From sleep medicine to medicine during sleep – a clinical ...
Upload
khangminh22Category
view
0download
0
HAL Id: hal-01841771https://hal.archives-ouvertes.fr/hal-01841771
Submitted on 21 Aug 2018
HAL is a multi-disciplinary open accessarchive for the deposit and dissemination of sci-entific research documents, whether they are pub-lished or not. The documents may come fromteaching and research institutions in France orabroad, or from public or private research centers.
L’archive ouverte pluridisciplinaire HAL, estdestinée au dépôt et à la diffusion de documentsscientifiques de niveau recherche, publiés ou non,émanant des établissements d’enseignement et derecherche français ou étrangers, des laboratoirespublics ou privés.
Social innovation by design in mobile healthcare forsleep disorders
Marie-Julie Catoir-Brisson
To cite this version:Marie-Julie Catoir-Brisson. Social innovation by design in mobile healthcare for sleep disorders. De-sign as a catalyst for change, Design Research Society, Jun 2018, Limerick, Ireland. pp.2324-2333�10.21606/dma.2018.264�. �hal-01841771�

ThisworkislicensedunderaCreativeCommonsAttribution-NonCommercial-ShareAlike4.0InternationalLicense.https://creativecommons.org/licenses/by-nc-sa/4.0/
SocialinnovationbydesigninmobilehealthcareforsleepdisordersCATOIR-BRISSONMarie-Juliea*
aAssociateProfessorofDesignandCommunication,UniversityofNîmes,ProjektLab(EA7447)*Correspondingauthore-mail:[email protected]:10.21606/dma.2017.264
This project-grounded research aims at answering a need for research on sleepdisorders and connected objects, through an interdisciplinary dialogue betweenhumanandsocialsciences,medicalsciencesanddesign.Theobjectiveofthisarticleistoanswerthefollowingquestions:howcansocialinnovationbydesignsustainthedevelopmentof innovativemedicaldevices?Howcandesignwork tooptimize theprevention, the support and the follow-up in sleepmedicine? The project aims atcreating a digital platform optimizing the circulation of the data, the customer’sjourney and the communication between patients and care professionals. Theresearchhashadadoublescientificchallenge,carryingontherapeuticeducationinsleep and digital health literacy, especially in the field of medical computing andmobile devices for chronic diseases. First, the scientific roots andmethodology isexplained. Then, the methods of inquiry and the results are reported. Finally, acontribution todesign research forhealthcare isproposed, focusingon the roleofdesign in promoting sleep’s hygiene through the creation of suitable services,products,experiencesandhealthcareenvironments.
Keywords:m-Health;insomnia;servicedesign;digitalliteracy
1. IntroductionThisarticledealswithaproject-groundedresearchcurrentlybeingdevelopedatthePROJEKTLabattheUniversityofNîmes,onservicedesigninmobilehealthcare(especiallysleepdisorders),incollaborationwiththeUniversityHospitalinNîmes1.Basedonaninterdisciplinarydialoguebetweendesignsciences,informationandcommunicationsciencesandmedicalsciences,thisresearchinvolves,atthesametime,interactiondesign,servicedesignandsocialinnovationbydesign.Usingexperimentationsandprototyping,theobjectiveistoshowthatadigitalservicecanbeusefultoeducateandtofollowinsomniacpeopleup,ifitisintegratedinacarenetworkandsupportedby
1Theresearchisco-managedbyDrBeatrizAbril,NeurologistandSleepdisorderspecialist,DrGauthierBrisson,General
careprofessionals.ThefinancialcontributionoftheUniversityHospitalinNîmes(SecondawardwoninOctober2016attheInnov’actionsTrophy)hasmadethisone-yearstudypossible,toassessthefeasibilityoftheprojectandtomakeinquirieswithlocalstakeholders.Researchisneededonchronicinsomniaandconnectedobjects.InFrance,insomniaisapublichealthproblemthataffectsalmost20%ofthepopulation.InspiteoftherecommendationsoftheHAS(HauteAutoritédeSantéwhichisFrenchHealthHighAuthority),patientscareislimitedatanylevel:accesstohealthcare,availabilityoftheprofessionals,lackofeducationalkittools,reimbursementforhealthcare,andadversedrugreactions.Moreover,connectedobjectsandappsdedicatedtosleeparegrowingfasterandfaster.Theyareusedbythecitizens,withoutanymedicalsupervision,andareoftengivenupafterafewmonths(Kebs,Duncan,2015).Buttheiremerginguseimpliesthedevelopmentofhealthdigitalliteracy.Thesetechnologicalinnovationsandthesocialchangesaccompanyingthemmaketheparticipationofhealthprofessionals,designers,researchersandcitizensinthefieldofmobilehealthcareforsleepdisordersnecessary.Problematicsinthisstudyaimtoanswerthefollowingquestion:Howthedesignofmobilehealthtechnologiesinthefieldofinsomnialeadstorethinkthecooperation’smodelsbetweenhealthcareprofessionalsandpatients,thecarejourneyofthepatientsandtheroleofthedifferentstakeholders?Thisarticleconsistsinthreepartstocopewiththiscomplexissue.Inthefirstpart,thescientificrootsandthemethodologyarepresented.Inthesecondpart,thefirstresultsoftheresearcharediscussed.Inthethirdpart,acontributiontodesignresearchforhealthcareisproposed.
