Sleep Related Problems and Urological Symptoms: Testing the Hypothesis of Bidirectionality in a...
7
Voiding Dysfunction Sleep Related Problems and Urological Symptoms: Testing the Hypothesis of Bidirectionality in a Longitudinal, Population Based Study Andre B. Araujo,*,† H. Klar Yaggi, May Yang,† Kevin T. McVary,‡ Shona C. Fang† and Donald L. Bliwise§ From the New England Research Institutes, Inc., Watertown (ABA, MY, SCF), and Harvard School of Public Health, Boston (SCF), Massachusetts; Yale University School of Medicine, New Haven, Connecticut (HKY); Southern Illinois University School of Medicine, Springfield, Illinois (KTM); and Emory University School of Medicine, Atlanta, Georgia (DLB) Purpose: We evaluate the bidirectional association between urological symptoms (urinary incontinence, lower urinary tract symptoms and nocturia) and sleep related variables. Materials and Methods: Data were obtained from a prospective cohort study of 1,610 men and 2,535 women who completed baseline (2002 to 2005) and followup (2006 to 2010) phases of the BACH (Boston Area Community Health) Survey, a population based random sample survey. Sleep restriction (5 hours or less per night), restless sleep, sleep medication use and urological symptoms were assessed by self-report. Urinary incontinence was defined as weekly leakage or moderate/severe leakage, lower urinary tract symptoms (overall, obstructive, irritative) were defined by the AUA-SI (American Urological Association symptom index) and nocturia was defined as urinary frequency 2 or more times per night. Results: At the 5-year followup 10.0%, 8.5% and 16.0% of subjects newly reported lower urinary tract symptoms, urinary incontinence and nocturia, respectively, and 24.2%, 13.3% and 11.6% newly reported poor sleep quality, sleep restriction and use of sleep medication, respectively. Controlling for confounders, the odds of urological symptoms developing were consistently increased for subjects who reported poor sleep quality and sleep restriction at baseline, but only baseline nocturia was positively associated with incident sleep related problems at fol- lowup. Body mass index, a potential mediator, reduced selected associations between sleep and incident urinary incontinence and irritative symptoms, but C-reactive protein did not. Conclusions: These data suggest that self-reported sleep related problems and urological symptoms are linked bidirectionally, and that body mass index may be a factor in the relationship between sleep and the development of urological symptoms. Key Words: cohort studies, epidemiology, sleep, urologic diseases URINARY incontinence, lower urinary tract symptoms secondary to benign prostatic hyperplasia and nocturia are common disorders which affect quality of life. 1 At the same time, sleep disorders affect 50 to 70 million people in the United States, 2 with sleep deprivation increasing in prevalence. 3 It is implicitly assumed that uro- logical symptoms lead to sleep relat- ed problems and not vice versa. 4,5 Abbreviations and Acronyms BMI ¼ body mass index BPH ¼ benign prostatic hyperplasia CRP ¼ C-reactive protein LUTS ¼ lower urinary tract symptoms SES ¼ socioeconomic status UI ¼ urinary incontinence Accepted for publication July 10, 2013. Study received institutional review board approval. Supported by the awards R21MD006769 from the National Institute on Minority Health and Health Disparities (NIMHD), U01DK056842 from the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK), CDTA 150S829 from the VA Clinical Science Research and Development Career Development Program; the SIU Urology Endowment Fund and Havana Day Dreamers Foundation. The content is solely the responsibility of the authors, and does not necessarily represent the official views of the NIMHD, NIDDK, NIH, VA, SIU Urology Endow- ment Fund or Havana Day Dreamers Foundation. * Correspondence: New England Research Institutes, Inc., 9 Galen St., Watertown, Massa- chusetts 02472 (telephone: 617-972-3152; FAX: 617-673-9509; e-mail: [email protected] ). † Financial interest and/or other relationship with New England Research Institutes. ‡ Financial interest and/or other relationship with Lilly/ICOS, NxThera, Watson Pharmaceuticals, Neotract, NIDDK and GSK. § Financial interest and/or other relationship with Ferring, New England Research Institutes and Vantia. See Editorial on page 15. 100 j www.jurology.com 0022-5347/14/1911-0100/0 THE JOURNAL OF UROLOGY ® © 2014 by AMERICAN UROLOGICAL ASSOCIATION EDUCATION AND RESEARCH,INC. http://dx.doi.org/10.1016/j.juro.2013.07.011 Vol. 191, 100-106, January 2014 Printed in U.S.A.
