The challenge for the designer in pharmaceutical packaging – Designing for an improved level of...
55
1 The challenge for the designer in pharmaceutical packaging – Designing for an improved level of patient compliance. Ashley Wiltshire Royal College of Art Innovation Design Engineering 04 October 2013 Word Count 9931
Transcript of The challenge for the designer in pharmaceutical packaging – Designing for an improved level of...

1
The challenge for the designer in pharmaceutical packaging – Designing for an improved level of patient compliance. Ashley Wiltshire Royal College of Art Innovation Design Engineering 04 October 2013 Word Count 9931

2
Contents List of Illustrations 1.0 The Industry 1.1 Patient Compliance - Introduction 1.2 The pharmaceutical industry and the cost of non-compliance 1.3 NHS Effect 1.4 Regulation 2.0 The stakeholders 2.1 The person/patient 2.1.1 The Engaged Patient 2.1.2 The power of patient empowerment 2.2 The Doctor/GP 2.3 The Nurse 2.4 The Friendly pharmacist 2.5 Hierarchal Decisions 3.0 Design philosophy 3.1 Assumptions 3.2 Foundations 3.3 Implications 4.0 Design Process 4.1 Current process approach 4.2 What is missing? 4.3 Marketing power 5.0 Design delivery 5.1 Typo – Point Size & Language 5.2 Similar Name Different Effect 5.3 The Information Problem 6.0 Recommendations 6.1 Relevant to the industry 6.2 Relevant to the stakeholders 6.3 Co-creation - change the game 6.4 How the process can change 6.5 Interactive ways designers can improve adherence 7.0 Conclusion Bibliography Appendix
3
List of Illustrations
Figure 1: Pharmaceutical Packaging Rack Photograph by Martin Lewin (2012) http://www.projectfreerange.com/wp-content/uploads/2012/10/Processed-9220.jpeg (28 February 2013) Figure 2: Reasons for Medication Non-Adherence Graph part of the study by P. Micheal Ho (2009) http://circ.ahajournals.org/content/119/23/3028/T1.expansion.html (8 April 2013) Figure 3: Self-Managed Patient Image provided by Ernst & Young (2012) Beyond Borders 2012 Ernst & Young (2 June 2013) Figure 4: Plastic Pill Box Photograph by Julia Losa (2013) Figure 5: ALMUS medication packaging Photograph by Maria Florio (2013) Figure 6: Multiple Medication Image Photograph by Maria Florio (2013) Figure 7: Daily intake print on foil packaging Photograph by Maria Florio (2013) Figure 8: Modern Prescribed Medication Packaging Photograph by Ashley Wiltshire (2013) Figure 9: Printed label Photograph by Ashley Wiltshire (2013) Figure 10: MWV’s Avive multiple medication dispenser Image provided by MWV (2013) http://www.meadwestvaco.com/mwv/groups/content/documents/image/mwv040456.gif (25 May 2013) Figure 11: Self-Expiring Packaging Image by Kanupriya Goel, Gautam Goel (2013) Self-Expiring http://www.red-dot.sg/en/online-exhibition/concept/?code=688&y=2012&c=14&a=0 Figure 12: Nike iD website customisation page Image by Brian Betschart (26 July 2007) http://www.sneakerfiles.com/wp-content/uploads/2007/07/nike-zoom-kobe-ii-hit-nike-id-1.gif (20 September 2013) Figure 13: Medication Instruction Icons Image by Haejin Song (June 4 2013) http://dribbble.s3.amazonaws.com/users/72948/screenshots/1099510/d.png (20 September 2013) Figure 14: Screenshot of Experientia Concept Video Image by Ashley Wiltshire (2013) Experientia, ‘Experientia - The Pharmacy of the Future - 03 Alison’ http://www.youtube.com/watch?v=jHuQazVO4AQ

4
1.0 The Industry
1.1 Patient Compliance - Intro
Patient compliance (also known as adherence) is the degree to which patients take their medication
‘as prescribed’. Globally, compliance is below 50%, meaning half of all pharmaceutical medications are
never taken or taken incorrectly. This problem contributes to a loss of £250 billion for the industry
and 200,000 deaths each year.1 This dissertation aims to demonstrate how a shift in design philosophy
and execution can help improve this massive problem for both the patient and pharmaceutical
companies.
Over the course of the last year I have become heavily involved in a start-up company focussed on
improving health and wellness of people in the United Kingdom. The aim is to bridge the gap between
the healthcare industry and the patient by making healthcare a more human experience. The research
and work conducted over the last year has led me to question the philosophies behind how
healthcare and pharmaceutical products (specifically pharmaceutical packaging of prescription drugs)
fail to appeal to and understand the consumer, the patient. (fig1).
Arriving at the Royal College of Art last October allowed me to step back from the zoomed in view I
had on healthcare and take a more balanced approach to what is a big problem for not only the NHS
but medication users as well. I see this dissertation as an opportunity to consider to what extent does
the graphic design of pharma (pharmaceutical) packaging impact on the users interpretation of
medication use.
Through interviews I aim to uncover:
• What are the challenges designers of packaging face on improving patient compliance?
• How do patients feel about the current state of medication packaging in the UK and what
are there concerns?
• How do people deal with handling multiple medications with multiple designs at one time?
1 Glen Giovannetti, Gautam Jaggi, Siegfried Bialojan, et al. “Beyond borders: Global Biotechnology Report 2012.”
Ernst & Young. 2012.

5
• Why has pharma failed thus far when other areas of design that deal with millions of people
have excelled?
Clarity on the above questions will help this research paper explore and understand the possibility of
enabling and empowering patients to take direct action when feeling confused or unsure with the
medication information provided by erroneous packaging design. This paper will encompass thoughts
and prospective views on the handling of graphic design of medical packaging in the future, whilst
taking into account the bigger picture of the pharmaceutical industry and looming changes to the
National Health Service in the United Kingdom.
Figure 1: Martin Lewin, Pharmaceutical packaging rack 2012
It is estimated that a third of medication errors in the NHS are caused by confusion over packaging
and labelling instructions2. This section will analyse how and why some modern medication packaging
fails to clearly communicate the use of its contents.
2 “Design for patient safety: A guide to the graphic design of medication packaging.” NHS.
http://www.nrls.npsa.nhs.uk/resources/?EntryId45=63053 (accessed 10 February 2013)

6
The Helen Hamlyn Centre has released two editions of a study titled ‘a guide to the graphic design of
medication packaging’. These studies are used as a guideline to gain an understanding of the
background material and subject matter surrounding pharmaceutical packaging. There are on average
900,000 recorded adverse events in the NHS every year.3 This is a substantial amount that could be
reduced through an increase in patient compliance of medication.
1.2 The Pharmaceutical Industry – cost of non-compliance
Looking across the Atlantic at the individual patient who does not take their medication or finds it
difficult to understand the directions, then we can see that patient non-adherence in the United States
is costing their healthcare system between $100-289 billion annually4. In the UK, primary studies have
been conducted by The Aston Medication Adherence study and initial reports claim that £300 million
is lost to medication misuse and non-use in the United Kingdom5 annually.
This is a remarkable statistic and raises questions as to why the problem exists, a graph6 created by P.
Micheal Ho as part of a study into the effects of non-adherence of medication and its importance in
cardiovascular outcome proposes reasons why. Low-literacy/language problems, vision problems, and
most integral to my study is the poor quality of provider-patient relations, something that Tomlinson
stated as well, as these can be directly related to the importance of packaging clarity and patient-
specific design, something I cover later in the paper.
3 “About patient safety.” NHS. http://www.nrls.npsa.nhs.uk/about-‐us (accessed 10 February 2013) 4 “Interventions to Improve Adherence to Self-‐administered Medications for Chronic Diseases in the United States: A
Systematic Review.” Meera Viswanathan. http://annals.org/article.aspx?articleid=1357338#r3-‐6 (Accessed April 10, 2013)
5 “Action on medicine wastage and improving medicine use.” Lord Howe. https://www.gov.uk/government/news/action-‐on-‐medicine-‐wastage-‐and-‐improving-‐medicine-‐use (Accessed 18 April 2013)
6 Ho, P. Michael, Bryson, Chris L. and Rumsfeld, John S. . “Key Issues in Outcomes Research: Medication Adherence: Its Importance in Cardiovascular Outcomes” Circulation, 2009 Jun 16; 119(23): 3028-‐35. Accessed April 10, 2013 http://circ.ahajournals.org/content/119/23/3028.full#cited-‐by

7
Figure 2: P. Micheal Ho, Reasons for medication non-adherence, 2009
To further rise this cost, patients have been oversubscribed medication, which just ends up as waste
and the BBC reported that around £300 million is wasted due to this every year7.
In response, doctors have been urged to stop over-prescribing with the article stating that
‘Pharmacists say this would be easy to do - if doctors offered more tailored, personal advice to
patients and stopped prescribing large amounts of drugs to cover long periods of time.’ Clearly, there
is a breakdown in communication and understanding across the channels from pharma company
down to the pharmacist.
1.3 NHS effect
The NHS is on its way to no longer being a free health service to the population of the UK. Changes
to the way services are conducted, funded and situated will come into effect as early as April 20148.
NHS Trusts will apply to become Foundation trusts, effectively privately run, privately funded
institutions which in turn affects the costing and opportunity for patients to receive care and
consistent care shall they need it.
7 Chittenden, Stephen. “Doctors urged to cut medicine prescription waste.” BBC. July 22, 2013.
http://www.bbc.co.uk/news/health-‐23374000 (Accessed September 21, 2013) 8 “Supporting all NHS Trusts to achieve NHS Foundation Trust status by April 2014.” DoH, NHS.
http://www.wsh.nhs.uk/AboutUs/TrustBoardMeetingsandPapers/2011/July29th2011/Item13bWestSuffolkTFAFinal.pdf (Accessed September 20, 2013)

8
The challenge for the designer here becomes additional layers of complexity and decision-making.
There is no longer one governing body to approach to make changes made to existing packaging
design. Before this break and redistribution of services in the NHS, uniform change may have been
harder to convince the MHRA of but it would have taken affect throughout the service with greater
fluency. With for-profit care institutions such as Virgin Care and CARE UK already operating many
general practices9 it will add further distance from the end user; patient and the drug producer, GSK
for example.
1.4 Regulation
It is known that advertising pharma goods in the public domain is banned, as it cannot be seen to
entice the patient. In contrast to this point, there is a difference between advertising and empowering
a patient to want to get better by taking their medication. Though the strict regulations regarding
usability are also a reason why there haven’t been radical changes to the way packaging has become
more personable.
I enquired about the process that a pharmaceutical company has to go through when they want to
change an aspect of their packaging. It all depends on whether it was in the licence initially granted by
the governing body, in the UK it is the Medicines and Healthcare Products Regulatory Agency
(MHRA). Wilson gives a clear, extensive example of the process required to make changes to existing
packaging design.
“As a global company the design of the packaging has been rolled out on a global level and follows
strict branding guidelines, which is then adapted to suite the individual countries regulations.
In the UK, if you want to make a change on a National level, UK only, then a variation must be
submitted to the MHRA. Depending on the extent of the change and which category it falls under,
this can take anywhere from a few weeks to years to be assessed and approved by the MHRA.
Also, depending on the category of variation, a fee is paid for each product licence that the change
affects.
9 Davis, Jacky, and Raymond Tallis. NHS SOS: How the NHS was betrayed – and how we can save it. London, One World,
2013, p.191-‐192