2. Scientificrootsandmethodology:socialinnovationbydesignanddigitalsocialinnovation
Tostartwith,let’sintroducethedifferentconceptandvaluesofthedesignresearch,inordertodefinethespecificityofthemethodology.
First,thisproject-groundedresearchispartofaspecificmethodologycalledrecherche-projet(Findeli,2003),characterizedbythefactofarticulatingaresearchprojectandaservicedesignproject.Itisakindofaction-research2(Rapoport,1973)tomaketheexperienceoftheparticipantsbetter.Consideredatthesametimeasexpertsoftheirownexperienceandbeneficiariesoftheproject,theyareinvolvedinthesearchforsolutions.
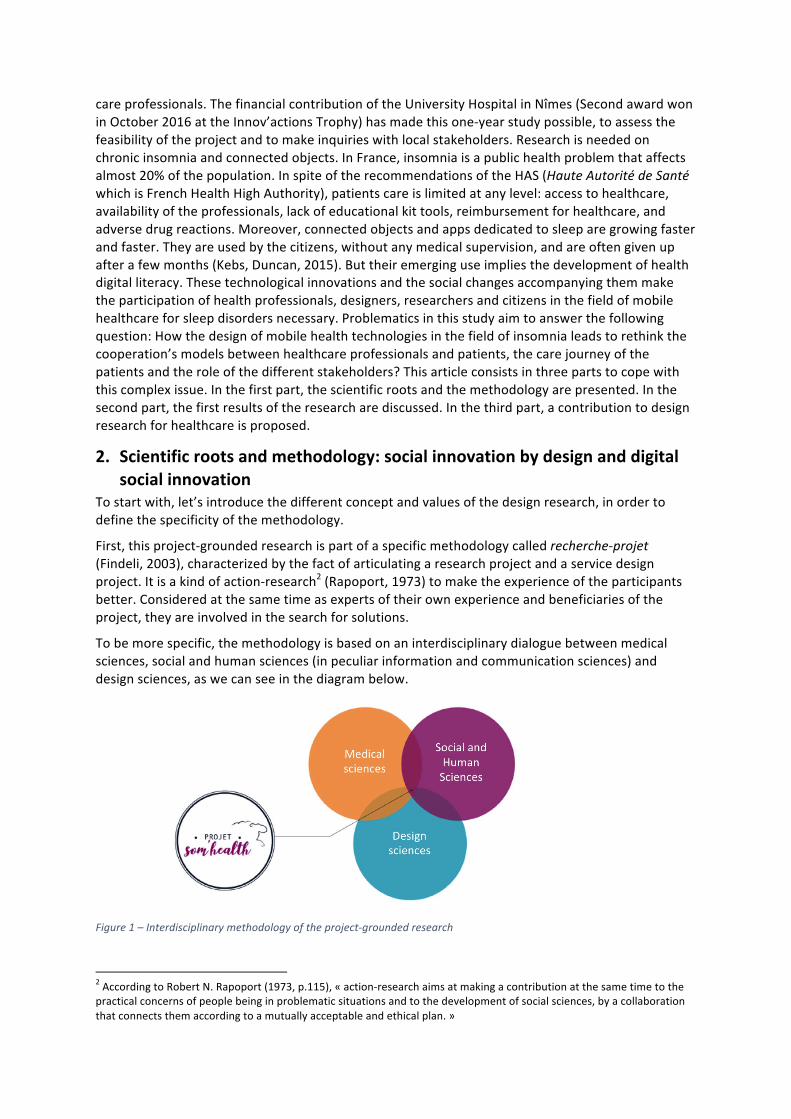
Tobemorespecific,themethodologyisbasedonaninterdisciplinarydialoguebetweenmedicalsciences,socialandhumansciences(inpeculiarinformationandcommunicationsciences)anddesignsciences,aswecanseeinthediagrambelow.
Figure1–Interdisciplinarymethodologyoftheproject-groundedresearch
2AccordingtoRobertN.Rapoport(1973,p.115),«action-researchaimsatmakingacontributionatthesametimetothepracticalconcernsofpeoplebeinginproblematicsituationsandtothedevelopmentofsocialsciences,byacollaborationthatconnectsthemaccordingtoamutuallyacceptableandethicalplan.»

