
Survey of surgical emergencies in a rural population in the Northern Areas of Pakistan
12
Tropical Medicine and International Health volume 4 no 12 pp 846–857 december 1999 © 1999 Blackwell Science Ltd 846 Survey of surgical emergencies in a rural population in the Northern Areas of Pakistan Mushtaq Ahmed 1 , Mehboob Ali Shah 2 , Stephen Luby 2 , Philomena Drago-Johnson 3 and Sifat Wali 4 1 Department of Surgery, The Aga Khan University, Karachi, Pakistan 2 Department of Community Health Sciences, The Aga Khan University, Karachi, Pakistan 3 Kunri Christian Hospital, Kunri, Pakistan 4 Aga Khan Health Services (AKHS), Gilgit, Pakistan Summary objective To determine the incidence of specific surgical emergencies in a mountainous rural community in the Northern Areas of Pakistan and to assess use of existing health services, and outcomes related to acute surgical illness events. method A cross-sectional population-based survey was conducted. Interviewers visited each of 118 villages in the study area (population 100000), selected a random sample from a total of 9900 households, and inter- viewed the oldest premenopausal female member (n 5 836). Questions were focused on injury, acute abdomen, and/or maternal morbidity occurring in the past year. Cases were included as surgical emergencies when one or more index clinical features indicating a potential for surgical intervention were present. Mortality from a wider range of surgical emergencies was also elicited based on the respondent’s lifetime knowledge of the household. results The incidence rates were 1531/100000 persons per year for injuries; 1364/100000 for acute abdomen, and 16462/100000 for maternal morbidity. The rate of injuries was 2.7 times higher and that of acute abdomen twice as high in males as in females. The injury rate decreased with advancing age, being 13 times higher in children , 5 years than in adults . 40. By contrast, the rate for acute abdomen showed a rise with advancing age, being 8 times higher in the . 40 age group than in under-fives. Burns, falls and road accidents, in that order, were the commonest forms of injury accounting for 82% of 138 cases. Of 43 burn casualties, 46% were in the age group , 5 years; there was no gender bias. Of 71 casualties from falls and road accidents, 85% were aged 6–40 years; there was 6 : 1 male predominance. The maternal morbidity rate was highest in the age group 25–35 years and may be attributed to the high pregnancy rate in this age bracket. Of 408 patients with acute surgical illness, 85% were managed initially at home or close to home in a health centre, dispensary or civil hospital; 32% eventually sought specialist surgical care. The overall rate for minor and major surgical procedures was 411/100000 persons per year (lowest estimate), and appeared to be low. The rate of operative deliveries at 11.8/1000 deliveries (lowest estimate) was particularly low. The mortality rates were correspondingly high: 55/100000 persons per year for injuries and for acute abdomen (lowest estimates). The maternal mortality ratio was particularly high at 8.9/1000 deliveries (lowest esti- mate). Annual mortality rates derived from deaths recalled during the respondent’s lifetime in the household (mean period 5 26 years), tended to corroborate the results of the 1-year survey. conclusion The incidence rates for broad categories of serious acute surgical illness in the study popula- tion far exceeded the rates of acute surgical intervention. Mortality rates were correspondingly high. Such evidence points to a large unmet surgical need and ought to spur improvements in the health service. keywords cross-sectional studies, surgical emergencies, rural populations, Pakistan correspondence Dr Mushtaq Ahmed, Department of Surgery, The Aga Khan University, Karachi, Pakistan. E-mail: [email protected] Introduction In Pakistan, rural communities do not have adequate access to emergency surgical care. In 1983, Blanchard et al. (1987) conducted a survey of 12 district hospitals providing 100% of the surgical cover for the entire population of Northern TMIH490
Transcript of Survey of surgical emergencies in a rural population in the Northern Areas of Pakistan
Tropical Medicine and International Health
volume 4 no 12 pp 846–857 december 1999
© 1999 Blackwell Science Ltd846
Survey of surgical emergencies in a rural population in theNorthern Areas of Pakistan
Mushtaq Ahmed1, Mehboob Ali Shah2, Stephen Luby2, Philomena Drago-Johnson3 and Sifat Wali4
1 Department of Surgery, The Aga Khan University, Karachi, Pakistan
2 Department of Community Health Sciences, The Aga Khan University, Karachi, Pakistan
3 Kunri Christian Hospital, Kunri, Pakistan
4 Aga Khan Health Services (AKHS), Gilgit, Pakistan
Summary objective To determine the incidence of specific surgical emergencies in a mountainous rural community
in the Northern Areas of Pakistan and to assess use of existing health services, and outcomes related to acute
surgical illness events.
method A cross-sectional population-based survey was conducted. Interviewers visited each of 118 villages
in the study area (population 100000), selected a random sample from a total of 9900 households, and inter-
viewed the oldest premenopausal female member (n 5 836). Questions were focused on injury, acute
abdomen, and/or maternal morbidity occurring in the past year. Cases were included as surgical emergencies
when one or more index clinical features indicating a potential for surgical intervention were present.
Mortality from a wider range of surgical emergencies was also elicited based on the respondent’s lifetime
knowledge of the household.
results The incidence rates were 1531/100000 persons per year for injuries; 1364/100000 for acute
abdomen, and 16462/100000 for maternal morbidity. The rate of injuries was 2.7 times higher and that of
acute abdomen twice as high in males as in females. The injury rate decreased with advancing age, being 13
times higher in children , 5 years than in adults . 40. By contrast, the rate for acute abdomen showed a rise
with advancing age, being 8 times higher in the . 40 age group than in under-fives. Burns, falls and road
accidents, in that order, were the commonest forms of injury accounting for 82% of 138 cases. Of 43 burn
casualties, 46% were in the age group , 5 years; there was no gender bias. Of 71 casualties from falls and
road accidents, 85% were aged 6–40 years; there was 6 : 1 male predominance. The maternal morbidity rate
was highest in the age group 25–35 years and may be attributed to the high pregnancy rate in this age
bracket. Of 408 patients with acute surgical illness, 85% were managed initially at home or close to home in
a health centre, dispensary or civil hospital; 32% eventually sought specialist surgical care. The overall rate
for minor and major surgical procedures was 411/100000 persons per year (lowest estimate), and appeared to
be low. The rate of operative deliveries at 11.8/1000 deliveries (lowest estimate) was particularly low. The
mortality rates were correspondingly high: 55/100000 persons per year for injuries and for acute abdomen
(lowest estimates). The maternal mortality ratio was particularly high at 8.9/1000 deliveries (lowest esti-
mate). Annual mortality rates derived from deaths recalled during the respondent’s lifetime in the household
(mean period 5 26 years), tended to corroborate the results of the 1-year survey.
conclusion The incidence rates for broad categories of serious acute surgical illness in the study popula-
tion far exceeded the rates of acute surgical intervention. Mortality rates were correspondingly high. Such
evidence points to a large unmet surgical need and ought to spur improvements in the health service.
keywords cross-sectional studies, surgical emergencies, rural populations, Pakistan
correspondence Dr Mushtaq Ahmed, Department of Surgery, The Aga Khan University, Karachi,
Pakistan. E-mail: [email protected]
Introduction
In Pakistan, rural communities do not have adequate access
to emergency surgical care. In 1983, Blanchard et al. (1987)
conducted a survey of 12 district hospitals providing 100% of
the surgical cover for the entire population of Northern
TMIH490

Tropical Medicine and International Health volume 4 no 12 pp 846–857 december 1999
M. Ahmed et al. Survey of surgical emergencies in rural Pakistan
Sindh, Northern Balochistan, and the Hazara district of the
North-west Frontier Province, totaling 11 million. The
overall rate of surgery in these rural areas of Pakistan was
124/100000 persons per year. The operations were related to
the specialties of general surgery, urology, orthopaedics, and
obstetrics-gynaecology. By comparison the rate of operations
in similar specialties in the USA in 1978 was 8,253/100000
persons per year. (Rutkow & Zuidema 1981). The situation in
rural Pakistan is not unique and has also been observed in
rural Kenya (Nordberg et al. 1996) and rural Mozambique
(McCord 1987).
A comparison of the rates of specific operations such as
caesarian section and groin hernia repair is perhaps more
valid. The annual rates per 100000 persons for caesarian sec-
tion were 9 in rural Pakistan, 129 in rural Kenya, 42 in rural
Mozambique and 236 in the USA (Rutkow & Zuidema 1981;
Blanchard et al. 1987; McCord 1987; Nordberg et al. 1996).
