Skye, Lochalsh and South West Ross Independent External ...
305
Skye, Lochalsh and South West Ross Independent External View |Out of Hours Urgent Care Briefing Pack Panel Session, 17 th April 2018 Jans Conference and Training Centre , 5-6 Broom Place Portree, Isle of Skye IV51 9HL
-
Upload
khangminh22 -
Category
Documents
-
view
2 -
download
0
Transcript of Skye, Lochalsh and South West Ross Independent External ...
Skye, Lochalsh and South West Ross Independent External View |Out of Hours Urgent Care
Briefing Pack
Panel Session, 17th April 2018
Jans Conference and Training Centre, 5-6 Broom Place
Portree, Isle of Skye IV51 9HL

Skye, Lochalsh and South West Ross Independent External View |Out of Hours Urgent Care
Briefing Pack
2 | P a g e
Skye, Lochalsh and South West Ross Independent External View |Out of Hours Urgent Care
Briefing Pack
3 | P a g e
NHS Highland ‘problem statement’
We welcome the panel’s insight and assistance in helping us move forward with our communities on a number of difficult questions, particularly:
• How do we provide unscheduled care to meet the need, and make best use of resources, locally and across Highland?
• How do we keep people safe and feel safe?
• How do we build a more innovative and ambitious working environment for staff?
• How do we make best use of all local assets to create greater resilience?
• What is the role of communities and community leaders in co-creating and delivering solutions?
Skye, Lochalsh and South West Ross Independent External View |Out of Hours Urgent Care
Briefing Pack
4 | P a g e
This pack accompanies the presentation to be given by the NHS Highland team on 17 April and comprises:
1. Programme and Participants for 17 April 2018
2. Terms of Reference
3. NHS Highland Organisational Structure and Governance
4. Slides to be presented on 17 April 2018
5. Position statements on:
Access and Definitions eHealth, Technology, Research & Development Glenelg & Arnisdale Feedback from NHS Highland to OOH Peer Review Team, February 2016 Housing Island Provision Major Service Change and Public Consultation Maternity Services Portree Hospital | Current and Future Services Portree Hospital | Summary Timeline | Unscheduled Care Raasay Rural Support Team Workforce
6. Data summary | Unscheduled Care in Skye, Lochalsh and South West Ross
7. NHS Highland Public Health Statistical Appendix
8. Advanced Nurses and Paramedics | Competency Framework and Training Toolkit
9. Communications

Skye, Lochalsh and South West Ross Independent External View |Out of Hours Urgent Care
Briefing Pack
1 | P a g e
Panel Members | 17 April 2018
Charlie Siderfin is the Lead GP for NHS Orkney and has lived and worked there,
with his family, for the last 17 years. As part of the role, he works as a 24/7 single-handed GP on the outer island of Westray for 3 out of 9 weeks and 6 weeks in Kirkwall. In 2009 he was involved in redesigning the delivery of services to the outer islands of Orkney, working with individual island communities to develop and refine systems of care. He has worked closely with the island communities to recruit and retain staff to the islands. Prior to taking up his current role, he worked for 14 years in the Balfour Hospital providing A&E and acute medical inpatient care, in combination with General Practice work in the community. He has a particular interest in the development of systems to support the recruitment and retention of practitioners to challenging remote and rural practice.
Linda Harper has worked in the community for many years, firstly as a district
nurse, midwife and health visitor. Linda then became a practice nurse progressing to an Advanced Nurse Practitioner. In 2000 Linda took up the post of Associate Nurse Director for Practice Nursing and the lead for Non-Medical Prescribing in NHS Grampian whilst maintaining a clinical role. In 2004 Linda was asked to develop a team of practitioners to work in the Out of Hours service, she started with 5 nurse and paramedic practitioners. Linda now has a team of 23 substantive staff and 14 bank staff working OOH across NHS Grampian alongside the GP's. Linda is now lead nurse for the Moray Health & Social Care Partnership. Linda has enjoyed secondments with the Scottish Government and the Royal College of Nursing!
David Pedley is a consultant in Emergency Medicine and Clinical Director of
emergency care in Dumfries and Galloway. Training as a registrar in Tayside and Grampian, David spent a year working as a rural fellow helping to establish one of the UK’s first telemedicine networks. He represents Emergency medicine to the Royal College of Physicians of Edinburgh and, until recently was a member of the Scottish board of the Royal College of Emergency Medicine representing the rural district general hospitals.
Garry Fraser joined the ambulance service in 1997 as an ambulance care assistant
moving to Technician and becoming a Paramedic in 2001 which he has maintained. Garry worked as an air ambulance Paramedic out of Glasgow serving remote and rural communities around Scotland. He became an Area Service Manager for Clyde, Head of Service for Argyll and Clyde and onto General Manager for South West Scotland. Garry is now undertaking the role of Regional Director for the the West of Scotland and is an executive team member.
Margaret Anderson is from Ayr and has been volunteering with NHS Ayrshire
& Arran since 2003 and NHS24's Public Participation Forum since 2008. Margaret has been
Skye, Lochalsh and South West Ross Independent External View |Out of Hours Urgent Care
Briefing Pack
2 | P a g e
involved in some key projects as a public representative during this time, including the creation of NHS Inform and the 111 number change. Margaret recently completed a three year term of office as Vice-chair of the NHS24 PPF, having served as Chair for the preceding three years. She was the Public Representative on the Public Holiday Review published in December 2017. Margaret joined the Board of NHS Ayrshire & Arran as a Non-Executive Director and she also serves on her local Integrated Joint Board in that capacity. Margaret takes a very keen interest in how services are delivered ensuring that ‘person-centeredness’ is at the heart of all discussions.
Kate Bell is Head of Service Change & Transformation at NHS Lanarkshire. Kate has
worked in the public sector for over 30 years in local authorities and the national health service. Her background is in child care social work carrying out case work, child protection and groupwork with adolescents. Kate is currently a senior manager in NHS Lanarkshire and continues to enjoy the challenges, complexity and the diverse portfolio of work. Kate’s work engages all stakeholders in complex service, change management, systems and process improvement and involve working with a range of people at different levels and across a mix of organisations.
Laura Ryan has been a doctor for 20 years. She has worked in Scotland since 2001.
She is the Medical Director for NHS 24 and works in the Out of Hours Service in NHS Borders. She was the Clinical Lead for OOH in NHS Borders for 7 years and is well versed in the challenges of covering a large area of diverse geography. She chaired the National OOH Operational Group for three years and was part of Professor Sir Lewis Ritchie’s reviews of Urgent care OOH and covering OOH during the Public Holiday period. Recognizing the need for joint working to best serve our communities, as part of her OOH work in Borders she developed a professional to professional line for SAS staff (supporting a safe alternative to admission in 85% of cases) and also developed the OOH Nursing staff to allow them to carry out home visiting.
Angus McKellar completed his GP training in Stornoway, then worked in Nepal
for eight years, involved in service development and clinical leadership. He became a GP partner in North Harris in 2002, delivering GP training, chaired the AMC and served on the Area Clinical Forum, taking up the post of NHS Western Isles Medical Director in 2014. He does occasional GP sessions, retains an interest in overseas work, and serves on a number of Regional and National committees.
Lewis Ritchie is presently James Mackenzie Professor of General Practice,
University of Aberdeen and Honorary Professor of Primary Care and Public Health, University of the Highlands and Islands, Honorary Professor of General Practice, University of Edinburgh and Honorary Consultant in Public Health, NHS Grampian. Sir Lewis recently retired as a Principal General Practitioner, Peterhead Health Centre and Community Hospital. He has also held posts as Director of Public Health, NHS Grampian and Consultant in Public Health Medicine, Grampian Health Board.
Skye, Lochalsh and South West Ross Independent External View |Out of Hours Urgent Care
Briefing Pack
3 | P a g e
Fergus Millan joined the civil service in 1997 following a career as a scientist. He
has held a number of posts across education, local government and health. He recently moved from Public Health Division in the SG where he had responsibility for policy on a wide range of subjects including national screening programmes, obesity and health inequalities. In his current role he leads one of three teams in the Primary Care Division with responsibility for the sponsorship of the Scottish Ambulance Service and NHS 24. In addition he is responsible for policy on Out of Hours and optometry.
Sian Tucker is a GP, she has been Clinical Director of Lothian Unscheduled care
service for the last 5 years. Other roles include National Clinical Lead Urgent Care program for NHS Health Improvement Scotland. Sian is co-chair of the National Operations Group for OOH and RCGP Scotland's executive officer for OOHs and interface. She works clinically one session a week in OOHs.

Skye, Lochalsh and South West Ross Independent External View |Out of Hours Urgent Care
17th April 2018
1 | P a g e
Programme
Time Activity09.00 Panel Members Assemble
09:30 - 10:30 NHS Highland Overview and Scene Setting (60 minutes)Professor Elaine Mead, Chief Executive Maimie Thompson, Head of Public Relations and Engagement Dr Paul Davidson, Associate Medical Director (Primary Care) Tracy Ligema, Deputy Director of Operations (North & West) David Park, Chief Officer
In attendance Ross Mackenzie, Area Manager (West) Dr Hugo van Woerden, Director of Public Heath Dr Rod Harvey TBC
10:40 - 11:25 SOSNHS Skye Representatives (45 minutes)Catriona MacDonald (Chair) Martin Waller (Secretary) Isobel MacDonald Mairi MacDonald Malcolm Henry
11.35 - 12:20 Glenelg & Arnisdale Representatives (45 minutes)Jenny Munro John Maclean Peter Jones
12:20 -13:00 Lunch
13:00 - 14.00 NHS clinical Staff (60 minutesDr Will Nel Clinical Lead for Skye, Lochalsh and South West Ross Kathy Shaw, Lead Unscheduled Care Practitioner, Rural Support Team Ross Mackenzie (Area Manager) Representatives from Portree Medical Practice
14:10 - 14.55 Raasay Representatives (45 minutes)Anne Gilles Norman Gillies Ann MacLeod Tekela Koek
15:05 -15:50 Community Council representatives (45 minutes)Anne Gilles, Raasay Bill Edgar, Portree and Braes
Skye, Lochalsh and South West Ross Independent External View |Out of Hours Urgent Care
17th April 2018
2 | P a g e
Finella MacKinnon, Struan Isobel Newall & Mairi MacDonald (Staffin) Margaret MacPhee, Glendale Rob Ware, Sleat + 2 TBC
16:00 -16:50 Emergency Services (50 minutes)Inspector Lynda Allan, Skye and Lochalsh, Police Scotland Graham MacLeod, Head of Service, Highland, Scottish Ambulance Service Mike Collier, Scottish Fire and Rescue Service Dave Phillips, HM Coastguard – TBC RNLI - TBC
17:00 - 17:30 NHS Highland | Immediate Issues and Feed-back
19:30 Panel Debrief and Next Steps
Terms of Reference
External view of arrangements for Unscheduled Care
(urgent primary care out-of-hours provision)
in Skye, Lochalsh and South West Ross
Background
Primary Care out of hours and urgent care is of key importance to the board of NHS
Highland. It has been continuously evolving following the GMS contract in 2004.
Most recently, NHS Highland Board agreed an approach and direction of travel for out of
hours and urgent care services in 2015.
This was considered to be in line with the multi-disciplinary approach and recommendations
set out in Sir Lewis Ritchie’s report Pulling Together -Transforming Urgent Care for the People of
Scotland.
A more detailed paper was presented and agreed at the NHS Board meeting in September
2016Work to implement the recommendations continues.
Specifically, in Skye, Lochalsh and South West Ross, work on building a sustainable model
has most recently been ongoing since 2014. Significant effort has gone into developing
Advanced Practitioners to be part of a multi-disciplinary service (including Rural
Practitioners and GPs) to address these challenges. Nevertheless, some significant concerns
remain from members of the public, NHS Save Our Services (SOS) and elected members, particularly
in North Skye. In particular these concerns relate to aspects of delivery, and access to,
emergency care, urgent primary care out of hours care, minor injuries and illness.
Taking these concerns into account, the Chair of NHS Highland has invited a team, led by Sir
Lewis Ritchie to provide an external professional view of the urgent care services in the
area.
Remit
The specific remit is to assess the resilience of urgent primary care out-of-hours provision.
Out of scope
The remit will not cover the redesign of wider health and social care services currently
underway, with Ministerial approval, which will progress to an Outline Business Case for a
Hub and Spoke model incorporating a new-build facility in Broadford as part of a wider
redesign.
Objective
To ensure that the present and planned delivery of urgent primary care out-of-hours
provision is in line with the recommendations set out in Sir Lewis Ritchie’s report Pulling
Together -Transforming Urgent Care for the People of Scotland.
Governance
Sir Lewis Ritchie, assisted by a small team of independent colleagues, including
representation from NHS 24 and the Scottish Ambulance Service, will report to the Chair
of NHS Highland, David Alston, and the Chair of the Highland Health and Social Care
Partnership, Melanie Newdick.
Administration
David Park, Chief Officer for Highland Health and Social Care Partnership, will ensure
appropriate support is in place to:
o make any arrangements for visits and meetings
o facilitate any data required and make available to the team in a timely manner
o ensure stakeholders are aware of the work and how they can get in touch
o arrange venues and any catering required
Work Plan
A work plan will be created for the external view including meetings with:
representatives of the local community including action group, SOS-NHS
local clinical staff who provide the service, service managers and any other staff as
deemed necessary.
with local GPs and other clinicians in the area,
As part of the work plan, meetings will be arranged with service users and providers including
political representatives.
The external view team will be asked to provide peer opinion on the safety, sustainability
and organisation of the service and be invited to make recommendations if necessary for
further action or developments.
Deliverables
A report of the external view will be produced by Sir Lewis Ritchie for NHS Highland by
the end of April 2018.
16 January 2018
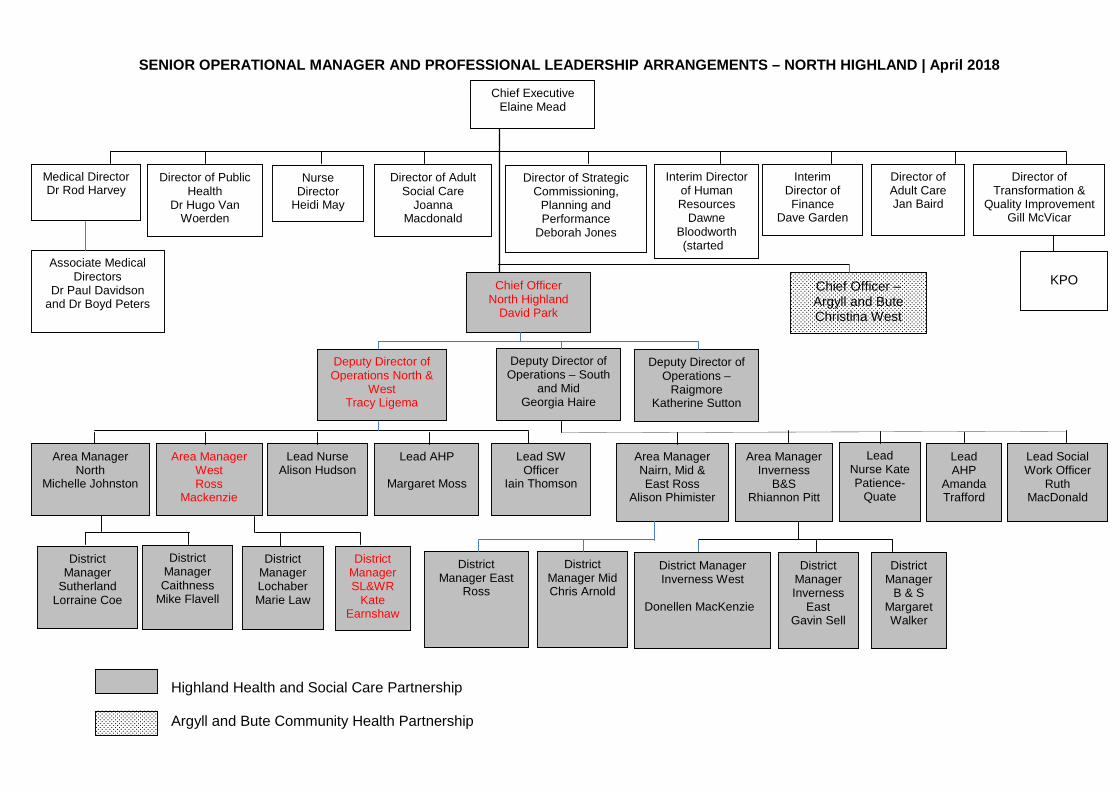
SENIOR OPERATIONAL MANAGER AND PROFESSIONAL LEADERSHIP ARRANGEMENTS – NORTH HIGHLAND | April 2018
Highland Health and Social Care Partnership
Argyll and Bute Community Health Partnership
District Manager Mid Chris Arnold
Associate Medical Directors
Dr Paul Davidson and Dr Boyd Peters
Chief Executive Elaine Mead
Medical Director Dr Rod Harvey
Director of Public Health
Dr Hugo Van Woerden
Nurse Director
Heidi May
Director of Strategic Commissioning,
Planning and Performance
Deborah Jones
Interim Director of Human Resources
Dawne Bloodworth (started 3/1/18)
Interim Director of Finance
Dave Garden
Director of Adult Care Jan Baird
Director of Adult Social Care
Joanna Macdonald
Director of Transformation &
Quality Improvement Gill McVicar
Deputy Director of Operations – South
and Mid Georgia Haire
Area Manager North
Michelle Johnston
Area Manager West Ross
Mackenzie
Lead Nurse Alison Hudson
Lead AHP
Margaret Moss
Lead SW Officer
Iain Thomson
Area Manager Nairn, Mid & East Ross
Alison Phimister
Area Manager Inverness
B&S Rhiannon Pitt
Lead Nurse Kate Patience-
Quate
Lead AHP
Amanda Trafford
Lead Social Work Officer
Ruth MacDonald
Chief Officer North Highland
David Park
District Manager
Sutherland Lorraine Coe
District Manager Lochaber Marie Law
District Manager SL&WR
Kate Earnshaw
District Manager Inverness
East Gavin Sell
District Manager
B & S Margaret Walker
District Manager East
Ross
District Manager Inverness West
Donellen MacKenzie
District Manager Caithness
Mike Flavell
KPO Chief Officer – Argyll and Bute Christina West
Deputy Director of Operations North &
West Tracy Ligema
Deputy Director of Operations –
Raigmore Katherine Sutton

EXTRACT FROM OUTLINE BUSINESS CASE FOR MAJOR SERVICE REDESIGN
PROJECTS | SKYE, LOCHALSH AND SOUTH WEST ROSS
8 MANAGEMENT CASE
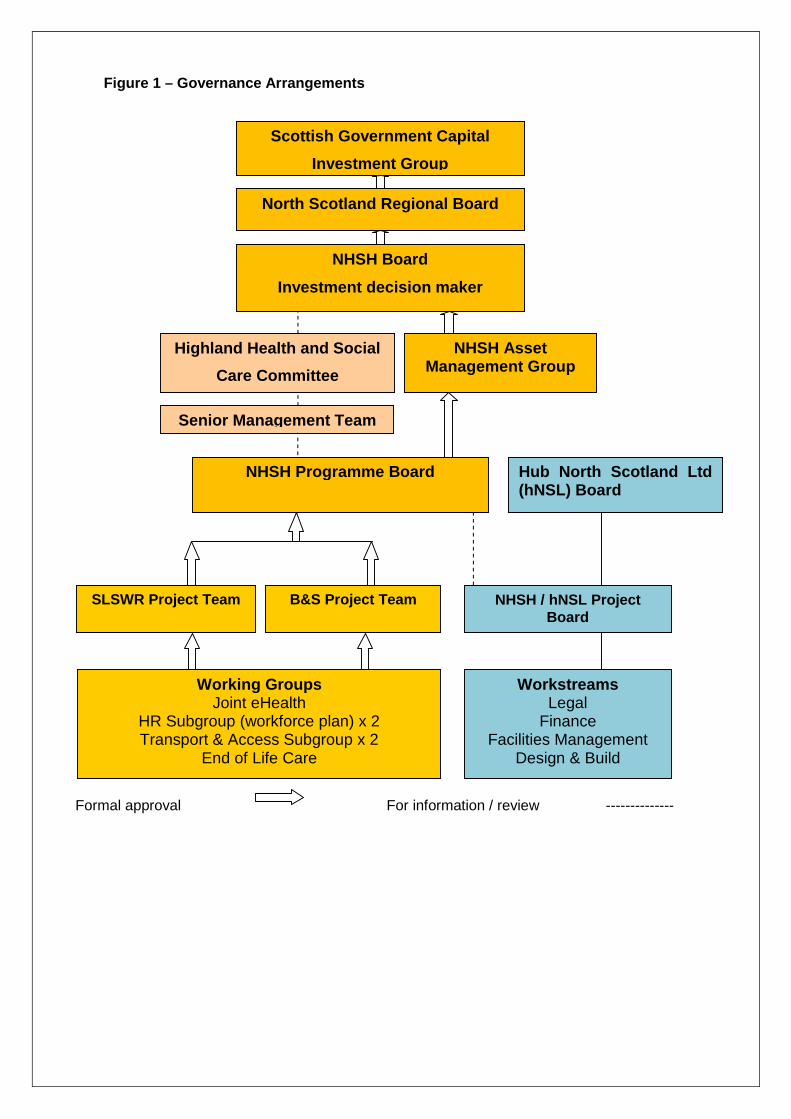
The Management Case sets out the governance arrangements in place to deliver this programme of major service change and associated infrastructure. It evidences the appropriate leadership, senior management, project management and internal governance structures.
8.1 Project Management Proposals
8.1.1 Reporting Structure and Governance Arrangements
At Initial Agreement the two service redesign projects were managed by separate Project Boards, but chaired by the same Senior Responsible Officer (SRO), as the need to bundle the projects as a single procurement under the Scottish Futures Trust (SFT) hub initiative was anticipated.
In January 2017 in advance of the submission of the New Project Request (NPR) to hubCo a single Joint Programme Board was formed.
The governance arrangements for the Programme bundle are set out (Figure 1).
Further information on the role, remit and membership of the Programme Board and Project Teams is provided (Appendix 7). This remains largely unchanged from the two Initial Agreements with the exception of some of the membership.
Most notably the membership of the Programme Board now reflects that this is a joint board for the two service redesigns, and the Project Team membership has expanded slightly in view of more detailed work associated with Outline Business Case (OBC).
The project work streams and arrangements for the management of the hubCo contract are included (Appendix 8). There is a joint NHS Highland / hub North Scotland Project Board responsible for delivery of the two community hospital new builds. NHS Highland membership of this Project Board includes the Senior Estates Lead, Lead Project Manager, Project Managers, Commercial Lead and a Senior Project Lead from each of the service redesign Project Teams. This ensures that the delivery of the new build community hospitals is embedded in to the overall service redesign programme.
The designation of Senior Responsible Officer, Project Directors, Senior Estates Lead and Lead Project Manager is identified (Figure 2).
Scottish Government Capital
Investment Group
North Scotland Regional Board
NHSH Board
Investment decision maker
Highland Health and Social
Care Committee
NHSH Asset Management Group
Senior Management Team
NHSH Programme Board
B&S Project Team SLSWR Project Team
Working GroupsJoint eHealth
HR Subgroup (workforce plan) x 2 Transport & Access Subgroup x 2
End of Life Care
NHSH / hNSL Project Board
WorkstreamsLegal
Finance Facilities Management
Design & Build
Hub North Scotland Ltd (hNSL) Board
Figure 1 – Governance Arrangements
Formal approval For information / review --------------

21/06/2018
1
welcomes
Sir Lewis Ritchie & Expert PanelTo Skye, Lochalsh and South West Ross
Tuesday 17th April 2018
Overview
• NHS Highland Context & Sustainability: Elaine Mead, Chief Executive
• Local Context : Maimie Thompson, Head of Public Relations and Engagement
• Local Engagement: Tracy Ligema, Deputy Director of Operations
• Out of Hours Primary Care overview: Paul Davidson, Associate Medical Director
• Summing Up: David Park, Chief Officer
21/06/2018
2
Demographic impact on the sustainability of servicesin remote and rural areas
Elaine Mead
Chief Executive
Aims
To maintain high standards of patient and client care (Highland Quality Approach)
To continue to sustain, develop and
deliver integrated services across the
Highland and Argyll & Bute areas
whilst
living within our financial allocation, without compromise to access or quality
21/06/2018
3
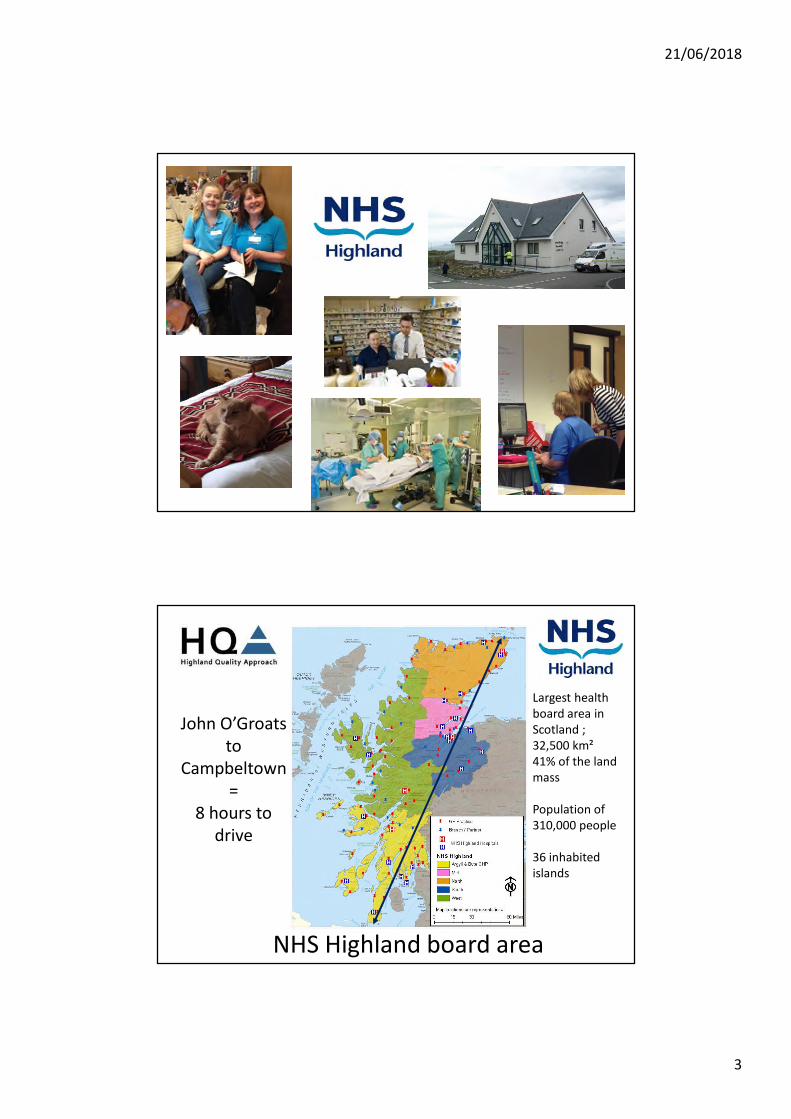
NHS Highland board area
Largest health board area in Scotland ;32,500 km² 41% of the land mass
Population of 310,000 people
36 inhabited islands
John O’Groats to
Campbeltown=
8 hours to drive
21/06/2018
4
Remote and Rural
Visit Scotland logoPoor weather slide
Inverness, Scotland’s newest city
Population 72,000,
fastest growing city in Western Europe
21/06/2018
5
Challenging times
• Demographics
• Workforce sustainability
• Maintaining skills
• Rising costs
– Targets and standards
– New drugs and therapies
– Adult Social Care
– Locums
• Expectations
• Geography
• History
Sustainability
(workforce)
Safety
Quality & Performance
Finance
(Affordability)
Balance

21/06/2018
6
Rising Costs
2012/13 2013-14 2014-15 2015-16 2016-17
Total 77354 79160 83227 90905 93585
75000
77000
79000
81000
83000
85000
87000
89000
91000
93000
95000£
000
'sNHS Highland Drugs Spend
£77m
£94m
Money Matters?
2017/18
Reporting £15m deficit on £810m integrated budget
£34m on locum and supplementary staffing
30 consultant posts and 21 GP posts vacant.
Responsibility to break even
21/06/2018
7
NHS Highland also has a social, economic and environmental responsibility
The image part with relationship ID rId4 was not found in the file.
2283 – SLSWR Community Hospital
External View Across Bay
21/06/2018
8
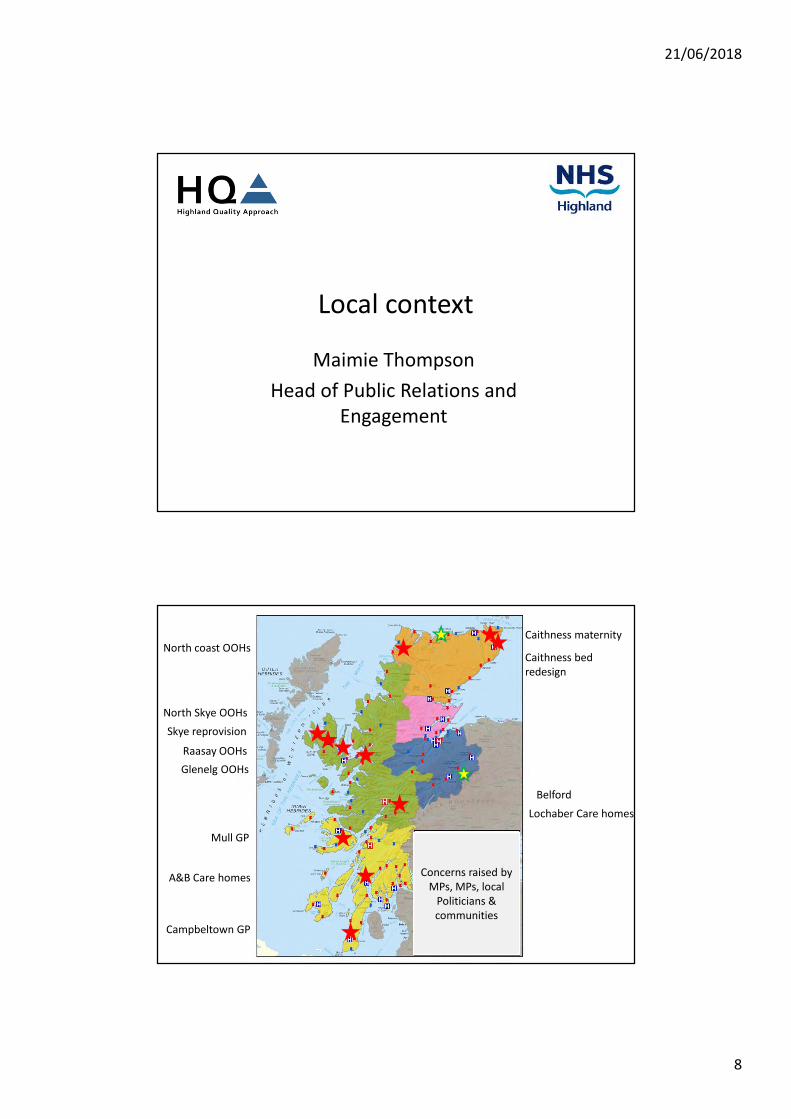
Local context
Maimie Thompson
Head of Public Relations and Engagement
Mull GP
Caithness maternity
Caithness bed redesign
North coast OOHs
Skye reprovision
Raasay OOHs
A&B Care homes
Campbeltown GP
Glenelg OOHs
North Skye OOHs
Concerns raised byMPs, MPs, local
Politicians & communities
Lochaber Care homes
Belford

21/06/2018
9
Concerns
• Changes to Out of Hours (Highland) – Historic and more recent
• Workforce and HR challenges
• Lack of trust in local managers and NHS Highland leadership
Political Change
Move from strong political support
to strong opposition
21/06/2018
10
Backdrop
Area the size of Belgium!
Largest geographic Health Board in Scotland ;32,500 km² from Kintyre in the south-west to Caithness in the north-east
Population of 310,000 people
John O’Groats to
Campbletown
History more important than geography
21/06/2018
11
History
1950s
Local engagement
Tracy Ligema
Deputy Director of Operations
21/06/2018
12
Improvement and Co-Production
Health
Social
Care
3rd
Sector
Issues inGlenelg and Raasay
• These communities request a return to models where there is a professional in the community 24/7.
21/06/2018
13
Glenelg & Arnisdale
• Population 260
• Previously covered by local GP + locums
• Identified as single-handed low volume location that could be safely covered from Broadford
• Change August 2017
• All cases 36 reviewed by two doctors – seen as safe and appropriate. We included patients who self-presented OOHs at Broadford (as most have always done)
• Emergency planning exercise held with community and multi-agency partners, December 2017.
Raasay
• Population 200• Inability to sustain 24/7 nurse cover for planned
and unscheduled care provision.• Continued provision of planned community
nursing.• Discussion with community regarding provision of
support OOHs.• Agreed rural health care support worker
recruitment with emergency responder skills supported by SAS training and third party agreement.

21/06/2018
14
Out of Hours Urgent Care
Dr Paul Davidson
Associate Medical Director
Primary Care
OOHs RedesignHighland |2014 -2018
• In line with principles outlined in ‘Pulling Together'
• Particular issue for Highland: high number of sites/doctor hours and high costs.
• Based on traditional models – reliant on lots of doctors on call. Difficult to sustain or afford (recognised in ‘Pulling Together’)
• Recommended reduction in 5 sites, and increase in training and development of ANPs.
• No increase to size of patches/populations covered compared to what already happens elsewhere in Highland.
21/06/2018
15
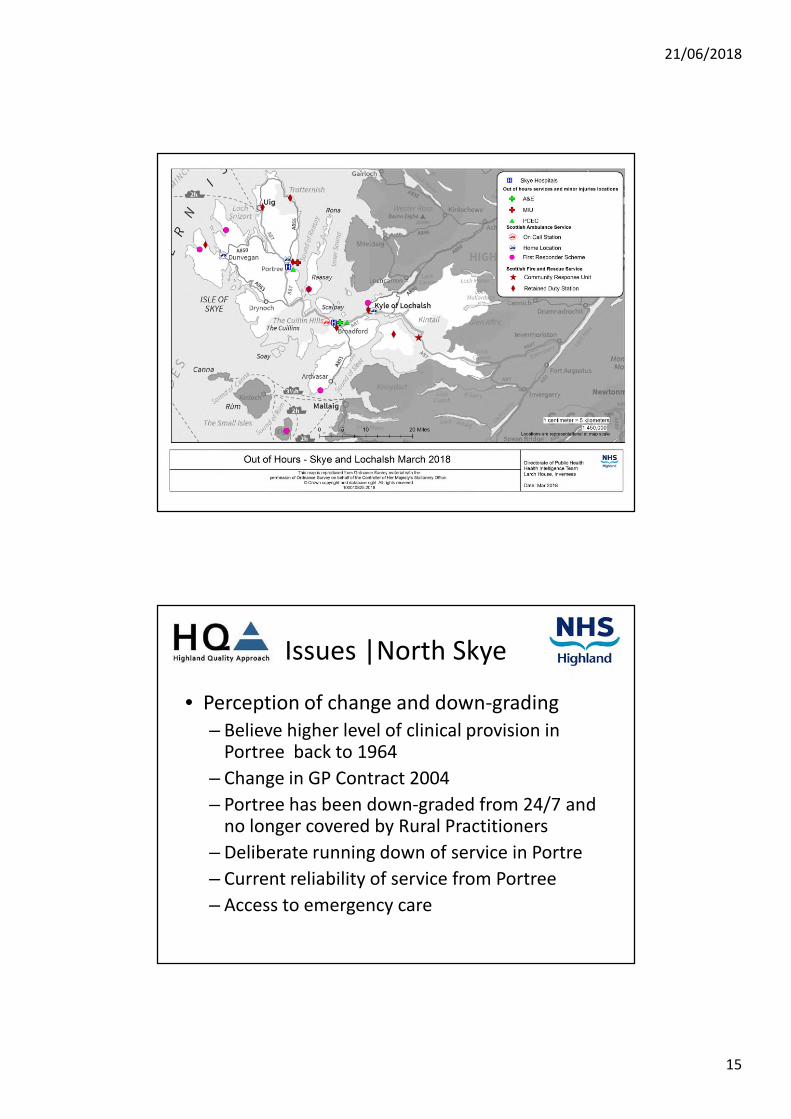
Issues |North Skye
• Perception of change and down-grading– Believe higher level of clinical provision in
Portree back to 1964
– Change in GP Contract 2004
– Portree has been down-graded from 24/7 and no longer covered by Rural Practitioners
– Deliberate running down of service in Portre
– Current reliability of service from Portree
– Access to emergency care
21/06/2018
16
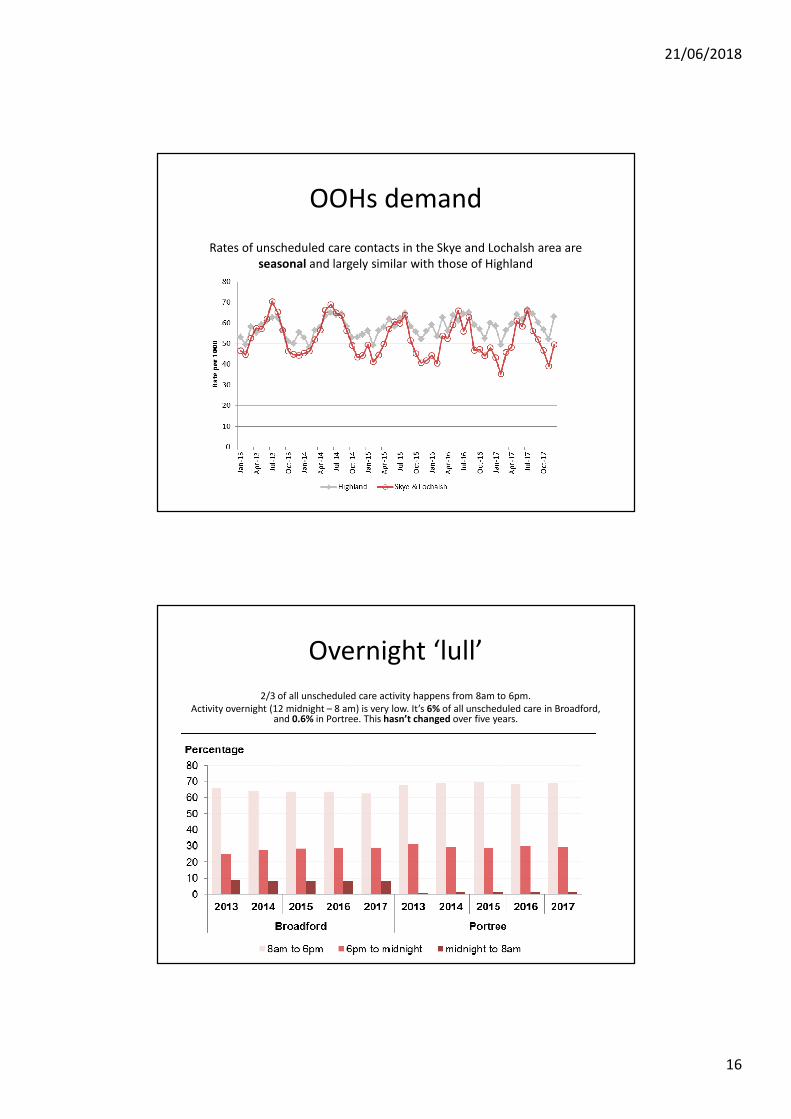
OOHs demand
Rates of unscheduled care contacts in the Skye and Lochalsh area are seasonal and largely similar with those of Highland
Overnight ‘lull’
2/3 of all unscheduled care activity happens from 8am to 6pm.Activity overnight (12 midnight – 8 am) is very low. It’s 6% of all unscheduled care in Broadford,
and 0.6% in Portree. This hasn’t changed over five years.
21/06/2018
17
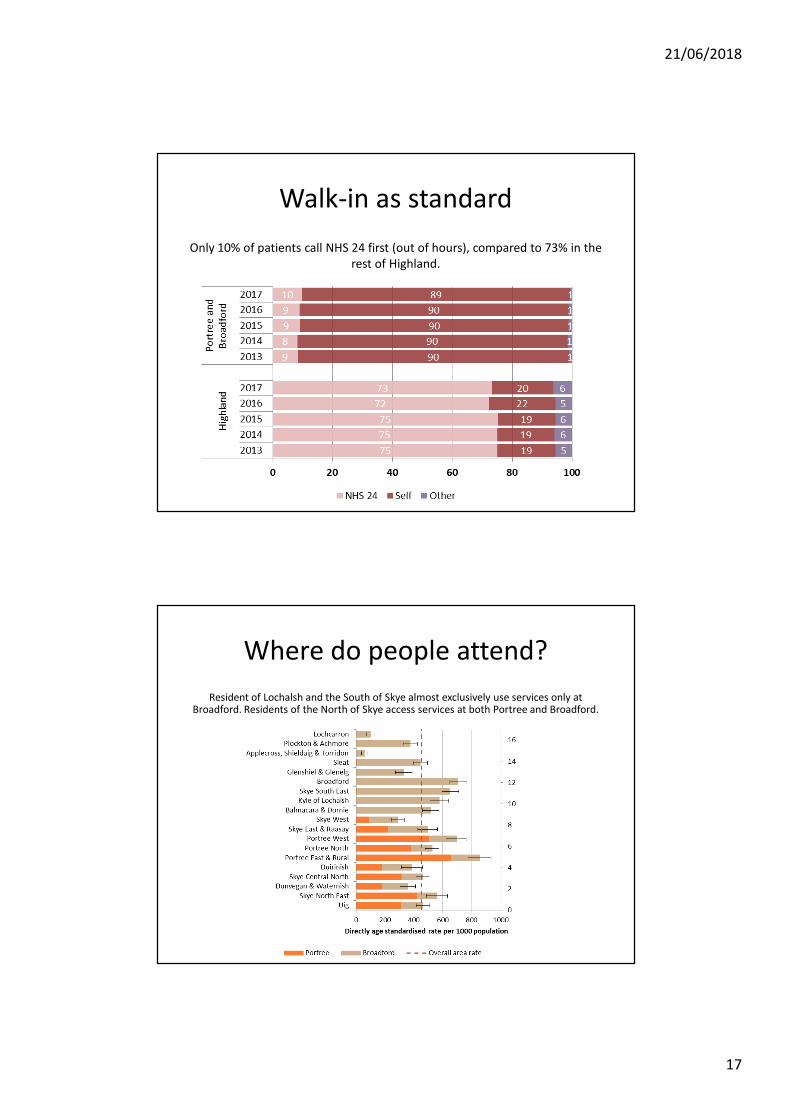
Walk-in as standard
Only 10% of patients call NHS 24 first (out of hours), compared to 73% in the rest of Highland.
Where do people attend?
Resident of Lochalsh and the South of Skye almost exclusively use services only at Broadford. Residents of the North of Skye access services at both Portree and Broadford.

21/06/2018
18
Who attends most?
If you live closer to Portree or Broadford, you are more likely to use unscheduled care.
Challenges
• Retention to Rural Support Team
– On call – sustainability issue Portree– Skills retention with low volume of patients– Addressing lone working in Portree for future– Addressing on call working – work-life balance and having
fulfilling roles
• Capacity of Rural Practitioner Team• Currently difficult atmosphere to work in• Affordable accommodation
21/06/2018
19
Summing up
David Park
Chief Officer
Convenience
Feeling SafeSafe
Balance
21/06/2018
20
Questions
• How do we provide unscheduled care to meet the need, and make best use of resources, locally and across Highland?
• How do we keep people safe and feel safe?
• How do we build a more innovative and ambitious working environment for staff?
• How do we make best use of all local assets to create greater resilience ?
• What is the role of communities in co-creating and delivering solutions?
Sustainability is key
21/06/2018
21
Thank you!
Skye, Lochalsh and South West Ross Independent External View |Out of Hours Urgent Care
Position Statement | Rural Support Team| 12 April 2018
1 | P a g e
Position Statement | Access and Terminology
Background It is very clear that terminology (i.e. how services are described) and how these should be accessed is a source of contention and possibly confusion. Not unreasonably the public confidence in the services provided will hinge on whether the manner they are described and the reality of the service provision are closely matched.
The available data demonstrates that, while the Service in Portree closes at 11pm, people do turn up without prior contact with NHS 24 and will invariably be seen. Therefore unsurprisingly, the public feel they already have 24/7 access.
Notably, most patients in Skye and Lochalsh do not use NHS24 to access unscheduled care. During the Out of Hours period, 10% of contacts were via NHS 24, compared to 73% in the rest of Highland (2017 data).
Sign-Posting and Definitions Further adding to public confusion was that until April 2016 the service at Portree was sign-posted as A&E, although the service was not an A&E by most definitions. It is now described as a “Minor Injury Unit” during the day and “Primary Care Emergency Centre” during the out of hour’s period.
While NHS Highland sought to address consistency in terminology across their community hospital sites by standardising signage to Minor Injury Unit, the situation is not helped by virtue of the fact that standard definitions for commonly used terms (e.g. Casualty, Accident and Emergency, Emergency Department, Minor Injuries Unit, Primary Care Emergency Centre, Urgent Care Centre) either do not exist or are not applied consistently.
Information Statistical Division (ISD) provide the following definitions:
Emergency Departments (ED): larger A&E services that typically provide a 24-hour consultant led service; MIU/Other: sites including minor injuries units (MIU), small hospitals and health centres in rural areas that carry out Emergency Department related activity and are GP or nurse led. They may or may not be open 24 hours.
Under ISD definitions both Portree and Broadford are classified as Minor Injury Unit. The clinical capability of staff at Dr MacKinnon Hospital in Broadford is above that of the majority of community hospitals and functions as intermediate facility somewhere between a community hospital and a District General Hospital.
Though outside the scope of this specific piece of work there are implications for data recording and reporting of performance around emergency four hour target which is something that NHS Highland is working on.
Communications NHS Highland has made various attempts to clarify terminology and how to access services. In 2015 NHS Highland and Scottish Ambulance in 2015 issued information to all homes and businesses across the
Skye, Lochalsh and South West Ross Independent External View |Out of Hours Urgent Care
Position Statement | Rural Support Team| 12 April 2018
2 | P a g e
redesign area setting out a description of services and how these should be accessed. This was prepared by local clinical staff and was in line with national guidelines ‘Know Where to Turn To’.
In July 2017 the Portree Medical Practice also issued a statement to the Local Newspaper The West Highland Free Press in a bid to provide reassurances to the public. The article stated that: “arrangements for accessing medical emergencies, urgent care and minor injuries are not changing” and went onto explain the arrangements (Appendix 3b).
In October 2017 NHS Highland included the Practice statement in a Newsletter issued to all homes in the area. Unfortunately it was not long after these statements were issued, that due to staffing difficulties, service provision from Portree started to be unreliable further undermining trust and confidence.
Know Who to Turn To
http://www.nhshighland.scot.nhs.uk/Publications/Documents/Leaflets/SLSWR%20know%20who%20to%20turn%20to.pdf
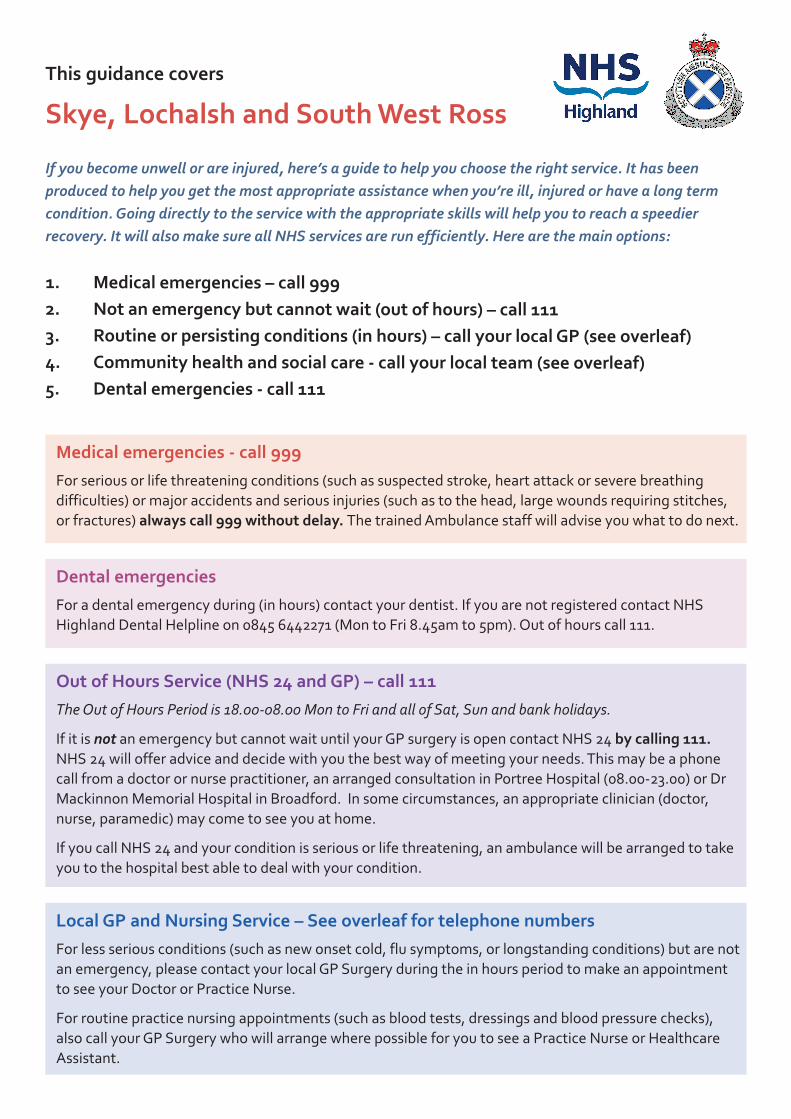
This guidance covers
Skye, Lochalsh and South West Ross
If you become unwell or are injured, here’s a guide to help you choose the right service. It has beenproduced to help you get the most appropriate assistance when you’re ill, injured or have a long termcondition. Going directly to the service with the appropriate skills will help you to reach a speedierrecovery. It will also make sure all NHS services are run efficiently. Here are the main options:
Medical emergencies - call 999For serious or life threatening conditions (such as suspected stroke, heart attack or severe breathingdifficulties) or major accidents and serious injuries (such as to the head, large wounds requiring stitches,or fractures) always call 999 without delay. The trained Ambulance staff will advise you what to do next.
Out of Hours Service (NHS 24 and GP) – call 111The Out of Hours Period is 18.00-08.00 Mon to Fri and all of Sat, Sun and bank holidays.
If it is not an emergency but cannot wait until your GP surgery is open contact NHS 24 by calling 111.NHS 24 will offer advice and decide with you the best way of meeting your needs. This may be a phonecall from a doctor or nurse practitioner, an arranged consultation in Portree Hospital (08.00-23.00) or DrMackinnon Memorial Hospital in Broadford. In some circumstances, an appropriate clinician (doctor,nurse, paramedic) may come to see you at home.
If you call NHS 24 and your condition is serious or life threatening, an ambulance will be arranged to takeyou to the hospital best able to deal with your condition.
1. Medical emergencies – call 9992. Not an emergency but cannot wait (out of hours) – call 1113. Routine or persisting conditions (in hours) – call your local GP (see overleaf)4. Community health and social care - call your local team (see overleaf)5. Dental emergencies - call 111
Local GP and Nursing Service – See overleaf for telephone numbersFor less serious conditions (such as new onset cold, flu symptoms, or longstanding conditions) but are notan emergency, please contact your local GP Surgery during the in hours period to make an appointmentto see your Doctor or Practice Nurse.
For routine practice nursing appointments (such as blood tests, dressings and blood pressure checks),also call your GP Surgery who will arrange where possible for you to see a Practice Nurse or HealthcareAssistant.
Dental emergenciesFor a dental emergency during (in hours) contact your dentist. If you are not registered contact NHSHighland Dental Helpline on 0845 6442271 (Mon to Fri 8.45am to 5pm). Out of hours call 111.

NHS Inform For up to date information on health, call NHS Inform 0800 22 44 88 or visit www.nhsinform.co.uk
Dr MacKinnon Memorial Hospital (MMH), Broadford A&E (24/7)This is the main emergency care unit for the area, open 24hrs per day. The doctors in the hospital – RuralPractitioners - have enhanced skills with additional training in anaesthetics, trauma and emergencies.Across all specialities these hospital doctors are trained (and the hospital is equipped) to providestabilisation, assessment, initial management and treatment or transfer as required.
The hospital team also provides the overview for the majority of the out of hours care for the area. Theywill ensure all patients are dealt with safely and promptly.
Portree Community Hospital, minor injury unit (8am – 11pm)There is a minor injury unit which runs from 8am until 11pm, seven days per week. If your injury cannotbe dealt with by your GP Practice during the in-hours period, you may be seen and assessed by anAdvanced Nurse Practitioner, Paramedic Practitioner or a Doctor and treated or transferred as required.Access to non emergency services in Portree after 11pm is via NHS 24. As appropriate NHS24 will contactthe doctors based in Mackinnon Memorial Hospital in Broadford who provide a key coordination role toensure all patients are dealt with safely and promptly. They will deploy the most appropriate responsebased on the clinical need.
Looking after yourselfKeep a well-stocked medicine cabinet to deal with minor injuries or illness such as cuts, grazes, sorethroat, coughs, colds, indigestion and constipation. You can get advice on minor ailments and what tostock in your medicines cabinet from any Pharmacy or via NHS Inform - see below.
Community health and social care
North Skye – 01478 613113South Skye and Lochalsh – 01471 820174West Ross – 01854 613911
Other
Community Mental Health – 01478 613772or via Portree Hospital 01478 613200Midwifery – 01471 822190Emergency – 999Dental Emergency – 111Dental Helpline - 0845 6442271NHS24 – 111NHS Inform – 0800 22 44 88
Local GP Surgeries:Telephone lines are open 8am to 6pm, Mon-Fri(times might vary slightly)
Applecross - 01520 744252Broadford Health Centre - 01471 822460Carbost Medical Centre Practice - 01478 640202Dunvegan Medical Practice - 01470 521203Glenelg Health Centre - 01599 522272Kyle of Lochalsh Surgery - 01599 534257Lochcarron - 01520 722215Portree Medical Centre - 01478 612013Sleat Medical Practice - 01471 844283Torridon - 01445 791223
Community health and social care servicesA range of community services including nursing, midwifery, social work, physiotherapy, occupationaltherapy, community mental health and care at home are also available. These can be accessed throughany health care professional or by self referral to the teams - see below.
Skye, Lochalsh and South West Ross Independent External View |Out of Hours Urgent Care
Position Statement | Rural Support Team| 12 April 2018
1 | P a g e
Letter from Portree Medical Practice to local newspaper
IONAD SLAINTE THRONDAIRNIS PORTREE MEDICAL CENTREPORT-RIGH, AN T-EILEAN SGITHEANACH PORTREE
ISLE OF SKYE, IV51 9BZ
Dr Stephen D McCabe Dr Shirley Potts Telephone: 01478 612013 Dr Sarah Clancy Facsimile: 01478 612340 Dr Hannah M MacLeod Dr Ishbel K MacDougall Practice Ref No: 55573 Dr Richard A Moss www.portreemedical.scot.nhs.ukDr Helen McArdle Dr Louise E Lankston
Mr Ian McCormack Editor, West Highland Free Press Unit 1B, Pairc nan Craobh Broadford Isle of Skye, IV49 9AP 19th July 2017
Dear Mr McCormack
As Doctors at Portree Medical Centre, we are becoming increasingly concerned about the perception local residents and visitors may have regarding the clinical care available in the north end. There have been a number of incidents over the last few weeks where individuals delayed seeking medical attention because they didn’t think that Portree had an evening or weekend out of hours service.
In an emergency, whatever the day or time, never delay in dialling 999 for an ambulance. The ambulance crew may provide initial emergency care in your home, in the ambulance or get you straight to a care centre. They can also get immediate support remotely if it is required. The crew will decide where the most appropriate centre to take you to is, as they know the services available at every location.
Portree Medical Centre’s clinical staff provides minor injury services at Portree Hospital from 8am – 6pm Monday to Friday (excluding public holidays).
Unscheduled Care Practitioners, based at Portree Hospital provide clinical care between 6pm and 11pm on Weeknights and 8am and 11pm at weekends. If you think you might need medical treatment out of hours, and it’s not an emergency, dial NHS24 on 111. Depending on your clinical need, NHS 24 can arrange; a non-emergency ambulance or for you to attend the most appropriate centre, which may be Portree. They can give self-care advice until the practice re-opens. It depends on your clinical need. Please be assured that if you attend Portree Hospital out of hours service without contacting NHS 24 you will be seen, however contacting NHS24 before attending ensures that you are directed to the most appropriate centre.
Skye, Lochalsh and South West Ross Independent External View |Out of Hours Urgent Care
Position Statement | Rural Support Team| 12 April 2018
2 | P a g e
It is important that the residents of North Skye know that the Doctors at Portree Medical Centre have full confidence in the Unscheduled Care Practitioners to manage anyone attending Portree Hospital. They provide an excellent service, backed up by the Rural Practitioners at Broadford Hospital.
Overnight medical care is provided by Broadford Hospital between 11pm and 8am. During this time there is a qualified clinical person on call in the north of the Island who can be called upon if the need arises.
General medical advice is available 24 hours a day, 7 days a week from NHS Inform either by phoning 0800 22 44 88 or going to www.nhsinform.scot.
As independent contractors in the NHS, we are independent advocates for our patients. Our primary concern is the safe, appropriate clinical care for all patients. It is essential that all patients and visitors are aware of the services available and that they will continue to be available.
Yours sincerely,
The Partners of Portree Medical Centre
Skye, Lochalsh and South West Ross Independent External View |Out of Hours Urgent Care
Position Statement | eHealth, Technology, R&D | 12 April 2018
1 | P a g e
Background
The current models to deliver health and social care across our complex and changing environment in Highland are not sustainable. Meeting the needs of the population has become increasingly difficult and now requires changes to parts of the service to ensure sustainable and affordable models are in place for future generations. These challenges were most recently set out in the boards Quality and Sustainability Vision and Plan which builds on the Health and Social Care Delivery Plan for Scotland published in December 2016.
e-Health
The eHealth Delivery Plan covers six items
• The Regional Clinical Portal
• Mobile Electronic Patient Records for Community Staff
• Support for TEC
• Implementation of the ‘view;’ products (Wardview, Admissionview, Paediatricview, Pharmacyview)
• Paper to Digital
• Clinical Dialogue
All of these will have an impact on the way we delivery services across NHS Highland including Skye. In addition there are other elements such as NHS Near Me which is being led by Technology Enabled Care; ECHO by the Highland Hospice and Capsule Endoscopy via R&D. All are supported by eHealth.
Hub and Spokes
The most established Hub and Spoke models relate to Renal, Paediatrics and Obstetrics and Gynaecology. They are set-up to provide a mix of visiting service but also support via VC from consultants in Raigmore.
The local redesign for Skye, Lochalsh and South West Ross is also moving to a local ‘Hub’ and ‘Spoke’ between Broadford and Portree. Links between these two centres are already well established with Rural Practitioners s providing clinical advice to the Rural Support Team over the telephone. The plan is also to develop Portree as the Hub for North Skye.
NHS Near Me
Work is underway to strengthen arrangements to reduce the need for travel to avoid outpatient appointments or hospital admissions. NHS Near Me captures a number of strands:
Using technology to support clinical decision making through enhanced communications between clinicians across secondary and primary care.
Skye, Lochalsh and South West Ross Independent External View |Out of Hours Urgent Care
Position Statement | eHealth, Technology, R&D | 12 April 2018
2 | P a g e
Attend Anywhere is using technology to carry out outpatient consultations remotely. It is the same approach as using VC but the quality of images is superior and the way patients are ‘called’ to a virtual waiting room is more organised and standardised. Moreover it also lends itself to consultations taking place in patients own home or more local facility (eg GP Practice). This is being rolled out during 2018.
3 minute animated film: youtu.be/SVxE1-iALdw
Project ECHO (Extension for Community Healthcare Outcomes), which is being led by the Highland Hospice is a way to meet local healthcare needs, when for whatever reason, access to specialist care is remote,
The heart of the ECHO model is its hub-and-spoke knowledge-sharing networks, led by expert teams who use multi-point videoconferencing to conduct virtual clinics with community providers. In this way, primary care doctors, nurses, and other clinicians learn to provide excellent specialty care to patients in their own communities.
Project ECHO Highland Hospice Scotland has adopted the ECHO model and is currently running two pilot networks; Nurse Specialists in Palliative Care and Palliative Care for Care Homes, throughout the Highlands and Islands. A new network is being developed involving practitioners to support management of urgent care.
There is potential for this approach to be rolled out in Skye subject to the findings of the Pilot.
Capsule endoscopy or pillcam is being tested to provide easy access to diagnostic endoscopy. Using some novel technology, instead of having to travel to hospital for invasive procedures a pill, which includes a tiny camera, can now be taken. As well as being less invasive the pillcam can be taken at home and the results discussed at the local GP surgery, or indeed in the persons own home.
This test is for diagnostic scopes only. Anyone requiring biopsies and treatment scopes would still have to travel to Belford or Raigmore Hospital, as currently happens
Connectivity
One of the biggest challenges around the provision of Urgent Care in remote and rural areas concerns the low level of connectivity outside the Urgent Care Centre. This includes the difficulty of accessing Adastra remotely (including access to ECS/KIS/SciStore), but also relates to the basics of phone/text connectivity. This means call dispatch/alert to ‘emergencies’ back at base can be unreliable.
Work is ongoing to provide a laptop solution that can connect to the NHS network from external connections, and to provide enhanced connectivity in remote and rural areas.
Skye, Lochalsh and South West Ross Independent External View |Out of Hours Urgent Care
Position Statement | Glenelg & Arnisdale | 12 April 2018
1 | P a g e
Glenelg and Arnisdale
Context
Glenelg and Arnisdale has a population of around 260 with road access via a hill pass over from the Glen Shiel road (the Mam Ratagan pass). The community is focussed in Glenelg, but with some residents in outlying areas (e.g. Arnisdale). When describing the delivery of services it is important to the community that it is referred to as Glenelg and Arnisdale.
Daytime Medical Care is provided by Glenelg Medical Practice (salaried). Until recently (September 2017) this practice was open five days per week. This has been reduced to four day opening, with one day cover provided by an Advanced Nurse Practitioner (ANP) based in Glenelg. On Tuesdays urgent cover is provided by South Skye in Broadford. Access to primary care is good, with only 30% utilisation of available appointments.
NHS Highland has particular challenges around staffing. Last year we spent £15m on locums and £19m on supplementary staffing. Currently we have 30 consultant posts vacant and 21 GPs based on current models of care.
Out of Hours Urgent Care | Background
Prior to August 2017 NHS Highland provided a doctor 24/7 in Glenelg. From August 2017, and in line with proposals submitted to the NHS Highland Board (September 2016), NHS Highland moved out of hours primary care cover to Broadford (35 miles).
Strategically, this was driven by: a) a move towards a smaller number of better-resourced OOH bases (Highland has a disproportionate number of doctors on overnight compared to the rest of Scotland), b) a move away from single-handed on-call practitioners; c) a move away from excessive locum usage in favour of stable local teams and d) a move away from a doctor-only model of OOH to a multi-disciplinary one.
This change affected urgent care (presentations that need seen by a GP but can’t wait until morning), not emergency care (serious and life threatening). Emergency care remains the responsibility of Scottish Ambulance Service. However, it is clear that the community see their GP as part of the emergency response because this has been the case in the past, with the GP often being called out by SAS as first person on scene. Development of a local emergency response (i.e. a community responder scheme) and development of a local evacuation plan have been encouraged but not yet achieved.
Out of Hours Activity and drive time analyses
In Glenelg and Arnisdale the new arrangements mean that roughly 20 calls per year will be dealt with differently (all advice calls will remain the same). Patients now either need to travel to Broadford, or will receive a home visit from staff based in Broadford (Table 1).
Skye, Lochalsh and South West Ross Independent External View |Out of Hours Urgent Care
Position Statement | Glenelg & Arnisdale | 12 April 2018
2 | P a g e
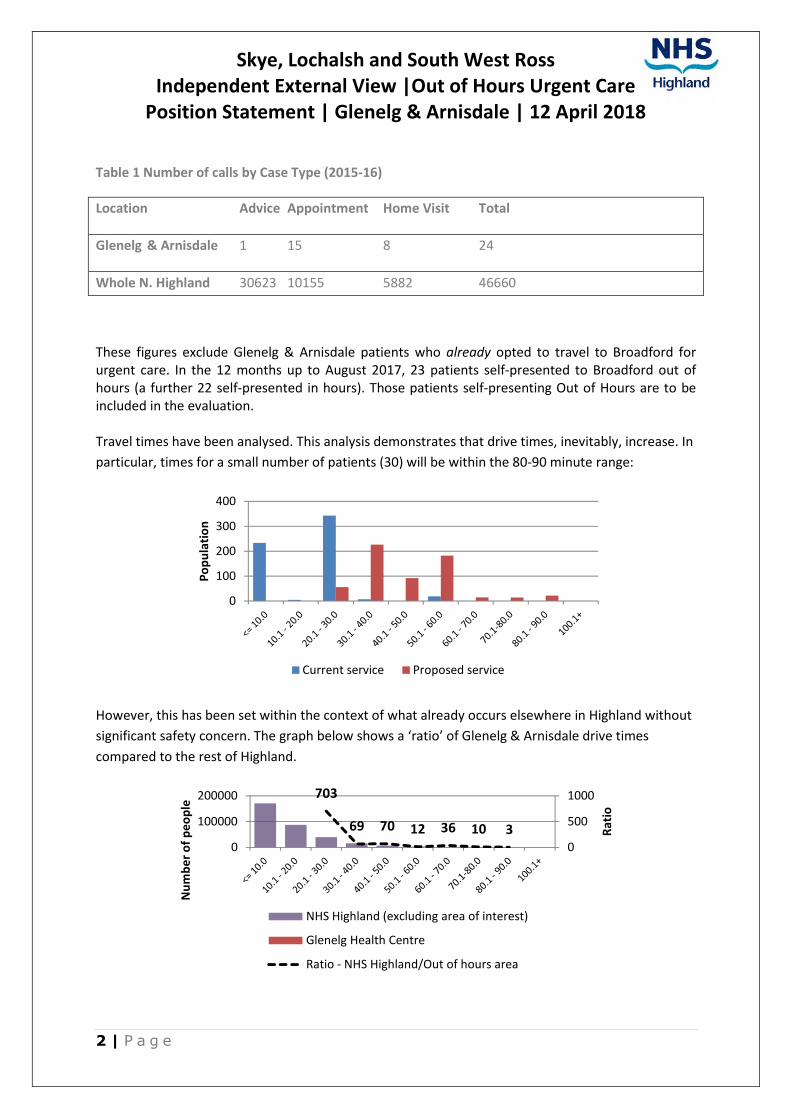
Table 1 Number of calls by Case Type (2015-16)
Location Advice Appointment Home Visit Total
Glenelg & Arnisdale 1 15 8 24
Whole N. Highland 30623 10155 5882 46660
These figures exclude Glenelg & Arnisdale patients who already opted to travel to Broadford for urgent care. In the 12 months up to August 2017, 23 patients self-presented to Broadford out of hours (a further 22 self-presented in hours). Those patients self-presenting Out of Hours are to be included in the evaluation.
Travel times have been analysed. This analysis demonstrates that drive times, inevitably, increase. In
particular, times for a small number of patients (30) will be within the 80-90 minute range:
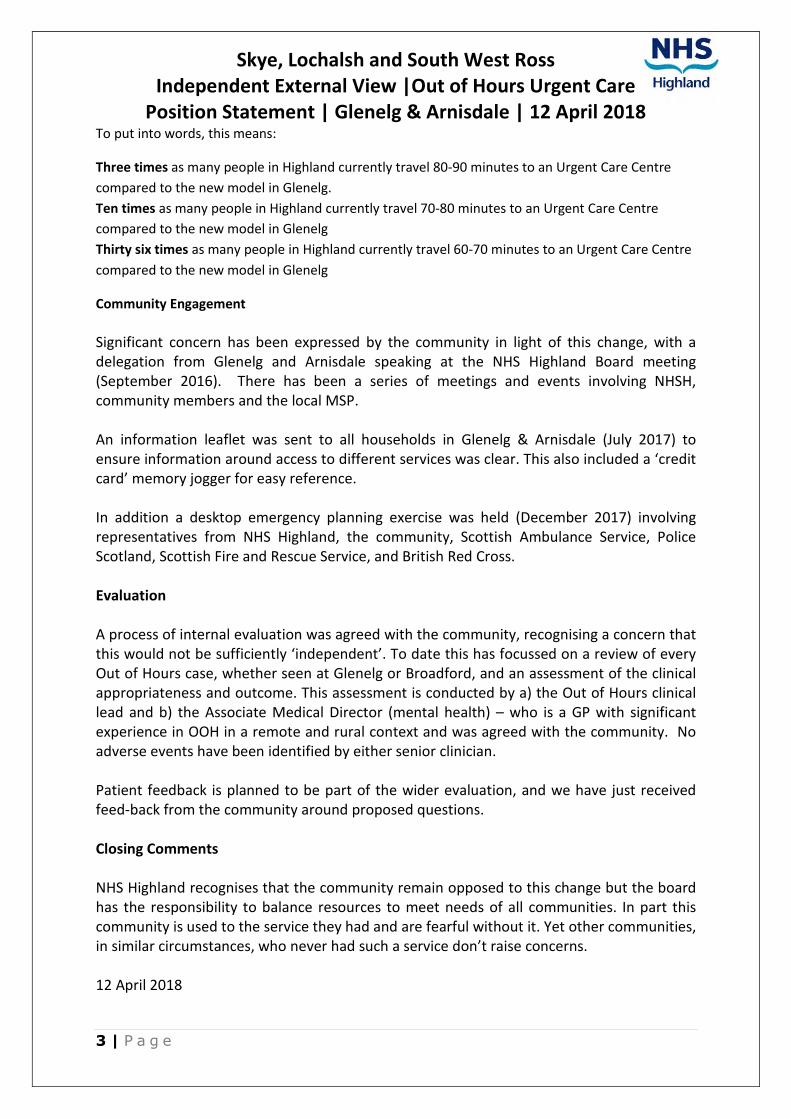
However, this has been set within the context of what already occurs elsewhere in Highland without
significant safety concern. The graph below shows a ‘ratio’ of Glenelg & Arnisdale drive times
compared to the rest of Highland.
0
100
200
300
400
Po
pu
lati
on
Current service Proposed service
703
69 70 12 36 10 30
500
1000
0
100000
200000
Rat
io
Nu
mb
er
of
pe
op
le
NHS Highland (excluding area of interest)
Glenelg Health Centre
Ratio - NHS Highland/Out of hours area
Skye, Lochalsh and South West Ross Independent External View |Out of Hours Urgent Care
Position Statement | Glenelg & Arnisdale | 12 April 2018
3 | P a g e
To put into words, this means:
Three times as many people in Highland currently travel 80-90 minutes to an Urgent Care Centre
compared to the new model in Glenelg.
Ten times as many people in Highland currently travel 70-80 minutes to an Urgent Care Centre
compared to the new model in Glenelg
Thirty six times as many people in Highland currently travel 60-70 minutes to an Urgent Care Centre
compared to the new model in Glenelg
Community Engagement
Significant concern has been expressed by the community in light of this change, with a delegation from Glenelg and Arnisdale speaking at the NHS Highland Board meeting (September 2016). There has been a series of meetings and events involving NHSH, community members and the local MSP.
An information leaflet was sent to all households in Glenelg & Arnisdale (July 2017) to ensure information around access to different services was clear. This also included a ‘credit card’ memory jogger for easy reference.
In addition a desktop emergency planning exercise was held (December 2017) involving representatives from NHS Highland, the community, Scottish Ambulance Service, Police Scotland, Scottish Fire and Rescue Service, and British Red Cross.
Evaluation
A process of internal evaluation was agreed with the community, recognising a concern that this would not be sufficiently ‘independent’. To date this has focussed on a review of every Out of Hours case, whether seen at Glenelg or Broadford, and an assessment of the clinical appropriateness and outcome. This assessment is conducted by a) the Out of Hours clinical lead and b) the Associate Medical Director (mental health) – who is a GP with significant experience in OOH in a remote and rural context and was agreed with the community. No adverse events have been identified by either senior clinician.
Patient feedback is planned to be part of the wider evaluation, and we have just received feed-back from the community around proposed questions.
Closing Comments
NHS Highland recognises that the community remain opposed to this change but the board has the responsibility to balance resources to meet needs of all communities. In part this community is used to the service they had and are fearful without it. Yet other communities, in similar circumstances, who never had such a service don’t raise concerns.
12 April 2018
Skye, Lochalsh and South West Ross Independent External View |Out of Hours Urgent Care
Position Statement | Feedback to OOH Peer Review Team| February 2016
1 | P a g e
NHS Highland: Feedback following peer review visit (1-2 Feb 2017) Following the visit by Sir Lewis Ritchie and the peer review team, NHS Highland were requested to
pull together priorities for areas where regional or national change would support our ability to
deliver quality, sustainable urgent primary care. The following list is largely reflective of issues which
were discussed over the course of the two day visit. They have been ordered by priority.
Acute Mental Health
Key contact: Boyd Peters, Associate Medical Director (Mental Health): [email protected]
We would strongly suggest that some solutions around mental health emergencies may need to be
provided regionally or nationally (though others are within our gift locally, and are being taken
forward).
North Highland, Argyll & Bute, NHS Western Isles and presumably other island health boards have
issues around emergency transfer of acute mental health patients. There are issues with both air
ambulance and sea transportation both in terms of the risks when they are used in this way and also
in terms of what the providers will or won’t do. It is felt that this is something which would need
influence centrally.
Highland now has a PEP (psychiatric emergency plan). The document is a working document
describing the current state which will be continually improved as we address some of the long term
challenges (often logistical) which we face.
Agenda for Change
Key contact: Evan Beswick, Project Manager, OOH: [email protected]
It is very clear that our ability to recruit, retain and support nurses and paramedics working at
advanced level is hampered by the restrictions of Agenda for Change. While there are some things
we can do to incentivise roles (e.g. enhanced levels of CPD time), other elements of the terms and
conditions are less flexible.
Specifically, there are issues with the restrictions imposed by the job banding process (lack of B7 job
outlines for Advanced Paramedics; difficulty of employing a lead practitioner at 8a to provide
educational support); on call payment (the £18 per session rate has already attracted a grievance
from staff we can ill afford to lose); disparity between doctors and nurses working alongside each
other but at vastly different pay rates. A national discussion that recognises the need to attract more
experienced individuals into these roles would be helpful.

Skye, Lochalsh and South West Ross Independent External View |Out of Hours Urgent Care
Position Statement | Feedback to OOH Peer Review Team| February 2016
2 | P a g e
Training and education
Key contact: Alison Hudson, Lead Nurse, North and West: [email protected]
There is an urgent need for standardization of educational requirements for the advanced
practitioner role. Furthermore, the Remote and Rural work environment needs to be recognised as
far as funding education is concerned.
A national accredited generic clinical supervisor training programme (for all professions eg: doctors,
nurses, paramedics, & AHP, and pharmacy) is a priority.
Consideration of the role of GPs providing urgent care as part of the new
contract discussions
Key contact: Antonia Reed, Clinical Lead OOH: [email protected]
The focus on quality as part of the new GP contract is very welcome. Despite the contractual
separation between in hours and out of hours, it would be disappointing if this were to become a
deeper separation in terms of responsibility, service provision and quality. We would be keen to
understand how out of hours is being considered in the context of the new contract, and the
development of quality clusters. We would suggest that daytime practice and out of hours can and
should support and learn from each other.
Maternity services
Key contact: Sarah McLeod, Lead Midwife, North and West: [email protected]
Key challenges around maternity services include:
• Fewer midwives attracted to rural posts, partly due to the lack of financial incentive around
Agenda for Change
• Lack of career structure for rural midwifery posts i.e. recognising it as a speciality
• Lack of really meaningful engagement with HEI’s especially around post grad opportunities.
Is there an opportunity to build on this with UHI on door step
• Unrealistic expectation re OOH’s cover – midwives on call night after night especially in
community midwifery units
• We are not using ageing workforce proactively – not just maternity services
• We are expecting too much of older midwives – as above
• We have midwives working in isolation from other health care professionals – this is historic,
and presents a need for more collaborative working
• There is a challenge in being able to utilise eHealth more effectively
Skye, Lochalsh and South West Ross Independent External View |Out of Hours Urgent Care
Position Statement | Feedback to OOH Peer Review Team| February 2016
3 | P a g e
• All of above making succession/workforce planning so challenging
Scottish Ambulance Service
Key contact: Milne Weir, General Manager, North Division, SAS: [email protected]
Integrated pathways of care and changes to patient flows for patients at a local, health board and
regional level will require ongoing investment in the Scottish Ambulance Service. The Scottish
Ambulance Service is fully committed to supporting changes to patient flows and is working closely
with IJBs, Health Boards, Regional and National Groups to identify what is required and how this will
be delivered. Road and or Air Ambulances are regularly required to transfer patients long distances
from remote and rural areas to definitive care at a local, regional and national level. There is a real
challenge around responding within 30 minutes in remote and rural areas.
The Scottish Ambulance Service is continuing to develop Specialist Paramedics who are contributing
to enhanced see and treat at home or in a community setting as well as reducing conveyances to
hospital. There are opportunities to further developing paramedics and specialist paramedics as an
integrated part of health and social care teams at a local level and there are opportunities to scale
up transformational change in this area. A strategic approach to supporting the training and
development of these specialist paramedics across SAS and territorial boards is required.
A further remaining issue concerns the ongoing requirement for communities to fundraise for
Community First Responder schemes. We see these resilience schemes, including higher-level
schemes such as emergency responders, as a strategic priority and one for which it is neither
feasible nor desirable to rely on fundraising to progress.
Support for technology that supports connectivity into NHS systems
Key contact: Iain Ross, Head of eHealth: [email protected]
With discussions around replacement of the Adastra software, consideration for the
hardware/devices which mobile practitioners need to access clinical systems on the move is
important. Adastra offer a ‘toughbook’ which natively connects to Adastra, but is very expensive.
The replacement of ageing toughbooks is, we presume, a national issue, and NSS support for mobile
connectivity into NHS systems would be extremely helpful.
What do doctors, nurses and paramedics do in the urgent care setting?
Key contact: Maimie Thompson, head of PR and engagement, [email protected]
One of the key messages for us from Pulling Together concerned multi-disciplinary teams, and the
reality that it will not necessarily be a doctor who sees patients requiring urgent care. Work is
ongoing locally to foster understanding around the excellent care delivered by doctors, nurses and
paramedics, and that they all have different, though often overlapping roles to play in the urgent
care network. Coordinated national messaging around this would be helpful.

Skye, Lochalsh and South West Ross Independent External View |Out of Hours Urgent Care
Position Statement | Feedback to OOH Peer Review Team| February 2016
4 | P a g e
National consistency around terminology
Key contact: Evan Beswick, Project Manager, OOH: [email protected]
We recognise this is happening, but would wish to emphasise the importance of this. Our
consultation with communities has indicated significant confusion around the different
requirements of urgent/emergency care. A timely move towards terminology (e.g. Urgent Care
Centres) which emphasises the non-emergency element of OOH primary care would be beneficial.
Paramedic Prescribing
Key contact: Graham MacLeod, Head of A&E Services, SAS: [email protected]
An application was rejected by the Royal College of Paramedics to allow paramedics to train as independent prescribers. We believe that paramedics have a significant role to play in the provision of urgent primary care (particularly in remote locations where their experience in driving distances and seeing patients in their homes is crucial). However, their inability to prescribe restricts this development. A timescale of 2 years has been cited for this to move forward. Any ability to shorten this timescale would be a help.
Skye, Lochalsh and South West Ross Independent External View |Out of Hours Urgent Care
Position Statement | Housing | 13 April 2018
1 | P a g e
Context
Housing is a significant problem across the West Highlands, with new and prospective staff frequently reporting to us that they are struggling to find suitable family accommodation.
On top of this, particularly on Skye, the tourism boom has been having an increasing adverse impact staffing on three fronts:
• Greater competition for catering and domestic staff
• Lack of affordable housing for staff moving into the area
• Individuals able to achieve higher incomes from providing Airbnb’
This has meant we have struggled to find long term rents as accommodation, and in all cases staff have not been in a position to buy as property is generally very expensive. Currently no priority is given to incoming workers in the Highland Housing register Allocations Policy.
Some of the issues are summarised in an article recently published by Lesley Riddoch Forget tourism Skye's housing crisis is the real emergency ( 1st March 2018). Facts and Figures quoted in the article include:
• There are no long-term lets any more
• 200 properties listed on one short-term letting website alone in Portree
• Average home on the Isle of Skye Property Centre website is around £185k – higher than almost everywhere else in rural Scotland
Naturally NHS Highland is not the only organisation/company struggling. The Council and local hotels for example are experiencing similar difficulties. The police built a hostel on Skye to try and counter the issue. Alongside these challenges there is, of course, the priority to house homeless people.
Local MSP Kate Forbes says: “I think rural homelessness, like rural poverty, largely goes unnoticed and is considered an urban problem. Yet, in the rural Highlands, the number one issue is lack of housing. House prices are higher than average, driven by low supply of land, holiday homes and increased construction costs.
“At the same time, average incomes are lower than the Scottish average. That means there is a greater affordability gap here”.
It is important to recognise that in starting to develop solutions around accommodation for staff, this is a new area for NHS Highland. We do not yet have the facts and figures around the scale of the issue, the financial implications and the impacts for sustainability. In particular we don’t know if it’s likely to be a short-term problem.
Skye, Lochalsh and South West Ross Independent External View |Out of Hours Urgent Care
Position Statement | Housing | 13 April 2018
2 | P a g e
There are others issues in relation to housing such as supported housing, housing adaptations which will support more people to live at home for longer but these issues are not the subject of this briefing.
Lochalsh and Skye Housing Association
Lochalsh and Skye Housing Association five year business plan 2018/2023 sets out the following Local Housing Analysis
• There is high demand for Highland Council and Association affordable rented housing. The housing list and transfer list of The Highland Housing Register (HHR) for Skye and Lochalsh contains more than 400 applicants consistently throughout the year. Approximately 19% (85) of Council and Association re-lets occur each year.
• Access to home ownership is chronically difficult due to high prices, high living costs and relatively low incomes.
• The total dwelling stock in Skye and Lochalsh is 7,103 of which 5,746 are permanently occupied. It is estimated that 17.2% of the dwellings are second/holiday homes and vacant dwellings account for 1.9% of the stock. There are 1089 social rented stock and 438 applications held on the housing lists. It is projected that an additional 350 housing units of all tenures are required by 2022.
• The abolition of the priority need test and the requirement to provide settled accommodation for homeless applicants presents significant challenges both in Skye and Lochalsh and across Highland.
• The Association is committed to working with partners to consider solutions that increase housing options, particularly in the private rented sector. However, there is growing evidence that private rented sector solutions may be constrained by the considerable recent increase in properties being used for tourism purposes and by the new requirements of the Private Residential Tenancy legislation which may deter private owners from making properties available for homelessness purposes. Increasing the supply of affordable housing is the preferred solution to homelessness.
Approval of the five year Business Plan which will result in more than 200 new houses being built by the Association across the area by 2023.
Forty four of the properties are already under construction or being purchased and a further seventy houses and flats will start on site during 2018. The anticipated cost of the development programme is in the region of £25 million.
Announcing the new programme, the Association's Chief Executive, Lachie MacDonald, said:-
"This is a massive and unprecedented investment in Skye and Lochalsh and, in addition to being excellent news for jobs in the construction industry, it demonstrates our commitment to meeting the housing needs of individuals and families in the area as quickly as possible. We believe that the best approach to dealing with housing need pressures is to increase the supply of housing and our development programme will certainly achieve that aim.
Skye, Lochalsh and South West Ross Independent External View |Out of Hours Urgent Care
Position Statement | Housing | 13 April 2018
3 | P a g e
We very much welcome the tremendous support and backing we are receiving from The Scottish Government, Highland Council and our lenders which we believe will allow us to achieve our ambition of eliminating homelessness in Skye and Lochalsh. We will be providing new affordable rented homes for those in priority need including those affected by overcrowding, damp, temporary and poorly repaired properties."
The Association's Business Plan also includes a commitment to partnership working with NHS Highland and other organisations working in the care sector to meet their specific housing needs. In addition, the Association's highly successful Handyperson, Care and Repair and Energy Advice Services will continue to be fully supported by the Association.
Implications for Service Redesign and sustainability and NHS Highland Actions
It remains to be seen how much of an impact and how quickly the new investment will impact on addressing some of the housing challenges. There are some immediate actions NHS Highland are taking as follows:
• Encouraging all new recruits to register with the HA so that they are on the list, that way if opportunities arise they are in with a chance – that could be rental or affordable housing scheme. This will ensure that their housing need is identified and assessed: if they are not eligible for social housing, Housing Options advice will be provided.
• The Association is currently represented at all the Skye and Lochalsh Health, Housing and Social Care Forum meetings and the Community Based Health and Housing Solutions Group meetings, both of which are meeting on a two-monthly basis.
• A meeting was held on 8th March with colleagues from the Highland Council and Lochalsh and Skye Housing Association to begin to scope out some of these issues. A further meeting is scheduled for June.
• Working in Partnership with the Association to look at Staff Accommodation relating to the proposed new Broadford Hospital
Proposed new hospital in Broadford
There are some opportunities around what we do with the old Dr Mackinnon Memorial Hospital and the rest of the undeveloped site owned by NHS Highland in Broadford. We have been looking at the potential for housing once the old hospital is demolished. There is significant potential for some housing with the idea being that we work with the Association to build the units then we get a proportion for key worker housing in exchange for the site.
This would need support from the Highland Council from a planning and policy perspective. The Council’s first priority for housing is homeless people and secondly it is people living in unsuitable accommodation. Key workers is at best third on the list but is not actually a housing priority they are actively working on.
Skye, Lochalsh and South West Ross Independent External View |Out of Hours Urgent Care
Position Statement | Housing | 13 April 2018
4 | P a g e
Therefore strategically we need to build to influence policy to seek to prioritise key worker housing a higher priority or we circumvent this entirely and build our own key worker housing with the local housing association.
The immediate step is to quantify the problem and get consensus around a way forward based on the evidence.
Skye, Lochalsh and South West Ross Independent External View |Out of Hours Urgent Care
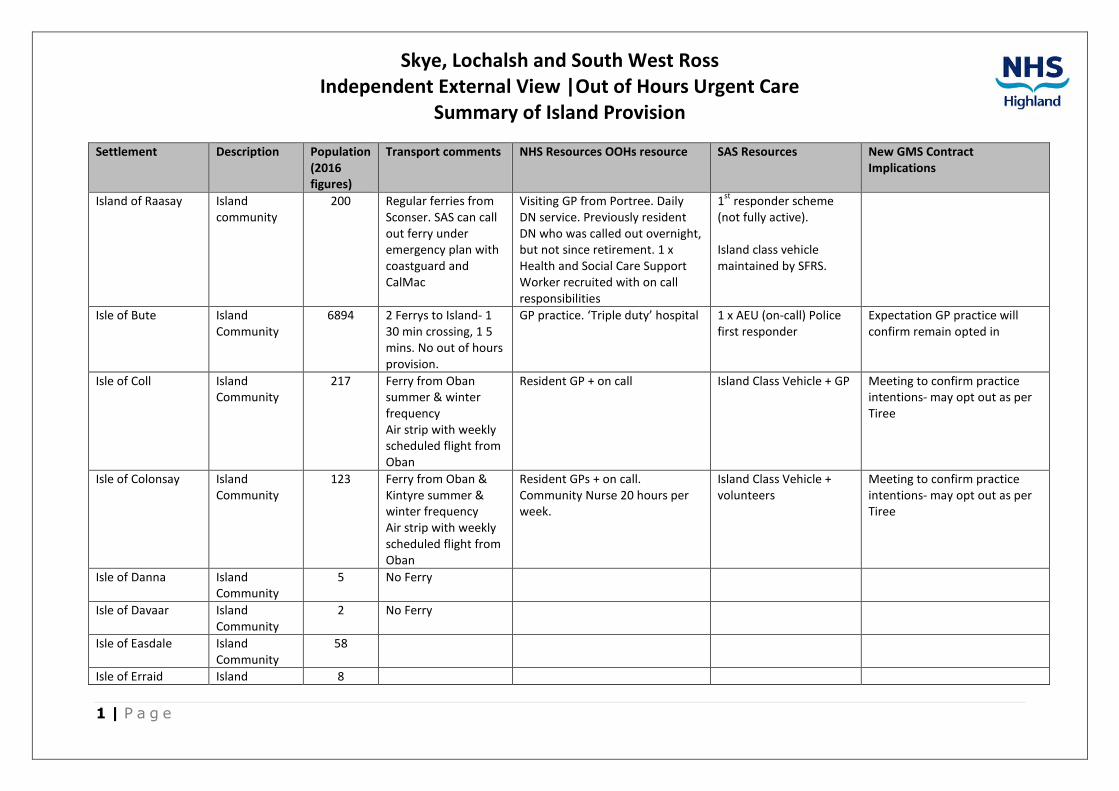
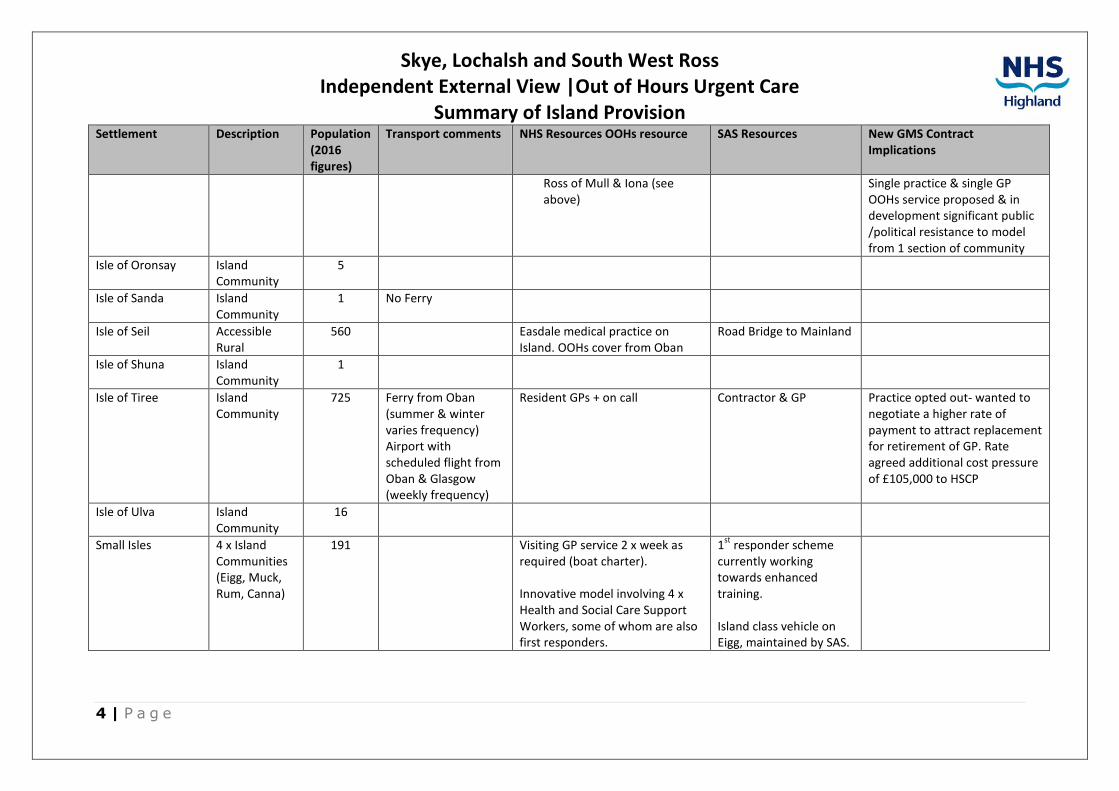
Summary of Island Provision
1 | P a g e
Settlement Description Population (2016 figures)
Transport comments NHS Resources OOHs resource SAS Resources New GMS Contract Implications
Island of Raasay Island community
200 Regular ferries from Sconser. SAS can call out ferry under emergency plan with coastguard and CalMac
Visiting GP from Portree. Daily DN service. Previously resident DN who was called out overnight, but not since retirement. 1 x Health and Social Care Support Worker recruited with on call responsibilities
1st
responder scheme (not fully active).
Island class vehicle maintained by SFRS.
Isle of Bute Island Community
6894 2 Ferrys to Island- 1 30 min crossing, 1 5 mins. No out of hours provision.
GP practice. ‘Triple duty’ hospital 1 x AEU (on-call) Police first responder
Expectation GP practice will confirm remain opted in
Isle of Coll Island Community
217 Ferry from Oban summer & winter frequency Air strip with weekly scheduled flight from Oban
Resident GP + on call Island Class Vehicle + GP Meeting to confirm practice intentions- may opt out as per Tiree
Isle of Colonsay Island Community
123 Ferry from Oban & Kintyre summer & winter frequency Air strip with weekly scheduled flight from Oban
Resident GPs + on call. Community Nurse 20 hours per week.
Island Class Vehicle + volunteers
Meeting to confirm practice intentions- may opt out as per Tiree
Isle of Danna Island Community
5 No Ferry
Isle of Davaar Island Community
2 No Ferry
Isle of Easdale Island Community
58
Isle of Erraid Island 8
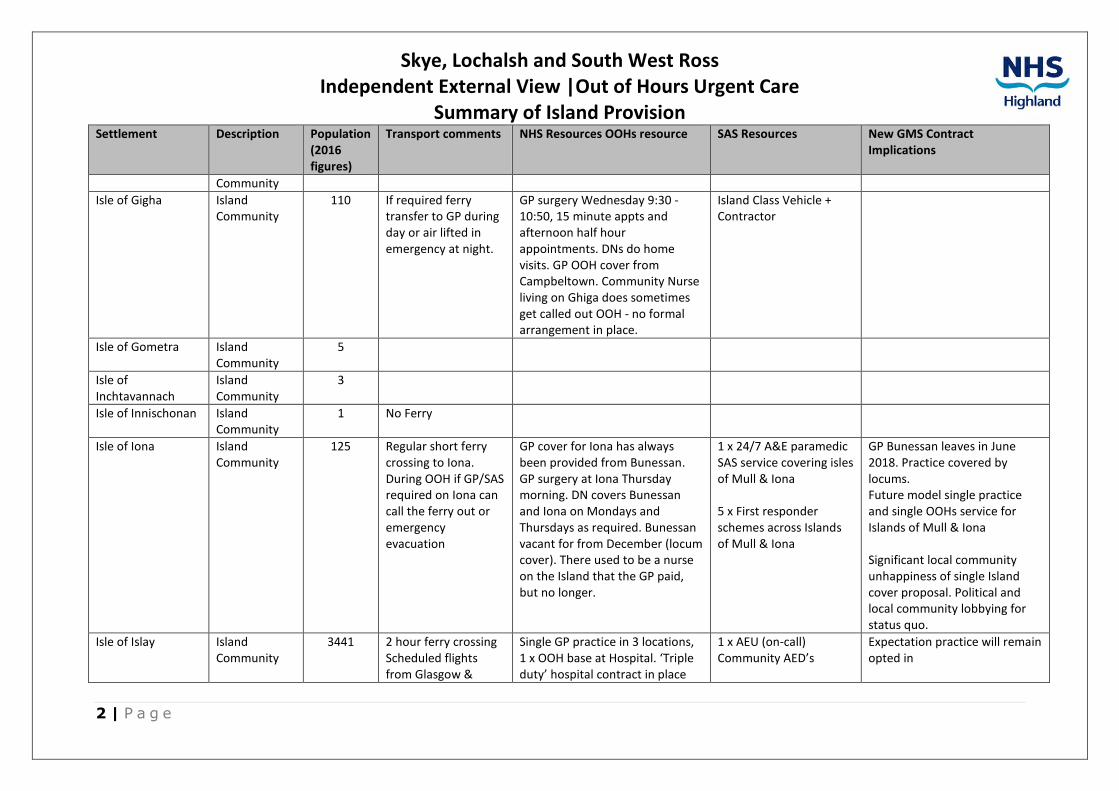
Skye, Lochalsh and South West Ross Independent External View |Out of Hours Urgent Care
Summary of Island Provision
2 | P a g e
Settlement Description Population (2016 figures)
Transport comments NHS Resources OOHs resource SAS Resources New GMS Contract Implications
Community
Isle of Gigha Island Community
110 If required ferry transfer to GP during day or air lifted in emergency at night.
GP surgery Wednesday 9:30 - 10:50, 15 minute appts and afternoon half hour appointments. DNs do home visits. GP OOH cover from Campbeltown. Community Nurse living on Ghiga does sometimes get called out OOH - no formal arrangement in place.
Island Class Vehicle + Contractor
Isle of Gometra Island Community
5
Isle of Inchtavannach
Island Community
3
Isle of Innischonan Island Community
1 No Ferry
Isle of Iona Island Community
125 Regular short ferry crossing to Iona. During OOH if GP/SAS required on Iona can call the ferry out or emergency evacuation
GP cover for Iona has always been provided from Bunessan. GP surgery at Iona Thursday morning. DN covers Bunessan and Iona on Mondays and Thursdays as required. Bunessan vacant for from December (locum cover). There used to be a nurse on the Island that the GP paid, but no longer.
1 x 24/7 A&E paramedic SAS service covering isles of Mull & Iona
5 x First responder schemes across Islands of Mull & Iona
GP Bunessan leaves in June 2018. Practice covered by locums. Future model single practice and single OOHs service for Islands of Mull & Iona
Significant local community unhappiness of single Island cover proposal. Political and local community lobbying for status quo.
Isle of Islay Island Community
3441 2 hour ferry crossing Scheduled flights from Glasgow &
Single GP practice in 3 locations, 1 x OOH base at Hospital. ‘Triple duty’ hospital contract in place
1 x AEU (on-call) Community AED’s
Expectation practice will remain opted in
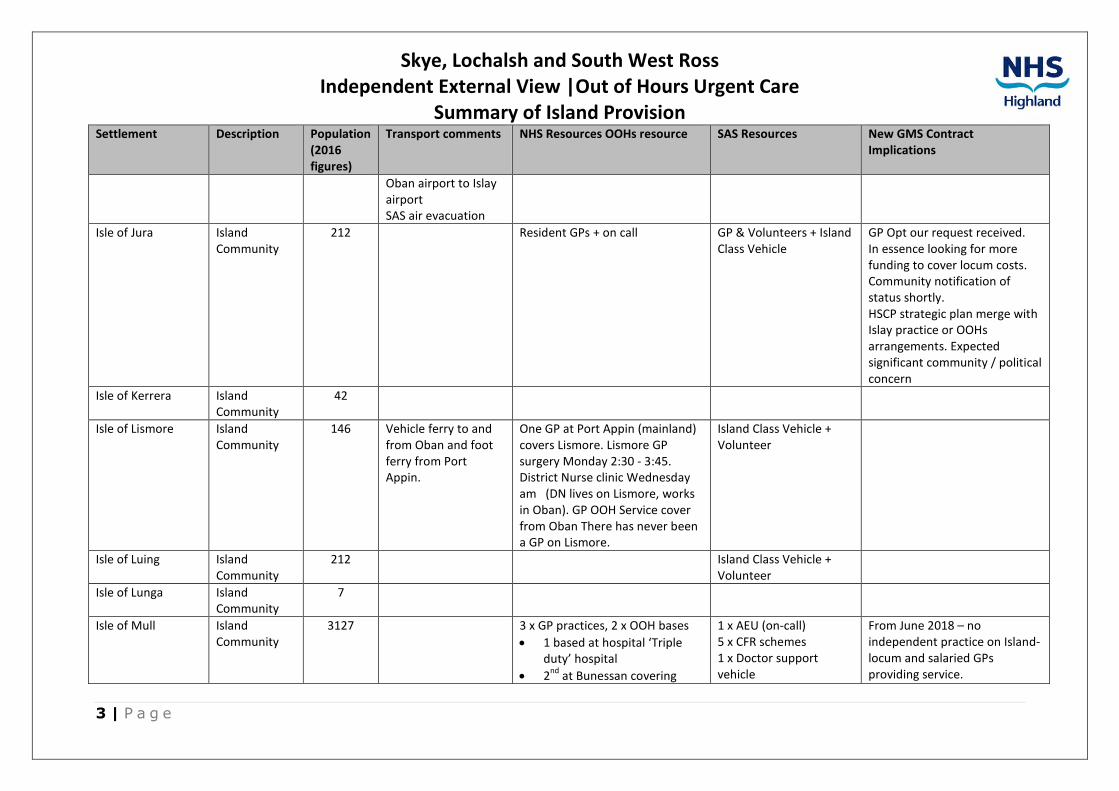
Skye, Lochalsh and South West Ross Independent External View |Out of Hours Urgent Care
Summary of Island Provision
3 | P a g e
Settlement Description Population (2016 figures)
Transport comments NHS Resources OOHs resource SAS Resources New GMS Contract Implications
Oban airport to Islay airport SAS air evacuation
Isle of Jura Island Community
212 Resident GPs + on call GP & Volunteers + Island Class Vehicle
GP Opt our request received. In essence looking for more funding to cover locum costs. Community notification of status shortly. HSCP strategic plan merge with Islay practice or OOHs arrangements. Expected significant community / political concern
Isle of Kerrera Island Community
42
Isle of Lismore Island Community
146 Vehicle ferry to and from Oban and foot ferry from Port Appin.
One GP at Port Appin (mainland) covers Lismore. Lismore GP surgery Monday 2:30 - 3:45. District Nurse clinic Wednesday am (DN lives on Lismore, works in Oban). GP OOH Service cover from Oban There has never been a GP on Lismore.
Island Class Vehicle + Volunteer
Isle of Luing Island Community
212 Island Class Vehicle + Volunteer
Isle of Lunga Island Community
7
Isle of Mull Island Community
3127 3 x GP practices, 2 x OOH bases
• 1 based at hospital ‘Triple duty’ hospital
• 2nd
at Bunessan covering
1 x AEU (on-call) 5 x CFR schemes 1 x Doctor support vehicle
From June 2018 – no independent practice on Island- locum and salaried GPs providing service.
Skye, Lochalsh and South West Ross Independent External View |Out of Hours Urgent Care
Summary of Island Provision
4 | P a g e
Settlement Description Population (2016 figures)
Transport comments NHS Resources OOHs resource SAS Resources New GMS Contract Implications
Ross of Mull & Iona (see above)
Single practice & single GP OOHs service proposed & in development significant public /political resistance to model from 1 section of community
Isle of Oronsay Island Community
5
Isle of Sanda Island Community
1 No Ferry
Isle of Seil Accessible Rural
560 Easdale medical practice on Island. OOHs cover from Oban
Road Bridge to Mainland
Isle of Shuna Island Community
1
Isle of Tiree Island Community
725 Ferry from Oban (summer & winter varies frequency) Airport with scheduled flight from Oban & Glasgow (weekly frequency)
Resident GPs + on call Contractor & GP Practice opted out- wanted to negotiate a higher rate of payment to attract replacement for retirement of GP. Rate agreed additional cost pressure of £105,000 to HSCP
Isle of Ulva Island Community
16
Small Isles 4 x Island Communities (Eigg, Muck, Rum, Canna)
191 Visiting GP service 2 x week as required (boat charter).
Innovative model involving 4 x Health and Social Care Support Workers, some of whom are also first responders.
1st
responder scheme currently working towards enhanced training.
Island class vehicle on Eigg, maintained by SAS.
Skye, Lochalsh and South West Ross Independent External View |Out of Hours Urgent Care
Position Statement | Major Service Change | 12 April 2018
1 | P a g e
Background
Following extensive public consultation in 2014, a proposal for enhanced community services and a 'hub' and 'spoke' model was approved by the board of NHS Highland. This would see a new build hospital facility to be located in Broadford and a ‘spoke’ in Portree as part of wider redesign of health and social care services. Summary of services to be provided by the ‘Hub’ and ‘Spoke’ are provided below. But one of the most significant changes in the new arrangements are that all hospital inpatient services would be provided from the ‘Hub’.
This was approved by the Cabinet Secretary in February 2015 and since then work is on going to develop the business case (see below for time-table.
The write up of the public consultation is available Consultation Report 2014
Summary of findings from Public Consultation
Through the options appraisal process three options were consulted
Option 1 Do minimum
Option 2 Community Hospital ‘Hub’ in either Broadford or Portree and the ‘Spoke’ in the other location (preferred option)
Option 3 Community Hospital ‘Hub’ in one location either in Broadford or Portree
The location of the Hub and Spoke were also consulted upon
Results
Of those who completed NHS Highland’s consultation response survey (2,273 = 20% of adult population) there was wide-spread support for the case for change.
99% of the population, who responded, supported a move away from current arrangements.
Moreover almost nine out of ten (86%) supported the preferred model of service i.e Hub and Spoke.
In terms of location, overall, the majority, 57%, favoured the preferred option 2a, ‘Hub in Broadford and ‘Spoke’ in Portree, whereas 29% supported Portree as the ‘Hub’ (option 2b).
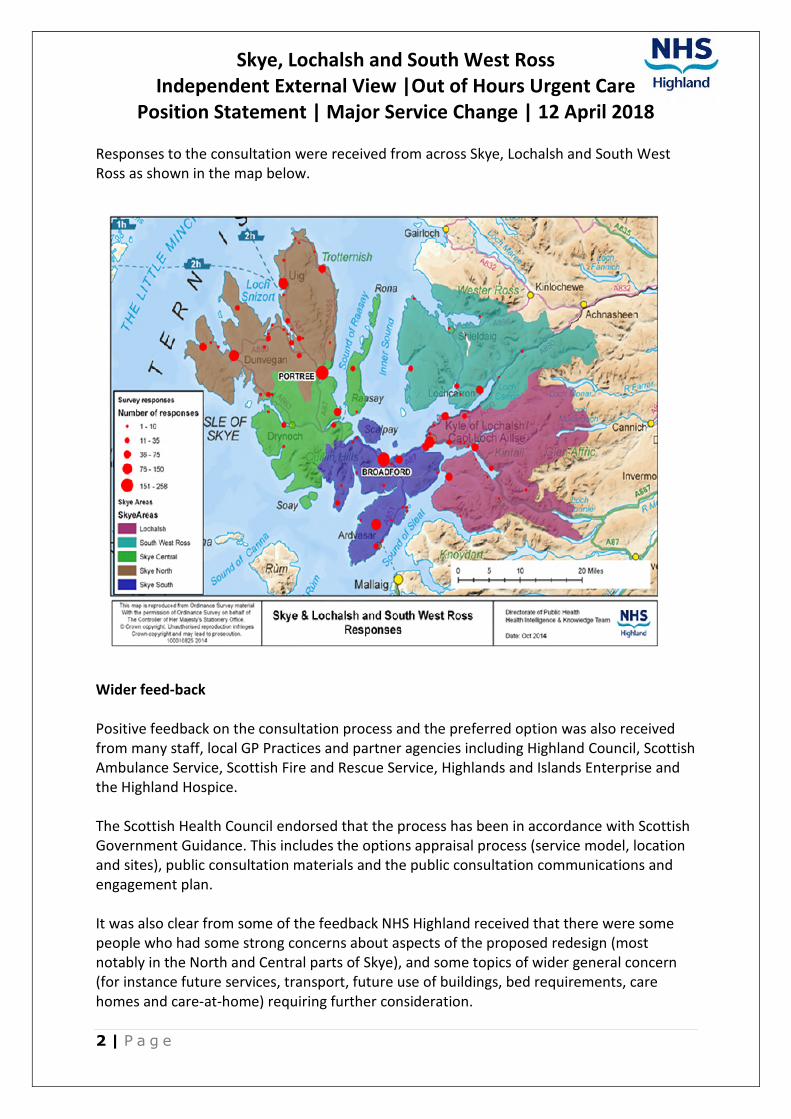
Skye, Lochalsh and South West Ross Independent External View |Out of Hours Urgent Care
Position Statement | Major Service Change | 12 April 2018
2 | P a g e
Responses to the consultation were received from across Skye, Lochalsh and South West Ross as shown in the map below.
Wider feed-back
Positive feedback on the consultation process and the preferred option was also received from many staff, local GP Practices and partner agencies including Highland Council, Scottish Ambulance Service, Scottish Fire and Rescue Service, Highlands and Islands Enterprise and the Highland Hospice.
The Scottish Health Council endorsed that the process has been in accordance with Scottish Government Guidance. This includes the options appraisal process (service model, location and sites), public consultation materials and the public consultation communications and engagement plan.
It was also clear from some of the feedback NHS Highland received that there were some people who had some strong concerns about aspects of the proposed redesign (most notably in the North and Central parts of Skye), and some topics of wider general concern (for instance future services, transport, future use of buildings, bed requirements, care homes and care-at-home) requiring further consideration.