Secondly,itisimportanttoexplainthemeaningofsocialinnovationthroughinthisresearch.Socialinnovationbydesignisatopicalissueinhumanandsocialsciencesespeciallyinthedesignsciences.Nevertheless,itisnotreallynewandthistrendtakesupwiththeoriginsofdesignhistory(forinstance,theworksoftheBauhaus,thenV.Papanek,A.Findeli).Designsciencesmayseizetheproblemofsocialinnovationtodaybecausethesetwofieldshaveincommontostudytheproblematicofuses,andtrytostandoutfromtechnologyandproduct-centeredinnovation.Thisapproachgivesthepatientsapowertodesignandact,besidehealthcareprofessionalsandadministrations.Thus,digitalproductsandservicescanbedesignedforsocialchange,asfarastheyaredesignedtocreateusesandbehavioursdedicatedtosocialinnovation(Tromp,Hekkert,Verbeek,2011).Itisimportanttounderlinetheimplicationofbothpatientsandprofessionalsinthisproject,toexplainhowitispossibletoreframepatientsaspersonswithactiveparticipationintheirownhealthcare.Theobjectiveoftheprojectistobuildahumananddigitalnetworkinwhichthepatientscandeveloptheirhealthcareanddigitalskillsbasedontheexpertiseoftheirownexperienceofpatients.Inaddition,healthcareprofessionalscandeveloptheirknowledgeinthefieldofinsomniaaswellastheirdigitalliteracy,bytakingpartintheservicenetwork.
Thespecificityofthisproject-groundedresearchisalsobasedonhuman-centered-design(Buchanan,2001).Theobjectiveistogofurthertotheproblematicofusetoreachsocialissuesinvolvingthedesigner’sresponsibility3.Human-centered-design“isanon-goingsearchforwhatcanbedonetosupportandstrengthenthedignityofhumanbeingsastheyactouttheirlivesinvariedsocial,economic,political,andculturalcircumstances.”Asaconsequence,“thequalityofdesignisdistinguishednotmerelybytechnicalskillofexecutionorbyaestheticvisionbutbythemoralandintellectualpurposetowardwhichtechnicalandartisticskillisdirected.4”Inthisperspective,theobjectiveoftheproject-groundedresearchistodevelopacreativeethicsoftechnologythatisclosetoethicsbydesign,basedontheresponsibilityoftheactofdesignintheproposalofanexperience-à-vivre(Vial,2015)fromfivekeystepsinthedesignprocess:understandingtheexperienceoftheusers,usingparticipativemethods,relyingonasystematicapproach(tocreateasynergybetweenalltheactors),makingworkshopsinordertopracticeideation,co-creationorco-designservicesandprototypeswiththebeneficiaries,inaniterativewayofthinking.
Atlast,digitalsocialinnovation5isalsopartofthemethodologyofthisproject.Thisapproachoftechnologymakesthemovementfromtechnological-centeredinnovationtosocialanddigitalinnovationpossible,inwhichdigitaltechnologyisputintheserviceofthecommongoodforpublichealthinterventions.
3. Methodsofinquiry:aqualitative,participativeandcreativeresearchThefirststepofthedesignprocesswasdedicatedtoinquiry,inthefieldofthepublichospitalinNîmesbutalsoinofficepractice(generalpractitioner).Thismethodologywasusefultounderstandandthentomakemanyactors(patients,healthcareprofessionalsandadministrations)takepartinthehealthcareproject.Itcanbeconsideredasacontributioninbothresearchandpracticeoninsomniabecause“nostudywasfocusedonthecross-personalviewsoftheseactors.6”Thequalitativemethodswereusedtocollectdataontherepresentations,thepracticesandtheexpectationsoftheparticipants.
3TrompN.,HekkertP.,VerbeekP-P.,«DesignforSociallyResponsibleBehavior:AClassificationofInfluenceBasedonIntendedUserExperience»,DesignIssuesVol.27,N°3,2011,p.3-19.4BuchananR.,«HumanDignityandHumanRights:ThoughtsontheprinciplesofHuman-CenteredDesign»,inDesignIssues,Vol15,n°3,2001,p.35.5OurresearchleadsonthevaluesdevelopedintheEuropeancommunityresearchofDSI:https://digitalsocial.eu6GaboreauY.,PricazF.,Cote-ReyA.,RoucouI.,ImbertP.(2017)«Consensus,controversesetdissensionsentremédecinsgénéralistesetpatientsautourdel’insomniechroniqueprimaire»,RevueExercer#130Volume28,CollègeNationaldesGénéralistes,février2017,p.52.

