The Alteration of Autonomic Function in Multiple Organ Dysfunction Syndrome
15
The Alteration of Autonomic Function in Multiple Organ Dysfunction Syndrome Hendrik Schmidt, MD a, * , Dirk Hoyer, PhD b , Joachim Wilhelm a , Gerold So¨ffker, MD a , Konstantin Heinroth, MD a , Kuno Hottenrott, PhD a , Samir M. Said, MD a , Michael Buerke, MD a , Ursula Mu¨ller-Werdan, MD a , Karl Werdan, MD a a Martin-Luther-University Halle-Wittenberg, Klinikum Kro ¨llwitz, Ernst-Grube-Strasse 40, D-06097 Halle/Saale, Germany b Friedrich-Schiller-University, Jena 07744, Germany In the last decade of the twentieth century, it became evident that therapies directed at inflammatory mediators failed to decrease the high mortality in sep- sis and multiple organ dysfunction syndrome (MODS), indicating that new pathophysiologic hypotheses needed to be explored, including a consideration of the role of autonomic dysfunction [1]. The following questions were raised: Does sepsis or MODS alter autonomic function? If so, can alterations in autonomic function predict mortality in MODS? Is the autonomic dysfunction observed in MODS confounded by age or pharmacologic agents? Can pharmacologic treatment strategies improve autonomic dysfunction? New insights have been gleaned regarding the complex interplay of car- diovascular reflexes mediating the autonomic dysfunction seen in MODS and sepsis, providing answers to at least some of these questions. Drs. Schmidt, Mu¨ller-Werdan, and Hoyer are supported by grants of the ‘‘Deutsche Forschungsgemeinschaft’’ (SCHM 1398/3-1,-2; HOY 1634/8-1,2). * Corresponding author. Department of Medicine III, Martin-Luther-University Halle- Wittenberg, Klinikum Kro¨llwitz, Ernst-Grube-Strasse 40, D-06097 Halle/Saale, Germany. E-mail address: [email protected] (H. Schmidt). 0749-0704/08/$ - see front matter Ó 2008 Elsevier Inc. All rights reserved. doi:10.1016/j.ccc.2007.10.003 criticalcare.theclinics.com Crit Care Clin 24 (2008) 149–163
Transcript of The Alteration of Autonomic Function in Multiple Organ Dysfunction Syndrome
The Alteration of Autonomic Functionin Multiple Organ Dysfunction
Syndrome
Hendrik Schmidt, MDa,*, Dirk Hoyer, PhDb,Joachim Wilhelma, Gerold Soffker, MDa,
Konstantin Heinroth, MDa,Kuno Hottenrott, PhDa,
Samir M. Said, MDa, Michael Buerke, MDa,Ursula Muller-Werdan, MDa, Karl Werdan, MDa
aMartin-Luther-University Halle-Wittenberg, Klinikum Krollwitz,
Ernst-Grube-Strasse 40, D-06097 Halle/Saale, GermanybFriedrich-Schiller-University, Jena 07744, Germany
In the last decade of the twentieth century, it became evident that therapiesdirected at inflammatorymediators failed todecrease the highmortality in sep-sis and multiple organ dysfunction syndrome (MODS), indicating that newpathophysiologic hypotheses needed to be explored, including a considerationof the role of autonomic dysfunction [1]. The following questions were raised:
� Does sepsis or MODS alter autonomic function?� If so, can alterations in autonomic function predict mortality in MODS?� Is the autonomic dysfunction observed in MODS confounded by age orpharmacologic agents?� Can pharmacologic treatment strategies improve autonomicdysfunction?
New insights have been gleaned regarding the complex interplay of car-diovascular reflexes mediating the autonomic dysfunction seen in MODSand sepsis, providing answers to at least some of these questions.
Crit Care Clin 24 (2008) 149–163
Drs. Schmidt, Muller-Werdan, and Hoyer are supported by grants of the ‘‘Deutsche
Forschungsgemeinschaft’’ (SCHM 1398/3-1,-2; HOY 1634/8-1,2).
* Corresponding author. Department of Medicine III, Martin-Luther-University Halle-
Wittenberg, Klinikum Krollwitz, Ernst-Grube-Strasse 40, D-06097 Halle/Saale, Germany.
E-mail address: [email protected] (H. Schmidt).
0749-0704/08/$ - see front matter � 2008 Elsevier Inc. All rights reserved.
doi:10.1016/j.ccc.2007.10.003 criticalcare.theclinics.com

150 SCHMIDT et al
Assessment of autonomic function in the critically ill
A basic feature of the healthy human body is a continuous communica-tion between all vital organs through signals of the autonomic nervoussystem. One of the major tasks of the autonomic nervous system is the ad-justment of the cardio-respiratory and the cardio-circulatory interactions tomaintain appropriate oxygen delivery and a proper adaptation of heart rateand blood pressure to changing physiologic demands. Although the inter-play of cardiovascular and ventilatory mechanisms in regulating oxygen de-livery to the tissues is well known and described in healthy controls [2,3],knowledge of the cardio-respiratory reflex behavior in ICU-relevant diseasestates is more limited. Relevant cardiovascular reflex arcs (chemo- and bar-oreflexes) are summarized in Table 1.
Methods for assessing autonomic function
Heart rate variability
Heart rate and rhythm are never constant but fluctuate under the influ-ence of changing sympathetic and parasympathetic tone (Fig. 1). Thereare numerous studies of heart rate variability (HRV) in patients with heartdisease. A depressed HRV predicts mortality and arrhythmic complicationsafter acute myocardial infarction (MI) [4] and in heart failure [4].
Analysis of HRV is a promising noninvasive method to assess patientswith MODS and sepsis [1,5–8]. It is a reflection of cardio-respiratory inter-action; therefore, changes in HRV are indicative of decoupling of the heartfrom other organs such as the lung and brain.
