Attitudes toward the integration of smoking cessation treatment into drug abuse clinics
Upload
khangminh22Category
view
4download
0
Alexandra Geusau
Department of Dermatology, Division of
Immunology, Allergy and Infectious Diseases,
Medical University of Vienna
Syphilis in the Brain – Clinics
and Management of
Neurosyphilis
ESCMID eLibrary
©
by author
Does neurosyphilis (NS) still exist ??
At which stage does NS manifest ??
How do you diagnose NS ??
How can NS be treated ??
Questions
ESCMID eLibrary
©
by author
0
5
10
15
20
25
1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014
EU gesamt*
Deutschland*
Österreich*
Schweiz*
UK*
USA primär/sek.
USA alle Stadien
USA all stages
Austria
Switzer-
and
Germany
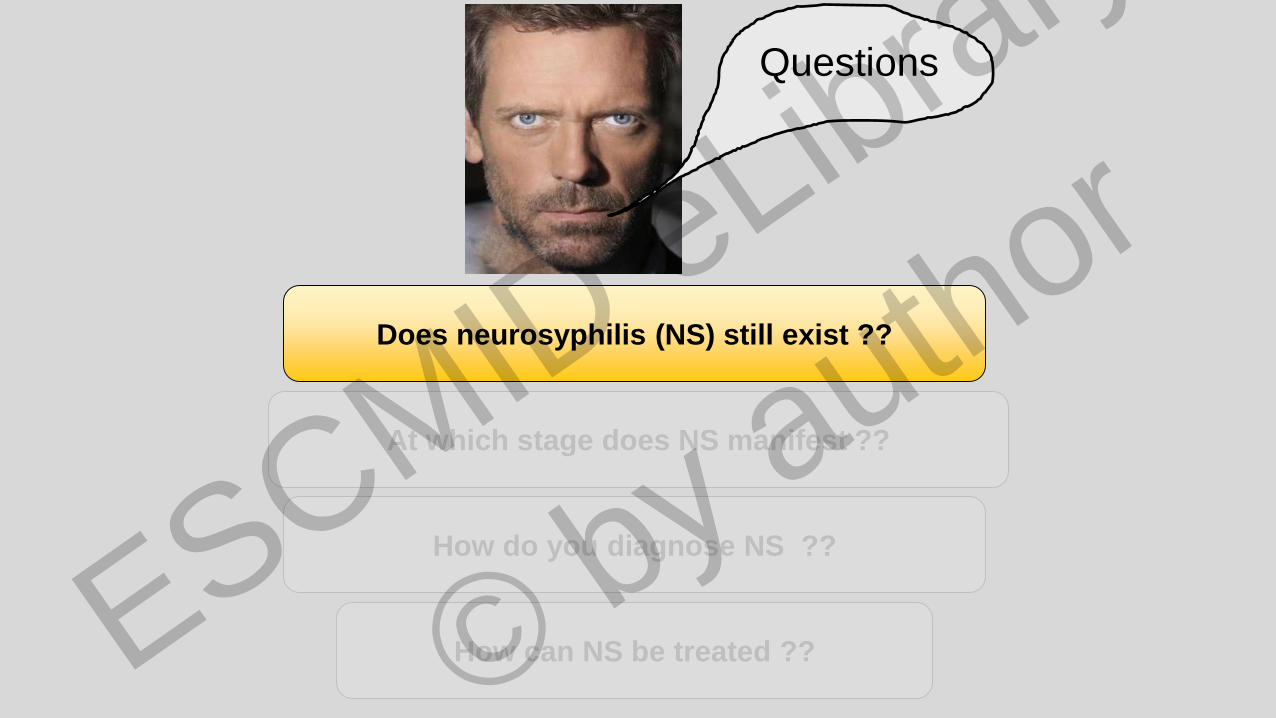
Trends of the incidence of syphilis (cases / 100.000 inhab.); no comparison
possible due to different case definitions and notification systems
Incidence rates of Syphilis in Europe / USA
Trend 1999-2014
ESCMID eLibrary
©
by author
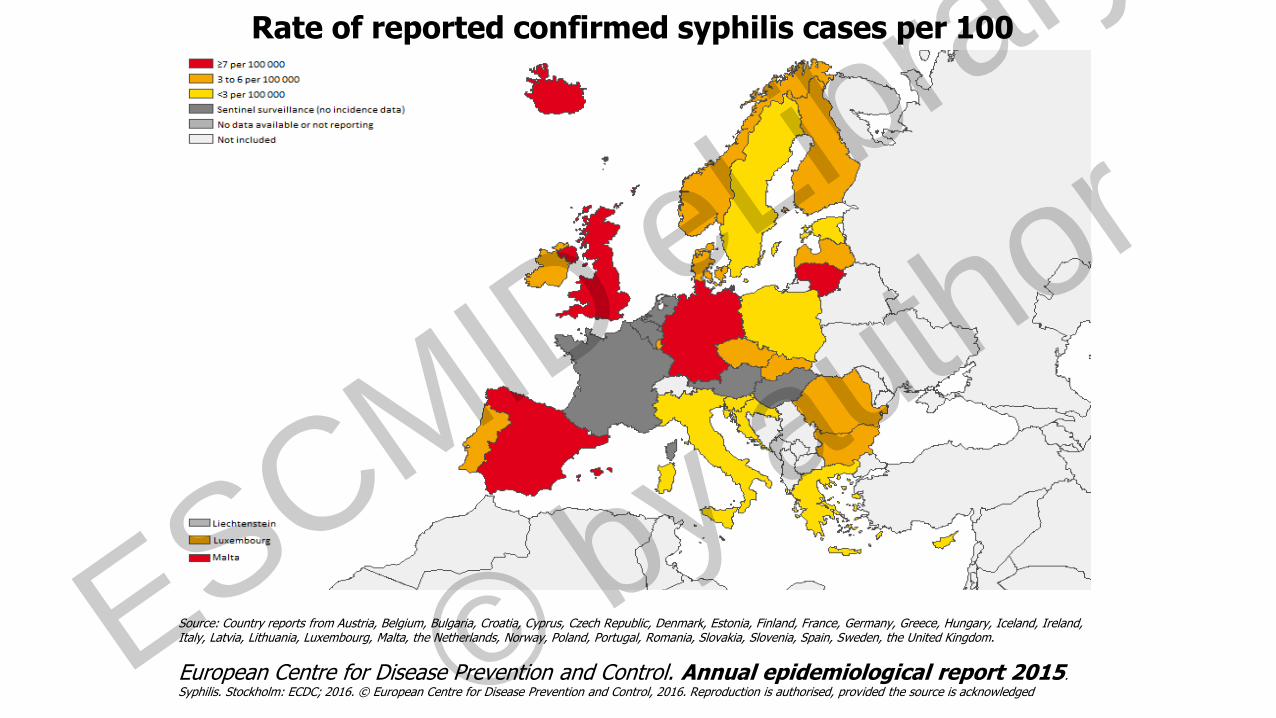
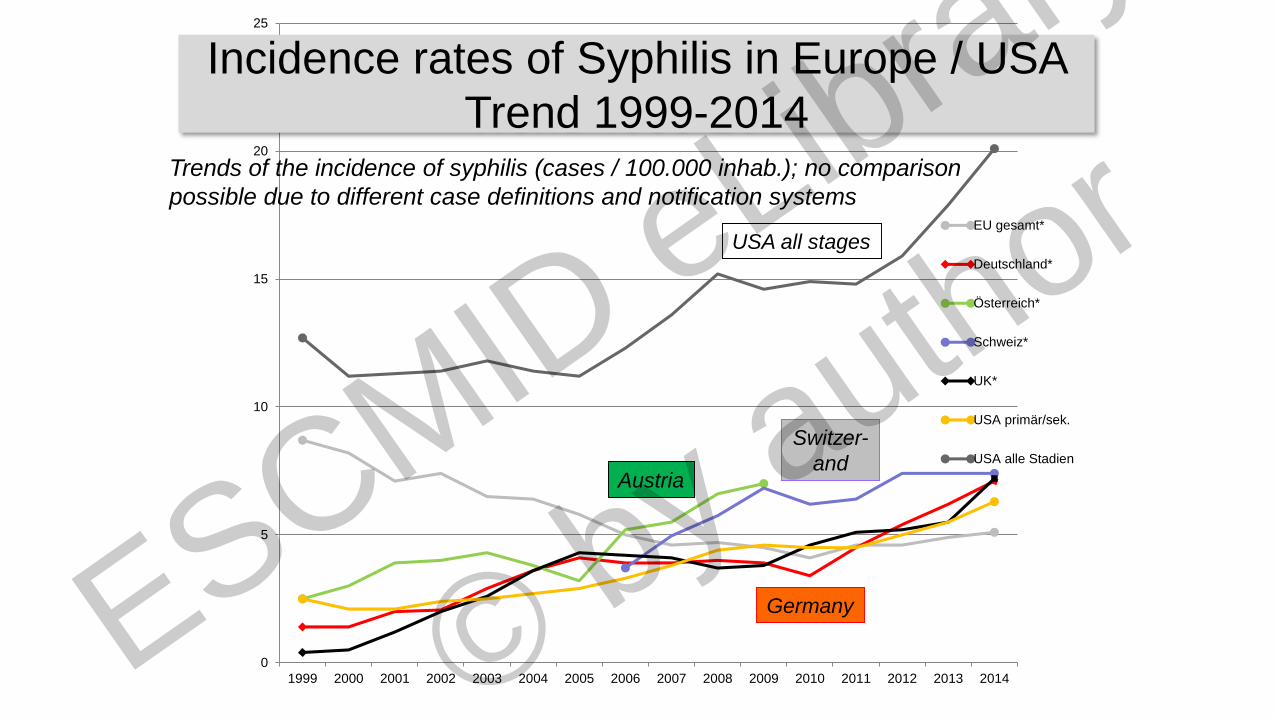
Rate of reported confirmed syphilis cases per 100 000 population, EU/EEA, 2014
Source: Country reports from Austria, Belgium, Bulgaria, Croatia, Cyprus, Czech Republic, Denmark, Estonia, Finland, France, Germany, Greece, Hungary, Iceland, Ireland, Italy, Latvia, Lithuania, Luxembourg, Malta, the Netherlands, Norway, Poland, Portugal, Romania, Slovakia, Slovenia, Spain, Sweden, the United Kingdom.
European Centre for Disease Prevention and Control. Annual epidemiological report 2015.
Syphilis. Stockholm: ECDC; 2016. © European Centre for Disease Prevention and Control, 2016. Reproduction is authorised, provided the source is acknowledged ESCMID eLibrary
©
by author

• In the past decades, the incidence has
been on the rise, largely because of an
increasing pool of patients infected with
syphilis and HIV at increased risk for
neurosyphilis
• Neurosyphilis is more commonly noted in
patients infected with HIV, with a
prevalence of 23.5% in HIV-positive
patients with untreated late-latent syphilisChen XS, Lancet 2013
Neurosyphilis
ESCMID eLibrary
©
by author

Does neurosyphilis (NS) still exist ??
At which stage does NS manifest ??
How do you diagnose NS ??
How can NS be treated ??
