Small, homelike care environments for older people with dementia: a literature review
13
International Psychogeriatrics (2009), 21:2, 252–264 C 2008 International Psychogeriatric Association doi:10.1017/S104161020800820X Printed in the United Kingdom REVIEW Small, homelike care environments for older people with dementia: a literature review ......................................................................................................................................................................................................................................................................................................................................................................... Hilde Verbeek, Erik van Rossum, Sandra M. G. Zwakhalen, Gertrudis I. J. M. Kempen and Jan P. H. Hamers School for Public Health and Primary Care, Faculty of Health, Medicine and Life Sciences, Maastricht University, Maastricht, The Netherlands ABSTRACT Background: There is large cross-national variation in the characteristics of small, domestic-style care settings which emphasize normalized living. However, a systematic overview of existing types is lacking. This study provides an international comparison of the care concepts which have adopted a homelike philosophy in a small-scale context. Insight into their characteristics is vital for theory, planning and implementation of such dementia care settings. Method: A literature search was performed using various electronic databases, including PubMed, Medline, CINAHL and PsycINFO. In addition, “gray” literature was identified on the internet. Concepts were analyzed according to five main characteristics: physical setting, number of residents, residents’ characteristics, domestic characteristics and care concept. Results: 75 papers were included covering 11 different concept types in various countries. Similarities among concepts reflected a focus on meaningful activities centered around the daily household. Staff have integrated tasks and are part of the household, and archetypical home-style features, such as kitchens, are incorporated in the buildings. Differences among concepts were found mainly in the physical settings, numbers of residents and residents’ characteristics. Some concepts have become regular dementia care settings, while others are smaller initiatives. Conclusion: The care concepts are implemented in various ways with a changing staff role. However, many aspects of these small, homelike facilities remain unclear. Future research is needed, focusing on residents’ characteristics, family, staff and costs. Key words: small-scale housing, group living, nursing home facilities, deinstitutionalization, long-term care Introduction The majority of people with dementia are cared for at home (de Vugt et al., 2006). However, when home care becomes inadequate, institutional care is necessary. Traditionally, institutional care for older people with dementia has been arranged according to the medical model (Finnema et al., 2000). In this model, emphasis is given to the treatment of the underlying pathology that causes the disease (Taft et al., 1997). However, the medical model provides little guidance in the care of dementia patients since there is no cure for Correspondence should be addressed to: Hilde Verbeek, School for Public Health and Primary Care, Faculty of Health, Medicine and Life Sciences, Maastricht University, P.O. Box 616, 6200 MD Maastricht, The Netherlands. Phone: +31 433 881513; Fax: +31 433 884162. Email: [email protected]. Received 4 Jun 2008; revision requested 3 Jul 2008; revised version received 10 Sep 2008; accepted 15 Sep 2008. First published online 23 December 2008. dementia yet. Nowadays, the medical approach has become outmoded and a shift towards a psychosocial model of care has been developed (Finnema et al., 2000). In this approach, the care is person-centered and aimed at the well-being of the individual. The therapeutic milieu is arranged to support the remaining strengths of older people with dementia. Together with interest in this new care approach, it is increasingly recognized that the design of the physical environment has an important influence on dementia care (Day et al., 2000). Some studies have suggested that a small, homelike environment is beneficial for older people with dementia (Calkins, 2001; Day et al., 2000; Judd et al., 1998; Sloane et al., 1998). As a result of these developments, new therapeutic environments have been created for older people with dementia, emphasizing normalization of daily life: the environment is 252
-
Upload
independent -
Category
Documents
-
view
4 -
download
0
Transcript of Small, homelike care environments for older people with dementia: a literature review

International Psychogeriatrics (2009), 21:2, 252–264 C© 2008 International Psychogeriatric Associationdoi:10.1017/S104161020800820X Printed in the United Kingdom
R E V I E W
Small, homelike care environments for older peoplewith dementia: a literature review
.........................................................................................................................................................................................................................................................................................................................................................................
Hilde Verbeek, Erik van Rossum, Sandra M. G. Zwakhalen, Gertrudis I. J. M. Kempenand Jan P. H. HamersSchool for Public Health and Primary Care, Faculty of Health, Medicine and Life Sciences, Maastricht University, Maastricht, The Netherlands
ABSTRACT
Background: There is large cross-national variation in the characteristics of small, domestic-style care settingswhich emphasize normalized living. However, a systematic overview of existing types is lacking. This studyprovides an international comparison of the care concepts which have adopted a homelike philosophy in asmall-scale context. Insight into their characteristics is vital for theory, planning and implementation of suchdementia care settings.
Method: A literature search was performed using various electronic databases, including PubMed, Medline,CINAHL and PsycINFO. In addition, “gray” literature was identified on the internet. Concepts were analyzedaccording to five main characteristics: physical setting, number of residents, residents’ characteristics, domesticcharacteristics and care concept.
Results: 75 papers were included covering 11 different concept types in various countries. Similarities amongconcepts reflected a focus on meaningful activities centered around the daily household. Staff have integratedtasks and are part of the household, and archetypical home-style features, such as kitchens, are incorporatedin the buildings. Differences among concepts were found mainly in the physical settings, numbers of residentsand residents’ characteristics. Some concepts have become regular dementia care settings, while others aresmaller initiatives.
Conclusion: The care concepts are implemented in various ways with a changing staff role. However, manyaspects of these small, homelike facilities remain unclear. Future research is needed, focusing on residents’characteristics, family, staff and costs.
Key words: small-scale housing, group living, nursing home facilities, deinstitutionalization, long-term care
Introduction
The majority of people with dementia are caredfor at home (de Vugt et al., 2006). However,when home care becomes inadequate, institutionalcare is necessary. Traditionally, institutional carefor older people with dementia has been arrangedaccording to the medical model (Finnema et al.,2000). In this model, emphasis is given to thetreatment of the underlying pathology that causesthe disease (Taft et al., 1997). However, themedical model provides little guidance in the careof dementia patients since there is no cure for
Correspondence should be addressed to: Hilde Verbeek, School for Public Healthand Primary Care, Faculty of Health, Medicine and Life Sciences, MaastrichtUniversity, P.O. Box 616, 6200 MD Maastricht, The Netherlands. Phone:+31 433 881513; Fax: +31 433 884162. Email: [email protected] 4 Jun 2008; revision requested 3 Jul 2008; revised version received 10Sep 2008; accepted 15 Sep 2008. First published online 23 December 2008.
dementia yet. Nowadays, the medical approachhas become outmoded and a shift towards apsychosocial model of care has been developed(Finnema et al., 2000). In this approach, the care isperson-centered and aimed at the well-being of theindividual. The therapeutic milieu is arranged tosupport the remaining strengths of older people withdementia.
Together with interest in this new care approach,it is increasingly recognized that the design of thephysical environment has an important influence ondementia care (Day et al., 2000). Some studies havesuggested that a small, homelike environment isbeneficial for older people with dementia (Calkins,2001; Day et al., 2000; Judd et al., 1998; Sloaneet al., 1998). As a result of these developments,new therapeutic environments have been createdfor older people with dementia, emphasizingnormalization of daily life: the environment is
252

Homelike care environments for older people with dementia: a review 253
small and homelike and the care is person-centered with respect for residents’ needs andchoices. In the literature, these environments aresometimes referred to as a “housing model”(Marshall and Archibald, 1998) or “home model”(Briller and Calkins, 2000) as opposed to the“hotel”, “resort” or “medical” models of care.In Sweden, almost 20% (14,000) of people withdementia residing in institutional care lived in groupliving facilities in 2000 (Wimo and MorthensonEkelof, 2004). Estimates indicate that in theNetherlands around 25% of the long-term nursinghome care in 2010 will be realized in thesesmall-scale, homelike facilities (te Boekhorst et al.,2007).