There are two methods of analysis to evaluate the sympathetic/parasym-pathetic influence on variations in heart rate. Time domain measurementsare simple to use but usually require a longer period of recording (24 hours).Short time recordings (5–20 minutes) can be used for a spectral analysis ofheart rate variations (frequency domain measurements), providing fourmain components for evaluation: high frequency (HF, 0.15–0.4 Hz), low fre-quency (LF, 0.04–0.15 Hz), very low frequency (VLF, 0.003–0.04 Hz), andultra-low-frequency (ULF, !0.003 Hz) (Table 2) [4].
Efferent vagal activity mainly contributes to the HF and VLF compo-nents, whereas LF, expressed in normalized units, is a marker of sympa-thetic or both vagal and sympathetic activity [9] and is influenced byseveral physiologic variables such as endocrine function, temperature, andvasomotion [4,10].
Nonlinear analysis of heart rate variability
Under physiologic conditions, the heart behaves in a nonlinear manner[1,5–7], meaning that cardiovascular variables may be superimposed ina non-additive rather than additive manner. Nonlinear measures may be su-perior to the classic linear variables in prediction of mortality [11–13], and
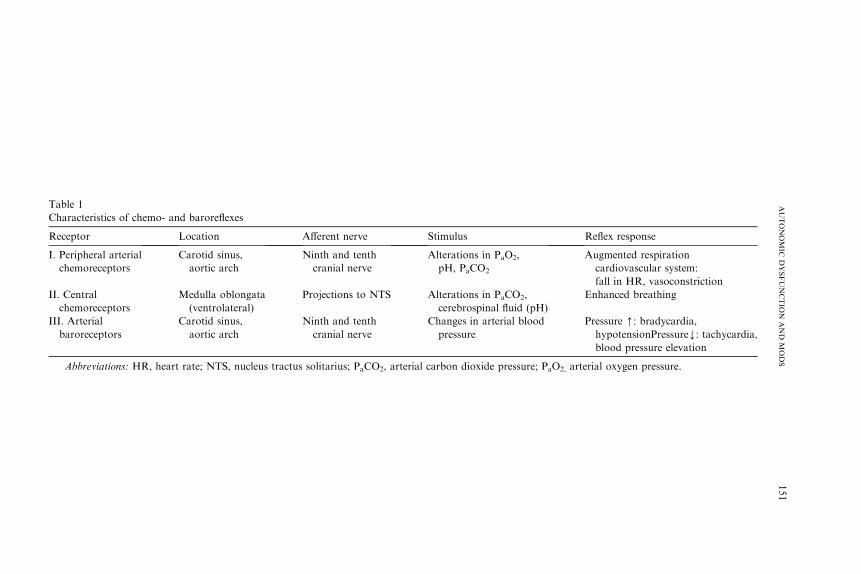
Table 1
Characteristics of chemo- and baroreflexes
Receptor Location Afferent nerve Stimulus Reflex response
I. Peripheral arterial
chemoreceptors
Carotid sinus,
aortic arch
Ninth and tenth
cranial nerve
Alterations in PaO2,
pH, PaCO2
Augmented respiration
cardiovascular system:
fall in HR, vasoconstriction
II. Central
chemoreceptors
Medulla oblongata
(ventrolateral)
Projections to NTS Alterations in PaCO2,
cerebrospinal fluid (pH)
Enhanced breathing
III. Arterial
baroreceptors
Carotid sinus,
aortic arch
Ninth and tenth
cranial nerve
Changes in arterial blood
pressure
Pressure [: bradycardia,hypotensionPressureY: tachycardia,
blood pressure elevation
Abbreviations: HR, heart rate; NTS, nucleus tractus solitarius; PaCO2, arterial carbon dioxide pressure; PaO2, arterial oxygen pressure.
151
AUTONOMIC
DYSFUNCTIO
NAND
MODS
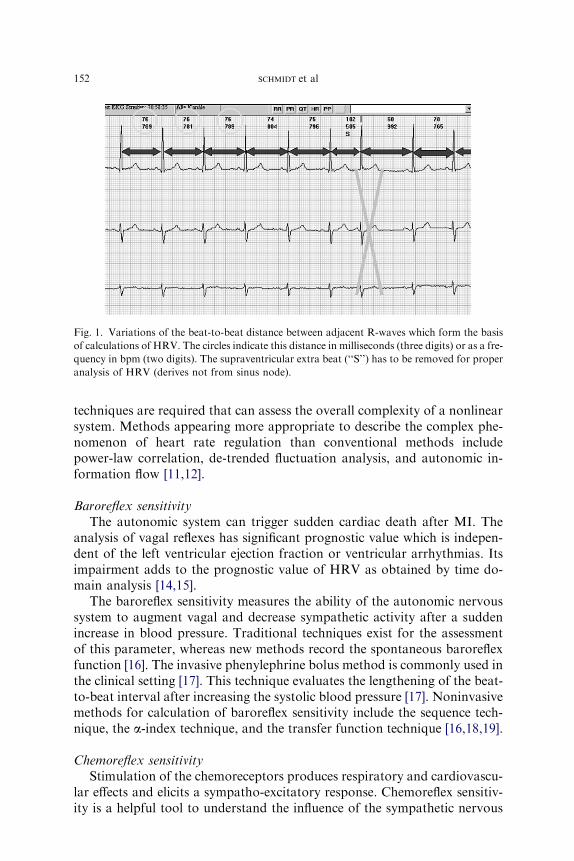
Fig. 1. Variations of the beat-to-beat distance between adjacent R-waves which form the basis
of calculations of HRV. The circles indicate this distance in milliseconds (three digits) or as a fre-
quency in bpm (two digits). The supraventricular extra beat (‘‘S’’) has to be removed for proper
analysis of HRV (derives not from sinus node).
152 SCHMIDT et al
techniques are required that can assess the overall complexity of a nonlinearsystem. Methods appearing more appropriate to describe the complex phe-nomenon of heart rate regulation than conventional methods includepower-law correlation, de-trended fluctuation analysis, and autonomic in-formation flow [11,12].
Baroreflex sensitivity
The autonomic system can trigger sudden cardiac death after MI. Theanalysis of vagal reflexes has significant prognostic value which is indepen-dent of the left ventricular ejection fraction or ventricular arrhythmias. Itsimpairment adds to the prognostic value of HRV as obtained by time do-main analysis [14,15].
