
Sexual behaviour and diagnosis of people over the age of 50 attending a sexual health clinic
18
For Review Only Sexual behaviour and diagnoses of people over 50 years of age attending a public sexual health clinic Journal: Australasian Journal on Ageing Manuscript ID: AAJA-2008-047 Manuscript Type: Research Keywords: Sexual health, sexually transmitted infections, sexuality, sexual behaviour Australasian Journal on Ageing
Transcript of Sexual behaviour and diagnosis of people over the age of 50 attending a sexual health clinic

For Review O
nlySexual behaviour and diagnoses of people over 50 years of age attending
a public sexual health clinic
Journal: Australasian Journal on Ageing
Manuscript ID: AAJA-2008-047
Manuscript Type: Research
Keywords:Sexual health, sexually transmitted infections, sexuality, sexual behaviour
Australasian Journal on Ageing

For Review O
nly
1
Sexual Behaviour and Diagnoses of People Over 50 Years of Age Attending a Public Sexual Health Clinic During a Ten Year Period
ABSTRACT
Objectives: To investigate the sexual health and behaviour of older Australians
attending a sexual health clinic. Methods: We undertook a retrospective patient
record data base extraction of people aged 50 years and over attending Sydney Sexual
Health Centre (SSHC) between 1993-2003. Results: 2438 people aged 50 years and
over, including 611 aged 60 years or more, attended SSHC. The proportion of these
men (7.4%) and women (1.7%) attending the clinic remained relatively unchanged
during the study period. The main reasons for attending were assessment of genital
symptoms (40%), testing for STIs (23%), and HIV testing or HIV care (13%); more
than 50% of the clients had a previous sexual health problem and more than 50% had
not been tested for HIV. Men reported more life time sexual partners than women and
25% of the men had had sex with another man; men were significantly more likely to
report using condoms (p<0.05), although condom use was variable; previous sexual
health problems and sex of the sexual partner did not influence recent condom use.
Genital herpes (10% women, 6% men) and non-gonococcal urethritis (9% men) were
the most commonly diagnosed STIs. Conclusions: High levels of unsafe sex and
many important sexual health problems were identified which provide direction for
public health interventions for older sexually active Australians.
Page 1 of 17 Australasian Journal on Ageing
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Review O
nly
2
INTRODUCTION
It is now a well known and widely recognised fact that the number of Australians
older than 65 years has increased significantly over the past 50 years and that active
life expectancy is enjoyed by a majority of seniors [1,2]. Older Australians are
remaining healthy, independent and sexually active, and, despite claims to the
contrary, are increasingly willing to discuss sexual matters and view sex as an
important part of their lives.[3,4] However, the sexual health needs, sexual risk
behaviours and epidemiology of sexually transmissible infections (STI) amongst older
Australians have received limited attention in the literature.
Opportunities to understand the sexual behavior and attitudes of older people in
national population studies have been largely missed in Australia [5], Britain [6],
France [7] and the United States of America [8] because of a resistance to sample
older populations, although increasingly national sex surveys are including samples of
people over the age of 50 and even 60. National sexual health strategies have also not
specifically included older people and usually target the sexual risk of young people
and other specific groups at high risk (UK [9], Australia [10,11]. However, clinic-
based studies in the United Kingdom have explored the reasons for attendance [12],
delays in health seeking behaviour [13], and characteristics of older people at
genitourinary medicine clinic.[14,15]. Many of these studies have focused on people
over the age of 50 years - the ‘baby boomers’ generation who have less conservative
attitudes, higher expectations of and tolerance for sexuality [16]. A small Australian
study has explored the patterns of access to a sexual health clinic for clients aged 60
or more year.[17].
Page 2 of 17Australasian Journal on Ageing
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Review O
nly
3
We sought to investigate the sexual health and behavior of people over 50 years of
age attending a public sexual health clinic in Sydney. While society can make it
difficult for older people to divulge personal details, sexual health clinics may provide
a legitimate place to openly and frankly talk about their sexual health experiences.
METHODS
Study subjects
All people aged 50 years or older attending Sydney Sexual Health Centre (SSHC) for
the first time between 1993-2003 who had a complete clinical assessment by a doctor
or nurse were included in the study. A cut off of 50 years was chosen to allow
comparison with the few studies of people of this age and because others have
identified that people of this age have been ignored by sexual health researchers [18].
