September 2018 - California Dental Association
68
Andrew Young, DDS, MSD Journa CALIFORNIA DENTAL ASSOCIATION Online Research Appraising Dental Literature Dental Statistics September 2018
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of September 2018 - California Dental Association

Andrew Young, DDS, MSD
JournaC A L I F O R N I A D E N T A L A S S O C I A T I O N
Online Research
Appraising Dental Literature
Dental Statistics
September 2018

Price comparison based on an actual customer who purchased a comparable product within the past six months. Prices rounded to the nearest dollar. All trademarks used herein are the property of their respective owners in the United States and abroad.
Sure, you could pay 36% more for a pack of CaviWipes1 Disinfectant Wipes.
$13
elsewhere
$8CaviWipes1™
Disinfectant
Wipes
160/package
Start now at tdsc.com/pricecompare.
Or, you could shop tdsc.com and have more to spend on
things you care about – whether it’s more dental supplies or
donuts for your team.
The DentistsSupply
Company

C DA J O U R N A L , V O L 4 6 , Nº 9
S E P T E M B E R 2 0 1 8 535
Enhancing Patient Care Through Evidence-Based Dentistry
An introduction to the issue.Andrew Young, DDS, MSD
Searching for Research Articles on the Internet
This practically oriented article covers several methods that can be used to make online searches more effective and efficient.Steve Kirk, PhD
The Anatomy of a Clinical Study
This article explains the different parts of a clinical study and why each part is important.Andrew Young, DDS, MSD
How To Critically Appraise the Dental Literature
This article guides the reader in critically appraising several common study designs.Terrence Shaneyfelt, MD, MPH
Statistics for Practicing Dentists
This article provides definitions and examples of some entry-level statistical concepts.Eric S. Salmon, DDS
Where the Rubber Meets the Road: Incorporating Evidence-Based Dentistry
This article proposes some solutions to integrating evidence-based dentistry at different dental career stages.Andrew Young, DDS, MSD, and Des Gallagher, BDS, MA
553
555
561
569
577
583
Sept. 2018
D E PA R TM E N T S
F E AT U R E S
541
The Associate Editor/DIY: A Fading Fad?
Letter to the Editor
Impressions
Winners of the 2018 Table Clinic Competition
RM Matters/Whodunit? Subrogation Determines Responsibility in Property Claims
Regulatory Compliance/Radiation and Pregnancy
Tech Trends
537
539
541
547
589
593
598

C DA J O U R N A L , V O L 4 6 , Nº 9
536 S E P T E M B E R 2 01 8
Volume 46, Number 9 September 2018
JournaC A L I F O R N I A D E N T A L A S S O C I A T I O N
CDA classifieds work harder to
bring you results. Selling a practice
or a piece of equipment? Now you
can include photos to help buyers
see the potential.
And if you’re hiring, candidates
anywhere can apply right from
the site. Looking for a job? You can
post that, too. And the best part—
it’s free to all CDA members.
All of these features are designed to
help you get the results you need,
faster than ever. Check it out for
yourself at cda.org/classifieds.
CDA Classifieds. Free postings.Priceless results.
CDA classifieds work harder to
bring you results. Selling a practice
or a piece of equipment? Now you
CDA Offi cersNatasha A. Lee, DDSPRESIDENT
R. Del Brunner, DDSPRESIDENT-ELECT
Richard J. Nagy, DDS VICE PRESIDENT
Judee Tippett-Whyte, DDS SECRETARY
Steven J. Kend, DDSTREASURER
Craig S. Yarborough, DDS, MBASPEAKER OF THE HOUSE
Clelan G. Ehrler, DDSIMMEDIATE PAST PRESIDENT
ManagementPeter A. DuBoisEXECUTIVE DIRECTOR
Carrie E. GordonCHIEF STRATEGY OFFICER
Kristine AllingtonVICE PRESIDENT, MARKETING
AND MEMBERSHIP
Alicia MalabyCOMMUNICATIONS
DIRECTOR
EditorialKerry K. Carney, DDS, CDEEDITOR-IN-CHIEF
Ruchi K. Sahota, DDS, CDEASSOCIATE EDITOR
Brian K. Shue, DDS, CDEASSOCIATE EDITOR
Gayle Mathe, RDHSENIOR EDITOR
Andrew Young, DDS, MSDGUEST EDITOR
Andrea LaMattina, CDEPUBLICATIONS MANAGER
Kristi Parker JohnsonEDITORIAL SPECIALIST
Blake EllingtonTECH TRENDS EDITOR
Jack F. Conley, DDSEDITOR EMERITUS
Robert E. Horseman, DDSHUMORIST EMERITUS
ProductionVal B. MinaSENIOR GRAPHIC DESIGNER
Randi TaylorSENIOR GRAPHIC DESIGNER
Upcoming Topics October/PeriodonticsNovember/General TopicsDecember/Biomaterials
AdvertisingSue Gardner ADVERTISING SALES
Permission and ReprintsAndrea LaMattina, CDEPUBLICATIONS MANAGER
Manuscript Submissionswww.editorialmanager.com/jcaldentassoc
Letters to the Editorwww.editorialmanager.com/jcaldentassoc
SubscriptionsSubscriptions are available only to active members of the Association. The subscription rate is $18 and is included in membership dues. Nonmembers can view the publication online at cda.org/journal.
Manage your subscription online: go to cda.org, log in and update any changes to your mailing information.Email questions or other changes to [email protected].
published by the California Dental Association 1201 K St., 14th Floor Sacramento, CA 95814 800.232.7645 cda.org
Journal of the California Dental Association (ISSN 1043–2256) is published monthly by the California Dental Association, 1201 K St., 14th Floor, Sacramento, CA 95814, 916.554.5950. Periodicals postage paid at Sacramento, Calif. Postmaster: Send address changes to Journal of the California Dental Association, P.O. Box 13749, Sacramento, CA 95853.
The California Dental Association holds the copyright for all articles and artwork published herein. The Journal of the California Dental Association is published under the supervision of CDA’s editorial staff . Neither the editorial staff , the editor, nor the association are responsible for any expression of opinion or statement of fact, all of which are published solely on the authority of the author whose name is indicated. The association reserves the right to illustrate, reduce, revise or reject any manuscript submitted. Articles are considered for publication on condition that they are contributed solely to the Journal.
Copyright 2018 by the California Dental Association. All rights reserved.
Stay Connected cda.org/journal

C DA J O U R N A L , V O L 4 6 , Nº 9
S E P T E M B E R 2 0 1 8 537
Assoc. Editor
The DIY (or do-it-yourself) trend has taken over. With Google and YouTube in our lives, we can learn how to do anything on our own. The willingness
to try a new trend matches well with the easy access of the internet.
One such trend is buzzing around our offi ces. Multiple start-ups are selling orthodontic aligners directly to patients. In most cases, the consultation and treatment planning for the aligners occur from the comfort of the patient’s home. A DIY impression is mailed into the company. Selfi e photos taken with a smartphone are electronically transmitted. And fi nally, an orthodontist or dentist, usually from hundreds or maybe thousands of miles away, evaluates and treatment plans a set of aligners for an average of $1,500. The process is simple, cost-effective and on trend with our current obsession of living life via the internet and our cellphone apps.
The idea of trend marketing, virtual communication and e-commerce is at the core of the treatment. Imagine this: A patient is browsing BuzzFeed or other internet sites in the middle of the night (which many of us may be guilty of — namely, me). Curiosity is piqued. Media coverage of a website or app that allows you to attain straight teeth from the convenience of your own home is enticing. An avid Amazon.com addict whose trigger fi nger is always ready to click “buy” will easily succumb to this seemingly effortless opportunity to fi x a smile.
Perhaps this is a good thing. The more people think about fi xing their smile, the more they will ask the questions needed to make good choices for their oral health. They may learn about why dentistry is important. Anything that increases oral health literacy and engagement is a good thing.
Alternatively, a seemingly streamlined process leading to a better smile is enticing. But is it too good to be true? Taking the time to think through options, explore the risks and benefi ts of the treatment and investigate the long-term impact on our oral health can seem cumbersome and unnecessary. Danger ensues if patients concentrate solely on the potential result and forget about the necessary processes or intricacies involved in the means of obtaining that straight-smile result.
While a few of these companies ask for at least one in-person visit with an orthodontist or dentist, most allow patients to complete treatment completely from the comfort of their own home — never setting foot in a dentist’s offi ce. While one company pays for and arranges the Uber ride to the orthodontist’s offi ce, most of the companies accept selfi e photos as the “clinical” pictures for the exam needed to diagnose and create an orthodontic treatment plan.
It sounds unfathomable. Are selfi es and DIY impressions all that are needed? Can it become legal to provide tooth-straightener treatments entirely without a doctor involved? The next question, of course, is what else can an app diagnose using just a selfi e without a dentist involved at all? What other dental treatment could be delivered to a patient’s home with a laminated card listing DIY directions? These questions may sound
crazy or far-reaching. But did the world think Uber or Lyft could so quickly replace taking a taxi? The way a simple app started prevailing over the private transportation industry was shocking. Now the concept of hailing a ride using an app is typical. But not all trends last. Let’s face it, most of our attempts at DIY projects do not end in the perfection portrayed in a Pinterest post. Will the direct-to-consumer form of dentistry have similar imperfect results? Will this cause patient dismay and fi nally cause the fad to dwindle away on its own? When even criminal cases and lawsuits did not defeat the disruptors of the taxi business, how likely is it that liability lawsuits will potentially burst this new trend’s bubble?
Football great Lou Holtz famously had three rules: Do the right thing, do the best you can and always show people you care. CDA dentists strive to do the same. Beauty is in the eye of the beholder, but good health and wellness comes from “doing things right.” So if we develop good relationships with our patients, will they still call us to receive our expert opinion before trying a new trendy treatment, even if we have not seen them in a long time? Or will the one-dimensional FAQ on the DIY aligner websites satisfy all of their questions? Will patients ask us for advice before they commit to a treatment plan from a dentist whom they have never met in person before?
Dentistry DIY: A Fading Fad?Ruchi K. Sahota, DDS, CDE
Let’s face it, most of our attempts at DIY projects do not end in the perfection portrayed in a Pinterest post. Will the direct-to-consumer form of dentistry have similar imperfect results?
C DA J O U R N A L , V O L 4 6 , Nº 9
538 S E P T E M B E R 2 01 8
S E P T . 2 0 1 8 A S S O C . E D I T O R
The new companies that are marketing directly to patients do not see themselves as “disruptors” like many startups in other industries may aspire to identify themselves. They attest that they are simply expanding access to care for patients who have “mild” orthodontic needs. They are reaching more people. Decreased costs and increased convenience will allow more people to straighten their teeth. The sense of nobility and of wearing the “white hat” that expands the access to more dental care is all too familiar. This notion is an “in” with the media, with the representatives in government and with sympathizers in the general public. However, it would be doubtful if such sentiments would sway a group of venture capitalists to give one of the new clear aligner companies $17 million.
It is not the outside-of-the-box use of technology that worries us. Technology has a place in our profession and we are thankful for it. One unconventional success in the last six years has been the teledentistry project headed by Paul Glassman, DDS, of the University of the Pacifi c, Arthur A. Dugoni School of Dentistry.1 The virtual dental home is a system that the Pacifi c Center for
Special Care created where people receive preventive and simple dental treatment services in settings like Head Start preschools, elementary schools, community centers, residential care facilities for people with disabilities, senior centers and nursing homes. This has brought treatment to those who would not otherwise be able to reach it. This story that Dr. Glassman told DentistryIQ is the perfect example: “A 7-year-old boy in San Diego came to see the dental hygienist working in his school. His teeth were covered with orange, caked-on material. She cleaned his teeth and encouraged him to brush his teeth regularly. He told her he did not have a toothbrush. He said he had previously had one but it was stolen by his siblings. Her ‘treatment’ for him was to give him a toothbrush whenever she saw him. This is a child who now has healthy teeth but would never have made it into a dental offi ce.”
Pieces of dentistry may be able to be sold directly to patients. But it is important to note that preventing and treating dental disease can be challenging in the four walls of our offi ces. It is hard to understand how these things could be accomplished using just the
internet. However, as Steve Jobs said, “Innovation is the ability to see change as an opportunity — not a threat.” Dentistry always continues to evolve. Time will tell whether the venture capitalist-funded companies that sell dentistry straight to the consumers for them to DIY are here to stay. But they are not our competition. They are not a threat. Dentists will be here, no matter what. We will need to be there for our patients. Hopefully we will only need to help maintain the pretty smiles the aligner companies help shape and nothing more. We will be here for our patients, in person, nonetheless. ■
REFERENCE
1. www.dentistryiq.com/articles/2017/01/california-teledentistry-program-virtual-dental-home-continues-success-with-recent-grant-and-further-growth.html.
Ruchi K. Sahota, DDS, CDE, practices family dentistry in Fremont, Calif., and serves as faculty at the University of the Pacifi c, Arthur A. Dugoni School of Dentistry. She is also a certifi ed dental editor, a consumer advisor for the American Dental Association, past president of the Southern Alameda County Dental Society and a fellow of the American College of Dentists, International College of Dentists and the Pierre Fauchard Academy.
e ve
able
T
VA ©
ev
The Original E-VAC TipPREVENT PAINFUL TISSUE PLUGSPROTECT YOUR EQUIPMENT
FROM COSTLY REPAIRS
Contact Your LocalDental Supply Company

C DA J O U R N A L , V O L 4 6 , Nº 9
S E P T E M B E R 2 0 1 8 539
Letter
The June issue of the Journal contains six articles by six very young dentists talking about what it means to be a young dentist. The articles are outstanding.
These millennials seem to be comfortable with themselves and perhaps a bit dismissive of the notion that they can be made to fi t into existing categories.
Generation watchers have long known that it isn’t the astrological year of one’s birth that matters. There are two temporal patterns: A personal life stage one and a larger one of societal progress. It is the interaction that produces what we think of as generational effects. We learn the habits of where to fi nd things, how others respond when we ask for something, taste in music, how to work with others, what it means to have a job or a career, how long a planning horizon should be and family and community stuff at predictable stages in our lives. We incorporate, unrefl ectively, the best of the big changes in society that are offered at the time we need them. In the 1960s, we read journals and met interesting others in libraries; today one skims abstracts picked by computer algorithms and meets interesting others on the small screen. There are really only two generations: Those who stay with whatever they fi rst learned, the Past Generations, and the Pioneers who are learning new ways of doing things.
It is partially true that today’s pioneers are defi ned by technology. The car was the technology of the 1930s. It invented the teen by allowing youths of that age to form their own groups independent of father and mother. The cellphone has created a new class, the preteen, complete with its own norms, market niche and chauffer class. What counts is how technology defi nes the way we interact with each other.
Today, a users’ group for a new technology, patient condition, economic scheme or political purpose can form,
Organizations or Networks
Christian Piers, DDS, MFA
MILLENNIAL DENTISTS: How They Work, How They Learn and What It Means for the Practice of the Future
JournaC A L I F O R N I A D E N T A L A S S O C I A T I O N
Educating Millennials
Practicing in Remote Areas
Confronting the Dental Generation Gap
June 2018
function and fade digitally before an existing organization can work the proposal through its committee structure. In 2002, Howard Rheingold said in Smart Mobs that participants do not belong to digital networks — they are the networks and both networks and identity are fl uid, multiple and overlapping. Choice regarding participation is critical. Even earlier, University of Chicago researcher Ronald Burt wrote in Structural Holes that where one is in the network determines power and success. Organizations are no longer the network; they are links that may or may not be relevant in defi ning some of the networks dentists use to fulfi ll their professional identities. Organizations with membership committees are probably in trouble.
Organizations on the formal model were the right thing in a slower and more confi dent time. They offered the stability and sense of place we needed then. Robert Putnam’s classic, Bowling Alone, documents the decade’s-long decline in American “joining.” Falling membership numbers in professional organizations do not mean dentists are disengaged. It means they are self-engaging in networks with easy entrance and exit and very active in defi ning both networks and their place in them.
Everyone in the dental profession should be proud of the contributions of these young individuals who contributed to the theme issue on millennials. They were not shy about looking to the future and we should not be shy about going along with them; they are closer to it than we are. It’s just a click away and requires no membership dues. Pass this link on to participate: www.cda.org/portals/0/journal/journal_062018.pdf.
DAV I D W. C H A M B E R S , E D M, M B A, P H D
San Francisco
The Journal welcomes lettersWe reserve the right to edit all
communications. Letters should discuss an item published in the Journal within the last two months or matters of general interest to our readership. Letters must be no more than 500 words and cite no more than fi ve references. No illustrations will be accepted. Letters should be submitted at editorialmanager.com/jcaldentassoc. By sending the letter, the author certifi es that neither the letter nor one with substantially similar content under the writer’s authorship has been published or is being considered for publication elsewhere, and the author acknowledges and agrees that the letter and all rights with regard to the letter become the property of CDA.

Unsure how to handle patients who are experiencing prolonged numbness following dental procedures? The Dentists Insurance Company’s new Risk Management
seminar is designed to build your confidence in these interactions.
Participate in the Pain & Perception seminar and learn how to: • Institute communication protocols when multiple dentists are involved in treatment.
• Recognize the importance of complete and appropriate documentation.
• Communicate unexpected treatment outcomes to patients and know when to refer.
• Understand that informed consent is a process, not a form.
Get expert advice while earning C.E. credits and a5% Professional Liability premium discount* for two years.
Save your spot today at tdicinsurance.com/seminarsor explore convenient eLearning options.
Protecting dentists. It’s all we do.®
800.733.0633 | tdicinsurance.com | CA Insurance Lic. #0652783
*TDIC policyholders who complete a seminar or eLearning option will receive a two-year, 5 percent Professional Liability premium discount effective their next policy renewal. To obtain the two-year, 5 percent Professional Liability premium discount, Arizona, California and Nevada dentists must successfully complete the seminar by April 26, 2019. Alaska, Hawaii, Illinois, Minnesota, New Jersey, North Dakota and Pennsylvania dentists must successfully complete the seminar by October 26, 2018. Any eLearning tests received after the deadline will not be eligible for the discount. Non-policyholders who complete a seminar or eLearning option and are accepted for TDIC coverage will also be eligible for this discount.

C DA J O U R N A L , V O L 4 6 , Nº 9
S E P T E M B E R 2 0 1 8 541
Impressions
The nub:
1. Where one practices determines how one practices.
2. It is good business to segment the market, but it may not be good ethics.
3. The poor get less care and of poorer quality.
David W. Chambers, EdM, MBA, PhD, is a professor of dental education at the University of the Pacifi c, Arthur A. Dugoni School of Dentistry, San Francisco, and the editor of the American College of Dentists.
Ethics of Practice LocationDavid W. Chambers, EdM, MBA, PhD
Practice location is perhaps the single largest ethical decision a dentist will ever make. It affects what patients expect and will accept, thus how one practices. The impact of that single decision is repeated day after day.
Wait a minute! Isn’t where one lives a personal choice? Yes, but ethical choices are personal ones. Where we practice becomes part of our professional identity.
Surveys of graduating seniors have consistently revealed a small tendency to establish practices in one’s own ethnic community. There are lifestyle issues that draw graduates to remote areas for the quality of small-town or outdoor living. One’s spouse has a say.
But economic factors have a strong pull. One can assuage anxieties about practicing on the least
needy by volunteering. These are temporary, selective interventions — almost always in areas remote from
one’s own practice. There are dentists, and they deserve respect and credit, who prefer to give back in their own communities. There are some who actively work to extend the range of potential patients to include a broader range of their neighbors. Bravo for them, but we need more.
Practice location is not randomly distributed across California. If it were, the ratio of dentists to population would be similar across counties. Instead, there are more than 50 dentists per 50,000 population in Marin, Santa Clara, San Francisco and around Lake Tahoe. By contrast, there are six per 50,000 in Yuba County and none in Alpine.
I recently checked the median household incomes by ZIP code around the state. The average in 2015 was $61,818 per household. We would expect that dentists, on average, would practice in ZIP codes where the average was close to that fi gure. Instead, dentists concentrated in areas where the median household income was $79,094. That is a 28 percent step up in potential economic support for practitioners.
That in and of itself suggests that practice location might be an ethical issue. But if we look farther at how dentists practice, the concern grows. Some dentists have their licenses disciplined in California (about 50 per year). Some of this is because of life issues such as drugs or tax evasion. There are cases of failure to diagnose cancer or placing implants where they are unjustifi ed. Dentists guilty of these infractions are likely to locate in upscale neighborhoods just like their colleagues do.
But there are many disciplined licenses resulting from overtreatment, overbilling and insurance fraud, failure to inform patients of their treatment options and patient abandonment. These dentists practice in communities where the median household income is 10 percent below the state average. That is certainly an ethical issue. ■

C DA J O U R N A L , V O L 4 6 , Nº 9
542 S E P T E M B E R 2 01 8
Gum Disease May Initiate RA-Related AutoimmunityThe results of a study presented at the Annual European Congress of
Rheumatology (EULAR) 2018 demonstrates increased levels of gum disease and disease-causing bacteria in individuals at risk of rheumatoid arthritis (RA).
“It has been shown that RA-associated antibodies … are present well before any evidence of joint disease. This suggests they originate from a site outside of the joints,” said study author Kulveer Mankia, PhD, of Leeds Institute of Rheumatic and Musculoskeletal Medicine and the Leeds Biomedical Research Centre. “Our study results support the hypothesis that local inflammation at mucosal surfaces, such as the gums in this case, may provide the primary trigger for the systemic autoimmunity seen in RA.”
The prevalence of gum disease is increased in patients with RA and could be a key initiator of RA-related autoimmunity. This is because autoimmunity in RA is characterized by an antibody response to citrullinated proteins, according to the study, and the oral bacterium Porphyromonas gingivalis (Pg) is the only human pathogen known to express an enzyme that can generate citrullinated proteins.
In study results, dentists diagnosed clinical gum disease in significantly more at-risk individuals than in healthy controls. In addition, the percentage of sites with clinical attachment level, pocket depth, bleeding on probing, periodontal disease and active periodontal disease were all significantly greater in the at-risk individuals compared to controls.
The study included 48 at-risk individuals, 26 patients with RA and 32 healthy controls. DNA was isolated from the subgingival plaque of each participant and used to measure the levels of three types of bacteria, Pg, Aggregatibacter actinomycetemcomitans (Aa) and Filifactor Alocis. Results showed that there was increased abundance of both Pg and Aa in at-risk individuals. However, in at-risk individuals, only Pg was significantly increased at healthy dental sites and was associated with the overall extent of gum disease.
S E P T . 2 0 1 8 I M P R E S S I O N S
the protocol in February 2016, 2,792 opioid prescriptions were written — a 47.1 percent overall decrease.
“There has been a linear decrease in the number of opioid prescriptions written since the introduction of the protocol in the fi rst quarter of 2016,” said Chad Lowell Wagner, a second-year dental student at UM School of Dentistry, who
presented the poster. “Our results support the hypothesis that an opioid prescribing protocol would be successful in decreasing the total number of opioid prescriptions written and number of tablets dispensed per prescription while appropriately addressing postoperative pain.”
Learn more about the AADR at aadr.org.
Protocol Reduces Number of Opioid Prescriptions Written By Dentists
Opioid abuse continues to cause harm in epidemic proportions, and dental providers are leading prescribers to individuals under age 18. To address this issue, the University of Minnesota department of oral and maxillofacial surgery implemented an opioid-prescribing protocol for the treatment of postsurgical pain.
The results of the protocol were presented in a poster titled “Effect of an Opioid Prescribing Protocol on Provider Prescribing Behavior” at the 47th Annual Meeting of the American Association for Dental Research (AADR), held in conjunction with the 42nd Annual Meeting of the Canadian Association for Dental Research in March 2018.
For the study, retrospective analysis was used to evaluate the use of opioid analgesics at the UM School of Dentistry, prior to and following implementation of the opioid-prescribing protocol. Using prescription data collected from institutional electronic health record software for FDA-schedule opioids written within the School of Dentistry, the analysis compared the number of total opioid prescriptions and the number of tablets per prescription in the previous 10 quarters.
Results showed that more than 5,000 opioid prescriptions were written across all departments in the fi ve quarters prior to the introduction of the opioid protocol on Oct. 1, 2016. In the fi ve quarters following the introduction of

C DA J O U R N A L , V O L 4 6 , Nº 9
S E P T E M B E R 2 0 1 8 543
Researchers analyzing the teeth of Britons from the Iron Age to the modern day have unlocked the potential for using proteins in tooth tartar to reveal the diet of our ancestors. The study was published in the July 2018 issue of the journal Proceedings of the Royal Society B.
Archaeological tooth tartar has previously been shown to preserve milk
proteins, but this international study, led by researchers at the University of York and the Max Planck Institute for the Science of Human History, has proved for the fi rst time that it can also reveal more precise information about a wider range of food proteins, including those from plants.
Analyzing 100 archaeological samples from across Britain and 14 samples from living dental patients and recently deceased
individuals, the research team found that potential dietary proteins could be found in about a third of the analyzed samples.
“In the teeth we look at from individuals who lived around the Victorian era, we identifi ed proteins related to plant foods, including oats, peas and vegetables in the cabbage family,” said senior author Camilla Speller, PhD, from the department of archaeology at the University of York. “Occasionally, we fi nd evidence of milk and oats in the same mouth. I like to think it’s from eating porridge.”
In the modern samples, the researchers found proteins that refl ected a global British diet, such as those related to potatoes, soybeans and peanuts, as well as milk proteins.
The research team plans to use the results of this study to help refi ne their protein-detection methods and to explore particular problem areas of ancient diet research.
“This approach may be particularly useful in the detection of understudied vegetative crops, especially in regions where macrobotantical remains are not preserved,” Dr. Speller said. “It may offer a more precise way of identifying foodstuffs compared to other methods such as ancient DNA and isotope analysis as it can distinguish between different crops and indicate whether people were consuming dairy products, like milk or cheese.”
Learn more about this study in Proceedings of the Royal Society B(2018); doi: 10.1098/rspb.2018.0977.
Research on British Teeth Off ers Insights Into Ancient Diets
Review of Improvements in Neutron TomographyA comprehensive overview of neutron-based imaging processes, published
recently in the journal Materials Today, reported on the latest developments in neutron tomography, which has facilitated breakthroughs in diverse areas such as dentistry, art history, battery research, energy materials, industrial research, magnetism, palaeobiology and plant physiology.
Neutrons can penetrate deep into a sample without destroying it and can also distinguish between light elements such as hydrogen, lithium and substances containing hydrogen. Because neutrons themselves have a magnetic moment, they react to the smallest magnetic characteristics inside the material, making them a versatile and powerful tool for materials research. Neutron tomographs, also known as 2D and 3D images, can be calculated from the absorption of the neutrons in the sample.
In their review paper, the authors describe the latest improvements in neutron imaging and outstanding applications. Improvements in recent years have extended the spatial resolution down into the micrometer range, which is more than 10 times better than with typical medical X-ray tomography, according to the study. Faster images are also possible now, which makes observing processes in materials feasible. This provides important information for optimizing the design of the cell, according to the study.
Applications range from observing the transport of lithium ions in batteries and strength analyses of industrial components, to examinations of teeth, bones and the roots of plants, to nondestructive analyses of historical objects such as old swords and knights’ armor in order to obtain information on historical manufacturing methods.
Read more of this study in Materials Today (2018); doi.org/10.1016/j.mattod.2018.03.001.
Fossils like this 250 million-year-old skull of a lystrosaurus can be examined very carefully by neutron tomography. (Credit: MfN Berlin)
Skeleton sampled for the study, dating to the postmedieval period in Britain. (Credit: Camilla Speller, University of York)