The baroreflex sensitivity measures the ability of the autonomic nervoussystem to augment vagal and decrease sympathetic activity after a suddenincrease in blood pressure. Traditional techniques exist for the assessmentof this parameter, whereas new methods record the spontaneous baroreflexfunction [16]. The invasive phenylephrine bolus method is commonly used inthe clinical setting [17]. This technique evaluates the lengthening of the beat-to-beat interval after increasing the systolic blood pressure [17]. Noninvasivemethods for calculation of baroreflex sensitivity include the sequence tech-nique, the a-index technique, and the transfer function technique [16,18,19].
Chemoreflex sensitivity
Stimulation of the chemoreceptors produces respiratory and cardiovascu-lar effects and elicits a sympatho-excitatory response. Chemoreflex sensitiv-ity is a helpful tool to understand the influence of the sympathetic nervous

Table 2
Indices of heart rate variability
Method of analysis Definition
Indexes of time domain
SDNN Standard deviation of all normal-to-normal
RR intervals (ms)
SDANN Standard deviation of the averages of NN intervals in
all 5-min segments of the entire recording (ms)
rMSSD Root mean square of successive
differences of N-N intervals (ms)
pNN50 Percentage of differences of successive RR intervals
differing R50 ms (%)
Indexes of frequency domain
VLF Very low frequency power (0.003–0.04 Hz, ms2)
LF Low frequency power (0.04–0.15 Hz, ms2)
HF High frequency power (0.15–0.4 Hz, ms2)
TP Total power (0.0–0.4 Hz, ms2)
153AUTONOMIC DYSFUNCTION AND MODS
system on the cardio-respiratory system, helping to elucidate the pathophys-iology of several disorders, including congestive heart failure (CHF), suddencardiac death, acute respiratory distress syndrome, and MODS. The respi-ratory chemoreflex sensitivity (peripheral hypoxic, peripheral hypercapnic,and central hypercapnic) must be distinguished from the cardiac chemore-flex sensitivity.
The respiratory chemoreflex sensitivity is typically assessed by a hypoxicstimulus, with most data obtained in patients with advanced CHF. Chuaand colleagues [20–22] reported an enhanced ventilatory response secondaryto a hypoxic or hypercapnic stimulus in stable CHF patients that was asso-ciated with an attenuation of baroreflex sensitivity and an increased inci-dence of nonsustained ventricular tachycardias. Of note, hyperoxiaameliorated autonomic function; the chemoreflex sensitivity decreased,whereas the baroreflex sensitivity was enhanced [20–22].
The cardiac chemoreflex sensitivity is a parameter that can be calculatedeither as the ratio between heart interval alterations and the decrease of ar-terial oxygen tension (D heart interval/D arterial PO2) or the lengthening ofthe heart interval versus the increase in venous oxygen saturation (D heartinterval/D venous SO2) [23]. Respiration impairs the assessment of this pa-rameter via activation of the pulmonary stretch receptors; therefore, itshould be obtained under controlled ventilation or corrected for this effect[23]. Cardiac chemoreflex sensitivity describes the cardio-respiratory interac-tion, which is otherwise difficult to quantify in intensive care patients.
Cardiac chemoreflex sensitivity has been used to assess interorgan com-munication in chronic heart failure (CHF), MI [24–28], and MODS. Car-diac chemoreflex sensitivity provides potentially useful prognostic andpathophysiologically relevant information; however, the use of a hypoxicstimulus may be problematic in the critically ill population. The induction
154 SCHMIDT et al
of hyperoxia is less hazardous but has the disadvantage of producing onlya small change in heart rate by deactivation of the peripheral chemorecep-tors [29]. In addition, an influence of spontaneous heart rate fluctuationson the calculation of the cardiac chemoreflex sensitivity cannot be excluded.In a recent report [29], a new method was proposed for calculating the car-diac chemoreflex sensitivity in critically ill patients. This method overcomesthe disadvantages of other methods because it uses an activation and deac-tivation of the peripheral arterial chemoreceptors, characterizing a dynamicresponse pattern in a range encompassing the resting state. In this study, thecardiac chemoreflex sensitivity was related to the severity of illness; the moresevere the MODS, the more the cardiac chemoreflex sensitivity was blunted.The study did not show a significant relationship between chemoreflex sen-sitivity and age.
Chemoreflex sensitivity can measured more safely in other disease statessuch as CHF or MI. Chemoreflex sensitivity has a significant prognosticvalue in CHF and is related to the severity of illness in this disease entity[25–29]. The assessment of chemoreflex sensitivity is also applicable to pa-tients who undergo resuscitation for cardiac arrest after MI; this subset ofpatients has a significantly lower chemoreflex sensitivity in comparisonwith infarction patients who do not have to be resuscitated [28].
Autonomic dysfunction and disease severity
The development of MODS is associated with a systemic inflammatoryresponse syndrome (SIRS) and dysregulated release of inflammatory medi-ators leading to cell damage and organ failure. Because autonomic dysfunc-tion is inherent in SIRS, it may be postulated that uncoupling of theneurally mediated organ interactions in sepsis and in non-infectious inflam-matory response syndromes contributes to the development of MODS [1].Godin and Buchman [1] proposed that bacterial toxins and sepsis mediatorsalter the neural reflexes and cytokine pathways and cause a defect in inter-organ communication, enabling single organ dysfunction to progress toMODS. In support of this hypothesis, it has been shown that administrationof endotoxin can decrease HRV in healthy subjects [1]. Others have notedthat a reduction in HRV, which characterizes a loss of autonomic balance,occurs in sepsis and MODS [29–31]. A reduction in HRV among critically illpatients is associated with an increase in mortality [29–31] and correlateswith the severity of illness [32].