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Sleep Related Problems and Urological Symptoms: Testing the Hypothesis of Bidirectionality in a...

Voiding Dysfunction
Sleep Related Problems and Urological Symptoms: Testingthe Hypothesis of Bidirectionality in a Longitudinal,Population Based Study
Andre B. Araujo,*,† H. Klar Yaggi, May Yang,† Kevin T. McVary,‡Shona C. Fang† and Donald L. Bliwise§
From the New England Research Institutes, Inc., Watertown (ABA, MY, SCF), and Harvard School of Public Health,Boston (SCF), Massachusetts; Yale University School of Medicine, New Haven, Connecticut (HKY); Southern IllinoisUniversity School of Medicine, Springfield, Illinois (KTM); and Emory University School of Medicine, Atlanta, Georgia (DLB)
Purpose: We evaluate the bidirectional association between urological symptoms(urinary incontinence, lower urinary tract symptoms and nocturia) and sleeprelated variables.
Materials and Methods: Data were obtained from a prospective cohort study of1,610 men and 2,535 women who completed baseline (2002 to 2005) and followup(2006 to 2010) phases of the BACH (Boston Area Community Health) Survey,a population based random sample survey. Sleep restriction (5 hours or lessper night), restless sleep, sleep medication use and urological symptoms wereassessed by self-report. Urinary incontinence was defined as weekly leakage ormoderate/severe leakage, lower urinary tract symptoms (overall, obstructive,irritative) were defined by the AUA-SI (AmericanUrological Association symptomindex) and nocturia was defined as urinary frequency 2 or more times per night.
Results: At the 5-year followup 10.0%, 8.5% and 16.0% of subjects newly reportedlower urinary tract symptoms, urinary incontinence and nocturia, respectively,and 24.2%, 13.3% and 11.6% newly reported poor sleep quality, sleep restrictionand use of sleep medication, respectively. Controlling for confounders, the odds ofurological symptoms developing were consistently increased for subjects whoreported poor sleep quality and sleep restriction at baseline, but only baselinenocturia was positively associated with incident sleep related problems at fol-lowup. Body mass index, a potential mediator, reduced selected associationsbetween sleep and incident urinary incontinence and irritative symptoms, butC-reactive protein did not.
Conclusions: These data suggest that self-reported sleep related problems andurological symptoms are linked bidirectionally, and that body mass index may bea factor in the relationship between sleep and the development of urologicalsymptoms.
Key Words: cohort studies, epidemiology, sleep, urologic diseases
URINARY incontinence, lower urinarytract symptoms secondary to benignprostatic hyperplasia and nocturiaare common disorders which affectquality of life.1 At the same time,sleep disorders affect 50 to 70 million
people in the United States,2 withsleep deprivation increasing inprevalence.3
It is implicitly assumed that uro-logical symptoms lead to sleep relat-ed problems and not vice versa.4,5
Abbreviationsand Acronyms
BMI ! body mass index
BPH ! benign prostatichyperplasia
CRP ! C-reactive protein
LUTS ! lower urinary tractsymptoms
SES ! socioeconomic status
UI ! urinary incontinence
Accepted for publication July 10, 2013.Study received institutional review board
approval.Supported by the awards R21MD006769
from the National Institute on Minority Healthand Health Disparities (NIMHD), U01DK056842from the National Institute of Diabetes andDigestive and Kidney Diseases (NIDDK), CDTA150S829 from the VA Clinical Science Researchand Development Career Development Program;the SIU Urology Endowment Fund and HavanaDay Dreamers Foundation. The content is solelythe responsibility of the authors, and does notnecessarily represent the official views of theNIMHD, NIDDK, NIH, VA, SIU Urology Endow-ment Fund or Havana Day Dreamers Foundation.
* Correspondence: New England ResearchInstitutes, Inc., 9 Galen St., Watertown, Massa-chusetts 02472 (telephone: 617-972-3152; FAX:617-673-9509; e-mail: [email protected]).
† Financial interest and/or other relationshipwith New England Research Institutes.
‡ Financial interest and/or other relationshipwith Lilly/ICOS, NxThera, Watson Pharmaceuticals,Neotract, NIDDK and GSK.
§ Financial interest and/or other relationshipwith Ferring, New England Research Institutesand Vantia.
See Editorial on page 15.