Currently, a common and desirable policyprinciple in many countries is to delay residencyin an institution by enabling older people withdementia to remain at home for as long as possible(Moise et al., 2004). Furthermore, when institu-tional care is required, this should be as home-like as possible. In addition, present health careethics emphasizes respect for residents’ autonomy(Hertogh et al., 2004). Small-scale, homelike careconcepts for older people with dementia are in linewith these policy and moral principles. Althoughtheir underlying core philosophy is similar, thereseems to be a large cross-national variation incharacteristics of such care settings with little insightinto the requirements of the physical and socialenvironment. A systematic international overviewof small-scale homelike concepts for older peoplewith dementia is lacking. Marshall (1993) hasreported several small-scale domestic style facilities.Since then, various new developments have beenreported in this rapidly changing field of care.Moreover, Warren et al. (2002) describe someresidential-style facilities but they focus on theimpact of the environment on residents, not oncharacteristics. Insight into these characteristicsis essential to improve our understanding of theconcept, planning and implementation of small-scale homelike facilities in dementia care.
The aim of this study is to present an interna-tional overview of small-scale and homelike facilitiesfor older people with dementia. It seeks to compareand describe them in terms of five main character-istics: the physical setting, number of residents, res-idents’ characteristics, domestic characteristics andcare philosophy. Overall similarities and differencesamong and within the concepts are emphasized.An overview of concepts and their characteristicsprovides tools for scientists as well as clinicians toimprove dementia care settings. This is relevantto the ongoing debate on enhancing domesticityin dementia care and for future planning of caresettings.
Methods
Search procedureTo identify the possible concepts, different searchstrategies were performed systematically. First,various electronic databases were searched for refer-ences, including Medline, PsycINFO, CumulativeIndex to Nursing and Allied Health Literature(CINAHL) and PubMed. English, German andDutch publications from 1970 until May 2008were included in the review. Search terms includeddementia, group living, group home, collectiveliving, group dwelling, small units, special careunit, special care facility, homelike environment.Because of the large amount of publications foundin PubMed, the key word “nursing home” wasadded to limit the results of the search in thisdatabase. Articles were screened for relevance basedon title and abstract. Furthermore, reference listswere explored to identify additional relevant studies.Finally a “gray” literature search was performedusing the internet. All types of publications wereincluded in the search procedure, i.e. articles,books, chapters, reports, non-empirical studies andcommentaries.
Selection criteriaPublications needed to fulfill three criteria to beeligible for this review. First, they had to describeprojects specifically designed for older people withdementia. Second, publications needed to describeprojects which were small scale, i.e. a maximum of15 residents living together in one group or unit(Zeisel et al., 1994; van Audenhove et al., 2003).Third, the philosophy of care as well as the design ofthe therapeutic milieu had to emphasize a homelike,normalized way of living. Those studies of group-living concepts which did not include all of thesethree criteria were excluded from the review.
AnalysesConcepts were analyzed and described according tothe following five main characteristics:
• physical setting: description of location and buildingfeatures (e.g. physical design, positioning of rooms);
• number of residents per house or unit;• residents’ characteristics: specification of the
project’s target group (e.g. level of dementia,activities of daily living (ADL) capacities andbehavioral disturbances);
• domestic characteristics: features which constitutea homelike environment;
• care concept: description of the project’s philosophyof care, including organizational and social aspectsof care.

254 H. Verbeek et al.
These five characteristics are based on aconceptual framework for organization of a person-environment system (Cohen and Weisman, 1991).In this framework, the environment for olderpeople with dementia is conceptualized accordingto different components, including characteristicsof the patient population, the physical setting andorganizational and social aspects. These last twoaspects are represented in the care concept. Inaddition, international recurring themes includingsmallness of the environment (reflected in thenumber of residents per house or group) andfamiliarity (reflected in domestic characteristics)are included in the analyses (Judd et al., 1998;Marshall and Archibald, 1998). Finally, a timescale of concepts was constructed and costs wereanalyzed.
Results
The search of the electronic databases yielded 859publications. Based on title and abstract, 77 wereselected for further reading, of which 46 wereincluded in the final selection of publications (seeFigure 1). Reference tracking yielded another 18relevant publications. The gray literature searchresulted in another 11 publications. Altogether, 75publications were included in the review.
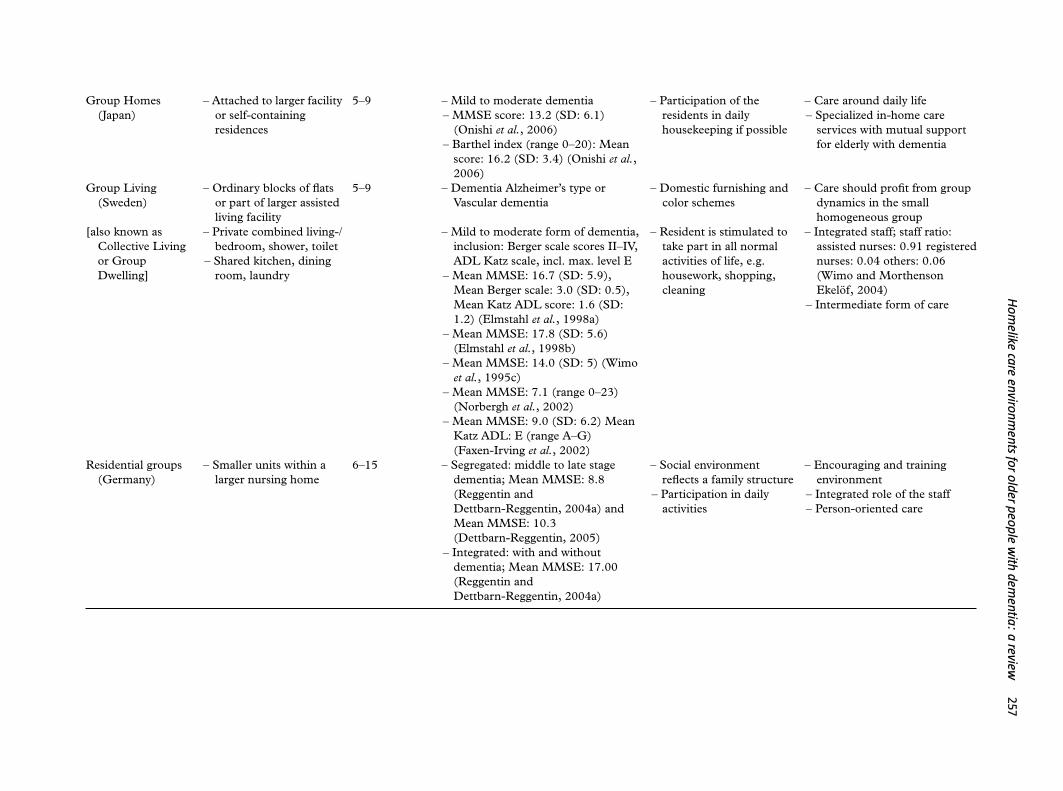
The 75 publications describe 11 types ofconcepts in 11 countries: “CADE units” (Aus-tralia), “Cantou” (France), “Care Housing”(Scotland), “Domuses” (U.K.), “Green Houses”(U.S.A.), “Group Home” (Japan), “Group Liv-ing” (Sweden), “Residential groups” (Germany),“Small-scale Living” (Netherlands/Belgium), “Spe-cial Care Facility” (Canada) and “Woodside place”(U.S.A./Canada). Concepts were identified basedon name, country and characteristics as provided inthe publications. Table 1 provides a short summaryof the 11 concept types, based on the five maincharacteristics.