Godin and Buchman [1] introduced HRV and approximate entropy,a measure characterizing dynamic-nonlinear coordinations (for a definition,please refer to the previous section on nonlinear analysis of HRV), as pa-rameters to quantify interorgan communication in MODS. They revealeda reversible attenuation of these parameters in healthy subjects 3 to 4 hoursafter intravenous infusion of endotoxin [33]. Endotoxin can also elicit anattenuation of the beating rate variability of spontaneous contracting

155AUTONOMIC DYSFUNCTION AND MODS
cardiomyocytes, whereas tumor necrosis factor-a does not [34]. Tibby andcolleagues [35] have shown that a power-law model (nonlinear measure ofself-similarity) is an appropriate measure of HRV, and that loss of HRV oc-curs with increasing organ failure.
Changes in cardiac chemoreflex sensitivity may characterize one aspect ofMODS. The cardio-respiratory system is not able to vary the heart rate inresponse to a hyperoxic stimulation, as is true in healthy subjects. A recentstudy [29] showed that the impairment of the cardiac chemoreflex sensitivityis related to the APACHE II score. According to these results, the more se-vere the physiologic disturbance, the more the heart and lung coupling isimpaired.
Neurologic dysfunction such as encephalopathy, polyneuropathy, or my-opathy is frequently seen among septic patients [36,37] and can prolong theprocess of weaning from mechanical ventilation [38,39]. In patients withMODS, the authors noted that the decrease in the cardiac chemoreflex sen-sitivity was associated with a decrease in the Glasgow coma scale [29]. Thedecrease in chemoreflex sensitivity could be due to critical illness polyneur-opathy, which also affects the neural cardio-respiratory reflex arcs.
Autonomic dysfunction in critical illness
Because autonomic dysfunction is inherent in SIRS, uncoupling of theneurally mediated organ–organ interactions in sepsis and in non-infectiousinflammatory response syndromes may contribute to the development ofMODS.
MODS has been associated with a significant suppression of vagal activ-ity [40]. In an intriguing set of observations, Tracey and colleagues [40–42]elucidated the role of parasympathetic efferent pathways in regulating sys-temic inflammatory processes [40–42]. This group proposed an ‘‘anti-inflam-matory cholinergic reflex’’ mediated essentially by the vagal nerve whichmight be a critical counterbalancing mechanism to the overwhelming proin-flammatory surge observed in sepsis and MODS. According to this hy-pothesis, depressed vagal activity could then be a critical factor in thepathophysiology of MODS.
By applying a comprehensive spectrum of available tests, the authors re-cently showed [43] that, in MODS, there is not merely a reduction in a singlecomponent of autonomic activity but an impairment of the full spectrum ofautonomic function as described by HRV and baro- and chemoreflex sensi-tivities (Fig. 2) [43]. Moreover, these alterations have prognostic implica-tions. In our cohort, a single HRV variable derived from continuouslyrecorded ECG (VLF) predicted 28-day mortality as accurately as the goldstandard in outcome prediction, the APACHE II score.
Reduced vagal tone (baroreflex) after MI has a significant prognosticvalue independently of the left ventricular ejection fraction or ventricular ar-rhythmias [14]. Baroreflex sensitivity in CHF patients is depressed and the
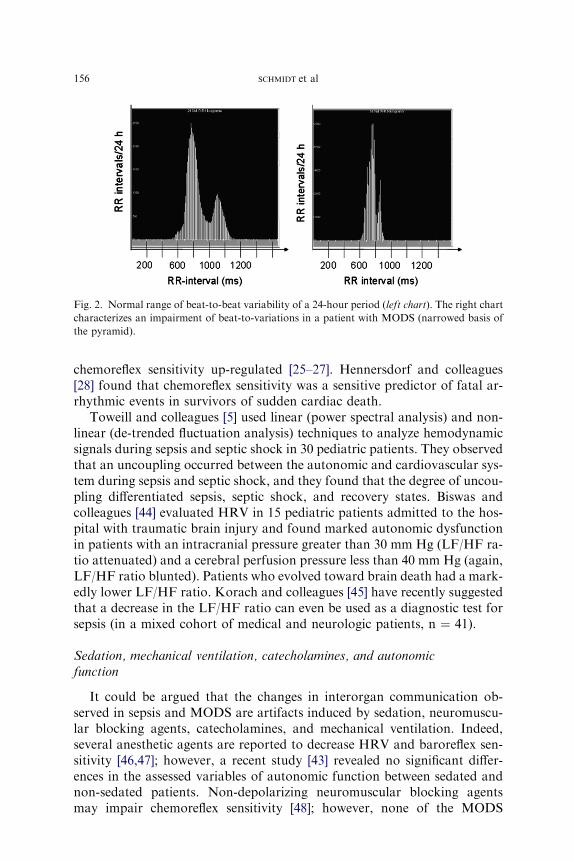
Fig. 2. Normal range of beat-to-beat variability of a 24-hour period (left chart). The right chart
characterizes an impairment of beat-to-variations in a patient with MODS (narrowed basis of
the pyramid).
156 SCHMIDT et al
chemoreflex sensitivity up-regulated [25–27]. Hennersdorf and colleagues[28] found that chemoreflex sensitivity was a sensitive predictor of fatal ar-rhythmic events in survivors of sudden cardiac death.
Toweill and colleagues [5] used linear (power spectral analysis) and non-linear (de-trended fluctuation analysis) techniques to analyze hemodynamicsignals during sepsis and septic shock in 30 pediatric patients. They observedthat an uncoupling occurred between the autonomic and cardiovascular sys-tem during sepsis and septic shock, and they found that the degree of uncou-pling differentiated sepsis, septic shock, and recovery states. Biswas andcolleagues [44] evaluated HRV in 15 pediatric patients admitted to the hos-pital with traumatic brain injury and found marked autonomic dysfunctionin patients with an intracranial pressure greater than 30 mm Hg (LF/HF ra-tio attenuated) and a cerebral perfusion pressure less than 40 mm Hg (again,LF/HF ratio blunted). Patients who evolved toward brain death had a mark-edly lower LF/HF ratio. Korach and colleagues [45] have recently suggestedthat a decrease in the LF/HF ratio can even be used as a diagnostic test forsepsis (in a mixed cohort of medical and neurologic patients, n ¼ 41).