100 j www.jurology.com
0022-5347/14/1911-0100/0THE JOURNAL OF UROLOGY®
© 2014 by AMERICAN UROLOGICAL ASSOCIATION EDUCATION AND RESEARCH, INC.
http://dx.doi.org/10.1016/j.juro.2013.07.011Vol. 191, 100-106, January 2014
Printed in U.S.A.

However, it is plausible that sleep related problemslead to the development of urological symptoms,mainly through their associations with obesity,6
metabolic dysregulation7,8 and systemic inflamma-tion.9 While studies have examined the bidirectionalassociation between other health conditions andurological outcomes,10,11 to our knowledge nostudies have explored the bidirectional relationshipbetween sleep and urological symptoms.
Therefore, we tested the 5-year longitudinal re-lations between sleep related variables at baselineand incident urological symptoms at followup, be-tween urological symptoms at baseline and incidentsleep related variables at followup, and investigatedwhether body composition or inflammatory statushas a role in mediating these associations.
MATERIALS AND METHODS
Overall Design and Overview of Data CollectionData were obtained from the BACH Survey, an observa-tional, longitudinal cohort study of men and women.12
The BACH Survey recruited a random sample of 5,502Boston men and women 30 to 79 years old from 3 racial/ethnic groups (black, Hispanic, white) to complete an in-person interview at baseline (2002 to 2005) and approxi-mately 5 years later (2006 to 2010). Home visits wereconducted for anthropometric measurements, and in-terviews were conducted regarding urological symptoms,health and lifestyle factors. Followup interviews werecompleted on 4,144 individuals (1,610 men and 2,534women with a conditional response rate of 80.5%). Allsubjects provided written informed consent and the studyreceived institutional review board approval.
Measurement of Sleep ParametersSleep quality. Subjects had poor sleep quality if theyendorsed yes in response to the statement, “Much of thetime during the last week... my sleep was restless.”
Restricted sleep. Sleep restriction was assessed by thequestion, “How much do you usually sleep?” (5 hours orless vs more than 5 hours per night). Data on sleep re-striction were not collected from women at baseline,mainly because the sleep data on men were obtained inthe context of a previously developed set of symptomspertaining to male hypogonadism.
Sleep medication use. The use of prescription, over-the-counter and supplemental medications was capturedusing self-report (prompts by indication) and directobservation/recording of medication labels by theinterviewer, which were coded using the Slone DrugDictionary.13 Medications in the sedative hypnotic classthat are used to induce sleep were considered primarysedation medications (see supplementary Appendix,http://jurology.com/).
Measurement of Urological SymptomsLower urinary tract symptoms. LUTS were assessed bythe AUA-SI.14 The AUA-SI was developed and validated
for BPH in men,14 but has been validated to captureLUTS in women.15 Given that we were interested inseparately examining the relationship between nocturiaand sleep related problems, we created a summaryAUA-SI score that excluded the nocturia item. Thismodified score could range from 0 to 30, with higherscores indicating more (frequent) symptoms and withLUTS defined as score 7 or greater (moderate/severesymptoms) on this modified AUA-SI. We also examinedLUTS obstructive symptom subscores (voidingsymptoms, 5 or more for incomplete bladder emptying,straining, weak urinary stream, hesitancy symptoms)and irritative symptom subscores (storage symptoms, 4or more for frequency, urgency, nocturia).
Urinary incontinence. UI was defined using Sandvik’sseverity index (frequency and quantity of urineleakage),16 with presence defined as weekly or moderate/severe leakage.
Nocturia. Nocturia was defined as needing to get up tourinate more than once during the night (fairly often,usually, almost always), or experiencing 2 or more uri-nations at night after falling asleep.17
Potential Confounding VariablesSeveral baseline variables were considered a priori con-founding variables including age (decades), gender (male/female), race/ethnicity (black/Hispanic/white), SES (low/medium/high), type 2 diabetes mellitus (yes/no), heartdisease (yes/no), alcohol use (0/less than 1/1 to 3/3" drinksper day), physical activity (low/medium/high), smoking(current/former/never) and antidepressant use (yes/no).In addition, the use of sedating (eg antihistamines) andstimulating (eg amphetamines) medications not indicatedfor sleep disorders were considered as covariates. Allvariables were included in all regression models withminor exceptions noted.
Potential Mediating VariablesBased on prior literature we studied the mediationalpathways of body composition assessed by weight, waistcircumference and BMI, and circulating CRP, a marker ofinflammation measured with an immunoturbidimetricassay on the Hitachi 917 analyzer (Roche Diagnostics,Indianapolis, Indiana).