Physical settingThe concepts’ location varies between units situatedwithin a larger nursing home (e.g. “Residentialgroups” in Germany) to stand-alone facilities (e.g.“Green Houses” in the U.S.A. or “Special CareFacility” in Canada; Dettbarn-Reggentin, 2005;Rabig et al., 2006; Reimer et al., 2004). Inaddition, there are differences within projects. Forinstance, “Small-scale Living” in the Netherlands/Belgium and “Group Living” in Sweden can belocated in ordinary houses in the community ormay be part of a larger, assisted-living facility(te Boekhorst et al., 2007; Wimo and MorthensonEkelof, 2004). Stand-alone facilities may prevent
institutional characteristics from gaining hold inthe project (Rabig et al., 2006; Reimer et al.,2004). However, such facilities are often not feasibleowing to pressures of financing arrangements andthe organization of health care. Some concepts,such as “CADE units” in Australia, are locatedin the local community because this increasesresidents’ opportunity to maintain their socialnetwork (Atkinson, 1995).
The buildings themselves are intended to offera homelike environment with archetypical featuressuch as a kitchen, dining room, living room and alaundry area (Rabig et al., 2006; Annerstedt, 1994).The kitchen often has an important function as ameeting center (Leichsenring et al., 1998). Almostall residents have private rooms and, in some cases,a private bathroom. In addition, some concepts usetechnology to support care in many different ways.For instance, “Green Houses” in the U.S.A. use“smart house” technology consisting of prosthetic,communication and educational devices (Rabiget al., 2006). This includes an interactive televisionto keep distant family and residents in contact witheach other.
Numbers of residentsThe number of residents per house or unit variesfrom 5–9 (e.g. “Group Homes” in Japan, “Groupliving” in Sweden and “Small-scale Living” inthe Netherlands/Belgium) to 13–15 residents (e.g.“CADE units” in Australia, “Cantou” in France)(Atkinson, 1995; Onishi et al., 2006; te Boekhorstet al., 2007; Ritchie et al., 1992). The main purposeof a small group is to promote social activitiesand to create an environment resembling a family(Dettbarn-Reggentin, 2005). There is opportunityfor staff, residents and family members to becomefamiliar with each other and thereby allow closecontact and communication (Leichsenring et al.,1998). The group dynamics of a small group seemto be beneficial for the care of residents (Annerstedt,1993). In practice, however, group size is oftendetermined by practical considerations, such asbudget, available space and staffing (Cohen andWeisman, 1991).
Residents’ characteristicsResidents’ characteristics are very heterogeneous,both between and within projects (see Table 1).Mean MMSE scores range from 7.1 to 17.8,although many studies do not report such objectiveparameters. Some concepts are designed forresidents in the early stages of their disease(e.g. “Woodside” in Canada/U.S.A. and “GroupLiving” in Sweden). Admission criteria may

Homelike care environments for older people with dementia: a review 255
Figure 1. Flow chart of the publication search.
include a sufficient level of participation inactivities, communication skills or being ambulatory(Annerstedt, 1993; Janzen, 2000). In theseconcepts, residents are usually transferred toanother care setting when these criteria are nolonger met. They manifest themselves as anintermediate form of care between the residents’own home and the nursing home. One concept(“CADE units” in Australia) is specifically aimedat residents with behavioral problems and nosignificant physical problems (Atkinson, 1995). It is
perceived as a complement to existing facilities andservices. In contrast, concepts such as “Domuses”in the U.K. and “Cantou” in France have a “home-for-life” principle, with residents being able tostay there until they die (Lindesay et al., 1991;Ritchie et al., 1992). “Care Housing” in Scotlandis intended as a home for life, except for thoseresidents who disturb the group living experience ofother residents or those residents who do not benefitfrom the household approach (Carr and Marshall,1993).

256H
.Verbeeketal.
Table 1. Concept characteristics (concepts are presented in alphabetical order)
C O N C E P T a P H Y S I C A L S E T T I N GN O . O FR E S I D E N T S
R E S I D E N T S ’C H A R A C T E R I S T I C S
D O M E S T I CC H A R A C T E R I S T I C S C A R E C O N C E P T
........................................................................................................................................................................................................................................................................................................................................................................................................................................................
CADE units(Australia)
– Purpose built “prostheticenvironment”
– Proximity to localcommunity
8–10/14 – Moderate to severe dementia– Ambulant, with no significant
physical problems– Behaviorally disturbed– Few psychiatric problems
– Opportunity to participatein household activities
– Familiar decor
– Based on normalization– Staff work patiently at the
resident’s pace– Needs of the resident take
precedence over needs of theunit
– Staff: registered nurses,enrolled nurses and residentialcare assistants
Cantou (France) – Community living in aseparate enclosed area
– Large kitchen and livingroom, with adjacentindividual rooms
12–15 – Senile dementia– Mean MMSE score: 9.29 (SD 8.17)
(Ritchie et al., 1992)
– Resident’s own furniture– Activities centered around
tasks of daily living– Activities participation of
family in daily life
– Non-medical, communal care– Stable multipurpose staff– Home for life
Care Housing(Scotland)
– Located in residentialhome / part of shelteredaccommodation
8–12 – Mild to moderate dementia– Mean MMSE score: 13,4 (range
6–20) (Roscrow, 1996)– Modified Crichton Royal Behavior
Rating Scale (MCRBRS, range0–38
Total score: 12.5 (range 8–16)(Roscrow, 1996)
– Participation in dailyactivities
– Flexible and individual tailoredcare
– Maximizing independence
Domus philosophy(U.K.)
– Purpose built facility orconversion of existingwards
– Private bedroom– Shared bathroom, toilet
and living room
9–12 – Dementia, requiring intensivenursing care
– Elderly psychiatric patients– Mean Organic Brain Syndrom
(OBS) score 7.1 (SD 2.6)(Lindesay et al., 1991)
– Active participation in life – “Home-for-life” principle– Psychological / emotional
needs above physical aspects– Emphasis on maintaining
independence and residualcapacities
Green House(U.S.A.)