C DA J O U R N A L , V O L 4 6 , Nº 9
544 S E P T E M B E R 2 01 8
a total of 211,393,167 people — had access to fl uoridated water, according to the CDC. However, access to fl uoridated water varies greatly between states. According to 2014 CDC data, in 27 states, 75 percent or more of the population had access to fl uoridated water, while in eight states less than half of the population had the same access.
Learn more about the U.S. study in the Journal of Dental Research (2018); doi.org/10.1177/0022034518774331 and the Australian study in the journal Community Dentistry and Oral Epidemiology (2018); doi.org/10.1111/cdoe.12384.
detailed national child oral health study conducted in 2012–14 and found caries prevalence and experience higher among children in Australia with lower lifetime exposure to fl uoridated water.
“Considered together, these studies provide dynamic contemporary evidence regarding the effectiveness of fl uoridation, which is often requested by policy decision-makers,” said Bonita Neighbors, DDS, chair of the American Dental Association National Fluoridation Advisory Committee.
Nationwide, in 2014, 74.4 percent of the U.S. population on public water systems —
Studies Underscore Effi cacy of Water Fluoridation
Children and adolescents in the U.S. with greater access to fl uoridation were less likely to experience dental caries, according to a study published in June 2018 in the Journal of Dental Research.
For the article, “Water Fluoridation and Dental Caries in U.S. Children and Adolescents,” researchers evaluated associations between the availability of community water fl uoridation and dental caries experience in children and adolescents.
Study authors used estimates from the Centers for Disease Control and Prevention’s (CDC) Fluoridation Reporting System of the percentage of population with fl uoridation. The information was merged with dental examination data from 10 years of National Health and Nutrition Examination Surveys (NHANES), from 1999–2004 and 2011–2014.
Researchers discovered a 30 percent reduction in dental caries experience in the primary dentition in counties where more than 75 percent of the population had access to community water fl uoridation when compared to communities where less than 75 percent had access. They also noted a 12 percent reduction in dental caries in the permanent dentition.
Another report, also published in June 2018, has similar conclusions. For the article, “Contemporary Evidence on the Effectiveness of Water Fluoridation in the Prevention of Childhood Caries,” researchers in Australia analyzed a
Warning Labels Deter Sugary-Drink ConsumptionPeople are less likely to buy sugary drinks if they see warning labels that
include graphic pictures of health consequences such as obesity, diabetes and tooth decay, according to a Harvard University study published online in June 2018 in the journal Psychological Science.
Researchers conducted a study in the cafeteria of a hospital in Massachusetts where three different types of labels were displayed one at a time for a few weeks near the bottled and fountain beverages. The labels included text warnings on the health risks of sugary drinks, graphic warnings on those health risks or a listing of calories in the drinks.
“Warning labels have been around a long time for tobacco products, but they’re a new concept for sugary drinks,” said study co-lead author Grant Donnelly, a former doctoral student at Harvard Business School.
When the graphic warning labels were posted, there was a nearly 15 percent drop in sugary drink sales and consumers appeared to substitute bottled water for sugary drinks. The average calories per drink sold decreased from 88 calories to 75, according to the study. The text-only warning labels and calorie labels had no effect on sales of sugary drinks.
“As policymakers search for ways to reduce excess consumption of sugary drinks, graphic warning labels merit consideration as a tool that can empower consumers with salient information to encourage healthier choices,” said study co-lead author Laura Zatz, a doctoral student at Harvard’s School of Public Health.
Learn more about this study in Psychological Science (2018); doi.org/ 10.1177/0956797618766361.
S E P T . 2 0 1 8 I M P R E S S I O N S

C DA J O U R N A L , V O L 4 6 , Nº 9
S E P T E M B E R 2 0 1 8 545
A plaster that sticks to the inside of the mouth is revolutionizing the treatment of painful recurring ulcers, according to a study published recently in the journal Biomaterials.
Scientists from the University of Sheffi eld’s School of Clinical Dentistry, working in close collaboration with Dermtreat A/S from Copenhagen, have
developed a unique patch using special polymers that are able to stick to moist surfaces. The patch successfully administers steroids directly to oral ulcers or lesions while also creating a protective barrier around the affected area, accelerating the healing process.
The novel plaster is a breakthrough therapy for the treatment of mucosal
conditions such as oral lichen planus (OLP) and recurrent aphthous stomatitis (RAS). Until now, ulcers and lesions inside the mouth have been treated using either creams or mouthwashes, which are used in the whole mouth rather than targeting the specifi c area, making them less effective. However, the biodegradable Rivelin patch has a long adhesion time and a high fl exibility that conforms to the surface inside the mouth, according to the study.
Craig Murdoch, BSc (Hons), PhD, reader in the Oral Bioscience School of Clinical Dentistry and lead author of the research, said the patch acts like a plaster inside the mouth, which means it is very effective at directly targeting the specifi c area as well as forming a protective barrier.
“Chronic infl ammatory conditions such as OLP and RAS, which cause erosive and painful oral lesions, have a considerable impact on quality of life,” Dr. Murdoch said. “Patients who have trialed the patch found it to be very comfortable to wear and they were really pleased with the length of adhesion, which makes it particularly effective and effi cient.”
Dermtreat A/S was recently awarded $17.7 million from the venture capital fi rm Sofi nnova. The funding will take the patches into phase two clinical trials, which will run at several sites in both the U.S. and the U.K. In addition, Dermtreat is funding further research at the University of Sheffi eld dental school to develop the next generation of patches that contain other useful drugs.
Learn more about this study in Biomaterials (2018); doi.org/10.1016/j.biomaterials.2018.06.009.
Plaster Patch Treats Oral Ulcers and Lesions
Mouth Bacteria Increase Risk of Dental Decay in Youths Born With HIV
A study led by a team of scientists from The Forsyth Institute found that differences in the mouth bacteria of youths born with HIV may increase their risk of cavities. The study published in the journal Microbiome in May 2018 found that HIV-infected youths, compared with uninfected youths, had lower numbers of Corynebacterium, a microbe that is abundant in dental plaque of healthy individuals.
Researchers followed two groups of youths — those born with HIV and a comparison group of youths who were not infected but were born to HIV-infected mothers — enrolled in a study that investigates the long-term outcomes of HIV infection and its treatment among children who acquired HIV from their mothers. The research demonstrated that bacterial composition was similar in both testing groups, implying that pediatric HIV infection and its treatment are not causing large-scale imbalances in the bacteria found in dental plaque.
The HIV-infected youths, however, had fewer corynebacteria in their dental plaque. This type of bacterium can help prevent the lactic acid produced by cavity-causing bacteria from reaching healthy teeth, which may help protect teeth from dental decay. Thus, the lower amounts of corynebacteria may explain why the HIV-positive youths also had more cavities.
“This may guide us in developing new therapies to prevent dental decay in these youths,” said Bruce Paster, PhD, senior member of staff at The Forsyth Institute and professor in oral medicine, infection and immunity at the Harvard School of Dental Medicine.
Read more about this study in Microbiome (2018);doi.org/10.1186/s40168-018-0484-6.
C. ulcerans colonies on a blood agar plate.
(Credit: University of Sheffield’s School of Clinical Dentistry)

WE HAVE ANSWERS.When it comes to managing your practice, you’re
not alone. Our smart analysts have dentistry-focused
expertise in leadership, ownership, patient
management, practice systems and transitions.
Tap into one-on-one guidance by phone or explore
an online library of tools and guides.
OVERWHELMED BY PRACTICE
MANAGEMENT?
800.232.7645cda.org/practicesupport
®
Practice ManagementEmployment PracticesDental Benefit PlansRegulatory Compliance
PRACTICE SUPPORT

C DA J O U R N A L , V O L 4 6 , Nº 9
S E P T E M B E R 2 0 1 8 547
Dental, dental hygiene and dental assistant students and military/residents from across the state competed in the California Dental Association’s annual Table Clinic Competition at CDA Presents in Anaheim May 17–19. The Journal is pleased to publish abstracts from the fi rst-place winners in each category. CDA continues to collaborate with the California Dental Hygienists’ Association for the RDH portion of the competition.
Winners of the 2018Table Clinic Competition
Abstracts
Alexander Zaykov and Trent Gillard accept their award from Drs. Natasha A. Lee and Mark J. Romanelli for winning the clinical dental student category. Their research evaluated elastomeric impression materials.
Eff ect of Disinfection on Two Elastomeric Impression Materials Over Time
Alexander Zaykov and Trent Gillard,Loma Linda University School of Dentistry
Objectives: To evaluate the effects of an immersion disinfectant on two elastomeric impression materials as a function of storage for up to 14 days.
Methods: Tests were performed in accordance with ANSI/ADA Specifi cation No. 19. Forty vinyl polyether siloxane and vinyl polysiloxane impressions were fabricated and examined
for surface detail reproduction and surface roughness (Ra) before and after disinfection with a complex phenol-based solution. Linear dimensional stability (LDS) was evaluated at four time points (0b, 0a, 7 and 14 days). Nonparametric Mann-Whitney U test and Freidman’s two-way analysis were conducted.
Results: All impressions clearly reproduced the 20μm line. No signifi cant differences were found for Ra (p>.05). All groups revealed signifi cant differences from the control at 14 days (p<.05) for LDS. Between-group comparisons revealed signifi cant differences at all time points (p<.05). All materials were within acceptable limit for LDS.
Conclusion: Within the limitations of the present study, both materials demonstrated acceptable accuracy for clinical use with this immersion disinfection solution.THE CORRESPONDING AUTHOR, Alexander Zaykov, can be reached at [email protected].
CLINICAL DENTAL STUDENT WINNERS

C DA J O U R N A L , V O L 4 6 , Nº 9
548 S E P T E M B E R 2 01 8
Integrating Teledentistry To Augment Clinical Outcomes and Access to Care
Corey D. Stein, MS, Western University of Health Sciences, College of Dental Medicine
Abstract: The rapid expansion of teledentistry applications is bridging gaps that limit underserved communities from accessing oral health care. In partnership with a Southern California city school district, teledentistry was implemented to support a web-based dental communication platform, which collected and electronically exchanged
COMMUNITY/EDUCATION DENTAL STUDENT WINNER
SCIENTIFIC DENTAL STUDENT WINNERS
S E P T . 2 0 1 8 A B S T R A C T S
patient-reported data to remotely located dentists. Providing patients the ability to electronically convey clinically meaningful information allows dentists to triage patient needs and allocate the appropriate resources for treatment. We will discuss how the teledental application, DentaCom, was integrated to create a network of health care providers for augmenting access to care while expediting oral health interventions.THE AUTHOR, Corey Stein, MS, can be reached at [email protected].
Eff ect of UV-Light Activation on Oxidation Potential of Titanium Oxide Nanofi bers Compared to Nanoparticles
Christina Chi, Loma Linda University School of Dentistry
Abstract: Photocatalytic oxidation with titanium-dioxide nanoparticles is well-established. The objective was to synthesize TiO2 nanofi bers (NFs) and evaluate the oxidation potential of TiO2 NFs compared to manufactured TiO2 nanoparticles (NPs) when activated with UV-light. TiO2 NFs were synthesized and characterized with scanning electron microscopy. Three dyes (50 μM of acid yellow, allura red and acid blue) were used to test oxidation potential of TiO2 NPs, TiO2 NFs, 3% hydrogen peroxide (HP) and distilled water (NC). Absorbance (A) was monitored with a microplate reader in duplicates at: T0 (baseline), T1 (post-30 minutes), T2 (post-90 minutes) and T3 (post-120 minutes). A0/AUV ratios were calculated and analyzed with Kruskal-Wallis test with adjustments for multiple comparisons. Tests were two-sided with α = 0.05. At T3, there was a signifi cant difference in A0/AUV ratio among the groups for all dyes (P < 0.001). It can be concluded that TiO2 NFs have applicability as an oxidizing agent.
THE AUTHOR, Christina Chi, can be reached at [email protected].
Drs. Natasha A. Lee and Mark J. Romanelli present Corey D. Stein, MS, with his award for the community/education dental student category for his work implementing a teledentistry application to improve access to care in underserved communities.
Christina Chi accepts congratulations from Drs. Natasha A. Lee and Mark J. Romanelli for winning the scientifi c dental student category. She researched the eff ect of UV-light activation on oxidation potential of titanium-oxide nanofi bers compared to nanoparticles.

C DA J O U R N A L , V O L 4 6 , Nº 9
S E P T E M B E R 2 0 1 8 549
RDA STUDENT WINNERS
RDH INFORMATIONAL STUDENT WINNERS (CDA IN COLLABORATION WITH CDHA)
Piercings — Jewelry or Medical Appliance?Bianca Hidalgo, Citrus College
Abstract: Body modifi cations have evolved into a normalized risk-taking experience in popular culture. However, the ADA advises against these practices because they are invasive with negative health consequences that outweigh any potential benefi t. Likewise, body jewelry piercers must obtain licenses before practicing their art, but it must come to question that regardless of training and skill, should these professionals be deemed educated enough to handle vital body parts that could interfere with detrimental health complications? For example, a surgeon is rarely questioned when performing
Crystal Relay Keeps Sensitivity AwayEsther Bucher and Marina Maslov,
Cypress CollegeBackground: Dentinal hypersensitivity
(DHS) is a condition that causes pain from exposed dentinal tubules. It affects up to half the population and commonly occurs in recession, periodontal treatment and bleaching.
surgery because their license validates that they have received years of proper practical, clinical and textbook education. Piercers’ educational requirements include a minimum of three months learning sterilization and disinfection, one CPR and blood-borne pathogens class and a four-day seminar in anatomy, techniques and hygiene.
In my presentation, my objective is to identify body piercings as a medical procedure. As such, I discuss the medical training that should be required of a piercer. My focus is on piercings in the oral cavity that can be rejected by the body and provoke damage, which is the fault of the piercer.THE AUTHOR, Bianca Hidalgo, can be reached at [email protected].
According to the hydrodynamic theory, when fl uid in dentinal tubules moves, pain receptors are activated. Mouthrinse containing potassium-oxalate compounds effectively reduces DHS by occluding exposed dentinal tubules from allowing hydraulic movement.
Methods: Reviewed clinical trials and academic journals.
Results: Compared to products available, over-the-counter mouthrinse with potassium-oxalate 1.4% provides a more effi cient and sustainable method of relief from DHS. Potassium-oxalate binds to calcium in saliva to form crystals and is deposited in and on exposed tubules.
Conclusion: The method in which oxalate deposits bind to dentinal tubules provides protection against acid exposure and daily home care routines. A 60-second swish is an effortless way to bring relief and a higher quality of life.THE CORRESPONDING AUTHOR, Esther Bucher, can be reached at [email protected].
Drs. Natasha A. Lee and Mark J. Romanelli present the RDA student winner, Bianca Hidalgo, with her award for her study on body piercings.
Esther Bucher and Marina Maslov receive their award for winning the RDH informational student category for their review on dentinal hypersensitivity. They are congratulated by CDHA President Lory Laughter, RDH, MS, and Drs. Mark J. Romanelli and Natasha A. Lee.

C DA J O U R N A L , V O L 4 6 , Nº 9
550 S E P T E M B E R 2 01 8
S E P T . 2 0 1 8 A B S T R A C T S
RDH RESEARCH STUDENT WINNERS (CDA IN COLLABORATION WITH CDHA)
Unveiling the Power of Charcoal-Containing Toothpastes
Rachel Andra; Mohammed Shaikh; Tery Lopez; and Brett McKean, Loma Linda University School of Dentistry
Objectives: Charcoal has gained increased interest due to its stain-removing properties and has recently been added to toothpastes. The purpose was to evaluate the whitening effi cacy of charcoal-containing toothpaste compared to hydrogen peroxide-containing toothpaste. Our hypothesis was that there would be no difference in whitening effi cacy among the different toothpastes used.
Methods: Bovine teeth (n=64) were cleaned and stored in sodium azide solution. Teeth were stained in tea solution for fi ve days, sectioned into 6 mm by 4 mm by 3 mm slabs and embedded in acrylic resin with the enamel surface facing up. Specimens were randomized into four experimental groups of 16 specimens each. Colgate
CDHA President Lory Laughter, RDH, MS, and Drs. Mark J. Romanelli and Natasha A. Lee congratulate Rachel Andra, Mohammed Shaikh, Brett McKean and Tery Lopez on winning the RDH research student category for their study on charcoal-containing toothpastes.
Cavity Protection (Colgate-Palmolive) was our negative control group (NC). The whitening toothpastes used were Optic White (OW) (Colgate-Palmolive) containing 2% hydrogen peroxide, Curaprox black toothpaste (CP) (Curaden AG) and My Magic Mud activated-charcoal toothpaste (MM) (Carbon and Clay Company). Slabs were mounted on an automated toothbrushing machine controlled for two minutes at a speed of 40. Color measurements were performed using a spectrophotometer at baseline (T1), one week postbrushing (T2), four weeks postbrushing (T3) and one-month follow-up (T4). The Kruskal-Wallis procedure was performed to compare changes in color among the different treatment groups. All post hoc comparisons were conducted with Bonferroni corrections. All tests were two-sided and conducted at an alpha level of 0.05 with SPSS v25.
Results: There was no signifi cant difference for baseline color parameters L*, a* and b*(p>0.05). The overall color change ΔE* was not signifi cantly different among the groups at one week postbrushing and at one-month follow-up. However, OW had a signifi cantly higher color change when compared to groups NC and CP at four weeks postbrushing (p<0.05).
Conclusion: The greatest whitening effect was observed with the hydrogen peroxide-containing toothpaste after four weeks of brushing.THE CORRESPONDING AUTHOR, Rachel Andra, can be reached at [email protected].

C DA J O U R N A L , V O L 4 6 , Nº 9
S E P T E M B E R 2 0 1 8 551
MILITARY/RESIDENT WINNER
Oral Appliance Therapy for Obstructive Sleep Apnea
Capt. John Lorenz, DDS, United States Air Force
Abstract: This table clinic reviews the use of oral appliances in the treatment of obstructive sleep apnea. It presents important background information relating to the prevalence, risk factors, signs, symptoms and adverse health outcomes associated with obstructive sleep apnea. Proper diagnosis and referral as it relates to available treatments is also stressed. The anatomical basis for how an oral appliance works is reviewed, and several demo models are displayed to show the variety of devices available. Oral appliances and CPAP are compared with regard to advantages, disadvantages and side effects. Lastly, a step-by-step implementation of oral appliance therapy into private practice is discussed in detail. Prominent conclusions are that oral appliances are an effective way to manage both mild and moderate forms of obstructive sleep apnea, while CPAP remains the fi rst-line therapy for more severe forms of disease.
THE AUTHOR, Capt. John Lorenz, DDS, can be reached at [email protected].
Drs. Natasha A. Lee and Mark J. Romanelli present Capt. John Lorenz, DDS, with his award for winning the military/resident category. His research focused on oral appliance therapy for obstructive sleep apnea.
Thank you to the following judges for the annual Table Clinic Competition:
RDA CompetitionPatricia Alvarez, RDAIzabella Ambartsumyan, RDAShari Becker, RDALisa Bocanegra, RDAMaleah Brooks, RDABenson Dimaranan, RDARobert McIntosh, RDAMelrose Nabua, RDAMiriam Ramirez, RDAClaudia Ritholz, RDAAlejandro Saravia, RDAKaren Schroeder, RDAManolita Teh, RDATobi Trotta, RDAGeorgina Vargas-Burket, RDA
RDH CompetitionMonica Bruce, DDSHoward Richmond, DDSDavid Rothman, DDS
Dental Students CompetitionMarileth Coria, DDSArthur Gage, DDSRamesh Gowda, DDSPradip Patel, DDSLeonard Raimondo, DDSAnn Steiner, DDSJudith Strutz, DDSArnold Valdez, DDSDale Wagner, DDS
Military/Resident CompetitionKai Chiao Chang, DDSHemant Joshi, DDSMadhavi Joshi, DDSChristopher Nuttall, DDSAnn Steiner, DDSKen Yaros, DDS

C DA J O U R N A L , V O L 4 6 , Nº 9
S E P T E M B E R 2 0 1 8 553
i n t r o d u c t i o n
GUEST EDITOR
Andrew Young, DDS, MSD, directs the University of the Pacifi c, Arthur A. Dugoni School of Dentistry orofacial pain curriculum and patient care. He has an MSD and board certifi cation in orofacial pain. He has published several studies in peer-reviewed journals and heads UOP’s evidence-based dentistry curriculum.Confl ict of Interest Disclosure: None reported.
Research literature is like whole wheat. It should be consumed regularly for its fundamental value, but unless substantial creative effort is mixed into
it, it tends to taste dry and boring. For that reason, this issue’s tone differs slightly from most scientifi c literature. Examples are used as often as possible and at times concepts are explained through narrative, but the reader will be learning about science in the process. The style is not scientifi c, but you will become more scientifi cally literate.
Evidence-based dentistry (EBD) is “an approach to oral health care that requires the judicious integration of systematic assessments of clinically relevant scientifi c evidence, relating to the patient’s oral and medical condition and history, with the dentist’s clinical expertise and the patient’s treatment needs and preferences,”1 according to the American Dental Association (ADA). It is well-summarized in the FIGURE.
Most of us actually use evidence-based practice on a daily basis. Before purchasing a bike, for example, we read and even assess the reviews.
This particular bike is rated with an average of fi ve stars … but that is based on only three reviews (sample size of three).
Enhancing Patient Care Through Evidence-Based DentistryAndrew Young, DDS, MSD
This bike earned 4.8 stars, based on 122 reviews, but many of the high ratings are for “great value” before the price doubled last week. Thirty-one others say, “Just got this today — can’t wait to try it out!” or something similar (assessing the evidence).
The one with 4.5 stars is a mountain bike, which you’ve found with your previous bike to be too heavy for your urban commute (experience/expertise). It also compromises on components to achieve a lower price, but you personally would rather pay more for the best components than accept lesser ones to save money (values).We engage in evidence-based
practice because it makes sense for decision-making. Online star ratings are not terribly accurate (the many reasons why will be clear by the end of this issue), but they are usually all that is available and the decisions are not of utmost importance. Patients’ health is. And for that, much more accurate “ratings” are available: research. Rarely would someone decide on an important purchase without fi rst reading the reviews. Yet clinicians often make clinical decisions (highly important) on materials, techniques and diagnoses without ever looking at the research,2,3 often just based on one person’s opinion.

