
























































th e mpm 1000 system availab le through - Forgotten Books
332
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of th e mpm 1000 system availab le through - Forgotten Books



MANAGE YOUROFFICEMORE EFFECTIVELYW ITHTH EMPM 1000 SYSTEMAVAILABLETHROUGH
SOUTHERNMEDICALASSOCIATIONSPHYSICIANS PURCHASING PROGRAM
Manage your office mor e
effect ive ly w ith the MPM1000System ava i lab lethrough the Phy s ic ianPu rchas ing Program .
Manag ing your officeshou ldn ’
t be hard ;how eve r , w ith the cu r rentin surance requ i rements and
MPM 1000 S i mp l if i e s Your Pape rw o rkYou w i l l be ab le to reduce the mou n ta i n s of paperwork by u s ing your MPM 1000 system to process a l lyour i n surance , complete your b i l l ing p lus instan f
taneously sort and fi le necessary informa t ion .
MPM 1000 Spe ed s Up Your Ca sh F l owThe MPM 1000 system w i l l increase your dai ly bankdepos its by p rocess i ng a ll your insurance and p a »
t ients’ rece ivab les qu ick ly .
MPM 1000 Imp r o v e s You r Pra c t i c e Mana gem e n tWith the MPM 1000 system you can eas i ly and inte ll igently manage your p ract ice w i th computer gene f
rated reports . Trends and prob lem s a re eas i ly identified so you can take correct ive act io n before theybecome ser ious .
ElYES ! I wou ld l ike more informatio n onMPM 1000
My interests are : D Immed iate D Lo ng term D Please co n tact me for a su rvey1 am a member ofSMAD
Name (Please Pr i n t)Add r ess
Spec i a l t y Off i ce PhoneMail to: CURTIS 1000 lNFORMATlON SYSTEMS
2296 H ende r sonM i ll RoadS u i te 402At la n t a , G eo rg i a 3034 5
the impend ingMed ica r echange s loom ing on theho r izon , it w i l l get mor
d ifficu lt . You shou ld ca l lCu rt is 1000 Info rmat ionSy stems or Southe rn
Med ica l As soc iat ion to findout how theMPM 1000 can
he lp mak e your pract icerunmore effect ive ly .
ON IBMA/TMPM 1000 I s AOne So u rc e So lut ionThe MPM 1000 is a one sou rce so l u t io n . With you rsystem you rece ive al l hardware (IBM or Tex as Instruments) , software , complete five day t ra i n i ng p rogram and respons ive after sale support .
I BM PC /ATAt D i sc o un tBest of al l , these system s are ava il ab le through SMAServ ices , Inc .
, Phys ic ia n s ’ Purchas i ng Program w ithsubstan t ia l d iscoun ts on IBM and Tex as Instrumentequ ipment .
FORMORE INFORMATION , p lease fi l l out the
coupon be low and mail it to Sou thern Med ical Association , or for faster serv ice cal l Sou thern Medica l at(205) 9454 840 or Curtis 1000 Informatio n Systems atBOO-2414 780.

Pub l ished Month ly as the Offic ial Organ of The North Caro l ina Med ical Soc iety ( ISSN -0029- 25 5 9 )

F inancia l new s you have been w ai ting to hear/l
CW ncreas e ml S O
ncome
Ava i lab le to ig ible Members Under Age 5 0Regardles s O ther D isabi l i Insurance
Offic ia l North Caro l ina Med ica l Soc ietyDis ab il ity Income Plan
Endors ed and Recommended S ince 193 9
Protect your“
mos t va luab le as s et, your profes s iona l income
For deta ils or claims se rvice call orwrite :
CRUMPTON COMPANYPROFESS IONAL GROUP INSURANCE
To ll free - 1 6 7 4
ACADEMY CENTERPOST OFFICE BOX 8 5 00DURHAM, NC 2 7 7 07
Account executives : J . S lade Crumpton and Gene G ree r, DurhamJack Feathe rs ton, CharlotteDan Ha ley , G reens boro
390 VOL . 46 , No . 7

naMEDICAL JOURNALfor d octors and the i r patients
Cover photo tak en by Jeremy Sugarman at the hote l Europa
CONTENTSEven Speci a l ist-s Can Be U sefulA Dermato logist Picks Up the Marb lesH emochromatos is An Unusual Arthropath yIntermittent Claud icat ion Due to
Cauda Equina Compress ionAn Unusual Cause of Recurrent Trans ientNeuro logic Defic it
Specia l Ar ticlesA B ig Pai n Between the Smal l ToesMycobacterium Av ium- Intrace l lu l are and
L ung Disease : More of a Prob lem forThose of U s i n the Southeast
Ear ly Diagnos is of Test icu lar CarcinomaSe lf-Examinat ion of the Testic le
Socioeconomic I ssuesNorth Caro l ina Hospital U t i l izat ion
We Can Change !L ea rning Exper iences from UNC.
Renal Autoregulat ion, Drugs ,
and Acute Renal Fai lureL earning About Word sUnderstanding the Pat ient : Med ical Words
the Doctor May Not KnowCa rol ina H is toryConscient ious Objec t ion and C l in ical Care :
A H istory of C iv i l ian Pub l ic Serv iceCamp No . 6 1 at Duke Univers ity , 194 2 - 194 6
Pub l ic H ea l t hProject Ipecac : An Acc ident Preven t ion Program
of the Robeson County Departmen t of H ealthToxic Encoun tersS isyphus on the Rocks Monoamine Ox idaseInh ib itorsBul letin BoardCont inu ing Med ical Educat ionNew Members
L etters to the Edi tor
Cl assified Adver t isementsIndex to Ad vertisers
JUL Y 1985 , NCMJ
vo lume 4 6 , no 7 , July 1985
Claude S . BurtonJohn R. Rice
James 0 . McNamara ,
Lori Pierce and Doug las Sla ter
Marvin P . Rozear and Wa lter G . Wolfe
Richa rd D . Goldner
NormanAda ir
E . Everett Anderson
Wil l iam W. Fore
Wi l l iam B . B lythe
Jeremy Suga rman and Rona ld R. Butters
Louis E . Swanson
and James F . G ifford , Jr .
Thad B . Wes ter
Rona ld B . Mack
393
3 95
3 98
399
403
405
407
4 10
4 13
4 15
4 19
4 2 5
4 29

392
Because you wan tto en t rus t you r pa t ien t s tothe best profess ional care ,
Sa i n t Albans is a log ica lchoice for you r psychiatrirefe rra ls .
Since 1916 , Sa intAlbans Psychia tri c Hospi talhas prov ided a spec trumof ca re for emo t iona ld isorde rs .
Today, we al so offe rspecial ized , ful ly accrediteprograms for adolescents ,a lcoho l ics , and s ubs tanceabusers .We have spec ialprograms for sen ior ad u l tsand t rea tmen t of ea t ingd isorders .And we offe r dayt reatmen t as anal ternat iveto hospi tal iza t ion.
Ca re is prov ided by oumode rn hospi ta l sec l uded al24 hours a day.And al l prog rams and serv ices are approved for B lue Cross ,Med icare , Champus , and mos t comme rc ia l insu rance carrie rs .
At Saint Albans , we ’ve bu i l t our repu tat ion on the t rus t of refe rr i ngphysic ians who wan t the bes t for tpa t ien ts . Tha t
’
s why you can refe rSa i n t Albans w i th confidence .
ged
VOL . 4 6 , No . 7
Private, Not For ProfitPsychiatric CarePO . Box 3608 Rad ford , V irginia 24 1431-800-368 -3468
Active Medical StaffRo l fe B . F i n n .MD . Bas il E. Roebu ck.MD .
Med ica l D i rec to r 0 . LeRoyce Roya l .MD .Dav is G ~ G a r re t t .M-D Mo rgan E. Sco t t . MD .
Hal 0 G i l lespie .M-D Don L .Wes ton , M.D.
0 Pau l H lusko. M-D' Psy chia tric Cons u l tan tRon a ld L .Mye rs.M.D. D.W i l fred Abse .MD .

SCIENTIFICARTICLE
ADermatolog ist Picks Up the Marb les
Claude S . Burton , MD .
“In thefields of observation [ in this instance , afie ld ofpoison ivy] , chancefavors only the mind tha t is prepared .
Quoted by Rene’
Va l lery-Radot in
The L ife of Pasteur ( 192 7 )I see nomore thanyou do , but I have tra inedmyse lf to notice what I see .
Sherlock H olmes
young lady presen ted to our emergency room w ithA dermat it is of both feet and d istal lower extremit ies .
The left ankle was swo l len and hurt w i th mot ion . The rashwas fire engine red and rare petech i ae were scattered hereand there in the ery thematou s les ions . No obv ious ves ic leswere noted but the rash was very wet to touch .
Petech iae and arthri t is suggested co l lagen vascu lar disease . Ah ankl e film was obtained , laboratory stud ies wereordered , and preparat ions were made for jo in t asp irat ion Iwas asked to see the pat ient .The moist , fire- engine red erythema suggested a spon
giotic process such as al lergic contac t dermat itis rather thana vasenl-it ic process . Though there was pain on flexion ofthe ankle , pound ing on the heal and pressure on the jo intspace produced no symptoms , suggest ing that the d iscomfort was in the sk in , not the jo int .H istory revealed the pat ient had been target shoot ing in
the woods over the weekend approx imate ly 24 -4 8 hoursbefore the rash appeared . Due to the warm weather , she hadbeen weari ng open sandals .
From the Divi sion of Derm a tology , Duke Universi ty Medical Center,Durham 27 7 10.
JUL Y 1985 , NCMJ
My d iagnos is of po ison ivy dermat i t is met w ith somesuspic ion in the emergency room . H av ing Ieamed fromA lexander Fisher that the tox ic catecho lamines in po isonivy ox id ize to an inde l ib le b lack ink , I exami ned her jeansand asked if she were wearing them on her shoot ing exped it ion . She said that th is was not the pair and when I explained why I asked ,
she and her girl friend said that the pairshe had been wearing wh i le shoot ing over '
the weekendwere covered w i th b lack spots d istal ly wh ich they hadassumed to be tar ! V igorou s wash ings had fai led to removethe stains
.
H er testimony conv inced the consu lt i ng phys i c i ans ; thel aboratory stud ies and jo int aspirat ion were deferred . She
was treated w ith a short prednisone taper and cal aminelot ion topical ly w i th prompt re l ief .Catecholarnines ox id ize to inde l ib le b lack inks , a discov
ery used w ide ly in the l aundry bus iness . Ind i a marking inkis a good example . The catecho ls of po ison ivy also do th is ,part icu lar ly when the humid ity is low s ince water rap id lyhydrol izes the mo lecu le . When the b lack ox id ized catecho lis found on the sk in or c loth ing of a pat ient w ith al lergiccontact dermat it is , one can be fairly certain of the offend ingagent .

Add itiona l informationava i lab le to the profes s ionon request.
Dlsta Products CompanyDivis ion of Eli Li l ly and CompanyInd ianapol is , Ind iana 4 6 2 8 5
4 201 13 Mid . by El i Li l ly Industrie s , Inc .
Carol ina , Puerto Rico 006 3 0

SCIENTIFICARTICLE
Hemochromatosis An Unusual Arthropa’
thy
John R. Rice , MD .
0 Afte r 12 years with arthritis . the pa tient is found to ha vehemochroma tos is .
THE day
- to-day c l inical prac t ice of med ic ine is at t imested ious and occas ional ly graced w ith the exc i t ing or theunusual . The poss ib i l ity of find ing an exot ic d isease amongthe mundane , the pear l among the oysters , is part of the funand the chal lenge of our profess ion as i l lustrated by thefo l low ing case .A 5 3 -year-old wh i te male insurance broker presentedw i th a complaint of “ art hrit is of twe lve years durat ion .H e had been in exce l lent general heal th unt i l 197 2 at wh icht ime he deve loped acu te , painful swe l l ing in the right knee .
The knee was aspirated , w ithou t examinat ion of the jo intfluid for crystals , and injected w ith cort icostero ids w ithimmed iate re l ief of symptoms . H yperu ricemia was foundon laboratory test ing , a d iagnos is of gou t was presumed andal lopurino l therapy was in i t iated . One year later an effus iondeve loped in the left knee and was treated in s imi lar fash ionw ith sat isfactory results .
Five years after the episodes of knee effus ion , painfu lswe l l ing deve loped in the metacarpophalangeal jo ints ofthe midd le and ring fingers on h is right hand . The painresponded in it ial ly to local inject ion bu t recurred and pers isted in spi te of attempts at therapy w ith al lopuri no l ,a sp ir i n and v ar iou s non - s te ro ida l an t i - i n fl amma toryagents . A l lopurino l was even tual ly d iscont inued . In 1982 ,
ten years after the onset of symptoms , h is ank les becamesomewhat swo l len and painfu l , pers istent knee st iffnessbecame an increas ing prob lem and the pat ient complainedof st iffness and d iscomfort in the left hand in a patterns imilar to that seen in the ri ght .L aboratory stud ies by his phys ic ians at home had lnc luded a rheumato id factor of 1 12 80 (RA latex ) and milde levation s of l iver funct ion stud ies were attributed to lowgrade alcoho l consumpt ion . Other than a h istory of recurring prostat it is and non- specific urethri t is in the past therewas no h istory to spec ifical ly suggest rheumato id arthri t is ,other connect ive t issue d isease or spondy loarthr it is . Thepat ient ’ s family h istory included an episode of podagra inh is father and a brother w ith a d iagnos is of hypoparathyroidism estab l ished at the Mayo C l in ic .Phys ical find ings were normal w ith the except ion of the
jo ints . Minimal fu l lness was present over the index andmiddle metacarpophalangeal jo ints of the right more thanthe left hand and a suggest ion of soft tissue fu l lness waspresent in the left ank le . Other peripheral jo ints and theFrom the D i v i s ion of Rhe uma tology and Immu no logy . D u ke Un i vers i tySchool of Med i c i ne , D urham 27 7 10 .
JULY 1985 , NCMJ
Approx imate ly 50% of pat ients w ith hemochromatos isdeve lop an arthropathy in conjunc t ion w ith other manifestations of the d isease . Jo int symptoms most commonlypresent s imultaneous ly w ith other manifestat ions of thed isease but may occur a decade or more in advance of othersymptoms ? 3
Cl inical and rad io logical features of thed isease are d ist inc t ive enough to al low the alert phys ic ian tosuspect the d iagnos is of hemochromatos is and order tests toestabl ish the d iagnos is .
H emochromatos is i s an uncommon d isorder characterized by excess ive iron absortion in the gu t . Ev idencepo ints to an au tosomal recess ive mode of inher itance w i than est imated gene frequency of C l in ical man ifestat ions deve lop as a result of the gradual accumulat ion of iron
spine were unremarkab le . There were no subcutaneousnodules present and no sk in or nai l fi nd ings to suggestpsorias is .
L aboratory stud ies usual ly obtained in pat ien ts w itharthri t is were normal , inc lud ing a repeat rheumato id factor .
The serum ur ic ac id had been reduced to mgm% byaspirin . L iver func t ion stud ies were remarkab le for a s l ighte levat ion in SGOT and SGPT .
H and x-rays ( see fi gure 1 ) showed smal l osteophytes atthe metacarpophalangeal art icu lat ions of the second and
th ird d ig its b i lateral ly . S l ight jo int space narrow ing waspresent at the th ird metacarpOphalangeal jo int b i l ateral lyw i th a suggest ion of assoc iated increase in subchondralbone dens ity in the respect ive prox imal phalanges . Ank le
fi lms ( not shown ) showed minimal degenerat ive change atthe calcaneonav icular art icu lat ions b i l ateral ly ; the sub talarand t ib iotalar jo ints were normal . Knee fi lms were not fe ltto be ind icated .
Subsequen t stud ies inc luded a serum ferr it in value greater than 2000 ng% ( normal range in adul t males 3 1-294ng%) and a serum iron of 2 3 8 mcg% w ith a total ironb ind ing capacity of 240 mcg% . L iver b iopsy ( see fi gure 2 )showed marked iron depos it ion w ith in hepatocytes , mostprominent in the portal areas , w ith only sparse amounts ofiron w ith in Kuppfer ce l ls . The changes were cons isten tw i th hemochromatos is . A t the t ime of d iagnos is there wasno sk in hyperpigmentat ion and no ev idence of endocrine ormyocard i a l dys func t ion . Therapy wa s i n i t i a ted w i thb iweek ly ph lebotomy and non - stero idal ant i- inflammatorydrugs were con t inued in hopes of min imiz ing jo in t complaints .
Discu s sion

in the parenchymal ce l ls of various organs inc lud ing thel iver , endocrine organs , sk in , jo ints and heart . 5 ' 6 Approximate ly 90% of c l in ica l ly apparent d isease deve lops inmen ; menstrual b lood loss has been postulated to de l ay orame l iorate the deve lopmen t of recognizab le d i sease inwomen . A lcoho l consumpt ion or heavy d ietary ingest ion ofiron may hasten the onset of symptoms . Most pat ientspresent between 40 and 60 years of age w ith bronze ors late- gray cu taneous hyperpigmentat ion , c irrhos is and endocrine dysfunct ion , inc lud ing d iabetes and hypogonadism . Myocard ial invo lvemen t may produce congestiveheart failure . Diagnos is is made by l iver b iopsy show ing , asin the case described above , an abnorm al accumulat ion ofiron in hepatocytes . B iopsy late in the course of untreatedd isease may show c irrhos is . Managemen t centers on thereduct ion of iron stores through regular ph lebotomy w ith agoal of normal iz ing serum iron leve ls and maintain ing ahemoglob in leve l of approx imate ly 1 1 gm% .
7 If in it iated atan early stage of the d isease , therapy may prevent hepat ic ,endocrine and myocard ial dysfunct ion or improve funct ionin affected organs .
The arthropathy of hemochromatos is has been we l l described by several authors” s ince the orig inal report bySchumacher in 1964 .
‘ 2 The characte rist ic c l in ical pic ture isessent ial ly that of osteoarthri t is w i th an atypical and characteri stic pattern.
8 Involvement of the 2nd and 3rdmetacarpophalangeal jo ints w ith loss of jo int space , subchondralsc leros is and osteophyte format ion is the s ingle most suggestive fi nd ing . Subcort ical cyst- l ike changes may occurand d iffuse osteopenia may deve lop bu t the characterist icper iart icu lar osteoporos is of rheumato id and other ihfl ammatory forms of arthr it is is lack ing as are marginaleros ions . H ypertroph ic arthr it is of the interphalangealjo ints , lack ing en tire ly in some pat ients , is indistinguishab le from other more common form s of degenerat ive jo intd isease but tends to invo lve the prox imal rather than thed istal interphalangeal jo ints . L arge jo ints inc lud ing thewrists , e lbows , shoulders , h ips , knees and ank les may be
affected although the earl iest changes are usual ly seen inthe smal l jo ints of the hand .
The arthropathy of hemochromatos is is s imi lar in manyrespec ts to that seen in calc ium pyrophosphate depos it iond isease (CPPD) , both the “ id iopath ic” form and that seenin assoc iat ion w i th a variety of metabo l ic d isorders . Inapp rox ima te l y 5 0% o f pa t ie n t s w i t h a rth r i t i s and
hemochromatos is , chondrocalc inos is may be found on xray in locat ions characterist ic of CPPD the hyal ine andfibrocanilage in the knees , the tr iangul ar cart i l age d istal tothe ulnar sty lo id , the fibrocart i lage at the symphys is pub isand occas ional ly in the h ips or intervertebral d iscs .
8 ' 9 Notal l of these pat ients have jo int symptoms . Acute episodes ofpseudogout may occur , most frequen tly in the knees , andhemochromatos is should be part of the d i fferent ial diagnos is oi any pat ient w i th e ith er chondrocalc inos is or pseudogout even ih the absence of obv ious changes in the smal lhand jo ints .
The pathophys io logy of the jo int d isease in hemochromatosis has not been we l l defined . Iron depos i t ion in thesynov ium is a re l at ive ly non- spec ific find ing , hav ing beendescribed in rheumato id arthri t is , transfus ion hemosideros is
,hemoph i l i a
,pigmen ted v i l lonodul ar synov i t is and
other d isorders .
8 Iron accumulat ion in hemochromatos isoccurs
,however
,in Type B synoviocytes and poss ib ly in
chondrocytes in d ist inct ion from the above l isted d iseasesin wh ich the depos its accumulate primari ly in the phagocytic Type A synov ial ce l l s . The occurrence of s imi lar jointd isease in experimenta l animals given a sustained ironoverload and in some pat ients w ith transfus ion hemosideros is supports the putat ive ro le of excess ive iron stores inproducing the art hropathy of hemochromatos is .
9
Therapy,as noted above , cons ists of a removal of exces
s ive iron stories v ia repeated ph lebotomy . Prevent ion of orimprovement in organ dysfunc t ion can be ach ieved w ithappropriate management bu t there is l itt le effect on theassociated jo in t d iseases .
” L oss of chondrocytes , ce l lsw ith l itt le or no regenerat ive propert ies , as a result of the
F igure 1 .X-rays of the right hand showing sma l l osteophytes at the second and third
metacarpopha langea l j oints (arrows) with narrowing of the third metacarpopha
langea l j oint space .
396 VO L . 46 , No . 7

F igure 2 . L iver biopsy showing mass ive accumulation of iron in hepatocytes with sparing of Kuppfer cel ls . Specia l sta ins (not shown)confirmed the ferrous na ture of the deposits .
toxic effects of iron may accoun t in part for th is observat ion . Iron inh ib it ion of pyrophosphatase has been proposedas an explanation for the occurrence of chondrocal cinos isand pseudogout in some patients .
13
References
1 . Dymock IW, Hami l ton EBD, Laws JW , et a] .Arthropa thyof hemochromatos i s .Ann RheumDis -4 76 .
2 . M'
SeffarA, Fornas ier VL , Fox IH . Anhropath y as th emajor cl i n ical i nd icatorof occul t iron s torage d i sease . JAMA l 97 7 ;2 38 : 1825 - 1828 .
3 . Rosner 1A, As kari AD, McLaren GD . et al . Arthropa thy . hypouri cemi a andnorma l serum i ron s t ud i es in hered i tary hemochroma tos i s . Am J Med198 1 -87 4 .
4 . Cartwri gh t GE , Edwards CQ .Krav i tz K , etal . Hered i tary hemochromatos is . NEng] J Med - l 79 .
5 . Finch SC , Fin ch SA. Idiopa thic hemochroma tosis. an iron storage disease .Med195 5 3 4 13 8 14 30 .
JULY 1985 , NCMJ 397
6 . Milder SM. Cook JD, Ranch CA. Idiopa thic hemochroma tosis , an in terimreport . Med 19805 93 44 9 .
7 . FreyWG , M i lne J , Johnson GB , et a] . Manageme n t of fami l ial hemochromatosis . N Engl J Med l 96 1 ;265 :7 - 12 .
8 . Hirsch IH . Kil l ien PC , Troupin RH . The arthropa th y of hemochromatos is .Radiology 1976 ;1 18 :59 l -596 .
9 . Twersky J . Jo in t changes in idiopathic hemochroma tos is . Am J Roentgenoll 97 5 ;124 : 139- 144 .
Askari AD.Mu ir WA, Rosner 1A, et a] . Arthri ti s of hemochroma tos i s . Clinicalspec trum. re la t ion to his tocompa tib i l i ty antigens and effecti veness of earlyphlebotomy . Am J Med -965 .
Fox IH .Arthropathywith iron storage di sease . InKellyWN , Harris ED , RuddyS . et al (eds) . Textbook of Rheumatology . W.B . Saunders Co Phi ladelphia .
- 1544 .SchumacherHR J r . Hemochromatos is and arthriti s .Arthri ti s Rheum50 .
McCarty DJ , Pepe PF , Solomon SD et a] . Inhibition of human erythrocytepymphosphatase acti v ity by calcium. cupn
'
c and ferrous ions Arthri tisRheum l 970; l 3 :3 36 .

SC IENTIF IC ARTICLE
Intermittent Claud ication Due to
Cauda Equ ina Compression
James O . McNamara , M .D. , L ori Pierce , MD . and Douglas S later , MD .
0 Apatientwithpa in in his legs when he s tood , rel ieved complete ly when hesat, is cured .
e recent ly evaluated a 60- year-old man w ith an intriW guing conste l lat ion of symptoms . He was we l l un t i lone year prev ious ly when he deve loped dul l ach ing pain inh is h ips prec ipitated by walking 6 -9 b locks . The pain remitted w ith rest . During the fol low ing three months he not icedthe pain after walking shorter d istances and even tual ly aftermere ly stand ing for as long as one minute . The pain wouldinvariab ly remi t w ith in 20- 30 seconds after he sat down .The pain was always b i lateral
,occas ional ly progressed
from the h ips to the th ighs and even the calves . On oneoccas ion the pat ient cont inued to walk in spite of the painand experienced weakness of both legs and fe l l . There wasno h istory of pa in or weakness e lsewhere
,nor of bowe l or
b ladder incont inence . There was no h istory of hypertens ion , d iabetes , or myocard ia l infarc t ion . The past med icalh istory , family h istory , and rev iew of systems prov ided noinformat ion essent ial to understand ing the present i l lness .
The pat ient ’ s v ital s igns were w ith in normal l imits . H is
general phys ical and neuro logical examinat ions were alsow ith in normal l imits . In part icul ar , al l of h is pulses . werefu l l inc lud ing the femoral
,popl iteal
,posterior t ib ial
, and
dorsal is ped is pulses . No bru its were detec ted . The sk in ofthe lower extremit ies showed no atr0phic changes . Analsph incter tone was normal . Motor and sensory examinat ions of the lower extremi t ies were also w ith in norm all imits . H is musc le stretch refl exes were 2 and symmet
rical and no Bab insk i s igns were present . The responses toboth Patrick ’ s maneuver and straight leg rais ing were normal . At the request of the phys ic ian , the pat ient walkedsuffi c ient ly far to precipitate h is pain ; the vascu lar andneuro logic examinat ions of the lower extremit ies remainedw ith in normal l imi ts in the presence of the pain .The presence of pain induced by standing and its re l iefbychange in posture together w ith the negat ive find ings on thevascular and neuro logic examinat ions suggested the diagnos is of in termittent Claud icat ion due to compress ion ofthe cauda equina . A CT scan of the Iumbosacral spined isc losed a spinal stenos is mainly at L 3 -4 ; the stenos is wasdue to narrow ing of the bony canal w ith hypert rophy of thel igamen tum flavum poster iorly , and a marked posteriorbulging of the L 3 -4 intervertebral d isc an terior to the canal .From the D i v i s ion of Ne urology , D u ke Un iversi ty Med i c a l Center,D u rham 27 7 10.
398 VO L . 46 , No . 7
A mye logram was performed after introduc t ion ofmetrizamide at the L l - 2 interspace . The caudal flow of metrizamide was complete ly b locked at the L 3 -4 interspace w iththe pat ient in the stand ing pos ition . The contrast did fl owcaudal ly past the b lock after the pat ient was placed in thes i tti ng pos it ion .The rad iograph ic find ings were confirmed at the time of
surgery . A lumbar laminectomy was performed at L 3 -4
together w ith removal of the intervertebral d isc . The patient
’
s symptoms remitted prompt ly after surgery .
The term “ c laud icat ion ’ is derived from the L at in verb ,claud ica re , wh ich means to l imp . The intermittent natureof the symptoms is str iking and crucial to the d iagnos is , andt he re fore the te rm inte rmi ttent C l aud i c a t ion s eem sappropriate . The vast majori ty of cases of in termittentC laud icat ion of nervous system or ig in (versus vascul ar intermittent Claud ication ) are re lated to compress ion of thecauda equina . Thus the term “ intermittent Claud icat ion dueto cauda equina compress ion seems the most appropriatet it le of th is syndrome and preferab le to the popular altema
tive , neurogen ic Claud icat ion .The precise pathophys io logy of the symptoms is unknown . The striki ng re lat ionsh ip of the symptoms to posture and the stereotyped temporal reso lut ion of symptomsfo l low ing change in posture are cr it ical c lues not only to aneurogenic rather th an a vascular orig in , but al so to theunder ly ing pathophys io logy . A var iety of degenerat ivebony and cart i laginous abnormal it ies superimposed on adeve lopmental ly narrow canal lumbar spinal stenos is ) comb ine to marked ly narrow the lumbar spinal canal .
The erect posture presumab ly prec ipitates the symptomsbecause the sagittal d iameter of the l umbar canal normal lynarrows in the extended pos it ion and w idens in the flexedpos it ion . The interac t ion of phys io logic narrow ing re latedto posture together w ith the patho logic narrow ing due to thefactors l isted above is suffic ient to compress the caudaequina . Perhaps compress ion of the arterial or venous c irculat ion of the root together w ith the increased vascu lardemands of nerve t issue ( re lated to exercise or maintenanceof the erect pos it ion) may interact to produce the symptoms . In any even t , surgical decompress ion leads to promptreso lut ion of the symptoms in properly d iagnosed cases .
Th is outcome prov ides a happy end ing for the pat ient , thed iagnost ician , and the surgeon .

SC IENTIF IC ARTICLE
An Unusual Cause of Recurrent Transient
Neurolog ic Deficit
Marv in P. Rozear , MD . and Walter G . Wo l fe , MD .
0 A rheuma tolog ist uncovers a rare card ia c condition in a woman with
TIAs .
fifty- year-old'
,right- handed bookkeeper was in exce l
lent health unt i l the fi rst week in January 1985 . Wh i lechanging clothes she noted an ach ing pain in her left armfo l lowed by a rash on the palm and forefinger , wh ich d idnot b lanch . A few days later wh i le talk ing on the phone , herleft hand fe l t weak and c lumsy w ith t ingl ing wh ich spreadinto the leg
,lasted several minutes and abated spontaneous
ly . The next dayl she had a splotchy red rash on her handagain . The fo l low ing week wh i le eat ing breakfast her ent ireri ght s ide fe lt numb and weak , her speech became s lurred ,
and she had d iffi cu lty gett ing the ri ght word out for 4 5minutes . She had d i fficu lty walk ing x
for several hou-rsz—Thenext day she had a s l ight rash on
"
her ri ght hand . Her
internist obtained an EKG ,head CT, and an M-mode
‘echocard iogram . She was d iagnosed as hav ing vascul it isand was started onDipyramidole and aspirin . A neuro logistexamined her and agreed w ith the treatment . A few dayslater wh i le dress ing she noted z igzag l ines” to her left fora few seconds fo l lowed by a left- s ided headache . Th isrecurred . She noted rash in both hands wh ich came andwent , last ing for a few days . On the day of admiss ion shewas eat ing breakfast when she suddenly passed out w ithoutwarn ing
,convuls ive ac t iv ity or any other specific features .
At her local hospital shortly thereafter her examinat ion wasnormal and she was transferred to Duke Hospital . H er pastmed ical h istory was unremarkab le . She was a nonsmokerand had had no prior symptoms of any card iac , vascu lar ,pulmonary or neuro logic d isease .
On examinat ion b lood pressure was 1 in both arms .
From the D i v is ion of Neurology and Department of S urgery , D u ke University Medic al Center, D urham 2 7 7 10.
JUL Y 1985 ,NCMJ 399
Pul se was 7 0 and regu lar . She was afebri le . Generalphys ical exam was normal except for a cluster of nontender , nonblanching erythematous spots measuring three tofour mil l imeters over the ulnar border of the left palm .
Neuro logic exam showed mi ld c lums iness of the left fingers and no other s ign ifican t find ings .
Short ly after the admiss ion she experienced another spe l lof c lums iness of her right hand and had d ifficu lty speak ingwh ich lasted one to two minu tes . The rheumato logy consultant recommended a 2 -D echocard iogram wh ich re
vealed a 2 x 3 x 2 cm left atri al mass w ith ge lat inouscons istency
,compat ib le w i th a left atrial myxoma .
Because she had experienced another TIA on that day ,
surgery was recommended immed iate ly , and the myxomawas removed w ith in 6 hours of its d i agnos is . The pat ientto lerated the procedure we l l , and was d ischarged w ith nofurther d ifficu lt ies .
Frequent ly in the evaluat ion of cerebrovascu lar insufficiency the workup focuses en t ire ly on the carot id system .
There is some reason for th is , as carot id stenos is/ulcerationis certainly the most common treatab le cause for carot idsystem TIA . H owever , when attacks involve both hemispheres intermittent ly in an otherw ise heal thy , re lat ive lyyoung
,nonsmok ing person w ith or w ithout carot id b ruits ,
other causes must be sought . Cerebral vascu l it is is certain lyone of these rare causes of cerebrovascu lar insufficiency iAtri al myxoma is among the rarest of causes of cerebrovascular insufficiency . In fac t it is so rare that some havestated that in a pat ient w ith TIAs , if the card i ac exam isnormal , echocard iography is not cost effect ive in the workup . The proponents of th is type of th ink ing might haved ifficulty conv inc ing th is patient or her fami ly of th is ph ilosophy .

TH IS SPACE CONTRIBUTEDAS APUBL IC SERVICE
There is evidence that dietand cancer are related . Somefoods may promote cancer, whileothers may protect you from it .
Foods related to lowering the risk of cancer of thelarynx and esophagus all havehigh amounts of carotene ,a form ofVitaminAwhichis in can tal oupes
,peaches
,
broccoli,spinach
,al l dark
green leafy vegetables,sweet
potatoes,carrots
,pumpkin
,
winter squash and tomatoes ,citrus fruits and brusselssprouts .
Foods that mhelp reduce the riskof gas trointestinaland respiratorytract cancer are
cabbage,broccoli
,
brussels sprouts,
hlrab i , cauliflower.
Fruits,vegetables
,and whole
grain cereal s such as oatmeal,bran
and wheatmay help lower the riskof colorectal cancer.
Foods high in fats,salt or
ni trite- cured foods like ham,and
fish and
types of sausages smoked by traditional methods should beeaten inmoderation .
Be moderate inconsumption of alcohol al so .
Agood rule ofthumb is cut down onfat and don ’ t be fat.
Weight reductionmaylower cancer risk . Our
2 year study ofnearly amillionAmericans uncoveredhigh cancer risks particularly
among people 40% ormoreoverweight .Now ,
more than ever,we
know you can cook up your owndefense agains t cancer. So eatheal thy and be healthy
N0 one faces

5 mg 10mg 2 0mg
Chewab le Tab le ts Oral Swa l low"Tab le ts
© 1985 IC Im emo sme See following pag e [or br ief summary ofp r escr ib i ng i nforma t ion.

(ISOSORBIDEDINITRATE)Pian ooom lt full prescribing infommlonbefore use .Asummary folkmo
INGCATIONSANDUSAGE: SORBI‘TRATE ( isosorb ide d in itra te) is ind icated forthe tre atmentand prevention of ang ina pectoris All dosage formsof isosorb ide d in itratemay be usedprophyl act ica l ly todec re ase freq uencyand seve r ityof ang ina l attacks and can be expec ted todec rease the need forSub l ingual n i trog lycerin.The Sub l ing ua l and chewable lorrns ofthe d ru g are ind ica ted foracute pro phy lax is of ang ina
pec tor iswhen taken a fewminutes be fore situat ions l ike ly toprovoke ang inal at ta cks. Becauseof aslower onse tofeffec t , th e ora l formsof isosorb ide d in itrate are not ind icated foracuteprophylax is.OON
'
TRAINDfCATIONS : SORB ITRATE is contra ind icated inpatien tswhohave shownpu rported hypersen si tivi tyor id iosyncrasy toit orothe r n itra tesorn i tri tes.Epinephrine andre lated compounds are ineffec t ive in re vers ing the severe hypotens ive events assoc iated wi thoverdose and are contraind ica ted in th is s ituationWARN INGS: The benefits ofSORB ITRATE du ri ng the early daysof an acmemyocard ia linfa rct ion have notbeen establ ished . Ifone e lects to use org an ic nitrates in early infarc tion.
hemod ynamicmonitor ing and f re quent c l in ica l assessment shou ld be used bec ause ofthepoten t ia l de le teriousef fec ts ofhypotens ion.PRECAUTIONS: Gene ral: Seve re hypotens ive response.pa rticu larlywi th upright postu re .mayoccurwi th even sma l l doses ofSORBI‘ ITlATE. The d rug shou ld therefore be used with caut ion inSubiecls whomay have blood volume deple t ion fromd iure tic therapyor in subjec tswhohavelow systol ic blood presswe (eg .below90mmHg). Para dox ica l b radycard iaand increasedang inapec tor ismay accompany n i trate-induced hypotension.N i trate thera pymay aggra vatethe ang ina caused by hypertroph ic card iomyopalhy.Mark ed symptomat ic.or thostat ic hypotension has been report ed when ca lc iumchanne l
blocke rs and organ ic nit rateswere used in comb inat ion.Dose adjustmen t ofe i ther c lass ofagents may be necessary.Tolerance to this d rug and cro ss-tolerance toother n itrates and n itri tesmayoccur.Tolerance
toth e vascu lar and antianginal ef fec ts of isosorb id e d in itrate orn itrog lycerin has beendemons trated in clin ical trials, experience throughoccupational exposwe. and in isolatedt issue experimen ts in the laboratory.The impor tance of tolerance tothe appropriate use ofisosorbide d in i tra te in themanagement ofpatientswith ang inapec toris has notbeendeterm ined However.one c l in ica l tri a l using treadmfil exerc ise tolerance (as an end point) foundan 8-hour du ration of ac tion ofora l isosorb id e d in i tra te fol lowi ng the first dose (af ter a 2 -weekplacebowashout) and on ly a 2 -hou rdu ra t ion ofe f fec t ofthe same dose af ter 1week ofrepe t itive dos in at convent iona l dos ing in te rva ls.Onthe other hand , severa l tr ials have beenable tod if fere n iaie isosorbide d initra te f romplaceboafter4 wee ksof therapy and . inopentrial s. aneffec t se ems detec tab le foras long as severa lmonths.Tolerance c learlyoccurs in industrialworkers cont inuous lyexposed ton i troglyceri n.Moreover.phys ica l dependence a lsooccurs s ince chestpa in.acutemyocard ai infarc t ion , andeven Sudden dea th have occu rred during tempora rywithd rawalof n i trog lycerin fromthe
workers. Inc l in ica l tr ia l s in ang ina pat ien ts. the re are repor ts of ang ina l at tacks be ingmoreeashy provoked and ofre bound in the hemodynamic ef fec ts soon after n itra tewithd rawal .There lat ive impor tanceof the se obse rvat ions toth e routine, c l in ical use of isosorb id e d in itrate isnotknown.However, it seems prudent tog radual lywithd rawpat ients fromisosorb id e d in itratewhen the therapy is be ing term inated . ra ther than stopping the d ru g ab ru pt ly.Information forPatients : Headachemayocc ur dur ing init ial therapywith SOFlBITFtATE.
Head ache rs usua l ly re l ieved by the use of s tand ard head ache remed ies orby lower ing thedose and tends tod isappear a ft er the firstwee k ortwoof use.!Drug Interactions : Alcoholmay enhance anymarked sensitMty tothe hypotensive effect of
mra teS.
Isosorb ide d initra te acts d i rectlyonvascu lar smoothmusc le: there fore. anyother agent thatdepends onvascu lar smoothmusc le as the f ina l common path can be expec ted tohavedec re ased or increa sed effec t depend ing onthe agent.Ca rcinog enesis.Mutagenes ls , lmpeirmemof Fe rti l ity :No long-term stud ies in an imals
have been per formed toeva luate the carc inog en icpotential of this drug.Amod if ied two~ litterre produc t ion study in rats fed isosorb id e d in i tra te at 25 or100mg/kg/dayd id nol reveal anyef fec tson fe rti l ityorgestat ion oranyremark able g rosspa thology in anyparentorof fspri ng fedisosorb ide d in i tra te as compared wi th rats fed a basa l-contro l led diet.Preg nancy CategoryC: lsosorb ide d in i trate has been shown tocause adose-re latedincrease in embryotoxlcriy (i nc re ase inmummified pups) in rabb i ts at ora ldoses 35 and 150t imes themax imumrecommended human dai lyclose. There are no adequate and
welhcontrolled stud ies in preg nan twomen. SORBITRATE shou ld be used du ring preg nancyon ly if the poten t ia l benefi t just ifies the potentia l risk tothe fe tus.NursingMothers: It isnotknownwhether this drug is exc re ted in humanmi lk . Becausemany d rug s are exc re ted in humanmi l k , cau t ion shou ld be exerc ised when SOFlBITRATE isadmin iste re d to a nurs ingwoman.Ped iatric Ib o: The safetyand effectivenessofSORB ITRATE in ch i ld re n has notbeenesta bl ished .
ADVERSE Rem us Adverse re actions.par t icu larly headache and hypotens ion. aredose re lated. Incl in ical tr ials at variouscloses. the followrn have bee n ob served :Headache is th emost common (re por ted inc id ence va eswide ly, apparent lybe ing
dose re lated .with an average occu rence of about adverse react ion andmaybe severeand pe rs istent.Cutaneous vasod i lat ionwi th f lush ingmayocom.Trans ient episodesofd izz iness andweak ness. aswe l l as other signsofcerebral ischemia assoc iated wi thpostu ra lhypotension ,mayoccas ional lydeve lop (the inc id ence of repor ted symptomat ic hypotensionranges from2% to Anoccasiona l ind ualwi l l exh ibitmarked sensi t ivity tothehypotens ive e f fec tsofn itra tes and seve re re sponses (nausea.vomit ing.weakness. re st lessness.pal lor.perspi ra t ion , and col lapse)mayoccur evenwith th e usua l therapeut ic dose.Dru grash and/or exloliative dermat i t ismayoccas iona l lyoccu r. Nausea and vomit ing appear tobeuncommonCase reportsofc l in ica l lys ign ificantmelhem ‘ nemia are ra re at convent iona ldosesoforg an ic nitrates.The form at ion ofmethemog lobin sdose-re lated and. in th e case ofgenet ic abnorma l i t iesofhemog lob in that favormethemog lobin forrnal ion. even convent ionaldosesoforg an ic n i trate cau ld produce harmful concentra t ionsofmethemog lob in.DOSAGEANDADMIN ISTRATION: Forthe treatment ofang ina pec tori s. the usua l star ti ngdose forSub l ingua l SORBITRATE is to5 m
gérl
rg‘rchewab le tab lets.5 mg: forora l (swa l lowed )tab le ts. 5 to20mg: and forcontrol led -re lease s, 40mg.
SORBFTRATE shou ld be ti tra ted upward unt il ang ina is re l ieved ors ide ef fec ts l imi t the dose.Inambu latory pat ients. themagn itude ofthe incrementaldose increase shou ld be gu id ed bymeasu remen tsofs tand ing blood pres swe .
The in it ial dosageofsubi in ua l orchewable SORB ITRATE forprophylactic therapy in ang inapector ispalients is genera l lygor 10mg every 2 lo 3 hours.Ad eq uate contro l led cl in ica l stud iesdemonstrating the effec t ivenessofch ro n icmaintenance th erapywi th these dosage formshave notbeen repor ted .
SORBfi FlATE inora l dosesof 10to40mg g iven every6 hoursor inora l control led -re leasedosesof40 to80mg g iven every8 10 12 hours isgenera l ly recommended . The ex tent towhichdeve lopmen t of tolerance should mod ify the dosage prog ramhas notbeen def ined .The oralcon tro l led -re lease forms of isosorbid e d initra te should notDOSAGEM MSAVAILABLE: Subl ingua lTab lets 5 . 10mg):Chewab leTab lets (5 10mg):Ora l Tab le ts (5 . 10.20. 30. 40mg).SustainedAc t ionTab le ts (40mg )
STR-22 8 2

Figure 2 .A. This represents the soft corn ( reactive prol iferation of epidermis) that ha s formed as a response to pressure and irrita tion
between irregular bony prominences at thefourth andfifth toes . B . Asma l l pad , pos itioned dista l to the clavus , rel ievespressure over the
bony prominence and can decrease symptoms in early les ions . C . Bony prominence at the base of the prox ima l pha lanx of thefourth toe
(shaded) canbe surgica l ly excised to rel ievepressure causing the clavus . The clavus itself on the l ittle toe) wil l usua l ly disappear after thisofiend ing prominence is removed . D . Ultima te treatment is to excise the exos toses a t both toes (shaded) , to remove the involved skin
between the toes and to suture the skin so as to close the involved portion of the web .
rigid , more painful . The ultimate treatment is to excise theirregular bony prominence caus ing the pressure , to removean el ipse of skin containing the clavus often between theinner border of the l ittle toe and the inner border of thefourth toe , and to suture the remaining sk in (figure 2D) .Thus a portion of the web between the two toes is joined(partial syndactyly) . By ex'cis ing the bony prominences andby removing the compressed skin between the two toes , noclavus can form and pain is el iminated .
Al though not a complex procedure , the operation should
be done when the p'
atient canavoid a greatdeal ofwalk ing ,
jogg ing , or wearing snug shoes for at least three month s .
Discussion
Treatment is sometimes delayed by failure to recognizethe les ion as a clavus . In feet with excess ive moisture ,
404 VOL . 46 , No . 7
maceration canoccur betweenthe toes and the soft corncanbe mistaken for a fungal infection. F issures and other skinproblems can result from improper use of a variety of
drugs . Scar tissue and infection from improper treatment
can al so compl icate the diagnosis .
Although its surgical treatment is not complex , cautionmust be used in patients with such prob lems as peripheralvascular disease or d iabetes mel l itus because heal ing maybe delayed and the ri sk of infection increased .
The clavus , or soft com , canbe apainful les ion thatdoesnot require elaborate diagnostic tests or procedures . It is an
entity that should be able to be diagnosed initial ly by thefami ly physician . If el imination of the les ion is desired anorthopaedic surgeon shoul d be consul ted . Although
seemingly inconsequential , the d iagnos is and treatmentrequire care and caution.




(PROPRANOLOLHCI)L
assie
BRIEF SUMMARY (FOR FULL PRESCRlB /NG INFORMATION. SEE PACKAGE C IRCULAR )INDERAU LA brand of propranolol hyd roch loride ( Long Ac ting Ca ps ule s )DESCRIPTION. tnderal LA is formulated to provide a Sustained re lease 01 propranolol
hyd roch l0 rid e Inderal LA is avai lab le as 80 mg 120 mg and 160mg capsules .
C L INICAL PNANMACOLOGY. INDERAL is a nonse lective be ta ad rene rg ic receptor
b loctung agent possess ing no other autonomic nerv0 us sys tem activity. It speCi l ically com
petes with beta-
_
ad renerg ic receptor stimulating agents tor ava i lab le receptor S ites . Whenaccess to beta-receptor s ites is b locked by INDERAL the chro notropic inotropic and
vasodilator re sponses to beta ad renerg ic stimulation are decreased proportionate ly.INDERAL LACapsmes (80. 120 , and 160mg ) re lease propranolol HCIata controlled and
pred ictab le rate . Peak blood leve ls lotlowmg dos ing W ith INDERAL LAoccmatabout6 hours
and the apparentp lasma halt- lite is a00 ut tohours .Whenmeasured ats tead y State overa 2 4h0 urperiod the areas under the propranolol plasma concentration-time curv e (AUGS ) tor thecapsules are approximate ly 60% to 65% oi the AUCS tora comparab le d ivided da i ly dose ofINDERAL tab lets . The lowe rAuCs tor the capsules are due to g reater hepatic metabol ismol
propranolol , re SUIIing tromthe s lowerrate ofab sorption0 1propranolol Overa twenty-Ig or (24 )hour pe riod . b lood leve ls are Ia i rly constant Ior about twe lve ( 12 ) home then dec l ineexponentially.INDERAL LA should not be cons idered a s imple mg tormg Sub s titute tor conventional
propranolol and the blood leve ls ach ieved do notmatch (are lower than) those attwo to lowtimes da ily dosing with the same dose When chang ing to INDERAL LA trom conventiona l
propranolol. a poss-b le need IOr retitration upward s should be cons idered espec ial ly to
ma intain e l lectiveness at the end of the dos ing interv a l Inmost c linical setting s however.Such as h penenS ion or ang ina where the re is little corre lation between plasma leve ls andclinical e ect INDERAL LA has been therapeutically equiva lent to the same mg dose of
conventiona l INDERAL as assessed by 2 4 hour ettects on b lood pressure and on 2 4 howexercise re sponses of heart rate . sys tolic presswe and rate pressure product. INDERAL LAcan prowde e l lective beta b lockade tor a 2 4
-hour period .
The mechanismol the antihypert ens ive e l lect oi INDERAL has not been estab l ished .
Among the factors thatmay be involved incontributing to the antihype rtens ive actionare ( 1)decreased card iac Output. (2 ) inh ib itionoi renin re lease by the kidneys. and (3 ) d iminutiona!tonic sympathetic nerv e outl low tromvasomotorcente rs in the brain. Although total peripheral
res is tance may increase initially it re ad jus ls to or be low the pretreatment leve l With chronicuse . Eltects on plasma volume appear to be minor and somewhat variab le . INDERAL hasbeen shown to cause a small increase in serumpotass ium concentrationwhen used in the
treatment 0 1 hypertens ive patientsInang ina pectoris propranolol generally reduces the oxygen requirementof the heart at
any g iven leve l 0 ! ettort by blocking the catecholamine induced increases in the heart rate
systolic b lood presswe . and the ve locity and extentol myocard ial contraction. Prop_
ranol_
ol
may increase oxyg en requirements by increasmg left ventricular l iber leng th end d iastolic
pressure and systolic erectionperiod The netphysiologic effect01beta-adrenerg ic b lockade
is usually ad vantageous and is manifested during exe rc ise by de layed onset of pain and
increased work capac-tyIn dosages gre ater than re Quired lor beta b lockade INDERAL also exert s a gum-d ine-like
or anesthetic l ike membrane actionwh ich al lects the card iac action potential The S igni l icance ot the memb rane action in the treatmentol arrhythmias is uncert a in.
Themechanismof the antimigra ine e l lectotpropranolol has notbeenestab lished Betaadrenerg ic receptors have been demonstrated in the pial vesse ls ol the b rain
Beta receptor b lockade can be use lul in conditions inwh ich. because ol patholog ic or
lunctional changes sympathetic activity is detrimental to the patient. But there are also
S ituations in wh ich sympathetic stimulation is vital. For example . in patients With severe lydamaged heart s . adequate ventricular lunction is maintained by virt ue of sympathetic d rivewh ich Should be pre served In the presence ol Av b lock , g reater than first degree . be ta
b lockademay pre vent the necessary lac ililal ing e l lectol sympathetic actwrty onconduction,
Beta b lockad e results in b ronch ial constriction by intertering With adre nergic bronchod i lator
activity wh ich should be preserv ed in patients Sub iect to bronchospasm.
Propranolol is not significantly d ialyzab leINDICATIONS ANDUSAGE. Hype rtens ion: INDERAL LA is ind icated
“
in the managementofhypertens ion: itmay be used alone 0rused incomb inationW ith otherantihypert ensweagents . particularly a th iazide d iuretic. INDERAL LA is not ind icated in the management othypert enswe emergenc ies
Ang ina Pe c toris Due to Coronary Athe ros c le ros is : INDERAL LA IS ind icated
for the long-termmana
gement 01 patients With ang ina pectoris
Mig ra ine : INDER L LA is ind icated lor the prophylaxis otcommonmig raine headache .
The e tticac ol propranolol in the treatmentol amig raine attack thathas start ed has not beenes tab lishe and propranolol is not ind icated for such use .
Nype rtroph lc Sub aort ic S tenos is : iNDERAL LA is use lul in the management ofhypert roph ic
_
Subaort ic Stenos IS .especially lot tre atmeq l otexertiona l orotherstress induced
ang ina palp itations . and Syncope INDERAL LA also improves exercise perlormance . The
etlectiveness oi propranolol hyd rochloride inthis disease appears to be due toa reductionol
the e levated cutl low pressure grad ient which is exacerbated by beta-receptor s timulation.
Clinical improvementmay be temporaryCONTRAINDICATIONS . INDERAL IS contra ind icated in t) cardiogenic shock; 2 ) S inusbrad ycard ia and gre ate r than l irs t degree b lock , 3 ) bronchial asthma: 4 ) congestive heartI
ta
l
i
‘
l
pée
flfiee WARN INGS) unless the lailure is secondary to a tachyarrhythmia treatab le with
l AL .
WARN INGS . CARDIAC FAILURE Sympathetic s timulationmay be a Vital component supporting Circulatory lunction inpatients wrth congestive heart tailure . and its inh ib itionby betab lockade may prec ipitate more severe tailure Althoug h beta b lockers should be avoided inOvert congestive heart lai lure itnecessary . they can be used With c lose tol low u- p in patients
With a h is tory ol tai lure who are we ll compensated and are rece iving d igita lis and d iuretics .
Be la-ad renergic b lock ing agents do not abolish the inotropic action or d ig ital is on heartmuscle
IN PATIENTSWITHOUTAH ISTORY OF HEARTFAILURE, continued use ol beta b lockers
can. in some cases . lead to card iac lai lure Therefore . at the first s ign or symptomot heart‘i i lure , the patient should be d ig italized and /or treated With d iuretics , and the response
ob served close ly, 0r INDERAL should be d iscontinued (g radually. itposs ib le ).
Nons tl e rg ic B ronc ho s a sm c h ronic b ronch iti s , emph s ome )PATIENTSWITH BRONCHOSPA TICDISEASES SHOULDINGENERAL NOTRE EIVEBETA
BLOCKERS INDERAL should be adminis te red with caution S ince itmay b lock b ronchod i lation produced b
yendo encus and exogenous catecholamine s timulationol beta re ceptors .
MAJOR SU GER The necess ity or des irab i lity ol W ithd rawal ot beta-b lock ing therapyprior tomater Surgery is controverS ial. It Should be noted , however, that the impaire d ab i l ity olthe bean to re spond to retlex ad renerg ic stimuli may augment the ris ks 0 ! genera l anes the
s ra and Surg ical procedures .
The appearance ol these capsules160 is a re g istered trademarkmg otAye rst Laboratories
Copyright 198 4 AYERSTLABORATORIESDiViS lonoi AMERICAN HOMEPRODUCTS CORPORATION
INDERAL (propranolol HCI) , l ike other beta b lockers is a competitive inhibitor ot betareceptor agonists and its ettects can be reversed by administration of such agents 9 .g .
dobutamine or isoprotere nol Howeve r. Such patients may be Sub iect to protracted seve re
hypotenS ion. Drt1iCulty in start ing and maintaining the heart beat has also been re ported withbeta b lockers .
DIABETES AND HYPOG LYCEMIA: Beta ad rene rgic b lockade may prevent the appearance 0 1 cert ain premonitory S igns and symptoms (pulse rate and pressure changes ) 01acute hypog lycemia in lab i le insulin d ependent diabetes . In these patients itmay be mored il lrcult to aGIUS l the dosage ot insulin
THYROTOXICOS IS: Be la b lockade may mask certain clinical S igns 0 1 hypert hyroid ismTherelore . abruptWithdrawal of propranololmay be fol lowed by anexacerbationof Symptomsothyyperthy
roidism includ ing h rOrd s torm Propranolol does nol d rstort thyroid function testsIN PA IENTS WITH WOLF -PARK INSON-WH ITE SYNDROME. several cases have been
reported in which al ter propranolol. the tachycard ia was replaced by a seve re b radycard rarecurring a demand pacemaker. In one case th is resulted alter an initia l dose 01 5 mgpropranolol.PRECAUTIONS . General Propranolol should be used with caution inpatients with impairedhepatic or renal lunction. INDERAL (propranolol HCI) is not ind icated lor the tre atment 01hypert ens ive emergenc ies .
Be la ad renoreceptor b lockade can cause reduction 01 intraocular pressure. Patientsshould be told that INDERAL
_
may interlere with the g laucoma screening test.Withd rawalmaylead to a return at increased intraOCUlar pressure
Clinical Laboratory Tests Elevated b lood urea leve ls in patients with severe heart d isease .
e levated serum transaminase . alkal ine phosphatase lactate dehyd rogenaseDRUG INTERACTIONS fi tients re ce iving catecholamine-depleting drug s such as re ser
pine should be c lose ly observed it INDERAL is administered . The added catecholamineb lock ing actionmay pro duce an exces s ive reduction ol resting sympathe tic nerv 0us activitywh ichmay reSult inhypotens ion marked bradycard ia.vert igo syncopal attacks orort hos tatichypotens ion
Carcinogenesrs ,Mutagenes i
’
s Impai rmentof Ferlrlrty Long-termstud ies inanimals havebeen conducted to evaluate toxic e l lects and carcinogenic potential In 18 month stud ies in
both rats andmice employ ing doses up to 150mg / kg /day. there was noevid ence 01s ignificantd rug
- induced toxi_
c ity There were no d rug -re lated tumorigenic e l lects at any01 the dosage
levels Reproductive stud ies in animals d id not Show any impa irment at ert ility that wasattributab le to the d rug
Pregnancy: Pregnancy Category C. INDERAL has been shown to be embry otoxrc in
animal studies atdoses ab0ut 10 times g reate r than themaximumre commended humandose .
There are no adequate and we ll-controlled stud ies in pregnantwomen. INDERAL Shouldbe used during pregnancy only it the potential bene tit ius tities the potentia l ris k to the Ietus .
Nurs ing Mothers' INDERAL is excreted in humanmi lk . Cautionsh0uld be exercised when
INDERAL rs administered to a nurs ing woman.
Ped iatric Use Se lety and ettectiveness in child ren have not been es tab lishedADVERSE REACTIONS . Mos t adverse etlects have been mi ld and trans ient and haverare ly re curre d the Withd rawal ot therapy
Card iovascwar. bradycard ia . congestive heart lailure . intens ification 01AV b lock: hypotens ion. paresthes ia 01 hands : thrombocytopenrc purpura; art erial insultrcrency. usua lly ol theRaynaud type.
Central Nervous Sys tem. lig htheadedness : menta l depress ionmanitested by insomnia .Iass itude. weakness tatrgue: reve rs ib le mental depress ion prog ressmg to catatonia. visual
d isturbances : hal lucinations : anaCute revers ib le synd rome characterized by d isorientation tortime and place ShOrt termmemory loss . emotional lab i l ity s l ightly clouded sensorium anddecreased pertormance on neuropsychometrrcs
Gastromlestrnal ' nausea . vomiting . epigastric d istress . abdominal cramping . d iarrhea ,
constipation mesenteric arterial thrombos is ischemic col itis .
Allerg ic phary ngitis and agranulocl S Is erythematous rash . Ievercomb ined wrth achingand Sore throat. lary ngospasm and respiratory d istress .
Respiratory. b ronchospasm.
H ematolog ic: ag ranulocytosis . nonthrombocytopenic purpura . thrombocytopenicpurpura .
Auto-lmmune. In extremely rare instances . systemic lupus ery thematosus has beenreported
Miscellaneous . alopec ia. LE-Iike reactions . psorias ilorm rashes . d ry eyes . male impotence , and Peyronie
'
s d isease have been reported rare ly Oculomucocutaneous reactions
involving the sk in, serous membranes and con|unctivae report ed tora beta b locker (practolol )have not been assoc iated wrth propranolol
DOSAGE ANDADMIN ISTRATION. INDERAL LAprovides propranolol hydroch loride inaSustained -re lease capSule loradminis trationonce daily. Itpatients are Swnched lrom INDERALtab lets to INDERAL LAcapSules. care should be taken to assure that the desired therapeutice l lect is maintained INDERAL LAshould not be considered a S implemg tormg
Substitute tor
INDERAL . INDERAL LAhas d rl terent k inetics and produces lowerb lood leve ls etrtra lronmaybe necessary especially toma intain e l lectrveness at the end ol the 24 how dos ing interv al
HYPERTENS ION Dosage must be ind i vrdualrzed The usual initia l dosage is 80 mgINDERAL LA once da i ly. whether used alone or added to a d iure tic The dosage may beincreased to 120 mg once d aily or hig her until ad ecwate b lood pressure control is ach ieved .
The uSUalmaintenance dosage is 120 to 160mg once dai ly. Insome instances a dosage 016 40mg may be re quired The time needed lor tutl hypertens ive response to a given dosage IS
variab le and may ran e trom a tew days to several weeksANG INARECTO IS—Dosage mus t be indrvrdualrzed . Start ing with 80mg iNDERAL LA
once da i ly. dosage should be gradually increased atthree to seven d ay interv als untiloptimumresponse is obta ined Although indivrdual patients may respond at any dosage leve l. the
average Optimum dosage appears to be 160 mg once da ily In ang ina pectoris . the value and
salety of dosage exceed ing 320mg per day have not been es tab l ishedIttreatment is to be d iscontinued .
reduce dosage g radually Over a period 0 1a tewweeks
(see WARN INGS ).MIGRAINE Dosage must be individualized . The initial ora l dose rs 80mg INDERAL LA
once dai ly. The usua l e l lectrve dose range is_
160-2 40 mg once dai ly The dosage may beincreased g radually to achieve optimummigraine prophylaxis . Il a satis lactory response is not
obtained with in tour to S ix weeks a l ter reach ing the maximum dose . INDERAL LA therapyshould be d iscontinued . Itmay be advisab le to wrthd raw the d rug g radually ove ra period olSeveral weeks
HYPERTROPH IC SUBAORTIC STENOS lS—80-160 mg INDERAL LAonce daily.
PEDIATRIC DOSAGE—At th is time the data on the use 01 the d rug in th is age g roup are too
limited to permit adequate d irections tor use .
REFERENCES
1 . Holland OB NixonJV. Kuhnert L: Diuretic induced ventricularectopicactivity AmJ Med 198 1 70. 7 62 7 68 2 . Holme l.He lge land A HiermannI etal: Treatmentofmild hypertensionwith d iuretics . The importance 01ECG
abnorma lities in the Os lo study and'
inMRF lT. JAMA198 4 2 5 1 :12 98 1299 .
AYERSTLABORATORIESAye rs New York . N Y. 10017

SClENTlFlCARTICLE
Myocobacterium Avium- lntrace llulare and
Lung Disease : More of a Prob lem for Those
of Us in the Southeast
Norman Adair , MD .
0 Close re la tivesM . avium andM . intracel lula re a re pres entmost often inthe elderly and the immunocompromised , and a re very drfli cult to treat
successful ly .
ULMONARY tuberculos is has decreased markedlyover the last few decades . As result, there has been a
relative increase in the frequency of lung d isease caused bythe non- tuberculous mycobactena . Physicians in North
Carol ina and the southeastern states have long been familiar with non- tuberculous mycobacterial disease of the
lungs . In the early part of this century , an atypical”
mycobacteriumwas isolated frompatients being treated fgrtuberculosis at the Battey State Hospital ih Rome, Georg iaand carried the name of that institution for several decades .
We now know the“Battey
” bacil lus as Mycobacteriumintracel lulare ,
la close re lative of Mycobacterium avium.
These two are often grouped together as vari ants of a sing le
strain. Soil isolates from southeastern river areas y ie ld 100
fold higher concentrations of M . avium- intrace l lulare
(MAI ) when compared w ith soi l samples from the
northeast.
2Natives of the southeastern states have an ih
creased frequency of cutaneous reactivity toMAI 3 and an
increased incidence of disease due to th is organism.
M . avium- intracellulare and M . kansas ii account for the
majority of the“atypical mycobacterial lung infections .
In terms of human pathogenicity these organisms fal l be
tweenM . tuberculos is , an ob l igate pathogen, and the be
nign free l iving mycobacteria . M . avium- intracel lulare can
cause anoverwhe lming and often fatal disseminated infec
tion, especial ly in the immunocompri sed host, e . g . AIDS ;however, disease is usua l ly manifest as an indolent pul
monary infection in the elderly . The chest x- ray demon
strates infiltrates , often w ith cavitation, that are indistin
guishable from pulmonary tuberculosis .
A confident diagnosis of“atypical
”mycobacterial lung
disease is compl icated by the fact that the organismmay bea harmless colonizer in the oral cavity or the tracheobronchial tree , particularly in lungs damaged previous ly bychronic bronch itis or a fibrotic- inflammatory disorder.
Strict adherence to d iagnostic criteria is especial ly important when non- tuberculous mycobacterial lung d isease issuspected in order to prevent unnecessary and potential ly
From the Department of Medicine , Bowman Gray School of Medicine ,
Winston-Salem 27 103 .
JUL Y 1985 NCMJ
toxic therapeutic intervention. Essential diagnostic criteria
for lung d isease due toMAI include the repeated isolation
of large numbers of organisms from the same source ( spu
tum) , the absence of alternative pathogens , and the pres
ence of cl inical disease for which no other etiology isapparent. Ahn and co-workers have defined even more
rig id criteria4 based on the ir observation that patients with
_ ,sputum pos itive for MAI may convert to negative withbronch ial hygiene alone .
Chemotherapy of M . avium- intracel lulare lung disease
is often unsuccessful because of primary resistance tomostof the first and second l ine anti- tuberculous drugs . This has
prompted some physicians to treat w ith five and six drug
comb inations , 5 a strategy analogous to multiple agent
chemotherapy of cancer. Presumably , these drug combinations cause multiple metabol ic defects which can result in
an anti-mycobacterial effect despite high level s of resistance to the ind ividual drugs .
6 Drug toxicity is very com
mon with these reg imens . However, some reports suggest
that such aggressive therapy may not be required in al l
cases . Dutt and Stead7have reported an initial 80% sputum
conversion rate using primari ly four-drug chemotherapy .
More recent reports from Wales8and Denmark9 indicate
60- 70% sputum conversionw ith a conventional three-drug
anti- tuberculous regimen employ ing isoniaz id , rifampin,
and ethambutol .Therapeutic success equal to that currently achieved in
pulmonary tuberculosis is not presently in s ight and wil lrequire improved know ledge of the immunology and
b iochemistry ofM . avium- intrace l lulare , the deve lopment
of new drugs , val id in vitro susceptib il ity testing of drug
comb inations , and additional cl inical trials . Current know l
edge indicates that initial treatment should include isoniaz id , ri fampin, and ethambutol . Supplemental chem
otherapy should be instituted if there is no sputum conver
sion in three months or if the cl inical situation is deterioraring . Ethionamide and cycloserine are frequently recom
mended for supplemental reg imens . Drug susceptib i l itytesting has not been shown to improve therapeutic responsebut is often used as a guide for drug se lection.In vitro
studies and pre l iminary observations suggest that two ex

perimental drugs , clofaz imine and ansamycin, may be
active against M . avium- intrace l lulare . The latter may be
obtained on a research bas is from the Centers for Disease
Control .'2
Because of the often indolent nature of these infections ,
the advanced age Of those afflicted , the frequent presenceof b ilateral involvement, and the coex istence of underlyinglung disease , surgery wi ll only occas ional ly be indicated .
However, resection of we l l—local ized lesions , includ ingcavity bearing areas , may be definitive in some cases and
should be carried out at a time when available drug effectsare presumed to be greatest.
References
l . Runyon EH . Mycobacterium intracel lulare . AmRev Respir Dis
867 .
2 . Brook sRW . ParkerBC . GraftH , Fal kenhamJO. Epidemiology of infectionbynontuberculous mycobacteria. Am Rev Respir Dis l 984 ; l 30;630
-633 .
3 . Edwards L B . Acquaviva FA. L ivesay VT. Cross FW , PalmerCE. An atlas of
406 VOL . 46 , No . 7
sensitivity to tubercul in. PPD-B . and histoplasmin in theUnited States . AmRev
Respir Dis 1969199l l - l 3 l .
Ahn CH . McLarty JW , Ahn SS . Ahn SI , Hurst GA. Diagnostic criteria for
pulmonary disease caused by Mycobacteri um kansasi i and Mycobacteriumintracel lulare. AmRev Respir Dis l 982 : l 25 : 388-893 .
DavidsonPT.KhanijoV , Goble M.Moulding TS . Treatmentof disease due to
Mycobacteri um intracel lulare. Rev Inf Dis 198 1z3 : 105 2 - 1059.
Heifets L B . Synergistic effect of ri fampin, streptomycin ethionamide . and
ethambutol onMycobacterium intr acel lulare . AmRevRespirDis4 8
Dutt AK and SteadWW . Long term re sults ofmedical treatment inMycobacterium intrace l lulare infection. Am J Med l 979:67 ;44 9-4 5 3 .
Hunter AM. Campbel l IA. Jenkins PA. Smith AP. Treatment of pulmonaryinfections caused by mycobactena oi
'
th e Mycobacterium avium-intracel lulare
complex. Thorax l 98 1:3 6; 3 26- 329 .
Engbaek HC , VergmannB . BentzdnMW. Aprospective study of lung disease
caused by Mycobacterium avium/Mycobacten'
um intracel lulare . Eur J Respir
Dis l 984 ;65 :4 l l -4 18 .
GangadharamPR, Pratt PF . Darnle PB , DavidsonP’
l‘
. Dynamic aspects of the
activity of c lofaz imine against Mycobacterium intrace l lulare. Tubercle
198 1 -206 .
Perumal VK , KimChuc N , IsemanM.GangadharamPR. Dynamic and in viva
chemotherapeutic aspects of ansamycin onMycobacterium intracel lulare . Am
Rev Respir Dis
CDC . Ansamyc in LM 4 2 7 . Morbidi ty and Morta l ity Wee k ly Report
l 985 ;34 :7 6.

COMMON PAINFUL SCROTAL MAS S ESIncarcerated
Inguina l He rnia
Tors ion of Te s tis
Tors ion of
Append ix Tes tiste Epid id ymitis
F igure l . Pa inful Scrota l Masses
COMMON PAINLES S SCROTAL MAS S ES
Ind ire ct Inguina l Her
Cy s t of Epid idymis
Varicoce le
Hydroce le
( Sac Opened )
Te s tis Tumor
F igure 2 . Pa inless Scrota l Masses
408 VOL . 4 6 , No . 7
An indirect inguinal hernia is the only scrotal mass that isintermittently present. The mass may be reducible and a
thumb and forefinger applied around the spermatic cord atthe external ring wi l l not confine the mass to the scrotum.
Auscultation of this scrotal mass may reveal bowe l soundsand the mass wi l l not transi l luminate .
Cysts of the epididymis usual ly involve the globusmajorof the epididymis ( superiorpole ) and al though they contain
fluid they are often fi rm . If these cysts contain sperm , theyare appropriate ly des ignated as sperrnatoceles . These scro
tal masses onphys ical examination caneasily be separatedfrom the testicle and they w il l transil luminate .
Testis tumors present as a symmetrical , smooth , firm
enlargement of the testicle or a fi rm nodular mass wh ich
arises from the testicle . On physical examination it is the
only common scrotal mass wh ich can not be separated
manual ly fromthe testicle . Rare ly if there has beennecrosisand hemorrhage w ithin the testicle , the testicular mass w il l
be painful .
Self-Examination of the Testicle
S ince the testic les are readi l y avai lab le for se l f
examination and testicular carc inoma is the most common
sol id tumor inmen between the ages of 15 and 40 , itwould
seemappropriate that the ind ividuals at risk be instructed inself-examination of the ir scrotal contents .
Manual self-examination of the testicle is performed
with the thumb on the anterior surface of the testicle and theremaining fingers behind . Back and forth movement of the
thumb over the anterior surface of the testicle wil l de l ineate

any mass protruding from the surface of the testicle . Ex
tratesticularmasses canbe identified by interpositionof the
thumb and forefinger between the mass and the testicle
proper . Any scrotal mass outs ide of the testicle is not a
testis tumor.
Self-examination of the testicle should be initiated at the
loth grade leve l and re-emphasized during subsequentroutine school physical examinations or on office vis its for
other complaints . Audiovisual presentations and mode ls
demonstrating abnormal scrotal masses would enhance thisClearly prior to patient education, there must be
TEGA-CORT FORTE 1 °/o
phys icianeducation. This would have to be initiated duringmedical school training and continued through residency
programs . There has already been general publ ic accept
ance Of se lf-examination of the female breast, and se l f
examination of the testicle would seem a log ical step for
ward .
References
1 . H igby DJ, Wal lace HJ Jr, Albert DJ. et al . Diaminodichloroplatinum: a phase Istudy showing responses in testicular and other tumors. Cancer
2 . Donohue JP. Surgical managementof testis cancer.TesticularTumors .Edited byEinhom. LH . New York . Masson. 1980t29.
TEGA CORT(Ava i lab le at a l l d rug s tores Rx Only)
SQUEEZE TYPE DISPENSER BOTTLESTega
-Cort Forte'
and Tega-Cort lotions are offered in a nice smooth non- s ta ining
water so lub le base .
Ind ications For re l ief of the inflammatory manifes tations of corticos terorrd
respons ive dermatoses inc lud ing Poison Ivy , and sunburn.
Contraind ications : Topica l s teroids have not been reported to have an adverse
effect on pregnancy , the safety of the ir use in pregnant. fema les has not absolute ly
been estab l is hed . Therefore , they s hould not be us ed extens ive ly on pregnant
patients , or in large amounts , or for pro longed period s of time .
Dosage and Adminis tration: Apply to affected area 3 or 4 times da ily as d irected
by your phys ic ian.
Caution: Federa l law proh ib its d ispens ing without prescription. For externa lus e only . Store in a cool place but do not freeze .
PLEASE CONSULT INSERT SUPPLIEDWITH EACH BOTTLE FOR MOREDETAILED IN FORMATION
WEFEATUREONEOFTHEMOSTCOMPLETELINEOF INJECTI'BLES INTHESOUTHEASTATTHEVERYBESTPRICE, CONS ISTENTWITH QUALITY.
ORTEGAPHARMACEUTICAL CO
JUL Y 1985 , NCMJ
INC. JACKSONVILLE, FLORIDA32205

SOCIOECONOMIC ISSUES
North Carolina Hospital Utilization
We Can Change !
W i l l iamW . Fore , MD .
0 Phys icians who want fee -for -service med icine to rema in an option in
North Carol ina are we l l advised to look at their hospita l util iza tion ra tes .
OSPITAL util ization is decreasing in North Carol ina .
H The change began before the implementation of payment by diagnos is re lated groups (DRG s) for Medicare
patients , and the rate of decrease has increased since DRG s
have been ineffect. Evenwith our 1 1% decrease inhospital
util ization, there is sti l l room for improvement. The problem is thatduring this period ofchange there remains awide
range of util ization over the one hundred counties in our
State . This difference between the counties with high andlow rates of util ization is Is it going to be necessaryfor al l of the negative incentives such as preadmission
certification, peer review contract quotas , and prepaid
medical care to be in place for the phys icians in our state to
lower medical costs by decreas ing hospital util ization?
This journal recently reviewed the history of the 20-
year
progress ionof Federal regulation of our practices while we
enjoyed the best incomes primary care physicians ever hadin th is country . Duri ng these years the high costofmedical
care was careful ly stud ied and analyzed . Control escaped
the purchasers ofmedical care and the med ical profess ion.
Ourpatients got the ir care when they wanted itorneeded it ,
and on the whole got the best med ical care in the world .
There were no incentives for physicians or patients to
decrease cost because two- thirds of the medical care b il ls inour State are paid by the Federal and State Governments
and bus iness corporations . The health care b il l has ihcreased by 15% to 30% a year, and in 1983 and 1984 we
saw the concern over cost turned into action. The ideal
s ituation to have positive incentives for change d id
not happen. Our behavior is be ing shaped by competition,
denial of payment, preadmiss ion certification, prepaid
medical care , and fi xed reimbursement. The majority of uspractice in anhonestmanner and have a s incere concern for
our patients . We do so in a fashion shaped by the commit
ment that strengthened us through the long years of school ,our training , and the expegtations of our patients .
There is a great deal of information on hospital util iza
tion in North Carol ina . Information on hospital ization in
1982 , 1983 , and 1984 is availab le from B lue Cross/B lue
Shie ld .
2 ' 3 These figures inc lude an over- 65 -
year-old
population of less than In 1982 , North Carol ina aver
aged 802 hospital days per subscribers . An 1 1%
From the Department ofMedicine . East Carol ina University . G reenvi l le
2 7 834 .
4 10 VOL . 46 . No . 7
decrease to 685 hospital days per subscribers occurred ih 1984 . Approximate ly 2 5
- 30% of North Carol inacounties are above this average figure . Health maintenance
organizations have uti l ization rates of 300-600 days per
el igible H ealthAmerica , a prepaid plan
expanding rapidly in North Carol ina , states that the ir hos
pital util ization is 20% below the HMO figures and 40%below al l BC/BS plans .
7Patients in the 65 -
year or older
category are not in plans with these lowest figures nor are
they the target population of HealthAmerica . An annual
util ization rate of 500- 600 hospital days per patients
(under 65 ) is not an unreasonable goal in North Carol ina .
Less than20 counties have hospital uti l ization inthis range .
There is room for improvement.
Since 197 9 , the difference in practice patterns in our
State has been recognized by the North Carol ina B lue
Cros s /B lue Shie l d ( B C/B S ) Corporation and state
agenciesz ’ 3 ‘ 8 ‘ 9 There is a 136% difference in hospital
util ization over our state . If we look at the extremes of
hospital util ization in the counties in North Carol ina with
the 1983 data for admiss ion rates , there is 12 5% d ifferencein admissions and 14 6% d ifference in hospital days per
subscribers . If one thenmatches the county popula
tionand the physician-
patient ratio in a comparisonof thesecounties , there are stil l large differences: 8 1% and
respectively . Does this w ide range of hospital util izationoccur in a population other than that of the North Carol ina
BC/BS population? It does ! The med ical program for the
aged ,b l ind , and disabled has a 3 30% d ifference inhospital
util ization over our state . The State Center for Health
Statistics has 17 9% difference in discharge rates betweentwo counties of similar size . We therefore have a difference
across our state of at least 100% in the way we use our
hospitals forpatient care . If one looks at hospital availabil
ity , county population s ize , and numbers ofphysicians , it is
difficult to general ize as to why th is situationexists . One is
left w ith the conclusion that it is due to the d ifference in
practice patterns .
2Therefore , it is due to physician be
havior. Education in the best of worlds should mod ify
physician behavior. Does it?
The North Carol ina 8 0 8 8 organization selected coun
ties with high admiss ion rates for respiratory diseases and
found l ittle change in admissionrates afterextensive educa
tion efforts in the target counties . A recent article shows
that education does not change hospital util ization or de

crease cost.
1°Dr . Carl L yle et al showed at 3 l decrease in
physician initiated charges by an intensive cost awarenessprogram at the Charlotte Memorial Hospital .“They analyzed inpatient and outpatient lab charges and length of
stay , and their physician group was residents in a city
hospital teaching service . This study did not address cost
saving by decreasing admission rate . It is difficult, with theabove facts inmind and physicians ’
characteristics of individual ity , to approach each countywith the facts and expectthat practice patterns w il l change and that the des ired decrease inhospital util izationwi l l result. I recently spoke toa county medical society about its high rate of hospital
uti l ization. This county has two hospita ls with an adequatenumber ofphysicians . The doctors had two excuses . One
was ,“My hospital has a lower per day cost than Duke
Hospital or the Raleigh hospitals . Regardless of the daily
cost a hospital saves money if unnecessary admi ssions do
not occur. The second excuse was that their patients werebe ing admitted by doctors in another county . The county
with the highest hospital util izationhas hospital days
per year per subscribers , and sends most of its pa
tients to an adjacent county hospital which has 8 18 hospitaldays/ 1000 for their res idents . Arecent study by BC/BS has
shown that inour state 6 1% of our patients are hospital izedin the county in wh ich they reside .
3 W ith these facts it ishard to blame higher uti l ization entirely on the doctors inthe next county . Excuses such as these only delay the
changes that need to be made ,
The fee-for-service practice ofmed icine inNorth Carol ina has provided a h igh level of care . Patients and doctors
prefer a strong patient-doctor relationship . Our current
system of medical care , however , with a strong doctor
patient relationship, has not control led the rapid escalationof medical care costs . The fee-for- service system is worth
saving and should not l ightly be abandoned . If the State and
Federal Government and the bus iness corporations of
North Carol ina see that fee- for-service doctors can effec
l ively containcosts there would be less pressure tomove to
prepaid heal th care .
Diagnosis re lated groups have only been in effect sinceOctober 1983 , and this has certainly had an effect, but the
largest decrease in hospital util ization is probably due tooutpatient surgery . In Pitt County for 1983
- 1984 , there
were approximately 4 30 outpatient surg ical proceduresdone eachmonth . This is 38% of the surgery being done inPitt County . This surg ical rate alone could account for a
20% decrease in hospital admissions and thus exceed theaverage decrease of Fourteen counties have remark
ably high hospital util ization. There are two counties thatexceed the average state hospital util ization figures by130% from al l three sources in al l parameters reviewed ,
*
there are e ight that exceed the 130% of the average from at
least one '
source, and there are four additional counties that
exceed th e average hospital ization util ization rates by 1444% from the State Center of H ealth Statistics . These
B lue Cross and B lue Shield of North Carol ina 1982 , 1983 ; Pediatric
hospital util ization, hospital ization for injury and poisoning , hospital iza
tion for il l -defined il lness , hospital ization for genitourinary d isease and
respiratory disease . DivisionofMedical Assistance Administrators Letter1983 ; data onmedical patientpopulation. StateCenter forHealth Statistics
1982 ; discharge rates per populations .
JUL Y 1985 , NCMJ
‘
l Myringotomy with tubes ; removal of tons ils and adenoids ; abdominalhernia repairs ; excision of breast masses; D& C ; laparoscopy; Bartholin
gland surgery ; therapeutic abortion; insertion of intraocular lens ; arthros
COPY; carpal tunnel decompress ion; excision of gangl ion; excision of
Mortons neuromas ; sk in grafts; cystoscopy ; bronchoscopy ; endoscopy ;colonoscopy .
counties also have two problems : a greater number of
surgical procedures per unitof population and fewerproce
dures done in ambulatory units . F ive of these 14 counties
have very low outpatient rates for the 18 surg ical proce
duresi‘ being monitored by BC/BS . Therefore , an effective
decrease in hospital ization wi l l occur only if the practicepatterns of the North Carol ina surgeons in these counties
change as they select the patients to have surgery and the
site where the surgery is performed .
The 14 counties with high hospital util ization are geo
graphical ly spread al l over the state . The populationof the
counties varies from to The physician :
population ratio varies from to It is im
possible to say that this high hospital util ization is due to thefact that the physicians and surgeons are overloaded . There
is no general ization that can be made regarding the population they serve . The high uti l ization practices cross al l
socioeconomic groups since the same information is available from BC/BS and the Med icaid program. The reason
our util ization varies greatly is due to the way we as phys icians practice and util ize our hospitals .
Why do anything about hospital util ization? Hospitalutil ization is the primary target of cost containment effort s
in our state at this time . If fee- for—service phys icians inNorth Carol inamake a dramatic change inhospital ization it
would show that our concern about the ri sing cost ofmedical care is sincere . Any county that lowers its util ization
rate dramatical lyw il l be looked onvery favorably by industry seeking future s ites for plant construction. The various
prepaid medical care programs are moving rapidly into
North Carol ina and the nation. They wil l not replace these
fee-for- service phys ic ians if we compete w ith a reduced
level of hospital ization. If we do not lower our hospital
util iz ation, then al l of the programs with the ir negativeincentives , such as the ones inplace at the present time , wil l
be extended by government, industry , and insurance com
panics to obtain lower med ical care costs . We wil l be the
pawns not the players inthis coming game to ‘
trimthe fat’
from the high costs of medical care .
How doe s one accompl ish lower hospital util ization?F irst, let
’
s admit there is a prob lem. Second , let’
s throw
away the excuses and not put it on the doctors in the next
county . Third , let’
s analyze whatwe can do to change our
community to provide qual ity outpatient care for those
problems we now admit to our hospital s . Fourth , let’
s stopusing hospital izationas amethod of postponing the history ,
phys ical , and diagnostic planning for our patients to the
evening hours to be performed by ourselves or our consultants .
Some spec ific areas to cons ider are :Do you know that businesses evaluate statistics onprac
tice patterns when choosing a community for a plant site?
Counties with high hospital uti l ization wil l have troub legetting new industry .
Does your radiologist provide instruction to prepare pa

tients for outpatient examinations?Does your Home Health Service provide hospital ser
vices such as intravenous therapy and parenteral med ica
tions?
Does your county medical society conduct a program of
publ ic education as to the necess ity of doing as an outpa
tientmany things that in the pastwere done in the hospital?
Are you referring your patient to a surgeonwho uses an
ambulatory surg ical unit?
Does the ophthalmolog ist who sees your patient do lens
surgery in an outpatient faci l ity?
Have you identified patients with pneumoniawho canbe
seen in the offi ce and treated at home with close office
fol low-up?
Do you treat urinary tract infections without nausea and
vomiting at home and get appropriate studies as an outpa
tient?
Do you have patient instruction sheets regarding home
care already prepared for your patients?Does a d ifficult diagnostic prob lem real ly need admis
sion for lab , consultation, and x- rays?
Do you encourage a mother to stay home w ith her sickchild rather than compete with hospital aides?
Is your local hospital deve loping a wel lness program?
When you order diagnostic tests on a patient, do youconsider cost?
Each of us must answer these questions and have the
4 12 VOL . 4 6 , No . 7
des ire to change our practice patterns . Change is upon us
and wil l come either because we participated and continuedto be advocates forourpatients or let itpass upby . Wemust
e ither change or resign ourse lves to be moved by forces
fromoutside ourprofession. Ifwe canpracticemedicine in
a concerned and most cost-effective way , then we can get
our patients , the bus iness world , the ir insurers , and the
governmental agencies to focus onothermajor reasons forincreased health care costs such as the care of the term inal lyil l , the aging population, inflation, and the proper util iza
tion of new technology .
REFERENCES
l . S ilberman HR . An insight into the uti l ization review: beyond re spons ibil ity and
towards accountabil ity“(amini history of th e developmentand evolutionofpeer
re view) . NC Med J —7 .
2 . Gre ene SB , DeMariaWJ. Hospita l uti l ization patterns in North Carolina: 1m
pl ications for cost of care. NC Med J 1983 314 25 8 14 .
3 . Greene SB . Personal communication.
4 . Gaus CR. Cooper BS , H irs chman CG . Contrast in HMO and fee for service
performance . Soc ial Sec Bul l 197613923 .
5 . Alternative Health Care De l ivery Systems , (The HMO Concept) . American
Medical AssociationDec 197 8:
6. Egdahl RH , Taft CH , Friedland J. Linde K . The potential of organizations of
fee- for- service physicians for achieving significantdecreases inhospital ization.
Ann Surg -99 .
7 . Heal th America Brochure . p. 6 .
8 . Sta te Center for Health Statistics . 1982 Summary Data .
9 . Matula BD. DMAAdministrative Letter. No. 34 -83 . July 6 . 1983 .
0. Schroeder SA et al . The failure of physician education as a cost containment
strategy . JAMA 1984 2 5 2 1225 8 0.
11 . Lyle CD. Bianchi RF . Teaching costcontainment to house officers atCharlotte
Memorial Hospital . J Med Educ -62 .

LEARNING EXPERIENCES FROM UNC
Renal Autoregulation, Drugs , and
Acute Renal Failure
Wil l iam B . B lythe , MD .
0 Aprimer on rena l autoregulationfor the cl inician .
F they recol lect it at al l , most physicians remember theI phenomenon of autoregulation of renal b lood fl ow and
glomerular filtration rate as a rather mysterious , perhaps
pedantic , principle which was sole ly the domain of the
renal physiolog ist in his animal laboratory , one wh ich wasbereft of any cl inical usefulness and never to be consideredagain after the bas ic-science years of med ical school .
As a resultof the development of certain classes of drugs
in recent years , renal autoregulation has moved squarelyinto the cl inic , and at least an awareness of it, how it canbe
deranged , and the serious consequences that can ensue
when it is interfered with , can he lp keep the physicianout
of trouble .
Renal hemodynamic autoregulation is concerned with
keeping renal blood fl ow and glomerular filtration rate
relatively constant over a w ide range of renal perfusion
pressures . Changes in renal vascular resistance effected bychanges in resistance in either the afferent or efferent arte
rioles or both , depending upon the circumstance keeprenal blood and glomerular fi ltration rate from ri sing drasti
cal ly when the renal perfus ionpressure is greatly increasedand , converse ly , keep them from fal l ing drastical ly when
perfusion pressure is low .
Consider the latter state . It is of particular cl inical im
portance . In settings of reduced renal perfusion pressure ,
such as might occur in salt depletion, hemorrhage , endo
toxin shock , severe congestive heart failure , and certainforms of chronic renal fai lure , renal vasoconstrictor and
vasodilator systems are activated simultaneously , and the
final setting of renal resistance represents the net effect ofthese excitatory and inhib itory influences . Although there
are numerous complex facets in the process , there are two
hormones that are involved that are important inourconsid
eration. These are angiotensin II. and the renal prostag land ins . Ang iotensin II produces constri ctor effects and the
prostaglandins antagonize these effects .
If ang iotensin II production is b locked , efferent arterio
lar constri ction cannot be effected and g lomerular filtr ationrate wil l fal l and renal failure may ensue as a consequence .
i f , on the other hand , prostaglandin synthesis is inhibited ,
efferent arteriolar constriction is unable to preserve glomerular filtrationrate because the fal l inglomerular plasma
From the Division of Nephrology , The University of North Carol ina ,
Chape l H il l 27 5 14 .
JUL Y 1985 , NCMJ
flow that results from afferent arteriolar constriction out
weighs the increase ih g lomerular capil lary pressure med i
ated by the increased efferent arteriolar resistance , and
acute renal failure may occur in this circumstance al so .
Thus , inhib ition of synthesis of e ither angiotensin IIthe renal prostaglandins may result in acute renal failure in
any cl inical setting in wh ich renal perfus ion pressure isreduced .
Three classes of drugs which have been deve lopedrecent years and for varying c l inical purposes fi t the b il l .F irst came the non- steroidal anti - inflammatory drug s .
These drugs are used in the treatment of al l sorts of dis
orders . It has been estimated that over five mil l ion peopleare exposed to them daily , a conservative fi gure that doesnot take into account the use of aspirin. They actby inhib iting prostagland in synthesis and , al though the prevalence of
acute renal failure associated with the ir use is re lative lylow , one mustbe alert to the possib il ity that itmay occur insituations where renal perfusion pressure is reduced .
Next came the angiotensin converting enzyme inhib itorssuch as Captopril , which are used primari ly in tr eatinghypertension and occas ional ly congestive heart failure .
It has been shown clearly that the use of this drug inpatients with fi xed b ilateral renal artery stenosis , a s ituationinwhich renal perfusionpressure is reduced , can lead to the
deve lopment of acute renal failure .
"2 Here the phys icianshould be particularly alert for this possibil ity in treatingolder patients with hypertension who may have bilateralrenal artery stenosis as a consequence of arteriosclerosis .
The last class of drugs to be indicated are the calcium
channel blockers . These new agents , wh ich are now beingwidely used in the treatment of ischemic heart d isease andhypertens ion, block the flux of calcium ions across variousexcitatory cel l membranes and thereby have a potent vasodilator action.
Diamond and col leagues recently reported that nifedi
pine , one of the slow calcium channel block ing agents ,
caused acute , reversible deterioration in renal function in
four patients with chronic renal insufficiency .
3
There was no evidence in the patients of any of the usual
causes of acute renal fai lure ; thus the authors postulated
that the nifedipine produced deterioration in renal function
by perturbing renal autoregulation through one or both ofthe mechanisms under discuss ion. One possibi l ity is thatnifedipine , by b locking slow calcium channels , prevents


No , Doc , ain’
t no fleas in my house*very
-close- ve ins Varicose ve ins
V irginia [REW ] Vag inavultures [REW] Convuls ions
*wound Wombwrecked fi stoola [REW ] Rectal fistula
ye l low jaunders [REW ] Jaund ice
Another source of confused communication may result
when the patient uses s lang or nonstandard d ialect to de
scribe symptoms , i l lness , or behavior vernacular that the
non-native doctormay not be famil iar with . Such terms are
often consistent w ith med ical theory , but they may also
hold subtleties that correspond to the patient’ s conceptionof i l lness .
9 As w ith malapropisms , some of these terms
have been described by others previous ly . A few of the
terms l isted here have apparently fal len from currentusage ,
yet others have a surpris ing permanence high blood‘
hypertension’
and low blood‘
anemia ,
’
described by bothSnow and Whalen) . The items that fol low were found in
folk speech primari ly in the southeastern United States .
S lang and Nonstandard Dia lect
agures chil l [JFB ] V iolent chi l l possib ly indicatingsepsis
*asthmy [REW ] Asthma
*al l -nervoused up [REW] Anxious
*bad b lood [REW , L FS] Syph i l is (See also
numbers in the bloodb l ind staggers [JFB ] Dizz iness , l ightheadedness
*blood wart s [REW ] Hemorrhoidscascading [REW] Vomiting
*changes Depression
corded [JFB ] Stiff , tight
deathly sick [JFB ] Nauseated*deep study In a depression
drawing spe l l [JFB ] Hyperventilation*fal l out [REW] Syncopal episode , fainting*fal l ing off the roof Menstruation*flick To have sexual intercourse*getting an attitude hostile , angry
*hark [JFB ] Cough or clear the throat
hassle ( l ike a dog) [JFB ] Dyspnea
haven’
t seen anything yet [JFB ] Fear of pregnancyas wel l as de layed menstruation
*heart drop Syncopal episode resulting from
Stokes-Adams Syndrome*high b lood [REW , LFS] Hypertension (But see
“low blood”
)*hunker [EWM] To get into a squatting pos ition
$ 9 6 6
Anemia (But see high
Syphil is ( see also bad
Septicemia , bacteri a in the
VOL . 46 , No . 7
* ln a deep study Depression (See changes*j immies Nervousness , anxietykernels [REW ] L ymph nodes
locked bowe l s [REW] Constipation
loss of courage [JFB ] Loss of sexual desire or
potency*low blood [REW , L FS]blood”
)*mak ing water Urination
my head rose [JFB ] Purulent otitis med ia*nature 1 . l ib ido , 2 . impotence , 3 . bowel s
*nerve aggravation Sciatica
nervous rigor [JFB ] Anxiety attack manifested byan alternating tensing and relaxing of the musclesover the body
*numbers in the b loodb lood”
)
peart , pyert [JFB ] L ive ly , in good health
pieted [JFB ] B lotched*piss hard (on) Erection common to young menupon wak ing
poison blood [LFS]blood stream
pone [JFB ] L ump or swel l ing , usual ly a harmlessaccumulating of fatquick ie [JFB ] H aving sharp pains
regina [JFB ] Vag inarisius [REW] Furuncles , boilsrunnin
’
off (at) the bowe l s Diarrhea
sal ivated [JFB ] Devastated by an il lness
shortness at the breast [JFB ] Dyspnea ( see also“hassle
*stretched out Nervous , anxious
stomach is torn up [JFB ] Diarrhea ( see also“runnin
’
off the bowe lsstubborn [JFB ] Constipated ( see al so locked
bowe ls , torpid l iver”
)strutted feet Swol len feet
suage down [REW] Lose weight*sugar diabetes Adult onset diabetes mel l itustorpid l iver, l iver is not k ick ing off just right[JFB ] Constipated (see also
“stubborn
locked bowels” )washing out the main nerve [REW ]Pneumoencephalography
*Terms previously reported by Whalen ( 196 1) are indicated by hisinitials [REW] ; those reported by Snow ( 197 4 ) are ind icated by [LFS] ;those reported by Bumham ( 1984 ) are indicated by [JFB ] ; by Massey
[EWM] ; and by Kol in [PCK] . Items actual ly attested inourown investigation are marked with an asteri sk .

References
I . Shuy RW . Unexpected by-
products of fieldwork . AmSpeech 1983 z5 8 13 4 5 -5 8 .
2 . West C. Routine Compl ications : Troubles w ith Talk Between Doctors and
Patients . B loomington: Ind iana UP. 1985 .
Kol in PC . The language of nursing . Am Speech l 97 3 :4 8 : l 92 -2 l0.
Kolin PC . More nursing term s. Am Speech -5 3 .
Huk i l l PB . The spoken language of medicine! argot, slang . cant. Am Speech
Pound L . Hospital lingo. Am Speech 193 8tl 3 122 7 -9 .
JUL Y 1985 , NCMJ
Bumbam JF. Dialect is diagnostic. Ann Intern Med l 984 :899-901 .
K leinmanA. Eisenberg L , Good B . Culture . il lness . and care? cl inical lessons
fromanthropologic and cross-cultura l research . Ann lntemMed l 97 8 :88 ; 25 1-8 .
Snow LF . Fol k medical be l iefs and their impl ications for care of patients: a
review based on studies among B lack Ameri cans . Ann lntemMed 1974 t8 1782
Whalen RE. Medical malaprops . JAMA l 96 l zl 7 7 315 8 -60.
Massey EW .Trofatter LP, Hartwig GB . Hunkering and peroneal palsy. Musc le
Nerve 198 1 . 44 5 .