For groin hernia repair the rates were 9, 6, 124 and 236 per
100000 persons per year, respectively. Nordberg et al. (1996)
concluded that the surgical output of a rural hospital in the
developing world does not reflect the true burden of surgical
disease in its catchment population. Barriers exist to seeking
health care including lack of education and awareness, cul-
tural factors, poverty, and inadequate health sector capacity.
The establishment of primary health care in a region cre-
ates the need for a first-level referral centre for management
of clinical conditions including those requiring surgery. In
1986, the Aga Khan Health Services, an NGO, established
a primary health care program in the Northern Areas of
Pakistan. Following introduction of the programme, the
infant mortality rate (IMR) decreased from 158 at baseline to
52 per 1000 live births by 1997 in the population served (Aga
Khan Health Services 1997). In 1992, a first-level referral cen-
tre with a surgical facility was established in the Ghizar dis-
trict of the Northern Areas of Pakistan (population 100000).
The aim was to meet essential needs such as obstetrical and
gynaecological emergencies, trauma, and other surgical emer-
gencies. A trained surgeon was posted at Singal Medical
Centre (SMC), the referral centre. The surgeon imparted clin-
ical training by rotation to Lady Health Visitors (LHV)
staffing the 13 Health Centres in the district, which in coordi-
nation with 2 field modules are responsible for providing pri-
mary health care to the entire Ghizar population.
The government, which is the only other health care
provider in the region, does not offer surgical facilities. Its
health personnel in 12 first aid posts, 12 dispensaries, and 4
civil hospitals were informed about the surgical facilities
available at SMC. With the institution of primary health care
in the region, along with health education and clinical train-
ing of paramedical staff, it was fair to expect an improved
referral of patients for emergency surgical care. Yet despite
these measures, the number of emergency surgical procedures
for Ghizar inhabitants remained low; 19 caesarian sections
were performed at SMC in 1993. Two additional patients
from Ghizar underwent caesarian section at the District
Headquarters (DHQ) Hospital in Gilgit, which is a sec-
ondary-level hospital in the adjacent district, 2.5 h away by
jeep ride from SMC.
It was obvious that there were large unmet surgical needs
in the Ghizar community. As knowledge of the burden of sur-
gical disease in the community is important for organizing a
cost-effective service, we undertook a population-based sur-
vey in Ghizar in 1995. Our objectives were to estimate
• the prevalence of specific surgical emergencies;
• use of existing health services;
• outcomes related to acute surgical illness.
We focused on emergency surgical conditions that would
represent the commonest risk of death or disability to the
population, and that a surgical centre in a remote rural area
should be able to address (Nundy 1984).
Methods
Study area and population
Ghizar is one of 5 districts in the Northern Areas of Pakistan
situated amid the Hindu Kush, Karakoram, and Himalayan
mountain ranges. The region, which is situated at 9000 feet
above sea level, has been called ‘the rooftop of the world’. Its
scenic splendor is matched only by the inhospitability of its
living conditions: the terrain is extremely rough and winters
are severe. The majority of the people are subsistence farmers
whose annual per capita income is $200, half the national per
capita income. The population is scattered in small clusters of
10–400 households connected by dirt tracks, jeep roads and
makeshift motor vehicles. The inaccessibility of the area had
been a strong impediment to development until the construc-
tion of the Karakoram Highway in the late 1970s linked
Pakistan to China through the Northern Areas. Further
development has taken place as a result of the establishment
of community institutions and the promotion of income-
generating activities, beginning in the early 1980s, by the Aga
Khan Rural Support Programme, an NGO.
Sampling
AKHS provided the baseline information for the study: the
total population of Ghizar is distributed in 118 villages and
9900 households. The main study variable was the proportion
of inhabitants who had suffered an acute surgical illness
during one year. The estimated prevalence of acute surgical
illness was 0.9 based on knowledge of the number of de-
liveries during one year (2994 in 1992); an assumed 10% rate
© 1999 Blackwell Science Ltd 847
Tropical Medicine and International Health volume 4 no 12 pp 846–857 december 1999
M. Ahmed et al. Survey of surgical emergencies in rural Pakistan
© 1999 Blackwell Science Ltd848
of caesarian sections and an assumed rate of procedures for
other acute surgical illnesses estimated to be twice that of
caesarian sections. Accepting 0.02 as the tolerable range of
error and a 95% level of confidence, it was necessary to enroll
850 households for the study. The actual number of house-
holds enrolled was 836.
Interviewers visited each of the 118 villages in the Ghizar
district. To select the households, a map of the village with
important landmarks was prepared. Shops, schools and
mosques served as landmarks. A landmark in each village was
randomly selected as the starting point where the study team
placed a soda bottle on its side on the ground and spun it.
They approached the closest house in the direction where the
mouth of the bottle pointed. After completing the interview,
the study team then approached every third house and con-
tinued this process until a sufficient number of houses were
enrolled proportionate to the size of the village.
Measurement
The incidence of acute surgical illnesses was assessed by
administering a structured questionnaire to the oldest woman
in the study household who was still in her reproductive
years. In the extended families that characterize the study vil-
lages, these women would be most likely to know the health
conditions of the family members in the preceding year. If an
appropriate respondent could not be identified, the house-
hold was not enrolled in the study. The Lady Health Visitors
(LHV) who were trained to administer the questionnaire had
a minimum of 3 years experience of providing maternal and
childcare in the region. The LHVs visited the women in their
homes and conducted the interviews in the language of the
respondents.
Section 1 of the questionnaire was related to demographic
details: number of people in the household and their age and
sex distribution. Section 2 sought to elicit deaths from surgi-
cal causes in the household during the respondent’s lifetime
in the household. Respondents were asked whether death had
occurred in association with injury including burn injury,
acute abdomen, a complication of pregnancy or childbirth,
gastro-intestinal haemorrhage, acute groin-scrotal swelling,
superficial spreading infection, limb gangrene or airway
obstruction by a foreign body. Section 3 was divided into 5
modules: injury, burns, acute abdomen, complication of preg-
nancy and complication of childbirth. This section of the
questionnaire was designed to capture only those acute surgi-
cal illness events that had occurred during the past year. The
survey was conducted around Eid-ul-Baqr, an Islamic feast,
and the previous Eid-ul-Baqr was taken as the reference point
marking one year. Once it was established that an acute ill-
ness event had occurred, respondents were asked whether
any of the index clinical features from a predetermined list
had been observed indicating the potential for surgical inter-
vention. Cases were included in the study only if one or more
index clinical features were present. Additionally, in each
module, questions were asked about risk factors, care
received, and outcome of illness.
An interview took approximately 30 min to complete. Five
percent of completed interviews were checked for reliability
by one of the authors (MAS), who re-visited the home of the
respondent and asked a few questions from the questionnaire
to verify the accuracy of the responses. No fake interviews
were detected.
To determine rates related to injury and acute abdomen
based on the 1-year survey, we totaled the number of persons
living in the visited households for denominator (n 5 9012).