C DA J O U R N A L , V O L 4 6 , Nº 9
554 S E P T E M B E R 2 01 8
Some say, “I think my own experience has taught me how to be a really good dentist — better than what some isolated academic observed in a lab.” Yes, learning from our experiences is a critical part of practice, and that is why it is one of the three components of EBD. But we can only see so much with our two eyes. We can only try so many materials, instruments and techniques. We can only make so many mistakes to learn from and would actually prefer to make fewer. Clinical research is really practicing dentists, just like you and me, reporting on their fi ndings while taking many precautions to make sure they are not being biased in what they see and report. Another advantage of research — we can learn from others’ mistakes instead of our own!
There are numerous, signifi cant reasons why we rarely consult the evidence. One reason is a natural trust in professors and speakers — some of the most common sources of our information. In dental school, we are given a complete set of information to start practicing. In the years following, we take continuing education courses for the purpose of staying updated. If all that information is regularly given to us, why read research literature?
Another reason is that looking at the research is so much more challenging. Finding potential articles, obtaining the full texts and analyzing the quality of those studies are each discouragingly diffi cult steps in which most dentists have not been trained. And if one can fi nd a study to support any opposing viewpoint, what is the point of reading studies?
But the need for EBD is unavoidable, because we all regularly fi nd ourselves in situations where the correct answer is best found in the research literature.
■ One “expert” says in a book that this is how to treat this particular condition. Is he right? And another “expert” says the exact opposite in a continuing education course. Who is right?
■ An article reports surprising results from a study. So should you start applying that to your practice?
■ Your colleagues recently started using a new composite and love it. You’ve been contemplating switching out your old composite system. Should you try theirs on your patients?
When we have the best information available, we have the greatest likelihood of the best clinical outcomes — so long as our skills are equally good. That means more successful treatments, happier patients and fewer redos.
All three of the previous bullet points can be answered well by reading the research literature. But like all skills, reading the research without training is similar to patients reading dental literature without training. A large percentage of temporomandibular disorder (TMD) patients read TMD articles online and, with their lay knowledge, come to erroneous and frightening conclusions. Likewise, clinicians can read studies and come to erroneous conclusions about their accuracy or scope of application.
For that reason, this issue aims to help you fi nd information, determine how trustworthy that information is and if it is trustworthy, apply it to your practice. That is evidence-based dentistry. You owe it to yourself and to your patients. And fortunately, it does not take nearly as long to become adept at EBD as it does to become adept at dentistry.
This issue is far from a comprehensive review of EBD. Undoubtedly some readers will opine this issue over emphasized irrelevant topics and omitted important ones. We encourage the reader to visit a number of other excellent EBD resources, such as the ADA website on EBD, the Journal of the American Dental AssociationEBD series (published 2014–2015), live EBD courses offered by the ADA, the Oxford Centre for Evidence-Based Medicine website and free online courses offered by Cochrane, to name only a few. There are many different ways to serve up whole wheat — the key is fi nding one that suits your taste. ■
REFERENCES
1. ADA Center for Evidence-Based Dentistry. ebd.ada.org/en/about.2. Warren JI, McLaughlin M, Bardsley J, et al. The Strengths and Challenges of Implementing EBP in Healthcare Systems. Worldviews Evid Based Nurs 2016;13(1):15–24. doi:10.1111/wvn.12149.3. Iqbal A, Glenny AM. General dental practitioners’ knowledge of and attitudes towards evidence based practice. Br Dent J 2002;193(10):587–591. doi:10.1038/sj.bdj.4801634.
i n t r o d u c t i o n
FIGURE. The American Dental Association defi nes evidence-based dentistry (EBD) as “an approach to oral health care that requires the judicious integration of systematic assessments of clinically relevant scientifi c evidence, relating to the patient’s oral and medical condition and history, with the dentist’s clinical expertise and the patient’s treatment needs and preferences.” (Reprinted with permission from ebd.ada.org.)
EBD
Dentist’s expertise
Scientifi c evidence
Patient needs and preferences

C DA J O U R N A L , V O L 4 6 , Nº 9
S E P T E M B E R 2 0 1 8 555
o n l i n e r e s e a r c h
AUTHOR
Steve Kirk, PhD, is an assistant professor at Nippon Medical School in Tokyo where he teaches English to future Japanese doctors. He has a master’s degree in teaching English to speakers of other languages from the University of Washington and a doctorate in applied linguistics from the University of Nottingham, U.K. He researches the development of second-language-spoken fl uency, as well as educational methods such as fl ipped learning.Confl ict of Interest Disclosure: None reported.
Searching for Research Articles on the InternetSteve Kirk, PhD
A B S T R AC T While reading original research articles is important for keeping up with recent developments in dentistry, locating the articles to read can be a frustrating experience. This practically oriented article covers several methods that can be used to make online searches more effective and effi cient and discusses methods for accessing the full text of those articles.
Most of the scientific or medical articles that people commonly read on the internet are secondary sources
of information, which means that the author based the article on someone else’s research, maybe discussing it and comparing it to other research or just summarizing it. On the other hand, primary sources are the original papers written by the researchers who carried out the research themselves. As anybody who has read original research papers knows, those research papers tend to be harder to read than the summaries that appear in news articles. So what is the value of reading primary sources? When you read a secondary source, you have to trust that the writer properly understood the primary sources and correctly reported them. Primary sources are required to follow certain standards for publication, such as a blind peer review process, which helps to ensure their reliability. Because they are written by the
researchers themselves, they show the researchers’ own certainty and uncertainty about the conclusions reached. They also show the details of the methodology used and the exact results obtained, which allows readers to evaluate the conclusions for themselves. Looking at the original research papers can help to clarify what can sometimes seem like flip-flopping conclusions in science. For example, Cooper, Bandelow and Nevill1 claim that eating breakfast improves accuracy on cognitively demanding tasks, while another paper2 claims that eating breakfast has no effect. Both studied children who were around the ages of 8–12, but one compared breakfast consumption versus breakfast omission while the other compared a “confectionery snack” (an unspecified Mars product) versus a noncalorie snack. This detail of the methodology could be the cause of the difference in results, and in fact, this is discussed in the discussion section of the article itself.1

C DA J O U R N A L , V O L 4 6 , Nº 9
556 S E P T E M B E R 2 01 8
One of the diffi culties with reading primary sources, however, is actually locating them. Getting access to a dental school library on a university campus is not an option for most people, and in any case, walking through the stacks to get a journal article is becoming a thing of the past. Most journal articles can be accessed online, but fi nding them easily requires a few techniques. This article goes over some practical steps that can be used to locate and download research papers.
How To Search for Papers
Searching GoogleProbably one of the most commonly
used solutions to the need to fi nd something online is to do a search on Google. The question of whether to recommend a dental implant or a fi xed bridge is a question that most dentists can relate to, and the answer to this question may change over time due to advances in technology and the related research results. When the term dental implant vs. bridge was entered into the Google search bar, the fi rst result, from a website connected to the magazine Dear Doctor — Dentistry and Oral Health,3 is a question from a patient about implants and bridges, as well as the answer from the doctors running the website. This is not unrelated, but clearly geared toward patients rather than practicing dentists. Most of the other results are explanations of the differences between implants and bridges, aimed at inquisitive patients. This demonstrates the problem with Google: Most of the search results will not be primary sources of research but rather websites aimed at ordinary people, including Wikipedia entries, blog posts, newspaper articles and YouTube videos. Even though there were 455,000 results for this search, all of the results at the top of the list are secondary sources. In fact,
o n l i n e r e s e a r c h
FIGURE 1. First page of results of a Google Scholar search for dental implant vs. bridge.
there is only one research paper in the fi rst 10 pages of results (on page 4), and most of the results are from the websites of private dental practices. Depending on the particular search, it is sometimes possible to locate primary sources through a regular search like this. However, Google offers another method, Google Scholar, which can be used to directly search for primary sources.
Google ScholarIn the same way that Google can
be tailored to search only for images or videos by selecting Images or Videos on the search page, there is also an option to search only for research papers, although it is not obvious to fi nd it. This is called “Google Scholar” and can be found at scholar.google.com4 or by simply searching for Google Scholar in a regular Google search. On Google Scholar’s initial search screen, make sure that the radio button for “Articles” is selected, and generally it is better to remove the check from the box next to “Include patents” so that the search results will only contain research papers.
Searching for dental implant vs. bridge in Google Scholar yields quite different results (FIGURE 1). Although there are fewer hits (44,800), all of the results shown are research papers. For each result, the title, some author information, the year of publication and part of the abstract is shown. On the right side of the search results are direct links to access the full text of the articles. Most of these will be PDF fi les that can be downloaded, however sometimes they may be links to a webpage with the full text of the article. Some of the results shown in FIGURE 1 have no links because they are behind a paywall, which means that the document cannot be downloaded or read in full without a subscription or paying a fee. Whether there are links or not for particular articles depends on the network your computer is connected to. On the campus network of a university that subscribes to many journals, most of the results will have links. At home or at a private clinic, the results will have fewer links. What to do about this will be discussed in more detail in the following section.

C DA J O U R N A L , V O L 4 6 , Nº 9
S E P T E M B E R 2 0 1 8 557
Search TermsThe most diffi cult but important
technique to locate papers easily and effectively is to refi ne the terms that are used in the search. This can help to eliminate many results that are not related to your chosen topic. Google has several advanced search techniques that can be accessed by clicking the three horizontal bars icon in the upper left corner of the search page or by using special characters or terms to modify the search. The advanced search window is shown in F I G U R E 3 . For example, searching for dental implant will fi nd articles that include the words dental and implant, resulting in 574,000 hits. Searching for dental implant by entering this into the box labeled “with the exact phrase” in the advanced search window, or by placing the phrase in quotations marks,
Clicking on any of the titles of the papers will usually open a page with the details of the article on the journal’s website. Here you will be able to read the abstract for the research paper (FIGURE
2), and you will also fi nd links to access the full article (usually by downloading the PDF version). An abstract is a short summary of the article, written by the authors, which contains the purpose, scope and primary results of the study. Reading the abstract can help you decide if the article is about what you were expecting, and generally whether or not it is worth reading in detail. Abstracts are always freely available online, while the full papers are often not. Reading the abstract can help you avoid spending time or money trying to get the full article, however, they don’t contain enough of the details or specifi cs to really be useful for clearly understanding the study and the results.
searches for these words occurring as a phrase, resulting in 86,000 hits. If you are interested in papers that research the effectiveness of dental implants, adding the word effectiveness to the search narrows it down to 21,400 hits. However, there are several ways of describing effectiveness, so the word effective and the word failure could be added to the search to include these options. The resulting search is for the phrase dental implant and any of the words effectiveness, effective or failure (using the various boxes in the advanced search window or by manually entering effective OR effectiveness OR failure “dental implant”) and results in 44,200 hits. At the bottom of the advanced search window, the search can be restricted to a particular author, a particular journal or certain dates. Refi ning the previous search to articles published since 2010 narrows the search to 19,500 hits. Finally, one of the results shown in F I G U R E 3 seems to discuss smoking as a risk factor for dental implant failure. If you are interested in further pursuing this particular topic, adding smoking to the previous search narrows the results down to 5,600 hits.
How To Find More Papers on the Same Topic
Reference ListsAnother technique to fi nd more
articles on the same topic is to use the list of references at the end of a paper that you already have. For example, Simonis et al.6 studied the long-term results of dental implants by looking at 55 patients at 10 to 16 years after receiving the implant. In the method section of their paper, they explain that part of the data collected involved:
FIGURE 2. Example of a webpage for a scholarly article — “Cost-eff ectiveness modeling of dental implant vs. bridge” from the journal Clinical Oral Implants Research.5 In this case, the link to download the full article (after logging in or paying) is in the center.

C DA J O U R N A L , V O L 4 6 , Nº 9
558 S E P T E M B E R 2 01 8
‘Cited by’ LinksGoogle Scholar also has some built-
in means of fi nding articles related to the one you are currently reading. Looking back at FIGURE 1 , each article listed in the search results has, below it, fi ve or six links. In the case of the second result in FIGURE 1 , “Cost-effectiveness modeling of dental implant vs. bridge,”5 the fi rst link is “Cited by 51” meaning that there are (at the time of writing) 51 research papers that cite that paper. Clicking this link will bring up a list of those 51 papers. All of these papers will, of course, be more recent than the original 2009 article.
Similarly, the next link under each search result is “Related articles.” In this case, clicking this link for “Cost-effectiveness modeling of dental implant vs. bridge” results in 101 articles, including some that are older than the original article. In my experience, the “Related articles” link tends to output more relevant articles than the “Cited by” link because many of the papers that cite the original paper may only mention it in passing and not actually deal with the topic of dental implants specifi cally.
A clinical examination in which the following parameters were evaluated for all implants: plaque index (Silness and Löe, 1964), gingival index (Löe and Silness, 1963), sulcular bleeding index (Mühlemann and Son, 1971), probing pocket depth (PPD) in millimeters, distance between the implant shoulder and the mucosal margin (DIM) in millimeters and probing attachment level in millimeters (calculated by adding the PPD and DIM).6
If you want to know more detail about how plaque index was measured, you could check the source that they cite, which is the paper by Silness and Löe.7 You can then locate this paper in the list of references to get the full title and other information about the paper. Then, it is easy enough to search for this title in Google Scholar to locate it. Of course, the articles listed will necessarily be older than the paper you have, but the references can be useful for fi nding more about topics mentioned only briefl y in the article or checking up on whether you agree with the summary statements given by the authors you are currently reading.
The other three links are not useful for fi nding more research papers. For “Cost-effectiveness modeling of dental implant vs. bridge,” the “All 6 versions” link outputs the same paper located at six different places on the internet. This could be useful for fi nding alternative sites where you can download the paper in cases where you cannot download it on the fi rst site, but I have yet to see this work. The “Cite” link (the quotation mark icon) outputs the full reference list information for the paper. This could be useful if you are writing a paper or want to cite it in a PowerPoint presentation, but generally reference management software such as Zotero8 can import this information with a single click. Finally, the “Save” link (the star icon) saves the item to “My library” located on the left pane of the Google Scholar search results after clicking the three horizontal bars icon. Again, reference management software such as Zotero would be a better tool for storing references, but for those who are not planning to write articles, it could be faster and more convenient to use the Google Scholar My Library.
How To Use Online DatabasesAnother useful way to search for
articles is to use online databases, such as PubMed,9 which is part of the U.S. National Library of Medicine National Institute of Health and can be found at ncbi.nlm.nih.gov/pubmed. Like Google Scholar, the databases will only output journal articles and scholarly books, but unlike Google Scholar, the scope is limited to biomedical literature. A search for pulpal necrosis resulted in 2,999 articles, while an identical search with Google Scholar resulted in 30,000. In general, a smaller output is better, and it would certainly take a long time to look through 30,000 results. PubMed is also useful in that the term pulpal necrosis
FIGURE 3 . Google Scholar advanced search window. Advanced search options can be entered here in the various input boxes. The search can also be done manually with special characters and terms as shown in the search box at the top.
o n l i n e r e s e a r c h

C DA J O U R N A L , V O L 4 6 , Nº 9
S E P T E M B E R 2 0 1 8 559
was recognized by the website after only typing pulpal. Clicking on any of the results will take you to the abstract for that article, which often has links to sites where the full paper can be downloaded, although it may be behind a paywall.
How To Download the PapersUsing Google Scholar or PubMed,
fi nding articles can be quite easy. Actually being able to download them to read is another story. Many journals require a subscription to be able to access the full text of the paper or they require paying an expensive fee. Most university libraries have subscriptions to a large number of journals, which enables students and staff to access the journals through the campus network or off-campus with a university login. The general public is required to pay a fee for each paper, which is generally on the order of $20–$40. Paying even $20 for a single PDF copy of a 12-page research paper is unreasonable for most people and results in a big disincentive to read primary sources. These days, there seem to be more and more open-access journals, but most publishers follow the traditional pay-to-read model. According to Laakso and Bjork,10 approximately 17 percent of articles published in 2011 were open access, and the trend seems to be toward more open access. However, traditional publishers argue that this will undermine editorial quality.11 At the time of this writing, I was able to access only two of the fi rst seven articles shown in FIGURE 1 on my personal computer.
There are, however, some other options (legal and otherwise) for locating papers. One useful legal option is the browser extension “Unpaywall.”12 Researchers often upload their own papers to their own websites or researcher-oriented social media like ResearchGate.13 These can often be located by searching for the name of the
article, but the “Unpaywall” extension for Firefox and Chrome automates this by giving the user a notifi cation if there is a legal, free version of the article somewhere else on the internet. In some cases, the version that can be downloaded could be a prepublication version and might lack fi nal editing.
Finding Primary Sources Through Other Sites
As a fi nal note, secondary sources on the internet sometimes contain links to the primary sources that support their summaries. Wikipedia always has citations marked with numbers in the text and a full list of those references at the bottom of the page. If the author did not put a citation, editors will usually add [needs citation] to the end of the sentence. For example, in the Wikipedia entry for “dental implant,” it is written that prosthetic teeth have a 10- to 15-year lifespan and Bozini et al.14 is cited as the source of this information. Similarly, websites like Science Daily15 have a link at the bottom to the paper being discussed.However, many secondary sources, such as newspapers and most of the patient-oriented websites discussed above, do not usually include links to the primary sources, which can make checking their information a bit of a scavenger hunt.
ConclusionWith resources like Google Scholar
and PubMed, fi nding primary sources of research is not as diffi cult as it might seem. In some cases, careful tweaking of search terms can help to make the articles you want move to the fi rst few pages of the search results. Downloading the papers can still be a problem for those without access to a university library; but open-access journals are becoming increasingly mainstream, so this may become easier in the future. ■
REFERENCES
1. Cooper SB, Bandelow S, Nevill ME. Breakfast consumption and cognitive function in adolescent schoolchildren. Physiol Behav 2011;103(5):431–439.2. Busch CR, Taylor HA, Kanarek RB, Holcomb PJ. The eff ects of a confectionery snack on attention in young boys. Physiol Behav 2002;77(2):333–340.3. Spektor M, Spektor W. Dental Implants Versus Bridgework. Dear Doctor — Dentistry and Oral Health. www.deardoctor.com/inside-the-magazine/issue-2/implants-vs-bridgework. Accessed Aug. 23, 2017.4. Google Scholar. scholar.google.co.jp. Accessed Aug. 23, 2017.5. Bouchard P, Renouard F, Bourgeois D, Fromentin O, Jeanneret MH, Beresniak A. Cost-eff ectiveness modeling of dental implant versus bridge. Clin Oral Implants Res 2009;20(6):583–587.6. Simonis P, Dufour T, Tenenbaum H. Long-term implant survival and success: A 10–16-year follow-up of nonsubmerged dental implants. Clin Oral Implants Res 2010;21(7):772–777.7. Silness J, Löe H. Periodontal Disease in Pregnancy II. Correlation Between Oral Hygiene and Periodontal Condition. Acta Odontol Scand 1964;22(1):121–135. 8. Zotero | Home. www.zotero.org. Accessed July 6, 2017.9. pubmeddev. Home — PubMed-NCBI. www.ncbi.nlm.nih.gov/pubmed. Accessed July 6, 2017.10. Laakso M, Björk B-C. Anatomy of open-access publishing: A study of longitudinal development and internal structure. BMC Med 2012;10:124.11. Van Noorden R. Open access: The true cost of science publishing. Nat News 2013;495(7442):426. 12. Unpaywall. unpaywall.org. Accessed July 2, 2017.13. ResearchGate — Share and discover research. ResearchGate. www.researchgate.net. Accessed July 2, 2017.14. Bozini T, Petridis H, Garefi s K, Garefi s P. A meta-analysis of prosthodontic complication rates of implant-supported fi xed dental prostheses in edentulous patients after an observation period of at least fi ve years. Int J Oral Maxillofac Implants 2011;26(2):304–318.15. ScienceDaily. Your source for the latest research news. ScienceDaily. www.sciencedaily.com. Accessed July 6, 2017.
THE AUTHOR, Steve Kirk, PhD, can be reached at [email protected].

TOTOTOTOTOTOTOGEGEGEGGEGEGEGETHTHTHTHTHHEREREREREREWEWEWEWEWEWEW AAAAREREREREE
LILILILILILIL MIMIMIMIMIMIM TLTLTLTLT ESESESESSSSSS
®
CDA. THIS IS WHERE VISION MEETS VALUE.
Member-exclusive savings from
The Dentists Supply Company
through a shopping site designed
to help your practice be competitive
and efficient. Just one of the limitless
member benefits at cda.org.
Costs, controlled.

C DA J O U R N A L , V O L 4 6 , Nº 9
S E P T E M B E R 2 0 1 8 561
AUTHOR
Andrew Young, DDS, MSD, directs the evidence-based dentistry curriculum at the University of the Pacifi c, Arthur A. Dugoni School of Dentistry. He also directs the orofacial pain curriculum and patient care, which involves temporomandibular disorders and neuropathic pain. He received an MSD in orofacial pain and is board certifi ed with the American Board of Orofacial Pain. He has published several studies in peer-reviewed journals.Confl ict of Interest Disclosure: None reported.
The Anatomy of a Clinical Study — In Everyday TermsAndrew Young, DDS, MSD
A B S T R AC T This article explains the different parts of a clinical study (including blinding, controls and randomization) and why each part is important. They are explained by examples through two fi ctitious stories that lead to a randomized controlled trial, a case report, a retrospective case-control study and a prospective cohort study.
The intention of this issue is not to make the readers into researchers. However, to recognize a trustworthy study, one needs to know
how a strong study should look. When reading an article, to know which specifi c aspects of that study are strong, which are weak and how those affect the reader’s application of the study to clinical practice, the reader needs to know how all the parts of a study should look and why each part is needed.
For fi ve years at the Arthur A. Dugoni School of Dentistry, University of the Pacifi c, we have used the following approach to teach the key components of a clinical study and why they are needed. These components are in italics and the TABLE defi nes the terms.
The Randomized Controlled TrialSuppose dentist Dr. John noticed that
when he drank Boost decaffeinated tea, his energy improved. He recommended to his colleagues that they give it to any of their patients who complain of low energy. But his colleagues said they could not
recommend it simply because one person said it works. One of them, Dr. Sarah, pointed out that she had tried Boost tea with no change in her energy levels.
What the members were essentially saying is that Dr. John’s conclusion was subject to random error.
Random error,1 also known as variability, refers to the fact that the population has a certain amount of variability for a given topic. Dr. John’s initially small sample size1 was so small that he had a considerable chance of not representing the actual percent of people who gain energy when drinking the tea. His study result concluded that 100 percent of patients do. That could not refl ect the actual population, because Dr. Sarah said she did not experience that effect. If Dr. John included her in the calculation, the results would then say that 50 percent of people will have more energy after drinking the tea. Would that then be the correct percentage? Most would not be confi dent with that answer either, because only two people were tested. The sample size was too small, putting the study at great risk for random error.
c l i n i c a l s t u d y p a r t s

C DA J O U R N A L , V O L 4 6 , Nº 9
562 S E P T E M B E R 2 01 8
c l i n i c a l s t u d y p a r t s
TABLE
Definition of Terms Used in This Article
Bias: A fl aw in the study design or the method of collecting or interpreting information. Biases can lead to incorrect conclusions about what the study or clinical trial showed.5
Blinding: A clinical trial design strategy in which one or more parties involved in the trial, such as the investigator or participants, do not know which participants have been assigned which interventions.5
Case-control study: Case-control studies begin with the outcomes and do not follow people over time. Researchers choose people with a particular result (the cases) and interview the groups or check their records to ascertain what diff erent experiences they had. They compare the odds of having an experience with the outcome to the odds of having an experience without the outcome.9
Case report: A report on a patient; no control group involved.6
Cohort study: A clinical research study in which people who currently have a certain condition or receive a particular treatment are followed over time and compared with another group of people who are not aff ected by the condition.9
Control: In a clinical trial, the group that does not receive the new treatment being studied. This group is compared to the group that receives the new treatment to see if the new treatment works.5
Double blinding: A method of studying a drug or procedure in which both the subjects and investigators are kept unaware of who is actually getting which specifi c treatment.9
Dropouts: Subjects who withdraw from a study after the study has commenced, but before completing the study.1
Experimental/interventional: A type of clinical study in which participants are assigned to groups that receive one or more intervention/treatment (or no intervention) so that researchers can evaluate the eff ects of the interventions on biomedical or health-related outcomes. The assignments are determined by the study’s protocol. Participants may receive diagnostic, therapeutic or other types of interventions.5
Generalizability/external validity: The extent to which the results of a study are generalizable or transferable to the general population or a population of interest.4
Observational studies: A type of clinical study in which participants are identifi ed as belonging to study groups and are assessed for biomedical or health outcomes. Participants may receive diagnostic, therapeutic or other types of interventions, but the investigator does not assign participants to a specifi c interventions/treatment.5
Power analysis: How likely a statistical test will be able to detect eff ects of a given size in a particular situ ation.2
Random error: Statistical fl uctuations (in either direction) in the measured data due to the precision limitations of the measurement device. Random errors usually result from the experimenter’s inability to take the same measurement in exactly the same way to get the exact same number. Random errors can be evaluated through statistical analysis and can be reduced by averaging over a large number of observations.7,8
Random sampling: A process used in research to draw a sample of a population strictly by chance, yielding no discernible pattern beyond chance.4
Randomized allocation: A type of allocation strategy in which participants are assigned to the arms (such as type of treatment) of a clinical trial by chance.5
Randomized controlled trial: A controlled clinical trial that randomly (by chance) assigns participants to two or more groups. There are various methods to randomize study participants to their groups.9
Sample size calculation: How large a sample is needed to enable statistical judgments that are accurate and reliable.2
Selection bias: An error in choosing the individuals or groups to take part in a study. Ideally, the subjects in a study should be very similar to one another and to the larger population from which they are drawn (for example, all individuals with the same disease or condition). If there are important diff erences, the results of the study may not be valid.5
Self-selection bias: The problem that very often results when survey respondents are allowed to decide entirely for themselves whether or not they want to participate in a survey. To the extent that respondents’ propensity for participating in the study is correlated with the substantive topic the researchers are trying to study, there will be self-selection bias in the resulting data. In most instances, self-selection will lead to biased data, as the respondents who choose to participate will not well represent the entire target population.3
Sponsorship: Funding or provision of free drugs, materials or devices.9
Systematic review: A literature review that typically involves a detailed and comprehensive plan and search strategy derived a priori, with the goal of reducing bias by identifying, appraising and synthesizing all relevant studies on a particular topic. Often, systematic reviews include a meta-analysis component that involves using statistical techniques to synthesize the data from several studies into a single quantitative estimate or summary eff ect size.10

C DA J O U R N A L , V O L 4 6 , Nº 9
S E P T E M B E R 2 0 1 8 563
Dr. John realized he needed a larger sample size. But how large? If he has too few subjects, his study would be invalid and he would have wasted time and funds. If he has too many subjects, he would have wasted money and time on the extra tea and subjects. So he performed a power analysis and sample size calculation,2 which is a calculation to determine the necessary sample size to detect an effect (if there is one), and concluded that 100 samples were needed.
Boost tea is expensive, so he requested a free supply for his study. Seeing an excellent marketing opportunity, Boost replied enthusiastically by sending him boxes of tea — much more than he needed for the study — and a voucher for free Boost tea for life.
Dr. John’s colleagues were skeptical.Question: What are you going to
do with the excess tea you have?Answer: Sell it.Concern: So you have vested
interest in this study favoring the tea. If the results are negative, people will not buy your excess.
Concern: You also need the product line to last, because if it ends, so does your voucher for free tea.
The study had a high risk of being biased. Readers would wonder if the study was designed to favor the brand because of this sponsorship.
Bias is any process that systematically (rather than randomly — random error is called imprecision) misguides one’s conclusions.1 It can be intentional (sometimes in cases of sponsorship) but usually is unintentional. Unintentional bias is a major cause of inaccuracy in research and the reason for many of the elements of study design that will be described shortly.
To avoid the perception of bias through sponsorship, Dr. John bought his own supply. Now he had to start
recruiting 100 subjects. Where could he conveniently fi nd 100 people in one place? That weekend he would be attending his daughter’s varsity volleyball conference. There would be at least 100 volleyball players there. He could give out 100 bags of tea and ask them if they felt more energy after they drink it, and his study could be done by the time he left.
His colleagues pointed out that they would still consider his study to be at risk for bias. Technically, this is a type of selection bias1 where the bias stems from the selection process. And the type of
selection bias that would happen here is what can happen with convenience sampling,3 where the individuals are selected because they’re easy to obtain. The generalizability or external validity (the degree to which the fi ndings of this study can be applied to the general population)4 would be limited when the fi ndings here were from only 15- to 17-year-old females. Adolescent females overall have different metabolism and hormonal proportions than adult males, for example, making it harder to apply this study to them.
Dr. John then proposed posting an ad online that said “Energy-elevating tea study: Participants welcome.” The problem with that, said his colleagues, is another type of selection bias called self-selection bias.3 He would likely attract more people with low energy levels
who feel a need for an energy-elevating tea. Their metabolism and hormone levels may not be representative of the general population, again limiting the external validity of the study unless his objective is to demonstrate Boost tea’s effect on those lacking energy. But he wanted to shows its effect on the average consumer like himself.
One colleague suggested, “You have a busy dental practice with a broad variety of patients. And dentistry has little connection to energy levels. Recruit consecutive patients into your study until you have 100 participants.” This would allow for random sampling.4
Dr. John proceeded as suggested. He gave a cup of tea to each patient at the front desk. After they drank it, he asked them if they felt more energy and then tallied the answers. At the end of the fi rst day, he had 24 responses. Many of the subjects reported feeling more energy. But to Dr. John’s dismay, he realized his staff accidentally put a bag of generic decaffeinated tea — the kind he normally buys for the offi ce—into the last patient’s cup. And that last patient said the tea made him feel “a little more energetic.” So was it Boost tea specifi cally that made people feel more energetic or was it just tea in general that had that effect?
The only way he could know for sure was to also test the generic tea. That would be a control,5 which helps determine if other factors may be infl uencing their answers. The next day, they restarted the study, this time aiming for 200 consumed cups (100 of each type of tea). But sometime that morning, he noticed that his staff was leaving the tea bag tag hanging out of the cup. People knew that his generic tea was an inferior tea, so that may have biased the answers in favor of Boost tea. He told his staff to conceal the label. This is called blinding.5
The study had a high risk of being biased. Readers would wonder if the study was designed to favor the brand because of this sponsorship.