Statistical AnalysisThe incidence of sleep related problems and urologicalsymptoms at 5 years was defined as the percentage ofthose with the relevant condition at followup among thosewithout the condition at baseline. The normal approxi-mation to the binomial distribution was used to compute95% CIs on incidence. The association of baseline char-acteristics with incident urological and sleep outcomeswas tested with Wald-type tests.
Odds ratios (ORs) and 95% CIs were estimated frommultivariate logistic regression models of the associationbetween sleep variables/urological symptoms assessed atbaseline and the incidence of urological symptoms/sleepvariables at followup, adjusted for covariates. The multi-variate models controlled for all covariates except for theprimary stimulant coalition medication, which wasredundant with the secondary stimulation coalition.
SLEEP AND UROLOGICAL SYMPTOMS 101

Interactions between gender and exposures of interestand multicollinearity among medication coalitions weretested. Of 24 interactions with gender tested, only 1 wasstatistically significant, thus allowing us to pool data onmen and women. We determined that followup time wassimilar in subjects with/without incident outcomes, thusfollowup time was not adjusted in final models.
Mediation was tested by examining whether bodycomposition variables and CRP induced a 10% change inthe exposure OR.18 Preliminary modeling identified BMI(vs weight and waist) as more strongly related to out-comes of interest and, thus, we examined BMI only inmediation analyses.
Multiple imputation (15 data sets) was used to imputeplausible values for missing observations using SAS!9.1.3. Missing data for the variables of interest (sleep andurological symptoms) were missing in less than 1% ofsubjects. Observations were weighted inversely to theirprobability of selection and weights were post-stratified tothe Boston population in 2000. Analyses were conductedin SUDAAN! 9.0.1.
Analytical SamplesAnalyses of outcomes were restricted to at risk samples, iethose without the relevant condition at baseline. Samplesizes for incident LUTS, UI and nocturia were 3,423,3,724 and 2,765, respectively. Sample sizes for incidentpoor sleep quality, sleep medication use and sleeprestriction (men only) were 2,449, 3,529 and 1,279,respectively.
RESULTS
Demographic ProfileThe mean baseline age of the BACH Survey popu-lation who completed followup (4,144) was 49 years.A total of 1,610 men and 2,534 women completedthe followup assessment, with women being slightlyolder than men at baseline (50 vs 48 years).
Incident Urological SymptomsAt the 5-year followup LUTS, UI and nocturia werereported by 10.0%, 8.5% and 16.0% of subjects,respectively, who did not have these symptoms atbaseline (supplementary table 1, http://jurology.com/). The incidence of obstructive symptoms was7.0% (95% CI 5.6, 8.6) and the incidence of irritativesymptoms was 20.7% (95% CI 18.2, 23.6) (data notshown). The crude incidence of urological symptomswas related to increasing age (p <0.001) and severalother factors.
Incident Sleep OutcomesNewly reported poor sleep quality, sleep restrictionand use of sleep medication was observed in 24.2%(95% CI 21.3, 27.3), 13.3% (95% CI 10.6, 16.4)and 11.6% (95% CI 10.0, 13.4), respectively, of sub-jects at the 5-year followup (supplementary table 2,http://jurology.com/). Compared with urologicalsymptoms, the crude incidence of sleep variables
exhibited fewer associations with confoundingvariables of interest. Selected results showed thatincident poor sleep occurred most commonly insubjects with low SES (32.2%; 95% CI 26.7, 38.2) andincident sleep restriction occurred most commonlyin black subjects (20.9%; 95% CI 16.3, 26.3).
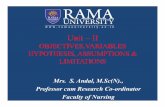
Association between Sleep and IncidentUrological SymptomsControlling for confounders, poor sleep quality wasassociated with incident LUTS (OR 1.73, 95% CI1.20, 2.51), including irritative (OR 1.55, 95% CI1.06, 2.27) and obstructive (OR 2.15, 95% CI 1.39,3.32) LUTS (fig. 1), as well as nocturia (OR 1.42,95% CI 1.02, 1.97; table 1). Sleep restriction wasassociated with incident LUTS (OR 1.98, 95% CI1.03, 3.78), including incident irritative symptoms(OR 2.58, 95% CI 1.41, 4.73) but not obstructivesymptoms. Findings from models that included thenocturia item in the total LUTS score were compa-rable. Sleep restriction was also associated with UI(OR 2.42, 95% CI 1.07, 5.48) but not with nocturia.Sleep medication use was unrelated to incidenturological symptoms. BMI reduced the relationshipbetween sleep restriction and incident UI and irri-tative symptoms, with 19% and 12% reductions inthe ORs, respectively. Closer examination of BMI
Figure 1. Multivariate regression models of sleep variablespredicting incident obstructive and irritative LUTS, BACHSurvey (2002 to 2010). Exposures (sleep) were assessed atbaseline. Black boxes represent ORs obtained frommultivariate logistic regression models with incidenturological symptoms, obstructive (A) and irritative (B),predicted by the sleep exposure variable, and controlling forage, gender, race, SES, diabetes, heart disease, alcohol use,physical activity, smoking, antidepressant use, secondarysedation and secondary stimulation. Gray boxes representORs obtained with further adjustment for BMI. Multivariatelogistic regression models for sleep restriction did not controlfor gender as this measure was collected only in men.