For maternal morbidity only the population of women
between the ages of 15 and 44 (n 5 1713) was used as de-
nominator. The numerator in relation to incidence, mortality
and operative procedure rates in each module included cases
with unequivocal answers. If answers were left blank or the
respondent answered ‘don’t know’, cases were not included in
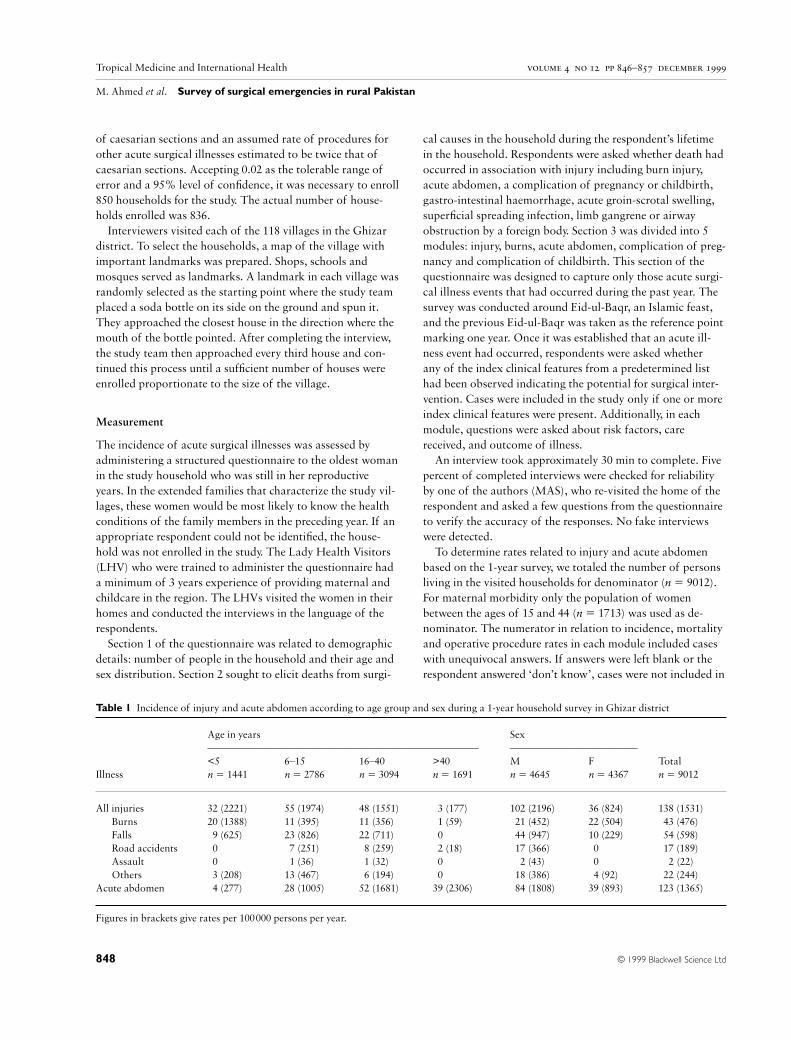
Table 1 Incidence of injury and acute abdomen according to age group and sex during a 1-year household survey in Ghizar district
Age in years Sex
––––––––––––––––––––––––––––––––––––––––––––––––––– ––––––––––––––––––––––––
<5 6–15 16–40 >40 M F Total
Illness n 5 1441 n 5 2786 n 5 3094 n 5 1691 n 5 4645 n 5 4367 n 5 9012
All injuries 32 (2221) 55 (1974) 48 (1551) 03 (177) 102 (2196) 36 (824) 138 (1531)
Burns 20 (1388) 11 (395) 11 (356) 01 (59) 021 (452) 22 (504) 043 (476)
Falls 09 (625) 23 (826) 22 (711) 00 044 (947) 10 (229) 054 (598)
Road accidents 00 07 (251) 08 (259) 02 (18) 017 (366) 00 017 (189)
Assault 00 01 (36) 01 (32) 00 002 (43) 00 002 (22)
Others 03 (208) 13 (467) 06 (194) 00 018 (386) 04 (92) 022 (244)
Acute abdomen 04 (277) 28 (1005) 52 (1681) 39 (2306) 084 (1808) 39 (893) 123 (1365)
Figures in brackets give rates per 100000 persons per year.

Tropical Medicine and International Health volume 4 no 12 pp 846–857 december 1999
M. Ahmed et al. Survey of surgical emergencies in rural Pakistan
© 1999 Blackwell Science Ltd 849
the numerator. As a result the lowest rate estimates were
obtained.
To calculate annual mortality rates based on the respon-
dents’ lifetime experience in study households, we determined
the mean period of recall for 836 respondents (26 years) and
the total number of deaths recalled in each acute surgical ill-
ness category. Annual mortality was the total number of
deaths in a given category divided by 26; the annual mortality
rate was annual mortality times 100000 divided by the rel-
evant population denominator. The mean 26-year recall
period included the last year of study, during which the inci-
dence rates of acute surgical illness were established.
Results
Demographic composition of the study population
The demographic composition of the study population con-
formed to the pyramidal shape identified for developing
countries (Figure 1). However, the relative sizes of the first
two age-groups, , 5 years and 5–9 years, suggests a decreas-
ing fertility rate and reduced IMR.
Geographical distribution of acute surgical illness
A total of 549 acute surgical illness events occurred during
one year. A single event occurred in 448 households (54%), 2
events in 40 households (4.8%), and 3 events in 7 households
(0.8%). There was no acute surgical illness event in 341
households (41%). There was a uniform distribution of
affected households throughout the district. Adequate
documentation was available of 543 illness events in as many
patients, forming the material for further analyses.
Incidence of acute surgical illness events
Table 1 shows the incidence of injuries and acute abdomen.
The incidence of burns decreased with age, being highest in
the age group , 5 years. However, falls, road accidents and
other forms of injury were more common between 6 and
40 years of age. There was male predominance in all forms of
injury except burns, which had affected both sexes equally.
The majority of the burn injuries in young children were
scalds sustained accidentally in their homes. In contrast to
injuries, there was a rising incidence of acute abdomen with
increasing age. There was also a male bias for acute abdomi-
nal pain.
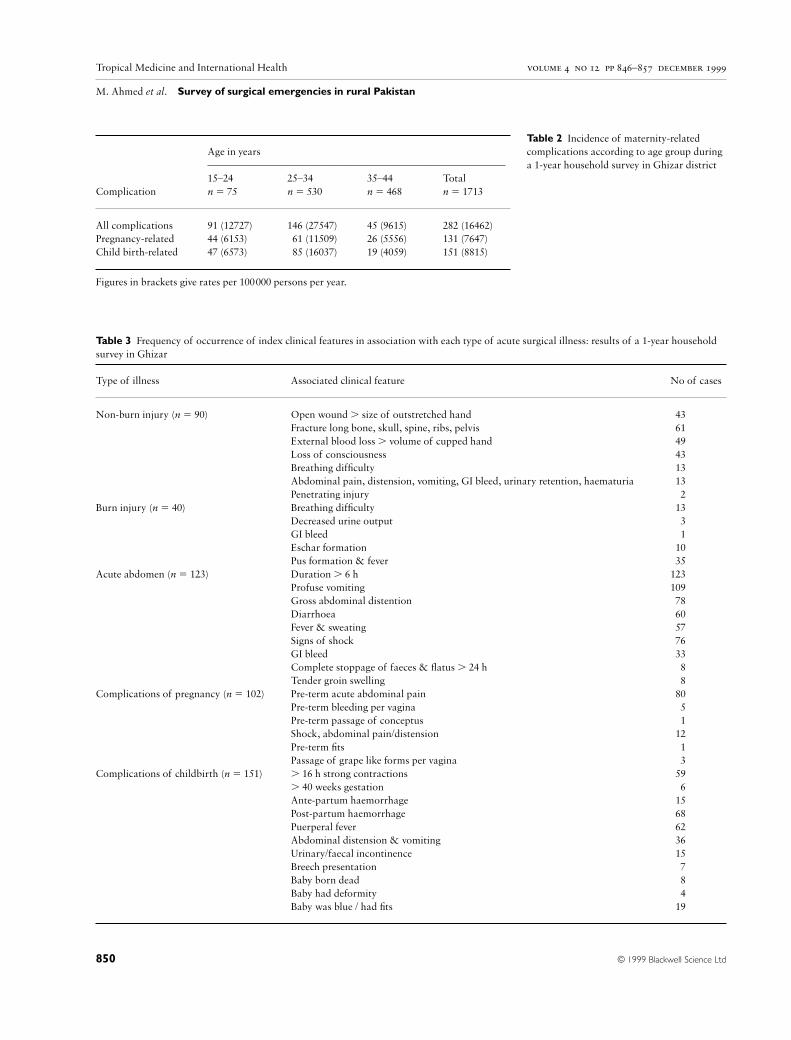
The incidence of pregnancy and childbirth related compli-
cations seemed particularly high in the age group 25–34 years
(Table 2). However, this simply reflected a higher incidence of
pregnancies in this age group. A little more than half (51%)
of the women who were pregnant (n 5 493) or had delivered
a child (n 5 338) were between 25 and 34 years of age; 31%
were 15–24 and 18% were . 35 years old. The complication
rate did not differ significantly between the different age
groups. The parity status of the women also did not seem to
significantly influence predisposition to complications.
Severity of acute surgical illness
Details of associated clinical features indicating a potential
for surgical intervention were available in 90 of 95 patients
0 200Female
400 600 8000200Males
400600800
>65
0–55–9
10–1415–1920–2425–2930–3435–3940–4445–4950–5455–5960–65
Number of population
Figure 1 Demographic structure of the
study population in Ghizar district,
Northern Areas, Pakistan (1996).
