
Tom Hoeg e Book: Child Abuse Victims, Combat Veterans and PTSD
Upload
independentCategory
view
0download
0
Journal of Traumatic StressDecember 2012, 25, 665–674
Sleep Quality Among U.S. Military Veterans With PTSD: A FactorAnalysis and Structural Model of Symptoms
Kimberly A. Babson,1,2 Daniel M. Blonigen,1 Matthew Tyler Boden,1,3 Kent D. Drescher,3
and Marcel O. Bonn-Miller1,3,4
1Center for Health Care Evaluation, VA Palo Alto Health Care System, Menlo Park, California, USA2Department of Psychiatry and Behavioral Sciences, Stanford University School of Medicine, Stanford, California, USA
3National Center for PTSD, VA Palo Alto Health Care System, Menlo Park, California, USA4Center of Excellence in Substance Abuse Treatment and Education, Philadelphia VAMC, Philadelphia, Pennsylvania, USA
Poor sleep quality among individuals with posttraumatic stress disorder (PTSD) is associated with poorer prognosis and outcomes. Thefactor structure of the most commonly employed measure of self-reported sleep quality, the Pittsburgh Sleep Quality Index (PSQI), hasyet to be evaluated among individuals with PTSD. The current study sought to fill this gap among a sample of 226 U.S. military veteranswith PTSD (90% with co-occurring mood disorders, 73.5% with substance use disorders). We evaluated the factor structure of the PSQIby conducting an exploratory factor analysis (EFA) in approximately half of the sample (n = 111). We then conducted a second EFA inthe other split half (n = 115). Lastly, we conducted a path analysis to investigate the relations between sleep factors and PTSD symptomseverity, after accounting for the relation with depression. Results suggested sleep quality can best be conceptualized, among those withPTSD, as a multidimensional construct consisting of 2 factors, Perceived Sleep Quality and Efficiency/Duration. After accounting for theassociation between both factors and depression, only the Perceived Sleep Quality factor was associated with PTSD (β = .51). The resultsprovide a recommended structure that improves precision in measuring sleep quality among veterans with PTSD.
Poor sleep quality is the most common presenting con-cern among veterans with posttraumatic stress disorder (PTSD;Geuze & Vermetten, 2004; Ohayon & Shapiro, 2000). Recentresearch has indicated that 74%–90% of currently deployedand postdeployed veterans report poor sleep quality (Lewis,Creamer, & Failla, 2009; Peterson, Goodie, Satterfield, & Brim,2008), with up to 91% of Vietnam era veterans reporting poorsleep quality (Neylan et al., 1998). In comparison, up to 50%of healthy adults of the same age range (over 50 years) reportpoor sleep quality (Vitiello, Moe, Larsen, & Prinz, 1997). Thesehigh rates are particularly troubling as poor sleep quality hasbeen shown to predict the onset of PTSD in several prospective
This work was supported, in part, by the following: A VA Clinical ScienceResearch and Development (CSR&D) Career Development Award-2 (Bonn-Miller), a VA HSR&D SUD-QUERI grant (RRP 10-192; Bonn-Miller), andHealth Services Research and Development Service funds provided to the firstauthor. Daniel M. Blonigen was supported by a Career Development Award-2from The VA Office of Research and Development (Clinical Sciences Research& Development). The expressed views do not necessarily represent those ofthe Department of Veterans Affairs.
Correspondence concerning this article should be addressed to Kimberly Bab-son, 795 Willow Road (152-MPD), Menlo Park, CA 94025. E-mail: [email protected]
Published 2012. This article is a US Government work and is in the publicdomain in the USA. View this article online at wileyonlinelibrary.comDOI: 10.1002/jts.21757
studies (Koren, Anon, Lavie, & Klein, 2002; Mellman et al.,1995), and in cross-sectional research, has been linked to greaterdaytime PTSD symptoms, increased suicidality and substanceabuse, poorer treatment outcomes, and the development andmaintenance of co-occurring psychopathology (Clum, Nishith,& Resick, 2001; Krakow et al., 2000; Nishith, Resick, Muser,2001; Picchioni et al., 2010; Saladin, Brady, Dansky, & Kirk-patrick, 1995; Wright et al., 2011).
Based on the significant consequences and implications ofpoor sleep quality, there have been increasing efforts targetedat the assessment of sleep quality among individuals withPTSD (Wright et al., 2011). The most widely used measureof self-reported sleep quality is the Pittsburgh Sleep QualityIndex (PSQI; Buysse Reynolds, Monk, Berman, & Kupfer,1989). Though the PSQI was originally developed and evalu-ated among “good sleepers” (healthy controls) and two groupsof “poor sleepers” (depressed patients and patients with sleepdisorders; Buysse et al., 1989), there have been 16 subsequentempirical investigations that have assessed the validity of thePSQI among other populations.
Psychometric evaluations of the PSQI have primarily in-volved the development of translated versions (e.g., French;Farrahi, Nakhaee, Sheibani, Garrusi, & Amirkafi, 2012),and/or validation among specialized populations (e.g., el-derly Caucasian and African American women, older adultswith and without depression; Beaudreau et al., 2012; Cole
665