The South Eastern Sydney Area Health Service Ethics Committee approved the study.
All data was de-identified and only group data was analysed. Individual consent was
therefore not obtained.
Data collection
All patients attending SSHC have a sexual history recorded on a standardised medical
record, which is subsequently entered onto a database after verification by trained
clinical staff. A random audit of 5% of the records of patients who have recently
attended is routinely undertaken to ensure data completeness. Detailed patient
information was retrospectively extracted from the SSHC database for people 50
years or older. The extracted information included demographics (age, gender, marital
status, country of birth), reasons for attendance, past and present sexual behaviour
(including number and sex of partners in 3 months, 12 months and life time periods),
Page 3 of 17 Australasian Journal on Ageing
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Review O
nly
4
past sexual health problems and tests for sexually transmitted infections, including
hepatitis B and HIV, and, for women, parity and contraceptive use. Categorical
variables were created for age (50-59 and >60 years) and condom use – one,
sometimes (<50% of times), usually (>50% of times), always (100% of times). Past
sexual health problems included gonorrhoea, chlamydia, genital herpes, genital warts,
syphilis, candidiasis, urinary tract infection, trichomoniasis and pelvic inflammatory
disease.
Statistical methods
Data cleaning and statistical analysis were undertaken using Microsoft Access version
2002 and SPSS version 11.5. Proportions were compared using Pearson χ2 test with
significance set at p<0.05.
Patient characteristics
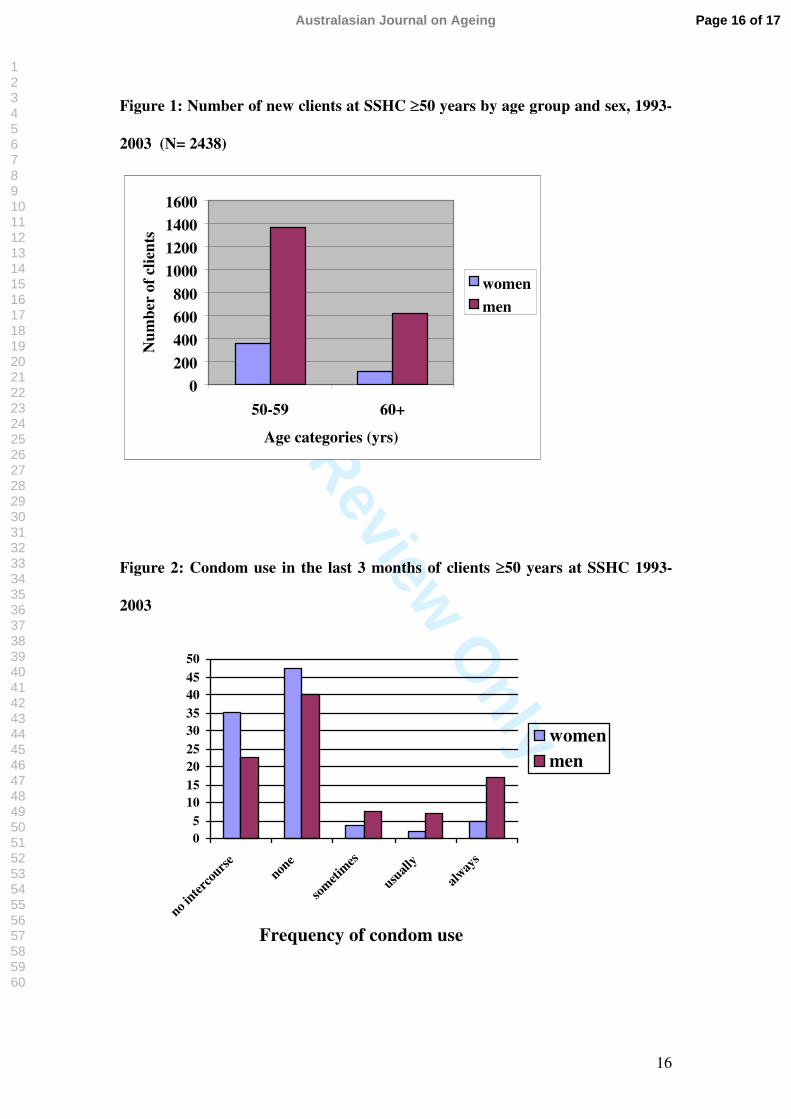
Between 1993 and 2003 there were 2438 people aged 50 years or older who attended
SSHC for the first time. Of these, 1976 (81%) of attendees were men and 1719
(70.5%) were aged 50-59 years. Compared with men, a significantly higher
proportion of women were aged 50-59 (82.4% vs. 72.9%, χ2 =, p=0.001) (see Figure
1).