– Stand alone quality– Self-contained semi
attached bungalows– Private bedrooms with
en-suite bathroom
7–10 – Dementia-specific or generalnursing home level of care
Minimum Data Set scores (MDS)(Kane et al., 2007):
– Cognitive Performance Scale (CPS;range 0–6) Mean: 2.8 (SD: 1.92)
– ADLs (range 0–16), Mean: 7.0(SD: 5.7)
– Garden / Fireplace– Participation in typical
home activities
– Social model with necessaryclinical care
– Emphasis on competence– Universal workers
Hom
elikecare
environments
forolder
peoplew
ithdem
entia:a
review257
Group Homes(Japan)
– Attached to larger facilityor self-containingresidences
5–9 – Mild to moderate dementia– MMSE score: 13.2 (SD: 6.1)
(Onishi et al., 2006)– Barthel index (range 0–20): Mean
score: 16.2 (SD: 3.4) (Onishi et al.,2006)
– Participation of theresidents in dailyhousekeeping if possible
– Care around daily life– Specialized in-home care
services with mutual supportfor elderly with dementia
Group Living(Sweden)
– Ordinary blocks of flatsor part of larger assistedliving facility
5–9 – Dementia Alzheimer’s type orVascular dementia
– Domestic furnishing andcolor schemes
– Care should profit from groupdynamics in the smallhomogeneous group
[also known asCollective Livingor GroupDwelling]
– Private combined living-/bedroom, shower, toilet
– Shared kitchen, diningroom, laundry
– Mild to moderate form of dementia,inclusion: Berger scale scores II–IV,ADL Katz scale, incl. max. level E
– Mean MMSE: 16.7 (SD: 5.9),Mean Berger scale: 3.0 (SD: 0.5),Mean Katz ADL score: 1.6 (SD:1.2) (Elmstahl et al., 1998a)
– Mean MMSE: 17.8 (SD: 5.6)(Elmstahl et al., 1998b)
– Mean MMSE: 14.0 (SD: 5) (Wimoet al., 1995c)
– Mean MMSE: 7.1 (range 0–23)(Norbergh et al., 2002)
– Mean MMSE: 9.0 (SD: 6.2) MeanKatz ADL: E (range A–G)(Faxen-Irving et al., 2002)
– Resident is stimulated totake part in all normalactivities of life, e.g.housework, shopping,cleaning
– Integrated staff; staff ratio:assisted nurses: 0.91 registerednurses: 0.04 others: 0.06(Wimo and MorthensonEkelof, 2004)
– Intermediate form of care
Residential groups(Germany)
– Smaller units within alarger nursing home
6–15 – Segregated: middle to late stagedementia; Mean MMSE: 8.8(Reggentin andDettbarn-Reggentin, 2004a) andMean MMSE: 10.3(Dettbarn-Reggentin, 2005)
– Integrated: with and withoutdementia; Mean MMSE: 17.00(Reggentin andDettbarn-Reggentin, 2004a)
– Social environmentreflects a family structure
– Participation in dailyactivities
– Encouraging and trainingenvironment
– Integrated role of the staff– Person-oriented care

258H
.Verbeeketal.
Table 1. Continued.
C O N C E P T a P H Y S I C A L S E T T I N GN O . O FR E S I D E N T S
R E S I D E N T S ’C H A R A C T E R I S T I C S
D O M E S T I CC H A R A C T E R I S T I C S C A R E C O N C E P T
........................................................................................................................................................................................................................................................................................................................................................................................................................................................
Small-scale Living(Netherlands /Belgium)[also known as“Group Living”]
– Variety in location– Shared kitchen and
living area; privatebedrooms
6–8 – Middle to late stage dementia – Participation in dailyactivities
– Familiar decor
– Emphasis on normalization ofliving
– Integrated staff; education:nursing assistants: 11%;certified nursing assistants:79%; registered nurse: 10%(te Boekhorst et al., 2008)
Special Care Facility(SCF) (Canada)
– 6 bungalows, purposebuilt
– Private bedrooms withen-suite bathrooms
10 – Middle to late stage dementia– Mean score Global Deterioration
Scale (GDS): 6.1 (range 5–7)(Reimer et al., 2004)
– Biodiverse environment:multigenerational, live-inpets, plants
– Physical environment,daily activities like atypical home
– Integrated role of the staffincluding personal care, leisureand rehabilitation activity
“Woodside place”(Canada / UnitedStates)
– Main buildingconnected to threeindividual houses
– Each house has a sharedkitchen and living room,private bed-/bathrooms
8–15 – Mild to moderate dementia– Mean MMSE: 11.1 (SD 6.1)
(Saxton et al., 1998)– Mean MMSE: 15.4 (SD: 5.0)
(Warren et al., 2001)
– Maximum engagement inactivities
– Home-like sitting spaces(e.g. kitchen, library)
– Program and staffing patternsaround social modelEmphasis on independence
– No physical and minimalpsychotropic restraints
a Publications:CADE units: Carr and Marshall, 1993; Atkinson, 1995; Fleming and Bowles, 1994; Marshall, 1993; Marshall and Archibald, 1998.Cantou: Ritchie et al., 1992; Ritchie and Ledesert, 1992; Marshall, 1993.Care Housing: Roscrow, 1996; Judd et al., 1998; Marshall, 1993; Carr and Marshall, 1993.Domus: Beecham et al., 1993; Dean et al., 1993a; 1993b; Macdonald et al., 2004; Radzey et al., 2001; Skea and Lindesay, 1996; Lindesay et al., 1991; Marshall, 1993.Green House: Rabig et al., 2006; Angelelli, 2006; Kane et al., 2007.Group Home: Funaki et al., 2005; Hirakawa et al., 2006; Nakanishi and Honda, 2008; Yokota et al., 2006; Onishi et al., 2006.Group Living: Annerstedt, 1993; 1994; 1997; Annerstedt et al., 1993a; 1993b; 1996; 2000; Andren and Elmstahl, 2002; 2007; Ahlund, 1999; Alfredson and Annerstedt, 1994; Elmstahl et al.,1997; 1998a; 1998b; Faxen-Irving et al., 2002; Jensen et al., 2002; Kihlgren et al., 1992; Kuremyr et al., 1994; Malmberg and Zarit, 1993; Marshall, 1993; Norbergh et al., 2001; 2002; Radzey et al.,2001; Sandman and Wallblom, 1996; Svensson et al., 1996; Wimo et al., 1991; 1995a; 1995b; 1995c; Wimo and Morthenson Ekelof, 2004.Residential groups: Radzey et al., 2001; Reggentin and Dettbarn-Reggentin, 2004a; 2004b; Leichsenring et al., 1998; Dettbarn-Reggentin, 2005.Small-scale Living: Depla and te Boekhorst, 2007; Leichsenring et al., 1998; te Boekhorst, 2007; te Boekhorst et al., 2007; 2008; Peters and Duine, 1987; van Audenhove et al., 2003;Fahrenfort, 1997; van Waarde and Wijnties, 2007; Marshall, 1993.Special Care Facility: Reimer et al., 2004; Slaughter et al., 2006.“Woodside”: Arehart-Treichel, 2001; Danes, 2002; Janzen, 2000; McAllister and Silverman, 1999; Nagy, 2002; Saxton et al., 1998; Warren et al., 2001; 2002.ADL = activities of daily living; CPS = Cognitive Performance Scales; GDS = Global Deterioration Scale; MDS = minimum data sets; MMSE = Mini-mental State Examination.

Homelike care environments for older people with dementia: a review 259
In practice, the principle of a home for lifemay vary within projects. In “Group Living” inSweden, for example, residents have become moredependent over the years than initially was intended(Norbergh et al., 2001;Wimo and MorthensonEkelof, 2004). Nevertheless, in Sweden increasedcare needs and demanding behavior, such asaggression, are the most common reasons forrelocations from non-specialized group-living intodementia care units (Horttana et al., 2007; Wimoet al., 1995b). In “Small-scale Living” in theNetherlands, a home for life is seen as a basicprinciple, but many projects nevertheless useinclusion and exclusion criteria for selection oftheir residents (te Boekhorst et al., 2007). Often,extreme behavioral problems are an exclusioncriterion, since this is seen as especially problematicamong a small group of residents (Verbeek et al.,2008). In many parts of the Netherlands “Small-scale Living” is a relatively new concept and,due to inexperience, detailed information regardingeveryday practice is often lacking. Some “GroupHomes” in Japan provide end-of-life care, makingthem true “homes for life”, while others focus onproviding accommodation for elderly people in theearly stages of dementia (Hirakawa et al., 2006).Hirakawa et al. (2006) found that 76% of “GroupHome” facilities considered it possible to provideend-of-life care, if necessary. However, only 17%had actual experience in providing such services.Furthermore, a survey by the Institute for HealthEconomics and Policy reported that in practice only5.4% of “Group Homes” in Japan provided end-of-life care to their residents (Nakanishi and Honda,2008).