102 SLEEP AND UROLOGICAL SYMPTOMS

with sleep restriction and incident UI and irritativesymptoms (data not shown) revealed that sleeprestriction and incident outcomes were morecommonly observed in obese subjects. CRP did notmediate any associations.
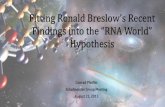
Association between Urological Symptoms andIncident Sleep OutcomesOverall, LUTS were not associated with incidentsleep related problems. However, obstructivesymptoms were inversely associated with incidentsleep medication use (OR 0.59, 95% CI 0.35, 0.99)and were positively associated with incident sleeprestriction (OR 2.20, 95% CI 1.11, 4.33, fig. 2), withno mediation by BMI or CRP. Nocturia was associ-ated with poor sleep quality (OR 1.98, 95% CI 1.38,2.85; table 2). Unexpectedly, UI was associated witha reduced risk of incident sleep restriction (OR 0.31,95% CI 0.11, 0.87).
DISCUSSIONIn this population based, longitudinal study of morethan 4,000 men and women, there was a bidirec-tional relationship between self-reported sleeprelated variables and urological symptoms, withBMI but not CRP possibly mediating the associationbetween restricted sleep and urological symptoms.Although these observational data did not demon-strate causality, they suggested that improvingsleep health may be a novel means of improvingurological symptoms. It is known that improvingurological function improves sleep outcomes.
The literature is replete with reports showingthat urological symptoms, particularly nocturia,have profound effects on sleep. However, to ourknowledge few if any studies have shown thatsleep related variables predict incident urologicalsymptoms, despite the known influence of sleepdisturbance on factors which tend to cluster with
urological symptoms, including obesity,19 systemicinflammation,20 type 2 diabetes21 and other comor-bidities.22 In this study sleep restriction (measuredonly in men) was associated with incident LUTSand UI, and poor sleep quality in men and womenwas associated with incident LUTS and nocturia.Poor sleep quality increased the risk of obstructiveand irritative LUTS, while sleep restriction wasassociated with a more than twofold risk of irrita-tive symptoms. The latter is of interest in light ofprevious studies showing impaired cardiometabolicfunction in sleep deprived individuals,7,8 and fitsconceptually with storage/irritative LUTS resultingfrom altered sensory innervation of the bladder orautonomic hyperactivity, which is noted in thosewith LUTS or sleep disturbances.
Our results are consistent with cross-sectionalstudies showing that urological symptoms areprevalent in patients with sleep disorders (egobstructive sleep apnea)23 and with a longitudinalstudy showing that improvements in LUTS leadto improvements in sleep disturbance.5 Voiding iscited as the main reason for waking at night24 andsleep disturbance mediates the effect of nocturia onquality of life.25 Nocturia and urgency correlatenegatively with direct measures of sleep efficiency26
and sleep quality.27 What has been debated iswhether patients are awakened because of the urgeto void, or whether they are awakened for someother reason and then sense the need to void.28
The current study was not designed to addressthis issue.
