
The c.-1639G>A polymorphism of the VKORC1 gene in Serbian population: retrospective study of the...
8
CE: Swati; MBC/200710; Total nos of Pages: 6; MBC 200710 The c.-1639G>A polymorphism of the VKORC1 gene in Serbian population: retrospective study of the variability in response to oral anticoagulant therapy Mirjana K. Kovac a , Aleksandar R. Maslac a , Ljiljana B. Rakicevic b and Dragica P. Radojkovic b Background A single nucleotide polymorphism c.-1639G>A in the promoter region of vitamin K-epoxide reductase (VKORC1) gene has been found to account for most of the variability in response to oral vitamin K antagonist (VKA). Objective Our aim was to study the effect of c.-1639G>A polymorphism on the acenocoumarol dosage requirements in a group of patients under stable anticoagulation, and to estimate the variability in response to VKA. Patients and methods We conducted a retrospective cohort analysis of 200 stable anticoagulation patients followed from the initiation of VKA. Results Out of 43 low-dose patients, 40 (93%) carried the A allele. The A allele was less frequent in the group of 30 patients requiring high VKA dose among these patients 13 (43.3%) carried the A allele in the heterozygous form and none of them carried AA genotype. Patients with GG genotype required 2.6 times higher dose than patients carriers of AA genotype (P < 0.0001). Carriers of AA genotype were more likely to be overanticoagulated during follow up after initiation of VKA when compared with carriers of GA and GG genotype (P < 0.0001). Patients with GG genotype spent more time below therapeutic range compared with patients carriers of AA (P U 0.0328) and GA genotype (P < 0.0001). Conclusion VKORC1 c.-1639G>A polymorphism significantly influenced VKA dose and represented a good predictor of individuals predisposed to unstable anticoagulation. Pharmacogenetic testing could predict a high risk of overdose among 28.5% of our patients, carriers of AA genotype, before the initiation anticoagulation. Blood Coagul Fibrinolysis 21:000–000 ß 2010 Wolters Kluwer Health | Lippincott Williams & Wilkins. Blood Coagulation and Fibrinolysis 2010, 21:000–000 Keywords: acenocoumarol dose, c.-1639 G>A polymorphism, variability in response to VKA, VKORC1 a Blood Transfusion Institute of Serbia, Svetog Save 39a and b Institute of Molecular Genetics and Genetic Engineering, Vojvode Stepe 444a, Belgrade, Serbia Correspondence to Ljiljana Rakicevic, Institute of Molecular Genetics and Genetic Engineering, Vojvode Stepe 444a, P.O. Box 23, 11010 Belgrade, Serbia e-mail: [email protected] Received 2 February 2009 Revised 20 April 2010 Accepted 27 April 2010 Introduction Oral vitamin K antagonist (VKA), including warfarin and acenocoumarol, are the most widely prescribed drugs for the prevention and treatment of patients with arterial and venous thromboembolic disorders [1]. The effectiveness and safety of VKA depend on maintaining the prothrom- bin time, expressed as the international normalized ratio (INR) within the therapeutic range [2]. Clinical use of VKA is further complicated by substantial risk for hae- morrhagic side effects, which is increased in patients with low-dose requirements [3]. The required dose of VKA for maintaining the prothrombin time is variable, and depends on several acquired factors such as age, dietary intake, interaction with other drugs and intercurrent ill- ness [2,4]. In addition to acquired factors, it is well known that response to VKA is genetically determined. The first gene documented to influence VKA dose requirement was CYP2C9. It encodes the enzyme cyto- chrome P450 2C9 – the main enzyme responsible for the hepatic metabolism of VKA [5]. Two common variants of the CYP2C9 gene, 2 and 3 are associated with reduced enzyme activity, resulted in deficient VKA clearance. Individuals who carry deficient CYP2C9 alleles are sen- sitive and have lower VKA dose requirements. Never- theless, only a small part (7–10%) of the interindividual variation could be explained by these polymorphisms [6]. Vitamin K epoxide reductase (VKORC1) is the key enzyme of the vitamin K cycle and the molecular target of coumarin derivates and it was found to determine up to 40% of individual coumarin dose requirement. VKORC1 recycles vitamin K 2,3-epoxide to vitamin K-hydro- quinone. Vitamin K-hydroquinone is the cofactor for the carboxylase that adds a molecule of carbon dioxide to glutamic acid, producing g-carboxyglutamic acid (g- Glu). The g-Glu residues are essential for some clotting factors, such as factors II, VII, IX, X and protein C, S Z, to bind phospholipids and thus be functional [5]. Mutations in VKORC1 cause two distinctive phenotypes. Those affecting VKORC1 function lead to vitamin K dependent coagulation factors deficiency type 2 Original article 1 0957-5235 ß 2010 Wolters Kluwer Health | Lippincott Williams & Wilkins DOI:10.1097/MBC.0b013e32833c2988
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of The c.-1639G>A polymorphism of the VKORC1 gene in Serbian population: retrospective study of the...