Domestic characteristicsTo create a homelike environment, the careconcepts incorporate physical as well as social andorganizational domestic characteristics. Physicaldomestic characteristics include allowing residents’own furniture, as in the “Cantou” in France or“Small-scale Living” in the Netherlands/Belgium(Ritchie et al., 1992; te Boekhorst et al., 2007),pets, gardens and a fireplace. In addition, someconcepts, such as the “Green House”, specificallyexclude traditional institutional features such aslong corridors, a nurses’ station and medicationcarts (Rabig et al., 2006). These are all attemptsto make the physical environment familiar andappealing to the residents. However, the physicalsetting alone is not sufficient to create a homelikeenvironment, it can only facilitate this (Cohen andWeisman, 1991). Organizational and social aspectsof the environment are necessary components inthe development of a small, homelike therapeutic
setting. In all concepts, residents are encouraged toparticipate in the household as far as possible (e.g.“Care Housing” in Scotland; Carr and Marshall,1993), with activities of daily life being plannedaccording to the residents’ wishes. They have theopportunity to choose their meals, sleep, rest,personal care and activities whenever they want(Onishi et al., 2006; Rabig et al., 2006), and arethereby able to maintain their own lifestyle tovarying degrees (te Boekhorst et al., 2007).
Social care conceptIn all concepts a social model of care is applied,focusing on residents’ psychosocial wellbeing ratherthan their physical needs. To realize this, thephysical and organizational environment has beenfundamentally changed in comparison with thetraditional setting in nursing homes (Kane et al.,2007). Improvement of residents’ quality of life isthe main priority (Rabig et al., 2006), with thefamily often being involved in the care program(e.g. the “Woodside”, “Cantou”, and “Small-scale Living” concepts; Janzen, 2000; Ritchieet al., 1992; te Boekhorst et al., 2007). Carestaff have integrated tasks and are part of thehousehold (e.g. “Residential Groups” in Germany;Dettbarn-Reggentin, 2005). They live togetherwith the residents and provide individually tailoredcare. Residents are stimulated, encouraged andsupported, emphasizing autonomy and choice.Daily life is organized around meaningful activities,such as cooking, with a lot of personal contact.This requires the care staff to have specific skills,such as high levels of social and communicationskills (te Boekhorst et al., 2007). The care staffusually comprises nursing assistants and a limitednumber of nurses. Detailed information regardingeducation and staff ratio was only available from theNetherlands and Sweden (see Table 1). Involvementof other staff members varies among projects.Some concepts (e.g. the “Green House”) use amultidisciplinary team, including a medical doctor,social worker, dietician and activity workers, whileother projects (e.g. the “Cantou”) are essentiallynon-medical, providing additional care only ifnecessary (Rabig et al., 2006; Ritchie et al., 1992). In“Domuses”, special attention and training is givento anxieties and attitudes that staff may experienceto improve quality of care (Lindesay et al., 1991).
Concepts over timeThe “Cantou”, developed in France in 1968, wasidentified in this study as the first small, homelikeconcept for older people with dementia (Ritchieet al., 1992). During the 1980s similar conceptsappeared, such as “Group Living” in Sweden

260 H. Verbeek et al.
(Annerstedt, 1993), “Small- scale Living” in theNetherlands (Depla and te Boekhorst, 2007) and“Domuses” in the U.K. (Lindesay et al., 1991).Some of these have become regular dementiacare settings, such as “Group Living” in Swedenand “Small-scale Living” in the Netherlands. Inboth countries, the government has stimulatedthe development of small, homelike facilitiesby adjusting their policy and financial support(Annerstedt et al., 1996; Verbeek et al., 2008). Incontrast, other facilities, such as “Domuses” inthe U.K., are smaller initiatives (Macdonald et al.,2004). “Domuses” appear to be a more costly formof care (Beecham et al., 1993) and in the U.K.a more widespread model of care is the “multi-purpose nursing home”, in which long-term careas well as shorter stay, day and/or respite care areprovided (Macdonald et al., 2004). This suggeststhat government policies may have a large influenceon dissemination of the concept.
Over time, there are some indications that theconcept of “Group Living” in Sweden has changedwith regard to the residents’ characteristics andphysical design. Originally, it was developed forresidents with mild to moderate forms of dementiaand sufficient ADL-capacities, situated in ordinaryflats, as a form of intermediate care (Annerstedt,1993; 1994). Nowadays, group living facilities tendto become part of larger assisted-living facilitiesand residents’ functional dependence is increasing(Wimo and Morthenson Ekelof, 2004; Norbergh etal., 2001), which implies that these are more likelyto become “homes for life”. This shift is also seenwithin the concept of “Small-scale Living” in theNetherlands.
CostsConcept costs were analyzed in only four studies.Costs of “Group Living” in Sweden were analyzedin three studies (Wimo et al., 1991; 1995c; Svenssonet al., 1996), while another study investigated thecosts of “Domuses” in the U.K. (Beecham et al.,1993). The latter concluded that Domus care ismore costly than regular hospital care. However, adetailed evaluation was not possible due to a smallsample size and lack of variation in individual costs.
The study by Wimo et al. (1991) suggests that“Group Living” is cheaper compared to the costsof nursing home care. However, this study is basedon a small population (two group living facilitieshousing 24 residents) and regards “Group Living”primarily as a non-institutional form of care. Costssuch as hospital days and extra support from socialservices were not included. In addition, residentsof both settings were not comparable in terms ofcare dependency. According to Wimo et al. (1995c),
“Group Living” seems a cost-effective form ofdementia care, although the differences were small.If residents’ care dependency levels increase, thecosts of “Group Living” would increase as well sinceinstitutional care would be required. Svensson et al.(1996) suggests that the average costs per patientmight be higher in “Group Living” than in oldpeople’s homes, although the costs of care vary bothwith the physical design and functional ability ofresidents. Cost comparisons are therefore difficultto make. Svensson et al. (1996) investigated 106“Group Living” units, housing 765 residents. Herecosts tend to be lower when the number of residentsper unit increases and when units are attachedto other institutional facilities. In addition, unitshousing residents with a higher level of functionaldisability have a higher staff ratio.
Discussion
This study is the first to present a comparativeinternational overview of concepts that haveimplemented small-scale homelike facilities forolder people with dementia. Based on our reviewof the literature, 11 concepts were identified in 11different countries. Some concepts have becomeregular dementia care facilities, while others aresmaller initiatives. Similarities among conceptsreflect a common social care concept, with a focuson meaningful activities based around the dailyhousehold. The implementation among concepts,however, varies with differences in residents’characteristics, numbers of residents and physicalsettings and might be influenced by cultural andorganizational differences among countries.
This review has some limitations. It is likelythat not all initiatives will have been identifiedfor different reasons. A standard definition of asmall-scale, homelike concept of dementia care islacking. We used many search terms that relateto the topic of small-scale, home like facilities,but this does not guarantee that all studies andprojects were identified. In addition, the searchwas restricted to publications in German, Dutchor English only, and some initiatives, particularlysmaller ones, may not have been reported at all andtherefore not identified. However, where initiativesare widespread within a country, it is likely thatthey have been included in this review. Since thisresearch is solely based on a literature search, itis difficult to assess to what extent a concept’sphilosophy is implemented in practice and thereforeto what extent differences exist among concepts indaily practice. With regard to objective parameters,such as residents’ characteristics (e.g. scores on
Homelike care environments for older people with dementia: a review 261
cognition, ADL functioning, and behavior) verylimited data were available.