9
So, the Regulatory Affairs team within in the company will prepare the submission package and submit
the change to the MHRA. During the time the MHRA asses the change they may have questions or
request further changes that Regulatory Affairs team will need to respond to.
Once the MHRA approve the change they will notify us of the approval and the date it was approved.
We, the pharmaceutical company will then have 6 months to implement that change. The 6 months is
deemed as the date the first batch is released following approval. So, if the implementation date was
30/09/2013. Any batches released after this date must include new artwork.
To implement the new artwork we have a change procedure we must follow. This requires
generating a change document and tracking the change with the suppliers who are located throughout
the EU. We liaise with them to communicate when the new artwork must be used depending on our
orders and demand.
Finally when the product is release onto the market with the new artwork we can close out the
change to make sure the artwork has been implemented within the six month timeframe.”10
This extremely, extensive process is clear to see that any change made would be very time consuming
and I imagine cost consuming as well. With this knowledge in mind I will move on to discuss and
explore the stakeholders I believe are integral to the designing taking new routes and methods in this
field.
10 Wiltshire, A; “Questions on the challenges designers face in improving patient compliance through pharmaceutical
packaging.” Interview. September 2013

10
2.0 The stakeholders
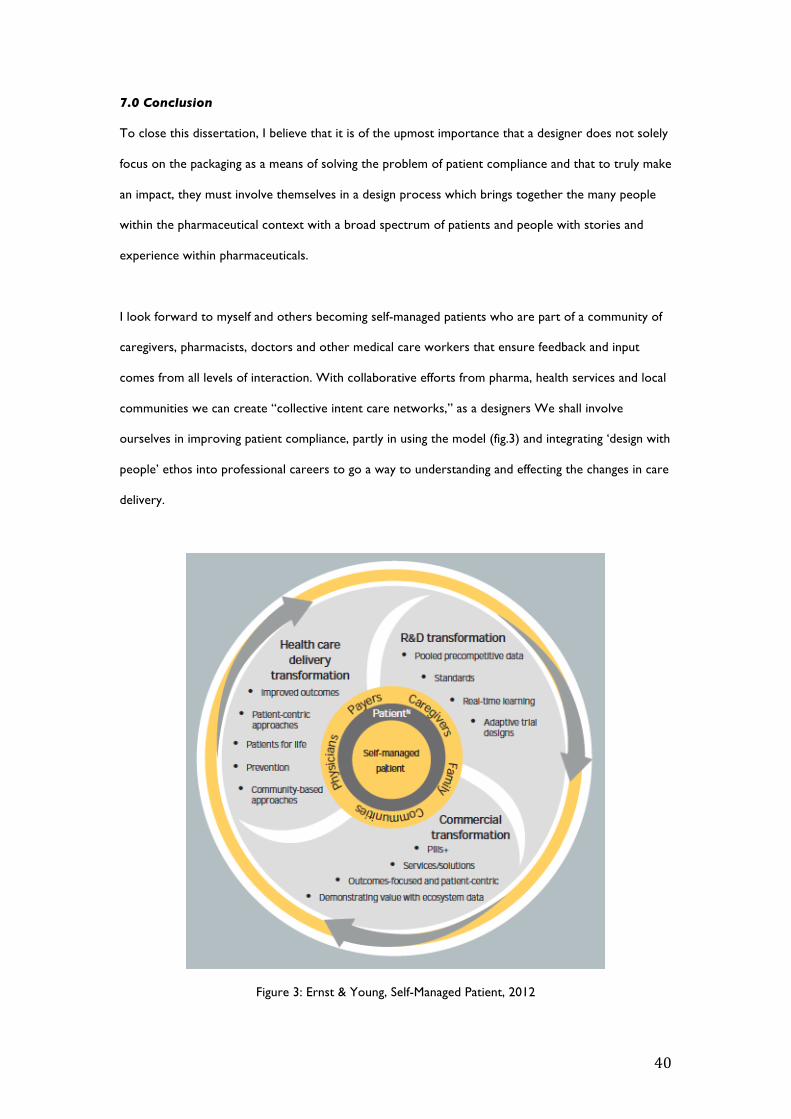
The company that I work for place patients and people at the centre of all we do, this shift in how
healthcare is delivered is part of a growing paradigm described in Ernst & Youngs – Beyond Borders
study. The ultimate goal of this, is the self-managed patient who is part of a community of caregivers,
pharmacists, doctors and other medical care workers to ensure that feedback and input comes from
all levels of interaction. These kind of networks are described as “collective intent care networks”
and if the designer is truly interested in involving themselves in improving patient compliance, the use
of the model (Fig. 3) would go a long way to understanding the prospective changes in care delivery.
Figure 3: Ernst & Young, Self-Managed Patient, 2012

11
2.1 The person/patient
2.1.1 Engaged patients
The Kings Fund UK ran a project into inquiring the quality of general practices and on the subject of
patient engagement and states that:
‘It is used to describe patients’ engagement in primary care consultations regarding their own health,
care and treatment.’11
Through working for the healthcare start-up I can comment on my experience in meeting engaged
patients that they have the self-efficacy to maintain their treatments, as well as have the confidence to
share their experience with others, help friends and family in understanding their own ailments and
problems as well as feel empowered about their lives in a way that has rarely been seen before.
2.1.2 Power of patient empowerment
The potential for patients to gain control over their compliance of medication has never been more
exciting. The range of products that aim to give the user an understanding of their health, their sleep
patterns, their dietary needs have all been welcomed with open arms, yet there is nothing to really
combat the chance of human error, forgetting to take your medication, or not having the knowledge
at hand or the confidence to gain the knowledge about the medication. This is why patient
empowerment is critical to improving patient compliance. The designer is suitably positioned to
create an intervention and it excites me to see how this approached in the coming years.
2.2 The Doctor/GP
I have conducted several interviews enquiring patients aged over fifty to begin to understand what
they feel is missing from their medication experiences and to what extent they feel their GP plays a
role in their adherence. In response to three questions this is what they had to say.
Is it clear what each medication aids with?
11 Parsons, Suzanne and Winterbottom, Anna and Cross, Peter and Redding, Don. “The quality of patient engagement and
involvement in primary care.” 2010. http://www.kingsfund.org.uk/sites/files/kf/field/field_document/patient-‐engagement-‐involvement-‐gp-‐inquiry-‐research-‐paper-‐mar11.pdf (Accessed September 21, 2013)

12
‘Most of the time its clear but the explanation could be clearer as not all patients understands the
Medical terms.’ And ‘Yes, as GP explains to me what each medicine is for.’
Do you read the small print information that comes with the medication?
‘No I don’t read the small print as I don’t understand all the English and rely on my daughters to
explain.’ And ‘Yes I always read the small print but at times can be quite difficult to understand due to
the technical terms that are used, so that could be simplified.’
If you are confused or do not understand the medication, what support do you get?
‘If at anytime I need further support I will go back to see my GP or go to pharmacy.’ And ‘If I am
confused about aspect of my medication I would return to see my doctor.’
It was clear to me when speaking with Vincenzo that some patients rely heavily on their GP if there is
any confusion and to couple this with their busy lifestyles and fear of embarrassment, the likelihood of
them returning to the GP is time consuming to get an appointment and the chance of non-adherence
rises with the feeling of pressure to get their point across in a short appointment time.
This is something that I consider as an outcome of the system failing earlier in its cycle and that it is
important to look at what potentially is the root cause.
‘With an average slot of 5-8 minutes per patient, doctors protest that there is not enough time for
the increasing number of tasks involved in routine consultations. Shortage of time is considered a
major obstacle to the realisation of a more patient centred medical practice that actively involves
patients in treatment decisions.’12
12 Pollock, Kristian and Grime, Janet. “Primary carePatients' perceptions of entitlement to time in general practice
consultations for depression: qualitative studyCommentary: Managing time appropriately in primary care.” BMJ 2002;325. September 28, 2002. http://dx.doi.org/10.1136/bmj.325.7366.687 (Accessed September 19, 2013)
13
It may be beyond the call of the packaging designer but the chance to improve compliance through
GP notes on medicinal packaging could further improve user understanding and trust in medication.
2.3 The Nurse
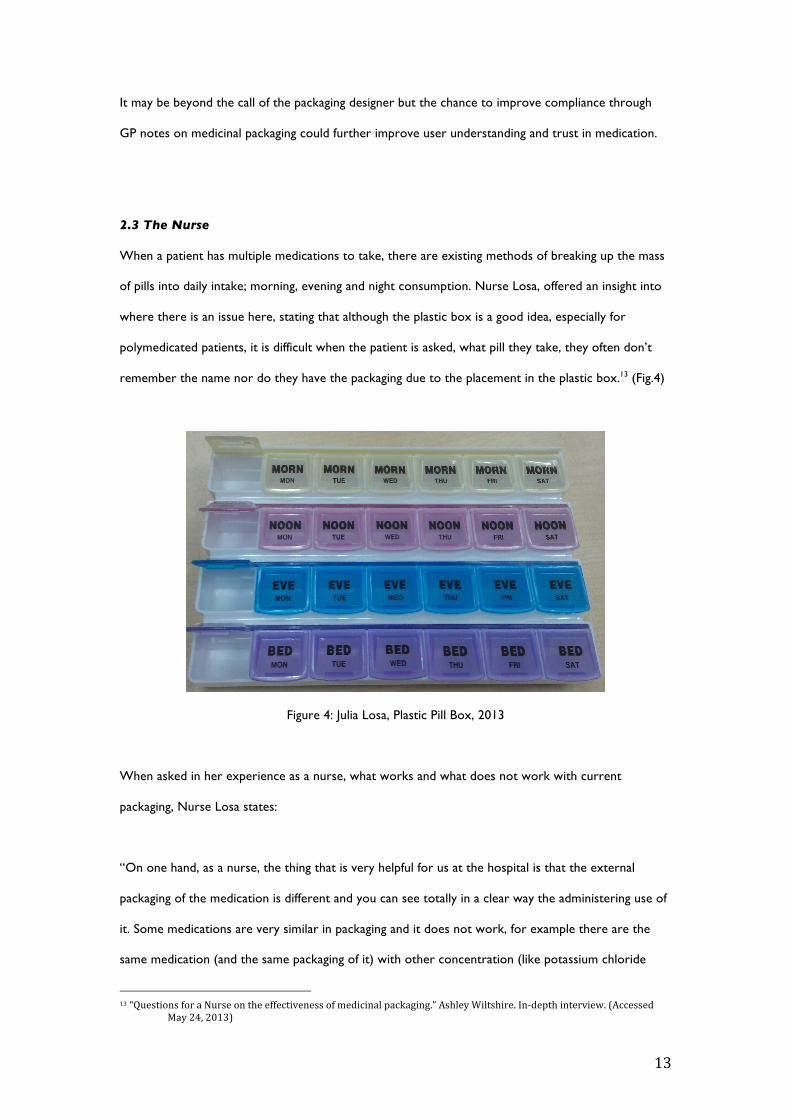
When a patient has multiple medications to take, there are existing methods of breaking up the mass
of pills into daily intake; morning, evening and night consumption. Nurse Losa, offered an insight into
where there is an issue here, stating that although the plastic box is a good idea, especially for
polymedicated patients, it is difficult when the patient is asked, what pill they take, they often don’t
remember the name nor do they have the packaging due to the placement in the plastic box.13 (Fig.4)
Figure 4: Julia Losa, Plastic Pill Box, 2013
When asked in her experience as a nurse, what works and what does not work with current
packaging, Nurse Losa states:
“On one hand, as a nurse, the thing that is very helpful for us at the hospital is that the external
packaging of the medication is different and you can see totally in a clear way the administering use of
it. Some medications are very similar in packaging and it does not work, for example there are the
same medication (and the same packaging of it) with other concentration (like potassium chloride
13 “Questions for a Nurse on the effectiveness of medicinal packaging.” Ashley Wiltshire. In-‐depth interview. (Accessed
May 24, 2013)