CE: Swati; MBC/200710; Total nos of Pages: 6;
MBC 200710
The c.-1639G>A polymorphism of the VKORC1 gene inSerbian population: retrospective study of the variability inresponse to oral anticoagulant therapyMirjana K. Kovaca, Aleksandar R. Maslaca, Ljiljana B. Rakicevicb
and Dragica P. Radojkovicb
Background A single nucleotide polymorphism
c.-1639G>A in the promoter region of vitamin K-epoxide
reductase (VKORC1) gene has been found to account for
most of the variability in response to oral vitamin K
antagonist (VKA).
Objective Our aim was to study the effect of c.-1639G>A
polymorphism on the acenocoumarol dosage requirements
in a group of patients under stable anticoagulation, and to
estimate the variability in response to VKA.
Patients and methods We conducted a retrospective
cohort analysis of 200 stable anticoagulation patients
followed from the initiation of VKA.
Results Out of 43 low-dose patients, 40 (93%) carried the A
allele. The A allele was less frequent in the group of 30
patients requiring high VKA dose among these patients 13
(43.3%) carried the A allele in the heterozygous form and
none of them carried AA genotype. Patients with GG
genotype required 2.6 times higher dose than patients
carriers of AA genotype (P < 0.0001). Carriers of AA
genotype were more likely to be overanticoagulated during
follow up after initiation of VKA when compared with
carriers of GA and GG genotype (P < 0.0001). Patients with
GG genotype spent more time below therapeutic range
compared with patients carriers of AA (P U 0.0328) and GA
genotype (P < 0.0001).
Conclusion VKORC1 c.-1639G>A polymorphism
significantly influenced VKA dose and represented a good
predictor of individuals predisposed to unstable
anticoagulation. Pharmacogenetic testing could predict a
high risk of overdose among 28.5% of our patients, carriers
of AA genotype, before the initiation anticoagulation. Blood
Coagul Fibrinolysis 21:000–000 � 2010 Wolters Kluwer
Health | Lippincott Williams & Wilkins.
Blood Coagulation and Fibrinolysis 2010, 21:000–000
Keywords: acenocoumarol dose, c.-1639 G>A polymorphism, variability inresponse to VKA, VKORC1
aBlood Transfusion Institute of Serbia, Svetog Save 39a and bInstitute ofMolecular Genetics and Genetic Engineering, Vojvode Stepe 444a,Belgrade, Serbia
Correspondence to Ljiljana Rakicevic, Institute of Molecular Genetics andGenetic Engineering, Vojvode Stepe 444a, P.O. Box 23, 11010 Belgrade, Serbiae-mail: [email protected]
Received 2 February 2009 Revised 20 April 2010Accepted 27 April 2010
IntroductionOral vitamin K antagonist (VKA), including warfarin and
acenocoumarol, are the most widely prescribed drugs for
the prevention and treatment of patients with arterial and
venous thromboembolic disorders [1]. The effectiveness
and safety of VKA depend on maintaining the prothrom-
bin time, expressed as the international normalized ratio
(INR) within the therapeutic range [2]. Clinical use of
VKA is further complicated by substantial risk for hae-
morrhagic side effects, which is increased in patients with
low-dose requirements [3]. The required dose of VKA for
maintaining the prothrombin time is variable, and
depends on several acquired factors such as age, dietary
intake, interaction with other drugs and intercurrent ill-
ness [2,4]. In addition to acquired factors, it is well known
that response to VKA is genetically determined.
The first gene documented to influence VKA dose
requirement was CYP2C9. It encodes the enzyme cyto-
chrome P450 2C9 – the main enzyme responsible for the
hepatic metabolism of VKA [5]. Two common variants of
the CYP2C9 gene, �2 and �3 are associated with reduced
enzyme activity, resulted in deficient VKA clearance.
Individuals who carry deficient CYP2C9 alleles are sen-
sitive and have lower VKA dose requirements. Never-
theless, only a small part (7–10%) of the interindividual
variation could be explained by these polymorphisms [6].
Vitamin K epoxide reductase (VKORC1) is the key
enzyme of the vitamin K cycle and the molecular target
of coumarin derivates and it was found to determine up to
40% of individual coumarin dose requirement. VKORC1
recycles vitamin K 2,3-epoxide to vitamin K-hydro-
quinone. Vitamin K-hydroquinone is the cofactor for
the carboxylase that adds a molecule of carbon dioxide
to glutamic acid, producing g-carboxyglutamic acid (g-
Glu). The g-Glu residues are essential for some clotting
factors, such as factors II, VII, IX, X and protein C, S Z, to
bind phospholipids and thus be functional [5].
Mutations in VKORC1 cause two distinctive phenotypes.