Clinical implicationsDuring the implementation process of a concept’score philosophy, it is very important to translatethe care concept into every day practice clearlyand unambiguously (Carr and Marshall, 1993;Marshall and Archibald, 1998). Appropriate stafftraining and education is essential (Annerstedt,1993). There is, however, a tension between thefocus on everyday life and the medical needs of olderpeople with dementia (Leichsenring et al., 1998).When too much emphasis is given to normalizationof living for older people with dementia, there isa risk that professionalism in dementia care maybe lost (Annerstedt, 1993). This aspect of careshould not be neglected when implementing small,homelike settings.
Furthermore, the role of care giving staff ischanging. In small-scale projects care is personor resident oriented, with emphasis on individualwell-being. This requires different capacities andskills, for example social and communicationskills, compared with traditional task-oriented care(te Boekhorst et al., 2007). Moreover, the respon-sibility of care staff increases (Reggentin andDettbarn-Reggentin, 2004b). Living together witholder people with dementia and creating ahousehold is a very intensive and complex process.The use of technology may support staff in thisprocess and may increase job satisfaction (Engstromet al., 2005).
Research implicationsAlthough the interest in small-scale, homelikefacilities in dementia care has increased, manyaspects regarding this development remain unclear.The characteristics of residents in these facilities arerelatively unknown. We have tried to collect databased on the literature, but this was insufficientto gain a complete understanding of objectiveparameters concerning residents’ characteristicssuch as cognition, ADL functioning, quality oflife and behavioral patterns. Some studies report afew such measures, but they frequently suffer frommethodological limitations, such as the inclusionof a limited number of residents. Moreover,outcomes are not comparable due to the useof different measurement scales. Future researchshould investigate characteristics of residents insmall-scale and homelike facilities and regular large-scale nursing homes in a longitudinal context,focusing on outcome measures such as behavior,functional status, quality of life and medication use.A comparison of characteristics in both settings
provides insight into suitable accommodation forolder people with dementia, and how to meet theneeds of possible subgroups. In addition, follow-up measurements allow comparison of the develop-ment and course of characteristics among residents.In this way, knowledge about effects of the conceptwill be obtained. Recent studies by Kane et al.(2007), Onishi et al. (2006) and Depla and teBoekhorst (2007) are a first attempt to realize this.However, organizational structures of dementia carevary across countries and probably have an effect onthese evaluations. Therefore, such comparisons areonly valuable when they are placed in the context ofthe wider structures and organization of dementiacare.
Besides residents’ characteristics, attentionshould also be paid to the experiences of thefamily and care staff. Family members appearmore satisfied with the provided care, althoughno differences in burden and health are reported(Depla and te Boekhorst, 2007). Positive outcomesfor staff have been suggested, such as increasedjob satisfaction, but negative results, for instancea higher workload, have also been reported(Reggentin and Dettbarn-Reggentin, 2004b). Arecent study by te Boekhorst et al. (2008) proposesthat nursing staff in small-scale living are moresatisfied with their jobs and report lower burnoutsymptoms than staff working in traditional nursinghomes. However, the skills and competences of staffworking in small-scale and homelike facilities havenot yet been investigated. Since the role of carestaff is changing in this concept, further researchis needed.
A final important aspect that needs furtherinvestigation relates to the costs of small-scale,homelike facilities. In this overview, a few costanalyses have been reported showing contrastingresults (Svensson et al., 1996; Wimo et al., 1991;1995c; Beecham et al., 1993). However, thereis little understanding as yet of the interplay ofcosts and financial structures on these concepts,particularly in terms of the services provided,staff education, residents’ care dependency andthe organization of care provision. The conceptsidentified in our overview lack a detailed descriptionof these factors. A cost-based comparison wouldbe valuable, though difficult, given the diversefinancial structures of health care systems acrosscountries, and particularly in dementia care.Comparisons should provide a detailed descriptionof the organization of dementia care and residents’characteristics in relation to costs.
Conflict of interest
None.

262 H. Verbeek et al.
Description of authors’ roles
All authors critically reviewed the manuscript, readand approved the final manuscript.
References
Ahlund, O. (1999). Group living for elderly with Alzheimer’sdisease: the importance of environmental design. STRIDE –Excellence in Long Term Care, Fall/Winter, 4–7.
Alfredson, B. B. and Annerstedt, L. (1994). Staff attitudesand job satisfaction in the care of demented elderly people:group living compared with long-term care institutions.Journal of Advanced Nursing, 20, 964–974.
Andren, S. and Elmstahl, S. (2002). Former family carers’subjective experiences of burden: a comparison betweengroup living and nursing home environments in onemunicipality in Sweden. Dementia, 1, 241–254.
Andren, S. and Elmstahl, S. (2007). Relationships betweenincome, subjective health and caregiver burden incaregivers of people with dementia in group living care: across-sectional community-based study. InternationalJournal of Nursing Studies, 44, 435–446.
Angelelli, J. (2006). Promising models for transforminglong-term care. The Gerontologist, 46, 428–430.
Annerstedt, L. (1993). Development and consequences ofgroup living in Sweden: a new mode of care for thedemented elderly. Social Science Medicine, 37,1529–538.
Annerstedt, L. (1994). An attempt to determine the impactof group living care in comparison to traditional long-termcare on demented elderly patients. Aging (Milan), 6,372–380.
Annerstedt, L. (1997). Group-living care: an alternative forthe demented elderly. Dementia and Geriatric CognitiveDisorders, 8, 136–142.
Annerstedt, L. et al. (1993a). Group Living for People withDementia. Stirling: Dementia Services DevelopmentCentre, University of Stirling.
Annerstedt, L., Gustafson, L. and Nilsson, K. (1993b).Medical outcome of psychosocial intervention in dementedpatients: one-year clinical follow-up after relocation intogroup living units. International Journal of GeriatricPsychiatry, 8, 833–841.
Annerstedt, L., Sanada, J. and Gustafson, L. (1996). Adynamic long-term care system for the demented elderly.International Psychogeriatrics, 8, 561–574.
Annerstedt, L., Elmstahl, S., Ingvad, B. andSamuelsson, S. M. (2000). Family caregiving indementia: an analysis of the caregiver’s burden and the“breaking-point” when home care becomes inadequate.Scandinavian Journal of Public Health, 28, 23–31.
Arehart-Treichel, J. (2001). Innovative Alzheimer’sresidence tries new models of care. Psychiatric News, 36,14–57.
Atkinson, A. (1995). Managing people with dementia:CADE units. Nursing Standard, 9, 29–32.
Beecham, J., Cambridge, P., Hallam, A. and Knapp, M.(1993). The costs of domus care. International Journal ofGeriatric Psychiatry, 8, 827–831.
Briller, S. H. and Calkins, M. (2000). Defining place-basedmodels of care: conceptualizing care settings as home,resort or hospital. Alzheimer’s Care Quarterly, 1, 17–23.
Calkins, M. P. (2001). Creating Successful Dementia CareSettings, Baltimore: Health Professions Press.
Carr, J. S. and Marshall, M. (1993). Innovations inlong-stay care for people with dementia. Reviews in ClinicalGerontology, 3, 157–167.
Cohen, U. and Weisman, G. (1991). Holding on to Home.Designing Environments for People with Dementia. London:John Hopkins University Press.
Danes, S. (2002). Creating an environment for community.Alzheimer’s Care Quarterly, 3, 61–66.
Day, K., Carreon, D. and Stump, C. (2000). Thetherapeutic design of environments for people withdementia: a review of the empirical research. Gerontologist,40, 397–416.
de Vugt, M. E. et al. (2006). Cognitive functioning in spousalcaregivers of dementia patients: findings from theprospective MAASBED study. Age and Ageing, 35,160–166.