Skye, Lochalsh and South West Ross Independent External View |Out of Hours Urgent Care
Position Statement | Major Service Change | 12 April 2018
3 | P a g e
History
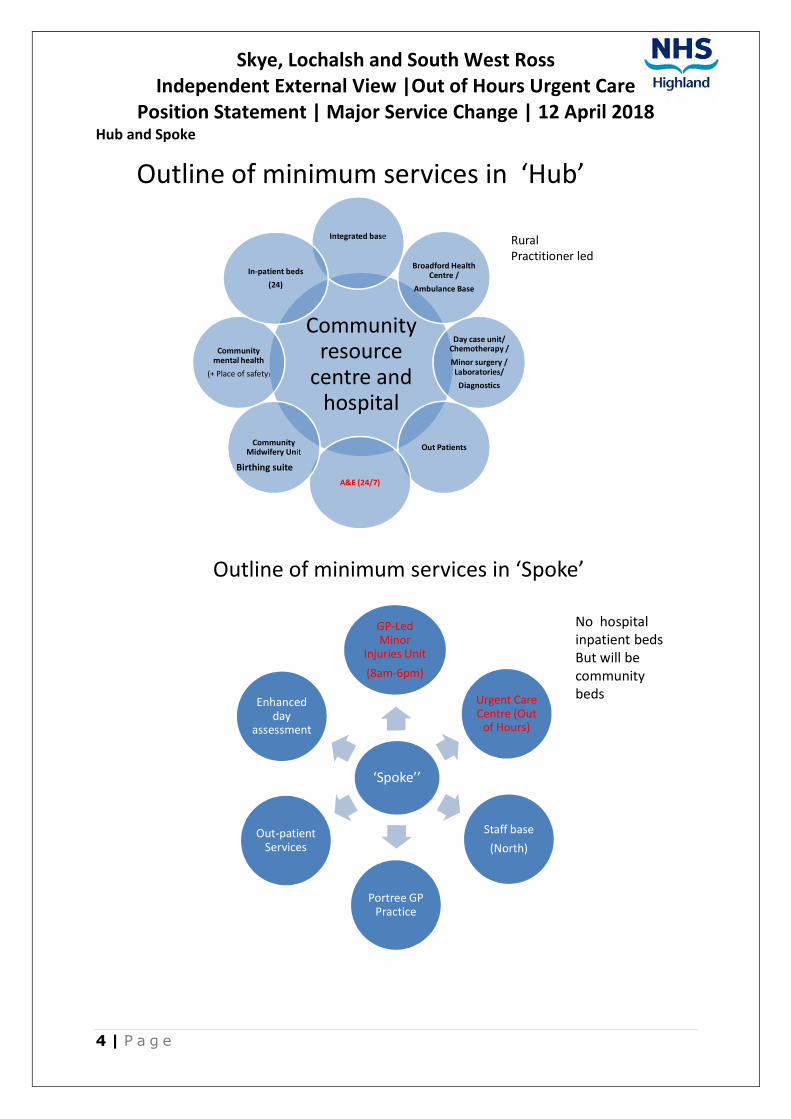
Skye, Lochalsh and South West Ross Independent External View |Out of Hours Urgent Care
Position Statement | Major Service Change | 12 April 2018
4 | P a g e
Hub and Spoke
Outline of minimum services in ‘Hub’
Community resource
centre and hospital
Integrated base
Broadford Health Centre /
Ambulance Base
Day case unit/ Chemotherapy /
Minor surgery / Laboratories/
Diagnostics
Out Patients
A&E (24/7)
Community Midwifery Unit
Community mental health
(+ Place of safety)
In-patient beds
(24)
Birthing suite
Rural Practitioner led
Outline of minimum services in ‘Spoke’
‘Spoke’’
GP-Led Minor
Injuries Unit
(8am-6pm)
Urgent Care Centre (Out
of Hours)
Staff base
(North)
Portree GP Practice
Out-patient Services
Enhanced day
assessment
No hospital inpatient bedsBut will be community beds
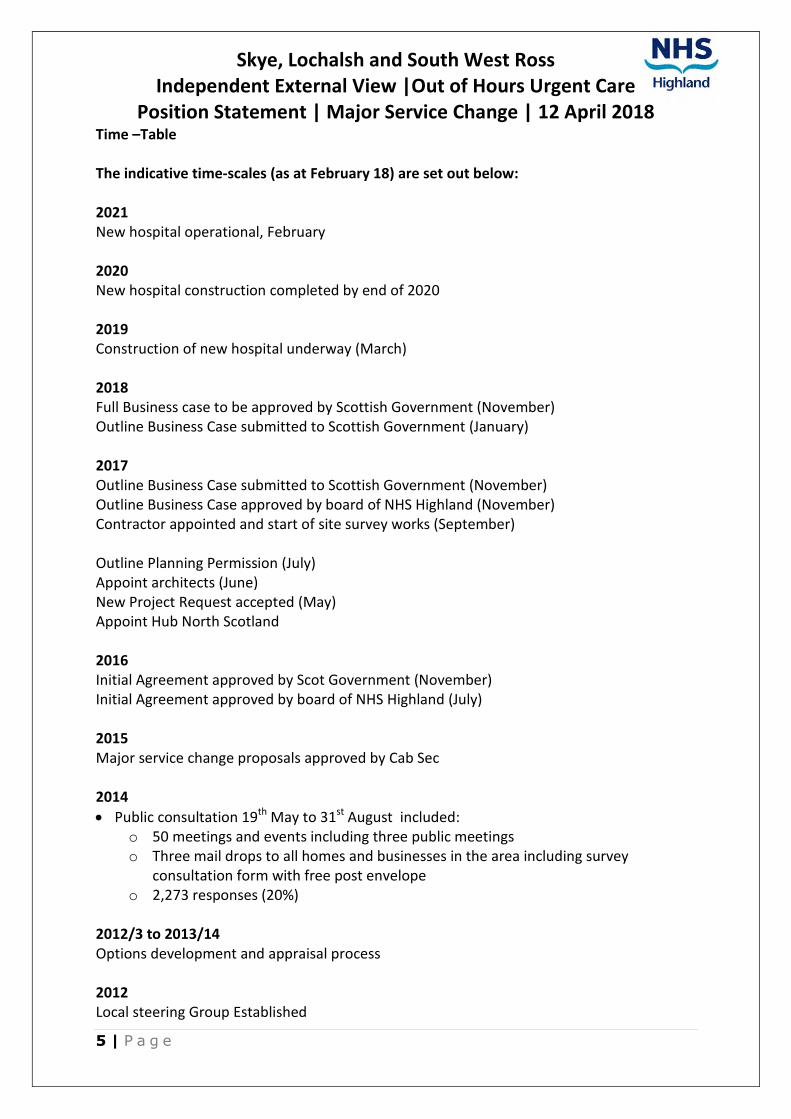
Skye, Lochalsh and South West Ross Independent External View |Out of Hours Urgent Care
Position Statement | Major Service Change | 12 April 2018
5 | P a g e
Time –Table
The indicative time-scales (as at February 18) are set out below:
2021New hospital operational, February
2020New hospital construction completed by end of 2020
2019Construction of new hospital underway (March)
2018Full Business case to be approved by Scottish Government (November) Outline Business Case submitted to Scottish Government (January)
2017Outline Business Case submitted to Scottish Government (November) Outline Business Case approved by board of NHS Highland (November) Contractor appointed and start of site survey works (September)
Outline Planning Permission (July) Appoint architects (June) New Project Request accepted (May) Appoint Hub North Scotland
2016Initial Agreement approved by Scot Government (November) Initial Agreement approved by board of NHS Highland (July)
2015 Major service change proposals approved by Cab Sec
2014
• Public consultation 19th May to 31st August included: o 50 meetings and events including three public meetings o Three mail drops to all homes and businesses in the area including survey
consultation form with free post envelope o 2,273 responses (20%)
2012/3 to 2013/14 Options development and appraisal process
2012 Local steering Group Established

Skye, Lochalsh and South West Ross Independent External View |Out of Hours Urgent Care Position Statement | Maternity Services| 14 April 2018
1 | P a g e
Summary
There are a number of matters making succession/workforce planning challenging. In the interest of sustaining and maintaining vibrant communities it is important that we continue to have safe maternity. Midwives play a crucial role in this.
Central to our local challenge is this: how do we provide holistic maternity care in a remote and rural context where midwives need to maintain additional competencies and skills given the distance from other professionals; where on call commitments make recruitment and retention difficult; where financial challenges mean pressure on establishments, and securing local accommodation for staff problematic.
Context
Rural maternity services differ to those in urban centres. They are provided from Community Midwifery Units (CMUs) rather than hospital obstetric departments. Community Midwives in remote and rural areas such as Skye, Lochalsh and South West Ross provide routine care to expectant mothers and to mothers and newborn babies in the postnatal period. Midwives work on call overnight for planned births and unscheduled maternity care.
It is important to note that maternity care is becoming more complex. Women on caseloads often have co-morbidities prior to becoming pregnant and therefore their needs during pregnancy often require multi professional care. In Skye & Lochalsh this is mainly co-ordinated by the named Midwife.
In more urban areas there would be more support from Obstetricians and generally a greater pool available expertise. Notably, however, in Skye & Lochalsh, Midwives have the benefit of the support of Rural Practitioners based in Dr MacKinnon Memorial.
There are also more women with complex social needs, requiring multi agency collaboration with the Midwife at the centre of the coordination role. Again this is easier in urban areas.
More generally, it would be fair to say that all maternity services across Highland and Argyll and Bute are stretched with a number of workforce issues and in particular during the Out of Hours (OOH) Period. All of these factors make succession workforce planning very challenging.
Recent History | Staffing Models and Establishments
Prior to 2004 Midwifery Care was provided by a collection of Midwives, all of whom had a dual sometimes triple role (i.e. were Nurses, Midwives & Health Visitors). Practitioners were spread across the Skye & Lochalsh locality and women with low risk pregnancies had an option to birth locally in both Portree and Broadford.
Following national and local reviews, along with emerging issues around skill maintenance, underpinned by the NMC registration, requirements for Midwives to undertake 450 hours of midwifery practice over three years, it was necessary to develop a single duty Midwifery Service. This development was combined with opening a Community Midwifery Unit (CMU) at Dr MacKinnon Memorial Hospital in Broadford.
Skye, Lochalsh and South West Ross Independent External View |Out of Hours Urgent Care Position Statement | Maternity Services| 14 April 2018
2 | P a g e
The funded establishment was set at 7.2 WTE. This provided enough cover in relation to OOHs with two Midwives on call per night (for planned births). If fully staffed, Midwives do not have to be on call on time off into days off.
In the intervening years the establishment reduced to 6.5 WTE. The routine daily workload and caseload size indicated staffing establishment of approx 6 WTE. Maternity workload tool runs in 2015 and 2017 showed an outcome requirement of 6.9 WTE and 6 WTE respectively.
Mapping professional judgement tool outcomes into this process and applying working time regulations demonstrates that a greater staffing establishment (in line with the original service set up of 7.2 WTE) is required if aiming to maintain the local birth service, on call working rota and 24/7 service provision. Findings from running national workload tools indicate that there is a requirement for 7.2 WTE.
Current Situation and Challenges with Sustainability
At the present time Midwifery cover OOH has been suspended due to significant staff shortage. Recruitment is ongoing with an additional two team members being required. This will bring funded establishment up to 6.5 WTE Midwives. Challenges with future sustainability include:
• Fewer midwives are attracted to rural posts, partly due to the lack of financial incentive around Agenda for Change
• There is a lack of career structure for rural midwifery posts i.e. recognising it as a speciality
• There is a lack of meaningful engagement with Higher Education Institutes especially around post graduate opportunities.
• There can be unrealistic expectation re OOHs cover especially when staffing levels are low due to vacant posts and sickness absence
• Historically there has been a tendency for midwives to work in isolation from other health care professionals during OOHs working
• There are some ongoing challenges to utilise eHealth more effectively
Positive Developments
In recent years within Skye and Lochalsh we have seen successful collaborative working with local medical, nursing and Scottish Ambulance colleagues. All have shown great willingness to support their midwifery colleagues in the event of unscheduled / emergency maternity incidents. Nevertheless it should be recognised that if there is no midwife available on call triage and assessment of unscheduled maternity cases is carried out by the Out of Hours clinicians.
We have ensured that there are telemedicine facilities available to be used in unforeseen obstetric or neonatal emergencies and for routine work
Women are also being reviewed virtually by consultant colleagues. This works well and will be expanded upon as it is also supports efficient use of consultant time.
University of the Highland and Islands (UHI) has been successful in gaining Scottish Government approval for a three to five year pilot, to provide a post-graduate shortened midwifery programme. Delivered in conjunction with NHS Highland it will offer places for registered nurses to undertake midwifery training.
Skye, Lochalsh and South West Ross Independent External View |Out of Hours Urgent Care Position Statement | Maternity Services| 14 April 2018
3 | P a g e
UHI are also looking to develop and run a three year direct entry, undergraduate programme and Return to Practice programme. This will give more opportunities for students and nurses living and working in Highland and who don’t want to move out of area for placements and training. This will hopefully offer longer term solution for the current and ongoing recruitment challenges.
NHS Highland is supporting a follow-up to the Channel 5 observational documentary series on Highland Midwives.
The first series was shown over three one hour episodes (5th, 12th an 19th July) and featured midwives from NHS Highland working in Ross-shire and Argyll and Bute. The second series has broadened out to cover other parts of Highland. Our focus for participating is to raise the profile to work in NHS Highland and hopefully enhance recruitment opportunities.
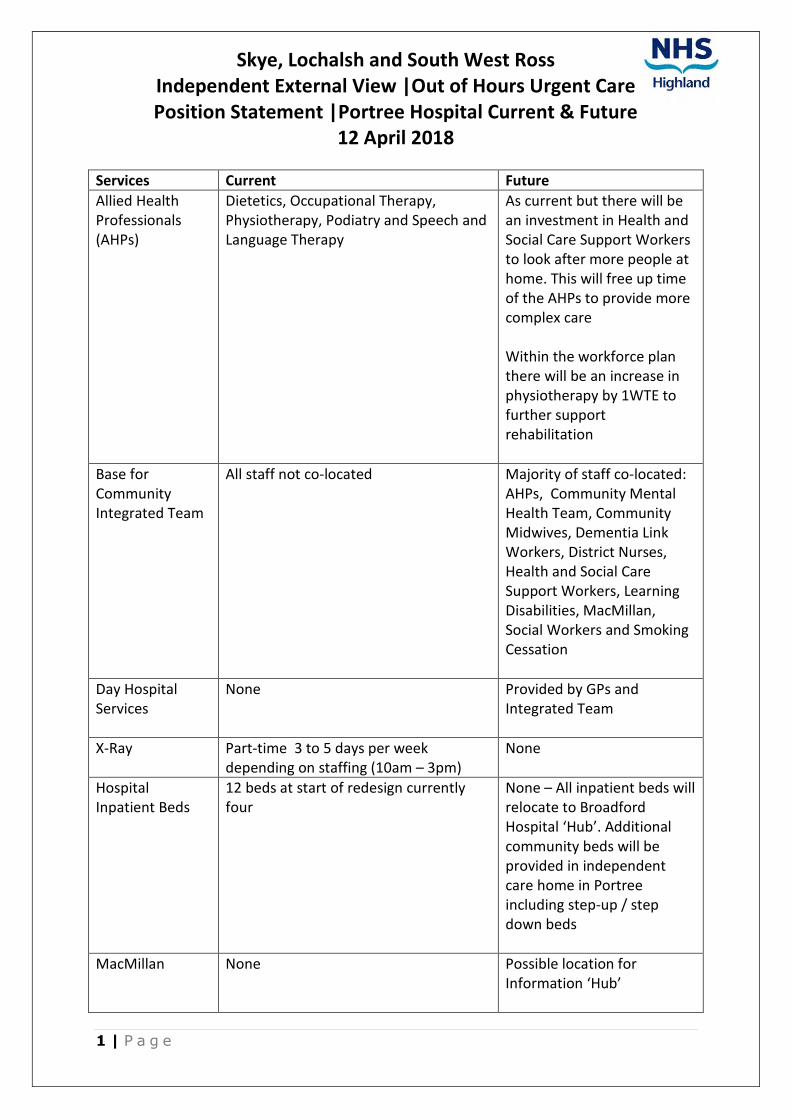
Skye, Lochalsh and South West Ross Independent External View |Out of Hours Urgent Care Position Statement |Portree Hospital Current & Future
12 April 2018
1 | P a g e
Services Current Future
Allied Health Professionals (AHPs)
Dietetics, Occupational Therapy, Physiotherapy, Podiatry and Speech and Language Therapy
As current but there will be an investment in Health and Social Care Support Workers to look after more people at home. This will free up time of the AHPs to provide more complex care
Within the workforce plan there will be an increase in physiotherapy by 1WTE to further support rehabilitation
Base for Community Integrated Team
All staff not co-located Majority of staff co-located: AHPs, Community Mental Health Team, Community Midwives, Dementia Link Workers, District Nurses, Health and Social Care Support Workers, Learning Disabilities, MacMillan, Social Workers and Smoking Cessation
Day Hospital Services
None Provided by GPs and Integrated Team
X-Ray Part-time 3 to 5 days per week depending on staffing (10am – 3pm)
None
Hospital Inpatient Beds
12 beds at start of redesign currently four
None – All inpatient beds will relocate to Broadford Hospital ‘Hub’. Additional community beds will be provided in independent care home in Portree including step-up / step down beds
MacMillan None Possible location for Information ‘Hub’
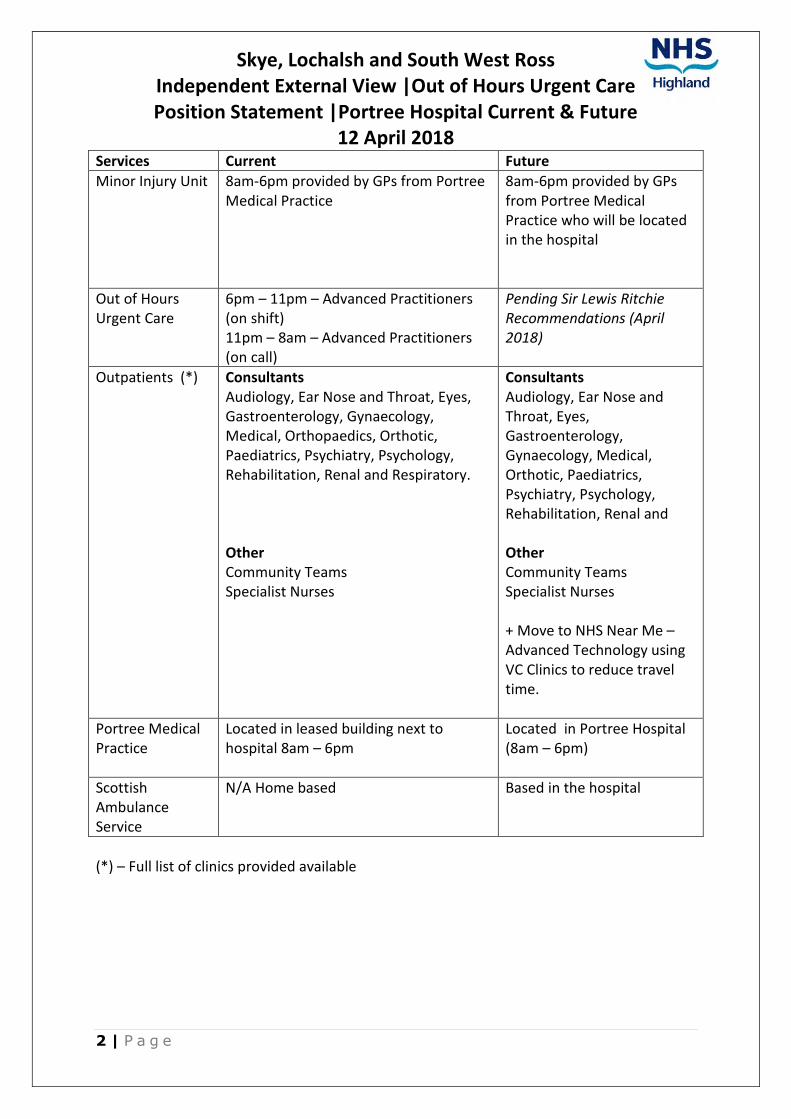
Skye, Lochalsh and South West Ross Independent External View |Out of Hours Urgent Care Position Statement |Portree Hospital Current & Future
12 April 2018
2 | P a g e
Services Current Future
Minor Injury Unit 8am-6pm provided by GPs from Portree Medical Practice
8am-6pm provided by GPs from Portree Medical Practice who will be located in the hospital
Out of Hours Urgent Care
6pm – 11pm – Advanced Practitioners (on shift) 11pm – 8am – Advanced Practitioners (on call)
Pending Sir Lewis Ritchie Recommendations (April 2018)
Outpatients (*) Consultants Audiology, Ear Nose and Throat, Eyes, Gastroenterology, Gynaecology, Medical, Orthopaedics, Orthotic, Paediatrics, Psychiatry, Psychology, Rehabilitation, Renal and Respiratory.
Other Community Teams Specialist Nurses
Consultants Audiology, Ear Nose and Throat, Eyes, Gastroenterology, Gynaecology, Medical, Orthotic, Paediatrics, Psychiatry, Psychology, Rehabilitation, Renal and
Other Community Teams Specialist Nurses
+ Move to NHS Near Me – Advanced Technology using VC Clinics to reduce travel time.
Portree Medical Practice
Located in leased building next to hospital 8am – 6pm
Located in Portree Hospital (8am – 6pm)
Scottish Ambulance Service
N/A Home based Based in the hospital
(*) – Full list of clinics provided available
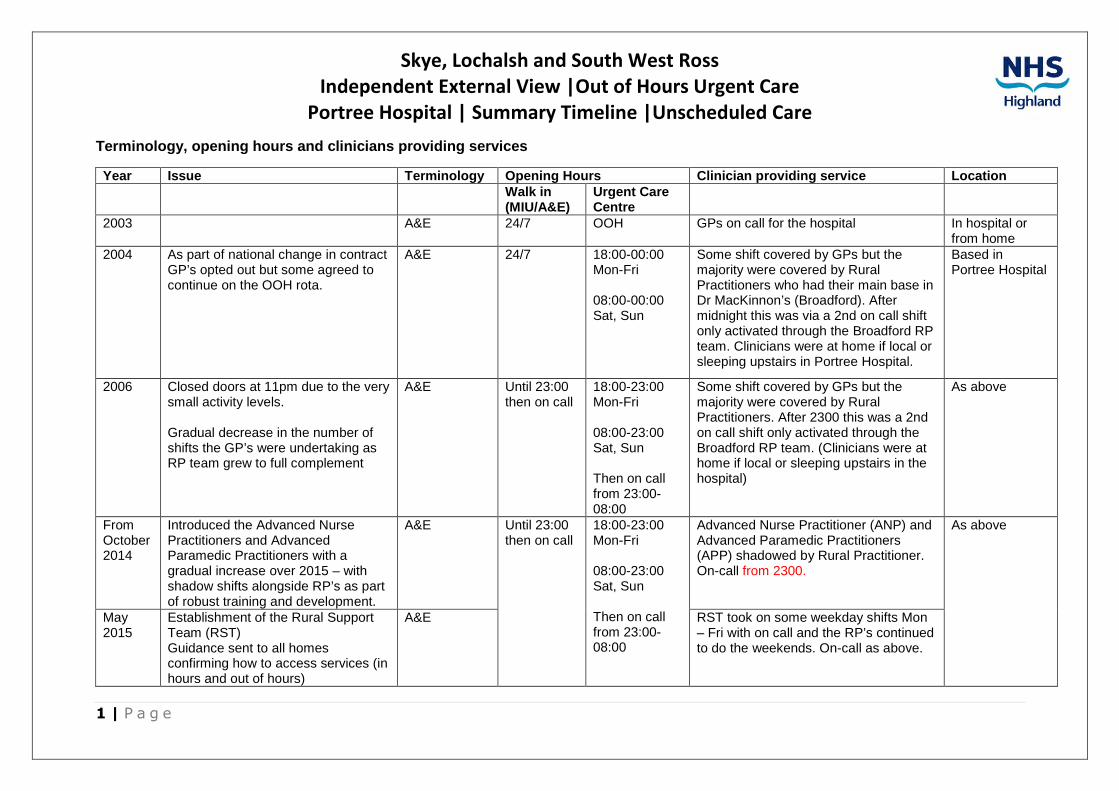
Skye, Lochalsh and South West Ross Independent External View |Out of Hours Urgent Care
Portree Hospital | Summary Timeline |Unscheduled Care
1 | P a g e
Terminology, opening hours and clinicians providing services
Year Issue Terminology Opening Hours Clinician providing service Location Walk in (MIU/A&E)
Urgent Care Centre
2003 A&E 24/7 OOH GPs on call for the hospital In hospital or from home
2004 As part of national change in contract GP’s opted out but some agreed to continue on the OOH rota.
A&E 24/7 18:00-00:00 Mon-Fri
08:00-00:00 Sat, Sun
Some shift covered by GPs but the majority were covered by Rural Practitioners who had their main base in Dr MacKinnon’s (Broadford). After midnight this was via a 2nd on call shift only activated through the Broadford RP team. Clinicians were at home if local or sleeping upstairs in Portree Hospital.
Based in Portree Hospital
2006 Closed doors at 11pm due to the very small activity levels.
Gradual decrease in the number of shifts the GP’s were undertaking as RP team grew to full complement
A&E Until 23:00 then on call
18:00-23:00 Mon-Fri
08:00-23:00 Sat, Sun
Then on call from 23:00-08:00
Some shift covered by GPs but the majority were covered by Rural Practitioners. After 2300 this was a 2nd on call shift only activated through the Broadford RP team. (Clinicians were at home if local or sleeping upstairs in the hospital)
As above
From October 2014
Introduced the Advanced Nurse Practitioners and Advanced Paramedic Practitioners with a gradual increase over 2015 – with shadow shifts alongside RP’s as part of robust training and development.
A&E Until 23:00 then on call
18:00-23:00 Mon-Fri
08:00-23:00 Sat, Sun
Then on call from 23:00-08:00
Advanced Nurse Practitioner (ANP) and Advanced Paramedic Practitioners (APP) shadowed by Rural Practitioner. On-call from 2300.
As above
May 2015
Establishment of the Rural Support Team (RST) Guidance sent to all homes confirming how to access services (in hours and out of hours)
A&E RST took on some weekday shifts Mon – Fri with on call and the RP’s continued to do the weekends. On-call as above.
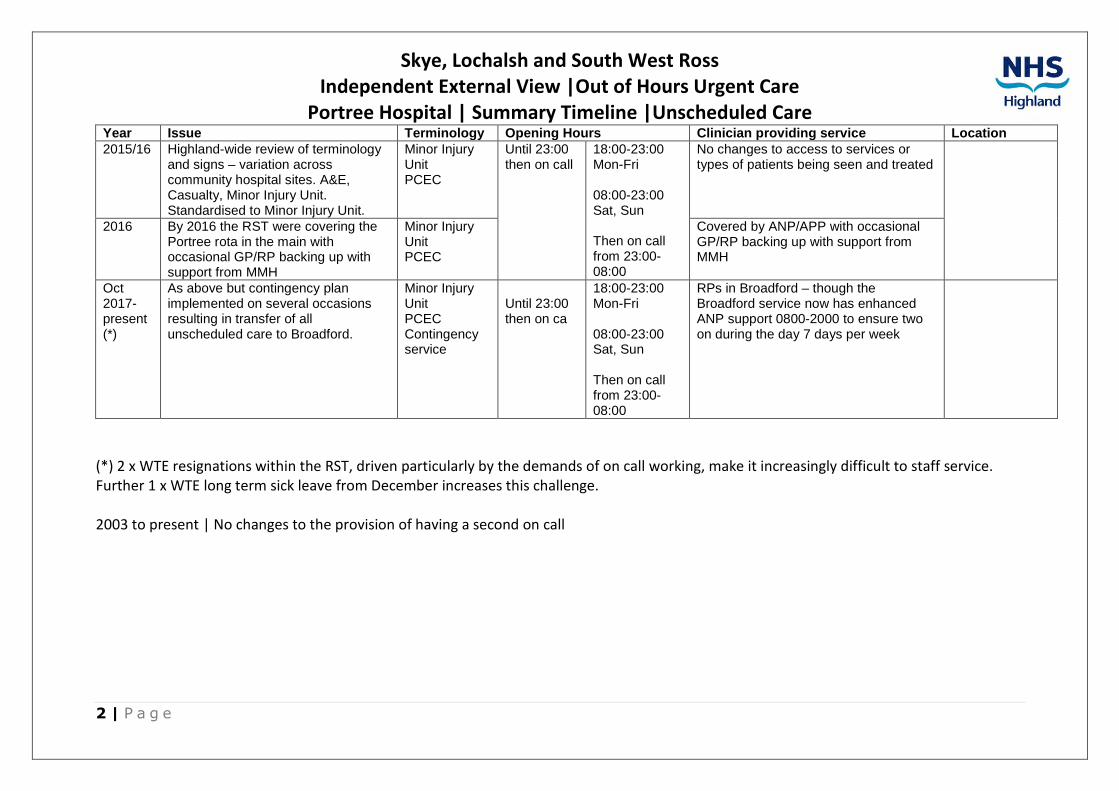
Skye, Lochalsh and South West Ross Independent External View |Out of Hours Urgent Care
Portree Hospital | Summary Timeline |Unscheduled Care
2 | P a g e
Year Issue Terminology Opening Hours Clinician providing service Location 2015/16 Highland-wide review of terminology
and signs – variation across community hospital sites. A&E, Casualty, Minor Injury Unit. Standardised to Minor Injury Unit.
Minor Injury Unit PCEC
Until 23:00 then on call
18:00-23:00 Mon-Fri
08:00-23:00 Sat, Sun
Then on call from 23:00-08:00
No changes to access to services or types of patients being seen and treated
2016 By 2016 the RST were covering the Portree rota in the main with occasional GP/RP backing up with support from MMH
Minor Injury Unit PCEC
Covered by ANP/APP with occasional GP/RP backing up with support from MMH
Oct 2017-present (*)
As above but contingency plan implemented on several occasions resulting in transfer of all unscheduled care to Broadford.
Minor Injury Unit PCEC Contingency service
Until 23:00 then on ca
18:00-23:00 Mon-Fri
08:00-23:00 Sat, Sun
Then on call from 23:00-08:00
RPs in Broadford – though the Broadford service now has enhanced ANP support 0800-2000 to ensure two on during the day 7 days per week
(*) 2 x WTE resignations within the RST, driven particularly by the demands of on call working, make it increasingly difficult to staff service. Further 1 x WTE long term sick leave from December increases this challenge.
2003 to present | No changes to the provision of having a second on call
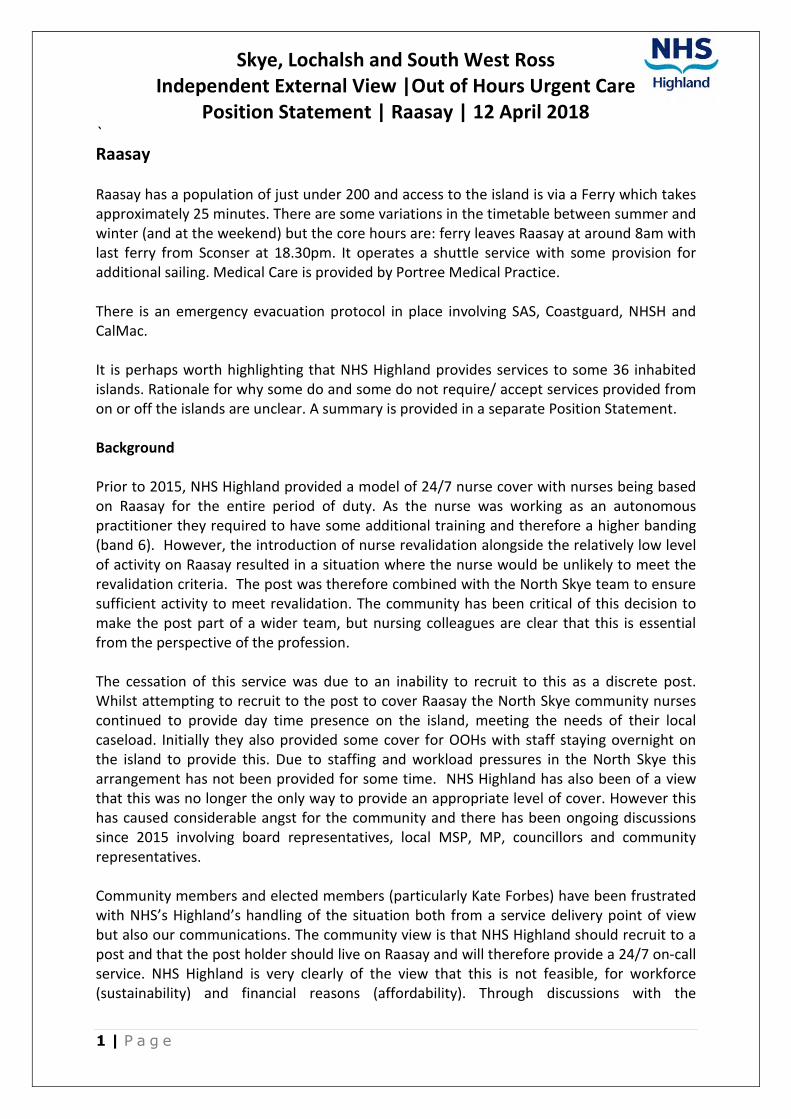
Skye, Lochalsh and South West Ross Independent External View |Out of Hours Urgent Care
Position Statement | Raasay | 12 April 2018
1 | P a g e
`
Raasay
Raasay has a population of just under 200 and access to the island is via a Ferry which takes approximately 25 minutes. There are some variations in the timetable between summer and winter (and at the weekend) but the core hours are: ferry leaves Raasay at around 8am with last ferry from Sconser at 18.30pm. It operates a shuttle service with some provision for additional sailing. Medical Care is provided by Portree Medical Practice.
There is an emergency evacuation protocol in place involving SAS, Coastguard, NHSH and CalMac.
It is perhaps worth highlighting that NHS Highland provides services to some 36 inhabited islands. Rationale for why some do and some do not require/ accept services provided from on or off the islands are unclear. A summary is provided in a separate Position Statement.
Background
Prior to 2015, NHS Highland provided a model of 24/7 nurse cover with nurses being based on Raasay for the entire period of duty. As the nurse was working as an autonomous practitioner they required to have some additional training and therefore a higher banding (band 6). However, the introduction of nurse revalidation alongside the relatively low level of activity on Raasay resulted in a situation where the nurse would be unlikely to meet the revalidation criteria. The post was therefore combined with the North Skye team to ensure sufficient activity to meet revalidation. The community has been critical of this decision to make the post part of a wider team, but nursing colleagues are clear that this is essential from the perspective of the profession.
The cessation of this service was due to an inability to recruit to this as a discrete post. Whilst attempting to recruit to the post to cover Raasay the North Skye community nurses continued to provide day time presence on the island, meeting the needs of their local caseload. Initially they also provided some cover for OOHs with staff staying overnight on the island to provide this. Due to staffing and workload pressures in the North Skye this arrangement has not been provided for some time. NHS Highland has also been of a view that this was no longer the only way to provide an appropriate level of cover. However this has caused considerable angst for the community and there has been ongoing discussions since 2015 involving board representatives, local MSP, MP, councillors and community representatives.
Community members and elected members (particularly Kate Forbes) have been frustrated with NHS’s Highland’s handling of the situation both from a service delivery point of view but also our communications. The community view is that NHS Highland should recruit to a post and that the post holder should live on Raasay and will therefore provide a 24/7 on-call service. NHS Highland is very clearly of the view that this is not feasible, for workforce (sustainability) and financial reasons (affordability). Through discussions with the
Skye, Lochalsh and South West Ross Independent External View |Out of Hours Urgent Care
Position Statement | Raasay | 12 April 2018
2 | P a g e
community, some common ground has been reached over these joint concerns, with a shared view that we should provide “a suitably trained person” on the island 24/7.
Community nursing for Raasay caseload is provided from the North Skye & Raasay team but we are unable to secure OOHs cover from within this team. It is not contractually possible to oblige them to remain on the island overnight.
In light of this, work with the community in 2017 identified a possible model based on the Health & Social Care Support worker role modelled on the retained roles in the Small Isles. The new job description includes an on-call element which will be accessed via NHS24 and at the direction of the Rural Practitioners in Broadford. These jobs have already been advertised without the on-call element and without success. The current Job Description includes the on-call element. Interviews were held at the start of March with one out of two posts recruited to.
Once the postholder starts, First Responder training will be provided by SAS and there is a formal third party agreement with SAS to utilise NHSH staff to provide the SAS First Responder service on Raasay. This is now included as a core part of the job description. However the community is looking for this to be at emergency responder level which we will try and work towards. The First Responder is generally a precursor to progressing to Emergency Responder but Scottish Ambulance Service is not presently supportive of the development of more of these schemes, and are working to progress governance arrangements and training that need to be in place first.
There is a low level of confidence that there will be interest from local residents to be First Responders. However, Scottish Fire and Rescue Service have intimated support for development of their local retained service on Raasay.
12 April 2018
Skye, Lochalsh and South West Ross Independent External View |Out of Hours Urgent Care
Position Statement | Rural Support Team| 13 April 2018
1 | P a g e
Background The Rural Support Team (RST) was set up for areas of Skye, Lochalsh and Lochaber as part of the “Being Here” Action Learning project.
The original strategy was tied to the “Being Here” project, funded by the Scottish Government. This came out of the recommendations of ‘Delivering for Remote and Rural Healthcare’, and the project was built around that delivery plan, with an ‘Action Research’ methodology. This was seen as appropriate for an innovative model as it meant that the project would change based on continuous learning. The project had several pilot sites including Skye, the Small Isles, Acharacle, Kintyre and Lochgilphead. Decisions (in relation to Skye) were made were through the RST working group, full papers of which can be provided.
Skye Team Central to the project was innovation in recruitment and multi-disciplinary team working in rural primary care. Portree was one pilot site, with a plan of moving towards a multi-disciplinary out of hours model.
From October 2014 Advanced Practitioners (Nurses and Paramedics) were introduced with a gradual increase over 2015. It was very quickly ascertained that these practitioners would not come ‘off the shelf’. Recruitment, via open processes, was undertaken of experienced individuals who had some but not all of the required skills. Initially there were shadow shifts alongside Rural Practitioners (RP) as part of robust training and development. That training programme developed as per the action research method, but within a short space of time a detailed competency framework and training plan was developed, and is publicly available. A copy if also included in the Briefing Pack for the Panel Meeting on 17th April 2018.
By 2016 the RST were covering the Portree rota in the main with occasional GP/RP backing up with support from staff in Dr MacKinnon Memorial Hospital (Broadford). The Advanced Nurses and Paramedics work on shift until 24:00 and then are on call.
Most recently contingency plans have had to be implemented on several occasions resulting in transfer of all unscheduled care patients (who need be seen) to Broadford. This has been due to staff shortages prompted by 3 x WTE resignations and 1 x WTE long term sick leave from December.
Evaluation of performance We have used case note review (in addition to the case based observations and assessment that are part of the training) to evaluate the clinical performance of Advanced Nurses and Advanced Paramedics. In short, this has been excellent, with most cases managed autonomously and clinical advice sought appropriately. We are extremely confident in the care these professionals provide. There is no evidence to suggest they work less efficiently than GPs, and they can manage most but not all of the cases a GP could. The small amount of feedback we have had from patients has been very positive. There have been no complaints and there is no evidence that patients do not wish to be seen by these practitioners.
However, what has become apparent is that, in contrast to GPs who usually work in daytime practice also, the low number of patients seen by OOH practitioners in rural locations has impacts in terms of job satisfaction and skills erosion.
Skye, Lochalsh and South West Ross Independent External View |Out of Hours Urgent Care
Position Statement | Rural Support Team| 13 April 2018
2 | P a g e
Recruitment & Retention Seven AP staff initially recruited to the wider RST (i.e across all of West Highland) left to work elsewhere (one to Portree Medical Practice and another to Gairloch Medical Practice). Of these seven, three were Portree-based staff.
There are three existing APs in post; one new start and three new post holders to commence in May 2018.
Dispute Linked to issues around recruitment and retention, there is an ongoing employment dispute between four practitioners and NHS Highland. This focuses around working hours and on-call hours (paid on shift 16:00 – 00:00 then on-call until 08:00). The Advanced Practitioners case is based on the following argument:
• APs feel they were never told at interview about being on-call;
• They argue they should be paid all hours as working hours;
• Though activity is low, APs feel they could be providing other services during the night;
• APs expected to be working in the community more and supporting SAS;
• They have to provide the on-call from the hospital (*)
• The rota prevents a reasonable work / life balance (this is specific to the remaining ANP (**)
Notes * APs were told 18 months ago they can be on call from home, but have opted not to with the ongoing grievance. ** The team were self-rostering and had elected to go on call immediately after working a shift. However there are other options for the configuration of the rota which the team have not tested.
Agenda for Change A further challenge around retention has been the constraints imposed by Agenda for Change Ts&Cs. It may be argued that these are not fit for these advanced and sought after roles, and NHS Highland raised this as part of the feedback requested following the peer review visit to NHS Highland by Sir Lewis Ritchie and his team (Feb 2017). Refer also to Position Statement on the feed-back.
In particular:
• NHS Highland can’t commit staff who we’ve invested training in to remain in our employment for a minimum period;
• NHS Highland can’t pay non-agenda for change wages, so practices can always outbid boards on salary;
• NHS Highland can’t pay a reasonable on-call rate (agenda for change is £18 for the whole night on call, plus sleep in rate of 2 hours basic living wage if sleeping on site, or full hourly rate – no sensible middle ground).
Understandably, daytime practices who are able to offer better terms for 9-5 work have had success in attracting these well trained individuals. We’ve made some difference offering good training and development leave/opportunities, which is the one contractual flexibility we do have.
Skye, Lochalsh and South West Ross Independent External View |Out of Hours Urgent Care
Position Statement | Rural Support Team| 13 April 2018
3 | P a g e
Lessons Learned Understandably a number of lessons have been learned from the experience to date with the RST. These are being put into action locally and on the north coast, and where a new rural support team is in development.
The following reflections are qualitative, and are informed by team discussions and formal exit interviews. In particular:
• A recognition that ‘Action Learning’ may not be the best approach for such a project.In some ways this approach worked very well, enabling us to continuously adapt and ‘knock down’ barriers which we could not have conceived at the start (e.g. the very particular governance implications of paramedics using their own skills framework, JRCALC, within an NHS Highland context). However, this had significant downsides, with staff finding that, in reality, this made work life unpredictable and the development of models unplanned. Because evaluation was ongoing rather than formal and time-limited, the team felt they didn’t know whether they had a future or not, and what that future might be. This led to frustration and conflict. We need to be clearer on new models before we commence recruitment, or recruit to fixed term contracts when experimenting with new ways of working. Of course, fixed term contracts bring their own complexities and challenges in terms of being able to attract practitioners to posts.
• Don’t take staff flexibility for granted. During the recruitment phase, the Rural Support Team was promoted as an innovative, dynamic idea for flexible cover across a large and remote geographical area – the idea being a similar approach to a multi-disciplinary internal locum agency. The reality is that, once staff are in post, they desire the same routine and work life balance as most do, with expectations around shift patterns and work locations. In new models, we need to ensure that flexibility rotation to other locations is part of the job, but that it is specified and quantified as part of the job, not the whole job and that this understood from the outset.
• Get Ts&Cs right at the start. This is very challenging, particularly with models that are new and evolving. But, unless spelled out in detail, patterns of work, hours and on-call become very fixed very quickly. We found that if we took people on as trainees, and their training occurred mostly in hours, this became very quickly the expectation for their work. Once they ‘graduated’ to their advanced practice roles and were rostered at weekends and on call, this became a source of dissatisfaction. On call remains a big challenge, which we have not resolved.
• ‘Dynamic’ and ‘innovative’ mean different things to different people. We described the models as dynamic and innovative at recruitment. For us, this meant working flexibly across different areas and times. Some of the staff who left felt they had been ‘mis-sold’ and for them that meant working more as part of the emergency teams than delivering primary care. We have since ensured that people expressing an interest in these roles are offered ‘shadowing’, and are wary of ‘overselling’ the roles.
• Single line management. We did not have enough line management capacity at the start. We now have a single senior line manager/professional lead for all of the team members, who supports their current and continuing education and manage staff operationally. This has had a huge positive impact, though we need to recognise that as the team expands this will become unmanageable for one individual. Put simply, there needs to be a recognition that management and professional leadership support is not an optional cost.
Skye, Lochalsh and South West Ross Independent External View |Out of Hours Urgent Care
Position Statement | Rural Support Team| 13 April 2018
4 | P a g e
• The importance of teamwork. These roles can be professionally isolating, as people work autonomously, often alone, and often in rural locations. We have learned that this is completely unsustainable, and models which have professionals working on their own for long periods are ‘off the table’. We also now place a greater emphasis on informal team meetings and get-togethers – even if only via VC. We did hold many meetings under the auspices of the RST working group, but these were more formal meeting and perhaps did not meet their informal team working needs.
• The importance of political context. This is very hard to quantify and to rectify, but we recognise that the particular relationship between NHS and the community in North Skye made for a poor atmosphere for a new team to flourish and gain in confidence. A useful comparison between Skye and Acharacle may be drawn. We are unsure how best to resolve this moving forward in Skye and is another reason we welcome the external peer opinion
• We got a lot right. In spite of the challenges, it is important to note that we got some things very right. In particular, the competency based training and development programmes, which have created very highly skilled, confident practitioners. This was accompanied by strong mentorship from named education leads, clinicians, and individualised educational needs assessments.
Strong links with the GP practice in Acharacle has been very positive (though, of course, this is easier with salaried practices). New rotational models into Dr Mackinnon hospital have been very successful for those staff members who have agreed to participate (not all), and the additional skilled input has been supported by the RP team. We are quite confident that our approach to clinical governance has been excellent. RST working group papers document key decisions around the clinical scope and function of team members, particularly around paramedics (prescribing, emergency skills).
Clinical Guardian is a genuinely innovative and high-quality approach to ensuring both oversight and feedback to clinicians working across a huge patch who cannot be observed constantly. The operational handbook and clinical protocols for OOHs are well documented and available to all staff on the intranet.
Further information on Clinical Governance is provided in the SBAR

SBAR: Clinical Governance for Out of Hours Consultations
Situation NHS Highland has the single largest out of hours service in Scotland. There are 62 out of hours
centres in Scotland with 32 of these being in Highland. In addition there are 14 minor injury units
which are increasingly nurse led with no GP available on site. Work is ongoing to look at recording of
information in MIUs, currently Adastra is the likeliest system to be implemented.
Each year in Highland around 75,000 primary care consultations occur out of hours. There are
320,000 patients in NHS Highland. Nearly all of these consultations are recorded on the Adastra
computer system, with the exception of some very small out of hours bases, and Nairn (around 3500
consultations).
There is minimal oversight or clinical support available to clinicians delivering this care, except for
when complaints are received. We cannot demonstrate that consultations are of a consistently high
quality, or that where standards of decision-making or record-keeping fall short, appropriate
feedback is available to clinicians. This issue has been raised by the SPSO for Advanced Nurse
practitioners.
A system for achieving this has been identified, namely, ‘Clinical Guardian’.
After feedback from Clinical Governance group alternative model based on the NHS Lothian model
has also been described and costed.
An electronic survey of staff attitudes to this was carried out. The majority were positive about the
proposed model. There were reservations about ‘big brother’, quality of feedback and whether this
should be a priority for OOH at this time. Since raising this idea there has been considerable positive
interest and support for it from ANPs and nursing leadership with more of the reservations coming
from the GP workforce.
Background Since the contract change in 2004, NHS Highland has become increasingly responsible for the direct
delivery of OOH primary care. With minor exceptions, NHS Highland now either directly delivers or
contracts delivery of OOH services. Most of this activity comes via NHS24. Most calls then go to the
local ‘Highland Hub’ for despatch to a local Urgent Care Centre for a consultation. This is all managed
and recorded using the Adastra system.
Clinical Guardian is a standalone system which takes an export from Adastra and creates a list of
cases to review. It was developed in response to the joint RCGP/RCPCH/RCEM Audit Toolkit from
2010. A copy of which is available on request. Reviewers work through this list, scoring the cases as
good, satisfactory or unsatisfactory, with feedback sent via email to the relevant clinician. Cases
deemed unsatisfactory are progressed to a group review. There is an add on system (no additional
charge) called Educational Guardian whereby all GP Registrar cases are reviewed and can then be
directly uploaded into their e-portfolio. Currently in Highland there is no clear system for clinical
supervision for GP registrars in OOH. This is not in line with recommendations from GMC.
Not all cases are reviewed. The system takes a risk stratified approach dependent on our
requirements. For instance, we may review 100% of the cases for a new clinician, but only a 10%
sample for an experienced clinician.
The cost of this system includes a 3 month trial, and is as follows (+VAT):
Setup fee £1000 One off payment Payable at the beginning of the 3 month
trial period
First year fee £800/month £7,200/annum Based on 9 months remaining in the first
year
Second year £717/month £8,600/annum Full annual fee discounted by £1000
This comes to £9840 for the first year.
Clinician time to review cases is additional to this, with a recommendation of £1 per case. The next
step would be to identify a team of clinicians to form the core reviewing team.
Below is a link to an article on Clinical Guardian on RCGP website.
http://www.rcgp.org.uk/clinical-and-research/bright-ideas/clinical-guardian.aspx
NHS Lothian model NHS Lothian has 860,000 patients with 5 OOH sites. Staffing is multidisciplinary with 30 salaried GPs, 19 WTE ANPs, 256 sessional GPs. There are no lone workers and ANPs never work at a site without GP cover. No Minor Injury Units. There is a full time Clinical Director, @ approx £124,000 p/a pro rata 4 Associate Clinical Directors given total of 28 hrs per week @ approx £115,000 p/a pro rata
• Quality improvement, interface between Lothian Unscheduled Care Service (LUCS), ED and SAS
• Complaints, education,
• Appraisals GP Registrars, Doctors in Difficulty
• NHS24 interface and feedback, ‘blue on blue’ feedback, Hub The 30 salaried GPs all have an annual face to face review as do the 19 ANPs. The sessional GPs can request a review.
NHS Highland Model NHSH has 320,000 patients with 32 OOH sites. Staffing is multidisciplinary with 50 nurses and 150 GPs engaged over the course of a month. There are 14 MIUs. The majority of staff are lone workers and ANPs work without direct GP cover in at least 6 sites and are first line contact with on call GP cover in at least 5 more. One Clinical Lead, 24 hours per week @ approx £85,000 p/a pro rata, temporary contract to expire March 2018. Responsible for service redesign, implementation of redesign (including public consultation), clinical governance, quality improvement, interface between NHSH, NHS24 and SAS, education events, complaints, evaluation of service changes. There is no system for reviews with either GP or ANPs.
Assessment It is clear that there needs to be a clear clinical governance structure for the NHS Highland OOH service. NHS Highland is providing services using different models of care to elsewhere in Scotland. In the spirit of this innovative approach a new model of governance and review is suggested.
With the geographical spread of staff and sites in the Highlands the most efficient system would be an electronic system with the ability to provide face to face or telephone/VC discussion with staff for those either identified as having a need or at their request for revalidation reasons.
GP Appraisal Lead is clear that this system in addition to some reflection and discussion of feedback would be acceptable under Quality Improvement section of appraisal.
• Benefits Step change in ability to support clinicians providing OOH primary care through regular feedback. Ability to identify problems which may impact patient safety and make decisions around future employment. Clinicians can use feedback for revalidation. Iron out inconsistencies in recording of data in Adastra Support new model of care in MIU
• Risks
Lack of buy in from clinicians who may see it as a threat.
Seen as being in competition with existing appraisal/education processes (see above).
Cost of reviewing cases exceeds budget. We will need to stratify the reviewing strategy to
ensure the number of cases is kept within budget.
Confidentiality for clinicians
• Evaluation Number o f cases reviewed and classification in each quarter Number of cases that cannot be reviewed due to technical issues in each quarter Survey of individual staff groups to classify differences in their views after taking part Number of people who have submitted reports as part of appraisal Survey of reviewers as to their view of system Estimation of total cost per case actually reviewed.
A survey was submitted to all clinicians (doctors and nurses and paramedics) working in OOH. 67% of
respondents answered positively to the question ‘would an audit of case notes and feedback be
useful to you’ (based on 82 responses). There were a number of concerns and uncertainties
expressed so a FAQ sheet could be useful. Reviewers will need to work to a recognised system for
constructive feedback whilst following the values of NHSH and HQA. This would also fulfil both the
clinician and managerial commitment to giving and receiving feedback in the Highland Clinical
Pledge.
50% of those who replied would be interested in taking part in reviewing.

Recommendation Support is requested to progress to a year’s trial for all nursing staff, locum agency GPs, GP registrars
and salaried GPs in North Highland, for which funding is available (via the Scottish Government
Transforming Primary Care fund - £14,000 received)
Antonia Reed
Evan Beswick
August 2017
Urgent care on Skye: a summary from routine patient management data
There are two Urgent Care Centres on Skye at Dr Mackinnon Memorial Hospital in Broadford and at Portree Hospital. Portree Hospital has a Minor Injuries Unit (MIU) that operates between 8am and 11 pm seven days a week. Staff are on call from 12pm-8am. The MIU on weekdays (8am-6pm) has a GP who provides care and at weekends the service is run by OOHs staff that will also include Advanced Nurse Practitioners (ANP).
There is an Accident and Emergency (A&E) Unit at Broadford providing a 24 hour service on 7 days of the week. The service is delivered by Rural Practitioners who are specialist hospital medical staff, supported on occasion by an ANP
Out of Hours (OOHs) Primary Care Services are located at both sites. OOHs operates 6pm to 8am weekdays and from 6pm Friday to 8am Monday at both sites. At both sites all patients are seen in A&E/MIU rooms and there is no recording distinction between patients coming in as OOH’s attendees or as A&E/MIU attendees. In both locations most patients present without coming via NHS 24.
The ADASTRA patient management system is used in Broadford and Portree to manage and record all urgent care activity in A&E, MIU and OOHs settings. The graphics and tables in this report are based upon an extract of data from this source and the term ‘unscheduled care’ is used to summarise the activity. We use the term contact to refer to the total of all types of unscheduled care activity. The primary types of contact are appointments, advice and homes visit. Over 90 percent of contacts at Broadford and Portree are appointments.
We use the postcode of residence of patient contacts with services to highlight the variation in unscheduled care activity by area, site and by time of day. A limitation of the way that the ADASTRA system is used at Broadford and Portree is that it is not possible to distinguish care provided as OOHs from that which occurred in A&E/MIU. This is due to the clinical integration between these services – they are delivered by the same teams. Our primary analysis is therefore based upon the time activity occurred. The local recording method limits the possibilities of benchmarking OOHs activity against other areas in Highland that record OOHs and A&E/MIU data separately.
The area referred to in the analysis as Skye, Lochalsh and South West Ross (SLsWR) is shown in Map 2. The current location of services related to the Urgent Care Centres and unscheduled activity in SLsWR is shown in Map 1.
Report prepared for Evan Beswick, Project Lead, Out of Hours and Acting Primary Care Manager North & West (GMS)
Date extract provided by NHS Highland Planning and Performance Team
Analysis and mapping by NHS Highland Health Intelligence Team, Directorate of Public Health
April 2018

Summary of key messages
1. Rates of unscheduled care contacts in the Skye and Lochalsh area are largely similar with those of Highland (based upon resident population).
2. Activity at Broadford and Portree is highly seasonal, with up to 30% of contacts in summer months being with ‘out of area’ patients.
3. This seasonal variation is evident in the whole of Highland, though is more marked in Skye and Lochalsh.
4. Most patients in Skye and Lochalsh do not use NHS24 to access unscheduled care. During the Out of Hours period, 10% of contacts were via NHS 24 in Skye, compared to 73% in the rest of Highland (2017 data).
5. 90 percent of unscheduled care contacts at Broadford and Portree are appointments.
6. The majority (two thirds) of unscheduled care is required between 8am and 6pm. This is consistent across the locality and over the past five years.
7. Activity overnight (12 midnight to 8am) at both sites makes up 6% of all unscheduled care activity.
8. Overnight (12 midnight to 8am) activity at Portree represents around 0.6% of all unscheduled care activity. This has remained consistent over the past five years.
9. Rates of resident use of unscheduled care services are observed to be higher closer to either the A&E or MIU.
10. Resident of Lochalsh and the South of Skye almost exclusively use services only at Broadford. Residents of the North of Skye access services at both Portree and Broadford.
11. Admissions in the OOHs period following a contact at Broadford are higher than the Highland average.
12. The majority of patients admitted to hospital are admitted locally (71%).
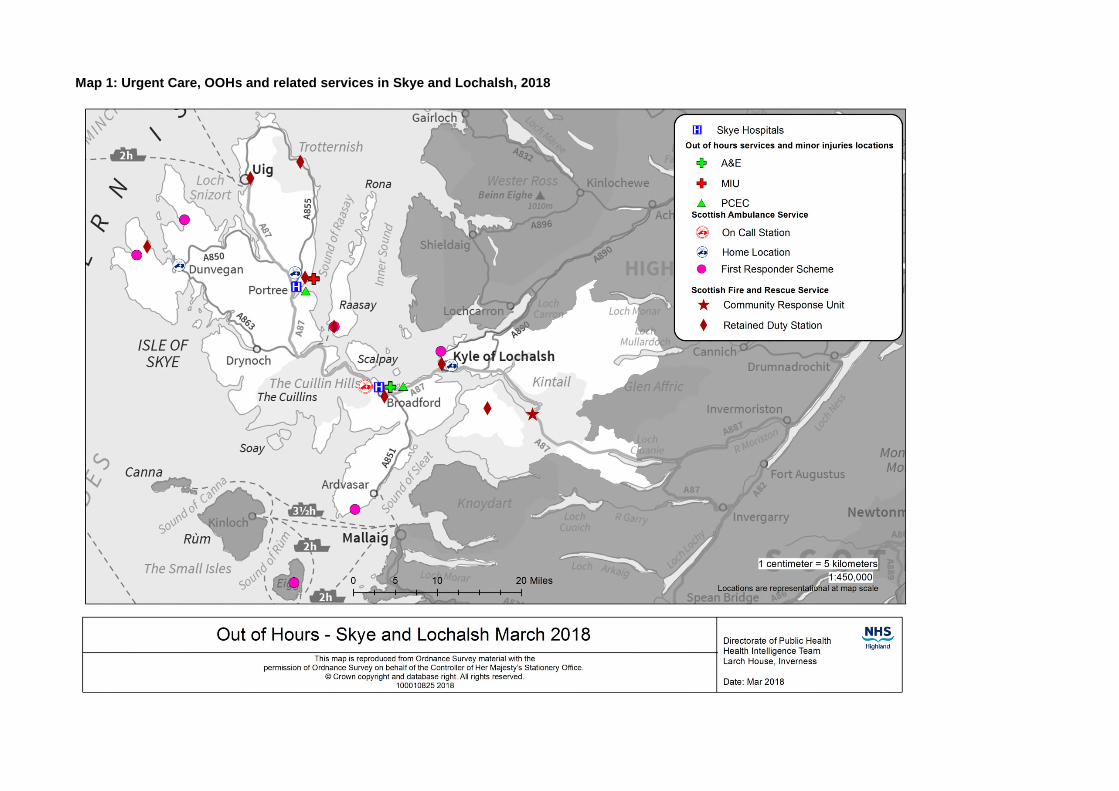
Map 1: Urgent Care, OOHs and related services in Skye and Lochalsh, 2018
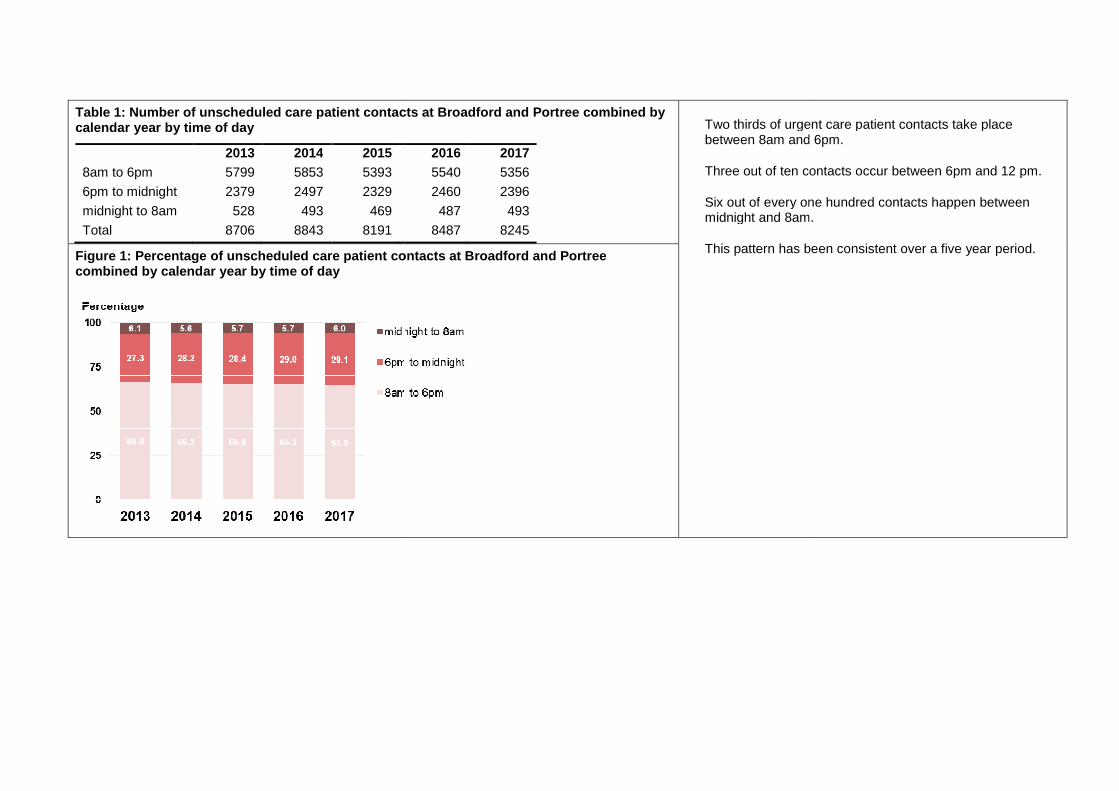
Table 1: Number of unscheduled care patient contacts atcalendar year by time of day
2013 2014 2015
8am to 6pm 5799 5853 5393
6pm to midnight 2379 2497 2329
midnight to 8am 528 493 469
Total 8706 8843 8191
Figure 1: Percentage of unscheduled care patient contacts at Broadford and Portreecombined by calendar year by time of day
: Number of unscheduled care patient contacts at Broadford and Portree combined by
2016 2017
5540 5356
2460 2396
487 493
8487 8245
Two thirds of urgent care patient contacts take place between 8am and 6pm.
Three out of ten contacts occur between 6pm and 12 pm.
Six out of every one hundred contacts happenmidnight and 8am
This pattern has been consistent over : Percentage of unscheduled care patient contacts at Broadford and Portree
Two thirds of urgent care patient contacts take place between 8am and 6pm.
Three out of ten contacts occur between 6pm and 12 pm.
Six out of every one hundred contacts happen between midnight and 8am.
This pattern has been consistent over a five year period.
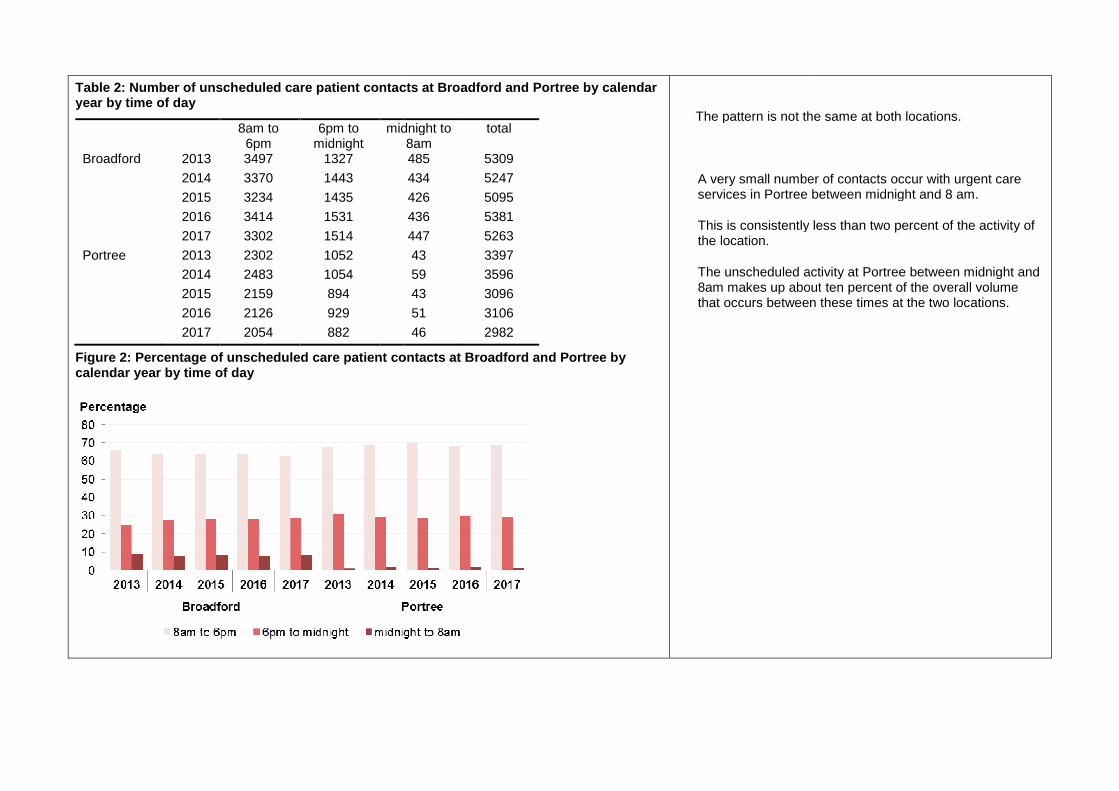
Table 2: Number of unscheduled care patient contacts at Broadford and Portree by calendar year by time of day
8am to 6pm
6pm to midnight
midnight to
Broadford 2013 3497 1327
2014 3370 1443
2015 3234 1435
2016 3414 1531
2017 3302 1514
Portree 2013 2302 1052
2014 2483 1054
2015 2159 894
2016 2126 929
2017 2054 882
Figure 2: Percentage of unscheduled care patient contacts at Broadford and Portree by calendar year by time of day
: Number of unscheduled care patient contacts at Broadford and Portree by calendar
midnight to 8am
total
485 5309
434 5247
426 5095
436 5381
447 5263
43 3397
59 3596
43 3096
51 3106
46 2982
care patient contacts at Broadford and Portree by
The pattern is not the same at both locations.
A very small number of contacts occur with urgent care services in Portree between midnight and 8 am
This is consistently the location.
The unscheduled activity at Portree between midnight and 8am makes up aboutthat occurs between these times
The pattern is not the same at both locations.
A very small number of contacts occur with urgent care services in Portree between midnight and 8 am.
This is consistently less than two percent of the activity of
The unscheduled activity at Portree between midnight and 8am makes up about ten percent of the overall volume that occurs between these times at the two locations.
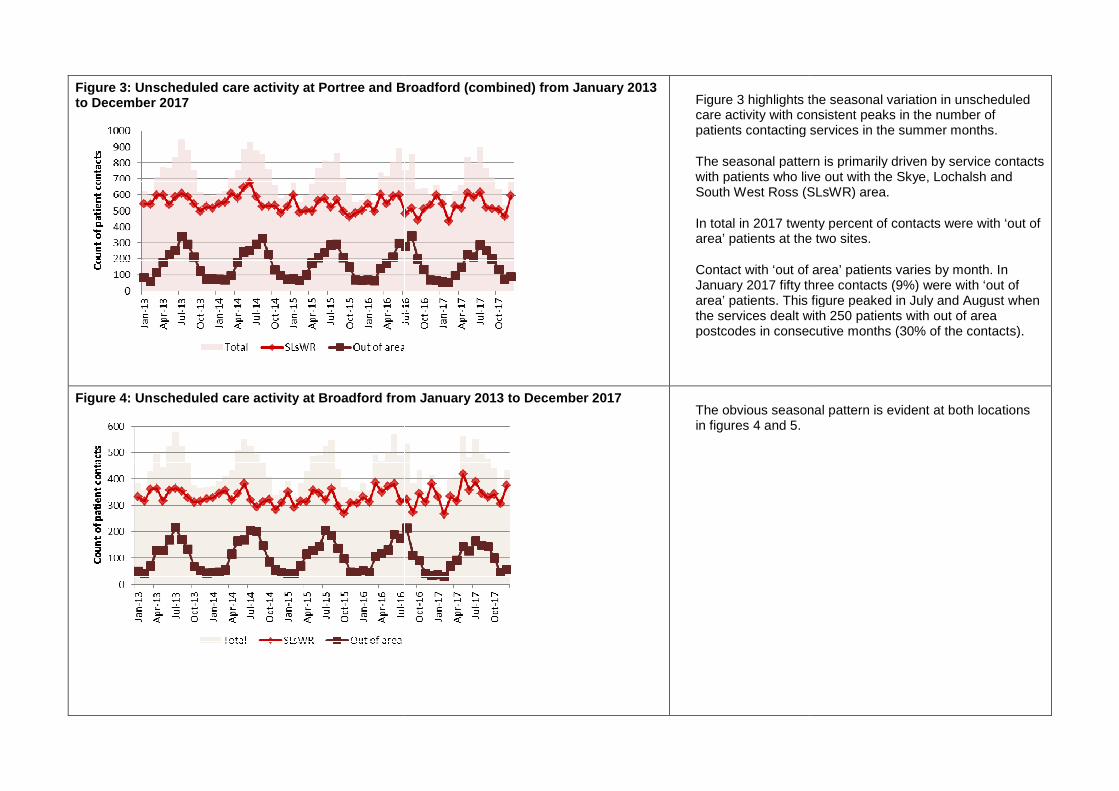
Figure 3: Unscheduled care activity at Portree and Broadford (combined) from January 2013 to December 2017
Figure 4: Unscheduled care activity at Broadford from January 2013 to De
Unscheduled care activity at Portree and Broadford (combined) from January 2013 Figure 3 highlights the seasonal variation in unscheduled care activity with consistent peaks in the number of patients contacting services in the summer months.
The seasonal pattern is primarily driven by service contacts with patients who live out with the Skye, South West Ross (SLsWR)
In total in 2017 twenty percent of contacts were with ‘out of area’ patients at the two sites.
Contact with ‘out of area’ patients varies by month. In January 2017 fifty three contacts (9%) were with ‘out of area’ patients. This figure peaked in July and August when the services dealt with 250 patients with out of area postcodes in consecutive months (30% of the contacts).
: Unscheduled care activity at Broadford from January 2013 to December 2017 The obvious seasonal pattern is evident at both locationsin figures 4 and 5.
the seasonal variation in unscheduled care activity with consistent peaks in the number of patients contacting services in the summer months.
The seasonal pattern is primarily driven by service contacts who live out with the Skye, Lochalsh and
South West Ross (SLsWR) area.
In total in 2017 twenty percent of contacts were with ‘out of area’ patients at the two sites.
Contact with ‘out of area’ patients varies by month. In January 2017 fifty three contacts (9%) were with ‘out of
ts. This figure peaked in July and August when the services dealt with 250 patients with out of area postcodes in consecutive months (30% of the contacts).
The obvious seasonal pattern is evident at both locations
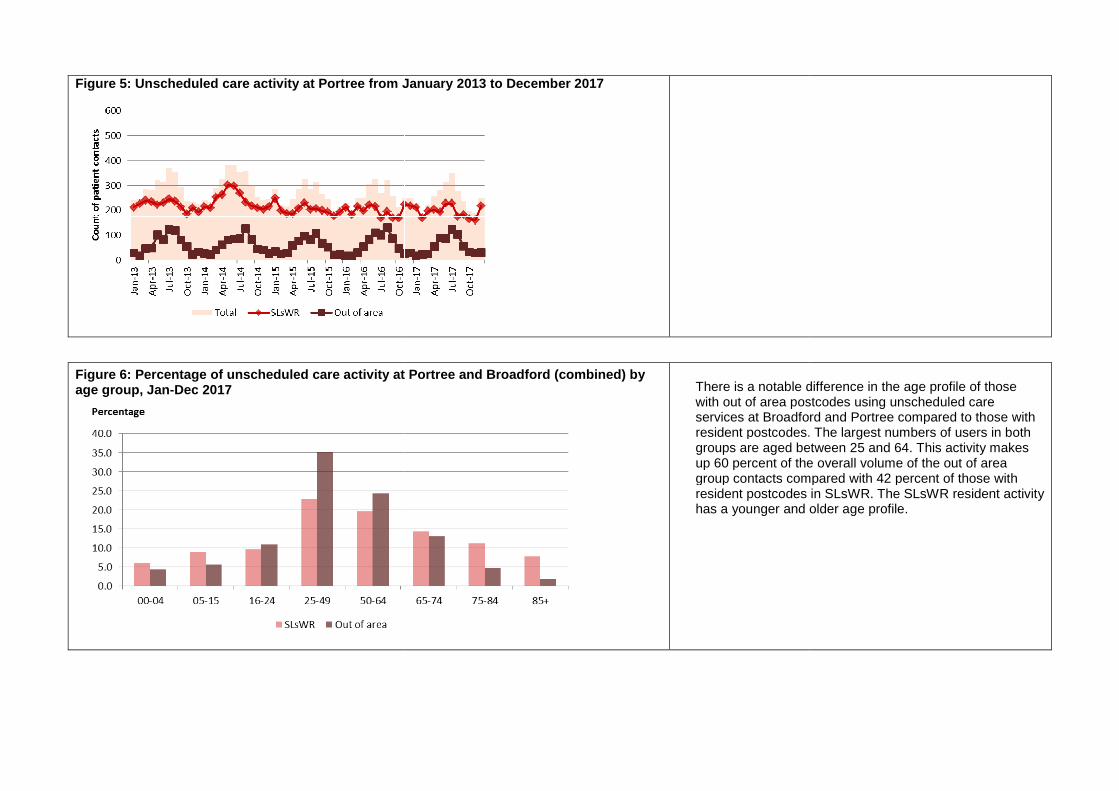
Figure 5: Unscheduled care activity at Portree from January 2013 to December 2017
Figure 6: Percentage of unscheduled care activity at Portree and Broadford (combined) by age group, Jan-Dec 2017
: Unscheduled care activity at Portree from January 2013 to December 2017
unscheduled care activity at Portree and Broadford (combined) by There is a notable difference in the age profile of those with out of area postcodes using unscheduled care services at Broadford and Portree compareresident postcodes. groups are aged between 25 and 64. Tup 60 percent of the overall volume of the out of area group contacts compared with 42 percent of those with resident postcodes has a younger and older age profile.
There is a notable difference in the age profile of those with out of area postcodes using unscheduled care services at Broadford and Portree compared to those with resident postcodes. The largest numbers of users in both
ed between 25 and 64. This activity makes up 60 percent of the overall volume of the out of area group contacts compared with 42 percent of those with resident postcodes in SLsWR. The SLsWR resident activity has a younger and older age profile.
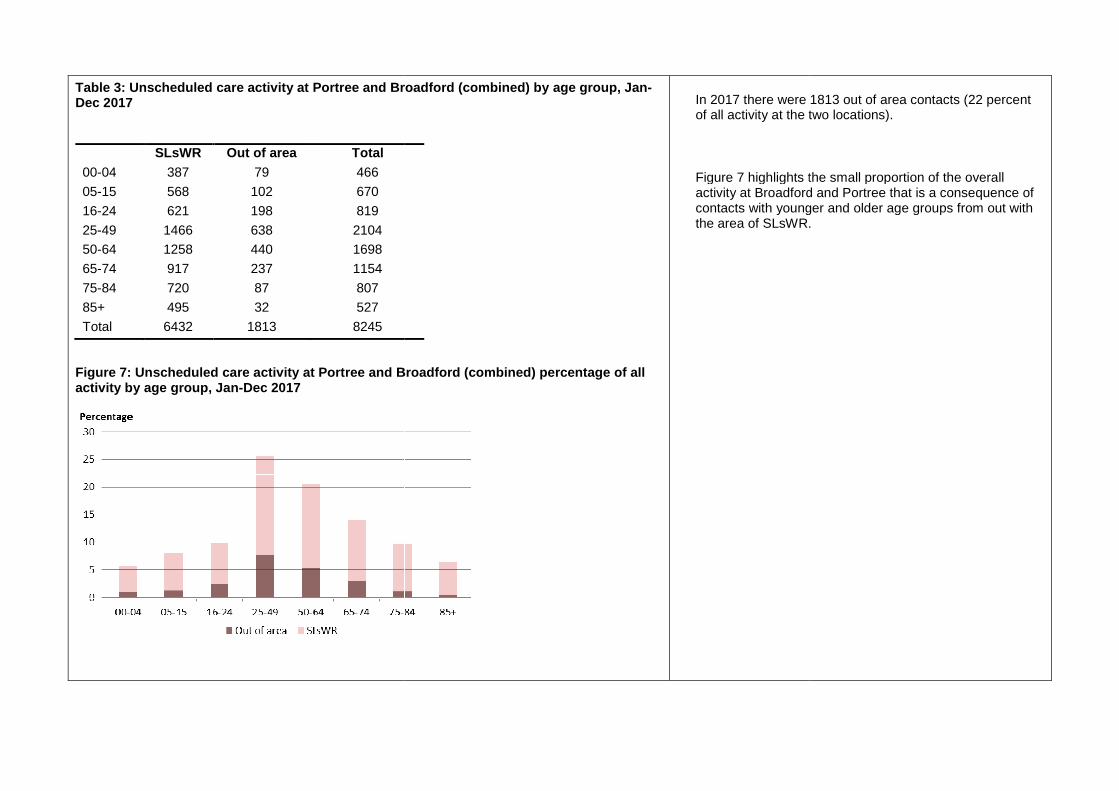
Table 3: Unscheduled care activity at Portree and Broadford (combined) by age group, JanDec 2017
SLsWR Out of area Total
00-04 387 79 466
05-15 568 102 670
16-24 621 198 819
25-49 1466 638 2104
50-64 1258 440 1698
65-74 917 237 1154
75-84 720 87 807
85+ 495 32 527
Total 6432 1813 8245
Figure 7: Unscheduled care activity at Portree and Broadford (combined) percentage activity by age group, Jan-Dec 2017
: Unscheduled care activity at Portree and Broadford (combined) by age group, Jan-
: Unscheduled care activity at Portree and Broadford (combined) percentage of all
In 2017 there were 1813 out of area contacts (22 percent of all activity at the two locations).
Figure 7 highlights the small proportion of the overall activity at Broadford and Portree that is a consequence contacts with younger and older age groups from out with the area of SLsWR.
In 2017 there were 1813 out of area contacts (22 percent of all activity at the two locations).
Figure 7 highlights the small proportion of the overall activity at Broadford and Portree that is a consequence of contacts with younger and older age groups from out with the area of SLsWR.
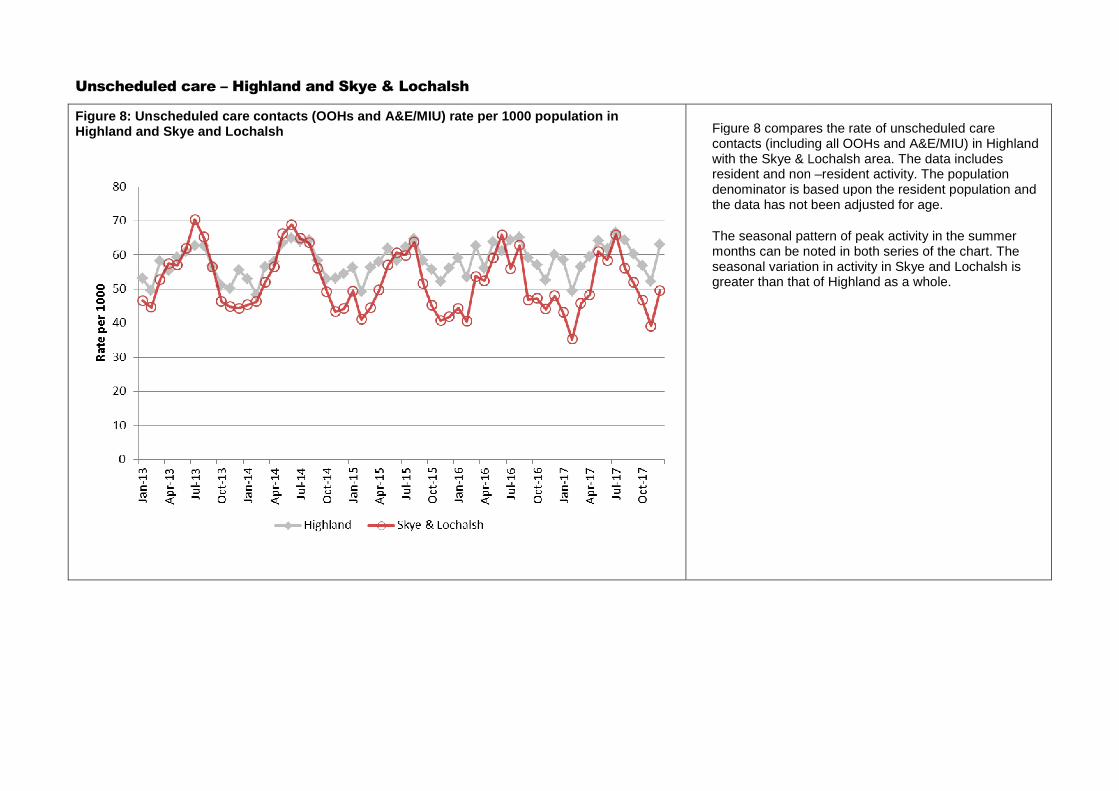
Unscheduled care – Highland and Skye & Lochalsh
Figure 8: Unscheduled care contacts (OOHs and A&E/MIU) rate per 1000 population in Highland and Skye and Lochalsh
Highland and Skye & Lochalsh
: Unscheduled care contacts (OOHs and A&E/MIU) rate per 1000 population in Figure 8 compares the rate of unscheduled care contacts (including all OOHs and A&E/MIU) in Highland with the Skye & Lochalsh area. The data includes resident and non denominator is based upon the the data has not been adjusted for age.
The seasonal pattern of peak activity in the summer months can be noted in both series of the chart. The seasonal variation in activity in Skye and Lochalsh is greater than that of Highland as
Figure 8 compares the rate of unscheduled care contacts (including all OOHs and A&E/MIU) in Highland with the Skye & Lochalsh area. The data includes resident and non –resident activity. The population denominator is based upon the resident population and the data has not been adjusted for age.
The seasonal pattern of peak activity in the summer months can be noted in both series of the chart. The seasonal variation in activity in Skye and Lochalsh is greater than that of Highland as a whole.
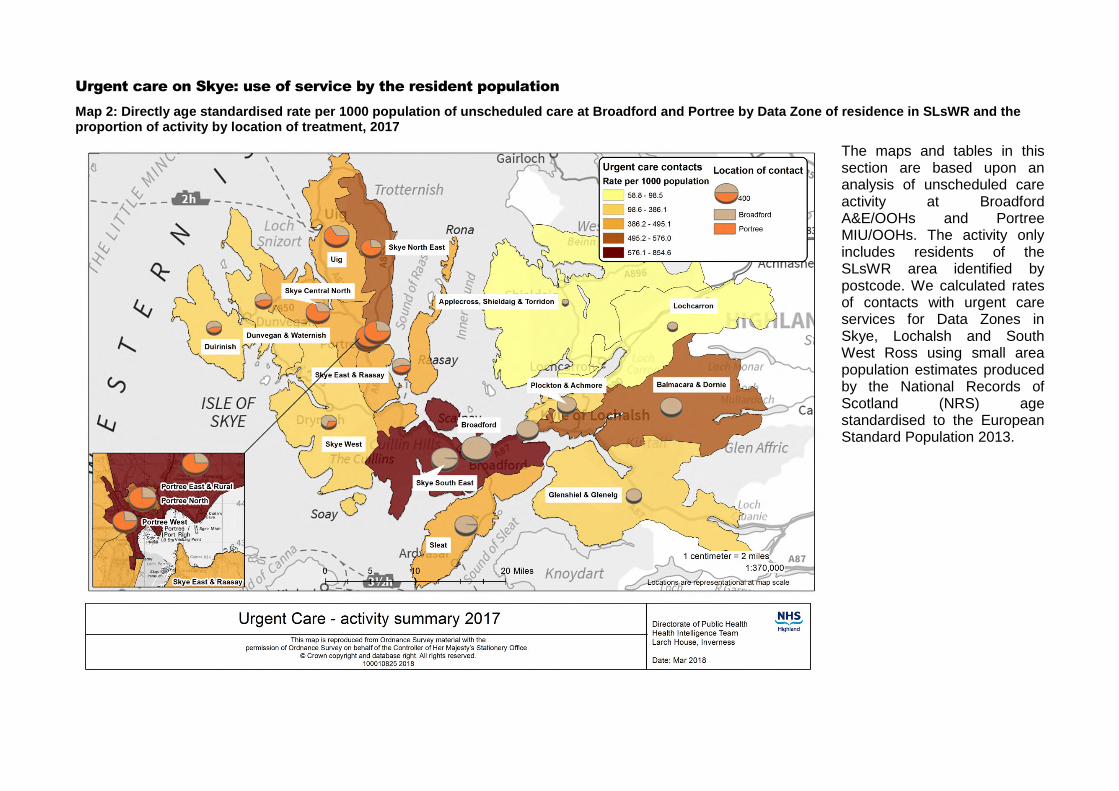
Urgent care on Skye: use of service by the resident population
Map 2: Directly age standardised rate per 1000 population of unscheduled care at Broadford and Portree by Data Zone of residence in SLsWR and the proportion of activity by location of treatment, 2017
The maps and tables in this section are based upon an analysis of unscheduled care activity at Broadford A&E/OOHs and Portree MIU/OOHs. The activity only includes residents of the SLsWR area identified by postcode. We calculated rates of contacts with urgent care services for Data Zones in Skye, Lochalsh and South West Ross using small area population estimates produced by the National Records of Scotland (NRS) age standardised to the European Standard Population 2013.
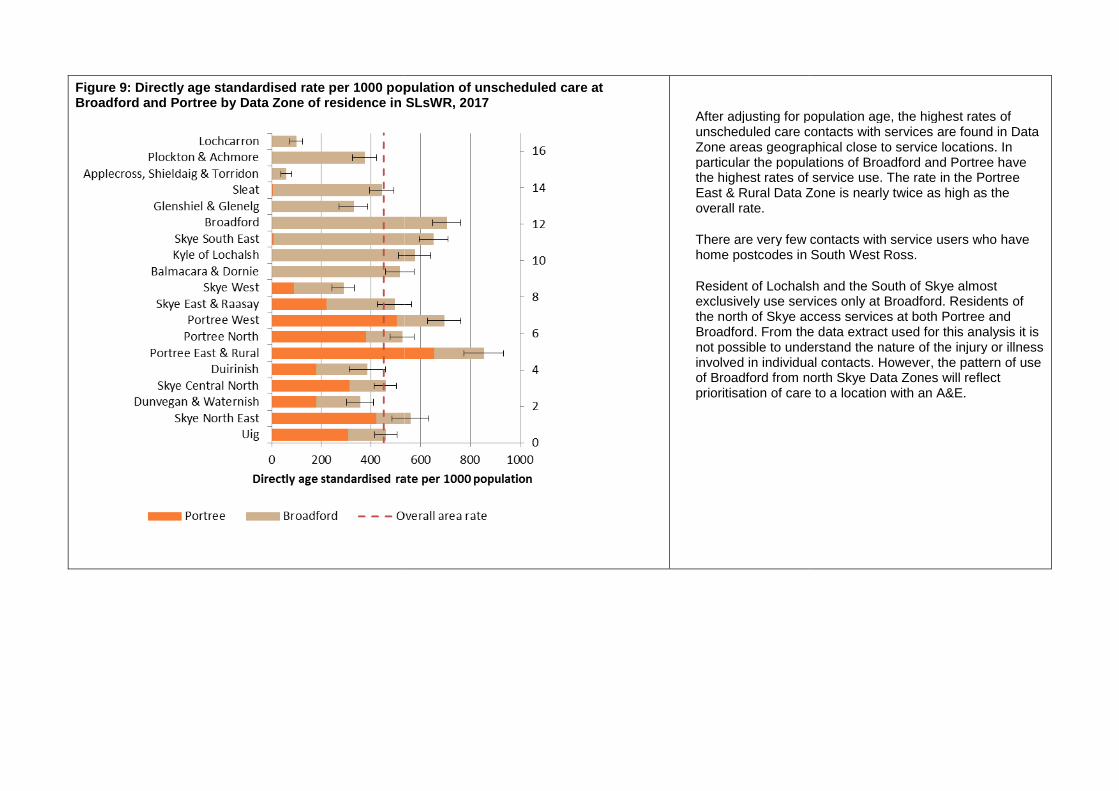
Figure 9: Directly age standardised rate per 1000 population of unscheduledBroadford and Portree by Data Zone of residence in SLsWR
te per 1000 population of unscheduled care at Broadford and Portree by Data Zone of residence in SLsWR, 2017
After adjusting for population age, the highest rates of unscheduled care contacts with services are found in Data Zone areas geographical close to service locations. In particular the populations of Broadford and Portree have the highest rates of service use.East & Rural Data Zone is neoverall rate.
There are very few contacts with service users who have home postcodes in South West Ross.
Resident of Lochalsh and the South of Skye almost exclusively use services only at Broadford. Residents of the north of Skye access services at both Portree and Broadford. From the data not possible to understand the nature of the injury or illness involved in individual contactsof Broadford from north Skyeprioritisation of care to a location with an A&E.
After adjusting for population age, the highest rates of unscheduled care contacts with services are found in Data Zone areas geographical close to service locations. In particular the populations of Broadford and Portree have the highest rates of service use. The rate in the Portree East & Rural Data Zone is nearly twice as high as the
There are very few contacts with service users who have home postcodes in South West Ross.
Resident of Lochalsh and the South of Skye almost exclusively use services only at Broadford. Residents of
access services at both Portree and Broadford. From the data extract used for this analysis it is not possible to understand the nature of the injury or illness involved in individual contacts. However, the pattern of use
north Skye Data Zones will reflect prioritisation of care to a location with an A&E.
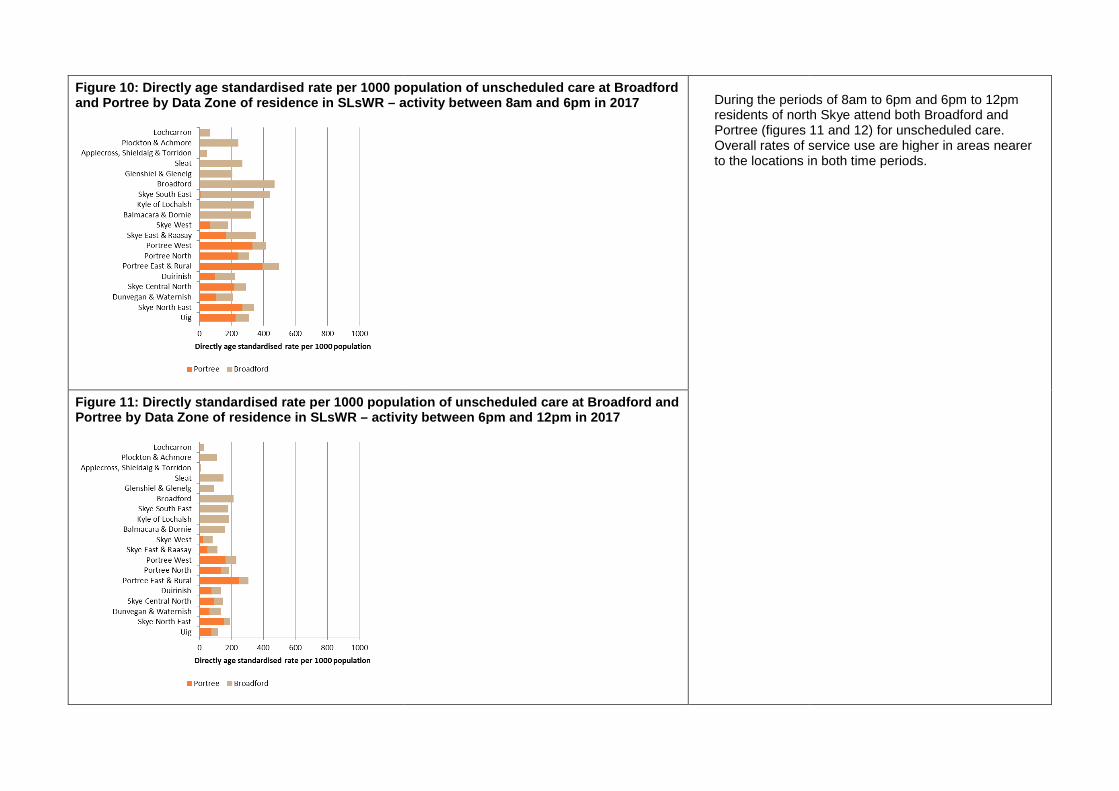
Figure 10: Directly age standardised rate per 1000 population of unscheduled care at Broadford and Portree by Data Zone of residence in SLsWR – activity between 8am and 6pm
Figure 11: Directly standardised rate per 1000 population of unscheduled care at Broadford and Portree by Data Zone of residence in SLsWR – activity between 6pm and 12pm
: Directly age standardised rate per 1000 population of unscheduled care at Broadford activity between 8am and 6pm in 2017 During the periods of 8am to 6pm and 6pm to 12pm
residents of north Skye attend both Portree (figures 11 and 12Overall rates of service use are higherto the locations in both time periods.
: Directly standardised rate per 1000 population of unscheduled care at Broadford and activity between 6pm and 12pm in 2017
During the periods of 8am to 6pm and 6pm to 12pm residents of north Skye attend both Broadford and Portree (figures 11 and 12) for unscheduled care.
erall rates of service use are higher in areas nearer in both time periods.
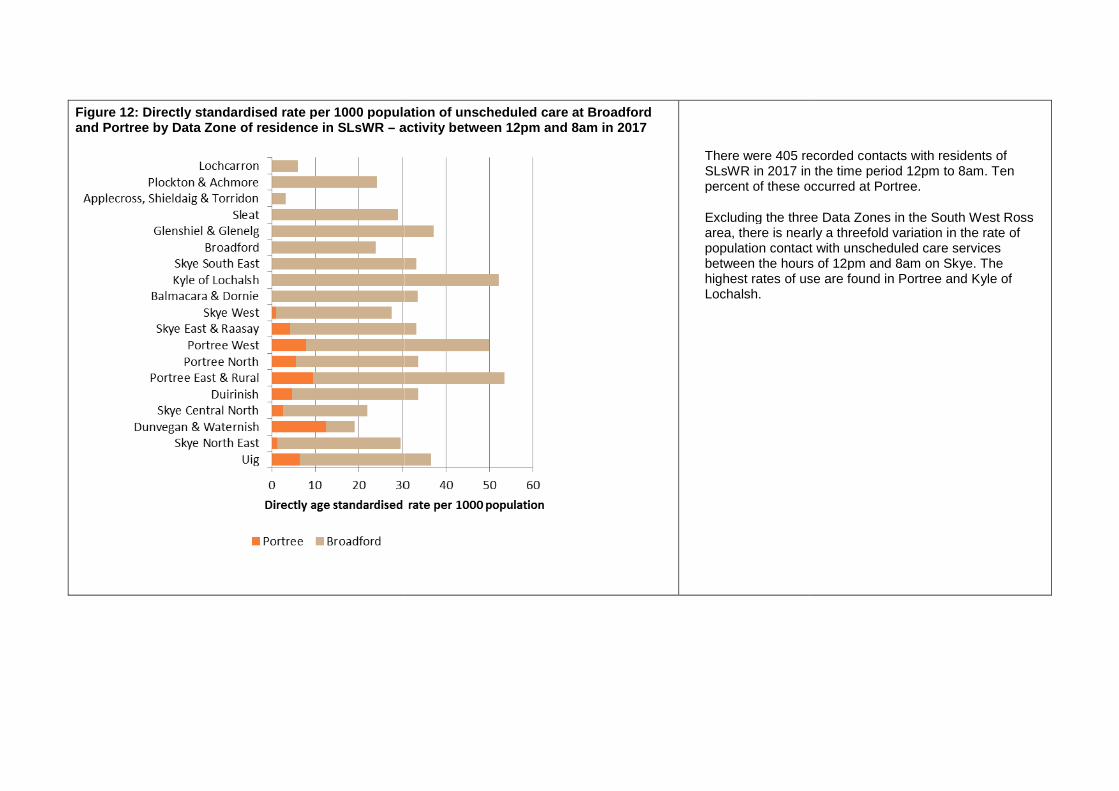
Figure 12: Directly standardised rate per 1000 population of unscheduled care at Broadford and Portree by Data Zone of residence in SLsWR – activity between 12pm and 8am
: Directly standardised rate per 1000 population of unscheduled care at Broadford activity between 12pm and 8am in 2017
There were 405 recorded contacts with residents of SLsWR in 2017 in the time period 12pm to 8am. Ten percent of these occurred at Portree.
Excluding the three Data Zonearea, there is nearly a threefold variation in the rate of population contact with unscheduled care services between the hours of 12pm and 8am on Skye. The highest rates of use are found in Portree and Kyle of Lochalsh.
There were 405 recorded contacts with residents of SLsWR in 2017 in the time period 12pm to 8am. Ten percent of these occurred at Portree.
Excluding the three Data Zones in the South West Ross area, there is nearly a threefold variation in the rate of
ulation contact with unscheduled care services between the hours of 12pm and 8am on Skye. The highest rates of use are found in Portree and Kyle of