Those affecting VKORC1 function lead to vitamin K
dependent coagulation factors deficiency type 2
Original article 1
0957-5235 � 2010 Wolters Kluwer Health | Lippincott Williams & Wilkins DOI:10.1097/MBC.0b013e32833c2988

CE: Swati; MBC/200710; Total nos of Pages: 6;
MBC 200710
(VKCFD2), confirming critical role of that enzyme in
vitamin K dependent coagulation factors function [5]. On
the contrary, several genetic variations of the VKORC1
gene have been found to influence sensitivity to VKA [5,7].
Twenty-eight polymorphisms have been described, con-
stituting three main haplotypes covering almost the whole
genetic variability of VKORC1, with the following distri-
bution in Caucasians VKORC1�2, 42%, VKORC1�3, 38%
and VKORC1�4, 20% [6]. Haplotype VKORC1�2includes a single nucleotide polymorphism in the promo-
ter region (c.-1639G>A) and has been found to account for
most of the variability in response to VKA [6,7]. Several
studies clearly showed a strong association of initial varia-
bility in the INR response to VKA with VKORC1 genetic
variability. Carriers of AA genotype had decreased time to
the first INR within therapeutic range and also to the first
INR above 4 [8,9].
Our aim was to study the effect of c.-1639G>A poly-
morphism on the acenocoumarol dosage requirements in
a group of patients under stable anticoagulation. We also
aimed to estimate the rate of bleeding during initiation of
the VKA, and variability in therapeutical response, in
regard to the presence of c.-1639G>A polymorphism.
Materials and methodsData collectionA total of 200 outpatients attending the Hemostasis
Department of the Blood Transfusion Institute of Serbia,
who had maintained stable anticoagulation with aceno-
coumarol for at least 3 months, were included in the
study. We considered a patient on stable anticoagulation
whose acenocoumarol dose requirement had remained
constant for at least three previous months, and was
enough to keep the INR within therapeutic ranges,
according to the indication for VKA treatment. In order
to minimize the possible influence of hepatic, renal or
malignant disease, which could have pharmacodynamic
influence, on increased prothrombin time (INR) and
possible bleeding complications, patients with hepatic,
renal or malignancy were excluded from the study. Like-
wise, all patients treated with amiodaron, which have
synergistic influence due to pharmacokinetic mechan-
isms on increased INR were excluded. In total, 116 male
and 84 female patients were included in the study,
median age 61 years (range 20–82).
On the arrival in the laboratory, a blood sample was taken
for INR measurement and genotyping. Genotyping was
performed by polymerase chain reaction followed by
digestion with MspI (New England Biolabs) as previously
described [10].
Furthermore, a retrospective analysis of medical records
was performed to investigate the potential influence of
VKORC1 genotype on oral anticoagulants response in the
initiation phase and during a follow up from the start of
VKA administration. Complete data on acenocoumarol
doses and INR were registered from medical records, as
well as the data on age, sex, indication for treatment,
concomitant medications and medications potentially
interacting with VKA.
Patients were subjected to the VKA treatment according
to standard care without specific warfarin dosing algor-
ithms. The average initial acenocoumarol dose was 3.7 �0.6 mg. Therapeutic INR was defined as INR between
two and three irrespective of the individual target range.
A minimum of three consecutive therapeutic INR
measurements denoted stable anticoagulation. Mainten-
ance dose was defined as the mean of all doses given to a
patient during stable anticoagulation. Stable mainten-
ance dose was calculated from weekly doses that were
unchanged over a minimum of three consecutive
measurements of three therapeutic INR. INR was
checked in all patients three times in the first, twice in
the second week, and weekly during the achievement
therapeutic INR. Upon the achievement of stable antic-
oagulation dose, the INR was measured less frequently,
usually every 4 weeks. Follow up period ranged from one
to 8 years per patient, average 3.9 years.
Considering the present maintenance dose, study popu-
lation consisted of 43 consecutive patients requiring low
(7 mg per week or less), 127 consecutive patients requir-
ing medium (7–28 mg per week) and 30 consecutive
patients requiring high-acenocoumarol dose (28 mg per
week or more). Number of bleeding complications, as
well as the size and localization of bleeding recorded
during the first 3 months of VKA initiation, were
analyzed completely.
The variability of INR regarding INR more than four and
INR less than two were evaluated during follow up from
initiation of VKA. We calculated number of INR more
than four or less than two from the first stable antic-
oagulation, and took in consideration only patients who
had change of INR without change of VKA doses as well
as possible influence of dietary change, intercurrent ill-
ness or interaction with other drugs.
All individuals had signed informed consent to partici-
pate in the study and the local ethics committee approved
the study.