Tropical Medicine and International Health volume 4 no 12 pp 846–857 december 1999
M. Ahmed et al. Survey of surgical emergencies in rural Pakistan
© 1999 Blackwell Science Ltd850
Table 3 Frequency of occurrence of index clinical features in association with each type of acute surgical illness: results of a 1-year household
survey in Ghizar
Type of illness Associated clinical feature No of cases
Non-burn injury (n 5 90) Open wound . size of outstretched hand 043
Fracture long bone, skull, spine, ribs, pelvis 061
External blood loss . volume of cupped hand 049
Loss of consciousness 043
Breathing difficulty 013
Abdominal pain, distension, vomiting, GI bleed, urinary retention, haematuria 013
Penetrating injury 002
Burn injury (n 5 40) Breathing difficulty 013
Decreased urine output 003
GI bleed 001
Eschar formation 010
Pus formation & fever 035
Acute abdomen (n 5 123) Duration . 6 h 123
Profuse vomiting 109
Gross abdominal distention 078
Diarrhoea 060
Fever & sweating 057
Signs of shock 076
GI bleed 033
Complete stoppage of faeces & flatus . 24 h 008
Tender groin swelling 008
Complications of pregnancy (n 5 102) Pre-term acute abdominal pain 080
Pre-term bleeding per vagina 005
Pre-term passage of conceptus 001
Shock, abdominal pain/distension 012
Pre-term fits 001
Passage of grape like forms per vagina 003
Complications of childbirth (n 5 151) . 16 h strong contractions 059
. 40 weeks gestation 006
Ante-partum haemorrhage 015
Post-partum haemorrhage 068
Puerperal fever 062
Abdominal distension & vomiting 036
Urinary/faecal incontinence 015
Breech presentation 007
Baby born dead 008
Baby had deformity 004
Baby was blue / had fits 019
Age in years
————————————————————————————
15–24 25–34 35–44 Total
Complication n 5 75 n 5 530 n 5 468 n 5 1713
All complications 91 (12727) 146 (27547) 45 (9615) 282 (16462)
Pregnancy-related 44 (6153) 061 (11509) 26 (5556) 131 (7647)
Child birth-related 47 (6573) 085 (16037) 19 (4059) 151 (8815)
Figures in brackets give rates per 100000 persons per year.
Table 2 Incidence of maternity-related
complications according to age group during
a 1-year household survey in Ghizar district
Tropical Medicine and International Health volume 4 no 12 pp 846–857 december 1999
M. Ahmed et al. Survey of surgical emergencies in rural Pakistan
© 1999 Blackwell Science Ltd 851
with nonburn injuries, 40 of 43 with burn injuries, all 123
with acute abdomen, 102 of 131 with complications of preg-
nancy and all 151 with complications of childbirth (Table 3).
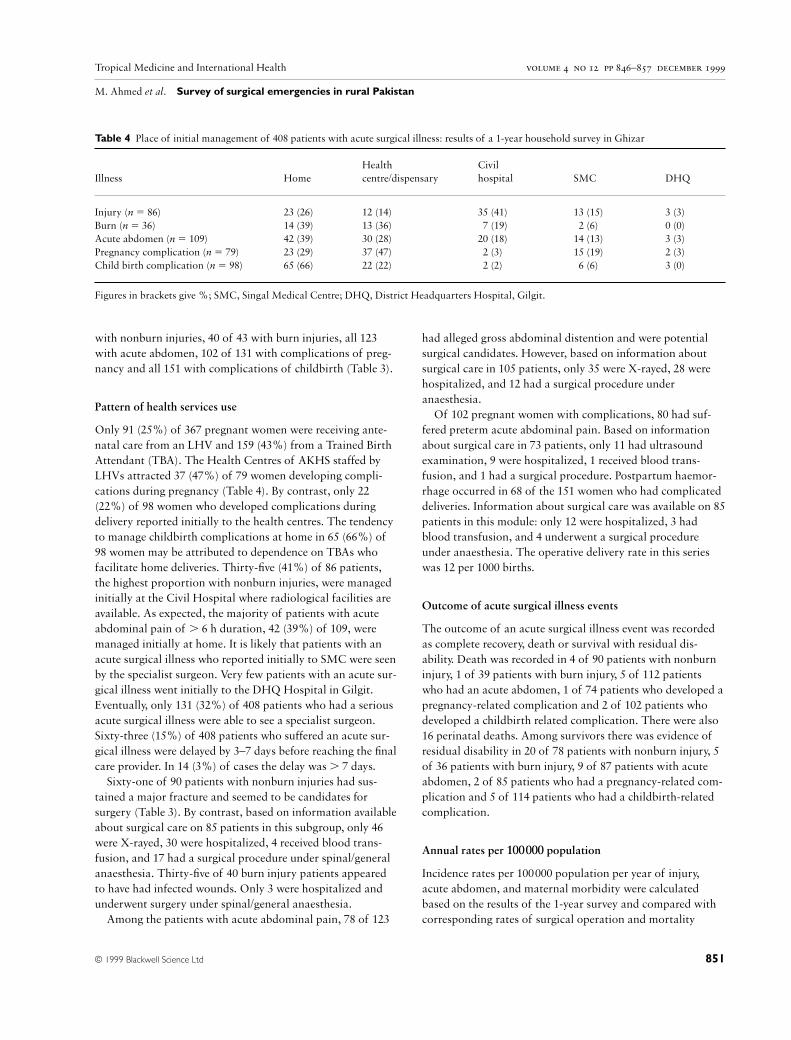
Pattern of health services use
Only 91 (25%) of 367 pregnant women were receiving ante-
natal care from an LHV and 159 (43%) from a Trained Birth
Attendant (TBA). The Health Centres of AKHS staffed by
LHVs attracted 37 (47%) of 79 women developing compli-
cations during pregnancy (Table 4). By contrast, only 22
(22%) of 98 women who developed complications during
delivery reported initially to the health centres. The tendency
to manage childbirth complications at home in 65 (66%) of
98 women may be attributed to dependence on TBAs who
facilitate home deliveries. Thirty-five (41%) of 86 patients,
the highest proportion with nonburn injuries, were managed
initially at the Civil Hospital where radiological facilities are
available. As expected, the majority of patients with acute
abdominal pain of . 6 h duration, 42 (39%) of 109, were
managed initially at home. It is likely that patients with an
acute surgical illness who reported initially to SMC were seen
by the specialist surgeon. Very few patients with an acute sur-
gical illness went initially to the DHQ Hospital in Gilgit.
Eventually, only 131 (32%) of 408 patients who had a serious
acute surgical illness were able to see a specialist surgeon.
Sixty-three (15%) of 408 patients who suffered an acute sur-
gical illness were delayed by 3–7 days before reaching the final
care provider. In 14 (3%) of cases the delay was . 7 days.
Sixty-one of 90 patients with nonburn injuries had sus-
tained a major fracture and seemed to be candidates for
surgery (Table 3). By contrast, based on information available
about surgical care on 85 patients in this subgroup, only 46
were X-rayed, 30 were hospitalized, 4 received blood trans-
fusion, and 17 had a surgical procedure under spinal/general
anaesthesia. Thirty-five of 40 burn injury patients appeared
to have had infected wounds. Only 3 were hospitalized and
underwent surgery under spinal/general anaesthesia.
Among the patients with acute abdominal pain, 78 of 123
had alleged gross abdominal distention and were potential
surgical candidates. However, based on information about
surgical care in 105 patients, only 35 were X-rayed, 28 were
hospitalized, and 12 had a surgical procedure under
anaesthesia.
Of 102 pregnant women with complications, 80 had suf-
fered preterm acute abdominal pain. Based on information
about surgical care in 73 patients, only 11 had ultrasound
examination, 9 were hospitalized, 1 received blood trans-
fusion, and 1 had a surgical procedure. Postpartum haemor-
rhage occurred in 68 of the 151 women who had complicated
deliveries. Information about surgical care was available on 85
patients in this module: only 12 were hospitalized, 3 had
blood transfusion, and 4 underwent a surgical procedure
under anaesthesia. The operative delivery rate in this series
was 12 per 1000 births.
Outcome of acute surgical illness events
The outcome of an acute surgical illness event was recorded
as complete recovery, death or survival with residual dis-
ability. Death was recorded in 4 of 90 patients with nonburn
injury, 1 of 39 patients with burn injury, 5 of 112 patients
who had an acute abdomen, 1 of 74 patients who developed a
pregnancy-related complication and 2 of 102 patients who
developed a childbirth related complication. There were also
16 perinatal deaths. Among survivors there was evidence of
residual disability in 20 of 78 patients with nonburn injury, 5
of 36 patients with burn injury, 9 of 87 patients with acute
abdomen, 2 of 85 patients who had a pregnancy-related com-
plication and 5 of 114 patients who had a childbirth-related
complication.