C DA J O U R N A L , V O L 4 6 , Nº 9
564 S E P T E M B E R 2 01 8
Later in the morning, he noticed that his staff was giving the generic tea to his more tired patients. And when a patient drank the generic tea and wavered between “more energetic” and “no change,” the staff circled “no change.” On the other hand, when a patient wavered for Boost tea, the staff circled “more energetic.”
Dr. John brought this to his staff’s attention, telling them they were biasing the data against the generic tea. They didn’t realize they had been doing this. It may have stemmed from their assumption, conscious or subconscious, that Boost tea was more effective at boosting energy levels.
He took two corrective measures. First, he randomly assigned the tea to the subjects. This is called randomized allocation5 and prevented the lethargic patients from all being in one tea group. It also helped prevent disproportionate distributions of other characteristics, even ones he had not thought of — such as tolerance to the energy-enhancing ingredient, metabolic conditions, etc.
Secondly, he needed to make sure he and his staff (the investigators) were unaware of which tea was being tested on a subject. With this he would achieve double blinding — both the subjects and the investigators would be blind to which tea they received.5 Then neither those giving the data (the subjects) nor those recording the data (the investigators) would artifi cially perceive more energy just because they knew Boost tea was being administered.
To randomize and blind his samples, he did the following: Using a die, he decided that rolling an odd number would indicate Boost tea and an even number would indicate generic tea. Then he labeled each cup, starting with A–Z, then AA–ZZ and so on. For cup A, he rolled a three and therefore fi lled cup A with Boost tea. He made 200 cups this way and
recorded on a sheet of paper what kind of tea went into each labeled cup. He gave the tea cups to his staff but kept the paper in his desk, hidden from him and his staff, until the study was concluded.
After eight days, he had 100 results per tea. The results were mediocre. Few people were more lethargic after drinking the tea, but not too many were more energetic either.
His colleagues pointed out that digestion takes more than a few minutes and suggested he have them mail back the questionnaires to him. So he gave
his patients prestamped envelopes, questionnaires and a week’s supply of tea. He passed 200 out over the course of the week, and the next week the questionnaires came back. Not all of them were returned, but the results were good. Eighty-fi ve percent of them experienced higher energy levels.
He eagerly presented the fi ndings to his colleagues.
Question: How many questionnaires were returned?
Answer: 40Question: Out of 200?Answer: Correct.Concern: Then you can’t trust this data.
You don’t know anything about three-quarters of the samples that were tested.
Answer: I don’t see why it should matter all that much.
Concern: It may matter a lot. What if people did not return it because they felt it was ineffective, so after a few days they just forgot about the study?
So Dr. John decided to call those subjects the next day and acquire the results from them verbally. His colleagues’ speculations were right. The majority of subjects who didn’t return the questionnaire did so for exactly those reasons. Less than a quarter of the participants actually completed the study. The rest were dropouts1 who felt the tea was ineffective. His study therefore was quite incomplete, and the portion that had been completed was at great risk for bias in favor of Boost tea.
Sometime later, a better-designed multicenter study was done in several workplaces, where the subjects’ consumption could be verifi ed on a daily basis. There was also funding to give the subjects a small compensation for completing the study over two weeks. This time, the dropout rate was only 10 percent and results showed no difference between Boost tea and the generic tea.
That was a randomized controlled trial,5 the gold standard for studies of treatments because of the numerous procedures done to minimize bias and random error. It is a robust, time-consuming and expensive type of study. However, it is not always the appropriate type of study for a given question.
Case ReportsSuppose the following situation:Dentists in a private practice
encountered a previously unseen case of rampant dental caries. Their patient for the last 45 years had no history of dental decay, but she did have recession. To help with the dentinal hypersensitivity, she had been using additional fl uoride. During her routine exam six months earlier, she still had no decay. But she returned for her routine dental exam with 12 new caries, many of them large and fi ve of them approaching the pulp.
c l i n i c a l s t u d y p a r t s
That was a randomized controlled trial, the gold standard for studies of treatments because of the numerous procedures done to minimize bias and random error.

C DA J O U R N A L , V O L 4 6 , Nº 9
S E P T E M B E R 2 0 1 8 565
The dentist decided to publish this in a case report.6 While a case report is not a study, it is valuable in that it alerts the health fi eld to previously largely unknown or emerging conditions. The entire process from writing to publishing the report took one year. Following this publication, four more dentists noted that they saw the same presentation with their patients. The broader dental community was realizing an investigation was needed to determine the cause of these caries as quickly as possible.
Would an RCT have been appropriate here? It is the gold standard for experimental/ interventional5 studies, but there was no intervention to test in this case. They were not interested in testing a drug or procedure. They needed to fi nd out what was happening to these patients. In such situations, observational studies5 are done.
Case-Control StudiesThorough histories were taken on
these fi ve patients, and it was discovered that they all had recently gone on vacations (at separate times) booked through an expensive touring company to a remote island in the Pacifi c.
Perhaps they had been infected by an unusual organism during the trip? The trip was three weeks long with numerous experiences novel to the travelers. The quickest way to narrow down the causative experience would be to compare the itineraries of those who had the rampant decay to those who did not.
The span of travel dates among those infected was four months. So it was decided that in addition to the fi ve infected patients, fi ve noninfected people who also went on the same tour during those same dates would also be investigated to serve as comparisons. The infected patients were called cases and the noninfected comparison individuals were called controls. Thus, this was a case-control study.5
When comparing the itineraries, it was discovered that all fi ve cases had eaten at the same small remote establishment during a day-long hike, but only one of the controls did. All who had eaten at that establishment were interviewed regarding what they ate. All fi ve cases had dishes with shellfi sh, as this was the specialty of the place, but the single control was allergic to shellfi sh so he ordered the ham sandwich. Ensuing studies of the shellfi sh on the menu found that during those fi ve months, a shellfi sh called Crabster was in season and served. It had just appeared
in the area and quickly became a popular dish because it had the tail of a lobster and the legs of a crab. And it harbored a bacteria called Antipulp that was found later in cultures of all the patients’ abscesses. This case-control study played a crucial role in solving this dental question.
Cohort StudiesA sparsely studied shellfi sh and a
bacteria previously unknown: Investigators wondered what other diseases it could cause. They advised the establishment to stop serving that fi sh (which the establishment ignored) and set up a station on the island. During that time, they advertised that they were doing a study that would include periodic medical and dental exams with a small cash incentive at each exam. Eight-hundred
of the islanders agreed to participate (90 percent of the island population) among whom 450 had eaten Crabster. Baseline medical information was collected, and it was explained that for the next 10 years they would re-examine the subjects. Those who were exposed to the shellfi sh in this study were a cohort. They were compared to controls — an equal number of islanders who did not eat the shellfi sh. This type of study is called a cohort study.5
Notice the similarities and differences between the previous two scenarios and how that affected what type of study the investigators chose. In a case-control study, the disease has already been identifi ed but the cause is unknown; it is a retrospective study where the investigator is trying to fi gure out what caused the disease.
In a prospective cohort study, the investigator knows the patients have already been exposed (or will be exposed) and is watching to see what will happen to them. What other health effects, both good and bad, will Crabster have on those who eat it?
In general, the reliability of these different types of studies can be ranked according to the evidence pyramid (see “How To Critically Appraise the Dental Literature” on page 569). RCTs, because they use random allocation, controls and blinding (often double blinding), are more reliable and thus sit higher on the pyramid. Cohort studies do not use random allocation and often have less or no blinding, so they sit below RCTs on the pyramid. Because case-control studies are retrospective, typically from past clinical records rather than studies designed from the very beginning, they are less reliable than prospective cohort studies.
Systematic reviews are articles that examine, combine and summarize all the available evidence on a specifi c topic. They do so using a system for the search and a system for rating the studies and deciding which to include in the
In a prospective cohort study, the investigator knows the patients have already been exposed (or will be exposed) and is watching to see what will happen to them.

C DA J O U R N A L , V O L 4 6 , Nº 9
566 S E P T E M B E R 2 01 8
combining and summarizing. The use of a system, universally applied to all studies being included in the review, helps maintain objectivity in the review process. The reviewers must also describe the system in detail so the reader can decide how trustworthy the review is. Because systematic reviews combine the results of multiple studies, they are higher on the evidence pyramid. Narrative reviews do not use a systematic approach and are therefore more prone to bias.
Case reports and case series (similar to case reports but with more than one patient being reported) are not actually studies, so they lack the components of a study and are relatively low levels of evidence.
Expert opinion, which includes lectures and textbooks that are not evidence based, and opinion articles (rather than studies) are also not actually studies and therefore are low on the evidence pyramid. Some lectures and textbooks are evidence based. It is important to clarify though that citing references does not automatically make a lecture or textbook evidence
based, because the audience will not be able to assess the evidence from those citations. Consistent with the standards in systematic reviews, study articles and evidence-based guidelines, lectures and textbooks should explain the studies that they base their conclusions on so the audience can make an educated decision of whether to agree. This is not to say that there is no use for lectures and textbooks that don’t explain the studies. There are many situations when such evidence-based formats are not necessary, not appropriate or not ideal. In such situations, the expert opinion serves as a stimulus for the dentist to go himself or herself to the research literature to make the fi nal decision on whether that opinion was correct.
This was a small glimpse of some of the pertinent principles of research. When reading research manuscripts, look for these basic elements to determine whether the study was appropriate and well-done to minimize the effects of bias and random error. A study that did that is more likely to have found a truth. ■
c l i n i c a l s t u d y p a r t s
REFERENCES
1. Gerstman B. Epidemiology Kept Simple: An Introduction to Traditional and Modern Epidemiology. Chichester: Wiley-Blackwell; 2013.2. Lewicki P. STATISTICS: Methods and Applications. Tulsa: Statsoft.3. Lavrakas P. Self-Selection Bias. In: Encyclopedia of Survey Research Methods. SAGE Publications; 2008.4. Research Glossary, University of Southern California Libguide. libguides.usc.edu/writingguide/researchglossary. Published 2017. Accessed Oct. 12, 2017.5. Glossary of Common Site Terms: NIH U.S. National Library of Medicine. clinicaltrials.gov/ct2/about-studies/glossary. Published 2018.6. Gopikrishna V. A report on case reports. J Conserv Dent 2010;13(4):265–271. doi:10.4103/0972-0707.73375.7. Southeastern University. www2.southeastern.edu/Academics/Faculty/rallain/plab193/labinfo. Accessed July 5, 2018.8. University of California at Berkeley Statistics Glossary. www.stat.berkeley.edu/~stark/SticiGui/Text/gloss.htm. Accessed July 5, 2018.9. Georgia State University Library. research.library.gsu.edu. Accessed July 5, 2018.10. Uman LS. Systematic reviews and meta-analyses. J Can Acad Child Adolesc Psychiatry 2011;20(1):57–59. www.ncbi.nlm.nih.gov/pubmed/21286370. Accessed May 7, 2018.
THE AUTHOR, Andrew Young, DDS, MSD, can be reached at ayoung@pacifi c.edu.
usbank.com/practicefinance
Financial options tailored to your practice.Whether you are establishing your career or have an existing
practice, U.S. Bank Practice Finance is your provider for
customized practice financing that may help your business grow.
Advantages of U.S. Bank Practice Finance
• Competitive fixed rates
• Term up to 10 years
• 100% financing options on acquisitions
• No prepayment penalty options
Contact a practice finance specialist today.
Jeramie Eimers | 605.681.7371 | [email protected]
Financing maximums and terms are determined by borrower qualification and use of funds. Credit products offered by U.S. Bank National Association and are subject to normal credit approval and program guidelines. See a banker for details. Deposit products offered by U.S. Bank National Association. Member FDIC. ©2018 U.S. Bank. 36901 6/18

®
ENDORSEDPROGRAMS
CDA has leveraged the strength of our large membership to
deliver even more value. As part of our resources to support
members in the business side of practice, Endorsed Programs provide money-saving solutions from vendors
that have been vetted by a team of CDA dentists.
cda.org/endorsedprograms
STRENGTH.SAVINGS.CONFIDENCE.
Grow your patient base, sustain your current base and manage your practice’s reputation with expert consulting and a broad range of marketing services. As a CDA member, you benefit from free assessments and discounted start-up costs from WEO Media.
WEO’s consultants apply the unique needs and goals of practicesof every size in developing custom marketing plans. Services include responsive websites, premium SEO, PPC, reviewgeneration, social media, video and more.
F E AT U R E D E N D O R S E D P R O G R A M

Give health, hope and happiness. By contributing your time and talent, you relieve pain, restore
dignity and create smiles for thousands of people who face
barriers to care. Volunteer at CDA Cares Modesto to help
provide essential dental care to those in need.
CDA Cares Modesto
October 26–27, 2018
Modesto Centre Plaza
Join us. cdafoundation.org/cdacares

C DA J O U R N A L , V O L 4 6 , Nº 9
S E P T E M B E R 2 0 1 8 569
L i t e r a t u r e A p p r a i s a l
The aim of any study is to determine the truth — the effectiveness of a treatment, the relationship between a chemical and a disease, the percentage of
the population with dental pain, etc. Yet studies vary greatly in their quality. While assessing the quality of a study can seem challenging, it is helpful to bear in mind the underlying principle that four factors can explain all fi ndings in a study: truth, chance, bias and confounding. The more a given study reduces the effects of chance, bias and confounding, the more we can assume its fi ndings are in fact the truth.
Chance: Sometimes the fi ndings of a study are purely due to chance and do not accurately refl ect reality. In such cases, when the study is repeated by others, they are unable to replicate the fi ndings. Statistics such as p-values and confi dence intervals can help readers determine the role of chance for a fi nding (for help with understanding this and other statistical concepts, see “Statistics for the Practicing Dentist” on page 577).
How To Critically Appraise the Dental LiteratureTerrence Shaneyfelt, MD, MPH
A B S T R AC T Four things can explain all fi ndings in a study: truth, chance, bias and confounding. When reading a study, it is incumbent upon the reader to determine which ones have the greatest impact on the results. This article will guide you in critically appraising several common study designs.
AUTHOR
Terrence Shaneyfelt, MD, MPH, is a professor of medicine in the division of general internal medicine at the University of Alabama School of Medicine and the Department of Veterans Aff airs. He is an expert in evidence-based medicine.Confl ict of Interest Disclosure: None reported.
l i t e r a t u r e a p p r a i s a l
Confounders: Confounders are factors other than those being examined in a given study, which affect the outcome. For example, in a patient comparing the survival rates of various dental implant systems, smoking would be a confounder.
Bias: Bias is systematic (rather than random) error. It can be thought of as a directional error, where data is steered in a particular direction, usually unintentionally. It is often the result of doing something different in one group in a study than is done in the other groups in a study. Different study types are susceptible to different biases. Several examples are given in “The Anatomy of a Clinical Study” on page 561.
In assessing the level of reliability of a study, readers often use the evidence-based medicine pyramid (FIGURE). This pyramid orders the various types of studies and publications based on their likelihood for bias, with the peak being the least prone to bias. This tool is a handy and rapid tool for initial assessment. However, within each level individual

C DA J O U R N A L , V O L 4 6 , Nº 9
570 S E P T E M B E R 2 01 8
publications can vary greatly in quality. For example, a very well-designed case-control study may surpass the reliability of a very poorly executed cohort study. Also, particular study designs are most appropriate for some clinical questions and less appropriate for others. For example, a randomized controlled study would not be appropriate for most research on potential carcinogens, because it would be unethical to expose subjects to carcinogens. Case-control studies, or even prospective cohort studies, would be more appropriate. It is therefore important to be able to appraise individual publications.
This article guides the reader in critically appraising several common study designs. Tools can be found at the Scottish Intercollegiate Guidelines Network (sign.ac.uk/checklists-and-notes.html) and the Centre for Evidence-Based Medicine (cebm.net/2014/06/critical-appraisal), to name a few. I have also developed an Android app (EBM Rater in the Google Play store) to aid critical appraisal and making clinically relevant calculations (note: I receive no funds for the download of this app). The goal of critical appraisal is to determine the validity of a study by scrutinizing it for bias in the design, conduct or analysis of the study. Each study design has a unique set of critical appraisal questions to answer while reading the study. It is assumed readers are familiar with basic study design. If not, they should read “The Anatomy of a Clinical Study” on page 561.
Reading a Study About HarmA 26-year-old mother of one presents
to your offi ce. She is 36 weeks pregnant with her second child. She inquires about preventing dental caries in her next child as her 3-year-old has had numerous caries. She wonders if the frequency or method of feeding has any effect on dental caries.
Studies about the potentially harmful effects of an exposure are usually case-control or cohort studies. Both study designs are observational where investigators observe patients for the effects or outcomes of various exposures. Observational studies are more prone to bias than experimental studies (where researchers are actually experimenting with treatments on subjects), largely because subjects are not randomly assigned to treatment groups. For example, an observational study that compares caries rates between high-frequency and low-frequency eaters would put the subjects into two groups depending on their eating frequency. But subjects might be eating more frequently because of their ethnic or social culture. Those very cultures may also infl uence what kinds of food they eat, what kinds of drinks they consume, how much attention they give to their oral health and their oral genetics. A randomized experimental study would have randomly distributed all of those factors through the random assignment steps. However, experimental studies are
not always appropriate. In this example, it would be unethical to make subjects eat more frequently simply to see if it causes more caries. Therefore, an observational study would be more appropriate.
You fi nd a cohort study by Feldens et al.1 (for help with fi nding articles, see “Searching for Articles on the Internet” on page 555), which you think will help answer the question posed by your patient. TABLE 1
includes the questions readers should answer as they read studies about harm. If signifi cant bias is detected, the study should be rejected as untrustworthy and an alternative source of evidence should be sought.
Feldens et al. performed a prospective cohort study in which they enrolled pregnant women at 20 health centers in Brazil. The “exposure” was “feeding frequency,” with “unexposed” subjects being babies who had lower feeding frequency and “exposed” subjects being those with higher feeding frequency. The “exposed” and “unexposed” groups were compared for the amount of early childhood caries (the “outcome” of interest) they developed.
l i t e r a t u r e a p p r a i s a l
FIGURE. Evidence-based medicine is the integration of best research evidence with clinical expertise and patient values. (Credit: EBM Pyramid and EBM Page Generator, copyright 2006 Trustees of Dartmouth College and Yale University. All Rights Reserved. Produced by Jan Glover, David Izzo, Karen Odato and Lei Wang.)
Background information/expert opinion
Case-controlled studies/case series/reports
Cohort studies
Randomized controlled trials (RCTs)
Critically appraised individual articles (article synopses)
Critically appraised topics
(evidence syntheses)
Systematic reviews
Qua
lity o
f evid
ence
Filtered information
Unfi ltered information

C DA J O U R N A L , V O L 4 6 , Nº 9
S E P T E M B E R 2 0 1 8 571
Applying the critical appraisal questions for cohort studies revealed some evidence of possible bias in the study:
■ Were the exposed and unexposed cohorts of patients similar in all important ways other than exposures? Unknown. There are no demographic data reported for the exposed and unexposed cohorts. There is thus potential for susceptibility bias, because we do not know whether other caries risk factors were affecting the results, such as oral hygiene, medication usage and medical conditions.
■ Were exposures and outcomes measured in the same way in the exposed and unexposed cohorts? Yes. Feeding habits were assessed in all participants via two 24-hour diet recall interviews in which mothers recalled all breastfeeding episodes and all foods and drinks consumed by the child the day before the study visit. Dental caries were assessed at a specifi ed time interval on all participants by trained and calibrated dentists following World Health Organization (WHO) guidelines.
■ Were the assessment of exposures and outcomes reasonable and objective? Yes, as they followed WHO guidelines and the criteria for decay seem reasonable.
■ Were the study personnel assessing exposures and outcomes blinded to exposure and outcome status? Yes, the dentists were masked to the child’s feeding habits.
■ Was the follow-up of the study patients suffi ciently long (for the outcome to occur) and complete (few losses to follow-up)? Yes, dental exams were performed at 38 months,
TABLE 1
Critical Appraisal Questions for Harm Studies2
Questions Explanation
Cohort studies
Were the exposed and unexposed cohorts of patients similar in all important ways other than exposures?
Besides the exposure being studied, many other factors can aff ect health, such as age, income, race and other medical conditions. Therefore, researchers should assure such relevant factors are similarly distributed between the cohorts (demographics table).It is unlikely they will be similar in an observational study. Any diff erences should be dealt with in the analysis phase, usually by doing a multivariable analysis controlling for baseline diff erences.
Were exposures and outcomes measured in the same way in the exposed and unexposed cohorts?
Disease incidence can increase simply through more thorough detection practices and vice versa. To prevent such artifi cial diff erences, researchers should use identical methods for all cohorts.
Were the assessment of exposures and outcomes reasonable and objective?
Using your clinical judgment, did the researchers do a good job of determining who was exposed and who developed outcomes? Was the method they used objective or subjective?
Were the study personnel assessing exposures and outcomes blinded to exposure and outcome status?
Knowing the exposure status can bias the assessment of outcomes, especially if they are subjective. You don’t want researchers looking for an outcome harder in one cohort than the other.
Was the follow-up of the study patients suffi ciently long (for the outcome to occur) and complete (few losses to follow-up)?
The follow-up time must be long enough for the outcome to occur. All patients entered in the study need to be accounted for at its conclusion. More than 10–20 percent loss to follow-up typically is too much.
Case-control studies
Were the cases and control patients similar to each other in all important ways other than the exposure of interest?
Cases and controls should have the same possibility of exposure. Cases will usually have more exposures, but controls should have the possibility of being exposed. This requires clinical judgment of who the controls are.
Did the case and control patients have a similar chance of being exposed to the exposure of interest?
If they don’t have a similar chance of exposure, that could be due to other medical, lifestyle or environmental factors that could also impact the outcome of interest.
Were exposures measured in the same way in both the case and control populations?
See explanation under cohort studies.
Were the study personnel assessing exposures and outcomes blinded to outcome status?
See explanation under cohort studies.
Both studies
Were all important potential confounders identifi ed and taken into account either in the design or analysis phase of the study?
When diff erences between cohorts or cases and controls are seen, the researchers must control for the eff ect of these diff erences. This can be done in the design phase (randomization, stratifi cation, matching) or analysis phase (most commonly via multivariable analysis).
Adapted from Levine M, Walter S, Lee H, Haines T, Holbrook A, Moyer V. Users’ guides to the medical literature. IV. How to use an article about harm. Evidence-Based Medicine Working Group. JAMA 1994 May 25;271(20):1615–1619.
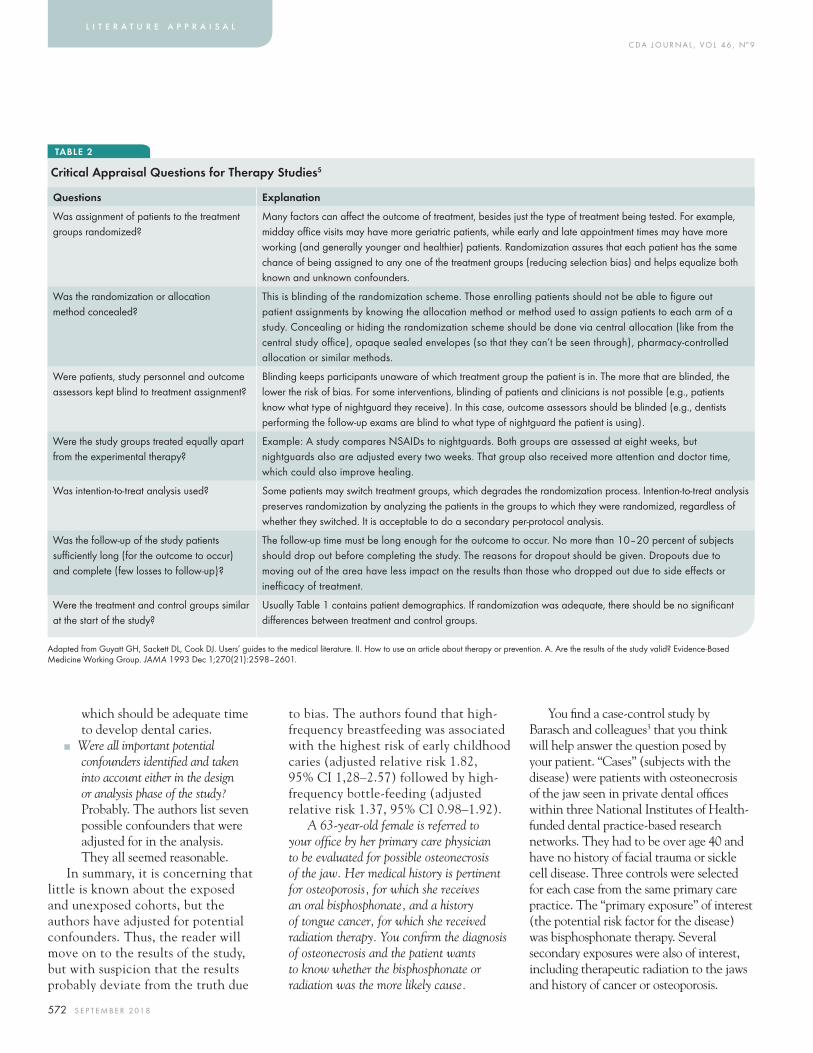
C DA J O U R N A L , V O L 4 6 , Nº 9
572 S E P T E M B E R 2 01 8
which should be adequate time to develop dental caries.
■ Were all important potential confounders identifi ed and taken into account either in the design or analysis phase of the study? Probably. The authors list seven possible confounders that were adjusted for in the analysis. They all seemed reasonable.
In summary, it is concerning that little is known about the exposed and unexposed cohorts, but the authors have adjusted for potential confounders. Thus, the reader will move on to the results of the study, but with suspicion that the results probably deviate from the truth due
to bias. The authors found that high-frequency breastfeeding was associated with the highest risk of early childhood caries (adjusted relative risk 1.82, 95% CI 1,28–2.57) followed by high-frequency bottle-feeding (adjusted relative risk 1.37, 95% CI 0.98–1.92).
A 63-year-old female is referred to your offi ce by her primary care physician to be evaluated for possible osteonecrosis of the jaw. Her medical history is pertinent for osteoporosis, for which she receives an oral bisphosphonate, and a history of tongue cancer, for which she received radiation therapy. You confi rm the diagnosis of osteonecrosis and the patient wants to know whether the bisphosphonate or radiation was the more likely cause.
You fi nd a case-control study by Barasch and colleagues3 that you think will help answer the question posed by your patient. “Cases” (subjects with the disease) were patients with osteonecrosis of the jaw seen in private dental offi ces within three National Institutes of Health-funded dental practice-based research networks. They had to be over age 40 and have no history of facial trauma or sickle cell disease. Three controls were selected for each case from the same primary care practice. The “primary exposure” of interest (the potential risk factor for the disease) was bisphosphonate therapy. Several secondary exposures were also of interest, including therapeutic radiation to the jaws and history of cancer or osteoporosis.
l i t e r a t u r e a p p r a i s a l
TABLE 2
Critical Appraisal Questions for Therapy Studies5
Questions Explanation
Was assignment of patients to the treatment groups randomized?
Many factors can aff ect the outcome of treatment, besides just the type of treatment being tested. For example, midday offi ce visits may have more geriatric patients, while early and late appointment times may have more working (and generally younger and healthier) patients. Randomization assures that each patient has the same chance of being assigned to any one of the treatment groups (reducing selection bias) and helps equalize both known and unknown confounders.
Was the randomization or allocation method concealed?
This is blinding of the randomization scheme. Those enrolling patients should not be able to fi gure out patient assignments by knowing the allocation method or method used to assign patients to each arm of a study. Concealing or hiding the randomization scheme should be done via central allocation (like from the central study offi ce), opaque sealed envelopes (so that they can’t be seen through), pharmacy-controlled allocation or similar methods.
Were patients, study personnel and outcome assessors kept blind to treatment assignment?
Blinding keeps participants unaware of which treatment group the patient is in. The more that are blinded, the lower the risk of bias. For some interventions, blinding of patients and clinicians is not possible (e.g., patients know what type of nightguard they receive). In this case, outcome assessors should be blinded (e.g., dentists performing the follow-up exams are blind to what type of nightguard the patient is using).
Were the study groups treated equally apart from the experimental therapy?
Example: A study compares NSAIDs to nightguards. Both groups are assessed at eight weeks, but nightguards also are adjusted every two weeks. That group also received more attention and doctor time, which could also improve healing.
Was intention-to-treat analysis used? Some patients may switch treatment groups, which degrades the randomization process. Intention-to-treat analysis preserves randomization by analyzing the patients in the groups to which they were randomized, regardless of whether they switched. It is acceptable to do a secondary per-protocol analysis.
Was the follow-up of the study patients suffi ciently long (for the outcome to occur) and complete (few losses to follow-up)?
The follow-up time must be long enough for the outcome to occur. No more than 10–20 percent of subjects should drop out before completing the study. The reasons for dropout should be given. Dropouts due to moving out of the area have less impact on the results than those who dropped out due to side eff ects or ineffi cacy of treatment.
Were the treatment and control groups similar at the start of the study?
Usually Table 1 contains patient demographics. If randomization was adequate, there should be no signifi cant diff erences between treatment and control groups.
Adapted from Guyatt GH, Sackett DL, Cook DJ. Users’ guides to the medical literature. II. How to use an article about therapy or prevention. A. Are the results of the study valid? Evidence-Based Medicine Working Group. JAMA 1993 Dec 1;270(21):2598–2601.