14
blisters) or some medications which at first view you can confuse because they are the same blisters, I
mean, you must read it for differentiate it (for example, the potassium chloride blisters and the
smaller saline solution blisters)
For me that is essential when we have an emergency, for take action fast. Moreover it works for us
for not commit a mistake.
On the other hand, in my opinion, a good and clear packaging works with patients as well, above all
when we are talking about polymedicated patients. Things like the days of the week in the metal film
that cover the pills are important in some drugs that they have to take day by day.”
2.4 The Friendly Pharmacist
Designers must look beyond just the patient to product compliant packaging, the pharmacist has a
growing role in the say of how pharmaceutical medicine is distributed and their insights and
experience cannot be overlooked, they are often the bridge between the patient, their medication
and the doctor or GP. If the designer took the approach of ‘designed with people’ and included
pharmacists in the design process I believe that outcome would tackle the issue with stronger insights.
Rob Darracott states that,
“Although we would like to see pharmacists on the governing bodies of clinical commissioning groups,
we are pleased that the important role of pharmacy has been acknowledged by the Government..
..Pharmacists see more people, more often, even more than GPs do so the advice and support they
will give to commissioners will be vital.14”
‘In addition, the research suggests that pharmacists can play a greater role in mitigating the
occurrence of error, through reviewing patients with complex medicines regimens at a practice level,
and in identifying and informing the GP of errors at the point of dispensing.15’
14 Darracott, Rob. Government acknowledges pharmacists role as an important source of expert advice. Pharmacy Voice.
June 21, 2011. http://www.pharmacyvoice.com/press/government-‐acknowledges-‐pharmacists-‐role-‐as-‐an-‐important-‐source-‐of-‐expert-‐a. (Accessed May 20, 2013)
15 Avery, Tony P., et al. “Investigating the prevalence and causes of prescribing errors in general practice: The PRACtICe

15
2.5 Hierarchal Decisions
By looking at a series of four different medications from the same supplier, ALMUS, in Fig. 5 it is
evident that consideration has been made to the order of information, at close inspection, the
audience for the medication is clear, GPs and Pharmacists as elements such as the name, dosage and
colour bands are the clearest attributes, not when or how often they should be taken.
There is however some consideration for the end user to differentiate between medications through
several indications. There is an image of the tablet type on the box, which serves as an aid if patients
keep their medication in a day-use box, and the colour of the tablet and also the name of the
medication in a white semi-bold typeface. In Fig. 5 the bottom right packaging, the label indicating the
most important information for the user is miniscule actually covers the dosage reflecting the lack of
attention to placement for end user instructions in this instance.
Study (PRevalence And Causes of prescrIbing errors in general practiCe) A report for the GMC.” GMC. May 2012.http://www.gmcuk.org/Investigating_the_prevalence_and_causes_of_prescribing_errors_in_general_practice___The_PRACtICe_study_Reoprt_May_2012_48605085.pdf (Accessed May 20, 2013)

16
Figure 5: Maria Florio, ALMUS medication packaging, 2013

17
3.0 Design Philosophy
3.1 Assumptions
Pharma packaging companies have many considerations to take into account when researching and
designing their packaging and there are five modern trends to help create the best all round
packaging. These areas have a major impact and often cause much of the limitation to the packaging,
restricting designers from making change. The five areas include unit-dose packaging for greater
dosage control, packaging against counterfeiting, non-invasive permeation testing, child-resistant
packaging and eco-friendly pharma packaging.
Some would argue that having to include so much into a design of a product makes the packaging
companies some of the most innovative and in credit to the general success of the evolution and
development of packaging, it has been achieved. The change to single dose dispensing of medication
users is a big part of the shift towards self-managed care.
‘ "With more of a focus on outpatient care and the self-regulation of medicine, there's greater onus
on patients to take the right medications in the right amount," said Dow Chemical senior research
scientist Jill Martin at a medical devices conference on 13 February 2012, in Anaheim, California, laying
out the future trends of pharmaceutical packaging.’16
The US National Center for Biotechnology Information released an in depth study of the future
trends and future of pharmaceutical packaging17 which covers the five modern trends previously
mentioned. It goes into detail about how the graphics, printing and outer-carton packaging play a huge
role in keeping the medication secure from counter-fitting. Providing a wealth of information on
techniques a company may use but very little on how the future of packaging will effect or attempt to
effect patient compliance. The mention of how the rise of care managed at home will mean packaging
will take on a different form, such as prefilled syringes but nothing about creating engaging products.
16 Butschli, Jim. “Dosage control, biologics, driving material considerations.” Pack World. February 13, 2012.
http://www.packworld.com/applications/healthcare/dosage-‐control-‐biologics-‐driving-‐materials-‐considerations. (Accessed September 22, 2013)
17 Zadbuke, Dr. Nityanand, et al. “Recent trends and future of pharmaceutical packaging technology,” J Pharm Bioall Sci, no. 5 (April-‐June 2013): 98-‐110. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3697200/. (Accessed September 23, 2013)

18
The concluding thoughts of the study make clear a challenge for the designer in self-administered
therapies stating ‘When self-administered drugs are in lyophilized or dry powder form, manufacturers
must find methods or packaging systems that help prevent accidental needle stick injuries, inaccurate
dosing, and drug spray-back. Manufacturers familiar with the drug administration process must
provide delivery systems that simplify drug reconstitution, especially for non-professional caregivers.’18
3.2 Foundations
‘Healthcare is delivered in many different contexts and patients’ sensory, physical and mental
capabilities vary greatly. Design solutions have to address these factors.19’ This is the opening
statement from the guide to design for patient safety. Designers have tackled issues with medication
packaging by employing the international type language, often known as Swiss design. The potential
users for medication packaging have extended and the requirements of them as well.
The guide to patient safety highlights the potential problem with coloured packaging stating that ‘if a
single colour is used for a whole range of medicines it can be difficult to identify a specific product.
This is compounded if medicines with similar names are stored next to one another. If a patient is
prescribed a number of medicines with the same colour packaging, there is an increased chance of
them taking the wrong one.20’
3.3 Implications
The use of the international type style has given medication packaging a grid and a hierarchy to its
information ordering. This has made for easier reading and tackled the main issues of distinguishing
medication from other similar types. The use of this style has removed the feeling of empowerment
to the product which could be found in the design of cosmetic or cologne industry, this lack of
personality and drive for clean simplistic visuals may be a cause for patient non-compliance (Fig.2).
18 Zadbuke, Dr. Nityanand, et al. “Recent trends and future of pharmaceutical packaging technology.” J Pharm Bioall
Sci, no. 5 (April-‐June 2013): 98-‐110. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3697200/. (Accessed September 23, 2013)
19 “Design for Patient Safety.” National Patient Safety Agency. 2007. Pg.7 http://www.hhc.rca.ac.uk/CMS/files/NPSA-‐
Design-‐for-‐patient-‐safety-‐.pdf, pg.7, (Accessed April 18, 2013) 20 “Information design for patient safety: A guide to the graphic design of medication packaging.” HHRC. 2007.
http://www.nrls.npsa.nhs.uk/EasySiteWeb/getresource.axd?AssetID=129650& pg.55(Accessed May 20, 2013)

19
It is well known that medical packaging cannot be seen to advertise directly to people but an emotive
reaction or belief in health improvement counts for a lot21. This is a question I raise, whether
disrupting and re-imagining the entire style used for medication may be a drastic move, it could raise
the opportunity to re-categorise the hierarchy, bring about a new sense of confidence in patients and
focus on improving patient compliance.
As the baby-boom generation ages, the likelihood of quick killers like cancer and heart attacks has
dropped22 and the biggest fear for the seniors of our time is the degradation of their mental health.
The increased likelihood of degradation of mental and physical health in later life in turn leads to an
increase in medication intake. ‘The average 75 year old has three chronic conditions and uses five
different prescription drugs.23’ This not only causes the patient to have a schedule to stick to but to
feel confident that taking five different drugs can help improve their health. In Fig. 6 you can see all the
medication that Vincenzo, the elderly gentlemen I interviewed takes everyday, eight different
medications, a day.
Figure 6: Maria Florio, Multiple medication use, 2013
21 Boskey, Elizabeth Dr. . “Health Belief Model: Use of a condom may hinge on perceived risk.” About. March 24, 2010.
http://std.about.com/od/education/a/healthbelief.htm (Accessed September 20, 2013) 22 “The Concern With Aging.” BBC. Audio Programme. March 2, 2013. http://www.bbc.co.uk/programmes/p014wlnp
(Accessed May 20, 2013) 23 Moore, Margaret J., Moir, Phyllis, et al. “The State of Aging and Health in America 2004.” MIAH, CDC. 2004.
http://www.cdc.gov/aging/pdf/State_of_Aging_and_Health_in_America_2004.pdf, (Accessed May 20, 2013)

20
4.0 Design Process
4.1 Current process approach
To be able to deconstruct the problems with patient compliance, it is helpful to understand how
packaging design works currently. Packaging plays an important role in the self-efficacy of a patient.
The language, the design including the colours, form, shapes are the patients first interaction with
their medication before consuming. Better understanding of packaging and a more positive interaction
with their medication can lead to better compliance.
This section encompasses two in-depth interviews with packaging designers and how they feel about
the history of packaging as well as their views on the room for innovation in packaging design. They
shares their opinions on the future of medicinal packaging and why it may not be as easy as changing
the packaging of a typical commercial product.
The interview started by raising questions over why patient non-compliance is on the rise and who is
to blame if any. Tomlinson’s response was that patients and the GP’s are to blame. Dispensers of
packaging should be accountable for the some of the issues raised with patient’s problems with taking
multiple medications. He states that there could be more done to differentiate the products under
current laws and legislation.
Further questioning in to why pharma packaging fails to engage with the end user as effectively as
progressive areas of design such as airport services or online shopping was explained as being two
fold. ‘Drugs aren’t packaged for the benefit of the end user’ with the dispenser as the main audience.
Pharma packaging has been ahead of the curve in regards to their efficient colour coding and symbol
systems but it in Tomlinsons words ‘it is unfair to suggest that drug packaging hasn’t progressed when
one looks at old pharmacies where the products might have been snake oil rather than a cure for
anything.’
Whilst Wilson argues that by stating “I believe this is because of how heavily regulated it is. The
patients safety is the number one priority for pharmaceutical companies and the MHRA (Medicines
and Healthcare products Regulatory Agency) who regulate medicines in the UK.