Sedation, mechanical ventilation, catecholamines, and autonomicfunction
It could be argued that the changes in interorgan communication ob-served in sepsis and MODS are artifacts induced by sedation, neuromuscu-lar blocking agents, catecholamines, and mechanical ventilation. Indeed,several anesthetic agents are reported to decrease HRV and baroreflex sen-sitivity [46,47]; however, a recent study [43] revealed no significant differ-ences in the assessed variables of autonomic function between sedated andnon-sedated patients. Non-depolarizing neuromuscular blocking agentsmay impair chemoreflex sensitivity [48]; however, none of the MODS
157AUTONOMIC DYSFUNCTION AND MODS
patients in the cited study [43] received neuromuscular blocking agents whileautonomic function was tested. Korach and colleagues [45] found that theuse of catecholamines, sedation, and mechanical ventilation was not associ-ated with a decrease in HRV (LF/HF ratio). When this finding is consideredwith the observation that autonomic function is reduced in relation to theseverity of illness [29], the data collectively indicate that MODS is a moreprominent factor in impairing autonomic function than are sedation, cate-cholamine administration, and mechanical ventilation.
Autonomic function and age
In healthy subjects, HRV declines with age [4,49,50]. An attenuated HRVhas been shown after MI and in chronic heart failure, which partly masksthe age-dependent attenuation of HRV [4,51,52]. The authors’ recent study[43] showed a decrease in HRV variables in MODS patients but no differ-ences in HRV when patients were stratified by age groups.
Baroreflex sensitivity in healthy subjects also decreases with age, and thisreduction is also potentiated in acutely ill elderly patients [53]. The authors’recent study [43] of MODS patients found no measurable differences in bar-oreflex sensitivity between the younger and middle-aged groups and betweenthe younger and older age groups. This finding indicates that MODS is theprevailing factor and dominates the impairment.
Fewdata describe the chemoreflex sensitivity in healthy subjects [54]; there-fore, it is difficult to differentiate between age and disease effects in changes inchemoreflex sensitivity. Some evidence suggests that age-related declines inchemoreflex sensitivity have no significant role in MODS patients [54].
These studies suggest that the observed decreases in autonomic functionare principally related to the severity of illness rather than to age. The degreeto which autonomic function recovers in response to treatment of MODS isnot well understood, nor is it known whether age may influence the degreeof autonomic restoration.
Possible mechanisms of impaired heart rate variability in sepsis
and multiple organ dysfunction syndrome
Godin and colleagues [33] have shown that intravenous administration ofendotoxin can induce a reversible reduction in HRV in healthy volunteers,suggesting that endotoxin and proinflammatory mediators contribute tothe impaired cardiac autonomic function seen in patients with MODS.What are the mechanisms behind this phenomenon?
The efferent sympathetic and vagal cardiac signals to the heart run fromthe medulla oblongata in a crossed reticulospinal projection innervating theheart, blood vessels, and respiratory muscles. The sympathetic neurotrans-mitter norepinephrine and the parasympathetic neurotransmitter ace-tylcholine bind the cardiac adrenoceptors and muscarinergic receptors,

158 SCHMIDT et al
respectively, triggering signal transduction pathways in the pacemaker cellsthat result in a modulation of the pacemaker current. The pacemaker cur-rent is mainly mediated by the HCN channel (hyperpolarization-activatedcyclic nucleotide-gated channel) activity (If current, where f denotes ‘‘funny’’because the current occurs during hyperpolarization). In principle, sepsis- orMODS-associated cardiac autonomic impairment can occur at all levelsmentioned. The described experiments of Godin and colleagues [13] donot answer the question of whether HRV narrowing is related to endo-toxin-induced changes in brain autonomic centers (neuronal and glial apo-ptosis as described by Sharshar and colleagues [55,56]), the efferentautonomic fibers, or the pacemaker cells themselves.
A potential target at the cellular level is the pacemaker current If, which ismainly driven by HCN channels. In the authors’ whole patch–clamp exper-iments with isolated human myocytes from right atrial appendages, endo-toxin (1 and 10 mg/mL) significantly impaired If by suppressing thecurrent at membrane potentials positive to �80 mV and slowing down cur-rent activation, but without affecting maximal current conduction [57]. Fur-thermore, in endotoxin-incubated cells, the response If to b-adrenergicstimulation (1 mM of isoproterenol) was significantly larger in a comparisonwith control cells (shift of half-maximal activation voltage to more positivepotentials amounted to �10 and �14 mV in untreated and treated cells, re-spectively). Simulations using a spontaneously active sino-atrial cell modeldemonstrated that endotoxin-induced If impairment reduces the responsive-ness of the model cell to fluctuations of autonomic input [57]. These datademonstrate a direct impact of endotoxin on the cardiac pacemaker currentIf which may contribute to the clinically observed reduction in HRV inMODS patients. It indicates that autonomic dysfunction is triggered notonly by an alteration of the autonomous nervous itself but also by changesin cellular ion channel/signal transduction pathways mediating autonomousnervous signals in target organs.
Autonomic function and survival
A reduction of HRV predicts mortality and fatal arrhythmic events afterMI [4]. Kleiger and colleagues [51] first reported that a decrease in the stan-dard deviation of all normal-to-normal RR intervals (SDNN) of less than 50milliseconds after a MI is associated with a higher risk for mortality than anSDNN of greater than 100 milliseconds. The UK-Heart study [58] founda higher risk in overall mortality for patients with chronic heart failureand an SDNN less than 50 milliseconds when compared with patientswith an SDNN greater than 100 milliseconds. In the ATRAMI trial [14],an SDNN less than 70 milliseconds combined with reduced baroreflex sen-sitivity (!3 ms/mm Hg) was associated with a sevenfold higher relative riskfor cardiac death after MI. These findings suggest that the overall variability
159AUTONOMIC DYSFUNCTION AND MODS
of HRV (SDNN) seems to be an accurate predictor of mortality for cardiacpatients. This observation is consistent with the authors’ recent study of pa-tients with MODS [43] in which an attempt was made to find a simple set ofvariables derived from the continuously recorded ECG which could predict28-day mortality. The lnVLF was found to be the best predictor.
