
sports physical therapy - IJSPT
156
I J SPT INTERNATIONAL JOURNAL OF SPORTS PHYSICAL THERAPY VOLUME TEN issue THREE APRIL 2015
-
Upload
khangminh22 -
Category
Documents
-
view
4 -
download
0
Transcript of sports physical therapy - IJSPT

I JSP
T INTERNATIONAL JOURNAL OF SPORTS PHYSICAL THERAPY
VOLUME TEN issue THREEAPRIL 2015


Editor in ChiefMichael L. Voight, PT, DHSc, OCS, SCS, ATC, CSCSBelmont UniversityNashville, Tennessee – USA
Senior Associate EditorBarbara Hoogenboom, PT, EdD, SCS, ATCGrand Valley State UniversityGrand Rapids, Michigan - USA
Manuscript CoordinatorAshley Campbell
Managing EditorMary Wilkinson
Editorial Board:
Scott Anderson, PT, Dip Sport PTNorthgate Physical TherapyRegina, Saskatchewan – Canada
Lindsay Becker, PT, DPT, SCS, CSCSThe Ohio State University Sportsmedicine CenterColumbus, Ohio – USA
Barton Bishop, PT, DPT, SCS, CSCSSport and Spine Rehab of RockvilleRockville, Maryland – USA
Turner A. “TAB” Blackburn, Jr., MEd, PT, ATCClemson Sports Medicine and RehabilitationManchester, Georgia – USA
Robert J. Butler, PT, DPT, PhDDuke UniversityDurham, NC – USA
Rick Clark, PT, DScPT, CCCEAir Force AcademyColorado Springs, CO – USA
George J. Davies, PT, DPT, SCS, ATC, FAPTAArmstrong Atlantic State UniversitySavannah, Georgia – USA
Mark S. De Carlo, PT, DPT, MHA, SCS, ATCAccelerated RehabilitationIndianapolis, Indiana – USA
Todd S. Ellenbecker, DPT, SCS, OCSPhysiotherapy Associates Scottsdale Sports ClinicScottsdale, Arizona – USA
John A. Guido, Jr., PT, MHS, SCS, ATC, CSCSOchsner Health SystemsNew Orleans, Louisiana – USA
Elizabeth L. Harrison, PT, PhD, Dip Sport PTUniversity of SaskatchewanSaskatoon, Saskatchewan – Canada
Walter L. Jenkins, PT, DHS, ATCEast Carolina UniversityGreenville, North Carolina - USA
Daniel S. Lorenz, PT, DPT, ATC, CSCSProvidence Medical CenterKansas City, Kansas - USA
Lorrie Maffey, PT, MPT, Dip Manip PTUniversity of CalgaryCalgary, Alberta – Canada
Terry Malone, PT, EdD, ATC, FAPTAUniversity of KentuckyLexington, Kentucky – USA
Peter J. McNair, PT, PhDAuckland University of TechnologyAuckland – New Zealand
Grethe Myklebust, PT, PhDOslo Sport Trauma Research CenterNorwegian School of Sports SciencesOslo – Norway
IJSPT INTERNATIONAL JOURNAL OF
SPORTS PHYSICAL THERAPY
Associate Editors, Thematic Issues:Robert Manske, PT, DPT, Med, SCS, ATC, CSCSWichita State UniversityWichita, Kansas – USA
Associate Editors:Mario Bizzini, PT, MScSchulthess ClinicZürich – Switzerland
Henning Langberg, PT, PhD, MScInstitute of Sports MedicineCopenhagen – Denmark

Phil Page, PT, PhD, ATC, CSCSThe Hygenic CorporationAkron, Ohio – USA
Mark Paterno, PT, PhD, MBA, SCS, ATCCincinnati Children’s Hospital Medical CenterCincinnati, Ohio – USA
Michael P. Reiman, PT, DPT, OCS, SCS, ATC,FAAOMPT, CSCS
Duke University School of MedicineDurham, North Carolina – USA
Mark F. Reinking, PT, PhD, SCS, ATCSaint Louis UniversitySt. Louis, Missouri – USA
Jill Robertson, PT, MSc (PT), Dip Manip PTBeaverbank Orthopaedic and Sport PhysiotherapyHalifax, Nova Scotia – Canada
Kevin Robinson, PT, DSc, OCSBelmont UniversityNashville, Tennessee – USA
Barbara Sanders, PT, PhD, SCS, FAPTATexas State University-San MarcosSan Marcos, Texas – USA
Teresa L. Schuemann, PT, DPT, SCS, ATC, CSCSColorado Physical Therapy SpecialistsFort Collins, Colorado – USA
Patrick Sells, DA, ESBelmont UniversityNashville, Tennessee – USA
Laurie Stickler, MSPT, OCSGrand Valley State UniversityGrand Rapids, Michigan – USA
Steven R. Tippett, PT, PhD, SCS, ATCBradley UniversityPeoria, Illinois – USA
Timothy F. Tyler, PT, ATCNISMAT Lenox Hill HospitalNew York, New York – USA
Timothy Uhl, PT, PhD, ATCUniversity of KentuckyLexington, Kentucky – USA
Mark D. Weber, PT, PhD, SCS, ATCUniversity of Mississippi Medical CenterJackson, Mississippi – USA
Kevin Wilk, PT, DPTChampion Sports MedicineBirmingham, Alabama – USA
Erik Witvrouw, PT, PhDGhent UniversityGhent – Belgium
EDITORIAL STAFF & BOARD
S P O R T S P H Y S I C A L T H E R A P YS E C T I O N
Executive CommitteeTim Tyler, PT, MS, ATC
President
Robert Manske, PT, DPT, Med, SCS, ATC, CSCSVice President
Teresa L. Schuemann, PT, DPT, SCS, ATC, CSCSSecretary
Bryan Heiderscheit, PT, PhD Treasurer
Stacey J. Pagorek, PT, DPT, SCS, ATCRepresentative-At-Large
AdministrationMark S. De Carlo, PT, DPT, MHA, SCS, ATC
Executive Director
Tammy JacksonExecutive Assistant
Mary WilkinsonDirector of Marketing
WebmasterManaging Editor, Publications
Contact Information9002 N. Meridian Street, Suite 112AIndianapolis, Indiana 46260
877.732.5009 Toll Free • 317.829.5790 Voice317.829.5791 Faxwww.spts.org
IJSPT is a bimonthly publication, with release dates inFebruary, April, June, August, October and December.
ISSN 2159-2896
IJSPT international JOURNAL OF
SPORTS PHYSICAL THERAPY
I N T E R N AT I O N A L J O U R N A LO F S P O R T S P H Y S I C A L T H E R A P Y
Editorial Staff
Michael L. Voight, PT, DHSc, OCS, SCS, ATCEditor-in-Chief
Barbara Hoogenboom, PT, EdD, SCS, ATCGrand Valley State UniversityGrand Rapids, Michigan - USA
Senior Associate Editor
Robert Manske, PT, DPT, Med, SCS, ATC, CSCSWichita State UniversityWichita, Kansas – USA
Associate Editor, Thematic Issues
Associate EditorsMario Bizzini, PT, MScSchulthess ClinicZürich – Switzerland
Henning Langberg, PT, PhD, MScInstitute of Sports MedicineCopenhagen – Denmark
Ashley CampbellManuscript Coordinator
Mary WilkinsonManaging Editor
Advertising SalesThe International Journal of Sports Physical Therapyaccepts advertising on its website, www.ijspt.org.
Log on to http://www.ijspt.org/advertisers for moreinformation about rates and placement opportunities.You may also email Mary Wilkinson, Marketing Director,
at [email protected] or contact by phone at317.501.0805.
I N T E R N AT I O N A L J O U R N A LO F S P O R T S P H Y S I C A L T H E R A P Y
is a publication of the Sports Physical Therapy Section ofthe American Physical Therapy Association.IJSPT is also an official journal of theInternational Federation of Sports PhysicalTherapy (IFSPT).

Page Number Article Title
Original Research
272 Relationship between Isokinetic Knee Strength and Jump Characteristics Following Anterior Cruciate Ligament ReconstructionAuthors: Laudner K, Evans D, Wong R, Allen A, Kirsch T, Long B, Meister K
281 Demographic and Epidemiological Trends in Patellofemoral Pain Authors: Glaviano NR, Kew M, Hart JM, Saliba S
291 The Effect of a Pelvic Compression Belt on Functional Hamstring Muscle Activity in Sportsmen With and Without Previous Hamstring Injury Authors: Arumugam A, Milosavljevic S, Woodley S, Sole G
303 Functional Movement Screen Normative Values and Validity in High School Athletes: Can the FMSTM be used as a Predictor of Injury? Authors: Bardenett SM, Micca JJ, DeNoyelles JT, Miller SD, Jenk DT, Brooks GS
309 A Comparison of Change in 3D Scapular Kinematics with Maximal Contractions and Force Production with Scapular Muscle Tests Between Asymptomatic Overhead Athletes with and without Scapular DyskinesisAuthors: Seitz AL, McClelland RI, Jones WJ, Jean RA, Kardouni JR
319 Total Arc of Motion in the Sidelying Position: Evidence for a New Method to Assess Glenohumeral Internal Rotation Deficit in Overhead AthletesAuthors: Cieminski CJ, Klaers H, Kelly SM, Stelzmiller MR, Nawrocki TJ, Indrelie AJ
332 An Elastic Exercise Band Mounted with a Bandcizer™ can Differentiate Between Commonly Prescribed Home Exercises for the Shoulder.Authors: McGirr K, Harring SI, Kennedy TSR, Pedersen MFS, Hirata RP, Thorborg K, Bandholm T, Rathleff MS
341 Impact Shoulder Angles Correlate with Impact Wrist Angles in Standing Back Handsprings in Preadolescent and Adolescent Female GymnastsAuthors: McLaren K, Byrd E, Herzog M, Polikandriotis J, Willimon SC
Case Report
347 Silent Deltoid Atrophy in Beach Volleyball Players: A Report of Two Cases and Literature ReviewAuthor: Monteleone G, Gismant M, Stevanato G, Tiloca A
354 Improved Pressure Pain Thresholds and Function Following Noxious Electrical Stimulation on a Runner with Chronic Achilles Tendinopathy: A Case ReportAuthors: Eckenrode BJ, Stackhouse SK
363 Cuboid Manipulation and Exercise in the Management of Posterior Tibialis Tendinopathy: A Case ReportAuthor: Patla C, Lwin J, Smith L, Chaconas E
371 Reactive Neuromuscular Training Results in Immediate and Long Term Improvements in Measures of Hamstring Flexibility: A Case Report Author: Loutsch RA, Baker RT, May JM, Nasypany AM
378 The Management of Iliotibial Band Syndrome with a Multifaceted Approach: A Double Case ReportAuthor: Shamus J, Shamus E
Clinical Commentary
391 Performance Optimization and Injury Prevention Strategies for the Army Physical Fitness Test: Technique MattersAuthors: Thelen M, Koppenhaver S
402 Dry Needling for Myofascial Trigger Point Pain: A Clinical Commentary402Authors: Unverzagt C, Berglund K, Thomas JJ
TABLE OF CONTENTS
VOLUME 10, NUMBER 3

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 272
ABSTRACTBackground: Clinicians are often challenged when making return-to-play decisions following anterior cruciate liga-ment reconstruction (ACL-R). Isokinetic strength and jump performance testing are common tools used to make this decision. Unfortunately, vertical jump performance standards have not been clearly established and many clinicians do not have access to isokinetic testing equipment.
Purpose: To establish normative jump and strength characteristics in ACL-R patients cleared by an orthopedic physi-cian to return-to-play and to determine if relationships exist between knee isokinetic strength measurements and jump characteristics described using an electronic jump map system.
Study Design: Descriptive laboratory study.
Methods: Thirty-three ACL-R patients who had been cleared to return to athletic competition participated in this study. Twenty-six of these ACL-R participants were also matched to 26 asymptomatic athletes based on sex, limb, height, and mass to determine isokinetic strength and jump characteristic differences between groups. Jump tests consisted of single leg vertical, double leg vertical, and a 4-jump single leg vertical jump assessed using an electronic jump mat system. Independent t-tests were used to determine differences between groups and multiple regression analyses were used to identify any relationships between jump performance and knee strength (p<0.05).
Results: The ACL-R group had lower vertical jump capabilities and some bilateral knee strength deficiencies com-pared to the matched control group. The ACL-R group also showed several moderate-to-strong positive relationships for both knee extension and flexion strength with several jump performance characteristics, such as single and double leg vertical jump height.
Conclusion: The current results indicate that ACL-R patients present with several knee strength and vertical jump differences compared to a matched control group at the time of return-to-play. Also, ACL-R patient’s performance on an electronic jump mat system is strongly related to isokinetic knee strength measures.
Keywords: Anterior cruciate ligament, functional tests, isokinetic strength, jump mat, return-to-play, vertical jump.
Level of Evidence: 2b
IJSP
TORIGINAL RESEARCH
RELATIONSHIP BETWEEN ISOKINETIC KNEE
STRENGTH AND JUMP CHARACTERISTICS
FOLLOWING ANTERIOR CRUCIATE LIGAMENT
RECONSTRUCTION
Kevin Laudner, PhD, ATC1
Daniel Evans, PT2
Regan Wong, PT2
Aaron Allen, CSCS2
Tom Kirsch, PT2 Brian Long, PT2
Keith Meister, MD2
1 Illinois State University, Normal, IL, USA2 Texas Metroplex Institute for Sports Medicine and
Orthopedics, Arlington, TX, USA
Investigation performed in the School of Kinesiology and Recreation at Illinois State University, Campus Box 5120 Normal, IL, 61790, USA
CORRESPONDING AUTHORKevin G. Laudner, PhD, ATCPhone: 309-438-5197Fax: 309-438-5559 E-mail: [email protected]

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 273
Table 1. Descriptive participant demographics
INTRODUCTIONOne of the challenges during the rehabilitation of athletes recovering from anterior cruciate ligament reconstruction (ACL-R) is gauging their functional ability and when it is safe to return to competitive sports. Post-operative assessment often includes lax-ity, flexibility, proprioception, strength, and func-tional testing.1-4 Functional testing has been reported to show how patient’s performance during physical tests, such as laxity and range of motion, correlate to more functional physical performance, such as those used in specific sports.2,3,5
Knee extension and flexion strength deficits have been reported to place unnecessary stress on the ACL due to a loss in lower extremity control.6-8 Knee extension and flexion strength are often assessed during the various stages of an ACL rehabilitation protocol and used as a gauge of functional ability and subsequently in the decision of when to return to participation.1-4,9-11 A survey of 40 international knee experts suggested that “adequate leg extension power” needs to be accomplished prior to return to play.11 Unfortunately, isokinetic testing systems that can measure extension/flexion power among other aspects of strength and endurance are not readily available for many clinicians due to limited space and budget.
Jump specific training has been used in various populations for the purpose of improving functional strength and power.13,14 Researchers have shown significant relationships between knee strength testing and jump testing, such as hop tests for distance.15, 16 Jumps for distance have been recom-mended to be useful for determining functional abil-ity among ACL deficit patients.17-21 However, little research has investigated the relationship between isokinetic testing and vertical jump tests among athletes. Although Petschnig et al22 did investigate the relationship between strength and jump tests, these authors did not use athletes or faster isokinetic speeds, which may be more indicative of athletic performance.
The purpose of this study was twofold. The first was to establish normative jump and strength charac-teristics in ACL-R patients cleared by an orthope-dic physician to return-to-play. The second purpose was to determine the relationship between knee
isokinetic strength and several jump characteris-tics determined using an electronic jump map sys-tem among ACL-R patients who had been cleared to return-to-play. An improved understanding of the usefulness of these jump mat systems may provide clinicians an additional means for making return-to-play decisions.
METHODSThirty-three participants volunteered for the ACL-R group (17 females, 16 males; age: 18.1±3.5 yrs; height: 176.0±9.9 cm; mass: 71.8±11.5 kg; involved limb: 14 dominant leg, 19 non-dominant leg). The same orthopedic surgeon performed all of the partic-ipants’ reconstructive surgeries using a bone-patellar tendon-bone autograft technique. These participants also completed a standardized therapeutic rehabilita-tion protocol at the same outpatient clinic under the guidance of a physical therapist. The rehabilitation protocol utilized is a combination of various evidence based programs and includes the use of modalities, open and closed chain strengthening exercises, patel-lar mobilizations, flexibility exercises, proprioceptive exercises, and functional activities, such as shuttle runs and forward and lateral jumps. At the time of testing, all of the ACL-R participants were at least six months post-operative (7.8±1.9 months) and had been cleared by an orthopedic physician to return-to-play. All return-to-play decisions were based on a combination of factors which include isokinetic strength testing, full pain free ROM, arthrometry testing, as well as physical therapist input based on biomechanical deficiencies and satisfactory comple-tion of the rehabilitation program.
Twenty-six of the ACL-R participants (11 females, 15 males; 7.8±1.9 months post-operative, involved limb: 10 dominant leg, 16 non-dominant leg), were matched to 26 control participants based on limb, sex, height, and mass (Table 1). Dominant leg was defined as the preferred leg to kick a ball. The control group had

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 274
no recent history of lower extremity injury (past six months) and no history of lower extremity surgery. All participants were members of an organized sports team (e.g. basketball, soccer, football, volleyball).
The Just Jump system (Probotics, Huntsville, AL) was used to assess jump performance. This system con-sists of a 27 x 27 inch mat interfaced with a handheld computer (Figure 1) capable of measuring several leg strength characteristics, such as vertical jump height, lateral movement times, and ground contact time (i.e. quickness). Kenny et al.23 has shown that electronic jump mats are valid when compared to force plate data, while Nuzzo et al.24 showed good intratester reliability for using this system (ICC=0.90-0.93; SEM=1.6-2.3 cm).
The Biodex 2 Multi-Joint Testing and Rehabilitation System (Biodex Medical Systems, Shirley, NY) uti-lizes a specialized software package, combined with a dynamometer containing strain gages, potentiom-eter, and remote range of motion set switches, along with several limb attachments, for testing, rehabili-tation, and diagnostic purposes of a variety of joints and muscle groups. The system allows for several resistance and speed options for individualizing test-ing procedures, including isometric, concentric, and eccentric modes in speeds of 0-500°/sec.
All participants attended one testing session. All par-ticipants signed an informed consent form approved
by the university institutional review board prior to all data collection and these participants rights were protected throughout the study. Anthropometric data (i.e. age, height, mass) for all participants was collected. The first phase of testing consisted of three jump tests using the electronic jump mat system (i.e. double leg vertical jump, four repeated single-leg vertical jumps, single leg vertical jump). Follow-ing a five minute rest period, the second phase of testing began and consisted of measuring bilateral isokinetic knee extension and flexion strength at two speeds. All tests were conducted by the same investigators. Investigators provided instructions for all testing procedures; however no verbal feedback was given during testing.
For the first phase of testing, participants warmed up for five minutes on a stationary bike using a self-determined pace. Following this warm-up, the participants completed three different jump tests: double-leg vertical jump, one-legged vertical jump, and four repeated single-leg vertical jump tests using the electronic jump mat system. Subjects were allowed to move their arms during the jump tests in whatever fashion felt most comfortable and natural. Subjects were allowed three practice trials for each procedure to ensure familiarity with the tasks. All practice trials and tests were followed by a 1 minute rest prior to the next test to minimize fatigue.
For the double-leg vertical jump test participants were asked to complete a total of three maximum effort vertical jumps using both legs. For the single-leg jump test participants also completed maximum effort jumps bilaterally; however, only the test leg was used for analysis. For both the double- and single-leg tests participants were allowed one minute of rest between each maximum vertical jump to minimize fatigue. The vertical jump heights for each jump test were displayed on the electronic jump mat system’s handheld computer, expressed in inches, and the average of the three jumps was used for data anal-ysis. For the four repeated single-leg vertical jump test each participant was instructed to jump as high and as fast as they could for four repeated jumps on the test limb. After the four consecutive single leg vertical jumps the averages of ground reaction time, power ratio consisting of air time divided by ground time, and vertical jump height expressed in inches
Figure 1. The Just Jump system used to assess jump perfor-mance.

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 275
were calculated by the jump mat system hand held computer. Failure to land the test limb(s) on the mat during any test resulted in discarding of that trial and the participant was allowed to re-test. Investiga-tors also instructed each participant to use their nat-ural jumping motion and visually monitored each for any variations in their jump mechanics.
For the second phase of testing participants were seated on the Biodex system and secured with pad-ded straps around the thigh, pelvis, and torso to minimize accessory and compensatory movements during testing. The test limb femoral condyle was aligned with the Biodex axis of rotation as per the manufacturer instructions. To ensure familiarity with the procedures participants performed five sub-maximal knee extension/flexion repetitions prior to each of the strength tests. To measure knee strength at 180°/sec, participants performed five maximal concentric contractions consecutively. To measure knee strength at 300°/sec, participants performed fif-teen maximal concentric contractions consecutively. Knee strength at 180°/sec was always tested prior to 300°/sec. Thirty seconds of rest were provided between the two strength tests in order to minimize fatigue and the averages of the repetitions were used for data analysis. Specific variables for knee strength consisted of peak torque-to-body weight (PT/BW) and percent bilateral difference in PT/BW.
Independent t-tests were used to determine dif-ferences in jump performance and knee strength between the ACL-R and matched control groups. These variables were determined for both knee extension and flexion at speeds of 180°/sec and 300°/sec. Effect sizes were determined to provide an indica tion of clinical meaningfulness of differences between groups. Effect size was calculated as ACL-R group mean – control group mean / control group standard deviation. Effect sizes were interpreted according to Cohen’s guidelines.25 Findings were considered significant at an alpha level of p<0.05.
Multiple regression analyses were used to deter-mine the strength of the relationships between knee strength and the jump performance tests within the ACL-R participants. Relationships were interpreted as follows: r=0.10-0.29 (weak); r=0.30-0.49 (moder-ate); r=0.50-1.0 (strong). The independent variables for the single leg and double leg vertical jump tests
were jump height and percent bilateral difference in jump height. The independent variables for the 4-jump single leg vertical jump test were vertical jump height, ground contact time, and the ratio of air time divided by ground time. Knee extension and flexion strength characteristics (PT/BW and percent bilateral difference in PT/BW) were the dependent variables.
RESULTSIndependent t-tests showed there were no demo-graphic group differences other than a difference in age with the control group being 3.2±5.0 years older than the ACL-R group (p=0.003). Between group differences in jump performance can be viewed in Table 2. The ACL-R group had significantly lower single leg vertical jump height in the involved knee than the control group (p=0.02). The inter-limb dif-ference in the single leg vertical jump height was also found to be greater in the ACL-R group when compared to the controls (p=0.001). Similarly, the ACL-R group had less vertical jump height (p=0.009) and air time-to-ground time ratio (p=0.01) in the involved leg during the 4-jump test compared to the control group.
Between group differences in knee extension and flexion strength can be viewed in Table 3. There was a significant bilateral difference in knee exten-sion strength at 180°/sec (p=0.001), with the ACL-R group having a larger differential than the control group. There was a similar bilateral difference in knee extension strength at 300°/sec (p=0.001) again with the ACL-R group having the larger differential. The ACL-R group also had significantly more PT/
Table 2. Between group descriptive statistics for jump tests (mean ± standard deviation)

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 276
ble leg jump height variables (r=.74 , p=.001) with single leg jump height accounting for the largest por-tion of this relationship (r=.39, p=.003). Thirty-four percent of peak torque flexion strength at 180°/sec was explained by the summation of the single and double leg jump height variables (r=.59 , p=.002); however neither single or double leg jump height significantly contributed to this relationship (p>.10). Twenty-five percent of peak torque flexion strength at 300°/sec was explained by the summation of the single and double leg jump height variables (r=.50, p=.01); however no single variable contributed sig-nificantly to this relationship. No other strength variables (bilateral difference in extension strength at 300°/sec, bilateral difference in flexion strength at 180°/sec, bilateral difference in flexion strength at 300°/sec) showed any relationship with the jump test variables (p>.07).
Several relationships were found between the vari-ous isokinetic strength tests and the summation of the 4-jump test variables. Forty percent of PT/BW extension strength at 180°/sec was explained by the summation of the 4-jump test variables (r=.64, p=.002) with vertical height contributing the most to this relationship (r=.61, p=.001). Fifty-five per-cent of PT/BW extension strength at 300°/sec was explained by the summation of the single and dou-ble leg jump height variables (r=.74, p=.001) with vertical height contributing the most to this relation-ship (r=.71, p=.001). Thirty-four percent of PT/BW flexion strength at 180°/sec was explained by the summation of the single and double leg jump height variables (r=.58, p=.007) with vertical height accounting for the largest portion of this relationship (r=.52, p=.002). No other strength variables (bilat-eral difference in extension strength at 180°/sec, bilateral difference in extension strength at 300°/sec, bilateral difference in flexion strength at 300°/sec) showed any relationship with the 4-jump tests variables (p>.17).
The independent relationships between jump perfor-mance with knee extension and flexion strength for the ACL-R group can be viewed in Tables 4 & 5, respec-tively. The ACL-R group showed moderate-to-strong positive relationships for both knee extension and flexion PT/BW with single leg vertical jump height (p<=0.004) (Tables 4 & 5). Similar positive relation-
BW extension strength in the non-involved knee at 300°/sec compared to the controls (p=0.008). No other extension strength differences existed between groups (p>0.06). Group differences for flexion strength showed that the ACL-R group had greater PT/BW in the involved limb at 180°/sec (p=0.04) and 300°/sec (p=0.03) as compared to the control group. No other flexion strength differences existed between groups (p>0.08).
Several relationships were found between the vari-ous isokinetic strength tests and the summation of single and double leg vertical height. Fifty-one per-cent of PT/BW extension strength at 180°/sec was explained by the summation of the single and dou-ble leg jump height variables (r=.71 , p=.001) with single leg jump height contributing the most to this relationship (r=.32, p=.02). Twenty-five percent of the bilateral difference in knee extension strength at 180°/sec was explained by the summation of the single and double leg jump height variables (r=.50, p=.01). Although, double leg jump height accounted for the largest portion of this relationship (r=.50, p=.004) single leg jump height also made a large contribution (r=.44, p=.009). Fifty-five percent of peak torque extension strength at 300°/sec was explained by the summation of the single and dou-
Table 3. Between group descriptive statistics for knee strength tests (mean ± standard deviation)

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 277
ACL-R patients.2, 3, 22, 26, 27 Although isokinetic knee strength testing is often viewed as an effective stan-dard for determining various stage progressions during ACL-R rehabilitation,3, 10, 26, 28 many clinicians do not have access to these expensive and bulky devices. Because of this, jump training and the use of electronic jump mat systems have become increasingly popular as an assessment tool.22 This study was the first to investigate the usefulness of a jump assessment system among athletes who had completed an ACL-R rehabilitation program and had been cleared to return-to-play by an orthopedic phy-sician. The results of this study show that ACL-R patients have less vertical jump capabilities and some bilateral knee strength differences when com-pared to matched controls. The ACL-R group also showed several moderate-to-strong positive relation-ships for both knee extension and flexion strength with several jump performance characteristics.
ships were found between knee extension and flex-ion PT/BW with double leg vertical jump (p<0.009) (Tables 4 & 5). The same positive relationships were found between knee extension and flexion PT/BW with the single leg vertical jump during the 4-jump test (p=<0.02) (Tables 4 & 5). Only two significant relationships were found between bilateral difference in knee strength and jump characteristics. Bilateral difference in knee flexion strength at 180°/sec had a moderate negative relationship with the double leg jump (r=-0.39, p=0.02). Also, the bilateral difference in knee flexion strength at 300°/sec had a moderate positive relationship with ground contact time during the 4-jump test (r=0.37, p=0.03).
DISCUSSIONJump and isokinetic strength testing are commonly utilized during therapeutic rehabilitation programs and used to determine functional capabilities among
Table 4. Relationships between involved knee extension strength and jump tests among ACL-R participants expressed as r-value (p-value)
Table 5. Relationships between involved knee fl exion strength and jump tests among ACL-R participants expressed as r-value (p- value).

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 278
cal jumps, as well as the vertical jump height and air time-to-ground time ratio during the 4-jump test when compared to a matched control group. Charac-teristics such as single leg vertical jump height and bilateral difference in vertical jump height, as well as air time-to-ground time ratio and vertical height dur-ing the repeated jump task differ when compared to a matched control group. These findings emphasize the need for vertical jump training and testing dur-ing ACL-R rehabilitation.
Although isokinetic testing has been proven to be beneficial when assessing ACL-R patients’ progress following rehabilitation,38 some clinicians may not have access to such equipment. Several studies have investigated the relationship between isokinetic knee strength testing and various jump for distance tests. Greenberger and Paterno16 reported that isokinetic knee extension strength had a significant correlation with a single leg hop for distance among an asymp-tomatic group. Paasuke et al39 showed a relationship between jump height and knee extension strength at 0°/sec and 60°/sec among asymptomatic partici-pants. However, Wilk et al,15 conducted one of the only studies to investigate and show a relationship between knee strength and hop tests among ACL-R patients. These investigators showed that knee extension peak torque correlated positively with three hop tests (hop for distance, timed hop, cross-over triple hop). The results of the current study are the first to show that a similar relationship exists among ACL-R patients during various jump tests for height. Thus, the use of these inexpensive and eas-ily portable and storable electronic jump mats may be an effective alternative to isokinetic testing as a means of determining functional performance.
There are a few limitations to the current study worth mentioning. First, the jump tests used in this study do not take into consideration side-to-side move-ments or rotation, which must also be considered during ACL-R rehabilitation. Second, the participants in this study were athletes which make comparison to non-athletes who sustain an ACL injury difficult. Also, the ACL-R participants were placed into a sin-gle group rather than separated by gender. Due to the known physical differences between genders, especially among incidence of ACL injuries, future research should investigate potential gender differ-
Numerous studies have shown diminished knee strength during various periods following ACL-R. Mattacola et al,29 reported that at 18 months post-surgery the involved knee extension isokinetic strength is not within the normal limits of the con-tralateral knee. Similarly, Giampietro30 reported several strength deficits among ACL-R patients approximately 25 months post-surgery when com-pared to a control group. Several investigations have also shown strength deviations around the time of return-to-play clearance. Thomas et al,8 showed that during this time period (approximately 212.5 days post-surgery), ACL-R patients had greater bilateral strength differences compared to a control group. Hsiao et al,31 reported that ACL-R patients had exces-sive weakness at six months post-surgery when com-pared to the contralateral knee. Similarly, Xergia et al,32 stated that knee extension deficits persist six to nine months following ACL-R. The isokinetic exten-sion strength results of the current study support these previous findings and provide further insight into deficiencies that occur at faster testing speeds such as 300°/sec. Conversely, the current results demonstrate that ACL-R patients actually have more knee flexion strength compared to a control group at speeds of 180°/sec and 300°/sec. As such, strength testing at speeds which more closely mimic func-tional activities should also be addressed in ACL-R rehabilitation programs.
Much of the previous research that has investigated jump characteristics among ACL-R patients has focused on hop tests for distance17-20, 34-36 with limited research on vertical jump performance.22, 27, 37 In one of the few studies that assessed a single one-legged jump for height among ACL-R patients, the inves-tigators reported less jump height in the involved side compared to the contralateral side.22 In another study investigating jump height, Myer et al27 found that repeated single leg jumps for height over a ten second span were less in an ACL-R group com-pared to controls. Based on these findings, Myer et al suggested that persistent side to side differences may increase risk of injury and that jump height should be considered in the return-to-play decision. The results of the current study support those of Petschnig et al and Myer et al and demonstrate that other jump characteristic deficiencies exist, such as the inter-limb difference during single leg verti-
The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 279
6. Vairo GL, Myers JB, Sell TC, Fu FH, Harner CD, Lephart SM. Neuromuscular and Biomechanical Landing Performance Subsequent to Ipsilateral Semitendinosus and Gracilis Autograft Anterior Cruciate Ligament Reconstruction. Knee Surg Sports Traumatol Arthrosc. 2008;16:2-14.
7. Lephart SM, Ferris CM, Riemann BL, Myers JB, Fu FH. Gender Differences in Strength and Lower Extremity Kinematics During Landing. Clin Orthop Relat Res. 2002:162-169.
8. Thomas AC, Villwock M, Wojtys EM, Palmieri-Smith RM. Lower Extremity Muscle Strength after Anterior Cruciate Ligament Injury and Reconstruction. J Athl Train. 2013.
9. Seto JL, Orofi no AS, Morrissey MC, Medeiros JM, Mason WJ. Assessment of Quadriceps/Hamstring Strength, Knee Ligament Stability, Functional and Sports Activity Levels Five Years after Anterior Cruciate Ligament Reconstruction. Am J Sports Med. 1988;16:170-180.
10. Jamshidi AA, Olyaei GR, Heydarian K, Talebian S. Isokinetic and Functional Parameters in Patients Following Reconstruction of the Anterior Cruciate Ligament. Isokin Ex Sci. 2005;13:267-272.
11. Paulos L, Noyes FR, Grood E, Butler DL. Knee Rehabilitation after Anterior Cruciate Ligament Reconstruction and Repair. J Orthop Sports Phys Ther. 1991;13:60-70.
12. Tsaklis P, Abatzides G. Acl Rehabilitation Program Using a Combined Isokinetic and Isotonic Strengthening Protocol. Isokin Ex Sci. 2002;10:211-219.
13. Miura K, Yamamoto M, Tamaki H, Zushi K. Determinants of the Abilities to Jump Higher and Shorten the Contact Time in a Running 1-Legged Vertical Jump in Basketball. J Strength Cond Res. 2010;24:201-206.
14. Carlock JM, Smith SL, Hartman MJ, Morris RT, Ciroslan DA, Pierce KC, et al. The Relationship between Vertical Jump Power Estimates and Weightlifting Ability: A Field-Test Approach. J Strength Cond Res. 2004;18:534-539.
15. Wilk KE, Romaniello WT, Soscia SM, Arrigo CA, Andrews JR. The Relationship between Subjective Knee Scores, Isokinetic Testing, and Functional Testing in the Acl-Reconstructed Knee. J Orthop Sports Phys Ther. 1994;20:60-73.
16. Greenberger HB, Paterno MV. Relationship of Knee Extensor Strength and Hopping Test Performance in the Assessment of Lower Extremity Function.J Orthop Sports Phys Ther. 1995;22:202-206.
17. Borsa PA, Lephart SM, Irrgang JJ. Comparison of Performance-Based and Patient-Reported Measures
ences in the same parameters. Lastly, although rela-tively fast speeds of isokinetic testing were chosen in an attempt to replicate athletic functional move-ments the authors understand that creating similar speeds and forces in a clinic is not possible.
CONCLUSIONThe results of this study indicate that ACL-R patient’s performance (e.g. jump height during single leg, double leg, and 4-jump tasks) assessed using an elec-tronic jump mat system have a moderate-to-strong positive relationship with isokinetic knee strength measures. Thus, jump height performance may be considered a partial predictor of knee strength. The ACL-R participants in this study also presented with several knee strength and vertical jump differences compared to a matched control group, suggesting that even at the time of return-to-play ACL-R athletes may not have full restoration of strength and verti-cal jump capabilities. The findings of this study may prove useful throughout an ACL-R rehabilitation protocol and when making return-to-play decisions.
REFERENCES 1. Lentz TA, Tillman SM, Indelicato PA, Moser MW,
George SZ, Chmielewski TL. Factors Associated with Function after Anterior Cruciate Ligament Reconstruction. Sports Health. 2009;1:47-53.
2. Neeter C, Gustavsson A, Thomee P, Augustsson J, Thomee R, Karlsson J. Development of a Strength Test Battery for Evaluating Leg Muscle Power after Anterior Cruciate Ligament Injury and Reconstruction. Knee Surg Sports Traumatol Arthrosc. 2006;14:571-580.
3. Bjorklund K, Skold C, Andersson L, Dalen N. Reliability of a Criterion-Based Test of Athletes with Knee Injuries; Where the Physiotherapist and the Patient Independently and Simultaneously Assess the Patient’s Performance. Knee Surg Sports Traumatol Arthrosc. 2006;14:165-175.
4. Tagesson S, Oberg B, Good L, Kvist J. A Comprehensive Rehabilitation Program with Quadriceps Strengthening in Closed Versus Open Kinetic Chain Exercise in Patients with Anterior Cruciate Ligament Defi ciency: A Randomized Clinical Trial Evaluating Dynamic Tibial Translation and Muscle Function. Am J Sports Med. 2008;36:298-307.
5. Manske R, Reiman M. Functional Performance Testing for Power and Return to Sports. Sports Health. 2013;5:244-250.

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 280
29. Mattacola CG, Perrin DH, Gansneder BM, Gieck JH, Saliba EN, McCue FC, 3rd. Strength, Functional Outcome, and Postural Stability after Anterior Cruciate Ligament Reconstruction. J Athl Train. 2002;37:262-268.
30. Vairo GL. Knee Flexor Strength and Endurance Profi les after Ipsilateral Hamstring Tendons Anterior Cruciate Ligament Reconstruction. Arch Phys Med Rehabil. 2014;95:552-561.
31. Hsiao SF, Chou PH, Hsu HC, Lue YJ. Changes of Muscle Mechanics Associated with Anterior Cruciate Ligament Defi ciency and Reconstruction. J Strength Cond Res. 2014;28:390-400.
32. Xergia SA, Pappas E, Zampeli F, Georgiou S, Georgoulis AD. Asymmetries in Functional Hop Tests, Lower Extremity Kinematics, and Isokinetic Strength Persist 6 to 9 Months Following Anterior Cruciate Ligament Reconstruction. J Orthop Sports Phys Ther. 2013;43:154-162.
33. Morrissey MC, Harman EA, Johnson MJ. Resistance Training Modes: Specifi city and Effectiveness. Med Sci Sports Exerc. 1995;27:648-660.
34. Gustavsson A, Neeter C, Thomee P, Silbernagel KG, Augustsson J, Thomee R, et al. A Test Battery for Evaluating Hop Performance in Patients with an Acl Injury and Patients Who Have Undergone Acl Reconstruction. Knee Surg Sports Traumatol Arthrosc. 2006;14:778-788.
35. Hopper DM, Goh SC, Wentworth LA, Chan D, Chau J, Wootton GJ, et al. Test–Retest Reliability of Knee Rating Scales and Functional Hop Tests One Year Following Anterior Cruciate Ligament Reconstruction. PT Sport. 2002;3:10-18.
36. Thomee R, Neeter C, Gustavsson A, Thomee P, Augustsson J, Eriksson B, et al. Variability in Leg Muscle Power and Hop Performance after Anterior Cruciate Ligament Reconstruction. Knee Surg Sports Traumatol Arthrosc. 2012;20:1143-1151.
37. Risberg MA, Ekeland A. Assessment of Functional Tests after Anterior Cruciate Ligament Surgery. J Orthop Sports Phys Ther. 1994;19:212-217.
38. Ericsson YB, Roos EM, Frobell RB. Lower Extremity Performance Following Acl Rehabilitation in the Kanon-Trial: Impact of Reconstruction and Predictive Value at 2 and 5 Years. Br J Sports Med. 2013;47:980-985.
39. Paasuke M, Ereline J, Gapeyeva H. Knee Extension Strength and Vertical Jumping Performance in Nordic Combined Athletes. J Sports Med Phys Fitness. 2001;41:354-361.
of Function in Anterior-Cruciate-Ligament-Defi cient Individuals. J Orthop Sports Phys Ther. 1998;28:392-399.
18. Noyes FR, Barber SD, Mangine RE. Abnormal Lower Limb Symmetry Determined by Function Hop Tests after Anterior Cruciate Ligament Rupture. Am J Sports Med. 1991;19:513-518.
19. O’Donnell S, Thomas SG, Marks P. Improving the Sensitivity of the Hop Index in Patients with an Acl Defi cient Knee by Transforming the Hop Distance Scores. BMC Musculoskelet Disord. 2006;7:9.
20. Paterno MV, Hillary B, Greenberger HB. The Test-Retest Reliability of a One Legged Hop for Distance in Young Adults with and without Acl Reconstruction Isokin Ex Sci. 1996;6.
21. Barber SD, Noyes FR, Mangine RE, McCloskey JW, Hartman W. Quantitative Assessment of Functional Limitations in Normal and Anterior Cruciate Ligament-Defi cient Knees. Clin Orthop Relat Res. 1990:204-214.
22. Petschnig R, Baron R, Albrecht M. The Relationship between Isokinetic Quadriceps Strength Test and Hop Tests for Distance and One-Legged Vertical Jump Test Following Anterior Cruciate Ligament Reconstruction. J Orthop Sports Phys Ther. 1998;28:23-31.
23. Kenny IC, A OC, Comyns TM. Validation of an Electronic Jump Mat to Assess Stretch-Shortening Cycle Function. J Strength Cond Res. 2012;26:1601-1608.
24. Nuzzo JL, Anning JH, Scharfenberg JM. The Reliability of Three Devices Used for Measuring Vertical Jump Height. J Strength Cond Res. 2011;25:2580-2590.
25. Cohen J. Statistical Power Analysis for the Behavioral Sciences. Hillsdale, NJ; 1988.
26. Keays SL, Bullock-Saxton JE, Newcombe P, Keays AC. The Relationship between Knee Strength and Functional Stability before and after Anterior Cruciate Ligament Reconstruction. J Orthop Res. 2003;21:231-237.
27. Myer GD, Martin L, Jr., Ford KR, Paterno MV, Schmitt LC, Heidt RS, Jr., et al. No Association of Time from Surgery with Functional Defi cits in Athletes after Anterior Cruciate Ligament Reconstruction: Evidence for Objective Return-to-Sport Criteria. Am J Sports Med. 2012;40:2256-2263.
28. Patel RR, Hurwitz DE, Bush-Joseph CA, Bach BR, Jr., Andriacchi TP. Comparison of Clinical and Dynamic Knee Function in Patients with Anterior Cruciate Ligament Defi ciency. Am J Sports Med. 2003;31:68-74.

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 281
ABSTRACTBackground: Understanding the demographics of patellofemoral pain is important to determine the best practices in diagnosis and treatment of this difficult pathology. The occurrence of patellofemoral pain has been reported from isolated sports medicine clinics and from within the military, but its incidence has never been examined in the general population within the United States.
Purpose: The purpose of this study was to examine the reported occurrence of patellofemoral pain for those individuals seeking medical care and to compare that to all other pathologies that result in anterior knee pain, such as tendinopathies, patella sublux-ation, osteoarthritis, or meniscal and bursal conditions. Occurrence rates were examined across sex, age and region within a large healthcare provider database that contains over 30 million individuals.
Methods: Data were queried with the PearlDiver Patient Record Database, a national database containing orthopedic patient records. Two common International Classification of Disease, Ninth Revision (ICD-9) codes for patellofemoral pain (717.7 – Patella Chondromalacia and 719.46 – Pain in joint, lower leg) were utilized and were searched from the years 2007-2011. The top twenty additional ICD-9 codes that were concurrently coded with 717.7 and 719.46 were removed from the data. Chi-squared and Mantel-Haenszel tests were utilized to identify statistically significant differences in the diagnosis of patellofemoral pain between sex, age, and year.
Results: During this five-year period, there were 2,188,753 individuals diagnosed with patellofemoral pain. The diagnosis was more common in females compared to males with 1,211,665 and 977,088 cases respectfully (p<0.001). Statistically significant dif-ferences between ages was found, with 50-59 year olds having the most cases with 578,854, p<0.001. And, during the five-year examination period, there was a steady increase between 2007-2011, p<0.01.
Conclusion: Patellofemoral pain was diagnosed between 1.5% and 7.3% of all patients seeking medical care within the United States. Females experienced patellofemoral pain more often than males and there was a steady increase of cases in the United States during the 2007-2011 examination period. The diagnosis of patellofemoral pain increased with age and the 50-59 year old age group had the most cases.
Keywords: Anterior knee pain, chondromalacia, epidemiology
Level of Evidence: 2b
IJSP
TORIGINAL RESEARCH
DEMOGRAPHIC AND EPIDEMIOLOGICAL TRENDS IN
PATELLOFEMORAL PAIN
Neal R. Glaviano, MEd, ATC1
Michelle Kew, BS2
Joseph M. Hart, PhD, ATC1,3
Susan Saliba, PhD, ATC, PT1
1 Department of Kinesiology, Exercise and Sport Injury Laboratory, University of Virginia, Charlottesville, VA, USA
2 School of Medicine, University of Virginia, Charlottesville, VA, USA
3 Department of Orthopedic Surgery, University of Virginia, Charlottesville, VA,USA
CORRESPONDING AUTHORNeal R. Glaviano, MEd, ATC Department of Kinesiology, Exercise and Sport Injury Laboratory, University of Virginia, Memorial Gymnasium P.O. Box 400407 Charlottesville, VA Offi ce Phone Number: (434) 924-6184. Fax Number: (434) 924-1389E-mail: [email protected]

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 282
INTRODUCTIONPatellofemoral Pain (PFP) is an overuse condition that increases pain and compressive force on the patello-femoral joint with activity and is generally not linked to trauma or known intra-articular damage to the knee.1-6 PFP is also commonly referred to as anterior knee pain or chondromalacia patella, however while these conditions often present with similar symptoms and are exacerbated by similar activities, the subtitle differences in improper interchanging nomenclature creates difficultly in the description of this pathol-ogy.7,8 Anterior knee pain is a generic term that can incorporate PFP as well as anterior knee pathologies such as a plica, fat pad fibrosis or bursitis compared to chondromalacia patella which requires softening or damage to the cartilage under the patella.9-11 PFP is specifically pain to the retro- or peri-patellar area during an array of activities ranging from prolonged sitting, squatting, to jumping and running.12-17 Those experiencing PFP often have major limitations of daily activities, work, and athletic participation. It has been reported that 74% of individuals experiencing PFP will limit or stop sport participation due to their painful symptoms.18-20 Emerging evidence suggests that PFP may also contribute to the development of patellofemoral osteoarthritis, which not only creates long-term implications for these individual’s health but also increases healthcare costs.21,22
PFP is often described as one of the most common knee conditions seen by sports medicine providers. Incidence rates have been reported to vary between 8% and 33% of all knee related injuries in small-scale epidemiological studies.23-26 It has also been reported that PFP not only occurs within physically active individuals and military personnel, but is also seen throughout the general population.25,27 While PFP is commonly believed to be experienced by ado-lescent and younger individuals, results of some of the earliest epidemiological studies suggest that PFP is one ofthe most frequently reported pathologies in individuals into their 60’s.24,28 Females have been reported to experience PFP two to ten times more often than their male counterparts.25,29
Previous studies provide some insight into the inci-dence rate of this chronic condition; however, the accuracy of these numbers has been called into ques-tion. Ireland et al,30 McConnell et al,31 and Witvrouw
et al32 have all referenced incidence rates of PFP within the general population, yet there currently is insufficient data to support these claims.7 These studies only provide data collected within individual sports medicine clinics, military populations and running clinics, which decreases the generalizability of their findings.23-26,33 Such practices or sites typi-cally provide care to specific populations and there-fore there is minimal data on the occurrence of PFP across the lifespan.7,23-26 It is important to appreci-ate the incidence of PFP and who may be suscep-tible to developing the condition in order to provide early interventions. The true understanding of the epidemiology of the pathology and its long-term consequences will influence appropriate care from healthcare professionals and help develop mecha-nisms to ultimately improve outcomes.
Since previous research has only provided incidence data from isolated sports medicine centers, single military academies and small epidemiological stud-ies, such research offers limited information and may represent only a narrow population. Therefore, the purpose of this study was to examine current trends in the diagnosis of patellofemoral pain by physicians within the general population by utiliz-ing two International Classification of Disease, Ninth Revision (ICD-9) codes commonly used to diagnose PFP. The authors hypothesized that the incidence rate of patellofemoral pain would be lower than previously published incidence rates. The current data set included diagnoses from visits to orthope-dic physicians while previous researchers examined smaller cohorts of potentially more physically active individuals. Based on previous literature, the authors also hypothesized that females would present with higher incidence rates of PFP compared to males, and that the majority of PFP cases would be seen in the younger active population, particularly in the 10-19 year old age group.
METHODSThe Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement recom-mendations to report the study methods and results was utilized.34 Data were collected with the PearlDiver Patient Record Database (PearlDiver Inc., Fort Wayne IN). The PearlDiver Database is an online database that is commercially available for retrospective reviews of

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 283
all data submitted to private insurance companies. The largest provider within the database is the Unit-edHeath Group (UnitedHealth Group, Minnetonka, MN). Patients who are insured via Medicare, Medic-aid or uninsured are not included within the Pearl-Diver database. The database contains over 1.1 billion patient records on over 30 million individual patients records between 2007 and 2011. The database can be used to identify ICD-9 codes and Current Procedural Terminology (CPT) codes.
The methodology of the current study is represented as a flow chart and is reported in Figure 1. The database was queried for patients who had been diagnosed with ICD-9 codes for patellofemoral pain (717.7 – Chondro-malacia of patella and 719.46 – Pain in joint, lower leg). These two ICD-9 codes were selected since previ-ous research identified them as the two most common diagnostic codes for PFP that does not involve struc-
tural damage or patellar tendinitis.25 Additionally, other common pathologies that may have been coded in conjunction to the 719.46 were also removed. For example, if a patient also concurrently had diagnoses corresponding to osteoarthritis, knee meniscal tears, cruciate ligament sprains, collateral ligament sprains, tendonitis, bursitis, or fractures to the patella, proxi-mal tibia or proximal fibula, they were removed from the analysis. The authors also searched seven other possible sources of anterior knee pain using nine com-mon ICD-9 codes and removed those diagnoses from the analysis as well. (Table 1, Figure 1) The decision to removed these pathologies and corresponding ICD-9 codes were related to the exclusion criteria of these pathologies seen within current PFP literature. 15,35
The remaining data were considered to be the PFP group, yet the authors chose to split the diagnoses of chondromalacia patella and pain in the lower leg
Figure 1. Flow Diagram.

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 284
in order to distinguish the prevalence of each ICD-9 code. Within those two sub-diagnoses, the number of total visits to physician’s offices by sex (male and female) and age (in ten year increments) were examined. Those data were also evaluated by region within the United States (South, Midwest, West and Northeast) and by year (2007, 2008, 2009, 2010, 2011) within the dataset.
Chi-square analyses were used to examine differ-ences between stratifications by sex and age groups. A Mantel-Haenszel test was utilized to evaluate dif-ferences in each year that was examined within the dataset. Incidence proportions were calculated by comparing the number of individuals with PFP by the total number of individuals reported in the data-base. Statistical analyses were conducted using SPSS (Version 20; SPSS Inc., Chicago, IL) with an alpha level set a priori at p≤0.05.
This study was approved by the University of Vir-ginia Institutional Review Board for Human Science Research. The review board granted access to utilize the aggregated data from the database without per-sonal informed consent from the patients included within the study.
RESULTS
Patellofemoral PainThe PearlDiver database contains a total of 30,108,510 patients with valid ICD-9 diagnosis or procedure codes during the years of 2007-2011. During this five-year period, there were 2,188,753 individuals diag-nosed with PFP as defined by using the two selected ICD-9 codes, or 7.3% of all individuals within the database. There were 437,711 cases of Chondromala-cia patella, (20% of the patients with PFP) and 1.5% of all diagnoses of individuals seeking care. There were 1,751,042 cases of joint pain of the lower limb
(80% of the patients with PFP) and representing 5.8% of all diagnoses.
Within the dataset of PFP, those with the diagnosis of joint pain of the lower limb were seen a total of 16,498,162 times while there were 2,803,842 physi-cian visits for chondromalacia. Therefore, individu-als with joint pain of the lower limb were seen by medical providers on average of 10.6 times, while those with chondromalacia were seen 6.4 times. When examining the location where medical provid-ers diagnosed these individuals, the top three were medical healthcare office, 64%, outpatient hospital, 23%, and ambulatory surgical center, 3%. When comparing the percentage of PFP cases by region, the South resulted in 925,395 cases, followed by the Midwest region at 565,085, West region at 397,695 and Northeast region at 300,578. (Figure 2)
The total PFP incidence, and subcategories were compared by sex using Chi Square analyses and revealed that females accounted for 1,211, 665 cases
Table 1. ICD-9 codes for the patellofemoral pain group and anterior knee pain pathologies
Figure 2. PFP breakdown by Region (In Percentages).

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 285
division as well. (Table 2) Within most age groups, females reported PFP more often than males.
Of the total 2,188,753 cases reported between 2007 and 2011, there appeared to be an increase in the condition over this five-year period. (Table 3) The smallest percentage of those experiencing PFP occurred in 2007 at 18.7% from 410,852 cases, while 2011 had the largest percentage at 22.7% including 496,816 cases. Mantel-Haenszel test identified a sta-tistically significant difference in the condition over the five-year period, p<.001.
Additional Sources of Anterior Knee Pain:The incidence of other sources of anterior knee pain totaled 173,896 individuals during this 5-year period. (Figure 1) Osgood-Schlatters disease, patellar ten-donitis, dislocation, bursitis and subluxations were most common diagnoses. There were 375,798 cases of other pathologies that were diagnosed on the same day the 719.46 ICD-9 codes and were removed from the analysis.
Females were more likely to present with Osgood-Schlatter, patellar dislocation, and patellar sublux-ation, with statistically significant differences in both patellar dislocation and subluxation as com-pared to males (p<0.001) (Figure 4). Statistically significant differences between sexes were also found with males having greater incidence of patel-lar tendonitis, patellar bursitis, and patellar tendon rupture, (p<0.001). Statistical differences between the seven additional sources of anterior knee pain could not be computed within age groups in order
(55%) compared to males who had 977,088 cases (45%) (p<.001). Females accounted for 262,754 cases or 60% of all chondromalacia patella com-pared to 174,957 cases in males or 40% (p<.001). Joint pain of the lower limb had a similar trend, with females tallying 55% with 948,911 cases compared to males who had 45% with 802,131 cases (p<.001).
Comparison by age group demonstrated that the occurrence of PFP increased within the age groups and peaked within the 50-59 year old group. The age groups of 50-59, 40-49, and 30-39 had the greatest incidence, respectively, followed by the 10-19 year old group. (Figure 3) Chi-squared testing identi-fied statistically significantly differences between ages for both total and subcategories of PFP cases, p<0.001. Differences between the sexes were exam-ined within the age groups for the combined and sub-
Table 2. Breakdown of Joint Pain in Lower Leg, Chondromalacia and total PFP by age
Figure 3. Percentage of PFP by Age Group.

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 286
patellofemoral pain. They found that PFP accounted for 25% of all knee related injuries within a 4 1/2 year study performed in a single sports medicine clinic.37 This reported rate is similar to other data from other sports medicine clinics during a compa-rable time period.26 These values do differ slightly from previously collected data examining mili-tary personnel, which have been reported to range between 12- 15%.25,36 PFP was also identified by Baquie et al as the most common orthopedic condi-tions treated during a single year in Australia sports medicine clinic.38 While Baquie et al38 did not pro-vide an exact incidence rate, these findings suggest PFP is a common pathology presenting in patients from multiple countries.
PFP has also been studied in multiple sports, with a focus on female participants due to their higher suggested prevalence and incidence rates.25,39 Nejati et al found prevalence rates of between 13 – 26% in females participating in soccer, volleyball, run-ning, fencing and rock climbing.39 This incidence is higher than the current results, which ranged from 1.5 – 7.3% of those seeking orthopedic care. The dif-ference is likely attributed to the wider age group, varied activity levels, the much larger sample size, and where/how the data was collected in the cur-rent study. (Table 4)
Females presented with PFP more often than males in the combined PFP data and the isolated ICD-9 code analysis in the majority of age groups. The largest dif-ferences between sex within age groups was the chon-dromalacia subdivision in the 10-19 age group, with 66.6% of all cases being females compared to 33.4%
to maintain patient confidentiality, as PearlDiver would not provide exact numbers if fewer than 10 patients existed in a subdivision. This occurred in multiple age group subdivisions in all of the lower incidence pathologies.
DISCUSSIONThe purpose of this study was to examine trends in diagnosis of PFP using two common ICD-9 codes in the general population based on age, sex, and region for those individuals within the United States seek-ing orthopedic medical care. Over 30 million cases were used to determine the diagnosis rates. The incidence rate of PFP was approximately 7.3% of all orthopedic visits and that there were differences in age and sex and an increase in the rate of PFP over the five-year period that was examined. The authors believed that these data are representative of the occurrence of PFP in the general population, com-pared to the previous studies that only examined sports medicine clinics, military settings or small epidemiological samples.23-26,36
Whitman et al 37 conducted one of the first studies to provide incidence rates of individuals experiencing
Table 3. Number of PFP cases and percentage during 2007-2011
Figure 4. Breakdown of all sources of AKP by Sex

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 287
Table 4. Previous PFP incidence and prevalence studies
used data from insurance company reported ICD-9 codes, so high school and college aged athletes being treated or evaluated in athletic training settings or direct access physical therapy clinics would not be included unless they sought medical attention at a physicians office. Other researchers have reported that females seek medical care more often with trau-matic knee pain compared to when they experience insidious knee pain28 The current data indicates that PFP is experienced by a wide age range, which is supported by DeHaven et al who reported that the condition was one of the most commonly treated conditions seen in their sports medicine clinic in patients between the ages of 10 and 60.24
The increased number of older individuals being diagnosed with PFP may actually represent those experiencing patellofemoral osteoarthritis (PFOA) or osteoarthrosis. The recognition of PFOA has increased over past years, and has been recently labeled a sub-group of knee osteoarthritis.22 Isolated PFOA has been studied over the last 20 years, with linear trends in occurrence rates identified between the ages of 50-70, which is similar to the findings of this study.44 It has been estimated that 25% of all individuals over the age of 50 who experience knee pain have isolated PFOA.45 Wood et al collected PFP disorder rates from a database of 57,555 patients representing eight gen-eral practitioner clinics over a single year and found high rates of PFP between 15-44 year olds and an increased rate in 75+ individuals.46 They also found a gradual increase in PFOA between the ages of 30 and 75+, which is similar to this study’s findings and
in males. Females had significantly higher prevalence of chondromalacia in all age groups except the 70+ group. For joint pain in the lower leg, females pre-sented with significantly more diagnoses in the 40-69 age groups. When the ICD-9 codes were combined, there were more females diagnosed within 10-19 and 30-69 age groups. These findings support other claims that females present with PFP more than males.25,40 Boling et al reported that females in the United States Naval Academy were 2.23 times more likely to develop PFP than males.25 PFP has also been studied in running clinics and of the 331 cases reported, 62% were by female runners.33 The higher PFP rates in females have also been a reason they are often solely enrolled in studies examining screening methods, muscle function, electromyography, and kinematic alteration during functional tasks.40-43
Perhaps the most surprising finding of the current research was that the highest percentage of a PFP diagnosis occurred in the 50-59 year age group and that the 10-19 year age group was the fourth highest percentage. The frequency of PFP was 13.5% and 10% in the 10-19 and 20-29 age groups respectively, while previous research has reported that 70% of all PFP is found in individuals between the ages of 16 and 25.26 Age has also been previously identified as a risk for developing PFP, as those under the age of 34 years were considered at a greater risk than older individuals.33 The current conflicting findings may be due to the previous study only examining athletes in a sports medicine clinic over a 5-year period. The current methodology of retrospective chart review

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 288
related, current research does not support the asso-ciation. 47 The treatments of each may be different as well, supporting the notion that clinicians need accurate diagnoses to provide optimal care. The fre-quency of patellar tendonitis, the next most common anterior knee pathology, is also very low at .25% of all individuals over the 5-year period. Rutland et al found that overuse tendon injuries accounted for 7% of all orthopedic physician visits, but they did not provide a specific categorical analysis.48
There are limitations to this retrospective chart review that should be considered; specifically, a lack of a true, stand-alone ICD-9 code for PFP. The ICD-9 codes of 719.46 (general joint pain in the lower leg) and 717.7 (chondromalacia patella) are the two most frequent codes used to classify PFP. 25 Boling et al used these two ICD-9 codes in previous pub-lished PFP epidemiological research in addition to a screening process for concurrent ligamentous and meniscal injuries.22 While this study was modeled for data extraction to also remove these pathologies; there may be the concern for improper or mistaken coding. While advancement and evolution of ICD-9 codes has occurred culminating in the recent release of ICD-10 codes, there is still no true PFP code for clinicians to use for the diagnosis of this condition. Differentiating between PFP and patellofemoral osteoarthritis in the older population is also diffi-cult, as it is not possible to identify true PFP versus PFOA. Removal of concurrent osteoarthritis codes was performed, however there is still a chance that improper diagnostic codes were utilized. Another limitation is the distribution of insurance providers who provide data for PearlDiver. UnitedHealthcare is the largest contributor to the PearlDiver system and is primarily utilized within the southern states, which may explain the higher occurrence in that region. These values also only include individuals who have received care through their insurance pro-vider. High school and college aged athletes may receive care from their athletic trainers, patients treated by physical therapists via direct access and military personnel who utilized TriCare insur-ance were not included in this database which may account for the lower values in the younger popula-tion. However, with over 30 million data points, this database represents the largest general population sample that has been evaluated.
may explain the increase in reported cases in the 50-59 year old group.46 While there were increased cases reported within the 50-59 year old age group, it is not possible to truly ascertain which individuals presented with PFP or PFOA. While individuals with concurrent osteoarthritic ICD-9 codes were removed, the challenge in calculating the occurrence of PFP within this dataset is dependent on proper ICD-9 cod-ing from the medical healthcare provider. It is also difficult to use the findings gleaned from this data-set without the benefit of a movement based assess-ment or physical evaluation which are commonly needed to diagnose this condition and to differentiate between PFP and additional pathologies that present with pain to the anterior knee.
Seven additional pathologies were included within the database search in order to provide a picture of all potential anterior knee pain sources. Since there is no true ICD-9 code for PFP, there are multiple possible diagnoses that medical providers can clas-sify the condition. Due to this limitation, inspect-ing other possible diagnoses of anterior knee pain can provide insight into what pathologies healthcare providers are commonly evaluating and treating within the population who seek medical care. This information can help clinicians become aware of the frequency of multiple pathologies they commonly treat. If there are high numbers of individuals devel-oping PFP pain severe enough to receive treatment, a specific ICD-9 code would be vital to provide the accurate diagnosis. As medicine advances to a more evidence based approach, proper evaluation and coding of diagnoses will be vital in providing optimal treatment plans.
It is of interest that diagnoses of patellar maltrack-ing and Osgood-Schlatter each had fewer than 100 cases over a five-year period, which is extremely low. The frequency of patella maltracking may actu-ally be underreported as physicians may view it as a mechanism that leads to the pathological process for PFP, but not an actual diagnosis. However, when the incidence of patella maltracking with a concurrent diagnosis of chondromalacia or lower extremity joint pain, there was an increase to 13% of all reported cases, indicating a prevalence of medical care pro-viders that use multiple ICD-9 codes. While there is empirical evidence PFP and patella maltracking are

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 289
10. Tuna B, Semiz-Oysu A, Pekar B, Bukte Y, Hayirlioglu A. The association of patellofemoral joint morphology with chondromalacia patella: A quantitative MRI analysis. Clinical Imaging. 2014;38(4):495-498.
11. Rothermich MA, Glaviano NR, Li J, Hart JM. Patellofemoral pain: Epidemiology, pathophysiology, and treatment options. Clin Sports Med. 2015;34(2):313-327.
12. Willson JD, Binder-Macleod S, Davis IS. Lower extremity jumping mechanics of female athletes with and without patellofemoral pain before and after exertion. Am J Sports Med. 2008;36(8):1587-1596.
13. Willson JD, Davis IS. Lower extremity mechanics of females with and without patellofemoral pain across activities with progressively greater task demands. Clin Biomech (Bristol, Avon). 2008;23(2):203-211.
14. Hewett TE, Myer GD, Ford KR, et al. Biomechanical measures of neuromuscular control and valgus loading of the knee predict anterior cruciate ligament injury risk in female athletes: A prospective study. Am J Sports Med. 2005;33(4):492-501.
15. Nakagawa TH, Moriya ET, Maciel CD, Serrao FV. Trunk, pelvis, hip, and knee kinematics, hip strength, and gluteal muscle activation during a single-leg squat in males and females with and without patellofemoral pain syndrome. J Orthop Sports Phys Ther. 2012;42(6):491-501.
16. Brindle TJ, Mattacola C, McCrory J. Electromyographic changes in the gluteus medius during stair ascent and descent in subjects with anterior knee pain. Knee Surg Sports Traumatol Arthrosc. 2003;11(4):244-251.
17. Kernozek TW, Torry MR, Van Hoof H, Cowley H, Tanner S. Gender differences in frontal and sagittal plane biomechanics during drop landings. Med Sci Sports Exerc. 2005;37(6):1003-12; discussion 1013.
18. Heintjes E, Berger M, Bierma-Zeinstra SM. Exercise therapy for patellofemoral pain syndrome. Cochrane Database Syst Rev. 2003;4(CD003472).
19. Fairbank JC, Pynsent PB, van Poortvliet JA, Phillips H. Mechanical factors in the incidence of knee pain in adolescents and young adults. J Bone Joint Surg Br. 1984;66(5):685-693.
20. Blond L, Hansen L. Patellofemoral pain syndrome in athletes: A 5.7-year retrospective follow-up study of 250 athletes. Acta Orthop Belg. 1998;64(4):393-400.
21. Utting MR, Davies G, Newman JH. Is anterior knee pain a predisposing factor to patellofemoral osteoarthritis? Knee. 2005;12(5):362-365.
22. Thomas MJ, Wood L, Selfe J, Peat G. Anterior knee pain in younger adults as a precursor to subsequent
CONCLUSIONThis study provides evidence that PFP accounts for 1.5 - 7.3% of the diagnoses of those who seek orthopedic care by physicians in the United States. Females experienced PFP more often than males and that PFP is experienced within the general popula-tion at high rates in all age groups, with an increase in the ages of 50-59. Due to the large percentage of individuals who require medical treatment for this condition, risk factors to prospectively identify those susceptible to develop PFP should be examined. Effective interventions should also be studied to decrease the long-term care needed to minimize the possible progression of PFP into PFOA and decrease health costs associated with this condition.
REFERENCES 1. Aminaka N, Gribble PA. Patellar taping,
patellofemoral pain syndrome, lower extremity kinematics, and dynamic postural control. J Athl Train. 2008;43(1):21-28.
2. Bolgla LA, Boling MC. An update for the conservative management of patellofemoral pain syndrome: A systematic review of the literature from 2000 to 2010. Int J Sports Phys Ther. 2011;6(2):112-125.
3. Crossley K, Bennell K, Green S, McConnell J. A systematic review of physical interventions for patellofemoral pain syndrome. Clin J Sport Med. 2001;11(2):103-110.
4. Davis IS, Powers CM. Patellofemoral pain syndrome: Proximal, distal, and local factors, an international retreat, April 30-May 2, 2009, Fells Point, Baltimore, MD. J Orthop Sports Phys Ther. 2010;40(3):A1-16.
5. Duffey MJ, Martin DF, Cannon DW, Craven T, Messier SP. Etiologic factors associated with anterior knee pain in distance runners. Med Sci Sports Exerc. 2000;32(11):1825-1832.
6. Fulkerson JP. Diagnosis and treatment of patients with patellofemoral pain. Am J Sports Med. 2002;30(3):447-456.
7. Callaghan MJ, Selfe J. Has the incidence or prevalance of patellofemoral pain in the general population in the united kingdom been properly evaluated? Phys.Ther.Sport. 2007;8:37-43.
8. Crossley K, Bennell K, Green S, Cowan S, McConnell J. Physical therapy for patellofemoral pain: A randomized, double-blinded, placebo-controlled trial. Am J Sports Med. 2002;30(6):857-865.
9. Thomee R, Augustsson J, Karlsson J. Patellofemoral pain syndrome. A review of current issues. Sports medicine (Auckland, N.Z.). 1999;28(4):245-262.