Annual rates per 100000 population
Incidence rates per 100000 population per year of injury,
acute abdomen, and maternal morbidity were calculated
based on the results of the 1-year survey and compared with
corresponding rates of surgical operation and mortality
Table 4 Place of initial management of 408 patients with acute surgical illness: results of a 1-year household survey in Ghizar
Health Civil
Illness Home centre/dispensary hospital SMC DHQ
Injury (n 5 86) 23 (26) 12 (14) 35 (41) 13 (15) 3 (3)
Burn (n 5 36) 14 (39) 13 (36) 07 (19) 02 (6) 0 (0)
Acute abdomen (n 5 109) 42 (39) 30 (28) 20 (18) 14 (13) 3 (3)
Pregnancy complication (n 5 79) 23 (29) 37 (47) 02 (3) 15 (19) 2 (3)
Child birth complication (n 5 98) 65 (66) 22 (22) 02 (2) 06 (6) 3 (0)
Figures in brackets give %; SMC, Singal Medical Centre; DHQ, District Headquarters Hospital, Gilgit.
Tropical Medicine and International Health volume 4 no 12 pp 846–857 december 1999
M. Ahmed et al. Survey of surgical emergencies in rural Pakistan
© 1999 Blackwell Science Ltd852
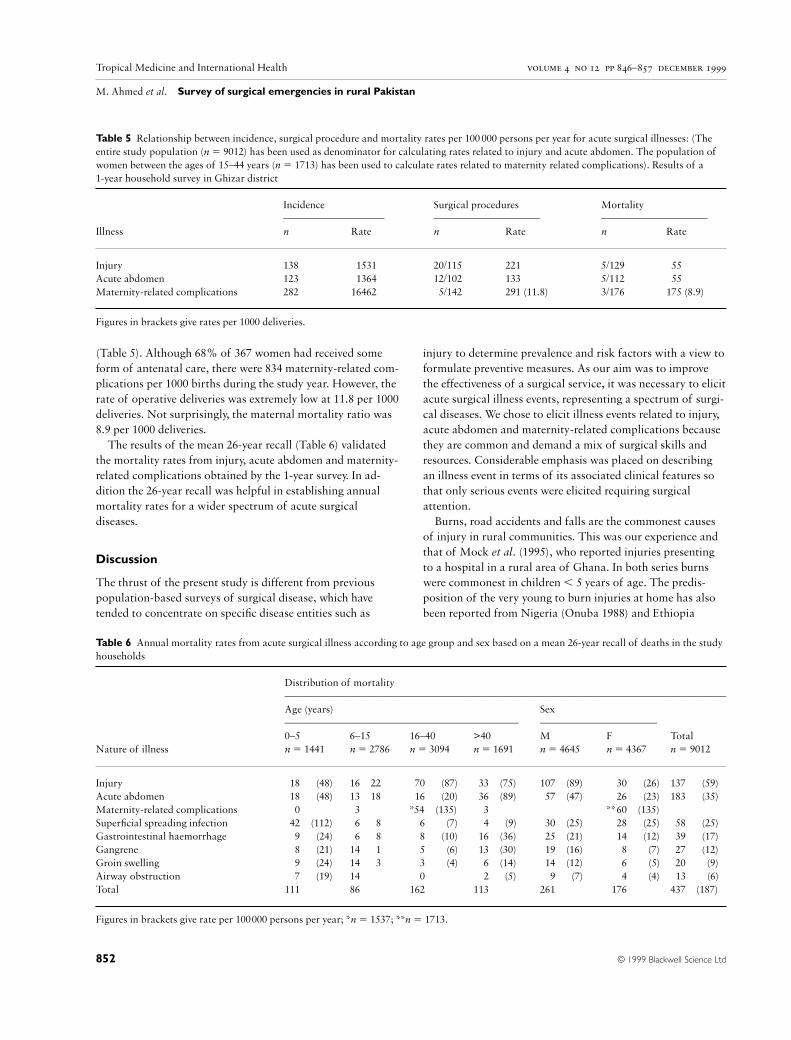
(Table 5). Although 68% of 367 women had received some
form of antenatal care, there were 834 maternity-related com-
plications per 1000 births during the study year. However, the
rate of operative deliveries was extremely low at 11.8 per 1000
deliveries. Not surprisingly, the maternal mortality ratio was
8.9 per 1000 deliveries.
The results of the mean 26-year recall (Table 6) validated
the mortality rates from injury, acute abdomen and maternity-
related complications obtained by the 1-year survey. In ad-
dition the 26-year recall was helpful in establishing annual
mortality rates for a wider spectrum of acute surgical
diseases.
Discussion
The thrust of the present study is different from previous
population-based surveys of surgical disease, which have
tended to concentrate on specific disease entities such as
injury to determine prevalence and risk factors with a view to
formulate preventive measures. As our aim was to improve
the effectiveness of a surgical service, it was necessary to elicit
acute surgical illness events, representing a spectrum of surgi-
cal diseases. We chose to elicit illness events related to injury,
acute abdomen and maternity-related complications because
they are common and demand a mix of surgical skills and
resources. Considerable emphasis was placed on describing
an illness event in terms of its associated clinical features so
that only serious events were elicited requiring surgical
attention.
Burns, road accidents and falls are the commonest causes
of injury in rural communities. This was our experience and
that of Mock et al. (1995), who reported injuries presenting
to a hospital in a rural area of Ghana. In both series burns
were commonest in children , 5 years of age. The predis-
position of the very young to burn injuries at home has also
been reported from Nigeria (Onuba 1988) and Ethiopia
Table 5 Relationship between incidence, surgical procedure and mortality rates per 100 000 persons per year for acute surgical illnesses: (The
entire study population (n 5 9012) has been used as denominator for calculating rates related to injury and acute abdomen. The population of
women between the ages of 15–44 years (n 5 1713) has been used to calculate rates related to maternity related complications). Results of a
1-year household survey in Ghizar district
Incidence Surgical procedures Mortality
––––––––––––––––––– –––––––––––––––––––– ––––––––––––––––––––
Illness n Rate n Rate n Rate
Injury 138 01531 20/115 221 5/129 055
Acute abdomen 123 01364 12/102 133 5/112 055
Maternity-related complications 282 16462 05/142 291 (11.8) 3/176 175 (8.9)
Figures in brackets give rates per 1000 deliveries.
Table 6 Annual mortality rates from acute surgical illness according to age group and sex based on a mean 26-year recall of deaths in the study
households
Distribution of mortality
–––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––––
Age (years) Sex
–––––––––––––––––––––––––––––––––––––––––––– ––––––––––––––––––––––
0–5 6–15 16–40 >40 M F Total
Nature of illness n 5 1441 n 5 2786 n 5 3094 n 5 1691 n 5 4645 n 5 4367 n 5 9012
Injury 018 (48) 16 22 070 (87) 033 (75) 107 (89) 0030 (26) 137 (59)
Acute abdomen 018 (48) 13 18 016 (20) 036 (89) 057 (47) 0026 (23) 183 (35)
Maternity-related complications 000 03 *54 (135) 003 **60 (135)
Superficial spreading infection 042 (112) 06 8 006 0(7) 004 (9) 030 (25) 0028 (25) 058 (25)
Gastrointestinal haemorrhage 009 (24) 06 8 008 (10) 016 (36) 025 (21) 0014 (12) 039 (17)
Gangrene 008 (21) 14 1 005 (6) 013 (30) 019 (16) 0008 (7) 027 (12)
Groin swelling 009 (24) 14 3 003 (4) 006 (14) 014 (12) 0006 (5) 020 (9)
Airway obstruction 007 (19) 14 000 002 (5) 009 (7) 0004 (4) 13 (6)
Total 111 86 162 113 261 0176 437 (187)
Figures in brackets give rate per 100000 persons per year; *n 5 1537; **n 5 1713.

Tropical Medicine and International Health volume 4 no 12 pp 846–857 december 1999
M. Ahmed et al. Survey of surgical emergencies in rural Pakistan
(Courtright et al. 1993). In our study and in the Ghanian and
Nigerian series, burns from scalds were commoner, while in
the Ethiopian series flame burns predominated. The urban
burn pattern in developing countries appears to be different.
In a burns study in Karachi (Marsh et al. 1996), young
women were observed to be most commonly affected and
were predisposed to flame burns sustained while cooking.
In the present study, falls caused injury three times more
often than road accidents. Both forms of injury were com-
monest in males in the age group 6–40 years. The predis-
position of young men to road accidents and falls reflects
their involvement with activities such as travel and climbing
trees in order to stack hay. Falls from trees have been reported
as the leading cause of serious injury in rural areas of other
developing countries, where the products of tall trees are
important sources of food and income (Smith & Barss 1991).