Figure 13: Number of contacts with unscheduled care services at between 12pm and 8am by month, 2013- 2017
Figure 14: Histograms of unscheduled care contacts a month at Portree and Broadford between 12pm and 8am, 2013-2017
0
10
20
30
40
50
60
70
80
90
100
0
2
4
6
8
10
12
14
16
0 1 2 3 4 5 6 7 8
Cu
mu
lati
ve
%
Fre
qu
en
cy
Number of contacts a month
Portree
Frequency Cumulative Percent
0
1
2
3
4
5
6
7F
req
ue
ncy
: Number of contacts with unscheduled care services at Broadford and Portree
: Histograms of unscheduled care contacts a month at Portree and Broadford
Figures 13 and 14(resident and non-pm and 8 am.
The number of contacts by month at Portree little over time. The average number of contacts a month is 4 and the mode is 3.
The number of contacts at Broadford varies between 21 and 51 per month. The mean number of contacts a month is 37 and the mode 34
0
10
20
30
40
50
60
70
80
90
100
21 26 30 32 34 36 38 41 43 45 47 49 51
Cu
mu
lati
ve
%
Number of contacts a month
Broadford
Frequency Cumulative Percent
4 include all unscheduled care activity -resident) at the locations between 12
of contacts by month at Portree has deviated little over time. The average number of contacts a month is 4 and the mode is 3.
The number of contacts at Broadford varies between 21 and 51 per month. The mean number of contacts a month s 37 and the mode 34
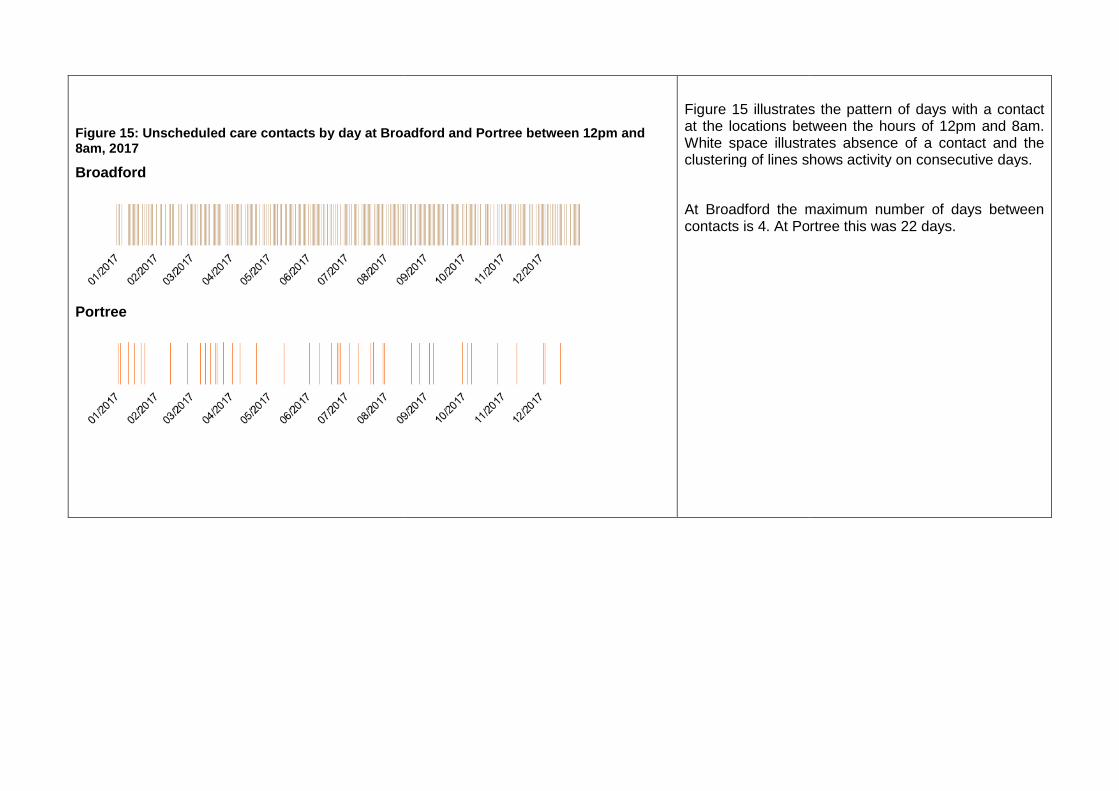
Figure 15: Unscheduled care contacts by day at Broadford and Portree between 12pm and 8am, 2017
Broadford
Portree
eduled care contacts by day at Broadford and Portree between 12pm and
Figure 15 illustrates the at the locations between the hours of 12pm and 8am.White space illustrates absence of a contact and the clustering of lines shows activity on consecutive days.
At Broadford the maximum number of days between contacts is 4. At Portree this was 22 days.
illustrates the pattern of days with a contact at the locations between the hours of 12pm and 8am.White space illustrates absence of a contact and the clustering of lines shows activity on consecutive days.
maximum number of days between contacts is 4. At Portree this was 22 days.

Map 3: Directly age standardised rate per 1000 population of unscheduled care at Broadford and Portree by Data Zone of residence in SLsWR and the proportion of activity by time of contact, 2017
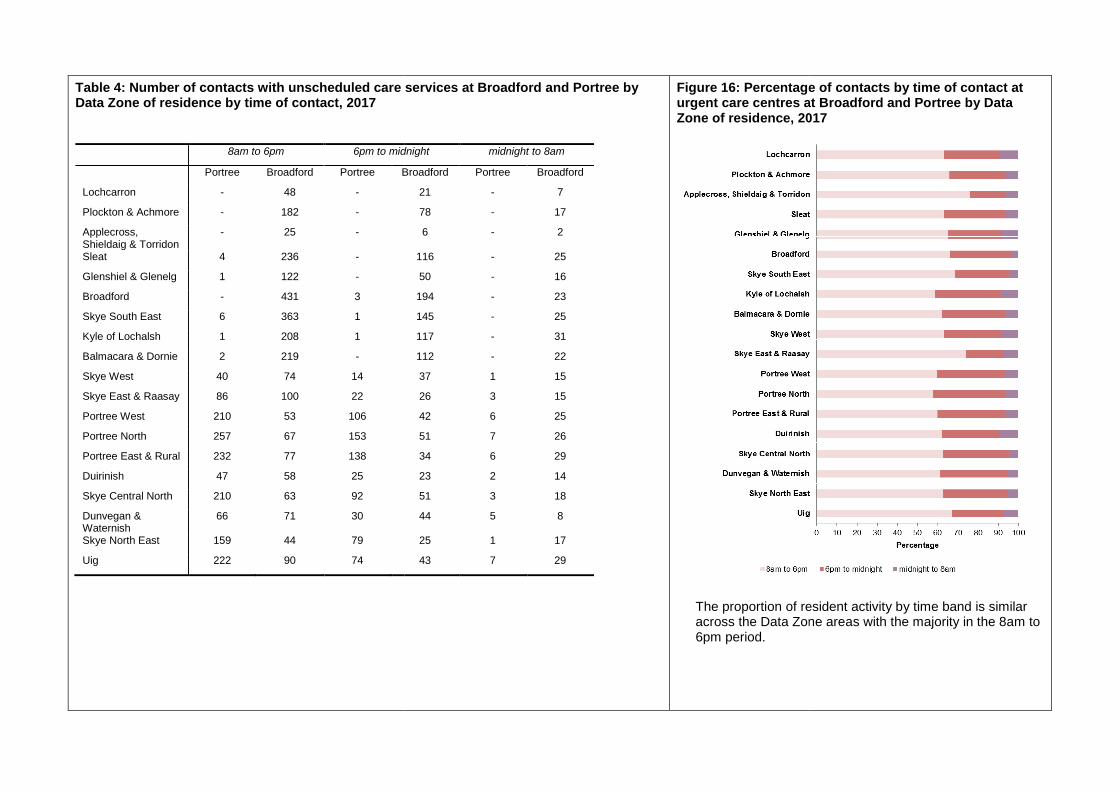
Table 4: Number of contacts with unscheduled care services at Broadford and Portree by Data Zone of residence by time of contact, 2017
8am to 6pm 6pm to midnight
Portree Broadford Portree Broadford
Lochcarron - 48 -
Plockton & Achmore - 182 -
Applecross, Shieldaig & Torridon
- 25 -
Sleat 4 236 -
Glenshiel & Glenelg 1 122 -
Broadford - 431 3
Skye South East 6 363 1
Kyle of Lochalsh 1 208 1
Balmacara & Dornie 2 219 -
Skye West 40 74 14
Skye East & Raasay 86 100 22
Portree West 210 53 106
Portree North 257 67 153
Portree East & Rural 232 77 138
Duirinish 47 58 25
Skye Central North 210 63 92
Dunvegan & Waternish
66 71 30
Skye North East 159 44 79
Uig 222 90 74
: Number of contacts with unscheduled care services at Broadford and Portree by
6pm to midnight midnight to 8am
Broadford Portree Broadford
21 - 7
78 - 17
6 - 2
116 - 25
50 - 16
194 - 23
145 - 25
117 - 31
112 - 22
37 1 15
26 3 15
42 6 25
51 7 26
34 6 29
23 2 14
51 3 18
44 5 8
25 1 17
43 7 29
Figure 16: Percentage of contacts by urgent care centres at Broadford and Portree by Data Zone of residence, 2017
The proportion of resident activity by time band isacross the Data Zone areas6pm period.
: Percentage of contacts by time of contact at urgent care centres at Broadford and Portree by Data Zone of residence, 2017
proportion of resident activity by time band is similar across the Data Zone areas with the majority in the 8am to
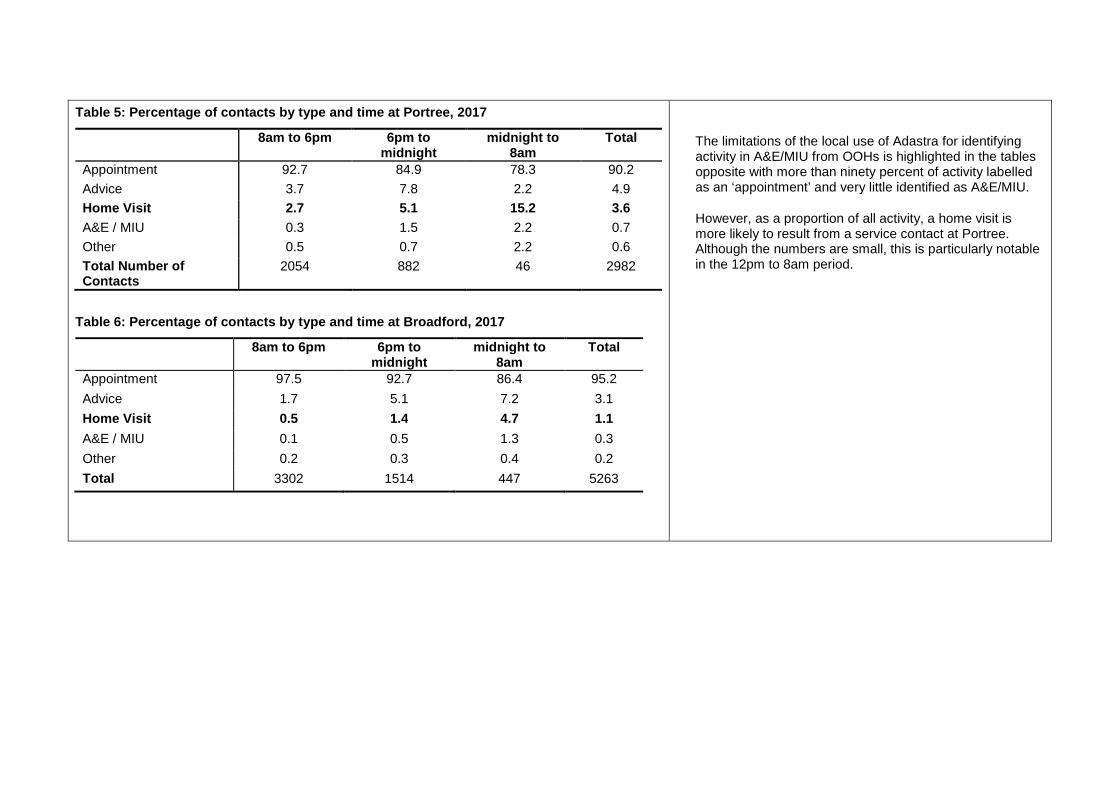
Table 5: Percentage of contacts by type and time at Portree, 2017
8am to 6pm 6pm to midnight
midnight to 8am
Total
Appointment 92.7 84.9 78.3 90.2
Advice 3.7 7.8 2.2 4.9
Home Visit 2.7 5.1 15.2 3.6
A&E / MIU 0.3 1.5 2.2 0.7
Other 0.5 0.7 2.2 0.6
Total Number of Contacts
2054 882 46 2982
Table 6: Percentage of contacts by type and time at Broadford, 2017
8am to 6pm 6pm to midnight
midnight to 8am
Total
Appointment 97.5 92.7 86.4 95.2
Advice 1.7 5.1 7.2 3.1
Home Visit 0.5 1.4 4.7 1.1
A&E / MIU 0.1 0.5 1.3 0.3
Other 0.2 0.3 0.4 0.2
Total 3302 1514 447 5263
The limitations of the local use of Adastra for identifying activity in A&E/MIU from OOHs is highlighted in the tables opposite with more than ninety percent of activity labelled as an ‘appointment’ and very little identified as A&E/MIU.
However, as a proportion of all activity, a home visit is more likely to result from a service contact at Portree. Although the numbers are small, this is particularly notable in the 12pm to 8am period.
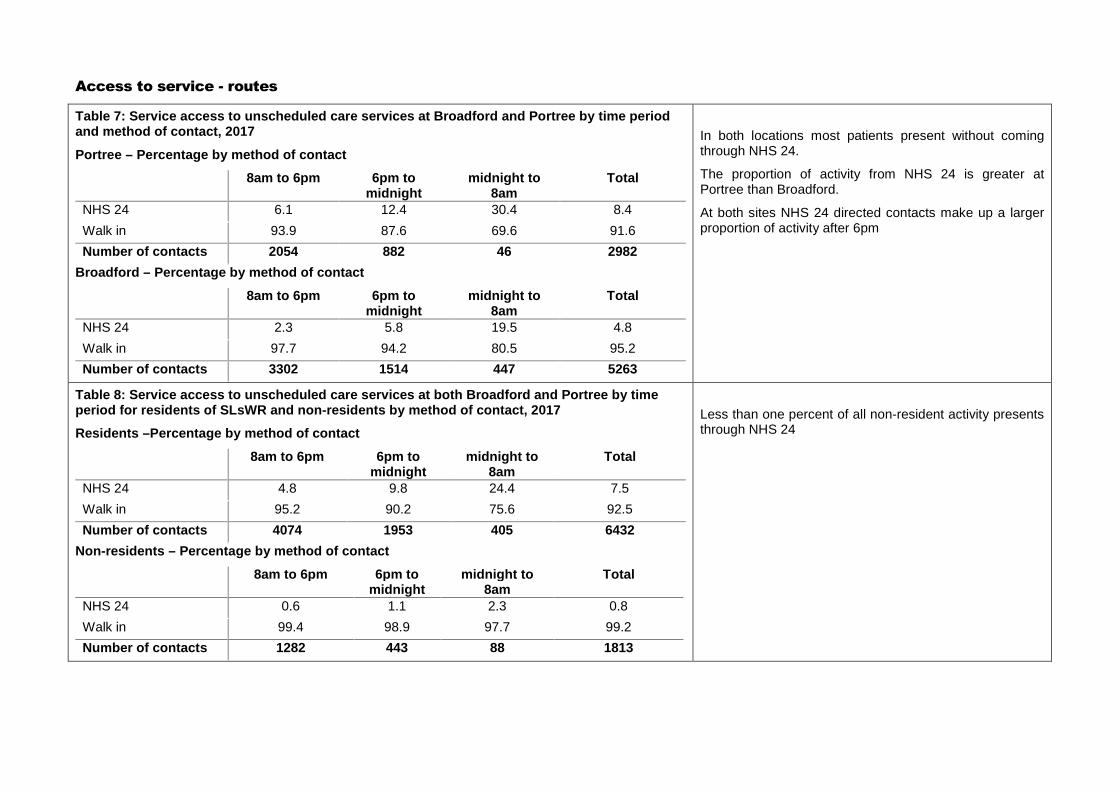
Access to service - routes
Table 7: Service access to unscheduled care services at Broadford and Portree by time period and method of contact, 2017
Portree – Percentage by method of contact
8am to 6pm 6pm to midnight
midnight to 8am
Total
NHS 24 6.1 12.4 30.4 8.4
Walk in 93.9 87.6 69.6 91.6
Number of contacts 2054 882 46 2982
Broadford – Percentage by method of contact
8am to 6pm 6pm to midnight
midnight to 8am
Total
NHS 24 2.3 5.8 19.5 4.8
Walk in 97.7 94.2 80.5 95.2
Number of contacts 3302 1514 447 5263
In both locations most patients present without coming through NHS 24.
The proportion of activity from NHS 24 is greater at Portree than Broadford.
At both sites NHS 24 directed contacts make up a larger proportion of activity after 6pm
Table 8: Service access to unscheduled care services at both Broadford and Portree by time period for residents of SLsWR and non-residents by method of contact, 2017
Residents –Percentage by method of contact
8am to 6pm 6pm to midnight
midnight to 8am
Total
NHS 24 4.8 9.8 24.4 7.5
Walk in 95.2 90.2 75.6 92.5
Number of contacts 4074 1953 405 6432
Non-residents – Percentage by method of contact
8am to 6pm 6pm to midnight
midnight to 8am
Total
NHS 24 0.6 1.1 2.3 0.8
Walk in 99.4 98.9 97.7 99.2
Number of contacts 1282 443 88 1813
Less than one percent of all non-resident activity presents through NHS 24

Access to service – routes in the out of hours period
Figure 17: Out of hours contacts at both Broadford and Portree and Highland by method of contact, 2013- 2017
in the out of hours period
: Out of hours contacts at both Broadford and Portree and Highland by method of Figure 17 includes contacts in out of honly (includes activity between 6pm Friday, weeken
The route of contact is very different at Broadford and Portree from Highland with a very small proportion of activity presenting through NHS 24.
Figure 17 includes contacts in out of hours periods only (includes activity between 6pm - 8am Monday to Friday, weekends and Bank Holidays).
The route of contact is very different at Broadford and Portree from Highland with a very small proportion of activity presenting through NHS 24.
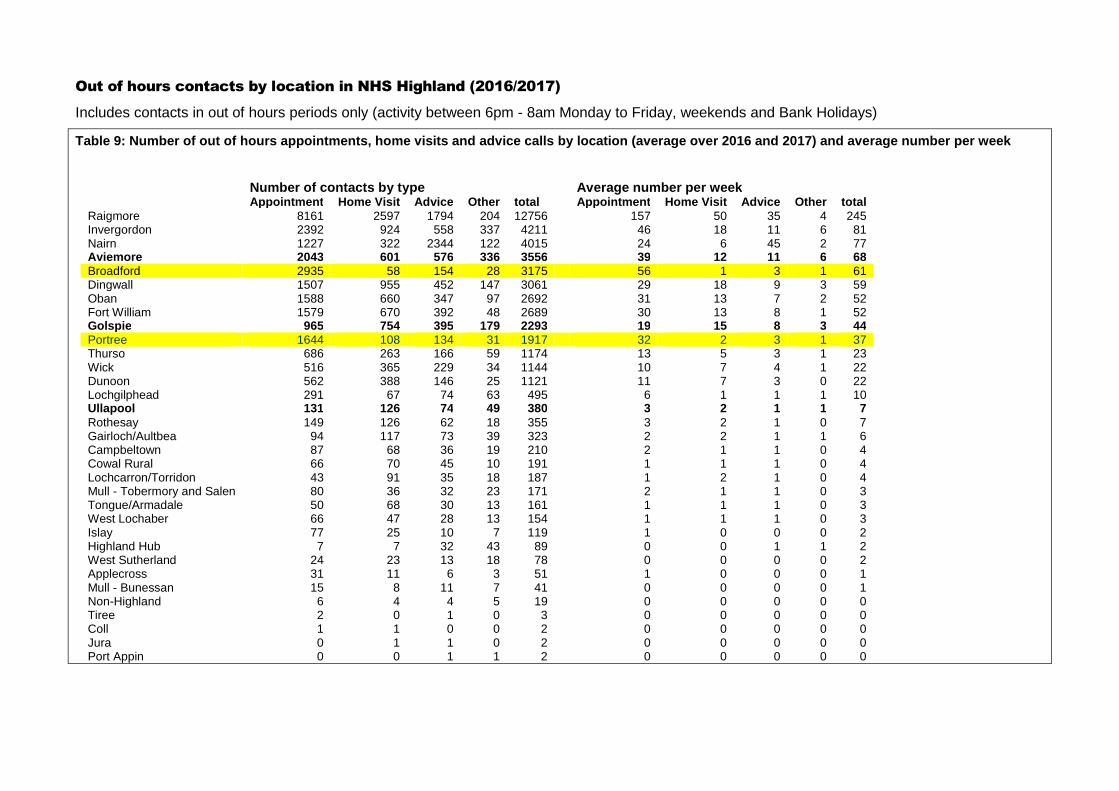
Out of hours contacts by location in NHS Highland (2016/2017)
Includes contacts in out of hours periods only (activity between 6pm - 8am Monday to Friday, weekends and Bank Holidays)
Table 9: Number of out of hours appointments, home visits and advice calls by location (average over 2016 and 2017) and average number per week
Number of contacts by type Average number per weekAppointment Home Visit Advice Other total Appointment Home Visit Advice Other total
Raigmore 8161 2597 1794 204 12756 157 50 35 4 245 Invergordon 2392 924 558 337 4211 46 18 11 6 81 Nairn 1227 322 2344 122 4015 24 6 45 2 77 Aviemore 2043 601 576 336 3556 39 12 11 6 68Broadford 2935 58 154 28 3175 56 1 3 1 61 Dingwall 1507 955 452 147 3061 29 18 9 3 59 Oban 1588 660 347 97 2692 31 13 7 2 52 Fort William 1579 670 392 48 2689 30 13 8 1 52 Golspie 965 754 395 179 2293 19 15 8 3 44Portree 1644 108 134 31 1917 32 2 3 1 37 Thurso 686 263 166 59 1174 13 5 3 1 23 Wick 516 365 229 34 1144 10 7 4 1 22 Dunoon 562 388 146 25 1121 11 7 3 0 22 Lochgilphead 291 67 74 63 495 6 1 1 1 10 Ullapool 131 126 74 49 380 3 2 1 1 7Rothesay 149 126 62 18 355 3 2 1 0 7 Gairloch/Aultbea 94 117 73 39 323 2 2 1 1 6 Campbeltown 87 68 36 19 210 2 1 1 0 4 Cowal Rural 66 70 45 10 191 1 1 1 0 4 Lochcarron/Torridon 43 91 35 18 187 1 2 1 0 4 Mull - Tobermory and Salen 80 36 32 23 171 2 1 1 0 3 Tongue/Armadale 50 68 30 13 161 1 1 1 0 3 West Lochaber 66 47 28 13 154 1 1 1 0 3 Islay 77 25 10 7 119 1 0 0 0 2 Highland Hub 7 7 32 43 89 0 0 1 1 2 West Sutherland 24 23 13 18 78 0 0 0 0 2 Applecross 31 11 6 3 51 1 0 0 0 1 Mull - Bunessan 15 8 11 7 41 0 0 0 0 1 Non-Highland 6 4 4 5 19 0 0 0 0 0 Tiree 2 0 1 0 3 0 0 0 0 0 Coll 1 1 0 0 2 0 0 0 0 0 Jura 0 1 1 0 2 0 0 0 0 0 Port Appin 0 0 1 1 2 0 0 0 0 0

Table 10: Number and rates of out of hours appointments, home visits and advice calls by for select Highland locations (based upon average over the two year period 2016-2017)
Number of contacts by type
Appointment Home Visit Advice Other All contacts Population
Aviemore 2043 601 576 336 3556 13750Broadford 2935 58 154 28 3175 6320Golspie 965 754 395 179 2293 9790Portree 1644 108 134 31 1917 7150Ullapool 131 126 74 49 380 2460
Rate per 1000 population
Appointment Home Visit Advice Other All contacts
Aviemore 148.5 43.7 41.9 24.4 258.6Broadford 464.0 9.2 24.3 4.4 502.0Golspie 98.6 77.0 40.4 18.3 234.3Portree 229.9 15.1 18.7 4.3 268.1Ullapool 53.1 51.1 30.0 19.9 154.2
Table 10 highlights the rates of OOH contacts for select comparable centres using the resident population of their service areas.
All these locations serve relatively discrete rural populations with small settlements with access to MIUs. All the locations use Raigmore Hospital as their primary A&E.
There is a Community Hospital located in Golspie. The Badenoch & Strathspey area that includes Aviemore has Community Hospitals at Grantown-on-Spey and Kingussie. Ullapool has no local hospital facility and the smallest resident population.
It is not possible to adjust the populations to account for seasonal activity related to visitors. In addition to the Skye locations, Aviemore and Ullapool are recognised centres for visitors.
All these selected sites collect OOHs and MIU data on Adastra.
The rate of all contacts in the OOHs period is notably high at Broadford. This results from the high number of appointments.
As highlighted above in figure 17 a very small proportion of OOHs activity at Broadford and Portree comes through NHS 24.
Both sites on Skye have low rates of home visits. Again, this is because the majority of patients self-present.
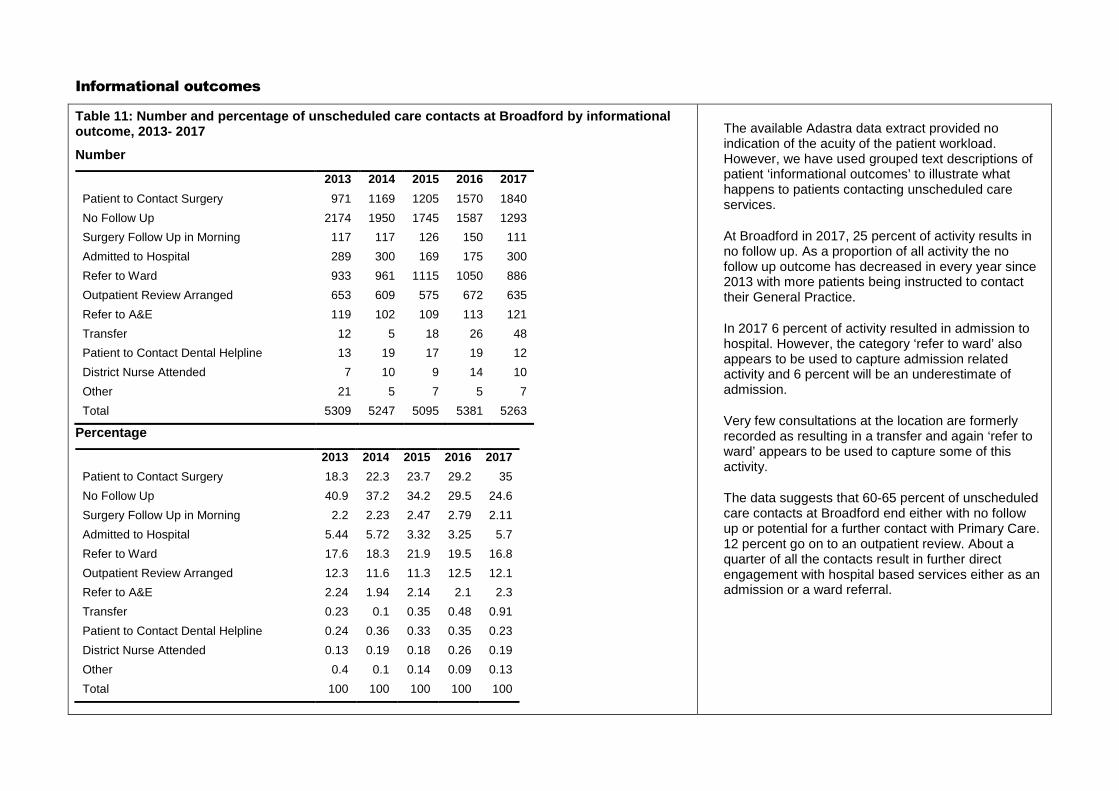
Informational outcomes
Table 11: Number and percentage of unscheduled care contacts at Broadford by informational outcome, 2013- 2017
Number
2013 2014 2015 2016 2017
Patient to Contact Surgery 971 1169 1205 1570 1840
No Follow Up 2174 1950 1745 1587 1293
Surgery Follow Up in Morning 117 117 126 150 111
Admitted to Hospital 289 300 169 175 300
Refer to Ward 933 961 1115 1050 886
Outpatient Review Arranged 653 609 575 672 635
Refer to A&E 119 102 109 113 121
Transfer 12 5 18 26 48
Patient to Contact Dental Helpline 13 19 17 19 12
District Nurse Attended 7 10 9 14 10
Other 21 5 7 5 7
Total 5309 5247 5095 5381 5263
Percentage
2013 2014 2015 2016 2017
Patient to Contact Surgery 18.3 22.3 23.7 29.2 35
No Follow Up 40.9 37.2 34.2 29.5 24.6
Surgery Follow Up in Morning 2.2 2.23 2.47 2.79 2.11
Admitted to Hospital 5.44 5.72 3.32 3.25 5.7
Refer to Ward 17.6 18.3 21.9 19.5 16.8
Outpatient Review Arranged 12.3 11.6 11.3 12.5 12.1
Refer to A&E 2.24 1.94 2.14 2.1 2.3
Transfer 0.23 0.1 0.35 0.48 0.91
Patient to Contact Dental Helpline 0.24 0.36 0.33 0.35 0.23
District Nurse Attended 0.13 0.19 0.18 0.26 0.19
Other 0.4 0.1 0.14 0.09 0.13
Total 100 100 100 100 100
The available Adastra data extract provided no indication of the acuity of the patient workload. However, we have used grouped text descriptions of patient ‘informational outcomes’ to illustrate what happens to patients contacting unscheduled care services.
At Broadford in 2017, 25 percent of activity results in no follow up. As a proportion of all activity the no follow up outcome has decreased in every year since 2013 with more patients being instructed to contact their General Practice.
In 2017 6 percent of activity resulted in admission to hospital. However, the category ‘refer to ward’ also appears to be used to capture admission related activity and 6 percent will be an underestimate of admission.
Very few consultations at the location are formerly recorded as resulting in a transfer and again ‘refer to ward’ appears to be used to capture some of this activity.
The data suggests that 60-65 percent of unscheduled care contacts at Broadford end either with no follow up or potential for a further contact with Primary Care. 12 percent go on to an outpatient review. About a quarter of all the contacts result in further direct engagement with hospital based services either as an admission or a ward referral.
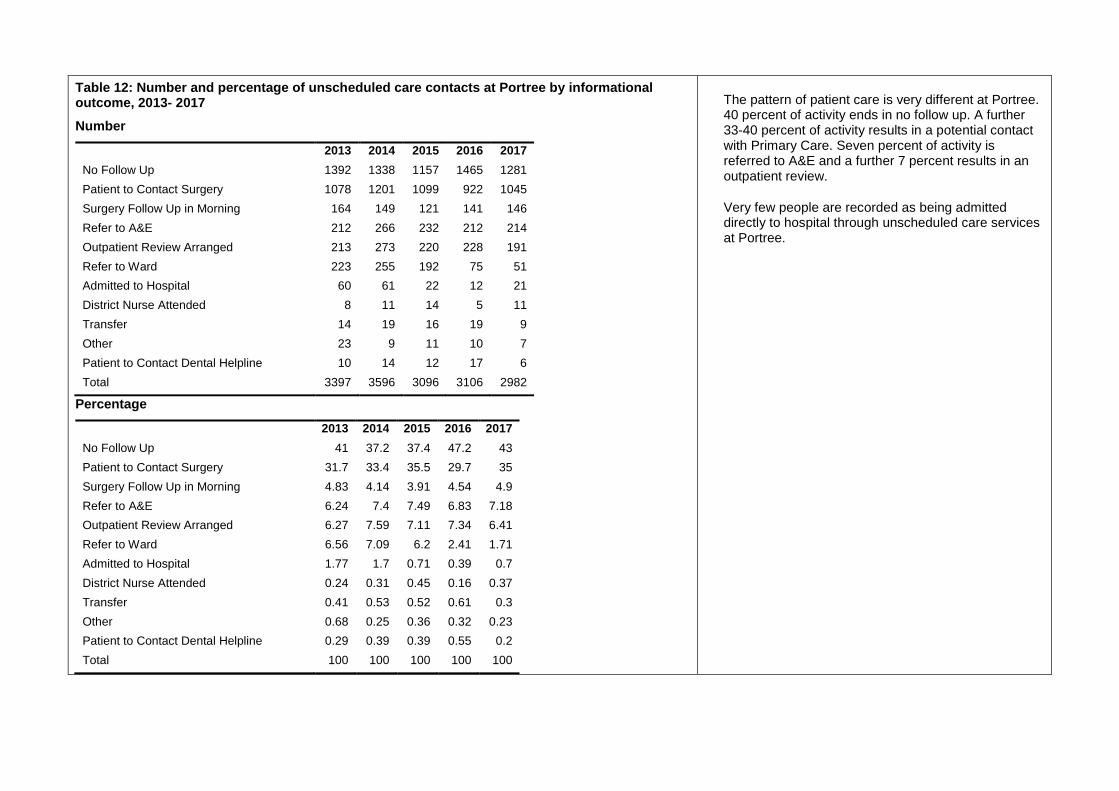
Table 12: Number and percentage of unscheduled care contacts at Portree by informational outcome, 2013- 2017
Number
2013 2014 2015 2016 2017
No Follow Up 1392 1338 1157 1465 1281
Patient to Contact Surgery 1078 1201 1099 922 1045
Surgery Follow Up in Morning 164 149 121 141 146
Refer to A&E 212 266 232 212 214
Outpatient Review Arranged 213 273 220 228 191
Refer to Ward 223 255 192 75 51
Admitted to Hospital 60 61 22 12 21
District Nurse Attended 8 11 14 5 11
Transfer 14 19 16 19 9
Other 23 9 11 10 7
Patient to Contact Dental Helpline 10 14 12 17 6
Total 3397 3596 3096 3106 2982
Percentage
2013 2014 2015 2016 2017
No Follow Up 41 37.2 37.4 47.2 43
Patient to Contact Surgery 31.7 33.4 35.5 29.7 35
Surgery Follow Up in Morning 4.83 4.14 3.91 4.54 4.9
Refer to A&E 6.24 7.4 7.49 6.83 7.18
Outpatient Review Arranged 6.27 7.59 7.11 7.34 6.41
Refer to Ward 6.56 7.09 6.2 2.41 1.71
Admitted to Hospital 1.77 1.7 0.71 0.39 0.7
District Nurse Attended 0.24 0.31 0.45 0.16 0.37
Transfer 0.41 0.53 0.52 0.61 0.3
Other 0.68 0.25 0.36 0.32 0.23
Patient to Contact Dental Helpline 0.29 0.39 0.39 0.55 0.2
Total 100 100 100 100 100
The pattern of patient care is very different at Portree. 40 percent of activity ends in no follow up. A further 33-40 percent of activity results in a potential contact with Primary Care. Seven percent of activity is referred to A&E and a further 7 percent results in an outpatient review.
Very few people are recorded as being admitted directly to hospital through unscheduled care services at Portree.
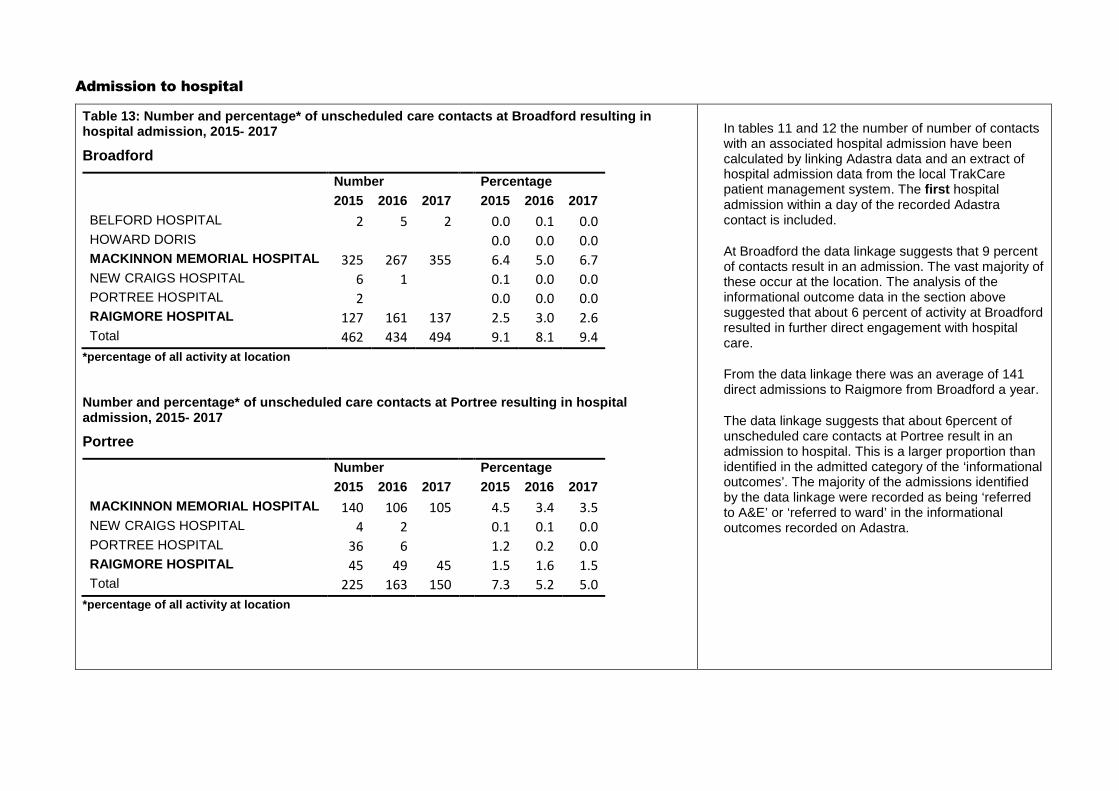
Admission to hospital
Table 13: Number and percentage* of unscheduled care contacts at Broadford resulting in hospital admission, 2015- 2017
Broadford
Number Percentage
2015 2016 2017 2015 2016 2017
BELFORD HOSPITAL 2 5 2 0.0 0.1 0.0HOWARD DORIS 0.0 0.0 0.0MACKINNON MEMORIAL HOSPITAL 325 267 355 6.4 5.0 6.7NEW CRAIGS HOSPITAL 6 1 0.1 0.0 0.0PORTREE HOSPITAL 2 0.0 0.0 0.0RAIGMORE HOSPITAL 127 161 137 2.5 3.0 2.6Total 462 434 494 9.1 8.1 9.4
*percentage of all activity at location
Number and percentage* of unscheduled care contacts at Portree resulting in hospital admission, 2015- 2017
Portree
Number Percentage
2015 2016 2017 2015 2016 2017
MACKINNON MEMORIAL HOSPITAL 140 106 105 4.5 3.4 3.5NEW CRAIGS HOSPITAL 4 2 0.1 0.1 0.0PORTREE HOSPITAL 36 6 1.2 0.2 0.0RAIGMORE HOSPITAL 45 49 45 1.5 1.6 1.5Total 225 163 150 7.3 5.2 5.0
*percentage of all activity at location
In tables 11 and 12 the number of number of contacts with an associated hospital admission have been calculated by linking Adastra data and an extract of hospital admission data from the local TrakCare patient management system. The first hospital admission within a day of the recorded Adastra contact is included.
At Broadford the data linkage suggests that 9 percent of contacts result in an admission. The vast majority of these occur at the location. The analysis of the informational outcome data in the section above suggested that about 6 percent of activity at Broadford resulted in further direct engagement with hospital care.
From the data linkage there was an average of 141 direct admissions to Raigmore from Broadford a year.
The data linkage suggests that about 6percent of unscheduled care contacts at Portree result in an admission to hospital. This is a larger proportion than identified in the admitted category of the ‘informational outcomes’. The majority of the admissions identified by the data linkage were recorded as being ‘referred to A&E’ or ‘referred to ward’ in the informational outcomes recorded on Adastra.
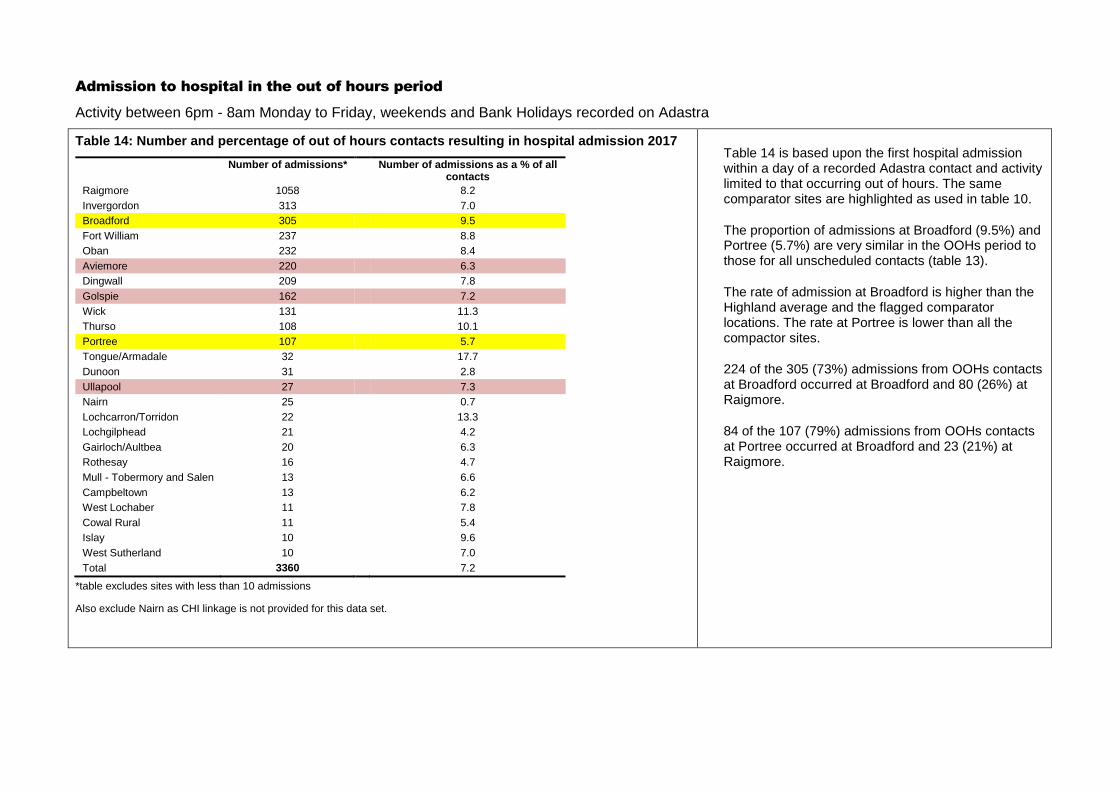
Admission to hospital in the out of hours period
Activity between 6pm - 8am Monday to Friday, weekends and Bank Holidays recorded on Adastra
Table 14: Number and percentage of out of hours contacts resulting in hospital admission 2017
Number of admissions* Number of admissions as a % of all contacts
Raigmore 1058 8.2
Invergordon 313 7.0
Broadford 305 9.5
Fort William 237 8.8
Oban 232 8.4
Aviemore 220 6.3
Dingwall 209 7.8
Golspie 162 7.2
Wick 131 11.3
Thurso 108 10.1
Portree 107 5.7
Tongue/Armadale 32 17.7
Dunoon 31 2.8
Ullapool 27 7.3
Nairn 25 0.7
Lochcarron/Torridon 22 13.3
Lochgilphead 21 4.2
Gairloch/Aultbea 20 6.3
Rothesay 16 4.7
Mull - Tobermory and Salen 13 6.6
Campbeltown 13 6.2
West Lochaber 11 7.8
Cowal Rural 11 5.4
Islay 10 9.6
West Sutherland 10 7.0
Total 3360 7.2
*table excludes sites with less than 10 admissions
Also exclude Nairn as CHI linkage is not provided for this data set.
Table 14 is based upon the first hospital admission within a day of a recorded Adastra contact and activity limited to that occurring out of hours. The same comparator sites are highlighted as used in table 10.
The proportion of admissions at Broadford (9.5%) and Portree (5.7%) are very similar in the OOHs period to those for all unscheduled contacts (table 13).
The rate of admission at Broadford is higher than the Highland average and the flagged comparator locations. The rate at Portree is lower than all the compactor sites.
224 of the 305 (73%) admissions from OOHs contacts at Broadford occurred at Broadford and 80 (26%) at Raigmore.
84 of the 107 (79%) admissions from OOHs contacts at Portree occurred at Broadford and 23 (21%) at Raigmore.
1
Public Health Statistical Appendix
Out of Hours Care in Skye, Lochalsh
and South West Ross
Hugo van Woerden, Director of Public Health and Policy, NHS Highland
Andrew Rideout, Public Health Speciality Registrar, NHS Dumfries and Galloway
April 2018

2
Executive Summary
The aim of the briefing is to present epidemiological information that will inform the
recommendations that the panel will make, whilst minimising any overlaps with sources of
epidemiological information that are provided by other reports to the panel.
The briefing considers: who receives care, who delivers care, what care is delivered, where is the
care delivered and when is care utilised?
The population of Skye is scattered with relatively long travel distances. It is an aging population,
with a falling proportion of working age, who can provide care services, although the elderly in Skye
place relatively low demands on Out of Hours services. There are areas of rural deprivation, which
may result in greater levels of Out of Hours care.
Out of Hours care has historically been provided by GPs and hospital based facilities including units
in both Portree and Broadford that did not fall into a typical description of emergency departments
or minor injury units. Unscheduled care is increasingly being provided by nurses, paramedics, NHS
24, other emergency services and first responders. Care is also provided for island populations on
Raasay and Eigg.
The delivery of care draws on community services, primary care, local intermediate care, NHS 24, a
general hospital in Fort William and a large general hospital1 in Inverness, which is the main source
of visiting outpatient services to the island. Service redesign plans around facilities in Broadford and
Portree are underway, with a new hospital planned in Broadford.
Out of Hours services display expected diurnal variation and an annual seasonal pattern associated
with the very large influx of tourists each summer. It is anticipated that complementary data on
ambulance and NHS 24 services will be provided by these services.
In conclusion, the Isle of Skye is a challenging environment in which to provide Out of Hours care,
given its geography. There is a need to build on emerging models of care to make Skye a place
which is internationally recognised as leading the way in providing solutions that work in such a
context. This is likely to require cross organisational working and increasing use of technology to link
local services with specialist input.
1 ISD Hospital classification: http://www.isdscotland.org/Health-Topics/Finance/Costs/Reference-Information.asp
3
Table of Contents
1. Introduction 7
1.1 Defining Out of Hours Care 7
2. Who receives care? 8
2.1 Demography 8
2.2 Deprivation 11
2.3 Patients with Long Term Limiting Illness 19
2.4 End of Life Care 19
3. Who delivers care? 24
3.1 NHS staff 24
3.2 Unpaid carers 27
4. What care is delivered? 30
4.1 Historic changes to services 30
4.2 Out of Hours Services 34
4.3 Unscheduled care contact outcomes 36
4.4 Admission to hospital after unscheduled care contact 37
4.5 Outpatient Care 38
4.6 District Nursing 43
4.7 Allied Health Professionals 44
4.8 Hospital services 48
4.9 Midwifery Care 60
4.10 Ambulance Services 61
5. Where is the care delivered? 66
5.1 Travel 70
5.2 Care Homes 74
5.3 Projections of future need 76
6. When is care utilised? 78
7. Conclusion 85
7.1 Limitations 85
7.2 Main findings 85
8. Acknowledgements 86
9. References 87
4
Tables
Table 1: Income deprivation in Skye, Lochalsh and South West Ross by data zone 17
Table 2: Proportion of deaths by Locality and District geographies and place of death, 2010-2012 (NHS
Highland residents only) 20
Table 3: Number of deaths by Locality and District geographies and place of death, 2010-2012 (NHS Highland
residents only / 3 year number of events) 21
Table 4: Unscheduled care contacts at Broadford and Portree by outcome, 2013- 2017 36
Table 5: Unscheduled care contacts at Broadford and Portree resulting in hospital admission, 2015- 2017 37
Table 6: Admission to hospital in the Out of Hours period after contact with the Out of Hours service 2017 38
Table 7: Summary of outpatient services at Portree Hospital and the MacKinnon Memorial Hospital 39
Table 8: Allied Health Professional Appointments, Portree Hospital 45
Table 9: Allied Health Professional Appointments, Mackinnon Memorial Hospital 46
Table 10: Allied Health Professional Appointments, other Skye and Lochalsh locations 47
Table 11: Summary of services in Portree Hospital and the Mackinnon Memorial Hospital, Broadford 48
Table 12: Mean and Median length of stay for Skye Hospitals, 2008/9 to 2012/13 55
Table 13: Pattern of delayed discharges by length of delay, Skye, Lochalsh and South West Ross, 2011-14 58
Table 14: Age specific delayed discharge rates per 1000 population, Skye, Lochalsh and South West Ross, 2011-
14 59
Table 15: Annual rates of SAS call-out attendances during 2014 by Ambulance station 61
Table 16: Annual rates and numbers of SAS call-out attendances during 2014 by area of attendance 62
Table 17: Patients transferred by ambulance from Portree Hospital/Medical Centre to Broadford Hospital
during 2014 by emergency status 62
Table 18: Community Health Index Practice list population of Skye and Lochalsh (excluding South West Ross)
within 60 minutes drive time from Portree and Broadford 71
Table 19: Summary of bus services to and from Broadford or Portree 73
Table 20: Summary of Ferry Services for Raasay-Sconser 74
Table 21: Number of unscheduled care patient contacts at Broadford and Portree by calendar year by time of
day 79
Table 22: Number of unscheduled care patient contacts at Broadford and Portree combined, by calendar year
by time of day 82
Table 23: Number of contacts with unscheduled care services at Broadford and Portree by Data Zone of
residence by time of contact, during 2017 82
Table 24: Percentage of contacts by type and time at Portree, 2017 83
Table 25: Percentage of contacts by type and time at Broadford, 2017 83
Table 26: Service access to unscheduled care services at both Broadford and Portree by time period for
residents of SLsWR and non-residents by method of contact, 2017 84
5
Figures
Figure 1: Trend in population estimates (2003 to 2013) and projections to 2037 by age band, Skye, Lochalsh
and South West Ross 8
Figure 2: Population over time – Skye, Lochalsh & West Ross 9
Figure 3: Community Health Index population distribution in the Skye, Lochalsh and South West Ross area 10
Figure 4: Population pyramid for Skye and Lochalsh, 2013 and 2026 11
Figure 5: Overview of the NHS Highland Board 1st
and 2nd
Quintiles of deprivation using SIMD 2012 12
Figure 6: Model of potentially fragile areas in Scotland 14
Figure 7: Economically fragile areas in Scotland 16
Figure 8: Distribution of income deprivation by data zone area in Skye, Lochalsh and South West Ross 18
Figure 9: Age and sex specific rates of Long Term Limiting Illness, Skye and Lochalsh, 2001 & 2012 19
Figure 10: Place of death by data zone, combined years 2013-17 (hospital deaths) 22
Figure 11: Place of death by data zone, combined years 2013-17 (deaths at home) 23
Figure 12: Proportion of Out of Hours cases seen by different professionals, Skye, 2013 to 2017 24
Figure 13: Summary of current Whole Time Equivalent (WTE) establishments in Skye, Lochalsh and South West
Ross Workforce Plan 25
Figure 14: Provision of unpaid care by category by Highland geography 2011 27
Figure 15: Unpaid care and formal care provision in Highland at 2011 Census 28
Figure 16: Estimated and projected number of older people in Highland receiving informal care 29
Figure 17: Location of Out of Hours Care, Skye and Lochalsh, 2018 34
Figure 18: Percentage of unscheduled care activity at Portree and Broadford (combined) by age group and
residence, Jan-Dec 2017 34
Figure 19: Directly age standardised rate per 1000 population of unscheduled care at Broadford and Portree by
Data Zone of residence in SLsWR, 2017 35
Figure 20: Directly age standardised outpatient attendance rates by data zone of residence in SLsWR, all
specialties and all locations, 2010-2011 – 2012-2013 40
Figure 21: Directly age standardised outpatient attendance rates by data zone of residence in SLsWR, all
specialties at MacKinnon Hospital, 2010-2011 – 2012-2013 41
Figure 22: Directly age standardised outpatient attendance rates by data zone of residence in SLsWR, all
specialties at Portree Hospital, 2010-2011 – 2012-2013 42
Figure 23: Directly age standardised outpatient attendance rates by data zone of residence in SLsWR, all
specialties at Raigmore Hospital, 2010-2011 – 2012-2013 43
Figure 24: Number of inpatient admissions and available beds at Portree Hospital, 2011-18 49
Figure 25: Number of inpatient discharges and length of stay at Portree Hospital, 2011-18 49
Figure 26: Percentage occupancy and available beds at Portree Hospital, 2011-18 50
Figure 27: Number of inpatient admissions and available beds, MacKinnon Memorial Hospital, 2012-18 51
Figure 28: Number of inpatient discharges and length of stay, MacKinnon Memorial Hospital, 2012-18 51
Figure 29: Occupancy and number of available beds, MacKinnon Memorial Hospital, 2012-18 52
Figure 30: Trends in admissions and bed day rates for Skye hospitals, 2003 - 13 53
Figure 31: Summary of bed changes identified in the Mackinnon Memorial Hospital, Broadford, 2006/07 to
2013/14 54
Figure 32: Summary of bed changes identified in the Portree Hospital, 2006/07 to 2013/14 54
Figure 33: Monthly percentage bed occupancy at Skye Hospitals, 2009/10 to 2013/14 55
Figure 34: Length of stay in Skye Hospitals, including inter-quartile data, maximum and minimum data,
2008/09 to 2012/13 (GP beds only) 56
Figure 35: Trends in admission rates per 1000 population by GP practice, Skye Hospitals, 2009-13 57
Figure 36: Top 25 primary diagnoses for admissions to Skye Hospitals, 2009-13 58
Figure 37: Reasons for delayed discharges, Skye, Lochalsh and South West Ross, 2011-14 60
6
Figure 38: Births to mothers resident in Skye and Lochalsh in calendar years 2006 - 2016 60
Figure 39: Number of patients conveyed from Skye and Lochalsh in 2017 by receiving hospital 63
Figure 40: Average time spent conveying patients to Raigmore Hospital, 2017 64
Figure 41: Average time spent on incidents in Inverness, when ambulances were detained in Inverness, by
home despatch point, 2017 65
Figure 42: Health Services across NHS Highland 66
Figure 43: Health care facilities in Skye and Lochalsh and South West Ross 67
Figure 44: Geography covered by Integrated Care teams (nursing and social care) 68
Figure 45: GP practices in Skye and Lochalsh 69
Figure 46: Population registered with General Practices in April 2014 and October 2017 70
Figure 47: Area within 30 and 60 minutes drive from Portree Hospital 71
Figure 48: Area within 30 and 60 minutes drive from MacKinnon Memorial Hospital 72
Figure 49: Care home places in Skye, Lochalsh and South West Ross 75
Figure 50: Care Home places and Hospital beds per 1000 population aged 75+, NHS Highland 76
Figure 51: Summary of bed models using Skye, Lochalsh and South West Ross population projections and 85%
bed occupancy 77
Figure 52: Cumulative number of Out of Hours cases seen per hour over a week, totalled over 12 months 78
Figure 53: Percentage of unscheduled care patient contacts at Broadford and Portree combined by calendar
year by time of day 78
Figure 54: Percentage of unscheduled care patient contacts at Broadford and Portree by calendar year by time
of day 79
Figure 55: Unscheduled care activity at Portree and Broadford (combined), Jan 2013 to Dec 2017 80
Figure 56: Unscheduled care activity at Broadford from January 2013 to December 2017 81
Figure 57: Unscheduled care activity at Portree from January 2013 to December 2017 81
Figure 58: Out of Hours contacts at both Broadford and Portree and Highland by method of contact, 2013-
2017 84

7
1. Introduction
The terms of reference for the Out of Hours work being led by Sir Lewis Ritchie state that, “The
specific remit is to assess the resilience of urgent primary care out-of-hours provision” and “to
provide an external professional view of the urgent care services in the area”2 . This briefing is
designed to support that review and provide epidemiological information for consideration by the
Panel who are supporting the review.
The aim of the briefing is, therefore, to present epidemiological information that will inform the
recommendations that the panel will make, whilst minimising any overlaps with sources of
information that are provided by other reports to the panel. It is anticipated that any
recommendations that the panel may make may wish to take into consideration: who receives
care?; who delivers care?; what care is delivered?; where is the care delivered?, and when is care
utilised? Available evidence which addresses these questions is provided below.
The primary focus of this briefing is the Isle of Skye. Data related to Lochalsh & South West Ross is
also provided where it is thought that this may be relevant and is easily available. Given the tight
timescale, the briefing draws primarily on available data, as opposed to undertaking fresh analyses.
This briefing has not been underpinned by a literature review, as relevant literature on Out of Hours
services and models of care are available as part of the recent Scottish Government National Review
on Out of Hours care published in 2015 by Sir Lewis Ritchie, ‘Pulling together: transforming urgent
care for the people of Scotland. The Report of the Independent Review of Primary Care Out of Hours
Services’.3
1.1 Defining Out of Hours Care
Out of Hours care can be defined in a recent review as “care provided between 18.30 and 08.00 on
weekdays, all weekend and Bank Holidays”4. The review goes on to say, “Care provided in the OOH
time period is unscheduled, i.e. there has been no forward planning (either by patient or professional)
or appointment made in advance. However, such care may or may not be regarded as urgent care.”
The report also states that, “in practice, out-of-hours care provision often starts at 6pm.” This is the
standard hand over time in NHS Highland.
2 NHS Highland, 2018. Terms of Reference, External view of arrangements for Unscheduled Care (urgent primary care out-
of-hours provision) in Skye, Lochalsh and South West Ross. Available online: http://www.nhshighland.scot.nhs.uk/News/PublicConsultation/Skye/Documents/1%20OOHs%202018/SkyeNHS%20HighlandReviewTOR160118_Final.pdf 3 Ritchie, L., 2015. Pulling together: Transforming Urgent Care for the People of Scotland. The Report of the Independent
Review of Primary Care Out of Hours Services. Edinburgh: Scottish Government. Available online: http://www.gov.scot/Resource/0049/00490526.pdf 4 O’Donnell, C., Foster, H., Macdonald, S., Burns, N. & Gannon, M., 2015. Out-of-Hours Primary Medical Care: What Can
Research Tell Us? Findings From a Rapid Systematic Review and Qualitative Study. University of Glasgow. Available online: http://www.gov.scot/Resource/0049/00492082.pdf [Accessed 9 April 2018].
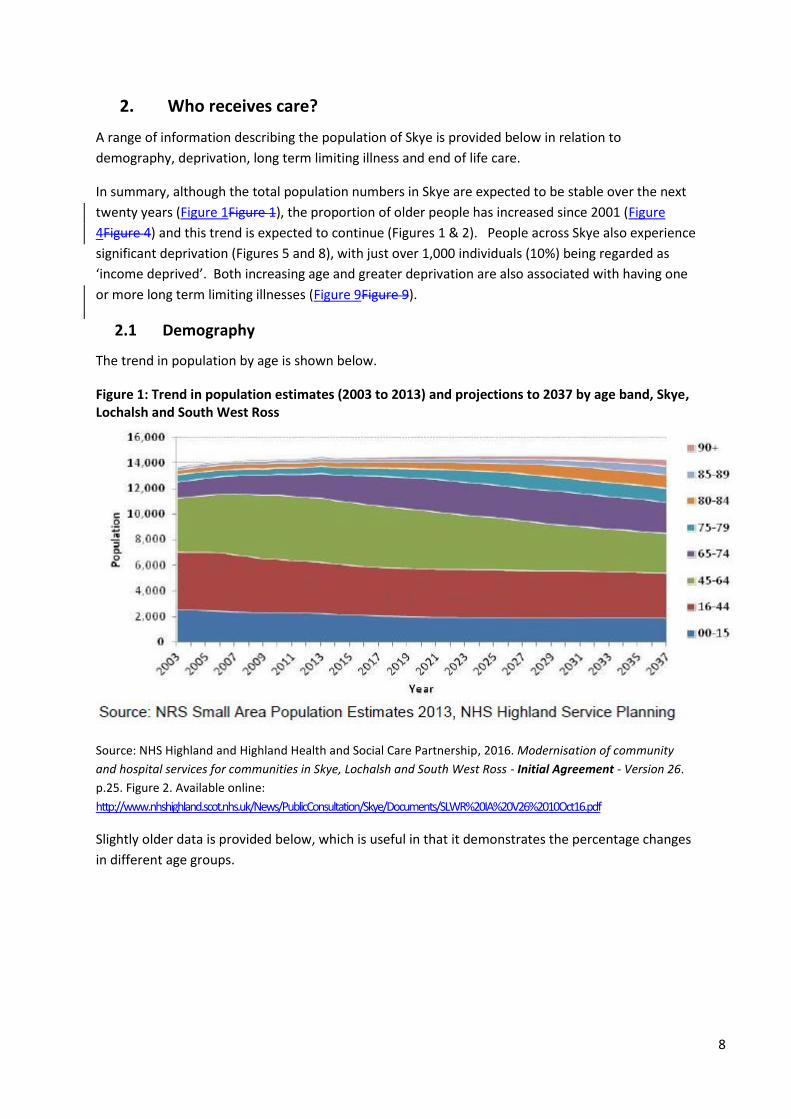
8
2. Who receives care?
A range of information describing the population of Skye is provided below in relation to
demography, deprivation, long term limiting illness and end of life care.
In summary, although the total population numbers in Skye are expected to be stable over the next
twenty years (Figure 1Figure 1), the proportion of older people has increased since 2001 (Figure
4Figure 4) and this trend is expected to continue (Figures 1 & 2). People across Skye also experience
significant deprivation (Figures 5 and 8), with just over 1,000 individuals (10%) being regarded as
‘income deprived’. Both increasing age and greater deprivation are also associated with having one
or more long term limiting illnesses (Figure 9Figure 9).
2.1 Demography
The trend in population by age is shown below.
Figure 1: Trend in population estimates (2003 to 2013) and projections to 2037 by age band, Skye, Lochalsh and South West Ross
Source: NHS Highland and Highland Health and Social Care Partnership, 2016. Modernisation of community
and hospital services for communities in Skye, Lochalsh and South West Ross - Initial Agreement - Version 26.
p.25. Figure 2. Available online:
http://www.nhshighland.scot.nhs.uk/News/PublicConsultation/Skye/Documents/SLWR%20IA%20V26%2010Oct16.pdf
Slightly older data is provided below, which is useful in that it demonstrates the percentage changes
in different age groups.
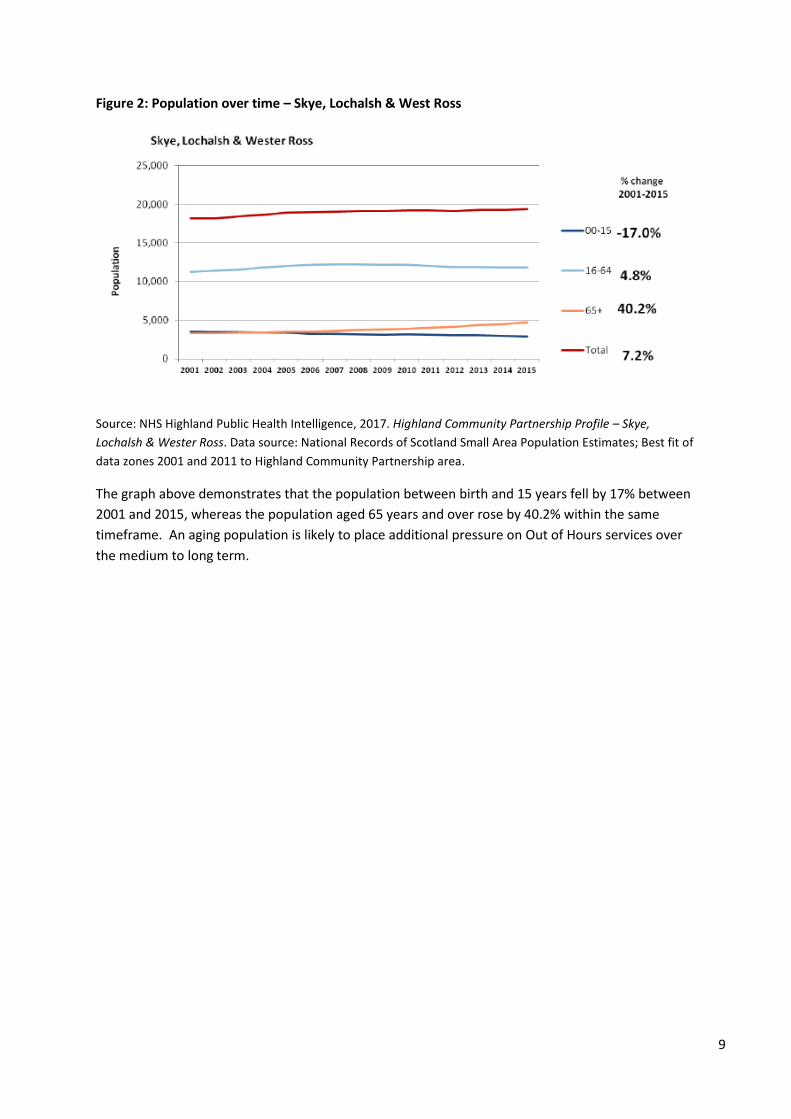
9
Figure 2: Population over time – Skye, Lochalsh & West Ross
Source: NHS Highland Public Health Intelligence, 2017. Highland Community Partnership Profile – Skye,
Lochalsh & Wester Ross. Data source: National Records of Scotland Small Area Population Estimates; Best fit of
data zones 2001 and 2011 to Highland Community Partnership area.
The graph above demonstrates that the population between birth and 15 years fell by 17% between
2001 and 2015, whereas the population aged 65 years and over rose by 40.2% within the same
timeframe. An aging population is likely to place additional pressure on Out of Hours services over
the medium to long term.
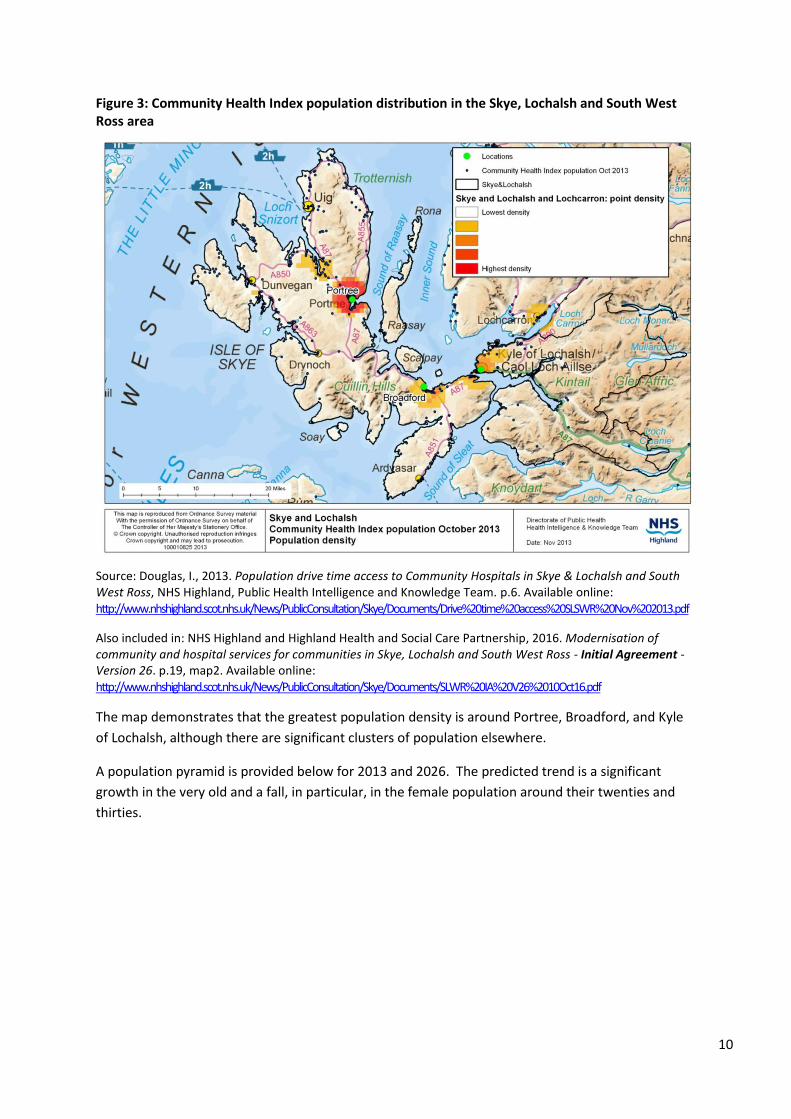
10
Figure 3: Community Health Index population distribution in the Skye, Lochalsh and South West Ross area
Source: Douglas, I., 2013. Population drive time access to Community Hospitals in Skye & Lochalsh and South West Ross, NHS Highland, Public Health Intelligence and Knowledge Team. p.6. Available online: http://www.nhshighland.scot.nhs.uk/News/PublicConsultation/Skye/Documents/Drive%20time%20access%20SLSWR%20Nov%202013.pdf
Also included in: NHS Highland and Highland Health and Social Care Partnership, 2016. Modernisation of community and hospital services for communities in Skye, Lochalsh and South West Ross - Initial Agreement - Version 26. p.19, map2. Available online: http://www.nhshighland.scot.nhs.uk/News/PublicConsultation/Skye/Documents/SLWR%20IA%20V26%2010Oct16.pdf
The map demonstrates that the greatest population density is around Portree, Broadford, and Kyle
of Lochalsh, although there are significant clusters of population elsewhere.
A population pyramid is provided below for 2013 and 2026. The predicted trend is a significant
growth in the very old and a fall, in particular, in the female population around their twenties and
thirties.
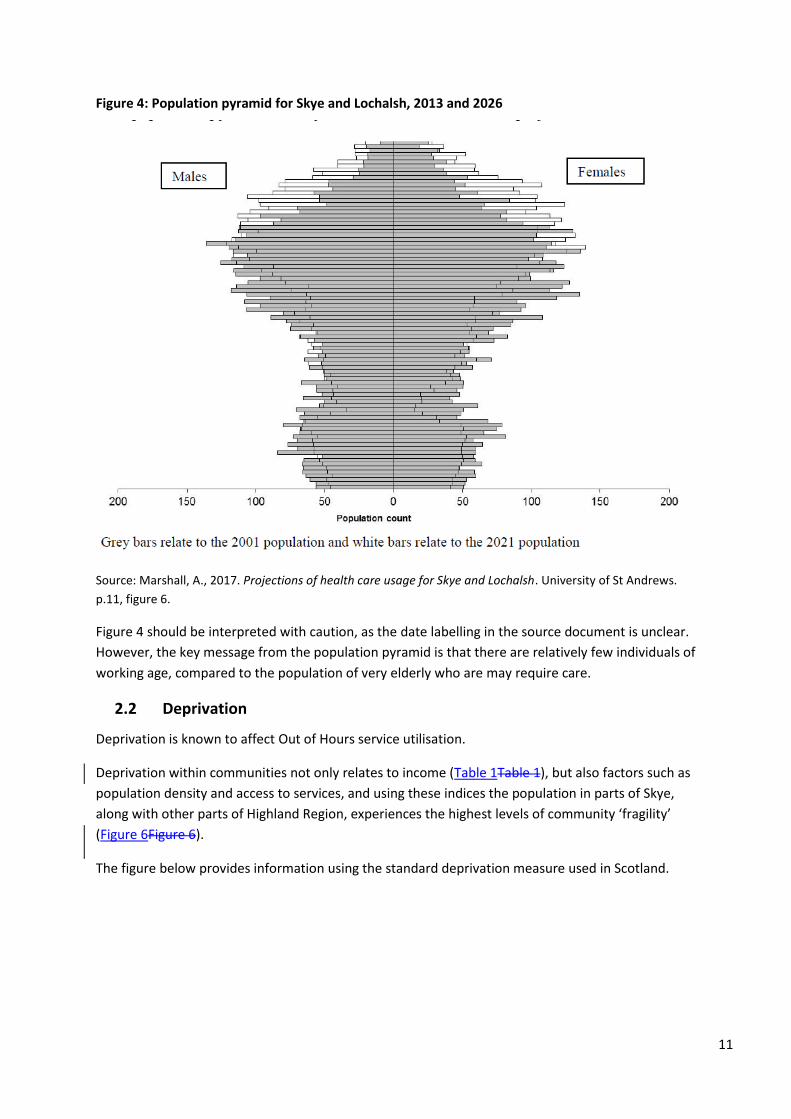
11
Figure 4: Population pyramid for Skye and Lochalsh, 2013 and 2026
Source: Marshall, A., 2017. Projections of health care usage for Skye and Lochalsh. University of St Andrews.
p.11, figure 6.
Figure 4 should be interpreted with caution, as the date labelling in the source document is unclear.
However, the key message from the population pyramid is that there are relatively few individuals of
working age, compared to the population of very elderly who are may require care.
2.2 Deprivation
Deprivation is known to affect Out of Hours service utilisation.
Deprivation within communities not only relates to income (Table 1Table 1), but also factors such as
population density and access to services, and using these indices the population in parts of Skye,
along with other parts of Highland Region, experiences the highest levels of community ‘fragility’
(Figure 6Figure 6).
The figure below provides information using the standard deprivation measure used in Scotland.
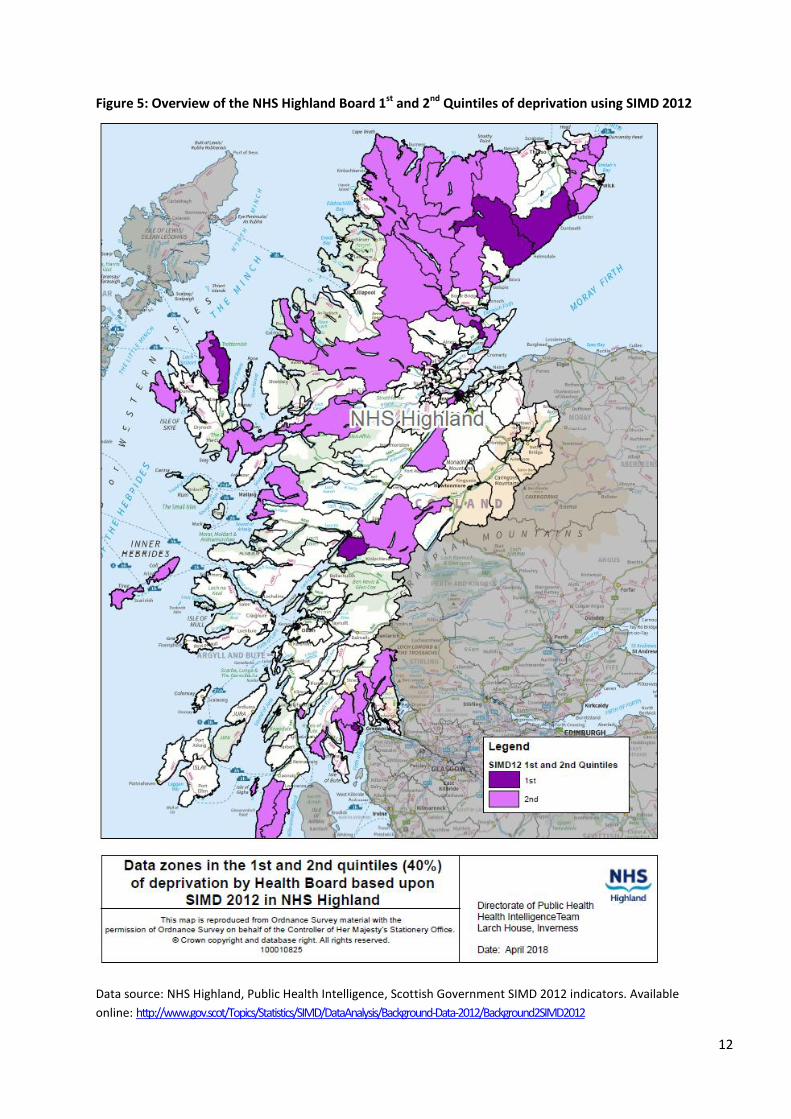
12
Figure 5: Overview of the NHS Highland Board 1st and 2nd Quintiles of deprivation using SIMD 2012
Data source: NHS Highland, Public Health Intelligence, Scottish Government SIMD 2012 indicators. Available
online: http://www.gov.scot/Topics/Statistics/SIMD/DataAnalysis/Background-Data-2012/Background2SIMD2012
13
The map above indicates that a number of data zones in the Skye, Lochalsh and South West Ross
area are in the 40% of most deprived areas within NHS Highland. One data zone, representing Skye
North East, is in the 20% of most deprived areas in the study area. If the national rather than health
board ranks of deprivation are considered, no areas in Skye, Lochalsh and South West Ross are
ranked in the 20% of most deprived areas.
Deprivation in remote and rural areas is poorly reflected in standard deprivation indices and,
therefore, two models which use alternative approaches5 are shown below, based on the concept of
fragility. In rough outline the first model included the following factors:
1. Depopulation related to young working age adults
2. Population density
3. Rates of claim for Department of Work and Pensions benefits
4. Estimated median gross total household income £ per week
5. Access to nine core services
6. Drive time to a major retail centre
5 Douglas, I. and Thomas, C., 2015. Supporting the Highland Community Planning Partnership to identify areas of rural
population need. NHS Highland and Highland Council. Published within: Highland Community Planning Partnership (CPP)
Board meeting 3 June 2015 – Item 8: Deprivation and Inequalities – Rural Analysis; Annex 2. Available online:
https://www.highland.gov.uk/meetings/meeting/3466/highland_community_planning_partnership_board
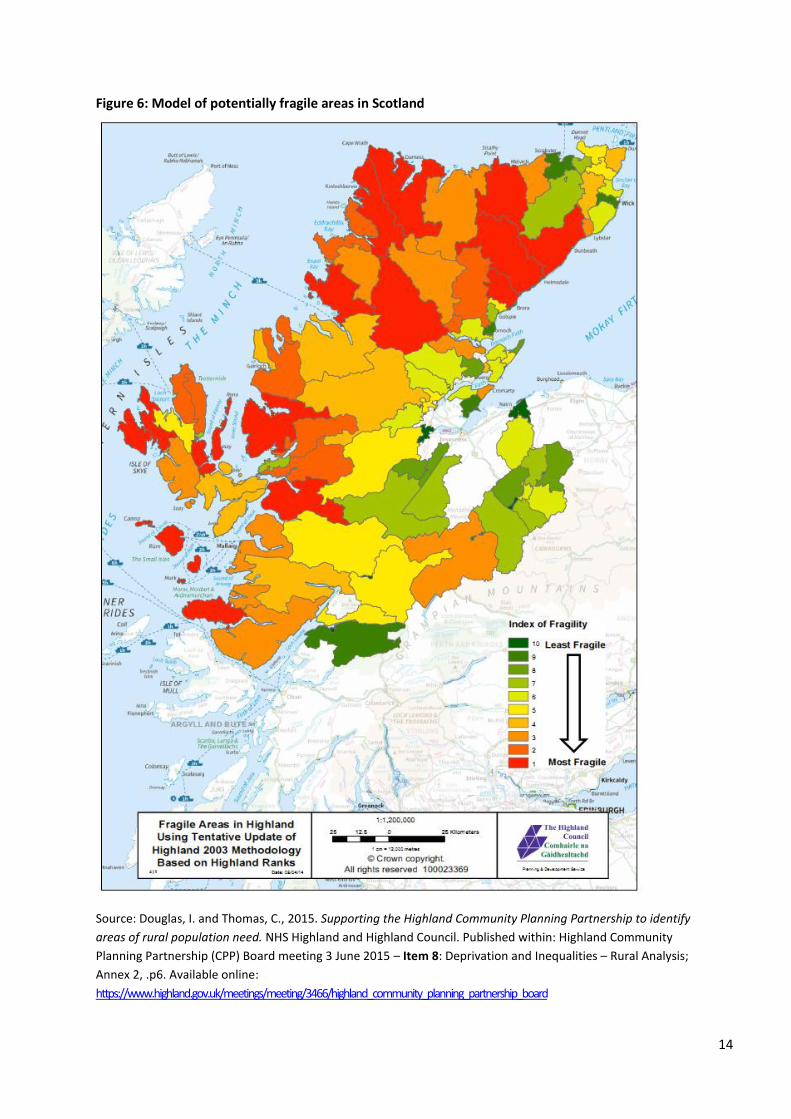
14
Figure 6: Model of potentially fragile areas in Scotland
Source: Douglas, I. and Thomas, C., 2015. Supporting the Highland Community Planning Partnership to identify
areas of rural population need. NHS Highland and Highland Council. Published within: Highland Community
Planning Partnership (CPP) Board meeting 3 June 2015 – Item 8: Deprivation and Inequalities – Rural Analysis;
Annex 2, .p6. Available online:
https://www.highland.gov.uk/meetings/meeting/3466/highland_community_planning_partnership_board
15
Fragile areas were “characterized by a number of factors including weakening of communities
through population loss; low incomes; limited employment opportunities; poor infrastructure;
inadequate housing and remoteness”, based on four indicators:
1. Population decline 2001 to 2005, three bands identified (Small Area Population Estimates)
2. Population density 2005, two bands identified (Small Area Population Estimates)
3. Drive time to a mid-sized service centre, three bands identified (SNS, Google Maps
4. Income per household, two bands identified (CACI Paycheck).
Although the map above and map below produce quite distinct patterns, both maps indicate that
parts of Skye, Lochalsh and South West Ross include economically fragile areas.
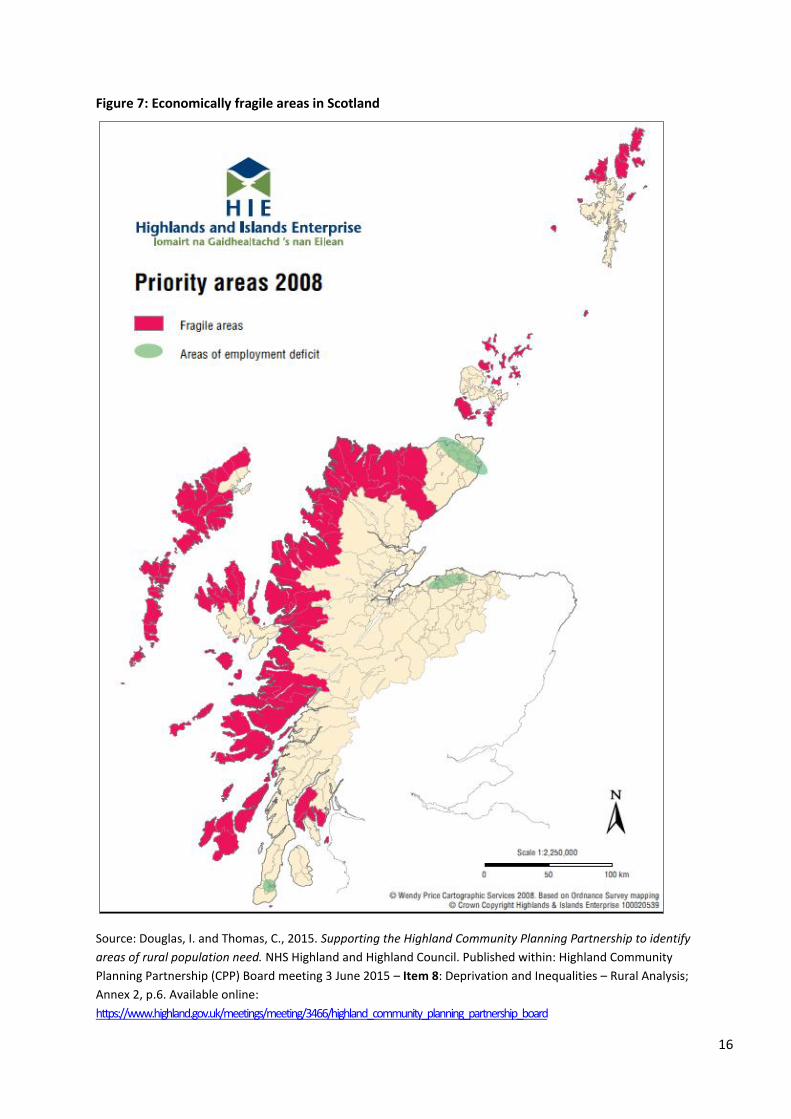
16
Figure 7: Economically fragile areas in Scotland
Source: Douglas, I. and Thomas, C., 2015. Supporting the Highland Community Planning Partnership to identify
areas of rural population need. NHS Highland and Highland Council. Published within: Highland Community
Planning Partnership (CPP) Board meeting 3 June 2015 – Item 8: Deprivation and Inequalities – Rural Analysis;
Annex 2, p.6. Available online:
https://www.highland.gov.uk/meetings/meeting/3466/highland_community_planning_partnership_board