One straightforward explanation for our findingsis the commonly observed phenomenon of patientswith sleep disorders awakening from sleep andrealizing that they have to void, quite apart fromany particular urinary dysfunction.28 However, it isnot likely that this fully accounts for our observa-tions, since other LUTS (not specifically nocturia)were also significantly related to poor sleep. So even
Table 1. Multivariate associations between baseline sleep variables and incidence of urological symptoms at followup
Exposure/Model*
LUTS UI Nocturia
OR (95% CI) p Value† OR (95% CI) p Value† OR (95% CI) p Value†
Poor sleep quality:Multivariate adjusted‡ 1.73 (1.20, 2.51) 0.004 1.50 (0.98, 2.31) 0.06 1.42 (1.02, 1.97) 0.04Multivariate adjusted " BMI 1.64 (1.14, 2.35) 0.008 1.39 (0.94, 2.05) 0.10 1.42 (1.02, 1.97) 0.04
Sleep restriction:§Multivariate adjusted‡ 1.98 (1.03, 3.78) 0.04 2.42 (1.07, 5.48) 0.03 1.03 (0.61, 1.77) 0.90Multivariate adjusted " BMI 1.89 (0.98, 3.65) 0.06 1.96 (0.95, 4.04) 0.07 1.02 (0.59, 1.76) 0.93
Sleep medications:Multivariate adjusted‡ 1.21 (0.70, 2.07) 0.50 0.68 (0.37, 1.24) 0.20 1.05 (0.69, 1.58) 0.83Multivariate adjusted " BMI 1.21 (0.69, 2.13) 0.50 0.68 (0.38, 1.22) 0.20 1.05 (0.69, 1.59) 0.83
*Exposures assessed at baseline.†p Value testing the null hypothesis that OR!1.00.‡Multivariate logistic regression model of incident urological symptoms as a function of baseline presence of sleep parameters controlling for age, gender, race, SES,diabetes, heart disease, alcohol use, physical activity, smoking, antidepressant use, secondary sedation medication use and secondary stimulation medication use.§Multivariate logistic regression models did not control for gender as sleep restriction was collected only in men at baseline.
SLEEP AND UROLOGICAL SYMPTOMS 103

if repeated awakenings among subjects with sleeprelated problems constitute a risk for a nocturnalvoid (which may be reported by the subject as noc-turia), they should not constitute a risk for non-nocturia LUTS including incomplete emptying,weak stream and other symptoms.
A common underlying mechanism(s) may linkthese 2 disorders. Obesity and metabolic dysfunc-tion are emerging areas of interest in urology andsleep medicine. There are strong epidemiologicaldata showing linkages between LUTS/BPH and themetabolic syndrome,21 likely mediated via path-ways not assessed in the current study, includingaltered estrogen-to-androgen ratios, increasedautonomic nervous system activation, vasopressinsecretion, and impaired smooth muscle functioningas a result of impaired nitric oxide synthase,cyclic guanosine monophosphate and RhoA/ROCKsignaling.
Furthermore, metabolic disturbances accompanyacute7 and chronic8 sleep deprivation. These path-ways impact the regulation of smooth muscle toneand, thus, are fundamental to healthy urologicalfunction given the requirements for coordinatedrelaxation/contraction of the detrusor and bladdermusculature. These factors may interact in aninterrelated manner, eg sleep disturbance is knownto result in increased autonomic nervous systemactivation, which has been shown to be related toLUTS secondary to BPH,29 which may feed back toinfluence sleep and so on. If obesity or metabolicdysfunction is involved in this relationship, as sug-gested by our data showing BMI as a potentiallyrelevant mediating variable, this would indicatethat weight loss or exercise could be an effectivemeans to improve sleep problems and urinarysymptoms simultaneously.
Limitations and strengths of the current studymerit consideration. The BACH Survey focusedon symptoms of urinary function, not diagnosedconditions, and certain measurements of interest(eg urine flow volume, prostate volume or prostatespecific antigen levels in men) were not available.The focus on symptoms was appropriate given theprimacy of symptoms in the LUTS/BPH complex.The measures of sleep were by self-report and wehad no specific questions regarding obstructive sleepapnea at baseline. Furthermore, the current designdid not address the dynamic nature of urologicalsymptoms or sleep related problems because interimmeasurements were not available for either. Pre-sumably this would have had the effect of increasingmeasurement error, thus reducing the chance ofrejecting null hypotheses. Finally, to our knowledge,the Sandvik index has not been formally validated inmen, but our prior publications showing differencesin the prevalence of UI between known groups
Figure 2. Multivariate regression models of irritative andobstructive LUTS predicting incident sleep variables, BACHSurvey (2002 to 2010). Exposures (LUTS) were assessed atbaseline. Black boxes represent ORs obtained from multivariatelogistic regression models with incident sleep outcomes of poorsleep quality (A), sleep restriction (B) and sleep medications(C ) predicted by urological symptom exposure variable, andcontrolling for age, gender, race, SES, diabetes, heart disease,alcohol use, physical activity, smoking, antidepressant use,secondary sedation and secondary stimulation. Gray boxesrepresent ORs obtained with further adjustment for BMI.Multivariate logistic regression models for sleep restriction didnot control for gender as this measure was collected only in men.