The highest risk group is young boys, and in some areas,
young adult males (Ebong 1978; Barss et al. 1984). In the
Ghanaian series (Mock et al. 1995) however, road accidents
were 2.5 times as common as falls and while road accidents
occurred at all ages beyond 5 years, falls were most commonly
observed in the age group . 60 years; males predominated in
both types of injury. Falling in the elderly has a different
aetiology and is known to be associated with reduced daily
physical activity (Cooper et al. 1988; Lau et al. 1988, 1990;
Wickham et al. 1989). Injuries related to assault were uncom-
mon in the Ghanian series and ours. By contrast, assault was
the leading cause of injury in an urban hospital based series
in Eldoret, Kenya (Odero & Kibosia 1995).
It is difficult to explain the predominance of older men in
acute abdominal pain cases. In neighbouring districts of
northern Pakistan, volvulus of the sigmoid colon was ob-
served to be a common surgical emergency, particularly dur-
ing Ramzan, which is the holy month of fasting (Blanchard
& Maguire 1985; Bokhari 1985). In Bokhari’s series the
majority of the patients were males between 40 and 80 years
of age.
With respect to maternal morbidity it seemed from the
clinical descriptions that complications such as haemorrhage,
obstructed labour and sepsis, which are amenable to surgical
intervention, frequently occurred in our patients. These three
complications together accounted for 43% of 77.6 million
obstetric morbidity events and 47% of 0.5 million obstetric
deaths occurring worldwide during 1993 (WHO 1994). It
seemed that complications such as obstetric fistulae and
pelvic inflammatory disease also occurred in our patients.
However, we did not elicit complications from unsafe
abortion, which are surgical in nature, probably reflecting a
weakness in questionnaire design.
The injury incidence rate of 1531/100000 persons per year
in the current study is likely to be an underestimate because it
did not take into account injuries which were not serious. In
addition, events such as poisoning, drowning, suffocation and
animal and insect bites, which are included under the rubric
of injury in the ICD 9 code, were not given specific import-
ance in our questionnaire. By comparison, Gordan et al.
(1962), who included all forms of external injury in their
community-based survey, determined the incidence rate to be
116/1000 persons per year in 11 rural villages in northern
India (study population 12022). These authors defined injury
quite simply as causing a disruption of normal daily activity.
Only 4% of the injuries in their study resulted in permanent
disability, a rate of 5/1000 persons per year. A comparable
rate of injury in the United States is about 270/1000 persons
per year allowing for some variation in injury definition
(Collins 1990). Most studies of distribution of injury in a
population focus on hospital admissions or attendances (Zwi
1993). Hospital-based rates of injury are much lower than
those based on community survey (Bangdiwala et al. 1990). In
the Ghanian series, the rate of serious injuries in a rural
population requiring hospital admission was 0.6/1000 per-
sons per year (Mock et al. 1995). In the Eldoret series (Odero
& Kibosia 1995), the rate of injuries in an urban population,
based on injured persons registering at a hospital, was
2.6/1000 persons per year. Only 20% of the injured persons
required hospital admission. The Eldoret study represents an
urban injury pattern with a predominance of motor vehicle
and assault-related injuries. The incidence rates of uninten-
tional injury, excluding injury caused by motor vehicles, are
said to be relatively similar across developing countries, even
though the importance of specific injuries varies from
country to country and from one area to the next (Smith &
Barss 1991).
Our incidence rate for acute abdomen was 1,364/100000
persons, per year. It is more difficult to compare the incidence
rates for acute abdomen, as there is a greater possibility of
geographical variation in disease pattern and diagnostic
capability. There is an estimated minimum need for 133
appendicectomies (Rutkow & Zuidema 1981) and 30 strangu-
lated inguinal hernia repairs (Nordberg 1984) per 100000
persons per year. For every person requiring operative inter-
vention for acute abdomen, many more require to be
screened. In one study (Thompson & Jones 1986), only 39%
of 220 admissions for acute abdomen resulted in operative
intervention. There was a 5% negative laparotomy rate. In
another study (Irvin 1989), 47% of 1190 admissions for acute
abdomen resulted in surgery with a 16% rate of unnecessary
appendicectomy. Ambulatory patients with acute abdominal
pain have a much lower rate of surgical intervention (White
et al. 1975; Wasson et al. 1981; Britt et al. 1994).
The maternal morbidity ratio of 834/1000 births during the
current study year seemed excessive. The maternal mortality
ratio was correspondingly high at 8.9/1000 births per year.
Unpublished estimates of worldwide maternal complications
© 1999 Blackwell Science Ltd 853

Tropical Medicine and International Health volume 4 no 12 pp 846–857 december 1999
M. Ahmed et al. Survey of surgical emergencies in rural Pakistan
and deaths in 1993 were 77.6 million and 0.5 million, respect-
ively (WHO Maternal Health and Safe Motherhood
Program, unpublished estimates 1994). There were 33 million
complications related to haemorrhage, sepsis and obstructed
labour. The ratio of the number of surgical type compli-
cations to death was 137:1 in the worldwide estimate com-
pared to 94:1 in our study.
Incongruity between the occurrence of serious acute surgi-
cal illness events and the surgical care patients receive has
also been observed by others in developing countries. Delay
in reaching the final care provider is corroborated in the
Ghanian series on rural injuries (Mock et al. 1995). In our
study, 54% of 85 injured patients who were taken to hospital
had X-rays; 57% of 30 who were hospitalized underwent
surgery. To our knowledge, comparable population-based
data on rates of radiological investigation and surgical inter-
vention for injury are not available from any other rural area
in a developing country. However, in an urban hospital based
series from Eldoret, Kenya, only 27% of 1304 injured patients
brought to hospital had X-rays; only 4% of 275 patients who
were hospitalized underwent surgery (Odero & Kibosia
1995). It seems that in rural areas as compared with the city,
patients attend hospital for relatively serious injuries.
The rate of operative deliveries in our study seemed to be
low; there were only 12 minor and major interventions per
1000 births. In another population-based study in rural
Morocco, Belghiti et al. (1998) showed that only 111 of 21392
mothers who were expected to deliver during 1995 underwent
a major obstetrical intervention – a rate of 5.2 per 1000
expected births. Another 135 mothers with life-threatening
conditions did not benefit from the major obstetrical inter-
vention they required – a rate of 6.3 per 1000 expected births.
By contrast, in a hospital-based series from rural Nigeria
(Harrison 1985), the rate of surgical intervention was 60 per
1000 deliveries in booked healthy women, 250 per 1000 deliv-
eries in booked women with complications, and 310 per 1000
births in unbooked emergencies. It seems that in rural areas
an alarmingly large proportion of women with serious
maternal complications requiring surgery does not reach hos-
pital. Those that do, as in the Nigerian study, require a high
rate of operative intervention.
Outcomes such as mortality ought to shed more light on
the seriousness of the illness events elicited in our study. The
annual death rate of 55 per 100000 persons from acute
injuries was very high and suggests that we were successful in
identifying serious injuries. High death rates from injury have
been observed in other population-based surveys of rural
areas in developing countries. In 1959, Gordan et al. (1962)
reported an annual death rate from unintentional injury of 63
per 100000. The study population was 12022 from 11 rural
villages in northern India. Besides burns and falls, the causes
of fatal injury included injuries from animals, drowning,
poisoning, suffocation, and lack of infant care. In the Matlab
study in Bangladesh (Zimicki et al. 1985), the causes of death
were determined through verbal autopsies from relatives.
There were 51 injury-related deaths per 100000 persons per
year, the majority from drowning in the age group 1–4 years.
Barss (1991) in another verbal autopsy study in a remote area
of the highlands of Papua New Guinea (population 25000),
observed that injury was the leading cause of death in the age
group 15–44 years. The annual mortality rates per 100000
population in this age group were 105 for males and 79 for
females. The deaths included homicide, suicide, drowning
and poisoning in addition to those caused by burns, falls
and falling objects and motor vehicles. In contrast with
community-based mortality rates, the hospital-based mortal-
ity rate from rural Ghana was 4.5/100000 persons per year
(Mock et al. 1995). It can be assumed that many patients with
serious injury died before reaching hospital.
The maternal mortality ratio of 8.9 per 1000 deliveries we
observed was much higher than that reported by AKHS for
Ghizar district in 1997. According to the AKHS report there
were only 9 maternal deaths in 1997, giving a ratio of 2.4
deaths per 1000 deliveries. The causes of maternal death,
according to the report, were: retained placenta 3, post-
partum haemorrhage 3, sepsis 2, and postoperative death 1,
following prolonged labour. No deaths in early pregnancy,
especially as a result of abortion, were reported and none
from indirect causes. Most significantly, because of the
absence of a trained surgeon that year, there were no
caesarian sections conducted at Singal Medical Centre, while
there were 3661 deliveries in the district. The implication of a
low rate of caesarian section is a higher incidence of death
and disability. A 6–8% rate of caesarian sections should be
expected provided that known and agreed indications for the
operation are strictly observed (Francome & Savage 1993).