Questions
ESCMID eLibrary
©
by author

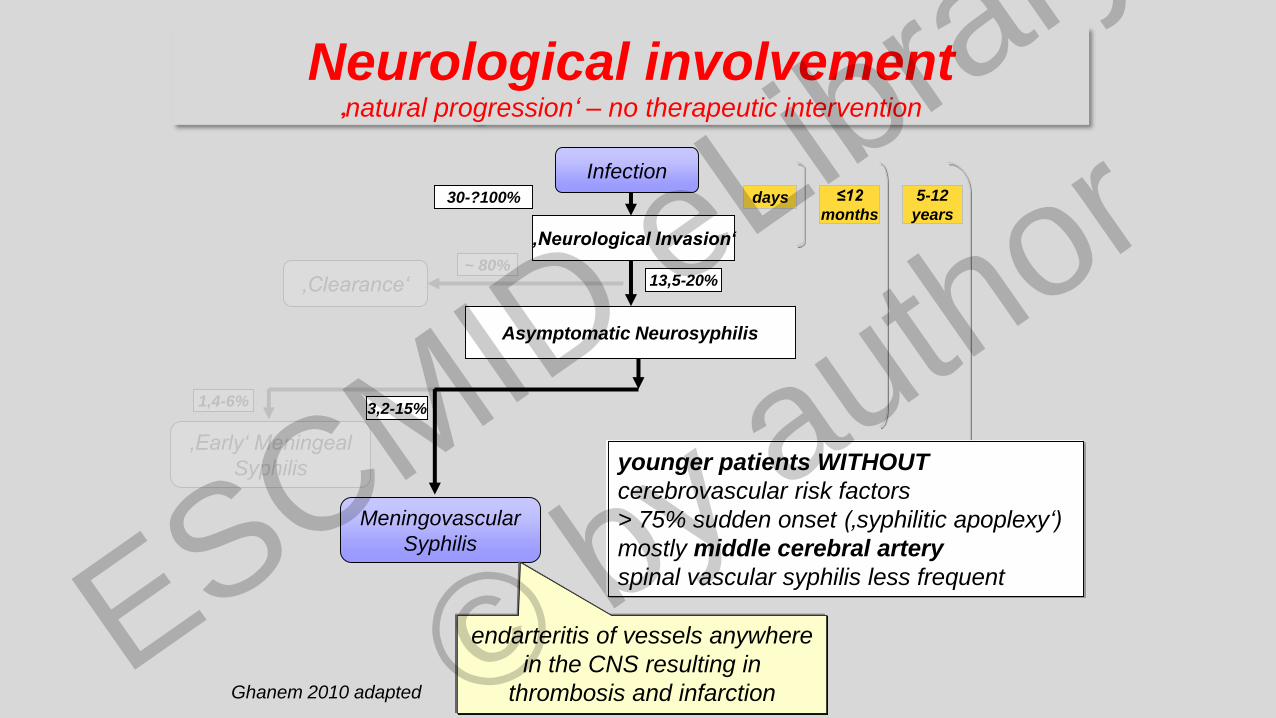
Infection
‚Neurological Invasion‘
‚Clearance‘
3,2-15% 5%
~ 80%
30-?100%
Ghanem 2010 adapted
Failure of the immune system to
clear the organism results in
neurological complications
days
Neurological involvement‚natural progression‘ – no therapeutic intervention
ESCMID eLibrary
©
by author

Infection
‚Neurological Invasion‘
Asymptomatic Neurosyphilis
‚Clearance‘ 13,5-20%~ 80%
30-?100% days ≤12
months
Ghanem 2010 adapted
The peak incidence of ANS
occurs 12-18 months after
infection and declines thereafter
Neurological involvement‚natural progression‘ – no therapeutic intervention
ESCMID eLibrary
©
by author
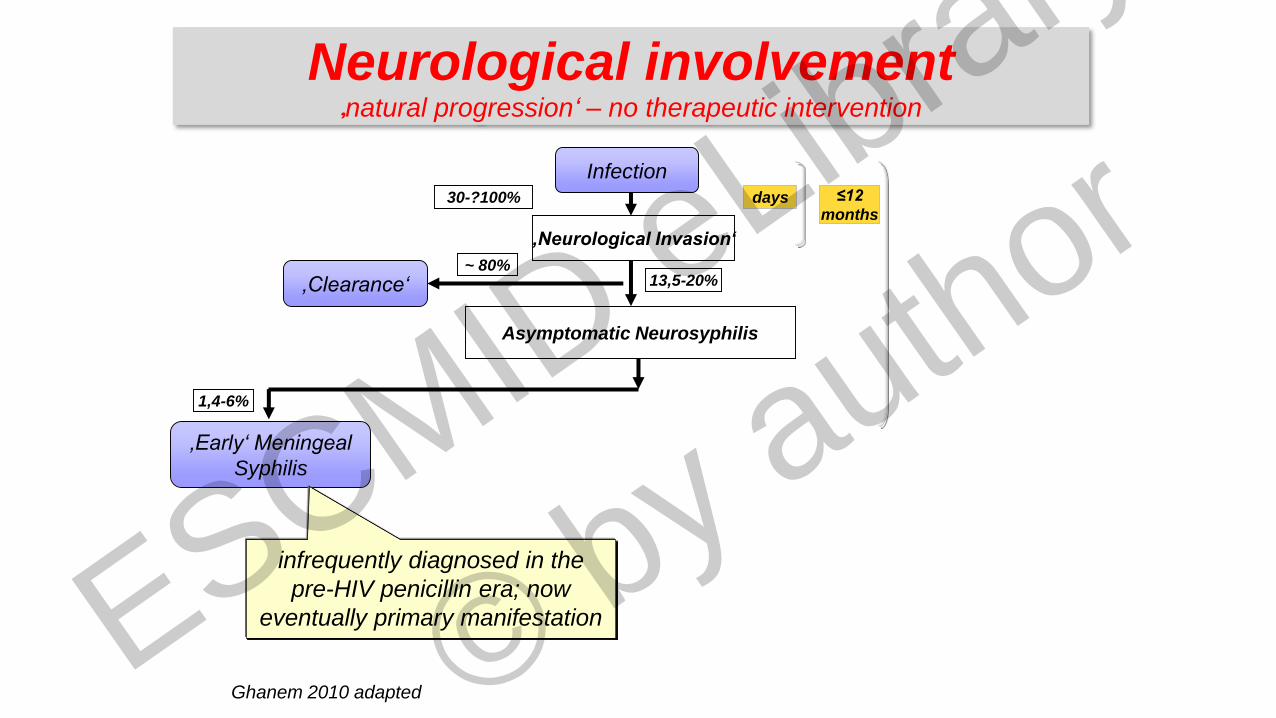
Infection
‚Early‘ Meningeal
Syphilis
‚Neurological Invasion‘
Asymptomatic Neurosyphilis
‚Clearance‘
1,4-6%
13,5-20%~ 80%
30-?100% days ≤12
months
Ghanem 2010 adapted
infrequently diagnosed in the
pre-HIV penicillin era; now
eventually primary manifestation
Neurological involvement‚natural progression‘ – no therapeutic intervention
ESCMID eLibrary
©
by author

• 29- year old male patient
• had recently acquired Human Immunodeficiency virus (HIV) infection
• for 6 months patchy hair loss and a history of a single self healing skin lesion in the anogenital area
• For 1 week acute loss of vision on left eye
• Diagnosis: Ischemic papillitis → high dose systemic corticosteroids ESCMID eLibrary
©
by author
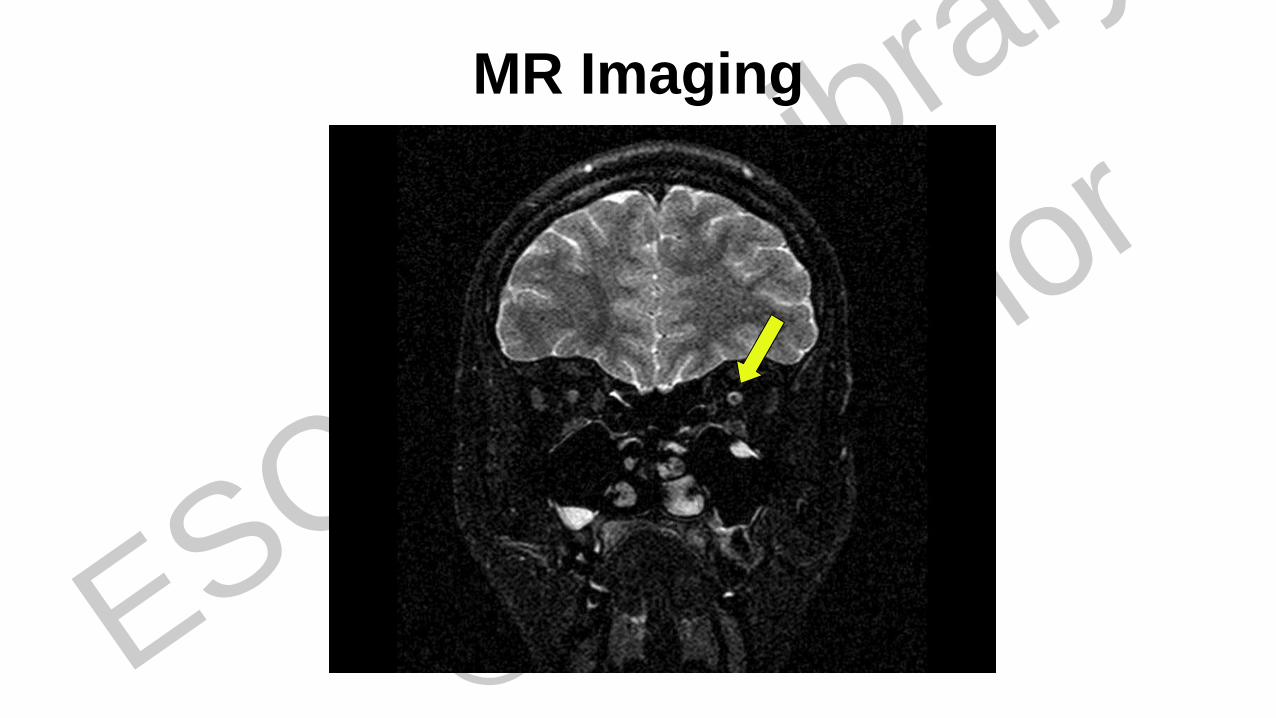
MR Imaging
ESCMID eLibrary
©
by author
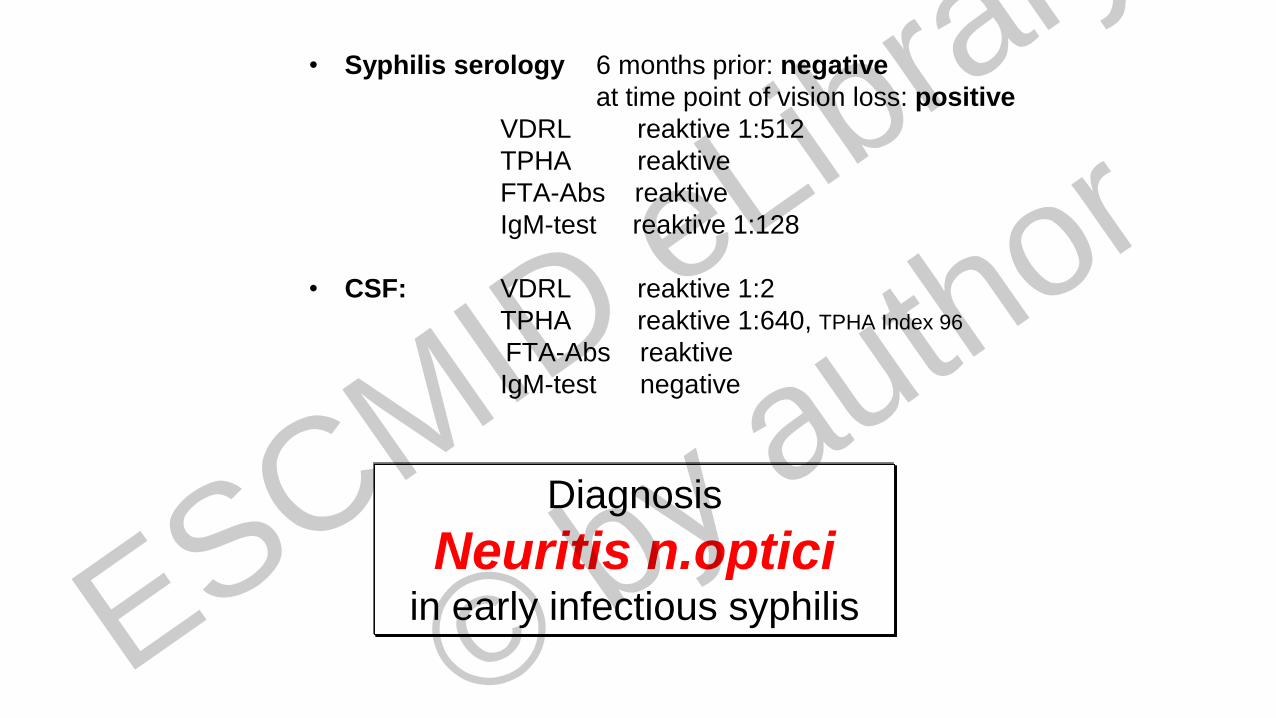
• Syphilis serology 6 months prior: negative
at time point of vision loss: positive
VDRL reaktive 1:512
TPHA reaktive
FTA-Abs reaktive
IgM-test reaktive 1:128
• CSF: VDRL reaktive 1:2
TPHA reaktive 1:640, TPHA Index 96
FTA-Abs reaktive
IgM-test negative
Diagnosis
Neuritis n.opticiin early infectious syphilis ESCMID eLibrary
©
by author
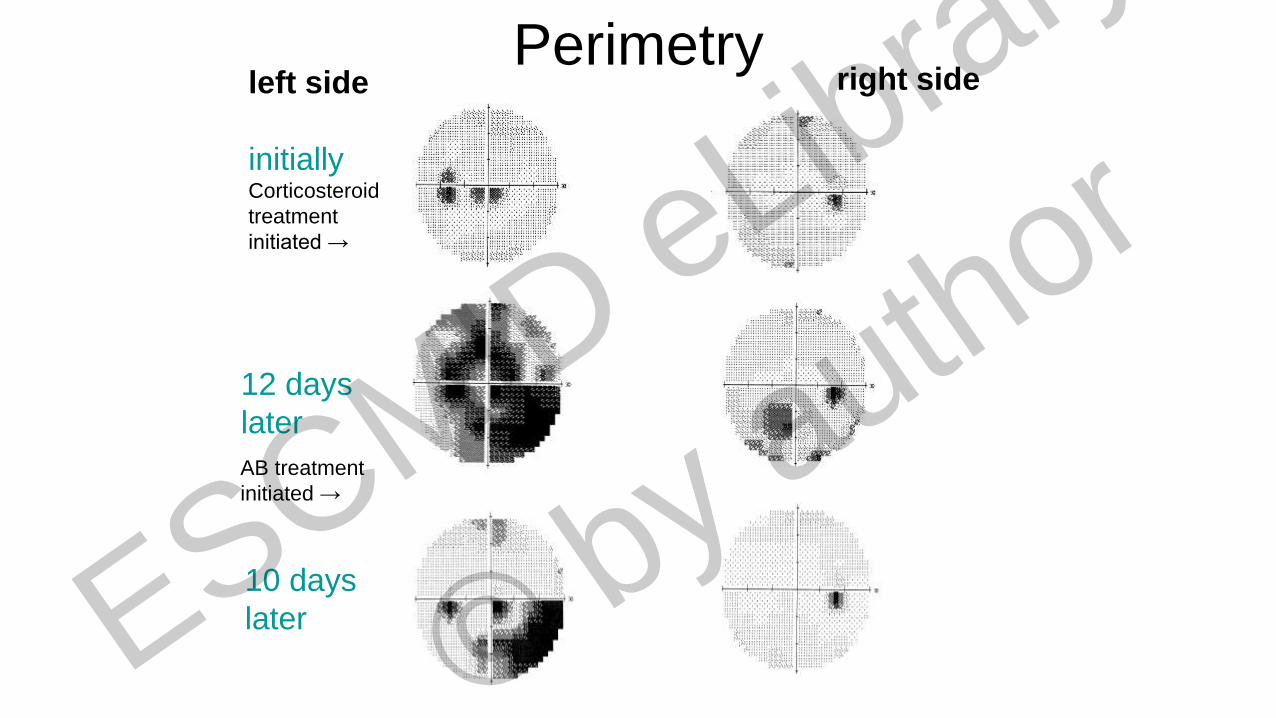
Perimetryleft side
initiallyCorticosteroid
treatment
initiated →
right side
12 days
later
10 days
later
AB treatment
initiated →
ESCMID eLibrary