Figure2Observationperiodsandinterviews
Theinquirywasbasedonthreesteps:observationperiods,interviewsandworkshops,fromFebruarytoJune,in2017.ObservationsofspecializedconsultationsintheSleepMedecineUnityoftheUniversityHospitalinNîmeswereundertakenwiththeagreementofthedoctorsandfifteenpatients.Then,semi-structuredindividualinterviewsandfocusgroupbasedonvisualandcreativemethodswereorganisedinthepublichospitalandintheofficeofageneralpractitioner(withdoctors,patients,medicalsecretaries,andalsolocalpublicadministrations(ARSOccitanie,CPAMduGard).Thisstepwasusefultounderstandthelimits,constraintsandthespecificitiesoftheconsultationinmedicalcityofficeandinthepublichospital.Itwasalsohelpfultovisualisethepatient’sjourneyinordertounderlinetheproblemsbetweenthepatientsandthetouchpointsoftheirhealthcarejourneybetweenpublichospitalandmanyhealthcareprofessionalsinthecity).TheanalysisofthedatacollectedduringtheobservationsperiodallowedustodesigntwoworkshopsinAprilandJunebasedoncreativemethodandco-design.
Thefirstworkshopwascomposedoftwelvehealthcareprofessionals(psychologist,generalandspecialistpractitioners)inordertocometogetherthemainactorsandtounderstandtheiractualproblemsintheinsomniacpatient’sjourneyandtheirusesofdigitaltoolsandmobiledevices.Visualandcreativemethodswereusedtomaketheexpressionoftheparticipantseasier.Visualmaterialscamefromtwodifferentsources.Theparticipants-especiallythegeneralpractitioners-wereinvitedtosendsomephotographsofthedigitaltoolstheymayuseintheireverydayprofessionalpractice.Forexample,twogeneralpractitionerssentusascreenshotoftheirmobilephonerepresentingthehomepageofKlepios(anappfordoctorswithasyntheticmedicalindexofthemainpathologies;seehttps://www.klepios.com)andUnivadis(freemedicalappandwebsitewithmedicalinformation,especiallyondruginteractions;seehttps://www.univadis.fr).Wealsogaveboardsandvisualcardsrepresentingvariousdigitaltoolsusedinmedicalcityoffice,madebythesocialservicedesigneroftheproject.Thevisualmethodsusedinthisinvestigationwerebasedatthesametimeontheparticipants’,thedesigner’sandtheresearcher’sproductions.Welettheparticipantsfreetocovertheboardswithnotesinordertorepresentthedigitaltoolsforwhichtheydidnothaveanypicture.Withthismethodology,wecollectedinformationontheindividualpracticesoftwelvehealthcareprofessionals.

Figure3Workshop#1April2017
Thesecondworkshopofco-designatthebeginningofJunewasmadewithpatients,healthcareprofessionalsandadministrators.Differentmethodscomingfromgamestormingwereused,basedonactivitiesmadetousespaceasanexpressionofopinions,andalsovisualandcreativemethods.Theparticipantswereinvitedtoworkinsmallgroupsofthreeorfourpeople,andeachteamhadtomixpatientswithdoctors,andasecretaryoranadministrator.Visualmaterials(suchasgameboard,cards,personas,patientcarejourney,map-tools,mapofthenetworketc.)werepreparedbythedesignerandresearcherandproposedtotheparticipantstosupporttheirexpressionbyplayfulandparticipativematerials.
Theresultsofthisco-designworkshopwereveryuseful,asthreemapsofthecareprofessionalsandinsomniacpatientsnetworkweresketched,inordertoexpressdifferentvisionsofthesleepinstituteimaginedbytheparticipants.Inaddition,morethantwentydigitaltoolsattheserviceofthehumannetworkwereproduced,allowingtoimaginethedigitalandhealthcareservicesoftheinstitute,thefunctionsofthewebsiteandtheconnectedobjectusedtooptimizetheprevention,thesupportandthemedicalfollow-upinsleepmedicine.
Figure4Workshop#2June2017

Thevisualmethodswererelevanttomakethevoicingofopinionseasierandtoincreasetheimplicationoftheparticipantsintheworkshops.«Thisimplicationcanbeexplainedbythefactthatvisualmethodsofferparticipantsthepossibilitytoexpressthemselvesfromseveralmaterialsthattheycanmobilizeinafreeway.7»Allthevisualandphysicalmaterialswereusedasmediation’ssupportintheworkshops,attheserviceofthemethodologyofthisproject-groundedresearch.Relyingonco-designandinclusivedesigncanbeausefulwayofleadingorganizationalchange-makingbasedonamethodtoinvolveparticipants,whocanbecareprofessionals,patientsandrelatives.Thissystemicdesignpracticeandresearchisnecessaryinthefieldofhealthcarebecausethisspecificfieldisacomplexfield,whichcombinestheinterventionsofmanydifferentstakeholders.