C DA J O U R N A L , V O L 4 6 , Nº 9
S E P T E M B E R 2 0 1 8 573
Applying the critical appraisal questions from TABLE 1 for case-control studies revealed some potential for bias in the study.
■ Were the cases and control patients similar to each other in all important ways other than the exposure of interest? No, but unless matching is used they rarely will be. Cases were older, smoked more, had more cancer, more osteoporosis, bisphosphonate use and extractions in the region. These differences are expected as cases have disease and thus have the risk factors for disease and commonly associated comorbid conditions. This is confounding. Confounding must be controlled for in some way so as to not skew the results. The confounding here appears to have been controlled for in the analysis phase of the study.
■ Did the case and control patients have a similar chance of being exposed to the exposure of interest? Probably. They were from a similar population as the cases. As best can be determined, they could have become a case had they developed osteonecrosis and could have been similarly exposed to the exposures of interest; they just weren’t as much.
■ Were exposures measured in the same way in both the case and control populations? Yes. Records were abstracted in the same way in cases and controls and both groups underwent the same structured telephone interviews.
■ Were the study personnel assessing exposures and outcomes blinded to outcome status? This was not reported, so the assumption is that they were not blinded. This could lead to some ascertainment bias.
■ Were all important potential confounders identifi ed and taken into account either in the design
or analysis phase of the study? Yes. The authors list multiple possible confounders of the association between exposures and osteonecrosis of the jaw. Confounders can skew the results of a study if not controlled for. They adjusted for each of these potential confounders in the analysis. They also used propensity score methods to control for confounding (propensity score methodology is beyond the scope of this article).
In summary, the lack of blinding is somewhat concerning, but this is not a fatal fl aw. Thus, we will move on to the results of the trial. The authors found that radiation to the head or neck was most strongly associated with osteonecrosis [OR 24.1 (95% CI 4.9-118.4)] followed by bisphosphonate use [OR 12.2 (95% CI 4.3-35.0)].
Reading a Study About TherapyA dental hygienist in your practice
recently attended a presentation at a meeting on the effect of a psychological technique called “motivational interviewing” (MI) on disease control in patients with periodontal disease. She comes to you suggesting that the practice hire a motivational interviewer or send the hygienists for MI training. What should you do?
When properly conducted, the most valid studies about a therapy are randomized controlled trials (RCTs) and systematic reviews of randomized controlled trials. RCTs are experimental studies in which the investigators randomly assign patients to various arms of the study. This contrasts with the observational studies discussed previously.
You fi nd an RCT by Stenman et al.4 that you think will help determine if you should hire a motivational interviewer or send your hygienist for training. TABLE 2 includes the questions readers should answer as they read studies about therapy.
Stenman et al. performed an RCT on patients with moderate chronic periodontitis who were treatment planned for nonsurgical periodontal therapy where one group (the “test group”) underwent a single session of MI. The primary outcome of interest was marginal gingival bleeding, with plaque scores being the secondary outcome of interest. The duration of the study was six months.
Applying the critical appraisal questions from TABLE 2 for therapy studies revealed some potential for bias in the study.
■ Was assignment of patients to the treatment groups randomized? While the authors name the randomization principle they adhered to, they did not describe the actual method (e.g., random-number generator, rolling of dice, fl ipping a coin, etc.) so the reader cannot be absolutely certain that random allocation occurred.
■ Was the randomization or allocation method concealed? Yes, the researcher who randomly assigned the patients to the treatment groups was not involved in the treatment or measurements.
When properly conducted, the most valid studies about a therapy are randomized controlled trials (RCTs) and systematic reviews of randomized controlled trials.

C DA J O U R N A L , V O L 4 6 , Nº 9
574 S E P T E M B E R 2 01 8
■ Were patients, study personnel and outcome assessors kept blind to treatment assignment? As best they could be. Because there was no sham intervention, such as a face-to-face discussion that does not use the principles of MI, the control patients would know they did not receive the intervention and also did not receive as much attention. The outcome (plaque and gingival bleeding) is objective and the outcome assessor was blinded to study group assignment.
■ Were the study groups treated equally apart from the experimental therapy? All patients followed the same treatment protocol for periodontal therapy. However, as stated above, the test group, by undergoing MI, did get more attention than the control group. And because the MI was aimed at improving oral hygiene compliance, the extra attention alone (regardless of psychological technique) may more strongly impress on the patient the importance of good oral hygiene.
■ Was intention-to-treat analysis used? Yes, as stated in the data analysis section.
l i t e r a t u r e a p p r a i s a l
■ Was the follow-up of the study patients suffi ciently long (for the outcome to occur) and complete (few losses to follow-up)? Follow-up was six months. This should be long enough for patients to change their infection control behaviors. A few patients [three (13 percent) in the experimental group and two (9 percent) in the control group] did not complete the study but were included in the analysis.
■ Were the treatment and control groups similar at the start of the study? Yes, there were no signifi cant differences between the groups.
In summary, the reader should be concerned somewhat about the increased attention that the test group received (compared to the control group), but this is not a fatal fl aw. Thus, the reader will move on to the results of the trial: The authors found no signifi cant effect of MI on marginal gingival bleeding and plaque.
Reading a Study About Diagnostic Testing
A 26-year-old male medical student is referred to your offi ce for evaluation of a temporomandibular disorder (TMD). For the past two months, he has felt popping and pain in the left temporomandibular joint (TMJ) when he eats. On examination
the pain is reproducible with maximum opening of his mouth. You inform him of your diagnosis and he asks how good clinical assessment is versus imaging?
You fi nd a study by Schiffman et al.6 that you think will answer the patient’s question. TABLE 3 includes the questions readers should answer as they read studies about diagnostic tests.
Schiffman et al. studied the new Axis I and Axis II diagnostic criteria for TMD. The patient population included 614 TMD cases and 91 controls. The reference standard for TMD was established by consensus between two TMD and orofacial pain experts at each study site using a comprehensive history, physical examination and imaging studies.
Applying the critical appraisal questions from TABLE 3 for diagnostic test studies revealed some potential for bias in the study.
■ Was the diagnostic test evaluated in the spectrum of patients who will receive the test in practice? Yes, cases were selected for each type of TMD of interest.
■ Does the reference standard test accurately determine the presence or absence of the target condition? Likely so, because experts using a variety of criteria made the diagnoses.
TABLE 3
Critical Appraisal Questions for Diagnostic Test Studies7
Questions Explanation
Was the diagnostic test evaluated in the spectrum of patients who will receive the test in practice?
The patient sample should include patients with whom you would use the test in practice. Patients should have various presentations and be in various stages of the disorder. Patients with other commonly confused diagnoses should also be included in the patient sample.
Does the reference standard test accurately determine the presence or absence of the target condition?
The reference standard is used to determine if the patient actually has the target condition or not. Judgment of the appropriateness of the reference standard relies on clinical judgment.
Did all study patients or a random sample of the study population undergo testing by the reference standard test regardless of the index test result?
All patients should receive the new test under study and the reference standard test (which establishes the diagnosis). The results of either the reference standard or the test under study should not infl uence who gets further testing (verifi cation bias). For example, a negative result on the new test should not infl uence getting the reference standard. How would you know if the negative result is a true negative or a false negative?
Were the test under study and the reference standard test interpreted in a blinded fashion?
Interpretation of test-under-study results can be infl uenced by knowledge of the reference standard and vice versa. Optimally, diff erent readers or labs will perform and interpret each test without knowledge of the other test result.
Adapted from Jaeschke R, Guyatt G, Sackett DL. Users’ guides to the medical literature. III. How to use an article about a diagnostic test. A. Are the results of the study valid? Evidence-Based Medicine Working Group. JAMA 1994 Feb 2;271(5):389–391.

C DA J O U R N A L , V O L 4 6 , Nº 9
S E P T E M B E R 2 0 1 8 575
■ Did all study patients or a random sample of the study population undergo testing by the reference standard test regardless of the index test result? Yes, all patients, regardless of the index test result, underwent testing by the reference standard.
■ Was the reference standard independent of the test under study (i.e., the test under study did not form part of the reference standard)? No. The diagnostic criteria under study contain elements that were used to diagnose TMD. Thus, there is incorporation bias. This is a challenging problem as TMD diagnoses are often made on clinical grounds that are part of the new diagnostic criteria.
■ Were the test under study and the reference standard test interpreted in a blinded fashion? Yes. Patients were examined three times by three examiners: Once by an examiner using the reference standard and by two examiners (each examining separately) using the next diagnostic criteria. All examiners were blinded to each other’s diagnoses.
Overall, this study is trustworthy. Focusing on arthralgia of the TMJ, the criteria studied had a sensitivity of 89 percent and specifi city of 98 percent.
Reading a Systematic ReviewA 22-year-old pregnant female returns
to your offi ce for a six-month check-up and cleaning. You counsel her on general dental health. She smokes one pack of cigarettes per day. You counsel her to stop smoking for her health, her baby’s health and because there might be an association between cigarette smoking and early childhood caries. She seems skeptical and asks for “proof” of this association.
You fi nd a study by Kellesarian et al.8 that you think will answer the patient’s question. TABLE 4 includes the questions readers should answer as they read systematic reviews. Another tool is the “a measurement tool to assess systematic reviews” (AMSTAR) checklist available at amstar.ca/amstar_checklist.php.
Kellesarian et al. performed a systematic review of observational studies to determine if there is an association between prenatal maternal cigarette smoking and early childhood caries.
Applying the critical appraisal questions from TABLE 4 for systematic reviews revealed minimal potential for bias in the review.
■ Was a comprehensive literature search performed? Yes. The reviewers searched four electronic databases and hand-searched the references of identifi ed studies to fi nd further potential studies. The search parameters were provided so the reader can evaluate if an adequate literature search was done.
■ Was there duplicate study selection and data extraction? Yes. Two reviewers independently screened articles for inclusion and independently extracted data using standardized forms. Disagreements were resolved by discussion and Kappa statistics (comparison of the judgements of the two reviewers) were good.
■ Was a list of the studies (included and excluded) provided? Only the included studies were listed.
■ Were the characteristics of the included studies provided? Yes. TABLE 1 includes information on the included studies. It would have been helpful to have seen more about the study populations included in the table.
TABLE 4
Critical Appraisal Questions For Systematic Reviews9
Questions Explanation
Was a comprehensive literature search performed?
The reviewers need to fi nd all the evidence about the question at hand. At least two electronic databases should be searched. In addition, searches should include references of other reviews and retrieved articles, trial registers and experts. If some studies are not included in the review, there is no way to know whether they would have altered its conclusions.
Was there duplicate study selection and data extraction?
There should be at least two independent decisions on which studies meet inclusion criteria and two independent data extractors. This prevents bias from aff ecting study selection and data inclusion.
Was a list of the studies (included and excluded) provided?
Studies included and excluded should be listed or referenced so that the reader can judge the comprehensiveness of the search. Often excluded studies can be obtained from the authors or an online appendix is provided.
Were the characteristics of the included studies provided?
Usually a table of included studies will be provided. The table should include study characteristics (design, patient population) and outcomes.
Was the scientifi c quality/validity of the included studies assessed and documented?
Included studies should be critically appraised using a validated instrument or methods. Readers need to know the limitations of the included studies.
Were the methods used to combine the fi ndings of studies appropriate?
Most commonly, random eff ects (when heterogeneity is present) and fi xed eff ects (when heterogeneity is minimal or absent) methods are used to combine data from individual studies into a summary result.
Was the likelihood of publication bias assessed?
Negative studies tend not to get published (publication bias). The goal of a systematic review is to fi nd and summarize all the literature on a topic. Reviewers should use both graphical (e.g., funnel plot) and statistical tests (e.g., Egger regression test) to assess for publication bias.
Adapted from Shea BJ, Grimshaw JM, Wells GA, et al. Development of AMSTAR: A measurement tool to assess the methodological quality of systematic reviews. BMC Med Res Methodol 2007 Feb 15;7:10. doi:10.1186/1471-2288-7-10.

C DA J O U R N A L , V O L 4 6 , Nº 9
576 S E P T E M B E R 2 01 8
■ Was the scientifi c quality/validity of the included studies assessed and documented? Yes. The Newcastle-Ottawa Scale was used to grade the methodological quality of the studies and was done independently by two reviewers. The authors report on the fi ndings of the quality assessment in TABLE 2. They report it as good but note inaccurate measurement of exposures and outcomes in all studies.
■ Were the methods used to combine the fi ndings of studies appropriate? This was a qualitative systematic review, meaning no statistical methods were
used to combine results of individual studies into a summary estimate of effect. The authors report there was signifi cant heterogeneity and thus it would have been inappropriate to combine results.
■ Was the likelihood of publication bias assessed? No. Overall, this is a fairly well-conducted systematic review. The limitations are not in the methods used but in the studies themselves. The authors report that the evidence is insuffi cient to justify an association between prenatal maternal cigarette smoking and early childhood caries.
ConclusionWhen reading any study, your job is
to determine if the results are true or due to chance, bias or confounding. Critical appraisal criteria exist for every study design to help detect various biases that could be present. If a study is found to have important biases, then it should be rejected and alternative evidence sought to answer your clinical question. ■REFERENCES
1. Feldens CA, Rodrigues PH, de Anastácio G, Vítolo MR, Chaff ee BW. Feeding frequency in infancy and dental caries in childhood: A prospective cohort study. Int Dent J 2018 Apr;68(2):113–121. doi:10.1111/idj.12333. Epub 2017 Sep 3.2. Levine M, Walter S, Lee H, Haines T, Holbrook A, Moyer V. Users’ guides to the medical literature. IV. How to use an article about harm. Evidence-Based Medicine Working Group. JAMA 1994 May 25;271(20):1615–1619. www.ncbi.nlm.nih.gov/pubmed/8182815. Accessed May 4, 2018.
3. Barasch A, Cunha-Cruz J, Curro FA, et al. Risk Factors for Osteonecrosis of the Jaws. J Dent Res 2011 Apr; 90(4):439–444. doi:10.1177/0022034510397196.4. Stenman J, Wennström JL, Abrahamsson KH. A brief motivational interviewing as an adjunct to periodontal therapy — A potential tool to reduce relapse in oral hygiene behaviors. A three-year study. Int J Dent Hyg 2018 May;16(2):298–304. doi: 10.1111/idh.12308. Epub 2017 Aug 24.5. Guyatt GH, Sackett DL, Cook DJ. Users’ guides to the medical literature. II. How to use an article about therapy or prevention. A. Are the results of the study valid? Evidence-Based Medicine Working Group. JAMA 1993 Dec 1;270(21):2598–2601. www.ncbi.nlm.nih.gov/pubmed/8230645. Accessed May 4, 2018.6. Schiff man EL, Velly AM, Look JO, et al. Eff ects of four treatment strategies for temporomandibular joint closed lock. Int J Oral Maxillofac Surg 2014 Feb;43(2):217–226. doi:10.1016/j.ijom.2013.07.744.7. Jaeschke R, Guyatt G, Sackett DL. Users’ guides to the medical literature. III. How to use an article about a diagnostic test. A. Are the results of the study valid? Evidence-Based Medicine Working Group. JAMA 1994 Feb 2;271(5):389–391. www.ncbi.nlm.nih.gov/pubmed/8283589. Accessed May 4, 2018.8. Kellesarian SV, Malignaggi VR, de Freitas P, Ahmed HB, Javed F. Association between prenatal maternal cigarette smoking and early childhood caries. A systematic review. J Clin Exp Dent 2017 Sep 1;9(9):e1141–e1146. doi:10.4317/jced.54064. doi: 10.4317/jced.54064.9. Shea BJ, Grimshaw JM, Wells GA, et al. Development of AMSTAR: A measurement tool to assess the methodological quality of systematic reviews. BMC Med Res Methodol 2007;7(1):10. doi:10.1186/1471-2288-7-10.
THE AUTHOR, Terrence Shaneyfelt, MD, MPH, can be reached at [email protected].
l i t e r a t u r e a p p r a i s a l
LIMITLESSMEMBERBENEFITS
®
cda.org
C DA J O U R N A L , V O L 4 6 , Nº 9
S E P T E M B E R 2 0 1 8 577
AUTHOR
Eric S. Salmon, DDS, has a background in data science and currently teaches the topics of treatment planning and statistics at the University of the Pacifi c, Arthur A. Dugoni School of Dentistry.Confl ict of Interest Disclosure: None reported.
Statistics for the Practicing DentistEric S. Salmon, DDS
A B S T R AC T Statistics can be intimidating, but basic statistical knowledge is critical for understanding the primary research that informs our clinical decisions. Knowing a few basic terms and concepts, such as p-value and confi dence interval, allows the clinician to critically evaluate the literature and make evidence-based clinical decisions. This article provides defi nitions and examples of some entry-level statistical concepts.
A case for statistics: You invite a new friend over for dinner. After some pleasant conversation, you’re surprised to discover
that you both have the same birthday. What are the odds of that? You quickly determine that the odds are approximately 1 in 365. That’s 0.27 percent chance … a very unlikely coincidence!
Let’s take this a step further: How many people would you have to have at your dinner party for there to be a 50 percent chance of two people having the same birthday? This scenario is commonly known as the birthday paradox and is where intuition usually fails us. The correct answer is 23 people, but most people answer much higher than that. In fact, it only takes 75 people at your party for there to be a 99.9 percent chance of two people having the same birthday.
If you got close to the right answer, you’re in the small minority. For most of us, the intuitive answer is much
s t a t i s t i c s
higher than the correct, mathematical answer. This illustrates why we, as people dependent upon research to inform our clinical practice, need statistics.
Our human intuition is one of the most powerful tools that nature has provided us. But it’s far from perfect. From the Will Rogers phenomenon to the gambler’s fallacy, comedians and mathematicians have supplied many examples of how our intuition can fail us. Statistics help us bridge the gap between intuition and reality. And here’s a secret: The bulk of statistical methods used in dental research isn’t that tough to grasp. As dentistry becomes progressively more dependent upon primary research to inform our clinical decisions, accurate assessment of that research is increasingly critical. While many (including myself) are sometimes intimidated by the arcane terminology and notation, knowing just a few statistical concepts can quickly cut through the noise.

C DA J O U R N A L , V O L 4 6 , Nº 9
578 S E P T E M B E R 2 01 8
Sample Size Before the scientifi c method,
humans relied almost exclusively on their personal experience to explain the world. If one person ate a berry and got sick, it was completely reasonable to conclude that the berry was poisonous. But what if that person just had a rare allergy to the berry? We are literally hardwired to take our personal experiences and extrapolate them in an effort to understand how the world works.
This kind of anecdote is on one extreme side of the sample-size scale, a sample size of one. The research equivalent is the case study: one clinician’s experience with one patient. The ideal experiment would have a sample size on the far other end of the scale, the size of the entire population being studied.1 If we knew every single person’s reaction to a drug, we would know how to ideally administer it to each person.
Most studies have a sample size somewhere between “one” and “all of them.” But how big is big enough? Intuition can help us a bit here. It’s intuitively obvious that testing a drug on fi ve people probably won’t get us results that accurately represent how the overall population will respond to the drug. It’s also easy to see that the bigger the sample size, the better, though this must be balanced with the cost, time and personnel required for larger sample sizes. But again, how do we know when it’s big enough?
Luckily, most of the commonly used statistical tests take sample size into consideration to some degree and it is represented in the mathematical equations. Often, if the sample size isn’t big enough, the statistical test will show the results are not signifi cant. But be careful. This can sometimes be deceptive. If the researcher gets results that are very unlikely due to
poor study design or random chance, a statistical test might show that result as signifi cant. For example, if all patients in a small sample coincidentally have the same, rare reaction to a drug, the results of the experiment might show as statistically signifi cant even though a larger, more diverse sample likely wouldn’t have. Sample size is one area where we really need both statistics and intuition to know if the study results are valid. You can usually trust your gut when it comes to sample size. If it doesn’t seem big enough, it likely isn’t.
Hypothesis/Null HypothesisEveryone understands what the
hypothesis of a research project is. It’s the core of what we do when we engage in research and propose a theory that we’re trying to prove. What’s a little less intuitive is the importance of the null hypothesis and its important relation to statistical tests.
The null hypothesis isn’t simply the opposite of the hypothesis. For example, we design a study with the hypothesis that a new endodontic technique will result in less postoperative pain than the old technique. The null hypothesis isn’t that the new technique will cause more pain. That’s one possibility if our hypothesis isn’t valid, but there are others that are equally important.
The null hypothesis should describe a result that shows no relationship between experimental action and the results or no signifi cant difference between two groups. With the example above, the null hypothesis would be: A new endodontic technique does not result in less postoperative pain than the old technique. There could be more pain, equivalent pain or just not enough data to prove the hypothesis. It really doesn’t matter because in all cases, we simply don’t have the evidence to show that our hypothesis is true.
When the statistical test shows that we haven’t proven our hypothesis, you might see this stated in a bit of a backward way. Often, instead of saying that the hypothesis must be rejected, the author will state that we “can’t reject the null hypothesis.” This is often considered the proper way to state results and is important because it doesn’t necessarily mean that our hypothesis is proven wrong. It could be wrong, but it also could be that we just didn’t have a large enough sample size to prove our hypothesis. Or our study design might have been fl awed. In any case, the statistical goal in most research is to determine if we can reject the null hypothesis.2
P-valueSo how do we know if we can reject
the null hypothesis? Some of the most commonly used statistical tests use the p-value approach to answer this question. A description of how the p-value is calculated will quickly get us deep into the statistical weeds, but don’t hesitate to explore this if you have interest. Understanding the relationship between the p-value and population distribution can be fascinating for those who are mathematically inclined. Several excellent online tutorials are available to guide you through this exploration.
s t a t i s t i c s
Sample size is one area where we really need both statistics and intuition to know if the study results are valid.