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 290
patellofemoral osteoarthritis: A systematic review. BMC Musculoskelet Disord. 2010;11:201-2474-11-201.
23. Kannus P, Aho H, Jarvinen M, Niittymaki S. Computerized recording of visits to an outpatient sports clinic. Am J Sports Med. 1987;15(1):79-85.
24. DeHaven KE, Lintner DM. Athletic injuries: Comparison by age, sport, and gender. Am J Sports Med. 1986;14(3):218-224.
25. Boling M, Padua D, Marshall S, Guskiewicz K, Pyne S, Beutler A. Gender differences in the incidence and prevalence of patellofemoral pain syndrome. Scand J Med Sci Sports. 2010;20(5):725-730.
26. Devereaux MD LS. Patellofemoral arthralgia in athletes attending a sports injury clinic. Br J Sports Med. 1984;18:18-21.
27. Witvrouw E, Callaghan MJ, Stefanik JJ, et al. Patellofemoral pain: Consensus statement from the 3rd international patellofemoral pain research retreat held in vancouver, september 2013. Br J Sports Med. 2014;48(6):411-414.
28. Rathleff MS, Skuldbol SK, Rasch MN, Roos EM, Rasmussen S, Olesen JL. Care-seeking behaviour of adolescents with knee pain: A population-based study among 504 adolescents. BMC Musculoskelet Disord. 2013;14:225-2474-14-225.
29. Myer GD, Ford KR, Barber Foss KD, et al. The incidence and potential pathomechanics of patellofemoral pain in female athletes. Clin Biomech (Bristol, Avon). 2010;25(7):700-707.
30. Ireland ML, Willson JD, Ballantyne BT, Davis IM. Hip strength in females with and without patellofemoral pain. J Orthop Sports Phys Ther. 2003;33(11):671-676.
31. McConnell J. Management of patellofemoral problems. Man Ther. 1996;1(2):60-66.
32. Witvrouw E, Cambier D, Danneels L, et al. The effect of exercise regimens on refl ex response time of the vasti muscles in patients with anterior knee pain: A prospective randomized intervention study. Scand J Med Sci Sports. 2003;13(4):251-258.
33. Taunton JE, Ryan MB, Clement DB, McKenzie DC, Lloyd-Smith DR, Zumbo BD. A retrospective case-control analysis of 2002 running injuries. Br J Sports Med. 2002;36(2):95-101.
34. von Elm E, Altman DG, Egger M, et al. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: Guidelines for reporting observational studies. Int J Surg. 2014;12(12):1495-1499.
35. Souza RB, Powers CM. Differences in hip kinematics, muscle strength, and muscle activation between subjects with and without patellofemoral pain. J Orthop Sports Phys Ther. 2009;39(1):12-19.
36. Milgrom C, Finestone A, Eldad A, Shlamkovitch N. Patellofemoral pain caused by overactivity. A prospective study of risk factors in infantry recruits. J Bone Joint Surg Am. 1991;73(7):1041-1043.
37. Whitman P, Melvin M, Nicholas J. Common problems seen in a metropolitan sports injury clinic. Phys.Sportsmed. 1981;9:105-108.
38. Baquie P, Brukner P. Injuries presenting to an australian sports medicine centre: A 12-month study. Clin J Sport Med. 1997;7(1):28-31.
39. Nejati P, Forogh B, Moeineddin R, Baradaran H, Nejati M. Patellofemoral pain syndrome in iranian female athletes. Acta Medica Iranica. 2011;49(3):169-172.
40. Grenholm A, Stensdotter AK, Hager-Ross C. Kinematic analyses during stair descent in young women with patellofemoral pain. Clin Biomech (Bristol, Avon). 2009;24(1):88-94.
41. Kaya D, Citaker S, Kerimoglu U, et al. Women with patellofemoral pain syndrome have quadriceps femoris volume and strength defi ciency. Knee Surg Sports Traumatol Arthrosc. 2011;19(2):242-247.
42. Powers CM, Landel R, Perry J. Timing and intensity of vastus muscle activity during functional activities in subjects with and without patellofemoral pain. Phys Ther. 1996;76(9):946-55.
43. Dolak KL, Silkman C, Medina McKeon J, Hosey RG, Lattermann C, Uhl TL. Hip strengthening prior to functional exercises reduces pain sooner than quadriceps strengthening in females with patellofemoral pain syndrome: A randomized clinical trial. J Orthop Sports Phys Ther. 2011;41(8):560-570.
44. McAlindon TE, Snow S, Cooper C, Dieppe PA. Radiographic patterns of osteoarthritis of the knee joint in the community: The importance of the patellofemoral joint. Ann Rheum Dis. 1992;51(7):844-849.
45. Duncan RC, Hay EM, Saklatvala J, Croft PR. Prevalence of radiographic osteoarthritis--it all depends on your point of view. Rheumatology (Oxford). 2006;45(6):757-760.
46. Wood L, Muller S, Peat G. The epidemiology of patellofemoral disorders in adulthood: A review of routine general practice morbidity recording. Prim Health Care Res Dev. 2011;12(2):157-164.
47. Narkbunnam R, Chareancholvanich K, Hanroongroj T. Sagittal plane evaluation of patellofemoral movement in patellofemoral pain patients with no evidence of maltracking. Knee Surg Sports Traumatol Arthrosc. 2013.
48. Rutland M, O’Connell D, Brismee JM, Sizer P, Apte G, O’Connell J. Evidence-supported rehabilitation of patellar tendinopathy. N Am J Sports Phys Ther. 2010;5(3):166-178.

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 291
ABSTRACTBackground: There is evidence that applying a pelvic compression belt (PCB) can decrease hamstring and lumbar muscle electromyographic activity and increase gluteus maximus activity in healthy women during walking. Increased isokinetic eccentric hamstring strength in the terminal range (25° - 5°) of knee extension has been reported with the use of such a belt in sportsmen with and without hamstring injuries. However, it is unknown whether wearing a pelvic belt alters activity of the hamstrings in sportsmen during walking.
Purpose: To examine the effects of wearing a PCB on electromyographic activity of the hamstring and lumbopelvic muscles during walking in sportsmen with and without hamstring injuries.
Study design: Randomised crossover, cross-sectional study.
Methods: Thirty uninjured sportsmen (23.53 ± 3.68 years) and 20 sportsmen with hamstring injuries (22.00 ± 1.45 years) sustained within the previous 12 months participated in this study. Electromyographic amplitudes of the ham-strings, gluteus maximus, gluteus medius and lumbar multifidus were monitored during defined phases of walking and normalised to maximum voluntary isometric contraction. Within-group comparisons [PCB vs. no PCB] for the normalised electromyographic amplitudes were performed for each muscle group using paired t tests. Electromyo-graphic change scores [belt – no belt] were calculated and compared between the two groups with independent t tests.
Results: No significant change was evident in hamstring activity for either group while walking with the PCB (p > 0.050). However, with the PCB, gluteus medius activity (p ≤ 0.028) increased in both groups, while gluteus maximus activity increased (p = 0.025) and multifidus activity decreased (p < 0.001) in the control group. The magnitude of change induced by the PCB in gluteus medius activity was similar between groups (p = 0.760). No statistically signifi-cant baseline differences in no belt scores were evident between groups for the investigated muscles (p ≥ 0.050).
Conclusion: Application of a PCB had individual-specific effects on electromyographic activity of injured and unin-jured hamstrings during walking, resulting in no significant changes within or between the two groups. Future studies investigating effects of the PCB on hamstring activity in participants with acute injury and during a more demanding functional activity such as running are warranted.
Key words: Athletic injury, hamstring, orthotic, surface electromyography, walking
Level of evidence: Level 3
IJSP
TORIGINAL RESEARCH
THE EFFECT OF A PELVIC COMPRESSION BELT ON
FUNCTIONAL HAMSTRING MUSCLE ACTIVITY IN
SPORTSMEN WITH AND WITHOUT PREVIOUS
HAMSTRING INJURY
Ashokan Arumugam, BPT, MPT (Ortho & Manual Therapy), PhD1,2
Stephan Milosavljevic, BAppSc (Physio), MPhty (Manips), PhD3
Stephanie Woodley, BPhty, MSc, PhD4
Gisela Sole, BSc (Physio), MSc (Med), PhD1
1 Centre for Health, Activity and Rehabilitation Research, School of Physiotherapy, University of Otago, New Zealand
2 RVS College of Physiotherapy, Tamil Nadu, India3 School of Physical Therapy, University of Saskatchewan,
Canada4 Department of Anatomy, University of Otago, New Zealand
CORRESPONDING AUTHORAshokan ArumugamSchool of PhysiotherapyUniversity of OtagoNew ZealandFax: 64 3 479 8367E-mail: [email protected]

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 292
INTRODUCTIONHamstring strain injuries are one of the most com-mon injuries in sports such as football and rugby that involve acceleration, sprinting and kicking.1,2 A number of risk factors for occurrence and recur-rence of hamstring injuries have been considered, including age, ethnicity, prior history of hamstring injury, hamstring weakness, poor flexibility, inad-equate sports-related skills, altered lumbopelvic biomechanics, and altered lumbopelvic neuromotor control.3-5 Clinical approaches and research findings have considered the hamstrings role in eccentrically decelerating the tibia during the terminal swing phase of sprinting as a critical function in the mech-anism of these injuries.6 However, despite various treatment and preventative interventions based on eccentric strengthening, the incidence and recur-rence rate of hamstring injuries have not decreased substantially over the past 20 years.
In order to advance the current understanding of factors that contribute to hamstring injuries, other functions of this muscle group require consideration. It has been argued that, in general, the hamstrings contribute to knee joint stability during stance and loading response phases,7-8 and that biceps femoris specifically aids in tensioning the sacrotuberous liga-ment, helping to prepare the sacroiliac joint (SIJ) for impact during initial foot contact.9-10 Therefore, this muscle group is also considered to have a role in sta-bilising the lower limb.3 In addition, the hamstring muscles extend the hip following initial foot contact during stance phase8,10-12 with the medial hamstrings contributing to internal rotation of the hip during the loading response phase during forward progres-sion of the contralateral pelvis.8 The hamstring mus-cles thus have considerable functional complexity which may be a factor in their high injury rates.
Peak hamstring lengthening occurs at the terminal swing phase during sprinting, when the hip is flexed (≈ 55˚to 65˚) and the knee is also slightly flexed (≈ 30˚to 45˚). Furthermore, maximal hamstring loading occurs just before peak musculotendinous stretch, and perhaps contributes to an increased injury risk during the terminal stance phase while sprinting.13-14 A small but significant reduction in the peak hip flexion angle of hamstring-injured limbs during ter-minal swing phase has been observed previously,
reflecting either a mechanical deficit resulting from injury or a compensatory mechanism to protect from further injury.15 In addition, with experimentally-induced hamstring pain, gait patterns demonstrate an unloading pattern of the limb, which is apparent in decreased internal hip extensor moments pres-ent during early stance, and internal knee flexor and lateral rotator moments during the terminal stance phase.16 However, the evidence for compara-tive alterations in neuromotor control of the ham-strings following injury or experimentally-induced pain during gait (walking or running) remains equivocal.15-17 An aberrant increase in the activity of injured hamstrings during functional tasks has been argued to contribute to reinjury.3 If application of a pelvic compression belt (PCB) can reduce electro-myographic (EMG) activity of the hamstrings dur-ing functional tasks, this might provide a plausible direction for future investigation of the PCB as a treatment option for those who have sustained ham-string injury.
Application of external pelvic compression by wear-ing a PCB just below the anterior superior iliac spines,at the level of the pubic symphysis or above the greater trochanter has been explored as a potential intervention for patients with lumbopelvic pain, and has been shown to alter EMG recruitment patterns of the lumbopelvic and hamstring muscles.18-20 Wear-ing a PCB has been hypothesized to reduce EMG activity of injured hamstrings during weight-bearing activities such as walking, based upon a number of hypothetical mechanisms related to anatomical and functional links between the hamstrings and pel-vis.21 The authors have recently reported the effects of application of a PCB on isokinetic thigh muscle strength22 and EMG activity of the hamstrings dur-ing transition from bipedal to unipedal stance23 in a group of sportsmen with a history of hamstring injuries. Terminal range eccentric hamstring strength was significantly increased22 while no sig-nificant change in hamstring activity23 was noted during transition from bipedal to unipedal stance with application of the PCB compared to the control condition. The immediate improvement in eccen-tric hamstring strength with application of the PCB suggests that neuromotor control influences torque production of these muscles during maximal con-tractions. No similar changes were evident during

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 293
the weight-bearing task with submaximal functional demands.23 Moreover, a decrease in EMG activity of the biceps femoris with application of a PCB has been reported during treadmill walking in healthy nulligravidae females19 and during standing in both sexes.20 Whether the application of a PCB will alter EMG activity of injured or uninjured hamstrings of sportsmen during gait (walking/running) remains unknown.
The aim of the current study was to investigate whether application of a PCB alters EMG activity of the hamstrings during over ground walking in individuals with and without hamstring injuries. In addition to the hamstrings, the lumbar multifidi and gluteal muscles were also examined by EMG analy-sis to better understand the changes occurring with the PCB in the lumbopelvic and proximal lower limb kinetic chain during walking.
METHODSStudy designThis was a laboratory based cross-over study in which the order of PCB conditions was random-ized using computer generated numbers. Ethical approval was granted by the University of Otago Human Ethics Committee (Reference no. 11/115). All participants provided written informed consent before data collection.
Study participants Sportsmen aged between 18 and 35 years, who par-ticipated regularly in sports at least twice weekly, were recruited in an urban setting through word of mouth, emails, flyers and adverts. As the ability to recall the occurrence of injury within the past year is reported to be reliable,24 sportsmen were included based on their self-declaration of prior hamstring injury diagnosed by a health professional. Eligibil-ity criteria have been described in prior published research involving the same group of sportsmen.22,23 In brief, sportsmen with unilateral or bilateral, first-time or recurrent hamstring injury were included. A hamstring injury was defined as a sudden onset of pain in the posterior thigh during a match, competi-tion or training session within the past year, but not less than four weeks prior to testing. Sportsmen with-out any previously diagnosed hamstring injury were recruited for the control group. Men with a history
of diagnosis and treatment for any injury or disease of the lumbopelvic spine or lower limb (other than hamstring injury for the hamstring-injured group) within the past six months, as confirmed by clinical examination,25 were excluded from both groups.
ElectromyographyEMG data were recorded at a sampling frequency of 1500 Hz using the MyoResearch XP Master-Edi-tion softwareTM 1.06.54 of a 16 channel, telemetric, Noraxon TelemyoTM 2400 T G2 system (Noraxon Inc., Scottsdale, AZ, USA). EMG signals were regis-tered from both sides (randomly ordered for testing) for the hamstring-injured participants and left or right side (randomly selected) for the uninjured par-ticipants. The EMG active leads had an input imped-ance of more than 100 MΩ, a base gain of 500, and a common mode rejection ratio more than 100 dB; other properties included an input of ± 3.5 mV and a baseline noise less than 1μV RMS.
Recommendations from the Surface Electromyo-graphy for the Non-Invasive Assessment of Mus-cles (SENIAM) committee were followed for skin preparation and the placement of surface electrodes (Table 1).26-27 Two silver/silver chloride surface elec-trodes (Ambu® Blue Sensor SP, AMBU A/S, Den-mark) were placed over the lumbar multifidus, gluteus maximus, gluteus medius, biceps femoris and semitendinosus at an inter-electrode distance of 2 cm, and the ground electrode was positioned on the spinous process of L2.
Standard manual muscle testing positions28 were used to record EMG activity during three trials of maxi-mum voluntary isometric contraction (MVIC) of the multifidus, gluteus maximus, gluteus medius, and hamstrings (Table 2). Once the EMG signals appeared stable on the display of EMG system’s monitor, EMG was recorded for three seconds per trial for three tri-als. Participants rested for one minute between trials.
Motion captureGround reaction forces were recorded with two force plates (BP2436 and OR6-5, Advanced Medical Tech-nologies, Newton, MA, USA), sampling at 1050 Hz. Three-dimensional kinematic data were recorded at a frequency of 100 Hz (12 EagleDigital-EGL-500RT cameras, Cortex - Motion Analysis CorporationTM,

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 294
Santa Rosa, CA, USA) using a set of 23 retro-reflec-tive skin markers.29 To enable the use of the PCB, markers were placed over each posterior superior iliac spine (PSIS) instead of a single sacral marker. The heel, toe (head of the fifth metatarsal) and PSIS (virtual mid-PSIS) markers were used to define the gait phases. Kinematic events were analysed based on a co-ordination algorithm.30 Orthogonal coordi-nate systems were aligned with the x axis pointing antero-posteriorly, the y axis pointing medio-later-ally and the z axis pointing supero-inferiorly.
Pelvic compression beltA PCB (SI-brace neoprene-ADL-anatomisch, 3200202; Rafys, The Netherlands) was manually applied below
the anterior superior iliac spines (Figure 1), with maximal tension without inducing any discomfort to the participant. The mean value of PCB tension that could be achieved without self-reported discomfort in healthy male participants during walking (method similar to the present study) has been found to range between 32 N and 55 N.31
Walking task Participants were asked to walk at a selected cadence of 120 steps per minute,32 controlled by a metronome, over a 7 m walkway. A custom-made stand with two lights (one green and one red) was placed in the vicinity of the walkway (Figure 2). The light signal was used to trigger the EMG recording
Table 1. Guidelines for placement of surface EMG electrodes27
Muscle Site of electrode placement* Alignment of electrodes*Bicepsfemoris
Halfway between the ischial tuberosity and the lateral condyle of the tibia
Along a line joining the ischial tuberosity and the lateral condyle of the tibia
Medial hamstrings
Midway between the ischial tuberosity and the medial condyle of the tibia
In the direction of a line joining the ischial tuberosity and the medial condyle of the tibia
Gluteus maximus
At the centre of a line connecting the sacral vertebrae and the greater trochanter corresponding to the greatest prominence of the gluteal region
Along a line running from the PSIS to the posterior mid-thigh region
Gluteus medius
At 50% of the distance between the iliac crest and the greater trochanter
Along a line drawn from the iliac crest to the greater trochanter
Lumbar multifidi
2 to 3 cm lateral to the midline at the level of L5 spinous process
Along a line connecting the PSIS to the interspace between L1 and L2
*Retrieved from SENIAM guidelines (www.seniam.org).
Table 2. Guidelines for eliciting maximum voluntary isometric contraction28
Muscle Participant’s position Researcher’s position Location of manual resistance
Movement performed
Lumbar multifidi
Prone with hands held behind the occiput
Standing to stabilise the legs using body weight and one hand
Upper thoracic spine
Extension of the lumbar spine
Gluteus maximus
Prone with knee flexed to 90˚
Standing near the pelvis on the side to be tested and stabilising the pelvis near the lumbopelvic junction with one hand
Distal part of the posterior high
Extension of the hip joint
Gluteus medius
Side lying on the contralateral side with leg to be tested uppermost
Standing behind the participant and stabilising the pelvis with one hand
Above the ankle Abduction of the hip joint
Hamstrings Prone lying with knee flexed between 50˚ and 25˚*
Standing near the limb to be tested
Above the ankle Flexion of the knee joint
*Maximum voluntary contraction of the hamstrings has been reported to occur between 24˚ to 48˚.44

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 295
with wireless sync trigger and receiver units (234 Inline-wireless-sync-receiver and 232 Transmitter, Noraxon, Scottsdale, AZ, USA), and the participants were asked to start walking in synchrony with the metronome after the green light was switched on. Kinematic (sampling rate -100 Hz), force plate (1050 Hz) and EMG data (1500 Hz) were collected from a minimum of five successful walking trials, for each belt condition (PCB vs. no PCB) following four prac-tice trials. Each trial lasted up to 7 s. Each success-ful trial consisted of walking in synchrony with the metronome beats without any obvious lag in speed and simultaneous capturing of motion with all 23 retro-reflective markers clearly visible in CortexTM software (Version 2.0.2.917) for at least three strides.
CortexTM software was used to register the ground reaction force and light signal.
Participants also performed two other tasks with and without the PCB: 1) a bipedal to unipedal stance task23 and 2) isokinetic strength testing of the knee.22 Data for walking were collected following the unipedal stance task during the same session, while isokinetic testing was carried out in a separate session. This paper reports the findings of the walking task only.
Data processing Kinematic data were processed using a Butter-worth filter with a frequency cut-off of 6Hz using CortexTM software version 2.0.2.917 (Motion Anal-ysis Corporation, Santa Rosa, CA, USA). A pilot analysis was performed with the various methods described in Table 3 using MATLAB® software (Ver-sion 12.0.0.58851, The Mathworks, Inc.; Natick, MA, USA). The algorithm described by Zeni Jr et al.30 was found to detect heel strike (HS) and toe off (TO) events more accurately than the other meth-ods trialled for the current data. Further, this algo-rithm was validated with that of visually tracked HS and TO events (frame by frame analysis) with the aid of Cortex software, with or without verti-cal ground reaction force data for 55 gait cycles randomly selected from five participants. Pilot analyses indicated that this algorithm30 detected HS by 10 ms (± 7 ms) before and TO by 7 ms (± 8 ms) after each event was identified by the visually tracked data, and was considered acceptable for the purpose of this study. Corresponding EMG data for each muscle were synchronised with the HS and TO events for each gait cycle.
EMG data were band-pass filtered within 10 to 500 Hz through a fourth order Butterworth filter. Fur-ther, the filtered EMG data were analysed with root mean square (RMS) in 50 ms epochs using MAT-LAB®. The mean EMG RMS value of the three MVIC trials (3 s each) for each muscle was used to nor-malise respective EMG amplitudes17 and expressed as a percentage of MVIC16 for all five muscles dur-ing the following two phases: terminal swing (20% before HS) and loading response (12% following HS). For the purpose of this study, terminal swing phase was defined as the last 20% of the gait cycle as EMG onset of the hamstrings has been reported
Figure 1. Application of the pelvic compression belt below the anterior superior iliac spines. This fi gure has been reused from the authors’ previous article23 after obtaining permission from Elsevier Limited.
Figure 2. Participant performing a walking trial after appli-cation of the pelvic compression belt.

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 296
to occur during the (late) mid-swing phase.8 Each participant walked at least five strides per trial, and the laboratory set-up allowed capture of two or three strides per trial following the first stride, depending on stride length. To counteract for acceleration and deceleration effects of walking at the start and the end of each trial respectively, only the middle stride was used for analysis. Thus, one gait cycle per trial resulting in five gait cycles per belt condition (PCB vs. no PCB) were analysed.
A customised MATLAB® program (Version 12.0.0.58851, The Mathworks, Inc.; Natick, MA, USA) was developed to synchronize kinematic and EMG data by using the start of the light signal as the synchro-nizer which triggered the EMG recording. The start of the light signal was identified from the synch channel column of force plate data (analog ASCII row column file). From that point, HS and TO events were defined with tracked kinematic data (track row column file) using the alogorithm of Zeni Jr et al.30 and corresponding EMG data of each muscle were synchronized for each gait cycle.
Data analysisTerminal swing and loading response phases were included for statistical analyses of the hamstring and gluteal muscle EMG data, respectively, as max-imum/most activity was observed during these periods. In addition, terminal swing was chosen as hamstring injuries are considered to occur during this phase of gait.6 Multifidus activity was averaged during these two phases as EMG peak values were observed during HS, with initiation and cessation occurring prior to and after HS, respectively.
Data were explored for normal distribution using both the Shapiro-Wilk test and histograms, while homogeneity of variances was determined using Levene’s test. Paired t tests were used to analyse within-group differences for: 1) PCB vs. no PCB tri-als for all the investigated muscles in each group, and 2) injured hamstring vs. uninjured hamstring EMG activity [no PCB trials] in participants with unilateral hamstring-injury. Independent t tests were used to 1) compare the change scores (PCB score - no PCB score) between groups and 2) to
Table 3. Various algorithms trialled for kinematic data in the current study to detect heel strike and toe-off eventsAlgorithms used to identify HS:
1.) HS occurs at a point where the jerk (the rate of change of acceleration) is equal to zero and the
acceleration is maximum for the vertical component (z coordinate) of the heel marker33.
2.) The velocity vector of horizontal (x coordinate) component of the heel marker changes from positive
to negative at HS30.
3.) The timing of HS (tHS) can be detected using the following formula:–
tHS = (xHeel – xSacrum)maximum
where the sacral (virtual mid-PSIS) marker’s x coordinate is subtracted from the heel marker’s x
coordinate at each corresponding frame and the maximum value of the resulting curve is taken as HS30.
Algorithms used to identify TO:
1.) TO occurs at a point where the jerk is equal to zero and the acceleration is maximum for the x
coordinate of the heel marker33.
2.) TO can be defined by a change in the vertical component (z coordinate) of the toe marker by more
than 0.2cm at two consecutive time frames34.
3.) The velocity vector of the x component of the toe marker changes from negative to positive at the
TO30,35.
4.) TO occurs when the velocity vector of the z coordinate of the toe marker reaches maximum 36.
5.) Timing of TO (tTO) can be detected using the following formula:
tTO = (xToe – xSacrum)minimum
where the sacral (virtual mid-PSIS) marker’s x coordinate is subtracted from the toe marker’s
x coordinate at each corresponding frame and the minimum value of the resulting curve istaken as TO30.
HS= heel strike; PSIS= posterior superior iliac spine; TO= Toe-off.

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 297
explore baseline differences in hamstring EMG activity between groups based on no PCB tri-als (hamstring-injured group vs. control group). Spearman’s ρ correlation coefficient was used to correlate the change scores ([with PCB – no PCB]/no PCB %) of injured hamstring muscles and respective time since (recent) injury of the corresponding limb for all hamstring-injured participants. A p value < 0.05 was decided a priori as the level of significance.
RESULTSA total of 37 participants for the hamstring-injured group and 36 for the healthy group volunteered between September 2011 and November 2012 for the study (Figure 3). Of these, 20 hamstring-injured vol-unteers (mean age, 22.00 ± 1.45 years; mean body weight, 85.52 ± 14.40 kg; mean body mass index, 25.89 ± 3.38 kg/m2) with (n = 2) or without (n = 18) imaging investigation and 30 healthy volunteers (mean age, 23.53 ± 3.68 years; mean body weight, 70.86 ± 11.01 kg; mean body mass index, 22.92 ± 2.68 kg/m2) fulfilled the eligibility criteria and participated in this study. Additional anthropometric characteris-tics of participants including height, body fat [%], and
sit-and- reach values have been published previously.23 Three participants in the hamstring-injured group had bilateral injuries and ten participants in this group had recurrent hamstring injuries. The number of injuries on the preferred side (leg self-preferred to kick a ball) and the non-preferred side were 13 and 10, respec-tively. The mean time since the recent injury was 4.85 (± 3.97) months and the mean time of absence from sports involvement due to injury was 3.55 (± 2.24) weeks. Four sportsmen were still undergoing some form of clinical intervention at the time of data collec-tion. The characteristics of hamstring-injured sports-men such as history of injury and treatment, and severity of injuries have been previously reported.22
A total of 22 injured limbs, including both limbs of two sportsmen with bilateral hamstring injury, and 30 uninjured limbs from healthy participants were included for analysis. One hamstring-injured limb of a participant with bilateral hamstring injury was excluded from analysis as the injury was sustained more than 12 months prior to data collection.
As data were not normally distributed, they were log transformed before conducting statistical tests.
Included after screening for eligibility – hamstring-injured
group (n = 20); soccer/football: 8, rugby: 9, hockey: 1, Sprinting: 1,
racquet sports: 1.
Included after screening for eligibility - control group (n = 30);
soccer/football: 11, rugby: 2, hockey: 4, long distance running: 2, sprinting: 1, triathlon: 1, ice hockey: 1, weight-lifting: 2, racquet sports: 2,
basketball: 2, cricket: 2.
Sportsmen volunteered for study
Hamstring-injured group (n = 37) Control group (n =36)
During walking, EMG was recorded from the lumbar multifidus, gluteus maximus, gluteus
medius and hamstrings (n = 20)
11 did not meet eligibility criteria: Hamstring injury < 1 month – 1 Hamstring injury > 12 months – 1 Hamstring injury not treated by a health professional - 4 Hamstring injury during an accident -1 Concussion – 1 Low back pain – 2 Iliotibial band syndrome - 1
4 unavailable due to time constraints
2 did not respond to follow-up emails
6 did not meet eligibility criteria: Low back pain – 3 Not participating in sports regularly - 3
With PCB (n = 9) No PCB (n = 11) With PCB (n = 18) No PCB (n = 12)
No PCB (n =9) With PCB (n = 11) With PCB (n =12) No PCB (n =18)
During walking, EMG was recorded from the lumbar multifidus, gluteus maximus, gluteus
medius and hamstrings (n = 30)
Figure 3. Design and fl ow of participants through the study. In those conditions where the task was performed fi rst with the pelvic compression belt (PCB), participants walked for 5 min after removing the belt to allow an adequate washout effect before performing the task without the belt.
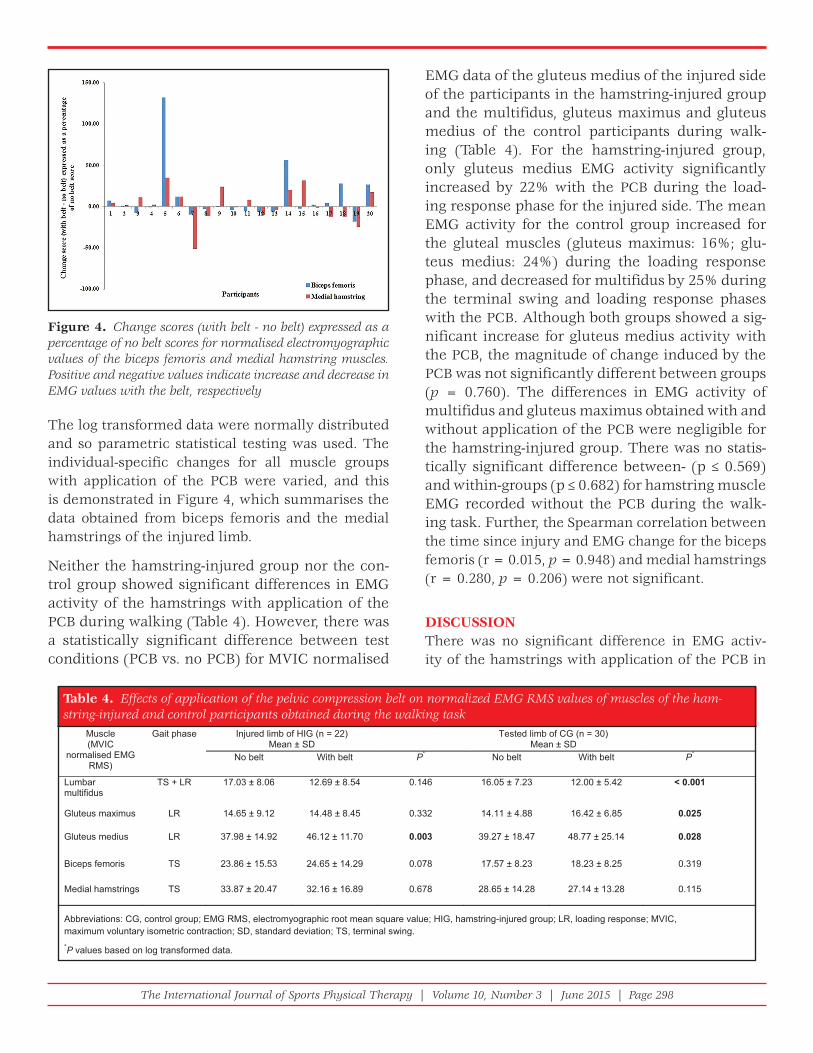
The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 298
The log transformed data were normally distributed and so parametric statistical testing was used. The individual-specific changes for all muscle groups with application of the PCB were varied, and this is demonstrated in Figure 4, which summarises the data obtained from biceps femoris and the medial hamstrings of the injured limb.
Neither the hamstring-injured group nor the con-trol group showed significant differences in EMG activity of the hamstrings with application of the PCB during walking (Table 4). However, there was a statistically significant difference between test conditions (PCB vs. no PCB) for MVIC normalised
EMG data of the gluteus medius of the injured side of the participants in the hamstring-injured group and the multifidus, gluteus maximus and gluteus medius of the control participants during walk-ing (Table 4). For the hamstring-injured group, only gluteus medius EMG activity significantly increased by 22% with the PCB during the load-ing response phase for the injured side. The mean EMG activity for the control group increased for the gluteal muscles (gluteus maximus: 16%; glu-teus medius: 24%) during the loading response phase, and decreased for multifidus by 25% during the terminal swing and loading response phases with the PCB. Although both groups showed a sig-nificant increase for gluteus medius activity with the PCB, the magnitude of change induced by the PCB was not significantly different between groups (p = 0.760). The differences in EMG activity of multifidus and gluteus maximus obtained with and without application of the PCB were negligible for the hamstring-injured group. There was no statis-tically significant difference between- (p ≤ 0.569) and within-groups (p ≤ 0.682) for hamstring muscle EMG recorded without the PCB during the walk-ing task. Further, the Spearman correlation between the time since injury and EMG change for the biceps femoris (r = 0.015, p = 0.948) and medial hamstrings (r = 0.280, p = 0.206) were not significant.
DISCUSSIONThere was no significant difference in EMG activ-ity of the hamstrings with application of the PCB in
Figure 4. Change scores (with belt - no belt) expressed as a percentage of no belt scores for normalised electromyographic values of the biceps femoris and medial hamstring muscles. Positive and negative values indicate increase and decrease in EMG values with the belt, respectively
Table 4. Effects of application of the pelvic compression belt on normalized EMG RMS values of muscles of the ham-string-injured and control participants obtained during the walking task
Abbreviations: CG, control group; EMG RMS, electromyographic root mean square value; HIG, hamstring-injured group; LR, loading response; MVIC, maximum voluntary isometric contraction; SD, standard deviation; TS, terminal swing. *P values based on log transformed data.
Muscle (MVIC
normalised EMG RMS)
Gait phase Injured limb of HIG (n = 22)Mean ± SD
Tested limb of CG (n = 30)Mean ± SD
No belt With belt P* No belt With belt P*
Lumbar multifidus
TS + LR 17.03 ± 8.06 12.69 ± 8.54 0.146 16.05 ± 7.23 12.00 ± 5.42 < 0.001
Gluteus maximus LR 14.65 ± 9.12 14.48 ± 8.45 0.332 14.11 ± 4.88 16.42 ± 6.85 0.025
Gluteus medius LR 37.98 ± 14.92 46.12 ± 11.70 0.003 39.27 ± 18.47 48.77 ± 25.14 0.028
Biceps femoris TS 23.86 ± 15.53 24.65 ± 14.29 0.078 17.57 ± 8.23 18.23 ± 8.25 0.319
Medial hamstrings TS 33.87 ± 20.47 32.16 ± 16.89 0.678 28.65 ± 14.28 27.14 ± 13.28 0.115

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 299
sportsmen with and without hamstring injuries. Simi-larly, the authors’ have recently shown no significant difference for such activity during a task entailing a transition from bipedal to unipedal stance.23 The lack of differences between the belt conditions dur-ing walking and transition from bipedal to unipedal stance23 contrasts with other data from this group of participants whereby isokinetic eccentric hamstring strength (injured and uninjured) in the terminal range increased with the PCB.22 Thus, while there is evidence for alteration in motor control of the hamstrings based on increased maximal eccentric strength, there appears to be no evidence for EMG changes during sub-maximal weight-bearing tasks. However, individual-specific changes with applica-tion of the PCB were noted (Figure 4). This indicates that changes in motor control of the hamstrings with the PCB could be individual- and task- specific (depending on the neuromotor demands of the task investigated) and also dependent upon the outcome variable measured.
The findings of this study contrasts with those of Hu et al19 who reported decreased activity of biceps fem-oris and increased activity of gluteus maximus with the PCB during treadmill walking in healthy nul-ligravidae females. These results supported hypoth-eses proposed by other researchers for patients with low back pain.37-38 Although both the present study and that undertaken by Hu et al19 investigated walk-ing, direct comparisons are limited due to various factors. Hu et al19 calculated median EMG activity per trial (per muscle) for the whole gait cycle but their data were not normalized, nor did they ran-domize the order of the belt conditions (PCB vs. no PCB), meaning results could be confounded by ordering and fatigue effects. Furthermore, in con-trast to the present study, Hu et al19 included female participants and this may have also contributed towards the difference, although it is unknown how sex would contribute to this effect.39-40
With application of the PCB there was an increase in gluteus medius activity (22 to 25%) in both groups of participants. Park et al documented a 31% increase in gluteus medius activity in healthy participants during hip abduction in side-lying while wearing the PCB.41 The increase noted during this non-weight bearing task appears similar to the response noted during the
loading response phase (weight-bearing task) in the current study. Peak EMG activity of the gluteal mus-cles occurs during the loading response phase when there is increased limb loading and a subsequent need for sacroiliac joint stability.7-8,37 Specifically, glu-teus medius stabilizes the pelvis in the coronal plane, preventing the pelvis dropping on the contralateral swinging limb.7 Application of a PCB has been hypoth-esized to provide proprioceptive input to facilitate gluteus medius recruitment owing to its neurophysi-ological (altered proprioception) and pseudofascial effects.21 However, there was no significant difference in the magnitude of change in gluteus medius activ-ity induced by the PCB in both groups, implying that similar neurophysiological mechanisms could have accounted for these effects in both groups.
A 25% decrease in multifidus activity with the PCB (compared to no PCB condition) during the termi-nal swing and loading response phases of walking in healthy participants was found. No similar changes were evident for the hamstring-injured group suggest-ing that this group responded differently with the PCB compared to uninjured participants. Similar to the cur-rent study, Hu et al reported an 8% decrease in erec-tor spinae activity in healthy women (nulligravidae) while wearing the PCB during treadmill walking.19 As both studies used similar EMG electrode placement, results appear to be similar for men and women for the low back muscles. A reduction in EMG activity of the multifidus may be due to increased force closure (forces other than the design of the articular surfaces providing sacroiliac joint stability) of the pelvic ring19 provided by the PCB, thus necessitating less multi-fidi activity to augment force closure. Application of a PCB may also influence hip and knee joint angles, inducing an altered gait pattern which could affect multifidus activity. However, these putative changes require substantiation in future studies.
The heterogeneous study sample, in terms of dif-ferent grades of injury and recovery, may have contributed to lack of effect of the PCB on injured hamstrings during walking. The results also indicate that the time since injury was not correlated with changes in biceps femoris and medial hamstring EMG activity with the application of the PCB. Thus, the EMG response with application of the PCB could not be predicted by the recovery phase.

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 300
This study has some limitations which require consid-eration. The results of this study cannot be extrapolated to the acute injury phase as all the injured sportsmen were recruited at least four weeks after injury occur-rence. In addition, pain was not a major limiting factor for participants, therefore examining participants with acute hamstring injury during walking would help to determine the effects of application of the PCB on pain as well as neuromotor control. It should be noted that between group differences (p > 0.05) in terms of age (borderline significance), height, weight and BMI, but not for body fat measurements (p = 0.941) were demonstrated. However, as the mean difference in age was only 1.5 years, it is unlikely that this factor would influence EMG activity. Furthermore, as there was no significant difference between the groups for body fat measurements, it is also unlikely that the anthropo-metric differences would have influenced the data. Only men were investigated in the current study, thus, the findings of the study cannot be extrapolated to women. It was assumed that walking velocity was not significantly different between test conditions for both groups, though this was not objectively analyzed. As the participants walked in synchrony with a met-ronome for both conditions, the step length was not monitored. Thus, changes in step length affecting the EMG results would be of less significance. PCB ten-sion was not directly measured in participants of the current study. PCB tension can change constantly during walking because of variations occurring in intra-abdominal pressure, lumbopelvic mobility and muscle activity.31 Therefore, maintaining a constant PCB tension is not possible; however, range of values indicating optimal PCB tension that could be achieved during over ground walking was measured in a sepa-rate study on 10 healthy male participants.31 Previ-ous research has demonstrated that participants with pelvic girdle pain42-43 present with altered neuromotor control of the lumbopelvic and hamstring muscles. Investigating the role of the PCB on sportspeople with more acute/subacute and severe hamstring injuries, with and without signs and symptoms of impaired pelvic stability, may help to further improve the cur-rent understanding of neuromotor control of the lum-bopelvic and thigh muscles.
The neuromotor demands/control of the hamstrings during walking may be well below any threshold
of detection for effect of injury on functional ham-strings muscle activity. Thus, future research may also require a similar EMG method and analysis that clearly focuses on running at various velocities in similarly injured participants and the effects of application of a PCB derived thereof.
CONCLUSIONWhile application of the PCB led to an increase in EMG activity of gluteus medius in participants with and without hamstring injuries, no significant effect was found for the hamstrings during the terminal swing phase of over ground walking. Therefore, such an orthotic may have limited applicability for altering hamstring activity, at least in this injured and uninjured population sample during walking. Although individual-specific responses may exist, the hamstrings may need a more demanding form of loading, or activity, in order to explore this puta-tive phenomenon.
REFERENCES1. McManus A, Stevenson M, Finch CF, Elliott B,
Hamer P, Lower A, et al. Incidence and risk factors for injury in non-elite Australian Football. J Sci Med Sport 2004;7:384-39.
2. Brooks JHM, Fuller CW, Kemp SPT, Reddin, DB. Incidence, risk, and prevention of hamstring Muscle Injuries in Professional Rugby Union. Am J Sports Med 2006;34:1297-1306.
3. Fyfe JJ, Opar DA, Williams MD, Shield AJ. The role of neuromuscular inhibition in hamstring strain injury recurrence. J Electromyogr Kinesiol 2013;23:523-530.
4. Hoskins W, Pollard H. The management of hamstring injury - Part 1: Issues in diagnosis. Man Ther 2005;10:96-107.
5. Sole G, Milosavljevic S, Sullivan SJ, Nicholson H. Running-related hamstring injuries: A neuromuscular approach. Phys Ther Rev 2008;13:102-110.
6. Thelen DG, Chumanov ES, Sherry MA, Heiderscheit BC. Neuromusculoskeletal models provide insights into the mechanisms and rehabilitation of hamstring strains. Exerc Sport Sci Rev 2006;34:135-141.
7. Levine D, Richards J, Whittle MW. Whittle’s Gait Analysis. 5th ed. Edinburgh/New York: Churchill-Livingstone; 2012.
8. Perry J, Burnfi eld JM. Gait Analysis: Normal and Pathological Function. 2nd ed. New Jersey: Slack Incorporated; 2010.

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 301
23. Arumugam A, Milosavljevic S, Woodley S, Sole G. Effects of external pelvic compression on electromyographic activity of the hamstring muscles during unipedal stance in sportsmen with and without hamstring injuries. Man Ther 2015;20:412-419.
24. Gabbe B, Finch C, Bennell K, Wajswelner H. How valid is a self reported 12 month sports injury history? Br J Sports Med 2003;37:545-547.
25. Petty N J. Principles of Neuromusculoskeletal examination and assessment: a handbook for therapists. 2 edn. Chruchill Livingstone/Elsevier; 2011
26. Hermens HJ, Freriks B, Disselhorst-Klug C, Rau G. Development of recommendations for SEMG sensors and sensor placement procedures. J Electromyogr Kinesiol 2000;10:361-374.
27. Hermens, H. J., Freriks, B., Merletti, R., Stegeman, D., Blok, J., Rau, G., et al. SENIAM 8: European Recommendations for Surface Electromyography, deliverable of the SENIAM project. Enschede, Netherlands: Roessingh Research and Development; 1999.
28. Daniels L, Worthingham C, Hislop HJ, Montgomery J. Daniels and Worthingham’s Muscle Testing: Techniques of Manual Examination. 8th edn. Philadelphia (PA): WB Saunders; 2007.
29. Davis RB, Ounpuu S, Tyburski D, Gage JR. A gait analysis data collection and reduction technique. Hum Mov Sci 1991;10:575-587.
30. Zeni Jr JA, Richards JG, Higginson JS. Two simple methods for determining gait events during treadmill and overground walking using kinematic data. Gait Posture 2008;27:710-714.
31. Arumugam A, Milosavljevic S, Woodley S, Sole G. Evaluation of changes in pelvic belt tension during 2 weight-bearing functional tasks. J Manipulative Physiol Ther 2012;35:390-395.
32. Oberg T, Karsznia A. Basic gait parameters: Reference data for normal subjects, 10-79 years of age. J Rehabil Res Dev 1993;30:210-223.
33. Hreljac A, Marshall RN. Algorithms to determine event timing during normal walking using kinematic data. J Biomech 2000;33:783-786.
34. Alton F, Baldey L, Caplan S, Morrissey MC. A kinematic comparison of overground and treadmill walking. Clin Biomech 1998;13:434-440.
35. Fusco N, Crétual A. Instantaneous treadmill speed determination using subject’s kinematic data. Gait Posture 2008;28:663-667.
36. Pantall A, Gregor RJ, Prilutsky BI. Stance and swing phase detection during level and slope walking in the cat: Effects of slope, injury, subject and kinematic detection method. J Biomech 2012;45:1529-1533.
9. Lee D. The Pelvic Girdle. 3rd ed. Edinburgh: Elsevier/Churchill Livingstone; 2004.
10. Kroll PG, Raya MA. Hamstring muscles: an overview of anatomy, biomechanics and function, injury etiology, treatment, and prevention. Crit Rev Phys Rehabil Med 1997;9:191-203.
11. Best TM, Garrett Jr WE. Hamstring strains: Expediting return to play. Phys Sportsmed 1996;24:37-44.
12. Agre JC. Hamstring injuries. Sports Med 1985;2,21-33.
13. Higashihara A, Nagano Y, Ono T, Fukubayashi T. Potential risk factors for hamstring muscle strain injury during the late swing phase of sprinting. Br J Sports Med 2014;48:608.
14. Thelen DG, Chumanov ES, Hoerth DM, Best TM, Swanson SC, Li L, et al. Hamstring muscle kinematics during treadmill sprinting. Med Sci Sports Exerc 2005;37:108-114.
15. Lee MJC, Reid SL, Elliott BC, Lloyd DG. Running biomechanics and lower limb strength associated with prior hamstring injury. Med Sci Sports Exerc 2009;41:1942-1951.
16. Henriksen M, Rosager S, Aaboe J, Bliddal H. Adaptations in the gait pattern with experimental hamstring pain. J Electromyogr Kinesiol 2011:21,746-753.
17. Silder A, Thelen DG, Heiderscheit BC. Effects of prior hamstring strain injury on strength, fl exibility, and running mechanics. Clin Biomech 2010;25:681-686.
18. Arumugam A, Milosavljevic S, Woodley S, Sole G. Effects of external pelvic compression on form closure, force closure, and neuromotor control of the lumbopelvic spine – A systematic review. Man Ther 2012;17:275-284.
19. Hu H, Meijer OG, van Dieen JH, Hodges PW, Bruijn SM, Strijers RL, et al. Muscle activity during the active straight leg raise (ASLR), and the effects of a pelvic belt on the ASLR and on treadmill walking. J Biomech 2010;43:532-539.
20. Snijders CJ, Ribbers MTLM, de Bakker HV, Stoeckart R, Stam HJ. EMG recordings of abdominal and back muscles in various standing postures: Validation of a biomechanical model on sacroiliac joint stability. J Electromyogr Kinesiol 1998;8:205-214.
21. Arumugam A, Milosavljevic S, Woodley S, Sole G. Can application of a pelvic belt change injured hamstring muscle activity? Med Hypotheses 2012;78:277-282.
22. Arumugam A, Milosavljevic S, Woodley S, Sole G. Effects of external pelvic compression on isokinetic strength of the thigh muscles in sportsmen with and without hamstring injuries. J Sci Med Sport 2015; 18:283–288.
The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 302
lumborum, and lumbar multifi dus activities during side-lying hip abduction. J Electromyogr Kinesiol 2010;20:1141-1145.
42. Hungerford B, Gilleard W, Hodges P. Evidence of altered lumbopelvic muscle recruitment in the presence of sacroiliac joint pain. Spine 2003;28:1593-1600.
43. Jung HS, Jeon, HS, Oh DW, Kwon OY. Effect of the pelvic compression belt on the hip extensor activation patterns of sacroiliac joint pain patients during one-leg standing: A pilot study. Man Ther 2013;18:43-148.
44. White KK, Lee SS, Cutuk A, Hargens AR, Pedowitz RA. EMG power spectra of intercollegiate athletes and anterior cruciate ligament injury risk in females. Med Sci Sports Exerc 2003;35:371-376.
37. Hossain M, Nokes LD. A biomechanical model of sacro-iliac joint dysfunction as a cause of low back pain. J Bone Joint Sur Br 2008;90B:222-223.
38. Hossain M, Nokes LD. A model of dynamic sacro-iliac joint instability from malrecruitment of gluteus maximus and biceps femoris muscles resulting in low back pain. Med Hypotheses 2005;65:278-281.
39. Abt J, Sell T, Laudner K, McCrory J, Loucks T, Berga S, et al. Neuromuscular and biomechanical characteristics do not vary across the menstrual cycle. Knee Surg Sports Traumatol Arthrosc 2007;15:901-907.
40. Eiling E, Bryant A, Petersen W, Murphy A, Hohmann E. Effects of menstrual-cycle hormone fl uctuations on musculotendinous stiffness and knee joint laxity. Knee Surg Sports Traumatol Arthrosc 2007;15:126-132.
41. Park KM, Kim SY, Oh DW. Effects of the pelvic compression belt on gluteus medius, quadratus

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 303
ABSTRACT
Background: Limited information exists regarding injury risk factors for high school athletes. The Func-tional Movement Screen (FMSTM) has been used to identify functional movement impairments and asym-metries, making it a potential predictor of injury.
Hypothesis/Purpose: To determine if the FMSTM is a valid predictor of injury in high school athletes and to identify a potential new FMSTM cutoff score for this population.
Study Design: Prospective Cohort
Methods: 167 high school athletes among several sports were scored using the FMSTM and were monitored for injury during a single season. Likelihood ratios were calculated to determine how much a subject’s total FMSTM score influenced the post-test probability of becoming injured.
Results: Of the 167 participants, 39 sustained a musculoskeletal injury. Of all component scores, the in-line lunge scores were significantly higher for injured players. For shoulder mobility, scores were signifi-cantly lower for injured players. No statistically significant associations were found between total FMSTM scores and injury status.
Conclusion: The FMSTM may be useful for recognizing deficiency in certain movements, however this data suggests that the FMSTM should not be used for overall prediction of injury in high school athletes through-out the course of a season. Normative data from a large sample size is now available in the high school athlete demographic.
Level of Evidence: Level 3
Key words: Functional Movement Screen (FMSTM), high school athlete, injury risk factors, sports injury
IJSP
TORIGINAL RESEARCH
FUNCTIONAL MOVEMENT SCREEN NORMATIVE
VALUES AND VALIDITY IN HIGH SCHOOL ATHLETES:
CAN THE FMSTM
BE USED AS A PREDICTOR OF INJURY?
Sean M. Bardenett, PT, DPT1
Joseph J. Micca, PT, DPT1
John T. DeNoyelles, PT, DPT, CSCS1
Susan D. Miller, PT, DPT, MS1
Drew T. Jenk, PT, DPT2
Gary S. Brooks, PT, DrPH1
1 SUNY Upstate Medical University, Syracuse, New York, USA2 Sports Physical Therapy of New York, Syracuse, New York,
USA
CORRESPONDING AUTHORDrew Jenk, DPTSports Physical Therapy of New York5320 W. Genesee StreetCamillus, NY 13031Phone: (315) 469-5400Fax: (315) 469-5724 E-mail: [email protected]

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 304
INTRODUCTIONHi gh school athletics involve an estimated 7.7 million participants each year as reported by the National High School Sports-Related Injury Surveil-lance Study, 2011-2012.1 This participation results in an estimated 1.4 million injuries at a rate of 2.2 inju-ries per 1,000 athletic exposures (practices or com-petitions). Limited data exists regarding injury risk factors for high school athletes. Previous authors have suggested that more years of playing experi-ence, previous history of being injured, and being involved in a greater number of coached sports are risk factors for injury in adolescent athletes, whereas physical characteristics such as height, weight, and strength are poor pr edictors.2,3,4 Although BMI is a poor predictor, authors of a previous study found that overweight high school football players were at an increased risk for ankle injuries, particularly in those who had previously sprained their ankle.5 Qualifications of the coach, in terms of level of experience and additional training and education, have been associated with a decreased risk of injury in adolescent athletes.6 Asymmetries, including mobility, range of motion and strength differences between sides, have also been identified as possible factors.7,8,9,10
The movement patterns examined in the Functional Movement Screen (FMSTM) place the athlete in posi-tions where functional movement limitations and asymmetries may be identified, making it a poten-tial predictor of injury.2 The FMSTM consists of seven tests, each scored between zero and three points with three representing the best possible score. The composite score, or total screen score, ranges from 0 to 21 points. The seven tests include the deep squat, hurdle step, inline lunge, shoulder mobility, active straight-leg raise, trunk stability pushup, and rotary stability tests. Descriptions of the tests and scoring criteria have been described previously.11,12,13,14
Pr evious research by Kiesel, et al15 suggested that the total FMSTM score could identify National Foot-ball League (NFL) players at risk for serious injury. Chorba et al16 found a significant correlation between low-scoring female collegiate athletes and injury. Both studies identified a cutoff score of 14 or less as a positive predictor of injury. Similarly, a study conducted on collegiate NCAA Division I and club
athletes involved in swimming/diving, rugby, and soccer found that subjects with composite scores of 14 or less and a self-reported history of previous injury were 15 times more likely to incur an injury versus those scoring above 14.17 To the knowledge of the authors, the FMSTM has not been validated for use in high school athletes, although normative values in physically active adolescent school-aged children have been reported.18 Using this tool could provide physical therapists, athletic trainers, coaches and other clinicians with the necessary information to have the injury risk in high school athletics reduced. Identifying at-risk athletes in pre-season screening with the use of a low cost, time efficient, and low physical risk screen can potentially decrease the number of injuries, decrease medical costs to par-ents and schools, and keep athletes from injury related school absences.
The purpose of this study was to determine if the FMSTM is a valid predictor of injury in high school athletes. It was hypothesized that those with lower FMSTM scores were at a higher risk of injury. Results of the study would also be used to examine if a score of 14 out of 21, as determined by Kiesel et al6 in NFL players, is an appropriate cutoff score in predicting injury in high school athletes.
METHODSOne hundred eighty-five student athletes (97 female, 88 male) from one public high school were recruited for the study during the 2012 fall season. All fall sport athletes were educated on the study design and participation was voluntary. Parental consent was obtained if the athletes were under the age of 18. The athletes or their guardians had the oppor-tunity to opt out of participation at any point in the screening process and throughout data collection during the season. Represented sports included boys and girls cross-country, boys football, boys and girls soccer, girls swimming, girls tennis, and girls volley-ball. Inclusion criteria included those ages 13-18 in good academic standing. Exclusion criteria included those not cleared by the school or their physician in a pre-participation physical exam and those who had reported any health contraindications to exercise and athletic activity including current musculoskel-etal injury. The study was approved by the SUNY Upstate Medical University Institutional Review

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 305
Board. Volunteers and their parents/legal guardians were required to provide written informed consent prior to participation in the study.
Testing occurred within the first week of the fall sports season. Four examiners, including one licensed physical therapist with 20+ years experi-ence and three third year doctor of physical therapy candidates, conducted the testing. All examiners held Functional Movement Screen certification through Functional Movement Systems, Inc. (Chatham, VA). Prior to data collection, each examiner participated in pilot study screening of at least 10 participants each, in addition to online training and formal class-room education of the FMSTM. The FMSTM has been reported to have high interrater composite score reliability (ICC = .98) between an experienced and novice tester,19 and moderate to good interrater and intrarater composite score reliability (ICC = .74 and ICC = .76, respectively) among novice testers.4 Prior to testing, subjects were familiarized to the FMSTM and study protocol, and examiners utilized the same verbal instructions provided by Cook, et al5 during testing. Scores were recorded at this pre-season screening session and the athletes were then monitored by the school’s certified athletic trainer (ATC) in order to obtain injury information through-out the fall season. All participating coaches were briefed on the study and were required to uphold policy that all injuries be reported to the ATC. The ATC was blinded from each subject’s FMSTM score. Based on previous research,16 injury was defined as a musculoskeletal injury that occurred as a result of participation in an organized high school practice or competition setting that required medical atten-tion in which the athlete sought care from an ATC, physical therapist, physician, or other health care provider, and was restricted from complete partici-pation for one or more exposures (practice or game). A single incidence of injury in accordance with this definition was considered an adequate inclusion in the injured group. Multiple injuries to the same ath-lete were not counted. Exclusion criteria included any neurological or non-musculoskeletal injury, such as a concussion, eye injury, or skin disorder. The identity of the subjects was protected and only the injury information was recorded and disclosed to the examiners. All injury data was collected for analysis at the conclusion of each team’s season.
The distributions of FMSTM scores and participant age were evaluated and found to be non-Gaussian. Accordingly, Wilcoxon signed-rank tests were per-formed to determine associations between total and component FMSTM scores and injury status (any injury versus no injury), and between age and injury status. Statistical significance was set at p (alpha) < 0.05. To assess the predictive validity of the FMSTM, sensitivity and specificity were calculated at differ-ent cut-off points. A receiver operator characteris-tics (ROC) curve was created to determine a cut-off score that maximized both sensitivity and specificity of total FMSTM scores. Likelihood ratios were calcu-lated to determine how much a subject’s total FMSTM score influenced the post-test probability of becom-ing injured.
RESULTSA total of 185 students underwent screening using the FMSTM prior to beginning the season. Over the course of the season, 39 participants sustained a musculoskeletal injury. Eleven students were lost to academic ineligibility, radiographic evidence of injury prior to testing, or not qualifying for partici-pation on a varsity or junior varsity level team. In addition, seven subjects incurred a concussion, and one sustained an eye injury. These 18 participants were excluded from analyses, leaving a sample of 167 participants, 90 females and 77 males, with com-plete data. Table 1 shows the distribution of partici-pants by sport and gender.
Mean (SD) age of the sample was 15.2 years, while the median age was 15 years. Median ages of injured participants was 16 years, and of non-injured par-ticipants was 15 years (p=.024, Wilcoxon rank-sum test). Mean (SD) total and component FMSTM scores
Table 1. Distribution of Partici-pants by Sport and Gender
Sport Female Male Total
Cross Country 10 16 26
Football 0 40 40
Soccer 37 21 58
Swimming 18 0 18
Tennis 9 0 9
Volleyball 16 0 16

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 306
are displayed in Table 2. Among the component FMSTM scores, in-line lunge and shoulder mobility were significantly different according to injury sta-tus. For in-line lunge, scores were higher for injured players, for shoulder mobility, scores were lower for injured players. The average score for males was 13.0 and 13.1 for females, while those injured scored a 13.0 compared to the non-injured group score of 13.1. Total FMSTM scores were not associ-ated with injury status. Sensitivity, specificity, posi-tive likelihood ratio and negative likelihood ratio are displayed in Table 3. Figure 1 displays a ROC curve based on this analysis.
DISCUSSION The results of the current investigation demon-strated that the FMSTM screening tool was not a valid
predictor of injury in male and female high school athletes participating in various sports over one sea-son of competition. Participants who sustained mus-culoskeletal injuries were more likely to be older than participants who were not injured. This is con-sistent with previous research regarding high school football players.2 It has been shown that the greatest risk factor for injury is sustaining a previous injury,20
thus older athletes have likely been playing for lon-ger amounts of time than younger athletes and have had more opportunities for injury. In addition, the nature of higher “varsity” level athletics and the increased exposure time in older athletes over more years of participation could result in more injuries and therefore greater risk for future injury.
Si gnificant findings included lower scores on the shoulder-mobility movement in injured athletes (p=.001). This finding may support the regional inter-dependence model, in which “seemingly unrelated impairments in a remote anatomical region may con-tribute to, or be associated with, the patient’s primary complaint.”21 Though the type of injuries sustained by these athletes varied in terms of body region, pub-lished research supports the notion of regional inter-dependence and how it could be used to potentially explain the lower scores that were found in shoulder
Table 2. Component and Total FMS Scores by Injury Status
FMS Component Not Injured (n = 128)
Injured (n = 39) p
Deep Squat 1.86 +0.67 1.79 +0.66 .522
Hurdle Step 1.91 +0.38 1.82 +0.39 .188
In-line Lunge 1.97 +0.55 2.21 +0.61 .022
Shoulder Mobility 2.67 +0.55 2.23 +0.84 .001
Active SLR 1.98 +0.68 1.97 +0.58 .850
Pushup 1.20 +0.49 1.41 +0.72 .100
Rotary Stability 1.51 +0.53 1.56 +0.55 .701
Total 13.11 +1.69 13.00 +2.32 .954 Values are mean (SD) p-values are derived from Wilcoxon signed-rank tests
Table 3. Validity Indices for Total FMS Scores at Various Cut-off Points
FMS Cut-off Score*
Sensitivity Specificity Positive
Likelihood Ratio
Negative Likelihood
Ratio 11 .15 .94 2.46 0.90
12 .21 .84 1.31 0.94
13 .41 .62 1.07 0.96
14 .56 .38 0.91 1.14
15 .74 .23 0.96 1.13
16 .87 .09 0.96 1.37
17 .95 .02 0.96 3.28
* At risk status is below the indicated cut-off score
Figure 1. Receiver Operator Characteristic Curve for Total FMS Scores at Different Cut-off Points.