Theobservations,theinterviewsandthetwoworkshopsallowedtodrawandtoproposesomesolutionsthatcanbeusefultotheresearchandtotheproject.Themainresultsaccentuatedthenecessityof1/creatingapatientsandhealthcareprofessionalsnetworktodeveloptherapeuticeducationandtooptimizethepatient’scarejourney;2/improvethecommunicationbetweenhealthcareprofessionals,patientsandadministrations.Thisnetworkwouldbebasedonadigitaltoolallowingtocollectdataonthepatient,whichwouldservetodeveloptheresearchonsleepingdisorderswithinalivinglab8(ENoLL,2008).Thedatawouldbevisualized,afteraworkofinformationdesign,toinformthepatientsontheirownmechanismsofsleepandimprovetheunderstandingandthefollow-upoftheirpathology.Ahumancareprofessionalnetworkinthelocalcommunitywouldsupportthedigitalnetwork.Theseresultsinviteustothinkaboutthewaythedigitaltechnologyre-configuresthemedicalpracticeandthecommunicationbetweendoctorsandpatients.Theyalsoopenthereflectiononthemutualcontributionsbetweeninformationandcommunicationsciencesanddesignsciences.
Moreover,wecanlistthevariousprojectdeliverablesthatweproducedduringthisfirstyearofstudy.Abook-includingtheresultsoftheenquiry,somerecommendationsforthedesignoftheinstitutededicatedtoinsomnia,morethantwentydigitalandeducationaltoolsforpatientsandcareprofessionals,andusersscenarios-wasprinted.ApedagogicalprojectwasalsomanagedwiththestudentsoftheMaster’sprogramme“DesignInnovationSociety”(MasterDIS)intheUniversityofNîmes,fromOctober2017toJanuary20189todevelopthepossibledeliverablesoftheproject.Theobjectiveofthepedagogicalprojectwastomakestudentsunderstandthecomplexityofthefieldofhealthcare,andimaginesolutionsabletochangecustomer’sjourney,landscapeandexperienceinhealthcarethroughsocialinnovationbydesign.Thestudent’spropositionswereusefultogiveformtothehumannetworkthatcanimprovethepatient’scarejourneyandtodeveloptheinteractiondesignbetweenthedigitalnetworkandtheconnectedobjectdedicatedtothedatacollectiononsleep(includingaprototypeofthewebapplication).Ashortdocumentarywasproducedtoexplaintheprojectmethodologybasedonsocialdesign.Awebsiteisalsoproposedtofollowthecurrenteventsoftheproject(see:https://projetsomhealth.org).
Itisimportanttofinishwiththemainlimitsofthisexperienceofproject-groundedresearchinthefieldofhealthcare.Wecanlistthreelimits:1/politicallimitsbothinthelocalandnationalcontextaschronicinsomniaisnotconsideredasapriorityinFrenchhealthpolicyduringthisone-yearstudy;2/limitsinrelationwiththestakeholderssuchasrepresentationsofpatientsandcareprofessionalsoninsomniaanditstreatment,fearsofchangeandoftechnology,accesstoprofessionals;3/limitations
7Catoir-BrissonM-J.,JankeviciuteL.,«Entretienetméthodesvisuelles:unedémarchederecherchecréativeensciencesdel’informationetdelacommunication»,Sciencesdelasociété,92,2014,p.125.8AccordingtotheEuropeanNetworkofLivingLabs(http://openlivinglabs.eu):“aLivingLabisaboutexperimentationandco-creationwithrealusersinreallifeenvironments,whereuserstogetherwithresearchers,firmsandpublicinstitutionslooktogetherfornewsolutions,newproducts,newservicesornewbusinessmodels.”9ThispedagogicalprojectwassupervisedbyMarie-JulieCatoir-Brisson,incollaborationwithLucileHauteandSandrinePirolles.Participatingstudentswere:YounesGzouli,MarylouPlanchon,EmelineTiteux-Flores,TiphaineRosier,AlanShammas,CamilleSoulier.

ofthemethodology,inpeculiarfortheparticipativeaction-research:difficultytomakecareprofessionals(especiallydoctorsandhealthadministrations)participateintheworkshops.