C DA J O U R N A L , V O L 4 6 , Nº 9
S E P T E M B E R 2 0 1 8 579
For those of us more interested in the clinical applications, the more important piece is understanding how to interpret the p-value. If the p-value method is used, it is often listed and discussed in the manuscript text. Sometimes you’ll only find it in the arcane statistical tables in the appendix. Either way, find it! The p-value will help you determine whether the author’s claims are valid.
P-value is essentially a probability that we can accurately reject the null hypothesis and thereby accept our hypothesis as true. For the hypothesis, the smaller the p-value, the better. The smaller it is, the more confidently we can reject the null hypothesis. For example, if the p-value is 0.10, that means we can reject the null hypothesis with 90 percent certainty. If the p-value is 0.01, we can do so with 99 percent certainty. An alternate term you might hear for this concept is “significance level.”
Another way to think about p-value is to remember that it tells us the odds that our research results were real or just due to random chance and are not significant. With almost any research, there’s a chance your experimental results are just the result of dumb luck. If your hypothesis is that a pair of dice are loaded, you might test that by rolling them 10 times and observing the results. But even if the dice are completely fair, there’s still a very small chance that you’ll roll 10 sevens in a row, thus making you incorrectly think that your hypothesis was correct. A p-value of 0.02 tells us that there’s a 98 percent chance that our results are significant evidence for our hypothesis and a 2 percent chance that our results were just the lucky equivalent of rolling 10 sevens in a row with fair dice.
Before starting a research project, the investigator should set what p-value will allow her to reject the null hypothesis and thereby confi rm the hypothesis. Setting the cutoff value ahead of time is one step that’s sometimes skipped. A researcher might wait until after the results are in and the statistical tests are run and then say, “well … that’s a good enough p-value.” This is a signal that they might be biasing their results.
Different research disciplines and methods sometimes set wildly different signifi cance level thresholds. In dental
research, it’s not uncommon to see p-value thresholds set at 0.05 or 0.01. A p-value of 0.05 has been recommended for general use since the early 1900s.3 In theoretical physics, they have different standards. When the Higgs boson was discovered, the p-value was 0.0000003.
One more critical point about significance: Just because a study shows that a result was statistically significant doesn’t mean the result was clinically significant. If research showed that a detergent significantly decreased the population of a certain bacterium in dental office water lines, you might be impressed. But how do we know that specific bacterial species cause harm to our patients? That species could be completely harmless and using the detergent has no clinical impact at all.
Confi dence IntervalInvestigators sometimes describe a
result and tack a “confi dence interval” to the reported metric. Conceptually, there’s some overlap between p-value and confi dence interval. Both describe how “confi dent” you are in your results. Where p-value defi nes how confi dent you are in rejecting your null hypothesis, a confi dence interval defi nes how precise your data is.
The mean of a population is probably the most common value that is given a confi dence interval. We almost always determine a population mean by taking a sample and measuring the mean of that sample (such as “21 percent of Americans never fl oss”). How confi dent are we that the mean of that sample is similar to the true mean of the entire population? This is typically expressed as mean ± margin of error, something like 12 mm ± 2 mm. In this case, the confi dence interval would be the range from 10 mm to 14 mm. The standard in most medical research is to use a 95 percent confi dence interval, meaning that there is a 95 percent chance that the true population mean falls within that range around the sample mean. Unless otherwise stated in a manuscript, a 95 percent confi dence interval should be your assumption. In general, the larger the 95 percent confi dence interval, the less precise/certain our data. Also, within that confi dence interval, values closer to the upper or lower limit are less probable.4 Imagine a bell curve (normal distribution) that is centered on the mean and that tapers down to the edges of the confi dence interval. The edges of the confi dence interval represent something close to the best and worst case scenarios, which we can communicate to our patients for informed consent.
P-value is essentially a probability that we can accurately reject the null hypothesis and thereby accept our hypothesis as true.

C DA J O U R N A L , V O L 4 6 , Nº 9
580 S E P T E M B E R 2 01 8
Suppose a study fi nds that 16 percent of children in Town A have early childhood caries, and 8 percent of children in Town B have early childhood caries. Readers may conclude that there is a large difference between these towns. However, if the readers also notice that the 95 percent confi dence interval for town A is ± 14 percent, or 2–30 percent, and for Town B is ±6 percent, or 2–14 percent, they would notice that there is a signifi cant chance that there is actually no difference between towns or the difference may be smaller than they thought. The difference could also be larger than they thought (2 percent of Town A and 30 percent of Town B has early childhood caries). This is why it is so important to look at the confi dence intervals.
Distribution and Standard DeviationSuppose we’re happy with the
p-value and the study has shown that we can reject the null hypothesis. What does that mean for your patient? If a study shows that 5 mg of a drug is safe for the average patient, what does that mean for the patient sitting in your chair and waiting for you to give her a prescription? If she responds like most patients do, she’ll be safe. But there’s a chance that she’s an outlier and doesn’t respond like most patients, potentially creating a dangerous situation for her. Understanding how a given procedure or drug could affect your patient is the key goal when translating research to clinical practice.
When we measure anything, there’s always a distribution of results. Even if we measure the same thing multiple times, the results will usually vary. If you measure a board three times, you might get 71.11 inches, 71.10 inches and 71.13 inches for your measurements. The same
is true when measuring a response in different people. If we perform the same procedure on several patients, their postoperative pain level will always vary. In most cases we deal with in dentistry, this variation is spread out in a “normal distribution” also called a bell curve. Most people respond somewhere in the middle of the bell curve and this is represented by the bump in the middle. As you move left or right on the curve, fewer and fewer people respond like that. Many classical biological phenomenon have a normal distribution.1
Let’s say an investigator does a new procedure on a group of patients and asks them to report their pain level the next day on a scale of 1 to 10. The average response might be a 5 and this tells us quite a bit about how much pain the procedure causes. But just as important is the breadth of responses, such as how the responses are distributed along that 10-point scale. A bell curve can be tall and skinny or short and wide. In this example, a tall, skinny bell curve means that most patients’ pain levels were around 5 and didn’t deviate very much from that number. A short, wide curve means that there was a wide variety of responses and any given patient might report a lot of pain or very little.
When we’re looking at research, the standard deviation (σ) is what’s used to describe the shape of the normal distribution curve. A low standard deviation means what it sounds like: There’s not that much variation between patients and we have a high, narrow curve. Any given patient is likely to respond in a way more similar to the average patient. A high standard deviation means that more patients deviate from the mean and we have a low, wide curve. In this situation, we have to be careful because patient response is more variable.
What is a high or low standard deviation? It depends upon your units and tolerance for variation. Approximately 95 percent of all patients will fall within two standard deviations of the middle of the bell curve (the mean). Using the above pain scale example, if our average was 5 and our standard deviation was 0.5, then about 95 percent of all patients reported pain levels between 4 and 6 on a 10-point scale, which is a pretty narrow range. If our standard deviation was 1.5, that describes a much higher level of variation with 95 percent of patients reporting pain from 2 to 8. Nearly all patients (99.7 percent) will fall within three standard deviations of the mean.
Odds Ratio vs. Relative RiskThese two concepts are both commonly
used and easily confused. Both use the chances of an event to describe a population. The main differences are given away in their names, odds versus risk. The “odds” of something happening is the number of times that thing happens compared to the number of times it didn’t happen. For example, if you roll a die, the odds of rolling any given number is 1:5, also expressed as 1/5. There’s one chance that you’ll get that number and fi ve chances that you won’t get that number.
s t a t i s t i c s
Approximately 95 percent of all patients will fall within two standard deviations of the middle of the bell curve (the mean).

C DA J O U R N A L , V O L 4 6 , Nº 9
S E P T E M B E R 2 0 1 8 581
So an odds ratio is defi ned as the odds of an event in the experimental group divided by the odds of the same event in the control group. If the experimental intervention actually does something, we’d usually expect the odds ratio to be signifi cantly less than or greater than 1. If it’s close to 1, that means the odds of the event occurring in the experimental group are roughly the same as the odds of it occurring in the control group, and we can’t reject the null hypothesis.
Relative risk is a very similar concept, except that it uses probability instead of odds. Probability (or risk) is calculated by taking the number of times something happened and dividing by the total number of samples in the group. So if we rolled a die six times and got a three just once, the probability is 1/6. Just like with an odds ratio, relative risk is risk in the experimental group divided by risk in the control group.
Because we usually use probability in statistical modeling and are more used to thinking about probability as opposed to odds, relative risk is usually the preferred calculation. In addition, if odds ratios aren’t interpreted properly, they can sometimes lead one to overestimate risk, which is usually what we are interested in studying.5
ConclusionWill Rogers was said to have quipped,
“When the Okies left Oklahoma and moved to California, they raised the average intelligence level in both states.” While this seems impossible at fi rst glance and is obviously offensive to Californians, it math-ematically could have been true. Believe it or not, the Will Rogers phenomenon is now an important concept in epidemiology, which helps limit bias when shifting subjects between groups and comparing experimen-tal results to historical controls. It’s puzzles like this that show us our need for statistics to complement our intuition when describ-ing the world and treating our patients. ■
REFERENCES
1. Bulmer M. Principles of Statistics. Dover Publications; 1967.2. Travers JC, Cook BG, Cook L. Null hypothesis signifi cance testing and p-values. Learn Disabil Res Pract 2017;32(4):208–215.3. Wright EF, Manuel A, Fischer JR. Usefulness of Posture Training For Patients With Temporomandibular Disorders. 2011.4. du Prel J-B, Hommel G, Röhrig B, Blettner M. Confi dence interval or p-value?: Part 4 of a series on evaluation of scientifi c publications. Dtsch Arztebl Int 2009;106(19):335-339. doi:10.3238/arztebl.2009.0335.5. Davies HT, Crombie IK, Tavakoli M. When can odds ratios mislead? BMJ 1998;316(7136):989–991. www.ncbi.nlm.nih.gov/pubmed/9550961. Accessed March 5, 2018.
Have a job opening or need a temp?
Join Swiss Monkey and let us match you up!(916) 500-4125 [email protected] www.swissmonkey.io
CONTACT US TODAY AND GET CONNECTED TO THE BEST TALENT!

800.752.7461
With scores of Buyers, profiles of their practice interests and financial ability,
is able to find the right buyer for your practice.
Experience the difference. Call Lee Skarin and Associates for responses to all of your questions - No obligation!
Visit our website for current listings: www.LeeSkarinandAssociates.comDental Practice Brokers CA DRE #00863149
Lee Skarin and Associates has been serving the dental profession since 1959. Kurt Skarin has over 30 years experience in dental practice sales. We have sold more practices than any broker in the state within
the last 12 months. Our experienced practice appraisals are backed with
credentials unequaled among dental practice brokers. We provide in-house legal counsel to advise you in all
aspects of the sale and purchase, including the tax consequences of the sale.
Excellent financing is available, in most cases for 100% of the purchase price.
With a reputation for experienced, conscientious, and ethical performance, we give our clients personal attention in all aspects of the purchase.

C DA J O U R N A L , V O L 4 6 , Nº 9
S E P T E M B E R 2 0 1 8 583
Des Gallagher, BDS, MA, is an assistant professor and a group practice leader at the University of the Pacifi c, Arthur A. Dugoni School of Dentistry. He recently completed a master’s degree in dental education and is a new fellow of the American Dental Education Association Leadership Institute.Confl ict of Interest Disclosure: None reported.
AUTHORS
Andrew Young, DDS, MSD, directs the University of the Pacifi c, Arthur A. Dugoni School of Dentistry orofacial pain curriculum and patient care. He has an MSD and board certifi cation in orofacial pain. He has published several studies in peer-reviewed journals and heads UOP’s evidence-based dentistry curriculum.Confl ict of Interest Disclosure: None reported.
Where the Rubber Meets the Road: Incorporating Evidence-Based DentistryAndrew Young, DDS, MSD, and Des Gallagher, BDS, MA
A B S T R AC T Different career stages in dentistry have unique challenges for incorporating evidence-based dentistry (EBD). Practicing dentists, the majority group, have daily time constraints. Students, the future of dentistry, need to become quick and profi cient at EBD if they are to practice it after graduation, as with any procedural skill. Faculty, the shepherds of the future, have widely different schedules that make universal training diffi cult. This article proposes some solutions for those challenges.
“Doctor, what would you recommend for this missing front tooth?”
“You’ve made it pretty clear that you don’t want anything removable, that aesthetics is a high priority and that cost is not a signifi cant factor. That leaves us with two general options, but your adjacent teeth, your bruxism and your medications will have an effect on each of those options differently. Let me explain that to you, and then we can come to a decision.”
The endpoint of evidence-based dentistry (EBD) is the dentist giving the most appropriate care to the patient. But the route to this endpoint involves many steps, each of which can either promote or hinder the pathway.
DentistsIn the course of their practice,
dentists will have many questions — is silver diamine fl uoride safe and effective? Which bonding agent should I use? For each question, the other articles in this issue teach dentists how to fi nd the
i n c o r p o r a t i n g e b d
literature that answers that question and how to evaluate each of those articles to determine which is the most trustworthy.
But consulting the evidence takes time — a commodity that is in short supply. Several tools exist that can make the EBD process more effi cient. For each of these tools, authors have already done much or all of the legwork to fi nd and assess the articles relevant to your topic.
Review ArticlesThese are described in more detail
in this issue in the article titled “The Anatomy of a Clinical Study,” but briefl y, in review articles, the authors (reviewers) do a high-quality EBD exercise (thoroughly searching the literature and carefully evaluating the articles) and summarize their fi ndings for the reader. These articles also tend to cover a broader topic — usually more similar to what the dentist is looking for. For example, while an individual study article may present fi ndings on one particular NSAID in

C DA J O U R N A L , V O L 4 6 , Nº 9
584 S E P T E M B E R 2 01 8
one population, a review article may summarize the data on multiple NSAIDs across many populations. For the above reasons, review articles are a more logical starting point than individual studies. The reader should bear in mind though that systematic reviews and meta-analyses are more reliable (and will describe themselves as such, usually in the title, but sometimes only in the methods section of the text) than narrative reviews. To fi nd a review article, use the methods described in the article “Searching for Research Articles on the Internet” on page 555 and request review articles in the search parameters.
American Dental Association (ADA) Evidence-Based Guidelines
The ADA has done the analysis already on several dental topics. Their recommendations are also much more succinct than review articles and much easier to search, making the time investment minimal. Their fi ndings can be found at ebd.ada.org/en/evidence/guidelines.
Specialty Board GuidelinesMany specialty boards publish
evidence-based clinical guidelines. Like the ADA guidelines, their recommendations are also much more succinct than review articles and thus easier to search. Some boards cover a fairly large scope of topics. But read carefully — not all guidelines are stringently evidence based.
To maximize effi ciency, consider this approach: For questions related to general dentistry, check the ADA Evidence-Based Guidelines and/or the appropriate specialty board guidelines. If the answer is not found there, consult review articles (the ADA Evidence-Based Guidelines webpage also has a link for many review articles on many topics), because just about every clinical
topic has review articles written for it. If review articles cannot be found, read the actual studies. Yet with the many demands of life both in and out of the offi ce, EBD does not need to be done for all decisions. Prioritize the procedures/materials of greater consequence before looking into the more benign. When purchasing patient bibs, dentists can purchase whatever suits their fancy. When deciding on a new bonding system for the practice, on which thousands of teeth will rely, the EBD homework should be done upfront, rather than risk redoing, apologizing and refunding afterward. The ADA Library and Archives (accessible online) is an excellent resource, with four full-time librarians to help member practitioners with a range of tasks including picking and acquiring articles.
StudentsFor EBD to become the norm in
the fi eld of dentistry, it must be the norm in the dental school curriculum. Students have many subjects competing for their attention. Restorative topics have no problem getting priority in their minds, in school and in their future practice. Other topics, such as infection control and ergonomics, require a bit more work on the educators’ part to become the norm — something every dentist should do. And educators have achieved that (to varying degrees of success) with students for decades.
For EBD to become the norm in dental school and beyond, a few steps are needed.
First, students must be convinced of the value of EBD. There must be buy-in. The logic, the ethical and professional responsibility, the improvement in clinical outcomes, the possible fi nancial benefi t (from better outcomes) and the legal responsibility should all be explained, with examples.
Second, a large amount of instruction and practice must be done. Any procedural skill (extractions, crowns, root canal therapy, EBD) takes time to learn and more time and practice to become competent. A lecture, or even a lecture series, on root canal therapy will not enable students to perform root canal therapy. Students also need practice. With one or two cases, those students would not be competent and most would not have the speed or confi dence to elect to do root canal therapy after graduation. EBD is the same. Students need adequate didactics and frequent practice.1
Ideally, instruction should begin early in their curriculum, because typically a number of other courses will also have assignments that require fi nding and assessing articles. An early start also allows for prolonged reinforcement and progressive improvement in EBD skills. One way of sequencing the steps of EBD in dental school curriculum is as follows:
1. How to fi nd articles. This requires minimal EBD background knowledge and will be needed for many other courses that require literature searches (see “Searching for Research Articles on the Internet” on page 555 for a very brief version). It is therefore a logical fi rst step.
2. Reasons for EBD. Read the introduction on page 553 of this issue for a very brief version.
3. Elements of study design. This includes blinding, controls, random allocation, etc., as well as the different types of studies (see “The Anatomy of a Clinical Study” on page 561 for a very brief version). Knowing how such elements should look and when and why they are needed is a prerequisite for appraisal (step 4).
4. Appraisal of studies. Steps 3 and 4 can be sequenced in either of two ways:
i n c o r p o r a t i n g e b d

C DA J O U R N A L , V O L 4 6 , Nº 9
S E P T E M B E R 2 0 1 8 585
• All elements and all types of studies are fi rst taught, followed by instruction on appraisal for all types of studies.
• One study design (e.g., case-control study) is taught, followed by instruction in appraisal on that type of study (e.g., case-control study). Next, another study design (e.g., randomized controlled trial) is taught, followed by instruction in appraisal of that type of study (e.g., randomized controlled trial) and so on.
• See “How To Critically Appraise the Dental Literature” on page 569 for a very brief version.
5. Critically appraised topics (CATs). These are small projects that pull together everything learned so far and apply those skills clinically2 (FIGURE). Students first lay out a clinical question that they want to find an answer to (e.g., Do resin-modified glass ionomers have superior survival in class V lesions compared to composite resins?) and then search the existing literature and choose two or three of the highest quality articles they can find. In one to two pages, they summarize the findings of those articles, describe their strengths and weaknesses, articulate the “clinical bottom line” of what those two to three articles concluded as a whole and explain how they would apply that conclusion to their patient care. CATs have a number of benefits including the following:• They keep EBD clinically
relevant.• They encourage keeping EBD
tasks short and manageable.
• The CAT template can serve as components of other assignments or as stand-alone assignments for many different departments’ curricula. This reduces instructional time and confusion.They can also be modifi ed to suit specifi c needs. For example, a shorter version may only require one or two articles (they can even be called “kittens;” a longer version could be called a “lion”).
• Frequent CAT assignments help students develop speed in EBD, in a format that can be used for all their future clinical questions (though once in practice, they’ll do a shorter version solely in their heads).
• CATs of high quality can be put into a searchable database as a resource for others. University of Texas Health Science Center, School of Dentistry, San Antonio has such a database at cats.uthscsa.edu.
6. Use in clinics. CATs can be used as graded assignments to provide evidence-based content for clinical questions that arise during the course of their patients in clinic.
Third, faculty must be the examples. When faculty also practice EBD and show this in the classroom and clinic, it reinforces its value to students.3,4
FacultyThe other reason for faculty to
practice EBD is that it yields the most up-to-date and reliable information (while factoring in the instructor’s clinical expertise) from which students should be taught. Yet the daily clinical workload for faculty can be demanding. With limited time at the school, they sometimes feel they cannot afford to invest in learning
about and doing something that they see as just another form to complete.5
So how can faculty be encouraged and trained to practice more EBD in general?
First, faculty must be convinced of the value of EBD, just like students, as discussed previously.
Second, widespread faculty training should be done. And unlike students, faculty training has the challenge of widely different personnel schedules, with some on campus every day of the week and some coming in once a month or only certain months of the year or only certain times of the day. Therefore, sequential lectures would result in only a fraction of the faculty receiving full training. Instead, training should be available at a variety of times. Online modules (that offer continuing education credit — another great motivator) with quizzes have the advantage of being the most accessible but the disadvantage of usually not being amenable to questions and being easier for the participant to completely skip the module content while still passing the quiz. Another option to reduce those disadvantages is to teach the modules as live lectures/seminars multiple times (mornings, lunches, evenings, various days, student breaks), though this can be expensive. The ADA also provides training sessions in EBD, both at their facilities and at dental schools.
Because faculty training time is tighter than student educational time, faculty training must be especially effi cient. The ultimate goals should be that all faculty can fi nd the most reliable articles that address a given question, assess the strengths and weaknesses of those articles and decide how to apply that new knowledge to patient care. Training sessions should only include content that would help achieve those goals. Advanced statistics, for example, would not be needed in those training

C DA J O U R N A L , V O L 4 6 , Nº 9
586 S E P T E M B E R 2 01 8
i n c o r p o r a t i n g e b d
FIGURE. Sample of a critically appraised topic by Armita Fartash, second-year dental student at the University of the Pacifi c, Arthur A. Dugoni School of Dentistry.
Title Effi cacy of Mandibular Advancement Device for Sleep Bruxism
Clinical question In a patient with obstructive sleep apnea (OSA) who is also a sleep bruxer, can a mandibular advancement device (MADs) manage both OSA and sleep bruxism?
Clinical bottom line The evidence at this time is inconclusive on whether MADs are eff ective in controlling sleep bruxism.
Evidence search (“mandibular advancement”[MeSH Terms] OR (“mandibular”[All Fields] AND “advancement”[All Fields]) OR “mandibular advancement”[All Fields]) AND (“equipment and supplies”[MeSH Terms] OR (“equipment”[All Fields] AND “supplies”[All Fields]) OR “equipment and supplies”[All Fields] OR “device”[All Fields]) AND (“bruxism”[MeSH Terms] OR “bruxism”[All Fields])
PubMed ID Author/year Patient group/number of studies and types Study type
Arti
cle
1
27422230 Solanki et al. 2017 Thirty participants, fi nal sample size 25; no controls. Uncontrolled prospective clinical trial.
Key results There was a decrease in the mean number of sleep bruxism episodes per hour at 15 days (42.5 percent) and at 30 days (59.9 percent). There was a signifi cant (P<.001) reduction in occlusal force at 15 days (30.4 and 33.1 percent) and 30 days (31.9 and 35.7 percent) on the right and left sides, respectively.
Arti
cle
2
26004173 Singh et al. 2015 Thirty-six participants, fi nal sample size 28, 14 wore MAD, 14 wore MOS. Randomized controlled trial.
Key results When compared to the participants wearing maxillary occlusal splints (MOS), the participants wearing MADs showed a greater reduction (statistically signifi cant) in bruxism episodes and bursts per hour at three months. However, the MAD was associated with discomfort involving tooth sensitivity, drooling and poorer aesthetics.
Arti
cle
3
23643652 Carra et al. 2013 Eight girls and eight boys (mean age 15 years), MAA worn in three positions for one week each, in a random order: free splints (FS), neutral position (NP) and advanced to 50 percent of maximum protrusion (A50).
Randomized, controlled, crossover study.
Key results Short-term use of MAD in all three positions signifi cantly reduced rhythmic masticatory muscle activity (RMMA), but there was no signifi cant diff erence between the three positions.
Appraisal of the evidence
Solanki et al.: This study did not have a control group, so the results may not conclusively be attributed to the MAD therapy. The originally small sample size further decreased because two participants did not follow up and three withdrew due to TMJ pain. The inclusion criteria relied heavily on the word of family members, who heard grinding sounds from the participant at least three times a week for six months. This criterion for inclusion was less reliable because a family member could think that any type of noise from the participant could be classifi ed as “grinding.” Sleep recordings are more reliable in this case but were not utilized.
Singh et al.: The 36 participants were reduced to 28 because of discomfort and not showing up to the follow-up examination. The inclusion criteria was tooth-grinding sounds that occurred three times a week for six months, but they did not state how this was recorded or determined. Block randomization was done by a computer-generated chart, and allocation concealment was achieved by separating the device-fabrication personnel from the examining personnel. Video recording was used to eliminate the potential for counting nonspecifi c orofacial activities as sleep bruxism. A larger sample size studied over a longer period of time is needed in the future.
Carra et al.: Candidates were fi rst screened and diagnosed with sleep bruxism before being included as participants. After a certain MAA position was tested for one week, it was followed by a fi ve- to seven-day washout period. There were no dropouts. This study would be strengthened if participants were monitored for compliance when wearing the appliance at home, such as with a compliance chip. The study reports random allocation of subjects to particular sequences but does not tell what randomization method was used. The same examiner was used for each participant when scoring the sleep report. These examiners were blind to which position the MAA was being worn. A longer study is needed to determine the long-term eff ects.
Application For my patients with obstructive sleep apnea who qualify for a MAD and who also have sleep bruxism, I would explain to them that the evidence does not currently specify whether a MAD will reduce sleep bruxism.
C DA J O U R N A L , V O L 4 6 , Nº 9
S E P T E M B E R 2 0 1 8 587
sessions. It may have value for a smaller group of faculty, but when the challenge is universally training all faculty, the content should be as effi cient as possible.
As often as possible, the most effective methods for a given subject should be used for students and faculty. Some content can be adequately delivered in lecture format, which is also the most effi cient. But small group seminars, which foster questions between the instructor and attendees (in both directions) and involve plenty of exercises, can be more engaging and enjoyable for the participants, with participants achieving superior understanding and retention of the information.6 Examples of the exercises that can be done include:
■ Searching for articles: “Please obtain three articles that address the question of the effi cacy in geriatric caries reduction for silver diamine fl uoride.” Ideally, participants individually would perform this search in a small group setting with an instructor ready to assist when needed.
■ Elements of study design: “Please design a hypothetical study to answer the question of whether using loupes results in superior clinical outcomes in restorative dental procedures, and share your design with the class.” The purpose of this exercise is not to turn the participants into researchers. But as they go through this exercise and receive constructive criticism from the group when they present their design, they learn the practical reasons why blinding, random allocation, controls, etc., are necessary to reduce bias and how each of those elements would look in a real study.
■ Appraisal: Research and review articles are given to students, as well as appraisal checklists (the Scottish Intercollegiate Guidelines Network has a very user-friendly set of appraisal checklists). Participants assess the articles for their specifi c strengths and weaknesses, present this to the class and discuss how those fi ndings affect their application of the article to patient care.
As stated, student schedules allow more of the ideal teaching methodology mentioned previously than faculty schedules.
AdministrationThird, administration must take
concrete action on EBD. Carving out time in student and faculty schedules for training and funding the cost of training both allows the training to occur and demonstrates to the dental community that this content is a priority. Setting aside time for faculty and giving credit for students, who actually want to become involved in research (which in reality is a relatively small percentage), are also necessary to nurture those budding careers, because time is often a major limiting factor in dental schools.
The Commission on Dental Accreditation (CODA), which should be acknowledged for its role in the increasing incorporation of EBD, states in its Accreditation Standards for Dental Education Programs:
“Curricular content and learning experiences must incorporate the principles of evidence-based inquiry and involve faculty who practice EBD and model critical appraisal for students during the process of patient care. As scholars, faculty contribute to the body of evidence supporting oral health care strategies by conducting research and guiding students in learning and practicing critical appraisal of research evidence.”7
CODA then further specifi es that students must be competent in EBD (standard 2-21) and patient care must be evidence based (standard 5-2).
In summary, for students, our next generation of dentists, to use EBD, they must become quick and competent at it, which is achieved through frequent practice. They must also see it as the norm, through the practice of their faculty (their examples) and through the support of administration.
All of this takes a signifi cant amount of time, but the investment is worthwhile. While much of what we learn is skills or information with expiration dates, EBD trains us to be true lifelong learners — continually updating our knowledge with the most reliable information.8 ■
REFERENCES
1. Straub-Morarend CL, Wankiiri-Hale CR, Blanchette DR, et al. Evidence-Based Practice Knowledge, Perceptions and Behavior: A Multi-Institutional, Cross-Sectional Study of a Population of U.S. Dental Students. J Dent Educ 2016;80(4):430–438. www.ncbi.nlm.nih.gov/pubmed/27037451. Accessed Jan. 16, 2018.2. Wyer PC. The critically appraised topic: Closing the evidence-transfer gap. Ann Emerg Med 1997;30(5):639–640. www.ncbi.nlm.nih.gov/pubmed/9360576. Accessed March 14, 2018.3. Irby DM. Faculty development and academic vitality. Acad Med 1993;68(10):760–763. www.ncbi.nlm.nih.gov/pubmed/8397601. Accessed March 14, 2018.4. Ciancio MJ, Lee MM, Krumdick ND, Lencioni C, Kanjirath PP. Self-Perceived Knowledge, Skills, Attitudes and Use of Evidence-Based Dentistry Among Practitioners Transitioning to Dental Educators. J Dent Educ 2017;81(3):271–277. www.ncbi.nlm.nih.gov/pubmed/28250032. Accessed March 14, 2018.5. Olatunbosun OA, Edouard L, Pierson RA. Physicians’ attitudes toward evidence-based obstetric practice: A questionnaire survey. BMJ 1998;316(7128):365–366. www.ncbi.nlm.nih.gov/pubmed/9487175. Accessed March 14, 2018.6. Springer L, Stanne ME, Donovan SS. Eff ects of Small-Group Learning on Undergraduates in Science, Mathematics, Engineering and Technology: A Meta-Analysis. Rev Educ Res 1999;69(1):21–51. doi:10.3102/00346543069001021.7. Accreditation Standards for Dental Education Programs. 2015. www.ada.org/~/media/CODA/Files/predoc.ashx.8. Iqbal A, Glenny AM. General dental practitioners’ knowledge of and attitudes towards evidence-based practice. Br Dent J 2002;193(10):587–591. doi:10.1038/sj.bdj.4801634.
THE CORRESPONDING AUTHOR, Andrew Young, DDS, MSD, can be reached at ayoung@pacifi c.edu.