666 Babson et al.
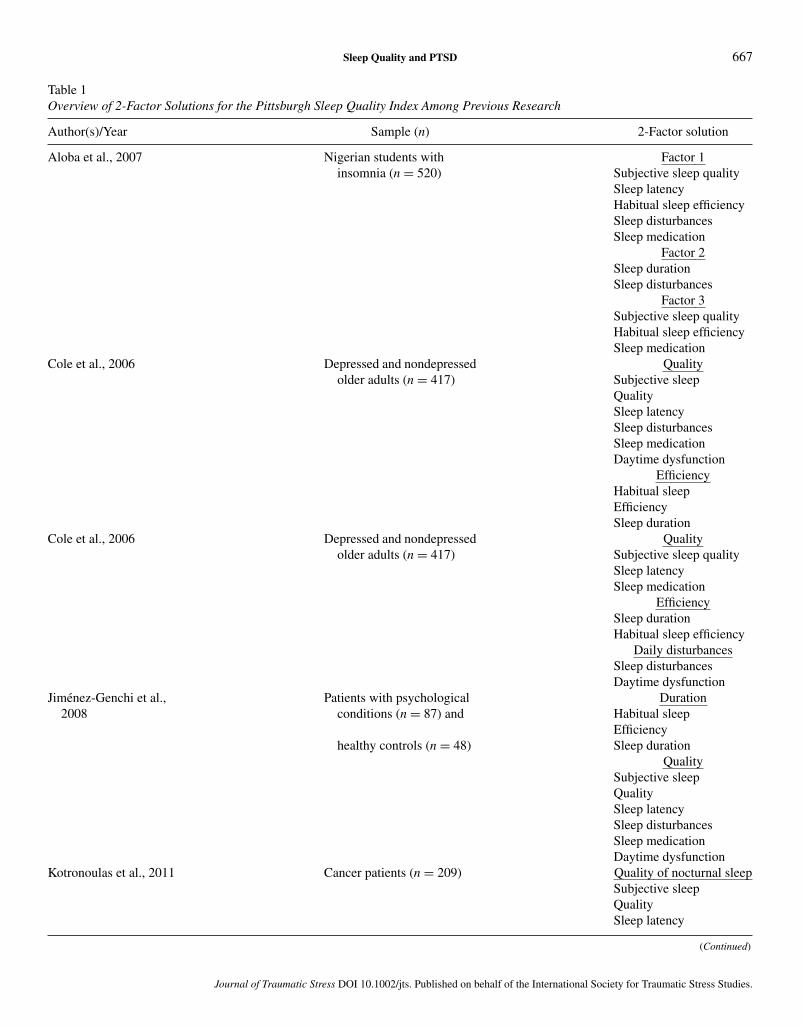
et al., 2006). Among the extant investigations of the PSQIfactor structure (i.e., Aloba, Adewuya, Ola, & Mapayi,2007; Jimenez-Genchi, Monteverde-Maldonado, Neclares-Portocarrero, Esquivel-Adame, & de la Vega-Pacheo, 2008;Kotronoulas, Papadopoulou, Papapetrou, & Patiraki, 2010; Sk-outeris, Wertheim, Germano, Paxton, & Milgrom, 2009), therehas been support for both 2- (Jimenez-Genchi et al., 2008;Kotronoulas et al., 2011; Skouteris et al., 2009) and 3-factor(Aloba et al., 2007; Cole et al., 2006) models (see Table 1).
As prior empirical work has shown alternative factor struc-tures of the PSQI among other populations, it is striking thatthe factor structure of the PSQI has not been evaluated amongindividuals with PTSD, particularly given its wide use amongthis population (e.g., Belleville, Guay, & Marchand, 2011; Ca-paldi, Guerrero, & Killgore, 2011; Ulmer, Edinger, & Calhoun,2011). The majority of research using the PSQI among in-dividuals with PTSD has used the global score. Use of thisglobal score, however, may obscure identification of the mostsalient sleep disturbances that would otherwise be observed byutilizing a multidimensional scoring system. For example, ev-idence suggests that sleep among individuals with PTSD maybe unique from sleep among other poor sleepers (Ohayon &Shapiro, 2000). Here, research has demonstrated that the sleepof individuals with PTSD is often characterized by trouble ini-tiating and maintaining sleep, as well as nightmares and violentbehaviors during sleep.
Using a sample of 226 U.S. military veterans with PTSD, thepresent study sought to fill the existing gap in the literature byinvestigating the factor structure of the PSQI, and examining thespecific relations between sleep quality and PTSD. Exploratoryfactor analyses (EFA) were used to address the first aim, and alatent variable structural modeling approach was used to exam-ine the relations between the underlying factors of sleep qual-ity and PTSD. In addition, given the significant interrelationsamong sleep quality, PTSD, and depression (Woodward, Fried-man, & Bliwise, 1996) structural links between sleep qualityand PTSD were examined after accounting for the associationbetween sleep quality and depression. Examining this questionrepresents a unique contribution by (a) providing improvedprecision in measuring sleep quality among individuals withPTSD, (b) refining our understanding of the relation betweensleep quality and PTSD, and (c) informing debates regardingthe comorbidity of PTSD and depression.
Method
Participants
Participants were admitted for PTSD treatment at the resi-dential rehabilitation programs of a VA Medical Center. Thisprogram admits clinician-referred U.S. military veterans withPTSD symptoms that have not been successfully amelioratedwith outpatient treatment. Exclusion criteria for enrollment inthe program included (a) current psychotic symptoms, (b) sub-stance use within 15 days of start of treatment, and (c) medi-
cal conditions with high probability of significantly interferingwith or preventing psychological treatment (i.e., those unableto move about independently). Data for the current study werebased on assessments administered to all veterans in the residen-tial treatment program for the purposes of program evaluationand as part of routine care. All data were obtained from ques-tionnaires and interviews administered during the first weekof treatment (treatment intake), with doctoral-level staff fromthe PTSD treatment program responsible for the conduct ofall Clinician Administered PTSD Scale (CAPS; Blake et al.,1995) interviews. Procedures were approved by the StanfordInstitutional Review Board.
Potential participants included 303 predominately male(86%) U.S. military veterans admitted to a VA 90-day res-idential rehabilitation program for PTSD between 2000 and2008. Of this sample, 77 individuals had more than 10% miss-ing data across individual items on the PSQI and were excludedfrom analyses, resulting in a final sample of 226 (mean age =51.78 years, SD = 6.23; range = 24–70 years) veterans. Theracial/ethnic composition of the sample was as follows: 60.6%Caucasian, 19.9% African American, 12.3% Hispanic/Latino,9.0% multiracial, 7.0% Asian, 4.0% identified as “other,” 0.7%Native American, and 0.3% did not report ethnicity. Psycho-logical comorbidities included the following: mood disorders(90.1%), substance use disorders (73.5%), and anxiety disor-ders (20.1%). Regarding general sleep patterns reported by thissample, mean time to sleep onset was 60.34 minutes (SD =70.10), time in bed was 8.24 hours (SD = 3.67), and meansleep efficiency was 63.94 (SD = 46.00).
Measures
Sleep quality. The Pittsburgh Sleep Quality Index (PSQI;Buysse et al., 1989) is a 19-item questionnaire designed to as-sess sleep quality. Participants indicate their usual bedtime, howlong it takes them to fall asleep, their usual waking time, andtheir usual hours of sleep per night, as well as respond to ques-tions such as, “During the past month, how often have you hadtrouble sleeping because you cannot get to sleep within 30 min-utes?” and “During the past month, how often have you takenmedicine (prescribed or over the counter) to help you sleep?”on a 4-point Likert-type scale (0 = not during the past month,3 = three or more times a week). All questions are assessedin relation to the past month. Items are coded through the useof various algorithms to generate seven component scores anda global total score (see Buysse et al., 1989 for the scoringalgorithms). These components include subjective sleep quality(defined as the overall quality of sleep), sleep latency (amountof time to fall asleep), sleep duration (number of hours of actualsleep per night), habitual sleep efficiency (number of hours ofsleep divided by number of hours spent in bed), sleep distur-bances (a nonspecific index of nighttime disturbances includingsymptoms of sleep apnea, middle insomnia, disturbing dreams,and physical conditions such as pain), sleep medication (use ofprescribed or over-the-counter sleep medication), and daytime
Journal of Traumatic Stress DOI 10.1002/jts. Published on behalf of the International Society for Traumatic Stress Studies.
