work for the 1987-88 studies. Nevertheless, for diarrhea prevalence the data show sufficient consistency with the previous results and between centers that it was decided to include them in the interest of increasing the total body of data available.
This gave two values for each month, one for each study, representing the overall experience of all visits by all centers for that study, as seen in Table 14 below. The value for each month is taken as the midpoint of the two values 'n' in the table. The general prevalence level for all months combined was calculated as the mean of the 24 (12 × 2) individual monthly values ('k').
To obtain adjustments factors for each month, this general mean (12.44%) was divided by the overall value for the month. If the monthly value was lower than the general mean, then the adjustment factor was less than one. These values can thus be multiplied by the actual prevalence level if the survey had been done at an 'average' time of year.
These estimates can be applied to one-week or two-week prevalence or incidence estimates, as well as day-point prevalence, since any corrections for longer periods could be expected to be trivial. In any case, these multipliers cannot be taken as terribly precise values; they are simply the best we have. They follow the general known patterns of seasonality according to hospital data, NCDDP service and sentinel area data and CAPMAS mortality data.
Copyright © 2022 FDOKUMEN