21
Also, with so many guidelines on what can and cannot be done, you are limited with the design. Not
only does the packaging need to be easily readable and identifiable for the patient, but also for the
pharmacist dispensing the medicine to ensure the patient safety.”
I questioned Wilson and Tomlinson on the current process of designing packaging and Tomlinson
started by offering an insight, stating,
“Unfortunately it has been quite a while since I worked on packaging. So can only really talk
accurately about marketing the drugs. The biggest ones are the amount of information that must be
displayed dependent on the type of advert produced.
All text must also be above 1mm in x-height and the language used on the ad can't say what the
product treats or encourage people to buy it. The adverts are therefore more intended to inform
pharmacists of its existence rather than promote it over competitors products.”
With Wilson responding by stating, “I have only worked in the industry for 6 years and haven’t seen
too much change in that time. Some of the key guidelines to follow are; to make sure the font size is
not below the minimum, ensure the correct space is allocated for the dispensing label, braille is
positioned correctly, pharmaceutical form and dosage is clearly identifiable and key warnings are
highlighted.”
There has been an increased interest in the analysis of pharmaceutical packaging over the last fifteen
years and the Helen Hamlyn Centre for design has produced two studies that cover the common
problems of legibility and clarity of information printed on packaging. These studies have helped
disseminate the existing challenges and have highlighted areas of improvement for interested parties in
pharmaceutical medication adherence. In recent years the media has brought to light the problem of
patient non-adherence24 and shown a greater interest in potential solutions25 to the issues faced.
24 Ledwith, Mario. “One in three patients does not take medication properly putting their health at risk and costing the
NHS half a billion pounds every year.” Daily Mail. February 18, 2013. http://www.dailymail.co.uk/health/article-‐2280363/One-‐patients-‐does-‐medication-‐properly-‐putting-‐health-‐risk-‐costing-‐NHS-‐half-‐billion-‐pounds-‐year.html, (Accessed May 20, 2013)
25 Andrews, Michelle. “New ideas to help people take medications correctly.” LA Times. March 21, 2011.

22
This investigation aims to question the role designers can create for themselves in pharmaceutical
packaging by deconstructing medication aesthetics, medication information and multiple medication
use. Understanding a patient’s position in all of this is essential to the study and will be referred to at
given stages of the case studies. Given that there is a minimal amount of user studies that have been
conducted regarding packaging interpretation, the approach taken by Helen Hamlyn’s studies will be
used as a guide. My aim is to learn first hand, where has it been going wrong and why, and to look at
the potential for how designers can create user-focussed solutions for individual medication
adherence.
The areas of focus for the issues are chosen with the intention of instigating direct changes or swift
alterations to existing design and investigative thoughts for long-term benefit to the patients of the
National Health Service.
‘Packaging design should take into account the needs and capabilities of the widest possible range of
potential users, and in particular older and partially sighted users, and how they interact with the
medicine in the home.26’ This point coupled with the aging baby-boom generation will only increase
pressure on pharmaceutical dispensers to provide a more bespoke medication experience and ensure
patient compliance.
Medication packaging has changed and has responded to feedback from patients, such as the
introduction of daily consumption labels on the foil seal (Fig. 7) and enlarged consumption
instructions printed onto the front and back of outer packaging. So where can these changes be
further improved? What could a designer implement to the design to raise patient compliance? Why
have improvements been limited to these minor changes, why such a conservative approach?
http://articles.latimes.com/2011/mar/21/health/la-‐he-‐medication-‐labels-‐20110314. (Accessed May 20, 2013)
26 “Design for Patient Safety.” National Patient Safety Agency. 2007. Pg.10 http://www.hhc.rca.ac.uk/CMS/files/NPSA-‐ Design-‐for-‐patient-‐safety-‐.pdf, (Accessed April 18, 2013)

23
Figure 7: Maria Florio, Daily use print on medication film, 2013
Fig. 8 is an example of the contemporary packaging provided by dispensers for a months’ use of a
drug. This is a relatively new form of packaging for a long dosage of a drug. Noticeably there is a use
of different colours for each week, as well as the strength labelled above the pills. The black bar to
the right gives indication of the dosage and is one of the clearer examples of prescribed drug for long-
term use.
Figure 8: Ashley Wiltshire, Modern Prescribed Medication Packaging, 2013

24
4.2 What is missing?
What is missing from the packaging that is currently causing errors, miss-use or disuse of
pharmaceuticals? ‘Errors may occur when key information appears in an inconspicuous place on the
label, is presented in an ambiguous manner, or is overshadowed by less important information .The
print may be less than optimal in size, boldness, or contrast. Highly stylized graphics, superiorly
positioned corporate names, or logos may distract from the primary purpose of the label’27 This
uncovers an underlying problem that the priorities of information display and layout could be
considered to be in an ineffective order for the pharmacist and consumer.
Cohen also comments that, ‘complicating the situation is that labels are often read under less-than-
ideal conditions (e.g., in a patients room at night when lights are dimmed, or by paramedics working
on an accident victim).’28
The ISMP recommend that the drug name and strength are the most important pieces of information
and should appear close to one another in the same field of view. This recommendation is of huge
importance when considering the layout of information. But this does not account for consumer
scenarios. Pharmacy stock rooms and shop shelves are well lit and the medication is displayed in an
ordered fashion. This may not be the case with a home pharmacy cupboard or bathroom shelf.
There appears to be a lack of consideration for the situations, which the medication will be used
beyond the shelf or pharmacy shelf. This could be challenged with the use of colour, paper stock of
packaging and treatment of packaging.
With any changes made to the packaging, Dr Ted Lithgow comments stating ‘Pharmaceutical
packaging must adhere to stringent regulations that require material traceability, good manufacturing
practices (GMPs), consistent quality, product protection, and often child-resistance.29’
27 Cohen, Michael R., The role of Drug Packaging and labeling in medication errors, Washington, D.C. American Pharmacists
Association, 2007, p.111 28 Cohen, Michael R., The role of Drug Packaging and labeling in medication errors, Washington, D.C. American Pharmacists
Association, 2007, p.111 29 Lithgow, Dr. Ted. “Six steps to pharmaceutical packaging sustainability: Through proactive planning, regulations need

25
The main objective of pharmaceuticals in general is ‘Sustaining positive patient outcomes. Being
socially sustainable also includes developing packaging that is effective, safe, and promotes medication
adherence.’
‘Effective adherence packaging has a positive impact on health outcomes. For example, convenience
blister packs are designed to remind patients to take medications correctly and on time, reducing
patient medication omissions and errors, and enhancing the treatment outcomes of those
medications.30’
When raising the question of whether there is room for innovation within pharma packaging and
improving patient compliance Tomlinson31 replied by talking about how more effort could go into
differentiating drug packets once they are out of their boxes. Suggesting that coloured foil could be
used on to break up the dosage of pills. Although he goes on to state that this would not work for
the demographic of hard of sight and blind so the solution would need to be more broad.
Designers must make the decision whether to follow the route of research and development, looking
at the short-term future, or to work through research, looking outside the contained principles of
existing products, with the ambition of creating something beyond.
4.3 Marketing power
Outside the realm of a designer’s role in creating compliance based packaging is the power of
marketing. Since the 1940s direct-to-consumer advertising has been banned for the simple reason
that it works: adverts distort doctors prescribing behaviour – by design – and increase costs
unnecessarily.32 After the relaxing of rules to allow side effects of drugs to be abbreviated, there was a
not be a hindrance to environmentally friendly pharmaceutical packaging practices.” Healthcarepackaging. June 2009. http://www.healthcarepackaging.com/sustainability/strategy/six-‐steps-‐pharmaceutical-‐packaging-‐sustainability. (Accessed May 25, 2013)
30 Lithgow, Dr. Ted. “Six steps to pharmaceutical packaging sustainability: Through proactive planning, regulations need not be a hindrance to environmentally friendly pharmaceutical packaging practices.” Healthcarepackaging. June 2009. http://www.healthcarepackaging.com/sustainability/strategy/six-‐steps-‐pharmaceutical-‐packaging-‐sustainability. (Accessed May 25, 2013)
31 Wiltshire, Ashley. Questions on the challenges designers face in improving patient compliance through pharmaceutical packaging. In-‐depth interview. September 2013. 32 Goldacre, Ben. "Bad Pharma: How Drug Companies Mislead Doctors and Harm Patients." London. Fourth State. 2012.