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 307
mobility correlating to missed exposures. In the base-ball literature, Scher et al determined that decreases in hip internal rotation in the non-dominant hip highly correlated with predisposition to shoulder injuries in the non-pitching baseball players.22 This is an example of how impairments in a remote anatomi-cal region such as the hip could have profound effects on a distant structure and correlate to injury. This is one of few significant findings in the data set and it is understood that a limitation of the current study may deem these results a spurious finding.
The other statistically significant finding was that higher scores for the in-line lunge were exhibited in athletes who were injured (2.21 +0.61), as compared to lower scores in uninjured athletes (1.97 +0.55) (p=.022). The authors cannot explain this counter-intuitive finding. Ultimately, the conclusion from this data is that in this particular population total FMSTM scores were a poor predictor of injury status in high school athletes. It is possible that younger athletes present with varying levels of maturity, development and motor control, and the FMSTM is not an appropriate test battery to detect those at risk for injury in this population. Future research is needed to further validate an association between age and FMSTM scores in younger populations.
The authors feel that this research has provided a basis for normative data for high school aged athletes performing the FMSTM. The deep squat, hurdle step and active straight leg raise trended towards lower scores in injured athletes compared to higher scores in uninjured athletes, without reaching statistically significant differences. The authors are unable to propose a cutoff score for high school athletes as the ROC curve indicates that there is no cutoff point that might be considered predictive of injury. Further research is necessary to identify if an alternate cut-off score other than 14 (as determined by Kiesel et al6 in NFL players) is appropriate for high school ath-letes. The trend does indicate, however, that in this population a cutoff score of 13 may warrant closer examination, as those injured had a slightly lower score of 13 while those uninjured scored just above 13. Other additional research in the future may com-pare FMSTM in fatigued to non-fatigued athletes, as multiple sources indicate a loss of motor control in a fatigued state.23,24,25,26
Study LimitationsThere are inconsistencies across the literature in terms of definition of injury. The definition for this study was limited to a single incidence of a muscu-loskeletal injury and was not specified to contact or non-contact. Further research may be more specific in defining this. The authors were not able to capture exposures in this study. Those with a higher score may have better movement quality and patterns, and consequently be better athletes. Better athletes are more likely to be starters in competitions and have more exposures, which may in turn lead to an increased risk of injury. It was difficult to keep track of exposures, and although the ATC did try to iden-tify who started versus who did not, however, this was not an accurate enough means of measurement and was therefore not included in the data analysis. Athlete side-to-side asymmetries were not collected during testing due to time constraints. The authors’ acknowledge that this was a potential limitation for the study, and further studies could examine if there is a correlation of asymmetrical scoring on FMSTM tests to injury risk. It was thought that the FMSTM could potentially identify athletes who sustained noncontact injuries, but this detail was not recorded in the injury reporting. Further studies may try to focus on tracking exposure and nature of injury.
CONCLUSIONPrevious studies using the FMSTM as a screening tool investigated performance in college age or profes-sional athletes, and in these studies, the FMSTM had some predictive validity for injury.6,7 According to the results of this study, the FMSTM is not a predic-tor of injury in high school age athletes. Normative data now exists on each of the seven movements of the FMSTM for clinicians to access when evaluating athletes of a similar demographic. The authors con-clude that the FMSTM does have benefits in recog-nizing deficiency in certain movements, and with further training the performance of these particular movements could improve, but it should not be used for overall prediction of injury in high school ath-letes throughout the course of a season.
REFERENCES1. Comstock RD, Collins CL, Corlette JD, Fletcher EN.
National High School Sports-Related Injury
The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 308
Surveillance Study - 2011-12 school year. Columbus, OH: Nationwide Children’s Hospital; 2012. Available at http://www.nationwidechildrens.org/cirp-rio-study-reports/2011-12HighSchoolRIOSummaryReport.pdf. Accessed February 27, 2013.
2. Turbeville SD, Cowan LD, Owen WL, Asal NR, Anderson MA. Risk factors for injury in high school football players. Am J Sports Med. 2003; 31(6):974-980.
3. Emery CA, Tyreman H. Sports participation, sport injury, risk factors and sport safety practices in Calgary and area junior high schools. Paediatr Child Health. 2009; 14(7): 439-444.
4. Knowles SB, Marshall SW, Bowling MJ, et al. Risk factors for injury among high school football players. Epidemiology. 2009; 20(2):302-310.
5. Tyler TF, McHugh MP, Mirabella MR, Mullaney MJ, Nicholas SJ. Risk factors for noncontact ankle sprains in high school football players: The role of previous ankle sprains and body mass index. Am J Sports Med. 2006; 34(3);471-475.
6. Schulz, MR, Marshal SW, Yang J, Mueller FO, Weaver NL, Bowling JM. A prospective cohort study of injury incidence and risk factors in North Carolina high school competitive cheerleaders. Am J Sports Med. 2004; 32(2):396-405.
7. Knapik JJ, Bauman CL, Jones BH, Harris JM, Vaughan L. Preseason strength and fl exibility imbalances associated with athletic injuries in female collegiate athletes. Am J Sports Med. 1991; Jan-Feb;19(1):76-81.
8. Nadler SF, Malanga GA, Feinberg JH, Prybicien M, Stitik TP, DePrince M. Relationship between hip muscle imbalance and occurrence of low back pain in collegiate athletes: a prospective study. Am J Phys Med Rehabil. 2001; 80(8):572-577.
9. Plisky PJ, Rauh MJ, Kaminski TW, Underwood FB. Star Excursion Balance Test as a predictor of lower extremity injury in high school basketball players. J Orthop Sports Phys Ther. 2006; 36(12):911-919.
10. Shanley E, Rauh MJ, Michener LA, Ellenbecker TS, Garrison JC, Thigpen. Shoulder range of motion measures as risk factors for shoulder and elbow injuries in high school softball and baseball players. Am J Sports Med. 2011; 39(9):1997-2006.
11. Cook G, Burton L, Hoogenboom B. Pre-Participation screening: The use of fundamental movements as an assessment of function—part 1. North Am J Sports Phys Ther. 2006; 1(2):62-72.
12. Cook G, Burton L, Hoogenboom B. Pre-Participation screening: The use of fundamental movements as an assessment of function—part 2. North Am J Sports Phys Ther. 2006; 1(3):132-139.
13. Teyhen DS, Shaffer SW, Lornson CL, et al. The Functional Movement Screen: a reliability study. J Orthop Sports Phys Ther. 2012; 42(6): 530-540.
14. Cook G, Burton L, Kiesel K, Rose G, Bryant MF. Movement: Functional Movement Systems: Screening-Assessment-Corrective Strategies. Aptos, CA: On Target Publications; 2010.
15. Kiesel K, Plisky JP, Voight ML. Can serious injury in professional football be predicted by a preseason functional movement screen? North Am J Sports Phys Ther. 2007; 2(3):147-158.
16. Chorba RS, Chorba DJ, Bouillon LE, Overmyer CA, Landis JA. Use of a functional movement screening tool to determine injury risk in female collegiate athletes. North Am J Sports Phys Ther. 2010; 5(2):47-54.
17. Garrison M, Westrick R, Johnson MR, Benenson J. Association between the Functional Movement Screen and injury development in college athletes. Int J Sports Phys Ther. 2015; 10(1):21-28.
18. Abraham A, Sannasi R, Nair R. Norative values for the Functional Movement ScreenTM in adolescent school aged children. Int J Sports Phys Ther. 2015; 10(1):29-36.
19. Onate, JA, Dewey, T, Kollock, RO, Thomas, KS, Van Lunen, BL, DeMaio, M, and Ringleb, SI. Real-time intersession and interrater reliability of the functional movement screen. J Strength Cond Res. 2012; 26(2):408–415.
20. Emery CA, Meeuwisse WH, Hartmann SE. Evaluation of risk factors for injury in adolescent soccer: Implementation and validation of an injury surveillance system. Am J Sports Med. 2005; 33(12):1882-1891.
21. Wainner RS, Whitman JM, Cleland JA, Flynn TW. Regional interdependence: a musculoskeletal examination model whose time has come. J Orthop Sports Phys Ther. 2007; 37(11):658-60.
22. Scher S, Anderson K, Weber N, Bajorek J, Rand K, Bey MJ. Associations among hip and shoulder range of motion and shoulder injury in professional baseball players. J Athl Train. 2010; 45:191-197.
23. McLean SG, Samorezov JE. Fatigue-induced ACL injury risk stems from degradation in central control. Med Sci Sports Exerc. 2009; 41(8):1661-1672.
24. Mathers JF, Grealy MA. Motor control strategies and the effects of fatigue on golf putting performance. Front Psychol. 2013; 4:1-10.
25. Lees A. Science and the major racket sports: a review. J. Sports Sci. 2003; 21:707-732.
26. Forestier N, Nougier V. The effects of muscular fatigue on the coordination of a multijoint movement in human. Neurosci Lett. 1998; 252(3):187-190.

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 309
ABSTRACTBackground: The significance of scapular dyskinesis is being challenged due to a lack of the association with pain and ability to predict injury in athletic populations. However, it is unknown whether asymptomatic overhead athletes with dyskinesis cope by normalizing scapular position with higher demand activities.
Hypothesis/Purpose: The purpose of this study was to compare change in scapular kinematics from an active unweighted contraction to a maximal isometric contrac-tion in asymptomatic overhead athletes with and without scapular dyskinesis. Secondarily, force generated with manual muscle tests were explored for differences and relationships with kinematics.
Study Design: Cross-sectional laboratory study
Methods: Twenty-five matched asymptomatic overhead athletes with (n=14) and without (n=11) scapular dyskinesis, defined with a reliable and validated clinical method, participated in this study. Three-dimensional scapular kinematics were evaluated in an active unweighted condition, and during maximal isometric contractions at 90° of shoulder flexion. Isometric force produced with lower trapezius and serratus anterior manual muscle tests were assessed with a dynamometer. Changes in scapu-lar kinematics were compared between groups. Differences in force generated with manual muscle tests between groups and relationships with kinematics were explored.
Results: Athletes with dyskinesis demonstrated greater deficits in scapular upward rotation with maximal contraction (p=<0.001), less external rotation (p=0.036) and weaker lower trapezius manual muscle test strength (p=0.031). Lower trapezius (p=0.003;r=0.57) and serratus anterior (p=0.042;r=0.41) manual muscle test strength deficits were fair to moderately associated with a lack of scapular upward rotation during maximal contraction.
Conclusion: Small to moderate changes in scapular kinematics are normal responses to a maximal contraction, but with scapular dyskinesis this response is accentuated. Athletes with dyskinesis generate less force with lower trapezius manual muscle testing compared to athletes without dyskinesis. Decreased strength with lower trapezius and serratus anterior manual muscle testing was also related to a lack of upward rotation in all athletes.
Keywords: Shoulder, biomechanics upper extremity, scapula, strength testing
Level of Evidence: 3
IJSP
TORIGINAL RESEARCH
A COMPARISON OF CHANGE IN 3D SCAPULAR
KINEMATICS WITH MAXIMAL CONTRACTIONS AND
FORCE PRODUCTION WITH SCAPULAR MUSCLE TESTS
BETWEEN ASYMPTOMATIC OVERHEAD ATHLETES
WITH AND WITHOUT SCAPULAR DYSKINESIS
Amee L. Seitz, PT, PhD, DPT, OCS1 Rebecca I. McClelland, ATC, MS2
W. Justin Jones, PT, DPT, OCS3
Randy A. Jean, PT, DPT, CSCS4
Joseph R. Kardouni, PT, DPT, PhD, OCS, SCS5
1 Department of Physical Therapy and Human Movement Sciences, Feinberg School of Medicine, Northwestern University, Chicago Illinois, USA
2 Department of Athletic Training, Boston University, Boston, Massachusetts, USA
3 Department of Physical Therapy, Simmons College, Boston, Massachusetts, USA
4 South Shore Hospital, Center for Orthopedics, Spine and Sports Medicine, Hingham, Massachusetts, USA
5 U.S. Army Research Institute of Environmental Medicine, Natick, Massachusetts, USA
Funding: none
The Institutional Review Board at Northeastern University approved this study protocol.
The opinions or assertions contained herein are the private views of the author(s) and are not to be construed as offi cial or refl ecting the views of the Department of the Army or the Department of Defense.
Any citations of commercial organizations and trade names in this report do not constitute an offi cial Department of the Army endorsement or approval of the products or services of these organizations.
CORRESPONDING AUTHORAmee L. SeitzDepartment of Physical Therapy & Human Movement SciencesFeinberg School of MedicineNorthwestern University645 N Michigan Ave, Suite 1100, Chicago IL 60611E-mail: [email protected]

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 310
INTRODUCTIONAbnormal movement of the scapula, termed scap-ular dyskinesis,1 is common among athletes who participate in overhead sports2,3 and has been theo-rized to predispose athletes to shoulder injury. In a prospective study of asymptomatic rugby players, players identified with scapular dyskinesis during preseason had a high incidence of in-season shoul-der injury.4 However, there is also evidence to sup-port the contrary.2,5 Additionally, the presence of clinically observed scapular dyskinesis exists inde-pendent of shoulder pain in athletes participating in overhead sports. As such, the significance of clini-cally observed scapular dyskinesis and need for scap-ular stabilization programs are being scrutinized.
Underlying conflicting study results is the fact that scapular motion is complex, occurring three-dimen-sionally (3D). This has challenged the clinician’s ability to reliably detect, much less subcategorize abnormal movement into types such as inferior angle prominence versus excessive shoulder shrug6-8 without sophisticated laboratory measures.9 Sev-eral clinical methods to evaluate scapular motion have been described with good reproducibility,10-14 but few have been validated.11,15 Visual observation of scapular motion during shoulder flexion with a light resistive load, termed the scapular dyskinesis test16, has been shown to be both a reliable and vali-dated method to clinically identify the presence of dyskinesis in overhead athletes in terms of either dysrhythmia or inferior/medial boarder promi-nence.3,7,16 Clinical measures should demonstrate both acceptable reliability and validity to be useful, and research that does not utilize such measures to identify dyskinesis should be taken in this context.
One possible reason for the conflicting evidence examining relationships between the presence of scapular dyskinesis and injury risk in overhead athletes may be due to the load used during test-ing. Studies investigating pain3 or injury risk2 in overhead athletes with dyskinesis have used visual observation methods which incorporate the use of light external load during repeated arm elevation. Clinically, scapular dyskinesis is often attributed to scapular muscle weakness, but evidence to sup-port this relationship using the visual observation method to define dyskinesis is lacking. It is possible
that asymptomatic overhead athletes with scapular dyskinesis with light external loads may respond dif-ferently with heavier external loads.
Previous investigations demonstrate that varying external resistance loads change 3D scapular motion during humeral elevation with inconsistent results.16-22 Discrepancies have been attributed to the varying loads used.17 However, only one study evaluated par-ticipants for scapular dyskinesis.17 To the authors’ knowledge, whether changes in 3D scapular kine-matics differ in overhead athletes with and without scapular dyskinesis in response to a higher demand activity, such as a maximal contraction, is unknown. If scapular dyskinesis is related to impaired scapular muscle strength contributing to the lack of scapu-lar stability, then scapular alterations in individuals with scapular dyskinesis would persist or worsen with greater loads. However, it is possible that over-head athletes with scapular dyskinesis detected with light loads may uniquely possess adequate scapular muscle strength and scapular stability with higher demand activities due to their specific sport training.
Therefore, the primary aim of this study was to compare change in 3D scapular kinematics with a maximal contraction between asymptomatic over-head athletes with and without scapular dyskinesis. It was hypothesized that compared to asymptomatic overhead athletes without dyskinesis, athletes with scapular dyskinesis would demonstrate alterations in 3D scapular kinematics during unweighted arm elevation, but those alterations would be less pro-nounced with a maximal isometric elevation contrac-tion. It was also hypothesized that overhead athletes without scapular dyskinesis would demonstrate smaller changes in scapular kinematics between the unweighted and maximum contraction arm elevation because these individuals are able to sufficiently sta-bilize the scapula during both contraction conditions. The secondary aims of the study were to explore scapular muscle strength as a potential explanatory factor for differences between groups.
METHODS
SubjectsThe University institutional review board approved this study. Overhead athletes were recruited to par-ticipate in this cross-sectional study from local college

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 311
and university populations. Twenty-eight asymp-tomatic overhead athletes agreed to participate and signed the university-approved informed consent. Subjects were eligible if they were currently partici-pating without restrictions in a club or varsity level overhead sport, defined as baseball, swimming, ten-nis, water polo, or volleyball. The dominant shoul-der was tested in all eligible participants. Exclusion criteria are listed in Table 1. The scapular dyskinesis test3 was used to define scapular motion as normal, subtle, or obvious dyskinesis, by two independent examiners. The examiners were physical therapists and an athletic trainer professional with experience ranging from 2-19 years. Examiners completed stan-dardized training in the dyskinesis visual observation method.16 The test consists of five repetitions of bilat-eral, active, shoulder flexion and abduction holding 1.4kg (3lb) or 2.3kg (5lb) weights, 2.3kgs was used for athletes weighing over 68.1kgs.16 Obvious dyskinesis was defined as dysrhythmia or inferior angle/medial boarder prominence of at least 2.5cm during at least 3 repetitions. Athletes classified with normal scapu-lar motion were included and matched by age (±5 years), laterality, and gender to participants with obvious dyskinesis (Figure 1). Three subjects with normal scapular motion were excluded due to a rat-ing of subtle dyskinesis by at least one of the two independent examiners. Thus, twenty-five subjects were included in the final analysis, fourteen subjects with scapular dyskinesis and eleven subjects with
normal motion (Table 2). Prior to initiating the study, a sample size of 16 total subjects was deemed neces-sary to provide 90% power, with α=0.05, to detect a 5° difference in change in 3D scapular kinematics with a maximal contraction between groups using effect size estimates from prior work.3,23,24
Manual Muscle TestingShoulder strength during manual muscle testing (MMT) was defined as peak isometric force measured with a handheld dynamometer. Assessment of shoulder strength with a handheld dynamometer has demon-strated excellent inter-rater and intra-rater reliability.25 The order of the muscle testing was randomized by blinded drawing prior to testing. For the serratus anterior muscle, the subject was seated upright in a chair posi-tioned with feet flat on the floor, shoulder-width apart. Subjects were asked to look straight ahead and flex the
Table 1. Participant study exclusion criteria
Athletes with any of the following were excluded: shtnom6tsalehtniniapredluohs
pain or limitations in shoulder or cervical spine active range of motion esaesidlateleksolucsumcimetsys
erutcarfroyregrusredluohsfoyrotsihecivedcinortceledetnalpmi
pain or instability with anterior apprehension23,24 or empty can25 tests
Table 2. Overhead athlete participant characteristics With Dyskinesis (n=14) Without Dyskinesis (n=11)
Gender (male/females) 5 (35.7%) / 9 (64.3%) 5 (38.5%) / 6 (54.5%) Age (mean ± SD), years 20.3±1.4 20.5±1.2 Height (mean ± SD), cm 175.5±13.9 175.3±9.0 Mass (mean ± SD), kg 67.0±12.4 71.6±10.3 Arm Dominance 1 left; 13 right 1 left; 10 right Participant Sport (n) 3 Swimming 2 Swimming
9 Volleyball 6 Volleyball 2 Water Polo 3 Water polo
Figure 1. An athlete classifi ed with scapular dyskinesis (right shoulder) with the visual observation method.

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 312
dominant shoulder to 120°, confirmed with a goniom-eter, with the thumb facing upward. For the lower tra-pezius muscle, the subject was prone on a plinth with the dominant arm in 120° of abduction and thumb fac-ing upward. With both tests, the pad of a handheld force dynamometer was placed at the distal aspect of the wrist, just proximal to the radial styloid process, and held sta-tionary by the examiner with two hands. Subjects were asked to push as hard as possible into the dynamometer pad for a verbal 5-second count. Before maximal test-ing of each muscle, a sub-maximal (50%) effort trial was performed to minimize learning effects. Maximum force output (kg) of two separate 5-second maximal isometric contractions was recorded. A 30-second rest period was provided between trials. The peak force of the two tri-als was averaged, normalized to the subject’s bodyweight (kg) and expressed as a percentage. These muscle testing positions have been validated to produce the maximum surface EMG activity of the primary agonist and the least involvement of surrounding muscles with electromyog-raphy.26 Therefore, the authors’ took force production in these positions to represent strength of the respective muscle. Within session, test-retest reliability was estab-lished for the examiners in this study. Intraclass correla-tion coefficients (ICC), standard error of measurement SEM=SD 1−( )ICC , and minimal detectable change
Mdc=SEM 2( ) , were calculated. The MMT mea-
surements showed excellent reliability (ICC 0.95-0.98). The lower trapezius MMT showed SEM=0.4% of body weight and MDC=0.5%, while the serratus anterior MMT showed SEM=0.6% and MDC=0.8%.
3D Scapular KinematicsThe Ascension Trakstar electromagnetic-based motion capture system (Ascension Technology Cor-poration, Milton, VT, USA) with a sampling rate of 240 Hz was used with Motion Monitor software (Innovative Sports Training, Inc., Chicago, IL, USA) to collect 3D kinematic data of the scapula, humerus, and trunk. The system consists of a transmitter that emits a magnetic field detected by 4 receivers. The reported accuracy of the electromagnetic tracking device is 1.4 mm and 0.5° 27 and mean errors for skin mounted receivers are 3.56° for scapular rota-tion below 120° of humeral elevation.28
Electromagnetic receivers were placed on the tho-rax over the spinous process of T3, the posterior-
lateral acromion, and the posterior aspect of the dis-tal humerus of the dominant arm using double-sided tape (3M HealthCare, St Paul, MN). The humeral receiver was further secured with PreWrap (Mueller, Prairie du Sac, WI). The fourth receiver was used to digitize anatomical landmarks on each segment fol-lowing International Society of Biomechanics (ISB) recommendations.29 Digitization allowed transfor-mation of the sensor position and orientation into anatomically-based position and orientation data of the humerus and scapula with respect to the tho-rax. Euler angle sequences for humeral (Y-X’-Y”) and scapular (Y-X’-Z”) rotations were used.29 Scap-ular upward/downward rotation occurs around a horizontal axis perpendicular to the plane of the scapula, anterior/posterior tilting occurs around a horizontal axis parallel to the scapular spine, and internal/external rotation occurs around a vertical axis through the plane of the scapula.30,31 Scapular movements into the directions of upward rotation, posterior tilt, and external rotation were defined as posi tive values for clinical interpretation. Three-dimensional kinematic data were collected during two 5-second trials of shoulder flexion (humeral ele-vation in the sagittal plane) at 90° under each con-traction condition. Kinematic data collected during a one second interval identified by the midpoint in each of the two separate 5-second trials were aver-aged and used for analysis. The three scapular rota-tions showed excellent reliability (ICC 0.98-0.99). The measurement error for the scapular rotations were: upward rotation SEM=3.0°, MDC=4.2°; pos-terior tilt SEM=1.9°, MDC=2.7°; external rotation SEM=2.0°, MDC=2.8°.
Elevation Contraction ConditionsTwo repetitions each of two contraction conditions (unweighted active contraction; maximal contrac-tion) were performed, with the order assigned by random drawing. During both contraction condi-tions, subjects were positioned with a non-elastic strap under both feet, standing shoulder-width apart, and over the distal aspect of both arms, proximal the radial styloid process at the wrist, thumbs facing upward. Both elbows were fully extended and shoul-ders flexed to 90°, confirmed with a goniometer. The length of the strap was adjusted so no slack was pres-ent maintaining the testing position (Figure 2). Once

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 313
contraction condition, standardized verbal encour-agement with a series of four sequential, loud cues of “push” was provided by the second examiner. During either contraction condition, if the subject’s position was not properly maintained, the trial was discarded and another trial was performed.
Statistical AnalysisDescriptive statistics were computed for all demo-graphic variables. Independent t-tests were used to compare age, height and mass between groups. Sep-arate 2x2 factorial mixed-model analysis of variance (ANOVAs) were used to compare mean 3D scapu-lar kinematics between groups with factors of group (dyskinesis; normal), contraction condition (active; maximum), and interactions. With a statistical sig-nificance, post hoc comparisons were made using linear contrasts with a Bonferroni adjusted alpha for a priori comparisons of interest to include main effects contraction condition, group, or interactions. To explore potential explanatory factors for MMT differences between the groups, independent t-tests were used. Bivariate correlation analyses were used to determine the relationships between lower tra-pezius and serratus anterior MMT and change in scapular kinematics with maximal contraction. For all statistical analyses, significance was set at α=.05. All analyses were performed using SAS Software (JMP 9.0.3;SAS Institute Inc., Cary, NC, USA).
RESULTSThere were no significant differences (p>0.05) in age, height and mass characteristics between groups. Scapular upward rotation showed both within group (contraction main effect) and between group (group-by-contraction interaction) differences during the two contraction conditions (Table 3 and Figure 3). The change in upward rotation between the unweighted and maximal contraction conditions was 6.3° (p<0.001; 95%CI=5.0°,7.6°) greater in athletes with-out dyskinesis. Athletes with dyskinesis demonstrated a smaller but significant 4.3° (p= 0.018; 95%CI=0.4°, 8.2°) increase in scapular upward rotation from unweighted to maximal contraction conditions com-pared to a 10.3° (p< 0.001; 95%CI=6.3°,14.2°) sig-nificant increase in athletes without dyskinesis. With scapular posterior tilt, there were no significant inter-actions or group main effect, but a significant main
the strap was properly tensioned, the subject relaxed both arms at his/her side for 30-seconds. The sub-ject would then assume this testing position with the strap with each of the contraction conditions.
During the unweighted active condition, subjects actively raised both arms to 90° in the sagittal plane, verified with a goniometer, taking up the slack in the strap and avoiding additional force. Three-dimen-sional kinematic data were recorded for a 5-second verbal count. During the maximum contraction con-dition, subjects assumed the testing position then were asked to push both arms upward into the strap at 50% effort for verbal 5-second count, maintaining a straight spine. This submaximal trial was used to gain familiarity with the procedure and make any necessary adjustments to the length of strap by veri-fying the 90° shoulder position with a goniometer. During this submaximal trial, additional verbal cues were provided to avoid substitutional movements such as trunk hyperextension. Two maximal con-tractions were then performed. During the maximal
Figure 2. Subject positioned with a non-elastic strap during both the active and maximal isometric contraction testing con-ditions.
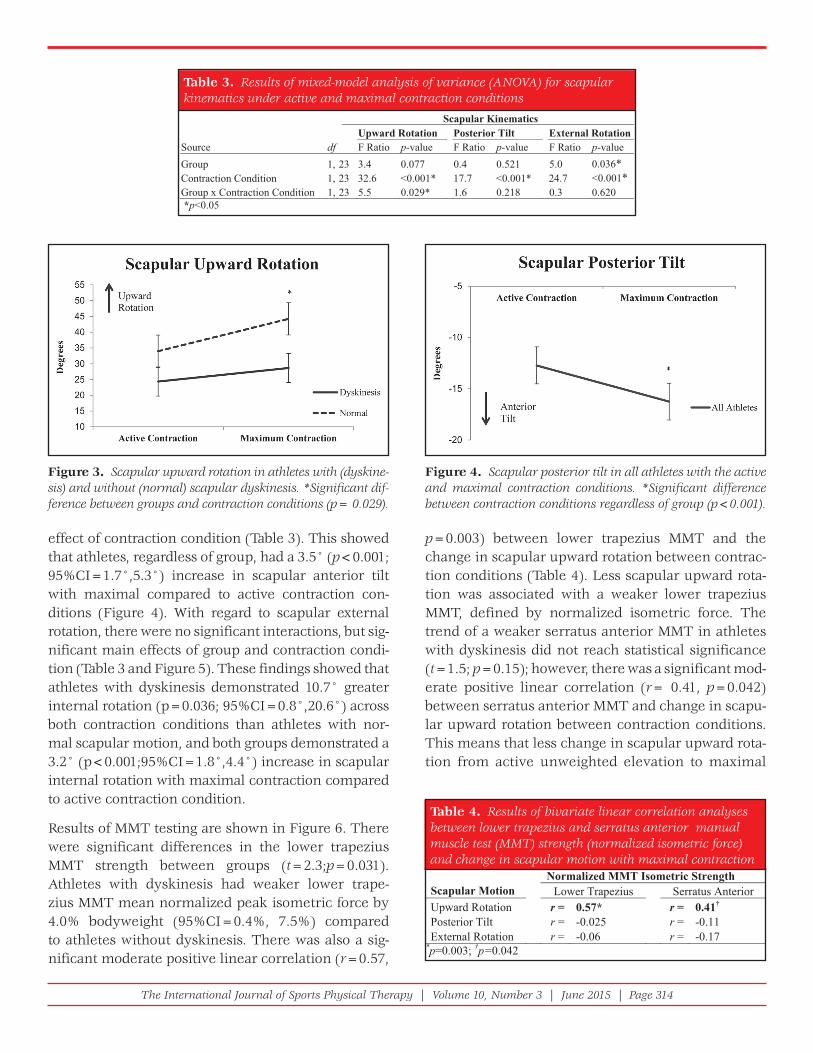
The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 314
p=0.003) between lower trapezius MMT and the change in scapular upward rotation between contrac-tion conditions (Table 4). Less scapular upward rota-tion was associated with a weaker lower trapezius MMT, defined by normalized isometric force. The trend of a weaker serratus anterior MMT in athletes with dyskinesis did not reach statistical significance (t=1.5; p=0.15); however, there was a significant mod-erate positive linear correlation (r= 0.41, p=0.042) between serratus anterior MMT and change in scapu-lar upward rotation between contraction conditions. This means that less change in scapular upward rota-tion from active unweighted elevation to maximal
effect of contraction condition (Table 3). This showed that athletes, regardless of group, had a 3.5° (p<0.001; 95%CI=1.7°,5.3°) increase in scapular anterior tilt with maximal compared to active contraction con-ditions (Figure 4). With regard to scapular external rotation, there were no significant interactions, but sig-nificant main effects of group and contraction condi-tion (Table 3 and Figure 5). These findings showed that athletes with dyskinesis demonstrated 10.7° greater internal rotation (p=0.036; 95%CI=0.8°,20.6°) across both contraction conditions than athletes with nor-mal scapular motion, and both groups demonstrated a 3.2° (p<0.001;95%CI=1.8°,4.4°) increase in scapular internal rotation with maximal contraction compared to active contraction condition.
Results of MMT testing are shown in Figure 6. There were significant differences in the lower trapezius MMT strength between groups (t=2.3;p=0.031). Athletes with dyskinesis had weaker lower trape-zius MMT mean normalized peak isometric force by 4.0% bodyweight (95%CI=0.4%, 7.5%) compared to athletes without dyskinesis. There was also a sig-nificant moderate positive linear correlation (r=0.57,
Table 3. Results of mixed-model analysis of variance (ANOVA) for scapular kinematics under active and maximal contraction conditions
Scapular Kinematics Upward Rotation Posterior Tilt External Rotation
Source df F Ratio p-value F Ratio p-value F Ratio p-value0.5125.04.0770.04.332,1puorG 0.036*
Contraction Condition 1, 23 32.6 <0.001* 17.7 <0.001* 24.7 <0.001*Group x Contraction Condition 1, 23 5.5 0.029* 1.6 0.218 0.3 0.620 *p<0.05
Table 4. Results of bivariate linear correlation analyses between lower trapezius and serratus anterior manual muscle test (MMT) strength (normalized isometric force) and change in scapular motion with maximal contraction
*p=0.003; †p=0.042
Normalized MMT Isometric Strength Scapular Motion Lower Trapezius Serratus Anterior Upward Rotation r = 0.57* r = 0.41†
Posterior Tilt r = -0.025 r = -0.11 External Rotation r = -0.06 r = -0.17
Figure 3. Scapular upward rotation in athletes with (dyskine-sis) and without (normal) scapular dyskinesis. *Signifi cant dif-ference between groups and contraction conditions (p= 0.029).
Figure 4. Scapular posterior tilt in all athletes with the active and maximal contraction conditions. *Signifi cant difference between contraction conditions regardless of group (p<0.001).

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 315
have significantly greater (15°) scapular upward rota-tion deficits. Athletes with dyskinesis also had sig-nificantly greater (10.7°) scapular internal rotation under both contraction conditions, while only trends of this were found in the prior study.3 Greater differ-ences between groups found in the current study are attributed to using a higher demand activity. Also, the prior study included athletes with shoulder pain, which may have influenced their results.
The second hypothesis was that overhead athletes with normal scapular motion would demonstrate small changes in scapular kinematics with a maximum contraction because these individuals are able to suf-ficiently stabilize the scapula. This was partially con-firmed. Athletes without dyskinesis had small changes in scapular anterior tilt (3.5°) and internal rotation (3.2°) with maximal isometric contraction, but larger increases in scapular upward rotation (10.3°). Camci et al17 found similar changes in scapular upward rota-tion (1.4° increase) and in scapular anterior tilt (4.3° increase) at 90° flexion during concentric sagittal plane elevation with an external load of elastic resis-tance compared to an unloaded condition. The authors of the current study attribute the larger changes in upward rotation to the use of a higher demand maxi-mal contraction. It is difficult to compare our results to the other previous research examining the effects of load on scapular kinematics16-22 since previous stud-ies may have included a heterogeneous mix of partici-pants with and without dyskinesis.
Athletes with scapular dyskinesis had impaired force generation with manual muscle tests used to test lower trapezius activity (Figure 6). Athletes
contraction was related to less serratus anterior MMT strength. There were no other significant relation-ships (Table 4) between change in scapular muscle MMT strength and change in scapular kinematics.
DISCUSSIONThe authors hypothesized that asymptomatic over-head athletes with dyskinesis have the ability to correctively stabilize their scapula during higher demand activities, explaining why athletes are able to participate in overhead sports without higher risk of injury. Contrary to the stated hypotheses, results suggest asymptomatic overhead athletes with visu-ally observed scapular dyskinesis do not correctively stabilize the scapula with a maximal contraction. Specifically, athletes with dyskinesis demonstrated a lack of scapular upward rotation from active to maximal contraction (Figure 3) and less external rotation with both contractions (Figure 5) compared to athletes with normal scapular motion.
While no prior study has examined the effect of a max-imal load in individuals with dyskinesis for compari-son, the current study results are in agreement with Tate et al3 who found athletes with scapular dyskine-sis had a statistically significant 9° deficit in scapular upward rotation during concentric humeral elevation below 90° in the sagittal plane while holding light weights (1.4/2.3kgs) compared to athletes with nor-mal scapular motion. In the current study, the authors utilized a higher demand activity, maximal isometric contraction, and found athletes with dyskinesis to
Figure 5. Scapular external rotation in athletes with (dyski-nesis) and without (normal) scapular dyskinesis *Signifi cant difference between groups (p=0.036) and contraction condi-tions (p<0.001).
Figure 6. Lower trapezius and serratus anterior normalized peak isometric muscle force (strength).

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 316
tion with a higher demand activity. A limitation of studying clinically identified scapular dyskinesis is that examiners may identify cases of dyskinesis with a heterogeneous mix of underlying factors, so future biomechanical studies may benefit from subgrouping scapular dyskinesis based on specific identifiable bio-mechanical factors such as specific muscle strength imbalance or aberrant muscle co-contraction patterns. A limitation specific to this study is that the authors measured scapular kinematics isometrically at 90° of shoulder flexion, which provides only a snapshot of overall scapular kinematics across the range of shoul-der motions and muscular contractions. Further study is warranted to determine whether a cluster of impair-ments, beyond the presence of dyskinesis, may increase injury risk in overhead athletes. Lastly, while athletes who experienced shoulder pain in the last 6 months were excluded, participants’ history of pain before the research timeframe was unknown.
CONCLUSIONSIn overhead athletes with normal scapular motion, a maximal isometric elevation contraction at 90° results in small increases (<3.5°) in scapular inter-nal rotation and anterior tilt, but moderate increases in scapular upward rotation (10°) compared to an unloaded active elevation condition. Athletes with scapular dyskinesis showed less upward rotation and greater internal rotation of the scapula at rest than those without dyskinesis. These scapular kine-matic alterations are accentuated with a maximal isometric contraction in individuals with dyskinesis. Therefore, clinicians could consider using a maxi-mal isometric contraction at 90° flexion to clarify the presence of dyskinesis or assess scapular stabiliza-tion in overhead athletes. Lastly, this study provides evidence that links lower trapezius MMT strength deficits with alterations in scapular motion in over-head athletes, and specifically identifies deficits in scapular muscle MMT strength in overhead athletes with clinically identified scapular dyskinesis.
REFERENCES 1. Kib ler WB, McMullen J. Scapular dyskinesis and its
relation to shoulder pain. J Am Acad Orthop Surg. 2003;11(2):142-151.
2. Mye rs JB, Oyama S, Hibberd EE. Scapular dysfunction in high school baseball players sustaining throwing-related upper extremity injury:
with dyskinesis were able to generate force with the manual muscle test of the lower trapezius equal to 6.3% bodyweight, a 40% deficit compared to ath-letes without dyskinesis. Scapular muscle MMT was also related to change in scapular upward rotation with maximal resistance. Weaker lower trapezius (r=0.57) and serratus anterior (r=0.41) MMT val-ues were related to a lack of scapular upward rota-tion from the active to maximal contraction. Thus, strength during manual muscle tests of the lower trapezius and serratus anterior accounted for 32.5% and 16.8% of the variance (r2) in scapular upward rotation, respectively. These findings are consistent with those of Laudner et al,32 who reported a mod-erate positive relationship between lower trapezius strength and scapular upward rotation (r2=0.56) at 90° of humeral elevation in the scapular plane (scap-tion). In contrast to Laudner et al.,32 the current authors found a moderate relationship between ser-ratus anterior strength and scapular upward rotation at 90° of shoulder flexion, whereas they reported a poor relationship (r2=0.16) at 90° of scaption. The current study strength results should be tempered since multiple shoulder muscles are activated dur-ing manual muscle testing intended to target one specific muscle. Specific to this study, the MMT used for the serratus anterior was modeled after the study by Ekstrom et al26 and did not involve stabilization of the lateral border of the scapula, as proposed by Kendall.33 This could have led to greater involve-ment of the anterior deltoid during the MMT used in this study. The results of these MMT tests show a moderate relationship between a lack of scapular upward rotation and normalized MMT strength defi-cits of the lower trapezius in overhead athletes and identify deficits of lower trapezius MMT strength in asymptomatic athletes with dyskinesis.
While this study provides new insight, the results are limited to asymptomatic overhead athletes. Fur-ther study in athletes with shoulder pain is neces-sary in order to determine if a distinct subgroup of athletes with pain have similar deficits in scapular muscle strength and a lack of scapular upward rota-tion. Additionally, no inferences can be made with regard to these athletes’ injury risk given the cross-sectional study design. Results of this study were in conflict with the authors’ hypothesis that overhead athletes may normalize scapular stabilization or posi-

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 317
16. Mc Clure P, Tate AR, Kareha S, Irwin D, Zlupko E. A clinical method for identifying scapular dyskinesis, part 1: reliability. J Athl Train. 2009;44(2):160-164.
17. Ca mci E, Duzgun I, Hayran M, Baltaci G, Karaduman A. Scapular kinematics during shoulder elevation performed with and without elastic resistance in men without shoulder pathologies. J Orthop Sports Phys Ther. 2013;43(10):735-743.
18. de Groot JH, van Woensel W, van der Helm FC. Effect of different arm loads on the position of the scapula in abduction postures. Clin Biomech.(Bristol., Avon.). 1999;14(5):309-314.
19. Fo rte FC, de Castro MP, de Toledo JM, Ribeiro DC, Loss JF. Scapular kinematics and scapulohumeral rhythm during resisted shoulder abduction--implications for clinical practice. Phys Ther Sport. 2009;10(3):105-111.
20. Mc Quade KJ, Smidt GL. Dynamic scapulohumeral rhythm: the effects of external resistance during elevation of the arm in the scapular plane. J Orthop Sports Phys Ther. 1998;27(2):125-133.
21. Mi chiels I, Grevenstein J. Kinematics of shoulder abduction in the scapular plane. On the infl uence of abduction velocity and external load. Clin Biomech (Bristol, Avon). 1995;10(3):137-143.
22. Pa scoal AG, van der Helm FF, Pezarat CP, Carita I. Effects of different arm external loads on the scapulo-humeral rhythm. Clin Biomech.(Bristol., Avon.). 2000;15 Suppl 1:S21-S24.
23. Se itz AL, McClure PW, Finucane S, et al. The scapular assistance test results in changes in scapular position and subacromial space but not rotator cuff strength in subacromial impingement. J Orthop Sports Phys Ther. 2012;42(5):400-412.
24. Se itz AL, McClure PW, Lynch SS, Ketchum JM, Michener LA. Effects of scapular dyskinesis and scapular assistance test on subacromial space during static arm elevation. J Shoulder Elbow Surg. 2012;21(5):631-640.
25. Ag re JC, Magness JL, Hull SZ, et al. Strength testing with a portable dynamometer: reliability for upper and lower extremities. Arch Phys Med Rehabil. 1987;68(7):454-458.
26. Ek strom RA, Soderberg GL, Donatelli RA. Normalization procedures using maximum voluntary isometric contractions for the serratus anterior and trapezius muscles during surface EMG analysis. J Electromyogr Kinesiol. 2005;15(4):418-428.
27. An KN, Browne AO, Korinek S, Tanaka S, Morrey BF. Three-dimensional kinematics of glenohumeral elevation. J Orthop Res. 1991;9(1):143-149.
28. Ka rduna AR, McClure PW, Michener LA, Sennett B. Dynamic measurements of three-dimensional
a prospective study. J Shoulder Elbow Surg. 2013;22(9):1154-1159.
3. Tat e AR, McClure P, Kareha S, Irwin D, Barbe MF. A clinical method for identifying scapular dyskinesis, part 2: validity. J Athl Train. 2009;44(2):165-173.
4. Kaw asaki T, Yamakawa J, Kaketa T, Kobayashi H, Kaneko K. Does scapular dyskinesis affect top rugby players during a game season? J Shoulder Elbow Surg. 2012;21(6):709-714.
5. Str uyf F, Nijs J, Meeus M, et al. Does Scapular Positioning Predict Shoulder Pain in Recreational Overhead Athletes? Int J Sports Med. 2014;35(1):75-82.
6. Ell enbecker TS, Kibler WB, Bailie DS, Caplinger R, Davies GJ, Riemann BL. Reliability of scapular classifi cation in examination of professional baseball players. Clin Orthop Relat Res. Jun 2012;470(6):1540-1544.
7. Uhl TL, Kibler WB, Gecewich B, Tripp BL. Evaluation of clinical assessment methods for scapular dyskinesis. Arthroscopy. 2009;25(11):1240-1248.
8. Kib ler WB, Uhl TL, Maddux JW, Brooks PV, Zeller B, McMullen J. Qualitative clinical evaluation of scapular dysfunction: a reliability study. J Shoulder Elbow Surg. 2002;11(6):550-556.
9. War ner MB, Whatling G, Worsley PR, et al. Objective classifi cation of scapular kinematics in participants with movement faults of the scapula on clinical assessment. Comput Methods Biomech Biomed Engin. 2015;18(7):782-9.
10. Di Veta J, Walker ML, Skibinski B. Relationship between performance of selected scapular muscles and scapular abduction in standing subjects. Phys Ther. 1990;70(8):470-476.
11. Jo hnson MP, McClure PW, Karduna AR. New method to assess scapular upward rotation in subjects with shoulder pathology. J Orthop Sports Phys Ther. 2001;31(2):81-89.
12. Od om CJ, Taylor AB, Hurd CE, Denegar CR. Measurement of scapular asymetry and assessment of shoulder dysfunction using the Lateral Scapular Slide Test: a reliability and validity study. Phys Ther. 2001;81(2):799-809.
13. Pe terson DE, Blankenship KR, Robb JB, et al. Investigation of the validity and reliability of four objective techniques for measuring forward shoulder posture. J Orthop Sports Phys Ther. 1997;25(1):34-42.
14. Wa tson L, Balster SM, Finch C, Dalziel R. Measurement of scapula upward rotation: a reliable clinical procedure. Br J Sports Med. 2005;39(9):599-603.
15. Ki bler WB. The role of the scapula in athletic shoulder function. Am J Sports Med. 1998;26(2):325-337.

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 318
32. La udner KG, Stanek JM, Meister K. The relationship of periscapular strength on scapular upward rotation in professional baseball pitchers. J Sport Rehabil. 2008;17(2):95-105.
33. Ke ndall FP, McCreary EK, Provance PG. Muscles, testing and function: with Posture and pain. 4th ed. Baltimore, Md.: Williams & Wilkins; 1993.
34. Gu anche CA, Jones DC. Clinical testing for tears of the glenoid labrum. Arthroscopy. 2003;19(5):517-523.
35. Ki m SH, Ha KI, Han KY. Biceps load test: a clinical test for superior labrum anterior and posterior lesions in shoulders with recurrent anterior dislocations. Am J Sports Med. 1999;27(3):300-303.
36. Jo be FW, Moynes DR. Delineation of diagnostic criteria and a rehabilitation program for rotator cuff injuries. Am J Sports Med. 1982;10(6):336-339.
scapular kinematics: a validation study. J Biomech Eng. 2001;123(2):184-190.
29. Wu G, van der Helm FC, Veeger HE, et al. ISB recommendation on defi nitions of joint coordinate systems of various joints for the reporting of human joint motion--Part II: shoulder, elbow, wrist and hand. J Biomech. 2005;38(5):981-992.
30. Mc Clure PW, Bialker J, Neff N, Williams G, Karduna A. Shoulder function and 3-dimensional kinematics in people with shoulder impingement syndrome before and after a 6-week exercise program. Phys Ther. 2004;84(9):832-848.
31. Mc Clure PW, Michener LA, Karduna AR. Shoulder function and 3-dimensional scapular kinematics in people with and without shoulder impingement syndrome. Phys Ther. 2006;86(8):1075-1090.

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 319
ABSTRACTBackground: Total arc of motion (TA) measured in a supine position has been utilized as a method to detect the presence of gle-nohumeral internal rotation deficit (GIRD) in overhead athletes. A component of supine TA is supine internal rotation (IR) range of motion (ROM), which has many variables including the amount and location of manual stabilization. A sidelying position for gathering IR ROM has recently been proposed and, when combined with supine external rotation (ER) ROM, constitutes a new method of quantifying TA. This new sidelying TA method, however, has no normative values for overhead athletes.
Purpose: The purposes of this study were to develop normative values for sidelying TA in overhead athletes, determine any ROM difference between supine and sidelying TA, and examine side-to-side differences within the two TA methods. A secondary pur-pose of the study was to examine for any effect of gender or level of competition on the two TA methods.
Study Design: Cross-sectional study.
Methods: Passive supine IR ROM, supine ER ROM, and sidelying IR ROM were gathered on bilateral shoulders of 176 collegiate and recreational overhead athletes (122 male [21.4±4.7 years, 71.7±2.7 inches, 25.3±2.7 BMI] and 54 female [21.4±5.4 years, 67.6±3.0 inches, 22.5±2.37 BMI]).
Results: Sidelying TA mean for the dominant shoulder was 159.6°±15.0°; the non-dominant shoulder was 163.3°±15.3°. Sidely-ing TA for both shoulders (p < 0.0001) was 14° less than supine TA. Both TA methods exhibited a 4° dominant-shoulder deficit (p < 0.0001). For the dominant and non-dominant shoulder, respectively, there was no gender (p = 0.38, 0.54) or level of competition (p = 0.23, 0.39) effect on sidelying TA.
Conclusion: In overhead athletes, sidelying TA is a viable alternative to supine TA when examining for the presence of GIRD. Gender and level of competition does not significantly affect sidelying TA, so the mean of 160° on the dominant shoulder and 163° on the non-dominant shoulder can be used by clinicians.
Level of Evidence: Level 3
Keywords: Bubble inclinometer, range of motion, shoulder internal rotation, shoulder reliability, total arc of motion
IJSP
TORIGINAL RESEARCH
TOTAL ARC OF MOTION IN THE SIDELYING POSITION:
EVIDENCE FOR A NEW METHOD TO ASSESS
GLENOHUMERAL INTERNAL ROTATION DEFICIT IN
OVERHEAD ATHLETES
Cort J. Cieminski, PT, PhD, ATC1
Hugo Klaers, PT2,3 Shannon M. Kelly, PT2,3 Michael R. Stelzmiller, PT2,4 Tatia J. Nawrocki, PT, DPT2,5 Alisse J. Indrelie, PT, DPT2,6
1 Professor – St. Catherine University - Doctor of Physical Therapy Program, Minneapolis, MN, USA
2 at the time of the study the author was a student physical therapist at St. Catherine University - Doctor of Physical Therapy Program, Minneapolis, MN, USA
3 Physical Therapy Resident - Fairview Health Services, Minneapolis, MN, USA
4 Staff Physical Therapist - Genesis Rehab Services, Eau Claire, WI, USA
5 Staff Physical Therapist - Aegis Therapies, New Hope, MN, USA
6 Staff Physical Therapist - HealthEast Optimum Rehabilitation, Maplewood, MN, USA
CORRESPONDING AUTHORCort J. Cieminski, PT, PhD, ATCSt. Catherine University – Doctor of Physical Therapy ProgramMinneapolis, MN, USAE-mail: [email protected]

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 320
INTRODUCTIONAthletes who participate in overhead sports often develop a chronic adaptation in the available range of motion (ROM) of the dominant shoulder, result-ing from repetitive exposure to these overhead activ-ities.1-7 This adaptation typically involves a loss of dominant shoulder internal rotation (IR) ROM, com-monly known as glenohumeral internal rotation deficit (GIRD). The presence of GIRD is often bal-anced with a concomitant increase in external rota-tion (ER) ROM of the same shoulder.1-5
Manske1 has described two types of GIRD. First, ana-tomical GIRD is a necessary adaptation of the domi-nant shoulder, resulting from repetitive exposure to overhead activities in which there is a loss of IR ROM, along with an equivalent increase in ER ROM. The total arc of motion (TA), however, which is defined as the sum of IR ROM and ER ROM, remains relatively sym-metrical when compared to the non-dominant shoul-der. This side-to-side TA symmetry has been observed in several studies of overhead athletes, ranging from youth to professional levels.2-7 The shift in dominant shoulder rotational motion with a TA that is equal to the non-dominant shoulder is considered a normal osse-ous adaptation and has been attributed to an increase in humeral retroversion (HRV) seen in the dominant shoulder of overhead athletes.6-8 The increase in HRV allows greater shoulder ER ROM during the cocking phase in overhead sports, such as baseball, softball, volleyball, and tennis, assisting the shoulder in reach-ing its extremely high rotational velocities during the acceleration phase of these sports.9-10 Increased HRV has also been purported to be a protective mechanism to minimize anterior shoulder laxity in overhead ath-letes,7,8,11,12 while also minimizing the risk of develop-ing internal impingement.12-16
Conversely, pathologic GIRD is present when a greater amount of IR ROM loss than ER ROM gain on the dominant shoulder exists, resulting in a TA defi-cit on the dominant shoulder compared to the non-dominant shoulder.1 This loss of TA or greater loss of IR ROM on the dominant shoulder has been associ-ated with higher risk of injury in the throwing shoul-der and elbow of overhead athletes.9,17-21 In studies by Wilk et al, baseball pitchers who demonstrated a TA deficit of 5° or more on their throwing shoulder were 2.5 times more likely to sustain a shoulder injury20
and 2.6 times more likely to sustain an elbow injury21 compared to pitchers without a TA deficit of their throwing shoulder. It has been suggested that over-head athletes who have a TA deficit of 5° or more on the dominant shoulder likely present with posterior shoulder soft tissue restrictions, namely posterior gle-nohumeral joint capsule thickening13,22-24 or increased posterior rotator cuff muscle stiffness,1,25-28 with these adaptations occurring secondary to chronic exposure to overhead sports.
While there is agreement that GIRD, whether ana-tomical or pathologic, occurs in overhead athletes, the techniques used to assess this deficit are not uni-versally agreed upon. The supine position with the arm abducted to 90° has traditionally been utilized to assess IR and ER ROM, as well as TA.6-8,11,29-33 Authors have noted, however, a lack of consistent stabiliza-tion of the scapula may be present when utilizing the supine position to assess the glenohumeral con-tribution to shoulder IR ROM.3,5,9,34,35 In the supine position, a posteriorly-directed manual stabilization force is typically applied to the anterior acromion and coracoid process, while simultaneously allow-ing humeral head rotation during IR ROM assess-ment. The amount of stabilization force provided is subjective in nature, and may vary between exam-iners. This lack of consistent stabilization has been implicated in the lower intra-35 and inter-rater reli-ability34,35 noted for the supine IR ROM position.
Attempts to evaluate supine IR ROM utilizing vari-ous methods of stabilization have been undertaken in recent years. Wilk et al36 examined the reliabil-ity and IR ROM of three supine IR ROM methods that differed in the location and application of sta-bilization. It was determined that the method that included stabilization of the scapula to minimize its accessory motion of anterior tilting produced the greatest intra-rater reliability of 0.62, but also the lowest inter-rater reliability of 0.43. These low reli-ability values for the supine method with scapular stabilization lend further evidence to its potential drawback as a reliable clinical measure of IR ROM.
Moreover, numerous studies have investigated IR ROM differences in the supine position between the dominant and non-dominant shoulders in over-head athletes. These results indicate that significant differences exist between sides, with the dominant

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 321
shoulder having less IR ROM than the non-dominant side.4,5,7,24,28,37-41 Based upon this difference, previous authors suggest not using the non-dominant shoul-der for comparison when assessing IR ROM loss of the dominant shoulder.42-46
Researchers have recently examined the sidelying position as an alternative for measuring IR ROM.27,35,41 In healthy subjects with non-impaired shoulders, as well as those with shoulder pathology, Lunden and colleagues35 found the full sidelying position to have greater intra- and inter-rater reliability when assess-ing shoulder IR ROM, as compared to the supine position. In a small sample of Division I baseball and softball athletes, Kevern and associates27 found that the sidelying position had the highest intra- and inter-rater reliability for measuring IR ROM, as com-pared to a supine position both with and without scapular stabilization. It has been purported that the sidelying position allows the scapula to be stabilized by the individual’s own body weight,26,27,35 thus IR ROM measurements taken in this position are likely not influenced by variations in stabilization force provided by the examiner. Also, in contrast to the supine position, the sidelying position may limit the scapular accessory motion of anterior tilting that occurs during IR, leading to a more distinct capsular end-feel35 and likely isolating IR ROM to the gleno-humeral joint.27,35
While Kevern27 defined sidelying TA as the sum of sidelying IR and sidelying ER, it may be more appropriate to consider a hybrid definition of side-lying TA. This hybrid sidelying TA is defined as the sum of sidelying IR and supine ER and may pro-vide a more functional assessment of the IR and ER motion extremes that occur in overhead sports. Spe-cifically, the assessment of IR ROM in the sidelying position places the shoulder in a combined position of flexion and horizontal adduction, positions that the shoulder assumes during the arm deceleration phase of throwing,47,48 where a lack of IR ROM may be problematic. Dillman et al47 noted that maximal IR ROM occurs at the end of the deceleration phase and is accompanied by horizontal adduction of the shoulder. The amount of horizontal adduction in this phase is more closely replicated in the sidelying IR position, as compared to the supine IR position. The assessment of ER ROM in the supine position,
with the shoulder abducted to 90º, mimics the cock-ing phase of many overhead sports where maximal ER ROM occurs.
Since GIRD is present in overhead athletes and research exists supporting the use of the sidelying position to assess IR ROM, a new method of quanti-fying total arc of motion, one that utilizes the sidely-ing position to assess IR ROM along with supine ER ROM, could be used to further differentiate between anatomical and pathologic GIRD in overhead ath-letes. Therefore, the primary purposes of this study of collegiate and recreational overhead athletes were to: 1) establish both dominant and non-dominant shoulder normative values for sidelying TA; 2) com-pare sidelying TA to the traditional supine TA for both the dominant and non-dominant shoulder; and 3) compare side-to-side differences for both supine and sidelying TA. A secondary purpose of this study was to determine if gender and level of competition affect the amount of sidelying TA. The hypotheses of this study were: 1) sidelying TA would be signifi-cantly smaller than supine TA for both shoulders; and 2) there would be no significant side-to-side dif-ference for either supine or sidelying TA.
METHODSAll testing procedures were completed in a single session lasting approximately 30 minutes, except for the reliability portion of this study, which took place over two testing sessions on consecutive days. A cross-sectional study design was employed in order to calculate mean values for supine and sidelying TA. Independent variables in the study included gender, level of competition in overhead sports, and upper extremity dominance, which was defined as the arm used by the participant to throw a ball. The dependent variables were supine and sidelying TA. This study was approved by the Institutional Review Board of St. Catherine University. Participants were recruited through a sample of convenience and were asked to review and sign a written consent and HIPAA autho-rization form prior to participating in the study.
ParticipantsParticipants were included in this study if they were: 1) 18 years or age or older; 2) a current Division I or Division III collegiate athlete or a current recre-ational athlete participating in the overhead sports of

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 322
baseball, softball, volleyball, or javelin throwing; and 3) symptom-free in at least one shoulder. Participants were excluded from this study if they: 1) had a history of shoulder surgery, fracture, or dislocation; 2) had pain that limited ROM in both shoulders; 3) were cur-rently participating in a medically-supervised shoul-der rehabilitation program; or 4) were unable to lie on their back or side. Participants were identified as overhead athletes based on their self-report and also from information gathered on a demographics form that inquired about history of participation in over-head sports. In order to be enrolled in the study, rec-reational athletes had to have a history of competitive overhead sport participation prior to age 18 and also have participated in overhead sports at least twice per week for the previous five years prior to participation in the study. After inclusion and exclusion criteria were determined, 176 participants were enrolled in the study (Table 1), including 33 Division I, 81 Divi-sion III, and 62 recreational overhead athletes. Two athletes had a painful non-dominant shoulder at the time of data collection, so only dominant shoulder data was collected and utilized for those participants. Therefore, this study included data from 176 domi-nant and 174 non-dominant shoulders.
RatersAll ROM measurements were taken by five Doctor of Physical Therapy (DPT) student investigators from St. Catherine University or their faculty research advi-sor. In order to ensure consistency among raters, the student investigators were instructed in the correct technique and end-feel assessment of shoulder IR ROM in supine and sidelying and shoulder ER ROM in supine. Instruction and training was provided by the faculty research advisor, a clinician with 25 years of physical therapy experience, who also had signifi-cant expertise in sidelying IR ROM assessment.
InstrumentationMeasurements of ROM were obtained using a bub-ble inclinometer (Johnson Level & Tool Manufactur-
ing Company Inc. Mequon, WI) that was placed on the participant’s distal forearm just proximal to the wrist, on the dorsal aspect for all IR ROM measure-ments (Figure 1) and on the ventral aspect for ER ROM measurements.
ProceduresAfter providing written informed consent, each sub-ject was asked to complete a brief questionnaire that included demographic information of age, gender, self-reported height and weight, history of participa-tion and current level of competition in overhead sports, as well as previous shoulder injuries or sur-geries. Arm dominance was determined by asking the subject which arm they would use to throw a ball.
All ROM measurements were taken on a standard treatment table. Supine IR ROM was gathered with the subject in a supine position. Investigators pas-sively abducted the humerus to 90°, with the elbow flexed to 90º and the forearm was maintained in a neutral rotation position. A small towel roll was placed under the distal humerus to limit any hori-zontal abduction of the humerus. Investigators used their thenar mass to apply a posteriorly-directed stabilization force to the acromion and coracoid pro-cesses, thus limiting anterior tilting of the scapula; care was taken to avoid any contact over the humeral head. Investigators passively moved the shoulder into IR (Figure 2) and when a firm capsular end-feel was noted or the scapula began to anteriorly tilt, the IR ROM measurement was obtained by placing the bubble inclinometer just proximal to the wrist joint on the dorsal forearm.
For sidelying IR ROM measurements, participants were positioned lying on the side to be measured and the humerus was passively flexed to 90º to place it in a position of horizontal adduction. The elbow was placed in 90º of flexion and the forearm was maintained in a neutral rotation position. In order to standardize the sidelying position, investigators
Table 1. Characteristics of study participants (mean ± standard deviation)Age
(years)
Age range
(years)
Height
(inches)
Weight
(pounds)BMI
Males (n=122) 21.4 ±4.7 18-47 71.7 ±2.7 184.9 ±23.1 25.3 ±2.7
Females (n=54) 21.4 ±5.4 18-56 67.6 ±3.0 145.9 ±18.1 22.5 ±2.3

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 323
scapular stabilization was provided over the anterior shoulder. The shoulder was passively moved into ER and upon achieving a capsular end-feel the measure-ment was obtained by placing the bubble inclinom-eter just proximal to the wrist joint on the ventral aspect of the forearm.
Prior to data collection, the order of the two IR ROM positions was randomized to minimize any possible order effect on the IR ROM values. Measurements in these two IR ROM positions were performed first, followed lastly by ER ROM. Range of motion was assessed first on the dominant shoulder and then on the non-dominant shoulder, using the same order of positions for both shoulders. Two measure-ments were obtained for each ROM position and the mean was used for subsequent data analysis. The ROM values were not blinded to the investigator, as they recorded the values onto a data form for each subject. Supine TA was operationally defined in this study as the sum of supine IR ROM and supine ER ROM, while sidelying TA was defined as the sum of sidelying IR ROM and supine ER ROM.
In order to pool data from all investigators for analy-sis, intra-rater and inter-rater reliability were deter-mined using 18 subjects. This took place prior to any data collection for the main part of the study. Measurements of supine IR ROM, sidelying IR ROM, and supine ER ROM were collected as previ-ously described on two consecutive days, with two measurements taken each day for all three ROM positions. Both the order of raters and the three measurement positions were randomized for each
visually aligned the bilateral acromion processes in a vertical plane (Figure 3), using methods described by Lunden et al.35 The scapula was then protracted slightly by the investigator pulling gently on the dis-tal humerus, stopping when the vertical alignment of the acromion processes first began to be altered. The pelvis not contacting the table was aligned in a neutral position (neither protracted or retracted) relative to the opposite side pelvis. Investigators passively moved the shoulder into IR (Figure 3) and when a firm capsular end-feel was noted that stopped shoulder motion, the IR ROM measurement was obtained by placing the bubble inclinometer just proximal to the wrist joint on the dorsal forearm. For the sidelying position there was no manual stabiliza-tion force applied by the investigators to the scapula.
For supine ER ROM the humerus was positioned similar to the supine IR ROM position, although no
Figure 1. Placement of bubble inclinometer for all IR ROM mea-surements.
Figure 2. Supine IR ROM position.
Figure 3. Sidelying IR ROM position.