One of the lowest rates of caesarian section achieved in an
urban community in the USA was 11.5 per 1000 live births
(Myers & Gleicher 1988).
The preliminary results of the community-based maternal
and infant mortality survey undertaken by the Community
Health Sciences department of Aga Khan University suggests
variation in maternal mortality ratio depending on access to
health care facilities in rural Balochistan and North-west
Frontier provinces of Pakistan (Midhet 1994). In rural
Balochistan (4 districts; 20 486 households in all), rates varied
between 3.64 and 6.30/1000 live births. In rural North-west
Frontier Province (3 districts; 7500 households in all),
rates varied between 3.60 and 5.23/1000 live births. In a
population-based survey in urban squatter settlements in
Karachi, Fikree et al. (1994) estimated a maternal mortality
ratio of 2.8 per 1000 live births. A report from the obstetrics
and gynaecology department of the Jinnah Postgraduate
Medical Centre in Karachi (Jaffery & Korejo 1993), which
© 1999 Blackwell Science Ltd854

Tropical Medicine and International Health volume 4 no 12 pp 846–857 december 1999
M. Ahmed et al. Survey of surgical emergencies in rural Pakistan
delivers 7000 indigent women per year (60% unbooked) was
in striking contrast. The centre acknowledged that 23% of all
maternal deaths occurred in women before they arrived at the
hospital and another 26% died within half an hour of arrival.
Its estimate of maternal mortality was 7.1 per 1000 deliveries.
Maternal mortality estimates from rural population-based
surveys are also available from other developing countries. In
rural Burkina Faso, the maternal mortality ratio declined
from 5.7 to 3.0 per 1000 live births during the period 1941–87
(Garenne et al. 1997). In coastal Kenya it was 6.6 (Boerma &
Mati 1989), in rural Bangladesh 5.5–6.2 (Koenig et al. 1988),
in southern India 8.3 (Bhatia 1986), and in The Gambia 10.2
per 1000 live births (Billewicz & McGregor 1981).
The perinatal mortality rate in our survey was 48 per 1000
deliveries (16/335). Awan (1979) in a prospective investigation
of pregnant women residing in an area of Lahore cantonment
in Pakistan, had observed a perinatal mortality rate of
61/1000 births. In the hospital-based Zaria study (Harrison
1985), the perinatal mortality rate per 1000 singleton births
was 22 in booked healthy women, 74 in the booked compli-
cation group, and 243 in unbooked emergencies. It seems that
maternal and child health in Ghizar was infinitely better than
in a section of the Zaria community producing a high pro-
portion of unbooked emergencies, but it did not compare
favourably with the healthier and better attended section of
that community. Birth asphyxia and birth trauma cause 32%
of newborn deaths in developing countries and can poten-
tially be prevented through improved surgical access (WHO
Maternal Health and Safe Motherhood Program; unpub-
lished estimates 1994).
An important limitation of our study was that elicitation
of an acute surgical illness depended entirely on the ability of
the interviewer to describe the event, and of the respondent
to comprehend and recall the occurrence of such an event.
Careful selection of interviewer and respondent may have
reduced the chances of error. However, no attempt was made
to corroborate the occurrence of every illness event in the
household with its detection and management by a health
care provider. Nor was there an attempt to obtain objective
evidence of an illness event in the form of a residual deform-
ity or debility. A 12-month recall period was used to produce
higher frequencies of events for analyses, but had the draw-
back of possible memory decay (Harel et al. 1994). To reduce
recall bias, the inquiry was limited to specific illness events of
serious import. Repeated surveys of study households at fre-
quent intervals during the study period may have further
reduced inaccuracies resulting from memory decay, but were
not feasible.
The validity of the death rate estimates obtained from the
mean 26-year recall should also be examined. It is highly
likely that the respondents would accurately recall circum-
stances of death of a household member unless the event had
occurred during the respondents’ childhood in the household.
In the latter case, the death could potentially be either
wrongly classified or forgotten. A forgotten death would tend
to lower the rate estimate. The likelihood of misclassification
of a maternal or injury-related death seems low, even though
a maternal death preventable by surgical intervention would
not be differentiated. On the other hand, misclassification of
deaths from acute abdomen and other categories of acute
surgical illness seems more likely. Yet despite these reser-
vations, there was considerable consistency between the
results of the mean 26-year recall and the 1-year survey in our
study in relation to death rates from injury, acute abdomen
and maternal causes.
Our community-based survey of surgical need, undertaken
with a view to streamline a surgical service, prevented us from
using standardized definitions of injury and maternal mor-
bidity which include nonsurgical conditions. This is partly
responsible for the differences in incidence rates compared
with other community-based studies. Acute abdomen does
not have a standardized definition. However, its inclusion
from the viewpoint of the study’s objective was important.
While mortality rates from injury and pregnancy elicited in
our study broadly agree with other studies, death rates from
the other categories of acute surgical illness, lacking standard
definitions, could not. However, the relatively high death
rate from superficial spreading infection in the age group
, 5 years can be explained by the high rate of home deliveries
and prevalent unsterile home delivery practices leading to
umbilical stump sepsis. The high death rate from tetanus
neonatorum in Pakistan, the highest in the eastern
Mediterranean region (EMRO & WHO 1995), reflects such
practices. Umbilical stump sepsis is also known to cause por-
tal venous thrombosis leading to death from GI haemorrhage
in the young, as observed in our study. Although frostbite
might account for the limb gangrene observed in the young in
our study, it does not generally cause death (Hashmi et al.
1998). Neglected strangulated hernias can certainly explain
deaths associated with acute groin swellings at all ages. The
high death rate from acute abdomen in the present study is
reminiscent of the 85% mortality from secondary peritonitis
observed in the west at the turn of the century, when surgery
was not indicated for this condition (Kirschner 1926).
Lastly, our limitation is also that we derived the lowest rate
estimates of mortality and operative procedures in each
module because of missing data. However, in a way, under-
estimation of mortality rates is likely to compensate for
underestimation of surgical procedure rates.
Conclusion
We have shown that a population-based survey can provide
valid estimates of the incidence of broad categories of acute
© 1999 Blackwell Science Ltd 855

Tropical Medicine and International Health volume 4 no 12 pp 846–857 december 1999
M. Ahmed et al. Survey of surgical emergencies in rural Pakistan
surgical illness in a rural community. Such estimates from
rural areas in developing countries are hard to come by in the
literature. Yet, population-based estimates are much more
sensitive than hospital-based information in eliciting the bur-
den of acute surgical illness. Estimates of acute surgical inter-
vention rates based on population studies are even harder to
find. Along with estimates of acute surgical mortality rates,
they are important for understanding the burden of unmet
emergency surgical needs. From our study, it was clear that
the incidence rates of injury, maternal complications and
acute abdomen in the Ghizar community far exceeded the
rates of acute surgical intervention for these conditions; the
mortality rates were correspondingly high. The evidence
clearly points to a significant deficiency in emergency surgical
care in Ghizar.
Such evidence could provide the stimulus for an organized
provider like AKHS to improve the health service. For in-
stance, it would be necessary to introduce injury-preventive
measures, enhance the quality of antenatal care, encourage
family planning, and train LHVs at the health centres to deal
effectively with obstetrical complications and refer appropri-
ate cases in a timely fashion to SMC. It would also be neces-
sary to remove cultural, physical and fiscal barriers to seeking
surgical care, ensure continuous posting of a surgeon at
SMC, who is trained to manage general surgical, orthopedic,
and obstetrical emergencies, and make arrangements for the
transfer of complex cases to a secondary care facility.
Acknowledgements
This project was funded by a seed money grant from the Aga
Khan University. The authors are grateful to Dr Imam Yar
Baig, General Manager AKHS, Northern Areas for facili-
tating the survey, to Dr Agha Jamil for help with data
analyses and Messers Sarwat Hussain and Nizar Nooruddin
for assistance in preparing the manuscript.
References
Aga Khan Health Services (1997) Annual report. Northern Areas
Health Care Program, Pakistan.
Awan AK (1979) Perinatal mortality. In Proceedings of the confer-
ences on child health. 17–22 February 1979. Ministry of Health
Social Welfare and Population, Government of Pakistan in collab-
oration with WHO and UNICEF, Geneva, pp. 70–73.