The average proportion of men (7.4%) and women (1.7%) over the age of 50
attending each year remained relatively unchanged during the study period. A similar
proportion of men (38%) and women (32%) were married or in de-facto relationships,
while 58% of women were separated, widowed or divorced compared to 35% of men.
About half of both women and men were currently with a self-defined ‘regular’
Page 4 of 17Australasian Journal on Ageing
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Review O
nly
5
partner. Over half (55%) of all clients were born in Australia and about half of
patients where employed (46% women, 56% men).
RESULTS
Reasons for attending
The main reasons for attending the clinic were for assessment of genital symptoms
(40%), testing for sexually transmissible infections (23%), HIV testing or care (13%),
Hepatitis tests or vaccination (6% as Hepatitis B, 3.2%, Hepatitis A, 2.4%, Hepatitis
C, 0.5%) and issues related to sexual function (4%) Over half of women and men had
a previous sexual health problem; while over 60% of women (277) and 50% of men
(988) had not been previously tested for HIV. Sixty three percent of women had
borne children, 25% had had prior termination of pregnancy and 19% miscarriages.
8% of women had never been pregnant.
Number of sexual partners
In the last 3 and 12 months, both women and men had a median of one opposite sex
partner, respectively. The median number of lifetime opposite sex partners was three
for women and 10 for men. There was a larger range of partner numbers for men than
women in all time periods.
Four hundred and ninety four (25%) of the older men had had sex with another man,
while only 5% of women reported same sex behaviour. For men, the median number
of same sex partners in the last 3 and 12 months was one and three, respectively. The
median number of lifetime partners for men with same sex partners was 40. Twenty
one percent of men had had sex overseas in the last 12 months and 17% of the men
Page 5 of 17 Australasian Journal on Ageing
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Review O
nly
6
had had sex with a female sex worker in Australia. Thirteen percent of the women
reported having had sex with a male partner who had had multiple partners.
Condom use
Of people having sexual intercourse in the previous 3 months, men were significantly
more likely to report any condom use than women (54% vs 19%, χ2=63.3; p<0.05),
although frequency of condom use was variable (see Figure 2).
However, there was no significant difference between the 50-59 and 60 years and
older age groups for any use of condoms in the last 3 months (χ2=0.79; p=0.8). Prior
sexual health problems did not influence recent use of any condoms (χ2=4.48;
p=0.04), while those older people who were single (62%) were more likely than either
those who were in married/defacto relationships (29%) or
separated/widowed/divorced (41%) to have used any condoms in the last three
months (χ2=99; p<0.05). Similarly, people who had had sex overseas in the last 12
months were more likely to have recently used condoms at all than those who had not
travelled overseas (χ2=26.9; p<0.05). The significance of condom use variables were
not affected by the sex of the sexual partners.
Page 6 of 17Australasian Journal on Ageing
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Review O
nly
7
Common diagnoses
Table 1 shows the ten most common diagnoses for men and women over 50 years at
SSHC. Bacterial STIs (gonorrhoea, chlamydia, trichomoniasis, NGU, PID and
epididymitis) were more often diagnosed in men than women (14% vs 6.3%, χ2
=20.6; p<0.05), although viral STIs (genital herpes, genital warts, Hepatitis B, HIV)
were found in similar proportions (9.2% men vs 11.0% women, χ2 =1.82; p=0.18).
‘No specific diagnosis and negative STI/HIV tests’ were found in up to 15% of men
and women. When compared with homosexual men, heterosexual men were more
likely to have been diagnosed with genital herpes (7.3% vs 3.7%, χ2 =7.79;p<0.05)
and balanoposthitis (8.3% vs 4.1%, χ2 =9.62;p<0.05). Homosexual men, however,
were more likely to have an HIV diagnosis (6.1% vs 0.5%, χ2 =62.3; p<0.05).
DISCUSSION
This large, clinic-based study is one of the first descriptions of the sexual health
problems of older people in Australia to assess reasons for attendance, sexual
behaviour and diagnoses. High levels of unsafe sex and many important sexual health
problems were identified.