104 SLEEP AND UROLOGICAL SYMPTOMS

(eg men vs women, young vs old, healthy vs un-healthy) support the concept that UI as measured bythe Sandvik severity index possesses constructvalidity.30
Significant strengths of the study include thepopulation based longitudinal design, large samplesize and relatively low 20% loss to followup rate.The breadth of questions on urological symptomsincluded allowed probing for different symptom re-lationships. Importantly, the loss to followup ratewas unrelated to urological symptoms and so ourresults are not subject to attrition bias.
CONCLUSIONSIn this population based longitudinal study of menand women, self-reported sleep related problemsand urological symptoms were linked bidirection-ally, and BMI may have a role in the relationshipbetween sleep restriction and the development ofurological symptoms. Thus, sleep may be a novelrisk factor for urological symptoms and, as such,patients with sleep disorders should be screenedand appropriately treated for urological symptoms,which may positively benefit quality of life outcomesin patients with sleep related problems.
REFERENCES1. Kupelian V, Wei JT, O’Leary MP et al: Prevalence
of lower urinary tract symptoms and effect onquality of life in a racially and ethnically diverserandom sample: the Boston Area CommunityHealth (BACH) Survey. Arch Intern Med 2006;166: 2381.
2. Colten HR and Altevogt BM: Sleep Disorders andSleep Deprivation: An Unmet Public HealthProblem. Washington, D.C.: The National Acad-emies Press 2006.
3. Knutson KL, Van Cauter E, Rathouz PJ et al:Trends in the prevalence of short sleepers in theUSA: 1975-2006. Sleep 2010; 33: 37.
4. Helfand BT, McVary KT, Meleth S et al: Therelationship between lower urinary tract symp-tom severity and sleep disturbance in theCAMUS trial. J Urol 2011; 185: 2223.
5. Helfand BT, Lee JY, Sharp V et al: Associationsbetween improvements in lower urinary tractsymptoms and sleep disturbance over time in theCAMUS trial. J Urol 2012; 188: 2288.
6. Patel SR and Hu FB: Short sleep duration andweight gain: a systematic review. Obesity (SilverSpring) 2008; 16: 643.
7. Spiegel K, Leproult R and Van Cauter E: Impactof sleep debt on metabolic and endocrine func-tion. Lancet 1999; 354: 1435.
8. Yaggi HK, Araujo AB and McKinlay JB: Sleepduration as a risk factor for the development oftype 2 diabetes. Diabetes Care 2006; 29: 657.
9. Simpson N and Dinges DF: Sleep and inflam-mation. Nutr Rev, suppl., 2007; 65: S244.
10. Hakkinen JT, Shiri R, Koskimaki J et al:Depressive symptoms increase the incidence ofnocturia: Tampere Aging Male Urologic Study(TAMUS). J Urol 2008; 179: 1897.
11. Shiri R, Koskimaki J, Tammela TL et al: Bidirec-tional relationship between depression anderectile dysfunction. J Urol 2007; 177: 669.
12. McKinlay JB and Link CL: Measuring the urologiciceberg: design and implementation of theBoston Area Community Health (BACH) Survey.Eur Urol 2007; 52: 389.
13. Kelley KE, Kelley TP, Kaufman DW et al: TheSlone Drug Dictionary: a research driven phar-macoepidemiology tool. PharmacoepidemiolDrug Saf 2003; 12: 168.
14. Barry MJ, Fowler FJ Jr, O’Leary MP et al: TheAmerican Urological Association symptom indexfor benign prostatic hyperplasia. The Measure-ment Committee of the American UrologicalAssociation. J Urol 1992; 148: 1549.
15. Okamura K, Nojiri Y, Osuga Y et al: Psychometricanalysis of International Prostate SymptomScore for female lower urinary tract symptoms.Urology 2009; 73: 1199.
16. Sandvik H, Hunskaar S, Seim A et al: Validationof a severity index in female urinary incontinenceand its implementation in an epidemiologicalsurvey. J Epidemiol Community Health 1993; 47:497.
17. Tikkinen KA, Johnson TM 2nd, Tammela TL et al:Nocturia frequency, bother, and quality of life:how often is too often? A population-basedstudy in Finland. Eur Urol 2010; 57: 488.