Sleep Quality and PTSD 667
Table 1Overview of 2-Factor Solutions for the Pittsburgh Sleep Quality Index Among Previous Research
Author(s)/Year Sample (n) 2-Factor solution
Aloba et al., 2007 Nigerian students with Factor 1insomnia (n = 520) Subjective sleep quality
Sleep latencyHabitual sleep efficiencySleep disturbancesSleep medication
Factor 2Sleep durationSleep disturbances
Factor 3Subjective sleep qualityHabitual sleep efficiencySleep medication
Cole et al., 2006 Depressed and nondepressed Qualityolder adults (n = 417) Subjective sleep
QualitySleep latencySleep disturbancesSleep medicationDaytime dysfunction
EfficiencyHabitual sleepEfficiencySleep duration
Cole et al., 2006 Depressed and nondepressed Qualityolder adults (n = 417) Subjective sleep quality
Sleep latencySleep medication
EfficiencySleep durationHabitual sleep efficiency
Daily disturbancesSleep disturbancesDaytime dysfunction
Jimenez-Genchi et al., Patients with psychological Duration2008 conditions (n = 87) and Habitual sleep
Efficiencyhealthy controls (n = 48) Sleep duration
QualitySubjective sleepQualitySleep latencySleep disturbancesSleep medicationDaytime dysfunction
Kotronoulas et al., 2011 Cancer patients (n = 209) Quality of nocturnal sleepSubjective sleepQualitySleep latency
(Continued)
Journal of Traumatic Stress DOI 10.1002/jts. Published on behalf of the International Society for Traumatic Stress Studies.

668 Babson et al.
Table 1Continued.
Author(s)/Year Sample (n) 2-Factor solution
Sleep durationHabitual sleepEfficiencySleep disturbancesManagement of sleepSleep medicationDaytime dysfunction
Skouteris et al., 2009 Pregnant women (n = 252) Sleep efficiencySleep latencyHabitual sleep efficiencySleep duration
DisturbancesSleep disturbanceDaytime dysfunction
Overall sleep qualitySubjective sleep quality
Note. Sleep medication was removed from the factor structure within the Skouteris et al., 2009. Cole et al., 2006 is listed twice as they report both a 2- and 3-factorsolution.
dysfunction (trouble staying awake and/or decreased energyduring the day). Component scores were used as observed in-dicators in all factor analyses.
PTSD symptoms. The Clinician Administered PTSDScale (CAPS; Blake et al., 1995) is a semistructured clinicalinterview that indexes traumatic event exposure as defined bythe Diagnostic and Statistical Manual of Mental Disorders (4th
ed.; DSM-IV; American Psychiatric Association, 1994), as wellas diagnostic status and severity of PTSD. The CAPS pro-vides a measure of the frequency and intensity of 17 symptomsof PTSD allowing for the determination of symptom severity,as well as a dichotomous diagnosis of PTSD. The CAPS haswell-established psychometric properties (Weathers, Keane, &Davidson, 2001; α = .84 in the current study). To ensure par-ticipants met – criteria for PTSD, the “1–2 rule” was imple-mented such that individuals had to have at least a 1 on fre-quency and 2 on intensity for each symptom to qualify as anendorsed symptom (Weathers, Ruscio, and Keane, 1999). DSM-IV criteria were then used to determine diagnostic status. Basedon this assessment, 100% of the sample met DSM-IV criteriafor PTSD. For the path models, a 4-factor model correspond-ing to the four symptom clusters of PTSD (reexperiencing,avoidance, numbing, hyperarousal) was employed. Within thismodel, the avoidance/numbing symptom cluster is split intoavoidance symptoms (i.e., avoiding trauma reminder includingpeople, places, and activities, and avoiding thoughts or feelingsof the event) and numbing symptoms (i.e., difficulty remember-ing the event, loss of interest, feeling distant or cutoff, feelingemotionally numb, and foreshortened future). This model waschosen, instead of the DSM-IV 3-factor model as factor analytic
research has indicated that a 4-factor solution consistently fitsPTSD symptom measures better than the traditional 3-factorsolution among a variety of trauma samples, including militaryveterans (King, Leskin King & Weathers, 1998; Mansfield,Williams, Hourani, & Babeu, 2010). Importantly, sleep items(nightmares and insomnia) were removed from the reexperi-encing and hyperarousal symptom clusters, respectively, forthe path analysis.
Depression symptoms. The Beck Depression Inventory(BDI-II; Beck, Steer, & Brown, 1996) is a 21-item self-reportmeasure of depression symptoms. Research on the latent struc-ture of the BDI-II suggests a 3-factor model best represents theoverall construct of depression (Beck, Steer, Brown, & van derDoes, 2002). As such the three factors of the BDI (i.e., cogni-tive, somatic, and cognitive) were used to generate a depressionlatent variable for the path analysis. Importantly, the sleep itemwas removed. (α = .88)
Data Analysis
We first examined descriptive statistics and correlations be-tween the PSQI component scores, PTSD, and depression. Wethen employed three analytic methods, with all models con-structed using Mplus 5.2 (Muthen & Muthen, 1998–2008).First, our overall sample was randomly split into two halves(n = 111 and 115, respectively). Random splitting of the sam-ple was conducted through SPSS V.20 in which an algorithmcalculates two random samples, each consisting of approxi-mately 50%. An EFA was conducted in the first split sample toinvestigate the fit of 1-, 2-, and 3-factor models. To determineif the resulting factor structure was replicable, we conducted a
Journal of Traumatic Stress DOI 10.1002/jts. Published on behalf of the International Society for Traumatic Stress Studies.

Sleep Quality and PTSD 669
second EFA (testing the 1-, 2-, and 3-factor models) in the othersplit sample. Consistent with previous research (Cole et al.,2006), component scores, instead of the individual items, ofthe PSQI were used as observed indicators due to the nonlineartransformations from item responses to component scores. Fi-nally, a latent variable structural modeling approach was usedto construct a path model to examine the associations betweenthe sleep quality factors, PTSD, and depression within theentire sample. The following indices were used to evaluate theoverall model fit: The chi-square goodness of fit test (χ2), thecomparative fit index (CFI; Bentler, 1990), the Tucker-Lewisindex (TLI; Tucker & Lewis, 1973), the root-mean-square er-ror of approximation (RMSEA; Browne & Cudeck, 1993), andthe standardized root-mean-square residual (SRMR; Bentler,1995). Consistent with recommendations (Hu & Bentler, 1999),CFI and TLI values > .95 and RMSEA and SRMR values <
.06 indicate adequate model fit. Due to missing data at the item-level, the maximum-likelihood estimator (MLE) was used in allmodels to allow for missing data estimation.