MedicalMutual is pleased to offeryou Crisis : Then and Now ,the
latest in a series ofphysician loss preventionworkshops .
Th is innovative program w ill he lpyou:
Identify potential prob lem areas inyourpractice .
Reduce exposure in these areas .
Rece ive 5 percent d iscount onMMICpremiums for
EarnContinuingMedical EducationCred it.
Crisis : Then and Now is open to all physicians in convenient
locations across the state . Be sure tomark yourcalendar now for this
important session:
June 2 0, 198 5 at pm. Eli zabeth C ityColl ege of theAlbemarle ( LectureAud z
’
torium— B ldg .
“
B"
)
Jul y 1 1 , 198 5 at pm . H ickoryCatawbaMemorial Hospital (AHECAudi torium)Jul y 1 6 , 198 5 at pm. Wil sonWi lsonMemorial Hospital (Aud itori um)September 1 7 , 198 5 at pm. Ashevi lle
MountainAB EC ( Lecture H a l l)
September 2 4 , 198 5 at pm. Greenville
East Caro linaUnivers ity, School ofMed ic ineOctober 2 , 198 5 at pm. Kinston
LenoirMemorial Hospital (Aud itorium)October 2 9 , 198 5 at pm . W inston-SalemForsyth Memorial Hospital (Meeting Rooms 1 G 11)
MedicalMutual Insurance NorthCarolina2 2 2 N . Person Sr. , Rale igh , NC 2 7 6 1 1

CAROLINAHISTORY
Conscientious Obj ection and Clinical Care
A H istory of Civilian Pub lic Service Camp No. 6 1
at Duke Unive 194 2 - 194 6
Louis E . Swanson and James F . G ifford , I r . , Ph .D.
0 Conscientious obj ectors inWorld War 11 became an integra l part of theDuke H ospita l workforce .
wORLDWar II produced serious shortages of cl inical
ly trained manpower in hospitals across America .
While the cal l ing-up of physicians was careful ly planned ,
the more random drafting of attendant staff seriously curtai led the operation of many institutions . Beginning in
194 2 , the Se lective Service began effort s to rel ieve these
shortages by ass igning units of conscientious objectors toserve as attendants inmental health facil ities .
1Conversa
tions between Dr. Richard S . L yman, Chairman of—theDepartment of Neuropsychiatry at Duke ,
"
and Charles F .
Boss , Executive Secretary of the Commiss ion on World
Peace of theMethod istChurch , led to the estab l ishment ofCivil ianPubl ic Service CampNo . 6 1 atDuke inDecember1942 . The result was an experiment , unplanned by theorganizers of the unit, in the util izationof highly educatedlaypersons for
“
cl inical duties and responsib i l ities we l lbeyond the minimum requirements of the attendant’ s job .
The service of the s ixty-e ightmenwho rotated throughCPSNo . 6 1 made a major contri bution to keeping Duke Hospital running during the war , contri buted also to a constructive national critique of health care for the mental ly il l andprepared a number of these men for health-related careers .
Twenty years after deactivation in 1946 , appreciation of
their achievementhelped prepare acceptance atDuke of thedesignof a new answer tocl inical manpower shortages , the
physician’
s assistant.
Back ground
The strong peace movement in the United States duringthe 19305 accounted for inclus ion in the Selective ServiceAct of 1940 of provis ions for al ternative service for those
who were conscientiously opposed to war . Men who, for
rel igious reasons , were Opposed to al l mil itary service wereclassifi ed
“ IV-E and inducted into the C ivil ian Pub l icService program to perform work deemed national ly important under civil ian direction. Unwri tten guidel ines included that the work should notbe too vis ible to the pub l ic ,
should not be too easy and should not support the war
effort. In meeting these objectives Selective Service offiFrom the Medical H istory Program and the Department of Health Administration, Duke University Medical Center, Durham 27 7 10 .
JUL Y 1985 NCMJ
cial s sought and received the cooperationof church leaders
through a coordinating agency cal led the National Service
Board for Re l igious Objectors (NSBRO) . Its task was tomanage C ivi l ian Pub l ic Service Camps under regulationsdrawn by the Selective Service System.
2
The earl iest camps were organized for outdoor activityunder sponsorship of the Forest Service , National Park
Service , General L and Office , and similar agencies . L ater ,
special service camps were authorized under nonfederal
sponsorship forwork ingeneral andmental hospital s , training schools , publ ic heal th agencies and state agriculturaldepartments . There were more requests for special serviceunits than could be manned , so there was competition forthem despite the fact that financing the units was the te
sponsibi l ity of the sponsoring church or insti tution.
CPS No . 6 1 atDuke was a general hospital camp. Great
care was taken to insure that the unitwas accepted initial lyat the host site : negotiations to establ ish CPS No . 6 1 even
tual ly included Dr . Richard L yman, DeanW ilbert C . Davi
son of the Medical School , representatives of Selective
Service and NSBRO , official s of the Methodist Church ,
members of the univers ity and hospital administrations ,officers of the local Ameri canLeg ionpost, studentgovemment leaders and hospital staff.
The first unit complement was to be twenty men, ten to
serve on Meyer Ward , the psychiatry inpatient ward at
Duke Hospital , and ten to serve at H ighland Hospital , an
affi l iated psychiatri c hospital inAshevi l le . Dr . Deryl Hart ,
Chairman of the Department of Surgery at Duke , then
requested an additional ten men to serve as orderl ies inoperating rooms . Se lective Service agreed and authorizedCPS No . 6 1 onOctober 27 , 194 2 . Notice of the new campwas circulated through the CPS system. Thirty men were
chosen from an initial appl icant pool of seventy- five men
already serving atmore thana dozencamps in the East andMidwest.
3
As a group these men knew l ittle about Duke , often
confus ing it with other univers ities . A few knew of the
parapsychology experiments of Dr . J. B . Rh ine ; a fewothers recognized the name of a national ly ranked footbal lteam. One had heard that a Mr . Duke had g iven fortymi l l ion dol lars to bui ld a univers ity in a forest. Coming to a

university hospital was a major incentive , however , for a
group ofmenwho , on average , were much better educatedthan those who normal ly held attendant and orderly posi
tions . A number of the inductees had col lege degrees and
many others some col lege experience . The ir personal con
victions about l ife ,which led them to refuse mi l itary ser
vice , strongly supported working ih the areas of medicine
and health .
Duty and Development
In general terms the mission of the unit was to staff the
psychiatric cal l units and the operating rooms . Its first
official exposure to Duke Hospital was a meeting in the
traditional medical school teaching amphitheater , which
was somewhat intimidating to the newcomers . VernonAltvater , Superi ntendent of Duke Hospital , extended an
official welcome which stil l is vividly remembered . The
menwere spread around the arena in the first row of seats .
Saying he wanted to make h is position perfectly clear ,
Altvater began by draw ing a l ine on the floor.
“When I amon this side of the l ine I can talk to you as individual s ,
whether or not I agree with the position you have taken asCOs . When I am on the other side of this l ine I am the
administrator of Duke Hospital and enforce the rules and
tel l youwhat“
to do . L et’
s notmix the two . We are glad you
are here ; we need your help.
” 4
Thereafter the men served in three distinct groups . The
Meyer Ward contingent was supervised by Dr. L yman,
who al so was the unit’
s overal l director . Dr . Robert S .
Carrol l supervised the tenmen assigned to H ighland Hos
pital and Dr.Max Rogers was responsible for the operatingroom group. R . Paul B rotsman, a member of the unit,
served as ass istant director responsib le for l iaison amongSe lective Service , the sponsoring Methodist Commission
forWorld Peace , and the administrationofDuke Hospital .
In 194 3 , whenDr . Lyman entered active mil itary service ,
he was replaced as unit director by Dr. R. Burke Suitt.
The work week for al l groups was 4 8 hours , including s ix
F igure l . Pos itioning a pa tient. Note the C0’
s uniformwith its distinctive diamond
shaped pa tch on both s leeves . (Photograph courtesy of Robert B lake . )
VOL . 46 , No . 7
Of instruction, plus an additional six hours of training in the
evenings . Pay was permonth plus room and board .
This stipend compared to the per hour, or approx
imate ly permonth , paid to GermanPows work ing
at amental hospital fifteenmiles northeast ofDurham, but
the COS accepted the differential in good humor and with
out il l fee l ings .
In the operating rooms the trad itional task s of orderl ies
were not difficult to learn, ranging from janitorial duties tonursing care . The men prepared equipment, transferredpatients to the operating suites , positioned patients for
surgery ( figure and returned them to their rooms . They
located and positioned equipment, transported instrumentsand suppl ies , mopped floors , wal ls and cei l ings , sorted
l inen and laundry , and ingeneral Ieamed to anticipate what
needed to be done without instruction. They staffed the
Operating rooms from AM to PM , earning from
Margaret Pinkerton, Dean of the School of Nursing , this
comment:“The operating room has had to handle more
cases this year than ever before: Our subsid iary he lp hasgrownprogressive ly poorer andmore unre l iab le . The oper
ating group (CPS) has worked hard and under a goodmanydifficulties . Due to their superior intel l igence , they are of
greater he lp in placing patients in position, l ifting , etc .
” 5
On Meyer Ward patients were admitted for intensive
treatment pointed toward recovery and release . The aver
age stay was 30 to 40 days . The men fed , clothed , and
bathed patients and part icipated in the ir recreation. They
administered wet sheetpacks to excited patients and nursed
others through shock treatments . They took TPRs (temper
ature , pulse , and respiration) and charted patient behavior.
Miss Pink erton noted splend id results in carry ing out
occupational therapy measures planned by the doctors .
This heretofore had been impossible due to “
inferior
help.
AtH ighland Hospital the work s ituationwas quite different . Therapy programs were long term. More thanone-hal f
of the employees had been at some time psychiatric pa

Figure 2 . Artist at work . (Photog raph courtesy of Robert B lake . )
tients . Some stil l were il l , whi ch made l ife interesting forattendants . Exercise and phys ical exhaustionwere used tomaintain the physical cond ition and rel ieve the nervous
tension Of the patients , and both insul in shock therapy andelectri c shock therapy were more frequent than_
onMeyerWard . Patients were at ri sk during these treatments and theattendantsworked closelywith the nursing staff tomeet anyemergencies . Dr . Carrol l commented that the male depart
ment of the hospital might we l l have closed but for the
coming of the CPS group. He al so noted that
Practical ly without exception themembers of this unitwho came to us directly from camp l ife fel l into the
unique routine Of respons ibil ities and activities here witha minimum of disruptance , indeed with an unexpectedmax imum of efficiency . Those who came to us after
Figure 3 . Working with EEG machine . (Photograph courtesy of Robert B lake . )
JUL Y 1985 , NCMJ 4 2 1
some months at Duke were definitely more difficult. Itwould seem that to the advantages Of the H ighland Hos
pital regime they expected to find the atmosphere of
Univers ity surroundings and so considerable gratuitousadvice was g ivenus , and fromcertain sources , cri ticismof conditions was apparent.
By the end of the first year the excel lentperformance ofthe inductees in the ir day
- to-day routines and the highpercentage of col lege graduates among them led Dr. Lyman to consider what more these men could do for his
patients .
“My major interest in the unit , he wrote , has
long since moved from the realmof the once needed hospi
tal routine to that of poss ib il ities of personal and groupdevelopment, which have been started but by no means
ful ly attained as yet. Encouraging the men to pursue their

personal and professional developmentmight save time for
physicians on wards and in labs . The point has beenreached where I would enjoy being chal lenged toprove thatwe can fulfi l l some of these possib il ities , creating values
which were not even recognized to l ie within the scope of
this project at first.
6
The values real ized were remarkab ly varied . One man
w ith previous experience in personnel work , assigned to
type patients’
social histories for psychiatry residents part
time , moved on to tak ing the histori es ful l - time , thus
freeing the residents for other work . A background in art
and photography led another to work preparing charts ,
drawings , and photographs for research articles and ex
hibits and , afterdeactivation, to a l ifetime career inmedical
art and i l lustration at Duke ( figure Two COS with
eng ineering backgrounds were assigned to the EEG (e lectroencephalogram) lab to help keep the only EEG machinein the reg ion running (figure In the process they madeseveral modifications of the machine that improved its
performance . Other unit members maintained colonies of
experimental research animals , became laboratory techni ~cians and assistants , deve loped courses of physical therapyto assistpatients preparing fordischarge from the hospitals ,and participated inresearch on insul in therapy , b lood banking , motion sickness and recreational therapy for children.
By 194 3 the complement of the Duke unitwas raised to 4 5to accommodate transfers to ful l time special duty . These
contributions , and the savings in trained manpower that
they represented , greatly benefited Duke Hospital . As VernonAltvater later noted , Although your unit is small in
size when it is compared to the total number of us workinghere , it has at times seemed to mark the dividing l inebetween this hospital
’
s running or be ing part ial ly shut
down.
” 7 At least five men took the MD . degree after the
war .
Diversion
L iving and working conditions general ly were betterthan inotherCPS camps . Initial ly the men atDuke l ived inlog cab ins fi rst built as hous ing for law students . At H ighland Hospital they l ived in smal l cottages . Beginning in
194 3 married couples could l ive Off s ite at the ir own ex
pense . There was l ittle publ ic reaction to the unit, and noreported or known incidents Of harassment other than the
loud ly voiced opinions of a few ind ividuals who resented
the ir presence atDuke . Wives who worked inDurham fe ltthemse lves somewhat different from the ir coworkers but,
in part because they usual ly chose not to d iscuss their
husbands ’
work , fe lt l ittle negative social pressure . In
comes were meager, but as th is was true formany fami l iesduring wart ime , few fe lt victimized . Ne ither did the CO
status impose undue pressures on the marri ages , except in
cases when the fami l ies of prospective w ives objected tothe mani ages beforehand . Unitmembers and the ir famil iessocial ized w ith each other , and other hospital staff, during
picnics in the Duke forest , b icyc le and bus trips , and in
softbal l and footbal l games , but social contact in the larger
communities was l imited .
The emphas is oneducation thatwas prominenton the jobcontinued during Off-duty hours . Some evenings were
spent in formal training , with lectures and demonstrations
4 22 VOL . 46 , No . 7
on patient problems and hospital procedures . Others were
spent in rap sessions”on topics such as the meaning of
conscientious Objection, the use of force in the manage
ment Of patients , and issues of international concern. Stil l
others were devoted to independent classes organized bythe men, including language study inFrench , German, and
Chinese , reconstruction in the South , and re l ief work
motivation. At H ighland Hospital , Dr. Carrol l conducted
classes inpsychiatric theory , d iagnosis and practice , noting
the outstanding inte l lectual capacity and seriousness of
purpose of the men.
Those who worked in the Meyer Ward and Highland
Hospital groups , in communication with COS serving at
othermental health facil ities , gradual ly developed a senseOf
“responsib il ity to contri bute to the improvement of the
standards of patient care in the hospitals and later in l ife to
contribute to the fie ld ofMental Hyg iene inone capacity or
another .
8This intentionemerged outof sess ions inwhich
the menmeasured the ir work experience against the ir personal principles , noting conditions that should be changed
and others that could be improved . Contrasting the Meyer
Ward and H ighland H ospital experiences led to the“
gra
tuitous advice”and
“criticism of conditions
”
at H ighland
noted by Dr . Carrol l , but al so to a shared conviction that“we shouldn
’
tjustpointoutvarious deficiencies and gripesbut that we should do something in the l ine of concrete
suggestions and detailed plans . Areas targeted for te
search included the use Of force , restraint and sedatives in
treatment, upgrading the role of attendant, the need to
reduce publ ic fear Of mental i l lness , improvement of lawsto safeguard patients , promotionof improved conditions ofmental health in local communities and preparation for
contri buting to the fie ld ofmental hyg iene , vocational ly or
avocational ly , after d ischarge from Civil ian Pub l ic Service .
Conditions at theDuke and H ighland hospitals innowayresemb led those discovered by COS stationed in somemental institutions ,
9wherepatients were poorly fed ,
il l housed ,
supervised by unqual ified attendants , occasional ly beatenor choked into unconsciousness , and often left for days at a
time wi th nothing to do . As the intention of CPS inductees
to improve cond itions inmental health facil ities became anationwide movement, CPS No . 6 1 members made usefulcontributions because of the ir exposure to more enl ight
ened standards of treatment. They col lected and shared
their experience through an in-house b imonthly pub l ication
cal led Service , wh ich also presented pertinent excerpts
from other pub l ications . NSBRO pub l ished The Reporter ,
which kept the men abreast of issues and events in other
camps . National ly , CPS men organized as the Mental
Hygiene ProgramofCivil ianPubl ic Service and pub l ishedThe Attendant, wh ich was devoted to publ ishing information describ ing appropriate attitudes and procedures in patient care and to improving the role of attendants to the
semi-professional status of psychiatric aides .
IOThis jour
nal’
s cal l for al l readers to become contributors d irectlyrefl ected the efforts of individual units l ike CPS No . 6 1 to
improve conditions at the ir host s ites . Some were d irectlyinvolved , beg inning in 194 6 , in the work of the National
Mental Health Foundation which , with five former Cos
serving as the executive committee and sponsorship from

lmes
Sa turn 3000 0 full d isc losure ca sse tte Holte r scanne r
offe rs your practice newly created profe ssiona l andeconomic Opportunitie s.
Sa turn 3000 is fully ed ita b le , comple te ly ve rifia b le a nd
six ( 6 ) fina l reports offe r you O we a lth of hig h ly interpreta b le d iag nostic informa tion.
Be st of a ll it'
s simple to ope ra te a nd ea sy to ma inta in.
It ta ke s le ss than 15 minute s to complete Cl study, a llowing you immed iate patienta sse ssmentand pe rsc ription.
Lewis Med ica l Instruments, e xc lusive d ea le rs of Sa turn3000, ha s ove r 20 ye a rs of sa le s and se rvice e xpe rienceto the North Ca rolina med ica l community.
Ourknowled g ea b le sa les representative s a nd expe rtlyequipped technica l se rvice depa rtment a ssure tha t youwill rece ive qua lity instrumenta tion a nd continuous se rvice support to provide you witht he be stva lue foryour inve stment. LewlsInc re a se d Opportunity , h ig hquo lity instrumentation and e xce l gets tolent se rvice is why you should ca ll the heart( 919 ) 84 8 -4 3 3 3 tod ay for your no
Ob lig a tion prod uct d emonstra tion. Of thematter
L EW IS ME D IC A L IN S TR UME N T S IN C .

PUBLIC HEALTH
PROJECT iPECAC
AnAccident Prevention Program of the
Robeson Coun epartment of Health
Thad B . Wester, MD .
0 Thad Wes ter has had a d istinguished ca reer as a ped ia tricpractitioner inLumberton. H e moved to the other s ide of the table to direct the Department of H ea lth of Robeson County . Knowing tha t
“where you s it deter
mines wha t you see , I have encouraged Thad to g ive the rest of us hisviewof our activitiesfromhis newperspective . I hope thathe wi l l continue
to publ ish in the Journal . E .A.S
HE most common health risk to children and youngTadults is accidents . In the preschool child , the mostfrequent accident-related risk is accidental ingestion of
poisonous and noxious substances .
Trad itional ly , ped iatricians and’
fami ly.
practitioners
have advised parents to keep syrupof ipecac on hand to be
used to induce vomiting as early intervention. Often this
advice is notheeded , leaving the family unprepared to reactin an emergency s ituation. In such instances , over-the
phone emergency counse l ing from phys ic ians and
emergency roompersonnel who suggest the use of ipecac isuseless , because ipecac is not readi ly at hand .
The program described , albeit fundamental ly very simple , provides a solution for a community with such a
problem. It also requires minimal continuous involvement,is cost effective and automatical ly accompl ishes its objectives . In addition, it is a testimonial to the advantage of
using the pub l ic health system in cooperation w ith community efforts to effectively accompl ish a result that the
private sector’
s one-on-one activity had been unable toobtain.
Obj ective
The ultimate goal of the project was to provide a oneounce bottl e of syrupof ipecac , along with instructions and
educational material s , to each household in the county witha preschool child .
An estimate of the number of households can be determined by multiplying the county b irthrate by five (representing the five preschool years) . To this estimatewe addeda fudge factorof 20percent to al low distributionto day-care
facil ities and fami ly households where day care was pro
vided by friends and members of the fami ly .
Depending on the availab i l ity of funds , the projectcanbeFrom the Robeson County Department of Health , Lumbenon 2 83 5 8 .
JUL Y 1985 , NCMJ 4 2 5
accompl ished , as in Robeson County , through a crash
program. In such a program, the initial distribution of
ipecac and the other material s occurs over a two or three
month period .
An al ternative would be a phased program that would
cost less but would require four or five years to reach the
desired saturation. The use of a phased program is stil l a
critical component of the ongoing program and wil l be
described separate ly .
Crash Program
We sol icited ass istance from the fol lowing groups :
pharmacists , ped iatri cians and general practitioners , daycare center operators , areamedical centers and cl inics , theDepartmmt of Social Services , school nurses , volunteerorganizations and hospital nursery and emergency room
personne l . The purpose of the ipecac program and the
distribution process were explained to these groups . Sup
port for“Project Ipecac was unanimous fromeach group.
Preliminary Results
The success ofour program, although based onfigures ofl imi ted numbers and for very short periods , sti l l appears
impressive . We have seen a reduction of 2 5 percent in
emergency room vis its for the ingestion of potential ly
poisonous substances during the six months immediate lyfol lowing the advent of
“Project Ipecac , compared with
the same six-month period in the previous year .
We have also real ized more than a 50 percent reduction
in hospital izations . Of the four hospital admissions duringthe most recent six-month peri od , twopatients were admit
ted for kerosene ingestion. The other two were admi tted
only for observation and were re leased w ithin 12 hours .
( Inone case , syrupof ipecac had beengivenappropri ately and vomiting had been induced , but the attending physi
eian felt admi ss ion for observation was worthwhile . The
chi ld was released in less than six hours . )

EMERG EN CY ROOM V IS ITSIN GES T IO N O F NO X IOUS S U BS TAN CES
1 9 8 3 i 9 8 4.
( J ULY necemaen 3 1 )
H OS P ITAL ADMIS S IONSING ES YION O F NO X IO US S UB STAN CES
1 9 8 3 1 9 8 4
( JULY t—OECEM B E R 3 1 )
F igure 1 . Emergency room vis its ( top ) and hosp ita l admis s ions
(bottom) in the years before and during the Proj ect Ipecac crash
program.
4 26VOL . 46 , No . 7
Cost B enefit
The cost of syrup of ipecac in quantity is approximate ly7 5 cents per one-ounce bottle . The cost of educational
material is approximate ly 60 cents , most of which is print
ing costs for the book let, “Your Child and Household
Safety . The staff time to deve lop and implement the
program came from with in the health department. Other
volunteer and professional time was contri buted as we l l .
The total costof the crash program inRobesonCounty wastimes or
The cost of the continuing (or phased ) program wil l be
d irectly related to the number of del iveries per year . In
Robeson County there are approximately de l iveries
each year for an annual cost of approximatelyIn the year prior to the program, there were 20 hospital
admissions for poison ingestions in the local hospital , two~
thirds of which might have been prevented by the timelyuse of syrup of ipecac . The estimated dol lar cost of these
hospital izations was approx imate ly According to
prel iminary data , these hospital izations have decreased by
50 percent s ince the advent of the Ipecac program ( figureThe cost of the crash programwould be s l ightly greater
than that saved in the first year of the project.
Our annual operation cost in the ensuing years is only
one- fi fth the cost of the crash program, yie lding a
savings to cost ratio each year . The value of the other
obvious benefits of preventive med ic ine , avoiding the
stresses , handicaps and even the loss of l ife resulting fromaccidental poisonings , is incalculable .
We recommend this program to other communities if anactive , efficient poison prevention program is not alreadyinplace . It is simple inconcept, is cost efficient and works .

ounce
IS WOI'
OWmucSound financial planning canhe lpprevent financiald isas ter inthe future if a s ickness or injury everkept youfromworking . If youcould notwork , howwould you
yourregularmonthly expenses both personallyand profess ionally?As amemberof the North CarolinaMed ica l Society,youare e lig ible forDisability Income Protect ionatAssociationGroup rates . This plancanhe lpreplace
los t income ifa covered accidentor illness keepsyoufromyourpractice .
The month ly benefits payable underthis planmaybe used tocoverre nt, utilities , medica l bills , houseorcarpayments , groceries any of your
expenses thatwill continue during yourd isability.
If youare underage 5 5 and are active full timeinyourpractice , find outmore about thisvaluable protectionby returning the couponbe low. Mutua lof Omaha underwriterof this
plan will provide prompt, courteousservice infurnis hing youwith full deta ils onthis fine coverage . Mail yourreques t forinformationtoday.Afterall, anounce
People youcancountl ife Insurance AffiliateUnited ofOmaha
MutualofOmaha InsuranceCompany 0 Home Offi ce: Omaha , Nebraska
Mutua l ofOmahaGeorge RichardsonPO. Box 2 1 1 3
Winston-Sa lem, NC 2 7 10 2
Pleas e provideme complete informationonthe Disability Income ProtectionPlanavailable tomembers of the North CarolinaMedica l Societywho are underage 5 5 .
JUL Y 1985 , NCMJ 4 2 7



B rie f Summary of Prescribing InformationNORLESTRIN l (nore ih ind rone acetate and eth iny l estrad iol tab le ts .USP)
See section und er Spec ia l Note s onAdminis tration and HOW SUPPL IED.
Before prescrib ing , please see lull presc rib ing infOrmal ion. ABriefSummary follows .
DESCRIPTIONNorles lnn Produc ls are proges logen
-es trogencomb ina l ions .
iNDlCATIONS ANDUSAGENorles i rin Products are ind icated for the preventionofpregnancy inwomenwho e lect to use
Ora l caniracepiives as a method ofcomi acepl ion.
Inc l inica l tria ls with NOrlesuin involvmg the rapy Cycles . lhe re was a pregnancy rate of0 05 per 100woman
-
years ; in cl inica l tria ls with NOi les l rin 2 involvingCyc les . lhere was a preg nancy rate ofO2 2 pe r 100woman
-
years .
Dose-Re lated Ris k ofThromboembolism fromOral Contraceptives : Studies haves hown a DOS l l lve assoa a lron beiween the dose of es trogens in oral contraceptives and the
ris k of lh romboembolism. If is prud entand in keeping wungood prinC iples of therapeutic s to
minimize e xposwe lo estrogen. The oral contraceptive preSOribed forany g iven pal ie ri l
s hould be me tproductwh ich conta ins the lee s l amountof estrogen that is compatib le withanacceptab le pregnancy rate and pa l ienl acceptance .
CONTPAINDICATIONSt. Thromboph leb itis Or th romboembolic d isorders2 . Apas t history of d eep
-ve in ih romboph lebil is or lhromboembolic d isorde rs3 Ce reb ral vascularorcoronary artery disease
4 . Knownorsuspected carcinoma of the b reas i5 KnownorSuspected es trog en-d epend entneoplas ia
6 Und iag nos ed abnormal genita l b leed ing7 . Knownorsuspected pregnancy (See WARN ING No. 5 )8 . Benignormalignant l ive r tumorwhich deve loped during the use ofOra l contraceptives
Orolhar estrogen-containing products
1 . Thromboembolic Disord ers and Other VascwarProb lems An increased ris k of lhromboembolic and th rombotic d isease as sociated wrl h the use Ofora l contraceptives is we lles lab lished S lud ies have d emons trated an increased ris k of la ia l and nonfatal ven0usl h romboembolismand s troke . boib hemorrhag ic and thrombotic .
Cerebrovas cularDisorders : In a collaborative stud y inwomenwith and wrlhoul pred isposing causes .
II was es timated that the ris k of hemorrhag ic stroke was limes g reater inusers thannonuse rs . and the ris k of thrombotic s troke was 4 0 lo 9 5 limes g reate rMyocard ial Infarction: An increased risk ofmyocard ia l infarction assoa aled wuh ora lcontraceptives has been reponed confirming a previous ly suspected association. These
s lud ies found that the greater the numberofunderlying ris k factors (cigarette smoking .
hypertension. hypercholes lerolemia . obes ity. d iabete s. h istory ofpreec lamptic toxemia ) forcoronary artery d isease . the h ig he r lhe risk ofdeve loping myocard ial infarction,
regard les s
ofwhethe r the patientwas anora l contraceplive userornot. Oral contraceptives . however.we re found lobe a c learad d itional risk factor.It has been es timated l ha l use rs who do notsmoke (smoking is cons idered a majorpre
d ispos ing cond ition tomyocard ia l infarc tion) are ab0ul lwice as like ly to have a fatalmyocard ial infarctionas nonusers who do not smoke . Oral contraceptive use rs who are smoke rshave aboma twofold increased ris k of laia l infarctioncompared to users who do not smoke .
bul abd ul a tenfold lo iwe lve lold increased ris k compared to nonusers who do not smoke .
The amountof smoking is also an important factorRis k of Dos e : Inan analys is of d ata. British inves tigators concluded that the ris k of lhrOm
boembolism,inc lud ing coronary thrombos is . is d irectly re lated to the dose of estrogenused
inoral contraceptives . howe ver, the quanlily ofes trogenmay not be the sole factor involved .
Pers is tence ofRis k : Two stud ies have sugges ted l ha l an increased ris kmay pers ist for aslong as 6 years afte rd iscontinuationofora l contraceptive use forcere brovas culard isease
and 9 years formyocard ia l infarction. Inad d ition. a prospecrive s tudy Suggested the per
s is lence of risk for subarachnoid hemorrhageEs timate of Exces s Morta l ity fromCirculatory Diseas es : The risk ofd iseases of the CI ! ‘
Cula lory Sys tem is concentrated inolderwomen. in inose with a long durationof use. and in
cigarette smokers .
As tudy ofavailab le data from a varie ly ol sources concluded that the morta lity as soma ledwnh a ll method s of b irth control IS low and be low that as sociated with chi ld birth. with the
exceptionoforal contraceptives inwomenover 40 who smoke .
The ris k of th romboembol ic and thrombotic d iseas es assoo aled wrlh ora l contraceptivesincreases wrlh age afte rapprOximale ly age 30 and , formyocard ia l infarction. is further
increased by hypenens ron. hype i choles le iolemia . obes ily. d iabetes .or h is tory ofpre
ec lampl ic toxemia. and espec ially by crgare l le smoking .
The phys iCianand the patient snOuld be a lerl lo the earliestmanifes tations ofrh romboembolic and thrombolic d isord ers . ShOuld any OcCw or be Suspected .
the d rug should be d is
continued immediate lyA fourf old lo s ixfold increased ris k ofpos lswgery ihromboembolic complications has
been reported in users . If feas ib le.ora l contraceptives shouid be d iscontinued a l leas l lOur
wee ks be fore Surg ery ofa type assOCialed wrlh an increased ris k of l hromboembolismor
prolonged immobi lization.
2 . Ocular Les ions . NeurO-Ocular les ions . Such as optic neuritis or retinal thrombos is . have
been as soc iated with the use ofora l contraceptives . Discontinue the oral contraceptive if
lhere is une xplained Suddenorg radua l. parl ia l. orcomplete loss ofViSlOn. onsetof proplo‘
s is or d iplopia : papi lled ema: Or re l inal vascular les ions3 . Carcrnoma. Long-termcontinuous administration ofestrogen in certa inanima l specres
increas es the frequency ofcarcinoma of the b reas l . ce rwx , vag ina . and l iver.
In humans , an increased ris k ofendome lrial carcmoma assoc iated wilh the prolongeduse ofexogenous es trog en in pos tmenopausa l women has been reboi led However, lhere
is no evid ence suggesting increased ris k ofendomel ria l cancer in use rs ofconventional
comb inationorproges logen-only ora l comiacepl ives .
Stud ies found no ewd ence of increase in b reas tcancer inwomen tak ing oral contracepi ive s : howeve r, an exce ss ris k in use rs W ith dOCUmenied benign breas t d iseas e wasreportedThe re IS no confirmed evidence ofan increase d ris k ofcancer assocraled with oral conira ~
captives . Close c l inica l surve i llance ofusers is .neverihe le s s . essential Incas es 0 | und iag
nosed perS isrenl or recnrreni abnormal vag ina l b lee d ing . appropriate d iagnos iic meas uress hould be taken to rule Oul mal ignancy.Womenwrlh a s trong family h is iory of b reas tcance r.orwho have breas tnodules .
lib rOCys lic d is eas e . orabnormal mammog rams . should be
monitored W l ih particularcare4 . Hepatic Tumors Benign hepatic adenomas have been found lo be as sociated with oral
conlracepl ives . Because hepa l ic ad enomas may rupture and may cause death throughinfra-abdominal hemorrhage . they should be conS id ered inwomenpresenl ing abdominal
pa in and lend erness . abdomina l mas s . or shock .
A few case s of heparoce llularcarcmoma have been reported inwomen taking oral contracep l ives . The re lationsh ip of these d rug s lo th is lype ofmalignancy IS nol known a l th is time .
5 Usa e in or Immed iate ! Preced ing Pregnancy. B irth De fects in Offspring , and Manynancy In emele Offspring .During early pregnancy. female sex hormones may serious lyd amage the off springAn increased risk ofcongenita l anoma l ies . inc lud ing heart defec ls and limb d e fecls . has
been reponed W ith the use ofOra l contraceptives in pregnancy.There is SOrn e evid ence that triploidy and pos s ib le olher types of polyploid y are increased
among aboi l uses fromwomenwho b ecome pregnani soon after ceas ing ora lconiracepi ive s
Pregnancy should be ruled OUI before cominumg anOra l comracep l ive inany pa lieri l who
has mis sed twoconseCui ive mensl rual periods ll lhe patient has notadhered lo the schod 0 1985 Wa rne r-Lamb ertCompany PD-21-JA-2 56 3 -P-tf11-84 ]
ule . the poss ib i l ity ofpregnancy should be cons idered at the time of the firs tmis sed period .
and oral contraceptives should be withhe ld unti l pregnancy has been ruled Out Ifpregnancy is confi rmed . the patients hould be apprised of the potential risks to the fetus and theadvis ab i lity of Continuationof the pregnancy should be d iscuss edWomenwho diSCOntinue oral contraceptives W ith the intentof becoming pregnant s hould
us e ana lternate form ofcontraception tora period of time before attempting to conce ive .
Adminis trationofprogestogen-only Orproges togen-es trogencombinations to induce
withd rawal b leed ing should not be us ed a s a tes tof pregnancy6 Ga llb lad d erDisease Stud ies report an increased ris k of Surg ica lly confirmed gallb lad
de r d is ease in us ers ofora l contraceptives .
7 Carbohydrate and Lip id Me tabolic Effects . Becaus e d ecreased g lucose tolerance hasbeen ob served in 3 S ignificantpercentag e ofpatients . pred iabetic and diabe tic patientsshould be care fully ob se rved wh ile rece iwng oral contraceptives .
An increase in trig lycerides and total phospholipid s has beenobserv ed .
8 . Elevated B lood Pres sure An increas e in b lood pressure has been reported in patientsrece iving Ora l contraceptives . The preva lence inusers increases W ith long e re xposwe .Ageis also s trong ly corre lated W ith deve lopmentof hype rtens ion.Womenwho previous ly havehad hypertens ion during pregnancymay be more like ly to d eve lop e levationofb loodpresSure
9 . H eadache . Onsetorexace rbationofmig ra in e ord eve lopmentof headache ofa new
pa tte rnwhich is recurrent. pers istent.orsevere . requires d iscontinuationoforalContraceptives
10 B leed ing lrregularitie s Breakthrough b leed ing . spotting . and amenorrhea are trequent reasons for patients d iscontinuing ora l contraceptives . In breakth roug h b leed ing .
nonfunctiona l causes should be borne inmind . tnund iag nosed abnorma l b leed ing from the
vag ina , ade quate d iag nos tic measures are ind icated to rule Outpregnancy ormal ignancy.Womenw ith a pas th is tory ofoligomenorrhea Or second ary amenorrhea . Or young women
without regularcycles should be adv ised that theymay have a tend ency to remain anovulatory or to b ecome amenorrhe ic after d iscontinuationol ora l contraceptives11. Ectop ic Pregnancy. Ectopic as we ll as intraute rine pregnancymay occur incontracep
tive fai lures
12 Breas t-Feeding . Ora l contraceptives may interfere with lactation Furthe rmore . a smallfractionof the hormonal agents in Oral contraceptive s has been id entified in the milk ofmothe rs rece iving these d rug s .
PRECAUTIONSl . Acompletemedica l and family h istory should be taken prior to the initiationoforal con
traceptives . The pretreatmentand period ic phys ical examinations should inc lude spec ia lreference to b lood pressure . breasts . abdomen. and pe lvic organs inc lud ing Papanicolaousmearand re levant laboratory tes ts. As a g eneral rule ora l contraceptives should not be
prescribed for longer thanone yearwithoutanother examination.
2 . Preexis ting uterine le iomyomatamay increase in S ize .
3 Patients with a his tory ofpsych ic depression should be carefully observed and the drugd iscontinued ifdepress ion recms toa se rious deg ree4 . Ora l contraceptives may cause fluid re tention and should be prescribed with caution.
and only with care fulmonitoring . in patients W ith cond itions wh ich mig ht be agg ravated .
5 Patients with a pasth is tory of jaund ice during pregnancy have an inc reased ris k ofrecurrence oI iaund ice . ll iaund ice deve lops . the med ication should be d iscontinued .
6 . Ste roid hormones may be poorly metabolized and should be adminis tered W ith cautionin patients W ith impaired liver function.
7 . Us ers may have d is turbances in norma l tryptophanmetabolism.wh ich may result inare lative pyridoxine de fic iency.8 . Se rum lotate leve ls may be depressed .
9 The patholog is t should be adwsed oforal contraceptive the rapy when re levantspeci
mens are Submitted .
10 Certain endocrine and liver function tests and b lood components may be affected( 3 ) Increased sutlobromophtha le in retention. (b ) Increased prothromb inand factors VII.VI I I. Ix. and X: decreased antithromb in 3 : increased norepineph rine - induced plate letaggre
gab ility (c ) Increased thyroid -b ind ing g lobulin (TBG ) lead ing to increased circula ting tota lthyroid hormone (d ) Decreased preg naned iol excretion. (e ) Red uced response tometyra
pone tes t.
Drug Inte ractions : Reduced e fficacy and increased inc idence ofbreakthroug h b leedinghave beenassoc iated with concomitantuse of rifampin As imi larassociation has been Sugg es ted W ith b arb iturates , phenylbutazone . phenytoin sod ium. tetracyc line . and ampic illinADVERSE REACTIONSAn increased risk of the fol lowing serious adverse reactions has been associated with oral
contraceptives thrombophteb itis : pulmona ry embolism: coronary th rombos is : cerebra lthrombos is : cereb ral hemorrhag e . hypertens ion: gallb ladderd isease : benign hepatomaszcong enita l anomalies .
The re is evidence ofanassoc iation between the following cond itions and the use oforal
contraceptives , a lth0ug h ad d itional confirmatory stud ies are needed ; mesenteric thrombos is. neuro
-ocular les ions . eg . re tinal thrombos is and optic neuritis .
The following adverse reactions have been reported in patients rece iving oral contracepl ives and are be l ieved to be d rug re lated : nausea and / orvomiting . usual ly the mostcommon adve rse reactions , occur inapproximate ly 10% or les s ofpatients d uring the firstcycle .
Other reactions . as a general rule. are seenmuch less frequently oronly occas ional ly:gas tromtes tinatSymptoms : breakthroug h b leed ing : spotting : chang e inmenstrua l flow:d ysmenorrhea. amenorrhea during and a fte r treatment. temporary infertility afte rd iscon~
tinuance of treatment: edema: ch loasma orme lasma: b reas tchanges : change inweig ht:change in cervica l a mmo and cervica l secre tion: pos s ib le d iminution in lactationwhen
g iven immed iate ly postpartum.cholestatic taund ice migraine ; increase in s ize ofuterinele iomyomata. ras h (alle rg ic ) :mental d epres s ion: reduced tolerance to carbohyd rates.vag ina l cand id iaS i5 : change
“
in cornea l Curvature; intole rance to contact lenses .
The followmg adverse reactions have beenreported and the assomation has beenne itherconfirmed norrefuted : premens trua l like synd rome : cataracts. Changes in libido: chorea:changes
“
inappetite. cystitis like Synd rome: headache: nervousness : d izz iness : h irSutisnt:loss of sca lp ha ir: erythema multi forme : e rythema nodosum: hemorrhag ic eruption: vag init
porphyria.
Spec ia l Notes onAdministrationMens truation usually beg ins two or three days . butmay beg inas late as the f0 urth or fifthday, afte rd iscontinuing med ication.
After severalmonth s on treatment. b leeding may be reduced to ammofvirtual absence :
reduced l lowmay be a resultofmed ication and not ind icative of pregnancyHOW SUPPL IEDNorle strin t/ so is availab le incompacts each containing 2 t tab lets Each tab letconta ins1mg ofnore th ind rone ace tate and 50mcg of eth inyl es trad iol.Ava i lab le inpackages of fivecompacts and oackages of l ive refills .
Norles trin is availab le incompacts each containing 2 1 tab lets Each tab letconta ins 2 5 mg ofnore th ind rone ace tate and 50mcg ofeth inyl es trad iol. Ava i lab le inpack
ages ot l ive compacts and packages of five re fills .
Norlestrin t/ so'
is availab le“
incompacts each containing 2 1 ye llow tab le ts and 7b rown tab lets Each ye llow tab le tcontains 1mg ofnore th ind rone acetate and 5 0mcg ofeth iny l es trad iol. Each b rown tab letconta ins 7 5 mg of ferrous fumarate . USP. Availab le in
packages of five compacts and packag es of five refills .
Norlestrin 2 is ava ilab le in compacts each conta ining 2 1 pink tab lets and 7brown tab le ts Each pink tab le tcontains mg ofnoreth ind rone ace tate and 50mcg ofe th iny l es trad iol. Eac h brown tab letcontains 7 5 mg of team s fumarate.USP.Availab le in
packages of l ive compacts and packag es of l ive refills .
Nones trin is availab le“
in compac ts each conta ining 2 1 ye llow tab le ts and 7 wh itemen tab lets . Each ye llow tab letconta ins 1mg ofnore th ind rone acetate and 5 0mcg ofeth iny l es trad iol. Availab le in pac kages of live compacts and packages of five refi lls .
090tG l 3 f
PARKE-DAVISDivis ionofWarner-LambertCompany
Morris Plains .NewJersey 07 950

what the cl inical features of a MAOI overdose would bel ike . The early adverse cl inical effects are those of remark
able stimulation of the nervous system. Therefore , tachy
cardia and hypertens ion are to be expected . Hyperpyrex ia
is quite common. Of course , you canexpect complaints ofdry mouth , nausea and vomiting . The hypertension can
occur in cris is form with severe occipital headache radiat
ing frontal ly , nuchal rig idity and photophobia . The hyper
pyrexia is often quite severe and can be associated w ith
diaphoresis and cold , clammy hands . The hypertens ion and
fever are often accompanied by twitching and myoclonic
fibri l lation of ske letal muscles at times leading to a
genera l ized rig idity and coma . Inmany patients with this
overdose the neuromuscular effects canbe outstanding and
it is useful to check for hypertonicity . The presence of
s e izures should not be a surpri se either. Di lated pupi ls are
de rigueur. In one recent series fasciculations , tw itching ,
tremor or rig idity was present in 92% of patients . Severe
ag itation and hal lucinations are part of this overdose nightmare . One ratherpecul iar and frightening cl inical feature isthe presence of a hypertensive cri s is occurring contemporaneous ly with postural hypotension.
The cl inical features of a MAOI overdose may not
appear for as long as 12 hours after ingestion; s igns of
overdose can persist for as long as 8- 10 days . Those pa
tients whose course leads to eventual recovery begin the irupward course (to health , not Heaven) by the third day and
are real ly wel l by one week after overdose . When death
occurs it is usual ly secondary to respiratory failure , circulatory fai lure or intracranial b leeding probably secondary to ahypertens ive crisis . Very bad prognostic signs are extremehyperpyrexia 4 2
°
C) and irreversible hypotension.
The CNS and peripheral nervous system signs youw il l we l l
recognize as manifestations of excess catecholamines described by some authors as a “
catecholamine storm This
cl inical syndrome is also seen, as you might expect, in
overdoses of cocaine , amphetamines , other psychostimu
lants such as pheny lpropanolamine as wel l as a pheochro
mocytoma . L etme draw you an analogy it’
s the sensa
tions you felt in my old neighborhood in Chicago whensomeone del ivered to you a fish wrapped innewspaperwith
4 30
a note that said s leep w ith the fishes ( translation) . In a
recent series of reported deaths from this drug the mean
time of demise was 16 hours after ingestionw ith a range of
8 to 24 hours . As you probab ly have already guessed ,
laboratory findings in this overdose are not real ly specific;if youhave access toepinephrine and norepinephrine levels
they probably would be elevated .
The treatment of overdose ofmonoamine ox idase inhibitor is not specifi c , in fact it
’
s quite non- specific . Patients
who are seen early and who are without symptoms should
have syrup of ipecac and activated charcoal administered .
Symptomatic patients should receive activated charcoal
and skip the ipecac especial ly if it is 2 hours or so post
ingestion. Many authors advise hospital iz ing apatientwithcl inical features ofMAOI overdose , even ifmild , for 12 - 24
hours . There are somany drugs that interactadverse ly with
MAOI thatdiscretion is often the betterpart ofvalorhere . If
the patient is hypertensive enough to be dangerous you
might try sod ium nitropruss ide or phentolamine . I f
hypotens ion seems to be the prob lem try IV fluids initial lyand if thatmaneuver fai ls use very smal l , titrated doses of
dopamine . Seizures and excessive neuromuscular activitycan be treated w ith a benzodiazepine such as diazepam. A
beta adrenerg ic b lock ing agent has been suggested as a
method to block the excessive sympathetic nervous systemstimulation. The hypertherrnia that can occur with thisoverdose is particularly worri some and can become mal ignant, best treated by cool ing blankets , acetaminophen or
sal icylate therapy . Some authors recommend the use of
chlorpromazine (Thoraz ine) for this purpose , but don’
t you
be tempted ; don’
t use this drug for this purpose uncon
trol led hypotension can ensue . If the temperature won’
t
come down and al l s implermeasures fai l youmay want toparalyze the patient w ith curare or succinylchol ine to re
ducemuscle activity and to reduce shivering . Forced d iuresis or hemodialysis have not been shown to favorab ly alterthe cl inical course .
Excuseme for leaving so abruptly , but I must have donesomething wrong Mary , the Chief
’
s secretary , justcal led and said that he has sentenced me to push a box of
Pampers up PilotMountain unti l next St. Sw ithin’
s Day .
VOL . 46 , No . 7
Bulletin BoardDianne L . Wil lard, BowmanGray ,
Winston- Salem 27 103 , 9 19/Continuing Med i cal 7 4 8- 4 5 050
Education
Please note: 1 . The Continuing Med ical Education Programs at BowmanG ray , Duke , EastCarolina and UNC Schoo ls ofMed icine DorotheaDix , New Membersand Burroughs Wel lcome Company are accredited by the AmericanMedical Association. Therefore CME programs Sponsored or cospon
sored by these schools automatical ly qual ify forAMACategory I credittoward the AMA
‘
s Phys icianRecognitionAward , and for North Carol ina
Medical Society Category A credit. Where AAFP cred it has been
obtained , this also is indicated .
IN STATE
July 11
Cri sis Then Now
Place : H ickoryInfo: Wayne Parker, MMlC , Box 27 444 , Raleigh 27 6 1 1 .
7 9 17
Jul y 15 -19
Sonography of the AbdomenPlace : Winston-SalemCredit: 35 hours Category 1 AMAInfo: Dianne L . Wi l lard , BowmanGray , Winston-Salem 2 7 103 . 9 19/
7 4 8-4 505
July 16
Cri sis Then Now
Place : W ilsonInfo: Wayne Parker, MMlC , Box 2 7 444 , Raleigh 27 6 1 1 .
7 9 17
July 17
Diabetes/New Care ConceptsPlace : Sanford
Info: Robert S . Cl ine , M.D. , Central Carol ina Hospital , Sanford27 3 30.
-65 18
July 29-August 3
Diagnostic Imag ingPlace : Atlantic BeachFee : $3 50Credit: 18 hours Category 1 AMAInfo: Carl E . Ravin, M .D. , Box 3 808 . Duke University Medical
Center, Durham 2 7 7 10.-5 268
August 2 1
Seizure Disorders in Pediatric PracticePlace : Sanford
Info: Robert S . Cline , M.D Centr al Carol ina Hospital , Sanford2 7 3 30 .
-65 18
OUT OF STATE
Jul y 19-2 1
5 th Annual MCV Cardiology ConferencePlace : Hot Springs , VAFee: $2 7 5
Info: Kathy Martin, Box 4 8 , MCV Station Richmond , VA 2 3 298 .
-04 94
September 5 -7
Doppler Echocardiography SeminarPlace Is le of Palms , SC
Credit: 16 hours Category 1 AMAInfo: Dianne L . Wil lard , BowmanGray , Winston-Salem 27 103 . 9 19/
7 4 8-4 505
September 12 - 14
Advanced Appl ied Ultrasound in Obstetri cs SeminarPlace : Myrt le Beach , SC
Credit: 12 hour-s Category 1 AMA
JUL Y 1985 , NCMJ
BLADEN
Betty B ruton B radley (FP) , Box 998 . B ladenboro 2 83 20BUNCOMBEAnn Meredith L ansing ( IM) , 203—A Doctors B ldg . , Ashevi l le
2 8801
CALDWEL LThomas Winfi e ld Gore (FP) , Col lettsvi l le Medical Center , Col
lettsvi lle 2 86 1 1
CL EVELANDThomas Karl B arton (PTH ) , Pathology Dept. Cleve land Memorial Hospital , Shelby 2 8 15 0
COLUMBUSPhi l l ipMabon W il l iford (HM) , Box 124 9 , Whitevi l le 2 84 7 2
DAVIDSONDeborah Barbara Cabral (FP) , 208 -B W . Center Sr. , L exington
2 7 292
DURHAM-ORANGE
George Eric Alexander ( student) , 2 7 06 H il lsborough Road ,
Durham 2 7 7 05
StephenJoseph B ick ston ( student) , 301- 1 Pinegate Circle , Chape l
H i l l 2 7 5 14
JonPhil ipB ris ley (student) , 201 Howell St. Apt. D—3 .Chape l H il l
2 7 5 14
Carol Ann Churchil l (student) , 4 7 15—B E . Cornwal l is Road ,
Durham 2 7 7 13
Jack Mart-ih Cole ( student) .D—7 BerkshireManorApts . Carrboro
2 7 5 10
Stanley Adolph Gal l , Jr . ( student) , 2907 Monroe Ave . , Durham2 7 7 07
Georg ia Lei la G il l iam ( 1M) , Dept. of IM , Duke Univ . Med ical
Center, Durham 2 7 7 10
Carol AnnG ioannini- Brown (FTH ) , 5 009 N . G lenDrive , Rale igh
2 7 609
David Chri stopher H abel (student) , 3 06 B riar B ridge Val ley ,
Chapel H il l 2 7 5 14
Michae l John Koriwchak ( student) , 19 13 Erwin St. Apt. C ,
Durham 2 7 7 05
Ritsu Kuno (student) , Chalet 1 , Greene St Chapel H il l 2 7 5 14
Wil l iam Todd Obremskey ( student) , 10 Durbin Place , Durham
2 7 7 05
Robert Derek Prentice (PP) , 2 7 16 Old Sugar Road , Durham2 7 707
KarenGipsonSeaton (student) , Rt. #2 , Box 5 7 7—B , H i l l sborough
Road , Durham 2 7 7 05
L isaMarie Stone ( student) , 1015 W . TrinityAve . Durham 2 7 701David Timothy Woodley (D) , Dept . of Dermatology , NC Mem.
Hosp. Room 13 7, Chapel H il l 2 7 5 14
FORSYTH -STOKES-DAVIEJohnHomer Barton, Jr. (student) , l 608 -L NorthwestB lvd . ,
W inston-Salem 27 104

Agreat way of lite.
JeffreyAl lenCleveland ( student) , 234 9-D SalemCourt , Winston
Salem 2 7 103Gary Brent Copeland ( student) , BowmanGray Med . Studt. Box
101 , 300 S . Hawthorne Rd . , Winston-Salem 2 7 103
John Doug las Davis ( student) , 17 2 1 Queen St. ,Winston-Salem
2 7 103
Lee PotterDresser ( student) , 163 1-C Northwest B lvd WinstonSalem 2 7 104
Robin Dawn Ifft ( student) , 1820 Ardsley St . ,W inston- Salem
2 7 103
Diana A. Jensen ( student) , 208 Eden Terrace , W inston—Salem
2 7 103
Chri stopher Carl Price (student) , 208 Eden Terrace ,Winston
Salem 27 103
Lawrence XavierWebb (ORS) , 300 S . H awthorne Rd . Winston
Salem 2 7 103
GASTON
JohnWesley Weeks (OBG ) , 902 Cox Road , Gastonia 2805 4
4 3 2
HAL IFAXRobert Decpc (GS) , 9 15 W . Third St. , Roanoke Rapids 2 7 870
HENDERSON
Charles Henrichs (FP) , 205 ThompsonSt. Hendersonvil le 2 87 39
IREDEL L
SteveMalone McKinnon (OPH ) , 1622 DavieAvenue , Statesvi l le
2 867 7
JACKSON
Moon Soog Choi-Chung (PM) , Eastgate Centre , Sy lva 2 87 7 9
L EE
L arry StephenButler (OBG ) , 109 -AS . Vance St. Sanford 2 7 3 30
MECKL ENBURGValyaEl izabeth Visser (PD) , Dept. of Pediatrics , CharlotteMem.
Hosp. Box 3 2 86 1 , Charlotte 282 3 2
MITCHEL L -YANCEY
KathleenMary Santi (FP) , 3 20PensacolaRoad , Bumsvil le 2 87 14
PITT
Deanna Marie Boyette ( student) , Doctors Pk . Apt. R-3 , Green
vil le 2 7 834
L inda Eves Brinkman ( student) , 10 Palmetto Place , Greenvi l le
27 834
Frank Cecchin (student) , 909 Forbes St. , Greenvi l le 27 834
John Parker Goforth ( student) , 108-B Paul Circle , Greenvil le
2 7 834
Joseph Peter Harris (FDC) , 701 Daventry Dr . , G reenvil le 27 834
Robert Mitchel l James (student) , 2 7 04 JeffersonDr . , Greenvil le
2 7 834
Michael Barry Kodroff (PDR) , Dept. of ECU School
of Medicine , Greenvil le 27 834
ScottAlanRodger ( student) , Rt. # 13 , Box 1 17 , Greenvil le 2 7 834
ROBESON
JosephMartinThomas (AN ) , 300W isteriaDr. Lumberton2 83 5 8SURRY-YADKIN
Tom Jimison Vaughn, Jr. (OBG ) , 708 S . South S i . , MountAiry2 7030
WAYNEG ilbert Joseph Garcia , Jr . (GS) , 1008 E . Ash Street, Goldsboro2 7 5 30
VO L . 46 , No . 7
GUI L FORD
Eric Lynn Dean ( 1M) , 102 3 Professional V il lage , Greensboro
27 401
David Goddard Dye (ORS) , 200 E . Northwood St. , Ste . 4 10,
G reensboro 2 7 401Haywood Me lton Ingram (GS) , 13 17 N . Elm St. , Ste . #5 , Box
1003 7 , Greensboro 27 404Timothy Walter L ane (1D) , 1200 N . Elm St Greensboro 2 7 401
Charles Stewart Rogers ( IM ) , 1200 N . Elm Street, Greensboro
2 7 4 10
Robert Van Cleve Sypher, Jr . (ORS) , Box 295 2 3 , Greensboro
27 4 29

Letters to the Editor
Bouquets for Ba l loonsTo the Editor
“Bal loons on theCCU by Charles Shunior is one of thebest articles I have read in the North Carol ina Med ica l
Journa l (NCMJ It typifies what is great
about med icine a learning , caring and loving rela
tionshipbetween the patientand those whoprovidemedicalcare .
Congratulations .
Joseph B . McCoy , MD .
15 0 Providence Road
Charlotte 2 8207
To the Editor
It’
s nice when writing opens the door for the reader to
step into another people’
s worlds . Specifical ly , I think it’ shelpful when we lay people are g iven a gl impse into the
l ives of med ical practitioners , as in B al loons on the
CCU in your Apri l issue .
I thought the piece was a tremendously effective , and
affecting , discussion of what it means to be a de l iverer of
health care the brains and hearts that govern al l that
technology and of the matter ofmaking the most_ outofone
’
s last days .
Thank s for the good article .
About Beard
To the Editor
It has been some time since I have had the pri vilege ofreading such a nice tribute asDr . B ridges
’
recentone onJoe
Beard (NCMJ 1985 ;46z303 It carri es a strong and im
portant message and is a landmark summary of the real
background of the Duke University Med ical Center .
I thoroughly enjoyed it!David C . Sab iston, I r . , MD .
Duke University Medical Center
Durham 2 7 7 10
To the Editor
I have just read the memorials to Dr . Joe B eard in the
NCMJ I worked with Dr . B eard for about three years in anarrangement made between him and Dr . Forbus so that 1could get some research training . My career in
'
research
started there even though I did not remain in the field ofvirus neoplasia . He was one of the three people that I thinkare extraordinary in the etymolog ic sense of the word , here
at Duke . Another one is Dr . Kempner with whom I havehad some memorable exchanges only recently for the firsttime since I have been at Duke .
Dr . Beard did have a very warm heart once one suc
ceeded in penetrating his gruff ways . Once I told him,
exuberantly as it were , that I had just purchased a lot in
Duke Forest, dreaming about owning a house and , aboveJUL Y 1985 , NCMJ
Each Person Can Mak e a Difference
al l, a work shop in which to bui ld things , furniture most of
al l . He immediate ly askedme when I was going to build thehouse and how I was going to finance it, knowing mybackground . I suggested that I was not worried about thatbecause I had two years unti l I had toputup the edifice . H e
offered me just l ike that, and I started bui ldingwithin a month or two . I have heard over the years that hedid that with many . 1 saw Mrs . Beard shortly after her last
Operation atDuke . She was in superb shape , but she toldme
thather l ife had come to an end with her husband ’
s demise .
Within a few week s she was dead . Not exactly w ithout
precedence that, among ind ividuals made for each other asDotty and Joe were .
Dr. B eard was an extraordinary man. When I saw Dr .
Forbus for the last time atDuke hospital , Dr . B eard asked
me if I had thank ed him for what he surely must have beentome . I said yes . A fewmonths before he died ,
I wrote Dr .
B eard a letter say ing the same to him. I am lucky .
No , I don’
t adulate Dr . Beard , nor anybody for thatmatter . But I am most comfortable to have l ived in the
presence of people l ike him, whose presence is real and ,
almost by definition, justifies the joy of l iving this l ife .
Joachim R. Sommer , M .D .
Box 3 7 12 DUMCDurham 2 7 7 10
To the Ed itor
To discuss abortions withoutmentioning overpopulationis l ike d iscussing fish without observing that fish l ive inwater .
Abortions are not performed in operating rooms in thesky . They take place in societies which have l imited capacities to raise , care for , and provide a satisfactory l ife for newoffspring .
The Chinese do notpromote abortions because they l iketo destroy Chinese fetuses . Instead , the Chinese are com
pass ionate and inte l l igent . They real ize the ir capacity toprovide a satisfactory l ife for children is l imited . Regard
less of how intensively cultivated , their land can grow onlysomuch food . Abort ions are better thanhaving infants andsmal l children die of starvation and related diseases .
The United States already has evidence of severe over
population. We have a twin deficitof budget and trade . We
l ive partly on borrowed resources , oi l produced in other
countries . We have a drug problem. We have a growing
prisonpopulation, many ofwhom could not find a place in
society . Some old people l ive in poverty and financialinsecurity .
F ish do l ive in water . Abortions do . take place in
societies . To properly evaluate abortions , we should ex
amine the entire picture , not just an isolated part of it.
Albert D. Warshauer, MD .
1608 East F ifth Street
G reenvil le 2 7 83 4

F rom The Medica l Journal of Austra l ia
Warts and a l l
To the Ed itor
InDecember an anxious mother brought tome a de l ightful five-
year-old , who had a d ig ital wart . I offered to buy
the wart from him. H e was de l ighted when I gave him 20cents , te l l ing him he could keep the wart for three or four
weeks , after which it would drop off, come to me and bemine . If this d id not happen he was to return the 20 cents !I thought nomore about it until 1 had a letter three week slater from the mother , stating that the wart had gone . Two
days after this I noticed the development of a s ingle digitalwart onmysel f!I write to warn your readers of yet another danger ofgeneral practice . (PS : F or sa le , one d ig ita l wart, price 5 0
cents yes , 5 0 cents you see . I have these overheads . )John Trol ler, FRACGP
Kab le Avenue ,
Tamworth , NSW 2 340
Pear ls for Perfect Practice Under PRO
To the Editor
Think ing about how to study a patient’
s problem is now(and always has been) an out-patient procedure .
Reviewing data , including sl ides , x-rays , op notes , path
reports , and d ischarge summaries , is an out-patient pro
cess .
Whenapatient requests time indays to think things over,
4 34
they mustbe informed that such a process should be carriedon out-of—hospital .
Coming from a d istance , even a greatone , is notby itse lf
an indication for hospital ization.
One shouldn’
tuse the hospital to obtaina consultation inorder to determine whether a particular invas ive procedureis indicated .
If you can conclude that what you want to do for/to a
patient could be accompl ished in the cl inic provided : that
ind ividual l ived near by ; youweren’
t real busy ; youweren’
t
going on the road; and you had time to review the studies/
advise the person, then the chances are a review special istfor PRO would deny such an admission even when those
descriptors do not obtain.
Whenever poss ible , a physician should mental ly walkthrough the hospital stay of an elective admission, focus ingupon inter
-relationsh ips between invasive studies , days ofthe week , and the anticipated next steponce the outcome ofsuch studies is known.
The telephone is not always dependab le , therefore when
in doubt about the need for hospital ization, see the patient
in cl inic/office fi rst.
Don’
t turn over complete respons ib il ity for sanctioningadmi ssions to your secretary review the new referral or“old patient
’
s cl inical descriptors yourself.
H arold R. S ilberman , M .D.
Duke Univers ity Medical Center
Durham 2 7 7 10
VO L . 46 , No . 7

Class ified Ads
PATIENT B IL L ING SERV ICES for Physicians and
Radiolog ists . Comprehensive computer ized patient
accounts management and bi ll ing services available
on a contract bas is . Physician Data Services , Inc. ,
P.O . Box 1026 , Mount Airy .-6962 .
GENERAL SURGEON OPEN ING : to replace retir ingsurgeon. Excel lent location, financia l assistance and
cal l exchange avai lable . Contact G rady K . Howard ,
Administrator , P .O . Box 2 3 2 , K ings Mounta in
28 086 .-3 601 .
FAMI L Y PRACTICE PHYS IC IAN OPEN ING : Family phys ician for hospita l satel l ite offi ce in Southern
PiedmontNorth Carol ina in the footh i l ls 30mileswestof Charlotte . G uaranteed salary or 50% of
net whichever is greater 5 days per week . Contact
G rady K . H oward , Administrator , P.O . Box 23 2 ,Kings Mounta in 2 8086 .
-3 601 .
CONSIDER the cost-effective potential of adding a
physician assistant toyour practice. theNorth Carol i
na Academy of Physician Assistants wi l l help y6uadvertise to a large pool of qual ified PAs at no cost toyou. For information on how you can advertise yourPA employment opportunity , contact: Charles Kober , PA-C , NGAPA Employment Chairman, 108Occoneechee St. , H il lsborough 2 7 2 7 8 . Day Phone:
-1 101 , H ome Phone -8823 .
URGENT CARE facil ity needs add itional phys ician
staffing , part-time/fuII-time , three days per week .
Twelve hour sh ifts . L ow volume practice in comfortab le setting . Competitive compensation with mal
practice provided . Contact: PiedmontWal k -In Cl in
ic, 6005 Russel l Road , Durham 2 7 7 12 . 919-47 7 -3008 .
CARY : Ful ly furnished solo phys ician’s office avai l
able . Used one year .-4 7 18 or -47 10.
BIOLOG ICAL SAF ETY CABINET FOR SAL E : L abconco Model 5 027 5 . Never used . Sold for
Ask ing or best reasonab le offer . Contact
James McCarthy , 13 25 Sycamore , Raleigh 2 7 604 .
-1408 .
JUL Y 1985 , NCMJ
NORTH CAROL INA: Director and ful l-time emergen
cy phys ician, independent contractor , needed for new
42 -bed hospita l located in lovely community with in 30
minutes of Chapel H i l l . annual ED vis its . 24
hour shifts . Excel lent med ical back -up. Competitivecompensation with malpractice provided . Contact:
Coastal Emergency Services , Inc. , Box 25 08 , Durham
2 7 705 .-03 67 , -1665 in NC ,
3 306 in US .
NORTH CAROL INA: Ful l -time emergency phys icians
needed for 160-bed hospita l with good med ica l staff
support. Located close to Charlotte and V2 hour from
the world famous Pinehurst and Southern Pines golfcourses . ED visits annual ly . 2 4 hour shifts
Competitive compensation with malpractice provided . Contact: Coasta l Emergency Services , Inc .
Box 2 508 , Durham 2 7 7 05 .-0367 ,
1665 in NC ,-3 306 in US .
300MA XONICS X-RAY MACH INE , complete with
floating top tab le and chest board , and a H ope Industr ies F i lm Processor for sa le at bargain prices . G ive
your office or cl inic almostnew, very rel iab le diagnos
tic x-ray capab il ity formore than off retai l !Write
Box 1 17 6 , Jamestown 2 7 2 82 .-1 166 .
GREENSBORO : Wanted , phys ician for estab l ished
Fami ly-Internal Medicine practice , to share and/or
buy . Dr . Joe H enson, 1 107 W . F r iend lyAve. , G reens
boro 2 7 401 .-15 67 .
FOR SAL E : B io-Dynamics Cel ltrak . Does CBC , HCB
HCT, MCV, RBC on fingerstick sample. L ik e new .
Al l accessories . Suppl ies for 100 tests . Cal l Dr . L ari
more col lect at -923 3 .
CABARRUS COUNTY H EAL TH DEPARTMENTseeks F ami ly Practice physician to work in areas of
prenata l care, family planning , child health , and
communicab le d isease control . Sa lary range is
Successful appl icant should be
available by September 1 , 1985 . C los ing date for ap
pl ications is July 15 , 1985 . Please reply toWil l iam F .
Pil k ington , H eal th Dir ector , Cabarrus CountyH ealth Department, Box 1 149 , Concord 2802 6-1 149.

Index to Advertisers
Army ReserveAyerst L aboratoriesCampbel l L aboratories , Inc .
CHAPS
Crumpton CompanyCurtis 1000 Information SystemsLewis Medical Instruments , Inc .
El i L il ly Co .
Guesthouse
Mac Thrift Office Furniture
Medical Mutual Insurance Company of NC
Mutual of Omaha
4 36 VOL . 4 6 , No . 7
National Staffing Services CorporationOffice Support Systems , Inc .
Ortega Pharmaceutical Company , Inc
Parke-Davis
Roche L aboratoriesSaint Joseph
’
s Hospital
St. Albans Psychiatri c HospitalStuart PharmaceuticalThe Upjohn CompanyU. S . Air ForceWil l ingway , Inc .
Winchester Surg ical Supply Co . , Inc .


The Offic ial Journal of the NORTH CAROL INA MEDICAL SOC IETY September 1985 ,Volume 4 6 , Number 9


Pub l ished Monthly as the Official Organ of The North Carol ina Medical Soc iety ( ISSN -0029-2 5 5 9 )
SEPTEMB ER 1985 , NCMJ 4 3 7

F inancia l new s you have been w a i ting to hea r!!
CW ncreas e
ncome
Ava i lable to ig ible Members Under Age 5 0Rega rdles s Other D is abi l i Insurance
Offic ia l North Carol ina Med ica l Soc ietyDis ab ility Income Plan
Endors ed and Recommended S ince 193 9
Protect your mos t va luab le as s et, your profes s iona l income
For deta ils or cla ims s ervice ca ll orwrite :
CRUMPTON COMPANYPROFESS IONAL GROUP iNSURANCE
Toll free - 1 67 4
ACADEMY CENTERPOST OFF ICE BOX 8 5 00DURHAM, NC 2 7 7 07
Account executives : J . S lade Crumpton, Gene Greer and CliffMos her, DurhamiJack Feathe rston, Charlotte
Dan Ha ley , G reensboro
VOL . 4 6 , No . 9

naMED ICAL JOURNALfor doctors and th e ir patients
volume 46 , no . 9 , September 1985
CONTENTS
Ed itorials
Ashevil le 1985 Danie l L . Dolan 44 1
Family Medicine at Duke : A Fol lowup E . H arvey Es tes , Jr . 44 3
Carol ina H istoryThe Mountain Area H ealth Education Center: Thomas J . Bacon
A Unique Univers ity/Community Partnership and F . MaxtonMauney , Jr . 44 5
Physicians’Forum
B lue Cross/B lue Shield’
s Personal Care Plan ed ited by Danie l L . Dolan 4 5 1
Specia l Article
Ashevil le : The Tuberculosis Era I rby Stephens 4 5 5
PharmacotherapySerum Digoxin Levels and Renal Failure Daniel L . Dolan and C . Edwin Webb 465
Features for Patients
Accidental Veratrum Viride Poisoning in Three Daniel Crummett, Deborah B ronste in“Ramp
”
Foragers and Zebulon Weaver III 4 69
Removing a Tick Daniel L . Dolan and John J . McKinsey 4 7 1
Scientific Articles
Sebaceous G land Carcinoma of the Eyel id :
Complete Response to Sequential Comb ination‘
Chemotherapy Ba rton R . Pascha l and Carter S . B ag ley 4 7 3
Cardiac Surgery in Ashevi l le : Review of 3 26
Consecutive Cases during 1983 Kent W. Sa l isbury 4 7 5
Cancer Immunology Is a Rapid ly Deve loping Field Warren H . Cole 4 7 9
F ine-Needle Aspiration An Aid to B reast Diagnos is Peter A. Gent/ing 4 8 1
Socioeconomic IssuesA Cost-Effective Community Mode l for Treating J . Paul Ma rtin, El l is Edney . Dan I . Gerber ,
Alcohol Withdrawal Syndrome : A Prel iminary Report Wi l l iamMeagher and David Si lver 4 87
Bul letin Board
Continuing Medical Education
L etters to the Editor
Classified Advertisements
Index to Advertisers
Sem rvrraea 1985 , NCMJ 4 39

Brings youToday’
s Technologywith the
B E N N ETTAWO-TEG ‘T
S Y S T EM
Amicroproces sor controlled
generator for cons istency,
accuracy, and cost efficiency.
The BennettAUTO-TECH System has thirteen preset technique stations forwhich anatomica l partsare automatica lly measured and converted into optimum kVp and mAs us ing the shortest exposuretime and the h ighestmAposs ible . AUTO-TECH saves time and money byproducing betterrad iog raphs with fewer retakes . 8 8 8 X Ray offers the BennettAUTO-TECH Systemwith a 5 -year
warranty inc lud ing tube , collimator, and hig h voltage cables . B 8 B X- Ray and the BennettAUTO
TECH System lets today’
s technology work for you.
working for the end result— optimum qua lity rad iographs
B BXRAY PO . Box 802 Matthews , NC 2 8 105 in NC Ca ll 1 - 800- 2 2 2 - 9262
In SC Ca ll Collect 7 04 - 84 7 - 8 5 2 1

a lead ing test for feca l occult blood
The‘
Hemoccult'
guaiac papertest for fecal occultblood
is a convenient, dependable , virtuallyodorlesspreliminary screenforabnormal g . i. bleed ing often
associated with colorectal cancer.
HemoccultII® S lides Hemoccult® Two-Hole S ing le S lides
Available in Available in
o Dispensapak": 100 patient kits . Each kitcontains 0 Boxes of 100 s lides
three‘
Hemoccult11’
s lides inmailing envelope with Cartons of 1000 s lidesinstructions , applicators and deve loping solution.
Also availab lea B
0
oxes of 100 s lides “Hemoccult
'
Tape
Cartons of 1000 s lides
34 5 1 W. Lawrence Ave .
e Smt line Diag nos tics . 19 8 1
Surg ca Supp y Co . Charlotte : -2 2 40

EDITORIAL
Fami Medicine at Duke : A Followup
E . H arvey Estes Jr . , MD .
Dr . Robert Sul l ivan’
s review of the F amily_
Med icine Program a tDuke ,
publ ished in the June 1985 issue of the North Carol ina Medical Journal
(NCMJ l 985 4 6 3 2 9-3 1 cited some of the environmenta l problemsfacingsuch a program within a tertia ry med ica l center .
I t was written at a point in time when the demise of the Duke F amilyMed icine Program seemed imminent and inevitable . F ortuna tely (from the
writer’
s viewpoint) , circumstances changed . and on Thursday , July 1 1 ,
1985 , Durham County Genera l H ospita l and Duke Univers ity Med ica l
Center , co-Sponsors of theDuke F ami lyMed icineProgram, announced tha t
they would continue sponsorship of the program, and that recruitment ofnew res idents for July 1986 would beg in immed ia te ly .
Thus , F amilyMed icine wil l continue atDuke , at both the undergraduate
and the res ident level , but the events a tDuke have sparked a nationa l deba te
over the necess ityfor an educationa lprogram inF amilyMed icine within the
increas ing ly comp lex tertiary hospita ls a ssocia ted with med ica l schools .
I t is interes ting to review the reasons g iven for initia ting a F amilyMedicine Programat early 1 970s . These are as va l id in 1985 as
they were then These reasons , as presented in 1973 , are reprinted be low .
The economic reasonsfor afami ly med ic ine presence aremuchmore urgentin 1985 than they were then. F ami ly phys icians a re stil l in short supply , in
spite of a growing surplus in other specia lties . They are actively sought byHMOs . especia l ly those emphas iz ing the casemanager approach . Since
HMOs are rapidly increas ing in number and in patient enrol lment. and
s ince a l l specia lty-based institutions need an ever -widening primary care
base , it is urgent tha t they tra in phys icians for these roles , and ma inta in
contact with themfol lowing the ir tra ining .
Those respons iblefor recons idera tion of the role of F ami ly Med icine at
Duke are to be commended for their dec is ion !
great variety of reasons why Duke should
have a strong , we l l supported Fami ly Practice Program.
These reasons can be grouped into four categories ethi
cal , educational , economic and pol itical . I would l ike tod iscuss each in turn .
A. Ethical
As a med ica l school , we have an obl iga tion to meet themedica l needs of the people we serve .I can present a strong case that medical schools havebecome autonomous to the pointof becoming self-serving .
The Flexnerian mode l of a strong b iolog ic base for med icine has been used as a justification for creating and maintaining a gross imbalance in the qual ity-quantity tradeoff inmedical services . Whenthe citizens of Pinetops , BatCave ,and even Durham complain that they cannot get med ical
From 407 Crutchfi eld Street, Durham 2 7 704 .
Presentationmade at the Quail RoostConference An annual conference
forreview of educational programs formedical students atDuke .May 15 ,
197 3 .
SEPTEMB ER 1985 , NCMJ
help, our answer is that it is impractical expect that
medicine can be dispersed so widely and that theyshould , instead , come to Duke , or some other center offer
ing specialty services . This is the medical equivalent ofMarie Antoinette
’
s“Let them eat cake !
”
I would not argue that we should provide a brand ofquackery and cal l itmedicine , but I do contend that a broadbased general ist, who is not “turned off by see ing com
mon il lnesses , who is wi l l ing to be concerned about convenience , access and cost, and who is wi l l ing to train and
use a team of ass istants is a much needed product moreso than many of the products we are now training .
The usual answer is‘
But that’
s notDuke’
s role ! L etEast
Carol ina do it. It is a difficultj ob , but that should certainlybe no justification for ass igning that task to a schoo l less
capab le than Duke .
1 do not say that we have been wrong for the past 40years , but I do say that times have changed , and that we
should change with them. We no longer have a state fil led
with variably trained general ists and no special ists as wasthe case in 1930. We have the oppos ite many special ists

and few general ists and we should have the courage to
face the facts and change our course accordingly .
B . Educationa l
Duke has an obl iga tion toprovide a spectrumof modelsof practice for its s tudents , a l l of high qua l ity , and each
trea ted with equa l respect, bothphilosophica l ly and ma te
ria l ly .
We have not met this obl igation. We do have a fami ly
practice program, which is doing very wel l , considering its
environment. If you infer from this remark that the environment is not a healthy one , you are right! I hasten to add thatit is not finances and/or space that stunt healthy growth
though both are indeed needed . Money alone is not enough
without a change in attitude . At the present time , medical
students and young doctors are often discouraged from
considering family medicine as a career because of the
comments made about it by respected and seniormembersof other branches ofmedicine . I am sorry to say that s imilarremarks are then used , without objective evidence , as a
justifi cation for lack of support for such programs . S ince
so few of our students go into fami ly medicine , we don’
t
need to seri ously cons ider attention to th is field of trainmg .
I accept the fact that a teaching medical center, especially a private school , should not accept a larger service
obl igation than it needs to support its teach ing and researchneeds . On the other hand , we do need an example of
continuous , high qual ity , convenient primary care so that
our students can see fi rst hand that such a thing exists ! 1
therefore include such a mode l under the rubric of education rather than service .
C . EconomicAmedical center is the apex of a broadly based pyramid
of facil ities doctors’
offices , cl inics , community hospi
ta l s , area hospitals etc . We must continua l ly protect,rebui ld , and expand our referra l base .
For twenty or thirty years , Duke has engaged in a canni
bal istic educational process . We have trained highly com
petent special ists and subspecial ists , who have gone to thelarger towns and hospital s in the state , and immediate lybegun to s iphon off those cl inical problems which once
were sent toDuke . I suspect that this is a subjectof concernwith several cl inical sectional chiefs ! I propose that a
healthy , expanding referral network , based inhigh volume ,
high qual ity fami ly practice settings is a viab le counter
balance to this trend .
Curiously , the economics of rural medicine have beenused as an argument against family med icine : Doctors
just won’
t go to smal ler towns , therefore we should onlytraingeneral internists , ped iatric ians and surgeons whowil lpractice in multispecialty groups . This is in many ways
s imilar to the argument that our students don‘
t go into
family medicine , therefore we should not train them.
The internist, pediatrician, surgeon comb ination musthave the support of a fairly sophisticated hospital , whichl imits ch oice of location. But there is more ! Doctors
want to practice in groups , and groups of three seem to be
the ideal size . An internist, pediatrician, surgeon comb ination is not a group, since no one can cover for anyone else .
Ideal ly there must be three internists , three pediatriciansand three surgeons .
Forpractical purposes , th is l imits such groups tocities ofat least people , s ince this is the population
VOL . 46 , No . 9
needed to support both the hospital and patient volumeneeds of such a group. There are only 14 towns in North
Carol inawhichmeet such specifications . There are only 36
towns of over in North Carol ina . Towns such as
H i l lsborough , Roxboro , Oxford ,Warrenton, Pittsboro are
in the be low group. My point is we have trained
people who , for economic and profess ional survival , must
go to larger towns , so it is not surpri sing that they have not
gone to rural areas . General ist/ spec ial ist ( Internal Medicine , Ped iatrics , Surgery ) teams must go to towns of
and up inorder to survive , and subspecial ists probably require a population base of and up, but
general ist ( family practice ) groups can thrive in towns of5 000 , a suitable base for a rural ambulatory center .
The importance of this is close ly re lated to the point
previouslymade . If it is ourethical duty , as I be l ieve it is , tofit our product to the needs of the population, then we
should concernourse lves with the problemof rural medicalcare . This is a huge prob lem, nationwide in its scope , and
terribly d ifficult to solve . I bel ieve strongly that the provision of a cadre of doctors who can , if they choose , go to
smal ler towns and survive is anobl igationwhichwe shouldaccept . If this is an unattractive job for a doctor, then wehave an obl igation to find out why , and to learn to correct
this problem new organizations , teams of individuals ,new fund ing patterns , etc . To say that we should not con
cem ourselves with the problem is ne ither constructive orresponsib le .
D. Pol itica l
This category is the area inwhich al l the other categoriesbecome translated into action on a publ ic pol icy level andon the leve l of expenditure of pub l ic funds . If we expect
continuedpubl icmoneta ry support, we must answerpubl icneeds .I recently attended a conference on ethical issues in
med ic ine . The head of a major institute , in which ethical
issues are under intense study , was asked who shoul d make
the final decisions regarding certain major ethical issues .
I-I is statement was that he would far rather trust
average men from Kansas to make wise decisions for thebenefi t of mankind than to entrust this to 100“experts
”
who have studied the prob lems in detail .Pol itics is the way in wh ich these “
average men make
theirwil l known. In this arena , you should note the fact that
several state legis latures have now required their state
schools to produce fami ly practitioners . In states in which
the state“
school has ignored this cal l , newmedical schoolshave been created , and the state dol lars are now spl it
several ways . East Carol ina derives most of its support
from those who do not have access to primary , general ist
care . The NC . L egis lature now has a b il l before it whichwould set as ide one mi l l ion dol lars for the private medicalschools in this state , if they are wi l l ing to establ ish a
co-equal Department of Fami ly Practice . This b i l l wil lprobab ly not pass , but is should be noted as a strongindicatorof thewi l l of the people , as read by the legislature .
The message is clear: If we wish the support of the
pub l ic , and pub l ic funds , we must l isten to the message .
The message is people want access to medical care .
They want easy access , re latively inexpens ive access , andcontinuous access . We , as a medical school , should be
l istening . I contend that a strong family practice program isa necessary part of that responsib il ity !




Once -da ily
Convenience without compromiseOne capsule
—Once da ily
The appearance oi these cap5 ules is a reg istere d trademark oi Ayerst Laboratories .B R I EF SUMMA R Y (FORFULL PRESCR IBING iNFORMAT/ON. SEEPACKAGEC IRCULAR.)INDERIDEG LA B rand oi P RO P R A NO LO L H YD ROCH LO R IDE ( IND E R A L0 LA) andHYDROCHLOROTHIAI IDE (Long Acting Caps ules )No. 4 5 5—Each INDEFI IDEo LA Cap5 ule containsPropranolol hyd roch loride ( iNDERAL® LA)Hyd roch lor0thiazide
No 4 5 7 - Each INDERIDE‘a LA Capsule contains .
Propranolol hyd roch lorid e t DERAL®LA)Hyd roch loroth iaZide
No ASS—Each INDERIDEe LA Capsule contains.
Propranolol hydroch loride ( INDERAL® LA)Hyd roch loroth iaZIdeI NDER ID E LA is ind icated in the management 01 hypertens ion.
Th is titted -comb inationd rug is not Ind icated tor initia l therapy oi hype rtens ion. Itthe fixed combination re pre s ents the dose titrated to the ind ivid ua l patient
'
s nee d s .
therapy with the tixed combinationmay be more convenient than with the separatecomponents .CON T R A IND ICAT ION SPropranolol hyd roch loride ( INDERALG)Propranolol is contra ind icated in: t) card iogenic shock: 2 ) S inus b radycardia and greater thantirstdegree b lock: 3 ) b ronch ial asthma; 4 ) congestive heart lailure (seeWARN INGS ) unless thetal lote is second ary to a tachyarrhythmia treatab le with propranololHyd roch loroth iaz ideHyd iOCNOfOlh laZlde is contraindicated inpatients wrth anuriaorhypersensitivity to this orotherSuttonamide-derived d rugs .
WA RN ING SPro renoloi hyd roch loride ( IND E RA L®)CA D IAC FA ILURE Sympathetic stimulationmay be a vital component supporting circulatorylunction in patients w-th congestive hean lailure . and its inhibition by beta b lockade mayprecipitate more seve re lai lure . Although be ta b lockers should be avoid ed inovert congestiveheart lailure . it necessary. they can be used with ctose tollow-ao in patients With a h is tory ol
lailure who are we ll compensated . and are rece iwng d igita lis and diure tics . Beta-ad renerg icb lock in agents do not abolish the inotropic action oi d ig ita lis on heartmuscle.
iN ATIENTSWI THOUT A H I STORY OF HEART FA ILURE. continued use oi beta b lockerscan. in some cases. lead to card iac lailure There lore. at the i i l s i S ign or Symptom ol heartlai lure. the patient should be d ig ita lized and /or treated With d iure tics . and the responseobserv ed close ly. orpropranolol should be d iscontinued (gradual ly. it poss ib le ) ,
report ed inwhich. a lter propranolol. the tachycard ia was re p laced by a severe brad ycard iarequiring a demand pacemaker. in One case this re sulted alter an initia l dose at 5 mgpropranolol.
MAJOR SURGERY: The necess ity or desirab ility oi withd rawal oi beta-b locking therapyprior tomajor surgery is controvers ial It should be noted . however. that the impaired ab i lity oithe heart to re spond to re l lex ad renergic s timulimay augment the ris ks ol genera l anesthesiaand Surgical procedures .
None l ler Io Bronchos earn (e chronic b ronch itis , emph s erum—PATIENTS WITHBRONCHDSPASTIC DIS ASES S OULD.L I N GEN ERAL. NOT R CEIVE BE TA BLOCKERS.INDERAL sh0utd be administered Wl lh cautions ince itmay b lock bronchod ilationproduced byendogenous and exogenous catecholamrne stimulationoi beta receptorsD IABE TES AND HYPOGLYCEMIA: Beta-ad re nergic b lockade may pre vent the appearance ol certain premonitory signs and Sym toms (pulse rate and pre ssure chang es ) ol aCuIehypog lycemia in lab ile insulin-dependentd iabetes . Inthese patients itmay bemore dilticmttoad jus t the dosage oi insulin. Hypog lycemic attacks may be accompanied by a pre c ipitouse levation 01 b lood pre SSure .
Hyd roch loroth iez ideThiazides should be used with caution in severe renal d iseas e . Inpatients with renal d isease.
lhtal ldeS may pre c-pilate azotemia. Inpatients with impaire d renal lunction. Cumulative el lectsoi the d rug may deve lop
Thiazides should also be used with caution inpatients with Impaired hepatic lunctionorprogresswe liver d isease . since minoralterations offluid and electrolyte balancemay precipitate hepatic coma.
Thiaz id esmayadd toorpotentiate the actionoi otherantihypert ensive drugs . Potentiationoccurs with gang l ionic or peripheral ad renergic
-blocking drugs .
Sens itivny reactions may occw in patients With a h is tory atallergy or bronchial asthmaThe poss ib i l ity ol exacerbationor activation 01 systemic lupus erythematosus has been
reported .P RECAUT IONSPropranoloi hyd roch loride ( INDERAN )GENERAL ' Propranolol should be used with caution in patients with impaired hepatic or re nallunction. Propranolol is not ind icated tor the tre atment 01 hypert ens ive emergenc ies.
Beta-ad re nore ceptor b lockade can cause reducfion oi intraocmar pressure Patientsshould be told thatpropranololmay interlerewrth the g laucoma screening test Withdrawalmaylead to a return ot increased intraocmar pres sure .CL I N ICAL LABORATORY TESTS: Elevated b lood urea leve ls inpatients with severe heartdisease. e levated serum transaminase. alkaline phosphatase. lactate dehyd rogenase.DRUG I N TERAC T IONS. Patients rece ivmg catecholamine-depleting d ru s . Such as reser
gine . should be close ly observed it propranolol is adminis tere d . The adde catecholamineIock ing actionmay produce anexcessive reduction of resting sympathetic nervous activity.wh ichmay resultin hypotension, marked bradycardia. vert igo. syncopal attacks .orort hostatichypotens ion.
12015 0
AYERSTLABORATORIESNew York . NY 10017
5 112 198 5
CARC I NOGENES IS . MUTAGENES I S. IMPA IRMEN T OF FERT IL I TY : Long -term studies inanimals have been conducted to evaluate t0xic e l lects and carcinogenic potential. In 18month s tud ies . in both rats and mice . employing doses up to 15 0mg / kg l day. there was noevidence oi s ignil icant d rug
- induced toxicity. There were no drug-re lated tumorigenic e l lects
at any ol the dosage leve ls. Reproductive stud ies inanimals d id not show any impairmentoilertility thatwas attributab le to the d rugPREGNANCY Pregnancy Category C. Propranolol has been shown to be embryotoxic inanimal s tud ies atdoses about totimes g reater than the maxima l recommend ed humandoseThere are noad equate and wel l-controlled studies inpre gnantwomen. Propranolol should beused during pregnancy only it the potential benefit justi l ies the potential risk to the Ietus.NURS I NGMOTHERS Propranolol is excreted inhumanmilk Cautionshould be exercisedwhen propranolol is adminis tered to a nurs ing motherPED IATR IC USE: Salaty and etiectiveness in child ren have not been estab lishedH d roch loroth laz ide :G NERAL Period ic d etermination 01 serum e lectrolytes to detect poss ib le e lectrolyte imbalance should be perlormed at appropriate interva ls .
All patients receiwng lh laZlde therapy should be ob serv ed tor clinical signs 01 fluid ere lectrolyte imbalance . name ly: Hyponatremia. hypoch loremic alka los is . and hypoka lemia.
Serum and urine e lectrolyte d eterminations are Dart icularly important when the patient isvomiting excess ive ly or rece iving parentera l ltuids . Med ication such as d ig ital is may alsoinl luence serume lectrotYi es .Warning S igns irrespective oi cause are: Dry ness oimauth. thirst.weakness . lethargy. d rows iness . restlessness. muscle pa ins or cramps . muscular latigue .
hypotens ion. oliguria. tachycard ia. and gastiomtes tinal disturbances Such as nausea andvomiting
Hypokalemiamay deve lop, espec iallywith b risk d iures is.when severe Cirrhos is is present.or during concomitant use atcorticosteroid s or ACTH
lnterterence with adequate oral e lectrolyte intake Wi ll also contribute to hypokalemia .
H ypokalemia can sens itize or exaggerate the response at the heart to the toxic el lect old ig italis (eg . increased ventricular irritabi lity ) Hypokalemia may be avoided or treated by useol potass ium Supplements . Such as lood s with a h igh DolaSS Ium content.
Any ch loride de l ictt is generally mild and usual ly does not reduire specific tre atment.except under extraord inary circumstances (as in l iver or renal disease ) Dilutional hyponatremia may occm in edematous patients
r i hot weather; appropriate therapy IS waterrestriction. ratherthanadministration0 ! sa lt. exc p in rare instances whenthe hyponatre mia islite-threatening . Inactual sa lt depletion, appro pri te replacement iS the therapy ol chOIce
H yperurice'miag tay occurpr frank gourmey be preC ipitaled incertainpatients receiving
thiazide therapy. L.Insulinre‘
Quirerr'
i ents in d iabetic patients may be increased. decreased. p r unchanged .
Diabelesmellitus wli ich-hasb een latentmay :becorn emani lestduring th iaz ide administrationitprogre ss ing re nal impai
‘
rn'
tenti become evident. cons iderwithhold ing or d iscontinuing.d iuretic th rapy "_ x SThiazides may decrease
'
s'
eruni_PB l lev Is without signs 01 thyroid d isturbance.
_Calc
’
rumexcretion is d ecreased'by thiazides . Patnotog ic changes in the parathyroid g land.with hypercalcemia and h p
'
ophosphatemia have been ob served in a lew patients on prolongbd lhiaé ide therapy The comhlion comp lications ol hyperparathyroid ism. Such as re nallith ias is. bgh
'
e resorption, and pepue'
ti lce iatlon have not been seen. Th iaz IdeS should bed iscontinued be lore carry ing d uti ests loruparathyroid lunct n
O‘Rt-J
lG I NT ERAC T IONS’ Thiazid e d rugsmay increase the respons iveness to tubocurarine.
The antihypertensive e llects oi th iazides may b e enhanced in the Dostsympalhect0mypa tient ThiaZide s
’may decrease arterial respons iveness to norepinephrine Th is d iminution IS,not Sul l icient' to rectud e el lectiveness oi the pre ssor agent Ior therapeutic use .PREGNAN Y: Pregnancy Category C. Thiaz ides cross the placental barrierand appearincord b lood . The use 01 thiaz ides inpregnancy requires that the anticipated benel itbe weighedagainst poss ib le hazard s to the Ietus These hazard s include letal or neonatal |aund ice.
th romboc topenia. and poss ibly other adverse reactions which have occwred in the adult.NUR tNG MOTHERS Thiazides appear in human milk. It use oi the d rug IS deemed
essentia l. the patient should st0p nurs ing .PED IATR IC USE: Salety and e l lectiveness in ch ildre n have not been estab lished .
ADVE R S E R EAC T ION SProprano lo l h d roch loride ( INDERALO)Mostadverse e lects have beenmi ld and trans ient and have rare ly re quire d the withdrawal oitherapy.
Card iovascwar: Bradycard ia'
congestive heart lai lure. intens ification 01AV b lock; hypotens ion: paresthesia oi hand s . thrombOCytopenic purpura: art erialmsul lrcrency. usually ol theRaynaud type
Central Nervous System: L ightheadednes s : mental depre ssionmanilested by insomnia.Iassnude. weakness. latigue: revers ib le mental depre ssion progressmg to catatonia: y iSual
d is turbances : ha llucinations : anacute reversib le syndrome characterized by drsofientationtorlime and place. short-termmemory loss . emotional lab i lity, s lightly clouded sensorium. anddecre ased perlormance onneuropSychometrics .
Gastromtes trnal. Nausea , vomiting . epigastric d istre ss . abdomina l cramping . d iarrhea.constipation, mesenteric arterial thrombos is. ischemic col itis .
Al lergic Phary ng itis and ag ranuIOCyIOS is: ery thematous rash; levercombined with achingand sore throat. lary ngospasmand respiratory d is tre s s
Respiratory: Bronchospasm.
Hematolog ic: AgranuIOCytos is . nonthrombocytopenic purpura. thrombocytopenicpurpura
Auto- Immune: In extreme ly rare instances. systemic lupus erythematosus has beenreperted .
Miscellaneous: Alopecia. LE-like re actions : psorias ilorm rashes : d ry eyes : male impotence: and Peyronie
'
s d isease have been reported rare ly. Oeulomucocmaneous reactionsinvolving the sk in. ser0usmembranes.and conjunctivae re ported tora beta b locker (practolol)have not been associated with propranolol.Hyd roch loroth laz ldeGastromlestrnal Anore xia. gastric irritation. nausea. vomiting . cramping : d iarrhea: constipation: iaundice (intrahe atic cholestatic jaund ice ) : pancre atitrsf s ialadenitis
Central Nervous ys iem: Dizz iness . vert igo; pare sthesias : headache. xanthopsra.
Hematolog ic: Leukopenia. ag ranulocyIOS is; thrombocytopenia: aplastic anemia.
Card iovascular Onhostatic hypotens ion (may be agg ravated by alcohol. barb iturates.ornarcotics )
Hypersensmwiy' Puipura: photosens itivity: rash : urt icaria: necrotizing angiitis (vascwitis.Cutaneous vascul itis ): lever; respiratory d is tre ss . including pneumonitis : anaphylacticreactions
Other . Hyperg lycemia: g lycoswia: hyperuricemia: muscle spasm: weakness: re stlessness. trans ient b lurred y i5 ion.
Wheneveradverse reactions aremoderate or seve re. thiazide dosage should be reducedor therapy Withd rawn.

County Med ical Society . These persons eventual ly establ ished the H ealth EducationCommissionofWesternNorth
Carol ina which remained active unti l the Mountain Area
Health Education Center was further organized .
The Health Education Commission of Western North
Carol ina obtained pilot fund ing in 197 2 of approximate lythrough the Veterans Administration headquarters
with the endorsement and close col laboration of the OteenVA Hospital . Both Memorial Mission and St. Joseph
’
s
Hospitals contributed “in-kind
”facil ity and staff support .
With theassistance ofmany local governmental and educational institutions , the ex isting but fragmented health
educationprograms throughout the l 6-county region were
inventoried and analyzed . Contemporary reg ional health
manpower demographics were gathered and updated . A
medical consultant was hired for assistance in writing and
submitting several grant appl ications toprivate foundationsand to the Bureauof HealthManpowerEducationof HEW .
The federal grant appl ication received a favorable review
by the Bureau of H ealth Manpower Education but funding
was not approved . This aggressive , tenacious , and frus
trated Health Education Commission of Western North
Carol ina provided fertile ground indeed for nurturing the
expansion to Ashevi l le of the AHEC Program .
Even though the H ealth EducationCommissionofWest
ern North Carol ina was work ing d il igently on the projectand rely ing heavily on its physician members who wererepresenting organized medicine in the community , there
was a notab le lack of unanimity amongst doctors inAshevil le and environs concerning the AHEC concept. Inmid
197 2 , the Buncombe County Medical Society Executive
Committee formal ly endorsed the AHEC project and recommended that the County Society mount a col laborativeeffort with the two major private hospital s . At this point,Dr . Wayne Montgomery , Pre sident of the BuncombeCounty Med ical Society , contacted the AHEC Division of
the Dean’
s Office atUNC -CH to explore the feasib i l ity ofexpand ing the ex isting pi lot state AHEC Program toAshe
vi l le . Local physicians took a strong leadership role at this
point and the initial meetings were exclusively withMedi
cal Society members at the Medical Society’
s express ih
vitation.
Dr . G lennWi lson, the first state AHEC ProgramDirce
tor and Dr. Eugene Mayer , Deputy Director (now Direc
tor) , led the discussions ih Ashevi l le in the early part of
197 2 and again in November-December of 197 2 . S low lyand steadily , support and understand ing of the AHEC con
cept expanded . Unfortunately , there were no monies to
expand to Ashevil le immediately , but in early 197 3 the
University ofNorth Carol ina Board ofGovernors adopted a
statewide plan formedical educationand recommended the
expans ion of the AHEC Program to encompass the entire
state . The Ashevil le groundwork was in place and the twoyears of , intensive planning paid off , for the speed with
which the Mountain AHEC was organized , funded , and
implemented was impress ive .
Inearly 197 3 there existed a Buncombe CountyMedical
Society Advisory Committee , which formed the core of
what would eventual ly become the Board of Directors of
the Mountain Area H ealth Education Foundation, Inc .
(Membership: three members of the Buncombe County
Program Activities
F amily Practice Res idency Program
As one of the cornerstones of the AHEC Program
statew ide , the training of fami ly phys icians has been a highpriority of the MountainAHEC from its inception. Found
ed as a department in 197 5 , the Family Practice Residency
VOL . 46 , No . 9
Medical Society and two members each from Memorial
Miss ion and St. Joseph’
s Hospital s the ChiefAdminis
trative Officer and aTrustee fromeach hospital ) . There was
also a letter of agreement with the University of North
Carol ina at Chape l H il l , and in the words of Henry S . M .
Uhl , M .D . , first director of the Mountain AHEC , there
were“h igh hopes sustained by Optimism and a vision.
The Mountain Area H ealth Education Center Charter
Board was authorized in 197 3 to recruit a Director . Dr.
H enry Uhl was appointed and assumed his duties on
September 1 , 197 3 , when the Mountain AHEC offices
were establ ished and space made avai lab le at Memorial
Miss ion Hospital .The MountainArea H ealth Education Foundation , Inc .
was incorporated inFebruary 197 4 , w ith Dr. JohnMcL eod
elected as the first Board Chairman. Operational and capi
tal grant contracts between the Foundation and UNC
Chapel Hil l were signed in Jul y 197 4 . The basic design forthe educational building , a unique bridge structure joiningthe two hospitals , was approved. in June 197 4 . The con
struction plans were approved in February 197 5 , and con
struction contracts were signed inMay of the same year .
Recruitmentof a dynamic and highly competenteducation
al staffwas begun inearly 197 4 and continued over the nexttwo years as continuing medical education programs wereinitiated and the framework was completed for im
plementing a free - standing Fami ly Practice ResidencyProgram and Fami ly Nurse Practitioner Program. Both of
these were approved in late 197 5 .
While the initial thrust of the program development of
necessity was centered inAshevi l le and Buncombe County , the reg iona l hospital and med ical manpower educational needs of the entire 16 -county reg ion has always been aparamount goal of the Mountain AHEC . To that end ,
its
board of directors , its outreach programs , and its reg ionalpriorities have expanded in a stepwise fashionover the past
decade . TheMountainArea H ealth EducationCenter owes
much to the countless volunteers who nourished a dream
and persevered in hundreds of committee sessions until thebits and pieces of this complex organization came togetherand amalgamated .
S ince 197 5 the MountainAHEC has grown into a large
and complex education institution for health professionals .
The educational activities span the entire array of health
care discipl ines and involve undergraduate , graduate , and
continuing education. W ith a staff of some 65 professional
and support personne l and a budget in excess of three
mil l iondol lars , theMountainAHEC has become an institutional force in the health care system of the western part of
the state . The programs described be low remain consistent
w ith the overal l goal s and structure of the North Carol ina
AHEC program, yet are respons ive and unique to the
changing health care needs of the providers and institutionsin western North Carol ina .

Program is an exce l lent example of the partnership that
exists between the University of North Carol ina at ChapelH il l School ofMedicine and the regional health care institu
tions inwesternNorth Carol ina . F ive of the ful l -time facul
tymembers are tenure track professors in the Department ofFamily Medicine or Department of Internal Medicine at
UNC-CH . At the same time , an add itional twe lve are
part- time community—based faculty who part icipate in a
signifi cantway in the teaching program. Inaddition, nearly
100 other community-based physicians in the Ashevi l le
area contribute the ir time to the res idency program.
Since its beg inning , the Fami ly Practice Residency Pro
gram at the Mountain AHEC has graduated 4 8 family
phys icians as of the summer of 1984 . These graduates are
now practicing throughout the western part of the state as
we l l as elsewhere in the United States .
The residency program in Ashevil le has developed a
national reputation for its innovative cuni culum, which
includes a strong ori entation to fami ly systems , an emerging emphasis in geriatrics , and an increasing focus on
health promotion and disease prevention. Through its highqual ity faculty , a curriculum responsive to national andregional trends , and a commitment to place its graduates in
the underserved towns of the region, the residency is now
recognized as a national mode l of a community -based family practice training program .
F amily Nurse Practitioner Program
The Fami ly Nurse Practitioner Program was founded at
the Mountain AHEC in 197 5 , in close col laboration w iththe School of Nursing at UNC-Chape l H il l . As the onlyd iploma program remaining in the state , the Mountain
AHEC’
s FNP Program fi l ls a unique need for registerednurses from al l educational backgrounds seek ing to expandtheir practice as nurse practitioners .
The program continues to rece ive substantial fund ingfrom the Division of Nursing with in the Bureau of Heal thProfessions of the US . Department of Health and Human
Services . Since its inception, 96 students have graduated
from the program. Of these , 62 are now practicing inwestern North Carol ina in a vari ety of settings , includingrural free-standing cl inics , heal th departments , private
medical practices , hospitals , and other sites . Increas inginterest is being shown by industry in employ ing nurse
practitioners to manage and staff occupational heal th and
heal th promotion programs at industri al sites .
The Nurse Practitioner Program at the MountainAHEChas a strong orientation to both behavioral sciences and
geriatrics . The curriculum involves eightmonths of didac
tic training at the AHEC , fol lowed by four months of astructured preceptorship in a practice setting .
Student Support
One of themajor elements of anAHEC as envisioned bythe Carnegie Commissionwas the rotationof students fromuniversity heal th sc iences centers into regional AHEC cen
ters . As a priori ty of the North Carol ina AHEC Program
from its inception, the MountainAHEC has seen a steady
growth over the years in the number of students seek ingcl inical placements in western North Carol ina . Approximately 250 students spend a portion of their cl inical time
SEPTEMBER 1985 NCMJ 44 7
on rotation to one of a number of cl inical facil ities in themountain region each year .
An excel lent example of a high- qual ity student experi
ence involves the rotationof seniorpharmacy students from
the School ofPharmacy atUNC Chapel H il l . Each year , ten
to fourteen senior pharmacy students spend an entire
semester work ing in the Mountain AHEC region. These
students are placed in hospital and community pharmacies ,
and are closely supervised by the AHEC Pharmacy facultymember housed at the Mountain AHEC . Students come
together each week for seminars , and al so participate in
structured learning experiences in the cl inical setting . Ser
vices provided to students on rotation to the mountain
reg ion include housing , l ibrary and media services , other
log istical support such as trave l , and assistance inexplori ngopportunities for future practice .
Information and Med ia Services
Amajor service provided to al l health sciences students
and practicing health professionals in the regionare l ibraryand audiovisual services under the auspices of the Department of Information and Media Services at the Mountain
AHEC . The l ibrary has a col lection of some twentythousand volumes and offers a comprehensive array of
information services including reference , on- l ine comput
erized bibl iographic searching , inter- l ibrary loan, consulta
tion and technical assistance , and audiovisual production.
The total number of services provided to the reg ion fromthe AHEC l ibrary in was approximatelyThese services were provided not only to students and
practitioners in the Ashevil le area , but reached heal th care
providers inal l 16 counties served by theMountainAHEC .
As a matter of fact, 4 5% of the services were provided topractitioners in counties other than Buncombe .
Continuing Education
Another major educational priori ty of the Mountain
AHEC is continuing education for al l practicing health
professionals in the region. Organized primari ly around themajor health care d iscipl ines , theMountainAHEC offers a
comprehensive array of continuing education programs
from one-hour lectures to courses of a month or more in
length . Approximately 3 50 continuing educationprogramsare put on each year , approximately half in Ashevil le and
hal f throughout the other 15 counties in the region. This
enables health practitioneis to have access to h igh qual itycontinuing education w ithout having to incur the expenseof travel to a univers ity heal th science center or a majormetropol itan area . Faculty from the university health sci
ence centers as we l l as other constituent universities and
two-
year col leges active ly teach in these programs . Re
g ional and national speak ers are al so invited to part icipateon a regular basis . Survey data and anecdotal evidencesuggest that the availab i l ity of such a leve l of continuingeducation has had amajor impact on reducing professionalisolation among health professionals in the mountain re
g ion.
Consultation and Technica l Ass istance
As part of the overal l goal of improving the practiceenvironment for al l health professional s in the region, the
faculty and staff of theMountainAHEC provide consultation and technical ass istance upon request. These services

provide many individual physicians as we l l as health care
agencies with access to the professional resources of the
Mountain AHEC for solving problems relating to personne l , financial management, human
"
resource development,and a host of cl inical ly
-related issues . The consultation is
des igned to augment the formal continuing education pro
grams provided throughout the reg ion.
The education programs described above are intended
both to stand alone as services offered by the AHEC , and
also to serve as an integrated and comprehens ive approachto improving the educational environment for health pro
fess ional s inwesternNorthCarol ina . There are a number ofexamples of the way oneAHEC programre lates to another.
Many of the graduates of the Fami ly Practice ResidencyProgram regularly contribute time teaching and preceptingcurrent residents . They are also often the ind ividuals tak ingthe lead in the ir respective counties in organiz ing active
continuing education programs in col laboration with thestaff of the MountainAHEC . In addition, their util ization
of the resources available through the l ibrary and media
center further strengthen the practice environment in the
smal l towns in the region.
Program ImpactThe Mountain AHEC has had a major impact on the
availab il ity of highly trained health professionals in westernNorth Carol ina . For example , of the 4 8 graduates of the
Family Practice Res idency Program since its inception, 40
have stayed in North Carol ina to practice and 7 5%
have remained in the 16 western counties of the MAHEC
reg ion (tab le This rate of retention exceeds that of al lotherprograms inNorth Carol ina , and may be unsurpassed
in the entire US .
The intent of the AHEC-based residency programs wasto place primary care physicians in the smal l towns in the
regions that have heretofore been underserved . Tab le 2demonstrates the success of theMountainAHEC ’
s residen
cy program in this regard . Again, of the 4 8 graduates
through 1984 , 2 7 have settled in towns w ith a
populationof less than and an additional 19% haveestabl ished practices in towns of under population.
Thus , three-fourths of the graduates are practicing in townsof a size that historical ly has had d ifficulty inattracting and
retaining primary care physicians . In addition, of the 3 6
graduates who have settled in towns of under
population, only one has not remained there permanently as
of March 1985 .
VOL . 4 6 , No . 9
In 197 5 , there was approximate ly one primary care
physician for every residents in themountain reg ion.
At the end of 1984 , the ratio was approximate ly
population. Although a variety of factors have contri butedto the improved availabi l ity of primary care phys icians , theAHEC residency program has had a s ignificantly favorableimpact on this ratio .
The second major program to address shortages of pri
mary care providers in rural areas is the Family Nurse
Practitioner Program. Since it was estab l ished in 197 5 ,
MAHEC’
s FNP program has graduated 96 students . The
data presented in table 3 show that nearly one-half of the
FNP graduates are now located in the 16 counties served bythe Mountain AHEC and an add itional l 6% are in other
counties inwesternNorth Carol ina . Although not shown in
the tab le , a substantial port ionof the graduates have settledinvery smal l towns or rural communities that either had no
physician or were clearly medical ly underserved .
As described above , the MountainAHEC sponsors over
300 continuing education programs per year in the region,
and targets these programs to al l health profess ionals .
Table 4 demonstrates the growth in the numberof programsover the past four years , and ind icates the balance of programming betweenBuncombe County and the other counties ih the reg ion.
Attendance at continuing education programs has risenstead i ly over the years as we l l . Although phys icians
’
attendance in continuing education continues to far exceed
that forother d iscipl ines , its absolute s ize and percentage ofthe total has decl ined s l ightly in the past three years (tableAttendance by nurses has increased steadily during the
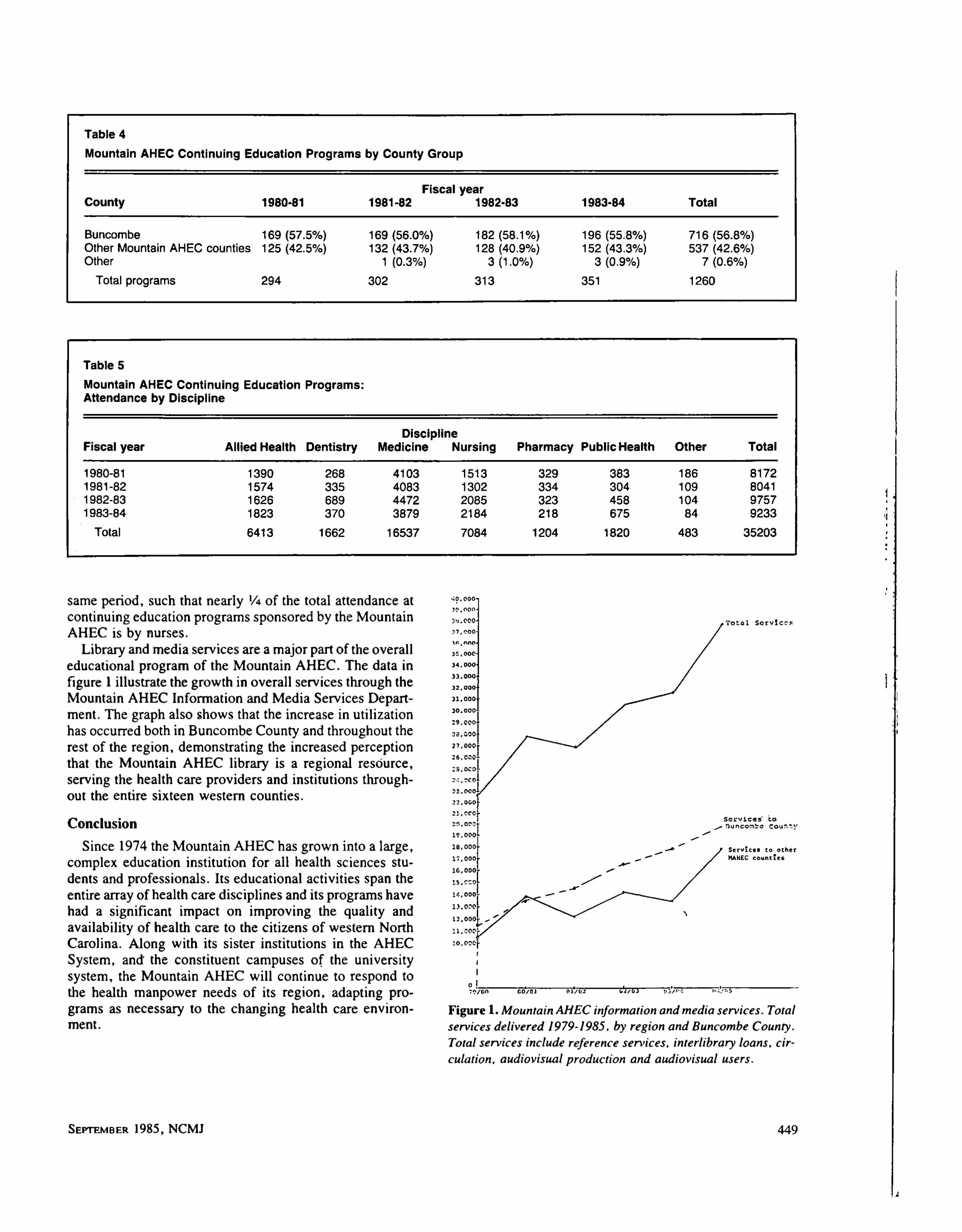
same period , such that nearly of the total attendance at
continuing educationprograms sponsored by the Mountain
AHEC is by nurses .
L ibrary andmed ia services are amajorpartof the overal leducational program of the MountainAHEC . The data in
figure 1 il lustrate the growth inoveral l serv ices through the
MountainAHEC Information and Media Services Depart
ment. The graph also shows that the increase in uti l ization
has occurred both inBuncombe County and throughout therest of the reg ion, demonstrating the increased perceptionthat the Mountain AHEC library is a regional reso
‘
urce
serving the health care providers and institutions through
out the entire sixteen western counties .
Conclusion
Since 197 4 theMountainAHEC has grown into a large ,
complex education institution for al l health sciences stu
dents and profess ional s . I ts educational activities span the
entire array of health care d iscipl ines and its programs havehad a significant impact on improving the qual ity and
avai lab il ity of health care to the citizens of western North
Carol ina . Along w ith its s ister institutions in the AHEC
System, and“
the constituent campuses of the universitysystem, the Mountain AHEC wil l continue to respond to
the heal th manpower needs of its region, adapting programs as necessary to the changing health care environ
ment.
SEPTEMBER 1985 NCMJ
O 000
To t a l Se r v i c e s
J 7 ,ooo
Tl : 0 0 0
9 000
7 2 0 5 0
COO
Buncomb e Cou
Se rv i ce . to o ther
MAREC count i e s
1 2 00
F igure 1 .Mounta inAH EC informa tion andmedia services . Tota l
services del ivered 1979- 1985 , by reg ion and Buncombe County .
Tota l services include reference services , interl ibrary loans , cir
cula tion, aud iovisua l production and aud iovisua l users .