Specialist sexual health clinics are used for the sentinel surveillance of sexual
behaviour and sexually transmitted infection because the services specifically
encourage the attendance of people at high risk [19]. The clinics employ staff who can
accurately assess sexual health in a highly confidential manner. And, in Australia,
people with symptoms or specific high-risk behaviour are usually given priority
access to care.
Page 7 of 17 Australasian Journal on Ageing
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Review O
nly
8
Over 2000 older people chose to attend a public sexual health clinic even though they
were socialised when ‘venereal disease’ clinics and their patients were stigmatised
and sexual matters were not discussed openly. Similar to other clinic reports[15,20]
men were over-represented compared with women. While women consult doctors
more often than men [21], have an established relationship with a general practitioner,
are usually more aware of their health and display different prevention strategies to
HIV [22], men may prefer the anonymity of a public sexual health clinic compared to
attending their general practitioner.
Differences in sexual risk behaviour among clinic attendees may also account for the
gender imbalance.[15]. Men were generally at greater risk of STIs than women – a
larger range of numbers of recent sexual partners, had paid for sex, had sex overseas
and had sex with a same sex partner/s. However, women attending also demonstrated
high but different sexual risk by being more likely to have had unprotected sex
recently than men. While much of this sex for women may have been within regular
relationships, less than 20% of recently sexually active women had used condoms
during sex.
Older people in relationships do not need contraception and perhaps consider
themselves protected from STIs by being in a relationship. Half of both older men and
women attending SSHC were in self-defined ‘regular’ relationships, including 35% of
attendees who were married, and (more) were widowed, separated or divorced.
However, ‘newly single’ older people who are most likely to be women [23], will
need to learn condom negotiation skills if they are to protect themselves from the
Page 8 of 17Australasian Journal on Ageing
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Review O
nly
9
sexual risk demonstrated by their male peers in this study. There is little research and
fewer programs to guide older women on how to even start a discussion about
condom use with their sexual partner.[24]. While it is reassuring that people who had
recently had sex overseas were more likely to use condoms then people sexually
active in Australia, the latter group had alarmingly low rates of condom use. This
should not surprise us given that condom promotion has only been directed a young
people in sexual health promotion campaigns in New South Wales [25].
Overall, the sexual risk of older people attending SSHC was significantly higher than
in previous UK reports [26]. Variations in approaches to patient triage, differences in
access to health care and the absence of safe sex campaigns directed at older people
might all contribute to the differences in sexual risk.
These older sexual health clinic attendees also appear to have a high level of access to
sexual health care if measured by previous HIV testing and sexual health diagnoses.
HIV testing rates (>50% men, 40% women) compare favourably with others of
similar ages in New South Wales (men 36%, women 27%) [27] and Sydney’s male
gay community (>80%) [28]. Over half of men and women had prior sexual health
problems suggesting some persistence of sexual risk into later life for these people.
Other studies have revealed very low rates of HIV testing among older sexual health
clinic attendees (15%) and relatively lower rates of prior sexual health problems
(29%) [26].
It might be expected that older people present to a sexual health centre because they
are concerned about their sexual health - 80% requesting either an assessment of
Page 9 of 17 Australasian Journal on Ageing
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Review O
nly
10
genital symptoms or specific STI/HIV testing or care - yet few older people presented
specifically for or were diagnosed with sexual function difficulties. All sexual
dysfunction diagnoses were made in men (4%). The impact of more widespread
availability and use of pharmacotherapy for sexual dysfunction on sexual health
services has been previously discussed in relation to pressure on sexual health
services [29]. However, the impact of greater discussion about sex, sexuality and
health has not been investigated and make sexual health promotion campaigns an
even more urgent priority.
Genital manifestations of skin problems or skin manifestations of genital problems
and non-sexual health problems accounted for six of the ten most frequent diagnoses
at SSHC-a similar finding to other studies [12,13]. It is unclear whether the
predominance of skin conditions is a result of biological changes in older people or
people seeking further opinions about undiagnosed problems. However, in contrast,
genital herpes in both older women and men, and NGU in older men were among the
top four most common diagnoses. Genital herpes research undertaken during the
study period, increased public awareness of genital herpes or differences in conditions
managed in general practise may account for the predominance of these diagnoses.
What all of the common diagnoses suggest is a keen interest by older people in their
sexual health.