26
rise in marketing budget from $200 million to $3 billion in just a space of a few years.33 With this huge
amount of money being put to marketing drugs opposed to the research and development of drugs it
is no wonder that there are many drugs misused. Almost twice as much is spent on marketing and
promotion as spent on research and development. 34
p.247
33 Goldacre, Ben. "Bad Pharma: How Drug Companies Mislead Doctors and Harm Patients." London. Fourth State. 2012. p.248
34 Goldacre, Ben. "Bad Pharma: How Drug Companies Mislead Doctors and Harm Patients." London. Fourth State. 2012. p.245

27
5.0 Design delivery
5.1 Typo – Point Size & Language
It is the responsibility of pharmacies, chemists and general practices to print the instructive directions
for medication use. These instructions are the most important part of the medication, for the patient.
Yet in all of my experience and time spent using prescribed medication, the legibility of the type has
always been on the small side (fig.9) the legal minimum being point size 1, it is also stated as a
suggestion in the study for patient study, claiming to ‘use bold or semi-bold type and avoid lightweight
type. It is important to note, however, that too much bold or semi-bold type can also impair
readability if in a very small point size.35’ This not just the case for me, "Health literacy is a big issue,"
says Allen Vaida, Pharm.D., executive vice president of the Institute for Safe Medication Practices
(ISMP) in Pennsylvania. "Even college grads can have trouble when it comes to understanding terms
that health-care workers use."36
Figure 9: Ashley Wiltshire, Printed Label, 2013
It is not just the legibility or the size of the typography, which causes confusion or misuse of
medication, it is the language used as well. A 2007 study in the journal Patient Education and
35 “Information design for patient safety: A guide to the graphic design of medication packaging.” HHRC. 2007
http://www.nrls.npsa.nhs.uk/EasySiteWeb/getresource.axd?AssetID=129650& pg.69(Accessed May 10, 2013) 36 “Can you read this drug label?” Consumer Reports. June 2011. http://www.consumerreports.org/health/best-‐buy-‐
drugs/prescription-‐labels/overview/index.htm (Accessed May 20,2013)

28
Counselling found that one-third of patients did not realize that "two tablets by mouth twice daily"
meant taking four pills in a 24-hour period. This is a clear indication of the gap between the
understanding of the medicinal organisations and the needs of patient themselves. Designers of
consumable products should always aim to communicate the product as clear as possible using the
most appropriate language, why has the MHRA responded to the rising waste of pills, material and
packaging? Why not focus on improving patient adherence to save not lives but precious millions the
NHS will be losing.37
5.2 Similar Name, Different Effect
I had the opportunity to interview a nurse to gain an insight and hear of medication handling by staff
for patients. Nurse Losa, told me of a tragic case where medication was needed in high pressure
situation and that through the similarity of aesthetic packaging, the wrong medication was
administered and the ultimate cost was paid in the loss of life of a baby. This was down to many
factors outside of the medication but right at the core was the painful reminder of human error and
in an environment like a hospital these cases cannot be allowed to happen, hence such a strict design
structure and storage system aimed at doctors, nurses and pharmacists to differentiate.
The PRACtICe study covered mis-prescribed medication and highlighted one potential development
in this field and that by ‘promoting the effective use of clinical computer systems for safe
prescribing,38’ the chances of misuse can be reduced. Doctors and nurses alike do not have the time
to administrate whole documents of personalised data but as I will go on to state, the future looks
prosperous if a humanised medication architecture is implemented, this is an interesting field for the
designer to become involved in, producing patient specific templates solely targeted at health-care
practitioners.
37 McDowell, Andrew and Barnett, Nina. How improved medication adherence can prevent costly medicine waste. HSJ.
February 9, 2012 http://www.hsj.co.uk/resource-‐centre/best-‐practice/qipp-‐resources/how-‐improved-‐medication-‐adherence-‐can-‐prevent-‐costly-‐medicine-‐waste/5041067.article#.UkSu1mTWH48 (Accessed September 20, 2013)
38 Avery, Tony P, et al. “Investigating the prevalence and causes of prescribing errors in general practice: The PRACtICe Study (PRevalence And Causes of prescrIbing errors in general practiCe) A report for the GMC.” GMC. May 2012.http://www.gmcuk.org/Investigating_the_prevalence_and_causes_of_prescribing_errors_in_general_practice___The_PRACtICe_study_Reoprt_May_2012_48605085.pdf (Accessed May 20, 2013)

29
5.3 The Information Problem
This leads on to “the problem of the modern world is not information poverty, after all, but
information overload, and even more precisely, what Clay Shirky calls ‘filter failure’…The exciting
future, for evidence based medicine, is an information architecture that can get the right evidence to
the right doctor at the right time.”39 Now what about getting the ‘right’ information to the ‘right’
patient on time?
Based on a study into how long it would take for a doctor to keep up to date with release of papers
on new drugs, it would take twenty-nine hours each weekday, which is, of course, not possible.40 This
in turn affects their knowledge of prescribing patients the most effective medication for their
condition. This missing information and potential knowledge could be a future pitfall for ensuring the
right medication is prescribed, without a designed information database for doctors, this simply will
not be possible.
Of course it isn’t just having a design system for all this information which could improve patient
compliance, there are ‘factors at a number of levels were identified as contributing to these errors.
These included a lack of training in the skill of prescribing, distractions and a failure to fully utilise
existing IT solutions for safer prescribing.41’
39 Goldacre, Ben. "Bad Pharma: How Drug Companies Mislead Doctors and Harm Patients." London. Fourth State. 2012.
p.241-‐242 40 Alper BS, Hand JA, Elliott SG, Kinkade S, Hauan MJ, Onion DK, et al. “How much effort is needed to keep up with the
literature relevant for primary care?” J Med Libr Assoc. 2004;92;429-‐37. (Accessed June 1, 2013) 41 Avery, Tony P., et al. “Investigating the prevalence and causes of prescribing errors in general practice: The PRACtICe
Study (PRevalence And Causes of prescrIbing errors in general practiCe) A report for the GMC.” GMC. May 2012.http://www.gmcuk.org/Investigating_the_prevalence_and_causes_of_prescribing_errors_in_general_practice___The_PRACtICe_study_Reoprt_May_2012_48605085.pdf (Accessed May 20, 2013)

30
6.0 Recommendations
6.1 Relevant to the Industry
Innovations aren’t necessarily just in the packaging of the medication but the makeup of the
medication itself. An Oxford Professor has been working on such a concept, proposing that it could
save the NHS and the pharma industry millions in waste medication.
“Professor Lionel Tarassenko CBE FREng FMedSci, from the Department’s Institute of Biomedical
Engineering, has been working with colleagues from the Medical Sciences Division on the first UK
clinical trials of a ‘texting pill’ that contains a tiny silicon sensor, which triggers the sending of a text to
say the pill has been swallowed. This follows a UK study, which found that £300 million a year is spent
on medicines that end up being thrown away. Part of the wastage is due to people not taking
medication, called ‘non-compliance’.”42
The product proposed may sound promising but there would need to be a system around it, who
pays for the texts, how to know if the pill was consumed and not placed in a glass of other liquid.
How to ensure an elderly person keeps their mobile charged. Many questions rise out of a product
that could be developed without working alongside the end-user themselves.
I believe that, a product will not solve the issue but a culmination of change, in attitude, dispensing
and consumption. There is however one product that has received a lot of praise recently, and that is
the Avive customized multi-medication 30 day dosing system goes some way to being a product that
starts to incorporate patient input, linking with doctors and dispensers and tackling the growing issue
of multi-medication dosages.
‘2012 Compliance Package of the Year: …Avive was developed with input from patients and
pharmacists, resulting in a patient-customized solution that simplifies daily dosing for patients on
multiple medications. The ready-to-dispense, script-filling pharmacy service is designed to increase
42 University of Oxford. “Tiny sensor in pills could save the nhs millions.” University of Oxford. 2013.
http://www.eng.ox.ac.uk/public-‐relations/news/tiny-‐sensor-‐in-‐pills-‐could-‐save-‐the-‐nhs-‐millions (Accessed September 21, 2013)

31
medication adherence, provide convenience for patients and allow more time for pharmacist-
customer counselling.43’
Figure 10: MWV, Avive Packaging, 2013
Observing the issues surrounding distinguishing medicine, it has been noted from the ALMUS figure
that packaging from the same company often uses different colours to distinguish between medicines
but the guide for patient safety covers the point that a colour coding system enables people to
memorise colour and match it to a function. ‘No colour coding system could differentiate between all
12,000 medicines authorised in the UK.. ..Furthermore, in the absence of a national or international
colour code, any UK system could become a barrier to trade.44’
Due to the effects of the drug, Warfarin, it is universally colour coded brown for strengths of 1mg,
blue for strengths of 3mg, and red for strengths of 5mg.45 Meaning that for the most important drugs,
designers should look to ‘use opposing, meaningless colours to distinguish between medicines with
similar names in a manufacturer’s range. An awareness of users with limited colour perception should
43 “HCPC Announces This Year's Compliance Package of the Year Winners!“ HCPC. 2013.
http://www.hcpconline.org/compliance-‐package-‐winner.html (Accessed April 19, 2013)
44 “Information design for patient safety: A guide to the graphic design of medication packaging.” HHRC. 2007 http://www.nrls.npsa.nhs.uk/EasySiteWeb/getresource.axd?AssetID=129650& pg.55(Accessed May 24,2013)
45 “Information design for patient safety: A guide to the graphic design of medication packaging.” HHRC. 2007. http://www.nrls.npsa.nhs.uk/EasySiteWeb/getresource.axd?AssetID=129650& pg.55(Accessed May 24, 2013)

32
be developed.46’ Highlighting older generations whose vision is more likely to deteriorate is an area
where specific settings could be applied to the label and directions, this sort of data could be stored
on the patients electronic record notifying the pharmacist of the users visual requirements.
A solution to helping the hard of sight visually understand when medication has past its expiry won
the reddot design award 2013 in the packaging category. It notifies users with limited sight and those
who aren’t when a medication is past expiry date, by using layers of film on top of the blister pack,
the ink slowly seeps through over time from the moment it is first packaged to a point where it
signals the expiration of the medication.47
Figure 11: Kanupriya Goel, Gautam Goel, Self-Expiring Packaging, 2013
Blister packs have proved to be an effective form of packaging, sealed and airtight from production,
they provide a sense of individual use and visual direction. It is important to account for the strength
of the medicine and that it is clearly labelled throughout the use of the medication to ensure safe
use.48 Because without this taken into account ‘mixing packages and blister strips up could lead to the
patient taking the wrong medication or even overdosing.49
The visual requirements of pharmacists and dispensers have been met through an effective use of
symbols and colour coding. With the progression of our health records becoming digital, could there
46 “Information design for patient safety: A guide to the graphic design of medication packaging.” HHRC. 2007.
http://www.nrls.npsa.nhs.uk/EasySiteWeb/getresource.axd?AssetID=129650& pg.59(Accessed May 24, 2013) 47 Goel, Kanupriya and Goel, Gautam. “Self-‐Expiring.” RedDot. 2013. http://www.red-‐dot.sg/en/online-‐
exhibition/concept/?code=688&y=2012&c=14&a=0 (Accessed September 20, 2013) 48 “Information design for patient safety: A guide to the graphic design of medication packaging.” HHRC. 2007.
http://www.nrls.npsa.nhs.uk/EasySiteWeb/getresource.axd?AssetID=129650& pg.70(Accessed May 24, 2013) 49 “Information design for patient safety: A guide to the graphic design of medication packaging.” HHRC. 2007.
http://www.nrls.npsa.nhs.uk/EasySiteWeb/getresource.axd?AssetID=129650& pg.70(Accessed May 25, 2013)

33
be the option to have a digital health account with a limited level of customisation to the labels that
are in preference to the users visual needs but meet MHRA regulations. A commercial example of
customisation system working effectively with constraint is the Nike iD franchise, whereby a
customer can change the colours, materials and type applied to the shoes.
Figure 12: Brian Betschart, Nike iD website customisation page, 2007
Packaging has been titled as the problem of patient adherence for the last decade and only last year
was news of Smart Packaging, posted on Pharmaceutical-technology.com ‘Another intelligent
packaging system already proving popular on the market is the GlowCap from Vitality. Winner of the
HCPC's innovative design in its compliance packages of the year awards in 2009, the design has
attracted a lot of attention. It can illuminate, play a melody, send a text message or call a phone over
a wireless network to prompt patients to take their medicine. It also has an embedded 'push-to-refill'
button that connects to the pharmacy to automate refills.’ This is a great example of a customisable
and multi-faceted packaging device that begins to connect with modern life’s social tools and an
attempt to break down boundaries.