Med ical Mutual is pleased to offeryou Crisis : Th en and Now,the
latest in a series ofphysician loss preventionworkshops .
Th is innovative programWill he lp you
Identify potentialproblem areas inyourpract ice .
Reduce exposure in these areas .
Rece ive 5 percent d iscount onMMIC premiums for
EarnContinuing Medical EducationCred it.
Crisis : Th en and Now is Open to all phys icians in convenient
loca tions across the state . Be sure tomark your calendarnow for th is
important session:
June 2 0, 198 5 at pm . Eli zabeth C ityColl ege of the Albemarle ( LectureAud z
'
ton’
um—B ldg .
”
B"
)
July 1 1 , 198 5 at pm . H ickoryCatawbaMemorial Hospital (AHECAudi torium)Jul y 1 6 , 198 5 at pm . W i lsonW ilsonMemorial Hospital (Aud i torium)Septembe r 1 7 , 198 5 at pm . Ashevi ll e
MountainAHEC ( Lecture Ha l l)
Septembe r 2 4 , 198 5 at pm . Greenvil le
Eas t CarolinaUnivers ity, School ofMed icine Bro dy Aud itorium)
October 2 , 198 5 at pm . Kinston
LenoirMemorial Hospital (Aud itorium)October 2 9 , 198 5 at pm. W inston-SalemForsyth Memorial Hospital (Meeting Rooms 1 G 11)
MedicalMutual Insurance NorthCarolina2 2 2 N . Person Sr. , Rale igh , NC 2 7 6 1 1

PHYSICIANS'
FORUM
Blue Cross/Blue Shie ld’
s
Personal Care Plan
ed ited by Danie l L . Dolan, MD .
The ed itor ha s queried phys icians in severa l d isc ip l ines who practice
under the rubric“Pr imary Care
"as to how they view the effects on the ir
practices of the newB lue Cross /B lue Sh ie ld ind ividua l practice associa tiontitled the Persona l Care P lan . In brief summary , a primary care phys ician
s igns a one-
year contract which canbe termina ted with 30-days noticefromyear to year . The phys ician agrees to a ccept up to 3 00 pa tients over a
three-
yea rperiod and be l isted as a pa rticipating phys ician in the d irectoryof the plan which is sold to subscr ibers . H e mus t ma inta in hospita l privi leges in at least one hospita l pa rticipa ting in the plan. H e agrees toprovide
afourpage l is t of servicesfree to a l l subscribers in exchangefor a monthlypayment per patient made to him by the plan va ry ing between to
$2 depend ing onfive ca tegories of age and sex . F or anadd itiona l three
pages of services , he wi l l be compensated between $ 16 to $1 .5 8 perpa tient
per month . Add itiona l ly , the plan cred its a second monthly payment to a
centra l Institution-and Referral F und between to perpa tient
to cover hosp ita l iza tion and consultants’
fees . If a t the end of one year , the
cashflow in the Ins titutiona l and Referra l F und is pos itive . the phys ician
reta ins I 00% of his prepa id s tipendp lus 5 0% of his surplus . If the cashflowis nega tive . he receives only 80% of his stipend . In no ins tance does he losemore s ince larger deficits are guaranteed by the p lan . Should he be unableto persona l ly provide a l l of the services on the l ist, he must obta in theseservicesfrom a consultant, butpayingfrom hisfirstfund H e ma inta ins thefreedom to continue other segments of h is practice a s he chooses . H e mus t
provide 2 4 hour per day , seven day per week coverage .
The question to the participants in th is Phys ician'
s Forum was , What doyou think of B lue Cross/B lue Sh ield
’s Persona l Care Plan?
F rom Dr . El len Boyd , a ped iatrician in Ashevil le
The Personal Care Plan presented by B lue Cross/B lue
Shie ld has the advantage over otherHMO type health plans
whereby consumers can choose the ir physician and main
tain an interpersonal re lationship w ith continuous fol low
up by this designated physician. It is anticipated that byhaving routine scheduled check
-ups , educationand preven
tive care can be taught with early screening of deve lopingproblems for the pediatric population. Under a pre
-
paid
plan, parents w il l bring the ir children in for acute care andhopeful ly prob lems canbemanaged on anout-patient basisbefore hospital ization is required .
The Personal Care Planmay benefit a new phys ician inan area by he lping th is physician get referrals and estab l isha practice . With this plan, the pediatrician needs reassur
ance that financial ly his/her practice w il l not be hindered
and wil l continue to have a pos itive growing balance .
Although emphasis is g iven to the fact thatpaperwork from
SEPTEMB ER 1985 NCMJ
process ing claims , bi l l ing and col lections w il l be minimized , it is a concern that the paper work completion of
encounter forms from patient vis its may require more timeand expense of the office personne l .
Pediatri c offices presently place anadd itional charge forafter hours visits . This encourages patients to bring the irchildren in during regular office hours . Under the prepaid
plan there is the guarantee of the standard twenty~ four hour
seven days per week availabi l ity of covered services to
participants at no additional costs . A concern is that this
may increase the demand for after hours vis its and that
financial incentive to come during regular office hours wi l lbe lost.
One major advantage of the Personal Care Plan is that itassures coordination and continuity of care of the part ici
pants by the ir personal phys ician. This physic ian is te
sponsib le formanaging the ir health care andmustauthorizeal l referrals to special ists and preauthorize al l e lective ih
patient and outpatient hospital admissions scheduled by
4 5 1

medical special ists . This plan wi l l encourage more coor
dination of care between the participant and al l medical
personne l involved w ith the personal care physician man
ag ing this care .
The estab l ishment of HMOs , industrial health care
plans , and personal care plans as presented by B lue Cross/
B lue Shie ld are proclaimed as the med ical care system of
the future . W ith the evaluationof heal th care expenses , theideal restraint to escalating costs would be practicing pre
ventive care . Stil l , med iocrity of medical care must be
guarded against. Phys icians need financial incentives and
there is nothing wrong with competition in the medical
arena . Competition serves as an advantage to themed ical lyserved population. Pediatricians are recognized as having
one of the lowest incomes among physicians . It would be
encourag ing to seemore equal ity of financial compensationfor services rendered , and more compensationgiven for the“thinking
”
primary care physicians . If health care plans
were to distribute the health care dol lars more across the
board for physicians , this would be an incentive to bri ngmore physicians into the primary care professionwhere the
medical need is greatest. F inancial incentives should be
placed among the primary care profession and it is hoped
that prepaid health care plans w il l reflect this need . The
payoff inpreventive primary health care would be anover
al l reduction in heal th care expenses .
F rom Dr . Robert H . Fabrey , I I , a familypractitioner in Weavervil le
At the present I do notparticipate in the B lue Cross/B lueShield Personal Care Plan,
because it is not offered in theAshevil le Area . However , when it becomes available , myassociates and I expect to participate . I am a family physi
oian in‘
a three man group.
I became a fami ly physician in part because I perce ivesome effi ciencies in the way I del iver medical care . Con
tinuity of care is one of the tenets of family practice .
Preventive medicine as manifested by risk factor control
and screening for il lness is an important part of our present
practice . We do it because we fee l it is cost effective interms of dol lars and personal suffering .
At the present time most health care insurance does not
provide financial incentives for health screening . The pres
ent system encourages care of higher cost acute il lness and
does not reward the low cost—high touch aspects of care .
The Personal Care Plan appears to address this issue , by
providing funds forwhatnowmight be uncovered services .
This wil l change my practice only in that services I alreadyprovide patients wil l now be re imbursed by the ir carrier .
I suspect that the Personal Care Plan w i l l change myrelationship w ith my consultants . It w i l l force me to bemore cost conscious for equal services . I expect there wi l lbe d ifficulties when a patient desires a consult or
“second
opinion?’
outside our office , when I can see no justificationfor it . I think that these are al l solvable problems , butmaychange my practice sty le .
From Dr . H arold D. Schutte , a ped iatrician in
Ashevi l le
Given the present cl imate of escalating health care costs
resulting in increased interest incost containmentby insur
VOL . 4 6 , No . 9
ance companies and government, the primary care phys i
cianmust take note of the trends thatwi l l affecthis practice
over the next decade . H e must also deal with a physician
surplus and a shrink ing patient population at the same time
that he copes w ith an uncertain economy . It is obvious thathe must have an anchor for economic and professional
survival .
The introduction of North Carol ina B lue Cross/B lue
Shie ld’
s Personal Care Plan has significant appeal . On the
surface, at least, it seems to work w ithin the framework of
the present health care de l ivery system . It accompl ishes
this by a prepaid plan for cost containment and the util iza
tion of primary care physicians already in private practice .
The plan also has provisions for early detection of disease
and preventive med icine education which ideal ly should
reduce health care costs and benefit the patient as wel l .
As a pediatrician in private practice I would l ike to haveoptions other thanone sing le plan to choose from inorder to
be able to choose the one most compatible withmy sty le ofpractice . The Personal Care Plan
,while stressing physician
involvement in peer review , does not mention the role of
the primary care physician on the governing board of its
plan. This type of re lationshipwould ensure that a specialtyl ike pediatrics would be given adequate emphasis . In myview if involvement at the board leve l is not an integral partof the plan it could we l l appropriate a large portion of its
funds and emphas is to surg ical procedures , with a smal l
amount for cognitive activities . As such , the primary care
physician again would end up on the low end of the finan
cial totempole . I t is somewhat reassuring to know that in its
formative stages the plan had significant physician input.
The plan’
s track record for accompl ishing its ideal goals of
ensuring qual ity care while reducing health costs and fairlycompensating participating physicians w i l l have to await
the verdict of time .
F rom Dr . L ewis C . Sommervil le , a general
practitioner in Ashevil le
If I d id not participate in such a plan, I am sure that there
would be a certain number of my patients from industryenrol l ing in such a plan, and I cannot, at this time , te l l
specifical ly whatpercentage of patients I am talk ing about.
However, because this would occur, I would probably feelsomewhat coerced into co-operating or participating in a
plan if it were very wide ly used in our area .
What would be the effect on my practice _
i_
f I did not
participate? I have looked , somewhat superfic ial ly of
course , at the cost. And I have looked at the total cost of
caring for patients in my office over the last year. The
impression I have gotten is that the “healthier patients ,
that is those in the work force who would be apt to be
covered by such a plan, actual ly take less cost for their care
during the year , and this se lect group then would be cov
ered by an IPA. The other type ofpatients olderpatients ,
those who take more care and have a higher costper year
would probably not be covered by an IPA because they arenot involved in industry , etc . It is my impression that 80%of the capitation fee does not quite cover the charges that Iammaking at the present time . This would , of course , be a
deterrent to my entering into th is k ind of plan.
The final thing , and this would seem to be the most

of a more comprehensive coverage being provided at whatis usual ly a reduced cost. The B lue Cross/B lue Shie ld
Personal Care Planprovides a very extensive and compre
hensive l istofmedical services which few traditional heal th
insurance pol icies can ri val .
There are , however , several disadvantages to the B lue
Cross/B lue Shie ld plan as we l l as most other IM OS no
matter whatmodel they are organized under. F irs t, for the
phys ician, I think there is a s ignifi cant loss of independence . Both the personal care physician and the med ical
subspecial ist lose the freedom to set their own fees . The
physician and the patient al so lose the ir freedom to choose
which medical special ist they want at the time of referral .
Any referral must be made to a medical special istwho is a
memberof the B lue Cross/B lue Shie ld Personal Care Plan.
The patient loses his abi l ity to choose any phys ician in the
community . I think inherent in th is type of heal th care
de l ivery system is a general loss of freedom of how the
individual wil l practice medicine .
I al so am greatly concerned about the issue of qual ity ofcare . Although each ofus would l ik e to drink that he would
refer any patientwithout hes itation if a referral was needed
or if a hospital izationwas necessary , under the B lue Cross/
B lue Shie ld program the physician is actual ly encouraged
financial ly not to refer to the medical special ists , not to do
VOL . 46 , NO . 9
vari ous tests , and not to admit the patient to the hospital .
Traditional ly , these dec isions have notaffected the primarycare physicianmonetari ly , butwith th is plan the physician
would be intimately involved and a confl ict of interest isalready estab l ished . Not only is there a reward for less
testing , less referrals , and less hospital ization, but there is
al so a reward for spending less time w ith the patient. I thinkthis type of plan would change the traditional way that
Internal Medicine is practiced . Traditional ly , Internistshave prided themselves in being able to spend an adequateamount of time to do a very thorough and complete assess
ment of a patient. The Personal Care Plan does notprovide
any financ ial reward for spending the time it sometimes
requires to complete a very thorough evaluation of a pa
tient’
s prob lems . This is perhaps themostd isturbing aspectof the Personal Care Plan. The financ ial pressure on each
primary care physician would be to see as many patients as
he could ina given amountof time . Another d isturb ing factabout the Personal Care Plan is that themed ical special ist ispaid on a fee-for-service basis . For every procedure he
performs he gets paid and the more procedures he does , the
more he gets paid , whereas the primary care physician’
s
fees are l imited and fixed . No matter how much time he
spends with the patient, he sti l l gets paid exactly the same
amount. This seems to again be a system that rewards
physic ians who perform procedures and specific tasks anddoes not reward cognitive ski l ls on the part of the primarycare phys ician. Al l the pressure seems to be laid on the
primary care physician to cut costs . He must cut costs byreducing referral s , reducing tests , reducing the amount of
time he spends with a patient, and reducing the number andlength of stay of hospital izations . None of this pressure is
placed on the medical special ist. He stil l gets a fee for
service , he has no incentive to do less procedures or less
testing , but infactwi l l getpaidmore foreach additional test
or procedure that is done .
I th ink the B lue Cross/B lue Sh ield Pers onal Care Plandoes address some of the problems of heal th care de l iverythat we face in our soc iety . It does stress reduction of the
overal l heal th care costs and does provide an increase in the
amount of coverage patients receive compared with tradi
tional health insurance pol icies . It furthermore returns the
primary care physician back to the entry point into the
health care system. However, I th ink many of the disadvantages of this program outwe igh the ‘
advantages . There is the
continued prob lem of providing l ittle re imbursement forcognitive ski l ls and yet continuing to reward the medical
spec ial istwho performs numerous procedures . There is the
very real questionof continuing toprovide a h igh qual ity ofcare to patients and yet be ing forced by the system to spendless time with patients . I fear that there mightbe a tendencynot to do tests which may be warranted , not to admit
patients who need hospital ization, and not to refer patients
who need referral . I general ly dis l ike the idea that we as
physicians are being forced to conform to the HMO brandof medicine just to provide for our continued surv ival in
years to come .

SPECIAL ARTICLE
Asheville : The Tuberculos is Era
Irby Stephens , MD .
0 Ashorthistory of the rise and decl ine of tuberculos is sanitaria and expertsinAshevi l le between 18 7 1 and the 195 0s .
oNE hundred years ago Ashevi l le was rapidly gaining
prominence as a vacation and health resort , and w ith
in the space of a few years became the nation’
s largest and
most famous center for the treatmentof tuberculos is . To the
medical historian, and to the student of tuberculos is inparticular , the transformationofAshevi l le from anobscuremountain vil lage to a world- renowned and major medicaltreatment center is a fascinating story .
At that time , tuberculosis was the most dreaded d iseasethroughout the world and the lead ing cause of death in the
United States . The ravages of the Wh ite Plague , as
tuberculosis was sometimes termed , were especial ly severe
in the crowded , rapid ly growing cities , re lative ly uncommon in the rural areas , and especial ly rare in the thinl y
populated mountain regions of Europe and the - .Uni ted
States . Patients with consumption placed“
at rest and ex
posed to the cool , pure mountain air began to gainweightand strength , the ir pulmonary lesions showed evidence of
heal ing , and the improvement was oftenmiraculous . This
gave rise to the cl imatic theory of the treatment of pulmo
nary disease , a theory orginating inGermany and Switzer
land and soon adopted and enthusiastical ly embraced byphysicians inAmerica . Physicians and patients everywhere
rejoiced that, for the firs t time , there was a reputabletherapeutic approach to pulmonary tuberculosis a bri ghtray of hope in a pre vious ly dismal scene . In al l the eastern
United States , Ashevil le offered the best combination of
al titude , atmosphere , and cl imate considered essential in
the treatmentof lung d isease . As a result, a groupof highlycompetent and ded icated phys icians found the ir way to
Ashevil le to devote themse lves to treating and study ingtuberculos is , spec ial iz ing in phthis iology . In a day when
special ization was extreme ly uncommon, these men and
their successors became the nation’
s most highl y regardedand most renowned experts in the fie ld of tuberculosis . For
50 years patients by the thousands flocked to Ashevil leseeking the promise of health offered there .
Beg inning about 100 years ago , there was a concurrent
andmore scientific approach to the treatment and control of
tuberculosis . In 1882 , Robert Koch discovered the tuberclebacil lus . Koch’
s discovery , paired with the introductionof
immunotherapy by Jenner and Pasteur, suggested the poss ibi l ity of spec ific method s for the treatment and control oftuberculosis , stimulating widespread re search in the fie ld .
One bf the early laboratori es engaged in this effort was
establ ished in Ashevil le .
From 54 Sunset Parkway . Ashevi l le 2880 1
SEPrEMB ER 1985 NCMJ
For 50 years , beg inning around 1885 , Ashevi l le served
as a stage for the dramatic triumph of med icine over the
foremost kil ler of the time . The stage setting and the actors
in th is drama wil l hold the attentionof any audience with an
interest in that s ingular epoch in the history of med icine .
The Pioneers : Gatchel l and G leitsmann
In 187 1 The V i l la , a sanitarium exclusive ly for patients
with tuberculosis , was estab l ished in the vil lage of ForestH i l ls (now the Keni lworth section of Ashevil le) by Dr.
H . P. G atche l l , a professor from Hahnemann Med icalSchool . He was joined by his brother, and the doctors
Gatchel l soon moved The V i l la to H aywood and Col lege
Sneets (now downtownAshevil le ) where they operated for
twoor three years , thenabruptly abondoned the project andmoved away . The reasons for the Gatche l ls
’
clos ing their
sanitariumare obscure , but the eventwas highly important
medical ly , as it was the first tuberculos is sanitari um in theUnited States , antedating the more famous Trudeau Sani
tari umat Saranac L ake , New York , by more than 12 years .
Very shortl y after the departure of the Drs . Gatche l l , a
second and more sustained effort to estab l ishAshevi l le as atuberculosis center was made by a highly capable and
enthus iastic pulmonary disease expert , Dr . Joseph W .
G le itsmann . Born and educated in Germany , G le itsmann
was a convinc ing exponentof the European- inspired theoryof the benefit of al titude and cl imate in the treatment of
tuberculosis . After a systematic study of the cl imatic fea
tures of the Uni ted States , he se lected Ashevi l le as havingan optimum comb ination of barometri c pressure , tempera
ture , humidity and sunl ight bel ieved to be conducive to theheal ing of the pulmonary lesions of the disease .
G leitsmannmoved from B al timore to Ashevi l le in 187 5and establ ished The Mounta in Sani tarium for PulmonaryDisease s located in the old Carol ina House on NorthMainStreet (now B roadway ) just south of Woodfin Street. He
later acquired an adjoining bui lding to\house his patients ,
who for the most part were referred by prominent physi
cians in the eastern and southeas tern United States . Withevangel istic zeal , G le itsmann (a remarkably vigorous andforceful personal ity) addressed medical gatherings and
publ ished scientific papers extol l ing the benefits of the
Ashevil le cl imate . He d istri buted copies of his papers publ ished in many of the leading med ical journal s by the
thousands to physicians and lay groups throughout the
eastern Uni ted States .
Dr. G leitsmann’
s accompl ishments , moreover, were ap
preciated and recognized by highly competent med ical

authorities of that day . Among these were Dr . Stanford E .
Chil le , Professor of Physiology and Patholog ical Anatomyin the Medical Department of the University of Louis iana .
Chil le himself on visits toAshevil le in the 18705 had beenimpressed that no tuberculosis had been found in the nativepopulation and had recommendedAshevil le to a numberofhis tubercular patients . He vis ited G le itsmann inAshevi l leand in a paper before the New OrleansMedical and Surgi
cal Society reported and extol led h is work . Dr. Fred
Loomis of New York , patron of Dr. Trudeau, referred
patients to G le itsmann’
s Mountain Sanitarium, and none
other thanDr. L awrason Brown, successor toDr. Trudeau
and recognized histori an of cl inical tuberculosis , creditsG leitsmannw ith establ ishing the first tuberculos is sanitarium in theUnited States . For five years , G le itsmannwork
ed unflaggingly , maintaining a census of 20 to 30 patientsin his smal l sanitarium, publ ishing enthusiastic progress
reports and d istributing them wide ly .
It appears , however, that G leitsmann'
s enthusiasm and
his dreamofconvertingAshevi l le into aMecca for tuberculosis sufferers were not shared by the local citizens . In 1880
when he attempted to expand his operation, he found his
effort s to obtainmore adequate quarters thwarted by localproperty owners who apparently feared the introduction oftuberculosis into the ir city and the poss ible adverse effecton property values . Unab le to procure a build ing suitablefor a sanitari um, he tried for one more year to house his
patients in the Eagle Hotel located on South Main (now
B iltmore Avenue) between Eagle and Sycamore Streets .
F ind ing this arrangement unsatisfactory , he gave up and
went toNew York , giving as his reason for leav ing the lackof facil ities . There are no records available that adequatelydocument these events , and we must re ly upon conjectureto explain the fai lures of these early ventures . It is very
possible that the Teutonic personal ities of Drs . Gatche l l
and G leitsmann did not mesh wel l with those of the pre
dominantly Scotch- Iri sh mountain people . Itmay be that,be ing homeopathic physicians , they were notwe l l receivedby theAshevil le doctors , but inthewords ofDr. Gail lard S .
Tennantwho recal ls that era , as itwas , G leitsmann probably did more than any other one man to bring th is placeinto notoriety , for s ince his time the stream of travel here
has been continuous .
The Beginnings : Battle and Von Ruck
Nothing is more characteristic of pioneers than that theyare ahead of their time . Pioneer efforts often fai l initial lybecause they are premature . This was undoubtedly true ofGatchel l and G leitsmann, forAshevil le in the 18708 was a
remote , relatively inaccessible mountain vi l lage wherecommunication was difficult and travel uncomfortable .
Th is was soon to change .
~
Emerging from the post-Civil
War depression years , Ashevil le in the 18805 was ri pe for
deve lopment. It was a smal l mountain vil lage of 7 00 in
1870 . On receiving its charter as a city in 1883 , it had
grown into a thri ving boom town of 3 87 4 ( 2 808 w ith 1066The stimulus for th is spurt of growth was the
advent of the railroad . The Western North Carol ina Rail
road , which in 187 1 had terminated at Old Fort , final lyreached Ashevil le in September 1880 , providing access
from Spartanburg , Atlanta , and Charleston. In 1883 the
Figure l . S . Westray Ba ttle , M.D outstanding Ashevi l le phys i
cian of the 1890 era whose enthus iasm and persona l cha rm
a ttractedmany influentia l ind ividua ls . contributing toAshevil le'
s
fame and growth .
VOL . 46 , No . 9
l ine was extended to Knoxvi l le , connecting with the rai l
road system serving east Tennessee , Georgia , V irginia ,
and Ohio . Trade immediate ly flouri shed and with sched
ules providing overnight service from points as distant asLouisvil le andAtlanta , visitors came in increasing numbersto enjoy the beautiful mountain scenery and incomparablesummer cl imate .
In this fert i le soil , the seeds planted by Gatche l l and
G leitsmann at last began to spring up and , tended by ca
pable men who soon fol lowed , began to thrive and to
transform Ashevil le into a medical center destined to be
famous for the next fifty years .
The years 1885 and 1886 were especial ly notable onesfor Ashevil le medicine in that they marked the arri val oftwo of the most influential men ever to appear on the localscene :Dr. S .Westray Battle andDr. Karl VonRuck . These
two outstanding phys icians were to pick up the pieces leftby Gatchel l and G le itsmann, and each in his own waybegan to build Ashevil le into a national ly knowncenter forthe treatment of tuberculosis .
The two men could not have been more different. Dr.
Battle (figure the very essence of the Southern aristo
erat, courtly , elegant, and strik ingly handsome in his grayVandyke beard and fash ionable attire , was endowed with
irres istible personal charm. Agraduate of the University of

V irginia , he studiedmedicine inNew York and attained anMD . degree from Be l lvueMedical Col lege . He started his
career as a naval surgeonbutwas forced to retire because ofinjuri es incurred on sea duty . He decided on a career in
private medical practice and became especial ly interestedin the field of tuberculosis . A firm bel iever in the theory ofcl imato- therapy , he had made his own study of the eastern
United States before selecting Ashevi l le as the ideal areafor the treatment of pulmonary disease . H av ing arrived inAshevil le in 1885 ,
within three years he had become hermost ardent promoter. Dr . Battle
’
s unreserved enthus iasm
forhis adopted home ismanifest inhis paper read before thecounty medical society in 1888 entitled “
Cl imate and the
Cl imatic Treatment of Diseases w ith Special Reference totheMerits of the Ashevil le Plateau. He stated that there is“noth ing l ike it East of the Rockies , and concluded that
Ashevil le ’
s cl imate is“tonic , invigorating , and bracing .
He al so attri buted an almost antiseptic qual ity to the air, inthat
“the cond itions which seem to favor germpropagation
and prolong the species of the genus Bacteriumdo notexisthere .
”
Battle’
s professional accompl ishments were modest buthis influencewas enormous . Aw idower formany years , hel ived at the old B attery Park Hote l where he was a highlyvisible and valuab le asset to the community :
“he was a
gifted speak er on any occasion. H is diction was pol ished ;
his phraseology careful ly chosen. Possessed of sparkl ingand pungent wit, he was at his best as an after-d innerspeaker. He was a raconteur blessed . with
‘
an unusual lyretentive memory . This portrait, quoted from the Ashe
vil leCitizenofApri l 30, 192 7 , at the time of Battle’
s death ,
reveals vividly the impactof the personal appearance of thisfascinating man: Strik ingly ind ividual in al l things , Dr.
Battle was particularly so in his attire . He never fol lowed
fashions ; he set his own, and no matter what he wore , it
always seemed a part of him, rather than an external dec
oration. H is favori te headgear, outside of the formal evening si lk topper , was a soft fe lt hatof the wide-brimmedvariety . In winter he wore a cape , reaching almost to his
knees . Awhite flanne l suit, with a black si lk sash in l ieuofa waistcoat , was his usual summer attire . In eveningclothes , ofmasterful cut and fit, he was in truth the glass of
fashion and the mold of form . Always he carri ed the smal l
rattan cane so popular with Engl ish and Indian army officers . Dressed with meticulous care , with pointed mustachios , carefully trimmed Vandyke , and a mi l itary air
withal . W ith a cape and cane sw inging as he came downBattery Park hil l , across H aywood and up the avenue , is it
any wonder that fe l low members sitting in the windows ofthe old Ashevil le Club watched him w ith admiring interest?
”
Dr . Battle’
s tremendous enthus iasm for Ashevi l le ,
which he communicated wide ly among his numerous influential connections throughout the eastern seaboard ,brought to Ashevil le many wealthy and enterprising individuals . These not only added lustre to theAshevi l le scene ,
butmany , captivated by the cl imate and scenery , returned
to become prominent residents and to use the ir wealth andvigor to enrich the area . Mrs . W . H . Vanderb ilt, sufferingfrom chronic malaria acquired on her travels , came to
Ashevil le under Dr. Battle’
s care . Her son, George H .
SEPTEMB ER 1985 , NCMJ
F igure 2 . Ka rl VonRuck . M .D a loof and controvers ia l physi
e ian-scientist who initiated the sanitarium era in Ashevi l le .
Vanderb ilt, fascinated by the area , returned to build theB iltmore House ;Dr . Battle is reported to have beenhelpfulin acquiring some of the land for Vanderbilt’ s B i ltmoreEstate . E . W . Grove of St. Louis , troubled by a bronchialcomplaint, was another ofDr. Battle
’
s patients whoplayed
amajor role in the growth and developmentof the city . Mr.
Grove was so impressed by the area thathe leve l led BatteryPark hil l , cons idered an eng ineering miracle of that day ,
and bui lt the present B attery Park Hotel . The street in frontof his new hotel , Grove named , appropri ate ly , Battle
Square for his esteemed physician and friend . G rove went
on to develop a new residential section in the north of the
c ity , the Grove Park section, and with his son- in- law , Fred
Seely , built the stil l famous Grove Park Inn.
Throughout a long career, Dr. Battle was Ashevil le ’
s
lead ing physician and a leader inmostof the city’
s civic and
social activities . He founded North Carol ina’
s first chapterof theAmericanRed Cross . After thewar , hewas chairmanofNorth Carol ina ’
s CommissionforRel ief inBe lg ium, and
was decorated by that country for his services . He was
active in North Carol ina’
s National Guard , served as its
SurgeonGeneral , and rose to the rank of brigad ier general .Stil l very active at seventy- two , he died while attend ing ameeting inRale igh , April 29 , 193 7 . H is impressive home
on Macon Avenue sti l l stands , now occupied by the
WLOS-TV station.
Dr. Karl Von Ruck , on the other hand , was a near
recluse , a dedicated scientist interested almost exclusively

in medical research . He was born in Constantinople , the
sonof a German d iplomat, and was educated inGermany ,
B .S . Univers ity of Stuttgart , MD . University of Tub ingen. He came to the United States and received a second
M .D. degree from the University of Michigan in 187 9 .
Interested in tuberculos is since his student days , he was
present at the famous 1882 meeting in Berl inwhenRobertKoch announced the discovery of the tubercle baci l lus .
VonRuck closed themed ical practice he had begun inOhioand thereafter devoted h imself entire ly to the study of
tuberculosis . Poss ib ly influenced by G le itsmann’
s reports ,
he came to Ashevi l le in 1886 to start a sanitarium and
conduct experimental work on tuberculosis . In 1888 , a
memorable date in Ashevi l le '
s med ical history , Karl Von
Ruck establ ished the W inyah Sanitarium (figure which
proved to be highly successful both professional ly and
financial ly . In 1902 , he was joined by his only son, Silvio ,
who had also become apulmonary disease special ist. S ilvio
took over the operationof the sanitariumand VonRuck was
able to devote himse lf entirely to his stud ies . Abri l l iant andeducated man, Von Ruck was not only a scientist but a
scholar as wel l . He founded and edited The Journa l ofTuberculos is , the first med ical journal devoted entire ly tothat disease . Publ ished quarterly , it contained papers con
tributed from leading experts in the fie ld from al l over the
world . He amassed a large l ibrary and careful ly abstractedon card fi les the entire world l iterature on tuberculosis ,mostof which at that time was inGerman. After his death ,
this invaluab le catalogue was purchased by the ArmyMedical L ibrary , thenAmerica
’
s largestmed ical reference
source .
Since his student days in Germany , VonRuck had beeninterested in research . Exciting andmomentous discoveries
emanating form the laboratories of Pasteur , Koch and
others in Europe gave promi se that infectious diseases
might be prevented and treated by injecting vaccines madefrom the newly discovered microbes found to be the causeof these diseases . In 1890 , on rece iving a cab legramannouncing the discovery of tubercul in, Von Ruck caught
the fi rstavailable steamer to Europe inorder to vis itKoch ’
s
F igure 3 . Winyah Sanitarium, I 896 . Artist'
s sketch of Von Ruck'
sfirst Ashevi llesanita rium.
VOL . 4 6 , No . 9
laboratory and to study his methods . Koch himself provided Von Ruck w ith a vial of tubercul in to bring back toAshevi l le and use in his own investigations . Von Ruck
real ized that if a potentvaccine could be perfected , tubercu
losis , the greatest scourge of the civil ized world , could be
prevented , possibly el iminated . Undeterred by Koch’
s ini
tial fai lure with tubercul in, Von Ruck devoted his entire
time and energy toward developing an effective anti
tuberculosis vaccine . In 1885 he formed the Von RuckResearch L aboratory and was joined by Dr . EdwinKlebs ,one of the world
’
s outstanding bacteriologists , who wasinvolved in a simi lar project. Klebs did come up with a
vaccine which he cal led antiphthis in, but he left Ashevil leafter two years to become the professor of pathology and
bacteri ology at Rush Medical Schoo l .Von Ruck worked on and succeeded in producing a
vaccine , a watery extract of tubercle bacil l i which hethought superi or to any of the previous preparations . He
and his son atonce set about to test its effectiveness both inpreventing tuberculosis in children and as an adjunct intreating adult tuberculosis . After more than ten years of
extensive but largely uncontrol led cl inical tri als , he pub
l ished his results in the Journa l of the AmericanMedica l
Assoc ia tionMay 8 , 19 1 1 , in a paper entitled“A Practical
Method of Prophylactic Immunization against Tuberculos is , claiming success not only in immuniz ing children
against tuberculos is but al so in using the vaccine to treat
those who had already conUacted the disease . He con
cluded his paper as fol lows:“These studies I am con
tinuing , and I hope that others w il l take themup also . Al l Ifeel justified in claiming at th is time is that I am the first tohave made a successful advent in this most important and
promising field ofprophylaxis in a disease that leads in themortal ity statistics of the human race .
In 19 14 he presented the results of his research to an
international conference in London and his ideas were
favorably received . Tragical ly , the outbreak ofWorldWar
I forced the cancel lation of cl inical tri al s of his vaccine inEngland and Europe , and in the turmoi l of a world at war
his work was shelved and forgotten.

Doggedl y he continued , and in 19 16 inconjunctionwithSilviopubl ished “
Studies on ImmunizationAgainstTuberculosis
”in which he described th e method of preparation
of the vacc ine and made further claims of benefit from themateri al . To his great disappointment and chagrin,
Von
Ruck’
s work fai led to find wide acceptance among his
col leagues . In fact, he was subjected to a great deal of
criticism and ridicule , difficult for a man of his nature to
tolerate .
In 19 18 SilvioVonRuck went toNew England to administer the vacc ine to chi ldren in a large orphanage as part ofthe ir study . He contracted influenza and d ied two days laterin New York City . Silvio
’
s daughter, Von Ruck’
s only
grandchil d , al so contracted the disease and died w ith inforty
-e ight hours on the train back to Ashevil le . Karl Von
Ruck never recovered fromth is blow , buthe l ived on in hisAshevil le mans ion another four years . H is w ife d ied in192 1 , and he d ied a year later of nephriti s at age seventythree . In 192 1 , one year before his death , two Frenchbacteriologists , Calmette and Guerin , using , as suggested
earlier by Klebs , an attenuated strainof the tubercle bacillus , produced BCG vaccine , the first real ly effective vac
c ine against tuberculos is and the one in widespread use
today . One cannot d iscount the value of VonRuck ’
s years
ofhardwork and hi s contri butionto the field of immunity totuberculosis . But forAshevil le , his great contributionwasthat he ushered in perhaps the greatest era in Ashevil le
med icine the eraof the great tuberculosis special is ts whocame to study under VonRuck , became master cl inicians ,and were the ones final ly respons ible forestabl ishing Ashevil le as the outstanding tuberculosis center in America .
Ashevi ll e ’s G reat Tuberculosis Special ists
The fruits of Battle’
s and VonRuck’
s laborwere not longin appeari ng . Several local physicians became students oftuberculosis , soon acquired a mass of experience , and
developed cons iderab le expertise in the fie ld . Notableamong these were Drs . J .M . Burroughs , L .B . McB rayer,
and John Hey Wi l l iams . Ashevil le’
s future , however, was
shaped primari ly by severa l young physicians who came to
study under Von Ruck atWinyah Sanitarium. These be
came the famous TB”special ists of Ashevi ll e .
The first was Dr . Chase P . Amb ler of Oh io. Amb lergraduated fromWestern Reserve Medical School in 1889 ,
and on the advice of his dean came to Ashevil le to work
with Von Ruck . Though trained in laryngology and
ophthalmology , Ambler was primari ly a special ist in pulmonary tuberculosis . Much later, in 1922 , he bui lt his ownfifty
-bed sanitari um cal led Amb ler_
He ights , which served
as amodel for similar institutions e lsewhere . Over the years
several phys icians were assoc iated in practice w ith him,
including his son, Arthur C . Amb ler , who joined him in
192 1 . He did not confine himse l f to his own sanitarium,
where be we lcomed the other‘
TB special ists asmembersof the staff, but also participated as a leading figure in theother Ashevi l le hospital s of his day . He reorganized the
Merriwether Hospital after its founder’
s death , serving as
Chief of Staff and dean of its nurses’
training school . He
was a consultant at St. Joseph’
s Sanitarium. In civic and
national affairs he achieved evengreater fame . Amblerwasa natural ist and an enthusiastic sport sman, enjoy ing hunt
SEPTEMBER 1985 , NCMJ
F igure 4 . Chase P . Ambler , M .D VonRuck'
sfirst res ident; oneof Ashevil le
’
s early TB specia l ists .
ing , fishing and al l aspects of outdoor l ife . He was a
founder ofAshevi l le ’
sAudubon Society and is givencreditfor initiating laws requiring hunting and fishing l icenses inNorth Carol ina and providing forwardens to enforce thoselaws . A National Park in western North Carol ina was
suggested by Amb ler as early as 1899 , and he thereafter
devoted a great deal of time and energy toward that end . He
pesonal ly organized the Appalachian National Park Associationwhich later became the Ameri canForestry Association. Mt. Amb ler, a foot peak in the Smokies alongthe Appalachian Trail near Newfound G ap is named forhim and a plaque in recognition of h is contri bution to theconservationmovement was appropriate ly placed in The
Crad le of Forestry”located in the love ly Pink Beds of hisbe loved Pisgah National Forest. H is outstanding contribu
tions in the National Park Movement an idea which he
proposed and pursued throughout his l ife , culminated in19 12 with the purchase by the Federal Government of
acres of the George Vanderb i lt estate to establ ishthe Pisgah National Forest. Dr . Ambler remained a leaderin professional and civic activities unti l the last year of his
l ife . He died of intestinal cancer at his home on H il ltopRoad , B i ltmore Forest, in June 1932 .
Von Ruck’
s second student, Dr . W il l iam L eroy Dunn
(figure was to achieve even greater th ings than hispredecessorAmbler. Dunn, also fromOhio , was a bri l l iantstudent. A near prod igy , he obtained a degree in phar
maceutical chemistry , then went on to receive an MD .
4 5 9

F igure 5 . W. L . Dunn, M .D ( left) and Charles L . Minor , M .D (right) . the two most outs tanding of Ashevi l le'
s many tuberculos is
specia l ists in the earlv 19005 .
degree atMichiganUniversity in 189 1 whenhe was only 20
years old . He was required towait a yearuntil he became 2 1to be l icensed to practice , so he spent that year and the next
as assistant to the Professor of Surgery at Michigan. In
1894 he came to Ashevi l le to work in VonRuck’
s laboratory bes ide the renowned Dr . Edwin K lebs for two years .
Upon Klebs ’
departure in 1897 , Dunn went to Europe to
study at the great univers ity centers of Leipz ig , Berl in,
V ienna , and Paris . 1900 found him back with VonRuck ashouse physician at W inyah , but shortly thereafter be en
tered practice for himse l f , estab l ishing the DunnCl inic . He
was soon recognized as an expert in tuberculosis and hisfame became widespread .
Dunnwas also a prominent figure inmedical circles and
he was associated with the leaders in his fie ld in national
and international organizations re lated to tuberculos is . He
was honored by e lection to the prestig ious Cl inical andCl imatolog ical Society and served as its pres ident. In 19 16
he was awarded an honorary degree by his alma mater.
During World War I , as a colone l in the Army MedicalCorps , he was sent on special assignment to Italy and wasdecorated by the Ital ianGovernment for his serv ices to thatcountry . After the war he was asked to serve on several
important commissions concerned w ith the rehab il itationof disab led veterans . He advised on the construction of
several veterans’
hospitals and it was due to his influenceand association with General H ines , chief of the Veteran’
s
VO L . 4 6 , No . 9
Administration, that apermanentcenter for the treatmentof
tuberculosis was located nearAshevil le atOteen. In 192 8 ,hospital ized with terminal cancer, Dr. Dunnwas unab le toattend the dedication of the permanent buildings at Oteenand d ied two week s later of lung cancer at the age of 5 7 .
Dr. Charles L aunce lotMinor ( figure a contemporaryand later an associate of Dr. Dunn, was a bri l l iant youngman who came to Ashevil le for health reasons and re
mained to become perhaps the most outstanding lung special ist of them al l . Dr . Minor
’
s credentials were impec
cable . Bom in New York , he was a descendent of an old
and il lustri ous Virginia fami ly . Educated atEpiscopal H igh
School and the University of V irg inia , he transferred from
academic studies to theMed ical School and graduated with
honors in 1888 . He served as house surgeon at St. Luke’
s
Hospital inNew York from 1888 to 1890: then, as was the
fashion in those days , he spent two years studying in the
hospita l s of V ienna , returning to beg in practice inWashington, D C . in 1892 . He contracted pulmonarytuberculosis , however, and came toAshevil le for treatmentin 1895 . After 18 months he was considered recovered , but
by this time , he had become interested in tuberculos is andspent the rest of his l ife in that fie ld . He was a remarkab lyable person, tal l , redheaded , impulsive , forceful , energetic
and impos ing with a bril l iantmind and studious hab its . He
rapidly achieved prominence as a tuberculos is special istand was a leader in the civic and social l ife ofAshevil le . He

F igure 6 . Paul H . Ringer , M .D . , an associa te of Drs . Dunn and
Minor and the last of the great specia l ists inAshevil le’
s tuberculo
s is era .
second generation tuberculosis experts . ANew Yorker.byb irth , his background was one of culture and learning . H is .
father was a professor of fore ign languages , his mother a .
distinguished musician. H e received his AB . and M .Df
degrees from Columb ia University and trained at the
Roosevelt Hospital . L ike so many of Ashevi l le’
s physi
eiaus of that day , he contracted tuberculosis and came to
Ashevil le for that reason. Witty ,charming ,
highly edu
cated , he was in the true traditionofDr. Minor,w ith whomhe became associated in 1906 . He enjoyed a long and
i l lustrious career spanning more than 40'
.years and was
accorded many honors . After serving'on the Board of
Medical Examiners , he was presidentof the North Carol ina
Med ical Society 193 5-3 6 and president of the Southern
Med ical Association 1940-4 1 . Among other honors , he
was , l ike Dr. Minor,’
amembcrof the Cl inical and Cl imatolog ical Association, Directoro f the North Carol ina Tuberculosis Association,
'
vice pre’
sident ofThe National Tuberculosis Association, and
'
regent of the American Association forThoracic Surgery . Hemarried anAshevil le girl , the
daughter of a prominent Ashevil le fami ly , and entered
actively into the civic and social l ife of the community . He
waS'
an Elder in the PresbyterianChurch , a member of theBoard
“
of the B iltmore Forest Country Club , a d irector ofVOL . 4 6 , No . 9
the and of the Good SamaritanMission, presi~
dentof the Community Chest, and the 193 7 -4 1 presidentofthe Ashevil le Music Association, now the Ashevi l le Sym
phony Society . In 1950 he retired for reasons ofpoor health
and is buried in Riverside Cemetery . At the time of his
retirement a resolution in praise of his achievements ,
passed by his fel low physicians in the Buncombe CountyMedical Society , characterized him most appropriately as“an ornament to our profession.
C . Hartwel l Cocke was the last of the second generation
phthisilog ists . H is story is remarkably simi lar in manyrespects toDr . CharlesMinor some fifteenyears earl ier. He
was born inMississ ippi , the son of the presidentof a smal lcol lege , and attended Episcopal H igh School where he was
the honor student for each ofh is three years . L ikeMinor, he
graduated from theUniversity of V irg inia , but thenwent to
Corne l l for his MD . degree . H e interned at the Presbyterian Hospital in New York City 1906 -07 , fol lowingwhich he studied in London, Pari s and Vienna . Just as had
Dr . Minor, Cocke trained initial ly _
in surgery and practicedbriefly in B irmingham, Alabama , but when he developed
tuberculosis he came to Ashevil le to be treated . Fol lowingrecovery , he decided to special ize in tuberculosis and inassociation with Dr. John W . Huston started the ZephyrH il l Sanitarium. Dr. Cocke fol lowed the footsteps of Dr .
Minor innational medical circles as we l l as in local affairs .
He became secretary of the section on tuberculosis in theA.M .A. and vice president of the American Col lege of
ChestPhys icians in 193 7 . He was a prominent figure in theAmerican Col lege of Physicians , serving as chairman of
the Board of Governors 1929-4 2 and Regent 193 6-4 2 . He
was a vestryman of Ashevil le’
s Trinity Episcopal Church
for 20 years and was one of the founders of B iltmore ForestCountry Club . He was a leading Ashevil le physician unti lhis death froma heart attack in 1944 . Dr. S . L . Crowe , who
came in 1926 as Dr . Cocke’
s associate , is stil l in active
practice in Ashevil le almost 60 years later.
Appropriate ly , it fel l to a nephew ofKarl VonRuck tobe
the last of the Ashevil le tuberculosis Special ists . Edward
W . Schoenheit, whose father, W . A. Schoenheit, was thebusiness manager at Winyah and whose mother , G raceMoore SchoenheitwasMr . VonRuck
’
s s ister , was born onthe sanitarium grounds atMt. Clare and Dortch Avenues .
He first went to the University of Tennessee to studyveterinary med icine but, chang ing careers , transferred to
the University ofMary land and was a pre-med ical student
when his cousin, Silvio Von Ruck , died . H e obtained hismedical degree from Jefferson, interned at the Pennsylva
nia Hospital , and returned to practice atWinyah in 192 1 ,just one year before Karl Von Ruck ’
s death . A principalheir of the Von Ruck estate , he inherited the sanitarium,
and after his marriage in 1924 , he and his wife , the formerEl izabeth Kimberl y , l ived in the Von Ruck mansion off
Charlotte Street unti l 193 7 when they built their presenthome in B iltmore Forest. About 1930, sens ing that thetuberculos i s era in Ashev i l l e was on the dec l ine ,
Schoenheit closed W inyah and spent a year in V iennastudying card iology . He returned to enjoy a long and successful career as an internist inAshevil le . H e was greatlyrespected by his col leagues , serving as president of the
North Carol ina Medical Society , and was the rec ipient of

theDistinguished Phys icianAward in 197 6 whenhe retired
after 5 3 years of practice . He d ied in 1980 and is buried inthe Von Ruck plot at Riverside Cemetery .
Ashevi l le ’s Sanitaria
In 1900 Ashevil le’
s only sanitarium, the Old Winyah ,
with a capacity of no more than 60 beds , had long since
become inadequate to accommodate the horde of tuberculosis patients who came to the now famous resort in ever
increasing numbers . Except for those inW inyah , patientswere housed in board ing houses , most ofwhich were Operated sole ly for the care of people with tuberculos is . In a
1901 brochure advertis ing Ashevil le , VonRuck mentionsthe numerous estab l ishments of th is nature available to
patients at a costof as l ittle as $4 perweek and ones with“better accommodations at rates of S IG A few
”
says Von Ruck ,
“refuse inval ids altogether, suggesting
thatmost of the boarding houses did accept “ tuberculars .
The number of “ boarding houses” rose from 5 5 in 1900 to13 7 in 19 10 and remained at that leve l for the next20years .
These were for the most part large houses converted intosmal l sanitaria providing room, board , and bedside nurs ingcare . The ever-presentopen air sleeping porch was a necessary feature common to al l . Usual ly the phys ic ians
arranged accommodations for their patients , which had theeffectof clustering patients inparticular locations , al l caredfor by one physician or his associates . Some phys iciansopened sanitari a of the ir own, some quite large and attractive two and three story buildingswi th the '
ub iquitous openair porches . In 1900 three nuns from B e lmontAbbey converted a former school house at 40North French Broad into“St. Joseph
’
s Retreat, which provided 18 beds for patients with tuberculos is . In 1905 it was moved to largerquarters on Stames Avenue and then in 19 16 to its presentlocation on B iltmore Avenue , where it became the St.
Joseph’
s Sanitarium with 95 beds , subsequently the St.
Joseph’
s Hospital of today .
The slopes of SunsetMountain quick ly became studdedwith sanitaria . By 1905 Dr . Dunn had added
“Sunnys ide”
operated by his parents on SunsetDrive . Miss AnnO’
con
nel , a retired Johns Hopk ins nurse , operated Edgewood
Cottage inDr . Porter’
s old summer home . The largest of
the group, Fairview , was run by a Mrs . Perk ins , whocared for as many as five hundred patients housed in smal l2 to 4 -bed shack s (a Trudeau Sanitarium term) : tinybuildings openon the sides above window level except forrol led down curtains . They were outfitted in Spartan
fashionwith only beds , a stove , and an enclosed bathroom.
Food was prepared in a large central bui lding and ‘ care was
provided by a staff of 50 or 60 nurses and attendants . Mrs .
Perkins was afforded great respect because she cared for
patients regardless of their financial status and admitted al lreferrals , many of whom were unable to pay . Other such
instal lations built in th is favorite area were Onteora Cot
SEr'rEMaER l 985 NCMJ
tage , SunsetHeights , and Roye Cottage , the latterofwh ich
was stil l in operation in the 19505 .
Because of the desire for open air (as we l l as the attitudeof the townspeople ) , the sanitaria were located at edges oftown, but as the city grew , many came to l ie w ithin thecorporate l imits ; for instance , the new W inyah on SpearsAvenue , the Wel l ington and the Elmhurst on EdgewoodRoad , and the Oak land on V ictoria Road al l original lylocated beyond the city l imits . With the advent of the
automobi le , additional facil ities were built further out,
such as Ambler Heights on the Swannanoa Road , H i l lcroft
and Abemathey Cottage south of B i ltmore V i l lage , VioletH i ll and Zephyr H il l inWest Ashevil le , and others as far
away as Fairview and B lack Mountain.
Ashevil le flourished in the good times of the 19205 , but
Dr. Schoenheit’
s estimate of the future of private sanitaria
proved to be accurate . In 1930 the business community ,
prompted by the economic reverses of the G reat Depres
sion, belatedly recognized the value of the tuberculosistrade . H ea lth and H appiness in the L and of the Sky , a
promotional magaz ine pub l ished in 1930 by the local
Chamber ofCommerce with the approval of the BuncombeCounty Medical Society , boasted twenty tuberculosis special ists and twenty
-five sanitari a providing 900 beds forpatients . The sanitarium rates in the depressed market ofthat day ranged from $ 15 to $3 5 a week while the moreluxurious Winyah and Ambler Heights commanded $50 aweek (phys ician’
s fees not included ) .
Times were chang ing rapidly , however. State sanitariamanned by ful ltime profess ional staffs had sprung upthroughout the nation, new and improved methods revolutionized the treatment of tuberculosis , and the days of theprivate sanitaria were over. In nearby Oteen, a thousand
bed modern sanitari um, the largest such faci l ity in the
nation, offered superior care at no cost forwar veterans . In
193 7 the state opened a branch of the North Carol ina
system in Swannanoa , later named the Western North
Carol ina Sanitarium, offering excel lent care at a rate of 50¢to per day including med ical fees .
One by one the Ashevi l le sanitaria closed . In 193 7 the
S isters of Mercy enclosed the sleeping porches at St.
Joseph’
s and converted it into a general hospital . A fewremaining cottage-s ized faci l ities remained as late as the
195 05 . Al l were gone by 1960 . By that time , with the
introductionof antib iotic therapy , sanitari umcarewas rare
ly needed . In 195 9 , with fewer than 60 patients with tuberculosis , Oteen itse lf was converted to a center for pulmonary and cardiac surgery , and by 197 9 the Western North
Carol ina Sanitarium, no longer needed for tuberculos is ,became a drug detox ification unit and a home for themental ly retarded . By the 19405 the only physicians spe
cial iz ing in tuberculosis were the ful l time staff of the
state- supported sanitarium. There were none inAshevil le .
The tuberculosis era had come to an end .

MANAGE YOUROFFICEMORE EFFECTIVELYWITHTH EMPM 1000 SYSTEMAVAILABLETHROUGH
SOUTHERNMEDICALASSOCIATIONSPHYSICIANS PURCHASING PROGRAM
Manage your Office moreeffect ively w ith the MPM1000 System ava i lablethrough the Phys ic ians ’Purchas ing Program.
Manag ing your officeshouldn
’
t be hard ;
however, w ith the currentinsurance requ irements and
MPM 1000 Simpl ifies Your Paperwork
You wil l be able to reduce the mountains of paper
work by using your MPM 1000 system to process al l
your insurance , complete your bill ing plus instan
taneously sort and file necessary information .
MPM 1000 SpeedsUp Your Cash F low
The MPM 1000 system w ill increase your daily bankdeposits by processing al l your insurance and pa
tients’
receivables quickly .
MPM 1000 Improves Your Pract ice Management
With the MPM 1000 system you can easily and intel
l igently manage your practice w ith computer gene
rated reports . Trends and problems are easily iden'
t ified so you can take corrective action before theybecome serious .
DYES ! I would l ike more information onMPM 1000
My interests are : D Immediate D Long term D Please contact me for a surveyI am a member ofSMAD
Name (Please Prim)
Address
Specia lty Office Phone
Mail to : CURTIS 1000 INFORMATION SYSTEMS2296 HendersonMi ll RoadSuite 402
Atlanta , G eorgia 3034 5
the impend ingMed icarechanges loom ing on thehor izon , it w il l get mord ifficult . You should cal l
Curt is 1000 Informat ionSystems or Southern
Medical Assoc iat ion to findout how theMPM 1000 can
he lpmake your pract icerun more effect ively .
ON IBMA/TMPM 1000 I sAOne Source So lution
The MPM 1000 is a one source solution . With yoursystem you receive all hardware (IBM or Texas In,
struments) , software , complete five day training pro
gram and responsive after sale support .
IBM PC /ATAt DiscountBest of al l , these systems are avai lable. through SMAServices , Inc . , Physicians
’
Purchasing Program with
substantial d iscounts on IBM and Texas Instrument
equipment .
FORMORE INFORMATION , please fill out the
coupon be low and mail it to Southern Med ical Asso
ciation , or for faster service call Southern Med ical at
(205 ) 945—1840 or Curtis 1000 Information Systems at800-241-4780.

PHARMACOTHERAPY
Serum Digoxin Leve ls and Renal Failure
Danie l L . Dolan, MD . and C . EdwinWebb , Pharm.D.
0 The authors measure and report serum d igoxin leve ls in pa tients with
rena l impa irment and compa re techiques for measuring digox in levels .
HE commonly employed methods for quantificationofserum digox in concentration include radioimmunoas
say , enzyme immunoassay and fluorescent polarizationimmunoassay . Measurement of the serum digoxin concentration is often he lpful in the management of certain pa
tients , is particularly important in young or e lderly patients
and in any patientwith significant renal impairment, since
these groups have been identified as be ing at ri sk fordigoxin toxicity .
"2
Recently , reports have appeared demonstrating e leva
tions of the serum digoxin concentration in patients withrenal impairment who were not rece iving digox in.
3 ‘ 5The
authors have suggested the possib il ity of a cross -reactivityof the assays w ith some unidentified digoxin- l ik e sub
stance , and have reported apparent varj ations inthi sEffect
from one assay method to another .
These reports prompted us to examine data onpatients in
our community having chronic renal failure who were not
taking digoxin. In add ition, since the twomajorhospitals inAshevil le employ d ifferent analytic techniques for digoxinmeasurement , we were able to study potential differences
in these two methods .
B lood was obtained from 26 patients in chronic renal
failure before and after routine outpatient hemodialysis .
S imultaneous serum creatinine determ inations were made
( tab le I ) . No serum creatinine value in any specimen fe l lbe low mg/dl . Each specimen was divided , then ana
lyzed by both the Fluorescence PolarizationTDX (Method
A) and the Gammacoat I 125 DigoxinRad ioimmunoassay(Method B ) . Patient 2 5 was tak ing digox in and served as acontrol . The remainder rece ived no d igox in, as determined
by analysis of chart records and medication history in
Under routine cl inical cond itions , the two hospital laboratories report quantitative values only when in excess of
ng/ml . Quantification below that leve l is poss ible w ithMethodAus ing simple dilution techniques , and values arereported here for interest. Values described as
“low in
Method A represent values S ng/ml . Method B em
ployed a ng/ml standard ; hence numerical values belowthat were reported as zero . Al l serum samples were im
med iately frozen upon col lection and al l analyses were
performed within 7 2 hours . No patients were receiving
From the Departments of Internal Medicine and Pharmacy , MountainAHEC , Ashevil le 28801 andThe Schools ofMedicine and Pharmacy , The
Univers ity of North Carol ina , Chape l H il l 2 7 5 14 .
SEPTEMBER 1985 , NCMJ
concurrent spironolactone , furosemide or steroid therapy at
the time of this study .
Results of the analysis are l isted in tab le 1 . Bothmethods
correctly identifi ed the patienton digoxin. W ith this exception, no value of any specimen exceeded a digox inconcentration of ng/ml .
G raves et al reported on serum digoxin concentrations inal iquots of sera from 5 4 patients w ith serum creatinine
values inexcess of 2 mg/dl and found considerable discrepancy among six radioimmunoassay methods .
4In this study
most values fel l below the usual cl inical ly report ab le leve lof ng/ml . However, the highest measured concentra
tion was ng/ml by radioimmunoassay and included

YOUCAN KEEP THEMmBALANCEvoun FAMILY LIFE AND YOURMEDICALPRACTICEWe
'
d like to he lpyouspendmore timewith yourfamilyyetrece ive profes s ional satisfactionfromyourmed icapractice . As a member of the Air Force hea lth careteam. you
’
ll be able to participate inourgrouppracticeconceptwh ichwill free youofmostofyouradministrative duties .
Air Force benefits are a lso very attractive . You andrfamilywill enjoy 3 0days ofvacationwith pay eachr, plus manymore Air Force advantages . Contact:
USAF Hea lth Profes s ions4 109 Wake Fores t Road , Suite 2 02Ra le igh , NC 2 7 609Ca l l col lect (91 9 ) 7 5 5 -4 1 30
Agreat’
way of lite.
values of and ng/ml in other sera by both this
method and EMIT-CAD, an enzyme immunoassay . One
level of ng/ml , along with a spread of levels between0and ng/ml was seenwith the G ammacoat assay . Use of
the RaimenDigoxin RIA K it resulted in levels between 0and ng/ml . The Digox inRadioimmunoassay Kit gave
leve ls be low ng/ml except forone value of ng/ml .
Leve ls measured by the Immunophase techniques also
clustered below ng/ml except for one value of
ng/ml .
Previous reports of spurious values have raised concerns
regard ing the interpretation of serum d igoxin concentra
tions inpatients with renal fai lure . Whi le the magnitude ofthese leve l s is frequently quite smal l and cl inical ly ins ignificant, the potential add ition of these values to true digoxin
content in a patient tak ing d igoxin could lead to amisinterpretation of the value with a correspond ing decision to
under-dose . The relatively few h igh spurious leve ls , when
present, could indeed lead to cl inical confus ion, and may
perhaps explain the rise in serum digoxin concentration
over an l l -day period reported by Gault et al fol lowing a
Acknowledgment
We wish to thank H . Denniston Crews , M.D Ashevil le KidneyCenter; John McCIeod , MD Memorial Miss ion Hospital ; and HenryGarfield , Ph .D. , St. Joseph
’
s Hospital for the ir technical assistance in this
study .
VOL . 4 6 , No . 9
total dose of 1 mg of d igoxin administered intravenouslyover 3 days in a patient with acute renal fai lure .
6S imilar
types of cross-reactivity have been reported in pregnant
patients ,7 '8
and neonates not tak ing digoxin. The d iffer
ences betweencommercial k its may be re lated to the specific antibody employed and its tendency toward cross
reactivity .
Our data in a series of 2 6 patients did not contain anyspurious serum digoxin concentrations above ng/mlby eithermethod , a value considerably below whatwouldbe routine ly reported . Yatschoff et al reported values by the
Abbott TDX and Kal lestad methods to be less than
ug/ml in 25 uremic patients , although a few false positiveswere seen in 30 neonates .
9Similar results inneonates have
been reported with the G ammacoat method .
10 We chose
not to include neonates in our evaluation.
We conclude that the ri sk of false pos itive serumd igoxin
levels by theAbbottTDX and Cl inical Assays Gammacoat
methods was acceptably smal l in our population with
chronic renal failure . While the possibi l ity exists that the
contribution of a spurious value may occasional ly lead to
pharrnacok ineticmisinterpretation and possib le inadequatedosing of d igox in in apatientwith renal fai lure , cl inical and
hemodynamic evaluation of the patient should provide the
additional data necessary to make appropriate therapeutic
decisions .
References
1 . SmithTW . Digital is toxicity : epidemiology and cl inical use of serumconcentr a
tion measurements . Am J Med l 97 5 ;5 8 :4 70-6 .
2 . Ke l ler F . Molzahn M. Ingerowsk i R. Digoxin dosage in renal insufficiency :
impractical ity ofbasing iton th e creatinine clearance . body weight. and volume
of d istribution. Eur J Clin Pharmacol -4 l .
3 . Craver IL . Valdes R. Anomalous serumd igoxinconcentrations inure mia. Ann
Intern Med l 983 ;98 :4 83 -4 .
4 . Graves SW , Brown 8 . Valdes R. An endogenous digoxin- li ke substance in
patients with renal impairment. Ann Intern Med l 983 ;99 :604 -8.
5 . Kl ingmul lerD. Weiler E. Dramer HH . Digoxin-li ke natri uretic activity in the
urine of sa lt- loaded healthy subjects . K linWochenschr l 982 z60; 1249—5 3 .6 . GaultM, Gal lway B , Fine A. Vasdev S . Ris ing serumdigoxinwith out furt her
dosage in acute renal fai lure . Nephron l 984 ;3 7 : l 90-4 .
7 . Drost RH , Plomp TA. Tennison AJ. Meas RA. A comparative study of the
homogeneous emzyme immunoassay (EMIT ) and two radioimmunoassays
(RIA) for d igoxin. C l in Chem Acta -67 .
8 . Bointk ABTJ , Kr0yswij k HH . Wil lebrauds AF , Maas AHJ . Some factors
affecting a commercial kit for radioimmunoassay of digoxin using tritiated
d igoxin. J Cl inChem 197 7 115 z26 1-6 .
9 . Yatscoff RW . Desj ardins PRE. Dalton JG . Digoxin- l ike immunoreactivity in
the serum of neonates and uremic patients as measured by the Abbott TDX
( letter) . C l in Chem l 984 :30 :5 88 .
lo. Valdes R, Graves SW. Brown B . LandtM. Endogenous substance in newborn
infants causing false positive digoxinmeasurements . J Peds l 983 : lO2 :94 7 -50.


Brief Summary of Presc rib ing Informat ionNORLESTRIN' (noreth ind rone acetate and ethinyl es tradiol tab lets.USP)See section under Spec ia l Notes onAdministration and HOW SUPPL IED.
Be fore prescribing please see lull prescrib ing information.ABriefSummary followsDESCRIPTIONNorles trin Products are prog estogen
-estrogencombinations .
INDICATIONS ANDUSAGENorlestrin Products are ind icated for the preventionofpregnancy inwomenwhoe lect touseora l contraceptives as amethod ofcontraception.
Inc linical tria ls with Norlestrin involving therapy cycles;there was a preg
nancy rate ol 0.05 per 100woman years : inclinical trials with Norles trin 2 . involving96.3 88 cyc les. there was a pregnancy rate of0 2 2 per ioowoman-years .
Dos e Reiated Ris k ofThromboembo l lsmfromOra l Contraceptives : Studies haveshowna posnive assoc iation between the dose ofes trogens inoral contraceptives and the
ris k of lh romboembolism. It'
is prudentand“
in keeping With good prinC iples o_f therapeutics tominimize exposwe to estrogen. The oral contraceptive prescribed forany g ivenpatient
should be thatproduc twh ich contains the leastamountofes trogen that is compatib le withanacceptab le pre nancy rate and patientacceptance .
CONTRAINDICA ONS1. Thrombophlebitis orthromboembolic disorders2 . Apasth istory ofdeep ve in thromboph leb itis or thromboembolic disorders3 . Cerebral vascularorcoronary artery d isease4 . Knownorsuspected carcin0ma of the breas t5 . KnownorS uspected estrogen dependentneoplas ia6 Und iagnosed abnormal genital b leed ing7. Knownor suspected pregnancy (SeeWARN ING No. 5 )8 Benignormal ignant liver tumorwhich deve loped during the use oforal contraceptivesorotheres trogen containing products .
1. Thromboembolic Disorders and OtherVascularProb lems . An increased risk ofthromboembolic and thrombotic d isease associated With the use oforal contraceptives is we llestab lished . Stud ies have demonstrated an increased ris k of fata l and nonfatal ven0usthromboembolismand stroke.both hemorrhagic and thrombotic .
Ce reb rovascularDis orders . Ina collaborative study'
inwomenwith and withoutpredisposing causes itwas es timated that the risk ofhemorrhag ic stroke was 2 .0 times greater inuse rs thannonusers . and the risk of thrombotic stroke was A.0 to times g reater.
ih child birth.with the
with ora l contraceptivesinfarction. is further
5 .or his tory ofpre
ec lamptic toxemia and especially by cigarette smoking .
The physician and the patient should be alert to the earliestmanifestations ol thromboem
bolic and th rombotic d isorde rs . Should any occurorbe suspected. the drug should be d is
continued immediate ly.Afourfold to
_
s ixfold increased ris k ofpos tsurgery thromboembolic complications hasbeen reported
'
inusers . If leaS ib le oral contraceptiy es should be discontinued at leas tfour
wee ks before Surg ery ofa type assoc iated with an increased risk of thromboembolismor
prolong ed immobilization.
2 . OcularLes ions . Neuro ocular les ions . such as optic neuritis orretinal thrombos is. havebeen
_
assouated with the use oforal contraceptives . Discontinue the oral contraceptive if
there is unexplained suddenorg radual partial.orcomplete loss ofvis ion; onsetofproptos is oi diplopia
‘
, papilledema: or retinal vascular leS ions .
3 . Carcrnoma . Long termcontinuous administrationof estrogen incertain animal specresincreases the freguency ofcarcinoma ofthe b i eas l. cerv ix. vag ina.and liver.
In humans. an increased ris k ofendometria l carc inoma as soc iated With the prolonged
_
use ofexog enous estrogen inpostmenopausalwomen has been reported However. there
is noevidence Sugg es ting increased ris k ofendometrial cancer inusers ofConventionalCombinationorprog estogen only ora l contraceptives .
Stud ies found no evidence of increase in breastcancer inwomentaking ora l contraceptives ; however an excess ris k
'
inusers with documented benign breas td isease wasreported .
There'
ts noconfirmed ewdence ofan increased ris k ofcancerassociated with oral contraceptives . Close clinical surv e illance ofusers is neverthe less. essential Incases oi und iagnosed persistentorrecmrentabnormal vagina l b leed ing . appropriale d iagnos tic measuresshould be taken to rule outmal ignancyWomenwrlh a s trong lamily h is tory of breastcancerorwho have b reastnodules fibrocystic d isease. orabnormalmammog rams should be
monitored with particularcare4 Hepatic Tumors . Benign hepatic adenomas have been lound to be associated with oral
gonlracepliv_
e .s Because hepatic ad enomas may ruplui e and may cause death throughintra abdominal hemorrhage they should be cons idered inwomenpresenting abdominal
pa in and tenderness . abdomina lmass .orshock .
A l_
ew cases ofhepatoce llularcarc inoma have been reported'
inwomen taking ora l contraceptives. The re lationsh ipof these d rugs to this type ofmalignancy is not known at th is time5 Use 9 inor Immed iatef Preced ing Pregnancy: Birth Defects
“
inOffspring and Malignancy in emale Offspring . uring early pregnancy. female sex hormones may serious lydamag e the offspring .
An increased ris k ofcongenita l anoma lies inc lud ing heartdefects and limb defects . has
been reqoned W ith the use oforal contraceptives inpregnancyThere
'
is some evidence that triploidy and poss ib le other types ofpolyploidy are increasedamong abortuses fromwomenwho become pregnant soonafterceas ing oralcontraceptives .
Pregnancy should be ruled outbefore continuing anoral contraceptive inany patientwho
has mis sed twoconsecutivemens trual periods . If the patienthas notadhered to the schad
ers receiving these d rugs .
PRECAUTIONS
0 1985 Wa rner-LambertCompany
ule. the possibility ofpregnancy should be conside red atthe time of the firs tmissed period.and ora l contraceptives should be W ithhe ld until pregnancy has been ruled OUI. Ifpregnancy is confirmed . the patientshould be apprised of the potential ris ks to the fetus and theadvisability ofc0ntinuati0nol the pregnancy sh0u|d be d iscus sed .
Womenwhod iscontinue oral contraceptives with the intentof becoming pregnant shoulduse ana lternate formofcontraceptiOn for a period oftime before attempting to conceive .
Administrationofproges togen-only orprog es togen-es trogencombinations to induce
withd rawal b leed ing should notbe used as a testofpregnancy.6 . Gallb ladderDisease. Stud ies reportan increased ris k ofsurg ically conl irmed gallb lad
der disease inusers oforal contraceptives .
7 Carbohydrate and Lipid Metabolic Effects . Because decreased g lucose tolerance hasbeenobserv ed ina s ignificantpercentage ofpatients . pred iabe l ic and d iabetic patients
should be carefully observed while receiving oral contraceptives .
An increase in trig lycerides and total phospholipids has beenobserved8 . Elevated Blood Pressure. An increase inb lood pressure has been reported in patients
receiving oral contraceptives The prevalence inusers increases with longerexposure .Ageis also strong ly corre lated with d eve lopmentofhypertens ion Womenwho previous ly havehad hypertens ionduring pregnancymay bemore like ly to deve lop e levationofb lood
presswe .
9. Headache. Onsetorexacerbationofmigraine ordeve lopmentof headache ofa new
patternwhich is recurrent. pers istent.orsevere. requires d iscontinuationoforalcontraceptives .
10. Bleed ing lrregularities . Breakthroug h b leed ing . spotting .and amenorrhea are frequent reasons forpatients d iscontinuing oral contraceptives . Inbreakthr0ugh b leed ing .nonfunctiona l causes should be borne inmind . Inundiagnosed abnorma l b leed ing from thevag ina . adequate d iagnosticmeasures are ind icated to rule 0ul pregnancy ormalignancy.WomenWith a pas l history ofoligomenorrhea orsecondary amenorrhea. ory0ung women
without regularcycles should be advised that theymay have a tendency to remainanovulatory or to become amenorrhe ic afterd iscontinuationofora l contraceptives .
i t. EctOpic Pregnancy. Ectopic as we ll as intrauterine pregnancymay eccm incontraceptive failures .
pone test.
Drug Interactions : Reduced efficacy and increased incidence of breakthroug h bleedinghave been assOC ialed with concomitantuse of rifampin.Asimilar association has
'
been sug
ges ted with barb iturates . phenylbutazone. phenytoin sodium. tetracycline. and ampici llin.ADVERSE REACTIONSAn increased ris k of the following serious adverse reactions has beenassociated with oral
comracepl ives : thromboph leb itis : pulmonary embolism: coronary thrombosis.cerebralthrombos is : cerebral hemorrhage: hypertension: gallb ladderd isease ; benign hepatomas :congenital anoma lies .
There is evidence ofanassociationbetween the following conditions and the use ofora l
contraceptives , although add itiona l confirmatory stud ies are needed .mesenleric thrombosis . neuro-Ocular lesions. 9 9 . retinal thrombos is and optic neuritis .
The lollowing adverse reactions have beenreported inpatients receiving oral contraceptives and are be lieved to be drug re lated : nausea and/ orvomiting . usual ly themostcommonadverse reactions.occur inapproximate ly 10% or le
'
ss of patients during the firs tcyc le.
Other reactions . as a general rule.are seenmuch less lrequeni ly oronly occas ionally:
gastrOinles l inal symptoms : breakthroug h b leeding : spotting , change inmenstrual flow:dysmenorrhea. amenorrhea during and altertreatment: temporary infertility a lter d isconlih uancoof treatment: edema; chloasma orme lasma: breas l changes: change inwe ig ht:change ince rvica l erosionand cervical secretion: possib le diminution in lactationwhen
g iven immed iate ly postpartum: choles tatic iaund ice;mig raine ; increase in s ize ofuterineleiomyomata: rash (allerg ic):mental depress ion: reduced tolerance tocarbohyd rates :vag inal cand id iasrs : change incorneal Curvature: intolerance to contact lenses .
The lollowmg adverse reactions have been reported and the associationhas been‘neither
confirmed nor refuted : premens truaklike synd rome: cataracts : changes in lib ido: chorea:changes inappetite: cystitis
-like syndrome: headache: nerv ousness : dizziness : hirsutism:loss of scalp hair: e rythemamultiforme : erythema nodosum: hemorrhagic eruption: vag initporphyria .
Special Notes onAdministrationMens truationusua lly beg ins twoor three days . butmay beginas late as the fourt h or lilthday.afterd iscontinuing med ication.
After severa lmonths on treatment. b leed ing may be reduced to a pointofvirtual absence;reduced l lowmay be a reSultofmedicationand not ind icative ofpregnancyHOWSUPPL IEDNorlestrin [E is availab le incompacts each containing 2 1 tab lets . Each tab letcontains1mg ofnore lh ind rone acetate and 5 0mcg ofethinyl estrad iol.Available inpackages of livecompacts and ackages of five refills
Norlestrin 2 is availab le incompacts each containing 2 1 tab lets . Each tablet
contains mg ofnore lh indrone acetate and 5 0mcg ofeth iny l estradiol Availab le inpac kages of five compacts and packages of live refil ls .
Norlestrin [B is avai lab le in compacts each containing 2 1 ye llow tab lets and 7brown tab lets . Each ye llow tab letcontains 1mg ofnorel hindrone acetate and 50mcg ol
eth inyl estrad iol. Each brown tab letcontains 7 5 mg of ferrous fumarate.USP.Ava ilab le in
packag es of live compacts and packages of five refillsNorlestrin is avai lab le incompacts each containing 2 1 pink tablets and 7
b rown tab lets . Each pink tab letcontains mg ofnore l hindrone acetate and 5 0mcg olethiny l estradiol. Each browntab letcontains 7 5 mg of ferrous fumarate .USP.Availab le in
packag es of live compacts and packages of five refills .
Norlestrin is availab le incompacts each containing 2 1 ye llow tablets and 7 whiteinerttab lets . Each ye llow tab letcontains 1mg ofnore lh indrone acetate and 5 0mcg 0 1ethiny l estrad iol Avai lab le in packages offive compacts and packages of live refills .
09016 11“PARKE-DAVIS
Divis ionofWarner-LambertCompanyMorris Plains .NewJersey 07 95 0
PD-2 1-JA-2 56 3 -P -84 )

ion gap 2 . Comple te b lood count a nd
urina lys is w e re unrema rka ble . Upon
a rriva l a t the eme rg e ncy room one
l ite r of la cta ted Ring e r'
s so lution w a s
infused ove r tw e nty minute s a nd IM
Compa z ine w a s g ive n to contro l
vomiting . Approx ima te ly one hour
a fte r a rriva l the pa tie nt'
s b lood pre s
sure became prompting a con
tinuous I.V. dopam ine infus ion a t 2
mg /kg /min w h ich quick ly ra ised the
b lood pre ssure to The pa tie nt‘
s
b lood pre ssure rema ined sta ble a fte r
the d iscontinua tion of dopamine . The
hea rt ra te , how eve r, d roppe d to 4 6
on seve ra l occa s ions . Atd ischa rg e the
pa tient'
s e lectrolyte s a nd a nion g a p
w e re norma l a nd the pea ked Twa ve s
ha d re so lved a nd w e re 5 mm in
he ig ht.
Discuss ion
Seve ra l of the p la nts in que stion
w e re re trie ve d in the eme rg e ncy
room . Althoug h w e w e re initia l ly un
a b le to ide ntify the p la nts w e we re
a b le to de te rmine tha t they we re not
ramps . The poss ib i l ity of d ig ita l is
tox icity from p la nt ing e stion wa s
strong ly cons ide red ; how e ve r, th is
wa s que stioned be ca use the deg ree
of hypote ns ion see n wou ld be uh
usua l ih d ig ita lis tox ic ity . We fe lt tha t
the deg ree of bra dyca rd ia could not
e xp la in the deg ree of hypo te ns ion .
Also , Foxg love a nd Li ly of the Va lley
VOL . 4 6 , No . 9
(know n d ig ita l is- conta ining pla nts)w e re e l im ina ted a s poss ib i l itie s be
ca use of morpho log ica l d iss imi la r
ities from the pla nts in que stion. It
w a sn'
t unti l seve ra l da ys la te r tha t
we we re a b le to correctly ide ntify the
pla nts a s Vera trum viride or more
commonly Fa lse He l le bore ) .
Vera trum viride is a pe re nnia l he rb
w h ich is w ide ly d istributed in we t or
sw a mpy g round th roug hout the
northe rn hemisphe re . The pha rma
colog y of Vera trum is complex a nd
conta ined w ith in the pla nt a re ma nytox ic a lka lo ids . G lycos id ic a nd e ste r
de riva tive s of a lkam ine a lka lo id s
ha ve be e n ide ntified ,the la tte r of
w h ich a re the principa l hypotens ive
a g ents .
1
Ve ra trum a l ka lo id s prod uce
hypote ns ion a nd a concom ita nt
bra dyca rd ia . Hypote ns ion is inde
pende nt of a cha nge in hea rt ra te .
Re f le x phe nome na w hose a ffe re nt
va ga l impulse s a re thoug ht to a rise in
the ca rotid s inuses , left ve ntricle a nd
lung s a re thoug ht to re su lt in
hypote ns ion seconda ry to va sod i la to
tion a nd bra dyca rd ia . Atropine w i l l
not comple te ly a bo l ish hypote ns ion,
but w i l l preve nt bra dyca rd ia , the re
fore , it a ppea rs tha t the va g i a re the
e ffe rent a rms of the reflex for the
hea rt, but the effe rentmecha nism for
hypote ns ion is more complex .
Veratrum a lka lo id s a lso produce a
d irect depre ssa nt e ffecton re spira tion
a nd a d irect bronchoconstrictor e ffect.
Vomiting is thoug ht to re sult from a
re fle x invo lving the nodose ga ng l ion .
Afte r ing e stion, Veratrum a lka lo id s
usua l ly a ct w ith in two hours a nd
e ffects ma y pe rs ist for four to s ix
hours . They a re deg ra ded in the l ive r
a nd e xcre ted in the fece s .
"2
Vera trum species have bee n used
for med icina l purpose s for hund reds
of yea rs . They w e re used in sorce ry
during the Midd le Ag e s a nd in fo lk
me d ic ine a s counte r i rrita nts in
neura lg ia , a s ca rd ia c tonics , a s eme t
ics a nd to trea t feve r.Veratrum viride
w a s a lso employed a s a n Ame rica n
Ind ia n potion to te st the stamina of
young Ind ia n bra ve s .
3"‘
In the ea rly - 19 5 05 Veratrum a lka
lo id s w e re among the f i rs t a nti
hy pe rte ns ive a g e nts used i h the
United Sta te s . The y have been used
in the trea tment of e sse ntia l , re na l ,
a nd ma l ig na nt hype rtens ion a s we l l
a s in preg na ncy- induce d hype rte n
s ion syndrome s . W ith new e r a nti
hype rte ns ive a g e nts the Vera trum
a lka loids fe l l into d isfa vor beca use of
the na rrow ra ng e betwee n the rape u
tic a nd tox ic dose s .
3
The ca se s pre se nte d ce rta in ly
typify the effe cts ofVeratrum a lka loid
poisoning . Of note , howeve r, a re the
pea ked T wave s of w h ich re
so lved a fte r a n incre a se in he a rt ra te
a nd blood pre ssure . Also of inte rest
a re the initia l decrea sed a nion g a ps

of a l l three pa tients . The rea son for
th is is unc le a r but ma y re pre se nt
la bora tory e rror.
Veratrum viride a nd Allium tricoc
cum (or ramps"
) a re both found in
southe rn Appa la ch ia a nd ha ve
a lmost ide ntica l d istribution pa tte rns ,
howeve r, the re should be l ittle d iffi
cu lty d iffe re ntia t ing be tw e en the
two . The most obv ious d iffe re nce is
the ve ry strong odor of le e ks w h ich“ramps posse ss , butw h ich Vera trum
viride la cks .
Morpho log ica l ly , the two p la nts
a re d iss imi la r whe n ma ture ; howev
e r, the re o re s imi la rities during ea rly
spring w he n ra mps"a re in sea son.
Vera trum viri'
de ha s de eply ve ined
lea ve s orig ina ting from a stem. The
ma ture pla nt is ve ry lea fy . The leng th
to w idth ra tio of le a ve s from a ma ture
pla nt is w h ich is le ss tha n the
le ng th to w id th ra tio of a young
p la nt. The bu lb of Vera trum viride is
s le nde r.
Al l ium tricoccum ha s on ly tw o
lea ve s , w h ich a re smooth . Leng th to
w idth ra tio of lea ve s is 4 The re is
no stem a nd the bu lb ha s a s l ig htlyfibrous coa t.
Remov ing a Tick
a nd eve n dea th . With ramps g o in
ing incre a s ing popu la rity , w e s te rn
North Ca ro l ina phy s icia ns shou ld be
susp ic ious of a cc ide nta l Ve ra trum
viride po isoning in pa tie nts a ppe a r
ing tox ic a fte r the ing e s t ion of"ramps .
"
We a re inde bted to Dr. Eva ns Whita ke r a ndDr. J . Lowe l l Orbison for the i r he lp in identifying Vera trum viri
’
de .
Da nie l L. Do la n, MD .
‘
a nd John J . McKinsey , M.D.
Ma ny me thod s of remov ing a n
embedded tick ha ve be e n dev ised .
Most ha ve proved fa l l ib le . Such pro
cedures a s burning the tick'
s poste rior
w ith a rece ntly lig hted ma tch he a d or
c ig a rette so tha t the tick would va lun
ta ri ly remove h imse lf, pa inting the
tick w ith nox ious a nd a ssumed pa in
ful ma te ria ls such a s na i l pol ish , e tc ,
ha ve met w ith only l imited succe ss .
Qui te ofte n once the se .approaches
fa i l , the tick is pu l le d off forcib ly ,
occa s iona l ly w ith d is lodg eme nt of
the he a d w h ich rema ins in the
wound , The fol low ing me thod ha s
be e n re l ia b le the ma iority of the
time
SEPTEMB ER 1985 , NCMJ
Refe rence
1 . O’
Too le K et a l . Removing cock roaches from the
a ud itory ca na l : contro l led tria l . N Eng l J Med
4 7 1
Conclus ion a nd Summa ry
As w ith a l l fora g ed foods , ramps
must be ca re fu l ly identified , prefe r
a b ly by a n e xpe rie nce d pe rson, prior
to ing e stion. Ide ntifica tion w i l l be
a ided by the strong odor of lee ks .
Mista ke n ing e stion of Veratrum viride
ca n ha ve se rious comp l ica tions ih
c lud ing f i rs t a nd se cond d e g re e
a triove ntricu la r b lock , s ig n if ica nt
hypote ns ion, re sp ira tory depre ss ion
1 . Sque e z e 2 °/o l idoca ine je l ly
(ava i la ble a t most d rug store s ; 5%
l idoca ine o intme nt is fa ste r, but re?
quires a. prescription) out of the tube
so a s to imme rse the embedded trick .
2 . Wa it approx ima te-Iy~ 10 m in.
ute s .
3 . Remove the tick w ith b lunt f'
or
ceps .
The me cha ni sm e mp loyed by“
the
tick to hold the hea d i ns ide the sk in
seems to become a ne sthe tized a nd
fla i l . At th is po int the tick w ith its
head may be ea s i ly removed .
In the Piedmontand w e ste rn se c
tions of .North Ca ro lina , the a ppea r
a nce of feve r or any fe bri le i l lne ss
Refe re nce s
1 . Ame rica n Hospi ta l Formu la ry Se rv ice , 19 8 3 .
Ame rica n Socie ty of Hospita l Pha rmacists , Hy
potens ive Age nts The Vera trumAlka lo id s .
2 . Goodma n LS, G i lman A. The pha rmaco log ica l
ba s is of therapeutics. New York : Ma cmi l la n Pub
l ish ing Compa ny , 19 7 5 .
3 . Kre ig MB. G reenmed icine . Chicago : Ra nd McNo l
ly a nd Compa ny , 196 4 .
4 . Pie rce RV. The people'
s common sense med ica l
a dv isor . Buffa lo : World'
s Di spensa ry PrintingOffice a nd Binde ry ,
18 8 2 .
5 . Re d ford AE, Ah les HE, Be l l RC. Ma nua l of the
va scula r flora of the Cora l ina s . Cha pe l H i l l : The
Unive rs ity of North Ca rol ina Pre ss , 19 6 8 .
3 - 12 da ys fo l low ing a tick b ite should
be promptly eva lua ted by a phys i
c ion. If no clea r- cut ca use is found ,
empiric te tra cycl ine the ra py shou ld
be strong ly cons ide re d s ince the
d ia g nostic ra sh of Rocky Mounta in
Spotted Feve r occa s iona l ly a ppe a rs
da ng e rous ly la te in its course .
Lidoca ine sprayed into the exte rna l
a ud itory ca na l“
ha s be e n faund to
ca use a“
cockroach to e'
x it ra pid ly . W i l l
wonde rs neve r ce a se !I


F igure 1 . CT scan of the head of our pa tient j ust before he started chemotherapy ( left) and after the fourth cycle ofchemotherapy ( right) . There was cons iderable regress ion of the tumor between the two scans .
for the fol lowing reasons : 1) sebaceous neoplasms can arisefrom sal ivary glands ; 2 ) adenoid cystic carcinoma some
times displays sebaceous differentiation; and 3 ) the naturalhistory of adenoid cystic carcinoma is similar in some
respects to that of8
Effective chemotherapy exists for patients with adenoid
cystic carcinoma . Johnson et al . reported two patients w ith
adenoid cystic carcinoma who responded to an intra
arteri al infusionof S-FU, one ofwhomultimately achieved
a complete response .
9 Doxorub ic inhas also shown activityin this Accordingly , we chose to treat our
patient w ith intravenous 5-FU and doxorub icin. Since 5
FU is more effective inpatients with head and neck cancerif administered as a continuous intravenous infus ion,
we
opted for this schedule .
12
When a head CT scan obtained after the fourth cycle ofS-FU and doxorub icin showed thatno further improvementhad occurred , we reasoned that a fifth cycle was unl ike ly tobe he lpful if cure had not already been achieved . This l ine
of thought stemmed from the col lective experience of a
numberof cl inical investigators who have util ized re latively brief durations of therapy to treatchemosensitive tumorsw ithout compromis ing cure rate s .
'3 ‘ ‘ 4 ' '5 ' 16Fur
thermore , our patient had already rece ived an add itional
course of chemotherapy after max imum tumor regression
had been documented on the head CT scan obtained between the third and fourth cycle of chemotherapy . F inal ly ,
we hoped to avoid the emergence of a doub ly resistant
tumor clone by using a second potential ly non- cross
resistant comb ination of drugs as soon as possible after
maximum tumor regression had been achieved with the
fi rst comb ination (Goldie -Coldman hypothesis )”
The use of cisplatin and vinb lastine (after doxorub icinand S-FU had failed to effect a complete remission) was
large ly empirical . The complete response observed w ith
Addendum
The patient recently experienced the onset of low backpain and lower extremity weakness . A mye logram shows
extradural'
compression of the spinal cord in the mid
thoracic spine . Cytologic examination of the spinal fluidshows mal ignant cel ls . Although re-b iopsy of the tempo
ral is muscle graft is unremarkab le , there is strong cl inical
suspicion of a local recurrence .
Acknowledgment
We are indebted toTheresaMil ler for secretarial assistance in the prepara
tion of the manuscript.
References
4 . RaoNA, H idayatAA.McLean lW ZimmermanLE. Sebaceous carcinomasof
the ocularadnexa: a clinicopathologrc study of 104 cases . with S-year fol low-up
data. Hum Pathol 1982 113 11 13 -22 .
I 7 . Caner SK . Some thoughts on res istance to cancer chemotherapy. CancerTre at
Rev 1984 ; I l (SuppI . A) :3 - 7 .
Complete reference l ist available from the NCMJ editorial office.
VOL . 46 , No . 9
cisplatin and vinb lastine , after a partial response was
obtained with doxorub icinand 5 -FU, impl ies that these two
comb inations are non-cross-res istant. Although it is im
possib le to discern which drug( s ) w ith in each combinationwas (were) respons ib le for our patient’ s response , it is
apparent that at leastone drug withineach comb inationwaseffective .
Th is case represents the first reported experience with
chemotherapy in the treatment of SGC . After two sequential courses of comb ination chemotherapy were adminis
tered , our patient not only responded to each combination,
but also achieved a complete response . We hope th is report
wi l l stimulate interest in further defining the role of chemotherapy in the treatment of th is d isease .

“hgmfmlk pnm
SCIENTIFICARTICLE
Cardiac Surgery in Asheville
Review of 3 2 6 Consecutive Cases During 198 3
KentW . Sal isbury , MD .
0 The results of this one-
year study comparefavorably with the CASS studyand the population is s icker , more symptoma tic and less stable .
THI S is a retrospective survey of the pre and post opera
tive status of 3 26 consecutive patients treated by Ashe
vil le Cardiology Assoc iates during 1983 .
Ashevi l le , North Carol ina is a city of approximate ly
people which serves as a referral center for cardiac
catheterization and card iac surgery for patients of western
North Carol ina . Geographical ly it is re lative ly remote .
Travel to the next closest catheterization and surgical
center in the state takes hours . The medical and referral
population of Ashevi l le is approximately ind i
viduals .
As a rural population the patient mix is predominantlyblue col lar with an enlarging percentage of refired citizensas the popularity of rural westernNorth Carol ina increases .
The e lderly Med icare population comprises approx imate ly35 of hospital izations atMemorial Miss ionHospital , oneof two general hospitals in Ashevi l le .
The card iology services program has steadily expandedover the past decade , and for several years has had enough
patients to meet the recommended national standards forcenters for catheterizationand cardiac surgery . Cardiologyservices are provided by the six board-certified cardiolo
g ists of Ashevi l le Cardiology Associates and surgical services by a s ingle cardiovascular surgery group of five
board -certified cardiac surgeons .
To avoid fragmentationof services and tomaintainquality and cost effectiveness , the medical staffs and admin
istrations of St. Joseph’
s and Memorial Mission HOSpitalshave agreed to perform al l invas ive card iology evaluationand cardiac surgery for the patients of both hospitals at
Memorial Miss ion H ospital . Both hospital s provide
noninvasive cardiology services .
For the purpose of this survey the fol lowing terms aredefined :1 . Elective Surgery : Surgery performed on elective ly
scheduled admission to hospital ( 14 5 patients2 . Urgent Surgery : Surgery performed during the same
hospital ization as catheterization general ly because of in
stabi l ity , the patient being cons idered in a high- risk subset(eg , signifi cant leftmain coronary stenosis) , or because ofrefractory symptoms or signs ( 164 patients3 . Emergency Surgery : Surgery performed on an
emergency basis within hours of consultation because of
From Ashevil le Cardiology Assoc iates , P.A. , I4 McDowe l l St Ashe
vil le
SEPTEMB ER 1985 NCMJ 4 7 5
acute and uncontrol lable decompensation ( 17 patients4 . Ventricular Dysfunction:
a . Normal : Ejection fraction (EF ) >5 0% and no
wal l -motion abnormal ities in RAO projection.
b . Mi ld : EF >5 0% with minor hypok inetic segments .
c . Moderate : EF >2 5 - 50% with significant wal lmotion abnormal ities .
d . Severe : EF <2 5% w ith marked wal l -motion
abnormal ities .
Valve SurgeryOf the 3 26 cardiac patients 30 required valve surgery
alone , 12 urgently . There were 14 mitral procedures (re
placements plus open valvulotomies ) , ten aortic valve re
placements and six combined mitral and aortic replace
ments . Fifteen add itional patients who had valve surgeryalso had coronary bypass grafts (ten were urgent or emergent) . Seven patients required one coronary ve in bypassgraft (CABG ) (five mitrals , one aortic and one aortic
mitral ) ; four required two grafts (two mitral s and two aor
tics) ; one required three grafts (mitral ) ; two required fourgrafts ( two mitrals) and one required five grafts (mitral ) .The patients who required three or more grafts had mitralvalve replacement because of mitral compl ications of
coronary disease .
Of these 4 5 patients undergoing valve surgery , four
required emergency surgery for acute hemodynamic compromise (one aortic and three mitral ) . Eighteen patients
required surgery urgently because of intractable Class IVsymptoms , refractory congestive heart failure or
_unre
solved seps is with endocarditis (ten mitrals , three aortics
and fivemitral aortic) . The remaining 2 3 patients underwent elective surgery ( 12 mitral , nine aortic and twomitral
aort ic) .There were no deaths in the elective surgery group.
There were four early deaths in the urgent group ( two
mitral and two aortic) . Three of these patients had signifi
cant left ventricular dysfunction and one had had recent
septic shock with hypotens ion and severe acute mitral insufficiency from papi l lary muscle infarction. Al l four of
these deaths had concomitant coronary bypass grafts .
There was no early mortal ity in the emergency surgical
group.

Overal l early mortal ity for valve surgery was thereforefour of 4 5 cases or mitrals , aortics al l
requiring CABG ) .
Nonva lve-Noncoronary Surgery
Seven patients underwent correction of atrial septal de
feets . One had l igationof a patent ductus arteriosus . There
was no mortal ity in this group. One patient died who
underwent attempted emergency pulmonary embolectomyfor refractory shock fol lowing saddle embol ization.
Coronary Bypass Surgery
Coronary artery bypass surgery was performed on 2 88patients . As mentioned above , 15 had concomitant valve
surgery leaving 27 3 with only CABG . Of the 2 88 patients
there were 64 women with an average age of
years . There were 2 24 men with an average age of
yaars .
In the CABG group there were 13 early deaths for an
operative mortal ity of However, if one excludes
valve replacement comb ined with CABG the mortal itydecreases to or l f emergency Operations are
excluded , the mortal ity is or Excluding urgent
Operations the mortal ity fal ls to or l . 7% .
As inmany publ ished studies the risks of cardiac surgeryin our center increase w ith the severity of coronary arterydisease , the severity Of leftventricular dysfunction, age and
sex of the patient and to a certain extent with non- specific
preoperative ri sk factors . The number of grafts placed inthis patientpopulation (mean defines this group as one
withmore severe atheroscleros is than inthe CASS randomized group (mean or in other publ ished studies .
Thirty~ three percent of our patients were hypertensive ,
4 5% were current or recent smokers and 10% were dia
betio. Of the 16 patients who had both diabetes and significant hypertension there were three deaths for amortal ity of
Patients with diabetes butnohypertens ionor smoking had nomortal ity . L ikew ise , there were no deaths in the
patients with diabetes who smoked but were not hypertens ive .
Seventeen percent (4 9 patients) had had acute myocar
dial infarctionwithin four weeks of surgery . There was no
morta l ity at surgery if there were no additional risk factors .
Old myocard ial infarctionwas present in 36% ( 104 patients) . Unstab le anginawas present in 3 8% ( 1 10 patients ) .
Eighteen percent of our patients ( 5 3 patients) had bothunstable angina and Old infarction. There were e ight earlydeaths in this group ( 15% mortal ity) .
Forty patients had congestive fai lure ; four
had early mortal ity .
Therefore in this series the hypertensive diabetic patientand the patient with unstab le angina superimposed upon
prior myocard ial infarctionr were at s ignificant risk . Con~
gestive heart failure also increased risk .
There were 2 3 men over age 7 0 , 40between 65 and 70 and 15 2 under 65 . Of 62
women, there were 12 over 70 , 14 be
tween 65 and 7 0, and 36 (5 8 . l%) under 65 .
When one looks at early mortal ity as a function of sex
and age , there were three deaths in the male group ( 1and six deaths in the female group There was one
VO L . 46 , No . 9
death in amanover 70 one death in the 65 - 7 0male
group and one death in the group under 65 ( lIn the female group there were two early deaths among the12 patients over 7 0 three in the 65 - 7 0 group
and one in the group younger than 65
In terms of left ventricular function the early deaths
occurred once among 80 normal ventricles four
times in 93 patients w ith mi ld LV dysfunction
twice in62 patients withmoderate dysfunction and
twice in 2 7 patients w ith severe dysfunction In 15
cases ventricular function was not l isted .
Attesting to the severity of il lness among the nine CABGpatients who had early death was an average graft numberof refractory and continuing unstable angina in al l ninepatients , pri or myocardial infarction in e ight and an average age Of 67 years .
Cons ideringmortal ity inrelationtourgency Of surgery inour entire series (val ves , CABG and comb ined) there were14 early deaths Of these , four occurred among 17emergency cases One was a pulmonary embolectomy , one doub le bypass w ith normal LV functionand two multiple CABG with severe LV dysfunction.
Of the 164 patients requiring urgent operation, there
were e ight early deaths In this group there were
twomitral valve replacements with CABG for severe mitralinsufficiency secondary to coronary disease , two aort ic
valve replacements and CABG for significant aortic insuffrciency and coronary disease and four patients with more
than three CABG , al l over age 60 (three women) .
Final ly , among the 14 5 patients undergoing elective
surgery there were two early deaths Both were
women (aged 69 and 7 1) and each had fi ve CABG .
Preoperative NYHA functional classification of our sur
g ical series identifies this group as a highly symptomatic
and incapacited population. With complete revascularization virtual ly al l our CABG patients returned toClass 1 . Of
the patients under age 65 , 15 4 were active ly employed , a
high rehab il itation rate . Patients who returned to work
tended to have had symptoms for a shorter period of time(days to months) than did those who did not (months to
years) .
Morb id ity of Card iac Surgery
Morbidity in card iac surgery is s ignifi cant even if a

The female patients inour series being comparable to otherpubl ished subsets , it seems l ikely that the high mort al ity inwomen inour smal l series is the resultof chance orof other
concurrent ri sk s such as age ,ventricular dysfunction, un
stable ang ina , etc .
Morb id ity and postoperative rehab il itation are also im
portant criteria for judg ing a program’
s qual ity . The recent
study by Kuan et al4summarized CABG morb idity in a
surgical series comparable in size to our own. The inc i
dence and type of major and minor compl ications in our
two series were s imi lar . Our patients required intra- aortic
bal loon pump insertion more frequently (nine cases com
pared with two cases) and additional compl ications of pan
creatitis (two cases) , brachial plexus injury (one case) ,
pleural empyema (one case) and non-A non-B hepatitis
( two cases) were noted . There seemed to be a higher inci
dence of respiratory d istress syndrome ( 13 cases or in
our series compared with none in the Kuan series and
in a Cleveland Cl inic Seri es .
5The incidence of
minor compl ications such as pericarditis , atrial fibri l lation,
cel lul itis and phrenic nerve pal sy were very s imilar in theKuan series and in ours The subsets of these
patients have already been discussed . In the ir series and
ours the major morb idities of renal failure , heart fai lure ,
shock and sepsis were prevalent among the patients who
died .
F inal ly , 82% ofourCABG patients under65 years of age
returned to work fol lowing their surgical convalescence .
Consideri ng that this group is we ighted toward a blue col lar
population this is a larger percentage than reported by some
studies , but similar to Others . The shorterdurationof symptoms ia the group that returned to work attests to the benefitof early CABG in the s ignificantly symptomatic patient in
achieving ful l rehab i l itation. Care in the patient'
s own
community or reg ion causes less social disruption and mayalso faci l itate rehab il itation.
Fo'
r samples tomakeCAMPBEM,u aom oares.
ION, NEW YORK, N.Y.
The Ed itor thought the author’
s summary was too longand repeated the substance of his artic le . The Ed itor
’
s
summary is :“If you l ive in western North Carol ina and
need card iac surgery , you are wel l off.
Acknowledgment
I wish to thankMr . Wil l iamLang . Phys ician'
s Ass istantforAshevi l le
CardiologyAssociates . P .A. a s we l l a sMs . AnnWelborn andMs . Denise
H ughes , R.N . for Drs . Kel ler . Mauney . Claxton. B i lbrey . Burton and
Associates , P .A. for their va luable ass istance in reviewing and abstract
ing records .
References
l . CASS Principal Investigators-
and Their Assoc iates : Coronary art ery surgery
study (CASS ) : A randomized trial of coronary anery bypass surgery . Survival
data . Circulation l 983 :68 :939 .
K ennedy JW , KaiserCC , Fisher LD, Maynard C . Fritz JK.MyersW.Mudd JG .
RyanTI . CogginJ. Multivariate discriminant anal ysis Of the cl inical and angio
graphic pred ictors ofoperative mortal ity from the col laborative study incoronaryartery surgery (CASS) . Thorac Cardiovasc SugSheldonWC . Loop FD. Coronary artery bypass surgery . The Cleve land Cl inic
experience , 1967 - 1982 . Postgrad MedKuan P, BemsieinSB . Ellestad MH . Coronary artery bypass surgery morbidity .
J Am Col l Card iol 1984 :3 : l 39 l .
Zapokanski A. Loop FD, Estafanous FG . She ltonWC . Myocardial revascular
ization at the Cleveland Cl inic Foundation 198 1 . Cleve Clin Q l 983 ;50:2 .