4. AcontributiontoDesignResearchforHealthcareInthisthirdandlastpart,acontributiontodesignresearchforhealthcareisproposed.Ourproject-groundedresearchcanbestudiedtodemonstratehowdesigncanimprovethepreventionandthepromotionofsleep’shygienethroughthecreationofservices,products,experiencesandhealthcareenvironments.Moreprecisely,themethodologybasedonsystemicdesignallowsustoopentheprojectfromaservicefocusedonmobiledevicestoaprojectofinstituteconsideredasacomplexofsystemsandservicedesigndedicatedtoinsomniapreventionandtreatment.Ahumananddigitalnetworkofpatientsandprofessionalscansupporttheinstitute.Inaddition,mobiledevicesandconnectedobjectscanbeusedtoservevariousstakeholders.Theglobalsolutionincludesoptimizingthepatientcarejourneyandthecommunicationbetweenpatientsandcaringprofessionalsthroughsecureinformationsystemsanddatabase.Accesstothepatient’sdatashouldbeco-definedbypatientsandcareprofessionals.Thispeculiarityisveryimportantfortheethicvalueoftheproject.Buttheaccesstothepatient’sdatawillalsoneedtoconsidertherecommendationsoftheFrenchHealthHighAuthority(HAS10)andthelegalregulationsondataprotectionintheEuropeanUnion.Theminimalequationofthedigitalplatformiscomposedofprofessionals+data+patients.Andthefinalformofthedigitalnetworkshouldbesuitabletotheconstraintofinformationsystem’sinteroperability(inpeculiarbetweenthesoftsusedinpublichospital,cityofficeandpublicadministrations).Thistechnologicalchallengewillbepossibleonlyifthesocialinteroperabilitybetweenthevariousactorsismadepossiblebythelocalandnationalpublichealthauthorities.Thisprojectofconnectedobjectsandsleepmedicineaffectshealthpublicpolicies.ThissupportedneedtoimprovethedevelopmentoftheprojectwasalsorecommendedbyoneofthegeneralpractitionersinthefirstAprilworkshop.Henoticedtheimportanceofa"politicalsupport"todevelopa"nationalinformationcampaign"onchronicinsomnia,tostrengthenourinitiativeofnetworkonthefieldwork.Thisiswheredesigncanbeusefultodevelopinformationandeducationalkittools,tosustainsleephygieneandpatients’andcareprofessionals’digitalhealthliteracy.
Theresultsofthisone-yeardesignresearchleadustothinkaboutmutualcontributionsbetweeninformationandcommunicationsciencesanddesign,andtofocusonthecontributionofdesigntothefieldofhumanandsocialsciences.
4.1Mutualcontributionbetweeninformationandcommunicationsciencesanddesign
Ontheonehand,wecanemphasizethelinksbetweenthesetohumanandsocialsciences.Indesignsciences,theprojectisseenas“theactofdesign”andtheactofdesignisan“actofcommunication”(Vial,2014).Itcanbeanalysedfrombothperspectives:conceptionandreception,thatistosay“thedesigngesture”and“theeffectofdesign”(Vial,2015).Theactofdesignreferstotheactofcommunicationinherenttoanymediadevice.Inthisproject-groundedresearch,thelinkbetweenthetwosidesoftheco-constructionofthemeaning(bydesigneranduser)isanalysedwiththreemainapproachesthatbuildthespecificityofthemainresearcher’sprofile:semiotics,communicationandanthropology.
Moreover,itisnecessarytoputthedesigner’sandresearcher’srolesinaproject-groundedresearchintoperspective,especiallyinthefieldwork.Ourexperienceofthisprojectmakesusthinkthatthesetwoapproachesarecomplementary.Withtheresearcher,thedesignercontributestothecreationofmediationdevicesthatarehelpfultothetransmissionandthecollectionofinformationbetweentheparticipants.Thevisualmaterialscanbeconsideredas“transitionalobjects”,usefulina“potentialenvironmentofskillsdevelopment11”.Thesematerialsbuildupanenvironmentallowing
10SeetheFrameofreferenceofthebestpracticesonhealthapplicationsandconnectedobjectspublishedin2016:http://webzine.has-sante.fr/portail/upload/docs/application/pdf/2016-11/has_ref_apps_oc.pdf11BertenA.,(1999),«Dispositif,médiation,créativité:petitegénéalogie»,Hermès25,Ledispositif,CNRS,p.41.

todevelopthenecessaryconditionstodevelopthecreativityoftheparticipants.Inaddition,thedesignercandrawvisualsynthesisoftheenquiry,whichcanenlightensomecharacteristicsofthequalitativeanalysis.
Ontheotherhand,themediationtoolsproducedinandfortheprojectcanbeconsideredascasestudiesininformationandcommunicationsciences.Thesecreativetoolsbasedonvisualmethodologycontributetotherenewalofthequalitativeinquiriesinhumanandsocialsciences,withdifferentobjectivesaccordingtothedifferentstepsoftheproject.Intheperiodsofobservation,thevisualmaterialscaneasethevoicingandtheexpressionoftheparticipants.Theyareusefultocollectrepresentations,experiencesanddataco-producedbystakeholders,designersandresearchers.Intheworkshops,thesemediationtoolscanbeusedtohelptheparticipantsgiveformtotheirideasandsolutions.Inthedevelopmentphaseoftheproject,visualmaterialscanbehelpfultocommunicatethesolutionstothebeneficiaries,andtosketchuser’sscenariostoexplainthefunctionsofthecomplexsystemofservicedesign,relyingonastorytellingfocusedonapatientexperience.