©
by author
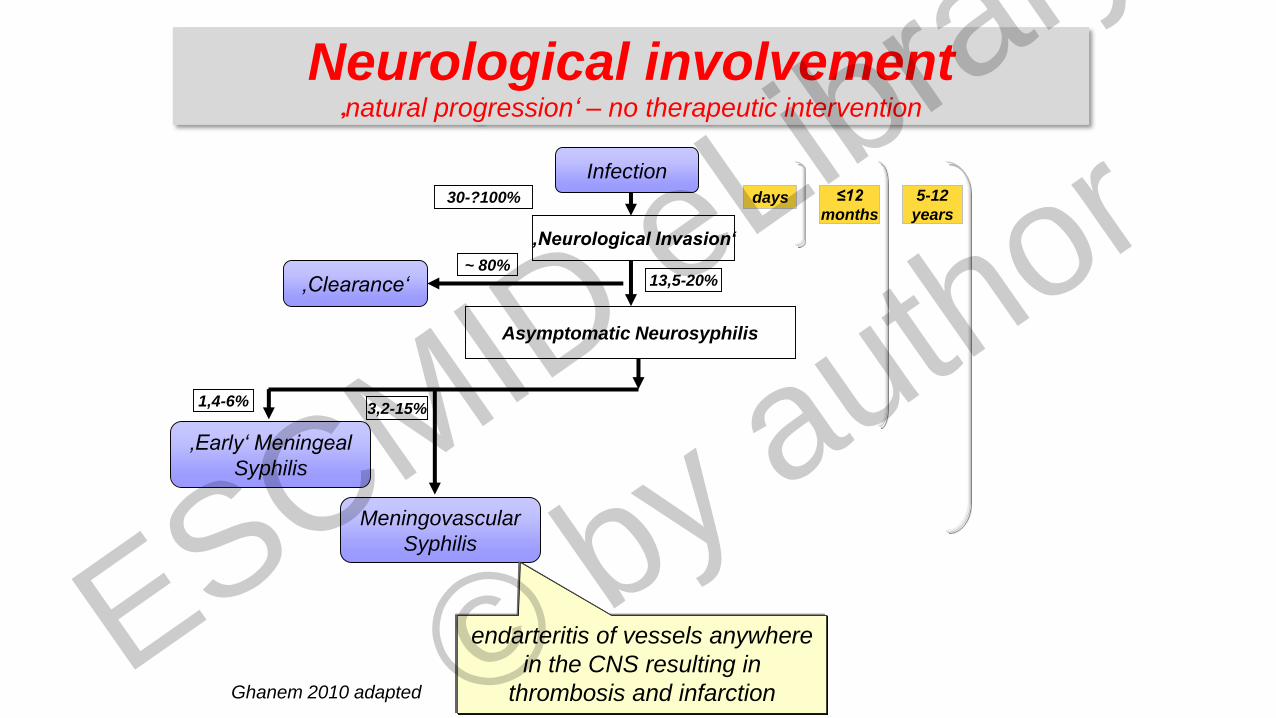
Infection
‚Early‘ Meningeal
Syphilis
‚Neurological Invasion‘
Asymptomatic Neurosyphilis
‚Clearance‘
Meningovascular
Syphilis
1,4-6% 3,2-15%
13,5-20%~ 80%
30-?100% days ≤12
months
5-12
years
Ghanem 2010 adapted
endarteritis of vessels anywhere
in the CNS resulting in
thrombosis and infarction
Neurological involvement‚natural progression‘ – no therapeutic intervention
ESCMID eLibrary
©
by author
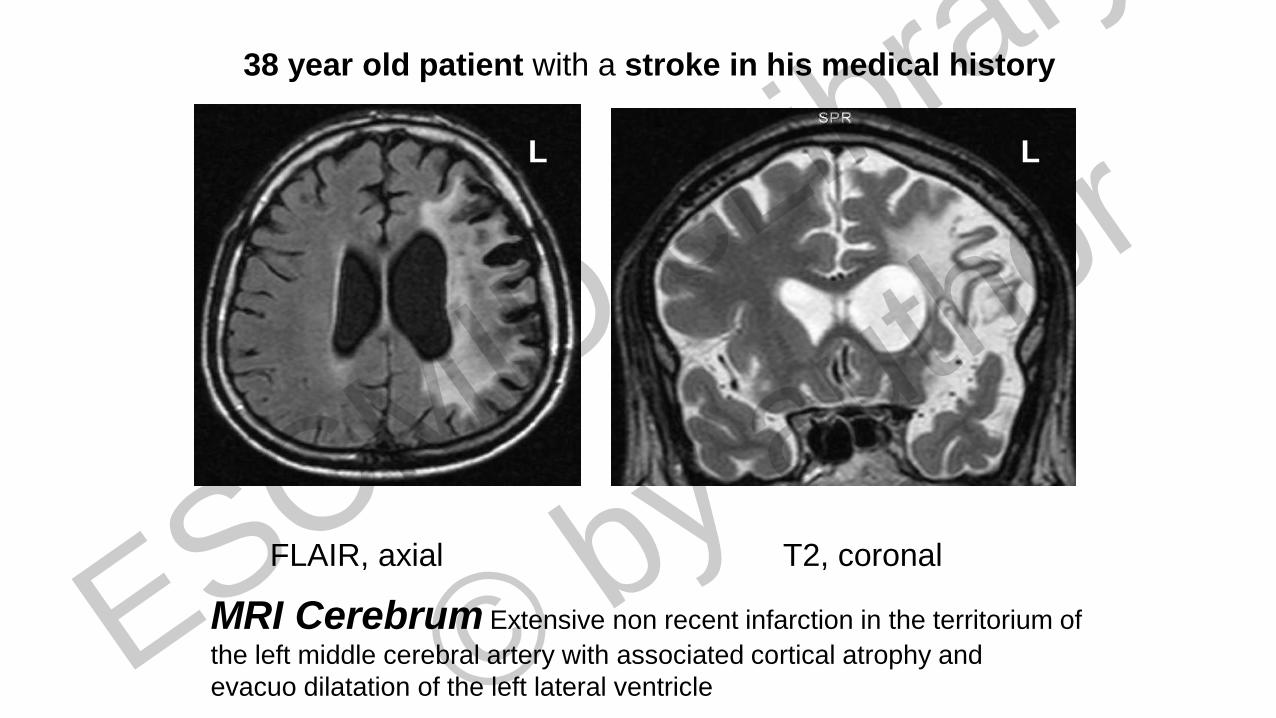
FLAIR, axial T2, coronal
L L
MRI Cerebrum Extensive non recent infarction in the territorium of
the left middle cerebral artery with associated cortical atrophy and
evacuo dilatation of the left lateral ventricle
38 year old patient with a stroke in his medical history
ESCMID eLibrary
©
by author
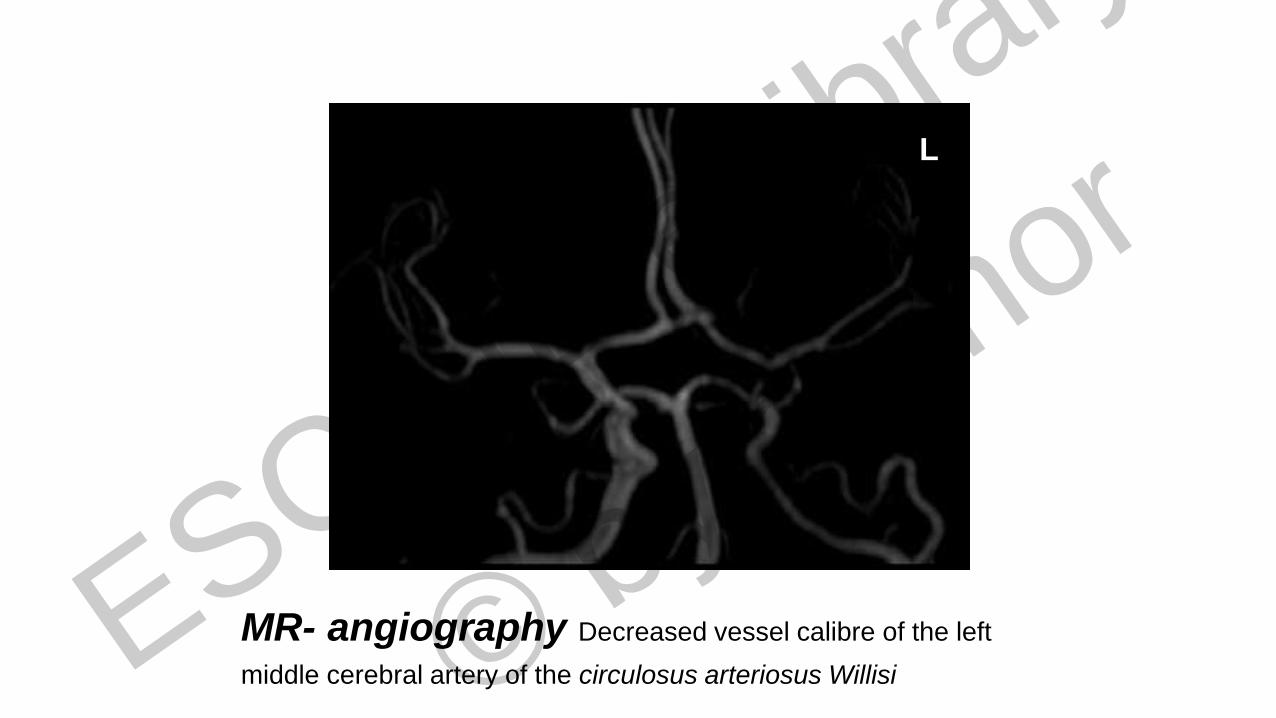
L
MR- angiography Decreased vessel calibre of the left
middle cerebral artery of the circulosus arteriosus Willisi ESCMID eLibrary
©
by author
Infection
‚Early‘ Meningeal
Syphilis
‚Neurological Invasion‘
Asymptomatic Neurosyphilis
‚Clearance‘
Meningovascular
Syphilis
1,4-6% 3,2-15%
13,5-20%~ 80%
30-?100% days ≤12
months
5-12
years
Ghanem 2010 adapted
endarteritis of vessels anywhere
in the CNS resulting in
thrombosis and infarction
younger patients WITHOUT
cerebrovascular risk factors
> 75% sudden onset (‚syphilitic apoplexy‘)
mostly middle cerebral artery
spinal vascular syphilis less frequent
Neurological involvement‚natural progression‘ – no therapeutic intervention
ESCMID eLibrary
©
by author

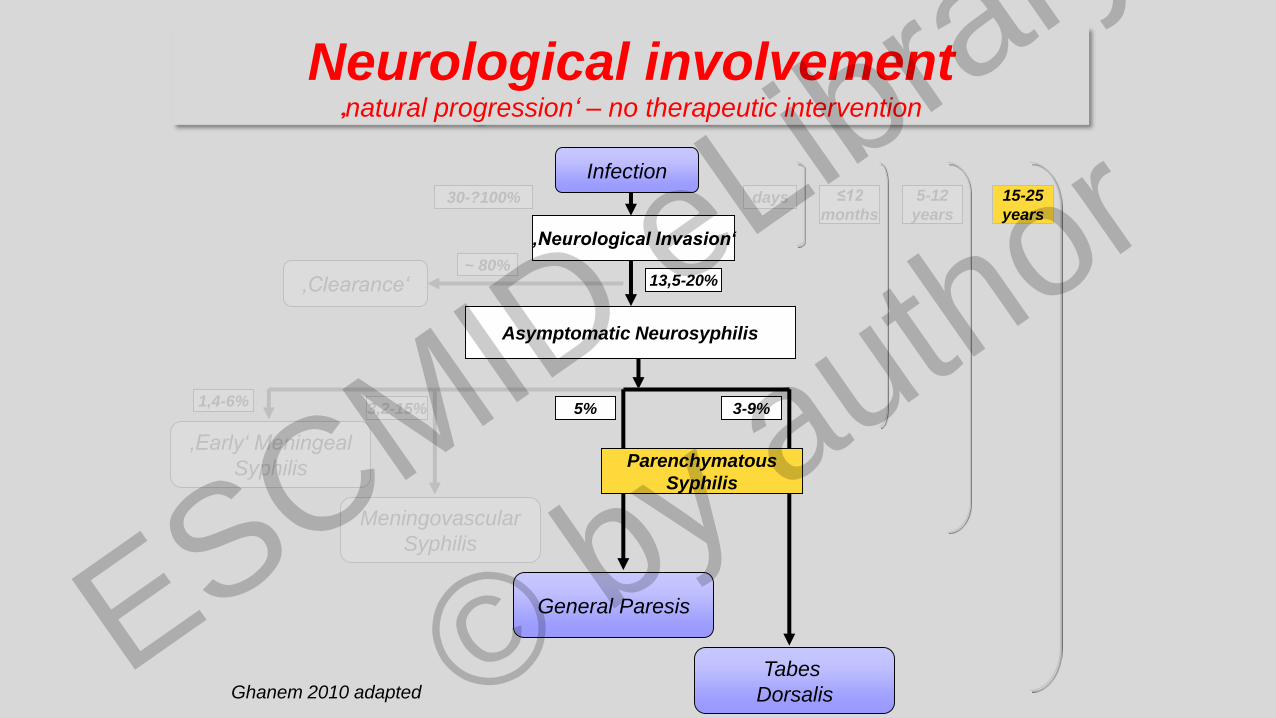
Infection
‚Early‘ Meningeal
Syphilis
‚Neurological Invasion‘
Asymptomatic Neurosyphilis
‚Clearance‘
Meningovascular
Syphilis
General Paresis
Tabes
Dorsalis
1,4-6% 3,2-15% 5% 3-9%
13,5-20%~ 80%
30-?100% days ≤12
months
5-12
years
15-25
years
Ghanem 2010 adapted
Parenchymatous
Syphilis
Neurological involvement‚natural progression‘ – no therapeutic intervention
ESCMID eLibrary
©
by author
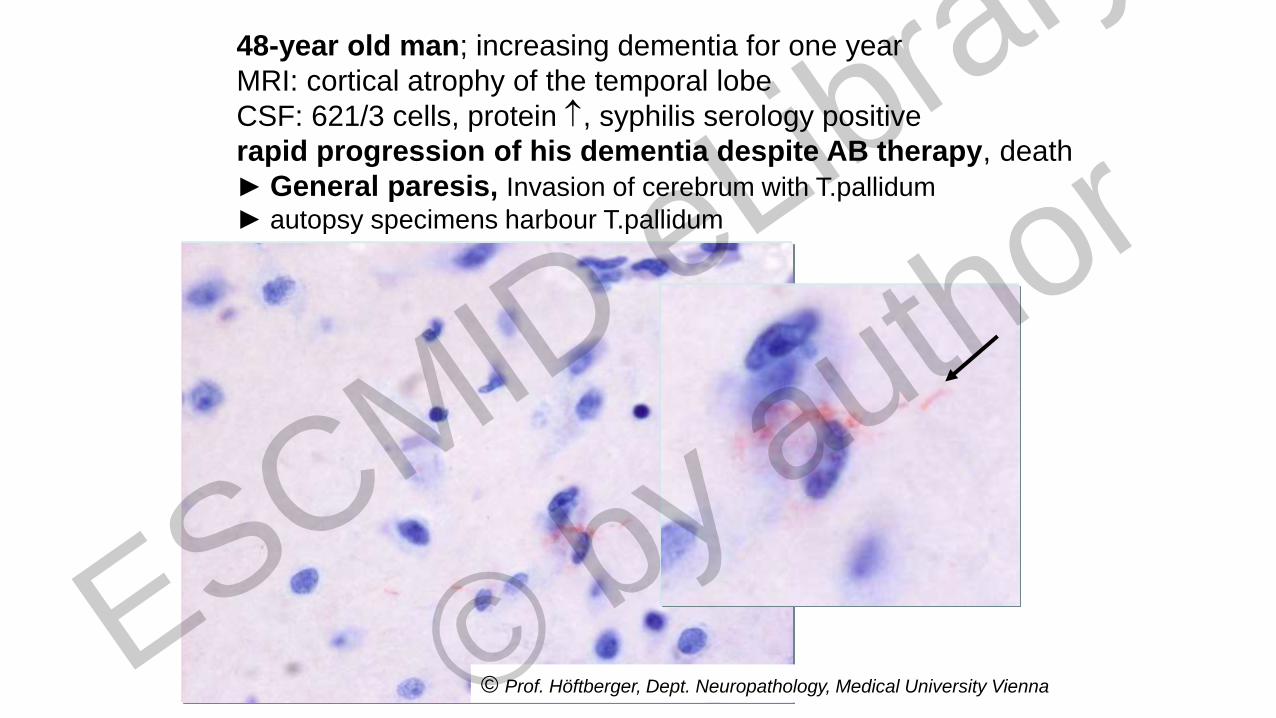
48-year old man; increasing dementia for one year