Bangdiwala SI, Anzola-Perez E, Romer C et al. (1990) The incidence
of injuries in young people: 1. Methodology and results of a col-
laborative study in Brazil, Chile, Cuba and Venezuela. Inter-
national Journal of Epidemiology 19, 115–124.
Barss P, Dakulala P & Doolan M (1984) Falls from trees and tree-
associated injuries in rural Melanesians. British Medical Journal
289, 1717–1720.
Barss PG (1991) Health impact of injuries in the highlands of Papua
New Guinea: A verbal autopsy study. Doctoral Dissertation, The
Johns Hopkins School of Hygiene and Public Health, Baltimore.
Belghiti A, De Brouwere V, Kegels G & Van Lerberghe W, (1998)
Monitoring unmet obstetric need at district level in Morocco.
Tropical Medicine and International Health 3, 584–591.
Bhatia JC (1986) A study of maternal mortality in Ananthpur
District, Andhra Pradesh, India. India Institute of Management,
Bangalore.
Billewicz WZ & McGregor IA (1981) The demography of two West
African (Gambian) villages. 1951–75. Journal of Biosocial Science
13, 219–240.
Blanchard RJW & Maguire D (1985) Intestinal obstruction during
Ramazan. Pakistan Journal of Surgery 1, 17–20.
Blanchard RJW, Blanchard MEE, Toussignant P, Ahmed M &
Smythe CM (1987) The epidemiology and spectrum of surgical
care in district hospitals of Pakistan. American Journal of Public
Health 77, 1439–1445.
Boerma JT & Mati JKG (1989) Identifying maternal mortality
through networking: results from coastal Kenya. Studies in Family
Planning 20, 245–253.
Bokhari H (1985) Volvulus of the sigmoid colon: pathogenesis and
review of treatment. Pakistan Journal of Surgery 1, 13–16.
Britt H, Bridges-Webb C, Sayer CP et al. (1994) The diagnostic diffi-
culties of abdominal pain. Australian Family Physician 23,
375–381.
Collins JG (1990) Type of injuries by selected characteristics, United
States 1985–87. US Department of Health and Human Services,
Hyattsville.
Courtright P, Haile D & Kohls E (1993) The epidemiology of burns
in rural Ethiopia. Journal of Epidemiology and Community
Health 47, 19–22.
Ebong WW (1978) Falls from trees. Tropical and Geographical
Medicine 30, 63–67.
EMRO & WHO (1995) Major child killers and handicapping condi-
tions. In The State of Child Health in the Eastern Mediterranean
Region (eds JK Harfouche & LJ Verhoestrate) 2nd edn. revised by
H Al-Shazali. Eastern Mediterranean Regional Organization.
Technical publication series 9. WHO Regional Office for the
Eastern Mediterranean, Alexandria. pp. 138.
Fikree FF, Gray RH & Berendes HW (1994) A community-based
nested case-control study of maternal mortality. International
Journal of Gynaecology and Obstetrics 47, 247–255.
Francome C & Savage W (1993) Caesarian section in Britain and the
United States 12% or 24%: is either the right rate? Social Science
and Medicine 37, 1199–1218.
Garenne M, Sauerborn R, Nougtara A, Borchert M, Benzler J &
Diesfeld J (1997) Direct and indirect estimates of maternal mortal-
ity in rural Burkina Faso. Studies in Family Planning 28, 54–61.
Gordan JE, Gulati PV & Wyon J (1962) Traumatic accidents in rural
tropical regions: an epidemiological field study in Punjab, India.
American Journal of Medical Science 243, 158–178.
Harel Y, Overpeck MD, Jones DH et al. (1994) The effects of recall
on estimating nonfatal injury rates for children and adolescents.
American Journal of Public Health 84, 599–605.
Harrison JA (1985) Childbearing, health and social priorities: a survey
of 22774 consecutive hospital births in Zaria, Northern Nigeria.
British Journal of Obstetrics and Gynaecology 92 (Suppl.), 1–119.
Hashmi MA, Rashid M, Haleem A, Bokhari SAH & Hussain T
© 1999 Blackwell Science Ltd856

Tropical Medicine and International Health volume 4 no 12 pp 846–857 december 1999
M. Ahmed et al. Survey of surgical emergencies in rural Pakistan
Nordberg EM (1984) Incidence and estimated need of caesarian sec-
tion, inguinal hernia repair and operation for strangulated hernia
in rural Africa. British Medical Journal 289, 92–93.
Nundy S (1984) How might we improve surgical services for rural
populations in developing countries? British Medical Journal 289,
71–72.
Odero WO & Kibosia JC (1995) Incidence and characteristics of
injuries in Eldoret. Kenya. East African Medical Journal 11,
706–710.
Onuba O (1988) Pattern of burns injury in Nigerian children.
Tropical Doctor 18, 106–108.
Rutkow IM & Zuidema GD (1981) Surgical rates in the United
States: 1966–78. Surgery 89, 151–162.
Smith GS & Barss P (1991) Unintentional injuries in developing
countries: the epidemiology of a neglected problem. Epidemi-
ological Review 13, 228–266.
Thompson HJ & Jones PF (1986) Active observation in acute ab-
dominal pain. American Journal of Surgery 152, 522–525.
Wasson KH, Sox HC Jr & Sox CH (1981) The diagnosis of abdomi-
nal pain in ambulatory male patients. Medical Decision Making 1,
215–224.
WHO (1994) Mother-baby package: Implementing safe motherhood
in countries. Safe motherhood practical guide. Maternal health
and safe motherhood program, Division of Family Health,
Geneva. WHO/FHE/MSM/94.11.
White JJ, Santillana M & Haller JA (1975) Intensive in-hospital
observation: a safe way to address unnecessary appendectomy.
American Surgery 41, 793–798.
Wickham C, Cooper C, Margett BM et al. (1989) Muscle strength
activity, housing and the risk of falls in elderly people. Age and
Ageing 18, 47–51.
Zimicki S, Nahar L, Sardar AM et al. (1985) Cause of death report-
ing in Matlab: scource book of cause-specific mortality rates
1975–81. International Centre for Diarrhoeal Disease Research,
Dhaka.
Zwi AB (1993) The public health burden of injury in developing
countries: a critical review of the literature. Tropical Diseases
Bulletin 90, 11.
© 1999 Blackwell Science Ltd 857
(1998) Frostbite: epidemiology at high altitude in the Karakoram
mountains. Annals of the Royal College of Surgeons of England
80, 91–95.
Irvin TT (1989) Abdominal pain: a surgical audit of 1190 emergency
admissions. British Journal of Surgery 76, 1121–1125.
Jaffery SN & Korejo R (1993) Mothers brought dead: an enquiry
into causes of delay. Social Science and Medicine 36, 371–372.
Kirschner M (1926) Die Behandlung der akuten eitrigen freien
Bauchfellentzuendung. Archives Klinikum Chirurgicum 142, 253.
Koenig MA, Fauveau V, Chowdhury AI, Chakraborty J & Khan MA
(1988) Maternal mortality in Matlab, Bangladesh: 1976–85.
Studies in Family Planning 19, 69–80.
Lau E, Donnan S, Barker DJP & Cooper C (1988) Physical activity
and calcium intake in fracture of the proximal femur in Hong
Kong. British Medical Journal 297, 1441–1443.
Lau EMC, Cooper C, Wickham C, Donnan S & Barker DJP (1990)
Hip fracture in Hong Kong and Britain. International Journal of
Epidemiology 19, 1119–1121.
Marsh D, Sheikh A, Khalil A et al. (1996) Epidemiology of adults
hospitalized with burns in Karachi, Pakistan. Burns 22, 225–229.
McCord C (1987) Use of surgical technicians to expand surgical ser-
vices in rural Mozambique. In USA for Africa proposal.
Midhet F (1994) Maternal mortality in rural Balochistan and the
Hazara division of North West Frontier Province. In Report of an
international workshop at the Aga Khan University on Maternal
and Infant Mortality Policy and Intervention, February 7–9, 1994.
National Institute of Health, Pakistan, UNICEF and World Bank,
pp. 43–46.
Mock CN, Adzotor E, Denno D, Conklin E & Rivara F (1995)
Admissions for injury at a rural hospital in Ghana: Implications
for prevention in the developing world. American Journal of Public
Health 85, 927–931.
Myers SA & Gleicher N (1988) A successful program to lower
caesarian section rates. Special Article. New England Journal of
Medicine 319, 1511–1516.
Nordberg E, Holmberg S & Kiugu S (1996) Rates of major surgery
by age and sex in a rural district in Kenya. Annals of Tropical
Medicine and Parasitology 90, 213–221.




