Results
Descriptive Information
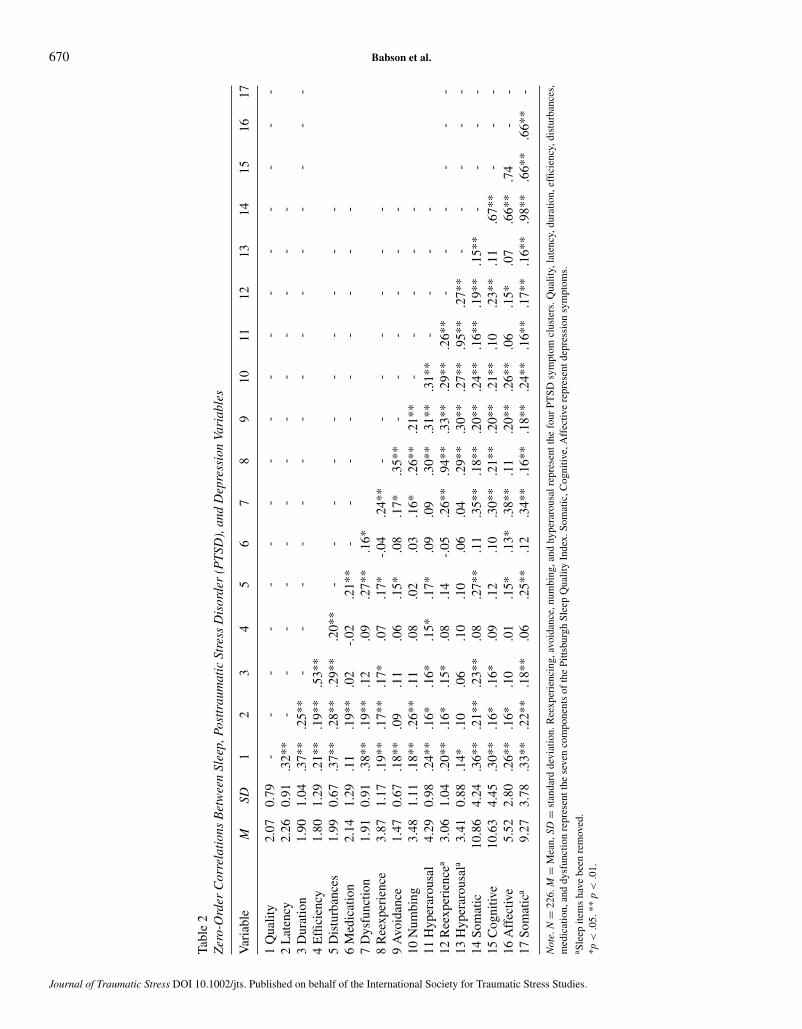
Among the entire sample, total PTSD symptoms severity (M =80.48, SD = 18.99) was indicative of severe PTSD; total depres-sion symptom severity (M = 26.99, SD = 10.25) was indicativeof moderate depression. Please see Table 2 for descriptive statis-tics for each variable as well as zero-order correlations betweenobserved indicators.
To assess the reliability of the PSQI scale we first conductedcorrelations between the PSQI global score and the componentscores. The component scores most highly correlated with theglobal score were sleep duration (r = .65) and subjective sleepquality (r = .61), while sleep medication exhibited the lowestcorrelation (r = .47). In addition, Cronbach’s α coefficientswere calculated for (a) the global PSQI score using the indi-vidual items (α = .78; α = .79 with sleep medication questionremoved), (b) the global PSQI score using component scales(α = .67; α = .68 with sleep medication removed), and (c) in-dividual items of the sleep disturbance scale on the componentscore (α = .72). Consistent with previous research (Carpenter &Andrykowski, 1998), αs were not calculated for the additionalindividual component scores due to the small number of itemson each component (one or two items).
Exploratory Factor Analysis
After randomly splitting our sample, an EFA was conducted toidentify the factor structure of the PSQI among veterans withPTSD. Results indicated good model-fit for both the 2- and 3-factor models (see Table 3). Evaluation of the factor loadings,however, demonstrated the sleep medication component did notreliably load onto any of the factors. Consistent with recommen-dations (Comrey & Lee, 1992) and previous research (Skouteriset al., 2009), the sleep medication factor was removed and the
1-, 2-, and 3-factor models were rerun. With the removal ofthe sleep medication factor, results indicated poor model fit forthe 1-factor solution and good model-fit for a 2-factor solution,while the 3-factor solution did not converge. Therefore, the2-factor model was retained. All factor loadings were selectedfrom a standardized Geomin rotation (see Table 4). The first fac-tor was composed of four components with salient loadings onindicators of sleep quality, sleep latency, sleep disturbance, anddaytime dysfunction. This factor was named Perceived SleepQuality. The second factor was composed of two components:sleep duration and habitual sleep efficiency, and was termedEfficiency/Duration. The correlation between these factors wasmoderate (r = .42). To determine the reliability of this factorstructure, we conducted a second EFA testing a 1-, 2-, and 3-factor model within the other split half of the overall sample(n = 115). Results demonstrated a poor model fit for a 1-factormodel, good model fit for the 2-factor model, and the 3-factormodel did not converge (see Table 3). In addition, the samecomponents loaded onto the same factors as in the other splithalf (see Table 4).
Path Analysis
To estimate the association between sleep quality and PTSDand depression, we conducted a path analysis among the en-tire sample. The following model-fitting procedures were used.First, consistent with current conceptualizations of the factorstructure of PTSD (King et al., 1998), four symptom clusters(i.e., reexperiencing, avoidance, numbing, and hyperarousal)were used as observed indicators of a PTSD latent variable.Next, based on results from the EFA conducted above, six com-ponents of the PSQI (without sleep medication) were used asindicators of two sleep factor latent variables (i.e., PerceivedSleep Quality and Efficiency/Duration). Finally, three compo-nents of depression (cognitive, somatic, affective; Beck et al.,2002) were used as observed indicators of a depression latentvariable. Covariances among all latent variables and residualerror terms were freely estimated.