The VLF power spectrum depends on parasympathetic outflow [9] butalso contains information on several physiologic variables, including changesin hormonal function, temperature, and vasomotion [4,10]. In a cohort of 52medical and neurologic ICU patients, Yien and colleagues [59] found that thetrend of changes in the power density values of the LF and VLF componentsof systemic arterial pressure and heart rate signals was comparable with dailyAPACHE II scores in predicting death. In 106 patients undergoing abdom-inal aortic surgery, the VLF on the first postoperative day was also the stron-gest predictor of length of stay at the ICU [13,60].
The finding that the lnVLF was the strongest predictor of mortality inMODS patients and had a predictive value similar to the APACHE II scorefor the survival of MODS patients reinforces the physiologic relevance ofthese measurements. Moreover, there is some evidence that decreases inHRV can be reversed by therapeutic intervention [61]. If the hypothesis ofuncoupled organ function is valid, one of the goals of therapy might be torestore autonomic function and thus improve survival in MODS [1].
Autonomic dysfunction in multiple organ dysfunction syndrome
and possible therapeutic implications
In addition to their cholesterol-lowering properties, HMG CoA-reduc-tase inhibitors (‘‘statins’’) have multiple other properties including a modu-lation of autonomic function by preserving parasympathetic tone andprominent anti-inflammatory actions [62]. Almog and colleagues [63]showed that prior therapy with statins was associated with a reduced rateof severe sepsis and ICU admission in patients hospitalized with presumedor documented acute bacterial infection. Hackam and colleagues [64] ana-lyzed 141,487 cardiovascular disease patients and found a lower incidenceof sepsis in patients receiving statins. Liappis and colleagues [65] retrospec-tively reviewed the records of patients who were admitted with gram-nega-tive bacillus or Staphylococcus aureus bacteremia and found that mortalitywas reduced in the group treated with statins. Kruger and colleagues [66]evaluated the association between statin administration and mortality in438 bacteremic patients and found that statins were linked to a significantreduction in mortality and death attributable to bacteremia.
In a recent retrospective cohort, the authors compared 40 patients withMODS (inclusion criteria of ICU admission and an APACHE II scoreR20 at admission) who were on statin therapy with 80 age- and gender-matched MODS patients without statin treatment [61]. The groups werecomparable in terms of demographic characteristics, APACHE II and

160 SCHMIDT et al
SOFA scores, and cholesterol levels on admission. During the analyzed 28-day period, there was a higher number of deaths in the group without statintreatment, suggesting that, in patients with MODS, statins may exert a pro-tective effect. Of note, the parasympathetically mediated variables lnVLFand lnpNN50 were better preserved in the statin group when comparedwith the non-statin group (lnVLF, 4.1 � 1.4 versus 3.2 � 1.3, P ¼ .02;lnpNN50, 0.09 � 1.8 versus 1.2 � 1.8, P ¼ .049). Hence, it might be hypoth-esized that statin therapy influences short-term mortality in MODS patientsby restoring parasympathetic tone, thereby reinforcing the cholinergic anti-inflammatory pathway [40–42].
The mechanisms explaining the associations found in these different stud-ies may be complex. The authors speculate that either or both of the follow-ing mechanisms could contribute to these observations: (1) statins haveanti-inflammatory actions and can modulate coagulation processes duringseptic episodes [67,68]; (2) statins enhance (or mitigate the depression of)parasympathetic activity to limit the propagation of systemic proinflamma-tory responses [37–39,41].
These data and other studies evaluating beta-blockers and angiotensin-converting enzyme inhibitors indicate that the autonomic dysfunction andclinical outcomes in sepsis and MODS can be ameliorated by pharmacologictherapeutic interventions. Nevertheless, prospective trials are needed to con-firm these observations.
Summary
Autonomic dysfunction is associated with the severity of illness and withmortality in patients with MODS and may contribute significantly to thepathogenesis of this syndrome. The association between certain pharmaco-logic treatment approaches and improved outcomes related to sepsis andMODS may reflect modulation of autonomic dysfunction. Nevertheless,the following important questions remain unanswered:
� What are the cellular mechanisms associated with autonomic dysfunc-tion seen in MODS?� Do MODS patients benefit from spontaneous or deliberately inducedimprovements in autonomic dysfunction?� Will the pharmacologic approaches that have been associated with im-proved survival be validated in prospective studies?
The work needed to answer these questions promises to be a compellingfield of critical care research in the years to come.
Acknowledgment
The authors are indebted to D. Monning for her technical help in thepreparation of this manuscript.
161AUTONOMIC DYSFUNCTION AND MODS
References
[1] Godin PJ, Buchman TG. Uncoupling of biological oscillators: a complementary hypothesis
concerning the pathogenesis of multiple organ dysfunction syndrome. Crit Care Med 1996;
24:1107–16.
[2] Abboud FM, Thames MD. Interaction of cardiovascular reflexes in circulatory control. In:
Sheperd JT, Abboud FM, Geiger SR, editors. Handbook of physiology. Section 2: the
cardiovascular system, vol. III. Bethesda (MD): American Physiological Society; 1983.
p. 675–752.
[3] Eyzaguirre C, Fitzgerald RS, Lahiri S, et al. Arterial chemoreceptors. In: Sheperd JT, Ab-
boud FM, Geiger SR, editors. Handbook of physiology. Section 2: the cardiovascular sys-
tem, vol. III. Bethesda (MD): American Physiological Society; 1983. p. 557–62.
[4] Board of the European Society of Cardiology and North American Society of Pacing and
Electrophysiology. Heart rate variabilitydstandards of measurement, physiological inter-
pretation and clinical use. Eur Heart J 1996;17:354–81.
[5] Toweill D, SonnenthalK,Kimberley B, et al. Linear and nonlinear analysis of hemodynamic
signals during sepsis and septic shock. Crit Care Med 2000;28:2051–7.
[6] Seely AJE, Christou NV. Multiple organ dysfunction syndrome: exploring the paradigm of
complex nonlinear systems. Crit Care Med 2000;28:2193–200.