4.2Specificcontributionofdesigntohumanandsocialsciencesinthefieldofhealthcare
Attheendofthisone-yearstudyondesignandmobilehealthinthefieldofsleepmedicine,wecanunderlinetheadvantagesofourmethodologybasedonsystemicandinclusivedesign:implicationoftheparticipantscommittedintheco-designprocess,appropriationoftheprojectandthevaluesoftheproject,andempowermentintheprevention,thecareandthefollow-upofchronicinsomnia.
Theparticipativedesignpracticeandresearchalsoallowedtheparticipantstoseizetheprojectandtobecomesomecontactpersonsineachcommunityofthelocalterritory.Theyparticipatedinthedistributionoftheprojectintheirownnetworks.Tous,thisistheminimalconditiontomakeaprojectdedicatedtosocialinnovationinhealthcaresuccessful.Indeed,co-designcanimproveacceptabilityandadoptionofthesolutionsbythebeneficiariesasfarastheycantakepartinthedesignprocess.
Thequalitativeapproachallowedustoseizethefears,theexpectationsandtheaspirationsofthestakeholders,tobeabletoproposethemostadaptedsolutions.Thecontributionofdesigntohumanandsocialsciencesinthefieldofhealthcareistotaketime,withqualitativeandparticipativemethodstounderstandtheconstraintsandtherepresentationsofthestakeholders.Thisapproachisrelevanttoidentifytheirreluctanceandtofindsolutionstogowiththeculturalandsocialchange.Byunderstandingthefearsandthereluctancesoftheactors,andputtingoneselfinthemainbeneficiaries’shoes-whosometimesliveinnovationasanorder,thequalitativemethodologiescanaccompanytheinnovationinthefieldofhealthcaretoacculturatetheprofessionalsandthepatientsinthecollectiveintelligencebasedoncreativemethods,butalsointhedigitalhealthliteracy.
Atlast,wecandistinguishfivefiguresofthedesigner’smediationroleinaproject.Thedesignercanalsobea“competenceconnector”(Deni,2014),acoordinator,acommunicator,afacilitatorandatranslator,abletomanagetheinter-professionalandinterdisciplinarydialoguebetweenthemultiplestakeholders.Newrolesforthedesignercanbeidentifyinthecomplexfieldofhealthcare.Sleepmedicine,asanewcross-disciplinarydiscipline,offersgreatchallengesfordesignerstoleadmultidisciplinarygroupsandmakemajordecisionsthatwillinfluencebehaviourcontributingtolong-termpreventionandbetteroverallpopulationsleep’shygiene.
5. ConclusionToconclude,thisproject-groundedresearchondesignandm-Healthdedicatedtosleepdisorderscanbeconsideredasanattempttocontributetothedesignresearchonhealthcareandwellbeing.Thespecificcontributionisaboutthesystemicdesignoftheproject,includingmanystakeholdersandsomedigitaltoolsattheserviceofthepatientsandcareprofessionalsnetwork.Thesystemic

approachisusefultounderstandhowitisnecessarytore-designthewholeexperienceofthepatient’scarejourney,andtodesigneducationalkittoolsforpatientsandcareprofessionals,includingtelemedicineserviceandmobilehealth.
Thespecificityoftheprojectandofthecomplexfieldworkleadustobuildupamethodologybasedonsocialinnovationbydesign,togivesuitableanswerstothequestionsweidentifyonthefield.Inthisperspective,thisproject-groundedresearchgoesforwardtoobjectorservicedesigntoreachtosystemicdesignofsystemsandservicesbasedonsuitablesolutionsforthemainstakeholders.Thescientificrootsoftheresearch,basedonhuman-centered-designleadustoworkonsocialinteroperabilitybetweentheactors.Thesolutionsaredesignedtooptimizethecommunicationbetweeninsomniacpatientsandcareprofessionals,toimprovethepatient’scarejourney,todevelopthetrainingofprofessionalsinsleepmedicineandtherapeuticeducation,andtodevelopdigitalhealthliteracy.Theobjectiveoftheprojectisthustoconsiderthebenefitsformdesigningadigitalservicededicatedtoinsomnia,whichisintegratedinapatientandprofessionalnetwork,toimprovetheimplicationandsustaintheempowermentofinsomniacpatientsintheirownpathology.