Dean, R., Briggs, K. and Lindesay, J. (1993a). The domusphilosophy: A prospective evaluation of two residentialunits for the elderly mentally ill. International Journal ofGeriatric Psychiatry, 8, 807–817.
Dean, R., Proudfoot, R. and Lindesay, J. (1993b). Thequality of interactions schedule (QUIS): development,reliability and use in the evaluation of two domus units.International Journal of Geriatric Psychiatry, 8, 819–826.
Depla, M. and te Boekhorst, S. (2007). Kleinschalig Wonenvoor Mensen met Dementie: Doen of Laten? (Small-ScaleLiving for People with Dementia: Do or Don’t?). Utrecht:Trimbos-Institute.
Dettbarn-Reggentin, J. (2005). Studie zum Einfluss vonWohngruppenmilieus auf demenziell Erkrankte instationaren Einrichtungen. [Study of the influence ofenvironmental residential groups on demented old peoplein nursing home residents]. Zeitschrift fur GerontologieGeriatrie, 38, 95–100.
Elmstahl, S., Annerstedt, L. and Ahlund, O. (1997). Howshould a group living unit for demented elderly be designedto decrease psychiatric symptoms? Alzheimer Disease andAssociated Disorders, 11, 47–52.
Elmstahl, S., Ingvad, B. and Annerstedt, L. (1998a).Family caregiving in dementia: prediction of caregiverburden 12 months after relocation to group-living care.International Psychogeriatrics, 10, 127–146.
Elmstahl, S., Stenberg, I., Annerstedt, L. and Ingvad, B.(1998b). Behavioral disturbances and pharmacologicaltreatment of patients with dementia in family caregiving: atwo-year follow-up. International Psychogeriatrics, 10,239–252.
Engstrom, M., Ljunggren, B., Lindqvist, R. andCarlsson, M. (2005). Staff perceptions of job satisfactionand life situation before and 6 and 12 months afterincreased information technology support in dementia care.Journal of Telemedicine and Telecare, 11, 304–309.
Fahrenfort, M. (1997). In search of the best environment.Results of five experiments in the institutional organizationof care for demented people. In B. M. L. Miesen andG. M. M. Jones (eds.), Care-Giving in Dementia. Researchand Applications. London and New York: Routledge.

Homelike care environments for older people with dementia: a review 263
Faxen-Irving, G., Andren-Olsson, B., Af Geijerstam, A.,Basun, H. and Cederholm, T. (2002). The effect ofnutritional intervention in elderly subjects residing ingroup-living for the demented. European Journal of ClinicalNutrition, 56, 221–227.
Finnema, E., Droes, R. M., Ribbe, M. and van Tilburg,W. (2000). A review of psychosocial models inpsychogeriatrics: implications for care and research.Alzheimer Disease and Associated Disorders, 14, 68–80.
Fleming, R. and Bowles, J. (1994). Small, specialised longstay units for the dementing: their role and effectiveness.Paper presented at Alzheimers Disease InternationalConference, Edinburgh.
Funaki, Y., Kaneko, F. and Okamura, H. (2005). Study offactors associated with changes in quality of life ofdemented elderly persons in group homes. ScandinavianJournal of Occupational Therapy, 12, 4–9.
Hertogh, C. M., The, B. A., Miesen, B. M. and Eefsting,J. A. (2004). Truth telling and truthfulness in the care forpatients with advanced dementia: an ethnographic study inDutch nursing homes. Social Science and Medicine, 59,1685–1693.
Hirakawa, Y., Masuda, Y., Uemura, K., Kuzuya, M.,Kimata, T. and Iguchi, A. (2006). End-of-life care atgroup homes for patients with dementia in Japan: findingsfrom an analysis of policy-related differences. Archives ofGerontology Geriatrics, 42, 233–245.
Horttana, B. M., Ahlstrom, G. and Fahlstrom, G. (2007).Patterns of and reasons for relocation in dementia care.Geriatric Nursing, 28, 193–200.
Janzen, W. M. (2000). Family members caring for relativeswith Alzheimer Disease in long-term care facilities.Unpublished dissertation, University of Alberta.
Jensen, J., Lundin Olsson, L., Nyberg, L. and Gustafson,Y. (2002). Falls among frail older people in residential care.Scandinavian Journal of Public Health, 30, 54–61.
Judd, S., Marshall, M. and Phippen, P. (1998). Design forDementia. London: Hawker Publications.
Kane, R. A., Lum, T. Y., Cutler, L. J., Degenholtz, H. B.and Yu, T.-C. (2007). Resident outcomes in small-housenursing homes: a longitudinal evaluation of the initialGreen House Program. Journal of the American GeriatricsSociety, 55, 832–839.
Kihlgren, M., Brane, G., Karlsson, I., Kuremyr, D.,Leissner, P. and Norberg, A. (1992). Long-terminfluences on demented patients in different caring milieus,a collective living unit and a nursing home: a descriptivestudy. Dementia, 3, 342–349.
Kuremyr, D., Kihlgren, M., Norberg, A., Astrom, S.and Karlsson, I. (1994). Emotional experiences, empathyand burnout among staff caring for demented patientsat a collective living unit and a nursing home.Journal of Advanced Nursing, 19, 670–679.
Leichsenring, K., Strumpel, C. and Group, S. (1998). TheUse of Small Housing Units for Older Persons Suffering fromDementia. Eurosocial Reports. Vienna: European Centrefor Social Welfare Policy and Research.
Lindesay, J., Briggs, K., Lawes, M., Macdonald, A. andHerzberg, J. (1991). The domus philosophy: acomparative evaluation of a new approach to residentialcare for the demented elderly. International Journal ofGeriatric Psychiatry, 6, 727–736.
Macdonald, A., Philpot, M. and Briggs, C. (2004). Anattempt to determine the benefits of a “home-for-life”principle in residential care for people with dementia andbehavioural problems: a comparative cohort study.Dementia and Geriatric Cognitive Disorders, 18, 6–14.
Malmberg, B. and Zarit, S. H. (1993). Group homes forpeople with dementia: a Swedish example. TheGerontologist, 33, 682–686.
Marshall, M. (1993). Small Scale, Domestic Style, Long StayAccommodation for People with Dementia. Stirling: DementiaServices Development Centre, University of Stirling.
Marshall, M. and Archibald, C. (1998). Long-stay care forpeople with dementia: recent innovations. Reviews inClinical Gerontology, 8, 331–343.
McAllister, C. L. and Silverman, M. A. (1999).Community formation and community roles amongpersons with Alzheimer’s disease: a comparative study ofexperiences in a residential Alzheimer’s facility and atraditional nursing home. Qualitative Health Research, 9,65–85.
Moise, P., Schwarzinger, M. and Um, M. (2004). DementiaCare in 9 OECD Countries: A Comparative Analysis. Paris:OECD.
Nagy, J. W. (2002). Kitchens that help residents reestablishhome. Alzheimer’s Care Quarterly, 3, 74–77.
Nakanishi, M. and Honda, T. (2008). Process of decisionmaking and end-of-life care for patients with dementia ingroup homes in Japan. Archives of Gerontology andGeriatrics, doi: 10.1016/j.archger.2008.02.009 (e-publishedahead of print).
Norbergh, K. G., Nordahl, G., Sandman, P. O. andAsplund, K. (2001). A retrospective study of functionalability among people with dementia when admitted togroup-dwelling. Scandinavian Journal of Primary HealthCare, 19, 39–42.
Norbergh, K. G., Hellzen, O., Sandman, P. O. andAsplun, K. (2002). The relationship betweenorganizational climate and the content of daily life forpeople with dementia living in a group-dwelling. Journal ofClinical Nursing, 11, 237–246.