17
The map above indicates that the whole of the north-west coastline of the north of Scotland is
economically fragile. If it is assumed that this is potentially associated with an aspect of rural
deprivation, it would confirm the fact that north Skye is an area which would be of importance in
terms of public sector planning.
The data below relate to income deprivation, which is arguably the single domain that is most
generalisable as a marker of deprivation.
Table 1: Income deprivation in Skye, Lochalsh and South West Ross by data zone
Source: Douglas, I., 2014. Income deprivation in Skye, Lochalsh and West Ross. NHS Highland Public Health Intelligence and Knowledge Team. p.6. Available online: http://www.nhshighland.scot.nhs.uk/News/PublicConsultation/Skye/Documents/Skye_incomedep.pdf
There are clearly areas of low income in Skye, which are likely to impact on the need for Out of
Hours services. The most deprived areas by this metric are Portree North and Portree West.
The map below provides a graphical description of income, which is one of the indices included in
many assessments of deprivation.
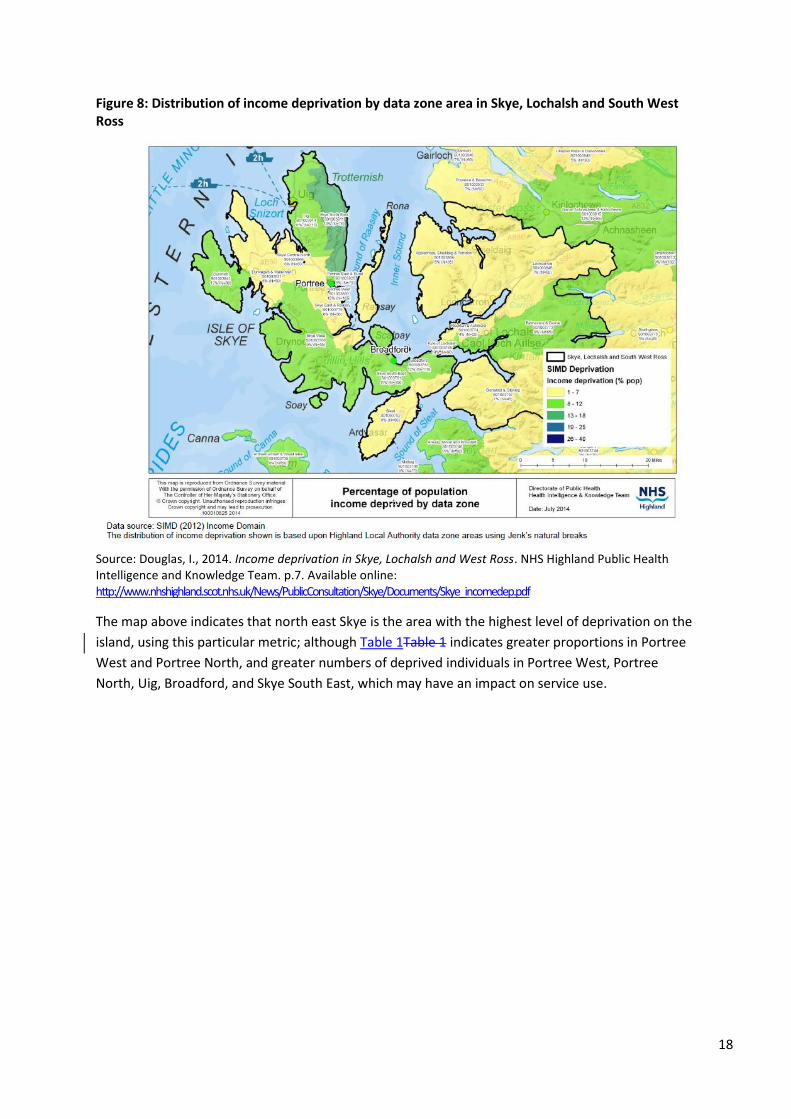
18
Figure 8: Distribution of income deprivation by data zone area in Skye, Lochalsh and South West Ross
Source: Douglas, I., 2014. Income deprivation in Skye, Lochalsh and West Ross. NHS Highland Public Health Intelligence and Knowledge Team. p.7. Available online: http://www.nhshighland.scot.nhs.uk/News/PublicConsultation/Skye/Documents/Skye_incomedep.pdf
The map above indicates that north east Skye is the area with the highest level of deprivation on the
island, using this particular metric; although Table 1Table 1 indicates greater proportions in Portree
West and Portree North, and greater numbers of deprived individuals in Portree West, Portree
North, Uig, Broadford, and Skye South East, which may have an impact on service use.
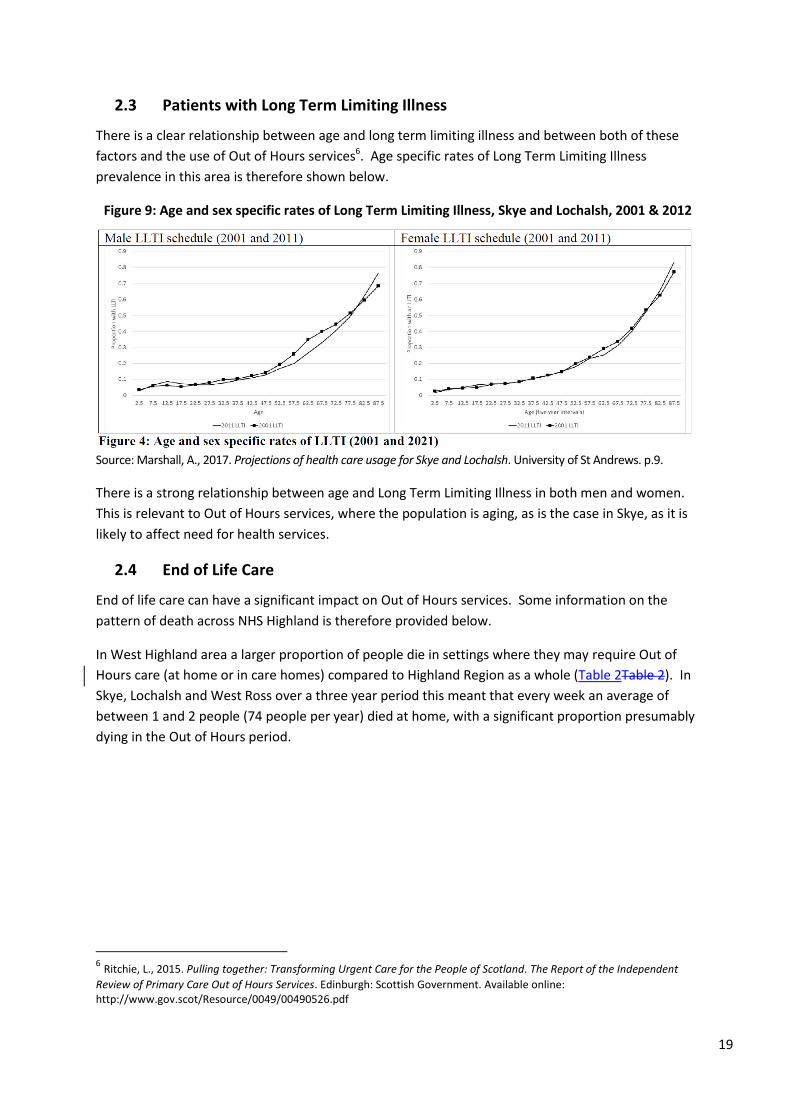
19
2.3 Patients with Long Term Limiting Illness
There is a clear relationship between age and long term limiting illness and between both of these
factors and the use of Out of Hours services6. Age specific rates of Long Term Limiting Illness
prevalence in this area is therefore shown below.
Figure 9: Age and sex specific rates of Long Term Limiting Illness, Skye and Lochalsh, 2001 & 2012
Source: Marshall, A., 2017. Projections of health care usage for Skye and Lochalsh. University of St Andrews. p.9.
There is a strong relationship between age and Long Term Limiting Illness in both men and women.
This is relevant to Out of Hours services, where the population is aging, as is the case in Skye, as it is
likely to affect need for health services.
2.4 End of Life Care
End of life care can have a significant impact on Out of Hours services. Some information on the
pattern of death across NHS Highland is therefore provided below.
In West Highland area a larger proportion of people die in settings where they may require Out of
Hours care (at home or in care homes) compared to Highland Region as a whole (Table 2Table 2). In
Skye, Lochalsh and West Ross over a three year period this meant that every week an average of
between 1 and 2 people (74 people per year) died at home, with a significant proportion presumably
dying in the Out of Hours period.
6 Ritchie, L., 2015. Pulling together: Transforming Urgent Care for the People of Scotland. The Report of the Independent
Review of Primary Care Out of Hours Services. Edinburgh: Scottish Government. Available online: http://www.gov.scot/Resource/0049/00490526.pdf
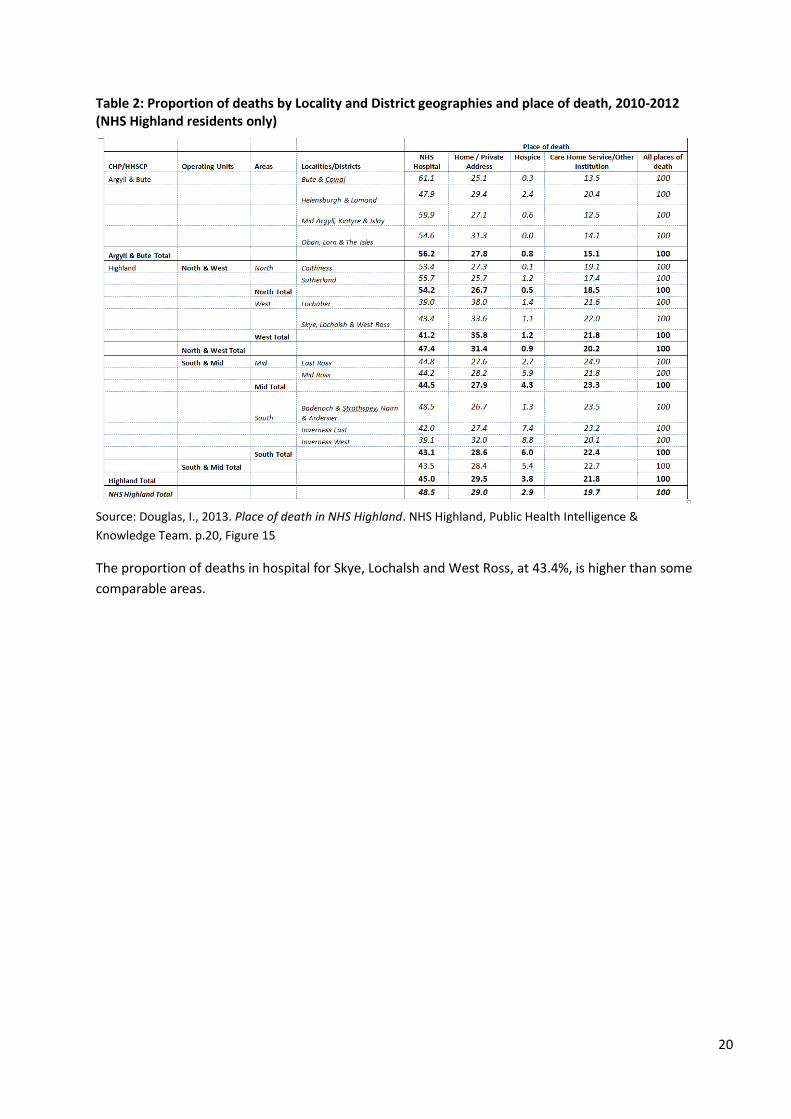
20
Table 2: Proportion of deaths by Locality and District geographies and place of death, 2010-2012 (NHS Highland residents only)
Source: Douglas, I., 2013. Place of death in NHS Highland. NHS Highland, Public Health Intelligence &
Knowledge Team. p.20, Figure 15
The proportion of deaths in hospital for Skye, Lochalsh and West Ross, at 43.4%, is higher than some
comparable areas.
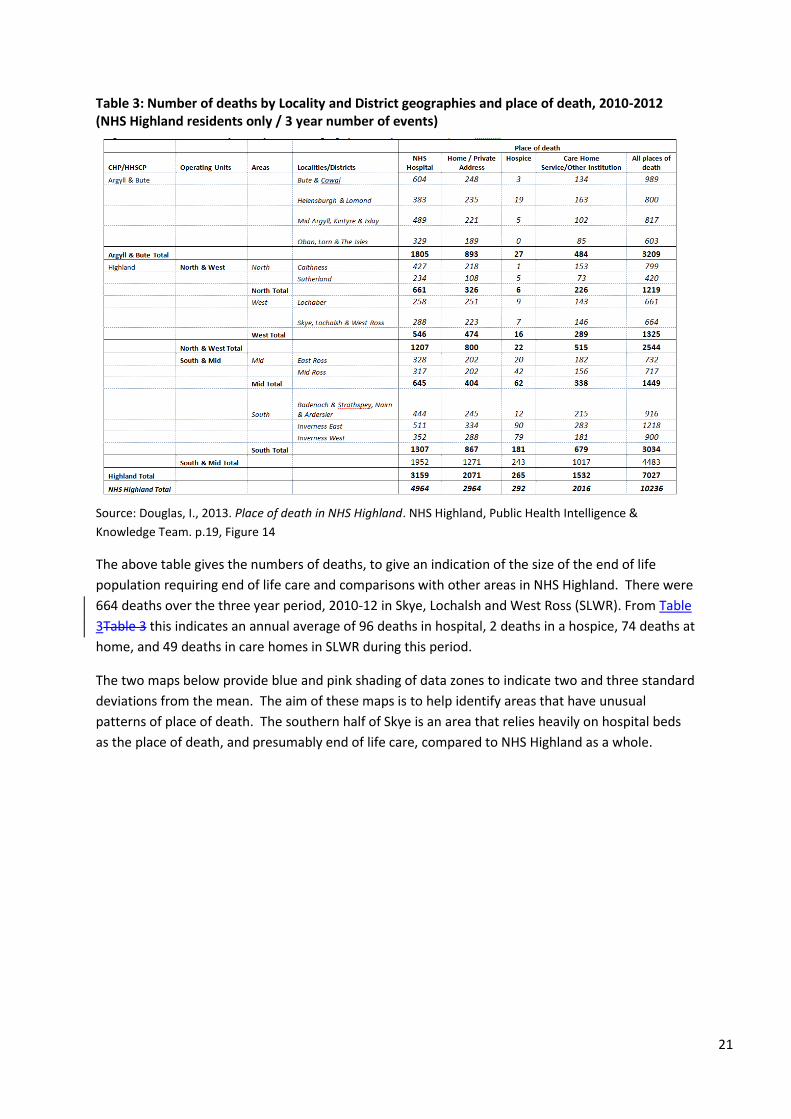
21
Table 3: Number of deaths by Locality and District geographies and place of death, 2010-2012 (NHS Highland residents only / 3 year number of events)
Source: Douglas, I., 2013. Place of death in NHS Highland. NHS Highland, Public Health Intelligence &
Knowledge Team. p.19, Figure 14
The above table gives the numbers of deaths, to give an indication of the size of the end of life
population requiring end of life care and comparisons with other areas in NHS Highland. There were
664 deaths over the three year period, 2010-12 in Skye, Lochalsh and West Ross (SLWR). From Table
3Table 3 this indicates an annual average of 96 deaths in hospital, 2 deaths in a hospice, 74 deaths at
home, and 49 deaths in care homes in SLWR during this period.
The two maps below provide blue and pink shading of data zones to indicate two and three standard
deviations from the mean. The aim of these maps is to help identify areas that have unusual
patterns of place of death. The southern half of Skye is an area that relies heavily on hospital beds
as the place of death, and presumably end of life care, compared to NHS Highland as a whole.
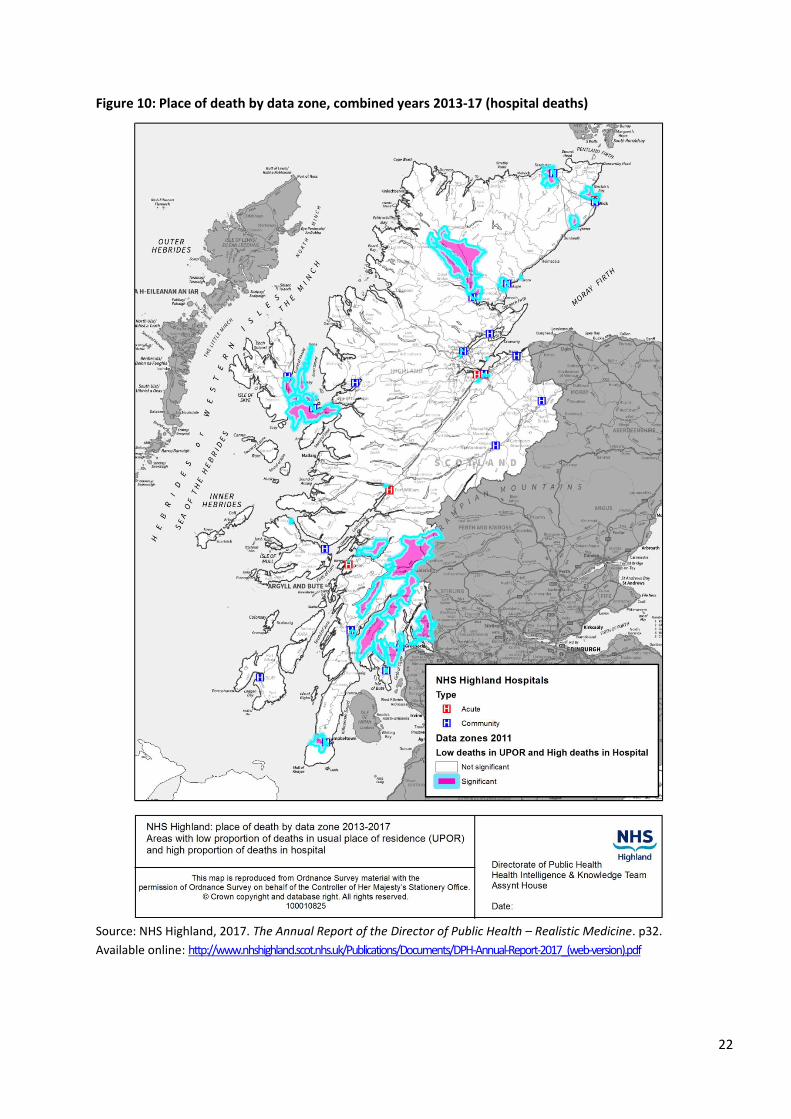
22
Figure 10: Place of death by data zone, combined years 2013-17 (hospital deaths)
Source: NHS Highland, 2017. The Annual Report of the Director of Public Health – Realistic Medicine. p32.
Available online: http://www.nhshighland.scot.nhs.uk/Publications/Documents/DPH-Annual-Report-2017_(web-version).pdf
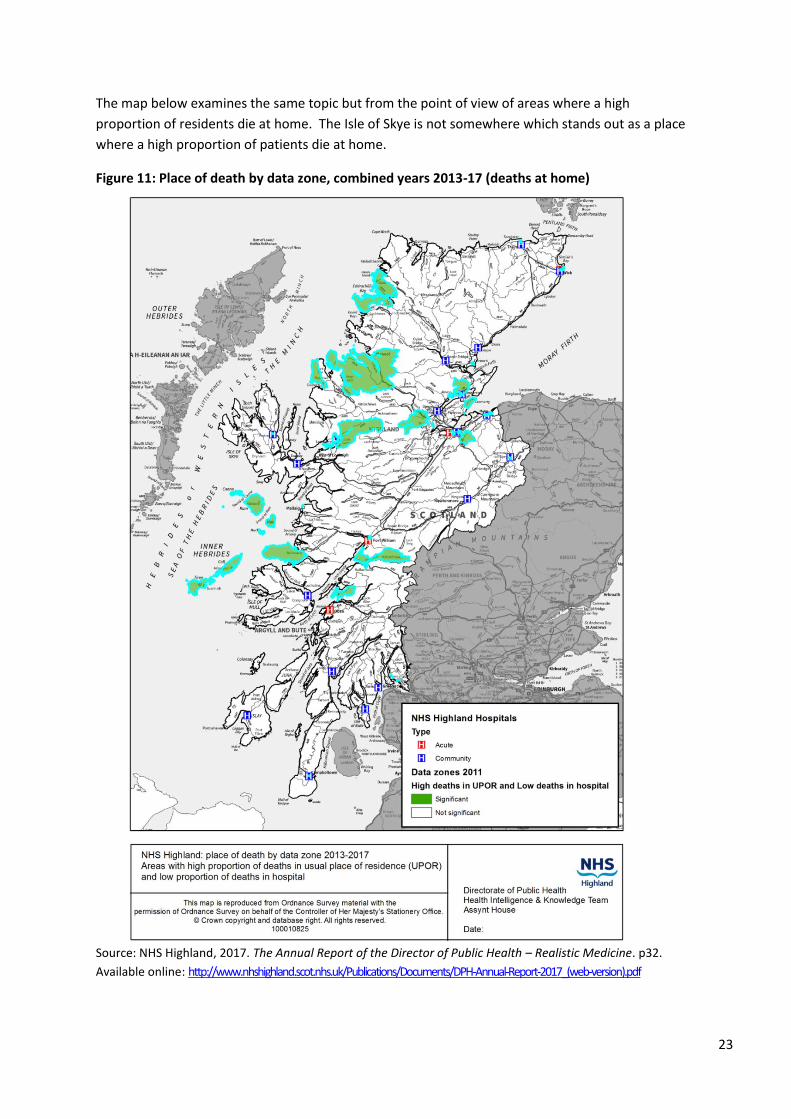
23
The map below examines the same topic but from the point of view of areas where a high
proportion of residents die at home. The Isle of Skye is not somewhere which stands out as a place
where a high proportion of patients die at home.
Figure 11: Place of death by data zone, combined years 2013-17 (deaths at home)
Source: NHS Highland, 2017. The Annual Report of the Director of Public Health – Realistic Medicine. p32.
Available online: http://www.nhshighland.scot.nhs.uk/Publications/Documents/DPH-Annual-Report-2017_(web-version).pdf

24
3. Who delivers care?
This section provides information on the workforce who deliver care. Some information is also
provided around informal carers.
3.1 NHS staff
In recent decades Out of Hours patients have been seen by GPs. However, parts of NHS Highland
are increasingly using a range of health professionals as is shown in the graph below.
Figure 12: Proportion of Out of Hours cases seen by different professionals, Skye, 2013 to 2017
Source: NHS Highland, 2017. Urgent Care – Data Summary for Skye. p.7.Prepared by Project Lead, Out of Hours
and Acting Primary Care Manager North & West (GMS) from ADASTRA patient management system.
The graph demonstrates the increasing use of nurses and paramedics to provide Out of Hours
services, with 40% of cases being seen by a professional other than a doctor by mid 2017. It is
anticipated that this trend will continue.
Several tables are provided below, which present available data on staff groups.
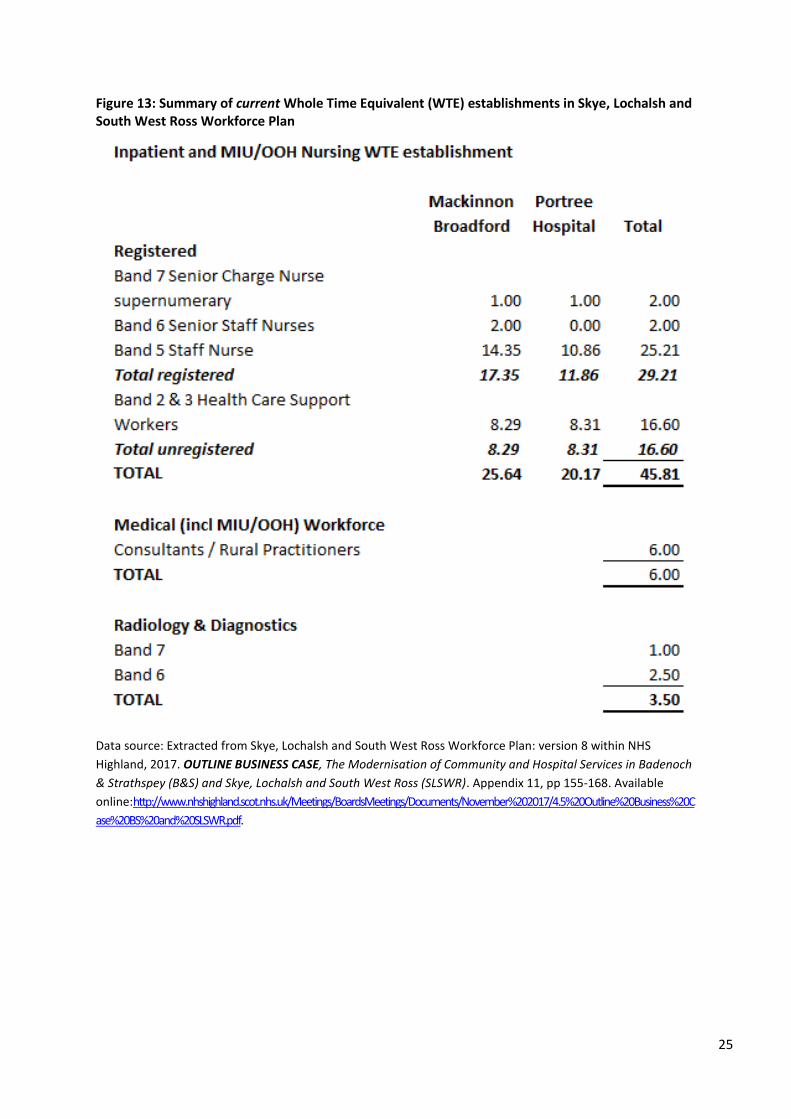
25
Figure 13: Summary of current Whole Time Equivalent (WTE) establishments in Skye, Lochalsh and South West Ross Workforce Plan
Data source: Extracted from Skye, Lochalsh and South West Ross Workforce Plan: version 8 within NHS
Highland, 2017. OUTLINE BUSINESS CASE, The Modernisation of Community and Hospital Services in Badenoch
& Strathspey (B&S) and Skye, Lochalsh and South West Ross (SLSWR). Appendix 11, pp 155-168. Available
online:http://www.nhshighland.scot.nhs.uk/Meetings/BoardsMeetings/Documents/November%202017/4.5%20Outline%20Business%20C
ase%20BS%20and%20SLSWR.pdf.
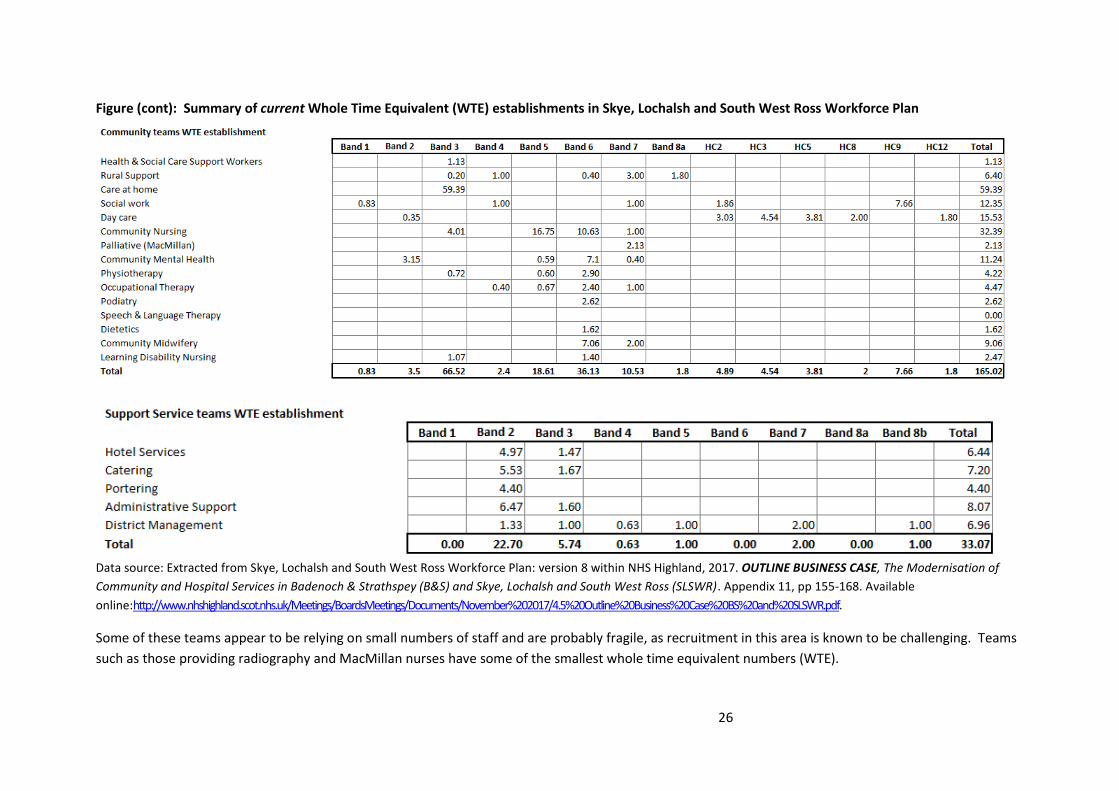
26
Figure (cont): Summary of current Whole Time Equivalent (WTE) establishments in Skye, Lochalsh and South West Ross Workforce Plan
Data source: Extracted from Skye, Lochalsh and South West Ross Workforce Plan: version 8 within NHS Highland, 2017. OUTLINE BUSINESS CASE, The Modernisation of
Community and Hospital Services in Badenoch & Strathspey (B&S) and Skye, Lochalsh and South West Ross (SLSWR). Appendix 11, pp 155-168. Available
online:http://www.nhshighland.scot.nhs.uk/Meetings/BoardsMeetings/Documents/November%202017/4.5%20Outline%20Business%20Case%20BS%20and%20SLSWR.pdf.
Some of these teams appear to be relying on small numbers of staff and are probably fragile, as recruitment in this area is known to be challenging. Teams
such as those providing radiography and MacMillan nurses have some of the smallest whole time equivalent numbers (WTE).
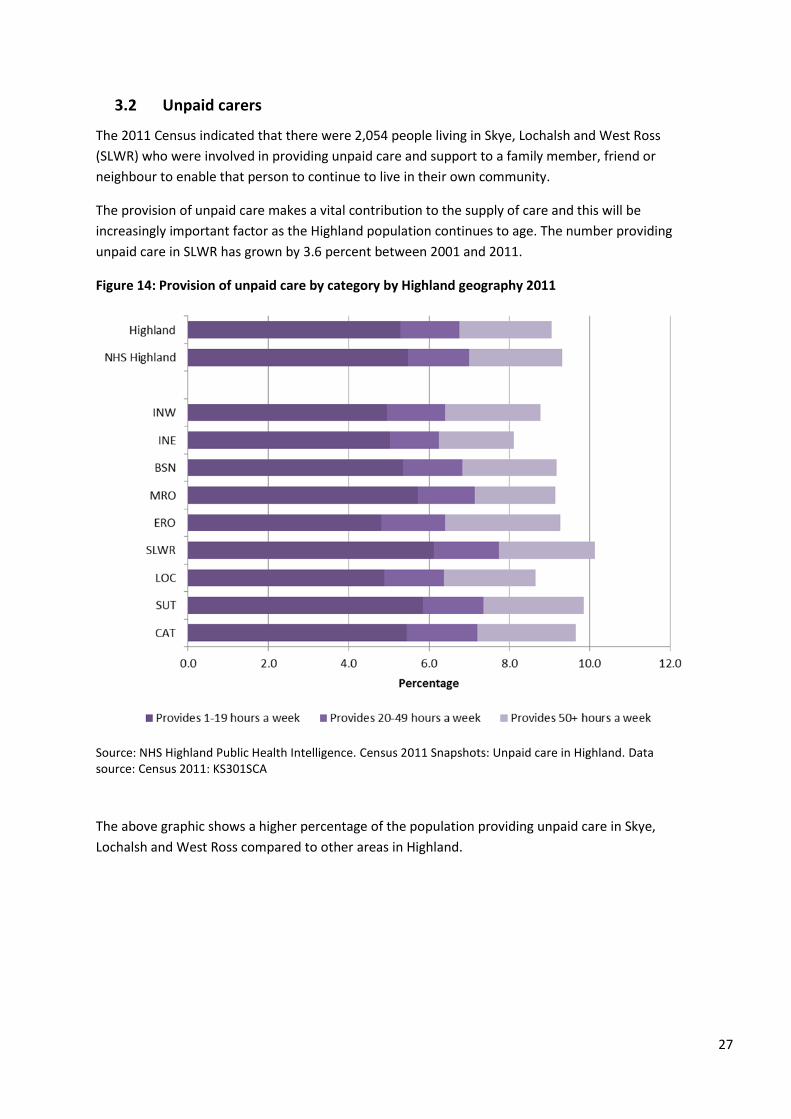
27
3.2 Unpaid carers
The 2011 Census indicated that there were 2,054 people living in Skye, Lochalsh and West Ross
(SLWR) who were involved in providing unpaid care and support to a family member, friend or
neighbour to enable that person to continue to live in their own community.
The provision of unpaid care makes a vital contribution to the supply of care and this will be
increasingly important factor as the Highland population continues to age. The number providing
unpaid care in SLWR has grown by 3.6 percent between 2001 and 2011.
Figure 14: Provision of unpaid care by category by Highland geography 2011
Source: NHS Highland Public Health Intelligence. Census 2011 Snapshots: Unpaid care in Highland. Data source: Census 2011: KS301SCA
The above graphic shows a higher percentage of the population providing unpaid care in Skye,
Lochalsh and West Ross compared to other areas in Highland.
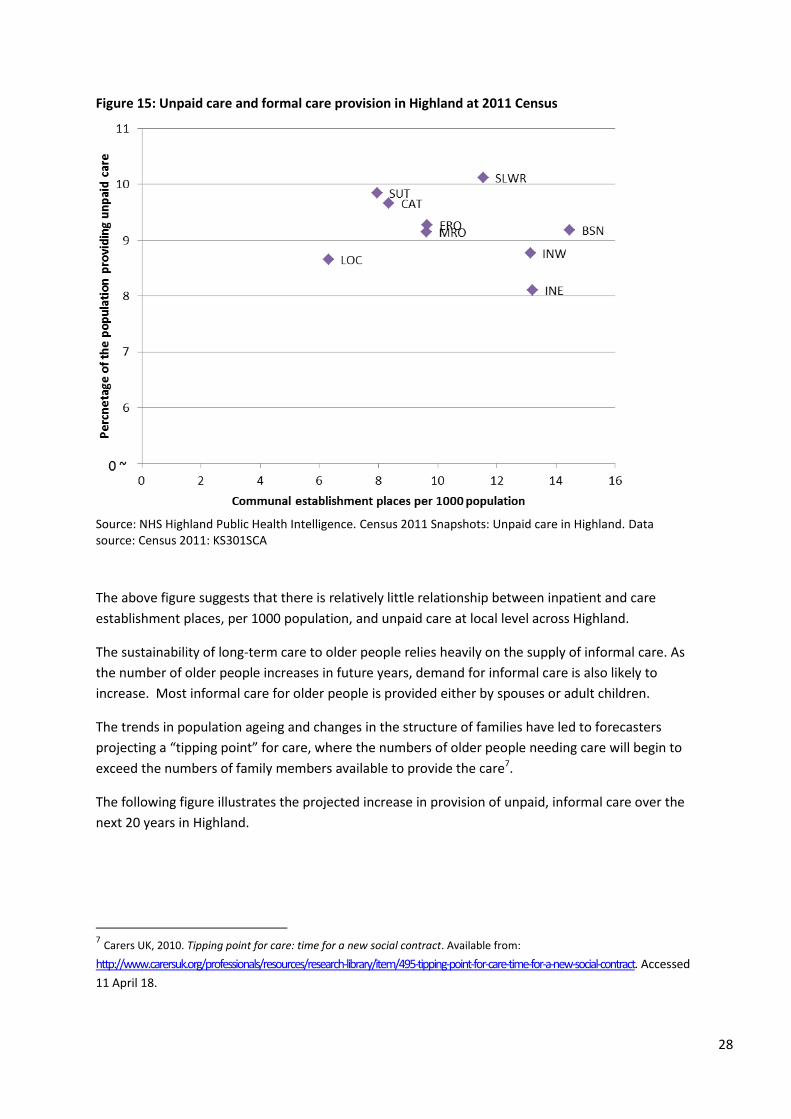
28
Figure 15: Unpaid care and formal care provision in Highland at 2011 Census
Source: NHS Highland Public Health Intelligence. Census 2011 Snapshots: Unpaid care in Highland. Data source: Census 2011: KS301SCA
The above figure suggests that there is relatively little relationship between inpatient and care
establishment places, per 1000 population, and unpaid care at local level across Highland.
The sustainability of long-term care to older people relies heavily on the supply of informal care. As
the number of older people increases in future years, demand for informal care is also likely to
increase. Most informal care for older people is provided either by spouses or adult children.
The trends in population ageing and changes in the structure of families have led to forecasters
projecting a “tipping point” for care, where the numbers of older people needing care will begin to
exceed the numbers of family members available to provide the care7.
The following figure illustrates the projected increase in provision of unpaid, informal care over the
next 20 years in Highland.
7 Carers UK, 2010. Tipping point for care: time for a new social contract. Available from:
http://www.carersuk.org/professionals/resources/research-library/item/495-tipping-point-for-care-time-for-a-new-social-contract. Accessed
11 April 18.
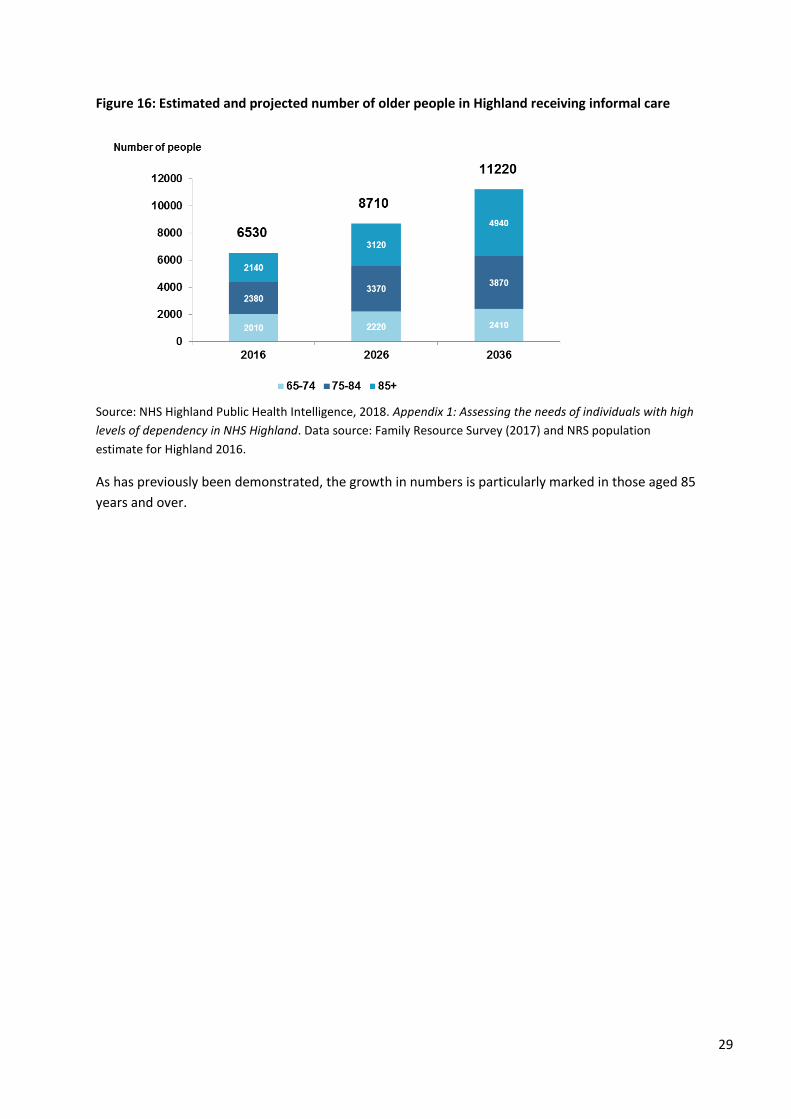
29
Figure 16: Estimated and projected number of older people in Highland receiving informal care
Source: NHS Highland Public Health Intelligence, 2018. Appendix 1: Assessing the needs of individuals with high
levels of dependency in NHS Highland. Data source: Family Resource Survey (2017) and NRS population
estimate for Highland 2016.
As has previously been demonstrated, the growth in numbers is particularly marked in those aged 85
years and over.
30
4. What care is delivered?
A number of aspects around what care is delivered is provided below including: historic aspects of
services, Out of Hours services, outpatient services, services delivered by Allied Health Professionals
in the community, and hospital services.
4.1 Historic changes to services
Some of the key changes to services that have happened in Skye are provided in box 1 and 2 below.
These are taken from the Full Public Consultation document for service redesign and provide a
snapshot of the services around 2014.
31
Box 1 Local context
The opening of the Skye Bridge in 1995, and removal of tolls in 2004, eased access onto and off the island.
Development of the Rural Practitioner Team based in Dr MacKinnon’s Memorial Hospital in Broadford. Rural Practitioners are mostly GPs with enhanced training in emergency care for rural settings. The team was established in 2004 to meet community needs following the withdrawal of local surgical consultant and anaesthesia cover (for safety reasons) plus the need to provide out-of-hours medical cover.
In May 2006, Gesto Hospital in Edinbane was closed.
New health centres were opened in Sleat in 2005, Kyle in 2008, and Broadford in 2012. Broadford Health Centre replaced the existing Broadford Medical Practice and serves patients from communities in Broadford, Strath, Kyleakin and Kyle Rhea communities. It is co-located with Dr MacKinnon’s Memorial Hospital.
There have been Care home closures – Staffin, Hilton (Broadford) and Graham House (Dornie).
An Acarsaid Care Home in Broadford was re-developed in 2010/11. There has been new supported housing in Dornie.
Teleneurology clinics, Telediabetes clinics and Telecardiac rehabilitation clinics got underway in both Portree and Broadford in 2011.
Various developments to community teams include redesign of community nursing team, community midwifery team and community midwifery Unit in Dr MacKinnon Memorial Hospital in Broadford.
A new dental clinic opened in Portree in 2012.
NHS Highland took on responsibility for adult social care (care-at-home, care homes, day care services) in April 2012, as part of integration.
The Broadford Ambulance station closed in 2013 and was re-located to Dr MacKinnon Memorial Hospital
Development of South Skye Practice (Broadford/Sleat/Carbost) – ongoing
Source: NHS Highland, 2014. Full public consultation document - Proposed modernisation of community and
hospital services in Skye, Lochalsh and South West Ross. p.14. Available online:
http://www.nhshighland.scot.nhs.uk/News/PublicConsultation/Skye/Documents/SLWR%20%20FINAL%20FULL%2019%20May%2014.pdf
32
A description of services, as included in the Public Consultation document, is provided below.
Box 2 Summary of some of the current services
Local GPs, nurses, allied health professionals8, community staff and others have been
working with an independent health care planner. They have been looking at current
services which are summarised below:
GP Practice
There are 14,680 registered patients in the area who are served by ten GP Practices
District General Hospital
The nearest district general hospital is Raigmore Hospital which is 120 miles away from
Portree, approximately three hours by road ambulance.
Dr MacKinnon Memorial Hospital, Broadford
This is a 20-bedded, intermediate care community hospital providing assessment,
resuscitation and stabilisation of acutely ill patients, supported by a small team of salaried
Rural Practitioners (RPs).
RPs are like GPs but with additional emergency training, allowing the hospital to function at
a higher level than most community hospitals. The hospital has 24-hour on-site medical and
nursing cover and 24 hour A&E and Primary Care Emergency Services (PCEC).
A small amount of planned day case surgery is carried out.
Radiology services, including ultrasound, are also on site.
There are a range of visiting specialist out-patient services from Raigmore (Inverness), New
Craigs Hospital (Inverness) and Belford Hospital (Fort William).
Portree Community Hospital
12-bedded community Hospital is located adjacent to the Portree Medical Centre. It is supported by 24-hour nursing cover and access to 24-hour medical cover. The medical cover is provided by GPs from the Portree Medical Centre from 0800-2300 every day, delivered by GPs and during the out-of-hours period by Rural Practitioners; after 2300 there is no on-site medical cover but is provided from Broadford RPs supported by a North Skye second on call doctor.
8 Allied Health Professionals or AHPs include a number of health care workers such as physiotherapists,
occupational therapists, podiatrists, dieticians, speech & language therapists and radiographers.
33
Box 2 Summary of services (contd) Portree Hospital (Contd) Radiology services are available four days per week to support out-patient clinics which include Orthopaedics, Ear, Nose and Throat, Ophthalmology, General Medicine, Renal, Chest, Rehabilitation and Psychiatry. Other services Midwifery services cover Skye and Lochalsh with a base in both hospitals and one community bed in Dr MacKinnon Memorial Hospital supporting 15-25 births per year. Multi-disciplinary teams (social workers, care-at-home workers, physiotherapists, occupational therapists, community nurses, and community mental health teams), currently work out of a number of different bases. Adult social care provided by NHS Highland includes care-at-home service, one Care Home (An Acarsaid) in Broadford, Day Care Services (Tigh na Drochaidh) in Portree and (Airdferry) in Dornie. There are also two privately run Care Homes (Budh Mhor) in Portree and (The Haven) in Idrigill, Uig. There is one private Nursing Home (Home Farm) in Portree. The Howard Doris Unit in Lochcarron is a privately run facility, providing residential and day services. Source: NHS Highland, 2014. Full public consultation document - Proposed modernisation of community and
hospital services in Skye, Lochalsh and South West Ross. pp15-16. Available online:
http://www.nhshighland.scot.nhs.uk/News/PublicConsultation/Skye/Documents/SLWR%20%20FINAL%20FULL%2019%20May%2014.pdf
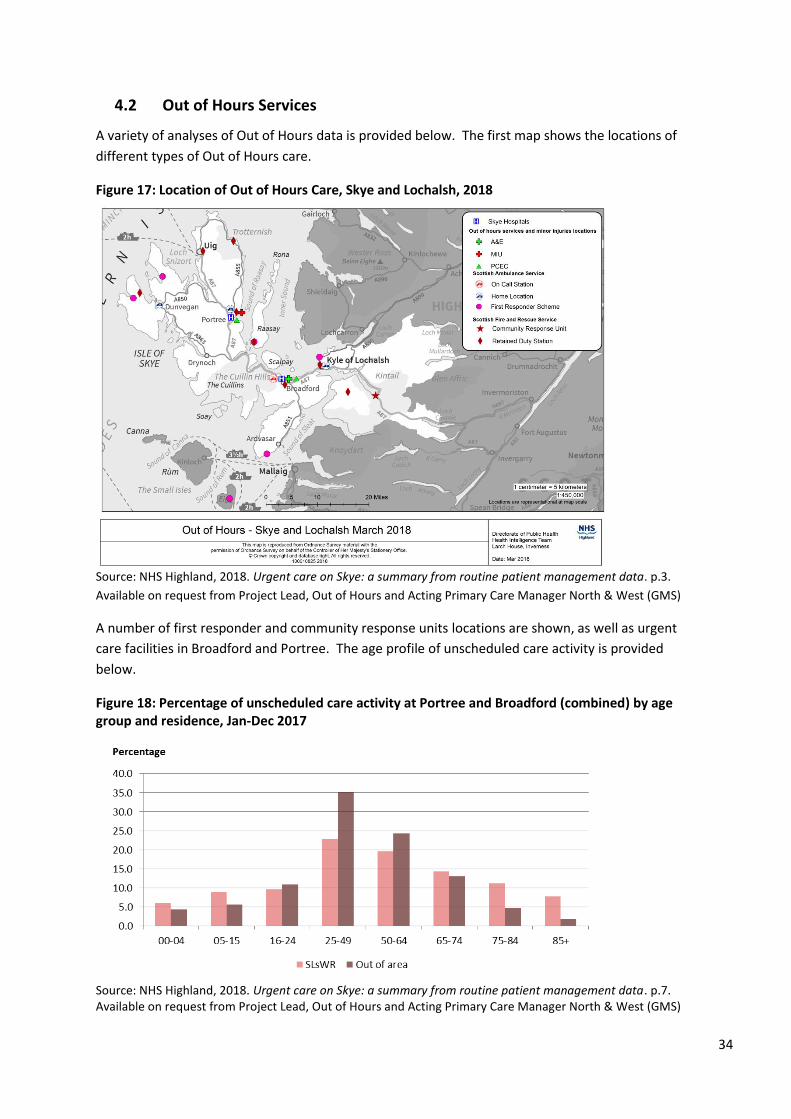
34
4.2 Out of Hours Services
A variety of analyses of Out of Hours data is provided below. The first map shows the locations of
different types of Out of Hours care.
Figure 17: Location of Out of Hours Care, Skye and Lochalsh, 2018
Source: NHS Highland, 2018. Urgent care on Skye: a summary from routine patient management data. p.3.
Available on request from Project Lead, Out of Hours and Acting Primary Care Manager North & West (GMS)
A number of first responder and community response units locations are shown, as well as urgent
care facilities in Broadford and Portree. The age profile of unscheduled care activity is provided
below.
Figure 18: Percentage of unscheduled care activity at Portree and Broadford (combined) by age group and residence, Jan-Dec 2017
Source: NHS Highland, 2018. Urgent care on Skye: a summary from routine patient management data. p.7. Available on request from Project Lead, Out of Hours and Acting Primary Care Manager North & West (GMS)
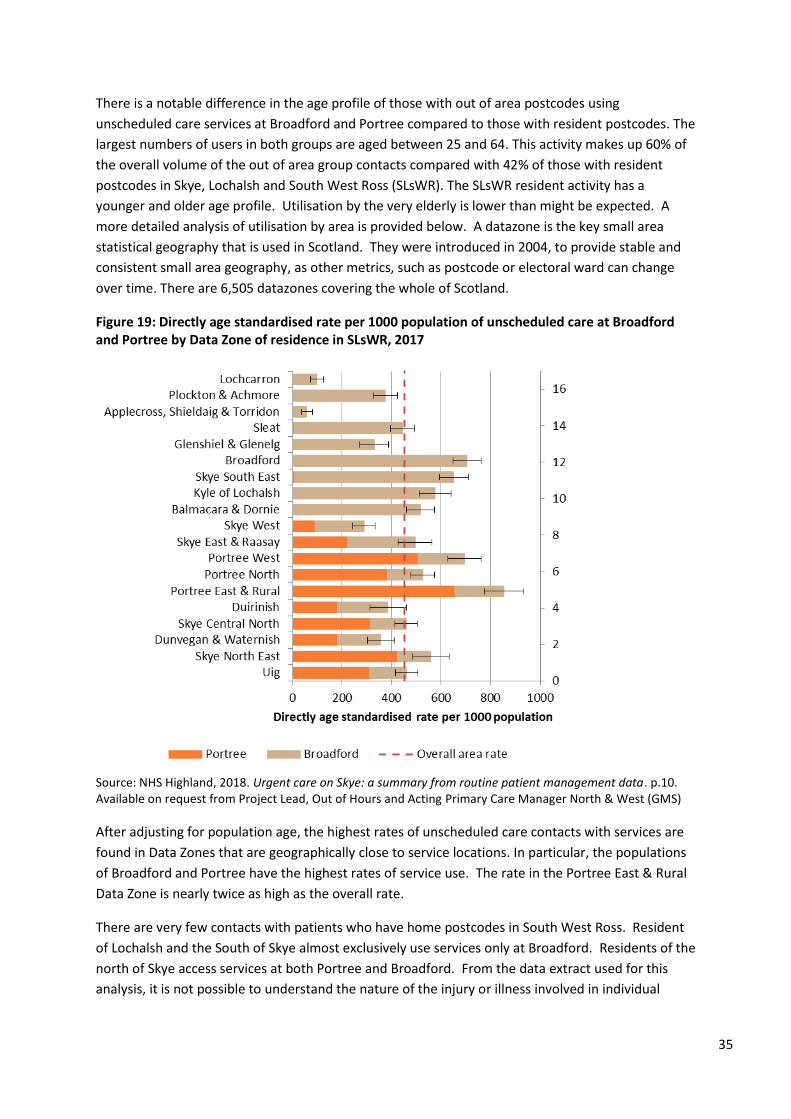
35
There is a notable difference in the age profile of those with out of area postcodes using
unscheduled care services at Broadford and Portree compared to those with resident postcodes. The
largest numbers of users in both groups are aged between 25 and 64. This activity makes up 60% of
the overall volume of the out of area group contacts compared with 42% of those with resident
postcodes in Skye, Lochalsh and South West Ross (SLsWR). The SLsWR resident activity has a
younger and older age profile. Utilisation by the very elderly is lower than might be expected. A
more detailed analysis of utilisation by area is provided below. A datazone is the key small area
statistical geography that is used in Scotland. They were introduced in 2004, to provide stable and
consistent small area geography, as other metrics, such as postcode or electoral ward can change
over time. There are 6,505 datazones covering the whole of Scotland.
Figure 19: Directly age standardised rate per 1000 population of unscheduled care at Broadford and Portree by Data Zone of residence in SLsWR, 2017
Source: NHS Highland, 2018. Urgent care on Skye: a summary from routine patient management data. p.10. Available on request from Project Lead, Out of Hours and Acting Primary Care Manager North & West (GMS)
After adjusting for population age, the highest rates of unscheduled care contacts with services are
found in Data Zones that are geographically close to service locations. In particular, the populations
of Broadford and Portree have the highest rates of service use. The rate in the Portree East & Rural
Data Zone is nearly twice as high as the overall rate.
There are very few contacts with patients who have home postcodes in South West Ross. Resident
of Lochalsh and the South of Skye almost exclusively use services only at Broadford. Residents of the
north of Skye access services at both Portree and Broadford. From the data extract used for this
analysis, it is not possible to understand the nature of the injury or illness involved in individual
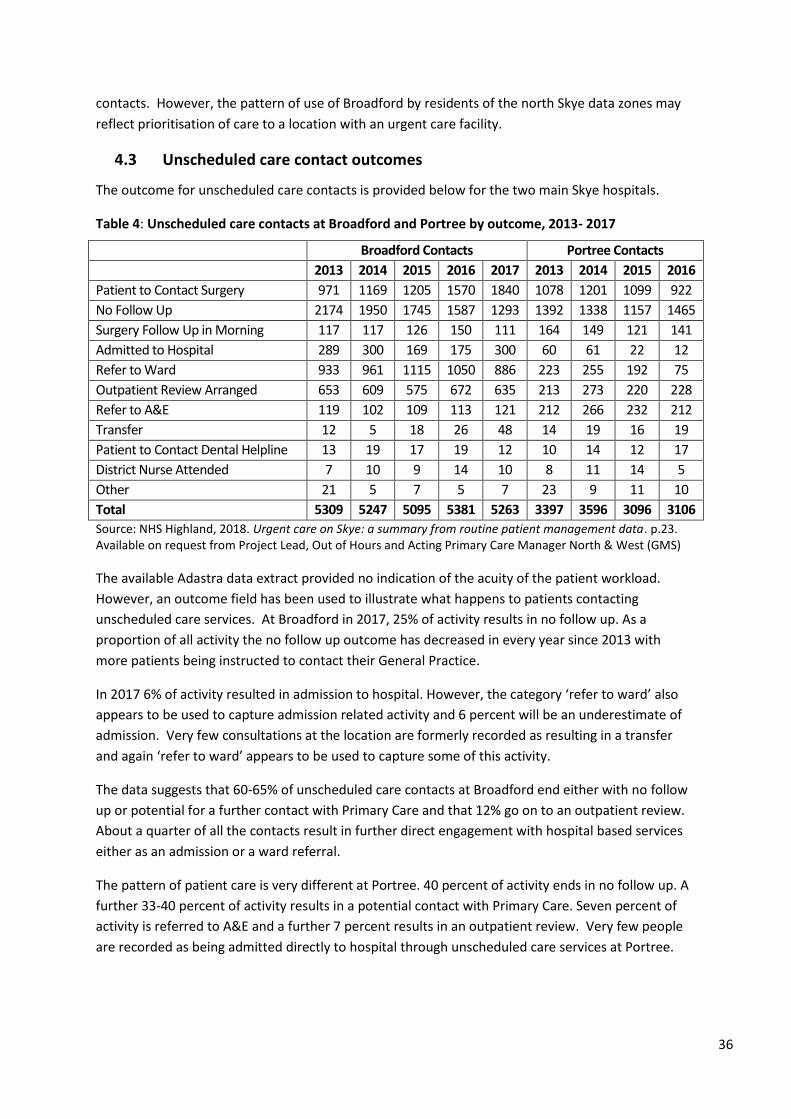
36
contacts. However, the pattern of use of Broadford by residents of the north Skye data zones may
reflect prioritisation of care to a location with an urgent care facility.
4.3 Unscheduled care contact outcomes
The outcome for unscheduled care contacts is provided below for the two main Skye hospitals.
Table 4: Unscheduled care contacts at Broadford and Portree by outcome, 2013- 2017
Broadford Contacts Portree Contacts
2013 2014 2015 2016 2017 2013 2014 2015 2016
Patient to Contact Surgery 971 1169 1205 1570 1840 1078 1201 1099 922
No Follow Up 2174 1950 1745 1587 1293 1392 1338 1157 1465
Surgery Follow Up in Morning 117 117 126 150 111 164 149 121 141
Admitted to Hospital 289 300 169 175 300 60 61 22 12
Refer to Ward 933 961 1115 1050 886 223 255 192 75
Outpatient Review Arranged 653 609 575 672 635 213 273 220 228
Refer to A&E 119 102 109 113 121 212 266 232 212
Transfer 12 5 18 26 48 14 19 16 19
Patient to Contact Dental Helpline 13 19 17 19 12 10 14 12 17
District Nurse Attended 7 10 9 14 10 8 11 14 5
Other 21 5 7 5 7 23 9 11 10
Total 5309 5247 5095 5381 5263 3397 3596 3096 3106
Source: NHS Highland, 2018. Urgent care on Skye: a summary from routine patient management data. p.23. Available on request from Project Lead, Out of Hours and Acting Primary Care Manager North & West (GMS)
The available Adastra data extract provided no indication of the acuity of the patient workload.
However, an outcome field has been used to illustrate what happens to patients contacting
unscheduled care services. At Broadford in 2017, 25% of activity results in no follow up. As a
proportion of all activity the no follow up outcome has decreased in every year since 2013 with
more patients being instructed to contact their General Practice.
In 2017 6% of activity resulted in admission to hospital. However, the category ‘refer to ward’ also
appears to be used to capture admission related activity and 6 percent will be an underestimate of
admission. Very few consultations at the location are formerly recorded as resulting in a transfer
and again ‘refer to ward’ appears to be used to capture some of this activity.
The data suggests that 60-65% of unscheduled care contacts at Broadford end either with no follow
up or potential for a further contact with Primary Care and that 12% go on to an outpatient review.
About a quarter of all the contacts result in further direct engagement with hospital based services
either as an admission or a ward referral.
The pattern of patient care is very different at Portree. 40 percent of activity ends in no follow up. A
further 33-40 percent of activity results in a potential contact with Primary Care. Seven percent of
activity is referred to A&E and a further 7 percent results in an outpatient review. Very few people
are recorded as being admitted directly to hospital through unscheduled care services at Portree.
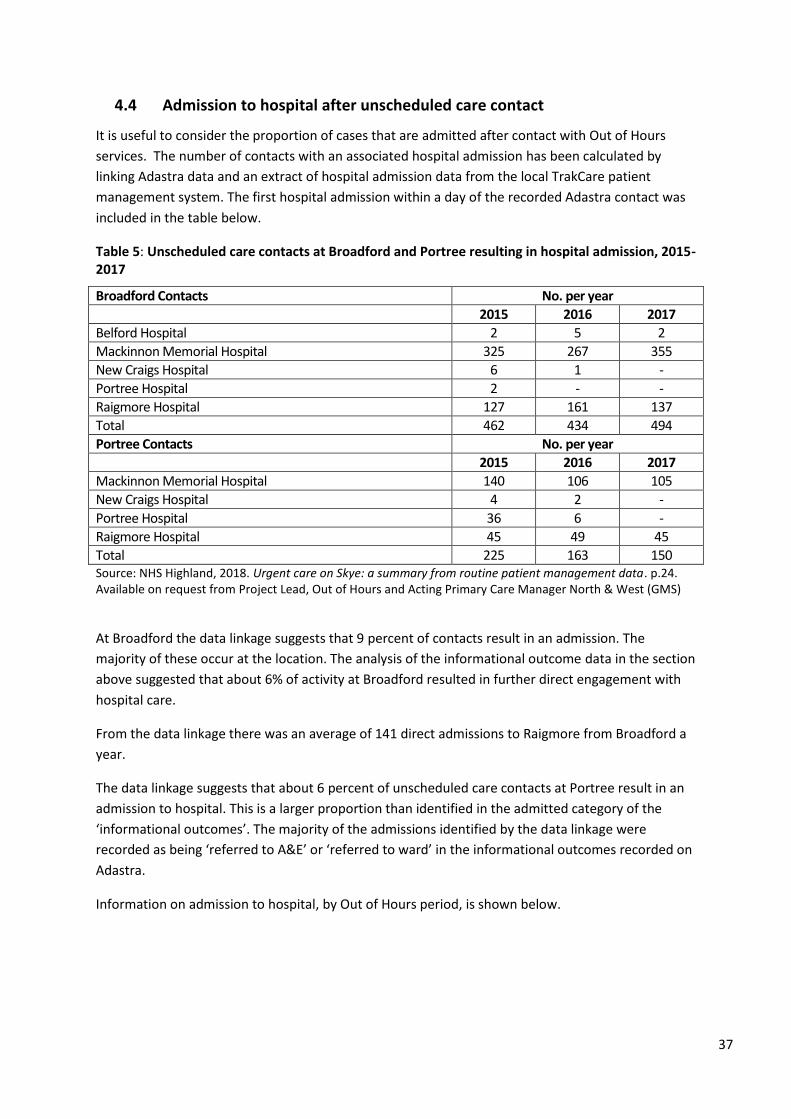
37
4.4 Admission to hospital after unscheduled care contact
It is useful to consider the proportion of cases that are admitted after contact with Out of Hours
services. The number of contacts with an associated hospital admission has been calculated by
linking Adastra data and an extract of hospital admission data from the local TrakCare patient
management system. The first hospital admission within a day of the recorded Adastra contact was
included in the table below.
Table 5: Unscheduled care contacts at Broadford and Portree resulting in hospital admission, 2015- 2017
Broadford Contacts No. per year
2015 2016 2017
Belford Hospital 2 5 2
Mackinnon Memorial Hospital 325 267 355
New Craigs Hospital 6 1 -
Portree Hospital 2 - -
Raigmore Hospital 127 161 137
Total 462 434 494
Portree Contacts No. per year
2015 2016 2017
Mackinnon Memorial Hospital 140 106 105
New Craigs Hospital 4 2 -
Portree Hospital 36 6 -
Raigmore Hospital 45 49 45
Total 225 163 150 Source: NHS Highland, 2018. Urgent care on Skye: a summary from routine patient management data. p.24. Available on request from Project Lead, Out of Hours and Acting Primary Care Manager North & West (GMS)
At Broadford the data linkage suggests that 9 percent of contacts result in an admission. The
majority of these occur at the location. The analysis of the informational outcome data in the section
above suggested that about 6% of activity at Broadford resulted in further direct engagement with
hospital care.
From the data linkage there was an average of 141 direct admissions to Raigmore from Broadford a
year.
The data linkage suggests that about 6 percent of unscheduled care contacts at Portree result in an
admission to hospital. This is a larger proportion than identified in the admitted category of the
‘informational outcomes’. The majority of the admissions identified by the data linkage were
recorded as being ‘referred to A&E’ or ‘referred to ward’ in the informational outcomes recorded on
Adastra.
Information on admission to hospital, by Out of Hours period, is shown below.
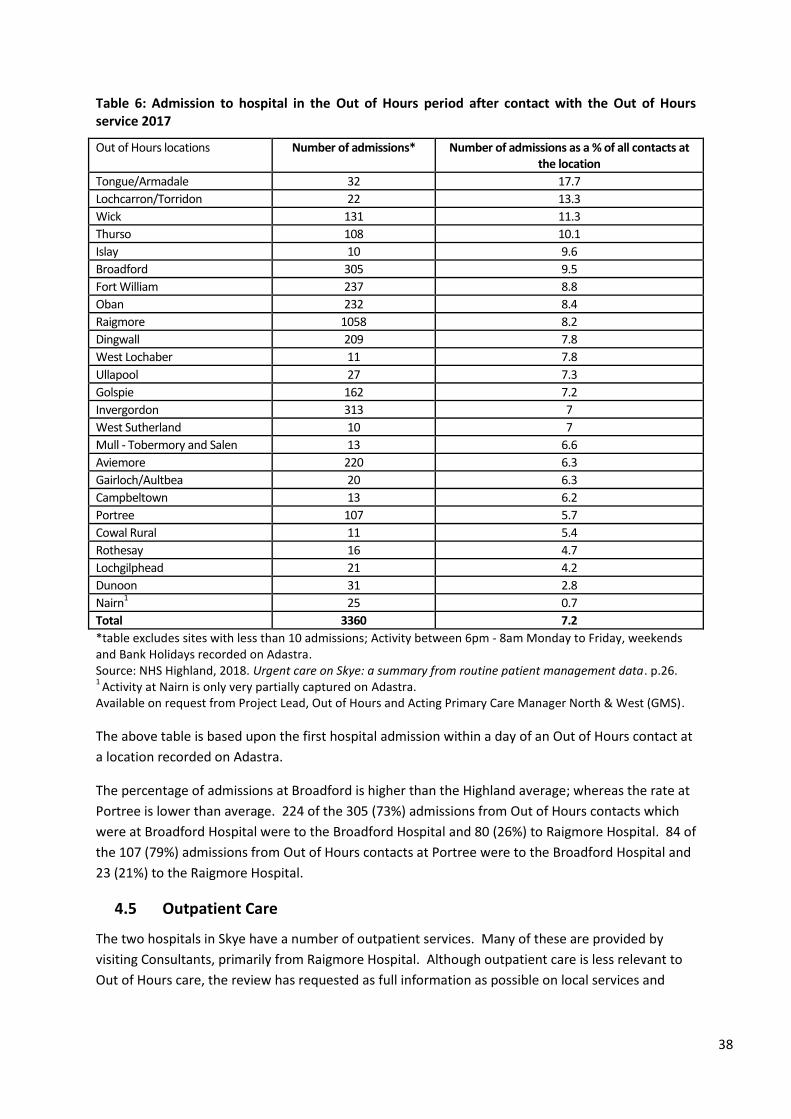
38
Table 6: Admission to hospital in the Out of Hours period after contact with the Out of Hours service 2017
Out of Hours locations Number of admissions* Number of admissions as a % of all contacts at the location
Tongue/Armadale 32 17.7
Lochcarron/Torridon 22 13.3
Wick 131 11.3
Thurso 108 10.1
Islay 10 9.6
Broadford 305 9.5
Fort William 237 8.8
Oban 232 8.4
Raigmore 1058 8.2
Dingwall 209 7.8
West Lochaber 11 7.8
Ullapool 27 7.3
Golspie 162 7.2
Invergordon 313 7
West Sutherland 10 7
Mull - Tobermory and Salen 13 6.6
Aviemore 220 6.3
Gairloch/Aultbea 20 6.3
Campbeltown 13 6.2
Portree 107 5.7
Cowal Rural 11 5.4
Rothesay 16 4.7
Lochgilphead 21 4.2
Dunoon 31 2.8
Nairn1 25 0.7
Total 3360 7.2
*table excludes sites with less than 10 admissions; Activity between 6pm - 8am Monday to Friday, weekends and Bank Holidays recorded on Adastra. Source: NHS Highland, 2018. Urgent care on Skye: a summary from routine patient management data. p.26. 1
Activity at Nairn is only very partially captured on Adastra. Available on request from Project Lead, Out of Hours and Acting Primary Care Manager North & West (GMS).
The above table is based upon the first hospital admission within a day of an Out of Hours contact at
a location recorded on Adastra.
The percentage of admissions at Broadford is higher than the Highland average; whereas the rate at
Portree is lower than average. 224 of the 305 (73%) admissions from Out of Hours contacts which
were at Broadford Hospital were to the Broadford Hospital and 80 (26%) to Raigmore Hospital. 84 of
the 107 (79%) admissions from Out of Hours contacts at Portree were to the Broadford Hospital and
23 (21%) to the Raigmore Hospital.
4.5 Outpatient Care
The two hospitals in Skye have a number of outpatient services. Many of these are provided by
visiting Consultants, primarily from Raigmore Hospital. Although outpatient care is less relevant to
Out of Hours care, the review has requested as full information as possible on local services and
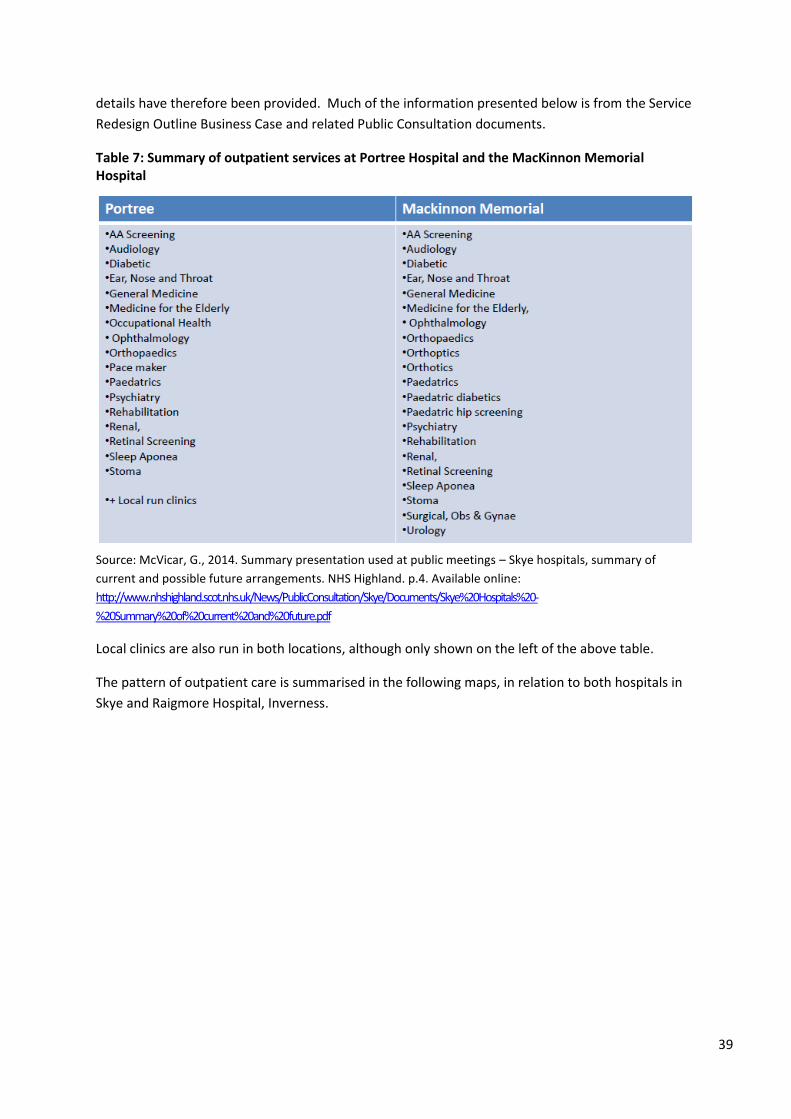
39
details have therefore been provided. Much of the information presented below is from the Service
Redesign Outline Business Case and related Public Consultation documents.
Table 7: Summary of outpatient services at Portree Hospital and the MacKinnon Memorial Hospital
Source: McVicar, G., 2014. Summary presentation used at public meetings – Skye hospitals, summary of
current and possible future arrangements. NHS Highland. p.4. Available online:
http://www.nhshighland.scot.nhs.uk/News/PublicConsultation/Skye/Documents/Skye%20Hospitals%20-
%20Summary%20of%20current%20and%20future.pdf
Local clinics are also run in both locations, although only shown on the left of the above table.
The pattern of outpatient care is summarised in the following maps, in relation to both hospitals in
Skye and Raigmore Hospital, Inverness.
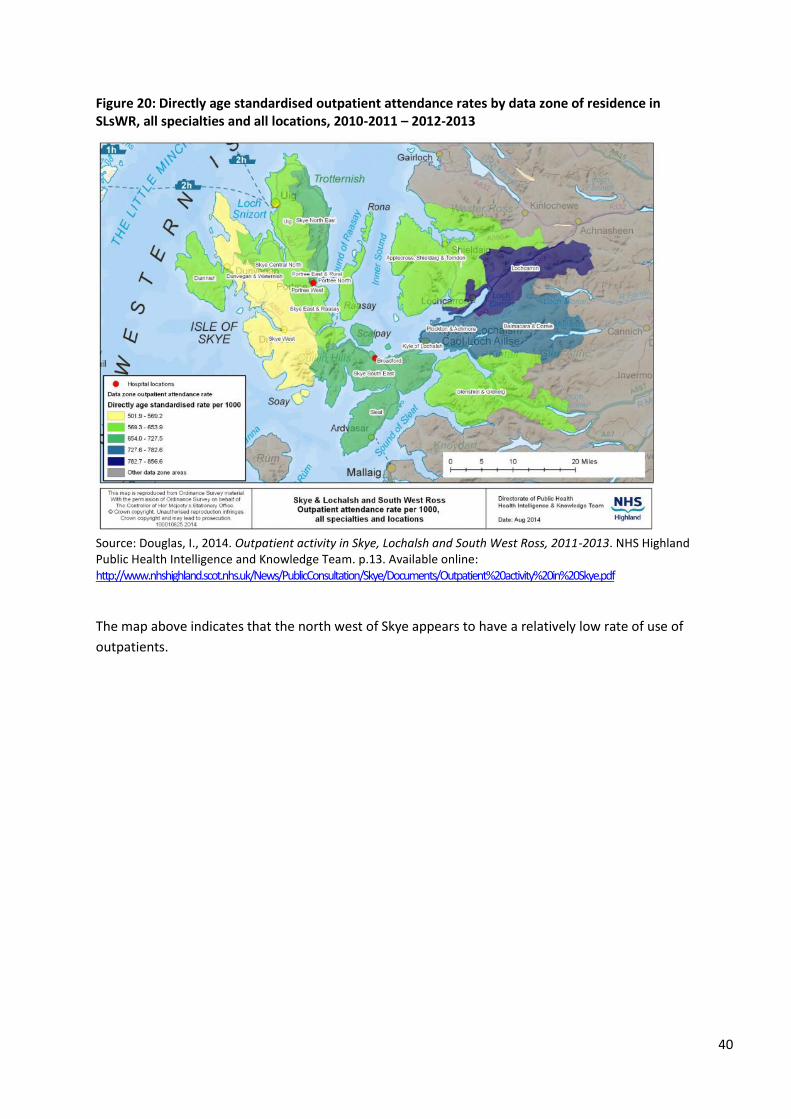
40
Figure 20: Directly age standardised outpatient attendance rates by data zone of residence in SLsWR, all specialties and all locations, 2010-2011 – 2012-2013
Source: Douglas, I., 2014. Outpatient activity in Skye, Lochalsh and South West Ross, 2011-2013. NHS Highland Public Health Intelligence and Knowledge Team. p.13. Available online: http://www.nhshighland.scot.nhs.uk/News/PublicConsultation/Skye/Documents/Outpatient%20activity%20in%20Skye.pdf
The map above indicates that the north west of Skye appears to have a relatively low rate of use of
outpatients.
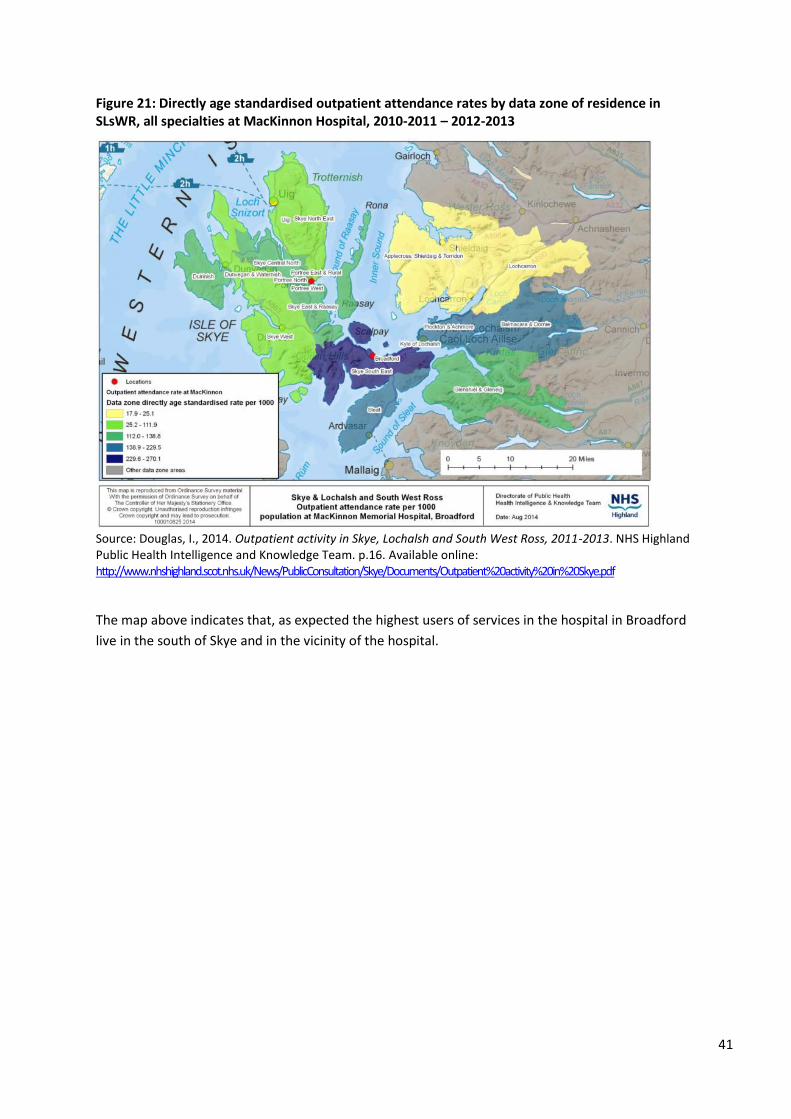
41
Figure 21: Directly age standardised outpatient attendance rates by data zone of residence in SLsWR, all specialties at MacKinnon Hospital, 2010-2011 – 2012-2013
Source: Douglas, I., 2014. Outpatient activity in Skye, Lochalsh and South West Ross, 2011-2013. NHS Highland Public Health Intelligence and Knowledge Team. p.16. Available online: http://www.nhshighland.scot.nhs.uk/News/PublicConsultation/Skye/Documents/Outpatient%20activity%20in%20Skye.pdf
The map above indicates that, as expected the highest users of services in the hospital in Broadford
live in the south of Skye and in the vicinity of the hospital.
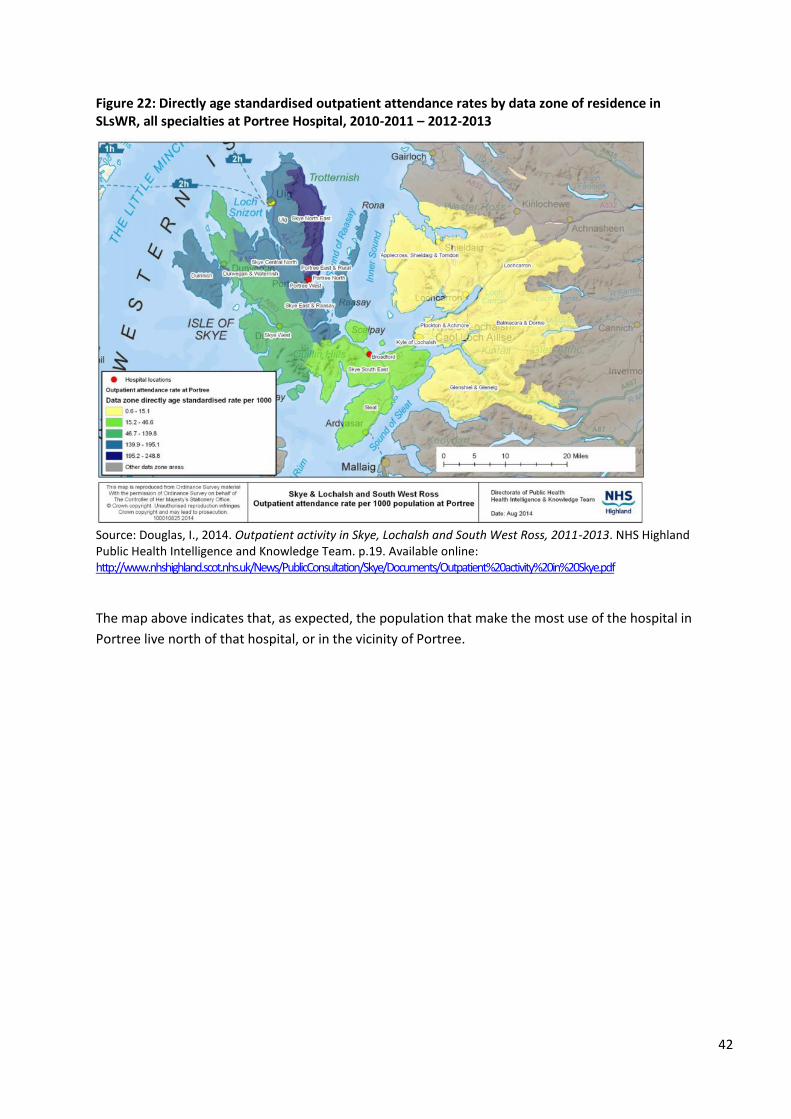
42
Figure 22: Directly age standardised outpatient attendance rates by data zone of residence in SLsWR, all specialties at Portree Hospital, 2010-2011 – 2012-2013
Source: Douglas, I., 2014. Outpatient activity in Skye, Lochalsh and South West Ross, 2011-2013. NHS Highland Public Health Intelligence and Knowledge Team. p.19. Available online: http://www.nhshighland.scot.nhs.uk/News/PublicConsultation/Skye/Documents/Outpatient%20activity%20in%20Skye.pdf
The map above indicates that, as expected, the population that make the most use of the hospital in
Portree live north of that hospital, or in the vicinity of Portree.
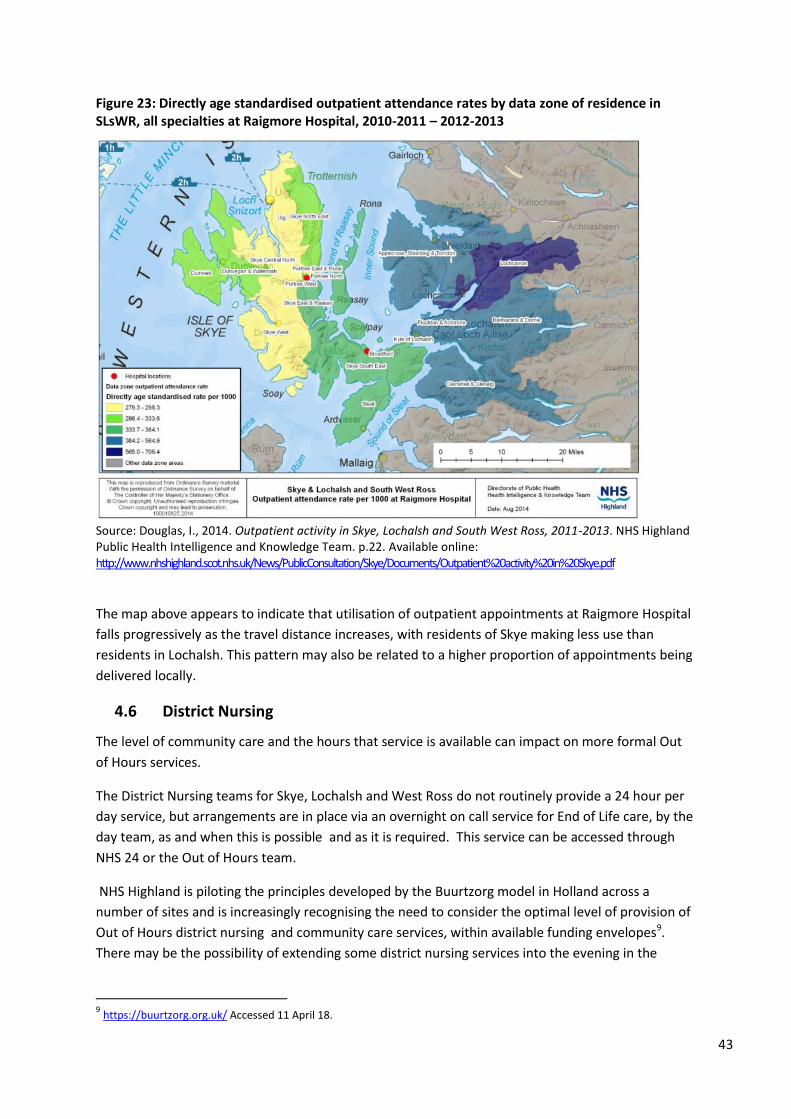
43
Figure 23: Directly age standardised outpatient attendance rates by data zone of residence in SLsWR, all specialties at Raigmore Hospital, 2010-2011 – 2012-2013
Source: Douglas, I., 2014. Outpatient activity in Skye, Lochalsh and South West Ross, 2011-2013. NHS Highland Public Health Intelligence and Knowledge Team. p.22. Available online: http://www.nhshighland.scot.nhs.uk/News/PublicConsultation/Skye/Documents/Outpatient%20activity%20in%20Skye.pdf
The map above appears to indicate that utilisation of outpatient appointments at Raigmore Hospital
falls progressively as the travel distance increases, with residents of Skye making less use than
residents in Lochalsh. This pattern may also be related to a higher proportion of appointments being
delivered locally.
4.6 District Nursing
The level of community care and the hours that service is available can impact on more formal Out
of Hours services.
The District Nursing teams for Skye, Lochalsh and West Ross do not routinely provide a 24 hour per
day service, but arrangements are in place via an overnight on call service for End of Life care, by the
day team, as and when this is possible and as it is required. This service can be accessed through
NHS 24 or the Out of Hours team.
NHS Highland is piloting the principles developed by the Buurtzorg model in Holland across a
number of sites and is increasingly recognising the need to consider the optimal level of provision of
Out of Hours district nursing and community care services, within available funding envelopes9.
There may be the possibility of extending some district nursing services into the evening in the
9 https://buurtzorg.org.uk/ Accessed 11 April 18.

44
future10. The ongoing review of district nursing services in the north and west operational unit
builds on the Scottish Government report, ‘Transforming Nursing, Midwifery and Health
Professionals Roles – Paper 3 - The district nursing role in integrated community nursing teams,11‘
published in December 2017, and on the ‘The Report of the Independent Review of Primary Care Out
of Hours Services’.12 Both of these documents highlight the challenges and opportunities for District
Nursing and Advanced Nurse Practitioners in remote and rural areas.
Virtual community wards are planned for Integrated Health and Social Care Teams in the North &
West NHS Highland unit. The aim of such virtual wards is to provide a high level of care in people’s
own homes for those most at risk from unscheduled hospital admissions. Work is also underway to
integrate Care at Home staff into such arrangements13.
4.7 Allied Health Professionals
Data on community services is generally poorly collected in Scotland and should be interpreted with
caution. Available data on Allied Health Professionals is provided below.
10
NHS Highland, 2017. Draft North Highland District Nursing Service Review. 11
http://www.gov.scot/Resource/0052/00529738.pdf 12
http://www.gov.scot/Resource/0049/00490526.pdf 13
North & West Operational Unit, Service Description, Virtual Community Ward (personal communication from Director of
Transformation and Quality Improvement to DPH 9/4/18)
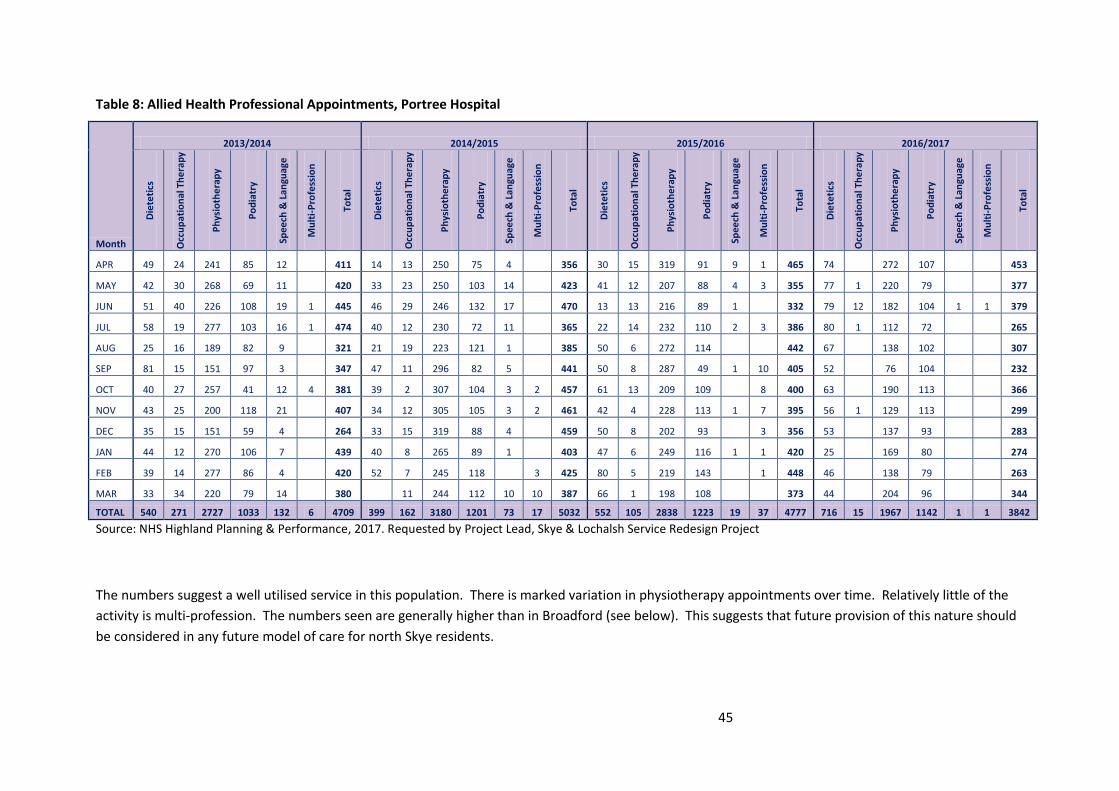
45
Table 8: Allied Health Professional Appointments, Portree Hospital
Month
2013/2014 2014/2015 2015/2016 2016/2017 D
iete
tics
Occ
up
atio
nal
Th
era
py
Ph
ysio
the
rap
y
Po
dia
try
Spee
ch &
Lan
guag
e
Mu
lti-
Pro
fess
ion
Tota
l
Die
teti
cs
Occ
up
atio
nal
Th
era
py
Ph
ysio
the
rap
y
Po
dia
try
Spee
ch &
Lan
guag
e
Mu
lti-
Pro
fess
ion
Tota
l
Die
teti
cs
Occ
up
atio
nal
Th
era
py
Ph
ysio
the
rap
y
Po
dia
try
Spee
ch &
Lan
guag
e
Mu
lti-
Pro
fess
ion
Tota
l
Die
teti
cs
Occ
up
atio
nal
Th
era
py
Ph
ysio
the
rap
y
Po
dia
try
Spee
ch &
Lan
guag
e
Mu
lti-
Pro
fess
ion
Tota
l
APR 49 24 241 85 12 411 14 13 250 75 4 356 30 15 319 91 9 1 465 74 272 107 453
MAY 42 30 268 69 11 420 33 23 250 103 14 423 41 12 207 88 4 3 355 77 1 220 79 377
JUN 51 40 226 108 19 1 445 46 29 246 132 17 470 13 13 216 89 1 332 79 12 182 104 1 1 379
JUL 58 19 277 103 16 1 474 40 12 230 72 11 365 22 14 232 110 2 3 386 80 1 112 72 265
AUG 25 16 189 82 9 321 21 19 223 121 1 385 50 6 272 114 442 67 138 102 307
SEP 81 15 151 97 3 347 47 11 296 82 5 441 50 8 287 49 1 10 405 52 76 104 232
OCT 40 27 257 41 12 4 381 39 2 307 104 3 2 457 61 13 209 109 8 400 63 190 113 366
NOV 43 25 200 118 21 407 34 12 305 105 3 2 461 42 4 228 113 1 7 395 56 1 129 113 299
DEC 35 15 151 59 4 264 33 15 319 88 4 459 50 8 202 93 3 356 53 137 93 283
JAN 44 12 270 106 7 439 40 8 265 89 1 403 47 6 249 116 1 1 420 25 169 80 274
FEB 39 14 277 86 4 420 52 7 245 118 3 425 80 5 219 143 1 448 46 138 79 263
MAR 33 34 220 79 14 380 11 244 112 10 10 387 66 1 198 108 373 44 204 96 344
TOTAL 540 271 2727 1033 132 6 4709 399 162 3180 1201 73 17 5032 552 105 2838 1223 19 37 4777 716 15 1967 1142 1 1 3842
Source: NHS Highland Planning & Performance, 2017. Requested by Project Lead, Skye & Lochalsh Service Redesign Project
The numbers suggest a well utilised service in this population. There is marked variation in physiotherapy appointments over time. Relatively little of the
activity is multi-profession. The numbers seen are generally higher than in Broadford (see below). This suggests that future provision of this nature should
be considered in any future model of care for north Skye residents.
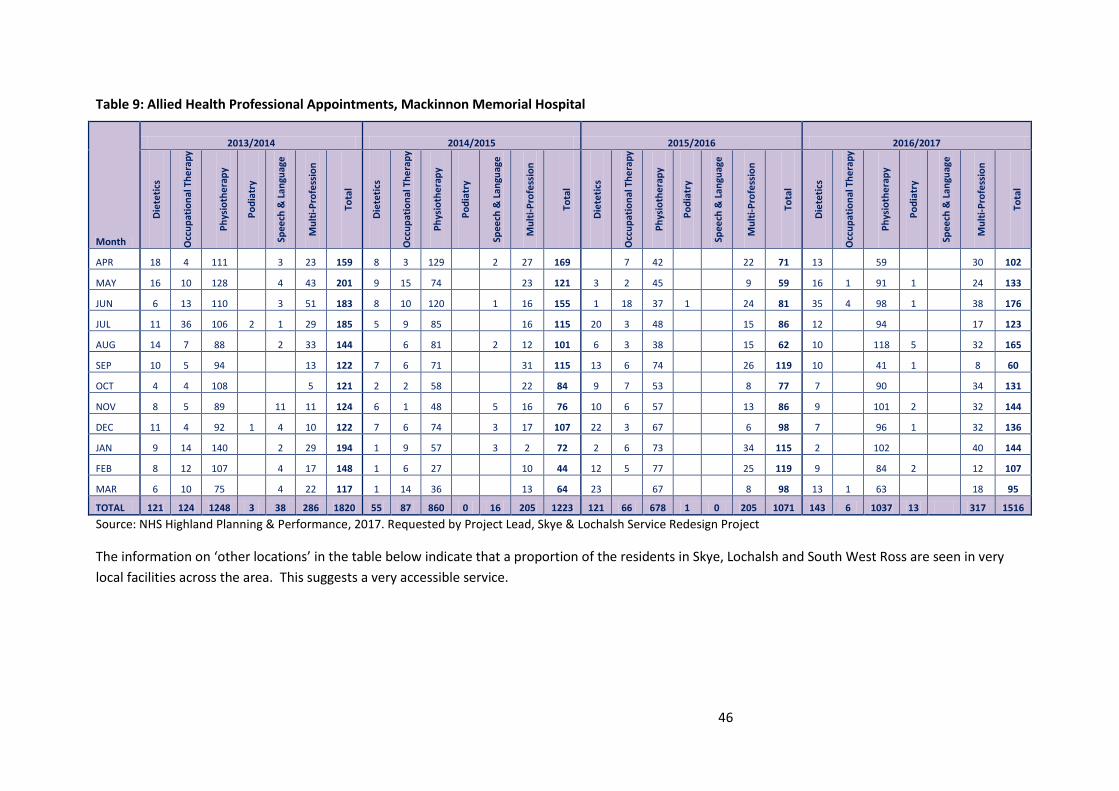
46
Table 9: Allied Health Professional Appointments, Mackinnon Memorial Hospital
Month
2013/2014 2014/2015 2015/2016 2016/2017 D
iete
tics
Occ
up
atio
nal
Th
era
py
Ph
ysio
the
rap
y
Po
dia
try
Spee
ch &
Lan
guag
e
Mu
lti-
Pro
fess
ion
Tota
l
Die
teti
cs
Occ
up
atio
nal
Th
era
py
Ph
ysio
the
rap
y
Po
dia
try
Spee
ch &
Lan
guag
e
Mu
lti-
Pro
fess
ion
Tota
l
Die
teti
cs
Occ
up
atio
nal
Th
era
py
Ph
ysio
the
rap
y
Po
dia
try
Spee
ch &
Lan
guag
e
Mu
lti-
Pro
fess
ion
Tota
l
Die
teti
cs
Occ
up
atio
nal
Th
era
py
Ph
ysio
the
rap
y
Po
dia
try
Spee
ch &
Lan
guag
e
Mu
lti-
Pro
fess
ion
Tota
l
APR 18 4 111 3 23 159 8 3 129 2 27 169 7 42 22 71 13 59 30 102
MAY 16 10 128 4 43 201 9 15 74 23 121 3 2 45 9 59 16 1 91 1 24 133
JUN 6 13 110 3 51 183 8 10 120 1 16 155 1 18 37 1 24 81 35 4 98 1 38 176
JUL 11 36 106 2 1 29 185 5 9 85 16 115 20 3 48 15 86 12 94 17 123
AUG 14 7 88 2 33 144 6 81 2 12 101 6 3 38 15 62 10 118 5 32 165
SEP 10 5 94 13 122 7 6 71 31 115 13 6 74 26 119 10 41 1 8 60
OCT 4 4 108 5 121 2 2 58 22 84 9 7 53 8 77 7 90 34 131
NOV 8 5 89 11 11 124 6 1 48 5 16 76 10 6 57 13 86 9 101 2 32 144
DEC 11 4 92 1 4 10 122 7 6 74 3 17 107 22 3 67 6 98 7 96 1 32 136
JAN 9 14 140 2 29 194 1 9 57 3 2 72 2 6 73 34 115 2 102 40 144
FEB 8 12 107 4 17 148 1 6 27 10 44 12 5 77 25 119 9 84 2 12 107
MAR 6 10 75 4 22 117 1 14 36 13 64 23 67 8 98 13 1 63 18 95
TOTAL 121 124 1248 3 38 286 1820 55 87 860 0 16 205 1223 121 66 678 1 0 205 1071 143 6 1037 13 317 1516
Source: NHS Highland Planning & Performance, 2017. Requested by Project Lead, Skye & Lochalsh Service Redesign Project
The information on ‘other locations’ in the table below indicate that a proportion of the residents in Skye, Lochalsh and South West Ross are seen in very
local facilities across the area. This suggests a very accessible service.