MRI: cortical atrophy of the temporal lobe
CSF: 621/3 cells, protein , syphilis serology positive
rapid progression of his dementia despite AB therapy, death
► General paresis, Invasion of cerebrum with T.pallidum
► autopsy specimens harbour T.pallidum
© Prof. Höftberger, Dept. Neuropathology, Medical University Vienna ESCMID eLibrary
©
by author
Infection
‚Early‘ Meningeal
Syphilis
‚Neurological Invasion‘
Asymptomatic Neurosyphilis
‚Clearance‘
Meningovascular
Syphilis
General Paresis
Tabes
Dorsalis
1,4-6% 3,2-15% 5% 3-9%
13,5-20%~ 80%
30-?100% days ≤12
months
5-12
years
15-25
years
Ghanem 2010 adapted
Parenchymatous
Syphilis
Neurological involvement‚natural progression‘ – no therapeutic intervention
ESCMID eLibrary
©
by author

Argyll-Robertson-pupils
42-year old patient (HIV-negative)
syphilis Serologie (serum)
VDRL 1:8
TPHA pos
FTA-Abs pos
IgM-test pos 1:16 ESCMID eLibrary
©
by author
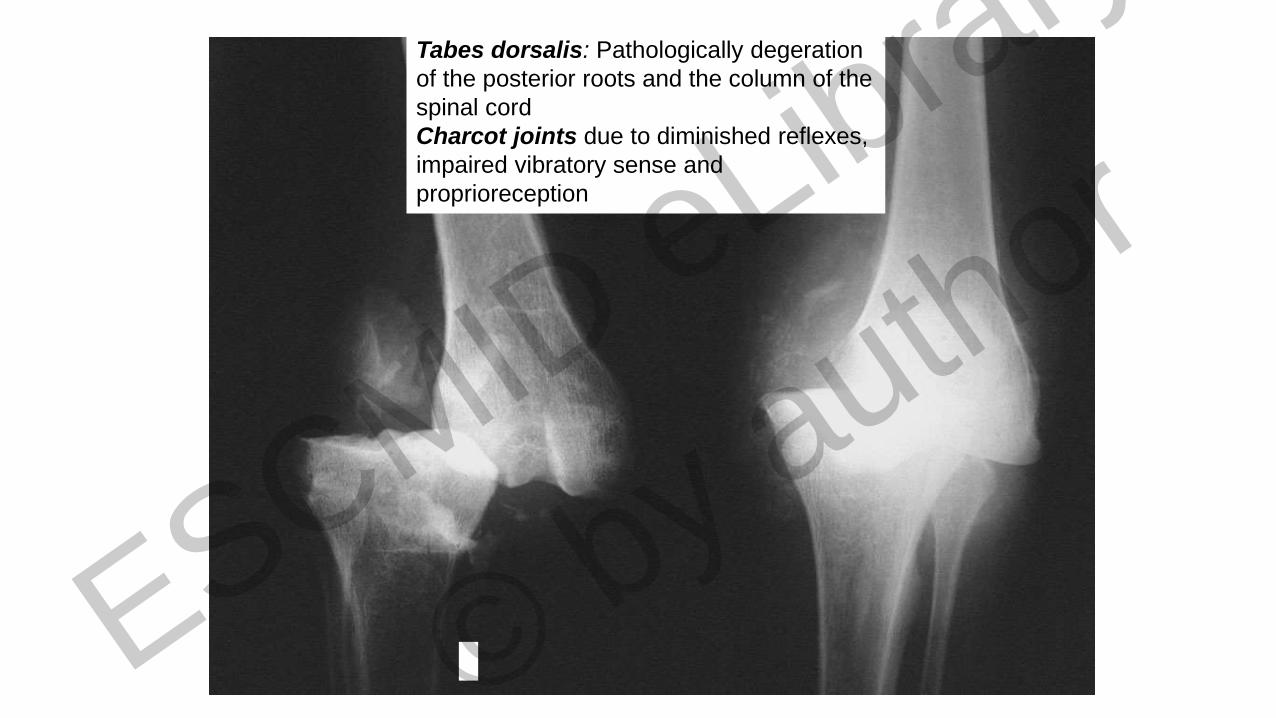
Tabes dorsalis: Pathologically degeration
of the posterior roots and the column of the
spinal cord
Charcot joints due to diminished reflexes,
impaired vibratory sense and
proprioreception
ESCMID eLibrary
©
by author

Infection
‚Early‘ Meningeal
Syphilis
‚Neurological Invasion‘
Asymptomatic Neurosyphilis
‚Clearance‘
Meningovascular
Syphilis
General Paresis
1,4-6% 3,2-15% 5%
13,5-20%~ 80%
30-?100% days ≤12
months
5-12
years
15-25
years
Ghanem 2010 adapted
Tabes
Dorsalis
Parenchymatous
Syphilis
3-9%
Neurological symptoms can occur at any stage of infection
therefore
ONLY LATE MANIFESTATIONS OF NEUROSYPHILIS SHOULD
BE ADDRESSED AS ‚TERTIARY SYPHILIS‘
Neurological involvement‚natural progression‘ – no therapeutic intervention
ESCMID eLibrary
©
by author
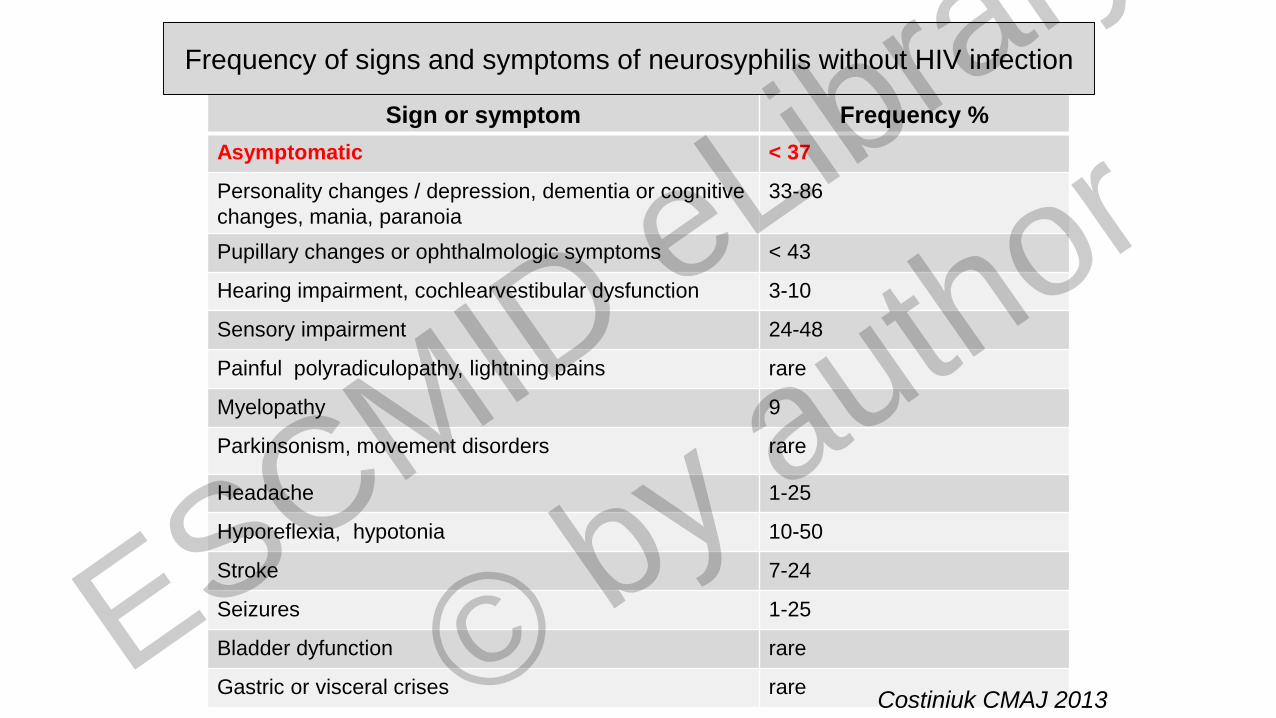
Sign or symptom Frequency %
Asymptomatic < 37
Personality changes / depression, dementia or cognitive
changes, mania, paranoia
33-86
Pupillary changes or ophthalmologic symptoms < 43
Hearing impairment, cochlearvestibular dysfunction 3-10
Sensory impairment 24-48
Painful polyradiculopathy, lightning pains rare
Myelopathy 9
Parkinsonism, movement disorders rare