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 324
athletes). For ANOVAs that were significant, a post-hoc analysis was performed using paired t-tests, with Bonferroni multiple comparisons correction applied to these t-tests.
The standard error of measurement (SEM) was also calculated for supine and sidelying TA on the domi-nant and non-dominant shoulder. The level of sig-nificance was set a priori at p ≤ 0.05 for all statistical analyses performed in this investigation. Number Cruncher Statistical Software (NCSS) was used for all statistical analyses.
RESULTS The results for intra-rater and inter-rater reliabil-ity, including 95% confidence intervals, appear in Tables 2 and 3, respectively. Intra-rater ICC values across the six raters for the three ROM positions that comprise supine and sidelying TA ranged from fair to excellent.49 The sidelying IR ROM position had the greatest intra-rater reliability with a range of values from 0.87-0.97 across the raters. Inter-rater ICC val-ues for the three ROM positions ranged from good to excellent,49 with the sidelying IR position having the highest inter-rater reliability value of 0.91.
Mean, standard deviation, and standard error of measurement for supine and sidelying TA of the dominant and non-dominant shoulders are noted in Table 4. The amount of supine TA of the dominant shoulder was 174.0º (±17.1°), while the non-domi-nant shoulder was 177.8º (±17.3°). The amount of sidelying TA of the dominant shoulder was 159.6º (±15.0°), while the non-dominant shoulder was
subject. All measurements for the reliability por-tion of this study were read and recorded by a stu-dent physical therapist who was not a part of the study, therefore allowing the raters to be blinded to the values of the measurements. The mean of these measurements was used for subsequent reliability determination.
Statistical AnalysisUsing the 18 subjects recruited for the reliability portion of this study, intraclass correlation coeffi-cients (ICCs) were calculated to quantify intra-rater reliability (ICC1,1) for each of the six raters for the supine IR, sidelying IR, and supine ER ROM posi-tions. Intraclass correlation coefficient values were also used to calculate inter-rater reliability (ICC2,k) using the mean of each rater’s two measurements taken on each subject in the three ROM positions. The faculty research advisor was used as the refer-ence standard for all inter-rater reliability calcula-tions. Intraclass correlation coefficient values were classified as: excellent (0.90-0.99); good (0.80-0.89); fair (0.70-0.79); and poor (<0.69).49 For both intra-rater and inter-rater reliability, 95% confidence intervals (CI) were also calculated.
The demographic variables of age, height, weight, and body mass index (BMI) were gathered for each subject and summary descriptive statistics (mean, standard deviation, range) were determined for each of these variables for the entire sample of subjects.
Means and standard deviations were determined for supine and sidelying TA on both the dominant and non-dominant shoulder. Within both supine and sidelying TA, paired t-tests were performed to com-pare the means of the dominant and non-dominant shoulder. Within both the dominant and non-dom-inant shoulders, paired t-tests were also utilized to compare the means of supine and sidelying TA. In addition, independent t-tests were used to examine the means of each gender within the supine and sidelying TA on both the dominant and non-domi-nant shoulder.
Repeated measures analyses of variance (ANOVAs) were calculated to examine the differences in means of supine and sidelying TA for both the dominant and non-dominant shoulder across the three levels of competition (Division I, Division III, recreational
Table 2. Intra-rater reliability range (95% CI) of the 6 raters for the three ROM positions that comprise supine and sidelying TA using ICC (model [1,1])
Supine IR Sidelying IR Supine ER
Intra-rater reliability0.78-0.92
(0.70-0.96)*0.87-0.97
(0.79-0.99)*0.79-0.95
(0.75-0.99)*
* p < 0.001
Table 3. Inter-rater reliability (95% CI) of the three ROM positions that comprise supine and sidelying TA using ICC (model [2,k])
Supine IR Sidelying IR Supine ER
Inter-rater reliability 0.84(.74-.91)*
0.91 0.84(.80-.90)*(.83-.96)*
* p < 0.001

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 325
a significantly smaller supine TA of 7.9° for males compared to females (171.4° vs. 179.3°, p = 0.004). Males also had a smaller sidelying TA of 2.2° on the dominant shoulder compared to females (158.7° vs. 160.9°), however the difference was not significant (p = 0.38). For the non-dominant shoulder, independent t-tests revealed a significantly smaller supine TA of 6.0° for males compared to females (173.5° vs. 179.5°, p = 0.01). Males also had a smaller sidelying TA of 1.5° compared to females (162.4° vs. 163.9°), but again, this difference was not significant (p = 0.54).
Results of repeated measures ANOVAs for supine and sidelying TA on the dominant shoulder across the three levels of competition are depicted in Fig-ure 4. Supine TA mean values ranged from 170.5°-174.8°, while sidelying TA values were smaller and ranged from 155.4°-159.1°. Recreational athletes demonstrated the smallest mean for both TA posi-tions on the dominant shoulder. There was no sig-nificant difference, however, across the levels of competition for either the supine TA (F2,175 = 0.77; p = 0.47) or sidelying TA (F2,175 = 1.5; p = 0.23) for the dominant shoulder. Figure 5 depicts the results of repeated measures ANOVAs for supine and side-lying TA on the non-dominant shoulder across the
163.3º (±15.3°). As depicted in Table 4, paired t-tests determined that the 3.8º and 3.7º loss in motion on the dominant shoulder for supine and sidelying TA, respectively, was statistically significant (p < 0.0001). When comparing the difference between the supine and sidelying TA values, results of paired t-tests revealed a significant difference of 14.4º on the dominant shoulder and 14.5º on the non-domi-nant shoulder, with sidelying TA having less motion than supine TA for each shoulder (Table 5).
Means and standard deviations for supine and sidely-ing TA of the dominant and non-dominant shoulders by gender are noted in Tables 6 and 7, respectively. When examining for possible gender differences on the dominant shoulder, independent t-tests revealed
Table 4. Supine and sidelying total arc of motion (mean ± standard deviation)
Table 5. Difference in total arc of motion (TA) positions by shoulder (mean ± standard deviation)
Dominant
shoulder
(° ±SD)
Non-dominant
shoulder
(º ±SD)
Mean
Difference
(º)
p
Dominant
shoulder
SEM (°)
Non-
Dominant
shoulder
SEM (°)
Supine TA 174.0 ± 17.1 177.8 ± 17.3 3.8 <0.0001* 4.2 4.2
Sidelying TA 159.6 ± 15.0 163.3 ± 15.3 3.7 <0.0001* 3.7 3.8
Dominant shoulder
(º ±SD)
Non-dominant shoulder
(º ±SD)
Supine TA 174.0 ± 17.1 177.8 ± 17.3
Sidelying TA 159.6 ± 15.0 163.3 ± 15.3 TA Difference 14.4° * 14.5° *
*p<0.001
Table 6. Dominant shoulder gender differences for supine and sidely-ing total arc of motion (TA) (mean ± standard deviation)
Male (° ±SD) Female (° ±SD) Difference (°) p
Supine TA 171.4 ±17.4 179.3 ±14.6 7.9 0.004*
Sidelying TA 158.7 ±15.9 160.9 ±12.9 2.2 0.38
Table 7. Non-dominant shoulder gender differences for supine and sidelying total arc of motion (TA) (mean ± standard deviation)
Male (° ±SD) Female (° ±SD) Difference (°) p
Supine TA 173.5 ±13.8 179.5 ±13.5 6.0 0.01*
Sidelying TA 162.4 ±12.8 163.9 ±12.6 1.5 0.54

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 326
DISCUSSIONA primary aim of this study was to establish nor-mative values for sidelying TA in overhead ath-letes using a novel technique to examine for GIRD. Results from the 176 participants revealed that the normative sidelying TA was 160° and 163° for the dominant and non-dominant shoulder, respectively. These values were lower than those obtained for supine TA, which were 174° for the dominant and
three levels of competition. Similar to the dominant shoulder, there was no significant difference across the levels of competition for either supine TA (F2,175
= 2.47; p = 0.09) or sidelying TA (F2,175 = 0.95; p = 0.39) for the non-dominant shoulder. Supine TA mean values ranged from 172.0°-180.3°, while side-lying TA values ranged from 160.5°-164.5°. Recre-ational athletes also had the smallest mean value for both TA positions on the non-dominant shoulder.
Figure 4. Dominant shoulder total arc of motion (TA) by level of competition (mean ± standard deviation).
Figure 5. Non-dominant shoulder total arc of motion (TA) by level of competition (mean ± standard deviation).

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 327
finding agrees with previous researchers who have noted increased supine IR ROM in females com-pared to males.51-53 In contrast to supine TA, there was no difference between genders for sidelying TA of the dominant shoulder, including no difference in the component motions of sidelying IR ROM and supine ER ROM. Our findings concur with those of Carcia and colleagues41 who found no gender differ-ence for sidelying IR ROM when examining both the dominant and non-dominant shoulder in a popula-tion of asymptomatic, collegiate, non-athletes. Due to no gender difference being observed for sidelying TA, rehabilitation professionals can have confidence in using the overall normative value of 160° for the dominant shoulder and 163° for the non-dominant shoulder of collegiate and recreational overhead athletes. These normative values, however, are not applicable to professional or youth athletes, as they were not represented in this sample of participants.
This study is also the first to examine the possible influence of level of competition on TA. There was no level of completion difference between Division I, Division III, or recreational overhead athletes for either supine or sidelying TA. This finding was noted for both the dominant and non-dominant shoulder. As in the gender discussion above, these findings lend further evidence that the sidelying TA normative value of 160° for the dominant shoulder and 163° for the non-dominant shoulder for can be used across Division I, Division III, and recreational overhead athletes. Again, caution is warranted when applying these norms to youth or professional ath-letes, as they were not examined in this study. Since this is the first study to examine sidelying TA using sidelying IR ROM and supine ER ROM, additional studies are warranted to further establish normative values for this new TA method.
The participants in this investigation had no diffi-culty assuming the sidelying position and did not complain of pain as the shoulder was internally rotated to its end-feel. This observation agrees with Lunden et al35, who found that less than 1% of their subjects, including both asymptomatic and those with various shoulder pathologies, were unable to assume a sidelying positon for IR ROM assessment. A possible reason for participants in the current study being able to assume a sidelying position and
178° for the non-dominant shoulder. These supine TA values are similar to those reported by previous authors who utilized this same position, with typical values ranging between 167° to 200°.2,6,7,20,21,25,29,31-33,50 Supine TA values in the present study are likely on the lower end of this range due to the care taken by the examiners to stabilize the scapula, thus limiting the amount of anterior tilting and effectively isolat-ing IR ROM to the glenohumeral joint.
The result for the dominant shoulder sidelying TA of 160° is in relative agreement with Kevern,27 who utilized two raters to examine the reliability of three methods to determine TA on the dominant shoulder of 38 Division I collegiate baseball and softball play-ers. These raters determined that the sidelying TA of the dominant shoulder was approximately 160° and 147°, respectively. While Kevern27 obtained sidelying IR ROM using the same position as the current study, they gathered ER ROM in the sidelying position. In contrast, the current study utilized a supine position to gather ER ROM, which was added to the sidelying IR ROM value for determination of sidelying TA. It appears that supine ER ROM may be greater than when measuring it in a sidelying position. Using the supine position to measure ER ROM places the shoulder in the same functional position where max-imal ER ROM is achieved during the cocking phase that occurs in overhead sports such as baseball, soft-ball, tennis serving, and volleyball spiking. It is the opinion of the current authors that gathering the two motions that comprised sidelying TA in this study, sidelying IR ROM and supine ER ROM, may provide a viable alternative when assessing the functional total arc of motion in overhead athletes.
To the authors’ knowledge, the effect of gender on TA in overhead athletes has yet to be examined. Results of this study indicate that there was a gender effect for supine TA, with females having 8° more motion on their dominant shoulder than their male coun-terparts. Further examination of the component motions of supine TA revealed that females had a non-significant 2° loss of supine ER ROM (females = 118.1°; males = 119.9°) and a significant 10° increase in supine IR ROM (females = 61.2°; males = 51.6°). It appears that the difference in supine IR ROM between genders was primarily responsible for the significant gender difference in supine TA. This

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 328
The smaller amount of IR ROM in sidelying is likely due to the tension placed upon the posterior shoul-der soft tissues structures, such as the glenohumeral joint capsule and posterior shoulder musculature. When IR ROM was assessed in a supine position, the shoulder was elevated to 90°. In sidelying, the shoul-der remained elevated to 90° but instead assumed a position of flexion/horizontal adduction. A posi-tion of horizontal adduction has been demonstrated to increase the strain on the posterior shoulder soft tissue structures when the shoulder undergoes IR,55 leading to a reduction in the available IR ROM in this horizontal adduction position.27,35 In addition, it is the experience of the investigators in the current study that the sidelying position yields a dramati-cally more distinct, capsular end-feel when assess-ing IR ROM, as compared to the supine position. This observation may be the result of the increased posterior shoulder soft tissue strain during IR in the sidelying position. Lastly, it has been suggested that the sidelying position limits the amount of scapular anterior tilting that typically accompanies shoulder IR ROM, thus isolating IR ROM in the sidelying posi-tion to that coming from the glenohumeral joint.26,27,35 In addition, the factors of increased posterior shoul-der soft tissue strain and limited anterior tilting of the scapula in the sidelying position may account for the increased reliability of sidelying IR ROM that was noted in this study, as well as by others.27,35
Sidelying TA may be a viable alternative to assess GIRD in overhead athletes, as opposed to the tradi-tional supine method. The primary osseous factor in GIRD is humeral retroversion and due to its bony nature, the impact of HRV on IR ROM likely does not depend on the position in which this motion is gathered. In contrast, the posterior shoulder soft tis-sue components of GIRD have significantly greater strain in a sidelying position compared to supine when the shoulder is undergoing IR.55 Therefore, sidelying TA may be a viable method to ascertain the soft tissue component of GIRD in overhead athletes.
When compared to the non-dominant shoulder, the dominant shoulder had a 4º deficit for both supine and sidelying TA. While the finding of this sidely-ing TA deficit is novel, the dominant-shoulder deficit for supine TA is similar to those found by previous authors.6,7 The supine TA deficit in the current study
undergo pain-free IR ROM is that the scapula was allowed to protract prior to undertaking IR ROM assessment. In effect, the positioning of the scapula into protraction allowed it to assume its scapular plane orientation. This positioning of the scapula is similar to a proposed sleeper stretch modification in which the trunk is allowed to rotate 20°-30° pos-terior to the coronal plane of the body, thus plac-ing the humerus in a scapular plane orientation and minimizing the risk of producing subacromial impingement during IR.54 In addition, during over-head sports the scapula protracts on the rib cage dur-ing the arm deceleration phase, during which time the shoulder is undergoing rapid internal rotation and horizontal adduction relative to the thorax.47-48 The current authors feel it is important to assess sidelying IR ROM with the scapula in some protrac-tion, simulating its functional position during the deceleration phase of overhead sports.
A significant 14° difference was noted on both the dominant and non-dominant shoulder when compar-ing supine and sidelying TA, with sidelying TA hav-ing less motion. The investigation by Lunden35 is the only previous study that examined sidelying TA using supine ER ROM. Results of their study revealed a sim-ilar difference between supine and sidelying TA, 12° and 18°, respectively, for the two raters. Since supine ER ROM was used in calculating both supine and side-lying TA values and was therefore a constant, the 14° difference in TA in the current study can be directly attributed to the difference in IR ROM between the two positions, with sidelying IR having less motion that supine IR (dominant shoulder IR ROM: supine = 54.5°; sidelying = 40.0°; non-dominant shoulder IR ROM: supine = 67.7°; sidelying = 53.2°). The domi-nant shoulder sidelying IR ROM value of 40° is the same as that reported by Lunden35 for their asymp-tomatic participants in the sidelying position, but is smaller than the 48° noted by Carcia,41 whose par-ticipants did not have a history of overhead athletic activity. This finding indicates that repetitive expo-sure to overhead sports may lead to a loss of IR ROM on the dominant shoulder. Interestingly, the current study’s non-dominant shoulder IR ROM value of 53° is the same as that reported by Carcia41 for their non-dominant shoulder, revealing that the non-dominant shoulder is likely to have similar IR ROM regardless of participation in overhead sports.

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 329
rent shoulder pathologies. Specifically, no data was gathered on youth or professional-level overhead athletes and the authors suggest additional supine and sidelying TA data be gathered for these groups. Second, multiple raters, including current DPT students, were utilized to collect data. While the authors acknowledge this potential limitation, care was taken to establish both intra- and inter-rater reli-ability for all raters prior to any supine or sidelying TA data collection. The reliability results have con-firmed those of previous authors who have investi-gated the sidelying position.27,35 Third, variations in the amount of scapular tilting in the resting position were not controlled for in this study and, therefore, they may have had an impact on the amount of IR ROM obtained in the supine and sidelying positions. Future studies should examine the effect of varia-tions in the resting or static position of the scapula on IR ROM, using three-dimensional motion analy-sis equipment. Lastly, the authors are aware that ath-letes with current shoulder pain or those who may be recovering from a surgical procedure may not be able to assume the sidelying position or have pain-free IR ROM during its assessment in this position.
CONCLUSIONThis investigation examined the differences between traditional supine TA and a newly proposed sidely-ing TA, one that is comprised of sidelying IR ROM and supine ER ROM. A normative value of 160° and 163° for sidelying TA was established for the dominant and non-dominant shoulder, respectively, regardless of gender or level of overhead athletic competition. There was also a difference between the two TA methods, with sidelying TA having 14° less motion than supine TA for both the dominant and non-dominant shoulder.
In addition, a dominant-shoulder deficit of 4° was noted for both supine and sidelying TA. When com-paring this 4° deficit to the calculated SEM for side-lying TA, it was revealed that this deficit indicated a meaningful clinical difference and suggests further investigation be performed for sideling TA to deter-mine the amount of TA deficit that places the dom-inant shoulder at greater risk for upper extremity injury. Youth and professional athletes should also be examined in future studies utilizing sidelying TA. Results of this investigation indicate that sidelying
fell within the 5° threshold suggested by Manske et al1 for an indication of anatomical GIRD, which is likely mediated by a difference in HRV between the domi-nant and non-dominant shoulder. Approximately 40% of our participants, however, exceeded this 5° domi-nant–shoulder deficit threshold for both supine and sidelying TA, and thus may be at risk for pathologic GIRD.1 While Wilk et al20,21 has demonstrated an asso-ciation between a supine TA deficit of 5° or more on the dominant side and increased risk of shoulder and elbow injuries in overhead athletes, similar studies need to be undertaken utilizing sidelying TA to deter-mine the dominant-shoulder deficit that increases the risk of upper extremity injuries in overhead athletes.
The SEM for sidelying TA was relatively low at 3.7° and 3.8° for the dominant and non-dominant shoul-der, respectively. This dominant-shoulder finding is similar to that found by Kevern27 and indicates that a true side-to-side difference was present for sidelying TA, as the difference between sidelying TA means of the dominant and non-dominant shoulder was 3.7° (Table 4). In addition, supine TA had a slightly higher SEM of 4.2° for both shoulders. Sidelying TA, therefore, had slightly less error associated with IR ROM measurements taken in the sidelying ver-sus supine position, as the supine ER position was common to both methods of TA determination. The lower SEM for sidelying TA is also likely linked to the higher intra- and inter-rater reliability values found for the sidelying IR position. Also, the SEM for supine TA was slightly greater than the dominant-shoulder deficit and, while statistically significant, this deficit may not indicate clinical significance using supine TA. In clinical practice it is important to use measurement positions that have small SEM and are therefore sufficiently accurate to evaluate for motion deficits in the shoulders of overhead ath-letes. Total arc of motion deficits of as little as 5°, for example, have been linked to upper extremity injures in overhead athletes.20,21
This investigation has some limitations. First, the mean values for supine and sidelying TA reported in this study were gathered on asymptomatic adults who were collegiate or recreational overhead ath-letes. The finding of this study, therefore, cannot be generalized to populations of varying ages, level of competition, or to those who are experiencing cur-

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 330
14. Meister K. Injuries to the shoulder in the throwing athlete. part one. biomechanics/pathophysiology/classifi cation of injury. Am J Sports Med. 2000;28:265-275.
15. Meister K. Internal impingement in the shoulder of the overhand athlete: pathophysiology, diagnosis, and treatment. Am J Orthop. 2000;29:433-439.
16. Riand N, Levigne C, Renaud E, Walch G. Results of derotational humeral osteotomy in posterosuperior glenoid impingement. Am J Sports Med. 1998;26:453-459.
17. Myers JB, Laudner KG, Pasquale MR, et al. Glenohumeral range of motion defi cits and posterior shoulder tightness in throwers with pathologic internal impingement. Am J Sports Med. 2006;34:385-391.
18. Laudner KG, Myers JB, Pasquale MR, et al. Scapular dysfunction in throwers with pathologic internal impingement. J Orthop Sports Phys Ther. 2006;36:485-494.
19. Dines JS, Frank JB, Akerman M, et al. Glenohumeral internal rotation defi cits in baseball players with ulnar collateral ligament insuffi ciency. Am J Sports Med. 2009;37:566-570.
20. Wilk KE, Macrina LC, Fleisig GS, et al. Loss of internal rotation and the correlation to shoulder injuries in professional baseball pitchers. Am J Sports Med. 2011;39:329-335.
21. Wilk KE, Macrina LC, Fleisig GS, et al. Defi cits in glenohumeral passive range of motion increase risk of elbow injury in professional baseball pitchers. Am J Sports Med. 2014;42:2075-2081.
22. Thomas SJ, Swanik CB, Higginson JS, et al. A bilateral comparison of posterior capsule thickness and its correlation with glenohumeral range of motion and scapular upward rotation in collegiate baseball players. J Shoulder Elbow Surg. 2011;20:708-716.
23. Tyler TF, Roy T, Nicholas SL, et al. Reliability and validity of a new method of measuring posterior shoulder tightness. J Orthop Sports Phys Ther. 1999;29:262-274.
24. Wang HK, McFarlane A, Cochrane T. Isokinetic performance and shoulder mobility in elite volleyball athletes from the United Kingdom. Br J Sports Med. 2000;34:39-43.
25. Reinold MM, Wilk KE, Macrina LC, et al. Changes in shoulder and elbow passive range of motion after pitching in professional baseball players. Am J Sports Med. 2008;36:523-527.
26. Kibler WB, Sciascia A, Thomas SJ. Glenohumeral internal rotation defi cit: pathogenesis and response to acute throwing. Sports Med Arthosc. 2012;20:34-38.
27. Kevern MA, Beecher M, Rao S. Reliability of measurement of glenohumeral internal rotation, external rotation, and total arc of motion in 3 test positions. J Athl Train. 2014;49:640-646.
TA may be a viable alternative to examine for GIRD in the overhead athlete.
REFERENCES 1. Manske R, Wilk KE, Davies G, et al. Glenohumeral
motion defi cits: friend or foe? Int J Sports Phys Ther.2013;8:537-553.
2. Shanley E, Rauh MJ, Michener LA, et al. Shoulder range of motion measures as risk factors for shoulder and elbow injuries in high school softball and baseball players. Am J Sports Med. 2011;39:1997-2006.
3. Meister K, Day T, Horodyski MB, et al. Rotational motion changes in the glenohumeral joint of adolescent/Little League baseball player. Am J Sports Med. 2005;33:693-698.
4. Hurd WJ, Kaplan KM, ElAttrache NS, et al. A profi le of glenohumeral internal and external rotation motion in the uninjured high school baseball pitcher: part I: motion. J Athl Train. 2011;46:282-288.
5. Ellenbecker TS, Roetert EP, Bailie DS, et al. Glenohumeral joint total rotation range of motion in elite tennis players and baseball pitchers. Med Sci Sports Exerc. 2002;34:2052-2056.
6. Hibberd EE, Oyama S, Myers JB. Increase in humeral retrotorsion accounts for age-related increases in glenohumeral internal rotation defi cit in youth and adolescent baseball players. Am J Sports Med. 2014;42:851-858.
7. Crockett HC, Gross LB, Wilk KE, et al. Osseous adaptation and range of motion at the glenohumeral joint in professional baseball pitchers. Am J Sports Med. 2002;30:20-26.
8. Reagan KM, Meister K, Horodyski MB, et al. Humeral retroversion and its relationship to glenohumeral rotation in the shoulder of college baseball players. Am J Sports Med. 2002;30:354-360.
9. Burkhart SS, Morgan CD, Kibler WB. The disabled throwing shoulder: spectrum of pathology part I: pathoanatomy and biomechanics. Arthroscopy. 2003;19:404-420.
10. Werner SL, Gill TJ, Murray TA, et al. Relationships between throwing mechanics and shoulder distraction in professional baseball pitchers. Am J Sports Med. 2001;29:354-358.
11. Osbahr DC, Cannon DL, Speer KP. Retroversion of the humerus in the throwing shoulder of college baseball pitchers. Am J Sports Med. 2002;30:347-353.
12. Pieper HG. Humeral torsion in the throwing arm of handball players. Am J Sports Med. 1998;26:247-253.
13. Harryman DT II, Sidles JA, Clark JM, et al. Translation of the humeral head on the glenoid with passive glenohumeral motion. J Bone Joint Surg Am. 1990;72:1334-1343.

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 331
42. Kibler WB, Chandler TJ, Livingston BP, Roetert EP. Shoulder range of motion in elite tennis players. Effect of age and years of tournament play. Am J Sports Med. 1996;24:279-285.
43. Witwer A, Sauers E. Clinical measures of shoulder mobility in college water-polo players. J Sport Rehabil. 2006;15:45-57.
44. Gunal I, Kose N, Erdogan O, et al. Normal range of motion of the joints of the upper extremity in male subjects with special reference to side. J Bone Joint Surg Am. 1996;78:1401-1404.
45. Conte AL, Marques AP, Casarotto RA, et al. Handedness infl uences passive shoulder range of motion in nonathlete adult women. J Manipulative Physiol Ther. 2009;32:149-153.
46. Yoshida M, Saho Y, Katayose M. Reliability of measuring humeral retroversion using ultrasound imaging in a healthy nonthrowing population. J Sport Rehabil. 2010;19:149-160.
47. Dillman CJ, Fleisig GS, Andrews JR. Biomechanics of pitching with emphasis upon shoulder kinematics. J Orthop Sports Phys Ther. 1993;18:402-408.
48. Pappas AM, Zawacki RM, Sullivan TJ. Biomechanics of baseball pitching. Am J Sports Med. 1985;13:216-222.
49. Blesh TE. Measurement in Physical Education. 2nd ed. New York, NY: The Ronald Press Company; 1974.
50. Wilk KE, Macrina LC, Arrigo C. Passive range of motion characteristics in the overhead baseball pitcher and their implications for rehabilitation. Clin Orthop Rel Res. 2012;470:1586-1594.
51. Barnes CJ, Van Steyn SJ, Fischer RA. The effects of age, sex, and shoulder dominance on range of motion of the shoulder. J Shoulder Elbow Surg. 2001;10:242-246.
52. Kronberg M, Brostrom LA, Soderlund V. Retroversion of the humeral head in the normal shoulder and its relationship to the normal range of motion. Clin Orthop Rel Res. 1990;253:113-117.
53. Clarke GR, Willis LA, Fish WW, et al. Preliminary studies in measuring range of motion in normal and painful stiff shoulders. Rheumatol Rehabil. 1975;14:39-46.
54. Wilk KE, Hooks TR, Macrina LC. The modifi ed sleeper stretch and modifi ed cross-body stretch to increase shoulder internal rotation range of motion in the overhead throwing athlete. J Orthop Sports Phys Ther. 2013;43:891-894.
55. Borstad JD, Dashottar A. Quantifying strain on posterior shoulder tissues during 5 simulated clinical tests: a cadaver study. J Orthop Sports Phys Ther. 2011;41:90-99.
28. Baltaci G, Johnson R, Kohl H. Shoulder range of motion characteristics in collegiate baseball players. J Sport Med Phys Fitness. 2001;41:236-242.
29. Myers JB, Oyama S, Wassinger CA, et al. Reliability, precision, accuracy, and validity of posterior shoulder tightness assessment in overhead athletes. Am J Sports Med. 2007;35:1922-1930.
30. Torres RR, Gomes JL. Measurement of glenohumeral internal rotation in asymptomatic tennis players and swimmers. Am J Sports Med. 2009;37:1017-23.
31. Borsa PA, Dover GC, Wilk KE, et al. Glenohumeral range of motion and stiffness in professional baseball pitchers. Med Sci Sports Exerc. 2006;38:21-26.
32. Downar JM, Sauers EL. Clinical measures of shoulder mobility in the professional baseball player. J Athl Train. 2005;40:23-29.
33. Chant CB, Litchfi eld R, Griffi n S, et al. Humeral head retroversion in competitive baseball players and its relationship to glenohumeral rotation range of motion. J Orthop Sports Phys Ther. 2007;37:514-520.
34. Riddle DL, Rothstein JM, Lamb RL. Goniometric reliability in a clinical setting: shoulder measurements. Phys Ther. 1987;67:668-673.
35. Lunden JB, Muffenbier M, Giveans MR, et al. Reliability of shoulder internal rotation passive range of motion measurements in the supine versus sidelying position. J Orthop Sports Phys Ther. 2010;40:589-594.
36. Wilk KE, Reinold MM, Macrina LC, et al. Glenohumeral internal rotation measurements differ depending on stabilization techniques. Sports Health. 2009;1:131-136.
37. Bigliani LU, Codd TP, Connor PM, et al. Shoulder motion and laxity in the professional baseball player. Am J Sports Med. 1997;25:609-613.
38. Borsa PA, Wilk KE, Jacobson JA, et al. Correlation of range of motion and glenohumeral translation in professional baseball pitchers. Am J Sports Med. 2005;33:1392-1399.
39. Brown LP, Niehues SL, Harrah A, et al. Upper extremity range of motion and isokinetic strength of internal and external rotators in major league baseball players. Am J Sports Med. 1988;16:577-585.
40. Baltaci G, Tunay VB. Isokinetic performance at diagonal pattern and shoulder mobility in elite overhead athletes. Scand J Med Sci Sports. 2004;14:231-238.
41. Carcia CR, Cacolice PA, Scibek JS. Sidelying glenohumeral passive internal rotation range of motion values in a healthy collegiate population. Int J Sports Phys Ther. 2013;8:793-799.

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 332
ABSTRACTBackground: Home-exercise is commonly prescribed for rehabilitation of the shoulder following injury. There is a lack of technol-ogy available to monitor if the patient performs the exercises as prescribed.
Purpose: The purpose of this study was to investigate the validity of using three dimensional (3D) gyroscope data recorded with the Bandcizer™ sensor to differentiate between three elastic band exercises performed in the shoulder joint: abduction, flexion, and external rotation.
Design: Concurrent validity study.
Methods: This study was performed over two phases. In the first phase, 20 subjects performed three sets of 10 of shoulder abduc-tion, external rotation and flexion exercises with a Thera-Band mounted with a Bandcizer, while supervised by a physical therapist. The Bandcizer has an inbuilt three-dimensional gyroscope, capable of measuring angular rotation. Gyroscope data were analyzed in Matlab, and a one-way ANOVA was used to test for significant differences between each of the three exercises. An algorithm was then created in Matlab based on the exercise-data from the gyroscope, to enable differentiation between the three shoulder exer-cises. Twenty new subjects were then recruited to cross-validate the algorithm and investigate if the algorithm could differentiate between the three different shoulder exercises.
Results: A blinded assessor using the Matlab algorithm could correctly identify 56 out of 60 exercise sets. The kappa agreement for the three exercises ranged between 0.86-0.91.
Conclusion: The ability to differentiate between the home exercises performed by patients after shoulder injury has great implica-tions for future clinical practice and research. When home exercises are the treatments-of-choice, clinicians will be able to quantify if the patient performed the exercise as intended. Further research should be aimed at investigating the feasibility of using the Bandcizer™ in a home-based environment.
Keywords: Adherence; Bandcizer; gyroscope; rehabilitation
Word count: 2429
Level of Evidence: 2
IJSP
TORIGINAL RESEARCH
AN ELASTIC EXERCISE BAND MOUNTED WITH A
BANDCIZER™ CAN DIFFERENTIATE BETWEEN
COMMONLY PRESCRIBED HOME EXERCISES FOR THE
SHOULDER
Kate McGirr, BSc (PT)1 Stine Ibsen Harring, BSc (PT)1
Thomas Sean Risager Kennedy, BSc (PT)1
Morten Frederik Schuster Pedersen, BSc (PT)1
Rogerio Pessoto Hirata, PhD Kristian Thorborg, PT, PhD3,4 Thomas Bandholm, PT, PhD4 Michael Skovdal Rathleff, PT, PhD1,2
1 Center for Sensory-Motor Interaction (SMI), Department of Health Science and Technology, Faculty of Medicine, Aalborg University, Denmark
2 Occupational Therapy and Physical Therapy Department Aalborg University Hospital, Aalborg, Denmark
3 Sports Orthopedic Research Center – Copenhagen (SORC-C), Arthroscopic Centre Amager, Copenhagen University Hospital, Copenhagen, Denmark
4 Physical Medicine & Rehabilitation Research – Copenhagen (PMR-C), Department of Occupational and Physical Therapy, Department of Orthopedic Surgery, and Clinical Research Center, Hvidovre Hospital, University of Copenhagen, Copenhagen, Denmark.
CORRESPONDING AUTHORKate McGirrDepartment of Health Science and TechnologyAalborg UniversityFredrik Bajers Vej 7DK-9220 AalborgTelephone: +45 61687345E-mail: [email protected]

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 333
INTRODUCTIONHome-based exercises are often a vital part of reha-bilitation for patients with shoulder impingement1 leading to improvements in pain intensity, quality of life and muscle strength, similar to supervised exer-cises.2,3 Home-based exercises are often performed with inexpensive, adjustable and transportable elastic exercise bands, which require little space compared to exercise machines.4 Despite the effectiveness of home-based exercises in shoulder rehabilitation, patient adherence to exercise programs has proven to be a challenge. Life-long adherence to exercise is required for many patient groups, however in many cases patient adherence is inadequate.5,6
It is often unknown if a patient’s lack of treatment response to an exercise program is due to reduced adherence, or if it is due to a problem with the exer-cise dose, type of exercise or simply because the patient does not perform the exercises correctly.6,7 Reliable and valid methods for quantifying adher-ence to home-exercise programs are sparse. One method widely used is self-reporting.7 This method is often unreliable, as patients can overestimate or underestimate how much exercise they have done.6 Even if the patient has been adherent to an exercise program, it is often uncertain whether the patient has performed a shoulder exercise as they were instructed.8 For example it may be relevant to dis-cern whether a patient performed abduction or a dif-ferent shoulder movement (e.g. shoulder extension or flexion), which would the likelihood that there will be optimal loading of the intended lateral mus-cle-tendinous structures of the shoulder (for exam-ple: the supraspinatus).
A new commercially available sensor has been developed, which automatically records and stores exercise data on a memory card or onto a mobile phone (the Bandcizer ™). The University of South-ern Denmark and the National Danish partnership UNIK developed Bandcizer™. This new sensor may enable clinicians and researchers to measure adher-ence to home-based shoulder exercises.9-11 Band-cizer™ is capable of automatically stamping training data with time-of-day and date, quantifying impor-tant aspects of exercise quality such as range of motion, and quantifying important exercise descrip-tors such as time under tension (TUT), based on the
Bandcizer’s™ recordings of changes in elastic band thickness.9 What it lacks, however, is the possibil-ity of determining which home-based exercises the patient has in fact performed while unsupervised. As the Bandcizer™ also contains a gyroscope, it is likely that gyroscope-data can be used to differen-tiate between commonly performed shoulder exer-cises, thus giving important information on which shoulder exercises/actions the patient actually per-formed at home.
The purpose of this study was therefore to inves-tigate the validity of using three dimensional (3D) gyroscope data recorded with the Bandcizer™ sensor to differentiate between three elastic band exercises performed in the shoulder joint: abduction, flexion, and external rotation. The authors’ hypothesized that it would be possible to differentiate between each of the three shoulder exercises using data from the 3D gyroscope.
MATERIAL AND METHODSEthics All participants included in the study received verbal and written information regarding the study. Writ-ten informed consent was obtained in accordance with the Declaration of Helsinki. The local Ethics Committee approved the study (2012-2410).
DesignThe design was a concurrent validity study, which investigated using the inbuilt 3D gyroscope in the Bandcizer™, attached to a standard elastic exercise band, to differentiate between three commonly per-formed shoulder exercises: abduction, flexion and external rotation. A physical therapist supervised the proper execution of the three shoulder exercises, ensuring that, for example, shoulder abduction was in fact performed as shoulder abduction. The study was designed with two Phases. Phase one involved collecting data from 20 participants, who each per-formed three sets of 10 exercise repetitions for each of the three exercises, with the Bandcizer™ attached to a Thera-Band. The position of the Bandcizer™ was standardized at 5cm from the Thera-Band handle.
Gyroscope data from the first Phase was used to cre-ate a Matlab algorithm with parameters designed to differentiate between the exercises. Phase two

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 334
included collecting data from 20 new participants who each performed one set of 10 repetitions of shoul-der abduction, flexion and external rotation, giving a total of 60 data sets. A blinded assessor was used then used to cross-validate the algorithm. The reporting of the study follows the Guidelines for Reporting Reli-ability and Agreement Studies (GRRAS).12
ParticipantsA convenience sample of 20 healthy volunteers (13 females), aged 21-48 without injury or operation to the shoulder, neck or back participated in the first phase to develop the algorithm and another 20 volun-teers aged 20-34 (13 females) also without injury or operation in the shoulder participated in the second phase of the study to cross-validate the developed algorithm. Participants were recruited from the stu-dent population of two local universities. The sample size in Phase 1 was based on getting at least 60 sets for each of the three exercises to allow Matlab to cal-culate an average dataset for each exercise based on data from the gyroscope. The sample size in Phase 2 was based on the amount of training a patient would perform during two weeks of home-based training, having received an initial supervised session with a physical therapist/rehabilitation specialist.
The Bandcizer™The Bandcizer™ measures the changes in thickness of the elastic band and has previously been validated for measuring TUT.9 The Bandcizer™ is equipped with a LSM330 3D digital gyroscope with a sample rate of 20 hz. The data recorded by the sensor is sent directly to a computer via Bluetooth in the form of text files.
Bandcizer’s™ 3D gyroscope measures rotation and angular velocity occurring around three axes: x, y and z. The positions of these axes are constant in the Bandcizer™ and cannot be altered. If rotational move-ment occurs, for example around a vertical axis, then the x-axis of the gyroscope will register and record this movement, under the condition that the x-axis of the gyroscope is always positioned on the Thera-Band to point vertically. This was an independent study, where none of the authors are affiliated with Bandcizer™.
Test setupA green Thera-Band was used in this study. The placement of Bandcizer™ on the Thera-Band was
standardized at 5cm from the handle and the 3D gyroscope was always in the same position. This was done by positioning the x-axis in a vertical direction.
The exercisesThe physical therapist responsible for observing the exercises determined the participants 12 repetition maximum (12RM) for each exercise, before data col-lection took place. The tension on the Thera-Band was adjusted according to each participant’s 12RM. The participants were then asked to perform three sets of 10 repetitions resembling a normal training load in the clinic.
Shoulder abduction, flexion and external rotation were performed with a three second concentric, two seconds isometric and three second eccentric contraction phase. There was a two second break between each repetition where there was no tension in the exercise band.
To assist the participants in maintaining the correct time under tension during the exercises, the partici-pants were shown a video of each exercise before testing took place. The same video also played dur-ing the exercises to assist with correct time under tension. A mirror was also provided to assist the par-
Figure 1. Exercise setup with Bandcizer™ placement on Thera-Band.

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 335
ticipant in reaching the required range of motion, as shown in Figure 2.
A two-minute break was held after each set of ten repetitions. If the exercises were not performed cor-rectly, the physical therapist would stop the test, allow the participant to take a break, and instruct the participant in the correct technique. Data from exercise sets not completed correctly were deleted, meaning that only correctly performed exercise data was collected and stored.
Data analysisData from the three gyroscope axes: x, y and z, was imported to Matlab (MATLAB and Statistics Toolbox Release 2013b, The MathWorks, Inc., Natick, Massa-chusetts, United States) in the form of text files. Each gyroscope axis was plotted separately as a function of time in Matlab, for every exercise set; a total of 180 plots. Data was filtered using a zero-lag, 4th order But-terworth IIR digital low-pass filter with a frequency of 5Hz. Plots were generated from the data in its fil-tered form and as a cumulative sum for each axis of
each exercise set. The plots were assessed visually to screen for the parameters most likely to differenti-ate between the exercises. The minimum and maxi-mum angular rates for the raw data and cumulative sum of the data for each axis appeared different between the exercises. These differences were then tested in SPSS using one-way analysis of variance, and Tukey’s test. There were two parameters, which were able to differentiate between the different exer-cises. These parameters were the minimum angular rate from the x-axis, which was significantly differ-ent between abduction and rotation (p < 0.001) and flexion and rotation (p < 0.001) and the cumulative sum maximum angular rate from the z-axis, which showed a significant difference between abduction and flexion (p < 0.001). These parameters were used to create a Matlab algorithm using conditional statements that could differentiate data from each of the exercises. The Matlab algorithm was then tested on data from 20 new participants (Phase 2).
The Matlab algorithm is attached as an appendix and is free to use. (Appendix 1)
Figure 2. Exercises used in the research, A=Abduction start position, B= Abduction end position; C=Flexion start position, D=Flexion end position; E=External rotation start position, F= External rotation end position.

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 336
which type of shoulder movement was being per-formed, due to the corresponding movements on the relevant axis. Using the Bandcizer™ it is possible to measure time under tension, range of motion and differentiate between three commonly used shoul-der exercises.9-11 In a practical scenario, the physical therapist would give the patient an initial instruc-tion in the relevant exercises. This could for example be three sets of 12 repetitions for shoulder abduc-tion and external rotation with a time under tension consisting of three seconds concentric, two seconds isometric and three seconds eccentric phases.13 The patient would then perform these exercises at home for two weeks, with the Bandcizer™, and then come to a follow up appointment with the physical therapist. During the follow up appointment, the therapist could review the exercise data and evalu-ate the patient’s adherence to the training program and check if the shoulder abduction was indeed performed as abduction and not as shoulder flex-ion instead. Data from the Bandcizer™ can be com-bined with the patient’s own reports of changes in pain and function, providing the physical therapist with a strong rationale for how the training dosage should be changed during the next phase of home-based training.
The algorithm developed for this study was cre-ated in Matlab, a software program that due to its expense, may not be a realistic tool for physical therapists to acquire. The principles used to develop the algorithm can however be easily adapted to other programming languages for example freeware such as Python. It would take the physical therapist approximately five minutes to apply the algorithm to the relevant data sets and read the results of the exercises performed. In order to combine this with training dosage (time under tension, number of rep-etitions and number of training sets it would take an additional 90 seconds per exercise set (see refer-ence9 for a more detail).
LimitationsThe three shoulder exercises tested in this study are performed across three different axes, allowing for successful differentiation when the positioning of the Bandcizer™ is standardized. This is likely to make it easier to differentiate between the three exercises. Challenges will arise when trying to differentiate
Statistical analysisCohen’s unweighted kappa statistic was used to calculate the agreement between the exercises performed under supervision by physical therapist and the answers that the Matlab algorithm gave for the new data.
RESULTSThe kappa agreement between the exercises per-formed under supervision by physical therapist and the answers that the Matlab algorithm gave was 0.90 (95%CI: 0.81-0.99) (Table 1). The algorithm correctly identified all 20 external rotation exercises but inter-preted one flexion and one abduction movement each as external rotation. Eighteen out of 20 abduc-tion and flexion exercises were correctly identified.
DISCUSSIONPatient adherence to home exercise programs is a vital step towards successful home-based rehabilitation after shoulder injury, yet adherence in many patient groups is inadequate.5,6 The Bandcizer™ has been proven to be a valid method for measuring time under tension,9 yet it was unknown if the inbuilt 3D gyroscope could be used to determine which type of movement direction the patient actually performed during their home-based unsupervised exercises. This study investigated the valid-ity of using 3D gyroscope data recorded with the Band-cizer™ sensor to differentiate between three elastic band exercises performed in the shoulder joint; abduction, flexion and external rotation. The results showed that the algorithm could correctly differentiate between 56 of the 60 exercises, corresponding to a kappa agreement of 0.86-0.91, demonstrating almost perfect agreement.
Practical usage of Bandcizer™By standardizing the position of the Bandcizer™ sen-sor on the Thera-Band, it was possible to distinguish
Table 1. Exercises performed in the second phase, com-pared to the answers returned by the Matlab algorithm from Phase 1, when used to differentiate between the exercises. The table depicts the number of times each exercise was identifi ed by the algorithm.
Answers Provided by Matlab Algorithm
Exercise Rotation Abduction Flexion Rotation 20 0 0 Abduction 1 18 1 Flexion 1 1 18

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 337
to quantify whether the patient performed the exer-cise as intended.
REFERENCES1. Camargo P, R., Haik MN, Ludewig PM,et.al. Effects of
strengthening and stretching exercises applied during working hours on pain and physical impairment in workers with subacromial impingement syndrome. Physiother Theory Prac.t 2008;25(7):463-475.
2. Vuorenmaa M, Ylinen J, Piitulainen K, et al. Effi cacy of a 12-month, monitored home exercise programme compared with normal care commencing 2 months after total knee arthroplasty: a randomized controlled trial. J Rehabil Med. 2014;46(2):166-172.
3. Thiebaud RS, Funk MD, Abe T. Home-based resistance training for older adults: A systematic review. Geriatr Gerontol Int. 2014;14(4):750-757.
4. Melchiorri G, Rainoldi A. Muscle fatigue induced by two different resistances: Elastic tubing versus weight machines. J Electromyogr Kinesiol. 2011;21(6):954-959.
5. Marks R. Knee Osteoarthritis and Exercise Adherence: A Review. Curr Aging Sci. 2012;5(1):72-83.
6. Bassett S. Measuring Patient Adherence to Physiotherapy. J Nov Physiother. 2012;2(7).
7. Bollen JC, Dean SG, Siegert RJ, Howe TE, Goodwin VA. A systematic review of measures of self-reported adherence to unsupervised home-based rehabilitation exercise programmes, and their psychometric properties. BMJ Open. 2014;4(6).
8. Andersen LL, Saervoll CA, Mortensen OS, et al. Effectiveness of small daily amounts of progressive resistance training for frequent neck/shoulder pain: randomised controlled trial. Pain. 2011;152(2):440-6.
9. Rathleff MS, Thorborg K, Rode LA, McGirr KA, Sørensen AS, Bøgild A, et al. Adherence to commonly prescribed, home-based strength training exercises for the lower extremity can be objectively monitored using the Bandcizer. J Str Condit Res. 2014;Epub ahead of print.
10. Rathleff MS, Thorborg K, Bandholm T. Concentric and Eccentric Time-Under-Tension during Strengthening Exercises: Validity and Reliability of Stretch-Sensor Recordings from an Elastic Exercise-Band. PLos One. 2013;8(6).
11. Rathleff M.S., Bandholm T, Ahrendt P, et al. Novel stretch-sensor technology allows quantifi cation of adherence and quality of home-exercises: a validation study. Br J Sports Med. 2014;48(8):724-728.
12. Kottner J, Audige L, Brorson S, et al. Guidelines for Reporting Reliability and Agreement Studies (GRRAS) were proposed. Int J Nurs Stud. 2011;48(6):661-671.
exercises, performed on the same axis, for example flexion and extension of the shoulder. In reality a patient is unlikely to perform a shoulder abduction instead of a flexion but rather a combination of the two exercises. This situation would call for a more advanced approach to differentiating between the exercises, where the gyroscope data would need to be more precise than that which can be recorded when attached to an elastic band.
3D gyroscopes have previously been used to assess ROM, gait and functional movement in several pre-vious studies 14-17 and are usually attached directly to limbs or other body parts. Attaching the gyro-scope directly to the body provides more precise data regarding movement, detecting even small variations 17 compared to that which can be detected when the gyroscope is placed on an elastic band. Despite the potential for tracking movement using 3D gyroscopes, it is not yet possible to combine the quantification of time under tension with more pre-cise measurements of movement using the Band-cizer™, due the fact that Bandcizer™ must be placed on an elastic band.
Further researchThe current study was performed under controlled supervised conditions. It can be expected that with-out supervision, a patient would perform the exer-cises with a larger variation in the quality, making it difficult to differentiate between the exercises. This could be, for example, because of the placement of the Bandcizer™ on the elastic exercise band. Future research should investigate if it is possible to differ-entiate between different exercises when the patient performs the exercises at home without supervision.
CONCLUSIONBy standardizing the positioning of Bandcizer’s™ 3D inbuilt gyroscope, it was possible to create an algorithm that could correctly distinguish between shoulder abduction, flexion and external rotation exercises, by correctly identifying 56 out of 60 exer-cise sets. The ability to differentiate between the home-exercises performed by patients after shoul-der surgery has great implications for future clinical practice and research, where home exercises are the treatments of choice, as they will enable clinicians

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 338
13. Ratamess NA, Alvar BA, Evetoch TK, et al. Progression Models in Resistance Training for Healthy Adults. Med Sci Sports Exerc. 2009;41(3):687-708.
14. El-Zayat BF, Efe T, Heidrich A W, U., Timmesfeld N, Heyse TJ, Lakemeier S, et al. Objective assessment of shoulder mobility with a new 3D gyroscope--a validation study. BMC Musculoskel Disord. 2011;21(12).
15. Penning LLF, Guldemond NA, de Bie RA, Walenkamp G. Reproducibility of a 3-dimensional
gyroscope in measuring shoulder antefl exion and abduction. BMC Musculoskelet Disord. 2012;13(135).
16. Wagenaar RC, Sapir I, Zhang Y, et al. Continuous monitoring of functional activities using wearable, wireless gyroscope and accelerometer technology. Conf Proc IEEE. Eng Med Biol Soc. 2011:4844-4847.
17. Patterson MR, Delahunt E, Sweeney KT, Caulfi eld B. An ambulatory method of identifying anterior cruciate ligament reconstructed gait patterns. Sensors (Basel). 2014;14(1):887-899.
APPENDIX 1
function [results, total] = bandcizerAlgorithm % BandcizerAlgorithm differentiates between shoulder abduction, flexion and % external rotation perfomed with an elastic band with Bandcizer device % attached. For more information, please visit www.bandcizer.dk % Bandcizer is equipped with a LSM330 3D digital gyroscope, data from the x % and z axes are used in the algorithm based on a standardized attachment % with the x-axis in the vertical direction. % The data was extracted using Matlab version R2013b % Input: % There is no input for the function, however it loads gyrodata from 2 % phases of data collection.(for details, see paper "Differentiation of % common shoulder elastic band exercises using the Bandcizer.") % Output: % results: exercises from the second phase are compared to data from the first % phase. 1. column: name of dataset. 2. column: correct exercises from second % phase. 3. column: recognition exercise from the BadcizerAlgorithm. % 4. column: proper recogniction = 1, incorrect recognition = 0. % total: number of correctly recognized exercises. % Authors: Stine Ibsen Harring, email:[email protected] and % Rogerio Hirata, email: [email protected] % Last update: 24/092014 %% Defining time window for analysis and sampling rate (Hz) time = 1:1900; samplingRate = 20; %% Defining parameters for butterworth filter: 2nd Order, low pass 5 Hz. [b,a] = butter(2,5/(samplingRate/2)); %% This loop extracts parameters acquired during the rotation exercises from the first phase files = dir('R*.txt'); for i = 1:length(files) filenames = files(i).name; gyroRotation = dlmread(filenames, ' ',1,12 ); x = gyroRotation(time,1); % Angular rate in the x direction x = filtfilt(b,a,x); % Filtering data minxRotation(i)= min(x); % Extracting the minimum value of x end clear x meanOfMinxRotation = mean(minxRotation);
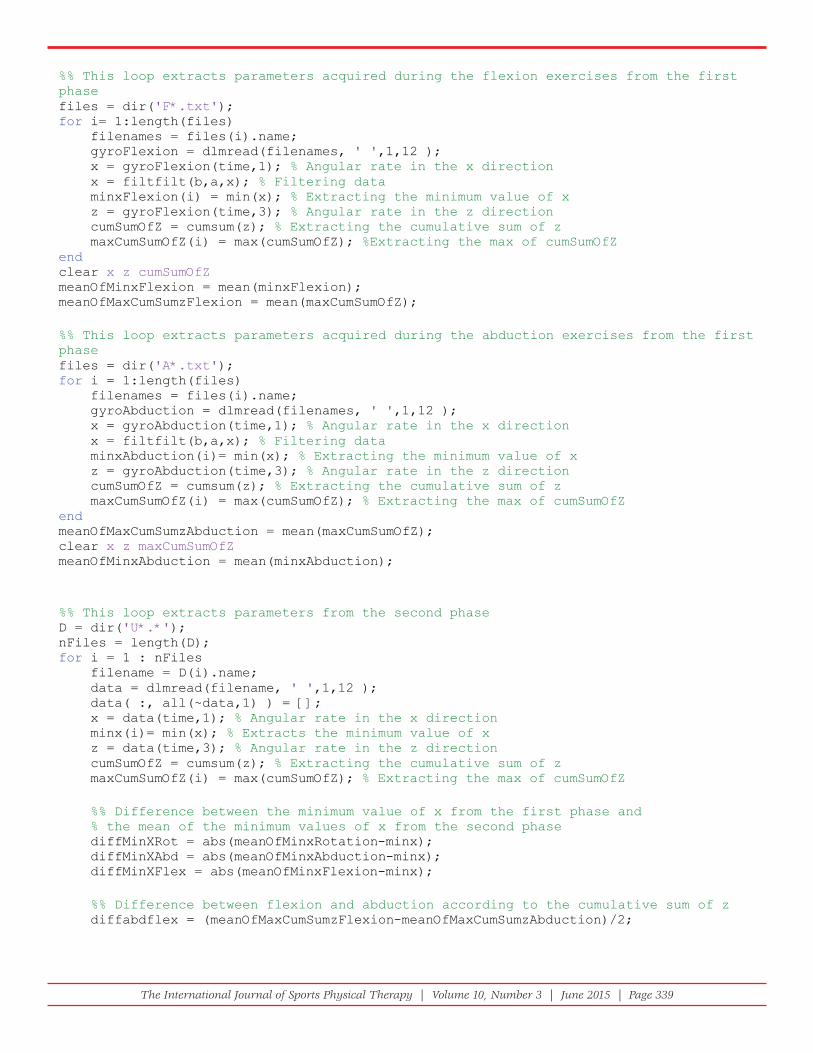
The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 339
%% This loop extracts parameters acquired during the flexion exercises from the first phase files = dir('F*.txt'); for i= 1:length(files) filenames = files(i).name; gyroFlexion = dlmread(filenames, ' ',1,12 ); x = gyroFlexion(time,1); % Angular rate in the x direction x = filtfilt(b,a,x); % Filtering data minxFlexion(i) = min(x); % Extracting the minimum value of x z = gyroFlexion(time,3); % Angular rate in the z direction cumSumOfZ = cumsum(z); % Extracting the cumulative sum of z maxCumSumOfZ(i) = max(cumSumOfZ); %Extracting the max of cumSumOfZ end clear x z cumSumOfZ meanOfMinxFlexion = mean(minxFlexion); meanOfMaxCumSumzFlexion = mean(maxCumSumOfZ); %% This loop extracts parameters acquired during the abduction exercises from the first phase files = dir('A*.txt'); for i = 1:length(files) filenames = files(i).name; gyroAbduction = dlmread(filenames, ' ',1,12 ); x = gyroAbduction(time,1); % Angular rate in the x direction x = filtfilt(b,a,x); % Filtering data minxAbduction(i)= min(x); % Extracting the minimum value of x z = gyroAbduction(time,3); % Angular rate in the z direction cumSumOfZ = cumsum(z); % Extracting the cumulative sum of z maxCumSumOfZ(i) = max(cumSumOfZ); % Extracting the max of cumSumOfZ end meanOfMaxCumSumzAbduction = mean(maxCumSumOfZ); clear x z maxCumSumOfZ meanOfMinxAbduction = mean(minxAbduction); %% This loop extracts parameters from the second phase D = dir('U*.*'); nFiles = length(D); for i = 1 : nFiles filename = D(i).name; data = dlmread(filename, ' ',1,12 ); data( :, all(~data,1) ) = []; x = data(time,1); % Angular rate in the x direction minx(i)= min(x); % Extracts the minimum value of x z = data(time,3); % Angular rate in the z direction cumSumOfZ = cumsum(z); % Extracting the cumulative sum of z maxCumSumOfZ(i) = max(cumSumOfZ); % Extracting the max of cumSumOfZ %% Difference between the minimum value of x from the first phase and % the mean of the minimum values of x from the second phase diffMinXRot = abs(meanOfMinxRotation-minx); diffMinXAbd = abs(meanOfMinxAbduction-minx); diffMinXFlex = abs(meanOfMinxFlexion-minx); %% Difference between flexion and abduction according to the cumulative sum of z diffabdflex = (meanOfMaxCumSumzFlexion-meanOfMaxCumSumzAbduction)/2;

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 340
%% These statements analyze the differences between the two sets of data and % recognize the exercise according to the minimum difference. results{i,1} = filename; if diffMinXRot(i) < diffMinXAbd(i) && diffMinXRot(i) < diffMinXFlex(i) results{i,2} = 'ROTATION'; end if diffMinXRot(i) > diffMinXAbd(i) && diffMinXRot(i) > diffMinXFlex(i) if maxCumSumOfZ(i) < diffabdflex; results{i,2} = 'ABDUCTION'; end if maxCumSumOfZ(i) > diffabdflex results{i,2} = 'FLEXION'; end end %% These variables show the correct exercises from the second phase. rotres = [5,9,13,14,18,20,21,25,29,33,35,36,40,43,44,46,49,54,56,60]; abdres = [3,4,6,7,8,12,15,16,22,23,30,31,32,37,42,45,50,52,53,55]; flxres = [1,2,10,11,17,19,24,26,27,28,34,38,39,41,47,48,51,57,58,59]; for i = 1 : length(rotres) results{rotres(i),3} = 'ROTATION'; end for i = 1 : length(abdres) results{abdres(i),3} = 'ABDUCTION'; end for i = 1 : length(flxres) results{flxres(i),3} = 'FLEXION'; end end %% This loop calculates the number of correctly recognized exercises. for i = 1 : length(results) total(i) = strcmp(results{i,2},results{i,3}); results{i,4} = total(i); end total = sum(total)

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 341
ABSTRACT
Background and Purpose: In gymnastics, the wrist is exposed to many different stresses including
increased extension, especially during back handsprings. Currently a wrist extension angle during impact
that places the wrist in danger has not been established. The purpose of this study was to: (1) determine
the mean impact wrist angle during a standing back handspring in female preadolescent and adolescent
gymnasts and (2) determine which factors predict impact wrist angles.
Methods: Fifty female gymnasts from six facilities, ages 8-15 were included in this study. Each gymnast
completed a questionnaire about gymnastics participation and history of wrist pain. Active range of motion
of the shoulder, elbow, wrist, hip, and ankle was measured. Each gymnast was asked to perform a standard
back handspring, which was videotaped. The wrist and shoulder flexion angles, at maximum impact, were
recorded and measured using motion analysis software. Two-sample t-test was used to assess the relationship
between impact wrist angle and wrist pain. Multiple linear regression was used to determine the association
between related variables and impact wrist angle.
Results: The mean back handspring impact wrist angle was 95º. Fifteen subjects (30%) reported wrist pain.
Years of participation (p=0.02) and impact shoulder angle (p=0.04) were predictive of impact wrist angles.
Conclusion: Shoulder angles and years of participation correlate with impact wrist angles during the perfor-
mance of a standing back handspring. Future studies are necessary to determine if addressing these factors can
affect the impact wrist angles.
Keywords: Back handspring, gymnastics, wrist
Level of Evidence: 3
IJSP
TORIGINAL RESEARCH
IMPACT SHOULDER ANGLES CORRELATE WITH
IMPACT WRIST ANGLES IN STANDING BACK
HANDSPRINGS IN PREADOLESCENT AND
ADOLESCENT FEMALE GYMNASTS
Kelli McLaren, PT, DPT, SCS1
Erin Byrd, PT, DPT, SCS, CSCS1
Mackenzie Herzog, BA1
John A. Polikandriotis, PhD, MBA, MPH1
S. C. Willimon, MD1
1 Children’s Healthcare of Atlanta Sports Medicine, Atlanta, GA, USA
CORRESPONDING AUTHOR
Kelli McLaren, PT, DPT, SCS
410 Peachtree Parkway
Suite 300
Cumming, GA 30041
E-mail: [email protected]

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 342
INTRODUCTION
USA Gymnastics reports that over 90,000 athletes
are currently registered participants in competi-
tive gymnastics in the United States.1 Gymnasts
are unique in that they weight-bear on their upper
extremities. This often results in joint injuries due to
increased loads at the shoulder, elbow, and wrist, and
these injuries often result in missed time from sport
and accumulated healthcare costs.2,3,4 The wrist is
the most frequently injured upper extremity joint in
female gymnasts,2 yet the body of research examin-
ing wrist angles during common impact gymnastic
skills and factors that affect the impact wrist angle
during dynamic gymnastic skills is limited.
It is theorized that development of correct technique
and attention to mechnaics are important early in a
gymnast’s career in order to minimize excessive forces
experienced through the wrist and subsequently lower
the potential for wrist injury. Gymnasts will build on
basic movements and positions as they progress in skill
level. In order to understand forces at the wrist, it is
important to examine a gymnast’s wrist angles during
activity. A hyperextended wrist angle during impact
centralizes and intensifies weight-bearing forces over
the distal radius and ulna.4 Hyperextension of the
wrist may result from decreased shoulder flexion and
increased elbow flexion at impact during a dynamic
skill, or failure of the shoulders to reach the fully open,
or fully flexed, position at time of impact. (Figures 1 & 2)
The back handspring, a basic skill that a gymnast will
build on throughout their career, is an excellent repre-
sentation of a dynamic skill that requires wrist motion
and will essentially pass through the basic handstand
position. The purpose of this study is to: (1) determine
the mean wrist angle during a standing back handspring
in female preadolescent and adolescent gymnasts; and
(2) determine if other factors, such as impact shoulder
angle, affect the impact wrist angle. For the purpose
of this study, glenohumeral shoulder flexion will be
measured in each gymnast. Discussion will consist of
addressing the shoulder complex as a whole as impact
during a back handspring is dynamic and is affected by
both the glenohumeral joint and the shoulder complex.
METHODS
This study was Institutional Review Board approved.
Between March 2013 and May 2013, participants
were prospectively recruited from six gymnastics
facilities in the metropolitan Atlanta area via phone
calls to the facilities. High-level female gymnasts
USAG level 6 or higher, USAG Platinum or higher,
or AAU Prep Op 3 who were between the ages of 8
to 15 years were invited to participate. Each level
listed is the minimum level in which a skilled back
handspring is required of the athlete, therefore the
inclusion competition levels were chosen to ensure
that the back handspring was not a novice skill for
the participant. Exclusion criteria were a history of
injury to the neck, shoulder, elbow, or wrist, a diag-
nosis of wrist pathology by a physician with or with-
out radiographs, and male sex.
Following consent to participate in the study from the
guardian and the athlete, each participant filled out
Figure 1. Greater shoulder fl exion angle with less acute
angle of wrist extension.
Figure 2. Decreased shoulder angle with greater angle of
wrist extension. (less optimal).