SCIENTIFICARTICLE
Cancer Immunology 15 a Rap id ly Deve lop ing Fie ld
Warren H . Cole , MD .
0 An overview of cancer immunology today .
E know many of the agents that can produce tumors
and are beg inning to understand how they alter cel lstomake them immortal . Tumor ce l ls carry surface markersnot present on normal ce l l s . These tumor markers act as
antigens and activate the immune system.
l Many tumorsmetastasize , and we are beg inning to understand how the
body mob i l izes its forces to resist metastasis . The role of
the immunolog ic system in resisting bacterial and viral
infections is we l l known to us .
2This paper summarizes the
evidence that this fami l iar immunological defense systemis used to destroy wandering cancer cel ls . A weakened
defense system, be it the result of hereditary defects , im
munosuppressive drugs , poor nutri tion, operative trauma ,
infections with virus or bacteri a or changes inmood , can
al ter the immune system and make metastasesmore l ikely .
I wi l l not describe the role of macrophages , the severaltypes of lymphocytes , the immunog lobul ins and Oth' er'
fea
tures of the immune system. This information is readilyavai lable in the recent l iterature .
”41 wil l stress that the
immune system is a dynamic and very changing system.
Tumors under favorab le conditions mob il ize the immunesystem for effective action.
1 Many environmental changesdepress the immune system and al ter the balance infavor Ofthe tumor .
5 ' 9
Each day the number of known tumor-specific antigensto which the body deve lops antibodies increases . The
tumor cel ls are not inert , and they may deve lop substancesthatmay result in non-specific suppressionof the patient’ simmune system. Surgery itse l f may set the stage for an
effective immune reaction.
’For example , when the tumor
is excised , the host’
s immune systemmay then be ab le todestroy a moderate number of tumor cel ls encountered inearly metastas is .
Unfortunately , the trauma of anesthes ia and surgery mayin itsel f cause immunosuppression.
” l lEvidence of sur
g ical immunosuppression was first described in 195 7 . In
this experiment 164 rats were divided into two groups . The
control group of 7 9 rats had inoculation of Walker
cel ls subcutaneously . The 85 rats in the other grouphad an
inoculation of Walker cel ls subcutaneously plus acel iotomy during which the intestines were stirred gently( s imulating a resection of a tumor) . The
“tak e
”in the
control group was compared with in the
experimental group.
‘ 2 We did not test human beings to seeif the immune resistancewas damaged by amajoroperationbecause at thatdate we had no lymphocyte count tests , etc .
avai lable to be used as a test for immune status .
A knowledge of the role of the immune system in deF rom 8 West Kens ington Road . Ashevi l le 28804 .
SEPTEMBER 1985 , NCMJ
Preface*
This is a time when advances in biochemistry and phys
iology permit us to cons ider , in experimenta l terms , the
role of the centra l nervous system (CNS) inmodulating thebehavior of the immune sys tem. The ex is tence of such
regula tion should not come as a surprise , g iven the genera l
role of the CNS in coord inating a l l sys tems of the organism.
H owever , the na ture , scope , and l imits of the regula tion
Reprinted with permission fromNeura l Modulation of Immunity , New
York , Raven Press , 1985 .
4 7 9
stroy ing tumor ce l ls has cleared up the mystery of why
radiation and chemotherapy cancure the orig inal cancerbut
induce the development of other cancers . The agents de
stroy ing the Cancer cel ls may alter other ce l ls in a way that
makes them cancerous and may have depressed the immune system to such a degree that the newly created cancer
cel ls are not destroyed .
The concept that clones ofmal ignant cel l s are constantlyari sing and that the body is constantly destroy ing them is animportant one . It al lows us to predict that whenever the
immune system is impaired by awide variety of causes , anincreased incidence of cancerwould be found . Al l series of
major organ transplants that require immunosuppressionhave shown an increased inc idence of a variety of
cancers .
”4 7 These include transplantation of k idneys ,hearts and bone marrow .
Each month more evidence is presented about the manyfactors that alter the immune system. In recent months ,evidence that the nervous system can alter the system hasbeen presented .
“2 1 We do not yet know the degree of
immunosuppress ionthatmay occur in each of our l ives as afunction of the way we l ive . The need for immune protec
tion against tumor cel ls must fluctuate . Many stimul i must
affect the way that tumor cel ls migrate . What is effectiveimmunity one day may be ineffective on another.
It is of interest that the genetic and acquired deficiencystates characteri zed by altered immunoglobul ins do not
lead to the same incidence of cancer as do immunodepres
sive drugs . These disturbances in immunog lobul ins do leadto severe and repeated infections . The physician caring for
such patients should careful ly examine changes in the hostthat permit bacteria ,
v iruses and protozoa to flourish .
Modulation of the immune system by the brain is a
rapid ly developing area of know ledge . We are reproducingthe preface of the book l isted as reference 2 1 to encourageyou to watch for developments in this area . RememberEugene Stead
’
s short summary of cl inical medicineNever underestimate the nervous sy
stem.
”

are far from be ing we l l und ers tood : What is known is thesubj ect of th is book .
Neural Modulation of Immunity is therefore addressedto those interested in the foundations of a ra tiona le for
psycholog ica l and pha rmacolog ica l attempts to modula teimmune respons iveness and , therefore , to a wide range ofbas ic and cl inica l investiga tors as wel l a s therapis ts and
phys icians who want an up- to-da te survey of the empirica l
a nd concep tua l s ta te of the burg eoning f ie l d ofpsychoneuroimmunology .
This is only the second book devoted entire ly to the new
fie ld (as ide from Mind and Immunity : Behavioral Immunology , the annota ted bibl iography ed ited by S . E .
Locke and M . H ornig-Rohan) . In the three years s ince the
publ ication of thefirst such book , Psychoneuroimmunolo
gy , ed ited by our contr ibutorDr . RobertAder , severa l new
aspects of neuroimmunomodula tion have been increas ingly s tud ied and are covered only in this book for example ,
the relationship of hemispheric latera l ity to immunity , and
the innerva tion of the thymus g land and other lymphoidtissues .
B efore commenting further on the contents of this book ,
we wish to distinguish its ma in subj ect from three other
important a spects of the rela tionships between the nervoussystem and the immune system .
F irst, this book is not about autoimmune d isease of thenervous system. Second , it is notabout the use of antibod iesto neurona l and g l ia l antigens in order to ana lyze the
ontogeny or circuitry of the nervous system. Third , it is not
about resemblances infunction or ana log ies between the
two systems , which are often described with s imilar terms ,
e .g . , memory , recognition, learning , redundancy , d ivers i
ty , etc .
This book is about the mechanism and role of regula torycommunication between the centra l nervous and immune
systems . The book opens with a tutoria l ana lys is of theessence of intrins ic immune regulation. Subsequent chapters work their wayfrompsycholog ica l through neuroanatomica l tomolecula r levels of ana lys is . Severa l conclud ingchapters dea l with conceptua l izing nervous - immune sys
tem relationships . Most of the chapters are reviewd byactive investiga tors in thefie ld of work in their laborato~
ries . The chapters are updated vers ions of presenta tionsmade a t a conference held in B russels in October , 1983 .
The princip les of these studies are stra ightforward : Welook for regulatory connections between the CNS and the
immune system tha t are coup led with relevant feedback
from connections between the immune and nervous sys
tems . F eedback is required because a regula tormustmonitor its own effect. The connectivity we seek must be bothCNS-regula ted and phys iolog ica l ly meaningful . I t can in~
va lve messenger molecules or direct innerva tion afi‘ecting
the ontogeny and respons iveness of the immune response .
The problem becomes ambiguous , but not less impor
tant, when we substitute“mind
”
for centra l nervous
system. The reason derives from the enormous d ifferences between our understanding of
“mind
"and the im
mune system. No one would measure the ve locity of an
a irplane by determining elapsed time with an atomic clockand traversed d is tance by dead reckoning . Yet we are
forced to do something l ike this when we study the re la
4 80
tionship between the immune system (dependent variable)and
“mind
”independent var iable The immune system is
understood in sufficient deta i l to measure the l imitingfactors in respons iveness with precis ion, while
“mind
"is a
col lectionof subj ective and obj ective events andprocesses :i .e . , emotions , stress , cognition (conscious and ancon
scious ) , cond itioning , vol ition. etc . This d isparity would be
sufficient reason to trea t the problem c ircumspectly werenot the effects of
‘
mind"on immune reactivity so dramatic
and paradoxica l that the urge to understand becomes irres istible . This , unfortunately , encourages the use of uneedata l and correlative da ta to support a conclus ion. Yet, quite
often, the mos tfundamenta l and genera l izable of conceptsin biology beg ins with such a tolera ted ambiguity which , in
time , becomes del inea ted with experimenta tion. In view ofthe med ica l and socia l importance of
“mind - rela ted
”
efi‘ects on immune respons iveness , as wel l as our scientifi c
curios ity concerning them, it is appropr iate tha t we should
undertake an ana lys is of the rela tionship by a ttempting toat leastde l ineate theproblem. This col lection of essays is amodes t s tep in tha t d irection.
BieberCP, Hunt SA. SchwinnDA. et al . Compl ications in long term survivors
of cardiac transplantation. Transplant Proc l 98 1: l 3 :207- l I .
Lanza RP. Cooper KC. Cassidy MJD, Barnard CN . Mal ignant neoplasms
occurring after cardiac transplanta tion. JAMA -83 .
Deeg IH , Sanders J , Martin P. FeferA. Ne imanP, Singer J, Sloth R. Thomas
ED. Secondary mal ignancies after marrow transplantation. Exp Hematol
1984 : -6 .
Blaloc k . I E. Smith EM. Acomplete regulatory loop betweenthe immune and
neuroendocri ne systems . Fed Proc - 1 1.
Wybran. J lntene gulations betweenthe immune systemand the central nervous
sy stem: phys iolog ica l and patholog ica l consequences . Acta Clin Be l
-5 .
Schle i fer SJ , Ke l ler SE. Camerino M, Thorton JC . Stein M. Suppre ssion of
lymphocyte stimulation fol lowing bereavement. JAMA l 983 :250:37 4-7 .
Gui l lemin R. CohnM. Melnechuk T (eds) . Neura l modulationof immunity .
New York: Raven Press. 1985 .
VOL . 46 , No . 9
References
l . MortonDL , Wel ls SA. Immunology of neoplastic disease . Davis-Christopher
Textbook of Surgery , ed ited by SabistonDC . Philadelphia, WB Saunders Co. ,
198 1 .
2 . G i l l i land BC . Introduction to cl inical immunology. Harrison'
s Pri nciples of
Internal Medicine l oth ed , ed ited by Petersdorf RG . Adams RJ et al . NY.
McGraw H ill , 1983 .
GuttmanRDet al . Cel lular immunology . K alamazoo.MI . UpjohnCo 198 1 .
Zwe iman B . Levinson Z. Cel l-med iated immunity . Allergy Principles and
Practice , edited by MeddletonE Jr. Reed CE , Ell is EF . St. Louis. CV MosbyCo. , 1983 .
5 . Purt iloDT, L inder I . Oncological consequences of impaired immune surveillance against ubiquitous viruses . J Cl in Irnmunol l 983 :3 : l 97 -206 .
6 . Sonnabend F .WitkinSS . Purt iloDT. Acquired immunodeficiency syndrome ,
opportunistic infections , and mal ignancies in male homosexuals . JAMA-4 .
7 . Gal lo RC , Sarin PS , Ge lmann EP, cl ai . Isolation of human T-c el l leukemia
virus in Acquired Immune De ficiency Syndrome ( AIDS ) . Sc ience
8 . Safai B .GroopmanJ.PopovicM .etal . Seroepidemiological studies ofhumanT
lymphotropic retrovirus type III in Acquired Immunodeficiency Syndrome .
Lance t l 984 zl 4 38-40.
9 . Anderson DW. Barre tt IT Ultrasound . a new immunosuppressant. Clin Im
munol Immunopath 197 9 : 14 : 18-29 .
10. Slade NS . S immons RL , Yunis E . et al . lmmunodepress ionaftermajor surgeryin normal patients . Surgery
- 37 2 .
l l . Lundy I Anesthesia and surgery ; a double-edged sword for the cancerpatient. J
Surg Oncol 1980:-5 .
12 . Buinauskas P. McDonald GO . Cole Wl-I . Role of Operative stress on the
resistance of the experimenta l animal to inoculated cancer cel ls . Ann Surgl 958 : 14 8 :64 2 .
13 . PennJ. Cancer in immunosuppressed patients . TransplantProc l 984 zl 6z492-4 .
14 . GuttmanRD, Jeakins I L . Associationof energy and the deve lopmentof cancer
in immunosuppressed renal al lograft recipients . Transplant Proc l 984 : l 6 :495
b
u


SCIENTIFIC ARTICLE
Fine -Need le Asp iration
AnAid to Breast Diagnos is
Peter A. Gentl ing , MD .
0 Results offine-needle aspira tion of breast lumps and masses .
HE breast is a particularly d ifficult organ to examine .
To have a secure d iagnostic understanding of benignversusmal ignant disease involves a comb inationof factors .
The only way to assure the patient that she has no cancer in
the breasts is to remove them and submit al l the tissue todetai led pathologic analysis . Needless to say , bi lateralprophylacticmastectomies are notpractical and are certainly not des irable . Therefore we must rely on al l diagnosic
modes to helpus detect the cancers thatare so very frequentin the breast. We must try to find themas early as poss iblewhile looking toward preserving non-mal ignant breast tissue and avoiding costly and multilating b iopsies whereposs ible .
The history and careful phys ical examinati on are stil l themost important features in breast d iagnosis . Various othermeans have been added to sharpend iagnostic acumen andto aid in earl ier d iagnosis . Mammography remains the
basic aid , but recently an older approach has been revived .
This involves cytologic evaluationof any area in the breastwhich feels pecul iar and wh ich the examiner is incl ined tocal l abnormal . F ine-needle aspiration for cytology has theadvantage of adding another diagnostic aid short of ex
cisional b iopsy . It has advantages in several ways . There
are al so some drawback s to its use .
The technique for fine-needle aspirationwas developedby Mart in and Ell is and presented in a paper pub l ished in
Soderstrom2 pointed out that the technique was notmeant to replace conventional b iopsy but to complement it.
Interest in the procedure waned but was revived by theScandinavians in the 19503 .
The advantages of fine-needle aspiration (PNA) include
its cheapness , its accuracy when positive , the add itionalinformation itprovides in lesions not suspicious enough forexcisional b iopsy and in les ions suspicious for cancer
where a pos itive diagnosis would aid in setting up stag ingtests and patient
-education discuss ions . Patients may al sobe reassured to know anegative cel l study has beendone . In
those having previous breast cancer the remaining breasttissue is always suspect for another cancer . Vague thickened areas may not require biopsy but bear observation.
Ce l l stud ies aid in these decis ions .
Disadvantages of FNA include mainly sampl ing error.
Fal se negative tests may be common. Pain, hematoma and
From Biltmore Surgical Associates , B iltmore Avenue .Ashevil le 28801.
SevrisMB ER i 985 , NCMJ
ecchymos is do occur but are minor. Cost of the procedure
varies from $50 to $ 100 .
The technique of PNA is eas ily Ieamed . Equipment forits use is readily avai lable and is inexpensive , but there is a
technique thatwi l l max imi ze cel l retri eval . If the procedureis poorly done , acel lular specimens wil l result, y ieldingunrel iable results . Some examiners use a special suction
‘
gun”
wh ich holds the syringe , butnormal ly-faci le peopledo not need this special apparatus . A 10 cc syri nge is used ,
attached to a #2 1 needle . No anesthes ia is injected . The
patient is supine w ith her armheld above her head to flattenthe breast. The tissue in question is firmly trapped against
“
the chest wal l by three fingers of the operator’
s non
dominant hand . Needle introduction fol lowing alcohol
swabb ing of sk in is accompanied by a warning that now
youwil l feel a smal l stick .
’
The needle is passed inand out
of the lesionwhile suction ismaintained onthe barrel of thesyringe . Once tissue-fluid is seen in the needle neck , an
adequate cel l specimen is present in the needle . The instru
ment is withdrawnwithout suction so that air is not suckedup, pul l ing the cel ls into the body of the syringe . Two g lass
microscope sl ides are prepared us ing a dropof albuminas aprotein fixative . The contents of the needle are squirtedforcibly into th is albumin. Occasional ly a core of tissue can
be removed in this way , but if l ittle material comes forth ,
the albumin drop can be aspirated into the needle bore andexpe l led onto the sl ide . The two sl ides are touched gentlytogether to spread the aspirate and placed directly in a
container of 95% ethanol . Processing by the pathologistcan fol low immediately .
Wemake a practice of us ing the same pathologist for al lour specimens s ince there is a knack of read ing these sl idesand consistency is important. Any agreed
-upon classifica
tion is acceptable . We have used a Class I through Class Vapproach . Class I and II smears are considered benign,
Class II I is suspicious , and Class IV and V are h ighlysuspicious and frankly mal ignant, respective ly .
Fal se negatives remain a problem. General ly cancers
w i l l shed cel l s read ily .When smeared , the sl ides are held to
l ight; the albumin wi l l be cloudy with cel lular material .However, operator error in aspirating the proper tissue orgetting considerable b lood or cystic fluid can dilute the
specimen and obscure mal ignant cel ls . Know ing whenthere is a good specimen is amatterof experience and is notdifficult to learn, but a negative result is not necessari ly aSign of benign disease . This must be constantly kept in

mind . On the other hand , a Class IV or V smear has never
been benign on subsequent b iopsy in our experience , and
under certain conditions , mastectomy has been performedwith no more evidence than a suspicious physicial examination, a condemning mammogram and aClass IV orVFNA.
The precise location of PNA is recorded on a patientbreast consultation sheet with a clear d iagram. Commentsare recorded about grittiness of tissue , cel lularity , associ
ated bleeding al l signs of presumptive mal ignancyand the presence of fluid with the disappearance of themasswith aspiration, re lative acel lularity , and softness of the
mass al l signs suggesting the les ion is benign.
In terms of time , much can be gained by the PNA. Atleast an hour and a hal f is required in our office to d iscusscancer of the breast, its treatment and implications . Muchof thismustbe done prior to any operative d iagnos is such asb iopsy . In a busy office practice such d iscuss ion periodswith the patient and her distraught relatives can needlesslyfrighten them while crippl ing an appointment schedule .
Therefore , while negative FNAs do not make a benigndiagnosis , they help, and pos itive FNAs al low for betterallotment of office time to instruct the patient and her
family . In add ition, a bone- scan , chest x-ray and SMA- 12
cost in excess of $200 and a half-day of the patient’ s time .
These can be more appropriately ordered us ing a positive
PNA and strong cl inical suspicion. Our pathologists can
give an answer to our FNA in two hours if takenearly in theday . The patient is anxious for th is news and grateful forany information.
During a three year period a total of 17 4 FNAs were
performed . Of these , 3 5 ( 20 . l%) were suspicious cl inical lyand 139 were benign cl inical ly . Tab le 1 shows theresults . Although al l lesions cl inical ly suspicious werebiops ied (as should be done) , those cons idered benigncl inical ly and b iops ied showed a surprise mal ignancy rateof and represented lesions thatmight not have beenb iopsied otherwise . The remaining 80 cases not b iopsiedwere fol lowed by returnoffice visits and/or repeatmammograms . The cost-benefitper unsuspected cancer showed an
expenditure of for those cancers that might nototherwise have beenb iopsied . We consider this costjustifiable . There were no compl ications in our PNA series , and
al l were easily tolerated by the patients without the use of
local anesthes ia .
We bel ieve fine needle aspiration to be a reasonab leadjunct to breast diagnos is which can be util ized by al l
cl inicians deal ing with breast disease . The technique is
VOL . 4 6 , No . 9
easily Ieamed , readily avai lable , and notvery expens ive . It
is safe and comfortable and adds anotherminimal ly invasive mode of d iagnos is . One must keep inmind the occasioual false-negatives (none in our series) so that an ex
cisional biopsy can be done if a question ar ises such as inany sol id dominant lump. Fal se ly pos itive findings are not aproblem.
The benefits of the test include reassurance for the pa
tient as wel l as the physician . They involve the more
appropriate use of time in counse l ing patients in a busyoffice practice setting as wel l as helping to minimize thed istress ing discussion of mal ignancy and its treatment
choices in those with benign disease . Occas ional ly PNAaids in finding mal ignancy early in the course of this
enigmatic process .
References
1. Martin ME, El l is E. B iopsy of needle puncture and aspiration. Ann Surgl 930;92 : 169-8 1 .
2 . Soderstrom N . Fine needle aspiration. New York , Grune Stratton, 1968 .
3 . K l in e TS et al . Fine need le aspirationof the breast: diagnosis and pitfal ls. Cancerl 979 ;44 : 14 5 8-64 .
4 . Bauermeister ES . Role and limitation of frozen section and needle aspiration
biopsy in breast cancer diagnosis . Cancer I980;4 6?94 7 -9.
5 Str awbridge HTG et al . Role of cytology inmanagementof lesions of the breast.
198 1: 15 2! I - 7 .
6 . Russ JE et al . Cytologic findings of aspiration of tumors of the breast.
197 8: l 46:4o7 - l l .


Whenhypertensioncontrol is complicated by the need fora beta-blocker plus a thiazide, CORZIDE® simplifies patientcompliancewith reliable once-a-day dosing ina s ingle tablet.
(nadolol-bendroflumethiazidetablets)

(nadolol -bendroflumethiazidetablets)
CORZ IDE° torsCORZ IDE"8015Nadolol -Bend rotlumeth laz lde Tab leta
DESCRIPTION: CORZ IDE (Nadolol-Bendroflumethiazide Tablets ) tor oral administrationcombines two antihypertens ive agents; CORGARD
°(nadolol) , a nonselective be tae drener
gic blocking agent. and NATURETIN0 (bend rotlume thiazide ) , a thiaz ide d iuretic -antihype r
tens ive . Formulations : 40mg and 80mg nadolol per tablet combined with 5 mg bendrol lumethiazide .
CONTRAINDICATIONS : Nadolol Bronchial asthma . sinus bradycard ia and greater thanfirstdegree conductionblock , card iogenic shock , and overtcard iac lailure (seeWARN INGS ).Bend rol lumeth laz lde Anurla , and in those with previous hypersensitivity to bendrol lumethiazlde orother sullonamlded erived drugs .
WARN INGS : Nadolol Card iac Failure Sympathetic stimulationmay be a vita l component supporting circulatory lunction inpatients with conges tive heart lailure . and its inh ibitionby betab lockademay precipitate more severe le itura .Although betab loc kers should beavoided in ove rt congestive heart iallure . it necessary , they can be used with caution In
patientswith a history ol la ilurewhoarewe ll compensated , usua llywith d igita lis and d iuretics .
Beta-adrenergic blocking agents do not abolish the Inotropic action 01 digita lis on heartmuscle . IN PATIENTS WITHOUTAH ISTORY OF HEART FAILURE. continued use oi be tab lockers can, insome cases , lead tocardiac lai lure . There lore .at the Iirs t signorsymptomatheart lailure . digital ize and /or g ive diuretics , and close ly observ e response , or d iscontinuenadolol (gradually. II poss ib le );
cemle Beta -ad renergic blockade may prevent the appearance ol premonitory signs andsymptoms tachycardia and b lood pressure changes ) oI acute hypog lycemia . This isespecial ly importantwith labi le diabetics . Beta-b lockade also reduces re lease of insulinIn re
nse to hype rg lycemia : there tore , itmay be necessary toad jus tdose oi antidiabe tic drugs .
oxlcoa le Be ta-adrenergic b loc kade may mas k certain clinica l signs tachycard ia ) ot hype rthyroid ism. To avoid abruptwithd rawal oi beta-adrenerg ic bloc kade whichmight precipitate a thyroid s torm, care lully manage patients suspected at developingthyrotoxicos is .
Bend rotlumethlaz lde Use with caution in severe renal d isease . In patients with renald isease , azotemiame be precipitated .With Impaired renal lunction.e l lects otthe drug maybe cumulative. Use w ih caution in impaired hepa tic lunction or prog ressive liver disease ,
s ince minora lterations ot tluld and electrolyte balancemay precipitate hepatic coma . Sens itivity reactions may occur inpatients with a his tory oi allergy orbronch ia l as thma . Poss ibilityoI exacerbationoractivationoi systemic lupus erythematosus has been reported .
PRECAUTIONS : General Nadolol Use with caution Inpa tients with impaired hepaticor renal lunction (see DOSAGEANDADMIN ISTRATION).Bend rotlumethlaz lde Atappropriate interva ls . ertormserume lectrolytes determinationto detectposs ible elec trolyte Imba lance warning 8 gns atwhich are dryness oi mouth , thirst.weakness , lethargy . drowsiness . restlessness . muscle pains or cramps . muscular tatigue ,
hypotens ion, oliguria . tachycardia . and G.I. d isturbances such as nausea and vomiting .
Observ e patients Ior clinical s igns oi l luid or e lectrolyte imba lance ; name ly , hyponatremia .
hypochloremic alkalos is .hypoka lemia . Serumand urine e lectrolyte determinations are particularly importantwhenthe patient is vomiting excess ive lyor receMng parentera l l luids . DrugsSuch as digitalismay inl luence serume lectrolytes . Hypokalemiamay develop, especiallywith
bris k d iures is . In presence ot severe cirrhos is . lnterterence with adequate ora l e lectrolyteIntake will also contribute to hypokalemia . Response oi the heart to toxic e l lects oi d igitalis
can be exaggerated with hypokalemia . Use potas siumsupplements such as high potass iumIood s toavoid or treathypokalemia.Any ch loride de l lcit is genera llymild and usua lly does notrequire specltic therapy except under extraordinary circumstances (as In liver or renaldisease ). Dilutional hyponatremia may occur in edematous patients in hotweather: approprlate therapy Is water restriction rather than salt adminis tration except In rare Ins tances
when the hyponatremia is Iile threatening . Inactua l saltdepletion.appropriate replacementisthe therapy oi choice .
Hype ruricemia may occur or trank goutmay be precipitated in certain thIaz Ide-treated
patients . Latent d iabetes me llitus may become manilest during th iaz ide therapy . Antihypertens ive e l lects ol bendrotlume th iazlde ma
ybe enhanced in the postsympathectomy patient.
Ca tetul reappraisa l oi therapy and cons deration g iven towithhold ing or stopping d iuretictherapy is necessary it rising nonproteinnitrogenorBUN ( Indica tive oi progressive renal Impairment) occurs . Thiazides maydecrease serumPBI leve ls without s lgns ot thyroid d isturbance . Th iaz ides decrease ca lc iumexcretion. Patholog ic changes Inparathyroid g land withhype rcaicemia and hypophosphatemia have been occas iona lly observ ed with prolongedtherapy . Commoncomplications oi hype rparathyroid ismhave not been seen.
© 1985 E. R. Squib b Sons . Inc Princeton. NJ 085 40
InformationforPatienta Warnpatients , especially thos ewith evidence oi coronary arteryinsul ticiency. against interruption or d iscontinuation ol nadolol without phys icran
'
s advice .
Although card iac lailure rarely occurs in prope rly se lected patients , advise patients be ingtreated with beta-ad renergic bloc king agents toconsultphysicianat the tirs ts i norsymptomcl impending la ilure.Advise patients oi proper course it dose inadvertently ms sed.
Laboratory Teete Regularlymonitor serumand urine electrolyte leve ls (see WARN INGS .
Bendroflumethrazr‘
de , and PRECAUTIONS , General , Bendrol lumethiaz ide) .Drug Interactions Nadolol When administered concurrently the lollowing drugs mayinteract with betaa d renerg ic b loc king agents : Anes thetica, general exaggeration oianes thetic-induced hypotens ion (see WARN INGS . Nadolot, Maior Surgery) . Antid labetlcd rug s (ora l agenta and Inaul ln) hypog lycemiaorhyperg lycemia : adlus tantidiabetlc d rugdosage accord ing ly (see WARN INGS . Nadolol, Diabetes and Hypog lycemia) . Ceamlned epletlng drug e reu rplne ) add itive all ect;monitor close ly tor evidence ofhypotens ionand /or excess ive bradycard ia .
Bend rol lurnethlazlde When administered concurrent! the tollowing drugs may Interactwrth thiaz ide diuretics : Alcohol , barb ituratee , or narcot may potentiate orthos tatichypotension. Ant ld labe tlc d rug e (ora l agenta and Insul in) thiaz ide-induced hype r lycemia may require ad jus tment oi antidiabetic drug dosage . Other antihypertenedmga add itive orpotentiated e l lect. Cod ieoeterolde.ACTH Intens itied elec trolyte de
pletion. particularly hypoka lemia . Ga Ilonlc or peripheral adre nerg ic blocking drugs
potentiated e l lect. Preaneathetlc a aneathettc agents e l lects may be potentia ted ;adius t dosage according ly . Preeeor aminee norepinephrine ) poss ible decreaseresponse butnot suItIc ient to preclude their use . Ske letal musc le relaxante.nondepolarlz lng tubocurarine ) poss ible Increased response .
Drug /Laboratory Tes t tnteractlona Discontinue thiazides betore tests tar parathyroidlunction (see PRECAUTIONS , General. Bend rol iume th iaz ide) .Carc inogeneela.Mutagenee le, Impairment ol Fertil ity Nadolol In t to 2 years oraltoxicolog ic stud ies inmice . rats , and dogs .nadolol did notproduce sig nii icant toxic ettects . In
2 y earora l carc inogenic stud ies inrats and mice .nadolol d id notproduce neoplastic.Dronao
plastic , or nonneoplas tic pa tholog ic les ions. Bendrol lumethiazl de Long‘ term s tud ies in
animals have not beenperlormed .
Pregnancy Teratogenlc El tecte Nadolol Category C. In animal reproductionstud ies with nadolol . evid ence oi embryo and Ietotoxlcity was lound inrabbits .butnot inrats
Or hams ters , at doses 5 to 10 times greater (onamg ik g bas is ) than the maximum ind icatedhumandose ;no teratogenic potentialwas seen inanyoi thes e species .There are nowe ll-c on
trolled stud ies Inpregnantwomen; there lore , use nadolol Inpregnantwomenonly itpotentialbene tlt Ius tiiies potential ris k to the Ietus . Bend rotlumethlad de Category 0 . Animalreproductionstudies have not beenconducted .This drug
‘
s effectonthe Ietus whenadministerad to a pregnantwomanor its effect on reproductive capacity is not known. Bendrotlumethiaz ide should be g iven to a pregnant woman only it clearly needed . NonteraEttecte S ince thiazides cross the placental barrierand appear incord blood ,we igh antici
pated benefit 0 1 the drug in preg nant women against poss ible hazards to the lotus : thesehaza rds include tota l orneonatal laundice . thrombocytopenia . and poss ib ly other reactionswh ich have occurred inadults .
Nurs ing Mothers Both nadolol and bendrol lumethiazide are excreted in human milk .
Because ol the potential tor serious adverse reactions in nursing intents either discontinuenursing or d iscontinue therapy . taking into account the importance oi CORZIDE (NadololBendrotlume lh laz ide Tablets ) to themother.Ped iatric Dee Sa lety and ettectiveness inchildren have not beenestab lished .
505 -502 Issued : March t985
oi 1000 pa tients : rash: pruritus ; headache : dry mouth , eyes .ors kin; impotence ordecreasedlibido; Iac ia l swelling :we ight ain: s lurred speech: coughrnasal stui l iness ; sweating : tinnitus ;blurred vis ion.Although re iatonship to drug usage is notc lear, s leepd is turbances have been
reported . The ocuiomucocutaneous syndrome associated with practolol has not been
reported with nadolol. The lollowing adverse reactions may also occur; Central Nervous
Sys tem reversb le mental depress ion prog ress ing to catatonia'visua l disturbances ;
halluc inations ; an acute revers ib le synd rome characterized by d isorientation lor time and
place . short-termmemory loss . emotiona l Iab ilitywith s ii htly clouded sensorium, decreased
Feriormance onneuropsychometrics. Gaelrolntes tina mesenleric arterial thrombos is:schemic colitis . Hematolog ic agranulocytos is : thrombocytopenic or nonthrombocytopanic purpura . Al lerg ic lever combined with aching and sore throat: lary ngospasm;respiratory d is tres s . Misce l laneous reve rs ib le a lopecia : Peyronie
'
s d isease:
erythematous rash ; arteria l inSui iiciency .
Bend rol lumethiazlde Gas trointes tina l Sys tem anorexia. as iric irritation. nausea .
vomiting . cramping , diarrhea , constipation, |aund ice ( intrahepatic c Iestatic iaundice ).pancreatitis . Central Nervous System d izz iness . vertigo , paresthes ia . headache . xanthops ia. Mama loi lo leukopenia , agranulocytos is . thrombocytopenia . aplastic anemia.
Dermatolog ic ypersens lt ivity purpura , photosensitivity . rash. urticaria. nec rotiz ingangiitis vasculitis . cutaneous vasculitis ). Card iovascular orthos tatic hypotensionmayoccur. r hyperg lycemia , g lycos uria . occas ional metabolic acidos is in d iabe tics .hype ruricemia . a llerg ic g iomerulonephritis .musc le spasm, wea kness , restlessness .Whenev
eradverse reactions aremoderate orseve re , thiaz ide dosage should be reduced ortherapy
wit drawn.
OVERDOSAGE: Nadololmay cause excess ive bradycardia , cardiac lailure , hypotension, or
bronchospasm ii ove rdosed . Overdosage oi thiaz ides may cause lethargy.wh ich may pro
gress to come with ina lew hours .with minima l depress ionoi respiration and ca rdiovas cularlunctionand withoutevidence oI serume lectrolyte changes ordehydration. Gas trorntes tinal
irritation and hypermotility may occur. Transitory increase In BUN and se rum e lec trolytechanges may occur, especially inpatients with rena l impairment.Treatment Nadolol canbe removed tromthe genera l circulationby hemod ialysis . Inde ter
mining dural ionoi corrective therapy . take note oI the long durationoi the e l lectoi nadolol . In
add ition to gas tric lavage employ the lollowing measures . as appropriate . Es cas
s ive Bradycard ia Administer atropine to mg ) . ii there is no response to vaga l
bloc kade . administer Isoproterenol cautious ly . Card iac Failure Adminis ter a d ig italis
g lycos ide and d iuretic. ithas beenreported thatg lucagonmay also be use lul inth is situa tion.
Hypotens ion Adminis ter vasopressors . e .g., epinephrine or levarterenol . (There is evidence that epinephrine may be the drug oi choice.) Bronchospaam Adminis ter a be ta,s timulating agentand /o ra theophylline de rivative. StupororComa Support ive therapy as
warranted . Gas trointes tina l El l ects Symptomatic treatment as needed . BUN andlor
SerumElectrolyte Abnorma l it ies Institute supportive measures as required toma inta inhydration. e lectrolyte ba lance , respiration. and ca rdiovascular and rena l lunction.
DOSAGE AND ADMINISTRATIO N: DOSAGE MUST BE INDIVIDUAL IZED. Patients with
renal lailure require adiustmeni in dosing interv al ; see package insert ior dosage in these
patients.
mult
lmckage Inse rt belore prescribing CORZIDE (Nadolol—Bendrol lumethlazlde
a ts
MowSUPPLIED: Availab le as scored tab le ts containing 40mg nadolol combinedwith 5 mg bendro l lumethiaz ide and 80 mg nadolol comb ined with 5 mg bendrol tumethiazide inbottles oi t00.

five days . From the day of admiss ion they are involved in a
support ive , but d irective , rehab i l itation process that ine ludes individual and group therapy , A.A. meetings , andarrangements for involvement of the patient and the patient
’
s family in aftercare . Patients are responsible forhousekeeping task s during the ir stay .
Those patients referred for medical evaluation are seen
by resident physicians from the MAHEC Family PracticeResidency Program in the emergency room at Memorial
Mission Hospital . Consultation is available from the resi
dent physicians 24 hours per day ; th is experience is anintegral part of the Residency Program
’
s curriculum in
addictions .
0 0
Pati ents requmng admi ssion to the hospital are placed on
the FamilyMed icine inservice and are superv ised by one offour rotating attend ing faculty . Al l patients admitted from
the social detox ificationcenter are placed onaprotocol thathas features that surprise many who were schooled in thetraditional medical detox ificationmodel . None of the patients receive intravenous med ications and none are givenbenzod iazepines .
The protocol is an adaptationof one util ized by Dr . John
Mooney at W il l ingway Hospital in Statesboro , GA ( see
Appendix A) . By avoiding intravenous treatment, costsand nursing time are reduced significantly . Although some
were cl inical ly volume depleted , al l our patients were ableto adequately rehydrate themselves oral ly . There is evi
dence to support the view that many cases of“DTs
”are
actual ly ianogenical ly- induced symptoms of cerebral ede
ma fromoverzealous intravenous hydration. Phenobarbitalhas multiple advantages over benzod iazepines8 includingantiseizure effects when administered oral ly .
The patients admitted to the hospital were begun on theprotocol and observed for progress ion or resolution of
symptoms . If symptoms of impending DTs quickly abated ,
the protocol was suspended , and fol lowing appropriate
observation the patient was returned to the social detox
ification unit on no mood- al tering drugs . If s igns andsymptoms ofDTs persisted orprogressed , the protocol was
continued . When the inpatient treatment forDTs was complete , the patient was referred to the soc ial detoxificationunit, without sedatives or other mood-altering drugsResults
BetweenSeptember 1984 and February 1985 there were400 admissions to the Dobb ins Center Residential SocialDetox ification Facil ity ( table 7 0% of the admissions
were“one- timers 30% of the admiss ions were “
rec idiVi sts .
The 400 admiss ions required 5 1 evaluations by a phys ician. Some of these involved s imple treatment of lacerations or refil l of prescription for chronic antihypertensivemedication. Twenty of thep atients evaluated were admit
ted for inpatient observation and treatment at MemorialMissionHospital . The average length of stay was l '/ z days ,for a comb ined total of 3 1 hospital days !None of the patients admitted to the hospital required
rehospital ization during the study period . There were no
deaths , no Intensive Care beds were util ized , and there
were no compl ications of therapy .
Of the 400 admissions to the Dobb ins Center, 3 20 indi
4 88
vidual s were involved in the study population; 127
of these were entered in alcohol ic rehabi l itation programsin add ition to Alcohol ics Anonymous .
Discussion
VOL . 46 , No . 9
Treatment of the alcohol w ithdrawal syndrome util iz ingthe trad itional med ical model is expensive , frustrating , and
fraught with complications of therapy and a h igh rate of
recidivism. Social setting detoxification has proven itselfeffective and cost efficient, but must have dependablemedical backup. Inour series 13% of the admiss ions to thesocial -setting detox ificationcenter required physician evaluation and 5% required hospital ization. These data are
consistent with the experience in Toronto as described inthe introduction.
1
The remarkably brief average length of hospital ization inth is study deserves further discussion. The populationadmitted to the hospital represented the 5% at h ighest risk ;among this group were patients w ith seizure disorders ,
marked coronary artery disease , prior documented historyofDTs , psychiatric disorders , intercurrent pye lonephritis ,and severe hypertens ion. H istori es were not always rel iable , and noncompl iance with prior med ical advice and
therapy was the norm.
The protocol as described in Appendix A minimizediatrogenic compl ications and effectively managed symptoms . No seizures occurred w ith th is protocol and al l patients were ambulatory within 18 hours of admiss ion.
The success of early transfer to the social-setting detox
ification center was made possible by the shared phi losophy tominimize drug administrationduring the withdrawal
phase . Hospital ized patients who would not have beenready ford ischarge home could be transferred to the socialsetting unit where sk il led observation and enforced abstincnoc occurred .
The medical aspects of alcohol withdrawal are only a
smal l part (albe it traditional ly expensive ) of the rehab il itationof the alcohol ic . Long
-term success is dependent upon
coordination of al l aspects of the rehab il itation process .
Drugs that inhib it or delay sobriety must be l imited to

treatment of l ife - threatening symptoms . Drugs used in
treating the withdrawal syndrome are dul l ing and have a
negative effect on sel fcare and sociab il ity of the alcohol icand may inhib it a clearheaded se lf-appraisal and accept
ance of rehab il itation. Drugs may become associated w iththe rel ief of painful symptoms in the alcohol ic ; this mayreinforce dependency ondrug s and especial ly on the use of
alcohol to cope with stressful situations .
9
The social setting detox ification program uti l izes the
d iscomfort associated w ith withdrawal in a pos itive fashionto re inforce the d isease conceptof alcohol ismand to under
score the alcohol ic’
s respons ib il ity for the consequences ofhis/her actions . This attitude that the alcohol ic is responsi
ble for his/her recovery mustpervade both the social settingand the medical setting . The patient should part icipate in
his/her recovery throughout the process , and should not be
excused to passively rece ive treatment in the hospital .
The fact that no patients required rehospital ization during the study period refiects admirab ly on the Dobb insCenter intervention. A high percentage of patients
were enrol led in specific aftercare programs to supplementinvolvement inA.A. ; 2 89 persons d id not require readmission to the Dobb ins Center . Early readmiss ion to the socialsetting unit cannot be construed as a failure if it obviateshospital ization.
The cooperation between the B lue Ridge Mental Health
social - setting detoxification unit and the MAHEC FamilyPractice Residency Program inpatient service has resulted;
in aneffective , cost-efficient alternative to treat
‘
t—he alcohol
withdrawal syndrome .
References
1 . V ictor M. Adams RD. Alcohol . In Ham'
son'
s Principles of internal medicine .
loth ed , Petersdorf ci al (eds) . NY?McGraw-Hi l l . 1983 .
2 . SchraederPL . Central nervous system intoxications. InFundamentals of internalmedicine . K aye D. Rose LF (eds ) . St. Louis: Mosby 1983 .
3 . Anderson RC . Alcohol ism. In Rake] R. Textboo k of family practice . 3rd ed .
Philadelphia , Saunders . 1984 .
4 . Sparedo FR, Zwic k WR, Rugg iero SD, Mee k DA. Carloni FA. S imone SS .
Evaluationof a social - setting detoxificationprogram. Studies Alcohol 1982 14 8.
5 . O'
Briant R. How safe is soc ial-setting detoxification? Alcohol Health and Re
SEPTEMB ER 1985 NCMJ
search World. Roc kvil le . Mary land?Winter Dept. of HEW .
6 . O'
BriantG . Social- setting detoxification. Alcohol Health and ReasearchWorld.
Roc kvil le . Mary land : Winter Dept. of HEW .
7 . Whitfield CL . Detoxification without dmgs . InWhitfie ld CL . The patient with
alcohol ism and other drug problems .
8 . Smith DE. Benzodiazepine dependence potential : current studies and trends .
Subst Abuse Treat I984 : I t l 63 - 7 .
9 . McGovernM. Comparative evaluationofmedical vs soc ial treatment of alcohol
withdrawal syndrome . J C l in Psych l 983z39179 l-803 .
Alcohol ism, alcohol w ithdrawal
orientation, pulse . respiration, temp. . BP, q_ J-I
*Adapted fromW il l ingway Hospital , Statesboro , GA
4 89
Append ix A
Routine Med ica l Detoxification Protocol"
!
a
l l .
12 .
13 .
I 4 .
15 .
I 6 .
17 .
Admit to medical floor. Dx .
syndrome . depress ion.
2 . Condition guarded .
3 .
4 . Darken room, night l ighton, bedrails up. urinal atbeds ide , ERPwith
Constant observation by attendant for hours .
assistance only
V ital signsH rs .
Diet as tolerated . F luids and snacks at bedside .
Admission L ab CBC with platelet count, e lectrolytes , glucose ,
UA STAT
CES-22 ; CXR and EKG when stable .
B lood alcohol leve l . Urine drug screen.
Phenergan 50mg [M on admission. Thiamine IOOmg IM on admis
sion.
MgSO4 1 g IM q 8 h 6 doses .
Phenobarbital 60 mg TID x 2 days . then
30 mg TID x 2 days . then
15 mg B ID x I day
Sodium Luminal Gr. II to IV IM PRN ag itation X 1 .
V istari l 50- 100 mg IM PRN anx iety x I .
Tylenol Gr x q 4 h PRN headacheRobaxin 7 50 mg qid PRN muscle cramps . P.O .
Nembutal 5 0mg P0 . or IMqHS PRN sleep. May repeat x 1 after 30
mm.
Cal l phys ician for:
( I ) marked agitation/change in mental status;
( 2 ) temp. greater than
(3 ) pulse greater than 100 on two occasions or for upward trend in
pulse or BP;
(4 ) BP gre ater than
No visitors


Because you want
to entrust your patients tothe best profess ional care .
Sa intAlbans is a log ica lcho ice foryourpsychiatricreferrals .
Since 1916 , Sa intAlbans Psychiatri c Hospitalhas provided a spectrumof care for emotiona ld isorders .
Today, we alsooffer
spec ial ized , ful ly accred itedprograms foradolescents ,a lcohol ics , and substanceabusers .We have spec ialprograms for senior adultsand treatment of eatingd isorders .And we offerdaytreatment as analternativeto hospital ization.
Care is provided by ourmedical and profess ional staffs in a beautimodernhospital secluded a long the NewRiver.Admiss ion can be arranged24 hours a day.And a ll programs and services are approved forBlue Cross ,Med icare , Champus , and most commerc ial insurance carriers .
At SaintAlbans , we ‘
ve bui lt our reputation on the trust of referringphysic ians who want the best for t
patients . That
’
s why you can refer
a intAlbans w ith confidence .
VOL . 46 . No . 9
Private, Not For ProfitPsychiatric CarePO . Box 3608 Radford .Virg inia 24 1431 -3468
Active Medica l Staff
Rol fe B . F inn.MD . Bas il E. Roebuck .MD .
Med ical Director 0 , LeRoyce Royal .M.D.
Davis 0 . Garrett.M.D. Morgan 5 , Scott.M,D.
Hal G . G il lespie.M.D. Don L .Weston.MD ,
0 . Paul H IUSkO M-D~ Ps ychiatric Consultant
Ronald L . Myers .M.D~ D.Wilfred Abse.M.D.

Letters to the Editor
To the Readersh ip from the Managing Ed itor
Youmay have noticed that the July NCMJ reached your
eager clutches just barely under the w ire July 30 if you
were lucky , July 3 1 otherwise . We do apolog ize . The July
issue was designed to include a 24 page central article ,
removable via a process that involves triple stapling w ith
three separate journeys through the b indery . Because of a
very great number of changes needed in that article at thevery lastminute , we had to pul l it from the July issue and
wi l l publ ish it inOctober. To accommodate the loss of 24
pages , our val iant printers had to repaste the entire issue ,
moving inserted ads to balance front and back , and , in
particular , moving the internal color to appear in the same
16 -
page signature to save money . The issue , printed and
bound , left our printer in Fulton, MO , on the afternoon of
July 22 . Where it spent the next seven or e ight days is a
mystery even the Postal Service cannot solve . We apolo
g ize for our part in the de lay . The Postal Service has no
comment.
An Open L etter to the Pres ident of R. J . Reynolds
Tobacco CompanyAs a retired physician who practiced for many years in
North Carol ina 1 am deeply committed , as I am sure you
are , to promoting the health of the people of our State . The
notable contri butions of the Duke Foundation to that endhave beena credit to your industry . However , a recent issue
of the Journa l of the American Medica l Associa tion con
tains a number of papers which refl ect the studied opinionofmy profess ionon the role of tobacco in serious diseases ,anopinionbased on th irty-five years of careful observationand research .
The grow ing , processing and sale of tobacco and its
products plays such an importantpart inthe economy of our
State that no one should damn it w ithout offering reasonable alternatives . As a starter, may I offer the fol low ingsuggestions
?
1 . That the R. J . Reynolds Tobacco Company take the
lead and establ ish a foundation to discover and deve lopan alternative crop to tobacco which our farmers couldprofitab ly grow;
2 . That your Company search out and deve lop an altemative industry , util iz ing the talents of yourmanagement
personnel and the energy of your workers with longterrn benefits to al l concerned ;
3 . That a time schedule be set up during which a gradualconversion could be completed , one that could be longenough to cover the l ife spanof persons already depen
dent on tobacco with immediate cessation of effort s toencourage use by the young ;
4 . And that this or a similarprogrambe active ly publ icizedSEPTEMB ER 1985 , NCMJ
in order to rece ive the we l l deserved good wil l and
support of the publ ic .
Please favor me with your reaction . I am taking the
l iberty of send ing you a copy of the recent Journa l of theAmericanMed ica l Associa tion.
Alex S . Moffett , MD .
7 0 West Luceme Circle
Orlando, FL 3 2 801
Editor ’s Comment
WW I I Duke: COs , Pows , V-12 , ASTP et al
The art icle about the conscientious objectors (NCMJ1985 ;4 6 :4 l 9-2 3 ) at Duke by Louis Swanson and James
G ifford brings back memories . We had an unusual con
g lomeration atDuke during that time . As noted , there were
the conscientious objectors . Most of the medical studentswere e ither in the V- l 2 Navy program or the ASTPArmy
program and were in respective mi l itary uniform s . Dr .
Robert (Daddy ) Ross continued hisOB practice , along w ith
commanding the Navy unit at Duke .
Another interesting groupwere the German soldiers who
worked at Duke Hospital during the last part of the war .
These prisoners of war were transported back and forth
from Camp Butner . Although I don’
t remember the exactwords , I do remember interesting conversations w ith theGermanPOWs whocould speak Engl ish , the conscientious
objectors , and we medical students who were in the Navyand the Army . The thing I remember,most is the inquisitiveness that each had about the other . A more exact,
detai led documentation of those encounters would be quiteinteresting .
Thomas B . Dameron, Jr . , MD .
Box 10707
Raleigh 2 7 605
Fami ly Medicine at Duke: Another V iewAs a Family Phys ician, I have read with great interest the
special art icle regarding Family Medicine written by Dr.
Robert Sul l ivan in the June 1985 issue of the North Carol i493
The insistence of the leaders in the tobacco companies
that there is no l ink between cigarette smok ing and cancerand emphysema does a great disservice to the image of
American industrial ists . They show us every day the force
of se lf- interest and mak e us distrust al l statements made byindustrial ists about safe work ing conditions and the safetyof their products .
Eisenhower’
s statement that we were not spy ing on the
Russians with our U2 airplane destroyed some of our sim
ple faith in statements by our government. The tobaccocompanies
’
refusal to face honestly the l inks between diseases and cigarette smok ing destroys our faith in industrialleadership. Until the tobacco companies face this issue
square ly , they wi l l do nothing to he lp our smal l farmers
create a new money crop.

na Med ica l Journa l (NCMJ It is obviousthat the article was written to present Duke Medical Cen
ter’
s viewpoint. Just enough historical data is presented to
make the casual reader be l ieve this to be an unb iased andfactual report .
Far from it. The author is from the Department ofMed i
c ine which presented the greatest opposition to Famil yMedicine and to a favorable solution to the prob lems . Many
of the statements in the article deserve comments .
The author states many are“skeptical that one person
can know enough to do the job we l l . Not al l graduates of
any spec ialty residency perform the ir jobwe l l , but the trackrecord of graduates of Family Practice Residency Programs
across the country has been a record of qual ity care . Fami ly
phys ic ians are required to obtain 150 hours of approvedpostgraduate education every three years tomaintainmem
bership in the American Academy of Family Phys icians .
Further, the cert ification by the American Board of FamilyPractice requires re -certification every six years . These
educational requirements contribute to the qual ity care ofFamily Phys icians .
Another statement in the article , Logic d ictated the new
program be placed in the local community hospital . This
move may have been good for the program but showed a
lack of commitment by Duke from the first . L ater. the
various departments accused the Famil yMedicine Program
of be ing d isloyal to Duke because they hospital ized the irpatients atDurhamCounty Hospital and used local consul
tants rather than the faci l ities at Duke Hospital . However,
the cl inical departments have consistently opposed admit
ting privi leges to Fami ly Physicians . How many phys icians
would be happy to admit their patients to a hospital where
they can have no part in the care of the ir patients?
Another statement, FamilyMedicine (hol istic , integra
tive , and humanistic) chal lenged deep- rooted trad itions in
academic med icine and cl inical practice . There are deep
philosophical d ifferences between the discipl ines , but if
academic med icine does not be l ieve in bond ing betweenpatient and doctor , and the continuity of care of patients ,
then in my Opinion,academic medicine is far off course .
This statement, inmy opinion, represents a groupof physi
cians who have not experienced on-
going contact w ith a
patient in years if ever .
The article deserves many more comments . but becausethis is a letter to the editor instead of a special article , I wi l linstead offer a few comments of my own.
The Lew in Associates External Review offered four
options :
1 . Status quo .
2 . Strengthen the Department of Community and FamilyMedicine , d irecting other departments to accept its role
and integrate it more ful ly into the Medical Center.
3 . El iminate FamilyMed ic ine as a primary care disc ipl ine ,
and replace itw ith a new integrated program inprimarycare under the Departments of Medic ine , Pediatrics ,
and OB -Gyn.
4 . El iminate al l primary care programs , and accept a ro le
as a pure ly tertiary institution.
Option 2 was recommended by the report . As we know ,
Option 3 was se lected by the Duke Med ical Center . I fail to494
understand how departments that have opted for sub
Specialty training and have no experience or understandingof primary care can run a program inprimary care . I mightfurther point out that Duke has never been known for itscooperative interaction between departments . This would
be another point against the success of a primary care
program under these Spec ialty departments .
Was Famil y Med ic ine“destructive to the fabric of the
organization? I hard ly think so . The Fami ly Practice
Res idency graduates have contributed greatly on a
statew ide bas is . The statement re lating to the destruction of
forces to the fabric is presented inpart because of economicprob lems resul ting from decis ions by se lf-centered departments . The cause of these prob lems is stil l present atDuke .
No , Dr . Sul l ivan this w il l notpass as did the decis ions
on the School of Nurs ing and Education. Today , we are
deal ing with the health needs of North Carol ina not the
se l fish interests of various departments in Duke MedicalCenter. The people ofNorth Carol ina wi l l not let this pass .
Duke should not let this pass . Did Duke truly make the
attempt to support the Family Medic ine Program or was it
just in name only?
We need sub- special ists in al l fie lds . No one , particular
ly Family Physicians , deny this fact. But we also need the
general ists the Family Phys ician, the general Internist.and the general Pediatrician. The people of North Carol ina
need these physicians for qual ity health care . We must put
aside personal differences and work together for the good
of North Carol ina . The citizens of North Carol ina deserve
qual ity health care inevery hamlet and county of the state . Ihope Duke wi l l recons ider.
G eorge T. Wol ff. MD .
10 16 A Professional V i l lageG reensboro 2 7 40 1
And Another
1 would l ike to take a second look at Dr. Robert Sul l ivan
’
s article (NCMJ l 985 ;46 :3 29-3 l ) justify ing Duke’
s
decis ion to terminate its Fami ly Medicine Program. Dr.
Sul l ivan pointed outmost of the pertinent facts of the casequite accurate ly . I would l ike to briefly re iterate those facts .
Fol lowing a nationw ide trend , Duke created a Depart
ment of Family Medicine in 197 2 , but“it was not done
with unanimous faculty acclaim. Duke Univers ity Hos
pital was already crowded with referral patients and did not
want the Family Practice Program. Durham County Hos
pital , the nearby community hospital , did want the pro
gram.
Not only was there lack of faculty acclaim for Fami ly
Medicine and lack ofDuke University Hospital support for
a Family Med icine Program. Duke went so far as to make
the medical center complete ly off l imits to Family Phys i
c lans . Family Phys ic ians . whether res idents or faculty , did
not have admitting priv i leges at the Duke Med ical Center.
S ince at Family Med icine’
s inceptionDuke had amonopo
ly on specialty care inDurhamCounty , atfirst res idents andfaculty had no choice but to send their patients to Duke .
However, in the fol lowing years , private subspecialty carefl ourished in Durham County . W ith the availab il ity of
VOL . 4 6 . No . 9

496
DOES YOUR LABORATORY OFFEREVERYTH ING WE DO?
0 RIA, Toxicology. S erology , Virology. Cytogenetics , Hematology andMicrobiology procedures
0 Routine results reported within 2 4 hours0 Customized profiles and preprinted test requis ition forms tailored toyour needs
0 Easy to read report formats
0 2 4 -hourC lient Services0 Free supplies0 Profes s ional consultation0 Courier pick-up and report de livery0 Interactive desktop termina l foryouroffice or home d irect accessto patient test results , drug information, d iagnostic data , clinica l abstracts , Continuing Medica l Education, and more .
MetPath offers youmoreFormore information dia l:
(9 19 ) 4 7 1 -64 95
VOL . 4 6 , No . 9
Practical informationonthemedical aspectsfitness and exercise.
Tennis e lbow : Joint re solution by
conse rva tive trea tment.
Hype rtrophic cord iomyopothyand the athle te .
Effects of sunscreenuse during
e xe rc ise in the he at.
Ove ruse injurie s to the kne e in
runne rs.
How Imanag e ing rown toena ils .



500
B & BXRAY
MAMMOGRAPHYCAN DETECTBREAST CANCER EVEN SMALLERTHAN THEHANDCAN FEEL.
The BennettMammography SystemM- 3000 is a heavyduty unit des igned for soft tissue d iagnos is of the
breast Optimum beamqua lity formammography isachieved by a 7 6 cm foca l film distance with amolybdenumx- ray tube . The BennettMammographySystemM-3000 is des igned for hospita l, c linic, privateoffice and screening facilities .
working for the end result—optimum qua lity rad iographs
PO . Box 802 Matthews , NC 2 8 105 In NC Ca ll 1 - 800- 2 2 2 -9262
In SC Ca ll Collect 7 04 - 84 7 -8 5 2 1
VOL . 46 , No . 9


Add itiona l informationava i lable to the profes s ionon reques t.
Dls ta Products CompanyDivis ion of El i Li l ly and CompanyInd ianapol is , Ind iana 4 6 2 8 5
4 20113 Mfd . by El i Li l ly Indus tries , Inc.
Carol ina , Puerto Rico 006 3 0

Index to Advertisers
Army Reserve
Ayerst L aboratories InsertB B X-Ray , Inc .
B lue Cross and B lue Shie ld of NC
Campbel l L aboratories , IncCHAPS
Crumpton CompanyCurtis 1000 lnforrnation Systems
GuestHouse
H ighland Hospital
H inrichs Financial G roupInfo Systems of N C , Inc .
Mark L eonard Assoc iates
El i L il ly Co .
Mac Thrift Office Furniture
TEGA-CORT FORTE 1% TEGA cont(Ava i lab le at a l l d rug s tores Rx Only)
SQUEEZE TYPE DIS PENS ER BOTTLESTega
-Cort Forte'
and Tega-Cort lotions are offered in a nice smooth non-s ta ining
water soluble base .
Ind ications : For re l ief of the inflammatory manifes tations of cort icos terond
respons ive dermatoses inc lud ing Poison Ivy , and sunburn.
Contraind ications Topica l steroids have not been reported to have an adverse
effect on pregnancy , the safety of the ir use in pregnant fema les has not abso lute ly
been es tab l ished . Therefore , they should not be used extens ive ly on pregnant
patients , or in large amounts , or for prolonged period s of time .
Dosage and Adminis tration: Apply to affected area 3 or 4 times da i ly as d irected
by your phys ic ian.
Caution: Federal law proh ib its d ispens ing without prescription. For externa l
use only . Store in a cool place but do not freeze .
PLEASE CONSULT INSERT SUPPLIEDWITH EACH BOTTLE FOR MOREDETAILED INFORMATION
WEFEATUREONEOFTHEMOSTCOMPLETELINEOF INJECTIBLES INTHESOUTHEASTATTHEVERYBESTPRICE, CONSISTENTWITH QUALITY.
ORTEGAPHARMACEUTICAL CO INC. JACKSONVILLE, FLORIDA32205
Medical Mutual Insurance Company of NCMetPathNational Staffing Services Corp.
Ortega Pharmaceutical Company Inc .
Parke-Davis
The Physician and Sportsmed icinePostgraduate MedicineRoche L aboratoriesSaint Albans Psychiatric HospitalE . R. Squibb Sons , Inc .
The Upjohn CompanyU. S . Air Force
U. S . ArmyWil l ingway , Inc .
Winchester Surg ical Supply Co .

EXCERPTS FROMASYMPOSIUM“THETREATMENTOFSLEEPDISORDERS"8
highly effectiveforboth s leep inductionands leepma intenance
SleepLaboratory InvestigatorPennsylvania
onsetofactionisrap id. . provides s leepwithno reboun
appears tohavethe bestsafety record ofanyofthe benzodiazep ines
PsychiatristCalifornia
After 15 years, the experts still concuraboutthecontinuing value ofDalmane (flurazepamHCI/Roche) . Itprovides s leepthatsatisfies patients .
and thewidemarginofsafety thatsatisfies you.
The recommended dose inelderlyordebilitatedpatients is 15 mg. Contraindicated inpregnancy.
flurazepam HC I/ Roche (iv:s leep tha t satisfie s
i s-mg/SO-mgcapsules
References: l . Kales J, ofof. l nPharmacol Ther 12 .
-691
697, JulAug 197 1. 2 . KalesA. efal: ClinPharmacol Ther-3 63 , Sep 197 5 . 3 . KalesA. erof. l nPharmacol
Ther 19 5 7 6-5 823 , May I976 . 4 . Kales A, eral: ClinPharmacol Trier -7 88 , Dec 198 2 . 5 . FrostJDJr, DeLucchiMR: JAmGeriarrSoc -5 46 , Dec 197 9. 6 . DementWC, eral; BehavMed, pp. 2 5 -3 1, Oct 197 8 . 7. KalesA,Kales JD: J ClinPsychopharmacol - 150, Apr1983 .
8 . TennantFS, eral. Symposiumonth eTreatmentofSleepDisorders , Teleconference, Oct 16 , 1984 . 9. GreenblattDJ,AllenMD, ShaderRI: ClinPharmacol Ther2 h 3 5 5 -3 61Mar 197 7,
Roche Products Inc.Manafi, PuertoRico0070]
DALMANE®
flurazepamHCl/Roche(llZBefore prescribing, please consultcomplete productinformation, a summary ofwhich follows :Indications: Effective inall types of insomnia characterizedby diff iculty infalling as leep, frequentnocturnal awakeningsand/orearlymorning awakening: inpatients with recurringinsomnia orpoors leeping habits ; inacute orchronicmedicasituations requiring restful s leep. Objective s leep laboratorydata have showneffectiveness forat least28 consecutivenights ofadministration. Since Il
'
ISOlTl I'
l IO is oftentransient
and intermittent, prolonged administrationis generally notnecessary orrecommended. Repeated therapy should onlybe undertakenwith appropriate patientevaluation.
Contraindications : Knownhypersens itivity to flurazepamHC :pregnancy. Benzod iazepines maycause fetal damagewhenadministered during pregnancy Several studies suggestanincreased risk ofcongenitalmalformations associatedwithbenzodiazepineuse during the firsttrimesterWarnpatientsofthe potential ris ks to the fetus should thepossibility ofbecoming pregnantexistwhile receiving flurazepam. Instructpatients todiscontinue drug priorto becoming pregnant. Cons iderthe possibility ofpregnancy priorto instituting therapy.
Warnings; Cautionpatients ab0utposs ible combined effectswith alcohol and otherCNS depressants. Anadditive effectmayoccurifalcohol is consumed the day followrng use fornighttime sedation. This potentialmay existforseveral daysfollowing discontinuation. Cautionagainsthazardous occu
pations requiring completemental alertness (e.g. , operatingmachinery, driving) . Potential impairmentofperformance ofsuch activities may occurthe day following ingestion. Not
recommended foruse inpersons under 15 years ofage.
Withdrawal symptoms rarely reported: abruptdiscontinuationshould be avoided with gradual tapering ofdosage forthose
patients onmedicationfora prolonged period of time. Usecautioninadministering toaddiction-
prone individuals orthosewhomight increase dosage.
Precautions : Inelderly and debilitated patients ,II is recom
mended thatthe dosage be limited to 15 mg toreduce risk ofoversedation, dizziness , confusionand/orataxia. Consider
potential additive effectswith otherhypnotics orCNS depressants. Employ usual precautions inseverely depressedpatients, orinthosewith latentdepreseonorsurcidal tendenc:es , or inthosewrth impaired renal orhepatic function.
Advers e Reactions: Dizziness, drowsiness , lightheadedness,
staggering, ataxia and falling haveoccurred, particularly in
elderly ordebilitated patients . Severe sedation, lethargy, CIISorientationand coma, probably indicative ofdrug intoleranceoroverdosage, have beenreported. Also reported: headache,
heart burn, upsetstomach, nausea, vomiting. diarrhea, con
stipation, GI pain, nervousness , talkativeness , apprehension,
irritability, weakness , palpitations , chestpains , body and jo1mpains and GUcomplaints . There have also beenrare occur
rences of Ieukopenia, granulocytopenia, sweating, flushes,difficulty infocusing, blurred vision, burning eyes, faintness,hypotension, shortness of breath, pruritus , s kinrash, drymouth, bittertaste, excessive salivation, anorexia, euphoria,
depress ion, s lurred speech, contuswn, restlessness , hallucinations , and elevated SGOT, SGPT, total and directbilirubins,and alkaline phosphatase; and paradoxical reactions , e.g.,excitement, stimulationand hyperactivity.
Dosage: Individualize formaximumbeneficial effect.Adults.
30mg usual dosage: 15 mgmay suffice insome patients.
Elderly ordebilitated patients; 15 mg recommended initiallyunti l response is determined.
Supplied: Capsules containing 15 mg or30mg flurazepamHCI.


Medical Mutual
We’
re H ere Because . ofYou .
Medical Mutual Insurance Companywas founded inOctober, 197 5 ,when the commercial professional liabilitymarket reached a peakof instabil ity . Recogniz ing the need for an altemative ,
the North
Carol inaMed ical Society created MedicalMutual as an independentcompany owned and d irected by physicians .
Today,MedicalMutual is North Carol ina’
s largest insurer of
physicians and surgeons, representing approx imate ly 80percentofall physicians inprivate practice . Our services extend to every
physician in the state , through competitive premium rates and
innovative riskmanagementprograms .
For these accomplishments ,we thankyou.Your support has made
our success poss ible ,and itw ill carry us forward into the future .
Medical Mutual .We’
ll be there whenyou need us .

Pub l ished Monthly as the Official Organ of The North Carol ina Medical Society ( ISSN -0029-2 5 5 9)
Oc roer-za l 985 , NCMJ
Practical informationonthemedical aspectsfitness and exercise.
Tennis e lbow : Joint re solution byconse rva tive tre a tnient .
Hype rtroph ic ca rd iomyopa thyand the a th le te .
Effects of sunscre en use duringe xe rc ise in the he at.
Ove ruse injurie s to the kne e inrunne rs .
How Imana g e ing rown toena ils .

F inancia l new s you have been w a i ting to hea r’
CW ncreas e ml S O
ncome
Ava i lable to ig ible Members Under Age 5 0Regardles s Other Dis abi l i Insurance
Offic ia l North Carol ina Med ica l Soc ietyDis ab ility Income Plan
Endors ed and Recommended S ince 193 9
Protect your mos t va luab le as s et, your profes s iona l income
For deta ils or cla ims service ca ll orwrite :
CRUMPTON COMPANYPROFESS IONAL GROUP INSURANCE
Toll free - 16 7 4
ACADEMY CENTERPOST OFFICE BOX 8 5 00DURHAM, NC 2 7 7 07
Account executives : J . S lade Crumpton, Gene Greer and CliffMas her, DurhamJack Feathe rs ton, Charlotte
Dan Ha ley , Greensboro
506 VOL . 46 , No . 10

MAMMOGRAPHYCAN DETECTBREAST CANCER EVEN SMALLERTHAN THEHANDCAN FEEL.
The BennettMammog raphy SystemM-3000 is a heavyduty unit des igned for soft tissue d iagnos is of the
breast. Optimum beamqua lity formammography isachieved by a 7 6 cm foca l fi lm d istance with amolybdenumx- ray tube . The BennettMammographySystemM- 3 000 is des igned for hospita l, c linic , private
office and screening facilities .
work ing for the end result—optimumqua lity radiographs
B BXRAY PO . Box 802 Matthews , NC 2 8 105 In NC Ca ll 1 -800- 2 2 2 -92 62
InSC Call Collect 704 - 84 7 - 85 2 1
508VOL . 46 , No . 10


need medical attent ion, they need to know that someone is
make certain all the finest care is given . And for just onemonthly payment through an employer thars exactly what our customers getThe Personal Care Plan from Blue Cross and Blue Shie ld ofNorth Carol ina prov ides
famil ies w ith the ir own Personal Care Phys ician who CAM”
IT-{ECARINC CARD‘
manages every aspect of the ir health care .
If you'
re a partic ipating phys ician in the Personal CarePlan , you
’
re working w ith us to offer the finest grouphealth care ava ilable . H igh qual ity health care in a plan
that'
s helping to hold back r ising costs .a ran
Ifyou'
re not a participating phys ician, butwould l ike tobe ,write or callDirector, Profess ional Re lations , Personal of: GE?“Care Plan , PO . Box 2291, Durham, North Carol ina27702 .Te lephone 919 489
-743 1.
°Blue Cross and Blue Shie ld ofNorth Carolina 1985 Fm“ Blue cm“and Blue Shie ld Of N°nhC3 01”
VOL . 46 , No . 10

cess tak es approximately 20 seconds and sl ides are ex
amined wet. The patholog istwil l then assess the adequacyof the sample and whether add itional aspirations need to beperformed . The patholog ist usual ly gives his prel iminarydiagnosis in person in the rad iology department procedureroom where he can review the x-rays and directly confer
with the radiolog ist. The immediate quick read”
proce
dure can eas ily be performed w ith in five minutes . At this
time , any add itional material can be al located for furtherstudies includ ing microbiolog ic examination, ce l l blockand electronmicroscopy . The remaining 95% alcohol fi xedsl ides are examined within one or two hours and the finaldiagnosis is rendered . The pathologist contacts both theradiologist and the patient
’
s phys ician. Fol lowing the b iopsy procedure , the patient is observed for any signs of
complications includ ing bleeding , and vital signs are re
corded . Ind ications for fine needle aspiration biopsy at
ECU/PCMH are outl ined in table 2 .
Results
Fifty-four patients underwent s ixty-two biopsies at Pitt
County Memorial Hospital in 1984 . The age range was 2 3
to 88 years old with a mean age of 62 . There were 26 men
and 28 women. Thirty-one Specific mal ignant diagnoseswere rendered . There were th irty -one negative cases . F iveof the negative cases were later shown to be mal ignant byhistologic examination for a fal se negative rate of l 4% .
There were no fal se pos itive d iagnoses . The sens itivity of
5 12
the procedure (true pos itive) was 86% and specificity ( truenegative ) was In fi fteen negative PNA biopsies
a specific non-mal ignant diagnos is was rendered .
There were no complications reported fol low ing any of thefine needle aspiration biopsies presented in th is study .
Discussion
References available from the authors .
VOL . 46 , No . 10
The main value of fine needle aspiration b iopsy of deepabdomen, retroperitoneum, soft tissue , and bone is in thediagnosis ofmal ignancy . An accuracy rate of 80 to 90% isreported inmost series which is exempl ified by our 1984
experience , where a diagnosis of mal ignancy was madewith a sensitivity of 86% and a specifi city of 100% for the
procedure .
H 3In addition, the procedure can serve as an
accuratemeans of diagnosing mal ignant lymphoma as evidenced by our experience with five cases inthis study . F ine
needle aspiration b iopsy is particularly useful in cases
where there is a question of recurrence of a previouslydiagnosed mal ignancy . Our results al so support the role of
FNA in diagnosing non-mal ignant cond itions . Forty-e ight
percentof our negative cases had a specific non-mal ignantdiagnosis .
Continued refinement of rad iologic guidance tech
niques , particularly the development of special aspirationtransducers for ultrasound which are capable of simul
taneous ly guid ing need le placement and imag ing regionalanatomy , should lead to continued improvement in accuracy of th is procedure .
Our experience in this study re-emphas izes that fineneedle aspiration b iopsy of deep abdomen, retroperi
toneum, soft tissue , and bone is a safe and quick means ofd iagnos ing both benign and mal ignant les ions and is bothless expensive and less invasive than other currently available modal ities . The procedure causes l ittle discomfort to
the patient and can be performed in both out-patient andhospital settings . PNA biopsy of deep, non
-
pal pable lesions util iz ing sophisticated radiologic technique offers anaccurate means of d iagnos is which minimizes delay intreatment. The procedure works bestwhen the experti se ofthe cytopathologist, radiologist, and primary physician arecomb ined in a team effort .


CGUSCI anisms
2 5 0-mgotters effectiveness aga inst
the ma jorcauses of bacte ria l b ronch itisH. influenzae , H. influenzae , S. pneumoniae , S. pyog ene s(ampic illin-susceptib le )
8rlal Summary.Consult the ou trage literature lot pmcrtblngInformation.indications andUsage: Ceclor
'
(celaclor.LIilyi is indicated inthetreatmentatthe loilowir
e
t
glniecrionswhencausedbysusceptible
strains oi therteSignal microorganisms:W impy includingpneumoniacaused by
Streptococcuspneumonraet ipiococcuspneumoniaeI.Haemopnflus tritiuerrrae. and S. pyogenes (groupAbela-hemolyttc v
streptococci)Appropriate culture and susce ttblllty studies should be
peréormed todetermine susceptl llltyoi thecausative organismto BC bi
Contraindical ion: Ceclor Is contraindicated inpatientswith Iinown
allergy tothe cephalosporrngroupatantlblotcs.
Warti lri 5 t PENIClLt -SENS ITIVEPATIENTS CEPHALOSPORl ANTIBtOi iCS SHOULDBEADMINISTEGEDCAUTIDUSLY.THERElSCLINICALANDLABORATORYEVIDENCEOF PARTIALCROSS-ALLERGENICITY OFTHEPENICILL INS ANDTHECEPHALOSPORINS, ANDTHEREARE INSTANCES INWHICHPATIENTS HAVEitADREACTIONS. INCLUDINGANAPHYLAXIS.
toBOTHDRUGCLASSES.
Antibiotics. lncludrnpsector, should beadministeredca utiouslytoanyp
atientwhohas demonstrated some lotmol allergy.panlcuarty todrugs.Pseudomembranous col itis has beenreportedwithvirtual! all
broad s l iumantibiotics ilncluding macroitdes.semlsynt lc
penicittns, and cephatosporinsi: lherelore. it Is important toconsider its diagnosis inpatients whodevelopdiarrhea Inassociationwith theuseoi antibiotics Such colitismayrange inseverity trommild to lite-threatening.Treatmentwith broad-spectrumantibiotics alters the n0rmal
l loraoi the colonand to permitovergrowthol clostrldia. Studiesindica te thata torin to uced byCiostridiumdittrcrie is oneprimary cause oi anti atic-associated colitis.Mild cases atpseudorh ernoranous colitis usually respond to
drug discontinuance alone. Inmoderate toseverecam.manage
(ampic illin-resislant)
ment should Include sigmoidoscopy.appropriate bacteriologicstudies. and Iluid, electrolyte. and proteinsupplementation.Whenthe col itis does not improve alterthe drug has beendiscontinued.orwhenIt is severe.oral vanto cmis the drugatchoice loi antibiotic-associatedpseudomem anous co l itis
ptpd
él ced byc. dl
'
i trciie. Othercauses 0! colitis should betue out.
Precautions: General Precautions ti analter loreactiontoCecloi
‘
icetaclor.Lillyl occurs .thedrug shout bediscontinued.and. II necessary.thepatient should be treatedwith appropriateagents. c.d., pressoi amines. antihistamines.orcorticosteroids.
Prolonged use 01Cecloi may term“intheovermmatnonsusceptible or
ganisms.Carelul observation0 thepatient ls
essential. Itso rniectlonoccurs duri ng therapy. appropriatemeasures shou0be taken.
PositivedirectCoombs' tests have beenreported during treatmentwith thecephalosporinantibiotics. inhematologic studiesor intransiusloncrossmaichlng procedures whenantlglobultntests are pertormed on theminorsideor inCoombs
'
testln oi
newborns whosemothers have received alosporlnanl l tics
beloreparturition. it should be recognize thatapositiveCoombs' test in be due tothe drug.Ceelot should administeredwithcautionInthepresence0!markedly impaired renal lunction.Undersuch conditions.carelulClinical observationand laboratory studies should bemadebecausesaledocoy
omay be lowerthanthat itSuaIly recommendedAs aresultata ministrationoi Cecior.aiatse-positlve reaction
torgluco se Intheuri nemayoccut This has beenobserved withBenedict
's and Fehling's solutions and alsowithCl lnltesl ‘
La
ggI
ltltutnotwith ies-Tape
'
(GlucoseEnzymatic test Strip.i l l.
Broad-spectrumantibiotics shouldbepres cribedwithcautioninIndividuals with a history oi gastrointes tinal disease.part icularlycoiltiS.Usage inPregnancy PregnancyCategory 8 Reproduction
studies have beenperiormed Inmiceand rats at doses upto l?times the humartdoseand inlurels giventhree times themaximum
humandoseand have revealed no evidence 0! lm l ied lertil ityorharmtothetetus due toCeclor‘ tcelaclor. Li lyi, Thereare.however. noadequateandwell-controlled studies inpregnantwomen. Becauseanimal reproductionstudies arenot alwayspredictive oi humanresponse, this drug shouldbeused duringor nancronly itclearlyneeded.
ts ingMothers Small amounts oiCec lorhavebeendetectediti mother smlitt toi iowi administrationoi Sin
gle 500mg doses.
Average levelswere (x20.omand mop/ml at two,three. tour.and live hours respectivel
'
y. i race amountsweredetected atonetrout The el iaci onnursing lntanls is notknown.Cautionshould beererclsed whenCectoris administered toanurs ing woman.Usage InChildren Saletyand etrectiveness orthisproductfor
use inrnlanls less thanmemonlhol agehmnotbemestabl lshed.Adverse Reactions:Adverse el lec ts considered related totherapywithCociorareuncommonand are listed below:Gastro intestinai symptoms occurinabout percentat
patients and Include diarrheai i inSymptoms oi pseudornombtanous col itismay appeareither
duringoral terantibiotictreatment.Nauseaandvomiting havebeenreported lately.tiraersensitrvlt reactions have beenreported inabout i .siceni oi patiens and include rnorb llltorrn eruptions It inrutilus.unlcarla,andpositiveCoomtts
‘tests eachoccurintess
than l in200 al ionis.Cases 01 seruni-s tcliness-titwreactions
erythemamull orthe above sli inmanltestatlons accompaniedirkearlhi ltls/ arthraig laand. treouently. leveri have beento ed.
T soreactions are apparently due tohypersens itivity an haveusuallyoccurred during or lollowing asecondcourse at l iterwithCectoi.Such reactions have beenreportedmore lreouenl yinchildrenthaninadults .Signs and symptoms usuallyoccura lewdays alter Initiationol therapy and subsidewithina lewdaysanarcecsationot th er .Noserious sapuelae havebeenreported.Antihistamines andconcosteioids appeartoenhance resolutionat the syndrome.Cases ol anaphylaii is have beenrationed, haltoiwhich have
occurred inpatients with a history orpenicillinatergy.Otherel lects considered related totherapy incuded
oosin Illa( I in50 patients) and genital pruritus orvaginitis|less t ant in100p
atientsi.Causal Relations inUncertain Transitory abnormalities in
clinical laboratory testresults have beenreport ed Although theywereoi uncertainottol y. they are listed belowtoserve asalert ing lnlormatlontort eoh ician.
Hepatic Slightelevations nSGDT.soet.oralkalinephosphatasevaluesj
l in
Hematopote tic ranslent l luctual lons inleukocytecount.predominantlyl
phoovtosls ocCurtIng tnInlanls and youngchlldrentl In4 l.Renal St htelevations inBUNorserumcreatinine (less than
t infromora ormal urinalysis ( less than i inmm.[06 1782RI
Nora; Coclor'tcetaclor, t lllyi is contraindicated Inpatients
with lrnownalle tothecephalosporins and should be givencautiousl
ytopencillin-allerg lc attents .
Pontcii in Is the usual dr 0 choice inthe treatmentandprevention01 streptococcal ntectlons , including theprophylaris
otrheumatic lever. See prescribing lnlorrnal ion.
0 i984.ELI LILLYANDCOMPANY

The causes ofNS are myriad . When evaluating a patientwith NS ( table 1) it is he lpful to try to distinguish whether itis
“secondary to another disease process , or
“
primary( that is , idiopathic) . Sources that lead to secondary neph
rotic syndrome should be ruled out first and include post
infectious sequelae , multisystemic d iseases such as di
abetes or lupus ; heredofami l ial d iseases l ike sickle ce l l
anemia; neoplasms ; and toxins such as gold or penicil la
mine. A partial l ist of specific causes of secondary NS is
found in tableAs in the patient be ing discussed , if there is no evidence
for secondary NS in an adult, renal b iopsy can be per
formed to class ify the type of primary NS based on histolog ic findings . Primary NS in the adult results fromminim
al change disease ( I S- 20% of cases ) , mesang ial prol ifera
tion (5 focal glomerular sclerosis id iopathic
membranous g lomerulopathy ( 30 membranoprol if
erative glomerulonephritis ( less than or chronic nonspec ific glomerulonephri tis ( 5 In many instances a
5 14
0 20 40 60 80 100KIDNEY FUNCTION (Percent of Norma l )
40 80 120 160 200CREATIN INE CLEARANCE (ml/min)
F igure l . The re lation between serum creatinine (broken l ine)and kidney function. As kidney function decl ines , the serumcreatinine rises in a nonl inear fashion. On the other hand , the
inverse of the serum creatinine ( sol id l ine) shows a direct and
l inear rela tion to kidneyfunction, decl ining by ha lf its va lue eachtime the kidney function decl ines by ha lf . (Da ta derived fromDoolan, Alpen and Tha i l .
6)
histolog ic diagnos is can aid in both determining the patient
’
s prognosis and establ ishing the most effective treatment plan; this information can not be re l iably predictedfrom the patient
’
s urine sediment or cl inical course . A
histolog ic diagnosis suggestswhich patients wil l respond to
g lucocorticoids . For example , glucocorticoids tend to be
pal l iative in minimal change d isease or membranousg lomerulonephritis , but seem to have l ittle beneficial effectin focal glomerular sclerosis or membranoprol iferativeglomerulonephritis .
3
It was clear that the patient’
s renal function was decl in
ing rapidly , but the ra te of the decl ine was not directlyobvious from themeasurementof serum creatinine alone . It
is helpful to remember that serum creatinine is curvi l inearlyre lated to renal function (figure 1) as measured by e ither
glomerular filtration rate or creatinine clearance .
5 ' 6 In
fact, the curve shown is a rectangular hyperbola fol lowingthe equation:
K idney Function l /Serum Creatinine
Thus , the inverse of the serum creatinine ( I /Scr) provides a
d irect estimate of k idney function (figure Although the
precise value of glomerular function in any given patient
requires calculation of the creatinine clearance (which in
turn requires col lection of a timed urine Specimen) , l /Scr
can be used to fol low patients with chang ing glomerular
fi ltration rates .
6
In order to get a picture of our patient’ s renal function,
we plotted the inverse of her serumcreatinines against time
( figure 2 ) in the manner suggested by Mitch et al .7In a
VOL . 4 6 , No . 10

sa me
NOV DEC FEB MAR APR MAY
MONTH
fi gure 2 . Changes in the patient’
s inverse serum creatinine
( 1/Scr) showa rapid and l inear decrease with time . Extrapolation
of the l ine backwards a l lows us to estima te that her disease began
sometime in Janua ry ; extrapolationforward predicts tha t. in the
absence of treatment, the serum creatinine would have been 10
mg /d l by July .
study of 34 patients w ith chronic renal insuffic iency causedby various d iseases , these authors showed
“that in most
cases reciprocal serum-creatinine decl ines l inearly with
time as renal failure progresses .
’ 7Inaddition, analysis of
th is relation in ind ividual patients g ives an estimate of the[rate of] progressionof the disease , may help to determine
the effects of therapy , and could be used to predict when
dialysis wil l become necessary .
” 7 We were fortunate to
have avai lab le a serum creatinine value of mg/dl
obtained when the patient underwent an e lective septoplasty in June of 1984 , and we assumed that to be the patient
’
s
OCTOBER 1985 , NCMJ
Acknowledgment
The authors express th eir gratitude to Dr. Rex Mahnensmith for his
generous , informative and helpful contri butions to the manuscript.
base l ine value . Figure 2 shows a strik ing l inear dec l ine in
renal function. We extrapolated the l ine backwards to getan ind ication of when the process causing the nephrotic
syndrome might have begun; the extrapolated l ine inter
cepts the patient’
s base l ine sometimes in early January ,
about three months before the onset of her symptoms . We
careful ly questioned the patient about il lnesses and med ications during early January . Unfortunate ly , she could not
provide any additional information. Nonethe less , the graph
as wel l as urinary prote in excretionwil l be useful tools w ithwhich to fol low th is patient ’ s response to treatment.
Progressive renal failure presents a chal lenge in diagno
sis and treatment. By plotting the inverse of serial serum
creatinine values versus time , the cl inician canmonitor the
progressionof the disease and the impactof any treatments .
References
l . Ackemecht EH . A short history of medicine , revised ed . Baltimore: Johns
Hopk ins Univers ity Press . 1982 . pp. 60- 1 .
2 . F i shman MC . Med icine . Phi lade lphia: 1. B . L ippincott. 198 1 . pp.-9 .
3 . Petersdorf , RG ci al . Harrison'
s principles of internal medicine , loth ed . NewYork : McGraw-Hi l l Book Company . 1983 .
4 . Earley LE , Gott schal k CW , eds . Strauss and Welt‘
s diseases of the k idney . 3 rd
ed . Boston: L ittle , Brown and Company . 197 9 .
5 . Pri ce SA,Wilson LMcC . Path ophysiology . zud ed . New York : McGraw-H i l l ,
1982 , p. 5 27 .
6 . Doo lanPD.AlpenEL , Thai] GB . Aclinical appraisal of the plasma concentration
and endogenous clearance of creatinine . Am J Med
7 . Mitch WE et al . A s imple meth od of estimating progression of chronic renal
fai lure . Lancet 197 6EI11 13 26 .

SCIENTIFICARTICLE
Purpura Fulminans Associated with
Haemophilus lnfluenzae lnfection
John Peter Santamaria , M .D . , Shannon Kenney , MD . and Alan D . Stiles , MD .
0 Threefa ta l cases demons trate the importance of prevention. Guidel ines
for va ccination of young ch ildren are g iven .
URPURA fulminans is a disorder characterized by
P progressive , symmetrical purpuric lesions of the sk in
in addition to laboratory evidence of disseminated intra
vascular coagulation (DIC) .
lThis disorder has beenassoci
ated with bacterial d iseases caused by streptococcus ,
meningococcus , and B ranhame l la ca tarrha l is , as we l l as
the exanthematous v ira l i l lne s se s of varice l l a and
measles .
”5H a emophi lus influenzae infections have been
descri bed w ith petechiae or redd ish-
purple cel lul itis butnot
with the pathognomonic features of purpura fulminans .
S ince the presence of this serious complication maysuggest other etiolog ic associations and inappropriate lynarrow treatment reg imens , the purpose of this paper is to
present three il lustrative cases treated on our service in a
six-month period . The deaths of al l three patients attest to
the severity of this problem. The need for adequate preventive measures and rapid and intensive therapy is clear .
Case 1
DE , a 9-month-old wh ite boy , presented at another hos
pital obtunded , convul sing , and cyanotic . Initial physicalexamination was remarkable for hypotension, fever, unre
sponsiveness , a tense fontane l le and right otitis med ia . A
lumbar puncture revealed purulent cerebrospinal fluid(CSP) which later grew H aemoph ilus influenzae type b ,sensitive to ampici l l in. H is coagulationprofi le onpresenta
tion included the fol lowing : Prothromb in time (PT) , 2 1
seconds (control , 1 1 seconds ) ; partial thromboplastin time(PTT) , 108 seconds (control , 3 2 seconds) ; fibrinogen 170mg/dl (normal , 170-4 20mg/dl ) ; and plate let count
ml .
The patient was treated with intravenous ampicil l in and
chloramphenicol , fresh frozen plasma , platelets , and vita
minK . Within several hours he deve loped marked purpuraof al l fingers and toes with no palpable pulses in the distalextremities . Repeat coagulation values were PTT of over
200 seconds (control , 5 6 seconds) and thromb in clotting
time (TGT) of 34 seconds (control , 12 . 1 seconds) . Ahepar
in infus ion (50 units/kg loading dose fol lowed by 15 units/
kg/hr) was added to h is therapy with no cl inical improvement. The heparin was discontinued when the patient de
veloped massive hematemes is . He d ied three days after his
From the School ofMedicine Univers ity of North Carol ina . Chape l H il l
27 5 14 .
5 16
initial presentationwith uncontrol lab le increase in intracranial pressure and hypotension.
Autopsy revealed purulent leptomeningitis , mul tiple
hemorrhag ic infarcts of the brainwith cerebral herniation,b ilateral adrenal cortical hemorrhage , and multiple hemor
rhag ic foci in the lungs , bladder and stomach . There was
purpura grossly of the hands , feet and calves . Microscopicexamof the sk in from the involved reg ions showed marked
vascular congestion and occlusion of the smal l capil laries
with hyal ine thrombi .Case 2
SC was a prev iously we l l , S I/ z-month-old white girl
admitted to a local hospital withmening itis which was later
shownby CSPculture to be due toH aemophilus influenzaetype b , sensitive to ampicil l in. She was initial ly treated
with ampicil l in, but developed general ized seizure activityand acidos is on the day of admission and was transferred to
the North Carol inaMemorial Hospital . Physical examwas
notab le for general ized seizures , bulg ing , tense fontane l le ,
and d iffuse purpuric lesions over the distal extremitiessymmetrical ly . Initial laboratory tests included the fol lowing : PT , seconds (control , seconds ) ; PTT,
(control , seconds ) ; TCT, seconds (control ,seconds) ; fibrinogen mg/dl ; Factor V111 3 5% of nor
mal , and a plate let count of 2 1 ,000/m1. The child was
maintained onmechanical ventilation and measures to con
trol intracranial pressure were instituted .
On the second hospital day purpura progressed despite
vitamin K , multiple plate let and fresh frozen plasma infu
sions , and laboratory evidence of coagulation improvementwith PT of seconds (control , seconds) . Heparin
therapy was begun (50 units/kg loading dose , then 15 -20
units/kg/hr infusion) with subsequent improvement in distal perfusion and some regre ssionof purpura . The patient’ sactivated PTT became equal to control , but the plate let
count could not be maintained greater than 20,000/m1. On
the fourth hospital day a massive pneumothorax occurred
and the child died . Autopsy was denied .
Case 3
PP, a 13 -month-old white boy , was admitted to a local
hospital with a diagnosis ofmening itis . H is b lood and CSPcultures grew H aemophi lus influenzae type b , sens itive toampicil l in. L aboratory tests on admission revealed PT ,
16
VOL . 46 , No . 10

TOXIC ENCOUNTERS
Play It Again, Voltaire
onkshood Poisoning
Ronald B . Mack , M .D.
sURELY you remember good old Voltaire . What a
stand-up guy he was ! ! Th is very provocative French
author and philosopher was a hero of the Enl ightenment
and inmy opinion was one of the real ly good things aboutthatperiod of history . H is writing was prodigious butmany
people remember him best for h is famous pronouncement:“ I may disagree with what you say , but I wi l l fight tomydeath your right to say it. I thoughtofVoltaire ’
s statement
recently whenanunsol icited journal came tome in themailand I began to experience intel lectual dysrrhythmia as a
result. No , I’
mnot talk ing about the ‘ journals ’
I rece ive inbrownpaperwrappers I l ike those the interviews are
simply marvelous .
The name of the journal that caused me to d issemble isAmerican H omeopa thy , Vol 2 , Number 3 , March 1985 ,
publ ished by the United States Homeopathic Association.
On page 4 there is an article entitled“Compari son of
homeopathicmed icines for treating tonsil l itis . The article
discusses this disease and then states“I f the condition is
ascertained very quickly , a dose or two of Aconite has an
excel lent chance of aborting tonsi l l itis .
word aconite I stopped reading for a moment and gulped .
Aconite was known to the ancient Greeks as an exce l lent
poison. Medea , of Greek mythology fame , was a very
tough lady . She was deserted by her husband , Jason (of the
Golden Fleece) ; he found a younger woman to dal ly with
(Excuse me , dal ly? Is that a euphemism for
Nevermind ! Medea was very angry and murdered al l of
herchildrenby Jasonexceptone . She thenmarriedAegeus ,K ing ofAthens . Aegeus had a son, Theseus , whomMedea
tr ied to k i l l w i th aconi te but she fai led . W i l l iam
Shakespeare knew plenty about this potential ly deadlyplant. InH enry I V, part 2 K ing Henry himse l f says
though it does work as strong as aconitum. In this
passage (Act IV , Scene IV ) the K ing speak s to his sons
concerning the strength of the love between brothers and
says itmust be so strong as to resist the force of a poison as
strong as aconite or of gunpowder. This plant has beenconsidered so poisonous ai td powerful throughout historythat it was used extens ive ly to coat arrows and daggers . In
H amlet, L aertes says And for that purpose I'
l l anointmysword . I bought an unctionof a mountebank somortal thatbut dip a knife in it, where it draws blood , no cataplasm so
rare can save the th ing fromdeath that is but scratched
From the Department of Ped iatrics , BowmanG ray School ofMedicine ,
W inston-Salem 27 103 .
5 18
When I read the
withal . Hamlet dies within half an hour after beingpoisoned thus and laments before dying ,
‘
Oh , I die , Hora
tio , the potent poison quite o ’
ercrows my spiri t.
”
Just what is th is plant that has been so popular for
mil lennia! ! Is it sti l l around? You bet your b ippy it is"Aconite has many synonyms , e .g . , it is probab ly betterknown these days asMonkshood but it isAKAFri ar
’
s Cap,
Helmet Flower, Sol dier’
s Cap and the everpopularWol fs
bane . There are 100 species of th is plant that are native tothe north temperate zone and they grow incultivated flowergardens and in the w ild throughout most of the UnitedStates and Canada except in the so
—cal led“deep South .
TheMonkshoods are perennial plants , mostly erect, sometimes branched , about two to six feet inheight. The characteristic upperpart of the plant is l ike a hood (no , not l ike the
guys who grow up inmy old ne ighborhood , but l ike a capor
cowl ) reflected in the various al iases that this flora enjoysFriars Cap, Sold ier
’
s Cap, etc . The flowers of most ofthe species are b lue but can be pink , white or flesh toned .
The seed pods contain numerous smal l seeds .
Probab ly the entire plant should be considered poi
sonous . The leaves , roots and seeds are particularly
troublesome if ingested (or if you happened to be hit by anarrow or stabbed with a dagger immersed in the plant’ scontents) because they contain aconitine and other poi
sonous alkaloids such as de lphinine and aj acine . These
chemicals are polycycl ic d iterpenoid alkaloids (of course
they are ! ! I knew Aconitine has been used ex
perimental ly by medical researchers to d isrupt the normalheartbeat so that new drugs that affect the heart can be
evaluated .
Gosh , I wonder what happens when you rece ive some
unwanted aconite l l The alkaloids are al leged to be so tox icthat mere ly pick ing the flowers of this plant can cause
prickl ing and/or numbness of the fingers . Poisoning does
occur, by ingestionusual ly accidental ly , ofcourse or
by eating the leaves as salad greens or by having it pre
scribed by uh , uh , uh practitioners . The symptoms of this
plant poisoning develop quite rapidly , usual ly within 30
minutes of ingestion, and are experienced initial ly as a
numbness or burning feel ing of the entire oral mucosa , l ips
and throat which may ultimately involve the entire dermal
surface inc lud ing the extremities . Speech , of course , maybe difficult and th is is often fol lowed by sal ivation, nausea
and vomiting , abdominal pain that is crampy innature anddiarrhea . G astrointestinal d istress seems to be the most
common denominator in a typical plant poisoning regard
VOL . 46 ,No . 10

less of species . With in l imits this is not necessari ly a
terribly destructive adverse effect as it he lps to rid the bodyof the plant part s and any unabsorbed toxins . Visual blurring can developw ith yel low-
green vis ion (as inoleander,fox glove, star-of-beth lehem poisonings) w ith mydrias is .
At this point the patient is dizzy , weak , uncoord inated and ,
if ab le to speak , complaining of paresthes ias , muscle
cramps , and general ized body pain. The worst is yet to
come ! ! Monk shood alkaloids fi rst stimulate then depressboth central and peripheral sensory nerves . The effects on
the heart are s imilar to quinidine . In the worst scenario ,
cardiac rhythm disturbances can lead to cardiac or respira
tory fai lure in as l ittle as 5 minutes or as long as four days .
The lethal dose is approximately 5 mg of the alkaloid or a
teaspoonful of the root; need less to say it is hard to stan
dard ize this substance .
So , you ask , just who are the se people the
homeopaths who , w ith in a few years of the 2 l st Cen
tury , recommend this substance , al leged ly , for acute tonsi l
l itis as wel l as decreas ing “heart action,
”decreasing e le
vated b lood pressure , treating neuralg ias , antipyresis , re
ducing rheumatic pains , etc . Our story goes back to thefather of homeopathy , the Germanphysician and theori st,Samuel C . Hahnemann ( 17 5 5 - 184 3 ) who was apparentlyrebel l ing against the so—cal led “
orthodox med ical systemof the day which often consisted ofwhat came to be known
as Heroic Medicine , e .g . , bleeding , purging , cupping ,bl isteri ng and sweating (wouldn’
t Galen have been proudthat his teachings from the F irst Century A.D. were sti l lpopular inthe 18th and 19th Hahnemann,
who
had conventional med ical training , formulated at the end of
the 18th Century the fundamental law of homeopathy :
s imi las , s imi l ibus , curantur (“l ike may be cured by
OC TOB ER 1985
l ike ) .IIn an explanatory brochure pub l ished under the
auspices of theU S . HomeopathicAssociation, it is stated ,
“The science of homeopathy rests on the principle that
i l lnesses result from natural causes , and that substancesanimal , vegetab le , mineral and chemical when given in
large doses to a healthy person wil l cause known i l lness
l ike reactions . In homeopathy , an i l lness is treated by
g iving the patientminute doses of a substance or substancesthat produce a set of symptoms identical to that of the
i l lness . (Wel l , somuch for that res ipsa loquitur. Keepquiet, Mack play it again,
The treatment ofMonk shoodAKAaconite poisoning is ,as you have guessed , symptomatic . Ingestion of anyamount of this quite tox ic compound should probably require you to administer ipecac syrup rather promptly (unless the conditionof the patient contraindicates this emetic)fol lowed by activated charcoal and a sal ine cathartic . It is
probab ly w ise to observe the patient via monitors , etc . for
cardiac or respiratory depression. More specific treatment
is directed toward the management of card iac arrhythmias
should they occur. Apparently bradycardia is quite common in th is poisoning and thus atropine assumes the role ofthe drug of choice if such an adverse effect occurs .
Th is is the 40th Anniversary of the end of WW II . Aslud icrous as it seems to me now , I can recal l vividly mytreatment for the sore throats incurred by my fel low shipmate s . Inmy role as a Pharrnacist
’
s Mate Third Class on asupply sh ip inthe Pacific 1 fol lowed the Navy
’
s instructionsand painted the ir throats with merthiolate (Oh H ippocrates ,
please forgive
References1 . Kaufman. M. Homeopath y InAmerica. Bal timore , Johns Hopk ins UniversityPre ss . 197 1. pp. 28-4 7 .