Analysis of fit indices indicated the model fit the data well:χ2(59, N = 226) = 74.62 p = .08, CFI = 0.98, TLI = 0.98,RMSEA = .03, SRMR = .04. Figure 1 provides a depiction ofthe model as well as the parameter estimates. First, results indi-cated that both Perceived Sleep Quality and Efficiency/Durationwere associated with depression. Second, after accounting forthe role of depression, Perceived Sleep Quality was uniquelyassociated with PTSD, whereas Efficiency/Duration was not.To determine if the sleep items from the CAPS impacted themodel, we conducted a second path analysis that included thesleep items from the CAPS (nightmares and insomnia). Resultsdemonstrated a similar pattern of findings. Analysis of fit in-dices indicated the model fit the data well: χ2(41, N = 226)= 40.97; p = .47, CFI = 1.00, TLI = 1.00, RMSEA = .00,SRMR = .04. Consistent with the main model, results indicatedthat Percieved Sleep Quality was significantly and uniquely as-sociated with PTSD. To determine if the sleep item from the
Journal of Traumatic Stress DOI 10.1002/jts. Published on behalf of the International Society for Traumatic Stress Studies.
670 Babson et al.
Tabl
e2
Zer
o-O
rder
Cor
rela
tion
sB
etw
een
Slee
p,Po
sttr
aum
atic
Stre
ssD
isor
der
(PT
SD),
and
Dep
ress
ion
Vari
able
s
Var
iabl
eM
SD1
23
45
67
89
1011
1213
1415
1617
1Q
ualit
y2.
070.
79-
--
--
--
--
--
--
--
--
2L
aten
cy2.
260.
91.3
2**
--
--
--
--
--
--
-3
Dur
atio
n1.
901.
04.3
7**
.25*
*-
--
--
--
--
--
--
--
4E
ffici
ency
1.80
1.29
.21*
*.1
9**
.53*
*5
Dis
turb
ance
s1.
990.
67.3
7**
.28*
*.2
9**
.20*
*-
--
--
--
--
-6
Med
icat
ion
2.14
1.29
.11
.19*
*.0
2-.
02.2
1**
--
--
--
--
-7
Dys
func
tion
1.91
0.91
.38*
*.1
9**
.12
.09
.27*
*.1
6*8
Ree
xper
ienc
e3.
871.
17.1
9**
.17*
*.1
7*.0
7.1
7*-.
04.2
4**
--
--
--
-9
Avo
idan
ce1.
470.
67.1
8**
.09
.11
.06
.15*
.08
.17*
.35*
*-
--
--
-10
Num
bing
3.48
1.11
.18*
*.2
6**
.11
.08
.02
.03
.16*
.26*
*.2
1**
--
--
-11
Hyp
erar
ousa
l4.
290.
98.2
4**
.16*
.16*
.15*
.17*
.09
.09
.30*
*.3
1**
.31*
*-
--
-12
Ree
xper
ienc
ea3.
061.
04.2
0**
.16*
.15*
.08
.14
-.05
.26*
*.9
4**
.33*
*.2
9**
.26*
*-
--
--
-13
Hyp
erar
ousa
la3.
410.
88.1
4*.1
0.0
6.1
0.1
0.0
6.0
4.2
9**
.30*
*.2
7**
.95*
*.2
7**
--
--
-14
Som
atic
10.8
64.
24.3
6**
.21*
*.2
3**
.08
.27*
*.1
1.3
5**
.18*
*.2
0**
.24*
*.1
6**
.19*
*.1
5**
--
--
15C
ogni
tive
10.6
34.
45.3
0**
.16*
.16*
.09
.12
.10
.30*
*.2
1**
.20*
*.2
1**
.10
.23*
*.1
1.6
7**
--
-16
Aff
ectiv
e5.
522.
80.2
6**
.16*
.10
.01
.15*
.13*
.38*
*.1
1.2
0**
.26*
*.0
6.1
5*.0
7.6
6**
.74
--
17So
mat
ica
9.27
3.78
.33*
*.2
2**
.18*
*.0
6.2
5**
.12
.34*
*.1
6**
.18*
*.2
4**
.16*
*.1
7**
.16*
*.9
8**
.66*
*.6
6**
-
Not
e.N
=22
6.M
=M
ean,
SD=
stan
dard
devi
atio
n.R
eexp
erie
ncin
g,av
oida
nce,
num
bing
,and
hype
raro
usal
repr
esen
tthe
four
PTSD
sym
ptom
clus
ters
.Qua
lity,
late
ncy,
dura
tion,
effic
ienc
y,di
stur
banc
es,
med
icat
ion,
and
dysf
unct
ion
repr
esen
tthe
seve
nco
mpo
nent
sof
the
Pitts
burg
hSl
eep
Qua
lity
Inde
x.So
mat
ic,C
ogni
tive,
Aff
ectiv
ere
pres
entd
epre
ssio
nsy
mpt
oms.
a Slee
pite
ms
have
been
rem
oved
.*p
<.0
5.**
p<
.01.
Journal of Traumatic Stress DOI 10.1002/jts. Published on behalf of the International Society for Traumatic Stress Studies.

Sleep Quality and PTSD 671
Table 3Model Fit Indices from Exploratory Factor Analysis
Model χ2 df p CFI TLI RMSEA SRMR
Sample 1: n = 1111 Factor 18.57 9 .02 .88 .80 .09 .062 Factor 1.05 4 .90 1.00 1.14 .00 .01
Sample 2: n = 1151 Factor 24.97 9 .00 .84 .73 .12 .072 Factor 1.66 4 .79 1.00 1.08 .00 .02
Note. The 2-factor model represents the best fitting model. χ2 (df) = chi-squareand degrees of freedom; p = significance level; CFI = comparative fit index;TLI = Tucker-Lewis index; RMSEA = root-mean-square error of approximation;SRMR = standardized root-mean-square residual.
BDI impacted the model, we conducted a third path analysisthat included the sleep item. Results demonstrated a similarpattern of results. Analysis of fit indices indicated the model fitthe data well: χ2(59, N = 226) = 78.71; p = .05, CFI = .98,TLI = .97, RMSEA = .03, SRMR =.05.
Table 4Factor Loadings from Exploratory Factor Analysis
EFA 1 (n = 111) EFA 2 (n = 115)
PSQI component PSQ E/D PSQ E/D
Sleep quality .68 .07 .78 .00Sleep disturbances .55 -.05 .41 .16Daytime dysfunction .55 -.11 .57 -.14Sleep latency .54 .01 .32 .12Sleep duration .00 1.03 .00 1.03Sleep efficiency .17 .42 .07 .51
Note. Factor loadings conducted from EFA using a standardized Geomin rotation.PSQ = Perceived sleep quality; E/D = efficiency/duration.