Headache 1-25
Hyporeflexia, hypotonia 10-50
Stroke 7-24
Seizures 1-25
Bladder dyfunction rare
Gastric or visceral crises rare
Frequency of signs and symptoms of neurosyphilis without HIV infection
Costiniuk CMAJ 2013 ESCMID eLibrary
©
by author
Does neurosyphilis (NS) still exist ??
At which stage does NS manifest ??
How do you diagnose NS ??
How can NS be treated ??
Questions
ESCMID eLibrary
©
by author
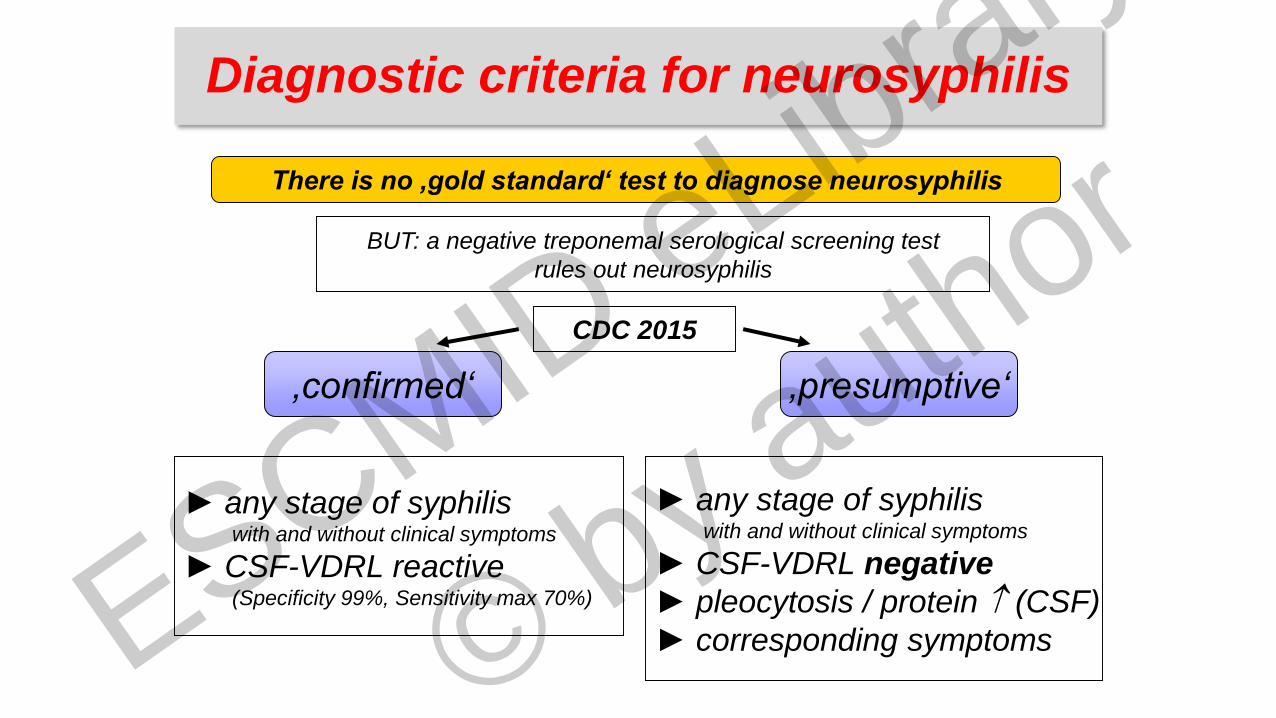
There is no ‚gold standard‘ test to diagnose neurosyphilis
CDC 2015
BUT: a negative treponemal serological screening test
rules out neurosyphilis
‚confirmed‘ ‚presumptive‘
► any stage of syphilis with and without clinical symptoms
► CSF-VDRL reactive(Specificity 99%, Sensitivity max 70%)
► any stage of syphilis with and without clinical symptoms
► CSF-VDRL negative
► pleocytosis / protein (CSF)
► corresponding symptoms
Diagnostic criteria for neurosyphilis
ESCMID eLibrary
©
by author
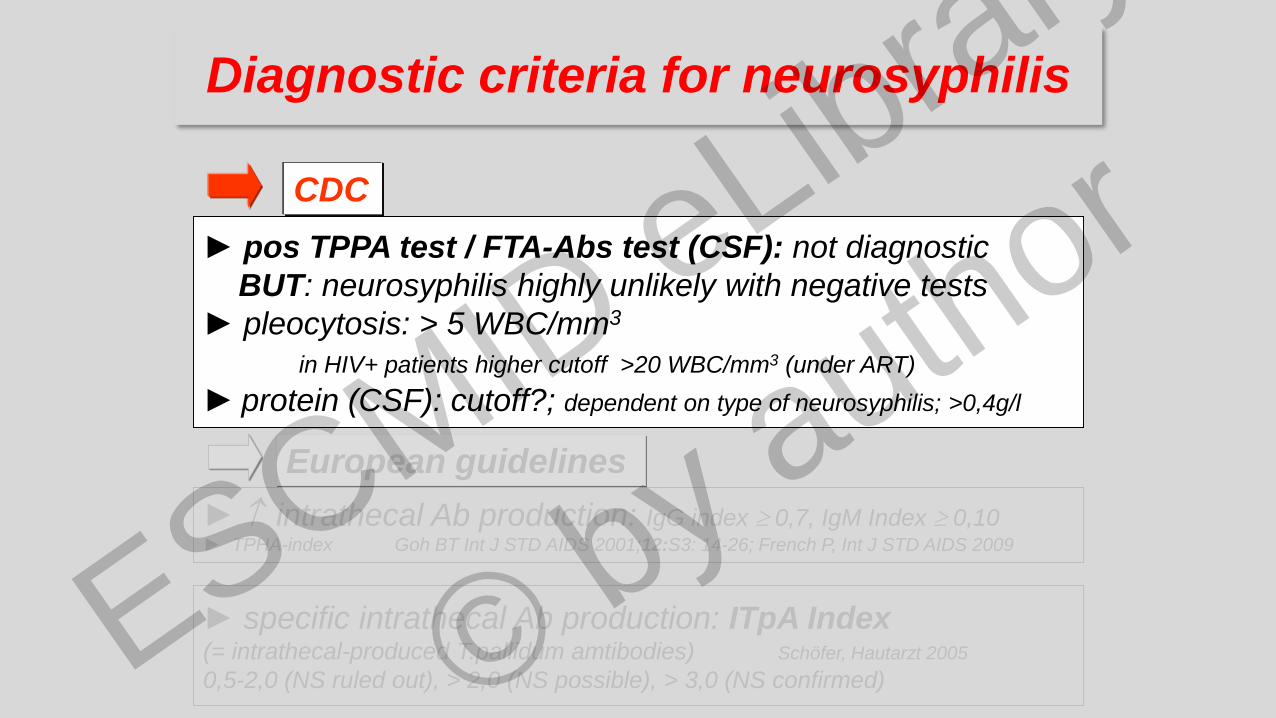
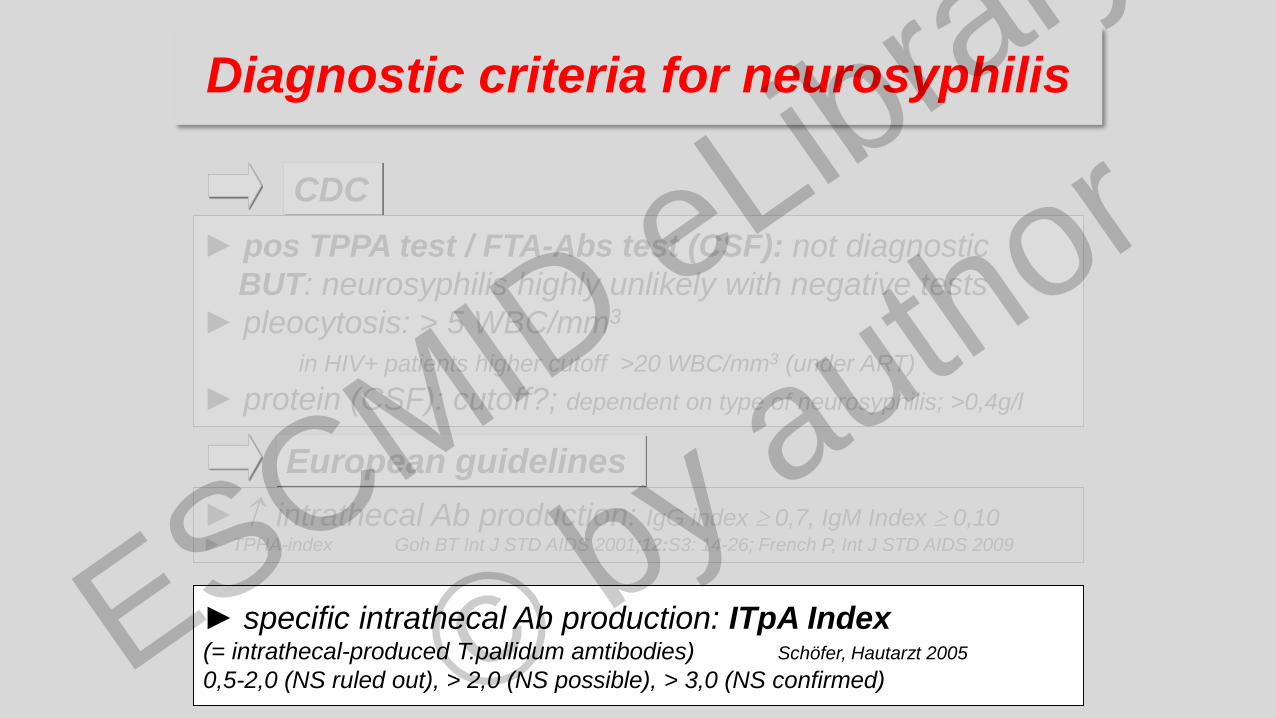
► pos TPPA test / FTA-Abs test (CSF): not diagnostic
BUT: neurosyphilis highly unlikely with negative tests
► pleocytosis: > 5 WBC/mm3
in HIV+ patients higher cutoff >20 WBC/mm3 (under ART)
► protein (CSF): cutoff?; dependent on type of neurosyphilis; >0,4g/l
CDC
European guidelines
Diagnostic criteria for neurosyphilis
► intrathecal Ab production: IgG index 0,7, IgM Index 0,10 ► TPHA-index Goh BT Int J STD AIDS 2001;12:S3: 14-26; French P, Int J STD AIDS 2009
► specific intrathecal Ab production: ITpA Index(= intrathecal-produced T.pallidum amtibodies) Schöfer, Hautarzt 2005
0,5-2,0 (NS ruled out), > 2,0 (NS possible), > 3,0 (NS confirmed) ESCMID eLibrary
©
by author

► pos TPPA test / FTA-Abs test (CSF): not diagnostic
BUT: neurosyphilis highly unlikely with negative tests
► pleocytosis: > 5 WBC/mm3
in HIV+ patients higher cutoff >20 WBC/mm3 (under ART)
► protein (CSF): cutoff?; dependent on type of neurosyphilis; >0,4g/l
► intrathecal Ab production: IgG index 0,7, IgM Index 0,10 ► TPHA-index Goh BT Int J STD AIDS 2001;12:S3: 14-26; French P, Int J STD AIDS 2009