Statistical analysisDifferences in the acenocoumarol requirement between
patients who were carriers, and noncarriers of c.-1639G>A
polymorphism in the low-dose, medium-dose and high-
dose group were assessed with chi-squared test. Differ-
ences between homozygotes (AA) and heterozygotes (GA)
regarding the overdosed patients and the presence of
bleeding complication were assessed using chi-squared
test or Fisher’s exact test. Differences between overdosed
patients with AA and GA genotype, regarding the level of
INR and age, were assessed with Student‘s t-test. All
the statistical analyses were performed according to the
2 Blood Coagulation and Fibrinolysis 2010, Vol 00 No 00
CE: Swati; MBC/200710; Total nos of Pages: 6;
MBC 200710
Statistical Package for Social Science SPSS software, Inc.
Chicago, Illinois, USA). A P value of less than 0.05 was
considered as statistically significant.
ResultsCharacteristics of the studied population and the distri-
bution of the G and A alleles of c.-1639G >A polymorph-
ism are shown in Table 1. In 57 (28.5%) patients AA
genotype was present, in 90 (45%) GA and 53 (26.5%)
patients were carriers of GG genotype. The frequencies of
genotypes of the c.-1639G>A polymorphism regarding the
requirement dose of acenocoumarol are shown in Table 2.
The allelic distribution was different across the various
acenocoumarol dosage groups. In the group of 43 patients
who maintained stable anticoagulation with the low dose
of acenocoumarol, 40 patients (93%) carried the A allele.
The A allele was less frequent in the group of 30 patients
requiring a high-acenocoumarol dose among these patients
13 (43.3%) carried the A allele in the heterozygous form
and none of them carried AA genotype. In groups with low
and high dose, we observed statistically significant differ-
ence among patients with different genotypes, whereas in
the group with medium dose, statistical difference
between patients carriers of different genotypes was not
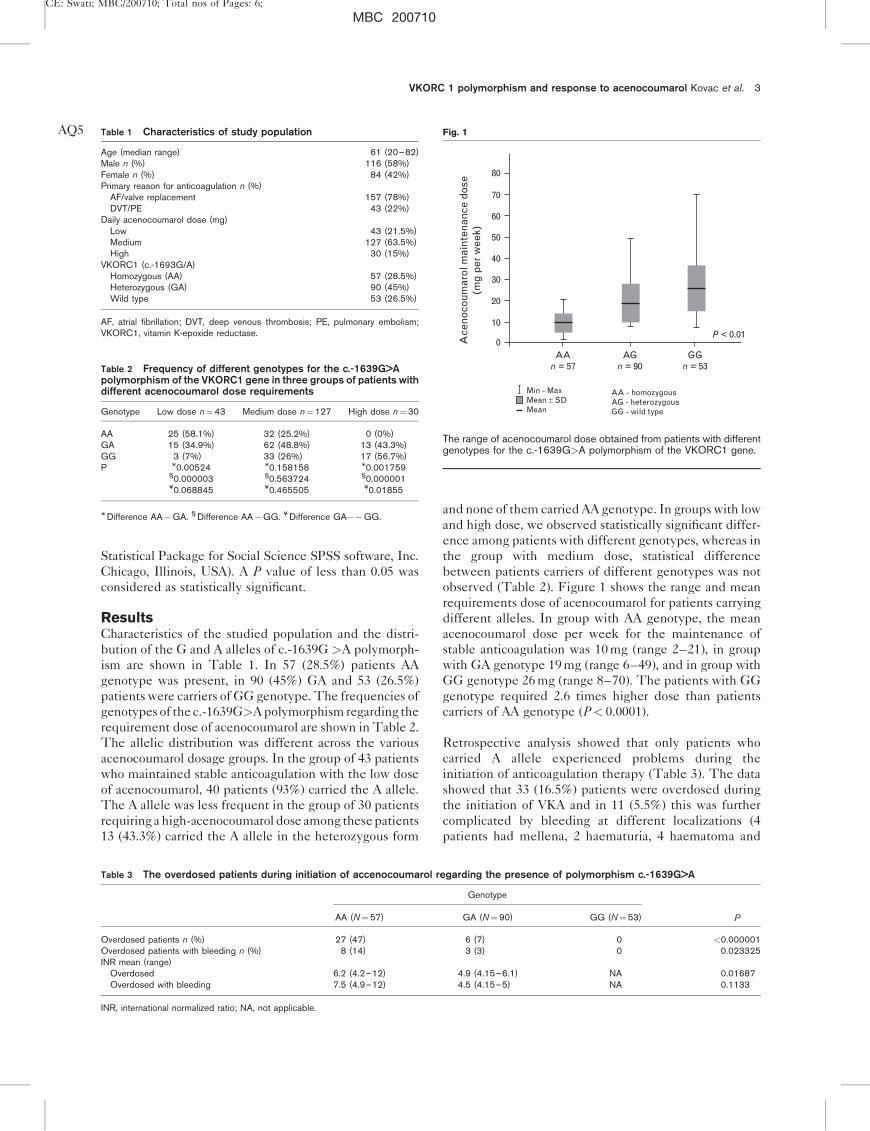
observed (Table 2). Figure 1 shows the range and mean
requirements dose of acenocoumarol for patients carrying
different alleles. In group with AA genotype, the mean
acenocoumarol dose per week for the maintenance of
stable anticoagulation was 10 mg (range 2–21), in group
with GA genotype 19 mg (range 6–49), and in group with
GG genotype 26 mg (range 8–70). The patients with GG
genotype required 2.6 times higher dose than patients
carriers of AA genotype (P< 0.0001).