Discussion
The present study was the first empirical investigation of thefactor structure of the PSQI among individuals with PTSDof which we are aware. Contrary to the 1-factor structure
PTSD
R 2 = .33***
Perceived sleep quality
Efficiency/Duration
Efficiency
Daytime dysfunction
Quality
Latency
Disturbance
Duration
Reexperiencing
Avoidance
Numbing
Hyperarousal
.47***
.52***
.51***
.72***
.57***
.55***
.48***
.55***
e1
e2
e3
e4
e5
e6
e7
e8
e9
e10
.61***
.87*** .51***
.01
Depression
Cognitive Affective Somatic
e11 e12 e13
.86*** .86*** .78***
.09
.55***
.21*
Figure 1. Structural model of the associations between PTSD symptom severity and Perceived Sleep Quality and Efficiency/Duration after accounting for depressionsymptoms. Parameter estimates shown are standardized beta coefficients. Solid lines indicate significant paths; dotted lines indicate nonsignificant paths. *p < .05.***p < .001.
Journal of Traumatic Stress DOI 10.1002/jts. Published on behalf of the International Society for Traumatic Stress Studies.

672 Babson et al.
commonly utilized (e.g., Belleville et al., 2011; Ulmer et al.,2011), the present study indicated a 2-factor solution for sleepquality among veterans with PTSD, with only one factor (Per-ceived Sleep Quality) showing significant associations withPTSD after accounting for depression symptoms.
Results from the EFA converge with prior work suggestingthat sleep quality is best evaluated, among those with PTSD, as amultidimensional construct consisting of two factors (PerceivedSleep Quality and Efficiency/Duration). As the observed factorstructure is consistent with that observed in other samples ofindividuals with psychopathology (Cole et al., 2006; Jimenez-Genchi et al., 2008), given the high rates of co-occurring psy-chopathology in the current sample, it is possible that this factorstructure could generalize to other forms of psychopathology orgeneral psychological distress. In fact, given the strong relationbetween PTSD and depression (Elhai et al., 2011) it is not sur-prising that we replicated a prior factor structure. In combina-tion with previous research (Cole et al., 2006; Jimenez-Genchiet al., 2008) results suggest that sleep quality among individ-uals with PTSD is best conceptualized as a multidimensionalconstruct.
Upon determining the association between sleep quality andPTSD and depression, we found that the proposed 2-factorsolution may also disentangle complex comorbid conditionssuch as PTSD and depression. Indeed, findings indicated thatPerceived Sleep Quality was associated with both PTSD anddepression. In comparison, the Efficiency/Duration factor wasuniquely associated with depression, but not PTSD. Resultsprovide a test of specificity and suggest that factors of sleepmay differentially relate to psychological symptoms; that is,individuals with PTSD may experience a disruption in theirsubjective feeling of sleep quality, rather than their actual sleeppatterns, whereas individuals with depression may experiencestructural changes in sleep as well as subjective feelings of poorsleep quality. These patterns are supported by prior research,which has demonstrated that individuals with PTSD report poorsleep subjectively, but show less evidence for changes in sleeppatterns (Dagan, Zinger, & Lavie, 1997; Pillar, Malhotra, &Lavie, 2000), whereas individuals with depression have shownboth self-reported and objectively assessed structural changesin sleep (Armitage, Trivedu, Hoffmann, & Rush, 1997). Theseresults suggest that evaluating sleep quality as a multidimen-sional construct may help identify differences between highlycomorbid forms of psychopathology.
Although this study has many strengths, including the struc-tured clinical assessment of PTSD, it is not without limitations.First, this study was conducted among a sample of predomi-nately male military veterans receiving inpatient treatment forPTSD, which may limit generalizability. Additional work isneeded to replicate this factor structure, and relations to PTSDand depression, among veterans receiving outpatient treatment,as well as civilian trauma samples that include a larger per-centage of women with varying severities of PTSD. Similarly,the current sample was generally older (50 years and greater).This may have impacted the findings, given that sleep tends to
decline with age (Vitiello et al., 1997). Replication of these find-ings among additional cohorts is a necessary next step. Second,we did not have an assessment of underlying sleep disorders(e.g., sleep apnea, periodic limb movements) or current medi-cation use. Additional work is needed to investigate the impactthat medication use and underlying sleep disorders may haveon the observed factor structure. Similarly, the Perceived SleepQuality factor assesses a broad range of possible disturbancesincluding symptoms of sleep apnea, pain, middle insomnia, andnightmares. Therefore, specific conclusions regarding the na-ture of elevations on this factor cannot be made. Third, causalinferences related to the association between sleep quality andPTSD symptom severity and depression symptoms cannot beascertained from the current results due to the cross-sectionalnature of the present data. Future work would benefit from in-clusion of prospective longitudinal designs to determine if thesleep factors predict differential treatment response. Fourth,the internal consistency of the PSQI within the current studywas slightly lower than anticipated. Therefore, inclusion of amultimethod assessment strategy, including physiological in-dices, would provide a more comprehensive assessment of sleepand PTSD. Fifth, the Efficiency/Duration factor was comprisedof two indicators. Although this is consistent with previous re-search (see Table 1), the small number of indicators comprisingthis factor may have impacted the results. Finally, the currentstudy did not include the PSQI-addendum for PTSD (Germain,Hall, Krakow, Shear, & Buysse, 2005), a 7-item addendum forthe PSQI that assesses disruptive nocturnal behavior specificto PTSD (e.g., hot flashes, nervousness, trauma nightmares).Although the purpose of the current study was to assess over-all sleep quality among individuals with PTSD, future researchwould benefit from inclusion of the PSQI-addendum as thiswould provide an opportunity to investigate if inclusion of theseitems impacts the factor structure of sleep quality among indi-viduals with PTSD.
Despite the early stages of this research, these initial findingshave many clinical implications. First, these results suggest po-tential benefit of modifying the 1-factor global scoring of thePSQI to a 2-factor solution among individuals with PTSD. Thismodification is important for two primary reasons. First, with-out such modification, it is possible that clinicians using a 1-factor scoring system may miss the most salient sleep problemsthat may only be present on one of the factors. For example,individuals with PTSD may not report impaired sleep dura-tion or sleep efficiency. This may artificially lower the globalscore, while their subjective quality of sleep and sleep distur-bances may be inflated; the multidimensional approach allowsfor differentiation of these symptoms. Second, use of a 2-factorsolution may help inform debates regarding the comorbidityof PTSD and depression, whether these are unitary or uniquedisorders, and if PTSD and general distress can be disentangled(Elhai et al., 2011). For example, among veterans with PTSD,factors of sleep quality differentially relate to PTSD and depres-sion. Therefore, individuals with elevations on both PerceivedSleep Quality and Efficiency/Duration may be suggestive of
Journal of Traumatic Stress DOI 10.1002/jts. Published on behalf of the International Society for Traumatic Stress Studies.