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 343
a self-administered subjective questionnaire about
her competition level, gymnastics experience, and
history of wrist pain developed by the researchers.
If the participant reported current or previous wrist
pain, she was asked the duration of symptoms and
any treatment she received. Next, range of motion
measurements were taken by two experienced clini-
cians using clinical standards of gonionmetric mea-
surements with a standard size goniometer. Motions
recorded included active shoulder flexion and exten-
sion, elbow flexion, extension and carrying angle,
wrist flexion and extension, hip extension and ankle
dorsiflexion.5
Biomechanical analysis was performed using a
Casio Ex-ZR200 camera for gathering video data, and
shoulder and wrist angles measured, documented,
and analyzed using Genesis motion analysis soft-
ware (EquineTec, Monroe, GA). Each gymnast was
allowed time to stretch and warm up with one back
handspring performed individually prior to perform-
ing the recorded back handspring. Each gymnast
was asked to perform one back handspring without
wrist guards or braces on a standard 1-inch (depth)
eight-panel mat. The gymnast was verbally cued to
“perform one back handspring.” A single investiga-
tor recorded each back handspring and measured
shoulder and wrist angles during the point of impact
for each back handspring. Impact angles were mea-
sured using standard goniometric landmarks. The
impact wrist and shoulder angle are defined as the
moment in time when a gymnast’s hands make con-
tact with the floor and the body absorbs its weight.
These measurements were captured simultane-
ously and were measured using the Genesis soft-
ware. Each wrist impact angle was measured with
the x-axis parallel to the floor and the y- axis through
the center of the wrist following the forearm. (Refer
to Figures 1 & 2) All angles were measured in the
right wrist. Angles that were measured to be less
than 90 degrees indicate closer proximity of the
fingers to the forearm and a greater (more severe)
extension angle at impact. Angles that are measured
to be greater than 90 degrees indicate a lesser (less
severe) extension angle at impact.
Statistical analyses were performed using SAS 9.3
(Cary, NC). A two-sample t-test was used to assess
the relationship between impact wrist angle and
wrist pain. Linear regression was used to identify
variables associated with impact wrist angle. Vari-
ables entered into the initial model included years of
participation, use of extension limiting wrist braces,
impact shoulder angle, age, and active range of motion
including shoulder flexion, shoulder extension,
elbow flexion, elbow extension, elbow valgus, wrist
flexion, wrist extension, hip extension, and ankle
dorsiflexion each measured separately. Backwards
elimination and forward selection were used to iden-
tify the best model and to determine which variables
should remain in the model for analysis (Table 1).
The final model was analyzed using linear regres-
sion to determine the association between related
variables and impact wrist angle. All statistics were
analyzed at the 95% level, and p<0.05 was consid-
ered statistically significant.
RESULTS
Fifty-seven female gymnasts from six gymnastics
facilities were examined. Participants were excluded
due to systemic pathology affecting joint mobility,
previous wrist, elbow, or shoulder surgery or previ-
ous wrist injury that required immobilization. Self
reported generalized wrist pain was not within exclu-
sion criteria. Fifty participants met the criteria for
this study and were included in the analysis. Mean
age of participants was 12.7 years (range: 8.1 to 15.0
years). Mean number of years of participation in
Table 1. Results of multivariate linear regression using
backward elimination

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 344
gymnastics was 8 (range: 3 to 15). Twenty-two (44%)
reported current usage of a wrist extension limiting
brace bilaterally.
Mean back handspring wrist angle was 95 degrees
(range: 77.0 to 119.0 degrees). Mean back hand-
spring glenohumeral shoulder flexion angle was 154
degrees (range: 126 to 174 degrees). There was a sig-
nificant difference between the mean impact wrist
angle and the measured active range of motion (95
degrees vs. 67 degrees; p=<0.001). Fifteen (30%)
reported current or recent history of wrist pain for
an average duration of 10.95 months (range: 0.25
to 24.00 months). Gymnasts with wrist pain had
a slightly different impact wrist angle compared
to those without wrist pain (97.8 degrees and 94.3
degrees, respectively; p=0.06), which approached
statistical significance. Multivariate linear regres-
sion analysis indicated that increased years of par-
ticipation decreases the amount of wrist extension
at impact (p=0.02), and that impact shoulder angle
(p=0.04) correlated with impact wrist angles. Back-
wards elimination and forward selection revealed
a final model where for every one degree increase
in impact shoulder angle (increased shoulder flex-
ion or a more open shoulder position), impact wrist
angle increases by 0.18 degrees (more wrist flexion
or less wrist hyperextension), after controlling for
the other variables in the model.
DISCUSSION
The mean impact wrist angle during a standing back
handspring was 95 degrees. While there was a differ-
ence in impact wrist angles for gymnasts with wrist
pain compared to gymnasts without wrist pain, this
difference was not significant due to sample size.
The results of the current study also indicate that
there is a relationship between impact wrist angle
and impact glenohumeral shoulder flexion angle
during a gymnast’s standing back handspring where
a decreased glenohumeral shoulder flexion angle at
impact results in an increased wrist extension angle.
A limitation in glenohumeral shoulder flexion dur-
ing impact results in an increase in elbow flexion,
creating excessive extension through the wrist. The
above summarizes what is described as a collapse
through the shoulders at impact. The results sug-
gest the development of strategies that increase
the angle of glenohumeral shoulder flexion during
a back handspring in gymnasts, possibly shoulder
strengthening and flexibility strategies in the shoul-
der complex could reduce increased wrist exten-
sion during impact. This could be useful for guiding
the clinical treatment of gymnasts and educating
coaches in prevention of wrist injuries.
A few studies have examined the shoulder complex
and wrist mechanics of a back handspring. Kamp-
schroeder et al7 and Penitente, Merni et al8 made
comparisons between “skilled” and “unskilled” gym-
nasts performance of back handsprings and reported
that a skilled gymnast performing a back handspring
had less ground reaction forces at the wrist and less
vertical displacement at the shoulders during the
back handspring.7 Henrichs reported that a back
handspring caused significantly more wrist exten-
sion than the gymnasts were able to obtain during
the active range of motion (AROM) measurement.9
This is in agreement with the findings of this study
(95 degrees during performance, versus 67 degrees
during AROM measurment; p=<0.001). In addi-
tion, Henrichs found that maximum wrist hyperex-
tension and maximum vertical force occur almost
simultaneously in the back handspring during
impact. The authors of the current study believe
that this requirement of a large increase in extension
of the wrist at the time of maximum vertical force is
one factor that may lead to injury of the wrist during
a back handspring.
The current results indicate that increased years of
particpation in gymnastics is correlated to decreased
wrist extension during impact. Upper extremity
weight-bearing in the skeletally immature gymnast
often leads to increased stress on the distal radial
physis and carpals, causing the wrist to be more
vulnerable to overuse injury.3,4,7,10 Overuse injuries
may include scaphoid impaction syndrome, dorsal
impingement syndrome3,4,7,10, 11 and arrest of growth
of the radius.8 The radius absorbs the majority
(roughly 80%) 4 of the stress during upper extrem-
ity weight bearing, which can be up to two times
the gymnast’s body weight during impact while per-
forming dynamic skills such as tumbling or vaulting.
With repeated stress to the distal radius, a condition
known as positive ulnar variance, where the ulna is
no longer 2.5mm shorter than the radius, can occur.3
Positive ulnar variance, caused by growth arrest at

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 345
were excluded from this study due to differences in
training, body structure and age of puberty. Recruit-
ment of female gymnasts within the ages of 8-15 who
had no history of upper extremity fracture requiring
immobilization or surgery proved to be a challenge.
Finally, the measurements derived using the motion
analysis software quantify glenohumeral motion
only in the sagittal plane. The blocking motion, which
takes place in multiple planes, as described above, is
a key component to a successful back handspring.
This complex, multi-planar blocking mechanism
was not analyzed. Strengths of this study include
recruiting gymnasts from multiple gymnastics facili-
ties in order to minimize the coaching effect and the
control of recruiting gymnasts who were not in the
process of learning a back handspring. Participants
in this study had competed a back handspring in a
tumbling pass for at least a year based on the level
of participation described in the inclusion criteria. In
addition, this study provides important groundwork
for future injury prevention studies among female
adolescent gymnasts.
CONCLUSION
To understand forces at the wrist, it is important
to examine a gymnast’s wrist angles and factors
that affect or predict these angles during dynamic
activity. Mean impact wrist angle during the back
handspring was determined to be 95 degrees in
this sample. This number provides a foundation for
future studies to examine what factors could pos-
sibly change this average impact wrist angle, and
establish a “dangerous” impact wrist angle. There
is a relationship between years of participation and
impact wrist angles and between shoulder angles
and impact wrist angles. These results indicate that
the longer a gymnast has been participating in gym-
nastics, the more practiced a back handspring will
become, resulting in less extension at the wrist dur-
ing impact. The results of the current study yield
valuable information that may relate to future
injury prevention efforts. These results suggest that
addressing any lack of shoulder flexion that exists
may be a strategy to decrease wrist hyperextension
during a back handspring, thereby reducing stress on
the wrist. Further avenues of study include examin-
ing the effects of strengthening proximally in order
to change wrist angle distally.
the radial physis, can also lead to other complex wrist
injuries that may require surgical intervention such
as triangular fibrocartilage complex (TFCC) repairs
and ulnar shortening procedures. Conversely, after
the closure of the growth plates, the injuries expe-
rienced by gymnasts differ. From repeated impact
forces, skeletally mature gymnasts are more likely
to present with TFCC tears, ulnar impaction syn-
drome, and lunotriquetral impingement.3 Correction
of wrist biomechanics in the skeletally immature
gymnast may lead to decreased chronic wrist condi-
tions that occur after skeletal maturity is reached.
Cools et al12 have described the characteristic pre-
sentation of elite female gymnasts as having greater
shoulder complex protraction than retraction, when
expressed as a ratio. This can alter the ability of the
serratus and trapezius to work together as a force
couple to stabilize the scapula during upward rota-
tion, and create an imbalance between bilateral
scapulae during upward rotation in order to accom-
modate the upper extremities in a weight bearing
position. Biomechanically, with insufficient scapu-
lar stabilizers and increased protraction force, it is
reasonable to conclude that the shoulders could col-
lapse at contact resulting in the inability to “block”,
or push off the hands and back on to the feet.13 The
blocking motion is a combination of simultaneous
shoulder complex protraction, elevation, and shoul-
der flexion. Addressing the strength and neuromus-
cular control in the shoulder complex including
the scapular stabilizers could potentially improve
the shoulder angle and therefore improve the wrist
angle at initial contact. When treating gymnasts
with wrist pain the function of the proximal kinetic
chain is important to consider as this population
bears weight through the upper extremities. Devel-
oping a gymnast’s strength and neuromuscular con-
trol proximally can affect the elbow and wrist in a
closed kinetic chain position.
A limitation of the current study is the small sam-
ple size; however, this study adds to the literature by
determining effect sizes, associations, and variability
in order to calculate sample size for a future studies
on this topic. Additionally, this study only included
youth and adolescent female gymnasts, and conse-
quently can only be generalized to the female gym-
nast population in this age range. Male gymnasts

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 346
performances in young female gymnasts. 15th
International Symposium on Biomechanics in Sports.
1997; 425-430
8. Penitente G, Merni F, and Sands WA Sands.
Kinematic Analysis of Centre of Mass in the Back
Handspring: A Case Study. Gym Coach. 2011;4:1-11.
9. Henrichs DK. A biomechanical comparison of
ground reaction force and wrist hyperextension
during the front and back handspring in gymnastics.
Western Washington University; 2005.
10. DiFiori JP, Caine DJ, Malina RM. Wrist pain, distal
radial physeal injury, and ulnar variance in the
young gymnast. Am J Sports Med. 2006; 34:840-849.
11. VanHeest AE, Luger NM, House JH. Extensor
retinaculum impingement in the athlete. A new
diagnosis. Am J Sports Med. 2007; 35:2126-2130.
12. Cools AM, Geerooms E, Van den Bergne DFM, et al.
Isokinetic Scapular Muscle Performance in Young
Elite Gymnasts. J Athl Train. 2007; 42: 458-463
13. Perrott L, Judge B. Posture for take-offs and landings.
Technique. 2011:21;7:8-10
REFERENCES 1. About USA Gymnastics. Available at http://usagym.
org/pages/aboutus/pages/about_usag.html.
Accessed March 30,2014
2. Amaral L, Claessens A, Ferreirinha J, Santos P. Ulnar
variance and its related factors in gymnasts: A
review. Science of Gym J. 2011;3:58-59.
3. Webb BG, Rettig LA. Gymnastic wrist injuries. Curr
Sports Med Rep. 2008;7:289-295.
4. DiFiori JP. Overuse injury and the young athlete: the
case of chronic wrist pain in gymnasts. Curr Sports
Med Rep. 2006;5:165-167.
5. Marsha GF, Sitler MR, Kozin SH, et al. Effect of
prophylactic brace on wrist and ulnocarpal joint
biomechanics in a cadaveric model. Am J Sports Med
. 2003; 31;736-743.
6. Norkin CC, White PJ. Measurement of Joint Motion: A
guide to Goniometry. 4th Edition. Philidelphia, PA; F.A.
Davis Company; 2009.
7. Kampschroeder D, Zebas C, Spina M. A comparison
of unskilled and skilled standing back handspring
The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 347
ABSTRACTWhile examining the shoulders of 91 professional and semi-professional beach volleyball players, the authors observed two cases of grave atrophy of the deltoid muscle following painless axillary neuropathy, not resulting from any trauma. The causes, the clinical history and the untreated history of the entrapment of the axillary nerve in the quadrilateral space in sportsmen, are discussed on the basis of the presentation of the two cases illustrated and from existing literature.
Keywords: axillary nerve entrapment; quadrilateral space syndrome; sport related axillary neuropathy
Level of Evidence: 4
IJSP
TCASE REPORT
SILENT DELTOID ATROPHY IN BEACH VOLLEYBALL
PLAYERS: A REPORT OF TWO CASES AND LITERATURE
REVIEW
Giovanni Monteleone, MD1,2,5
Marco Gismant, MD3
Giorgio Stevanato, MD4
Alessandra Tiloca, DAT5
1 Department of Biomedicine and Preventative Medicine, Faculty of Medicine and Surgery, University of Rome “Tor Vergata”, Rome, Italy
2 C.O.N.I. - Italian Olympic Committee, Sardinia, Italy3 S.I.U.M.B. - Italian Society for Ultrasound in Medicine and
Biology, Rome, Italy4 Neurosurgery Unit, Dell’Angelo Hospital, Mestre (Ve), Italy5 School of Sport and Exercise Sciences, University of Rome
“Tor Vergata”, Rome, Italy
CORRESPONDING AUTHORGiovanni Monteleone, MDUniversity of Rome “Tor Vergata”, Rome, Italy Via Montpellier n. 100133-Rome - ItalyPhone/fax: 0039-06-72596061E-mail: [email protected]

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 348
INTRODUCTIONThere is a high prevalence of cases of atrophy of the infraspinatus muscle of the hitting shoulder (30%) in athletes playing beach volleyball at the competi-tive level, arising from the damage to the suprascap-ular nerve.1 On the contrary, non-traumatic atrophy of deltoid muscle consequent to axillary neuropathy in overhead sports is a rare event.2
Some authors3 associate a compressive axillary nerve injury with the neuropathy of quadrilateral/quadran-gular space (or Velpeau space).4,5A space delimited superiorly by the inferior margin of the subscapularis, inferiorly by the superior margin of the teres major, medially by the external margins of the long head of the triceps, externally by the humerus surgical neck and the inferior portion of the glenohumeral joint.
The axillary nerve runs through the quadrilat-eral space together with the posterior circumflex humeral artery, and in its most common conforma-tion it innerves the anterior, middle and posterior deltoid with its anterior branch, and the teres minor and the lateral skin of the arm and the posterior deltoid with its posterior branch.6 Axillary nerve compression causes Quadrilateral space syndrome (QSS), which usually causes disabling, painful symp-toms causing the athlete to suspend any sport activ-ity for long periods.7 Duparc et al8 observed many anatomical variants of the axillary nerve related to different origins of collateral nervous branches, and this anatomical inconsistency may be a reason for frequent dissociation between sensitive and motor deficiency.
In the current case report series, the authors report two cases of deltoid muscle atrophy, caused by pain-less non-traumatic neuropathy of the axillary nerve, found while examining 91 professional and semi-professional beach volleyball players.
CASE 1A 49-year old player, who had been playing beach volleyball for over 15 years, presented a severe atrophy of the right deltoid (the hitting shoulder) (Figure 1). The athlete reported having noticed the localized loss of muscular volume approximately 12 years before, but had not considered the necessity to interrupt sport competition nor the necessity to have therapy because of the lack of shoulder pain.
At physical examination, rotator cuff tests, including the “hornblower’s” sign and the power of external rotation in 90° of abduction in the scapular plane exam for the teres minor,9 were negative. The Neer’s sign and the sulcus sign10,11 were also negative. Digi-tal pressure caused no pain at any point. A consider-able reduction of strength in forward flexion of the shoulder, grade 4 Medical Research Council (MRC) scale with slight resistance, was observed.
The results of electromyography (EMG) and electro-neurography (ENG) (Table 1) highlighted stabilized neurogenic damage of the right deltoid muscle; the Motor Unit Potential (MUP) were of increased aver-age amplitude and duration in the deltoid muscle, with reduced voluntary recruitment of an interme-diate/simple type. The compound Motor Action Potential (cMAP) of the right deltoid muscle for the stimulus of the axillary nerve at the point of Erb, showed symmetrical latency and amplitude in com-parison with the contralateral.
At the time of the evaluation, this athlete was among the top twenty players in the final phase of the Ital-ian championship.
CASE 2The second subject was a 26-year old female player, who had been playing competitive volleyball since
Figure 1. Subject 1: Clinical presentation at the examination.
Figure 2. Subject 2: Clinical presentation at the examination.
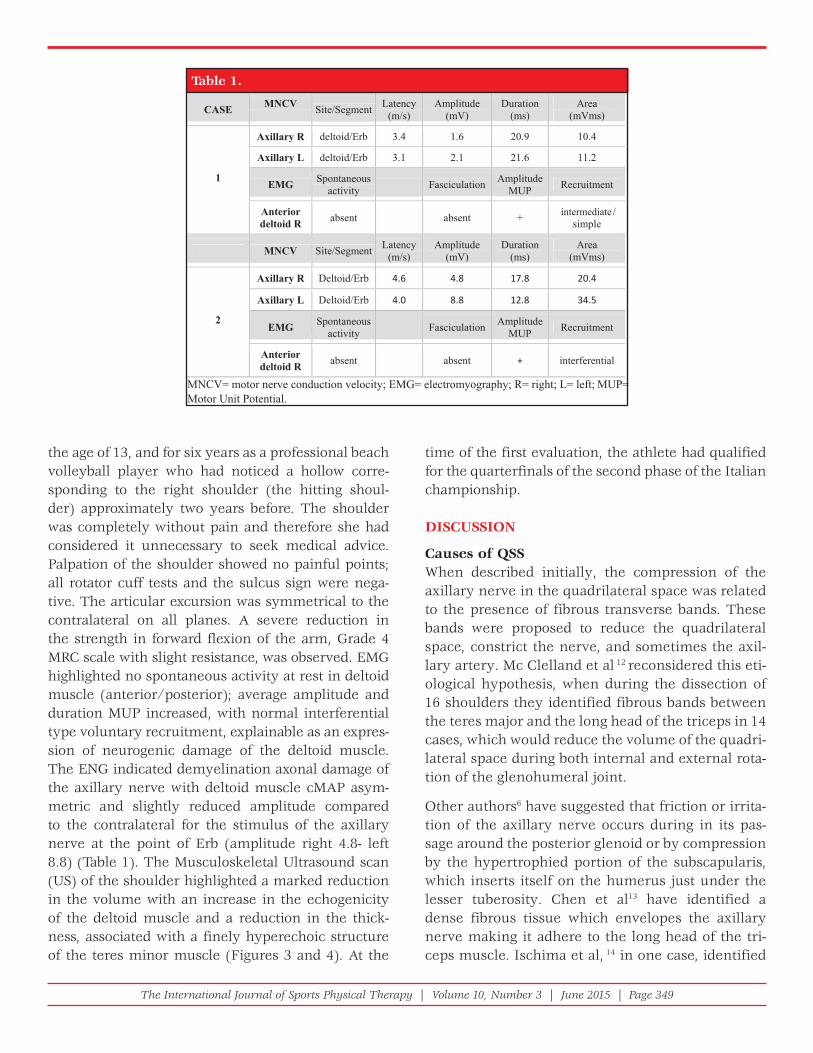
The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 349
the age of 13, and for six years as a professional beach volleyball player who had noticed a hollow corre-sponding to the right shoulder (the hitting shoul-der) approximately two years before. The shoulder was completely without pain and therefore she had considered it unnecessary to seek medical advice. Palpation of the shoulder showed no painful points; all rotator cuff tests and the sulcus sign were nega-tive. The articular excursion was symmetrical to the contralateral on all planes. A severe reduction in the strength in forward flexion of the arm, Grade 4 MRC scale with slight resistance, was observed. EMG highlighted no spontaneous activity at rest in deltoid muscle (anterior/posterior); average amplitude and duration MUP increased, with normal interferential type voluntary recruitment, explainable as an expres-sion of neurogenic damage of the deltoid muscle. The ENG indicated demyelination axonal damage of the axillary nerve with deltoid muscle cMAP asym-metric and slightly reduced amplitude compared to the contralateral for the stimulus of the axillary nerve at the point of Erb (amplitude right 4.8- left 8.8) (Table 1). The Musculoskeletal Ultrasound scan (US) of the shoulder highlighted a marked reduction in the volume with an increase in the echogenicity of the deltoid muscle and a reduction in the thick-ness, associated with a finely hyperechoic structure of the teres minor muscle (Figures 3 and 4). At the
time of the first evaluation, the athlete had qualified for the quarterfinals of the second phase of the Italian championship.
DISCUSSION
Causes of QSSWhen described initially, the compression of the axillary nerve in the quadrilateral space was related to the presence of fibrous transverse bands. These bands were proposed to reduce the quadrilateral space, constrict the nerve, and sometimes the axil-lary artery. Mc Clelland et al 12 reconsidered this eti-ological hypothesis, when during the dissection of 16 shoulders they identified fibrous bands between the teres major and the long head of the triceps in 14 cases, which would reduce the volume of the quadri-lateral space during both internal and external rota-tion of the glenohumeral joint.
Other authors6 have suggested that friction or irrita-tion of the axillary nerve occurs during in its pas-sage around the posterior glenoid or by compression by the hypertrophied portion of the subscapularis, which inserts itself on the humerus just under the lesser tuberosity. Chen et al13 have identified a dense fibrous tissue which envelopes the axillary nerve making it adhere to the long head of the tri-ceps muscle. Ischima et al, 14 in one case, identified
Table 1.
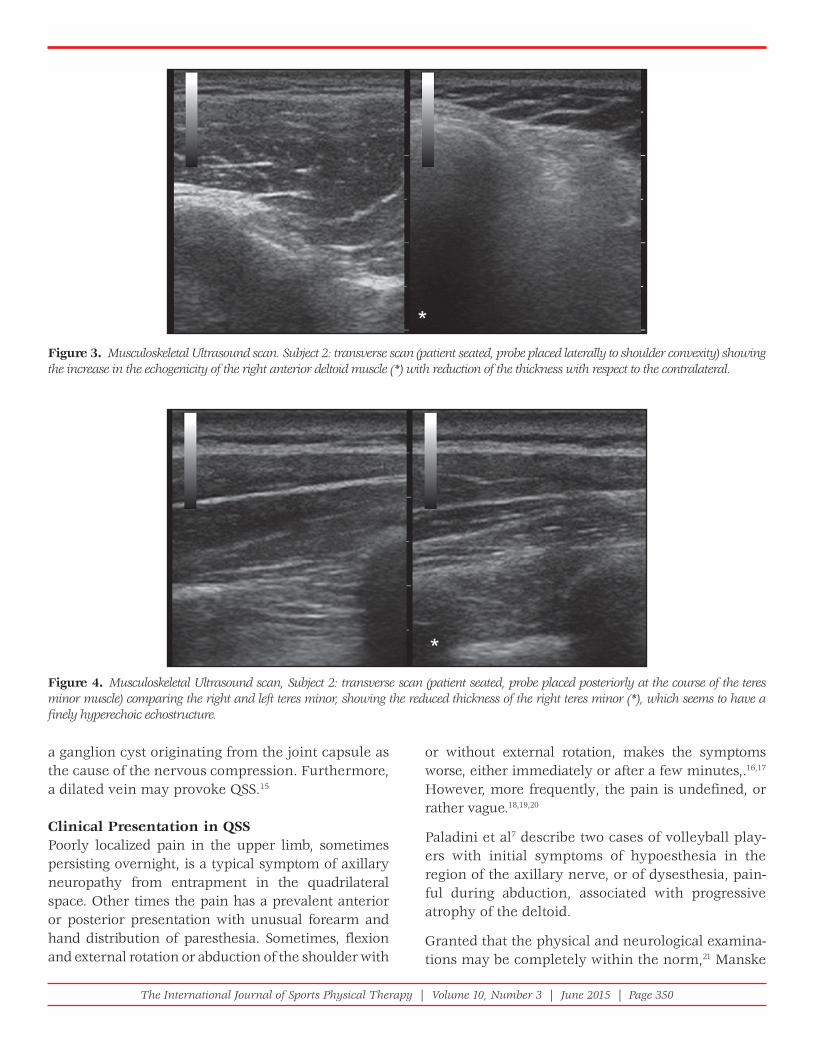
The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 350
a ganglion cyst originating from the joint capsule as the cause of the nervous compression. Furthermore, a dilated vein may provoke QSS.15
Clinical Presentation in QSSPoorly localized pain in the upper limb, sometimes persisting overnight, is a typical symptom of axillary neuropathy from entrapment in the quadrilateral space. Other times the pain has a prevalent anterior or posterior presentation with unusual forearm and hand distribution of paresthesia. Sometimes, flexion and external rotation or abduction of the shoulder with
or without external rotation, makes the symptoms worse, either immediately or after a few minutes,.16,17
However, more frequently, the pain is undefined, or rather vague.18,19,20
Paladini et al7 describe two cases of volleyball play-ers with initial symptoms of hypoesthesia in the region of the axillary nerve, or of dysesthesia, pain-ful during abduction, associated with progressive atrophy of the deltoid.
Granted that the physical and neurological examina-tions may be completely within the norm,21 Manske
Figure 3. Musculoskeletal Ultrasound scan. Subject 2: transverse scan (patient seated, probe placed laterally to shoulder convexity) showing the increase in the echogenicity of the right anterior deltoid muscle (*) with reduction of the thickness with respect to the contralateral.
Figure 4. Musculoskeletal Ultrasound scan, Subject 2: transverse scan (patient seated, probe placed posteriorly at the course of the teres minor muscle) comparing the right and left teres minor, showing the reduced thickness of the right teres minor (*), which seems to have a fi nely hyperechoic echostructure.

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 351
the teres minor which is examined using a nuclear magnetic resonance (NMR) scan, whether there is any alteration of the deltoid or not. Cothran et al26 state the extreme rarity of the isolated lesion of the teres minor, and in 2436 NMR examination scans of the shoulder, they identified 0.8% of the cases as atrophy or an abnormal sign of this muscle, attribut-able to QSS.
In a clinical case of QSS, Brestas et al27 observed lim-ited volume reduction and increased echogenicity of teres minor using Musculoskeletal US. Data was con-firmed by the EMG, NMR scan and by surgery. Simi-larly, the US scan described in case two highlighted a reduction in the volume and a finely hyperechoic structure of the teres minor.
Course of QSSThe course of the neuropathy does not always have the same characteristics and while surgical neuroly-sis is sometimes indispensable to treat a severe syn-drome, in other cases the painful symptomatology may cease after a period of rest and conservative treatment; in one case, the sportive arm movement was modified to decrease symptoms.17
Sometimes the dysfunction of the deltoid, even if only partial, causes a serious and non-tolerable loss of function of the shoulder, and therefore requires correction with a palliative surgical operation such as a tendinous transfer.28 According to Resch et al,29 the dysfunction of just the anterior portion may pre-clude any overhead activity, especially when this is associated with a damage to the rotator cuff. By acti-vating alternative biomechanical mechanisms, some subjects are able to raise their arm quite well despite the complete paralysis of the deltoid; 30 young ath-letes can compensate for the complete paralysis of the deltoid in their daily activities with limited disability.31
The subjects presented in these case reports demon-strated the athlete’s remarkable ability to compen-sate unconsciously for the serious deltoid atrophy, in order to maintain their competitive athletic per-formance. Therefore, axillary neuropathy in some athletes may represent a clinical event similar to that frequently occurring due to suprascapular nerve lesions. As reported by several authors, in the majority of cases, this neuropathy is asymptomatic
et al22 underlined the importance of examining for tenderness with digital pressure in the area corre-sponding to the quadrilateral space. In their clini-cal observation, baseball pitchers frequently have a thick band along the margin between the teres minor muscle and the infraspinatus muscle, which may be attributed to the hypertrophic connective tissue of the musculature of these athletes. Therefore, they report this thickening is frequently associated to QSS.
For QSS diagnosis McClelland et al12 suggest a pro-vocative test carried out by putting the arm to be examined in abduction at 90° and rotating it inter-nally and externally in order to attempt to reproduce the symptoms. Chautems et al,23 in one case report, reproduced the QSS with the Falconer maneuver. This test is performed asking the patient to retract and then depress the shoulder and to hold this posi-tion for one minute.
However, in all QSS cases reported in literature, there are descriptions of more or less disabling symptoms of which pain, and not atrophy of the deltoid muscle, is the predominant aspect in the array of symptoms: resulting in patients usually resorting to medical treat-ment and suspending sport activity for many months.
In the cases described herein, pain was completely absent in both subjects, however, the deltoid atrophy and the consequent reduction of strength in forward flexion of the shoulder were the only clear clinical manifestations of the axillary neuropathy.
Instrumental Diagnosis of QSSIn QSS, the electrodiagnostic exams are often com-pletely normal. Other times, the EMG and ENG identify damage to the axillary nerve of various seriousness with axonal involvement and/or long period persistent denervation.24 In order to confirm QSS diagnosis, some authors have suggested study-ing the posterior circumflex artery with angiography or NMR angiography in order to identify its oblit-eration when the limb is placed in abduction and extrarotation.3,20 Mochizuki et al25 however, have shown that, with the limb in this position, the occlu-sion of the posterior circumflex humeral artery is frequent even in completely asymptomatic patients.
Linker et al19 recognize an important diagnostic ele-ment of the syndrome with regard to the atrophy of

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 352
who participate in volleyball. The cases were identi-fied exclusively using physical examination of the shoulder and the athletes’ medical history, which was not selectively focused on the research of this neuropathy. The authors cannot exclude the possi-bility of finding a higher percentage of cases of silent or symptomatic axillary neuropathy in similar ath-letes in clinical epidemiological studies, considering that it is common for this type of athlete to compete despite pain or dysfunction that may be present in their shoulder.35
REFE RENCES 1. Lajtai G, Pfi rrmann C W A, Aitzetmüller G, et al. The
shoulders of professional beach volleyball players; high prevalence of infraspinatus muscle atrophy. Am J Sports Med. 2009; 37: 1375-82
2. Hoskins WT, Pollard HP, McDonald AJ. Quadrilateral space syndrome: a case study and review of the literature. Br J Sports Med. 2005; 39(2):e9
3. Cahill BR, Palmer RE. Quadrilateral space syndrome. J Hand Surg Am. 1983; 8: 65-9
4. Drez DJ Jr. Re: Surgical decompression of the quadrilateral space in overhead athletes. Am J Sports Med. 2008; 36: E8
5. Testut L, Laterjet A: Treaty of human anatomy. [Trattato di anatomia umana]. Trans. Bianchi L, (Original title: Traité d’anatomie humaine, 9e édition). Ed. Unione Tipografi co Editrice Torinese, Torino 1971, 4: 73-75
6. Safran MR. Nerve injury about the shoulder in athletes, part 1: suprascapular nerve and axillary nerve. Am J Sports Med. 2004; 32: 803-19
7. Paladini D, Dellantonio R, Cinti A, et al. Axillary neuropathy in volleyball players: report of two cases and literature review. J Neurol Neurosurg Psychiatry. 1996; 60: 345-7
8. Duparc F, Bocquet G, Simonet J, et al. Anatomical basis of the variable aspects of injuries of the axillary nerve (excluding the terminal branches in the deltoid muscle). Surg Radiol Anat. 1997; 19: 127-32
9. Walch G, Boulahia A, Calderone S, et al. The ‘dropping’ and ‘hornblower’s’ signs in evaluation of rotator-cuff tears. J Bone Joint Surg [Br]. 1998; 80-B: 624-8
10. Andrews J R, Wilk KE. The athlete’s shoulder. New York, Edimburgh, London. Madrid, Melbourne, Tokyo: Churchill Livingstone, 1994, 47-56
11. Clarnette RG, Miniaci A. Clinical exam of the shoulder. Med Sci Sports Exerc. 1998; 30 (4Suppl): S1-6
12. McClelland D, Paxinos A. The anatomy of the quadrilateral space with reference to quadrilateral
and causes no perception of any functional disabil-ity in athletes.32,33
This does not mean that the complete or partial loss of the deltoid muscle capacity can be ignored. Harm-ful effects on physical function of the limb may appear over a lifetime. For this reason, the medical and athletic staff who look after the players should pay particular attention to the earliest possible iden-tification of QSS.
Early Diagnosis and Treatment in Silent Deltoid AtrophyWith the absence of the standard symptomatologi-cal pattern, the suspicion of an axillary nerve injury may be due to a sudden reduction in the forward arm flexion ability or power; that may be perceptible but not considered disabling by the athlete. Meanwhile, medical and athletic staff should conduct a thorough examination, which can lead to proper diagnostic protocols that may include electrodiagnostic exam, and an NMR and/or US examination to evaluate the volume and structural changes present in the del-toid and teres minor muscles. US could be used even to monitor the pathology progression.34
Treatment must take into consideration the suspen-sion of sport activity and drug administration with physical therapy in order to support nerve and mus-cles regeneration. As reported by Steinmann et al, 30 in axillary injury surgical treatment may be considered if no evidence of recovery is noted on physical exami-nation or electrodiagnostic studies after a course of three months.
In volleyball disciplines, considering QSS multi form clinical expression, the authors cannot exclude the possibility that axillary neuropathy is more frequent than expected. Thus, considering the difficulty in making this diagnosis, QSS is often confused with other common pathologies of the shoulder and there-fore may be subject to incongruous treatment. 15
CONCLUSIONSThe two cases presented demonstrate the presence of deltoid atrophy in two of 91 competitive level beach volleyball athletes, representing a prevalence of 2.2% occurring from presumed neuropathy of the axillary nerve. This report presents the first epide-miological data related to this syndrome in athletes

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 353
with MR angiography in healthy volunteers and in a patient with quadrilateral space syndrome. AJR Am J Roentgenol. 1994; 163: 625-7
26. Cothran RL Jr1, Helms C. Quadrilateral space syndrome: incidence of imaging fi ndings in a population referred for MRI of the shoulder. AJR Am J Roentgenol. 2005; 184: 989-92
27. Brestas PS, Tsouroulas M, Nikolakopoulou Z, et al. Ultrasound fi ndings of teres minor denervation in suspected quadrilateral space syndrome. J Clin Ultrasound. 2006; 34: 343-7
28. Groh GI, Simoni M, Rolla P, et al. Loss of the deltoid after shoulder operations: An operative disaster. J Shoulder Elbow Surg. 1994; 3: 243-53
29. Resch H, Povacz P, Maurer H, et al. Pectoralis major inverse plasty for functional reconstruction in patients with anterolateral deltoid defi ciency. J Bone Joint Surg Br. 2008; 90: 757-63
30. Leffert RD: Neurologic problems, in Rockwood C A, Matsen III FA: The Shoulder 2nd Ed, 2 Volume. Philadelphia: WB Sounders, 1998, 982
31. Steinmann SP, Moran EA. Axillary nerve injury: diagnosis and treatment. J Am Acad Orthop Surg. 2001; 9: 328-35
32. Ferretti A, Cerullo G, Russo G. Suprascapular neuropathy in volleyball players. J Bone Joint Surg Am. 1987; 69: 260-3
33. Holzgraefe M, Kukowski B, Eggert S. Prevalence of latent and manifest suprascapular neuropathy in high level volleyball players. Br J Sports Med. 1994; 28: 177-179
34. Bailey LB, Beattie PF, Shanley E, et al. Current Rehabilitation Applications for Shoulder Ultrasound Imaging. J Orthop Sports Phys Ther. 2015 Jan 27:1-44. In press
35. Monteleone G, Tramontana A, Mc Donald K, Sorge R, et al. Ultrasonographic evaluation of the shoulder in elite italian beach volleyball players. J Sports Med Phys Fitness. 2014 May 27. In press
space syndrome. J Shoulder Elbow Surg. 2008; 17: 162-4
13. Chen D, Cai P, Lao G, et al. Quadrilateral space syndrome. Chin Med J (Engl). 1995; 108: 109-12
14. Ishima T, Usui M, Satoh E, et al. Quadrilateral space syndrome caused by a ganglion. J Shoulder Elbow Surg. 1998; 7: 80-2
15. McAdams TR, Dillingham MF. Surgical decompression of the quadrilateral space in overhead athletes. Am J Sports Med. 2008; 36: 528-32
16. Cormier PJ, Matalon TA, Wolin PM. Quadrilateral space syndrome: a rare cause of shoulder pain. Radiology. 1988; 167: 797-8
17. Redler MR, Ruland LJ 3rd, McCue FC 3rd. Quadrilateral space syndrome in a throwing athlete. Am J Sports Med. 1986; 14: 511-3
18. Duralde XA. Neurologic Injuries in the Athlete’s Shoulder. J Athl Train. 2000; 35: 316-28
19. Linker CS, Helms CA, Fritz RC: Quadrilateral space syndrome: fi ndings at MR imaging. Radiology. 1993; 188: 675-6
20. McKowen HC, Voorhies RM. Axillary nerve entrapment in the quadrilateral space. Case report. J Neurosurg. 1987; 66: 932-4
21. Baker CL Jr1, Liu SH. Neurovascular injuries to the shoulder. J Orthop Sports Phys Ther. 1993; 18: 360-4
22. Manske R C, Sumler A, Runge J: Quadrilateral Space Syndrome. ATT. 2009; 14: 45-47
23. Chautems RC, Glauser T, Waeber-Fey MC, et al. Quadrilateral space syndrome: case report and review of the literature. Ann Vasc Surg. 2000; 14: 673-6
24. Turker H, Sarica M, Bilgici A, et al. Axillary neuropathy mimicking quadrilateral space syndrome and its follow up for one year. Neurosciences (Riyadh). 2008; 13: 79-83
25. Mochizuki T, Isoda H, Masui T, et al. Occlusion of the posterior humeral circumfl ex artery: detection

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 354
ABSTRACTBackground and Purpose: Achilles tendinopathy is a common overuse injury sustained by athletes including run-ners. The use of noxious electrical stimulation for the treatment of chronic tendinopathies is a novel treatment inter-vention, which may alter pain perception and serve as adjunct technique in the recovery of painfree function. The purpose of this case report is to demonstrate the use of noxious electrical stimulation for the treatment of chronic, bilateral Achilles tendinopathy that was resistant to conservative treatment using plantarflexor eccentric exercise.
Case Description: A 27-year old male runner was referred to physical therapy with a 7-year history of bilateral Achil-les tendinopathy. He scored a 73/80 on the Lower Extremity Functional Scale (LEFS) and a 64% on the Victorian Institute of Sports Assessment-Achilles (VISA-A). Pain pressure threshold testing of the Achilles tendon was per-formed, followed by a single session of noxious electric stimulation to bilateral Achilles tendons, and the subject was instructed to continue with eccentric gastroc-soleus complex strengthening as previously performed.
Outcomes: Pain pressure threshold testing was performed to the mid-portion of the posterior Achilles tendon. The left Achilles tendon mean was 10.50kg and right Achilles tendon was 8.33kg prior to the noxious stimulation interven-tion. Twenty-four hours after the noxious stimulation treatment, improvements in mean pain threshold testing were found for both the left (16.31kg) and right (12.36kg) Achilles tendons. At one month after the physical therapy noxious stimulation session, the subject was able to progress his workouts to include sprints and interval training. His LEFS improved to 76/80 and his VISA-A improved to 96%.
Discussion: The case illustrates the successful pain reduction and return to progressive sports activity in a runner with chronic Achilles tendinopathy. The utilization of noxious electric stimulation may have altered the pain percep-tion of the nervous system as evidenced by the improvement in pain pressure threshold testing. Future studies on the application of noxious electric stimulation on chronic Achilles tendinopathy may help support the benefit of this intervention on pain and function.
Level of Evidence: Therapy, Level 4.
Keywords: Achilles tendinopathy, noxious electrical stimulation, pain, running
IJSP
TCASE REPORT
IMPROVED PRESSURE PAIN THRESHOLDS AND
FUNCTION FOLLOWING NOXIOUS ELECTRICAL
STIMULATION ON A RUNNER WITH CHRONIC
ACHILLES TENDINOPATHY: A CASE REPORT
Brian J. Eckenrode, PT, DPT, OCS1
Scott K. Stackhouse, PT, PhD1
1 Arcadia University, Department of Physical Therapy, Glenside, PA
For a single-subject case study, institutional IRB approval was not required. The authors certify that they have no affi liations with or fi nancial involvement in any organization or entity with a direct fi nancial interest in the subject matter or materials discussed in the article.
CORRESPONDING AUTHORBrian J. EckenrodeArcadia University450 S. Easton Road, Glenside, PA 19038E-mail: [email protected]

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 355
BACKGROUND AND PURPOSEAchilles tendinopathy is one of the more com-mon overuse injuries sustained by runners,1,2 with a reported approximate 52% lifetime incidence in recreational runners.3 Pain is localized to the mid-portion (2-6 cm proximal to the insertion) or inser-tion of the Achilles tendon.4 Symptoms are often provoked during tendon loading activities, which include running, jumping, walking uphill, or ascend-ing and descending stairs.5,6 No consensus on the eti-ology of Achilles tendinopathy exists. It is theorized to result from mechanical overuse with inflamma-tion during the acute stage6-8 and degeneration in the chronic stage.4,6 Aside from the physical damage to the tendon, there may be maladaptive changes to the nociceptive system that are part of the problem associated with chronic common wrist extensor9 and patellar tendinopathies.10,11 Maladaptive changes to the nociceptive system may also contribute to the symptoms of chronic Achilles tendinopathy.12,13
Current evidence and recommendations for the treatment of chronic Achilles tendinopathy supports the use of eccentric plantarflexor exercises, which has been shown to result in a clinically meaningful pain reduction and allow for return to activity when performed 2-3 times daily over several months;14-17 however recovery can be incomplete.18 A study by de Vos et al19 demonstrated Achilles tendon pain reduction prior to evidence of morphologic changes. Evidence also exists that the central substance of the Achilles tendon exhibits a low rate of collagen turn-over.20 Therefore, eccentric exercise may achieve a reduction in pain through changes in the local biochemical environment, or it may work to alter nociception through alternate pathways rather than through physical changes in tendon structure.
Electrical stimulation can affect nociception through segmental inhibition,21 descending central inhibi-tion,22,23 and several other neuromodulatory mecha-nisms.24-30 Transcutaneous electrical nerve stimulation (TENS), is a common modality used by rehabilitation clinicians and has been studied employing a variety of pulse frequencies, intensity-levels, and durations making it difficult to determine its effectiveness.31 The intensity level of TENS appears to mediate the analgesic response, with higher intensities result-ing in greater hypoalgesia in humans.32,33 Electrical
stimulation that is delivered at high intensities (just below motor threshold through pain threshold level stimulation) can reduce central sensitization in ani-mal models.34-36 In human studies of fibromyalgia and knee osteoarthritis, TENS can restore central inhibi-tion and increase pressure pain thresholds at the local treatment site and sites beyond,37,38 and may thus be useful in reversing some of the adaptations that the nervous system makes when confronted with chronic pain.
The purpose of this case report is to demonstrate the use of noxious electrical stimulation for the treat-ment of chronic, bilateral Achilles tendinopathy that was resistant to conservative treatment using plan-tarflexor eccentric exercise.
CASE DESCRIPTIONThe subject of this case report is a 27-year old male runner (height 1.8m, weight 65.8kg, BMI 20.8) who was referred to outpatient physical therapy by his sports medicine physician with a diagnosis of bilat-eral Achilles tendinopathy. He denied any significant medical history, was not taking any medications, and reported that he was in overall good health. The subject noted that his Achilles tendon pain began in college, and he continued to experience symptoms for the seven subsequent years. The subject was a former NCAA Division 1 collegiate runner compet-ing in both cross-country and distance track events. He reported running approximately 80 to 100 miles per week while in college, and had continued to run with bilateral Achilles tendon pain approximately 60-90 miles per week. The subject reported that the pain was consistent throughout his runs, and did not worsen unless he attempted to increase his pace faster than an 8.5 min/mile. His goal was to run pain-free and be able to increase the intensity of his training without pain symptoms. No Institutional Review Board approval was required for a single sub-ject case report. The subject granted approval for his participation in this study.
CLINICAL IMPRESSION #1Numerous conservative approaches were attempted in the past by the subject without resolution of his symptoms, including taking a full year off from all running activity, night splints, custom orthotics, and various modalities from his college athletic trainer

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 356
and previous physical therapists. He reported sev-eral courses of physical therapy in the past, includ-ing two months of eccentric exercise without any noticeable difference in his pain levels. The subject reported undergoing a prior Magnetic Resonance Imaging (MRI) which confirmed Achilles tendinopa-thy bilaterally. Given the subject’s MRI findings and failed conservative management, a thorough physi-cal therapy evaluation was performed to confirm the diagnosis and attempt to identify potential compen-satory impairments which may have contributed to this condition.
EXAMINATIONObjective data collected on the initial evaluation include pain at 8/10 on the numeric pain rating scale (NPRS) at worst (0/10 current) to bilateral Achilles tendons with running; right Achilles tendon pain equal to the left. He scored a 73/80 on the Lower Extremity Functional Scale (LEFS) and 64% on the Victorian Institute of Sports Assessment-Achilles (VISA-A). The NPRS has been shown to be a valid and reliable tool for assessing pain intensity,39-41 with a reported minimally clinical important difference (MCID) of between 1.7 points42 and 2 points43 for chronic musculoskeletal pain. The LEFS has been shown to have good reliability and validity with patients with lower extremity musculoskeletal prob-lems.44 This self-report questionnaire asks patients to rate their ability to perform 20 different activi-ties, with a score of 80 indicating maximal function. The minimum detectable change (MDC) and mini-mal clinically important difference (MCID) were both found to be 9 scale points for the LEFS.44 The VISA-A questionnaire has been shown to be a reli-able and valid disease-specific measure of function in patients with Achilles tendinopathy.45 This self-report measure consists of 8 questions that assess stiffness, pain, function, and sports training specific to Achilles dysfunction. The VISA-A is scored based on a percentage, with 100% indicating full pain-free function and sports. Based on reliability data pub-lished by Robinson and colleagues,45 the estimated MDC90% is 17.3 points.
The subject exhibited tenderness with palpation to bilateral Achilles tendons, approximately 3cm proxi-mal and 4cm proximal to the Achilles insertion on the calcaneus for the left and right ankles respec-
tively. A positive Arc sign was found to both Achil-les tendons.46 This test is performed by having the patient actively plantarflex and dorsiflex the ankle, and the examiner looks for movement of the visible area of swelling with the ankle motion in those with tendinopathy of the Achilles tendon.46 In addition, he presented with small painful nodules laterally along the painful portion of each Achilles tendon. A 0.5cm leg length discrepancy was measured from the anterior superior illiac spine to the medial mal-leous, with the right lower extremity being longer. The subject reported that this was previously iden-tified by prior practitioners and corrected for with both custom and over-the-counter orthotics.
Lumbar spine range of motion was full and pain-free with no deviations or aberrant movement patterns noted. SI joint provocative tests were negative and his lower quarter screen was unremarkable for any dermatomal or myotomal impairments. Neural ten-sion testing to the lower extremities was also unre-markable. In addition, there were no additional red flags through his medical history review.
The subject presented with decreased right ankle functional dorsiflexion ROM as measured in weight-bearing as described by Bennell et al47 with 14cm on the left and 11.5cm on the right. Bilateral ankle plantarflexion, inversion, and eversion ROM was within normal limits.48 Strength testing of the hips and knees was performed via hand-held dynamom-etry, but no major deficits were noted. Core strength was assessed through the double leg lowering test (65 degrees) and endurance with the side plank (60s right vs. 75s left). Flexibility and range of motion testing of bilateral lower extremities was with mini-mal to no restriction for the quadriceps, hip flexors, hamstrings, illiotibial band, and gluteal muscles. Strength testing of the ankle dorsiflexors, inverters, and everters demonstrated 5/5 manual muscle test grades and were painfree bilaterally. The subject was able to complete 20 single leg heel raises on each lower extremity, however these were accomplished with pain. He was limited to 4 single leg hops on each leg before the onset of the Achilles tendon pain symptoms (Table 1).
Pain pressure threshold (PPT) testing of bilateral Achilles tendons was performed to assess deep mechanical sensitivity. The subject was supine on a

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 357
treatment table, and a mobilization belt was placed around the metatarsal heads to stabilize the foot and bring the ankle joint into a neutral position of dor-siflexion (approximately 0 degrees via goniometric assessment) (Figure 1). A hand-held pressure algome-ter (Wagner; FDIX25) with a 1-cm2 in diameter rubber tip was used to apply increasing amounts of pressure (~1kg/sec) to the most painful portion of the Achilles tendon (previously noted). The distance from the cal-caneal attachment was measured so repeated testing could be performed at the same sites. Pressure was gradually applied with the algometer and the subject indicated when the pressure sensation first changed to pain, the pressure was immediately removed and the peak force recorded (done automatically by the algometer). The peak force from the trial was recorded by the clinician. The PPT test was performed two times on each Achilles tendon, with a minimum of 30-seconds of rest between bouts and the data were averaged (Table 1). Test-retest reliability for between day sessions for PPT of the Achilles is good (ICC(3,k) = 0.91) with the MDC90% CI of 2.05 kg.49
CLINICAL IMPRESSION #2The subject presented with minimal musculoskeletal impairments aside from his reported pain symptoms,
all while he continued participation in a high volume of running activity. Due to the multiple failed con-servative management attempts, the chronic nature of his Achilles symptoms, and the potential maladap-tive changes in the nociceptive system,12 the authors decided to incorporate a novel approach to address the pain aspect of this pathology in this runner by using noxious level electrical stimulation. On-going assessment would be performed as necessary based upon the response of the intervention and availabil-ity of the subject. Optimally, a reduction in subjective pain rating and improvement in outcome measures would be expected with a positive response to the electrical stimulation intervention.
INTERVENTIONDue to the chronic nature of the condition and lack of progress, a trial of noxious electrical stimulation to bilateral Achilles tendons was discussed with the sub-ject and implemented at the initial session. Noxious electrical stimulation was applied with the subject in the test position for PPT assessment with his ankles held in neutral. Self-adhesive electrodes were cut down to 1cm by 5cm and were placed on either side of the Achilles tendon to surround the site of maximal tenderness of each Achilles tendon. An Empi 300PV electrical stimulation unit (DJO Global, Vista, CA, USA) was utilized with the following parameters: 150 pulses per second; 2-second ramp-up time; 10-seconds on time: 10-seconds off time; 400-μs phase duration; 20-minute treatment duration. The electrical current was delivered at maximum tolerable intensity with instruction to maintain a “sharp, prickly” pain rating of 5-7/10 on the NPRS. The intensity was adjusted approximately every two minutes to maintain the 5-7/10 rating. Following the single noxious stimula-tion treatment, the subject refrained from activity for 24 hours and he returned the next day where the pain pressure threshold testing was repeated. No addi-tional treatment sessions were provided, due to the subject’s limited availability and travel schedule for work. The subject continued with his running pro-gram and an eccentric reloading program on his own.
Current evidence supports the use of eccentric exer-cise in the management of chronic Achilles ten-dinopathy.14-16 This exercise is described as being performed off a step with the eccentric phase per-formed by the involved lower extremity and the
Table 1. Improvement in Victorian Institute of Sports Assessment-Achilles (VISA-A) score over time
Baseline 1 month 2 months 9 months VISA-A Total 64% 96% 81% 94% Q5 Pain immediately after doing 10 single leg heel raises from a flat surface 5% (5/10)
10% (0/10) 10% (0/10) 9% (1/10)
Q6 Number of single leg hops without pain 4 10 6 8
Figure 1. Pain pressure threshold (PPT) testing set up.

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 358
he scored a 94% on the VISA-A, with an increased pace time with his running.
His LEFS score improved from a 73/80 to 74/80 over time, which is not significant but may be due to a ceiling effect of this outcome measure (Table 3). Self-reported pain rating via the NPRS was an 8/10 to bilateral Achilles tendons at worst prior to the intervention, which decreased to a 1/10 at worst at all testing sessions thereafter. Prior to the noxious electrical stimulation intervention, the subject was able to run, but only with sustained pain of 3-5/10. Any increase in running distance or intensity would increase his symptoms bilaterally. Post interven-tion, there was no Achilles pain with running at one and nine month follow-ups.
With running, the subject consistently ran approxi-mately 75 miles per week before and during the course of care (Table 4). However, he noted the inability to run faster than an 8.5 min/mile and had been unable to progress his workouts without exac-erbation of his symptoms. After the noxious electri-cal stimulation treatment, the subject reported no more than 1/10 pain to bilateral Achilles tendons
concentric phase performed only by the uninvolved side. Given that this subject had previously com-pleted the Achilles eccentric exercises in the past without success, he was encouraged to restart these. The author reviewed the performance of the eccen-tric exercises with the subject to ensure these were completed with correct form and dosage. Given the bilateral nature of these symptoms, the subject was instructed to complete this exercise bilaterally off a step. Recommended dosage was for the subject to perform 3 sets of 15 repetitions, two times per day.15 He was instructed to complete the eccentric phase over a five second time period, allow a two minute rest between sets, and to induce a pain level of no more than 2-3/10 in the Achilles tendon during the exercise. Once painfree during the bilateral eccen-trics, these exercises were progressed to unilateral eccentrics then unilateral eccentrics with a weighted backpack following the same dosage progression.
Follow-up testing sessions were completed at two months and nine months from the initial evaluation for a total of four sessions. Self-report outcome mea-sures were also collected at one month, but due to the subject’s work schedule he was unable to attend an onsite session for PPT.
OUTCOMESFollowing one treatment session of noxious electri-cal stimulation, the subject demonstrated Improve-ments in Achilles tendon PPT testing, pain levels, and function via the VISA-A, in addition to running progression gains (Tables 1-4). For PPT, the subject exhibited an increase in threshold for pain at 24-hours post noxious stimulation treatment to both Achilles tendons, with a sustained improvement seen at 9 months (Table 1). The increase in PPT at 24-hours exceeded the MDC90% CI of 2.05 kg.49 A small reduc-tion in PPT was observed between 24 hours and two months, which may be attributed to the increase in running intensity and pace during this time period as his tissues adapted to the new forces.
For the VISA-A, the subject scored a 64% at the ini-tial evaluation, then improved to 96% at one-month post intervention (Table 2). At his two-month follow-up, the subject scored an 81% on the VISA-A most likely due to the recent increase in his intensity and distance with running. At his nine month follow-up
Table 2. Improved Achilles tendon mean pain pressure threshold (PPT) measurements over timeAchilles Baseline 24 hours 2 months 9 months
Right (kg) 8.33 12.36 10.91 12.78
Left (kg) 10.5 16.31 10.96 14.9
Test-Retest Reliability Between Day49: ICC(3,k) = 0.91; MDC90% CI = 2.05 kg
Mean value 13.7 ± 4.9kg for PPT laboratory database mean in healthy controls49
Table 3. Lower Extremity Functional Scale over time Baseline 1 month 2 months 9 months LEFS Total Score 73/80 76/80 74/80 74/80 Q17 Running on uneven ground 3 3 2 3 Q18 Making sharp turns while running fast 2 3 3 3
Table 4. Subject progression of running Baseline 1 month 2 months 9 months Weekly Mileage 75mi/week 75mi/week 75mi/week 75mi/week Tempo Runs No No Yes Yes Track Work No No Yes Yes Mile Pace 8.5 min/mi 8.5 min/mi 8 min/mile 7 min/mile

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 359
chronic pain,9,54-56 and the authors have since gen-erated and presented evidence that central sensiti-zation also occurs in people with chronic Achilles tendinopathy (> 3 months duration).57 The authors of this case report hypothesize that noxious electri-cal stimulation reduced the mechanical responsive-ness of either the peripheral nociceptors or central neurons in the pain pathways as evidenced by the large change (> MDC90% CI) in pressure pain thresh-olds at 24-hours post-treatment. This is consistent with literature showing that high-frequency TENS can have both peripheral27 and central effects22,26,28 that can reduce pain sensitivity. Further research needs to address if signs of central sensitization are mitigated with treatment in people with Achilles tendinopathy.
For the VISA-A scores the subject demonstrated a significant improvement in function by one month via this self-report measure. The VISA-A is designed specifically for individuals with Achilles tendon pain, and features relevant questions on the ability to perform tasks and report on activities such as min-utes of Achilles stiffness in the morning, pain with heel raises, number of single leg hops without pain, and Achilles pain with sports. The subject exceeded the estimated MDC90% CI for the VISA-A at all testing time frames when compared with his initial score. He did experience a decrease from his initial post-treatment VISA-A score over the subsequent two months, which could be attributed to his increase in running activity (track workouts in spikes, tempo runs, and running pace).
While the subject’s mileage remained relatively unchanged, he was able to progress the intensity of his workouts over time. The authors did recommend that the subject reduce and or cease running for a period of time to allow for recovery according to tendinopathy treatment guidelines by Davenport et al.58 However, the subject was unwilling to back off from his running due to the fact that the last break from running provided no relief of his symptoms upon return to activity. He was comfortable with the current management of his pain through the maintenance of his current running routine without any changes in intensity or distance. This approach is supported by research from Silbernagel and col-leagues,18 who showed that Achilles tendon-loading
with running. He maintained this current training regimen during the first month, as he did not want to progress his running routine for fear of poten-tially redeveloping his pain. At two months post intervention, the subject was able to slowly increase his running pace to 8 min/mile without increased pain. He also noted the ability to add track work-outs and tempo runs, which he had been unable to progress to over the past several years. The sub-ject reported that his track workouts consisted of 6 to 12 400m runs at moderate to high intensity in track spikes. Tempo runs were approximately 20 to 30 minutes in length, designed to increase stamina through improvement of running rhythm meant to be performed at a “comfortably hard” pace. At his nine-month follow-up session, he continued to note no pain with his runs and that he was able to run a 7 min/mile pace consistently without symptoms bilat-erally. He also reported the ability to run a 4:14 mile, coming close to his personal record of a 4:04 mile as a collegiate runner. He was able to achieve one of his primary goals for physical therapy, which was to run close to his best college mile time for an upcom-ing reunion with his college cross-country and track teammates.
DISCUSSIONThis case illustrates the successful pain reduction and return to progressive sports activity in a run-ner with chronic bilateral Achilles tendinopathy. The utilization of noxious electrical stimulation may have decreased the sensitivity to mechanical stimuli as evidenced by the large increase in pain pressure thresholds at 24 hours post-treatment. The ability of noxious electrical stimulation to reduce pain sensi-tivity is supported by results from animal studies, which show that electrical stimulation delivered at an intensity that activated A-delta pain fibers, decreased dorsal horn neuron responsiveness.34,50,51 In humans, TENS delivered at painful intensities reduced somatosensory evoked cortical potentials and perceived pain,52 and in an osteoarthritis clini-cal trial, noxious intensity TENS (30% above pain threshold) produced a greater reduction in pain and stiffness after a treatment period (3x/wk for 4wks) than strong, comfortable level TENS.53 The pres-ence of central sensitization of pain has been shown to occur in other musculoskeletal conditions with
The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 360
8. Gao H, Fisher P, Lambi A, Wade C, Barr-Gillespie A. Increased serum and musculotendinous fi brogenic proteins following persistent low-grade infl ammation in a rat model of long-term upper extremity overuse. 8:e71875, 2013. PLOS One. 2013;8(8):e71875.
9. Fernandez-Carnero J, Fernandez-de-Las-Penas C, de la Llave-Rincon AI, Ge HY, Arendt-Nielsen L. Widespread mechanical pain hypersensitivity as sign of central sensitization in unilateral epicondylalgia: a blinded, controlled study. The Clinical journal of pain. 2009;25(7):555-561.
10. van Wilgen CP, Konopka KH, Keizer D, Zwerver J, Dekker R. Do patients with chronic patellar tendinopathy have an altered somatosensory profi le? A Quantitative Sensory Testing (QST) study. Scand J Med Sci Sports. 2013;23(2):149-155.
11. Lian Ø, Dahl J, Ackermann PW, Frihagen F, Engebretsen L, Bahr R. Pronociceptive and antinociceptive neuromediators in patellar tendinopathy. Am J Sports Med. 2006;34(11):1801-1808.
12. Rio E, Moseley L, Purdam C, et al. The pain of tendinopathy: physiological or pathophysiological? Sports Med. 2014;44(1):9-23.
13. Christensen J, Alfredson H, Andersson G. Protease-activated receptors in the Achilles tendon-a potential explanation for the excessive pain signalling in tendinopathy. Mol Pain. 2015;11(1):13.
14. Silbernagel KG, Thomeé R, Thomeé P, Karlsson J. Eccentric overload training for patients with chronic Achilles tendon pain--a randomised controlled study with reliability testing of the evaluation methods. Scand J Med Sci Sports. 2001;11(4):197-206.
15. Alfredson H, Pietila T, Jonsson P, Lorentzon R. Heavy-load eccentric calf muscle training for the treatment of chronic Achilles tendinosis. Am J Sports Med. 1998;26(3):360-366.
16. Carcia CR, Martin RL, Houck J, Wukich DK, Orthopaedic Section of the American Physical Therapy A. Achilles pain, stiffness, and muscle power defi cits: achilles tendinitis. J Orthop Sports Phys Ther. 2010;40(9):A1-26.
17. Kingma JJ, de Knikker R, Wittink HM, Takken T. Eccentric overload training in patients with chronic Achilles tendinopathy: a systematic review. British journal of sports medicine. 2007;41(6):e3.
18. Silbernagel KG, Thomee R, Eriksson BI, Karlsson J. Full symptomatic recovery does not ensure full recovery of muscle-tendon function in patients with Achilles tendinopathy. British journal of sports medicine. 2007;41(4):276-280; discussion 280.
19. de Vos RJ, Heijboer MP, Weinans H, Verhaar J AN, van Schie J TM. Tendon structure’s lack of relation
activity can be maintained during treatment of ten-dinopathy using a pain-monitoring model of activity.
CONCLUSIONSIn summary, the application of noxious electrical stimulation in a runner with chronic history of bilat-eral mid-portion Achilles tendinopathy resulted in a positive effect on pain level and activity where other conservative measures failed, including eccentric plantarflexor strengthening. Although the benefit of continued eccentric exercises may have contributed to the final outcome of this case, the incorporation of noxious electrical stimulation was a novel approach to pain management of this chronic injury. The authors hypothesize that noxious electrical stimulation may work to reduce pain in chronic tendinopathies via alter-ing central pain processing. Future directions include testing if central sensitization is present in individu-als with chronic Achilles tendinopathy and testing the effects of noxious electrical stimulation and eccentric exercise on pain processing in this pathology.
REFERENCES 1. Kujala UM, Sarna S, Kaprio J. Cumulative incidence
of achilles tendon rupture and tendinopathy in male former elite athletes. Clin J Sport Med. 2005;15(3):133-135.
2. Knobloch K, Yoon U, Vogt PM. Acute and overuse injuries correlated to hours of training in master running athletes. Foot Ankle Int. 2008;29(7):671-676.
3. Scott A, Huisman E, Khan K. Conservative treatment of chronic Achilles tendinopathy. CMAJ : Canadian Medical Association journal = journal de l’Association medicale canadienne. 2011;183(10):1159-1165.
4. Paavola M, Kannus P, Jarvinen TA, Khan K, Jozsa L, Jarvinen M. Achilles tendinopathy. J Bone Joint Surg Am. 2002;84-A(11):2062-2076.
5. Paavola M, Kannus P, Paakkala T, Pasanen M, Jarvinen M. Long-term prognosis of patients with achilles tendinopathy. An observational 8-year follow-up study. Am J Sports Med. 2000;28(5):634-642.
6. Abate M, Silbernagel KG, Siljeholm C, et al. Pathogenesis of tendinopathies: infl ammation or degeneration? Arthritis research & therapy. 2009;11(3):235.
7. Barbe MF, Gallagher S, Massicotte VS, Tytell M, Popoff SN, Barr-Gillespie AE. The interaction of force and repetition on musculoskeletal and neural tissue responses and sensorimotor behavior in a rat model of work-related musculoskeletal disorders. BMC Musculoskelet Disord. 2013;14:303.