LEARNING EXPERIENCES FROM UNC
Thirst , Dehydration, and Old Age
Wi l l iam B . B lythe , MD .
0 The e lderly may need more wa ter than they think they need .
AS both seasoned physiciana nd October intern unfortunate ly know too wel l , dehydration is more dangerous
and much more common in the e lderly patient than in
younger adults . Why?
The increased hazard of dehydration in the older group is
due to blunting of the cardiovascular reflexes which re
spond to , and minimize the effects of , depletion of the
plasma volume . Thus , for a g iven loss in plasma volume ,
the older patient is more apt to deve lop symptoms of or
thostatic hypotension and evidence of hypoperfusion of
virtual ly al l organ systems .
The higher prevalence of dehydration in the elderly is
usual ly ascribed to a comb ination of two factors . F irst , the
ag ing k idney is unab le to concentrate urine as wel l as the
youngerone . Thus , for a givendegree ofwaterdeprivation,
the older patient is more apt to sustain a greater loss of
plasma volume than a younger one . The only means bywhich dehydration can be natural ly corrected is by an
increased intake of fluid occasioned by thirst; and thus theneed for the second factor to explain the frequency of
dehydration in older people . The trad itional view has beenthat, as a consequence of the slugg ish cardiovascular re
sponse to dehydration or to il lness per s e , d iminishedmental awareness and confusion deve lop, thirst is abolished or decreased and dehydration thereby begets furtherdehydration.
From the Department of Med icine , UNC , Chapel H il l 2 7 5 14 .
5 20
Thus , in this construct, at least some s l ightening of
mental acuity is necessary for diminished thirst.
A recent important study suggests that even the latter is
not essential and mak es it even clearer as to why dehydra
tion is so common in the e lderly . Investigators in Oxford ,
England stud ied the effectofwater deprivation for 24 hours
on th irst sensation in a group of“
healthy , e lderly men and a
control group of healthy , young men. After the period of
water deprivation, both groups were asked to rate the de
gree of thirstoccasioned by the water depri vation and then,
during the fol lowing hour , to drink the amount of water
needed to assuage the ir thirst.
The results are fascinating . Despite the fact that the
stimul i for thirstwere stronger in the oldermen, they were
less thirsty and drank significantly less water during the
repletion period than did the younger men.
Those who care for the e lderly take heed ! F luid losses via
mild gastrointestinal i l lness ormodest diuretic therapy maynot invoke thirst in this group and dehydration and plasma
volume deficits may progress to a dangerous degree , even
though there is no change inmental acuity . There may be
times in the nursing home or hospital whenwater should be
prescribed ! It is cheaper and may save more l ives than
expens ive and fancier nostrums .
Reference
1. Phil lips PA, Rol ls BJ . LedinghamJGG , et al. Reduced thirst afterwaterdepriva
tion in healthy e lderly men. N Engl J Med 1984 23 1 -9 .
VOL . 4 6 ,No . 10

PROFESSIONAL USE INFORMATION
DESCRIPTIONCARDIZEIII ® Idiltlazemhydrochloride) Is a calciumIon Influx
inhibitor Islowchannel blockerorcalclumantagonist). Chemically.diltlazemhydrochloride is 1.S Benzoth IazepIMISHIone.3-Iacety loxy)-5 -IdimethylamInolethyI1 -dihydro-2-I4 -methoxyphenyI)monohydtochlmide.l+ ) -cis The chemical structure Is;
CHQCHQNICH 3 I2
Diltiazemhydrochloride Is awhile tooff-whitecry stallinepowderwith aoldertaste. It is soluble inwater.methanol. and chloroform.
It has amolecularweight of Each tablet of CARDI ZEMcontains eIther 30mg or 60mg diltlazemhydrochlorlde fororaladmlnislration.
CLINICAL PHARMACOLOGYThe therapeutic benefits achievedwithCARDIZEMare beIIeved
to be related to Its abIIIty to Int It the influx of calclum Ionsduringmembrane depolarizationof catdlac and vascular smooth
musce.Mochanlsms of Actlon. Although precisemechanisms of Its
antian
glnal actions arestill beingdelineated, CARDIZEMis believed
toact nthe lollowIn ways:1 . AngIna Due to monary Artery Spasm: CARDIZEMhas beenshowntobeapotentdilatorofcoronary anetles bothepicardIaIand subendocardlal. Spontaneous andergonovIne-Induced coronary artery spasmate Inhibited byCARDIZEM.
2 . Exenional Angina CARDIZEMhas been shown to produceincreases inexercise tolerance. probably due to Its ability toreducemyocardial oxygendemand. ThIs Is accomplished vIareductions inbeantaleandsystemlcbloodpressureatsubmaximalandmaximal exercisework loads.
Inanimal models . diltiazemInlexfetes wlth the slow Inward(depolarizing) cunentInexcitable tlssue. Itcauses excllatIon-conbactlonuncoupling Invarious myocardial tissues without changes Intheconfigurationof the actlonpotential . Diltiazemproduces relaxationof coronary vascularsmoothmuscle and dilationof both large andsmall coronary anerles at drug levels which cause“the or nonegative inol ioplceffect. The resultant Increases Incoronary bloodflowIepicardial and subendocatdlal)occurInIschemlcandnonischemicmodels and are accompanied by dose-dependentdecreases Insyslemlcbloodpressure and decreases inperipheral reslstance.Remodynamlc and Electrophys lolog le Effects . LIke other
calciumantagonists.diltiazemdecreases slncatrial andatrioventricuIat conductioninIsolated tissues andhasanegatlve lnohopIceffectInIsolatedpreparations. Inthe Intactanimal.prolongationof theAHinterval canbe seenat higherdoses.
Inman.dlItIazemprevents spontaneous andergonovine-ptovokedcoronary artery spasm. Itcauses adecrease Inperipheral vascqresistance and amodest fall Inblood pressure and, Inexercisetolerance studies inpatientswlth Ischemlcheart disease. reducesthe bean rate-blood pressure product for any givenwork load.Studies todate.primarily inpatIenlswithgoodventricularfunction.have not revealed evidence of anegative lnolropic effect: cardiacoutput. electionfraction. and leftventricularend diastolicpressurehavenotbeenal lectet ereare as yet fewdatacuthe Interactlonofdiltiazemandbeta-blockers.RestingheartrateIsusuallyunchangedorslightly reduced by diltlazem.
Intravenous dllfiazemIndoses of 20mgprolongsAll conductionllmeandAVnodefunctional andeffectlverefractory pei lods approxlmately 2096. Ina study involvlng slngle oral doses of 300 mg ofCARDIZEM In six normal volunteers , the average maximumPRprolongationwas 1496withnoinstances ofgreaterthanfirst-degreeAVblock.DIltIazem-assoclatedprolongationoftheAll Interval isnotmutepronounced Inpatientswithfirst-degreeheartblock. Inpatientswith sick sinus syndrome. diltiazemsignIIicantly prolongs sinuscycle length (upto5096 Insome cases).Chronicoral admInIstralIonofCARDIZEMIndoses ofupto240mg/day has resulted insmall Increases inPRInterval, bul has notusuallyproduced abnormal prolongation.Therewere. however. threeinstances of second-degree AV block and one instance of thIrddegreeAVblock Inagroupof 959 chronically treatedpatients.
Phannacoklnotlcs and Metabolls in. DilliazemIS absorbedfromthe tabletformulationtoabout8096ofareferencecapsuleandIs subIecl to an extensive Ilfst-pass el lect. givin an absolutebloavallabIlIty (compared toIntravenousdosInglol about CARDIZEMundergoes extensive hepaticmetabolismInwhlch 296 to496of theuncha ed dru
gappears Intheurlne. Inviltobinding studies show
CAROI EMIs 096 to8096 bound toplasmaproteins . Competitiveligand binding studies have alsoshownCARDIZEMbIndIng Is notaltered by therapeutlcconcentrations ofdigoxIn. hydrochlotothiazlde,
phenylbutazone. propranolol. sallcyIIc acid. Ofwarf ai in. Singleoral
doses of 30 lo 120mg ofCARDI EMresult Indelectable plasmalevelswithin30 lo60minutes andpeak plasma levels twotothreehours after drug admlnIsltatIon. The plasma ellminatlon hall -lifefollowing sIngleormultlpledrug adminlsl iallonIs approximatelyhours.Desacelyl diltiazemls alsopresent Intheplasmaat levels of1096 to 2096 of the parent drug and Is 2596 to 5096 as potent acoronary vasodilator as diltlazem. Therapeullc blood levels ofCARDIZEMappeartobe inthe rangeof 50 to200ng/ml.There is adeparture fromdose-linearity whenslngle doses above 60m are
given: a120-mgdosegaveblood levels three tlmes thatofthe6 -mgdose. There Is no Informationabout the effectof renal orhepaticImpairmentonexcretionOImetabollsmof dlll iazem.
INDICATIONS ANDUSAGE1. AnginaPoctorls Due toCoronaryArtery Spasm.CARDIZEM
Is lndIcated inthe treatmentofanglnapectorlsduetocoronaryartery spasm. CARDIZEMhas been shown effective in thetreatmentofspontaneous coronaryartery _
spasmpresenting asPrinzmelal
'
s variant anglna (resting anglnawlth SI -segmentelevationoccunlng durlng attacks).
2. ChronlcStableAngina (Cla sh: Elton-AssociatedAnglos ) .CARDIZEMIs Indicated inthemana ementof chronic stableangina. CARDIZEMhas beeneffectwe incontrolled trials inreducing anglna frequency and Increaslng exetclse tolerance.
Therearenocontrolled studles oftheeffectiveness oftheconcomietant use of dlltlazemand beta-blockers OI of the safety of thiscomblnationinpatientswith impalredventricularfunctionorconductlonabnormalities.
CONTRAINDICATIONSCARDIZEM is contraIndlcaled in (1) patients with sick slnus
s meexceptinthepresenceofaIunclloningventricularpawmaker.I I patients with second or thIrd-degreeAVblock except in thepresence of a Iunclloning ventricular pacemaker. and I3) patientswith hypotension(less than90mmHg systollc).
WARNINGS1. Canl lac Conductlon. CARDIZEMprolongs AVnode refractory periodswithoutsignificantlyprolonglng sinus node recove
qtime. except inpatlenls wlth sIck sinus syndrome. This
e ectmayrarelyresultInabnormallyslowheart rates“
cularlyinpatlentswlthslck sinus syndrome)orsecond orthrd-degieeAVblock Islxof 1243 patients for Concomitantuseofdlltiazemwithbeta-blockers ordigltalfsmay result inadditiveeffects oncardlac conductlon. Apatlenl wlth Prlnzmelal
'
s
anglnadeveloped periods of asystole I2 10 5 seconds) afterasingle doseof60mg of diltiazem.
2 . CongestlveRoanFallon .AlthoughdiltlazemhasanegativeInotroplceffectInisolated animal llssuepreparations , hemodynamicstudles Inhumans with normal venlrlcular functionhave notshowna reductionIncardiac indexnor consistent negativeeffects oncontractility Idp/ dt). Ex dance with lhe use ofCARDIZEMalone01 Incombinationw hbeta-blockers inpatlentswlth impalredventricularfunctlonIs very limlted.Cautlonshouldbe exercisedwhenusing the drug insuchpatIents.
3. Hypotension. Decreases inblood pressure associatedwithCARDIZEMtherapymay occasionally result Insymptomatichypotension.
4.Acute Repatle Inlury. Inrare Instances, patIents receivingCARDIZEMhave exhibited reverslble acute hepatic Injury asevidenced bymoderate toextremeelevations of liverenzymes.(SeePRECAUTIONS andADVERSEREACTIONS.)
PRECAUTIONSGeneral .CARDIZEMIdlItIazemhydrochloride) is extensivelymetab
olizedbythe liverandexcretedby the kidneys andInbile.Aswlthanynewdrugglvenoverprolongedperiods. laboratoryparameters shouldbe monitored at regular intervals. The drug should be used wlthcautionInpatients with ImpaIred renal orhepallc function. Insubacute and chronlcdog and ratstudies deslgned toproduce toxIcIty.high doses of diltIazemwere associatedwlth hepallc damage. Inspecial subacute hepatic studies. oral doses of 125 mg/ kg andhigher inratswereassociatedwithhIstological changes inthe liverwhich were reversible whenthe drug was dlscontlnued. Indogs.doses of 20mg/ kg were also associated wlth hepatic changes:however. these changeswere reversiblewlth continued dosing.Drug lntouctlon. Pharmacologic studies indicate that theremay be addltive effects Inprolonging AVconductlonwhenusingbeta-blockers or digitalls concomllantly wlth CARDIZEM. (SeeWARNINGS).Controlled anduncontrolled domestlc studies suggest that con
comIlantuseofCARDIZEMand beta-blockers OI digitalls lsusuallywell tolerated. Aval lable dataare not sufficient, however. topredicttheeffectsofconcomitanttreatment.particularlyInpatientswlth leftventriculardyslunctlonorcardiacconductionabnormalltlas . Inhealthyvolunteers. diltiazemhas beenshown to Increase serumdlgoxlnlevels upto2096.
Carclnogonos ls, Mutagonesls. Impairment of Fortll lty. A24-month study Inrats and a 21-monlh study inmice showed noevidenceofcarcinogenlcltyTherewas alsonomulagenicresponse
{it Invitrobactei lal tests .NoInhlnslceffectonlettillly wasobservedit rats.
Pregnancy. Category C. Reproductlonstudies have beenconducted inmice. rats. and rab ts. Administrationof doses tanglngfromflve to ten tlmes greater (on 3 mg/ kg basis) than the dailyrecommended therapeutic dose has resulted Inembryo and fetallethality.Thesedoses. insome studies.havebeenreportedtocauseskeletal abnormalities. IntheperInataI/poslnatal studies. therewassome reducllonInearly lndivldual pupwelghts and survival rates.
Therewas anIncreasedIncidenceofstIIIbInhs atdoses of20timesthe humandoseorgreater.Therearenowell-controlled studies Inpregnantwomen: therefore.
use CARDIZEMIn pregnant womenonly If the polenl lal benelltIustIe s thepotentlal ilsk tothe fetus.Nurs lngMothers . It Isnot knownwhetherthis drug Is excreted
inhumanmilk. Becausemany dru s are excreted Inhumanmilk ,
exerclse cautionwhenCARDIZE Is admlnlsteied to a nutslngwomanif lhe drug
‘
s benefits are thought tooutwelgh its potenllalrisks Inthis sItualIon.
Pedlatrlc Use. Safety and effectiveness inchildrenhave notbeenestablished.
ADVERSEREACTIONSSerlous adversereactions have beenrate instudies carriedoutto
dale.butItshouldberecognizedthal pal ienlswlthImpaltedventricularfunctionandcardiacconductlonabnmmalil les haveusuallybeenexcluded.Indomestic placebo-controlled trials. the incidence of adverse
reactions reported during CARDIZEMtherapywas not greater thanthat reported durlng placebotherapy.The followlng representoccurrences observed inclinical studies
whichcanbe at leastreasonablyassociatedwith thepharmacologyof calcium Influx inhibition. Inman cases. the relationship toCARDIZEMhas notbeenestabllshed. hemostcommonoccunences.as well as their frequency of presentation, are: edema
headache nausea dlzzlness rash II .396).asthenla AVblock Inaddition. the following eventswere reponed Infrequently (lessth an196)with theorderofpresentalIoncorresponding to the relative frequency ofoccunence.
Cardiovascular: Flushing. anhythmla, hypotension. bradycardia. palpitations. congestive heart Iallure.
syncope.
Paresthes ia, nervousness. somnolence,Nervous System:
tremor, Insomnla.hallucinations.andamnesiaGastiolntesllnal : Constlpation. dyspepsla. diarrhea. vomitlng ,
mildelevatlonsofalkalinephosphatase.SCOT.SGPT, and LOH.
Dermatologlc; Prurltus, petechiae.urtIcatIa, photosensltivity.Other: Polyui ia, occluda.
The followingaddItIonal experIences have beennoted;
Apatle_
ntwth Prlnzmetal‘
s anglna oxperlenclng episodes ofvasospastlc an Ina developed periods of tlansIenl asymptomaticasyslole approxmately flve hours after receiving a single 60mgdoseofCARDIZEM.
The following postmarketln events have been reported Infrequently Inpatients tece Ing C RDIZEM: erythemamultilonne; Ieukopenia; and extreme elevations of al kal ine phosphatase. SGOT.SGPT, LDIl .andCPK. However, adefinitivecauseandeffectbetweentheseevents andCARDIZEMtherapy is yet tobe established.
OVERDOSAGEOREXAGGERATEDRESPONSEOverdosage experience with oral dlltlazemhas been limlled.
Slngleoral doses of 300mgofCARDIZEMhavebeenwell toleratedby healthy volunleers. Inthe eventof overdosage or exaggeratedresponse. approptlate su
pportivemeasures should be employed In
additiontogastric lavage. be followingmeasure smaybeconsidered:Bradycatdla AdmInIslet atropine to mg). If there
is noresponse tovagal blockade. adminlsterIsomolerenol cautiousl
High-DegreeAV Treat as for bradycat 13 above. l ed high
Block degreeAVblock should be heatedwith catdIacpacing.AdministerIncltoplcagents Iisoptoterenol.dopamine. ordobutamlne) and diuretics.Vasopressors leg, dopamine or Ievarterenolbltartrale).
Actual treatmentand dosage shoulddependontheseverity oftheclinical sltuationand the judgment and experience of the tre ataphysiclan.The cial/LDSU
‘
s inmlce and rats range from415 to740mg/ kgand from560 to810mg/ kg. respectivelyThe Intravenous L0
'
s inthese specieswere60 and 38mg/ kg, respectivelyTheoral LIIsoindogs Is consldered tobe inexcess of 50mg/ kg.while Iethal lty wasseeninmonkeys a1380mg/ kg.The toxicdose inmanIs not known,butblood levels Inexcess of 800 ng/ml have not beenassoclatedwlth toxicity
DOSAGEANDADMINISTRATIONEn rtlonal Anglna Poetons Due toAthm sclerotlc Coro
naryArtery Disease orAngina PretorIs atRestDue tocoronary Artery Spam . Dosagemust be adiusled toeach pal lenl
'
s
needs. StartIng wlth 30mg four times dail beforemeals and atbedtlme, dosage should be Increased gt ually Iglven Indl deddoses three or four tlmes daily) at one to two-day Intervals untiloptimumresponse is obtained. Although lndivldual patients mayrespond to any dosage level. the average optImumdosage rangeappeal s tobe 180 to240mg/ dayTherearenoavailabledataconcernIng dosage requirements inpal ienls wlth Impaired renal OI hepal lclunctlon. Ifthedrugmustbeused insuchpatients.titrationshouldbecarriedOul withpartlcularcaution.ConcomltantUseWithOtherAntlanglnal Agents1. Subllngual NTGmay be taken as requlted toabonacuteanginal attacks during CARDIZEMtherapy.
2. Prophylactic NltratoTherapy—CARplZEMmay be safely
coadmlnlsteredwlth short and ong-actmg nitrates. but therehave beenno contro lled studies toevaluate the anllanginaletfecllveness of this combination.
3 . Beta-blockers . (SeeWARNINGS and PRECAUTIONS.)
ROWSUPPLIEDCatdizem30mg tablets are supplled Inbottles of 100 INDC
0088-1771-4 7 ) and inUnitDose IdentificationPaks of 100 INOC0088-1771 Eachgreentablet Is engravedwlthMARIONononeside and 17 71 e raved on lhe other. CARDIZEM60mg scoredtablets aresuppli Inbott les of 100INDC00884 7 724 7 )andInUnItDose ldenlIfIcatIonPaks of 100 INDC0088-1772 Each yellowtablet is engravedwithMARIONonone side and 17 72 ontheother.
Issued
CardiacFailureHypotension
AnotherpatIentbene l l l product from
PHARMACEUTICAL DIVISIONMAR IO NLABORATOR I ES . INC .
KAN SAS C ITY . M I S S OUR I 5 4 1 3 7
LEARNINGWITHOUTWORK
Peritonitis in a Patient on Continuous
Ambulatory Peritoneal Dialys is
Debra A. He ldman, MD .
0 Report of a case of peritonitis caused by the fungus F usa rr'
um oxysporum.
VER the past decade , continuous ambulatory peritoneal dialysis (CAPD) has become an accepted and
increasingly util ized method of treating patients w ith
chronic renal failure . Its advantages over hemod ialys is
include lower cost, increased patient mob i l ity , higher
hemog lob in concentration, fewer fluid and e lectrolyte re
strictions , better b iochemical balance , and better control ofblood pressure .
The most frequent seri ous compl ication of CAPD is
peritonitis which occurs every year or two in the average
patient. Vas et allrequire at least two of the fol lowing three
criteria to establ ish a diagnos is of peri tonitis . I ) abdominalpainor tenderness , 2 ) peritoneal fluid w ith greater than lOQ_
neutrophils/mm3, and 3 ) organisms in the peritoneal fluid .
G ram pos i tive org ani sms ( usual ly S taphy lococcus
epidermidis , Staph . aureus , or Streptococcus) cause 60
7 0% of cases and gramnegative organisms (usual ly E . col i ,
Pseudomonas , Klebsie l la , or Enterobacter) cause 15 ~
"3The remaining cases are caused by anaerobes , less
common bacterial species , or fung i .I recently cared for a patientonCAPDwho had peritonitis due to an unusual organism. This patientwas a 4 I
-
year
old b lack womanw ith chronic renal failure who had beenonCAPD for three years . Two week s before admission toour hospital , she deve loped d iffuse abdominal pain,
nausea , vomiting , and low-
grade fever. When she initial lydeveloped these symptoms , she was admitted to another
hospital and felt to have bacterial peritonitis . She was
treated for three days with intraperitoneal cephalothin but
her peritoneal fluid showed fewer than 100 neutrophi ls/
mm3 and cultures were negative . Her symptoms did not
improve and she came to us for another opinion. Her
temperature was C and she had bi lateral lower quadrant tenderness . The peri pheral white b lood cel l count was
the peritoneal fluid had 4 7 white ce l ls/mm3 with49% neutrophils . An abdominal echogram showed smal lk idneys ; there was no perinephric fluid col lection or evi
dence of loculation e lsewhere . She was admitted to our
hospital and was treated empirical ly w ith intravenous andintraperitoneal tobramycin. This was discontinued on the
third hospital day when peritoneal , b lood , and urine cul
tures were negative . Subsequently , the peritoneal fluid
From the Department of Med icine , Duke University Medical Center,Durham 27 7 10 .
Oc roaen 1985 , NCMJ
F igure 1 . F usarr'
um oxysporum growing on agar .
grew a fungus identified as Fusarium oxysporum. (See
figures I and
Fusarium is a mold found in the soi l and air throughout
the United States , especial ly in the Southeast. Human in
fections with Fusarium are uncommon but have been described in keratitis , endophthalmitis , burn infections , brainabscess , osteomye l itis , sk in infections , septic arthritis , and
disseminated opportunistic infection.
Three cases of peri tonitis caused by Fusarium have beenreported previous ly , al l tnpatients onCAPD.
4 5 Fusarium
i s or rapidly becomes resistant to antifungal agents .
4 6
McNee ly et al4described two cases of Fusariumperitonitis ,
one caused by F . moni l iforme , the other by F . oxysporum.
In both cases , the organism had or deve loped re sistance toamphotericin, 5 -fluorocytosine , and miconazole . Kerr et
alsdescribed one case of peritonitis caused by a Fusarium
species onwhich sensitivity testing was not done . In addi
tion to be ing resistant to antifungal agents , Fusarium hasbeen shown to adhere to and invade the wal l of the peri
toneal catheter of a patient.
4Both of these factors are
important considerations in determining the appropriate
therapy for Fusarium peritonitis .
4 McNee ly et al4treated

F igure 2 . F . oxysporum spores on lactophenol s l ide , unsta ined .
magnification x 13 00 .
the first of the ir patients with miconazole inuaperitoneal lyfor 2 1 days duri ng which time the peritoneal cultures re
mained positive for Fusarium. After removal of the section
of peritoneal catheter harboring a Fusarium “vegetation,
the cultures became negative . They successful ly treated
the ir second patient with catheter removal only . Kerr et al
treated their patient with Fusarium peritonitis with I .V .
amphotericin and catheter removal . 5
Since these three previously described cases showed
little or no benefit fromantifungal drugs , we elected to treat
our patient just by removing the Tenckhoff catheter. Cul
tures of the catheter tip and subcutaneous cuffwere positivefor Fusarium oxysporum . After catheter removal , the pa
tient did wel l w ith resolution of her symptoms . She was
hemodialyzed for three week s after which the catheter was
replaced . She has continued to do wel l three months aftercatheter replacement.
5 2 2 VOL . 46 , No . 10
Fusarium is one of several fung i thatcancause peritonitis
in patients onCAPD. Five to fifteenpercent of al l cases of
peritonitis in the se patients are caused by a fungal
organism .
3 ' 5 ' 7 In add ition to Fusarium , these organismshave included Candida alb icans , Cand ida paraspilosis ,Candida tropica l is , Torulops is g lubrata , Trichodermaviride , Exophiala jeanse lme i , Drechslera spicifera , Orech
slera austral iensis , Mucor sp. , Trichosporum sp.,Rhodo
torula rubra , and Asperg il lus fumigatus . Most cases have
been secondary toCandida with only a few cases caused byother species .
Thus , CAPD represents amajor advance inour ab il ity totreat chronic renal failure . An appreciation of the risk of
peritonitis and the organisms that cause it is necessary forsuccessful use of this form of dialysis . Symptoms of fungal
peritonitis mimic those of the more commonbacterial peritonitis (abdominal pain, fever , and cloudy peritoneal fluidwith increased neutrophils) . The management of fungal
peritonitis is controversial . Some favor early catheter temoval in al l cases . However , others have reported success
ful treatment of sensitive organisms with appropriate in
trapcritoneal (with or without intravenous) antifungal therepy .
References
I . Vas SI: Microbiologic aspects of chronic ambulatory peritoneal dialysis . K idneyInt l 983 :2 3 :83 -92 .
2 . Gokal R. Francis DMA. GoodshipTHJ. BintAI . Ramos 1M. c erRE. Proud
G .Ward MK . Ken DNS: Peritonitis in continuous ambulatory peritoneal dialysis. L ancet l 982 :2 : 13 88-9 l .
3 . Cecchin E. DeMarchi S . Panare l lo G FranceschinA. Chiaradia V . Santini G .
Tesio F: Torulopsis glabrata peritonitis complicating continuous ambulatoryperitoneal dialysis: successful management with oral 5 ~ fluorocytosine . Am J
K idney Dis l 984 :4 ;280-4 .
4 . McNee DJ. Vas SI . Dombros N . Oreopoulos DG : Fusarium peritonitis: an
uncommoncomplicationofcontinuous ambulatory peritoneal dialysis. Peritoneal
Dial Bul l l 98 1: 1194 -6.
S . K errCM. Perfect JR. CravenPC . JorgensenI H .Drutz DI . She lbumc JD. Gal lis
HA. Gutman RA.Fungal peritonitis In patients on continuous ambulatory peri~toneal dialysis. Ann Intern Med 1983 9 933 34 -7 .
6 . Jones DB . ForsterRK. Rebel laO: Fusarium solani keratitis treated with natamycin (pimaricin) . Arch Ophthal 197 2 t88314 7 -5 4 .
7 . CecchinE. Panarel loG .DeMarchi S : Fungal peritonitis inambulatory peritoneal
d ialysis ( letter) . Ann Intern Med

Agreat way of lite.
Hence , they periodical ly chal lenge themselves to do more
inthe way of provid ing value added”health care services
to their patients while keeping their fees below those of
most of the ir peers .
Another group practice in its initial formative stage of
assoc iation has created a work ing committee whose sole
ass ignment is to critical ly evaluate alternative de l ivery sys
tems . It is particularly on the lookout forwhere the“bl ind
side competition”w il l be coming from. The committee
members play devil 's advocates inprojecting how , if theywere various other competing prov iders , they wouldattempt to compete with their own entity .
,
Alert to Competitors
And a fami ly practice groupwe know ofmeets regularlyto discuss and hopeful ly discover competitive approaches
of which the ir“col leagues (who real ly are the ir competi
tors in the same service area) e ither are unaware or are
ignori ng . This group’
s forum is an informal“rap
"session
during which the doctors attempt, among other things , to
l ist as many consumer concerns as poss ib le for the k inds ofhealth services they provide . In other words , their orientation is not what services the doctors provide (a product
”
orientation) butwhat benefits the irpatients derive (a ‘
con
sumer”orientation) .
5 24 VOL . 4 6 , No . 10
This k ind of brainstorming led the family practice groupto begin marketing a
“heal th wel l -being education ser
vice to people who purchase home health care k its in theemerging self-care market. The doctors be l ieve they can
position themselves as the premier health care informationsource to consumers who remain apprehens ive about administering and understanding sel f-care products after the
purchase of such products .
Just as entrepreneurs who started vastly successful high
tech companies ( l ike Wang , Apple and lesser successes) ,these entrepreneurial ly
-minded famil y practitioners are
keeping the ir focus on the consumer . They fol low a“re in
vigoration process to be sure they stay close ly enough
attuned to the buyers of their services to keep theirmomentum going .
Risk Takers , But Adapters
Entrepreneuri al phys icians reflect a tension common toal l risk takers they are not that concerned over security .
That is , they are personal ly not afraid to fail or lose the ir
investment as part of the pri ce for special accompl ishment.
Indeed , they thrive on chal lenge and hard work so long as
they are part of something new . Family values caneasily be
shunted to the wayside by such people , but interesting lymost of these doctors we have seen appear blessed withcontinued good perspectives on the ir whole l ives .
Perhaps part of the ir sense of perspective , the entre
preneur doctors accept the need for thought processes that
mostphysicians reject as notwithin the ir training . They are
active in forecasting revenues and overal l budgeting , in
evaluating costs and capital requirements and in the harddiscipl ine of strategic planning . One group of just fourpartners in a nearby state , for example , has assembled a
200-
page prospectus describ ing the group; their avowed
purpose is to attract major corporate financing for theirexpansionplans w ithin the HMO , PFC , etc . environment.
F inal ly , entrepreneurial phys icians share supportive
value systems and anoptimistic corporate culture . Whereasmany others inmedicine see only negativism and external
meddl ing by outside forces in these turbulent times , theentrepreneurs seem to accept free enterprise and competition. They look upon the prob lems facing health care as
opportunities to be capital ized upon in hopes that these
opportunities w i l l result in better health care and increasedconsumer satisfaction, wh ile benefiting themse lves and
their groups .
Conclus ion
Today , we l ive in an era of innovation and entrepre
neurial drive . This fact is true in every other industry , and
there is no reason to exempt health care from the patterns .
As events seem to overwhe lmmost doctors , and in the longrun we fear that events wil l in fact do so , entrepreneurial
physicians promise to be the people who w il l adapt andprosper . Grouppractices with such people intheirmidst areindeed blessed , though poss ibly uneasy .

CONJOINT REPORT
The State of the State
Ronald H . L evine , M .D. , MPH
0 Dr . L evine reviewed the hea l th of North Carol ina in this address a t theAnnua lMeeting of the North Carol ina Med ica l Society onMay 3 1985 .
T is anhonor to once againcarry outmy statutory obl igaI tionof presenting to the phys icians ofNorth Carol ina as
we l l as themembers of the Health Commiss ion a review of
the major publ ic health accompl ishments of the year past.
Just last week the latest results of The North Carol ina
Citizen Survey became availab le . I was struck by the finding that over a third of our adult population indicated they
had one or more of the fol lowing diseases : h igh b loodpressure , heart disease , stroke or glaucoma . Add arthritis
and the percentage increases to The staggering futureeconomic burden that faces us as a state and nation as a
result ofmorbidity and mortal ity among tomorrow ’
s ag ing
population has led me to devote a sizab le section of this
d iscussion to the topic of health promotion efforts inNorth
Carol ina . F irst, however , let me review some of _the
achievements recently recorded , much of them with your
help and support .
During the last several years the provis ionof health careto tuberculos is patients has changed dramatical ly fromsaniton
’
um-dwel l ing to a community-based approach . Re
l iance upon the 12 acute care hospitals and our local healthdepartments , now our front l ine against th is disease , has not
compromised the control program.
We found that 4 1% of newly pos itive TB cases on
treatment converted their sputum to negative w ithin threemonths and that 7 1% had converted within six months .
Eighty- three percent of patients who were started on drugs
completed the prescribed course of therapy . Eighty-e ight
percent of close contacts of patients were examined within
14 days ofwhen the local heal th departmentwas notified .
F orty-seven percent who were on preventive therapywith INH completed the prescribed l Z-month course of
treatment.Although al l these ind ices fal l short of the idealthey do ind icate , as does our fal l ing incidence rate , that the
closure of the sanitoria has not led to a decrease inprogramqual ity . Ad isturb ing note is that there were two outbreaksof disease caused by drug
-resistantmycobacterium tuber
culos is in our state . One of these strains is the first ever
documented to be res istant to four drugs .
In the area of Sexual ly transmitted diseases , reported
gonorrhea cases ( including mi l itary morb idity) decreasedfor the second consecutive year. During 1984 , more thanone quartermil l ion women in fami ly planning cl inics andel sewhere were screened for gonorrhea and sl ightly less
than 5% were positive . This screening effort , coupled with
referral of sex partners for examinationand patientcounse l
From the Division of Health Services , Box 209 I , Raleigh 27 602 -209 1 .
OC TOB ER 1985 , NCMJ
ing and treatment, has played a large part inthe reductionof
this disease .
Drug resistance is a problem with this bacterium also .
We saw an increase from 24 cases with penici l l in- resistant
strains during 1983 to 62 cases during 1984 . These were
reported from 15 different counties during 1984 , compared
with only 10 counties the previous year .
Early syphil is cases decreased for the first time in fiveyears . Although the decrease was only l % , this reversal of
the upward trend is encourag ing . We only had two cases of
congenital syphil is in 1984 . We should not have any !
An area of present and future concern is the AIDS problem. The acquired immunodeficiency syndrome was firstdescribed in 198 1 and was quickly recognized as an almostuniversal ly fatal disease . North Carol ina has reported 7 5patients with the disease and 5 3 of those have already died .
A primary concern is that infected persons may con
taminate the nation’
s b lood supply . OnMarch 2 , the Food
and Drug Administration l icensed a test for b lood banks touse to detect antibodies to the presumed causative agent.
B lood showing a positive finding w i l l be d iscarded and the“
donor wi l l be informed .
"The”Centers for Disease Control is intent upon dis
couraging concerned high- risk individuals from donatingb lood just for the purpose of receiving a screening test atblood bank s and thereby increasing the danger to the blood
supply due to poss ib le false negative tests . They have
cal led upon us and we have agreed to set up alternative
diversionary testing sites across the state . The sites wil l be
located in most local health departments . [See NCMJ
l 985 ;46 :3 5 3 The North Carol ina State Laboratoryw il l perform the screening tests and obtain confirmatorytests , if indicated , onb lood specimens drawn at local heal thfacil ities . The individual w i l l rece ive pretest counsel ing ,
post- test counse l ing if test results are positive , and referral
for medical evaluation. Printed materials wi l l be madeavai lable to assist in these counse l ing ; sess ions . Personne l
from the Venereal Disease Control Program w il l be re
assigned in order to assist counties with this effort . Please
do not hesitate to cal l orwrite our agency if youwould l ike
more information on this effort .
In the area ofDental Health , we continue to improve ourfluoridation coverage throughout the state . The fluoridecontent ofwater suppl ies is being adjusted to the optimumlevel in 195 North Carol ina communities ; 26 additional
towns are served by natural ly fluoridated water. Thus 85%
of the population served by a municipal water system is
receiving fluoridated water. An add itional chi ldren

are served by rural school-water fluoridators , and
children in grades K-8 in over 1000 schools in 85 counties
participate in a week ly sodium fluoride mouthrinse program; 80% of these children l ive in non-fluoridated areas .
The 5 5% decrease in dental caries achieved in our state bythe country
’
s # l preventive dentistry program should be
readily recognizable to you when you look in your youngpatients
’
mouths .
Maternal and ch ild care continues to be amajoremphas isof your state and local publ ic health agencies . In 1983 ,
North Carol ina’
s infantmortal ity rate was deaths per
thousand l ive b irths , down from in 1982 . but reflect
ing an unmistak ab le leve l ing of what had been a rather
steady and significant drop in infant mortal ity over a con
s iderable time . The preventionof premature b irths is at thecore of our efforts to te - set inmotion the reduction in infant
mortal ity . As of this date 83 counties have implementedprematurity risk assessment and intervention systems . If
these efforts are successful we expect to see some impacton
the incidence of low b irthweight beginning in 1986 or
1987 . This year we completed the network of 2 1 reg ional
high risk maternity cl inics . Only nine counties remain that
have no publ icly- administered prenatal care for ind igentpregnant women. Unfortunate ly , some of these nine are
among those with the highest infant mortal ity rates in the
state .
Teen age pregnancies remain a prob lem. In 197 9 , North
Carol ina ranked e leventh national ly inthe percentof al l livebirths that occurred to women 19 and under. At that time
one in 13 adolescents aged 15 to 19 became pregnant. Since
then this statistic has worsened . In 1983 one in e leven
North Carol ina teens 15 - 19 became pregnant. Mothers
under 20produced 2 1 percentof al l pregnancies . 17 percent
of l ive b irths , 2 3 percent of low we ight bab ies and 24
percent of the neonatal deaths . Teens were less l ike ly tobeg in theirprenatal care early and less l ike ly to have at leaste ight prenatal v isits . Our Family Planning Program con
tinnes to provide cl inical services to these teenagers but i s
also initiating programs for parents and teenagers on the
subjectof postponing sexual activity . Over 200 ind ividuals
in this state have been trained to use the . Postponing
Sexual Involvement” curriculumdeveloped atEmory Uni
versity . Many of these trainees have inturnoffered trainingin the ir communities and . in some instances, have workedwith local education agencies to incorporate this into theschool curriculum.
Let us turn now to more ih -depth coverage of health
promotionprograms and services inour state . At the turnof
the century the leading causes of death were infectious and
communicable diseases . Gains against these once great
kil lers came as a result of improvements in sanitation,
housing and nutrition and the adventof immunizations and
antib iotics . Maintaining services to prevent infectious and
communicable d iseases among those at risk remains an
important task for pub l ic health .
Today’
s leading k i l lers and cripplers are chronic diseases
and accidents . New methods are needed to address these
causes of death and d isab i l ity . These methods unavoidab lyfocus on l ifesty le change and environmental enhancementas we l l as antic ipatory , h igh
- qual ity medical care .
To understand the need for successful preventive in
5 26
terventions in our state , it is useful to look at data on
premature adultmortal ity , i .e . those deaths occurring be
tween the ages of 18 and 64 . InNorth Carol ina each year
there are approx imate ly deaths from al l causes ,one- th ird of which occur during th is age Span. Thus , 4 5
North Carol inians d ie premature ly each day . This is a tragicwaste . These deaths are occurring during the
“
productive
years of l ife . In fact, in 198 1 almost person-
years
of the adult work ing population of North Carol ina were
lost. The economic impact of these deaths is estimated at
bi l l ion dol lars .
In comparing North Carol ina against the latest nationaldata , we found that age
-adjusted mortal ity rates for cere
brovascular disease are 2 7% higher in North Carol ina,
motor vehicle accidents 10% higher , al l other accidentsl 7% , higher and pneumonia and influenza and nephritis10% higher. Our age
-adjusted heart disease rate is almost9% higher than the nation. In addition. cancer mortal ityappears to be ris ing faster in North Carol ina than in the
United States . Between 197 9 and 198 1 , the state’
s age
adjusted cancer death rate rose by while the national
rate rose byAge
- adjustedmortal ity rates show wide gaps inthe overal l risk ofmortal ity for North Carol ina men versus womenand nonwhites versus whites . In 197 9-8 1 , the male mortality rate was nearly doub le the female rate . The nonwhite
age-adjusted mortal ity rate for both sexes remained more
than 40 percent above the white rate . Th is suggests thatpreventive interventions should be targeted to specific high
risk groups .
As much as 50% of mortal ity may relate to l ifestyle .
Individuals can make modest l ifestyle changes which cansubstantial ly reduce risks for several of the lead ing causesof death . Such measures include but are not l imited to:
reduction of alcohol misusemoderate d ietary changes to reduce excess intake ofcalories , fat, salt, and sugarel imination of cigarette smoking
participation in periodic , targeted screeningadherence to speed laws and seat be lt use
Agrowing number of interventionprograms are demonstrating pos itive health outcomes or impacts . From these
successes , certain characteristics which seem to be effec
tive in reducing heal th risks have been identified .
First is the use of a reasonab ly formal ized risk assess
ment to ass ist ind ividuals in identify ing elevated health
risks . The subsequent referral of those persons who w ish tomake changes in their health behavior via an appropriateintervention program is more l ike ly to lead to some mea
sure of success .
A second characteristic is the use of periodic selective
screening ; let me emphasize notmass multiphas ic screening but se lective screening (determined by age and sex) for
major disorders such as hypertens ion and certain forms ofcancer . This type of screening is much more cost
-effective
and more l ike ly to reveal s ignificant findings that can befurther clarified and diagnosed by the phys icianand lead to
successful early intervention.
A third characteristic of successful programs has beenthe de l iberate use of multiple interventions to address a
specific health problem inaspecific targetpopulation. This
VOL . 46 , No . 10

general population al l attesting to the importance of the
abil ity to understand and adapt th is concept . I think youwi l lbe part icularly interested in this next find ing . Twenty
- five
years ago white male Cal ifornia phys icians were dyingfrom coronary heart disease at a rate 15% higher than
aged-matched non-
physicians . They are now dy ing at a rate
3 1 lower than the control group. Trends inmortal ity from
lung cancer paral le l these findings . It wi l l not be a surprise
for you to hear that 2 5 years ago amajority of male physiclans were cigarette smokers . Today less than 10% of
physicians smoke as compared with 40% of white men
general ly .
Time prevents me from exploring issues of seat be lt use ,
5 28
sedentary l ife style , stress management and other health
behaviors , but I submit that the jury is in, its verd ict is
unassailable and it is now the job of the practitioner, the
university , the health department and anyone e lse who can
lend a hand to convert th is understanding into concerted ,
effective action.
I amconfident that the strong col laborative effort thatwehave demonstrated in the great victories we have together
won and enjoyed in the past over such enemies as com
municable disease , environmental contamination and
maternal mortal ity can and wil l be util ized as we intensifyour efforts to reduce preventable , premature death and
d isab il ity from today’
s major health prob lems .
VO L . 46 , No . 10





Once -da ily
Convenience without compromis eOne capsule
—Once da iiy
The appearance of these capsmes is a reg istere d trademark oi Ayerst Laboratories .
BRIEF SUMMARY {FORFULL PRESCRIB ING iNFORMATiON, SEEPACKAGEC IRCULAR. )
INDERIDEO LA Brand of PROPRANOLOL H YDROCHLOR IDE ( INDERALO LA) andHYDROCHLOROTH IAZ IDE (Long Acting Capsules )No. 4 5 5—Each INDERIDEo LA Capsule conta insPropranolol hyd rochloride ( iNDERAL®LA)Hyd roch IOtolh iaZIGe
No. 4 5 7 Each INDERIOEca LA Capsule containsPropranolol hyd roch loride ( INDERAL0 LA)Hyd roch lorol h iazide
No 4 59—Each INDERIDEO LA 160150 Capsule conta insPropranolol hyd roc h loride ( INDERALo LA) .
Hyd roch loroih iab de
INDERIOE LA is ind icated in the managementof hypert enS ionTh is fixed combination drug tonot ind icated tor Initial therapy oI hype rtens ion. It
the fixed combination repre s ents the dos e titrated to the Ind ividual atlent'
5 nee d s .the rapy with the fixed comb lnationmay be more convenient thanw tth the separate
components .
CONTRAINDICATIONSPropranolol hydroch loride ( INDERALO)Propranolol is contra ind icated ln 1) card iogenic shock . 2 ) s inus bradycard ia and re ater than
firs tdeg ree b lock: 3 ) bro nch ia l asthma. 4 ) congestive heart iatture (seeWARNINGSg) unless the
fa i lure IS second ary to a lachyarrhyl hmia tre atab le With propranololHyd roch loroth laz ideHyd rochloroth iamd e is contraind icated inpatientswith anuriaorhypersensrtivily to this orother
Sulionamide derived d rugs .
WARN INGSPro ranolol hyd roch loride ( INDERALO)CA DIAC FAILURE. Sympathetic stimulationmay be a vital component Support ing circulatoryfunction in patients With congestive heart lai lure and its inh ib ition by beta b lockade maypre cipitate more severe lai lure .Although beta b lockers should be avoided inovencongestiveheart lai lure . it necessary . they can be used with close Iollow-up in patients with a h istory or
la ilure who are we l l compensated . and are re ce iving or italis and d iuretics Be la-adrenerg icb lockih agents do not abol ish the inotropic actionof ig italis on heart muscle
IN ATIENTSW ITHOUTAH ISTORY OF HEARTFAILURE. continued use 01 beta b lockers
THYROTOXICOS IS : Be la b lockade may mask cert 'ain clinical Slgfl§ oi. hypert hyro id ismThere lore . abruptW ithd rawal oi propranololmay be followed by tan iaxacerbation0 1 symptomsol hypert h fOld ISm. includ ing ih ro id stomi Propranolol doe s nbt.d is lon1hyro-d lunction tests
IN PA IENTS WiTH WOLF -PARK INSON WH ITE SYNDROME. seve ral cases have been
re ported inwh ich . alter propranolol . the tachycard ia was rep laced by a severe bradycard iare gumng a demand pacemaker. In one case th is re sulted alter an initial dose of 5 mgpropranolol .
MAJOR SURGERY. The necess ity or des-rab il iiy oI withd rawa l ol beta-b loc k ing therapyprior toma |or Surgery 15 controverS iat It should be noted . however. that the impaire d abi lity orthe heart to respond to re flex ad renerg ic stimuli may augment the risks ol genera l anesthes iaand surg ical procedure s
None i ier Io Bronchos u m leg . chronic bronch itis . emph eeme )—PATIENTS WITHBRONCH SPASTIC DlS ASES SHOULD. IN GENERAL . NOT R CEIVE BETA BLOCKERSINDERAL should be administere d wrih cautionS ince l l may b lock b ronchod i lal ionproduced byendog enous and exogenous catecholamrne s timulationof beta re ceptors .
DIABETES AND HYPOGLYCEMIA Beta-adrenerg ic blockade may prevent the appearance 0 1 certain premoni lory signs and Symptoms (pulse rate and pre ssure changes ) oi acmehypog lycemia in lab ile insulin-dependentd iabetes Inthese patients. l lmay bemore d ili iCuIl toad just the dosage oi insul in Hypog lycemic attacks may be accompanied by a Dfe C Il OUS
e levation 0 ! b lood pre ssure .
Hydroch loroth lez lde :Th iazides s hould be used with caution in severe rena l d isease In patients wrth re nal d iseaseth iazidesmay pre cipitate azotemia Inpatients wunimpa ired renal luhotien. Cumulative e llectsoi the d rug may deve lop
Thiazides snOuld also be used with caution in patients with impaired hepatic lunctiono_
i
progresswe liver d isease S ince minor alteratlbns oi i luid and e lectrolyte balancemay pre cipitate hepatic coma
Th iazidesmay add toorpolenl iale the actionofotherantihypert ensive drug s . Potentiationoccws with gang l ionic orperipheral ad renerg ic b locking drugs
Sens itivity re actions may mom in patients With a h istory 01 allergy or bronchial asthmaThe pOSSibilily oi exacerbation Or activation 0 1 systemic lupus erythematosus has been
report ed .
PRECAUTIONSPropranolol hydroch loride ( INDERALO)GENERAL. Pinpranolol should be used W ith caution in patients W ith impaire d hepatic or re nallunction. Propranolol is not ind icated for the tre atment 0 ! hypertensive emerg encres .
Be ta-ad renoreceptor b lockade can cause re duction ol intraocwar pre ssure Patientsshould be told thatpropranololmay interl erewith the g laucoma scre ening test.Withdrawa lmaylead to a return 0 1 incre ased intraocularpressure .
CL INICAL LABORATORY TESTS' Elevated b lood ure a leve ls in patients with severe heart
d isease . e levated serum transaminase . alkal ine phosphatase. lactate dehydrog enase
DRUG INTERACTIONS: Patients re ce iving catecholamrne -depleting dru 3 . Such as re ser
pine . should be close ly ob serve d ii propranolol is administere d . The ad d catecholamineb locking actionmay produce an encessrve re ductionof re s ting sympathetic nervous acIiVIIy ,
wh ichmay result inhypotenS ion.marked bradycardia. vert igo. syncopal attacks oronhos ial ic
hypotens-onAye rs
AYERST LABORATORIESNew York , NY 1001 7
5 112 198 5
CARC INOGENES IS. MUTAGENES IS. IMPAIRMENTOF FERTIL ITY: Long-term stud ies inanimals have been conducted to evaluate texic e l lects and carcinogenic potential In 18month stud ies. in both rats and mice . employing doses up to 150mg / kg / day. there was noevidence oI s ignil icant d rug
-induced toxicity There were no dru -re lated tumorigenic e llectsat any 01 the dosage leve ls Reproductive studies in animals d i not Show any impairmentatlert i lity thatwas attributab le to the d rug .
PREGNANCY. Pre gnancy Category C Propranolol has been shown to be embryotoxic inanimal stud ies atdoses about 10 times gre ater than the maximal re commended human dose .
There are noadequate and we l l-controlled stud ies in pregnantwomen Pro pranolol Should beused during pre gnancy only it the potential benetti iustities the potential risk to the Ietus .
NURS ING MOTHERS Propranol0 I is excre ted inhumanmi lk.Cautionshould be exercisedwhen propranolol is administere d to a nursmg mother.
PEDIATRIC USE'
Se lety and e l lectiveness inch ild re n have not been estab lished .
It d roch lorothtaz ide :G NERAL Pe riod ic determination of serum electrolytes to detect poss ib le e lectrolyte imbalance should be pertormed at appropriate intervals .
Al l patients rece iving th iaz ide therapy should be observed for cl inical s igns ol fluid orelectro lyte imbalance name ly
"H yponatre mia. hypoch lore mic alkal0 5 is . and hypokalemia.
Se rum and urine e lectrolyte determinations are Dafllculai ly import ant when the patient isvomiting excess ive ly Or rece ivmg parenteral ltuid s . Med ication Such as d ig ital is may alsoinl luence se rum electrolytes Warning S igns irre spective oi cause are
“Dry ness ol mouth. thirst.weakness , lethargy. d rows iness . restlessness . muscle pa ins or cramps . muscular fatigue .
hypotension. otiguria. tachycard ia . and gastiomtestinal d isturbances such as nausea andvornIIing
Hypokalemiamay deve lop. espec ially with bris k d iure S is .whensevere cirrhos is is pre sent.or during concomitant use at COTI ICOSTe iOId S orACTH
lnterterence with ad equate oral e lectrolyte intake Wi ll also contribute to hypokalemia.
Hypokalemia can sens itize or exagg erate the response oI the heart to the toxic e l lect oId ig ita lis (eg incre ased ventricular irritab i lity ) Hypokalemia may be avoid ed or tre ated by use
thromboc openia. and poss ib ly other adverse reactions wh ich have Occurre d in the adultNUR tNG MOTHERS : Th iazides appear in human mi lk. It use 0 ! the d rug is deemed
essential the patient should step nurS ingPEDIATRIC USE. Salety and e l lectiveness in ch ild re n have not been estab lished
ADVERSE REACTIONSPropranolol hy
d roch loride ( INDERALO)Most adverse e ects have beenmi ld and transientand have rare ly re gutre d thewithdrawal oithera
ard iovascwar; Bradycard ia : congestive heart lai lure : intens il icationoI AVbloc k; hypotension: pare sthes ia oI hands . thrombocytopenic purpura; arterial insultiCiency. usual ly ol theRaynaud type
Centra l Nervous System Lightheadedness . mental depre ss ionmani lested by insomnia.Iass itude . weakness .latique . re ve rS ibte mental depre ss ion prog re ssmg to catatonia. viSual
d isturbances . haltucmations ; anacme re vers ib le Synd rome characterized by d isorientationfortime and place short -termmemory loss . emotional lab i lity _ s l ightly clouded sensorium, and
decre ased pertormance on neuropsychometricsGastromles l inai. Nausea. vomiting , epigastric d istre ss . abdominal cramping . diarmea.
constipation. mesenleric art erial IhrombOS ls , ischemic col itis.
Allerg ic Phary ng itis and ag ranulocytos is erythematous rash ; Ievercomb ined with ach ingand sore thro at. Iary ngospasm and re spiratory d is tre ss
Respiratory Bronchospasm.
Hematolog ic: Ag ranulocyIOS is : nonthrombocwopenic purpura . thrombocytopenicpurpura
Auto-immune In extreme ly rare instances . systemic lupus ery thematosus has beenreport ed .
Miscellaneous: Alopecra: LE-tike re actions; psorias ilorm rashes : d ry eyes : male impotence . and Peyronie
'
s d isease have been re port ed rare ly. Oeulomuc00utah e0us re actionsinvolving the sk in. ser0usmemb ranes.and coniunctivae reported tora beta b locker (practolol)have not been associated With propranolol
Hydrochlorothlaz ideGas lromtes tinai: Anore xia: gastric irritation. nausea . vomiting , cramping; d iarrhea. constipa
tion. aund ice ( intrahe atic cholestatic taund ice ); pancre atitis. S ia ladenitis .
entral Nervous ystem Dizz iness. vert igo: pare stheS ias: headache : xanthops ia.
Hematolog ic: Leukopenia , agranulocytosrs. thrombocytopenia: aplastic anemia.
Card iovascular: Ort hostatic hypotens ion (may be agg ravated by alcohol. barbiturates . or
narcotics ) .Hypersens itivity
“Purpura: photosens itiwly : rash: urt icaria: necrotiz ing ang i itis (vasculitis.cutane0us vasculitis ); lever; respiratory d is tre ss . including pneumonitis : anaphylacticreactions .
Other Hyperg lycemia : g lycosuria: hyperuricemia; muscle spasm; weakness : re stlessness . transient b lurre d viS ion
Wheneveradve rse re actions are moderate orsevere . th iazide dpsage should be re ducedor therapy Withd rawn.

by Dr. 7 . and it was mutual ly decided and supported that cardiac arrest and expired . Postmortem examination was“do not resuscitate
"orders be instituted . This was aecom not obtained .
pl ished although caradiac arrestwas not anticipated . Unex Fourteen physicians were directly or indirectly involvedpected ly at am . onMonday , the patient experienced a in this patient
’
s 7 2 hour acute i l lness .
Samples to make

ETHICS
Ethical uandaries for the Present Day
Med ical Institution
EbenAlexander, MD .
0 Phys icians seeking to do no ha rm in today'
s complex medica l institutionneed specia l leadership to guide them through the ethica l mazes that
confront them.
IT IS no great revelation that l ife is becoming more complex and more expensive . It costs more to heal people ,
to kil l people in warfare , to educate people , and to feed
people . Al l of these increasingly complex areas have cre
ated special problems and ethical cons iderations , butprobably none more so thanour own area the care of the sick
and the preservation of health .
It was not until about 19 13 that a patient could vis it aphysician and have a better than fifty-fifty chance of be ingimproved thereby . S ince then, the tools , the drugs , the
d iagnosticmethods , and the uniformity ofmedical tra ininghave improved so greatly that it is a rare patientwho cannot
expect some rel ief from such a visit. However , thatpatient
can also be hurt by il l-advised treatment, and there in l ies
some of the prob lem.
I read in the Chicago Tribune recently that the horse lesscarriage had just about gotten ri d of chivalry (and virginity ) ; that nuclear arms had just about gotten rid of war; andthat air conditioning was about to ruin the Old South . Of
course the writerwas referring to the fact that air condition
ing has made the cl imate bearable enough that people are
moving south in increas ing numbers and bringing withthem ethnic and reg ional characteri stics that dilute and
change the character of our area . Whether those changesare ruinous or not is debatable , and is not re levant here . Iuse the story to il lustrate how technological advances forcechange on a society . In the fie ld of medicine the rapid
advances in technology that have changed the character of
medicine have brought with them inord inately complexeth ical cons iderations .
1 have been told that the phi losophical study of eth ics inour higher educational institutions had hit a slough of
despond”until med ical eth ics came along to enl iven it
and certainly it has been enl ivened .
I know some ofwhat the ethicists say about the complexissues imposed onmedicine by modern technology , and it
is obvious that they view with disdain the“unsophisti
cated physician struggl ing with ethical decisions on a
day-to-day basis . That di sdain leads them to discuss ethics
in ph ilosophical terms d ifficult to understand . Their lan
From the SectiononNeurosurgery , Departmentof Surgery , Wake ForestUnivers ity Medical Center, Bowman Gray School ofMedicine , WinstonSalem 27 103 .
OC TOB ER 1985 NCMJ
guage is about as understandable to us as that we use is tothe patient who is told that he is going to have a cra
niotomy for a cerebel lar spong ioblastoma or“rece ive
3025 rets of Cobalt-60 through a lateral portal . Whenwephysicians clothe our expert ise in the complexity of our
language , we do not help our patients to understand their
condition, just as the eth ic ists do not he lp us with day-to
day decisions unl ess they can state the problems in day-to
day language . Until that time comes , we have to stumb lealong on our own.
Medical care was simpler before the tremendous ad
vances in technology and therapeutic drugs took place ,
advances thatenable us toprolong life under circumstancesthatmay ormay not be of value to the patient. When andhow to use these advances become increasing ly difficultdecisions tomak e asmore of thembecome availab le , and itbecomes increasingly difficult to remember the injunctionthat should always be appl ied inmedical practice
“F irst
of al l , to do no harm.
We can al l feel comfortable with that part icular injunetion, but how best to adhere to it is not always clear . I havefound two guides to be very useful : 1) the patient
’
s rights
must always be respected ; and 2 ) when values differ , the
patientusual ly should be takencare of according to his , not
the physician’
s ,values . Social and economic factors affectal l of these ethical decis ions , but if they become the mostwe ighty factors they wi l l surely d istortour ethical approachto med ical care .
The physicianmust constantly be aware thathe serves asthe patient
’
s advocate . No one e lse is trained to do it as
wel l ; no one else has a professional trad ition in that role; no
one else bel ieves h imself or hersel f as w i l l ing to do it. As
patient advocate , however , the physician wi l l invariablysometimes find himself atodds with the institutionofwhichhe is a part .
Institutional eth ical quandaries in the care of the patientare of such quantity that we can only touch on a few of
them. Warshauer recently discussed one aspectof the problem when he addressed the possib le confl icts betweenmedical and rel ig ious institutions .
‘He applied the term
“medical institution”
to the philosophy of the practice of
medicine ; throughout this paper I use the term in the senseof a medical center or hospital complex . Institutions thatprovide medical care are as necessary to our continued

existence as a civil ization as are our schools , our pol ice
departments , and ourfire departments . The prob lem is howto help medical institutions keep the proper perspective .
The word“institution, in the sense of a facil ity and those
who run it, unfortunate ly impl ies a cold , unfee l ing organization seek ing primari ly its own we l fare and survival .S ince the physician has been affil iated with a medical
institution frommedical school onward and is an essentialpart of a medical institution, he or she is probably betterable to judge what that institution can and should do on
behalfof the patients , and those things that it should not do .
This“inside
”knowledge demands that physicians be as
wise as serpents and harmless as doves”
(Matthew
Nothing inwhat I have just said should be taken to implythat al l those who run organizations providing patient careare unfee l ing persons or are unappreciative of the needs ofthepatients . However, by the nature of the irpos itions , the irinterests are primari ly in the stab il ity , the future , and , in
some instances , the very survival of the ir institutions .
The cost of modernmedical technology is so great that
certainprocedures can only be done if an institution electsto support their use . One institutionmay transplant baboonhearts into certain babies with congenital heart prob lems .
Another institution may decide to invest the mi l l ions ofdol lars necessary to implant mechanical hearts in certain
adults with heart disease . Stil l another institutionmay decide that heart transplantation is not sufficiently advancedfor the institution to part icipate in it and , even though the
institution’
s staff may have the highest technical ab i l ity ofany institution in the country , itmay choose to take another
direction.
These examples of experimental problems have profound ethical connotations fora committee of trustees , for acommittee of medical staff, and for an eth ics committee .
L et us look at some more practical examples .
Despite the relative ly generous federal support for the
people in theUnited States now onrenal dialys is ,some institutions may decide to forego dialys is for endstage renal d isease . As a consequence , those institutions
may have to agree not to participate in renal transplantatione ither, despite the fact the renal transplantation, while not
w ithout prob lems , has given victims of end-stage renal
disease a gratify ing qual ity and prolongation of l ife .
Or, an institutionmay e lect not to have an intens ive carenursery to take care of premature bab ies ornewborn bab ieswith congenital anomal ies . The level of expertise now
availab le to these chi ldren complicates that decis ion. If in
1960 the decision had not been made to resusc itate anyneonate we ighing under 1000 grams , the expertise that hasbeen developed since would be no further along now than itwas then. However, with that expertise , the 1000-
gramneonate now has a good chance of survival and anormal l ifeexpectancy .
It is'
necessary sometimes to invest in some of the ad
vances of medicine simply because of the increasing lyimpressive experience that has been gained . The reduction
of mortal ity after coronary artery bypass operations from18% to and to even less in selected groups of pa
l ich ts , is a very marked improvement. The testimony of
numerous patients who have been re l ieved of unstableang ina by the procedure and who feel that they have had
5 34
their l ives prolonged provides increasing vocal support for
the procedure .
Plasmapheresis is a complex procedure that is being usedfor d iseases thought to have immunologic connotations ,
such asmyasthenia gravis andmul tiple scleros is . It is new ,
and it is expens ive . However , it, and other such new and
experimental procedures , should continue tobe used if theyappear to be effective . They wi l l continue to be expensive ,
and wil l continue to be supported only if phys icians intel
l igently and articulately justify their use ,whether at the
experimental stage or only after the ir therapeutic benefithas been proved .
No longer can a s ingle institutionoffer al l services to al l
people . When should expens ive , complex , experimental
machines and procedures be covered by the institution’
s
own funds? How does thephys icianma inta inhis traditionalrole as patient advocate when the institution faces the
difficult choices ofwhatpatients to admit, what services tooffer, and what research to fol low?
No institutioncanexpect to anticipate al l the needs of thefuture or expect always to make the right decisions . Re
l iancemust therefore be placed on the expertise , the vision,
and the understand ing of physicians w ith in the institution.
The dangerof not being able to continue to improve patientcare is great, and wi l l be prevented only by the continuedeffort s of al l involved . The ethical quandaries of medicalprogress dictate that phys icians , while remaining patientadvocates , involve themse lves also in institutional pol itics ,management and financial prob lems , and the equitabledel ivery of medical care .
I was privi leged to be a professor of neurosurgery in achurch- re lated institution with a strong rel ig ious base , a
strong pastoral care program, and ministers of al l faiths
whowere interested incooperating with the institution andits physicians to assure the optimal care of patients . Over
my 20 years as the Chief ofProfessional Services I Ieamedsome valuab le concepts . I did not Ieam the ultimate answer
to the ethical quandaries facing medical institutions , but IIeamed the fol lowing relevant facts :
I Ieamed that an institution is only as good as the peoplewho run it, and therefore it is important to assure that the
right people are in charge .
I Ieamed that a good name and a good reputation aloneare not sufficient to keep even the best institution on the
right track .
I Ieamed that good working relationships need to be
achieved at al l levels by physic ians work ing in institutionsand only in that way can the phys icians be of value in
solving ethical questions and be assured of having the toolsw ith which to work for the future .
In conclusion,I Ieamed that the best patient care is
provided andmany of the ethical quandaries are diminishedwhenever compass ion, understand ing , technical sk il l , thebestpossible tools , recognitionof patient and fami ly roles ,the best ancil lary services , and the best trained physiciansand administrators are comb ined in a balanced potpourri ofwhat we know as a medical institution.
References
l . WarshauerAD. Thoughts on the bel iefs of re l ig ious andmedical institutions . NC
Med J I98 5 ;4 6 :29-32 .
VOL . 46 , No . 10

of us . But final ly , even as we savor this moment, let'
s not
forget the importance of the other smal l things inour l ives
those people and things wh ich are prone to be neglectedat the expense of our higher
”
goals . So rel ish themomentof becoming anMD . for a while . But when you go home
tonight, after you’
ve tucked the kids into bed and k issed
them goodnight, go back outside . Stop on the porch andbreathe the fresh night air . Savor the fragrance of roses in
the yard . Spend some time watching the squirrels as theyplay the ir balancing games in the branches above you. Cal l
for the dog and watch him bound upwith wagging tai l anddancing tongue . Think about the richness these smal l thingshave added to your l ife . Wander back ins ide . Read some
5 36
poetry . Tel l your spouse you love him or her. Better yet,
show your love by doing the dishes . Take some time tolaugh together.
The smal l things in l ife . L etus never forget them, lestwe
forget l ife itself. My w ish for al l of us is thatwe may findjoy in those things that do not make the news .
References
l . Relman AS . Men’ imon lecture . Chapel Hil l , Univers ity of North Carol ina.
October 19 , 1982 .
2 . Thomas L . The Youngest Science . New York : V ik ing Pre ss . 1983 .
3 . Sharkey F . A Parting Gift. New York : St. Martin'
s Press , 1982 .
4 . Dic kinson 5 . Not in Vain. as reprinted in One H undred and One FamousPoems . Roy Cook , ed itor. Chicago: Contemporary Books. Inc . , 195 8.
VOL . 46 , No . 10

"fl ush m
“M bj iomcwhenllie
DEMOGRAPHY
Distribution of Women and M inori icians
in North Carolina
Mary Anne Salmon and Jane Stein
0 Women phys icians are not, and minority phys ic ians a re , improvingequity of access to med ica l care across North Carol ina .
ORTH CAROL INA physicians1are not distributed
across the state in amanner comparable to the generalpopulation d istribution. They are proportionately over
represented ih the Piedmont and under-represented in the
Coastal Plainwhile the irnumbers in themountainous counties are approximate ly proportionate to the population. This
distribution largely reflects the location choices of white ,
male physicians who constituted percent of North
Carol ina’
s active , nonfederal physician population in
Does this same distribution apply to fer—ri al é and
minority physicians or are the ir practices moving NorthCarol ina closer to equitable access among the three regionsof the state?
Data on the sex , race , and county of practice3 for al ll icensed physicians , avai lable from the Health Manpower
statistics files of the Univers ity of North Carol ina’
s Health
Services Research Center were used to construct figures
1-4 . The racial category As ian in figures 3 and 4 in
e ludes phys icians who report ed themselves as AmericanIndian Oriental or As ian,
“Spanish Orig in or
“other on their appl ication for reg istration. Population
data in figure 5 were tak en frompubl ished data of the StateCenter forHealth Statistics .
4The assignmentof counties to
one of the three regions was made on the bas is of a majorterrain reg ionmap of the state ,
5and is shown in figure 6 .
North Carol ina‘
s female phys icians are more geographical ly concentrated than the ir male counterpart s . Nearlythree quarters of them practice in the Piedmont, and morethan half of those in the Piedmont practice in the three
Research Triangle counties Durham, Orange andWak e .
This concentrationmay be related to the d ifferent practice
patterns of female physicians . Whether by choice or be
cause of restricted opportunity , women physicians are
somewhat less l ikely thanmen to be in solo , self-employed
practice and much less l ikely to be in partnerships and
grouppractices . Less than hal f of North Carol ina’
s women
physicians are inone of these practice types compared withover 7 2 percent of the male phys icians .
6 The Research
Triang le with its univers ities , medical schools and state
From the Health Services Research Center, Chase Hal l l 3 2 -A, Univers ityof North Carol ina, Chape l H il l 27 5 14 .
OC TOB ER 1985 , NCMJ
F igure 1 . Proportion of phys icians , by gend er , forreg ions of North Carol ina , 1982 .

governmentprovides opportunities in those areas outs ide ofprivate practice where womenphys icians are more l ike ly to
be employed . Women doctors are only a l ittle less l ike lythanmen to work in the mountains and in the major citiesouts ide theTriang le but are considerab ly less l ikely toworkin the Coastal Plain or in Piedmont counties that do not
contain a city of or more .
7
While women doctors are more geographical ly coneen
trated than men, both b lack and Asian doctors are some
what less concentrated in the Piedmont thanwhite doctors .
Stil l the majority practice in that reg ion. Within the Pied
mont the practice patterns of the twoethnic groups are quitedifferent. B lack physicians are over- represented in the
counties that house the state’
s largest cities Meck len
burg , Gui lford and the Triang le while more than half of
Asian and other physicians practicing in the Piedmont are
in the smal ler , more rural counties .
Both b lack and Asian doctors are also more l ikely than
whites to practice in the Coastal Plainwhere over a third of
the population is not white and almost half of the state’
s
non-wh ite population l ives . B y contrast, they are very
much under- represented in the mountains though the As ian
doctors are more l ike ly to practice there than are b lackdoctors . Itmight be imagined that since the mountains are
HALE Pl l Sl ClA‘
fi-‘fi
I kI I I I I I I I I I I I I I I I I I I I I I I I I I I I I I I I I I I I L
FEUALE PHYSICIANS
F igure 2 . Reg iona l distribution of phys icians for each gender ,
North Carol ina . 1982 .
5 38
"( DMI NI
F igure 3 . Proportionofphysicians . by race .for the three reg ionsof North Carol ina . 1982 . The ca tegory As ian is over 90%As ian.
buta lso includesAmerican Indian, Spanish orig in, and‘
other .
Notes
I . This describes active . nonfederal phys ic ians and does not include those cum ntly
VOL . 4 6 , No . 10
home tomostof the state’
sAmerican Ind ianpopulation thatAmerican Ind ians would account for some of the “
others
in practice in the mountains . However only one of the
state’
s seven (al l male) non- federalAmerican Indianphysicians is in practice there .
8 As in the remainder of the state ,
more than 90% of the As ian category of doctors in the
mountains are , in fact, As ian.
From these data it can be seen thatminority phys iciansare helping to reduce North Carol ina
’
s geograph ic inequityin access to phys icians . Howeverwomenphys icians ,
percent of whom are white , remain concentrated near the
state’
s major med ical centers .

a lead ing test forfecal occult blood
The‘
Hemoccult'
guaiac paper test for fecal occultblood
is a convenient, dependable.virtually odorless
preliminary screenforabnormal g . i. bleed ing often
associated with colorectal cancer.
HemoccultII® S lides Hemoccult® Two-Hole S ing le S lides
Available in Available in
0 Dispensapak®z
.
100 patient kits . Each kitcontains Boxes of 100 s lidesthree
‘
HemoccuItII'
s lides inmailing envelope with Cartons of 1000 s lidesinstructions . applicators and deve loping solution.
0 Boxes of 100 s lidesCartons of 1000 s lides
Also available
0‘
Hemoccult'
Tape
34 5 1 W. Lawrence Ave .
0 8mithKline Diagnostics . 1 98 1
Surg ica l SUDDIV Co . Charlotte : -22 40

AUXILIARY
Pres ident’
s Report to the North Carolina
Medical Socie
L inda P. Nance
IHAVE looked forward to this day , for I am excited to
report to you that a tidal wave of actionhas rol led across
North Carol ina as auxi l ians have armed themse lves to
promote better health care , health education, health related
leg is lation, and programs to combat social issues that
undermine and destroy the health care which you work
tire lessly to produce .
A successful child sexual abuse awareness program presented at the annual meeting was the necessary impetus for
30 county auxi l iaries to present awareness programs for
their members .
Armed with facts , auxil ians have learned to discuss
openly a subject we once pretended did not exist. Catawbacounty
’
s leadership researched their community’
s -needs
and establ ished a child abuse awareness program in their
county’
s e lementary schools with a goal to reach
s tudents . H enderson, Cumberl and , G aston, N ash ,
Durham, and New H anover-Fender counties offered out
stand ing awareness programs for their communities in
coal itionwith many other agencies . Two of these counties
offered week - long programs in wh ich they promoted al l
aspects of child protection.
Through a grant from the Kate B . Reynolds Health Care
Trust, video tapes of‘
Funny Tummy Fee l ings ,”a training
program suitable for children inmany settings which promotes awareness and preventionof child sexual abuse ,
was
made available for training teaching volunteers . This pro
gram is available for any county aux i l iary thatw ishes to useit. We hope th is program wi l l make children free from
abuse , free to grow , free to develop, and free to becomeproductive citizens .
Two smal ler grants al lowed us to print healthy l ivingbrochures and“Buck le Up
”stickers . These have been
distri buted throughout the state to schools , at health fairs ,
and in physicians’
offices . These carry the clear messagethat the North Carol inaMedical Soc iety Auxi l iary wants topromote better health for its citizens .
At the directionof the Committee onPhysicians’
Heal th
and Effectiveness , the auxi l iary prepared , with the help of
the medical society staff, a new H elpl ine brochure thatbetter explains the purpose of this access l ine for phys icians
’
fami l ies . This service , staffed by an auxil ian, hasbeen successful in offering aid to members of physicians ’
fami l ies in need of support for impairment.
From 1922 Brookhaven Road , Wilmington 28403 .
OC TOB ER 1985 , NCMJ 54 1
Auxil ians have he lped to distribute the Med ical Society
’
s L iving Wi l l . It has been introduced at state meetingsthrough Ta rhee l Tandem, the
"President
’
s Newsletter,
and during presidential vis its to counties . It has been usedin conjunction with organ donor awareness programs , and
the GastonCounty Aux il iary d istributed copies to al l of thenurs ing homes in their communitv.
More members than ever before attended the state meetings atwhich part icipants were offered programs about notonly child abuse and neglect, but prenatal and postnatal
care , automobi le safety restraints , anorexia nervosa and
bul imia , leg islation, orderly financial planning , and par
l iamentary procedure .
Through the outstand ing efforts of county leaders and
members , exciting heal th projects are underway . Countyauxil iari es are work ing in coal ition with forty- s ix other
organizations to promote “Shape Up For L ife
"health
projects in their communities . There are awareness pro
grams des igned to combat drunk dri ving , drug abuse , and
chi l d abuse . The L enoir-G reene Aux i l iary was instrumental in establ ishing aMADD chapter for the county ,
and auxil iari es are active inprograms for cancer rehab il itation, foster parenting , organ donor awareness , cancer de
tection, and prenatal and postnatal care . Inaddition to these
programs , auxi l iaries promote CPR training , distribute“Shape Up For L ife pamphlets , contribute time and
money to hospice , support and staff hands-on health
museums , and produce health fairs . This year was
distri buted to these projects through auxi l iary efforts .
Mecklenburg County ’
s endowment exceeded al l ex
pectations . It grew to tenmonths ahead of sched
ule . An advisory board , composed ofmajorCharlotte personal ities was formed andMMAE
’
s Inn, aRonaldMcDon
ald type house , had its grand opening Apri l 29 . New
Hanover-PenderCounty’
s similar goal is in its early stages ,but is gaining active support among the citizens of thatcommunity .
North Carol ina auxil ians raised over for the
American Medical Association Education and Research
Foundation through hol iday sharing cards and other fund
raisers . To help assure thatmed ical education is not l imitedto the wealthy , counties contributed to the state
student loan fund . In addition, three percent of each member’
s dues was placed in this fund for North Carol inians
enrol led in North Carol ina’
s med ical school s . Thirteen
loans were made this year for a total of Plans are
underway to secure even larger sums ofmoney for loans in

the coming years .
Bes ides the student loan fund , counties have awarded
to sixty students study ing in al l ied health fie lds ,
and interest free loans to sixteen students have beenmadeby several counties .
To assure thatphys icians wi l l have a voice in the leg isla
tive process , counties have had outstand ing participation in
leg is lative programs and alerts . Twe lve counties partici
pated in the AMA’
s project Medvote in the fal l of 1984 .
Auxi l iary efforts made a d ifference in the voter turnout.
With so many outstand ing projects and programs underway ih the counties , the med ia has discovered this to be
newsworthy . B uncombe , Cumberland , G ui l ford -H igh
Point, Henderson, Nash and New H anover-Fender coun
ties thankedmembers of themedia for the irpart inpubl icizing the ir many projects and programs with very successful
5 4 2
med ia days .
Physicians’
spouses across North Carol ina have proven
thatmore th ings happenwhenwaters are stirred thanwhen
they are stil l . They accepted the chal lenge tomake a d iffer
ence in the ir communities . Our numbers grew as we
worked to keep the federation strong . Mak e certain that
your spouse is a member so we can push our membershiptoward the 100% mark of participation. The AMA
’
s ori g i
nal constitution, now more than a century old , stated its
objectives thusly ,
“to promote the science and art ofmed i
cine and the betterment of pub l ic health . Only our bestefforts and our support wil l assure that every Americanwi l l
continue to rece ive the best health care
The North Carol ina Medical Society Auxil iary is proudto be your partner in this cause .
VOL . 4 6 , No . 10

Bulletin Board
Continuing Med ica l
EducationPlease note: 1 . The Continuing Medical EducationPrograms at BowmanGray .Duke . EastCarol ina and UNC Schools ofMedicine , DorotheaDix ,
and Bum ughs Wel lcome Company are accred ited by the AmericanMedical Association. Th erefore CME programs sponsored or cospon
sored by these schools automatical ly qual ify forAMA Category I credittoward theAMA
’
s PhysicianRecognitionAward , and forNorth Carol ina
Medical Soc iety Category A credit. Where AAFP credit has been
obtained , this al so is indicated .
IN STATE
October 16
OxygenUse CO: Narcosis and Venti lator UsePlace: Sanford
Credit: 2 hours Category I AMAInfo: Robert S . Cl ine , M.D. , Central Carol ina Hospital , Sanford
2 7 3 30.-65 18
October 19-20
Jungian Techni ques of Analytic HypnotherapyPlace : Chape l Hill
Credit: 12 hours Category I AMA, NCMSInfo: W. B . Wood , M.D. , 2 3 1 MacNider 202H , UNC School of
Med icine , Chape l H il l 2 7 5 14 .-2 1 18
October 29
Crisis Then New
Place : Kinston
Info: Wayne Parker. MMIC , Box 27 444 , Raleigh 27 6 1 1 .
7 9 17
November 1 -2
Alcohol and Drug AbusePlace: Chape l H il l
Cred it: 10 hours Category I AMA, NCMSInfo: W . B . Wood , M.D. , 2 3 1 MacNider 202H , UNC School of
Med icine . Chapel H il l 2 7 5 14 . 9 191962 -2 1 18
November 1-2
Review of the Management of SIDS and Near-Miss SIDSPlace: Chape l Hill
Credit: 7 hours Category I AMA, NCMSInfo: W . B . Wood , M .D. , 2 3 1 MacNider ZO2H , UNC School of
Medicine. Chapel H il l 2 7 5 14 .-2 1 18
November 14 -15
Clinical Teaching and Evaluation of Cl inical PerformancePlace : Chape l Hil l
Credit: 12 hours Category 1 AMA, NCMSInfo: W . B . Wood , M.D. , 2 3 1 MacNider 202H , UNC , Chape l H il l
2 7 5 14 .-2 1 18
November 20
Endocrinology for the L ifetime of the FemalePlace : Sanford
Credit: 2 hours Category I AMAInfo: Robert S . C l ine , M.D. , Central Carol ina Hospital , Sanford
2 7 3 30 .-65 18
December 5 -7
Fourth Compre hensive Sympos ium on Breast Disease
Place: Winston-SalemCredit: 16 hours Category I AMAFee
Info: Center forMedical Ultrasound , BowmanGray ,W inston-Salem
2 7 103 .-4 5 05
December 5 -7
Microcomputers inMedical EducationPlace : Chape l H i l l
Credit: 18 hours Category I AMA, NCMSInfo: W . B . Wood , M.D. , 2 3 1 MacNider 202H , UNC. Chape l H i l l
27 5 14 .-2 1 18
5 44
December 7
UNC Ophthalmology Resident’
s DayPlace: Chape l H il l
Info: Baird S . Grimson.M .D. 6 17 Cl inical Sciences Building 2 29H .
UNC , Chapel H il l 2 7 5 14 .-5 296
December 12
Controvers ies in Transplantation
Place: Chape l H il l
Info: W . B . Wood . MD 23 1 MacNider 202H , UNC , Chape l H i l l
2 7 5 14 .-2 1 18
December 18
New Uses of Calcium Channel B lockersPlace: Sanford
Info: R. S . Cline , M.D Central Carol ina Hospital , 113 5 Carthage
Street, Sanford 27 3 30 .-65 18
OUT OF STATE
October 17 -24
Review of Clinical Chemistry for Practicing Pathologists and ClinicalChemistsPlace: San Diego, CAFee : $3 15Credit: 40 hours Category I AMAInfo: Office ofCME , ECUSchool ofMedicine , Box 7 224 , Greenvil le
2 7 83 5 -7 224 .-5 200 , ext. 208
October 29-November 2
Diagnostic ImagingPlace: Southampton, BermudaFee: $495Cred it: 25 hours Category I AMAInfo: Carl E . Ravin, M.D. , Box 3808 DUMC , Durham 27 7 10 . 9 19/
68 1-5 268
New MembersMichael Craig Whi te (D) , 8362 Rim L ine , San Antonio , TX
7 825 1
BEAUFORT-HYDE-MARTIN-WASH INGTON-TYRREL L
Phi l ipMarget Spiro (GP) , Box 65 9 , Columbia 27 925BLADEN
Peter Michae l Kindschuh (OBG ) , Box 2 14 1 , Cromart ie Road ,
El izabethtown 2 83 37
BRUNSWICKStephen Joseph Candela (ORS) , Doctor
’
s Complex #5 , The
Brunswick Hospital , Supply 2 8462
Mark David H il z (EM) , Brunswick Hospital , Box 139 , Supply
28462
Bernard Leroy Langston, 111 (GP) , Box 1934 , Shal lotte 284 59
VOL . 46 , No . 10
BUNCOMBEDavid Soule Bate , Jr. (FP) , Box 5 37 , Arden 28704
Richard Bruce Ke l ly (FP) , 4 9 1 B i ltmore Ave . , Ashevi l le 2 8801
J . Paul Mart in (FP) , 49 1 B iltmore Ave . , Ashevil le 2 8801
Robert Stanley Wel ls ( IM) , 44 5 B iltmore Ctr . , Ste . 407 , Ashe
vil le 2 8801
Evans Mccol lumWhitaker (Resident) , 5 9 G ibson Road , Ashe
vil le 28804
CABARRUS
David Wi l l is McMurry ( IM) , 888 Church St North , Concord
2 8025

CALDWEL LFrancis Theodore Ol iver (AN ) , 2 17 Mt. Circ le Dr Lenoir 2 864 5
JohnGarold Tye (OPH ) , 40 1 Mulberry St. S .W . , L enoir 2 864 5
DUPL IN
Ronald Burton Dietrick (GS ) , Box 501 , Kenansvil le 2 8349
DURHAM-ORANGEBerryl in June Ferguson (resident) , 23 10 Pri nce St Durham
2 7 707
Fred Freedman (resident) , Route #7 , Box 5 5 , Durham 2 7 707JosephMorri s Garfunkel (PD) , 229 HuntingtonDr. , Chape l H il l
2 7 5 14
Mari anna Matthews Henry (PD) , Unc . 63 5 Burnett-WomackB ldg . , Chape l H i l l 2 7 5 14
El izabeth Sumner Jokerst ( student) , 2 1 12 Broad Sr. , D- 8 ,
Durham 2 7 705Gary Roth L ichtenstein (resident) , 3 1 1 S . L aSaIle St. Apt. 15 -A,
Durham 2 7 705Paul Andrew Payne ( student) , Box 2 7 60 DUMC , Durham 27 7 10Ronnie H . Ruff (resident) , 2 7 5 2 MiddletonAve . #3OL , Durham
2 7 705
David Michael Schlossman ( IM) , 3800 Portsmouth St. , Durham2 7 704
Robert S . Toms ick (D) , Dept. of Dermatology , UNC School of
Medicine , Chape l H il l 2 7 5 14
Eric D. Weber (resident) , 105 BuckinghamAve . , Syracuse , NY
132 10
Tonja Miche lle Wynn (student) , E- 17 Carol ina Apts . , Carrboro
2 7 5 10
FORSYTH -STOKES-DAVIEGregory Steven Hardie (resident) , 9 15 Panola Road , WinstonSalem 27 106
Betty Winfield Joyce (student) , 2 2 1 LocklandAvenue , WinstonSalem 2 7 103
David Eugene Spivey , Jr . (student) , 8 13 Sunset Dr. , WinstonSalem 2 7 103
Debra L ynn Wul fhorst ( student) , 209-D New Drive , WinstonSalem 2 7 103
GUIL FORD
Paul W . F . Coughlin (U) , 62 4 Quaker L ane , D- 100 , H igh Point
2 7 262
Mark Thomas Shapiro (OPH ) , 13 1 1 N . Elm St. , Greensboro
2 7 401
HENDERSON
KennethT. Lenington (P) , 800-AN . Fleming St. Hendersonvil le2 87 3 9
OC TOB ER 1985 , NCMJ
MECKL ENBURGDanie l Wil l iam B lue (AN ) , 10009 Pinevil le—Matthews Rd . ,
Matthews 2 8 105
George Louis Radd (FP) , 2 12 5 Beny hil l Road , Charlotte 2 82 1 1
MOOREAlan Dean Davis (PD) , 2 17 0 Midland Road , Southern Pines
2 83 87
NASH
DonaldWeesner Bales , Jr. ( IM) , Box 4 7 7 7 , Rocky Mount 27 803Margaret Eva Sowerwine ( IM) , Box 4 7 7 7 , Rocky Mount 2 7 803
PITT
Ulrich Karl Alsentzer (PM) , Reg ional Rehabil itation Ctr. , Box
602 8 , Greenvi l le 2 7 834
Carol Ann Grolnick ( student) , 2007 -B E . 4 th St. , Greenvil le
2 7 834
Edward Wayne H aga ( student) , 207 H ardy C ircle , Greenvi l le
2 7 834
Kimberly Sue Norman ( student) , 200- 14 Rol l ins Drive , Green
vil le 2 7 834
JohnCarsonRounds ( student) , 104 Chesterfield Ct #26 , Green
vi l le 2 7 834
JohnGriffith Stee l (N) , 4 25 Stantonsburg Road , Greenvil le 2 7 834
WAYNEJosephDurhamGrant (ORS) , 2 801Medical Office Place , Golds
boro 2 7 5 30
WI L SONMichae l Robert Bohnsack (AN ) , 3 305 Mil lbrook Dr. ,
W il son2 7 893
54 5
POL K
NatashaThomasovna H ays (PD) , Route #3 , Box 3 15 BB , Forest
City 2 804 3
WAKERobert Carl Jacobson (AN ) , Box 18 139 , Rale igh 2 7 6 19
Robert EltonL ittl eton (OBG ) , 3 622 Haworth Dr. Raleigh 2 7 609
Jerome JosephMagolan, Jr . (resident) , 3 3 20 Executive Dr . , Ste .
2 10 , Rale igh 2 7 609
Edwin Scott Thomas ( IM) , 106 E . Park St. , Cary 27 5 1 1
David Cushman Thurber, Jr. (IM) , Med ical Dep. Dorothea Dix
Hosp , South Boylan Ave . , Raleigh 27 6 1 1
Anthony Thomas Zaldonis (GE) , 1 15 1 Kildaire FarmRoad , Cary2 7 5 1 1

TH IS SPACECONTRIBUTEDAS APUBL IC SERVICE
There is evidence that d iet
and cancer are related . Somefoods may promote cancer, wh ile
othersmay protect you from it.
Foods related to low er
ing the risk of cancer of th e
larynx and esophagus al l have
h igh amounts of carotene ,
a form ofVitaminAwhichis in cantaloupes , peaches ,broccoli , spinach ,
all dark
green leafy vegetables , sweet
potatoes , carrots , pumpk in,
w inter squash and tomatoes ,citrus fruits and brussels
sprouts .
Foods thatm
he lp reduce the risk
of gas trointestinal
and respiratorytract cancer are
cabbage ,broccoli
,
brussels sprouts ,hlrab i
,cauliflower.
Fruits,vegetables , and whole
grain cereal s such as oatmeal , branand wheatmay help lower the riskof colorectal cancer.
Foods h igh in fats , salt or
nitrite -cured foods like ham,and
fish and
types of sausages smoked by tradi
tional methods should beeaten inmoderation .
Bemoderate inconsumption of alcohol also .
Agood rule of
thumb is cut down on
fat and don’
t be fat .
Weigh t reductionmaylower cancer risk . Our
2 year study ofnearly a
mill ionAmericans uncovered
h igh cancer risks particularlyamong people 40% ormore
overweigh t.
Now ,more than ever, we
know you can cook up your own
defense against cancer. 80 eat
healthy and be healthy.
No one faces

U.S . Savings Bonds now offer h igher, variable interest rates and a guaranteed
return . Your employees w ill appreciate that . They’
ll also appreciate your giv ingthem the eas iest , surest way to save .
Formore informat ion , wr ite to : Steven R. Mead ,Execut ive Director , U.S. Sav ings Bonds Div is ion ,
Department of theTreasury,Wash ington ,DC 20226.
as SAVINGS BONDSL PayingBetterlhanEverApublic se rvice of this publication.



ropomil HCl/ Knoll80mg and 120mg scored , film- coated tab lets
Contraind icat ions : Severe left ventricular dysfunction (see Warnings) , hypotension (systolic pressure 90 mm Hg) or cardiogenic shock, sick sinus syndrome (except in patients with a functioning artificial ventricular pacemaker) ,2nd or 3 rd-deg reeAVblock.Warnings : ISOPTINshould be avoided inpatientswith severe left ventricular dysfunction e
'
ect ion fraction 30% or
moderate to severe symptoms of cardiac failure and in patients with anydeg ree of ventricular dysfunction if they are receiving a beta blocker. (SeePrecautions .) Patients withmilderventricular dysfunction should ,
if possible , be
controlled with optimum doses of dig ita lis and/or diuretics before ISOPTIN isused . (Note interactions with digoxin under Precautions.) ISOPTIN may occasionally produce hypotension (usually asymptomatic, orthostatic, mild and controlled by decrease in ISOPTIN dose) . Elevations of transaminases with andwithout concomitant elevations inalkaline phosphatase and bilirubinhave beenreported . Such e levationsma disappear evenwith continued treatment; however, four cases of hepatoce llii lar injury by verapamil have beenproven by rechallenge . Periodic monitoring of liver function is prudent during verapamiltherapy. Patients with atrial flutteror fibrillationand an accessory AV pathway(e .g .W-P-Wor L-G-L syndromes) may develop increased anteg rade conductionacross the aberrant pathway bypassing the AV node, producing a very rapidventricular response after rece iving ISOPTIN (or dig italis). Treatment is usuallyD.C.
-cardioversion, which has been used safe ly and effectively after ISOPTIN.
Because of verapamil'
s effect onAV conduction and the SAnode , 1° AV block
and transient bradycardia may occur. High grade block, however, has beeninfrequently observed . Marked 1
°
or prog ressive 2°or 3
°AV block requires a
dosage reduct ion or, rare ly, discontinuation and institution of appropriate
therapy de nding upon the clinical situation. Patients with hypertrophic car
diomyopat y (IHSS) received verapamil in doses up to 7 20 mglday. It must beappreciated that this group of patients had a serious disease with a high mortality rate and thatmostwere refractory or intolerant to propranolol. Avarietyof serious adverse effects were seen in this group of patients including sinusbradycardia , 2
°
AV block, sinus arrest, pulmonary edema and/or severe hypotension. Most adverse effects responded well to dose reduction and only rarelywas verapamil discontinued . Precautions : ISOFTIN should be givencautiouslyto patients with impaired hepatic funct ion ( in severe dysfunction use about30% of the normal dose) or impaired renal function, and patients should bemonitored forabnormal prolongationof the PRinterval orothersigns of excessive pharmacolog ic effects . Studies ina small number of patients suggest thatconcomitant use of ISOPTIN and beta blockers ma be beneficial in patientswith chronic stable ang ina. Combined therapy can a so have adverse effects oncardiac function. Therefore, until furtherstudies are completed , ISOPTIN shouldbe used alone , if poss ible . If combined therapy is used , close surveillance of vital
signs and clinical status should be carried out. Combined therapywith ISOPTINand propranolol should usually be avoided in patients with AV conduction
abnormalities and/orde ressed left ventricular function. Chronic ISOPTIN treatment increases serum i
goxin levels by 50% to 70°/ o during the firstwee k of
therapy, which can resur in digita lis toxicity. The digoxin dose should be re
duced when ISOPTIN is iven, and the patients should be carefullymonitored toavoid over or under ig ita lization. ISOPTIN may have an additive effect onlowering blood pressure in patients receiving oral antihypertensive agents.Disopyramide should not be given within 48 hours before or 24 hours after
ISOPTIN administration. Until further data are obta ined , combined ISOPTINandquinidine therapy in patients with hype rtrophic cardiomyopathy should probabl be avoided , since significant hypotension may result. Clinical experiencewit the concomitant use of ISOPTIN and short and long
-acting nitrates sug
gest beneficial interactionwithout undesirable drug interactions.Adequate animal carcinogenicity studies have not beenperformed . One study in rats d id not
suggest a tumorigenic potential, and verapamilwas notmutagenic in theAmestest. Pregnancy Category C: There are no adequate and well-controlled studiesin pregnant women. This drug should be used during pregnancy,
labor and
delivery only if clearly needed . It is not knownwhetherverapamil is excreted inbreast milk; therefore, nursing should be d iscontinued during ISOPTIN use .
Adverse Reactions : Hypotension peripheral edema ( 1 AVblock:3 rd deg ree bradycardia : HR 50/min CHF or pulmonaryedema dizz iness headache fatigue constipa
tion nausea e levations of liver enzymes have been reported .
(See Warnings . ) The following reactions , reported in less than occurredunder circumstances where a causa l relationship is not certain: ecchymosis,bruisin gynecomastia, psychotic symptoms , confusion, paresthesia , insomnia,
somnoence , equilibriumd isorder, blurred vision, syncope, muscle cramp, shaki
ness, claudication, hair loss , macules, spotty menstruation. How Supplied
ISOPTIN (verapamil HCI) is supplied in round, scored , film-coated tablets con
taining either 80mg or 120mg of verapamil hydrochloride and embossed withISOPTIN 80“ or "isoPTIN 120" onone side and with "KNOLL" on the reverseside . RevisedAugust, 1984 . 2 3 8 5
KNOLL PHARMACEUTICAL COMPANY3 0 NORTH JEFFERSON ROAD, WH IPPANY. NEW JERSEY0798 1

Letters to the Editor
Joe Beard
To the Editor
I was deeply moved by your tri bute to Joe Beard (NCMJ1985 ;46 z303 He was a surg ical resident at Vanderb iltwhen I entered medical school there , and wh ile I was neverprivi leged to know him personal ly , I admired him from
afar .
The regular appearance and read ing of theNorth Cara li
na Med ica l Journa l helps th is retiree feel he is not entirelyout of the medical world and his favorite state . Your edi
torship is appreciated .
Alex X . Moffett, MD .
7 0 W . Luceme Circle
Orlando, FL 3 2 801
Smokeless Tobacco: A Future H eal th Concern for
North Carol ina?
To the Editor
Snuff dipping and tobacco chewing are hab its that arerapidly gaining p0pulan
'
ty inour country .
1Moist'
snuff has
increased domestic sales from mi l l ionpounds in1 978 .
to mi l l ion pounds in 1984 wh ich is a‘
5 5% increase .
2
Sales for US . Tobacco more than quadrupled frommi l l ion dol lars in 197 3 to mi l l ion dol lars in 1984 .
One pub l ication claims there are 2 2 mi l l ion users of
smoke l ess tobacco in the Uni ted States .
3 Another
ind ication of the increase in dipping and chew ing isevidenced by the rise of “chewing clubs” spawned by this
new tobacco craze in h igh schools and col leges , completew ith charters , membersh ip cards and even t- shirts
emblazoned with mottos l ike “Don
’
t spit onme .
” 3
According to the tobacco industry , the typicaltobacco dipper or chewer involves a wide range of adult
menandmay come from any sectionof the country ; but the
Southeast , Southwest and Midwest are the primarymarkets .
4They claimthatdemand is greatest inthemale 18
to 30 year-old group in these areas of the country .
Currently , the tobacco industry is not a'
ctively promotingdipping and chewing for women.
Smokeless tobacco can produce significant detrimenta leffects on the soft and hard tissues of the mouth , includ ingbad breath , discolored teeth , decreased ab il ity to taste andsmel l
, gum recession, advanced periodontal destructionofthe soft and hard tissues , leukoedema and erythema of thesoft ti ssue , l eukopl ak ia , and for long
- term users ,
cancers .
"5 Fortunately , the poss ibi l ity of cancer at this
time appears relatively low ; however, a careful review of
the North Americanmed ical and dental l iterature disclosed64 6 documented cases of oral , pharyngeal , or laryngeal
cancer which have been l ink ed to smokeless tobacco .
6
Jayant et a] suggested that the re lative risk of deve lopingoral cancer is for smokers and for chewers .
7 Acase-control study of 2 5 5 womenwith oral and pharyngeal
cancer and 5 03 women control subjects in North Carol inaOCTOB ER 1985 NCMJ
byWinn et al reported a fifty- fold increased risk of cancerof the gum and buccal mucosa in snuff-d ipping , and
re lative risk of percent for al l mouth cancers in thesewomen.
8 A 1985 prevalence study in Pitt County , North
Carol ina revealed approx imately 15 percent of the adult
population res id ing in the county use smokeless tobacco ,
wh ich trans l ates into approx imate l y users
(unpub l ished observations) .
Due to the time lag of use and manifestation of cancer ,experts fear an epidemic ofmouth cancer in 40 years . Thi s
fear is reflected in the latest of several demonstrations ofconcern:
549
Rep. Tom Tauke (R- Iowa) introduced a b il l that wouldtax smokeless tobacco.
Rep. Mik e Synar (D-Oklahoma) introduced a b il l thatwould require warning label s on al l smokeless tobaccoand advertisements .
Rep. Samuel Stratton (D-NewYork ) introduced a bi l l thatproh ib its the advert i s ing of smokeless tobacco (al ltobacco) on any medium of e lectronic communication.
Rep. Card iss Col l ins (D- Il l inois) introduced a b il l thatwoul d set as ide funds to educate youth regardingsmokeless tobacco .
OnJuly 1 1 , 1985 , Massachusetts became the first state torequire health warn ing labels on a smokeless tobaccoproduct moist snuff .
0 Warning label b il ls are being considered in Delaware ,Il l inois , Michigan, New Jersey , New York , Oregon,
Pennsylvania and Utah .
In June , Surgeon General C . Everett Koop appointed a
pane l of scientists to review the heal th haz ards of these
products .
0 B etty Ann Marsee of Ada , Oklahoma , charged in a
mi l l ion suit against US . Tobacco Co . that her
19-
year-old son Sean d ied in 1984 of tongue cancer from
snuff use . The trial is scheduled for November 1985 .
Cons idering the adverse heal th consequenées associatedwith smokeless tobacco , the potential add ictiveness of
smokeless tobacco , the high prevalence of smokelesstobacco use in North Carol ina and the potenti al healthbenefits accruing from smokeless tobacco cessation, or
never initiating the hab it, and based onmy expertise in thearea of smokeless tobacco I recommend and support thatphysicians in North Carol ina cons ider the fol lowing :1 ) the implementation of a warning label on smokelesstobacco containers ;
2 ) the development of a smokeless tobacco cessationmodel for those currently addicted ;
3 ) the support of heal th education in the publ ic schools
regarding the dangers assoc iated w ith the use of
smokeless tobacco this education should beg inearly ,
when children are 7 and 8 years old ; and
4 ) the enforcement of l aws restricting minors frompurchasing/sel l ing smoke less tobacco products .

References
l . Christen AG . The case against smokeless tobacco: Five facts for the healthprofessional to consider. J AmDent Assoc l 980; l0 l :464—9.
2 . United States Department of Agri culture . 1984 .
3 . Harper S . In tobacco , when there‘
s smokeless fire . Advertising Age . June 2 3 ,
1980 .
4 . News article and interview w ith four tobacco executives . Pinkerton'
s fortunes
rise with soc ial acceptance of chewin g . US Tobacco J, May 29 . I9BO.
5 . Silverrnan S . Oral Cancer, American Cancer Society ; 6-35 . 198 1 .
6 . G loverED. ChristenAG . HendersonAH . Smokeless tobacco and the adolescent
male . J Early Adolescence l 982 ;2 ; l - l 3 .
7 . Jayant K . Balakrishnan V , Sanghvi LD, et al. Quantification of the role of
smoking and chewing tobacco inoral , pharyngeal , and oesophageal cancers . BrJ
Cancer l 97 7 ;3 5 :2 32—5 .
8 . WinnDM, B lotWJ , ShyCM, et ai . Snuffd ipping and oral cancer among women
in the south ernUnited States . New Eng J Med l 98 1;304 ; 7 4 5 -9 .
Elbert D. G lover, Ph .D.
East Carol ina UniversitySchool of Al l ied Health Social Work
G reenvil le 2 7 834
Bal loons on the CCU
To the Editor
We would l ike your permission to reproduce inour new
magaz ine , Med iScene , your art icle entitled“Bal loons on
the CCU”by Charles Shunior. BSN . which appeared in
Apri l 1985 (NCMJ
This article would be reprinted in our pi lot issue of
Med iScene which is a new magaz ine about medical caretrends and is directed toward the publ ic . We wil l be distrib
uting the magaz ine to doctors for their offices .
Judy Marr , Ed itor
MichiganMedicine Medigram
120 West Sag inaw StreetEast L ansing , MI 4 8823
Med ical Mystery and the Whistl e B lowerA letter to the author , Mebane Hol loman Burgwyn
Dear Mebane ,HelenDuganAl len, a classmate of yours , brought tomy
attention your art icle , Medical Mystery and the WhistleB lower, which appeared in the North Ca rol ina Med ica l
Journa l last September (NCMJI am so touched by your article that I would l ike to reprint
it in the fal l issue ofAlumni News . I request permission todo so .
Your article is so personal and so reveal ing . What youhave experienced w i l l be of great value to our alumnireaders . B less you for demystifying chemotherapy in suchan Open manner and with such good
-hearted charm . Irejoice with you that the outcome of your treatment hasbeen positive .
Questionable Med ica l Advertis ing
To the Editor
Dr. Maymandi , M.D. , Chairman of the State MedicalCommittee onEth ics , has informed me that he has taken itupon himse lf to inform each one of you of an ad that
5 50 VOL . 4 6 , No . 10
appeared three times in the Fayettevil le newspaper, The
F ayettevi l le Times , in Fayettevi l le , NC , concerning theopening of a mammography imaging center located at a
Doctor’
s Urgent Care Centre faci l ity in Fayettevil le , NC .
Although I do not have d irect involvement at this time withthe imag ing center and d id nothave prior know ledge of th isadvertising modal ity , I am the Medical Director for Doctor
’
s Urgent Care and feel that I must respond to the
advertisement, as we l l as toDr. Maymandi’
s letter to you.
It was , for me , a most unhappy experience to see this
form of advert isement in the paper. I immediately con
tacted Mr. SidWol insky , who is the President ofDoctor’
s
UrgentCare Centre , and informed himofmy deep concernthat the ad , with the schematic drawing of the lady , would
appear to be in very poor taste and placed in the paperwith
poor judgment. Mr. Wol insky immediate ly agreed and
stated thathe also had not had the Opportunity of see ing this
material before publ ication. We have had a board meetingconcerning this advertisement, and our board has beenequal ly unhappy . Unfortunately , because the advertise
ment does represent our imaging center , we must assume
the responsibi l ity . I would l ike to explain how this hap
pened but real ize that the blame must certainly be ours .
An exce l lent radiolog ist, Dr. Mart in Locey , M.D. ,
directs the new imag ing center at a facil ity managed byDoctor
’
s UrgentCare Centre . I personal ly know him to be
one of the finest trained rad iologists I’
ve had the pleasure of
meeting . As part of the imaging package , amammographyunit was establ ished , and Dr. Locey has put together a
patient educational program for self-examination with en
couragement to seek annual examinations by their own
phys icians . This educational experience is accompanied bythe newest mammography equipment availab le with thelowest yie ld of radiation. Itwas felt that th is was a service
needed in our community , as mammography had beenoffered by the only radiological team in the area at
per examination. They have subsequently reduced the ir feeto and 1 can only fee l that this was a result of the
competitive nature of this center.
An advertisement agency was h ired to announce to the
publ ic the establ ishmentof themammography cl inic . They
put together the advertisement that you have seen, and
unfortunate ly , no one on the Doctor’
s Urgent Care Centre
staff saw the ad prior to it be ing placed in the paper.
Apparentl y , the business component division felt that theprofess ional component was handl ing this , and the oppo
s ite al so had been thought to be true , but apparently not so.
When the ad came out, we did have ourmeeting , and itwas
requested to withdraw the ad from the paper. Unfortunate
ly , the ad was going to be in a Sunday edition and that
section of the paper had already been printed ; therefore , it
was unable to be w ithdrawn, so a second ad appeared . The
advertisement company was contacted and told the ad was
not fe lt to be appropriate , particularly the schematic draw
ing . The final insult to the situationwas that the advertis ingpeople did change the schematic , but certainly not enough
to make the ad tolerab le , and the ir change went into the
paper as the last and final advertisement.
This ad has been entirely and total ly withdrawn from thepaper, and I can assure you future publ icity wi l l be lookedat close ly by the medical staff of Doctor
’
s Urgent Care

nal insufficiency there is low cortisol and high ACTHlevels . ) b) low 17 OH -cort isosteroids , urinary free cortisols
and serum cortisol that increased stepwise during three
days of intravenous ACTH stimulation.
We do not understand the claim of Drs . Krestev and
Tersieva of hav ing cases of primary suprarenal insuffi
ciency who have increased the level of cortisol after synac
then stimulation. This , by definition, would inval idate
the diagnosis of primary adrenal insufficiency .
3 ) The different theoretical poss ib i l ities mentioned forpatient No . 2 are doubtful because of the normal thyroidhormone , testosterone and prolactin levels . Again, one
cannot postulate primary adrenal insufficiency in a patientwho shows a normal cortisol response to ACTH . Th istogether with failure to increase the cortisol level duringsymptomatic hypog lycemia has to be interpreted as a deficiency inACTH secretion. It is possible that the underly ing mechanism is an autoimmune one .
4 ) We agree that in case 3 there is an ongoing autoimmune process . We do not have definite proof that th isautoimmune process involves any other organ than the
thyroid . The presence of any adrenal antibodies wouldsuggest an autoimmune attack to the adrenals , but would
not be of help in decid ing if the patient had primary or
secondary adrenal insufficiency . This is a functional di
agnosis . The ACTH stimulation, the insul in tolerance andmetyrapone test al l suggest thatthe hypocorticismis causedby ACTH defi ciency .
F inal ly , we think that computerized tomography is an
exce l lent technique to visual ize the adrenals . Unfortunatelyit does not provide any information about the function of
the adrenal g lands .
Jorge J . Gonzalez , MD .
Emi l E . Werk , Jr. , MD .
New Hanover Memorial HospitalW ilmington 2 8402
Ole Doc
Recently a fel low phys ician agreed that we have been privileged topractice through what seems to be the final days Of the best days of thepractice of medicine despite the many new developments in drugs and
marvelous procedures . Nevertheless , refl ecting upon this , these l ines came
to me :
H is rickety buggyDown the muddy road he rode
H is patient’
s pain to ease
Now he has other thingsTo worry aboutNot only patientBut family , lawyer ,
Uncle Sam and PISRO to please .
There was a time when doctoring was more funWhen the horse , not the doctor , stayed on the run
When Ole Doc received thank s with respectEven when his treatment fai led
Twas sti l l the horse not Ole Doc
Who got the whip to the tai l .
5 5 2
John Fitzgerald , Jr. , MD .
VOL . 46 , No . 10


B rief Summary of Presc ribing InformationNORLESTRIN' (nore l h ind rone ace tate and eth inyl es tradiol tab lets . USP)
See sectionunder Spec ial Notes onAdministrationand NOWSUPPLIED.
Before prescrib ing . please see lull prescrib ing information ABrief Summary follows .
DESCRIPTIONNorlestrinProducts are prog estogen
-estrogencomb inations .
INDICATIONS ANDUSAGENorles trinProducts are ind icated for the preventionofpregnancy inwomenwho e lecl touseoral contraceptives as amethod ofcontraceptionInc linical tria ls with Norlestrin involving therapy cycles . there was a preg
nancy rate of0 05 per 100 woman-years : incl inical trials With Norlestrin involvingcyc les. there was a pregnancy rate of0 2 2 pe r 100woman
-
years .
Dose -Re lated Rlalt ofThromboembol lsmfromOral Contraceptives : Stud ies haveshowna pos rtive assoc iationbetween the dose ofes trogens inora l contraceptives and the
risk of th romboembolism It is prudentand in keeping with good prrncrples of therapeutics to
minimize exposure toestrogen. The oral contraceptive prescribed forany g iven patient
should be thatproductwhich contains the leas tamountofes trogen that is compatib le wrth
anacceptab le pr nanCy rate and patientacceptance .
CONTRAINDICAT ONSThromboph leb itis or thromboembolic d isord ersApas th istory of deep-ve inthromboph leb itis orthromboembolic d isordersCerebral vascmarorcoronary art ery d iseaseKnownor suspected carcinoma of the breas tKnownorsuspected estrogen-dependentneoplas
'
ia
Und iagnosed abnormal genital b leedingKnownorSuspected pregnancy (SeeWARN ING No. 5 )Benignorma lignant liver tumorwh ich deve loped during the use oforal contraceptivesOrothe restrogen
-containing products .
1. Thromboembolic Disorders and.Other VascularProb lems . An increased ris k of lhromboembolic and thrombotic d isease associated with the use oforal contraceptives IS we lles tab lished Stud ies have demonstrated an increased ris k of fatal and nonfata l ven0usthromboembolismand stroke . both hemorrhag ic and thrombotic.
CerebrovaecularDisorders : Ina collaborative s tudy inwomenwith and Withoutpred isposing causes . itwas es timated that the ris k ofhemorrhag ic stroke was times g reater inusers thannonusers . and the ris k of thrombotic s troke was 4 0 to times .greater
were found to be a clearadditional ris k factor.
'
ec lamptic toxemia. and espec ially by cigarette smoking .
The phys ic ian and the patient should be alert to the earlies tmanifestations ofthromboembolic and thrombotic disorders . Should any occurorbe suspected . the d rug should be d is
continued immed iate lyAfourfold Io s ixfold increased ris k ofpos lsurgerythromboembolic compl
ications has
been reported inusers . if feas ib le . oral contraceptives should be d iscontinued at least four
weeks be fore surgery ofa type assocra led With an increased ris k of thromboembolismor
prolonged immobilization2 . Ocular Les ions . NeurO-ocular lesions . Such as optic neuritis orretinal thrombos is. have
beenassoc iated with the use oforal contraceptive s . Discontinue the Oral contraceptive if
there IS unexplained suddenOrg radual . partial . orcomplete loss ofvrs ion. onseto propto
s is or d iplopia; papilledema: or retina l vascular Iesrons .
3 . Carcrnoma . Long-termcontinuous adminis trationofes trogen incertainanimal species
increases the frequency ofcarcmdma ofthe breas t.cervix. vag ina . and liver.Inhumans . an increased risk of endometrial carc inoma assomated with the prolonged
use ofexogenous es trogen inpos tmenopausa l womenhas been reported . However, thereis no evidence sugges ting increased ris k ofendome lria l cancer inusers ofconventionalcomb inationorproges togen-only oral contraceptives .
Stud ies found no evidence of increase in breas tcanoerinwomen tak ing oral contraceptives : however. anexcess ris k inusers With documented benign breast d isease wasreport ed .
There is noconfirmed evid ence ol an increased ris k ofcancer assoc iated With ora l contraceptives Close clinical surve i llance ofusers is . nevertheless . essential incases ofund iagnosed perSrs lentor recurrentabnormal vag inal b leed ing , appropriate d iagnos tic measuresshould be taken to rule outma lignancy Womenwrth a s lrong fami ly h istory of breas t cancer.orwho have breastnod ules .
Iibrocystic d isease . or abnormalmammog rams . should be
monitored with particularcare .
4 . Hepatic Tumors . Benignhepatic adenomas have been found to be assoc iated with oralcontraceptives . Because hepatic adenomas may rupture and may cause death throughinfra-abdominal hemorrhage . they should be cons idered inwomenpresenting abdominal
painand tenderness . abdominalmass , or shock.
Afewcases ofhepatoce llular carc inoma have been reported inwomen tak ing oral contraceptives The re lationsh ip of these d rug s to this type ofmal ignancy is not knownatth is time.
5 . Use 8 in or Immed iate! Preced ing Pregnancy: Birlh De fecls inOffspring . and Malignancy In emale Offspring .During early pregnancy. female sex hormones may serious lydamag e the offspring .
An increased ris k ofcongenital anomalies . includ ing heart defects and limb defects . has
been reported with the use oforal contraceptives in pregnancy.There IS some evidence thattriploidy and poss ib le other types ofpolyploidy are increased
among abortuses fromwomenwho become pregnant soonafterceas ing oralcontraceptives .
Pregnancy should be ruled outbefore continuing anoral contraceptive inany patientwhohas missed two consecwrve mens trual periods . If the patienthas notad hered to the sched
ule . the poss ib i lity of pregnancy should be cons idered at the time of the firs tmissed period .and oral contraceptives should be withhe ld unl itpregnancy has been ruled Out. Ifpregnancy is confirmed . the patient should be apprised of the potential risks to the fetus and theadvrsab ility of continuationof the pregnancy should be d iscus sedWomenwho d iscontinue oral contraceptives with the intentofbecoming pregnantshould
use an alternate formofcontracepe n fora period of time before attempting toconce ive .
Administrationofprogestogen-only orproges togen-es trogencombinations to inducewithd rawal b leed ing should notbe used as a testofpregnancy6 . Gallb ladderDisease. Stud ies report an increased risk ofsurgically confirmed gallb lad
der d isease inusers oforal contraceptives .
7 . Carboh yd rate and Lip id Metabolic Effects Because decreased g lucose tolerance hasbeenobserv ed in a s ignificantpercentage ofpatients . pred iabe l ic and d iabetic patientsshould be carefully observ ed wh ile rece iving oral contraceptives .
An increase in trig lycerides and total phospholipids has beenobserv ed .
8 . Elevated Blood Pressure . An increase in b lood pressure has been reported inpatients
rece iving oral contraceptives . The prevalence inusers increases with longerexposure . Ageis also strong ly corre lated with deve IOpmenl ol hypertens ion.Womenwhoprevious ly havehad hypertens ionduring pregnancy may be more like ly to deve lop e levationofb loodpressure .
9 Headache Onsetor exacerbationofmigraine ordeve lopmentof headache ofa newpatternwh ich is recurrent. pers is tent.orsevere . requires d iscontinuationoforalcontraceptives .
10 B leed ing Irregulari‘
i i'
es . Breakthrough b leed ing . spotting . and amenorrhea are Irequentreasons forpatients d iscontinuing oral contraceptives lnbreakthrough b leed ing .
nonfunctiona l causes should be borne inmind Inund iagnosed abnormal b leed ing from thevag ina . ade quate d iagnosticmeasures are ind icated to ru le outpregnancy ormalignancy.Womenwith a past h istory ofoligomenorrhea orsecondary amenorrhea . Oryoung women
without regularcycles should be advised that theymay have a tendency to remainanovulatory or to become amenorrhe rc alter d iscontinuationofora l contraceptives .
11
fEl
cfopic Pregnancy. Ectopic as well as intrauterine pregnancymay occur incontraceptive a i ures .
ers rece ivin these drug s .
PRECAUTI NS
pone test.
Drug Interactions : Reduced e ff icacy and increased incidence ofbreakthrough b leed inghave beenas soc iated with concomitantuse of rifampin.Asimilarassoualron has beensuggested with barb iturates . phenylbutazone . phenytoin sodium. te tracyc line . and ampicillin.
ADVERSE REACTIONSAn increased risk of th e followmg serious adverse reactions has beenassociated with oralcontraceptives . thromboph leb itis : pulmonary embolism: coronary thrombosis . cerebral
thrombos is; cereb ra l hemorrhage; hypertension; gallb ladderd isease : benignhepatomas :congenital anomal ies .
There is evidence ofanassoma lron be tween the following cond itions and the use oforalcontraceptives . althoug h add itional confirmatory stud ies are needed . mesenteric thromboS IS .
neuro-ocular leS ions . eg .retinal lhromDOS is and optic neuritis
The followmg adverse reactions have been reported inpatients receiving ora l contraceptives and are be lieved to be d rug re lated . nausea and/ orvomiting . usual ly themos tcommonadverse reactions , occur inapproximate ly 10% or less of patients during the firstcycle.
Olhe r reactions. as a g eneral rule . are seenmuch less frequently oronly occas ionally:gas trorntes trnal symptoms : breakthmug h b leed ing : spoi l ing ; change inmenstrual flow:dysmenorrhea . amenorrhea during and after treatment, temporary infertility after d iscontinuance of treatment. edema : ch loasma orme lasma. breastchanges : change inwe ig ht:change ince rvical eros ionand cerv ical secretion: poss-b le d iminution in lactationwhen
g iven immed iate ly pos tpartum: choles tatic jaund ice :mig raine , increase in s ize ofuterine
le iomyomata ; rash (allerg ic) :mental depreSSron: reduced tole rance to carbohydrates ;vag inal cand id ias is. change incorneal curvature : intolerance tocontact lense s .
The following adverse reactions have been report ed and the association has been‘ne ilher
c0nlirmed nor re futed : premens trua l-like synd rome : cataracts : changes in lib ido: chorea:changes inappetite : cys titis
-like syndrome : headache : nerv ousness : d izziness : h irsutism:loss of scalp hair. erythema multrforme , erythema nodosum: hemorrhag ic eruption; vag initis :porphyria
Spec ia l Notes onAdministratlonMens truationusually beg ins twoor three days . butmay beg inas late as the fourth or fifthday. after d iscontinuing med icationAfte r severalmonths on treatment. b leed ing may be reduced toa pointofvirtual absence:
reduced flowmay be a resultofmed icationand not ind icative of pregnancy.HOW SUPPL IEDNorles trin is availab le incompacts each containing 2 1 tab lets Each tab letcontains1mg ofnoreth ind rone acetate and 5 0mcg ol eth inyl es trad iol. Availab le inpackages of fivecompacts and ackages of live refills
Norlestrin 2 is availab le incompacts each containing 2 1 tab lets . Each tab let
conta ins mg ofnore lhind rone acetate and 5 0mcg Ofeth inyl estradiol . Avai lab le inpack
ages ol five compacts and packages of live refills .
Norle strinE ] is availab le incompacts each containing 2 1 ye llow tab le ts and 7
brown tab lets . Each ye llow tab letcomains 1mg ofnore lh indrone acetate and 5 0mcg ofeth inyl estrad iol Each browntab letcontains 7 5 mg of fe rrous fumarate . USP.Ava ilab le in
packag es of five compacts and packages of five refi lls .
Norles trin is availab le incompacts each containing 2 1 pink tablets and 7brown tab lets Each pink tab letconta ins mg ofnorethindrone acetate and 5 0mcg ol
eth inyl es trad iol. Each brown tab letconta ins 75 mg of ferrous fumarate .USPAva ilab le in
packag es of five compacts and packages of l ive refi lls .
Norles trin is ava i lab le incompacts each containing 2 1 ye llow tab lets and 7 wh ileinert tab lets Each ye llow tab letconta ins 1mg ofnore lh ind rone acetate and 5 0mc of
eth iny l es trad iol. Availab le in packages of five compacts and packages of live re lil s .
09016 13 1PARKE-DAVIS
Divis ionofWarner-LambertCom anyMorris Plains .New Jersey 0 95 0
O 1085 Wa rner-Lamb ertCompa ny PD-21-JA-2563 -P-1f11-84 )

index to Advert isers
Army ReserveAyerst LaboratoriesB B X-Ray , Inc .
B lue Cross/B lue Shie ld of North Carol ina
Campbel l L aboratories , IncCHAPS
Crumpton CompanyCurtis 1000 Information Systems
GuestHouse
EF Hutton Company Inc .
Info Systems of NC , Inc .
Knol l Pharmaceutical
El i L il ly Company
5 5 6 VOL . 46 , No . 10
Marion L aboratories , Inc .
Medical Mutual Insurance Company of NC
National Staffing Services Corporation
Ortega Pharmaceutical
Parke-Davis
The Physician and Sportsmedicine
Roche L aboratoriesSeabrook IslandSmith Kline BeckmanThe Upjohn CompanyU. S . Air Force
Wil l ingway , Inc .
Winchester Surgical Supply Co . , Inc .