34
The progression in packaging design with the end-user in mind is slowly becoming a bigger issue for
pharmaceutical manufacturers and health services alike.
Overall, it appears as though the pharma companies and the research associates will continue to re-
invent the existing products and pills they already have on the market and a fresh outlook or
approach to how to improve patient compliance may come from the rise of wearable computing,
something the designer will find more accessible initially but problems arise when data collecting and
sharing with companies put patient confidentiality at risk.
6.2 Relevant to the stakeholders
Designers have clearly played a role in the update of this packaging and taken measures to distinguish
one medication between another. But is there a way to incorporate the printed labels that come from
the pharmacy into the grid or format of the medication to provide a clearer understanding of the
purpose of the medication? These dot-printed labels could become a humanised part of the solution
by utilising the graphic language used in UX design. Web icons have become extremely useful and
familiar for users of the Internet so by taking inspiration from this language, could one be created for
labelling. For instance, introducing prompts or schedule icons for consumption (Fig. 13) could be used
to improve patient compliance.
Figure 13: Haejin Song, Medication Instruction Icons, 2013

35
From a patients’ perspective Ben Goldacre’s book, Bad Pharma, gives them a chance to grasp the not-
so-hidden agendas of pharmaceutical conglomerates like GSK and formulate their own opinion on
how to approach pharmaceutical use in the future. It shall be up to the designer to seek out
pharmaceutical companies that show willingness and an honesty to change current methods,
contribute funds to long-term benefits and give the minor and major changes suggested a chance to
flourish.
In the last few years we have seen electronic consumer products come on leaps and bounds with
improved wireless connectivity, increased tactile response in the products and more accurate
sensors. These progressions have brought a range of condition monitoring bands to the market.
Products like the JAWBONE UP and Nike Fuel are two popular examples of this where citizens
concerned with their health are taking an active decision to invest in a product to keep them on top
of their diet, sleep patterns and exercise plans. These devices also act as a clock, vibrating reminder
and data storage device to link with smartphones, PCs, etc.
Earlier this year, Jawbone launched an ecosystem for UP, letting other applications on the market
utilise the data collected by the fitness band50. This, in the first instance is extremely positive for the
cross-use of data in different products that has not been seen for much of the last decade in
consumer electronics. It also provides many opportunities for the designer to create and tailor an app
for medication adherence. Providing empowering tools for generations of smartphone users to track
their schedule and to keep them up to date when it slips the mind.
The team from the useful mobile application Med Helper Pill Reminder state that ‘Our belief is that
Better Healthcare Needs Better Tools... and better tools are best designed by those who use them.
Meaning YOU.’51 The application has been in use for over 2 years and has provided over 100,000
people with a way to track this information.
50 D'Orazio, Dante, “Jawbone launches an ecosystem for Up, lets other apps tap into your fitness data.” The Verge. April 30,
2013. http://www.nytimes.com/2013/01/24/us/pentagon-‐says-‐it-‐is-‐lifting-‐ban-‐on-‐women-‐in-‐combat.html. (Accessed September 21, 2013)
51 “Med Helper Pill Reminder.” Earthflare, Googleplay Store. http://play.google.com/store/apps/details?id=com.earthflare.android.medhelper.lite&hl=en (Accessed September 21, 2013)

36
The individual has to have the positive mentality and commitment to purchase these sorts of product
and invest the time and effort to make it truly beneficial in their life. Speaking with optimism these
products could be potential game changers if it is represented or is advocated by health services and
administrations. Their application in aiding with a patients recovery or health and diet could be tied in
with the electronic health records as well as pharmaceutical purposes. Serving as an on-the-body
reminder of when to take medication set up with the GP or dispenser.
6.3 Co-creation – change the game
The optimism shown towards designers role and place in healthcare changes will quite suddenly come
up against hurdles that may seem like mountains in the first place but it is important that the designer
shows a high level of understanding of the current situation to make any ground in the first place.
Participatory design techniques used by Experientia are promising signs of patient-centric changes
happening in the administration and dispensing of pharmaceuticals as well as a platform to come up
with ideas and systems of potentially higher percentage of patient compliance.
6.4 How the process can be changed
Experientia, an Italian consultancy focussed on putting people first, worked with CVS Pharmacy, the
biggest pharmacy chain in the world. Experientia and the pharmacy workers collaborated on how the
pharmacy of the future should look, function and operate for the workers and the people who used
it. The outcome video highlights the benefit of bringing together designers of different kinds, staff and
a creative environment. Personal health records displayed and medication notifications are just two of
the highlighted developments.52
52 Experientiasrl. "Experientia -‐ The Pharmacy of the Future -‐ 03 Alison ." YouTube. Flash video file.
http://www.youtube.com/watch?v=jHuQazVO4AQ (Accessed September 20, 2013).

37
Figure 14: Ashley Wiltshire, Screenshot of Experientia Concept Video, 2013
6.4 How the process can change
Rob Darracott, Chief Executive of Pharmacy Voice53 said: ‘There are lots of good ideas around for
how health professionals can provide better support for patients and the public to help them use
their medicines more effectively. What the NHS needs now is a real plan for embedding those ideas
in systems that historically have been more concerned with the product than the person.’
Darracotts statement that historically there has been more of a focus on the product than person, is
a case for why there is room for the designer to step in and not just create a packaging based heavily
on mid-century Swiss design, which is used for its high-clarity, readability and objective image54. But to
look at the innovation space within pharma packaging, where individualisation, a customisation of
printing labels, a combination package for multi-medication use could be implemented.
The issues posed on the designers’ role in medication packaging and what this means for the changing
face of healthcare are a few opportunities for the designer to have a greater influence on how
53 “Pharmacy Voice: Speaking up for community pharmacy.” Pharmacy Voice. http://www.pharmacyvoice.com (Accessed
April 18, 2013) 54 Meggs, Phillip B. “Postwar graphic design in Japan.” Britannica. April 4, 2012.
http://www.britannica.com/EBchecked/topic/1032864/graphic-‐ design/242775/Postwar-‐graphic-‐design-‐in-‐Japan (Accessed April 18, 2013)

38
pharmaceutical companies and health services tackle some of the biggest problems facing patient
compliance. With a supportive government, HMRA, Pharma authorities and packaging companies that
are willing to be part of a new paradigm towards a more holistic, patient-centric system the chances
for designer intervention will rise. It is looking unlikely that any of what was stated will happen any
time soon but first and foremost EU law on pharma packaging will have to be the first area of reform
before any minor changes to type, colour, size or major changes to packaging material, technologies
occur.
6.5 Interactive ways designers can improve adherence
Speaking as a designer, I have found by having the opportunity to work closely with those in the field
of healthcare and then to step back and speak with patients, it gives a more rounded understanding of
what is within my power at this current point and that by adopting the ‘design with people’ ethos.
‘One: Sharing knowledge and provoking new design thinking, Two: Providing practical resources for
different learning styles and levels and Three: Building an integrative platform for the future’ the
insights and ability to make a change seem much more achievable. 55
We as designers must not only follow in the footsteps of the guide to patient safety and provide
notes, suggestions and improved design for existing packaging but work alongside the different
channels and links of pharmaceuticals from the manufacturer, to the licenser, to the doctors and GPs
who prescribe to the dispenser to the end-user. By working along this line of contributors, we move
beyond solely visual communicators but a multi-faceted, multi-skilled leader in a field that is in danger
of its best interests becoming further corrupt and commercial, when the bottom line is, our health
and care should not be a for-profit opportunity.
Ken Loach’s foreword in NHS SOS asks the questions, ‘Who puts forward the idea of working
together for the common good? That we should be our brothers and sisters keeper? That we have
the technology and the knowledge to provide a decent life for all but we are in the grip of an
economic ideology that makes that impossible?’56
55 Lee, Yankee Dr., “Ethos, Designing With People.” http://designingwithpeople.rca.ac.uk/home/ethos. (Accessed
September 20,2013) 56 Loach, Ken. foreword to NHS SOS: How the nhs was betrayed – and how we can save it. by Jacky Davis & Raymond Tallis(UK: One World, 2013), xi.

39
As designers, we are sometimes labelled as trying to do too much, to advise and be involved in fields
we are not skilled or trained in. If we relate this to looming reform of the National Health Service of
the United Kingdom, it is fair to say that designers will have plenty of opportunity to impose their
ideas and thoughts for change. Designers can collaborate to be the bridge between corporate care
institutions in the UK and the publics’ needs and concerns with how they handle and review self-
medication.
Ultimately it is up to designer how much they want to challenge the existing paradigm of
pharmaceutical services. Creativity is integral to the introduction of ideas that can have a lasting effect
on the way people interact and use products. In Adrian Shaughnessy’s ‘How to be a graphic designer
without losing your soul’ he presents his creativity equation as
“Risk + discomfort + sweat (±inspiration) = creativity”57
This simple yet hard to implement equation should be understood and utilised in the design process
of challenging pharmaceutical paradigms.
57 Shaughnessy, Adrian . How to be a graphic designer without losing your soul. London. Laurence King. 2010. p.112
40
7.0 Conclusion
To close this dissertation, I believe that it is of the upmost importance that a designer does not solely
focus on the packaging as a means of solving the problem of patient compliance and that to truly make
an impact, they must involve themselves in a design process which brings together the many people
within the pharmaceutical context with a broad spectrum of patients and people with stories and
experience within pharmaceuticals.
I look forward to myself and others becoming self-managed patients who are part of a community of
caregivers, pharmacists, doctors and other medical care workers that ensure feedback and input
comes from all levels of interaction. With collaborative efforts from pharma, health services and local
communities we can create “collective intent care networks,” as a designers We shall involve
ourselves in improving patient compliance, partly in using the model (fig.3) and integrating ‘design with
people’ ethos into professional careers to go a way to understanding and effecting the changes in care
delivery.
Figure 3: Ernst & Young, Self-Managed Patient, 2012
41
Bibliography
Books
Cohen, Michael R. The role of Drug Packaging and labeling in medication error, 2nd edition,
Washington, D.C., American Pharmacists Association, 2007.
Davis, Jacky and Tallis, Raymond. NHS SOS: How the NHS was betrayed – and how we can save
it. London, One World, 2013.
Goldacre, Ben. Bad Pharma: How Drug Companies Mislead Doctors and Harm Patients. London.
Fourth State, 2013.
Shaughnessy, Adrian. How to be a graphic designer without losing your soul. London, Laurence King.
2010.
Audio
The Concern With Aging, BBC, http://www.bbc.co.uk/programmes/p014wlnp, 2013.
Online Articles/Documents
“About patient safety.” NHS. http://www.nrls.npsa.nhs.uk/about-us (Accessed February 10, 2013).
Andrews, Michelle. “New ideas to help people take medications correctly.” LA Times. March 21,
2011. http://articles.latimes.com/2011/mar/21/health/la-he-medication-labels-20110314. (Accessed May
20, 2013).
“Can you read this drug label?” Consumer Reports. June 2011.
http://www.consumerreports.org/health/best-buy-drugs/prescription-labels/overview/index.htm
(Accessed May 20,2013).