CDC
European guidelines
► spezifische intrathekale Ak Produktion: ITpA Index(= intrathekal-produzierte T.pallidum Antikörper)
0,5-2,0 (keine NS), > 2,0 (NS wahrscheinlich), > 3,0 (beweisend)
Diagnostic criteria for neurosyphilis
ESCMID eLibrary
©
by author
CDC
European guidelines
► specific intrathecal Ab production: ITpA Index(= intrathecal-produced T.pallidum amtibodies) Schöfer, Hautarzt 2005
0,5-2,0 (NS ruled out), > 2,0 (NS possible), > 3,0 (NS confirmed)
Diagnostic criteria for neurosyphilis
► pos TPPA test / FTA-Abs test (CSF): not diagnostic
BUT: neurosyphilis highly unlikely with negative tests
► pleocytosis: > 5 WBC/mm3
in HIV+ patients higher cutoff >20 WBC/mm3 (under ART)
► protein (CSF): cutoff?; dependent on type of neurosyphilis; >0,4g/l
► intrathecal Ab production: IgG index 0,7, IgM Index 0,10 ► TPHA-index Goh BT Int J STD AIDS 2001;12:S3: 14-26; French P, Int J STD AIDS 2009
ESCMID eLibrary
©
by author
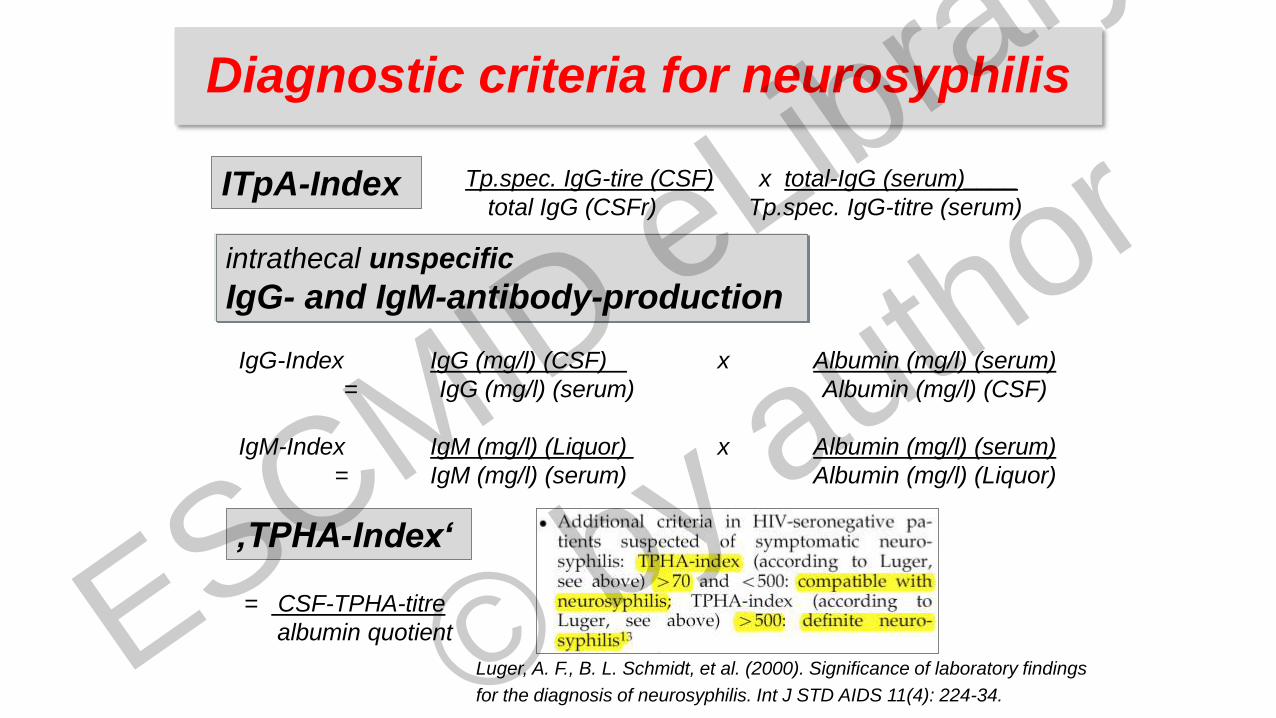
Tp.spec. IgG-tire (CSF) x total-IgG (serum)____
total IgG (CSFr) Tp.spec. IgG-titre (serum)
IgG-Index IgG (mg/l) (CSF) x Albumin (mg/l) (serum)
= IgG (mg/l) (serum) Albumin (mg/l) (CSF)
IgM-Index IgM (mg/l) (Liquor) x Albumin (mg/l) (serum)
= IgM (mg/l) (serum) Albumin (mg/l) (Liquor)
intrathecal unspecific
IgG- and IgM-antibody-production
Luger, A. F., B. L. Schmidt, et al. (2000). Significance of laboratory findings
for the diagnosis of neurosyphilis. Int J STD AIDS 11(4): 224-34.
‚TPHA-Index‘
ITpA-Index
= CSF-TPHA-titre
albumin quotient
Diagnostic criteria for neurosyphilis
ESCMID eLibrary
©
by author

• In patients who have syphilis and symptoms or signs
suggesting neurologic / psychiatric, or ophthalmic or
tertiary disease
• In patients who have treatment failure
• NOT in patients who have primary or secondary
syphilis as invasion of CSF by T. pallidum accompanied by CSF
laboratory abnormalities is common in these stages, unless clinical
signs or symptoms of neurologic or ophthalmic
involvement
• In patients with syphilis of > 1 year duration?
• In HIV+ patients?