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 361
in the spinal cord dorsal horn. Journal of neurochemistry. 2005;95(6):1794-1801.
31. Sluka KA, Bjordal JM, Marchand S, Rakel BA. What makes transcutaneous electrical nerve stimulation work? Making sense of the mixed results in the clinical literature. Phys Ther. 2013;93(10):1397-1402.
32. Moran F, Leonard T, Hawthorne S, et al. Hypoalgesia in response to transcutaneous electrical nerve stimulation (TENS) depends on stimulation intensity. The journal of pain : offi cial journal of the American Pain Society. 2011;12(8):929-935.
33. Pantaleao MA, Laurino MF, Gallego NL, et al. Adjusting pulse amplitude during transcutaneous electrical nerve stimulation (TENS) application produces greater hypoalgesia. The journal of pain : offi cial journal of the American Pain Society. 2011;12(5):581-590.
34. Liu XG, Morton CR, Azkue JJ, Zimmermann M, Sandkuhler J. Long-term depression of C-fi bre-evoked spinal fi eld potentials by stimulation of primary afferent A delta-fi bres in the adult rat. The European journal of neuroscience. 1998;10(10):3069-3075.
35. Ma YT, Sluka KA. Reduction in infl ammation-induced sensitization of dorsal horn neurons by transcutaneous electrical nerve stimulation in anesthetized rats. Experimental brain research. 2001;137(1):94-102.
36. DeSantana JM, Da Silva LF, De Resende MA, Sluka KA. Transcutaneous electrical nerve stimulation at both high and low frequencies activates ventrolateral periaqueductal grey to decrease mechanical hyperalgesia in arthritic rats. Neuroscience. 2009;163(4):1233-1241.
37. Dailey DL, Rakel BA, Vance CG, et al. Transcutaneous electrical nerve stimulation reduces pain, fatigue and hyperalgesia while restoring central inhibition in primary fi bromyalgia. Pain. 2013;154(11):2554-2562.
38. Vance CG, Rakel BA, Blodgett NP, et al. Effects of transcutaneous electrical nerve stimulation on pain, pain sensitivity, and function in people with knee osteoarthritis: a randomized controlled trial. Phys Ther. 2012;92(7):898-910.
39. Jensen MP, Karoly P, Braver S. The measurement of clinical pain intensity: a comparison of six methods. Pain. 1986;27(1):117-126.
40. Jensen MP, Turner JA, Romano JM. What is the maximum number of levels needed in pain intensity measurement? Pain. 1994;58(3):387-392.
41. Price DD, Bush FM, Long S, Harkins SW. A comparison of pain measurement characteristics of mechanical visual analogue and simple numerical rating scales. Pain. 1994;56(2):217-226.
to clinical outcome after eccentric exercises in chronic midportion Achilles tendinopathy. J Sport Rehabil. 2012;21(1):34-43.
20. Heinemeier KM, Schjerling P, Heinemeier J, Magnusson SP, Kjaer M. Lack of tissue renewal in human adult Achilles tendon is revealed by nuclear bomb (14)C. FASEB journal : offi cial publication of the Federation of American Societies for Experimental Biology. 2013;27(5):2074-2079.
21. Woolf C, Mitchell D, Barrett G. Antinocioceptive effect of peripheral segmental electrical stimulation in the rat. Pain. 1980;45:311-314.
22. Sluka KA, Christy MR, Peterson WL, Rudd SL, Troy SM. Reduction of pain-related behaviors with either cold or heat treatment in an animal model of acute arthritis. Archives of physical medicine and rehabilitation. 1999;80(3):313-317.
23. Kalra A, Urban MO, Sluka KA. Blockade of opioid receptors in rostral ventral medulla prevents antihyperalgesia produced by transcutaneous electrical nerve stimulation (TENS). The Journal of pharmacology and experimental therapeutics. 2001;298(1):257-263.
24. Han ZS, Gu GB, Sun CQ, Ju G. Convergence of somatosensory and baroreceptive inputs onto parabrachio-subfornical organ neurons in the rat: an electrophysiological study. Brain research. 1991;566(1-2):239-247.
25. Salar G, Job I, Mingrino S, Bosio A, Trabucchi M. Effect of transcutaneous electrotherapy on CSF beta-endorphin content in patients without pain problems. Pain. 1981;10(2):169-172.
26. Maeda Y, Lisi TL, Vance CG, Sluka KA. Release of GABA and activation of GABA(A) in the spinal cord mediates the effects of TENS in rats. Brain research. 2007;1136(1):43-50.
27. King EW, Audette K, Athman GA, Nguyen HO, Sluka KA, Fairbanks CA. Transcutaneous electrical nerve stimulation activates peripherally located alpha-2A adrenergic receptors. Pain. 2005;115(3):364-373.
28. Radhakrishnan R, Sluka KA. Deep tissue afferents, but not cutaneous afferents, mediate transcutaneous electrical nerve stimulation-Induced antihyperalgesia. The journal of pain : offi cial journal of the American Pain Society. 2005;6(10):673-680.
29. Rokugo T, Takeuchi T, Ito H. A histochemical study of substance P in the rat spinal cord: effect of transcutaneous electrical nerve stimulation. Journal of Nippon Medical School = Nippon Ika Daigaku zasshi. 2002;69(5):428-433.
30. Sluka KA, Vance CG, Lisi TL. High-frequency, but not low-frequency, transcutaneous electrical nerve stimulation reduces aspartate and glutamate release

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 362
51. Sjolund BH. Peripheral nerve stimulation suppression of C-fi ber-evoked fl exion refl ex in rats. Part 1: Parameters of continuous stimulation. Journal of neurosurgery. 1985;63(4):612-616.
52. Jung K, Rottmann S, Ellrich J. Long-term depression of spinal nociception and pain in man: infl uence of varying stimulation parameters. European journal of pain. 2009;13(2):161-170.
53. Defrin R, Ariel E, Peretz C. Segmental noxious versus innocuous electrical stimulation for chronic pain relief and the effect of fading sensation during treatment. Pain. 2005;115(1-2):152-160.
54. Gwilym SE, Oag HC, Tracey I, Carr AJ. Evidence that central sensitisation is present in patients with shoulder impingement syndrome and infl uences the outcome after surgery. J Bone Joint Surg Br. 2011;93(4):498-502.
55. Slater H, Arendt-Nielsen L, Wright A, Graven-Nielsen T. Sensory and motor effects of experimental muscle pain in patients with lateral epicondylalgia and controls with delayed onset muscle soreness. Pain. 2005;114(1-2):118-130.
56. Bajaj P, Bajaj P, Graven-Nielsen T, Arendt-Nielsen L. Osteoarthritis and its association with muscle hyperalgesia: an experimental controlled study. Pain. 2001;93(2):107-114.
57. Stackhouse S, Eckendrode B. Chronic Achilles tendinopathy is associated with signs of central sensitization. J Orthop Sports Phys Ther 2014;44(1):A21.
58. Davenport TE, Kulig K, Matharu Y, Blanco CE. The EdUReP model for nonsurgical management of tendinopathy. Phys Ther. 2005;85(10):1093-1103.
42. Farrar JT, Young JP, LaMoreaux L, Werth JL, Poole RM. Clinical importance of changes in chronic pain intensity measured on an 11-point numerical pain rating scale. Pain. 2001;94(2):149-158.
43. Salaffi F, Stancati A, Silvestri CA, Ciapetti A, Grassi W. Minimal clinically important changes in chronic musculoskeletal pain intensity measured on a numerical rating scale. European journal of pain. 2004;8(4):283-291.
44. Binkley JM, Stratford PW, Lott SA, Riddle DL. The Lower Extremity Functional Scale (LEFS): scale development, measurement properties, and clinical application. North American Orthopaedic Rehabilitation Research Network. Phys Ther. 1999;79(4):371-383.
45. Robinson JM, Cook JL, Purdam C, et al. The VISA-A questionnaire: a valid and reliable index of the clinical severity of Achilles tendinopathy. British journal of sports medicine. 2001;35(5):335-341.
46. Maffulli N, Kenward MG, Testa V, Capasso G, Regine R, King JB. Clinical diagnosis of Achilles tendinopathy with tendinosis. Clin J Sport Med. 2003;13(1):11-15.
47. Bennell KL, Talbot RC, Wajswelner H, Techovanich W, Kelly DH, Hall AJ. Intra-rater and inter-rater reliability of a weight-bearing lunge measure of ankle dorsifl exion. The Australian journal of physiotherapy. 1998;44(3):175-180.
48. Norkin C, White D. Measurement of Joint Motion: A Guide to Goniometry. Philadelphia, PA: F.A. Davis; 2003.
49. Stackhouse S, Carlin M, Fitzsimmons E, et al. Do Physical Therapy Interventions Affect Mechanical and Thermal Pain Processing Around The Healthy Achilles Tendon? J Orthop Sports Phys Ther. 2012;42(1):OPO3154.
50. Lee KH, Chung JM, Willis WD, Jr. Inhibition of primate spinothalamic tract cells by TENS. Journal of neurosurgery. 1985;62(2):276-287.

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 363
ABSTRACTBackground and Purpose: Posterior tibialis tendinopathy is a prevalent musculoskeletal condition often resulting in gait abnormalities along with medial ankle and foot pain. The purpose of this case report is to describe the treatment of a patient with a three year history of posterior tibialis tendinopathy utilizing a combination of cuboid manipulation and exercise.
Case Description: The patient was a 23-year old female recreational runner and collegiate basketball player reporting a three year history of chronic left ankle and lower leg pain. Outcome measures included the numeric pain rating scale, lower extremity functional scale, strength, passive joint mobility, and func-tional activities including running distance. Standard care for the treatment of tendinopathy was followed for six weeks with minimal functional improvements. Clinical reasoning skills were applied to redirect the hypothesis implicating limitations in cuboid-calcaneus internal rotation joint mobility contributing to a posterior tibialis tendinopathy. Manipulation at this joint was utilized to restore mobility. This intervention resulted in an immediate reduction in symptoms and improved functioning. Both muscle strengthening and functional task training were implemented post manipulation.
Outcomes: At discharge, the patient reported full recovery and no pain with running 14 miles. Her lower extremity functional score improved to 78/80, posterior tibialis strength increased to 4/5 and the patient was able to perform 12 single leg heel raises without pain.
Discussion: By restoring cuboid internal rotation mobility, associated midtarsal pronation, and lower extremity neuromuscular control, the posterior tibialis muscle was able to perform efficiently, thus resolv-ing the chronic tendinopathy and returning the patient to optimum functional ability of running.
Key Words: posterior tibialis tendon dysfunction, cuboid, manipulation, clinical reasoning.
Level of Evidence: 4
IJSP
TCASE REPORT
CUBOID MANIPULATION AND EXERCISE IN THE
MANAGEMENT OF POSTERIOR TIBIALIS
TENDINOPATHY: A CASE REPORT
Catherine Patla, PT, DHsc, OCS1
Janice Lwin, PT, DPT, OCS2
Laura Smith, PT, PhD, DPT, OCS3
Eric Chaconas, PT, DPT, CSCS1
1 University of St. Augustine for Health Sciences, St. Augustine, FL, USA
2 Kellaya Performance, San Diego, CA, USA 3 University of Michigan-Flint, Flint, MI, USA
CORRESPONDING AUTHOREric ChaconasUniversity of St. Augustine for Health Sciences1 University BlvdSt. Augustine, FL 32086E-mail: [email protected]: 904-826-0084

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 364
BACKGROUND AND PURPOSEPosterior tibialis tendinopathy is a prevalent muscu-loskeletal condition that includes a spectrum of tis-sue changes around the foot and ankle complex.1 The symptoms can vary and may include pain located on the medial lower leg, ankle, heel and medial foot.2,3 Common functional limitations include pain with pro-pulsion off the toes and abnormal gait due to pain.3,4 Posterior tibialis tendinopathy is referenced in the lit-erature with similar names including: posterior tibialis tendon dysfunction (PTTD), tibialis posterior tendon (TPT), or tibialis posterior myofascial tightness (TPMT). This manuscript will use the PTTD identifier.3,4
The reported etiology of PTTD varies from acute trauma to gradual onset micro-trauma including idio-pathic onset.3,4 Johnson & Strom5 initially described three distinct stages of posterior tibialis tendinopa-thy as Stage I with swelling, Stage II with a partial tear and Stage III identified as a complete tear. The three examination findings used to diagnose PTTD stage I include: swelling behind the malleoli, medial foot and ankle pain with single heel raise and pal-pable tenderness of the posterior tibialis tendon.5 Stage II is characterized by increased levels of func-tional limitation, inability to perform a single heel raise and a mid-foot pronation deformity.5 Stage III includes the above signs identified in Stage II and the hindfoot pronation deformity often becomes permanent.5 Advanced cases of Stage III PTTD can include lateral compression pain between the cal-caneous and distal fibula.5 Patla & Abbott3 further expanded this classification system to identify and describe a pre-stage I PTTD. Pre-stage I is devoid of tendon swelling although posterior tibialis muscle tightness, weakness, and functional activity limita-tions are present.3 It is proposed that Stages II and III may require surgical intervention while Stage I and pre-Stage I can be effectively treated with conser-vative management.5 Treatment varies dependent on the stage of injury healing and patient presenta-tion. Management in Stage I is primarily focused on the elimination of tendon swelling. Since swelling is absent with pre-Stage I PTTD, specific interventions to the posterior tibialis muscle addressing tightness and loss of strength may be the focus of treatment.
In addition to these interventions, manipulation of the mid-tarsal joints and ankle has been described
as an effective treatment for various lower leg condi-tions.6 Improvement in pain and function after joint manipulation to the foot has been described for vari-ous conditions including cuboid syndrome,7 iliotibial band friction syndrome,8 and plantar heel pain.9 A paucity of research exists relating joint manipulation to the foot and PTTD. The purpose of this case report is to describe the combination of cuboid-calcaneous joint manipulation and therapeutic exercise for a patient with a three year history of pre-Stage I PTTD.
CASE DESCRIPTIONThe patient was a 23-year old female collegiate basket-ball player and recreational runner who was informed that the data concerning her case would be submitted for publication. She had experienced a gradual onset of sharp pain over the medial lower leg and ankle that had persisted for three years. Aggravating factors included any activity increasing weight-bearing mid-tarsal pronation, especially walking without shoes and running. The patient was unable to ambulate with a normal gait due to pain. She reported the discomfort eventually became so intense that she walked on the outside of her foot to avoid pain. At the time of ini-tial examination, the patient was unable to run any distance due to 9/10 pain on the Numeric Pain Scale Rating (NPRS). The NPRS is a valid and reliable pain assessment tool that can be utilized in a variety of settings for musculoskeletal pain.10 The location of pain was on the medial lower leg and ankle within the first steps of running. Plain film radiographs were negative for fracture and ankle joint abnormalities. The patient denied a history of any similar injury on either extremity and she reported no other health problems. The patient failed an initial course of reha-bilitation with another healthcare provider which included cryotherapy, isotonic strengthening at the ankle and balance training. Despite ongoing symp-toms, the patient reported that she had continued to play collegiate basketball for a year beyond the initial onset of pain. Her pain worsened approximately two years after initial onset when she began running long distances. The patient provided her consent for use of her information for publication.
EXAMINATIONThe Lower Extremity Functional Scale (LEFS) is an 80-point patient reported functional outcome
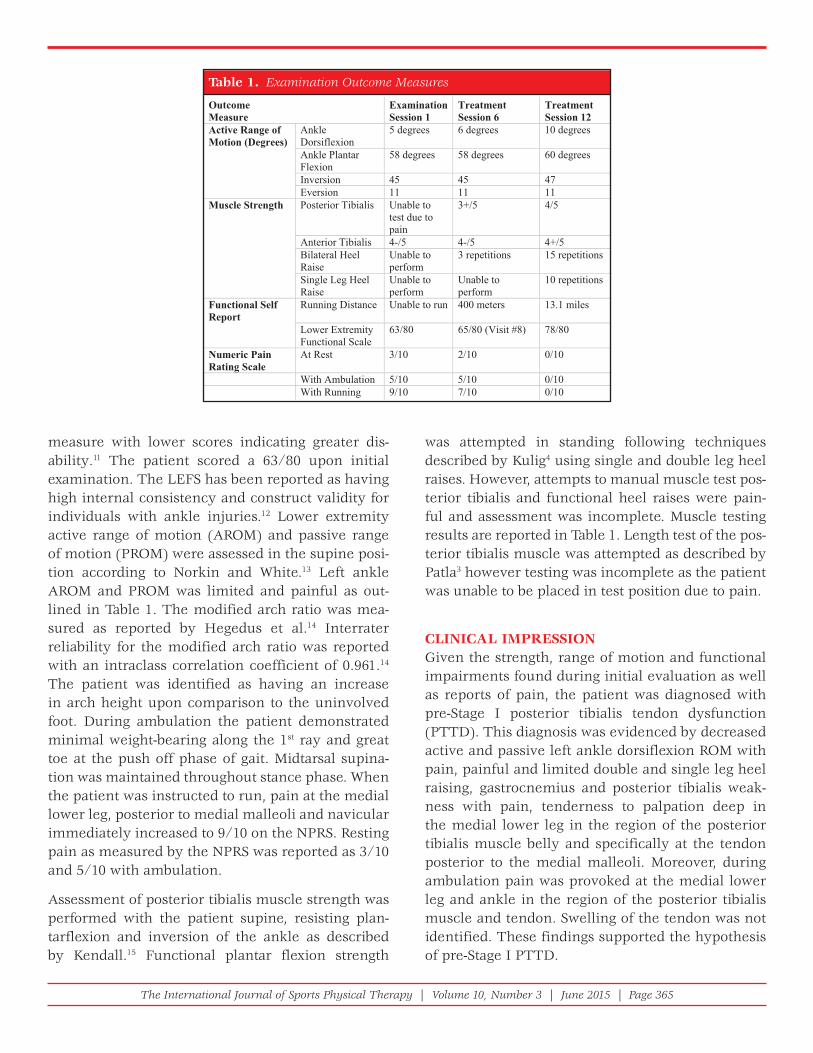
The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 365
measure with lower scores indicating greater dis-ability.11 The patient scored a 63/80 upon initial examination. The LEFS has been reported as having high internal consistency and construct validity for individuals with ankle injuries.12 Lower extremity active range of motion (AROM) and passive range of motion (PROM) were assessed in the supine posi-tion according to Norkin and White.13 Left ankle AROM and PROM was limited and painful as out-lined in Table 1. The modified arch ratio was mea-sured as reported by Hegedus et al.14 Interrater reliability for the modified arch ratio was reported with an intraclass correlation coefficient of 0.961.14 The patient was identified as having an increase in arch height upon comparison to the uninvolved foot. During ambulation the patient demonstrated minimal weight-bearing along the 1st ray and great toe at the push off phase of gait. Midtarsal supina-tion was maintained throughout stance phase. When the patient was instructed to run, pain at the medial lower leg, posterior to medial malleoli and navicular immediately increased to 9/10 on the NPRS. Resting pain as measured by the NPRS was reported as 3/10 and 5/10 with ambulation.
Assessment of posterior tibialis muscle strength was performed with the patient supine, resisting plan-tarflexion and inversion of the ankle as described by Kendall.15 Functional plantar flexion strength
was attempted in standing following techniques described by Kulig4 using single and double leg heel raises. However, attempts to manual muscle test pos-terior tibialis and functional heel raises were pain-ful and assessment was incomplete. Muscle testing results are reported in Table 1. Length test of the pos-terior tibialis muscle was attempted as described by Patla3 however testing was incomplete as the patient was unable to be placed in test position due to pain.
CLINICAL IMPRESSIONGiven the strength, range of motion and functional impairments found during initial evaluation as well as reports of pain, the patient was diagnosed with pre-Stage I posterior tibialis tendon dysfunction (PTTD). This diagnosis was evidenced by decreased active and passive left ankle dorsiflexion ROM with pain, painful and limited double and single leg heel raising, gastrocnemius and posterior tibialis weak-ness with pain, tenderness to palpation deep in the medial lower leg in the region of the posterior tibialis muscle belly and specifically at the tendon posterior to the medial malleoli. Moreover, during ambulation pain was provoked at the medial lower leg and ankle in the region of the posterior tibialis muscle and tendon. Swelling of the tendon was not identified. These findings supported the hypothesis of pre-Stage I PTTD.
Table 1. Examination Outcome Measures
OutcomeMeasure
Examination Session 1
TreatmentSession 6
TreatmentSession 12
Active Range of Motion (Degrees)
AnkleDorsiflexion
5 degrees 6 degrees 10 degrees
Ankle Plantar Flexion
58 degrees 58 degrees 60 degrees
Inversion 45 45 47 Eversion 11 11 11
Muscle Strength Posterior Tibialis Unable to test due to pain
3+/5 4/5
Anterior Tibialis 4-/5 4-/5 4+/5 Bilateral Heel Raise
Unable to perform
3 repetitions 15 repetitions
Single Leg Heel Raise
Unable to perform
Unable to perform
10 repetitions
Functional Self Report
Running Distance Unable to run 400 meters 13.1 miles
Lower Extremity Functional Scale
63/80 65/80 (Visit #8) 78/80
Numeric Pain Rating Scale
At Rest 3/10 2/10 0/10
With Ambulation 5/10 5/10 0/10 With Running 9/10 7/10 0/10
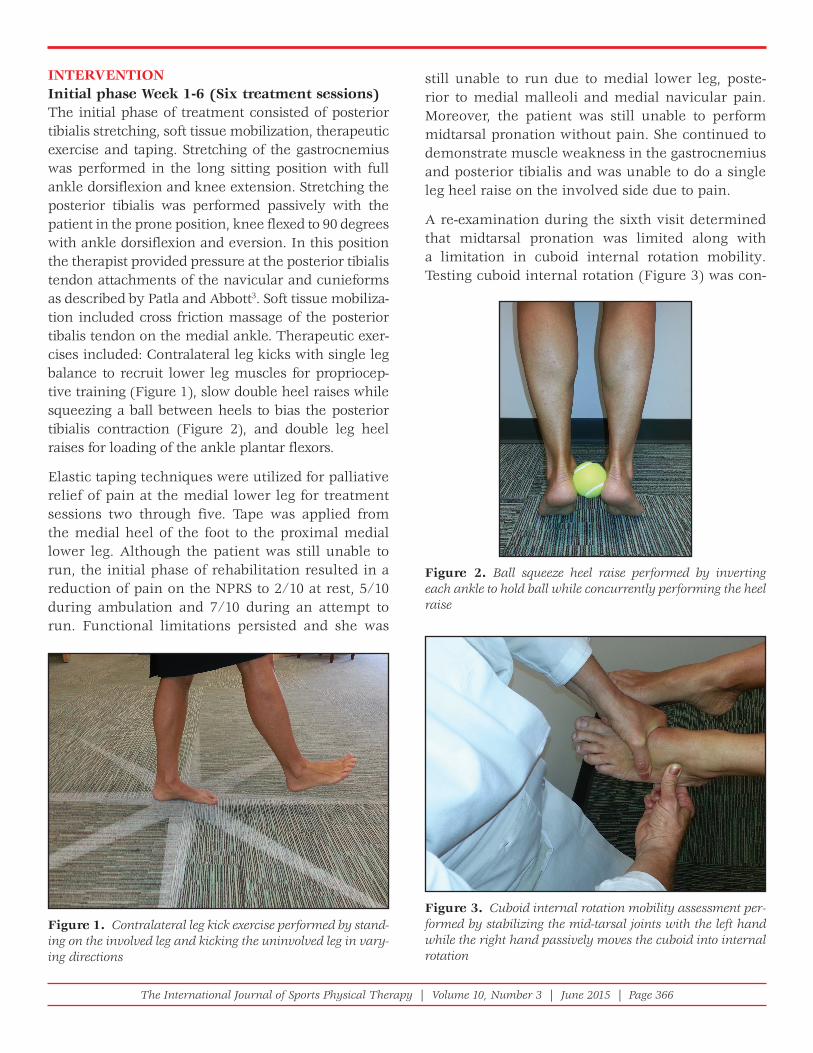
The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 366
INTERVENTIONInitial phase Week 1-6 (Six treatment sessions)The initial phase of treatment consisted of posterior tibialis stretching, soft tissue mobilization, therapeutic exercise and taping. Stretching of the gastrocnemius was performed in the long sitting position with full ankle dorsiflexion and knee extension. Stretching the posterior tibialis was performed passively with the patient in the prone position, knee flexed to 90 degrees with ankle dorsiflexion and eversion. In this position the therapist provided pressure at the posterior tibialis tendon attachments of the navicular and cunieforms as described by Patla and Abbott3. Soft tissue mobiliza-tion included cross friction massage of the posterior tibalis tendon on the medial ankle. Therapeutic exer-cises included: Contralateral leg kicks with single leg balance to recruit lower leg muscles for propriocep-tive training (Figure 1), slow double heel raises while squeezing a ball between heels to bias the posterior tibialis contraction (Figure 2), and double leg heel raises for loading of the ankle plantar flexors.
Elastic taping techniques were utilized for palliative relief of pain at the medial lower leg for treatment sessions two through five. Tape was applied from the medial heel of the foot to the proximal medial lower leg. Although the patient was still unable to run, the initial phase of rehabilitation resulted in a reduction of pain on the NPRS to 2/10 at rest, 5/10 during ambulation and 7/10 during an attempt to run. Functional limitations persisted and she was
still unable to run due to medial lower leg, poste-rior to medial malleoli and medial navicular pain. Moreover, the patient was still unable to perform midtarsal pronation without pain. She continued to demonstrate muscle weakness in the gastrocnemius and posterior tibialis and was unable to do a single leg heel raise on the involved side due to pain.
A re-examination during the sixth visit determined that midtarsal pronation was limited along with a limitation in cuboid internal rotation mobility. Testing cuboid internal rotation (Figure 3) was con-
Figure 1. Contralateral leg kick exercise performed by stand-ing on the involved leg and kicking the uninvolved leg in vary-ing directions
Figure 2. Ball squeeze heel raise performed by inverting each ankle to hold ball while concurrently performing the heel raise
Figure 3. Cuboid internal rotation mobility assessment per-formed by stabilizing the mid-tarsal joints with the left hand while the right hand passively moves the cuboid into internal rotation

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 367
ducted as described by Brandon and Patla.8 A disrup-tion in cuboid arthrokinematics has been described to be a part of cuboid syndrome and has been asso-ciated with foot and ankle pain.16 The impaired cuboid mobility resulted in an additional diagnosis of cuboid syndrome potentially contributing to pre-Stage I PTTD. Since cuboid internal rotation occurs with mid-tarsal pronation, a limitation in this motion may contribute to the lack of mid-tarsal pronation. As a result, a cuboid manipulation for internal rota-tion was indicated.
Week 7-17 (Six treatment sessions) The limitation of cuboid internal rotation was addressed with one treatment utilizing a cuboid whip manipulation technique (Figure 4) as described by Newell.17 Immediately following manipulation, pas-sive non-weight-bearing midtarsal pronation was full with a 0/10 NPRS score. Moreover, 20 repetitions of active mid-tarsal pronation in weight bearing was pain free. A novel exercise emphasizing the entire kinetic chain for lengthening the posterior tibialis was implemented (Figure 5). This exercise is per-formed in the standing position with the combined movements of active mid-tarsal pronation, rear foot eversion, tibial internal rotation and knee extension. This lengthening exercise for the posterior tibialis was added to the patient’s home exercise program. Immediately post treatment the patient was able to run 400 yards with a 0/10 NPRS score. Elastic taping
techniques were not used this session as the patient demonstrated significant functional pain relief after joint manipulation.
During follow up visit number eight the patient reported voluntarily increasing her running dis-tances resulting in an exacerbation of symptoms to a 6/10 on the NPRS. Soft tissue mobilization and manual stretching were performed for the posterior tibialis and gastrocnemius as described earlier. Upon re-assessment the cuboid internal rotation mobility remained symmetrical as well as passive midtarsal pronation. The patient continued active pain free weight-bearing muscular re-education movement exercises (Figure 5) to encourage midtarsal prona-tion in addition to previously assigned exercises as part of the home program. Although the patient had a reduction in symptoms and reports of pain during ambulation and activities with and without the use of elastic tape, she requested continued use of tap-ing techniques. However, to minimize unnecessary treatments, the patient was educated on the likely placebo effect of interventions and agreed to discon-tinue elastic taping techniques and focus efforts on
Figure 4. Cuboid whip manipulation performed with the patient in prone and the operator utilizing both hands to deliver a high velocity low amplitude internal rotation force through the cuboid-calcaneus joint
Figure 5. Weight bearing pronation exercise while actively assuming knee extension and lower leg internal rotation in the standing position creates pronation of the rear and mid-foot to lengthen the posterior tibialis in a weight bearing position

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 368
the home exercise program. Strength improvements are reported in Table 1. LEFS improved to a 65/80.
During visit number nine the patient presented with only slight 1/10 discomfort at rest and with ambula-tion on the NPRS at the medial navicular. Remain-ing limitations included limited arch ratio without pain, inability to perform more than four single heel raises and 2/10 pain during running. Soft tis-sue mobilization, the cuboid whip, posterior tibialis stretching and the home exercise program were con-tinued for three visits in order to maintain mobility. Pain and tenderness to palpation along the lower leg and medial malleoli was resolved. LEFS revealed a score of 69/80.
OUTCOMEThe patient was seen for 12 visits over 28 weeks. During the final session the patient reported a 0/10 NPRS score at rest, with ambulation and while run-ning 13.1 miles. Push off during gait was pain free along with a normalized arch ratio and 10 single leg heel raises. The LEFS score decreased to 78/80 resulting in an overall improvement of 15 points. The patient exceeded the nine point reported mini-mal detectable change for the LEFS as determined in prior studies.18
DISCUSSIONThis case report highlights several important aspects of clinical reasoning contributing to the successful outcomes for this patient. Although examination of this patient’s symptoms suggested a diagnosis of pre-Stage I PTTD, an uncommon impairment of limita-tions in cuboid joint mobility may have contributed to this patient’s PTTD. Re-assessment of impair-
ments during the course of treatment was crucial in achieving successful outcomes. The importance of monitoring functional progress and re-evaluating impairments to achieve the goal of full pain free patient activity was described.
This patient demonstrated signs and symptoms consistent with pre-Stage I chronic posterior tibi-alis tendon dysfunction. Posterior tibialis tendon dysfunction is often accompanied by increased mid-tarsal pronation which causes a lengthening of the posterior tibialis with weight-bearing activities leading to irritation and pain.3,5 Prior investigations have reported optimal outcomes with the combina-tion of orthoses wear and exercise to diminish the midtarsal overpronation.4 However, the uncommon finding in this case report was a lack of midtarsal pronation due to a limitation of cuboid internal rotation.8 It is important that clinicians assess joint mobility because clinically it is more common for a midtarsal hypermobility to be present.19 During weight-bearing activities, this patient was unable to functionally utilize midtarsal pronation due to a lack of cuboid internal rotation joint mobility. The authors theorized that the limitation of this joint mobility resulted in the inability for the posterior tibialis to function effectively and hence PTTD “pre-Stage I” condition ensued.
Although the patient was appropriately treated for PTTD “pre-Stage I” for the first five visits, functional gains were minimal. The reflective practice of the physical therapist in recognizing minimal gains after six weeks and re-assessing impairments after the fifth visit was instrumental in identifying an additional treatment approach. The use of clinical reasoning skills is based on two guiding principles
Table 2. Home Exercise Program Progression
Exercise Early Phase (Week 1-6)
Middle Phase (Week 7-16)
Late Phase (Week 17-19)
Single leg stance with clock kicks
15 sec x 3 rep 20 sec x 3 rep 20 sec x 4 rep
Heel raises with ball squeeze
2 sets x 10 rep 3 sets x 10 rep 3 sets x 15 rep
Weight bearing mid-tarsal supination/pronation
2 sets x 20 rep 2 sets x 30 rep 2 sets x 40 rep
Double heel raise up with single lowering
Not performed 15 rep 2 sets x 15 rep
Abbreviations: Seconds (sec) Repetitions (rep)

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 369
proposed in this case report. These are: (1) mobil-ity is needed for full function of the muscle and (2) full length is needed of the muscle to gain functional strength. The presence of the long-standing painful dysfunction was likely perpetuated as the muscle/ tendon was unable to function normally due to a lack of mobility at the midtarsal joint. Once midtar-sal pronation mobility was restored, strength deficits were addressed and full function could be achieved.
Although soft tissue mobilization, stretching and taping techniques provided some pain relief during the course of treatment, cuboid manipulation was the most significant treatment factor resulting in the greatest level of immediate pain reduction and improved ability to run. The dramatic improvement in pain free running following a cuboid manipula-tion could be related to several mechanisms. The traditional mechanism lends merit to the hypothesis that the cuboid mobility impairment is restored after the manipulation resulting in improved mechanics for the posterior tibialis. Another mechanism could be that a reverse neurological sensitization occurs post cuboid manipulation as a result of neurophysi-ological effects.20
This case report also provides evidence of the value of the physical therapist’s individualized home exercise program and long-term supervision. The physical therapist selectively chose supportive home exercises with rigid activity parameters. The exercise of lengthening the posterior tibialis while standing provided a stretching intervention to the impaired muscle tissue while simultaneously facili-tating the mid-foot pronation movement. The the-ory supporting this weight bearing exercise is that muscle lengthening can occur in a manner specific to the posterior tibialis function. Moreover, when the patient was prescribed these movement re-education exercises very strict activity limitations were imposed for running. Patient independence with management of this chronic condition was emphasized. During the six-week break, the patient remained in communication with the physical ther-apist regarding home exercises and running param-eters to ensure progress was maintained. While a six week break in a traditional physical therapist plan of care is uncommon, this case report demonstrates the value in consistent physical therapist/ patient
communication and independent patient manage-ment through a well-defined home exercise program to decrease symptoms in patients who experience pain or limitation from chronic conditions.
Several limitations to this case report exist. Utilizing the LEFS may not have been the most specific self-report measure for this patient. A region specific outcome measure such as the foot function index could be more sensitive to change in individuals experiencing medial ankle and foot pain.21 Another limitation is the lack of a valid and reliable test for cuboid mobility assessment.16 While mobility of the cuboid is commonly assessed in clinical practice fur-ther research is needed to establish the diagnostic accuracy of this examination test.
CONCLUSIONIn conclusion, standard physical therapist practice should include reflective decision-making and altera-tions of intervention selection when outcomes are not favorable. This case report identifies the impor-tance of looking beyond common factors contributing to a dysfunction as well as the significance of re-eval-uation of impairments when functional gain is mini-mal. By following these aspects of clinical reasoning, this patient was able to progress from an inability to run without pain to running over 13 miles pain free.
REFERENCES 1. Geideman WM, Johnson JE. Posterior tibial tendon
dysfunction. J Orthop Sports Phys Ther. 2000;30(2):68-77.
2. Durrant B, Chockalingam N, Hashmi F. Posterior tibial tendon dysfunction: a review. J Am Podiatr Med Assoc. 2011;101(2):176-186.
3. Patla CE, Abbott JH. Tibialis posterior myofascial tightness as a source of heel pain: diagnosis and treatment. J Orthop Sports Phys Ther. 2000;30(10):624-632.
4. Kulig K, Reischl SF, Pomrantz AB, Burnfi eld JM, Mais-Requejo S, Thordarson DB, Smith RW. Nonsurgical management of posterior tibial tendon dysfunction with orthoses and resistive exercise: a randomized controlled trial. Phys Ther. 2009;89(1):26-37.
5. Johnson KA, Strom DE. Tibialis posterior tendon dysfunction. Clin Orthop Relat Res. 1989(239):196-206.
6. Dananberg HJ. Manipulation of the ankle as a method of treatment for ankle and foot pain. J Am Podiatr Med Assoc. 2004;94(4):395-399.

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 370
7. Jennings J, Davies GJ. Treatment of cuboid syndrome secondary to lateral ankle sprains: a case series. J Orthop Sports Phys Ther. 2005;35(7):409-415.
8. Brandon K, Patla C. Differential diagnosis and treatment of iliotibial band pain secondary to a hypomobile cuboid in a 24-year-old female tri-athlete. J Man Manip Ther. 2013;21(3):142-147.
9. Cleland JA, Abbott JH, Kidd MO, Stockwell S, Cheney S, Gerrard DF, Flynn TW. Manual physical therapy and exercise versus electrophysical agents and exercise in the management of plantar heel pain: a multicenter randomized clinical trial. J Orthop Sports Phys Ther. 2009;39(8):573-585.
10. Hjermstad MJ, Fayers PM, Haugen DF, Caraceni A, Hanks GW, Loge JH, et al. Studies comparing Numerical Rating Scales, Verbal Rating Scales, and Visual Analogue Scales for assessment of pain intensity in adults: a systematic literature review. J Pain Symptom Manag. 2011;41(6):1073-1093.
11. Binkley JM, Stratford PW, Lott SA, Riddle DL. The Lower Extremity Functional Scale (LEFS): scale development, measurement properties, and clinical application. Phys Ther.1999;79(4):371-383.
12. Lin CW, Moseley AM, Refshauge KM, Bundy AC. The lower extremity functional scale has good clinimetric properties in people with ankle fracture. Phys Ther. 2009;89(6):580-588.
13. Norkin CC, White DJ. Measurement of joint motion: a guide to goniometry: FA Davis; 2009.
14. Hegedus EJ, Cook C, Fiander C, Wright A. Measures of arch height and their relationship to pain and dysfunction in people with lower limb impairments. Physiother Res International. 2010;15(3):160-166.
15. Kendall FP ME, Provance P, Rodgers M, Romanill W. Muscles: Testing and Function with Posture and Pain. 5th ed. Hagerstown, MD: Lippincott Williams and Wilkins; 2005.
16. Durall CJ. Examination and treatment of cuboid syndrome: a literature review. Sports Health. 2011;3(6):514-519.
17. Newell SG WA. Cuboid syndrome. Phys Sports Med. 1981;9(4):71-76.
18. Shultz S, Olszewski A, Ramsey O, Schmitz M, Wyatt V, Cook C. A systematic review of outcome tools used to measure lower leg conditions. Int J Sports Phys Ther. 2013;8(6):838-848.
19. Remvig L, Jensen DV, Ward RC. Epidemiology of general joint hypermobility and basis for the proposed criteria for benign joint hypermobility syndrome: review of the literature. J Rheumatol. 2007;34(4):804-809.
20. Matthews ML, Claus AP. Two examples of ‘cuboid syndrome’ with active bone pathology: why did manual therapy help? Man Ther. 2014;19(5):494-498.
21. Budiman-Mak E, Conrad KJ, Roach KE. The Foot Function Index: a measure of foot pain and disability. J Clin Epidemiol. 1991;44(6):561-570.

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 371
ABSTRACTBackground and Purpose: Hamstring tightness is a common complaint among active individuals and patients are traditionally classified with tight hamstrings based on commonly accepted clinical exams including the active knee extension, active straight leg raise, and passive straight leg raise tests. Apparent hamstring tightness is a condition that is present in patients who have the perception of hamstring tightness and are classified with a tissue extensibility dysfunction but demonstrate immediate gains in hamstring range of motion following an intervention that does not address a tissue length dysfunction. Reactive neuromuscular training can be used as part of the evaluative process used to classify and treat patients with apparent hamstring tightness. The purpose of this case report was to identify, treat, and report the outcomes experienced when using a reactive neuromuscular training technique on a patient who was classified with hamstring inflexibility based on traditional testing methods.
Case Description: A 20 year-old female softball player presented with a chief complaint of hamstring tightness of more than four years duration. The patient tested positive for hamstring inflexibility based on traditional testing methods. The patient was then treated using a reactive neuromuscular training technique in which the patient resisted a manual anterior to posterior force at the abdomen, sternum and across the hips while simultaneously bend-ing forward at the hips in an attempt to touch her toes.
Outcomes: Following one reactive neuromuscular training treatment session the patient tested negative for ham-string inflexibility based on traditional testing methods and maintained those results at a five-week follow-up appointment.
Discussion: The subject in this case report demonstrated the effectiveness of reactive neuromuscular training in identifying and treating apparent hamstring tightness. Based on these findings, clinicians should consider using reac-tive neuromuscular training to properly classify and treat patients with a chief complaint of hamstring “tightness.”
Level of Evidence: 4 (single case report)
Keywords: Apparent hamstring tightness, patient classification, treatment based classification
IJSP
TCASE REPORT
REACTIVE NEUROMUSCULAR TRAINING RESULTS IN
IMMEDIATE AND LONG TERM IMPROVEMENTS IN
MEASURES OF HAMSTRING FLEXIBILITY: A CASE
REPORT
Rick A. Loutsch, MS, ATC1
Russell T. Baker, DAT, AT2
James M. May, DAT, AT2
Alan M. Nasypany, EdD, AT2
1 Northwestern College, Orange City, IA, USA2 University of Idaho, Moscow, ID, USA
CORRESPONDING AUTHORRick Loutsch, MS, ATCAthletic Training Clinical Coordinator, Northwester College 208 8th St. SWOrange City, IA 51041E-mail: [email protected] ce: 712-707-7319Fax: 712-707-7305

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 372
BACKGROUND AND PURPOSEHamstring tightness is a common complaint among active individuals.1 In the clinical setting, patients who present with limited range of motion (ROM) on the active knee extension (AKE), passive straight leg raise (PSLR), and active straight leg raise (ASLR) tests are commonly classified with tight hamstrings and treated with traditional stretching techniques.2–5 Stretching activities are commonly used in health-care to improve joint ROM,6–10 and the American College of Sports Medicine recommends routine flexibility exercises to maintain and improve joint ROM.11 The current literature on the most effective methods to improve ROM via stretching is inconsis-tent,7 and recent evidence suggests increases in ROM following a stretching program may not be due to increases in tissue length, but rather, are caused by an increase in stretch tolerance.12–14 In addition, there is evidence to suggest that some types of stretching may negatively impact muscle strength and power under specified stretching parameters.15–17 Given the proposed effects of stretching and the current method of classifying hamstring tightness, clinicians must ensure the cause of the apparent “tightness” warrants the application of stretching interventions prior to recommending any stretching program.
Apparent hamstring tightness is a provisional clas-sification for those patients who have been identi-fied as having hamstring tightness using traditional measures (e.g., AKE, PSLR). The importance of a provisional classification of apparent hamstring tightness is that testing may lead to a more defini-tive classification of tissue extensibility dysfunction (TED), which is a dysfunction in the length or exten-sibility of multi-articular soft tissue structures (i.e., muscle, fascia, nervous tissue) identified through the Selective Functional Movement Assessment (SFMA).4 However, recent clinical practice findings demonstrate that these apparent hamstring tight-ness or TEDs (based on special test findings) can often be resolved in a single treatment session that does not directly involve lengthening structures. If one follows the current accepted classification path-way based on exam findings (i.e., hamstring tight-ness or TED), then this classification would lead the clinician to a local treatment (e.g., stretching, instrument assisted soft tissue mobilization) which may or may not resolve the “tightness.” The prob-
lem with assuming local tightness or TED, is that the clinician may wrongly lengthen a normal tis-sue (e.g. hamstrings), when the results (e.g., nega-tive special tests) may be gained by using non-local, non-structural lengthening techniques. An alternate hypothesis is that the apparent tightness may be a low level contraction of some fibers of a muscle (e.g., non-local stability motor control dysfunction, trigger point), which presents with similar symp-toms of a TED during a traditional clinical exam. In many cases, non-traditional treatment options, such as a stability motor control intervention (e.g., reac-tive neuromuscular training) at a proximal or distal segment, a regional interdependence approach (e.g., Total Motion Release18), or slacking the local tissue instead of stretching it (e.g., positional release ther-apy19), will immediately resolve the apparent tissue tightness.
One proposed method to differentially diagnose a true TED from apparent hamstring tightness is to use a treatment based classification (TBC) system to classify patients prior to treatment. One potential component of a TBC system for hamstring tightness is reactive neuromuscular training (RNT). The term RNT was first introduced by Voight and Cook20 and is utilized to restore functional stability about the joint and enhance motor control skills. Individualized RNT techniques are thought to correct motor pat-tern dysfunctions by applying a light external load to exaggerate the dysfunctional movement and cause the patient to reactively correct the subconscious dysfunctional movement pattern.4 Current literature on the use of RNT is lacking, but the results of one case report suggested that a rehabilitation program utilizing RNT that consisted of exercises that focused on promoting proper body positioning and posture by having the patient react to an outside force (e.g., elastic tubing) that promoted an unwanted move-ment pattern quickly improved apparent strength deficits in a patient with an anterior cruciate liga-ment deficient knee.21
It is hypothesized that patients who present with hamstring tightness may be experiencing a dysfunc-tional motor control pattern in which the normal firing pattern of the postural (i.e., static) muscles is delayed or sub-optimal causing the hamstring muscle group to function as a stabilizer versus their

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 373
normal function as a prime mover. Therefore, this alteration of the hamstring muscle group’s func-tion results in the presentation of apparent ham-string tightness. The proposed use of a specific RNT technique may help classify and correct this dysfunctional motor control pattern by reflexively inhibiting the hamstring muscle group and activat-ing the postural stabilizers. While variations exist, the recommended application begins with the cli-nician applying a manual anterior-posterior (AP) force to the center of a patient’s abdomen (i.e., umbilicus), sternum, and/or across the hips bilater-ally at the level of the anterior superior iliac spine while instructing the patient to prevent the clinician from pushing him/her backwards. Once the patient “stops” the AP force provided by the clinician, the patient reacts simultaneously by bending forward at the hips in an attempt to “touch” his/her toes (Multi-segmental forward flexion) (Figure 1). The patient should complete five to ten reactive forward flexion bends with the clinician applying the AP force prior to each repetition. Multiple sets of this maneuver can be performed in a single treatment session and the clinician may adjust the location (superior or inferior) of the AP force throughout the treatment session. The clinician can choose to adjust the loca-tion of the AP force in an attempt to find the location
that produces the greatest increase in forward flex-ion by producing the optimal motor control pattern for performing forward flexion.
Patients who do not have a true hamstring TED, and have a possible motor control pattern dysfunction, will quickly improve their multi-segmental forward flexion ROM during the initial RNT treatment ses-sion. As a result of this change, the patient can be classified as having apparent hamstring tightness and would not be indicated to receive a treatment protocol designed at increasing tissue extensibility (e.g., stretching). The purpose of this case report was to identify, treat, and report on the patient out-comes while using this RNT technique on a patient who demonstrated hamstring inflexibility based on the traditional testing methods.
CASE DESCRIPTIONA 20-year-old, female softball player agreed to partici-pate after she was informed of the purpose of this case study. The patient denied any recent history of lower extremity, lumbar, or thoracic injury. She did report chronic hamstring tightness of more than four years duration despite the use of traditional warm-up and stretching techniques. The patient reported no addi-tional health history that would have affected trunk or lower extremity ROM and was otherwise healthy.
Figure 1. Reactive Neuromuscular Training (RNT) technique used to identify and treat apparent hamstring tightness. (A) Clinician applies an anterior-posterior force and (B) the patient simultaneously reacts by reaching for his/her toes.

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 374
INITIAL CLINICAL IMPRESSIONThe cause of the patient’s chief complaint of chronic hamstring tightness was hypothesized to be a result of apparent hamstring tightness since the patient reported no improvement following traditional warm-up and stretching interventions. Further ROM testing was performed in order to identify whether the patient could be classified with hamstring tight-ness based on traditional evaluation techniques.
EXAMINATIONPrior to beginning the clinical examination the patient performed a warm up which consisted of five consecutive standing toe touches in order to reduce the potential mobilizing effect from performing repetitive hip flexion measurements.22 Immediately after the warm up, the following ROM measurements were taken: (a) ASLR, (b) PSLR, (c) AKE, (d) finger to floor distance test (FFD), (e) sit and reach (SnR), (f) modified Shober (mShober), (g) seated sacral angle (SA), and (h) standing SA. Range of motion measure-ments for the ASLR, PSLR, AKE, and SA were taken using an iPhone 5s with the Clinometer (Plaincode, http://www.plaincode.com/products/clinometer/)
application which has previously been shown to be reliable at measuring ROM in the shoulder23 and cer-vical spine.24 The FFD, SnR and mSchober were mea-sured using a cloth measuring tape.
Normal ROM on the ASLR and PSLR tests has been suggested as 70� or more and 80� or more of hip flex-ion respectively.4 For the AKE test, a knee flexion angle of 20� or less has been used to define normal ROM.3 During the clinical examination, the patient’s ROM measurements (Table 1) on the ASLR (R=60�, L=58� ), PSLR (R=67�, L=70�), and AKE (R=30�, L=34� ) tests all fell outside of the normal ROM limits.
CLINICAL IMPRESSION AFTER EXAMINATIONBased on the ROM measurements during the clinical examination, the patient was classified as having a potential TED. The clinical examination results were consistent with the patient’s chief complaint of ham-string tightness, but had remained despite regular stretching techniques applied as part of her pre-sport warm-up. As such, the use of RNT as a screening and intervention technique to identify if the patient has apparent hamstring tightness was warranted.
Table 1. Clinical evaluation range of motion measurements pre-and post- reactive neuromuscular treatment including 5 week follow-up testing and total change in range of motion

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 375
week follow up. The patient did not demonstrate any change in the mSchober following treatment; however, her SA measurements improved (10� sit-ting, 11� standing) at the initial post-measurements, but were not maintained at the five week follow up.
DISCUSSIONPrior to RNT treatment, ROM measurements on the ASLR, PSLR, and AKE tests would classify the patient as having had tight hamstrings resulting from a TED.2,10,21 Following one treatment session with a RNT exercise intervention, the movement improved and her hamstrings were within normal ROM limits21 on each of the above tests. At the five week follow up appointment, the patient’s ROM measurements on the ASLR, PSLR, and AKE remained within the normal limits and had increased from the initial post-treatment measurements. The patient denied making any changes to her physical activity level or training program following initial treatment and did not receive any additional treatments aimed at increasing hamstring flexibility.
While only one patient, these findings indicate superior results compared to stretching studies that have assessed similar outcome measures. De Weijer, Gorniak, and Shamus25 found patients achieved an immediate increase in ROM on the AKE test of about 13� following a single session of three sets of 30 sec-ond passive static stretches; however, after 24 hours the post-stretch increase in ROM decreased to just under 8� and no additional follow-up testing was per-formed. Bandy, Irion, and Briggler10 reported similar results following a six-week stretching program. In their study, patients in the stretching groups gained, on average, between 10.5� and 11.5� of knee exten-sion on the AKE test. Similarly, Cipriani, et al26 reported an 18.1� increase in ROM on the PSLR test following a four-week static stretching program, but also reported a steady decrease in ROM in the same patients during the subsequent four weeks after dis-continuing the stretching program. The patient in this case study demonstrated a greater increase in ROM on the AKE test immediately following a single treatment session of RNT (R=19�, L=16�) without utilizing any treatment designed to directly elongate tissue. More importantly, the patient demonstrated further increases in ROM at a five-week follow up (R=30, L=34) without any additional RNT treat-
INTERVENTIONThe patient was treated with an RNT technique immediately following ROM measurements. Treat-ment began by having the patient stand with her feet together while the clinician provided a mild AP force to the patient’s abdomen. The patient resisted this force and simultaneously completed the multi-segmental forward flexion pattern while the clinician maintained application of the force. Upon completion of the repetition, the clinician re-applied the force and the process was repeated for a set of 10 repetitions with the force being re-applied prior to each repetition. The clinician then provided the AP force on the superior portion of the sternum for approximately five repetitions and an additional five to eight repetitions were performed with the clinician providing the AP force at the level of the anterior superior iliac spines. The clinician paused treatment between each set to inform the patient of the change in location of the AP force but no additional rest was given. Total treatment time was less than three minutes. Immediately follow-ing the RNT treatment, ROM measurements were repeated. After the initial treatment was complete, the patient was instructed to resume normal daily and sport activities. The patient returned to the ath-letic training clinic five weeks after initial treatment for follow-up testing. The patient reported she did not participate in any additional RNT treatments or additional stretching activities outside of her normal sport activities between the initial treatment session and follow-up testing.
OUTCOMESAll post-treatment and follow-up ROM measure-ments are included in Table 1. The patient had an increase in post-treatment ROM on the ASLR (R=15�, L=22�), PSLR (R=16�, L=14�), and AKE (R=19�, L=16�) from the initial treatment. At the five week follow up, the patient further increased ROM com-pared to initial measurements on the ASLR (R=25�, L=32�), PSLR (R=25�, L=23�), and AKE (R=30�, L=34�). In addition, FFD post-treatment improved 4.5 cm from the single treatment and the patient maintained that improvement at the five week fol-low up. Sit and reach measurements were similar to the FFD measurements with a 4 cm improvement post-treatment and a 3.5 cm improvement at the five

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 376
as a treatment for patients who present with signs of hamstring tightness. The use of such interventions may lead to the development of an efficient and effective treatment based classification system for improving outcomes in patients who present with hamstring flexibility issues.
REFERENCES 1. Wang SS, Whitney SL, Burdett RG, Janosky JE.
Lower extremity muscular fl exibility in long distance runners. J Orthop Sports Phys Ther. 1993;17(2):102-107.
2. Davis DS, Ashby PE, McCale KL, Mcquain JA, Wine JM. The effectiveness of three stretching techniques on hamstring fl exibility using consistent stretching parameters. J Strength Cond Res. 2005;19(1):27-32.
3. Davis DS, Quinn RO, Whiteman CT, Williams JD, Young CR. Concurrent validity of four clinical tests used to measure hamstring fl exibility. J Strength Cond Res. 2008;22(2):583-588.
4. Cook G. Movement: Functional Movement Systems: Screening, Assessment, and Corrective Strategies. Santa Cruz, CA: On Target Publications; 2010.
5. Gajdosik RL, Rieck MA, Sullivan DK, Wightman SE. Comparison of four clinical tests for assessing hamstring muscle length. J Orthop Sports Phys Ther. 1993;18(5):614-618.
6. Sainz de Baranda P, Ayala F. Chronic Flexibility Improvement After 12 Week of Stretching Program Utilizing the ACSM Recommendations: Hamstring Flexibility. Int J Sports Med. 2010;31(06):389-396. doi:10.1055/s-0030-1249082.
7. Decoster LC, Cleland J, Altieri C, Russell P. The effects of hamstring stretching on range of motion: a systematic literature review. J Orthop Sports Phys Ther. 2005;35(6):377-387.
8. DePino GM, Webright WG, Arnold BL. Duration of maintained hamstring fl exibility after cessation of an acute static stretching protocol. J Athl Train. 2000;35(1):56-59.
9. Spernoga SG, Uhl TL, Arnold BL, Gansneder BM. Duration of maintained hamstring fl exibility after a one-time, modifi ed hold-relax stretching protocol. J Athl Train. 2001;36(1):44-48.
10. Bandy WD, Irion JM, Briggler M. The effect of time and frequency of static stretching on fl exibility of the hamstring muscles. Phys Ther. 1997;77(10):1090-1096.
11. Garber CE, Blissmer B, Deschenes MR, et al. Quantity and Quality of Exercise for Developing and Maintaining Cardiorespiratory, Musculoskeletal, and Neuromotor Fitness in Apparently Healthy Adults: Guidance for Prescribing Exercise. Med Sci Sports
ment sessions, as opposed to the decrease in ROM that was seen in the stretching studies.25,26
The gains in ROM seen in this patient immediately following RNT treatment and the increased gains in ROM at a five-week follow up meet or exceed the increases in ROM identified in traditional stretch-ing literature.8,10,25,26 The results may be explained by a change in motor pattern function as a result of the RNT intervention and suggests it is unlikely the patient had a hamstring length deficit prior to treatment despite the positive tests for hamstring tightness. More importantly, the results of this case report identify a potential flaw in the current think-ing regarding evaluation and treatment of ham-string tightness. Current evaluation techniques may be unable to differentiate between true and appar-ent hamstring tightness; therefore, patients may often be incorrectly prescribed stretching interven-tions which may be contraindicated if the clinician is lengthening tissue that does not require tissue elongation. Clinicians should consider using treat-ment based assessment techniques to differentiate between true and apparent hamstring tightness. Future research needs to be conducted on a larger population in order to determine the reliability and validity of using the proposed RNT treatment as an individual treatment for apparent hamstring tight-ness, as well as using it as part of a more comprehen-sive hamstring tightness TBC system. In addition, further research needs to identify if a true change in motor control occurs with RNT, and if that change correlates with improved athletic performance and/or injury prevention.
CONCLUSIONThe results of this case report demonstrate that the subject did not have a TED despite fitting that clas-sification based on the use of traditional evaluation techniques to assess hamstring flexibility. The use of an RNT intervention allowed for quick identification of the apparent hamstring tightness and improved all of the patient’s ROM measurements in only three minutes of treatment. The improvements were maintained at a five-week follow-up appointment without any further treatment being applied. Based on these results, clinicians should consider utiliz-ing the described RNT intervention as a screening tool within the differential diagnostic process, and

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 377
20. Voight M, Cook G. Clinical application of closed kinetic chain exercise. J Sport Rehabil. 1996;5:25-44.
21. Cook G, Burton L, Fields K. Reactive neuromuscular training for the anterior cruciate ligament-defi cient knee: A case report. J Athl Train. 1999;34(2):194.
22. Atha J, Wheatley DW. The mobilising effects of repeated measurement on hip fl exion. Br J Sports Med. 1976;10(1):22-25.
23. Shin SH, Ro DH, Lee O-S, Oh JH, Kim SH. Within-day reliability of shoulder range of motion measurement with a smartphone. Man Ther. 2012;17(4):298-304. doi:10.1016/j.math.2012.02.010.
24. Tousignant-Lafl amme Y, Boutin N, Dion AM, Vallée C-A. Reliability and criterion validity of two applications of the iPhoneTM to measure cervical range of motion in healthy participants. J NeuroEngineering Rehab. 2013;10(1):69.
25. De Weijer VC, Gorniak GC, Shamus E. The effect of static stretch and warm-up exercise on hamstring length over the course of 24 hours. J Orthop Sports Phys Ther. 2003;33(12):727-733. doi:10.2519/jospt.2003.33.12.727.
26. Cipriani DJ, Terry ME, Haines MA, Tabibnia AP, Lyssanova O. Effect of stretch frequency and sex on the rate of gain and rate of loss in muscle fl exibility during a hamstring-stretching program: a randomized single-blind longitudinal study. J Strength Cond Res. 2012;26(8):2119-2129.
Exerc. 2011;43(7):1334-1359. doi:10.1249/MSS.0b013e318213fefb.
12. Weppler CH, Magnusson SP. Increasing muscle extensibility: a matter of increasing length or modifying sensation? Phys Ther. 2010;90(3):438-449. doi:10.2522/ptj.20090012.
13. Magnusson SP, Simonsen EB, Aagaard P, Sørensen H, Kjaer M. A mechanism for altered fl exibility in human skeletal muscle. J Physiol. 1996;497(Pt 1):291-298.
14. Magnusson S, Aagard P, Simonsen E, Bojsen-Møller F. A Biomechanical Evaluation of Cyclic and Static Stretch in Human Skeletal Muscle. Int J Sports Med. 1998;19(05):310-316. doi:10.1055/s-2007-971923.
15. Costa PB, Herda TJ, Herda AA, Cramer JT. Effects of Dynamic Stretching on Strength, Muscle Imbalance, and Muscle Activation. Med Sci Sports Exerc. 2014;46(3):586-593.
16. Samuel MN, Holcomb WR, Guadagnoli MA, Rubley MD, Wallmann H. Acute effects of static and ballistic stretching on measures of strength and power. J Strength Cond Res. 2008;22(5):1422-1428.
17. Haddad M, Dridi A, Chtara M, et al. Static stretching can impair explosive performance for at least 24 hours. J Strength Cond Res. 2014;28(1):140-146.
18. Baker T. Total Motion Release. https://tmrseminars.com/tmr-home/. Accessed April 20, 2015.
19. D’Ambrogio KJ, Roth GB. Positional Release Therapy: Assessment & Treatment of Musculoskeletal Dysfunction. St. Louis: Mosby; 1997.