47
Table 10: Allied Health Professional Appointments, other14 Skye and Lochalsh locations
Month
2013/2014 2014/2015 2015/2016 2016/2017 D
iete
tics
Occ
up
atio
nal
Th
era
py
Ph
ysio
the
rap
y
Po
dia
try
Spee
ch &
Lan
guag
e
Mu
lti-
Pro
fess
ion
Tota
l
Die
teti
cs
Occ
up
atio
nal
Th
era
py
Ph
ysio
the
rap
y
Po
dia
try
Spee
ch &
Lan
guag
e
Mu
lti-
Pro
fess
ion
Tota
l
Die
teti
cs
Occ
up
atio
nal
Th
era
py
Ph
ysio
the
rap
y
Po
dia
try
Spee
ch &
Lan
guag
e
Mu
lti-
Pro
fess
ion
Tota
l
Die
teti
cs
Occ
up
atio
nal
Th
era
py
Ph
ysio
the
rap
y
Po
dia
try
Spee
ch &
Lan
guag
e
Mu
lti-
Pro
fess
ion
Tota
l
APR 43 68 102 172 23 18 426 21 24 85 193 26 5 354 4 26 88 103 6 17 244 47 22 82 205 19 375
MAY 51 70 106 220 49 53 549 45 34 75 200 20 17 391 2 10 69 164 6 13 264 38 16 70 288 1 9 422
JUN 53 31 68 205 43 5 405 29 27 56 214 42 10 378 5 13 72 188 3 20 301 57 12 80 263 1 9 422
JUL 41 66 106 195 25 4 437 24 45 68 198 25 1 361 20 33 63 189 12 11 328 44 3 64 182 2 295
AUG 56 31 111 203 27 8 436 14 46 52 171 10 39 332 49 28 58 171 1 27 334 61 79 178 318
SEP 42 45 85 201 29 3 405 35 58 84 241 27 93 538 63 39 78 208 5 33 426 46 73 232 1 352
OCT 27 48 135 143 31 4 388 47 34 64 177 25 62 409 43 34 62 207 2 19 367 64 104 180 348
NOV 77 68 92 217 42 1 497 31 26 76 185 16 55 389 28 36 69 271 1 27 432 29 129 201 359
DEC 27 37 70 167 24 1 326 42 19 63 181 8 35 348 42 19 65 219 2 16 363 41 85 178 304
JAN 57 52 76 69 34 21 309 39 36 84 136 15 34 344 25 43 54 218 2 7 349 39 111 162 312
FEB 27 27 56 240 35 21 406 42 29 63 107 8 52 301 23 18 64 183 12 300 44 108 168 320
MAR 40 37 71 225 29 11 413 1 35 80 111 13 28 268 52 32 86 286 15 471 76 88 138 302
TOTAL 541 580 1078 2257 391 150 4997 370 413 850 2114 235 431 4413 356 331 828 2407 40 217 4179 586 53 1073 2375 3 39 4129
Source: NHS Highland Planning & Performance, 2017. Requested by Project Lead, Skye & Lochalsh Service Redesign Project
14 NB: Other centres included: An Acarsaid Community Care Centre, Applecross Primary School, Applecross Surgery, Auchtertyre Nursery, Auchtertyre Primary School, Broadford Medical Centre, Broadford Nursery, Broadford Primary School,
Budmhor House, Carbost Medical Practice, Carbost Nursery, Carbost Surgery, Domiciliary Visit, Dundonnell Community Clinic, Dunvegan Health Centre, Dunvegan Nursery (Gaelic), Dunvegan Primary School, Ferguson Medical Centre, Gairloch
Health Centre, Glenelg Primary School, Glenelg Heath Centre, Glenelg Surgery, Graham House, Home Farm Nursing Home, Howard Doris Centre, Kilmuir Primary School, Kyle Church Rd Surgery, Kyle Nursery, Kyle Primary School, Kyleakin Clinic,
Kyleakin Primary School, Loch Duich Primary School, Lochalsh Healthcare Centre, Lochcarron Playgroup, Lochcarron Primary School, Lochcarron Surgery, MacDiarmid Nursery, Macdiarmid Primary School, None, Nurses Cottage, Raasay, Other
Community Setting, Plockton High School, Plockton Primary School, Portree High School, Portree Medical Centre, Portree Primary School, Raasay Nursery, Raasay Primary School, Sleat Medical Practice, Sleat Primary School, Staffin Nurse Base,
The Haven Care Home, To Be Confirmed, Torridon Surgery, Uig Surgery, Ullapool Health Centre.
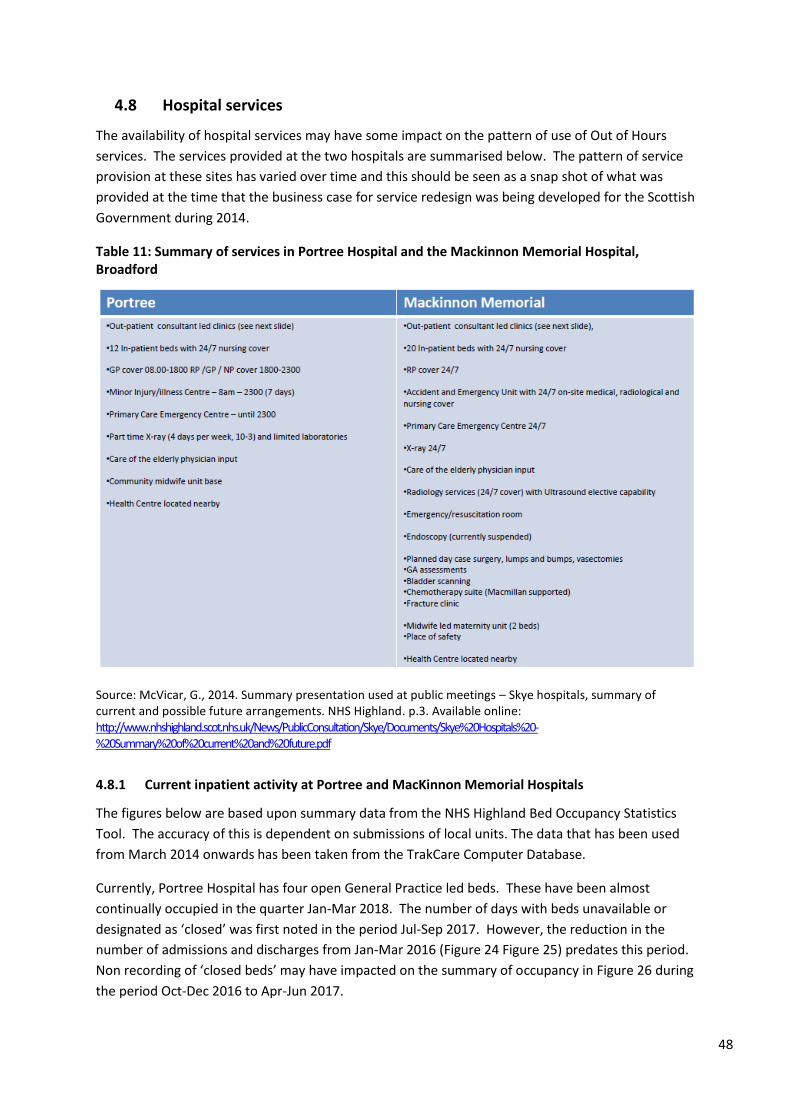
48
4.8 Hospital services
The availability of hospital services may have some impact on the pattern of use of Out of Hours
services. The services provided at the two hospitals are summarised below. The pattern of service
provision at these sites has varied over time and this should be seen as a snap shot of what was
provided at the time that the business case for service redesign was being developed for the Scottish
Government during 2014.
Table 11: Summary of services in Portree Hospital and the Mackinnon Memorial Hospital, Broadford
Source: McVicar, G., 2014. Summary presentation used at public meetings – Skye hospitals, summary of current and possible future arrangements. NHS Highland. p.3. Available online: http://www.nhshighland.scot.nhs.uk/News/PublicConsultation/Skye/Documents/Skye%20Hospitals%20-%20Summary%20of%20current%20and%20future.pdf
4.8.1 Current inpatient activity at Portree and MacKinnon Memorial Hospitals
The figures below are based upon summary data from the NHS Highland Bed Occupancy Statistics
Tool. The accuracy of this is dependent on submissions of local units. The data that has been used
from March 2014 onwards has been taken from the TrakCare Computer Database.
Currently, Portree Hospital has four open General Practice led beds. These have been almost
continually occupied in the quarter Jan-Mar 2018. The number of days with beds unavailable or
designated as ‘closed’ was first noted in the period Jul-Sep 2017. However, the reduction in the
number of admissions and discharges from Jan-Mar 2016 (Figure 24 Figure 25) predates this period.
Non recording of ‘closed beds’ may have impacted on the summary of occupancy in Figure 26 during
the period Oct-Dec 2016 to Apr-Jun 2017.
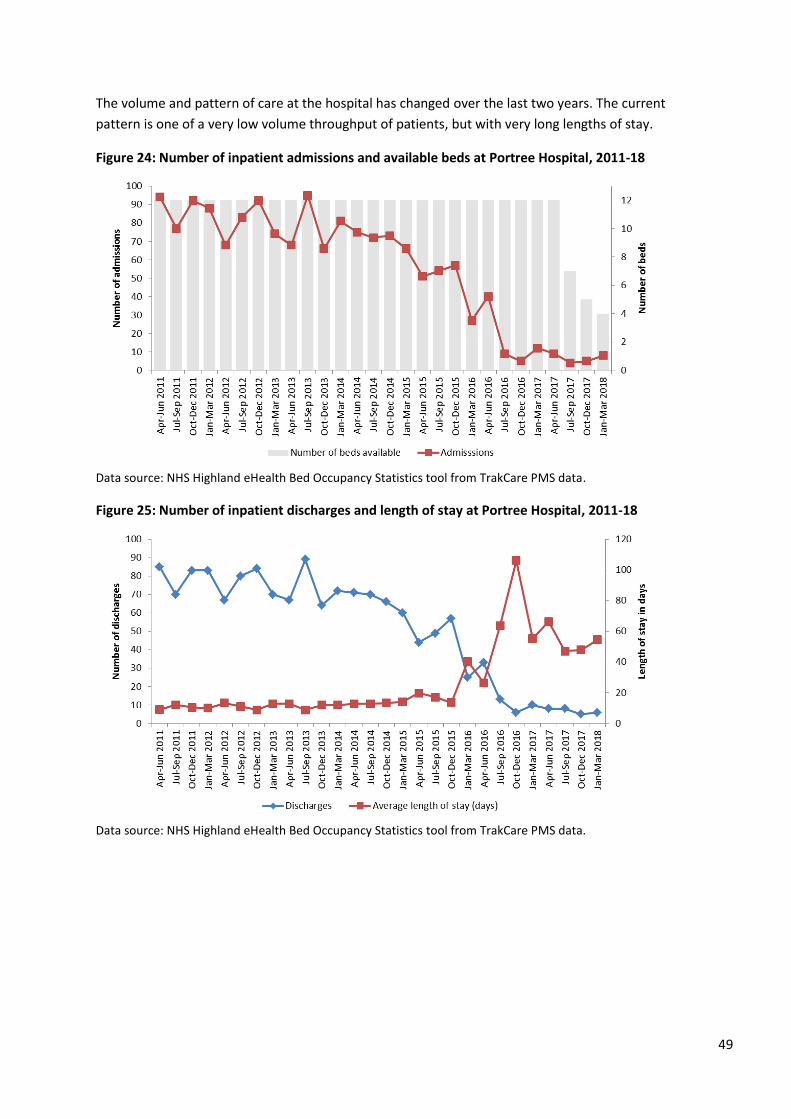
49
The volume and pattern of care at the hospital has changed over the last two years. The current
pattern is one of a very low volume throughput of patients, but with very long lengths of stay.
Figure 24: Number of inpatient admissions and available beds at Portree Hospital, 2011-18
Data source: NHS Highland eHealth Bed Occupancy Statistics tool from TrakCare PMS data.
Figure 25: Number of inpatient discharges and length of stay at Portree Hospital, 2011-18
Data source: NHS Highland eHealth Bed Occupancy Statistics tool from TrakCare PMS data.
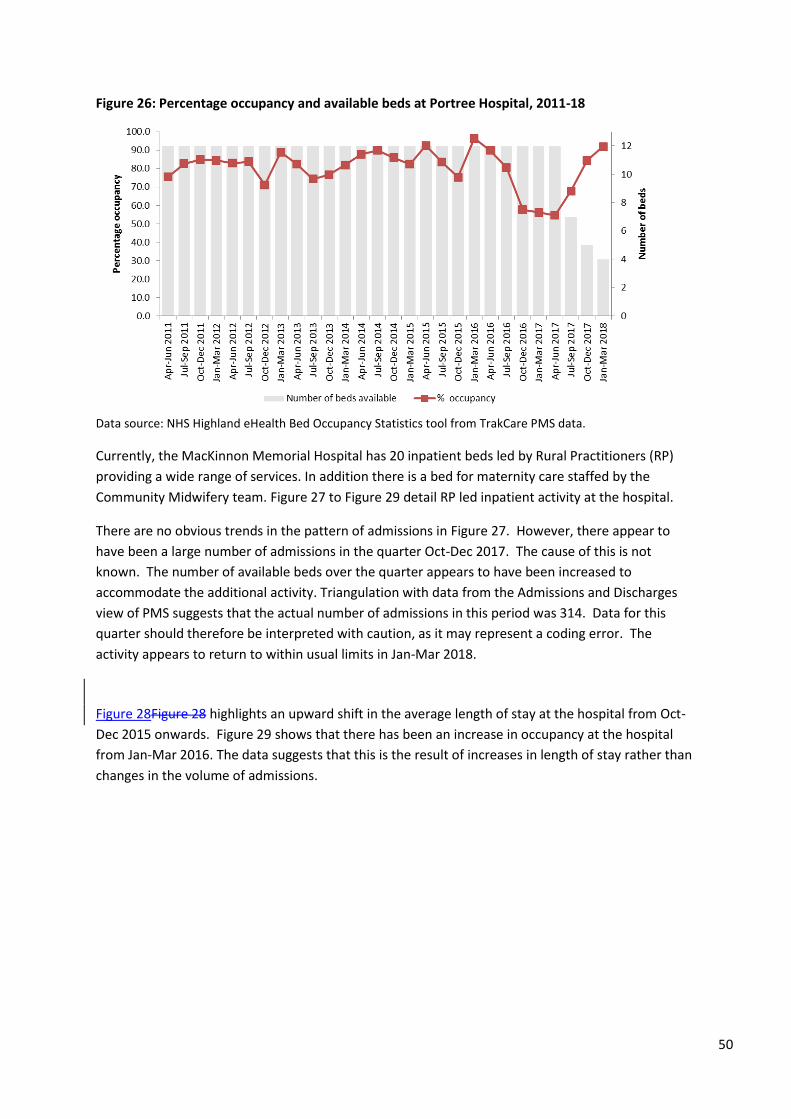
50
Figure 26: Percentage occupancy and available beds at Portree Hospital, 2011-18
Data source: NHS Highland eHealth Bed Occupancy Statistics tool from TrakCare PMS data.
Currently, the MacKinnon Memorial Hospital has 20 inpatient beds led by Rural Practitioners (RP)
providing a wide range of services. In addition there is a bed for maternity care staffed by the
Community Midwifery team. Figure 27 to Figure 29 detail RP led inpatient activity at the hospital.
There are no obvious trends in the pattern of admissions in Figure 27. However, there appear to
have been a large number of admissions in the quarter Oct-Dec 2017. The cause of this is not
known. The number of available beds over the quarter appears to have been increased to
accommodate the additional activity. Triangulation with data from the Admissions and Discharges
view of PMS suggests that the actual number of admissions in this period was 314. Data for this
quarter should therefore be interpreted with caution, as it may represent a coding error. The
activity appears to return to within usual limits in Jan-Mar 2018.
Figure 28Figure 28 highlights an upward shift in the average length of stay at the hospital from Oct-
Dec 2015 onwards. Figure 29 shows that there has been an increase in occupancy at the hospital
from Jan-Mar 2016. The data suggests that this is the result of increases in length of stay rather than
changes in the volume of admissions.
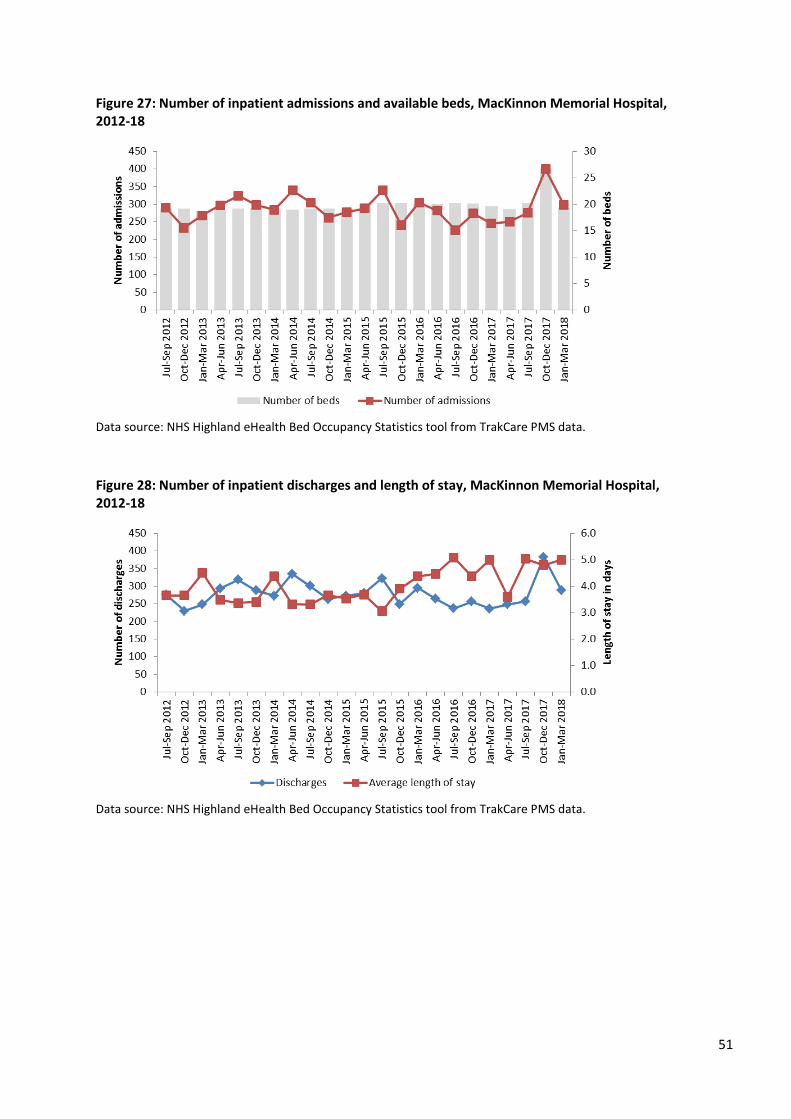
51
Figure 27: Number of inpatient admissions and available beds, MacKinnon Memorial Hospital, 2012-18
Data source: NHS Highland eHealth Bed Occupancy Statistics tool from TrakCare PMS data.
Figure 28: Number of inpatient discharges and length of stay, MacKinnon Memorial Hospital, 2012-18
Data source: NHS Highland eHealth Bed Occupancy Statistics tool from TrakCare PMS data.
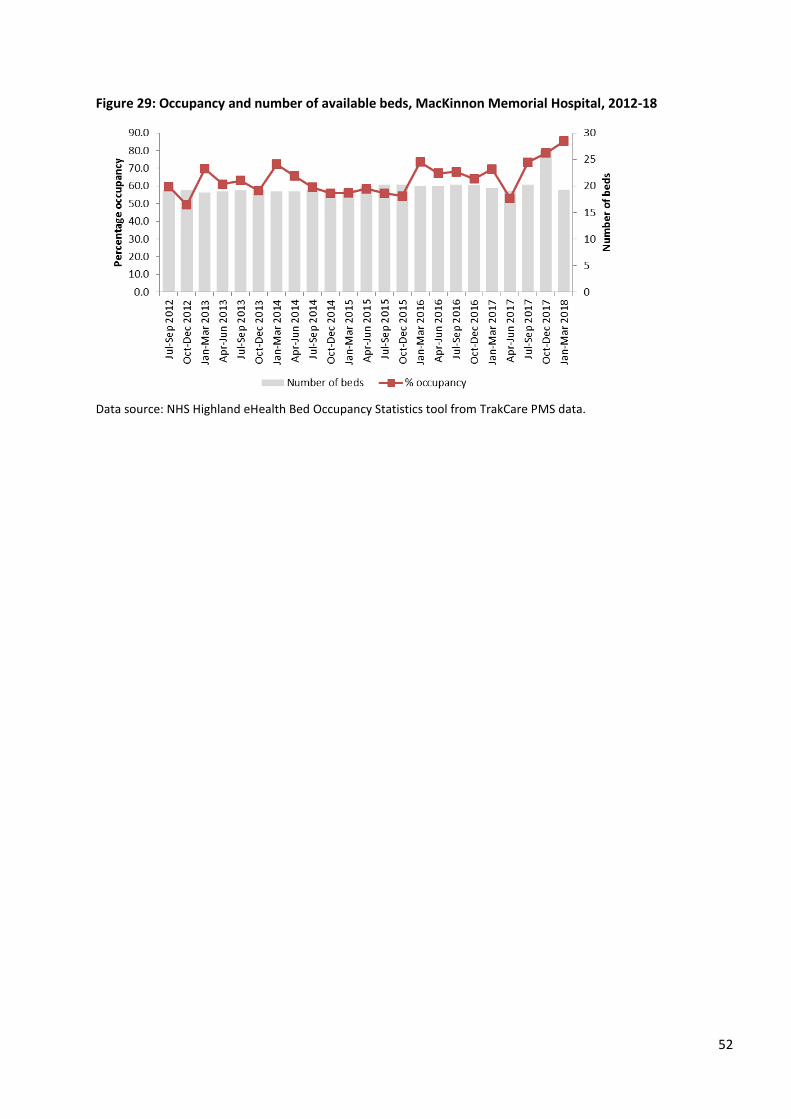
52
Figure 29: Occupancy and number of available beds, MacKinnon Memorial Hospital, 2012-18
Data source: NHS Highland eHealth Bed Occupancy Statistics tool from TrakCare PMS data.
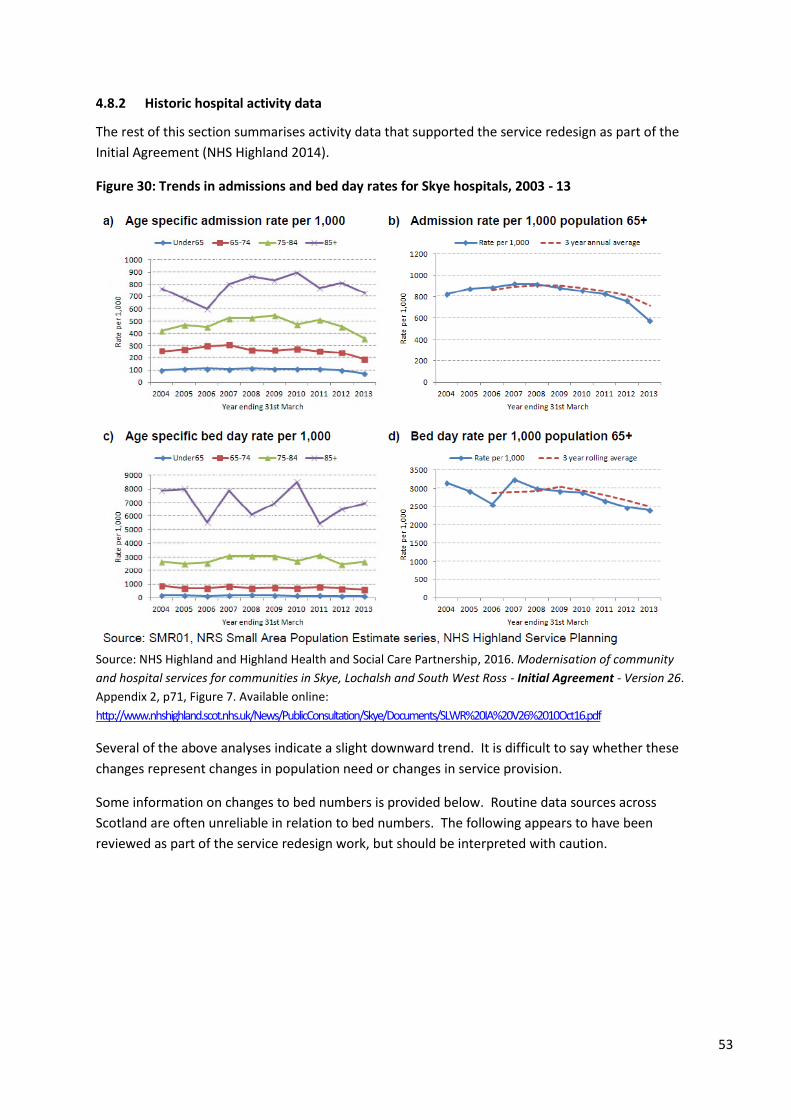
53
4.8.2 Historic hospital activity data
The rest of this section summarises activity data that supported the service redesign as part of the
Initial Agreement (NHS Highland 2014).
Figure 30: Trends in admissions and bed day rates for Skye hospitals, 2003 - 13
Source: NHS Highland and Highland Health and Social Care Partnership, 2016. Modernisation of community
and hospital services for communities in Skye, Lochalsh and South West Ross - Initial Agreement - Version 26.
Appendix 2, p71, Figure 7. Available online:
http://www.nhshighland.scot.nhs.uk/News/PublicConsultation/Skye/Documents/SLWR%20IA%20V26%2010Oct16.pdf
Several of the above analyses indicate a slight downward trend. It is difficult to say whether these
changes represent changes in population need or changes in service provision.
Some information on changes to bed numbers is provided below. Routine data sources across
Scotland are often unreliable in relation to bed numbers. The following appears to have been
reviewed as part of the service redesign work, but should be interpreted with caution.
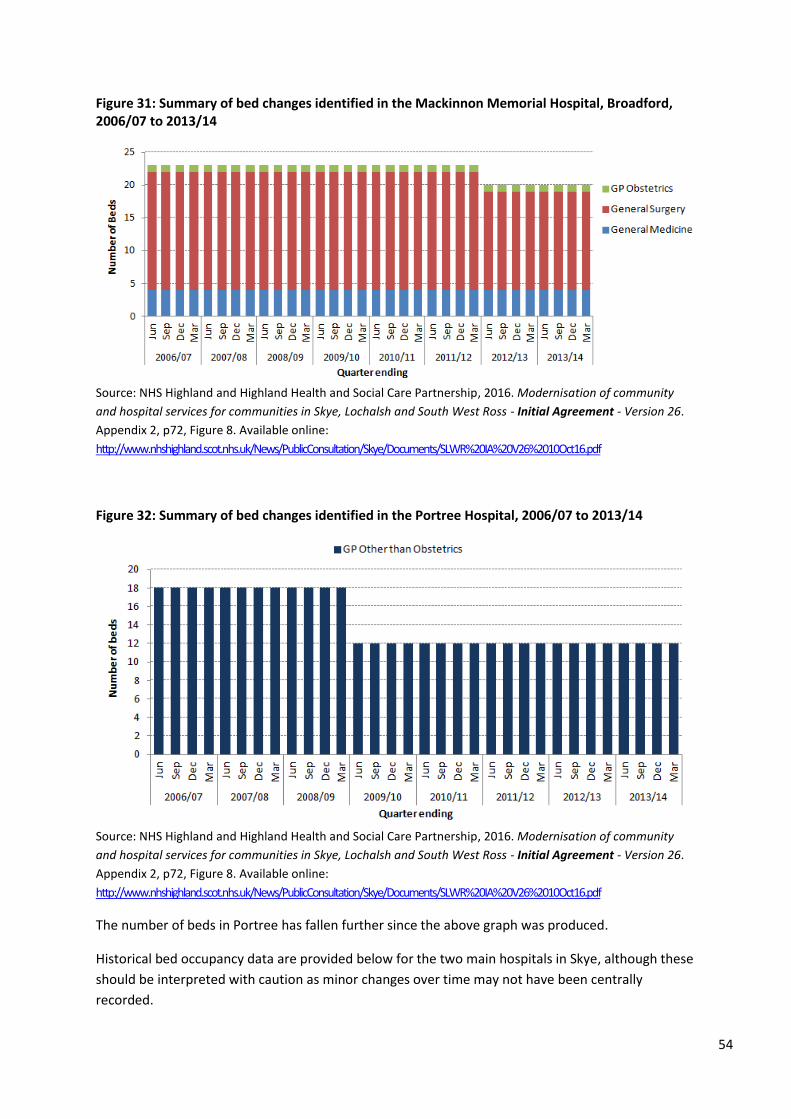
54
Figure 31: Summary of bed changes identified in the Mackinnon Memorial Hospital, Broadford, 2006/07 to 2013/14
Source: NHS Highland and Highland Health and Social Care Partnership, 2016. Modernisation of community
and hospital services for communities in Skye, Lochalsh and South West Ross - Initial Agreement - Version 26.
Appendix 2, p72, Figure 8. Available online:
http://www.nhshighland.scot.nhs.uk/News/PublicConsultation/Skye/Documents/SLWR%20IA%20V26%2010Oct16.pdf
Figure 32: Summary of bed changes identified in the Portree Hospital, 2006/07 to 2013/14
Source: NHS Highland and Highland Health and Social Care Partnership, 2016. Modernisation of community
and hospital services for communities in Skye, Lochalsh and South West Ross - Initial Agreement - Version 26.
Appendix 2, p72, Figure 8. Available online:
http://www.nhshighland.scot.nhs.uk/News/PublicConsultation/Skye/Documents/SLWR%20IA%20V26%2010Oct16.pdf
The number of beds in Portree has fallen further since the above graph was produced.
Historical bed occupancy data are provided below for the two main hospitals in Skye, although these
should be interpreted with caution as minor changes over time may not have been centrally
recorded.
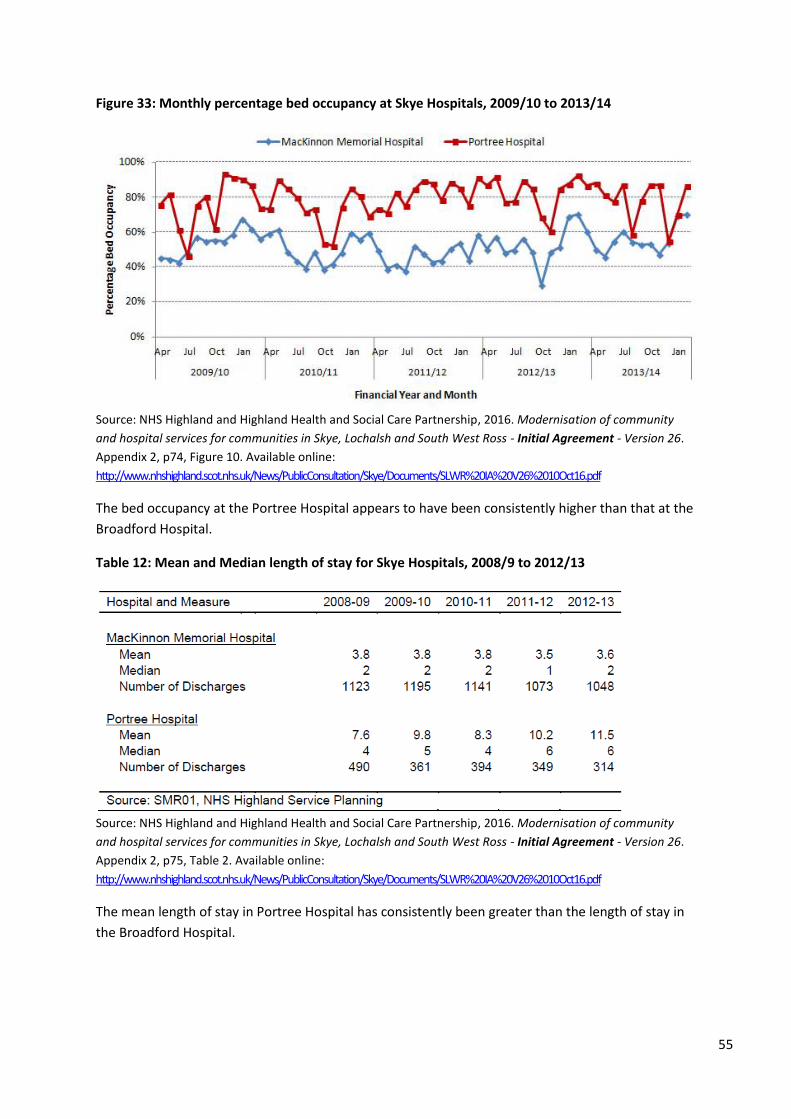
55
Figure 33: Monthly percentage bed occupancy at Skye Hospitals, 2009/10 to 2013/14
Source: NHS Highland and Highland Health and Social Care Partnership, 2016. Modernisation of community
and hospital services for communities in Skye, Lochalsh and South West Ross - Initial Agreement - Version 26.
Appendix 2, p74, Figure 10. Available online:
http://www.nhshighland.scot.nhs.uk/News/PublicConsultation/Skye/Documents/SLWR%20IA%20V26%2010Oct16.pdf
The bed occupancy at the Portree Hospital appears to have been consistently higher than that at the
Broadford Hospital.
Table 12: Mean and Median length of stay for Skye Hospitals, 2008/9 to 2012/13
Source: NHS Highland and Highland Health and Social Care Partnership, 2016. Modernisation of community
and hospital services for communities in Skye, Lochalsh and South West Ross - Initial Agreement - Version 26.
Appendix 2, p75, Table 2. Available online:
http://www.nhshighland.scot.nhs.uk/News/PublicConsultation/Skye/Documents/SLWR%20IA%20V26%2010Oct16.pdf
The mean length of stay in Portree Hospital has consistently been greater than the length of stay in
the Broadford Hospital.
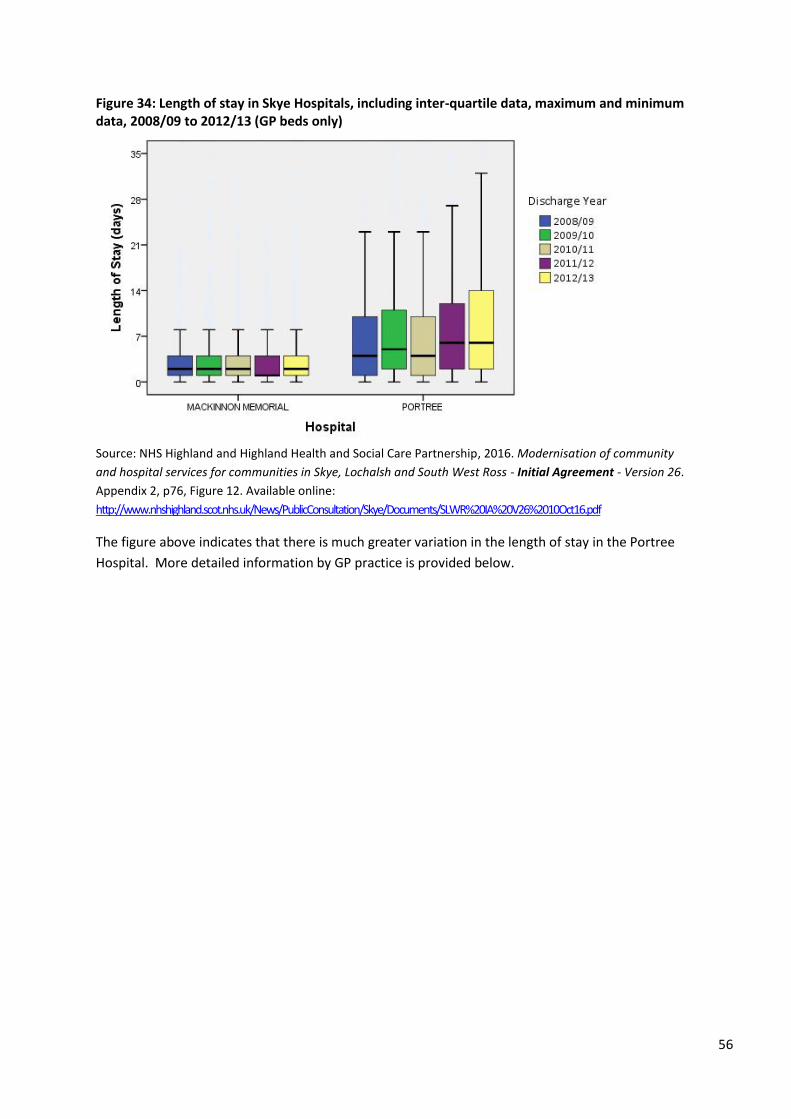
56
Figure 34: Length of stay in Skye Hospitals, including inter-quartile data, maximum and minimum data, 2008/09 to 2012/13 (GP beds only)
Source: NHS Highland and Highland Health and Social Care Partnership, 2016. Modernisation of community
and hospital services for communities in Skye, Lochalsh and South West Ross - Initial Agreement - Version 26.
Appendix 2, p76, Figure 12. Available online:
http://www.nhshighland.scot.nhs.uk/News/PublicConsultation/Skye/Documents/SLWR%20IA%20V26%2010Oct16.pdf
The figure above indicates that there is much greater variation in the length of stay in the Portree
Hospital. More detailed information by GP practice is provided below.
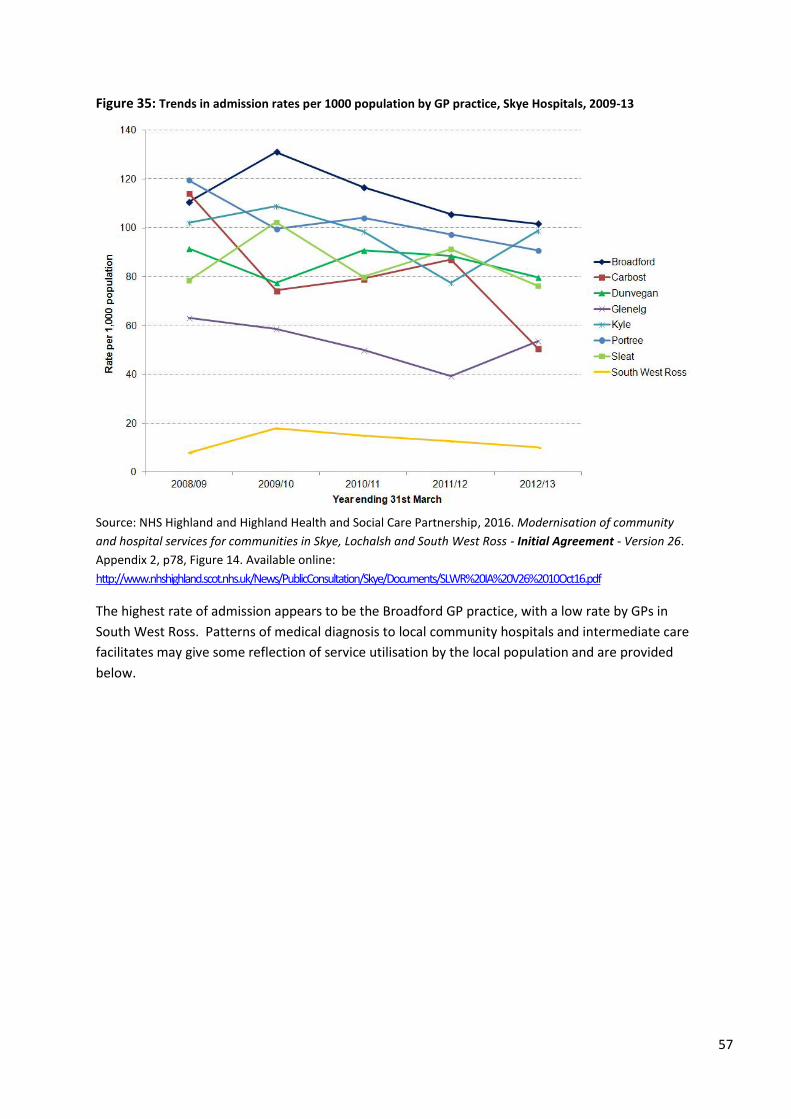
57
Figure 35: Trends in admission rates per 1000 population by GP practice, Skye Hospitals, 2009-13
Source: NHS Highland and Highland Health and Social Care Partnership, 2016. Modernisation of community
and hospital services for communities in Skye, Lochalsh and South West Ross - Initial Agreement - Version 26.
Appendix 2, p78, Figure 14. Available online:
http://www.nhshighland.scot.nhs.uk/News/PublicConsultation/Skye/Documents/SLWR%20IA%20V26%2010Oct16.pdf
The highest rate of admission appears to be the Broadford GP practice, with a low rate by GPs in
South West Ross. Patterns of medical diagnosis to local community hospitals and intermediate care
facilitates may give some reflection of service utilisation by the local population and are provided
below.
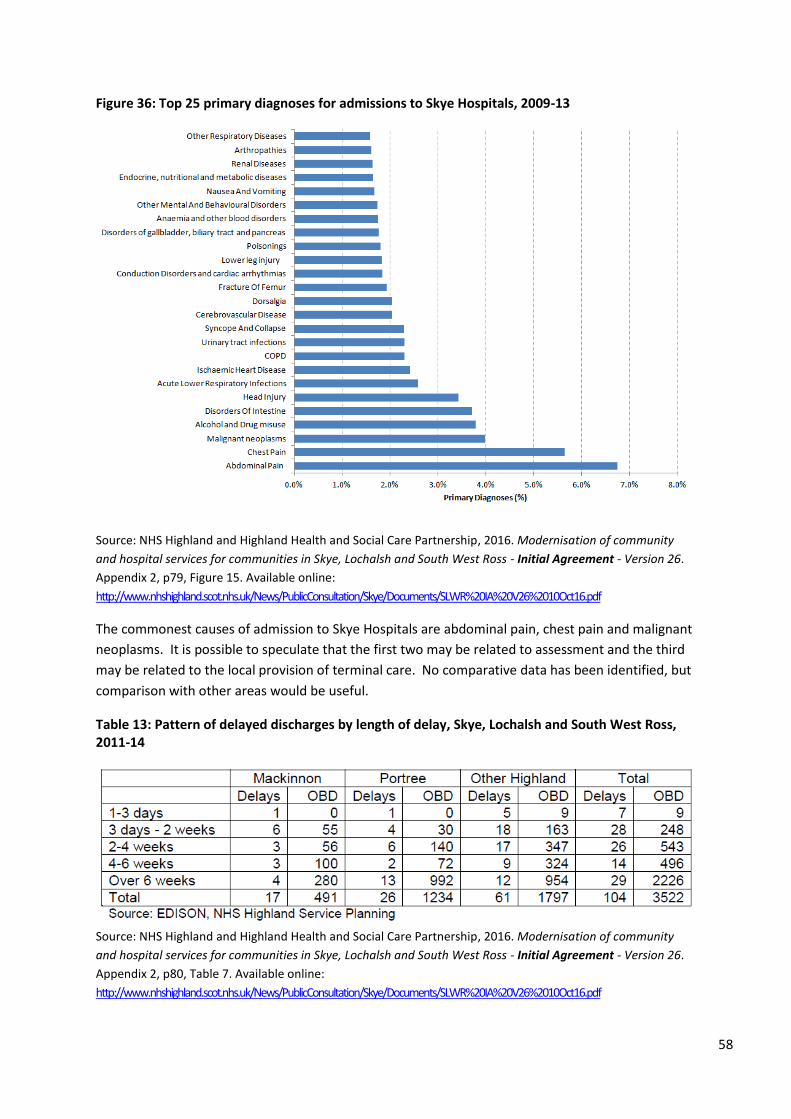
58
Figure 36: Top 25 primary diagnoses for admissions to Skye Hospitals, 2009-13
Source: NHS Highland and Highland Health and Social Care Partnership, 2016. Modernisation of community
and hospital services for communities in Skye, Lochalsh and South West Ross - Initial Agreement - Version 26.
Appendix 2, p79, Figure 15. Available online:
http://www.nhshighland.scot.nhs.uk/News/PublicConsultation/Skye/Documents/SLWR%20IA%20V26%2010Oct16.pdf
The commonest causes of admission to Skye Hospitals are abdominal pain, chest pain and malignant
neoplasms. It is possible to speculate that the first two may be related to assessment and the third
may be related to the local provision of terminal care. No comparative data has been identified, but
comparison with other areas would be useful.
Table 13: Pattern of delayed discharges by length of delay, Skye, Lochalsh and South West Ross, 2011-14
Source: NHS Highland and Highland Health and Social Care Partnership, 2016. Modernisation of community
and hospital services for communities in Skye, Lochalsh and South West Ross - Initial Agreement - Version 26.
Appendix 2, p80, Table 7. Available online:
http://www.nhshighland.scot.nhs.uk/News/PublicConsultation/Skye/Documents/SLWR%20IA%20V26%2010Oct16.pdf
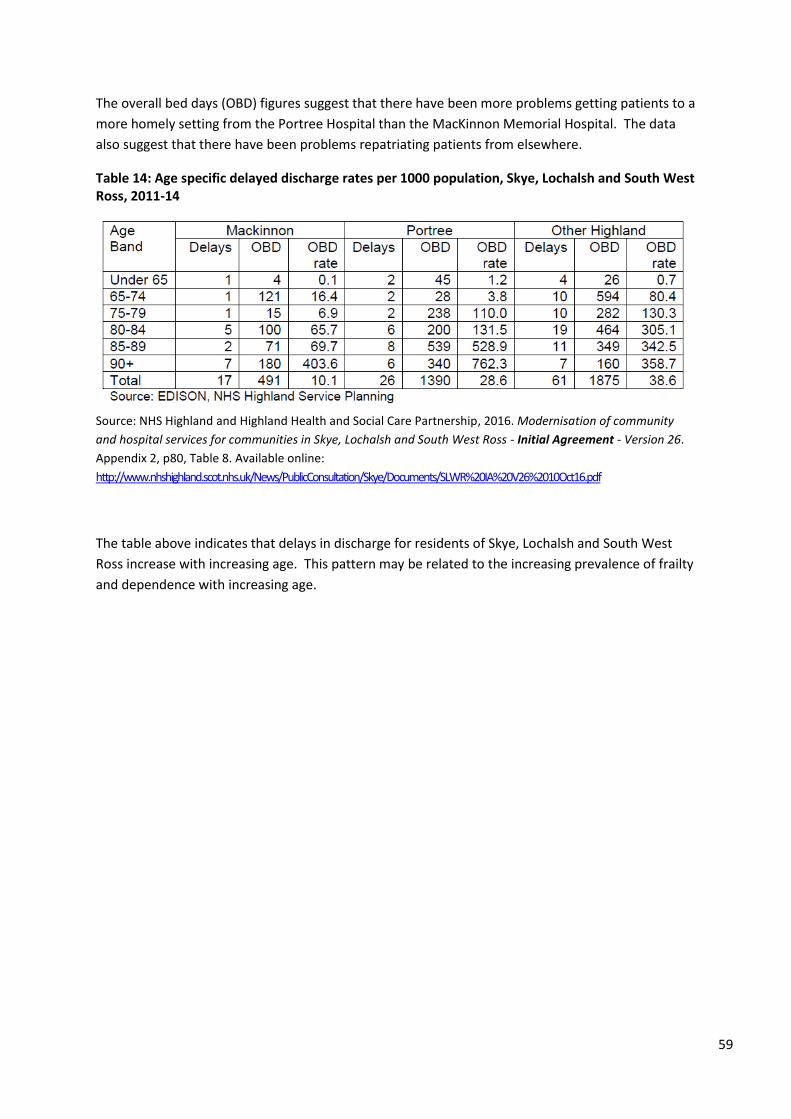
59
The overall bed days (OBD) figures suggest that there have been more problems getting patients to a
more homely setting from the Portree Hospital than the MacKinnon Memorial Hospital. The data
also suggest that there have been problems repatriating patients from elsewhere.
Table 14: Age specific delayed discharge rates per 1000 population, Skye, Lochalsh and South West Ross, 2011-14
Source: NHS Highland and Highland Health and Social Care Partnership, 2016. Modernisation of community
and hospital services for communities in Skye, Lochalsh and South West Ross - Initial Agreement - Version 26.
Appendix 2, p80, Table 8. Available online:
http://www.nhshighland.scot.nhs.uk/News/PublicConsultation/Skye/Documents/SLWR%20IA%20V26%2010Oct16.pdf
The table above indicates that delays in discharge for residents of Skye, Lochalsh and South West
Ross increase with increasing age. This pattern may be related to the increasing prevalence of frailty
and dependence with increasing age.
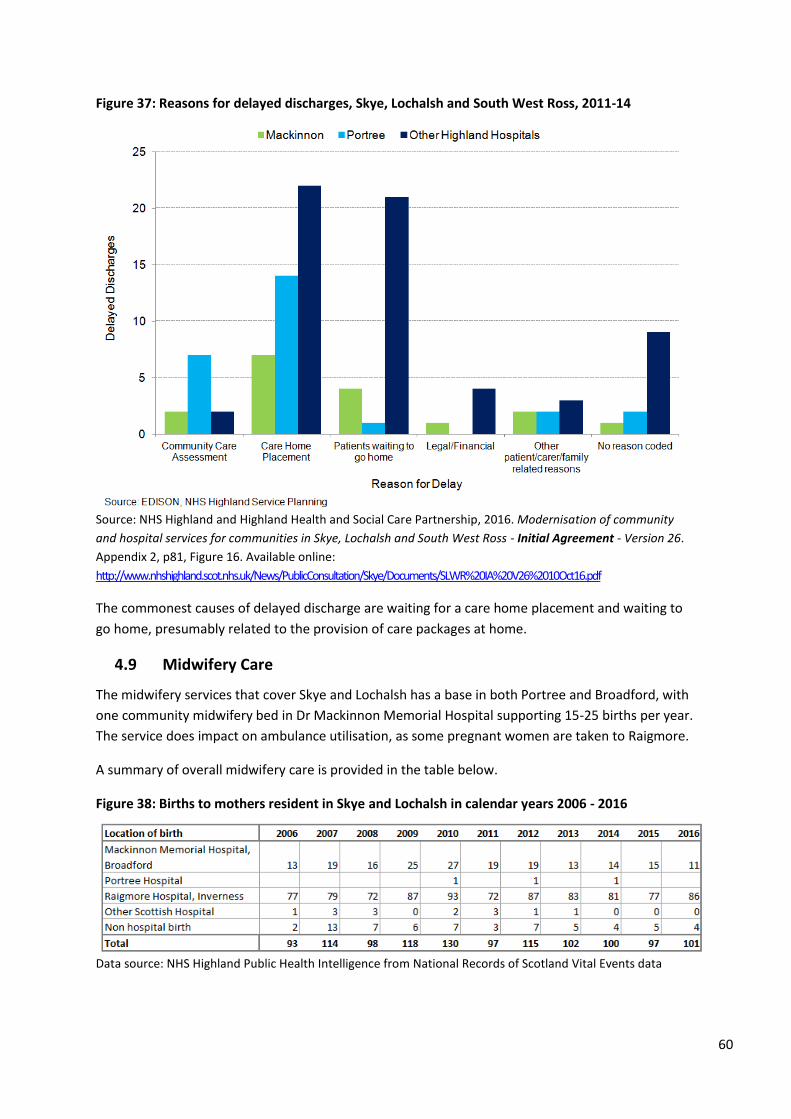
60
Figure 37: Reasons for delayed discharges, Skye, Lochalsh and South West Ross, 2011-14
Source: NHS Highland and Highland Health and Social Care Partnership, 2016. Modernisation of community
and hospital services for communities in Skye, Lochalsh and South West Ross - Initial Agreement - Version 26.
Appendix 2, p81, Figure 16. Available online:
http://www.nhshighland.scot.nhs.uk/News/PublicConsultation/Skye/Documents/SLWR%20IA%20V26%2010Oct16.pdf
The commonest causes of delayed discharge are waiting for a care home placement and waiting to
go home, presumably related to the provision of care packages at home.
4.9 Midwifery Care
The midwifery services that cover Skye and Lochalsh has a base in both Portree and Broadford, with
one community midwifery bed in Dr Mackinnon Memorial Hospital supporting 15-25 births per year.
The service does impact on ambulance utilisation, as some pregnant women are taken to Raigmore.
A summary of overall midwifery care is provided in the table below.
Figure 38: Births to mothers resident in Skye and Lochalsh in calendar years 2006 - 2016
Data source: NHS Highland Public Health Intelligence from National Records of Scotland Vital Events data
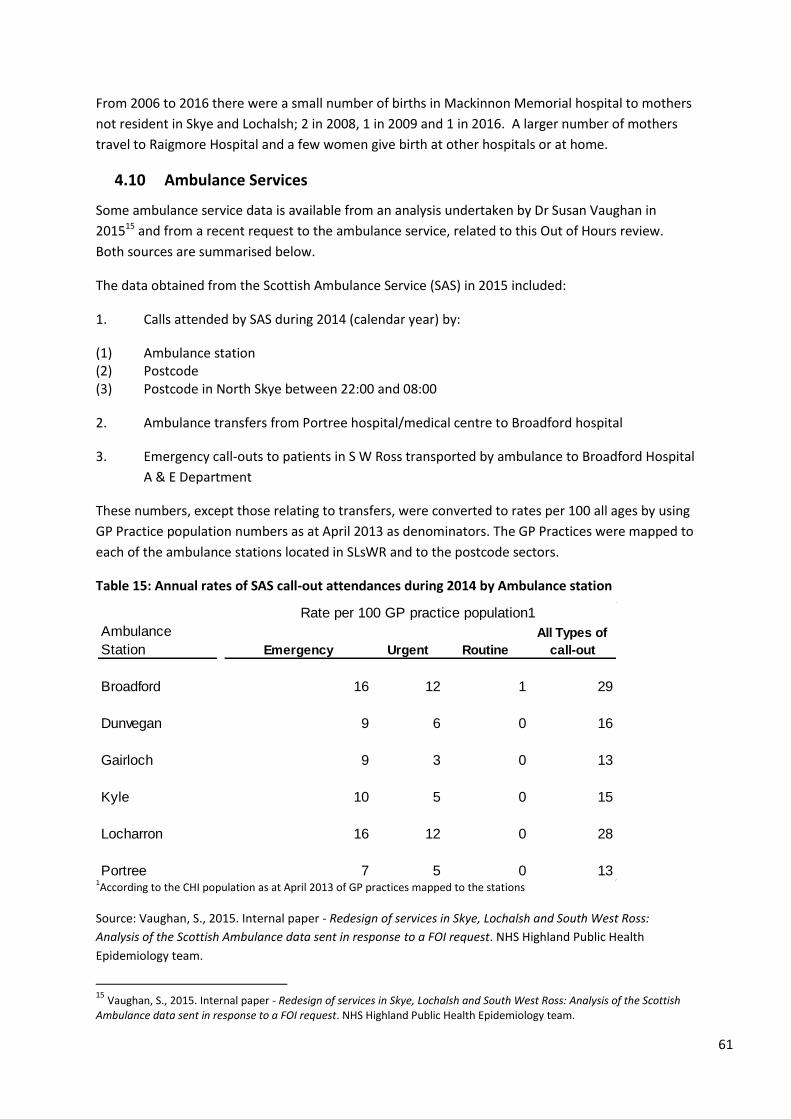
61
From 2006 to 2016 there were a small number of births in Mackinnon Memorial hospital to mothers
not resident in Skye and Lochalsh; 2 in 2008, 1 in 2009 and 1 in 2016. A larger number of mothers
travel to Raigmore Hospital and a few women give birth at other hospitals or at home.
4.10 Ambulance Services
Some ambulance service data is available from an analysis undertaken by Dr Susan Vaughan in
201515 and from a recent request to the ambulance service, related to this Out of Hours review.
Both sources are summarised below.
The data obtained from the Scottish Ambulance Service (SAS) in 2015 included:
1. Calls attended by SAS during 2014 (calendar year) by:
(1) Ambulance station (2) Postcode (3) Postcode in North Skye between 22:00 and 08:00
2. Ambulance transfers from Portree hospital/medical centre to Broadford hospital
3. Emergency call-outs to patients in S W Ross transported by ambulance to Broadford Hospital
A & E Department
These numbers, except those relating to transfers, were converted to rates per 100 all ages by using
GP Practice population numbers as at April 2013 as denominators. The GP Practices were mapped to
each of the ambulance stations located in SLsWR and to the postcode sectors.
Table 15: Annual rates of SAS call-out attendances during 2014 by Ambulance station
1According to the CHI population as at April 2013 of GP practices mapped to the stations
Source: Vaughan, S., 2015. Internal paper - Redesign of services in Skye, Lochalsh and South West Ross:
Analysis of the Scottish Ambulance data sent in response to a FOI request. NHS Highland Public Health
Epidemiology team.
15
Vaughan, S., 2015. Internal paper - Redesign of services in Skye, Lochalsh and South West Ross: Analysis of the Scottish Ambulance data sent in response to a FOI request. NHS Highland Public Health Epidemiology team.
Broadford 16 12 1 29
Dunvegan 9 6 0 16
Gairloch 9 3 0 13
Kyle 10 5 0 15
Locharron 16 12 0 28
Portree 7 5 0 13
Rate per 100 GP practice population1
Ambulance
Station Emergency Urgent Routine
All Types of
call-out

62
The ambulance station in Broadford appears to have had a higher call out rate than did the
ambulance station in Portree.
Table 16: Annual rates and numbers of SAS call-out attendances during 2014 by area of attendance
1Areas aggregated from post code sectors;
2CHI populations as at April 2013 of GP Practices making up the areas of
attendance
Source: Vaughan, S., 2015. Internal paper - Redesign of services in Skye, Lochalsh and South West Ross:
Analysis of the Scottish Ambulance data sent in response to a FOI request. NHS Highland Public Health
Epidemiology team.
The rate of attendance appears to be highest in South West Ross and South Skye, although in terms
of absolute numbers, the greatest number of call outs was in north Skye.
The number of patients transferred between Portree Hospital or Portree medical centre to
Broadford Hospital by ambulance during 2014 is tabulated below.
Table 17: Patients transferred by ambulance from Portree Hospital/Medical Centre to Broadford Hospital during 2014 by emergency status
Source: Vaughan, S., 2015. Internal paper - Redesign of services in Skye, Lochalsh and South West Ross:
Analysis of the Scottish Ambulance data sent in response to a FOI request. NHS Highland Public Health
Epidemiology team.
The total number represents an average of just over 3 per week.
During 2014, the number of call-out attendances made by SAS to the North Skye area was almost
twice that to South Skye area (1002 versus 530 respectively). When the numbers of people residing
in these two areas are considered, the rates from postcode sectors in South Skye were 1.5 times
higher than North Skye. The rates of call-out from the various Ambulance stations also reflected this
difference, with the Broadford station rate being over twice that of the Portree station.
The number of ambulance call-outs to South West Ross resulting in transport to Broadford Hospital
was low (22 per year; data not shown) and represented a small proportion of the total call-out
attendances made by SAS to this area during the same year (approx. 6% of 396). It is assumed that
emergencies amongst this population result in transport to other hospitals, most likely Raigmore.
South Skye 6 13 1 20 152 354 24 530
North Skye 7 6 0 13 549 441 12 1002
Lochalsh 8 2 0 10 229 61 0 290
South West Ross 16 8 0 25 259 134 3 396
Urgent
Rate per 100 GP practice population2 Number of attendances
Routine Routine
All Types of
call-out
Area of
attendance1Emergency Urgent
All Types
of call-out Emergency
Emergency Urgent Sum:
PORTREE HOSPITAL 12 153 165
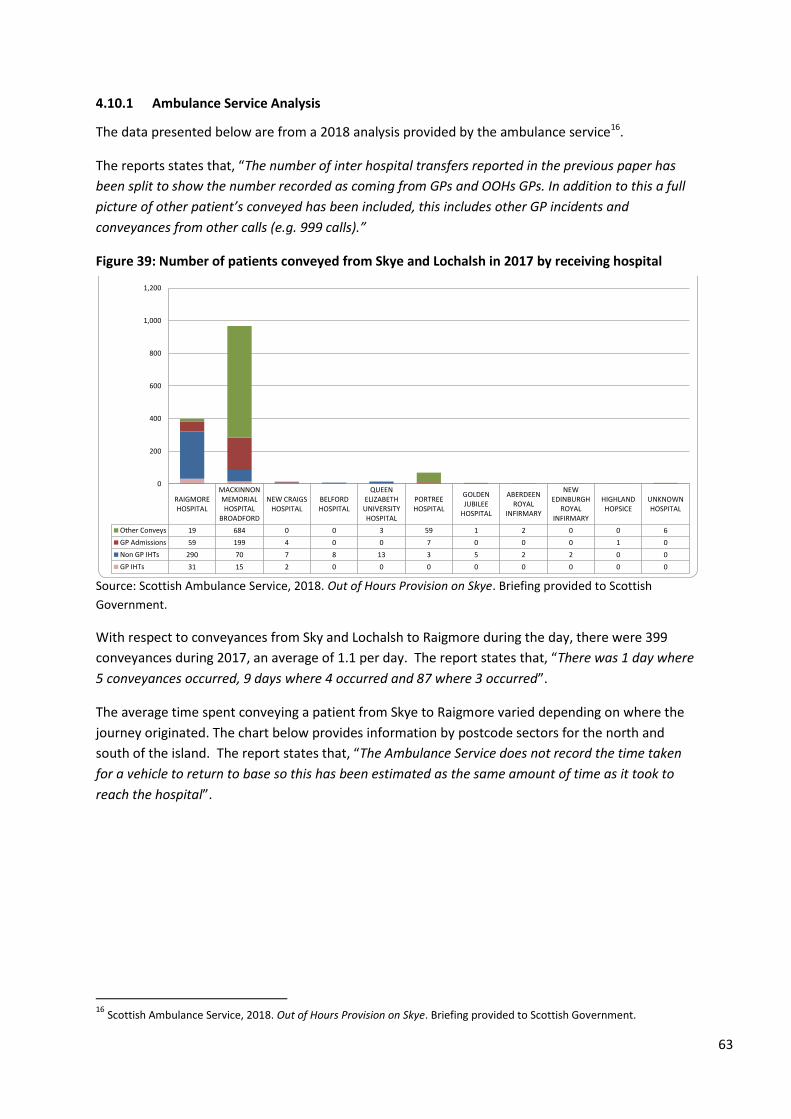
63
4.10.1 Ambulance Service Analysis
The data presented below are from a 2018 analysis provided by the ambulance service16.
The reports states that, “The number of inter hospital transfers reported in the previous paper has
been split to show the number recorded as coming from GPs and OOHs GPs. In addition to this a full
picture of other patient’s conveyed has been included, this includes other GP incidents and
conveyances from other calls (e.g. 999 calls).”
Figure 39: Number of patients conveyed from Skye and Lochalsh in 2017 by receiving hospital
Source: Scottish Ambulance Service, 2018. Out of Hours Provision on Skye. Briefing provided to Scottish
Government.
With respect to conveyances from Sky and Lochalsh to Raigmore during the day, there were 399
conveyances during 2017, an average of 1.1 per day. The report states that, “There was 1 day where
5 conveyances occurred, 9 days where 4 occurred and 87 where 3 occurred”.
The average time spent conveying a patient from Skye to Raigmore varied depending on where the
journey originated. The chart below provides information by postcode sectors for the north and
south of the island. The report states that, “The Ambulance Service does not record the time taken
for a vehicle to return to base so this has been estimated as the same amount of time as it took to
reach the hospital”.
16
Scottish Ambulance Service, 2018. Out of Hours Provision on Skye. Briefing provided to Scottish Government.
RAIGMOREHOSPITAL
MACKINNONMEMORIALHOSPITAL
BROADFORD
NEW CRAIGSHOSPITAL
BELFORDHOSPITAL
QUEENELIZABETH
UNIVERSITYHOSPITAL
PORTREEHOSPITAL
GOLDENJUBILEE
HOSPITAL
ABERDEENROYAL
INFIRMARY
NEWEDINBURGH
ROYALINFIRMARY
HIGHLANDHOPSICE
UNKNOWNHOSPITAL
Other Conveys 19 684 0 0 3 59 1 2 0 0 6
GP Admissions 59 199 4 0 0 7 0 0 0 1 0
Non GP IHTs 290 70 7 8 13 3 5 2 2 0 0
GP IHTs 31 15 2 0 0 0 0 0 0 0 0
0
200
400
600
800
1,000
1,200
All Conveyed Patients from Skye and Lochalsh (2017)by Receiving Hospital

64
Figure 40: Average time spent conveying patients to Raigmore Hospital, 2017
Source: Scottish Ambulance Service, 2018. Out of Hours Provision on Skye. Briefing provided to Scottish
Government.
The average time spent conveying patients is higher in north Skye (5 hrs 56 min) versus south Skye (5
hrs 17 min).
Concern has been expressed that ambulances are used to cover emergency calls when they are in
the vicinity of Raigmore Hospital, prolonging the time that they are away from the Isle of Skye.
Anecdotally, the priority for the Scottish Ambulance Service is to meet its 18 minute repose target,
even if this could potentially put more pressure on Out of Hours services on Skye.
The SAS report states that, “In 2017 vehicles from Skye and Lochalsh attended 71 incidents in
Inverness (IV1, IV2 and IV3). They spent an average of 61 minutes on these calls, however if the
estimated travel back to base is added this rises to 188 minutes. As stated above, the Ambulance
Service does not record the time taken for a vehicle to return to base so this has been estimated
using the same criteria as above”.
20 20
30 20
121 148
2521
121
148
0
50
100
150
200
250
300
350
400
IV40 to IV49 IV51 to IV61
Avg
Tim
e (
min
s)Average Time Spent Conveying Patient to Raigmore (2017)
Average Resource Time to Scene Average Resource Time On Scene Average Resource Time to Hospital
Average Resource Turnaround Time at Hospital Estimated Return Time to Base
Number of Patients: 328Avg Time: 5 hours 17 minutes
Number of Patients: 71Avg Time: 5 hours 56 minutes
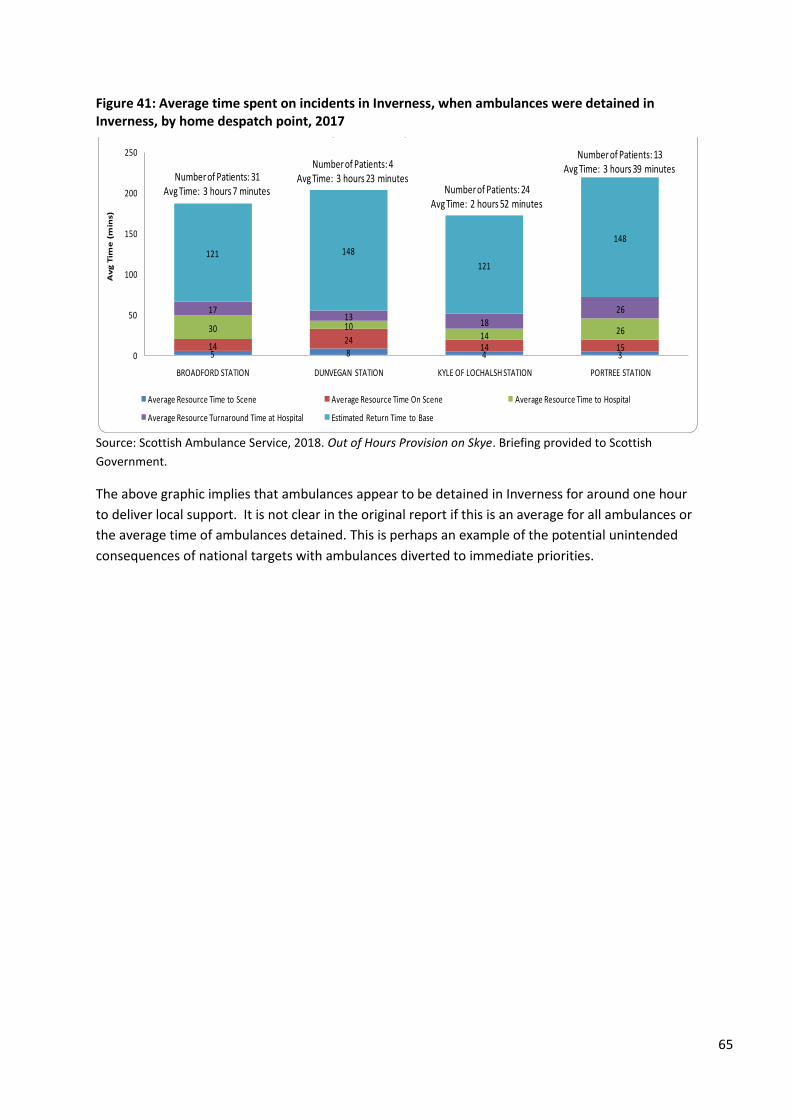
65
Figure 41: Average time spent on incidents in Inverness, when ambulances were detained in Inverness, by home despatch point, 2017
Source: Scottish Ambulance Service, 2018. Out of Hours Provision on Skye. Briefing provided to Scottish
Government.
The above graphic implies that ambulances appear to be detained in Inverness for around one hour
to deliver local support. It is not clear in the original report if this is an average for all ambulances or
the average time of ambulances detained. This is perhaps an example of the potential unintended
consequences of national targets with ambulances diverted to immediate priorities.
5 8 4 314
2414 15
30 1014 26
1713
18
26
121 148
121
148
0
50
100
150
200
250
BROADFORD STATION DUNVEGAN STATION KYLE OF LOCHALSH STATION PORTREE STATION
Av
g T
ime
(m
ins)
Average Time Spent on Incidents in Inverness (2017)By Home Despatch Point
Average Resource Time to Scene Average Resource Time On Scene Average Resource Time to Hospital
Average Resource Turnaround Time at Hospital Estimated Return Time to Base
Number of Patients: 31Avg Time: 3 hours 7 minutes
Number of Patients: 13Avg Time: 3 hours 39 minutesNumber of Patients: 4
Avg Time: 3 hours 23 minutesNumber of Patients: 24
Avg Time: 2 hours 52 minutes

66
5. Where is the care delivered?
This section provides some information on where care is delivered. The map below provides an
overall view of locations where care is provided across NHS Highland.
Figure 42: Health Services across NHS Highland
Source: NHS Highland, 2017. OUTLINE BUSINESS CASE, The Modernisation of Community and Hospital Services
in Badenoch & Strathspey (B&S) and Skye, Lochalsh and South West Ross (SLSWR). p11, Map 1. Available
online:http://www.nhshighland.scot.nhs.uk/Meetings/BoardsMeetings/Documents/November%202017/4.5%20Outline%20Business%20C
ase%20BS%20and%20SLSWR.pdf
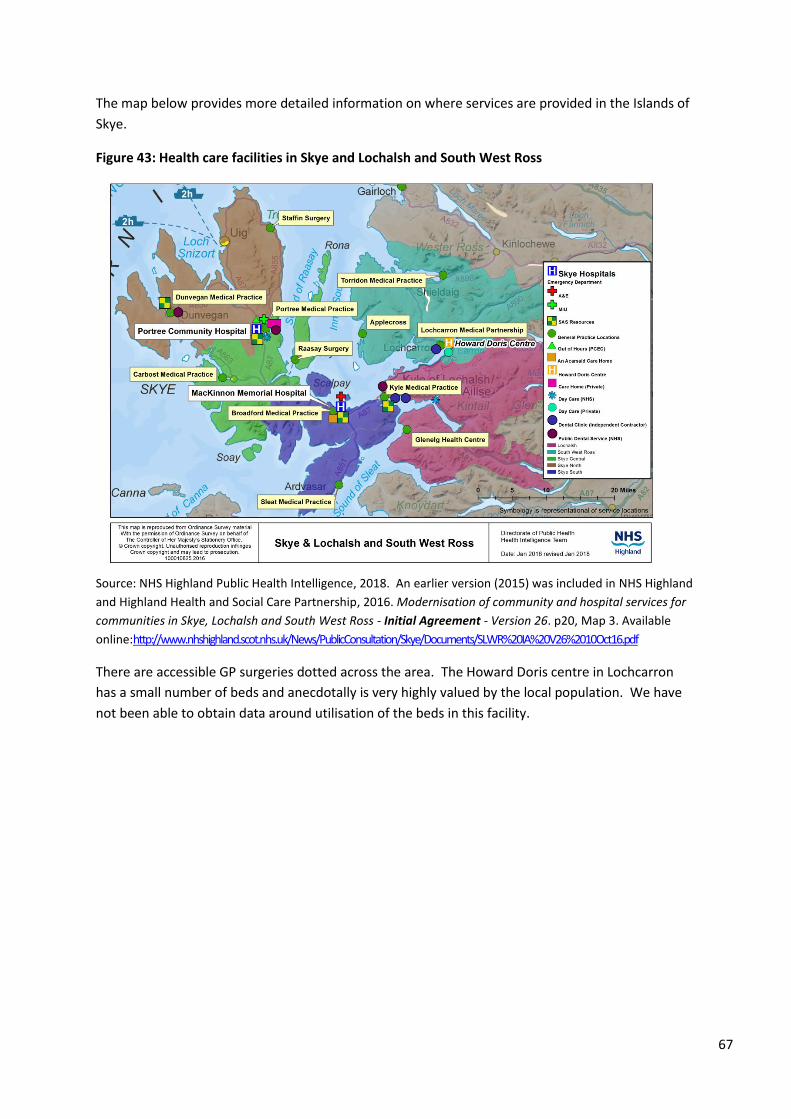
67
The map below provides more detailed information on where services are provided in the Islands of
Skye.
Figure 43: Health care facilities in Skye and Lochalsh and South West Ross
Source: NHS Highland Public Health Intelligence, 2018. An earlier version (2015) was included in NHS Highland
and Highland Health and Social Care Partnership, 2016. Modernisation of community and hospital services for
communities in Skye, Lochalsh and South West Ross - Initial Agreement - Version 26. p20, Map 3. Available
online:http://www.nhshighland.scot.nhs.uk/News/PublicConsultation/Skye/Documents/SLWR%20IA%20V26%2010Oct16.pdf
There are accessible GP surgeries dotted across the area. The Howard Doris centre in Lochcarron
has a small number of beds and anecdotally is very highly valued by the local population. We have
not been able to obtain data around utilisation of the beds in this facility.
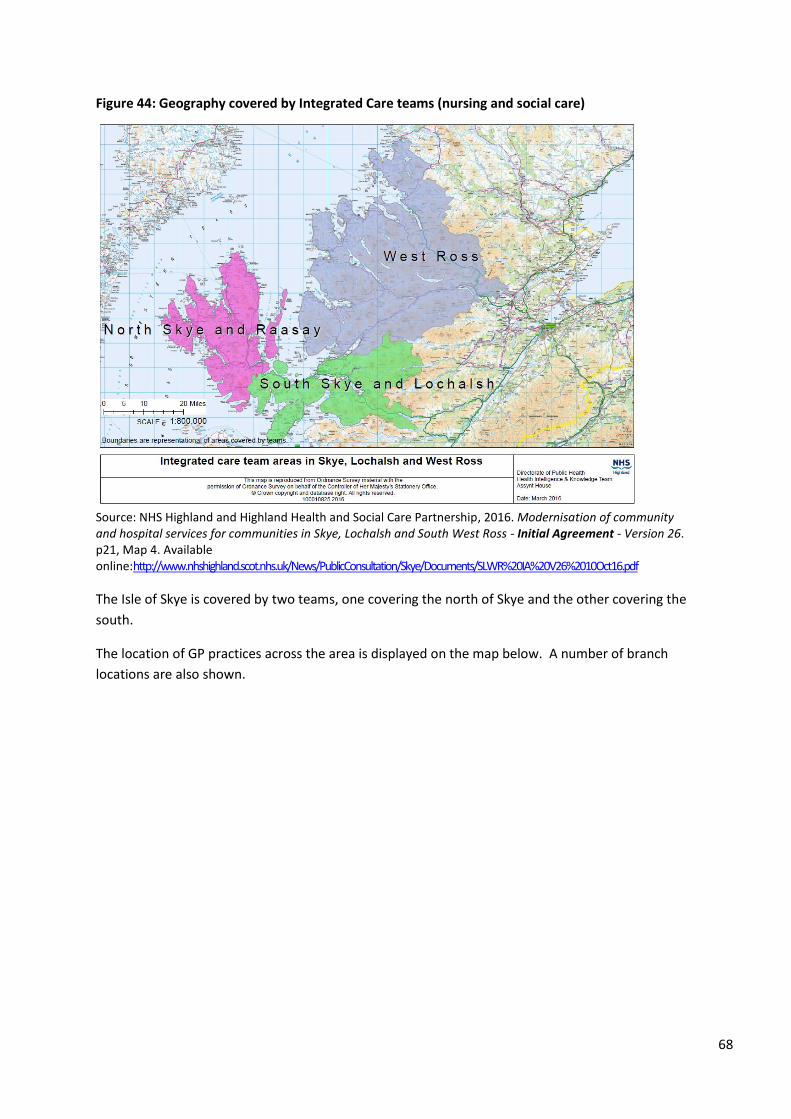
68
Figure 44: Geography covered by Integrated Care teams (nursing and social care)
Source: NHS Highland and Highland Health and Social Care Partnership, 2016. Modernisation of community and hospital services for communities in Skye, Lochalsh and South West Ross - Initial Agreement - Version 26. p21, Map 4. Available online:http://www.nhshighland.scot.nhs.uk/News/PublicConsultation/Skye/Documents/SLWR%20IA%20V26%2010Oct16.pdf
The Isle of Skye is covered by two teams, one covering the north of Skye and the other covering the
south.
The location of GP practices across the area is displayed on the map below. A number of branch
locations are also shown.
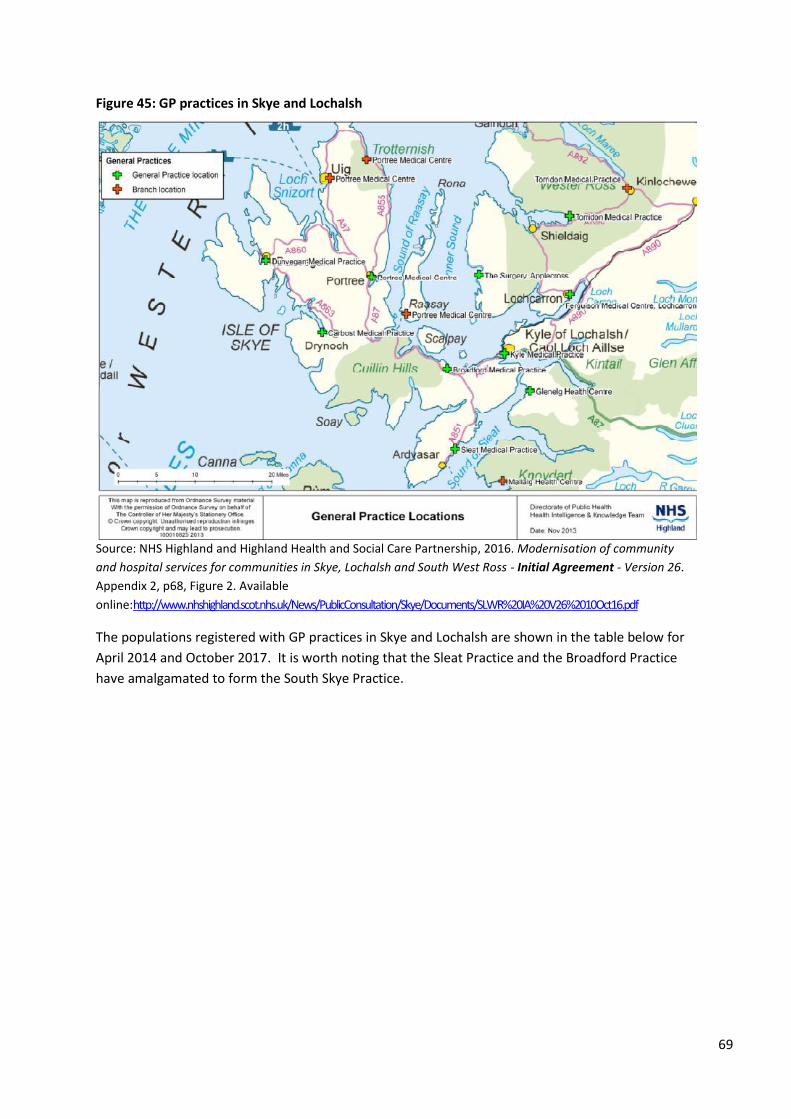
69
Figure 45: GP practices in Skye and Lochalsh
Source: NHS Highland and Highland Health and Social Care Partnership, 2016. Modernisation of community
and hospital services for communities in Skye, Lochalsh and South West Ross - Initial Agreement - Version 26.
Appendix 2, p68, Figure 2. Available
online:http://www.nhshighland.scot.nhs.uk/News/PublicConsultation/Skye/Documents/SLWR%20IA%20V26%2010Oct16.pdf
The populations registered with GP practices in Skye and Lochalsh are shown in the table below for
April 2014 and October 2017. It is worth noting that the Sleat Practice and the Broadford Practice
have amalgamated to form the South Skye Practice.
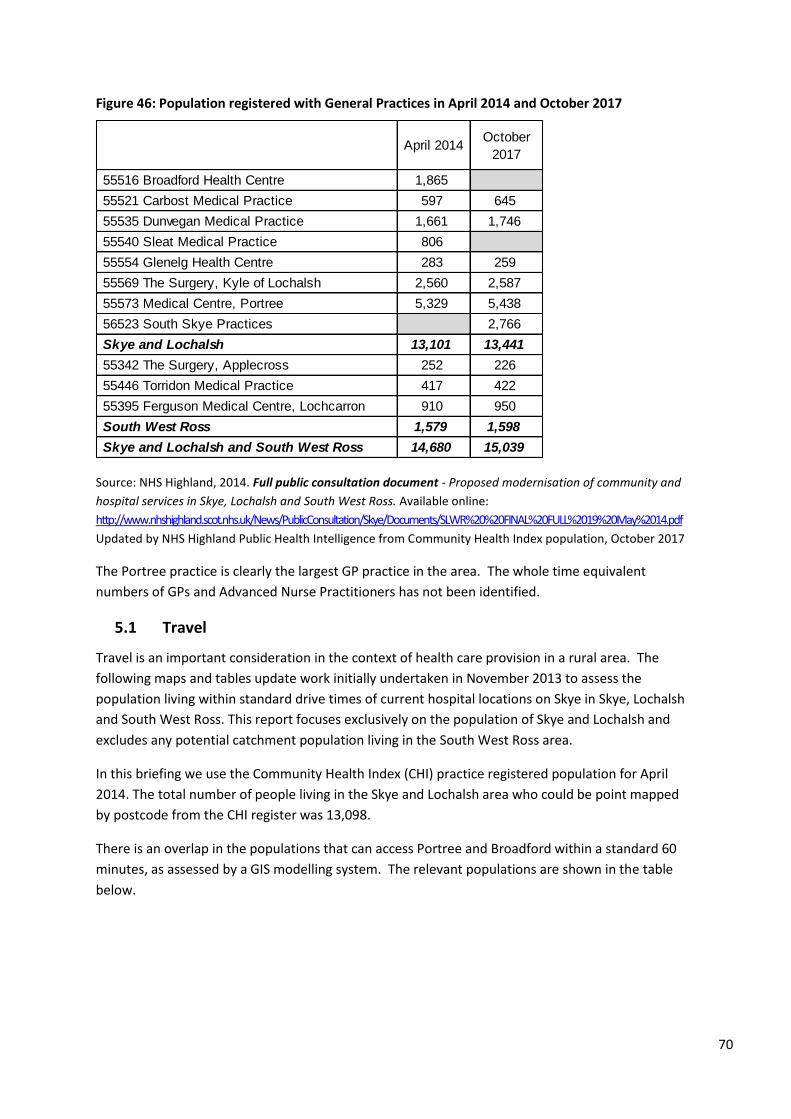
70
Figure 46: Population registered with General Practices in April 2014 and October 2017
Source: NHS Highland, 2014. Full public consultation document - Proposed modernisation of community and
hospital services in Skye, Lochalsh and South West Ross. Available online:
http://www.nhshighland.scot.nhs.uk/News/PublicConsultation/Skye/Documents/SLWR%20%20FINAL%20FULL%2019%20May%2014.pdf
Updated by NHS Highland Public Health Intelligence from Community Health Index population, October 2017
The Portree practice is clearly the largest GP practice in the area. The whole time equivalent
numbers of GPs and Advanced Nurse Practitioners has not been identified.
5.1 Travel
Travel is an important consideration in the context of health care provision in a rural area. The
following maps and tables update work initially undertaken in November 2013 to assess the
population living within standard drive times of current hospital locations on Skye in Skye, Lochalsh
and South West Ross. This report focuses exclusively on the population of Skye and Lochalsh and
excludes any potential catchment population living in the South West Ross area.
In this briefing we use the Community Health Index (CHI) practice registered population for April
2014. The total number of people living in the Skye and Lochalsh area who could be point mapped
by postcode from the CHI register was 13,098.
There is an overlap in the populations that can access Portree and Broadford within a standard 60
minutes, as assessed by a GIS modelling system. The relevant populations are shown in the table
below.
April 2014October
2017
55516 Broadford Health Centre 1,865
55521 Carbost Medical Practice 597 645
55535 Dunvegan Medical Practice 1,661 1,746
55540 Sleat Medical Practice 806
55554 Glenelg Health Centre 283 259
55569 The Surgery, Kyle of Lochalsh 2,560 2,587
55573 Medical Centre, Portree 5,329 5,438
56523 South Skye Practices 2,766
Skye and Lochalsh 13,101 13,441
55342 The Surgery, Applecross 252 226
55446 Torridon Medical Practice 417 422
55395 Ferguson Medical Centre, Lochcarron 910 950
South West Ross 1,579 1,598
Skye and Lochalsh and South West Ross 14,680 15,039