Retrospective analysis showed that only patients who
carried A allele experienced problems during the
initiation of anticoagulation therapy (Table 3). The data
showed that 33 (16.5%) patients were overdosed during
the initiation of VKA and in 11 (5.5%) this was further
complicated by bleeding at different localizations (4
patients had mellena, 2 haematuria, 4 haematoma and
VKORC 1 polymorphism and response to acenocoumarol Kovac et al. 3
Table 1 Characteristics of study populationAQ5
Age (median range) 61 (20–82)Male n (%) 116 (58%)Female n (%) 84 (42%)Primary reason for anticoagulation n (%)
AF/valve replacement 157 (78%)DVT/PE 43 (22%)
Daily acenocoumarol dose (mg)Low 43 (21.5%)Medium 127 (63.5%)High 30 (15%)
VKORC1 (c.-1693G/A)Homozygous (AA) 57 (28.5%)Heterozygous (GA) 90 (45%)Wild type 53 (26.5%)
AF, atrial fibrillation; DVT, deep venous thrombosis; PE, pulmonary embolism;VKORC1, vitamin K-epoxide reductase.
Table 2 Frequency of different genotypes for the c.-1639G>Apolymorphism of the VKORC1 gene in three groups of patients withdifferent acenocoumarol dose requirements
Genotype Low dose n¼43 Medium dose n¼127 High dose n¼30
AA 25 (58.1%) 32 (25.2%) 0 (0%)GA 15 (34.9%) 62 (48.8%) 13 (43.3%)GG 3 (7%) 33 (26%) 17 (56.7%)P M0.00524 M0.158158 M0.001759
§0.000003 §0.563724 §0.000001¥0.068845 ¥0.465505 ¥0.01855
M Difference AA�GA. § Difference AA�GG. ¥ Difference GA��GG.
Table 3 The overdosed patients during initiation of accenocoumarol regarding the presence of polymorphism c.-1639G>A
Genotype
PAA (N¼57) GA (N¼90) GG (N¼53)
Overdosed patients n (%) 27 (47) 6 (7) 0 <0.000001Overdosed patients with bleeding n (%) 8 (14) 3 (3) 0 0.023325INR mean (range)
Overdosed 6.2 (4.2–12) 4.9 (4.15–6.1) NA 0.01687Overdosed with bleeding 7.5 (4.9–12) 4.5 (4.15–5) NA 0.1133
INR, international normalized ratio; NA, not applicable.
Fig. 1
80
70
60
50
40
Ace
noco
umar
ol m
aint
enan
ce d
ose
(mg
per
wee
k)
30
20
10
0AA
n = 57
Min - MaxMean ± SDMean
AA - homozygousAG - heterozygousGG - wild type
AGn = 90
GGn = 53
P < 0.01
The range of acenocoumarol dose obtained from patients with differentgenotypes for the c.-1639G>A polymorphism of the VKORC1 gene.

CE: Swati; MBC/200710; Total nos of Pages: 6;
MBC 200710
1 epistaxis). In the group of 33 overdosed patients, 27 had
AA genotype, and six carried GA genotype
(P< 0.000001). In the group of patients who carried
AA genotype, the mean value of INR level in overdosed
patients was 6.2 (4.2–12), whereas in the group with GA
genotype the mean INR was 4.9 (4.15–6.1). A statistically
significant difference (P¼ 0.01687) was observed
between groups.
The mean age of overdosed patients with bleeding
complication, was 69 years, (range 50–81) and in the
group of overdosed patients without bleeding, 59 years
(26–71) representing statistically significant difference
(P¼ 0.0312).
In the follow up period from initiation of VKA, INR more
than four was recorded 149 times in 31 (54%) carriers of
AA genotype. In 14 (16%) patients with GA genotype
INR more than four were recorded 72 times, whereas in
four (8%) patients with GG genotype INR more than four
was recorded 11 times. Patients carriers of AA genotype
were more likely to be overanticoagulated during follow
up after initiation of VKA compared with GA genotype,
P< 0.0001 and respectively with GG genotype,
P< 0.0001 (Table 4).
Patients with GG genotype spent more time below
therapeutic range compared with patients carriers of
AA (P¼ 0.0328) and GA genotype (P< 0.0001). In 11
patients (19%) with AA genotype, INR less than two was
recorded 62 times. In seven (8%) patients with GA, INR
less than two was recorded 51 times, and in 21 (40%) with
GG genotype, INR less than two was recorded 73 times
during follow up of initiation of VKA (Table 5).