Onishi, J. et al. (2006). Behavioral, psychological andphysical symptoms in group homes for older adults withdementia. International Psychogeriatrics, 18, 75–86.
Peters, H. J. and Duine, T. J. (1987). [The NormalizedLiving Project at the De Landrijt nursing home inEindhoven: various results of an experiment inpsychogeriatric care]. Tijdschrift voor Gerontologie enGeriatrie, 18, 187–191.
Rabig, J., Thomas, W., Kane, R. A., Cutler, L. J. andMcalilly, S. (2006). Radical redesign of nursing homes:applying the green house concept in Tupelo, Mississippi.Gerontologist, 46, 533–539.
Radzey, B., Kuhn, C., Rauh, J. and Heeg, S. (2001).Qualitatsbeurteilung der institutionellen Versorgung undBetreuung dementiell Erkrankter (Literatur-Expertise).Stuttgart: Bundesministerium fur Familie, Senioren,Frauen und Jugend.
Reggentin, H. and Dettbarn-Reggentin, J. (2004a).[Group homes for patients with dementia: the possibility ofsocial interaction]. Pflege Zeitschrift, 57, 181–184.
Reggentin, H. and Dettbarn-Reggentin, J. (2004b).Wohngruppen fur Menschen mit Demenz: Belastung wird

264 H. Verbeek et al.
durch Motivation kompensiert. (Group homes for patientswith dementia: stress is compensated by motivation). PflegeZeitschrift, 57, 489–492.
Reimer, M.-A., Slaughter, S., Donaldson, C., Currie, G.and Eliasziw, M. (2004). Special care facility comparedwith traditional environments for dementia care: alongitudinal study of quality of life. Journal of the AmericanGeriatrics Society, 52, 1085–1092.
Ritchie, K. and Ledesert, B. (1992). The families of theinstitutionalized dementing elderly: a preliminary study ofstress in a French caregiver population. InternationalJournal of Geriatric Psychiatry, 7, 5–14.
Ritchie, K., Colvez, A., Ankri, J., Ledesert, B., Gardent,H. and Fontaine, A. (1992). The evaluation of long-termcare for the dementing elderly: a comparative study ofhospital and collective non-medical care in France.International Journal of Geriatric Psychiatry, 7, 549–557.
Roscrow, S. (1996). Small units specialising in dementia carein West Lothian. Health Bulletin, 54, 294–300.
Sandman, P. O. and Wallblom, A. (1996). Characteristicsof the demented living in different settings in Sweden. ActaNeurologica Scandinavica, 168 (Suppl.), 96–100.
Saxton, J., Silverman, M., Ricci, E., Keane, C. andDeeley, B. (1998). Maintenance of mobility in residentsof an Alzheimer special care facility. InternationalPsychogeriatrics, 10, 213–224.
Skea, D. and Lindesay, J. (1996). An evaluation of twomodels of long-term residential care for elderly people withdementia. International Journal of Geriatric Psychiatry, 11,233–241.
Slaughter, S., Calkins, M., Eliasziw, M. and Reimer, M.(2006). Measuring physical and social environments innursing homes for people with middle- to late-stagedementia. Journal of the American Geriatrics Society, 54,1436–1441.
Sloane, P. D., Mitchell, C. M., Preisser, J. S., Phillips,C., Commander, C. and Burker, E. (1998).Environmental correlates of resident agitation inAlzheimer’s disease special care units. Journal of theAmerican Geriatrics Society, 46, 862–869.
Svensson, M., Edebalk, P. G. and Persson, U. (1996).Group living for elderly patients with dementia: a costanalysis. Health Policy, 38, 83–100.
Taft, L. B., Fazio, S., Seman, D. and Stansell, J. (1997).A psychosocial model of dementia care: theoretical andempirical support. Archives of Psychiatric Nursing, 11,13–20.
te Boekhorst, S. (2007). Kleinschalig wonen voor ouderenmet dementie: een kwaliteitsverbetering? [Small-scale livingfor older people with dementia: a quality improvement?].Kwaliteit in Beeld, 3, 8–9.
te Boekhorst, S., Depla, M. F. I. A., De Lange, J., Pot, A.M. and Eefsting, J. A. (2007). Kleinschalig wonen voorouderen met dementie: een begripsverheldering.[Small-scale group living for elderly with dementia: aclarification]. Tijdschrift voor Gerontologie en Geriatrie, 38,17–26.
te Boekhorst, S., Willemse, B., Depla, M. F. I. A.,Eefsting, J. A. and Pot, A. M. (2008). Working in groupliving homes for older people with dementia: the effects onjob satisfaction and burnout and the role of jobcharacteristics. International Psychogeriatrics, 20, 927–940.
van Audenhove, C., Declercq, A., De Coster, I.,Spruytte, N., Molenberghs, C. and van den Heuvel,B. (2003). Kleinschalig Genormaliseerd Wonen voor Personenmet Dementie [Small-scale normalized living for personswith dementia]. Antwerp/Apeldoorn: Garant.
van Waarde, H. and Wijnties, M. (2007). De Toekomst vanKleinschalig Wonen voor Mensen met Dementie. Utrecht:Aedes-Actiz Kenniscentrum Wonen-Zorg.
Verbeek, H., van Rossum, E., Zwakhalen, S. M. G.,Kempen, G. I. J. M. and Hamers, J. P. H. (2008).Kleinschalig Wonen voor Ouderen met Dementie. EenBeschrijvend Onderzoek naar de Situatie in de ProvincieLimburg. [Small-scale living for older people with dementia.A descriptive study of the situation in the province ofLimburg]. Maastricht: Maastricht University Press.
Warren, S., Janzen, W., Andiel-Hett, C., Liu, L., Mckim,H. R. and Schalm, C. (2001). Innovative dementia care:functional status over time of persons with Alzheimerdisease in a residential care centre compared to special careunits. Dementia and Geriatric Cognitive Disorders, 12,340–347.
Warren, S., Janzen, W. M. and McKim, R. (2002).Innovative dementia care: the impact of residential carecenters on the functional status of residents. Annals ofLong-Term Care, 10, 51–56.
Wimo, A. and Morthenson Ekelof, C. (2004). OECD CaseStudy on Dementia. Stockholm: Stiftelsen Stockholms IansAldrecentrum.
Wimo, A. et al. (1991). Group living, an alternative fordementia patients: a cost analysis. International Journal ofGeriatric Psychiatry, 6, 21–29.
Wimo, A., Adolfsson, R. and Sandman, P. O. (1995a).Care for demented patients in different living conditions:effects on cognitive function, ADL-capacity and behaviour.Scandinavian Journal of Primary Health Care, 13, 205–210.
Wimo, A., Asplund, K., Mattsson, B., Adolfsson, R. andLundgren, K. (1995b). Patients with dementia in groupliving: experiences 4 years after admission. InternationalPsychogeriatrics, 7, 123–127.
Wimo, A., Mattson, B., Krakau, I., Eriksson, T., Nelvig,A. and Karlsson, G. (1995c). Cost-utility analysis ofgroup living in dementia care. International Journal ofTechnology Assessment in Health Care, 11, 49–65.
Yokota, O. et al. (2006). Effects of group-home care onbehavioral symptoms, quality of life, and psychotropic druguse in patients with frontotemporal dementia. Journal of theAmerican Medical Directors Association, 7, 335–337.
Zeisel, J., Hyde, J. and Levkoff, S. (1994). Best practices:an environment behavior (E-B) model for Alzheimerspecial care units. American Journal of Alzheimer’s Diseaseand Other Dementias, 9, 4–21.