71
Table 18: Community Health Index Practice list population of Skye and Lochalsh (excluding South West Ross) within 60 minutes drive time from Portree and Broadford
Location Population with 60 minutes drive
Portree Hospital 11,261
MacKinnon Memorial Hospital (Broadford) 11,448
Source: NHS Highland, 2014. Report to Board Item 4.1: Proposed redesign of services in Syke, Lochalsh and
South West Ross. Appendix 13. p.96. Available online:
http://www.nhshighland.scot.nhs.uk/Meetings/BoardsMeetings/Documents/Board%20Meeting%202%20December%202014/4.1%20Redes
ign%20of%20Services%20SLSWR.pdf
There has been debate as to whether populations within a drive time of thirty or sixty minutes
should be considered in relation to service provision. The notional ‘drive times’ for both 30 and 60
minutes from each base are shown graphically in the maps below for both centres. Further
information on the proportion of the population within different drive times of Broadford and
Portree is available in other reports and has not been presented here.
Figure 47: Area within 30 and 60 minutes drive from Portree Hospital
Source: NHS Highland, 2014. Report to Board Item 4.1: Proposed redesign of services in Syke, Lochalsh and
South West Ross. Appendix 13. p.97. Available online:
http://www.nhshighland.scot.nhs.uk/Meetings/BoardsMeetings/Documents/Board%20Meeting%202%20December%202014/4.1%20Redes
ign%20of%20Services%20SLSWR.pdf
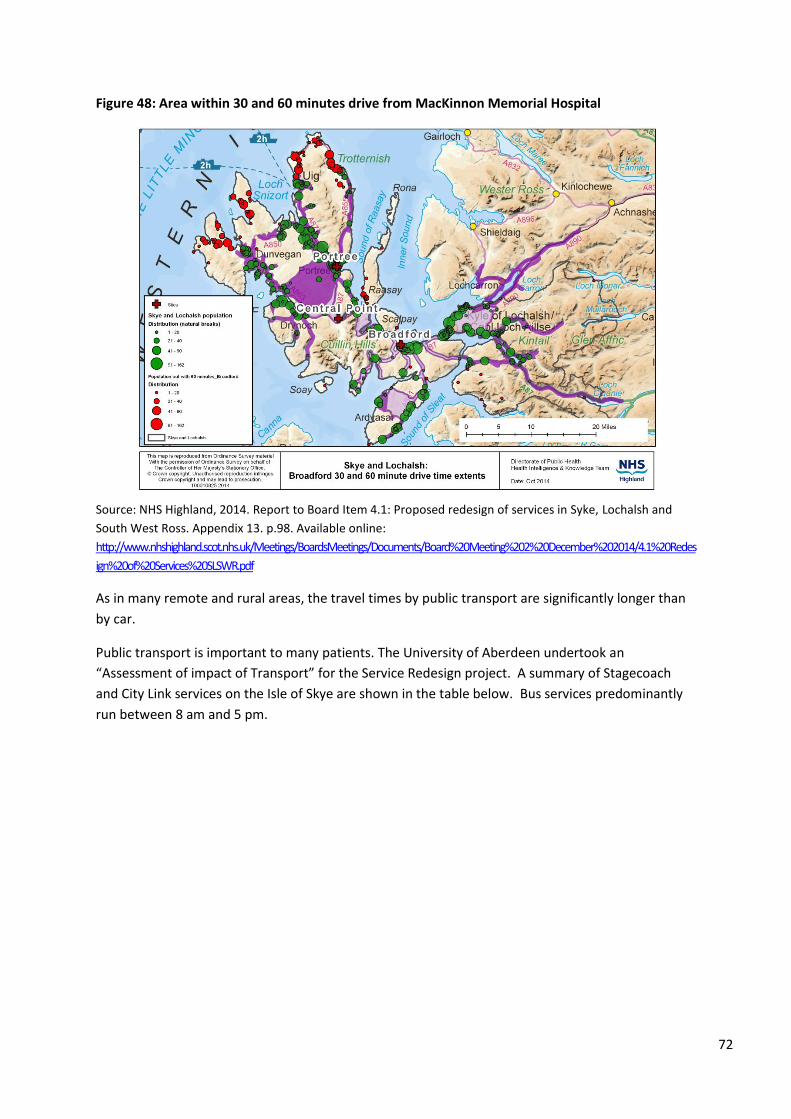
72
Figure 48: Area within 30 and 60 minutes drive from MacKinnon Memorial Hospital
Source: NHS Highland, 2014. Report to Board Item 4.1: Proposed redesign of services in Syke, Lochalsh and
South West Ross. Appendix 13. p.98. Available online:
http://www.nhshighland.scot.nhs.uk/Meetings/BoardsMeetings/Documents/Board%20Meeting%202%20December%202014/4.1%20Redes
ign%20of%20Services%20SLSWR.pdf
As in many remote and rural areas, the travel times by public transport are significantly longer than
by car.
Public transport is important to many patients. The University of Aberdeen undertook an
“Assessment of impact of Transport” for the Service Redesign project. A summary of Stagecoach
and City Link services on the Isle of Skye are shown in the table below. Bus services predominantly
run between 8 am and 5 pm.
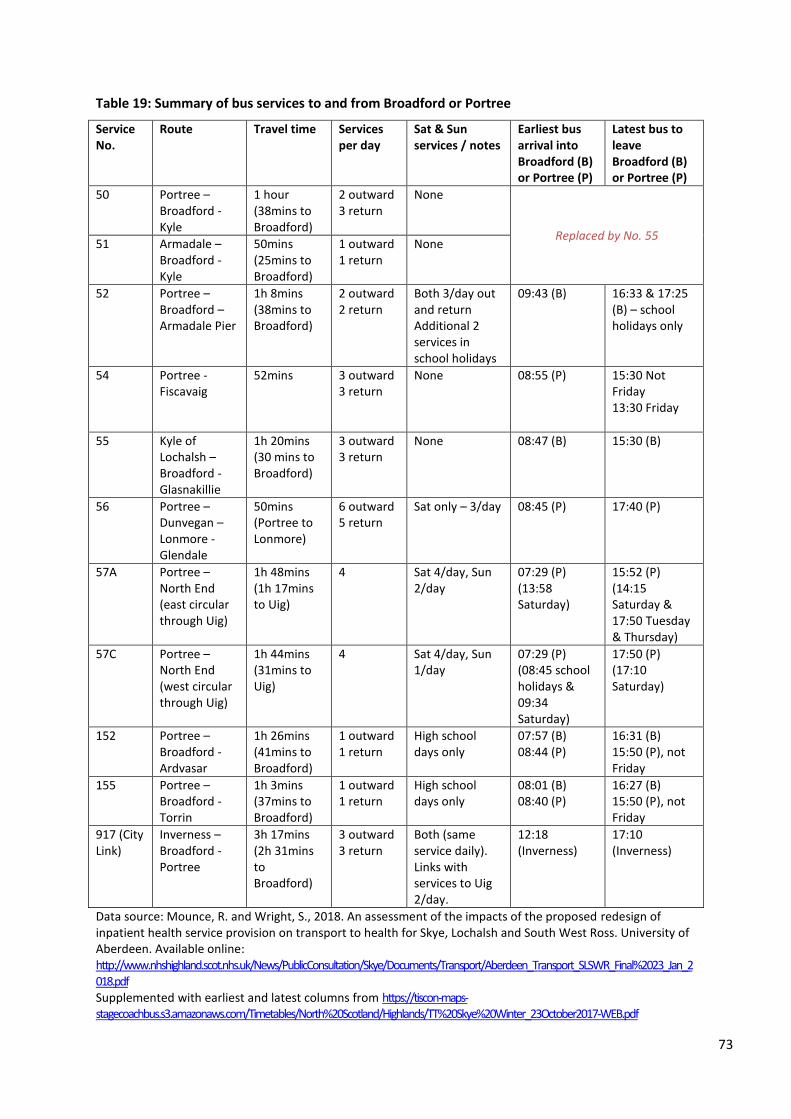
73
Table 19: Summary of bus services to and from Broadford or Portree
Service No.
Route Travel time Services per day
Sat & Sun services / notes
Earliest bus arrival into Broadford (B) or Portree (P)
Latest bus to leave Broadford (B) or Portree (P)
50 Portree – Broadford - Kyle
1 hour (38mins to Broadford)
2 outward 3 return
None
Replaced by No. 55 51 Armadale –
Broadford - Kyle
50mins (25mins to Broadford)
1 outward 1 return
None
52 Portree – Broadford – Armadale Pier
1h 8mins (38mins to Broadford)
2 outward 2 return
Both 3/day out and return Additional 2 services in school holidays
09:43 (B) 16:33 & 17:25 (B) – school holidays only
54 Portree - Fiscavaig
52mins 3 outward 3 return
None 08:55 (P) 15:30 Not Friday 13:30 Friday
55 Kyle of Lochalsh – Broadford - Glasnakillie
1h 20mins (30 mins to Broadford)
3 outward 3 return
None 08:47 (B) 15:30 (B)
56 Portree – Dunvegan – Lonmore - Glendale
50mins (Portree to Lonmore)
6 outward 5 return
Sat only – 3/day 08:45 (P) 17:40 (P)
57A Portree – North End (east circular through Uig)
1h 48mins (1h 17mins to Uig)
4 Sat 4/day, Sun 2/day
07:29 (P) (13:58 Saturday)
15:52 (P) (14:15 Saturday & 17:50 Tuesday & Thursday)
57C Portree – North End (west circular through Uig)
1h 44mins (31mins to Uig)
4 Sat 4/day, Sun 1/day
07:29 (P) (08:45 school holidays & 09:34 Saturday)
17:50 (P) (17:10 Saturday)
152 Portree – Broadford - Ardvasar
1h 26mins (41mins to Broadford)
1 outward 1 return
High school days only
07:57 (B) 08:44 (P)
16:31 (B) 15:50 (P), not Friday
155 Portree – Broadford - Torrin
1h 3mins (37mins to Broadford)
1 outward 1 return
High school days only
08:01 (B) 08:40 (P)
16:27 (B) 15:50 (P), not Friday
917 (City Link)
Inverness – Broadford - Portree
3h 17mins (2h 31mins to Broadford)
3 outward 3 return
Both (same service daily). Links with services to Uig 2/day.
12:18 (Inverness)
17:10 (Inverness)
Data source: Mounce, R. and Wright, S., 2018. An assessment of the impacts of the proposed redesign of inpatient health service provision on transport to health for Skye, Lochalsh and South West Ross. University of Aberdeen. Available online: http://www.nhshighland.scot.nhs.uk/News/PublicConsultation/Skye/Documents/Transport/Aberdeen_Transport_SLSWR_Final%2023_Jan_2018.pdf Supplemented with earliest and latest columns from https://tiscon-maps-stagecoachbus.s3.amazonaws.com/Timetables/North%20Scotland/Highlands/TT%20Skye%20Winter_23October2017-WEB.pdf
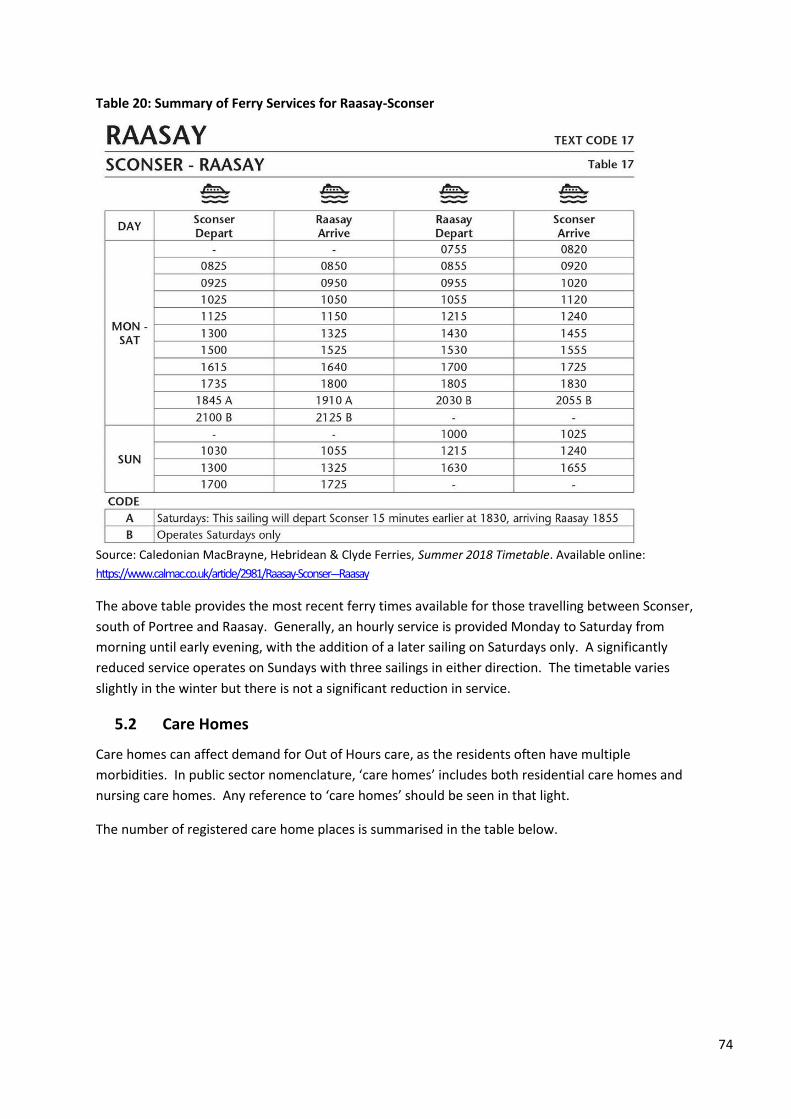
74
Table 20: Summary of Ferry Services for Raasay-Sconser
Source: Caledonian MacBrayne, Hebridean & Clyde Ferries, Summer 2018 Timetable. Available online:
https://www.calmac.co.uk/article/2981/Raasay-Sconser---Raasay
The above table provides the most recent ferry times available for those travelling between Sconser,
south of Portree and Raasay. Generally, an hourly service is provided Monday to Saturday from
morning until early evening, with the addition of a later sailing on Saturdays only. A significantly
reduced service operates on Sundays with three sailings in either direction. The timetable varies
slightly in the winter but there is not a significant reduction in service.
5.2 Care Homes
Care homes can affect demand for Out of Hours care, as the residents often have multiple
morbidities. In public sector nomenclature, ‘care homes’ includes both residential care homes and
nursing care homes. Any reference to ‘care homes’ should be seen in that light.
The number of registered care home places is summarised in the table below.
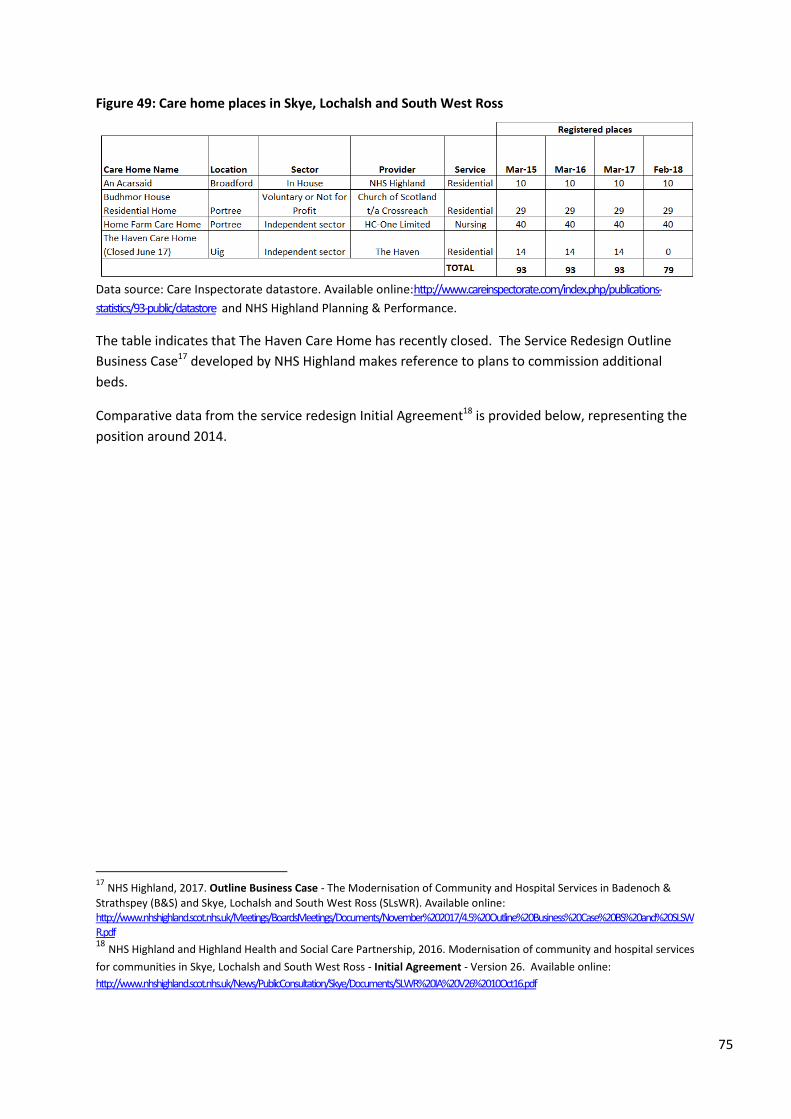
75
Figure 49: Care home places in Skye, Lochalsh and South West Ross
Data source: Care Inspectorate datastore. Available online:http://www.careinspectorate.com/index.php/publications-
statistics/93-public/datastore and NHS Highland Planning & Performance.
The table indicates that The Haven Care Home has recently closed. The Service Redesign Outline
Business Case17 developed by NHS Highland makes reference to plans to commission additional
beds.
Comparative data from the service redesign Initial Agreement18 is provided below, representing the
position around 2014.
17
NHS Highland, 2017. Outline Business Case - The Modernisation of Community and Hospital Services in Badenoch &
Strathspey (B&S) and Skye, Lochalsh and South West Ross (SLsWR). Available online: http://www.nhshighland.scot.nhs.uk/Meetings/BoardsMeetings/Documents/November%202017/4.5%20Outline%20Business%20Case%20BS%20and%20SLSWR.pdf 18 NHS Highland and Highland Health and Social Care Partnership, 2016. Modernisation of community and hospital services
for communities in Skye, Lochalsh and South West Ross - Initial Agreement - Version 26. Available online:
http://www.nhshighland.scot.nhs.uk/News/PublicConsultation/Skye/Documents/SLWR%20IA%20V26%2010Oct16.pdf
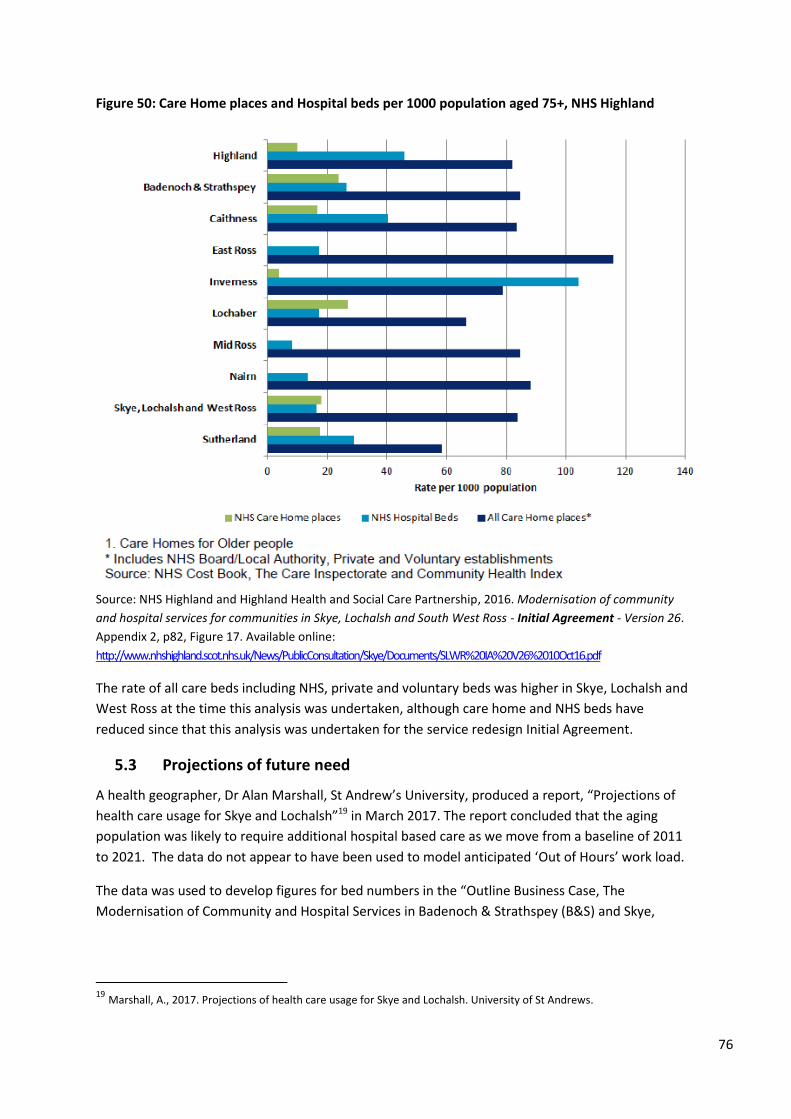
76
Figure 50: Care Home places and Hospital beds per 1000 population aged 75+, NHS Highland
Source: NHS Highland and Highland Health and Social Care Partnership, 2016. Modernisation of community
and hospital services for communities in Skye, Lochalsh and South West Ross - Initial Agreement - Version 26.
Appendix 2, p82, Figure 17. Available online:
http://www.nhshighland.scot.nhs.uk/News/PublicConsultation/Skye/Documents/SLWR%20IA%20V26%2010Oct16.pdf
The rate of all care beds including NHS, private and voluntary beds was higher in Skye, Lochalsh and
West Ross at the time this analysis was undertaken, although care home and NHS beds have
reduced since that this analysis was undertaken for the service redesign Initial Agreement.
5.3 Projections of future need
A health geographer, Dr Alan Marshall, St Andrew’s University, produced a report, “Projections of
health care usage for Skye and Lochalsh”19 in March 2017. The report concluded that the aging
population was likely to require additional hospital based care as we move from a baseline of 2011
to 2021. The data do not appear to have been used to model anticipated ‘Out of Hours’ work load.
The data was used to develop figures for bed numbers in the “Outline Business Case, The
Modernisation of Community and Hospital Services in Badenoch & Strathspey (B&S) and Skye,
19 Marshall, A., 2017. Projections of health care usage for Skye and Lochalsh. University of St Andrews.
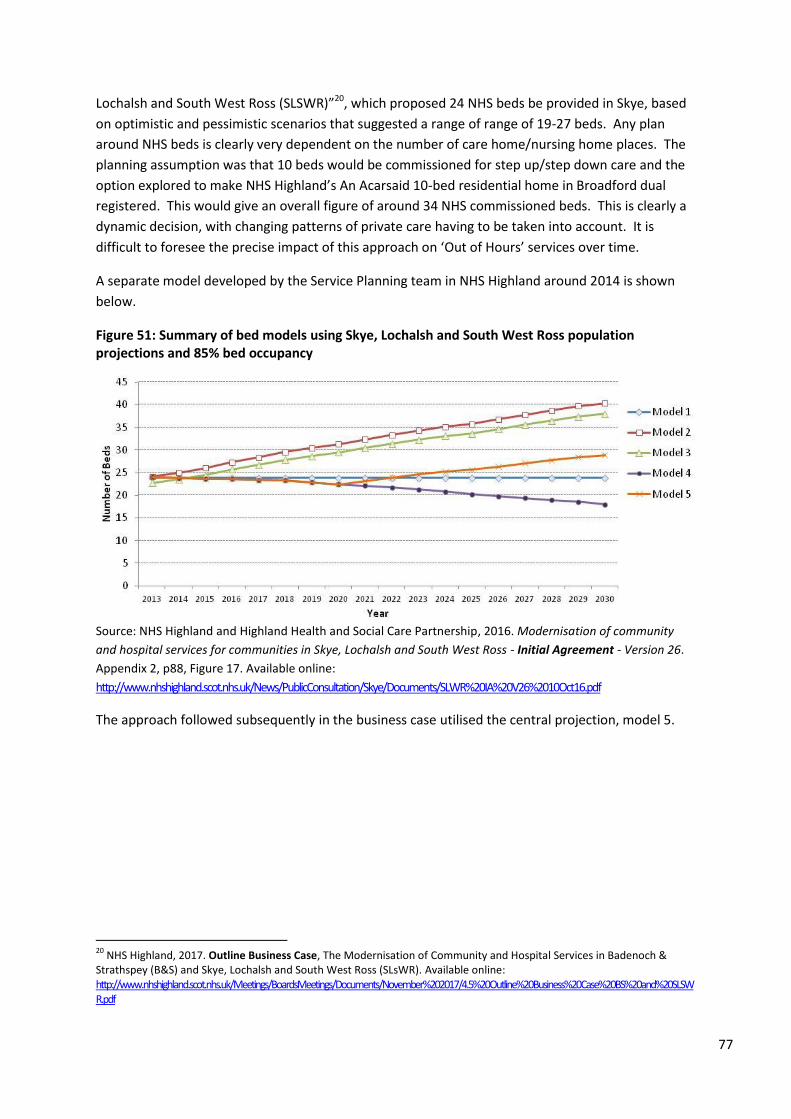
77
Lochalsh and South West Ross (SLSWR)”20, which proposed 24 NHS beds be provided in Skye, based
on optimistic and pessimistic scenarios that suggested a range of range of 19-27 beds. Any plan
around NHS beds is clearly very dependent on the number of care home/nursing home places. The
planning assumption was that 10 beds would be commissioned for step up/step down care and the
option explored to make NHS Highland’s An Acarsaid 10-bed residential home in Broadford dual
registered. This would give an overall figure of around 34 NHS commissioned beds. This is clearly a
dynamic decision, with changing patterns of private care having to be taken into account. It is
difficult to foresee the precise impact of this approach on ‘Out of Hours’ services over time.
A separate model developed by the Service Planning team in NHS Highland around 2014 is shown
below.
Figure 51: Summary of bed models using Skye, Lochalsh and South West Ross population projections and 85% bed occupancy
Source: NHS Highland and Highland Health and Social Care Partnership, 2016. Modernisation of community
and hospital services for communities in Skye, Lochalsh and South West Ross - Initial Agreement - Version 26.
Appendix 2, p88, Figure 17. Available online:
http://www.nhshighland.scot.nhs.uk/News/PublicConsultation/Skye/Documents/SLWR%20IA%20V26%2010Oct16.pdf
The approach followed subsequently in the business case utilised the central projection, model 5.
20
NHS Highland, 2017. Outline Business Case, The Modernisation of Community and Hospital Services in Badenoch & Strathspey (B&S) and Skye, Lochalsh and South West Ross (SLsWR). Available online: http://www.nhshighland.scot.nhs.uk/Meetings/BoardsMeetings/Documents/November%202017/4.5%20Outline%20Business%20Case%20BS%20and%20SLSWR.pdf
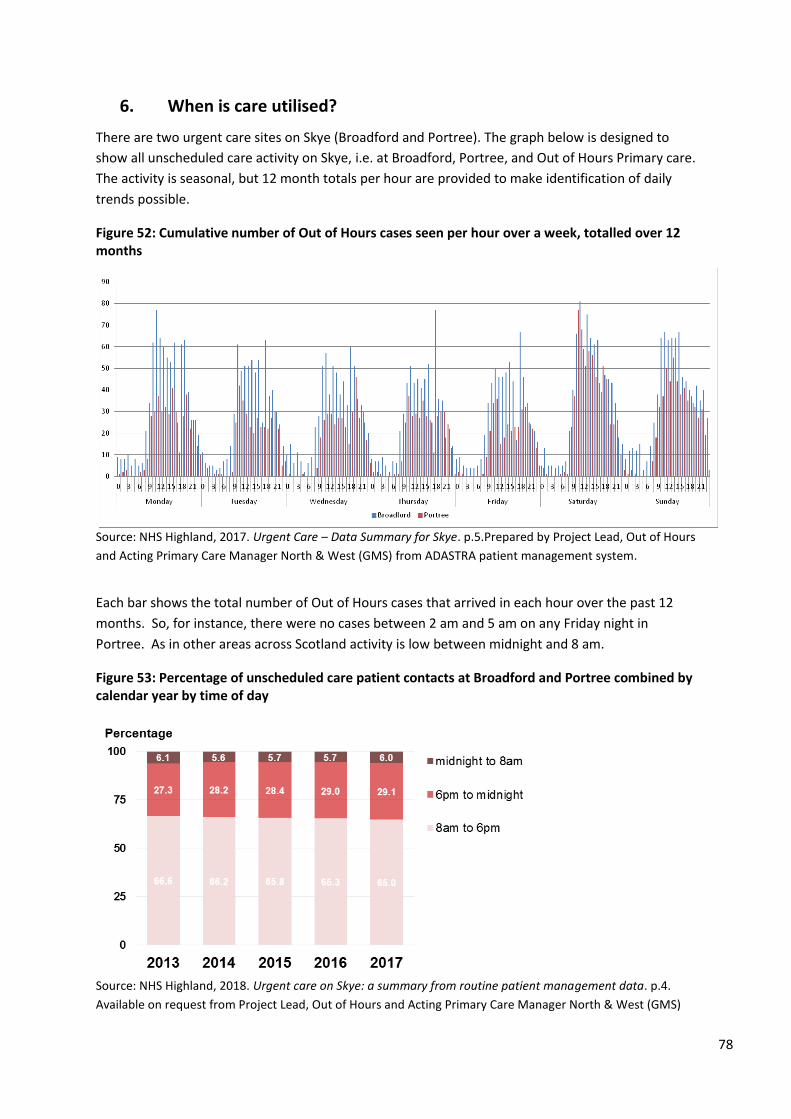
78
6. When is care utilised?
There are two urgent care sites on Skye (Broadford and Portree). The graph below is designed to
show all unscheduled care activity on Skye, i.e. at Broadford, Portree, and Out of Hours Primary care.
The activity is seasonal, but 12 month totals per hour are provided to make identification of daily
trends possible.
Figure 52: Cumulative number of Out of Hours cases seen per hour over a week, totalled over 12 months
Source: NHS Highland, 2017. Urgent Care – Data Summary for Skye. p.5.Prepared by Project Lead, Out of Hours
and Acting Primary Care Manager North & West (GMS) from ADASTRA patient management system.
Each bar shows the total number of Out of Hours cases that arrived in each hour over the past 12
months. So, for instance, there were no cases between 2 am and 5 am on any Friday night in
Portree. As in other areas across Scotland activity is low between midnight and 8 am.
Figure 53: Percentage of unscheduled care patient contacts at Broadford and Portree combined by calendar year by time of day
Source: NHS Highland, 2018. Urgent care on Skye: a summary from routine patient management data. p.4.
Available on request from Project Lead, Out of Hours and Acting Primary Care Manager North & West (GMS)
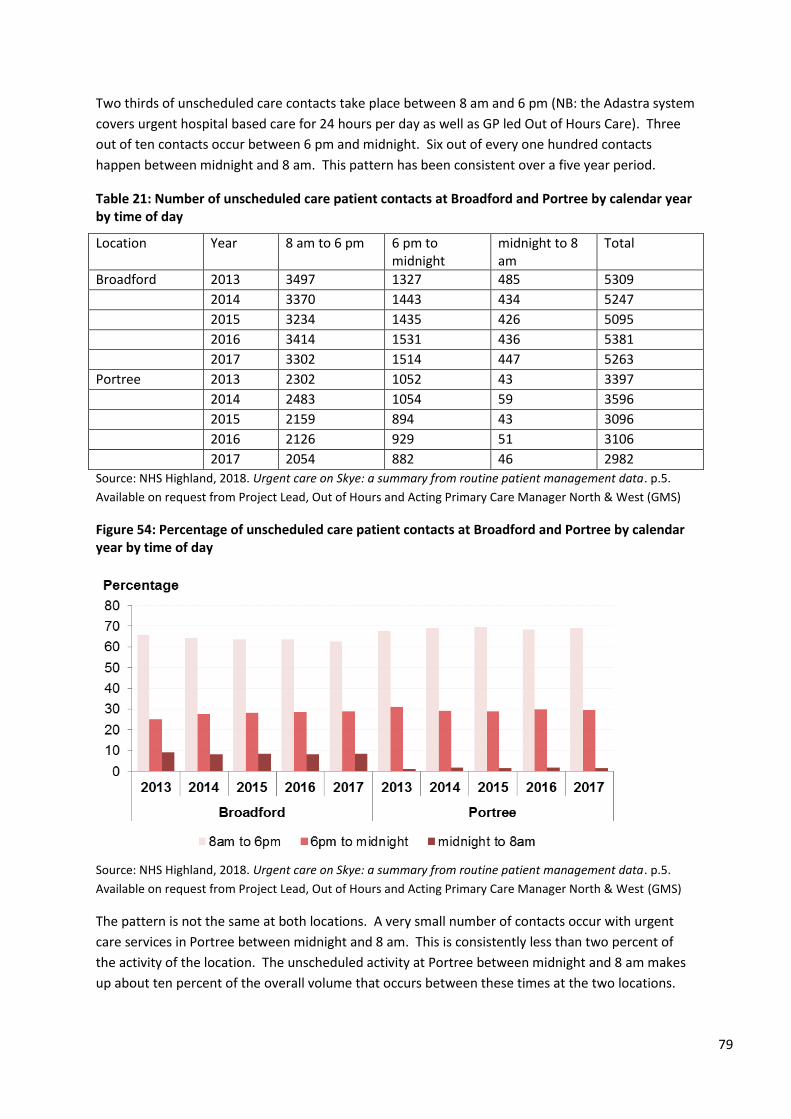
79
Two thirds of unscheduled care contacts take place between 8 am and 6 pm (NB: the Adastra system
covers urgent hospital based care for 24 hours per day as well as GP led Out of Hours Care). Three
out of ten contacts occur between 6 pm and midnight. Six out of every one hundred contacts
happen between midnight and 8 am. This pattern has been consistent over a five year period.
Table 21: Number of unscheduled care patient contacts at Broadford and Portree by calendar year by time of day
Location Year 8 am to 6 pm 6 pm to midnight
midnight to 8 am
Total
Broadford 2013 3497 1327 485 5309
2014 3370 1443 434 5247
2015 3234 1435 426 5095
2016 3414 1531 436 5381
2017 3302 1514 447 5263
Portree 2013 2302 1052 43 3397
2014 2483 1054 59 3596
2015 2159 894 43 3096
2016 2126 929 51 3106
2017 2054 882 46 2982
Source: NHS Highland, 2018. Urgent care on Skye: a summary from routine patient management data. p.5.
Available on request from Project Lead, Out of Hours and Acting Primary Care Manager North & West (GMS)
Figure 54: Percentage of unscheduled care patient contacts at Broadford and Portree by calendar year by time of day
Source: NHS Highland, 2018. Urgent care on Skye: a summary from routine patient management data. p.5.
Available on request from Project Lead, Out of Hours and Acting Primary Care Manager North & West (GMS)
The pattern is not the same at both locations. A very small number of contacts occur with urgent
care services in Portree between midnight and 8 am. This is consistently less than two percent of
the activity of the location. The unscheduled activity at Portree between midnight and 8 am makes
up about ten percent of the overall volume that occurs between these times at the two locations.
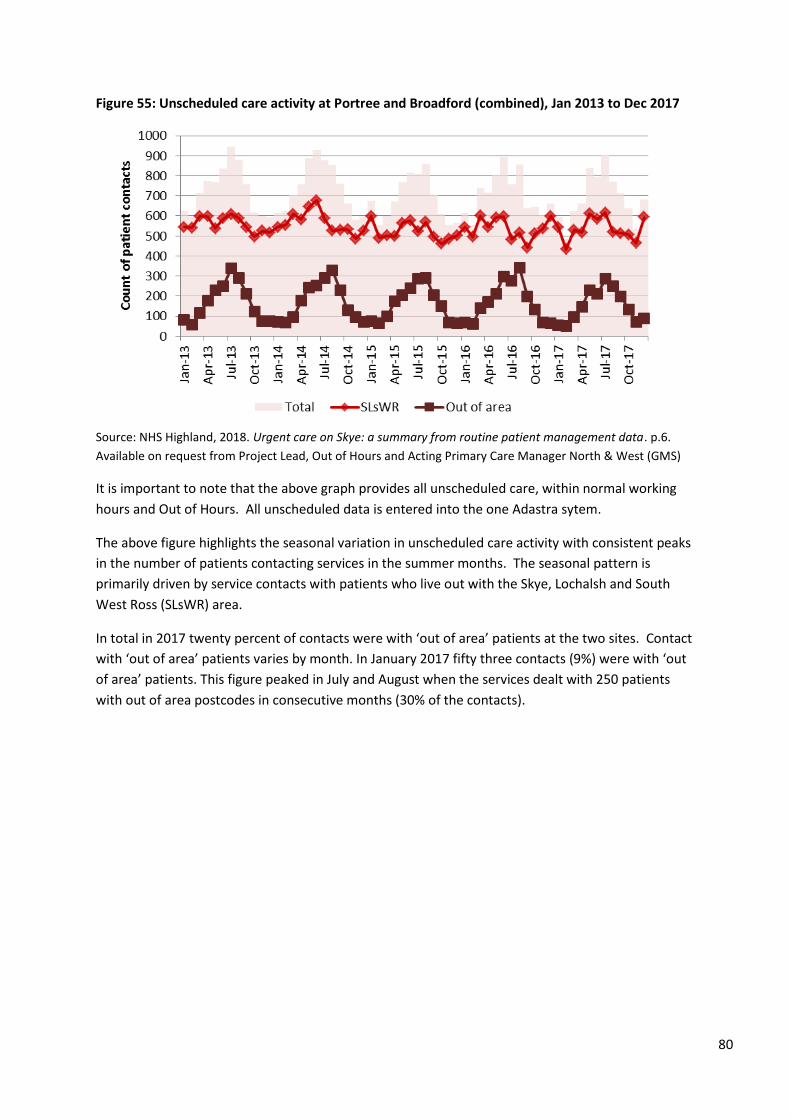
80
Figure 55: Unscheduled care activity at Portree and Broadford (combined), Jan 2013 to Dec 2017
Source: NHS Highland, 2018. Urgent care on Skye: a summary from routine patient management data. p.6.
Available on request from Project Lead, Out of Hours and Acting Primary Care Manager North & West (GMS)
It is important to note that the above graph provides all unscheduled care, within normal working
hours and Out of Hours. All unscheduled data is entered into the one Adastra sytem.
The above figure highlights the seasonal variation in unscheduled care activity with consistent peaks
in the number of patients contacting services in the summer months. The seasonal pattern is
primarily driven by service contacts with patients who live out with the Skye, Lochalsh and South
West Ross (SLsWR) area.
In total in 2017 twenty percent of contacts were with ‘out of area’ patients at the two sites. Contact
with ‘out of area’ patients varies by month. In January 2017 fifty three contacts (9%) were with ‘out
of area’ patients. This figure peaked in July and August when the services dealt with 250 patients
with out of area postcodes in consecutive months (30% of the contacts).
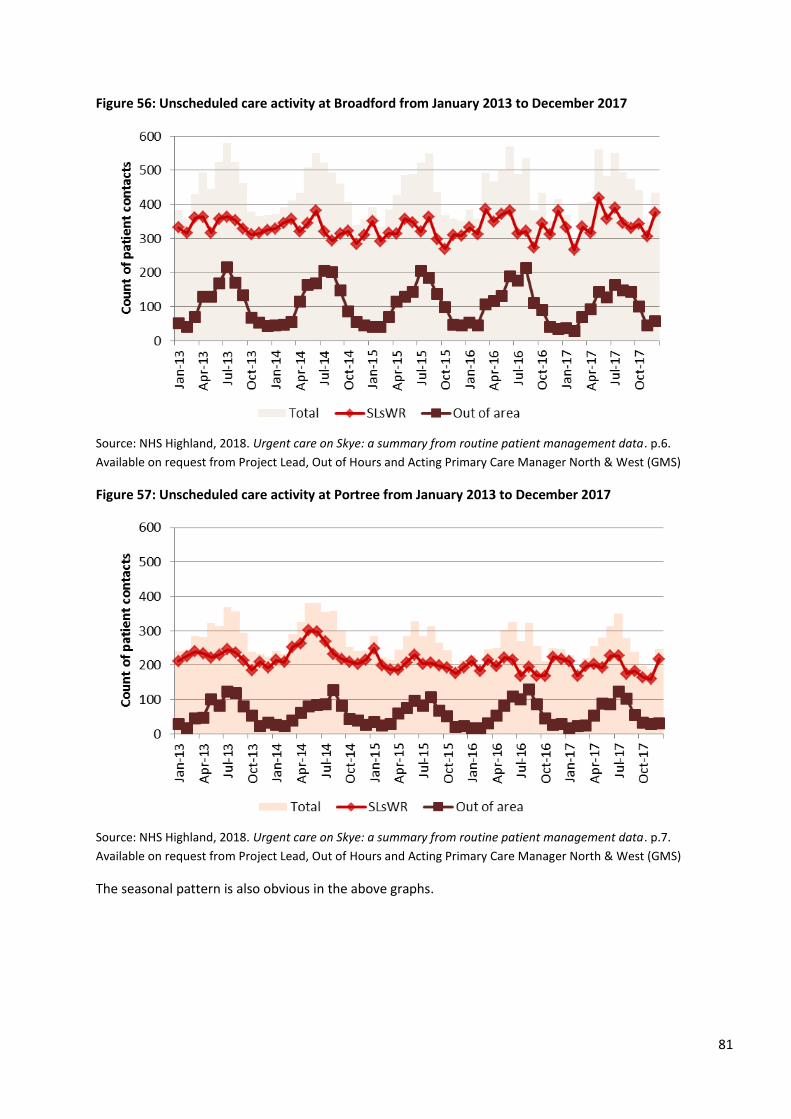
81
Figure 56: Unscheduled care activity at Broadford from January 2013 to December 2017
Source: NHS Highland, 2018. Urgent care on Skye: a summary from routine patient management data. p.6.
Available on request from Project Lead, Out of Hours and Acting Primary Care Manager North & West (GMS)
Figure 57: Unscheduled care activity at Portree from January 2013 to December 2017
Source: NHS Highland, 2018. Urgent care on Skye: a summary from routine patient management data. p.7.
Available on request from Project Lead, Out of Hours and Acting Primary Care Manager North & West (GMS)
The seasonal pattern is also obvious in the above graphs.
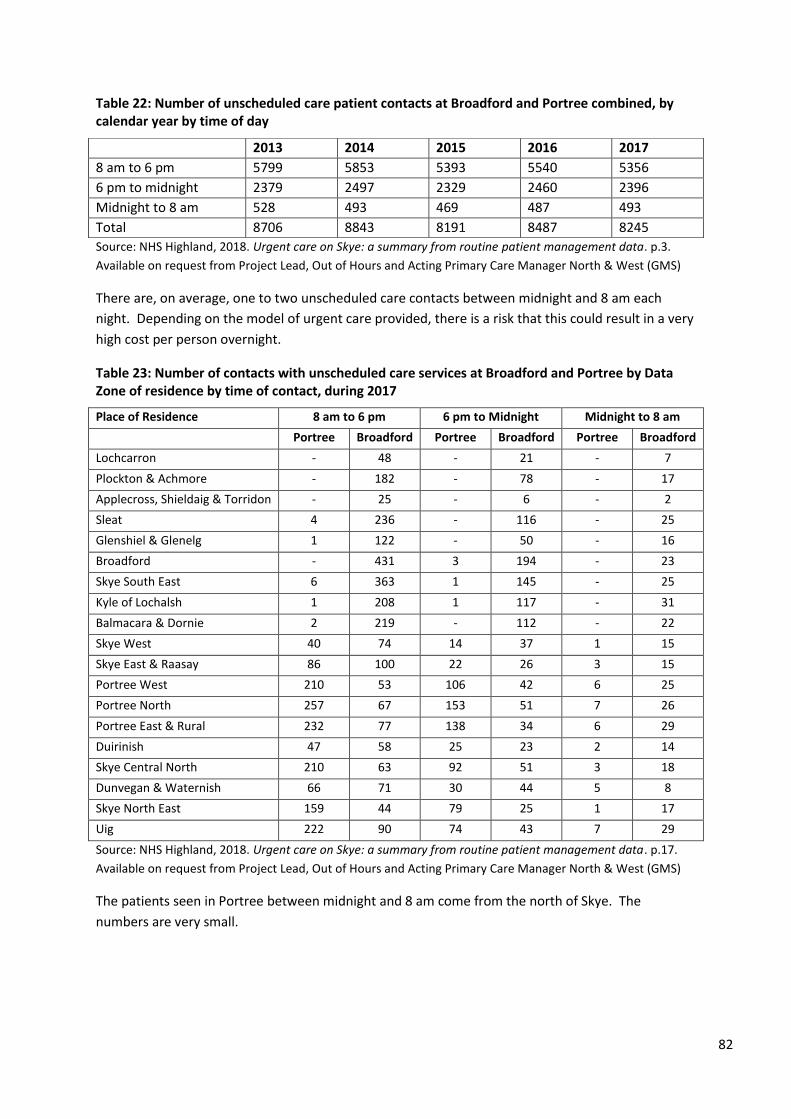
82
Table 22: Number of unscheduled care patient contacts at Broadford and Portree combined, by calendar year by time of day
Source: NHS Highland, 2018. Urgent care on Skye: a summary from routine patient management data. p.3.
Available on request from Project Lead, Out of Hours and Acting Primary Care Manager North & West (GMS)
There are, on average, one to two unscheduled care contacts between midnight and 8 am each
night. Depending on the model of urgent care provided, there is a risk that this could result in a very
high cost per person overnight.
Table 23: Number of contacts with unscheduled care services at Broadford and Portree by Data Zone of residence by time of contact, during 2017
Place of Residence 8 am to 6 pm 6 pm to Midnight Midnight to 8 am
Portree Broadford Portree Broadford Portree Broadford
Lochcarron - 48 - 21 - 7
Plockton & Achmore - 182 - 78 - 17
Applecross, Shieldaig & Torridon - 25 - 6 - 2
Sleat 4 236 - 116 - 25
Glenshiel & Glenelg 1 122 - 50 - 16
Broadford - 431 3 194 - 23
Skye South East 6 363 1 145 - 25
Kyle of Lochalsh 1 208 1 117 - 31
Balmacara & Dornie 2 219 - 112 - 22
Skye West 40 74 14 37 1 15
Skye East & Raasay 86 100 22 26 3 15
Portree West 210 53 106 42 6 25
Portree North 257 67 153 51 7 26
Portree East & Rural 232 77 138 34 6 29
Duirinish 47 58 25 23 2 14
Skye Central North 210 63 92 51 3 18
Dunvegan & Waternish 66 71 30 44 5 8
Skye North East 159 44 79 25 1 17
Uig 222 90 74 43 7 29
Source: NHS Highland, 2018. Urgent care on Skye: a summary from routine patient management data. p.17.
Available on request from Project Lead, Out of Hours and Acting Primary Care Manager North & West (GMS)
The patients seen in Portree between midnight and 8 am come from the north of Skye. The
numbers are very small.
2013 2014 2015 2016 2017
8 am to 6 pm 5799 5853 5393 5540 5356
6 pm to midnight 2379 2497 2329 2460 2396
Midnight to 8 am 528 493 469 487 493
Total 8706 8843 8191 8487 8245
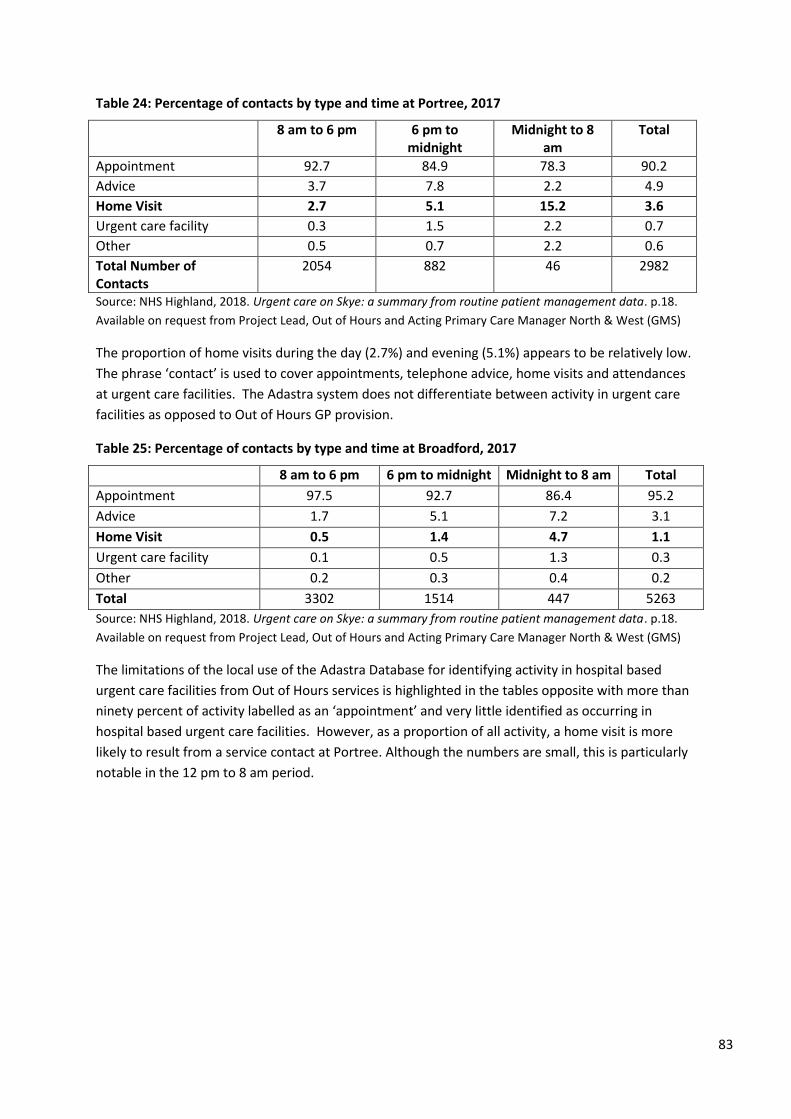
83
Table 24: Percentage of contacts by type and time at Portree, 2017
8 am to 6 pm 6 pm to midnight
Midnight to 8 am
Total
Appointment 92.7 84.9 78.3 90.2
Advice 3.7 7.8 2.2 4.9
Home Visit 2.7 5.1 15.2 3.6
Urgent care facility 0.3 1.5 2.2 0.7
Other 0.5 0.7 2.2 0.6
Total Number of Contacts
2054 882 46 2982
Source: NHS Highland, 2018. Urgent care on Skye: a summary from routine patient management data. p.18.
Available on request from Project Lead, Out of Hours and Acting Primary Care Manager North & West (GMS)
The proportion of home visits during the day (2.7%) and evening (5.1%) appears to be relatively low.
The phrase ‘contact’ is used to cover appointments, telephone advice, home visits and attendances
at urgent care facilities. The Adastra system does not differentiate between activity in urgent care
facilities as opposed to Out of Hours GP provision.
Table 25: Percentage of contacts by type and time at Broadford, 2017
8 am to 6 pm 6 pm to midnight Midnight to 8 am Total
Appointment 97.5 92.7 86.4 95.2
Advice 1.7 5.1 7.2 3.1
Home Visit 0.5 1.4 4.7 1.1
Urgent care facility 0.1 0.5 1.3 0.3
Other 0.2 0.3 0.4 0.2
Total 3302 1514 447 5263
Source: NHS Highland, 2018. Urgent care on Skye: a summary from routine patient management data. p.18.
Available on request from Project Lead, Out of Hours and Acting Primary Care Manager North & West (GMS)
The limitations of the local use of the Adastra Database for identifying activity in hospital based
urgent care facilities from Out of Hours services is highlighted in the tables opposite with more than
ninety percent of activity labelled as an ‘appointment’ and very little identified as occurring in
hospital based urgent care facilities. However, as a proportion of all activity, a home visit is more
likely to result from a service contact at Portree. Although the numbers are small, this is particularly
notable in the 12 pm to 8 am period.
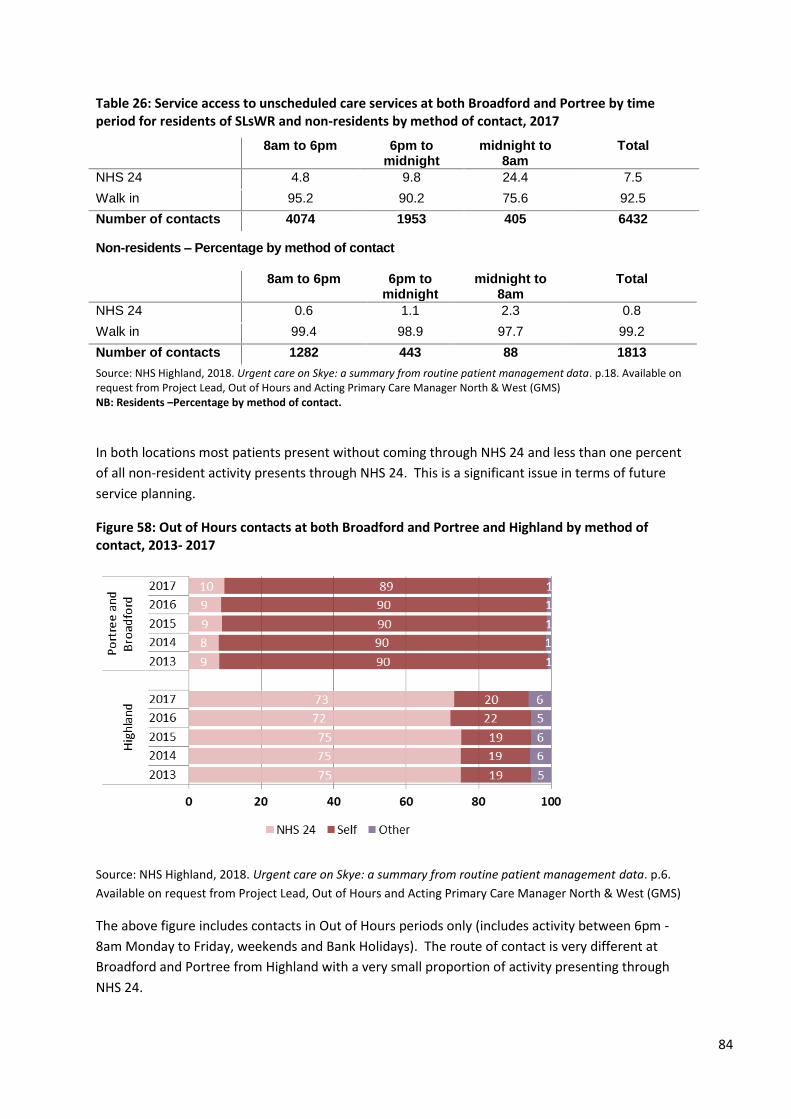
84
Table 26: Service access to unscheduled care services at both Broadford and Portree by time period for residents of SLsWR and non-residents by method of contact, 2017
8am to 6pm 6pm to midnight
midnight to 8am
Total
NHS 24 4.8 9.8 24.4 7.5
Walk in 95.2 90.2 75.6 92.5
Number of contacts 4074 1953 405 6432
Non-residents – Percentage by method of contact
8am to 6pm 6pm to midnight
midnight to 8am
Total
NHS 24 0.6 1.1 2.3 0.8
Walk in 99.4 98.9 97.7 99.2
Number of contacts 1282 443 88 1813
Source: NHS Highland, 2018. Urgent care on Skye: a summary from routine patient management data. p.18. Available on request from Project Lead, Out of Hours and Acting Primary Care Manager North & West (GMS) NB: Residents –Percentage by method of contact.
In both locations most patients present without coming through NHS 24 and less than one percent
of all non-resident activity presents through NHS 24. This is a significant issue in terms of future
service planning.
Figure 58: Out of Hours contacts at both Broadford and Portree and Highland by method of contact, 2013- 2017
Source: NHS Highland, 2018. Urgent care on Skye: a summary from routine patient management data. p.6.
Available on request from Project Lead, Out of Hours and Acting Primary Care Manager North & West (GMS)
The above figure includes contacts in Out of Hours periods only (includes activity between 6pm -
8am Monday to Friday, weekends and Bank Holidays). The route of contact is very different at
Broadford and Portree from Highland with a very small proportion of activity presenting through
NHS 24.
85
7. Conclusion
The aim of this briefing has been to provide epidemiological information that will help the Panel
meeting on 17 April 2018 to assess the resilience of urgent primary care out-of-hours provision and
to make recommendations in that regard. The briefing has considered: who receives care?; who
delivers care?; what care is delivered?; where is the care delivered?, and when is care utilised?
7.1 Limitations
As with all analysis of data, analysis often raises more questions than it answers. The focus of this
rapid compilation has been on existing data, which inevitably affects the areas that are covered. We
have not had access to raw ambulance data, which is key to understanding the pattern of Out of
Hours provision, but understand that the Scottish Ambulance Service may provide a report to the
panel. There is a need to triangulate analysis in relation to this service, as it can be argued that
primary responsibility for the delivery of out of hours emergency care rests with that service.
7.2 Main findings
In common with other rural areas, the Isle of Skye has an aging and scattered population. There is
some evidence of rural deprivation, based on a variety of metrics, which is likely to be associated
with raised levels of healthcare need.
It is difficult to recruit staff in Skye, as there is a relatively small working age population. Some
services lack resilience as they are dependent on small numbers of staff.
The area has a wide range of services, including primary care, community care and care based at
hospital faculties in both Broadford and Portree. Services face the challenge of providing 24 hour a
day care for relatively small numbers of patients spread over a very large geographic area, including
remote populations such as those on the mainland (e.g. Glenelg) and island communities (e.g.
Raasay).
Service utilisation between midnight and 8 am is relatively low, and the cost per case for such care is
likely to be very high whatever model of care is used. Innovative solutions may be required to
address this, involving working across traditional boundaries with other emergency services, using a
range of professionals, with high quality support from larger centres. There may also be a role for
first responders and community based responses, such as those developed in the Isle of Eigg.
86
8. Acknowledgements
I am grateful for input from Dr Cameron Stark, Liz Smart, Ian Douglas, Fiona MacPherson and
Michael Robb, all of whom work in the NHS Highland Public Health Directorate and who have helped
extensively with the development of this report. I am also grateful for input from Maimie
Thompson, Evan Beswick and colleagues in the operational units who contributed information.
The briefing draws heavily on previous reports developed within NHS Highland and the team who
have worked on the redesign of services for the population of Skye, Lochalsh and South West Ross.
I am grateful for the use of the picture on the front page under a creative commons licence. It is
taken from https://commons.wikimedia.org/wiki/File:Skye_Road_Sign_Sheep_01.jpg
Version control
For version control purposes this is version 0.94 of:
Van Woerden HC, Rideout RA. Public health statistical appendix, Out of Hours care in Skye, Lochalsh
and South West Ross. Inverness: NHS Highland. 16 April 21082018.

87
9. References
Carers UK, 2010. Tipping point for care: time for a new social contract. Available from:
http://www.carersuk.org/professionals/resources/research-library/item/495-tipping-point-for-care-time-for-a-new-social-
contract. Accessed 11 April 18.
Douglas, I. and Thomas, C., 2015. Supporting the Highland Community Planning Partnership to
identify areas of rural population need. NHS Highland and Highland Council. Published within:
Highland Community Planning Partnership (CPP) Board meeting 3 June 2015 – Item 8: Deprivation
and Inequalities – Rural Analysis; Annex 2. Available online:
https://www.highland.gov.uk/meetings/meeting/3466/highland_community_planning_partnership_board
Douglas, I., 2013. Place of death in NHS Highland. NHS Highland, Public Health Intelligence and
Knowledge Team. p.20, Figure 15
Douglas, I., 2013. Population drive time access to Community Hospitals in Skye & Lochalsh and South
West Ross. NHS Highland, Public Health Intelligence and Knowledge Team. Available online:
http://www.nhshighland.scot.nhs.uk/News/PublicConsultation/Skye/Documents/Drive%20time%20access%20SLSWR%20Nov%202013.pdf
Douglas, I., 2014. Income deprivation in Skye, Lochalsh and West Ross. NHS Highland Public Health
Intelligence and Knowledge Team. Available online:
http://www.nhshighland.scot.nhs.uk/News/PublicConsultation/Skye/Documents/Skye_incomedep.pdf
Douglas, I., 2014. Outpatient activity in Skye, Lochalsh and South West Ross, 2011-2013. NHS
Highland Public Health Intelligence and Knowledge Team. Available online:
http://www.nhshighland.scot.nhs.uk/News/PublicConsultation/Skye/Documents/Outpatient%20activity%20in%20Skye.pdf
Marshall, A., 2017. Projections of health care usage for Skye and Lochalsh. University of St Andrews.
McVicar, G., 2014. Summary presentation used at public meetings – Skye hospitals, summary of
current and possible future arrangements. NHS Highland. p.3. Available online:
http://www.nhshighland.scot.nhs.uk/News/PublicConsultation/Skye/Documents/Skye%20Hospitals%20-
%20Summary%20of%20current%20and%20future.pdf
NHS Highland and Highland Health and Social Care Partnership, 2016. Modernisation of community
and hospital services for communities in Skye, Lochalsh and South West Ross - Initial Agreement -
Version 26. Available online:
http://www.nhshighland.scot.nhs.uk/News/PublicConsultation/Skye/Documents/SLWR%20IA%20V26%2010Oct16.pdf
NHS Highland Public Health Intelligence, 2017. Highland Community Partnership Profile – Skye,
Lochalsh & Wester Ross. Data source: National Records of Scotland Small Area Population Estimates;
Best fit of data zones 2001 and 2011 to Highland Community Partnership area.
NHS Highland, 2014. Full public consultation document - Proposed modernisation of community and
hospital services in Skye, Lochalsh and South West Ross. Available online:
http://www.nhshighland.scot.nhs.uk/News/PublicConsultation/Skye/Documents/SLWR%20%20FINAL%20FULL%2019%20May%2014.pdf
88
NHS Highland, 2014. Report to Board Item 4.1: Proposed redesign of services in Syke, Lochalsh and
South West Ross. Available online:
http://www.nhshighland.scot.nhs.uk/Meetings/BoardsMeetings/Documents/Board%20Meeting%202%20December%202014/4.1%20Redes
ign%20of%20Services%20SLSWR.pdf
NHS Highland, 2017. Outline Business Case, The Modernisation of Community and Hospital Services
in Badenoch & Strathspey (B&S) and Skye, Lochalsh and South West Ross (SLsWR). Available online:
http://www.nhshighland.scot.nhs.uk/Meetings/BoardsMeetings/Documents/November%202017/4.5%20Outline%20Business%20Case%20B
S%20and%20SLSWR.pdf
NHS Highland, 2017. The Annual Report of the Director of Public Health – Realistic Medicine. p32.
Available online: http://www.nhshighland.scot.nhs.uk/Publications/Documents/DPH-Annual-Report-2017_(web-version).pdf
NHS Highland, 2017. Urgent Care – Data Summary for Skye. Prepared by Project Lead, Out of Hours
and Acting Primary Care Manager North & West (GMS) from ADASTRA patient management system.
NHS Highland, 2018. Terms of Reference, External view of arrangements for Unscheduled Care
(urgent primary care out-of-hours provision) in Skye, Lochalsh and South West Ross. Available online:
http://www.nhshighland.scot.nhs.uk/News/PublicConsultation/Skye/Documents/1%20OOHs%202018/SkyeNHS%20HighlandReviewTOR160
118_Final.pdf
NHS Highland, 2018. Urgent care on Skye: a summary from routine patient management data.
Available on request from Project Lead, Out of Hours and Acting Primary Care Manager North &
West (GMS)
O’Donnell, C., Foster, H., Macdonald, S., Burns, N. & Gannon, M., 2015. Out-of-Hours Primary
Medical Care: What Can Research Tell Us? Findings From a Rapid Systematic Review and Qualitative
Study. University of Glasgow. Available online: http://www.gov.scot/Resource/0049/00492082.pdf [Accessed 9
April 2018].
Ritchie, L., 2015. Pulling together: Transforming Urgent Care for the People of Scotland. The Report
of the Independent Review of Primary Care Out of Hours Services. Edinburgh: Scottish Government.
Available online: http://www.gov.scot/Resource/0049/00490526.pdf
Scottish Ambulance Service, 2018. Out of Hours Provision on Skye. Briefing provided to Scottish
Government.
Vaughan, S., 2015. Internal paper - Redesign of services in Skye, Lochalsh and South West Ross:
Analysis of the Scottish Ambulance data sent in response to a FOI request. NHS Highland Public
Health Epidemiology Team.
1
Advanced Nurses and Advanced Paramedics
Competency Framework and Training Toolkit
WARNING: Document uncontrolled when printed
Policy reference: Advanced Practice Date of Issue: May 2017
Prepared by: Claire Savage Date of Review:
Lead Reviewer: Version: 1
Authorised by: NMAHP Workforce Planning Steering Group
Date: 24th April 2017
EQIA(Equality Impact Assessments): EQIA Date:
Distribution: NHSH OOH Education Working Group NHSH NMAHP Leadership Group Director of Operations for Unit wide management distribution OOH Guiding Team UCP/AP Network
Method: CD-Rom Email Paper Intranet
Please consider your environmental responsibility
before printing this document.
Unscheduled Care
2
Contents
Introduction ........................................................................................................................................................ 4
Overview ......................................................................................................................................................... 5
Getting Started: Checklist for Employing Managers/Mentors ....................................................................... 6
Getting Started: Checklist for New Practitioners ........................................................................................... 7
Learning Agreement ........................................................................................................................................... 8
What, why and how: The NHS Highland Advanced Practice Education Plan ................................................... 10
Building a Portfolio ....................................................................................................................................... 13
Skills/Training matrix for Advanced Practitioners ........................................................................................ 15
Capability Framework ................................................................................................................................... 20
The Induction Process ...................................................................................................................................... 23
The Core Elements of Induction ................................................................................................................... 25
Induction Checklist for Managers ................................................................................................................. 27
Induction Checklist for Employees ............................................................................................................... 34
Continuing Professional Development ............................................................................................................. 41
Appendix 1: NHS Highland Portfolio Assessment............................................................................................. 44
Appendix 2: Self Assessment Tool .................................................................................................................... 47
The Highland Competency Framework ........................................................................................................ 48
Appendix 3: Action Planning Tool ..................................................................................................................... 58
Appendix 4: Learning Log ................................................................................................................................. 60
Learning Log: Template ................................................................................................................................ 63
Appendix 5: Consultation Observation Tool .................................................................................................... 64
Appendix 6: Case-Based Discussion Tool ......................................................................................................... 67
Appendix 7: 360 Degree Multisource Feedback.............................................................................................. 68
Appendix 8: 360 Degree Multisource Patient Feedback ................................................................................. 70
Appendix 9: Significant Event Analysis (SEA) .................................................................................................... 71
Appendix 10: Assessment of Practitioner Attachments ................................................................................... 72
Appendix 11: Structured Reflection ................................................................................................................. 78
Appendix 12: Standard Offer Letter ................................................................................................................. 82
Appendix 13: Example Job Descriptions ........................................................................................................... 86
North & West, Advanced Nurse Practitioner (Unscheduled Care) .............................................................. 86
IMFOU: Unscheduled Care Nurse ................................................................................................................. 93
3
Introduction
4
Introduction
NHS Highland is working towards achieving the ambitions set out in “Better Health Better Care” in seeking to develop the capability, capacity and competence of their non-medical workforce. This Toolkit has been designed around the changing needs of delivering healthcare in the Highlands, specifically around the need to enable experienced nurses and paramedics to practice at advanced level. It is envisaged that this Toolkit will be used to guide Supervisors and support staff employed by NHS Highland as they identify, undertake and record appropriate learning experiences. Central to the thinking behind this toolkit is that the Advanced Nurse/Advanced Paramedic level of practice in Highland is consistent and accredited across a range of roles/settings.
Purpose The purpose of the toolkit is to support supervisors to facilitate staff working as, or towards, the Advanced Nurse or Advanced Paramedic role within NHS Highland, to demonstrate that they have achieved the level of capability & competence required by NHSH. Although the tool is primarily for supervisors, a checklist is provided to signpost the Advanced Nurse/Paramedic Practitioner to relevant sections. It is suggested that parts of the tool should be used alongside any more formal, academic learning that the Advanced Nurse/Paramedic may be undertaking, to underpin the achievement of clinical capability & competence.
Who will use the tool?
Mentors/Supervisors
Those involved in mentoring or supervising staff working as, or towards Advanced Nurse/Paramedic roles, to help assess, plan and structure individual learning experiences for these staff.
Staff working towards the Advanced Nurse/Paramedic role
These staff should use parts of the tool in conjunction with their planned learning experiences. The process of self assessment, action planning and achievement of competence will guide their journey towards achievement.
Staff already working as Advanced Nurses/Paramedics but not yet accredited as such
These staff can use the tool to demonstrate that they already perform at the required practice level.
Managers
Managers will be able to use the tool to identify learning needs within their team and to forward plan learning activities to address these. The tool will also be of value in ongoing and annual e KSF and PDP processes.
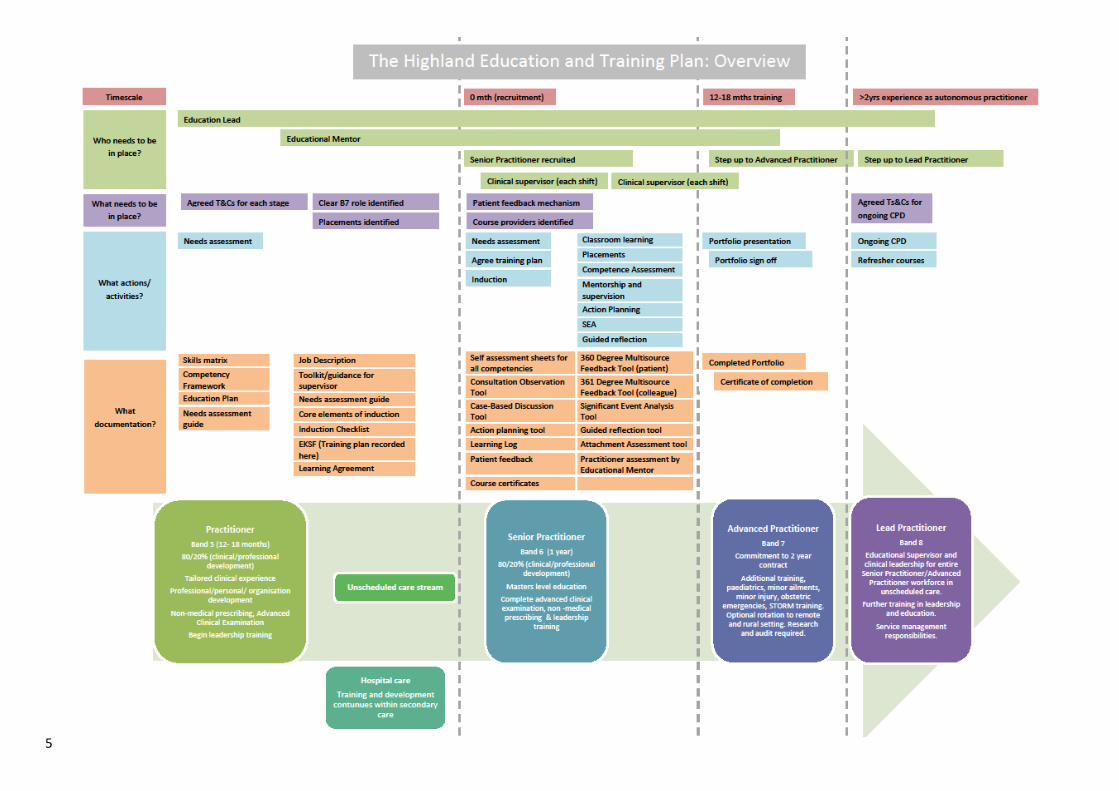
5
Overview

6
Getting Started: Checklist for Employing Managers/Mentors There is a lot to consider when supporting an employee through this training plan from recruitment, to portfolio sign-off. This checklist should help you get started.
Do you have…?
A mentor identified? Mentoring from a clinician is essential for individuals to progress through this plan.
An offer letter agreed? This should include e.g relevant Ts&Cs, on call requirement, base. An agreed standard offer letter is provided in Error! Not a valid result for table., page 64.
The correct Job Description Standard Job Descriptions for a range of roles are provided in Error! Reference source not found., Page 4
A current future job role identified Recruitment to training posts should be inkeeping with local workforce plans. We should not be training people unless they have a) current substantive roles in which they can continue to practice while training and b) identified Advanced level roles to enter once training/sign off is complete.
Next Steps With the above in place, here’s where you should start: Before Practitioner starts, or immediately after start:
1. Self assessment sent to practitioner for completion The start of the training process is for the practitioner to assess where they are in relation to the competency framework. There’s a Appendix 2: Self Assessment Tool on Page 47 to support this.
2. Practitioner returns self assessment 3. Induction
See Error! Reference source not found., Page Error! Bookmark not defined. As soon as possible after practitioner starts:
4. Practitioner and mentor and Education Lead agree a Training Action Plan This is the start of an ongoing discussion around how to meet training or experience needs. There’s an Appendix 3: Action Planning Tool on page 58 to support this. It’ll be a live document for the entirety of their training unless
a. The practitioner is employed in a B7 role, in which case this needs to be completed at least within the first three months
5. Practitioner begins Learning Log This supports the Action Planning Tool, and enables practitioners to begin collection reflections and evidence. There’s a template and guidance for keeping a Appendix 4: Learning Log on page 60.

7
Getting Started: Checklist for New Practitioners There is a lot to consider when embarking on the process towards accreditation as a Highland Advanced Nurse/Paramedic. This checklist should help you get started.
Do you have…?
A clear idea of your job role, banding and plan for a future role? You’ll either be employed as a Band 6 in a training post, or directly into a Band 7 role. Part of your training role may also be a substantive post e.g. in community nursing, to ensure your skills remain in use. You should agree this before you start.
Next Steps This gives you an overview. Relevant chapters are given so you can investigate requirements in more detail as required: Before you start, or immediately after you start
1. The first stage for any practitioner is a self assessment This enables practitioners to compare their skills and experience against the Highland Competency Framework. There’s a Appendix 2: Self Assessment Tool on Page 47 to support this.
2. Induction See Error! Reference source not found., Page Error! Bookmark not defined.
If you are in a training (band 6) role:
3. Discuss the self assessment with your mentor and Education Lead and agree a Training Action Plan This is the start of an ongoing discussion around how to meet training or experience needs. There’s an Appendix 3: Action Planning Tool on page 58 to support this. It’ll be a live document for the entirety of your training
4. Begin training activities and supervised practice
5. Collate evidence of learning and achievement to populate a portfolio This will include: Certificates; COTs; 360 feedback; Case Based Discussions; Reflective Log; an SEA; Assessment Forms.
6. Portfolio submitted and signed off This means you have fulfilled all of the requirements of accrediting as an Advanced Nurse/Paramedic in Highland. Ongoing CPD and yearly review.
If you are employed directly into an Advanced Nurse/Advanced Paramedic (band 7) role:
3. Discuss the self assessment with your mentor and Education Lead and identify any gaps There should be very few of these as you are already experienced and nearly ‘ready to go’
4. Collate evidence of learning and achievement to populate a portfolio This should be done at within your first three months or sooner. It will include evidence that your prior experience demonstrates that you fulfil the criteria.
5. Complete any missing training/experience 6. Portfolio submitted and signed off 7. Ongoing CPD and yearly review
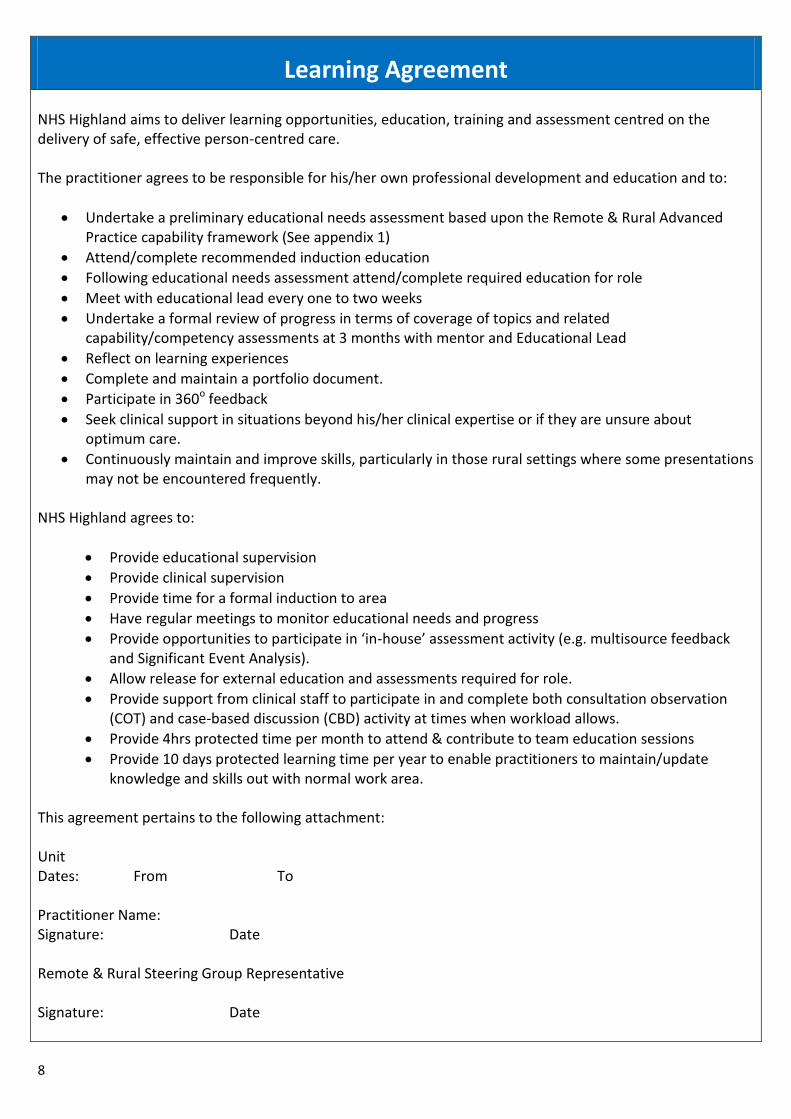
8
Learning Agreement NHS Highland aims to deliver learning opportunities, education, training and assessment centred on the delivery of safe, effective person-centred care. The practitioner agrees to be responsible for his/her own professional development and education and to:
Undertake a preliminary educational needs assessment based upon the Remote & Rural Advanced Practice capability framework (See appendix 1)
Attend/complete recommended induction education
Following educational needs assessment attend/complete required education for role
Meet with educational lead every one to two weeks
Undertake a formal review of progress in terms of coverage of topics and related capability/competency assessments at 3 months with mentor and Educational Lead
Reflect on learning experiences
Complete and maintain a portfolio document.
Participate in 360o feedback
Seek clinical support in situations beyond his/her clinical expertise or if they are unsure about optimum care.
Continuously maintain and improve skills, particularly in those rural settings where some presentations may not be encountered frequently.
NHS Highland agrees to:
Provide educational supervision
Provide clinical supervision
Provide time for a formal induction to area
Have regular meetings to monitor educational needs and progress
Provide opportunities to participate in ‘in-house’ assessment activity (e.g. multisource feedback and Significant Event Analysis).
Allow release for external education and assessments required for role.
Provide support from clinical staff to participate in and complete both consultation observation (COT) and case-based discussion (CBD) activity at times when workload allows.
Provide 4hrs protected time per month to attend & contribute to team education sessions
Provide 10 days protected learning time per year to enable practitioners to maintain/update knowledge and skills out with normal work area.
This agreement pertains to the following attachment: Unit Dates: From To Practitioner Name: Signature: Date Remote & Rural Steering Group Representative Signature: Date
9
The Highland Advanced Practice Education
Plan
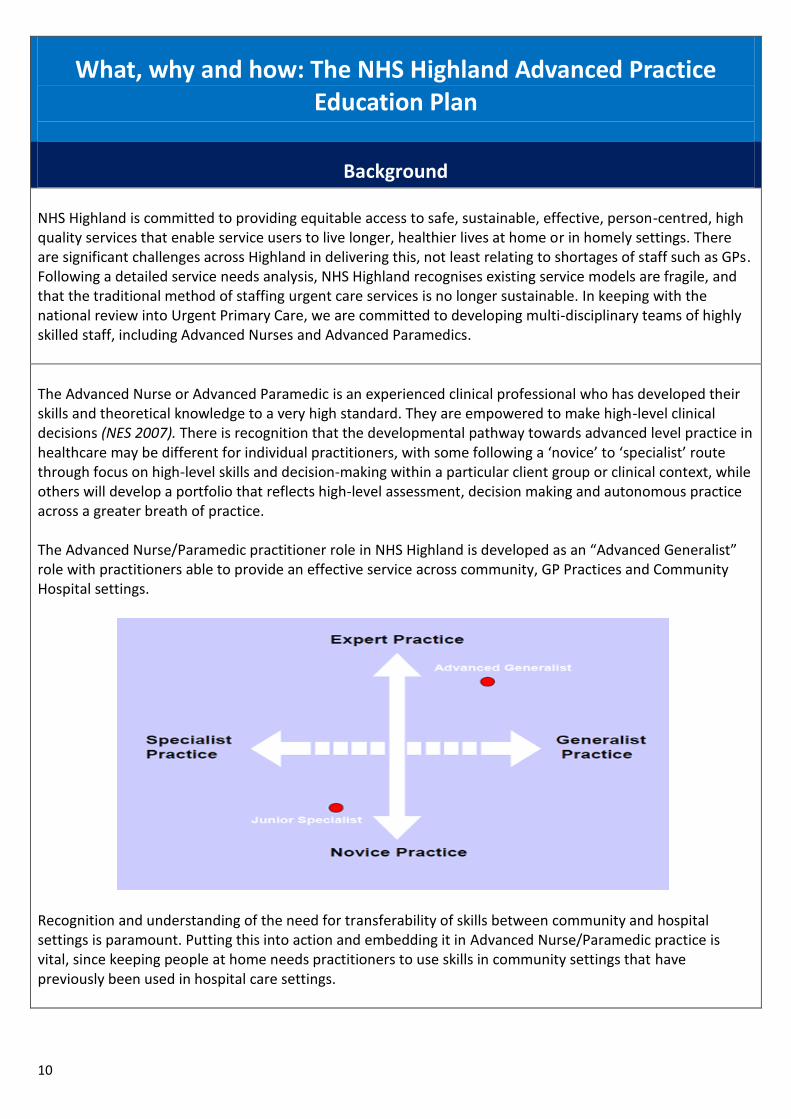
10
What, why and how: The NHS Highland Advanced Practice Education Plan
Background NHS Highland is committed to providing equitable access to safe, sustainable, effective, person-centred, high quality services that enable service users to live longer, healthier lives at home or in homely settings. There are significant challenges across Highland in delivering this, not least relating to shortages of staff such as GPs. Following a detailed service needs analysis, NHS Highland recognises existing service models are fragile, and that the traditional method of staffing urgent care services is no longer sustainable. In keeping with the national review into Urgent Primary Care, we are committed to developing multi-disciplinary teams of highly skilled staff, including Advanced Nurses and Advanced Paramedics.
The Advanced Nurse or Advanced Paramedic is an experienced clinical professional who has developed their skills and theoretical knowledge to a very high standard. They are empowered to make high-level clinical decisions (NES 2007). There is recognition that the developmental pathway towards advanced level practice in healthcare may be different for individual practitioners, with some following a ‘novice’ to ‘specialist’ route through focus on high-level skills and decision-making within a particular client group or clinical context, while others will develop a portfolio that reflects high-level assessment, decision making and autonomous practice across a greater breath of practice. The Advanced Nurse/Paramedic practitioner role in NHS Highland is developed as an “Advanced Generalist” role with practitioners able to provide an effective service across community, GP Practices and Community Hospital settings.
Recognition and understanding of the need for transferability of skills between community and hospital settings is paramount. Putting this into action and embedding it in Advanced Nurse/Paramedic practice is vital, since keeping people at home needs practitioners to use skills in community settings that have previously been used in hospital care settings.
11
An Advanced Nurse/Paramedic is a highly skilled professional who can:
Take a comprehensive patient history.
Carry out physical examinations.
Use their expert knowledge and clinical judgment to identify the potential diagnosis.
Refer service users for investigations where appropriate.
Make a final diagnosis.
Decide on and carry out treatment, including the prescribing of medicines, or refer patients to an
appropriate specialist
Use their extensive practice experience to plan and provide skilled and competent care to meet
Service user’s health and social care needs, involving other members of the integrated team as
appropriate
Ensure the provision of continuity of care including follow-up visits.
Assess and evaluate, with service users, the effectiveness of the treatment and care provided and
make changes as needed
Work independently, and also as part of a Team/ Rural Support team
Provide leadership
Make sure that each service user’s treatment and care is based on current best practice. Nursing & Midwifery Council Definition of the Advanced Nurse Practitioner (NMC, 2005)
It is acknowledged that potential Advanced Nurses/Paramedics may already have a wide range of relevant skills, knowledge and experience. Education and development will be based on the role requirements. Individual Personal Development Plans (PDP’s) will be key in identifying the appropriate learning and development required. Within NHS Highland relevant Masters level education is recommended (or equivalent experience). Advanced Practice is a level of practice rather than a specific role. For individuals currently working in or towards Advanced practice roles (that do not have a formal Masters level qualification), compiling a portfolio of learning and competence assessment can help practitioners to demonstrate their competence and capability. Or they may wish to put together a portfolio of evidence to demonstrate master’s level learning (mapping against the SCQF Masters level descriptors) and submit to a Higher Education institution for Recognition of Prior Learning. Crucially, NHSH recognises that educational provision supports the development and recognition of advanced practice capability in a practitioner. It prepares the practitioner to be able to fulfil the requirements and expectations of such a level of practice, but does not in itself grant the practitioner advanced practitioner ‘status’. Achieving and demonstrating competence, confidence and expertise in practice are also vital. NHSH Advanced Nurses/Paramedics will be required to demonstrate capability, competence, confidence and expertise in practice though the use of an Advanced Practice capability framework.
Aim By promoting person-centred, outcome-focused, safe, effective, quality care, and self-management, the education plan aims to develop multi-skilled Advanced Nurses/Paramedics. It will:
Utilise the Career Framework for Health (2008) at level 7. (People at this level have a critical awareness
12
of knowledge issues in the field and at the interface between different fields. They are innovative, and have a responsibility for developing and changing practice and /or services in a complex and unpredictable environment).
Create, or source, accessible training and appropriate education at Scottish Credit and Qualification Framework level 11 (MSc level).
Develop new, and utilise a collation of relevant advanced practice competency documents (NES 2013).
Link to the NHS Scotland Quality Strategy, the (NHS) Highland Quality Approach, NHS Highland Advanced Practice for Nurses, Midwives & Allied Health Professionals Policy, and is mapped to the NHS Career Framework & Knowledge and Skills Framework, the NMC Code of Conduct and the HCPC standards of conduct, performance, ethics and standards of continuing professional development.
Accredited Advanced Nurses/Paramedics will evidence previous experience and/or consolidation of practice, or can evidence an appropriate level of knowledge, demonstrating understanding and ability to deliver care in which:
Health and social care are integrated.
There is a major focus on prevention, anticipation and supported self-management.
Care is person centred and is provided to the highest standard of quality and safety.
Care is provided in the community unless hospital treatment is required.
If admitted to hospital, people get back to their home as soon as appropriate with minimal risk of re-admission.
Advanced Nurses/Paramedics will possess -- or have the opportunity to attain within an agreed timeframe (which will be agreed within the first 6 months) -- education at SCQF Level 11.
Outcomes/Results The Highland Education plan:
Supports Advanced Nurses/Paramedics education and role development within national guidelines and standards.
Effectively contributes toward meeting local health and social care needs.
Appropriately develops staff to enable effective opportunities for optimal independence within the service users’ environment.
Enables access to quality-assured transferable learning.
Enables application and consolidation of learning to practice.
Definitions of Clinical Supervision and Educational Mentor Clinical Supervisor “The clinical supervisor facilitates learning and supervises and assesses Practitioners/Learners in the practice setting". The clinical supervisor is an experienced practitioner who is willing and able to share their professional knowledge whilst working in partnership with a Practitioner/learner, and to guide and support the learner throughout the period of their particular learning with the intention of ensuring the well-being of patients/clients and the professional development of their learner. It is neither practical nor desirable for a clinical supervisor to work with the practitioner all the time.
13
However, the clinical supervisor should be familiar with the current progress and stage of development of the practitioner across the range of activity outlined in any learning needs assessment. The practitioner should aim to work with their clinical supervisor 1 to 2 days per week in order to assess progress and evaluate appropriately. Educational Lead The role of the educational mentor is to support and challenge the practitioner (through case-based discussion and reflection on practice) to deliver safe, effective, person-centred outcome focused care. The educational mentor supports the principles of clinical and educational governance and is an integral component of staff support and development. The educational mentor will also support staff in thinking and reflecting systematically on the contribution they can make to leading continuous service improvement that facilitates personal and community resilience.
Process You will be allocated a clinical supervisor who, for a period of time, will observe you doing specific clinical tasks/examinations, or consulting with specific patients using the skills checklist or the Consultation Observation Tool (COT). You will be required to discuss specific cases with your clinical supervisor and/or your educational mentor, or Clinical Lead. Keep an anonymised copy of the patient information (remove name, address, postcode and substitute age for date of birth) and ask that you discuss the case with the practitioner completing the Case Based Discussion (CBD). You will have designated time with your educational mentor on a regular basis. Using these methods it should be possible, over the course of the training period, to cover the range of skills, conditions and patient presentations. These assessments will build up into a portfolio of evidence that you are seen to be professionally competent by your peers. Should an assessment or review not be satisfactory in all areas, you will be required to discuss this with your educational mentor. This discussion should indicate a need for more training, more specific experience or additional reading/preparation. Within an agreed timeframe or once you feel confident you should arrange for that area to be reassessed.
Building a Portfolio Key to the progression of practitioners through the framework is the compilation, and presentation, of a portfolio demonstrating competence in all of the elements outlined in the competency framework. As practitioners undergo training courses, workplace learning, and their own reflection, this should be documented and collated for presentation. Portfolios are submitted to the NHS Highland Unscheduled Care Education and Training Group, who have governance responsibility for the process. A subgroup will assess the portfolio and provide feedback.
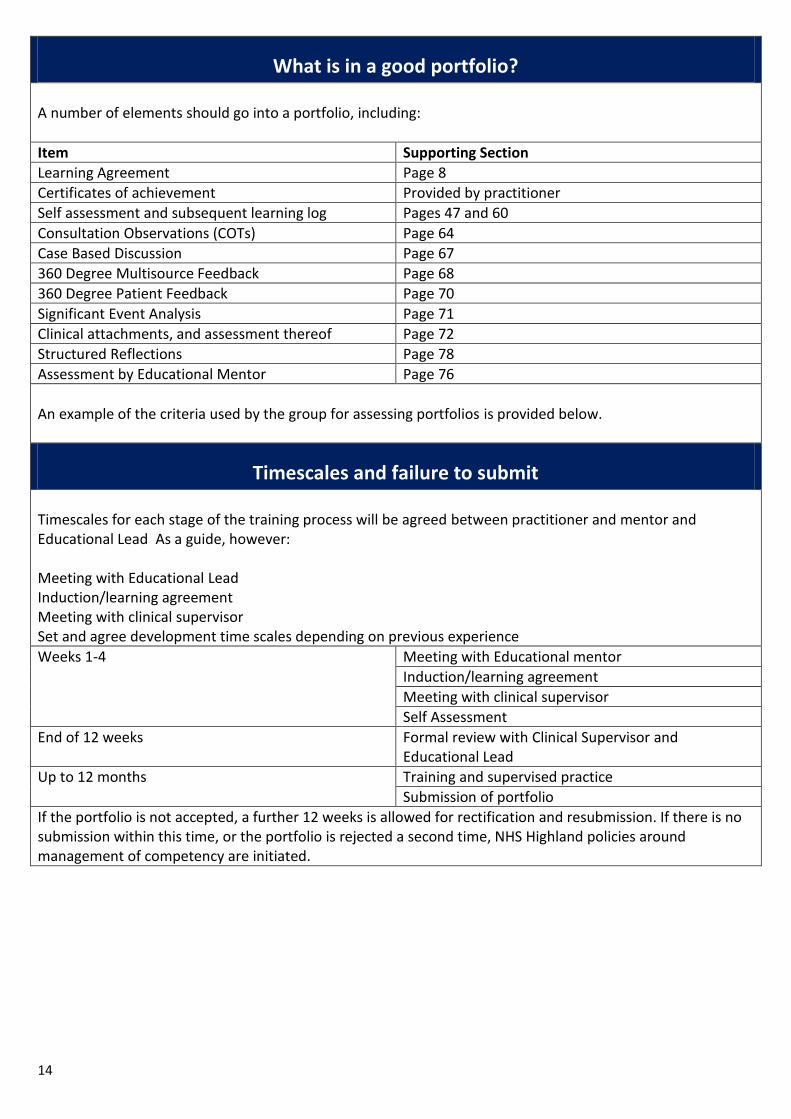
14
What is in a good portfolio? A number of elements should go into a portfolio, including:
Item Supporting Section
Learning Agreement Page 8
Certificates of achievement Provided by practitioner
Self assessment and subsequent learning log Pages 47 and 60
Consultation Observations (COTs) Page 64
Case Based Discussion Page 67
360 Degree Multisource Feedback Page 68
360 Degree Patient Feedback Page 70
Significant Event Analysis Page 71
Clinical attachments, and assessment thereof Page 72
Structured Reflections Page 78
Assessment by Educational Mentor Page 76
An example of the criteria used by the group for assessing portfolios is provided below.
Timescales and failure to submit Timescales for each stage of the training process will be agreed between practitioner and mentor and Educational Lead As a guide, however: Meeting with Educational Lead Induction/learning agreement Meeting with clinical supervisor Set and agree development time scales depending on previous experience
Weeks 1-4 Meeting with Educational mentor
Induction/learning agreement
Meeting with clinical supervisor
Self Assessment
End of 12 weeks Formal review with Clinical Supervisor and Educational Lead
Up to 12 months Training and supervised practice
Submission of portfolio
If the portfolio is not accepted, a further 12 weeks is allowed for rectification and resubmission. If there is no submission within this time, or the portfolio is rejected a second time, NHS Highland policies around management of competency are initiated.