Specializing in selling and appraising dental practices for over 40 years!
CONTACT US FOR A FREE CONSULTATION Phone: (800) 697-5656
WWW.CALPRACTICESALES.COM CA BRE #00283209
youtube.com/mycpsteam faceboook.com/mycpsteam
Visit our Website and Social Media pages for Prac ce Photos and Videos
LOS ANGELES COUNTY
CARSON— Long established GP in a small shopping center. Grossed $277K in 2017. Net $128K. Has 3 eq ops & 2 plmbd not eq. Re ring seller work 3 days/wk. Great street visibility. Property ID #5181.
ENCINO - GP w/ 4 eq ops in a prof. bldg. w/ widow views to the mountain. Fee for service. Net $144K. Gross. $488K in 2017. Property ID #5210.0
GLENDALE—Beau ful office w/ 3 eq ops in a 850 sq . LH & Equip Only! Great starter office. Near resi-
den al & commercial area. Property ID #5208.
GLENDALE - GP located in a med bldg w/3 eq ops in a 1,123 sq ste. Ins & Cash Only! Est. in 1994. Grossed $473K in 2017. Prop. #5216.
LANCASTER (GP + Bldg) Long established prac ce w / 4 eq ops in a 1,600 sq office. Grossed $693K in 2017. NET $220K. Property ID #5222.
MONTEREY PARK— GP in shopping center. Absen-tee owner. Grossed approx. $636K in 2017. Net $183K. 5 eq ops / 3 plumbed not eq ops. Property ID #5201.
MOTEBELLO—Grossed approx. $1M in 2017, locat-ed in a free standing bldg w/ 5 eq ops. Established in 2002. Property ID #5168
SANTA CLARITA—GP w/ 36 yrs of goodwill in prof. bldg. w/ 5 eq ops. Grossed $449K in 2017. Property ID #5207.
TARZANA - Established in 1929 w/ 5 eq ops in a 1,552 sq suite. Delta Premier and Cash Only! Grossed $681K in 2017. Buyer’s Net $211K. Proper-ty #5226.
KERN, VENTURA, & SAN LUIS OBISPO COUNTIES
FRESNO— GP 4 eq ops in a retail shopping center. Grossed $448K in 2017. NET $202K. Prop. #5214.
GOLETA—GP w/ 27 yrs of gdwll in a 2 story mix bldg. 4 eq ops. Grossed $572K. Prop. #5205.
OXNARD—Est, in 1973 w/ 4 eq ops in a 1,100 sq suite. Grossed $585K Net $186K. Prop. #5206.
SIMI VALLEY— GP + Real Estate. Prac ce has 4 eq ops & 2 plmbd not eq ops. Net of $92K. ID #5185.
ORANGE COUNTY
COSTA MESA - Est. in 1952 in a sing bld w/ 3 eq ops. Cash & Delta Premier Only!! Proj. approx. $373K for 2017. Property #5202.
IRVINE - Well established Cash Only GP w/ 5 eq ops in a1,915 sq office . Grossed approx. $482K in 2017. Property ID #5193.
LA PALMA— With 60 years of goodwill this GP prac ce is located in 2 story dental bldg w/ 4 eq ops. Grossed $443K in 2017. Property ID # 5234.
NEWPORT BEACH—Long established GP in mul story bldg w/ great views to the coast. Has 3 eq ops and 2 plumbed not eq. Grossed approx. $560K in 2017. Net $241K. Property ID #5211.
ORANGE— Est. in 1978 GP in one story free stand-ing duplex w/ 3 eq ops. Grossed approx. $386K in 2017. Property ID #5213.
ORANGE— Beau ful office w/ 4 eq ops in a 1,300 sq office in single free standing bldg. Property ID #5229.
PLACENTIA— Turn-Key GP in one story medical bldg w/ 2 eq ops & 2 plmbed not eq. Estab. in 2009. Grossed $129K in 2017. Property ID #5227.
SANTA ANA— Well established prac ce. PPO & Cash only. Gross. approx. $500K. Prop. ID #5113.
RIVERSIDE & SAN BERNARDINO COUNTIES
BANNING—LH & Equipment only! Consists of 3 eq ops in a 925 st suite. Property ID #5184.
CHINO HILLS— GP in busy shopping center. Grossed $352K . NET $141K. PPO & Cash Only! Has 3 eq ops and 1 plmbed op. Established in 1992. Property ID #5219.
CORONA— Beau ful GP w/ 6 eq ops / 4 plmbd not eq for expansion in a 3,700 sq office. Located on a one story free standing building next to a busy shop-ping center. Grossed $346K in 2017. Great poten al for a full me den st. Property ID #5224.
DESERT HOT SPRINGS— GP + Real Estate! Two partners one office. Consists of 4 eq ops / 1 plmbd not eq. Est. in 1986. Proj. approx. $802K for 2017. Property ID #5198.
FONTANA— GP + Real Estate!! Premier office with 50 years of goodwill. In a 3,000 sq bldg with 8 eq ops. Has the latest technology. Grossed approx. $2.3M in 2016. Net of $968K. Property ID #5140.
PALM DESERT— Beau ful GP located in a single story corner building. Heavy traffic flow. Consists of 4 eq ops in a 1,800 sq office. Reasonable rent. Monthly revenues of $132K. Grossed $1.4M in 2017. NET $383K. Property ID #5217.
PALM SPRINGS – General prac ce with 3 equipped ops located in a free standing bldg. Established in 2005. Suite is approx. 1,200. Seller work 5 days/wk. BUYER’S NET OF $115K. Property ID #4487.
RANCHO CUCAMONGA— GP established in 2004 in busy shopping center. Consists of 3 eq ops in a 1,200 sq suite. Grossed $422K in 2017. Net $149K. Prop-erty ID #5169.
UPLAND—Pediatric dental prac ce located in a medical bldg with 40 years of goodwill. Consists of 4 chairs in open with Alpha-Dent so ware. Grossed $271K in 2016. Property ID #5188.
COMING SOON IN CANOGA PARK, GARDEN GROVE, LA JOLLA,
LOS ANGELES, SAN DIEGO, TEMECULA, TUSTIN, & UPLAND
SAN DIEGO COUNTY
LA JOLLA— 4 eq ops in 2 story med building. PPO & Cash Only! Grossed approx. $1.1M in 2017. Property ID #5220.
LA MESA— Beau ful GP office in shopping center w/ 5 eq ops & 1 plumbd not eq. Sees 80-100 new pa ents/mo. Grossed $1.5M in 2017. Net $368K. Prop.#5228.
OCEANSIDE— Orthodon c prac ce w/4 chairs in open bay in a 1,550 sq office. Grossed $263K in 2017. Property ID #5225.
SAN DIEGO— GP in med/dent bldg. w/ 3 eq ops. Fee for service. Estab. circa 1950. Grossed $301K in 2017. Net $129K. Property ID # 5212.
SOLD
SOLD
SOLD
SOLD
SOLD
SOLD
SOLD
SOLD
SOLD SOLD
C DA J O U R N A L , V O L 4 6 , Nº 9
S E P T E M B E R 2 0 1 8 589
RM Matters
From electrical fi res to leaky roofs to failed equipment — suffering property damage can be an unfortunate part of dental practice ownership. As any dentist who has
experienced a loss can attest, the goal is to minimize downtime and get back to work as soon as possible. After all, patients depend on dentists to keep their oral health in good order and a disruption in practice operations can prevent them from receiving the care they need.
The ProcessLet’s say you’ve been away for a
long weekend and return to work early Monday morning to fi nd your offi ce fl ooded with water. Or the back window broken. Or the compressor nonfunctional. First things fi rst: Notify your commercial property insurer (and the police, in criminal incidents), who will walk you through the process of fi ling a claim. On the outside, the process seems relatively straightforward: You fi le a claim, your case is evaluated, a determination is made, a check is sent for your covered damages and the case is closed. But there’s much more that goes on behind the scenes than you may realize.
Determining ResponsibilityAt the heart of any claim is the
determination of the cause of the damage and who, exactly, is responsible for causing it. Sometimes this is simple: A staff member fails to turn off a faucet in a sink when watering the offi ce plants and closes up for the night, allowing the sink to overfl ow and fl ood the offi ce. But oftentimes, the problem is far less cut and dried: A water supply line to the cavitron springs a leak. The loss raises questions about whether the tubing or connections are defective or whether the unit was property assembled
Whodunit? Subrogation Determines Responsibility in Property Claims
TDIC Risk Management Staff
You are not a sales goal.
You are a dentist deserving of an insurance company relentless
in its pursuit to keep you protected. At least that’s how we see
it at The Dentists Insurance Company, TDIC. Take our Risk
Management program. Be it seminars, online resources or our
Advice Line, we’re in your corner every day. With TDIC,
you are not a sales goal or a statistic. You are a dentist.
Protecting dentists. It’s all we do.®
800.733.0633 | tdicinsurance.com | CA Insurance Lic. #0652783
and installed. Or the failure of the water line may be the result of a broken water pressure regulator managed by the building.
The same questions can be asked of many common property claims. For example, in the case of a fi re, was any recent electrical work done? Any new equipment installed? Or was it caused by a careless employee? And in the case of vehicle claims, investigators must fi nd out who was driving the vehicle, whether the driver was possibly impaired or whether there was an issue with the overall operation of the vehicle or parts that caused the accident.
You fi le a claim, your case is evaluated, a determination is made, a check is sent for your covered damages and the case is closed. But there’s much more that goes on behind the scenes than you may realize.

C DA J O U R N A L , V O L 4 6 , Nº 9
590 S E P T E M B E R 2 01 8
S E P T . 2 0 1 8 R M M A T T E R S
What Is Subrogation?Technically speaking, subrogation
is the legal right of one party to recover monies from a responsible party, usually between two insurance companies. According to attorney Daniel Watkins, in cases of property damage, subrogation involves the insurance company stepping in the shoes of the dentist and seeking recovery from the responsible party for the money paid by their insurer to repair the dental suite after the loss. It should be noted that an insurance provider like The Dentists Insurance Company (TDIC) does not subrogate against the dentist if the dentist is responsible for the loss. Subrogation results in recovery of the dentist’s deductible and potentially lower premiums.
Policyholders can play an important role in maximizing recovery in subrogation claims. There are steps they can take to prevent the loss or destruction of critical evidence that may conclusively show who is the responsible party.
Preservation of PropertyOne of the most important
steps a practice owner can take to ensure the claim and/or subrogation process goes smoothly is to keep any damaged or defective items until they have been instructed by their claims representative to dispose of them. Occasionally, dentists — desperate to get their practice up and running again — dispose of the failed or damaged equipment or allow a vendor or contractor to take it off their hands when they replace it.
However, it is important that the practice owner retains the equipment in question so that it can be evaluated for potential subrogation recovery. Failure to retain the
equipment can result in a delay in payment or, even worse, denial of the claim. TDIC Claims Representative James Dunham says evaluating a loss and inspecting damaged property or failed equipment is a standard procedure in the insurance industry.
“It is critical to determine the cause of the loss to a reasonable degree of certainty from both a coverage and subrogation standpoint,” Dunham said. “From a subrogation standpoint, that information is invaluable in determining the viability and the percentages of recovering our paid claims.”
In addition to retaining failed or damaged equipment after a loss, dentists have certain responsibilities to fulfi ll. For TDIC policyholders, that means notifying the company immediately. It also means reporting any injuries, obtaining names of witnesses and refraining from offering to cover losses suffered by a neighboring tenant or other parties. The practice owner should never admit fault or speculate to others over why the loss occurred. Other duties for the policyholder include the following:
■ Take reasonable steps to prevent potential safety risks or further damage.
■ Secure property such as windows, doors and roofs as necessary.
■ Notify the police if a crime has been committed.
■ Alert banks and credit card companies about any missing debit or credit cards.
■ Photograph damaged property prior to repairs.
■ Keep accurate records and receipts for what you spend on securing or repairing your property.
■ Separate items that may be restored through cleaning or repair.
Your patients depend on you to maintain their oral health and you depend on the smooth operation of your practice to keep them healthy. Any disruption in operation trickles down to patients so when faced with a loss the goal is to get back to work as quickly as possible. The negative impact of property loss can be minimized by taking a few prudent steps and fulfi lling your responsibilities as a policyholder. ■
To schedule a confi dential consultation with an experienced risk management analyst, visit tdicinsurance.com/RM consult or call 800.733.0633. TDIC’s Risk Management Advice Line is a benefi t of CDA membership.

4248 MENLO PARK FACILITY Remodeled, 930 sq. ft. dental facility with2 fully equipped ops. and plumbed for 2 additional ops, reception area,doctor's office, sterilization, lab, storage and restroom. Medical/Dentalbuilding in highly desirable location. Asking $135K.
4246 SUNNYVALE GP Retiring seller offering a well est. general practicewith loyal staff in organized office with 3 fully-euipped ops. Located in highlydesirable neighborhood. 2017 Gross Receipts $540K+. Asking $390K.
4269 SAN JOSE GP Well established practice offering 46 yrs of goodwill.Excellent West San Jose location. 7ops, 5 fully equipped in 2,000 sq. ftfacility. Approx 3,000 active patients, all fee-for-service. 9 days of hygiene/week. Outstanding staff. Average annual GR $1.3M with an adjusted net of$473K. Asking price $1,015,000. Potential to purchase bldg interest, priceto be determined. Owner willing to help in the transition.
4217 WEST SAN JOSE GP Seller retiring, offering 35+ years of goodwill inwell-established practice with loyal staff and stable patient base. 10-15 newpatients a month. Excellent location on busy thoroughfare. Asking $509K.
4237 SAN JOSE GP Busy general practice in state-of-the-art 1,500 sq. ft.office with 5 fully-equipped operatories. Approx. 1,900 active patients andapprox. 19 new patients per month. Average Gross Receipts $1.3M+.
4267 SAN JOSE GP 36-year established 4 op practice near Willow Glenarea grossing $650K average. 950+ active patients. Beautifully maintainedand updated 1,450 sq. ft. facility. 3-day doctor week, 3 hygiene days.Asking $450K.
4233 SF GP Seller offering 26+ year general practice in SF Financial district.Ground floor office with high volume foot traffic. Approx. 1,200 sq. ft. facilitywith 4 fully-equipped ops. $930K+ avg. annual GR. Seller willing to help for asmooth transition. Asking $640K.
4241 SF ENDO Seller transitioning into retirement and offering 41 yearpractice in premier downtown building. 1,190 sq. ft. modern office. 4 doctor-days per week with seasoned & loyal staff and excellent referral sources.Asking $463K.
4271 SOUTH SF DENTAL FACILITY Turnkey facility in well knownbeautiful, professional building with dedicated parking lot. Incredible locationwith EZ freeway access to Hwys 280, 380 and 101. Asking only $45K.
4198 PETALUMA DENTAL BUILDING Condominiumized dental officeconveniently located close to Petaluma Valley Hospital and nearby shops,with easy access to Highway 101 and with ample, dedicated parking.Approximately 1,600+ square feet with five (5) fully-equipped operatories setup for right hand delivery. There is a reception area, business office, consultroom, staff lounge, lab, sterilization area, private office and separate storagearea. Asking $495K.
4178 SONOMA COUNTY PERIO Seller retiring from 21 year practice withtrained, seasoned staff and great location. Exceptional 2,100 sq. ft. ampleoffice with 6 fully equipped ops. Majority of equipment purchased in 2002. 4doctor-days & 3 hygiene days per week. Average gross receipts $1M+.Asking $677K.
4191 SONOMA COUNTY ENDO Seller retiring from 38 year endodonticpractice located in attractive ground floor office (remodeled in 2011) withupdated modern equipment and cabinetry. Close to several regular referralsources. Doctor sees an average of 7-8 patients per day. 5 year averageGross Receipts $700K+. Asking $447K.
4225 EUREKA GP & BUILDING Established since 1981 in charmingNorthern California port city. Retiring doctor is offering practice and building.Practice has approximately 1,200 active patients with new patients acceptedon a selective basis. Average Gross Receipts of $765K+ with 61% averageoverhead. Beautiful 1,400 square foot office with four (4) fully-equippedoperatories. Asking price for practice $468K.
4216 SIERRA NEVADA FOOTHILLS 23 year practice located in the heartof the Sierra Nevada foothills in modern building close to downtown area.1,024 square foot office with 4 fully- equipped ops., upgraded majorequipment and digital radiography. Average Gross Receipts $890K+ with56% average overhead. Asking price for practice $604K. Seller is offeringreal estate for sale to the buyer of his practice.
4172 NAPA GP Amazing opportunity to own the practice of your dreams inone of the world’s premier wine destinations! Situated in a primeneighborhood close to many amenities. 1,200 square foot office with 4 fully-equipped and updated operatories. Over 1,000 active patients. Averageannual gross receipts over $700K. Asking price for practice $484K. Buildingavailable for purchase.
4322 MENLO PARK GP Practice in seller owned facility in desireablecorner location in the heart of Menlo Park, 1 block fron Santa Cruz Ave. 60%of patients are private pay. Great upside potential from retiring seller. Asking$25K.
4326 SANTA CLARA GP Practice with an emphasis on Restorativedentistry with over 1,000 active patients located in sought-afterneighborhood close to major routes, shopping centers and hospitals.Approximately 850 sq. ft. facility with 3 fully-equipped ops. pljus a seasonedand loyal staff. Avg. Gross Receipts $617K. Asking $433K.
4324 SF GP Seller offering 33 year in busy financial district building.Gorgeous 890 sq. ft. office with 3 fully equipped operatores, 3 parkingspaces and panoramic views. Average Gross Receips for the past 5 yearsapprox. $419K. Asking price to be determined.
4210 UNION CITY GP Retiring GP offering 40+ years of goodwill. 5 ops in1,100 sq. ft. 350 active patients, all fee-for-service. 2 yr average GR$177K. Asking $85K.
UPCOMING: Saratoga, San Jose & Santa Cruz GPs
carroll.company [email protected] (650) 362-7004 (650) 362-7007
CARROLL& C O M P A N YV “Matching the Right Dentist to the Right Practice”
SOLD
SOLD
SOLD
Mike Carroll Pamela Carroll-Gardiner Mary McEvoy Carroll
Carroll & Company2055 Woodside Road, Suite 160Redwood City, CA 94061BRE #00777682
PENDING
SOLD

Making your transition a reality.
www.henryscheinppt.com 1.888.685.81001.800.519.3458
Dr. Lee Maddox
LIC #01801165(949) 675-5578
Dr. Thomas Wagner
Dr. Russell Okihara
Jim Engel
Kerri McCullough
Gina Miller
Steve Caudill
Thinh Tran
Jaci Hardison
• • • ••

C DA J O U R N A L , V O L 4 6 , Nº 9
S E P T E M B E R 2 0 1 8 593
This article reviews the obligations a dentist-employer or supervising dentist has with regard to informing pregnant employees of the risks
associated with operating radiography equipment and how to reduce those risks. A dentist should inform any female employee in her childbearing years that the fi rst three months of pregnancy are the most important as the embryo/fetus is most sensitive to radiation at this time. Once an employee provides written notice of her pregnancy to a dentist-employer or supervising dentist, it becomes the dentist’s responsibility to ensure that the embryo/fetus is not exposed to occupational radiation exceeding 0.5 rem (5mSv).
The dentist must inform a pregnant employee that:
■ In most cases of occupational exposure, the actual dose received by the embryo/fetus is less than the dose received by the mother because the mother’s body absorbs some of the dose.
■ At the current occupational dose equivalent limits, the risk to the unborn baby is considered small but experts disagree on the exact amount of risk.
■ There is no need for women to be concerned about sterility or loss of ability to bear children because of occupational exposure.
■ Once a pregnancy is known, occupational radiation dose of the embryo/fetus shall be no greater than 0.5 rem (5mSv) for the entire pregnancy. The dose to any embryo/fetus shall be taken as the deep-dose equivalent to
Radiation and PregnancyCDA Practice Support
Regulatory Compliance
the declared pregnant woman. Deep-dose equivalent, which applies to external whole-body exposure, is the dose equivalent at a tissue depth of 1 cm (100 mg/cm2). Special circumstances apply if the pregnant employee has already exceeded this dose prior to declaring her pregnancy.
The dentist should be able to inform the pregnant employee that on-site radiation monitoring or the calculations
A dentist should inform any female employee in her childbearing years that the fi rst three months of pregnancy are the most important as the embryo/fetus is most sensitive to radiation at this time.
C DA J O U R N A L , V O L 4 6 , Nº 9
594 S E P T E M B E R 2 01 8
of a health physicist have demonstrated that radiation exposure at the practice is not likely to exceed 0.5 rem. If it is likely that the employee during the pregnancy will receive a deep dose equivalent in excess of 0.1 rem, then the dentist should provide her with a personal monitoring device (dosimeter).
The dentist and employee can consider and utilize one or more of the following options for protecting the embryo/fetus:
■ Temporary assignment to tasks that involve less risk of being exposed to radiation.
■ Use of a protective apron (full-size, half-size, wrap-around or
SEPT. 2018 REGUL ATORY COMPL IANCE
any other protective clothing appropriate to the situation) while actually exposing patients.
■ Use of monitoring devices such as a fi lm badge worn at the abdomen.
■ Staying out of the X-ray room and behind the protective barrier during exposure.
■ Abiding by the following regulatory prohibitions.
Regulations prohibit dental personnel during patient exposure from:
■ Holding the patient. ■ Holding the image receptor, i.e.,
fi lm, phosphor plate (PSP), CCD or CMOS, in the patient’s mouth.
■ Holding X-ray tube housing, unless a valid exemption is on fi le at the dental facility. An exemption letter for handheld X-ray units can be found on the California Department of Public Health Radiological Health Branch website, cdph.ca.gov/Programs/CEH/DRSEM/Pages/RHB.aspx.
■ Holding the aiming cylinder (also known as PID or pointer cone).
■ Standing in the path of the useful X-ray beam.
■ Standing closer than 6 feet from the patient being radiographed.
Dental personnel must not expose any individual to the useful beam for training or demonstration purposes without a valid X-ray prescription from a licensed dentist or a medical doctor stating a diagnostic need for the exposure.
A sample form to document an employee’s declaration of pregnancy and that she has been informed by the dentist of the potential risks of occupational radiation exposure is available on the CDA Practice Support website. ■
Regulatory Compliance appears monthly and features resources about laws that impact dental practices. Visit cda.org/practicesupport for more than 600 practice support resources, including practice management, employment practices, dental benefi ts plans and regulatory compliance.