18. Rothman KJ and Greenland S: Modern Epide-miology, 2nd ed. Philadelphia: Lippincott-Raven1998.
19. Link CL, Steers WD, Kusek JW et al: The asso-ciation of adiposity and overactive bladderappears to differ by gender: results from theBoston Area Community Health survey. J Urol2011; 185: 955.
Table 2. Multivariate associations between baseline urological symptoms and incident sleep outcomes at followup
Exposure/Model†
Poor Sleep Quality Sleep Restriction* Sleep Medications
OR (95% CI) p Value‡ OR (95% CI) p Value‡ OR (95% CI) p Value‡
LUTS:Multivariate adjusted§ 0.90 (0.61, 1.32) 0.58 1.29 (0.68, 2.45) 0.43 0.87 (0.53, 1.42) 0.57Multivariate adjusted " BMI 0.90 (0.61, 1.32) 0.58 1.30 (0.68, 2.47) 0.43 0.85 (0.52, 1.39) 0.51
UI:Multivariate adjusted§ 0.70 (0.40, 1.25) 0.23 0.31 (0.11, 0.87) 0.03 1.25 (0.69, 2.27) 0.46Multivariate adjusted " BMI 0.71 (0.40, 1.25) 0.23 0.31 (0.11, 0.87) 0.03 1.29 (0.71, 2.35) 0.40
Nocturia:Multivariate adjusted§ 1.98 (1.38, 2.85) <0.001 1.12 (0.66, 1.89) 0.67 1.27 (0.82, 1.97) 0.29Multivariate adjusted " BMI 1.98 (1.38, 2.85) <0.001 1.12 (0.67, 1.89) 0.67 1.32 (0.85, 2.04) 0.21
*Multivariate logistic regression models for sleep restriction did not control for gender as this measure was collected only in men.†Exposures assessed at baseline.‡p Value testing the null hypothesis that OR!1.00.§Multivariate logistic regression model with incident sleep disorder predicted by urological symptom exposure variable, and controlling for age, gender, race, SES, diabetes,heart disease, alcohol use, physical activity, smoking, antidepressant use, secondary sedation and secondary stimulation.
SLEEP AND UROLOGICAL SYMPTOMS 105

20. Kupelian V, McVary KT, Barry MJ et al: Associ-ation of C-reactive protein and lower urinarytract symptoms in men and women: results fromBoston Area Community Health survey. Urology2009; 73: 950.
21. Kupelian V, McVary KT, Kaplan SA et al: Asso-ciation of lower urinary tract symptoms and themetabolic syndrome: results from the BostonArea Community Health survey. J Urol 2009; 182:616.
22. Fitzgerald MP, Link CL, Litman HJ et al: Beyondthe lower urinary tract: the association ofurologic and sexual symptoms with commonillnesses. Eur Urol 2007; 52: 407.
23. Parthasarathy S, Fitzgerald M, Goodwin JLet al: Nocturia, sleep-disordered breathing, and
cardiovascular morbidity in a community-basedcohort. PLoS One 2012; 7: e30969.
24. Bing MH, Moller LA, Jennum P et al: Prevalenceand bother of nocturia, and causes of sleepinterruption in a Danish population of men andwomen aged 60-80 years. BJU Int 2006; 98: 599.
25. Yoshimura K, Oka Y, Kamoto T et al: Night-timefrequency, sleep disturbance and general health-related quality of life: is there a relation? Int JUrol 2009; 16: 96.
26. Tsujimura A, Takao T, Miyagawa Y et al: Urgencyis an independent factor for sleep disturbance inmen with obstructive sleep apnea. Urology 2010;76: 967.
27. Asplund R: Nocturia in relation to sleep, somaticdiseases and medical treatment in the elderly.BJU Int 2003; 91: 302.
28. Pressman MR, Figueroa WG, Kendrick-MohamedJ et al: Nocturia. A rarely recognized symptom ofsleep apnea and other occult sleep disorders.Arch Intern Med 1996; 156: 545.
29. McVary KT, Rademaker A, Lloyd GL et al: Auto-nomic nervous system overactivity in men withlower urinary tract symptoms secondary tobenign prostatic hyperplasia. J Urol 2005; 174:1327.
30. Tennstedt SL, Link CL, Steers WD et al: Preva-lence of and risk factors for urine leakage in aracially and ethnically diverse population ofadults: the Boston Area Community Health(BACH) Survey. Am J Epidemiol 2008; 167: 390.
106 SLEEP AND UROLOGICAL SYMPTOMS