Sleep Quality and PTSD 673
co-occurring depression and PTSD, whereas elevations solelyon Perceived Sleep Quality may be more indicative of PTSDwithout depression. Gaining this knowledge through a sleepassessment is beneficial as individuals may be more likely torespond in an open manner to sleep questions because of lessstigma associated with these questions as compared to questionstargeting psychopathology, and response patterns observed onthese factors could inform additional targeted specialized as-sessment (i.e., depression) and inform treatment. Specifically,interventions that target underlying distress (i.e., PTSD symp-toms and depression symptoms) are important in treating sleepproblems. For example, providers may prioritize behavioral in-terventions aimed at reducing PTSD and depression within thecontext of sleep treatment, instead of prescribing sleep medica-tions which are costly, have little evidence for their long-termeffectiveness, and have potential adverse side effects includ-ing worsening of depression and addiction potential (Kupfer &Reynolds, 1997).
ReferencesAloba, O., Adewuya, A., Ola, B., & Mapayi, B. (2007). Validity of the Pitts-
burgh Sleep Quality Index (PSQI) among Nigerian university students. SleepMedicine, 8, 266–270. doi:10.1016/j.sleep.2006.08.003
American Psychiatric Association. (1994). Diagnostic and statistical manualof mental disorders (4th ed.). Washington, DC: Author.
Armitage, R., Trivedi, M., Hoffmann, R., & Rush, A. (1997). Rela-tionship between objective and subjective sleep measures in depressedpatients and healthy controls. Depression and Anxiety, 5, 97–102.doi:10.1002/(SICI)1520–6394(1997)5:2<97::AID-DA6>3.0.CO;2-2
Beaudreau, S., Spira, A., Stewart, A., Kezirian, E., Lui, L. . . . Stone, K.(2012). Validation of the Pittsburgh Sleep Quality Index and the EpworthSleepiness Scale in older black and white women. Sleep Medicine, 13, 36–42. doi:10.1016/j.sleep.2011.04.005
Beck, A., Steer, R., & Brown, G. (1996). Manual for the Beck DepressionInventory-II. San Antonio, TX: Psychological Corporation.
Beck, A., Steer, R., Brown, G., & van der Does, A. (2002). BDI-II-NL. Lisse,the Netherlands: Psychological Corporation.
Belleville, G., Guay, S., & Marchand, A. (2011). Persistence of sleepdisturbances following cognitive-behavior therapy for posttraumaticstress disorder. Journal of Psychosomatic Research, 70, 318–327.doi:10.1016/j.jpsychores.2010.09.022
Bentler, P. (1990). Comparative fit indexes in structural models. PsychologicalBulletin, 107, 238–246. doi:10.1037/0033-2909.107.2.238
Bentler, P. (1995). EQS structural equations program manual. Encino, CA:Multivariate Software.
Blake, D., Weathers, F., Nagy, L., Kaloupek, D., Gusman, F., Charney, D., &Keane, T. (1995). The development of a clinician-administered PTSD scale.Journal of Traumatic Stress, 8, 75–90. doi:10.1002/jts.2490080106
Browne, M., & Cudeck, R. (1993). Alternative ways of assessing model fit.In K. Bollen & J. Long (Eds.), Testing structural equation models (pp.136–162). Newbury Park, CA: Sage.
Buysse, D., Reynolds, C., Monk, T., & Berman, S. (1989). The PittsburghSleep Quality Index: A new instrument for psychiatric practice and research.Psychiatry Research, 28, 193–213. doi:10.1016/0165-1781(89)90047-4
Capaldi, V., Guerrero, M., & Killgore, W. (2011). Sleep disturbances amongreturning combat veterans from Iraq and Afghanistan. Military Medicine,176, 879–888.
Carpenter, J., & Andrykowski, M. (1998). Psychometric evaluation of thePittsburgh Sleep Quality Index. Journal of Psychosomatic Research, 45,5–13. doi:10.1016/S0022-3999(97)00298-5
Clum, G., Nishith, P., & Resick, P. (2001). Trauma-related sleep disturbanceand self-reported physical health symptoms in treatment-seeking femalerape victims. Journal of Nervous and Mental Disorders, 189, 618–622.doi:10.1097/00005053-200109000-00008
Cole, J., Motivala, S., Buysse, D., Oxman, M., Levin, M., & Irwin, M. (2006).Validation of a 3-factor scoring model for the Pittsburgh Sleep Quality Indexin older adults. Sleep, 29, 112–116.
Comrey, A., & Lee, H. (1992). A first course in factor analysis (2nd ed.).Hillsdale, NJ: Erlbaum.
Dagan, Y., Zinger, Y., & Lavie, P. (1997). Actigraphic sleep monitoring inposttraumatic stress disorder (PTSD) patients. Journal of PsychosomaticResearch, 42, 577–581. doi:10.1016/S0022-3999(97)00013-5
Elhai, J., Carvalho, L., Miguel, F., Palmieri, P., Primi, R., & Frueh, B. (2011).Testing whether posttraumatic stress disorder and major depressive disorderare similar or unique constructs. Journal of Anxiety Disorders, 25, 404–410.doi:10.1016/j.janxdis.2010.11.003
Farrahi, M., Nakhaee, N., Sheibani, V., Garrusi, B., & Amirkafi, A. (2012).Reliability and validity of the Persian version of the Pittsburgh Sleep Qual-ity Index (PSQI-P). Sleep Breath, 16, 79–82. doi:10.1007/s11325-010-0478-5
Germain, A., Hall, M., Krakow, B., Shear, K., & Buysse, D. (2005). A briefsleep scale for posttraumatic stress disorder: Pittsburgh Sleep Quality In-dex Addendum for PTSD. Journal of Anxiety Disorders, 19, 233–244.doi:10.1016/j.janxdis.2004.02.001
Geuze, E., & Vermetten, E. (2004). Disordered sleep in posttraumatic stressdisorder: Clinical presentation, research, findings, and implications for treat-ment. In A. Golbin, H. Kravitz, & L. G. Keith (Eds.), Sleep psychiatry (pp.247–269). New York: Taylor & Francis.
Hu, L., & Bentler, P. (1999). Cutoff criteria for fit indexes in covariance struc-ture analysis: Conventional versus new alternatives. Structural EquationModeling, 6, 1–55. doi:10.1080/10705519909540118
Jimenez-Genchi, A., Monteverde-Maldonado, E., Nenclares-Portocarrero, A.,Esquivel-Adame, G., & de la Vega-Pacheco, A. (2008). Reliability andfactorial analysis of the Spanish version of the Pittsburgh Sleep QualityIndex among psychiatric patients. Gaceta Medica de Mexico, 144, 491–496.