DiscussionRecently, genetic variations within the gene encoding for
a subunit of the vitamin K epoxide reductase complex,
have been found to predict sensitivity to anticoagulant
therapy. The c.-1639G>A polymorphism marks the
VKORC1�2 haplotype [5], and its association with
increased response to acenocoumarol has been shown
in a group of healthy individuals [6], as well as in a group
of patients treated with warfarin or acenocoumarol [7–
15].
The aim of our study, which represents the first one ever
performed in our population, was to evaluate the effect of
the c.-1639G>A polymorphism on the acenocoumarol
dosage requirements in a group of patents under stable
anticoagulation. The rate of bleeding during the
initiation of VKA and variability in response during follow
up, considering the presence of this polymorphism, were
also evaluated.
Our study supports the importance of the role of c.-
1639G>A in the sensitivity to acenocoumarol. In the
group of patients who maintained stable anticoagulation
with low doses of acenocoumarol, 93% carried the A
allele, whereas this allelic variant was present in 43.3%
patients requiring high doses and in 74% patients in the
medium-dose group. None of the patients who carried
AA genotype was in the group requiring high-acenocou-
marol dose, and statistically significant difference was
observed only in groups with low and high dose, among
patients with different genotypes.
Similar results were demonstrated by Montes et al. [10].
They found that more than 90% of the patients required
low doses of acenocoumarol, and less than 30% of the
patients who needed a high dose carried the A allele.
Likewise, in the study performed by Geisen et al. [7], 93%
patients with the increased coumarin sensitivity and none
of the patients with partial coumarin resistance, were
found to be homozygous for the A allele (representing
VKORC 1�2).
In our study, the mean acenocoumarol dose per week in
the group with AA genotype, required for the maintenance
of stable anticoagulation was 10 mg, in the group with GA
genotype 19 mg, and in the group with GG genotype
26 mg. The data show that patients with GG genotype
required 2.6 times higher dose than patients who were
carriers of AA genotype. In a similar study by Qazim et al.[13] the mean phenprocoumon dosage per week to achieve
therapeutic VKA was 15.3 mg in patients without the
VKORC1 c.-1639G>A gene polymorphism, 10.9 mg in
patients carrying the heterozygous and 7.8 mg in patients
carrying the homozygous c.-1639G>AVKORC1 poly-
mprphism. Sonce et al. [14] also showed that the mean
warfarin dose was the highest in patients with GG geno-
type compared with the GA and AA genotype patients, and
in patients who are homozygous AQ1wild type for CYP2C9. In
order to estimate the optimum initial warfarin dose needed
to maintain stable and optimum anticoagulation they
proposed dosing algorithm that incorporate the contri-
bution of genetic (VKORC-1639, 2C9�3) and nongenetic
variables (age, height) [14].
4 Blood Coagulation and Fibrinolysis 2010, Vol 00 No 00
Table 4 Patients with INR more than four during follow upfrom initiation of VKA regarding the presence of polymorphismc.-1639G>A
AA (N¼57) GA (N¼90) GG (N¼53)
Patients n (%) 31 (54) 14 (16) 4 (8)Number of INR > 4 149 72 11Num. of INR > 4 per patient 4.8 5 2.7Patients with bleeding n (%) 1 (1.8) 1 (1) 0
P<0.0001 M, P<0.0001 §, P¼0.2571 ¥.
Table 5 Patients with INR less than two during follow upfrom initiation of VKA regarding the presence of polymorphismc.-1639G>A
AA (N¼57) GA (N¼90) GG (N¼53)
Patients n (%) 11 (19) 7 (8) 21 (40)Number of INR < 2 62 51 73Num. of INR < 2 per patient 5.6 7.2 3.5
P¼0.1139 M, P¼0.0328 §, P<0.0001 ¥.
Ljiljana Rakicevic
Cross-Out
Ljiljana Rakicevic
Replacement Text
Sconce

CE: Swati; MBC/200710; Total nos of Pages: 6;
MBC 200710
Oral anticoagulant therapy, particularly during the
initiation period, is associated with the overanticoagula-
ton that may result in bleeding. Therefore, we estimated
the rate of overanticoagulation patients regarding the
presence of c.-1639G>A polymorphism during the first
3 months of the initiation. Our results showed that only
patients who carried A allele were at risk of overanticoa-
gulation. In the group of 33 overdosed patients, 27 carried
AA genotype, and six carried GA genotype. From those in
the overdosed group, 11 patients (5.5%) had overanticoa-
gulation further complicated with bleeding and five of
them had to be transfused with fresh frozen plasma to
stop the bleeding and reverse the INR to therapeutic
range. Our results suggest that performing of pharmaco-
genetic testing for the presence of c.-1639G>A prior to
the initiation of VKA, could minimize the risk of over-
anticoagulation and subsequent bleeding complications
in our patients.