[7] Marshall JC. Complexity, chaos, and incomprehensibility: parsing the biology of critical
illness. Crit Care Med 2000;28:2646–8.
[8] Haji-Michael PG, Vincent JL, Degaute JP, et al. Power spectral analysis of cardiovascular
variability in critically ill neurosurgical patients. Crit Care Med 2000;28:2578–83.
[9] Stauss HM. Heart rate variability. Am J Physiol Integr Comp Physiol 2003;285:R927–31.
[10] Taylor JA, Deborah LC, Myers CW, et al. Mechanisms underlying very-low-frequency
RR-interval oscillations in humans. Circulation 1998;98:547–55.
[11] Lombardi F. Chaos theory, heart rate variability and arrhythmic mortality. Circulation
2000;101:8–10.
[12] HoyerD,FriedrichH,SteinPK,et al.Autonomic informationflow improvesprognostic value
of heart rate patterns after abdominal aortic surgery. Journal of Critical Care 2008, in press.
[13] HoyerD, Frank B, Gotze C, et al. Interactions between short-term and long-term cardiovas-
cular control mechanisms. Chaos 2007;17:015110–1, -015110-8.
[14] La Rovere MT, Bigger JT Jr, Marcus FI, et al. Baroreflex sensitivity and heart rate variabil-
ity in prediction of total cardiac mortality after myocardial infarction. Lancet 1998;351:
478–84.
[15] Bigger JT Jr, La RovereMT, Steinmann RC, et al. Comparison of baroreflex sensitivity and
heart rate variability after myocardial infarction. J Am Coll Cardiol 1989;14:1511–8.
[16] DiRienzoM,Castiglioni P,ManciaG, et al. Advancement in estimating baroreflex function.
IEEE Engineering in Medicine and Biology 2001;20:25–32.
[17] Schmidt H, HeinrothK,WerdanK. Autonomic dysfunction in critically ill patients. In: Vin-
cent JL, editor. Yearbook of intensive care and emergency medicine 1999. Heidelberg (NY):
Springer, Berlin; 1999. p. 519–36.
[18] Maestri R, Pinna GD, Mortara AM, et al. Assessing baroreflex sensitivity in post-myocar-
dial infarction patients: comparison of spectral and phenylephrine techniques. J Am Coll
Cardiol 1998;31:344–51.
[19] PitzalisMV,Mastropasqua F, Passantino A, et al. Comparison between noninvasive indices
of baroreceptor sensitivity and the phenylephrine method in post-myocardial infarction
patients. Circulation 1998;97:1362–7.
[20] ChuaTP, ClarkAL,AmadiAA, et al. Relation between chemosensitivity and the ventilatory
response to exercise in chronic heart failure. J Am Coll Cardiol 1996;27:650–7.
[21] Chua TP, Coats AJS. The reproducibility and comparability of tests of the peripheral che-
moreflex: comparing the transient hypoxic ventilatory drive test and the single-breath carbon
dioxide response test in healthy subjects. Eur J Clin Invest 1995;25:887–92.
162 SCHMIDT et al
[22] Chua TP, Harrigton D, Ponikowski P, et al. Effects of dihydrocodeine on chemosensitivity
and exercise tolerance in patients with chronic heart failure. J Am Coll Cardiol 1997;29:
147–52.
[23] Schmidt H, Rauchhaus M, Francis DP, et al. Assessment of chemoreflex sensitivity in free
breathing young subjects by correction for respiratory influence. Int J Cardiol 2001;78:
157–65.
[24] Schmidt H,WerdanK,Muller-WerdanU. Autonomic dysfunction in the ICU patient. Curr
Opin Crit Care 2001;7:314–22.
[25] Ponikowski P, Banasiak W. Chemosensitivity in chronic heart failure. Heart Fail Monit
2001;1:126–31.
[26] Ponikowski P, ChuaTP, PiepoliM, et al. Augmented peripheral chemosensitivity as a poten-
tial input to baroreflex impairment and autonomic imbalance in chronic heart failure.
Circulation 1997;96:2586–94.
[27] Ponikowski P, Chua TP, Piepoli M, et al. Chemoreceptor dependence of very low frequency
rhythms in advanced chronic heart failure. Am J Physiol 1997;272:H438–47.
[28] HennersdorfM, Perings C,NiebichV, et al. Chemoreflex sensitivity in patients with survived
sudden cardiac arrest and prior myocardial infarction. Pacing Clin Electrophysiol 2000;23:
457–62.
[29] Schmidt H,Muller-WerdanU, Nuding S, et al. Impaired chemoreflex sensitivity in adult pa-
tients with Multiple Organ Dysfunction Syndrome–the potential role of disease severity.
Intensive Care Med 2004;30:665–72.
[30] Hoyer D, Friedrich H, Zwiener U, et al. Prognostic impact of autonomic information in
Multiple Organ Dysfunction Syndrome patients. Int J Cardiol 2006;108:359–69.
[31] Winchell RJ, Hoyt DB. Spectral analysis of heart rate variability in the ICU: a measure of
autonomic function. J Surg Res 1996;63:11–6.
[32] Garrard CS, Kontoyannis DA, PiepoliM. Spectral analysis of heart rate variability in sepsis
syndrome. Clin Auton Res 1993;3:5–13.
[33] Godin PJ, Fleisher LA, EidsathA, et al. Experimental human endotoxemia increases cardiac
regularity: results from a prospective, randomized crossover trial. Crit Care Med 1996;24:
1117–24.
[34] SchmidtH,Muller-WerdanU, Saworski J, et al. Beating rate variability of cardiomyocytes is
narrowed by LPS but not by TNF-alpha [abstract]. Intensive CareMed 1999;25(Suppl 1):59.
[35] Tibby SM, Frndova H, Durward A, et al. Novel method to quantify loss of heart rate var-
iability in pediatric multiple organ failure. Crit Care Med 2003;31:2059–67.
[36] EidelmanLA, PuttermanD, PuttermanC, et al. The spectrumof septic encephalopathy: def-
initions, etiologies, and mortalities. JAMA 1996;275:470–3.