EXCERPTS FROMASYMPOSIUM“THETREATMENTOF SLEEPDISORDERS"8
highly effectiveforboth s leep inductionands leep ma intenance
SleepLaboratory InvestigatorPennsylvania
onsetofactionisrap id. . provides s leepwithno rebound effectto
patientthe fol lowing
PsychiatristCalifornia
. . appears tohavethe bestsafety record ofanyofthe benzod iazep ines
PsychiatristCalifornia
After 15 years, the experts still concuraboutthecontinuing value ofDalmane (flurazepamHOI/Roche) . Itprovides s leepthatsatisfies patients .
and thewidemarginofsafety thatsatisfies you.
The recommended dose inelderlyordebilitatedpatients is 15 mg. Contraindicated inpregnancy
flura zepam HC I/Roche as leep tha t satisfies
i S-mg/30-mgcaps
References : l . Kales J, atat: ClinPharmacol Ther 12 :69 l
69 7, Jul-Aug 19 7 1. 2 . KalesA, efal: ClinPharmacol Ther—3 63 , Sep 197 5 . 3 . Kales A, atof: ClinPharmacol
Ther -583 , May ig 7 6 . 4 . Kales A, efal: ClinPharmacol Ther3 2 : 78 t-7 88 , Dec 198 2 , 5 . FrostJDJr, DeLucchiMR: JAmGeriatrSoc - 5 4 6 , Dec 197 9 . 6 . DementWC, efal; BehavMed, pp. 2 5 Oct l 97 8 . 7. KalesA.
Kales JD: J ClinPsychopharmacol —150, Apr l 983 .
8 . TennantFS, 9! al. SymposiumontheTreatmentofSleepDisorders , Teleconference, Oct is, 1984 . 9. GreenblattDJAllenMD, ShaderRI: ClinPharmacol Ther -36 l ,Mar 197 7.
DALMANE"
flurazepamHCI/RocheCttZ
Before prescri bing , please consultcomplete productInformation. a summaryofwhich follows :Indications: Effective inal l types of insomnia characterizedby d ifficulty in fall ing asleep,
frequentnocturnal awakeningsand/orearlymorning awakening, inpatients with recurringinsomnia orpoors leeping habits ,
inacute orchronicmedicalS ituations requiring restful steep. Objective s leep laboratorydata have showneffectiveness forof least28 consecwivenights ofadministration. Since insomnia is oftentronsrenfand intermittent, prolonged administration is generally notnecessaryorrecommended Repeated therapy should onlybe undertakenWith appropriate patientevaluation.
Controlndicotions : Knownhypersensitivity to flurazepamHCI.pregnancy. Benzodiazeprnes may cause fetal damagewhenodmrnrstered during pregnancy. Several stud les suggestanincreased risk ofcongenitalmalformations associated Withbenzodiazepine use during the firsttrimesterWornpatientsofthe potential risks to the fetus should the possibility ofbecoming pregnantexistwhile receiving tlurazepom Instructpatients todiscontinue drug priortobecoming pregnant. Considerthe poss ibil ity ofpregnancy priorto instituting therapy.
Warnings : Cautionpatients aboutpossible combined effectswith alcohol and otherCNS depressants. Anadd itive effectmay occurifalcohol rs consumed the day following use fornighttime sedation. This potentialmay existforseveral daysfol lowrng discontinuation. Cautionagainsthazardous accu
patrons recurring completemental alertness ( e g operatingmachinery, drivmg) . Potential impairmentofperformanceofsuch activities may occw the day fol lowmg ingestion. Not
recommended foruse inpersons under 15 years ofageWithdrawal symptoms rarely reported , abruptdiscontinuation
should beovorded With gradual tapering ofdosage forthose
patients onmed icationfora prolonged period of time Usecaution inadministering toaddiction-
prone rndiwduols or
thosewhomight increase dosage.
Precautions : Inelderly and debilitated patients. it is icccmmended thaf the dosage be limited to 15 mg to reduce risk ofoversedation, dizziness, confusronand/orataxia. Cons ider
potential additive effects with otherhypnotics orCNS depres
sants Employ usual precautions inseverely depressedpatients, or inthosewith latentdepressionorsurcidal tenden~
eres, or inthosewith impaired renal orhepatic function
Adverse Reactions : Dizziness . drowsiness ,lightheadedness .
staggering, ataxia and fall ing haveoccurred , part icularly inelderly ordebi litated patients Severe sedation, lethargy, d isorientationand coma, probably ind icative of drug intoleranceoroverdosage, have beenreported Also reported. headache,
heartburn, upsetstomach, nausea, vomiting, d iarrhea . con
stipation, GI pain, nervousness , talkativeness, apprehensron,
irritability, weakness , palpitations , chestpa ins , body and jOlt'
l l
pains and GUcomplaints . There have also been rare occur
rences of Ieukopenia, granulocytopenia, sweating,flushes,
difficulty rnfocus ing, blurred vis ion, burning eyes . fa intness.hypotension, shortness of breath, pruritus , s k inrash, drymouth, bittertaste, excessive salivation, anorexia. euphoria,
depreSSron, s lurred speech, confusion, restlessness. halluo
notions , and elevated SGOT. SGPT. total and d irectbil irub ins,and alkaline phosphatase; and paradoxical reactions , 9 g. .
excitement, stimulationand hyperactivity.
Dosage: Individualize formaximumbeneficial effect Adults30mg usual 005 099: 15 mgmay suff ice insome patientsElderlyordebilitated palienls: 15 mg recommended initiallyunti l response rs determined .
Supplied: Capsules containing 15 mg or30mg flurazepamHCI.



Pub l ished Monthly as the Official Organ of The North Carol ina Medical Society ( l SSN -0029 - 2 5 5 9 )
NOVEMB ER 1985 , NCMJ

F inancia l new s you have been w a i ting to hearl.
’
ew ncreas e
ncome
Ava i lable to ig ible Members Under Age 5 0Rega rd les s Other D is abi l i Insurance
Offic ia l North Carol ina Med ica l Soc ietyDis abil ity Income Plan
Endors ed and Recommended S ince 193 9
Protect your mos t va luab le as s et, your profes s iona l income
For details or cla ims s ervice ca ll orwrite :
CRUMPTON COMPANYPROFESS IONAL GROUP INSURANCE
Toll free - 16 7 4
ACADEMY CENTERPOST OFFICE BOX 8 5 00DURHAM, NC 2 7 7 07
Account executives : J . S lade Crumpton, Gene G reer and CliffMasher, DurhamJack Featherston, Charlotte
Dan Ha ley , G reensboro
VOL . 46 , No . 1 1

Roche salutes
its many aspectsIt is estimated that2 5 millionpeople ( l 1% ofthe
population) are overage 65 , and representthefastest-growing segmentof the populationby far. It isfurtherestimated thatthis groupcurrently spendsapproximately 7 5 bi lliondollars annually forpersonalhealth care, and accounts forsome 5 5% atall federa
health dollars .
‘ Forthese reasons alone, studiesconcernedwith various aspects ofaging are ofvitalimportance to the entire nation. Muchmajorresearch inthis complex area is being conducted inNorth Carolina,
at its severalmedical centers and univers ities , oftenundergrants fromthe National Institute onAging.
Studies coverawide rangeRecentstudies have reported onthe phys iologicaldynamics ofaging as related tocirculatory diseasesand circulatory risk factors ofadvanced ages (over85 ) as compared to findings ina study populationwith ameanage ofover7 0 years .
2 Anotherstudy,stemming fromthe comprehensive Duke FirstLongitudinal Study, evaluatedWechslerMemory Scale scoresas related todistance fromdeath and the potential useoftheWMS as a predictorof survival inboth normaland demented elderly populations , 3 while yetanothercompared young and old adults inthe spontaneoususe ofcontextto learnand recall information.
4
Copyright 1985 byRoche Products Inc. All rights reserved.
Deal ingwithAmerica’
s
fourth leading kil lerdiseaseResearchers atDukeUniversity Centerforthe StudyofAging are focus ing onthe study ofAlzheimer’ sdisease, a type ofprimary neuronal degenerationthat is themostcommonformof dementia. Estimatesvary but indicate thatas many as 4 millionolderAmericans ‘ are afflictedwith this illness, which hasbeen labeled
“the disease of the century( '5 Concurrent
with its medical research onAlzheimer’ s disease, theDukeUniversity Center is providing innovative supportmechanisms forafflicted families and othercaretakers .
Ahotline provides callers with telephone consultations,introductions toothers close by ins imilarcircumstances, and practicalmedical, legal and psychologicaliriformation. The Centerhas alsoaided inthe establishmentof 19 local supportgroups statewide, andregularlymakes avai lable informationonAlzheimersdisease to health providers, nursing homes and hospitals, and others responsible forprograms and servicesdirected toward the victims of this killerdisease.
6
References : 1. MasonMK Slack ML, Mooney RP: WVaMed J 79 98 -102 ,
May 1983 . 2 . MantonKG, Woodbury MA: J Gerontal 3834064 13 , Apr 1983 .
3 . Sieg ler IO, Mccarty SM, Logue PE: J Gerontol-18 1, Feb 1982 .
4 . Hess TM, Higgins JN: J Gerontol-7 1, Jan 1983 . 5 . RoachM: NY
Times Mag, Jani e, 1983 , p. 22. 6 . (MytherLTNCMed J 44 ;4 34 -4 3 6, Jul 1983 .

Arational approach, combiningThe standard antidepressant
amitriptylineThe provenanxiolytic actionofLibrium® (chlordiazepoxide HCI/Roche) @
Marked improvementoftenoccurs_
asearly as the firstweek
Headache, insdmniaor'
Gl upsets associatedwithmixed depress ionandanxiety oftenrespond quickly
Feeling better, patients feel encouraged tostay the course—therefore,fewerdropouts : P:
.006 compared toamitriptyline*
Convenients ingle h.s . dos ing sufficient insome patients; helps patientswithmixed depressionand anxiety s leepthrough the night. Patientsshould be cautioned aboutthe combined effects ofLimbitrolwith alcoholand otherCNS depressants, and aboutactivities requiring completemental alertness such as operatingmachineryordriving a car.
Inmoderate depress ionand anxiety
IN PLACEOFLIMBITROL 5 WRITE:
Each tabletcontains 5 mg chlordiozepoxide and mg amitripty line ( as the hydrochloride salt)
INPLACEOFLIMBITROL IO- 25 WRITE:
Each tabletcontains 10mg chlordiazepoxide and 2 5 mg amitripty line ( as the hydrochloride salt)
Eas ierto remember. eas iertoprescribe



LEARNINGWlTHOUTWORDS
That Addisonian Tan
The Healthy Looks that May Deceive
Mark L inzer, MD .
0 Amanfrom Buffa lo whofeels poorly , craves sa lty foods , and looks in
December as if he j ust stepped ofl'
the beach but didn’
t mus t beviewed with a skeptical eye .
HATa tan!’
The phrase canbe heard frequentlyaround the swimming pool s , backyards , and
beaches of North Carol ina . But phys icians have becomeincreasingly aware that solar energy can produce seriousand long
- lasting destructive dermal and epidermal changesas well as markedly increase the risk of developing mal ignant melanoma . Thus , the medical l iterature has recentlybeenfill ed with warnings forour patients towearprotectiveclothing , uti l ize sunscreens and even beware the reflectionfrom sand , snow or water.
W ith the plethora of recent reminders concerning theevil s of suntanning , phys icians may begin to V iew the
From the Department of Medicine , Duke Univers ity Medical Center,Durham 27 7 10 .
Figure 1 . Patient (on left) with excessive hyperpigmentation. Author’
s chest is included for comparison.
NOVEMB ER 1985 , NCMJ
excess ively tanned personas someonenotunl ike the chronia smoker individual s whomeri t a serious lecture on thedangers of their
“hab it. ” The fol lowing case report wi l l
serve as a reminder that excess ive suntanningmay be a s ignof the l ife-threatening but treatable d isorder described byThomas Addison 130 years ago; it il lush ates that a patientwith th is d isorder may appear deceptively healthy .
I recently saw a 2 7 -year—old former carpenterwho com
plained of two months of weakness , anore x ia , nausea ,dizz iness and a 10pound we ight loss . He al sonoted thathis
suntan from the previous summer had not faded . In fact, he
felt thathis tanwas evendarker inDecember (wh ile he wasl iving inBuffalo) than it had been the previous July . Over
the past six months he had deve loped a craving forDoritossuch that he consumed over one large bag (containing

F igure 2 . Patient'
s suntanned ax i l la .
approximately 4 g of sod ium) per day . The patient had had
no trauma , recent surgery or exposure to tuberculosis . H e
had always been in good heal th before the present il lness .
The fami ly history was remarkable for hypothyroidism inhismother and adult onset diabetes mel l itus in an aunt. He
was a tal l , healthy appeari ng , lean and muscular person
with a dark tan that was most prominent in sun-exposedareas ( figure The fanwas sharply demarcated at the l ine
where he wore his swimsuit. There was no hyperpigmenta
tion of the palms or buccal mucosa , and no accentuationof
tanning at the elbows , knees or metacarpophalangeal
joints . There was some excessive tanning in the ax il lae( figure
H is blood pressure was supine and dropped to
wh ile standing . H is heart rate was 80 supine and 108standing . He was afebri le and breathing comfortably at
rest. Cardiac examination showed normal heart sounds
w ith amid-systol ic cl ick .
‘
Due to the comb inationof orthostasisand the excess ive tanning , the diagnosis ofAdd ison’
s
disease was considered . Th is diagnosis was supported byfinding that the serum sod iumwas 12 1 mm/ l (normal 13 514 5 mm/ 1) and the potassium was mm/ l (normal
VOL . 46 , No . 1 1
mm/ l ) . Serum glucose was 7 6 mg/ 100 ml (normal7 5 - 100 mg/ 100 ml ) .The patient was placed in the hospital for further d iag
nostic evaluation, including a 4 8 hour cosyntropin stimulation test. Although a
“one shot cosyntropin stimulation
test mi ght have been sufficient in the eyes of some , Iperformed the ful l 4 8 hour test in order to unequivocal lydocument a diagnos is which , once made , would re legate
the patient to a l ifetime of medications for an endocrine
insufficiency disease that is potential ly l ife threatening .
Amorning serumcortisol wasmarkedly low at ug/dl
(normal 12 - 2 5 ug/dl ) and a simultaneous ACTH level waselevated at 12 1 pg/ml (normal 10-50 pg/ml ) . Continuouscosyntropin stimulationproduced no rise in serum cortisolafter 4 8 hours (normal response 50 ug/dl ) . A sk in testfor tuberculosis was negative at 4 8 hours , and an abdominalCT scan showed no evidence ofmetastases , calcifi cation,
or adrenal hemorrhage . A d iagnos is of primary adrenal
insuficiency was made , and the patient was started on
cortisone acetate and fl udrocort isone by mouth . After onlytwo weeks the patient was feel ing markedly improved .
There a sharp decrease in his consumption ofDoritos , and
his tan had already begun to fade .
FromAddison’
s orig inal descriptionof his patients withadrenal fai lure , one might not expect the vigorous , sun
tanned appearance of the patient reported above to be a signof Addison
’
s disease . Indeed , the“anaemia , general lan
guor and deb il ity , remarkable feebleness of the heart’
s
action, irr itab i l ity of the stomach and pecul iar change of
color in the skin”noted by Addison,
l might lead one toexpect a sal low and debil itated individual . Although mypatient feltunwe l l , there was nothing inhis general appear
ance that gave a clue to this . Perhaps this is why he waitedso long before seeking med ical attention. Not al l patients
with Add ison’
s disease are hyperpigmented ,
2but the vast
majority are excessively tanned ,
3often in unusual loca
tions . In our patient, the tanning in the ax il lae (espec ial lyduring a Buffalo winter) was a clue thatpathologic tanningwas tak ing place . The association of mitral valve prolapse
with Addison’
s disease has not previously been reported
and atpresent can only be V iewed as a chance assoc iation.
Chronic sunl ight exposure is associated with several
derrnatopathologic changes including wrink les , te langiectasiae , Favre-Racouchot Syndrome (yel low facial skincolor w ith cysts and comedones) and the poik iloderrna of
C ivatte (prominent hair fol l icles in brown te langiectatic
skin) . Excessive suntanning , while clearly a common sign
of longstanding exposure to ultraviolet l ight, should al so
raise the specter of primary adrenal insuffi ciency , even in
the“glowingly
”healthy patient.
References
l . AddisonT. On th e constitutional and local effects of disease of the supra-renal
capsules . London: Highley. 185 5 .
2 . BarnettAH , EspinerEA, Donal d RA. Patients presentingwith Addison'
s disease
need not be pigmented . Postgrad Med J l 982z5 8z690-2 .
3 . Nerup .l . Addison'
s disease cl inical studies . A report of [ 08 cases . Acta
Endocrinol l 97 4 ;7 6 : 127 -39 .

SCIENTIFICARTICLE
Triiodothyronine Therapy : An Iatrogenic Bait
Jorge J. Gonzalez , MD .
0 There are thyroid pi l ls and thyroid pi l ls .
THE alterati ons of the class ical thyroid function test
produced by T3 replacement or suppress ion therapyare wel l known. Despite thi s fact condoned mi sinterpreta
tionof the resul ts of thyroid functiontests of patients onT3therapy occur . Some patients donot know the type orname
of the ir thyroid pill s . The fol lowing exchange il lustrates thehi story of several patients I have seen in the last two years .
“How long have you been taking the thyroid pil ls , Ms .
Smith , asked Doctor One .
“oh , three or four years ,
”
said Ms . Smith .
“Do you know why you were started on
the thyroid pill s?’
DoctorOne asked .
‘
TheDoctor toldme
my thyroid was low or something like that,”repl ied Ms .
Smith .
“Well , we'
l l check that out,”said Doctor One .
Two days laterT4 is free thyroxine index equals(those values are quite low) . Phone cal l : “Ms . Smith , are
you taking your thyroid pil ls?”
From the Department of Internal Medicine , New Hanover Memorial
Hospital , Wilmington 28402 .
Effe ct of Thyroid Suppre s s ion The rapy
on Thy rox ine Le ve ls
Normal
Serum T4
Normal
Serum T4 Serum T4
Figure l . A s impl ified scheme of thyroid suppression by T3 or T4 .
VOL . 46 , No . 1 1
Yes , Doctor One , every day , she said . Wel l , yourblood level s are very low so double your tablets , okay?”retaned Doctor One .
One month later Ms . Smi th is talking to Doctor Twoand my thyroid level was very low so he told me to
double my pil l s . I sti ll fee l quite bad , as a matter of fact,worse .
”Thyroid functions are checked again. T4 is now
less than 1 . Doctor Two phones Ms . Smith .
“Are you
tak ing your pil ls , Ms . SmithMs . Smith ends on a fairly mass ive dose of tri iodothy
ronine (Cytomel ) replacement and with a beautiful case ofiatrogenical ly- induced hyperthyroid ism.
The class ical “thyroid function test” used in the great
majority ofhospitals and pri vate offices includes a total T4 ,
a T3 res inuptake and a free thyrox ine index . Ingestion oftn
'
iodothyronine in doses greater than 50 pg per day sup
pressesTSH secretionby the hypothalamus-pituitary complex . This suppress ionof theTSH induces amarked hypofunction of the thyroid gland . (This was recognized quite

early and was the bas is for the now somewhat d isplaced“thyroid suppression test. The hypofunction of the thy
roid gland produces amarked decrease in the circulating T4
level ( figure Neither the total T4 nor the resin uptake
measure the circulating T3 . The conventional package of
thyroid function tests wil l show numbers that wil l suggesthypothyroid ism. If the
'
Ueating physician is notaware of the
exact type of thyroid pill s the patient is tak ing ,-he may
commit the mi stake of asking the patient to increase the
ui iodothyronine . The increase of the dose ofT3 is fol lowed
by a more profound depression of the T4 leve l and , too
frequently , an additional increase of the “thyroid replace
ment.
Patients on T3 replacement or suppression therapyshould be fol lowed using measurements of T3 by rad ioim
munoassay , TSH , and in some cases TRH stimulation
tests .
So next time you see a patient on thyroid pil ls with a
low total T4 , ask her or h im to look at the prescri ptionbottle : You may be in for a surprise !

SCIENTIFICARTICLE
Overwhe lming InfectionAfter SplenectomyA Challenge to Preventive Medicine
Johnny B . Craig , MD . and B ayard L . Powel l , MD .
0 This is a case of overwhe lming post splenectomy infectionfromwhich the
pa tient d ied 20 years afier remova l of her spleen.
sPLENECTOMIZED patients are at increased ri sk for
infections; themost dramatic and cl inical ly significantis overwhe lming post splenectomy infection (OPSI ) , a syn
drome of documented bacterial septicemia and/ormening itis more than s ix week s after splenectomy .
A67 -
year-old white womanpresented after three days of
nonproductive cough , myalgias , andmalaise . Twenty-four
hours before admission she had noted fever of 102°F , a
shaking chi l l , nausea , vomi ting , diarrhea , and discolora
tionof the skinof her face , hands and feet. She was treated
with intravenous ampicil l in and tobramycin in the referringemergency room and transferred to our institution. H er
spleen had been removed 20 years earl ier because of
trauma .
Upon arri val she was alert and oriented , but tachypneic ,
febri le (oral temperature 1O2 .S°
F ) and hypotensive
mmHg) w ith general ized purpura and ecchymoses . Whiteblood cel l (WBC) count was 20, 300/mm with 5 6% segmented neutrophils and 3 1% band forms . Dohle bodies(pale blue intracyCIOplasmic inclusion bodies ) were notedand intrace l lular encapsulated diplococc i were obviousw ith inWBCs on routine b lood smear. Urine and serum
counter immunoelectrophoreses were positive for Streptococcus pneumoniae . Prolongationof the prothrombin time
seconds ) , partial thromboplastin time
seconds) , thrombocytopenia mm3 ) , hypofibri
nogenemia ( 2 6 mg/dl ) and elevated fibrin spl it products
and <5 12 ug/ml ) cons istent w ith d isseminated intravascular coagulation were al l present. Arterial b loodgases revealed hypoxemia and a profoundmetabol ic acidosis (ph pCOz 2 2 ; p0 2 5 3 ; HCO3
Despite aggressive respiratory , cardiovascular (volume
replacement and vasopressor agents) , chemotherapeutic
(hi gh dose penicil l in, high dose steroids) , and hematolog ic
(platelet, red blood ce l l , and fresh frozen plasma transfusion) therapy , the patient rapidly deteri orated and d ied 36
hours after admiss ion. Premortem b lood cultures were
positive forpneumococci exquisitely sens itive to both penicil l in-G and ampici l l in. Autopsy findings were consistent
with septicemia , disseminated intravascular coagulation,
and adrenal hemorrhage .
From the Department of Medicine , BowmanG ray School of Med icine ,
Winston-Salem 2 7 103 .
5 70
Discussion
VOL . 4 6 . No . l l
This case is a definitive example of the dramatic pre
sentationand cl inical course associated with overwhelming
postsplenectomy infection. The incidence of this syndrome
is re lated to age , interval after splenectomy , and the pres
ence or absence of an underlying medical il lness . The
overal l mortal ity from sepsis in splenectomized patients is30-200 times higher than in a population with normal
splenic function. OPSI is most common in the pediatri c
population with the majority of cases (7 0 occurringw ith in three years after splenectomy ; however, cases
occurring up to 3 1 years postsplenectomy have been re
ported .
" Children whose spleens are surgical ly re
moved before 12 months of age have the greatest chance ofdeve loping OPSI ; risk gradual ly decreases until age 17
after which the incidence is relatively independent of age3 ' 4 ' 6 ' 7 In ch i ldren the risk of developing
OPSI is increased in those w ith anunderlying hematologicor mal ignant disease when compared w ith patients w ithsplenectomies after trauma . The highest risk in this population occurs in association w ith thalassernia ( 16 and
Iymphoreticular neoplasms the lowest after
trauma-re lated splenectomy ( l . 53In contrast to
the ped iatri c population, in adults the syndrome is less
common, occurs more than 3 years after splenectomy inupto 7 5 of cases , and incidence shows l ittle correlationw ith
age or underlying disease .
“7
The cl inical syndrome is most frequently caused by
encapsulated bacteria ; pneumococcal infections are the
most common ( 50 However, Hemophilus influen
zae , Ne isseria meningitidis , staphy lococci , Salmonel lae ,
Escherichia col i , Pseudomonas aerug inosa , other strepto
coccal species , and L isteria monocytogenes have been teported to be the causal organism incase reports .
"7There is
often a prodromal period characterized by symptoms s imilar to those of
“viral syndromes
”
for 3 6 - 7 2 hours beforethe onset of the acute fulminant i l lness described in our
patient. The fulminant i l lness is characterized by dissemi
nated intravascular coagulation in greater than 5 0% of
cases (especial ly in cases caused by pneumococcal organ
isms ) , Waterhouse-Friderichsen syndrome and vis i
ble organisms on peripheral smear The mortal ityrate is 50- 80% despite appropriate therapy . Recurrences
are common among survivors (40

SCIENTIFICARTICLE
Snakeb ite Treatment in the 805
Theodore R. W inneberger, M .D . , E . Jackson Al l ison, I r . , MD/MPH , Joyce M. Mitche l l , M D . ,
Mark R. Pierce , M .D . , George Podgomy , MD . and J . Jeffrey Tope , MD .
0 This paper outl ines the sens ible steps to take , and some of thecontrovers ies , when a victim encounters a poisonous snake .
SNAKE envenomations , although not a frequent event inmost physicians
’
med ical practices , are nonethe less amedical emergency requiring an organized approach to
treatment for a successful outcome .
In the U. approximately people are b itteneachyear , and 12
- 15 of these result in death .
1North Carol ina
has been found to have the highest incidence of poisonoussnak e envenomations ; they occur here at a rate of 18 cases
per of the population.
2
There are 20 species ofpoisonous snakes intheU. S . the
majori ty of which are pit v ipers (crotal ids) which includethe rattle snakes , copperheads and water moccasins .
Another group, the e lapidae , includes the coral snake ,
wh ich wil l be discussed later in this paper .
Poisonous snakes are endemic in every state except
Maine , Alaska and Hawaii . Identifying features of the pitvipers include the pit between the eye and nostri l b ilaterally . Th is is apparently a heat
-sensing organ used in findingprey . Pit vipers have tri angular
- shaped heads and e l l iptical
pupils if you get close enough to observe them. On their
underside , they have a s ing le row of caudal plates , most
safely observed when the snake is dead . Pit vipers de l iver
their venom through fangs suppl ied by venom g lands , each
of which has an ind ividual muscle and nerve . Th is systemal lows the snake to inject variable amounts of venom or
none at al l . Of ind ividuals b itten by crotal ids , up to 30%
may not have been envenomated .
3 ' 4
In North America b ites are predominantly inflicted bythe crotal ids and rarely by the e lapidae .
5Other more rare
poisonous snakes in North America wil l most l ikely befound in the zoo where identification is already known.
Distinguishing which snake has infl icted the b ite should bestraightforward , and treatment with antivenin wi l l consistof a single antivenin for the crotal ids and a single antiveninfor the e lapidae , removing much confus ion about whichantivenin should be used .
The pit viper’
s strik ing range may be as much as one
third to two- th irds of its body length . Some rattlesnakes
have been known to attain lengths of seven to eight feet,
and anecdotes have reported them over nine feet long .
Rattlesnakes account formostof themortal ity andmorb idity from envenomations .
From the Department of Emergency Medicine . East Carol ina Univers itySchool of Medicine , Greenvil le 2 7 834 .
VOL . 46 , No . 11
The copperheads are reportedly the least poisonous ofthe pit vipers , with some authors stating that the treatment
of copperhead envenomations should be undertakenonly in
the young , the old and the chronical ly il l .6 Most experts
would recommend simple observation of other patients
except in the case of apparently significant envenomation.
Pit v iper venom is very destructive to mammal ian
structures .
3 '
Cl inical manifestations of envenomations can vary , but
the most common initial reaction is .buming pain fol lowedby local ized tissue swel l ing . Some of the more common
systemic symptoms include nausea ,vomiting , paresthe
sias , hypotension andmuscle fasiculations . The deaths that
occur secondary to envenomations are not infrequently dueto coagulopathies .
Treatment
Prehospital treatment has been the subject of much discussionand controversy for a number of years . After beingb itten, the first thing to do is tomove away from the snake .
Some authors recommend k il l ing and bringing the snake infor identification; l o s ince few people have any experienceinhandl ing snak es , however, this does not seem tobe w ise .
B ites have been known to occur even from a disembod iedhead .
Another commonly recommended procedure in prebospital care of snake envenomations is incis ion and suction,
popularized in the 19205 and restudied several times in
more recent years . The more recent l iterature suggests that
if the patient has signs and symptoms of envenomation, if
transport to a hospital wil l take longer than an hour, and ifthe procedure can be performed safely w ithout damage to
underlying structures , then it should be done .
9 ' It is
doubtful that this recommendation is safe for the lay publ ic ,
mostofwhomhave neverout another human therapeutically . Incision and suction has been shown to remove some ofthe venom from the wound and some victims having it
performed tend to have a less severe reaction to the irb ite .
” 13 Incision and suction should be done 15 minutes
after the b ite and continuous suction should be applied for30 to 4 5 minutes .
3 ' 4 ' ‘ 4 ' 15 The incisions should be shorter
than one centimeter, just through the subcutaneous layer,and across the bite marks . Incis ion and suction should onlybe used if the patient is showing signs of s ignificant envenomation, is more than anhour from the hospital , and if
thepersontoperform the procedure is comfortab le doing it.

The use of a tourniquet is a controversial first aid recommendation. Wh ile the tourniquet has fal len into d isfavor,the new terminology be ing used is that of a loose ly con
strictive band to occlude only the lymphatics . Many au
thors bel ieve that the venom is disseminated via the Iym
phatics and that slowing its dissemination wi l l lessen the
severity of the patient’
s reaction in the fie ld .
3 ' 4 ’ 9 MSome
authors disagree with the use Of any band , even a looselyconstrictive band ,
” because the tourniquet can exacerbatethe swe l l ing and edema of the extremity and can quickl ybecome even more hazardous secondary to progressive
ischemia to that extremity .
Ice and cool ing of the site of the b ite is condemned by thevastmajority of physicians because of increased morb idityin cases treated w ith
Commonly accepted recommendations , felt at least to donoharmand possibly to he lp infirstaid , include immobil iz
ing the affected extremity , keeping the patient from tak inganyth ing by mouth while transporting , and always be ingaware of the ABCs of resuscitation while en route .
Depend ing on location of the heal th care facil ity , the
patient may be confronted w ith either of two schools of
thought regard ing definitive treatment. Most agree w ithstarting at least one I .V . of a crystal loid solution and
draw ing routine labs includ ing type and crossmatch ,
prothromb in time , part ial thromboplastin time , fibrinogen,
fibrinogen degradationproducts , plate lets , complete bloodcount, creatinine and urinal ysis . The most common
~ d ~is
agreement concerns whetheror not surgical treatment has a
place inthemanagement of snakebites . Enbloc excisionofthe b ite s ite and frequent, ifnot routine , use of fasciotomieswere popularized by G lass and are supported by someauthors in the current l iterature .
7 ' ‘ 7 Most cl inicians todayfavor antivenin as the definitive treatment and only use
fasc iotomie s in a documented compartment syn
drome s“ Some authors concede that en bloc excisionmay have a place in snak eb ite treatment, but only undervery se lective and stil l controversial situations : when the
bite has occurred within 30 minutes ; when the patient isshowing significantmanifestations of envenomation;whenthe patient has a history of be ing al lerg ic to the antiveninorhas a pos itive skin test to the antivenin.
2 l
The administration of antivenin is wel l - covered inOtten
’
s article in the American Journa l of EmergencyMed icine and wil l not be restated here .
‘5Once the decision
ismade touse antivenin, which is any situationwhere signs
and symptoms of envenomation occur , enough should be
used to arrest the signs and symptoms .
6 ' 2"2 2F inal ly ,
cover the patient with appropriate tetanus prophylaxis anduse a broad spectrum antib iotic .
4 ' 2 3
Coral snakes , which are members of the elapidae , tequire separate d iscuss ion from the crotal ids due to their
many differences . These snakes are usual ly smal l , shy ,
slender, and very colorful . To distinguish a coral snake
from s imi lar looking butnon-
poisonous snakes , such as the
king snake , observe the arrangement of the colored bands
NO VEMB ER 1985 , NCMJ
on itsmainbody . As the saying goes , red on yel low , k il ls
a fe l low; red on black , venom lack s . These band characteristics are consistent only on the mid-body . Coral snakes
can be found along the eastern seaboard as far north as
North Carol ina , and there is a Sonoran or Ari zona coralsnake found in the southwestern United States . The del iv
ery systemof the elapids’
venom ismuch less efficient thanthe crotal ids . The elapidae havemuch smal ler fangs , which
require the snak e to hold on longer in order to envenomatethe victim. The venomof the elapidae is very different fromthe crotal ids , with the exceptionof theMojave rattlesnak e ,
and has beenrecognized as be ing primari ly neurotox icwithsystemic manifestations appearing five hours ormore afterthe bite . The earl iest manifestations may be cranial nervedysfunction such as ptos is , slurred speech and mydrias is .
Respiratory musculature is affected last and is the mostfrequent cause of death .
Because of the vari ab le period betweenb ite and systemicmanifestations , and the seriousness of the sequelae , al l
suspected coral snak eb ite patients (alsoMojave rattlesnak ebites) should be admitted to the hospital and receive five
vials of antivenin, even in the absence of symptoms .
5 7 3
References
I .
2 .
3 .
4 .
5 .
10.
l l .
12 .
13 .
14 .
15 .
16 .
17 .
18 .
19 .
20 .
2 1 .
22 .
2 3 .
Treatment of snakebite in the USA. Med Lett Drugs Ther l 982 ;24 :87 -9.
Parri sh HM. Incidence of treated snakebites in the United States. Publ ic Heal thReports l 966 ;8 1:8.
Russel l FE . Snake venompoisoning . Phi ladelphia . J . B . L ippin cott Company.
1980 .
Russel l FE . Snake venompoisoning in th e United Sta tes . Ann RevMed 1980;-59 .
Arnold RE . Tre atment of venomous snakebites in the Western Hemisphere .
Milit Med l 984 ; 149 :36 1-5 .
Otten El . Antivenin therapy in the emergency department. Am J Emer Med1983 ; l :83 -93 .
Huang TT, B lackwel l SJ , Lewid SR. Ti ssue necrosis in snakebite . JAMAl 98 1 ;7 7 :5 3 -8 .
Kunkel DB .Curry SC , VanceMV. Ryan PI . Reptile envenomations . JToxicol
C l inToxicol 1983 - 84 2 15 03 -26 .
W ingertWA, PattabhiramanTR. Effects of crotal id venoms on humancel ltissue cultures . Proc West Phannacol Soc -402 .
Watt CH . Poisonous snakebite treatment in the United States. JAMA-6 .
JacksonD. Treatment of snakebite . So Med J - 8 .
Jackson D. Harrison WT. Mechanical treatment of experimental rattlesnakevenompoisoning . JAMA l 928 ;90 : l 928-9 .
Parri sh HM . Early incision and suctionof snakebite wounds indogs . NCMed J195 5 ; l 6 :93 -6 .
Garfin SR, Mubarak SJ. DavidsonTM. Rattlesnake bites. Cl inOrt ho Related
Res 1979 ; l 40:50- 7 .
Meni amTW. Leopold RS . Evaluationof incisionand suction invenom removal . Cl inRes
StewartME .Greenland S .HoffmanJR. Firs t-aid treatmentofpoisonous snakebite : are currently recommended procedures justified? Ann Emerg MedG lass TG . Early debridement in pit viper bites . JAMA l 97 6 ;2 35 :2 5 l 3 - 6 .
Garfin SR. Rattl esnake bites : current hospi tal therapy . West J Med1982 ;13 7 :4 l 1-2 .
Garfin SR. Cas tilonia RR, Mubarak SJ et al . Ratt lesnake bites and surgical
decompression: re sults us ing a laboratory mode l . Toxicon l 984 ;22 : 17 7 - 82 .
Garfin SR. Cas ti lonia RR , Murbarak S] cl al . Role of surgical decompression intreatment of rattlesnake bites . Surg Forum 19793 025024 .
Boyden TW . Snake venom poisoning : diagnosis and treatment. Ariz Medl 980;37 :639-4 1 .
BuntainWL . Successful venomous snak ebite neutr al izationwithmassive antivenin infusion in a chi ld . J Trauma l 983 ;2 3 : 1012-4 .
GoldsteinEJ CitronDM.Gonzalez H , etal . Bacteriology of rattlesnake venom
and impl ications for therapy . J Infect Dis l 97 9 ; l 40 :8 l 8-2 1 .


and neck primaries while lower neck nodes ari se from an
infraclavicular site . A left supraclavicular node (“Vir
chow’
s node”
) raises the question of an abdominal primary . Midl ine orparatracheal sites suggest larynx , thyroid ,
orpulmonary s ites . B ilateral nodes canmean lymphoma or
a suprag lottic , base of tongue , or anterior oral cavity pri
mary s ince these structures have bi lateral lymph drainage .
In our patient the mass appeared to be beneath the sternocleidomastoid and did not feel l ike a node .
A second important observation is whether or not themass moves with swal low ing . Structures belong ing to , or
attached to , the upper aerodigestive tract move up and
downwith swal low ing . The upper aerodigestive tract is the
funnel -shaped group of organs (pharynx , larynx , trachea ,
and thyroid) suspended from the hyoid bone . The onlynodes in this tract are the delphian nodes in the thyrohyoid
membrane , which canbe enlarged with thyroid or laryngeal
cancer . Since the mass in our patient d id not move withswal low ing , we concluded that it was not part of the aero
digestive tract.
Nextonemustdecide whether themass is of blood vesselorig in. These are peri pheral to the visceral funnel , are
usual ly pul satile , occasional ly are associated with a bruit,and can usual ly be moved side to side , but notup and downbecause they are attached to the carotid sheath . Carotid
body tumors and chemodectomas occur frequently at the
b ifurcationof the common carotid . The lump in our patient
had displaced the left carotid anteriorly but the artery itself
did not appear to be enlarged and contained no bruit.
Although it appeared intimate ly involved with the carotid
artery , it could be moved side to side and up and down.
The nasopharynx and base of the tongue must also beexamined . Tumors of the tongue canbe submucosal and bemissed by visual inspection, even with mirrors . Some of
these can be fe lt with a d igital examination. If a node
contains metastatic cancer for which no primary source is
found , bl ind b iopsy of the base of the tongue may be
indicated .
At the end of the h istory and physical , we were certain
only that our patient had a mass beneath the left stemo
cleidomastoid muscle in the middle third of the neck . It
seemed close to but distinct from the thyroid gland and
close to but d istinct from the carotid artery . Because of the
uncertainty , x-ray and laboratory tests were performed .
Thyroid scan did not demonstrate the mass . There was
decreased uptake in the left lower pole but itwasn’
t certain
that this was due to the lump inquestionas nomass could befelt in the thyroid .
Ultrasonography was considered butomitted because themass lay deep in the neck and ultrasonography works betterfor lesions closer to the surface .
5Computed tomograph ic
(CT) scan can define the extent of soft tissue involvement
and altered anatomical relationships inmany patients withneck masses ; when used w ith contrast it can define re la
tionships to the major vessels .
6In this case , al though the
extentwas we l l defined by CT scan, the orig in of the mass
could not be clearly defined , especial ly whether or not it
arose from the throid g land . It did appear vascular and an
arteriogram confirmed this . Its b lood supply came from theleft inferi or and superior thyroidal arteries but onphysical
examination it fe lt clearly distinct from the thyroid . S ince it
5 7 6
did not appear to be ametastatic node , but rather a primarytumor , the next step was an excis ional b iopsy which re
vealed a benign paragang l ioma .
VOL . 4 6 , NO . 1 1
Case 2
A 7 5 -
year—old woman came to the medical cl inic com
plaining of severe cough , especial ly when supine , and
difficulty swal lowing sol ids and l iquids . She had some painin her throat hoarseness , we ight loss , and a ful lness in her
neck but no fever, chil l s , abdominal pain, nausea , vomiting , diarrhea , constipation, or sk in changes . On physical
examination she was anxious and chronical ly i l l - appeari ng .
V ital signs were normal except for tachypnea (24 breathsper minute) . H ead , eyes , nose , and throat were normal .Neck examination revealed a ful lness in the area of the
thyroid . The thyroid was easi ly palpab le , firm , non
nodular , and minimal ly enlarged . The thyroid and larynx
were pushed forward . H er voice was hoarse . Lung ex
amination revealed stridorous breath ing and a brassycough , especial ly when recumbent. H igh pitchedwheez ing
primari ly on inspiration but al so on expiration was heard
over the larynx , but the lungs were clear . The remainder ofthe examination was normal .
Comments
Table 1 l ists clues deri ved from a patient history that can
help to local ize the probable site of a neck mass and its
nature . Careful questioning is imperative but not alwayseasy . Patients may not always formulate their complaintwith precision and phys icians may not always critical lyevaluate the complaint . When questioned careful ly , our
patient demonsd ated several of the class ic symptoms of
head and neck disease . She complained of difficulty swallowing both sol id and l iquid meals but not sal iva betweenmeals . This latterpointhe lps to differentiate true dysphagia
from globus hystericus or postnasal dripwhich can cause avague sensation of d ifficult swal lowing but tends to occurbetweenmeal s . Of course ,
w ith nearly complete obstruc
tion of the es0phagus the patient can have difficulty swallowing even oral secretions . Our patient local ized her siteof obstruction to the back of her throat rather than the lower

esophagus or stomach . Patients can often local ize we l l thearea of disease when the site is above the upper esophagealsphincterbutnot as wel l when below . She had some we ight
loss , ate s lowly , and tended to choke on her food which
supported the interpretation of true dysphagia . Painful
swal lowing (odynophagia) al so helps to distinguish local
structural disease from globus hystericus . It suggests con
d itions such as l ingual tonsi l l itis or neoplasms of pharynx ,larynx , oral cavity , or tongue . B ecause of the distri butionof cranial nerves V , IX , and X , painful swal lowing can be
fe lt in the car , but our patient did not have this problem.
Hoarseness w ith a mass in the neck strongly suggests
cancer (causing vocal cord or recurrent laryngeal nerve
dysfunction) . Inspiratory stridor, d iagnostic of upper airway obstruction, is produced whena soft tissue obstructioncol lapses into the airway on inspiration and vibrates . In
expiration the positive air pressure forces soft tissues apartand decreases the vibration. Lower airway obstructionsbehave oppositely in that on inspiration the airways open,
wh ile on expiration they tend to col lapse lead ing to increased vibration and stri dor. Tracheal stri dor tends to be
present on both inspiration and expiration. Ourpatient hadinspiratory stri dor placing the lesion in the laryngeal area .
The symptoms strongly suggested cancer.
Indirect laryngoscopy revealed a paralyzed vocal cord ,
but no mass , thus impl icating recurrent laryngeal nerve
pressure . Soft tissue lateral x-ray of the neck confirmed the
presence of a mass in the area of the thyroid , beh ind thetrachea (figure Bari um swal low showed a marked extrinsic obstructionof the upper esophagus (figure Chest
x- ray was normal . Thyroid scan showed no uptak e in the
left lobe , suggesting th at the mass might be of thyroidorigin. Wh ile the evaluation was in progress , the patient
had a cardiac arrest and died . Autopsy showed anaplastic
carcinoma of the thyroid withmetastases to bone and liver,skul l , and lymph nodes .
F igure 5 . Sofi tissue x -ray of neck demonstra ting ma ss (arrows ) .
NO VEMBER 1985 , NCMJ
F igure 6 . Barium swa l low of patient 2 demonstra tes near ob
s truction of esophagus a t leve l of thyroid .
Case 3
A 3 5 -
year—old woman was noted by fri ends to have a
s l ightly asymmetri cal neck . She then noted a sl ight, pain
less swel l ing below the left stemocleidomastoid muscle .
She had no symptoms . She had been treated with 113“forhyperthyroidism several years previously and now took
standard doses of thyroxine to maintain euthyroid ism.
On phys ical examination the left stemocleidomastoidwas more prominent than the right . No definite marg inscould be palpated and there was no discoloration, ecchymoses , or erythema . No thyroid tissue could be felt. Ultra
sonography of the neck showed a cystic mass , compatible
F igure 7 . Computed tomogram of neck inpatient 3 demonstrating cystic mass (arrows ) in posterior
'
triang le .

w ith a branchial cleft cyst orposs ib ly with a d ilated jugularvenous structure .
Comment
Indistinction to our other two patients , ne ither h istory or
physical examination gave specific clues as to the etiologyof the prominent stemocle idomastoid in this patient. The
lack of symptoms and findings suggested a benignprocess ,such as thyroglossal duct cyst , branchial cleft cyst, sialol ithiasis , s ialadenitis , cervical adenopathy , chemodecto
ma , laryngocoe le or pharyngocoele .
CT scan of the neck (figure 7 ) showed a cystic structurebeneath the stemocleidomastoid which appeared to be a
cystic hygroma . This was removed surg ical ly ; the pathol
og ist confirmed the d iagnosis of a cystic hygroma . The
patient has done we l l s ince .
Summary
Primary care physicians see most adult patients with a
lump in the neck . Knowledge of the epidemiology of neckmasses , the anatomy of the neck , the appropri ate use of
history and physical examination, and the capab il ities ofimag ing techniques is essential to choosing appropriate
d iagnostic strateg ies for these patients .
References
1 . Simpson GT. The evaluation and management of neck masses of unknown
etiology. Otol Cl in North Am 1980713 24 89-98 .
2 . Keene WM , Atk ins JP , Wetmore R. V idas M. Epidemiology of head and neck
cancer. The Laryngoscope 198 119 12 03 7 4 5 .
3 . SalemBS , SchraderKE.Mair IWS.Differential-diagnosis of amass in the upper
lateral neck . J Laryngol Otol-4 7 .
4 . Dec ker J Goldstein JC . Risk factors in head and neck cancer. N Eng l J Med
1982 z3063 1 15 1-5 4 .
5 . Pogrel MA. The use of ultrasonogra phy in the diagnosis of nec k lumps . J Oral
Max il lofacial Surg-6.
6 . MancusoAA, HamsbergerHR.Murah i AJ StevensMH . Computed tomographyof cervical and retropharyngeal lymph nodes. Norm al anatomy , variants of
normal , and applications in staging head and neck cancer. Part II : Pathology.
Radiology 1983zl 4 8t7 15 -2 3 .
‘
7 . Moloy P. How to (and how not to) manage the patientwith a lump in th e neck .
Prim Care l 982 ;9:269- 89.
VOL . 4 6 , No . 1 1


ing buckshot. Rather than performing kitchen tablesurgery as described inN icholas Senn’
s Practica l Surgery
for the Genera l Practitioner (Philade lphia , he re
ferred patients toDrs . Wesley Long and Reeves ofGreensboro .
No diagnostic aids l ike a microscope ( to examine urinedepos its and Sputum for tuberculos is organisms ) or
Sphygmomanometers have been found in the office ; on theother hand , records of his stock ofmedicines , a few surviv
ing prescri ptions and the numerous bottles in the officesuggest a sense of eclectic ism and a w il lingness to try new
remedies . H is notes recordmany polypharrnaceutical preparations , then decl ining in popularity . One was a
“tonic
cholagogue containing quinine sulphate , extract Of leptandrin, tincture of stil l ingia , extract of podophyl l in, oil of
sassafras , oi l of gaultheria al l in cinnamon water .
El l ingtonpurchased his medic ines from such local com
panics as the RichardsonDrug Co . of G reensboro , famed
for the manufacture of V ick ’
s products , and from majorpharmaceutical companies l ik e Massengil l of Tennessee .
From the latterhe bought large quantities ofone of themostinteresting ofmed ic ines , the obnoxious , garl icky- sme l l ingasafetida . However, he bought it as “
taste less”
pil ls and
probably employed it as a mild sedative for“nervous
complaints”and as a general antispasmodic . Much of its
local popularity was probably l inked with its reputationamong many Southerners as a cure- al l . Childrenoftenhunga smal l lump in a sack around the neck .
El lington’
s considerable range"
of medicines certainlyal lowed him to tai lorprescriptions to the whims ofpatients .
Judging from the number of housecal l s he made averag
ing three to four a day for long periods he probably knewhis patients we l l . Personal consideration for patients is
considered one of the hal lmark s of country doctors , im
plying , often unfairly , that other attributes such as cl inicalsk il l s in diagnos is and therapy were commonly behind thetimes . While the richness of El l ington
’
s surviving persona
l ia is frustratingly bare of cl inical detail s abouthis practice ,
it suggests that his reputation rested on more than goodbedside manners .
Fromal l the available evidence , commentsmade in 19 12
about El l ington themanmay reflect the attitudes of El l ington the physician concerned with keeping up with med ical
progress during the progressive era:“Dr. El l ington hasbeen, and is yet, one of our most valuab le assets to
citizenship. H e has seen the dawn of a better day in our
country . For th is condition he has worked faithful ly formany years . Nothing daunts him yet when it comes to
publ ic- spirited work . H e is just as eager to see our countryprogress as he ever was , and lends his influence in that
d irection. Constructive in his views and progress ive in his
acts , he is an invaluableman, doing his fel lows anunspeak
able amount of good .
*Biographical note: The l ibrary of the Country Doctor Museum has a
pol icy of col lecting the scattered autobiography and biography ofCountryDoctors .
Acknowledgment
I wish to thank Mr. John Ell ington and Mrs . Magg ie El l ington for
generous access to the El lingtonmanuscri pts and artifacts . Mrs . El l ington
’
s hospital ity added much tocapturi ng the ethos of country doctoring in
Sandy Ridge . Access to the material was facil itated by accession l ist
prepared by Dr. David Hal l when a medical student atDuke Univers ity .


cannot be a standing order and the PA must write the
prescription as a“verbal order of the physician. For
example , the signature area would look l ike this :“J . H il l ,
P.A.-C . per verbal order of J . B ak er , M .D. Of course ,
this procedure cannot be done for control led substancess ince they require a physician
’
s signature .
4 ) Don’
t permit your PA employee to replace you as a
supervis ing physician for PA students fromDukeUniversi
ty Medical Center or Bowman G ray Schoo l of Medicine .
Both have exce l lent programs and both programs use
physicians in private practice across the state as precep
torships for the cl inical phase of training . Some of these
practices already have graduate PAs work ing in them. The
BME has d iscovered that sometimes the graduate PA is
primary supervisor of the PA student. The physician em
ployer sees only the complicated cases of the student. Just
as the decision to add a graduate PA to the staff must be
made w ith the best interests of the patient and practice inmind , the decision to add PA students to the practice setting
mustbemade only if the physicianhas the time and interestto adequately supervise the student’ s activities . This is not
to say that a graduate PA in the practice cannot be used as a
role model for a student , al lowing him to witness the real
world of a physician/PA team at work .
5 ) Don’
t al low your PA to s ign prescriptions for PAstudents ormed ical students . The author has been activelyinvolved as anofficer or committee chairman inour state
’
s
professional academy since 197 7 and has worked as aPA in
th is state’
s largest emergency department since 197 6 .
Those of us whometw ith the BME this spring thought thatwe had seen and heard it al l but the Board reported to us an
activity that surprised me . It seems that an occas ional PA
graduate working with PA students provided them with
prescriptions for commonly used antib iotics and other
medicines . They ignored the requirement that each prescription has to be signed at the time the patient is seen.
This is a rare occurrence but the fact that it happens at al l
suggests that some PAs are not taking the privi lege of
prescription wri ting as serious ly as they should . Although
some situations and practices fal l in an ethical gray zone ,
th is one is definitely b lack and should not be tolerated byphysician or PA.
The Do’s
1) Do review and countersign promptly those medical
records written by your PA. Chart review is one of the
primary methods phys icians use to supervise theirPAs . It’
s
also an excel lent opportunity to give your PA feedback ,
both positive and negative . The rule is that this reviewmusttake place w ith in 24 hours of the PA/ patient contact. To
address a special problem posed by some practices , the
BME let us know that they’
re understanding enough to
recognize the difficulty met by physicians and PAs when aPA sees a patient in the office late Friday afternoon whilethe physician is mak ing rounds in the hospital . If the teamdoesn
’
tmeet againuntilMondaymorning , then the 24 hour
l imit is“understood tomean by the nextwork ing day . A
weekend stops the clock , in other words .
2 ) Do register your PAwith the North Carol ina Board of
Pharmacy if you are going to have the PA d ispense any
med ications (OTC medications can be d ispensed by PAs
American Academy of PhysicianAss istantsSuite 300
1 1 17 North 19th Street
Arl ington, VA 2 2 209-4 200
6 ) Do encourage your PA to seek and maintain professioual competency by participating in national cert ificationexaminations for PAs . The 2 4 -month- long PA training
programprepares a student in the basics ofmedicine , just asmedical school provides the basics for postgraduate res
VOL . 4 6 , NO . 1 1
w ithout Board of Pharmacy permi t) . An occasional phar
maceutical sample may be dispensed by a PAprovided it is
entered on the med ical record , is not a control led substanceor an excludedmed ication, and you countersign the record .
B e aware of the definitions of “administering ,
” “d ispens
ing ,
”and
“
prescrib ing ”as defined by the North Carol ina
Board of Pharmacy .
3 ) Do insist that the PAwhowork s foryourpractice wear
a name tag whichw il l prevent the PA frombe ing misidentified as a physician. If l ife and the practice ofmedicine are
considered a game in which the rules must be fol lowed toplay , then this next rule might sound a lot l ike the game of“tri vial pursuit. The rule is that every PAmust wear a
name tag identifying himse l f as a“
physician assistant,
not just a “PA.
”Considering myse lf anempathetic obser
ver of PA regulators , I can understand the strong feel ingsfor this requirement. PAS perform traditional physician
task s and while most people know what“MD . and
“RN .
”stand for, many people stil l don
’
t know what
PA”means . The rule insures . that patients and other
involved parties do not confuse a PAwith a physician. No
PA should be permitted to avoid weari ng his phys icianassistant name tag because of the fl imsy excuse that nametags put holes in shirts , especial ly when cl ip
-on name tags
are available .
4 ) Do supervise your PA so that both you and your PA
are comfortab le and within safe and ethical medical prac
tice standards in your community or hospital setting , and
within the regulations of the BME and Board ofPharmacy .
5 ) Do encourage yourPAtopart icipate in local , state and
national phys ician ass istant organizations . Often, the
annual cost of membership in such professional organizations can be offset by lowermember rates at CME confer
caces and by having your PA sensitive to standards and
changes inthe PA profession.
More information about regulations ormemberships canbe easily obtained by writing to these addresses :
North Carol ina Board of Med ical ExaminersSuite 2 14 , 2 22 North Person Street
Rale igh 27 601-5 3 2 1
North Carol ina Academy of Physician Ass istantsBox 2 7 84 3
Raleigh 27 6 1 1
North Carol ina Board of PharmacyP O . Box H
Carrboro 2 7 5 10-44 5 4

idency training . The secret to success as a knowledgableand wel l - informed graduate PA
'
l ies in the ab il ity to be a
continual student and to build on the bas ics taught in thedidactic and cl inical training of the PA school . There is a
difference betweenhaving 10 years ’
experience and having
one year’
s experience 10 times over. If PAS are to grow as
cl inicians they must read , attend conferences , view
videotapes , l isten to col leagues ; in short, they must Ieamevery day . One method of testing basic knowledge isthrough the national certification examination, given after
graduation and at six year intervals for recertification. PAS
and those physicians who employ PAs Should emphasize
EDITORIAL
Thoughts on the PA/P
F . MaxtonMauney , Jr . MD .
THE practical and timely paper by James E . H il l Jr. ,
P .A.
-C , M .Ed . , concerning the Do’
s_
and -Don -ts o f
Responsible PA Practice , is worth -
tak ing a minute to
review whether youuse physic ian “extenders or not. For
those who do use e ither nurse practitioners or PAs it servesto point out the most common pitfal ls in this importantarena of health care de l ivery and , in a practical , common
sense manner , suggests some useful tips about strengthening and building uponwhat has for the most part proved tobe a beneficial and effective re lationship. There are cur
rently more than 500 PAS registered under the phys icians ’
l icense in North Carol ina , and an add itional 406 nurse
practitioners are also work ing with physicians inour state .
Approximately one out of every ten phys icians l icensed inthe state has either d irect or secondary supervision of a
physician assistant .
At the time the editor of th is Journa l embarked on the
formal training of ass istants to the physician, I doubt thatanyone would have predicted the success that this program
has had , not only inNorth Carol ina but across the country .
While many are greatly concerned about the upcoming
physician“
glut, there are no s imi lar concerns about classsize in the 50 or so PA training programs nationwide .
Several PA schools have closed in the past couple of years
as manpower training grants have phased out and as the
perceived needs for these talented men and women havedecreased . At the same time , as Chairman of the Joint
Review Committee for Physician Ass istants , which re
views and accredits al l PA training programs nationwide ,I
know that three or four prominent schools across the nationare considering establ ishing new PA training programs .
The success that“
primary care providers” and special ists
in almost every field have real ized with the uti l ization of
From 25 7 McDowel l Street, Ashevi l le 2 8803 .
NO VEMBER 1985 , NCMJ
continuingmed ical educationand national certificationas arequirement for continued employment. We cannot afford
to ask less of ourse lves .
Resolving these problem areas wil l domuch to make al l
of us better physician/PA teams . For those who fee l it’
s al l
much too picky , perhaps a thought from S irWi l l iamOs ler
wil l convince you.
Things cannot always go yourway . L earn to accept in
silence the minor aggravations , cultivate the gift of taci
turnity and consume your own smoke with anextra draught
of hard work , so that those about youmay not be annoyedwith the dust and soot of your complaints .
ician Team
PAS has been enormous and far-reaching , touching al l
levels of the health care del ivery system.
Unfortunatel y , as is inevitable , there have been abusesand misuse of the physician extender concept not onl y by
the PAs and nurse practitioners themse lves , but also byphysicians who eithermisunderstand the role of the supervising physician or improperly use the
“extender.
”
Those who have not been directly involved in this teamplay hear only the loud voices of critics of the system,
who
are usual ly quite vocal . l have beenprivileged toparticipatein the deve lopment and use of the PA concept as a faculty
member at Duke in the Department of Surgery in the late19605 , as a physician and supervising employer in Ashe
vil le of a number of physician ass istants since 197 0 , and as
a representative of the American Col lege of Surgeons on
the Accred itation Review Committee for Training Programs nationwide for PAS s ince 1980 . I have al so had theopportuni ty of chairi ng the North Carol inaMedical SocietyCommittee onAl l ied Heal th , meeting with th is Committee
as a commissioner, and working with the North Carol inaAcademy of Phys icianAssistants as aphysician advisor forseveral years . The commitment of the majority of PAs to
maintaining excel lent standards , fostering continuing
medical education, and solving problems in the practicearena has beenexemplary . Very few groups of al l ied heal thprofessional s stri ve any harder to develop close , col laborative and dependent re lationships with physicians th an the
PAs in th is state . We as physician employers and supervising doctors need to be pro
- active and understanding in
learning how touse PAs appropriately w ithoutputting themout on a l imb with the bad hab its l isted under the don
’
ts”
in this time ly paper .
JimH il l and his col leagues are to be commended for theirhonesty and openness in communicating the issues to al l
physicians .




LONG ACTINGCAPSULES
BRIEF SUMMARY (FOR FULL PRESCRIB ING INFORMATION. SEE PACKAGE CIRCULAR.)IN IDEIIAU l LA brand of propranolol hydroch loride ( Long Ac ting Capsule s )DESCRIPTION . lnderal LA is lormula led to provide a sus tained re lease of pro pranololhyd roch loride. Ind eral LA is ava ilab le as 80 mg , 120 mg . and 160 mg cap5ules .
C L INICAL PHARMACOLOGY. INDERAL rs a nonse lective be ta -ad re nerg ic receptor
b lock in agent pos ses s ing no othe r autonomic ne rvous system activity . It Specifically compe tes h be ta ‘ ad re nerg ic receptor s timulating agents Ior availab le rec eptor s ites . Whenacces s to be ta-receptor s ites is b loc ked by INDERAL , the chronotro pic. inotro pic. andvasod i lator res ponses to beta-adre nergic s timulationare d ec re ased proport ionate ly.
INDERAL LACapsules (80 . 120. and 160mg ) re lease pro pranolol HCl ata controlled andpred ictab le rate . Peak b lood leve ls lollowing dosmg with INDERAL LAoccuratabout6 howsand the appare ntplasma ha ll- lite is about 10 hours .Whenmeasured ats teady s tate overa 2 4hourperiod the are as underthe pro pranolol plasma concentration-time curve (AUCS) lor theca ules are approxima te ly (50% to 65 96 of the AUCS Iora compara b le d ivided dai ly dose 0 1IN ERAL tab lets . The lowerAuCs lor the capsules are due to gre ater hepaticmetabolismof
pro pranolol. re sulting tromthe s lowe rrate ol absorption0 1propra nolol.Ove ra twenty -tour (2 4 )hour pe riod . b lood leve ls are lairly cons tant for about twe lve ( 12 ) hours then dec lineexponentia lly.
INDERAL LA should not be cons idered a s imple mg Iormg subs titute Ior conventionalpro pranolol and the blood leve ls achieved do notmatch (are lowe r than) those 01 two to lourtimes d aily dos ing with the same dose . When changing to INDERAL LA ltom conventional
propranolol . a poss ib le need Ior re titration upward s should be cons idered espec ially tomaintain eff ectiveness at the end 01 the dos ing interv al. Inmos t c linical sett ing s ,
however.such as
hypert ensionor angina where there Is little corre lation between plasma leve ls and
clinica l e ec t, INDERAL LA has been therapeutica lly equiva lent to the same mg dose ol
conventiona l IN DERAL as asses sed by 2 4 -h0 ur e llec ts on b lood pre ssure and on 2 4 ~ hour
exercise responses of heart rate . systolic pre ssure and rate pressure product. INDERAL LAcan provide e l lective be ta b lockad e Ior a 2 4 -hour pe riod .
The mechanism 01 the antihypertens ive al lec t 01 INDERAL has not been es tab lished .
the lectors thatmay be involved incontributing to the antihype rt ensive actionare ( 1)decre ased card iac output. (2 ) inhib itionof re ninre lease by the kidneys . and (3 ) d iminutionoltonic sympathetic nerve outl lowlromvasomotorcenters inthe brain.Although tota lperipheralres is tance may incre ase initia lly, it re ad |usts to or be low the pre treatment leve l Wl lh chro nicuse . Effec ts on plasma vo lume appear to be minor and somewhat variab le. INDERAL hasbeen shown to cause a sma ll incre ase in serumpotassiumconcentrationwhenused in thetreatment of hypert ensive patients .
Inang ina pectoris . propranolol generally reduces the oxyg en require ment0 1 the heart atany given leve l ol e llort by b loc king the catecholamine -induced incre ases in the heart rate.
sys lollc b lood pre ssure , and the ve loc ity and extentofmyocard ial comraction. Propranololmay incre ase oxygen re quirements by incre asing le ltventricular llber leng th . and diastolic
pres sure and sy stolic ejectionperiod . The ne tphys rolog rc e ll ec tol beta-adre nerg ic b loc kade
rs usually advantageous and IS manilested during exerc ise by de layed onset ol pain andincre ased work capac ity .
In dosages greater than required for beta b lockade , INDERAL also exert s a outnld ine likeor anesthetic- like membrane action which al lects the cardiac action potential. The significance of the membrane action in the tre atment 01 arrh ythmias is uncert ain.
Themechanism0 1th e antlmig raine eff ectofpropranolol has notbeenestab lished . Betaadre nergic receptors have been demonstrated in the pial vess e ls ol the brain.
Beta receptor b loc kade can be use lul incond itions inwh ich . because 0 1 patholog ic or
functional changes . sympathetic activity is detrimental to the patient. But there are also
situations inwh ich sympathetic s timulation is vital. For example. in patients with sevemdamaged heart s . adequate ventricular lunction is maintained by virtue of sympathetic d rivewhich should be pre served . In the pre sence of AV b loc k. gre ater than lirst degree . betab loc kadema preventthe necessary lacilitaling e ll ec toi sympathetic activity onconduction.Beta b locka e re sults inb ronchial cons triction by Interf ering with adre nerg ic bronchod ilatoractivity which Should be pre served In patients sub ject to bronchospasm.
Propranolol is not significant! dialyzab le .
INDICATIONS ANDUSAG E. m nens ion: INDERAL LA is ind icated in the managementol hype rtension.“may be used alone orused incombinationwith otherantihypert ensiveagents. part ic ularly a lhiaz rde d iure tic. INDERAL LA IS not ind icated in the management 0 !hype rt ens ive eme rg encies .
Ang ina M orinDue to Corona ry Ath e ros c le ros is : INDERAL LA Is ind icatedtor the long-termmanag
ementOl palienls wrth ang ina pec toris.Mig ra ine : lNDER L LAis ind lcated lorthe prophylaxis 01commonmig raine headache .
The etl rcacyol propranolol inthe treatment0 1amig raine attack lhal has s latt ed has notbeenestab lished and propranolol is not indicated Ior such use.
Nypomoph ie Subaortic S teno s is : INDERAL LA Is use lul in the management 01hypenroph lc Subaort ic stenos rs . especia ll lortre atment01exert rona l orotherStress -inducedang lna. palpitations. and syncope . INDE AL LA also improves exercise peri ormance. Thee ll ectivenes s ol pro pranolol hyd rochloride in this disease appears to be due to a re ductionof
the e levated Outflow pre ssure grad ientwhich is exacerbated by beta-re ceptor stimulation.
Clinical improvementmay be temporary.
CONTRAINDICATIONS. INDERAL rs contraind icaled in 1) card iogenic shoc k: 2 ) s inusbradycard ia and g reater than firs t deg ree b loc k; 3 ) bronchial asthma; 4 ) congestive heartlaIl
Du
‘r
Ee
R(see WARN INGS ) unless the lai lure is secondary to a tachyarrhyrhmia tre atab le with
IN AL.
WARN INGS. CARDIAC FAILURE; Sympathetic stimulationmay be a vital component support ing circulatory lunctioninpatients with conges tive heart lailure. and its inhib ition by betab lockade may prec ipitate more severe lailure . Although beta b loc kers should be av0 |ded inovencongestive heart failure . ifnecessary . they can be used with close letlow-noinpatientswith a history of lai lure who are we ll compensated and are re ceiving d igita lis and d iure ticsBe la-ad renerg ic b loc king agents do not abolish the inotro pic action 01 d ig italis on heartmuscle.
IN PATIENTSWITHOUTAH ISTORY OF HEARTFAILURE, continued use ofbeta b lockerscan. in some cases . lead to card iac lailure. There lore. at the l irs l Sign or symplomof heart
lai lure . the patient should be d igitalized and /or tre ated with diure tics. and the re sponse
Ob served closely, or INDERAL should be d iscontinued (g radua lly, rl poss ib le).
Nona l l e rg lc S ronc h os pa sm c h ronic b ronc h it is , s mph s ome )PATIENTSWITH BRONCHOSPASTICDISEASES SHOULD INGENERAL NOTRE EIVEBETABLOCKERS . INDERAL should be administered wrlh caution S ince itmay b lock b ronchod ilationproduced by.
endogenous and exog enous catecholamrne stimulationol beta re ceptors.MAJOR SU GERY' The necessily or des rrability ol withdrawal ol beta-block in lherapy
pnor lomajor Surgery is controvers ial. It should be noted , however. thatthe imparte ab i lity ol
the heart to re spond to rel lex ad renerg ic stimuli may augment the ris ks 01 general anesthes ia and Surg ical procedures .
_
The appearance 0 1 these capsules160 IS a reg istered trademarkmg orAyers tLaboratories .
Copyright 1984 AYERSTLABORATORIESDivrs ion01AMERICAN HOMEPRODUCTS CORPORATION
INDERAL_(propran9lol HCI) . like other beta b loc kers . is a competitive inhibitor 0 ! beta
receptor -agonis
_
ts and its e l lects can be re versed by adminis tration ol Such agents . e .g. .
dobutamine or isopro le re nol. However. such patients may be sub iec t to pro tracted seve re
hypotension. Dill iculty in start ing and maintaining the heart beat has a lso been re port ed withbe ta b loc kers .
DIABETES AND HYPOGLYCEMIA: Beta-ad rene rg ic b lockade may pre vent the aopearance ol cert ain pre monitory signs and symptoms (pulse rate and pre ssure changes) 01acute hypog lycemia in lab ile insulin -d ependent diabetes . In these patients . it may be moredilticutt lo ad iust the dosage ol insulin.
THYROTOXICOS IS: Be ta b loc kade may mask certain c linical signs of hypert hyro id ism.
There lore . abruptwithdrawa lol pro pranololmay be lollowed by anexacerbationof symptoms01hypert hyrord ism. including thyroid storm . Propranolol does notd istort thyro id lunction tes ts .
IN PATIENTS WITH WOLFE-PARK INSON-WH ITE SYNDROME. seve ra l cases have beenre port ed inwhich . after pro pranolol . the tachycardia was re placed by a severe b radycard iare quiring a demand pacemaker. In one case this re sulted alter an initial dose 01 5 mgpro pranolol.PRECAUTIONS . General: Propranolol should be used with cautioninpatients with impairedhepatic or re nal lunction. INDERAL (propranolol HCI) is not ind icated lor the tre atment ofhypert ens ive emergencies .
Beta adre noreceptor b loc kade can cause red uction of intraocular pre ssure . Patientsshould be told that INDERAL may interl ere with the g laucoma scre ening test.Withd rawalmaylead to a re turn ol incre ased intraocular pre ss ure .
Cl inical Laboratory Tests . Elevated b lood ure a leve ls inpatients with seve re heart disease .
e levated serum transaminase. alkaline phosphatase . lactate dehydrog enase.
DRUG INTERACTIONS: Patients rece iving catecholamine -depleting d rug s such as re serpine should be close ly observed il INDERAL is administere d. The added catecholamineb loc king actionmay pro duce an excessive re duction 01 re sting sympathetic nervous activitywh ichmay re sult inhypotension.marked bradycard ia . vert igo. syncopal attacks .orort hos tatichypotens ion.
Carcinogenes is .Mutagenes is . ImpairmentofFertility. Long-term studies inanimals have
been conducted to evaluate toxic e l lects and carcinog enic potential. In ta-month stud ies inboth rats andmice.employ ing doses up to 150mg l kg /day.there was noevidence ofsignilicantd rug
-induced toxicity . There were no drug-re lated tumorigenic ellects at any ol the dosage
leve ls . Reproductive s tudies in animals d id not show any impairm ent at lertility that wasattributab le to the d rug.
Pre gnancy: Pregnancy Category C. INDERAL has been shown to be embryotOxic inanimal studies atdoses about 10 times g re aterthan themaximumrecommended humandose.
There are noadequate and we ll-controlled s tudies inpregnantwomen. INDERAL shouldbe used during preg nancy only it the potential benel it jus tifies the potential ris k to the Ietus.
Nurs ing Mothers : INDERAL is excre ted inhumanmilk. Caution should be exercised whenINDERAL is administere d to a nursing woman.
Ped iatric Use: Se lety and ettectiveness in child re n have not been estab lished .
ADVERSE REACTIONS . Most adve rse e l lects have been mild and trans ient and haverare ly re quire d the withdrawal of therapy.
Card iovascular: bradycard ia: congestive heart lailure : intens ification 01AV b lock; hypotension: pare sthesia 01 hands: thrombocytopenic purpura: art eria l insufficiency.usually 01 theRaynaud ty pe.
Central Nervous Sys tem: lightheadedness : mental depre ss ionmanilested by insomnia.Iass itude. weakness. latigue : reversib le mental depre ssion prog re ssing to catatonia : visuald is turbances : hallucinations: anacute re vers ib le syndrome characterized by disorientation Iortime and place. short-termmemory loss . emotiona l lability . s lig htly clouded sensorium, anddecre ased pertormance on neuro psychometrics .
Gas trointes tinal: nausea , vomiting . epigastric d istre ss abdominal cramping . d iarrhea.cons tipation. mesenleric arterial thrombosis. ischemic coliti
Al lerg ic: phary ng itis and agranulocytos is . e hematous rash. leve rcombined with achingand sore throat. lary ngospasmand re spiratory istre ss .
Respiratory. b ro nchospasm.
Hematolog ic: ag ranulocylos is . nonth rombocytopenic purpura . thrombocytopenicpurpura .
Auto-Immune: In extre me ly rare instances . systemic lupus ery thematosus has beenre port ed .
Misce llaneous : alopecia . LE- Iike re actions. psoriasilorm rashes. dry eyes . male impotence. and Peyronie
‘s d isease have been re port ed rare ly. Oculomucocutaneous re actionsinvolving the s k in. sero us membranes and ceniunctivae re poned tora beta b locker (practolol)have not been as soc iated with propranolol.DOSAG E ANDADMINISTRATION. INDERAL LAprovides propranolol hydro chloride inaSus tained -re lease capswe Ioradministrationonce daily. Itpatients are switched trom INDERALtab lets to INDERAL LAcapsules . care should be taken to assure that the des ire d therapeutice ll ect is maintained . INDERAL LAshould not be cons idere d a simple mg Iormg
substitute IorINDERAL. INDERAL LAhas dittere nt kinetics and produces lowerb lood leve ls . etitrationmaybe necessa especially tomaintain e llectiveness at the end orthe 2 4 -hour dosing interv al.
HYPERiyENS ION—Dosage must be individualized. The usual initial dosage is 80 mgINDERAL LA once daily. whether used alone or added to a d iure tic . The dosage may beincre ased to 120mg once dai ly orh igheruntil ad equate b lood pre ssure contro l is ach ieved .
The usua lmaintenance dosage is 120 to 160mg once daily. Insome instances a dosage oi 640mg may be re quire d . The time needed Ior lull hypert ens ive re sponse to a given dosage IS
variab le and may ran e troma lew days to seve ra l weeks.ANG INAPECTO lS—Dosage must be ind ividualized . Start ing with 80mg INDERAL LA
once daily. dosage should be g radually incre ased atthre e tosevend ay interva ls until optimumre sponse is obtained . Although ind ividual patients may re spond at any dosage level. theaverage optimum dosage appears to be 160mg once dai ly. Inang ina pectoris. the value andsa lety ol dosag e exceed ing 3 20 mg per day have not been estab lished .
It tre atment is to be d iscontinued . re duce dosage g radually overa period ata lewweeks
(see WARN INGS).MIGRAINE—Dosage mus tbe individualized . The initial oral dose is 80 mg INDERAL LA
once daily. The usual ellective dose range is 160-2 40 mg once dai ly The dosag e may be
incre ased gradually toach ieve optimummigraine pro phylaxis. Ita sa lis lactoryire sponse is not
obtained W lihin tour to six weeks alter re aching the maximum dose . INDE AL LA therapyshould be discontinued . Itmay be advisab le to withdraw the drug gradually over a period oiseveral weeks .
HYPERTROPH IC SUBAORTIC STENOS IS—SO- IGOmg INDERAL LAonce daily.PEDIATRIC DOSAGE—At th is time the data on the use ol the d rug in this age g ro up are t
limited to permit adequate d ire ctions toruse.
REFERENCES
1 . Holland OB . NixonJV. Kuhnert L: Diuretic-induced ventricularectopic
activity. Am J Med - 7 68 . 2 . Holme I. Helgeland A. HiermannI. etal; Treatmentofmild hypertensionwith d iuretics.The importance ofECGabnorma lities in the Os lo study and inMRFlT. JAMA -1299 .
A AYERSTLABORATORIESYG I
’
S at NewYork. N.Y, 10017

MAMMOGRAPHYCAN DETECTBREAST CANCER EVEN SMALLERTHAN THEHANDCAN FEEL.
The BennettMammography SystemM- 3000 is a heavy
duty unit des igned for soft tis sue d iagnos is of thebreast. Optimumbeamqua lity formammography isachieved by a 7 6 cm foca l film d istance with amolybdenumx- ray tube. The BennettMammographySystemM-3000 is des igned for hospita l, c linic, privateoffice and screening faci lities .
work ing for the end re sult—optimumqua lity rad iographs
B BXRAY PO . Box 802 Matthews , NC 2 8 105 InNC Ca ll 1 -800- 2 2 2 - 9262
In SC Ca ll Collect 704 -84 7 - 85 2 1
6 12VOL . 4 6 , No . 1 1



(nadolol-bendroflumethiazidetablets)
OORZIDE. 405
M T.“DESCRIPTION : OORZlDE (Nadolot-Bend ro flume th iazide Table ts ) lor ora l adrh inis trationcombines two antihypertensive agents OORGARD’
(nadolol ). a nonse lec tive be ta -a d rene r
gic blocking agent. and NATURETIN’(bendrotlume thiazide ) . a thiazide diuretic -a ntihype r
tens ive . Form ulations ; 40 mg and 80mg namlol per table t combined with 5 mg bend rol lu
CONTRN NDICA'
HONS : Nadolol Bronchia l as thma . sinus bradycardia and grea ter than
firs tdeg ree conductionblock , cardiogenic shock.and overt ca rd ia c lailure (see WARN INGS ) .Bortdrotim othlt zido Anuria . and in those with previous hypersensitiv ity to bend rol lu
me th iazide orothe r sultonamided erived drugs .WARNlNGS : Nadolol Cardiac Falim W thetic stimulationmay be a vita l component supporting circulatory lunction inpatients with conges tive heart failure . and its inhibi
tionby be ta b lockade mayprecipitate more seve re lai lure . Although beta-blocke rs s hould beavoided In ove rt conges tive heart fai lure . it neces sary . they can be used with caution in
patients with a his tory ol lai lurewhoarewe ll compensated .usua lly with dig ita lis and d iuretics .
Beta—ad rene rgic blocking agents do not abolish the inotropic action of d ig ita lis on heart
mus c le . IN PATIENTS WITHOUTAH ISTORY OF HEART FAILURE. continued use of be ta
blockers can. insome cases . le ad toca rdiac lailure .There lore . atthe l irstsig norsymptomot
hea rt lai lure . dig ita liz e and/or give d iuretics . and c lose ly observe response . or discontinuenadolol (gradua lly , itposs ib le ) .
00min Beta-ad rene rgic b loc kade may prevent th e appearance ol premonitory signs andsymptoms tachycardia and blood pressure changes ) 0 ! acute hypog lycemia . Th is is
especia lly importantwith labi le diabe tics . Beta b lockade a lso reduces re lease at insulin inrense to hyperglycemia: there lore . itmay be necessary toad justdose atantid iabe tic drug s.M Betae drenergic blockade may mas k certa in clinica l sig ns tachy
ca rdia) ol hype rthyroid ism. To avoid ab ruptWithd rawa l oi be ta-a drenerg ic bloc kade whichmig ht prec ipitate a thyroid storm. care lulty manage patients suspec ted of developingthyrotoxicos is.Bondmflumothiazldo Use with caution in severe renal disease . In patients with renal
disease .azotemiamaybe precipitated .With impaired renal lunction.e l lects of the d rug maybe cumulative . Use wrth caution in impaired hepatic lunction or
prog ress ive liver d isease .
since minoralterations oi l luid and e lectrolyte ba lancemay precip tate hepatic coma. Sensitivity reactions may occur inpatientswith a history ofa llergy orbronchial as thma . Poss ibilityoi exace rbationor activationof systemic lupus erythematosus has been reported .
PRECAUTIONS: Genera l Nadolol Use with caution inpatients with impaired hepaticor renal lunc tion (see DOSAGEANDADMIN ISTRATION).Bondrotlumothlazido At ropriate interv als , performserume lectrolytes determinationtodetec tposs ible e lec trolyte mba lance warning s igns ofwhich are dryness ofmouth , thirst.weakness , lethargy , drowsiness . restlessness . musc le pains or cramps , muscular latl ue ,
hypotens ion, oliguria . tachycard ia , and S .I. disturbances such as nausea and vomitng.Obse rv e patients for c linical s igns of fluid or e lectrolyte imba lance ; name ly. hyponatremia,
hypochloremic alka losis .hypokalemia.Serumand urine e lec trolyte determinations are pa lt lcularly Importantwhenthe patient is vomiting excess ive ly or rece iving parentera l l luids.Drugssuch as d ig italismay inl luence serume lectrolytes . Hypoka lemiamay deve lop.especiallywithbris k diuresis , in presence of severe clrrhosrs . lnterterence with adequate ora l e lectrolyteintake will a lso contribute to hypoka lemia. Response oi the heart to toxic e ll ec ts oi digitaliscan be exaggerated with hypokalemia. Use potass iumsupplements such as high potass iumloods toavoid ortreathypokalemia.Any ch loride de lic it is gene rallymild and Usually does notrequire specil lo therapy except under extraordinary circums tance s (as in liver or renald isease ). Dilutional hyponatremia may occur in edematous patients in hotweather: appropriate therapy is water restriction rather than sa lt administration except in rare instanceswhen the hyponatremia is lite threatening. Inactual sa ltdepletion, appropriate replacement isthe therapy atchoice.
Hyperuricemia may occur or l rank goutmay be precipitated in certa in thiazide -treated
patients . La tent d iabe tes me llitus may become manlies t during thiazide therapy.Antihyperlenslve e l lec ts otbendrol lumethiaz ide maybe enhanced in the pos tsympathectomy patient.Ce retul reappraisa l ol therapy and conS rderationgiven towithhold ing ors topping d iuretic
therapy is necessary it rising nonprote innitrogenor BUN (i ndica tive oi prog ress ive renal impairment) occurs . Thiaz ides may decrease se rumPS I leve ls without s igns of thyroid disturbance. Thiaz ide s decrease ca lc iumexcretion. Patholog ic changes inparathyroid g land withhyperca lcemia and hypophosphatemia have been occasional ly obse rved With prolongedtherapy . Common complications ol hype rpa rathyroidismhave not been seen.
0 1985 E. R. Squibb 8 Sons . Inc Princeton. NJ 085 40 505 -602 Issued ! March 1985
N ormatlonforPatients Warnpatients .especially thosewith evidence ofcoronary arteryinsuffic iency . aga ins t interruption or d iscontinuationof nadolol without phys ician
'
s advice.Al thoug h ca rdiac failure rare ly occurs in prope rly se lec ted patients . advise patients beingtreated with beta
—a drenerg ic b loc king agents toconsultphysicianatthe first s l norsymptomof impending fa ilure.Advise patie nts of proper course if dose inadvertentlymssed .
la boratory Teete Regularlymonitor serumand urine e lectrolyte leve ls (see WARN INGS .
Bend roflumeth iazr‘
de . and PRECAUTIONS .General . Bend roflumethrazide) .Drug Interactions Nadolol When adminis tered concurrently the following drugs mayinteract with be taa drene rg ic b loc king agents : Aneetttetlce , genera l exa garefion ofanes thetic-i nduced hypotens ion (see WARN INGS . Nadolol, Meier Sargent) labetlcdrugs (ora l agents and lneul ln) hypog lycemia orhype rglycemia: adiustantidiabetlc drudosage accordmg l (see WARN INGS . Nadolol. Diabe tes and Hypog lycemia) . Cand l erarnlned epletlng reeerplne ) additive effect:monitorclose ly for evidence ofhypotensionand /or excess ive bradycard ia.
Bendrol ltl nethlazlde Whenadministered concurrent! the following drugs may interactwith th iaz ide d iuretics : Alcohol . barbituratee , or na may potentrate orthos tatichypotens ion. Antid labetlc druge (oral agente and Insul in) thiaz ide -i nduced hyper Iyoemia may require adjustment of antid iabetic drug dosage. Other anti
gringo additive or
tpotent
iated ci
ao
-ct.
Corticoetere lda.Am Inle
'r
ésl l led electrolyte de
etion. particularly ypoka emia . lonlc or periphere renerg block ! drugepotentiated effect. Preaneathetlc a aneethetlc agents eft ects may beg temra ted :ad iust dosage accord ing ly . Preaaor amlnea norepinephrine ) poss ible decreaseresponse but not suffic ie nt to preclude their use . Skeletal muecle re laxante.nondepolarizing hb ocurarfne ) poss ible inc reased response .
Drugfla boratory Teet interaction. Discontinue thiaz ides before tests for parathyroidfunction (see PRECAUTIONS .Gene ral , Bend roflume th iaz ide) .Carc inogeneale, Mutageneala, Impa irment of Ferti l ity Nadolol In 1 to 2 yea rs oral
toxicolog rc stud ies inmice . rats .and dogs .nadolol did notproduce sig nificanttoxic effects . In
2—y ea rora l ca rcinogenic stud ies inrats and mice .nadolol did notproduce neoplastic.preneo
plas tic. ornonneoplas tic patholog ic les ions . Bendroflumethlaztde Long-term studies in
anima ls have not beenperformed .
nancy Teratogenic Effects Nadolol Category C. In animal reproductionst ies v/ ith nadolol .evidence ofemb ryo and fetotoxic ity was found inrabb its .butnot inratsor hamsters . at doses 5 to 10 times greater (on a mgri tg bas is ) than the maximum indicatedhumandose: no teratogenic potentia lwas seen Inany of these species .There are nowe llc ontrolled s tudies inpregnantwomen: the reIOre .use nadolol inpregnantwomenonly ifpotentialbene fit jus tifies potential risk to the fetus . Bendroflumethlazlde Category C. Animalreproduction studies have notbeenconducted . This drug
'
s eff ectonthe fetus whenadministered to a pregnantwomanor its effec t on reproductive capacity is not known. Bendroflwmethiazide should be g iven to a pregnantwoman only It c learly needed . NonteraEffects Since thiaz ides cross the placental barrierand appearincord blood ,weig h antlci
pa ted benefit of the drug in pregnant women against poss ible hazards to the fetus : thesehazards include fetal or neonata l jaund ice . thrombocytopenia. and possibly other reactionswhich have occurred inadults .
Nurelng Mothera Both nadolol and bend roflumethiaz ide are excreted in humanmi lk.
Because of the potential for serious adverse reactions innursing infants either discontinue
nurs ing or discontinue therapy . taking into account the importance of CORZ IDE (NadololBend rol lume thiaz lde Tab lets ) to the mother.Ped iatric Uee Safety and effectiveness inchildren have not beenestab lished .
of 1000 patients : rash: pruritus: headache: dry mouth .eyes , ors kin: impotence ordecreasedlibido: facial swe lling:weight ain: s lurred speech ; cough ;nasa l stuffiness : sweating ; tinnitus:b lurred vision. Although re latonship to drug usage is notclear. s leep disturbances have been
report ed . The oculomucocutaneous synd rome associated with practolol has not been
report ed with nadolol . The following adverse reactions may also occur: Centra l Nervone
Syetem revers ible menta l depression prog ressing to catatonia: visual disturbances:hallucinations : an acme reversible syndrome characterized by d isorientation for time and
place . short-termmemory loss : emotional Iab ilitywith s lightly clouded sensorium, decreased
performance on neuropsychometrics. Gaetrolnteatlna mesenleric art erial thrombos is :ischemic colitis. Hematolog lc agranulocytos is : thrombocytopenic or nonthrombocyto
penic purpura. Al lerg ic lever'
combined with aching and sore throat: laryngospasm:respiratory d istress . Mlace l laneoua revers ib le alopecia : Peyronie
'
s d isease:erythematous rash: arterial insufficiency .
Bendroflumethlazide Gaetrd nteatlna l Syatem anorexia . gas tric Irritation, nausea .
vomiting .cramping , d iarrhea .constipation. jaund ice (intrahepatic cholestatic laund lce) , pancreatitis. Central Nervoua Syalam dizz iness . vertigo. paresthes ia . headache . xanlhopsia . Home to Ieukopenia , agranulocytosis . thrombocytopenia . aplas tic anemia .
Dermatolog lc yperaene ltlvl ty purpura . photosensitlvity . rash . urticaria , necrotizingangmis (
vascul itis . cutaneous vasculitis ). Card iovaecular orthos tatic hypotens ionmayoccur. hype rg lycemia , g iycosuria. occas iona l metabolic acidosis in diabetics .
hype ruricemia . a llergic g lomerulonephritis , musc le spasm. weakness , res tlessness .Wheneve radverse reactions aremode rate orsevere .thiazide dosage should be reduced ortherapywithdrawn.
OVERDOSAGE: Nadololmay cause excess iVe bradycardia .cardiac fai lure . hypotens lon.or
bronchospasm if overdosed . Overdosage of thiaz ides may cause lethargy.which may pro
gress tocomawithina few hours .with minima l depress ionof respirationand cardiovascularfunc tionand withoutevidence of serume lec trolyte changes ordehydration. Gastrointes tinal
irritation and hype rmotility may occur. Transitory increase in BUN and serum e lectrolytechanges may occur. especially in patients with renal impairment.Trea tment Nadolol canbe removed l romthe genera l circulationby hemod lalys ls. Inde termining durationofcorrective therapy. take note ofthe long durationof the effectofnadolol . In
add ition to gas tric lavage . employ the following measures . as appropriate. Excee
alve Bradycard la Adminis ter atropine to mg ) . If there is no response to vagal
bloc kade . administer isoproterenol cautious ly. Card iac Fe llure Administer a digitalis
mosida and diuretic . Ithas beenreported thatglucagonmay a lso be useful in th is s ituation.
potene lon Adminis ter vasopressors . e.g .. epinephrine Or levarterenol. here is evi~
dence that epinephrine may be the drug of choice.) Bronchoepaem Admin s tar 8 be ta ,stimulating agentand /ora theophylline derlvative.S orComa Supportive therapy as
warranted . Gaatrolnteetlna l Effecta Symptomal c treatment as need ed . BUN and/or
SerumElectrolyteAbnorma l ltlea Institute support ive measures as required tomaintainhyd ration. e lectrolyte ba lance . respiratlon. and card iovascular and renal function.
DOSAGE ANDADMINIS TRATION: DOSAGE MUST BE INDIVIDUAL IZED. Patients with
ren
tal failure require adius lment in dosing interv al: see package insert for dosage In these
patents.
Conan“.
lt package Ineert before preecrlblng CORZIDE (Nadolol-Bendroflumeth lazldeTa ta).
HOWSUPPLIED:Available as scored tab lets containing 40 mg nadolol combined with 5 mg bendroflumethiazide and 80 mg nadolol combined with 5 mg bend roflumethiaz ide inbott les of IOO.