Regarding the mean INR in overdosed patients, a stat-
istically significant difference was observed between
carriers of AA and GA genotype (P¼ 0.01687), whereas
between carriers of AA and GA genotype who had bleed-
ing complications, no statistical difference was observed
regarding the mean INR, possible due the small number
of patients carriers of GA genotype.
Schwartz et al. [8] reported thatAQ2 patients carriers of AA
genotype, had significantly higher INR values in the first
week than non-A homozygotes. They also found that the
patients with one or two VKORC1 haplotype A alleles
had shorter times to the first INR more than four. They
reported the association of an increase in the anticoagu-
lant response in these patients, as indicated by an INR
above the therapeutic range, and an increased risk of
bleeding [8].
Contrary to our findings, Wadelius et al. [9] did not find an
association between VKORC1 polymorphism and risk of
bleeding, but they emphasized that homozygosity for
VKORC1 c.-1639G>A variant alleles increased the risk
of early INR over four. They showed the strongest
association with dose, which was observed for VKORC1,
and significantly lower for CYP2C9 [9]. The mean age of
overdosed patients with bleeding complications in our
study was 69 years, (range 50–81), whereas in overdosed
group without bleeding it was 59 years (range 26–71).
P¼ 0.0312, supports the early investigation stating that
elderly patients were at a higher risk of bleeding [16]. Our
findings were similar to study by Schwartz et al. [8] in
which patients with bleeding events older (median age,
71 years) than the ones in studied population (median
age, 61 years) were included.
In our study after initiation of VKA, INR more than 4
were recorded in 54% carriers of AA genotype, 16% with
GA genotype and in 8% with GG genotype. Patients
carriers of AA genotype were more likely to be over-
anticoagulated during follow up after initiation of VKA
compared carriers of GA genotype and GG genotype, Pless than 0.0001. Osman et al. [12] also reported more
variations in INR in patients with VKORC1�2 than those
with VKORC1�3 or VKORC1�4 haplotypes, in the
initiation phase which could be connected with an
increased risk of bleeding complications. Our patients
with GG genotype spent more time below therapeutic
range compared with patients carriers of AA (P¼ 0.0328)
and GA genotype (P< 0.0001). Similarly, Meckley et al.[17] showed in a retrospective study that patients with
GG genotype spent more time below therapeutic INR
compared with patients carriers of A allele.
In summary, even with careful monitoring, initiation of
VKA is associated with highly variable responses between
individuals and maintaining levels within the narrow
therapeutic range that can lead to adverse-drug events.
For that reason, the use of every tool that contributes to
properly estimation of VKA dosage is a considerable asset.
In planning of optimal initial and maintenance doses, in
addition to the age, height and intercurrent illness, geno-
type plays an important role, especially if the using of
computer dosing software is not available and patients are
subjected to treatment according to standard care without
specific dosing algorithm. Testing for VCKORC1 c.-
1639G>A polymorphism predicts high risk of overdose
among third of our patients. Therefore, on the basis of the
results obtained from this study, testing for VCKORC1 c.-
1639G>A may be considered as a preliminary examination
before starting anticoagulation in order to increase effec-
tiveness and safety of anticoagulation therapy.
AcknowledgementsThis work supported by grant 143051 from Ministry of
Science, Republic of Serbia.
References1 Hirsh J. Oral anticoagulant drugs. N Engl J Med 1991; 324:1865–1875.
2 Baglin TP, Keeling DM, Watson HG. Guidelines on oral anticoagulation(warfarin): third edition–2005 update. Br J Haematol 2006; 132:277–285 AQ3.
3 Dentali F, Ageno W, Crowter M. Treatment of coumarin-associatedcoagulopathy: a systemic review and proposed treatment algorithms. JThromb Haemost 2006; 4:1853–1863.
4 Wittkovsky AK. Drug interactions with oral anticoagulants. In: Colman RW,Clowes AW, Goldhaber SZ, Marder VJ, George JN, editors. Hemostasisand Thrombosis, 5th ed. Philadelphia: Lippincott Williams & Wilkins; 2006.pp. 1699–1709.
5 Oldenburg J, Watzka M, Rost S, Muller R. VKORC1: molecular target ofcoumarins. J Thromb Haemost 2007; 5 (suppl1):1–6.
6 Bodin L, Verstuyft C, Tregouet DA, Robert A, Dubert L, Funck-Brentano C,et al. Cytochrome P450 2C9 (CYP2C9) and vitamin K epoxide reductase(VKORC1) genotypes as determinants of acenocumarol sensitivity. Blood2005; 106:135–140.
7 Geisen C, Watzka M, Sittinger K, Steffens M, Daugela L, Seifried E, et al.VKORC1 haplotypes and their impact on the inter-individual and inter-ethnical variability of oral anticoagulation. Thromb Haemost 2005;94:773–779.
8 Schwartz UI, Ritchie MD, Bredford Y, Chun L, Dudec S, Frye-Anderson,et al. Genetic determinants of response to warfarin during initialanticoagulation. N Engl J Med 2008; 358:999–1008.