15
Skills/Training matrix for Advanced Practitioners
A Skills Matrix has been devised which provides an overview of the different levels and scenarios of practice and, broadly, the elements of training which meet the needs of these roles. It enables read-across and recognises that different settings require different skills – though, largely, it demonstrates that many similar skills are required. The Capability Framework (see below) provides a much greater level of detail, and is used for assessment of practitioner capability.
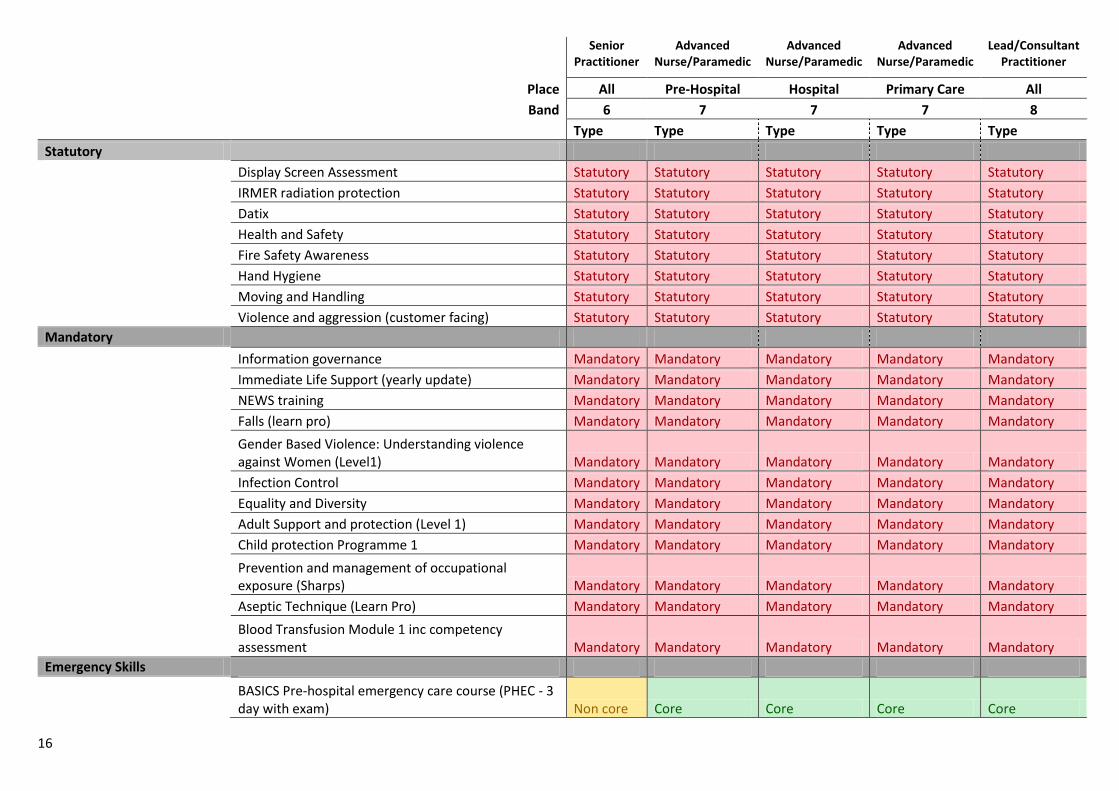
16
Senior Practitioner
Advanced Nurse/Paramedic
Advanced Nurse/Paramedic
Advanced Nurse/Paramedic
Lead/Consultant Practitioner
Place All Pre-Hospital Hospital Primary Care All
Band 6 7 7 7 8
Type Type Type Type Type
Statutory
Display Screen Assessment Statutory Statutory Statutory Statutory Statutory
IRMER radiation protection Statutory Statutory Statutory Statutory Statutory
Datix Statutory Statutory Statutory Statutory Statutory
Health and Safety Statutory Statutory Statutory Statutory Statutory
Fire Safety Awareness Statutory Statutory Statutory Statutory Statutory
Hand Hygiene Statutory Statutory Statutory Statutory Statutory
Moving and Handling Statutory Statutory Statutory Statutory Statutory
Violence and aggression (customer facing) Statutory Statutory Statutory Statutory Statutory
Mandatory
Information governance Mandatory Mandatory Mandatory Mandatory Mandatory
Immediate Life Support (yearly update) Mandatory Mandatory Mandatory Mandatory Mandatory
NEWS training Mandatory Mandatory Mandatory Mandatory Mandatory
Falls (learn pro) Mandatory Mandatory Mandatory Mandatory Mandatory
Gender Based Violence: Understanding violence against Women (Level1) Mandatory Mandatory Mandatory Mandatory Mandatory
Infection Control Mandatory Mandatory Mandatory Mandatory Mandatory
Equality and Diversity Mandatory Mandatory Mandatory Mandatory Mandatory
Adult Support and protection (Level 1) Mandatory Mandatory Mandatory Mandatory Mandatory
Child protection Programme 1 Mandatory Mandatory Mandatory Mandatory Mandatory
Prevention and management of occupational exposure (Sharps) Mandatory Mandatory Mandatory Mandatory Mandatory
Aseptic Technique (Learn Pro) Mandatory Mandatory Mandatory Mandatory Mandatory
Blood Transfusion Module 1 inc competency assessment Mandatory Mandatory Mandatory Mandatory Mandatory
Emergency Skills
BASICS Pre-hospital emergency care course (PHEC - 3 day with exam) Non core Core Core Core Core
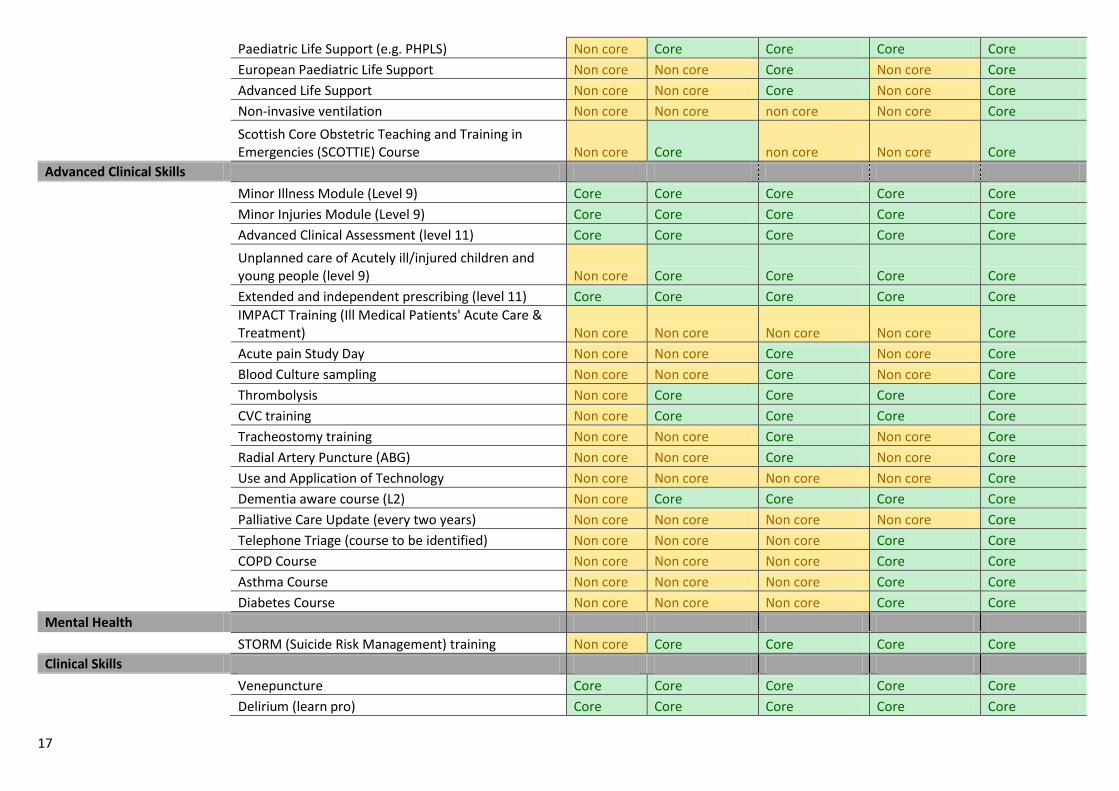
17
Paediatric Life Support (e.g. PHPLS) Non core Core Core Core Core
European Paediatric Life Support Non core Non core Core Non core Core
Advanced Life Support Non core Non core Core Non core Core
Non-invasive ventilation Non core Non core non core Non core Core
Scottish Core Obstetric Teaching and Training in Emergencies (SCOTTIE) Course Non core Core non core Non core Core
Advanced Clinical Skills
Minor Illness Module (Level 9) Core Core Core Core Core
Minor Injuries Module (Level 9) Core Core Core Core Core
Advanced Clinical Assessment (level 11) Core Core Core Core Core
Unplanned care of Acutely ill/injured children and young people (level 9) Non core Core Core Core Core
Extended and independent prescribing (level 11) Core Core Core Core Core
IMPACT Training (Ill Medical Patients' Acute Care & Treatment) Non core Non core Non core Non core Core
Acute pain Study Day Non core Non core Core Non core Core
Blood Culture sampling Non core Non core Core Non core Core
Thrombolysis Non core Core Core Core Core
CVC training Non core Core Core Core Core
Tracheostomy training Non core Non core Core Non core Core
Radial Artery Puncture (ABG) Non core Non core Core Non core Core
Use and Application of Technology Non core Non core Non core Non core Core
Dementia aware course (L2) Non core Core Core Core Core
Palliative Care Update (every two years) Non core Non core Non core Non core Core
Telephone Triage (course to be identified) Non core Non core Non core Core Core
COPD Course Non core Non core Non core Core Core
Asthma Course Non core Non core Non core Core Core
Diabetes Course Non core Non core Non core Core Core
Mental Health
STORM (Suicide Risk Management) training Non core Core Core Core Core
Clinical Skills
Venepuncture Core Core Core Core Core
Delirium (learn pro) Core Core Core Core Core
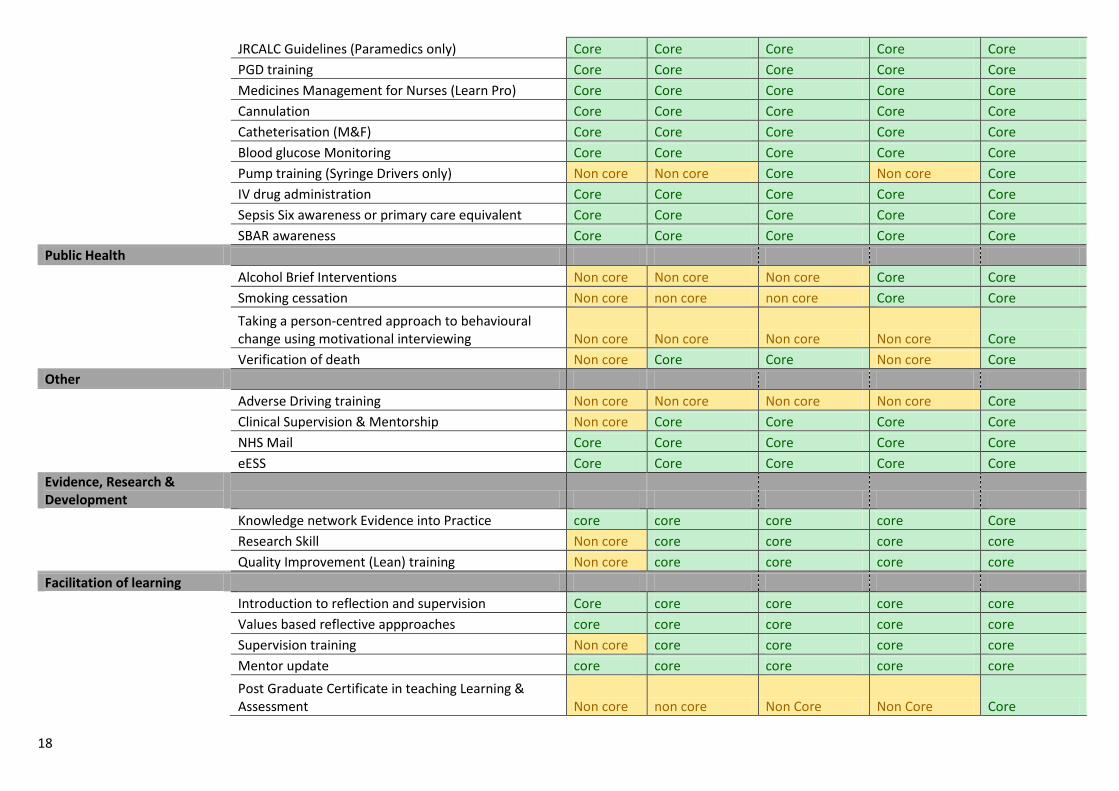
18
JRCALC Guidelines (Paramedics only) Core Core Core Core Core
PGD training Core Core Core Core Core
Medicines Management for Nurses (Learn Pro) Core Core Core Core Core
Cannulation Core Core Core Core Core
Catheterisation (M&F) Core Core Core Core Core
Blood glucose Monitoring Core Core Core Core Core
Pump training (Syringe Drivers only) Non core Non core Core Non core Core
IV drug administration Core Core Core Core Core
Sepsis Six awareness or primary care equivalent Core Core Core Core Core
SBAR awareness Core Core Core Core Core
Public Health
Alcohol Brief Interventions Non core Non core Non core Core Core
Smoking cessation Non core non core non core Core Core
Taking a person-centred approach to behavioural change using motivational interviewing Non core Non core Non core Non core Core
Verification of death Non core Core Core Non core Core
Other
Adverse Driving training Non core Non core Non core Non core Core
Clinical Supervision & Mentorship Non core Core Core Core Core
NHS Mail Core Core Core Core Core
eESS Core Core Core Core Core
Evidence, Research & Development
Knowledge network Evidence into Practice core core core core Core
Research Skill Non core core core core core
Quality Improvement (Lean) training Non core core core core core
Facilitation of learning
Introduction to reflection and supervision Core core core core core
Values based reflective appproaches core core core core core
Supervision training Non core core core core core
Mentor update core core core core core
Post Graduate Certificate in teaching Learning & Assessment Non core non core Non Core Non Core Core
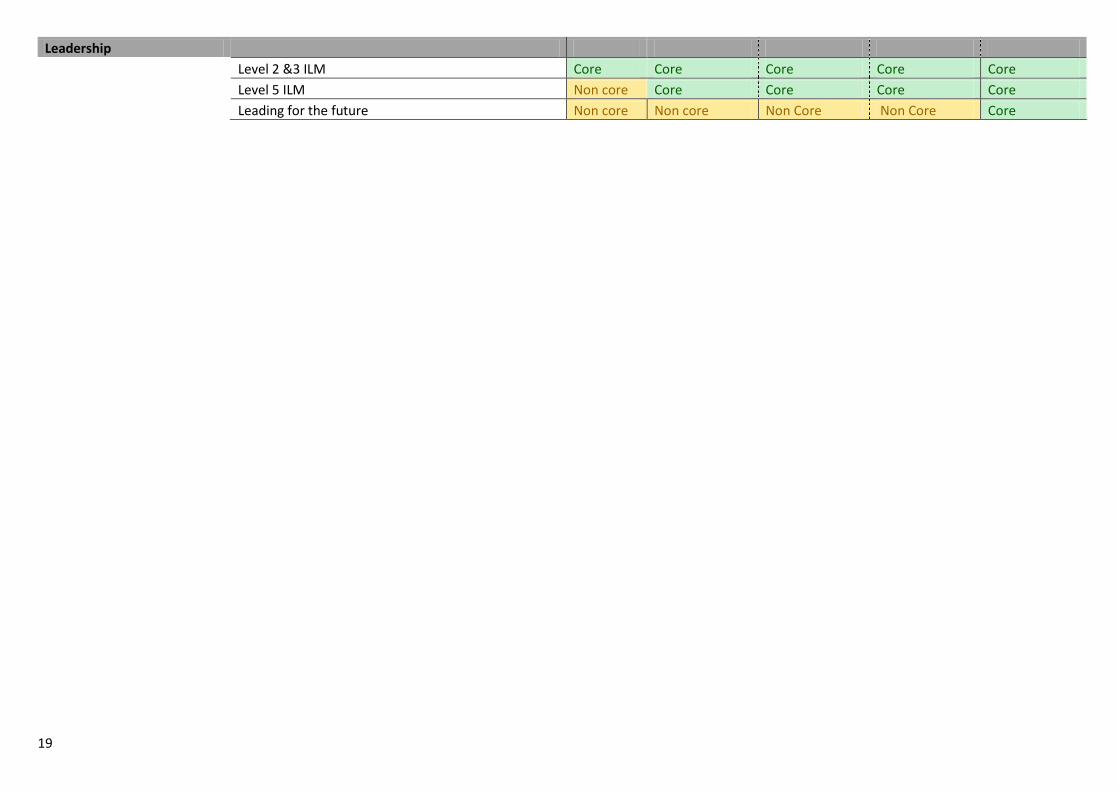
19
Leadership
Level 2 &3 ILM Core Core Core Core Core
Level 5 ILM Non core Core Core Core Core
Leading for the future Non core Non core Non Core Non Core Core
20
Capability Framework “Capability is associated with facilitating the continuous development of practitioners’ ability and potential and is an essential element of life-long learning and personal and professional development... The framework incorporates practice competencies to detail what practitioners should be able to achieve and to capture the notion of capability as current competence combined with the development of future potential competence.” P.2, RRHEAL (2014)
A The Highland Competency Framework, page 48, has been produced, devised from a collation of relevant advanced practice competency documents produced by (NES 2013). The capability framework consists of 4 Pillars of practice (See Appendix 2: Self Assessment Tool, p. 47) 1: Advanced clinical/professional practice. 2: Leadership. 3: Research & Development. 4: Facilitating Learning. A range of principles (adapted from the NES advanced practice succession planning programme 2007) run through and support the capability framework and competencies these are:
Autonomous practice: involves the freedom to exercise judgement about actions, in turn accepting responsibility for them, and being held to account.
Critical thinking: practising autonomously requires higher-level critical thinking skills. Critical thinking allows advanced practitioners to explore and analyse evidence, cases and situations in clinical practice, enabling a high level of judgement and decision-making.
High levels of decision-making and problem solving: an advanced practitioner is expected to demonstrate expertise in complex decision-making in relation to their role, including determining what to include in the decision-making process and making a decision based on judgement and critical thinking.
Values-based care: the advanced practitioner is required to have a high level of awareness of their own values and beliefs. Care is negotiated with service users, carers and families as equal partners.
Improving practice: it is important that advanced practitioners deliver advanced practice that is evidence based while acting as positive role models who enable change and practice/service improvement.
Types of Learning The elements which Advanced Nurses/Paramedics need to know for their current post and for development may fall into a range of categories including: Essential: Statutory/mandatory learning. Core: Education identified by NHSH as key to the Advanced role; needs identified through assessment of
21
capability using the capability framework, and the KSF development review. Non-Core: Education depending on setting, need or context, identifying what is needed for safe and appropriate role development.
References
Development of Rural Generic (Health and Social Care) Support Worker Roles May 2014 http://www.rrheal.scot.nhs.uk/what-we-do/reports/rgsw-orkney-.aspx RRHEAL Quality Assurance Guide http://www.rrheal.scot.nhs.uk/what-we-do/resources/quality-assurance-(qa)-guide-for-distributed-education.aspx NES (2007) Visible Accessible and Integrated Care Capability Framework for the Advanced Practitioner: Nursing in the community NES (2013) Remote & Rural Advanced Nurse Practitioner: Mapping of advanced level nursing competencies to support the development of the Rural Nurse Practitioner Role February 2013 NHS Education for Scotland (2007) Emergency Care in Scotland: A framework for Practice. NHS Education for Scotland (2009) Out of Hours Unscheduled Care Advanced Clinical Practice. NHS Highland Advanced Practice for Nurses, Midwives & Allied Health Professionals Policy 2012 NHS Highland Mandatory & Statutory Prospectus http://intranet.nhsh.scot.nhs.uk/Training/LearningAndDevelopment/Induction/Documents/Statutory%20and%20Mandatory%20Training%20Prospectus%20V5.0.pdf
22
The Induction Process
23
The Induction Process The following details the induction process in general and highlights the key responsibilities and actions necessary for an effective induction. The induction process begins with recruitment, continues into employment and ‘kick-starts’ the personal development planning and review process. All necessary forms are available on the intranet.
1. The Recruitment Process The Manager completes both Vacancy Form and Health Declaration Form and Job Specification and sends to Employment Services The vacancy is approved by the Workforce Group and the recruitment process commences The recruitment process takes place; a job offer is made subject to satisfactory employment checks as per NHS Highland Safer Pre and Post Employment Checks Policy Employment Services sends an Appointment Pack including Health Declaration Form and Job Specification and Staff Handbook to the successful candidate Successful candidate completes and returns the necessary paperwork including Health Declaration Form and Job Specification to Employment Services Employment Services sends Health Declaration Form and Job Specification to Occupational Health to establish fitness for employment
2. The Pre-Employment Process Occupational Health paper screen the health information declared on the Health Declaration Form and recommend appropriate vaccination, screening and baseline health surveillance work to the employee as required by Scottish Government directives (Note: On-going Occupational Health vaccination work may be required) Manager plans for the new employees arrival and: Notifies existing employees of new employee including start date Agrees roles and responsibilities of Buddy/ Mentor and others supporting the induction process Arranges key meetings, events and on the job training Identifies and books all necessary Statutory and Mandatory Training Produces employee induction plan Orders essential equipment and supplies Requests user name and passwords for systems
3. The first day of employment Manager welcomes new employee, provides introductions to immediate colleagues and to the working environment, discusses induction requirements, and provides information regarding basic policies and conduct. This should include the following health and safety information: Fire evacuation procedures Names and locations of first aiders The smoking policy Any job-specific health and safety information needed by employees immediately in order to carry out their tasks without risk Manager advises employee of statutory and mandatory requirements, and agrees necessary arrangements
24
with the employee to support their attendance at training and appointments with Occupational Health Manager discusses job role requirements using Job Description and NHS KSF Post Outline (where relevant
4. Within the first week of employment Manager to ensure the employee receives further information on the safe systems of work applicable to their job, essential policies and procedures, learn about the work of the department, meet key people and discuss their work programme and priorities. This should include the following in terms of health and safety:
The fundamentals of the Health and Safety Policy
Basic information on safe systems of work applicable to job role
Names and locations of staff with key health and safety responsibilities
Manager identifies and agrees learning and development needs with employee and buddy/mentor in line with appropriate framework, e.g. NHS Knowledge and Skills Framework (NHS KSF) and/or Health Care Support Workers Mandatory Induction Standards
5. Within the first month of employment Manager to ensure the employee has a fuller understanding of their job role within the department and NHS Highland, aware of the standards expected, and attends necessary statutory and mandatory training
6. Within three months of employment Employee to complete induction process Employee to complete Induction Evaluation Questionnaire and send to the Learning and Development Team Manager and employee to discuss and agree a personal development plan in line with appropriate system, e.g. NHS KSF Manager to continue to provide guidance on areas with which the employee is still not familiar Employee to sign up to Code of Practice where appropriate, e.g. Health Care Support Workers
7. Within six months of employment Employee to meet all statutory and mandatory requirements Manager and Employee to have an informal development review discussion of the employees work against the requirements of their post
8. At the end of the first year Manager and employee to discuss and agree a personal development plan in line with appropriate system, e.g. NHS KSF
25
The Core Elements of Induction
1. Core Elements The following identifies the core elements that should be the focus of induction. Each element emphasises the entitlement of the employee to a robust, fit for purpose, induction programme. Provide a welcoming environment for the employee Provide an introduction to Manager and colleagues Explanation of management structure Explanation of tasks, duties and responsibilities Explanation of relationship of job to others Explanation of learning opportunities and the development review process Physical tour of premises and location of facilities Explanation of terms and conditions of employment Explanation of the culture and values of the NHS Explanation of communication channels Explanation of effective team working Explanation of emergency arrangements including fire, first aid, spillages etc. Explanation of accident and incident reporting procedures Explanation of hazard reporting and obtaining help on health and safety matters Explanation of relevant personal protective equipment Explanation of what is expected in terms of employee conduct Explanation of statutory and mandatory training requirements and how these are to be met Explanation of Occupational, Health and Safety requirements and how these are applied to the workplace/job role Explanation of policies, procedures, guidelines and protocols that guide the employees practice Explanation of Confidentiality and Data Protection guidelines Explanation of European Working Time Directive This list is not exhaustive and others will also need to be considered. It is the manager’s responsibility to decide what level of information and instruction is necessary to ensure the core elements of induction are sufficiently covered in relation to the individual’s job role and working environment.
2. Methods of delivery There is a degree of judgement of the most appropriate method and level of delivery required. The range of methods generally considered effective in providing successful induction includes the following: One to one briefings Visits and tours Meeting with key people Group events Formal presentations Literature/documentation Computer based, e.g. e-learning Workbooks Self-directed learning
Shadowing Coaching Supervision Mentoring Practical skills Checklists Self and Peer Review Buddy
26
It is the manager’s responsibility to decide which methods are appropriate to ensure induction is both successful and effective.
3. Criteria for choosing methods Research indicates that induction is most successful if a variety of methods are available to take account of: Physical location, whether urban or remote and rural or a mixture of both The nature of the job Whether the inductee is new to the job, department, and/or organisation Differing learning styles Availability, especially for part-time workers or people working ‘unsocial’ hours If there are any equal opportunities or accessibility issues, e.g. representatives from ethnic minorities may have different cultural issues, there may be language issues for those with English as a second language, or there may be physical access issues or specific communication requirements If there is a group intake of new staff If a new team is being set up The manager is responsible for an employee's induction, but would not be expected to cover all the elements personally. A typical allocation of induction tasks could be: Manager/supervisor: explain the departmental organisation, requirements of the job, limitations of the role, health and safety, terms and conditions of employment, the personal development review process, and then help to develop a personal development plan and provide details of other sources of information and support during induction Supervisor or a nominated colleague: provide an escorted tour of the department and introduce colleagues; then give day-to-day guidance in local procedures for the first couple of weeks Senior manager(s): give an overview of the organisation and its values, quality systems and culture Mentor or 'buddy': an experienced colleague to act as point of contact, to support and enhance the induction process and the personal development of the employee.
27
Induction Checklist for Managers
This checklist considers the induction process from start to finish; beginning with the recruitment process, continuing into employment, through to the development review process. It includes examples of tasks that you should complete at each stage of the process to ensure an effective and robust induction.
Section 1: Pre-employment Checklist Section 2: The first day checklist Section 3: The first week checklist
Section 4: The first month checklist Section 5: The first three months checklist
The timescales have been identified as a guide only. These can be amended depending on individual requirements based on local risk assessment. Elements of health and safety should be covered as a priority to minimise risk to staff, patients and other people affected by the employees work. Ultimately you as the Manager will decide what is required to meet all statutory and mandatory requirements, ensuring individuals are supported to undertake the induction process and take forward any reasonable adjustments required. Once complete, this form must be retained in the employee’s personal file for future reference.
Employee Details Name: ………………………………………………………………………… Job Title: ……………………………………………………………………………….. Department: ……………………………………………………………………………………………… Start Date: ……………………………………………….. Buddy / Mentor Details Name: ………………………………………………………………………… Job Title: ………………………………………………………………………………..
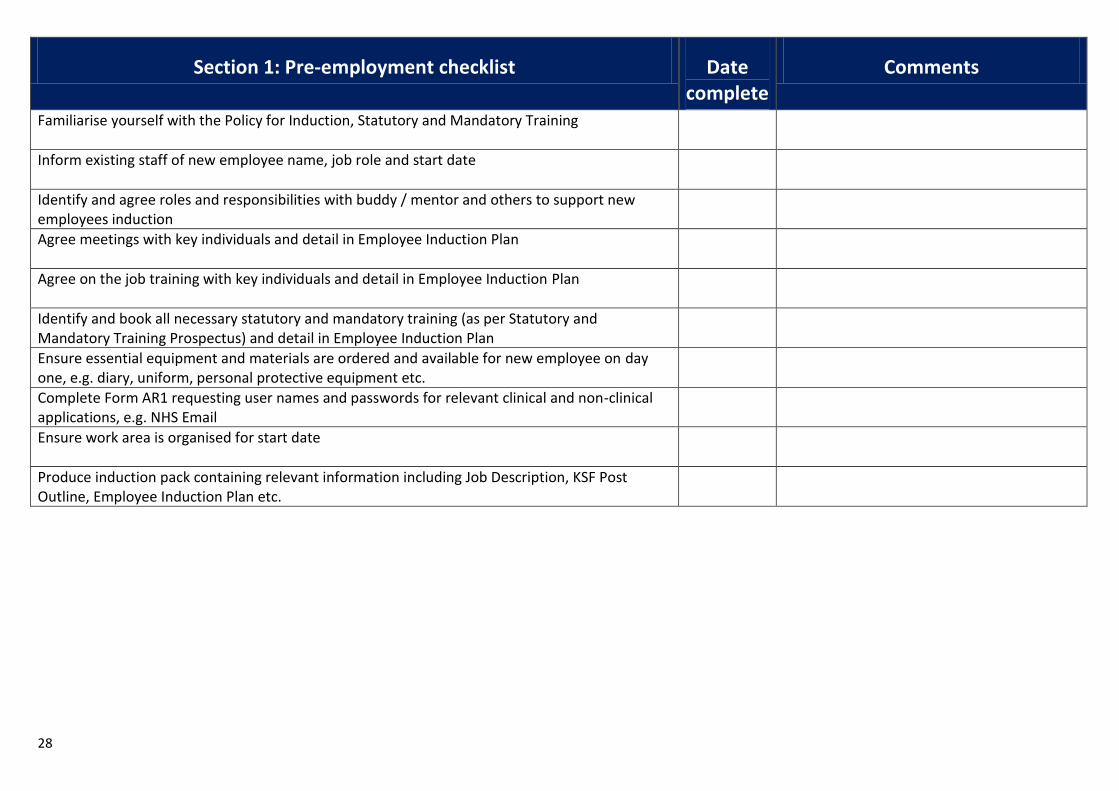
28
Section 1: Pre-employment checklist Date complete
Comments
Familiarise yourself with the Policy for Induction, Statutory and Mandatory Training
Inform existing staff of new employee name, job role and start date
Identify and agree roles and responsibilities with buddy / mentor and others to support new employees induction
Agree meetings with key individuals and detail in Employee Induction Plan
Agree on the job training with key individuals and detail in Employee Induction Plan
Identify and book all necessary statutory and mandatory training (as per Statutory and Mandatory Training Prospectus) and detail in Employee Induction Plan
Ensure essential equipment and materials are ordered and available for new employee on day one, e.g. diary, uniform, personal protective equipment etc.
Complete Form AR1 requesting user names and passwords for relevant clinical and non-clinical applications, e.g. NHS Email
Ensure work area is organised for start date
Produce induction pack containing relevant information including Job Description, KSF Post Outline, Employee Induction Plan etc.
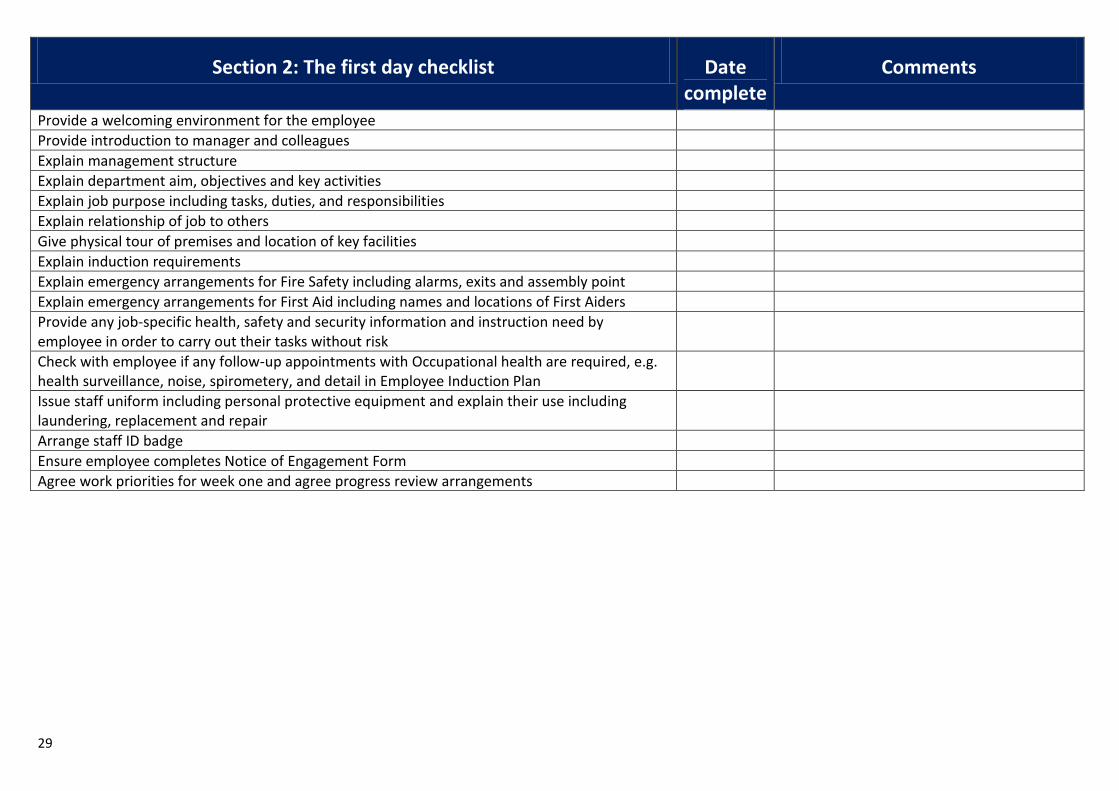
29
Section 2: The first day checklist Date complete
Comments
Provide a welcoming environment for the employee
Provide introduction to manager and colleagues
Explain management structure
Explain department aim, objectives and key activities
Explain job purpose including tasks, duties, and responsibilities
Explain relationship of job to others
Give physical tour of premises and location of key facilities
Explain induction requirements
Explain emergency arrangements for Fire Safety including alarms, exits and assembly point
Explain emergency arrangements for First Aid including names and locations of First Aiders
Provide any job-specific health, safety and security information and instruction need by employee in order to carry out their tasks without risk
Check with employee if any follow-up appointments with Occupational health are required, e.g. health surveillance, noise, spirometery, and detail in Employee Induction Plan
Issue staff uniform including personal protective equipment and explain their use including laundering, replacement and repair
Arrange staff ID badge
Ensure employee completes Notice of Engagement Form
Agree work priorities for week one and agree progress review arrangements
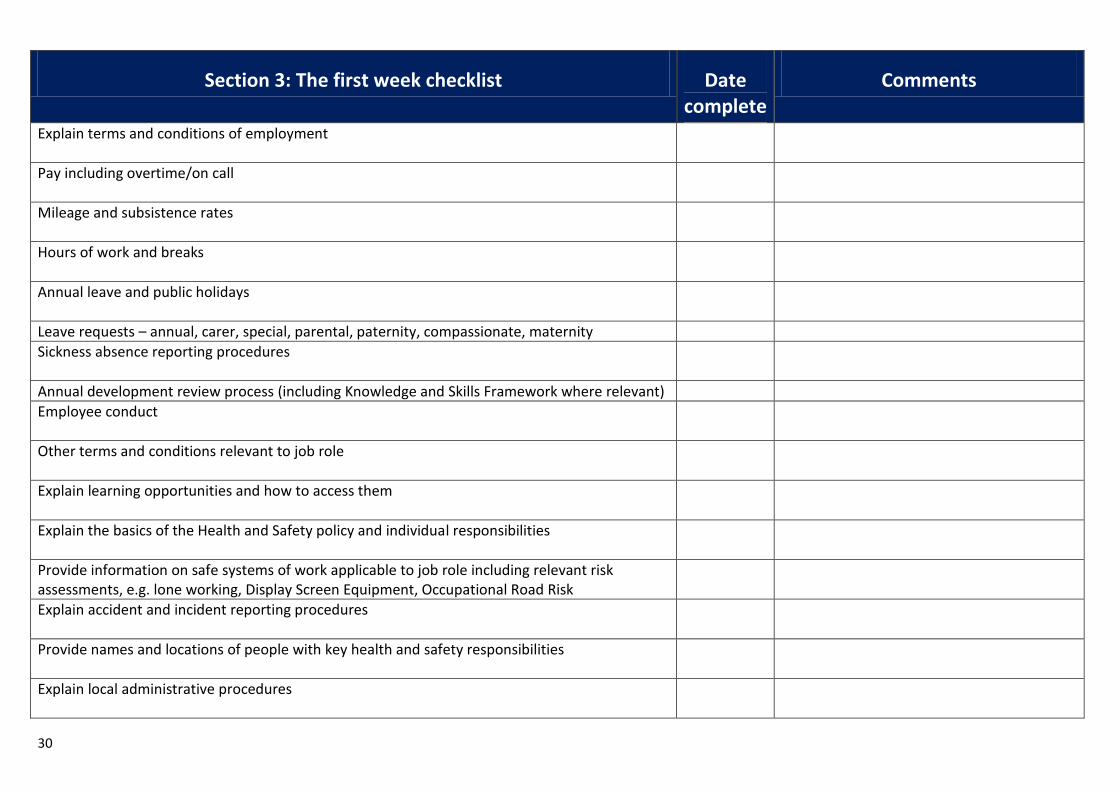
30
Section 3: The first week checklist Date complete
Comments
Explain terms and conditions of employment
Pay including overtime/on call
Mileage and subsistence rates
Hours of work and breaks
Annual leave and public holidays
Leave requests – annual, carer, special, parental, paternity, compassionate, maternity
Sickness absence reporting procedures
Annual development review process (including Knowledge and Skills Framework where relevant)
Employee conduct
Other terms and conditions relevant to job role
Explain learning opportunities and how to access them
Explain the basics of the Health and Safety policy and individual responsibilities
Provide information on safe systems of work applicable to job role including relevant risk assessments, e.g. lone working, Display Screen Equipment, Occupational Road Risk
Explain accident and incident reporting procedures
Provide names and locations of people with key health and safety responsibilities
Explain local administrative procedures
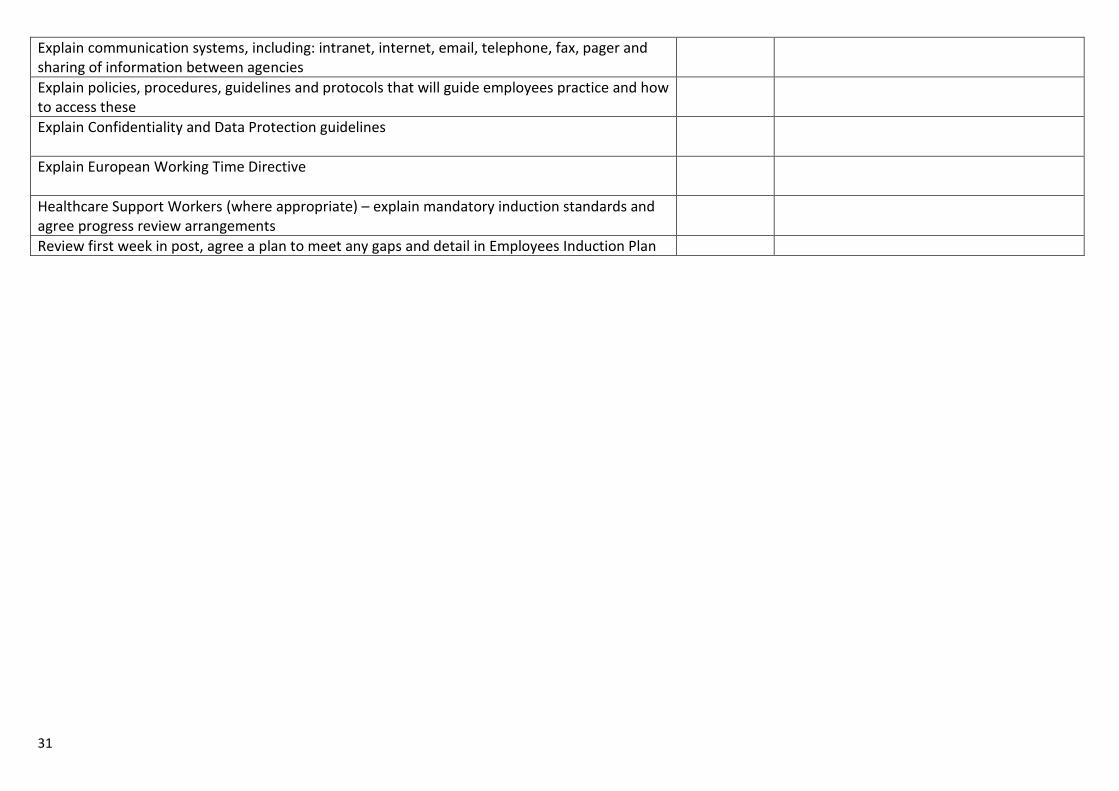
31
Explain communication systems, including: intranet, internet, email, telephone, fax, pager and sharing of information between agencies
Explain policies, procedures, guidelines and protocols that will guide employees practice and how to access these
Explain Confidentiality and Data Protection guidelines
Explain European Working Time Directive
Healthcare Support Workers (where appropriate) – explain mandatory induction standards and agree progress review arrangements
Review first week in post, agree a plan to meet any gaps and detail in Employees Induction Plan

32
Section 4: The first month checklist Date complete
Comments
Explain effective team working
Explain sources of information including, intranet, newsletters, notice boards, web sites etc.
Check with buddy/mentor how the employee has been progressing, and that the buddy/mentor has been providing relevant feedback and facilitating reflection on practice, performance and experiences of the employee and amended the Employees Induction Plan as necessary
Check employee has a fuller understanding of their role within the department and aware of the standards expected and provide guidance on areas with which employee is unfamiliar
Check employee is attending statutory and mandatory training and discuss how they may apply the learning in the workplace
Agree date for first development review meeting (3 months in post)
Explain complaints management procedure
Explain how to raise employees concerns
Explain Fraud Policy
Explain how to access translation and interpretation services
Review subsequent weeks in post, agree a plan to meet any gaps and detail in Employees Induction Plan
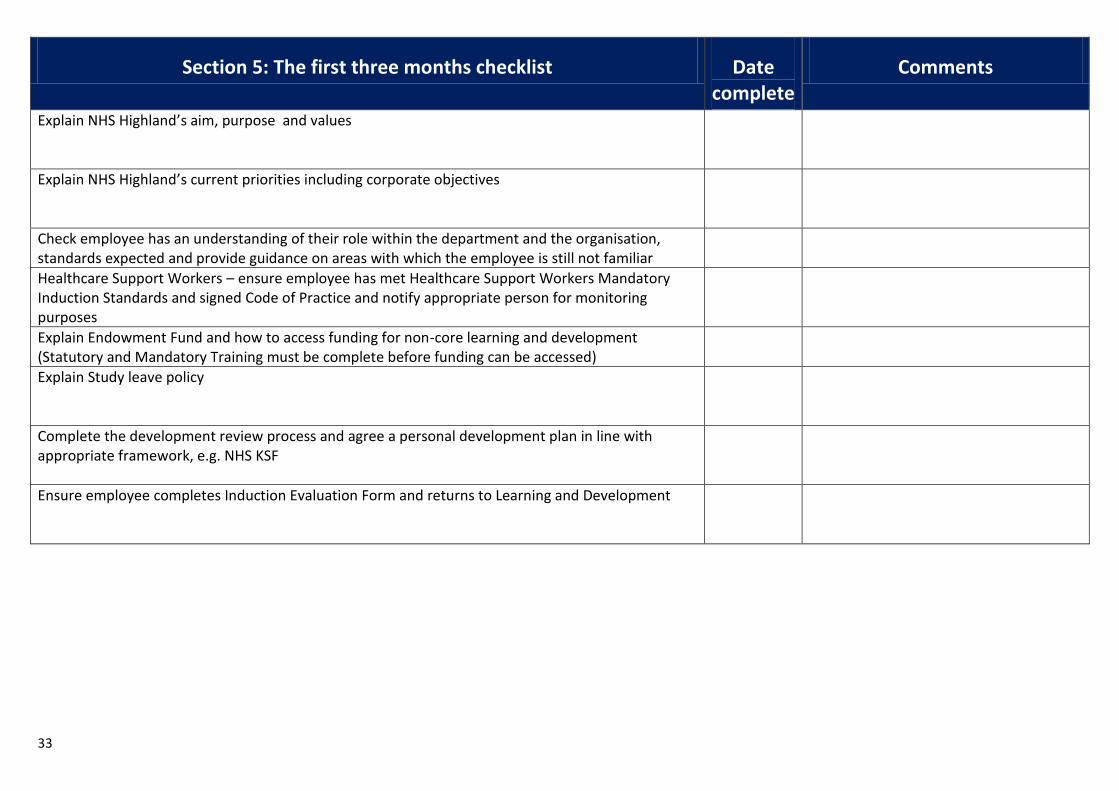
33
Section 5: The first three months checklist Date complete
Comments
Explain NHS Highland’s aim, purpose and values
Explain NHS Highland’s current priorities including corporate objectives
Check employee has an understanding of their role within the department and the organisation, standards expected and provide guidance on areas with which the employee is still not familiar
Healthcare Support Workers – ensure employee has met Healthcare Support Workers Mandatory Induction Standards and signed Code of Practice and notify appropriate person for monitoring purposes
Explain Endowment Fund and how to access funding for non-core learning and development (Statutory and Mandatory Training must be complete before funding can be accessed)
Explain Study leave policy
Complete the development review process and agree a personal development plan in line with appropriate framework, e.g. NHS KSF
Ensure employee completes Induction Evaluation Form and returns to Learning and Development
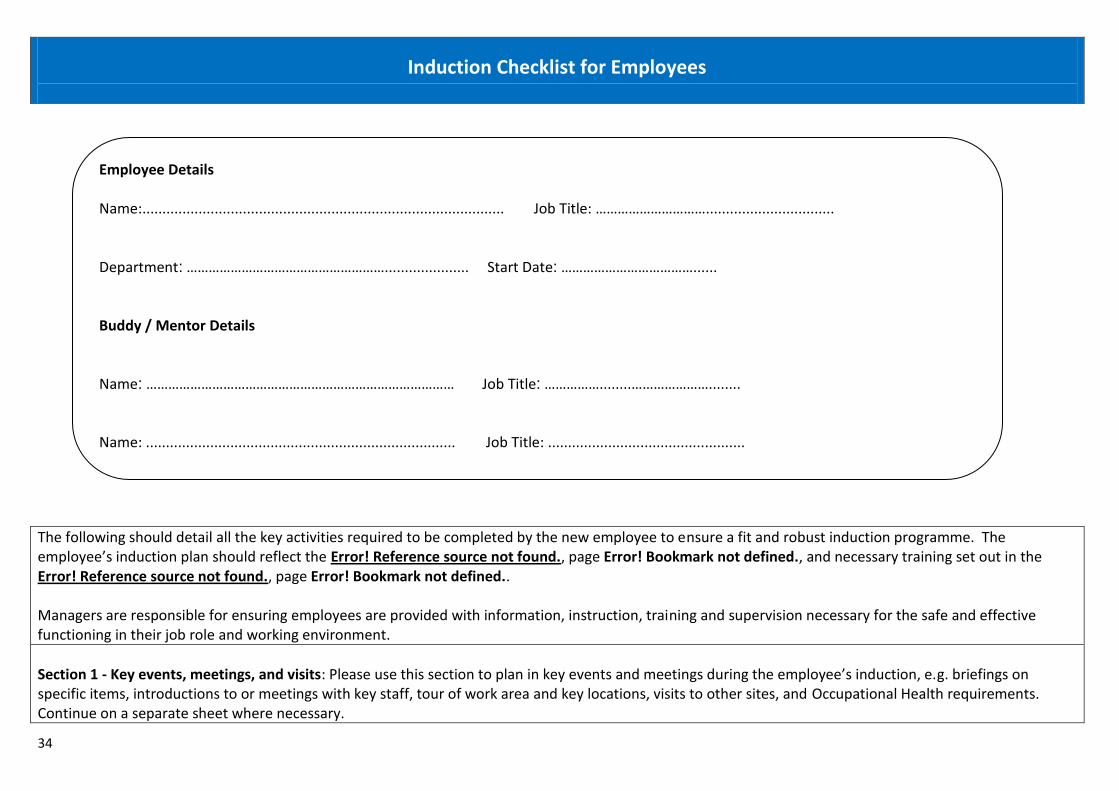
34
Induction Checklist for Employees
The following should detail all the key activities required to be completed by the new employee to ensure a fit and robust induction programme. The employee’s induction plan should reflect the Error! Reference source not found., page Error! Bookmark not defined., and necessary training set out in the Error! Reference source not found., page Error! Bookmark not defined.. Managers are responsible for ensuring employees are provided with information, instruction, training and supervision necessary for the safe and effective functioning in their job role and working environment.
Section 1 - Key events, meetings, and visits: Please use this section to plan in key events and meetings during the employee’s induction, e.g. briefings on specific items, introductions to or meetings with key staff, tour of work area and key locations, visits to other sites, and Occupational Health requirements. Continue on a separate sheet where necessary.
Employee Details Name:.......................................................................................... Job Title: …………………………................................ Department: ………………………………………………..................... Start Date: ………………………………...... Buddy / Mentor Details Name: ………………………………………………………………………… Job Title: ……………........…………………........ Name: ............................................................................. Job Title: .................................................
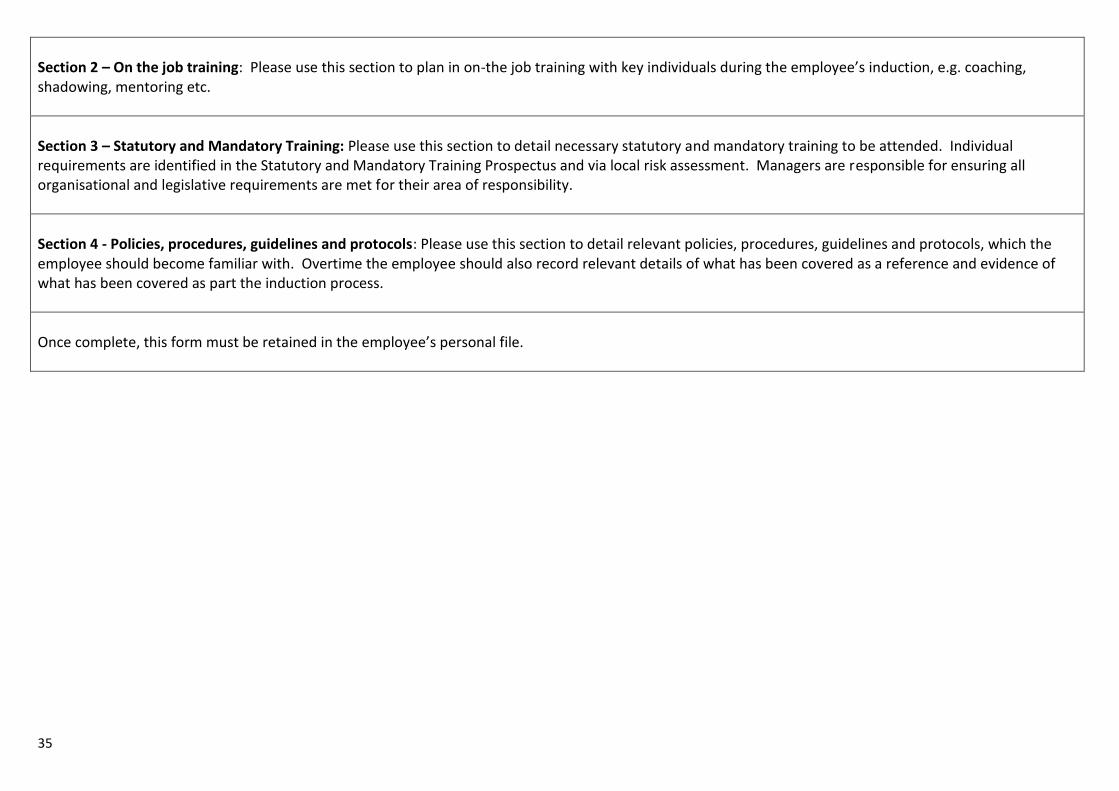
35
Section 2 – On the job training: Please use this section to plan in on-the job training with key individuals during the employee’s induction, e.g. coaching, shadowing, mentoring etc.
Section 3 – Statutory and Mandatory Training: Please use this section to detail necessary statutory and mandatory training to be attended. Individual requirements are identified in the Statutory and Mandatory Training Prospectus and via local risk assessment. Managers are responsible for ensuring all organisational and legislative requirements are met for their area of responsibility.
Section 4 - Policies, procedures, guidelines and protocols: Please use this section to detail relevant policies, procedures, guidelines and protocols, which the employee should become familiar with. Overtime the employee should also record relevant details of what has been covered as a reference and evidence of what has been covered as part the induction process.
Once complete, this form must be retained in the employee’s personal file.
36
Section 1: Key events, meetings, and visits
Date Time Who Where What

37
Section 2: On the job training
Date Time Who Where What
38
Section 3: Statutory and Mandatory Training
Date Time Where What Comments
Fire Safety
Moving and Handling
Violence and Aggression
Hand Hygiene
39
Section 4: Policies, procedures, guidelines and protocols
Date
Name of policy, procedure, guideline and protocol
Information given by: Comments

40
Continuing Professional Development
41
Continuing Professional Development NHS Highland recognises the important role that Advanced Nurses/Paramedics play in the delivery and support of quality health and social care. This Education and Training CPD guidance has been developed to support managers, supervisors and staff to continue to provide services of the highest quality. This ultimately inspires confidence in patients and communities, as well as staff. A key aim of education and training is to ensure that all Advanced Nurses/Paramedics are equipped to meet required standards and that good practice is carried out across NHS Highland in relation to Person-Centered, Safe, and Effective care. The areas of competence are applicable to all settings where Advanced Nurses/Paramedics deliver services and should be at the heart of induction and ongoing CPD education and training (See Error! Reference source not found., page Error! Bookmark not defined., and The Highland Competency Framework, page 48).
CPD will also support Nurses & Paramedics Preparing for Revalidation and PDPs Revalidation is the new process by which nurses and midwives demonstrate that they practice safely. All nurses and midwives are currently required to renew their registration every three years. Provisional requirements
450 Practice hours
35 hours of CPD
5 pieces of practice-related feedback
5 reflections and discussion
Health and character declaration
Professional indemnity arrangement
Confirmation from a third party To help you prepare for the Revalidation process Register online with the NMC - http://www.nmc.org.uk/registration/nmc-online/ This allows you to check your registration status, find out your renewal date, update your information, etc.
Think about your portfolio and review those available – NMC are currently strongly recommending an e-portfolio (currently not mandatory). There are various available (some may have a cost attached) including
o NES e-portfolio (free): http://www.nes.scot.nhs.uk/education-and-training/by-discipline/nursing-and-midwifery/careers-and-recruitment/nursing-midwifery-career-long-eportfolio.aspx
o RCN: https://www.rcn.org.uk/development/learning/learningzone/my_portfolio o RCM: https://www.rcm.org.uk/news-views-and-analysis/analysis/the-rcms-new-eportfolio-for-
members
Think about reflective practice and look at the templates o This website may help with this: http://www.effectivepractitioner.nes.scot.nhs.uk/learning-
and-development/recording-learning-and-development.aspx
Visit the NMC revalidation site for information and updates: http://www.nmc.org.uk/standards/revalidation/
Check your NMC renewal date – as this date will be key in knowing when you will go through the revalidation process
Read the new NMC Code: http://www.nmc.org.uk/standards/code/
Visit the NES Revalidation Community of Practice for information on all aspects of preparing evidence : http://www.knowledge.scot.nhs.uk/revalidation.aspx

42
If you need help, or further information, please liaise with your line manager or your local Practice Education Facilitator
Accessing Education and Training Learning activities to support the contents of the framework relating to Statutory / Mandatory and Core training will be accessible through two key resources:
1. NHS Highland Statutory/Mandatory Training Prospectus 2. NHS Highland Out of Hours Unscheduled Care – A Framework for Practice
43
Appendices

44
Appendix 1: NHS Highland Portfolio Assessment
Criteria used for sign-off of practitioners Practitioner name: ...........................................................................
1) Self-Assessment / Learning Needs Analysis / Evidence
Local Clinical Lead OOH Clinical Lead Education Lead Lead Nurse
Satisfactory Unsatisfactory Satisfactory Unsatisfactory Satisfactory Unsatisfactory Satisfactory Unsatisfactory
YES/NO YES/NO YES/NO YES/NO YES/NO YES/NO YES/NO YES/NO
Comments
2) Supervisor Assessment Consultation Observations / Evidence
Local Clinical Lead OOH Clinical Lead Education Lead Lead Nurse
Satisfactory Unsatisfactory Satisfactory Unsatisfactory Satisfactory Unsatisfactory Satisfactory Unsatisfactory
YES/NO YES/NO YES/NO YES/NO YES/NO YES/NO YES/NO YES/NO
Comments
3) Case-based Discussions / Evidence Local Clinical Lead OOH Clinical Lead Education Lead Lead Nurse
Satisfactory Unsatisfactory Satisfactory Unsatisfactory Satisfactory Unsatisfactory Satisfactory Unsatisfactory
YES/NO YES/NO YES/NO YES/NO YES/NO YES/NO YES/NO YES/NO

45
Comments
4) Multi-Source Feedback Local Clinical Lead OOH Clinical Lead Education Lead Lead Nurse
Satisfactory Unsatisfactory Satisfactory Unsatisfactory Satisfactory Unsatisfactory Satisfactory Unsatisfactory
YES/NO YES/NO YES/NO YES/NO YES/NO YES/NO YES/NO YES/NO
Comments
5) Significant Event Analysis Local Clinical Lead OOH Clinical Lead Education Lead Lead Nurse
Satisfactory Unsatisfactory Satisfactory Unsatisfactory Satisfactory Unsatisfactory Satisfactory Unsatisfactory
YES/NO YES/NO YES/NO YES/NO YES/NO YES/NO YES/NO YES/NO
Comments
6) Evidence of Practitioner-structured Reflection following Education sessions
Local Clinical Lead OOH Clinical Lead Education Lead Lead Nurse
Satisfactory Unsatisfactory Satisfactory Unsatisfactory Satisfactory Unsatisfactory Satisfactory Unsatisfactory
YES/NO YES/NO YES/NO YES/NO YES/NO YES/NO YES/NO YES/NO
Comments
46
Educational Governance Group Chair
Pass: YES/NO Refer: YES/NO
General Comments Signature: Date:
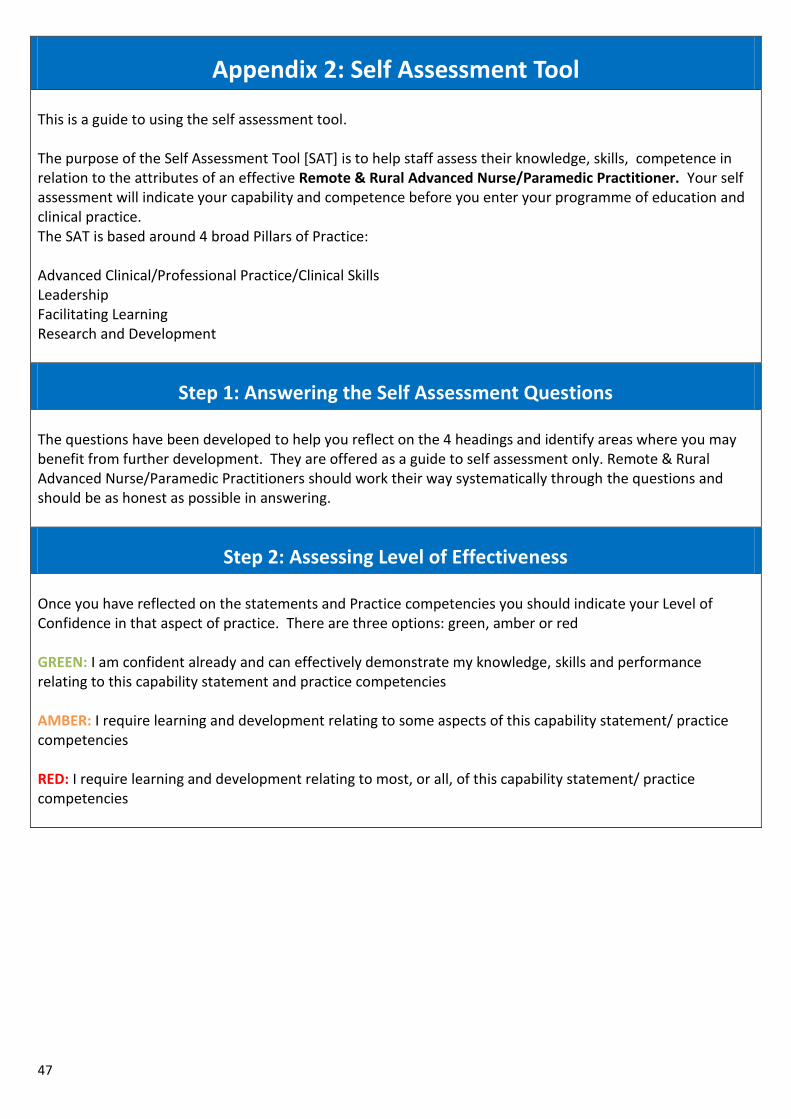
47
Appendix 2: Self Assessment Tool This is a guide to using the self assessment tool. The purpose of the Self Assessment Tool [SAT] is to help staff assess their knowledge, skills, competence in relation to the attributes of an effective Remote & Rural Advanced Nurse/Paramedic Practitioner. Your self assessment will indicate your capability and competence before you enter your programme of education and clinical practice. The SAT is based around 4 broad Pillars of Practice: Advanced Clinical/Professional Practice/Clinical Skills Leadership Facilitating Learning Research and Development
Step 1: Answering the Self Assessment Questions The questions have been developed to help you reflect on the 4 headings and identify areas where you may benefit from further development. They are offered as a guide to self assessment only. Remote & Rural Advanced Nurse/Paramedic Practitioners should work their way systematically through the questions and should be as honest as possible in answering.
Step 2: Assessing Level of Effectiveness Once you have reflected on the statements and Practice competencies you should indicate your Level of Confidence in that aspect of practice. There are three options: green, amber or red GREEN: I am confident already and can effectively demonstrate my knowledge, skills and performance relating to this capability statement and practice competencies AMBER: I require learning and development relating to some aspects of this capability statement/ practice competencies RED: I require learning and development relating to most, or all, of this capability statement/ practice competencies
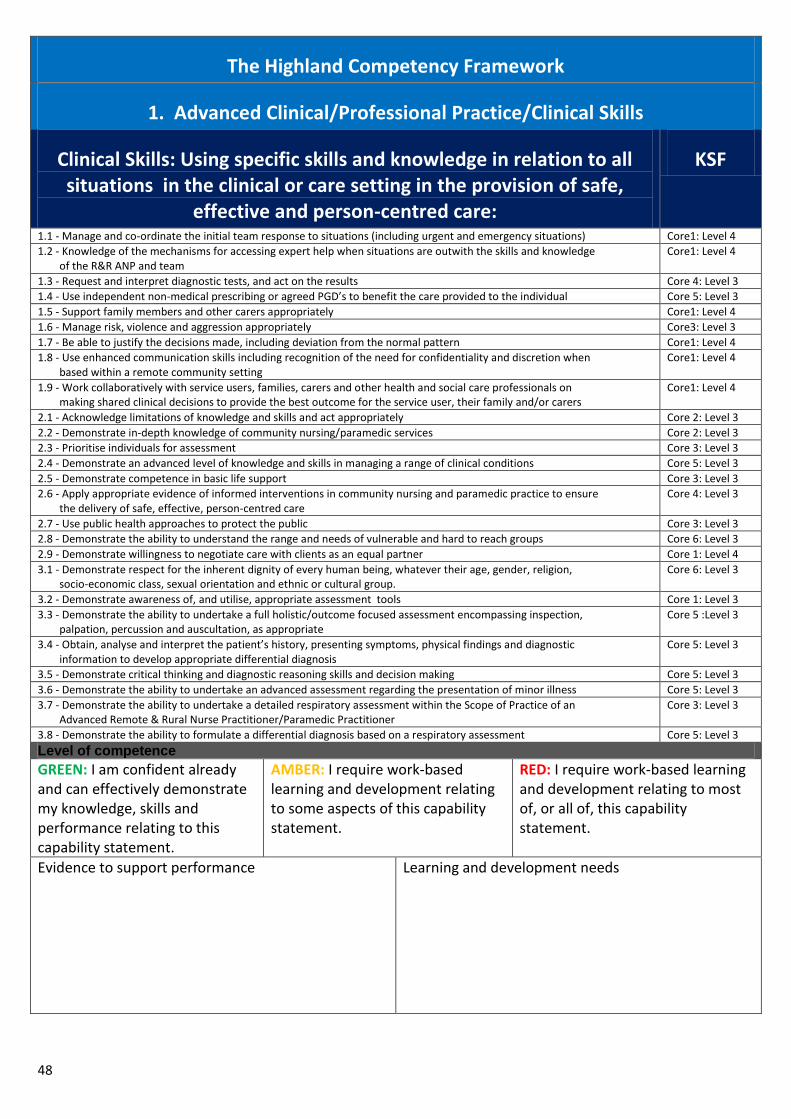
48
The Highland Competency Framework
1. Advanced Clinical/Professional Practice/Clinical Skills
Clinical Skills: Using specific skills and knowledge in relation to all situations in the clinical or care setting in the provision of safe,
effective and person-centred care:
KSF
1.1 - Manage and co-ordinate the initial team response to situations (including urgent and emergency situations) Core1: Level 4
1.2 - Knowledge of the mechanisms for accessing expert help when situations are outwith the skills and knowledge of the R&R ANP and team
Core1: Level 4
1.3 - Request and interpret diagnostic tests, and act on the results Core 4: Level 3
1.4 - Use independent non-medical prescribing or agreed PGD’s to benefit the care provided to the individual Core 5: Level 3
1.5 - Support family members and other carers appropriately Core1: Level 4
1.6 - Manage risk, violence and aggression appropriately Core3: Level 3
1.7 - Be able to justify the decisions made, including deviation from the normal pattern Core1: Level 4
1.8 - Use enhanced communication skills including recognition of the need for confidentiality and discretion when based within a remote community setting
Core1: Level 4
1.9 - Work collaboratively with service users, families, carers and other health and social care professionals on making shared clinical decisions to provide the best outcome for the service user, their family and/or carers
Core1: Level 4
2.1 - Acknowledge limitations of knowledge and skills and act appropriately Core 2: Level 3
2.2 - Demonstrate in-depth knowledge of community nursing/paramedic services Core 2: Level 3
2.3 - Prioritise individuals for assessment Core 3: Level 3
2.4 - Demonstrate an advanced level of knowledge and skills in managing a range of clinical conditions Core 5: Level 3
2.5 - Demonstrate competence in basic life support Core 3: Level 3
2.6 - Apply appropriate evidence of informed interventions in community nursing and paramedic practice to ensure the delivery of safe, effective, person-centred care
Core 4: Level 3
2.7 - Use public health approaches to protect the public Core 3: Level 3
2.8 - Demonstrate the ability to understand the range and needs of vulnerable and hard to reach groups Core 6: Level 3
2.9 - Demonstrate willingness to negotiate care with clients as an equal partner Core 1: Level 4
3.1 - Demonstrate respect for the inherent dignity of every human being, whatever their age, gender, religion, socio-economic class, sexual orientation and ethnic or cultural group.
Core 6: Level 3
3.2 - Demonstrate awareness of, and utilise, appropriate assessment tools Core 1: Level 3
3.3 - Demonstrate the ability to undertake a full holistic/outcome focused assessment encompassing inspection, palpation, percussion and auscultation, as appropriate
Core 5 :Level 3
3.4 - Obtain, analyse and interpret the patient’s history, presenting symptoms, physical findings and diagnostic information to develop appropriate differential diagnosis
Core 5: Level 3
3.5 - Demonstrate critical thinking and diagnostic reasoning skills and decision making Core 5: Level 3
3.6 - Demonstrate the ability to undertake an advanced assessment regarding the presentation of minor illness Core 5: Level 3
3.7 - Demonstrate the ability to undertake a detailed respiratory assessment within the Scope of Practice of an Advanced Remote & Rural Nurse Practitioner/Paramedic Practitioner
Core 3: Level 3
3.8 - Demonstrate the ability to formulate a differential diagnosis based on a respiratory assessment Core 5: Level 3
Level of competence
GREEN: I am confident already and can effectively demonstrate my knowledge, skills and performance relating to this capability statement.
AMBER: I require work-based learning and development relating to some aspects of this capability statement.
RED: I require work-based learning and development relating to most of, or all of, this capability statement.
Evidence to support performance
Learning and development needs

49
1. Advanced Clinical/Professional Practice/Clinical Skills
Clinical Skills: Using specific skills and knowledge in relation to all situations in the clinical or care setting in the provision of safe,
effective and person centred care:
KSF
3.9 - Recognise common indications for requiring necessary diagnostic tests Core 5: Level 3
4.1 - Demonstrate detailed knowledge and practical skills to interpret pulse oximetry and in relation to individual assessment
Core 5: Level 3
4.2 - Demonstrate appropriate knowledge when spirometry should be conducted Core 5: Level 3
4.3 - Demonstrate appropriate knowledge reference values for spirometry and interpret results Core 5: Level 3
4.4 - Assess and provide treatment for a patient with breathlessness Core 5: Level 3
4.5 - Recognise referral indicators for assessment for oxygen therapy Core 5: Level 3
4.6 - Demonstrate the ability to conduct a detailed cardiovascular examination within the Scope of Practice of a Remote & Rural Advanced Nurse Practitioner/Paramedic Practitioner
Core 5: Level 3
4.7 - Demonstrate the ability to formulate a differential diagnosis based on a cardiovascular assessment Core 5: Level 3
4.8 - Recognise common indications for requesting a 12-lead ECG Core 5: Level 3
4.9 - Evaluate potential causes of abnormal reading Core 5: Level 3
5.1 - Demonstrate the ability to conduct a detailed clinical gastrointestinal examination (including percussion, palpation and auscultation) within the Scope of Practice of a Remote & Rural Advanced Nurse/Paramedic Practitioner
Core 5: Level 3
5.2 - Demonstrate the ability to formulate a differential diagnosis based on a gastrointestinal assessment Core 5: Level 3
5.3 - Demonstrate the ability to recognise abnormal findings and refer, if appropriate Core 5: Level 3
5.4 - Demonstrate the ability to conduct a sufficiently detailed musculoskeletal examination within the Scope of a Remote & Rural Advanced Nurse/Paramedic Practitioner
Core 5: Level 3
5.5 - Demonstrate the ability to formulate a differential diagnosis based on a musculoskeletal examination Core 5: Level 3
5.6- Demonstrate the ability to recognise abnormal findings and refer, if appropriate Core 5: Level 3
5.7 - Demonstrate the ability to conduct a sufficiently detailed ENT examination within the Scope of Practice of a Remote & Rural Advanced Nurse/Paramedic Practitioner
Core 5: Level 3
5.8 - Demonstrate the ability to formulate a differential diagnosis based on an ENT examination Core 5: Level 3
5.9 - Demonstrate the ability to recognise abnormal findings and refer, if appropriate Core 5: Level 3
6.1 - Demonstrate the ability to conduct a detailed clinical renal examination within the Scope of Practice of a Remote & Rural Advanced Nurse/Paramedic Practitioner
Core 5: Level 3
6.2 - Demonstrate the ability to formulate a differential diagnosis based on a renal examination Core 5: Level 3
6.3 - Demonstrate the ability to assess common biochemistry results and outline the significance of common electrolyte abnormalities
Core 5: Level 3
Level of competence
GREEN: I am confident already and can effectively demonstrate my knowledge, skills and performance relating to this capability statement.
AMBER: I require work-based learning and development relating to some aspects of this capability statement.
RED: I require work-based learning and development relating to most of, or all of, this capability statement.
Evidence to support performance
Learning and development needs
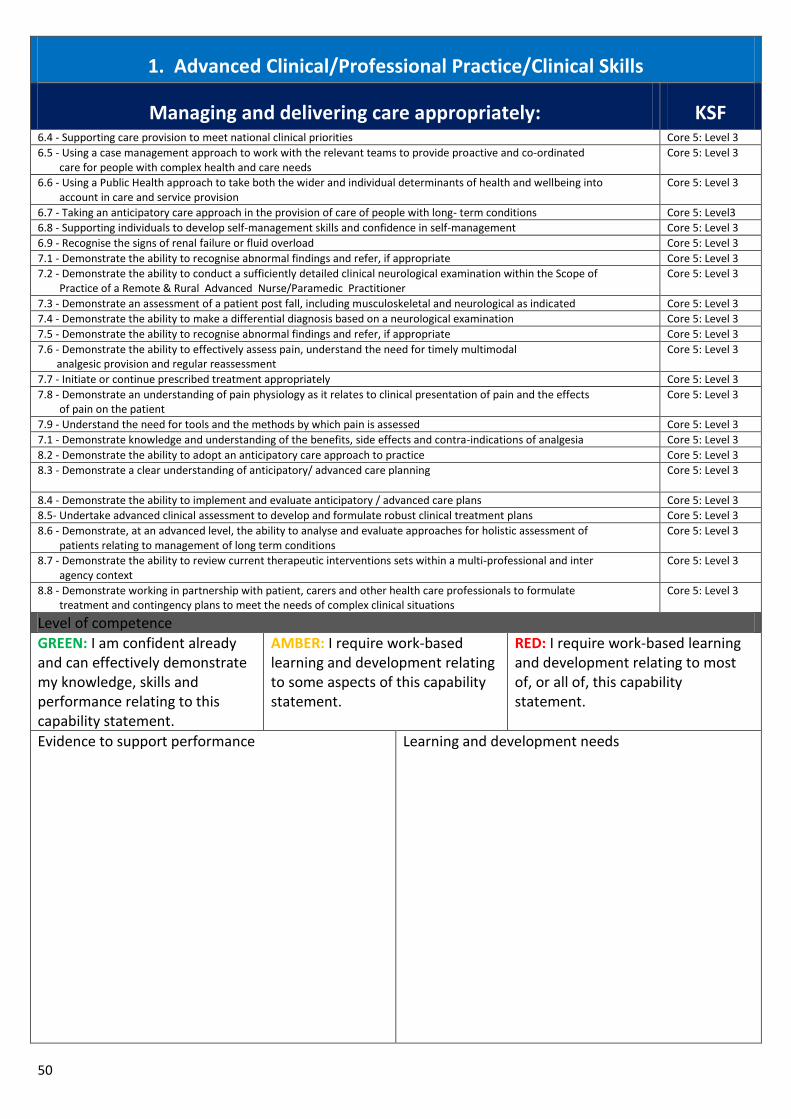
50
1. Advanced Clinical/Professional Practice/Clinical Skills
Managing and delivering care appropriately: KSF 6.4 - Supporting care provision to meet national clinical priorities Core 5: Level 3
6.5 - Using a case management approach to work with the relevant teams to provide proactive and co-ordinated care for people with complex health and care needs
Core 5: Level 3
6.6 - Using a Public Health approach to take both the wider and individual determinants of health and wellbeing into account in care and service provision
Core 5: Level 3
6.7 - Taking an anticipatory care approach in the provision of care of people with long- term conditions Core 5: Level3
6.8 - Supporting individuals to develop self-management skills and confidence in self-management Core 5: Level 3
6.9 - Recognise the signs of renal failure or fluid overload Core 5: Level 3
7.1 - Demonstrate the ability to recognise abnormal findings and refer, if appropriate Core 5: Level 3
7.2 - Demonstrate the ability to conduct a sufficiently detailed clinical neurological examination within the Scope of Practice of a Remote & Rural Advanced Nurse/Paramedic Practitioner
Core 5: Level 3
7.3 - Demonstrate an assessment of a patient post fall, including musculoskeletal and neurological as indicated Core 5: Level 3
7.4 - Demonstrate the ability to make a differential diagnosis based on a neurological examination Core 5: Level 3
7.5 - Demonstrate the ability to recognise abnormal findings and refer, if appropriate Core 5: Level 3
7.6 - Demonstrate the ability to effectively assess pain, understand the need for timely multimodal analgesic provision and regular reassessment
Core 5: Level 3
7.7 - Initiate or continue prescribed treatment appropriately Core 5: Level 3
7.8 - Demonstrate an understanding of pain physiology as it relates to clinical presentation of pain and the effects of pain on the patient
Core 5: Level 3
7.9 - Understand the need for tools and the methods by which pain is assessed Core 5: Level 3
7.1 - Demonstrate knowledge and understanding of the benefits, side effects and contra-indications of analgesia Core 5: Level 3
8.2 - Demonstrate the ability to adopt an anticipatory care approach to practice Core 5: Level 3
8.3 - Demonstrate a clear understanding of anticipatory/ advanced care planning Core 5: Level 3
8.4 - Demonstrate the ability to implement and evaluate anticipatory / advanced care plans Core 5: Level 3
8.5- Undertake advanced clinical assessment to develop and formulate robust clinical treatment plans Core 5: Level 3
8.6 - Demonstrate, at an advanced level, the ability to analyse and evaluate approaches for holistic assessment of patients relating to management of long term conditions
Core 5: Level 3
8.7 - Demonstrate the ability to review current therapeutic interventions sets within a multi-professional and inter agency context
Core 5: Level 3
8.8 - Demonstrate working in partnership with patient, carers and other health care professionals to formulate treatment and contingency plans to meet the needs of complex clinical situations
Core 5: Level 3
Level of competence
GREEN: I am confident already and can effectively demonstrate my knowledge, skills and performance relating to this capability statement.
AMBER: I require work-based learning and development relating to some aspects of this capability statement.
RED: I require work-based learning and development relating to most of, or all of, this capability statement.
Evidence to support performance
Learning and development needs
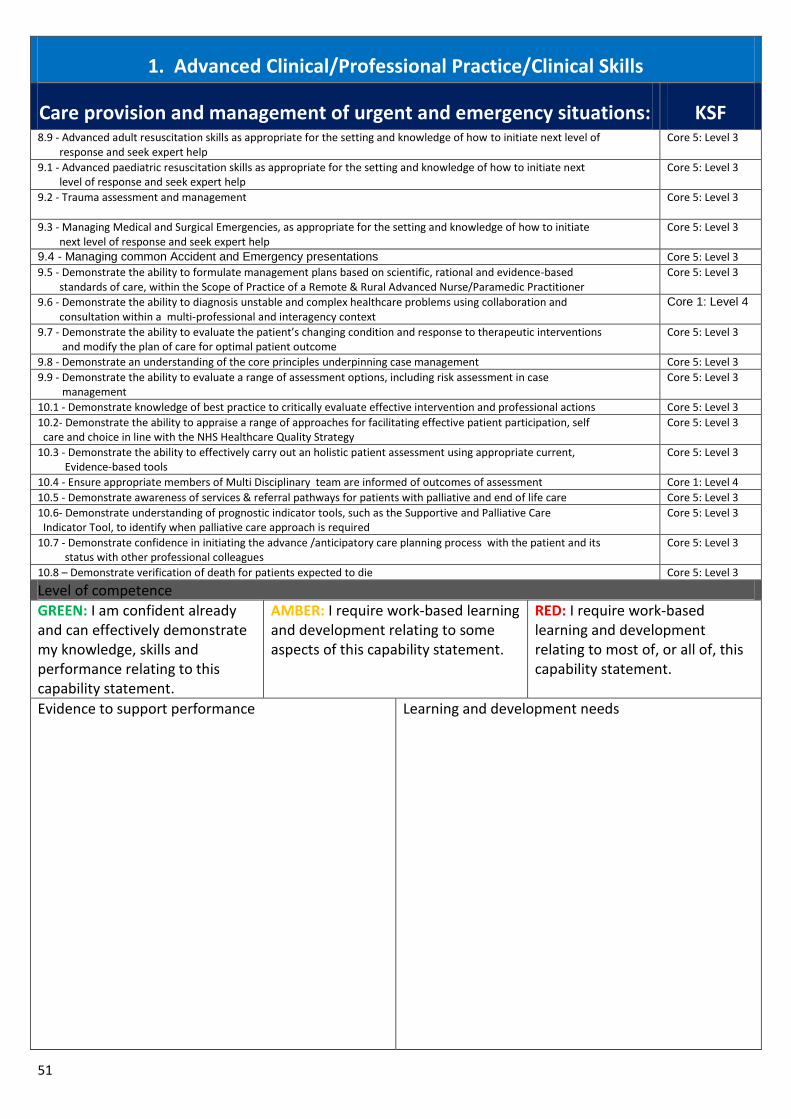
51
1. Advanced Clinical/Professional Practice/Clinical Skills
Care provision and management of urgent and emergency situations: KSF 8.9 - Advanced adult resuscitation skills as appropriate for the setting and knowledge of how to initiate next level of response and seek expert help
Core 5: Level 3
9.1 - Advanced paediatric resuscitation skills as appropriate for the setting and knowledge of how to initiate next level of response and seek expert help
Core 5: Level 3
9.2 - Trauma assessment and management Core 5: Level 3
9.3 - Managing Medical and Surgical Emergencies, as appropriate for the setting and knowledge of how to initiate next level of response and seek expert help
Core 5: Level 3
9.4 - Managing common Accident and Emergency presentations Core 5: Level 3
9.5 - Demonstrate the ability to formulate management plans based on scientific, rational and evidence-based standards of care, within the Scope of Practice of a Remote & Rural Advanced Nurse/Paramedic Practitioner
Core 5: Level 3
9.6 - Demonstrate the ability to diagnosis unstable and complex healthcare problems using collaboration and consultation within a multi-professional and interagency context
Core 1: Level 4
9.7 - Demonstrate the ability to evaluate the patient’s changing condition and response to therapeutic interventions and modify the plan of care for optimal patient outcome
Core 5: Level 3
9.8 - Demonstrate an understanding of the core principles underpinning case management Core 5: Level 3
9.9 - Demonstrate the ability to evaluate a range of assessment options, including risk assessment in case management
Core 5: Level 3
10.1 - Demonstrate knowledge of best practice to critically evaluate effective intervention and professional actions Core 5: Level 3
10.2- Demonstrate the ability to appraise a range of approaches for facilitating effective patient participation, self care and choice in line with the NHS Healthcare Quality Strategy
Core 5: Level 3
10.3 - Demonstrate the ability to effectively carry out an holistic patient assessment using appropriate current, Evidence-based tools
Core 5: Level 3
10.4 - Ensure appropriate members of Multi Disciplinary team are informed of outcomes of assessment Core 1: Level 4
10.5 - Demonstrate awareness of services & referral pathways for patients with palliative and end of life care Core 5: Level 3
10.6- Demonstrate understanding of prognostic indicator tools, such as the Supportive and Palliative Care
Indicator Tool, to identify when palliative care approach is required
Core 5: Level 3
10.7 - Demonstrate confidence in initiating the advance /anticipatory care planning process with the patient and its status with other professional colleagues
Core 5: Level 3
10.8 – Demonstrate verification of death for patients expected to die Core 5: Level 3
Level of competence
GREEN: I am confident already and can effectively demonstrate my knowledge, skills and performance relating to this capability statement.
AMBER: I require work-based learning and development relating to some aspects of this capability statement.
RED: I require work-based learning and development relating to most of, or all of, this capability statement.
Evidence to support performance
Learning and development needs
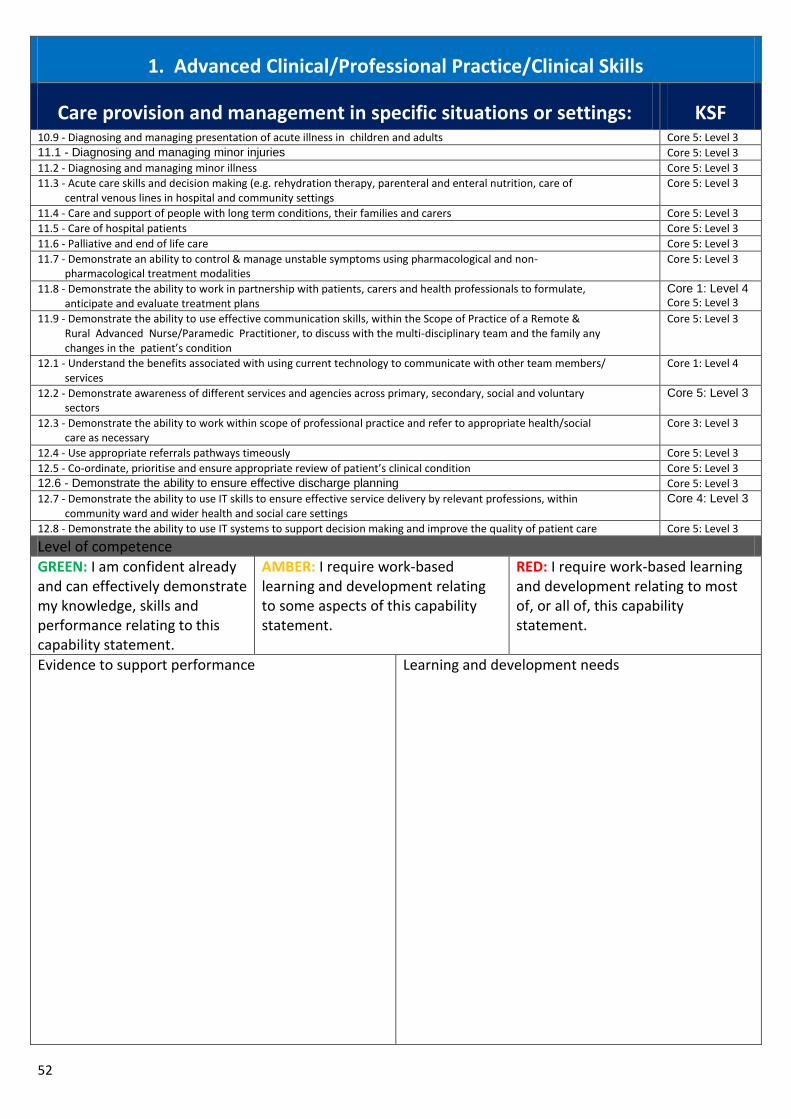
52
1. Advanced Clinical/Professional Practice/Clinical Skills
Care provision and management in specific situations or settings: KSF 10.9 - Diagnosing and managing presentation of acute illness in children and adults Core 5: Level 3
11.1 - Diagnosing and managing minor injuries Core 5: Level 3
11.2 - Diagnosing and managing minor illness Core 5: Level 3
11.3 - Acute care skills and decision making (e.g. rehydration therapy, parenteral and enteral nutrition, care of central venous lines in hospital and community settings
Core 5: Level 3
11.4 - Care and support of people with long term conditions, their families and carers Core 5: Level 3
11.5 - Care of hospital patients Core 5: Level 3
11.6 - Palliative and end of life care Core 5: Level 3
11.7 - Demonstrate an ability to control & manage unstable symptoms using pharmacological and non- pharmacological treatment modalities
Core 5: Level 3
11.8 - Demonstrate the ability to work in partnership with patients, carers and health professionals to formulate, anticipate and evaluate treatment plans
Core 1: Level 4 Core 5: Level 3
11.9 - Demonstrate the ability to use effective communication skills, within the Scope of Practice of a Remote & Rural Advanced Nurse/Paramedic Practitioner, to discuss with the multi-disciplinary team and the family any changes in the patient’s condition
Core 5: Level 3
12.1 - Understand the benefits associated with using current technology to communicate with other team members/ services
Core 1: Level 4
12.2 - Demonstrate awareness of different services and agencies across primary, secondary, social and voluntary sectors
Core 5: Level 3
12.3 - Demonstrate the ability to work within scope of professional practice and refer to appropriate health/social care as necessary
Core 3: Level 3
12.4 - Use appropriate referrals pathways timeously Core 5: Level 3
12.5 - Co-ordinate, prioritise and ensure appropriate review of patient’s clinical condition Core 5: Level 3
12.6 - Demonstrate the ability to ensure effective discharge planning Core 5: Level 3
12.7 - Demonstrate the ability to use IT skills to ensure effective service delivery by relevant professions, within community ward and wider health and social care settings
Core 4: Level 3
12.8 - Demonstrate the ability to use IT systems to support decision making and improve the quality of patient care Core 5: Level 3
Level of competence
GREEN: I am confident already and can effectively demonstrate my knowledge, skills and performance relating to this capability statement.
AMBER: I require work-based learning and development relating to some aspects of this capability statement.
RED: I require work-based learning and development relating to most of, or all of, this capability statement.
Evidence to support performance
Learning and development needs
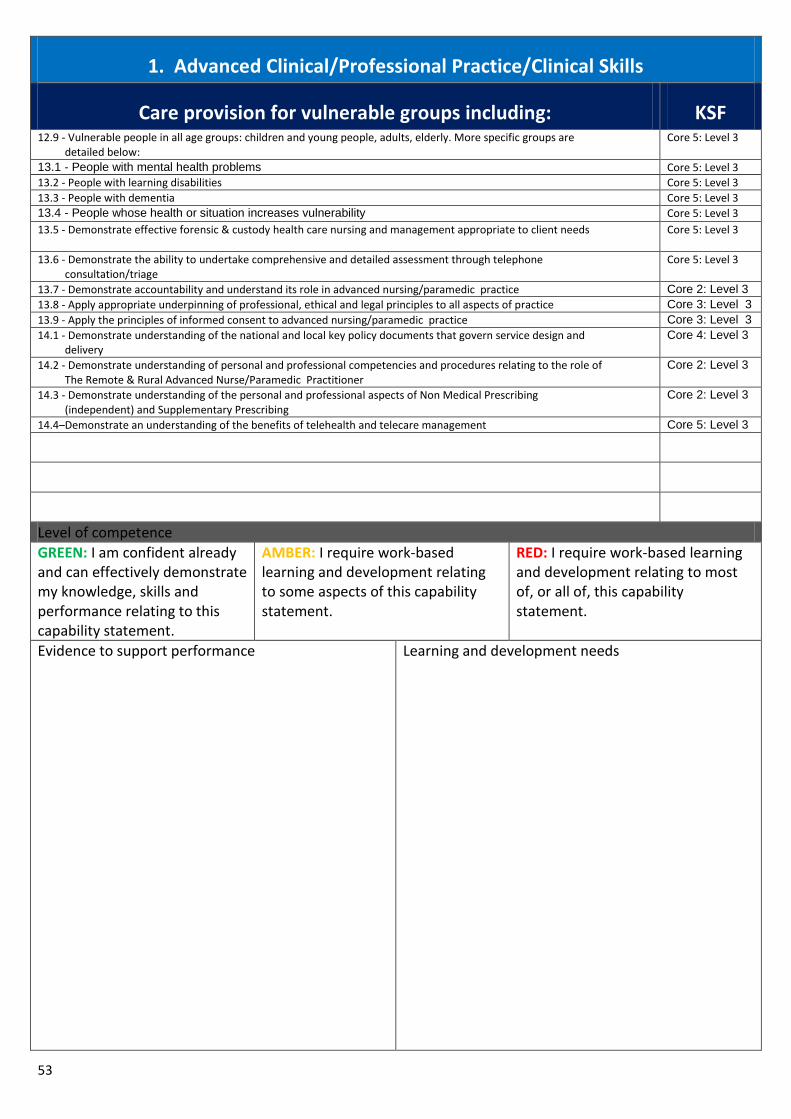
53
1. Advanced Clinical/Professional Practice/Clinical Skills
Care provision for vulnerable groups including: KSF 12.9 - Vulnerable people in all age groups: children and young people, adults, elderly. More specific groups are detailed below:
Core 5: Level 3
13.1 - People with mental health problems Core 5: Level 3
13.2 - People with learning disabilities Core 5: Level 3
13.3 - People with dementia Core 5: Level 3
13.4 - People whose health or situation increases vulnerability Core 5: Level 3
13.5 - Demonstrate effective forensic & custody health care nursing and management appropriate to client needs
Core 5: Level 3
13.6 - Demonstrate the ability to undertake comprehensive and detailed assessment through telephone consultation/triage
Core 5: Level 3
13.7 - Demonstrate accountability and understand its role in advanced nursing/paramedic practice Core 2: Level 3
13.8 - Apply appropriate underpinning of professional, ethical and legal principles to all aspects of practice Core 3: Level 3
13.9 - Apply the principles of informed consent to advanced nursing/paramedic practice Core 3: Level 3
14.1 - Demonstrate understanding of the national and local key policy documents that govern service design and delivery
Core 4: Level 3
14.2 - Demonstrate understanding of personal and professional competencies and procedures relating to the role of The Remote & Rural Advanced Nurse/Paramedic Practitioner
Core 2: Level 3
14.3 - Demonstrate understanding of the personal and professional aspects of Non Medical Prescribing (independent) and Supplementary Prescribing
Core 2: Level 3
14.4–Demonstrate an understanding of the benefits of telehealth and telecare management Core 5: Level 3
Level of competence
GREEN: I am confident already and can effectively demonstrate my knowledge, skills and performance relating to this capability statement.
AMBER: I require work-based learning and development relating to some aspects of this capability statement.
RED: I require work-based learning and development relating to most of, or all of, this capability statement.
Evidence to support performance
Learning and development needs

54
2. Leadership
Demonstrate a wide range of leadership skills and knowledge to support the provision of person-centred care and to provide leadership at strategic and practice levels across the settings
KSF
1.1 - Utilisation of advanced communication skills at all levels: interpersonal, inter-professional and interagency Core1: Level 4
1.2 - Leadership and management of the team, and wider multi professional and multiagency teams ( including working across a range of settings)
Core 2: Level 3
1.3 - Leading and managing change (including monitoring the impact and effectiveness of change) Core 2: Level 3
1.4 - Leading and supporting team working Core 2: Level 3
1.5 - Leading and managing on quality improvement and patient safety Core4,5: Level3
1.6 - Utilising evidence in implementing change Core2,4: Level3
1.7 - Clinical practice and care development Core 4: Level 3
1.8 - Promote and influence others to incorporate non-judgmental, values-based care and spiritual care into practice Core 6: Level 3
1.9 - Risk management Core3: Level 3
2.1 - Policy development Core4: Level 3
2.2 - Resource management (including finance) Core4,5: Level3
2.3 - Negotiation and influencing Core1: Level 4
2.4 - Demonstrate strong and effective clinical leadership across professional and organisational teams/ boundaries Core 2: Level 3
2.5 - Actively encourage involvement of service users to influence and improve person-centred care Core 5: Level 3
2.6 - Demonstrate knowledge and understanding of clinical governance frameworks within own organisation and take responsibility for clinical governance within a defined setting
Core 5: Level 3
2.7 - Contribute to the development, implementation and monitoring evaluation of standards of care to ensure the delivery of safe and effective, person-centred care and act on the results
Core 5: Level 3
2.8 - Demonstrate the ability to contribute to policy and strategy development at departmental, organisational and, where appropriate, national level
Core 5: Level 3
Level of competence
GREEN: I am confident already and can effectively demonstrate my knowledge, skills and performance relating to this capability statement.
AMBER: I require work-based learning and development relating to some aspects of this capability statement.
RED: I require work-based learning and development relating to most of, or all of, this capability statement.
Evidence to support performance
Learning and development needs
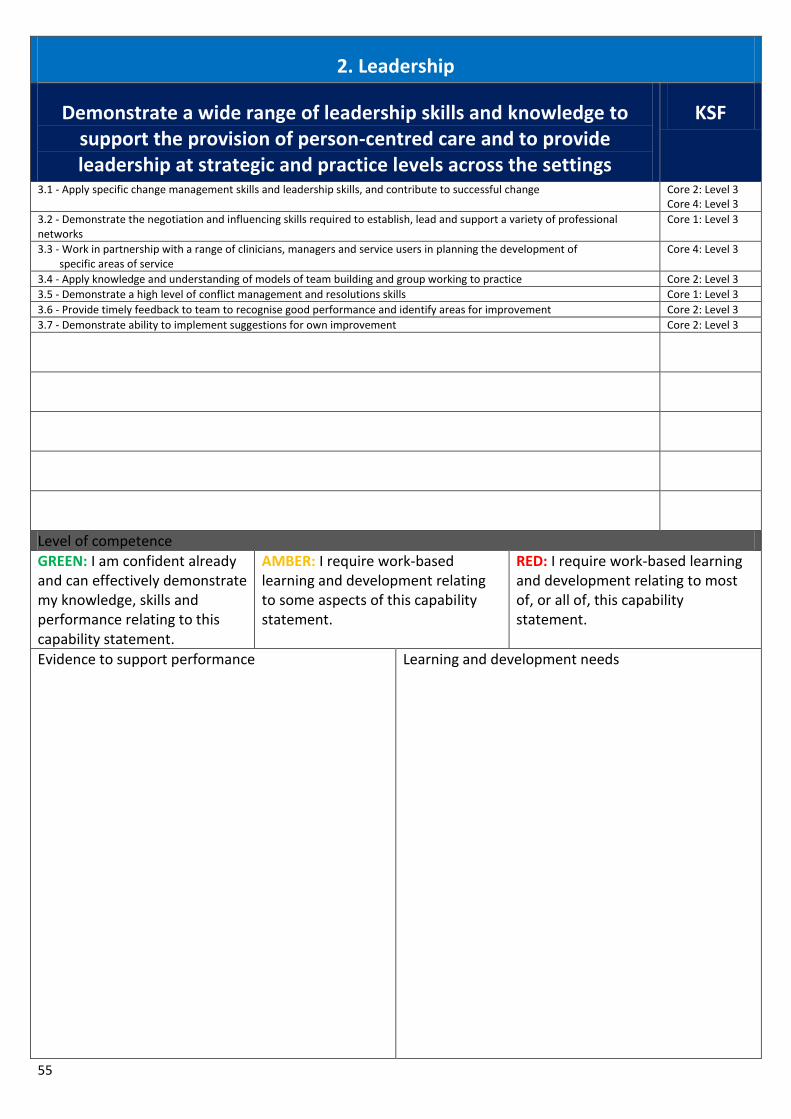
55
2. Leadership
Demonstrate a wide range of leadership skills and knowledge to support the provision of person-centred care and to provide leadership at strategic and practice levels across the settings
KSF
3.1 - Apply specific change management skills and leadership skills, and contribute to successful change Core 2: Level 3 Core 4: Level 3
3.2 - Demonstrate the negotiation and influencing skills required to establish, lead and support a variety of professional networks
Core 1: Level 3
3.3 - Work in partnership with a range of clinicians, managers and service users in planning the development of specific areas of service
Core 4: Level 3
3.4 - Apply knowledge and understanding of models of team building and group working to practice Core 2: Level 3
3.5 - Demonstrate a high level of conflict management and resolutions skills Core 1: Level 3
3.6 - Provide timely feedback to team to recognise good performance and identify areas for improvement Core 2: Level 3
3.7 - Demonstrate ability to implement suggestions for own improvement Core 2: Level 3
Level of competence
GREEN: I am confident already and can effectively demonstrate my knowledge, skills and performance relating to this capability statement.
AMBER: I require work-based learning and development relating to some aspects of this capability statement.
RED: I require work-based learning and development relating to most of, or all of, this capability statement.
Evidence to support performance
Learning and development needs
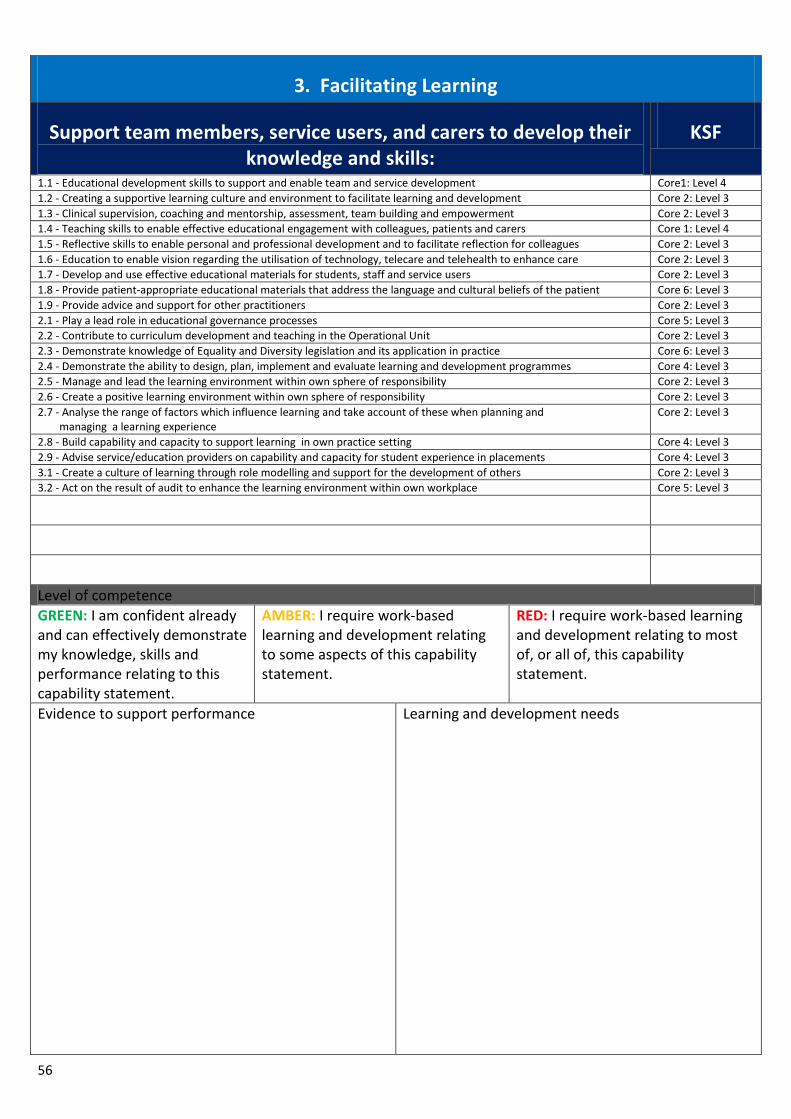
56
3. Facilitating Learning
Support team members, service users, and carers to develop their knowledge and skills:
KSF
1.1 - Educational development skills to support and enable team and service development Core1: Level 4
1.2 - Creating a supportive learning culture and environment to facilitate learning and development Core 2: Level 3
1.3 - Clinical supervision, coaching and mentorship, assessment, team building and empowerment Core 2: Level 3
1.4 - Teaching skills to enable effective educational engagement with colleagues, patients and carers Core 1: Level 4
1.5 - Reflective skills to enable personal and professional development and to facilitate reflection for colleagues Core 2: Level 3
1.6 - Education to enable vision regarding the utilisation of technology, telecare and telehealth to enhance care Core 2: Level 3
1.7 - Develop and use effective educational materials for students, staff and service users Core 2: Level 3
1.8 - Provide patient-appropriate educational materials that address the language and cultural beliefs of the patient Core 6: Level 3
1.9 - Provide advice and support for other practitioners Core 2: Level 3
2.1 - Play a lead role in educational governance processes Core 5: Level 3
2.2 - Contribute to curriculum development and teaching in the Operational Unit Core 2: Level 3
2.3 - Demonstrate knowledge of Equality and Diversity legislation and its application in practice Core 6: Level 3
2.4 - Demonstrate the ability to design, plan, implement and evaluate learning and development programmes Core 4: Level 3
2.5 - Manage and lead the learning environment within own sphere of responsibility Core 2: Level 3
2.6 - Create a positive learning environment within own sphere of responsibility Core 2: Level 3
2.7 - Analyse the range of factors which influence learning and take account of these when planning and managing a learning experience
Core 2: Level 3
2.8 - Build capability and capacity to support learning in own practice setting Core 4: Level 3
2.9 - Advise service/education providers on capability and capacity for student experience in placements Core 4: Level 3
3.1 - Create a culture of learning through role modelling and support for the development of others Core 2: Level 3
3.2 - Act on the result of audit to enhance the learning environment within own workplace Core 5: Level 3
Level of competence
GREEN: I am confident already and can effectively demonstrate my knowledge, skills and performance relating to this capability statement.
AMBER: I require work-based learning and development relating to some aspects of this capability statement.
RED: I require work-based learning and development relating to most of, or all of, this capability statement.
Evidence to support performance
Learning and development needs
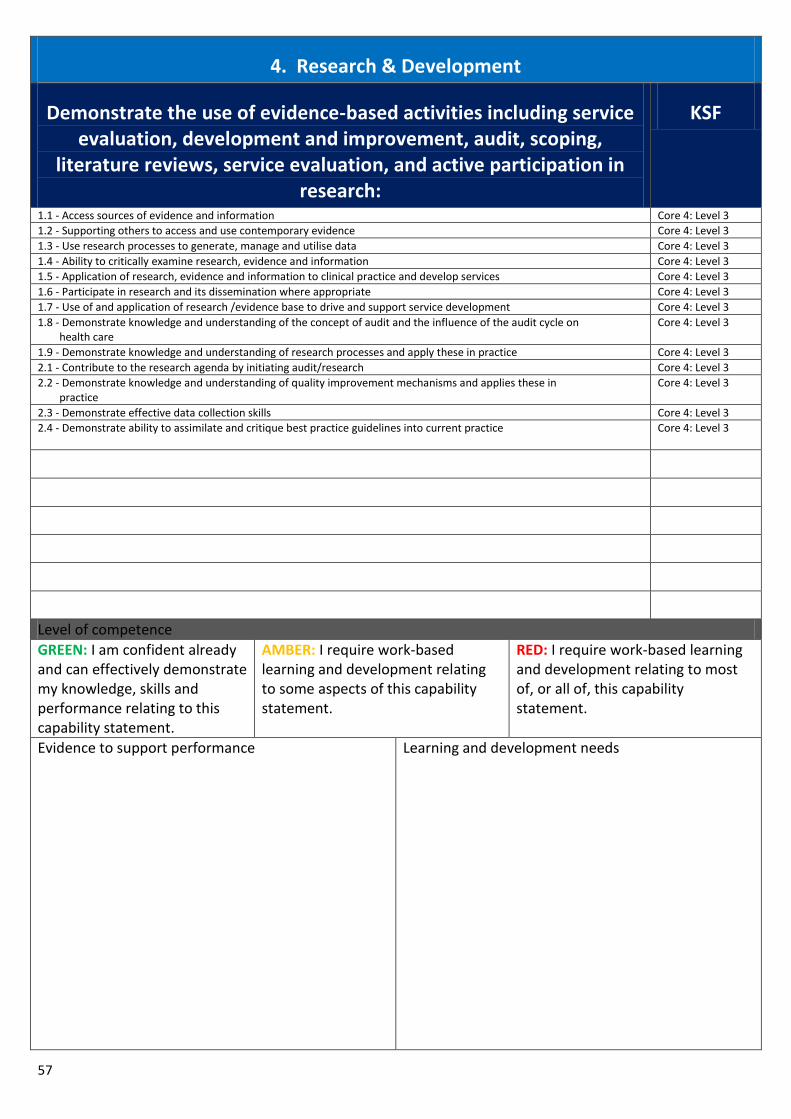
57
4. Research & Development
Demonstrate the use of evidence-based activities including service evaluation, development and improvement, audit, scoping,
literature reviews, service evaluation, and active participation in research:
KSF
1.1 - Access sources of evidence and information Core 4: Level 3
1.2 - Supporting others to access and use contemporary evidence Core 4: Level 3
1.3 - Use research processes to generate, manage and utilise data Core 4: Level 3
1.4 - Ability to critically examine research, evidence and information Core 4: Level 3
1.5 - Application of research, evidence and information to clinical practice and develop services Core 4: Level 3
1.6 - Participate in research and its dissemination where appropriate Core 4: Level 3
1.7 - Use of and application of research /evidence base to drive and support service development Core 4: Level 3
1.8 - Demonstrate knowledge and understanding of the concept of audit and the influence of the audit cycle on health care
Core 4: Level 3
1.9 - Demonstrate knowledge and understanding of research processes and apply these in practice Core 4: Level 3
2.1 - Contribute to the research agenda by initiating audit/research Core 4: Level 3
2.2 - Demonstrate knowledge and understanding of quality improvement mechanisms and applies these in practice
Core 4: Level 3
2.3 - Demonstrate effective data collection skills Core 4: Level 3
2.4 - Demonstrate ability to assimilate and critique best practice guidelines into current practice Core 4: Level 3
Level of competence
GREEN: I am confident already and can effectively demonstrate my knowledge, skills and performance relating to this capability statement.
AMBER: I require work-based learning and development relating to some aspects of this capability statement.
RED: I require work-based learning and development relating to most of, or all of, this capability statement.
Evidence to support performance
Learning and development needs

58
Appendix 3: Action Planning Tool
Action Planning - five step guide An Action Plan is exactly what is says it is – a plan outlining actions to be taken in order to achieve a set goal or target. Actions Plans are very useful for clarifying exactly what a practitioner needs to do in order to achieve a specific goal or aim. They can also be a valuable tool for using with a mentor to plan how to structure clinical experiences. You may have identified, from your self assessment, that there are areas of your practice that you need to develop further. A detailed Action Plan will help structure and guide your development.
Step 1: Aim – Exactly what is it that you hope to achieve? The first step in the process is to set a clear and specific aim/goal. Your aim also needs to be achievable and realistic. When using this capability tool, your aim/goal may be to achieve a specific capability statement or practice learning outcome.
Step 2: Structure – Exactly what do you need? Once you have defined your aim/goal, you need to think about what it is that you need to have in order to achieve it. This could be, for example, access to learning resources or opportunities, dedicated time for learning, or specific learning opportunities.
Step 3: Process – Exactly what are you going to do? Having detailed what you need in order to achieve your aim/goal, you need to think about how you are going to achieve it. The Process stage of action planning requires you to outline the specific actions you will need to take.
Step 4: Outcome – How will you know that you have achieved your goal? You also need to think about how you are going to demonstrate to yourself and others that you have achieved your goal or aim. In order to do this, you should include measurable outcomes in your action plan.
Step 5: Timescale – Exactly when will you have achieved your aim/goal This is the final stage in the process and it involves you setting defined timescales for when you are going to achieve your goal or aim. You need to be realistic about this and set timescales that are achievable within the parameters of your clinical practice.