Inaddition,wecansaythatfurtherresultscouldbepresentedtotheDRSCongressinJune2018,asthecurrentdevelopmentphasehasledthescientificteamtomeetpotentialpartnerstodevelopaprototypeofthedigitalnetworkandtheconnectedobjectsinthefollowingtwoyears.
Tofinishwith,thesetwoinitiativescanalsobeconsideredasanattempttounderlinetheroleofdesigninpreventionandwellbeinginsleepmedicine.
6. ReferencesAlDahdah,M.(2014).MHealth:l’informationdesantéubique?,LeTempsdesmédias2014/2(n°23),52-65.Bartlett,eDJ.Marshall,NS.Williams,A.Grunstein,RR.(2008).Predictorsofprimarymedicalcareconsultation
forsleepdisorders.Sleepmed,9,123-130.BertenA.(1999).Dispositif,médiation,créativité:petitegénéalogie,Hermès25,CNRS,33-47.Caccamo,E.,Catoir-BrissonM-J.(2016).Métamorphosesdesécrans:invisibilisations,Interfacesnumériques
n°5/Vol2,Editionsdesignnumérique,juin2016.Catoir-Brisson,M-J.(2017).Dudesignd’interactionau«textilesocial»:approchescommunicationnelleet
sémiotiqued’unmédiatangible,MEI41,Designetcommunication.Retriewedfromhttp://mei-info.com/revue/40/209/
Catoir-BrissonM-J.,JankeviciuteL.(2014).Entretienetméthodesvisuelles:unedémarchederecherchecréativeensciencesdel’informationetdelacommunication,Sciencesdelasociété,92,111-127.
ConseilNationaldel’OrdredesMédecins.(2015).Santéconnectée:delae-santéàlasantéconnectée,LivreblancduCNOM,janvier2015.
D.ReayS.,CollierG.,DouglasR.,HayesN.,Nakarada-KordicI.,NairA.&Kennedy-GoodJ.(2017).Prototypingcollaborativerelationshipsbetweendesignandhealthcareexperts:mappingthepatientjourney,DesignforHealth,Vol1,65-79.
Deni,M.(2014).Ledesigndeservices:projeterlebien-être,Communication&organisation2/2014(n°46),129-142.
DuretF.,FloriotD.(2012).Attentesdespatientssurlapriseenchargedeleurinsomniechroniqueauseindel’arcalpin.Thèsedemédecine:UniversitédeGrenoble.
EuropeanNetworkofLivingLabs(2008):‘OpenLivingLabs’,availableonlineathttp://openlivinglabs.eu.E.WildevuurS.(2017).Couldhealthlearnfromdesign?,DesignforHealth,1/2017,59-64.Findeli,A.(2015).Larecherche-projetendesignetlaquestionderecherche:essaideclarification
conceptuelle,SciencesduDesign#1,43-55.GaboreauY.,PricazF.,Cote-ReyA.,RoucouI.,ImbertP.(2017),Consensus,controversesetdissensionsentre
médecinsgénéralistesetpatientsautourdel’insomniechroniqueprimaire,RevueExercer#130Volume28,CollègeNationaldesGénéralistesEnseignants,2017,p.52-59.Retriewedfromhttps://www.exercer.fr/numero/130/page/52/
JonesP.(2013).Designforcare:innovatinghealthcareexperience,NewYork,RosenfeldMedia,Retriewedfromhttp://tandfonline.com/doi/full/10.1080/24735132.2017.1295541

Krebs,P.,DuncanDT.(2015).HealthAppUseAmongUSMobilePhoneOwners:ANationalSurvey»,JMIRMHealthUHealth,Retriewedfromhttps://www.ncbi.nlm.nih.gov/pmc/articles/PMC4704953/
Lagger,G.Pataky,Z.Golay,A.(2010).Efficacyoftherapeuticpatienteducationinchronicdiseasesandobesity.PatientEducCouns,79,283-286.
Moggridge,B.(2007).DesigningInteractions,TheMITPress.NormanD.(2012).Designémotionnel,Bruxelles,DeBoeck.RapoportR.N.(1973),“Lestroisdilemnesdelarecherche-action”,Connexionsn°7,115-131.TrompN.,HekkertP.,VerbeekP.(2011).DesignforSociallyResponsibleBehavior:AClassificationofInfluence
BasedonIntendedUserExperience,DesignIssuesVol.27,N°3,2011,.3-19.Vial,S.(2014)Ledesign,unactedecommunication?Hermès#70,174-180.Vial,S.(2015).Ledesign.Quesais-je?Paris:PUF.
AbouttheAuthor:
Marie-Julie Catoir-Brisson works on mHealth and social innovation. Her recentworks deal with digital interfaces, connected objects, information and interactiondesign, which she approaches on a critical perspective, from several knowledges:design,semiotics,intermediality,communication’santhropology,visualmethods.
Copyright © 2022 FDOKUMEN