This study provides a description of the sexual behaviour and sexual health of people
over the age of 50 - a generally neglected age group in sexuality studies. Further
studies comparing people above and below 50 years of age may be useful in order to
Page 10 of 17Australasian Journal on Ageing
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Review O
nly
11
better target services and education programs to meet special needs of different age
groups.
While the strength of this study is the large sample of older people over a ten year
period, the limitation is that the data is from a clinic-based sample that are self-
selected and triaged patients who may not represent the broader community. It is
critical that population based studies on sexuality and sexual health include larger and
more representative cohorts of older persons (70 years and older) in their sampling as
future generation of older persons will be in relationships and sexually active [30].
Responsive education and public health campaigns must be informed by appropriate
knowledge of this population gained through research.
ACKNOWLEDGEMENTS
We would like to thank Richard Rohrsheim for data set extraction from the SSHC
database and for Kate Tribe for her assistance with data cleaning and analysis.
Page 11 of 17 Australasian Journal on Ageing
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Review O
nly
12
Key Points
Older people have sexual health needs that need greater recognition.
Older people present to a sexual health centre because they are concerned about their sexual health - 80% requesting either an assessment of genital symptoms or specific STI/HIV testing or care
In the last 3 and 12 months, both women and men had a median of one opposite sex partner, respectively. The median number of lifetime opposite sex partners was three for women and 10 for men.
Condom use is an issue for older people and this has implications for sexual health.
Over 60% of women and 50% of men had not been previously tested for HIV, despite being sexual active and sometimes with more than one partner.
Over half of men and women had prior sexual health problems suggesting some persistence of sexual risk into later life for these people.
Page 12 of 17Australasian Journal on Ageing
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Review O
nly
13
REFERENCES
1 Australian Bureau of Statistics. Population by Age and Sex, Australian States and
Territories. Cat No 3201.0, June 2004.
2 Minichiello V, Coulson I. The challenge of promoting positive ageing. In:
Minichiello V, Coulson I, eds. Contemporary Issues in Gerontology: Promoting
Positive Ageing. Sydney: Allen & Unwin, 2005.
3 Minichiello V, Plummer D, Seal A. The “asexual” older person? Australian
evidence. Venereology, 1996; 9:180-188.
4 Minichiello V, Plummer D, Loxton D. Knowledge and beliefs of older Australians
about sexuality and health. Australasian Journal on Ageing 2000; 19:190-194.
5 Smith AMA, Rissel CE, Richters J, Grulich A, de Visser R. Sex in Australia: The
rationale and methods of the Australian Study of Health and Relationships. Aust N Z J
Public Health 2003; 27: 106-117.
6 Johnson AM, Mercer CH, Erens B, Copas AJ, et al. Sexual behaviour in Britain:
Partnerships, practices, and HIV risk behaviours. Lancet 2001; 358: 1835-1842.
7 ACSF Investigators. AIDS and sexual behaviour in France. Nature 1992; 360: 407-
409.
8 Laumann E, Gagnon J, Michael R, Michaels S. The Social Organization of
Sexuality: Sexual Practices in the United States. Chicago: University of Chicago
Press, 1994.
9 Department of Health. The national strategy for sexual health and HIV. London:
DOH, 2001. http://www.dh.gov.uk/assetRoot/04/05/89/45/04058945.pdf. Accessed
29 June 2006.
10 Department of Health and Ageing. The National Sexually Transmissible Infections
Strategy 2005-2008. Canberra: Commonwealth of Australia, 2005.
Page 13 of 17 Australasian Journal on Ageing
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Review O
nly
14
11 Department of Health and Ageing. The National HIV/AIDS Strategy, Revitalising
Australia’s Response 2005-2008. Canberra: Commonwealth of Australia, 2005.
12 David N, Rajamanoharan S, Tang A. Sexually transmitted infections in elderly
people (letter). Sex Transm Infect 2000; 76: 222.
13 Tobin JM, Harindra V. Attendance by older patients at a genitourinary medicine
clinic. Sex Transm Inf 2001; 77: 289-291.
14 Jalell H, Allan PS, Wade AAH. Sexually transmitted infections in elderly people
(letter). Sex Transm Inf 2000; 75: 448-455.
15 Gott CM, Ahmed-Jusuf I, McKee K, Morgan K, Riley V, Rogstad KE.
Characteristics of older patients attending genitourinary medicine clinics. Health Care
in Later Life 1998; 3: 252–257.