42
“Department of Health, NHS, Supporting all NHS Trusts to achieve NHS Foundation Trust status by
April 2014.” DoH, NHS. June 29, 2011.
http://www.wsh.nhs.uk/AboutUs/TrustBoardMeetingsandPapers/2011/July29th2011/Item13bWestSuff
olkTFAFinal.pdf , (Accessed September 2013).
“Design for patient safety: A guide to the graphic design of medication packaging.” NHS.
http://www.nrls.npsa.nhs.uk/resources/?EntryId45=63053 (Accessed February 10, 2013).
Darracott, Rob. “Government Acknowledges Pharmacists Role As An Important Source of Expert
Advice.” Pharmacy Voice. June 21, 2011. http://www.pharmacyvoice.com/press/government-
acknowledges-pharmacists-role-as-an-important-source-of-expert-a. (Accessed May 20, 2013).
“HCPC Announces This Year's Compliance Package of the Year Winners!” HCPC. 2013.
http://www.hcpconline.org/compliance-package-winner.html (Accessed April 19, 2013).
Ledwith, Mario, “One patients does medication properly putting health risk costing NHS half a billion
pounds a year.” Daily Mail. February 18, 2013. http://www.dailymail.co.uk/health/article-2280363/One-
patients-does-medication-properly-putting-health-risk-costing-NHS-half-billion-pounds-year.html.
(Accessed May 20 2013).
Lee, Yankee Dr. “Ethos, Designing With People.” HHRC. 2013.
http://designingwithpeople.rca.ac.uk/home/ethos. (Accessed September 20, 2013).
Lithgow, Dr Ted. “Six steps to pharmaceutical packaging sustainability Through proactive planning,
regulations need not be a hindrance to environmentally friendly pharmaceutical packaging practices.”
Healthcarepackaging. June 2009. http://www.healthcarepackaging.com/sustainability/strategy/six-steps-
pharmaceutical-packaging-sustainability. (Accessed May 25, 2013).
Lord Howe. “Action on medicine wastage and improving medicine use.” GOV UK. August 8, 2011.
43
https://www.gov.uk/government/news/action-on-medicine-wastage-and-improving-medicine-use.
(Accessed May 25, 2013).
McDowell, Andrew and Barnett, Nina. “How improved medication adherence can prevent costly
medicine waste.” HSJ. February 9, 2012. http://www.hsj.co.uk/resource-centre/best-practice/qipp-
resources/how-improved-medication-adherence-can-prevent-costly-medicine-
waste/5041067.article#.UkSu1mTWH48 (Accessed September 20, 2013).
Meggs, Philip B. “Postwar graphic design in Japan.” Britannica. April 4, 2012.
http://www.britannica.com/EBchecked/topic/1032864/graphic-design/242775/Postwar-graphic-design-
in-Japan (Accessed 18 April 2013).
Zinnagl, Lucas. “Package Design For Drugs Does Matter.” MedCrunch. January 18, 2011.
http://www.medcrunch.net/package-design-for-drugs-does-matter/ (Accessed February 10, 2013).
Youtube Videos
experientiasrl " Experientia - The Pharmacy of the Future - 03 Alison " YouTube. Flash video file.
http:// http://www.youtube.com/watch?v=jHuQazVO4AQ (Accessed 20 September 2013).
Studies
Alper BS, Hand JA, Elliott SG, Kinkade S, Hauan MJ, Onion DK, et al. “How much effort is needed to
keep up with the literature relevant for primary care?” J Med Libr Assoc 2004;92;429-37.
Glen Giovannetti, Gautam Jaggi, Siegfried Bialojan, Scott Morrison, Jurg Zurcher, Sanjeev Wadhwa,
Ulrike Trauth, Eva-Marie Hilgarth, Claudia Pantke, Paul Karamanoukian; “Beyond borders: Global
Biotechnology Report 2012.” Ernst & Young. 2012.
Online Studies
Meera Viswanathan, PhD; Carol E. Golin, MD; Christine D. Jones, MD, MS; Mahima Ashok, PhD;
Susan J. Blalock, MPH, PhD; Roberta C.M. Wines, MPH; Emmanuel J.L. Coker-Schwimmer, MPH;

44
David L. Rosen, MD, PhD; Priyanka Sista, BA; and Kathleen N. Lohr, PhD; “Interventions to Improve
Adherence to Self-administered Medications for Chronic Diseases in the United States: A Systematic
Review.” Annals of Internal Medicine. 4 December 2012.
http://annals.org/article.aspx?articleid=1357338#r3-6. (accessed May 20, 2013)
“National Patient Safety Agency, Information design for patient safety: A guide to the graphic design of
medication packaging.” HHRC. 2007.
http://www.nrls.npsa.nhs.uk/EasySiteWeb/getresource.axd?AssetID=129650&. (Accessed May 2013)
Moore, Margaret J., Moir, Phyllis, et al. “The State of Aging and Health in America 2004.” MIAH,
CDC. 2004. http://www.cdc.gov/aging/pdf/State_of_Aging_and_Health_in_America_2004.pdf,
(Accessed May 20, 2013)
Professor Tony Avery, Professor Nick Barber, Dr. Maisoon Ghaleb, Professor Bryony Dean Franklin,
Dr. Sarah Armstrong, Dr. Sarah Crowe, Professor Soraya Dhillon, Dr. Anette Freyer, Dr Rachel
Howard, Dr. Cinzia Pezzolesi , Mr. Brian Serumaga, Glen Swanwick, Olanrewaju Talabi; Investigating
the prevalence and causes of prescribing errors in general practice: The PRACtICe Study (PRevalence
And Causes of prescrIbing errors in general practiCe) A report for the GMC.” GMC. May 2012.
http://www.gmcuk.org/Investigating_the_prevalence_and_causes_of_prescribing_errors_in_general_p
ractice___The_PRACtICe_study_Reoprt_May_2012_48605085.pdf (Accessed May 20, 2013)
Parsons, Suzanne and Winterbottom, Anna and Cross, Peter and Redding, Don. “The quality of
patient engagement and involvement in primary care.” 2010.
http://www.kingsfund.org.uk/sites/files/kf/field/field_document/patient-engagement-involvement-gp-
inquiry-research-paper-mar11.pdf (Accessed September 21, 2013)
P. Michael Ho, Chris L. Bryson, and John S. Rumsfeld. “Key Issues in Outcomes Research: Medication
Adherence: Its Importance in Cardiovascular Outcomes.” 2009;119:3028-3035,
doi:10.1161/CIRCULATIONAHA.108.768986
http://circ.ahajournals.org/content/119/23/3028.full#cited-by (Accessed April 2013).

45
Pollock, Kristian and Grime, Janet. “Primary carePatients' perceptions of entitlement to time in
general practice consultations for depression: qualitative studyCommentary: Managing time
appropriately in primary care.” BMJ 2002;325. September 28, 2002.
http://dx.doi.org/10.1136/bmj.325.7366.687 (Accessed September 19, 2013)
Zadbuke, Dr. Nityanand, et al. “Recent trends and future of pharmaceutical packaging technology,” J
Pharm Bioall Sci, no. 5 (April-June 2013): 98-110.
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3697200/. (Accessed September 23, 2013)
Interviews
Wiltshire, A; Questions on Medication use, May 2013.
Wiltshire, A; Questions for a Nurse on the effectiveness of medical packaging, May 2013
Wiltshire, A; Questions on the challenges designers face in improving patient compliance through
pharmaceutical packaging, September 2013
Appendix
Interview on Medication Use
Vincenzo Florio
1. Is it clear to you what each medication aids with?
Yes, as gp explains to me what each medicine is for.
2. Do you know whether one can be mixed with another?
I trust my doctor to prescribe me medication which cannot be mixed, but if it was up to me i
wouldn’t know as I don’t read English.

46
3. Do you read the small print information document that comes with the medication?
No I don’t read the small print as I don’t understand all the English and rely on my daughters to
explain.
4. How do you ensure you do not mix up one medication with another?
I arrange my medication so that it is in order i.e. morning, lunchtime and evening and have them
sorted in my pill box.
5. If you are confused or do not understand the medication, what support do you get?
If I am confused about aspect of my medication i would return to see my doctor.
6. Are there any clear problems with packaging or defining the difference between medications?
The packaging is fine and marked clearly but as a suggestion a small picture on front of box could
make it clearer i.e. if a heart was printed on my heart medication i would know that it was for my
heart especially as I have to take lots of medication.
7. And finally, as it is usually the doctor who prescribes you with the drug, do you ever look beyond
their opinion or do you own study of the drug?
Yes my doctor prescribes all my medication, I don’t tend to look beyond as I trust my doctor to
prescribe me the correct drugs for my condition therefore I do not feel the need to carry out my
own studies, as a suggestion I personally think it would be a good idea if the leaflet enclosed with the
medication was in other languages just a brief explanation on medication and dosage would be most
helpful.
Maria Florio
1. Is it clear to you what each medication aids with?