[37] Bolton CF, YoungGB, ZochodneDW. The neurological complications of sepsis. AnnNeu-
rol 1993;33:94–100.
[38] Tobin MJ, Laghi F, Jubran A. Respiratory muscle dysfunction in mechanically ventilated
patients. Mol Cell Biochem 1998;179:87–98.
[39] Hussain SNA. Respiratory muscle dysfunction in sepsis. Mol Cell Biochem 1998;179:
125–34.
[40] Borovikova LV, Ivanova S, ZhangM, et al. Vagus nerve stimulation attenuates the systemic
inflammatory response to endotoxin. Nature 2000;405:458–62.
[41] Tracey KJ. The inflammatory reflex. Nature 2002;420:853–9.
[42] Libert C. A nervous connection. Nature 2003;421:328–9.
[43] Schmidt H, Muller-Werdan U, Hoffmann T, et al. Autonomic dysfunction predicts mortal-
ity in patients withMultiple OrganDysfunction Syndrome of different age groups. Crit Care
Med 2005;33:1994–2002.
[44] Biswas AK, Scott WA, Sommerauer JF, et al. Heart rate variability after acute traumatic
brain injury in children. Crit Care Med 2000;28:3907–12.
[45] Korach M, Sharshar T, Jarrin I, et al. Cardiac variability in critically ill adults: influence of
sepsis. Crit Care Med 2001;29:1380–5.
163AUTONOMIC DYSFUNCTION AND MODS
[46] Agelink MW, Majewski TB, Andrich J, et al. Short-term effects of intravenous benzodiaze-
pines on autonomic neurocardiac regulation in humans: a comparison between midazolam,
diazepam and lorazepam. Crit Care Med 2002;30:997–1006.
[47] Sellgren J, Biber B, Henriksson BA, et al. The effects of propofol, methohexitone and iso-
fluorane on the baroreflex in the cat. Acta Anaesthesiol Scand 1992;36:784–90.
[48] Eriksson LI. Reduced hypoxic chemosensitivity in partially paralyzed man: a new property
of muscle relaxants? Acta Anaesthesiol Scand 1996;40:520–3.
[49] Colosimo A, Giuliani A, Mancini AM, et al. Estimating cardiac age by means of heart rate
variability. Am J Physiol 1997;273:H1841–7.
[50] Pikkujamsa SM, Makikallio TH, Sourander LB, et al. Cardiac interbeat interval dynamics
from childhood to senescence: comparison of conventional and newmeasures based on frac-
tals and chaos theory. Circulation 1999;100:393–9.
[51] Kleiger RE, Miller JP, Bigger JT, et al. Decreased heart rate variability and its association
with increased mortality after acute myocardial infarction. Am J Cardiol 1987;59:256–62.
[52] Mili�cevic G, Lakusic N, Szirovicza L, et al. Different cut-off points of decreased heart rate
variability for different age groups of cardiac patients. J Cardiovasc Risk 2001;8:93–102.
[53] Smyth H, Sleight P, Pickering G. Reflex regulation of arterial pressure during sleep in man.
Circ Res 1969;24:109–21.
[54] Schmidt H, Muller-Werdan U, Hoffmann T, et al. Attenuated autonomic function in mul-
tiple organ dysfunction syndrome across three age groups. Biomed Tech 2006;51:264–7.
[55] Sharshar T, Gray F, Lorin de la Grandmaison G, et al. Apoptosis of neurons in cardiovas-
cular autonomic centres triggered by inducible nitric oxide synthase after death from septic
shock. Lancet 2003;362:1799–805.
[56] Sharshar T, Annane D, de la Grandmaison GL, et al. The neuropathology of septic shock.
Brain Pathol 2004;14:21–33.
[57] Zorn-Pauly K, Pelzmann B, Lang P, et al. Endotoxin impairs the human pacemaker current
If. Shock 2007;28(6):655–61.
[58] Nolan J, Batin PD,AndrewsR, et al. Prospective study of heart rate variability andmortality
in chronic heart failuredresults of the United Kingdom Heart Evaluation and Assessment
of Risk Trial (UK-Heart). Circulation 1998;98:1510–6.
[59] Yien HW, Hseu SS, Lee LC, et al. Spectral analysis of systemic arterial pressure and heart
rate signals as a prognostic tool for prediction of patients’ outcome in the intensive care
unit. Crit Care Med 1997;25:258–66.
[60] Stein PK, SchmiegRE, El-FoulyA, et al. Association between heart rate variability recorded
on postoperative day 1 and length of stay in abdominal aortic surgery patients. Crit Care
Med 2001;29:1738–43.
[61] SchmidtH,HennenR,Keller A, et al. Association of statin therapy and increased survival in
patients with Multiorgan Dysfunction Syndrome. Intensive Care Med 2006;32:1248–51.
[62] Welzig CM, Shin DG, Park HJ, et al. Lipid lowering by Pravastatin increases parasympa-
thetic modulation of heart rate: G alphai2, a possible molecular marker for parasympathetic
responsiveness. Circulation 2003;108:2743–6.
[63] Almog Y, Shefer A, Novack V, et al. Prior statin therapy is associated with a decreased rate
of severe sepsis. Circulation 2004;110:880–5.
[64] HackamDG,MamdaniM, Li P, et al. Statins and sepsis in patients with cardiovascular dis-
ease: a population-based cohort analysis. Lancet 2006;367:413–8.
[65] Liappis AP, Kan VL, Rochester CG, et al. The effect of statins on mortality in patients with
bacteraemia. Clin Infect Dis 2001;33:1352–7.
[66] Kruger P, Fitzsimmons K, Cook D, et al. Statin therapy is associated with fewer deaths in
patients with bacteraemia. Intensive Care Med 2006;32:75–7.
[67] Merx MW, Liehn EA, Janssens U, et al. HMG-CoA reductase inhibitor Simvastatin pro-
foundly improves survival in a murine model of sepsis. Circulation 2004;109:2560–5.
[68] Pruefer D, Makowski J, Schnell M, et al. Simvastatin inhibits inflammatory properties of
Staphylococcus aureus alpha-toxin. Circulation 2002;106:2104–10.