CSF examination is indicated I
ESCMID eLibrary
©
by author

265 patients with late latent
syphilis at the Medical University Vienna
+/- neurological symptoms
Neurosyphilis + - S
Sex
female [n] 5 (11.6%) 74 (33.3%) 79 (29.8%)
male [n] 38 (88.4%) 148 (66.7%) 186 (70.2%)
Mean age [y] ± SD 46.7 ± 14.8 48.5 ± 17.2 48.2 ± 16.8
HIV positive [n] 7 65 72
S 43 222 265(16%)
ESCMID eLibrary
©
by author
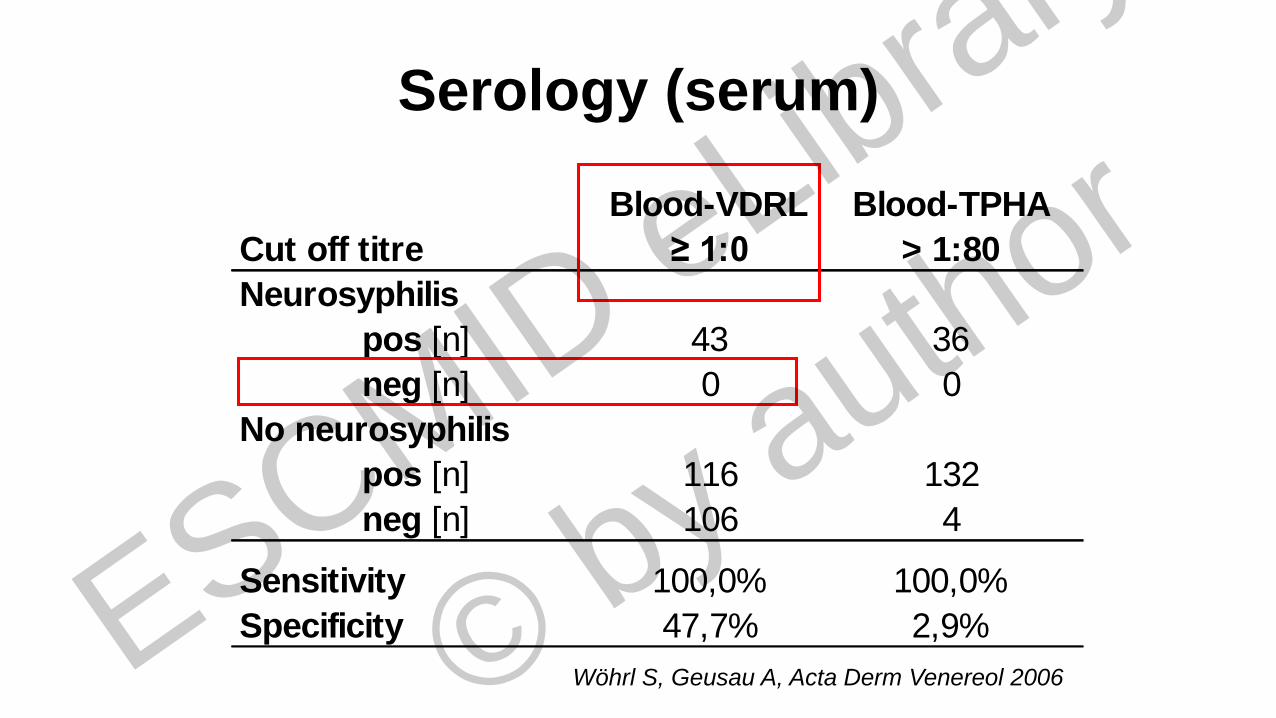
Serology (serum)
Cut off titre
Blood-VDRL
≥ 1:0
Blood-TPHA
> 1:80
Neurosyphilis
pos [n] 43 36
neg [n] 0 0
No neurosyphilis
pos [n] 116 132
neg [n] 106 4
Sensitivity 100,0% 100,0%
Specificity 47,7% 2,9%
Wöhrl S, Geusau A, Acta Derm Venereol 2006 ESCMID eLibrary
©
by author
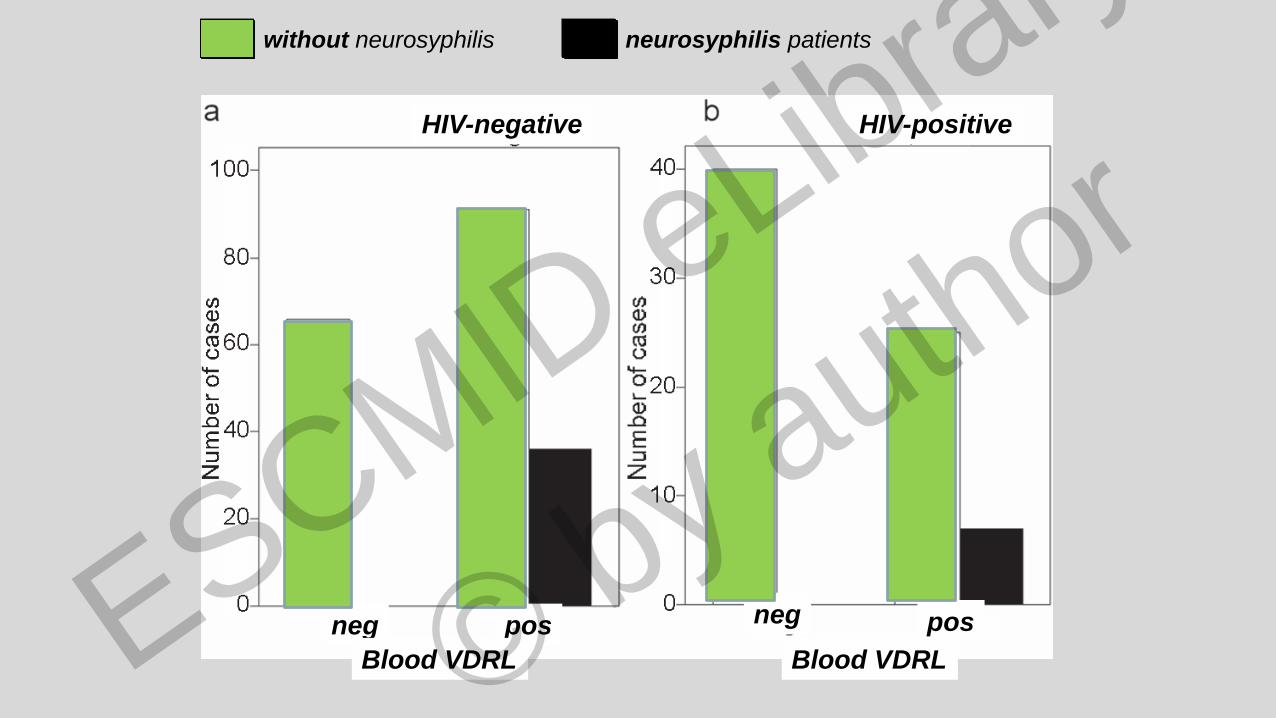
without neurosyphilis neurosyphilis patients
HIV-negative HIV-positive
negneg pos
Blood VDRL
pos
Blood VDRL ESCMID eLibrary
©
by author
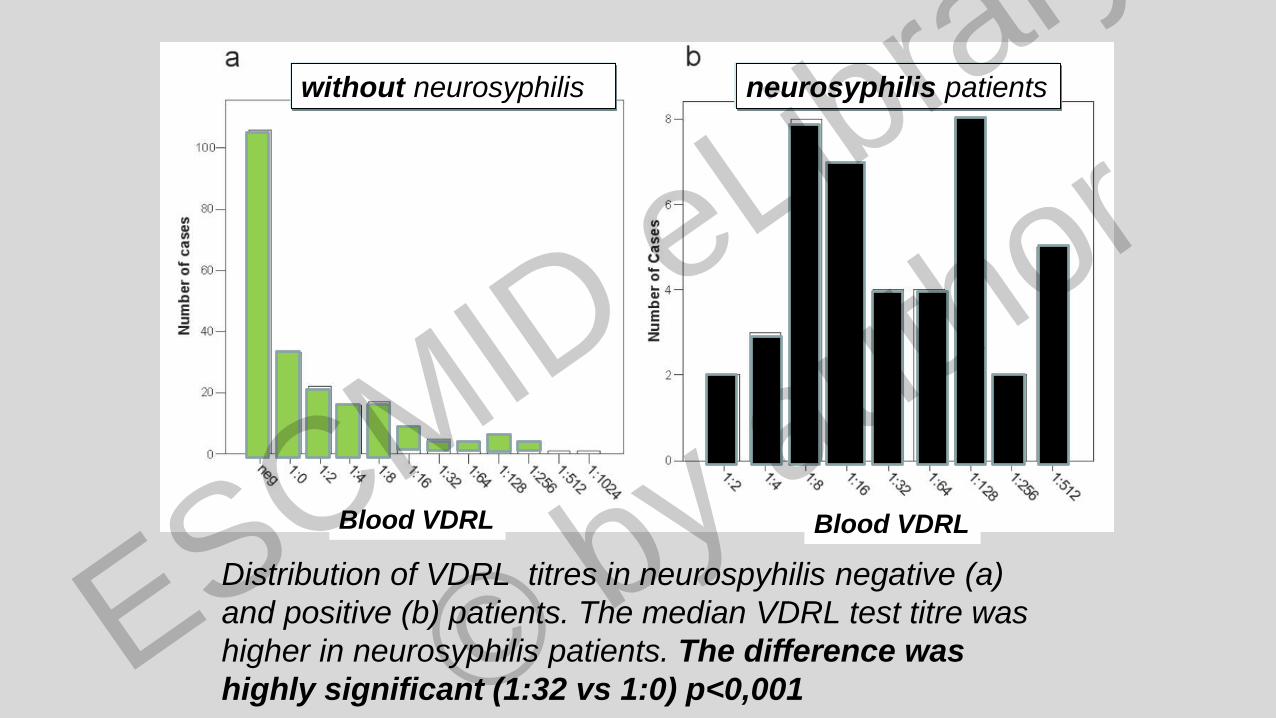
Distribution of VDRL titres in neurospyhilis negative (a)
and positive (b) patients. The median VDRL test titre was
higher in neurosyphilis patients. The difference was
highly significant (1:32 vs 1:0) p<0,001
Blood VDRL Blood VDRL
neurosyphilis patientswithout neurosyphilis
ESCMID eLibrary
©
by author
• In patients with syphilis of > 1 year
duration? RPR 1:32 in late latent syphilis
Marra et al; JID 2004
• In HIV+ patients?? (according to CDC 2015)
same criteria as in HIV-neg patients; exception:
CD4<350/ul; RPR32) Marra Clin Infect Dis 2004
CSF examination is indicated II
ESCMID eLibrary
©
by author
Risk factors for neurosyphilis: ≤350 CD4/ul cell count , RPR>128
- use of ART before syphilis infection reduces odds ratio of
neurosyphilis by 65% and the risk of serological ‚failure‘
- most of them (>60%) early manifestations within 9 months
- 66% symptomatic (33% Uveitis), 34% ANS
Ghanem AIDS 2008 (231 co-infected patients)
• Current guidelines for the treatment of syphilis among HIV-infected subjects
are based on limited objective data. The optimal antimicrobial regimen to treat
syphilis in HIV-infected subjects is unknown
Blank et al, Sex Transm Infect 2011
…..and in
HIV+ patients??
ESCMID eLibrary
©
by author
Does neurosyphilis (NS) still exist ??
At which stage does NS manifest ??
How do you diagnose NS ??
How can NS be treated ??