Bulletin Board
Continuing Med ica l
Education
Please note: I . The Continuing Med ical EducationPrograms at BowmanG ray , Duke , EastCarol ina and UNC Schools ofMedicine . DorotheaDix ,
and Burroughs Wel lcome Company are accredited by the AmericanMed ical Association. Therefore CME programs sponsored or cosponsored by these schoo ls automatical ly qual ify for AMACategory 1 cred ittoward the AMA
‘
s PhysicianRecognitionAward , and forNorth Carol inaMedical Soc iety Category A credit. Where AAFP cred it has beenobtained , this also is indicated .
IN STATE
November 14-15
Clinical Teaching and Evaluation of Cl inical Perform ance
Place: Chapel H il lCredit: 12 hours Category I AMA, NCMSInfo: W . B . Wood , M.D. , 2 3 1 MacNider 202H , UNC. Chape l H il l
2 7 5 14 .-2 1 18
November 20
Endocrinology for the L ifetime of the Fema lePlace: SanfordCredit: 2 hours Category I AMAInfo: Robert S . Cl ine , M.D. , Central Carol ina Hospital , Sanford
2 7 3 30.-65 18
December 5 -7
Fourth Comprehensive Symposium on Breast DiseasePlace : Winston-SalemCredit: 16 hours Category I AMAFee :
Info: Center forMedical Ultr asound , BowmanGray , Winston-Salem2 7 103 .
-4 5 05
December 5 -7
Microcomputers inMedical EducationPlace: Chape l H il lCred it: 18 hours Category 1 AMA, NCMSInfo: W. B . Wood , M .D. , 23 1 MacNider 202H , UNC , Chape l H il l
2 7 5 14 .-2 1 18
December 7
UNC Ophthalmology Res ident'
s DayPlace : Chape l Hi l lInfo: Baird S . Grimson, MD 6 17 Cl inical Sciences Building 229H ,
UNC , Chape l H i l l 27 5 14 .-5 296
December 12
Controversies in TransplantationPlace: Chapel H il lInfo W . B . Wood , MD 2 3 1 MacNider 202H , UNC , Chape l H il l
2 7 5 14 .-2 1 18
December 18New Uses of Cal cium Channel BlockersPlace: SanfordInfo: R. S . Cline , M .D. , Central Carol ina Hospital , 1 13 5 Carthage
Street, Sanford 27 3 30.-65 18
January 10-1 1 , 1986
Advanced Cardiac L ife SupportPlace : Chapel H i l lInfo: W . B . Wood . M.D. , 2 3 1 MacNider 202H , UNC , Chape l H il l
2 7 5 14 .-2 1 18
January 30, 1986
Controvers ies in TransplantationPlace: Chapel H il lCredit: 7 hours Category I AMAInfo: W . B . Wood , M .D. , 23 1 MacNider 202H , UNC , Chapel Hil l
2 7 5 14 . 9 191962 -2 1 18
NO VEMB ER 1985 NCMJ
OUT OF STATE
December 5
A Seminar on Legal MedicinePlace : Johnson City , TNCredit: hours Category I AMA, 7 hours AAFPFee: $7 5Info: Sue Hutchinson. Box l 9660A, Qui l len-Dishner Col lege of
Med icine , Johnson City , TN 37 6 14 .-64 26 , ext. 204
January 24 -26
Winter Conference onGeriatricsPlace : Hot Springs , VAInfo: Mary Anna Hendley , NC Academy of Family Physicians , Box
20146 , Raleigh 2 76 19 .-6467
New Members
Almond JerkinsDrake , II I ( IM ) , 4 963 CaminoDavid , Boni ta , CA92002
Paul Edward Viser, 6704 Rockwood Rd . L ittle Rock , AR 72 207
BUNCOMB EDan
'
lyn HeddcnDealy ( ID) , 44 5 B iltmore Ctr . , Ste . 404 , Ashevil le 28801
Rex Arthur Henderson (EM) , 36 Wembley Road , Ashevil le2 8804
Michael Phi l l ip Hooker (AN) , Rt. 5 , Box 7 7 1 , Ashevil le 2 8803
CHOWAN-PERQUM ANSJohn Arl ie Francis (OBG ) , Box 150, Currituck 27929
DUPL IN
Doris Bans-Murray (FP) , Rt. 1 , Box 4 , Kenansvil le 28349
DURHAM-ORANGEMichae l Armstrong , Jr. ( student) , 13 15 Moreene Rd . Apt. 25 -F ,
Durham 2 7 705
Peter Tannahil l Beatty ( student) , 2 205 Cranford Rd . , Durham2 7 7 06
KarenEl izabeth Bel iles (student) , 3 3 8 Ashley Forest, Chape l H il l2 7 5 14
Eli zabeth Anne Bel l (student) , 5 2—B Davie Circle , Chape l H il l
2 7 5 14
Miche l le Louise B leynat ( student) , H -5 Tarheel Manor, Carrboro2 7 5 10
Pame la Eaton Bond ( student) , 806 Demerius St. , Apt. T5 ,
Durham 2 7 701
David Brodeur (student) , 1505 Duk e Univers ity Rd . Apt. 5K ,
Durham 2 7 701
Francis Gregory Brusino (resident) , Fl int Ridge Apts . # 15 1 ,Hi l lsborough 27 2 7 8
BenuChatterjee (resident) , B -8 Stone Vil lage Ct. Durham 2 7 704Myron Scott Cohen, ( ID) , UNC . 5 4 7 Bumett-Womack , 229-H ,
Chapel H il l 2 7 5 14
El izabeth Jo Conrad (student) , 601 Jones Ferry Rd . Apt. N-S ,
Carrboro 2 7 5 10
David Wil l iam Cooke ( student) , 2 7 16 Middleton St. Apt. 3-D,
Durham 2 7 7 05
Jonathan Baldridge Covey ( student) , 2 14 Cedarwood Ln. , Carr
boro 2 7 5 10
6 17

Kri stin Leah Dutrow ( student) , 204 -A Howel l St. , Chape l H i l l
2 7 5 14
KarenDiane Fairchi ld ( student) , 2920Chape l H il l Rd . Apt. 168
Durham 2 7 7 07Mark Stuart Forman (student) , 301 Swift St. , Apt. 17 , Durham2 7 705
Frederick Alexander Frohbose (student) , Rt. 1 , Box 93 -E , Chapel
H il l 27 5 14
Thomas Funcik ( student) , 17 04 N . Roxboro St Durham 2 7 701
Jeffrey Wil l iam Furman (FP) , 1 10 S . Estes Dr . , Chape l H il l
2 7 5 14
George Scott Goodwyn ( student) , 705 -A N . Greensboro St. ,
Carrboro 27 5 10Dan T. Goulson ( student) , 102 Kel ly Ct. , Chape l H il l 2 7 5 14B ruce Lee Hal l (student) , 19 1 1 Erwin Rd . , Apt. K , Durham2 7 705
James Rene Herlong (student) , 1907 ErwinRd . Apt. G , Durham
2 7 705
Jeffrey Dale Hoffman ( student) , UNC . Box 460, Craige Hal l ,
Chape l H il l 2 7 5 14
GeorgeThomas Hol land ( student) , 15 1 1Robinhood Rd . Durham
2 7 701
Daniel Phil ipp Holschneider ( student) , 87 5 Airport Rd . # 16 ,
Chape l H il l 2 7 5 14
Barbara Sorenson Hulka (GPM) , Dept. of Epidemiology , UNC ,
Roseman H al l B ldg . 201 , Chape l H il l 27 5 14
Donal d Leland Ives ( student) , 4 13 Pritchard Ave . , Chape l H i l l
2 7 5 14
Rosemary Jack son (student) , 2405 University Dr. Durham27 707
PeterWitham Just (resident) , 15 7 Cedar L ake Rd . Chapel H il l
2 7 5 14
James ChristopherKaregeannes ( student) , 1901 ErwinRd . Apt
F , Durham 2 7 7 05
Charles Michae l L eCroy , Jr. ( student) , 134 L andsbury Dr. ,
Durham 2 7 707
Noe l David L ist (Ger) , Box 3003 , DUMC , Durham 27 7 10
MargaretE . Ferri terMarsden (student) , 200WoodcroftParkway ,
#40-B , Durham 27 7 13
James Cicero Manin, Jr . (resident) , 9 10 ConstitutionDr . , Apt
1009 , Durham 2 7 705
SharonMavros ( student) , 4 1 1- 1 Downing St. , Durham 2 7 7 05
Kenneth Paul McDonnel l (student) , 19 1 1 Erwin Rd . , Apt. B ,
Durham 2 7 705
Wil l iam Frederi ck McGuirt , Jr. ( student) , 601 Jones Ferry Rd . ,
Apt E- l , Carrboro 27 5 10Jeffrey Roy Medoff (GE) , Box 3 3 84 , DUMC , Durham 27 7 10
Roger Niles Mennil lo ( student) , 8 1 1 Vickers Ave . , Durham
2 7 701
Charles Edward Parke ( student) , 6 14 Caswel l Rd . , Chape l H il l
2 7 5 14
Suzanne El izabeth Patton ( student) , Box 2 7 86 , DUMC , Durham
2 7 7 10
Loe l Zachary Payne ( student) , 2 19 Mccauley St. , Chape l H il l
2 7 5 14
Dwight Dean Perry (OPH ) , 5 12 Simmons St Durham 27 707
Jeffrey McBrayer Peterson (student) , 2 Spring Garden, Hol land
Dr . , Chape l H il l 27 5 14
Marcus Plescia ( student) , 102 Ke l ly Cl . , Chape l H il l 27 5 14
John Bradford Pracyk ( student) , 6 10 Douglas St. , Apt. 3 12—B ,
Durham 2 7 7 05
Charles David Scheil ( student) , 24 -F Stratford H il ls , Chape l H il l
2 7 5 14
Rick Paul Sessions (student) , 2 10 Westbrook Dr. , Carrboro2 7 5 10
Spencer Marion Smith (student) , 206 Alexander St. , Apt. E ,
Durham 2 7 7 05
6 18
GRANVI L L EAlfred Dadee L aminMassaquoi (GEG ) , 1030 Col lege St. , Box15 13 , Oxford 27 5 65
GUl L FORD
Ernesto Miguel Botero (NS) , 200 E. Northwood St. Ste . 504 ,
Greensboro 2 7 401
VOL . 4 6 , No . 1 1
JeffreyDavid Snedeker ( resident) , 303 1Weymouth St. Apt-G ~ 6 ,
Durham 2 7 7 07John Haddon Stephenson ( student) , 500 Umstead Rd . 201-E ,
Chape l H il l 27 5 14
T. Scott Stroup ( student) , A- l Oak Terrace Apts Chapel H il l
2 7 5 14
Sylvia Sutton (student) , H - 5 Tarheel Manor, Carrboro 2 7 5 10
Wal lace Clements Tarry ( student) , 208 E . Knox St. , Durham27 7 02
Grace Emerson Terre l l ( student) , 2920 Chape l Hil l Rd . Apt.5 4—D , Durham 2 7 707
Jayne Fel icia Trachman ( student) , 105 -4 2 Avenue K , Brookl yn,
NY 1 12 36
Charles Barnes Watson, NCMH , Dept. An. 2 162 -A 2ud Pl . ,Chapel H il l 2 7 5 14
Michael StephenWebb , Jr. ( student) , 3 1 1 S . L a Sal le St # 18-D ,
Durham 2 7 705
Th eresa L ynWhee ler ( student) , 0-6 Kingswood Apts . , Chape l
Hi l l 2 7 5 14
Daniel BaxterWhi tesides (res ident) , 4 404 Cheshire Ct. Durham2 7 705
FORSYTH -STOKES-DAVIEL isa Kay Christensen ( student) , 4 5 2 Corona St. Winston-Salem2 7 103
Roger Dale Cole ( student) , 407 Corona St. , Winston-Salem27 103
Robert Kent Dyer, Jr. ( student) , 5 20 West End B lvd . , Apt. B ,
Winston-Sal em 2 7 102Kimberlee Eastman F ish ( student) , l 4o7 -D Seneca St. WinstonSalem 2 7 103
Kevin S . Harboume ( student) , 25 64 Mil ler Park Cir. , WinstonSalem 2 7 103
Ziaol lah Hashemi (student) , 14 39-L Hutton St. Winston-Salem27 103
David Montgomery Hunter (student) , 16 15 Northwest Blvd . ,
Winston-Salem 27 104Brantley Tilman Jol ly , Jr. (student) , 2401 Fairway Dr . WinstonSalem 27 103
Douglas Evan Kaye ( student) , 405 Corona St Winston-Salem27 103
Robert Edward Leyrer ( student) , 300 S . H awthome Rd . , Winston-Salem 27 103
Coy Randolph Matthews (student) , 120 Eden Terrace # 1 , Winston-Salem 2 7 103
Michael C . Maxwel l (student) , 4 18 Lockland Avenue , WinstonSalem 2 7 103
Charles Carmen Miragl ia ( student) , 105 7 S . Hawthorne Rd
Winston-Sal em 2 7 103
Wendy Elaine Murphy ( student) , 205 7 Bethabara Rd . , Apt. 17 ,
Winston-Salem 2 7 106
Joseph Edward Robert s (student) , 1608-F Northwest B lvd . Winston-Salem 27 104
Thomas Anthony Schroeter ( student) , 1008 S . Hawthorne Rd . ,
Winston-Salem 27 103
Barbara Anne Smi th ( student) , 607 -B S . H awthorne Rd . , Winston-Salem 2 7 103
Robert G regory Stout ( student) , 601 Mil ler Street, WinstonSalem 2 7 103


Letters to the Editor
What To Do About Tobacco?
To the Ed itor
I congratulate Dr. Moffett and Dr . Stead on their excellent L etter and Comment regarding tobacco in the September issue of the NCMJ Phys icians final ly havestopped al low ing the pretense that the l ink betweencigarette smoking and disease is doubtful . The proof of theassociation is overwhelming .
Dr . Moffett’
s suggestions to the tobacco companies
would be wonderful if the changes were l ike ly . But as
lawyers remark :“Tobacco companies are not e leemosy
nary institutions . Industri es seldom act in the publ ic interest when such actions oppose their own economic interests .
There is a s imple way to decrease our dependence on
tobacco . Provide such high price support s for cotton, corn ,
vegetables , fruits , and other valuable crops that any efficient farmer can mak e a good l iving by planting them.
Discontinue al lotments and pri ce support s for tobacco .
Prohibit publ ic b il lboard advertisements for tobacco . ln
crease the tax ontobaccoproducts yearly until consumption
5 5 0m» i mu
NO VEMB ER 1985 , NCMJ
More on Coccydynia
To the Ed itor
Another cause of coccydynia was recently reported byE . A. Mortimer, M .D. : two teenage g irls developed coc
cyx pain when slouch ing in hard classroom seats while
wearing tight blue jeans (Pediatrics One of
the patients was concerned enough to seek orthopedic eval
uation, but Dr . Mortimer recognized that the stiff rein
forced jean seams caused coccyx trauma .
B ased on this experience , Dr. Mortimer has an interesting comment about our Case 3 , the young man on the
motorcycle who suffered from tai lbone pain (NCMJ1985 ;46 z209
“ I notice that the guy sitting on the motorcycle and
holding a beer (Case 3 ) is wearing b lue jeans : inhis instancethe etiology may be multi—factorial . It would then have tobe cal led the Har ley
-Davidson-Jordache Syndrome .
L inda Fraz ier, MD .
Divis ion of General lntemal Medicine
Duke Univers ity Medical Center
Durham 2 7 7 10
Duke ’s Fami ly Med icine
To the Ed itor
I read w ith interest Dr. Robert Sul l ivan’
s review of the
Fami ly Medicine program at Duke (NCMJDr . H arvey Estes , Jr .
’
s Family Medicine at Duke : A
fol low up (NCMJ -4 ) and George T. Wol lf’
s
andWil l iamA. Hense l’
s letters to the editor about the same62 1
fal ls significantly , but do not make the tax so high thatpeople begin to bootleg tobacco .
An extra advantage of this course of action would be to
lessen the g laring governmental incons istency wh ichmakes marijuana il legal and growing it a crime , wh iletobacco receives pri ce supports and beer advertisements
rule the TV screens . We cannot teach our youth to respect
prohibitions that seem arbitrary and il logical comparedwith the incentives and freedoms g iven rather simi lar prod
ucts .
Of course , my suggestions have l ittle chance of be ingaccepted in the next few years . Inanoverpopulated society ,
such as theUSA, many people have few al ternativeways ofmak ing a l iving . The leaders and people in favorab le positions become afraid of proposed changes wh ich mightjeopardize the ir economic securi ty . In North Carol ina to
day , a pol iticianwho ran on the above platform regardingtobacco would be lucky to rece ive 5% of the votes . Never
theless , the preced ing suggestions (or something similar)eventual ly are almost sure to be adopted . Tobacco, once a
mighty King , wil l become a weed in the farmer’
s garden.
Albert D. Warshauer , MD .
1608 East F ifth Street
Greenvi l le 27 834

subject (NCMJ 1985 ;4 6 z4 93 They outl ined many
powerful currents that have affected this watershed event . Ishould l ike to suggest another angle that I think is bothsupplementary and complementary of the ideas presented
by these writers .
Much of the struggle that Fami ly Med icine departments
and Family Medicine practitioners face in the intemecine
warfare of the tertiary medical center revolves around our
own fai lure to earn our academic spurs . We can easily
demonstrate the fami ly physician’
s superiori ty at del iver
ing medical care , and this de l ivery includes the efficient
and effective util ization of the sk i l l s and talents of our
subspecial ist col leagues . We may successful ly rest our
future existence on th is strength , and as this strength de
velops , itwil l enhance our re lationshipw ith our subspecial
istcol leagues . But, we wil l not successful ly stand toe to toe
with them in academe until we do research on disease
processes that is better then theirs .
Intel lectual strength belongs to those who break new
ground .
And we have several characteri stics of family practice
that present us with the opportunity to do exactly that.
The first of these is that we often deal with a re latively
stable patient population, stable as compared with that
which passes through the tertiary care cl inics . We aremuch
more able to present research done in a longer time frame .
62 2
We are much more ab le to analyze in depth as opposed tobroad statistical guesswork .
Secondly , such diseases as the sexual ly transmitted dis
eases should be almost the exclusive province of the family
physician. The internist and infectious disease special ist
has to move out of his usual age group to deal with these
diseases . Syphil is is obviously no longer the province of thedermatolog ist. The urolog istmay know a bitaboutprostatitis , but is often unfamil iar with the cervix . The gynecolo
g ist knows a great deal about the cervix , butalmostnothingabout the prostate . The pediatri cian beg ins to blush whenhis patients reach this age .
Andmost importantly , fami ly physic ians should be least
guilty of al l physicians of think ing in pigeon holes . We
shoul d understand the interre lationsh ips between the
psychopharmacology of depression and the pharmaco ther
apeutics of hypertens ion, for example . The internist is sobusy treating the high b lood pressure that he has l ittle
interest in depression, and the psychiatrist is so busy withthe depressionthathe has l ittle interest inhypertension.We
see both!Family physicians should be prepared to undertake these
explorations and to break new ground .
John R. Dykers , Jr . , MD .
Box 565
S iler City 2 7 344
VOL . 4 6 , No . 1 1

Index to Advert isers
Army ReserveAyerst L aboratoriesB& B X Ray , Inc .
B lue Cross/B lue Shie ld of North Carol ina
Burroughs-Wel lcome
Campbel l L aboratories , IncCHAPS
Crumpton CompanyCurtis 1000 Information SystemsEastWoods Press
GuestHouse
E . F . Hutton Company , Inc .
Info Systems of NC . Inc .
624 VOL . 4 6 , No . 1 1
Eli L il ly Co . 5 64
MacThri ft Office Furniture 5 62
Medical Mutual Insurance Company 5 67
National Staffing Services Corp. 5 5 7
Ortega Pharmaceutical Company , Inc . 624
Roche L aboratories 5 60 , 5 6 1 , 5 62 , Cover 3 , 4
Saint Albans Psychiatric Hospital 5 63
Seabrook Island 6 19
E . R. Squibb Sons , Inc . 6 13 , 6 14 , 6 15 , 6 16
The Upjohn Company 6 10- 6 1 1
U S Air Force 5 62
Wi l l ingway , Inc . 5 7 8
Winchester Surgical Supply Co . Cover 2

EXCERPTS FROMASYMPOSIUMTHETREATMENTOFSLEEPDISORDERS"8
highly effectiveforboth s leep inductionands leepma intenance
SleepLaboratory investigator
Pennsylvania
onsetofaction israp id. . provides s leepwithno rebound effecttoag itatepatientthe fol lowing day
Psychiatrist
California
. . appears tohavethe bestsafety record ofanyofthe benzod iazep ines
Psychiatrist
California
After 15 years, the experts still concuraboutthecontinuing value ofDalmane (flurazepamHCI/Roche) . Itprovides s leepthatsatisfies patients .
and thewidemarginof safety thatsatisfies you.
The recommended dose inelderlyordebilitated
patients is 15 mg. Contraindicated- inpregnancy.
tlura zepom HC I/ Roches leep tha t sa tisfies
l 5 —mg/30—mgcaps
Retere nces : 1. Kales J, aral: CllnPharmacol Ther 12 .
-691
697, Jul-Aug 197 1. 2 . KalesA, etal: ClinPharmacol Ther-363 , Sep 197 5 . 3 . KalesAeta/. Cli'nPharmacol
7179! - 5 83 , May 19 76 . 4 . KalesA, arat; ClinPharmacol Ther -7 88 , Dec 198 2 . 5 . FrostJDJr, DeLucchiMR; JAmGeriatrSoc - 5 4 6 , Dec 197 9 . 6 . DementWC, etol: BehavMed, pp. 2 5
-3 1, Oct 197 8. 7. Kales A,Kales JD: J ClinPsychopharmacol - 15 0,
Apr 198 3 .
8 . TennantFS, etal: SymposiumontheTreatmentofSleepDisorders , Teleconference, Oct 16 , 1984 . 9. GreenblattDJ
AllenMD, ShaderRI: ClinPharmacol The/ 2 13 5 5 43 6 1,Mar 197 7.
DALMANEG‘
flurazepamHCl/Roche
Before prescribing, please consultcomplete productInformation, a summary ofwhich follows:Indications: Effective inall types of insomnia characterizedby d iff iculty infalling as leep, frequentnocturnal awakeningsand/orearlymorning awakening. inpatientswith recmringinsomnia orpoorsleeping habits; inacuteorchronicmedical
S ituations requuing restful s leep. Objective s leep laboratorydata have showneffectiveness forat least28 consecutive
nights ofadministration. Since insomnia is oftentransientand intermittent, prolonged administrationis generally notnecessary orrecommended. Repeated therapy should only
be undertakenwith appropriate patientevaluation.
Contraindicatians: Knownhypersensnivity lo flurazepamHCI;pregnancy. Benzod iazepinesmay cause fetal damagewhenadministered during pregnancy. Several studies suggestanincreased risk ofcongenitalmalformations ossocmted Withbenzodiazepine use during the firsttrimesterWarnpatientsofthe potential risks to the fetus should the pOSS ibi lify ofbe
coming pregnantexistwhile receiving flurazepam. Instructpatients todiscontinue drug prior tobecoming pregnant. ConS iderthe possibility ofpregnancy priorto instituting therapy.
Warnings; Cautionpatients aboutpossible combined effectsWith alcohol and otherCNS depressants. Anadditive effect
may acourifalcohol is consumed the day following use fornighttime sedation. This potentialmay existforseveral daysfollowing discontinuation Cautionagainsthazardous occu
pations requiring completemental alertness ( e.g operatingmachinery, drivmg) . Potential impairmentofperformance ofsuch activitiesmay occurthe day fol lowmg ingestion. Not
recommended foruse inpersons under 15 years ofageWithdrawal symptoms rarely reported , abruptdiscontinuation
should be avoidedwith gradual tapering ofdosage forthose
patients onmedicationfora prolonged period of lime. Use
caution inadministering toaddiction—prone individuals or
thosewhomight increase dosage.
Precautions: Inelderly and debilitated patients ,it is recom
mended thatthe dosage be limited to 15 mg to reduce risk ofoversedation, dizziness , confusronand/orataxia. Consider
potential additive effects with otherhypnotics orCNS depres
sants . Employ usual precautions inseverely depressed
patients , or inthosewith latentdepressionorSUICIOO| tenden
cies. orinthosewith impaired renal orhepatic function.
Adverse Reactions: Dizziness , drowsiness, lightheadedness ,
staggering, ataxia and fall ing have occurred , particularly in
elderly ordebilitated patients. Severe sedation,lethargy. dis
orientationand coma, probably indicative ofdrug intolerance
oroverdosage,have beenreported. Also reported: headache.
heartburn, upsetstomach, nausea, vomiting,diarrhea. can
stipation, GIpain,nervousness. talkativeness, apprehens ion,
irritability, weakness , palpitations, chestpains. body and JoInl
pains and GUcomplaints. There have alsobeenrare occur
rences of Ieukopenia, granulocytopenia, sweating, flushes.
difficulty inmous ing, blurredVision, burning eyes ,faintness,
hypotensron, shortness of breath. pruritus , s kinrash, drymouth, bittertaste, excessive salivation, anorexia, euphoria,
depression, s lurred speech, confus ion, restlessness, halluci
nations , and elevated SGOT, SGPT, total and d irectbilirubins
and alkaline phosphatase: and paradoxrcol reactions , e.g. ,
excitement. stimulationand hyperactivity.
Dosage: Individualize formaximumbeneficial effect. Adults30mg usual dosage; 15 mgmay suff ice insome patients .
Elderlyordebilitated patients: 15 mg recommended initiallyuntil response is determined .
Supplled: Capsules containing ISmg or30mg flurazepam


Because you want
to entrust your patients tothe bestprofess ional care ,
Sa intAlbans is a log icalcho ice foryourpsych iatricreferrals .
Since 1916 , Sa intAlbans Psychiatri c Hospita lhas provided a spectrumof care for emotionald isorders .
Today, we al so offer
spec ial ize d , fully accredite
programs foradolescents ,
alcohol ics , and substanceabusers .We have spec ialprograms for senior adultsand treatment of eatingd isorders .And we offerdaytreatment as analternativeto hospital ization.
Care is provided by oumodern hospital secluded al ( 1
24 hours a day.And al l programs and services are approved forBlue Cross ,Med icare , Champus , and most commerc ial insurance carriers .
At Sa int Albans , we ’
ve bui lt our reputation on the trust of referringphys ic ians who want the best for tatients . That
’
s why you can refer
a intAlbans with confidence .
Private, Not For ProfitPsychiatric CarePO. Box 3608 Radford.Virginia 24 1431-800-368 -3468
Active Medica l Staff
Ro lfe B . Finn.M.D. Bas il E. Roebuck . M.D.
Med ical Director 0 . LeRoyce Royal .M.D.
Davis G . G arrett, M.D. Morgan E. Scott.M.D.
Hal G . G i llespie .M.D. Don L .Weston, M.D.
0 ~ Paul H lus lto , M-D Psy chiatric ConsultantRonald L Myers .M-0 0 .Wil fred Absc .M.D.

Publ ished Monthly as the Official Organ of The North Carol ina Medical Society ( ISSN -OO29- 2 5 5 9)
DECEMB ER 1985 , NCMJ 625

F inancia l new s you have been w a i ting to hea r! !
ew ncreas e ml S O
ncome
Ava i la ble to ig ible Members Age 5 0Rega rdles s O ther D is abi l i Insurance
Offic ia l North Caro l ina Med ica l Soc ietyDis ab il ity Income Plan
Endors ed and Recommended S ince 193 9
Protect your mos t va luab le as s et, your profes s iona l income
For deta ils or cla ims s ervice ca ll orwrite :
CRUMPTON COMPANYPROFESS IONAL GROUP INSURANCE
Toll free - 1 6 7 4
ACADEMY CENTERPOST OFFICE BOX 8 5 00DURHAM, NC 2 7 7 07
Account executives : J . S lade Crumpton, Gene Greer and CliffMasher, DurhamJack Featherston, Charlotte
Dan Ha ley , Greensboro
626 VOL . 4 6 , No . 12

MANAGEYOUROFFICEMORE EFFECTIVELYW ITHTH EMPM 1000 SYSTEMAVAILABLETHROUGH
SOUTHERNMEDICALASSOCIATIONSPHYSICIANS PURCHASING PROGRAM
Manage your Office moreeffect ively w ith theMPM1000System ava i lablethrough the Phys ic iansPurchas ing Program .
Manag ing your officeshouldn
’
t be hard ;
however, w ith the currentinsurance requ irements and
MPM 1000 Simpl ifie s Your Paperwork
You will be able to reduce the mountains of paper
work by using your MPM 1000 system to process al l
your insurance , complete your bil l ing plus instan
taneously sort and file necessary information .
MPM 1000 Spe ed sUp Your Cash F low
The MPM 1000 system w i ll increase your daily bank
deposits by processing all your insurance and pa
tients’
receivables quickly .
MPM 1000 Improve s Your Pract ice Management
With the MPM 1000 system you can easily and inte l
l igently manage your practice w ith computer gene
rated reports . Trends and problems are eas i ly iden
tified so you can take corrective action before theybecome serious .
DYES ! I would l ike more information onMPM 1000
My interests are : D Immed iate D Long term D Please contact me for a surveyI am a member ofSMAD
Address
Specia lty Office Phone
Ma il to : CURTIS 1000 INFORMATION SYSTEMS2296 H endersonMill RoadSu ite 402
Atlanta , G eorgia 30345
the impend ingMed icarechanges loom ing on thehor izon , it w i ll get mor
d ifficult . You should cal l
Curt is 1000 Informat ionSystems or Southern
Med ical Assoc iat ion to findout how theMPM 1000 can
helpmake your pract icerun more effect ive ly .
ON IBMA/TMPM 1000 I sAOne Source So lution
The MPM 1000 is a one source solution . With yoursystem you rece ive al l hardware (IBM or Texas In
struments) , software , complete five day training pro
gram and respons ive after sale support .
IBM PC /ATAtD iscountBest of all , these systems are ava ilable. through SMAServices , Inc . , Physicians
’
Purchasing Program with
substantial d iscounts on IBM and Texas Instrument
equipment .
FORMORE IN FORMATION , please fi ll out the
coupon below and mail it to Southern Med ical Asso'
ciation , or for faster service call Southern Med ical at
(205) 9454 840 or Curtis 1000 Information Systems at
800—241—4780.

MODERN MEDICINE
On Dating , Marriage and Other Strange
Re lationships : The Future of Singular Hosp itals
Harry A. Nurk in, Ph .D.
0 The dating game turns serious when the parties a re hosp ita ls and the
product is hea lth care .
N the world of business , corporate marriages are a familI iar phenomenon. Often industrial mergers occur for
purposes of diversification of product l ine , improved mar
ketpenetration, economies of scale , strength and/or surviv
al . While some industri al mergers are characterized as
unfriendly takeovers , for the most part the joining of
two businesses or the merger of smal ler businesses intolarger corporate structures is considered to be routine and
oftenhealthy . One also seesmarriages occur inother stab leinstitutions and enterpri ses in our society . For example ,
institutions of higher learning join together for economicreasons as wel l as for more effective provision ( i f—the
process of learning and the deve lopment of new knowl
edge . Churches and rel ig ious orders marry for the purpose
of creating stronger congregations in order to carry out
more effectively themissionof the part icular denominationor church . Human be ings marry for a vari ety of purposes ,
but such unions are general ly based on a mutual desire tol ive , to work and to love together so that the parties of the
union benefit far greater than they would have as separate
individual s .
Butwhen hospita ls considermarry ing , or other types of
symbiotic relationships , unusual emotions erupt. Perhaps
such mergers , marriages and other strange relationshipsinvolving hospital s engender emotion and lengthy d iscussion because such activity is a relatively new phenomenonin the hospital bus iness .
Hospital s have been created for social and scientificpurposes in over locations in the United States .
Hospitals are the most unique of modern enterprises
accord ing to management theorist Peter Drucker . They
provide services that most recipients would prefer not toneed . With the exception of normal b irth s , most activitiescarried on in hospitals place the recipients of care in an
atypical and unnatural environment where the ir bodies ,internal chemistri es , organs , and personal ity are examined ,
probed , punctured , and excised , in an attempt to resolve
and/or cure affl ictions that cause great anx iety and fear. In
addition, hospitals are unique enterpri ses because of the
myriad of formal and informal re lationships brought to bearat the point of service . Physicians , w ith the exception of
teaching physicians and hospital-based special ists , are pri
FromThe Charlotte-Mecklenburg Hospital Authori ty , Box 32 86 1 Char
lotte 2 82 32 .
DECEMB ER 1985 NCMJ
vate entrepreneurs whopractice voluntari ly at hospitals . In
this capacity , physicians interface with a potpourri ofworkers inheal th profess ional and support capacities to carry out
the directions of the phys ician in order to d iagnose , ex
amine and provide therapeutic modal ities for the care andtreatment of patients .
Hospitals are also the prime example of a service industry . General ly the products of hospital activity are human
to- human serv ices as compared with manufacturi ng or
sales of products in the typical industrial setting . Most
patients leave the hospital experience without tangible evidence of the experience , other thana general feel ing ofwe llbe ing and el iminationof anxiety and fear related to diseaseand injury . Unl ike institutions of higher education, d iplo
mas are not awarded . Unl ike sales companies , no productcan be viewed , used or worn by the purchaser of the
hospital service .
Although hospitals are unique enterprises , communitiesregard them not only as necess ities , but also as symbol s ofpride . Yet there ex ists in the midst of the pride in commumity hospital s an identifiable love-hate re lationship. Gener
al ly , community citizens are prideful about the resourcesand technology and buildings cal led hospitals , yet the emotions of fear and anx iety and the potential for death also are
apparent in the identification w ith hospital s .
Inrecentyears , hospitals have also become the subjectofmuch discuss ion related to the cost of care . Headlines
proclaimthathealth care cost, ofwhich a sizable proportionrelates to hospital cost, has risen at an infl ationary rate inexcess of 18% annual ly , to the extent that almost 12% of
the gross national product of our country can be related to
expenditures for keeping our populous heal thy . Of course
such dramatic increases in the cost of health care create
additional anx iety on the part of citizens in communitiesthroughout our country , as we l l as business leaders whobuy insurance for employees , tax payers who sponsor
health care through taxation, insurance companies who
provide various types of health care insurance , and others
who are general ly concerned about the rapid increase in
heal th care cost.
In addition to such broad and varied emotional responsesto hospital s as necessary but troubl ing enterprises , a broader social view ofhospitals and heal th care inourcountry hasbeen difficult to define . Because of the increas ing cost toprovide care through hospitals , we have wrestled w ith how

this soc ietal need should be balanced against other needs inl ight of available financial resources . General ly , Amer
icans accept a social philosophy that supports the“highest
possible qual ity”and unl imited access
”but al so bel ieve
that such qual ity and access be provided at reasonablecosts .
In a strained economy individual emotional responses tohospital s and the health care provided therein cause us to
examine our col lective soc ial and ph i losophical conscienceregarding whether the traditional system of hospitals
should continue or whether new corporate formats should
be created to prov ide necessary services at the highest
poss ible qual ity with unl imited access , but at a control ledcost. These are difficult and oftenunanswerable dilemmasthat we face .
Those who serve as members of Boards of Trustees ofhospitals and managers of such faci l ities currently face a
troubled environment. Uniformly , such persons are buf
feted with complaints about the high cost of care providedby hospitals . Simultaneously , communities des ire to havethe mostmodern, up
—to-date technology and facil ities and
the most ski l led health profess ional and support personne lavailable . Na citizen wants to bel ieve that when he needshospital care there wi l l be inadequate physical facil ities ,outdated diagnostic and therapeutic equipment or too few
health professional and support personnel . As the scienceand art ofmedicine progress , physicians desire to have themostmodern and effective diagnostic and therapeutic tools
available to assist in the care of the physician’
s patient inthe laboratory or cl inical environment known as a hospital .
Phys icians are al so be ing buffeted by complaints and concerns on the part of business and industry and indiv idualpatients regarding the high cost of health care and the
apparent inab i l ity of the health care system to work effi
ciently and effectively .
Our desire for super- special ization has developed to the
extent that not every hospital is capable of deal ing with al ld iseases and injuries . In earl ier times hospitals provided al ltypes of care and al l types of equipment necessary for thephys ician to practice his trade . Today , inmany communi
ties a broad range of specialty faci l ities exists in addition togeneral facil ities that cancare for al l maladies . Patients and
physicians are forced to make decisions regarding the
appropriate hospital to use depend ing on the disease or
injury affl icting the patient. The re lationships among thehospitals , patients , phys icians , trustees , providers , insarers , administrators and other health profess ional s are indeed strained because of these compel l ing pressures of
societal need ,qual ity , access , competition and cost.
The most press ing issue facing the family of heal th carere lationships today is the issue of cost. If, indeed , appropriate health care is a bas ic human right in America , how
much can we afford to spend on this right as opposed toother human necess ities and societal needs?One of the ways to address the dilemma we al l face is to
determine whethermore efficient, alternative del ivery systems can replace what we have known to be the hospitalsystem in our country . Alternative de l ivery systems can
take the forms of mergers , partnerships and other intimate
re lationships among and between hospitals . In the decade
of the 905 , we wi l l see a change in the corporate structure of
630 VOL . 46 , No . 12
hospital s throughout the State ofNorth Carol ina as we l l asother states in our country . B ecause most hospital s have
operated as singular corporate entities , l ittle in the way of
economies of scale to contain costs has been availab le . In
essence , hospital s have beenas self centered and jealous ofthe ir singular enterprises as have been communities .
Until the burden of regulated payment systems and theadvent of for-profit multiple hospital systems emerged in
the decade of the 7 05 , singular hospital units bel ieved theycould survive financial ly and provide al l elements needed
by physicians and patients on a continuing basis . The
decade of the 905 w i l l w itness aprol iferationof new corpo
rate designs as hospital s d iscover that “
going it alone”
does not work , and they begin to maneuver for secure
positions in a highl y competitive marketplace fi l led withincreased risks and continuing complaints aboutefficiency ,
effectiveness , and the high cost of care .
Multiple hospital systems are already growing rapidly .
Central ly managed chains of heal th del ivery facil ities nowprovide services to patients in over facil ities . This
number combines hospital s , ambulatory centers , nurs inghomes , rest homes and other institutional sites for healthcare . It has been predicted that by 1990 investor-ownedhospital chains wil l constitute 19% ofour nation
’
s hospital s
and 2 3% by 1995 , upfrom 14% in 1982 . Singular , not- for
profit hospitals , once 100% of the market, wil l fal l to less
than 50% by 1995 . It is estimated that over 40% of non
governmental hospitals wi l l be owned , leased ar control led
bymulti -hospital systems by 1995 an increase ofone-third
over 1982 . Much of the growth in multi-hospital systems
wil l be generated by investor-owned or for-profit hospital
chains , butnot-for-profit systems wil l merge , marry or l ive
together stri ctly for survival purposes by the decade of the
905 .
Mergers , mani ages and other strange relationships wil lbe based on the need of singular hospital units toprotectorexpand the irmarket areas to achieve economies of scale byspreading
“
the high cost of personnel and technology in
order to survive in the next decade .
The reasons are easy to understand . Inadditionto cconamies of scale , singular hospitals that merge into larger
corporate entities wi l l also have greater access to capital ,
increased reimbursement from cost-based payors , reducedregulatory constraints , and to a lesser degree l imited l iabi lity for certainoperations w ithin the hospital organization.
In addition, hospital s in multi-hospital systems wi l l begin
to enter non-traditional bus iness ventures as a way to offsetthe high costof health care and l imited re imbursement fromregulated governmental agencies and commercial insur
ance companies .
S imilar to humanbonding throughmarriage , suchmergers , marriages and other affi l iations wi l l not occur w ithouttrauma . For centuri es hospitals have been singularly ownedand operated , and the community pride and spiri t of thosesingular units wil l be forced to give way to the good o
f a
greater need and to provide high qual ity and access at
reasonable costs . There are examples in the State of NorthCarol ina ofmulti-hospital systemmarri ages . InCharlotte ,
the Charlotte-Meck lenburg Hospital Authori ty was createdby an act of the leg islature in 194 3 to al low for economies
of scale ,e l imination of dupl ication and protection against

MODERN MEDICINE
ADukeAdministratorSurveys the Current Scene
Duncan Yaggy , Ph .D
R. Nurkin has put his finger on a problem thatworries
many communities inNorth Carol ina , for the survival
of rural , independent hospitals is threatened on four s ides at
once :
0 Pressures to l imit the growth in expenditures for
health care are reducing hospital ization. Hospital uti l iza
tion has dropped sharply the last three years , and it wi l l
continue dropping for several years more .
0 Pub l ic and phys ic ian perception that large urbanhospital s can provide more comprehensive serv ices is taking patients outof rural hospitals . Rapid deve lopment in thePiedmont, along the coast, and in other parts of the state
wil l bring more residents of rural areas to the cities and
accelerate the trend .
0 It is hard to raise the capital required to renovate
hospitals and keep them up to date . Many of our rural
h0 5pital s were built during the 19405 and 195 05 and requirereconstruction
"
or extensive renovation s imply to operate
efficiently . Decl ining occupancies make it seem essential
From Duke Univers ity Medical Center, Durham 27 7 10 .
63 2
that they renovate , but they wil l alsomake itmore d ifficultto find the funds .
0 The growth of health maintenance organizations , pre
ferred provider organizations , and other prepaid plan
arrangements wi l l bri ng into the health care market buyerswho wil l use the competitionbetweenhospitals with emptybeds to compel substantial discounts .
Whether to hold on to the ir patients , protect their revenues , gain access to the capital they require , or share in the
economies of scale that come w ith participation in a largersystem, independent hospitals are entering al l manner of
new relationships . Some are joining multi-hospital systems , while others are joining with their physicians to
create prepaid plans , and sti l l others are creating ties w ithambulatory care providers , nurs ing homes , and home
health agencies to create health care service organizationsproviding a ful l range of services .
As Dr . Nurk in points out, the difficulty of developingnetwork ing arrangements is formidab le , and hospitalboards accustomed to concernwith acute inpatient servicesand to independence may find the trans ition awkward anddifficult. But for many hospitals , large and especial lysmal l , there is no choice .
VOL . 46 , NO . 12


PROFESSIONAL USE INFORMATION
DESCRIPTIONCARDIZEM' Idlitiazemhydrochloride) Is a calciumIon Influx
inhibitor Islowchannel blockerorcalciumantagonist). Chemically,diltiazemhydrochloride is I .S Benzotfi iazepIn4 I5H)one.3-I acetyioxy)-5 -dihydro-2 -I4 -methoxyphenyI)monohydrochloride,l+ ) -cIs The chemical structure is:
Diltiazemhydrochloride is awhite tooff-white crystallinepowderwith abittertaste. It is soluble inwater.methanol. andchloroform.
It has amolecularweight of Each tablet of CARDIZEMcontains either 30 mg or 60mg diltiazemhydrochloride fororaladministration.
CLINICAL PHARMACOLOGYThe therapeutic benefits achievedwithCARDIZEMare believed
to be related to its ability to inhibit the Influx of calciumionsduri membrane depolarizationof cardiac and vascular smoothmusce.
Mechanisms of Action. Although precisemechanisms of itsantianginal actions arestill being delineated.CARDIZEMis believed
toact nthe fol low) ways:i . AnginaDue to ronaryArtery Spasm: CARDIZEMhas beenshowntobeapotemdilatorofcoronaryarteriesbothepicardlaland subendocardial . Spontaneousand e novine lnducedcoronary artery spasmare inhibited byCAR IZEM.
2. Exertional Angina: CARDIZEMhas been shown to produceincreases Inexercise tolerance. probably due toits ability toreducemyocardial oxygendemand. This is accomplished viareductions lnheartrateandsystemlcbloodrxessmeatsubnaxlmaandmaximal exercisework loads.
Inanimal models. diltiazeminterferes with the slowinward(depolarizing) currentinexcitable tissue. Itmuses excitationmntractionuncoupling invarious myocardial tissues without changes Intheconfigurationof the actionpotential . Diitiazemproduces relaxationof coronary vascular smooth muscle and dilationof both large andsmal l coronary arteries at drug levels which cause little or nonegative lnotroplc effect.The resultantincreases incoronary bloodflowIepicardlal andsubendocardal)occurinischemicandnonischemlcmodels and are accompanied by dose-dependentdecreases insystemic bloodpressure and decreases Inperipheral resistance.hemodynamic and Electrophys lologlc Effects. Like other
calciumantagonists .diltiazemdecreases sinoatrial andabioventricularconductioninisolated tissues andhas anegative inotropiceffectinisolated preparations. Inthe intactanimal.prolongationof theAHinterval canbe seenat higherdoses.
Inman.diltiazemprevents spontaneous andergonovine provokedcoronary artery spasm. Itcauses adecrease Inperipheral vascularresistance and amodest fall inblood pressure and. Inexercisetolerance studies inpatientswith Ischemicheart disease. reducesthe heart rate-blood pressure product for any givenwork load.Studies todate, primarily Inpatientswith goodventricularfunction.have not revealed evidence of anegative inotropic effect: cardiacoutput, ejectionfraction, and Ieh ventricularend diastolicpressurehavenotbeenaffected.There areas yetfewdataonthe interactionofdiltiazemandbeta-blockers.Restingheart rate isusual lyunchangedorslightly reduced by diltiazem.
Intravenous diltiazemIndoses of 20mgprolongsAHconductiontimeandAVnode functional andeffectiverefractory periodsapproximately Ina study Involving single oral doses of 300mg ofCARDIZEM In six normal volunteers. the average maximumPRprolongationwas 14%withnoinstances ofgreaterthanfirst-degreeAVblock .Diltiazem-associatedprolongationoftheAll interval Isnotmorepronounced inpatientswith first-d egreeheartblock. Inpatientswith sick sinus syndrome. diltiazemsignificantly prolongs slnuscycle length Iupto50% insome cases).Chronicoral administrationofCARDIZEMindoses ofupto240mg/day has resulted insmal l increases inPRinterval. but has notusuallyproducedabnormal prolongationt i herewere.however. threeInstances of second-degree AVblock and one Instance of thirddegree AVblock inagroupof959 chronicall
tytreatedpatients.
Pharmacoitlnetlcs and Metabolism. lltlazem s absorbedfromthe tabletionnulatlontoabout80%ofareferencecapsuleandis subiect to an extensive first-pass effect. givi an absolutetrioavallabilitylmmpaedto inbaverms lotabout CARDIZEMundergoes extensive hepaticmetabolismnwhich 296 to496oftheunch d dm
gappears Intheurine. Invitrohindhostudies show
CARD) EMis 096 to80%bound toplasma oteins. Competitiveligand binding studies have alsoshownCAR IZEMbindin Is notaltered by therapeuticconcentrations ofdigoxin.hydrochloro Iazlde.
phenylbulazone. propranolol , sali IIc acid. orwarfarin. Single oraldoses of 30 to 120mg ofCARDI EMresult Indetectable plasmalevelswithin30 to60minutes and
Rgak plasma levels twotothree
hours after drug administration. T plasma elimination half-lifefollowing singleormultipledrug administrationis approximatelyhours, Desacety l diltiazemIs alsopresent inthe plasmaat levels of1096 to20% of the parent drug and is 2596 to 50%as potent acoron vasodilator as diltiazem. Therapeutic blood levels ofCARD) EMappear tobe Inthe rangeof 50to200ng/ml.There is adeparture fromdose-Iinearl whensin
gl
edoses above 60m are
given;a IZDmgdosegave ood levels t 90 times thatofthe mgdose.There is no informationabout the effect of renal orhepaticImpairmentonexcretionormetabolismof diltiazem.
INDICATIONS ANDUSAGEi . AnginaPectoris DuetoCoronaryArtery Spears .CARDIZEM
Is Indicated Inthe treatmentofanginapectori s due tocoronaryartery spasm. CARDIZEMhas beenshowneffective in thetreabnentofspontaneous coron artery spasmpresenting asPrinzrnetal
'
s variant angina Irestng anginawith STsegmentelevationoccurring durfn attacks).
2 ChroucSta leAnl naf laselcEliortM ecimdAngina) .CARDI ZEMis indicated Inthemanagementof chronic stableina CARDIZEMhas beeneffective Incontrolled trials In
re clng anginafrequency and Increasing exercise tolerance.
Therearenocontrolled smdiesoftheeffeaivenessoftheconcomltant use of diltiazemand beta-blockers or of the safety of thiscombinationInpatientswith impairedventricularhrnctlonorconductionabnormalities.
CONTRAINDICATIONSCARDIZEM is conbaindicated in If) patients with sick sinus
exwptinthepresenceol ahrnctioni ventriwlarpacemarer.patients with second or third-degree A block except inthe
presence of a functioning ventricular pacemaker. and I3 ) patientswithhypotension(less th an90mmHg systol ic).
WARNINGS1. cardiac Conduction. CARDIZEMprolongs AVnode refrac~
toryperiodswithoutsignificantlyprolonging sinus node rocov
gyegme. except In atients wih sick sinus syndrome. Thismayrarelyresu Inabnormaily slowheatrates fpabcularfy
in tientswithsick sinus syndrome)orsecond orthirddegreeA block {sixof 1243 patients for Concomitantuseofdiltiazemwith betablockers orIII Ital ismay result Inadditiveeffects oncardiac conduction. patient with Prinzmetal
'
s
anglnadevelo 0periods of asystole (2 to 5 seconds) afterasingle dose 0 60m ofdiltiazem.
2 Congestivetleart llrrre.Althoughdiltiazemhas anegativemoppiceffectlnlsolatedanhnd dss lepepaabons.henodynanlcstudies Inhumans with normal ventricular functionhave notshowna reduction Incardiac Indexnor consistent negativeeffects oncontractility Idp/dt). Ex ence with the use ofCARDIZEMaloneorincombination beta-blockers Inpatientswith ImpairedventricularfunctionIsvery limited.Cautionshouldbe exercisedwhenusing the drug insuchpatients.
3 II enslon. Decreases inblood pressure associatedwithC DI ZEMtherapymay occasionally result Insymptomatichypotension.
4. Acute Hepatic Injury. inrare instances. patients receivingCARDI ZEMhave exhibited reversible acute hepatic Injury asevidencedbymoderate toextremeelevations of liverenzymes.
(SeePRECAUTIONS andADVERSEREACTIONS.)
PRECAUTIONSGeneral .CARDIZEM(diltiazemhydrochloride) Is extensivelymetab
olizedbythe liverandexcretedbythe kidneys and inbile.Aswith anynewdruggivenoverprolongedperiods. Iaborato
s
r
tyoparameters should
bemonitored‘
at regular Intervals . The drug uId be used withcautionInpatients with impaired renal orhepatic function. Insubacute and chronicdog and rat studies designed toproduce toxicity,high doses of diltiazemwere associated with hepatic damage. Inspecial subacute hepatic studies. oral doses of 125 mal koandhi her Inratswereassociatedwith histological Inth e liverw ich were reversiblewhenthe drug was discontinued. Indogs.doses of 20mol kawere also associated with hepatic changes;however. these changes were reversiblewith continued dosing.
Drug Interaction. Pharmacol Ic studies Indicate that theremay be additive effects Inprolong noAVconductionwhenusingbeta-blockers or digitalis concomitantly with CARDIZEM. {SeeWARNINGS).Controlled and uncontrolled domesticstudies suggest that con
comitantuse ofCARDIZEMand betablockers ordigitalis Is usuallywell tolerated. Availabledataare not sufficient, however, to predicttheeffectsofconcomitanttreabnent. articularlyinpatientswith leftvenbiculardysfunctionorcardiaccon ctionabnormal ities. Inhealthyvolunteers. diltiazemhas beenshown to increase serumdigoxinlevels uptoCarcinogenesis.M nes ls, Impairment of Fertl l A
24month study Inrats an aZimonth study Inmice showe no
evidenceof carcinogenici Therewas alsonomutagenicresponse
inInvitrobacterial tests. 0 Intrinsiceffectonfertilitywasobservedit rats.
Pregnancy. Category C. Reproduction studies havewenconducted inmice. rats. and rabbits. Administrationof doses r Ingfromfive to tentimes greater Ionamo/ kobasis) thanthe al lyrecommended therapeutic dose has resulted inembryoand fetallethality.Thesedoses, Insome studies, have beenreported tocauseskeletal abnormalities. Intheperinatal/postnatal studies, therewassome reduction inearly lndivldual pupweights and survival rates .
There was an Increased incidenceof stlllbirths atdosesof20timesthe humandose orgreater.Therearenowell—controlled studies Inpregnaitwomen: therefore.
use CARDIZEM inpregnant womenonly If the potential benefitIustifles the potential risk tothe fetus.
Nurs ingMothers . It Is not knownwhetherthis dru Is excretedInhumanmilk . Because in s are excreted in manmilk.exercise cautionwhenCAR IZE Is administered toa nursingwoman if the drug
‘
s benefits are thought tooutweigh its potentialrisks inthis situation.
Pediatric Il se. Safety and effectiveness Inchildrenhave notbeenestablished.
ADVERSEREACTIONSSerious adversereactionshavebeenrare Instudies carriedoutto
date.butItshouldberecognizedthatpatientswith Impairedventricularflur
t
i
'r
éEonandcardiacconductionabnormalities haveusuallybeen
cxcu
Indomestic placebo-controlled trials. the Incidence of adversereactions reported during CARDIZEMtherapywas notgreaterthanthat reported during placebotherapy.The following representoccurrences observed Inclinical studies
whichcanbe at leastreasonably associatedwiththepharmacologyof calcium influx Inhibition. Inman cases, the reiatlonsh‘nIoCARDIZEMhas notbeenestablished. mostcommonoccurrences.as well as their frequency of presentation, are; edema
Anotherpatientbe ne fit productfrom
PHARMACEUTICAL DIVISIONM AR IO NLABORATOR I ES . INC .
KAN SAS c rt v . M I S SOUR I 6 4 1 3 7
headache nausea dizz iness rashasthenia (1 Avblock Inadd it ion the fol lowing eventswere reported infrequentfy (less th an196)with theorderofpresentationcorrespond ing tothe relative frequency ofoccurrenceCardiovascular: Flushing, arrhythmia hypotens ion. bradycar
dia. palpitations , congestive heart fai lure,syncope.
Paresthes ia nervousness somnolencetremor insomnia, hal lucinations andamnesiaConstipation dyspepsia. diarrhea vomitin
gmi ldelevations ofalkal inephosphatase SOOSGPT. and LOHDennatofoglc: Pruritus.petechiae.urticaria.photosensitivltyOther; Polyuria.nocturiaThe fol lowing additional experiences have beennoted:Apat ientwith Prinzmetal s ang ina experiencing episodes of
vasospastlc angina developed periods of transient asymptomaticasystole ao roxrmately l ive hours alter receiving a single 60mgdose ofCADIZEMThe fol lowing postmarketingevents have been ed inhequently inpatients receiving C HOIZEM: erythemamutlforme; Ieu
k nia and extreme elevations of alkal ine phosphatase SGOT8 PTLDil andCPK However.adefinitivecauseandeffectbetweerithese events andCARDIZEMtherapy is yet tobe establ ished.
DVEIIDDSASEDI! EXAGSEIIATEDRESPONSEOverdos 0 experience with oral di ltiazemhas been l imited.
Singieoral ses ofSOOm ofCARDIZEMhavebeenweIl toleratedby healthy volunteers. Int event of overdo or exaggeratedmouse, appropriate su measures shouabe employed inltlontogastric lavage. fol lowingmeasuresmaybeconsidered:
Bradycardla Administeratropine to mg). if thereis noresponse tovagal blockade, administerisoproterenol cautiousl
gTreat as forbradycard a above. Fixed highdegree Avblock should be treated with cardiacpacingAdminister inotropic agents ( Isoproterenol.dopamine. ordobutarnlne) and diuretics .
Vasopressors (eg. dopamine or Ievarterenolbitartrate).
Actual treatmentanddosage shoulddependontheseverity of thecitinigais ituationand the judgment and experience of the beating
pncmTheoral/L0$0
‘
s Inmice and rats range from415 to740mg/ kgand from560 to“810mo/ko.respectivelyThe intravenous LO s Ill
th ese specieswere60and 38mgg/ kg speraspectiveiyTheoral LL050 indogs ls considered tobe inexcess o 50ma/ kawhi le lethal ity wasseeninmonk atmomg/k The tox icdose Inmanis notknown.but blood leve s inexcess9of no/mi have not beenassociatedwith tox icity.
DOSAGEANDADMINISTRATIONExertlm l Angina Poctorfe live toAtherosclerotlc Coro
naryArtery Dlsm oorAnglna Poetorfoat lImnue tocpnmy Artery 8mm. Dosagemust be adiusted toeach patient
‘
s
needs. Starting with 30mg four times dai beforemeals and atbedtime. dosage should be increased gra ual iy (given Individeddoses three or four times daily) at one to two~day intervals untiloptimumresponse is obtained Although individual patients mayrespond toany dosage level. the average optimumdosage rangewpears tobe 180m240mo/ tiaif i herearenoavallabledataconcerndosage requirements inpatients with impaired renal orhepaticfunction fthedrugmustbeusedinsuchpatients.titrationshouldbe
carriedoutwithparticularcaution.Cerisel w
pUseWith OtherAnia-glutAgents
1. Subl ime! NTGmay be takenas required toabort acuteangInal attacks duringa"CAFIOIZEM
_
theregy2mutate NitrateThem lZEMmay be safely
nisteredwith short and orig acting nitrates. but therehave beennocontrol led studies toevaluate the antiang inaleffectiveness of this combination.
3 .M iocene. (SeeWARNINGS and PRECAUTIONS.)HOWSUPPLIEDCardizem30-mg tablets are suppl ied inbottles of 100 (NOC
0088-17714 7 ) and InUnitDose Identif icationPaks of 100 (N000088 1771 Eachgreentablet is engravedwithMARIONononeside and 1771
eaved onthe other CARDIZEM60mg scoredinbotdesof 100 (N000088-17724 7 )and InUnit
Dose Identif icationPairs of 100 (N000088-1772-4 9) Each Iye iowtabletIs engravedwithMARIONonone s ideand 1772 ontheveother.Issued

state of consc iousness) , the attend ing phys ician must berespons ib le for recogniz ing th is deficit and for implementing appropriate corrective steps . The eth ical mandate is clear that the phys ic ian should assess the patient
’
s
capacity to enter into decision mak ing and should assure
that good choices are made on behalf of each patient whohas inadequate judgment capab il ities .
There are several alternateways inwh ich the patientmayindicate to the phys ician his/her capacity for participatingin decis ions aboutmedical care . First, the patientmay beable to demonstrate an appreciation of the seriousness ofthe choice thathe/ she ismaking . Areasonab le standard forthe patient
’
s dec is ion is the same as a prudent person in
s imi lar circumstances . Th is lay person standard is not thesame as the
“
prevai l ing standard”of medical practice .
S imi larly , psychiatric assessment for substantial deficits incognitive emotional functioning may be he lpful , but notdeterminative , because evenpeople with major psychosesmay be able tomake some decis ions that are unaffected bythe ir psychoses . Second , the patient may name his/her
preferred surrogate and g ive that person instructionsthrough a
“durab le powerof attorney ’
(to be defined in the
next section) . When the patient is not ab le tomake seri ousdecis ions about his/her own choices , the attending phys ician should identify a surrogate who can col laborate in thedecis ionmaking on behalf of the patient. F inal ly , the pa
tientmay wish to turn over s ignificant treatment choices tohis/her physician. As long as the patient real izes the impl ications of these dec is ions and real izes that he/she couldhave made them, and as long as the physician iswil l ing toaccept this role , delegation of the final decisions to thephysician is quite acceptab le and should be documented .
As in al l med ical care , physicians are wel l advised todocumentcareful ly the contentof the d iscuss ions with the irpatients and the processes uti l ized in mak ing these dec is ions . Both ideal ly and practical ly , these dec is ions shouldbemade before the patient is admitted to the nursing home .
Ways to Determine the Wishes of the Fami lyThe prognos is of patients admitted to nurs ing homes is
usual ly we l l known to their fami ly careg ivers long beforethe frai l patient is admitted to a nurs ing home . Consequently , these fami ly members oftendevelopopinions about therelative merits of supportive versus curative care . As
shown by Smal legan2and by Knight and Walker, 3 the
decis ion to admit a re lative to a nurs ing home is general lymade only after long del iberation and cons ideration byfami ly members . Most of the patients admitted to nurs inghomes have required a great deal of he lp (usual ly byspouses , daughters and/or sons) long before the patientswere admitted to the nurs ing home . Inat least two-thirds ofthe il l elderly patients , the breaking point general ly oc
curred when the leve l of care needed was high , particularlywhen'
supervis ion or care was needed 24 hours a day .
The major prob lems precipitating admiss ion to nurs inghomes were confusion and an inab i l ity to walk we l l . Atleast 60% of the patients needed some ass istance in fi ve ormore of the standard activities of dai ly l iving , particularlybath ing . Eighty-eight percent of the patients had recognized the ex istence of prob lems formore than a year;morethan half of them or the ir fami l ies had beenworried about
634 VOL . 4 6 , No . 12
these prob lems for a year or longer . Fami l ies and nursinghome staff reported an average of just over four heal thproblems for each person, with at least one of these problems having become more acute during the month preceding admission. Health problems that most often precipitated admiss ion to skil led nurs ing facil ities included fractures , strokes , cancer, pulmonary d isease and pain. For
intermediate care faci l ities the major precipitating problems were d ifficult behavior (2 5% of those admitted) , confus ion, incontinence , debi l ity , and unwi l l ingness to eat.
Fal ls were also a frequent precipitating complaint. From
the fami ly’
s standpoint, about a third of the admiss ionsoccurred when the fami ly fe lt that the new prob lems of
caring for the patient required too much work . Exhaustionor death of the careg iver accounted for about 20% of the
admiss ions .
Physic ians are also aware of the decl ine of these patientsbefore the ir admiss ions to nurs ing homes . As shown byLewis , Cretin, and Kane ,
45 4% of the patients admi tted to a
variety ofCal ifornia nursing homes over a two-
year periodwere transferred frequently between hospitals and nursinghomes . Phys icians were obviously responsib le for the patients during the ir care in hospital . In addition, the current
prospective re imbursement mechanism for hospital izedMed icare and Med ica id patients (Diagnos is Re latedGroups DRGs) fosters the tendency to send patients tonursing homes inorder topromote early d ischarge from thehospital . Paradox ical ly , the DRG mechanism is l ike ly toexacerbate the tendency to shuttle nurs ing home patientsback to hospitals for re latively minor problems , providedthat the interval between h0 5pital izations is sufficientlylong . In any case , the phys ician is usual ly ab le to inquire ofboth the patient and fami ly about the ir wishes for l ifesupport measures not only in the hospital , but also at the
time that they plan for transfer to the nurs ing home .
Legal Mechanisms for Documenting the Patient’ sWishes : Advance DirectivesMaking l ife or death decis ions becomes measurably
eas ier when the patient expresses his values and wishes .
Both the patient’ s fami ly and the physician or other healthcare givers fee l much more comfortab le mak ing such a
decision when the patient’
s w ishes are known. In our cul
ture , legal requirements mandate that the patient be presumed compe tent and ab le tomake informed decis ions . In
these matters , competency or decis ion-mak ing capacitycan be defined in terms of an ind ividual ‘ s capab il ity tounderstand information relevant to the med ical decis ion athand and to reason about re levant alternatives against thebackground of stab le personal values and l ife goals .
These decis ions canbemade before the fact as wel l as atthe time of a critical event. An “
advance d irective”is an
oral or written instruction prepared by an individual concerning his/her health care in the event of later loss of
competence or decis ion-making capacity .
5 Al l of thesemechanisms require legal consultation and need to be fi ledand/or approved by a court. The North Carol ina Right toNatural Death Act6 provides for patients to make legaldocuments , i .e . , l iving wi l ls , in which the nature andtype of l ife-supporting mechanisms to be l imited or usedcan be specifi cal ly stated . This Right to Natural Death Act

is , by its own language , not l imited to L iving Wi l ls . Thus ,other written mechanisms can be cons idered . For the pa
tient who wishes to insure that al l resuscitative options becons idered , it is poss ib le to write a
“Directive to Provide
Max imumCare" statementwhich specifical ly requests thephys ician to undertak e al l reasonab le mechanisms for provid ing l ife support in the event of card io-respiratoryfai lure .
7
Another mechanism, durab le power of attorney , is
embod ied in Chapter 3 2A of the North Carol ina GeneralStatutes: Powers ofAttorney .
aThe durab le power of attor
ney concept enables the surrogate designated by the patientto
“do all acts necessary for maintaining the customary
standard of l iving of the princ ipal , inc lud ing provid ingmedical , dental and surg ical care , hospital ization and
custod ial care for the princ ipal , spouse , and/or chi ldren.
A durab le power of attorney is superior to the usual powerof attorney , since the latter usual ly lapses when the person
granting it becomes incompetent. Thus , the usual power ofattorney is of l ittle legal merit in med ical treatment decis ions for incompetent patients . By contrast, the provisionsof the durable power of attorney al low it to become effective or to remain in effect duri ng incompetency . A lso, the
incompetency need not be determined in court if the document specifies another procedure .
5 ' 6
A less formal way of capturing the patient’ s wishes aboutlong-term care is to request that the patient s imply write a
letter of “ instructions to my physician”
(E,A .
.Ste ad Jr.,
M .D . , personal communication) . In this l etter, the patientcanexpress his or herwishes aboutways inwh ich hemightw ish to be cared for in the event of various outcomes basedon the patient
’
s current or anticipated medical prob lems .
Obviously , it would behoove the phys ic ian to note the
rece ipt of such a document in his own records and to
include it in the med ical record any time the patient isadmitted or transferred to anewmed ical institution, including a nurs ing home .
Regard less of the form of these advance directives , it isimportant to recognize that the process of d iscuss ing theseoutcomes may be as important as the dec isions and the
outcomes . Open, frank d iscuss ions of various treatment!care options between the physician and the patient andfami ly increase the l ikel ihood that good decisions w i l l bemade and that good outcomes wi l l be achieved . The bestoutcomes and decisions are those in which everyone feelsmutual ly satisfied .
Incorporating PatientWishes into Nursing Home PlansIdeal ly , a physician who has enjoyed a profess ional
re lationsh ip of substantial duration w ith an older patientshould continue to provide care even after that patiententers a nursing home . Accord ing to Kapp:9Phys icians who admit ind ividuals to nurs ing homesshould understand both the ir own legal and ethical responsibil ities and those ob l igations of the nurs ing home to
wh ich the patient is admitted . Personal phys icians , nurs inghome administrators , and med ical d irectors , must worktogether to insure that the ir separate and mutual duties arebe ing carried to the ultimate betterment of the res ident.
Where the nurs ing home already has a pol icy in effect
regard ing its expectations and requirements concerning
DECEMB ER 1985 , NCMJ
admitting physicians , the admitting phys icians should beaware of the pol icy , scrupulous ly obey it, and offer to ass istin amend ing portions that are unreasonable or otherwisei l l-advised . The phys ician should also strive to exert influence to encourage his or her students and peers to act
s imi larly regard ing the ir own nurs ing home patients .
Where the nursing home to which the phys ician sends
patients has not yet adopted a pol icy in this area , the
phys ician practicing in the community should help to des ign a pol icy that reflects his or her leg itimate needs andconcerns , wh i le adequate ly protecting the rights of the
res idents .
Phys icians with patients innurs ing homes should also beaware that the nursing homes themse lves are increasinglybe ing advised to adopt pol icies and procedures that specifythe mechanisms for dec is ion making in the ir institutions .
These include a descriptionof the roles and responsib i l itiesof the physician and mechanisms for reviewing these decis ions .
Overal l , fac i l ity pol icies concerning medical decis ionmaking general ly , and
‘ l ife and death’
decisionmak ing inpart icular , should be clear , expl ic it, and cons istently ap
pl ied . Whi le the professionals involved ih the actual decis ion mak ing process may understand the reasoning ihvolved , many staff members wi l l need spec ial he lp inunderstand ing why and how these decis ions are made .
Faci l ity pol icy should be flex ib le enough to account for
individual circumstances and staff should be g iven suffi
cient information to understand the d ifferences . Directcarestaff, inpart icular , wi l l need careful training and continuedsupport to carry out
‘
comfortmeasures only’
or supporti vecare plans . Phys ic ian orders that include detai led compo
nents of a supporti ve care plan for the ind ividual residentshould be required by the faci l ity ’
s procedures . Under noc ircumstances should itbe poss ib le to infer that the res identfor whom supportive care only is appropriate has beenabandoned by the health care team or the faci l ity .
Obviously , both the patient and the fami ly , as wel l as the
phys ician wi l l fee l much more comfortab le if the nurs inghome provides vigorous supportive care for the patientrather than simply orders for
‘
do not resuscitate ,
“do not
intubate , etc . The phys ic ian ( and/or nurs ing home )should supply a l ist of specific measures , in the form of
orders , thatclearly de l ineates the k ind of caremeasures thatare needed by the patient and are always medical ly appro
priate . As noted by Lynn10 these supportive orders shouldinclude cons ideration of symptom control , pain control(when necessary ) , mental function, gastrointestinal symptoms ( includ ing anorex ia , dysphas ia , nausea , vomiting ,
constipation, d iarrhea) , skin problems ( such as decubitusulcers , fistulas , s inuses) , fever , weakness , respiratorysymptoms . Also , the management of bereavement of thepatient, fami ly and staff should al so be g ivencons iderationin these orders . If al l of these orders are attended to , neitherthe patient nor the family should fee l abandoned .
As an add itional measure , both the attending phys iciansand the administrators of nurs ing homes should cons iderthe establ ishmentof advisory committees to prevent b iasedtreatment reg imens from be ing estab l ished by phys ic ians ,nurses , or administrators .
5 Attempts should be made toinvolve the res idents of the nurs ing home in general pol icy

issues whenever competent patients can be brought intosuch d iscuss ions . W ith regard to day
-to-day decis ions ,these should probab ly be rev iewed by a group of ind ividual s who come from a broad-based perspective , bothwithin the institution and from the community . Thus ,lawyers , ministers , phys icians , and other ind ividuals withan interest in the broad prospectus of patient care should beavai lable to he lp phys ic ians and fami l ies review management decis ions in which some confl ict may arise .
Other Ethical I ssues
Implementation of these pol icies w i l l not be easy . Goodtreatment wi l l require ind ividual ization of care plans .
These care plans must meet the needs of the patient andfami ly . However , ind ividual izationchal lenges (and sometimes negates ) the equitab le use of scarce resources such asnurs ing home personnel , services , and avai lab le dol lars .
Good supportmeasures forpatients who are truly fail ingmay mean only
“decent minimum of care .
” 10However ,
this may be truly caring care in much the same way that
Hospice provides care for the terminal ly i l l in their ownhomes . Itmay be much more appropriate to substitute anLPN instead of anRN when personal care is needed ratherthan h igh technology . Neverthe less ,
“
the phys icians and
nursing home personnel must be careful not to economizefor one patient at the expense of others . When it is deter
mined that l ife is no longermeaningful for a g ivenpatient,it would be reasonab le to withhold or restrict treatment tosave funds . However, th is would be eth ical in the realmof
patient care only so long as the heal th care profess ionalsreta in control of these funds and have alternate ways ofspend ing the money . Itwould be unreasonab le and unethical for the government to reclaim the money only to use itfor non-health care purposes (C . K . Casse l l , personal communication) .
Forphysicians to continue tobe involvedw ith the care oftheir patients innurs ing homes , it is important that they beappropri ately reimbursed for the time and effort spent
there . It is recognized that re imbursement from Medicareand Med icaid (the latter funds approx imate ly 65% of al l
nurs ing home res idents in North Carol ina) is usual ly s lowand sometimes contentious . Neverthe less , it is poss ible tob i l l Med icaid and Med icare for services rendered at intervals more frequent than once a month . To be el igible forreimbursement, the phys ic ian must document the problem(s) for which care is be ing given and use procedure
codes that are read i ly recognized and accepted byMedicaidand Medicare re imbursement agents . Appendix A showsresponses to questions I posed to EDS Federal regard ingMedicaid re imbursement forphysician services fornurs inghome care inMay 1985 . I bel ieve that these answers wi l l bevery he lpful to any phys icianwhoprovides care fornursinghome patients . In part icul ar , I would stress that the phys ician document (both in themedical record and in the b i l ltoMedicaid/Medicare) the reason for the vis itand (2 ) selecta procedure code from the 903 series that would beappropriate for the nature of the prob lemand the amountof
time spent with the patient.
Conclusion
Appropriate med ical care for nurs ing home res idents
636
remains a major med ical , ethical , moral , and economicchal lenge for the practicing phys ician. I bel ieve that caringphysicians can provide important leadersh ip for nurs inghomes and the ir administrators and staff , as wel l as comfortto patients and their fami l ies . Th is requires sagacious cons ideration of care needs and wise investment of time w iththese patients . Through some consol idated effort and planning , many important advances can be made in the care ofthese patients at l ittle additional cost and relatively smal lexpend iture of time by the phys ic ian. With a modest ih
crease ih the amount of time spent communicating effectively with patients and fami l ies particularly before eventsbecome critical , by encourag ing the use of advance directives , and by documenting these efforts , phys ic ians wi l l bemaking important contributions to the health care of frai l
patients and their fami l ies .
Append ix AResponses to questions d irected to EDS Federal regard ingMed icaid reimbursement for phys icians services for nursing home care .
1 . How are physicians reimbursed for nursing home
care?
Medicaid w i l l pay per vis it per CPT code , us ing codes90300-903 70 found in the CPT code book . Phys icians arereimbursed at 100% of the b i l led amount or the amount
al lowed for the part icularCPT code ona fee schedule basedon the doctor
’
s special ty , wh ichever is less .
VOL . 46 , No . l 2
2 . H ow often are physicians required to visit nursing
home patients?
For Skil led Nurs ing F aci l ity (SNP) Pa tients :
Med icaid patients must be initial ly cert ified by a physician at the time of admi ss ion, or if an ind ividual appl ies forass istance whi le in an SNP, before the Med icaid Agencyauthorizes payment. Phys ician recertification must bemade at 30 , 60 and 90 days after admiss ion and every 60days thereafter .
The phys ician is required to vis it and write a progress
note at least every 30 days . He/She is also required toreview and renew orders every 30 days . After the first 90days the physician can request approval of analternate vis itschedule from DMA/Util ization Control Section. . l f the
patient’
s cond ition does not require phys ician visits every30 days and it is approved , the alternate schedule cannotexceed 60 days between vis its .
Each Medicaid patientmust be reviewed by the Uti l ization Review Committee every 30 days from the day of
admissionup to the first 90 days and every 90 days thereafter for as long as the patient remains at the ski l led nurs ingleve l of care . Readmiss ion to the same level of care afterhospital ization would start the review process over again.
For Intermed ia te Care F acil ity (ICF ) Patients :
Med icaid patients must be initial ly certified by a phys ician at the time of admiss ion, or if an individual appl ies forass istance whi le in an ICF , before the Med icaid Agencyauthorizes payment. Phys ician recertification must bemade at 12 , 18 and 24 months after admiss ionand annual lythereafter.

Re imbursementwi l l be determined by the usual , customaryand reasonab le charge (as estab l ished by Med icare) of each
phys ician.
The phys ician service claim form, Heal th InsuranceC laimForm (HCFA- I SOO) must be used by nurs ing homeswhen b i l l ing for phys ic ian services .
As always , when fi l ing for services covered by bothMedicare and Med icaid , fol low b i l l ing procedures establ ished by Med icare . On crossover claims , Med icai d wi l lpay the coinsurance/deductible determined by the Med icare carrier.
References
1 . LynnJ. Legal and eth ical issues inpal l iative heal th care . Seminars in Oncology( in press ) .
MAMMOGRAPHY IS G IVING HOPE THATTHELEADING CAUSEOF CANCERDEATHAMONG WOMENWILL BE DIMINISHED.
Accord ing to the American Cancer Society. breas t cancer is the lead ingcause of cancer death among women in the United Sta tes . Mammographyhas been shown to de tect 90 percent of breas t cancer les ions before theygrow large enough to become palpab le . Because de tectionofminima lbreas t cancer, les ions sma ller than five mill imeters in diameter,marked ly improves pa tient surviva l , mammography is the procedure I Q
of choice in a lmos t all pa tients .
The Bennett Mammog raphy Sys temM- 3000 is a s imple to operate , low cos t,yet trul y sophis ticated ded icated mammography x- ray unit. Optimum beamqua l ity for.mammography is achieved by us ing a long foca l filmd istance , 7 6
centimeters , and a molybdenumx- ray tube . Use of the BennettMammog raphySystemM coupled with low dose film/ screen techniques , canprovide
optimum qua l ity images with as l ittle as 1 / soth the rad iation required only a fewyears ago by conventional x- ray equipment and d irect exposure methods .
working for the end result— optimumqua lity rad iographsPO . Box 802 Matthews , NC 2 8 105 InNC Call 1 - 800- 2 2 2 -9262
In SC Call Collect 7 04 - 84 7 - 85 2 1
VOL . 46 , No . 12
Smal leganM. There was noth ing else to do: Needs forcare before nurs in g homeadmiss ion. The Gerontolog ist l 985 ;25 :364—9 .
Knight 8 , WalkerDL , Toward a defin itionofal ternatives to institut ional izationfor the fra i l elderl y . The Gerontolog ist l 985 ;25 :3 5 8-63 .Lewis MA, Cretin S , Kane RL . Th e natural h istory of nursing home patients .
The Gerontolog ist l 985 z25 23 82 -8 .
Health care dec is ion-mak ing in the long te rm care facil ities . A pol icy recommendationof theAmericanHealth Care Association.Wash ington.DC . Reproduced inthe Sy l labus forthe course ,
“Legal and eth ical aspects ofheal th care forth e e lderl y , St. Petersburg Beach , March 7 -9 , 1985 . Sponsored by the American Soc iety of Law and Medicine (Boston, Mass ) .NorthCarol inaGeneral Sta tutes , Chapter90 : Right toNatural Death ; art icle 23 .
KappMB . Response to the living wil l furor: Directives formaximumcare . Am ]Med l 982 ;7 2 :85 5 -9 .
Nort h Carol ina General Sta tute s , Chapte r 3 2A. Powers of Attorne y .KappMB . Nurs ing home pat ients '
rights tophys ical care . Generat ions i 984 ;303 (Spri ng Issue) .LynnD. Care near the end of l i fe , inCasse l l CK ,
Walsh JR Geriatric
med ic ine ( volume New York : Springer-Verlag , 1984 23 32 -44 .

Med ical Mutual
MedicalMutual Insurance Companywas founded inOctober, 197 5 ,when the coM ercial professional l iabilitymarketreached apeakof instabil ity. Recogniz ing the need for an al temative ,
the NorthCarol inaMedical Society createdMed icalMutual as an independentcompany owned and directed by physicians .
Today,Medical Mutual is North Carol ina’
s largest insurerofphysicians and surgeons , representing approx imate ly 80percent ofall physicians inprivate practice . Our serv ices extend to everyphysician in the state ,
through competitive premium rates and
innovative riskmanagementprograms .
For these accomplishments ,we thankyou.Your support has made
our success poss ible , and itw ill carry us forward into the future .
MedicalMutual .We’
l l be therewhenyou need us .
DECEMBER 1985 NCMJ 639

a lead ing test for feca l occult blood
The‘
Hemoccult’
guaiac papertest for fecal occult blood
is a convenient, dependable , virtually odorless
preliminary screen forabnormal g . i. bleed ing often
associated with colorectal cancer.
Hemoccult l I®'
S lides Hemoccult® Two-Hole S ing le S lides
Available in Availab le in
o Dispensapak®z 100 patientkits . Each kitcontains Boxes of 100 s lides
three ‘
Hemoccultll'
s lides inmailing envelope with Cartons of 1000 slidesinstructions , applicators and developing solution.
Also available0 Boxes of 100 slides ‘
Hemoccult'Tape0 Cartons of 1000 s lides
OSmlthKllne Diagnostics . 1 98 1
Surg ca Supp y Co . Charlotte : 7 04 13 7 24 2 40



Convenience without compromiseOne capsule
—Once daily
The appearance ol l hese capswes 1s a re g istere d trademark ol Ayerst LaboratoriesBRIEF S UMMARY (FORFULL PRESCRIB ING INFORMATION , SEEPACKAGE CIRCULAR )INDER IDEG L A Brand of PROPRANO LOL HYDROCH LORIDE ( INDERALO L A ) andHYDROCH LOROTH IAZ IDE ( Long Act ing Capsules )No. 4 5 5—Each INDERIDEO LA 8015 0 Capswe contamS '
Propranolol hyd ro ch loride ( INDERAL ! ll LA)Hyd roch IOrolh iaZIOe
No. 4 5 7 Each INDERIOE!"LA Capsule contamsPropranolol h yd ro ch loride ( INDERAL G LA)Hyd roch loroth iamd e
No 4 5 9 Each INDERIDE® LA CapSule conta insPropranolol hyd roch loride ( INDERAUb LA ) .
Hyd rochloro lh1a2 1d eINDERIDE LA rs ind icated 1n the management ol hypertens ion.Th is f i xed comb lnatlond rug Is not lnd leated for lnltlal therapy of h ypertens ion. It
the fixed comb inat ion repre s ents the dos e t itrated to the ind iv idua l atlent'
s needs ,
the rapy wlth the flxed comb lnatlonmay be more convenient than w th the separatecomponents .
CONTRA INDICAT IONSPropranolol h yd roch lor ide ( INDERALG )Propranolol IS contramd icaled in: I ) card 1ogen1c shock : 2 ) s rnus b radyca1d 1a and g reater thanIns td eg re e b lock. 3 ) bronch ia l asthma 4 ) congestive heart la1lure (see WARN INGS ) unless thela ilure IS secondary to a lachyarrhylhmla tre atab le wilh propranololHyd roch loroth laz ldeHyd IOCh IOIOIh IaZIde is contra1nd 1caled inpalienls wunanunaorhypersensrt-vrty to th is orothersullonamide denved d rugs .WARN INGSRro ranolol h yd roch lor ide ( INDERALO)CA DlAC FA ILURE Sympathehc st1mulal ronmay be a vulal componentSupport ing circulatoryluncnon 1n patients w1lh congestwe heart Ia1lure . and us 1nhib rt1on by be ta b lockad e maypre C1pitale more severe la1|ure A lthough beta b lockers should be avorded inovert congestiveheart lailure . it necessary. they can be used wnh c los e IoIlow-up m panenls wnh a h istory of
tenure who are we l l compensated . and are re ce ivmg d 1g 11al1s and d iure lucs Be la-ad re nerg-cb lock rn agents do not abohsh the 1notropic action 01 d 1g 1lal1s on heartmusc le
N ATIENTS W I THOU T A H ISTORY OF HEART FA ILURE. conunued use of beta b lockerscan,
in some cases . lead to card iac Iarlure . There lore. at the nts l srgn or symptom oi heart
lai lure . l he par-ent sh0u|d be d rg rlahzed and /or treated wrth d iure tics . and the re sponse
observed c lose ly. or propranolol s hould be d 1scon11nued (g radua l ly. 11 pos 5 1b le l
TH YROTOXICOS IS. Beta b lockade may mask certa in cI1n1cal 5 1gns ol hypenhyroud 1smThere lore abruptwnhd rawal oI propranolol may be lol lowed by anexacerbationol Symptomsol hypenh ro1d 1sm, 1nclud ing th ro1d storm. Proprano lol does notd istort lhyro1d lunchon rests .
l PA IENTS W I TH WOLF -PARKINSON-WH I TE SYNDROME. severa l cases have beenreport ed mwh ich . a l ter propranolol , the tachycard 1a was rep laced by a severe brad ycard iareduiring a demand pacemaker In one case th is re smted alter an miha l dose 01 5 mgpropranolol ,
MAJOR SURGERY : The necessuy or desirab1l1ly oi w1thd rawal of beta b lock ing therapyprior tomayor surgery IS controvers ia l It should be noted however. that the impaire d ab1hly olthe heart to respond to retlex ad renerg ic s l1mu|1may augment lhe t1sks ol general anesthe 5 1aand Surg ica l procedures .
Nona l ler lc B ronchos cam (09 , chronic b ronch ltls , cmph sema)—PAT IENTS W I THBRONCH SPAS T IC DIS ASES SHOULD. IN GENERAL. NOT R CEIVE BETA BLOCKERS .INDERAL should be adm1n1s |ere d with cauluonsmee itmay b lock bronchod i latnonproduced byendogenous and exogenous catecholamme s imulation 0 ! beta receptors .
DIABETES AND HYPOGLYCEMIA: Be la-ad renerg 1c b lockade may prevent the appearance 01 cert a in premonitory $ 1gns and symptoms (pulse rate and pre sswe changes ) 01 aeuleh ypog lycemia in lab i le msulin depend entd 1ebe les In these pat1enl s 1l may bemore d 1lt1cu|t toad just l he dosage of msulin Hypog lycemic attacks may be accompamed by a pre cip itouse levahon ol b lood pressure .
Hyd rochloroth laz lde :Thraz id es should be used with caution in severe rena l disease In patients w ith renal d iseaseth iaz idesmay precrpula le azolemra. Inpa l ienls Wl lh Impa1red rena l lunchon. cumula l lve e l lecisol the d rug may d eve lop
Th IaZIdes should a lso be used with caution II'
l patients with impaued hepatic functionorpreg resswe l iver d 1se'
ase . smce m1noralleratrons ol Iluid and e lectrolyte ba lancemay premolla le heparlc comaTh ramd es mayadd toorpotenuale the actionofotheranhhyperrenswe d rugs Polentrahon
occurs wrth g ang liomc or penphera l ad renerg ic b lock ing d rugsSensnivity reactions may occw in patients W i l l“) a h istory of a l lergy or bronch ial asthmaThe poss ibnny ol e xacerbation or acl1val 1on of s ystemic lupus erythematosus has been
reported
PRECAU T IONSPropranolo l hyd roch lorlde ( INDERALG )GENERAL Propranolol s hould be used with caution inpatients wrth impaired hepahc or rena llunction Propranolol 15 not 1nd 1cated lor the treatmentol hypertens ive emergencres .
Be la-ad renoreceptor blocrrade can cause ledUCI IOn ol miraOCulaf preSSure Patientsshould be told thatpropranololmay interlere W ith the g laucoma screening test. W ithdrawa lmaylead to a returnol inoreased 1ntr3 0CuIar pre ssure
CL IN ICAL LABORATORY TESTS Elevated b lood urea leve ls inpal ienls wuh severe heartd 1sease . e levated serum transammase . alkahne phosphatase . lactate d eh yd rogenase
DRUG INTERACTlONS : Par1enls rece 1v1ng catecholamrne -deple lmg drug s . such as reser‘
p1ne. should be c lose ly observed it propranolol IS adminis tered . The added catecholamrneb lock ing aCI IOfl may produce an excesswe reductionof re sting sympalhe lrc nerv0us acl 1v1ly.wh ichmay reSull inhypotens-on.marked brad ycard ia. vert igo. syncopa l attacks , orort hostatich ypotensron
1 20150
AYERS T LABORATORIESNew York . NY 1001 7
CARC INOGENES IS . MUTAGENES IS. IMPA IRMENT OF FERTIL I TY : Long-term studies inanima ls have been conducted to eva luate tox ic e l lects and carc inogenic potentia l In ta.
month stud ies . in both rats and mice . emp loy ing doses up to 15 0 mg / kg /day. there was noewdence of S igml icant d rug - induced tox ic ity. There were no d rug
-re lated tumorigenic e llectsat any of the dosage leve ls . Reproductive stud ies in anima ls d id not show any impa irmentollertil ity thatwas-a ttributab le to the d rug
PREGNANCY : Pre gnancy Category C Propranolol has been s hown to be embryotoxic inanima l stud ies at doses abbot tOt1mes gre ater than the max ima l re commended human doseThere are no adequate and we l l -control led s tud ies in pre gnantwomen Propranolol should beused during pregnancy only it the potentia l benefit |ustifies the potentia l risk to the Ietus.
NURS INGMOTHERS' Propranolol is e xcreted inhumanmi lk . Cautionshould be exerc isedwhen pro pranolo l is administered to a nurs ing mother
PEDIATRIC USE Selety and e l lectiveness in ch i ld re n have not been estab l ishedH droch loroth laz ide :G NERAL : Pe riod ic determination of serum e lectrOIytes to detect possmle e lectrolyte 1mbalance should be performed at appropriate interv a ls
All patients re ce iving th iaz ide therapy should be ob serv ed for c l inica l S igns ol l luid ore lectro lyte imba lance . name ly; H yponatre mia. hypoch loremic a lka los is . and h ypoka lemiaSerum and urine e lectrolyte determinations are part icmarly important when the patient isvomiting excesswe ly or rece iving parentera l l lu1d s Med ication Such as d ig ita l is may a lsoinl luence serume lectro lytes Warning s 1gns irrespective ol cause we Dry ness otm0uth , th 1rst.we akness . letharg y. d rows iness . restlessness . musc le pa ins or cramps . muscwar latigue .
h ypotens ion. ol iguria. tachycard ia. and gastrointestina l d isturbances Such as nausea andvomiting .
Hypoka lemiamay deve lop. espec ia l ly with bris k d 1ure sis .whensevere cmhoss is present.
Or during concomitant use oI con-cos terOId s or ACTHlntertere nce with adeQUate oral e lectrolyte intake W i l l a lso contribute to h ypoka lemia
Hypoka lemia can sens itize or exaggerate the response ol the hean to the tox ic e llect ol
d ig ita l is (eg . increased ventricular irritab i l ity ) . Hypoka lemia may be avoided or treated by useot potasswm Supp lements . Such as Iood s with a h igh potas s iumcontent
Any ch loride defic it is genera l ly mi ld and usua l ly does not re qurre speCil ic tre atment.except under extraord inary C ircumstances (as in l iver 0 1 rena l d isease ). Di lutiona l hyponatremia may occur in edematous patients in hot weather. appropriate therapy is waterrestriction. rather thanadministrationofsa lt. except inrare instances when the hyponatrem1a lsl ite -th re atening In actual salt dep letion. appropriate re p lacement is the therapy of ch0 ice
H yperuricemiamay occuror frank goutmay be preCipitated in cert a inpatients re ce ivingth iamd e therapyInsul in re gunements in d iabetic patients may be incre ased . decre ased . or unchanged .
Diabetes me l l itus wh ich has been latentmay become manilestduring th iaz ide administrationIt progresswe re na l impa irment becomes evident. con5 1derW ithhold ing or d iscontinuing
d iuretic therapy.Th iaz ides may decrease serumPRI leve ls without s igns of thyroid d is turbanceCalcwmexcre tion is d ecre ased by th iaz ides . Patholog ic changes in the parathyroid g landW ith hyperca lcemia and hypoph0 5 phatem1a have been ob served in a lew patients on prolonged th 1a2 1de therapy. The common compl ications ot hyperparathe id ism. Such as re na ll 1th13 5 1s. bone resorption. and peptic ulceration have not been seen. Th iaz ides should be
d iscontinued before carry ing out tests for parathyroid lunctionDRUG INTERACT IONS : Th iaz ide d rugsmay increase the respons iveness totubocwarineThe antihypertens ive e l lects of th iaz id es may be enhanced in the pos t5 ympathectomy
patient. Th iaz ides may decre ase arteria l respons iveness to nore pinephrine . Th is d iminution isnot Sutticient to rectude e l lectiveness ol the pres sor agent for therapeutic use
PREGNAN Y PregnancyCategory C Th1a2 1des cross the placenta l barrierand appear incord b lood The use of th iaz ides inpregnancy re quue s that the antic ipated bene l itbe we 1ghedaga inst poss ib le hazards to the Ietus . These hazard s inc lude leta l or neonata l iaund ice.
thromboc topenia. and poss ib ly other adverse reactions wh ich have occwred in the adultNUR lNG MOTHERS Th iaz ides appear in humanmi lk It use 0 1 the drug is deemed
essentia l . the patient should stop nursmgPEDIATRIC USE. Sale ty and effectiveness in ch i ld ren have not been estab l ished .
ADVERSE REAC T IONSPropranolol hy
d roch loride ( INDERAW)Most adverse e lects have beenmi ld and IranS 1enl and have rare ly re quire d the W ithd rawa l oftherapy.
Card i'
ovascwar: Brad ycard ia: congestive heart fa i lure: intens ification 01AV b lock : hypo‘
tens ion: paresthes ia 0 1 hands: thrombocytopenic purpura: arter1al 1nsutt1C1enCy. usua l l y ol theRaynaud type
Centra l Nerv0us System: L ightheadedness: menta l depress ionmanilested by insomnia .
lassnude weakness . latique : revers ib le menta l depre ss ion prog re ss ing to catatonia. visua ld is turbances : ha l luc inations.anacme revers ib le syndrome characterized by d isorientation Iortime and p lace short-termmemory loss emotiona l Iab i l ity. s l ightly c louded sensorium, and
decreased performance on neuropsychometricsGastromtestinal. Nausea. vomiting . epigastric d istress . abdomina l cramping . d iarrhea .
constipation_ mesenteric art eria l thromboss . ischemic co l itis .
Al lerg ic . Pharyng itis and agranulocyIOS is . ery themaIOus rash: levercomb ined with ach ingand 5 0 re throat: lary ngospasm and resp iratory d istre ss
Resp iratory Bronchospasm.
Hematolog ic: Ag ranu locytos is : nonth rombocytopenic purpura . thrombocytopenicpurpura.
Auto-Immune In extreme ly rare instances . systemic lupus ery thematosus has beenreported
Misce llaneous : Alopeoa. LE- l ike re actions : psoriaS i lorm rashes. d ry eyes : mate impotence . and Peyronie '
s d isease have been re port ed rare ly. Ocutomucocmaneous re actionsinvolv ing the sk in, serousmembranes.and comunctivae reported tora beta b loc ker (practolol )have not been as soa ated W ith propranololHyd roch loroth laz ideGas tromtestinal. Anore x ia. gastric irritation. nausea. vomiting. cramping. d iarrhea: constipa~
tion: |aund ice ( intrahe atic cholestatic jaund ice ). pancre atitis. s ia ladenitisCentral Nerv 0us ystem. Dizzmess . vert igo; pare sthes ias. headache: xanthopsm.
Hematolog ic. Leukopenia . ag ranulOCyIOS is : thrombocytopenia: ap lastic anemia.
Card iovascular: Orthostatic h ypotens ion (may be agg ravated by a lcohol. barb iturates . or
narcotics ).H ypers ens itivity“Purpura: photosenS itivity : rash: urticaria: necrotiz ing ang i itis (vascul itis .
cutaneous vascul iti s ) . lever: resp iratory d is tres s . inc lud ing pneumonitis . anaph y lacticreactions
Other H yperg lycemia: g lycosuria: hyperurlcemia . musc le spasm: weakness : re stlessness. trans ient b lurred vis ionWheneve radverse re actions are moderate orsevere . th iaz ide dosage should be re ducedor therapy W ithd rawn

Speaking of Ecstasy , do any of you remember thefamousmovie of thatname w ith the ever-popular star HedyLamarr? When I was a young lad this was an adult’ s-onlyfllm (no
“R"rating or
“X
”rating in those days) . What a
fuss about nothing the movie shows Hedy , barefoot al lover, sw imming for a few nanoseconds”For shame l l My5 -
year-old grandson, Jeb , sees more nud ity than thatwhen
he goes to the sw imming pool or turns on cab le TV .
Now , what did OscarW ilde do to offend pub l ic moralsand land in jai l? In case you forgot, this dude was marriedand fathered two sons but he also indulged in other sexualoutlets thatwere not_pub l icly (or is itnotpubicly) accepted .
H ard to be l ieve , but the Marquis of Queensberry ( the boxing rules expert) who advocated not hitt ing below the be ltl iteral ly did so figurative ly by accusing ourWi lde man of
be ing a card-carry ing homosexual . Our anti-hero sued the
Marquis for l ibe l (bad move ) . Queensberry ’
s lawyersfound plenty of evidence and witnesses toprove thatOscarwas in fact gay . OscarW i lde was subsequently indicted forcommitting acts of gross indecency w ith othermale per
sons . He was found gui lty and sentenced to two years in
prison at hard labor . In pri son he wrote an incred ib le lettervery ,
very long andmoving cal ledDe Profound is that
is one of the most expl icit examples of a person’
s fee l ingsthat I have ever read . In 1897 he was released from prisonand wrote the famous poem, The Ba l lad of Read ing Gaol
“And al l men ki l l the thing they love , By al l let th is be
heard , Some do itwith a b itter look , Some with a flatteringword , The coward does itwith a ki ss , The bravemanwith asword !
”
64 2
Wel l , back to fee l ing good . If you get too muchMDMA oruse it forpro longed periods youcanget amphetamine- l ike side effects wh ich include tachycardia , card iacarrhythmias , hypertens ion, panic attacks , remarkab le diaphoresis , d iplopia , brux ism and someth ing more we ird :involuntary teeth clenching . The FDA has recently cried“Hold , Enough and placed an emergency ban on the use
of MDMA as of July l , 1985 . Th is drug was placed inSchedule I of the Control led Substances Act ( “ has highabuse potential , no acceptab lemedical use and no acceptedsafety for The Drug Enforcement Administrationc ites abuse of MDMA as a “
nationw ide prob lem. Thisrestri ctionmay cut down on some of the
“ leg itimate”use
of this drug by some psych iatri sts but cert ainly the i l l icitmanufacture , d istri bution and use w i l l flourish . I mustadmit that I have not seen a case ofMDMA abuse . We d id
have a patientwho said his fami ly burned al l the umb i l icalcord stumps of the ch i ldren born to them to preventenuresis . (He admitted upon questioning to two facts : ( 1 )the cord was not sti l l attached to the baby when burned ; (2 )it prevented bedwetting 100% of the time . )The management of an adverse reaction to MDMA
would seem to be very symptomatic , i .e . monitoring heartrate and rhythm and b lood pressure and using drugs l ik epropranolol for worrisome tachycard ia and severe hypertens ionw ith nitropruss ide orphentolamine . Maybe descretion is the better part of valor here . If any of your patientsfee l that they need th is drug to stay afloat, suggest insteadcannol i and a cupof expresso. Thatought to do it. Itworksfor me ! !
VO L . 4 6 , No . 12



not constitute a formal statement of award . Drs . Enge land Lee continued to correspond throughout the summer.
Dr. Engel continuously requested reassurance that the grantwould be funded , and Dr. Lee attempted to provide thatreassurance , without abandoning the stated caveat. On
October 17 , 1960 Dr. Enge l received a te legram stating“ Processing of award for cl inical research center in progress . What do you request as initial paymentwhichmay notexceedApparently the initial grant, OG -S , was funded based
sole ly on the written appl ication. At the present time , the
NIH customari ly vis its institutions apply ing for or renewing large center- type grants . Investigators make scientifi cpresentations at these
“s ite vis its the s ite vis itors inspect
laboratory facil ities and meet w ith institutional officials .
S ite visits become landmarks in the histories of large programs and theNIH conducted thematDuke whenthe CRUappl ied for renewal in 1966 ,
197 3 , 197 8 , and 1983 .
The October funding notice d id not al low time for theproposed renovations before investigators were ready to
beg in admitting patients . Therefore , three beds onWe lchWard , a general pediatric ward , were ded icated to the
center , which local ly was referred to as The Cl inical Research Unit (CRU) ; patients were admitted beg inning December I , 1960 . Four add itional beds for adult patientswere opened onOs lerWard on February 19 , 196 1 . Duringthe second fund ing year seven beds for both adult and
ped iatric patients were occupied onWe lch Ward , and the
unit achieved a true geograph ic identity . Later that year anadd itional e ight beds were opened , bri ng ing the total number to 15 . By that time construction of The C l inical Research Bui lding was wel l underway . Unexpended funds forrenovation actual ly were returned to the NIH .
James B . S idbury , Jr . was recruited from the Department
F igure 1 . The Cl inica l Research Bui lding in 1963 This extreme ly unusua l photograph shows afree-s tand ingstructure .
Within a few years this bui lding was connected to the ma in hospita l by a large administrative core ca l led The Woodha l lBuild ing . An addition to the north s ide , which opened in 1968 , further camouflaged thisfacade . I t is nearly imposs ible to
identify this structure in the east profile of the med ica l center at the present time . (Photog raph courtesy of the DukeUniversity Archives . )
VOL . 46 , No . 12
of Ped iatri cs at Johns Hopk ins to be the first director of theunit in 196 1 . Dr . S idbury was a native North Carol inian.
He rece ived his M .D . degree from Columb ia Univers ityCol lege of Phys icians and Surgeons , and he was trained inboth medic ine and ped iatrics , the latter at Johns Hopkins .
He was an instructor at Emory Univers ity , a staffmemberof the Communicab le Disease Center, and an ass istantprofessor of ped iatri cs at Johns Hopkins before be ing tecruited to Duke . He was appointed associate professor ofped iatri cs and Director of the CRU at Duke in 196 1 . H is
research interest was inborn errors of metabol ism.
In May 1963 The C l inical Research Bui ld ing opened
(figure and the CRU moved to its permanent home ,
named Rank inWard forWatsonRank in, the d istinguishedphys icianwho had been incharge of the Hospital Sectionofthe Duke Endowment. The new unit contained seventeenbeds in five s ing le rooms and six doub le rooms . A specialroom with a one-way mirror window was des igned forstudies on psychiatri c patients . A ki tchen on the ward
provided regular meal service as wel l as spec ial d iets forpatients on metabol ic protocols . Office and laboratorySpace for the d irector and a smal l core laboratory for samplehand l ing were included . TheWomen
’
s Aux i l iary providedfurniture for the patient lounge , includ ing a te levision set( stil l an uncommon amenity at the time ) . The entire unitwas air cond itioned , an important improvement over othersections ofDuke Hospital where the hotCarol ina summersbaked the wards .
By the mid - 1960s admini stration of the Unit hadassumed its contemporary form. At the NIH the DivisionofResearch Resources had assumed responsib i l ity for theGeneral C l inical Research Centers program, and grant
number OG - 5 had been reass igned number RR-30. AtDuke Dr. Anlyan was Dean of the Med ical School and

Pri ncipal Investigator of the grant. Dr . S idbury was ProgramDirector; andMortonBogdonoffwas Chairmanof theAdvisory Commi ttee , which included representatives fromal l cl inical departments and some bas ic science departments . Duri ng its first several years of operation, the di
vers ity of the unitpred icted by Dr . Engel was demonstratedby the range of investigators us ing the most bed days .
These inc luded two pediatri cians , Drs . S idbury and RobertStempfe l ; a cardiolog ist, H enryMcIntosh ; a neurosurgeon,B laine Nashold ; a gastroenterolog ist, Jul ian Ruffin; anendocrinolog ist, Harold Lebovitz ; and a hematolog ist,Wayne Rund les . Training was an important theme . In 1966
there were 2 5 separate training grants acti ve in the institution, and trainees from almost al l of them rotated through
the CRU.
In 1968 an add ition to the north s ide of The C l inicalResearch Bui ld ing opened and added one doub le room and
two s ingle rooms to the Unit. The s ingle rooms were
intended for patients requiring intens ive care unit” treatment, and both had the latestequipment for beds ide electrocardiogrammonitoring . About this time an isolation roomwith laminar air-flow control was built forneonatal patientswith immune deficiency diseases .
Dr . Samuel Wel ls , a general surgeon, was appo intedassociate d irector of the Unit in 197 2 . Dr . We l ls had te
ceived his M .D . degree from Emory Univers ity and then
did two years of tr aining in internal medicine at JohnsHopkins . H e rece ived add itionaltraining ih_ genera l s urg eryand add itional research experience at Wash ington Univers ity , Barnes Hospital , St. Louis ; The National CancerInstitute ; The Karol inska Institute , Stockholm; and DukeUnivers ity before be ing appointed ass istant professor ofsurgery at Duke in 197 0 . Dr . Wel ls used the CRU extensively as a s ite for stud ies of patients w ith medul lary carcinoma of the thyroid g land , multiple- endocrine neoplas iatype H , and parathyroid disorders .
When the renewal appl icationwas written in 197 3 , Drs .
S idbury , Nashold ,and Lebovitz remained among the most
active users . Drs . Stempfel and McIntosh had departed ,
and important new programs had emerged . Delford Stickel(general surgery ) and J . Caul ie Gunne l ls (nephrology)stud ied patients w ith renal d iseases . Wendel l Rosse (hematology) and John Tindal l (dermatology) became major users , as did W i l l iam Ke l ley , who stud ied abnormal ities ofpurine metabolism. Rebecca Buckl ey deve loped a strong
program study ing immune deficiency d iseases in chi ldren.
Dr . Buckley ’
s protocol # 15 0, submitted in 1965 , remainsthe longest continuous ly active protocol on the unit; andDr . Buckley has the d istinctionof be ing the only investigator to present at three CRU s ite vis its ( in 197 3 , 197 8 , and
Dr . S idbury departed in August 197 6 to become scien
tific directorof the chi ld heal th program at the NIH , andDr
We l ls was appointed Director. During Dr. Wel ls ’
tenure as
DECEMBER 1985 , NCMJ
AcknowledgmentThe authors appreciate the fol lowing individuals who lent their records
and the ir recol lections to us whi le we wrote thi s history : W il l iam G litz ,Mildred Engel H and leman, Leon Lack , June Perry , Eugene S tead , Jr . ,
R. Wayne Rund les , James B . S idbury , Jr . , and Samuel Wel ls . We also
acknowledge the contri bution of the Duke Univers ity Archives (Wil l iamKing ) and the Med ical Center Arch ives (James Gifford) .
Reference
1. Pri tchett ELC, AnlyanW0 .Ahistory of the Rankincl inical researchunitofDukeUnivers ity Medical Center. Arch lntem Med -4 8.
64 7
Director , the core laboratory was substantial ly expanded ,
and radioimmunoassays for parathorrnone ,calcitonin, and
cycl ic adenos ine monophosphate were instal led along w ithatomic absorption spectrophotometr ic assays for calc iumandmagnesium. These assays serviced a burgeoning groupof investigators interested in d isorders of calcium merabol ism. In add ition to Dr . We l ls , this group included GeorgeLe ight ( surgery) ; John Weinerth (urology) ; and Franc isNee lon, Marc Drezner , and Kenneth Ly les (endocrinology) .
In add ition to expand ing the core laboratory , the CLINFO computer system was acquired and a second isolationroom was bui lt by Dr . Wel ls . Drs . L ebovitz and Buckleycontinued to have large programs . A l lenRoses (neurology)begana new large program study ing patients withmyotonicmuscular dystrophy . Interd iscipl inary research evolved betweenDr . We l ls (general surgery ) and the associate director , Dr . Neelon (endocrinology) , and between Drs . JohnGal lagher and Edward Pritchett (card iology) andW il l Sealy (thoracic surgery ) .
In 198 1 Dr . Wel ls was appointed Professor and Chairman of theDepartmentof Surgery atWashingtonUnivers ity , St. Louis ;Dr . Pri tchett succeeded him as Director of theCRU. At that time Dr . Pri tchett was col laborating withDavid Shand (pharmacology) in study ing the cl inical pharmacology of antiarrhythmic drugs and calc ium channe lb locking drugs . Drs . Buckl ey and Roses continued to bemajorusers of unitresources ; and Hugh Sampson, who had
been trained by Dr . Buck ley , was appointed associated irector . Dr . Sampson stud ied patients with atopic eczemaand food al lergy in add ition to sharing respons ib i l ity withDr . Buckley for studying patients w ith immune deficiencyd iseases .
The compos ition of investigators us ing the CRU in themid- 19805 continued to confirmDr . Engel
’
s pred iction ofd ivers ity and the trad ition of col laboration between bas icand cl inical sciences . N inety-one investigators with 1 10academic departmental appointments were us ing the CRU.
C l inical investigators were active from the departments of
Medicine , Ped iatri cs , Surgery ,Psych iatry , Obstetrics andGynecology , Rad iology , and Community and Fami ly
Medicine ; and almost a quarter of the appointments were inbas ic science departments .