59
Action Plan (Clinical Practice) Structure Process Outcome Timescale
What do you need?
What are you going to do?
How will you know you have achieved what you set out to achieve?
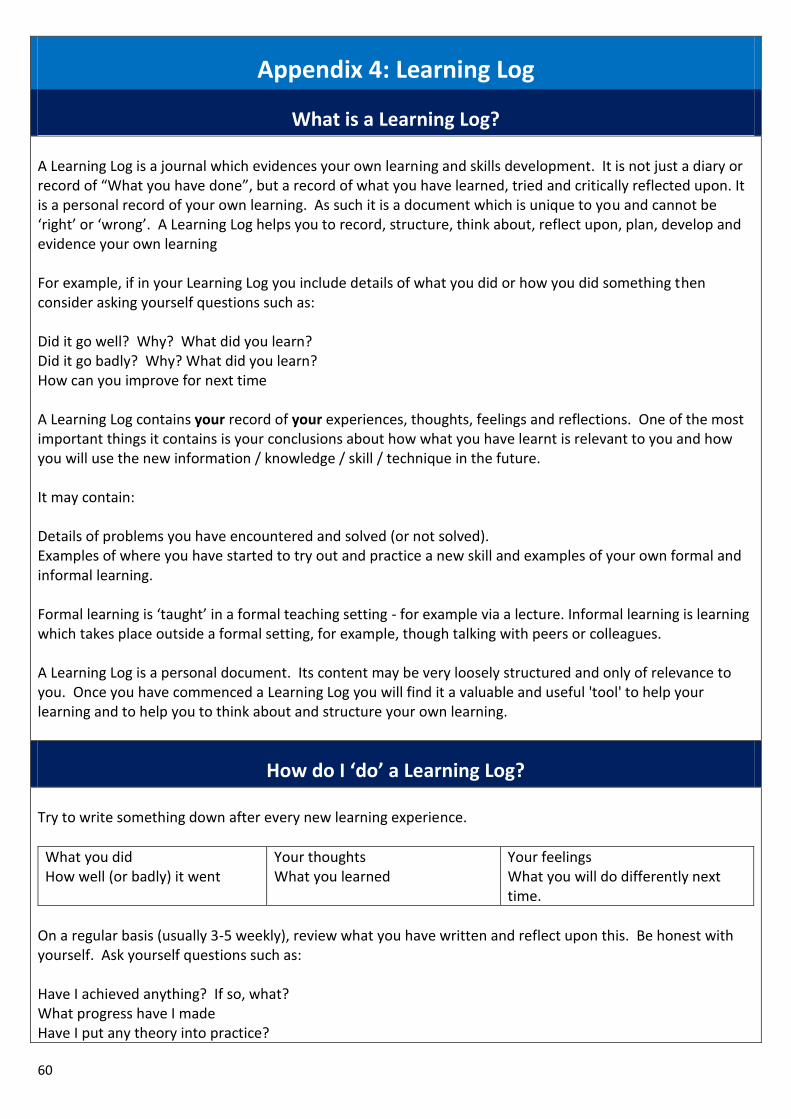
60
Appendix 4: Learning Log
What is a Learning Log? A Learning Log is a journal which evidences your own learning and skills development. It is not just a diary or record of “What you have done”, but a record of what you have learned, tried and critically reflected upon. It is a personal record of your own learning. As such it is a document which is unique to you and cannot be ‘right’ or ‘wrong’. A Learning Log helps you to record, structure, think about, reflect upon, plan, develop and evidence your own learning For example, if in your Learning Log you include details of what you did or how you did something then consider asking yourself questions such as: Did it go well? Why? What did you learn? Did it go badly? Why? What did you learn? How can you improve for next time A Learning Log contains your record of your experiences, thoughts, feelings and reflections. One of the most important things it contains is your conclusions about how what you have learnt is relevant to you and how you will use the new information / knowledge / skill / technique in the future. It may contain: Details of problems you have encountered and solved (or not solved). Examples of where you have started to try out and practice a new skill and examples of your own formal and informal learning. Formal learning is ‘taught’ in a formal teaching setting - for example via a lecture. Informal learning is learning which takes place outside a formal setting, for example, though talking with peers or colleagues. A Learning Log is a personal document. Its content may be very loosely structured and only of relevance to you. Once you have commenced a Learning Log you will find it a valuable and useful 'tool' to help your learning and to help you to think about and structure your own learning.
How do I ‘do’ a Learning Log? Try to write something down after every new learning experience.
What you did How well (or badly) it went
Your thoughts What you learned
Your feelings What you will do differently next time.
On a regular basis (usually 3-5 weekly), review what you have written and reflect upon this. Be honest with yourself. Ask yourself questions such as: Have I achieved anything? If so, what? What progress have I made Have I put any theory into practice?
61
How does what I have been doing lead to me becoming better at a skill? How can I use this to plan for the future? How can I use this to plan new learning? Experiences? In addition to 3-5 weekly reflection, you should also ask yourself these questions the next day or within 24-48 hours of each one of the taught sessions you attend or within 24-48 hours of having practiced a new skill. You will find that how you view something (your perception of something) changes over time. For example, you may have been trying to develop your communication skills and have had a bad or negative learning experience when something went wrong and you feel you have made little or no, or even backwards, progress. You may reflect upon this the next day and your thoughts and feelings may be mainly negative ones. If you reflect about the experience 3-5 weeks later on, you may find that you have now overcome the negative experience and have used it to develop further and improve yourself. Skills rarely suddenly develop or improve ‘overnight’. Learning new knowledge and applying it within a skills context usually takes time, effort and perseverance. A Learning Log will help you to become more aware of how you learn, what learning tasks you enjoy (and don't enjoy) and of your emotional and cognitive (thought) processes. At first it may seem difficult to start to critically reflect upon your own learning. Over time though, you will find that it becomes easier. The more often that you practice the skill of self-reflection, then the easier it will become. You can use your Learning Log to record courses you went on, books or papers you have read, discussions you have had, internet sites you have looked at, television programmes you have watched. Your log should become something that is directly relevant to you and your learning.
Is there a ‘best’ or ‘correct’ way of producing a Learning Log? The log should be relevant to you and your job / studies / role / activities. There is no ‘right’ or ‘wrong’ way of producing a Learning Log. Perhaps the 3 key questions when engaging in the process of producing a Learning Log are: Am I being honest with myself? Is this a useful process for me? Is this helping my own process of learning?
How can producing a Learning Log and developing the skill of critical self-reflection help me?
Again, that depends very much upon you. Some people will get more out of engaging in the process of producing a Learning Log than other people will. Research has identified that reflection can help people to change. Some of the changes which have been identified are listed below. Changes associated with reflection: From To Accepting Questioning
62
Intolerant Tolerant Doing Thinking Being descriptive Analytical Impulsive Diplomatic Being reserved Being more open Unassertive Assertive Unskilled communicator’s Skilled communicators Reactive Reflective Concrete thinking Abstract thinking Lacking self-awareness Self-aware
63
Learning Log: Template
Date of event What was the development activity?
What was I expecting to learn? What have I learned? How will I apply this learning?
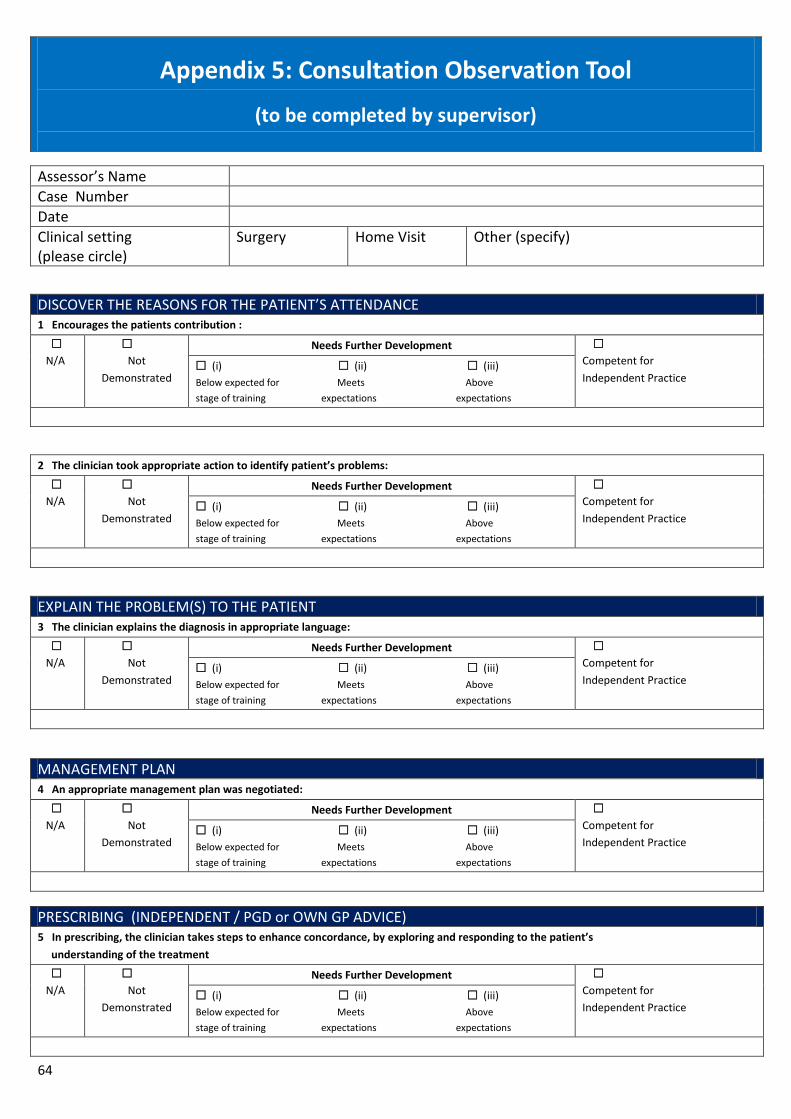
64
Appendix 5: Consultation Observation Tool
(to be completed by supervisor)
Assessor’s Name
Case Number
Date
Clinical setting (please circle)
Surgery Home Visit Other (specify)
DISCOVER THE REASONS FOR THE PATIENT’S ATTENDANCE 1 Encourages the patients contribution :
N/A
Not
Demonstrated
Needs Further Development
Competent for
Independent Practice (i) (ii) (iii)
Below expected for Meets Above
stage of training expectations expectations
2 The clinician took appropriate action to identify patient’s problems:
N/A
Not
Demonstrated
Needs Further Development
Competent for
Independent Practice (i) (ii) (iii)
Below expected for Meets Above
stage of training expectations expectations
EXPLAIN THE PROBLEM(S) TO THE PATIENT 3 The clinician explains the diagnosis in appropriate language:
N/A
Not
Demonstrated
Needs Further Development
Competent for
Independent Practice (i) (ii) (iii)
Below expected for Meets Above
stage of training expectations expectations
MANAGEMENT PLAN 4 An appropriate management plan was negotiated:
N/A
Not
Demonstrated
Needs Further Development
Competent for
Independent Practice (i) (ii) (iii)
Below expected for Meets Above
stage of training expectations expectations
PRESCRIBING (INDEPENDENT / PGD or OWN GP ADVICE) 5 In prescribing, the clinician takes steps to enhance concordance, by exploring and responding to the patient’s
understanding of the treatment
N/A
Not
Demonstrated
Needs Further Development
Competent for
Independent Practice (i) (ii) (iii)
Below expected for Meets Above
stage of training expectations expectations
65
EXPLAIN THE PROBLEM(S) TO THE PATIENT 5 The clinician specifies the conditions and interval for follow-up or review:
N/A
Not
Demonstrated
Needs Further Development
Competent for
Independent Practice (i) (ii) (iii)
Below expected for Meets Above
stage of training expectations expectations
ADDRESS THE PATIENT’S PROBLEMS 6 The patient’s problem was managed appropriately:
N/A
Not
Demonstrated
Needs Further Development
Competent for
Independent Practice (i) (ii) (iii)
Below expected for Meets Above
stage of training expectations expectations
UNDERSTANDING 7 The clinician understands the consultation process:
N/A
Not
Demonstrated
Needs Further Development
Competent for
Independent Practice (i) (ii) (iii)
Below expected for Meets Above
stage of training expectations expectations
ERRORS 8 There is/are no significant clinical error(s) in the consultation:
N/A
Not
Demonstrated
Needs Further Development
Competent for
Independent Practice (i) (ii) (iii)
Below expected for Meets Above
stage of training expectations expectations
THE CLINICIAN’S OVERALL PERFORMANCE
N/A
Not
Demonstrated
Needs Further Development
Competent for
Independent Practice (i) (ii) (iii)
Below expected for Meets Above
stage of training expectations expectations
66
Brief description of care – e.g. age, gender, presenting complaint:
Level of difficulty of challenge of consultation – Low / Average / High:
Practitioner’s own reflections:
Feedback and recommendations for further development:
Agreed action:
Assessor’s signature: Time taken for observation (minutes):
Time taken for feedback (minutes):
(Assessor’s) Surname: (Assessor’s) Forename:
67
Appendix 6: Case-Based Discussion Tool
(to be completed by Supervisor)
Clinician’s Surname
Forename
Case Descriptor Needs further
development
Competent Excellent Not
assessed
Practising holistically
Data gathering and interpretation
Making diagnoses / decisions
Clinical management
Managing medical complexity
Primary Care administrator / Multi disciplinary team referral
Working with colleagues and in teams
Community orientation
Maintaining an ethical approach
Fitness to practise
Overall assessment: Please tick Feedback and recommendations for further development:
Needs Competent Excellent
Agreed action:
Assessor’s signature:
Date:
Assessor’s name: Time taken for discussion:
Time taken for feedback:
Reflections:
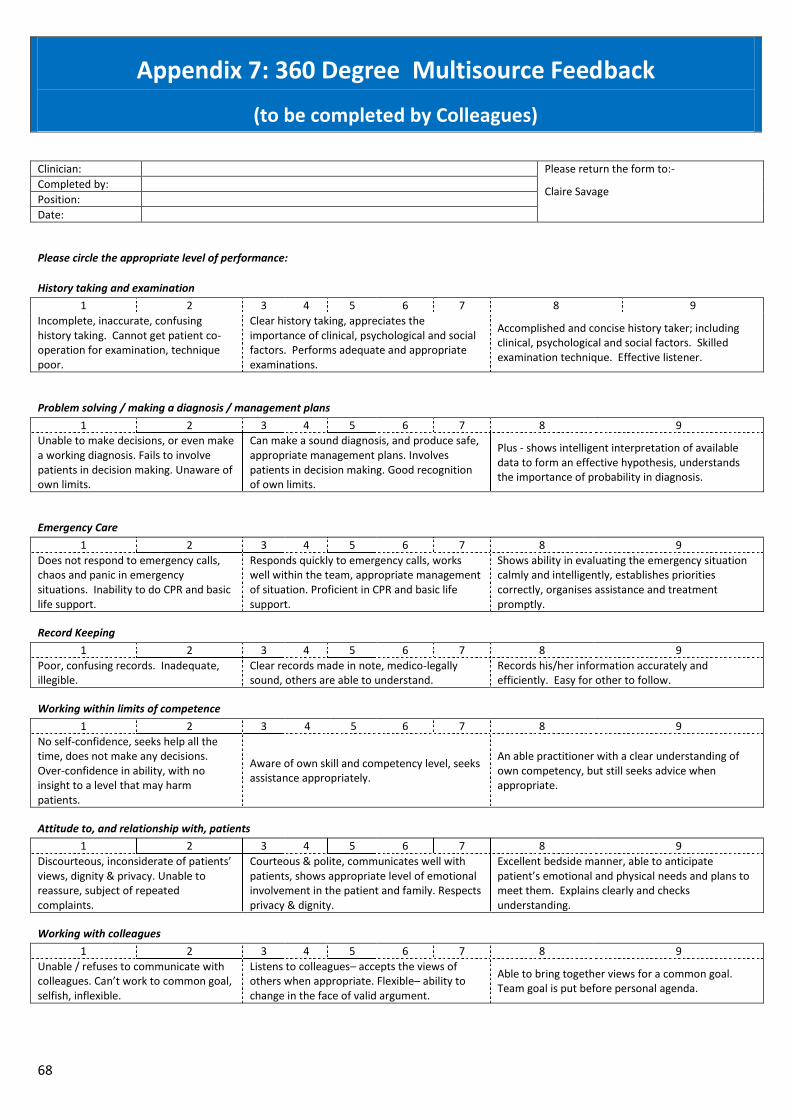
68
Appendix 7: 360 Degree Multisource Feedback
(to be completed by Colleagues)
Clinician: Please return the form to:-
Claire Savage Completed by:
Position:
Date:
Please circle the appropriate level of performance:
History taking and examination
1 2 3 4 5 6 7 8 9
Incomplete, inaccurate, confusing history taking. Cannot get patient co-operation for examination, technique poor.
Clear history taking, appreciates the importance of clinical, psychological and social factors. Performs adequate and appropriate examinations.
Accomplished and concise history taker; including clinical, psychological and social factors. Skilled examination technique. Effective listener.
Problem solving / making a diagnosis / management plans
1 2 3 4 5 6 7 8 9
Unable to make decisions, or even make a working diagnosis. Fails to involve patients in decision making. Unaware of own limits.
Can make a sound diagnosis, and produce safe, appropriate management plans. Involves patients in decision making. Good recognition of own limits.
Plus - shows intelligent interpretation of available data to form an effective hypothesis, understands the importance of probability in diagnosis.
Emergency Care
1 2 3 4 5 6 7 8 9
Does not respond to emergency calls, chaos and panic in emergency situations. Inability to do CPR and basic life support.
Responds quickly to emergency calls, works well within the team, appropriate management of situation. Proficient in CPR and basic life support.
Shows ability in evaluating the emergency situation calmly and intelligently, establishes priorities correctly, organises assistance and treatment promptly.
Record Keeping
1 2 3 4 5 6 7 8 9
Poor, confusing records. Inadequate, illegible.
Clear records made in note, medico-legally sound, others are able to understand.
Records his/her information accurately and efficiently. Easy for other to follow.
Working within limits of competence
1 2 3 4 5 6 7 8 9
No self-confidence, seeks help all the time, does not make any decisions. Over-confidence in ability, with no insight to a level that may harm patients.
Aware of own skill and competency level, seeks assistance appropriately.
An able practitioner with a clear understanding of own competency, but still seeks advice when appropriate.
Attitude to, and relationship with, patients
1 2 3 4 5 6 7 8 9
Discourteous, inconsiderate of patients’ views, dignity & privacy. Unable to reassure, subject of repeated complaints.
Courteous & polite, communicates well with patients, shows appropriate level of emotional involvement in the patient and family. Respects privacy & dignity.
Excellent bedside manner, able to anticipate patient’s emotional and physical needs and plans to meet them. Explains clearly and checks understanding.
Working with colleagues
1 2 3 4 5 6 7 8 9
Unable / refuses to communicate with colleagues. Can’t work to common goal, selfish, inflexible.
Listens to colleagues– accepts the views of others when appropriate. Flexible– ability to change in the face of valid argument.
Able to bring together views for a common goal. Team goal is put before personal agenda.
69
Probity: Has a responsible and professional attitude and approach to their work, in the following areas:- Trustworthiness
Honesty Confidentiality
Ethics Dress code Manners
Punctuality Time management
1 2 3 4 5 6 7 8 9
Poor attitude / approach in above areas, possible concerns…… Fails to make care of patient first concern, own beliefs prejudice care, abuses position as a practitioner.
Reasonable attitude / approach in above areas, a good practitioner.
Excellent attitude / approach in above areas, a credit to the profession. Patient care is the priority.
Health issues that may affect fitness to practice
Are there any health issues that are affecting or may affect the Practitioners fitness to practice? YES / NO
If you have any further comments, please add below:
Strengths:
Areas for development:
70
Appendix 8: 360 Degree Multisource Patient Feedback
(to be completed nearing the end of the supervised/training period)
Patient Assessment
Practitioner: Please return the form to:- Claire Savage Completed by:
Date:
As part of our quality assessment we need to assess how you were treated by the clinician/professional you have just seen.
Please think about your consultation with the practitioner and circle the appropriate level of performance.
How thoroughly did the practitioner ask you about your symptoms?
Unsatisfactory
Satisfactory Very good
How well did the practitioner listen to what you had to say?
Unsatisfactory
Satisfactory Very good
How well did the practitioner put you at ease during your physical examination?
Unsatisfactory
Satisfactory Very good
How well did the practitioner explain your problem or your treatment?
Unsatisfactory
Satisfactory Very good
Was the practitioner concerned for your welfare?
Unsatisfactory
Satisfactory Very good
Do you have any other comments on the practitioner?
71
Appendix 9: Significant Event Analysis (SEA) Record of Significant Event
(Patients must be identified by age and sex only)
What happened and where?
What were the contributing factors?
What have you learnt?
Further training / educational needs identified.
72
Appendix 10: Assessment of Practitioner Attachments
Section 1: To be completed by practitioner at the end of the attachment
NAME: ………………………………….…………….............................………….. POST: …………………….…...............…… SUPERVISOR: ………..……………………. DATE: ……………….. Attachment with GPs OOH Service Nurses
Poor Marginal Good Excellent
CRITERIA
01 02 03 04 05 06 07 08 09 10 11 12
1. Variety and relevance of clinical experience to OOH conditions
2. The teaching you received: (a) the quality
(b) the time
3. Conditions of work including time off, study leave etc.
4. Enjoyment of the appointment
5. Support/supervision by others in unit (a) Other staff (e.g. GPs/Partners/Team/Nurses)
(b) Supervisor
6. Portfolio (a) Usage in Teaching
(b) Overall Completion
7. Assessment (a) To what extent have you been assessed
(b) Quality of Assessment
73
RESPONSIBILITY: In this post please assess the responsibility you were given/allowed/or exposed to in terms of its appropriateness to your previous level of training and experience.
Much Too Little Too Little About Right Too Much A Lot Too Much
TEACHING TIME:
(i)
Informal teaching (hours per week)
(ii) Formal tutorials (hours per
week)
Main strengths of Post/Experience Main Weaknesses of Post/Experience
Would you recommend this post to a colleague? Yes/No Have you discussed this assessment with Clinical Supervisor? Yes/No
74
Section 2: To be completed by main clinical supervisor and two or three other clinicians
The Clinical Supervisor is requested to complete this assessment at the end of each attachment. NAME: POST: DATE: Attachment number: First Second Final (Please enter appropriate number)
Poor Marginal Good Excellent
In my opinion his/her 01 02 03 04 05 06 07 08 09 10 11 12
1.
Clinical history skills are
2.
Clinical examination skills are
3.
Clinical reasoning skills are
4.
Relationship with patients is
5.
Relationship with team is
6.
Relationship with medical colleagues is
7. Willingness to learn is
8.
Professional values are
9
Competence in portfolio areas and skills
Number of ‘sign offs’ completed:
Examination skills
Practical skills Symptoms Emergencies Chronic disease Patients
75
Please comment
Main strengths:
Main Weaknesses:
Future Learning Needs:
Assessment discussed with Practitioner? YES / NO
Signed: Name: (Clinical Supervisor) (Please Print)
Date:
76
Section 3: To be completed by Educational Lead NAME: POST: DATE: Attachment number: First Second Final (Please enter appropriate number)
Poor Marginal Good Excellent
In my opinion his/her 01 02 03 04 05 06 07 08 09 10 11 12
1.
Clinical history skills are
2.
Clinical examination skills are
3.
Clinical reasoning skills are
4.
Relationship with patients is
5.
Relationship with team is
6.
Relationship with medical colleagues is
7.
Willingness to learn is
8.
Professional values are
9
Competence in OOH portfolio areas and skills

77
Please comment
Main strengths:
Main Weaknesses:
Future Learning Needs:
Assessment discussed with Practitioner? YES / NO
Signed: Name: (Clinical Supervisor) (Please Print)
Date:

78
Appendix 11: Structured Reflection Guided reflection is a combination of techniques intended to enable the practitioner to reflect on their professional work experience in order to become increasingly effective, i.e. enabling them to utilise and learn through reflection on experiences, in a structured and supported way. Reflection is the process of internally examining and exploring an experience, which creates and clarifies its meaning and decisions made, resulting in changes to your knowledge and potentially your own perceptions. The practitioner needs to be able to use reflection in a meaningful way. For example, knowing what the essential learning areas are does not necessarily mean you will become a skilled practitioner. You need to consider your own performance and use the opportunities for learning in a pro-active way. Understanding the nature of assertiveness may help you to enact any difficulties you may have but unless you are able to transfer these skills to the learning environment, through reflection, you will not be able to make best use of the learning opportunities.
There are three elements to guided reflection:
Using a model of structured reflection
Supervision
Using a diary structure to support your portfolio development
A model of structured reflection Core Questions: • Description of experience • Describe the ‘here and know’ experience • What contributed to this experience? • What was the significant background to this experience?
Reflection • What was I trying to achieve? • Why did I behave as I did? • What were the consequences of my actions for – the patient, and myself? • How did I feel about this experience when it was happening?
Learning • How do I feel about this experience? • How have I made sense of this experience in light of past experience and future practice? • How has this experience changed my ways of knowing? • By observing/seeing? • By doing and applying principles • Understanding ethical considerations • Personally?
79
Influencing Factors • What internal and external factors influenced my learning • What sources of knowledge did/should have influenced my decision-making? • Could I have dealt with the experience differently? • What choices did I have? • What would have been the consequences of these choices?
Maintaining a Structured Diary Write up experiences on the same day, wherever possible. Use your own words to capture the situation for you. Make a habit of writing up a least one experience per day. Balance positive experiences with problematic or less positive experiences. Challenge yourself at least once a day to do something that you would normally do without thought or take for granted – ask yourself – ‘why do I do that.’ Always try to be open and honest with yourself. Use the above to develop a plan for further reflection, analysis, study or action.
80
To be completed following education sessions/courses, either by interview or questionnaire
Please rate the extent to which the statements below are true:
Strongly Disagree Disagree Agree Strongly Agree
The programme has had a positive impact on my practice
The programme improved my performance in the job
I have had sufficient opportunity to apply my learning
I have applied the knowledge taught on the programme to my job
I have applied the skills taught on the programme to my job
I have applied the attitudes taught on the programme to my job
I feel confident in applying what I have learnt to my job
I feel more effective in my job as a result of this programme
If you have implemented new knowledge as a result of the programme, please describe below, e.g. What new knowledge? How did you apply it to your job? What effect did this have on your practice?
If this programme has had an impact upon any of the skills you use in your job (either existing or new skills), please describe below, e.g. Which skills were affected? In what way did they change as a result of the programme? How has this affected your practice?
If this programme has had an impact on your attitude, please describe below, e.g. Has there been a change in your confidence and / or self-awareness? What effect has this had on your job?
81
82
Appendix 12: Standard Offer Letter
Dear New Employee, Post of Senior Practitioner / Advanced Practitioner (Primary Care) I refer to your recent interview for the above post and have pleasure in confirming our offer on the terms below. 1. Salary Scale: This post is offered at Band 6 / Band 7. The salary scale for this post is:- £31,696; £32,731; £33,895; £35,577; £36,612; £37,777; £39,070; £40,428; £41,787 (Band 7). Or £26,595; £27,635; £28,746; £29,626;£30,661; £31,696; £32,731; £33,895; £35,577 (Band 6). Your point of entry to the scale and your incremental date will be determined after verification of any reckonable previous service. 2. Work Base: Work location will be flexible, but mileage will be calculated from this base. Pool cars will be used where possible. 3. Hours of Work: 37.5 per week - actual hours may vary weekly due to service needs. Regular on call commitments away from home are required. 4. Appointment Effective from: 5. Notice: One month This offer of employment is subject to 2 satisfactory references, and satisfactory clearances from the Occupational Health Service and Disclosure Scotland in respect of substantial access to children and/or vulnerable adults. Please complete the attached Occupational Health Declaration Forms and return to me in the envelope provided. Fitness for work All new NHS Highland employees and recruits transferring into posts where statutory health surveillance is in place are required to provide information on their health to the Occupational Health Service so an assessment on fitness to work, any reasonable adjustment needed to support work, requirement for statutory health surveillance and need for immunisation can be made. If you are entering a post that involves Exposure Prone Procedures (EPP) there is very specific screening that requires to be done prior to you undertaking EPP tasks. This is based on explicit Scottish Government guidance on protecting patients. If you are aware you have any infectious disease or other health related condition that may impact on your work you have a responsibility to discuss this with the Occupational Health Service. ALL health care workers with direct clinical contact are required to provide information relating to their immunity to Tuberculosis, Rubella, Measles, Mumps and Varicella. Hepatitis B vaccination is recommended. Health care workers undertaking exposure prone procedures (EPP) must also provide documentary evidence of having undergone a validated blood test showing their Hepatitis B surface antigen status. Since 2002 EPP workers entering training or an EPP post are also required to provide validated blood test results for Hepatitis C and since 2006 results of an HIV antibody
83
test. This information is required before starting EPP work. Failure to do so may delay the Occupational Health clearance process and your manager will be advised that you cannot undertake EPP work until this information has been received. Have you had your immunity checked or been immunised against any of the following infectious diseases? All information is held in strict confidence and will not be divulged to any other party without your consent. An opinion on your fitness for work and any other needs to protect your health however will be given to the recruiting manager. NHS Highland Policies NHS Highland has a policy that all staff will be issued with and required to wear a NHS Highland Identity Badge at all times when on duty. All Identity badges are the property of NHS Highland and must be returned when you terminate your employment. NHS Highland's general employment relations policies and procedures are available for reference on the staff section of the Policies Library on the NHS Highland Intranet. The leave year runs from 1st April to 31st March and your annual leave entitlement and public holiday entitlement will be based on a proportion of the following:-
Length of Service Annual Leave and Public Holiday Allocation
On appointment 27 days + 8 public holidays
After 5 years service 29 days + 8 public holidays
After 10 years service 33 days + 8 public holidays
All of the above entitlements are based on a working day of 7.5 hours (5 days per week) and will be applied on a pro rata basis for part time staff. A list of the designated public holidays is available from your manager. The enclosed Induction Handbook will provide you with useful information prior to joining the organisation. Superannuation - Auto Enrolment All employees, eligible to join the NHS must be automatically included in the scheme from the first day of employment. Eligible employees will no longer be allowed to opt out of the scheme before they take up employment. They must be enrolled in the first instance. Training and development Your training and ongoing development will be governed by the Highland Competency Framework for Advanced Practice. You will be assigned an educational supervisor who will take you through the needs analysis element of this framework, and support you to develop appropriate skills and experience. [In order to progress from a development role (Band 6) to an autonomous Advanced Practitioner (Band 7), you will require to submit a portfolio demonstrating that you have met the levels of competency outlined in the framework. The competency framework details the process to be followed. It also details the point at which failure to submit a portfolio may result in termination of contract.] Recovery of Expenses where Voluntary Termination Occurs This role involves the supported development of a range of advanced skills and qualifications. In the event of an employee voluntarily terminating their employment with NHS Highland, costs relating to learning and
84
development activities may be required to be repaid by the employee if a financial investment has been made in the activities. Normally, repayment would be required up to two years after the completion of a training course or activity. Repayment will be based upon the direct cost to the organisation of the training activity. It will not include salary or backfill costs. Repayment will be based on the sliding scale show in the table following. This is in line with the NHS Highland Study Leave Policy:
No of Months since completion of a training activity/course
Percentage repayable by employee in event of resignation
0-6 (or if termination occurs before completion of training programme)
100 – Up to a maximum of £7000
7 95
8 90
9 85
10 80
11 75
12 70
13 65
14 60
15 55
16 50
17 45
18 40
19 35
20 30
21 25
22 20
23 10
24 NIL
When an employee terminates their contract of employment with NHS Highland, it is the manager’s responsibility to ensure, in accordance with the above criteria, the monies to be recovered. In the event that monies are to be recovered from an employee it is the manager’s responsibility to advise the pay unit of the amounts to be recovered. NHS Highland Out of Hours Part of your rota will involve the provision of Out of Hours Unscheduled care, both on shift and on call. NHS Highland’s Out of Hours service is governed by a suite of operational and clinical protocols. They are available on the Intranet (http://intranet.nhsh.scot.nhs.uk/Org/DHS/UnscheduledCare). A condition of your employment in out of hours settings is that you read and sign a copy of the handbook. [The Rural Support Team The Rural Support Team is a new multi-disciplinary model, providing primary care services in and out of hours using a team of professionals from different backgrounds. Led by GPs, the team also includes Advanced Nurse Practitioners and Advanced Paramedic Practitioners. These practitioners work autonomously to provide scheduled and unscheduled care across North Skye, Ardnamurchan and Wester Ross, often working alone in remote and rural locations of the Highlands.
85
Practitioners appointed to the Rural Support Team will be expected to work flexibly across this patch, with on-call arrangements applying for some Out of Hours shifts. Highland’s unique geography means that extensive travel to remote and rural locations is required. The development of this team has taken the form of an action learning project. This means the team is an evolving one, and team members will be asked to contribute to the development and improvement of the Rural Support Team.] Please confirm acceptance of this offer of appointment by signing the copy letter and returning it to me in the envelope provided within one week of its receipt. I hope that you will be happy in your new post and that you will find it both interesting and rewarding. Yours sincerely Employment Services Manager If you agree to accept this arrangement under the foregoing terms and conditions please sign the enclosed copy of this letter and return it to me along with the documents listed below in the enclosed stamped return envelope. Signed ......................................... Date ........................................
86
Appendix 13: Example Job Descriptions
North & West, Advanced Nurse Practitioner (Unscheduled Care)
1. Job Identification
Job Title: Advanced Nurse (Unscheduled Care) (Band 7) Managerial Reports to: District Manager Professional: Lead Nurse Department: North and West Operational Unit Job Reference: NWOUWESTNURSUNSC01 No of Job Holders: Last Update: 31st July 2014 (Revised 20 August 2014)
2. Job Purpose As a Nurse Practitioner (Unscheduled Care), you will be expected to provide expert clinical case management to children and young people, adults, carers, families and communities within a defined population in the most appropriate environment, whether in the community, on the telephone or in the Emergency Department. To undertake advanced level assessment in order to address undifferentiated illness and injury by using expert knowledge and clinical judgement to diagnose, initiating interventions and negotiate discharge, to refer or follow up arrangements. To provide health promoting, patient-centred, evidence-based clinically effective nursing care. To continually improve patient care pathways, in conjunction with other statutory and voluntary services, for patients and their carers. Will be working as part of the wider out of hour’s team but will mainly work in isolation without direct supervision. Responsible for the assessment, planning, delivery and evaluation of high quality health care. Using a proactive approach to promoting health and wellbeing, detection and prevention of vulnerability, preventing illness, reacting and responding to existing or potential ill health issues and contributing to reduction in unplanned hospital admissions.
3. Dimensions NHS Highland has a predominantly rural geographical area. The ANP post holder will work autonomously as first contact clinician to both patients requiring home visits and also attendees to the Primary Care Centre. This post is integral to ensuring safe, effective, high quality care is delivered as close to home as possible, by a sustainable and appropriately skilled workforce with a reduction in dependency on medical models of care provision.
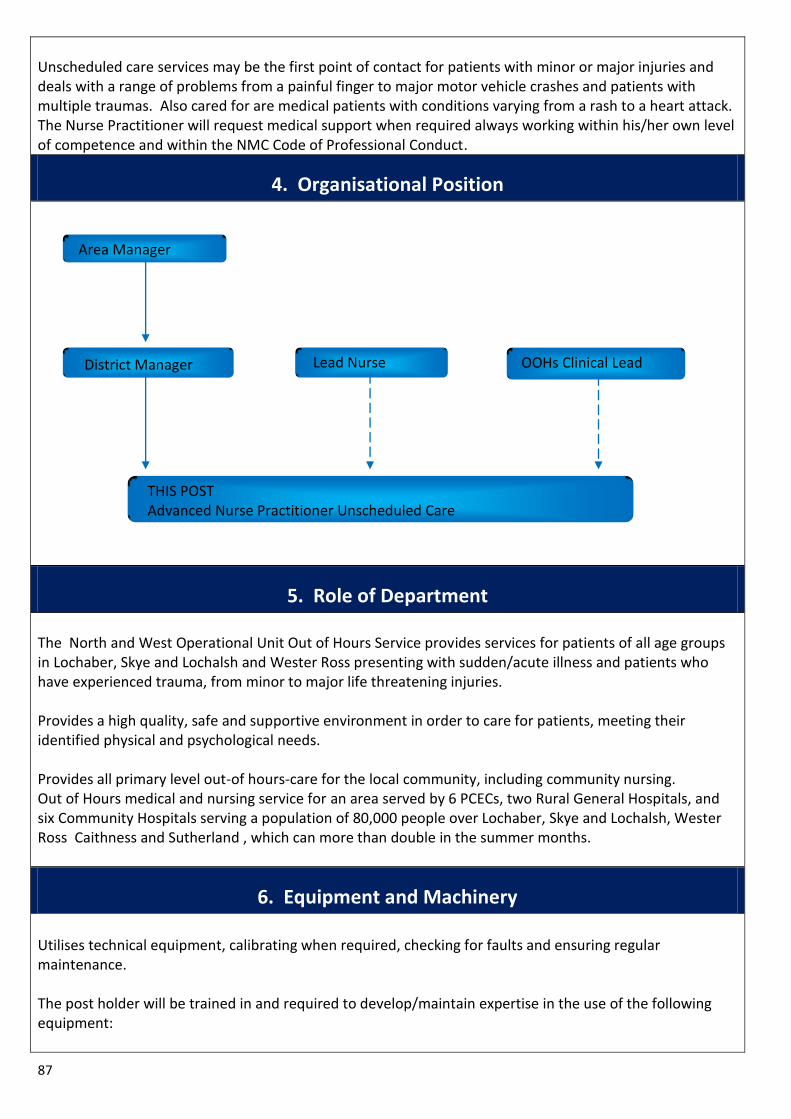
87
Unscheduled care services may be the first point of contact for patients with minor or major injuries and deals with a range of problems from a painful finger to major motor vehicle crashes and patients with multiple traumas. Also cared for are medical patients with conditions varying from a rash to a heart attack. The Nurse Practitioner will request medical support when required always working within his/her own level of competence and within the NMC Code of Professional Conduct.
4. Organisational Position
5. Role of Department The North and West Operational Unit Out of Hours Service provides services for patients of all age groups in Lochaber, Skye and Lochalsh and Wester Ross presenting with sudden/acute illness and patients who have experienced trauma, from minor to major life threatening injuries. Provides a high quality, safe and supportive environment in order to care for patients, meeting their identified physical and psychological needs. Provides all primary level out-of hours-care for the local community, including community nursing. Out of Hours medical and nursing service for an area served by 6 PCECs, two Rural General Hospitals, and six Community Hospitals serving a population of 80,000 people over Lochaber, Skye and Lochalsh, Wester Ross Caithness and Sutherland , which can more than double in the summer months.
6. Equipment and Machinery
Utilises technical equipment, calibrating when required, checking for faults and ensuring regular maintenance. The post holder will be trained in and required to develop/maintain expertise in the use of the following equipment:
Area Manager
District Manager Lead Nurse
THIS POST Advanced Nurse Practitioner Unscheduled Care
OOHs Clinical Lead
88
Moving and handling including Mangar Elk lifting equipment.
Patient assessment and monitoring equipment including tympanic thermometers, ECG machines, pulse oximeters.
Continuous Subcutaneous Infusion pumps.
Resuscitation equipment including defibrillators.
Digital imaging
Telehealth, telemedicine/video conferencing
7. Systems The post holder will be trained in and required to develop/maintain expertise in the use of the following systems:
Maintain accurate records in accordance with NMC and NHS Highland guidelines.
Work within NHS Highland and departmental policies, procedures and protocols.
Systems for risk identification, management and complaints.
Policies and procedures for child protection and the protection of adults at risk.
Use of Adastra and other administration system.
Laboratory and radiology results systems.
NHS Highland intranet and email.
Internet – able to source up to date clinical information and guidelines i.e. SIGN guidelines.
Maintaining stores and ordering system within funded financial footprint, supporting line manager with achievement of efficiency measures, whilst maintaining a quality service for patients.
Adhere to all hospital and office systems for example, reorganise rotas for sudden cover requirements, sickness / absence, change in workload, training etc
Utilise communication systems for example, meetings, communication book, and multi-disciplinary team meetings.
8. Assignment and Review of Work The post holder is expected to work autonomously, organising and prioritising their own workload in relation to meeting the needs of the service. The remit also includes responsibility for decision making regarding the assessment, subsequent diagnosis and management plan of patients presenting during the out of hours period. The post holder will:
Be able to analyse complex information on which, judgements and consequently sound decisions will be based.
Be accountable for professional conduct in accordance with NMC standards.
Be responsible for exercising professional judgement in relation to the clinical element of their role.
Make clinical decisions in partnership with patients and their families, other clinicians and members of the MDT.
The workload is determined by the needs of the service and the post holder will delegate / allocate work appropriately to the nursing team.
When undertaking Nurse Practitioner (Unscheduled Care) duties the post holder will seek clinical guidance from senior medical staff as appropriate.
Is expected to anticipate problems / needs and take steps to resolve them in the absence of Charge
89
Nurses, involving appropriate colleagues e.g. Nurse Manager, Consultant, Bed Manager, Duty Manager
Work within a duty rota developed for the department and Unscheduled Care Team.
9. Decisions and Judgments The ability to quickly assess and respond to patients needs in emergency situations. The post holder has to demonstrate rapid decision-making skills in an ever changing and unpredictable environment. Post holder will be responsible for ensuring that clinical practice meets the standard of care set by the NMC and NHSH, and that non compliance with these standards is managed in accordance with the appropriate policies and procedures. Provision of professional advice to registered/ unregistered staff and students and an ability to recognise own limitations and the requirement for appropriate referral. Judgments involving highly complex facts or situations, which require the analysis, interpretation and comparison of a range of options. Assessment of patients’ complex needs (physical, psychological, social and spiritual) to establish a change in condition, inform clinical decision making and plan care.
10. Most Challenging/Difficult Parts of the Job Developing a new and challenging clinical role to best meet the needs of the service. Working alone. Palliative Care: Difficult communication and decision making with patients and relatives. Managing an unpredictable and diverse workload Accountability whilst working as an autonomous practitioner. Geography of Highland – extended travelling times, potentially difficult to meet targets. Risk assessment in the community setting. Prioritising and meeting competing demands from patients, relatives and members of the multidisciplinary team. Working effectively, as an autonomous practitioner, with a variable and unpredictable workload. Ability to at the same time deal with patients and/or relatives who may be highly anxious, as well as meeting the needs of the patients of all ages and diverse conditions with time constraints and without the availability of the patients’ records. In urgent or emergency situations, being able to deliver quality, spiritually sensitive and culturally appropriate care to patients with communication problems. Ability to give direct quality patient care to all patients, prioritising and re-prioritising in the face of
90
changing demands. Supervision of inexperienced staff while they gain the necessary experience to enable them to work under minimal supervision. Maintaining up to date high standard of clinical knowledge and competences required to provide a breadth of care, in different settings for a very wide variety of presenting conditions. Maintain high levels of concentration with frequent interruptions. Have knowledge and skills to enable Child Protection and Vulnerable Adults needs to be recognised and managed as current policy states. Knowledge and skills required to perform telephone/telemedicine assessment / advice.
11. Communications and Relationships
Identifies potential and existing challenges in care options for patients, carers and staff, using negotiation and counselling skills to achieve reconciliation and the best outcomes for the patients. Communicates effectively verbally, in writing or electronically and non verbally. Ensures effective communication with all team members, which proves challenging due to various shift patterns across the 24 hour period, including all members of the MDT. Liaise with external agencies e.g. Police, SAS, Social Work, Armed Forces, Procurator Fiscal, mountain rescue, Press Officers and university educational staff. Participates in regular meetings with colleagues for the purpose of planning, managing and developing nursing services, improving patient care, discussing policy issues, amending, updating, implementing and evaluating them, discussing and problem solving challenges in clinical care and team development. Facilitates effective dissemination of information to all relevant staff. Demonstrate empathy, sensitivity and support when communicating with patients, relatives and staff, especially in relation to breaking bad news and dealing with emotionally challenging situations. Regularly demonstrates the ability to handle highly sensitive information in a manner not liable to offend or antagonise. Dealing with situations when patients do not easily understand their care packages, due to culture, language or learning difficulties. Maintain confidentiality in accordance with NMC and NHS Highland policies, including promoting compliance and adherence to the requirements of the Data Protection Act and the Caldicott Guidelines.
12. Physical, Mental, Emotional and Environmental Demands of the Job Physical Moving and handling of patients - in bed / trolley, on to and off trolleys, from bed/trolley to chair,
91
assistance with walking, transfer from ambulance trolley, undertake co-ordinated log rolls for patients with potential spinal injuries, assist injured/ill patients out of private transport. Frequently assessing the risk of violent / aggressive / challenging behaviour of patients and visitors and deal with it appropriately. Highly developed physical skills where a degree of precision or speed and high levels of hand, eye and sensory co-ordination are essential, e.g. take blood samples, administer injections, suture insertion and removal, insertion of venflon devices to set up IV access, calibrate equipment, use computer keyboard. Remove full outdoor clothing from unconscious / incontinent / uncooperative patients. Daily efforts to assist patients to move/talk/transfer. Risk assess to create a safe working environment whist being sensitive to patient’s environment and property – daily. Exposure to hazardous substances. Exposure to violence and aggression. Driving/accompanying a driver in unfamiliar geographical areas. Working in a patient’s home, where there may be reduced lighting and confined space. Mental / Emotional Concentration, decision-making and organisational skills to cope with competing demands. Recognising patients’ urgent health care needs and making appropriate instant decisions to provide appropriate clinical management, often without being in full receipt of patients’ full medical history. Dealing with emotional effects of caring for patients and their families who may be distresses anxious or worried. Dealing with emotional effects on patients, family and oneself when breaking bad news. Concentration required checking documentation / patient notes and calculating drug dosages. Autonomous lone working recognising patients urgent health care needs and making rapid decisions to provide appropriate clinical management – daily. Emotional demands of coping with colleagues diverse personalities. Emotional demands of working unsupervised in patients’ homes. Emotional demands of patients and relatives spiritual needs. Emotional demand in relation to family and human dynamics, dealing with people in high distress or crises such as dying and death. Environmental Coping with unpleasant materials and smells – bodily fluids, excreta, infected wounds – daily.
13. Knowledge, Training and Experience Required to do the Job Qualifications: Registered Nurse. Current NMC Registration. 1st level degree- preferred. Extended and Independent Nurse Prescriber. Advanced Clinical Assessment Module certificate at degree level. Completion of Common Presentation Module at degree level or to be completed within a mutually agreed timescale. Training and Experience: 4 years post registration experience. Community & Primary care experience. Evidence of relevant on-going professional development. Mandatory training as per NHSH.
92
Ability to manage minor illness and injury. PILS/ ILS/ Paediatric emergency care framework. BASICS Pre-hospital Care. (desirable) Experience of working in collaboration with other professionals across organisational boundaries. Experience or working with children and young people, adults, families, carers and communities. It is also an expectation that the post holder will undertake further education and study relevant to the post for service developmental purposes. Risk assessment/ incident reporting. Ability to work under own initiative and prioritise effectively and confidence and experience to act autonomously. Knowledge and Skills: Highly developed specialist knowledge across a wide range of work procedures and practices underpinned by theoretical knowledge and relevant practical experience. Knowledge and skills to work at an advanced level of practice within a generic / specialist area of clinical practice. Complex decision making skills. Knowledge and experience of mentorship within clinical practice. A broad range of knowledge and skill underpinned by theory, to deal with the full range of patients presentations and complexities of need including minor to urgent life threatening health needs. Knowledge and understanding of Health and Safety Policy, with evidence based practice i.e. Mental Health Act, and Incapacity of Adults Act. Capable and competent in a range of advanced level of clinical skills. A commitment to lifelong learning and evidence of continuing professional development. Ability to direct and coordinate programmes of care working collaborative and autonomously. Participation in audit data capture to evaluate service delivery and to inform future service planning. Clinical skills as follows: Cannulation Venepuncture Arterial blood gas sampling and interpretation Male and female urinary catheterisation Syringe driver operation Recording and interpreting 12 lead ECG’s IV drug administration Wound and skin care management including suturing.
14. Job Description Agreement
I agree that the above Job Description is an accurate reflection of my duties and responsibilities at the date of signing. Job Holder’s Signature: Manager’s Signature:
Date: Date:
93
IMFOU: Unscheduled Care Nurse
1. Job Identification Job Title: Nurse Practitioner (Unscheduled Care) (Band 7) Reports to: District Manager Department, Ward or Section: Emergency Department CHP, Directorate or Corporate Department: Medical Directorate Job Reference: SMOUNHSHNURSUNSC05 No of Job Holders: 4 Last Update: May 2013
2. Job Purpose
As a Nurse Practitioner (Unscheduled Care), you will be expected to provide expert clinical case management to children and young people, adults, carers, families and communities within a defined population in the most appropriate environment, whether in the community, on the telephone or in the Primary Care Emergency Centre (PCEC).
To undertake advanced level assessment in order to address undifferentiated illness and injury by using expert knowledge and clinical judgement to diagnose, initiating interventions and negotiate discharge, to refer or follow up arrangements.
To provide health promoting, patient focused, evidence based clinically effective nursing care.
To continually improve patient care pathways, in conjunction with other statutory and voluntary services, for patients, and their carers.
Will be working as part of the wider out of hour’s team but will mainly work in isolation without direct supervision. Responsible for the assessment, planning, delivery and evaluation of high quality health care.
Using a proactive approach to promoting health and wellbeing, detection and prevention of vulnerability, preventing illness, reacting and responding to existing or potential ill health issues and contributing to reduction in unplanned hospital admissions.
3. Dimensions The post holder will assist in providing an autonomous injury and illness service within their area/ department. This involves triage, assessment, requesting investigations and interpretation of results, diagnosis, treatment, discharge or onward referral to other medical specialties, without always referring to a doctor. Triage and institute care in the PCEC and community, referring to appropriate agencies within the care family. Comprehensive management of cases using specialized skills. Unscheduled care services may be the first point of contact for patients with minor or major injuries and deals with a range of problems from a painful finger to major motor vehicle crashes and patients with multiple traumas. Also cared for are medical patients with conditions varying from a rash to a heart attack. The Nurse Practitioner will request medical support when required always working within his/her own level of competence and within the NMC Code of Professional Conduct.
94
Expectations: Post holders will independently assess, treat and discharge a large proportion of patients attending. They will have medical clinical support available on request, and assist medical colleagues with clinical management of patients with major illness and injury. Provide nursing expertise and management of patients in Unscheduled Care. Provide unscheduled nursing care to patients in their own homes with immediate issues, e.g. medication management, wound care, urinary catheter management to prevent hospital admission. Assessing, planning and implemention of care of in-patients in Mid Area community hospitals. Planning and organisation of a broad range of complex activities, some of which are ongoing, which requires the formulation and adjustment of plans or strategies. To care for patients of all ages including paediatrics and elderly Provide care for bereaved relatives/carers/ friends Sudden, sometimes traumatic, death of adults and children Infection Control Leading/taking part in research projects within the department Leading/taking part in delivering teaching and training Awareness of staff rostering and ability to make best use of resources Awareness of departments supply levels and correct ordering procedures Initial care of patients presenting with mental health problems.
4. Organisational Position
Area Manager
District Manager Lead Nurse OOHs Clinical Lead
Nurse Practitioner Unscheduled Care (this post)
5. Role of Department The Mid Area Out of Hours Service provides services for patients of all age groups in Mid and East Ross presenting with sudden / acute illness and patients who have experienced trauma, from minor to major life threatening injuries. Provides a high quality, safe and supportive environment in order to care for patients, meeting their identified physical and psychological needs. Provides all primary level out-of hours-care for the local community, including community nursing. Out of hours medical and nursing service for 2 PCECs and 3 community hospital units serving a population of 100.000 people.
95
6. Main Tasks, Duties and Responsibilities 1. Works as an autonomous practitioner within the Statutes and Guidelines as laid down by the
Nursing and Midwifery Council. 2. Works autonomously as a Nurse Practitioner (Unscheduled Care) adhering to defined
unscheduled care guidelines. Assessment, history taking, examination, treatment, request/interpret tests, full comprehensive documentation, prescribe medication within the role of an extended and independent nurse prescriber.
3. Sets high standards of professional practice and clinical leadership 4. Involved with the setting and maintaining of standards of care within the agreed guidelines of
NHS Highland policies and procedures and ensures adherence to and delivery of a high quality service, whilst developing clinical leadership.
5. Responsible for assessment of health care needs of patients, involving families / carers and develops, plans, implements and evaluates programmes of care.
6. Has the ability to organise own workload and adjust priority of changing demands to ensure all needs are met in the care of Out of Hours patients.
7. With reference to NHS Highland and NMC guidelines, the post holder is accountable to initiate and maintain patient records e.g. Triage / assessment, Nursing Notes, Care Pathways, clinical notes.
8. Provide support and advice to patients and their families or carers, giving the knowledge required to help them understand and cope with their condition, offering psychological, physical and spiritual support, including health support and accident prevention.
9. Demonstrate skills within scope of Professional Practice with sound clinical knowledge e.g. ECG recording, I.V. drug therapy, basic plaster of Paris and splint application, urinary catheterisation, venepuncture, cannulation, arterial blood gases, wound management and closure including suturing, skin adhesives and steristrips. Able to identify own limitations and refer to more senior practitioners or medical staff when skill required is beyond scope of practice.
10. With knowledge and skills in unscheduled care, act as a clinical advisor to junior medical and nursing staff and encourage others to develop their skills ensuring staff are competent to deliver high standards of care e.g. develop role by using evidence based practice and continuously improve own knowledge.
11. Perform appropriate triage model to undertake an autonomous initial assessment of patient’s health and well being needs, identify care priorities and initiate appropriate treatment or first aid measures, administer analgesia and inform relevant personnel.
12. Provide nursing expertise and assist medical staff in management of the critically ill or major trauma victims (adults and paediatrics)
13. Maintain knowledge of Child Protection issues and guidelines. 14. Undertake appropriate training to administer an identified drug, essential for the Nurse
Practitioner (Unscheduled Care) role, within role of an extended and independent nurse prescriber.
15. To be familiar with the Hospitals’ Major Incident Plan and equipment, taking an active role in preparations and care of multiple casualties received in the event of a major incident or accident occurring.
16. In absence of reception staff, admit patient on to ADASTRA system once treatment is completed and patient has left department.
17. Initiate care and investigations of patients presenting with potential cardiac problems if doctor not immediately available i.e. O2 therapy, cannulate, obtain blood samples, ECG
18. Maintains Department supply and pharmacy levels, undertaking correct ordering procedures and ensure economic use of all resources.
19. Ensure there is a robust Discharge and Transfer Planning system in operation to ensure the smooth transition of the patient from hospital to home, community facilities, wards,
96
departments or other hospitals and onward referral to day time services. 20. Maintains effective communications with patients / families / carers and other members of the
multidisciplinary team to ensure appropriate information is shared and patient needs met. 21. Participates in developing and maintaining a positive learning environment. Undertake teaching
of students, nursing colleagues and other members of the multidisciplinary team and participate in orientation and student mentorship programmes, encourage staff with Personal Development Plans to facilitate ongoing development.
22. Work with all team members to ensure a high standard of cleanliness throughout the department promoting good standards of hygiene in conjunction with the Control of Infection Team to ensure infection rates are minimised.
23. Promote the health and safety of patient, staff and visitors within the ward area and during transfer to other wards and departments.
24. Ensure safe custody of patients’ valuables following NHS Highlands policies, with accurate and concise documentation
25. Seek medical decision making support within the department or via telephone when required within the community or request GP attendance, or ambulance transfer to hospital.
26. Participate, with the Charge Nurses, in the implementation and audit of standards of clinical care and comment on proposed changes to practices / procedures in own department to ensure high standard of patient care, promote evidence based practice and the attainment of healthcare governance requirements.
27. Adhere to NHS National, NHS Highland and NMC policies and codes of practice including record keeping / care planning, health and safety, infection control, PIN guidelines and standing financial instructions.
28. Demonstrate highly developed clinical nursing skills and act as a mentor for student nurses and clinical advisor and educator to unqualified team members.
29. Work in a professional and cooperative manner within a multi-disciplinary team, liaising with Social Work Department, District Nursing Service and other agencies as required.
30. Identifying/reacting to mechanical breakdown, fabric of building communications failures.
Managerial
1. Consultation with the Clinical Lead to develop and support initiatives in order to deliver enhanced levels of care and client satisfaction.
2. Supports managers and the Clinical Lead in managing and driving change and development through planning, communication and action within the multidisciplinary team to ensure objectives are met.
3. Consultation with regards to development and implementation of new local guidelines. 4. Facilitates the work of nurses and others through knowledge, support and advice, ensuring
standards of care are met, monitored and maintained. 5. Assist Clinical Lead in maintaining effective communication systems in the service ensuring staff
access relevant documented minutes and information and are involved and informed of all agreed decisions.
6. Assists in Health and Safety policies and procedures being maintained and accurate and up to date records are kept e.g. Completion of Risk assessments, Moving and Handling, Control of Substances Hazardous to Health, Mandatory training needs, completing of Datix forms.
7. In conjunction with Charge Nurses, actively involved in recruitment, by short-listing and interviewing junior staff.
8. Assists in implementing and managing PIN Guidelines and liaises with the Charge Nurses on particular issues / difficulties.
9. Actively develop and maintain a positive learning environment, participating in teaching programmes for nursing, allied health professionals, patient / carers using resources available.
10. Assists Charge Nurses to create an environment for research based nursing practice, participating
97
in and encouraging others to undertake audit and research to improve local practice as designated by the Lead Nurse following Clinical Effectiveness Guidelines.
11. Initiates informal critical incident debriefing after a stressful incident. 12. Promotes and maintains good relationships within the service and with staff of all disciplines
throughout the Area and NHS Highland. Actively participates in relevant meetings, promoting the department, unscheduled care nursing and the nursing profession in general.
13. Undertake staff rosters when required to ensure safe skill levels and effective use of resources. 14. Responsible for procurement and maintenance of all physical assets or supplies for the Out of
Hours service
7a. Equipment and Machinery Utilises technical equipment, calibrating when required, checking for faults and ensuring regular maintenance. Is expected to have knowledge of all equipment used in the department and will use equipment once provided with training but may not have daily clinical involvement.
EQUIPMENT USE Intravenous Pumps, syringe drivers, Deliver prescribed drugs / fluids safely I.V. lines, venflons, butterfly devices, Syringes, needles Arterial lines Invasive monitoring, essential for Central Venous Pressure lines acutely ill or trauma patient Non invasive monitoring equipment for: Measure and observe patients condition Blood pressure, temperature, pulse, Oxygen saturations, CO2, telemetry Blood Gas Analyser Accurate assessment of arterial blood Oxygen equipment: Deliver correct prescribed oxygen
Flowmeters, masks, humidification concentrations Nasal cannulae Pneupac IPPV ventilator Aid patient’s respiration / breathing BPAP machine Various suction devices Drain fluid – mouth / upper airway Chest Drains Drain fluid /air from thorax Nebulisers, Volumatic / spacers Deliver prescribed respiratory therapy Pulmo-aid Peak flow meter Guide measurement of lung function Entonox equipment and delivery system Deliver inhaled analgesia Resuscitation equipment including: Defibrillator, Laryngoscope, E.T tubes For use in resuscitation of acutely ill Ambu bag, laryngeal masks or trauma patient Difficult Intubation Trolley Specialist anaesthetic equipment
98
Nasogastric tubes Drain gastric contents Urinary catheters: Urethral, suprapubic Drain and measure urine ECG machine Record heart rhythm Patient Trauma Trolley, PAT slide Safe transfer and movement of patients Wheelchairs, Hoist, Slides sheets, Monkey poles, Underarm / elbow crutches Stiff cervical collars, head huggers Help protect neck after injury Major Incident Equipment including: Amputation sets Amputation of limbs at incident site Rucksacks Resuscitation equipment Documentation packs Essential documentation for M.I. use High visibility clothing, helmets etc Use by staff attending incidents Electric DeSouter saw Removal of plaster and synthetic casts Plaster scissors and shears Removal of plaster casts Slit lamp, ophthalmoscope Examination of eyes Auroscope Examination of ears Doppler machine Observe for arterial pulse Glucometer Monitor blood glucose Alcohol breathalyser monitor Monitor blood alcohol levels Ring cutters Removal of rings from injured fingers Ambulance radio transmitter Verbal contact with ambulances
Chute System Transportation of items Pregnancy testing kits Digital Camera Taking appropriate consented clinical photographs Patient call system Staff personal safety alarms Overhead operating/ portable examination lights Use in technical /delicate procedures Computers: PAS system, Intranet, Toxbase, ADASTRATA Information on effects of poisons Results Reporting Obtain patients clinical results Furniture:
99
Beds, bedside lockers, chairs Spenco mattresses Use on beds and trolley Help prevent pressure sores Fluid Warming Cupboard Warm I.V.fluids for resuscitation Blood Fridge Store blood for urgent use Heated Blanket cupboard Store warm bedding Car Travel to visit community based patients
7b. Systems Maintains patient records in accordance with the NMC guidelines and NHS Highland standards. Ensure correct use of computerised system for the out of hours services. Participates in clinical audit Assists in maintenance of accurate staff records relating to PIN guidelines e.g. leave through annual leave, sick leave, employee friendly policies, training, e-KSF and PDPs . Adhere to all service and office systems for example, reorganise rotas for sudden cover requirements, sickness / absence, change in workload, training etc Utilise communication systems for example, meetings, communication book, and multi-disciplinary team meetings.
8. Assignment and Review of Work The workload is determined by the needs of the service and the post holder will delegate / allocate work appropriately to the nursing teams. The Nurse Practitioner (Unscheduled Care) will look to the District Manager and Lead Nurse for guidance in their professional management, work review and formal appraisal of performance. When undertaking Nurse Practitioner (Unscheduled Care) duties the post holder will seek clinical guidance from senior medical staff as appropriate. Regularly discusses all aspects of OOHs management with managers, attends and participates in speciality meetings, staff meetings, nurse development meetings. Is expected to anticipate problems / needs and take steps to resolve them in the absence of more senior staff, involving appropriate colleagues e.g. , Consultant, Bed Manager, Duty Manager Support is available to and from all members of the multidisciplinary team as required. In conjunction with the Charge Nurses, ensures policies are initiated / revised, developed, implemented and reviewed regularly. When allocated to triage/manage patients within own sphere of competencies. Discuss if appropriate with medical colleagues, referrals from NHS 24 agreeing the most appropriate practitioner to respond to patients’ needs. In conjunction with the District Manager, Clinical Educator and OOH doctors taking the lead in unscheduled care, identify own education, training and support needs via the Personal Development Plan process, access clinical supervision and action learning and participate in in-service education. Works within a duty rota developed for the Mid Area OOH Service. Accountable for his / her own actions without direct supervision and for the care provided by unqualified staff.
9. Decisions and Judgements The ability to quickly assess and respond to patients needs in emergency situations. The post holder has to demonstrate rapid decision-making skills in an ever changing and unpredictable environment. Post holder will be responsible for ensuring that clinical practice meets the standard of care set by the
100
NMC and NHSH, and that non compliance with these standards is managed in accordance with the appropriate policies and procedures. Provision of professional advice to registered/ unregistered staff and students and an ability to recognise own limitations and the requirement for appropriate referral. Judgments involving highly complex facts or situations, which require the analysis, interpretation and comparison of a range of options. Assessment of patients’ complex needs (physical, psychological, social and spiritual) to establish a change in condition, inform clinical decision making and plan care.
10. Most Challenging/Difficult Parts of the Job Working effectively, as an autonomous practitioner, with a variable and unpredictable workload with fluid dynamic change where minor conditions may change to emergency care at a moments notice. Ability to at the same time deal with patients and/or relatives who may be highly anxious, as well as meeting the needs of the patients of all ages and diverse conditions with time constraints and without the availability of the patients’ records. The post holder has responsibility to provide leadership, supervision and guidance. Dealing with sudden, often traumatic death in adults, children and babies. Accountability whilst working as an autonomous practitioner. In urgent or emergency situations, being able to deliver quality, spiritually sensitive and culturally appropriate care to patients with communication problems e.g. non-English speaking, deaf, have learning difficulties, unidentified unconscious people. Managing the demands of the service within existing resources, whilst responding to and satisfying the varying needs of the patients and staff. Ability to give direct quality patient care to all patients, prioritising and re-prioritising in the face of changing demands. Working in a high-risk area for patients attending under the influence of drink and drugs, which are difficult to manage safely and not allowing it to impinge on the safety of other patients. Dealing with violence and aggression and disruptive / challenging behaviour, both verbal and physical from patients and member of the public. The aim is to have a safe environment for the staff patients and relatives but this is a very difficult task as violent incidents do occur. Establish and maintain effective communication with numerous individuals on complex potentially stressful issues. Making referrals to other specialities when there may be a difference of opinion between specialities as to the appropriateness of the referral for that service. Dealing with complaints directed at other services, agencies or situations out with the post holders control which can develop into confrontational or aggressive situations. Continue to work and deliver care after being involved in distressing resuscitation situations and ensuring staff are emotionally coping. Involved in the implementation of change (service and practice). Management of people, and coping with a range of personalities to maintain an efficient and effective team working environment. Supervise inexperienced staff while they gain the necessary experience to enable them to work under minimal supervision. Negotiating packages of care with other disciplines / agencies who work within different cultures, different response times and budgetary constraints. Managing unrealistic expectations of colleagues and patients. Maintain up to date high standard of clinical knowledge and competences required to provide a breadth of care, in hospital and community settings, for a very wide variety of presenting conditions. Able to cover a variety of shift patterns, including night duty, within team environment. Maintain high levels of concentration with frequent interruptions.
101
Have knowledge and skills to enable Child Protection and Adult Support and Protection needs to be recognised and managed as current policy states. Knowledge and skills required to perform telephone assessment / advice. Lone working.
11. Communications and Relationships Identifies potential and existing challenges in care options for patients, carers and staff, using negotiation and counselling skills to achieve reconciliation and the best outcomes for the patients. Communicates effectively verbally, in writing or electronically and non verbally Communicates with support departments e.g. Estates, Security, I.T., Supplies, Human Resources, Medical Physics, Health and Safety and Pharmacy, Catering, Ensures effective communication with all team members, which proves challenging due to various shift patterns across the 24 hour period, including all members of the MDT Liaise with external agencies e.g. Police, SAS, Social Work, Armed Forces, Procurator Fiscal, mountain rescue, Press Officers and university educational staff. Participates in regular meetings with colleagues for the purpose of planning, managing and developing nursing services, improving patient care, discussing policy issues, amending, updating, implementing and evaluating them, discussing and problem solving challenges in clinical care and team development. Facilitates effective dissemination of information to all relevant staff. Early identification of potential and actual complex and or conflicting perspectives of choice of care options between staff, patients and carers and using negotiation and counselling skills to achieve compromise and defuse possible volatile situations to achieve the best outcome for the patient referring to more senior colleagues where appropriate and reports and action as appropriate Demonstrate empathy, sensitivity and support when communicating with patients, relatives and staff, especially in relation to breaking bad news and dealing with emotionally challenging situations. Provides and receives complex, highly sensitive or contentious information where there are significant barriers to acceptance, which need to be overcome, using high levels of interpersonal and communication skills, such as would be required in a hostile, antagonistic or highly emotive atmosphere. Regularly demonstrates the ability to handle highly sensitive information in a manner not liable to offend or antagonise. Dealing with situations when patients do not easily understand their care packages, due to culture, language or learning difficulties. Maintain confidentiality in accordance with NMC and NHS Highland policies, including promoting compliance and adherence to the requirements of the Data Protection Act and the Caldicott Guidelines.
12. Physical, Mental, Emotional and Environmental Demands of the Job Physical Frequent moving and handling of patients - in bed / trolley, on to and off trolleys, from bed/trolley to chair, assistance with walking, transfer from ambulance trolley, undertake co-ordinated log rolls for patients with potential spinal injuries, assist injured/ill patients out of private transport. Hand washing / cleansing between each patient Washing and cleaning patients. Frequent wearing of disposable gloves. Frequent need to walk, stand and bend during shift to provide patient care Frequent transfer of patients and belongings to and from other wards and departments. Frequently assessing the risk of violent / aggressive / challenging behaviour of patients and visitors and deal with it appropriately. Highly developed physical skills where a degree of precision or speed and high levels of hand, eye and
102
sensory co-ordination are essential, e.g. take blood samples, administer injections, suture insertion and removal, insertion of venflon devices to set up IV access, calibrate equipment, use computer keyboard. Frequent checking of equipment attached to patients e.g. IV fluids, IV pumps, catheters, Cardiac monitors. Remove full outdoor clothing from unconscious / incontinent / uncooperative patients. Daily efforts to assist patients to move/talk/transfer Risk assess department and to be inventive to create a safe working environment whist being sensitive to patient’s environment and property – daily Adequate hearing – listening to chest/heart sounds Continuous need to talk throughout shift to provide patient care Daily moving and handling physically disabled/ill patient/equipment, e.g. beds, oxygen cylinders, wheelchairs – daily Exposure to hazardous substances Exposure to violence and aggression Driving/accompanying a driver in unfamiliar community areas Working in a patient’s home, where there may be reduced lighting and confined space Mental / Emotional Concentration, decision-making and organisational skills to cope with competing demands e.g. dynamic changes in patient condition, personnel issues with staff, sudden staff sickness, arrival of multiple trauma patient(s) or several patients arriving together requiring assessment and attention. Frequently recognising patients’ urgent health care needs and making appropriate instant decisions to provide appropriate clinical management, often without being in full receipt of patients’ full medical history. Dealing with emotional effects of caring for patients and their families who may be distresses anxious or worried. Dealing with emotional effects on patients, family and oneself when breaking bad news. Giving police statements / attending court over incidents. Possibility of attending Child Protection Case Conferences. Concentration required checking documentation / patient notes and calculating drug dosages whilst subject to frequent interruptions from patients, relatives and team members. Autonomous lone working recognising patients urgent health care needs and making rapid decisions to provide appropriate clinical management – daily Concentration, decisions making and organisational skills to cope with competing demands, (dynamic changes in patients conditions, personnel issues with staff, sudden staff absences, unpredictable nature of service demand, contracts from within and out with the organisation – managers, other departments, other agencies) daily. Negotiation skills to co-ordinate complex packages of care with a wide range of people and agencies, daily. Ensuring information is transferred accurately. Concentration to provide emergency care within a team that has frequent interruptions on a continuous basis. Emotional demands related to the implementation of change. Impact of colleague’s stressful personal circumstances e.g. family crisis, bereavement, illness, that impact on the individual’s ability to carry out expected role – on going. Emotional demands of involvement in patients complaints. Emotional demands of coping with colleagues diverse personalities. Emotional demands of working unsupervised in patients’ homes. Emotional demands of patients and relatives spiritual needs. Emotional demand in relation to family and human dynamics, dealing with people in high distress or crises such as dying and death.
103
Environmental High risk area with people presenting regularly under the influence of drink / drugs or psychiatric illness. Frequent exposure to infections e.g. MRSA, Airborne germs, communicable problems e.g. lice, scabies. Working in area with high noise levels e.g. phones, call bells, voices, monitoring equipment alarms. Considerable exposure to potential blood-borne infections e.g. Hepatitis, HIV. Exposure to the hospital environment: unnatural light, dry and hot conditions, VDU monitors. Coping with unpleasant materials and smells – bodily fluids, excreta, infected wounds – daily.
13. Knowledge, Training and Experience Required to do the Job Qualifications: Registered Nurse. Current NMC Registration. 1st level degree- preferred. Extended and Independent Nurse Prescriber. Advanced Clinical Assessment Module certificate at degree level. Completion of Common Presentation Module at degree level within a mutually agreed timescale. Training and Experience: 4 years post registration experience. Evidence of relevant on-going professional development. Mandatory training as per NHSH. PILS/ ILS/ Paediatric emergency care framework. Experience of working in collaboration with other professionals across organisational boundaries. Experience or working with children and young people, adults, families, carers and communities. It is also an expectation that the post holder will undertake further education and study relevant to the post for service developmental purposes. Ability to manage minor illness and injury. Risk assessment/ incident reporting. Knowledge and Skills: Highly developed specialist knowledge across a wide range of work procedures and practices underpinned by theoretical knowledge and relevant practical experience. Knowledge and skills to work at an advanced level of practice within a generic / specialist area of clinical practice. Knowledge and experience of mentorship within clinical practice. A broad range of knowledge and skill underpinned by theory, to deal with the full range of patients presentations and complexities of need including minor to urgent life threatening health needs. Knowledge and understanding of Health and Safety Policy, with evidence based practice i.e. Mental Health Act, and Incapacity of Adults Act. Capable and competent in a range of advanced level of clinical skills. A commitment to lifelong learning and evidence of continuing professional development. Ability to direct and coordinate programmes of care working collaborative and autonomously. Participation in audit data capture to evaluate service delivery and to inform future service planning. Clinical skills as follows: Cannulation Venepuncture Arterial blood gas sampling and interpretation Male and female urinary catheterisation
104
Syringe driver operation Recording and interpreting 12 lead ECG’s IV drug administration Wound and skin care management including suturing IT literate. High level decision making and prioritisation. Clinical audit. Presentation. Problem solving skills. Teaching, supervising, mentoring and supporting of junior staff.
14. Job Description Agreement I agree that the above Job Description is an accurate reflection of my duties and responsibilities at the date of signing. Job Holder’s Signature: Manager’s Signature:
Date: Date:

1
In this editionWhat’s not changing
Portree update
News in Brief
Business as usual for
emergencies
Major incident
response
Key Milestones
View from Cabinet
Secretary
Contact details
Skye, Lochalsh and South West Ross
O C T O B E R 2 0 1 7
Produced by NHS Highland
Commitment toimprove projectengagementRECENTLY I havebeen taking furthersoundings about theredesign and it is clearthat there remainsome concerns aboutprogress and timelycommunication. I amsorry about this andwish to assure all con-cerned that I take thisfeed-back very seri-ously.
To this end I havetasked the Project Teamoverseeing the redesign to strengthen com-munications and engagement. I have alsomade it clear that providing clarity on thedetail of the new arrangements needs totake place as matter of some urgency espe-cially in Portree.
However, I would in no way wish thisto down-play the significant work that hasalready taken place. Important milestonesare now being reached including appointingthe architects and the main contractor forthe hospital and submission of pre-planningapplication for the new hospital ‘Hub’ in
Broadford.Clearly in a project thatwill span the best part of adecade, there are going tobe times when things arequiet and it may seem thatlittle progress is beingmade. The options devel-opment and consultationwas very intensive in termsof engagement, whereasdeveloping the businesscase to secure the neces-sary funding and technicalexpertise has been less so.
I apologise if it wasn’t clear that quieterperiods should be expected.
Inevitably managers have had to priori-tise engagement efforts across Highland.This has been particularly challenging thispast few years with significant efforts alsorequired to meet unprecedented savingstargets requiring considerable managementattention and action.
I am pleased to confirm that we areentering a new phase which will again re-
THE REDESIGN of ser-vices including commis-sioning of the new hos-pital ‘Hub’ in Broadfordis now well underway.
However, it has notbeen without its chal-lenges and it is clearthat further efforts arerequired to improvecommunications andengagement with allconcerned.
Following recentmeetings, David Alston,chair of NHS Highland,sets out his support forthe redesign and hiscommitment to im-prove communicationsand engagement goingforward.
This newsletter isbeing sent to everyhome in the area toupdate on progress.Contact details are pro-vided at the back of thisnewsletter, please getin touch if you have anyqueries.
David Alston
Continued on next page
...as major milestones reached
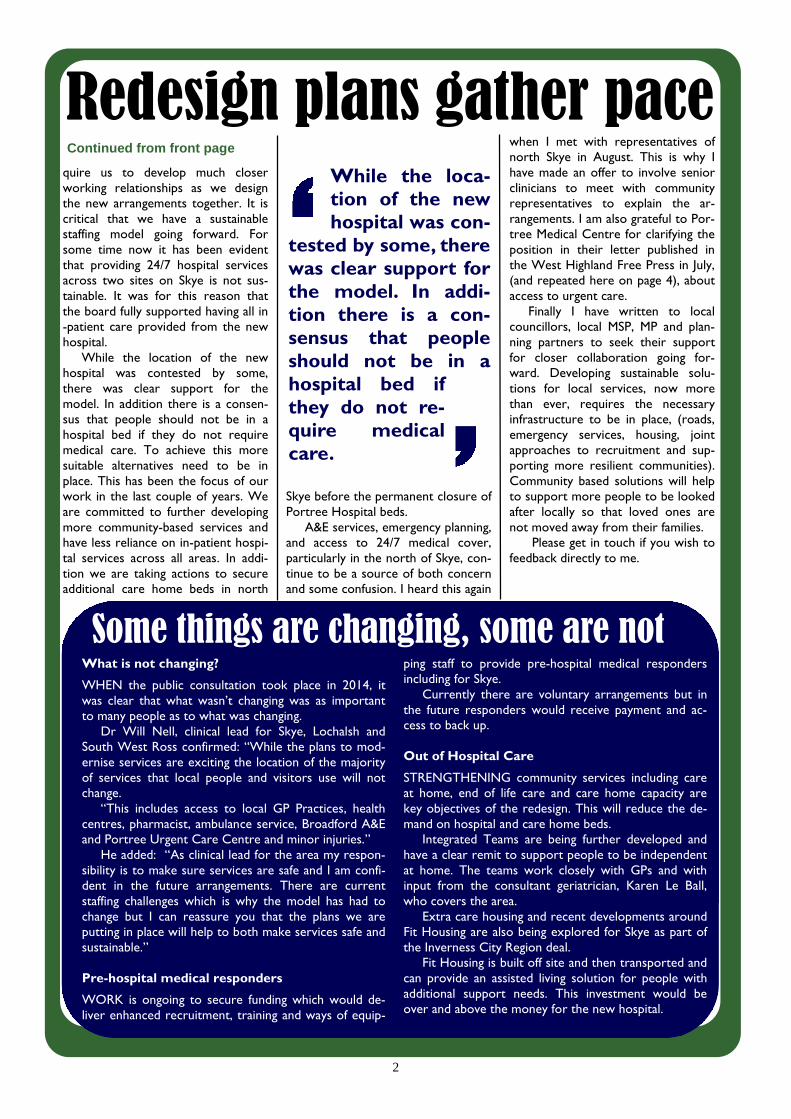
2
Redesign plans gather pacequire us to develop much closerworking relationships as we designthe new arrangements together. It iscritical that we have a sustainablestaffing model going forward. Forsome time now it has been evidentthat providing 24/7 hospital servicesacross two sites on Skye is not sus-tainable. It was for this reason thatthe board fully supported having all in-patient care provided from the newhospital.
While the location of the newhospital was contested by some,there was clear support for themodel. In addition there is a consen-sus that people should not be in ahospital bed if they do not requiremedical care. To achieve this moresuitable alternatives need to be inplace. This has been the focus of ourwork in the last couple of years. Weare committed to further developingmore community-based services andhave less reliance on in-patient hospi-tal services across all areas. In addi-tion we are taking actions to secureadditional care home beds in north
Skye before the permanent closure ofPortree Hospital beds.
A&E services, emergency planning,and access to 24/7 medical cover,particularly in the north of Skye, con-tinue to be a source of both concernand some confusion. I heard this again
when I met with representatives ofnorth Skye in August. This is why Ihave made an offer to involve seniorclinicians to meet with communityrepresentatives to explain the ar-rangements. I am also grateful to Por-tree Medical Centre for clarifying theposition in their letter published inthe West Highland Free Press in July,(and repeated here on page 4), aboutaccess to urgent care.
Finally I have written to localcouncillors, local MSP, MP and plan-ning partners to seek their supportfor closer collaboration going for-ward. Developing sustainable solu-tions for local services, now morethan ever, requires the necessaryinfrastructure to be in place, (roads,emergency services, housing, jointapproaches to recruitment and sup-porting more resilient communities).Community based solutions will helpto support more people to be lookedafter locally so that loved ones arenot moved away from their families.
Please get in touch if you wish tofeedback directly to me.
What is not changing?
WHEN the public consultation took place in 2014, itwas clear that what wasn’t changing was as importantto many people as to what was changing.
Dr Will Nell, clinical lead for Skye, Lochalsh andSouth West Ross confirmed: “While the plans to mod-ernise services are exciting the location of the majorityof services that local people and visitors use will notchange.
“This includes access to local GP Practices, healthcentres, pharmacist, ambulance service, Broadford A&Eand Portree Urgent Care Centre and minor injuries.”
He added: “As clinical lead for the area my respon-sibility is to make sure services are safe and I am confi-dent in the future arrangements. There are currentstaffing challenges which is why the model has had tochange but I can reassure you that the plans we areputting in place will help to both make services safe andsustainable.”
Pre-hospital medical responders
WORK is ongoing to secure funding which would de-liver enhanced recruitment, training and ways of equip-
ping staff to provide pre-hospital medical respondersincluding for Skye.
Currently there are voluntary arrangements but inthe future responders would receive payment and ac-cess to back up.
Out of Hospital Care
STRENGTHENING community services including careat home, end of life care and care home capacity arekey objectives of the redesign. This will reduce the de-mand on hospital and care home beds.
Integrated Teams are being further developed andhave a clear remit to support people to be independentat home. The teams work closely with GPs and withinput from the consultant geriatrician, Karen Le Ball,who covers the area.
Extra care housing and recent developments aroundFit Housing are also being explored for Skye as part ofthe Inverness City Region deal.
Fit Housing is built off site and then transported andcan provide an assisted living solution for people withadditional support needs. This investment would beover and above the money for the new hospital.
Continued from front page
Some things are changing, some are not
While the loca-tion of the newhospital was con-
tested by some, therewas clear support forthe model. In addi-tion there is a con-sensus that peopleshould not be in ahospital bed ifthey do not re-quire medicalcare.

3
Redesign of careat homeWORK is ongoing to strengthen theprovision of care at home services.NHS Highland’s care at home servicenow forms part of the wider integratedteam in the community. This means thatthe service benefits from closer links withother health and social care services ena-bling the teams to support each other toprovide care in people’s homes.
We are also working closely with theindependent and third sector providers tosupport them to further develop theircapability. This will bring additional capac-ity allowing more people to be cared forin their own communities.
Elsewhere in Highland communityenterprise solutions are progressing well.Excellent examples include Foyers(Boleskine), Black Isle and Port Appin.Local events are being arranged to look atwhether these approaches would work inSkye, Lochalsh and South West Ross.
Care Home SummitTHE future requirements for CareHomes across Highland are beinglooked into by NHS Highland andothers.
The strategic review, which is under-way, will look at the number, location andsize (beds) as well as types of beds. It willalso cover how to work more collabora-tively with all providers.
Specifically on the Skye the privatelyowned 12-bed home ‘The Haven’ in Uigclosed at the end of June 2017. At thetime of closing there were 10 residents.Nine were re-located locally and oneresident was placed in a home in Gairloch(Wester Ross) with a plan to bring themback to the island as soon as possible. Akey issue forcing the closure is under-stood to be due to staffing challenges,
further illustrating why new approachesare required.
Meanwhile, options to make the NHSHighland managed An Acarsaid 10-bedresidential home in Broadford dual regis-tered, are being considered. This wouldenable nursing level care to be providedin the home.
More paramedicsrecruited to SkyeWE invited Alan Knox, Area ServiceManager for Lochaber, Skye & Lo-chalsh District to update on localScottish Ambulance Service re-sources.
“Scottish Ambulance Service has re-cently recruited a relief paramedic forPortree, who took up post in August. Afurther three relief A&E staff for Broad-ford have been recruited with two al-ready in post and a third in training.
“I am also pleased to report that anew patient transport vehicle is in placeat Portree. In addition, A&E ambulancesacross Skye are being updated. Staff areundergoing training and the feed-back isthat the new vehicles are more spaciousand comfortable for patients.”
Location of SAS basesand staffingKyle – Five staff including two para-medics plus another who is training as aparamedic.Broadford – Three paramedics andthree technicians plus three relief A&Estaff have been recruitedDunvegan – Currently five qualifiedambulance technicians
Portree – An additional paramedichas been recruited increasing the numberof paramedics to four. There are alsotwo technicians in post.
This means there are 25 Ambulancestaff covering the area.
Temporary closureof hospital bedsTen of the 12 beds in the hospitalare currently closed due to severeshortages (nurses, catering staff,domestics).
Vacant posts are being advertised andfurther efforts are underway to recruit tothe nurse bank. There have been discus-sions with The Highland Council aroundcatering. NHS Highland is also looking ata range of other potential solutions.
Everything is being done to keep Por-tree Hospital in-patient beds open untilalternative arrangements are in place, butthis is proving increasingly challenging. Itfurther highlights the urgent need to putin place the additional investment forcommunity based models in the northincluding additional care home capacity.
The reason the new model was pro-posed in the first place was because thesignificant challenges faced around main-taining 24/7 services across two hospitalsites. Was recognised.
Building accessibilityNHS HIGHLAND has called on thetechnical expertise of Skye and Lo-chalsh Access Panel members andothers to make sure the architects,NHS Highland and others are fullyaware of the most up to date legisla-tion, guidance and good practice.
The Access Panel, who have qualifiedAccess Auditors have provided the fol-lowing advice to NHS Highland.
ALL the existing services (minus in-patient beds andx-ray) will continue to be delivered from PortreeHospital.
Discussions are also ongoing to develop dayassessment services for North of Skye. The aimwould be to provide access to the multidisciplinaryteam (GP, nurse, social work, physiotherapist, occu-pational therapist and so on) to address any pa-tients’ medical and social care needs in a singlevisit. This would reduce the likelihood of the patienthaving to be admitted to a hospital in-patient bed in
Broadford. In addition the Portree Medical Practicewill also move into the ’spoke’.
The building works to redesign the space in thehospital is being delivered through NHS Highland’scapital monies, and is over and above the moniesallocated for the new hospital in Broadford.
A working group will be established to overseethe development of the ‘spoke’ and other services inNorth Skye. It will also oversee the link in with the‘Hub’ and will have staff and community representa-tives from across the redesign area.
Portree Community Hospital ‘Spoke’
NEWS in brief
Continued on next page
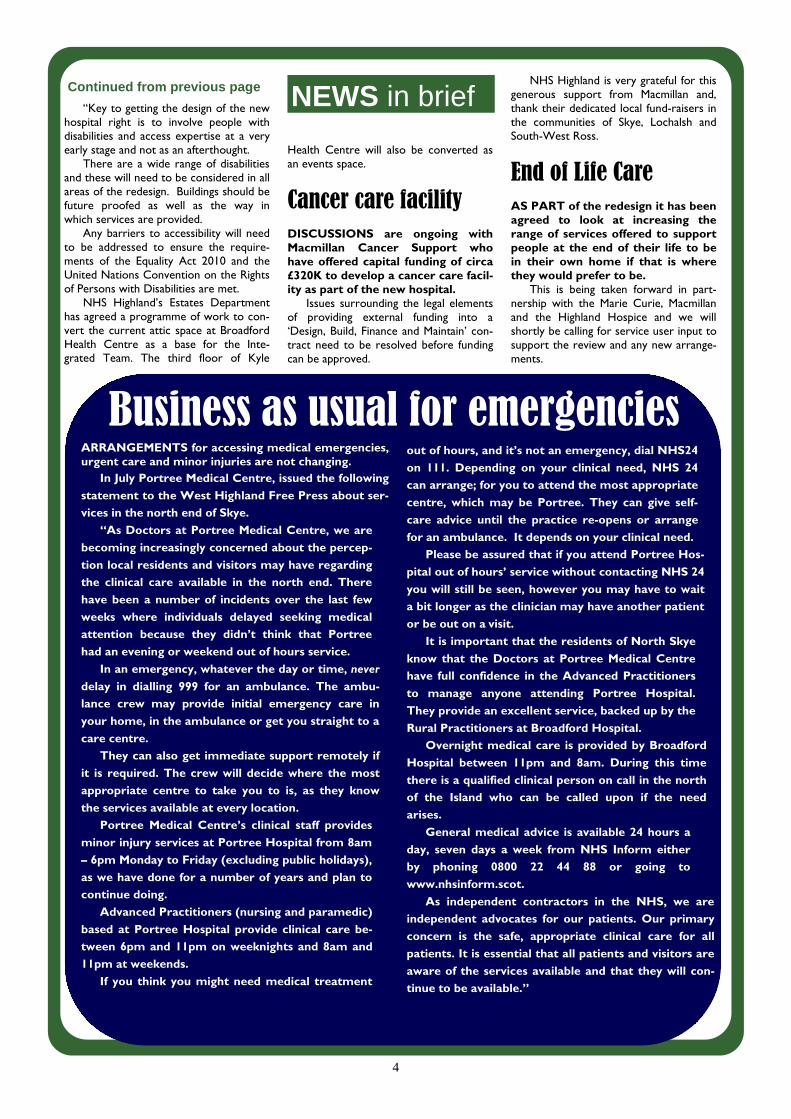
4
“Key to getting the design of the newhospital right is to involve people withdisabilities and access expertise at a veryearly stage and not as an afterthought.
There are a wide range of disabilitiesand these will need to be considered in allareas of the redesign. Buildings should befuture proofed as well as the way inwhich services are provided.
Any barriers to accessibility will needto be addressed to ensure the require-ments of the Equality Act 2010 and theUnited Nations Convention on the Rightsof Persons with Disabilities are met.
NHS Highland’s Estates Departmenthas agreed a programme of work to con-vert the current attic space at BroadfordHealth Centre as a base for the Inte-grated Team. The third floor of Kyle
Health Centre will also be converted asan events space.
Cancer care facilityDISCUSSIONS are ongoing withMacmillan Cancer Support whohave offered capital funding of circa£320K to develop a cancer care facil-ity as part of the new hospital.
Issues surrounding the legal elementsof providing external funding into a‘Design, Build, Finance and Maintain’ con-tract need to be resolved before fundingcan be approved.
NHS Highland is very grateful for thisgenerous support from Macmillan and,thank their dedicated local fund-raisers inthe communities of Skye, Lochalsh andSouth-West Ross.
End of Life CareAS PART of the redesign it has beenagreed to look at increasing therange of services offered to supportpeople at the end of their life to bein their own home if that is wherethey would prefer to be.
This is being taken forward in part-nership with the Marie Curie, Macmillanand the Highland Hospice and we willshortly be calling for service user input tosupport the review and any new arrange-ments.
ARRANGEMENTS for accessing medical emergencies,urgent care and minor injuries are not changing.
In July Portree Medical Centre, issued the following
statement to the West Highland Free Press about ser-
vices in the north end of Skye.
“As Doctors at Portree Medical Centre, we are
becoming increasingly concerned about the percep-
tion local residents and visitors may have regarding
the clinical care available in the north end. There
have been a number of incidents over the last few
weeks where individuals delayed seeking medical
attention because they didn’t think that Portree
had an evening or weekend out of hours service.
In an emergency, whatever the day or time, never
delay in dialling 999 for an ambulance. The ambu-
lance crew may provide initial emergency care in
your home, in the ambulance or get you straight to a
care centre.
They can also get immediate support remotely if
it is required. The crew will decide where the most
appropriate centre to take you to is, as they know
the services available at every location.
Portree Medical Centre’s clinical staff provides
minor injury services at Portree Hospital from 8am
– 6pm Monday to Friday (excluding public holidays),
as we have done for a number of years and plan to
continue doing.
Advanced Practitioners (nursing and paramedic)
based at Portree Hospital provide clinical care be-
tween 6pm and 11pm on weeknights and 8am and
11pm at weekends.
If you think you might need medical treatment
out of hours, and it’s not an emergency, dial NHS24
on 111. Depending on your clinical need, NHS 24
can arrange; for you to attend the most appropriate
centre, which may be Portree. They can give self-
care advice until the practice re-opens or arrange
for an ambulance. It depends on your clinical need.
Please be assured that if you attend Portree Hos-
pital out of hours’ service without contacting NHS 24
you will still be seen, however you may have to wait
a bit longer as the clinician may have another patient
or be out on a visit.
It is important that the residents of North Skye
know that the Doctors at Portree Medical Centre
have full confidence in the Advanced Practitioners
to manage anyone attending Portree Hospital.
They provide an excellent service, backed up by the
Rural Practitioners at Broadford Hospital.
Overnight medical care is provided by Broadford
Hospital between 11pm and 8am. During this time
there is a qualified clinical person on call in the north
of the Island who can be called upon if the need
arises.
General medical advice is available 24 hours a
day, seven days a week from NHS Inform either
by phoning 0800 22 44 88 or going to
www.nhsinform.scot.
As independent contractors in the NHS, we are
independent advocates for our patients. Our primary
concern is the safe, appropriate clinical care for all
patients. It is essential that all patients and visitors are
aware of the services available and that they will con-
tinue to be available.”
Business as usual for emergencies
NEWS in briefContinued from previous page
5
Major incidentresponse plansOVER recent months some concernshave been raised with NHS Highlandthat the redesign of services will im-pact on emergency planning particu-larly if there is a major incident inPortree.
Peter MacPhee, NHS Highland’s emer-gency planning officer has provided thisupdate.
“NHS Highland is classed as a Category1 Responder under Civil Contingency legis-lation and regulations. As such, this re-quires us to work with other respondingagencies and have plans in place to enableus to respond to major incidents. Thereare a number of multi-agency plans whichstipulate the roles and responsibilities ofNHS Highland, and these detail the majorincident response and co-ordination struc-tures including within hospitals.
“Raigmore Hospital in Inverness, is themain receiving hospital for major incidentcasualties in north Highland. There are alsoa number of hospitals within NHS Highlanddesignated as support hospitals, which cantake receipt of less seriously injured casual-ties or other patients. On Skye the desig-nated hospital is Dr Mackinnon MemorialHospital.
“Over the last 24 months, a MassCasualties Incident Plan for NHS Scotlandhas been under development, whichamongst others things, details the arrange-ments for casualty distribution from thescene or scenes being co-ordinated fromthe Scottish Ambulance Control Centre inCardonald.
“This is, to ensure that patients aretaken to the most appropriate hospital,based on clinical need and with a view tominimising the requirement for secondarytransfers.
“Whether it is a major incident ormass casualties incident, it is not necessar-ily the nearest hospital to which casualtieswill be conveyed.
“There is an ongoing programme ofexercising and training both internallywithin NHS Highland and within the High-lands & Islands Local Resilience Partner-ship. A number of major incident exercisesin Skye & Lochalsh have taken place inrecent years, with the most recent being inPortree in April 2017.
“A further major incident exercise isscheduled for Broadford Hospital in No-vember 2017, for which planning is wellunder way.”
...legislation and regulations outlined
In with the new: Revolutionising Rural Health Care...WORK is underway in Skye which is set to revolutionise rural health care.
Capsule endoscopy or pillcam is being tested to provide easy access to diagnos-tic endoscopy. Using some novel technology, instead of having to travel to hospitalfor invasive procedures a pill, which includes a tiny camera, can now be taken. Aswell as being less invasive the pillcam can be taken at home and the results dis-cussed at the local GP surgery, or indeed in the persons own home.
This test is for diagnostic scopes only. Anyone requiring biopsies and treatmentscopes would still have to travel to Belford or Raigmore Hospital, as currently hap-pens.
...Out with the oldTHE ENDOSCOPY service in Dr Mackinnon Memorial Hospital was stopped sev-eral years ago due to health and safety concerns. At that time, NHS Highland was ofthe view that the service could be resumed in the new facility.
However, a review conducted by Mr James Docherty, colorectal surgeon andNHS Highland Clinical Lead for Endoscopy, recommended that given the low levelof activity the unit would only warrant running for one session per week. This hesaid would question the sustainability. The current testing of capsule endoscopyoffers the best solution to allow more patients with Gastrointestinal (stomach andintestine symptoms to be investigated locally.
Helipad plansWork is underway to secure asite and funding for a new Heli-pad.
A report by the MissionCritical Services Onshore /Aviation Department of Bab-cock International Group, theair ambulance service opera-tors, identified safety concernsat the existing helipad at DrMackinnon Memorial Hospitalin Broadford and the servicewas discontinued.
Since then, Scottish Ambu-lance Service (SAS) and Bab-cock have been using theAshaig Airstrip 4.5 miles (7.25Kilometres) away.
Now SAS, Babcock Interna-tional, and NHS Highland Es-tates Department are lookingat options to re-provide a heli-pad as part of the new hospitalsite.
A bid for charitable fundingvia the County Air AmbulanceTrust, Helicopter EmergencyLanding Pad (HELP) appeal hasbeen made.
Contractor newsBALFOUR Beatty have beenannounced as the main con-tractor for the new hospital. InJune we announced that Archi-tectural firms Portree-basedRural Design and Oberlandersfrom Edinburgh had won thecontract for the design of thenew hospital.
Capital fundingCAPITAL funding of around£15million has been allocatedfor the 24 in-patient unit whichwill include 24/7 Accident &Emergency services, radiogra-phy, community maternity unitand outpatients clinics. In thenew arrangements the ScottishAmbulance will also being co-located at the new hospital.
Planning approvalANOTHER milestone wasreached in July when a pre-planning application for thenew hospital was submitted.
BROADFORD news
6
2017Outline Business Case due to submitted to Scottish
Government (SG) (November)Plans to strengthen engagement in place (October)Contractors appointed (September)Outline Planning Permission submitted (July)Architects appointed (June)
2018Outline Business Case to be approved by SG (January)Full Business Case to be approved by SG (November)Alternative arrangements to replace in-patient hospital
beds tested2019
New arrangements for ‘Spoke’ in placeConstruction of new hospital underway (March)
2020New hospital construction completed (December)
2021New hospital operational (February)
Key milestones
To find out more, contact...Ross Mackenzie, Area Manager; tel. 01349 869237;e-mail: [email protected]
Maimie Thompson, Head of PR ; tel. 01463 704722;e-mail: [email protected]
David Alston, Chair NHS Highland; tel, 01463 704811Email: [email protected]
NHS Highland, Assynt House, Beechwood Park, Inverness IV2 BW
Alternatively, visit the NHS Highland website via the home page:http://www.nhshighland.scot.nhs.uk/Pages/Welcome.aspx
Transport needs onSkye to be assessedby university teamTHIS year NHS Highland com-missioned Aberdeen Universityto carry out an IndependentTransport Needs Assessment ofthe impact of closing in-patientbeds at Portree CommunityHospital.
It included reviewing whattransport is currently available,feed-back from stakeholders andsurveys of in-patients, their rela-tives and visitors.
A draft report is being final-ised and will be available forcomment shortly.
While the research was tospecifically assess the impact ofclosing in-patient beds in Por-tree, it has also highlightedwider transport issues that willneed to be considered by localplanning partners.
Two local workshops arebeing planned initially in NorthSkye. Following on from this, anaction plan will be agreed withpartner agencies which will berequired to be implemented inadvance of the planned changes.
Maimie Thompson, Head ofPR and Engagement said; “Wewill continue to gather viewsfrom patients and visitors, par-ticularly around the implicationsof transferring in-patient bedsfrom Portree to Broadford.
“If you would like to feed-back any comments, please getin touch or complete an onlinesurvey available on NHS High-land website or hard copies alsoon request.”
Cabinet Secretary callsfor board to improveCommunications...AT a meeting held on 21st September with Margaret Davidson (Leader of HighlandCouncil ), Cllr Ronald MacDonald and NHS Highland’s Chair and Chief Executive, theCabinet Secretary made it clear she expects improved communications from NHSHighland.
She expects better mechanisms to be in place to ensure all communities are in-formed about the redesign and in particular about the “spoke” in Portree Hospital. MsRobison also emphasised that there needs to be more rapid and visible progress aroundfuture services in Portree.
Topics raised included out of hours and emergency care. Cllr MacDonald raisedconcerns about availability of ambulances and the Cabinet Secretary agreed to followthis up with the Scottish Ambulance Service.
The Cabinet Secretary was of a view that there needs to be greater clarity aboutwhat to do in different scenarios when people are unwell. For example, she questionedwhether it was clear that in an emergency the most appropriate response is to call 999and that this will not change in the future. To further promote this, NHS Highland hasagreed to set up a meeting for senior clinicians to meet with local elected members inthe first instance.
A local steering group to oversee the redesign going forward from the perspectiveof the North will be established. As a first step a facilitated event is being considered tobring together representatives including clinicians. One of the outputs will be to agreeTerms of Reference for the local steering group. The planning of this event will be dis-cussed with the local clinicians and local elected members.

7