Questions
ESCMID eLibrary
©
by author
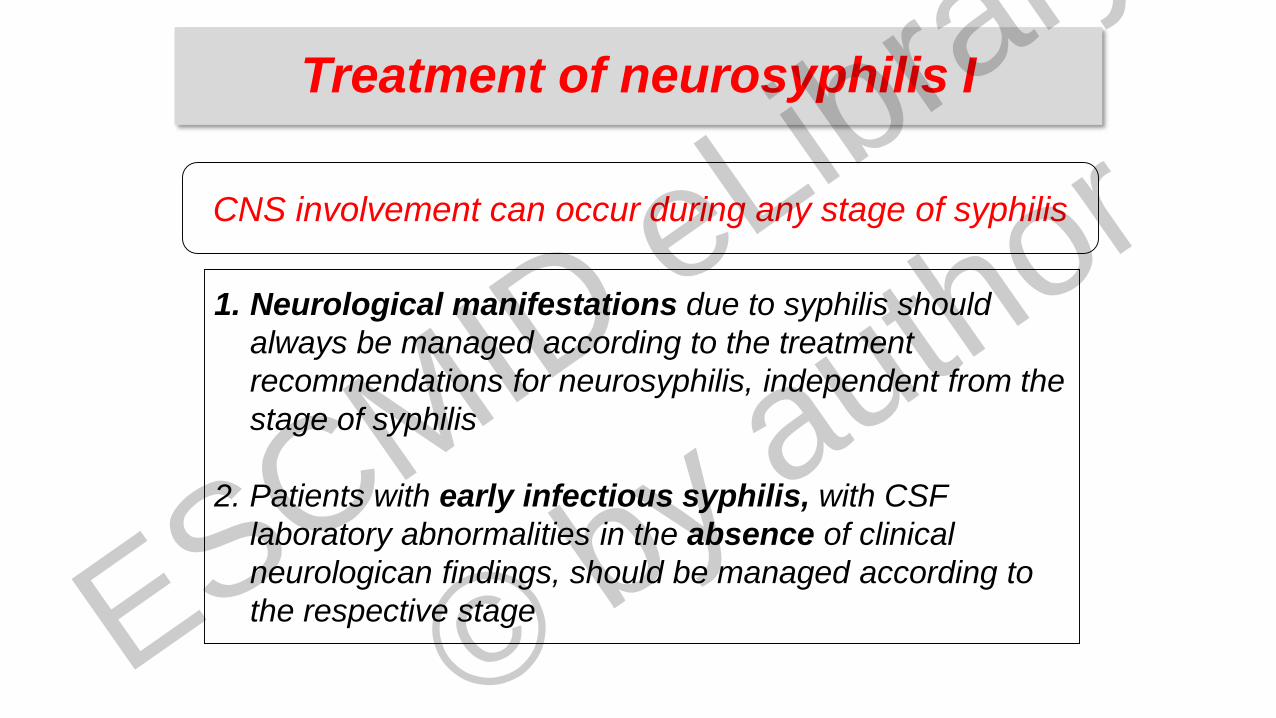
1. Neurological manifestations due to syphilis should
always be managed according to the treatment
recommendations for neurosyphilis, independent from the
stage of syphilis
2. Patients with early infectious syphilis, with CSF
laboratory abnormalities in the absence of clinical
neurologican findings, should be managed according to
the respective stage
CNS involvement can occur during any stage of syphilis
Treatment of neurosyphilis I
ESCMID eLibrary
©
by author
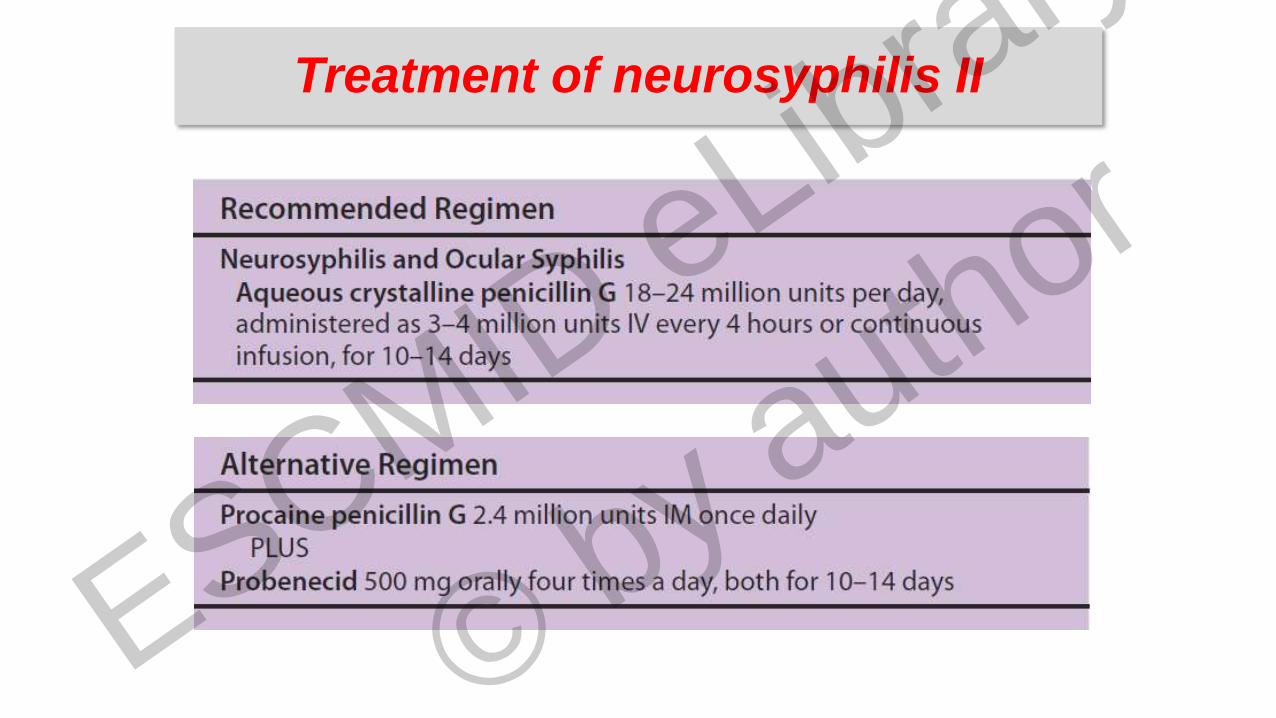
Treatment of neurosyphilis II
ESCMID eLibrary
©
by author
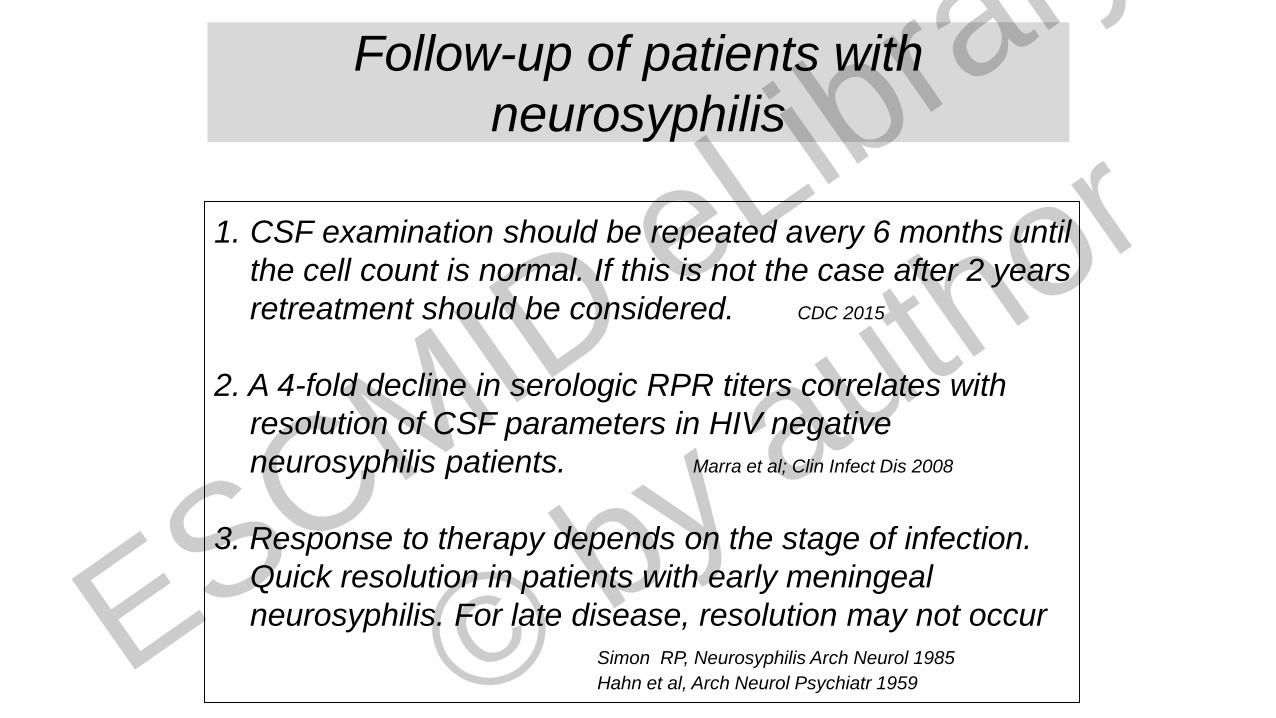
Follow-up of patients with
neurosyphilis
1. CSF examination should be repeated avery 6 months until
the cell count is normal. If this is not the case after 2 years
retreatment should be considered. CDC 2015
2. A 4-fold decline in serologic RPR titers correlates with
resolution of CSF parameters in HIV negative
neurosyphilis patients. Marra et al; Clin Infect Dis 2008
3. Response to therapy depends on the stage of infection.
Quick resolution in patients with early meningeal
neurosyphilis. For late disease, resolution may not occur
Simon RP, Neurosyphilis Arch Neurol 1985
Hahn et al, Arch Neurol Psychiatr 1959 ESCMID eLibrary
©
by author
….what
else?
ESCMID eLibrary
©
by author
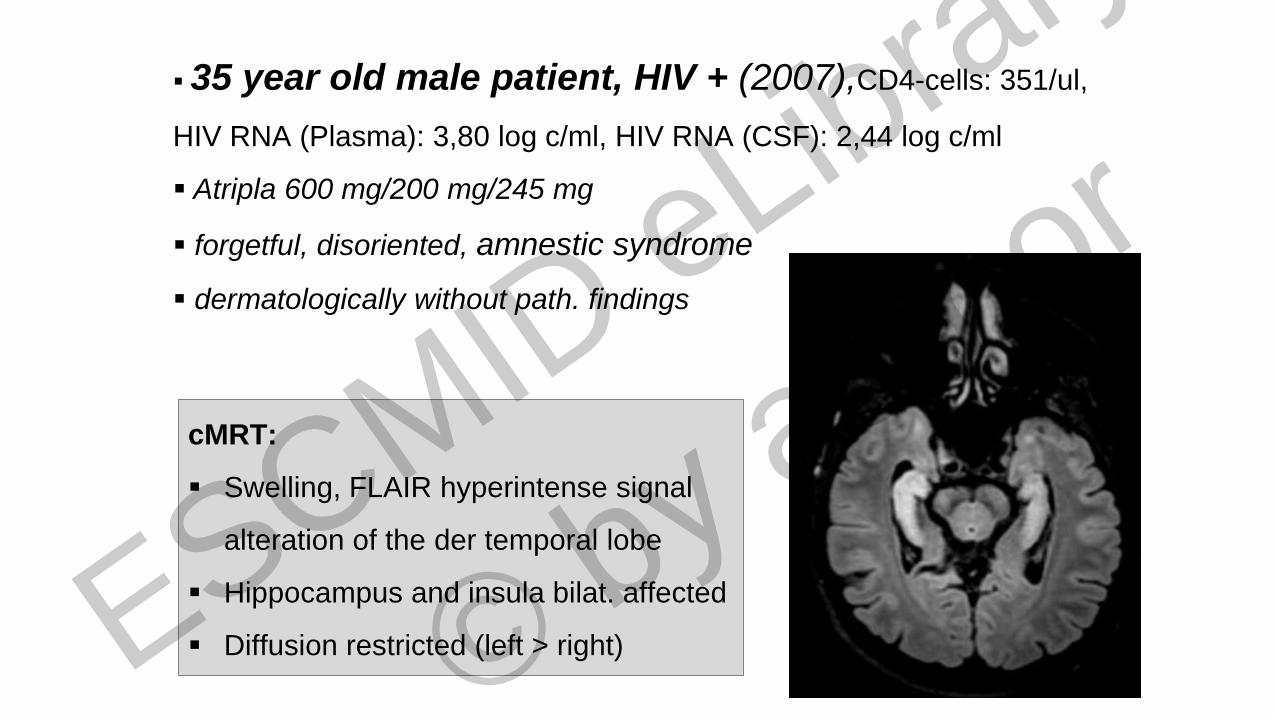
35 year old male patient, HIV + (2007),CD4-cells: 351/ul,
HIV RNA (Plasma): 3,80 log c/ml, HIV RNA (CSF): 2,44 log c/ml
Atripla 600 mg/200 mg/245 mg
forgetful, disoriented, amnestic syndrome
dermatologically without path. findings
cMRT:
Swelling, FLAIR hyperintense signal
alteration of the der temporal lobe
Hippocampus and insula bilat. affected
Diffusion restricted (left > right) ESCMID eLibrary
©
by author

Syphilis-Serology / Serum:
VDRL reaktive, titer 1:64
TPPA positive (titer 1:524.880)
IgM-ELISA positive
Syphilis Serology /CSF):
TPPA positive (titer 1:2621440)
FTA-Abs-Test positive
VDRL reaktive, titer 1:8
ITpA 13,6 (pos > 3)
Diagnosis
Syphilitic encephalitis ESCMID eLibrary
©
by author
- The clinical picture of NS often non-specific
and may develop at any time
- also in immunocompetent patients
- In HIV+ patients NS - more fulminant course
- Change in the interval early syphilis
and NS manifestations
- ? Standard BPG inefficient ?
- existence of ‚particularly‘
neuroinvasive T.pallidum strains
Changes in neurosyphilis (NS)
Drago et al, JEADV 2016 ESCMID eLibrary
©
by author
Thank you for your attention
ESCMID eLibrary
©
by author
Copyright © 2022 FDOKUMEN