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 378
ABSTRACTBackground and Purpose: Iliotibial Band Syndrome (ITBS) has commonly been thought of as an overuse injury in runners. The exact etiology of ITBS is not well understood and there is no consensus on how to properly manage it. The purpose of this case series is to present a comprehensive model that utilizes a review of the current literature and the concept of regional interdependence as a foundation for the treat-ment of ITBS in runners.
Case Descriptions: The first subject was a 36-year old female, referred from an orthopedic physician with the diagnosis of left iliotibial band friction syndrome. She reported a 9/10 stabbing pain on a visual analog scale (VAS) in the left lateral knee at mile two while running. The second subject was a 41-year old female with a referral to physical therapy from an orthopedic surgeon for left iliotibial band tendinitis. She reported the symptoms beginning one month prior to her presentation to therapy, and that she would get an 8/10 stabbing pain on a VAS in the left lateral knee at mile three while running. Both subjects complained of the onset of lateral knee pain at a consistent mileage that forced them to stop running. Neither of them initially reported pain in adjoining regions, but did recall some low back stiffness from time to time when ques-tioned further. The concept of regional interdependence, as well as neuromuscular re-education, and strengthening interventions in conjunction with addressing the contributing factors of training errors, shoe wear, running surface, and program design were utilized.
Outcomes: At a six-month follow-up, subject one had successfully completed a half marathon without knee pain. At a nine-month follow-up, subject two was able to run five miles, twice weekly and 10 miles once weekly without pain or symptoms.
Discussion: These case reports demonstrate the successful management of ITBS in two subjects using a multifaceted approach based on the current literature and the concept of regional interdependence.
Keywords: Iliotibial band syndrome, manual therapy, physical therapy, regional interdependence, running injuries
IJSP
TCASE REPORT
THE MANAGEMENT OF ILIOTIBIAL BAND SYNDROME
WITH A MULTIFACETED APPROACH: A DOUBLE
CASE REPORT
Jennifer Shamus, DPT, PhD1
Eric Shamus, DPT, PhD2
1 Select Physical Therapy, Pembroke Pines, Florida, USA2 Department of Rehabilitation Sciences, Florida Gulf Coast
University, Fort Myers, Florida, USA
Each subject was informed that the data concerning the case would be submitted for publication. Subject confi dentiality must be protected according to the U.S. Health Insurance Portability and Accountability Act (HIPPA).
CORRESPONDING AUTHOREric Shamus, DPT, PhDChair and Associate ProfessorDepartment of Rehabilitation SciencesCollege of Health Professions & Social WorkFlorida Gulf Coast UniversityMarieb Hall10501 FGCU Boulevard SouthFort Myers, FL 33965E-mail: [email protected]

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 379
BACKGROUND AND PURPOSEIliotibial Band Syndrome (ITBS)/Iliotibial Band Fric-tion Syndrome (ITBFS) is considered to be one of the most common overuse injuries in the lower extrem-ity, affecting anywhere from 7-14% of the running population.1,2 It not only affects runners, but it can decrease performance in cyclists, soccer players, field hockey players, basketball players, and row-ers.3 ITBS often leads to an inability to participate in a sport secondary to severe hip, lateral thigh, and knee pain.
Currently, the exact etiology of ITBS is not well understood. Orchard et al4 described an area of fric-tion occurring between the iliotibial band and the lateral femoral condyle when the knee is flexed to around thirty degrees. The friction is said to lead to inflammation and pain. However, findings of cadaver studies and biopsies of the area are leading researchers to challenge this theoretical model.5,6 Fairclough et al5,6 suggest that there is an illusion of movement of the ITB on the condyle due to chang-ing tension, and however, the tendon does not actu-ally have the capability to slide across the bone. It instead exerts a compressive force on the joint when the fascia tightens. In addition to fascial restrictions, Ferber et al7 studied three hundred recreational ath-letes and identified decreased iliotibial band and iliopsoas extensibility in recreational athletes. Surgi-cal examination of the area often reveals a lack of inflammatory response. In a few cases, there may be an underlying cyst or extension of the joint capsule laterally, but this has not been found consistently in all subjects. Even more infrequently, degeneration of the lateral femoral condyle has been discovered.3 On cadaver dissection, no bursa was seen distally at the knee in the region of where the iliotibial band inserts. There is a lateral recess of the knee that contains a highly vascularized fatty tissue vis-ible on magnetic resonance image (MRI). It is most likely that the iliotibial band is not transferring loads properly and friction is not likely responsible for the painful presentation.5,6
Abnormal kinematics of the lower extremity have also been suggested as a contributing factor to ITBS. Multiple authors have studied the hip, knee, and ankle kinematics in runners with and without ITBS and found conflicting results.7,8 Noehren et al studied
competitive female runners with a history of ITBS and found that they had increased hip internal rota-tion and adduction range of motion upon contact.8 Grau et al found that hip adduction at initial con-tact and maximal hip adduction in the control group were significantly less than in the group with ITBS.9 Orchard et al found that runners with ITBS landed with less knee flexion upon initial contact on the involved limb than uninjured runners.4 Noehren et al studied over 400 runners and found that the run-ners with ITBS had greater peak hip adduction, peak knee internal rotation and femoral external rota-tion moments and remained more adducted during stance.8 No difference was found in knee flexion and rearfoot eversion.8 Muscle weakness, specifically in the hip abductors, has also been suggested as a poten-tial contributing factor in ITBS. Grau et al studied ten individuals with ITBS compared to ten controls and found no difference in hip abductor strength.9 Fred-ericson et al, however, studied a group of 24 runners with ITBS against 30 matched controls and found that hip abductor torque was significantly lower on the involved side in those with ITBS.10
Due to these varied results, the optimal treatment for athletes with ITBS remains undescribed. In the initial stages, anti-inflammatory medications are frequently prescribed. However, this practice comes under question if the evidence from biopsies sup-ports the lack of inflammation in the area.3 Physical therapy is often recommended. Interventions such static stretching, strengthening, manual therapy and neuromuscular re-education have been researched. Pinshaw et al stressed the importance of address-ing shoe wear and training schedules.11 Deep fric-tion massage is often used, but outcomes research does not support it.12 In some chronic cases lasting greater than one year, resection of the lateral syno-vial recess have been performed. The purpose of this case series is to present a comprehensive model that utilizes a review of the current literature and the concept of regional interdependence as a foun-dation for the treatment of ITBS in runners.
CASE DESCRIPTION: SUBJECT HISTORY AND SYSTEMS REVIEW #1Subject HistoryThe subject was a 36-year old female, referred from an orthopedic physician with the diagnosis of left
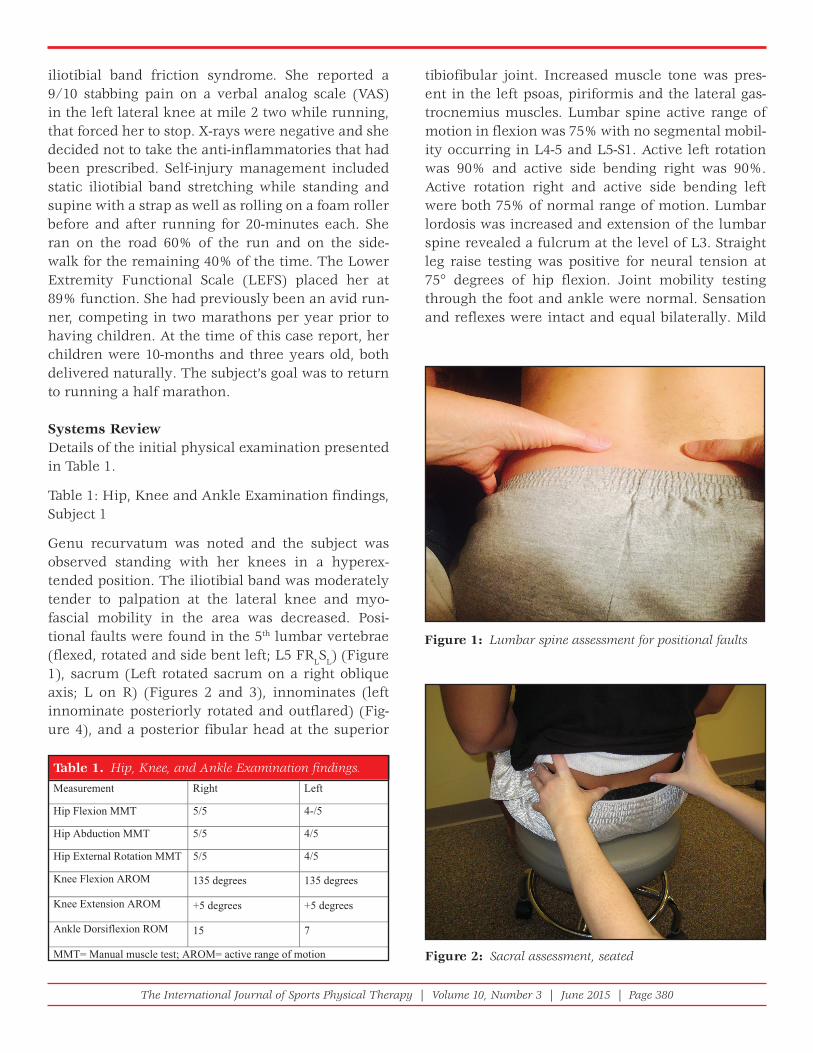
The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 380
iliotibial band friction syndrome. She reported a 9/10 stabbing pain on a verbal analog scale (VAS) in the left lateral knee at mile 2 two while running, that forced her to stop. X-rays were negative and she decided not to take the anti-inflammatories that had been prescribed. Self-injury management included static iliotibial band stretching while standing and supine with a strap as well as rolling on a foam roller before and after running for 20-minutes each. She ran on the road 60% of the run and on the side-walk for the remaining 40% of the time. The Lower Extremity Functional Scale (LEFS) placed her at 89% function. She had previously been an avid run-ner, competing in two marathons per year prior to having children. At the time of this case report, her children were 10-months and three years old, both delivered naturally. The subject’s goal was to return to running a half marathon.
Systems ReviewDetails of the initial physical examination presented in Table 1.
Table 1: Hip, Knee and Ankle Examination findings, Subject 1
Genu recurvatum was noted and the subject was observed standing with her knees in a hyperex-tended position. The iliotibial band was moderately tender to palpation at the lateral knee and myo-fascial mobility in the area was decreased. Posi-tional faults were found in the 5th lumbar vertebrae (flexed, rotated and side bent left; L5 FRLSL) (Figure 1), sacrum (Left rotated sacrum on a right oblique axis; L on R) (Figures 2 and 3), innominates (left innominate posteriorly rotated and outflared) (Fig-ure 4), and a posterior fibular head at the superior
tibiofibular joint. Increased muscle tone was pres-ent in the left psoas, piriformis and the lateral gas-trocnemius muscles. Lumbar spine active range of motion in flexion was 75% with no segmental mobil-ity occurring in L4-5 and L5-S1. Active left rotation was 90% and active side bending right was 90%. Active rotation right and active side bending left were both 75% of normal range of motion. Lumbar lordosis was increased and extension of the lumbar spine revealed a fulcrum at the level of L3. Straight leg raise testing was positive for neural tension at 75° degrees of hip flexion. Joint mobility testing through the foot and ankle were normal. Sensation and reflexes were intact and equal bilaterally. Mild
Table 1. Hip, Knee, and Ankle Examination fi ndings.
Measurement Right Left
5/-45/5TMMnoixelFpiH
5/45/5TMMnoitcudbApiH
5/45/5TMMnoitatoRlanretxEpiH
Knee Flexion AROM 135 degrees 135 degrees
Knee Extension AROM +5 degrees +5 degrees
Ankle Dorsiflexion ROM 15 7
MMT= Manual muscle test; AROM= active range of motion
Figure 1: Lumbar spine assessment for positional faults
Figure 2: Sacral assessment, seated

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 381
pronation bilaterally was noted during gait analy-sis. She used a mild motion control shoe with a dual density sole present in only the rearfoot. The clini-cal impression was that the iliotibial band pain was a result of biomechanical and neuromuscular dys-functions related to regional interdependence and that this subject would benefit from a multifaceted approach over a local approach that focused on the pain at the ITB only.
InterventionTable 2: Treatment Summary Subject 1
Session One
Following the evaluation, treatment was provided. First, the sacral torsion was treated with a muscle
energy technique in right sidelying (Figure 5). The lumbar spine was then treated with a muscle energy technique in left sidelying position utilizing hip adduction of the top leg (Figure 6). The left posterior innominate was addressed in right sidelying with hip flexion (Figure 7). Hip abduction strength was then retested and improved from 4/5 to 5-/5. The superior tibiofibular joint demonstrated a posterior fibular head and was mobilized with a Grade 3 joint glide anteriorly in a sidelying position followed by ligament articular strain fibular balance technique (Figure 8). The distal iliotibial band and lateral fascia were treated with grasping the fascia and gliding in a perpendicular anterior and posterior direction. A detonification technique consisting of grasping the muscle belly of the gastrocnemius and lengthen-ing it laterally over a period of seven seconds was used. This combination of interventions increased her ankle dorsiflexion to 15° degrees to match the opposite side. The left psoas tone was reduced using counterstrain (Figure 9). The piriformis tone was addressed by applying a moderate pressure on the muscle in a shortened position and as the thera-pist passively lengthens the muscle, the pressure eases up. Once joint and soft tissue mobility were improved, the subject was instructed to perform upper trunk and lower trunk rotation in sidelying to promote segmental mobility as well as circula-tion and nutrition in the facet joints. Isometric hip abduction and adduction exercises were performed in supine hooklying. Prone opposite arm and leg raises were introduced to increase recruitment of the hip and back musculature and to reinforce the new length of the psoas. Her straight leg raise was performed and showed a 20° degree increase in range of motion from 75° to 95° degrees with nega-tive neural tension. She was instructed how to stand with her knees in neutral and to maintain a neutral lumbar spine posture. The subject was advised to stop her static stretching and was taken through a walking warm up and dynamic stretching consist-ing of high knees, hip flexion with knee extension and hip internal and external rotation in midrange. While she was running on the treadmill, visual and verbal cues were used to normalize knee position, avoiding hyperextension and adduction. She was permitted to run 1.5 miles on even ground on the next day, but not on the cement.
Figure 3 Sacral assessment, prone
Figure 4: Innominate assessment, supine

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 382
ject reported that she no longer felt the need to use her foam roller. Sidelying hip abduction exercises and clam shells for hip external rotation strength were added. Lateral step (dip) downs off the edge of a step without the leg touching the ground were utilized for neuromuscular re-education of knee position. The subject was advised to run three times per week, every other day. She was to run three miles one more time and then increase by ½ mile increments up to five miles if there was no pain during or after the run.
Session Two: Two days later
The subject reported that she ran past the 1.5 miles that were recommended but stopped at three miles just to be safe. Subjective pain level on a visual ana-log scale (VAS) was 0/10. Her lumbar spine AROM was full and there was no muscle guarding in the piri-formis or gastrocnemius. Mild hypertonicity in the psoas with treated with counterstrain. The tender-ness at the distal iliotibial band had resolved. The sub-
Table 2.
Treatment Number
Day Interventions Exercises Added Response on that day or presentation on the next visit
1 1 Muscle energy to positional faults
Grade III joint mobilization superior tibiofibular joint
Myofascial release of the ITB
Detonification of the piriformis and lateral gastrocnemius muscle
Counterstrain to the psoas
Side lying: Upper trunk rotation and lower trunk rotation
Isometric hip abduction and adduction exercises
Prone opposite arm and leg raises
Standing postural re-education of knee position
Dynamic stretching
Running gait verbal retraining
L Hip abductionstrength 5-/5
L Dorsiflexion 15 degrees
Straight leg raise 95degrees
100% Lumbar spine active range of motion
No ITB tenderness
Subjective pain level (SPL) on a (VAS) 0/10
Ran 3 miles without pain the next day
2 3 Counterstrain psoas Side lying: hip abduction and external rotation exercises
Lateral step downs without contacting floor
Run 3x/week, increase by ½ mile increments
No positional faults
Normal muscle tone
Worked up to running 5 miles painfree
LEFS 100%
tahtnurgnoladdA313would not exceed 25% of the total weekly mileage
6 months
½adetelpmoCmarathon

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 383
Session Three: Ten days later
The subject reported that she had been compliant with her home program. She was gradually increas-ing her running mileage and had run five miles without lateral knee pain. Lower extremity func-tional scale (LEFS) score was 100%. She had full joint mobility in the spine and lower extremities. There was no abnormal tone. It was agreed that she would progress to one longer run on the weekend that was no more than 25% of her total weekly mileage. The long run could then progress every other week until her goal was met. The subject was discharged.
Figure 5: Muscle energy intervention for sacral torsion
Figure 6: Muscle energy technique for the lumbar spine, L5 positional fault
Figure 7: Muscle energy technique for posterior innominate
Figure 8: Fibular balance technique
Figure 9: Conterstrain technique for psoas

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 384
posterior. Lumbar spine active range of motion was 80% of flexion, 60% of rotation and side bending bilaterally and 40% of extension with pain. Straight leg raise testing was positive for neural tension at 65° degrees on the left. Palpation and special tests led to the conclusion that she had a left on right sacral torsion, a left anterior innominate, and L5-S1 flexed, rotated left, and sidebent left (L5 FRLSL). The proximal fibular head was posterior at the superior tibiofibular joint. There was increased tone in the bilateral psoas muscles, the left piriformis, the left erector spinae and the left lateral gastrocnemius. The subject lacked 30% of hip internal rotation PROM on the left compared to the right. Sensa-tion and reflexes were intact. Gait analysis revealed that she was a late midstance pronator. A single leg squat test on the left revealed poor eccentric control with excessive hip internal rotation and adduction, also present during her running visual analysis on the treadmill. The clinical impression was that the iliotibial band pain was a result of biomechanical and neuromuscular dysfunction related to regional interdependence and that this subject would benefit from a multifaceted approach over an approach that focuses on the pain at the ITB only.
Intervention
Table 4 Treatment Summary, Subject 2
Session One
After the evaluation, the positional faults in the sacral and lumbar spine were addressed with muscle energy techniques in sidelying and were followed by ten grade 3 oscillations to L5-S1 in prone until the surrounding soft tissue musculature softened. This resulted in increased passive hip internal rota-tion and active lumbar spine range of motion as well as an increase in the straight leg raise from 65° to 85° degrees with minimal neural tension. At supe-rior tibiofibular joint the fibular head was mobilized anteriorly with ligament articular strain balancing technique. The lateral gastroc and the left erector spinae were detonified with lateral bending/dis-placement, and the distal iliotibial band was treated with myofascial techniques. Detonification was per-formed on the psoas muscles using a counterstrain technique and the piriformis with a passive pump technique with the subject in prone. The subject was
Six-month follow up:
The subject had successfully completed a half mara-thon without knee pain. She was signed up to run a marathon within the subsequent four months.
CASE DESCRIPTION: SUBJECT HISTORY AND SYSTEMS REVIEW #2Subject HistoryThe subject was a 41-year old female referred for physical therapy by an orthopedic surgeon for left iliotibial band tendinitis. She reported the symptoms began one month prior and that she would experi-ence stabbing pain, rated at 8/10 on a visual analog scale (VAS) in the left lateral knee at mile three while running. X-rays of the left knee were negative. Self-injury management had included static stretching of the iliotibial band, hamstrings and gastroc-soleus complex. Once the pain had developed, she started using a foam roller along her iliotibial band, both before and after running. She had stopped running for two weeks, during which the pain subsided, but it returned the first time she tried to run after this break. She was running on the sidewalk. The subject reported a LEFS score of 86% function. After further questioning, the subject recalled a fall down her flight of stairs about three months prior to the onset of left knee pain. She had forgotten to mention it because the pain in her back pain had resolved. She reported that she was currently unable to exercise. Her goals included being able to run a 5k and to run for training multiple times a week without pain.
Systems ReviewPhysical examination summary findings are pre-sented in Table 3.
Table 3 Hip and Knee examination findings, Subject 2
The left distal iliotibial band was slightly tender to palpation and had decreased mobility anterior/
Table 3. Hip and Knee Examination fi ndings, Subject 2tfeLthgiR
5/+35/5TMMnoisnetxEpiH
5/45/5TMMnoitatoRlanretxEpiH
5/45/5TMMnoitcudbApiH
Knee Flexion AROM 140 degrees 140 degrees
Knee Extension AROM 0 degrees 0 degrees

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 385
Table 4. Treatment Summary, Subject 2
Treatment Day Intervention Exercises Added Response that day or presentation on the next visit
1 1 Muscle energy to the positional faults
Grade III mobilizations to the lumbar spine and superior tibiofibular joint
Detonification to the erector spinae, piriformis and gastrocnemius
Myofascial release to the ITB
Counterstrain psoas
Side lying: Upper trunk rotation, lower trunk rotation and hip external rotation
Supine: Isometric hip abduction and adduction
Squatting to ¼ depth
Postural education for sitting
No running at this time
SLR 85 degrees
Lumbar spine active range of motion 100% all planes
Symmetrical hip internal rotation
Pelvis was level
2 3 Muscle energy L5
Detonification of the erector spinae
Counterstrain of the psoas
Bridging
Running gait training on the treadmill
Dynamic stretching
Run 2 miles every other day
SPL on a verbal analog scale 0/10
Run 2 miles without pain the next day
No positional faults in the lumbar spine
3 10 Muscle energy to the innominate
Counterstrain psoas and iliacus
Detonification of the erector spinae
Prone opposite arm and leg raises
Resisted walk backs
Leg press
Run 3 miles every other day
Run 4 miles without pain
No positional faults
Normal tone
4 24 Side lying: hip Run 5 miles abduction
Lateral step downs without ground contact
Run 3 times a week increasing in ½ mile increments once a week
without pain
100% lumbar spine active range of motion
Hip and knee strength 4+/5
LEFS 100%
5 38 Increasing her mileage steadily
9 months
Run 5 miles 2x/week and 10 miles on Saturday

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 386
tile cues were used to improve trunk position and proprioception. Leg press exercises were added to increase strength of the quadriceps and gluteals, as well as to work on hip and knee position and to pro-vide equal weight bearing with symmetrical force through the pelvis. The subject was permitted to run three miles every other day until the next visit.
Session Four: Two weeks later
The subject reported that she was able to run three miles without pain and even went up to four miles without symptoms. She no longer felt the need to use her foam roller. Joint and soft tissue mobility had normalized. Hip abduction isolation exercises were advanced to the sidelying position, being care-ful to avoid sidebending of the lumbar spine. Squat-ting was advanced to lateral step (dip) downs off of the step without contacting the ground to repro-duce the mechanics of support phase during run-ning. A return to running program was discussed that included running only three days per week and increasing mileage only once weekly, by ½ mile increments.
Session Five: Two weeks later
The subject requested one additional visit to make sure that everything was progressing as expected. She was up to running five miles without pain. Her lumbar active range of motion was 100%, her hip and knee strength on the left had increased to 4+/5. LEFS score upon discharge was 100%.
Nine month follow–up
The subject was running five miles, twice weekly and 10 miles on Saturdays without pain or symp-toms. She had participated in one 5k and was satis-fied with her time.
DISCUSSIONBoth subjects had similar presentations. They each complained of the onset of lateral knee pain at a consistent mileage that forced them to stop running. Neither of them initially reported pain in adjoining regions, but did recall some low back stiffness from time to time when questioned further. They had lim-ited lumbar spine active range of motion, decreased superior tibiofibular joint mobility (posterior fibular head) and increased tone in the psoas, piriformis
instructed in sidelying upper trunk and lower trunk rotations to promote segmental mobility as well as joint circulation and joint nutrition. The subject was instructed in isometric hip abduction and adduction exercises supine. Hip external rotation strengthening was introduced with sidelying clam shells. Squatting with a focus on eccentric control and proper hip and knee position was used to re-educate the muscles in closed chain function. Sitting posture and transfers were reviewed for good form with an emphasis on keeping the lower extremities symmetrical and not crossing the legs. The subject was asked not to run until after the next visit.
Session Two: Two days later
The subject returned with a positional fault at L5 (FRLSL), but the pelvis was level. The L5 positional fault was addressed with a muscle energy technique in left sidelying. The erector spinae and psoas mus-cles were slightly hypertonic so they were again det-onified using the previously described techniques. Bridging was added to the home program in order to activate the gluteal muscles. Retraining neuromus-cular control of knee position was conducted on the treadmill to ensure carry over. The subject was per-mitted to run two miles every other day on asphalt until the next visit. Dynamic stretches of the lower extremities to be used prior to running included high knee marching, butt kicks, marching with knee exten-sion, and hip internal and external rotation walking.
Session Three: One week later
The subject reported that she had run pain free for two miles. The subject had slight increased psoas and iliacus tone on the left that was addressed using strain-counterstrain techniques. Lumbosacral mobil-ity was normal, however there was slight increase in tone of the left erector spinae. The increased tone was addressed with active pump techniques, com-bining soft tissue mobilization with active move-ment. The left anterior innominate was treated with a muscle energy technique. Isometric hip abduction and adduction strengthening were continued. Prone opposite arm and leg raises were added to the pro-gram to increase hip extensor and back musculature recruitment and to encourage a lengthened position of the psoas. The subject walked backwards while holding tubing at the chest level, and verbal and tac-

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 387
targeting these areas of joint restriction may trigger the endogenous descending pain inhibition system and create a hypoalgesic affect. Manual therapy techniques may not only work at a biomechanical level but also at the neurophysiological level provid-ing influence to the supraspinal level.13,14 It is also plausible that the cutaneous nerve distribution to the lateral knee is affected by the lumbosacral spine interventions.21 In our case series, this quick shift in symptoms also supports the notion that inflamma-tion may not be the driving force in iliotibial band syndrome. Selkow et al22 promote the concept of utilizing muscle energy techniques to provide an immediate decrease in non-specific low back pain. However, this effect is transient when used in isola-tion. Selkow et al22 felt that this subsequent decrease in pain levels lead to the ability to reeducate and strengthen inhibited muscles. Wilson et al23 had superior outcomes in their subjects with acute low back pain when muscle energy techniques were combined with neuromuscular reeducation and resistance training which is similar to the current suggested model of treatment.
In both cases, neuromuscular reeducation and strengthening exercises were introduced during the first visit. This approach is supported by Thein-Nis-senbaum et al24 who strengthened the core muscles and utilized treadmill retraining to alleviate hip and low back pain in a post partum runner. An eight-week program of hip abduction and external rotator strengthening was reported by Khayambashi et al to decrease knee pain and increase function in females with patellofemoral pain.25 A one-year follow up was provided that showed the positive results remained. An individual with piriformis syndrome was also successfully treated with an emphasis on hip muscle strengthening and movement reeducation instead of static stretching of the piriformis.26 A program of manual therapy, trunk and hip stabilization, and taping and orthoses led to positive outcomes in sub-jects with patellofemoral stress syndrome.27
Furthermore, on the first or second visit a running analysis was conducted with each of the two sub-jects, with cuing provided as needed. Providing same day feedback on running biomechanics was an important component to the successful long term return to running.28-30 Teran-Yengle et al uti-
or erector spinae, and gastrocnemius. There was decreased myofascial mobility in the distal one third of the iliotibial band. Strength of the involved lower extremity was decreased or inhibited in the hip flex-ors, external rotators, and abductors.
Muscle energy techniques and joint mobilization were the first interventions performed. Muscle energy was utilized to correct positional faults of the lumbosacral spine and Grade 3 mobilizations were used on the superior tibiofibular joint. This led to increased joint mobility, increased neural mobility and it contributed to reduced tone in the area. This is due to not only the biomechanical effect of man-ual therapy, but also the effects on the central ner-vous system.13,14 Additional soft tissue techniques were used by applying a moderate pressure on the muscles in a shortened position and as the muscle lengthens passively the pressure eased up to achieve normal tone throughout the lumbar spine and lower extremities.15 In both cases, utilizing the soft tissue techniques to normalize the tone led to a quick shift in pain levels.
Treatment that includes the lumbar spine and lower extremity below the knee is consistent with the model of regional interdependence for the treat-ment of iliotibial band syndrome. Joint dysfunction in the lumbar spine or extremities can precipitate or perpetuate injury regardless of how remote it is from the site of pain.16 Several authors17-20 reported success in subjects with lower extremity complaints when techniques to improve lumbosacral posi-tional faults have been utilized. Vaughn reported using lumbosacral mobilizations on a subject with isolated knee pain that eliminated all pain in one visit.17 High velocity, low amplitude (HVLA) lum-bopelvic manipulation has also been reported to not only decrease pain dramatically but to increase hip abductor and extension strength while increas-ing hip internal rotation range of motion on the affected side.18 Grassi et al reported they were able to normalize weight distribution through the lower extremities with a HVLA mobilization of the sacro-iliac joint.19 Additionally, it was not until treatment commenced on the lumbar spine that a 70-year old woman’s knee pain resolved.20 Although diagnos-tic tests have been unable to support the presence of a positional fault, it is apparent that techniques

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 388
demonstrated to be quite effective. Incorporating lumbosacral spine and lower quarter joint mobiliza-tion techniques as indicated improved muscle tone and myofascial mobility. Additional soft tissue mobi-lization, neuromuscular reeducation, strengthen-ing, and running form retraining with proper advice on surface, shoes and schedule, led to a successful return to running in these two subjects. These case reports demonstrate the successful management of ITBS using a multifaceted approach based on the cur-rent literature and regional interdependence. These two case reports present the rationale for the use of a multifaceted approach for not just this condition, but with the entire lower extremity. Physical therapists should incorporate a multifaceted approach with all of their subjects. Multiple individual techniques were performed which turned out to be effective. It is the authors’ opinion that the techniques are more effective combined then individually based on the reduced number of visits and the quick shift in pain levels that led to the return to pain free running. This quick shift in symptoms also supports the notion that inflammation may not be the driving force in this condition. Too often, in the clinical management of ITBS, the focus is ultrasound, static stretching, and myofascial techniques directly to the ITB. Physical therapists need to address underlying dysfunctions and compensatory patterns.
Future research needs to look at how Johansson described how the simulation of fascial mechano-receptors may primarily lead to changes in gamma motor tone regulation.36,37 The fascia may have some microscopic sympathetic or contractile properties that benefited from the techniques used in this case series. In addition, future research should continue to investigate the descending pain inhibitory system and the most effective way to activate it to decrease pain levels. This may lead to implementing neuro-muscular reeducation and strengthening interven-tions into the treatment plan, early on, for excellent outcomes.
RE FERENCES 1. McKean KA, Manson NA, Stanish WD. Musculoskeletal
injury in the master’s runners. Clin J Sports Med. 2006 Mar;16(2):149-54.
2. Taunton JE, Ryan MB, Clement DB, McKenzie DC, Llyod-Smith DR, Zumbo BD. A retrospective case-
lized treadmill training to significantly reduce sagit-tal plane knee extension.31 Crowell and Davis found that treadmill training could also reduce vertical ground reaction forces by over 30% and improve tib-ial and overall lower extremity position during run-ning.32 These studies illustrate that having proper flexibility and strength in the absence of neuromo-tor control will not automatically create normal run-ning mechanics.28-32
Also important to the long-term success of these two runners was the information and education pro-vided regarding training surface, shoes, and training schedules. All subjects were advised to run a sur-face that provided some shock absorption such as the road, a track, or grass (if level). They were to avoid cement at all times. Shoes were inspected for each subject in order to ensure that the footwear matched the foot type, they were not excessively worn and that foot position was stable and not exces-sively pronated during running. Kong et al deter-mined that as little as 200 miles on a running shoe can lead to altered biomechanics.33 Butler et al were able to demonstrate that motion control shoes were able to control rearfoot motion better than cushion shoes.34 Schedule was important to review second-ary to training errors accounting for at least 60% of all running related injuries.35 These subjects were provided with a program that outlined a four week progression, running three times weekly. Three times a week was chosen because of the correlation between the risk of injury and the number of days per week an individual runs.1,35
Case report research results are not generalizable. In addition, several factors were not controlled for or were not assessed using objective measures (e.g positional faults, MMT vs. hand-held dynamometry). The ability to reproduce the results seen in these case reports may relate to the skill of the therapist in order to identify positional faults and the ability to normalize tone.
CONCLUSIONTreating athletes can be a challenging task due to their dedication to a sport. Most athletes, how-ever, find that they cannot participate fully when they have ITBS. Utilizing a multifaceted treatment approach based on a review of the literature has been
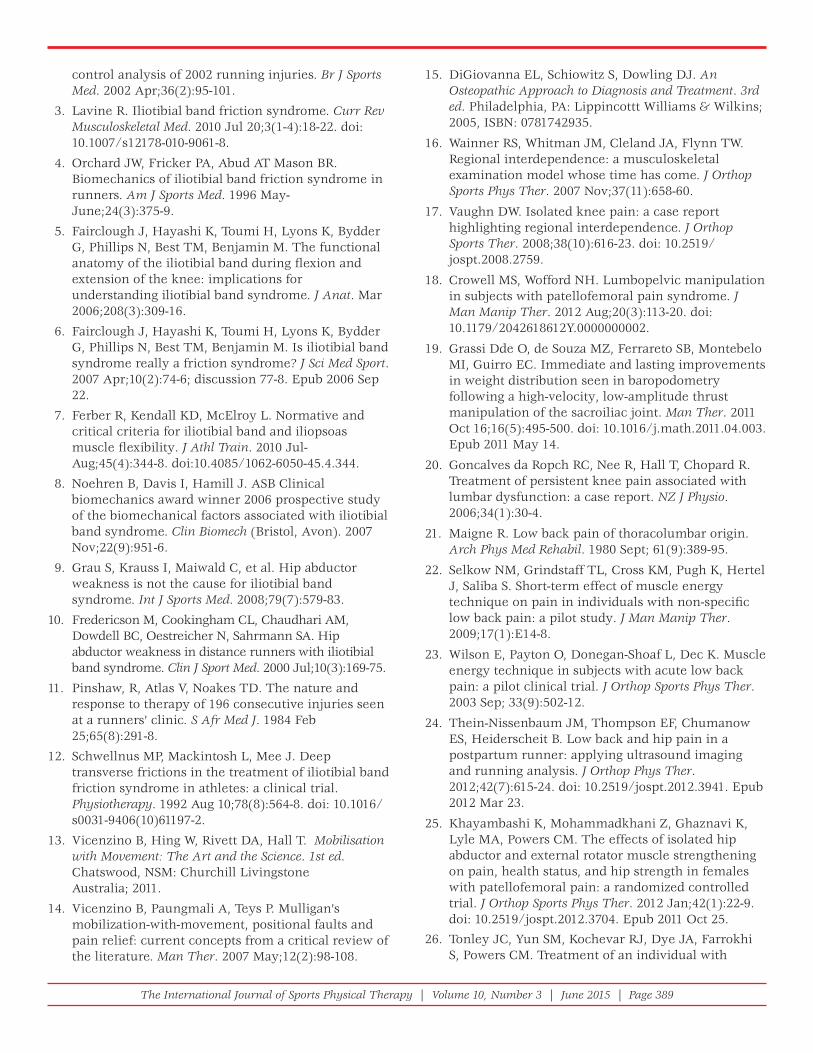
The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 389
control analysis of 2002 running injuries. Br J Sports Med. 2002 Apr;36(2):95-101.
3. Lavine R. Iliotibial band friction syndrome. Curr Rev Musculoskeletal Med. 2010 Jul 20;3(1-4):18-22. doi: 10.1007/s12178-010-9061-8.
4. Orchard JW, Fricker PA, Abud AT Mason BR. Biomechanics of iliotibial band friction syndrome in runners. Am J Sports Med. 1996 May-June;24(3):375-9.
5. Fairclough J, Hayashi K, Toumi H, Lyons K, Bydder G, Phillips N, Best TM, Benjamin M. The functional anatomy of the iliotibial band during fl exion and extension of the knee: implications for understanding iliotibial band syndrome. J Anat. Mar 2006;208(3):309-16.
6. Fairclough J, Hayashi K, Toumi H, Lyons K, Bydder G, Phillips N, Best TM, Benjamin M. Is iliotibial band syndrome really a friction syndrome? J Sci Med Sport. 2007 Apr;10(2):74-6; discussion 77-8. Epub 2006 Sep 22.
7. Ferber R, Kendall KD, McElroy L. Normative and critical criteria for iliotibial band and iliopsoas muscle fl exibility. J Athl Train. 2010 Jul-Aug;45(4):344-8. doi:10.4085/1062-6050-45.4.344.
8. Noehren B, Davis I, Hamill J. ASB Clinical biomechanics award winner 2006 prospective study of the biomechanical factors associated with iliotibial band syndrome. Clin Biomech (Bristol, Avon). 2007 Nov;22(9):951-6.
9. Grau S, Krauss I, Maiwald C, et al. Hip abductor weakness is not the cause for iliotibial band syndrome. Int J Sports Med. 2008;79(7):579-83.
10. Fredericson M, Cookingham CL, Chaudhari AM, Dowdell BC, Oestreicher N, Sahrmann SA. Hip abductor weakness in distance runners with iliotibial band syndrome. Clin J Sport Med. 2000 Jul;10(3):169-75.
11. Pinshaw, R, Atlas V, Noakes TD. The nature and response to therapy of 196 consecutive injuries seen at a runners’ clinic. S Afr Med J. 1984 Feb 25;65(8):291-8.
12. Schwellnus MP, Mackintosh L, Mee J. Deep transverse frictions in the treatment of iliotibial band friction syndrome in athletes: a clinical trial. Physiotherapy. 1992 Aug 10;78(8):564-8. doi: 10.1016/s0031-9406(10)61197-2.
13. Vicenzino B, Hing W, Rivett DA, Hall T. Mobilisation with Movement: The Art and the Science. 1st ed. Chatswood, NSM: Churchill Livingstone Australia; 2011.
14. Vicenzino B, Paungmali A, Teys P. Mulligan’s mobilization-with-movement, positional faults and pain relief: current concepts from a critical review of the literature. Man Ther. 2007 May;12(2):98-108.
15. DiGiovanna EL, Schiowitz S, Dowling DJ. An Osteopathic Approach to Diagnosis and Treatment. 3rd ed. Philadelphia, PA: Lippincottt Williams & Wilkins; 2005, ISBN: 0781742935.
16. Wainner RS, Whitman JM, Cleland JA, Flynn TW. Regional interdependence: a musculoskeletal examination model whose time has come. J Orthop Sports Phys Ther. 2007 Nov;37(11):658-60.
17. Vaughn DW. Isolated knee pain: a case report highlighting regional interdependence. J Orthop Sports Ther. 2008;38(10):616-23. doi: 10.2519/jospt.2008.2759.
18. Crowell MS, Wofford NH. Lumbopelvic manipulation in subjects with patellofemoral pain syndrome. J Man Manip Ther. 2012 Aug;20(3):113-20. doi: 10.1179/2042618612Y.0000000002.
19. Grassi Dde O, de Souza MZ, Ferrareto SB, Montebelo MI, Guirro EC. Immediate and lasting improvements in weight distribution seen in baropodometry following a high-velocity, low-amplitude thrust manipulation of the sacroiliac joint. Man Ther. 2011 Oct 16;16(5):495-500. doi: 10.1016/j.math.2011.04.003. Epub 2011 May 14.
20. Goncalves da Ropch RC, Nee R, Hall T, Chopard R. Treatment of persistent knee pain associated with lumbar dysfunction: a case report. NZ J Physio. 2006;34(1):30-4.
21. Maigne R. Low back pain of thoracolumbar origin. Arch Phys Med Rehabil. 1980 Sept; 61(9):389-95.
22. Selkow NM, Grindstaff TL, Cross KM, Pugh K, Hertel J, Saliba S. Short-term effect of muscle energy technique on pain in individuals with non-specifi c low back pain: a pilot study. J Man Manip Ther. 2009;17(1):E14-8.
23. Wilson E, Payton O, Donegan-Shoaf L, Dec K. Muscle energy technique in subjects with acute low back pain: a pilot clinical trial. J Orthop Sports Phys Ther. 2003 Sep; 33(9):502-12.
24. Thein-Nissenbaum JM, Thompson EF, Chumanow ES, Heiderscheit B. Low back and hip pain in a postpartum runner: applying ultrasound imaging and running analysis. J Orthop Phys Ther. 2012;42(7):615-24. doi: 10.2519/jospt.2012.3941. Epub 2012 Mar 23.
25. Khayambashi K, Mohammadkhani Z, Ghaznavi K, Lyle MA, Powers CM. The effects of isolated hip abductor and external rotator muscle strengthening on pain, health status, and hip strength in females with patellofemoral pain: a randomized controlled trial. J Orthop Sports Phys Ther. 2012 Jan;42(1):22-9. doi: 10.2519/jospt.2012.3704. Epub 2011 Oct 25.
26. Tonley JC, Yun SM, Kochevar RJ, Dye JA, Farrokhi S, Powers CM. Treatment of an individual with

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 390
32. Crowell HP, Davis IS. Gait retraining to reduce lower extremity loading in runners. Clin Biomech (Bristol, Avon). 2011 Jan;26(1):78-83. doi: 10.1016/j.clinbiomech.2010.09.003.
33. Kong PW, Candelaria NG, Smith DR. Running in new and worn shoes: a comparison of three types of cushioning footwear. Br J Sports Med. 2009 Oct; 43(10):745-9. doi: 10.1136/bjsm.2008.047761. Epub 2008 Sep 18.
34. Butler RJ, Davis IS, Hamill J. Interaction of arch type and footwear on running mechanics. Am J Sports Med. 2006 Dec;34(12):1998-2005.
35. Buist I, Bredeweg SW, Lemmink KA, Van Mechelen W, Diercks RL. Predictors of running-related injuries in novice runners enrolled in a systematic training program: a prospective cohort study. Am J Sports Med. 2010 Feb;38(2):273-80. doi: 10.1177/0363546509347985. Epub 2009 Dec 4.
36. Johansson H, Sjolander P, Sojka P. Receptors in the knee joint ligaments and their role in the biomechanics of the joint. Crit Rev Biomed Eng. 1991;18(5):341-68.
37. Schleip R. Fascial plasticity – a new neurobiological explanation. Journal of Bodywork and Movement Therapies. 2003;7(1):11-9. doi:10.1016/S1360-8592(02)00067-0.
piriformis syndrome focusing on hip muscle strengthening and movement reeducation: a case report. J Orthop Sports Phys Ther. 2010 Feb; 40(2):103-11. doi: 10.2519/jospt.2010.3108.
27. Lowry CD, Cleland JA, Dyke K. Management of subjects with patellofemoral pain syndrome using a multimodal approach: a case series. J Orthop Sports Phys Ther. 2008 Nov;38(11):691-702. doi: 10.2519/jospt.2008.2690.
28. Willy RW, Scholz JP, Davis IS. Mirror gait retraining for the treatment of patellofemoral pain in female runners. Clin Biomech (Bristol, Avon). 2012 Dec;27(10):1045-51. doi: 10.1016/j.clinbiomech.2012.07.011. Epub 2012 Aug 20.
29. Willy RW, Davis IS. The effect of a hip-strengthening program on mechanics during running and during a single leg squat. J Orthop Sports Phys Ther. 2011 Sep;42(9):625-32. doi: 10.2519/jospt.2011.3470. Epub 2011 Jul 12.
30. Davis IS. Gait Retraining in Runners. Orthopaedic Practice. 17;2:05. Accessed April 24, 2015.http://www.udel.edu/PT/PT%20Clinical%20Services/journalclub/caserounds/07_08/Dec07/GaitRetrain_OP.pdf
31. Teran-Yengle P, Emrick A, Hare K, Yack J, Cole K. CSM 2012 Orthopaedic section platform presentations: Effects of Internal and External Focus of Attention in Correcting Knee Hyperextension in Young Women. J Orthop Sports Phys Ther. Jan 2012;42(1)A14-40, OPL 4. doi:10.2519/jospt.2012.42.1.A14

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 391
ABSTRACTThe Army Physical Fitness Test (APFT) is a biannual training requirement for all soldiers. The Army has made significant overall fitness gains by developing functional and comprehensive Physical Readiness Training (PRT) programs, but more emphasis on individualized physical fitness test taking technique is warranted in order to optimize performance. The purpose of this clinical commentary is to provide clini-cians with several examples of APFT performance enhancement techniques that can potentially be applied not only in the Army, but throughout the military and in the sports community where general fitness assessments are routinely administered.
Keywords: Fitness assessments, Army Physical Fitness Test, human performance optimization
Level of Evidence: 5
IJSP
TCLINICAL COMMENTARY
PERFORMANCE OPTIMIZATION AND INJURY
PREVENTION STRATEGIES FOR THE ARMY PHYSICAL
FITNESS TEST: TECHNIQUE MATTERS
Mark Thelen, DSc, PT1
Shane Koppenhaver, PhD, PT1
1 U.S. Army-Baylor University Doctoral Program in Physical Therapy, San Antonio, TX, USA
Disclaimer: The views expressed in this article are those of the authors and do not refl ect the offi cial policy or position of the Department of the Army, Department of Defense, or the United States government.
CORRESPONDING AUTHORMark Thelen3630 Stanley Road, Bldg 2841, Suite 1301Fort Sam Houston, TX 78234-6100E-mail: [email protected]

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 392
BACKGROUNDThe concept of human performance optimization has garnered a lot of attention within the military in recent years.1 While there are multiple facets (physical, nutrition, cognitive, psychological, etc.) that have to be addressed for an individual to attain the highest level of performance, physical training and functional fitness is definitely a key component. Periodic generalized physical fitness assessments are a commonly utilized tool in the military, in addi-tion to numerous sports organizations.2,3 The Army Physical Fitness Test (APFT) is aimed at measur-ing cardiorespiratory endurance, upper and lower body muscular endurance and currently serves as a unit commander’s generalized fitness assessment of his/her soldiers.4 The events making up the APFT include: two minutes of push-ups, two minutes of sit-ups, and a two-mile run. Each event is worth a maxi-mum of 100 points and is based on an age and gender based scoring system. A minimum score of 60 points in each event is required to receive a passing grade. The test itself has remained relatively unchanged for well over 30 years.5 During that time a common performance improvement strategy has revolved around increasing the training volume and inten-sity of the events where improvement was desired, with the “prevailing thought” being, if you do enough push-ups, sit-ups, and running, scores will eventu-ally improve. More recently, the Physical Readiness Training (PRT) program was implemented in order to provide a more balanced training stimulus, prevent musculoskeletal injuries, and improve physical fit-ness.6–8 Improving muscular endurance and aerobic capacity is undoubtedly the most important aspect of improving APFT scores. Moreover, several stud-ies have provided research support for cross train-ing and the greater variety of exercises found in the revised PRT program.9–11 In some cases, a high level of baseline physical conditioning is enough to help individuals to achieve acceptable and occasionally even maximum scores. Other components that are essential for maximizing performance on the APFT have been recently stressed as a part of the Army Performance Triad initiative including proper sleep and performance nutrition.12
However, just like the technique aspect of any sports performance, technique likely matters for optimiz-ing APFT scores as well. It might seem reasonable
to assume that soldiers will self-select an exercise strategy for each of the APFT events, be it for prac-ticing or testing, that will likely yield optimal results if training occurs on a consistent basis. This is not always the case, some choose an exercise strategy based on ease of movement or comfort, regardless of how biomechanically or physiologically efficient it may be. To the authors’ knowledge, no published research or even expert guidance has addressed specific techniques aimed at improving APFT per-formance. The purpose of this commentary is to highlight some of the common deficiencies that can be observed in soldiers performing the APFT and provide technique recommendations to opti-mize performance. Since minimal research or data is available to frame this discussion, some of these recommendations are based off of commonly rec-ognized biomechanical and physiologic principles along with the clinical experience of the authors. Given the advanced knowledge of biomechanics, functional movement analysis, and exercise physiol-ogy that sports physical therapists possess, they are ideally suited to provide this kind of service.
APFT EVALUATION
Principles of PerformancePerhaps the most relevant biomechanical principle to APFT technique concerns the concept of “torque”, which is simply the force (or weight) applied mul-tiplied by the length of the lever arm (i.e. torque = force x lever arm).13 A simple example can be illus-trated by holding a gallon of milk. If held close to the body, a gallon of milk doesn’t feel excessively heavy because it’s exerting a fairly small “torque” on the shoulder due to a small lever arm. However, if held with an outstretched arm, the same gallon of milk feels quite heavy (larger torque) due to the increased lever arm. Similarly, from an exercise physiology perspective, the amount of “work” that a muscle per-forms is determined by the forces exerted (weight) multiplied by the distance moved (i.e. work = force x distance).13 Therefore, it will take much more work for the shoulder muscles to lift a gallon of milk 10 times with the arm outstretched than it will to lift it 10 times close to the body. Additionally, the amount of “work” that a muscle expends during repetitive lifts is the sum of the work that occurs during the lifting phase (concentric contraction) and that which

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 393
occurs during the lowering phase (eccentric con-traction). Although eccentric contraction may pro-tect the muscle, joints, tendons, and ligaments from stress of ballistic deceleration, it requires substantial muscle work without contributing to higher num-ber of repetitions. The ability to produce and sus-tain mechanical work done by the musculoskeletal system is facilitated through the conversion of met-abolic energy. Physical fitness and nutrition status play a key role in developing an efficient system of energy utilization to fuel physical performance. Fur-ther, choosing movement strategies that minimize unnecessary energy expenditure will likely lower the metabolic cost associated with that activity.
Two Minute Push-up EventSoldiers are required to descend while maintaining the trunk and lower extremities in a generally straight line until the upper arms are parallel to the ground in order for a repetition to be counted. They are allot-ted two minutes for this event, which is a significant amount of time to continuously perform push-ups. It has been anecdotally observed that some soldiers do not utilize the full two minutes because they reach fatigue and/or they choose to conserve energy for a subsequent event. Those who do utilize the full time allotment typically expend an excessive amount of energy particularly within the last 30 seconds or so to only produce a handful of repetitions that may not all end up counting. A common reason for repetitions to not be counted is failure to descend low enough. Sol-diers should attempt to achieve their maximal score within the first 90 seconds. The primary ingredient to achieve this is proper pacing. Repetitions during the test need to be done quickly, but not so quickly that a grader cannot determine if the performance stan-dards were met, potentially resulting in a repetition not counting. Soldiers should strive to never have a repetition be uncounted as it becomes a waste of energy that could have downstream effects on the cur-rent or a later event. Given a 10-minute rest period is prescribed between each event, this time period may result in suboptimal recovery.14 This can adversely affect performance on the sit-up event which is also a local muscle endurance event that maximally chal-lenges anaerobic endurance of the core musculature. Those who struggle with this event, often expend too much energy by lowering themselves too slow during
the down phase, which requires increased eccentric muscle action.15 This can lead to premature fatigue and is a less than optimal test performance strategy. The down phase should be led by the chest, not the head or the abdomen and should require little to no muscular work. Often, soldiers will allow the head to flex and lead the down phase which gives the false appearance of going farther down than the body actually travels, possibly resulting in one or more uncounted repetitions.
Generally, the up phase is easier to sustain16 and is more quickly achieved than the down position.15 The up phase can be made more difficult by the selection of hand position. The hands should be just slightly more than shoulder width apart. Positioning the hands too narrowly will cause excessive work of the triceps and pectoralis major muscles17 leading to premature fatigue. Positioning the hands too wide, depending on arm length, can increase the lever arm possibly requiring more work of the pectoral mus-cles and increase anterior strain at the glenohumeral joint. Seek to find a hand position that will allow the upper arms to be positioned less than 60 degrees abducted away from the body when viewed from the top and the forearms oriented vertically. (Figures 1 and 2) This positioning is preferred to avoid scapu-lar positioning that could lead to shoulder impinge-ment.18 In the presence of hypothenar wrist pain a wider hand position may be better tolerated, and conversely, a narrower hand position may be more comfortable if a soldier has some thenar wrist pain.19
The position of the foot and ankle can also serve to make this event more challenging. For example,
Figure 1. Recommended arm position during the push-up event.

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 394
those who perform push-ups in any degree of ankle plantar flexion are expending more energy than nec-essary. (Figure 3) This ankle motion results in a lon-ger lever arm of the body causing more weight to be borne through the upper extremities.20 The individ-ual should seek to maintain the ankle in some degree of dorsiflexion throughout the event if the range of motion is available and comfortable. (Figure 4) Per regulation,4 the foot contact points can be placed together or up to 12 inches apart. Some soldiers keep their feet separated during the push-up event, which challenges the lower extremities to achieve a station-ary position with only minimal surface area contact that is provided by the distal aspect of the shoes. To increase the active and passive stability of the lower
extremities and trunk, place the feet about 3-4 inches apart and then allow the heels come into contact with one another. When viewed from the rear it will form a triangle shape (Figure 5). The authors refer to this position as the “stability triangle”, because it allows the lower extremities to brace against one another serving as an anatomic splint. Further, when the heels and medial thighs push into one another with mild to moderate force it creates muscle activ-ity in the powerful gluteal musculature, the pelvic floor, lumbar paraspinals, and even the periscapular musculature which should assist in maintaining the trunk in a proper plank position.21
Figure 3. Ankle plantarfl exion results in more weight being borne through the upper extremities. Figure 5. The stability triangle position.
Figure 4. Ankle dorsifl exion helps to better distribute weight-bearing between the upper and lower extremities.
Figure 2. Vertical orientation of forearms during push-up event.

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 395
the event. Consistent and purposeful breathing and avoidance of Valsalva maneuver is again of para-mount importance during this test.24 The first step is to ensure that the entire testing area, particularly when outdoors, is inspected to ensure that there is not a disadvantageous slope present, but also to make sure there is no portion of the terrain that will interfere during the test (i.e. sticks, rocks, ants, etc.). Ensure that the soldier tasked with holding the feet has a firm and comfortable hold whether a heel con-tact or foot flat contact is preferred. Understand that a heel contact will require more muscular work from the front part of the lower leg, and a foot flat posi-tion requires more muscular work from the thighs.25 Both can have consequences during the two mile run event, so some experimentation may be needed to determine which does not adversely affect leg drive and muscular endurance during the run. That said, a foot flat position is easier for a holder to stabilize and should result in less inefficient lower extremity rotational motion during the up phase of the sit-up. Regardless of the foot hold technique, it is recom-mended to keep the feet approximately four to six inches apart during the test. Soldiers should visual-ize that they are lying on a pair of railroad tracks with the goal being to appropriately align the shoul-der with the thigh and the foot for both the right and left side. (Figure 7) The rationale for this stems from the notion that hip flexor musculature is very active during the sit-up event.26 Maintenance of uniplanar motion could prevent unnecessary energy expendi-ture particularly on the up phase when some Sol-diers allow their thigh(s) to move inward toward one another or outward away from one another. Ensure that the fingers remain tightly interlaced as low on the neck as possible. Keeping the hands low should
Breathing is another aspect that is often overlooked and can result in diminished performance. Remem-bering to breathe consistently and purposefully to ensure adequate oxygenation for the working mus-cles is important. Trying to exhale during the up phase is generally recommended in order to avoid a Valsalva maneuver.22
Soldiers are authorized to rest at one or more points during the event. Short rests will potentially help achieve more repetitions as long as the primarily fatiguing muscles (pectorals and triceps) are allowed to mostly relax. There are only two authorized rest posi-tions: flexing or arching the back while maintaining the original position of the four points of contact. Rest-ing in the flexed position while sticking the buttocks as high in the air as possible (i.e. “tenting”) is the position that allows the sternocostal portion of pectoralis major and rectus abdominis muscles to be the more relaxed23 and presumably would result in the lower extremities bearing more weight. Additionally, by resting in this flexed position, it will be easier to lower the trunk back to the starting position, as opposed to actively raising your trunk back up from an arched low back position to the starting position. On a final note, any soldier that struggles to adequately recover following the push-up event should seek to be in the front of the respective testing line in order to maximize rest periods.
Two Minute Sit-Up EventWith the feet held in place, soldiers are required to perform as many sit-ups as possible while maintain-ing the knees at a 90-degree angle and ensuring the shoulder blades touch the ground at the end of each repetition. A key checkpoint is to ensure that the vertical position is achieved, that is when the base of the neck is above the base of the spine. (Figure 6) Additionally, soldiers are not permitted to lift their buttocks off the ground at any point during the event. Unlike the push-up event, when done cor-rectly and consistently, the sit-up event can be usu-ally done with proper form for the entire allotted time. Again pacing is very important in this event, as a quick yet sustainable pace is preferred. Many try to go too fast and burn-out within a minute and struggle significantly in the second half of the event resulting in fewer counted repetitions and marked energy expenditure. Soldiers should seek to do an equal amount of repetitions during each minute of
Figure 6. The vertical position of the sit-up event.

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 396
An alternative to this would be to somewhat, but not completely, relax the abdomen to allow a quick down phase that can be stopped at the point of shoulder blade-ground contact followed with a rapid reversal of direction. This again will require some training to become comfortable with, but the use of a rolled hand towel placed perpendicular to and at the level of the middle of the scapulae to provide an inexpensive form of biofeedback is recommended. Soldiers should avoid allowing the elbows to move rapidly outward during the transition from the down phase to the up phase. This is commonly referred to as winging and results in unnecessary energy expenditure, a static position where the elbows are angled slightly to the outside of the thighs is recommended.
The last point to make is for the individual hold-ing the tested soldier’s feet. Most soldiers sustain a position that has a majority of their bodyweight being borne through the upper extremities for the duration of the event. This is not needed, so con-sider shifting the weight forward toward the upper extremities when the tested Soldier goes down and then shift toward the feet as the tested Soldier comes up. (Figures 8 and 9) By staying in rhythm with the tested Soldier in this manner the end result is less energy expended by the holder.
Two Mile Run EventThis is the culminating event of the APFT and requires a reasonable amount of cardiopulmonary and muscular endurance to meet or exceed the standard. In many cases, a planned and periodized increase in training volume is a large part of the solu-tion for this event. However, self-selected running
minimize the torque (weight) of the trunk being lifted, thereby potentially increasing the number of repetitions possible. Placing the hands too high can potentially cause soldiers to pull on their head and strain their neck. Also, a common reason for stopping the test is due to the fingers slipping off the neck. Next, ensure that the knee angle is main-tained at 90 degrees throughout the event. If the but-tocks are allowed to slide closer to or further away from the heels that will result in sit-ups that may not count and/or be more unnecessarily difficult to perform due a mechanical disadvantage.
Ensure that the necessary amplitude of movement for both the up and down phase of the sit-up is not exceeded. Some soldiers choose to move so far up such that their chest nearly touches the thighs. This exceeds the standard vertical position and is not neces-sary; further it results in more energy and time being required to complete each repetition. Another poten-tial pitfall, especially from soldiers taking their first APFT, is choosing how to expend the least amount of energy on eccentric contraction during the lowering phase. Some choose to completely relax their abdom-inal muscles during the down phase, which requires a rapid concentric contraction in the down position and sometimes a lifting of the buttocks off the ground in order to reverse direction back into the up position.
Figure 7. Recommended thigh alignment during the sit-up event.
Figure 8. Recommended foot holding technique during the down phase of the sit-up event.

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 397
There is a significant amount of research regard-ing the relative value of the various foot strike pat-terns.31–34 A majority of runners today utilize a heel strike pattern in which the heel of their running shoe strikes the ground first. There is some evidence to suggest that this results in increased ground reac-tion forces being absorbed within the lower extremi-ties and could increase risk for injury.35 Other less common foot strike patterns are mid-foot strike and forefoot strike. These landing strategies can result in decreased joint reaction forces but also result in increased muscle activation within the plantarflex-ors, particularly during early stance phase.32 It is unclear at this point, if there is a preferred foot strike pattern that should be considered to either increase running performance or decrease risk for running related overuse injury. It has been reported that individuals are not that reliable at self-reporting the type of foot strike pattern they utilize, nor does the type of shoe worn dictate the type of foot strike pattern that is utilized.36,37
styles are not always the most efficient or comfort-able method available to the soldier. A brief but thor-ough evaluation of running form can easily be done utilizing a commercial treadmill and a smartphone with a native camera. It is ideal, but not essential, to have the ability to view the runner using slow-motion video as well (preferably at a minimum rate of 120 frames per second). First, while there is no one ideal way to run there are some basic principles that most will agree upon. When running the head should be upright and the shoulders back to allow for more efficient breathing. Elbows should be bent at about 90 degrees and the fingers gently curled. There should be a very minimal amount of forward trunk lean on level surfaces. It is recommended to first look at the soldier running real time without videotaping in order to get a general sense of the running gait. Different aspects of running form can be revealed by looking from different angles, so at a minimum a lateral and posterior view should be obtained. From the lateral aspect, one can easily dis-cern the relative stride length, foot strike pattern, and vertical displacement. Stride length will vary by individual, however, assess for those who over stride. This occurs when the foot strikes the ground forward of a line drawn straight from the trunk to the ground. (Figure 10) The result of this is a less efficient running gait and an increase in ground reaction forces being absorbed by the lower extremi-ties.27,28 While it may take some practice and prob-ably the use of a metronome, shortening the stride length slightly and increasing the cadence slightly may help to overcome this issue and decrease load-ing in the lower extremities.29,30
Figure 9. Recommended foot holding technique during the up phase of the sit-up event.
Figure 10. An example of excess vertical displacement and over striding.
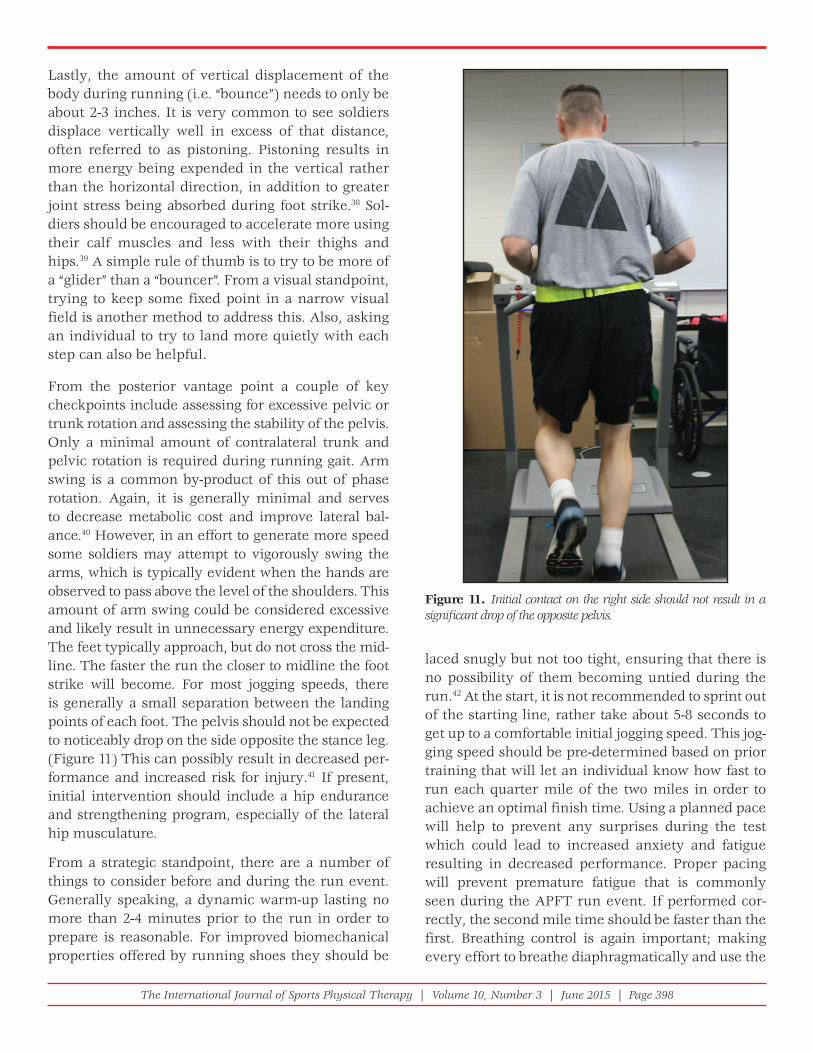
The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 398
laced snugly but not too tight, ensuring that there is no possibility of them becoming untied during the run.42 At the start, it is not recommended to sprint out of the starting line, rather take about 5-8 seconds to get up to a comfortable initial jogging speed. This jog-ging speed should be pre-determined based on prior training that will let an individual know how fast to run each quarter mile of the two miles in order to achieve an optimal finish time. Using a planned pace will help to prevent any surprises during the test which could lead to increased anxiety and fatigue resulting in decreased performance. Proper pacing will prevent premature fatigue that is commonly seen during the APFT run event. If performed cor-rectly, the second mile time should be faster than the first. Breathing control is again important; making every effort to breathe diaphragmatically and use the
Lastly, the amount of vertical displacement of the body during running (i.e. “bounce”) needs to only be about 2-3 inches. It is very common to see soldiers displace vertically well in excess of that distance, often referred to as pistoning. Pistoning results in more energy being expended in the vertical rather than the horizontal direction, in addition to greater joint stress being absorbed during foot strike.38 Sol-diers should be encouraged to accelerate more using their calf muscles and less with their thighs and hips.39 A simple rule of thumb is to try to be more of a “glider” than a “bouncer”. From a visual standpoint, trying to keep some fixed point in a narrow visual field is another method to address this. Also, asking an individual to try to land more quietly with each step can also be helpful.
From the posterior vantage point a couple of key checkpoints include assessing for excessive pelvic or trunk rotation and assessing the stability of the pelvis. Only a minimal amount of contralateral trunk and pelvic rotation is required during running gait. Arm swing is a common by-product of this out of phase rotation. Again, it is generally minimal and serves to decrease metabolic cost and improve lateral bal-ance.40 However, in an effort to generate more speed some soldiers may attempt to vigorously swing the arms, which is typically evident when the hands are observed to pass above the level of the shoulders. This amount of arm swing could be considered excessive and likely result in unnecessary energy expenditure. The feet typically approach, but do not cross the mid-line. The faster the run the closer to midline the foot strike will become. For most jogging speeds, there is generally a small separation between the landing points of each foot. The pelvis should not be expected to noticeably drop on the side opposite the stance leg. (Figure 11) This can possibly result in decreased per-formance and increased risk for injury.41 If present, initial intervention should include a hip endurance and strengthening program, especially of the lateral hip musculature.
From a strategic standpoint, there are a number of things to consider before and during the run event. Generally speaking, a dynamic warm-up lasting no more than 2-4 minutes prior to the run in order to prepare is reasonable. For improved biomechanical properties offered by running shoes they should be
Figure 11. Initial contact on the right side should not result in a signifi cant drop of the opposite pelvis.

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 399
ing in order to be incorporated correctly, others may be readily correctable and could theoretically lead to immediate improved performance. The goal of any periodized training program is to deliver peak performance at the right time in the training cycle, and this should be taken under consideration when making any technique modifications.
Lastly, it has been well documented that physical training results in a large number of musculoskeletal injuries.50 The level of physical effort provided dur-ing the APFT typically reaches maximal exertion not encountered during typical physical readiness train-ing sessions. As a result, more serious injuries and illnesses have been reported during the conduct of the APFT.24,51–53 This provides even more incentive to ensure that soldiers are using the most biomechani-cally and physiologically sound techniques to com-plete the APFT.
REFERENCES 1. Deuster PA, O’Connor FG, Henry KA, et al. Human
performance optimization: an evolving charge to the Department of Defense. Mil Med. 2007;172(11):1133-1137.
2. Ebben WP, Carroll RM, Simenz CJ. Strength and conditioning practices of National Hockey League strength and conditioning coaches. J Strength Cond Res Natl Strength Cond Assoc. 2004;18(4):889-897.
3. Ebben WP, Blackard DO. Strength and conditioning practices of National Football League strength and conditioning coaches. J Strength Cond Res Natl Strength Cond Assoc. 2001;15(1):48-58.
4. Headquarters, Department of the Army. Army Physical Readiness Training: Field Manual 7-22.; 2012.
5. Knapik JJ, East WB. History of United States Army physical fi tness and physical readiness training. US Army Med Dep J. 2014:5-19.
6. Knapik JJ, Hauret KG, Arnold S, et al. Injury and fi tness outcomes during implementation of physical readiness training. Int J Sports Med. 2003;24(5):372-381.
7. Knapik J, Darakjy S, Scott SJ, et al. Evaluation of a standardized physical training program for basic combat training. J Strength Cond Res Natl Strength Cond Assoc. 2005;19(2):246-253.
8. Knapik JJ, Rieger W, Palkoska F, Van Camp S, Darakjy S. United States Army physical readiness training: rationale and evaluation of the physical training doctrine. J Strength Cond Res Natl Strength Cond Assoc. 2009;23(4):1353-1362.
accessory muscles of the chest and neck minimally. A rhythmical breathing pattern where inhalation occurs over two to three steps and exhalation then occurs over the next two to three steps is a common practice.43,44 Deeper breathing or pursed lip breathing for a few breathing cycles may help to restore a com-fortable and consistent breathing pattern as needed during the run.43,45 Breathing through the nose as much as possible, particularly during cold weather, helps avoid possible airway irritation.
DISCUSSIONThis clinical commentary was specifically intended to address individual performance during the APFT. However, the other military services and various sports organizations that utilize similar generalized physical fitness assessments could also potentially benefit from the implementation of a program that exploits the functional movement analysis skill set of the physical therapists that support those cli-ent populations. Further, excelling on the APFT is a common long-term rehabilitation goal for many injured soldiers. Therefore, the information con-tained in this commentary can assist sports physi-cal therapists conducting advanced rehabilitation in addition to optimizing human performance. In addition to the PRT program, it should be noted that there are several comprehensive functional physical fitness programs that have shown promise regard-ing the ability to improve physical fitness measures to include the APFT.46–48 The authors believe if the technique-specific training presented in this com-mentary is incorporated into the aforementioned programs, there is the possibility of a synergistic effect. When available, attempts to draw upon avail-able research evidence have been made with regard to making the aforementioned recommendations. However, field trials are now warranted to validate the effectiveness of these suggested performance techniques.
An evaluation of APFT technique can easily be com-pleted during one 30-minute clinical session. At that time, the appropriate technique modification(s) can then be incorporated into an existing regimen assuming that there is an appropriate level of train-ing volume and intensity.49 Whereas, some training modifications may require additional time and train-

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 400
23. Kang D-H, Jung S-Y, Nam D-H, Shin S-J, Yoo W-G. The Effects of Push-ups with the Trunk Flexed on the Shoulder and Trunk Muscles. J Phys Ther Sci. 2014;26(6):909-910.
24. Uber-Zak LD, Venkatesh YS. Neurologic complications of sit-ups associated with the Valsalva maneuver: 2 case reports. Arch Phys Med Rehabil. 2002;83(2):278-282.
25. Parfrey KC, Docherty D, Workman RC, Behm DG. The effects of different sit- and curl-up positions on activation of abdominal and hip fl exor musculature. Appl Physiol Nutr Metab Physiol Appliquée Nutr Métabolisme. 2008;33(5):888-895.
26. Szasz A, Zimmerman A, Frey E, Brady D, Spalletta R. An electromyographical evaluation of the validity of the 2-minute sit-up section of the Army Physical Fitness Test in measuring abdominal strength and endurance. Mil Med. 2002;167(11):950-953.
27. Seay JF, Frykman PN, Sauer SG, Gutekunst DJ. Lower extremity mechanics during marching at three different cadences for 60 minutes. J Appl Biomech. 2014;30(1):21-30. doi:10.1123/jab.2012-0090.
28. Thompson MA, Gutmann A, Seegmiller J, McGowan CP. The effect of stride length on the dynamics of barefoot and shod running. J Biomech. 2014;47(11):2745-2750.
29. Heiderscheit BC, Chumanov ES, Michalski MP, Wille CM, Ryan MB. Effects of step rate manipulation on joint mechanics during running. Med Sci Sports Exerc. 2011;43(2):296-302.
30. Hobara H, Sato T, Sakaguchi M, Sato T, Nakazawa K. Step frequency and lower extremity loading during running. Int J Sports Med. 2012;33(4):310-313.
31. Daoud AI, Geissler GJ, Wang F, Saretsky J, Daoud YA, Lieberman DE. Foot strike and injury rates in endurance runners: a retrospective study. Med Sci Sports Exerc. 2012;44(7):1325-1334.
32. Goss DL, Gross MT. A review of mechanics and injury trends among various running styles. US Army Med Dep J. 2012:62-71.
33. Lieberman DE, Venkadesan M, Werbel WA, et al. Foot strike patterns and collision forces in habitually barefoot versus shod runners. Nature. 2010;463(7280):531-535.
34. Ogueta-Alday A, Rodríguez-Marroyo JA, García-López J. Rearfoot striking runners are more economical than midfoot strikers. Med Sci Sports Exerc. 2014;46(3):580-585.
35. Milner CE, Ferber R, Pollard CD, Hamill J, Davis IS. Biomechanical factors associated with tibial stress fracture in female runners. Med Sci Sports Exerc. 2006;38(2):323-328.
9. Baxter RE, Moore JH, Pendergrass TL, Crowder TA, Lynch S. Improvement in sit-up performance associated with 2 different training regimens. J Orthop Sports Phys Ther. 2003;33(1):40-47.
10. Childs JD, Teyhen DS, Benedict TM, et al. Effects of sit-up training versus core stabilization exercises on sit-up performance. Med Sci Sports Exerc. 2009;41(11):2072-2083.
11. Kraemer WJ, Vescovi JD, Volek JS, et al. Effects of concurrent resistance and aerobic training on load-bearing performance and the Army physical fi tness test. Mil Med. 2004;169(12):994-999.
12. Horoho PD. A system for health: essential element of national security. US Army Med Dep J. 2013:4.
13. Levangie P, Norkin CC. Joint Structure and Function: A Comprehensive Analysis Fifth Edition. 5 edition. Philadelphia: F.A. Davis Company; 2011.
14. Association NS and C. Essentials of Strength Training and Conditioning - 3rd Edition. 3 edition. Champaign, IL: Human Kinetics; 2008.
15. Yoo W-G. Effect of Exercise Speed and Isokinetic Feedback on the Middle and Lower Serratus Anterior Muscles during Push-up Exercises. J Phys Ther Sci. 2014;26(5):645-646.
16. Suprak DN, Dawes J, Stephenson MD. The effect of position on the percentage of body mass supported during traditional and modifi ed push-up variants. J Strength Cond Res Natl Strength Cond Assoc. 2011;25(2):497-503.
17. Cogley RM, Archambault TA, Fibeger JF, Koverman MM, Youdas JW, Hollman JH. Comparison of muscle activation using various hand positions during the push-up exercise. J Strength Cond Res Natl Strength Cond Assoc. 2005;19(3):628-633.
18. Suprak DN, Bohannon J, Morales G, Stroschein J, San Juan JG. Scapular kinematics and shoulder elevation in a traditional push-up. J Athl Train. 2013;48(6):826-835.
19. Chuckpaiwong B, Harnroongroj T. Palmar pressure distribution during push-up exercise. Singapore Med J. 2009;50(7):702-704.
20. Gouvali MK, Boudolos K. Dynamic and electromyographical analysis in variants of push-up exercise. J Strength Cond Res Natl Strength Cond Assoc. 2005;19(1):146-151.
21. Kim M-H, Yoo W-G. Effects of Push-up Exercise with Hip Adduction on the COP Deviation and the Serratus Anterior and L1 Paraspinal Muscles. J Phys Ther Sci. 2013;25(7):783-784.
22. Linsenbardt ST, Thomas TR, Madsen RW. Effect of breathing techniques on blood pressure response to resistance exercise. Br J Sports Med. 1992;26(2):97-100.