King, D., Leskin, G., King, L., & Weathers, F. (1998). Confirmatory factoranalysis of the Clinician-Administered PTSD Scale: Evidence for the di-mensionality of posttraumatic stress disorders. Psychological Assessment,10, 90–96. doi:10.1037/1040-3590.10.2.90
Koren, D., Arnon, I., Lavie, P., & Klein, E. (2002). Sleep complaints as earlypredictors of posttraumatic stress disorder: A 1-year prospective study of in-jured survivors of motor vehicle accidents. American Journal of Psychiatry,159, 855–857. doi:10.1176/appi.ajp.159.5.855
Kotronoulas, G., Papadopoulou, C., Papapetrou, A., & Patiraki, E. (2011). Psy-chometric evaluation and feasibility of the Greek Pittsburgh Sleep QualityIndex (GR-PSQI) in patients with cancer receiving chemotherapy. SupportCare Cancer, 19, 1831–1840. doi:10.1007/s00520-010-1025-4
Krakow, B., Germain, A., Tandberg, D., Koss, M., Schrader, R., Hollifield,M., & Edmond, T. (2000). Sleep breathing and sleep movement disordersmasquerading as insomnia in sexual assault survivors. Comprehensive Psy-chiatry, 41, 49–56. doi:10.1016/S0010-440X(00)90131-7
Journal of Traumatic Stress DOI 10.1002/jts. Published on behalf of the International Society for Traumatic Stress Studies.

674 Babson et al.
Kupfer, D., & Reynolds, C. (1997). Management of insomnia. TheNew England Journal of Medicine, 336, 341–346. doi:10.1056/NEJM199701303360506
Lewis, V., Craemer, M., & Failla, S. (2009). Is poor sleep in veterans a functionof post-traumatic stress disorder? Military Medicine, 174, 948–951.
Mansfield, A., Williams, J., Hourani, L., & Babeu, L. (2010). Measurementinvariance in posttraumatic stress disorder symptoms among US militarypersonnel. Journal of Traumatic Stress, 23, 91–99. doi:10.1002/jts.20492
Mellman, T., David, D., Kulick-Bell, R., Hebding, J., & Nolan, B. (1995).Sleep disturbance and its relationship to psychiatric morbidity after hurricaneAndrew. American Journal of Psychiatry, 152, 1659–1663. Retrieved from:ajp.psychiatryonline.org/data/Journals/AJP/3652/1659.pdf
Muthen, B., & Muthen, L. (1998–2008). Mplus 5.2. Los Angeles, CA: Author.
Neylan, T., Marmar, C., Metzler, M., Weiss, D., Zatzick, D., Delucchi, K.,& Schoenfeld, F. (1998). Sleep disturbances in the Vietnam generation:Findings from a nationally representative simple of male Vietnam Vet-erans. American Journal of Psychiatry, 155, 929–933. Retrieved from:http://ajp.psychiatryonline.org/data/Journals/AJP/3690/929.pdf
Nishith, P., Resick, P., & Mueser, K. (2001). Sleep difficulties and alcohol usemotives in female rape victims with posttraumatic stress disorder. Journalof Traumatic Stress, 14, 469–479. doi:10.1023/A:1011152405048
Ohayon, M., & Shapiro, C. (2000). Sleep disturbances and psychiatric disor-ders associated with posttraumatic stress disorder in the general population.Comprehensive Psychiatry, 41, 469–478. doi:10.1053/comp.2000.16568
Peterson, A., Goodie, J., Satterfield, W., & Brim, W. (2008). Sleep disturbanceduring military deployment. Military Medicine, 173, 230–235.
Picchioni, D., Cabrera, O., McGurk, D., Thomas, J., Castro, C., Balkin, T.,& Hoge, C. (2010). Sleep symptoms as a partial mediator between combatstressors and other mental health symptoms in Iraq war veterans. MilitaryPsychology, 22, 340–355.
Pillar, G., Malhotra, A., & Lavie, P. (2000). Post-traumatic stress disor-der and sleep—what a nightmare! Sleep Medicine Reviews, 4, 183–200.doi:10.1053/smrv.1999.0095
Saladin, M., Brady, K., Dansky, B., & Kirkpatrick, D. (1995). Understand-ing comorbidity between PTSD and substance use disorders: Two prelim-inary investigations. Addictive Behaviors, 20, 643–655. doi:10.1016/0306-4603(95)00024-7
Skouteris, H., Wertheim, E. H., Germano, C., Paxton, S., & Milgrom, J. (2009).Assessing sleep during pregnancy. A study across two time points exam-ining the Pittsburgh Sleep Quality Index and associations with depressivesymptoms. Women’s Health Issues, 19, 45–51. doi:10.1016/j.whi.2008.10.004
Tucker, L., & Lewis, C. (1973). A reliability coefficient for maximum likeli-hood factor analysis. Psychometrika, 38, 1–10. doi:10.1007/BF02291170
Ulmer, C., Edinger, J., & Calhoun, P. (2011). A multi-component cognitive-behavioral intervention for sleep disturbances in veterans with PTSD:A pilot study. Journal of Clinical Sleep Medicine, 7, 57–68. Retrievedfrom: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3041620/pdf/jcsm.7.1.57.pdf
Vitiello, M., Moe, K., Larsen, L., & Prinz, P. (1997). Age-related sleepchange: Relationships of objective and subjective measures of sleep inhealthy older men and women. Sleep Research, 26, 220.
Weathers, F., Keane, T., & Davidson, J. (2001). Clinician-Administered PTSDScale: A review of the first ten years of research. Depression and Anxiety,13, 132–156. doi:10.1002/da.1029
Weathers, F., Ruscio, A., & Keane, T. (1999). Psychometric properties ofnine scoring rules for the Clinician-Administered Posttraumatic Stress Dis-order Scale. Psychological Assessment, 11, 124–133. doi:10.1037/1040-3590.11.2.124
Woodward, S., Friedman, M., & Bliwise, D. (1996). Sleep and depressionin combat-related PTSD inpatients. Biological Psychiatry, 39, 182–192.doi:10.1016/0006-3223(95)00104-2
Wright, K., Britt, T., Bliese, P., Adler, A., Picchioni, D., & Moore, D. (2011).Insomnia as predictor versus outcome of PTSD and depression amongIraq combat veterans. Journal of Clinical Psychology, 67, 1240–1258.doi:10.1002/jclp.20845
Journal of Traumatic Stress DOI 10.1002/jts. Published on behalf of the International Society for Traumatic Stress Studies.
Copyright © 2022 FDOKUMEN




