CONTENTSWha t is a ca ta ract?
Wha t ca use s a ca ta ra ct?
How ma ny people ha ve ca ta ra cts?
How ra pid ly do ca ta ra cts de ve lop?Is v i sua l loss f rom a ca ta ra ct pe rma ne nt?
Wha t a re the symptoms of a ca ta ra ct?
How is a ca ta ra ct d ia g nosed ?How is a ca ta ra ct trea ted?
How succe ss ful is ca ta ra ct surg e ry ?Ca n a la se r be used i nstea d of surg e ry to remove a ca ta ra ct?
When w i l l I be ready for ca ta ra ct surg e ry?
Am I too o ld for ca ta ra ct surg e ry?
Wha t a re the d i f fe rent wa y s in w hich ca ta ra cts a re removed?
Wha t is a lens impla nt?If I don
'
t wa nt a n impla nt, how ca n my v i s ion be re stored a fte r ca ta ract surg e ry ?How long have le ns impla nts be e n used ?
How common is ca ta ra ct surg e ry w ith le ns impla nta tion?Are the re d i ffe rent type s of le ns impla nts?Wh ich type of impla nt is be st for me ?Wha t is a
“seconda ry impla nt"?
Wha t type of te st i ng do I ha ve to go throug h before hav ing ca ta ract surg e ry w i th lens impla nta t ion?Ca n I ha ve a n impla nt if I have g la ucoma ?Is it poss ible tha t a n imp la ntw i l l not be put into my eye duri ng ca ta ra ct surg e ry eve n thoug h I w a s to ld to e xpect
one ?
Will I ha ve pa in during the ope ra t ion?W i ll I ne ed to use my g la ucoma med ica t ions a fte r ca ta ra ct surg e ry ?ls the impla nt put into my e ye a t the same t ime tha t my ca ta ra ct is removed?
Dur ing the ope ra t ion, w i ll I be a b le to see w i th the e ye be ing ope ra ted on?
Wi l l both of my eye s be ope ra ted on a t the same time ?
Do I need to stop a sp i r i n, coumad in, or othe r blood - th inne rs be fore surg e ry?
Should I cont i nue othe r med ic i ne s unt i l the da te of surg e ry ?Wha t ha ppens immed ia te ly be fore ca ta ra ct surg e ry
?
Who w i ll be in the ope ra t ing room w i th me ?How w i l l I fee l a nd w ha t should I do dur i ng the ope ra t ion?How long w i l l the surg e ry ta ke ?Wha t type of a nesthe s ia is be st for me ?
How w i ll I fee l immed ia te ly a fte r surg e ry ?Wha t ca n I do immed ia te ly afte r surg e ry?
Wha t w i ll my eye look l ike rig ht a fte r surg e ry?Wi ll ca ta ra ct Surg e ry in a ny wa y cha nge the a ppea ra nce of my eye ?
W i ll the re be st i tche s in my eye a fte r surg e ry?W i ll the st i tche s have to come out?
How long w ill it ta ke for my e ye to hea l?W i ll my vis ion be pe rfe ctly clea r immed ia te ly a fte r surg e ry
?
How soon a fte r surg e ry ma y I use the ope ra ted e ye?
W i ll I need to use eyedrops a fte r surg e ry?W i ll I ha ve to wea r e y eg la sse s a fte r surg e ry ?Wha t a re some cond i t ions tha t ma y ex i st in my eye be fore surg e ry wh ich ma y prevent good vis ion a fte rwa rd sa lthoug h pe rfect ca ta ra ct surge ry is done ?Wha t a re some of the poss ible comp l ica tions of ca ta ra ct surg e ry even thoug h pe rfect surg e ry is done ?
Wha t w i ll my eye fee lJ ike during the f irst few da ys a fte r surge ry ?Do I have to keep my eye cove red a fte r surg e ry?Haw often w i l l I ha ve to see my surg eon afte r the ope ra tion
?
Wha t a bout phys ica l a ctiv i ty a fte r surg e ry?Ca n I rub or pre ss my eye a fte r ca ta ra ct surge ry?Ca n I d rink a lcohol a fte r surg e ry ?When ca n I show e r a nd wa sh my ha i r?When ca n I resume d riv i ng ?When ca n I go ba ck to work?How much w ill the surg e ry cost?
650 VOL . 4 6 , No . 12

1 Wha t is a ca ta ra ct?
In order to understa nd w ha t a ca ta ra ct i s , one need s to know a l i tt le bi t a bout theeye a nd how i t works . The eye i s a lmos t spherica l in sha pe a nd conta ins w i th in i t alens w h ich i s clea r a nd co lorless l i ke g la ss (see Fig ure l ) . The lens i s s l ig ht ly sma l lertha n a l imo bea n a nd l ies beh ind the i ri s . The i ri s i s the pa rt of the eye w h ichma kes a person blue eyed or brow n eyed .
nerve Cornea
The lens of the e ye i s surrounded by a thin, sa ra n-w ra p l i ke membra ne ca l led theca psule (see Fig ure I ) . The lens _ ha s the funct ion of focus ing l ig ht on the ret ina w h ichi s a l ig ht- sens i t i ve l i ri l-ng ins ide the eye . The ret ina i s connected to the opt ic nervewh ich in turn i s connected to the bra in. When l ig ht fa l l s in the ret ina , v i sua lmessa g es a re tra nsmi tted to the opt ic nerve a nd fina l ly to the bra in ena bl ing us to
see .
Norma l ly , l ig ht pa sses throug h the clea r cornea (the tra nspa rent dome- l i ke s tructurein the front port ion of the eye ) , throug h the pupi l (w hich i s the round openingformed by the i ri s) a nd throug h the co lorless lens w hich focuses i t on the re t ina (seeFig ure
EYEWITH NORMAL LENS EYEWITH CATARACT
When a colorless lens a cqui res color, becomes cloudy or s l ig ht ly Opa que , i t i s ca l leda ca ta ract . Wh i le a c lea r lens i s a ble to let ra ys of l ig ht pa ss throug h i tse lf, aca ta ra ct prevents l ig ht ra y s from pa ss ing throug h a s they should . Th i s ca uses ablurred ima g e to fa l l on the ret ina a nd , a s a resul t , ca uses a person to ha ve b lurredv i s ion (see Fig ure
DECEMB ER“
1985 , NCMJ 65 1

A ca ta ract i s not a fi lm over the eye . If i s a l so not a g row th or tumor. I t does notsprea d from one eye to a nother l i ke a n infect ion . It deve lops independent ly in eacheye , a l thoug h both eyes a re usua l ly a ffected . One eye ma y a cqui re a ca ta ra ctmonths or even yea rs before the other eye does .
2 Wha t ca use s a ca ta ra ct?
Most ca ta ra cts a re due to increa s ing a g e . Other less common ca uses a re iniurie s tothe eye , inflamma t ion w i thin the eye , certa in types of med ica t ion, x
- ra y s , a ndd i sea ses such a s d ia be tes .Ca ta racts do not occur due to poor ea t ing ha bi ts , smok ing or d rink ing too much , or
overus ing your eyes . Ha v ing a ca ta ract does not mea n tha t the rest of your body i sdeteriora t ing a nd not in good sha pe . You ca n be very hea l thy a nd s t i l l ha veca ta ra cts . Even ba bies a re occa s iona l ly born w i th ca ta racts .
3 How ma ny peop le ha ve ca ta ra cts?
More tha n 5 0% of a l l America ns ca n expect to ha ve ca ta racts by the t ime they a re
6 5 yea rs of ag e .
4 How ra p id ly do ca ta ra cts deve lop?Ca ta ra cts usua l ly deve lop s low ly over ma ny yea rs or even deca des a l thoug h somemay deve lop more ra pid ly .
5 Is v isua l loss from a ca ta ra ct pe rma ne nt?
No . Unl i ke certa in other d i sea ses of the eye , for example g la ucoma , the v i s ion los tfrom a ca ta ract ca n be res tored .
6 Wha t a re the symptoms of a ca ta ra ct?
They ca n va ry from person to person. Blurred v i s ion or a d imming of v i s ion i scommon. You ma y a so ha ve d ifficul ty read ing sma l l print a nd d ri v ing a t nig ht .
SL IT LAMP MICROSCOPE
65 2 VOL . 46 , No . 12

1 3 Wha t a re the d i ffe re nt w a y s in w h ich ca ta ra cts a re
remove d?Ba s ica l ly , there a re two wa y s in w hich a ca ta ra ct ca n be removed . In bothtechniques , the eye i s surg ica l ly opened .
I In the Intra ca psula r technique , a n enzyme i s iniected into the front port ion of
the eye w h ich w ea kens the zonules (see Fig ure I ) w hich hold the lens in pla ce . The
ent i re ca ta ra ct i s then removed from the eye w i th a co ld probe w h ich i s broug ht intocontact w i th the lens ca psu le (see Fig ure The probe freezes a port ion of the
ca ta ra ct w h ich then st icks to i t a nd ena bles the surg eon to pul l the ent i re ca ta ra ct outof the eye .
"Intra ca psu la r mea ns ins ide the ca psule a nd intra ca psu la r ca ta ra ctex tra ct ion“ mea ns tha t the ca ta ra ct i s ta ken out wh i le i t i s ins ide the ca psule .
INTRACAPSULAR EXTRACAPSULAR
Entire lens removed Back of capsule
rema ins
2 In the Ex tra ca psula r technique , a n opening i s ma de in the front pa rt of the lensca psule a nd the contents of the ca psu le a re g ent ly removed from the eye lea v ing a n
inta ct ba ck ca psule in the eye (see Fig ure The ca psule i s clea r a nd a l low s l ig ht topa ss throug h norma l ly . Ad va nta g es of lea v ing the back ca psule in the eye a re tha t i tma y he lp prevent ret ina l deta chment a nd macula r edema (sw e l l ing of the ret ina ) . Ad i sa d va nta g e of ex tra ca psula r ex tra ct ion i s tha t the ba ck ca psule in some eyes ma ybecome cloudy months or yea rs a fter surg ery a nd reduce a person's v i s ion. However,w i th the use of a la ser, v i s ion ca n be res tored by a pa in less procedure ta k ing only a
few minutes a nd done in your doctor's office . Phacoemul s ifica t ion i s a va ria t ion on
the e x traca psula r technique in w hich a need le- l i ke dev ice producing h ig h frequencysound w a ves i s used to brea k up the ca ta ra ct w hi le a t the same t ime suck ing i t outof the eye .
At present , i t i s g enera l ly thoug ht tha t the e x traca psula r technique i s the best wa y toremove a ca ta ract . However, there a re except ions to thi s a nd your surg eon w i l ldecide w hich i s bes t for your pa rt icula r eye .
1 4 Wha t is a le ns imp la nt?A lens impla nt ( intraocula r lens or IOL) i s a ma n-ma de , t iny , c lea r, pla st ic dev icew hich i s pla ced ins ide the eye a t the t ime the ca ta ra ct i s removed . It replaces thena tura l lens a nd rema ins perma nent ly w i th in the eye .
654 VOL . 46 , NO . 12

1 5 If I don’
t w a nt a n imp la nt, how ca n my v i s ion bere store d a fte r ca ta ra ct surg e ry?If a n impla nt i s not pla ced in the eye , ca ta ra ct g la sses or conta ct ense s a re two
opt ions by w h ich v i s ion ca n be res tored a fter surg ery .
A l thoug h ca ta ra ct g la sses a re a tried a nd true w a y to restore s ig ht a fter surg ery , theyha ve severa l d raw backs (see Fig ure They ma ke th ing s a ppea r c loser to you a nd
a bout one - th i rd la rg er tha n they rea l ly a re . In a dd i t ion, they ma y ma ke obiects seemcurved a nd d i s tort s ide v i s ion so tha t to see th ing s clea rly to the left or rig ht , youha ve to turn your head instea d of iust g la ncing in tha t d i rect ion. You ma y a l so ha vetrouble doing s imple thing s l i ke putt ing a key in a lock or go ing up a nd dow n s ta i rs .Dri v ing ca n a l so be d ifficul t . How ever, ma ny people g e t a long qui te w e l l w i thca ta ra ct g la sses .
Contact lenses prov ide more na tura l v i s ion tha n do ca ta ra ct g a sses . Ob j ects a ppea ronly s l ig ht ly la rg er tha n they a ctua l ly a re , a nd s ide v i s ion i s more norma l . How ever,conta ct lenses l ie on the outer surfa ce of the e ye (see Fig ure 8 ) a nd mos t types ha veto be removed , c lea ned a nd re inserted re la t i ve ly frequent ly . O lder people ma y findthem somew ha t d iff icul t to ha nd le .
Lens imp la nts a re opt ica l ly superior to ca ta ra ct eyeg la sses . Vi s ion w i th a n impla nt i sa s close a s poss i b le to the norma l v i s ion you had w i th your ow n na tura l lens . Lensimpla nts a re a l so more convenient tha n conta ct lenses .
1 6 How long ha ve le ns imp la nts be e n used?The fi rst lens impla nts were used over 3 0 yea rs a go . More recent ly the des ig n of
impla nts ha s been improved a nd perfected a nd ca ta ract surg ery w i th lensimpla nta t ion i s now a common procedure .
1 7 How common is ca ta ra ct surg e ry w ith le nsimp la nta t ion?In 19 8 3 , ca ta ra ct ex tra ct ions w ere performed in the Uni ted Sta tes . Over
or 7 0% of these pa t ients rece i ved lens impla nts .DECEMB ER 1985 , NCMJ 65 5

1 8 Are the re d i ffe re nt type s of le ns imp la nts?Yes . They come in va rious sha pes a nd s i zes , but ba s ica l ly ,
there a re two types Ofimpla nts w hich a re in common use toda y : (see Fig ure 9 )l Anterior chamber impla ntsThese impla nts a re inserted into the a nterior chamber of the e ye w h ich i s the spa cebetween the i ri s a nd the cornea ( see Fig ure l 0) . They a re usua l ly used w henintra ca psula r ca ta ra ct surg ery i s done .
2 Posterior chamber impla ntsThese impla nts a re inserted into the pos terior chamber w hich i s the spa ce beh ind thei ri s (see Fig ure l I ) . They a re used w hen ex tra ca psula r ca ta ra ct surg ery i s done . The
ba ck of the lens ca psule tha t i s left a t the t ime of ex tra ca psula r ca ta ra ct ex tra ct ionprov ides a support for these impla nts .
ANTERIOR CHAMBER IMPLANT POSTER IOR CHAMBER IMPLANT
These d iagrams are much larger thanactua l s ize of implants .
1 9 Wh ich type of imp la nt is be st for me?
A l thoug h there ha s been a n increa se in the use of posterior chamber lens impla ntsin recent yea rs , your surg eon w i l l use h is iudgment in decid ing w hich type i s bestfor your pa rt icula r eye .
2 0 Wha t is a se conda ry imp la nt?”
If a person ha s a ca ta ra ct removed w i thout lens impla nta t ion, h is v i s ion i s correctedw i th ca ta ra ct eyeg la sses or a conta ct lens . If ne i ther ca n be to lera ted , i t i s poss i b le toput a n impla nt in the eye even yea rs a fter the ca ta ra ct i s removed . In such a n
insta nce , the impla nt used i s ca l led a seconda ry impla nt .
2 1 Wha t type of te st ing do I have to g o throug hbe fore ha v ing ca ta ra ct surg e ry w ith lens imp la nta t ion?The tests ment ioned be low a re done in your ophtha lmolog i st ’ s office a few weeksbefore your ca ta ra ct surg ery . Your v i s ion w i l l be tested a nd the pressure in your eyesw i l l be checked . Your pupi l w i l l be ma de la rg er w i th eyed rops so tha t the ba ck ofyour eye ca n be checked thoroug h ly for d i sea ses tha t ca n a ffect the success of theopera t ion, such a s d ia betes a nd macu la r deg enera t ion. You should remember tha ta fter d i la t ion, your v i s ion for rea d ing w i l l be blurred for a few hours . A l so w hen yougo into the sun l ig ht , the l ig ht ma y be very brig ht beca use more l ig ht i s nowentering the eye . So i t i s a d v i sa ble to bring sung la sses w i th you .
65 6 VOL . 4 6 , No . 12

2 6 Is the imp la nt put into my ey e a t the same t ime
tha t my ca ta ra ct is remove d?Yes .
2 7 During the ope ra t ion , w i l l I be a ble to se e w ith theeye be ing ope ra ted on?
No . The a nesthet ic so lut ion w hich i s iniected a round the eye iust before ca ta ra ctsurg ery prevents the opt ic nerve (the nerve w hich ca rries v i sua l messa g es ) fromfunct ioning for a few hours . 5 0 during surg ery , you don
’ t see a ny l ig ht , the surg eon’ sha nd s , or the surg ica l ins truments w i th the eye tha t i s be ing opera ted on. Your othereye w i l l be a ble to see a s usua but w i l l be covered w i th s teri le d ra pes to a void
infect ion in the opera ted e ye .
2 8 W i l l both of my eye s be ope ra ted on a t the same
t ime?
No . It i s bes t to do one eye a t a t ime , so tha t you a lwa y s ha ve the use of one of
your eyes w h i le the other one hea ls . The second eye ca n be opera ted on a few
months la ter.
2 9 Do I ne e d to stop a sp i rin, couma d in, or othe rb lood -th inne rs be fore surg e ry?
Yes . Aspi rin a nd other blood - thinners prevent your blood from clott ing a nd ca n
produce excess i ve bleed ing during your opera t ion . 5 0 i t i s importa nt tha t you te llyour
‘
surg eon tha t you a re ta k ing these med icines . Mos t l i ke ly , he w i l l ha ve you s topi t severa l days before surg ery . You should a lso inform your interni st a bout th i s . Aftersurg ery , you ma y s ta rt ta k ing them a g a in.
3 0 Shou ld I cont inue othe r med icine s unt i l the da te ofsurg e ry?
Yes . Med icines tha t you ma y be ta k ing for cond i t ions such a s hig h blood pressureshould be cont inued unt i l the da te of surg ery . It i s importa nt to te l l your surg eon or
ULTRASOUNDSCANNER
65 8 VOL . 46 , No . 12

his or he r nurse a l l the med ica t ions you a re us ing so tha t you ca n be a d v i seda ppropria te ly .
3 1 Wha t ha ppe ns immed ia te ly be fore ca ta ra ct
surg e ry?
Before surg ery , certa in rout ine blood a nd urine tests , a ches t x- ra y , a nd a n
e lectroca rd iog ram a re done . These he lp to ensure tha t a l l w i l l go w e l l for you dua nd a fter surg ery .
It i s importa nt to remember not to ea t or d rink a ny th ing a fter midnig ht on the da ybefore surg ery . On the morning of surg ery , d i la t ing eye drops a nd a nt i b iot ic eyed rops w i l l be g i ven to the eye be ing opera ted on .
After you a re ta ken to the opera t ing room,a n intra venous tube i s connected to
your a rm . Throug h thi s tube a seda t i ve i s g i ven. Thi s w i l l ma ke you qui te d row sy .
During thi s period , a n a nesthet ic so lut ion i s in jected a round the eye .
After a few minutes , the s k in of the eye l id s , forehea d a nd cheek on the s ide of theeye to be opera ted a nd the eye i tse lf a re numb . The s k in i s then wa shed w i th soa p,
wa ter, a nd a lcoho l to ma ke i t steri le a nd he lp prevent the eye from be ing infectedduring surg ery . Steri le cloth d ra pes a re then placed over your ent i re hea d (except forthe eye to be opera ted on) a nd body to further minimi ze the cha nces of a n infect ionoccurring . There i s no rea son to fee l suffoca ted under the d ra pes beca use a tubebring ing fresh a ir or oxyg en w_
i lLb_e rig ht nex t to you under the d ra pes .
Beca use of the de l ica te na ture of the opera t ion a nd the t iny a rea be ing opera ted on,
your surg eon w i l l use a microscope to do your surg ery . The m icroscope ma g nifiesa nd i l lumina tes the t iny opera t ing a rea in your eye . After the microscope i s pla cedin pos i t ion, your surg eon i s rea dy to sta rt the procedure .
3 2 Who w i l l be in the ope ra t ing room w ith me?
Your surg eon, the' surg eon's a ss i s ta nt , a nd a nurse w ho ta kes ca re of the ins truments .
Other nurses w i l l a l so be in the opera t ing room to he lp w i th the va rious de ta i l s ofyour surg ery , a nd a n a nes thes io log i st w i l l be there in ca se more med ica t ion i sneeded .
3 3 How w i l l I fe e l a nd w ha t shou ld I do during theope ra t ion?You w i l l fee l comforta ble during surg ery . You ma y be aw a ke or s l ig ht ly d row sy a nd
mig ht hea r some unfami l ia r sound s . If there i s someth ing tha t you finduncomforta ble , you w i l l be a ble to te l l your surg eon a bout i t throug h the d ra pes overyour hea d . He w i l l then correct the problem . Your g rea tes t contri but ion to the successof the surg ery w i l l be to ho ld st i l l a nd rema in quiet . If you need to sneeze or coug hte l l your surg eon before do ing so .
3 4 How long w i l l the surg e ry ta ke?
Thi s va ries but usua l ly ta kes from 4 5 minutes to a n hour.
3 5 Wha t type of a ne sthe s ia is be st for me?
Ba s ica l ly , there a re two types of a nesthes ia used for eye surg ery . Your surg eon w i l ldecide w hich i s best for you .
DECEMBER 1985 NCMJ 65 9

1 G ene ra l Ane sthe s iaIn th i s type of a nesthes ia a seda t i ve i s in jected into the intra venous tube connectedto your a rm . Thi s w i l l ma ke you lose consciousness complete ly . Wh i le you a re
a s leep, a tube i s pa ssed throug h your mouth into the tra chea or w indpipe , thepa ssa g ew a y lea d ing to the lung s . One e nd of th i s tube i s connected to a ma chinefrom w h ich a m i x ture of a nesthet ic ga s a nd oxyg en i s pumped into your lung s bythe a nesthes iolog i st . Long opera t ions such a s re tina l surg ery a re best done w i thg enera l a nesthes ia . A lso , s ince ch i ld ren find i t d ifficul t to ho ld s t i l l during surg ery ,g enera l a nesthes ia i s best for them. A d i sa d va nta g e w i th g ene ra l a nesthes ia i s tha ti t usua l ly ta kes you severa l hours to become aw a ke a nd a lert a fter surg ery . In
a dd ition , you ma y ha ve a m i ld sore throa t a nd perha ps na usea a nd vom i t ing . W i ththi s type of a nes thes ia , you w i l l know nothing a bout w ha t too k place duringsurg ery . How ever, g i ven the d i scomfort , g enera l a nesthes ia ma y not be a g rea tad va nta g e .
2 l oca l Anesthe s iaIn th i s type of a nesthes ia , a seda t i ve i s in jected throug h the intra venous tubeconnected to your a rm . Thi s w i l l only ma ke you d row sy . An a nesthet ic solut ion i sthen in j ected a round your eye . The need le of the sy ring e conta ining the a nesthet icma y hurt a l i tt le but most pa t ients don’ t find i t pa inful beca use they a re qui ted row sy w hen the in j ect ion i s be ing g i ven. When loca l a nes thes ia i s g i ven, on ly the
eye to be opera ted on a nd tha t s ide of the face i s numb . During the opera t ion, you
w i l l be a l i tt le d row sy but awa ke a nd ca lm a nd w i l l fee l no pa in . A lmos t a l l typesof eye surg ery a re done us ing loca l a nes thes ia . An a d va nta g e w i th loca l a nesthes iai s tha t rig ht a fter surg ery , you ca n s i t up, e a t, d rink or ta ke a w a l k . In add i t ion,
there i s no na usea a nd vomi t ing . Mos t eye surg eons prefer to do ca ta ract surg eryus ing loca l a nes thes ia .
3 6 How w i l l I fe e l imme d ia te ly a fte r surg e ry?You may be a li tt le d row sy a nd ma y not remember much a bout the opera t ion or you
ma y be qui te awa ke a nd a lert . Th i s pa rt ia l ly depend s on the type of med ica t ion tha twa s used to ma ke you d row sy before the opera t ion. After surg ery , mos t pa t ients a resurpri sed a t how ea sy the w ho le experience wa s .
3 7 Wha t ca n I do imme d ia te ly a fte r surg e ry?You ma y ea t a nd d rink , s i t up in a cha i r, a nd a lso w a l k a nd go to the ba throomw i th a ss i sta nce .
3 8 Wha t w i l l my eye look l i ke rig ht a fte r surg e ry?Your eye lid s ma y be a l i tt le swo l len,
s l ig ht ly droopy a nd a l i tt le d i scolored . In a few
da y s , the l id s w i l l a ppea r complete ly norma l . The eye i tse lf ma y be a l i tt le red fora bout a w eek or two . Th i s redness w i l l a l so clea r comple te ly .
3 9 W i l l ca ta ra ct surg e ry in a ny w a y cha ng e thea ppea ra nce of my eye?
After the eye hea ls , your friend s a nd fami ly , looking a t your eye , w i ll proba bly not
be a ble to detect a ny cha ng e in i ts a ppea ra nce .
VOL . 46 , No . 12

w i l l only restore the v i s ion you lost due to the ca ta ra ct . The v i s ion lost fromg la ucoma i s perma nent a nd w i l l not be restored by ca ta ra ct surg ery .
Ma cula r deg e ne rtion i s a n a g ing cha ng e in the ret ina w h ich ca uses you to lose c lea rv i s ion in the centra l pa rt of your v i sua l fie ld . If you ha ve severe ma cula rdeg enera t ion a nd ca ta ract , the improvement of v i s ion a fter surg ery ma y be minima l .D ia betes ca n a ffect your ret ina a nd produce poor centra l v i s ion if i t a ffects thema cula . Remova l of a ca ta ra ct w i l l not e l imina te th i s poor v i s ion a l thoug h the pa rtof v i s ion los t due to the ca ta ract w i l l be restored .
4 8 Wha t a re some of the poss ib le comp l ica t ions of
ca ta ra ct surg e ry eve n thoug h pe rfect surg e ry is done?Infect ion i s a serious compl ica t ion w hich ca n s ig nifica nt ly reduce v i s ion a fter surg ery .
To he lp prevent thi s poss i b i l i ty , a n a nt i b iot ic w i l l be prescri bed by your surg eon .
Fortuna te ly , such infect ions a re very ra re , occurring once in a thousa nd ca ses .
Hemorrha g e or bleed ing i s a compl ica t ion tha t ra nges from mi ld to very serious . Theworst type i s ca lled a n e xpuls i ve hemorrha g e a nd ca n lea ve the eye w i thout v i s ion .
Fortuna te ly , i t i s ex treme ly ra re a nd the cha nces of i t occurring a re less tha n one in
fi ve thousa nd .
A ret ina l deta chment i s a compl ica t ion tha t occurs in l to 2% of people w ho ha veca ta ract surg ery . If you a re very nea rs ig hted or myopic, you ha ve a 4 to 5% cha nceof deve loping a ret ina l deta chment a fter surg ery . If you ha ve ha d a prev ious ret ina ldetachment w hich ha s been surg ica l ly rea tta ched , there i s a n increa sed cha nce ofthe ret ina rede ta ch ing a fter ca ta ra ct surg ery . How ever, if the deta chment i s de tectedea rly , i t ca n be rea ttached surg ica l ly w i th l i tt le loss in v i s ion. It i s importa nt toremember tha t in some people , even if ca ta ra ct surgery i s not done , the ret ina ca n
deta ch .
Ma cula r edema or sw e l l ing of the ma cula w i th fluid ca n occur in a bout 2 0% of
people w ho ha ve ca ta ra ct surg ery . Fortuna te ly , in a lmost a l l ca ses the fluid i sa bsorbed by the eye a nd g ood v i s ion returns . However, the t ime ta ken for th i s toha ppen i s va ria ble a nd ma y ta ke from a few w eeks to a yea r.
G la ucoma ma y occur a fter ca ta ract surg ery , but ca n be usua l ly contro l led w i thmed icines .
4 9 Wha t w i l l my eye fe e l l ike during the f i rst fewda y s a fte r surg e ry?lt i s norma l for you to fee l tha t you ha ve a sma l c inder in the eye for a few da y s toa few w eeks a fter surg ery . As the t i ssues of the e ye hea l , th i s fore ig n body sensa t ionw i l l g e t less a nd '
l ess a nd fina l ly d i sa ppea r.
l t ' i s importa nt to rea l i ze tha t the symptoms ment ioned a bove ma y va ry in deg ree . If
the fore ig n body sensa t ion or tea ring i s very mi ld , there i s no rea son to beconcerned . How ever, if they a re severe , you should bring i t to the a ttent ion of your
surg eon .
662 VOL . 46 , No . 12

5 0 Do I ha ve to ke e p my eye cove red a fte r surg e ry?Yes . Immed ia te ly fo l low ing surg ery , a soft eye pa d made of cotton a nd a fi rm me ta leye sh ie ld a re pla ced over the opera ted eye a nd secured w i th a dhes i ve ta pe w h ichst icks to the s k in of the forehea d a nd cheek (see Fig ure
On the da y fol low ing surg ery , you ma y omi t the soft eye pa d a nd use only the
meta l eye sh ie ld . Wi th the opera ted eye , you ca n then look throug h the ho les in theshie ld . If the eye fee ls more comforta b le w i th the lid s closed , you ca n cont inue to use
the eye pa d in a dd i t ion to the meta l sh ie ld .
If you w ea r eyeg la sses , you cou ld omi t the meta l sh ie ld w henever you ha ve yourg la sses on. How ever, w hen the g la sses a re ta ken off for a ny rea son, the meta lshie ld should be put ba ck on a t once . In other word s , you should a lw a y s ha ve e i theryour g la sses on or the me ta l sh ie ld covering the eye a t a l l t imes for a bout 6 w eeksa fter surg ery beca use i t ta kes tha t long for the eye to hea l complete ly .
The importa nt po int i s tha t there should be something fi rm in front of your eye toprov ide protect ion a g a ins t a nything tha t mig ht a ccidenta l ly h it or push on i t . Youshould remember tha t w hen you go to s leep a t nig ht or if you l ie dow n to ta ke a na fternoon na p, the me ta l sh ie ld must be on the eye . You shou ld a l so try to s leepe i ther fla t on your back or on the s ide of the unopera ted eye to a vo id press ing on
the opera ted eye w i th your pi l low . Ha v ing the me ta l shie ld on the opera ted eye w i l l
prevent dama g e to the eye even if you accidenta l ly turn to the other s ide durings leep. These restrict ions only a pply for the fi rs t s i x weeks a fter surg ery .
DECEMBER 1985 NCMJ 663

5 1 How ofte n w i l l I ha ve to se e my surg eon a fte r theope ra t ion?Thi s va ries s l ig ht ly betw een pa t ients , but g enera l ly , you w i l l be examined three orfour t imes during the fi rs t two months a fter your opera t ion.
5 2 Wha t a bout phy s ica l a ct iv ity a fte r surg e ry?Due to a d va nces in surg ica l technique , your phys ica l a ct i v i ty a fter ca ta ract surg ery i snot a s restricted a s i t w a s in the pa s t . There i s no res trict ion on l ig ht a ct i v i t ies such a s
wa l k ing . You should a vo id l ift ing hea vy ob jects , bend ing over so tha t your hea d i sbe low the leve l of your wa i s t , jog g ing or do ing other v igorous phy s ica l exerci se fora bout 6 w eeks a fter surg ery . You ma y pick up ob jects from the floor but knee l w hendoing so ins tea d of bend ing over.
5 3 Ca n I rub or pre ss my eye a fte r ca ta ra ct surg e ry?No , not for a t lea st s i x w eeks .5 4 Ca n I d rink a lcoho l a fte r surg e ry?Yes . A lcohol in modera t ion i s permi tted a fter surg ery .
5 5 When ca n I show e r a nd w a sh my ha i r?You may ta ke a show er from the neck dow n rig ht a fter surg ery . It i s importa nt tha tsoa p a nd shampoo do not conta ct the opera ted eye for s i x w eeks . Thi s w i l l he lpa vo id i rri ta t ion a nd infect ion of the eye . During th i s t ime , a fam i ly member, afriend , or your ha i r dresser ca n wa sh your ha i r w h i le you a re ly ing back , but youshould wea r your meta l sh ie ld over the opera ted eye . S ix w eeks a fter surg ery , you
ma y ta ke show ers a s you d id before surg ery .
5 6 When ca n I re sume driv ing ?Since the v i s ion in the unopera ted eye va ries from one pa t ient to a nother, i t i s bestto a sk your surg eon w ha t i s a ppropria te for you.
5 7 When ca n I g o ba ck to w ork?
Th i s depend s on the type of work you do . If you ha ve a des k job, you ma y re turn towork in a bout a w ee k or two a fter surg ery . If you ha ve a job tha t invol ves l ift inghea vy ob jects , you should w a i t a t lea s t s i x w eeks .5 8 How much w i l l the surg e ry cost?
The cost of ca ta ra ct surg ery va ries from one pa rt of the country to a nother a nd a l sobetween surg eons . Mos t insura nce pla ns cover a port ion of the cost . As k yoursurg eon or h is bi l l ing c lerk w ha t the fees a re .
A Note from the Ed itorDoctors do ta lk to the ir pa tie nts . We ha ve a sked doctors in North Ca rol ina to provide us w ith
doctor—pa tient ta lk for our Fe a ture s for Pa tients . Our first re sponse come not from North Ca rol ina , but
from Ma ssa chuse tts . Dr. Thoma s ha s Ta r He e l roots , how eve r; he wa s ra ised in Cha rlotte , a nd he
g radua ted from UNC med ica l school in 19 7 3 .
VOL . 4 6 . No . 12

med ical care , but primari ly a function of technologyintens ive d iagnostic services , is seen as amajor contributorto the rise in health care costs . Spurred on by the mass ivefederal budget defic it, Congress and the Administrationhave already implemented cost cuttingmeasures , includ ingDRG s and the phys ician
’
s fee freeze . Industry and such
insurance programs as HMOs and PPOs have attempted tol imit health care costs by other means .
One of the criticisms of the current methodology of
payment forphysicians’
services , based onUCRs , is that itrewards physicians who order (and whomay perform) hightechnology procedures wh i le penal izing those whopracticehigh qual ity but conservative med ic ine .
It is entire ly feas ible that a new Relati ve Value Scale(RVS ) may be developed uponwh ich phys ician re imbursement wi l l be based . The American Society of InternalMed icine has advocated a change from the charge
-basedsystem, wh ich is a reflection of present phys ic ians
’
charges , to a resource cost”
approach . Factors to be
considered include the time spent by a phys ic ian in performing a procedure or in anoffice visit, the complex ity ofthe service rendered ( the intens ity of the phys ical and
mental effort involved , includ ing the risk of intraoperativecompl ications , the d iagnostic ski ll s and cl inical judgmentsrequired to choose appropriate procedures , and the technical ski l ls required to perform the procedure) , the phys ician
’
s investment inprofess ional training and the overheadexpenses ofphys icians ’
practices . (H s iao and Stason, para
phrased from the ASIM “wh ite paper
”on an alternative
RVS based on resource costs . )In response , then, to the question, my answer is Yes ,
part ly . I bel ieve a resource cost-based RVS for physicians ’
services , of wh ich time is but one factor , w i l l he lpreward the conservative , cost conscious but effective
phys ic ian, and wi l l not interfere with the appl ication of
high technology services and procedures when ind icated ,
whi le at the same time he lping curb the rate of rise of thenation’
s health care costs . Of interest, HCFA has recentlyawarded a contracttoHarvard University , with the AMA asa subcontractor, to construct such a cost-based RVS .
F romDr . Joseph D. Russel l , an internist fromW i lson.
The questionof an hourly rate for phys icians ’
services isa question which often comes up but leaves those in the
med ical profess ionwith an immed iate , emotional , No,it
just wouldn’
t work .
” Why wouldn’
t it? We assume it
works wel l for plumbers and electricians . How can we
defend a negative response to this question?Bas ical ly plumbers and e lectri c ians figure the cost of ajob based on materials , equipment, labor, overhead , and
profit. Materials costs may vary accord ing to the s ize of thejob , specifications , and competition among manufacturers
or d istributors . The equipr’
nent required to complete a certainjob alsomay affect cost, especial ly if amortized over aperi od of time , the number of uses , and depreciation.
Labor for a given job may also vary accord ing to theavailab i l ity of trained electricians orplumbers in the area orcommunity . These rates might also vary accord ing to thetime of day , i .e . weekends , hol idays , etc . and the numberand type of personne l required on a part icular job and the irrespective wages .
666
Overhead is a fixed cost which may vary according tofixed operating and support services and the volume of
services provided by the bus iness , and its phys ical plantrequirements .
F inal ly profit is calculated based on an acceptable scalefor the industry and competition within the marketplace .
S ince physic ians trad itional ly have ex isted as owners ofthe ir bus iness rather than employees , al l of the above factors would need to be addressed inorder to come upwith anacceptab le hourly rate . Us ing current cost estimates formaterials , equipment , overhead , labor, and profit, wewould assume that an hourly rate could be cal culated forphysicians
’
services wh ich would be defens ib le . Guarantees of outcome would be d ifficult to project and wouldthen create the add itional prob lem of how long serviceswould be mainta ined , especial ly in cases of chronic disease , variab le responses to therapy , and frequency of follow-up for maintenance or surve i l lance of therapy or dis
ease .
The initiationof an hourly rate for re imbursementwouldl ikely lead to col lective bargaining and poss ib le unionization with in the med ical profession. The potential cousequences of such actions would no doubt have extremenegative effects on the doctor-patient relationship not tomention the overal l we l l - be ing of this nation and its
c itizens . Controls would most l ike ly fal l under the juri sd ictionof the Federal Trade Commiss ionand/or the Fair LaborStandards Act. Questions regard ing antitrust as wel l asovertime compensation would be matched by prob lemsconcerning continuity of care and payment for cognitiveservices .
So , I fee l re imbursement of phys icians by the hour isopening Pandora ’
s box and would use the above argumentsto defend the answer,
“No, it just wouldn’
t work .
VOL . 46 , No . 12
F rom Dr . Phill ip A. Sellers , an internist from
H endersonvi l le .
Two bas ic issues re lated to phys ic ian re imbursement areraised by this question. ( I ) Should re imbursementbe basedsole ly ontime spentand ( 2 ) Should phys ic ians be organizedas labor unions to obtain the advantages of unionization?Time alone is inadequate to describe phys ic ians ’
ser
vices . Rig id appl ication of time-based guide l ines for re imbursement should be opposed . However, time should be alarge and important e lementof any re imbursement system.
Several other factors such as complex ity , overhead ,
training ofphysician and risk al l need tobe considered inre imbursement formulas .
Though physician income is dropping and re imbursement for physicians
’
services by third part ies both governmental and corporate is decreasing , the medical
profess ion at present general ly sti l l has its autonomy . The
physician’
s relationship is sti l l primari ly with the patient,not w ith the third-
party payor . We don’
t need to be em
ployees with a“John L . Lew is ” leader; nor do we need to
be able to strike . We do need to maintainour profess ionalrelationshipwith our patients ; this relationship, accordingto recent words of Dr . James Todd of the AMA , includesconcern, competence , communication, consc ience withmoral respons ibi l ity and compass ion.
There is no question that phys ician re imbursement sys

tems are going to changemore in the next one to two yearsthan they have in the last 20- 30 years , when
“usual , cus
tomary and reasonab le (UCR) insurance reimbursementsystems were put inplace . There is no question that there isa need for change . For example , the Medicare phys ic ianre imbursement system is far too complex and compl icated .
It is an administrative nightmare and over the years hasbuiltupmany unfair inequities for the physicians as wel l asfor patients .
A new system of reimbursement needs to be developed .
0 EDITOR'S NOTE :
The bas ic ingredients should include an indemnity feeschedule based on a relative value scale of al l phys icianservices . The phys ician could accept this as ful l payment.
The other necessary feature of the system should g ive thephys ic ian the option to balance bi l l . Inother words , the
phys ic ian would be ab le to b i l l more than the fee scheduleal lows .
No , I would not l ike to be paid as a union e lectri cian ispaid .
Once again I thank al l ofour respondents for the irOpinions . I know it isd ifficult tofind time for something extra when you are already very busy .
If I am read ing these opinions correctly , time spent on the patient’
s
problem is only one of several important parts of the re imbursementformula . A s imple hourly rate for phys icians might be inflex ible and
certainl y would change the doctor-
patient relationsh ip.
A broaderbut re lated question for a later issue of the Forum is ,Wi ll feefor service survive the pressure from al ternative heal th care deliverysystems , e.g . , HMOs , PPOs , l PAs? Shoul d it? I would apprec iate youropinions .
DECEMB ER 1985 , NCMJ 667

THlS SPACECONTRIBU TEDAS A PUBLiC SERVICE
There is evidence that dietand cancer are related . Somefoods may promote cancer, whileothersmay protect you from it.
Foods related to low er
ing the risk of cancer of thelarynx and esophagus all havehigh amounts of carotene ,
a form ofVitaminAwhichis in cantaloupes , peaches ,broccol i
,spinach ,
all darkgreen leafy vegetables , sweetpotatoes , carrots , pumpkin,
w inter squash and tomatoes ,citrus fruits and brusselsSprouts .
Foods thatmhe lp reduce the riskof gas tro intestinal
and respiratorytract cancer are
cabbage ,broccol i ,
brussels sprouts ,hlrab i
,caul iflower.
Fruits , vegetables , and wholegrain cereal s such as oatmeal
,bran
and wheatmay help lower the riskof colorectal cancer.
Foods h igh in fats , sal t orni trite -cured foods l ike ham
,and
fish and
types of sausages smoked by traditional methods should beeaten inmoderation .
Bemoderate inconsumption of al cohol also .
Agood rule ofthumb is cut down onfat and don ’
t be fat.
We ight reductionmaylower cancer risk . Our
2 year study ofnearly amill ionAmericans uncoveredhigh cancer risks particularly
among people 40% ormore
overwe ight.
Now ,more than ever
,we
know you can cook up your own
defense agains t cancer. 80 eat
heal thy and be heal thy.

ly defined onset of Reye syndrome compared with 2 8-5 9%of the control groups at any time during the ir matchedi l lnesses . The risk defined in this pi lot study was comparable to or greater than that determined in the previous lyreported studies . Fol lowing a review of these data , an
Institute of Medicine/National Academy of Sciences Review Committee recommended :
I . The PHS Task Force should proceed with the ful lstudy .
2 . Results of the pi lot study should be released promptlyto the pub l ic and to scientists for review and analysis .
3 . Analys is of the pi lot study data reveals a strong association between the Reye syndrome and the use of
aspiri n; considering data from previous stud ies al soshow an assoc iation of use of aspirin and Reye syndrome , the Committee recommends that steps shouldbe taken to protect the pub l ic health before the ful lstudy is completed .
4 . A lthough it is imposs ib le to know with certaintywhether the re lease of the pi lot study data wi l l harmthe ful l study , the Commi ttee suspects the effects ofthe attendantpubl ic ity wi l l be nomore damag ing thanthe current cl imate of pub l ic opinion,
which appearsnot to have impeded conduct of the pi lot study .
Inconcluding its presentation in the Morb id ity andMortal ity Weekly Report , the ed itors state , A report of thepilot study is currently be ing prepared for pub l ication. In
view of these prel iminary find ings , phys icians , parents , orolder ch il dren who se lf-med icate should continue to beadvised of the probab le increased risk of Reye syndrome
associated w ith the use of sal icylates forch i ldren, includingteenagers , with influenza- l ike i l lness or chickenpox .Thus , the saga of the association between aspirin and
Reye syndrome continues and may be far fromover. Greatcontroversy rage s over the adequacy of al l of the
670
References
1 4
2 .
10.
l l .
12 .
13 .
14 .
Sul l ivan-Bol yai IZ , Corey L . Epidemiology of Reye syndrome . EpidemRev
198 1 ;3 : l -25 .Lichtenstein PK. Henk i JE, Daughert y CC , et al . Grade I Reye ‘
s s yndrome : afrequent cause of vomiting and l iverd ysfunct ion fol lowing vari cella and upperrespir atory tr act infection. N Engl J Med 198313091 3 39Devivo DC . How common is Reye ’
s s yndrome? N Engl JMed 1983 3 09 : 17 98 1 .
StarkoKM, Ray CC .Dominguez LB . et al . Re ye Syndrome and sal icy late use .
Ped iatri cs 1980266z859- 64 .
Cente rs forDisease Control . Reye syndrome Ohio, Michigan.Morb id ity and
Mortal ity Weekl y Report l 980;29 :5 3 2 , 5 3 7 -9 .
Centers for D isease Control . National surve i ll ance for Re ye syndrome 198 ]
Update. Re ye syndrome and sal icy late use . Morb id ity and Mortal i ty Weekl yReport
-6 .
Waldman RS , Hal l WN . McGee H , et al . Aspirin as a ri sk factor in Reye '
s
s yndrome . JAMA l 982z24 7 z3089-94 .
HalpinTI HoltzhauerF ] Campbel l RI . etal . Reye ‘
s syndrome andmed icati onuse . JAMA -9 1 .
Nati onal Institutes of Heal th . The diagnosis and treatmentof Reye ’
s s yndrome .
Consensus development conference summary . Volume 4 . number 1 . March198 1 .
Centers for Disease Control . SurgeonGeneral ‘ s advisory on the use of sal icylates and Re y e s ynd rome . Morbidity and Mortal i ty Wee k l y Reportl 982 ;3 1 :289-90.
Committee on Infect ious Diseases . Aspirin and Reye syndrome . Ped iatricsl 982 ;69:8 10-12 .
Department of Heal th and Human Services . Food and Drug Administrat ion.Labe l ing for sal icy late -containing drug products . Federal Reg i ster December2 8 . l 982 ;4 7 :5 7 886-901 .Sta tement by Executive Committee. American Academy of Pediatrics . datedNovember 8 , 1982 .
Centers forDisease Control . Reye s yndrome Unite d States , 1984 . Morb idityand Mortal ity Weekl y Report i 985 ;34 : l 3 -6 .
VOL . 46 , No . 12
epidemiolog ical stud ies reported up to th is time . The in
terested reader is advised to observe careful ly future publ ications and news releases thatmightclarify th is issue . It is
of interest to note that fewer cases of Reye syndrome werereported in 1985 than in recent years (CDC , personal communication) ; the number of cases occurri ng now may preclude further epidemiolog ical stud ies . The cause for this isunknoivn. Unti l a final answer is obta ined it would seem
prudent for phys icians , parents and chi ldren al ike to becautious in the use of aspirin invarice l la and viral infectionsof the respiratory and gastrointestinal tracts .

EDITOR IAL
Confused About Advert is ing?
Thomas V . Bennett
0 Advertis ing by doctors is increas ing . The North Carol inaMed ical Journalcan rej ect or a ccept advertis ing as itwishes . TheNorth Carol inaMed ica l
Society cannotprevent ads from be ing placed in any of the publ icmed ianewspapers , magaz ines . rad io , te levis ion. This subj ect has recently
been covered in the Bul letin of the North Carol ina Medica l Society . I t is
being republ ished in the Journal because many persons missed it. The
Ed itor be l ieves tha t thefirs t rule of tea ching is repetition.
PHYS ICIAN advertising used to cons ist of a name on as ign and a l isting in the te lephone d irectory . Phys ic iansbuilt the ir practices through referrals from col leagues or
word-of-mouth“advertis ing by patients . It was consid
ered unprofess ional and uneth ical to do more .
But th ings have changed .
In the words of the North Carol ina Medical Soc iety ’
s
legal counse l , Jul ian D. Bobb itt , Jr. The Federal TradeCommiss ion continues to take an aggressive pos ition—re-
e
gard ing any l imitations on professional advert ising .
”The
American Medical Assoc iation is operating under an FTCinjunction that l imits the restri ctions that a professionalgroup can place on advertis ing .
Some phys icians want to advertise ; others strong ly disapprove of it. To clear the air and ease the controversy , the
NCMS House of Delegates has directed that the Soc ietyreport to members on the laws that define the l imits of
phys ician advertis ing .
The current status of the law is reflected in sectionof the 1984 ed ition of Current Op inions of the Judicia lCounci l of the AmericanMed ica l Associa tion. An AMAspokesman summari zed the section by say ing , Essentially , a physician can advertise as much as he wants , as oftenas he wants , through any med ium he wants , as long as heisn’
t deceptive or mis lead ing .
Section offers some noteworthy specifics :“There are no restri ctions on adverti s ing by phys icians
except those that can be spec ifical ly justified to protect thepubl ic fromdecepti ve practices . A phys icianmay publ icizeh imself as a phys ician through any commerc ial publ icity orother form of pub l ic communication ( includ ing any newspaper, magaz ine , telephone d irectory , rad io , televis ion orother advertising) provided that the communication shal lnot be mislead ing because of the omi ss ion of necessarymateri al information, shal l not contain any false or mi slead ing statement, or shal l not otherw ise Operate to de
ce ive .
The fortn of communication should be des igned tocommunicate the information contained there in to the pub
Reprinted from the Bul letin of the North Carol ina Medical Society .
November 1984 .
DECEMB ER 1985 , NCMJ 67 1
l ic in a direct, d ignified and read i ly comprehens ib le manner . Aggress ive , high pressure advertis ing and pub l ic itymay create unjustified med ical expectations . Any adver
tisement or pub l icity , regard less of format or content
should be true and not mis lead ing .
“The communication may include : (a) the educational
background of the phys ician; (b) the bas is onwhich fees aredetermined ( includ ing charges for specifi c services) ; (c)avai lab le cred it or othermethods of payment; and other
information about the phys icianwh ich a reasonable personmight regard as re levant in determining whether to seek thephysician
’
s services .
“Testimonials of patients , however, as to the physician
’
s ski l l or the qual ity of his profess ional services shouldnot be pub l icized . Statements re lating to the qual ity of
med ical services are extremely d ifficult, if not imposs ib le ,
to veri fy ormeasure by objective standards . Claims regarding experience , competence and the qual ity of the phys ic ian
’
s services may be made if they can be factual ly supported and if they do not imply that he has an exclus ive andunique ski l l or remedy . A statement that a phys ician hascured or successful ly treated a large number of cases involving a particular serious ai lmentmay imply a certaintyof result and create unjustified andmi sleading expectationsin prospective patients .
Cons istent with Federal regulatory standards whichapply to commerc ial advertis ing , a phys ician who is cons idering the placement of an advertisement or pub l icityrelease , whether in print, rad io or televis ion, should determine ih advance that his communication or message isexpl ic itly and impl icitly truthful and notmi slead ing . Thesestandards require the advertiser to have a reasonab le bas isfor claims before they are used in advert ising . The reason
able bas is must be estab l ished by those facts known to theadvert iser, and those which a reasonab le , prudent advertiser should have discovered .
“As used here in, references to a
‘
physician’
apply al soto informationrelating to the phys ic ian
’
s group, partners or
assoc iates . Any communication or message with in the
scope of th is opinion should inc lude the name ofat leastonephys ician responsib le for its content.
“Noth ing in any Opinion of the Jud icial Counci l is ih

tended or shal l be construed to discourage or to l imit adver The law is permiss ive . Itopens the door forprofessionaltis ing and representations wh ich are not false or deceptive advertising , and Mr . Bobbitt noted that attempts to l imit aw ithin the meaning of Section 5 of the Federal Trade physician
’
s advertis ing create a legal ri sk .
Commiss ion Act.
"my treatment of choice forGP, NV,
N-L appears tous ed soon enough.
”
N a conservative approach,
sklh igh-benefits.
” MD, FL
5
For samples to make



ropomil HCI/ Knoll80mg and 120mg scored , film- coated tablets
Contraind ications : Severe left ventricular dysfunct ion (see Warnings) , hypotens ion (systol ic pressure 90 mm Hg) or cardiogenic shock , sick sinus syndrome (except in pat ients with a funct ioning artificial ventricular pacemaker) ,2nd or 3 rd—degreeAVb lock .Warning s : ISOPT IN should be avoided inpat ientswith severe le ft ventricular d ys funct ion e
'
ection fract ion 3 0% or
moderate to severe symptoms of card iac failurel and in patients w ith anydeg ree of ventricular dysfunction if the y are rece iving a beta b locker.’ (SeePrecautions.) Patients with mi lderventriculardysfunct ion should , if poss ible, becontrol led with optimum doses of digita l is and/or d iuretics before ISOPT IN isused . (Note interactions with digoxin under Precautions.) ISOPT IN may occasionally produce hypotens ion (usua l l y asymptomatic, orthostatic, mi ld and control led by decrease in I SOP T IN dose) . Elevations of transaminases with andwithout concomitant e levations ina l ka line phosphatase and bi lirubinhave beenreported . Such e levat ions may d isappearevenwith continued treatment; however, four cases of hepatoce l lular iniury by verapami l have been proven by recha l lenge. Periodic monitoring of l iver function is prudent during verapami ltherapy. Patients with atria l f lutteror f ibri l lationand an accessory AV pathway(e.g . W-P-W or L-G-L syndromes) may deve lop increased antegrade conduct ionacross the aberrant pathway bypass ing the AV node , producing a very rapidventricular response after receiving ISOPT IN (or d ig ita l is) . Treatment is usua l l yD.C.
-card iovers ion, which has been used safe l y and effect ive l y after isoPTIN.
Because of verapami l ’s effect onAV conduction and the SAnode , 1°
AV b lockand trans ient brad ycardia ma occur. High grade b lock , however, has beeninfrequentl y observed. Marke 1
°orprogressive 2
°or 3
° AV b lock requires adosage reduction or, rare l y, discontinuation and institution of appropriatetherapy depending upon the clinica l situation. Pat ients with hypertroph ic cardiomyopathy (IHSS) received verapami l in doses up to 7 20 mg/day. it must beappreciated that th is groupof patients had a serious disease with a high morta l ity rate and that most were refractory or intolerant to propranolol . Avarietyof serious adverse e ffects were seen in this group of patients inc luding sinusbradycard ia , 2
°
AV block , s inus arrest, pulmonary edema and/or severe hypotens ion. Most adverse effects responded we l l to dose reduct ionand onl y rare l ywas verapami l d iscontinued. Precautions : ISOPT IN should be g iven cautious l yto patients with impa ired hepatic function (in severe dysfunct ion use about30% of the normal dose ) or impa ired rena l funct ion, and patients should bemonitored forabnorma l prolongationof the PR interva l orother signs of excess ive pharmaco logic effects . Stud ies in a sma l l numberof patients suggest thatconcomitant use of ISOPT IN and beta b lockers may be beneficia l in patientswith chronic stable angina . Comb ined therapycan also have adverse e ffects oncardiac function. Therefore, unti l further stud ies are completed, ISOPT IN shouldbe used a lone, if possib le . if comb ined therapy is used , close surve i l lance ofvitals igns and c linica l status should be carried out. Combined therapy w ith ISOPT INand propranolol should usua l l y be avoided in patients with AV conductionabnorma lities and/ordepressed left ventricular funct ion. Chronic ISOPT IN treatment increases serum d igoxin leve ls by 50% to 70°/e during the f irst week oftherapy, wh ich can result in digita lis toxicity. The digoxin dose should be re
ducedwhen ISOPT IN is given, and the patients should be careful lymonitored toavo id over or under-d igita lization. ISOPT IN may have an add itive ef fect onlowering b lood pressure in patients receiving ora l antihypertensive agents.Disopyramide should not be iven with in 4 8 hours before or 24 hours afterISOPTINadministration. Unti l urtherdata are obtained , combined iSOPTiN andquinid ine therapy in patients w ith hypertrophic cardiomyopathy should probabl y be avoided, since significant hypotension may result. Clinical experiencewith the concomitant use of ISOPT IN and short and long -acting nitrates suggest beneficial interactionw ithout undesirab le drug interactions.Adequate animal carc inogenicity studies have not beenperformed. One study in rats did notsuggest a tumorigenic potentia l , and verapami l was notmutagenic inthe Amestest . Pregnancy Category C: There are no adequate and we l l -control led studiesin pregnant women. This drug should be used during pregnancy, labor andde l ivery onl y if clearl y needed. It is not knownwhetherverapami l is excreted inbreast mi l k : therefore. nurs ing should be discontinued during ISOPT IN use.
Adverse Reactions : Hypotens ion periphera l edema ( i AVblock :3 rd degree bradycard ia: HR 5 0/min CHF or pulmonaryedema d i z z iness headache fatigue constipation nausea e levat ions of l iver enzymes have been reported .
(See Warnings . ) The fol low ing react ions, reported in less than occurred
under circumstances where a causa l re lat ionsh ip is not certa in: ecchymosis ,bruisin g ynecomastia , psychotic symptoms, confus ion, paresthes ia , insomnia,
somno ence, equi libriumdisorder, b lurred vis ion, syncope, muscle cramp, shak iness. claudicat ion, hair loss, macules , Spotty menstruation. How SuppliediSOPTIN (verapami l HCI) is supplied in round , scored , f i lm-coated tablets conta ining e ither 80 mg or 120mg of verapami l hydrochloride and embossed withISOPT IN 80 Or
”
iSOPTIN 120"onone side and with
"KNOLL
"on the reverse
side . RevisedAugust, 1984 . 2 3 8 5
e KNOLL PHARMACEUTICAL COMPANV30 NORTH JEFFERSON ROAD.WHIPPANV, NEW JERSEY07981

ICAL
AMPULLARY
OVARlAN
ABDOMINAL
INFUNDIBULAR
Figure 2 . Implanta tion sites in ectopic pregnancy . Arrow indica tes pregnancy s ite in this pa tient.
This dec l ine may largely be due to earl ier detect ionresu l ting from improved d iagnost ic techniques . Even so ,
one recent report estimated that 7 5% of maternal deathscou ld be prevented by prompt treatment . 4Ectop ic pregnanc ies commonly present w ith m i ld or
subtle symptoms so the phys ic ian must maintain a h ighindex of susp ic ion . Breast soreness , nausea and othersymptoms of early pregnancy may be absent . Regu larmenses may persi st i n 20—40% of patients ! 3 due to theinabi l ity of the abnormal embryo to stimu late the hormona lchanges necessary to prevent endometrial shedd ing .
Abdominal pain is near ly always present in ectop ic pregnancy , but the pain is uni lateral in only Our patientwas unusual because she had minimal adnexal tendernessand because her abdominal pai n reso lved .
It may be d ifficu l t to d ifferentiate between ectop ic andin trauterine pregnancy . In one series , abdom inal pain andamenorrhea were found in 8 1% of women who were foundto have in trau teri ne pregnanc ies . 3Ectopic pregnanc ies have been reported in patients us ingevery form of con traception . 6 Patients us ing lUDs are notat greater ri sk for ectop ic pregnancy than patients us i ng noform of con traception , 6 but use of .ah IUD does not preventectopic pregnanc ies ei ther. Patients who have had tuball igations or who use barrier methods have the lowest cctopic pregnancy rates . Patients us ing contracept ives , wh ichprevent ovu lation , have rates simi lar to patients us ing barrier methods .
6
The cause of ec top ic imp lan tat ions rema i ns poorlyunders tood . A h i story of pelv ic inflammatory. d isease is animportant risk factor because tubal patency and peri stals i smay be impaired . A h istory of pe lv ic infection or microscopic evidence of prior infection is present in approximate ly 20-40% of patients w ith ec top ic pregnancy ? 6
Tubal b lockage is not the only cause of ectop ic imp lantation because the embryo is often found in the oviductcontral ateral to the side where ovu lation occurred :6 Otheretiolog ic hypotheses inc lude delayed ovu lation , retrogrademenstrual flow and abnormal hormonal mechanisms z ' 6 In
VOL . 46 , No . 12
approx imate ly one th ird of ec top ic pregnanc ies , thekaryotype of the zygote is abnormal , suggesting that cctopic imp lantat ion may also be caused by non-matemalfactors .
Ec top ic pregnancy shou ld be suspected in women ofch i ld bearing age who deve lop pelv ic pain . The presentcase shows that lack of an adnexa l mass or tendernessshou ld not d issuade the physic ian from considering thed iagnosis . Use of serum hcG tes ting i n conjunction w ithpelvic u ltrasonography accurately pred icts ectop ic pregnancy in 93% of cases . 3 The hCG may be negative if thezygote has degenerated or if the laboratory thresho ld for apositive hCG is too h igh . If th i s occurs , quant itative hCGtests and laparoscopy general ly make the d iagnos is . Someauthors recommend the use of cu ldocentesis but th is is apainfu l procedure wh ich is nond iagnostic in 2 3% of patients w ith surg ical ly-proven ectop ic pregnanc ies . 3In our patient , the d iagnosi s of ectop ic pregnancy was
suspected on the bas is of uni lateral abdominal pain andmenstrual irregu larity . H er course was unusual because thepe lvic tenderness reso lved , but the d iagnos i s was confirmed by ri s ing quantitative hcG values and laparoscopy .Subacute manifestations are common in ectop ic pregnancy , so the d iagnosis shou ld be suspected on the bas is of theh istory even when the abdominal examination is “
s i lent . ”AcknowledgmentS upported in part b y aDaland Fe l low sh i p of the Ameri can Phi losophi
cal S oc ie ty .
Referencesl . Leads from theMMWR. Ec top ic pregnanc ies Un i ted Sta tes. 1970-80. JAMA1984 2 5 12 3 2 7 .
2 . Green TH . G yneco logy : essen ti als of c l in ica l prac tice . 3rd ed . Boston : L i tt le ,
Brown and Company . l 97 7 :2 85 -96 .
3 . Weckstein LN . Boucher AR . Tucker H . G ibson D, Rett enmaierMA. Accurated iagnos is of earl y ec topic pre gnancy. Obste t G ynecol —7 .
4 . Schne iderJ BergerCI Cart el C. Maternal mortal i ty due to ec top ic pregnancy ; are v iew of 102 deaths . Obstet Gynecol I 97 7 :49;SS7 -6 1 .
5 . BrennerPF , Sub irR , Mishe l l DR. Ec top ic pregnancy : a s tudy of 300 consecu t ivesurg ical ly ureated cases . JAMA l 980:24 3 :67 3 -6 .
6. BarnesAB , Wennberg CN. Barnes BA. EctOpic pregnancy : inc idence and rev iewof de terminan t fac tors . Obstet Gyneco l Survey l 983 ;3 8 :34 5—56 .

Bulletin Board
New Members
Bax terColumbus J . Leonard (FP) , 2 3 30Rol l inghil l Rd . Fayettevil le 2 8304
AL AMANCE-CASWELLHenry Joseph Van Pala (GE) , Graham-Hopedale Rd . Burlington2 7 2 15 .
BERTIEDexter Levi t icus Bacote (FP) , Box 7 29 , Lew iston-Woodvil le27 849
BUNCOMBETerry Ce ly Chi lders (PD) , 13 1 McDowel l St Ashev il le 28803Kim James Masters ( P) , Appalachian Hal l , Box 5 5 34 ,
Ashe v il le288 13
CATAWBALe land James Cook (GS) , 4 20 N . Center St. , H ickory 28601Carlos Arturo De L a Garza (FP) , 24 Second Ave . NE, H ickory28601
Ted Steven Kel ler (NS) , 4 20 N . Center St. , H ickory 2 8601Wil liam Martin Pekman (HS ) , 1985 Tate B lvd . SE , H ickory2 8601
Kent Alan Robertson (AN) , 4 20 N . Center St. , H ickory 28601Wil liam Leonard S ims (NS ) , 4 20 N . Center Sr. , H ickory 2860 1Walter Rex Stah ly (FP) , 24 Second Ave . , NE , H ickory 2860 ]El izabeth Ann Wri ght (N ) , 4 20 N . Center Sr. , H ickory 2 8601CH OWAN-PERQUIMANSLance Dewitt Potocki (FP) , Box 4 29 , Edenton 27 932CUMBERLANDBruce Wayne B lackwel l (FP) , 160 1-B Owen Dr. ,
Fayette v i l le ,
2 8304
DURHAM-ORANGEJeffrey Char les Acker ( STUDENT) , 1909 Yearby Sr. , Apt. A ,
Durham 2 7 705
MaryElizabeth Aitken (STUDENT) 308 Briarbri dge Val leyRd .
Chape l H il l 2 7 5 14Robert Wi l liam Andrews (U) , 92 3 Broad St Durham 27 705
Eliot Anthony Atstupenas ( STUDENT) , 200 Westminster Dr.
#F -64 , Chapel H i l l 2 7 5 14Ed ward Francis Barbano , Jr. ( STUDENT) , 1909-A Yearby St. ,
Durham 2 7 7 05
Wil liam James Barwick (PS ) , Box 3098 , DUMC ,Durham2 7 7 10
Kyra Jo Becker (STUDENT) , Box 2 87 6 , DUMC ,Durham2 7 7 10
Laurie Owen Beitz ( STUDENT) , 201 Westbrook Dr. Apt . B - l ,
Carrboro 27 5 10Wil l iamMonroe Boyd , V ( STUDENT) , # 1 Spring GardenApts .
Chape l H il l 2 7 5 14Carolyn Heri Chang ( STUDENT) , 19 1 1 Erw in S t #J , Durham2 7 7 05
DECEMBER 1985 , NCMJ 67 5
Thomas Boyle Clark , 111 (RESIDENT) , Box 295 1 , Durham2 7 7 05
DebraLynnColes ( STUDENT) 804 ShadyLawnDr Chapel H il l27 5 14
Donald Scott Co v ington ( STUDENT) , 13 6-A Purefoy Rd . ,
Chape l H il l 2 7 5 14RichardCraig Eamhardt ( STUDENT) , 3903 Neal Rd . Apt . #4 ,
Durham 2 7 705
Jay Marshal l Ede lberg ( STUDENT) , 3 1 1 S . Lasal le St. , Apt .34 -E, Durham 27 705
Robert Douglas Fitch (ORS ) , Box 2 9 1 1 , DUMC , Durham 2 7 7 10Mary Elizabeth Herbert ( STUDENT) , 3 1 1 S . Lasal le St. , Apt.
8- I , Durham 2 7 705Miche l le Marianna Heng (STUDENT) , 13 15 Morreene Rd
#26-F , Durham 27 705
Joe l Doug las MacDonal d ( STUDENT) , 308 Carol S t . Carrboro2 7 5 10
Che t Law rence Nasta la ( STUDENT) , Box 2 7 7 9 , DUMC ,
Durham 2 7 7 10John Christie N icholson ( STUDENT) , 803 Green S t Durham2 7 701
James Robert Oleson (R) , Box 3085 , DUMC , Durham 27 7 10Thomas Arthur Payne ( STUDENT) , E- 18 Ridgewood Apts . ,
Carrboro 27 5 10Jacque lyn Lorraine Redd (STUDENT) , UNC , 650 Craige H al l ,Chapel H il l 2 7 5 14
Parvata Chinna P . Reddy (AN) . 4 1 15 Cobblestone Pl Durham2 7 7 07
Michae l Andrew Sav itt (STUDENT) , 3 1 1 S . LaSal le Sr. , Apt.
4 0-J, Durham 27 705
Robert Andre w Schmaltz ( STUDENT) , 13 15 Morreene Rd . Apt .3K , Durham 27 705
Arthur James Shepard , III ( STUDENT) , 130—N East Long v iewChape l H il l 2 7 5 14
G ary Bradley Sherri l l (STUDENT) , 134 . Beechwood Dr. , Carrboro 2 7 5 10Win fie ld Strickland S ims (RESIDENT) , 507 MorganCreek Rd .
Chape l H il l 2 7 5 14Wil l iam Ross Ste vens ( STUDENT) , 3903 Neal Rd Apt. #4 ,
Durham 27 705
Lisa Carol Sykes ( STUDENT) , 204—A Howel l St. , Chapel H il l2 7 5 14
Catherine M . Minock Wilfert (PD) , Box 295 1 , DUMC , Durham2 7 7 10
FORSYTH -STOKES-DAVI EMelanie Adams ( STUDENT ) , 300 S . Haw thorne Rd . Box 44 7Winston- Salem 2 7 103Joseph Taylor Bel l , II ( STUDENT) , 3 26 Crafton Sr. , WinstonSalem 2 7 103
Brian Clifford Carty (STUDENT) , 120-4 Rainridge Dr. , Winston- Salem 2 7 104
Pame la S . De Luca (STUDENT) , 1068 -G Northwest B lvd . Winston- Salem 2 7 103
Miche l George Haddad (STUDENT ) , 3 00 S . Hawthome Rd . Box4 87 , Winston- Salem 2 7 103

EleanorCarswe l l Hoots ( STUDENT) , 2 2 1 LocklandAve . Win
s ton-Salem 2 7 103Danie l Joseph Ke l ley ( STUDENT) , 44 8 S . H aw thorne St. , Winston—Salem 2 7 103
Timothy Frances Kel ley ( STUDENT) , 44 8 S . Haw thorne Rd . ,
W inston- Salem 2 7 103Edward Norman Lamay ( STUDENT ) , 44 8 Haw thorne Rd Win
ston-Sal em 27 103
George H enry L impert (RESIDENT) , 1 124 Fenimore St. , Winston-Salem 2 7 103Y vonneMack ( STUDENT) , 2 2 1 LocklandAve Winston-Salem2 7 103
Gregory Don Mears (RESIDENT) , 905 Camden Ct. , WinstonSalem 2 7 103
Ste ven H art Mishki nd ( STUDENT) , 2 5 00-C Mil ler Park Circle ,
Winston-Salem 27 103
Jeffrey Dove O lsen (STUDENT) , 2 4 5 1 Boone Ave WinstonSalem 2 7 103
Michae l A l len Olympio (RESIDENT) , 5 26 Osborne Rd Winston- Salem 27 103
Cynthia Lee Reid (RESIDENT) , 505 Brookside Court , Kemersvil le 2 7 284
Gary Lee Roark (STUDENT) , 1 106Me lrose St . Winston-Salem27 103
Claudia Pri chard Shepard (STUDENT) , 1406 Jarvis St Winston- Salem 2 7 101
Mary Claire Skrzynski (STUDENT) , 270 G loucestershire Rd . ,
Winston- Salem 2 7 104
Jennifer Celeste Snowhite (STUDENT) , 1 116 Ebert St. , Winston-Salem 2 7 103
Anne Elizabeth Stephenson ( STUDENT) , 7 25 Gal es Ave . #B ,
Winston- Salem 27 103
Grace Janine Stonerock ( STUDENT) , 164 1-E Northwest B l vd . ,
Winston-Salem 27 104Douglas Paul Wil liams (RESIDENT) , 3924 O ld Vineyard Rd .
# 107 , Winston—Salem 27 104GASTONVincent Eugene Voc i (PS) , 902 Cox Rd . Ste . B , Gas tonia 28054HAYWOODWil liamM . Cal laghan (OBO) , 1600 N . Main Sr. , Waynesvi l le2 87 86
George Randal l Dixson (DR) , 90 Hospital Dr. , Clyde 2 87 2 1NASHJohn Raymond Ste inbaugh (D) , 1 12 Nash Medical Arts B ldg ,
Rocky Mount 27 801NEW HANOVER-PENDERMichae l Rocco Mas trange lo (GE) , 15 15 Doctor’ s Circle , Wilmington 2 8401
ONSLOWTimothy Roy Oman (FP) , 267 Kings Landing Rd Hampstead2 844 3
PITTScott Douglas Beane ( STUDENT) , 3000 Golden Rd . , Apt . #7 ,
Greenvil le 2 7 83 4Mark Lee B inion (STUDENT) , 106 Scales PI . , Apt. A- 7 , Greenvil le 2 7 834Joy Louise Boone (RESIDENT) , 1 104 W . Main St . Wi l l iamston27 892
SAMPSONCarolyn Rose Tatum, 603 Beaman St. , Clinton 2 8328
VOL . 46 , No . 12
Chris Richards Bowman (STUDENT ) , Route #5 , Box 5 4 6-B ,
G reenv il le 27 834Anthony Thomas Burnett (STUDENT) , Rt. #4 , Box 62 , Greenvil le 2 7 834
Donald Keith Clarke ( STUDENT) , 1085 Cheyenne Ct. , Apt.# 13 . Greenv il le 2 7 834
Timothy Lee Dagenhart (STUDENT ) , 322 Springh il l Rd Greenv il le , 2 7 834
Margaret Bleick D i l lard (RESIDENT) , 206 Commerce St. ,
Greenv i l le 2 7 834Sharon Kay Foster ( STUDENT) , M-4 Doctor ’
s Park Apts . ,
Greenv il le 27 834Wil l iam Edward Fowler (STUDENT) , 106 Scales Pl . , B - l ,
Greenv i l le 27 834She l ley Faye G lenn ( STUDENT) , E-5 Doctor’
s Park Apts . ,
Greenv il le 27 834Brent Dwayne Hal l (STUDENT) , Doctor’ s Park Apts . #P—7 ,
Greenv il le 2 7 834Joseph AI Hodges , Jr. (STUDENT) , 1 108 E. l oth St. , Apt. 3
-H ,
Greenv il le 2 7 834Al len Daniel Johnson (STUDENT) , D- 15 Doctor’
s Park , Greenvil le 27 834
Samuel Andrew Johnson ( STUDENT) , Apt . #4 , Carriage House ,
Greenvil le 2 7 834Wil l iamMi l ler Johnstone , Jr . (STUDENT) , 408 S . Harding Sr. ,G reenvil le 27 834Yate s Alton Apt . 13 -E Courtney Square ,
Greenvil le 2 7 834Mari lyn Jean Leonard ( STUDENT) , # 18 G lenwood Apts . ,
Greenvil le 2 7 834Mark Ed w ard MacDonal d (STUDENT) , 1046 E . Rock SpringsRd . , Greenvil le 2 7 834
Barbara Annette Martin (STUDENT) , 13 Upton Court , Greenvil le 27 834Pene lope Jane McDonald ( STUDENT) , M-4 Doctor's ParkApts . , Greenvil le 2 7 834
Ervin Lamar Phipps ( STUDENT) , 15 00 W i l low S t . Apt. #3 ,
Greenv il le 27 834Richard Phi l ip Rizzuti (RES IDENT) , 504 Lancelot Dr. , Greenv il le 27 834John Robert Smith , Jr ( STUDENT) , 3 14 Roundtree Dr . , Gre env i l le 27 834GeorgeMichae l Spencer (STUDENT) , 3000 GoldenRd . Condo#7 , Greenv i l le 27 834Frankie Edward S tanley ( STUDENT) , 24 10-B E. Third St. ,
Greenvi l le 27 834Lawrence Francis Supik ( STUDENT) , 206 -B L indbeth Dr. ,
Greenv il le 27 834Jerry Jurgen Taylor ( STUDENT) , 2402 -B E . Third St. , Greenvil le 2 7 834Phil l ipZachary Timmons (STUDENT) , D-6 Doctors Park AptsGreenv il le 2 7 834
Charles Amon Trant , Jr . ( STUDENT) , 106 Scales Pl . , A-8 ,
Greenv il le 2 7 834Mart in Keith Wi l liams (STUDENTJ) , B -5 Doctor’
s Park Apts . ,
Greenv i l le 27 834Garret Pinkney Young (STUDENT) , L - 13 Beas ley St. , Greenvil le 27 834

With market—basedinterest rates , Sav ingsBonds are a secure
With a guaranteedminimum ofthere is no risk to
and competitive savings instrument .
”
—Suzanne O ’
Toole
principal and app
recia
tion is assured .
—Mark Young
U.S . Savings Bonds now offer h igher , var iable interest rates and a guaranteedreturn . Your employees wi l l appreciate that . They ’l l also appreciate your givingthem the eas iest , surest way to save .
For mone information , wr ite to : Steven R. Mead ,Executive Director , U.S . Savings Bonds Divi sion ,
Department of theTreasury ,Washington ,DC 20226 .
as SAVINGS BONDSL PayingBetterThanEverA public service of this publicat ion .

Letters to the Ed itor
More Med ical WordsTo the Edi torA few months agowe catalogued a co l lection of patients ’
med ica l malaprop i sms , nons tandard d ialec t and s langterms . ‘ A number of readers subsequently forwarded to ussome of the terms they have heard being used in med icalsettings . * Several contr ibutors independently suggested anadd it ional subclassification: medical transcri pt ion malapr0pisms , perinea l plastic syndrome and H ighland membrane d isease , for examp le . Another phys ic ian proposedthe topic of horrors emerg ing from punc tuat ion- free nursing notes (e .g .
“Large fou l green stoo l seen walki ng downthe hal l We have not , however, investigated any ofthese subclassifications further .
S ince the preparation of our ini tial lex icon , James D .
Thomas has wri tten about some of the prob lems faced bymembers of the American subcu lture of Gyps ies as theyinteract w ith the heal th care system and some of the particular med ical terms used by them .
2 Thomas ’ work comp lements that of Snow , who focuses on the prob lems germaneto some B lack Americans in simi lar sett ings . 3 We have al soread an essay by F . Gonzalez-Crussi wh ich mak es reference to several hundred col loquia1\ter[ns used to describemale genital ia .
4 It i s our purpose here to present the termssubmi tted to us along w ith some add itional ones recentlyd iscovered by the first author . As i n the prev ious co l lectionof medical terms , patien t med ical talk i s div ided i nto thetwo categories of Ma lapropism and Slang and Nonstan
da rd Dia lect . In the former , s tandard med ical term ino logyi s mispronounced , becomi ng confused w ith other items ofstandard Eng l i sh vocabu lary ; i n the latter , terms may bepart icu lar to a certai n reg ion or subcul ture .MalapropismsArticle ArteryArthuritis Art hri tisBabygel Basogel
gonreh GoutIns ens itive Care Unit Intensive Care Uni tIntentiona l Care Intensive Carej anitor VaginaOld Timers
'
Disease A lzheimer’
s D iseasepaj ama ! i tch Vag inal itchpenici l l ium Penic i l l i npinwheels Pinworrns
Prima vera Proverapuls e Pus
subscription Prescriptionsulfur Su lfonam ideTAP smear PAP smeartechnica l shot Tetanus shot*Con tr i bu tors were th e fo l l ow ing pe op le: Juni u s W . Dav is , Hes ter G id '
di ngs , Jared Go lds tein , James L . Mathis , Bru ce K . Morgan , George Olt,James G . Pede n , Adrena J . Perry , Mary lin Te le n , John L . Weinerth ,J . W . Wri gh t , and Richard C . Zahn.
DECEMB ER 1985 , NCMJ
tenderl itis Tendoniti stenta cles Testic lesthrash Thrushwheazels in the chest Wheezes ; spec ifical ly asthmaticwhelps Welts or urt icari awound Womb
Referencesl . Sugarrnan J Butt ers RR. Unders tand in g th e patien t : med ical words th e doc tormay not know . NCMJ 1985 ;4 6z4 l S- I 7 .
2 . Thomas JD . Gyps ies and Americanmedi cal care . Ann lntemMed l 985 ;102 :84 24 S .
3 . Snow LF . Folkmedical be l iefs and the ir imp l ications forcate of pat ien ts : a re v iewbased on stud ies among B lack Americans. Ann lntemMed4 . Gonzal ez-Crussi F . Note s of an anatomi st . San Diego: Harcourt Brace Jovanov ich Pub , l 985 : 1 10~ 29 .
To the Ed itorYou have probab ly received hundreds of these since the
pub l ication of the l i st of unusual words used to describemed ical cond itions . I had heard mos t of them before
,but
came across one yesterday that I had never heard before .You may w ish to keep th is in your fi les .
An eighty-year-o ld lady who had grown up down on theeas tern coast was describ ing al lerg ic symptoms of pos tuasal dri p . In describ ing th i s , she said that sometimes she felther
“ Sunday tongue was down al l the way to the bottomof her throat . We d iscussed th is a l i tt le whi le longer and i t
67 9
S lang and Nonstandard Dial ec tclap Urethral d ischarge due to gonorrheacold Mucusgrimes Gro inha ir cut Chancreheart dropsy Swe l l ing of the ank les due to heart fai lurehunya Herniakidney hurting Dysuriaknots Lymph nodeslambooda Lib idoleaders Tendons or l igaments , espec ial ly i n the neckloose bowels D iarrheamigram heada ches Migraine headachesphlegm Upper resp iratory trac t infectionpocke tbook Vag inapoor in blood Anem iapunish Pain (as in It puni shes me ri ght smartsex in To have sexual intercourse w iths ide p leurisy Any thorac ic wal l painsuage down 1 . Loss of edema or swel l i ng 2 . Lose weightsump in
’
tee Anorex ia (perhaps from , something to eat” )tired blood Malaisewhi tes , the Vaginal d ischarge

was perfectly c lear that what she was descri b ing was a
boggy uvula related to al lergic s inus i ti s .
I have enj oyed the Journa l very much over the years , andin part icu lar the recent immense improvement in the ent ireoperation . Keep up the good work and thank you for devoting so much of your t ime to th i s concern .
Margare t Nelsen Harker, M .D .
Morehead C ity 2 85 5 7I t ’ s Sti l l H ard to Make a LivingTo the EditorNot that long ago the Journa l ‘ was kind enough , perhapslacking copy shortly before dead l ine , to pub l i sh some
medi tations of mine about how hard it can be for somepeop le to make a l iv ing . F loyd Rogers , a ta lented reporterfor theWins ton-Sa lemJourna l , read the artic le and dec idedthat it held promise for a news story . We d iscussed thematter by phone and then over coffee and I deluged h imw i th repri nts about obscure occupational hazards and thel ike as wel l as tel l ing himmore about the h i story of occupational di sease than he real ly needed to know .
A few Sundays later h i s story appeared ,
2rather less
pedant ic and more spright ly than becomes a med ica lacademic but as it turned out be tter attuned to the vu lgarear . That very night , someone from a press serv ice in thenorth cal led me about midnight for an interv iew s ince I nowapparently qual ified as a medical expert . S trugg l ing out ofs leep I sought , w ithout sound ing surly , to answer questionswh ich he real ly seemed to have a lready answered h imself.During the next few weeks I received phone cal l s from
friends , c l ippings from ourOffice of Information and fromother fri ends and even a copy of an ed itorial from thenewspaper i n my w ife ’ s home town
,She lby
, accusi ng meever so gently of pu l l ing the pub l ic leg . S ince some of thecal l s came from peop le I had never heard of who hadsuffered from Honda h ip and other anatomic insu lts , Iwrote a letter to the ed i tor so that my w ife ’ s friendswou ldn ’ t th ink that I made a hab it of perpetrati ng hoaxes .
And when a Honda dealer reported that he had had customers complain of simi lar troub les I felt even better about thematter. My patient who suffered that syndrome in the firstp lace recently re turned for h i s annual phys ical and reportedthat he is sti l l symptom- free and that he enjoyed v icarious ,if anonymous , p leasure in recognizing his med ical past inprint . He al so reminded me that i t had been a H ondaAccord , not a C iv ic , wh ich had led to h i s di s tress .Others cal led too , seeking med ical adv ice for themse lvesand their friends , v ictims of a variety of pedestrian difficulties . A hel ic0ptor designer even cal led from Fort Worthbecause the story had appeared in a Dal las newspaper. Itseems that cockp its of he l icoptors are in need of beingredesigned because of techno log ical advances and becauseveteran helicopter p i lots get al l sorts of aches and painsfrom s itting at the contro l s for long peri ods . Sad ly I cou ldoffer no cons tructive sugges tions al though it occurred tome later that med ical institutions featuring heliports mightrequ ire expert personne l , or personnel wh ich wou ld become expert in a short time , and wou ld be happy to pub l ic ize their efforts in the air by trotti ng out their authori tiesfor h im .
To my know ledge vers ions of the story appeared in
References1 . Fe l ts JH . Sometimes it‘ s tough to make a l iv ing . NC Med J2 . Rogers F . Honda hip no fun, bu t ch icken packer's hands is serious . W instonSalem Journal May 5 , l 985 zA17 .
Kenneth E . O l ive , M .D.
Ch ief Med ical ResidentWright-Patterson AFB , Oh io 4 5 4 3 3
newspapers in Ashev i l le , Charlotte , S tatesv i l le , RockyMount , Sal isbury , Boone , Shelby , Greenv i l le , New Bern ,Chapel H i l l , Durham , Henderson , and Gastonia , NC ; C0Iumbia and Myrtl e Beach , SC ; B irmi ngham , Houston ,Dal las , Richmond , Cinc innati , Read ing , PA and Jonesboro , AR . So for a bri ef moment both the Journa l and I hada b igger aud ience than usual . My transient celebri ty wasp leasant but I wou ldn ’ t want to mak e it a hab it .
John H . Felts , M .D.
Bowman Gray Schoo l of Medic ineW ins ton- Salem 27 103
Stil l Fol lowing Family Med icineTo the Editor :
I read w ith interest Dr . Estes ’ ed itorial Fami ly Med ic ine at Duke : A Fo l lowup” in the September 1985 issue ofthe NCMJ . I am p leased that the subsequent developmentof the East Caro l ina Univers i ty Schoo l ofMed ic ine provesDr . Estes ’ chauv in is tic 197 3 comments wrong : The usualanswer i s ‘ But that ’ s not Duke ’ s role ! Let Eas t Caro l ina doit . ’ It is a d ifficu lt job
,but that shou ld certainly be no
justification for ass igning that task to a schoo l less capab lethan Duke .North Caro l ina is fortunate to have four excel lent med i
cal school s w ith d ifferent attributes . East Caro l inamay notperform some activ ities such as basic sc ience research , atthe same level as Duke . However , East Caro l ina has fi l ledneeds that Duke and other inst itutions were unab le to fi l l , inpart by estab l ish ing a reg ional med ical center in a prev iousIy underserved area . And i t has done so w ith excel lence . Asan alumnus of both Duke and East Caro l ina , I have seen thes trengths of both institut ions , wh ich are different . I amproud to have attended both schoo l s and do not feel that myyears at East Caro l ina were spent at “a school less capab lethan Duke , just at a schoo l serv ing a much d ifferentpurpose than Duke .
To the EditorThe ed itorial by Dr . E . Harvey Estes , I r . , Fami ly
Medic ine at Duke : A Fo l low-Up, in your journal ofSeptember 85 causes me some concern . About two monthsago in your journal under the c lass ified ads , there was aso l ic itat ion for a fami ly practice physic ian to jo in a c l inic inthe midd le part ofour state w ith a starting salary ofper year or 50% of the gross , wh ichever wou ld be thelarger. To support the pro l iferation of fami ly medic inephys ic ians on a financ ial basi s i s rather lud icrous . I havebeen in med ic ine for th irty years and in private practice fornine and one half years . I am one of three neuro log ists whopractice toge ther at the Durham C l inic . 1 do not make
a year after th irty years in practice and being in asubspec ialty . Are they real ly going to try and tel l me thatstarting a brand new fam i ly pract itioner at a year is
VOL . 46 , No . 12

creases ; to improve our pos it ion in a h igh ly competitivemarket; and to maintain the integri ty of the private heal thsector.
In ini tiating the program , we emp loyed me thods to ensure a fair and equ itab le method of reimbursement . B lueCross and B lue Sh ie ld of North Caro l ina so l ic ited inputfrom practic ing North Caro l ina doctors and from s imi larreimbursement programs in operation in 6 1 other B lueShield P lans .To maintain the program , we wil l conduct regu lar rev iews of Spec ial needs of doctors , inc lud ing malpracticeinsurance , through adv isory groups of partic ipating doctors , and cons ider appropriate changes based upon theirrecommendations . In addition , these groups w i l l rev iew theP lan ’ s fairness in admin istering the partic ipating doctorprogram .
Previous cost contai nment programs have not sacrificedthe qual ity of care in our state . Likew ise , the part ic ipatingdoctor program does not affect the level of benefits forheal th care serv ices or l imit med ical ly necessary health careserv ices .The partic ipating doctor program , as a reimbursement
system , only affects the mechanism of benefit payment .Though our program seemingly shares s imi larities w ithother systems affecting the financ ing of health care , i t mustbe rev iewed on its own merits .Inc luded in those meri ts is the method for determi ning
Thomas A . RosePresident , B lue Cross B lue Sh ie ld
Box 2 29 1Durham 2 7 7 02
VOL . 4 6 , No . 12
the max imum al lowab le . We computed thi s max imum at
the 9oth percenti le of al l doctors ’ charges . We l inked feeincreases to the al l - items Consumer Pri ce Index (CPI) tosustain the pred ictab i l i ty of reimbursement increases as
wel l as increases in rates for health insurance premiums . Asnoted above , spec ial cons ideration w i l l be given thosefactors which wou ld impose unique costs upon doctors .We have estab l i shed a team of profess ional relations
representatives across the s tate whose primary funct ion w i l lbe to serve partic ipating doctors by addressing any admi nistrative concerns they may have . _
As part of the P lan ’ s contract , we prov ided a cancel lationc lause so doctors are not locked into partic ipation . Tosupport the success and sav ings potential of the program ,
we necessari ly inc luded a d irec t payment incentive forpart ic ipation .The dec i sion to part ic ipate is an individual choice of the
state ’ s doc tors . Each doctor shou ld judge the program ’ simpact on h is or her practice . We invi te North Caro l inadoctors to assi st inmak inga ffordable heal th care protectionavai lab le for the subscribers of B lue Cross and B lue Sh ieldof North Caro l ina .

Volume 46
January -December , 1985
SUBJECT INDEXAconi te poison ing . 5 18Acquired immunodefic iency syndrome
effec t on b lood donat ions. 35 3information abou t , 3 56Addison 's d isease , 565Advertis ing. med ical . 67 1
AHEC , Moun ta in , 44 5AIDSimpac t on b lood donat ion , 3 5 3informati on abou t , 3 56Al cohol w i th drawaltreatment of, 4 87ALS un i ts in NCemergency pro toco ls for, 5 79Army med ical reserve , 167Arthropa th yhemochromatosis as an, 395Ashev il le 1985 , 44 1card iac surgery in 1983 , 4 7 5tu bercu losis era , 4 5 5Asparaguseffec t on urine odor, 3 32Asp irinand Reye syndrome , 669Auxi l iaryincomin g Pres iden t ’ s address , 5 4 3Pres ident 's report to NCMS , 5 4 1
Beard , Joseph W . , 303B iopsyus in g fin e need le asp ir ati on , 5 1 1B lood replacement
for C-se ction . 139 , 14 1B lue Cross/B lue Shie ldpersonal care p lan , 4 5 1Book re v iew , 3 1 1Bre ast
hno-needle asp iration of, 4 8 1Cancer immunology , 4 79care of th e patient , 85early d iagnos is of tes t icu lar , 407
Candies . die te ticand d iarrhea. 1 14
Carc inoma of eye l id , 4 7 3Card iac surgery
in Ashev i l le in 1983 , 47 5Ca taracts and lens implants , 649Cauda equinacompress ion of, 398CCUbal loons on the , 197Cefurox ime sod ium, 17 3Cert ificationpreadmiss ion , 23 3Cesarean section
repeat. 139blood re p lacemen t for. 14 1C ircumcis ion
and d iabetes in adul ts , 109C laud ication . in te rm i tt en t. 398Coccydyn ia , 209Commencemen t address
UNC May 1985 , 5 3 5Consc ient ious objectors
at Duke in WWII , 4 19Cooper, George M. , Jr.obi tuary , 5 36Cost-effec tive med ic ine
al coho l w ithdrawal syndrome , 4 87Country doc toring in NC , 603Coverage , 5 3 1Crohn 's d isease , 199DNR orders
in nurs ing homes , 633Dehydrati on
in old age , 5 20Dental prac tices
'
and fluoride , 7 7Dermatologis t. 393Diabetes
and c ir cumcis ion in adu l ts , 109Dial ys iscontinuous ambu latory peri toneal , and peri ton itis ,DECEMB ER 1985 , NCMJ
683
Diarrheal inked to d iete tic cand ies . 1 14Dig i ta l isinteract ions , 25Digox in
and re nal fai lure , 465Disulfiram tox ic i ty , 2 7 7Di zz iness , 156Drugs
antiarrh ythmic , 25how they work , 14 7
Dukefamil y med ic ine at, 329famil y med ic ine fo l lowup , 44 3avuls ion inj uries to , 5 1Eco logyand po l lut ion , 37 3
Economicsmedical . 129
Ec top ic pregnancys i lent , 67 3
Educationmed ical , 129
E l li ng ton . Dr. J . H . . 603Embo l ismpu lmonary , 19Emergency Med ical Serv icesin rural NC , 2 7 1
Emergency transportuse of hel icopters , 93
Emergency treatmentpro tocols for, 5 7 9Emphysema
med iastinal , 2 1Entrepreneur phys ic ian , 5 23Eth ical quandaries
for med ical inst itu tions , 5 3 3E th icsmed ical , 129
Exerc ise te s tingand card iac rehab i l i ta t ion , 340Eyel idsebaceous gland carc inoma of,
Fami ly med ic in e at Dukefol lowup , 44 3at Duke , 3 29
Federal regu lat ionsfor critical ly i l l infants , 265
Fees , phys ic ianprospec ti ve paymen t and . 27 5Fine needle as p irationb iopsy . 5 1 1
of breas t , 4 8 1F luoride
use in chi ldren , 7 7G oals
short term, 195Grief, good , 15 3Gri ev ing
stages of, 15 3Haemophi lus in fluenzae type B in fectionw i th purpura fulminans , 5 16Hea l th profess ional sincrease in NC. 3 36Heal th reporton th e s ta te of NC , 5 25He l icopter wars
Bowman Gray and . 99Duke and. 98ECU and . 93UNC and . 99
Hemlock , waterpo ison in g , 163Hemochromatos is, 395Hepati tis . de lta , 1 13Hip replacemen t book le t , 285Home care , 3 3
Hosp i tal u ti l izat ionin NC , 4 10Hosp i talscri s is in , 3 7 9

LECl-INER , Debb ie , So you are go ing to have a total hip rep lacementLEE , Aus tin . Cefurox ime sod iumLEVINE , Ronald H . , The proper use of systemic fl uoride supplemen ts w i thchi ldren in med ical and denta l pract icesThe state of th e StateLEVY Steven M. , The proper use of sys temi c fluoride supplements w i thch i ldre n in med ical and den tal prac t ices
LINFORS . EugeneW . , ed i tor Respond ing to pat ients who re fuse l ife savingtreatmented i tor, Preadmiss ion cert ificat ioned i tor, Ecology and po l lu t ionedi tor. Pay ing phys ic iansNeck mas sesLINZER , Mark , That Add ison ian tan. The heal thy looks that may dece iveL IPTON , Morris A. , Eco logy and po l lut ionLYNCH . John F , Med ical re volution hosp i tal cris is
MaccoRMACK , J . N A IDS information for doc tors arid pat ien tsMACK , Ronald B . , Ju l 1us Se i zure Carbamazep ine (Tegretol ) poison ingPervas ive procrustianism isopropyl alcohol in tox icationKeats Socrates and foo l ‘ s pars ley water heml ock po ison ing
Talj anbu k i la dawa isifal : yohimb ine intox icat ionThe dark n ight of the sou l disul l
'
i ram tox ic i tyAquari us redux lyserg ic ac id d ie thylamideSisyphus on the rocks monoamine ox idase inhibi torsP lay i t agai n , Vol ta ire acon i te (monkshood ) po ison ingA b i t on th e Wi lde s ide: MDMA abuse
MANSF IELD, Chris topher J The deve lopmen t of a hel icopter emergencymed ical serv ice for eas tern North Carol ina
MARR , Judy , Le tter to the ed i torMASSEY E Wayne . Common mononeuropathiesLetter to the ed i tor: responseMAUNEY F Max ton Jr. , Le tter to the ed i tor
The Mounta in Area Heal th Education Cen ter: a un ique university/cornmunity partnership .
Thoughts on the PA/physiciari teamMAY , W Joseph , Maternal mortal i ty in North Caro linaMccoLLUM. Donal d . So you are go ing to have a to tal hip rep lacementMCCOY , Joseph Le tt er to the ed i torMcKINSEY , John J. . Remov ing a t ickMcNAMARA. James O . lntenni ttent c laud icat ion due to cauda equ ina compre ss ionMcwHORTER. John Henry , O ld tobaccoMEASE , E l i zabe th . The d iagnos is of viral pneumon i t is in a compromisedMITCHELL , Joyce M Snakeb i te treatmen t in the 805 .
MOELLER . Arlyn M , Le tter to th e ed i torMOFFETT Al ex Le tter to the ed i torLe tter to th e ed i torMULROW , Cynth ia D Peri card ial pseudoeffusion due to s tero id inducedl ipomatos isMUNSON Eric North caro l ina Memori al Hospi tal ‘ 5 pos i t ionNANCE ,Ke i th V . , Percutaneous fine needle asp irat ion b iopsy of deep abdo
men, re troperi toneum, soft tissue and bone under rad iologic gu idanceNANCE , Linda P Pres iden t's report to the North Caro li naMed ical Soc ietyNEELON . Franc is A. , The management of bee h ivesLe tter to th e ed i tor: responseYou 're in for a tre at : asparagusLook ing at renal fa i lure ups ide down
Neck massesNEISH , Donald D Short term goals for young heal th care prov idersNEWBORG , Barbara . The ro le of oxygen pre ssure in the fight agains t th ech ief ki l lers in th e firs t and in the las t hal f of the 201h Cen turyNICHOLS , Stephen R . The managemen t of bee hivesNORTHCROSS . Grayce P , Le tt er to the ed i torNURKIN . Harry A. , On da ting , marriage and other s trange re lationships : thefu ture of s ingu lar hosp i talsO 'RAND. Michae l , In v i tro ferti l i zation at the North Carol ina MemorialHosp i tal in Chape l H i l lOLDS , Roben, better to the ed i torOLIVE , Kenneth E. , Let ter to the ed i torOSTERHOUT, Shirley K American Assoc iat ion of Poison Contro l Centerscertifies the Duke programOUTLAND, Robert Sr. , Le tter to the ed i torPARKER . Roy T. , B lood re placement for repeat cesarean sect ionPASCl-IAL , Barton R. , Sebaceous g land carc inoma of the eye l idPEDEN. James G Jr Le tter to the edi torPHI LLIPS , Charles A Speas , Termi nal i l lness managemen t e lec tivesestab l ishment of a TIME commi t teePIERCE , Lori , In termi tten t c laud icati on due to cauda equ ina compress ionPIERCE , Mark R , Snakeb i te tr eatment in the 805PODGORNY . George , Snakebi te tre atmen t in the 805POWELL , Bayard L . , Overwhe lming infection afte r sp lenec tomy
PRITCHEI'
I , Edward L . C The Rankin Cl in ical Research Un i t of DukeUn ivers i ty Med ical Cen ter commemorates 2 5 1h ann iversaryPROCTOR , H. J Respond ing to patien ts who refuse l ife sav ing treatmen t
QUIGLESS , Mi l ton D. . I r. , Let ter to the ed i torREDICK . L loyd F Letter to the ed i torRENUART, A W Le tter to the ed i torR ICE , John R . Hemochro matos is an unusual arthropathyROGERS Wal ter R. , Jr., The top heavy p lan ru lesROSE , Thomas A. , Le tt er to the ed i torROZEAR, Marv in P . When to see your doc tor about vert igo and d i zz inessAn unusual cause of re curre nt trans ien t neurolog ic defic i tRUPP . Sharon L Premens tru al syndromeSAB ISTON , Dav id C Jr Le tter to the ed i torSALISBURY . Ken t W Card iac sureerv in Ashev i l le
Phys ic ians can and shou ld offer d irect ion for the 1985 leg is latureLette r to the ed i torS ILVERMAN , Jan F Percu taneouus fine need le aSpir-at ion b iopsy of deepabdomen , re troperi toneum, soft tissue and bone under rad iolog ic gu idanceSLATER . Doug las , In termitten t c laud ication due to cauda equ ina compresSLOAN , Carol , In v i tr o ferti l i zat ion at the North Caro l inaMemori al Hosp i ta lin Chape l H il lSOMMER , Joachim R . Letter to the ed i torSOMMERVIL LE . Lewis G . , B lue Cross/B lue Sh ie ld“5 Personal Care PlanSQUIRES , Jerry E. , The impac t of AIDS on blood donationSTEAD, Eugene A I r. , Le tter to the ed i tor: responseAl ive bu t not l iv ingLe tter to th e ed i tor: responseSTEEGE . John F , Premenstrual syndromeSTEEL J Griffi th .The impact of prospective payment for phys ic ian fee s orimed ical spec ial istsSTEIN . Jane , Distri bu tion of women andminori ty phys ic ians inNorth Caro l iSTEPHENS , Irb y , Ashev il le: th e tubercul os is eraSTILES , AlanD. , Purpura fu lminans assoc iated w i th Haemoph i lus influenz aetype b infectionSTOUT. Anna L Premensu'ual svndromeSTRAUSS , Harold C Interac t ions be tween d ig i tal is and antiarrhy thmic
WEBB , C Edw in , Serum d igox in levels and re nal fai lureWELLS . Robert , B lue Cross/B lue Shie ld 's Pers onal Care P lWENGER , Thomas L In terac tions between d ig i tal is and ant iarrhy thmicdrugsWERK Emi l E . Jr. , be tter to the ed i tor: responseWESTER . Thad B . Project Ipecac : an acc iden t pre vent ion program of th e
Robe son Coun ty Departmentof Heal thWESTON , George W . , A vu ls ion inj uries of the ex te rnal earWHITLEY Theodore W . , Le tter to the ed i torWILKINS , Luc ien S Respond ing to pa t ients who re fuse l ife sav ingthemWINNEBERGER , Theodore R Snakeb i te treatmen t in the 805WOLFE , Wal ter G . An unusual cause of recurre nt trans ient neuro logicWOLFF , George T Le t ter to the ed i torWOODWORTH . Torn , Le tter to the ed itorYAGGY . Duncan . Duke takes the p lungeA Duke admin istr ator surveys the curre nt sceneYOUNG , Dar lene , Pres iden t ’ s speechYOWELL , Robert K Le tter to th e ed i tor
5 11
33 8
4 33
4 5 2
35 3
63
27 7
3 85
2 2 1
VOL . 4 6 , No . 12
3 101
1
16220 1
:n Anne. Increase in heal th profess ional s in North Caro l ina '
I
Distribut ion of women and minori ty phys ic ians in North Carol inaSALMON. Patri c ia M A check l ist of prac tice marke t ing ideasSALTZMAN , Herbert A . The patien t fromwhom I have Ieamed th e mostSANTAMARIA John Peter. Purpura fulminans assoc iated w i th Haemoph i lusinfluenzae type b infec t ionSARGENT , Dale , The d iagnos is of v ir al pneumon i tis in a compromised hostSAYERS . Dan ie l G . Statew ide pre hosp i tal mob i le intensi ve care treatmen tpro tocols for advanced l ife support un i ts in NC
SCHAFERMEYER, RobertW Statew ide prehosp i tal mob i le intens ive caretre atment protocols for advanced l ife support un i ts in NC
SCHU’
ITE . Haro ld D B lue Cross/B lue Shield ‘ 5 Pers onal Care P lanSCHWARTZ. Robert P Screen ing for congen i tal hypothyroid ism 111 NorthCaro l ina 197 9- 1984SHEAFFER , Charles l . . Ecology and pol lutronSHEAR IN , J . Conne l l , Avu ls ion inj uri es of the external earSHEPHERD, SuzanneM. Statew ide prehosp i tal mob i le intens ive care treatmen t pro tocols for advanced l ife support un i ts in NC
SHUNIOR, Charles . Bal loons on the CCU .S ILBERMAN . Haro ld R. , Respond ing to patien ts who refuse l ife savrng
STRAWCU’
ITER, H Letter to the ed i torSTUART. John J. , Fami l ial thrombo tic d isordersSUGARMAN . Jeremy , You 're in for a treat: asparagusUnderstand ing the pat ien t: med ical words the doc tor may not knowLooking at renal fai lure ups ide downLe tter to the ed i torSULL IVAN . Robert J Fami ly med ic ine at DukeSWANSON ,Lou is E Consc ientious objec t ion and cl in ical care : a history of
C iv i l ian Publ ic Serv ice Camp No. 6 ] at Duke Un ivers i ty , 194 2- 194 6 .
TALB ERT, LutherM In v i tro fert i l i zation at the North Caro l inaMemori alHosp i tal in Chape l H i l l
TARRY , W i l l iam B Jr. Le tt er to th e ed i torTERZIEVA, Tsvetanka , Letter to the ed i torTHOMAS , John V . , Catarac t and lens imp lan t surgeryTHRASH , V irg il . B lue Cross/B lue Sh ie ld 's Personal Care P lanTOPE , J . Jeffrey , Snakebi te treatment in th e 805TRACY , Margueri te K , Coal i tion on sexual ly transmi tted d iseasesLetter to th e ed i torTROLLER , John , Le tter to the ed i torTROMBETI
‘
A. Wi ll iam L . , The entrepre neur physic ianWALKER . Andrew W headmission cert ificat ionWAL L , Thomas C When t u
'
5 d isease is not Crohn ’s d iseaseWARSHAUER , Albert D Th oughts on the bel iefs of relig ious andmed icalinsti tu tionsLet ter to the ed i torLe tter to the ed i torLetter to the ed i tor
WEAVER , Zebu lon . lI l , Accidenta l veratrum V iride po ison ing in three

index toAdvertisers
Ayerst LaboratoriesB B X -Ray , Inc .
Campbel l Laboratories , Inc .
CHAPSCrumpton CompanyCurt is 1000 Inform ation SystemsGuestHouse
EF Hutton Company , Inc .
Info Systems of NC , Inc .
Kno l l PharmaceuticalLew is Med ical Instruments Inc .
El i Li l ly Company
VOL . 46 , No . 12
Marion Laboratories ,Inc .
Medical Mutual Insurance Company ofNational S taffing Services Corp .
Newtron of V irginiaNorth Caro l ina- Sou th Caro l inaSoc ieti es of Patho logyOrtega Pharmaceutica l Company , Inc .
Roche LaboratoriesSaint A lbans Psych iatric H osp italU . S . Air ForceWil l ingway ,
Inc .
W inchester Surg ical Supp ly Co .

EXCERPTS FROMASYMPOSIUMTHETREATMENTOF SLEEPDISORDERS"8
h igh ly effect ivefor both s leep i nduct ion ands leepma i ntenance
SleepLaboratory InvestgatorPennsylvania
onset of act ion israp id. p rovides s leepwithno rebound effect topat ient the fo llowi ng
Psychiatrist
Cal ifornia
. . appea rs to havethe best safety record of anyof the benzod iazep i nes
Ps chiatrist
Ca fornia
After 15 years, the experts sti l l concurabout thecontinuing va lue ofDalmane (flurazepamHCI/Roche) . Itprovides s leepthat satisfies patients .
and thewidemarg inof safety that sat isfies you.
The recommended dose inelderlyordebi l i tatedpatients is 15 mg. Contra ind icated inpregnancy.
flura zepam HC I/ Roches le ep tha t sa tisfies
i s-mg/3 0-mgcaps
References : l . Kales J, etat. ClinPharmacol Ther 12 .
-691
69 7. Jul-Aug 197 1. 2 . KalesA, eral; ClinPharmacol Ther-363 , Sep IE)?5 . 3 . Kales A, et01: Clin Pharmacol
Ther - 5 83 ,May 197 6 . 4 . KalesA, etol: ClinPharma
col Iner3 2 7 8 1-7 138 , Dec 1982 . 5 . Frost JDJt DeLucchiMRrJAmGeriatrSoc - 5 46 , Dec 197 9 . 6 . DementWC, etol: BenovMed, pp. 2 5 -3 1, Oct 197 8 . 7. KalesA,Kales JD; J Clin Psychophormacot - 150, Apr 1983 .
8 . Tennant FS, eta/. Sympos iumon theTreatment ofSleepDisorders , Teleconference, Oct 16. 1984 . 9 . Greenblatt DJ.Allen MD, ShaderRt; ClinPharmacol Ther -3 5 5 -3 6 1
Mar 197 7.
DALMANE”flurazepamHCl/RocheBefore prescribing. please consu l t complete produc tinformation , a summary ofwhich fol lows:Ind ications; Effect ive in all types of insomnia characteri zedby d iff iculty in fal ling as leep, frequent nocturnal awaken ingsand/orearlymorn ing awakening,
inpatients With recurringinsomnia orpoors leeping habits; in acute orchron ic med ica lsituations requ iring restfu l s leep. Objective sleep laboratorydata have shown effectiveness forat least 28 consecutivenights ofadministrat ion . S ince insomn ia is oftentransientand intermittent, prolonged administration is general ly notnecessary orrecommended. Repeated therapy shou ld onlybe undertakenw ith appropriate patient evaluation .Con traind ications; Knownhypersens itivity to flurazepamHCl;pregnancy Benzod iazepines may cause fetal damage whenadministered during pregnancy. Several s tud ies Suggest anincreased risk of congen italmalformations associated w ithbenzod iazepineuse during the firs t trimester. Warnpatientsofthe potential risks to the fetus shou ld the possrbility ofbecoming pregnant ex ist whi le receiving flurazepam. Instructpatients to discontinue drug prior to becoming pregnant. Consrderthe possibil ity of pregnancy priorto instituting therapyWarnings: Caution patients about possible combined effectswith alcohol and otherCNS depressants . Ari add itive effectmay occurifalcohol is consumed the day lol lowmg use forn ighttime sedation. This potential may exist forseveral daysfollowing d iscontinuation Caut ion against hazardous occu~
pations requ iring completemental alertness ( e g. , operatrngmachinery, drlvmg) Potential impairment ofperf ormance ofsuch activitiesmay acourthe day tallow ing ingestion. Not
recommended foruse in persons under 15 years ofage.
Withdrawal symptoms rarely reported , abrupt d iscontinuat ionshou ld be avoided with gradual tapering ofdosage forthosepatients onmed icationfora prolonged period of time Usecaution inadminis tering toadd iction- prone individuals arthosewhomight increase dosage.Precau tions: Inelderly and debi litated patients,
it IS recommended that the dosage be limited to 15 mg to reduce risk ofoversedation , d iz z iness , confUS ionand/or0 l0Xl0 Considerpotential add itive effects with otherhypnotics orCNS depressants . Employ usual precautions in severely depressedpatients, or inthose with latent depress ionorsu icidal tendencies , orinthose with impaired renal orhepat ic functionAdverse Reactions; Dizz iness, drowsiness , lightheadedness.
staggering, atax ia and falling have occwred , part icu larly inelderly ordebil itated patients. Severe sedation, lethargy. disorientation and coma,
probably indicat ive ofdrug intoleranceoroverdosage. have been reported. Also reported: headache,
heart burn , upset stomach. nausea, vomiting, d iarrhea, constipation, GI pain , nervousness, talkativeness , apprehens ion ,irritab ili ty, weakness, palpitat ions , chest pains , body and jointpains and GUcomplaints. There have also beenrare occurrences of Ieukopen ia, granu locytopenia, sweating,
flushes ,d iff iculty in f00usmg,blurred vrs ion, burn ing eyes , faintness,
hypotens ion , shortness of breath,pruritus. Sklnrash, dry
maulh, bitter taste, excessrve salivation , anorexia, euphoria,depression, slurred speech , confus ion, restlessness.halluci
nations , and elevated SGOT, SGPT, total and d irect b il irub ins,and alkaline phosphatase: and paradoxical reactions, e.g .
exc itement, stimu lation and hyperactivity.
Dosage: Ind ividualize formaximumbeneficial effect. Adu lts.
30mg usual dosage: i 5 mgmay suffice insome patients .
Elderlyordebilitated patients; I5 mg recommended in itial lyunti l response IS determined.Suppl ied; Capsu les contain ing 15 mg or3 0mg tlurazepomHCI.