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 401
46. Sell TC, Abt JP, Crawford K, et al. Warrior Model for Human Performance and Injury Prevention: Eagle Tactical Athlete Program (ETAP) Part II. J Spec Oper Med Peer Rev J SOF Med Prof. 2010;10(4):22-33.
47. Kelly TK, Masi R, Walker B, Knapp S, Leuschner KJ. An Assessment of the Army’s Tactical Human Optimization, Rapid Rehabilitation and Reconditioning Program. 2013. http://www.rand.org/pubs/technical_reports/TR1309.html. Accessed April 22, 2015.
48. CrossFit program improves APFT scores� | Article | The United States Army. http://www.army.mil/article/103460/. Accessed April 22, 2015.
49. Garber CE, Blissmer B, Deschenes MR, et al. American College of Sports Medicine position stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fi tness in apparently healthy adults: guidance for prescribing exercise. Med Sci Sports Exerc. 2011;43(7):1334-1359.
50. Bullock SH, Jones BH, Gilchrist J, Marshall SW. Prevention of physical training-related injuries recommendations for the military and other active populations based on expedited systematic reviews. Am J Prev Med. 2010;38(1 Suppl):S156-S181.
51. Statler JD, Ronsivalle JA, Depper MH, Rao KC. Bilateral carotid artery dissection during the Army physical fi tness test. Mil Med. 1998;163(12):857-860.
52. McHale KM, Prahinski JR. Acute exertional compartment syndrome occurring after performance of the army physical fi tness test. Orthop Rev. 1994;23(9):749-753.
53. Munter DW, Charles JA. Exertional rhabdomyolysis following an Army physical fi tness test. Mil Med. 1989;154(11):579-581.
36. Goss DL, Lewek M, Yu B, Ware WB, Teyhen DS, Gross MT. Lower Extremity Biomechanics and Self-Reported Foot-Strike Patterns Among Runners in Traditional and Minimalist Shoes. J Athl Train. 2015.
37. Willson JD, Bjorhus JS, Williams DSB, Butler RJ, Porcari JP, Kernozek TW. Short-term changes in running mechanics and foot strike pattern after introduction to minimalistic footwear. PM R. 2014;6(1):34-43; quiz 43.
38. Halvorsen K, Eriksson M, Gullstrand L. Acute effects of reducing vertical displacement and step frequency on running economy. J Strength Cond Res Natl Strength Cond Assoc. 2012;26(8):2065-2070.
39. Schache AG, Dorn TW, Williams GP, Brown NAT, Pandy MG. Lower-limb muscular strategies for increasing running speed. J Orthop Sports Phys Ther. 2014;44(10):813-824.
40. Arellano CJ, Kram R. The effects of step width and arm swing on energetic cost and lateral balance during running. J Biomech. 2011;44(7):1291-1295.
41. Noehren B, Hamill J, Davis I. Prospective evidence for a hip etiology in patellofemoral pain. Med Sci Sports Exerc. 2013;45(6):1120-1124.
42. Hagen M, Hennig EM. Effects of different shoe-lacing patterns on the biomechanics of running shoes. J Sports Sci. 2009;27(3):267-275.
43. How To Breathe When Running | Runner’s World. http://www.runnersworld.com/running-tips/lung-power?page=2. Accessed April 22, 2015.
44. Breathing During Exercise | Military.com. http://www.military.com/military-fi tness/workouts/breathing-during-exercise. Accessed April 22, 2015.
45. Cabral LF, D’Elia TDC, Marins DDS, Zin WA, Guimarães FS. Pursed lip breathing improves exercise tolerance in COPD: a randomized crossover study. Eur J Phys Rehabil Med. 2015;51(1):79-88.

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 402
ABSTRACTSports and orthopaedic physical therapists have long used a multitude of techniques in order to address pain and dysfunction associated with myofascial trigger points. One technique in particular has recently received overwhelming attention: trigger point dry needling (DN). Despite its efficacy and low risk, ques-tions remain as to its effectiveness, safety, and whether the technique is within the scope of practice of physical therapists. Therefore, the purpose of this clinical commentary is to summarize the current litera-ture related to the associated mechanisms of action of DN, the safety of DN, as well as to discuss relevant scope of practice concerns.
Keywords: Dry needling, TDN, DN, Trigger point dry needling
Level of Evidence: 5
IJSP
TCLINICAL COMMENTARY
DRY NEEDLING FOR MYOFASCIAL TRIGGER POINT
PAIN: A CLINICAL COMMENTARY
Casey Unverzagt, DPT, DSc, OCS, SCS, CSCS1
Kathy Berglund, PT, DSc, FAAOMPT, OCS, ATC2
J.J. Thomas, MPT, CMTPT3
1 Wise Physical Therapy and Sports Medicine, Slippery Rock, PA, USA
2 Andrews University Department of Physical Therapy, Berrien Springs, MI, USA
3 Primal Physical Therapy, Havertown, PA, USA
CORRESPONDING AUTHORCasey Unverzagt215 Grove City RoadSlippery Rock, PA 16057E-mail: [email protected]

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 403
Table 1. Precipitating & perpetuating factors of MTrPs
INTRODUCTIONDry needling (also known as intramuscular manual stimulation, or intramuscular needling) is a treat-ment technique that has been utilized by physiother-apists in Canada, Chile, Ireland, Spain, South Africa and the United Kingdom since the 1980’s, and in the United States since 1984.1 While the technique is typ-ically not taught in entry-level education, there has been a dramatic increase in dry needling (DN) certi-fication programs and continuing education courses in recent years. Additionally, the practice of DN has received significant attention at the federal level, as the Federation of State Boards of Physical Therapy (FSBPT) has released four editions of a resource paper between 2010 and 2013, all regarding physical therapist use of DN.1 The American Physical Therapy Association (APTA) and the American Academy of Orthopaedic Manual Physical Therapists (AAOMPT) have both created position statements supporting physical therapists’ use of the technique.2,3 With the increase in exposure to the practice of DN, thera-pists should question its efficacy, as well its associ-ated risks. In order to appreciate both, it is vital to have a robust understanding of the various models for DN, as well as the proposed associated outcomes when treating pain of myofascial trigger point origin. Lastly, physical therapists must fully understand the scope of practice challenges that are associated with the performance of DN.
Myofascial Trigger Point PainMyofascial trigger point pain is defined as “pain arising from one or more myofascial trigger points (MTrPs), which are hyperirritable spots in skeletal muscle that are associated with hypersensitive pal-pable nodules in taut bands.”4 With MTrPs, the entire muscle is not hard, cramped, nor tender; the tender-ness is strictly limited to the taut band.5 Typically, MTrPs are painful on compression and can give rise to referred pain and/or tenderness, as well as autonomic phenomena (localized sweating, vaso-constriction or vasodilation, and pilomotor activ-ity).1,4,6 Additionally, they can be divided into active and latent types. These must be differentiated from tender points found in a muscle, which in contrast to MTrPs, only cause local pain upon compression.7 These differences underscore the need for the diag-nosis of MTrP’s to be classified not only as a motor or architectural abnormality, but as also including painful sensory dysfunction.
Several theories of precipitating and perpetuating factors responsible for creating MTrPs have been proposed (Table 1). The leading belief is that MTrPs are caused from an excessive release of acetylcho-line (Ach) from motor endplates.8,9 The prolonged release of Ach results in chronic shortening and contractures of sarcomeres, coupled with decreased circulation leading to hypoxia and local ischemia.7,10

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 404
As a result, prostaglandins, bradykinins, cytokines, and histamine are released, which then sensitize the sensory afferent nerve fibers of the muscle, likely accounting for the specific point tenderness commonly seen with MTrPs.10-12 Furthermore, the bombardment of nociceptors by the endogenous chemicals often leads to central sensitization of the dorsal horn neurons.11,12
Central sensitization is “an increase in the excitabil-ity of neurons within the central nervous system” that elicits pain hypersensitivity, so that normal inputs begin to produce abnormal responses.13,14(p.
205) The underlying neurobiological basis for central sensitization relates to the fact that most synaptic input to neurons is subthreshold, acting sublimi-nally either because synaptic input is too weak, or membrane excitability is restrained by inhibitory inputs.13 These subthreshold inputs can be elevated to suprathreshold action potentials by increasing synaptic response to the transmitter, by reducing inhibition, or by increasing membrane excitability.13 Central sensitization has been observed during cuta-neous inflammation as well as during inflammation of a joint, muscle or viscera.15 Typical changes of the individual neurons include, but are not limited to: 1) increased response to noxious stimulation of inflamed tissue; 2) lowered threshold of nociceptive specific spinal cord neurons; 3) increased response to stimuli applied to non-inflamed tissue surround-ing the inflamed site; and 4) expansion of the receptive field.15 Furthermore, it has recently been appreciated that in addition to activity-dependent synaptic plasticity, changes to microglia, astrocytes, gap junctions, membrane excitability, and gene transcription all can contribute to the continuation of central sensitization.13 This “ramped up” nervous system perpetuates chronic muscular hypertonicity, and the development of MTrPs.
In contrast to central sensitization, peripheral sensi-tization occurs due to an increase in responsiveness, and reduced threshold of activation of the peripheral ends of nociceptors.13,14,16,17 Sensitization arises sec-ondary to inflammatory mediators released around the site of tissue damage.16 Specifically, peripheral nociceptive terminals become ‘‘sensitized” after injury, secondary to an influx of neutrophils. The neutrophils create Cox-2 enzyme, which leads to
the production and secretion of prostaglandin E2 (PGE2).16 The PGE2 acts as a sensitizer, thus altering pain sensitivity. This hypersensitivity is localized to the site of injury, also known as the zone of primary hyperalgesia.13,16,17 Because peripheral sensitization represents a form of pain elicited by activation of nociceptors, it generally requires ongoing peripheral pathology in order for it to continue.16
It has been estimated that myofascial pain is respon-sible for 30-85% of patients who present to a pri-mary care setting or pain clinic with a complaint of pain.18-21 Gerwin et al5 noted that MTrPs were the primary source of pain in 71 of 96 patients who were referred to a neurologist with musculoskeletal pain. Similar results have been found in patients with chronic head and neck pain seeking dental care.20 In a study of musculoskeletal disorders in rural Thai-land, it was found that pain arising from one or more myofascial trigger points was the primary cause for 36% of 431 individuals who had pain in the previ-ous seven days.22 Despite the prevalence of MTrPs causing musculoskeletal pain, they often go undiag-nosed, and therefore untreated.
Recent advances in medical imaging allow for the visualization of MTrPs.23 Sikdar et al24 recently intro-duced sonoelastography, a unique ultrasound appli-cation, which allows visualization of MTrPs. They noted that MTrPs in the upper trapezius were ellipti-cally shaped focal areas of hypoechogenicitiy (ultra-sound waves did not reflect back to sound head) that corresponded with the palpable nodule (Figure 1).23,24 The authors were able to identify retrograde blood flow during diastole which suggests a highly restrictive vascular bed. Additionally, magnetic reso-nance elastography (MRE) has recently been used to quantify asymmetries in muscle tone, and localize MTrPs.23,25 MRE has the ability to measure stiffness of soft tissues by measuring the propagation of shear waves introduced by a standard MRI.
While particular imaging methods can assist in identifying specific locations of MTrPs, their avail-ability and cost currently prohibit their widespread use. Thus, a systematic approach to palpating trig-ger points is vital prior to treatment. Not only is it essential to palpate MTrPs in the primarily affected muscle, but also in the synergist and antagonist as well (secondary MTrPs). Baldry26 suggests practitio-

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 405
ners first draw their palpating finger perpendicular to the muscle using a flat finger. A pincer palpation is not advised. In addition, if the practitioner does not palpate with sufficient pressure (approximately 4 kilograms), it is very difficult to elicit the charac-teristic ‘jump’ sign (involuntary flexion withdrawal) that confirms the presence of the MTrP.26 If the lesion is superficial, the MTrP should feel like a taut band; this can be confirmed by “snapping” the trigger point similar to how one would pluck a violin string. A local twitch response that frequently produces the associated referred pain will confirm the presence of the trigger point; both responses are not neces-sary, however, as either is sufficient for diagnosis.26
As Lucas et al27(p. 80) note: “pivotal to the appropri-ate and accurate prescription of any treatment is accurate diagnosis.” Therefore, both intra and inter-rater reliability should be established. Various tech-niques have been employed attempting to establish a reference standard for identifying MTrPs, though none have been accepted as definitive.27 Microdialy-sis, biopsy, imaging, and electromyography all fall short of qualifying as a gold standard in MTrP iden-tification.6,9,12,25 Gerwin et al28 attempted to establish inter-rater reliability with identifying MTrPs in the neck and upper quarter. The first phase of their study failed to establish a high degree of agreement between therapists when palpating MTrPs for tender-ness, taut bands, referred pain, local twitch response, or reproduction of pain. The authors extended the study into a second phase, which included a three-hour training session prior to patient examination. The features of a trigger point were reviewed dur-ing this training in order to be certain that the phy-sicians were interpreting their findings similarly.
Following Phase II, the authors concluded that the training period significantly increased their inter-rater reliability in the diagnosis of MTrPs. Addition-ally, they noted that inter-rater reliability of different clinical features tended to vary, with the local twitch response being the most difficult to identify and that reliability with all characteristics varied depending on the muscle being palpated.
The need for well-trained examiners in the identi-fication of MTrPs was further supported by several studies. Wolf et al29 found poor reliability between clinicians (k=0.38), which was similar to the results of Nice et al.30 However, in both studies, there was a lack of training standardization amongst clinicians. Njoo and Van der Does31 reported a kappa of 0.49 with well-trained examiners. Bron et al32 investi-gated reliability between three well-trained examin-ers as they assessed 40 subjects. The authors noted good reliability for referred pain and the jump sign.32 These improvements in reliability are consistent with the results from Phase II Gerwin et al28 suggest-ing that inter-rater reliability of trigger point iden-tification is adequate as long as the clinicians are properly trained.
There is a marked paucity of research related to intra-rater reliability of MTrP palpation. One of the only well designed studies investigating this utilized an experienced therapist (>10 years clinical practice, with extensive training with MTrP palpation) using the upper trapezius of 24 subjects with neck pain.33 Using the acromion angle of the scapula, and the C7 spinous process, a Cartesian coordinate system was utilized to record the locations of the MTrPs. Inter-class correlation coefficient (ICC) for the observed
Figure 1. Gray scale imaging of a trigger point in the upper trapezius. (A) An isolated MTrP appears as a well-defi ned focal hypoechoic nodule. (B) A series of four hypoechoic MTrPs in the upper trapezius. Reproduced with permission from Sikdar et al., 2009

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 406
philosophy to treat not only musculoskeletal dys-function, but also problems with fertility, smoking cessation, allergies, depression, and other non-mus-culoskeletal and neuromuscular conditions.
A more modern and alternate model to acupuncture recognizes that inserting a needle into the skin (not necessarily into a MTrP) stimulates A-delta nerve fibers, consequently releasing opioid peptides from interneurons in the dorsal horns.40 These peptides inhibit intradorsal horn transmission of nocicep-tive information conveyed to the cord via group IV sensory afferents from the MTrP.40 A-delta fibers are also stimulated with needle insertion secondary to a low-intensity monophasic current of injury being created secondary to the difference in electrical potential between the needle and the skin.40 The combination of the mechanical and electrical activa-tion of A-delta fibers is what likely drives the inhibi-tory pain response noted with TCA.41
While there are several philosophies of practice that differ between acupuncture institutes, all TCA is based on the Daoist concept of yin and yang.42 Dao-ism refers to a “philosophical system developed by Lao-tzu and Chuang-tzu advocating a simple honest life and noninterference with the course of natural events.”42 Yin and yang refers to two principles in Chinese philosophy and religion; yin is negative, dark and feminine, while yang is positive, bright and masculine.43 It is thought that the interaction between the two influences the destinies of man. TCA promotes diagnoses related to meridians, such as “kidney-yang deficiency, water overflowing” or “damp heat in the bladder.”37
While traditional Chinese Acupuncturists typically perform a multi-system case history, the focus of their evaluation is on the shape, coating and color of the tongue, as well as the color of the face, and the strength, rhythm and quality of the pulse.37 The quality of these markers is thought to be an indica-tor of the patient’s state of health. Typically between four and ten acupoints are needled during a ses-sion, with the needles being left in anywhere from 10-30 minutes.37 Traditional Chinese Acupuncturists often augment their practice with various adjunctive therapies as well, including the use of electrical cur-rent between the needles, moxibustion (burning of an herb just above the surface of the skin), massage,
values revealed a moderate to high correlation for both the x and y axis (ICC= 0.62 with a 95% CI of 0.30-0.81 for the x axis; ICC= 0.81 with a 95% CI of 0.61-0.91 for the y axis).33 This research must be reproduced with various muscle groups, and with varied levels of clinician training, before any clinical inferences should be drawn.
Trigger Point Dry Needling History & TheoryModern trigger point dry needling has its origins in the work of Karel Lewit of Czechoslovakia.23,34,35 In his classic work, he examined the short and long-term effects of dry needling in the treatment of myofas-cial pain in 241 patients with 312 painful MTrP sites. He reported an immediate analgesic affect without hypesthesia in 86% of cases when the most painful location was engaged by the needle. He popularized the phrase “needle effect,” where the analgesic affect of the needle is distinct from that of the injectable substance.23,35 This is similar to research published ~40 years prior (1941) by Kelly.36 Kelly36 noted that injections of local anesthetics did not achieve any better effect than the introduction of normal saline when treating myofascial pain.
To some, trigger point dry needling may appear synonymous with Traditional Chinese Acupuncture (TCA); nonetheless, the two are uniquely different. TCA is based on the theory that the workings of the human body are controlled by a vital force or energy called “Qi” (pronounced “chee”), which circulates between organs along channels called meridians.37 These meridians are networks of channels inside the body with acupoints (high density sites of polymodal and specific nociceptive receptors near neurovascu-lar structures and/or lymphatic vessels) on the skin and deeper tissues.38,39 TCA suggests that there are 12 primary meridians, each corresponding to major functions or organs of the body.37 In theory, these meridian channels provide migratory tracks for mast cells, fibroblasts, and other cells to carry out various physiological functions;38 Qi must flow in the correct strength and quality through each meridian in order to maintain optimal homeostasis. Therefore, if an acupuncturist detects any abnormal flow or quality of Qi about a meridian, he or she would needle the respective acupoint, theoretically normalizing the flow of Qi in the body.38 Acupuncturists utilize this

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 407
model. These differences include, but are not lim-ited to: 1) the use of injection needles by Fischer vs. acupuncture needles by Gunn; 2) Fischer’s rec-ognition of the MTrPs vs. Gunn who minimizes their importance; and 3) the integration of new research into Fischer’s model vs. Gunn’s which has not been developed much beyond its inception in 1973.48
The last, and most frequently utilized model for dry needling, is the trigger point model. This model was birthed from the research and observations of Janet Travell (1901-1997) (Figure 2).34 Clinicians who subscribe to this model specifically target myo-fascial trigger points in hopes of relieving the sen-sory, motor and autonomic abnormalities that can occur secondary to myofascial trigger points. The trigger point model advocates that inactivation of the MTrPs via dry needling is the fastest and most effective means to reduce pain, as compared to
cupping, and herbal preparations.37 A typical course of acupuncture will span 6-12 sessions over a three month period, followed by “maintenance” treatments approximately every 3-6 months.37
Several authors have noted that the scientific basis regarding pain neurophysiology and the mechanisms employed with dry needling supports its use.44-47 This technique is based on a different model than that of acupuncture, and is commonly broken down into three typical schemes: 1) a radicular model; 2) a spi-nal segmental sensitization model; and 3) a trigger point model.44 The radicular model is based on the empirical observations by Chan Gunn, a Canadian physician and early pioneer of dry needling.48,49 This technique is based on the hypothesis that myofas-cial pain is always the result of neuropathy or radic-ulopathy.48,49 This model is founded on the “Law of Denervation,” as written by Cannon & Rosen-bluth.50 According to this law, the health and integ-rity of innervated structures is dependent upon the unhindered flow of nervous impulses providing a regulatory or trophic affect.48 When this free flow of impulses is inhibited in a series of efferent neurons, “an increased irritability to chemical agents devel-ops in the isolated structure or structures, the effect being maximal in the part directly denervated.”50(p.
185) That being said, Gunn noted that treatment points are always located close to the muscle motor points, or musculotendinous junctions, and the dis-tribution is myotomal in nature, and thus, MTrPs do not play a vital role.48
The second model is called the spinal segmental sensitization model, and was developed by Andrew Fischer.51 He proposed that paraspinal muscle spasm is frequently responsible for compression of a nerve root, narrowing of a foraminal space, and a sprain of the supraspinous ligament.48 Hence, Fischer51 con-tends that the most effective treatment for musculo-skeletal pain includes preinjection blocks, dry and/or wet needling, infiltration (injection) of tender spots and trigger points, somatic blocks, spray and stretch methods, and relaxation exercises. Fischer51 contends that use of the needle and infiltration of a local anesthetic is optimal for achieving long term relief of muscle pain and normalization of tender-ness.51 Several key differences distinguish the spi-nal segmental sensitization model and the radicular
Figure 2. Janett Travell, MD (1901-1997). Compliments of Bachrach Studios. Used with permission from Virginia Street, daughter of Dr. Janet Travell

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 408
An ideal candidate for DN should possess the fol-lowing qualities: 1) a physical therapy diagnosis that will reasonably improve with DN; 2) the ability to understand what is being done and why; 3) the ability to effectively communicate his or her own response to treatment; 4) the ability to lie still dur-ing treatment; and 5) the ability to provide informed consent according to clinical guidelines.2,57 Once indications, contraindications and precautions have been examined, it is vital to obtain signed informed consent from the patient. This comes after discus-sion regarding the indication and aim of the treat-ment, a brief explanation of how the intervention works, and an open discussion concerning the risks involved.2,57
Treatment is commenced with the patient positioned in a relaxed posture suitable to expose the muscles being treated. Positions may include supine, prone, or sidelying, and pillows and bolsters may be utilized to help with patient positioning. Completion of DN in a seated position is not recommended given the risk of syncope. Ideally, the practitioner would be able to view the patient’s face, so as to receive regu-lar feedback during the intervention, though treat-ing the patient in prone is acceptable. According to the work of several authors, routine disinfection of visibly clean skin before needling is not neces-sary.26,55,56,58,59 However, current standards of care in the United States recommend preparing the skin with 70% isopropyl alcohol prior to needling, as well the practitioner utilizing gloves during the intervention.1 The trigger point is then identified using palpation methods previously described. A pincer grip tech-nique is employed to gently lift the skin. Addition-ally, flat palpation can be utilized to take up the slack of the skin. A high quality, sterile, disposable, solid filament needle is inserted directly through the skin, or using a guide tube that is then removed (Figure 3).2 The depth of needle penetration must be sufficient to engage the MTrP. Once the needle has penetrated the skin and is inserted into the muscle, techniques vary: the practitioner may utilize a slow, steady, lancing or pistoning motion in and out of the muscle (termed dynamic needling), he or she may leave the needle in situ (termed static needling), or the needle may be rotated several revolutions in order to draw the fas-cia or soft tissues.2 Baldry26 recommends leaving the needle in situ for 30-60 seconds for “average respond-
other conventional interventions. While the actual mechanism of dry needling continues to be debated, the localized twitch response commonly evoked with dry needling may interrupt motor end-plate noise, thus inducing an analgesic effect.52 This local-ized twitch response, when coupled with stretching, helps to relax the actin-myosin bonds restricting the tight bands.53 Additionally, dry needling of the MTrPs will help to normalize muscle tone and the neurological interface, and improve the flow of ace-tylcholinesterase, thus correcting bradykinin, calci-tonin gene-related peptide, and substance P levels in the affected muscle.52-54 Advocates of the trigger point model believe that treatment of the MTrPs should only be one facet of a patients plan of care: stretching, joint mobilizations, neuromuscular reed-ucation, strengthening, and other related interven-tions should still be employed. It is this model of trigger point dry needling that the remainder of this commentary will address.
Trigger Point Dry Needling TechniqueProper DN technique begins with identifying the appropriate patients, and eliminating those in whom it may lead to adverse affects. DN should not be administered in the following patient scenarios: 1) a patient with needle phobia; 2) an unwilling patient; 3) a patient who is unable or unwilling to give con-sent; 4) a patient with a history of abnormal reaction to needling or injection; 5) in a medical emergency; 6) a patient who is on anticoagulant therapy, or who has thrombocytopenia; and 7) into an area or limb with lymphoedema.2,55,56 Relative contraindications include, but are not limited to, abnormal bleeding tendencies, a severely compromised immune sys-tem (eg. cancer, HIV, hepatitis, etc.), vascular dis-ease, diabetes mellitus, pregnancy, frail patients, epilepsy, allergy to metals or latex, children, and individuals taking certain prescriptive medications (eg. significant mood altering medication, blood thinning agents, etc.). Additional relative contrain-dications include an altered psychological status, anatomic considerations (extreme caution must be taken over the pleura and lungs, blood vessels, nerves, organs, joints, prosthetic implants, implant-able electrical devices, etc.), needling near a surgical site within four months of the surgical procedure, and a decreased ability to tolerate the procedure.2,55,56

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 409
of the mid or low back, pelvis or abdomen during pregnancy;2 5) in the vicinity of the carotid sinus or near the recurrent laryngeal nerve;40 and 6) in an area of sensory denervation.56 The aforementioned contraindications are synonymous with those for all electrical stimulation, and are not exclusive when used with dry needling.
Whichever techniques are employed, the intensity of the treatment must suit the tolerance of the patient, and their pathologic presentation. After a needle is withdrawn, the tissue should be compressed for 5-10 seconds, or for 30-60 seconds using a cotton swab if there is any bleeding; this will help to ensure ade-quate hemostasis.2
It is important to note that gauge and length of nee-dles vary (Figure 4). A 0.30 x 50mm needle is appro-priate for most muscles. The 0.30 corresponds to the gauge, or diameter, of the needle, and the 50 cor-responds to length. .30 x 60mm is often utilized for the quadratus lumborum, and a .30 x 75mm for the psoas or for other muscles of similar depth. Smaller gauge needles are utilized for smaller tissues, includ-ing a .20 x 25mm for the forearm, .14 x 25mm for the face/head, and .12 x 25mm for the hands or feet.
ers,” or up to 2-3 minutes in “weak responders.” While there is no consensus as to which technique is ideal, it is the opinion of the author that dynamic needle is superior to static needling (without intramuscular electrical stimulation) in most cases.
If a static technique is utilized, it can be augmented by intramuscular electrical stimulation (IES) as well.26,49,56 Since electrotherapy has been shown to elicit muscle relaxation and increase local blood cir-culation, utilizing the modality in conjunction with dry needling can be used to further decrease muscle tone and improve motor recruitment.60 While there is very little research to support specific parameters, typically IES (often with an asymmetric biphasic square waveform) is utilized at the motor level of a muscle with the frequency set at a level sufficient to elicit repeated muscular contractions; this typically corresponds to between 2 and 4 Hz with as high intensity as tolerable.48 If the goal is to reduce neuro-pathic pain, frequencies between 80 and 100Hz are recommended, which can enhance the release of gamma-aminobutyric acid, galanin, and dynophin, which will ultimately function by modulating the pain response.61 While all standard precautions and contraindications should be followed for DN, unique contraindications must be followed when electrical stimulation is delivered via dry needling. Contrain-dications include, but are not limited to: 1) a patient who is not comfortable or phobic to electrical stimu-lation or needling;2 2) it is not recommended to con-nect needles across the spinal column; 56 3) patients with implanted electrical devices; 56 4) in the vicinity
Figure 3. Needle being inserted into the upper trapezius
Figure 4. Various lengths of dry needles within guide tubes

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 410
including twirling of the needle, or repeated lanc-ing motions. If the twitch is still not elicited, then the needle should be withdrawn and second attempt made. It is opinion of the author that if the twitch is not elicited after the second needle is inserted, the practitioner may not have correctly palpated the trigger point, the needle did not engage the palpated trigger point, or the trigger point will require IES in order to engage it.
Another frequent question relates to how many trig-ger point sessions should be utilized with patients. In order to answer this, it is imperative that the practi-tioner sees dry needling within the larger picture of an entire plan of care. Dry needling is often followed by stretching the affected muscle groups, coupled with neuromuscular re-education of new movement patterns. In subsequent visits (not the same day the DN was performed), strengthening of the once inhibited or painful muscle groups can then be ini-tiated. Therefore, the dry needling itself should be seen as a “springboard” in order to facilitate a rapid decrease in pain, thus facilitating improvements in mobility and function. It is this author’s opinion that most sub-acute conditions will improve after two to three needling sessions, with chronic MTrP’s requir-ing five to six sessions. Rarely will the author needle an individual fitting these parameters for more than six sessions, although the remainder of the rehabili-tation program may still be in progress.
Risk Management Despite the proven efficacy of DN when treating myofascial pain, utilization of the procedure must be balanced by the inherent risk that comes with employing the technique; this is especially true given the fact that the skin is violated. While a pau-city of research currently exists describing the risk of infection with dry needling, extensive data has been reported on infections and acupuncture. Con-sidering that both techniques employ dermal pene-tration with a solid filament to varying depths within the body for therapeutic indications, it appears rea-sonable to correlate the data.2 However, readers are encouraged to remember the key philosophical dif-ferences between acupuncture and DN, noting that many of the locations that a Traditional Chinese Acupuncturist would needle, a practitioner utilizing DN would not.
Please note that these are simply guidelines, and not standards; choosing the gauge and length of nee-dles should be left to the discretion of the treating practitioner.
The effectiveness of DN is largely dependent upon the skill of the therapist, and his or her own ability to accurately palpate MTrPs. Not only is superficial palpation key, but also the ability to picture the trig-ger point in 3-dimensions. This kinesthetic aware-ness helps assist in better localization of needling, and improved outcomes. Several authors have noted that a trained clinician should be able to perceive the end of the needle, the pathway or trajectory the needle takes inside the patient’s body and be able to decipher between skin, subcutaneous tissue, and the anterior and posterior lamina of the aponeurosis of the rectus abdominis, for example.44,62,63
Practitioners often inquire as to how many mus-cles should be treated in one session. This is highly dependent on the patients’ history, location of pain, reservations with needling, and chronicity of their symptoms. For example, if a patient consents to treatment, but displays obvious apprehension, then treating 1-2 muscles in the first session may be appropriate. After the patients’ reservations begin to decrease, then treating 3-4 muscles, or more, may be appropriate. As young practitioners will learn, every muscle will respond uniquely different to DN. For example, the medial gastrocnemius often becomes tonic and dysfunctional in young athletes. Obtaining more than one or two twitch responses of this mus-cle will undoubtedly cause excessive post needling soreness; hence, this muscle is often the only muscle needled in a session. Other muscles, such as muscles of the rotator cuff or the upper trapezius tend to pro-duce less post-needling soreness, and more can be treated in the same session. Rarely will the author needle more than 4-5 muscles in a given session.
Occasionally the practitioner will be unable to elicit a twitch response, commonly occurring when treating deep musculature (eg. gluteus minimus). Often with these deeper muscles, the patient will still receive a therapeutic effect, without a twitch response, if the needles are left in place for 5-10 minutes, with or without IES. If a twitch response is not elicited in a more superficial muscle, it is advised that the prac-titioner utilize more dynamic needling techniques,

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 411
needling provided by trained physicians or physical therapists can be considered a safe treatment. Seri-ous adverse effects of dry needling are very rare.”23(p.
411)
In order to place risk in perspective, one could com-pare the aforementioned data to that describing the risk of taking nonsteroidal anti-inflammatory drugs (NSAIDs). These drugs range from over the counter aspirin, ibuprofen or naproxen, to a whole host of prescription brands (Indocin®, Daypro®, Celebrex®, etc). Rarely do patients think twice about taking one of these medications. However, data suggests that patients are significantly more likely to have a serious adverse effect, or even die, after taking one of these medications, as compared to receiving trigger point dry needling.71 Another perspective can compare the risk of DN to driving to a physical therapy clinic. According to the Department of Transportation, the annual risk of dying in a transportation-related acci-dent is 1 in 6,800.72 This is 32% higher than the risk of catastrophic injuries noted by McCutcheon & Yel-land64 associated with acupuncture or DN. There-fore, while there is a risk to any physical therapy intervention, the risk associated with DN is minute in the hands of a skilled practitioner.73
Trigger Point Dry Needling OutcomesConsidering the invasive nature of DN, it is very difficult to execute a double blinded, randomized, controlled clinical trial.44,62,63 Nonetheless, there have been several case reports, review articles, and research studies that support the benefit of DN. A 2005 Cochrane review investigated the effects of DN in the treatment of myofascial pain syndrome in the lumbar spine.74 While the authors noted that there is a lack of high-quality literature related to DN, they also reported that “dry-needling appears to be a use-ful adjunct to other therapies for chronic low back pain.”74(p. 961)
Several systematic reviews have also been pub-lished related to needling therapies for the manage-ment of myofascial trigger point pain. Cummings & White4 reviewed 23 randomized controlled clinical trials investigating needling of myofascial trigger points with the use of various injectable medications (known as “wet needling”). They noted that nearly all the studies revealed that the beneficial effect of
Vulfsons et al23 summarized several adverse effects associated with dry needling, including post-nee-dling soreness, hemorrhages at the needling site, syncopal responses, and acute cervical epidural hematoma. On a catastrophic level, McCutcheon & Yelland64 recently documented several cases of pneumothorax secondary to acupuncture or dry nee-dling. Despite the relatively low incidence reported (<1/10,000), the authors did note over 100 cases of pneumothorax, with four subsequent deaths; all were secondary to acupuncture treatment.64 There is also a risk of damage to the central nervous sys-tem as well. In a review of the literature, Peuker and Gronemeyer65 noted ten cases of injuries to the spi-nal cord or spinal nerve roots. In four cases, frag-mented needles were responsible for the lesions, whereas six were caused from direct injury. The authors also describe several cases of arachnoiditis and subarachnoid hemorrhage as well.65 It is vital to note, however, that these cases were secondary to deep needling of BL11 to B20 (inner line of the bladder meridian), which are not typical locations for dry needling.65
There have been rare and isolated cases of serious bacterial skin infection associated with acupuncture, which have even led to death.66 Walsh67 reviewed several outbreaks of Hepatitis B in England, Wales, Germany, Israel and the United States between 1976 and 1997; he notes that nearly all infections could be attributed to negligence on the behalf of the admin-istering practitioner.67 The author goes on to note that as of 2001, there have been no cases reported in the UK of human immunodeficiency virus (HIV) transmission through acupuncture; the same is true with regards to Hepatitis C, and Variant Creutzfeldt-Jacob Disease.67
The incidence of infectious diseases with acupunc-ture has decreased dramatically since the 1980’s.67 Greater emphasis has been placed on the utiliza-tion of single use, disposable acupuncture needles, which is now the standard of care. The risk of infec-tion continues to decrease with the optimization of sharps containers, latex gloves, and universal pre-cautions, including regular hand washing.68 Two reviews investigating the risk of infections associated with acupuncture noted that the risk is “extremely low.”69,70 Furthermore, Vulfsons et al23 notes that “dry

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 412
and that there was poor consistency between spe-cific parameters of intervention (eg. depth of needle penetration, length of time needles were left in the skin, the number of needles being utilized, etc.).75 The authors concluded: “Whilst the result of the meta-analysis of needling compared with placebo controls does not attain statistical significance, the overall direction could be compatible with a treat-ment effect of dry needling on myofascial trigger point pain.”75(p. 3)
Most recently, Rainey76 described the case of a 30-year female on active military duty who injured her low back while weight lifting. 76 She was diagnosed with a lumbar segmental instability along with right hip sta-bility dysfunction. 76 She was treated for two sessions with DN and IES to the gluteus maximus and medius, as well as the bilateral L3 and L5 multifidus muscles.76 After two sessions, the patient reported no existing pain or disability on the Numerical Pain Rating Scale or the Oswestry Disability Questionnaire, and a large improvement on the Global Rating of Change. 76
Several case series have also been documented dem-onstrating the benefits of DN. Fernandez-Carnero et al77 found that the application of dry needling into active MTrPs in the masseter muscle of 12 females significantly increased their pressure pain threshold, as well as jaw active range of motion.77 Edwards78
conducted a pragmatic, single blind, randomized, controlled trial of 40 patients in order to assess if dry needling coupled with active stretching was more effective than stretching alone at deactivating trig-ger points and reducing myofascial pain. They con-cluded that dry needling followed by active stretching is more effective than stretching alone in reducing the sensitivity to pressure of MTrPs.78 They also noted that stretching without prior deactivation of the MTrP may actually increase pain and MTrP sensitivity.78
In summary, dry needling research is still in its infancy. However, there is mounting evidence that the procedure can be effective at decreasing pain, improving range of motion, reducing the sensitivity of MTrPs, and ultimately improving quality of life.
Scope of Practice & ReimbursementAs of March 2014, State Boards regulating the prac-tice of physical therapy in 32 jurisdictions have deter-mined that DN does indeed fall within a physical
the intervention was independent of the injectable substance.4 They concluded by stating that marked improvement was noted in all groups under investi-gation in which trigger points were directly needled. However, the hypothesis that this has any efficacy beyond placebo is “neither supported nor refuted by the evidence from clinical trials.”4(p. 986)
A second systematic review was performed by Teas-dale10 and focused on DN in athletes. The study exam-ined two systematic reviews, one meta-analysis, one case summary, four randomized clinical trials, and two clinical trials all published after 2000. Teasdale10 investigated four comparisons: 1) DN vs. placebo or no treatment; 2) DN vs. standard care; 3) DN vs. stan-dard acupuncture; and 4) DN vs. wet needling. She concluded that DN in athletes was more beneficial than sham acupuncture or no treatment, and that no safety problems were reported.10 She also noted no statistically significant benefit with dry needling compared to standard care. However, when compar-ing dry needling to standard acupuncture, Teasdale10
found a statistically significant benefit to dry nee-dling, and noted that dry needling has been shown to reduce pain, increase quality of life, and increase range of motion beyond that produced with standard acupuncture.10 She concluded, “For athletes, this treatment has the ability to have a positive impact on pain, performance, and quality of life,” especially if used in conjunction with stretching, exercise ther-apy, and other non-invasive treatments.10(p.7)
A recent meta-analyses conducted by Tough et al75 reviewed seven randomized clinical trials includ-ing DN and acupuncture for the management of MTrPs.75 The authors noted that only one study suggested that DN was effective in reducing pain, when compared with no intervention. Four stud-ies revealed that DN is superior to non-penetrating interventions aimed at decreasing myofascial trig-ger points.75 Lastly, two studies provided contradic-tory results when comparing outcomes with dry needling placed into the trigger point itself, versus another location in the muscle.75 However, Tough et al75 reported significant methodological flaws with the literature under investigation. The authors noted that the source of patients pain was not controlled in any of the studies, that sample sizes were small (thus increasing the risk of making a Type II error),

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 413
the public with a safe and effective product,” again implying that physical therapists should not per-form the intervention.81(p. 1)
In order to understand the complex issues related to a physical therapists’ scope of practice, and the “turf-battles” that cloud the issue, it is imperative to have a robust understanding of the many issues surrounding DN. These issues include, but are not limited to:
1) Understanding what is included in entry-level physical therapy education
2) Identifying the similarities and differences between trigger point dry needling and TCA
3) Defining clinical competence
4) Exploring the dynamics related to reimburse-ment practices
Is DN an Entry-level Skill?In the United States (US), DN is not commonly included in the physical therapy entry-level curricu-lum.44 As of 2011, Georgia State College is the only physical therapy program in the US that has DN included in their entry-level coursework.44 However, Mercer University and the University of St. Augus-tine for Health Sciences have both made significant strides towards adding intramuscular manual ther-apy to the curricula of their entry-level educational programs.1 Therefore, given the paucity of entry-level programs that include DN in their curricula, DN is not typically considered an entry-level skill; hence, DN should not be utilized without appropri-ate entry-level or post-graduate training.
The lack of training at the entry-level will likely con-tinue, given The Federation of State Boards of Physi-cal Therapy’s (FSBPT) recently released report.1 The report notes:
…it appears that there is a historical basis, avail-able education and training as well as an educa-tional foundation in the CAPTE criteria, and supportive scientific evidence for including intramuscular manual therapy in the scope of practice of physical therapists. The education, training and assessment within the profession of physical therapy include the knowledge base
therapists scope of practice. This view is shared by Canada, the United Kingdom, Ireland, the Nether-lands, Norway, Switzerland, Belgium, Spain, Chile, South Africa, Australia, and New Zealand, among other nations.79 Nine states have prohibited the prac-tice by physical therapists.1 Arizona and Pennsylvania are unique, as their state boards are legally prohibited from issuing an interpretive statement about their respective practice acts.79 In many states, the jurisdic-tion has made no definitive statements on the issue.
Several organizations have taken a stance on the sensitive issue of dry needling and physical therapy practice. The American Academy of Orthopaedic and Manual Physical Therapists (AAOMPT) released a position statement in October of 2009 stating:
Physical therapists are well trained to utilize dry needling in conjunction with manual physical therapy interventions. Research supports that dry needling improves pain control, reduces muscle tension, normalizes biochemical and electrical dysfunction of motor endplates, and facilitates an accelerated return to active rehabilitation.3(p. 1)
The APTA shares in this opinion, and supports the practice of trigger point dry needling by licensed physical therapists.2 In fact, the 3rd Edition of the Guide to Physical Therapy Practice includes dry needling as part of manual therapy techniques employed by physical therapists in order to “pre-vent, minimize, or eliminate impairments of body functions and structures, activity limitations, and participation restrictions.”80
Not all organizations share this view, however. The American Association of Acupuncture & Oriental Medicine stated that dry needling is, by definition, an acupuncture technique.81 This implies that the technique is outside of a physical therapists scope of practice. The statement also notes: “Trigger Point Dry Needling and Intramuscular Manual Therapy are re-titlings and re-packaging’s of a subset of the acupuncture techniques described in the field of Acupuncture as “ashi point needling.”81(p. 1) The orga-nization goes on to state that “no standards of edu-cation have been validly determined to assure that Physical Therapists (PT) using DN are providing

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 414
less is a risk to the general public. Nonetheless, this argument is fundamentally flawed. The hours acu-puncturists gain are not exclusive to the performance of acupuncture. Significant time must be spent on anatomy, physiology, diagnosis, as well as studying Eastern and Western theory long before a student ever inserts a needle into a patient.73 A similar, rig-orous preparation is required of entry-level physical therapists. Entry-level physical therapist education includes anatomy, histology, physiology, biome-chanics, kinesiology, neuroscience, pharmacology, pathology, clinical sciences, clinical interventions, medical screening and differential diagnosis. Much of the basic anatomical, physiological, and biome-chanical knowledge that dry needling uses is taught as part of the core or entry-level physical therapist education; the specific dry needling skills are sup-plemental to that knowledge.82
Currently there is no profession-wide standard that defines initial competence before being allowed to dry needle. To date, each state has been forced to define its own requirements. States have taken vastly differ-ent approaches to this. Some states have treated dry needling the same as any other tool that a therapist might use, and therefore require professionals to per-form only what they are trained and competent to do. Other states require that therapists have a predeter-mined number of years of experience before utilizing the technique. Still, others require a specific number of continuing education hours in order to be deemed “competent.” Whatever the requirement, the physical therapist is held to the practice act and laws in their respective state, and thus he or she must comply.
Reimbursement ConcernsCurrently there is no CPT code dedicated to dry needling. It appears as though CPT 20552 and 20553 (both for trigger point injection) would be appropri-ate. However, according to Medicare guidelines, this code requires that an injectable substance be admin-istered. Since dry needling is not acupuncture, CPT codes 97780-97781 (acupuncture codes) are not appropriate either. The APTA’s 2014 Official State-ment titled, “Billing of Dry Needling by Physical Therapists” recommends that practitioners check the payer’s coverage policy to determine if the pol-icy specifies which code should be used to report the service.”83
and skill set required to perform the tasks and skills with sound judgment. It is also clear; how-ever, that intramuscular manual therapy is not an entry-level skill and should require additional training.1(p. 15)
Is Trigger Point Dry Needling the Same as Acupuncture?Within practitioners or disciplines, a particular group does not own, or have the rights to, a particular tech-nique. Such restrictions, especially in medicine, would ultimately be disadvantageous to patients. For example, chiropractors do not possess an exclusive domain over the skill of manipulation; physical ther-apists and osteopathic physicians commonly utilize the skill as well, since they too have the prerequisite training necessary to effectively use the skill. Nei-ther naturopathic physicians nor homeopathic phy-sicians “own” herbal remedies, but they instead use them autonomously for the purpose of improving patient outcomes. Both a carpenter and a surgeon utilize a hammer; should one own the tool to the exclusion of the other? The vast difference between the two professionals relates to their underlying phi-losophy, thought processes, and decision making; the only thing they really have in common is the tool.73 The same argument applies to acupuncture versus dry needling: Traditional Chinese Acupuncturists and physical therapists utilizing DN use the same needles. However, just like the surgeon has a com-pletely different thought process compared to the carpenter, despite having the same tool, a physical therapist diagnoses and treats pain and dysfunction completely differently than an acupuncturist. There-fore, to prevent confusion on the part of the patient, it is imperative that physical therapists clearly com-municate they are not performing acupuncture. This is often done through utilizing consent forms, as well as during discussions with the patient.
Defi ning Clinical CompetenceEven though DN is not synonymous with acu-puncture, acupuncturists often argue that physical therapists lack sufficient training in order to safely perform the technique. The American Association of Acupuncture & Oriental Medicine reports that acu-puncturists must complete 3000 hours of education prior to being licensed; they contend that anything

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 415
8. Bron C, Dommerholt JD. Etiology of myofascial trigger points. Curr Pain Headache Rep. 2012;16:439-444.
9. Shah JP, Danoff JV, Desai MJ, et al. Biochemicals associated with pain and infl ammation are elevated in sites near to and remote from active myofascial trigger points. Arch Phys Med Rehabil. 2008;89:16-23.
10. Teasdale T. Safety, effectiveness and impact of dry needling trigger points in athletes: Asystematic review. SIRC. Available online from http://old.sirc.ca/research_awards/documents/TTeasdale.pdf .
11. Mense S. The pathogenesis of muscle pain. Curr Pain Headache Rep. 2003;7:419-425.
12. Shah JP, Danoff JV, Desai MJ, et al. Biochemicals associated with pain and infl ammation are elevated in sites near to and remote from active myofascial trigger points. Arch Phys Med Rehabil. 2008;89:16-23.
13. Woolf CJ. Central sensitization: Implications for the diagnosis and treatment of pain. Pain. 2011; S2-S15.
14. Dommerholt J, Bron C, Franssen J. Myofascial trigger points: An evidence-informed review. J Man Manip Ther. 2006;14:203-221.
15. Schaible HG. Peripheral and central mechanisms of pain generation. HEP. 2006; 177:3-28.
16. Latremoliere A, Woolf C. Central Sensitization: A generator of pain hypersensitivity by central neural plasticity. J Pain. 2009;10:895-926.
17. Vranken JH. Mechanisms and treatment of neuropathic pain. Central Nervous System Agents in Med Chem. 2009:9:71-78.
18. Kalichman K, Vulfsons S. Dry needling in the management of musculoskeletal pain. J Am Board Fam Med. 2010;23:640-646.
19. Fishbain DA, Goldberg M, Meagher BR, et al. Male and female chronic pain patients categorized by DSM-III psychiatric diagnostic criteria. Pain. 1986;26:181-197.
20. Fricton JR, Kroening R, Haley D, et al. Myofascial pain syndrome of the head and neck: a review of clinical characteristics of 164 patients. Oral Surg Oral Med Oral Pathol. 1985;60:615-623.
21. Skootsky SA, Jaeger B, Oye RK. Prevalence of myofascial pain in general internal medicine practice. West J Med. 1989;151:157–160.
22. Chaiamnuay P, Darmawan J, Muirden KD, et al. Epidemiology of rheumatic disease in rural Thailand: a WHO-ILAR COPCORD study. Community oriented programme for the control of rheumatic disease. J Rheumatol. 1998;25:1382-1387.
23. Vulfsons S, Ratmansky M, Kalichman L. Trigger point needling: Techniques and outcome. Curr Pain Headache Rep. 2012;16:407-412.
It is clear that the issue of reimbursement for dry needling is unresolved, and varies widely from state to state. It is also clear that third-party payer policies are rapidly changing with regards to DN. As such, therapists are encouraged to review these policies on a regular basis in order to accurately bill for the technique.
CONCLUSIONTrigger point dry needling is a technique rooted in medical science, and can be utilized to treat various musculoskeletal pathologies. It has been deemed safe, often effective, and consistent with the gen-eral scope of practice for a physical therapist. DN is not synonymous with acupuncture, which is a disci-pline and licensed profession. The technique of DN should be available to any profession provided they prove sufficient knowledge and training. As physical therapy moves forward as a profession, therapists must be able to engage in professional conversations with both colleagues and adversaries, in order to ele-vate the standard of care, in an ongoing attempt to improve patient outcomes.
REF ERENCES 1. Federation of State Boards of Physical Therapy. Dry
Needling Resource Paper (Intramuscular Manual Therapy): 4th Ed. Alexandria, VA: Federation of State Boards of Physical Therapy; 2013.
2. American Physical Therapy Association. Physical Therapists & the Performance of Dry Needling: An Educational Resource Paper. Alexandria, VA: American Physical Therapy Association; 2012.
3. American Academy of Orthopaedic Manual Physical Therapists. Position Statement: Dry Needling. Baton Rouge, LA: American Academy of Orthopaedic Manual Physical Therapists; 2009.
4. Cummings TM, White AR. Needling therapies in the management of myofascial trigger point pain: A systematic review. Arch Phys Med Rehabil. 2001;82:986-992.
5. Gerwin RD. A review of myofascial pain and fi bromyalgia – factors that promote their persistence. Acupunct in Med. 2005;23:121-134.
6. Simons DG. Diagnostic criteria of myofascial pain caused by trigger points. J Musculoskel Pain. 1999;7:111-120.
7. Yap, E. Myofascial pain – an overview. Ann Academy of Med. 2007;36:43-48.

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 416
38. Fung PCW. Probing the mystery of Chinese medicine meridian channels with special emphasis on the connective tissue interstitial fl uid system, mechanotransduction, cells durotaxis and mast cell degranulation. Chin Med. 2009:4:10.
39. Madsen MV, Gotzsche PC, Hrobjartsson A. Acupuncture treatment for pain: systematic review of randomized clinical trials with acupuncture, placebo acupuncture, and no acupuncture groups. BMJ. 2009;338:a3115.
40. Baldry P. Management of Myofascial Trigger Point Pain. Acupuncture in Med. 2002;20:2-10.
41. Gunn CC. Acupuncture and the Peripheral Nervous System. A Radiculopathy Model. 1998. Churchill Livingstone. Institute for the Study and Treatment of Pain - 2002.
42. “Daoism.” thefreedictionary.com/Daoism. Accessed May 12, 2014.
43. “Yin and Yang.” thefreedictionary.com/yin+and+yang. Accessed May 12, 2014.
44. Dommerholt J, Mayoral del Moral O, Grobli C. Trigger point dry needling. J Man Manip Ther. 2006;14:70-87.
45. Carlsson C. Acupuncture mechanisms for clinically relevant long-term effects – reconsideration and a hypothesis. Acupunct in Med. 2001;20:82-99.
46. Filshie J, Cummings M. Western medical acupuncture. In Ernst E & White A (Eds.) Acupuncture: A Scientifi c Appraisal. Oxford: Butterworth Heinemann; 1999:31-59.
47. Bradnam L. A proposed clinical reasoning model for western acupuncture. New Zealand J of Physio. 2003;31:4-45.
48. Dommerholt J. Dry needling in orthopedic physical therapy practice. Orthop Practice. 2004;16:15-20.
49. Gunn, CC. The Gunn Approach to the Treatment of Chronic Pain. 2nd ed. New York, NY: Churchill Livingstone; 1997.
50. Cannon WB, Rosenblueth A. The Supersensitivity of Denervated Structures: A Law of Denervation. New York, NY: MacMillan; 1949.
51. Fischer AA. Treatment of myofascial pain. J Musculoskeletal Pain. 1999;7:131-142.
52. Kietrys DM, Palombaro KM, Azzaretto E, et al. Effectiveness of dry needling for upper-quarter myofascial pain: A systematic review and meta-analysis. J Orthop Sports Phys Ther. 2013;43:620-634.
53. Chu J. Does EMG (dry needling) reduce myofascial pain symptoms due to cervical nerve root irritation? Electromyogr Clin Neurophysiol. 1997;37:259-272.
24. Sikdar S, Shah JP, Gebreab T, et al. Novel applications of ultrasound technology to visualize and characterize myofascial trigger points and surrounding soft tissue. Arch Phys Med Rehabil. 2009;90:1829-1838.
25. Chen Q, Bensamoun S, Basford JR, et al. Identifi cation and quantifi cation of myofascial taut bands with magnetic resonance elastography. Arch Phys Med Rehabil. 2007;88:1658-1661.
26. Baldry PE. Acupuncture, Trigger Points and Musculoskeletal Pain. Edinburgh: Churchill Livingstone; 2005.
27. Lucas N, Macaskill P, Irwig L, et al. Reliability of physical examination for diagnosis of myofascial trigger points. A systematic review of the literature. Clin J Pain. 2009;25:80-89.
28. Gerwin RD, Shannon S, Hong CZ, et al. Interrater reliability in myofascial trigger point examination. Pain. 1997;69:65-73
29. Wolfe F, Simons DG, Fricton J, et al. The fi bromyalgia and myofascial pain syndromes: a preliminary study of tender points and trigger points in persons with fi bromyalgia, myofascial pain syndrome and no disease. J Rheumatol. 1992;19:944-951.
30. Nice DA, Riddle DL, Lamb RL, et al. Intertester reliability of judgments of the presence of trigger points in patients with low back pain. Arch Phys Med Rehabil. 1992;73:893–898.
31. Njoo KH, Van der Does E. The occurrence and inter-rater reliability of myofascial trigger points in the quadratus lumborum and gluteus medius: A prospective study in non-specifi c low back pain patients and controls in general practice. Pain.1994; 58:317–323.
32. Bron C, Franssen J, Wensing M, et al. Interrater reliability of palpation of myofascial trigger points in three shoulder muscles. J Man Manip Ther. 2007;15:203-215.
33. Barbero M, Bertolia P, Cescon C, et al. Intera-rater reliability of an experienced physiotherapist in locating myofascial trigger point in the upper trapezius muscle. J Man Manip Ther. 2012;20:171-177.
34. Travell G, Simons DG. Myofascial Pain and Dysfunction: The Trigger Point Manual. Baltimore, MD: Williams & Wilkins; 1992.
35. Lewit K. The needle effect in the relief of myofascial pain. Pain. 1979;6:83–90.
36. Kelly M. The treatment of fi brositis and allied disorders by local anaesthesia. Med J Aust. 1941;1:294-298.
37. Vickers A, Zollman C. ABC of complementary medicine: Acupuncture. BMJ. 1999; 319:973-976.

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 417
000 treatments by traditional acupuncturists. BMJ. 2001; 323:486-487.
70. White A, Hayhoe S, Hart A, et al. Adverse events following acupuncture: Prospective survey of 32 000 consultations with doctors and physiotherapists. BMJ. 2001;323:485-486.
71. Singh G. Recent considerations in nonsteroidal anti-infl ammatory drug gastropathy. Am J Med.1998;105:31S-38S.
72. Savage I. Comparing the fatality risks in United States transportation across modes and over time. Res in Transport Econ. 2013;43:9-22.
73. Dommerhold J. The dry needling issue. Qi-Unity Report, AAAOM. July 2008.
74. Furlan AD, van Tulder M, Cherkin D, et al. Acupuncture and dry-needling for low back pain: An updated systematic review within the framework of the Cochrane Collaboration. Spine. 2005;30:944-963.
75. Tough EA, White AR, Cummings TM, et al. Acupuncture and dry needling in the management of myofascial trigger point pain: a systematic review and meta-analysis of randomized controlled trials. Eur J Pain. 2009;13:3–10.
76. Rainey CE. The use of trigger point dry needling and intramuscular electrical stimulation for a subject with chronic low back pain: A case report. IJSPT. 2013; 8:145-161.
77. Fernandez-Carnero J, LaTouche R, Ortega-Santiago R, et al. Short-term effects of dry needling of active myofascial trigger points in the masseter muscle in patients with temporomandibular disorders. J Orofacial Pain. 2010;24:106-112.
78. Edwards J, Knowles N. Superfi cial dry needling and active stretching in the treatment of myofascial pain – A randomised controlled trial. Acupunct in Med. 2003;21:80-86.
79. FitzGibbon S. Should dry needling for myofascial pain be within the scope of practice for physical therapists? Ortho Practice. 2011;23:212-218.
80. American Physical Therapy Association. Guide to Physical Therapist Practice (3rd ed). Alexandria, VA: American Physical Therapy Association; 2014.
81. American Association of Acupuncture & Oriental Medicine. American Association of Acupuncture and Oriental Medicine (AAAOM) Position Statement on Trigger Point Dry Needling (TDN) and Intramuscular Manual Therapy (IMT). Roseville, MN: American Association of Acupuncture & Oriental Medicine; 2011.
82. Edelman, George Edelman. On Behalf of Delaware Physical Therapy Association Letter to Grant, Jerry. Received 7 May 2014.
54. Kash H, Qerama E, Kongsted A, et al. Clinical assessment of prognostic factors for long-term pain and handicap after whiplash injury: A 1-year prospective study. Eur J Neurol. 2008;15:1222-1230.
55. Australian Society of Acupuncture Physiotherapists Inc. Guidelines for safe acupuncture and dry needling practice. Lismore, NSW: Australian Society of Acupuncture Physiotherapists; 2007.
56. White A, Cummings M, Filshie J. An Introduction to Western Medical Acupuncture. Edinburgh: Churchill Livingstone; 2008.
57. College of Physical Therapists of Alberta. Dry needling competency profi le for the physical therapist. Alberta, Canada: College of Physical Therapists of Alberta; 2007.
58. Hoffman P. Skin disinfection and acupuncture. Acupunct Med. 2001;19:112-116.
59. Hutin Y, Hauri A, Chiarello L, et al. Best infection control practices for intradermal, subcutaneous, and intramuscular needle injections. Bull World Health Org. 2003;81:491-500.
60. Cameron MH. Physical Agents in Rehabilitation: From Research to Practice. 3rd ed. St. Louis, MO: Elsevier. Saunders; 2008.
61. Lundeberg T, Lund I. Is there a role for acupuncture in endometriosis pain, or ‘endometrialgia.” Acupunct Med. 2008;26:94-110.
62. Dincer F, Linde K. Sham interventions in randomized clinical trials of acupuncture: A review. Complement Ther Med. 2003;11:235-242.
63. White P, Lewith G, Hopwood V, et al. The placebo needle: Is it a valid and convincing placebo for use in acupuncture trials? A randomised, single-blind, cross-over pilot trial. Pain. 2003;106:401-409.
64. McCutcheon LJ, Yelland M. Iatrogenic pneumothorax: safety concerns when using acupuncture or dry needling in the thoracic region. Phys Ther Rev. 2011;16:126-132.
65. Peuker E, Gronemeyer D. Rare but serious complications of acupuncture: Traumatic lesions. Acupunct in Medicine. 2001;19:103-108.
66. Pierik MG. Fatal Staphylococcal septicemia following acupuncture: Report of two cases. Rhode Isl Med J. 1982;65:251-253.
67. Walsh B. Control of infection in acupuncture. Acupunct in Med. 2001;19:109-111.
68. British Acupuncture Council. The British Acupuncture Council Code of Safe Practice. London, England: British Acupuncture Council; 2010.
69. MacPherson H, Thomas K, Walters S, et al. The York acupuncture safety study: Prospective survey of 34

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 418
88. Letchuman R, Gay RE, Shelerud RA, et al. Are tender points associated with cervical radiculopathy? Arch Phys Med Rehabil. 2005;86:1333-1337.
89. Hsueh TC, Yu S, Kuan TS, et al. Association of active myofascial trigger points and cervical disc lesions. J Formos Med Assoc. 1998;97:174-180.
90. Dimitriadis Z, Kapreli E, Strimpakos N, et al. Hypocapnia in patients with chronic neck pain: association with pain, muscle function, and psychologic states. Am J Phys Med Rehabil. 2013;92:746-754.
91. McLaughlin L, Goldsmith CH, Coleman K. Breathing evaluation and retraining as an adjunct to manual therapy. Man Ther. 2011;16:51-62.
83. American Physical Therapy Association. Billing of Dry Needling by Physical Therapists. Offi cial Statement. APTA Public Policy, Practice, and Professional Affairs Unit. Alexandria, VA: American Physical Therapy Association; 2014.
84. Borg-Stein J, Simons DG. Focused review: Myofascial pain. Arch Phys Med Rehabil. 2002;83:S40-S47.
85. Hong CZ, Simons DG. Pathophysiologic and electrophysiologic mechanisms of myofascial trigger points. Arch Phys Med Rehabil. 1998;79:863-872.
86. Friction JR. Myofascial pain. Baillieres Clin Rheumatol. 1994;8:857-880.
87. Gerwin RD. The management of myofascial pain syndrome. J Musculoskel Pain. 1993;1:83-94.

The International Journal of Sports Physical Therapy | Volume 10, Number 3 | June 2015 | Page 419
CORRIGENDUM
A NOVEL APPROACH TO TREATMENT FOR CHRONIC AVULSION FRACTURE OF THE ISCHIAL TUBEROSITY IN THREE ADOLESCENT ATHLETES: A CASE SERIES, Volume 9, Number 7, December 2014, Pages 974-990.
The original paper “A Novel Approach to Treatment for Chronic Avulsion Fracture of the Ischial Tuberosity in Three Adolescent Athletes: A Case Series” was originally published in IJSPT in December 2014, without the Appendix describing the specific rehabilitation progression used in the case series. The editorial staff of IJSPT apologizes for the oversight and the corrected paper appears here.
Appendix 1. Specifi c Rehabilitation Progression UtilizedPhase/Time Gait Sitting Manual Therapy/Exercise
Protection
Weeks: 0-2 Crutches: NWB
Protected (decrease weight on involved side)
Supine ankle dorsiflexion/plantarflexion for neuromobilization exercise to prevent possible symptoms of hamstring syndrome. Gait with crutches NWB* hip and knee flexed. Sitting emphasis weight-bearing on uninvolved ischial tuberosity.
Weeks: 2-4 TTWB- 50% Symptom dependent
Protected (decreased weight on involved side)
Same as above. Gentle soft tissue mobilization as needed to hamstring muscle belly not ischial tuberosity. Supine partial knee flexion/extension (straight leg raise with dorsiflexion) neuromobility exercise as needed for hamstring syndrome symptoms), Isometric exercises painfree: gluteal sets, quad sets, ankle pumps. Core exercises (crunches).
Weeks: 4-6 75%-WBAT
To pain tolerance
Same as above: progress home exercises (painfree exercise only) add hip abduction, gastroc-soleus stretching, bridging, progress core ex with ball, planks/ side planks with knees flexed to decrease load proximally.
Strengthening,eccentric loading at 6+ weeks
WBAT no crutches
To pain tolerance Continue above as pain tolerance allows progression.
Weeks: 8-12 FWB Unlimited Continued core exercises. Mini-squats, lateral step up/downs, Eccentric loading: prone leg only eccentric lowering, crab walkouts, supine active knee flexion/extension with concurrent hamstring stretching, hip abduction walk. Progressed gym exercise, running, functional activities, eccentric loading exercises May progress slower based on symptoms, size of fracture etc.
Weeks: 12-16+ FWBJogging- Running
Unlimited Return to sport criteria: no pain. Functional hop tests: 90% in bilateral comparison. Symptoms guide speed of progression.
NWB=Non weight bearing, TTWB=toe touch weight bearing, WBAT=weight bearing as tolerated, FWB= full weight bearing






