9 Wadelius M, Chen LY, Lindh JD, Eriksson N, Ghori M JR, Bumpstead S,et al. The largest prospective warfarin-treated cohort supports geneticforecasting. Blood 2008; 4:149070 AQ4.
VKORC 1 polymorphism and response to acenocoumarol Kovac et al. 5
Ljiljana Rakicevic
Cross-Out
Ljiljana Rakicevic
Replacement Text
Schwarz
Ljiljana Rakicevic
Cross-Out
Ljiljana Rakicevic
Replacement Text
Baglin TP, Keeling DM, Watson HG; British Committee for Standards.
Ljiljana Rakicevic
Cross-Out
Ljiljana Rakicevic
Replacement Text
2009;113:784-792
Ljiljana Rakicevic
Cross-Out
Ljiljana Rakicevic
Replacement Text
MJ
Ljiljana Rakicevic
Cross-Out
Ljiljana Rakicevic
Replacement Text
Li C
Ljiljana Rakicevic
Inserted Text
A

CE: Swati; MBC/200710; Total nos of Pages: 6;
MBC 200710
10 Montes R, Ruiz de Gaona E, Martinez-Gonzales MA, Alberca I, Hermida J.The c.-1639G>A polymorphism of the VKORC1 gene is a majordeterminant of the response to acenocoumarol in anticoagulated patients.B J Haematol 2006; 133:183–187.
11 D‘Andrea G, D‘Ambrosio LC, Di Perna P, Chetta M, Santacroce R,Brancaccio V, et al. A polymorphism in the VKORC1 gene is associatedwith an interindividual variability in the dose-anticoagulant effect of warfarin.Blood 2005; 105:645–649.
12 Osman A, Enstrom C, Arbring K, Soderkvist P, Lindhal TL. Main haplotypesand mutational analysis of vitamin K epoxide reductase (VKORC1) in aSwedish population: retrospective analysis of case records. J ThrombHaemost 2006; 4:1723–1729.
13 Qazim B, Stollberger C, Krugluger W, Dossenbach-Glaninger A, Finsterer J.Dependency of phenprocoumon dosage on polymorphisms in the VKORC1and CYP2C9 genes. J Thromb Thrombolysis 2008; 28:211–214.
14 Sonce E, Kahn T, Wynne H, Avery P, Monkhouse L, King B, et al. The impactof CYP2C9 and VKORC1 genetic polymorphism and patientcharacteristics upon warfarin dose requirement: proposal for a new dosingregimen. Blood 2005; 106:2329–2333.
15 Quteinech L, Verstuyft C, Descot C, Dubert L, Robert A, Jaillon P, et al.Vitamin K epoxide reductase (VKORC1) genetic polymorphism isassociated to oral anticoagulant overdose. Thromb Haemost 2005;94:690–691.
16 Levine MN, Beyth R, Kearon C, Schulman S. Hemorrhagic complications ofanticoagulant treatment. Chest 2004; 126:287S–310S.
17 Meckley LM, Wittkowsky AK, Rieder MJ, Rettie AE, Veenestra DL. Ananalysis of the relative effects of VKORC1 and CYP2C9 variants onanticoagulation related outcomes in warfarin-treated patients. ThrombHaemost 2008; 100:220–239.
6 Blood Coagulation and Fibrinolysis 2010, Vol 00 No 00
Ljiljana Rakicevic
Cross-Out
Ljiljana Rakicevic
Replacement Text
Sconce
Ljiljana Rakicevic
Cross-Out
Ljiljana Rakicevic
Replacement Text
RL

MBC Blood Coagulation & Fibrinolysis Typeset by Thomson Digital
for Lippincott Williams & Wilkins Manuscript No. 200710 Dear Author, During the preparation of your manuscript for typesetting, some queries have arisen. These are listed below. Please check your typeset proof carefully and mark any corrections in the margin as neatly as possible or compile them as a separate list. This form should then be returned with your marked proof/list of corrections to the Production Editor.
QUERIES: to be answered by AUTHOR/EDITOR QUERY NO. QUERY DETAILS RESPONSE <AQ1> Please check edit in this statement for
correctness. 'Sonce et al. [14] … for CYP2C9.'
<AQ2> Please check edit in the spelling of author name in this statement for correctness. 'Schwartz et al. [8] … homozygotes.
<AQ3> Please check edits in article title of Refs. [2,11] for correctness.
<AQ4> Please check details of Ref. [9] for correctness.
<AQ5> Please check edit in Tables [1–5] for correctness.
Ljiljana Rakicevic
Note
We have made required changes.
Ljiljana Rakicevic
Note
We have made required changes.
Ljiljana Rakicevic
Note
We have made required changes.
Ljiljana Rakicevic
Note
We have no suggestions relating to the tables and figure.
Ljiljana Rakicevic
Note
We have made required changes in the statement, and in reference 14, also.




