16 Johnson AM, Wadsworth J, Wellings K, Bradshaw S, Field J. Sexual lifestyles
and HIV risk. Nature 1992; 360: 410–412.
17 Wood K, Jacons S, Chuah J, Dixon B. A profile of older people accessing a sexual
health clinic. Venereology 1996; 9(3): 176-179.
18 Coates TA. Strategies for modifying sexual behaviour for the primary and
secondary prevention of HIV disease. Journal of Consulting and Clinical Psychology
1990; 58: 57-69.
19 Dore GJ, Kaldor JM. Sexually transmissible diseases surveillance in Australia:
Towards a coordinated national system. Comm Dis Intell 1998; 22: 49-52.
20 De Hertough DA. Sexually transmitted diseases in the elderly. Infect Med 1994;
11: 361–363.
21 Australian Bureau of Statistics, National Health Survey, Australia, 2001. Cat No
4364.0, June 2004.
Page 14 of 17Australasian Journal on Ageing
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Review O
nly
15
22 Gomez L, Martin B. Gender, culture and power: Barriers to HIV prevention
strategies for women, J Sex Res 1996; 33: 355-363.
23 Minichiello V, Ackling S, Bourne C, Plummer D. Sexuality, sexual intimacy and
sexual health in later life. In Minichiello V, Coulson I, eds. Contemporary Issues in
Gerontology: Promoting Positive Ageing. Sydney: Allen & Unwin, 2005.
24 Zablotsky D, Kennedy M. Risk Factors and HIV transmission to midlife and older
women, knowledge, options, and initiation of safer sexual practises. JAIDS(suppl)
2003; 33: S122-S130.
25 New South Wales Health Department. Safe sex, No Regrets Campaign. Sydney:
Department of Health, 2004.
26 Gott CM, Rogstad KE, Riley V, Ahmed-Jushufand I, Green T. Exploring the
sexual histories of older GUM clinic attenders. Int J STD & AIDS 2000; 11: 714-718.
27 Grulich A, Jin J. Sex in New South Wales: A report to New South Wales Health
Department. Sydney: National Centre in HIV Epidemiology and Clinical Research,
2003.
28 National Centre in HIV Social Research. HIV/AIDS, hepatitis and sexually
transmissible infections in Australia: Annual Report of Behaviour 2005. Sydney:
NCHSR, University of New South Wales, 2005.
29 Hillman J. Clinical Perspectives on Elderly Sexuality. New York: Kluwer
Academic/Plenum Publishers, 2000.
30 Gott M. Are older people at risk if sexually transmitted infections? A new look at
the evidence. Reviews in Clinical Gerontology 2005; 14: 5-13.
Page 15 of 17 Australasian Journal on Ageing
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Review O
nly
16
Figure 1: Number of new clients at SSHC ≥50 years by age group and sex, 1993-
2003 (N= 2438)
0
200
400
600
800
1000
1200
1400
1600
50-59 60+
Age categories (yrs)
Num
ber
of c
lient
s
women
men
Figure 2: Condom use in the last 3 months of clients ≥50 years at SSHC 1993-
2003
05
101520253035404550
no inter
cours
enon
e
som
etim
es
usuall
y
alway
s
Frequency of condom use
womenmen
Page 16 of 17Australasian Journal on Ageing
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Review O
nly
17
Table 1: The ten most common diagnoses amongst people ≥50 years attending
SSHC
N (%) Diagnosis in men N (%) Diagnosis in women
228 (12) Anogenital rash or lesion 45 (10) Genital herpes
173 (9) Non-sexual health conditions for
investigation &/or referral
40 (9) Non-specific vulvovaginal
conditions
169 (9) NGU 38 (8) Non-sexual health conditions for
investigation &/or referral
123 (6) Genital herpes 33 (7) Counselling issues*
141 (7) Balanoposthitis +/- candidiasis 28 (6) Anogenital rash or lesion
138 (7) Counselling issues* 20 (4) Menstrual disorder
114 (6) Genital warts 17 (4) Genital warts
74 (4) Dermatological conditions 16 (4) Vulvovaginal candidiasis
71 (4) Scrotal symptoms/signs 16 (4) Syphilis
71 (4) Sexual dysfunction 14 (3) Bacterial vaginosis
*Pychosocial &/or relationship issues
Page 17 of 17 Australasian Journal on Ageing
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960




