6147 SAN FRANCISCO BAY AREA – “OUT-OF-NETWORK” Extraordinary opportunity justifies selling current practice. Location shall realize cash paying patients in perpetuity. 2017 collected $2 Million. 2018 tracking $2.15 Million. Hygiene produces $1+ Million. Practice is rich in patients. Seller available for long transition. 6146 LOWER SACRAMENTO FOOTHILLS Highly regarded practice in great family community. 6-days of hygiene reflects practice’s strong patient foundation. Well laid out office. Great expansion possibilities. 2017 collected $880,000. 2018 projecting $950,000. 6145 MARIN COUNTY’S NOVATO Excellent foundation in this desirable family community. Best location. Beautiful office. Adec equipped throughout with everything new since 2014. 500-active files. 2018 tracking $250,000. Change in owner’s life dictates sale. Full rice $125,000.6144 SACRAMENTO AREA Deeply anchored in its community. Conservative philosophy. 14-days of Hygiene. 3,000 active patients. 2017 collected $1.85 Million. Strong staff. 7-ops in 2,500 sq.ft. suite. Great location. Condo optional purchase. 6143 BERKELEY’S ALTA BATES MEDICAL VILLAGE Perfect opportunity for nearby Delta Premier Dentist to relocate their practice into this stand-alone building on Webster Street. On 3-day week, collections totaled $550,000 in 2017. 4-days of Hygiene saw 1,558 hygiene appointments last 12-months. 4-ops. 6142 OAKLAND’S PIEDMONT - “OUT-OF-NETWORK” 3-ops
and Planmeca ProMax. 2017 collected $667,000. Profits of $300,000+. Successor should be proficient in rtho or willing to learn. Seller available to provide an orderly transition.6141 NAPA VALLEY’S ST. HELENA 3-day per week Delta PPO practice. 3-days of Hygiene. 2017 Collected $359,000. Attractive 3-op office. 15 new patients per month. Full rice $100,000.6140 SAN RAFAEL Dentist retiring after long career. Delta PPO provider. Has averaged $390,000 in annual collections on 26.5-hour week. $223,000+ in Profits in 2017. Full Price $125,000.6139 SAN FRANCISCO BAY AREA PROSTHODONTIC PRACTICE - “OUT-OF-NETWORK” 2017 billed $1.2 Million and collected $1.19 Million. 4-days of Hygiene. Owner can work back to help assist with transition. 6138 SILICON VALLEY Phenomenal opportunity. Best technology, perfectly designed suite and optimum stage to practice your craft. 2017 collected $900,000+ with Profits of $420,000. Perfect for skilled practitioner who seeks to create high-end brand.6135 SONOMA COUNTY’S ROHNERT PARK 2017 collected $1,067,000. Available Profits exceeded $500,000 for second year in a row. 6-days of Hygiene. There shall be no change in fees for Successor. Great family area.6129 FOSTER CITY – “OUT-OF-NETWORK” Wish to infuse your practice with quality patients? Collected $500,000+ in 2017 on part-time schedule. Seller and Hygienist shall relocate into Buyer’s practice to transition patients. Full Price $100,000.6122 SANTA CLARA - STARBUCKS "LIKE" LOCATION! Best exposure in beautiful strip center on El Camino Real. 5-Ops. Delta PPO practice currently trending $1+ Million in Collections on 4-days. Perfect platform to operate 6-days a week. Wants to do $1.5+ Million.
N FRANCISCO BAYAA AREA – “OUT-OF-NETTT
NORTHERN CALIFORNIA(415) 899-8580 – (800) 422-2818
Raymond and Edna [email protected]
California DRE License 1422122
SOUTHERN CALIFORNIA(714) 832-0230 – (800) 695-2732Thomas Fitterer and Dean George
California DRE License 324962
ALTA LOMA Shopping Center. Absentee Owner. Grossing $700,000. Can do $1 Million. BAKERSFIELD 3,000 sq.ft. building. Established 60-years. Can do $1 Million. F $650,000 includes BAKERSFIELD AREA Small City. Grosses $40
-days. 1,800 sq.ft. 5-ops with small apt. F $330,000.BELLFLOWER DDS doing $100,000. 3-ops. Full Price$65,000.CAPISTRANO BEACH Doing $200,000 part-time. Full Price$150,000COLTON Hispanic practice doing $350,000. Absentee Owner.Hands-on Owner will do $500,000 first year. F $285,000.DIAMOND BAR Korean / Chinese Shopping Center. Very busyuntil 9 PM. Owner works 1-day. Does $450,000. Should do $1+Million. F $450,000..GLENDALE / BURBANK Absentee Owner grossing $840,000.Beautiful corner building. Newly renovated. R includes small ap . $2 Million location.INLAND EMPIRE 3,000 sq.ft. building. 7- Adec ops, ConeBeam. Grossing $1.3 Million. F $2.5 Million includes real estate.INLAND EMPIRE DentiCal. Grosses near $300,000. 4-ops. F 150,000.IRVINE Female grossing $1.2 Million. 5-ops.LAKE FOREST Adec equipped. Female DDS grossing $325,000.Buyer shall do $500,000 first year. Option to purchase condo.LA MIRADA H identity shopping center. HMO pays rent. Like new 3-ops with 2-more available. Grossing $450,000.NORTH PASADENA Doing $1 Million. Beautiful. Includes
.ORANGE COUNTY BEACH CITY Absentee Owner. Grossing$550,000. Hands-on Owner will do $1+ Million first year. Valuable R possible.ORANGE COUNTY’S FASHION ISLAND Grossing $650,000.Rare opportunity.PEDO – CHINESE / HISPANIC Grossing $450,000. Longestablished. F $285,000.REDLANDS Long established. Has done $1 Million. Lots ofpotential. Grossing over $400,000.REDLANDS Rent only $1,250 per month.RIALTO HMO 4-to-5 Cap checks per month. Once did $1Million. Asking $285,000RIVERSIDE Grossing near $300,000. 3-ops. Full Price $150,000.SAN DIMAS Emergency Sale!SANTA CLARITA Endo wants to share with Perio or GP.SANTA CLARITA 70,000 autos pass daily. 8-ops. AbsenteeOwner. Full Price $250,000.TEMECULA HMO Grossing $500,000. Hi dentity , 5 ops. F 285UNION PRACTICE Shall do $1 Million. Full Price $775,000.
PracticesWanted
NORT
Specialists in the Sale and Appraisal of Dental PracticesServing California Dentists since 1966
How much is your practice worth??Selling or Buying, Call PPS today!

Largest Broker in Northern California
Over $34.5M in 2017 sales
Extensive Buyer Database &
Unsurpassed Exposure allows us to offer you
Better Candidate
Better Fit
Better Price
BAY AREA CONTINUED DG-844 SAN JOSE: Beloved prac ce delivers quality care and warm rela onships which pa ents have come to expect. 1500sf 3 ops + 1 add’l. $$195k DG-854 SUNNYVALE: Do your best den stry here to an educated, diverse, family-oriented, business-friendly popula on! 782sf w/ 3 ops $$875k DG-862 MID-PENINSULA: Prac ce is a rare gem with up to 7 operatories in the Bay Area!! 1800sf w/ 6ops + 1 add’l. $475k DG-865 SANTA MARIA: Live and prac ce in this desirable collegiate coastal community! 930sf w/ 3 ops $395k DN-771 SOQUEL Facility: The perfect place to sink down roots, raise a family & build an empire! 1100sf w/2 ops + 1 add’l. $$38,500 DG-785 SANTA CRUZ: Great price and cash flow for only 3 days a week!! 1000sf w/ 4 ops. Reduced Price: $190k DG-842 FREMONT: Imagine being able to live, prac ce and play here! 3200 sf w/ 10 ops $$395k DG-857 SAN JOSE: Do the math - this associate-driven prac ce with profitability consistently! 1709 sf w/5 ops $$595k DN-806 WATSONVILLE: This quality, family-oriented prac ce thrives $ focuses on delivering quality care. 1,182 SF W/ 4 OPS. $$495K/ Real Estate TBD DN-845 FREMONT Facility: Build your dream Prac-
ce! Primed for success in this proven loca on! 1800sf w/3 ops + 2 add’l. $$90k
NORTHERN CALIFORNIA EC-729 GREATER SACRAMENTO AREA: Seller re r-ing! FFS Prac ce and Real Estate Available! CCall for details! EN-664 SACRAMENTO Facility: Great corner loca-
on, excellent visibility & easy access! 2300sf w/ 4 ops. NNow Only: $30k EN-747 CITRUS HEIGHTS Facility: Be the only dental office in this a rac ve, popular Retail Shopping Center! 2200sf w/5 ops + 6 add’l. $$75k EN-749 LINCOLN: Come sink your roots down and enjoy a fantas c lifestyle which can’t be beat! 1877sf w/4 ops + 1 add’l. $$320k EN-755 FOLSOM: A perfect loca on, envied by all! Enjoy an amazing quality lifestyle in this thriving city. 1200sf w/ 4 ops. $$175k EN-791 SO. SACRAMENTO CO: Highly esteemed prac ce to an adoring & apprecia ve pa ent base! 1950sfw/ 5 ops. $$450k
BAY AREA AC-649 SAN FRANCISCO Facility: Richmond Dis-trict, 3 ops+1 add’l, Newer Equipment $$120k AC-782 SAN FRANCISCO: Well maintained, mul -level Professional Medical Complex. 1450 sf w/ 5 ops $195k AC-886 SAN FRANCISCO (Facility): Unsurpassed visibility & loca on! Poten al here is limitless! 850 sf w/ 3 ops $85k AG-852 SAN FRANCISCO: PRIME LOCATION! 600 sf w/ 2 fully equipped, computerized ops $$375k AG-871 SAN FRANCISCO: The LOCATION of this office is the envy of all! 600 sf w/ 2 ops $$88k AG-880 SAN FRANCISCO: Seller re ring a er 39 years! Remodeled in 2010. ~ 700 sf w/ 2 ops $$350k BC-710 WALNUT CREEK: Desirable location in stand-alone, single-story bldg. 1313sf w/ 3 ops $150k BC-741 DANVILLE (FACILITY): Move in Ready facility to build the practice of your dreams! ~ 1600sf w/ 3 fully equipped ops $$150k BC-789 OAKLAND (Facility): Perfect layout for Pedo or Ortho. 2800 sf w/ 6 fully equipped ops. Plumb-er for 2 add’l $$135k BG-734 ANTIOCH: The perfect place to work, live and play! Located in desirable professional neigh-borhood. 1,323 sf w/ 4 ops. $$315k BG 838 HAYWARD: If Alameda County is where you want to be, then THIS is the prac ce for you! 800sf w/ 2 ops. $$125k BG-839 PINOLE: Sink your roots into this community which retains many “turn-of-the-century” buildings! 1212sf w/ 3 ops + 1 add’l. $$350k CC-798 PETALUMA: Partially equipped dental office for lease. Only $2500/mo for 1400 sf! Call for De-tails! CC-802 SANTA ROSA: Retail shopping center w/ 1200 sf and 4 fully equipped ops $$220k or $260k w/CT Scanner CC-846 SAN RAFAEL: Prof/Retail Building Complex. 3 ops 640 sf Collections $433k in 2017 $$295k CG-616 NAPA: State-of-the-Art practice. Seller mov-ing out of state! $$425k CG-859 SONOMA: On track to collect over $700k in 2018! 2000sf w/ 4 ops highly esteemed FFS Practice $395k CN-878 VALLEJO: Highly desirable thriving communi-ty! 2 story prof bldg. 2000 sf w/4 ops $$315k DC-812 REDWOOD CITY Facility: Reasonable rent and great landlord! 740 sf w/ 3 fully equipped ops $65k
NORTHERN CALIFORNIA CONTINUED EG-788 ROSEVILLE:
. Reduce Price $275k/ Real Estate Available EG-849 AUBURN:
$350k EG-887 FOLSOM Facility:
Priced for quick Sale! $50k EN-800 SACRAMENTO:
Seller Mo vated! $150k EN-797 WOODLAND:
Prac ce $575k/ Real Estate TBD EN-831 SACRAMENTO“a cut above” Now Only: $650k EN-836 CITRUS HEIGHTS:
$188k EN-824 SIERRA FOOTHILLS:
$625 EN-858 ORANGEVALE:
Priced to Sell Only $70k! EN-885 ROSEVILLE Facility:
$95k FC-650 FORT BRAGG:
$350k for the Prac ce & $400k for the Real Estate FG-841 ARCATA:
$275k/Real Estate TBD FN-754 SO. HUMBOLDT:
Now $150k! FN-855 NO. HUMBOLDT:
$275kGG-769 REDDING AREA:
Prac ce $390k/ Real Estate $540k GN-799 PARADISE:
Prac ce $375k, Real Estate $325k GN-808 CHICO:
$395k/ Real Estate TBD GN-853 REDDING:
$595k GN-884 YUBA CITY Real Estate w/ Equip:
$400kHG-732 GRASS VALLEY:
$205kHG-815 SIERRA CO: Reduced Price: $165k/ Real Estate $437k HG-827 SO. LAKE TAHOE:
$310k HG-851 SO LAKE TAHOE:
$425k HN-618 SIERRA FOOTHILLS:
$65k HN-740 SHASTA CO:
$475k/ Real Estate $350k
NORTHERN CALIFORNIA CONTINUED HN-773 SUTTER CREEK: Seller Mo vated!
! $175k HN-816 CHESTER/ALMANOR AREA:
Prac ce $140k/ Real Estate TBD HN-879 SONORA:
$275k
CENTRAL VALLEY & SOUTHERN CALIFORNIA IC-468 SAN JOAQUIN VALLEY
$425k IG-832 OAKHURST:
$235k/ Real Estate 375kIG-881 TURLOCK:
$360K IN-764 STOCKTON:
$267.5k JC-811 FRESNO COUNTY:
$350kJC-823 LOS BANOS:
$80kJG-778 FRESNO:
$275k JG-807 FRESNO:
Seller Mo vated $99k KG-779 SAN CLEMENTE Ortho:
$325k/ Real Estate Available! Call for Details!
SPECIALTY PRACTICES AC-748 SAN FRANCISCO Perio:
$750kBC-784 CENTRAL CONTRA COSTA CO Perio:
$395kBG-843 WALNUT CREEK Perio:
$645kEG-826 ROSEVILLE Perio:
$150kEN-821 DAVIS Perio:
$385k EN-822 SACRAMENTO Perio:
$790k IC-543 CENTRAL VALLEY Ortho:
$125k JG-757 VISALIA Perio:
Reduced Price: $350k
800.641.4179 [email protected] “ASK THE BROKER” WWW.WESTERNPRACTICESALES.COM

Largest Broker in Northern California
Over $34.5M in 2017 sales
Extensive Buyer Database &
Unsurpassed Exposure allows us to offer you
Better Candidate
Better Fit
Better Price
BAY AREA CONTINUED DG-844 SAN JOSE:
$195kDG-854 SUNNYVALE
$875kDG-862 MID-PENINSULA:
$475k
DN-771 SOQUEL Facility:
$38,500 DG-785 SANTA CRUZ:
Reduced Price: $190k DG-842 FREMONT:
$395kDG-857 SAN JOSE:
$595k DN-806 WATSONVILLE:
$495K/ Real Estate TBD DN-845 FREMONT Facility:
$90k
NORTHERN CALIFORNIA EC-729 GREATER SACRAMENTO AREA:
Call for details!EN-664 SACRAMENTO Facility:
Now Only: $30k EN-747 CITRUS HEIGHTS Facility:
$75k EN-749 LINCOLN:
$320k EN-755 FOLSOM:
$175k EN-791 SO. SACRAMENTO CO:
$450k
BAY AREA AC-649 SAN FRANCISCO Facility:
$120k AC-782 SAN FRANCISCO:
$195kAC-886 SAN FRANCISCO (Facility):
$85k AG-852 SAN FRANCISCO:
$375k AG-871 SAN FRANCISCO:
$88k AG-880 SAN FRANCISCO:
$350kBC-710 WALNUT CREEK:
$150kBC-741 DANVILLE (FACILITY):
$150kBC-789 OAKLAND (Facility):
$135kBG-734 ANTIOCH:
$315k BG 838 HAYWARD:
$125k BG-839 PINOLE:
$350k CC-798 PETALUMA:
CC-802 SANTA ROSA:$220k or $260k w/CT
ScannerCC-846 SAN RAFAEL:
$295kCG-616 NAPA:
$425k CG-859 SONOMA:
$395kCN-878 VALLEJO:
$315kDC-812 REDWOOD CITY Facility:
$65k
Jon B. Noble, MBA Mona Chang, DDS John M. Cahill, MBA
NORTHERN CALIFORNIA CONTINUED EG-788 ROSEVILLE: Do not pass up on this remarkable opportunity! 2700sf w/ 6 ops.. Reduce Price $275k/ Real Estate Available EG-849 AUBURN: Peaceful, rural town that has an ideal climate and “big city” ameni es less than an hour away. 1400 sf w/ 4 ops $350k EG-887 FOLSOM Facility: Build the prac ce of your dreams here! 1200 sf w/ 2 ops Priced for quick Sale! $50k EN-800 SACRAMENTO: Awai ng your talent and skill to take it to the next level! 1200sf w/ 4 ops. SSeller Mo vated! $150k EN-797 WOODLAND: Do not hesitate or this enviable opportunity will fulfill someone else’s dream! 2316sf w/ 6 ops. PPrac ce $575k/ Real Estate TBD EN-831 SACRAMENTO: Loca on & prac ce philosophy make this opportunity “a cut above” others! ~1600sf w/4 ops. NNow Only: $$650k EN-836 CITRUS HEIGHTS: well-established, quality prac ce comes loaded W/ 30+ years of goodwill. 1300sf w/3 ops + 2 add’l. $$188k EN-824 SIERRA FOOTHILLS: well-known, well-loved, well-established prac-
ce focused on quality dental care! 1000sf w. 4 ops. $$625 EN-858 ORANGEVALE: Perfect for a second loca on or satellite situa on! 850 sf w/ 3 ops. PPriced to Sell Only $70k! EN-885 ROSEVILLE Facility: Looking for the ideal loca on, great visibility, and close to just about anything? Here it is! 1000sf w/3 ops. $$95k FC-650 FORT BRAGG: Family-oriented prac ce. 5 ops in 2000sf, 6 npts/mo $$350k for the Prac ce & $400k for the Real Estate FG-841 ARCATA: Live and own a little slice of heaven, when you practice here! 1114sf w/3 ops $$275k/Real Estate TBD FN-754 SO. HUMBOLDT: Sea air, a relaxed lifestyle & charm of coastal living, then look no further! 1500sf w/ 3 ops + 1 add’l. NNow $$150k! FN-855 NO. HUMBOLDT: This long-established, quality 100% fee-for-service prac ce could be yours! 1600sf w/ 3ops + 1 add’l. $$275k GG-769 REDDING AREA: Offering a full spectrum of general den stry and total care! 2700sf w/ 6ops. PPrac ce $390k/ RReal Estate $540k GN-799 PARADISE: This remarkable opportunity is undeniably too good to be true! 1800sf w/ 4 ops. PPrac ce $375k, Real Estate $325k GN-808 CHICO: It just doesn’t get any be er than this! Hesitate & you might miss out! 2800sf w/ 5 ops. $$395k/ Real Estate TBD GN-853 REDDING: A great place to visit…and an even be er place to live, work and play! 1450sf w/ 5 ops $$595k GN-884 YUBA CITY Real Estate w/ Equip: Designed specifically w/ pa ent flow &efficiency in mind. 1750sf w/ 5 ops. $$400k HG-732 GRASS VALLEY: Seller retiring. Well established practice. 1250sf w/ 3 ops. Real Estate also available. $$205k HG-815 SIERRA CO: Perfect location for outdoor enthusiast! 1000 sf w/ 3 ops Reduced Price: $165k/ Real Estate $437k HG-827 SO. LAKE TAHOE: Ski, live, play and prac ce here where your lifestyle can’t be beat! 1200sf w/4 ops. $310k HG-851 SO LAKE TAHOE: Don’t wait another day to start living your dream of a serene lifestyle! 2100 sf w/ 5 ops $$425k HN-618 SIERRA FOOTHILLS: Seller Retiring! Huge opportunity for growth by increasing office hours! 750sf w/ 2 ops $$65k HN-740 SHASTA CO: Well-established prac ce, excep onal long-term staff. 2400+sf w/5 ops + 1 add’l. $$475k/ Real Estate $350k
NORTHERN CALIFORNIA CONTINUED HN-773 SUTTER CREEK: Seller Mo vated! Loca on known for beau ful scen-ery, excellent wine & rich history! 1536sf w/4 ops + 1 add’l!! $175k HN-816 CHESTER/ALMANOR AREA: The perfect place to work, live and play! Do not hesitate, or this prac ce will be gone! 1250 sf w/ 4ops. Prac ce $140k/ Real Estate TBD HN-879 SONORA: Live and prac ce in the cap va ng beauty of this family-oriented, scenic town in Tuolumne County! 2950 sf w/ 3 ops $275k
CENTRAL VALLEY & SOUTHERN CALIFORNIA IC-468 SAN JOAQUIN VALLEY: High-end restora ve prac ce! 6 ops in 2500+sf office. Call for Details! $$425k IG-832 OAKHURST: Have you ever dreamed of living and prac cing by beau-
ful mountain ranges, surrounded by nature? 2048sf w/3 ops + 1 add’l. $235k/ Real Estate 375k IG-881 TURLOCK: Offering a philosophy to provide “Nothing but the Very Best” in dental care! 10 ops $$360K IN-764 STOCKTON: Well-established, fully computerized, paperless, digital-ized prac ce just wai ng for your talent & skill! 5,000sf w/10 ops $$267.5k JC-811 FRESNO COUNTY: Amazing Opportunity! Considerable Goodwill in Community! 3,000 sf w/ 6 ops $$350k JC-823 LOS BANOS: Unique opportunity. Heavy emphasis on hygiene. Growth poten al by increasing DDS days. 1000 sf w/ 3 ops $$80k JG-778 FRESNO: What a steal. Consistent collec ons over $600k with cash flow over $300k!! 1452 sf w/ 4 ops $$275k JG-807 FRESNO: Reasonable Overhead, Stellar Reputa on, Excellent Loca-
on! 1000 sf w/3 ops SSeller Mo vated $$99k KG-779 SAN CLEMENTE Ortho: Huge growth potential by expanding relaxed work week! 2896 sf w/ 6 open bay chairs $$325k/ Real Estate Available! Call for Details!
SPECIALTY PRACTICES AC-748 SAN FRANCISCO Perio: Reputable PERIO practice with million dollar Bay views! 980 sf w/ 3 ops $$750k BC-784 CENTRAL CONTRA COSTA CO Perio: Seasoned Staff. Office runs like well-oiled machine! 3 ops $$395k BG-843 WALNUT CREEK Perio: Collec ons over $1M! Desirable area w/20-30 new pts per month. Professional building on major thoroughfare $645k EG-826 ROSEVILLE Perio: Create your success story with this warm and car-ing, pa ent-centered prac ce! 1000sf w/3 ops + 1add’l $$150k EN-821 DAVIS Perio: Live, prac ce & play here! It’ll be the BEST decision you’ll ever make! 1700sf w/4 ops + 1 add’l. $$385k EN-822 SACRAMENTO Perio: This prac ce is known throughout Sacramento for its stellar reputa on! 2200sf w/ 5 ops + 1add’l. $$790k IC-543 CENTRAL VALLEY Ortho: 1650sf w/ 5 chairs in open bay & plumbed for 2 add’l. Strong referrals and PT base $$125k JG-757 VISALIA Perio: Keep implants in house and imagine the growth possibilities! 9 hygiene days per week! Rare Gem! 2,000 sf w/ 5 ops Reduced Price: $350k
Edmond P. Cahill, JD Timothy Giroux, DDS
800.641.4179 [email protected] “ASK THE BROKER” can now be found at WWW.WESTERNPRACTICESALES.COM

C DA J O U R N A L , V O L 4 6 , Nº 9
598 S E P T E M B E R 2 01 8
A look into the latest dental and general technology on the market
Tech Trends
Malwarebytes Mobile Security (Free 30-day trial period, $1.49 monthly, $11.99 annually, Malwarebytes)
Malicious software, otherwise known as malware, infects a multitude of computers daily as users check their email and view sites on the internet. Most users are unaware that malware can also aff ect mobile devices, including smartphones and tablet computers. Ransomware, phishing scams and other potentially dangerous threats may arise when users unknowingly visit fake websites. Recent security breaches have given scammers access to mobile phone numbers to spam and text unsuspecting individuals. Malwarebytes for iOS protects users and their privacy by preventing attempts to disrupt their mobile device experience.
Malwarebytes for iOS requires a premium, in-app subscription to enable web and call protection. Ad blocking and text message fi ltering are complimentary and do not require a subscription to enable. All protection features are prominently displayed on the main dashboard, where users can activate them by following simple provided instructions to enable in iOS settings. After the features have been activated, the protection works in the background seamlessly, requiring no user intervention. Websites visited in Safari no longer display ads, providing users with a faster browsing experience. Attempts to visit known fraudulent websites will display a blocked URL message. Users receiving calls from scammers or spoofed numbers will see a warning on their screen that a fraudulent call is suspected. Users can also customize settings to block any suspected fraudulent calls without warning. Suspicious texts from senders not in a user’s contact list are fi ltered in to a junk tab in the Messages app, where users can review them with caution.
As the threat of malware continues to increase, cybersecurity is essential to maintaining user privacy and experience on the internet. Malwarebytes for iOS is an invaluable tool for mobile device users to keep their experience focused on the content that matters to them the most.
— Hubert Chan, DDS
Unsplash (Free to join)
First impressions are lasting impressions. Appropriate, high-quality photographs can enhance the impact of a practice’s marketing material, especially when patients are inundated with options for dental providers through social media, online promotional ads and crowd-sourced review apps. Frustratingly, taking professional photographs that connect with patients is a challenging, time-consuming process. Furthermore, photographs taken from online sources like Google Images are often protected, opening those who use them without permission to potential litigation.
Fortunately, there is a solution to this issue.
Unsplash is one of the world’s leading photography websites, boasting more than a half million, completely free-to-use photographs. Since 2013, companies like Apple, Google and Adobe (as well as countless individuals worldwide) have used photos from the Unsplash website to support their presentations, convention booths and online presence. In April 2018, Unsplash launched its free iOS app, putting its formidable archive of pictures in the palm of users’ hands.
Unsplash’s iOS app is uncluttered and easy to navigate, reminiscent of its website. When the app is launched, users are greeted with a simple search bar and a list of interesting photos to scroll through. Recent searches are saved; trending images — popular searches by other Unsplash users — are shown below the recent search history. After inputting a search, photographs appear in a list for users to scroll through. To download a photograph, users can either drag an image to the lower left-hand corner of the screen (thereby never leaving the search list screen) or tap on the individual photo to see a full-screen preview, then tap on the download icon. At the full-screen preview, users also have a host of other options to share the picture, such as copying to Dropbox, sharing directly on Instagram, emailing, text messaging and more. The photographer’s name is displayed in the Unsplash application, allowing users to give credit and feedback to the photographer, a practice that is encouraged by Unsplash. By putting the Unsplash photo archive into a mobile platform, dental practitioners can readily incorporate high-quality, free-to-use images in their study club presentations, social media marketing campaigns or in-offi ce forms without fear of running afoul with copyright laws.
— Alexander Lee, DMD

[ FIND YOUR WONDER ]
REGISTER TODAY AT cdapresents.com
The Art and Science of Dentistry
EXPLORE
®
EXPLORE INNOVATIVE TECH. SHOP 400+ EXHIBITORS AND SAVE
WITH DEALS AND DISCOUNTS
EXCLUSIVE TO THE CONVENTION.

Haleigh, from the United States—a hairstylist, gamer, and athlete—
smiles because she loves to be herself. Opalescence Go® prefilled whitening
trays are the perfect way to whiten on her busy schedule. For many patients a
brighter, whiter smile is all they need to shine. That’s the power of a smile.
Find out more at ultradent.com/mysmileispowerful.
800.552.5512 | ultradent.com© 2018 Ultradent Products, Inc. All rights reserved.
RadiantM Y S M I L E I S
#MYSM I L E I S P OWER FU L