47
Most of the time its clear but the explanation could be clearer as not all patients understand the
Medical terms.
2. Do you know whether one can be mixed with another?
Yes I always read leaflet to make sure I am not taking medicines that cannot be mixed but then I
would expect my gp not to prescribe medicines that cannot be mixed.
3. Do you read the small print information document that comes with the medication?
Yes I always read the small print but at times can be quite difficult to understand due to the technical
terms that are used, so that could be simplified.
4. How do you ensure you do not mix up one medication with another?
I always keep my medication separate to ensure there is no mix up.
5. If you are confused or do not understand the medication, what support do you get?
If at anytime I need further support I will go back to see my gp or go to pharmacy.
6. Are there any clear problems with packaging or defining the difference between medications?
Personally I don’t have any issues as i am not taking any regular medication.
7. And finally, as it is usually the doctor who prescribes you with the drug, do you ever look beyond
their opinion or do you own study of the drug?
Yes my doctor prescribes my medicine and yes i do tend to carry out my own study of the drug as I
find it easier to understand than on the small printed information enclosed with the drug.
Interview questions for a Nurse on the effectiveness of pharmaceutical packaging
1. In your experience as a nurse, how understandable is pharmaceutical packaging?

48
It depends of the medication and how you are familiarized with it, some packaging’s medication are
very clear and some not as clear, also some medicaments are more common than others.
2. What works, and what does not work?
On one hand, as a nurse, the thing that is very helpful for us at the hospital is that the external
packaging of the medication is different and you can see totally in a clear way the administering use of
it. Some medications are very similar in packaging and it does not work, for example there are the
same medication (and the same packaging of it) with
other concentration (like potassium chloride
blisters) or some medications which at first view you
can confuse because they are the same blisters, I
mean, you must read it for differentiate it (for
example, the potassium chloride blisters and the
smaller saline solution blisters) /Photo/
For me that is essential when we have an emergency, for take action fast. Moreover it works for us
for not commit a mistake.
On the other hand, in my opinion, a good and clear packaging works with patients as well, above all
when we are talking about polymedicated patients. Things like the days of the week in the metal film
that cover the pills are important in some drugs that they have to take day by day.
3. Have patients ever asked you to explain what the drug does and how it works?

49
Yes. Some patients want to know the use, the reason and the effects of the drug that I am
administering.
4. What could be improved on the packaging of the drugs, either the cardboard package or the metal
film cover of the pills?
I think that a good idea for the patients to know how to take it would be personalized the cardboard
package of the drug with the personalized dosage of each patient in each case. I think in England you
have it sometimes putting a sticker on the package, but in Spain is not the same and I have seen a
handwritten (made it for the patient or for a relative) with the indication for what is the drug and the
recommended dosage for this person as well.
/Photo example/:
(1-1-1 = one pill in breakfast, one in lunch, one in dinner)
A good idea as well is the plastic box format for polymedicated people, it is a box with different
departments, usually divided in days of the week and times in the day (for example the food hours),
where you put inside the pills that you will need for each day. This is a great idea for ambulatory
polymedicated patients, because with some of these pillboxes the patients can take and bring “each
box day” in their bag.

50
About the format or the design, I think is obvious, but I would like to add than always is very
important the big letters with the most important things and the colours as well. Maybe the format of
the pills as well, because I had many patients that when I asked to them “which pills do you usually
take?” they replied to me “I don’t remember the name of that one but, the little white one” or “the
one with a stripe in the middle”.
5. Are there any stories or anecdotes you can share of yours or someone else's experience?
I know a story of a Spanish nurse that she made a terrible mistake, much of it because the packaging
of the medication, because the patients' nutrition is many times a very similar packaging.
She was doing the night shift in a Neonatal ward of a Hospital of Madrid and she confused the way
drugs are administered; she administered enteral nutrition by venous catheter, as a parenteral
nutrition, which the directions strictly say not to, and it cost the life of the baby.

51
Interview questions on the challenges designers face in improving patient compliance through pharmaceutical
packaging. – Alex Tomlinson
1. Increasingly in the UK, patient non-compliance has been on the rise, costing the National Health
Service around a £billion annually not taking into account medical costs of further treatment,
operations and consultations. Why is this so? Who is to blame if any?
Personally I would place the blame with patients themselves and GPs. Potentially pharmacists. The
question is whether or not the patient understands the amount of each prescribed drug that they
should take. Perhaps more could be done to differentiate the products with multiple prescriptions but
I think this is something that dispensers rather than producers should be looking at.
2. Why in your opinion has pharmaceutical packaging remained one of the only areas design to fall
behind in engaging its end user whilst others are excelling in user experience, e.g. airport services,
online shopping, GUI’s?
I think the issue is two fold. Drugs aren't packaged for the benefit of the end user. They are packaged
for the benefit of the dispenser. In that respect I think pharma packaging was probably ahead of the
curve with regards to colour coding and efficient coding systems for their packaging. Airports and
gui's by comparison to drug packaging are relatively new in the realm of human production. I think it
is unfair to suggest that drug packaging hasn't progressed when one looks at old pharmacies where
the products might just as easily have been snake oil rather than a cure for anything.
The second issue is regulation. Because packets for prescription only are banned from advertising to
patients they can't be seen to entice the end user. There are also usability constraints I.e. How big
and where Braille must appear, spaces for dispensing information etc.
3. What is the chain or process a pharmaceutical company has to go through to change an aspect of
its design, whether it is colour, shape, material used, productions, etc.?

52
Any change to a pharmaceutical product, whether it relates to packaging or production, that is not
included in the license already granted by the governing body (in the uk this is the MHRA) must be
submitted as a variation.
For instance if I wanted to change my box from blue to green I would have to draw up the artwork,
okay it with my production chain and then get relevant cutter guides etc. once the artwork is finalised
it would be submitted to the MHRA as a variation. Once this is approved the product is put into full
production with the changes applied. There is normally a time frame of around 6 months that any
required changes must be applied by depending on the change. I.e. If the company had moved
addresses a variation wouldn't need to be submitted to change the contact address on every product,
however it would need to be changed in a timely manner to keep products compliant.
4. What are some of the current guidelines a designer has to abide by when creating pharmaceutical
packaging? How do the guidelines differ from when you first worked on pharma packaging?
Unfortunately it has been quite a while since I worked on packaging. So can only really talk accurately
about marketing the drugs. The biggest ones are the amount of information that must be displayed
dependent on the type of advert produced.
All text must also be above 1mm in x-height and the language used on the ad can't say what the
product treats or encourage people to buy it. The adverts are therefore more intended to inform
pharmacists of its existence rather than promote it over competitors products.
5. Do you agree with the statement that currently, pharmaceutical packaging is predominantly aimed
at aiding the pharmacist and chemist as opposed to the patient/person who needs the medication?
Absolutely. The only part of a drug packet that is for the benefit of the end user is the space for
dispensing labels (which are often ignored by dispensers who put the label wherever they feel like it at
the time)
53
6. Where do you consider there to be room for innovation in improving patient compliance through
pharmaceutical drug packaging? Please answer with a short-term solution and if possible, a radical
change with money and regulation not as barriers.
More effort could go into differentiating drug packets once they are outside of their boxes. This could
help patients especially if prescription instructions were provided in a relevant way to coincide with
this difference. A simple example would be to colour the foils on each set of tablets, prescription
information would then be "take two blue foil pills and 3 green" of course this doesn't help for certain
demographics like blind people or colour blind people so a solution would need to be more broad.
Interview questions on the challenges designers face in improving patient compliance through pharmaceutical
packaging. – Daniel Wilson
1. Increasingly in the UK, patient non-compliance has been on the rise, costing the National Health
Service around a £billion annually not taking into account medical costs of further treatment,
operations and consultations. Why is this so? Who is to blame if any?
Couldn’t answer this one I’m afraid.
2. Why in your opinion has pharmaceutical packaging remained one of the only areas design to fall
behind in engaging its end user whilst others are excelling in user experience, e.g. airport services,
way finding, GUI’s?
I believe this is because of how heavily regulated it is. The patients safety is the number one priority
for pharmaceutical companies and the MHRA (Medicines and Healthcare products Regulatory
Agency) who regulate medicines in the UK.

54
Also, with so many guidelines on what can and cannot be done, you are limited with the design. Not
only does the packaging need to be easily readable and identifiable for the patient, but also for the
pharmacist dispensing the medicine to ensure the patient safety.
3. What is the chain or process a pharmaceutical company has to go through to change an aspect of
its design, whether it is colour, shape, material used, productions, etc.?
As a global company the design of the packaging has been rolled out on a global level and follows
strict branding guidelines, which is then adapted to suite the individual countries regulations.
In the UK, if you want to make a change on a National level, UK only, then a variation must be
submitted to the MHRA. Depending on the extent of the change and which category it falls under,
this can take anywhere from a few weeks to years to be assessed and approved by the MHRA.
Also, depending on the category of variation, a fee is paid for each product licence that the change
affects.
So, the Regulatory Affairs team within in the company will prepare the submission package and submit
the change to the MHRA. During the time the MHRA asses the change they may have questions or
request further changes that Regulatory Affairs team will need to respond to.
Once the MHRA approve the change they will notify us of the approval and the date it was approved.
We, the pharmaceutical company will then have 6 months to implement that change. The 6 months is
deemed as the date the first batch is released following approval. So, if the implementation date was
30/09/2013. Any batches released after this date must include new artwork.
To implement the new artwork we have a change procedure we must follow. This requires
generating a change document and tracking the change with the suppliers who are located throughout
the EU. We liaise with them to communicate when the new artwork must be used depending on our
orders and demand.
Finally when the product is release onto the market with the new artwork we can close out the
change to make sure the artwork has been implemented within the six month timeframe.
4. What are some of the current guidelines a designer has to abide by when creating pharmaceutical
packaging? How do the guidelines differ from when you first worked on pharma packaging?

55
I have only worked in the industry for 6 years and haven’t seen too much change in that time. Some
of the key guidelines to follow are; to make sure the font size is not below the minimum, ensure the
correct space is allocated for the dispensing label, braille is positioned correctly, pharmaceutical form
and dosage is clearly identifiable and key warnings are highlighted
5. Do you agree with the statement that currently, pharmaceutical packaging is predominantly aimed
at aiding the pharmacist and chemist as opposed to the patient/person who needs the medication?
Personally, I would say that I wouldn’t agree with that statement as at Sandoz we aim to aid all
interested parties, whether it be the pharmacist, patient or any other stakeholder that comes into
contact with our packaging. See our website for more information on this
http://www.uk.sandoz.com/site/en/quality_generics/packaging_design/index.shtml
Also, in recent years, the MHRA has ensured all packaging includes braille and that all patient
information leaflets undergo user testing. This highlights that even more focus is being put upon the
patient than was before.
6. Where do you consider there to be room for innovation in improving patient compliance through
pharmaceutical drug packaging? Please answer with a short-term solution and if possible, a radical
change with money and regulation not as barriers.
I believe with technology there is room for innovation, a lot of support materials for products come
in the form of apps and online learning portals, etc. However, I believe this to be more difficult for the
packaging itself as it is a requirement for patients to have access to critical safety information on the
medicine they are taking. Therefore, not everyone has access to the internet and such technologies.